User login
Expert tips for adnexal surgery through the laparoscope
The authors report no financial relationships relevant to this article.
CASE 1: Cystic mass in patient’s only remaining ovary
Mrs. R is a 29-year-old G1P1 who underwent a right oophorectomy, with a midline incision, for a dermoid cyst at the time of cesarean delivery. She now has a left ovarian cyst. Preoperative ultrasonography (US) reveals that it measures 3.5×4.2×3.7 cm and has both solid components and a multiloculated appearance, consistent with a dermoid cyst.
How common is this scenario?
Studies predict that one of every three women will undergo surgical management of an adnexal mass at some point in her life.1 This troubling statistic prompts several critical questions:
- How do we handle the workup for these women so that only appropriate patients undergo surgery?
- How often will a mass be malignant?
- How can we safely remove an adnexal mass to maximize patient safety, reduce overall recovery time, and prevent less favorable outcomes in women who are eventually found to have a malignancy?
A thorough workup and, sometimes, conservative management can prevent unnecessary surgery that may lead to early menopause or surgical complications. And maximizing the use of minimally invasive techniques in women who do require surgery can shorten hospital stay and recovery time. At the time of surgery, careful abdominal entry and meticulous surgical dissection and mass removal can limit the potential risks of laparoscopic excision in women who have an ultimate diagnosis of cancer.
In this article, we review the workup for women who have an adnexal mass, describe patient-selection criteria for laparoscopic surgery, including the risks and benefits of this approach ( TABLE 1 ), and present several techniques to safely manage a mass with potentially malignant histology via laparoscopy.
TABLE 1
There are benefits and risks to managing an adnexal mass laparoscopically
| Benefit | Risk |
|---|---|
| Shorter recovery Fewer adhesions Decreased overall cost Magnification Decreased pain and narcotic use Fewer wound complications | Expensive equipment* Loss of tactile sensation Concern for malignancy Risk of tumor dissemination/spillage/chemical peritonitis Trocar-site metastasis |
| *Though greater expense is not a risk per se, it does enter into decision making. | |
Begin with the physical
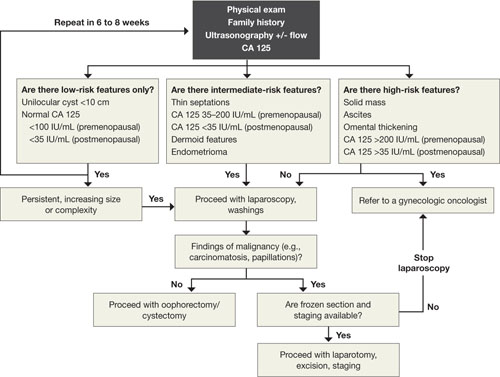
When a woman is known to have a pelvic mass, the aim of the office exam is to 1) identify characteristics that suggest malignancy and 2) rule out nongynecologic causes of the mass. Physical findings that are worrisome for a malignant process include:
- fixed or nodular pelvic mass
- bilateral masses
- nodular abdominal mass
- ascites
- pleural effusion on auscultation or percussion of the lung.
Although these findings can be present under benign conditions, they increase the risk that a malignancy will be detected at surgery.
Other causes of a pelvic mass should also be considered, including infection (pelvic abscess) and tumors of the colon, particularly when the pelvic mass occurs on the left side.
Some symptoms, though vague, are worth noting
Although ovarian cancer was once thought to be a silent disease, recent research has shown that bloating, pelvic or abdominal pain, early satiety, and urinary frequency and urgency are more common among women with ovarian cancer than among healthy controls and patients in high-risk screening clinics.2-4 Although these symptoms are generally nonspecific, they merit attention if they occur more than 12 times a month and have been present for less than 1 year. When they meet these criteria, the symptoms have a sensitivity for diagnosing early- and late-stage ovarian cancer of 56.7% and 79.5%, respectively.4
Sensitivity for the diagnosis of early-stage ovarian cancer may be as high as 80% when the symptom index score is combined with an elevated level of the tumor marker CA 125.3
Transvaginal US is crucial
Transvaginal US is now standard practice to obtain high-resolution images of an adnexal mass. Grayscale US has traditionally been used alone for evaluation.
Specificity is typically lower in women who are premenopausal because many benign lesions, such as endometrioma, have a similar sonographic appearance to cancer.
A number of US scoring algorithms have now been proposed to aid in the triage of women who have an adnexal mass. Sensitivity of these algorithms ranges from 65% to 100%; specificity, from 77% to 95%.5
CA 125 is the standard tumor marker
For the past two decades, CA 125 has been the standard serum marker in the screening of high-risk women for ovarian cancer and the triage of women who have an adnexal mass.
This blood test has been studied widely since its introduction in 1983. It typically has sensitivity of 75% to 85% and specificity of 85% to 95% in identifying women who have ovarian cancer. However, it is elevated in only 50% to 60% of women who have stage I ovarian cancer. Its lack of specificity and poor positive predictive value have kept researchers busy trying to identify other serum markers, for both ovarian cancer and identification of high-risk pelvic masses.
Our recommended workup and management of adnexal masses In postmenopausal women who had a pelvic mass, one study found that a CA 125 level above 65 IU/mL had sensitivity of 71% and specificity of 92.5% in the identification of ovarian cancer.6 Another group found that CA 125 levels above 65 IU/mL were more than 95% sensitive in the diagnosis of ovarian cancer in postmenopausal women.7
Several studies have combined CA 125 with other markers or with US to screen high-risk women or triage those who have an adnexal mass. These studies have shown modest improvements in sensitivity but usually lower specificity than with CA 125 testing alone.
Markers that may be used for suspected sex cord stromas and germ-cell tumors are:
- lactate dehydrogenase (LDH) for dysgerminomas
- alpha-fetoprotein (AFP) and human chorionic gonadotropin (hCG) for yolk sac tumors
- testosterone for Sertoli-Leydig cell tumors
- inhibin A and B for granulosa cell tumors.
An algorithm for working up and managing adnexal masses appears above.
How to gain abdominal access
In the opening case, the patient clearly has a benign mass. The treatment? Safe entry into the peritoneal cavity to remove the cyst and as little normal tissue as possible. This is critical in this patient because she has only one ovary.
Peritoneal access for abdominal and pelvic laparoscopy has been studied widely. Options include:
- direct insertion using a Veress needle
- open laparoscopy
- direct trocar insertion.
The technique usually depends on the preference of the surgeon. The primary goal of abdominal entry is to minimize the risk of injury, particularly unrecognized injury.
Data on complication rates show no definite benefit for open versus closed techniques in the prevention of injury to underlying viscera. However, evidence does suggest that the open technique may lower the risk of major vascular injury.8
We employ direct trocar insertion using radially expanding or optical trocars.
The Veress needle option
When the Veress needle is used to gain intraperitoneal access, data indicate that initial intraperitoneal pressure below 10 mm Hg is a reliable marker for peritoneal entry, even in obese patients.9 Insufflation pressure as high as 25 to 30 mm Hg prior to placement of the initial trocar is safe from a cardiopulmonary standpoint and may allow easier entry with a nonbladed trocar.10
Tests to confirm intraperitoneal placement of the Veress needle, such as the hanging-drop test or saline flush, do not appear to offer any additional useful information.11
Open laparoscopy is suitable when adhesions are unlikely
Open laparoscopy is typically performed by making a minilaparotomy incision at the umbilicus and then dissecting and entering the peritoneal cavity. A blunt-tip trocar is inserted.
The disadvantage of this approach is that there may be extensive adhesions under the umbilicus, and it is difficult to dissect such adhesions sufficiently to introduce a cannula and laparoscope. Adhesions left behind often obscure the field of view after introduction of the trocar.
Our preference? Left upper-quadrant insertion
In Case 1, the previous midline incision mandates an alternative approach. When abdominal entry at the umbilicus is unsuccessful or potentially difficult because of an earlier midline incision, umbilical hernia repair, or history of multiple lower abdominal or pelvic surgeries, a left upper-quadrant insertion is useful. It is, in fact, our preferred technique, and involves a small incision at the midclavicular line 5 cm below the left costal margin, at a site called Palmer’s point.
The direction of insertion usually ranges from 45° to 90°, depending on the patient’s body weight. If the trocar is placed properly, the closest organs are the stomach and the left lobe of the liver (4 to 6 cm).12 Given the stomach’s close proximity, it should be decompressed with an orogastric tube prior to trocar insertion.
Several studies have demonstrated the safety and efficacy of this entry technique.12-14 It can be helpful in cases that involve difficult access. We usually use a 5-mm primary trocar site for a 5-mm laparoscope. Modern optics allow for a pristine view with these small scopes, eliminating the need to close fascia and perhaps causing less pain at the incision.
Accessory trocar sites facilitate complex technique
We usually use three accessory sites. Two of them are lower-quadrant ports that are placed 2 cm medial and 2 cm cephalad to the anterior superior iliac spine. This area generally lies well away from the inferior epigastric vessels and remains above the area of the ilioinguinal and iliohypogastric nerves, making it a safer point of insertion.15 One trocar is 5 mm in size and the other is 10 mm. The larger one is used to extract the specimen.
We place an additional 5-mm port lateral to the rectus muscle at the level of the umbilicus. This allows the principal surgeon to use two instruments (a toothed forceps and scissors) comfortably while the assistant holds the laparoscope and assists with a grasper.
Does the type of trocar matter?
No randomized studies have directly compared all types of trocars. Options include:
- a pyramidal tip (as in reusable trocars) or shielded tip
- radial expansion
- visible entry
- blunt (Hasson-type) trocar.
Safety data on direct comparison of trocars are limited, but it appears that a radially expanding trocar may offer less port-site pain and potentially less bleeding than a traditional cutting trocar.16 Moreover, the rate of hernia at the port site appears to be relatively low with a radially expanding trocar, even when fascia is left unclosed at a 10-mm site.17
None of these trocars appears to be clearly superior at avoiding visceral or vascular injury.
Technique of laparoscopic cyst removal
A video clip of the surgery is linked to this article in the Video Library at www.obgmanagement.com. In this case, a trocar was inserted in the left upper quadrant, and a laparoscopic cystectomy was initiated using the trocars already specified.
The peritoneal cavity and adnexa were inspected, followed by pelvic washings, as detailed in TABLE 2 . Next, the ovarian cortex was incised ( FIGURE 1A ) with scissors using bipolar or unipolar energy, typically at a low power setting, such as 12 to 15 watts.
It was relatively easy to develop a tissue plane between the cortex and underlying dermoid cyst using simple or aqua-dissection ( FIGURE 1B and C ). The cyst was enucleated without rupture and inserted into a specimen bag through a 10-mm port ( FIGURE 1D ). (The specimen bags generally are available in 10-mm and 15-mm sizes.) Once the trocar was removed, the entire specimen was brought out through the incision ( FIGURE 1E ).
Cystic masses can generally be carefully aspirated using a laparoscopic needle or angiocath, or they can be incised and drained using a standard suction device. Manufacturers of most specimen bags do not recommend the morcellation of tissue within the bag because of the potential for rupture of the bag with tumor spillage or injury to underlying structures.
Occasionally, the mass remains too large to remove after drainage of the cyst fluid. Remedies include enlarging the port site with a scalpel or using a gallbladder speculum to increase the diameter of the port site ( FIGURE 1E ). If possible, the incision should be large enough to deliver the entire bag intact. Use of excessive force will rupture the bag and may cause the specimen to be lost or malignant cells to be inadvertently spilled (in the case of a cancer diagnosis).
TABLE 2
Take these 10 steps to safe laparoscopic surgery
| Examine the anesthetized patient |
| Enter the abdomen |
| Inspect the mass and peritoneal surfaces, including the diaphragm. Biopsy sites suspicious for metastasis and obtain frozen section |
| Perform pelvic and abdominal washings |
Closely inspect adnexa. If findings are not suggestive of malignancy, proceed with laparoscopy. If findings indicate obvious malignancy
|
Perform cystectomy or oophorectomy
|
| Inspect for hemostasis |
| Place cyst/ovary in endopouch |
| Open bag at abdominal wall and remove for frozen section |
| Reinspect and close |
Avoid:
|

FIGURE 1 Laparoscopic cyst removal
Begin by incising the cortex using scissors with or without an energy source. 
Dissect the cyst free from the cortex using sharp dissection. 
Remove the cyst from the ovary. 
Place the cyst in a specimen bag, and … 
… bring it to the surface for extraction. The abdominal incision may have to be enlarged to accommodate the specimen.
CASE 1: OUTCOME
The patient’s cyst is removed intact and she is discharged home. Rupture of a dermoid cyst is not associated with any problems as long as copious irrigation is used to aspirate the cyst content.18 Other cysts, such as endometriomas, may not be as easily dissected, and rupture is inevitable.
CASE 2: Symptoms suggestive of cancer
Mrs. B is a 47-year-old woman who reports abdominal bloating for the past 3 weeks. She also complains of early satiety and occasional constipation. She has no history of cancer, but her sister was given a diagnosis of breast cancer at 41 years of age, and her maternal aunt had breast cancer at 55 years.
Mrs. B is moderately obese, with a nontender abdomen and no palpable mass. Her pelvic exam also is negative for a mass or nodularity, but the extent of the exam is limited by body habitus. Her physician orders a transvaginal US, which reveals a 6-cm complex mass with thin septation and a 1-cm solid nodule, with no definite blood flow. The patient’s CA 125 level is 80 IU/mL, which we consider to be within the low-risk range for a premenopausal woman.
The patient is counseled about the need to have the mass removed and is scheduled for laparoscopic right salpingooophorectomy. Given the family history of breast cancer, the physician also requests consultation with a gynecologic oncologist, who agrees to assist with surgery and perform a laparotomy and staging in the event that a malignancy is diagnosed.
Is the mass likely to be malignant?
Given the patient’s family history of breast cancer, the recent onset of symptoms associated with ovarian cancer,2 and the characteristics of the mass (complex, with a nodule), malignancy is possible. This patient has an intermediate risk of cancer and requires additional counseling and planning.
However, most women who undergo laparoscopy for removal of an adnexal mass have benign pathologic findings.
What is the real risk of ovarian cancer?
The lifetime risk of developing ovarian cancer in the general population remains stable at approximately 1 in 70 women, with a mean age at diagnosis of 63 years.19 Ninety percent of ovarian cancer cases are sporadic, and less than 10% can be linked to genetic syndromes.
Women who have mutations in the BRCA1 gene carry a lifetime risk of ovarian cancer of up to 50%, and women who have mutations in BRCA2 have a lifetime risk of up to 25%.20,21 Women who have mutations associated with Lynch II syndrome or Hereditary Nonpolyposis Colorectal Cancer syndrome may have a lifetime risk of ovarian cancer of 12%.22,23
Some women who have a strong family history of breast and ovarian cancer do not carry a known mutation, but are likely to be at increased risk.
Additional risk factors known to be associated with ovarian cancer are nulliparity and infertility. However, the single most important risk factor for epithelial ovarian cancer is age.
Risk-reducing strategies include:
In the case of PBSO, it is imperative to ensure that all ovarian surface epithelium is removed. This means excising the infundibulopelvic ligament at least 1.5 cm above the proximal end of the ovary and excising any adjacent tissue to which the ovary is adherent (including pelvic sidewall peritoneum). Both requirements are easily achieved using the techniques outlined here.
Who should perform surgery?
The American College of Obstetricians and Gynecologists (ACOG) and the Society of Gynecologic Oncologists (SGO) have published guidelines for referral to a gynecologic oncologist ( TABLE 3 ). When Im and colleagues reviewed the records of more than 1,000 women who underwent surgery for a pelvic mass at six institutions over 12 months, they found that 70% of premenopausal women and 94% of postmenopausal women who were diagnosed with ovarian cancer were properly referred to a qualified subspecialist.27 “Over”-referral occurred in 30% to 40% of women who had a benign mass, but may be preferable given the importance of proper staging and debulking to survival.
ACOG and the SGO recommend referral for women who have:
- elevated tumor markers
- ascites
- a fixed or nodular mass
- a strong family history of breast or ovarian cancer.
Consider preoperative referral of all high-risk and, probably, intermediate-risk women, depending on the availability of qualified specialists for complete surgical staging.
In addition, women need to be counseled thoroughly about the possibility that a malignancy will be diagnosed by frozen section, necessitating additional surgical procedures.
TABLE 3
Your patient has a newly diagnosed pelvic mass. Should you refer her?
| Is she premenopausal? Then refer her when… | Is she postmenopausal? Then refer her when… |
|---|---|
| CA125 >200 IU/mL Ascites is present Evidence of abdominal or distant metastasis on exam or imaging Family history of breast or ovarian cancer in a first-degree relative | CA125 >35 IU/mL Ascites is present Nodular or fixed pelvic mass Evidence of abdominal or distant metastasis on exam or imaging Family history of breast or ovarian cancer in a first-degree relative |
Technique of laparoscopic adnexectomy
In Case 2, an umbilical site was chosen for the primary cannula. In general, the direction of insertion depends on the patient’s body habitus. Heavier patients have a thicker abdominal wall and an umbilicus below the level of the aortic bifurcation. In these women, the angle of insertion should be adjusted from the usual 45° (for patients of normal weight) to an angle nearer to 90°. Lateral ports are typical, as in Case 1.
Treat every mass like cancer
Laparoscopic excision of an adnexal mass can be safe and effective, with better outcomes and recovery than with laparotomy, provided the surgeon adheres to basic principles ( TABLE 2 ). This means treating every mass as though it is potentially malignant, and thoroughly inspecting the abdominal cavity before and after excision of the mass.
Know the retroperitoneal space
As with Case 1, successful laparoscopic excision of an adnexal mass begins with inspection of the peritoneal cavity, abdominopelvic washings, and identification of both the infundibulopelvic ligament and ureter. Knowledge of the retroperitoneal space can be of great value in difficult cases that involve significant pelvic adhesions or sidewall fibrosis. We generally use a retroperitoneal approach for laparoscopic adnexectomy ( FIGURE 2A ).
In our typical approach, we incise the peritoneum lateral to the uteroovarian ligament and continue the incision up the pelvic sidewall lateral to the infundibulopelvic ligament and up along the paracolic gutter, if needed ( FIGURE 2A ). We then mobilize the medial leaf of the broad ligament from the sidewall using blunt dissection between the external iliac vessels laterally and the ureter medially ( FIGURE 2B ).
Once we have identified the ureter, we use scissors to create a window in the medial leaf of the broad ligament just beneath the gonadal vessels. We then use an energy source to occlude and transect the pedicle. Using this technique, we secure the infundibulopelvic ligaments and safely mobilize the ureter before initiating more aggressive sidewall dissection distally for adhesions or fibrosis.
Once the ureter is mobilized, we excise the involved peritoneum along with the mass. We then seal and transect the uteroovarian ligament.

FIGURE 2 The retroperitoneal approach
Grasp and incise the peritoneum just lateral to the adnexal mass and enter the retroperitoneal space, where loose areolar tissue is visible, with the ureter seen on the medial leaf of the broad ligament. 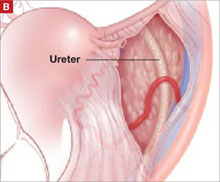
After dissecting this tissue, identify the ureter and internal iliac vessels.
Remove the mass in a bag
Once the mass is excised, we place it in a laparoscopic bag, as described for Case 1. Solid adnexal masses are problematic because they are not amenable to drainage, and morcellation is usually discouraged. Laparoscopic excision can still be carried out, and a minilaparotomy or posterior colpotomy can be used to extract the mass in a bag. Patients managed in this way still have a complication rate similar to or lower than that of patients undergoing laparotomy for oophorectomy; they also recover faster.
Risks in cases of malignancy
The risk of tumor spillage in laparoscopic surgery can be lowered using laparoscopically guided minilaparotomy techniques. Preoperative rupture appears to be more predictive of outcome.28
The concern about metastatic implants in a laparoscopic port site in patients who have gynecologic cancer is real, with an incidence ranging from 0.97% to 1.1%. The phenomenon usually affects women who had ovarian cancer and is most common after laparoscopy with findings of ascites, carcinomatosis, or persistent disease (in the case of second-look laparoscopy performed after completion of primary therapy for ovarian cancer).
These data suggest that port-site implantation is not a concern that should deter clinicians from laparoscopic evaluation of a suspected ovarian neoplasm unless a patient presents with ascites or carcinomatosis suggestive of advanced disease.29
Data are limited regarding delays in definitive therapy. One study suggests that definitive staging on the day of rupture does not influence overall outcome, but delay by more than 2 weeks may lead to poorer prognosis.30
CASE 2: OUTCOME
Laparoscopy is performed. On initial inspection, the peritoneal cavity is unremarkable. The right ovary is multicystic with normal surface anatomy. The mass is somewhat adherent to the pelvic sidewall. Adnexectomy is performed, and frozen section reveals the mass to be a serous cystadenoma.
1. Curtin JP. Management of the adnexal mass. Gynecol Oncol. 1994;55:S42-S46.
2. Goff BA, Mandel LS, Melancon CH, Muntz HG. Frequency of symptoms of ovarian cancer in women presenting to primary care clinics. JAMA. 2004;291:2705-2712.
3. Andersen MR, Goff BA, Lowe KA, et al. Combining a symptoms index with CA 125 to improve detection of ovarian cancer. Cancer. 2008;113:484-489.
4. Goff BA, Mandel LS, Drescher CW, et al. Development of an ovarian cancer symptom index: possibilities for earlier detection. Cancer. 2007;109:221-227.
5. Alcázar JL, Mercé LT, Laparte C, et al. A new scoring system to differentiate benign from malignant adnexal masses. Am J Obstet Gynecol. 2003;188:685-692.
6. Maggino T, Gadducci A, D’Addario V, et al. Prospective multicenter study on CA 125 in postmenopausal pelvic masses. Gynecol Oncol. 1994;54:117-123.
7. Malkasian GD, Jr, Knapp RC, Lavin PT, et al. Preoperative evaluation of serum CA 125 levels in premenopausal and postmenopausal patients with pelvic masses: discrimination of benign from malignant disease. Am J Obstet Gynecol. 1988;159:341-346.
8. Larobina M, Nottle P. Complete evidence regarding major vascular injuries during laparoscopic access. Surg Laparosc Endosc Percutan Tech. 2005;15:119-123.
9. Vilos GA, Vilos AG. Safe laparoscopic entry guided by Veress needle CO2 insufflation pressure. J Am Assoc Gynecol Laparosc. 2003;10:415-420.
10. Vilos GA, Vilos AG, Abu-Rafea B, Hollett-Caines J, Nikkhah-Abyaneh Z, Edris F. Three simple steps during closed laparoscopic entry may minimize major injuries. Surg Endosc. 2008 July 15. [Epub ahead of print]
11. Vilos GA, Ternamian A, Dempster J, Laberge PY. The Society of Obstetricians and Gynaecologists of Canada. Laparoscopic entry: a review of techniques, technologies, and complications. J Obstet Gynaecol Can. 2007;29:433-465.
12. Tulikangas PK, Nicklas A, Falcone T, Price LL. Anatomy of the left upper quadrant for cannula insertion. J Am Assoc Gynecol Laparosc. 2000;7:211-214.
13. Stepp KJ, Tulikangas PK, Goldberg JM, Attaran M, Falcone T. Laparoscopy for adnexal masses in the second trimester of pregnancy. J Am Assoc Gynecol Laparosc. 2003;10:55-59.
14. Tulikangas PK, Robinson DS, Falcone T. Left upper quadrant cannula insertion. Fertil Steril. 2003;79:411-412.
15. Whiteside JL, Barber MD, Walters MD, Falcone T. Anatomy of ilioinguinal and iliohypogastric nerves in relation to trocar placement and low transverse incisions. Am J Obstet Gynecol. 2003;189:1574-1578.
16. Yim SF, Yuen PM. Randomized double-masked comparison of radially expanding access device and conventional cutting tip trocar in laparoscopy. Obstet Gynecol. 2001;97:435-438.
17. Johnson WH, Fecher AM, McMahon RL, et al. VersaStep trocar hernia rate in unclosed fascial defects in bariatric patients. Surg Endosc. 2006;20:1584-1586.
18. Lin P, Falcone T, Tulandi T. Excision of ovarian dermoid cyst by laparoscopy and by laparotomy. Am J Obstet Gynecol. 1995;173:769-771.
19. Jemal A, Murray T, Samuels A, et al. Cancer statistics, 2003. CA Cancer J Clin. 2003;53:5-26.
20. Kauff ND, Satagopan JM, Robson ME, et al. Risk-reducing salpingooophorectomy in women with a BRCA1 or BRCA2 mutation. N Engl J Med. 2002;346:1609-1615.
21. King MC, Marks JH, Mandell JB. Breast and ovarian cancer risks due to inherited mutations in BRCA1 and BRCA2. Science. 2003;302:643-646.
22. Aarnio M, Sankila R, Pukkala E, et al. Cancer risk in mutation carriers of DNA-mismatch-repair genes. Int J Cancer. 1999;81:214-218.
23. Dunlop MG, Farrington SM, Carothers AD, et al. Cancer risk associated with germline DNA mismatch repair gene mutations. Hum Mol Genet. 1997;6:105-110.
24. Dowdy SC, Stefanek M, Hartmann LC. Surgical risk reduction: prophylactic salpingooophorectomy and prophylactic mastectomy. Am J Obstet Gynecol. 2004;191:1113-1123.
25. Narod SA, Risch H, Moslehi R, et al. Oral contraceptives and the risk of hereditary ovarian cancer. Hereditary Ovarian Cancer Clinical Study Group. N Engl J Med. 1998;339:424-428.
26. Whittemore AS, Balise RR, Pharoah PD, et al. Oral contraceptive use and ovarian cancer risk among carriers of BRCA1 or BRCA2 mutations. Br J Cancer. 2004;91:1911-1915.
27. Im SS, Gordon AN, Buttin BM, et al. Validation of referral guidelines for women with pelvic masses. Obstet Gynecol. 2005;105:35-41.
28. Vergote I, De Brabanter J, Fyles A, et al. Prognostic importance of degree of differentiation and cyst rupture in stage I invasive epithelial ovarian carcinoma. Lancet. 2001;357:176-182.
29. Ramirez PT, Wolf JK, Levenback C. Laparoscopic port-site metastases: etiology and prevention. Gynecol Oncol. 2003;91:179-189.
30. Lehner R, Wenzl R, Heinzl H, Husslein P, Sevelda P. Influence of delayed staging laparotomy after laparoscopic removal of ovarian masses later found malignant. Obstet Gynecol. 1998;92:967-971.
The authors report no financial relationships relevant to this article.
CASE 1: Cystic mass in patient’s only remaining ovary
Mrs. R is a 29-year-old G1P1 who underwent a right oophorectomy, with a midline incision, for a dermoid cyst at the time of cesarean delivery. She now has a left ovarian cyst. Preoperative ultrasonography (US) reveals that it measures 3.5×4.2×3.7 cm and has both solid components and a multiloculated appearance, consistent with a dermoid cyst.
How common is this scenario?
Studies predict that one of every three women will undergo surgical management of an adnexal mass at some point in her life.1 This troubling statistic prompts several critical questions:
- How do we handle the workup for these women so that only appropriate patients undergo surgery?
- How often will a mass be malignant?
- How can we safely remove an adnexal mass to maximize patient safety, reduce overall recovery time, and prevent less favorable outcomes in women who are eventually found to have a malignancy?
A thorough workup and, sometimes, conservative management can prevent unnecessary surgery that may lead to early menopause or surgical complications. And maximizing the use of minimally invasive techniques in women who do require surgery can shorten hospital stay and recovery time. At the time of surgery, careful abdominal entry and meticulous surgical dissection and mass removal can limit the potential risks of laparoscopic excision in women who have an ultimate diagnosis of cancer.
In this article, we review the workup for women who have an adnexal mass, describe patient-selection criteria for laparoscopic surgery, including the risks and benefits of this approach ( TABLE 1 ), and present several techniques to safely manage a mass with potentially malignant histology via laparoscopy.
TABLE 1
There are benefits and risks to managing an adnexal mass laparoscopically
| Benefit | Risk |
|---|---|
| Shorter recovery Fewer adhesions Decreased overall cost Magnification Decreased pain and narcotic use Fewer wound complications | Expensive equipment* Loss of tactile sensation Concern for malignancy Risk of tumor dissemination/spillage/chemical peritonitis Trocar-site metastasis |
| *Though greater expense is not a risk per se, it does enter into decision making. | |
Begin with the physical
When a woman is known to have a pelvic mass, the aim of the office exam is to 1) identify characteristics that suggest malignancy and 2) rule out nongynecologic causes of the mass. Physical findings that are worrisome for a malignant process include:
- fixed or nodular pelvic mass
- bilateral masses
- nodular abdominal mass
- ascites
- pleural effusion on auscultation or percussion of the lung.
Although these findings can be present under benign conditions, they increase the risk that a malignancy will be detected at surgery.
Other causes of a pelvic mass should also be considered, including infection (pelvic abscess) and tumors of the colon, particularly when the pelvic mass occurs on the left side.
Some symptoms, though vague, are worth noting
Although ovarian cancer was once thought to be a silent disease, recent research has shown that bloating, pelvic or abdominal pain, early satiety, and urinary frequency and urgency are more common among women with ovarian cancer than among healthy controls and patients in high-risk screening clinics.2-4 Although these symptoms are generally nonspecific, they merit attention if they occur more than 12 times a month and have been present for less than 1 year. When they meet these criteria, the symptoms have a sensitivity for diagnosing early- and late-stage ovarian cancer of 56.7% and 79.5%, respectively.4
Sensitivity for the diagnosis of early-stage ovarian cancer may be as high as 80% when the symptom index score is combined with an elevated level of the tumor marker CA 125.3
Transvaginal US is crucial
Transvaginal US is now standard practice to obtain high-resolution images of an adnexal mass. Grayscale US has traditionally been used alone for evaluation.
Specificity is typically lower in women who are premenopausal because many benign lesions, such as endometrioma, have a similar sonographic appearance to cancer.
A number of US scoring algorithms have now been proposed to aid in the triage of women who have an adnexal mass. Sensitivity of these algorithms ranges from 65% to 100%; specificity, from 77% to 95%.5
CA 125 is the standard tumor marker
For the past two decades, CA 125 has been the standard serum marker in the screening of high-risk women for ovarian cancer and the triage of women who have an adnexal mass.
This blood test has been studied widely since its introduction in 1983. It typically has sensitivity of 75% to 85% and specificity of 85% to 95% in identifying women who have ovarian cancer. However, it is elevated in only 50% to 60% of women who have stage I ovarian cancer. Its lack of specificity and poor positive predictive value have kept researchers busy trying to identify other serum markers, for both ovarian cancer and identification of high-risk pelvic masses.
Our recommended workup and management of adnexal masses In postmenopausal women who had a pelvic mass, one study found that a CA 125 level above 65 IU/mL had sensitivity of 71% and specificity of 92.5% in the identification of ovarian cancer.6 Another group found that CA 125 levels above 65 IU/mL were more than 95% sensitive in the diagnosis of ovarian cancer in postmenopausal women.7
Several studies have combined CA 125 with other markers or with US to screen high-risk women or triage those who have an adnexal mass. These studies have shown modest improvements in sensitivity but usually lower specificity than with CA 125 testing alone.
Markers that may be used for suspected sex cord stromas and germ-cell tumors are:
- lactate dehydrogenase (LDH) for dysgerminomas
- alpha-fetoprotein (AFP) and human chorionic gonadotropin (hCG) for yolk sac tumors
- testosterone for Sertoli-Leydig cell tumors
- inhibin A and B for granulosa cell tumors.
An algorithm for working up and managing adnexal masses appears above.
How to gain abdominal access
In the opening case, the patient clearly has a benign mass. The treatment? Safe entry into the peritoneal cavity to remove the cyst and as little normal tissue as possible. This is critical in this patient because she has only one ovary.
Peritoneal access for abdominal and pelvic laparoscopy has been studied widely. Options include:
- direct insertion using a Veress needle
- open laparoscopy
- direct trocar insertion.
The technique usually depends on the preference of the surgeon. The primary goal of abdominal entry is to minimize the risk of injury, particularly unrecognized injury.
Data on complication rates show no definite benefit for open versus closed techniques in the prevention of injury to underlying viscera. However, evidence does suggest that the open technique may lower the risk of major vascular injury.8
We employ direct trocar insertion using radially expanding or optical trocars.
The Veress needle option
When the Veress needle is used to gain intraperitoneal access, data indicate that initial intraperitoneal pressure below 10 mm Hg is a reliable marker for peritoneal entry, even in obese patients.9 Insufflation pressure as high as 25 to 30 mm Hg prior to placement of the initial trocar is safe from a cardiopulmonary standpoint and may allow easier entry with a nonbladed trocar.10
Tests to confirm intraperitoneal placement of the Veress needle, such as the hanging-drop test or saline flush, do not appear to offer any additional useful information.11
Open laparoscopy is suitable when adhesions are unlikely
Open laparoscopy is typically performed by making a minilaparotomy incision at the umbilicus and then dissecting and entering the peritoneal cavity. A blunt-tip trocar is inserted.
The disadvantage of this approach is that there may be extensive adhesions under the umbilicus, and it is difficult to dissect such adhesions sufficiently to introduce a cannula and laparoscope. Adhesions left behind often obscure the field of view after introduction of the trocar.
Our preference? Left upper-quadrant insertion
In Case 1, the previous midline incision mandates an alternative approach. When abdominal entry at the umbilicus is unsuccessful or potentially difficult because of an earlier midline incision, umbilical hernia repair, or history of multiple lower abdominal or pelvic surgeries, a left upper-quadrant insertion is useful. It is, in fact, our preferred technique, and involves a small incision at the midclavicular line 5 cm below the left costal margin, at a site called Palmer’s point.
The direction of insertion usually ranges from 45° to 90°, depending on the patient’s body weight. If the trocar is placed properly, the closest organs are the stomach and the left lobe of the liver (4 to 6 cm).12 Given the stomach’s close proximity, it should be decompressed with an orogastric tube prior to trocar insertion.
Several studies have demonstrated the safety and efficacy of this entry technique.12-14 It can be helpful in cases that involve difficult access. We usually use a 5-mm primary trocar site for a 5-mm laparoscope. Modern optics allow for a pristine view with these small scopes, eliminating the need to close fascia and perhaps causing less pain at the incision.
Accessory trocar sites facilitate complex technique
We usually use three accessory sites. Two of them are lower-quadrant ports that are placed 2 cm medial and 2 cm cephalad to the anterior superior iliac spine. This area generally lies well away from the inferior epigastric vessels and remains above the area of the ilioinguinal and iliohypogastric nerves, making it a safer point of insertion.15 One trocar is 5 mm in size and the other is 10 mm. The larger one is used to extract the specimen.
We place an additional 5-mm port lateral to the rectus muscle at the level of the umbilicus. This allows the principal surgeon to use two instruments (a toothed forceps and scissors) comfortably while the assistant holds the laparoscope and assists with a grasper.
Does the type of trocar matter?
No randomized studies have directly compared all types of trocars. Options include:
- a pyramidal tip (as in reusable trocars) or shielded tip
- radial expansion
- visible entry
- blunt (Hasson-type) trocar.
Safety data on direct comparison of trocars are limited, but it appears that a radially expanding trocar may offer less port-site pain and potentially less bleeding than a traditional cutting trocar.16 Moreover, the rate of hernia at the port site appears to be relatively low with a radially expanding trocar, even when fascia is left unclosed at a 10-mm site.17
None of these trocars appears to be clearly superior at avoiding visceral or vascular injury.
Technique of laparoscopic cyst removal
A video clip of the surgery is linked to this article in the Video Library at www.obgmanagement.com. In this case, a trocar was inserted in the left upper quadrant, and a laparoscopic cystectomy was initiated using the trocars already specified.
The peritoneal cavity and adnexa were inspected, followed by pelvic washings, as detailed in TABLE 2 . Next, the ovarian cortex was incised ( FIGURE 1A ) with scissors using bipolar or unipolar energy, typically at a low power setting, such as 12 to 15 watts.
It was relatively easy to develop a tissue plane between the cortex and underlying dermoid cyst using simple or aqua-dissection ( FIGURE 1B and C ). The cyst was enucleated without rupture and inserted into a specimen bag through a 10-mm port ( FIGURE 1D ). (The specimen bags generally are available in 10-mm and 15-mm sizes.) Once the trocar was removed, the entire specimen was brought out through the incision ( FIGURE 1E ).
Cystic masses can generally be carefully aspirated using a laparoscopic needle or angiocath, or they can be incised and drained using a standard suction device. Manufacturers of most specimen bags do not recommend the morcellation of tissue within the bag because of the potential for rupture of the bag with tumor spillage or injury to underlying structures.
Occasionally, the mass remains too large to remove after drainage of the cyst fluid. Remedies include enlarging the port site with a scalpel or using a gallbladder speculum to increase the diameter of the port site ( FIGURE 1E ). If possible, the incision should be large enough to deliver the entire bag intact. Use of excessive force will rupture the bag and may cause the specimen to be lost or malignant cells to be inadvertently spilled (in the case of a cancer diagnosis).
TABLE 2
Take these 10 steps to safe laparoscopic surgery
| Examine the anesthetized patient |
| Enter the abdomen |
| Inspect the mass and peritoneal surfaces, including the diaphragm. Biopsy sites suspicious for metastasis and obtain frozen section |
| Perform pelvic and abdominal washings |
Closely inspect adnexa. If findings are not suggestive of malignancy, proceed with laparoscopy. If findings indicate obvious malignancy
|
Perform cystectomy or oophorectomy
|
| Inspect for hemostasis |
| Place cyst/ovary in endopouch |
| Open bag at abdominal wall and remove for frozen section |
| Reinspect and close |
Avoid:
|
FIGURE 1 Laparoscopic cyst removal
Begin by incising the cortex using scissors with or without an energy source.
Dissect the cyst free from the cortex using sharp dissection.
Remove the cyst from the ovary.
Place the cyst in a specimen bag, and …
… bring it to the surface for extraction. The abdominal incision may have to be enlarged to accommodate the specimen.
CASE 1: OUTCOME
The patient’s cyst is removed intact and she is discharged home. Rupture of a dermoid cyst is not associated with any problems as long as copious irrigation is used to aspirate the cyst content.18 Other cysts, such as endometriomas, may not be as easily dissected, and rupture is inevitable.
CASE 2: Symptoms suggestive of cancer
Mrs. B is a 47-year-old woman who reports abdominal bloating for the past 3 weeks. She also complains of early satiety and occasional constipation. She has no history of cancer, but her sister was given a diagnosis of breast cancer at 41 years of age, and her maternal aunt had breast cancer at 55 years.
Mrs. B is moderately obese, with a nontender abdomen and no palpable mass. Her pelvic exam also is negative for a mass or nodularity, but the extent of the exam is limited by body habitus. Her physician orders a transvaginal US, which reveals a 6-cm complex mass with thin septation and a 1-cm solid nodule, with no definite blood flow. The patient’s CA 125 level is 80 IU/mL, which we consider to be within the low-risk range for a premenopausal woman.
The patient is counseled about the need to have the mass removed and is scheduled for laparoscopic right salpingooophorectomy. Given the family history of breast cancer, the physician also requests consultation with a gynecologic oncologist, who agrees to assist with surgery and perform a laparotomy and staging in the event that a malignancy is diagnosed.
Is the mass likely to be malignant?
Given the patient’s family history of breast cancer, the recent onset of symptoms associated with ovarian cancer,2 and the characteristics of the mass (complex, with a nodule), malignancy is possible. This patient has an intermediate risk of cancer and requires additional counseling and planning.
However, most women who undergo laparoscopy for removal of an adnexal mass have benign pathologic findings.
What is the real risk of ovarian cancer?
The lifetime risk of developing ovarian cancer in the general population remains stable at approximately 1 in 70 women, with a mean age at diagnosis of 63 years.19 Ninety percent of ovarian cancer cases are sporadic, and less than 10% can be linked to genetic syndromes.
Women who have mutations in the BRCA1 gene carry a lifetime risk of ovarian cancer of up to 50%, and women who have mutations in BRCA2 have a lifetime risk of up to 25%.20,21 Women who have mutations associated with Lynch II syndrome or Hereditary Nonpolyposis Colorectal Cancer syndrome may have a lifetime risk of ovarian cancer of 12%.22,23
Some women who have a strong family history of breast and ovarian cancer do not carry a known mutation, but are likely to be at increased risk.
Additional risk factors known to be associated with ovarian cancer are nulliparity and infertility. However, the single most important risk factor for epithelial ovarian cancer is age.
Risk-reducing strategies include:
In the case of PBSO, it is imperative to ensure that all ovarian surface epithelium is removed. This means excising the infundibulopelvic ligament at least 1.5 cm above the proximal end of the ovary and excising any adjacent tissue to which the ovary is adherent (including pelvic sidewall peritoneum). Both requirements are easily achieved using the techniques outlined here.
Who should perform surgery?
The American College of Obstetricians and Gynecologists (ACOG) and the Society of Gynecologic Oncologists (SGO) have published guidelines for referral to a gynecologic oncologist ( TABLE 3 ). When Im and colleagues reviewed the records of more than 1,000 women who underwent surgery for a pelvic mass at six institutions over 12 months, they found that 70% of premenopausal women and 94% of postmenopausal women who were diagnosed with ovarian cancer were properly referred to a qualified subspecialist.27 “Over”-referral occurred in 30% to 40% of women who had a benign mass, but may be preferable given the importance of proper staging and debulking to survival.
ACOG and the SGO recommend referral for women who have:
- elevated tumor markers
- ascites
- a fixed or nodular mass
- a strong family history of breast or ovarian cancer.
Consider preoperative referral of all high-risk and, probably, intermediate-risk women, depending on the availability of qualified specialists for complete surgical staging.
In addition, women need to be counseled thoroughly about the possibility that a malignancy will be diagnosed by frozen section, necessitating additional surgical procedures.
TABLE 3
Your patient has a newly diagnosed pelvic mass. Should you refer her?
| Is she premenopausal? Then refer her when… | Is she postmenopausal? Then refer her when… |
|---|---|
| CA125 >200 IU/mL Ascites is present Evidence of abdominal or distant metastasis on exam or imaging Family history of breast or ovarian cancer in a first-degree relative | CA125 >35 IU/mL Ascites is present Nodular or fixed pelvic mass Evidence of abdominal or distant metastasis on exam or imaging Family history of breast or ovarian cancer in a first-degree relative |
Technique of laparoscopic adnexectomy
In Case 2, an umbilical site was chosen for the primary cannula. In general, the direction of insertion depends on the patient’s body habitus. Heavier patients have a thicker abdominal wall and an umbilicus below the level of the aortic bifurcation. In these women, the angle of insertion should be adjusted from the usual 45° (for patients of normal weight) to an angle nearer to 90°. Lateral ports are typical, as in Case 1.
Treat every mass like cancer
Laparoscopic excision of an adnexal mass can be safe and effective, with better outcomes and recovery than with laparotomy, provided the surgeon adheres to basic principles ( TABLE 2 ). This means treating every mass as though it is potentially malignant, and thoroughly inspecting the abdominal cavity before and after excision of the mass.
Know the retroperitoneal space
As with Case 1, successful laparoscopic excision of an adnexal mass begins with inspection of the peritoneal cavity, abdominopelvic washings, and identification of both the infundibulopelvic ligament and ureter. Knowledge of the retroperitoneal space can be of great value in difficult cases that involve significant pelvic adhesions or sidewall fibrosis. We generally use a retroperitoneal approach for laparoscopic adnexectomy ( FIGURE 2A ).
In our typical approach, we incise the peritoneum lateral to the uteroovarian ligament and continue the incision up the pelvic sidewall lateral to the infundibulopelvic ligament and up along the paracolic gutter, if needed ( FIGURE 2A ). We then mobilize the medial leaf of the broad ligament from the sidewall using blunt dissection between the external iliac vessels laterally and the ureter medially ( FIGURE 2B ).
Once we have identified the ureter, we use scissors to create a window in the medial leaf of the broad ligament just beneath the gonadal vessels. We then use an energy source to occlude and transect the pedicle. Using this technique, we secure the infundibulopelvic ligaments and safely mobilize the ureter before initiating more aggressive sidewall dissection distally for adhesions or fibrosis.
Once the ureter is mobilized, we excise the involved peritoneum along with the mass. We then seal and transect the uteroovarian ligament.
FIGURE 2 The retroperitoneal approach
Grasp and incise the peritoneum just lateral to the adnexal mass and enter the retroperitoneal space, where loose areolar tissue is visible, with the ureter seen on the medial leaf of the broad ligament.
After dissecting this tissue, identify the ureter and internal iliac vessels.
Remove the mass in a bag
Once the mass is excised, we place it in a laparoscopic bag, as described for Case 1. Solid adnexal masses are problematic because they are not amenable to drainage, and morcellation is usually discouraged. Laparoscopic excision can still be carried out, and a minilaparotomy or posterior colpotomy can be used to extract the mass in a bag. Patients managed in this way still have a complication rate similar to or lower than that of patients undergoing laparotomy for oophorectomy; they also recover faster.
Risks in cases of malignancy
The risk of tumor spillage in laparoscopic surgery can be lowered using laparoscopically guided minilaparotomy techniques. Preoperative rupture appears to be more predictive of outcome.28
The concern about metastatic implants in a laparoscopic port site in patients who have gynecologic cancer is real, with an incidence ranging from 0.97% to 1.1%. The phenomenon usually affects women who had ovarian cancer and is most common after laparoscopy with findings of ascites, carcinomatosis, or persistent disease (in the case of second-look laparoscopy performed after completion of primary therapy for ovarian cancer).
These data suggest that port-site implantation is not a concern that should deter clinicians from laparoscopic evaluation of a suspected ovarian neoplasm unless a patient presents with ascites or carcinomatosis suggestive of advanced disease.29
Data are limited regarding delays in definitive therapy. One study suggests that definitive staging on the day of rupture does not influence overall outcome, but delay by more than 2 weeks may lead to poorer prognosis.30
CASE 2: OUTCOME
Laparoscopy is performed. On initial inspection, the peritoneal cavity is unremarkable. The right ovary is multicystic with normal surface anatomy. The mass is somewhat adherent to the pelvic sidewall. Adnexectomy is performed, and frozen section reveals the mass to be a serous cystadenoma.
The authors report no financial relationships relevant to this article.
CASE 1: Cystic mass in patient’s only remaining ovary
Mrs. R is a 29-year-old G1P1 who underwent a right oophorectomy, with a midline incision, for a dermoid cyst at the time of cesarean delivery. She now has a left ovarian cyst. Preoperative ultrasonography (US) reveals that it measures 3.5×4.2×3.7 cm and has both solid components and a multiloculated appearance, consistent with a dermoid cyst.
How common is this scenario?
Studies predict that one of every three women will undergo surgical management of an adnexal mass at some point in her life.1 This troubling statistic prompts several critical questions:
- How do we handle the workup for these women so that only appropriate patients undergo surgery?
- How often will a mass be malignant?
- How can we safely remove an adnexal mass to maximize patient safety, reduce overall recovery time, and prevent less favorable outcomes in women who are eventually found to have a malignancy?
A thorough workup and, sometimes, conservative management can prevent unnecessary surgery that may lead to early menopause or surgical complications. And maximizing the use of minimally invasive techniques in women who do require surgery can shorten hospital stay and recovery time. At the time of surgery, careful abdominal entry and meticulous surgical dissection and mass removal can limit the potential risks of laparoscopic excision in women who have an ultimate diagnosis of cancer.
In this article, we review the workup for women who have an adnexal mass, describe patient-selection criteria for laparoscopic surgery, including the risks and benefits of this approach ( TABLE 1 ), and present several techniques to safely manage a mass with potentially malignant histology via laparoscopy.
TABLE 1
There are benefits and risks to managing an adnexal mass laparoscopically
| Benefit | Risk |
|---|---|
| Shorter recovery Fewer adhesions Decreased overall cost Magnification Decreased pain and narcotic use Fewer wound complications | Expensive equipment* Loss of tactile sensation Concern for malignancy Risk of tumor dissemination/spillage/chemical peritonitis Trocar-site metastasis |
| *Though greater expense is not a risk per se, it does enter into decision making. | |
Begin with the physical
When a woman is known to have a pelvic mass, the aim of the office exam is to 1) identify characteristics that suggest malignancy and 2) rule out nongynecologic causes of the mass. Physical findings that are worrisome for a malignant process include:
- fixed or nodular pelvic mass
- bilateral masses
- nodular abdominal mass
- ascites
- pleural effusion on auscultation or percussion of the lung.
Although these findings can be present under benign conditions, they increase the risk that a malignancy will be detected at surgery.
Other causes of a pelvic mass should also be considered, including infection (pelvic abscess) and tumors of the colon, particularly when the pelvic mass occurs on the left side.
Some symptoms, though vague, are worth noting
Although ovarian cancer was once thought to be a silent disease, recent research has shown that bloating, pelvic or abdominal pain, early satiety, and urinary frequency and urgency are more common among women with ovarian cancer than among healthy controls and patients in high-risk screening clinics.2-4 Although these symptoms are generally nonspecific, they merit attention if they occur more than 12 times a month and have been present for less than 1 year. When they meet these criteria, the symptoms have a sensitivity for diagnosing early- and late-stage ovarian cancer of 56.7% and 79.5%, respectively.4
Sensitivity for the diagnosis of early-stage ovarian cancer may be as high as 80% when the symptom index score is combined with an elevated level of the tumor marker CA 125.3
Transvaginal US is crucial
Transvaginal US is now standard practice to obtain high-resolution images of an adnexal mass. Grayscale US has traditionally been used alone for evaluation.
Specificity is typically lower in women who are premenopausal because many benign lesions, such as endometrioma, have a similar sonographic appearance to cancer.
A number of US scoring algorithms have now been proposed to aid in the triage of women who have an adnexal mass. Sensitivity of these algorithms ranges from 65% to 100%; specificity, from 77% to 95%.5
CA 125 is the standard tumor marker
For the past two decades, CA 125 has been the standard serum marker in the screening of high-risk women for ovarian cancer and the triage of women who have an adnexal mass.
This blood test has been studied widely since its introduction in 1983. It typically has sensitivity of 75% to 85% and specificity of 85% to 95% in identifying women who have ovarian cancer. However, it is elevated in only 50% to 60% of women who have stage I ovarian cancer. Its lack of specificity and poor positive predictive value have kept researchers busy trying to identify other serum markers, for both ovarian cancer and identification of high-risk pelvic masses.
Our recommended workup and management of adnexal masses In postmenopausal women who had a pelvic mass, one study found that a CA 125 level above 65 IU/mL had sensitivity of 71% and specificity of 92.5% in the identification of ovarian cancer.6 Another group found that CA 125 levels above 65 IU/mL were more than 95% sensitive in the diagnosis of ovarian cancer in postmenopausal women.7
Several studies have combined CA 125 with other markers or with US to screen high-risk women or triage those who have an adnexal mass. These studies have shown modest improvements in sensitivity but usually lower specificity than with CA 125 testing alone.
Markers that may be used for suspected sex cord stromas and germ-cell tumors are:
- lactate dehydrogenase (LDH) for dysgerminomas
- alpha-fetoprotein (AFP) and human chorionic gonadotropin (hCG) for yolk sac tumors
- testosterone for Sertoli-Leydig cell tumors
- inhibin A and B for granulosa cell tumors.
An algorithm for working up and managing adnexal masses appears above.
How to gain abdominal access
In the opening case, the patient clearly has a benign mass. The treatment? Safe entry into the peritoneal cavity to remove the cyst and as little normal tissue as possible. This is critical in this patient because she has only one ovary.
Peritoneal access for abdominal and pelvic laparoscopy has been studied widely. Options include:
- direct insertion using a Veress needle
- open laparoscopy
- direct trocar insertion.
The technique usually depends on the preference of the surgeon. The primary goal of abdominal entry is to minimize the risk of injury, particularly unrecognized injury.
Data on complication rates show no definite benefit for open versus closed techniques in the prevention of injury to underlying viscera. However, evidence does suggest that the open technique may lower the risk of major vascular injury.8
We employ direct trocar insertion using radially expanding or optical trocars.
The Veress needle option
When the Veress needle is used to gain intraperitoneal access, data indicate that initial intraperitoneal pressure below 10 mm Hg is a reliable marker for peritoneal entry, even in obese patients.9 Insufflation pressure as high as 25 to 30 mm Hg prior to placement of the initial trocar is safe from a cardiopulmonary standpoint and may allow easier entry with a nonbladed trocar.10
Tests to confirm intraperitoneal placement of the Veress needle, such as the hanging-drop test or saline flush, do not appear to offer any additional useful information.11
Open laparoscopy is suitable when adhesions are unlikely
Open laparoscopy is typically performed by making a minilaparotomy incision at the umbilicus and then dissecting and entering the peritoneal cavity. A blunt-tip trocar is inserted.
The disadvantage of this approach is that there may be extensive adhesions under the umbilicus, and it is difficult to dissect such adhesions sufficiently to introduce a cannula and laparoscope. Adhesions left behind often obscure the field of view after introduction of the trocar.
Our preference? Left upper-quadrant insertion
In Case 1, the previous midline incision mandates an alternative approach. When abdominal entry at the umbilicus is unsuccessful or potentially difficult because of an earlier midline incision, umbilical hernia repair, or history of multiple lower abdominal or pelvic surgeries, a left upper-quadrant insertion is useful. It is, in fact, our preferred technique, and involves a small incision at the midclavicular line 5 cm below the left costal margin, at a site called Palmer’s point.
The direction of insertion usually ranges from 45° to 90°, depending on the patient’s body weight. If the trocar is placed properly, the closest organs are the stomach and the left lobe of the liver (4 to 6 cm).12 Given the stomach’s close proximity, it should be decompressed with an orogastric tube prior to trocar insertion.
Several studies have demonstrated the safety and efficacy of this entry technique.12-14 It can be helpful in cases that involve difficult access. We usually use a 5-mm primary trocar site for a 5-mm laparoscope. Modern optics allow for a pristine view with these small scopes, eliminating the need to close fascia and perhaps causing less pain at the incision.
Accessory trocar sites facilitate complex technique
We usually use three accessory sites. Two of them are lower-quadrant ports that are placed 2 cm medial and 2 cm cephalad to the anterior superior iliac spine. This area generally lies well away from the inferior epigastric vessels and remains above the area of the ilioinguinal and iliohypogastric nerves, making it a safer point of insertion.15 One trocar is 5 mm in size and the other is 10 mm. The larger one is used to extract the specimen.
We place an additional 5-mm port lateral to the rectus muscle at the level of the umbilicus. This allows the principal surgeon to use two instruments (a toothed forceps and scissors) comfortably while the assistant holds the laparoscope and assists with a grasper.
Does the type of trocar matter?
No randomized studies have directly compared all types of trocars. Options include:
- a pyramidal tip (as in reusable trocars) or shielded tip
- radial expansion
- visible entry
- blunt (Hasson-type) trocar.
Safety data on direct comparison of trocars are limited, but it appears that a radially expanding trocar may offer less port-site pain and potentially less bleeding than a traditional cutting trocar.16 Moreover, the rate of hernia at the port site appears to be relatively low with a radially expanding trocar, even when fascia is left unclosed at a 10-mm site.17
None of these trocars appears to be clearly superior at avoiding visceral or vascular injury.
Technique of laparoscopic cyst removal
A video clip of the surgery is linked to this article in the Video Library at www.obgmanagement.com. In this case, a trocar was inserted in the left upper quadrant, and a laparoscopic cystectomy was initiated using the trocars already specified.
The peritoneal cavity and adnexa were inspected, followed by pelvic washings, as detailed in TABLE 2 . Next, the ovarian cortex was incised ( FIGURE 1A ) with scissors using bipolar or unipolar energy, typically at a low power setting, such as 12 to 15 watts.
It was relatively easy to develop a tissue plane between the cortex and underlying dermoid cyst using simple or aqua-dissection ( FIGURE 1B and C ). The cyst was enucleated without rupture and inserted into a specimen bag through a 10-mm port ( FIGURE 1D ). (The specimen bags generally are available in 10-mm and 15-mm sizes.) Once the trocar was removed, the entire specimen was brought out through the incision ( FIGURE 1E ).
Cystic masses can generally be carefully aspirated using a laparoscopic needle or angiocath, or they can be incised and drained using a standard suction device. Manufacturers of most specimen bags do not recommend the morcellation of tissue within the bag because of the potential for rupture of the bag with tumor spillage or injury to underlying structures.
Occasionally, the mass remains too large to remove after drainage of the cyst fluid. Remedies include enlarging the port site with a scalpel or using a gallbladder speculum to increase the diameter of the port site ( FIGURE 1E ). If possible, the incision should be large enough to deliver the entire bag intact. Use of excessive force will rupture the bag and may cause the specimen to be lost or malignant cells to be inadvertently spilled (in the case of a cancer diagnosis).
TABLE 2
Take these 10 steps to safe laparoscopic surgery
| Examine the anesthetized patient |
| Enter the abdomen |
| Inspect the mass and peritoneal surfaces, including the diaphragm. Biopsy sites suspicious for metastasis and obtain frozen section |
| Perform pelvic and abdominal washings |
Closely inspect adnexa. If findings are not suggestive of malignancy, proceed with laparoscopy. If findings indicate obvious malignancy
|
Perform cystectomy or oophorectomy
|
| Inspect for hemostasis |
| Place cyst/ovary in endopouch |
| Open bag at abdominal wall and remove for frozen section |
| Reinspect and close |
Avoid:
|
FIGURE 1 Laparoscopic cyst removal
Begin by incising the cortex using scissors with or without an energy source.
Dissect the cyst free from the cortex using sharp dissection.
Remove the cyst from the ovary.
Place the cyst in a specimen bag, and …
… bring it to the surface for extraction. The abdominal incision may have to be enlarged to accommodate the specimen.
CASE 1: OUTCOME
The patient’s cyst is removed intact and she is discharged home. Rupture of a dermoid cyst is not associated with any problems as long as copious irrigation is used to aspirate the cyst content.18 Other cysts, such as endometriomas, may not be as easily dissected, and rupture is inevitable.
CASE 2: Symptoms suggestive of cancer
Mrs. B is a 47-year-old woman who reports abdominal bloating for the past 3 weeks. She also complains of early satiety and occasional constipation. She has no history of cancer, but her sister was given a diagnosis of breast cancer at 41 years of age, and her maternal aunt had breast cancer at 55 years.
Mrs. B is moderately obese, with a nontender abdomen and no palpable mass. Her pelvic exam also is negative for a mass or nodularity, but the extent of the exam is limited by body habitus. Her physician orders a transvaginal US, which reveals a 6-cm complex mass with thin septation and a 1-cm solid nodule, with no definite blood flow. The patient’s CA 125 level is 80 IU/mL, which we consider to be within the low-risk range for a premenopausal woman.
The patient is counseled about the need to have the mass removed and is scheduled for laparoscopic right salpingooophorectomy. Given the family history of breast cancer, the physician also requests consultation with a gynecologic oncologist, who agrees to assist with surgery and perform a laparotomy and staging in the event that a malignancy is diagnosed.
Is the mass likely to be malignant?
Given the patient’s family history of breast cancer, the recent onset of symptoms associated with ovarian cancer,2 and the characteristics of the mass (complex, with a nodule), malignancy is possible. This patient has an intermediate risk of cancer and requires additional counseling and planning.
However, most women who undergo laparoscopy for removal of an adnexal mass have benign pathologic findings.
What is the real risk of ovarian cancer?
The lifetime risk of developing ovarian cancer in the general population remains stable at approximately 1 in 70 women, with a mean age at diagnosis of 63 years.19 Ninety percent of ovarian cancer cases are sporadic, and less than 10% can be linked to genetic syndromes.
Women who have mutations in the BRCA1 gene carry a lifetime risk of ovarian cancer of up to 50%, and women who have mutations in BRCA2 have a lifetime risk of up to 25%.20,21 Women who have mutations associated with Lynch II syndrome or Hereditary Nonpolyposis Colorectal Cancer syndrome may have a lifetime risk of ovarian cancer of 12%.22,23
Some women who have a strong family history of breast and ovarian cancer do not carry a known mutation, but are likely to be at increased risk.
Additional risk factors known to be associated with ovarian cancer are nulliparity and infertility. However, the single most important risk factor for epithelial ovarian cancer is age.
Risk-reducing strategies include:
In the case of PBSO, it is imperative to ensure that all ovarian surface epithelium is removed. This means excising the infundibulopelvic ligament at least 1.5 cm above the proximal end of the ovary and excising any adjacent tissue to which the ovary is adherent (including pelvic sidewall peritoneum). Both requirements are easily achieved using the techniques outlined here.
Who should perform surgery?
The American College of Obstetricians and Gynecologists (ACOG) and the Society of Gynecologic Oncologists (SGO) have published guidelines for referral to a gynecologic oncologist ( TABLE 3 ). When Im and colleagues reviewed the records of more than 1,000 women who underwent surgery for a pelvic mass at six institutions over 12 months, they found that 70% of premenopausal women and 94% of postmenopausal women who were diagnosed with ovarian cancer were properly referred to a qualified subspecialist.27 “Over”-referral occurred in 30% to 40% of women who had a benign mass, but may be preferable given the importance of proper staging and debulking to survival.
ACOG and the SGO recommend referral for women who have:
- elevated tumor markers
- ascites
- a fixed or nodular mass
- a strong family history of breast or ovarian cancer.
Consider preoperative referral of all high-risk and, probably, intermediate-risk women, depending on the availability of qualified specialists for complete surgical staging.
In addition, women need to be counseled thoroughly about the possibility that a malignancy will be diagnosed by frozen section, necessitating additional surgical procedures.
TABLE 3
Your patient has a newly diagnosed pelvic mass. Should you refer her?
| Is she premenopausal? Then refer her when… | Is she postmenopausal? Then refer her when… |
|---|---|
| CA125 >200 IU/mL Ascites is present Evidence of abdominal or distant metastasis on exam or imaging Family history of breast or ovarian cancer in a first-degree relative | CA125 >35 IU/mL Ascites is present Nodular or fixed pelvic mass Evidence of abdominal or distant metastasis on exam or imaging Family history of breast or ovarian cancer in a first-degree relative |
Technique of laparoscopic adnexectomy
In Case 2, an umbilical site was chosen for the primary cannula. In general, the direction of insertion depends on the patient’s body habitus. Heavier patients have a thicker abdominal wall and an umbilicus below the level of the aortic bifurcation. In these women, the angle of insertion should be adjusted from the usual 45° (for patients of normal weight) to an angle nearer to 90°. Lateral ports are typical, as in Case 1.
Treat every mass like cancer
Laparoscopic excision of an adnexal mass can be safe and effective, with better outcomes and recovery than with laparotomy, provided the surgeon adheres to basic principles ( TABLE 2 ). This means treating every mass as though it is potentially malignant, and thoroughly inspecting the abdominal cavity before and after excision of the mass.
Know the retroperitoneal space
As with Case 1, successful laparoscopic excision of an adnexal mass begins with inspection of the peritoneal cavity, abdominopelvic washings, and identification of both the infundibulopelvic ligament and ureter. Knowledge of the retroperitoneal space can be of great value in difficult cases that involve significant pelvic adhesions or sidewall fibrosis. We generally use a retroperitoneal approach for laparoscopic adnexectomy ( FIGURE 2A ).
In our typical approach, we incise the peritoneum lateral to the uteroovarian ligament and continue the incision up the pelvic sidewall lateral to the infundibulopelvic ligament and up along the paracolic gutter, if needed ( FIGURE 2A ). We then mobilize the medial leaf of the broad ligament from the sidewall using blunt dissection between the external iliac vessels laterally and the ureter medially ( FIGURE 2B ).
Once we have identified the ureter, we use scissors to create a window in the medial leaf of the broad ligament just beneath the gonadal vessels. We then use an energy source to occlude and transect the pedicle. Using this technique, we secure the infundibulopelvic ligaments and safely mobilize the ureter before initiating more aggressive sidewall dissection distally for adhesions or fibrosis.
Once the ureter is mobilized, we excise the involved peritoneum along with the mass. We then seal and transect the uteroovarian ligament.
FIGURE 2 The retroperitoneal approach
Grasp and incise the peritoneum just lateral to the adnexal mass and enter the retroperitoneal space, where loose areolar tissue is visible, with the ureter seen on the medial leaf of the broad ligament.
After dissecting this tissue, identify the ureter and internal iliac vessels.
Remove the mass in a bag
Once the mass is excised, we place it in a laparoscopic bag, as described for Case 1. Solid adnexal masses are problematic because they are not amenable to drainage, and morcellation is usually discouraged. Laparoscopic excision can still be carried out, and a minilaparotomy or posterior colpotomy can be used to extract the mass in a bag. Patients managed in this way still have a complication rate similar to or lower than that of patients undergoing laparotomy for oophorectomy; they also recover faster.
Risks in cases of malignancy
The risk of tumor spillage in laparoscopic surgery can be lowered using laparoscopically guided minilaparotomy techniques. Preoperative rupture appears to be more predictive of outcome.28
The concern about metastatic implants in a laparoscopic port site in patients who have gynecologic cancer is real, with an incidence ranging from 0.97% to 1.1%. The phenomenon usually affects women who had ovarian cancer and is most common after laparoscopy with findings of ascites, carcinomatosis, or persistent disease (in the case of second-look laparoscopy performed after completion of primary therapy for ovarian cancer).
These data suggest that port-site implantation is not a concern that should deter clinicians from laparoscopic evaluation of a suspected ovarian neoplasm unless a patient presents with ascites or carcinomatosis suggestive of advanced disease.29
Data are limited regarding delays in definitive therapy. One study suggests that definitive staging on the day of rupture does not influence overall outcome, but delay by more than 2 weeks may lead to poorer prognosis.30
CASE 2: OUTCOME
Laparoscopy is performed. On initial inspection, the peritoneal cavity is unremarkable. The right ovary is multicystic with normal surface anatomy. The mass is somewhat adherent to the pelvic sidewall. Adnexectomy is performed, and frozen section reveals the mass to be a serous cystadenoma.
1. Curtin JP. Management of the adnexal mass. Gynecol Oncol. 1994;55:S42-S46.
2. Goff BA, Mandel LS, Melancon CH, Muntz HG. Frequency of symptoms of ovarian cancer in women presenting to primary care clinics. JAMA. 2004;291:2705-2712.
3. Andersen MR, Goff BA, Lowe KA, et al. Combining a symptoms index with CA 125 to improve detection of ovarian cancer. Cancer. 2008;113:484-489.
4. Goff BA, Mandel LS, Drescher CW, et al. Development of an ovarian cancer symptom index: possibilities for earlier detection. Cancer. 2007;109:221-227.
5. Alcázar JL, Mercé LT, Laparte C, et al. A new scoring system to differentiate benign from malignant adnexal masses. Am J Obstet Gynecol. 2003;188:685-692.
6. Maggino T, Gadducci A, D’Addario V, et al. Prospective multicenter study on CA 125 in postmenopausal pelvic masses. Gynecol Oncol. 1994;54:117-123.
7. Malkasian GD, Jr, Knapp RC, Lavin PT, et al. Preoperative evaluation of serum CA 125 levels in premenopausal and postmenopausal patients with pelvic masses: discrimination of benign from malignant disease. Am J Obstet Gynecol. 1988;159:341-346.
8. Larobina M, Nottle P. Complete evidence regarding major vascular injuries during laparoscopic access. Surg Laparosc Endosc Percutan Tech. 2005;15:119-123.
9. Vilos GA, Vilos AG. Safe laparoscopic entry guided by Veress needle CO2 insufflation pressure. J Am Assoc Gynecol Laparosc. 2003;10:415-420.
10. Vilos GA, Vilos AG, Abu-Rafea B, Hollett-Caines J, Nikkhah-Abyaneh Z, Edris F. Three simple steps during closed laparoscopic entry may minimize major injuries. Surg Endosc. 2008 July 15. [Epub ahead of print]
11. Vilos GA, Ternamian A, Dempster J, Laberge PY. The Society of Obstetricians and Gynaecologists of Canada. Laparoscopic entry: a review of techniques, technologies, and complications. J Obstet Gynaecol Can. 2007;29:433-465.
12. Tulikangas PK, Nicklas A, Falcone T, Price LL. Anatomy of the left upper quadrant for cannula insertion. J Am Assoc Gynecol Laparosc. 2000;7:211-214.
13. Stepp KJ, Tulikangas PK, Goldberg JM, Attaran M, Falcone T. Laparoscopy for adnexal masses in the second trimester of pregnancy. J Am Assoc Gynecol Laparosc. 2003;10:55-59.
14. Tulikangas PK, Robinson DS, Falcone T. Left upper quadrant cannula insertion. Fertil Steril. 2003;79:411-412.
15. Whiteside JL, Barber MD, Walters MD, Falcone T. Anatomy of ilioinguinal and iliohypogastric nerves in relation to trocar placement and low transverse incisions. Am J Obstet Gynecol. 2003;189:1574-1578.
16. Yim SF, Yuen PM. Randomized double-masked comparison of radially expanding access device and conventional cutting tip trocar in laparoscopy. Obstet Gynecol. 2001;97:435-438.
17. Johnson WH, Fecher AM, McMahon RL, et al. VersaStep trocar hernia rate in unclosed fascial defects in bariatric patients. Surg Endosc. 2006;20:1584-1586.
18. Lin P, Falcone T, Tulandi T. Excision of ovarian dermoid cyst by laparoscopy and by laparotomy. Am J Obstet Gynecol. 1995;173:769-771.
19. Jemal A, Murray T, Samuels A, et al. Cancer statistics, 2003. CA Cancer J Clin. 2003;53:5-26.
20. Kauff ND, Satagopan JM, Robson ME, et al. Risk-reducing salpingooophorectomy in women with a BRCA1 or BRCA2 mutation. N Engl J Med. 2002;346:1609-1615.
21. King MC, Marks JH, Mandell JB. Breast and ovarian cancer risks due to inherited mutations in BRCA1 and BRCA2. Science. 2003;302:643-646.
22. Aarnio M, Sankila R, Pukkala E, et al. Cancer risk in mutation carriers of DNA-mismatch-repair genes. Int J Cancer. 1999;81:214-218.
23. Dunlop MG, Farrington SM, Carothers AD, et al. Cancer risk associated with germline DNA mismatch repair gene mutations. Hum Mol Genet. 1997;6:105-110.
24. Dowdy SC, Stefanek M, Hartmann LC. Surgical risk reduction: prophylactic salpingooophorectomy and prophylactic mastectomy. Am J Obstet Gynecol. 2004;191:1113-1123.
25. Narod SA, Risch H, Moslehi R, et al. Oral contraceptives and the risk of hereditary ovarian cancer. Hereditary Ovarian Cancer Clinical Study Group. N Engl J Med. 1998;339:424-428.
26. Whittemore AS, Balise RR, Pharoah PD, et al. Oral contraceptive use and ovarian cancer risk among carriers of BRCA1 or BRCA2 mutations. Br J Cancer. 2004;91:1911-1915.
27. Im SS, Gordon AN, Buttin BM, et al. Validation of referral guidelines for women with pelvic masses. Obstet Gynecol. 2005;105:35-41.
28. Vergote I, De Brabanter J, Fyles A, et al. Prognostic importance of degree of differentiation and cyst rupture in stage I invasive epithelial ovarian carcinoma. Lancet. 2001;357:176-182.
29. Ramirez PT, Wolf JK, Levenback C. Laparoscopic port-site metastases: etiology and prevention. Gynecol Oncol. 2003;91:179-189.
30. Lehner R, Wenzl R, Heinzl H, Husslein P, Sevelda P. Influence of delayed staging laparotomy after laparoscopic removal of ovarian masses later found malignant. Obstet Gynecol. 1998;92:967-971.
1. Curtin JP. Management of the adnexal mass. Gynecol Oncol. 1994;55:S42-S46.
2. Goff BA, Mandel LS, Melancon CH, Muntz HG. Frequency of symptoms of ovarian cancer in women presenting to primary care clinics. JAMA. 2004;291:2705-2712.
3. Andersen MR, Goff BA, Lowe KA, et al. Combining a symptoms index with CA 125 to improve detection of ovarian cancer. Cancer. 2008;113:484-489.
4. Goff BA, Mandel LS, Drescher CW, et al. Development of an ovarian cancer symptom index: possibilities for earlier detection. Cancer. 2007;109:221-227.
5. Alcázar JL, Mercé LT, Laparte C, et al. A new scoring system to differentiate benign from malignant adnexal masses. Am J Obstet Gynecol. 2003;188:685-692.
6. Maggino T, Gadducci A, D’Addario V, et al. Prospective multicenter study on CA 125 in postmenopausal pelvic masses. Gynecol Oncol. 1994;54:117-123.
7. Malkasian GD, Jr, Knapp RC, Lavin PT, et al. Preoperative evaluation of serum CA 125 levels in premenopausal and postmenopausal patients with pelvic masses: discrimination of benign from malignant disease. Am J Obstet Gynecol. 1988;159:341-346.
8. Larobina M, Nottle P. Complete evidence regarding major vascular injuries during laparoscopic access. Surg Laparosc Endosc Percutan Tech. 2005;15:119-123.
9. Vilos GA, Vilos AG. Safe laparoscopic entry guided by Veress needle CO2 insufflation pressure. J Am Assoc Gynecol Laparosc. 2003;10:415-420.
10. Vilos GA, Vilos AG, Abu-Rafea B, Hollett-Caines J, Nikkhah-Abyaneh Z, Edris F. Three simple steps during closed laparoscopic entry may minimize major injuries. Surg Endosc. 2008 July 15. [Epub ahead of print]
11. Vilos GA, Ternamian A, Dempster J, Laberge PY. The Society of Obstetricians and Gynaecologists of Canada. Laparoscopic entry: a review of techniques, technologies, and complications. J Obstet Gynaecol Can. 2007;29:433-465.
12. Tulikangas PK, Nicklas A, Falcone T, Price LL. Anatomy of the left upper quadrant for cannula insertion. J Am Assoc Gynecol Laparosc. 2000;7:211-214.
13. Stepp KJ, Tulikangas PK, Goldberg JM, Attaran M, Falcone T. Laparoscopy for adnexal masses in the second trimester of pregnancy. J Am Assoc Gynecol Laparosc. 2003;10:55-59.
14. Tulikangas PK, Robinson DS, Falcone T. Left upper quadrant cannula insertion. Fertil Steril. 2003;79:411-412.
15. Whiteside JL, Barber MD, Walters MD, Falcone T. Anatomy of ilioinguinal and iliohypogastric nerves in relation to trocar placement and low transverse incisions. Am J Obstet Gynecol. 2003;189:1574-1578.
16. Yim SF, Yuen PM. Randomized double-masked comparison of radially expanding access device and conventional cutting tip trocar in laparoscopy. Obstet Gynecol. 2001;97:435-438.
17. Johnson WH, Fecher AM, McMahon RL, et al. VersaStep trocar hernia rate in unclosed fascial defects in bariatric patients. Surg Endosc. 2006;20:1584-1586.
18. Lin P, Falcone T, Tulandi T. Excision of ovarian dermoid cyst by laparoscopy and by laparotomy. Am J Obstet Gynecol. 1995;173:769-771.
19. Jemal A, Murray T, Samuels A, et al. Cancer statistics, 2003. CA Cancer J Clin. 2003;53:5-26.
20. Kauff ND, Satagopan JM, Robson ME, et al. Risk-reducing salpingooophorectomy in women with a BRCA1 or BRCA2 mutation. N Engl J Med. 2002;346:1609-1615.
21. King MC, Marks JH, Mandell JB. Breast and ovarian cancer risks due to inherited mutations in BRCA1 and BRCA2. Science. 2003;302:643-646.
22. Aarnio M, Sankila R, Pukkala E, et al. Cancer risk in mutation carriers of DNA-mismatch-repair genes. Int J Cancer. 1999;81:214-218.
23. Dunlop MG, Farrington SM, Carothers AD, et al. Cancer risk associated with germline DNA mismatch repair gene mutations. Hum Mol Genet. 1997;6:105-110.
24. Dowdy SC, Stefanek M, Hartmann LC. Surgical risk reduction: prophylactic salpingooophorectomy and prophylactic mastectomy. Am J Obstet Gynecol. 2004;191:1113-1123.
25. Narod SA, Risch H, Moslehi R, et al. Oral contraceptives and the risk of hereditary ovarian cancer. Hereditary Ovarian Cancer Clinical Study Group. N Engl J Med. 1998;339:424-428.
26. Whittemore AS, Balise RR, Pharoah PD, et al. Oral contraceptive use and ovarian cancer risk among carriers of BRCA1 or BRCA2 mutations. Br J Cancer. 2004;91:1911-1915.
27. Im SS, Gordon AN, Buttin BM, et al. Validation of referral guidelines for women with pelvic masses. Obstet Gynecol. 2005;105:35-41.
28. Vergote I, De Brabanter J, Fyles A, et al. Prognostic importance of degree of differentiation and cyst rupture in stage I invasive epithelial ovarian carcinoma. Lancet. 2001;357:176-182.
29. Ramirez PT, Wolf JK, Levenback C. Laparoscopic port-site metastases: etiology and prevention. Gynecol Oncol. 2003;91:179-189.
30. Lehner R, Wenzl R, Heinzl H, Husslein P, Sevelda P. Influence of delayed staging laparotomy after laparoscopic removal of ovarian masses later found malignant. Obstet Gynecol. 1998;92:967-971.
‘Night owls’: Reset the physiologic clock in delayed sleep phase disorder
Jason, age 16, has had difficulty with sleep initiation for 2 years. He describes going to bed at 10:30 PM on school nights but falling asleep no sooner than midnight and typically after 1:30 AM. He denies contributions from an “active mind” or environmental disturbances, and his bedroom contains no TV, computer, or other media devices. He does not sleep better with a change in environment. He denies pervasive low mood symptoms and believes his mood hinges predominantly on his ability to achieve sufficient sleep.
Once asleep, Jason generally enjoys good sleep consolidation until he needs to arise at 6:30 AM. His mother awakens him with difficulty, as he often sleeps through his alarm. He sleeps approximately 5 hours nightly during the school week, endorses impaired concentration, and often dozes during his first several classes. When he returns home from school, he finds it very difficult to resist napping.
On weekends he retires at 1 AM or later and typically falls asleep within 30 minutes. He usually awakens at noon but can sleep as late as 4:30 PM. He feels slightly more refreshed on weekends and describes his mood then as improved. During a recent spring break, he felt much better when allowed to sleep as much as he wanted.
Delayed sleep phase disorder (DSPD)—characterized by a pathological “night owl” circadian preference—is seen most commonly in adolescents and is associated with psychiatric morbidity, psychosocial impairment, and poor academic performance. Proper identification of the condition can be enhanced with a variety of assessment tools, and successful treatment requires an awareness of potential endogenous and exogenous contributors.
This article describes what is known about DSPD and uses the case example to illustrate diagnostic assessment and treatment choices. Intriguing data support various pathophysiologic explanations for DSPD (Box 1).1-6 Facilitating the adjustment of patients’ physiologic clocks is the overall goal in managing DSPD.
In individuals normally entrained to the light/dark cycle, circadian rhythms are:
- delayed by evening exposure to bright light (≥ 2,500 lux) prior to the core body temperature minimum (Tmin)
- advanced by morning light exposure after the Tmin.1
These opposing effects attune most people to the light/dark cycle, with sleep and wakefulness occurring on a conventional schedule. Persons with delayed sleep phase disorder (DSPD) live at a delayed phase that resists advancement and is incompatible with their personal and social obligations.
Theories have been proposed, but DSPD’s etiology has not been fully explained. Affected adolescents may exhibit an extreme in circadian preference. Case reports also describe DSPD emerging after traumatic brain injury.2
Intriguing evidence supports various pathophysiologic explanations for DSPD. An abnormally long intrinsic circadian period (>25 hours) was recently demonstrated during temporal isolation in 1 individual with DSPD.3 Both this case report and controlled studies describe deviations from expected relationships between the sleep/wake cycle and physiologic circadian markers. Most consistently described are longer intervals from Tmin4 to sleep offset (final rise time) in DSPD patients compared with controls.
Other research suggests:
Extreme ‘eveningness’
Because of their extreme seemingly innate preference to retire and arise at relatively late clock hours (an “eveningness” trait), school-aged patients with DSPD represent a high-risk population for problematic sleepiness. In a survey of 612 high school students, the 63% who felt they needed more sleep on school nights showed a strong eveningness preference (as assessed by questionnaire), compared with students who described getting sufficient sleep.7 Other studies have revealed psychiatric morbidity (including affective and personality disorders), psychosocial impairment, and poor academic performance associated with the condition.8-10
DSPD may affect 7% to 16% of patients presenting with insomnia complaints in sleep medicine clinics.11 The condition appears most common among young cohorts and has been reported to affect up to 7% of adolescents in the United States.12 Its high frequency in this age group may be a pathologic exaggeration of the normal tendency toward delayed timing of sleep and wakefulness linked with pubertal development.13
Sleep and wakefulness regulation
Conceptually, 2 processes govern sleep and wakefulness:
- The homeostatic drive to sleep (process S) is proportional to the duration of sleep restriction and becomes maximal at about 40 hours.
- Circadian regulation (process C) creates a drive for wakefulness that variably opposes process S and depends upon intrinsic rhythms.14
Neurons of the suprachiasmatic nucleus in the hypothalamus exert master coordination of this sleep/wake rhythm, along with other behavioral and physiologic variables.15 Because the typical intrinsic period is slightly longer than 24 hours, synchronization to the 24-hour day (entrainment) is accomplished by environmental inputs (zeitgebers, or “time givers”), the most important of which is exposure to light.16
Misalignment between endogenous circadian rhythms and the light/dark cycle can result in circadian rhythm sleep disorders, such as:
- delayed sleep timing (DSPD)
- advanced sleep timing (advanced sleep phase disorder)
- erratic sleep timing (irregular sleep/wake rhythm)
- complete dissociation from the light/dark cycle (circadian rhythm sleep disorder, free-running type).
These 4 conditions are thought to involve predominantly intrinsic mechanisms, but circadian dysrhythmias also can be induced by exogenous factors. Extreme work schedules or rapid travel across time zones can challenge the circadian system’s ability to acclimate and the individual’s ability to achieve a desired sleep schedule.17
Differential diagnosis
Because DSPD relates primarily to an aberration in timing of sleep, it is characterized as a disorder only if the individual’s preferred schedule interferes substantially with social or occupational functioning. The International Classification of Sleep Disorders (ICSD) provides detailed diagnostic criteria (Table).17
Table
Diagnostic criteria for delayed sleep phase disorder
A. Delay exists in the phase of the major sleep period in relation to desired sleep time and wake-up time, as evidenced by:
|
| B. When allowed to choose a preferred schedule, patients exhibit normal sleep quality and duration for age and maintain a delayed but stable phase of entrainment to the 24-hour sleep/wake pattern. |
| C. Monitoring with a sleep log or actigraphy (including sleep diary) for at least 7 days demonstrates a stable delay in the timing of the habitual sleep period. |
| D. The sleep disturbance is not better explained by another sleep disorder, medical or neurologic disorder, mental disorder, medication use, or substance use disorder. |
| Source: Adapted and reprinted with permission from International classification of sleep disorders. Diagnostic and coding manual. 2nd ed17 |
Depression and anxiety often manifest with sleep difficulties, as do inadequate sleep hygiene and other conditions associated with prolonged sleep initiation. According to ICSD criteria, primary insomnia can be differentiated from DSPD if the patient readily initiates and maintains sleep when allowed to sleep on his/her desired sleep/wake schedule. Accumulated evidence has largely debunked this notion, however, as polysomnographic studies have demonstrated both prolonged sleep latency and impaired sleep efficiency in DSPD patients versus matched controls.3
Assessment tools can complement the clinical history in diagnosing DSPD. Either a sleep log or actigraphy is required to demonstrate a stable phase delay, but actigraphy typically generates more reliable data.18 Actigraphs are compact “motion detectors” whose output while being worn by patients allows longitudinal assessment of sleep/wake parameters.
Eveningness tendencies of presumptive DSPD patients can be further verified with the Morningness-Eveningness Questionnaire (MEQ) (Box 2).19 Low scores are associated with evening types—felt to correspond to the endogenous circadian period—and can help narrow the differential diagnosis of sleep-initiation complaints.20
The Morningness-Eveningness Questionnaire (MEQ) developed by Horne and Ostberg19 can be used to verify eveningness tendencies of patients with presumptive delayed sleep phase disorder. The MEQ is a 19-item self-assessment tool with responses that are assigned values totaling up to 86 points. Examples of the questions include:
- Considering only your own ‘feeling best’ rhythm, at what time would you get up if you were entirely free to plan your day?
- Considering only your own ‘feeling best’ rhythm, at what time would you go to bed if you were entirely free to plan your day?
- How easy do you find it to get up each day?
- When you have no commitments the next day, how much later do you go to bed compared to your usual bedtime?
- One hears about ‘morning’ and ‘evening’ types of people. Which ONE of these types do you consider yourself to be?
Lower scores are associated with evening types—felt to correspond to the endogenous circadian period—and can help in narrowing the differential diagnosis of sleep-initiation complaints.20 Scores on the MEQ are interpreted as:
- 70 to 86: definite morning type
- 59 to 69: moderately morning type
- 42 to 58: neither type
- 31 to 41: moderately evening type
- 16 to 30: definite evening type
CASE CONTINUED: ‘Definite evening type’
Jason scores 28 on the MEQ, consistent with a “definite evening type.” Actigraphic monitoring is scheduled during a school holiday, when he is instructed to sleep according to his preferred schedule with the least possible restriction.
A clearly delayed sleep phase is evident, with the habitual sleep period occurring between 5 AM and 1 PM. Even on days when he was quite sleep-restricted because of an enforced wake time, sleep onset on the ensuing evening was substantially delayed, suggesting an obligate nature for the delayed sleep/wake schedule. Overall, Jason had few complaints with respect to impaired alertness while on this unrestricted schedule and experienced a much more stable mood.
Interventions
Without physiologic assessments, understanding the patient’s “natural” sleep schedule can allow for rational recommendations about using phototherapy and oral melatonin (Figure21). However, referral to a sleep specialist is required unless the general psychiatrist has experience in treating circadian rhythm sleep disorders.
Morning phototherapy. Properly timed morning bright light therapy (≥2,500 lux) has been shown to help DSPD patients achieve physiologically measured sleep phase advances, objective improvements in daytime alertness, and earlier reported bedtimes compared with controls.22 Unfortunately, the described 2-hour treatment duration make this research protocol clinically impractical, and most clinicians commence with a 30-minute duration of therapy, as described in the seasonal affective disorder literature.
Relatively new and widely available blue light boxes have been reported to exhibit at least equivalent efficacy to bright light devices (as reported in the literature pertaining to seasonal affective disorder), but with markedly decreased light intensity and fewer associated adverse effects.23 As the research addressing their use in the treatment of circadian rhythm sleep disorders is still emerging, their future role remains uncertain.
Precautions. Most psychiatrists would not perform a physiologic determination of a patient’s circadian phase, and further undesired phase delays can occur if phototherapy is administered before the core body temperature minimum (Tmin).24 Also, use caution if prescribing phototherapy to patients taking photosensitizing drugs and/or those with ocular or retinal pathology.20
Evening light avoidance. Whether or not you prescribe morning phototherapy, recommending that DSPD patients avoid evening light is essential to avoid further induction or exacerbation of phase delays. Protective eyewear is warranted in instances where these advisory precautions are insufficient (see Related Resources). Such an intervention has been shown effective in decreasing light exposure and undesired phase advances in studies involving subjects exposed to simulated shift work.25
Oral melatonin. Abundant evidence supports melatonin use in achieving phase advances in individuals with DSPD.26,27 A synergistic effect can be obtained when melatonin is combined with phototherapy.28
Proper timing of melatonin to achieve a maximal phase advance can be estimated based on the individual’s dim light melatonin onset (DLMO), which occurs approximately 14 hours after the habitual (unrestricted) wake time.29 Maximal phase advances appear to occur when melatonin is given approximately 6 hours before the DLMO.26 Thus, a rational practice is to recommend that patients take melatonin 8 hours after their natural wake time. Doses of ≤0.5 mg appear to achieve the maximal chronobiotic effect while avoiding an undesired hypnotic effect.30
Precautions. Verifying the purity of over-the-counter melatonin is difficult. A review by the National Academy of Sciences states that short-term use of melatonin, ≤10 mg/d, appears to be safe in healthy adults but recommends caution in children/adolescents and women of reproductive age. Doses recommended for circadian-based interventions are typically physiologic in nature (i.e., ≤0.5 mg), which may serve to mitigate these concerns.
Adverse effects such as headaches, somnolence, hypotension, hypertension, gastrointestinal upset, and exacerbation of alopecia areata have been reported at higher melatonin doses in healthy adults and at lower doses in persons with preexisting central nervous system, cardiovascular, gastrointestinal, or dermatologic conditions.31
Figure Light and melatonin phase response curves: Normal vs. delayed
This schematic compares ‘normal sleep’ phase response curves (PRCs) to light and exogenous melatonin with postulated PRCs for an individual with delayed sleep phase disorder (DSPD), presumed to be 5 hours ‘out of phase.’ Y-axis shows the direction and relative magnitude of phase shifts produced by light or melatonin at times shown on the x-axis. X-axis covers >24 hours to better illustrate the PRCs.
Relationships between ‘normal sleepers’ and DSPD patients are depicted by:
- rectangles (sleep period)
- triangles (core body temperature minimum [Tmin])
- arrows (dim light melatonin onsets [DLMOs]).
‘Normal’ sleep is shown to occur from midnight to 8 AM, and the DSPD patient’s sleep from 5 AM to 1 PM; DLMO and Tmin are similarly delayed by 5 hours in the DSPD patient. This schematic assumes that phase relationships are maintained in DSPD patients, which is not a certainty.
Source: Adapted from reference 21
CASE CONTINUED: Under the bright lights
Jason starts phototherapy treatment during his winter break, administering bright light daily upon natural awakening using a 10,000 lux light box for at least 30 minutes. As instructed, he gradually advances the time of administration by approximately 30 minutes every other day, striving for a nocturnal sleep period of 11 PM to 7 AM. He also wears protective eyewear to reduce light exposure during evening hours to avoid further delays in sleep phase. To further promote a phase advance, he takes oral melatonin, 0.5 mg/d at approximately 8 PM, as determined by his self-report and results of actigraphic recording.
Other options
Hypnotics. Little evidence supports the use of hypnotics in DSPD,32 and patients may show resistance to these drugs.33 Nevertheless, hypnotics can heighten confidence in the ability to initiate sleep in individuals with a concomitant conditioned insomnia.
With chronotherapy, patients are prescribed a sleep schedule that is delayed several hours incrementally until sleep is aligned to a target bedtime. The individual then is advised to rigorously maintain a regular sleep/wake schedule, repeating the process as necessary.
Although case reports have shown positive results with chronotherapy for DSPD,34 no controlled trials have demonstrated its efficacy or safety. One study reported high relapse rates,31 and 1 patient with DSPD developed free-running circadian rhythms.35 Clinical experience suggests chronotherapy is impractical for patients who must adhere to a fixed schedule.
Behavioral approaches
For an adolescent with DSPD, consider asking the school district to allow him or her a later school start-time. This alone often can substantially increase total sleep time and mitigate associated impairments.36 In all instances pursue and address external contributors to DSPD, such as poor sleep hygiene (including excessive caffeine use) and substance misuse.
Emphasize regular wake times, as arising later on weekends can cause phase delays.37 DSPD patients may have a concomitant conditioned insomnia that responds to evidence-based behavioral treatments.38
Whatever intervention you choose, schedule a follow-up appointment in approximately 2 months to evaluate patients’ progress and compliance. Encourage them to contact you with questions or concerns in the interim. Review sleep logs or actigraphy during this visit, and adjust the timing and/or nature of interventions as needed. Adolescents can be particularly noncompliant with clinical interventions, and therapeutic goals cannot be reached without their full investment.
Because no guidelines exist on how long to treat DSPD, stop on a “trial-and-error” basis when symptoms are controlled, and resume if they recur. Another approach is to maintain a desired sleep/wake schedule with bedtime melatonin and encourage continued adherence to other measures.
CASE CONTINUED: Maintenance therapy
Jason returns to the clinic approximately 10 weeks later. After an obviously concerted effort to adhere to treatment, his progress is quite remarkable. He rarely falls asleep later than 11 PM, so he is obtaining 2.5 hours more sleep each night before arising for school at 6:30 AM. Sleepiness at school is rarely problematic, and his mood is more stable.
He nevertheless describes a persistent tendency to retire and arise later and asks to continue melatonin and phototherapy. Because no guidelines exist for long-term therapy of DSPD, he is advised to switch melatonin to bedtime dosing (with a presumed phase-neutral “maintenance” effect), and to continue phototherapy as prescribed.
- Wyatt JK. Delayed sleep phase syndrome: pathophysiology and treatment options. Sleep. 2004;27(6):1195-1203.
- Crowley SJ, Acebo C, Carskadon MA. Sleep, circadian rhythms, and delayed sleep phase in adolescence. Sleep Med. 2007;8(6):602-612.
- National Sleep Foundation. Adolescent sleep needs and patterns: research report and resource guide. Washington, DC; 2000:1-30.
- Products designed to assist in the avoidance of light at improper times. www.lowbluelights.com.
Disclosure
Dr. Auger reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Khalsa SB, Jewett ME, Cajochen C, et al. A phase response curve to single bright light pulses in human subjects. J Physiol. 2003;549(Pt 3):945-952.
2. Quinto C, Gellido C, Chokroverty S, et al. Posttraumatic delayed sleep phase syndrome. Neurology. 2000;54(1):250-252.
3. Campbell SS, Murphy PJ. Delayed sleep phase disorder in temporal isolation. Sleep. 2007;30(9):1225-1228.
4. Uchiyama M, Okawa M, Shibui K, et al. Altered phase relation between sleep timing and core body temperature rhythm in delayed sleep phase syndrome and non-24-hour sleep-wake syndrome in humans. Neurosci Lett. 2000;294(2):101-104.
5. Aoki H, Ozeki Y, Yamada N. Hypersensitivity of melatonin suppression in response to light in patients with delayed sleep phase syndrome. Chronobiol Int. 2001;18(2):263-271.
6. Uchiyama M, Okawa M, Shibui K, et al. Poor compensatory function for sleep loss as a pathogenic factor in patients with delayed sleep phase syndrome. Sleep. 2000;23(4):553-558.
7. Mercer PW, Merritt SL, Cowell JM. Differences in reported sleep need among adolescents. J Adolesc Health. 1998;23(5):259-263.
8. Krahn LE, Pankratz VS, Harris AM, et al. Long-term outcome of adolescents with delayed sleep phase disorder [abstract]. Sleep. 2003;26:A115.-
9. Dagan Y, Stein D, Steinbock M, et al. Frequency of delayed sleep phase syndrome among hospitalized adolescent psychiatric patients. J Psychosom Res. 1998;45(1):15-20.
10. Thorpy MJ, Korman E, Spielman AJ, et al. Delayed sleep phase syndrome in adolescents. J Adolesc Health Care. 1998;9(1):22-27.
11. Regestein QR, Monk TH. Delayed sleep phase syndrome: a review of the clinical aspects. Am J Psychiatry. 1995;152(4):602-608.
12. Pelayo RP, Thorpy MJ, Glovinsky P. Prevalence of delayed sleep phase syndrome among adolescents [abstract]. Sleep Res. 1988;17:391.-
13. Gau SF, Soong WT. The transition of sleep-wake patterns in early adolescence. Sleep. 2003;26(4):449-454.
14. Beersma DG, Gordijn MC. Circadian control of the sleep-wake cycle. Physiol Behav. 2007;90(2-3):190-195.
15. Ralph MR, Foster RG, Davis FC, et al. Transplanted suprachiasmatic nucleus determines circadian period. Science. 1990;247(4945):975-978.
16. Waterhouse J, DeCoursey PJ. Chronobiology: biological timekeeping. Sunderland, MA: Sinauer Associates, Inc. Publishers; 2004:291-323.
17. American Academy of Sleep Medicine. International classification of sleep disorders. Diagnostic and coding manual. 2nd ed. Westchester, IL: American Academy of Sleep Medicine; 2005.
18. Bradshaw DA, Yanagi MA, Pak ES, et al. Nightly sleep duration in the 2-week period preceding multiple sleep latency testing. J Clin Sleep Med. 2007;3(6):613-619.
19. Horne JA, Ostberg O. A self-assessment questionnaire to determine morningness-eveningness in human circadian rhythms. Int J Chronobiol. 1976;4(2):97-110.
20. Sack RL, Auckley D, Auger RR, et al. Circadian rhythm sleep disorders: Part I. basic principles, shift work and jet lag disorders. Sleep. 2007;30(11):1460-1483.
21. Burgess HJ, Sharkey KM, Eastman CI. Bright light, dark and melatonin can promote circadian adaptation in night shift workers. Sleep Med Rev. 2002;6(5):407-420.
22. Rosenthal NE, Joseph-Vanderpool JR, Levendosky AA, et al. Phase-shifting effects of bright morning light as treatment for delayed sleep phase syndrome. Sleep. 1990;13(4):354-361.
23. Glickman G, Byrne B, Pineda C, et al. Light therapy for seasonal affective disorder with blue narrow-band light-emitting diodes (LEDs). Biol Psychiatry. 2006;59:502-507.
24. Czeisler C, Wright K, Jr. Influence of light on circadian rhythmicity in humans. New York, NY: Marcel Dekker; 1999:149-180.
25. Crowley SJ, Lee C, Tseng CY, et al. Combinations of bright light, scheduled dark, sunglasses, and melatonin to facilitate circadian entrainment to night shift work. J Biol Rhythms. 2003;18(6):513-523.
26. Mundey K, Benloucif S, Harsanyi K, et al. Phase-dependent treatment of delayed sleep phase syndrome with melatonin. Sleep. 2005;28(10):1271-1278.
27. Sack RL, Auckley D, Auger RR, et al. Circadian rhythm sleep disorders: Part II, advanced sleep phase disorder, delayed sleep phase disorder, free-running disorder, and irregular sleep-wake rhythm. Sleep. 2007;30(11):1484-1501.
28. Revell VL, Burgess HJ, Gazda CJ, et al. Advancing human circadian rhythms with afternoon melatonin and morning intermittent bright light. J Clin Endocrinol Metab. 2006;91(1):54-59.
29. Burgess HJ, Eastman CI. The dim light melatonin onset following fixed and free sleep schedules. J Sleep Res. 2005;14(3):229-237.
30. Lewy AJ. Clinical applications of melatonin in circadian disorders. Dialog Clin Neurosci. 2003;5:399-413.
31. Committee on the Framework for Evaluating the Safety of Dietary Supplements FaNB, Board on Life Sciences, Institute of Medicine and National Research Council of the National Academies. Dietary supplements: a framework for evaluating safety. Washington, DC: The National Academies Press; 2005.
32. Ito A, Ando K, Hayakawa T, et al. Long-term course of adult patients with delayed sleep phase syndrome. Jpn J Psychiatry Neurol. 1993;47(3):563-567.
33. Auger RR. Circadian rhythm sleep disorder, delayed sleep phase type (pediatric case). In: Winkelman JW (chair), Henderson JH, Kotagal S, et al, eds. Case book of sleep medicine. Westchester, IL: American Academy of Sleep Medicine; 2008:195-199.
34. Czeisler C, Weitzman E, Moore, et al. Chronotherapy: resetting the circadian clocks of patients with delayed sleep phase insomnia. Sleep. 1981;4:1-21.
35. Oren DA, Wehr TA. Hypernyctohemeral syndrome after chronotherapy for delayed sleep phase syndrome. N Engl J Med. 1992;327(24):1762.-
36. Wahlstrom K. Changing times: findings from the first longitudinal study of later high school start times. NASSP Bulletin. 2002;86(633):3-21.
37. Burgess HJ, Eastman CI. A late wake time phase delays the human dim light melatonin rhythm. Neurosci Lett. 2006;395(3):191-195.
38. Morgenthaler T, Kramer M, Alessi C, et al. Practice parameters for the psychological and behavioral treatment of insomnia: an update. An American Academy of Sleep Medicine report. Sleep. 2006;29(11):1415-1419.
Jason, age 16, has had difficulty with sleep initiation for 2 years. He describes going to bed at 10:30 PM on school nights but falling asleep no sooner than midnight and typically after 1:30 AM. He denies contributions from an “active mind” or environmental disturbances, and his bedroom contains no TV, computer, or other media devices. He does not sleep better with a change in environment. He denies pervasive low mood symptoms and believes his mood hinges predominantly on his ability to achieve sufficient sleep.
Once asleep, Jason generally enjoys good sleep consolidation until he needs to arise at 6:30 AM. His mother awakens him with difficulty, as he often sleeps through his alarm. He sleeps approximately 5 hours nightly during the school week, endorses impaired concentration, and often dozes during his first several classes. When he returns home from school, he finds it very difficult to resist napping.
On weekends he retires at 1 AM or later and typically falls asleep within 30 minutes. He usually awakens at noon but can sleep as late as 4:30 PM. He feels slightly more refreshed on weekends and describes his mood then as improved. During a recent spring break, he felt much better when allowed to sleep as much as he wanted.
Delayed sleep phase disorder (DSPD)—characterized by a pathological “night owl” circadian preference—is seen most commonly in adolescents and is associated with psychiatric morbidity, psychosocial impairment, and poor academic performance. Proper identification of the condition can be enhanced with a variety of assessment tools, and successful treatment requires an awareness of potential endogenous and exogenous contributors.
This article describes what is known about DSPD and uses the case example to illustrate diagnostic assessment and treatment choices. Intriguing data support various pathophysiologic explanations for DSPD (Box 1).1-6 Facilitating the adjustment of patients’ physiologic clocks is the overall goal in managing DSPD.
In individuals normally entrained to the light/dark cycle, circadian rhythms are:
- delayed by evening exposure to bright light (≥ 2,500 lux) prior to the core body temperature minimum (Tmin)
- advanced by morning light exposure after the Tmin.1
These opposing effects attune most people to the light/dark cycle, with sleep and wakefulness occurring on a conventional schedule. Persons with delayed sleep phase disorder (DSPD) live at a delayed phase that resists advancement and is incompatible with their personal and social obligations.
Theories have been proposed, but DSPD’s etiology has not been fully explained. Affected adolescents may exhibit an extreme in circadian preference. Case reports also describe DSPD emerging after traumatic brain injury.2
Intriguing evidence supports various pathophysiologic explanations for DSPD. An abnormally long intrinsic circadian period (>25 hours) was recently demonstrated during temporal isolation in 1 individual with DSPD.3 Both this case report and controlled studies describe deviations from expected relationships between the sleep/wake cycle and physiologic circadian markers. Most consistently described are longer intervals from Tmin4 to sleep offset (final rise time) in DSPD patients compared with controls.
Other research suggests:
Extreme ‘eveningness’
Because of their extreme seemingly innate preference to retire and arise at relatively late clock hours (an “eveningness” trait), school-aged patients with DSPD represent a high-risk population for problematic sleepiness. In a survey of 612 high school students, the 63% who felt they needed more sleep on school nights showed a strong eveningness preference (as assessed by questionnaire), compared with students who described getting sufficient sleep.7 Other studies have revealed psychiatric morbidity (including affective and personality disorders), psychosocial impairment, and poor academic performance associated with the condition.8-10
DSPD may affect 7% to 16% of patients presenting with insomnia complaints in sleep medicine clinics.11 The condition appears most common among young cohorts and has been reported to affect up to 7% of adolescents in the United States.12 Its high frequency in this age group may be a pathologic exaggeration of the normal tendency toward delayed timing of sleep and wakefulness linked with pubertal development.13
Sleep and wakefulness regulation
Conceptually, 2 processes govern sleep and wakefulness:
- The homeostatic drive to sleep (process S) is proportional to the duration of sleep restriction and becomes maximal at about 40 hours.
- Circadian regulation (process C) creates a drive for wakefulness that variably opposes process S and depends upon intrinsic rhythms.14
Neurons of the suprachiasmatic nucleus in the hypothalamus exert master coordination of this sleep/wake rhythm, along with other behavioral and physiologic variables.15 Because the typical intrinsic period is slightly longer than 24 hours, synchronization to the 24-hour day (entrainment) is accomplished by environmental inputs (zeitgebers, or “time givers”), the most important of which is exposure to light.16
Misalignment between endogenous circadian rhythms and the light/dark cycle can result in circadian rhythm sleep disorders, such as:
- delayed sleep timing (DSPD)
- advanced sleep timing (advanced sleep phase disorder)
- erratic sleep timing (irregular sleep/wake rhythm)
- complete dissociation from the light/dark cycle (circadian rhythm sleep disorder, free-running type).
These 4 conditions are thought to involve predominantly intrinsic mechanisms, but circadian dysrhythmias also can be induced by exogenous factors. Extreme work schedules or rapid travel across time zones can challenge the circadian system’s ability to acclimate and the individual’s ability to achieve a desired sleep schedule.17
Differential diagnosis
Because DSPD relates primarily to an aberration in timing of sleep, it is characterized as a disorder only if the individual’s preferred schedule interferes substantially with social or occupational functioning. The International Classification of Sleep Disorders (ICSD) provides detailed diagnostic criteria (Table).17
Table
Diagnostic criteria for delayed sleep phase disorder
A. Delay exists in the phase of the major sleep period in relation to desired sleep time and wake-up time, as evidenced by:
|
| B. When allowed to choose a preferred schedule, patients exhibit normal sleep quality and duration for age and maintain a delayed but stable phase of entrainment to the 24-hour sleep/wake pattern. |
| C. Monitoring with a sleep log or actigraphy (including sleep diary) for at least 7 days demonstrates a stable delay in the timing of the habitual sleep period. |
| D. The sleep disturbance is not better explained by another sleep disorder, medical or neurologic disorder, mental disorder, medication use, or substance use disorder. |
| Source: Adapted and reprinted with permission from International classification of sleep disorders. Diagnostic and coding manual. 2nd ed17 |
Depression and anxiety often manifest with sleep difficulties, as do inadequate sleep hygiene and other conditions associated with prolonged sleep initiation. According to ICSD criteria, primary insomnia can be differentiated from DSPD if the patient readily initiates and maintains sleep when allowed to sleep on his/her desired sleep/wake schedule. Accumulated evidence has largely debunked this notion, however, as polysomnographic studies have demonstrated both prolonged sleep latency and impaired sleep efficiency in DSPD patients versus matched controls.3
Assessment tools can complement the clinical history in diagnosing DSPD. Either a sleep log or actigraphy is required to demonstrate a stable phase delay, but actigraphy typically generates more reliable data.18 Actigraphs are compact “motion detectors” whose output while being worn by patients allows longitudinal assessment of sleep/wake parameters.
Eveningness tendencies of presumptive DSPD patients can be further verified with the Morningness-Eveningness Questionnaire (MEQ) (Box 2).19 Low scores are associated with evening types—felt to correspond to the endogenous circadian period—and can help narrow the differential diagnosis of sleep-initiation complaints.20
The Morningness-Eveningness Questionnaire (MEQ) developed by Horne and Ostberg19 can be used to verify eveningness tendencies of patients with presumptive delayed sleep phase disorder. The MEQ is a 19-item self-assessment tool with responses that are assigned values totaling up to 86 points. Examples of the questions include:
- Considering only your own ‘feeling best’ rhythm, at what time would you get up if you were entirely free to plan your day?
- Considering only your own ‘feeling best’ rhythm, at what time would you go to bed if you were entirely free to plan your day?
- How easy do you find it to get up each day?
- When you have no commitments the next day, how much later do you go to bed compared to your usual bedtime?
- One hears about ‘morning’ and ‘evening’ types of people. Which ONE of these types do you consider yourself to be?
Lower scores are associated with evening types—felt to correspond to the endogenous circadian period—and can help in narrowing the differential diagnosis of sleep-initiation complaints.20 Scores on the MEQ are interpreted as:
- 70 to 86: definite morning type
- 59 to 69: moderately morning type
- 42 to 58: neither type
- 31 to 41: moderately evening type
- 16 to 30: definite evening type
CASE CONTINUED: ‘Definite evening type’
Jason scores 28 on the MEQ, consistent with a “definite evening type.” Actigraphic monitoring is scheduled during a school holiday, when he is instructed to sleep according to his preferred schedule with the least possible restriction.
A clearly delayed sleep phase is evident, with the habitual sleep period occurring between 5 AM and 1 PM. Even on days when he was quite sleep-restricted because of an enforced wake time, sleep onset on the ensuing evening was substantially delayed, suggesting an obligate nature for the delayed sleep/wake schedule. Overall, Jason had few complaints with respect to impaired alertness while on this unrestricted schedule and experienced a much more stable mood.
Interventions
Without physiologic assessments, understanding the patient’s “natural” sleep schedule can allow for rational recommendations about using phototherapy and oral melatonin (Figure21). However, referral to a sleep specialist is required unless the general psychiatrist has experience in treating circadian rhythm sleep disorders.
Morning phototherapy. Properly timed morning bright light therapy (≥2,500 lux) has been shown to help DSPD patients achieve physiologically measured sleep phase advances, objective improvements in daytime alertness, and earlier reported bedtimes compared with controls.22 Unfortunately, the described 2-hour treatment duration make this research protocol clinically impractical, and most clinicians commence with a 30-minute duration of therapy, as described in the seasonal affective disorder literature.
Relatively new and widely available blue light boxes have been reported to exhibit at least equivalent efficacy to bright light devices (as reported in the literature pertaining to seasonal affective disorder), but with markedly decreased light intensity and fewer associated adverse effects.23 As the research addressing their use in the treatment of circadian rhythm sleep disorders is still emerging, their future role remains uncertain.
Precautions. Most psychiatrists would not perform a physiologic determination of a patient’s circadian phase, and further undesired phase delays can occur if phototherapy is administered before the core body temperature minimum (Tmin).24 Also, use caution if prescribing phototherapy to patients taking photosensitizing drugs and/or those with ocular or retinal pathology.20
Evening light avoidance. Whether or not you prescribe morning phototherapy, recommending that DSPD patients avoid evening light is essential to avoid further induction or exacerbation of phase delays. Protective eyewear is warranted in instances where these advisory precautions are insufficient (see Related Resources). Such an intervention has been shown effective in decreasing light exposure and undesired phase advances in studies involving subjects exposed to simulated shift work.25
Oral melatonin. Abundant evidence supports melatonin use in achieving phase advances in individuals with DSPD.26,27 A synergistic effect can be obtained when melatonin is combined with phototherapy.28
Proper timing of melatonin to achieve a maximal phase advance can be estimated based on the individual’s dim light melatonin onset (DLMO), which occurs approximately 14 hours after the habitual (unrestricted) wake time.29 Maximal phase advances appear to occur when melatonin is given approximately 6 hours before the DLMO.26 Thus, a rational practice is to recommend that patients take melatonin 8 hours after their natural wake time. Doses of ≤0.5 mg appear to achieve the maximal chronobiotic effect while avoiding an undesired hypnotic effect.30
Precautions. Verifying the purity of over-the-counter melatonin is difficult. A review by the National Academy of Sciences states that short-term use of melatonin, ≤10 mg/d, appears to be safe in healthy adults but recommends caution in children/adolescents and women of reproductive age. Doses recommended for circadian-based interventions are typically physiologic in nature (i.e., ≤0.5 mg), which may serve to mitigate these concerns.
Adverse effects such as headaches, somnolence, hypotension, hypertension, gastrointestinal upset, and exacerbation of alopecia areata have been reported at higher melatonin doses in healthy adults and at lower doses in persons with preexisting central nervous system, cardiovascular, gastrointestinal, or dermatologic conditions.31
Figure Light and melatonin phase response curves: Normal vs. delayed
This schematic compares ‘normal sleep’ phase response curves (PRCs) to light and exogenous melatonin with postulated PRCs for an individual with delayed sleep phase disorder (DSPD), presumed to be 5 hours ‘out of phase.’ Y-axis shows the direction and relative magnitude of phase shifts produced by light or melatonin at times shown on the x-axis. X-axis covers >24 hours to better illustrate the PRCs.
Relationships between ‘normal sleepers’ and DSPD patients are depicted by:
- rectangles (sleep period)
- triangles (core body temperature minimum [Tmin])
- arrows (dim light melatonin onsets [DLMOs]).
‘Normal’ sleep is shown to occur from midnight to 8 AM, and the DSPD patient’s sleep from 5 AM to 1 PM; DLMO and Tmin are similarly delayed by 5 hours in the DSPD patient. This schematic assumes that phase relationships are maintained in DSPD patients, which is not a certainty.
Source: Adapted from reference 21
CASE CONTINUED: Under the bright lights
Jason starts phototherapy treatment during his winter break, administering bright light daily upon natural awakening using a 10,000 lux light box for at least 30 minutes. As instructed, he gradually advances the time of administration by approximately 30 minutes every other day, striving for a nocturnal sleep period of 11 PM to 7 AM. He also wears protective eyewear to reduce light exposure during evening hours to avoid further delays in sleep phase. To further promote a phase advance, he takes oral melatonin, 0.5 mg/d at approximately 8 PM, as determined by his self-report and results of actigraphic recording.
Other options
Hypnotics. Little evidence supports the use of hypnotics in DSPD,32 and patients may show resistance to these drugs.33 Nevertheless, hypnotics can heighten confidence in the ability to initiate sleep in individuals with a concomitant conditioned insomnia.
With chronotherapy, patients are prescribed a sleep schedule that is delayed several hours incrementally until sleep is aligned to a target bedtime. The individual then is advised to rigorously maintain a regular sleep/wake schedule, repeating the process as necessary.
Although case reports have shown positive results with chronotherapy for DSPD,34 no controlled trials have demonstrated its efficacy or safety. One study reported high relapse rates,31 and 1 patient with DSPD developed free-running circadian rhythms.35 Clinical experience suggests chronotherapy is impractical for patients who must adhere to a fixed schedule.
Behavioral approaches
For an adolescent with DSPD, consider asking the school district to allow him or her a later school start-time. This alone often can substantially increase total sleep time and mitigate associated impairments.36 In all instances pursue and address external contributors to DSPD, such as poor sleep hygiene (including excessive caffeine use) and substance misuse.
Emphasize regular wake times, as arising later on weekends can cause phase delays.37 DSPD patients may have a concomitant conditioned insomnia that responds to evidence-based behavioral treatments.38
Whatever intervention you choose, schedule a follow-up appointment in approximately 2 months to evaluate patients’ progress and compliance. Encourage them to contact you with questions or concerns in the interim. Review sleep logs or actigraphy during this visit, and adjust the timing and/or nature of interventions as needed. Adolescents can be particularly noncompliant with clinical interventions, and therapeutic goals cannot be reached without their full investment.
Because no guidelines exist on how long to treat DSPD, stop on a “trial-and-error” basis when symptoms are controlled, and resume if they recur. Another approach is to maintain a desired sleep/wake schedule with bedtime melatonin and encourage continued adherence to other measures.
CASE CONTINUED: Maintenance therapy
Jason returns to the clinic approximately 10 weeks later. After an obviously concerted effort to adhere to treatment, his progress is quite remarkable. He rarely falls asleep later than 11 PM, so he is obtaining 2.5 hours more sleep each night before arising for school at 6:30 AM. Sleepiness at school is rarely problematic, and his mood is more stable.
He nevertheless describes a persistent tendency to retire and arise later and asks to continue melatonin and phototherapy. Because no guidelines exist for long-term therapy of DSPD, he is advised to switch melatonin to bedtime dosing (with a presumed phase-neutral “maintenance” effect), and to continue phototherapy as prescribed.
- Wyatt JK. Delayed sleep phase syndrome: pathophysiology and treatment options. Sleep. 2004;27(6):1195-1203.
- Crowley SJ, Acebo C, Carskadon MA. Sleep, circadian rhythms, and delayed sleep phase in adolescence. Sleep Med. 2007;8(6):602-612.
- National Sleep Foundation. Adolescent sleep needs and patterns: research report and resource guide. Washington, DC; 2000:1-30.
- Products designed to assist in the avoidance of light at improper times. www.lowbluelights.com.
Disclosure
Dr. Auger reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Jason, age 16, has had difficulty with sleep initiation for 2 years. He describes going to bed at 10:30 PM on school nights but falling asleep no sooner than midnight and typically after 1:30 AM. He denies contributions from an “active mind” or environmental disturbances, and his bedroom contains no TV, computer, or other media devices. He does not sleep better with a change in environment. He denies pervasive low mood symptoms and believes his mood hinges predominantly on his ability to achieve sufficient sleep.
Once asleep, Jason generally enjoys good sleep consolidation until he needs to arise at 6:30 AM. His mother awakens him with difficulty, as he often sleeps through his alarm. He sleeps approximately 5 hours nightly during the school week, endorses impaired concentration, and often dozes during his first several classes. When he returns home from school, he finds it very difficult to resist napping.
On weekends he retires at 1 AM or later and typically falls asleep within 30 minutes. He usually awakens at noon but can sleep as late as 4:30 PM. He feels slightly more refreshed on weekends and describes his mood then as improved. During a recent spring break, he felt much better when allowed to sleep as much as he wanted.
Delayed sleep phase disorder (DSPD)—characterized by a pathological “night owl” circadian preference—is seen most commonly in adolescents and is associated with psychiatric morbidity, psychosocial impairment, and poor academic performance. Proper identification of the condition can be enhanced with a variety of assessment tools, and successful treatment requires an awareness of potential endogenous and exogenous contributors.
This article describes what is known about DSPD and uses the case example to illustrate diagnostic assessment and treatment choices. Intriguing data support various pathophysiologic explanations for DSPD (Box 1).1-6 Facilitating the adjustment of patients’ physiologic clocks is the overall goal in managing DSPD.
In individuals normally entrained to the light/dark cycle, circadian rhythms are:
- delayed by evening exposure to bright light (≥ 2,500 lux) prior to the core body temperature minimum (Tmin)
- advanced by morning light exposure after the Tmin.1
These opposing effects attune most people to the light/dark cycle, with sleep and wakefulness occurring on a conventional schedule. Persons with delayed sleep phase disorder (DSPD) live at a delayed phase that resists advancement and is incompatible with their personal and social obligations.
Theories have been proposed, but DSPD’s etiology has not been fully explained. Affected adolescents may exhibit an extreme in circadian preference. Case reports also describe DSPD emerging after traumatic brain injury.2
Intriguing evidence supports various pathophysiologic explanations for DSPD. An abnormally long intrinsic circadian period (>25 hours) was recently demonstrated during temporal isolation in 1 individual with DSPD.3 Both this case report and controlled studies describe deviations from expected relationships between the sleep/wake cycle and physiologic circadian markers. Most consistently described are longer intervals from Tmin4 to sleep offset (final rise time) in DSPD patients compared with controls.
Other research suggests:
Extreme ‘eveningness’
Because of their extreme seemingly innate preference to retire and arise at relatively late clock hours (an “eveningness” trait), school-aged patients with DSPD represent a high-risk population for problematic sleepiness. In a survey of 612 high school students, the 63% who felt they needed more sleep on school nights showed a strong eveningness preference (as assessed by questionnaire), compared with students who described getting sufficient sleep.7 Other studies have revealed psychiatric morbidity (including affective and personality disorders), psychosocial impairment, and poor academic performance associated with the condition.8-10
DSPD may affect 7% to 16% of patients presenting with insomnia complaints in sleep medicine clinics.11 The condition appears most common among young cohorts and has been reported to affect up to 7% of adolescents in the United States.12 Its high frequency in this age group may be a pathologic exaggeration of the normal tendency toward delayed timing of sleep and wakefulness linked with pubertal development.13
Sleep and wakefulness regulation
Conceptually, 2 processes govern sleep and wakefulness:
- The homeostatic drive to sleep (process S) is proportional to the duration of sleep restriction and becomes maximal at about 40 hours.
- Circadian regulation (process C) creates a drive for wakefulness that variably opposes process S and depends upon intrinsic rhythms.14
Neurons of the suprachiasmatic nucleus in the hypothalamus exert master coordination of this sleep/wake rhythm, along with other behavioral and physiologic variables.15 Because the typical intrinsic period is slightly longer than 24 hours, synchronization to the 24-hour day (entrainment) is accomplished by environmental inputs (zeitgebers, or “time givers”), the most important of which is exposure to light.16
Misalignment between endogenous circadian rhythms and the light/dark cycle can result in circadian rhythm sleep disorders, such as:
- delayed sleep timing (DSPD)
- advanced sleep timing (advanced sleep phase disorder)
- erratic sleep timing (irregular sleep/wake rhythm)
- complete dissociation from the light/dark cycle (circadian rhythm sleep disorder, free-running type).
These 4 conditions are thought to involve predominantly intrinsic mechanisms, but circadian dysrhythmias also can be induced by exogenous factors. Extreme work schedules or rapid travel across time zones can challenge the circadian system’s ability to acclimate and the individual’s ability to achieve a desired sleep schedule.17
Differential diagnosis
Because DSPD relates primarily to an aberration in timing of sleep, it is characterized as a disorder only if the individual’s preferred schedule interferes substantially with social or occupational functioning. The International Classification of Sleep Disorders (ICSD) provides detailed diagnostic criteria (Table).17
Table
Diagnostic criteria for delayed sleep phase disorder
A. Delay exists in the phase of the major sleep period in relation to desired sleep time and wake-up time, as evidenced by:
|
| B. When allowed to choose a preferred schedule, patients exhibit normal sleep quality and duration for age and maintain a delayed but stable phase of entrainment to the 24-hour sleep/wake pattern. |
| C. Monitoring with a sleep log or actigraphy (including sleep diary) for at least 7 days demonstrates a stable delay in the timing of the habitual sleep period. |
| D. The sleep disturbance is not better explained by another sleep disorder, medical or neurologic disorder, mental disorder, medication use, or substance use disorder. |
| Source: Adapted and reprinted with permission from International classification of sleep disorders. Diagnostic and coding manual. 2nd ed17 |
Depression and anxiety often manifest with sleep difficulties, as do inadequate sleep hygiene and other conditions associated with prolonged sleep initiation. According to ICSD criteria, primary insomnia can be differentiated from DSPD if the patient readily initiates and maintains sleep when allowed to sleep on his/her desired sleep/wake schedule. Accumulated evidence has largely debunked this notion, however, as polysomnographic studies have demonstrated both prolonged sleep latency and impaired sleep efficiency in DSPD patients versus matched controls.3
Assessment tools can complement the clinical history in diagnosing DSPD. Either a sleep log or actigraphy is required to demonstrate a stable phase delay, but actigraphy typically generates more reliable data.18 Actigraphs are compact “motion detectors” whose output while being worn by patients allows longitudinal assessment of sleep/wake parameters.
Eveningness tendencies of presumptive DSPD patients can be further verified with the Morningness-Eveningness Questionnaire (MEQ) (Box 2).19 Low scores are associated with evening types—felt to correspond to the endogenous circadian period—and can help narrow the differential diagnosis of sleep-initiation complaints.20
The Morningness-Eveningness Questionnaire (MEQ) developed by Horne and Ostberg19 can be used to verify eveningness tendencies of patients with presumptive delayed sleep phase disorder. The MEQ is a 19-item self-assessment tool with responses that are assigned values totaling up to 86 points. Examples of the questions include:
- Considering only your own ‘feeling best’ rhythm, at what time would you get up if you were entirely free to plan your day?
- Considering only your own ‘feeling best’ rhythm, at what time would you go to bed if you were entirely free to plan your day?
- How easy do you find it to get up each day?
- When you have no commitments the next day, how much later do you go to bed compared to your usual bedtime?
- One hears about ‘morning’ and ‘evening’ types of people. Which ONE of these types do you consider yourself to be?
Lower scores are associated with evening types—felt to correspond to the endogenous circadian period—and can help in narrowing the differential diagnosis of sleep-initiation complaints.20 Scores on the MEQ are interpreted as:
- 70 to 86: definite morning type
- 59 to 69: moderately morning type
- 42 to 58: neither type
- 31 to 41: moderately evening type
- 16 to 30: definite evening type
CASE CONTINUED: ‘Definite evening type’
Jason scores 28 on the MEQ, consistent with a “definite evening type.” Actigraphic monitoring is scheduled during a school holiday, when he is instructed to sleep according to his preferred schedule with the least possible restriction.
A clearly delayed sleep phase is evident, with the habitual sleep period occurring between 5 AM and 1 PM. Even on days when he was quite sleep-restricted because of an enforced wake time, sleep onset on the ensuing evening was substantially delayed, suggesting an obligate nature for the delayed sleep/wake schedule. Overall, Jason had few complaints with respect to impaired alertness while on this unrestricted schedule and experienced a much more stable mood.
Interventions
Without physiologic assessments, understanding the patient’s “natural” sleep schedule can allow for rational recommendations about using phototherapy and oral melatonin (Figure21). However, referral to a sleep specialist is required unless the general psychiatrist has experience in treating circadian rhythm sleep disorders.
Morning phototherapy. Properly timed morning bright light therapy (≥2,500 lux) has been shown to help DSPD patients achieve physiologically measured sleep phase advances, objective improvements in daytime alertness, and earlier reported bedtimes compared with controls.22 Unfortunately, the described 2-hour treatment duration make this research protocol clinically impractical, and most clinicians commence with a 30-minute duration of therapy, as described in the seasonal affective disorder literature.
Relatively new and widely available blue light boxes have been reported to exhibit at least equivalent efficacy to bright light devices (as reported in the literature pertaining to seasonal affective disorder), but with markedly decreased light intensity and fewer associated adverse effects.23 As the research addressing their use in the treatment of circadian rhythm sleep disorders is still emerging, their future role remains uncertain.
Precautions. Most psychiatrists would not perform a physiologic determination of a patient’s circadian phase, and further undesired phase delays can occur if phototherapy is administered before the core body temperature minimum (Tmin).24 Also, use caution if prescribing phototherapy to patients taking photosensitizing drugs and/or those with ocular or retinal pathology.20
Evening light avoidance. Whether or not you prescribe morning phototherapy, recommending that DSPD patients avoid evening light is essential to avoid further induction or exacerbation of phase delays. Protective eyewear is warranted in instances where these advisory precautions are insufficient (see Related Resources). Such an intervention has been shown effective in decreasing light exposure and undesired phase advances in studies involving subjects exposed to simulated shift work.25
Oral melatonin. Abundant evidence supports melatonin use in achieving phase advances in individuals with DSPD.26,27 A synergistic effect can be obtained when melatonin is combined with phototherapy.28
Proper timing of melatonin to achieve a maximal phase advance can be estimated based on the individual’s dim light melatonin onset (DLMO), which occurs approximately 14 hours after the habitual (unrestricted) wake time.29 Maximal phase advances appear to occur when melatonin is given approximately 6 hours before the DLMO.26 Thus, a rational practice is to recommend that patients take melatonin 8 hours after their natural wake time. Doses of ≤0.5 mg appear to achieve the maximal chronobiotic effect while avoiding an undesired hypnotic effect.30
Precautions. Verifying the purity of over-the-counter melatonin is difficult. A review by the National Academy of Sciences states that short-term use of melatonin, ≤10 mg/d, appears to be safe in healthy adults but recommends caution in children/adolescents and women of reproductive age. Doses recommended for circadian-based interventions are typically physiologic in nature (i.e., ≤0.5 mg), which may serve to mitigate these concerns.
Adverse effects such as headaches, somnolence, hypotension, hypertension, gastrointestinal upset, and exacerbation of alopecia areata have been reported at higher melatonin doses in healthy adults and at lower doses in persons with preexisting central nervous system, cardiovascular, gastrointestinal, or dermatologic conditions.31
Figure Light and melatonin phase response curves: Normal vs. delayed
This schematic compares ‘normal sleep’ phase response curves (PRCs) to light and exogenous melatonin with postulated PRCs for an individual with delayed sleep phase disorder (DSPD), presumed to be 5 hours ‘out of phase.’ Y-axis shows the direction and relative magnitude of phase shifts produced by light or melatonin at times shown on the x-axis. X-axis covers >24 hours to better illustrate the PRCs.
Relationships between ‘normal sleepers’ and DSPD patients are depicted by:
- rectangles (sleep period)
- triangles (core body temperature minimum [Tmin])
- arrows (dim light melatonin onsets [DLMOs]).
‘Normal’ sleep is shown to occur from midnight to 8 AM, and the DSPD patient’s sleep from 5 AM to 1 PM; DLMO and Tmin are similarly delayed by 5 hours in the DSPD patient. This schematic assumes that phase relationships are maintained in DSPD patients, which is not a certainty.
Source: Adapted from reference 21
CASE CONTINUED: Under the bright lights
Jason starts phototherapy treatment during his winter break, administering bright light daily upon natural awakening using a 10,000 lux light box for at least 30 minutes. As instructed, he gradually advances the time of administration by approximately 30 minutes every other day, striving for a nocturnal sleep period of 11 PM to 7 AM. He also wears protective eyewear to reduce light exposure during evening hours to avoid further delays in sleep phase. To further promote a phase advance, he takes oral melatonin, 0.5 mg/d at approximately 8 PM, as determined by his self-report and results of actigraphic recording.
Other options
Hypnotics. Little evidence supports the use of hypnotics in DSPD,32 and patients may show resistance to these drugs.33 Nevertheless, hypnotics can heighten confidence in the ability to initiate sleep in individuals with a concomitant conditioned insomnia.
With chronotherapy, patients are prescribed a sleep schedule that is delayed several hours incrementally until sleep is aligned to a target bedtime. The individual then is advised to rigorously maintain a regular sleep/wake schedule, repeating the process as necessary.
Although case reports have shown positive results with chronotherapy for DSPD,34 no controlled trials have demonstrated its efficacy or safety. One study reported high relapse rates,31 and 1 patient with DSPD developed free-running circadian rhythms.35 Clinical experience suggests chronotherapy is impractical for patients who must adhere to a fixed schedule.
Behavioral approaches
For an adolescent with DSPD, consider asking the school district to allow him or her a later school start-time. This alone often can substantially increase total sleep time and mitigate associated impairments.36 In all instances pursue and address external contributors to DSPD, such as poor sleep hygiene (including excessive caffeine use) and substance misuse.
Emphasize regular wake times, as arising later on weekends can cause phase delays.37 DSPD patients may have a concomitant conditioned insomnia that responds to evidence-based behavioral treatments.38
Whatever intervention you choose, schedule a follow-up appointment in approximately 2 months to evaluate patients’ progress and compliance. Encourage them to contact you with questions or concerns in the interim. Review sleep logs or actigraphy during this visit, and adjust the timing and/or nature of interventions as needed. Adolescents can be particularly noncompliant with clinical interventions, and therapeutic goals cannot be reached without their full investment.
Because no guidelines exist on how long to treat DSPD, stop on a “trial-and-error” basis when symptoms are controlled, and resume if they recur. Another approach is to maintain a desired sleep/wake schedule with bedtime melatonin and encourage continued adherence to other measures.
CASE CONTINUED: Maintenance therapy
Jason returns to the clinic approximately 10 weeks later. After an obviously concerted effort to adhere to treatment, his progress is quite remarkable. He rarely falls asleep later than 11 PM, so he is obtaining 2.5 hours more sleep each night before arising for school at 6:30 AM. Sleepiness at school is rarely problematic, and his mood is more stable.
He nevertheless describes a persistent tendency to retire and arise later and asks to continue melatonin and phototherapy. Because no guidelines exist for long-term therapy of DSPD, he is advised to switch melatonin to bedtime dosing (with a presumed phase-neutral “maintenance” effect), and to continue phototherapy as prescribed.
- Wyatt JK. Delayed sleep phase syndrome: pathophysiology and treatment options. Sleep. 2004;27(6):1195-1203.
- Crowley SJ, Acebo C, Carskadon MA. Sleep, circadian rhythms, and delayed sleep phase in adolescence. Sleep Med. 2007;8(6):602-612.
- National Sleep Foundation. Adolescent sleep needs and patterns: research report and resource guide. Washington, DC; 2000:1-30.
- Products designed to assist in the avoidance of light at improper times. www.lowbluelights.com.
Disclosure
Dr. Auger reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Khalsa SB, Jewett ME, Cajochen C, et al. A phase response curve to single bright light pulses in human subjects. J Physiol. 2003;549(Pt 3):945-952.
2. Quinto C, Gellido C, Chokroverty S, et al. Posttraumatic delayed sleep phase syndrome. Neurology. 2000;54(1):250-252.
3. Campbell SS, Murphy PJ. Delayed sleep phase disorder in temporal isolation. Sleep. 2007;30(9):1225-1228.
4. Uchiyama M, Okawa M, Shibui K, et al. Altered phase relation between sleep timing and core body temperature rhythm in delayed sleep phase syndrome and non-24-hour sleep-wake syndrome in humans. Neurosci Lett. 2000;294(2):101-104.
5. Aoki H, Ozeki Y, Yamada N. Hypersensitivity of melatonin suppression in response to light in patients with delayed sleep phase syndrome. Chronobiol Int. 2001;18(2):263-271.
6. Uchiyama M, Okawa M, Shibui K, et al. Poor compensatory function for sleep loss as a pathogenic factor in patients with delayed sleep phase syndrome. Sleep. 2000;23(4):553-558.
7. Mercer PW, Merritt SL, Cowell JM. Differences in reported sleep need among adolescents. J Adolesc Health. 1998;23(5):259-263.
8. Krahn LE, Pankratz VS, Harris AM, et al. Long-term outcome of adolescents with delayed sleep phase disorder [abstract]. Sleep. 2003;26:A115.-
9. Dagan Y, Stein D, Steinbock M, et al. Frequency of delayed sleep phase syndrome among hospitalized adolescent psychiatric patients. J Psychosom Res. 1998;45(1):15-20.
10. Thorpy MJ, Korman E, Spielman AJ, et al. Delayed sleep phase syndrome in adolescents. J Adolesc Health Care. 1998;9(1):22-27.
11. Regestein QR, Monk TH. Delayed sleep phase syndrome: a review of the clinical aspects. Am J Psychiatry. 1995;152(4):602-608.
12. Pelayo RP, Thorpy MJ, Glovinsky P. Prevalence of delayed sleep phase syndrome among adolescents [abstract]. Sleep Res. 1988;17:391.-
13. Gau SF, Soong WT. The transition of sleep-wake patterns in early adolescence. Sleep. 2003;26(4):449-454.
14. Beersma DG, Gordijn MC. Circadian control of the sleep-wake cycle. Physiol Behav. 2007;90(2-3):190-195.
15. Ralph MR, Foster RG, Davis FC, et al. Transplanted suprachiasmatic nucleus determines circadian period. Science. 1990;247(4945):975-978.
16. Waterhouse J, DeCoursey PJ. Chronobiology: biological timekeeping. Sunderland, MA: Sinauer Associates, Inc. Publishers; 2004:291-323.
17. American Academy of Sleep Medicine. International classification of sleep disorders. Diagnostic and coding manual. 2nd ed. Westchester, IL: American Academy of Sleep Medicine; 2005.
18. Bradshaw DA, Yanagi MA, Pak ES, et al. Nightly sleep duration in the 2-week period preceding multiple sleep latency testing. J Clin Sleep Med. 2007;3(6):613-619.
19. Horne JA, Ostberg O. A self-assessment questionnaire to determine morningness-eveningness in human circadian rhythms. Int J Chronobiol. 1976;4(2):97-110.
20. Sack RL, Auckley D, Auger RR, et al. Circadian rhythm sleep disorders: Part I. basic principles, shift work and jet lag disorders. Sleep. 2007;30(11):1460-1483.
21. Burgess HJ, Sharkey KM, Eastman CI. Bright light, dark and melatonin can promote circadian adaptation in night shift workers. Sleep Med Rev. 2002;6(5):407-420.
22. Rosenthal NE, Joseph-Vanderpool JR, Levendosky AA, et al. Phase-shifting effects of bright morning light as treatment for delayed sleep phase syndrome. Sleep. 1990;13(4):354-361.
23. Glickman G, Byrne B, Pineda C, et al. Light therapy for seasonal affective disorder with blue narrow-band light-emitting diodes (LEDs). Biol Psychiatry. 2006;59:502-507.
24. Czeisler C, Wright K, Jr. Influence of light on circadian rhythmicity in humans. New York, NY: Marcel Dekker; 1999:149-180.
25. Crowley SJ, Lee C, Tseng CY, et al. Combinations of bright light, scheduled dark, sunglasses, and melatonin to facilitate circadian entrainment to night shift work. J Biol Rhythms. 2003;18(6):513-523.
26. Mundey K, Benloucif S, Harsanyi K, et al. Phase-dependent treatment of delayed sleep phase syndrome with melatonin. Sleep. 2005;28(10):1271-1278.
27. Sack RL, Auckley D, Auger RR, et al. Circadian rhythm sleep disorders: Part II, advanced sleep phase disorder, delayed sleep phase disorder, free-running disorder, and irregular sleep-wake rhythm. Sleep. 2007;30(11):1484-1501.
28. Revell VL, Burgess HJ, Gazda CJ, et al. Advancing human circadian rhythms with afternoon melatonin and morning intermittent bright light. J Clin Endocrinol Metab. 2006;91(1):54-59.
29. Burgess HJ, Eastman CI. The dim light melatonin onset following fixed and free sleep schedules. J Sleep Res. 2005;14(3):229-237.
30. Lewy AJ. Clinical applications of melatonin in circadian disorders. Dialog Clin Neurosci. 2003;5:399-413.
31. Committee on the Framework for Evaluating the Safety of Dietary Supplements FaNB, Board on Life Sciences, Institute of Medicine and National Research Council of the National Academies. Dietary supplements: a framework for evaluating safety. Washington, DC: The National Academies Press; 2005.
32. Ito A, Ando K, Hayakawa T, et al. Long-term course of adult patients with delayed sleep phase syndrome. Jpn J Psychiatry Neurol. 1993;47(3):563-567.
33. Auger RR. Circadian rhythm sleep disorder, delayed sleep phase type (pediatric case). In: Winkelman JW (chair), Henderson JH, Kotagal S, et al, eds. Case book of sleep medicine. Westchester, IL: American Academy of Sleep Medicine; 2008:195-199.
34. Czeisler C, Weitzman E, Moore, et al. Chronotherapy: resetting the circadian clocks of patients with delayed sleep phase insomnia. Sleep. 1981;4:1-21.
35. Oren DA, Wehr TA. Hypernyctohemeral syndrome after chronotherapy for delayed sleep phase syndrome. N Engl J Med. 1992;327(24):1762.-
36. Wahlstrom K. Changing times: findings from the first longitudinal study of later high school start times. NASSP Bulletin. 2002;86(633):3-21.
37. Burgess HJ, Eastman CI. A late wake time phase delays the human dim light melatonin rhythm. Neurosci Lett. 2006;395(3):191-195.
38. Morgenthaler T, Kramer M, Alessi C, et al. Practice parameters for the psychological and behavioral treatment of insomnia: an update. An American Academy of Sleep Medicine report. Sleep. 2006;29(11):1415-1419.
1. Khalsa SB, Jewett ME, Cajochen C, et al. A phase response curve to single bright light pulses in human subjects. J Physiol. 2003;549(Pt 3):945-952.
2. Quinto C, Gellido C, Chokroverty S, et al. Posttraumatic delayed sleep phase syndrome. Neurology. 2000;54(1):250-252.
3. Campbell SS, Murphy PJ. Delayed sleep phase disorder in temporal isolation. Sleep. 2007;30(9):1225-1228.
4. Uchiyama M, Okawa M, Shibui K, et al. Altered phase relation between sleep timing and core body temperature rhythm in delayed sleep phase syndrome and non-24-hour sleep-wake syndrome in humans. Neurosci Lett. 2000;294(2):101-104.
5. Aoki H, Ozeki Y, Yamada N. Hypersensitivity of melatonin suppression in response to light in patients with delayed sleep phase syndrome. Chronobiol Int. 2001;18(2):263-271.
6. Uchiyama M, Okawa M, Shibui K, et al. Poor compensatory function for sleep loss as a pathogenic factor in patients with delayed sleep phase syndrome. Sleep. 2000;23(4):553-558.
7. Mercer PW, Merritt SL, Cowell JM. Differences in reported sleep need among adolescents. J Adolesc Health. 1998;23(5):259-263.
8. Krahn LE, Pankratz VS, Harris AM, et al. Long-term outcome of adolescents with delayed sleep phase disorder [abstract]. Sleep. 2003;26:A115.-
9. Dagan Y, Stein D, Steinbock M, et al. Frequency of delayed sleep phase syndrome among hospitalized adolescent psychiatric patients. J Psychosom Res. 1998;45(1):15-20.
10. Thorpy MJ, Korman E, Spielman AJ, et al. Delayed sleep phase syndrome in adolescents. J Adolesc Health Care. 1998;9(1):22-27.
11. Regestein QR, Monk TH. Delayed sleep phase syndrome: a review of the clinical aspects. Am J Psychiatry. 1995;152(4):602-608.
12. Pelayo RP, Thorpy MJ, Glovinsky P. Prevalence of delayed sleep phase syndrome among adolescents [abstract]. Sleep Res. 1988;17:391.-
13. Gau SF, Soong WT. The transition of sleep-wake patterns in early adolescence. Sleep. 2003;26(4):449-454.
14. Beersma DG, Gordijn MC. Circadian control of the sleep-wake cycle. Physiol Behav. 2007;90(2-3):190-195.
15. Ralph MR, Foster RG, Davis FC, et al. Transplanted suprachiasmatic nucleus determines circadian period. Science. 1990;247(4945):975-978.
16. Waterhouse J, DeCoursey PJ. Chronobiology: biological timekeeping. Sunderland, MA: Sinauer Associates, Inc. Publishers; 2004:291-323.
17. American Academy of Sleep Medicine. International classification of sleep disorders. Diagnostic and coding manual. 2nd ed. Westchester, IL: American Academy of Sleep Medicine; 2005.
18. Bradshaw DA, Yanagi MA, Pak ES, et al. Nightly sleep duration in the 2-week period preceding multiple sleep latency testing. J Clin Sleep Med. 2007;3(6):613-619.
19. Horne JA, Ostberg O. A self-assessment questionnaire to determine morningness-eveningness in human circadian rhythms. Int J Chronobiol. 1976;4(2):97-110.
20. Sack RL, Auckley D, Auger RR, et al. Circadian rhythm sleep disorders: Part I. basic principles, shift work and jet lag disorders. Sleep. 2007;30(11):1460-1483.
21. Burgess HJ, Sharkey KM, Eastman CI. Bright light, dark and melatonin can promote circadian adaptation in night shift workers. Sleep Med Rev. 2002;6(5):407-420.
22. Rosenthal NE, Joseph-Vanderpool JR, Levendosky AA, et al. Phase-shifting effects of bright morning light as treatment for delayed sleep phase syndrome. Sleep. 1990;13(4):354-361.
23. Glickman G, Byrne B, Pineda C, et al. Light therapy for seasonal affective disorder with blue narrow-band light-emitting diodes (LEDs). Biol Psychiatry. 2006;59:502-507.
24. Czeisler C, Wright K, Jr. Influence of light on circadian rhythmicity in humans. New York, NY: Marcel Dekker; 1999:149-180.
25. Crowley SJ, Lee C, Tseng CY, et al. Combinations of bright light, scheduled dark, sunglasses, and melatonin to facilitate circadian entrainment to night shift work. J Biol Rhythms. 2003;18(6):513-523.
26. Mundey K, Benloucif S, Harsanyi K, et al. Phase-dependent treatment of delayed sleep phase syndrome with melatonin. Sleep. 2005;28(10):1271-1278.
27. Sack RL, Auckley D, Auger RR, et al. Circadian rhythm sleep disorders: Part II, advanced sleep phase disorder, delayed sleep phase disorder, free-running disorder, and irregular sleep-wake rhythm. Sleep. 2007;30(11):1484-1501.
28. Revell VL, Burgess HJ, Gazda CJ, et al. Advancing human circadian rhythms with afternoon melatonin and morning intermittent bright light. J Clin Endocrinol Metab. 2006;91(1):54-59.
29. Burgess HJ, Eastman CI. The dim light melatonin onset following fixed and free sleep schedules. J Sleep Res. 2005;14(3):229-237.
30. Lewy AJ. Clinical applications of melatonin in circadian disorders. Dialog Clin Neurosci. 2003;5:399-413.
31. Committee on the Framework for Evaluating the Safety of Dietary Supplements FaNB, Board on Life Sciences, Institute of Medicine and National Research Council of the National Academies. Dietary supplements: a framework for evaluating safety. Washington, DC: The National Academies Press; 2005.
32. Ito A, Ando K, Hayakawa T, et al. Long-term course of adult patients with delayed sleep phase syndrome. Jpn J Psychiatry Neurol. 1993;47(3):563-567.
33. Auger RR. Circadian rhythm sleep disorder, delayed sleep phase type (pediatric case). In: Winkelman JW (chair), Henderson JH, Kotagal S, et al, eds. Case book of sleep medicine. Westchester, IL: American Academy of Sleep Medicine; 2008:195-199.
34. Czeisler C, Weitzman E, Moore, et al. Chronotherapy: resetting the circadian clocks of patients with delayed sleep phase insomnia. Sleep. 1981;4:1-21.
35. Oren DA, Wehr TA. Hypernyctohemeral syndrome after chronotherapy for delayed sleep phase syndrome. N Engl J Med. 1992;327(24):1762.-
36. Wahlstrom K. Changing times: findings from the first longitudinal study of later high school start times. NASSP Bulletin. 2002;86(633):3-21.
37. Burgess HJ, Eastman CI. A late wake time phase delays the human dim light melatonin rhythm. Neurosci Lett. 2006;395(3):191-195.
38. Morgenthaler T, Kramer M, Alessi C, et al. Practice parameters for the psychological and behavioral treatment of insomnia: an update. An American Academy of Sleep Medicine report. Sleep. 2006;29(11):1415-1419.
Stimulus Offers Cash for Quality
The economic stimulus bill that became law last week includes several items on SHM's healthcare policy wish list.
"It clearly hits some key issues," Eric Siegal, MD, chair of SHM's Public Policy Committee, says in regard to the American Recovery and Reinvestment Act. "This is a step in the right direction."
The $787 billion stimulus package includes:
- $1.1 billion for comparative effectiveness research (CER). Funding for CER is one of SHM's top policy priorities, says Laura Allendorf, SHM's senior advisor for advocacy and government affairs. CER examines the effectiveness of multiple therapies for specific medical conditions, or for a specific set of patients, to determine the best care options. "Funding for this is long overdue and key to healthcare reform," Dr. Siegal says. CER money will be split among the major players in this research, including the National Institutes of Health (NIH) and the Agency for Healthcare Research and Quality (AHRQ).
- A 34% increase in NIH funding. This includes $8.5 billion for research grants and programs that will allow for as many as 15,000 additional grants. "We know that an investment in biomedical research is an investment in the future of healthcare," says David Meltzer, MD, PhD, chair of SHM's Research Committee.
- $19 billion for health information technology. Incentives—and penalties—will target adoption of electronic health records by hospitals and office-based practices. "This will help improve patient safety, as well as care coordination," Allendorf says.
Other healthcare provisions in the package include an additional $86.6 billion in federal Medicaid funds, as well as temporary Medicaid coverage for the recently unemployed.
To keep up with public policy initiatives, check out SHM's advocacy portal.
The economic stimulus bill that became law last week includes several items on SHM's healthcare policy wish list.
"It clearly hits some key issues," Eric Siegal, MD, chair of SHM's Public Policy Committee, says in regard to the American Recovery and Reinvestment Act. "This is a step in the right direction."
The $787 billion stimulus package includes:
- $1.1 billion for comparative effectiveness research (CER). Funding for CER is one of SHM's top policy priorities, says Laura Allendorf, SHM's senior advisor for advocacy and government affairs. CER examines the effectiveness of multiple therapies for specific medical conditions, or for a specific set of patients, to determine the best care options. "Funding for this is long overdue and key to healthcare reform," Dr. Siegal says. CER money will be split among the major players in this research, including the National Institutes of Health (NIH) and the Agency for Healthcare Research and Quality (AHRQ).
- A 34% increase in NIH funding. This includes $8.5 billion for research grants and programs that will allow for as many as 15,000 additional grants. "We know that an investment in biomedical research is an investment in the future of healthcare," says David Meltzer, MD, PhD, chair of SHM's Research Committee.
- $19 billion for health information technology. Incentives—and penalties—will target adoption of electronic health records by hospitals and office-based practices. "This will help improve patient safety, as well as care coordination," Allendorf says.
Other healthcare provisions in the package include an additional $86.6 billion in federal Medicaid funds, as well as temporary Medicaid coverage for the recently unemployed.
To keep up with public policy initiatives, check out SHM's advocacy portal.
The economic stimulus bill that became law last week includes several items on SHM's healthcare policy wish list.
"It clearly hits some key issues," Eric Siegal, MD, chair of SHM's Public Policy Committee, says in regard to the American Recovery and Reinvestment Act. "This is a step in the right direction."
The $787 billion stimulus package includes:
- $1.1 billion for comparative effectiveness research (CER). Funding for CER is one of SHM's top policy priorities, says Laura Allendorf, SHM's senior advisor for advocacy and government affairs. CER examines the effectiveness of multiple therapies for specific medical conditions, or for a specific set of patients, to determine the best care options. "Funding for this is long overdue and key to healthcare reform," Dr. Siegal says. CER money will be split among the major players in this research, including the National Institutes of Health (NIH) and the Agency for Healthcare Research and Quality (AHRQ).
- A 34% increase in NIH funding. This includes $8.5 billion for research grants and programs that will allow for as many as 15,000 additional grants. "We know that an investment in biomedical research is an investment in the future of healthcare," says David Meltzer, MD, PhD, chair of SHM's Research Committee.
- $19 billion for health information technology. Incentives—and penalties—will target adoption of electronic health records by hospitals and office-based practices. "This will help improve patient safety, as well as care coordination," Allendorf says.
Other healthcare provisions in the package include an additional $86.6 billion in federal Medicaid funds, as well as temporary Medicaid coverage for the recently unemployed.
To keep up with public policy initiatives, check out SHM's advocacy portal.
Model's Death Sheds Spotlight on Sepsis Treatment
The recent death of an up-and-coming Brazilian model due to sepsis has again drawn attention to the common disease and how hospitalists should be wary not to miss its diagnosis in hospitalized patients.
Mariana Bridi da Costa, a 20-year-old beauty queen who participated in international competitions, died Jan. 24 from septicemia that began with a urinary tract infection. The original diagnosis did not include the urinary tract infection, leading to severe sepsis. Septicemia kills about 1,400 people a day worldwide, according to the Society of Critical Care Medicine (SCCM). The sepsis mortality rate is on a similar scale to lung, breast, and colon cancer, SCCM data shows.
"When someone comes in with high fever, high heart rate, high respiratory rate, and low blood pressure, you have to begin thinking about how well their organs are working," says Jeffrey Dichter, MD, medical director of cardiovascular intensive care at Regions Hospital in St. Paul, Minn., and former HM program director. "How sick are they? ... Hospitalists should look for the source of infection and evidence of organ failure."
According to the Mayo Clinic, about 750,000 people in the U.S. contract severe sepsis each year, and more than 200,000 people die of it.
Dr. Dichter notes that hospitalists in any setting—from acute-care hospitals to off-site clinics—can run blood tests for kidney and liver functions, as well as electrolyte levels, that serve as quick windows into the presence of sepsis. He also promotes www.survivingsepsis.org, the SCCM's program that aims to reduce sepsis mortality by 25% in five years by defining the disease more clearly and improving its diagnosis.
"Sometimes the symptoms patients come in with seem subtle," Dr. Dichter says. "Sometimes they may come in with evidence of an infection or low blood pressure, but they're awake and alert and talking and seem very normal. … Hospitalists need to be attune."
The recent death of an up-and-coming Brazilian model due to sepsis has again drawn attention to the common disease and how hospitalists should be wary not to miss its diagnosis in hospitalized patients.
Mariana Bridi da Costa, a 20-year-old beauty queen who participated in international competitions, died Jan. 24 from septicemia that began with a urinary tract infection. The original diagnosis did not include the urinary tract infection, leading to severe sepsis. Septicemia kills about 1,400 people a day worldwide, according to the Society of Critical Care Medicine (SCCM). The sepsis mortality rate is on a similar scale to lung, breast, and colon cancer, SCCM data shows.
"When someone comes in with high fever, high heart rate, high respiratory rate, and low blood pressure, you have to begin thinking about how well their organs are working," says Jeffrey Dichter, MD, medical director of cardiovascular intensive care at Regions Hospital in St. Paul, Minn., and former HM program director. "How sick are they? ... Hospitalists should look for the source of infection and evidence of organ failure."
According to the Mayo Clinic, about 750,000 people in the U.S. contract severe sepsis each year, and more than 200,000 people die of it.
Dr. Dichter notes that hospitalists in any setting—from acute-care hospitals to off-site clinics—can run blood tests for kidney and liver functions, as well as electrolyte levels, that serve as quick windows into the presence of sepsis. He also promotes www.survivingsepsis.org, the SCCM's program that aims to reduce sepsis mortality by 25% in five years by defining the disease more clearly and improving its diagnosis.
"Sometimes the symptoms patients come in with seem subtle," Dr. Dichter says. "Sometimes they may come in with evidence of an infection or low blood pressure, but they're awake and alert and talking and seem very normal. … Hospitalists need to be attune."
The recent death of an up-and-coming Brazilian model due to sepsis has again drawn attention to the common disease and how hospitalists should be wary not to miss its diagnosis in hospitalized patients.
Mariana Bridi da Costa, a 20-year-old beauty queen who participated in international competitions, died Jan. 24 from septicemia that began with a urinary tract infection. The original diagnosis did not include the urinary tract infection, leading to severe sepsis. Septicemia kills about 1,400 people a day worldwide, according to the Society of Critical Care Medicine (SCCM). The sepsis mortality rate is on a similar scale to lung, breast, and colon cancer, SCCM data shows.
"When someone comes in with high fever, high heart rate, high respiratory rate, and low blood pressure, you have to begin thinking about how well their organs are working," says Jeffrey Dichter, MD, medical director of cardiovascular intensive care at Regions Hospital in St. Paul, Minn., and former HM program director. "How sick are they? ... Hospitalists should look for the source of infection and evidence of organ failure."
According to the Mayo Clinic, about 750,000 people in the U.S. contract severe sepsis each year, and more than 200,000 people die of it.
Dr. Dichter notes that hospitalists in any setting—from acute-care hospitals to off-site clinics—can run blood tests for kidney and liver functions, as well as electrolyte levels, that serve as quick windows into the presence of sepsis. He also promotes www.survivingsepsis.org, the SCCM's program that aims to reduce sepsis mortality by 25% in five years by defining the disease more clearly and improving its diagnosis.
"Sometimes the symptoms patients come in with seem subtle," Dr. Dichter says. "Sometimes they may come in with evidence of an infection or low blood pressure, but they're awake and alert and talking and seem very normal. … Hospitalists need to be attune."
Research Roundup
Question: Do blood transfusions in hospitalized cancer patients with anemia or thrombocytopenia affect thrombotic event and in-hospital mortality rates?
Background: Erythropoiesis-stimulating agents have recently been shown to increase thrombotic risk and decrease survival in cancer patients. Blood transfusions are a common alternative for anemic patients. However, there are no randomized trials demonstrating improved outcomes in cancer patients receiving transfusions. Furthermore, the safety of transfusions has not been clearly defined.
Study design: Retrospective, cohort study.
Setting: 60 U.S. medical centers.
Synopsis: Using discharge data from the University Health System Consortium, 504,208 hospitalizations of cancer patients revealed that 14% of patients received at least one RBC transfusion and 3% of patients received a platelet transfusion. RBC and platelet transfusions were associated with increased risk of arterial thrombosis (RBCs: OR 1.53; 95% CI 1.46-1.61; platelets: OR 1.55; 1.4-1.71, P<0.001) and venous thrombotic events (RBCs: OR 1.34; 1.29-1.38; platelets: OR 1.2; 1.11-1.29, P<0.001). Additionally, transfusions were associated with increased in-hospital mortality (RBCs: OR 1.34; 1.29-1.38; platelets: OR 2.4; 2.27-2.52, P<0.001). Study results are limited by several factors, including the observational nature and the use of administrative coding data. Information on venous thromboembolism prophylaxis was not available, and the timing of transfusions in relation to the diagnosis of thrombotic events is unknown. Finally, anemia-necessitating transfusions may be a surrogate for "sicker" patients, explaining the increased in-hospital mortality. Blood transfusions in hospitalized patients require further study to determine whether there is a causal relationship between transfusions and increased thrombotic events and mortality.
Bottom line: Blood transfusions in hospitalized cancer patients should be used cautiously, as they are associated with increased thrombotic events and in-hospital mortality.
Citation: Arch Int Med. 2008;168:2377-2381
—Reviewed for the eWire by Kerry Will, MD, Jayne Barr, MD, Kim Tartaglia, MD, Aaron Wenger, MD, Jonathan Wynbrandt, MD, Nathan J. O’Dorisio, MD, The Ohio State University Medical Center, Columbus, OH.
Question: Do blood transfusions in hospitalized cancer patients with anemia or thrombocytopenia affect thrombotic event and in-hospital mortality rates?
Background: Erythropoiesis-stimulating agents have recently been shown to increase thrombotic risk and decrease survival in cancer patients. Blood transfusions are a common alternative for anemic patients. However, there are no randomized trials demonstrating improved outcomes in cancer patients receiving transfusions. Furthermore, the safety of transfusions has not been clearly defined.
Study design: Retrospective, cohort study.
Setting: 60 U.S. medical centers.
Synopsis: Using discharge data from the University Health System Consortium, 504,208 hospitalizations of cancer patients revealed that 14% of patients received at least one RBC transfusion and 3% of patients received a platelet transfusion. RBC and platelet transfusions were associated with increased risk of arterial thrombosis (RBCs: OR 1.53; 95% CI 1.46-1.61; platelets: OR 1.55; 1.4-1.71, P<0.001) and venous thrombotic events (RBCs: OR 1.34; 1.29-1.38; platelets: OR 1.2; 1.11-1.29, P<0.001). Additionally, transfusions were associated with increased in-hospital mortality (RBCs: OR 1.34; 1.29-1.38; platelets: OR 2.4; 2.27-2.52, P<0.001). Study results are limited by several factors, including the observational nature and the use of administrative coding data. Information on venous thromboembolism prophylaxis was not available, and the timing of transfusions in relation to the diagnosis of thrombotic events is unknown. Finally, anemia-necessitating transfusions may be a surrogate for "sicker" patients, explaining the increased in-hospital mortality. Blood transfusions in hospitalized patients require further study to determine whether there is a causal relationship between transfusions and increased thrombotic events and mortality.
Bottom line: Blood transfusions in hospitalized cancer patients should be used cautiously, as they are associated with increased thrombotic events and in-hospital mortality.
Citation: Arch Int Med. 2008;168:2377-2381
—Reviewed for the eWire by Kerry Will, MD, Jayne Barr, MD, Kim Tartaglia, MD, Aaron Wenger, MD, Jonathan Wynbrandt, MD, Nathan J. O’Dorisio, MD, The Ohio State University Medical Center, Columbus, OH.
Question: Do blood transfusions in hospitalized cancer patients with anemia or thrombocytopenia affect thrombotic event and in-hospital mortality rates?
Background: Erythropoiesis-stimulating agents have recently been shown to increase thrombotic risk and decrease survival in cancer patients. Blood transfusions are a common alternative for anemic patients. However, there are no randomized trials demonstrating improved outcomes in cancer patients receiving transfusions. Furthermore, the safety of transfusions has not been clearly defined.
Study design: Retrospective, cohort study.
Setting: 60 U.S. medical centers.
Synopsis: Using discharge data from the University Health System Consortium, 504,208 hospitalizations of cancer patients revealed that 14% of patients received at least one RBC transfusion and 3% of patients received a platelet transfusion. RBC and platelet transfusions were associated with increased risk of arterial thrombosis (RBCs: OR 1.53; 95% CI 1.46-1.61; platelets: OR 1.55; 1.4-1.71, P<0.001) and venous thrombotic events (RBCs: OR 1.34; 1.29-1.38; platelets: OR 1.2; 1.11-1.29, P<0.001). Additionally, transfusions were associated with increased in-hospital mortality (RBCs: OR 1.34; 1.29-1.38; platelets: OR 2.4; 2.27-2.52, P<0.001). Study results are limited by several factors, including the observational nature and the use of administrative coding data. Information on venous thromboembolism prophylaxis was not available, and the timing of transfusions in relation to the diagnosis of thrombotic events is unknown. Finally, anemia-necessitating transfusions may be a surrogate for "sicker" patients, explaining the increased in-hospital mortality. Blood transfusions in hospitalized patients require further study to determine whether there is a causal relationship between transfusions and increased thrombotic events and mortality.
Bottom line: Blood transfusions in hospitalized cancer patients should be used cautiously, as they are associated with increased thrombotic events and in-hospital mortality.
Citation: Arch Int Med. 2008;168:2377-2381
—Reviewed for the eWire by Kerry Will, MD, Jayne Barr, MD, Kim Tartaglia, MD, Aaron Wenger, MD, Jonathan Wynbrandt, MD, Nathan J. O’Dorisio, MD, The Ohio State University Medical Center, Columbus, OH.
Discharge Development
A multidisciplinary pre-discharge intervention—one that hospitalists can advocate for and help lead—resulted in a 30% reduction in hospital utilization within 30 days, according to a single-center study published in the Feb. 3 Annals of Internal Medicine (2009;150(3):178-187).
Researchers, including hospitalist Jeffrey Greenwald, MD, followed 749 adult patients over 30-day periods at Boston Medical Center to test the effects of a nurse discharge advocate program. A nurse arranged follow-up appointments and confirmed medication, while a clinical pharmacist called patients two to four days after discharge to reinforce the discharge plan.
"It isn't realistic that the hospitalists become the primary-care doctors after the discharge," says Dr. Greenwald, director of HM at Boston Medical Center and associate professor of medicine at Boston University School of Medicine. "It's critical that the hospitalists take a lead role in taking responsibility for the pitfalls into which the patients are likely to fall."
Dr. Greenwald thinks hospitalists can push for interventions at their respective centers to reduce rehospitalizations. The research team already is working on a new study to determine which measures could be automated to ensure their completion.
"All we're asking is that, as a team, you put in place the common stopgaps. ... None of this is gene therapy," Dr. Greenwald says. "This is low brain activity. The problem is that it's not low resource intense, and it's not low culture change."
Dr. Greenwald plans to submit information about his study to SHM's Project BOOST (Better Outcomes for Older Adults through Safe Transitions), a mentoring program meant to help hospitalists redesign their discharge process to improve patient outcomes. He says programs like Project BOOST are helping to draw attention to post-discharge protocols at hospitals around the country.
A multidisciplinary pre-discharge intervention—one that hospitalists can advocate for and help lead—resulted in a 30% reduction in hospital utilization within 30 days, according to a single-center study published in the Feb. 3 Annals of Internal Medicine (2009;150(3):178-187).
Researchers, including hospitalist Jeffrey Greenwald, MD, followed 749 adult patients over 30-day periods at Boston Medical Center to test the effects of a nurse discharge advocate program. A nurse arranged follow-up appointments and confirmed medication, while a clinical pharmacist called patients two to four days after discharge to reinforce the discharge plan.
"It isn't realistic that the hospitalists become the primary-care doctors after the discharge," says Dr. Greenwald, director of HM at Boston Medical Center and associate professor of medicine at Boston University School of Medicine. "It's critical that the hospitalists take a lead role in taking responsibility for the pitfalls into which the patients are likely to fall."
Dr. Greenwald thinks hospitalists can push for interventions at their respective centers to reduce rehospitalizations. The research team already is working on a new study to determine which measures could be automated to ensure their completion.
"All we're asking is that, as a team, you put in place the common stopgaps. ... None of this is gene therapy," Dr. Greenwald says. "This is low brain activity. The problem is that it's not low resource intense, and it's not low culture change."
Dr. Greenwald plans to submit information about his study to SHM's Project BOOST (Better Outcomes for Older Adults through Safe Transitions), a mentoring program meant to help hospitalists redesign their discharge process to improve patient outcomes. He says programs like Project BOOST are helping to draw attention to post-discharge protocols at hospitals around the country.
A multidisciplinary pre-discharge intervention—one that hospitalists can advocate for and help lead—resulted in a 30% reduction in hospital utilization within 30 days, according to a single-center study published in the Feb. 3 Annals of Internal Medicine (2009;150(3):178-187).
Researchers, including hospitalist Jeffrey Greenwald, MD, followed 749 adult patients over 30-day periods at Boston Medical Center to test the effects of a nurse discharge advocate program. A nurse arranged follow-up appointments and confirmed medication, while a clinical pharmacist called patients two to four days after discharge to reinforce the discharge plan.
"It isn't realistic that the hospitalists become the primary-care doctors after the discharge," says Dr. Greenwald, director of HM at Boston Medical Center and associate professor of medicine at Boston University School of Medicine. "It's critical that the hospitalists take a lead role in taking responsibility for the pitfalls into which the patients are likely to fall."
Dr. Greenwald thinks hospitalists can push for interventions at their respective centers to reduce rehospitalizations. The research team already is working on a new study to determine which measures could be automated to ensure their completion.
"All we're asking is that, as a team, you put in place the common stopgaps. ... None of this is gene therapy," Dr. Greenwald says. "This is low brain activity. The problem is that it's not low resource intense, and it's not low culture change."
Dr. Greenwald plans to submit information about his study to SHM's Project BOOST (Better Outcomes for Older Adults through Safe Transitions), a mentoring program meant to help hospitalists redesign their discharge process to improve patient outcomes. He says programs like Project BOOST are helping to draw attention to post-discharge protocols at hospitals around the country.
Pin the Pinworm
An 84‐year‐old female patient with hypertension, osteoarthritis, hypothyroidism, and remote breast cancer was admitted with complaints of generalized abdominal pain of 2 months' duration. Pain was described as noncolicky in nature and was associated with diarrhea. She reported 78 daily episodes of watery, non‐foul‐smelling diarrhea. She denied any nausea, vomiting, fever, joint pains, oral ulcers, eye redness, stool incontinence, melena, hematochezia, or weight loss. There was no history of recent travel, antibiotic use, or exposure to sick contacts. She had no risk factors for HIV infection or other sexually transmitted infections. Her social history was significant for dining out on a regular basis and living in an assisted living facility. However, she denied any relationship between her abdominal symptoms and any particular food intake or with bowel movements. She denied any anal pruritis but reported seeing white squiggly things on tissue paper after bowel movements. She denied use of over‐the‐counter laxatives or herbal supplements. None of her prescription medications had diarrhea as a major side effect. Her social history was unremarkable for smoking, alcohol use, or illicit drug use. There were no prior abdominal surgeries. The patient's physical exam showed normal vitals on presentation and was unremarkable except for vague, generalized abdominal tenderness with no involuntary guarding or rebound pain. Her initial laboratory evaluation showed normal complete blood counts with no eosinophilia and normal serum electrolytes and liver and thyroid panel. Acute‐phase reactants, erythrocyte sedimentation rate, and C‐reactive protein were not elevated. Stool evaluation was unremarkable for Clostridium difficile toxin, fat droplets, leukocytes, erythrocytes, ova, parasites, or any bacterial growth on cultures. Computed tomography scans of the abdomen and pelvis were nonrevealing. Her colonoscopic examination 1 year prior was significant only for diverticulosis.1, 2
The patient was treated with loperamide as an outpatient with no relief. She was then admitted to the hospital for further diagnostic workup. Hospital workup included a Scotch tape test, which showed adult pinworms. She was treated with a single dose of 400 mg of albendazole with complete resolution of her symptoms within 2 days. No further workup was done. Patient was discharged with advice to contact her primary care doctor for reevaluation if symptoms recurred. However, the patient remained symptom free 1 year after discharge.
DISCUSSION
Enterobius vermicularis is a parasite that infects 2040 million people annually in the United States and about 200 million people worldwide. Equal infection rates are seen in all races, socioeconomic classes, and cultures.1 It is more prevalent among those in crowded living conditions. Humans are the primary natural host for the parasite, although it has been documented in cockroaches and primates. Transmission occurs via the feco‐oral route or via airborne eggs that are dislodged from contaminated clothing or bed linen. Its life cycle begins with parasite eggs hatching in the duodenum, usually within 6 hours of ingestion. They mature into adults in as little as 2 weeks and have a life span of approximately 2 months. Enterobius vermicularis normally inhabits distal small bowel including the terminal ileum, cecum, and vermiform appendix, as well as the proximal ascending colon. After copulation, an adult female will migrate to the perineum, often at night, and lay an average of 10,00015,000 eggs. These eggs mature in about 6 hours and are then transmitted to a new host by the feco‐oral route. The worms live mainly in the intestinal lumen and do not invade tissue. Hence, pinworm infections, unlike many other parasitic infections, are rarely associated with serum eosinophilia or elevated serum IgE levels.
E. vermicularis is generally considered to be an innocuous parasite. Perianal pruritis, especially during the nighttime, is the most common symptom. Patients may develop secondary bacterial infection of the irritated anal skin. Rarely, E. vermicularis infection may result in a life‐threatening illness. A literature review showed pinworm infection to be an infrequent cause of eosinophilic enterocolitis, appendicitis, intestinal obstruction, intestinal perforation, hepatic infection, urinary tract infection, sialoadenitis, salpingitis, enterocolitis, eosinophilic ileocolitis, vulvovaginitis, pelvic inflammatory disease, conditions mimicking inflammatory bowel diseases, perianal abscesses, and perianal granulomas. In a retrospective review of 180 colonoscopies done on patients with rectal bleeding or suspected inflammatory bowel disease, E. vermicularis was identified macroscopically in 31 cases (17.2%). Data collected on 23 of these cases showed that symptoms were present for a mean of 17 months; the symptoms with the highest frequency were abdominal pain (73%), rectal bleeding (62%), chronic diarrhea (50%), and weight loss (42%). None of these patients experienced perianal pruritis or developed inflammatory bowel disease during the follow‐up period of up to 5 years, although 21 patients demonstrated histopathological evidence of nonspecific colitis.6
The gold standard for diagnosing E. vermicularis infection is by visualizing the worms directly or by examination of the parasitic eggs under a microscope. The Scotch tape test is a simple, inexpensive, and quick way for confirming the infection. It is performed by doubling clear cellophane Scotch tape onto a wooden stick so that the sticky side points outward and pressing it against the perianal skin. The kidney‐bean‐shaped eggs (50 25 m) will stick to the tape and can then be directly visualized under a microscope. Pinworms are most active during the night, and eggs are deposited around the perianal region and are best recovered before defecation, early in the morning. The sensitivity of this test is 90% if done on 3 consecutive mornings and goes up to 99% when performed on 5 consecutive mornings.2, 3 Female adult worms are pin‐shaped, about 813 mm long, and white in color. They may be seen by direct visualization in the perianal region or more invasively by an anoscopic or colonoscopic examination. However, endoscopic examination may sometimes give false‐negative results as the worms are small, (ie, only a few millimeters in length) and may be missed if the endoscopist is not actively looking for them.
A single oral dose of benzimidazoles (100 mg of mebendazole or 400 mg of albendazole) results in a cure of rate of 95% and 100%, respectively. Despite the high initial cure rates, reinfection remains common; hence, a second dose 12 weeks after the initial treatment is often given to prevent it.4, 5 Pyrantel pamoate and piperazine are alternate treatments. However, they have lower efficacy and are more toxic than benzimidazoles.
Close contacts such as household members are often concurrently infected, and treatment of the remaining household members or of the group institution is also indicated. All bedding and clothes should be laundered. Personal hygiene such as fingernail clipping, frequent hand washing, and bathing should also be encouraged.
Although the pinworm's entire life cycle is in the human intestinal tract, gastrointestinal symptoms have seldom been reported. However, this may be because of underreporting. Given the increasing number of patients living in institutionalized environments such as nursing homes and assisted living, it is important to consider the possibility of E. vermicularis infection early on in a diagnostic workup of patients presenting with symptoms of colitis, even when not accompanied by anal pruritis. In a patient presenting with symptoms of inflammatory bowel disease with histopathological evaluation of nonspecific colitis should prompt clinicians to consider E. vermicularis infection.6 On the other hand, in patients who fail to respond to antiparasitic therapy or those who present with weight loss, change in bowel habits, or melena, colonscopic examination is warranted. Considering pinworm infection early during evaluation of nonspecific abdominal complaints may avoid an unnecessary and expensive diagnostic workup.
KEY POINTS
-
Recognize early on that Enterobius vermicularis infection is an important differential diagnosis for patients presenting with symptoms of colitis, thus avoiding unnecessary, expensive, and potentially harmful invasive testing.
-
Recognize that a simple and inexpensive Scotch tape test and/or direct visualization is an easy and effective way of confirming diagnosis and that stool examination may be unhelpful.
-
Recognize that reinfection may be prevented using a second dose of the antiparasitic drug.
- .The pinworm, Enterobius vermicularis.Prim Care.1991;18:13–24.
- ,,,,.Prevalence of intestinal parasites in three socioeconomically‐different regions of Sivas, Turkey.J Health Popul Nutr.2005;23:184–191.
- ,,,.Pinworm infection.Gastrointest Endosc.2001;53:210.
- ,,.Mebendazole (R 17635) in enterobiasis. A clinical trial in mental retardates.Chemotherapy.1975;21:255–260.
- ,,, et al.Field trials on the efficacy of albendazole composite against intestinal nematodiasis.Chung Kuo Chi Sheng Chung Hsueh Yu Chi Sheng Chung Ping Tsa Chih.1998;16:1–5.
- ,,.Enterobius vermicularis and colitis in children.J Pediatr Gastroenterol Nutr.2006;43:610–612.
An 84‐year‐old female patient with hypertension, osteoarthritis, hypothyroidism, and remote breast cancer was admitted with complaints of generalized abdominal pain of 2 months' duration. Pain was described as noncolicky in nature and was associated with diarrhea. She reported 78 daily episodes of watery, non‐foul‐smelling diarrhea. She denied any nausea, vomiting, fever, joint pains, oral ulcers, eye redness, stool incontinence, melena, hematochezia, or weight loss. There was no history of recent travel, antibiotic use, or exposure to sick contacts. She had no risk factors for HIV infection or other sexually transmitted infections. Her social history was significant for dining out on a regular basis and living in an assisted living facility. However, she denied any relationship between her abdominal symptoms and any particular food intake or with bowel movements. She denied any anal pruritis but reported seeing white squiggly things on tissue paper after bowel movements. She denied use of over‐the‐counter laxatives or herbal supplements. None of her prescription medications had diarrhea as a major side effect. Her social history was unremarkable for smoking, alcohol use, or illicit drug use. There were no prior abdominal surgeries. The patient's physical exam showed normal vitals on presentation and was unremarkable except for vague, generalized abdominal tenderness with no involuntary guarding or rebound pain. Her initial laboratory evaluation showed normal complete blood counts with no eosinophilia and normal serum electrolytes and liver and thyroid panel. Acute‐phase reactants, erythrocyte sedimentation rate, and C‐reactive protein were not elevated. Stool evaluation was unremarkable for Clostridium difficile toxin, fat droplets, leukocytes, erythrocytes, ova, parasites, or any bacterial growth on cultures. Computed tomography scans of the abdomen and pelvis were nonrevealing. Her colonoscopic examination 1 year prior was significant only for diverticulosis.1, 2
The patient was treated with loperamide as an outpatient with no relief. She was then admitted to the hospital for further diagnostic workup. Hospital workup included a Scotch tape test, which showed adult pinworms. She was treated with a single dose of 400 mg of albendazole with complete resolution of her symptoms within 2 days. No further workup was done. Patient was discharged with advice to contact her primary care doctor for reevaluation if symptoms recurred. However, the patient remained symptom free 1 year after discharge.
DISCUSSION
Enterobius vermicularis is a parasite that infects 2040 million people annually in the United States and about 200 million people worldwide. Equal infection rates are seen in all races, socioeconomic classes, and cultures.1 It is more prevalent among those in crowded living conditions. Humans are the primary natural host for the parasite, although it has been documented in cockroaches and primates. Transmission occurs via the feco‐oral route or via airborne eggs that are dislodged from contaminated clothing or bed linen. Its life cycle begins with parasite eggs hatching in the duodenum, usually within 6 hours of ingestion. They mature into adults in as little as 2 weeks and have a life span of approximately 2 months. Enterobius vermicularis normally inhabits distal small bowel including the terminal ileum, cecum, and vermiform appendix, as well as the proximal ascending colon. After copulation, an adult female will migrate to the perineum, often at night, and lay an average of 10,00015,000 eggs. These eggs mature in about 6 hours and are then transmitted to a new host by the feco‐oral route. The worms live mainly in the intestinal lumen and do not invade tissue. Hence, pinworm infections, unlike many other parasitic infections, are rarely associated with serum eosinophilia or elevated serum IgE levels.
E. vermicularis is generally considered to be an innocuous parasite. Perianal pruritis, especially during the nighttime, is the most common symptom. Patients may develop secondary bacterial infection of the irritated anal skin. Rarely, E. vermicularis infection may result in a life‐threatening illness. A literature review showed pinworm infection to be an infrequent cause of eosinophilic enterocolitis, appendicitis, intestinal obstruction, intestinal perforation, hepatic infection, urinary tract infection, sialoadenitis, salpingitis, enterocolitis, eosinophilic ileocolitis, vulvovaginitis, pelvic inflammatory disease, conditions mimicking inflammatory bowel diseases, perianal abscesses, and perianal granulomas. In a retrospective review of 180 colonoscopies done on patients with rectal bleeding or suspected inflammatory bowel disease, E. vermicularis was identified macroscopically in 31 cases (17.2%). Data collected on 23 of these cases showed that symptoms were present for a mean of 17 months; the symptoms with the highest frequency were abdominal pain (73%), rectal bleeding (62%), chronic diarrhea (50%), and weight loss (42%). None of these patients experienced perianal pruritis or developed inflammatory bowel disease during the follow‐up period of up to 5 years, although 21 patients demonstrated histopathological evidence of nonspecific colitis.6
The gold standard for diagnosing E. vermicularis infection is by visualizing the worms directly or by examination of the parasitic eggs under a microscope. The Scotch tape test is a simple, inexpensive, and quick way for confirming the infection. It is performed by doubling clear cellophane Scotch tape onto a wooden stick so that the sticky side points outward and pressing it against the perianal skin. The kidney‐bean‐shaped eggs (50 25 m) will stick to the tape and can then be directly visualized under a microscope. Pinworms are most active during the night, and eggs are deposited around the perianal region and are best recovered before defecation, early in the morning. The sensitivity of this test is 90% if done on 3 consecutive mornings and goes up to 99% when performed on 5 consecutive mornings.2, 3 Female adult worms are pin‐shaped, about 813 mm long, and white in color. They may be seen by direct visualization in the perianal region or more invasively by an anoscopic or colonoscopic examination. However, endoscopic examination may sometimes give false‐negative results as the worms are small, (ie, only a few millimeters in length) and may be missed if the endoscopist is not actively looking for them.
A single oral dose of benzimidazoles (100 mg of mebendazole or 400 mg of albendazole) results in a cure of rate of 95% and 100%, respectively. Despite the high initial cure rates, reinfection remains common; hence, a second dose 12 weeks after the initial treatment is often given to prevent it.4, 5 Pyrantel pamoate and piperazine are alternate treatments. However, they have lower efficacy and are more toxic than benzimidazoles.
Close contacts such as household members are often concurrently infected, and treatment of the remaining household members or of the group institution is also indicated. All bedding and clothes should be laundered. Personal hygiene such as fingernail clipping, frequent hand washing, and bathing should also be encouraged.
Although the pinworm's entire life cycle is in the human intestinal tract, gastrointestinal symptoms have seldom been reported. However, this may be because of underreporting. Given the increasing number of patients living in institutionalized environments such as nursing homes and assisted living, it is important to consider the possibility of E. vermicularis infection early on in a diagnostic workup of patients presenting with symptoms of colitis, even when not accompanied by anal pruritis. In a patient presenting with symptoms of inflammatory bowel disease with histopathological evaluation of nonspecific colitis should prompt clinicians to consider E. vermicularis infection.6 On the other hand, in patients who fail to respond to antiparasitic therapy or those who present with weight loss, change in bowel habits, or melena, colonscopic examination is warranted. Considering pinworm infection early during evaluation of nonspecific abdominal complaints may avoid an unnecessary and expensive diagnostic workup.
KEY POINTS
-
Recognize early on that Enterobius vermicularis infection is an important differential diagnosis for patients presenting with symptoms of colitis, thus avoiding unnecessary, expensive, and potentially harmful invasive testing.
-
Recognize that a simple and inexpensive Scotch tape test and/or direct visualization is an easy and effective way of confirming diagnosis and that stool examination may be unhelpful.
-
Recognize that reinfection may be prevented using a second dose of the antiparasitic drug.
An 84‐year‐old female patient with hypertension, osteoarthritis, hypothyroidism, and remote breast cancer was admitted with complaints of generalized abdominal pain of 2 months' duration. Pain was described as noncolicky in nature and was associated with diarrhea. She reported 78 daily episodes of watery, non‐foul‐smelling diarrhea. She denied any nausea, vomiting, fever, joint pains, oral ulcers, eye redness, stool incontinence, melena, hematochezia, or weight loss. There was no history of recent travel, antibiotic use, or exposure to sick contacts. She had no risk factors for HIV infection or other sexually transmitted infections. Her social history was significant for dining out on a regular basis and living in an assisted living facility. However, she denied any relationship between her abdominal symptoms and any particular food intake or with bowel movements. She denied any anal pruritis but reported seeing white squiggly things on tissue paper after bowel movements. She denied use of over‐the‐counter laxatives or herbal supplements. None of her prescription medications had diarrhea as a major side effect. Her social history was unremarkable for smoking, alcohol use, or illicit drug use. There were no prior abdominal surgeries. The patient's physical exam showed normal vitals on presentation and was unremarkable except for vague, generalized abdominal tenderness with no involuntary guarding or rebound pain. Her initial laboratory evaluation showed normal complete blood counts with no eosinophilia and normal serum electrolytes and liver and thyroid panel. Acute‐phase reactants, erythrocyte sedimentation rate, and C‐reactive protein were not elevated. Stool evaluation was unremarkable for Clostridium difficile toxin, fat droplets, leukocytes, erythrocytes, ova, parasites, or any bacterial growth on cultures. Computed tomography scans of the abdomen and pelvis were nonrevealing. Her colonoscopic examination 1 year prior was significant only for diverticulosis.1, 2
The patient was treated with loperamide as an outpatient with no relief. She was then admitted to the hospital for further diagnostic workup. Hospital workup included a Scotch tape test, which showed adult pinworms. She was treated with a single dose of 400 mg of albendazole with complete resolution of her symptoms within 2 days. No further workup was done. Patient was discharged with advice to contact her primary care doctor for reevaluation if symptoms recurred. However, the patient remained symptom free 1 year after discharge.
DISCUSSION
Enterobius vermicularis is a parasite that infects 2040 million people annually in the United States and about 200 million people worldwide. Equal infection rates are seen in all races, socioeconomic classes, and cultures.1 It is more prevalent among those in crowded living conditions. Humans are the primary natural host for the parasite, although it has been documented in cockroaches and primates. Transmission occurs via the feco‐oral route or via airborne eggs that are dislodged from contaminated clothing or bed linen. Its life cycle begins with parasite eggs hatching in the duodenum, usually within 6 hours of ingestion. They mature into adults in as little as 2 weeks and have a life span of approximately 2 months. Enterobius vermicularis normally inhabits distal small bowel including the terminal ileum, cecum, and vermiform appendix, as well as the proximal ascending colon. After copulation, an adult female will migrate to the perineum, often at night, and lay an average of 10,00015,000 eggs. These eggs mature in about 6 hours and are then transmitted to a new host by the feco‐oral route. The worms live mainly in the intestinal lumen and do not invade tissue. Hence, pinworm infections, unlike many other parasitic infections, are rarely associated with serum eosinophilia or elevated serum IgE levels.
E. vermicularis is generally considered to be an innocuous parasite. Perianal pruritis, especially during the nighttime, is the most common symptom. Patients may develop secondary bacterial infection of the irritated anal skin. Rarely, E. vermicularis infection may result in a life‐threatening illness. A literature review showed pinworm infection to be an infrequent cause of eosinophilic enterocolitis, appendicitis, intestinal obstruction, intestinal perforation, hepatic infection, urinary tract infection, sialoadenitis, salpingitis, enterocolitis, eosinophilic ileocolitis, vulvovaginitis, pelvic inflammatory disease, conditions mimicking inflammatory bowel diseases, perianal abscesses, and perianal granulomas. In a retrospective review of 180 colonoscopies done on patients with rectal bleeding or suspected inflammatory bowel disease, E. vermicularis was identified macroscopically in 31 cases (17.2%). Data collected on 23 of these cases showed that symptoms were present for a mean of 17 months; the symptoms with the highest frequency were abdominal pain (73%), rectal bleeding (62%), chronic diarrhea (50%), and weight loss (42%). None of these patients experienced perianal pruritis or developed inflammatory bowel disease during the follow‐up period of up to 5 years, although 21 patients demonstrated histopathological evidence of nonspecific colitis.6
The gold standard for diagnosing E. vermicularis infection is by visualizing the worms directly or by examination of the parasitic eggs under a microscope. The Scotch tape test is a simple, inexpensive, and quick way for confirming the infection. It is performed by doubling clear cellophane Scotch tape onto a wooden stick so that the sticky side points outward and pressing it against the perianal skin. The kidney‐bean‐shaped eggs (50 25 m) will stick to the tape and can then be directly visualized under a microscope. Pinworms are most active during the night, and eggs are deposited around the perianal region and are best recovered before defecation, early in the morning. The sensitivity of this test is 90% if done on 3 consecutive mornings and goes up to 99% when performed on 5 consecutive mornings.2, 3 Female adult worms are pin‐shaped, about 813 mm long, and white in color. They may be seen by direct visualization in the perianal region or more invasively by an anoscopic or colonoscopic examination. However, endoscopic examination may sometimes give false‐negative results as the worms are small, (ie, only a few millimeters in length) and may be missed if the endoscopist is not actively looking for them.
A single oral dose of benzimidazoles (100 mg of mebendazole or 400 mg of albendazole) results in a cure of rate of 95% and 100%, respectively. Despite the high initial cure rates, reinfection remains common; hence, a second dose 12 weeks after the initial treatment is often given to prevent it.4, 5 Pyrantel pamoate and piperazine are alternate treatments. However, they have lower efficacy and are more toxic than benzimidazoles.
Close contacts such as household members are often concurrently infected, and treatment of the remaining household members or of the group institution is also indicated. All bedding and clothes should be laundered. Personal hygiene such as fingernail clipping, frequent hand washing, and bathing should also be encouraged.
Although the pinworm's entire life cycle is in the human intestinal tract, gastrointestinal symptoms have seldom been reported. However, this may be because of underreporting. Given the increasing number of patients living in institutionalized environments such as nursing homes and assisted living, it is important to consider the possibility of E. vermicularis infection early on in a diagnostic workup of patients presenting with symptoms of colitis, even when not accompanied by anal pruritis. In a patient presenting with symptoms of inflammatory bowel disease with histopathological evaluation of nonspecific colitis should prompt clinicians to consider E. vermicularis infection.6 On the other hand, in patients who fail to respond to antiparasitic therapy or those who present with weight loss, change in bowel habits, or melena, colonscopic examination is warranted. Considering pinworm infection early during evaluation of nonspecific abdominal complaints may avoid an unnecessary and expensive diagnostic workup.
KEY POINTS
-
Recognize early on that Enterobius vermicularis infection is an important differential diagnosis for patients presenting with symptoms of colitis, thus avoiding unnecessary, expensive, and potentially harmful invasive testing.
-
Recognize that a simple and inexpensive Scotch tape test and/or direct visualization is an easy and effective way of confirming diagnosis and that stool examination may be unhelpful.
-
Recognize that reinfection may be prevented using a second dose of the antiparasitic drug.
- .The pinworm, Enterobius vermicularis.Prim Care.1991;18:13–24.
- ,,,,.Prevalence of intestinal parasites in three socioeconomically‐different regions of Sivas, Turkey.J Health Popul Nutr.2005;23:184–191.
- ,,,.Pinworm infection.Gastrointest Endosc.2001;53:210.
- ,,.Mebendazole (R 17635) in enterobiasis. A clinical trial in mental retardates.Chemotherapy.1975;21:255–260.
- ,,, et al.Field trials on the efficacy of albendazole composite against intestinal nematodiasis.Chung Kuo Chi Sheng Chung Hsueh Yu Chi Sheng Chung Ping Tsa Chih.1998;16:1–5.
- ,,.Enterobius vermicularis and colitis in children.J Pediatr Gastroenterol Nutr.2006;43:610–612.
- .The pinworm, Enterobius vermicularis.Prim Care.1991;18:13–24.
- ,,,,.Prevalence of intestinal parasites in three socioeconomically‐different regions of Sivas, Turkey.J Health Popul Nutr.2005;23:184–191.
- ,,,.Pinworm infection.Gastrointest Endosc.2001;53:210.
- ,,.Mebendazole (R 17635) in enterobiasis. A clinical trial in mental retardates.Chemotherapy.1975;21:255–260.
- ,,, et al.Field trials on the efficacy of albendazole composite against intestinal nematodiasis.Chung Kuo Chi Sheng Chung Hsueh Yu Chi Sheng Chung Ping Tsa Chih.1998;16:1–5.
- ,,.Enterobius vermicularis and colitis in children.J Pediatr Gastroenterol Nutr.2006;43:610–612.

Polymorphic Ventricular Tachycardia?
The medical team was called emergently from the telemetry station in response to the tracing shown in Figure 1. The patient was a 65‐year‐old woman with paroxysmal atrial fibrillation and no structural heart disease. The medical team arrived at the bedside to find the patient chatting with her family with a heart rate of 95 and blood pressure of 144/92. The patient had been awake and alert throughout the episode. Initial inspection of the rhythm strip (Figure 1) shows what appears to be nonsustained polymorphic ventricular tachycardia followed by normal QRS complexes. Upon careful inspection of the V1 (lower) tracing, the QRS complexes can be marched backward through the wide complexes to the beginning of the strip, as shown in Figure 2 (arrows), indicating that the wide complexes are artifact.


The presence of artifact is confirmed in Figure 3, in which the arterial blood pressure (ABP) waveform follows the QRS complexes. In polymorphic ventricular tachycardia, the ABP would have fallen and the waveform would have been chaotic. Failure to differentiate between artifact and ventricular tachycardia can lead to inappropriate management.1, 2 The artifact in this case is likely due to electrode motion and emphasizes the importance of using all the available data when evaluating rhythm strips. Critical evaluation of multiple electrocardiographic (ECG) leads is the cornerstone of diagnosis; continuous arterial monitoring, if available, can be useful for confirmation.
- ,,.Approach to the diagnosis and initial management of the stable adult patient with a wide complex tachycardia.Am J Cardiol.2008;101(10):1456–1466.
- ,,,,.Physician interpretation of electrocardiographic artifact that mimics ventricular tachycardia.Am J Med.2001;110(5):335–338.
The medical team was called emergently from the telemetry station in response to the tracing shown in Figure 1. The patient was a 65‐year‐old woman with paroxysmal atrial fibrillation and no structural heart disease. The medical team arrived at the bedside to find the patient chatting with her family with a heart rate of 95 and blood pressure of 144/92. The patient had been awake and alert throughout the episode. Initial inspection of the rhythm strip (Figure 1) shows what appears to be nonsustained polymorphic ventricular tachycardia followed by normal QRS complexes. Upon careful inspection of the V1 (lower) tracing, the QRS complexes can be marched backward through the wide complexes to the beginning of the strip, as shown in Figure 2 (arrows), indicating that the wide complexes are artifact.
The presence of artifact is confirmed in Figure 3, in which the arterial blood pressure (ABP) waveform follows the QRS complexes. In polymorphic ventricular tachycardia, the ABP would have fallen and the waveform would have been chaotic. Failure to differentiate between artifact and ventricular tachycardia can lead to inappropriate management.1, 2 The artifact in this case is likely due to electrode motion and emphasizes the importance of using all the available data when evaluating rhythm strips. Critical evaluation of multiple electrocardiographic (ECG) leads is the cornerstone of diagnosis; continuous arterial monitoring, if available, can be useful for confirmation.
The medical team was called emergently from the telemetry station in response to the tracing shown in Figure 1. The patient was a 65‐year‐old woman with paroxysmal atrial fibrillation and no structural heart disease. The medical team arrived at the bedside to find the patient chatting with her family with a heart rate of 95 and blood pressure of 144/92. The patient had been awake and alert throughout the episode. Initial inspection of the rhythm strip (Figure 1) shows what appears to be nonsustained polymorphic ventricular tachycardia followed by normal QRS complexes. Upon careful inspection of the V1 (lower) tracing, the QRS complexes can be marched backward through the wide complexes to the beginning of the strip, as shown in Figure 2 (arrows), indicating that the wide complexes are artifact.
The presence of artifact is confirmed in Figure 3, in which the arterial blood pressure (ABP) waveform follows the QRS complexes. In polymorphic ventricular tachycardia, the ABP would have fallen and the waveform would have been chaotic. Failure to differentiate between artifact and ventricular tachycardia can lead to inappropriate management.1, 2 The artifact in this case is likely due to electrode motion and emphasizes the importance of using all the available data when evaluating rhythm strips. Critical evaluation of multiple electrocardiographic (ECG) leads is the cornerstone of diagnosis; continuous arterial monitoring, if available, can be useful for confirmation.
- ,,.Approach to the diagnosis and initial management of the stable adult patient with a wide complex tachycardia.Am J Cardiol.2008;101(10):1456–1466.
- ,,,,.Physician interpretation of electrocardiographic artifact that mimics ventricular tachycardia.Am J Med.2001;110(5):335–338.
- ,,.Approach to the diagnosis and initial management of the stable adult patient with a wide complex tachycardia.Am J Cardiol.2008;101(10):1456–1466.
- ,,,,.Physician interpretation of electrocardiographic artifact that mimics ventricular tachycardia.Am J Med.2001;110(5):335–338.

CIPNM in Disseminated Cryptococcal Infection
Critical illness polyneuromyopathy (CIPNM) is frequent among critically‐ill patients.1, 2 CIPNM develops in critically‐ill patients with systemic inflammatory response syndrome, sepsis, or multiple organ failure. We report a case of disseminated cryptococcal infection in a critically‐ill patient who presented with treatment‐refractory cellulitis. His recovery was complicated by difficulty in weaning from mechanical ventilation due to CIPNM.
CASE REPORT
A 49‐year‐old man developed skin swelling and tenderness over his right thigh 1 month prior to admission at a local hospital. He was a pigeon breeder by profession. His medical history was significant for hypertension and poorly controlled diabetes mellitus. His medications included prednisolone (15 mg per day), which he was taking for his chronic arthritis for about 6 months. He was admitted for treatment of cellulitis. Despite antibiotic treatment with ampicillin and sulbactam, his skin lesion became necrotic and gangrenous. Wound healing remained poor even after wound debridement. Patient developed dyspnea 2 weeks after admission and was transferred to the intensive care unit (ICU) of National Taiwan University Hospital for further management.
On transfer to ICU, he was drowsy and had an ear temperature of 37.1C, pulse rate of 108 beats/minute, blood pressure of 132/82 mm Hg, and respiratory rate of 20 breaths/minutes. His pupils were isocoric with prompt light reflex. His right thigh wound was 6 cm in length with eschar formation and focal erythema. His total white blood cell count was 14.08 109 cells/L with 72.2% polymorphonuclear leukocytes. His blood glucose level was 326 mg/dL. Other blood work, including hemoglobin, coagulation studies, and renal and liver function tests, were within normal range. Urinalysis was positive for glucose, but there was no hematuria, pyuria, or ketonuria. The chest radiograph (Figure 1) showed small nodules and peripheral infiltrates in both lung fields. Chest computerized tomogram (CT) scans found multiple cavitated lung nodules (Figure 2A,B). Human immunodeficiency virus (HIV) screening test was negative.
Soon after transfer to the ICU, the patient developed respiratory distress and became hemodynamically unstable. He was intubated and resuscitation efforts were started to stabilize him. Yeast‐like organisms were found in the debrided tissue. CT‐guided biopsy of the pulmonary nodules also found yeast‐like organisms. Tissue cultures of skin wound and lung biopsy grew Cryptococcus neoformans. He was diagnosed with disseminated cryptococcal infection and Amphotericin B was started. His hemodynamic status stabilized 2 days after the start of Amphotericin B. Follow‐up chest radiograph 1 week after starting Amphotericin B treatment showed resolution of pulmonary nodules. His right thigh skin lesion also healed gradually.
Unfortunately, he developed severe weakness of all extremities on the fourteenth ICU day, and had difficulty weaning from mechanical ventilation. Neurological examination found diffuse hyporeflexia. The nerve conduction velocity (NCV) study showed decreased amplitude in nerve conduction, with normal velocity. Electromyogram (EMG) found diffuse muscular fibrillation. Based on these findings, CIPNM was diagnosed. Patient underwent tracheostomy on the twenty‐sixth ICU day due to the need for prolonged mechanical ventilation. His antifungal therapy was changed to intravenous fluconazole 600 mg per day. Blood glucose levels were controlled with continuous insulin infusion and insulin dose was titrated to keep the blood glucose below 120 mg/dL. He was finally weaned from mechanical ventilation on the forty‐seventh day of ICU admission, and was transferred to the general ward. With physical therapy, he resumed his daily activities and was discharged from the hospital.
DISCUSSION
Cryptococcus rarely causes disseminated infection in healthy individuals. The vast majority of patients with cryptococcosis are immunocompromised due to conditions such as acquired immunodeficiency syndrome, prolonged treatment with corticosteroids, organ transplantation, malignancy, or diabetes mellitus.3, 4 The patient in this report had 2 of the documented risk factors. In a study of 52 disseminated cryptococcosis patients, the most prevalent underlying condition was HIV infection (46%). Out of these 52 patients, 28 were HIV‐negative, and only 3 of them had no predisposing condition.4 Cutaneous cryptococcus infection could be a manifestation of disseminated cryptococcal infection, or may be a primary disease that would evolve into systemic disease several months later.5, 6 The incidence of primary cutaneous cryptococcosis is much lower than systemic disease with cutaneous manifestation. Cellulitis, which is refractory to treatment with traditional antibacterial agents, should lead to consideration of fungal cellulites, such as cutaneous cryptococcosis or aspergillosis. Once cryptococcal cellulitis is diagnosed, other foci of cryptococcal infection should be sought.
CIPNM includes myopathies, acute neuropathies, neuromuscular transmission defects, or any combination of these disorders.2, 7 CIPNM might arise in ICU patients who have systemic inflammatory response syndrome (SIRS), sepsis, or multiple organ failure. In patients with new onset limb weakness, disuse hyporeflexia, and difficulty in weaning from mechanical ventilation, CIPNM should be among the differential diagnoses. In 1 prospective trial, de Letter et al.8 found CIPNM incidence of 33% in 98 ICU patients. A high APACHE III score, SIRS, and the use of aminoglycoside antibiotics are significant risk factors for the development of CIPNM. In various studies, the incidence of CIPNM ranges from 13% to 76%.2, 710
The definitive diagnosis of CIPNM is established by EMG and NCV studies, which are characterized by (1) reduced amplitudes of compound muscles and sensory action potentials, (2) relatively normal conduction studies, and (3) widespread fibrillations and sharp waves.2 The mean mortality of patients who have developed CIPNM is 35%, with a range from 0% to 73%. About 45% of patients completely recover from CIPNM within 6 weeks to 12 months (with a mean duration of 4.5 months), with good supportive care, provided the underlying condition has been treated.2, 9 There is little evidence to support a specific treatment modality for CIPNM. Mohr et al.1 reported that intravenous immunoglobulin may prevent or ameliorate CIPNM in the ICU, but more prospective and placebo‐controlled studies are needed to confirm their result. In recent studies,11 strict blood glucose control with insulin was found to reduce the risk of CIPNM and duration of mechanical ventilation in both medical and surgical ICU patients.
In conclusion, CIPNM occurs frequently in ICU patients with SIRS, sepsis, or multiple organ failure, leading to prolonged ventilator dependence and increased morbidity and mortality. Risk factor prevention and intensive insulin treatment may reduce the incident of CIPNM and the duration of mechanical ventilation in ICU patients.
- ,,,,.Effects of early treatment with immunoglobulin on critical illness polyneuropathy following multiple organ failure and gram‐negative sepsis.Intensive Care Med.1997;23:1144–1149.
- .Critical illness polyneuropathy and myopathy: clinical features, risk factors and prognosis.Eur J Neurol.2006;13:1203–1212.
- .Cryptococcus neoformans. In:Mandell GL,Bennett JE,Dolin R, eds.Principles and Practice of Infectious Diseases.Philadelphia:Churchill Livingstone;2000:2707–2718.
- ,,, et al.Cryptococcameia: clinical features and prognostic factors.Q J Med.2002;95:511–518.
- ,,.Primary cutaneous cryptococcal cellulitis secondary to insect bite in an immunosuppressed patient after liver transplantation.Clin Exp Dermatol.2005;30:241–243.
- ,.Primary cutaneous cryptococcosis as the presenting manifestation of AIDS.Plast Reconstr Surg.1992;90:1065–1067.
- ,,,,.Effect of critical illness polyneuropathy on the withdrawal from mechanical ventilation and the length of stay in septic patients.Crit Care Med.2005;33:349–354.
- ,,, et al.Critical illness polyneuropathy and myopathy (CIPNM): evidence for local immune activation by cytokine‐expression in the muscle tissue.J Neuroimmunol.2000;106:206–213.
- ,.Critical illness neuromuscular abnormalities.Crit Care Clin.2002;18:553–568.
- ,,,,,.Neuromuscular disorders associated with failure to wean from the ventilator.Intensive Care Med.1995;21:737–743.
- ,,, et al.Impact of intensive insulin therapy on neuromuscular complications and ventilator‐dependency in MICU.Am J Respir Crit Care Med.2007;175:480–489.
Critical illness polyneuromyopathy (CIPNM) is frequent among critically‐ill patients.1, 2 CIPNM develops in critically‐ill patients with systemic inflammatory response syndrome, sepsis, or multiple organ failure. We report a case of disseminated cryptococcal infection in a critically‐ill patient who presented with treatment‐refractory cellulitis. His recovery was complicated by difficulty in weaning from mechanical ventilation due to CIPNM.
CASE REPORT
A 49‐year‐old man developed skin swelling and tenderness over his right thigh 1 month prior to admission at a local hospital. He was a pigeon breeder by profession. His medical history was significant for hypertension and poorly controlled diabetes mellitus. His medications included prednisolone (15 mg per day), which he was taking for his chronic arthritis for about 6 months. He was admitted for treatment of cellulitis. Despite antibiotic treatment with ampicillin and sulbactam, his skin lesion became necrotic and gangrenous. Wound healing remained poor even after wound debridement. Patient developed dyspnea 2 weeks after admission and was transferred to the intensive care unit (ICU) of National Taiwan University Hospital for further management.
On transfer to ICU, he was drowsy and had an ear temperature of 37.1C, pulse rate of 108 beats/minute, blood pressure of 132/82 mm Hg, and respiratory rate of 20 breaths/minutes. His pupils were isocoric with prompt light reflex. His right thigh wound was 6 cm in length with eschar formation and focal erythema. His total white blood cell count was 14.08 109 cells/L with 72.2% polymorphonuclear leukocytes. His blood glucose level was 326 mg/dL. Other blood work, including hemoglobin, coagulation studies, and renal and liver function tests, were within normal range. Urinalysis was positive for glucose, but there was no hematuria, pyuria, or ketonuria. The chest radiograph (Figure 1) showed small nodules and peripheral infiltrates in both lung fields. Chest computerized tomogram (CT) scans found multiple cavitated lung nodules (Figure 2A,B). Human immunodeficiency virus (HIV) screening test was negative.
Soon after transfer to the ICU, the patient developed respiratory distress and became hemodynamically unstable. He was intubated and resuscitation efforts were started to stabilize him. Yeast‐like organisms were found in the debrided tissue. CT‐guided biopsy of the pulmonary nodules also found yeast‐like organisms. Tissue cultures of skin wound and lung biopsy grew Cryptococcus neoformans. He was diagnosed with disseminated cryptococcal infection and Amphotericin B was started. His hemodynamic status stabilized 2 days after the start of Amphotericin B. Follow‐up chest radiograph 1 week after starting Amphotericin B treatment showed resolution of pulmonary nodules. His right thigh skin lesion also healed gradually.
Unfortunately, he developed severe weakness of all extremities on the fourteenth ICU day, and had difficulty weaning from mechanical ventilation. Neurological examination found diffuse hyporeflexia. The nerve conduction velocity (NCV) study showed decreased amplitude in nerve conduction, with normal velocity. Electromyogram (EMG) found diffuse muscular fibrillation. Based on these findings, CIPNM was diagnosed. Patient underwent tracheostomy on the twenty‐sixth ICU day due to the need for prolonged mechanical ventilation. His antifungal therapy was changed to intravenous fluconazole 600 mg per day. Blood glucose levels were controlled with continuous insulin infusion and insulin dose was titrated to keep the blood glucose below 120 mg/dL. He was finally weaned from mechanical ventilation on the forty‐seventh day of ICU admission, and was transferred to the general ward. With physical therapy, he resumed his daily activities and was discharged from the hospital.
DISCUSSION
Cryptococcus rarely causes disseminated infection in healthy individuals. The vast majority of patients with cryptococcosis are immunocompromised due to conditions such as acquired immunodeficiency syndrome, prolonged treatment with corticosteroids, organ transplantation, malignancy, or diabetes mellitus.3, 4 The patient in this report had 2 of the documented risk factors. In a study of 52 disseminated cryptococcosis patients, the most prevalent underlying condition was HIV infection (46%). Out of these 52 patients, 28 were HIV‐negative, and only 3 of them had no predisposing condition.4 Cutaneous cryptococcus infection could be a manifestation of disseminated cryptococcal infection, or may be a primary disease that would evolve into systemic disease several months later.5, 6 The incidence of primary cutaneous cryptococcosis is much lower than systemic disease with cutaneous manifestation. Cellulitis, which is refractory to treatment with traditional antibacterial agents, should lead to consideration of fungal cellulites, such as cutaneous cryptococcosis or aspergillosis. Once cryptococcal cellulitis is diagnosed, other foci of cryptococcal infection should be sought.
CIPNM includes myopathies, acute neuropathies, neuromuscular transmission defects, or any combination of these disorders.2, 7 CIPNM might arise in ICU patients who have systemic inflammatory response syndrome (SIRS), sepsis, or multiple organ failure. In patients with new onset limb weakness, disuse hyporeflexia, and difficulty in weaning from mechanical ventilation, CIPNM should be among the differential diagnoses. In 1 prospective trial, de Letter et al.8 found CIPNM incidence of 33% in 98 ICU patients. A high APACHE III score, SIRS, and the use of aminoglycoside antibiotics are significant risk factors for the development of CIPNM. In various studies, the incidence of CIPNM ranges from 13% to 76%.2, 710
The definitive diagnosis of CIPNM is established by EMG and NCV studies, which are characterized by (1) reduced amplitudes of compound muscles and sensory action potentials, (2) relatively normal conduction studies, and (3) widespread fibrillations and sharp waves.2 The mean mortality of patients who have developed CIPNM is 35%, with a range from 0% to 73%. About 45% of patients completely recover from CIPNM within 6 weeks to 12 months (with a mean duration of 4.5 months), with good supportive care, provided the underlying condition has been treated.2, 9 There is little evidence to support a specific treatment modality for CIPNM. Mohr et al.1 reported that intravenous immunoglobulin may prevent or ameliorate CIPNM in the ICU, but more prospective and placebo‐controlled studies are needed to confirm their result. In recent studies,11 strict blood glucose control with insulin was found to reduce the risk of CIPNM and duration of mechanical ventilation in both medical and surgical ICU patients.
In conclusion, CIPNM occurs frequently in ICU patients with SIRS, sepsis, or multiple organ failure, leading to prolonged ventilator dependence and increased morbidity and mortality. Risk factor prevention and intensive insulin treatment may reduce the incident of CIPNM and the duration of mechanical ventilation in ICU patients.
Critical illness polyneuromyopathy (CIPNM) is frequent among critically‐ill patients.1, 2 CIPNM develops in critically‐ill patients with systemic inflammatory response syndrome, sepsis, or multiple organ failure. We report a case of disseminated cryptococcal infection in a critically‐ill patient who presented with treatment‐refractory cellulitis. His recovery was complicated by difficulty in weaning from mechanical ventilation due to CIPNM.
CASE REPORT
A 49‐year‐old man developed skin swelling and tenderness over his right thigh 1 month prior to admission at a local hospital. He was a pigeon breeder by profession. His medical history was significant for hypertension and poorly controlled diabetes mellitus. His medications included prednisolone (15 mg per day), which he was taking for his chronic arthritis for about 6 months. He was admitted for treatment of cellulitis. Despite antibiotic treatment with ampicillin and sulbactam, his skin lesion became necrotic and gangrenous. Wound healing remained poor even after wound debridement. Patient developed dyspnea 2 weeks after admission and was transferred to the intensive care unit (ICU) of National Taiwan University Hospital for further management.
On transfer to ICU, he was drowsy and had an ear temperature of 37.1C, pulse rate of 108 beats/minute, blood pressure of 132/82 mm Hg, and respiratory rate of 20 breaths/minutes. His pupils were isocoric with prompt light reflex. His right thigh wound was 6 cm in length with eschar formation and focal erythema. His total white blood cell count was 14.08 109 cells/L with 72.2% polymorphonuclear leukocytes. His blood glucose level was 326 mg/dL. Other blood work, including hemoglobin, coagulation studies, and renal and liver function tests, were within normal range. Urinalysis was positive for glucose, but there was no hematuria, pyuria, or ketonuria. The chest radiograph (Figure 1) showed small nodules and peripheral infiltrates in both lung fields. Chest computerized tomogram (CT) scans found multiple cavitated lung nodules (Figure 2A,B). Human immunodeficiency virus (HIV) screening test was negative.
Soon after transfer to the ICU, the patient developed respiratory distress and became hemodynamically unstable. He was intubated and resuscitation efforts were started to stabilize him. Yeast‐like organisms were found in the debrided tissue. CT‐guided biopsy of the pulmonary nodules also found yeast‐like organisms. Tissue cultures of skin wound and lung biopsy grew Cryptococcus neoformans. He was diagnosed with disseminated cryptococcal infection and Amphotericin B was started. His hemodynamic status stabilized 2 days after the start of Amphotericin B. Follow‐up chest radiograph 1 week after starting Amphotericin B treatment showed resolution of pulmonary nodules. His right thigh skin lesion also healed gradually.
Unfortunately, he developed severe weakness of all extremities on the fourteenth ICU day, and had difficulty weaning from mechanical ventilation. Neurological examination found diffuse hyporeflexia. The nerve conduction velocity (NCV) study showed decreased amplitude in nerve conduction, with normal velocity. Electromyogram (EMG) found diffuse muscular fibrillation. Based on these findings, CIPNM was diagnosed. Patient underwent tracheostomy on the twenty‐sixth ICU day due to the need for prolonged mechanical ventilation. His antifungal therapy was changed to intravenous fluconazole 600 mg per day. Blood glucose levels were controlled with continuous insulin infusion and insulin dose was titrated to keep the blood glucose below 120 mg/dL. He was finally weaned from mechanical ventilation on the forty‐seventh day of ICU admission, and was transferred to the general ward. With physical therapy, he resumed his daily activities and was discharged from the hospital.
DISCUSSION
Cryptococcus rarely causes disseminated infection in healthy individuals. The vast majority of patients with cryptococcosis are immunocompromised due to conditions such as acquired immunodeficiency syndrome, prolonged treatment with corticosteroids, organ transplantation, malignancy, or diabetes mellitus.3, 4 The patient in this report had 2 of the documented risk factors. In a study of 52 disseminated cryptococcosis patients, the most prevalent underlying condition was HIV infection (46%). Out of these 52 patients, 28 were HIV‐negative, and only 3 of them had no predisposing condition.4 Cutaneous cryptococcus infection could be a manifestation of disseminated cryptococcal infection, or may be a primary disease that would evolve into systemic disease several months later.5, 6 The incidence of primary cutaneous cryptococcosis is much lower than systemic disease with cutaneous manifestation. Cellulitis, which is refractory to treatment with traditional antibacterial agents, should lead to consideration of fungal cellulites, such as cutaneous cryptococcosis or aspergillosis. Once cryptococcal cellulitis is diagnosed, other foci of cryptococcal infection should be sought.
CIPNM includes myopathies, acute neuropathies, neuromuscular transmission defects, or any combination of these disorders.2, 7 CIPNM might arise in ICU patients who have systemic inflammatory response syndrome (SIRS), sepsis, or multiple organ failure. In patients with new onset limb weakness, disuse hyporeflexia, and difficulty in weaning from mechanical ventilation, CIPNM should be among the differential diagnoses. In 1 prospective trial, de Letter et al.8 found CIPNM incidence of 33% in 98 ICU patients. A high APACHE III score, SIRS, and the use of aminoglycoside antibiotics are significant risk factors for the development of CIPNM. In various studies, the incidence of CIPNM ranges from 13% to 76%.2, 710
The definitive diagnosis of CIPNM is established by EMG and NCV studies, which are characterized by (1) reduced amplitudes of compound muscles and sensory action potentials, (2) relatively normal conduction studies, and (3) widespread fibrillations and sharp waves.2 The mean mortality of patients who have developed CIPNM is 35%, with a range from 0% to 73%. About 45% of patients completely recover from CIPNM within 6 weeks to 12 months (with a mean duration of 4.5 months), with good supportive care, provided the underlying condition has been treated.2, 9 There is little evidence to support a specific treatment modality for CIPNM. Mohr et al.1 reported that intravenous immunoglobulin may prevent or ameliorate CIPNM in the ICU, but more prospective and placebo‐controlled studies are needed to confirm their result. In recent studies,11 strict blood glucose control with insulin was found to reduce the risk of CIPNM and duration of mechanical ventilation in both medical and surgical ICU patients.
In conclusion, CIPNM occurs frequently in ICU patients with SIRS, sepsis, or multiple organ failure, leading to prolonged ventilator dependence and increased morbidity and mortality. Risk factor prevention and intensive insulin treatment may reduce the incident of CIPNM and the duration of mechanical ventilation in ICU patients.
- ,,,,.Effects of early treatment with immunoglobulin on critical illness polyneuropathy following multiple organ failure and gram‐negative sepsis.Intensive Care Med.1997;23:1144–1149.
- .Critical illness polyneuropathy and myopathy: clinical features, risk factors and prognosis.Eur J Neurol.2006;13:1203–1212.
- .Cryptococcus neoformans. In:Mandell GL,Bennett JE,Dolin R, eds.Principles and Practice of Infectious Diseases.Philadelphia:Churchill Livingstone;2000:2707–2718.
- ,,, et al.Cryptococcameia: clinical features and prognostic factors.Q J Med.2002;95:511–518.
- ,,.Primary cutaneous cryptococcal cellulitis secondary to insect bite in an immunosuppressed patient after liver transplantation.Clin Exp Dermatol.2005;30:241–243.
- ,.Primary cutaneous cryptococcosis as the presenting manifestation of AIDS.Plast Reconstr Surg.1992;90:1065–1067.
- ,,,,.Effect of critical illness polyneuropathy on the withdrawal from mechanical ventilation and the length of stay in septic patients.Crit Care Med.2005;33:349–354.
- ,,, et al.Critical illness polyneuropathy and myopathy (CIPNM): evidence for local immune activation by cytokine‐expression in the muscle tissue.J Neuroimmunol.2000;106:206–213.
- ,.Critical illness neuromuscular abnormalities.Crit Care Clin.2002;18:553–568.
- ,,,,,.Neuromuscular disorders associated with failure to wean from the ventilator.Intensive Care Med.1995;21:737–743.
- ,,, et al.Impact of intensive insulin therapy on neuromuscular complications and ventilator‐dependency in MICU.Am J Respir Crit Care Med.2007;175:480–489.
- ,,,,.Effects of early treatment with immunoglobulin on critical illness polyneuropathy following multiple organ failure and gram‐negative sepsis.Intensive Care Med.1997;23:1144–1149.
- .Critical illness polyneuropathy and myopathy: clinical features, risk factors and prognosis.Eur J Neurol.2006;13:1203–1212.
- .Cryptococcus neoformans. In:Mandell GL,Bennett JE,Dolin R, eds.Principles and Practice of Infectious Diseases.Philadelphia:Churchill Livingstone;2000:2707–2718.
- ,,, et al.Cryptococcameia: clinical features and prognostic factors.Q J Med.2002;95:511–518.
- ,,.Primary cutaneous cryptococcal cellulitis secondary to insect bite in an immunosuppressed patient after liver transplantation.Clin Exp Dermatol.2005;30:241–243.
- ,.Primary cutaneous cryptococcosis as the presenting manifestation of AIDS.Plast Reconstr Surg.1992;90:1065–1067.
- ,,,,.Effect of critical illness polyneuropathy on the withdrawal from mechanical ventilation and the length of stay in septic patients.Crit Care Med.2005;33:349–354.
- ,,, et al.Critical illness polyneuropathy and myopathy (CIPNM): evidence for local immune activation by cytokine‐expression in the muscle tissue.J Neuroimmunol.2000;106:206–213.
- ,.Critical illness neuromuscular abnormalities.Crit Care Clin.2002;18:553–568.
- ,,,,,.Neuromuscular disorders associated with failure to wean from the ventilator.Intensive Care Med.1995;21:737–743.
- ,,, et al.Impact of intensive insulin therapy on neuromuscular complications and ventilator‐dependency in MICU.Am J Respir Crit Care Med.2007;175:480–489.

Coding and Documentation
You admitted a patient to the hospital for an upper gastrointestinal bleed. At the time of admission, the patient's mucous membranes were dry, and he was mildly orthostatic and tachycardic. He was given several boluses of normal saline, and he improved. All of this was carefully documented in the medical record. Shortly after discharge, the following cryptic message arrives in your mailbox:
The patient was admitted with gastrointestinal bleeding and noted to have dry mucous membranes, orthostatic hypotension, and tachycardia. He was given intravenous saline. What diagnosis, if any, required treatment with 2 boluses of normal saline?
You remember the patient well but still pull the chart to review the case. It appears obvious that the patient was dry and needed fluid resuscitation. You are confused and do not know how to respond. Your response is just that: Patient was dry and needed fluid resuscitation.
Several days later, you get another message thanking you for your reply but describing what the coder actually needed to be able to code appropriately. Had you answered hypovolemia or dehydration, it would have changed the diagnosis‐related group (DRG) and reimbursement from gastrointestinal hemorrhage ($2700) to gastrointestinal hemorrhage with complications ($4600). Because you did not provide the right answer, the institution was reimbursed for the lesser amount. Now you are left with more questions. Hypovolemia is exactly what the patient had; you basically said so, and it was described throughout the chart, although not in so many words. Why did the coder not just say what was needed? Why can you not just answer again? Why are you being asked to play what appears to be a stupid game when you have sick patients to care for and never enough time? What can you do to prevent this from happening the next time? What other surprises are in store for you?
INTRODUCTION
Beginning October 1, 2007 the Centers for Medicare and Medicaid Services (CMS) implemented changes in the hospital inpatient prospective payment system that have profound implications for how physicians code and document hospital care. These changes were implemented in an effort to better recognize severity of illness,1 and the information will be used to plan for current and future needs of hospitals, insurers, caregivers, and patients. Severity of illness is a measure of the patient's overall health status reflected by the resources necessary for care and the risk of morbidity and mortality. Factors including the presenting illness, comorbid conditions, functional status, nutritional status, and age contribute to the severity of illness. From a physiologic perspective, factors reflecting loss of homeostatic control such as abnormal vital signs, poor oxygenation, and altered sensorium are determinants of severity of illness. For hospitals, severity of illness is generally reflected by the case mix of concomitant illness. Thus, a patient with community‐acquired pneumonia without other comorbidities requires fewer resources and has a greater chance of a good outcome than the same patient with complications such as acute congestive heart failure. In the context of this article, severity of illness should be considered an indication of the complexity of the patient's presentation. Reporting comorbidities and illness severity will help better define quality of care and medical necessity for that care.
The DRG system provided a set payment for a given hospitalization based on primary and sometimes secondary diagnoses. The new system, using Medicare severity diagnosis‐related groups (MS‐DRGs), accounts for all diagnoses present at the time of admission and all diagnoses made during the hospitalization.
This article discusses the value of appropriate documentation and outlines changes that physicians will need to make to ensure optimal coding. The value of appropriate documentation is described. Specific terminology is illustrated so physicians can document properly and coders can easily extract the necessary information from the medical record to code appropriately. Finally, specific strategies institutions can implement to support physicians and coders are suggested.
A PRIMER ON CODING AND MEDICAL DOCUMENTATION
Prior to October 1, 2007, the DRG for a given hospitalization was calculated from the principle diagnosis and in some cases 1 secondary diagnosis that represented a significant complication or comorbidity. For example, a patient admitted to the hospital with abdominal pain diagnosed as a peptic ulcer would have a DRG to reflect the ulcer. If the patient also had anemia secondary to blood loss from the ulcer, this would serve as a complication, and a DRG with a comorbidity or complication and a higher case weight would be assigned. Additional significant complications would not further alter the DRG.
The new guidelines recognize 3 levels of severity for secondary diagnoses. The DRG from the principal diagnosis can be associated with other diagnoses that recognize no complication or comorbidity, a complication or comorbidity, or a major complication or comorbidity. Thus, a patient admitted with a duodenal ulcer may have a secondary diagnosis such as hypertension, which is not considered significant enough to complicate the DRG, a complication such as ileus, or a major complication such as perforation or heart failure. Depending on the clinical circumstances, a patient admitted with a principal diagnosis of duodenal ulcer could have any of 3 DRGs.
Of all the information contained in the medical record, coders can use only documentation by physicians who are directly caring for the patient during that admission. This includes documentation by resident physicians, physician assistants, or nurse practitioners if the attending documents agreement. Notes of nurses and allied health professionals cannot be used. Consultants' notes can also be used for coding, except when their findings contradict those of the attending physician. In this case, 1 of 2 things can happen. The coder may use the documentation of the attending physician or, if clarification of the appropriate diagnosis or procedure is necessary, query the attending physician. Pathology and radiology reports and laboratory findings cannot be used unless the diagnoses are documented by the attending.
Because coders can use only documentation that follows universal terminology, physicians need to understand coding principles and learn to document using appropriate terminology.2, 3 This includes documentation of diagnoses, conditions, symptoms, or procedures defined by CMS. The large number of vagaries in the coding vernacular used by CMS sometimes makes this lexicon confusing and difficult for physicians. To ensure appropriate documentation, physicians must abandon doctorese, the shorthand vernacular that is commonly used for documentation. Even when a coder is able to correctly infer the diagnosis, he or she cannot use this information because the diagnosis was not specifically documented. It will either be lost or generate a query; both are negative consequences for the hospital and physician because reimbursement might be inappropriately low and the true level of severity of illness might not be appreciated.
Examples of this are myriad (see Appendix B) and include the following:
-
Shorthand notation, such as Na (hyponatremia) and plts, (thrombocytopenia) is not acceptable; the actual diagnosis must be written.
-
Often, there is no documentation of the diagnosis at all, but physicians read between the lines to glean the diagnosis. A note states dysuria followed by +U/A, leaving the assessment blank. The plan says ciprofloxin 500BID X 3d. Most physicians recognize this as shorthand for an uncomplicated urinary tract infection, but the documentation is incomplete because the assessment is omitted, and the coders will not be able to code.
-
A note documents an abnormal laboratory value that is intended to reflect a diagnosis (eg, Na+ = 117, restrict fluids). Coders likely understand that hyponatremia is the diagnosis, but they cannot code it because coding rules state it is only an abnormal laboratory value, not a diagnosis. Hyponatremia must be written in the medical record.
In most circumstances, a few simple guidelines will help:
-
Avoid abbreviations. Full diagnoses should be written in longhand rather than abbreviations or symbols. Use a diagnosis when appropriate, rather than just the symptom, such as hypoxia for dyspnea.
-
Write complete SOAP notes. Always document the diagnosis for which any treatment is rendered or evaluation performed. In other words, always write complete SOAP notes, not SOP notes.
-
Become familiar with rules and concepts of coding and documentation. Some peculiarities of coding rules make little sense to physicians and may appear arbitrary. Certain diagnoses, conditions, or descriptive terms that physicians commonly use cannot be used for coding purposes. These peculiarities will simply need to be learned or handled by queries from coders or real‐time chart review by coding personnel. For example, although exacerbation of chronic obstructive pulmonary disease is recognized in coding rules, exacerbation of congestive heart failure codes to a nonspecific code, and the physician must document it as acute on chronic or acute congestive heart failure. Likewise, the new terminology adopted by the National Kidney Foundation for acute renal failure, acute kidney injury, has no code. Because both of these diagnoses serve as major comorbidities, they have major financial implications for hospitals.
-
Be thorough. All clinically significant conditions noted should be documented and coded. According to CMS rules, a condition, whether major or minor, is clinically significant if it requires any of the following:4
-
Clinical evaluation
-
Therapeutic treatment
-
Diagnostic procedures
-
Extended length of hospital stay
-
Increased nursing care and/or monitoring.
-
Avoid rule‐out diagnoses. It is perfectly acceptable to qualify an uncertain diagnosis. For example, suspected pneumonia can be documented as probable or possible. If you document it as such and empirically treat for pneumonia, the coder may document pneumonia as the diagnosis. Diagnoses that have been ruled out should not be documented. For example, a patient is admitted with neutropenic fever and suspected sepsis. The patient may be given empirical therapy, but if sepsis is ruled out and the treatment is stopped, sepsis is not an appropriate diagnosis.
-
Identify the principal diagnosis. The principal diagnosis is defined as the condition responsible for the patient's admission to the hospital. All other diagnoses are secondary. If a patient enters the hospital because of sepsis of urinary origin but during the hospitalization develops pneumonia that extends the stay, the principal diagnosis from which the DRG is derived remains sepsis of urinary origin. The only exception is the patient with several conditions, any of which would have independently required hospitalization and treatment. In this case, the coders have the option of selecting the principal diagnosis from among the possible principal diagnoses if each is treated with essentially equal effort.
-
Include relevant secondary diagnoses. Another complexity and frustration regarding the coding rules is that they are often highly specific and follow a logic of their own. For coding purposes, upper gastrointestinal bleeding is a diagnosis without comorbidity. However, adding the secondary diagnosis of blood loss anemia increases the case weight by adding a comorbidity, and documenting esophageal hemorrhage adds a major comorbidity, further increasing the case weight. Coders may not, by Medicare rules, prompt or lead physicians to the proper term. If the physician documents upper gastrointestinal bleed, anemia, and esophagitis, the coder cannot ask, Was the esophagitis the cause of the anemia?
Other Considerations
Although coders cannot use documentation from nurses and allied health professionals, their notes often provide clues to issues that the physician may have failed to document. For example, a patient with significant postoperative nausea and vomiting may be treated and followed carefully by the physicians and improve despite no physician documentation. The information contained in the nursing notes can generate a query to the physician to clarify the diagnosis that required treatment for significant nausea and vomiting.
Under the new guidelines, diagnoses present on admission must be distinguished from diagnoses occurring after admission. CMS is very concerned about reducing the incidence of preventable nosocomial events such as decubitus ulcers and catheter‐associated infections. In an attempt to push hospitals to reduce or eliminate the incidence of these adverse events, CMS no longer reimburses certain diagnoses for the added cost of care when these events occur. If a patient leaves the hospital with a catheter‐associated urinary tract infection, CMS assumes that it was hospital‐acquired unless it was clearly documented as present on admission (see Appendix A). It is likely that the list will grow over time; in fact, CMS is considering adding ventilator‐associated pneumonia, Staphylococcus aureus septicemia, and deep venous thrombosis/pulmonary embolism in 2009. Thus, it is important to develop systematic methods to ensure that all diagnoses present on admission are captured and that diagnoses which developed during the hospitalization are acknowledged. A diagnosis present on admission but not recognized until after admission can be documented as present on admission. Another category will also be apparent occasionally in which it cannot be known whether a condition was present on admission or occurred following hospitalization.
PREPARING TO COMPLY WITH MS‐DRG GUIDELINES
Information from Maryland hospitals that have piloted the MS‐DRG methodology indicates that coders will be 25% to 50% less efficient (private communication), largely because of increased communication (queries) between coders and physicians to clarify medical documentation. Queries may be generated whenever the record lacks codable documentation or information is missing, conflicting, ambiguous, or illegible. Most hospitals will need to increase their coding staff and hire or develop educators to teach coders and physicians medical terminology. Many of these educators will need experience in both coding and medicine and will generally require at least an RN degree or the equivalent.5, 6 Hiring experienced coders with a medical background is currently a challenge as many hospitals are responding to the new guidelines, and they are in high demand. Many hospitals will need to upgrade the skills of existing coders or medical personnel to fill these roles. Hospitals that invest in additional coders to train physicians in coding terminology may eventually regain efficiency in the coding process; however, it seems likely that some degree of additional clarification will always be needed.
Hospitals should develop educational programs, including didactic presentations that define the new MS‐DRGs, outline the risks and benefits of the new rules, and provide examples of universal terminology. They should provide handouts, pocket guides, and electronic medical record prompts with coding terminology and frequently asked questions. Specific physician feedback may occur on an individual, departmental, or DRG basis or on the basis of the International Statistical Classification of Diseases and Related Health Problems, 9th edition. Coding specialists need to be available to provide real‐time chart review and answer specific physician inquiries on coding and documentation questions. Physician buy‐in is essential and can be encouraged through careful education, administrative support, and physician champions.
INCENTIVE AND DISINCENTIVES: HOW TO MAXIMIZE COMPLIANCE AMONG PHYSICIANS AND HOSPITALS (AND WHY IT IS SO IMPORTANT)
The new coding rules affect only hospital reimbursement, so physicians get no direct benefit from ensuring that hospitals obtain the maximum appropriate reimbursement. However, physicians indirectly benefit when hospitals have strong profit margins, which allow for improved staffing levels, capital expenditures, additional services, programs, and growth. Any physician who has worked in institutions that operate in the red and in the black fully understands how important hospital revenue is to morale, efficiency, and work satisfaction.
The importance of properly evaluating quality of care cannot be overestimated. CMS, the Joint Commission on the Accreditation of Healthcare Organizations, and other oversight bodies have emphasized this through guidelines, legislation, and financial incentives.7 Pay for performance, value‐based purchasing, and performance indicator data are terms commonly understood by physicians. Hospitals and physicians benefit from improved quality measurements, which are affected by coding and documentation. Without appropriate coding and documentation, institutions that care for the very sickest patients cannot demonstrate their true severity of illness. Increases in morbidity, mortality, and length of stay will not correlate with the documented severity of illness, adversely skewing quality data and affecting hospitals' reputations. Hospitals that do not adequately account for the severity of the patients that they treat and accurately adjust their performance measures for severity will face increasingly difficult challenges to their financial stability and reputation in the future.8 The ability to demonstrate favorable quality report cards2, 3 represents an increasingly important incentive for hospitals.9 Finally, it is important to realize the multitude of functions supported by good documentation in the medical record. The record is also important for quality measurement, protection from liability, evaluation of resource utilization, tumor and other medical data registries, and other uses (see Appendix A).
CONCLUSION
The MS‐DRG system has important implications for physicians and hospitals. The changes will allow CMS to understand more fully the severity of illness of hospitalized patients. It replaces a system that derived a DRG from a single principle diagnosis and in some cases a single comorbidity with one that reflects all conditions. Comorbidities and complications are designated as major, minor, or no complication. Because multiple parties use the medical record for many different functions, better documentation of specificity of severity of illness will affect hospitals in many ways. Importantly, one of these will be reimbursement. Hospitals that historically have had a higher level of severity will now see that reflected in their case mix and may actually see improved reimbursement. Another area that will be affected is quality measurement. If severity of illness is not appropriately documented and accounted for, hospitals could exhibit skewed outcomes of care. For example, if hospitals with sicker (on average) patients document a lower indicator of severity than the true severity of its patients, their mortality experience might appear to be abnormally high in comparison with other hospitals. This can damage reputations and thus affect many things such as patient referrals and utilization of services. This becomes particularly important in a competitive medical market and at a time when patients have increased access to hospital‐specific data on quality of care.
The new guidelines also require medical documentation to capture diagnoses present on admission as opposed to conditions that arise during hospitalization. If not recorded as present on admission, selected conditions will be considered iatrogenic complications and will not receive additional reimbursement. CMS intends this as an incentive for hospitals to improve quality of care by developing safeguards against complications.
It is likely that hospitals will take different approaches to ensuring that medical record documentation skills are taught and adopted by physicians. As different approaches evolve, hopefully best practices will emerge that can be disseminated. These efforts should be taken to ensure appropriate documentation prospectively rather than heavy reliance on a retrospective review and query process, which can be inefficient and expensive, intrusive to physician workflow, and possibly subject to third‐party criticism.
It is vital for hospital senior managers to gain physician input and involvement in both the design and implementation of the programs outlined in this article and to provide them with adequate resources and administrative support throughout the educational process. Ultimately, developing a program that enhances and sustains the medical record documentation skills of its medical staff is critical to the well‐being of any hospital. Accepting the new changes and making the changes necessary to ensure success is certainly an additional burden on physicians; many, if not most, of whom likely feel overworked and overburdened by the many demands on their time. Although they may not derive personal benefit for changing their behaviors, physicians should nevertheless understand the importance of appropriate documentation for the purposes of quality assessment, reimbursement, and resource allocation.
Appendix
APPENDIX A: SELECTED PENNSYLVANIA AND NATIONAL DATABASES USING MEDICAL RECORDS
| Joint Commission on Accreditation of Healthcare Organizations (JCAHO) |
| United Hospital Consortium (UHC) |
| Pennsylvania Health Center Cost Containment Council (PHC4) |
| United Network for Organ Sharing (UNOS) |
| National Cancer Data Base (NCDB) |
| National Database of Nursing Quality Indicators (NDNQI) |
| National Association of Children's Hospitals and Related Institutions (NACHRI) |
| Pennsylvania Trauma Systems Foundation (PTSF) |
| American College of Cardiology (ACC) |
| National Endoscopy Data Base (NEDB) |
| National Surgery Quality Improvement Program (NSQIP) |
| Society of Thoracic Surgery (STS) |
| Uniform Data System for Medical Rehabilitation (UDSMR) |
Appendix
APPENDIX B: NOTES TAKEN DIRECTLY FROM THE MEDICAL RECORD
| What the MDs Document (Doctorese) | What They Mean (Diagnosis/ Universal Terminology) | Coding Result |
|---|---|---|
| plts, Tx 4U plts | Thrombocytopenia | Coders cannot decipher |
| Na+ = 117, fluid restrict | Hyponatremia | Abnormal laboratory test; cannot code |
| O2 sat 80, NC @ 4 l/min | Hypoxia | Coders cannot decipher |
| Alb = 2.4, diet consult, start suppl | Malnutrition | Abnormal laboratory test; cannot code |
| IV NS 250/hr, 2U Tx, GI bleed | Hypovolemia, blood loss anemia | Coders cannot decipher |
| BP, fever, MS, +UA | Sepsis of urinary origin | Urinary tract infection |
Appendix
APPENDIX C: HOSPITAL‐ACQUIRED CONDITIONS OF FOCUS TO THE CENTERS FOR MEDICARE AND MEDICAID SERVICES FOR 2008
| Serious preventable event: object left in surgery |
| Serious preventable event: air embolism |
| Serious preventable event: blood incompatibility |
| Catheter‐associated urinary tract infections |
| Vascular catheterassociated infections |
| Surgical site infection: mediastinitis after coronary artery bypass surgery |
| Hospital‐acquired injuries: fractures, dislocations, intracranial injury, crushing injury, burn, and other unspecified effects of external causes |
Appendix
APPENDIX D: STRATEGIES FOR SUCCESS WITH MEDICARE SEVERITY DIAGNOSIS‐RELATED GROUPS
| Educational initiatives |
| Introductory didactic presentations |
| Online tutorial: coding and documentation |
| Periodic memos with coding tips (Tip of the Month) |
| Web site references on coding tips (comprehensive list) |
| Posters, announcements, and branding |
| Physician support services |
| Web site reference with FAQs |
| Direct contact with coding specialists |
| RN/coding specialist liaison |
| Computerized medical record |
| Staff feedback associated with query process |
| Physician champions |
| Coding department changes |
| Increased staffing |
| RN/coding specialist: real‐time chart reviews |
| Physician coding specialist |
| Standing Coding and Documentation Committee |
Appendix
APPENDIX E: SELECTED CODING TIPS FOR GENERAL MEDICINE
|
| Disease/condition specific tips |
| Gastrointestinal bleed with anemia does not mean that the patient is anemic from the hemorrhage: write blood loss anemia (chronic or acute). |
| Urosepsis codes to urinary tract infection site NOS: write sepsis with urinary origin. |
| CVA or stroke does not mean infarction: write CVA with infarction. |
| Common complications and comorbidities |
| Cardiac: acute myocardial infarction, congestive heart failure, atrial flutter, paroxysmal supraventricular tachycardia, heart block, and second‐degree heart block |
| Gastrointestinal: melena, ascites, hepatitis, and hematemesis |
| Genitourinary: urinary retention, hematuria, urinary tract infection, hydronephrosis, and renal failure |
| Nutritional: dehydration, malnutrition, cachexia, and volume overload |
| Gastrointestinal: peritonitis, perforation, bleeding esophageal varices, ascites, and ileus |
| Genitourinary: acute renal failure, end‐stage renal disease, urinary tract infection, and nephritic syndrome |
| Nutritional: severe malnutrition, body mass index > 40, malnutrition NOS, and cachexia |
| Pulmonary: respiratory failure, aspiration pneumonia, pneumothorax, atelectasis, and hemoptysis |
| General tips |
| A culture must be linked to the site of infection: write pseudomonas pneumonia. |
| Ambulatory dysfunction and deconditioning lack the required specificity to ensure accurate coding; when possible, use abnormal gait, difficulty walking, muscle weakness, and so forth. |
| If the patient appears to be septic, positive blood cultures are not necessary to document sepsis. |
| Discriminate between acute, chronic, and acute on chronic. |
| If the problem is active, do not write history of , which implies that the condition no longer exists: write PMH: chronic (diagnosis). |
| Be specific in documenting congestive heart failure (acute/chronic, systolic/diastolic failure, L/R). |
- Centers for Medicare and Medicaid Services. Medicare Program: Changes to the Hospital Inpatient Prospective Payment Systems and Fiscal Year 2008 Rates. Available at:http://www.cms.hhs.gov/acuteinpatientpps/downloads/cms‐1533‐fc.pdf. Accessed October2008.
- ,,,,.Straight talk: new approaches in healthcare. Rx for reimbursement woes: high‐quality medical documentation and coding. Panel discussion.Mod Healthc.2007;32(29):35–38.
- ,,.Optimizing hospital reimbursement through physician awareness: a step toward better patient care.Orthopedics.1998;21(1):79–83.
- ICD‐9‐CM Official Guidelines for Coding and Reporting (effective October 1, 2007). Available at:http://www.cdc.gov/nchs/datawh/ftpserv/ftpicd9/icdguide07.pdf. Accessed October2008.
- ,.Improving physician documentation through a clinical documentation management program.Nurs Adm.2003;27(4):285–289.
- .A primer for understanding diagnosis‐related groups and inpatient hospital reimbursement with nursing implications.Crit Care Nurs.2005;28(4):360–369.
- US Department of Health and Human Services. Report to Congress: Plan To Implement a Medicare Hospital Value‐Based Purchasing Program. Available at:http://www.cms.hhs.gov/acuteinpatientpps/downloads/hospitalvbpplanrtcfinalsubmitted2007.pdf. Accessed October2008.
- ,,, et al.Results of report cards for patients with congestive heart failure depend on the method used to adjust for severity.Ann Intern Med.2000;133:10–20.
- ,,, et al.Assessment of the Medicare quality improvement organization program.Ann Intern Med.2006;145(5):342–353.
You admitted a patient to the hospital for an upper gastrointestinal bleed. At the time of admission, the patient's mucous membranes were dry, and he was mildly orthostatic and tachycardic. He was given several boluses of normal saline, and he improved. All of this was carefully documented in the medical record. Shortly after discharge, the following cryptic message arrives in your mailbox:
The patient was admitted with gastrointestinal bleeding and noted to have dry mucous membranes, orthostatic hypotension, and tachycardia. He was given intravenous saline. What diagnosis, if any, required treatment with 2 boluses of normal saline?
You remember the patient well but still pull the chart to review the case. It appears obvious that the patient was dry and needed fluid resuscitation. You are confused and do not know how to respond. Your response is just that: Patient was dry and needed fluid resuscitation.
Several days later, you get another message thanking you for your reply but describing what the coder actually needed to be able to code appropriately. Had you answered hypovolemia or dehydration, it would have changed the diagnosis‐related group (DRG) and reimbursement from gastrointestinal hemorrhage ($2700) to gastrointestinal hemorrhage with complications ($4600). Because you did not provide the right answer, the institution was reimbursed for the lesser amount. Now you are left with more questions. Hypovolemia is exactly what the patient had; you basically said so, and it was described throughout the chart, although not in so many words. Why did the coder not just say what was needed? Why can you not just answer again? Why are you being asked to play what appears to be a stupid game when you have sick patients to care for and never enough time? What can you do to prevent this from happening the next time? What other surprises are in store for you?
INTRODUCTION
Beginning October 1, 2007 the Centers for Medicare and Medicaid Services (CMS) implemented changes in the hospital inpatient prospective payment system that have profound implications for how physicians code and document hospital care. These changes were implemented in an effort to better recognize severity of illness,1 and the information will be used to plan for current and future needs of hospitals, insurers, caregivers, and patients. Severity of illness is a measure of the patient's overall health status reflected by the resources necessary for care and the risk of morbidity and mortality. Factors including the presenting illness, comorbid conditions, functional status, nutritional status, and age contribute to the severity of illness. From a physiologic perspective, factors reflecting loss of homeostatic control such as abnormal vital signs, poor oxygenation, and altered sensorium are determinants of severity of illness. For hospitals, severity of illness is generally reflected by the case mix of concomitant illness. Thus, a patient with community‐acquired pneumonia without other comorbidities requires fewer resources and has a greater chance of a good outcome than the same patient with complications such as acute congestive heart failure. In the context of this article, severity of illness should be considered an indication of the complexity of the patient's presentation. Reporting comorbidities and illness severity will help better define quality of care and medical necessity for that care.
The DRG system provided a set payment for a given hospitalization based on primary and sometimes secondary diagnoses. The new system, using Medicare severity diagnosis‐related groups (MS‐DRGs), accounts for all diagnoses present at the time of admission and all diagnoses made during the hospitalization.
This article discusses the value of appropriate documentation and outlines changes that physicians will need to make to ensure optimal coding. The value of appropriate documentation is described. Specific terminology is illustrated so physicians can document properly and coders can easily extract the necessary information from the medical record to code appropriately. Finally, specific strategies institutions can implement to support physicians and coders are suggested.
A PRIMER ON CODING AND MEDICAL DOCUMENTATION
Prior to October 1, 2007, the DRG for a given hospitalization was calculated from the principle diagnosis and in some cases 1 secondary diagnosis that represented a significant complication or comorbidity. For example, a patient admitted to the hospital with abdominal pain diagnosed as a peptic ulcer would have a DRG to reflect the ulcer. If the patient also had anemia secondary to blood loss from the ulcer, this would serve as a complication, and a DRG with a comorbidity or complication and a higher case weight would be assigned. Additional significant complications would not further alter the DRG.
The new guidelines recognize 3 levels of severity for secondary diagnoses. The DRG from the principal diagnosis can be associated with other diagnoses that recognize no complication or comorbidity, a complication or comorbidity, or a major complication or comorbidity. Thus, a patient admitted with a duodenal ulcer may have a secondary diagnosis such as hypertension, which is not considered significant enough to complicate the DRG, a complication such as ileus, or a major complication such as perforation or heart failure. Depending on the clinical circumstances, a patient admitted with a principal diagnosis of duodenal ulcer could have any of 3 DRGs.
Of all the information contained in the medical record, coders can use only documentation by physicians who are directly caring for the patient during that admission. This includes documentation by resident physicians, physician assistants, or nurse practitioners if the attending documents agreement. Notes of nurses and allied health professionals cannot be used. Consultants' notes can also be used for coding, except when their findings contradict those of the attending physician. In this case, 1 of 2 things can happen. The coder may use the documentation of the attending physician or, if clarification of the appropriate diagnosis or procedure is necessary, query the attending physician. Pathology and radiology reports and laboratory findings cannot be used unless the diagnoses are documented by the attending.
Because coders can use only documentation that follows universal terminology, physicians need to understand coding principles and learn to document using appropriate terminology.2, 3 This includes documentation of diagnoses, conditions, symptoms, or procedures defined by CMS. The large number of vagaries in the coding vernacular used by CMS sometimes makes this lexicon confusing and difficult for physicians. To ensure appropriate documentation, physicians must abandon doctorese, the shorthand vernacular that is commonly used for documentation. Even when a coder is able to correctly infer the diagnosis, he or she cannot use this information because the diagnosis was not specifically documented. It will either be lost or generate a query; both are negative consequences for the hospital and physician because reimbursement might be inappropriately low and the true level of severity of illness might not be appreciated.
Examples of this are myriad (see Appendix B) and include the following:
-
Shorthand notation, such as Na (hyponatremia) and plts, (thrombocytopenia) is not acceptable; the actual diagnosis must be written.
-
Often, there is no documentation of the diagnosis at all, but physicians read between the lines to glean the diagnosis. A note states dysuria followed by +U/A, leaving the assessment blank. The plan says ciprofloxin 500BID X 3d. Most physicians recognize this as shorthand for an uncomplicated urinary tract infection, but the documentation is incomplete because the assessment is omitted, and the coders will not be able to code.
-
A note documents an abnormal laboratory value that is intended to reflect a diagnosis (eg, Na+ = 117, restrict fluids). Coders likely understand that hyponatremia is the diagnosis, but they cannot code it because coding rules state it is only an abnormal laboratory value, not a diagnosis. Hyponatremia must be written in the medical record.
In most circumstances, a few simple guidelines will help:
-
Avoid abbreviations. Full diagnoses should be written in longhand rather than abbreviations or symbols. Use a diagnosis when appropriate, rather than just the symptom, such as hypoxia for dyspnea.
-
Write complete SOAP notes. Always document the diagnosis for which any treatment is rendered or evaluation performed. In other words, always write complete SOAP notes, not SOP notes.
-
Become familiar with rules and concepts of coding and documentation. Some peculiarities of coding rules make little sense to physicians and may appear arbitrary. Certain diagnoses, conditions, or descriptive terms that physicians commonly use cannot be used for coding purposes. These peculiarities will simply need to be learned or handled by queries from coders or real‐time chart review by coding personnel. For example, although exacerbation of chronic obstructive pulmonary disease is recognized in coding rules, exacerbation of congestive heart failure codes to a nonspecific code, and the physician must document it as acute on chronic or acute congestive heart failure. Likewise, the new terminology adopted by the National Kidney Foundation for acute renal failure, acute kidney injury, has no code. Because both of these diagnoses serve as major comorbidities, they have major financial implications for hospitals.
-
Be thorough. All clinically significant conditions noted should be documented and coded. According to CMS rules, a condition, whether major or minor, is clinically significant if it requires any of the following:4
-
Clinical evaluation
-
Therapeutic treatment
-
Diagnostic procedures
-
Extended length of hospital stay
-
Increased nursing care and/or monitoring.
-
Avoid rule‐out diagnoses. It is perfectly acceptable to qualify an uncertain diagnosis. For example, suspected pneumonia can be documented as probable or possible. If you document it as such and empirically treat for pneumonia, the coder may document pneumonia as the diagnosis. Diagnoses that have been ruled out should not be documented. For example, a patient is admitted with neutropenic fever and suspected sepsis. The patient may be given empirical therapy, but if sepsis is ruled out and the treatment is stopped, sepsis is not an appropriate diagnosis.
-
Identify the principal diagnosis. The principal diagnosis is defined as the condition responsible for the patient's admission to the hospital. All other diagnoses are secondary. If a patient enters the hospital because of sepsis of urinary origin but during the hospitalization develops pneumonia that extends the stay, the principal diagnosis from which the DRG is derived remains sepsis of urinary origin. The only exception is the patient with several conditions, any of which would have independently required hospitalization and treatment. In this case, the coders have the option of selecting the principal diagnosis from among the possible principal diagnoses if each is treated with essentially equal effort.
-
Include relevant secondary diagnoses. Another complexity and frustration regarding the coding rules is that they are often highly specific and follow a logic of their own. For coding purposes, upper gastrointestinal bleeding is a diagnosis without comorbidity. However, adding the secondary diagnosis of blood loss anemia increases the case weight by adding a comorbidity, and documenting esophageal hemorrhage adds a major comorbidity, further increasing the case weight. Coders may not, by Medicare rules, prompt or lead physicians to the proper term. If the physician documents upper gastrointestinal bleed, anemia, and esophagitis, the coder cannot ask, Was the esophagitis the cause of the anemia?
Other Considerations
Although coders cannot use documentation from nurses and allied health professionals, their notes often provide clues to issues that the physician may have failed to document. For example, a patient with significant postoperative nausea and vomiting may be treated and followed carefully by the physicians and improve despite no physician documentation. The information contained in the nursing notes can generate a query to the physician to clarify the diagnosis that required treatment for significant nausea and vomiting.
Under the new guidelines, diagnoses present on admission must be distinguished from diagnoses occurring after admission. CMS is very concerned about reducing the incidence of preventable nosocomial events such as decubitus ulcers and catheter‐associated infections. In an attempt to push hospitals to reduce or eliminate the incidence of these adverse events, CMS no longer reimburses certain diagnoses for the added cost of care when these events occur. If a patient leaves the hospital with a catheter‐associated urinary tract infection, CMS assumes that it was hospital‐acquired unless it was clearly documented as present on admission (see Appendix A). It is likely that the list will grow over time; in fact, CMS is considering adding ventilator‐associated pneumonia, Staphylococcus aureus septicemia, and deep venous thrombosis/pulmonary embolism in 2009. Thus, it is important to develop systematic methods to ensure that all diagnoses present on admission are captured and that diagnoses which developed during the hospitalization are acknowledged. A diagnosis present on admission but not recognized until after admission can be documented as present on admission. Another category will also be apparent occasionally in which it cannot be known whether a condition was present on admission or occurred following hospitalization.
PREPARING TO COMPLY WITH MS‐DRG GUIDELINES
Information from Maryland hospitals that have piloted the MS‐DRG methodology indicates that coders will be 25% to 50% less efficient (private communication), largely because of increased communication (queries) between coders and physicians to clarify medical documentation. Queries may be generated whenever the record lacks codable documentation or information is missing, conflicting, ambiguous, or illegible. Most hospitals will need to increase their coding staff and hire or develop educators to teach coders and physicians medical terminology. Many of these educators will need experience in both coding and medicine and will generally require at least an RN degree or the equivalent.5, 6 Hiring experienced coders with a medical background is currently a challenge as many hospitals are responding to the new guidelines, and they are in high demand. Many hospitals will need to upgrade the skills of existing coders or medical personnel to fill these roles. Hospitals that invest in additional coders to train physicians in coding terminology may eventually regain efficiency in the coding process; however, it seems likely that some degree of additional clarification will always be needed.
Hospitals should develop educational programs, including didactic presentations that define the new MS‐DRGs, outline the risks and benefits of the new rules, and provide examples of universal terminology. They should provide handouts, pocket guides, and electronic medical record prompts with coding terminology and frequently asked questions. Specific physician feedback may occur on an individual, departmental, or DRG basis or on the basis of the International Statistical Classification of Diseases and Related Health Problems, 9th edition. Coding specialists need to be available to provide real‐time chart review and answer specific physician inquiries on coding and documentation questions. Physician buy‐in is essential and can be encouraged through careful education, administrative support, and physician champions.
INCENTIVE AND DISINCENTIVES: HOW TO MAXIMIZE COMPLIANCE AMONG PHYSICIANS AND HOSPITALS (AND WHY IT IS SO IMPORTANT)
The new coding rules affect only hospital reimbursement, so physicians get no direct benefit from ensuring that hospitals obtain the maximum appropriate reimbursement. However, physicians indirectly benefit when hospitals have strong profit margins, which allow for improved staffing levels, capital expenditures, additional services, programs, and growth. Any physician who has worked in institutions that operate in the red and in the black fully understands how important hospital revenue is to morale, efficiency, and work satisfaction.
The importance of properly evaluating quality of care cannot be overestimated. CMS, the Joint Commission on the Accreditation of Healthcare Organizations, and other oversight bodies have emphasized this through guidelines, legislation, and financial incentives.7 Pay for performance, value‐based purchasing, and performance indicator data are terms commonly understood by physicians. Hospitals and physicians benefit from improved quality measurements, which are affected by coding and documentation. Without appropriate coding and documentation, institutions that care for the very sickest patients cannot demonstrate their true severity of illness. Increases in morbidity, mortality, and length of stay will not correlate with the documented severity of illness, adversely skewing quality data and affecting hospitals' reputations. Hospitals that do not adequately account for the severity of the patients that they treat and accurately adjust their performance measures for severity will face increasingly difficult challenges to their financial stability and reputation in the future.8 The ability to demonstrate favorable quality report cards2, 3 represents an increasingly important incentive for hospitals.9 Finally, it is important to realize the multitude of functions supported by good documentation in the medical record. The record is also important for quality measurement, protection from liability, evaluation of resource utilization, tumor and other medical data registries, and other uses (see Appendix A).
CONCLUSION
The MS‐DRG system has important implications for physicians and hospitals. The changes will allow CMS to understand more fully the severity of illness of hospitalized patients. It replaces a system that derived a DRG from a single principle diagnosis and in some cases a single comorbidity with one that reflects all conditions. Comorbidities and complications are designated as major, minor, or no complication. Because multiple parties use the medical record for many different functions, better documentation of specificity of severity of illness will affect hospitals in many ways. Importantly, one of these will be reimbursement. Hospitals that historically have had a higher level of severity will now see that reflected in their case mix and may actually see improved reimbursement. Another area that will be affected is quality measurement. If severity of illness is not appropriately documented and accounted for, hospitals could exhibit skewed outcomes of care. For example, if hospitals with sicker (on average) patients document a lower indicator of severity than the true severity of its patients, their mortality experience might appear to be abnormally high in comparison with other hospitals. This can damage reputations and thus affect many things such as patient referrals and utilization of services. This becomes particularly important in a competitive medical market and at a time when patients have increased access to hospital‐specific data on quality of care.
The new guidelines also require medical documentation to capture diagnoses present on admission as opposed to conditions that arise during hospitalization. If not recorded as present on admission, selected conditions will be considered iatrogenic complications and will not receive additional reimbursement. CMS intends this as an incentive for hospitals to improve quality of care by developing safeguards against complications.
It is likely that hospitals will take different approaches to ensuring that medical record documentation skills are taught and adopted by physicians. As different approaches evolve, hopefully best practices will emerge that can be disseminated. These efforts should be taken to ensure appropriate documentation prospectively rather than heavy reliance on a retrospective review and query process, which can be inefficient and expensive, intrusive to physician workflow, and possibly subject to third‐party criticism.
It is vital for hospital senior managers to gain physician input and involvement in both the design and implementation of the programs outlined in this article and to provide them with adequate resources and administrative support throughout the educational process. Ultimately, developing a program that enhances and sustains the medical record documentation skills of its medical staff is critical to the well‐being of any hospital. Accepting the new changes and making the changes necessary to ensure success is certainly an additional burden on physicians; many, if not most, of whom likely feel overworked and overburdened by the many demands on their time. Although they may not derive personal benefit for changing their behaviors, physicians should nevertheless understand the importance of appropriate documentation for the purposes of quality assessment, reimbursement, and resource allocation.
Appendix
APPENDIX A: SELECTED PENNSYLVANIA AND NATIONAL DATABASES USING MEDICAL RECORDS
| Joint Commission on Accreditation of Healthcare Organizations (JCAHO) |
| United Hospital Consortium (UHC) |
| Pennsylvania Health Center Cost Containment Council (PHC4) |
| United Network for Organ Sharing (UNOS) |
| National Cancer Data Base (NCDB) |
| National Database of Nursing Quality Indicators (NDNQI) |
| National Association of Children's Hospitals and Related Institutions (NACHRI) |
| Pennsylvania Trauma Systems Foundation (PTSF) |
| American College of Cardiology (ACC) |
| National Endoscopy Data Base (NEDB) |
| National Surgery Quality Improvement Program (NSQIP) |
| Society of Thoracic Surgery (STS) |
| Uniform Data System for Medical Rehabilitation (UDSMR) |
Appendix
APPENDIX B: NOTES TAKEN DIRECTLY FROM THE MEDICAL RECORD
| What the MDs Document (Doctorese) | What They Mean (Diagnosis/ Universal Terminology) | Coding Result |
|---|---|---|
| plts, Tx 4U plts | Thrombocytopenia | Coders cannot decipher |
| Na+ = 117, fluid restrict | Hyponatremia | Abnormal laboratory test; cannot code |
| O2 sat 80, NC @ 4 l/min | Hypoxia | Coders cannot decipher |
| Alb = 2.4, diet consult, start suppl | Malnutrition | Abnormal laboratory test; cannot code |
| IV NS 250/hr, 2U Tx, GI bleed | Hypovolemia, blood loss anemia | Coders cannot decipher |
| BP, fever, MS, +UA | Sepsis of urinary origin | Urinary tract infection |
Appendix
APPENDIX C: HOSPITAL‐ACQUIRED CONDITIONS OF FOCUS TO THE CENTERS FOR MEDICARE AND MEDICAID SERVICES FOR 2008
| Serious preventable event: object left in surgery |
| Serious preventable event: air embolism |
| Serious preventable event: blood incompatibility |
| Catheter‐associated urinary tract infections |
| Vascular catheterassociated infections |
| Surgical site infection: mediastinitis after coronary artery bypass surgery |
| Hospital‐acquired injuries: fractures, dislocations, intracranial injury, crushing injury, burn, and other unspecified effects of external causes |
Appendix
APPENDIX D: STRATEGIES FOR SUCCESS WITH MEDICARE SEVERITY DIAGNOSIS‐RELATED GROUPS
| Educational initiatives |
| Introductory didactic presentations |
| Online tutorial: coding and documentation |
| Periodic memos with coding tips (Tip of the Month) |
| Web site references on coding tips (comprehensive list) |
| Posters, announcements, and branding |
| Physician support services |
| Web site reference with FAQs |
| Direct contact with coding specialists |
| RN/coding specialist liaison |
| Computerized medical record |
| Staff feedback associated with query process |
| Physician champions |
| Coding department changes |
| Increased staffing |
| RN/coding specialist: real‐time chart reviews |
| Physician coding specialist |
| Standing Coding and Documentation Committee |
Appendix
APPENDIX E: SELECTED CODING TIPS FOR GENERAL MEDICINE
|
| Disease/condition specific tips |
| Gastrointestinal bleed with anemia does not mean that the patient is anemic from the hemorrhage: write blood loss anemia (chronic or acute). |
| Urosepsis codes to urinary tract infection site NOS: write sepsis with urinary origin. |
| CVA or stroke does not mean infarction: write CVA with infarction. |
| Common complications and comorbidities |
| Cardiac: acute myocardial infarction, congestive heart failure, atrial flutter, paroxysmal supraventricular tachycardia, heart block, and second‐degree heart block |
| Gastrointestinal: melena, ascites, hepatitis, and hematemesis |
| Genitourinary: urinary retention, hematuria, urinary tract infection, hydronephrosis, and renal failure |
| Nutritional: dehydration, malnutrition, cachexia, and volume overload |
| Gastrointestinal: peritonitis, perforation, bleeding esophageal varices, ascites, and ileus |
| Genitourinary: acute renal failure, end‐stage renal disease, urinary tract infection, and nephritic syndrome |
| Nutritional: severe malnutrition, body mass index > 40, malnutrition NOS, and cachexia |
| Pulmonary: respiratory failure, aspiration pneumonia, pneumothorax, atelectasis, and hemoptysis |
| General tips |
| A culture must be linked to the site of infection: write pseudomonas pneumonia. |
| Ambulatory dysfunction and deconditioning lack the required specificity to ensure accurate coding; when possible, use abnormal gait, difficulty walking, muscle weakness, and so forth. |
| If the patient appears to be septic, positive blood cultures are not necessary to document sepsis. |
| Discriminate between acute, chronic, and acute on chronic. |
| If the problem is active, do not write history of , which implies that the condition no longer exists: write PMH: chronic (diagnosis). |
| Be specific in documenting congestive heart failure (acute/chronic, systolic/diastolic failure, L/R). |
You admitted a patient to the hospital for an upper gastrointestinal bleed. At the time of admission, the patient's mucous membranes were dry, and he was mildly orthostatic and tachycardic. He was given several boluses of normal saline, and he improved. All of this was carefully documented in the medical record. Shortly after discharge, the following cryptic message arrives in your mailbox:
The patient was admitted with gastrointestinal bleeding and noted to have dry mucous membranes, orthostatic hypotension, and tachycardia. He was given intravenous saline. What diagnosis, if any, required treatment with 2 boluses of normal saline?
You remember the patient well but still pull the chart to review the case. It appears obvious that the patient was dry and needed fluid resuscitation. You are confused and do not know how to respond. Your response is just that: Patient was dry and needed fluid resuscitation.
Several days later, you get another message thanking you for your reply but describing what the coder actually needed to be able to code appropriately. Had you answered hypovolemia or dehydration, it would have changed the diagnosis‐related group (DRG) and reimbursement from gastrointestinal hemorrhage ($2700) to gastrointestinal hemorrhage with complications ($4600). Because you did not provide the right answer, the institution was reimbursed for the lesser amount. Now you are left with more questions. Hypovolemia is exactly what the patient had; you basically said so, and it was described throughout the chart, although not in so many words. Why did the coder not just say what was needed? Why can you not just answer again? Why are you being asked to play what appears to be a stupid game when you have sick patients to care for and never enough time? What can you do to prevent this from happening the next time? What other surprises are in store for you?
INTRODUCTION
Beginning October 1, 2007 the Centers for Medicare and Medicaid Services (CMS) implemented changes in the hospital inpatient prospective payment system that have profound implications for how physicians code and document hospital care. These changes were implemented in an effort to better recognize severity of illness,1 and the information will be used to plan for current and future needs of hospitals, insurers, caregivers, and patients. Severity of illness is a measure of the patient's overall health status reflected by the resources necessary for care and the risk of morbidity and mortality. Factors including the presenting illness, comorbid conditions, functional status, nutritional status, and age contribute to the severity of illness. From a physiologic perspective, factors reflecting loss of homeostatic control such as abnormal vital signs, poor oxygenation, and altered sensorium are determinants of severity of illness. For hospitals, severity of illness is generally reflected by the case mix of concomitant illness. Thus, a patient with community‐acquired pneumonia without other comorbidities requires fewer resources and has a greater chance of a good outcome than the same patient with complications such as acute congestive heart failure. In the context of this article, severity of illness should be considered an indication of the complexity of the patient's presentation. Reporting comorbidities and illness severity will help better define quality of care and medical necessity for that care.
The DRG system provided a set payment for a given hospitalization based on primary and sometimes secondary diagnoses. The new system, using Medicare severity diagnosis‐related groups (MS‐DRGs), accounts for all diagnoses present at the time of admission and all diagnoses made during the hospitalization.
This article discusses the value of appropriate documentation and outlines changes that physicians will need to make to ensure optimal coding. The value of appropriate documentation is described. Specific terminology is illustrated so physicians can document properly and coders can easily extract the necessary information from the medical record to code appropriately. Finally, specific strategies institutions can implement to support physicians and coders are suggested.
A PRIMER ON CODING AND MEDICAL DOCUMENTATION
Prior to October 1, 2007, the DRG for a given hospitalization was calculated from the principle diagnosis and in some cases 1 secondary diagnosis that represented a significant complication or comorbidity. For example, a patient admitted to the hospital with abdominal pain diagnosed as a peptic ulcer would have a DRG to reflect the ulcer. If the patient also had anemia secondary to blood loss from the ulcer, this would serve as a complication, and a DRG with a comorbidity or complication and a higher case weight would be assigned. Additional significant complications would not further alter the DRG.
The new guidelines recognize 3 levels of severity for secondary diagnoses. The DRG from the principal diagnosis can be associated with other diagnoses that recognize no complication or comorbidity, a complication or comorbidity, or a major complication or comorbidity. Thus, a patient admitted with a duodenal ulcer may have a secondary diagnosis such as hypertension, which is not considered significant enough to complicate the DRG, a complication such as ileus, or a major complication such as perforation or heart failure. Depending on the clinical circumstances, a patient admitted with a principal diagnosis of duodenal ulcer could have any of 3 DRGs.
Of all the information contained in the medical record, coders can use only documentation by physicians who are directly caring for the patient during that admission. This includes documentation by resident physicians, physician assistants, or nurse practitioners if the attending documents agreement. Notes of nurses and allied health professionals cannot be used. Consultants' notes can also be used for coding, except when their findings contradict those of the attending physician. In this case, 1 of 2 things can happen. The coder may use the documentation of the attending physician or, if clarification of the appropriate diagnosis or procedure is necessary, query the attending physician. Pathology and radiology reports and laboratory findings cannot be used unless the diagnoses are documented by the attending.
Because coders can use only documentation that follows universal terminology, physicians need to understand coding principles and learn to document using appropriate terminology.2, 3 This includes documentation of diagnoses, conditions, symptoms, or procedures defined by CMS. The large number of vagaries in the coding vernacular used by CMS sometimes makes this lexicon confusing and difficult for physicians. To ensure appropriate documentation, physicians must abandon doctorese, the shorthand vernacular that is commonly used for documentation. Even when a coder is able to correctly infer the diagnosis, he or she cannot use this information because the diagnosis was not specifically documented. It will either be lost or generate a query; both are negative consequences for the hospital and physician because reimbursement might be inappropriately low and the true level of severity of illness might not be appreciated.
Examples of this are myriad (see Appendix B) and include the following:
-
Shorthand notation, such as Na (hyponatremia) and plts, (thrombocytopenia) is not acceptable; the actual diagnosis must be written.
-
Often, there is no documentation of the diagnosis at all, but physicians read between the lines to glean the diagnosis. A note states dysuria followed by +U/A, leaving the assessment blank. The plan says ciprofloxin 500BID X 3d. Most physicians recognize this as shorthand for an uncomplicated urinary tract infection, but the documentation is incomplete because the assessment is omitted, and the coders will not be able to code.
-
A note documents an abnormal laboratory value that is intended to reflect a diagnosis (eg, Na+ = 117, restrict fluids). Coders likely understand that hyponatremia is the diagnosis, but they cannot code it because coding rules state it is only an abnormal laboratory value, not a diagnosis. Hyponatremia must be written in the medical record.
In most circumstances, a few simple guidelines will help:
-
Avoid abbreviations. Full diagnoses should be written in longhand rather than abbreviations or symbols. Use a diagnosis when appropriate, rather than just the symptom, such as hypoxia for dyspnea.
-
Write complete SOAP notes. Always document the diagnosis for which any treatment is rendered or evaluation performed. In other words, always write complete SOAP notes, not SOP notes.
-
Become familiar with rules and concepts of coding and documentation. Some peculiarities of coding rules make little sense to physicians and may appear arbitrary. Certain diagnoses, conditions, or descriptive terms that physicians commonly use cannot be used for coding purposes. These peculiarities will simply need to be learned or handled by queries from coders or real‐time chart review by coding personnel. For example, although exacerbation of chronic obstructive pulmonary disease is recognized in coding rules, exacerbation of congestive heart failure codes to a nonspecific code, and the physician must document it as acute on chronic or acute congestive heart failure. Likewise, the new terminology adopted by the National Kidney Foundation for acute renal failure, acute kidney injury, has no code. Because both of these diagnoses serve as major comorbidities, they have major financial implications for hospitals.
-
Be thorough. All clinically significant conditions noted should be documented and coded. According to CMS rules, a condition, whether major or minor, is clinically significant if it requires any of the following:4
-
Clinical evaluation
-
Therapeutic treatment
-
Diagnostic procedures
-
Extended length of hospital stay
-
Increased nursing care and/or monitoring.
-
Avoid rule‐out diagnoses. It is perfectly acceptable to qualify an uncertain diagnosis. For example, suspected pneumonia can be documented as probable or possible. If you document it as such and empirically treat for pneumonia, the coder may document pneumonia as the diagnosis. Diagnoses that have been ruled out should not be documented. For example, a patient is admitted with neutropenic fever and suspected sepsis. The patient may be given empirical therapy, but if sepsis is ruled out and the treatment is stopped, sepsis is not an appropriate diagnosis.
-
Identify the principal diagnosis. The principal diagnosis is defined as the condition responsible for the patient's admission to the hospital. All other diagnoses are secondary. If a patient enters the hospital because of sepsis of urinary origin but during the hospitalization develops pneumonia that extends the stay, the principal diagnosis from which the DRG is derived remains sepsis of urinary origin. The only exception is the patient with several conditions, any of which would have independently required hospitalization and treatment. In this case, the coders have the option of selecting the principal diagnosis from among the possible principal diagnoses if each is treated with essentially equal effort.
-
Include relevant secondary diagnoses. Another complexity and frustration regarding the coding rules is that they are often highly specific and follow a logic of their own. For coding purposes, upper gastrointestinal bleeding is a diagnosis without comorbidity. However, adding the secondary diagnosis of blood loss anemia increases the case weight by adding a comorbidity, and documenting esophageal hemorrhage adds a major comorbidity, further increasing the case weight. Coders may not, by Medicare rules, prompt or lead physicians to the proper term. If the physician documents upper gastrointestinal bleed, anemia, and esophagitis, the coder cannot ask, Was the esophagitis the cause of the anemia?
Other Considerations
Although coders cannot use documentation from nurses and allied health professionals, their notes often provide clues to issues that the physician may have failed to document. For example, a patient with significant postoperative nausea and vomiting may be treated and followed carefully by the physicians and improve despite no physician documentation. The information contained in the nursing notes can generate a query to the physician to clarify the diagnosis that required treatment for significant nausea and vomiting.
Under the new guidelines, diagnoses present on admission must be distinguished from diagnoses occurring after admission. CMS is very concerned about reducing the incidence of preventable nosocomial events such as decubitus ulcers and catheter‐associated infections. In an attempt to push hospitals to reduce or eliminate the incidence of these adverse events, CMS no longer reimburses certain diagnoses for the added cost of care when these events occur. If a patient leaves the hospital with a catheter‐associated urinary tract infection, CMS assumes that it was hospital‐acquired unless it was clearly documented as present on admission (see Appendix A). It is likely that the list will grow over time; in fact, CMS is considering adding ventilator‐associated pneumonia, Staphylococcus aureus septicemia, and deep venous thrombosis/pulmonary embolism in 2009. Thus, it is important to develop systematic methods to ensure that all diagnoses present on admission are captured and that diagnoses which developed during the hospitalization are acknowledged. A diagnosis present on admission but not recognized until after admission can be documented as present on admission. Another category will also be apparent occasionally in which it cannot be known whether a condition was present on admission or occurred following hospitalization.
PREPARING TO COMPLY WITH MS‐DRG GUIDELINES
Information from Maryland hospitals that have piloted the MS‐DRG methodology indicates that coders will be 25% to 50% less efficient (private communication), largely because of increased communication (queries) between coders and physicians to clarify medical documentation. Queries may be generated whenever the record lacks codable documentation or information is missing, conflicting, ambiguous, or illegible. Most hospitals will need to increase their coding staff and hire or develop educators to teach coders and physicians medical terminology. Many of these educators will need experience in both coding and medicine and will generally require at least an RN degree or the equivalent.5, 6 Hiring experienced coders with a medical background is currently a challenge as many hospitals are responding to the new guidelines, and they are in high demand. Many hospitals will need to upgrade the skills of existing coders or medical personnel to fill these roles. Hospitals that invest in additional coders to train physicians in coding terminology may eventually regain efficiency in the coding process; however, it seems likely that some degree of additional clarification will always be needed.
Hospitals should develop educational programs, including didactic presentations that define the new MS‐DRGs, outline the risks and benefits of the new rules, and provide examples of universal terminology. They should provide handouts, pocket guides, and electronic medical record prompts with coding terminology and frequently asked questions. Specific physician feedback may occur on an individual, departmental, or DRG basis or on the basis of the International Statistical Classification of Diseases and Related Health Problems, 9th edition. Coding specialists need to be available to provide real‐time chart review and answer specific physician inquiries on coding and documentation questions. Physician buy‐in is essential and can be encouraged through careful education, administrative support, and physician champions.
INCENTIVE AND DISINCENTIVES: HOW TO MAXIMIZE COMPLIANCE AMONG PHYSICIANS AND HOSPITALS (AND WHY IT IS SO IMPORTANT)
The new coding rules affect only hospital reimbursement, so physicians get no direct benefit from ensuring that hospitals obtain the maximum appropriate reimbursement. However, physicians indirectly benefit when hospitals have strong profit margins, which allow for improved staffing levels, capital expenditures, additional services, programs, and growth. Any physician who has worked in institutions that operate in the red and in the black fully understands how important hospital revenue is to morale, efficiency, and work satisfaction.
The importance of properly evaluating quality of care cannot be overestimated. CMS, the Joint Commission on the Accreditation of Healthcare Organizations, and other oversight bodies have emphasized this through guidelines, legislation, and financial incentives.7 Pay for performance, value‐based purchasing, and performance indicator data are terms commonly understood by physicians. Hospitals and physicians benefit from improved quality measurements, which are affected by coding and documentation. Without appropriate coding and documentation, institutions that care for the very sickest patients cannot demonstrate their true severity of illness. Increases in morbidity, mortality, and length of stay will not correlate with the documented severity of illness, adversely skewing quality data and affecting hospitals' reputations. Hospitals that do not adequately account for the severity of the patients that they treat and accurately adjust their performance measures for severity will face increasingly difficult challenges to their financial stability and reputation in the future.8 The ability to demonstrate favorable quality report cards2, 3 represents an increasingly important incentive for hospitals.9 Finally, it is important to realize the multitude of functions supported by good documentation in the medical record. The record is also important for quality measurement, protection from liability, evaluation of resource utilization, tumor and other medical data registries, and other uses (see Appendix A).
CONCLUSION
The MS‐DRG system has important implications for physicians and hospitals. The changes will allow CMS to understand more fully the severity of illness of hospitalized patients. It replaces a system that derived a DRG from a single principle diagnosis and in some cases a single comorbidity with one that reflects all conditions. Comorbidities and complications are designated as major, minor, or no complication. Because multiple parties use the medical record for many different functions, better documentation of specificity of severity of illness will affect hospitals in many ways. Importantly, one of these will be reimbursement. Hospitals that historically have had a higher level of severity will now see that reflected in their case mix and may actually see improved reimbursement. Another area that will be affected is quality measurement. If severity of illness is not appropriately documented and accounted for, hospitals could exhibit skewed outcomes of care. For example, if hospitals with sicker (on average) patients document a lower indicator of severity than the true severity of its patients, their mortality experience might appear to be abnormally high in comparison with other hospitals. This can damage reputations and thus affect many things such as patient referrals and utilization of services. This becomes particularly important in a competitive medical market and at a time when patients have increased access to hospital‐specific data on quality of care.
The new guidelines also require medical documentation to capture diagnoses present on admission as opposed to conditions that arise during hospitalization. If not recorded as present on admission, selected conditions will be considered iatrogenic complications and will not receive additional reimbursement. CMS intends this as an incentive for hospitals to improve quality of care by developing safeguards against complications.
It is likely that hospitals will take different approaches to ensuring that medical record documentation skills are taught and adopted by physicians. As different approaches evolve, hopefully best practices will emerge that can be disseminated. These efforts should be taken to ensure appropriate documentation prospectively rather than heavy reliance on a retrospective review and query process, which can be inefficient and expensive, intrusive to physician workflow, and possibly subject to third‐party criticism.
It is vital for hospital senior managers to gain physician input and involvement in both the design and implementation of the programs outlined in this article and to provide them with adequate resources and administrative support throughout the educational process. Ultimately, developing a program that enhances and sustains the medical record documentation skills of its medical staff is critical to the well‐being of any hospital. Accepting the new changes and making the changes necessary to ensure success is certainly an additional burden on physicians; many, if not most, of whom likely feel overworked and overburdened by the many demands on their time. Although they may not derive personal benefit for changing their behaviors, physicians should nevertheless understand the importance of appropriate documentation for the purposes of quality assessment, reimbursement, and resource allocation.
Appendix
APPENDIX A: SELECTED PENNSYLVANIA AND NATIONAL DATABASES USING MEDICAL RECORDS
| Joint Commission on Accreditation of Healthcare Organizations (JCAHO) |
| United Hospital Consortium (UHC) |
| Pennsylvania Health Center Cost Containment Council (PHC4) |
| United Network for Organ Sharing (UNOS) |
| National Cancer Data Base (NCDB) |
| National Database of Nursing Quality Indicators (NDNQI) |
| National Association of Children's Hospitals and Related Institutions (NACHRI) |
| Pennsylvania Trauma Systems Foundation (PTSF) |
| American College of Cardiology (ACC) |
| National Endoscopy Data Base (NEDB) |
| National Surgery Quality Improvement Program (NSQIP) |
| Society of Thoracic Surgery (STS) |
| Uniform Data System for Medical Rehabilitation (UDSMR) |
Appendix
APPENDIX B: NOTES TAKEN DIRECTLY FROM THE MEDICAL RECORD
| What the MDs Document (Doctorese) | What They Mean (Diagnosis/ Universal Terminology) | Coding Result |
|---|---|---|
| plts, Tx 4U plts | Thrombocytopenia | Coders cannot decipher |
| Na+ = 117, fluid restrict | Hyponatremia | Abnormal laboratory test; cannot code |
| O2 sat 80, NC @ 4 l/min | Hypoxia | Coders cannot decipher |
| Alb = 2.4, diet consult, start suppl | Malnutrition | Abnormal laboratory test; cannot code |
| IV NS 250/hr, 2U Tx, GI bleed | Hypovolemia, blood loss anemia | Coders cannot decipher |
| BP, fever, MS, +UA | Sepsis of urinary origin | Urinary tract infection |
Appendix
APPENDIX C: HOSPITAL‐ACQUIRED CONDITIONS OF FOCUS TO THE CENTERS FOR MEDICARE AND MEDICAID SERVICES FOR 2008
| Serious preventable event: object left in surgery |
| Serious preventable event: air embolism |
| Serious preventable event: blood incompatibility |
| Catheter‐associated urinary tract infections |
| Vascular catheterassociated infections |
| Surgical site infection: mediastinitis after coronary artery bypass surgery |
| Hospital‐acquired injuries: fractures, dislocations, intracranial injury, crushing injury, burn, and other unspecified effects of external causes |
Appendix
APPENDIX D: STRATEGIES FOR SUCCESS WITH MEDICARE SEVERITY DIAGNOSIS‐RELATED GROUPS
| Educational initiatives |
| Introductory didactic presentations |
| Online tutorial: coding and documentation |
| Periodic memos with coding tips (Tip of the Month) |
| Web site references on coding tips (comprehensive list) |
| Posters, announcements, and branding |
| Physician support services |
| Web site reference with FAQs |
| Direct contact with coding specialists |
| RN/coding specialist liaison |
| Computerized medical record |
| Staff feedback associated with query process |
| Physician champions |
| Coding department changes |
| Increased staffing |
| RN/coding specialist: real‐time chart reviews |
| Physician coding specialist |
| Standing Coding and Documentation Committee |
Appendix
APPENDIX E: SELECTED CODING TIPS FOR GENERAL MEDICINE
|
| Disease/condition specific tips |
| Gastrointestinal bleed with anemia does not mean that the patient is anemic from the hemorrhage: write blood loss anemia (chronic or acute). |
| Urosepsis codes to urinary tract infection site NOS: write sepsis with urinary origin. |
| CVA or stroke does not mean infarction: write CVA with infarction. |
| Common complications and comorbidities |
| Cardiac: acute myocardial infarction, congestive heart failure, atrial flutter, paroxysmal supraventricular tachycardia, heart block, and second‐degree heart block |
| Gastrointestinal: melena, ascites, hepatitis, and hematemesis |
| Genitourinary: urinary retention, hematuria, urinary tract infection, hydronephrosis, and renal failure |
| Nutritional: dehydration, malnutrition, cachexia, and volume overload |
| Gastrointestinal: peritonitis, perforation, bleeding esophageal varices, ascites, and ileus |
| Genitourinary: acute renal failure, end‐stage renal disease, urinary tract infection, and nephritic syndrome |
| Nutritional: severe malnutrition, body mass index > 40, malnutrition NOS, and cachexia |
| Pulmonary: respiratory failure, aspiration pneumonia, pneumothorax, atelectasis, and hemoptysis |
| General tips |
| A culture must be linked to the site of infection: write pseudomonas pneumonia. |
| Ambulatory dysfunction and deconditioning lack the required specificity to ensure accurate coding; when possible, use abnormal gait, difficulty walking, muscle weakness, and so forth. |
| If the patient appears to be septic, positive blood cultures are not necessary to document sepsis. |
| Discriminate between acute, chronic, and acute on chronic. |
| If the problem is active, do not write history of , which implies that the condition no longer exists: write PMH: chronic (diagnosis). |
| Be specific in documenting congestive heart failure (acute/chronic, systolic/diastolic failure, L/R). |
- Centers for Medicare and Medicaid Services. Medicare Program: Changes to the Hospital Inpatient Prospective Payment Systems and Fiscal Year 2008 Rates. Available at:http://www.cms.hhs.gov/acuteinpatientpps/downloads/cms‐1533‐fc.pdf. Accessed October2008.
- ,,,,.Straight talk: new approaches in healthcare. Rx for reimbursement woes: high‐quality medical documentation and coding. Panel discussion.Mod Healthc.2007;32(29):35–38.
- ,,.Optimizing hospital reimbursement through physician awareness: a step toward better patient care.Orthopedics.1998;21(1):79–83.
- ICD‐9‐CM Official Guidelines for Coding and Reporting (effective October 1, 2007). Available at:http://www.cdc.gov/nchs/datawh/ftpserv/ftpicd9/icdguide07.pdf. Accessed October2008.
- ,.Improving physician documentation through a clinical documentation management program.Nurs Adm.2003;27(4):285–289.
- .A primer for understanding diagnosis‐related groups and inpatient hospital reimbursement with nursing implications.Crit Care Nurs.2005;28(4):360–369.
- US Department of Health and Human Services. Report to Congress: Plan To Implement a Medicare Hospital Value‐Based Purchasing Program. Available at:http://www.cms.hhs.gov/acuteinpatientpps/downloads/hospitalvbpplanrtcfinalsubmitted2007.pdf. Accessed October2008.
- ,,, et al.Results of report cards for patients with congestive heart failure depend on the method used to adjust for severity.Ann Intern Med.2000;133:10–20.
- ,,, et al.Assessment of the Medicare quality improvement organization program.Ann Intern Med.2006;145(5):342–353.
- Centers for Medicare and Medicaid Services. Medicare Program: Changes to the Hospital Inpatient Prospective Payment Systems and Fiscal Year 2008 Rates. Available at:http://www.cms.hhs.gov/acuteinpatientpps/downloads/cms‐1533‐fc.pdf. Accessed October2008.
- ,,,,.Straight talk: new approaches in healthcare. Rx for reimbursement woes: high‐quality medical documentation and coding. Panel discussion.Mod Healthc.2007;32(29):35–38.
- ,,.Optimizing hospital reimbursement through physician awareness: a step toward better patient care.Orthopedics.1998;21(1):79–83.
- ICD‐9‐CM Official Guidelines for Coding and Reporting (effective October 1, 2007). Available at:http://www.cdc.gov/nchs/datawh/ftpserv/ftpicd9/icdguide07.pdf. Accessed October2008.
- ,.Improving physician documentation through a clinical documentation management program.Nurs Adm.2003;27(4):285–289.
- .A primer for understanding diagnosis‐related groups and inpatient hospital reimbursement with nursing implications.Crit Care Nurs.2005;28(4):360–369.
- US Department of Health and Human Services. Report to Congress: Plan To Implement a Medicare Hospital Value‐Based Purchasing Program. Available at:http://www.cms.hhs.gov/acuteinpatientpps/downloads/hospitalvbpplanrtcfinalsubmitted2007.pdf. Accessed October2008.
- ,,, et al.Results of report cards for patients with congestive heart failure depend on the method used to adjust for severity.Ann Intern Med.2000;133:10–20.
- ,,, et al.Assessment of the Medicare quality improvement organization program.Ann Intern Med.2006;145(5):342–353.