User login
Double jeopardy: How to treat kids with comorbid anxiety and ADHD
Aaron, age 10, has been diagnosed with an anxiety disorder and attention-deficit/hyperactivity disorder (ADHD) but is not being treated with medication because his parents do not believe in psychopharmacology. They bring him to a specialized child anxiety clinic and ask for “urgent CBT” because his behavior at school is out of control.
Aaron rearranges the therapist’s office furniture during much of the assessment interview. He also acknowledges many anxiety symptoms. The therapist doubts that cognitive-behavioral therapy (CBT) would help without other interventions.
Children with anxiety disorders and ADHD—a common comorbid presentation—tend to be more impaired than those with either condition alone.1 Effective treatment usually requires 4 components (Table 1), including medication plus behavioral or cognitive-behavioral therapy. This article discusses clinical issues related to each component and describes how to successfully combine them into a treatment plan.
Table 1
Comorbid ADHD and anxiety: 4 treatment components
| Successful treatment usually involves combining 4 components: | |
| |
| Make individual adjustments as needed, depending on the child’s symptom profile, social context, and developmental level | |
| ADHD: attention-deficit/hyperactivity disorder | |
Medication options
Stimulants, atomoxetine, and selective serotonin reuptake inhibitors (SSRIs) have been advocated for children with anxiety and ADHD. Given the high risk of behavioral disinhibition with SSRIs in children,2 stimulants or atomoxetine are suggested as first-line medications.3,4
Stimulants target ADHD symptoms primarily, but anxiety decreases in some children (24% in a recent trial) as ADHD symptoms are controlled.4 Because it is a selective norepinephrine reuptake inhibitor (SNRI), atomoxetine may target both ADHD and anxiety symptoms. When initiating these medications, “start low and go slow.” Recommended dosing is no different for children with ADHD and anxiety than for those with ADHD alone (Table 2).5
Stimulant response rates for children with ADHD and anxiety vary among studies. Some report lower response rates than for children with ADHD alone and possibly more treatment-emergent side effects.6 The National Institute of Mental Health’s Multimodal Treatment Study of Children with ADHD (MTA) found that comorbid anxiety did not adversely affect behavioral response to stimulants but did moderate outcomes (Box 1).7,8 Adding intensive psychosocial intervention to stimulant treatment appeared to yield greater improvements in anxious children with ADHD, compared with stimulants alone.8
Cognitive impairments related to inattention do not consistently improve with stimulant treatment.9 This is clinically important because children with ADHD and comorbid anxiety disorders can be very cognitively impaired.10
Add an SSRI? Monotherapy is simpler and usually more acceptable to families, but a placebo-controlled study examined adding an SSRI (fluvoxamine) to methylphenidate treatment.4 Children with anxiety and ADHD who received adjunctive fluvoxamine did no better than those who received methylphenidate plus placebo.
Atomoxetine. A large, randomized, controlled trial of atomoxetine in this population found good tolerability and statistically significant reductions in ADHD and anxiety symptoms compared with placebo. Effect size was greater for ADHD symptoms than for anxiety symptoms,11 however, which supports smaller trials that show more consistent evidence of atomoxetine reducing ADHD symptoms than anxiety symptoms.
Similar to antidepressants with the SNRI chemical structure, atomoxetine’s effectiveness for a given child takes several weeks to determine. This can be a problem in children who are highly distressed or impaired and require rapid symptomatic improvement.
Recommendation. Consider a stimulant or atomoxetine initially for children with anxiety disorders and ADHD, and seek concurrent behavioral or cognitive-behavioral therapy. Caution families that:
- >1 medication trial might be needed, as response may not be as consistent as in children with ADHD alone
- medication-related improvements in ADHD symptoms will not necessarily be associated with reduced anxiety symptoms or improved academic ability
- improvements with atomoxetine might not be evident for several weeks.
Table 2
Medication dosing for children with ADHD*
| Medication | Recommended starting dosage | Recommended maximum dosage | 5 most common side effects in descending prevalence |
|---|---|---|---|
| Stimulants | |||
| Methylphenidate hydrochloride (Ritalin) | 5 mg tid | Total 60 mg/d | Insomnia, nervousness, decreased appetite, dizziness, nausea |
| Methylphenidate hydrochloride (Concerta) | 18 mg every morning | 54 mg every morning | Headache, abdominal pain, decreased appetite, vomiting, insomnia |
| Dextroamphetamine sulfate (Dexedrine) | 5 mg every morning | Total 40 mg/d | Palpitations, restlessness, dizziness, dry mouth, decreased appetite |
| Mixed amphetamine salts (Adderall) | 10 mg every morning | 30 mg every morning | Decreased appetite, insomnia, abdominal pain, emotional lability, vomiting |
| Nonstimulant | |||
| Atomoxetine (Strattera) | 0.5 mg/kg/d | 1.2 mg/kg/d | Decreased appetite, dizziness, stomach upset, fatigue, irritability |
| ADHD: attention-deficit/hyperactivity disorder | |||
| * Recommended dosing is no different for children with ADHD and anxiety than for children with only ADHD | |||
| Source: Reference 5 | |||
Psychological intervention
CBT has been shown effective for child-hood anxiety disorders in randomized controlled trials,12 but even those that included children with comorbid ADHD required that an anxiety disorder be the primary, most impairing diagnosis.13 Thus, little is known about CBT’s effectiveness for children with anxiety plus ADHD. Given the evidence for cognitive deficits in comorbid anxiety and ADHD10 and the challenge of working with highly distractible children, one would expect CBT to be more difficult in this population.
The potential for distraction to adversely affect learning of coping strategies is higher in group than in individual therapy, and children with anxiety and ADHD can be disruptive to other children in CBT groups. Consider individual CBT, and seek a therapist who has experience with this population. Having the child on medication for ADHD symptoms usually helps reduce these symptoms’ impact on sessions.
For children younger than about age 8 or too cognitively impaired to benefit from CBT, behavioral intervention alone may be helpful. The largely behavioral psychosocial intervention in the MTA study of ADHD children age 7 to 9 (Box 2)8,14 helped many of those with comorbid anxiety.
Although programs as intense as that used in the MTA study rarely are provided in community practice, consider behavior modification. For example:
- To reduce anxiety, have the child follow regular, predictable routines, and reward the child for gradually facing previously avoided situations.
- To reduce distractibility in class, have the child sit near the teacher, break work into small chunks, and reward completion of each chunk.
Even small improvements in the child’s home or school behavior may reduce negative interactions with others and the attendant effects on self-esteem.
CASE CONTINUED: Weighing the options
The therapist seeing Aaron’s family listens to their concerns about medication and reassures them that their son will not be denied psychotherapy. She tells them, however, that psychotherapy will not address his urgent school problems and is unlikely to work in the absence of medication, given Aaron’s behavior in the office. The therapist provides accurate information about the risks and benefits of medication and CBT, and the parents agree to think about all treatment options.
By the next office visit, the school has threatened to suspend Aaron. He and his parents agree to combined treatment with a stimulant medication and CBT and to having the therapist provide a behavioral consultation at the school.
shows best outcomes for ADHD with anxiety
The National Institute of Mental Health’s Multimodal Treatment Study of Children with ADHD—the largest study to date—found that comorbid anxiety did not adversely affect behavioral response to stimulants but did moderate outcomes.
In the parallel group design study, 579 ADHD children age 7 to 9 were enrolled at 6 treatment sites, thoroughly assessed, then randomly assigned to 4 groups: medication treatment alone, intensive psychosocial treatment alone, a combination of both treatments, or usual community care. The first 3 interventions were designed to reflect best practices for each approach, and these children were closely monitored and studied for 14 months. All 4 groups were reassessed periodically for 24 months, evaluating multiple outcomes.
For the total sample, combined and medication treatment were more effective than psychosocial treatment and community care. For ADHD children with comorbid anxiety disorders:
- combined treatment was more effective than either medication treatment alone or psychosocial treatment alone
- both monotherapies were superior to community care.
ADHD: attention-deficit/hyperactivity disorder
Family psychoeducation
With families of children with behavioral challenges, adopt a patient, educational approach rather than acquiescing to their wishes or arguing with them. Either can result in treatment failure. Discuss potential benefits and risks of all treatment options and the impact of comorbidity on treatment.
Parents’ rigid insistence on a particular course of action—such as refusing psychopharmacology—may be caused by anxiety or misinformation. Elicit the source of any anxiety, and provide realistic information and reassurance if possible.
Anxiety in family members may be constitutional—as anxiety is highly heritable15—or relate to aspects of treatment. Families may feel overwhelmed by:
- their child having 2 disorders rather than 1
- your suggestion to start medical and nonmedical intervention together
- hearing about the possibility of multiple medication trials.
Negotiating medication. Discuss with the family the difficulties of a child learning CBT strategies when ADHD is not well-controlled and the cognitive difficulties in many of these children that may necessitate individualized CBT. If the family remains reluctant to consider combining medication with CBT, try contracting for a limited number of CBT sessions (perhaps 3 or 4) before re-evaluating the need for medication.
The child’s perceptions (and potential anxieties) about his or her difficulties also must be understood, validated, and addressed. Children are more likely to engage in a treatment if they participate in the decision to adopt it.
Anxiety can heighten vigilance in the child or the parents to treatment-emergent side effects, which you may exacerbate by providing exhaustive lists of potential ad-verse events. Limit discussion to serious side effects—with emphasis on their rarity—and those that are common.
ADHD traits in families can affect treatment success. Because of their own distractibility and organizational difficulties, parents with ADHD traits may have difficulty ensuring the child’s medication adherence and treatment participation.16
Behavior modification can require a high degree of consistency in parents’ behavior toward the child. This may be difficult to achieve in families where:
- 1 or both parents are inattentive because of ADHD
- a high degree of conflict exists between parents.
To help these families, provide reminder calls about appointments and schedule sessions at a consistent time. To improve consistency of medication use:
- combine medication administration with an essential daily activity
- check adherence with pill counts or other means.
If the child participates in CBT, provide separate notebooks for in-session and homework exercises—anticipating some loss of homework notebooks.
Individualizing care
Individualized care is important to return each child to his or her best possible level of functioning. The child’s symptom profile, environment, and developmental level can affect treatment.
For example, in a child whose ADHD-related impairment is substantial but whose anxiety-related impairment is mild, pharmacotherapy for ADHD and some pa-rental guidance may be adequate to manage remaining anxiety symptoms.17 As mentioned, some children show decreased anxiety as their ADHD is better controlled.4 Conversely, if ADHD-related impairment is mild but the child is highly anxious, consider CBT alone—preferably on an individual basis—provided the child can manage the cognitive aspects of therapy.
School personnel can monitor change in relation to various interventions, as many of these children’s symptoms manifest in the classroom. Behavioral interventions are more likely to succeed if they are administered consistently across home and school environments8 and teachers participate in behavior modification.
To elicit cooperation from school personnel, listen to their concerns and observations and help them understand the child’s difficulties and the rationale for various treatments. This approach often reduces negative feedback toward the child, a benefit that may further improve outcomes.
Attention to peer relationships and social stressors is often needed. Because of their multiple difficulties, these children may lack social skills and be shunned by their peers.1 You may need to help them develop social skills and reconnect with their peers after symptoms are well-controlled.
Poverty or lack of social support can affect treatment. Children with ADHD and anxiety usually need multiple interventions, and it is difficult for families to at-tend to these consistently when struggling with social stressors.
The 14-month intensive behavioral intervention used in the National Institute of Mental Health’s Multimodal Treatment Study (MTA) of 579 children age 7 to 9 with ADHD included:
- weekly parent training initially, decreasing to monthly by the end
- biweekly teacher consultations in behavior management
- 8-week full-day therapeutic summer program for children, focusing on behavioral and cognitive behavioral intervention
- 12-week half-time behaviorally trained paraprofessional aide in the classroom to generalize gains from summer program
- parent coaching on collaborating with teacher long-term so therapeutic consultation could be faded.
ADHD: attention-deficit/hyperactivity disorder
Adolescent adjustments. ADHD and anxiety often are diagnosed in the early school years, so anticipate developmental effects on treatment as the child enters adolescence. Adolescents value autonomy and may need to be more involved in treatment decisions than younger children.
Ask about and address family disagreements about treatment options, which may reduce adherence. You may need to talk about peer pressure to “not take drugs” by clearly differentiating the reasons some people take street drugs and the reasons for taking prescribed medication. Also discuss in a frank, nonjudgmental manner the risks of experimenting with street drugs (especially with prescribed medication) or of “sharing” one’s medications with friends.
Increased cognitive sophistication in adolescence may increase the potential benefit of CBT, so explore this option with the teen, especially if it was not attempted in the past.
Related resources
- American Academy of Child and Adolescent Psychiatry. “ADHD—a guide for families,” under the Resources for Families tab. www.aacap.org.
- Watkins C. Stimulant medication and ADHD. www.ncpamd.com/Stimulants.htm.
- Manassis K. Keys to parenting your anxious child. 2nd ed. Hauppauge, NY: Barron’s Educational Series, Inc.; 2008.
Drug brand names
- Atomoxetine • Strattera
- Dextroamphetamine • Dexedrine
- Fluvoxamine • Luvox
- Methylphenidate • Ritalin, Concerta
- Mixed amphetamine salts • Adderall
Disclosures
Dr. Manassis reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Bowen R, Chavira DA, Bailey K, et al. Nature of anxiety comorbid with attention deficit hyperactivity disorder in children from a pediatric primary care setting. Psychiatry Res 2008;157:201-9.
2. Walkup JT, Labellarte MJ, Riddle MA, et al. Searching for moderators and mediators of pharmacological treatment in children and adolescents with anxiety disorders. J Am Acad Child Adolesc Psychiatry 2003;42:13-21.
3. Wiesegger G, Kienbacher C, Pellegrini E, et al. Pharmacotherapy of attention-deficit/hyperactivity disorder (ADHD) and comorbid disorders. Neuropsychiatr 2007;21:187-206.
4. Abikoff H, McGough J, Vitiello B, et al. Sequential pharmacotherapy for children with comorbid attention-deficit/hyperactivity and anxiety disorders. J Am Acad Child Adolesc Psychiatry 2005;44:418-27.
5. Compendium of pharmaceuticals and specialties. Ottawa, Canada: Canadian Pharmacists Association; 2008.
6. Goez H, Back-Bennet O, Zelnik N. Differential stimulant response on attention in children with comorbid anxiety and oppositional defiant disorder. J Child Neurol 2007;22:538-42.
7. Wells KC, Pelham WE, Kotkin RA, et al. Psychosocial treatment strategies in the MTA study: rationale, methods, and critical issues in design and implementation. J Abnorm Child Psychol 2000;28:483-505.
8. March JS, Swanson JM, Arnold EL, et al. Anxiety as a predictor and outcome variable in the Multimodal Treatment Study of Children with ADHD (MTA). J Abnorm Child Psychol 2000;28:527-41.
9. Tannock R, Ickowicz A, Schachar R. Differential effects of methylphenidate on working memory in ADHD children with and without anxiety. J Am Acad Child Adolesc Psychiatry 1995;34:886-96.
10. Manassis K, Tannock R, Young A, Francis-John S. Cognition in anxious children with attention deficit hyperactivity disorder: a comparison with clinical and normal children. Behav Brain Funct 2007;3-4.
11. Geller D, Donnelly C, Lopez F, et al. Atomoxetine treatment for pediatric patients with attention-deficit/hyperactivity disorder with comorbid anxiety disorder. J Am Acad Child Adolesc Psychiatry 2007;46:1119-27.
12. Compton SN, March JS, Brent D, et al. Cognitive behavioural psychotherapy for anxiety and depressive disorders in children and adolescents: an evidence-based medicine review. J Am Acad Child Adolesc Psychiatry 2004;43:930-59.
13. Manassis K, Mendlowitz SL, Scapillato D, et al. Group and individual cognitive-behavioral therapy for childhood anxiety disorders: a randomized trial. J Am Acad Child Adolesc Psychiatry 2002;41:1423-30.
14. Arnold LE, Abikoff HB, Cantwell DP, et al. National Institute of Mental Health Collaborative Multimodal Treatment Study of Children with ADHD (the MTA). Design challenges and choices. Arch Gen Psychiatry 1997;54:865-70.
15. Kagan J, Reznick JS, Snidman N. Biological basis of childhood shyness. Science 1990;240:167-71.
16. Van Cleave J, Leslie LK. Approaching ADHD as a chronic condition: implications for long-term adherence. Pediatr Ann 2008;37:19-26.
17. Manassis K, Monga S. therapeutic approach to children and adolescents with anxiety disorders and associated comorbid conditions. J Am Acad Child Adolesc Psychiatry 2001;40:115-7.
Aaron, age 10, has been diagnosed with an anxiety disorder and attention-deficit/hyperactivity disorder (ADHD) but is not being treated with medication because his parents do not believe in psychopharmacology. They bring him to a specialized child anxiety clinic and ask for “urgent CBT” because his behavior at school is out of control.
Aaron rearranges the therapist’s office furniture during much of the assessment interview. He also acknowledges many anxiety symptoms. The therapist doubts that cognitive-behavioral therapy (CBT) would help without other interventions.
Children with anxiety disorders and ADHD—a common comorbid presentation—tend to be more impaired than those with either condition alone.1 Effective treatment usually requires 4 components (Table 1), including medication plus behavioral or cognitive-behavioral therapy. This article discusses clinical issues related to each component and describes how to successfully combine them into a treatment plan.
Table 1
Comorbid ADHD and anxiety: 4 treatment components
| Successful treatment usually involves combining 4 components: | |
| |
| Make individual adjustments as needed, depending on the child’s symptom profile, social context, and developmental level | |
| ADHD: attention-deficit/hyperactivity disorder | |
Medication options
Stimulants, atomoxetine, and selective serotonin reuptake inhibitors (SSRIs) have been advocated for children with anxiety and ADHD. Given the high risk of behavioral disinhibition with SSRIs in children,2 stimulants or atomoxetine are suggested as first-line medications.3,4
Stimulants target ADHD symptoms primarily, but anxiety decreases in some children (24% in a recent trial) as ADHD symptoms are controlled.4 Because it is a selective norepinephrine reuptake inhibitor (SNRI), atomoxetine may target both ADHD and anxiety symptoms. When initiating these medications, “start low and go slow.” Recommended dosing is no different for children with ADHD and anxiety than for those with ADHD alone (Table 2).5
Stimulant response rates for children with ADHD and anxiety vary among studies. Some report lower response rates than for children with ADHD alone and possibly more treatment-emergent side effects.6 The National Institute of Mental Health’s Multimodal Treatment Study of Children with ADHD (MTA) found that comorbid anxiety did not adversely affect behavioral response to stimulants but did moderate outcomes (Box 1).7,8 Adding intensive psychosocial intervention to stimulant treatment appeared to yield greater improvements in anxious children with ADHD, compared with stimulants alone.8
Cognitive impairments related to inattention do not consistently improve with stimulant treatment.9 This is clinically important because children with ADHD and comorbid anxiety disorders can be very cognitively impaired.10
Add an SSRI? Monotherapy is simpler and usually more acceptable to families, but a placebo-controlled study examined adding an SSRI (fluvoxamine) to methylphenidate treatment.4 Children with anxiety and ADHD who received adjunctive fluvoxamine did no better than those who received methylphenidate plus placebo.
Atomoxetine. A large, randomized, controlled trial of atomoxetine in this population found good tolerability and statistically significant reductions in ADHD and anxiety symptoms compared with placebo. Effect size was greater for ADHD symptoms than for anxiety symptoms,11 however, which supports smaller trials that show more consistent evidence of atomoxetine reducing ADHD symptoms than anxiety symptoms.
Similar to antidepressants with the SNRI chemical structure, atomoxetine’s effectiveness for a given child takes several weeks to determine. This can be a problem in children who are highly distressed or impaired and require rapid symptomatic improvement.
Recommendation. Consider a stimulant or atomoxetine initially for children with anxiety disorders and ADHD, and seek concurrent behavioral or cognitive-behavioral therapy. Caution families that:
- >1 medication trial might be needed, as response may not be as consistent as in children with ADHD alone
- medication-related improvements in ADHD symptoms will not necessarily be associated with reduced anxiety symptoms or improved academic ability
- improvements with atomoxetine might not be evident for several weeks.
Table 2
Medication dosing for children with ADHD*
| Medication | Recommended starting dosage | Recommended maximum dosage | 5 most common side effects in descending prevalence |
|---|---|---|---|
| Stimulants | |||
| Methylphenidate hydrochloride (Ritalin) | 5 mg tid | Total 60 mg/d | Insomnia, nervousness, decreased appetite, dizziness, nausea |
| Methylphenidate hydrochloride (Concerta) | 18 mg every morning | 54 mg every morning | Headache, abdominal pain, decreased appetite, vomiting, insomnia |
| Dextroamphetamine sulfate (Dexedrine) | 5 mg every morning | Total 40 mg/d | Palpitations, restlessness, dizziness, dry mouth, decreased appetite |
| Mixed amphetamine salts (Adderall) | 10 mg every morning | 30 mg every morning | Decreased appetite, insomnia, abdominal pain, emotional lability, vomiting |
| Nonstimulant | |||
| Atomoxetine (Strattera) | 0.5 mg/kg/d | 1.2 mg/kg/d | Decreased appetite, dizziness, stomach upset, fatigue, irritability |
| ADHD: attention-deficit/hyperactivity disorder | |||
| * Recommended dosing is no different for children with ADHD and anxiety than for children with only ADHD | |||
| Source: Reference 5 | |||
Psychological intervention
CBT has been shown effective for child-hood anxiety disorders in randomized controlled trials,12 but even those that included children with comorbid ADHD required that an anxiety disorder be the primary, most impairing diagnosis.13 Thus, little is known about CBT’s effectiveness for children with anxiety plus ADHD. Given the evidence for cognitive deficits in comorbid anxiety and ADHD10 and the challenge of working with highly distractible children, one would expect CBT to be more difficult in this population.
The potential for distraction to adversely affect learning of coping strategies is higher in group than in individual therapy, and children with anxiety and ADHD can be disruptive to other children in CBT groups. Consider individual CBT, and seek a therapist who has experience with this population. Having the child on medication for ADHD symptoms usually helps reduce these symptoms’ impact on sessions.
For children younger than about age 8 or too cognitively impaired to benefit from CBT, behavioral intervention alone may be helpful. The largely behavioral psychosocial intervention in the MTA study of ADHD children age 7 to 9 (Box 2)8,14 helped many of those with comorbid anxiety.
Although programs as intense as that used in the MTA study rarely are provided in community practice, consider behavior modification. For example:
- To reduce anxiety, have the child follow regular, predictable routines, and reward the child for gradually facing previously avoided situations.
- To reduce distractibility in class, have the child sit near the teacher, break work into small chunks, and reward completion of each chunk.
Even small improvements in the child’s home or school behavior may reduce negative interactions with others and the attendant effects on self-esteem.
CASE CONTINUED: Weighing the options
The therapist seeing Aaron’s family listens to their concerns about medication and reassures them that their son will not be denied psychotherapy. She tells them, however, that psychotherapy will not address his urgent school problems and is unlikely to work in the absence of medication, given Aaron’s behavior in the office. The therapist provides accurate information about the risks and benefits of medication and CBT, and the parents agree to think about all treatment options.
By the next office visit, the school has threatened to suspend Aaron. He and his parents agree to combined treatment with a stimulant medication and CBT and to having the therapist provide a behavioral consultation at the school.
shows best outcomes for ADHD with anxiety
The National Institute of Mental Health’s Multimodal Treatment Study of Children with ADHD—the largest study to date—found that comorbid anxiety did not adversely affect behavioral response to stimulants but did moderate outcomes.
In the parallel group design study, 579 ADHD children age 7 to 9 were enrolled at 6 treatment sites, thoroughly assessed, then randomly assigned to 4 groups: medication treatment alone, intensive psychosocial treatment alone, a combination of both treatments, or usual community care. The first 3 interventions were designed to reflect best practices for each approach, and these children were closely monitored and studied for 14 months. All 4 groups were reassessed periodically for 24 months, evaluating multiple outcomes.
For the total sample, combined and medication treatment were more effective than psychosocial treatment and community care. For ADHD children with comorbid anxiety disorders:
- combined treatment was more effective than either medication treatment alone or psychosocial treatment alone
- both monotherapies were superior to community care.
ADHD: attention-deficit/hyperactivity disorder
Family psychoeducation
With families of children with behavioral challenges, adopt a patient, educational approach rather than acquiescing to their wishes or arguing with them. Either can result in treatment failure. Discuss potential benefits and risks of all treatment options and the impact of comorbidity on treatment.
Parents’ rigid insistence on a particular course of action—such as refusing psychopharmacology—may be caused by anxiety or misinformation. Elicit the source of any anxiety, and provide realistic information and reassurance if possible.
Anxiety in family members may be constitutional—as anxiety is highly heritable15—or relate to aspects of treatment. Families may feel overwhelmed by:
- their child having 2 disorders rather than 1
- your suggestion to start medical and nonmedical intervention together
- hearing about the possibility of multiple medication trials.
Negotiating medication. Discuss with the family the difficulties of a child learning CBT strategies when ADHD is not well-controlled and the cognitive difficulties in many of these children that may necessitate individualized CBT. If the family remains reluctant to consider combining medication with CBT, try contracting for a limited number of CBT sessions (perhaps 3 or 4) before re-evaluating the need for medication.
The child’s perceptions (and potential anxieties) about his or her difficulties also must be understood, validated, and addressed. Children are more likely to engage in a treatment if they participate in the decision to adopt it.
Anxiety can heighten vigilance in the child or the parents to treatment-emergent side effects, which you may exacerbate by providing exhaustive lists of potential ad-verse events. Limit discussion to serious side effects—with emphasis on their rarity—and those that are common.
ADHD traits in families can affect treatment success. Because of their own distractibility and organizational difficulties, parents with ADHD traits may have difficulty ensuring the child’s medication adherence and treatment participation.16
Behavior modification can require a high degree of consistency in parents’ behavior toward the child. This may be difficult to achieve in families where:
- 1 or both parents are inattentive because of ADHD
- a high degree of conflict exists between parents.
To help these families, provide reminder calls about appointments and schedule sessions at a consistent time. To improve consistency of medication use:
- combine medication administration with an essential daily activity
- check adherence with pill counts or other means.
If the child participates in CBT, provide separate notebooks for in-session and homework exercises—anticipating some loss of homework notebooks.
Individualizing care
Individualized care is important to return each child to his or her best possible level of functioning. The child’s symptom profile, environment, and developmental level can affect treatment.
For example, in a child whose ADHD-related impairment is substantial but whose anxiety-related impairment is mild, pharmacotherapy for ADHD and some pa-rental guidance may be adequate to manage remaining anxiety symptoms.17 As mentioned, some children show decreased anxiety as their ADHD is better controlled.4 Conversely, if ADHD-related impairment is mild but the child is highly anxious, consider CBT alone—preferably on an individual basis—provided the child can manage the cognitive aspects of therapy.
School personnel can monitor change in relation to various interventions, as many of these children’s symptoms manifest in the classroom. Behavioral interventions are more likely to succeed if they are administered consistently across home and school environments8 and teachers participate in behavior modification.
To elicit cooperation from school personnel, listen to their concerns and observations and help them understand the child’s difficulties and the rationale for various treatments. This approach often reduces negative feedback toward the child, a benefit that may further improve outcomes.
Attention to peer relationships and social stressors is often needed. Because of their multiple difficulties, these children may lack social skills and be shunned by their peers.1 You may need to help them develop social skills and reconnect with their peers after symptoms are well-controlled.
Poverty or lack of social support can affect treatment. Children with ADHD and anxiety usually need multiple interventions, and it is difficult for families to at-tend to these consistently when struggling with social stressors.
The 14-month intensive behavioral intervention used in the National Institute of Mental Health’s Multimodal Treatment Study (MTA) of 579 children age 7 to 9 with ADHD included:
- weekly parent training initially, decreasing to monthly by the end
- biweekly teacher consultations in behavior management
- 8-week full-day therapeutic summer program for children, focusing on behavioral and cognitive behavioral intervention
- 12-week half-time behaviorally trained paraprofessional aide in the classroom to generalize gains from summer program
- parent coaching on collaborating with teacher long-term so therapeutic consultation could be faded.
ADHD: attention-deficit/hyperactivity disorder
Adolescent adjustments. ADHD and anxiety often are diagnosed in the early school years, so anticipate developmental effects on treatment as the child enters adolescence. Adolescents value autonomy and may need to be more involved in treatment decisions than younger children.
Ask about and address family disagreements about treatment options, which may reduce adherence. You may need to talk about peer pressure to “not take drugs” by clearly differentiating the reasons some people take street drugs and the reasons for taking prescribed medication. Also discuss in a frank, nonjudgmental manner the risks of experimenting with street drugs (especially with prescribed medication) or of “sharing” one’s medications with friends.
Increased cognitive sophistication in adolescence may increase the potential benefit of CBT, so explore this option with the teen, especially if it was not attempted in the past.
Related resources
- American Academy of Child and Adolescent Psychiatry. “ADHD—a guide for families,” under the Resources for Families tab. www.aacap.org.
- Watkins C. Stimulant medication and ADHD. www.ncpamd.com/Stimulants.htm.
- Manassis K. Keys to parenting your anxious child. 2nd ed. Hauppauge, NY: Barron’s Educational Series, Inc.; 2008.
Drug brand names
- Atomoxetine • Strattera
- Dextroamphetamine • Dexedrine
- Fluvoxamine • Luvox
- Methylphenidate • Ritalin, Concerta
- Mixed amphetamine salts • Adderall
Disclosures
Dr. Manassis reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Aaron, age 10, has been diagnosed with an anxiety disorder and attention-deficit/hyperactivity disorder (ADHD) but is not being treated with medication because his parents do not believe in psychopharmacology. They bring him to a specialized child anxiety clinic and ask for “urgent CBT” because his behavior at school is out of control.
Aaron rearranges the therapist’s office furniture during much of the assessment interview. He also acknowledges many anxiety symptoms. The therapist doubts that cognitive-behavioral therapy (CBT) would help without other interventions.
Children with anxiety disorders and ADHD—a common comorbid presentation—tend to be more impaired than those with either condition alone.1 Effective treatment usually requires 4 components (Table 1), including medication plus behavioral or cognitive-behavioral therapy. This article discusses clinical issues related to each component and describes how to successfully combine them into a treatment plan.
Table 1
Comorbid ADHD and anxiety: 4 treatment components
| Successful treatment usually involves combining 4 components: | |
| |
| Make individual adjustments as needed, depending on the child’s symptom profile, social context, and developmental level | |
| ADHD: attention-deficit/hyperactivity disorder | |
Medication options
Stimulants, atomoxetine, and selective serotonin reuptake inhibitors (SSRIs) have been advocated for children with anxiety and ADHD. Given the high risk of behavioral disinhibition with SSRIs in children,2 stimulants or atomoxetine are suggested as first-line medications.3,4
Stimulants target ADHD symptoms primarily, but anxiety decreases in some children (24% in a recent trial) as ADHD symptoms are controlled.4 Because it is a selective norepinephrine reuptake inhibitor (SNRI), atomoxetine may target both ADHD and anxiety symptoms. When initiating these medications, “start low and go slow.” Recommended dosing is no different for children with ADHD and anxiety than for those with ADHD alone (Table 2).5
Stimulant response rates for children with ADHD and anxiety vary among studies. Some report lower response rates than for children with ADHD alone and possibly more treatment-emergent side effects.6 The National Institute of Mental Health’s Multimodal Treatment Study of Children with ADHD (MTA) found that comorbid anxiety did not adversely affect behavioral response to stimulants but did moderate outcomes (Box 1).7,8 Adding intensive psychosocial intervention to stimulant treatment appeared to yield greater improvements in anxious children with ADHD, compared with stimulants alone.8
Cognitive impairments related to inattention do not consistently improve with stimulant treatment.9 This is clinically important because children with ADHD and comorbid anxiety disorders can be very cognitively impaired.10
Add an SSRI? Monotherapy is simpler and usually more acceptable to families, but a placebo-controlled study examined adding an SSRI (fluvoxamine) to methylphenidate treatment.4 Children with anxiety and ADHD who received adjunctive fluvoxamine did no better than those who received methylphenidate plus placebo.
Atomoxetine. A large, randomized, controlled trial of atomoxetine in this population found good tolerability and statistically significant reductions in ADHD and anxiety symptoms compared with placebo. Effect size was greater for ADHD symptoms than for anxiety symptoms,11 however, which supports smaller trials that show more consistent evidence of atomoxetine reducing ADHD symptoms than anxiety symptoms.
Similar to antidepressants with the SNRI chemical structure, atomoxetine’s effectiveness for a given child takes several weeks to determine. This can be a problem in children who are highly distressed or impaired and require rapid symptomatic improvement.
Recommendation. Consider a stimulant or atomoxetine initially for children with anxiety disorders and ADHD, and seek concurrent behavioral or cognitive-behavioral therapy. Caution families that:
- >1 medication trial might be needed, as response may not be as consistent as in children with ADHD alone
- medication-related improvements in ADHD symptoms will not necessarily be associated with reduced anxiety symptoms or improved academic ability
- improvements with atomoxetine might not be evident for several weeks.
Table 2
Medication dosing for children with ADHD*
| Medication | Recommended starting dosage | Recommended maximum dosage | 5 most common side effects in descending prevalence |
|---|---|---|---|
| Stimulants | |||
| Methylphenidate hydrochloride (Ritalin) | 5 mg tid | Total 60 mg/d | Insomnia, nervousness, decreased appetite, dizziness, nausea |
| Methylphenidate hydrochloride (Concerta) | 18 mg every morning | 54 mg every morning | Headache, abdominal pain, decreased appetite, vomiting, insomnia |
| Dextroamphetamine sulfate (Dexedrine) | 5 mg every morning | Total 40 mg/d | Palpitations, restlessness, dizziness, dry mouth, decreased appetite |
| Mixed amphetamine salts (Adderall) | 10 mg every morning | 30 mg every morning | Decreased appetite, insomnia, abdominal pain, emotional lability, vomiting |
| Nonstimulant | |||
| Atomoxetine (Strattera) | 0.5 mg/kg/d | 1.2 mg/kg/d | Decreased appetite, dizziness, stomach upset, fatigue, irritability |
| ADHD: attention-deficit/hyperactivity disorder | |||
| * Recommended dosing is no different for children with ADHD and anxiety than for children with only ADHD | |||
| Source: Reference 5 | |||
Psychological intervention
CBT has been shown effective for child-hood anxiety disorders in randomized controlled trials,12 but even those that included children with comorbid ADHD required that an anxiety disorder be the primary, most impairing diagnosis.13 Thus, little is known about CBT’s effectiveness for children with anxiety plus ADHD. Given the evidence for cognitive deficits in comorbid anxiety and ADHD10 and the challenge of working with highly distractible children, one would expect CBT to be more difficult in this population.
The potential for distraction to adversely affect learning of coping strategies is higher in group than in individual therapy, and children with anxiety and ADHD can be disruptive to other children in CBT groups. Consider individual CBT, and seek a therapist who has experience with this population. Having the child on medication for ADHD symptoms usually helps reduce these symptoms’ impact on sessions.
For children younger than about age 8 or too cognitively impaired to benefit from CBT, behavioral intervention alone may be helpful. The largely behavioral psychosocial intervention in the MTA study of ADHD children age 7 to 9 (Box 2)8,14 helped many of those with comorbid anxiety.
Although programs as intense as that used in the MTA study rarely are provided in community practice, consider behavior modification. For example:
- To reduce anxiety, have the child follow regular, predictable routines, and reward the child for gradually facing previously avoided situations.
- To reduce distractibility in class, have the child sit near the teacher, break work into small chunks, and reward completion of each chunk.
Even small improvements in the child’s home or school behavior may reduce negative interactions with others and the attendant effects on self-esteem.
CASE CONTINUED: Weighing the options
The therapist seeing Aaron’s family listens to their concerns about medication and reassures them that their son will not be denied psychotherapy. She tells them, however, that psychotherapy will not address his urgent school problems and is unlikely to work in the absence of medication, given Aaron’s behavior in the office. The therapist provides accurate information about the risks and benefits of medication and CBT, and the parents agree to think about all treatment options.
By the next office visit, the school has threatened to suspend Aaron. He and his parents agree to combined treatment with a stimulant medication and CBT and to having the therapist provide a behavioral consultation at the school.
shows best outcomes for ADHD with anxiety
The National Institute of Mental Health’s Multimodal Treatment Study of Children with ADHD—the largest study to date—found that comorbid anxiety did not adversely affect behavioral response to stimulants but did moderate outcomes.
In the parallel group design study, 579 ADHD children age 7 to 9 were enrolled at 6 treatment sites, thoroughly assessed, then randomly assigned to 4 groups: medication treatment alone, intensive psychosocial treatment alone, a combination of both treatments, or usual community care. The first 3 interventions were designed to reflect best practices for each approach, and these children were closely monitored and studied for 14 months. All 4 groups were reassessed periodically for 24 months, evaluating multiple outcomes.
For the total sample, combined and medication treatment were more effective than psychosocial treatment and community care. For ADHD children with comorbid anxiety disorders:
- combined treatment was more effective than either medication treatment alone or psychosocial treatment alone
- both monotherapies were superior to community care.
ADHD: attention-deficit/hyperactivity disorder
Family psychoeducation
With families of children with behavioral challenges, adopt a patient, educational approach rather than acquiescing to their wishes or arguing with them. Either can result in treatment failure. Discuss potential benefits and risks of all treatment options and the impact of comorbidity on treatment.
Parents’ rigid insistence on a particular course of action—such as refusing psychopharmacology—may be caused by anxiety or misinformation. Elicit the source of any anxiety, and provide realistic information and reassurance if possible.
Anxiety in family members may be constitutional—as anxiety is highly heritable15—or relate to aspects of treatment. Families may feel overwhelmed by:
- their child having 2 disorders rather than 1
- your suggestion to start medical and nonmedical intervention together
- hearing about the possibility of multiple medication trials.
Negotiating medication. Discuss with the family the difficulties of a child learning CBT strategies when ADHD is not well-controlled and the cognitive difficulties in many of these children that may necessitate individualized CBT. If the family remains reluctant to consider combining medication with CBT, try contracting for a limited number of CBT sessions (perhaps 3 or 4) before re-evaluating the need for medication.
The child’s perceptions (and potential anxieties) about his or her difficulties also must be understood, validated, and addressed. Children are more likely to engage in a treatment if they participate in the decision to adopt it.
Anxiety can heighten vigilance in the child or the parents to treatment-emergent side effects, which you may exacerbate by providing exhaustive lists of potential ad-verse events. Limit discussion to serious side effects—with emphasis on their rarity—and those that are common.
ADHD traits in families can affect treatment success. Because of their own distractibility and organizational difficulties, parents with ADHD traits may have difficulty ensuring the child’s medication adherence and treatment participation.16
Behavior modification can require a high degree of consistency in parents’ behavior toward the child. This may be difficult to achieve in families where:
- 1 or both parents are inattentive because of ADHD
- a high degree of conflict exists between parents.
To help these families, provide reminder calls about appointments and schedule sessions at a consistent time. To improve consistency of medication use:
- combine medication administration with an essential daily activity
- check adherence with pill counts or other means.
If the child participates in CBT, provide separate notebooks for in-session and homework exercises—anticipating some loss of homework notebooks.
Individualizing care
Individualized care is important to return each child to his or her best possible level of functioning. The child’s symptom profile, environment, and developmental level can affect treatment.
For example, in a child whose ADHD-related impairment is substantial but whose anxiety-related impairment is mild, pharmacotherapy for ADHD and some pa-rental guidance may be adequate to manage remaining anxiety symptoms.17 As mentioned, some children show decreased anxiety as their ADHD is better controlled.4 Conversely, if ADHD-related impairment is mild but the child is highly anxious, consider CBT alone—preferably on an individual basis—provided the child can manage the cognitive aspects of therapy.
School personnel can monitor change in relation to various interventions, as many of these children’s symptoms manifest in the classroom. Behavioral interventions are more likely to succeed if they are administered consistently across home and school environments8 and teachers participate in behavior modification.
To elicit cooperation from school personnel, listen to their concerns and observations and help them understand the child’s difficulties and the rationale for various treatments. This approach often reduces negative feedback toward the child, a benefit that may further improve outcomes.
Attention to peer relationships and social stressors is often needed. Because of their multiple difficulties, these children may lack social skills and be shunned by their peers.1 You may need to help them develop social skills and reconnect with their peers after symptoms are well-controlled.
Poverty or lack of social support can affect treatment. Children with ADHD and anxiety usually need multiple interventions, and it is difficult for families to at-tend to these consistently when struggling with social stressors.
The 14-month intensive behavioral intervention used in the National Institute of Mental Health’s Multimodal Treatment Study (MTA) of 579 children age 7 to 9 with ADHD included:
- weekly parent training initially, decreasing to monthly by the end
- biweekly teacher consultations in behavior management
- 8-week full-day therapeutic summer program for children, focusing on behavioral and cognitive behavioral intervention
- 12-week half-time behaviorally trained paraprofessional aide in the classroom to generalize gains from summer program
- parent coaching on collaborating with teacher long-term so therapeutic consultation could be faded.
ADHD: attention-deficit/hyperactivity disorder
Adolescent adjustments. ADHD and anxiety often are diagnosed in the early school years, so anticipate developmental effects on treatment as the child enters adolescence. Adolescents value autonomy and may need to be more involved in treatment decisions than younger children.
Ask about and address family disagreements about treatment options, which may reduce adherence. You may need to talk about peer pressure to “not take drugs” by clearly differentiating the reasons some people take street drugs and the reasons for taking prescribed medication. Also discuss in a frank, nonjudgmental manner the risks of experimenting with street drugs (especially with prescribed medication) or of “sharing” one’s medications with friends.
Increased cognitive sophistication in adolescence may increase the potential benefit of CBT, so explore this option with the teen, especially if it was not attempted in the past.
Related resources
- American Academy of Child and Adolescent Psychiatry. “ADHD—a guide for families,” under the Resources for Families tab. www.aacap.org.
- Watkins C. Stimulant medication and ADHD. www.ncpamd.com/Stimulants.htm.
- Manassis K. Keys to parenting your anxious child. 2nd ed. Hauppauge, NY: Barron’s Educational Series, Inc.; 2008.
Drug brand names
- Atomoxetine • Strattera
- Dextroamphetamine • Dexedrine
- Fluvoxamine • Luvox
- Methylphenidate • Ritalin, Concerta
- Mixed amphetamine salts • Adderall
Disclosures
Dr. Manassis reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Bowen R, Chavira DA, Bailey K, et al. Nature of anxiety comorbid with attention deficit hyperactivity disorder in children from a pediatric primary care setting. Psychiatry Res 2008;157:201-9.
2. Walkup JT, Labellarte MJ, Riddle MA, et al. Searching for moderators and mediators of pharmacological treatment in children and adolescents with anxiety disorders. J Am Acad Child Adolesc Psychiatry 2003;42:13-21.
3. Wiesegger G, Kienbacher C, Pellegrini E, et al. Pharmacotherapy of attention-deficit/hyperactivity disorder (ADHD) and comorbid disorders. Neuropsychiatr 2007;21:187-206.
4. Abikoff H, McGough J, Vitiello B, et al. Sequential pharmacotherapy for children with comorbid attention-deficit/hyperactivity and anxiety disorders. J Am Acad Child Adolesc Psychiatry 2005;44:418-27.
5. Compendium of pharmaceuticals and specialties. Ottawa, Canada: Canadian Pharmacists Association; 2008.
6. Goez H, Back-Bennet O, Zelnik N. Differential stimulant response on attention in children with comorbid anxiety and oppositional defiant disorder. J Child Neurol 2007;22:538-42.
7. Wells KC, Pelham WE, Kotkin RA, et al. Psychosocial treatment strategies in the MTA study: rationale, methods, and critical issues in design and implementation. J Abnorm Child Psychol 2000;28:483-505.
8. March JS, Swanson JM, Arnold EL, et al. Anxiety as a predictor and outcome variable in the Multimodal Treatment Study of Children with ADHD (MTA). J Abnorm Child Psychol 2000;28:527-41.
9. Tannock R, Ickowicz A, Schachar R. Differential effects of methylphenidate on working memory in ADHD children with and without anxiety. J Am Acad Child Adolesc Psychiatry 1995;34:886-96.
10. Manassis K, Tannock R, Young A, Francis-John S. Cognition in anxious children with attention deficit hyperactivity disorder: a comparison with clinical and normal children. Behav Brain Funct 2007;3-4.
11. Geller D, Donnelly C, Lopez F, et al. Atomoxetine treatment for pediatric patients with attention-deficit/hyperactivity disorder with comorbid anxiety disorder. J Am Acad Child Adolesc Psychiatry 2007;46:1119-27.
12. Compton SN, March JS, Brent D, et al. Cognitive behavioural psychotherapy for anxiety and depressive disorders in children and adolescents: an evidence-based medicine review. J Am Acad Child Adolesc Psychiatry 2004;43:930-59.
13. Manassis K, Mendlowitz SL, Scapillato D, et al. Group and individual cognitive-behavioral therapy for childhood anxiety disorders: a randomized trial. J Am Acad Child Adolesc Psychiatry 2002;41:1423-30.
14. Arnold LE, Abikoff HB, Cantwell DP, et al. National Institute of Mental Health Collaborative Multimodal Treatment Study of Children with ADHD (the MTA). Design challenges and choices. Arch Gen Psychiatry 1997;54:865-70.
15. Kagan J, Reznick JS, Snidman N. Biological basis of childhood shyness. Science 1990;240:167-71.
16. Van Cleave J, Leslie LK. Approaching ADHD as a chronic condition: implications for long-term adherence. Pediatr Ann 2008;37:19-26.
17. Manassis K, Monga S. therapeutic approach to children and adolescents with anxiety disorders and associated comorbid conditions. J Am Acad Child Adolesc Psychiatry 2001;40:115-7.
1. Bowen R, Chavira DA, Bailey K, et al. Nature of anxiety comorbid with attention deficit hyperactivity disorder in children from a pediatric primary care setting. Psychiatry Res 2008;157:201-9.
2. Walkup JT, Labellarte MJ, Riddle MA, et al. Searching for moderators and mediators of pharmacological treatment in children and adolescents with anxiety disorders. J Am Acad Child Adolesc Psychiatry 2003;42:13-21.
3. Wiesegger G, Kienbacher C, Pellegrini E, et al. Pharmacotherapy of attention-deficit/hyperactivity disorder (ADHD) and comorbid disorders. Neuropsychiatr 2007;21:187-206.
4. Abikoff H, McGough J, Vitiello B, et al. Sequential pharmacotherapy for children with comorbid attention-deficit/hyperactivity and anxiety disorders. J Am Acad Child Adolesc Psychiatry 2005;44:418-27.
5. Compendium of pharmaceuticals and specialties. Ottawa, Canada: Canadian Pharmacists Association; 2008.
6. Goez H, Back-Bennet O, Zelnik N. Differential stimulant response on attention in children with comorbid anxiety and oppositional defiant disorder. J Child Neurol 2007;22:538-42.
7. Wells KC, Pelham WE, Kotkin RA, et al. Psychosocial treatment strategies in the MTA study: rationale, methods, and critical issues in design and implementation. J Abnorm Child Psychol 2000;28:483-505.
8. March JS, Swanson JM, Arnold EL, et al. Anxiety as a predictor and outcome variable in the Multimodal Treatment Study of Children with ADHD (MTA). J Abnorm Child Psychol 2000;28:527-41.
9. Tannock R, Ickowicz A, Schachar R. Differential effects of methylphenidate on working memory in ADHD children with and without anxiety. J Am Acad Child Adolesc Psychiatry 1995;34:886-96.
10. Manassis K, Tannock R, Young A, Francis-John S. Cognition in anxious children with attention deficit hyperactivity disorder: a comparison with clinical and normal children. Behav Brain Funct 2007;3-4.
11. Geller D, Donnelly C, Lopez F, et al. Atomoxetine treatment for pediatric patients with attention-deficit/hyperactivity disorder with comorbid anxiety disorder. J Am Acad Child Adolesc Psychiatry 2007;46:1119-27.
12. Compton SN, March JS, Brent D, et al. Cognitive behavioural psychotherapy for anxiety and depressive disorders in children and adolescents: an evidence-based medicine review. J Am Acad Child Adolesc Psychiatry 2004;43:930-59.
13. Manassis K, Mendlowitz SL, Scapillato D, et al. Group and individual cognitive-behavioral therapy for childhood anxiety disorders: a randomized trial. J Am Acad Child Adolesc Psychiatry 2002;41:1423-30.
14. Arnold LE, Abikoff HB, Cantwell DP, et al. National Institute of Mental Health Collaborative Multimodal Treatment Study of Children with ADHD (the MTA). Design challenges and choices. Arch Gen Psychiatry 1997;54:865-70.
15. Kagan J, Reznick JS, Snidman N. Biological basis of childhood shyness. Science 1990;240:167-71.
16. Van Cleave J, Leslie LK. Approaching ADHD as a chronic condition: implications for long-term adherence. Pediatr Ann 2008;37:19-26.
17. Manassis K, Monga S. therapeutic approach to children and adolescents with anxiety disorders and associated comorbid conditions. J Am Acad Child Adolesc Psychiatry 2001;40:115-7.
Study shows drug is safe and effective in cardiac patients
The direct thrombin inhibitor bivalirudin (Angiomax) reduces major bleeding and increases short-term survival in certain cardiac patients, according to a study published in the New England Journal of Medicine.
Bivalirudin was associated with a lower rate of major bleeding and death from cardiac and other causes at 30 days from treatment initiation. This was in comparison to treatment with heparin plus glycoprotein IIb/IIIa inhibitors.
Both therapies were tested in patients with ST-segment elevation myocardial infarction who were undergoing primary percutaneous coronary intervention (PCI).
Gregg Stone, MD, of Columbia University Medical Center, and colleagues randomized 3602 patients to receive either bivalirudin (n=1800) or heparin plus glycoprotein IIb/IIIa inhibitors (n=1802).
The 2 primary endpoints of the study were major bleeding and combined clinical events. Combined events included death, reinfarction, target-vessel revascularization for ischemia, and stroke.
Bivalirudin reduced the overall rate of combined events, as compared to heparin plus glycoprotein IIb/IIIa inhibitors (9.2% vs 12.1%, respectively). However, when evaluated separately, there were no significant differences in the incidence of these events between the 2 treatment groups.
The rate of reinfarction was the same in both groups (1.8%). The rate of stroke was insignificantly higher in the bivalirudin group (0.7% vs 0.6%). The same was true of target-vessel revascularization; the rate was 2.6% in bivalirudin patients and 1.9% in the other patient group.
Patients on bivalirudin experienced a lower rate of major bleeding than patients on heparin plus glycoprotein IIb/IIIa inhibitors (4.9% vs 8.3%, respectively). When large hematomas were excluded, the rates of major bleeding were reduced to 4.7% and 7.8%, respectively.
Bivalirudin also reduced the incidence of hemorrhagic complications, the development of thrombocytopenia, and the need for blood transfusions.
The rate of cardiac-related death at 30 days was significantly lower for bivalirudin patients than for patients who received heparin plus glycoprotein IIb/IIIa inhibitors (1.8% vs 2.9%, respectively). The rate of death from any cause was also lower in bivalirudin patients (2.1% vs 3.1%).
Bivalirudin increased the rate of acute stent thrombosis within 24 hours of treatment initiation (1.3% vs 0.3%). However, between 24 hours and 30 days, the incidence of acute stent thrombosis was lower in the bivalirudin patients than in those on heparin plus glycoprotein IIb/IIIa inhibitors (1.2% vs. 1.7%, respectively).
This study, known as HORIZONS-AMI, was sponsored, in part, by The Medicines Company, makers of bivalirudin (Angiomax). ![]()
The direct thrombin inhibitor bivalirudin (Angiomax) reduces major bleeding and increases short-term survival in certain cardiac patients, according to a study published in the New England Journal of Medicine.
Bivalirudin was associated with a lower rate of major bleeding and death from cardiac and other causes at 30 days from treatment initiation. This was in comparison to treatment with heparin plus glycoprotein IIb/IIIa inhibitors.
Both therapies were tested in patients with ST-segment elevation myocardial infarction who were undergoing primary percutaneous coronary intervention (PCI).
Gregg Stone, MD, of Columbia University Medical Center, and colleagues randomized 3602 patients to receive either bivalirudin (n=1800) or heparin plus glycoprotein IIb/IIIa inhibitors (n=1802).
The 2 primary endpoints of the study were major bleeding and combined clinical events. Combined events included death, reinfarction, target-vessel revascularization for ischemia, and stroke.
Bivalirudin reduced the overall rate of combined events, as compared to heparin plus glycoprotein IIb/IIIa inhibitors (9.2% vs 12.1%, respectively). However, when evaluated separately, there were no significant differences in the incidence of these events between the 2 treatment groups.
The rate of reinfarction was the same in both groups (1.8%). The rate of stroke was insignificantly higher in the bivalirudin group (0.7% vs 0.6%). The same was true of target-vessel revascularization; the rate was 2.6% in bivalirudin patients and 1.9% in the other patient group.
Patients on bivalirudin experienced a lower rate of major bleeding than patients on heparin plus glycoprotein IIb/IIIa inhibitors (4.9% vs 8.3%, respectively). When large hematomas were excluded, the rates of major bleeding were reduced to 4.7% and 7.8%, respectively.
Bivalirudin also reduced the incidence of hemorrhagic complications, the development of thrombocytopenia, and the need for blood transfusions.
The rate of cardiac-related death at 30 days was significantly lower for bivalirudin patients than for patients who received heparin plus glycoprotein IIb/IIIa inhibitors (1.8% vs 2.9%, respectively). The rate of death from any cause was also lower in bivalirudin patients (2.1% vs 3.1%).
Bivalirudin increased the rate of acute stent thrombosis within 24 hours of treatment initiation (1.3% vs 0.3%). However, between 24 hours and 30 days, the incidence of acute stent thrombosis was lower in the bivalirudin patients than in those on heparin plus glycoprotein IIb/IIIa inhibitors (1.2% vs. 1.7%, respectively).
This study, known as HORIZONS-AMI, was sponsored, in part, by The Medicines Company, makers of bivalirudin (Angiomax). ![]()
The direct thrombin inhibitor bivalirudin (Angiomax) reduces major bleeding and increases short-term survival in certain cardiac patients, according to a study published in the New England Journal of Medicine.
Bivalirudin was associated with a lower rate of major bleeding and death from cardiac and other causes at 30 days from treatment initiation. This was in comparison to treatment with heparin plus glycoprotein IIb/IIIa inhibitors.
Both therapies were tested in patients with ST-segment elevation myocardial infarction who were undergoing primary percutaneous coronary intervention (PCI).
Gregg Stone, MD, of Columbia University Medical Center, and colleagues randomized 3602 patients to receive either bivalirudin (n=1800) or heparin plus glycoprotein IIb/IIIa inhibitors (n=1802).
The 2 primary endpoints of the study were major bleeding and combined clinical events. Combined events included death, reinfarction, target-vessel revascularization for ischemia, and stroke.
Bivalirudin reduced the overall rate of combined events, as compared to heparin plus glycoprotein IIb/IIIa inhibitors (9.2% vs 12.1%, respectively). However, when evaluated separately, there were no significant differences in the incidence of these events between the 2 treatment groups.
The rate of reinfarction was the same in both groups (1.8%). The rate of stroke was insignificantly higher in the bivalirudin group (0.7% vs 0.6%). The same was true of target-vessel revascularization; the rate was 2.6% in bivalirudin patients and 1.9% in the other patient group.
Patients on bivalirudin experienced a lower rate of major bleeding than patients on heparin plus glycoprotein IIb/IIIa inhibitors (4.9% vs 8.3%, respectively). When large hematomas were excluded, the rates of major bleeding were reduced to 4.7% and 7.8%, respectively.
Bivalirudin also reduced the incidence of hemorrhagic complications, the development of thrombocytopenia, and the need for blood transfusions.
The rate of cardiac-related death at 30 days was significantly lower for bivalirudin patients than for patients who received heparin plus glycoprotein IIb/IIIa inhibitors (1.8% vs 2.9%, respectively). The rate of death from any cause was also lower in bivalirudin patients (2.1% vs 3.1%).
Bivalirudin increased the rate of acute stent thrombosis within 24 hours of treatment initiation (1.3% vs 0.3%). However, between 24 hours and 30 days, the incidence of acute stent thrombosis was lower in the bivalirudin patients than in those on heparin plus glycoprotein IIb/IIIa inhibitors (1.2% vs. 1.7%, respectively).
This study, known as HORIZONS-AMI, was sponsored, in part, by The Medicines Company, makers of bivalirudin (Angiomax). ![]()
Midlife Menopause Management
Supplement Editor:
Holly L. Thacker, MD, FACP
Contents
Assessing benefits and risks of hormone therapy in 2008: New evidence, especially with regard to the heart
Howard N. Hodis, MD
Update on nonhormonal approaches to menopausal management
Marjorie R. Jenkins, MD, and Andrea L. Sikon, MD, FACP
Case studies and clinical considerations in menopausal management: Putting the latest data into practice
Margaret McKenzie, MD, FACOG; Andrea L. Sikon, MD, FACP; Holly L. Thacker, MD, FACP; Margery Gass, MD; Howard N. Hodis, MD; and Marjorie R. Jenkins, MD
Supplement Editor:
Holly L. Thacker, MD, FACP
Contents
Assessing benefits and risks of hormone therapy in 2008: New evidence, especially with regard to the heart
Howard N. Hodis, MD
Update on nonhormonal approaches to menopausal management
Marjorie R. Jenkins, MD, and Andrea L. Sikon, MD, FACP
Case studies and clinical considerations in menopausal management: Putting the latest data into practice
Margaret McKenzie, MD, FACOG; Andrea L. Sikon, MD, FACP; Holly L. Thacker, MD, FACP; Margery Gass, MD; Howard N. Hodis, MD; and Marjorie R. Jenkins, MD
Supplement Editor:
Holly L. Thacker, MD, FACP
Contents
Assessing benefits and risks of hormone therapy in 2008: New evidence, especially with regard to the heart
Howard N. Hodis, MD
Update on nonhormonal approaches to menopausal management
Marjorie R. Jenkins, MD, and Andrea L. Sikon, MD, FACP
Case studies and clinical considerations in menopausal management: Putting the latest data into practice
Margaret McKenzie, MD, FACOG; Andrea L. Sikon, MD, FACP; Holly L. Thacker, MD, FACP; Margery Gass, MD; Howard N. Hodis, MD; and Marjorie R. Jenkins, MD
Intensivists and ICUs

Intensivists and ICUs
Question: What is your opinion on a closed ICU that already has a hospitalist program but now has a new intensivist program? Certainly some patients should be cared for by critical care physicians. However I feel we play an important role throughout the hospital, including the ICU. As physicians who specialize in hospital care, I do not want to lose opportunities to care for patients in the ICU. Do you feel medicine may move toward that, especially in the larger hospitals? Or have you found a happy medium?
Eric Marsh, MD,
Carolinas Healthcare System,
Charlotte, N.C.
Dr. Hospitalist responds: In many small and rural hospitals throughout the country, generalists remain the frontline providers for ICU patients.
There is a shortage of critical care physicians in this country. Many small and rural hospitals have a difficult time recruiting sufficient numbers of critical care physicians to their medical staffs. This is not the case in most academic tertiary care medical centers, where pulmonary/critical care providers routinely care for the ICU patients.
In fact, during the past two decades, many hospitals, particularly tertiary care medical centers, have “closed” their ICUs to generalists and now use specialty-trained physicians, such as pulmonary/critical care physicians, to care for ICU patients. The reason is quality. Evidence suggests intensivists provide higher-quality, more evidence-based care to ICU patients than generalists.
Quality organizations, such as the National Quality Forum and The Leapfrog Group have actively promoted the role of intensivists in the ICU and labeled them as a marker of quality care. Hospitals are under increasing scrutiny to increase the quality of care they give patients. Reimbursement is increasingly tied to performance and quality.
I expect to see more and more hospitals “close” their ICU to generalists. To be fair, the data comparing intensivists and generalists came out before the widespread role of hospitalists in our nation’s hospitals. It would be interesting to compare the care provided by hospitalists versus intensivists in the ICU. It may be we find hospitalists fare comparably to intensivists. Until that data exist, I agree with the quality organizations. Hospitals, and more importantly patients, should rely preferentially on physicians with additional critical care training to provide care for their ICU care.
If your hospitalists are interested in continuing to provide care for patients in the ICU, I suggest you speak with the leader of the intensivist group to see how your hospitalists can work with—not in lieu of—the intensivists in the care of ICU patients.
In Pursuit of More Pay
Question: I am writing to get your advice on how to go about negotiating base pay increases. I come from a four-physician hospitalist program at the New York Hospital of Queens that has tripled its annual number of discharges since 2005 without a commensurate increase in base pay and no bonus or incentive pay. If this keeps up, we’ll continue to have high turnover always manned by junior attendings. Also, what is reasonable pay for the director of a hospitalist program?
Anne Park, DO,
hospitalist faculty,
New York Hospital of Queens
Dr. Hospitalist responds: I am writing to you from the lovely Manchester Grand Hyatt in San Diego, where I am attending the SHM Annual Meeting. I am here with nearly 1,600 of my closest friends in hospital medicine.
Meeting attendees heard SHM Senior Vice President Joe Miller reveal the results of the latest “Society of Hospital Medicine 2007-08 Survey: The Authoritative Source on the State of the Hospitalist Movement.” I refer to this survey not only because I believe it is the latest, most accurate, and comprehensive data on hospitalist productivity and compensation, but also because I think it is the objective data you need before you start discussions about compensation for you and your hospitalist staff.
Before discussing compensation, I suggest you make sure your supervisor is well-informed of your hospitalists’ roles and responsibilities. Discussions will be more productive if your supervisor understands the value of your hospitalists. Be careful because how you go about informing your supervisor will influence the response you get.
It’s important for your supervisor to know the hospitalist marketplace is highly competitive. There are more jobs than hospitalists. Many hospitals are developing hospitalist programs, and existing programs continue to expand. There are many signs of this competition for hospitalists. For example, I counted 130 vendors exhibiting at this year’s SHM Annual Meeting. About two-thirds are vendors recruiting hospitalists. This suggests hospitalists are in higher demand then ever. I didn’t need to come to San Diego to figure this out. One glance at the numerous ads in the pages preceding this section of The Hospitalist is sufficient evidence. Another sign of the times is the rise in hospitalist compensation since the results of the last survey two years ago.
Try to present this information to your supervisor in a nonconfrontational manner. Discussions will start poorly if this information is viewed as a threat the hospitalists will depart the program if you do not get your way. You alluded to “high turnover” in your group. Let your supervisor know you are presenting this information because you are concerned the cost of replacing hospitalists may exceed the cost of retaining experienced staff. Before discussions, I also suggest you think about why hospitalists have left your program. Your comments about increased discharges suggest a mismatch between compensation and job description. It is possible the discussion should be about changing the job description rather than adjusting compensation.
Once discussions begin, your supervisor will consider several factors when entertaining your request for additional compensation. Aside from individual performance, your supervisor will consider how your groups’ compensation compares to other hospitalists with similar job descriptions in the same geographic region. This is where the survey data are helpful. Most hospitalist compensation contains some element of incentive compensation. Do your best to compare apples to apples by looking at the entire compensation package, including benefits.
Your supervisor also will ask you to compare your groups’ job description to others in the area. Your hospitalists have tripled the number of discharges they did in 2005. Did other groups in the area see the same rise in productivity? What happened to their staffing and compensation? Expect these types of questions from your supervisor.
After your preparation, you may find that your hospitalists are being paid more, less, or about the same as what others are being paid for a comparable level of productivity. The latest SHM survey will assist you in preparing for your discussion. But please remember the survey just reports data. It does not indicate how much SHM thinks you should be working or how much money you should be making. It is merely a snapshot of what the market bears for hospitalists in our country. TH
Intensivists and ICUs
Question: What is your opinion on a closed ICU that already has a hospitalist program but now has a new intensivist program? Certainly some patients should be cared for by critical care physicians. However I feel we play an important role throughout the hospital, including the ICU. As physicians who specialize in hospital care, I do not want to lose opportunities to care for patients in the ICU. Do you feel medicine may move toward that, especially in the larger hospitals? Or have you found a happy medium?
Eric Marsh, MD,
Carolinas Healthcare System,
Charlotte, N.C.
Dr. Hospitalist responds: In many small and rural hospitals throughout the country, generalists remain the frontline providers for ICU patients.
There is a shortage of critical care physicians in this country. Many small and rural hospitals have a difficult time recruiting sufficient numbers of critical care physicians to their medical staffs. This is not the case in most academic tertiary care medical centers, where pulmonary/critical care providers routinely care for the ICU patients.
In fact, during the past two decades, many hospitals, particularly tertiary care medical centers, have “closed” their ICUs to generalists and now use specialty-trained physicians, such as pulmonary/critical care physicians, to care for ICU patients. The reason is quality. Evidence suggests intensivists provide higher-quality, more evidence-based care to ICU patients than generalists.
Quality organizations, such as the National Quality Forum and The Leapfrog Group have actively promoted the role of intensivists in the ICU and labeled them as a marker of quality care. Hospitals are under increasing scrutiny to increase the quality of care they give patients. Reimbursement is increasingly tied to performance and quality.
I expect to see more and more hospitals “close” their ICU to generalists. To be fair, the data comparing intensivists and generalists came out before the widespread role of hospitalists in our nation’s hospitals. It would be interesting to compare the care provided by hospitalists versus intensivists in the ICU. It may be we find hospitalists fare comparably to intensivists. Until that data exist, I agree with the quality organizations. Hospitals, and more importantly patients, should rely preferentially on physicians with additional critical care training to provide care for their ICU care.
If your hospitalists are interested in continuing to provide care for patients in the ICU, I suggest you speak with the leader of the intensivist group to see how your hospitalists can work with—not in lieu of—the intensivists in the care of ICU patients.
In Pursuit of More Pay
Question: I am writing to get your advice on how to go about negotiating base pay increases. I come from a four-physician hospitalist program at the New York Hospital of Queens that has tripled its annual number of discharges since 2005 without a commensurate increase in base pay and no bonus or incentive pay. If this keeps up, we’ll continue to have high turnover always manned by junior attendings. Also, what is reasonable pay for the director of a hospitalist program?
Anne Park, DO,
hospitalist faculty,
New York Hospital of Queens
Dr. Hospitalist responds: I am writing to you from the lovely Manchester Grand Hyatt in San Diego, where I am attending the SHM Annual Meeting. I am here with nearly 1,600 of my closest friends in hospital medicine.
Meeting attendees heard SHM Senior Vice President Joe Miller reveal the results of the latest “Society of Hospital Medicine 2007-08 Survey: The Authoritative Source on the State of the Hospitalist Movement.” I refer to this survey not only because I believe it is the latest, most accurate, and comprehensive data on hospitalist productivity and compensation, but also because I think it is the objective data you need before you start discussions about compensation for you and your hospitalist staff.
Before discussing compensation, I suggest you make sure your supervisor is well-informed of your hospitalists’ roles and responsibilities. Discussions will be more productive if your supervisor understands the value of your hospitalists. Be careful because how you go about informing your supervisor will influence the response you get.
It’s important for your supervisor to know the hospitalist marketplace is highly competitive. There are more jobs than hospitalists. Many hospitals are developing hospitalist programs, and existing programs continue to expand. There are many signs of this competition for hospitalists. For example, I counted 130 vendors exhibiting at this year’s SHM Annual Meeting. About two-thirds are vendors recruiting hospitalists. This suggests hospitalists are in higher demand then ever. I didn’t need to come to San Diego to figure this out. One glance at the numerous ads in the pages preceding this section of The Hospitalist is sufficient evidence. Another sign of the times is the rise in hospitalist compensation since the results of the last survey two years ago.
Try to present this information to your supervisor in a nonconfrontational manner. Discussions will start poorly if this information is viewed as a threat the hospitalists will depart the program if you do not get your way. You alluded to “high turnover” in your group. Let your supervisor know you are presenting this information because you are concerned the cost of replacing hospitalists may exceed the cost of retaining experienced staff. Before discussions, I also suggest you think about why hospitalists have left your program. Your comments about increased discharges suggest a mismatch between compensation and job description. It is possible the discussion should be about changing the job description rather than adjusting compensation.
Once discussions begin, your supervisor will consider several factors when entertaining your request for additional compensation. Aside from individual performance, your supervisor will consider how your groups’ compensation compares to other hospitalists with similar job descriptions in the same geographic region. This is where the survey data are helpful. Most hospitalist compensation contains some element of incentive compensation. Do your best to compare apples to apples by looking at the entire compensation package, including benefits.
Your supervisor also will ask you to compare your groups’ job description to others in the area. Your hospitalists have tripled the number of discharges they did in 2005. Did other groups in the area see the same rise in productivity? What happened to their staffing and compensation? Expect these types of questions from your supervisor.
After your preparation, you may find that your hospitalists are being paid more, less, or about the same as what others are being paid for a comparable level of productivity. The latest SHM survey will assist you in preparing for your discussion. But please remember the survey just reports data. It does not indicate how much SHM thinks you should be working or how much money you should be making. It is merely a snapshot of what the market bears for hospitalists in our country. TH
Intensivists and ICUs
Question: What is your opinion on a closed ICU that already has a hospitalist program but now has a new intensivist program? Certainly some patients should be cared for by critical care physicians. However I feel we play an important role throughout the hospital, including the ICU. As physicians who specialize in hospital care, I do not want to lose opportunities to care for patients in the ICU. Do you feel medicine may move toward that, especially in the larger hospitals? Or have you found a happy medium?
Eric Marsh, MD,
Carolinas Healthcare System,
Charlotte, N.C.
Dr. Hospitalist responds: In many small and rural hospitals throughout the country, generalists remain the frontline providers for ICU patients.
There is a shortage of critical care physicians in this country. Many small and rural hospitals have a difficult time recruiting sufficient numbers of critical care physicians to their medical staffs. This is not the case in most academic tertiary care medical centers, where pulmonary/critical care providers routinely care for the ICU patients.
In fact, during the past two decades, many hospitals, particularly tertiary care medical centers, have “closed” their ICUs to generalists and now use specialty-trained physicians, such as pulmonary/critical care physicians, to care for ICU patients. The reason is quality. Evidence suggests intensivists provide higher-quality, more evidence-based care to ICU patients than generalists.
Quality organizations, such as the National Quality Forum and The Leapfrog Group have actively promoted the role of intensivists in the ICU and labeled them as a marker of quality care. Hospitals are under increasing scrutiny to increase the quality of care they give patients. Reimbursement is increasingly tied to performance and quality.
I expect to see more and more hospitals “close” their ICU to generalists. To be fair, the data comparing intensivists and generalists came out before the widespread role of hospitalists in our nation’s hospitals. It would be interesting to compare the care provided by hospitalists versus intensivists in the ICU. It may be we find hospitalists fare comparably to intensivists. Until that data exist, I agree with the quality organizations. Hospitals, and more importantly patients, should rely preferentially on physicians with additional critical care training to provide care for their ICU care.
If your hospitalists are interested in continuing to provide care for patients in the ICU, I suggest you speak with the leader of the intensivist group to see how your hospitalists can work with—not in lieu of—the intensivists in the care of ICU patients.
In Pursuit of More Pay
Question: I am writing to get your advice on how to go about negotiating base pay increases. I come from a four-physician hospitalist program at the New York Hospital of Queens that has tripled its annual number of discharges since 2005 without a commensurate increase in base pay and no bonus or incentive pay. If this keeps up, we’ll continue to have high turnover always manned by junior attendings. Also, what is reasonable pay for the director of a hospitalist program?
Anne Park, DO,
hospitalist faculty,
New York Hospital of Queens
Dr. Hospitalist responds: I am writing to you from the lovely Manchester Grand Hyatt in San Diego, where I am attending the SHM Annual Meeting. I am here with nearly 1,600 of my closest friends in hospital medicine.
Meeting attendees heard SHM Senior Vice President Joe Miller reveal the results of the latest “Society of Hospital Medicine 2007-08 Survey: The Authoritative Source on the State of the Hospitalist Movement.” I refer to this survey not only because I believe it is the latest, most accurate, and comprehensive data on hospitalist productivity and compensation, but also because I think it is the objective data you need before you start discussions about compensation for you and your hospitalist staff.
Before discussing compensation, I suggest you make sure your supervisor is well-informed of your hospitalists’ roles and responsibilities. Discussions will be more productive if your supervisor understands the value of your hospitalists. Be careful because how you go about informing your supervisor will influence the response you get.
It’s important for your supervisor to know the hospitalist marketplace is highly competitive. There are more jobs than hospitalists. Many hospitals are developing hospitalist programs, and existing programs continue to expand. There are many signs of this competition for hospitalists. For example, I counted 130 vendors exhibiting at this year’s SHM Annual Meeting. About two-thirds are vendors recruiting hospitalists. This suggests hospitalists are in higher demand then ever. I didn’t need to come to San Diego to figure this out. One glance at the numerous ads in the pages preceding this section of The Hospitalist is sufficient evidence. Another sign of the times is the rise in hospitalist compensation since the results of the last survey two years ago.
Try to present this information to your supervisor in a nonconfrontational manner. Discussions will start poorly if this information is viewed as a threat the hospitalists will depart the program if you do not get your way. You alluded to “high turnover” in your group. Let your supervisor know you are presenting this information because you are concerned the cost of replacing hospitalists may exceed the cost of retaining experienced staff. Before discussions, I also suggest you think about why hospitalists have left your program. Your comments about increased discharges suggest a mismatch between compensation and job description. It is possible the discussion should be about changing the job description rather than adjusting compensation.
Once discussions begin, your supervisor will consider several factors when entertaining your request for additional compensation. Aside from individual performance, your supervisor will consider how your groups’ compensation compares to other hospitalists with similar job descriptions in the same geographic region. This is where the survey data are helpful. Most hospitalist compensation contains some element of incentive compensation. Do your best to compare apples to apples by looking at the entire compensation package, including benefits.
Your supervisor also will ask you to compare your groups’ job description to others in the area. Your hospitalists have tripled the number of discharges they did in 2005. Did other groups in the area see the same rise in productivity? What happened to their staffing and compensation? Expect these types of questions from your supervisor.
After your preparation, you may find that your hospitalists are being paid more, less, or about the same as what others are being paid for a comparable level of productivity. The latest SHM survey will assist you in preparing for your discussion. But please remember the survey just reports data. It does not indicate how much SHM thinks you should be working or how much money you should be making. It is merely a snapshot of what the market bears for hospitalists in our country. TH
Value Your Practice

The issue of practice valuation is a sensitive one. Some hospitalist practices might have significant monetary value, which could make it reasonable to ask new doctors to buy in or enable selling the practice for a profit. Still, it’s risky to assume this is the case for your practice.
Let’s examine the issue using a pair of situations I encountered not long ago. I have changed some details of the practices to more clearly illustrate a point and conceal which practices I’m describing. Both situations would have gone smoother if it was clear what the hospitalist practice was worth. But how do you assess that value?
Case No. 1
During a couple of days in 2006, I consulted with a high-performing private practice hospitalist group on the East Coast. The group was led by one of the most energetic and thoughtful leaders I’ve encountered.
Like many other private practice groups, they divided physician members of the practice into partners and non-partners (sometimes referred to as shareholder and non-shareholders in the corporation). A hospitalist who had been a full-time member of the practice for a specified period of time (two years in this case) was eligible to become partner.
This entailed a “buy-in” requiring the doctor to pay money to the practice (usually the doctor would pay using a loan from the practice, which was repaid through deductions from his/her paycheck).
For this practice, the principal benefits of partner status were having a vote in group decisions (non-partners couldn’t vote) and receiving a portion of the distribution of all corporate profits each year. These profits came from two sources:
- Money remaining after all salaries and overhead were paid; and
- Buy-in money received by the practice.
Because the partners had this “upside potential” they agreed they would cover any staff shortages by working extra shifts instead of the non-partners.
Setting things up with a buy-in to achieve partner/shareholder status seemed to make a lot of sense. After all, it is the way nearly all private-practice medical groups in other specialties are structured.
Problems soon arose when they realized there wasn’t significant “profit” available unless there happened to be two or three doctors buying into the practice in a given year.
So, the partners became disenchanted because they shouldered the burden of covering any extra shifts but didn’t get a significant profit distribution in most years. Non-partners who became eligible for partnership were choosing not to buy in because it seemed like more responsibility without more income. The group’s system began breaking down.
Keep in mind they had a terrific practice. The docs liked each other and were pleased with the group leader, were highly regarded by hospital executives and other doctors, and had a growing patient volume.
Yet, the partners were unhappy they weren’t seeing extra compensation as a reward for buying into the practice with the money, time, and effort they invested.
Despite being a desirable practice in nearly every respect, new doctors were choosing to forgo partnership status. These things were creating significant morale issues that threatened the ongoing success of the group.
So why did these problems arise?
Case No. 2
Later in 2006, I worked with a different private-practice hospitalist group out West. Their practice had been started by, and was still owned by, a “parent” medical group. As the hospitalist practice grew, everyone (hospitalists and non-hospitalist doctors in the group) agreed it made sense to have the hospitalist practice separate into its own distinct corporation. Like the practice in the first case, all parties had high regard for one another.
The problem was the non-hospitalists who invested the time and energy to start the hospitalist practice wanted the departing hospitalists to compensate the larger group.
The hospitalists could understand why the other doctors proposed a buyout but wondered what the hospitalists would get in return for paying it. The answer seemed to be not much. They weren’t confident they could recoup their investment by having future hospitalists buy in to the practice (proposing this had scared off more than one recruit), or by selling the practice to another party.
Assess Your Value
The problems faced by both these practices are a result of uncertainty about what their practices are worth.
In the first case, doctors who had the opportunity to buy into the practice were choosing not to because they believed they weren’t going to get anything in return (and had the added burden of putting themselves on the schedule more often to cover open shifts).
Likewise, in the second case the hospitalists agreed it seemed reasonable to pay the other doctors in the parent group to go out on their own. But the hospitalists worried they would never be able to recoup that money by selling shares of the practice to new partner hospitalists or selling the whole group to another entity.
It’s tricky to value any medical practice. A common approach is to put a price on tangible assets owned by the practice (e.g., buildings and equipment like computers and lab apparatus, and the accounts receivable), and the patient base (or good will) the practice has developed.
It isn’t too difficult to come up with a value for tangible assets, and most hospitalist practices have little or nothing in this category (the only hard assets I can think of that I own are my pager, stethoscope, and a couple of lab coats I never wear). Patient lists and good will are particularly difficult to place a value on. Even for a primary care practice with thousands of patient charts, there is no guarantee patients will agree to transfer their care to a purchasing doctor.
For most any kind of medical practice, including a hospitalist group, good will mainly is a function of the referral relationships doctors have developed that ensure a steady flow of patients. Since a steady flow of patients is not a problem for most hospitalist practices (too many patients is more common than too few) the value of that referral stream may not be much.
Another asset many hospitalist practices own is their contract(s) with sponsoring organizations (usually hospitals, but sometimes health plans). They provide for supplemental payments over and above professional fees the practice collects.
This is often a hospitalist practice’s most valuable asset, and it may be worth investing money to acquire. It’s the primary reason large hospitalist staffing companies are willing to pay to acquire local hospitalist practices.
Usually these contracts cannot automatically be assigned to another party without the hospital’s consent. Most hospitals’ loyalty lies with the hospitalists who provide their coverage, not with the company that may hold the contract. For example, with the hospitalists in the second case, their hospital would have been willing to immediately sign a new contract with their spin-off group to maintain their existing hospitalist coverage. The parent group’s hospital contract wasn’t worth acquiring.
All this suggests hospitalist practices may not have much monetary value. That is, an outside party probably wouldn’t pay much to buy your practice. I think this is true for the two practices I describe above. For practices like these, it is probably best to avoid having a buy-in to achieve partner status, and not diverting some practice revenue that would otherwise be used to pay salaries into a “profit” pool from which distributions are made to partners/owners periodically.
Practices Worth A Lot
I’m aware my comments might seem insulting to a group of hospitalists who have worked long and hard for several years to build what they think is a great practice. Surely it’s worth something.
Maybe your practice really does have significant value over and above the salaries the doctors earn. Perhaps you have developed proprietary operational processes that are particularly valuable and would be difficult for others to replicate without knowing your “trade secrets.” These could include things such as particularly effective ways to document, code, and collect professional fees; methods to enhance hospitalist efficiency and/or quality; unusually effective recruitment strategies; or even the ability to negotiate highly favorable contracts with payers.
Even if your practice does have remarkably effective proprietary components, you still would have to convince a buyer these valuable assets would persist after the change in ownership and the departure of key individuals. For example, you might have the best practice in the country because you’ve been able to recruit the best doctors. If I buy your practice and those excellent doctors leave, I’ve lost the unique asset that was key to the practice’s value.
Clearly there is room for a lot of debate about hospitalist practice valuation. (Search the Internet for “medical practice valuation” for a number of good articles about this.) There are many practice management companies that rely on the notion that their ideas and operations provide greater value than other practices. One such company, IPC, had a successful initial public offering of stock that found a marketplace willing to pay for its perceived value. But keep in mind that this company has many practices in many states, and much of the value may lie in the fact that the value of the whole is greater than the sum of its parts. So, unless your practice is huge and has sites in many states, I don’t think you can assume IPC’s public offering means your practice might have a similar value.
Think critically about your practice. Challenge yourself to think about what you would pay for your practice and what you would get in return. If you have a hard time coming up with clear reasons your practice has significant intangible value, you should probably avoid structuring a buy-in for new doctors or a buy-out for departing doctors. TH
Dr. Nelson has been a practicing hospitalist since 1988 and is co-founder and past president of SHM. He is a principal in Nelson/Flores Associates, a national hospitalist practice management consulting firm. He is also part of the faculty for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. This column represents his views and is not intended to reflect an official position of SHM.
The issue of practice valuation is a sensitive one. Some hospitalist practices might have significant monetary value, which could make it reasonable to ask new doctors to buy in or enable selling the practice for a profit. Still, it’s risky to assume this is the case for your practice.
Let’s examine the issue using a pair of situations I encountered not long ago. I have changed some details of the practices to more clearly illustrate a point and conceal which practices I’m describing. Both situations would have gone smoother if it was clear what the hospitalist practice was worth. But how do you assess that value?
Case No. 1
During a couple of days in 2006, I consulted with a high-performing private practice hospitalist group on the East Coast. The group was led by one of the most energetic and thoughtful leaders I’ve encountered.
Like many other private practice groups, they divided physician members of the practice into partners and non-partners (sometimes referred to as shareholder and non-shareholders in the corporation). A hospitalist who had been a full-time member of the practice for a specified period of time (two years in this case) was eligible to become partner.
This entailed a “buy-in” requiring the doctor to pay money to the practice (usually the doctor would pay using a loan from the practice, which was repaid through deductions from his/her paycheck).
For this practice, the principal benefits of partner status were having a vote in group decisions (non-partners couldn’t vote) and receiving a portion of the distribution of all corporate profits each year. These profits came from two sources:
- Money remaining after all salaries and overhead were paid; and
- Buy-in money received by the practice.
Because the partners had this “upside potential” they agreed they would cover any staff shortages by working extra shifts instead of the non-partners.
Setting things up with a buy-in to achieve partner/shareholder status seemed to make a lot of sense. After all, it is the way nearly all private-practice medical groups in other specialties are structured.
Problems soon arose when they realized there wasn’t significant “profit” available unless there happened to be two or three doctors buying into the practice in a given year.
So, the partners became disenchanted because they shouldered the burden of covering any extra shifts but didn’t get a significant profit distribution in most years. Non-partners who became eligible for partnership were choosing not to buy in because it seemed like more responsibility without more income. The group’s system began breaking down.
Keep in mind they had a terrific practice. The docs liked each other and were pleased with the group leader, were highly regarded by hospital executives and other doctors, and had a growing patient volume.
Yet, the partners were unhappy they weren’t seeing extra compensation as a reward for buying into the practice with the money, time, and effort they invested.
Despite being a desirable practice in nearly every respect, new doctors were choosing to forgo partnership status. These things were creating significant morale issues that threatened the ongoing success of the group.
So why did these problems arise?
Case No. 2
Later in 2006, I worked with a different private-practice hospitalist group out West. Their practice had been started by, and was still owned by, a “parent” medical group. As the hospitalist practice grew, everyone (hospitalists and non-hospitalist doctors in the group) agreed it made sense to have the hospitalist practice separate into its own distinct corporation. Like the practice in the first case, all parties had high regard for one another.
The problem was the non-hospitalists who invested the time and energy to start the hospitalist practice wanted the departing hospitalists to compensate the larger group.
The hospitalists could understand why the other doctors proposed a buyout but wondered what the hospitalists would get in return for paying it. The answer seemed to be not much. They weren’t confident they could recoup their investment by having future hospitalists buy in to the practice (proposing this had scared off more than one recruit), or by selling the practice to another party.
Assess Your Value
The problems faced by both these practices are a result of uncertainty about what their practices are worth.
In the first case, doctors who had the opportunity to buy into the practice were choosing not to because they believed they weren’t going to get anything in return (and had the added burden of putting themselves on the schedule more often to cover open shifts).
Likewise, in the second case the hospitalists agreed it seemed reasonable to pay the other doctors in the parent group to go out on their own. But the hospitalists worried they would never be able to recoup that money by selling shares of the practice to new partner hospitalists or selling the whole group to another entity.
It’s tricky to value any medical practice. A common approach is to put a price on tangible assets owned by the practice (e.g., buildings and equipment like computers and lab apparatus, and the accounts receivable), and the patient base (or good will) the practice has developed.
It isn’t too difficult to come up with a value for tangible assets, and most hospitalist practices have little or nothing in this category (the only hard assets I can think of that I own are my pager, stethoscope, and a couple of lab coats I never wear). Patient lists and good will are particularly difficult to place a value on. Even for a primary care practice with thousands of patient charts, there is no guarantee patients will agree to transfer their care to a purchasing doctor.
For most any kind of medical practice, including a hospitalist group, good will mainly is a function of the referral relationships doctors have developed that ensure a steady flow of patients. Since a steady flow of patients is not a problem for most hospitalist practices (too many patients is more common than too few) the value of that referral stream may not be much.
Another asset many hospitalist practices own is their contract(s) with sponsoring organizations (usually hospitals, but sometimes health plans). They provide for supplemental payments over and above professional fees the practice collects.
This is often a hospitalist practice’s most valuable asset, and it may be worth investing money to acquire. It’s the primary reason large hospitalist staffing companies are willing to pay to acquire local hospitalist practices.
Usually these contracts cannot automatically be assigned to another party without the hospital’s consent. Most hospitals’ loyalty lies with the hospitalists who provide their coverage, not with the company that may hold the contract. For example, with the hospitalists in the second case, their hospital would have been willing to immediately sign a new contract with their spin-off group to maintain their existing hospitalist coverage. The parent group’s hospital contract wasn’t worth acquiring.
All this suggests hospitalist practices may not have much monetary value. That is, an outside party probably wouldn’t pay much to buy your practice. I think this is true for the two practices I describe above. For practices like these, it is probably best to avoid having a buy-in to achieve partner status, and not diverting some practice revenue that would otherwise be used to pay salaries into a “profit” pool from which distributions are made to partners/owners periodically.
Practices Worth A Lot
I’m aware my comments might seem insulting to a group of hospitalists who have worked long and hard for several years to build what they think is a great practice. Surely it’s worth something.
Maybe your practice really does have significant value over and above the salaries the doctors earn. Perhaps you have developed proprietary operational processes that are particularly valuable and would be difficult for others to replicate without knowing your “trade secrets.” These could include things such as particularly effective ways to document, code, and collect professional fees; methods to enhance hospitalist efficiency and/or quality; unusually effective recruitment strategies; or even the ability to negotiate highly favorable contracts with payers.
Even if your practice does have remarkably effective proprietary components, you still would have to convince a buyer these valuable assets would persist after the change in ownership and the departure of key individuals. For example, you might have the best practice in the country because you’ve been able to recruit the best doctors. If I buy your practice and those excellent doctors leave, I’ve lost the unique asset that was key to the practice’s value.
Clearly there is room for a lot of debate about hospitalist practice valuation. (Search the Internet for “medical practice valuation” for a number of good articles about this.) There are many practice management companies that rely on the notion that their ideas and operations provide greater value than other practices. One such company, IPC, had a successful initial public offering of stock that found a marketplace willing to pay for its perceived value. But keep in mind that this company has many practices in many states, and much of the value may lie in the fact that the value of the whole is greater than the sum of its parts. So, unless your practice is huge and has sites in many states, I don’t think you can assume IPC’s public offering means your practice might have a similar value.
Think critically about your practice. Challenge yourself to think about what you would pay for your practice and what you would get in return. If you have a hard time coming up with clear reasons your practice has significant intangible value, you should probably avoid structuring a buy-in for new doctors or a buy-out for departing doctors. TH
Dr. Nelson has been a practicing hospitalist since 1988 and is co-founder and past president of SHM. He is a principal in Nelson/Flores Associates, a national hospitalist practice management consulting firm. He is also part of the faculty for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. This column represents his views and is not intended to reflect an official position of SHM.
The issue of practice valuation is a sensitive one. Some hospitalist practices might have significant monetary value, which could make it reasonable to ask new doctors to buy in or enable selling the practice for a profit. Still, it’s risky to assume this is the case for your practice.
Let’s examine the issue using a pair of situations I encountered not long ago. I have changed some details of the practices to more clearly illustrate a point and conceal which practices I’m describing. Both situations would have gone smoother if it was clear what the hospitalist practice was worth. But how do you assess that value?
Case No. 1
During a couple of days in 2006, I consulted with a high-performing private practice hospitalist group on the East Coast. The group was led by one of the most energetic and thoughtful leaders I’ve encountered.
Like many other private practice groups, they divided physician members of the practice into partners and non-partners (sometimes referred to as shareholder and non-shareholders in the corporation). A hospitalist who had been a full-time member of the practice for a specified period of time (two years in this case) was eligible to become partner.
This entailed a “buy-in” requiring the doctor to pay money to the practice (usually the doctor would pay using a loan from the practice, which was repaid through deductions from his/her paycheck).
For this practice, the principal benefits of partner status were having a vote in group decisions (non-partners couldn’t vote) and receiving a portion of the distribution of all corporate profits each year. These profits came from two sources:
- Money remaining after all salaries and overhead were paid; and
- Buy-in money received by the practice.
Because the partners had this “upside potential” they agreed they would cover any staff shortages by working extra shifts instead of the non-partners.
Setting things up with a buy-in to achieve partner/shareholder status seemed to make a lot of sense. After all, it is the way nearly all private-practice medical groups in other specialties are structured.
Problems soon arose when they realized there wasn’t significant “profit” available unless there happened to be two or three doctors buying into the practice in a given year.
So, the partners became disenchanted because they shouldered the burden of covering any extra shifts but didn’t get a significant profit distribution in most years. Non-partners who became eligible for partnership were choosing not to buy in because it seemed like more responsibility without more income. The group’s system began breaking down.
Keep in mind they had a terrific practice. The docs liked each other and were pleased with the group leader, were highly regarded by hospital executives and other doctors, and had a growing patient volume.
Yet, the partners were unhappy they weren’t seeing extra compensation as a reward for buying into the practice with the money, time, and effort they invested.
Despite being a desirable practice in nearly every respect, new doctors were choosing to forgo partnership status. These things were creating significant morale issues that threatened the ongoing success of the group.
So why did these problems arise?
Case No. 2
Later in 2006, I worked with a different private-practice hospitalist group out West. Their practice had been started by, and was still owned by, a “parent” medical group. As the hospitalist practice grew, everyone (hospitalists and non-hospitalist doctors in the group) agreed it made sense to have the hospitalist practice separate into its own distinct corporation. Like the practice in the first case, all parties had high regard for one another.
The problem was the non-hospitalists who invested the time and energy to start the hospitalist practice wanted the departing hospitalists to compensate the larger group.
The hospitalists could understand why the other doctors proposed a buyout but wondered what the hospitalists would get in return for paying it. The answer seemed to be not much. They weren’t confident they could recoup their investment by having future hospitalists buy in to the practice (proposing this had scared off more than one recruit), or by selling the practice to another party.
Assess Your Value
The problems faced by both these practices are a result of uncertainty about what their practices are worth.
In the first case, doctors who had the opportunity to buy into the practice were choosing not to because they believed they weren’t going to get anything in return (and had the added burden of putting themselves on the schedule more often to cover open shifts).
Likewise, in the second case the hospitalists agreed it seemed reasonable to pay the other doctors in the parent group to go out on their own. But the hospitalists worried they would never be able to recoup that money by selling shares of the practice to new partner hospitalists or selling the whole group to another entity.
It’s tricky to value any medical practice. A common approach is to put a price on tangible assets owned by the practice (e.g., buildings and equipment like computers and lab apparatus, and the accounts receivable), and the patient base (or good will) the practice has developed.
It isn’t too difficult to come up with a value for tangible assets, and most hospitalist practices have little or nothing in this category (the only hard assets I can think of that I own are my pager, stethoscope, and a couple of lab coats I never wear). Patient lists and good will are particularly difficult to place a value on. Even for a primary care practice with thousands of patient charts, there is no guarantee patients will agree to transfer their care to a purchasing doctor.
For most any kind of medical practice, including a hospitalist group, good will mainly is a function of the referral relationships doctors have developed that ensure a steady flow of patients. Since a steady flow of patients is not a problem for most hospitalist practices (too many patients is more common than too few) the value of that referral stream may not be much.
Another asset many hospitalist practices own is their contract(s) with sponsoring organizations (usually hospitals, but sometimes health plans). They provide for supplemental payments over and above professional fees the practice collects.
This is often a hospitalist practice’s most valuable asset, and it may be worth investing money to acquire. It’s the primary reason large hospitalist staffing companies are willing to pay to acquire local hospitalist practices.
Usually these contracts cannot automatically be assigned to another party without the hospital’s consent. Most hospitals’ loyalty lies with the hospitalists who provide their coverage, not with the company that may hold the contract. For example, with the hospitalists in the second case, their hospital would have been willing to immediately sign a new contract with their spin-off group to maintain their existing hospitalist coverage. The parent group’s hospital contract wasn’t worth acquiring.
All this suggests hospitalist practices may not have much monetary value. That is, an outside party probably wouldn’t pay much to buy your practice. I think this is true for the two practices I describe above. For practices like these, it is probably best to avoid having a buy-in to achieve partner status, and not diverting some practice revenue that would otherwise be used to pay salaries into a “profit” pool from which distributions are made to partners/owners periodically.
Practices Worth A Lot
I’m aware my comments might seem insulting to a group of hospitalists who have worked long and hard for several years to build what they think is a great practice. Surely it’s worth something.
Maybe your practice really does have significant value over and above the salaries the doctors earn. Perhaps you have developed proprietary operational processes that are particularly valuable and would be difficult for others to replicate without knowing your “trade secrets.” These could include things such as particularly effective ways to document, code, and collect professional fees; methods to enhance hospitalist efficiency and/or quality; unusually effective recruitment strategies; or even the ability to negotiate highly favorable contracts with payers.
Even if your practice does have remarkably effective proprietary components, you still would have to convince a buyer these valuable assets would persist after the change in ownership and the departure of key individuals. For example, you might have the best practice in the country because you’ve been able to recruit the best doctors. If I buy your practice and those excellent doctors leave, I’ve lost the unique asset that was key to the practice’s value.
Clearly there is room for a lot of debate about hospitalist practice valuation. (Search the Internet for “medical practice valuation” for a number of good articles about this.) There are many practice management companies that rely on the notion that their ideas and operations provide greater value than other practices. One such company, IPC, had a successful initial public offering of stock that found a marketplace willing to pay for its perceived value. But keep in mind that this company has many practices in many states, and much of the value may lie in the fact that the value of the whole is greater than the sum of its parts. So, unless your practice is huge and has sites in many states, I don’t think you can assume IPC’s public offering means your practice might have a similar value.
Think critically about your practice. Challenge yourself to think about what you would pay for your practice and what you would get in return. If you have a hard time coming up with clear reasons your practice has significant intangible value, you should probably avoid structuring a buy-in for new doctors or a buy-out for departing doctors. TH
Dr. Nelson has been a practicing hospitalist since 1988 and is co-founder and past president of SHM. He is a principal in Nelson/Flores Associates, a national hospitalist practice management consulting firm. He is also part of the faculty for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. This column represents his views and is not intended to reflect an official position of SHM.
Safety, Salary, and Saints

I just returned from the SHM annual meeting, and I am brimming with new knowledge. While we’ve tried to capture the essence of the meeting in this edition of The Hospitalist, it’s hard to describe in print the excitement, energy, and edification I encountered during those three days in San Diego.
Nearly 1,600 hospitalists descended on the Grand Hyatt on the San Diego Harbor for the six pre-courses April 3 and the two-day meeting April 4-5, marking the biggest and widest-reaching hospitalist meeting to date. Here’s just a smattering of what I learned in southern California.
I learned that Don Berwick, MD, is a healthcare visionary. In his plenary address the founder of the Institute for Healthcare Improvement and national leader of the patient safety movement gave his insights on the quality of the healthcare system and offered a challenge for hospitalists. He started by deftly outlining how Americans pay $3,000 more per capita for healthcare than other industrialized countries only to receive less access, worse care, and higher mortality rates. Clearly, more money does not equate to better care.
After noting that every system is perfectly designed to achieve the results it gets, Dr. Berwick challenged hospitalists to debunk the romantic view of the “individual as the cause of excellence” in favor of creating multidisciplinary teams and systems of care whose results do not depend on the heroism of the individual.
I learned that hospitalists are getting paid more today for the same amount of work they provided in 2005. At the same time that the average salary is up 13% to $193,300 (compared with 2005) the average number of annual encounters per hospitalist is down 4% from 2,558 in 2005 to 2,447 in 2007.
I’ve seen several interpretations of these data. The most cynical take, generally from non-hospitalists, is that this is further proof that hospitalists are overpaid compared with our non-hospitalist generalist colleagues in internal and family medicine. While these changes obviously represent a free-market response to a shortage of hospitalists, I firmly believe these higher salaries are a more accurate valuation of the work hospitalists do—and the more appropriate interpretation is that we’ve been underpaid in previous years. Now it’s time for our healthcare system to more appropriately reward our outpatient colleagues as well.
I also learned that academic hospitalists are struggling with similar issues across the country. Drs. Adrienne Bennett, Brian Lucas, and Bob Wachter, led an enthralling but sobering session surveying the challenges facing academic hospitalist groups. In many cases the vision of developing a sustainable academic model around the core tenets of research, scholarly activity, and education is being undermined by the service mandate of non-teaching clinical work.
These tensions lead to profound challenges come promotion time, a topic that Drs. Scott Flanders, David Meltzer, and Sankey Williams covered in an afternoon session.
As a director of an academic program who recently went through the promotion process, I view these two issues as critical to the health of all segments of hospital medicine, not just academics. Community hospitalist groups will encounter even larger workforce deficiencies if future hospitalists (i.e., current residents) shy away from the field because they see academic hospitalists devalued as unpromotable resident extenders and academic second-class citizens.
Speaking of workforce shortages, I learned that several highly respect leaders in hospital medicine believe this to be one of the most significant factors threatening the field. In a plenary panel discussion, Drs. Ron Greeno, John Nelson, Mike Guthrie, and John Laverty, commented that overcoming the current and future hospitalist shortage requires rethinking the current model. Dr. Greeno highlighted the need to build more efficient care models whereby hospitalists could see more patients in the same time by reducing the high levels of busy work and administrative minutiae.
Other ideas centered on the development of midlevel provider hospitalists and limiting our scope of practice. To the latter point, there was a lively debate about just how much of the traditionally “non-medical” piece of the pie hospitalists should bite off. Eric Siegal, MD, tackled this issue in a later session challenging hospitalist groups to rethink the value of further expanding the co-management model to more surgical patients while we struggle to care for the patients for whom we currently care.
I learned that Drs. Nelson and Win Whitcomb, co-founders of SHM, showed tremendous vision in their founding of this society. I had the chance to have lunch with John, and I asked him if he ever imagined that the tiny group he brought together in San Diego 11 years ago would ever grow to this—20,000 hospitalists, 6,000 SHM members, an annual meeting with 1,600 people, and a hospitalist (Russell Holman, MD, past president of SHM) seated at the table of the most influential healthcare policy meetings in Washington, D.C.
Rather than being awestruck by the development of this field and SHM, he simply noted this is exactly what he and Win foresaw more than a decade ago; this is the reason they founded SHM. That’s the kind of vision that explains why the field of hospital medicine is the fastest-growing medical specialty.
I learned that the future of hospital medicine is being defined today. Nearly 200 posters were presented at the Research, Innovations and Clinical Vignettes (RIV) Competition. When we look back 10 years from now, we will see a mature field and wonder how we got there so quickly.
That future is being constructed today by folks like Ken Epstein, MD, who presented fascinating data on the effects of fragmentation of hospitalist care, and Param Dedhia, MD, who showed that a formalized discharge toolkit could reduce emergency visits and hospital readmissions in elderly patients.
Finally, while I was away in the city named after a saint, I learned that my wife, too, is a saint. Unable to travel with me, she was landlocked in Denver with our 6-month-old son. I, like many attendees, acknowledge the families who sacrificed so their loved ones could attend the meeting. While I was socializing, learning, networking, and teaching a session, my wife was home soothing tears, changing diapers, cleaning chinfuls of cereal, and answering 3 a.m. wakeup calls. On behalf of all attendees I say thanks to all the saints who enabled us to be away charting the course of hospital medicine at Hospital Medicine 2008. TH
Dr. Glasheen is associate professor of medicine at the University of Colorado at Denver, where he serves as director of the Hospital Medicine Program and the Hospitalist Training Program, and as associate program director of the Internal Medicine Residency Program.
I just returned from the SHM annual meeting, and I am brimming with new knowledge. While we’ve tried to capture the essence of the meeting in this edition of The Hospitalist, it’s hard to describe in print the excitement, energy, and edification I encountered during those three days in San Diego.
Nearly 1,600 hospitalists descended on the Grand Hyatt on the San Diego Harbor for the six pre-courses April 3 and the two-day meeting April 4-5, marking the biggest and widest-reaching hospitalist meeting to date. Here’s just a smattering of what I learned in southern California.
I learned that Don Berwick, MD, is a healthcare visionary. In his plenary address the founder of the Institute for Healthcare Improvement and national leader of the patient safety movement gave his insights on the quality of the healthcare system and offered a challenge for hospitalists. He started by deftly outlining how Americans pay $3,000 more per capita for healthcare than other industrialized countries only to receive less access, worse care, and higher mortality rates. Clearly, more money does not equate to better care.
After noting that every system is perfectly designed to achieve the results it gets, Dr. Berwick challenged hospitalists to debunk the romantic view of the “individual as the cause of excellence” in favor of creating multidisciplinary teams and systems of care whose results do not depend on the heroism of the individual.
I learned that hospitalists are getting paid more today for the same amount of work they provided in 2005. At the same time that the average salary is up 13% to $193,300 (compared with 2005) the average number of annual encounters per hospitalist is down 4% from 2,558 in 2005 to 2,447 in 2007.
I’ve seen several interpretations of these data. The most cynical take, generally from non-hospitalists, is that this is further proof that hospitalists are overpaid compared with our non-hospitalist generalist colleagues in internal and family medicine. While these changes obviously represent a free-market response to a shortage of hospitalists, I firmly believe these higher salaries are a more accurate valuation of the work hospitalists do—and the more appropriate interpretation is that we’ve been underpaid in previous years. Now it’s time for our healthcare system to more appropriately reward our outpatient colleagues as well.
I also learned that academic hospitalists are struggling with similar issues across the country. Drs. Adrienne Bennett, Brian Lucas, and Bob Wachter, led an enthralling but sobering session surveying the challenges facing academic hospitalist groups. In many cases the vision of developing a sustainable academic model around the core tenets of research, scholarly activity, and education is being undermined by the service mandate of non-teaching clinical work.
These tensions lead to profound challenges come promotion time, a topic that Drs. Scott Flanders, David Meltzer, and Sankey Williams covered in an afternoon session.
As a director of an academic program who recently went through the promotion process, I view these two issues as critical to the health of all segments of hospital medicine, not just academics. Community hospitalist groups will encounter even larger workforce deficiencies if future hospitalists (i.e., current residents) shy away from the field because they see academic hospitalists devalued as unpromotable resident extenders and academic second-class citizens.
Speaking of workforce shortages, I learned that several highly respect leaders in hospital medicine believe this to be one of the most significant factors threatening the field. In a plenary panel discussion, Drs. Ron Greeno, John Nelson, Mike Guthrie, and John Laverty, commented that overcoming the current and future hospitalist shortage requires rethinking the current model. Dr. Greeno highlighted the need to build more efficient care models whereby hospitalists could see more patients in the same time by reducing the high levels of busy work and administrative minutiae.
Other ideas centered on the development of midlevel provider hospitalists and limiting our scope of practice. To the latter point, there was a lively debate about just how much of the traditionally “non-medical” piece of the pie hospitalists should bite off. Eric Siegal, MD, tackled this issue in a later session challenging hospitalist groups to rethink the value of further expanding the co-management model to more surgical patients while we struggle to care for the patients for whom we currently care.
I learned that Drs. Nelson and Win Whitcomb, co-founders of SHM, showed tremendous vision in their founding of this society. I had the chance to have lunch with John, and I asked him if he ever imagined that the tiny group he brought together in San Diego 11 years ago would ever grow to this—20,000 hospitalists, 6,000 SHM members, an annual meeting with 1,600 people, and a hospitalist (Russell Holman, MD, past president of SHM) seated at the table of the most influential healthcare policy meetings in Washington, D.C.
Rather than being awestruck by the development of this field and SHM, he simply noted this is exactly what he and Win foresaw more than a decade ago; this is the reason they founded SHM. That’s the kind of vision that explains why the field of hospital medicine is the fastest-growing medical specialty.
I learned that the future of hospital medicine is being defined today. Nearly 200 posters were presented at the Research, Innovations and Clinical Vignettes (RIV) Competition. When we look back 10 years from now, we will see a mature field and wonder how we got there so quickly.
That future is being constructed today by folks like Ken Epstein, MD, who presented fascinating data on the effects of fragmentation of hospitalist care, and Param Dedhia, MD, who showed that a formalized discharge toolkit could reduce emergency visits and hospital readmissions in elderly patients.
Finally, while I was away in the city named after a saint, I learned that my wife, too, is a saint. Unable to travel with me, she was landlocked in Denver with our 6-month-old son. I, like many attendees, acknowledge the families who sacrificed so their loved ones could attend the meeting. While I was socializing, learning, networking, and teaching a session, my wife was home soothing tears, changing diapers, cleaning chinfuls of cereal, and answering 3 a.m. wakeup calls. On behalf of all attendees I say thanks to all the saints who enabled us to be away charting the course of hospital medicine at Hospital Medicine 2008. TH
Dr. Glasheen is associate professor of medicine at the University of Colorado at Denver, where he serves as director of the Hospital Medicine Program and the Hospitalist Training Program, and as associate program director of the Internal Medicine Residency Program.
I just returned from the SHM annual meeting, and I am brimming with new knowledge. While we’ve tried to capture the essence of the meeting in this edition of The Hospitalist, it’s hard to describe in print the excitement, energy, and edification I encountered during those three days in San Diego.
Nearly 1,600 hospitalists descended on the Grand Hyatt on the San Diego Harbor for the six pre-courses April 3 and the two-day meeting April 4-5, marking the biggest and widest-reaching hospitalist meeting to date. Here’s just a smattering of what I learned in southern California.
I learned that Don Berwick, MD, is a healthcare visionary. In his plenary address the founder of the Institute for Healthcare Improvement and national leader of the patient safety movement gave his insights on the quality of the healthcare system and offered a challenge for hospitalists. He started by deftly outlining how Americans pay $3,000 more per capita for healthcare than other industrialized countries only to receive less access, worse care, and higher mortality rates. Clearly, more money does not equate to better care.
After noting that every system is perfectly designed to achieve the results it gets, Dr. Berwick challenged hospitalists to debunk the romantic view of the “individual as the cause of excellence” in favor of creating multidisciplinary teams and systems of care whose results do not depend on the heroism of the individual.
I learned that hospitalists are getting paid more today for the same amount of work they provided in 2005. At the same time that the average salary is up 13% to $193,300 (compared with 2005) the average number of annual encounters per hospitalist is down 4% from 2,558 in 2005 to 2,447 in 2007.
I’ve seen several interpretations of these data. The most cynical take, generally from non-hospitalists, is that this is further proof that hospitalists are overpaid compared with our non-hospitalist generalist colleagues in internal and family medicine. While these changes obviously represent a free-market response to a shortage of hospitalists, I firmly believe these higher salaries are a more accurate valuation of the work hospitalists do—and the more appropriate interpretation is that we’ve been underpaid in previous years. Now it’s time for our healthcare system to more appropriately reward our outpatient colleagues as well.
I also learned that academic hospitalists are struggling with similar issues across the country. Drs. Adrienne Bennett, Brian Lucas, and Bob Wachter, led an enthralling but sobering session surveying the challenges facing academic hospitalist groups. In many cases the vision of developing a sustainable academic model around the core tenets of research, scholarly activity, and education is being undermined by the service mandate of non-teaching clinical work.
These tensions lead to profound challenges come promotion time, a topic that Drs. Scott Flanders, David Meltzer, and Sankey Williams covered in an afternoon session.
As a director of an academic program who recently went through the promotion process, I view these two issues as critical to the health of all segments of hospital medicine, not just academics. Community hospitalist groups will encounter even larger workforce deficiencies if future hospitalists (i.e., current residents) shy away from the field because they see academic hospitalists devalued as unpromotable resident extenders and academic second-class citizens.
Speaking of workforce shortages, I learned that several highly respect leaders in hospital medicine believe this to be one of the most significant factors threatening the field. In a plenary panel discussion, Drs. Ron Greeno, John Nelson, Mike Guthrie, and John Laverty, commented that overcoming the current and future hospitalist shortage requires rethinking the current model. Dr. Greeno highlighted the need to build more efficient care models whereby hospitalists could see more patients in the same time by reducing the high levels of busy work and administrative minutiae.
Other ideas centered on the development of midlevel provider hospitalists and limiting our scope of practice. To the latter point, there was a lively debate about just how much of the traditionally “non-medical” piece of the pie hospitalists should bite off. Eric Siegal, MD, tackled this issue in a later session challenging hospitalist groups to rethink the value of further expanding the co-management model to more surgical patients while we struggle to care for the patients for whom we currently care.
I learned that Drs. Nelson and Win Whitcomb, co-founders of SHM, showed tremendous vision in their founding of this society. I had the chance to have lunch with John, and I asked him if he ever imagined that the tiny group he brought together in San Diego 11 years ago would ever grow to this—20,000 hospitalists, 6,000 SHM members, an annual meeting with 1,600 people, and a hospitalist (Russell Holman, MD, past president of SHM) seated at the table of the most influential healthcare policy meetings in Washington, D.C.
Rather than being awestruck by the development of this field and SHM, he simply noted this is exactly what he and Win foresaw more than a decade ago; this is the reason they founded SHM. That’s the kind of vision that explains why the field of hospital medicine is the fastest-growing medical specialty.
I learned that the future of hospital medicine is being defined today. Nearly 200 posters were presented at the Research, Innovations and Clinical Vignettes (RIV) Competition. When we look back 10 years from now, we will see a mature field and wonder how we got there so quickly.
That future is being constructed today by folks like Ken Epstein, MD, who presented fascinating data on the effects of fragmentation of hospitalist care, and Param Dedhia, MD, who showed that a formalized discharge toolkit could reduce emergency visits and hospital readmissions in elderly patients.
Finally, while I was away in the city named after a saint, I learned that my wife, too, is a saint. Unable to travel with me, she was landlocked in Denver with our 6-month-old son. I, like many attendees, acknowledge the families who sacrificed so their loved ones could attend the meeting. While I was socializing, learning, networking, and teaching a session, my wife was home soothing tears, changing diapers, cleaning chinfuls of cereal, and answering 3 a.m. wakeup calls. On behalf of all attendees I say thanks to all the saints who enabled us to be away charting the course of hospital medicine at Hospital Medicine 2008. TH
Dr. Glasheen is associate professor of medicine at the University of Colorado at Denver, where he serves as director of the Hospital Medicine Program and the Hospitalist Training Program, and as associate program director of the Internal Medicine Residency Program.
Paying Doctors Differently

Something is happening out there. Can you feel it?
It is like a small tremor before an earthquake or a brief lightning flash before a thunderstorm. It’s the signal that alerts us something is coming without indicating what it might be—ominous, promising, or revolutionary.
Our ossified, dysfunctional nonsystem of incentivizing the behavior of healthcare professionals gradually is eroding, even as the haves—the over-rewarded—cling to the past or rush to create the next procedure or modality to run by the insurance industry guardians of the dollar. The days of the system of paying for care in an a la carte manner—by the unit of the visit or performance of the procedure without consequence or reward for appropriate indications or demonstration of expected outcomes—clearly are numbered.
What will replace the current imperfect approach is not clear or perfect, but there are discernible, inexorable trends.
Performance Will Matter
Few sectors of our economy have been so devoid of standards—or, more to the point, of rewards for better service or outcomes—than healthcare.
Could you imagine paying the same for a 2008 Lexus as you would for a 1995 Toyota? Could you imagine a pricing system that couldn’t recognize or properly reward the difference between Motel 6 and the Ritz Carlton, excusing the inability to differentiate them by saying they both have beds, sheets, towels, and indoor plumbing? Today, the worst orthopedist in the country and the best are paid the same fee for a hip replacement—whether it’s indicated or not. Most patients or purchasers of healthcare have no way to know which is which.
Performance measurement and standards are here, and while imperfect and evolving, they will be with us throughout the rest of our professional careers. Whether you are in the “process” or “outcomes” camp, you and your institution will be measured. The carrot or the stick can take many forms.
Right now, it is much more than about just reporting. Disturbingly, only 30% of physicians have participated in the first round of the Physician Quality Reporting Initiative (PQRI). Look for Medicare to apply financial pressure on physicians who do not report.
On the hospital side, reporting has focused as much on embarrassment as anything. In April, every hospital received its mortality statistics for pneumonia from the Centers for Medicare and Medicaid Services (CMS). In July, these numbers will be made public. Look for a flurry of indignation and activity as hospitals try to regain the trust of their patients and assure them they indeed can manage something as basic to their core mission as pneumonia. SHM will be developing strategies to help hospitalists help their hospitals improve their performance.
Much has been made of paying for performance—and this may drive change at the hospital level. Yet, it is doubtful individual physicians will substantially change their work flow or processes, or purchase new systems for measurement, just to get an extra dollar or two for better glycemic control of their patients. What may carry more weight is if lack of performance means some physicians, or even hospitals, are restricted from performing certain procedures or caring for certain illnesses.
Bundling Episodes of Care
A move is afoot to change the unit of healthcare delivery. SHM has been in discussions with MedPAC, which advises CMS on changes to the reimbursement system, about aggregating a continuum of care as a “bundled” episode of care.
More than 15 years ago, the implementation of diagnosis-related groups (DRGs) moved hospital thinking from a la carte charging for each aspirin to managing the use of resources for the entire hospital stay, since their reimbursement was fixed. The DRG payment system as much as anything has encouraged hospitals to develop and support hospital medicine groups. Bundling would extend and expand a DRG-like concept to physicians.
Think of a future where physicians are not reimbursed for an admission work-up, three daily visits, and a discharge summary. Instead, they’d receive a global fee that might include the hospital care, transitions to the outpatient provider, and measurement of performance that might include patient satisfaction and a low readmission rate.
If we look at healthcare from the patient’s viewpoint, this is the kind of service for which they’re crying out. They want to move away from a system that even with the best providers leads to each expert doing his or her individual part well, but with voltage drops and white spaces as the patient moves through an uncoordinated non-system.
Hospitalists are in a unique position to be successful, especially as we look for strategies that align our performance with strong and engaged outpatient physicians and when we fully engage the entire healthcare team.
A Team Sport
Bundling and rewards driven by demonstrable performance create interlinking responsibilities for care among multiple physicians (primary care physicians, emergency physicians, surgeons, subspecialists, and hospitalists), as well as allied health professionals (registered nurses, nurse practitioners, physician assistants, pharmacists, therapists, social workers, and case managers).
While the makeup of the team is important, the environment in which it performs is most crucial for success. A system of healthcare delivery that focuses on and supports best practices and nudges—or forces—providers to make the right choice is of prime importance. In the end, a good system of care and one or two members of the team can save the entire enterprise, leading to the best outcome for the patient.
By the same token, a dysfunctional outlier on the team can sink everyone, including the patient. Think of the “new” healthcare as a crew team that needs a well-made boat (i.e., the system of care), a good coxswain (accountable physician), and a group of rowers, each of whom know and execute their roles. One rower can sink seven Olympians.
We are all in the boat together. We need to be clear where the finish line is and how best to get there. The future is in sight, and we need to continue to shape our role in helping the rest of the team get there. We must do this for ourselves, our profession, and—most of all—our patients today and tomorrow. TH
Dr. Wellikson is CEO of SHM.
Something is happening out there. Can you feel it?
It is like a small tremor before an earthquake or a brief lightning flash before a thunderstorm. It’s the signal that alerts us something is coming without indicating what it might be—ominous, promising, or revolutionary.
Our ossified, dysfunctional nonsystem of incentivizing the behavior of healthcare professionals gradually is eroding, even as the haves—the over-rewarded—cling to the past or rush to create the next procedure or modality to run by the insurance industry guardians of the dollar. The days of the system of paying for care in an a la carte manner—by the unit of the visit or performance of the procedure without consequence or reward for appropriate indications or demonstration of expected outcomes—clearly are numbered.
What will replace the current imperfect approach is not clear or perfect, but there are discernible, inexorable trends.
Performance Will Matter
Few sectors of our economy have been so devoid of standards—or, more to the point, of rewards for better service or outcomes—than healthcare.
Could you imagine paying the same for a 2008 Lexus as you would for a 1995 Toyota? Could you imagine a pricing system that couldn’t recognize or properly reward the difference between Motel 6 and the Ritz Carlton, excusing the inability to differentiate them by saying they both have beds, sheets, towels, and indoor plumbing? Today, the worst orthopedist in the country and the best are paid the same fee for a hip replacement—whether it’s indicated or not. Most patients or purchasers of healthcare have no way to know which is which.
Performance measurement and standards are here, and while imperfect and evolving, they will be with us throughout the rest of our professional careers. Whether you are in the “process” or “outcomes” camp, you and your institution will be measured. The carrot or the stick can take many forms.
Right now, it is much more than about just reporting. Disturbingly, only 30% of physicians have participated in the first round of the Physician Quality Reporting Initiative (PQRI). Look for Medicare to apply financial pressure on physicians who do not report.
On the hospital side, reporting has focused as much on embarrassment as anything. In April, every hospital received its mortality statistics for pneumonia from the Centers for Medicare and Medicaid Services (CMS). In July, these numbers will be made public. Look for a flurry of indignation and activity as hospitals try to regain the trust of their patients and assure them they indeed can manage something as basic to their core mission as pneumonia. SHM will be developing strategies to help hospitalists help their hospitals improve their performance.
Much has been made of paying for performance—and this may drive change at the hospital level. Yet, it is doubtful individual physicians will substantially change their work flow or processes, or purchase new systems for measurement, just to get an extra dollar or two for better glycemic control of their patients. What may carry more weight is if lack of performance means some physicians, or even hospitals, are restricted from performing certain procedures or caring for certain illnesses.
Bundling Episodes of Care
A move is afoot to change the unit of healthcare delivery. SHM has been in discussions with MedPAC, which advises CMS on changes to the reimbursement system, about aggregating a continuum of care as a “bundled” episode of care.
More than 15 years ago, the implementation of diagnosis-related groups (DRGs) moved hospital thinking from a la carte charging for each aspirin to managing the use of resources for the entire hospital stay, since their reimbursement was fixed. The DRG payment system as much as anything has encouraged hospitals to develop and support hospital medicine groups. Bundling would extend and expand a DRG-like concept to physicians.
Think of a future where physicians are not reimbursed for an admission work-up, three daily visits, and a discharge summary. Instead, they’d receive a global fee that might include the hospital care, transitions to the outpatient provider, and measurement of performance that might include patient satisfaction and a low readmission rate.
If we look at healthcare from the patient’s viewpoint, this is the kind of service for which they’re crying out. They want to move away from a system that even with the best providers leads to each expert doing his or her individual part well, but with voltage drops and white spaces as the patient moves through an uncoordinated non-system.
Hospitalists are in a unique position to be successful, especially as we look for strategies that align our performance with strong and engaged outpatient physicians and when we fully engage the entire healthcare team.
A Team Sport
Bundling and rewards driven by demonstrable performance create interlinking responsibilities for care among multiple physicians (primary care physicians, emergency physicians, surgeons, subspecialists, and hospitalists), as well as allied health professionals (registered nurses, nurse practitioners, physician assistants, pharmacists, therapists, social workers, and case managers).
While the makeup of the team is important, the environment in which it performs is most crucial for success. A system of healthcare delivery that focuses on and supports best practices and nudges—or forces—providers to make the right choice is of prime importance. In the end, a good system of care and one or two members of the team can save the entire enterprise, leading to the best outcome for the patient.
By the same token, a dysfunctional outlier on the team can sink everyone, including the patient. Think of the “new” healthcare as a crew team that needs a well-made boat (i.e., the system of care), a good coxswain (accountable physician), and a group of rowers, each of whom know and execute their roles. One rower can sink seven Olympians.
We are all in the boat together. We need to be clear where the finish line is and how best to get there. The future is in sight, and we need to continue to shape our role in helping the rest of the team get there. We must do this for ourselves, our profession, and—most of all—our patients today and tomorrow. TH
Dr. Wellikson is CEO of SHM.
Something is happening out there. Can you feel it?
It is like a small tremor before an earthquake or a brief lightning flash before a thunderstorm. It’s the signal that alerts us something is coming without indicating what it might be—ominous, promising, or revolutionary.
Our ossified, dysfunctional nonsystem of incentivizing the behavior of healthcare professionals gradually is eroding, even as the haves—the over-rewarded—cling to the past or rush to create the next procedure or modality to run by the insurance industry guardians of the dollar. The days of the system of paying for care in an a la carte manner—by the unit of the visit or performance of the procedure without consequence or reward for appropriate indications or demonstration of expected outcomes—clearly are numbered.
What will replace the current imperfect approach is not clear or perfect, but there are discernible, inexorable trends.
Performance Will Matter
Few sectors of our economy have been so devoid of standards—or, more to the point, of rewards for better service or outcomes—than healthcare.
Could you imagine paying the same for a 2008 Lexus as you would for a 1995 Toyota? Could you imagine a pricing system that couldn’t recognize or properly reward the difference between Motel 6 and the Ritz Carlton, excusing the inability to differentiate them by saying they both have beds, sheets, towels, and indoor plumbing? Today, the worst orthopedist in the country and the best are paid the same fee for a hip replacement—whether it’s indicated or not. Most patients or purchasers of healthcare have no way to know which is which.
Performance measurement and standards are here, and while imperfect and evolving, they will be with us throughout the rest of our professional careers. Whether you are in the “process” or “outcomes” camp, you and your institution will be measured. The carrot or the stick can take many forms.
Right now, it is much more than about just reporting. Disturbingly, only 30% of physicians have participated in the first round of the Physician Quality Reporting Initiative (PQRI). Look for Medicare to apply financial pressure on physicians who do not report.
On the hospital side, reporting has focused as much on embarrassment as anything. In April, every hospital received its mortality statistics for pneumonia from the Centers for Medicare and Medicaid Services (CMS). In July, these numbers will be made public. Look for a flurry of indignation and activity as hospitals try to regain the trust of their patients and assure them they indeed can manage something as basic to their core mission as pneumonia. SHM will be developing strategies to help hospitalists help their hospitals improve their performance.
Much has been made of paying for performance—and this may drive change at the hospital level. Yet, it is doubtful individual physicians will substantially change their work flow or processes, or purchase new systems for measurement, just to get an extra dollar or two for better glycemic control of their patients. What may carry more weight is if lack of performance means some physicians, or even hospitals, are restricted from performing certain procedures or caring for certain illnesses.
Bundling Episodes of Care
A move is afoot to change the unit of healthcare delivery. SHM has been in discussions with MedPAC, which advises CMS on changes to the reimbursement system, about aggregating a continuum of care as a “bundled” episode of care.
More than 15 years ago, the implementation of diagnosis-related groups (DRGs) moved hospital thinking from a la carte charging for each aspirin to managing the use of resources for the entire hospital stay, since their reimbursement was fixed. The DRG payment system as much as anything has encouraged hospitals to develop and support hospital medicine groups. Bundling would extend and expand a DRG-like concept to physicians.
Think of a future where physicians are not reimbursed for an admission work-up, three daily visits, and a discharge summary. Instead, they’d receive a global fee that might include the hospital care, transitions to the outpatient provider, and measurement of performance that might include patient satisfaction and a low readmission rate.
If we look at healthcare from the patient’s viewpoint, this is the kind of service for which they’re crying out. They want to move away from a system that even with the best providers leads to each expert doing his or her individual part well, but with voltage drops and white spaces as the patient moves through an uncoordinated non-system.
Hospitalists are in a unique position to be successful, especially as we look for strategies that align our performance with strong and engaged outpatient physicians and when we fully engage the entire healthcare team.
A Team Sport
Bundling and rewards driven by demonstrable performance create interlinking responsibilities for care among multiple physicians (primary care physicians, emergency physicians, surgeons, subspecialists, and hospitalists), as well as allied health professionals (registered nurses, nurse practitioners, physician assistants, pharmacists, therapists, social workers, and case managers).
While the makeup of the team is important, the environment in which it performs is most crucial for success. A system of healthcare delivery that focuses on and supports best practices and nudges—or forces—providers to make the right choice is of prime importance. In the end, a good system of care and one or two members of the team can save the entire enterprise, leading to the best outcome for the patient.
By the same token, a dysfunctional outlier on the team can sink everyone, including the patient. Think of the “new” healthcare as a crew team that needs a well-made boat (i.e., the system of care), a good coxswain (accountable physician), and a group of rowers, each of whom know and execute their roles. One rower can sink seven Olympians.
We are all in the boat together. We need to be clear where the finish line is and how best to get there. The future is in sight, and we need to continue to shape our role in helping the rest of the team get there. We must do this for ourselves, our profession, and—most of all—our patients today and tomorrow. TH
Dr. Wellikson is CEO of SHM.
What is the best choice for prophylaxis against VTE in medical inpatients?
Case
A 76-year-old gentleman is admitted for progressively worsening dyspnea, cough, and bilateral leg edema. Upon admission, his blood pressure is 150/90 mm/Hg, pulse 90 beats per minute, and respiration is 24 per minute.
Pertinent physical findings include jugular venous distension, bilateral crackles, S3 gallop, and 2+ bilateral lower extremity edema. The chest radiograph shows cardiomegaly and pulmonary edema. He is admitted to the hospital with a diagnosis of acute decompensated heart failure and starts aggressive medical therapy.
Overview
Approximately 2 million cases of deep-vein thrombosis (DVT) occur annually in the United States. Based on studies utilizing ventilation-perfusion scanning, half these patients likely have a silent pulmonary embolism (PE); of these, approximately 250,000 die.
The spectrum of venous thromboembolism (VTE), which includes DVT and PE, can vary from being asymptomatic to sudden death. Autopsy studies suggest a leading cause of sudden death in hospitalized medical patients is often a PE. There also are sequelae, such as chronic pulmonary hypertension, occurring in approximately 5% of PE cases, and post-thrombotic syndrome, occurring in approximately 40% of patients with DVT at two years.1
A recent study suggests DVT occurs three times more commonly in the outpatient setting. However, more than half of these patients were hospitalized in the three months prior.2 This is likely due to inadequate in-hospital prevention because of absence of prophylaxis, use of an unsuitable modality, insufficient dose of the drug, or ineffective duration of therapy. Inadequate and omitted VTE prophylaxis for medical patients was clearly demonstrated in the DVT Free Registry. This registry was created by 183 U.S. hospitals and included 5,451 patients, inpatients, and outpatients with ultrasound-confirmed DVT.
The number of medical inpatients who received prophylaxis in the 30 days prior to diagnosis was 28%—lower than the 48% of surgical patients.3 In a recent international registry, IMPROVE, only approximately 50% of hospitalized patients received prophylaxis.4
Virchow’s triad describes three underlying etiologic factors for thrombosis: stasis of blood flow, endothelial injury, and hypercoagulability. Established VTE risk factors reflect these underlying pathophysiologic processes. Important risk factors for VTE include increasing age, prolonged immobility, malignancy, major surgery, multiple trauma, prior VTE, and chronic heart failure.5
However, the magnitude of risk conferred by these and other risk factors varies (see Table 1, p. 35). It is not known how these factors interact to determine a patient’s individual VTE risk, but there is evidence it increases in proportion to the number of predisposing factors present.
In a recent systematic review of nine studies, including approximately 20,000 patients, prophylaxis reduced the rate of symptomatic VTE in at-risk hospitalized medical patients without increasing major bleeding.6
Multiple healthcare organizations, such as the National Quality Forum (NQF), Joint Commission on Accreditation of Healthcare Organizations (JCAHO), and Agency for Healthcare Research and Quality (AHRQ) have identified VTE as a preventable condition in hospitalized patients. Formal risk assessment must be conducted as a first step, followed by the initiation of timely prophylaxis to improve patient safety.
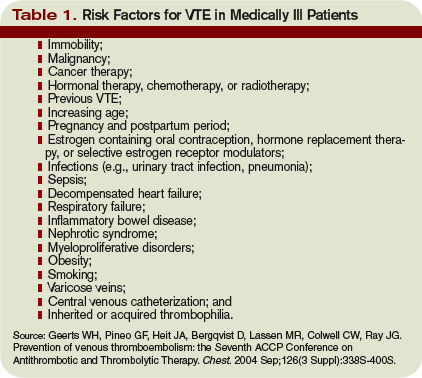
Review of the Data
Mechanical forms of prophylaxis, such as graduated compression stockings, have been evaluated in patients with stroke and myocardial infarction. Intermittent pneumatic compression stockings and venous foot pumps have not been studied in randomized controlled trials (RCTs) in general medical patients.
Although there is data supporting the efficacy of these devices in surgical patients, the American College of Chest Physicians’ (ACCP) guidelines recommend against the use of mechanical forms of prophylaxis in medical patients unless there is a contraindication to pharmacologic prophylaxis.7
The ideal prophylactic agent is cost-effective and has no side effects. Available pharmacologic options for prevention of VTE in medical patients include unfractionated heparin (UFH), low molecular weight heparins (LMWHs), and the synthetic pentasaccharide, fondaparinux. Oral anticoagulants, (e.g., vitamin K antagonists [VKA]), have not been adequately studied in medical inpatients. Since VKA take several days to achieve therapeutic anticoagulation, we do not recommend using them de novo as VTE prophylaxis.
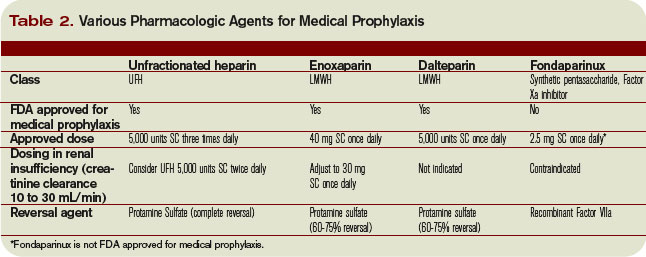
However, patients taking an oral VKA in the outpatient setting who have a therapeutic international normalized ratio (INR) during hospitalization probably are adequately protected from VTE and do not need additional pharmacologic prophylaxis. Newer anticoagulants in phase III testing for prevention of VTE in medically ill patients include oral direct thrombin inhibitors and anti-Xa inhibitors. ACCP guidelines recommend either low-dose UFH or LMWH as first-line agents for VTE prevention in medical inpatients.
Unfractionated heparin: UFH is a heterogeneous mixture of repeating polysaccharide chains of varying sizes, averaging about 15,000 Daltons. It binds anti-thrombin III (AT-III) and facilitates AT-III-mediated inactivation of factors IIa, IXa, Xa, and XIIa; of these, IIa and Xa are most responsive to inhibition.
Due to its large size, UFH only is partially absorbed from subcutaneous (SC) tissue, and it has a variable anticoagulant response due to interactions with plasma proteins, macrophages, and endothelial cells.8 However, in prophylactic SC doses (5,000 units two or three times daily), monitoring of the activated partial thromboplastin time (aPTT) is not required. In some cases, (e.g., frail or elderly patients), prophylactic SC doses may slightly prolong the aPTT.
UFH also binds to platelets and platelet factor 4 (PF4), and may precipitate heparin-induced thrombocytopenia (HIT). At least three clinical trials have compared the efficacy of SC UFH with a placebo and found prophylactic doses of UFH decrease the relative risk of DVT as detected by fibrinogen uptake test by about 70% without increasing the risk of bleeding.9-11
Low molecular weight heparins: LMWHs are derived from UFH through a chemical depolymerization, or fractionation, process. They are about one-third the size of UFH, with a molecular weight of approximately 5,000 Daltons.
These smaller molecules are readily absorbed from the SC tissue, eliciting a more predictable anticoagulant response than UFH. Unlike UFH, LMWHs have only minimal nonspecific binding to plasma proteins, endothelial cells, and monocytes, resulting in a predictable dose response. This obviates the need for lab monitoring, even when used in full, therapeutic dosing.
Compared with UFH, these agents have a longer plasma half-life, allowing them to be dosed SC once or twice daily. Also, they don’t bind platelets as readily as UFH resulting in a lower risk of HIT. Because they’re smaller, LMWHs tend to preferentially inhibit factor Xa, whereas UFH tends to inhibit factors Xa and IIa equally.
LMWHs have been evaluated in two large, placebo-controlled clinical trials for the prevention of VTE in medical inpatients.
In the first trial, MEDENOX, almost half the patients were older than 75 (mean age approximately 73). Inclusion criteria were NYHA class 3 or 4 heart failure, acute respiratory failure without mechanical ventilation, acute infection without septic shock, acute rheumatic disease, or inflammatory bowel disease. The primary outcome was assessed in 866 patients. Enoxaparin 40 mg SC once daily decreased the rate of VTE by two-thirds, from 15% to 5% (p=0.0002), without increased bleeding or thrombocytopenia compared with placebo.12 Enoxaparin 40 mg SC once daily is approved by the Food and Drug Administration (FDA) for VTE prophylaxis in medically ill patients.
PREVENT was an international, multicenter, randomized, double-blind, placebo-controlled trial evaluating dalteparin’s efficacy and safety. The inclusion criteria in this trial were acute congestive heart failure, non-ventilator-requiring acute respiratory failure, infection without septic shock, acute rheumatologic disorders, or inflammatory bowel disease. It studied 2,991 patients, and the primary outcome was VTE incidence and sudden death at day 21.
Dalteparin at 5,000 units decreased the rate of VTE, as detected by compression ultrasound, from 5% in the placebo group to 2.8%, a relative risk reduction of 45% (p=0.0015). The authors concluded the use of dalteparin reduced the incidence of VTE without increased risk of bleeding.13 Dalteparin is FDA approved for VTE prophylaxis in medical inpatients.
At least two meta-analyses have evaluated LMWHs compared with UFH. In the first, nine trials comparing LMWH to UFH (4,669 patients) were included. No significant effect was observed on DVT, clinical PE, or mortality. However, LMWH reduced the risk of major hemorrhage by 52% (p=0.049).14
In a more recent meta-analysis, 36 studies were included comparing placebos with UFH and LMWH. Both agents were associated with a reduced risk of VTE. A UFH dosage of 5,000 units three times daily was more effective in preventing DVT than a dosage of 5,000 units twice daily when compared with the control (risk ratio [RR], 0.27; 95% confidence interval [CI], 0.20-0.36; vs. RR, 0.52; 95% CI, 0.28-0.96). Neither UFH nor LMWH reduced mortality. When directly compared with UFH, LMWH was associated with a lower risk of DVT (RR, 0.68; 95% CI, 0.52-0.88) and injection-site hematoma (RR, 0.47; 95% CI, 0.36-0.62), but no difference was seen between the two agents in the risk of bleeding or thrombocytopenia.
This contemporary meta-analysis clearly illustrates that UFH and LMWH reduce VTE risk in hospitalized medical patients, but neither agent alters mortality. When directly compared, LMWH is more effective in preventing DVT.15
Despite the higher drug acquisition costs, LMWHs are more cost-effective than UFH for prophylaxis in medical patients because of their lower complication rates of HIT. LMWH reduces incremental costs by $13.88 per day compared with UFH.16, 17
Synthetic pentasaccharide: Fondaparinux is a synthetic analogue of the unique pentasaccharide sequence that mediates the interaction of heparin with antithrombin. It inhibits both free and platelet-bound factor Xa. It binds antithrombin with high affinity, has close to 100% bioavailability, and has a plasma half-life of 17 hours that permits once-daily administration.
The drug is excreted unchanged in the urine and therefore contraindicated in patients with severe renal impairment (e.g., creatinine clearance less than 30 mL/min). It does not bind PF4 in vitro and thus should not cause HIT.
Fondaparinux has been evaluated in medical inpatients in a randomized placebo controlled trial, ARTEMIS. Fondaparinux 2.5 mg SC once daily decreased the rate of venographically-confirmed DVT from 10.5% to 5.6% (p=0.029); there was also a decrease in fatal PE from 1.7% to 0.7% (p=0.029). A reduction in overall mortality from 6% to 3.3% (P=NS) was observed. Major bleeding occurred in 0.2% of patients in both groups. The drug is not FDA approved to prevent VTE in medical inpatients.18
Duration of therapy: Most clinical trials have used prophylaxis for seven to 14 days. The Extended Clinical Prophylaxis in Acutely Ill Medical Patients (EXCLAIM) trial evaluated duration of therapy, the results of which were presented recently at the 21st Congress of the International Society on Thrombosis and Haemostasis (ISTH).
Of the 5,105 patients who met inclusion criteria, 5,049, or 99%, received open-label prophylaxis with enoxaparin (10 ± four days); 2,013 patients subsequently received extended-duration enoxaparin; and 2,027 received placebo (each for 28 ± four days). Subjects were at least 40 years old, had been recently immobilized (for at least 3 days) and had a predefined acute medical illness. Mobility was defined as level 1 (total bed rest or sedentary) or level 2 (bathroom privileges). After a planned blinded interim analysis, the trial’s data safety monitoring board recommended an amendment to the inclusion criteria, changing level 2 mobility to include age >75 years, and/or prior VTE, and/or diagnosed cancer.
When compared with placebo, extended-duration enoxaparin following the open-label, standard-duration enoxaparin reduced the relative risk of VTE by 44% (2.8% vs. 4.9%; p=0.0011). There was major bleeding in 12 subjects who received extended-duration enoxaparin and three subjects receiving placebo (0.6% vs. 0.1%; p=0.0192).
There was no difference in all-cause mortality between the extended-duration enoxaparin and placebo groups at six months (10.1% vs. 8.9%, p=0.179). The authors concluded 38 days of enoxaparin 40 mg SC once daily significantly reduced the overall incidence of VTE compared with a 10-day regimen in acutely ill medical patients with reduced mobility. This reduction in overall risk for VTE was consistent with a reduction in risk for asymptomatic proximal DVT and symptomatic VTE.
Based on this trial, we would recommend five weeks of prophylaxis for those older than 75 years with prior history of VTE or with active cancer. In the absence of these criteria, we recommend up to 14 days of therapy.
For many patients, this will mean prophylaxis after discharge from the hospital. While this represents a change in practice for many and may significantly complicate some discharge care plans we believe the significant burden of post-hospital VTE mandates a more aggressive approach to peri-hospitalization prophylaxis.
Back to the Case
Our patient has acute decompensated heart failure and likely will be limited in his ability to ambulate. All the clinical trials discussed above included similar patients and support the use of pharmacological prophylaxis. All hospitalized medical patients should undergo VTE risk assessment and implementation of pharmacologic prophylaxis in the absence of contraindications. TH
Dr. Lenchus is an assistant professor of medicine at the University of Miami School of Medicine. Dr. Jaffer is an associate professor of medicine at the University of Miami School of Medicine, where he serves as the chief of the division of hospital medicine.
References
- Hirsh J, Hoak J. Management of deep vein thrombosis and pulmonary embolism. A statement for healthcare professionals. Council on Thrombosis (in consultation with the Council on Cardiovascular Radiology), American Heart Association. Circulation. 1996 Jun 15;93(12):2212-2245.
- Spencer FA, Lessard D, Emery C, Reed G, Goldberg RJ. Venous thromboembolism in the outpatient setting. Arch Intern Med. 2007 Jul 23;167(14):1471-1475.
- Goldhaber SZ, Tapson VF. A prospective registry of 5,451 patients with ultrasound-confirmed deep vein thrombosis. Am J Cardiol. 2004 Jan 15;93(2):259-262.
- Tapson VF, Decousus H, Pini M, et al. Venous thromboembolism prophylaxis in acutely ill hospitalized medical patients: findings from the International Medical Prevention Registry on Venous Thromboembolism. Chest. Sep 2007;132(3):936-945.
- Anderson FA, Jr., Spencer FA. Risk factors for venous thromboembolism. Circulation. 2003 Jun 17;107(23 Suppl 1):I9-16.
- Dentali F, Douketis JD, Gianni M, Lim W, Crowther MA. Meta-analysis: anticoagulant prophylaxis to prevent symptomatic venous thromboembolism in hospitalized medical patients. Ann Intern Med. 2007 Feb 20;146(4):278-288.
- Geerts WH, Pineo GF, Heit JA, et al. Prevention of venous thromboembolism: the Seventh ACCP Conference on Antithrombotic and Thrombolytic Therapy. Chest. 2004 Sep;126(3 Suppl):338S-400S.
- Hirsh J, Raschke R. Heparin and low-molecular-weight heparin: the Seventh ACCP Conference on Antithrombotic and Thrombolytic Therapy. Chest. 2004 Sep;126(3 Suppl):188S-203S.
- Cade JF, Andrews JT, Stubbs AE. Comparison of sodium and calcium heparin in prevention of venous thromboembolism. Aust N Z J Med. 1982 Oct;12(5):501-504.
- Gallus AS, Hirsh J, Tutle RJ, et al. Small subcutaneous doses of heparin in prevention of venous thrombosis. N Engl J Med. 1973 Mar 15;288(11):545-551.
- Belch JJ, Lowe GD, Ward AG, Forbes CD, Prentice CR. Prevention of deep vein thrombosis in medical patients by low-dose heparin. Scott Med J. 1981 Apr;26(2):115-117.
- Samama MM, Cohen AT, Darmon JY, et al. A comparison of enoxaparin with placebo for the prevention of venous thromboembolism in acutely ill medical patients. Prophylaxis in Medical Patients with Enoxaparin Study Group. N Engl J Med. 1999 Sep 9;341(11):793-800.
- Leizorovicz A, Cohen AT, Turpie AG, Olsson CG, Vaitkus PT, Goldhaber SZ. Randomized, placebo-controlled trial of dalteparin for the prevention of venous thromboembolism in acutely ill medical patients. Circulation. 2004 Aug 17;110(7):874-879.
- Mismetti P, Laporte-Simitsidis S, Tardy B, et al. Prevention of venous thromboembolism in internal medicine with unfractionated or low-molecular-weight heparins: a meta-analysis of randomised clinical trials. Thromb Haemost. Jan 2000;83(1):14-19.
- Wein L, Wein S, Haas SJ, Shaw J, Krum H. Pharmacological venous thromboembolism prophylaxis in hospitalized medical patients: a meta-analysis of randomized controlled trials. Arch Intern Med. 2007 Jul 23;167(14):1476-1486.
- McGarry LJ, Thompson D, Weinstein MC, Goldhaber SZ. Cost effectiveness of thromboprophylaxis with a low-molecular-weight heparin versus unfractionated heparin in acutely ill medical inpatients. Am J Manag Care. 2004 Sep;10(9):632-642.
- Creekmore FM, Oderda GM, Pendleton RC, Brixner DI. Incidence and economic implications of heparin-induced thrombocytopenia in medical patients receiving prophylaxis for venous thromboembolism. Pharmacotherapy. 2006 Oct;26(10):1438-1445.
- Cohen AT, Davidson BL, Gallus AS, et al. Efficacy and safety of fondaparinux for the prevention of venous thromboembolism in older acute medical patients: randomised placebo controlled trial. BMJ. 2006 Feb 11;332(7537):325-329.
Case
A 76-year-old gentleman is admitted for progressively worsening dyspnea, cough, and bilateral leg edema. Upon admission, his blood pressure is 150/90 mm/Hg, pulse 90 beats per minute, and respiration is 24 per minute.
Pertinent physical findings include jugular venous distension, bilateral crackles, S3 gallop, and 2+ bilateral lower extremity edema. The chest radiograph shows cardiomegaly and pulmonary edema. He is admitted to the hospital with a diagnosis of acute decompensated heart failure and starts aggressive medical therapy.
Overview
Approximately 2 million cases of deep-vein thrombosis (DVT) occur annually in the United States. Based on studies utilizing ventilation-perfusion scanning, half these patients likely have a silent pulmonary embolism (PE); of these, approximately 250,000 die.
The spectrum of venous thromboembolism (VTE), which includes DVT and PE, can vary from being asymptomatic to sudden death. Autopsy studies suggest a leading cause of sudden death in hospitalized medical patients is often a PE. There also are sequelae, such as chronic pulmonary hypertension, occurring in approximately 5% of PE cases, and post-thrombotic syndrome, occurring in approximately 40% of patients with DVT at two years.1
A recent study suggests DVT occurs three times more commonly in the outpatient setting. However, more than half of these patients were hospitalized in the three months prior.2 This is likely due to inadequate in-hospital prevention because of absence of prophylaxis, use of an unsuitable modality, insufficient dose of the drug, or ineffective duration of therapy. Inadequate and omitted VTE prophylaxis for medical patients was clearly demonstrated in the DVT Free Registry. This registry was created by 183 U.S. hospitals and included 5,451 patients, inpatients, and outpatients with ultrasound-confirmed DVT.
The number of medical inpatients who received prophylaxis in the 30 days prior to diagnosis was 28%—lower than the 48% of surgical patients.3 In a recent international registry, IMPROVE, only approximately 50% of hospitalized patients received prophylaxis.4
Virchow’s triad describes three underlying etiologic factors for thrombosis: stasis of blood flow, endothelial injury, and hypercoagulability. Established VTE risk factors reflect these underlying pathophysiologic processes. Important risk factors for VTE include increasing age, prolonged immobility, malignancy, major surgery, multiple trauma, prior VTE, and chronic heart failure.5
However, the magnitude of risk conferred by these and other risk factors varies (see Table 1, p. 35). It is not known how these factors interact to determine a patient’s individual VTE risk, but there is evidence it increases in proportion to the number of predisposing factors present.
In a recent systematic review of nine studies, including approximately 20,000 patients, prophylaxis reduced the rate of symptomatic VTE in at-risk hospitalized medical patients without increasing major bleeding.6
Multiple healthcare organizations, such as the National Quality Forum (NQF), Joint Commission on Accreditation of Healthcare Organizations (JCAHO), and Agency for Healthcare Research and Quality (AHRQ) have identified VTE as a preventable condition in hospitalized patients. Formal risk assessment must be conducted as a first step, followed by the initiation of timely prophylaxis to improve patient safety.
Review of the Data
Mechanical forms of prophylaxis, such as graduated compression stockings, have been evaluated in patients with stroke and myocardial infarction. Intermittent pneumatic compression stockings and venous foot pumps have not been studied in randomized controlled trials (RCTs) in general medical patients.
Although there is data supporting the efficacy of these devices in surgical patients, the American College of Chest Physicians’ (ACCP) guidelines recommend against the use of mechanical forms of prophylaxis in medical patients unless there is a contraindication to pharmacologic prophylaxis.7
The ideal prophylactic agent is cost-effective and has no side effects. Available pharmacologic options for prevention of VTE in medical patients include unfractionated heparin (UFH), low molecular weight heparins (LMWHs), and the synthetic pentasaccharide, fondaparinux. Oral anticoagulants, (e.g., vitamin K antagonists [VKA]), have not been adequately studied in medical inpatients. Since VKA take several days to achieve therapeutic anticoagulation, we do not recommend using them de novo as VTE prophylaxis.
However, patients taking an oral VKA in the outpatient setting who have a therapeutic international normalized ratio (INR) during hospitalization probably are adequately protected from VTE and do not need additional pharmacologic prophylaxis. Newer anticoagulants in phase III testing for prevention of VTE in medically ill patients include oral direct thrombin inhibitors and anti-Xa inhibitors. ACCP guidelines recommend either low-dose UFH or LMWH as first-line agents for VTE prevention in medical inpatients.
Unfractionated heparin: UFH is a heterogeneous mixture of repeating polysaccharide chains of varying sizes, averaging about 15,000 Daltons. It binds anti-thrombin III (AT-III) and facilitates AT-III-mediated inactivation of factors IIa, IXa, Xa, and XIIa; of these, IIa and Xa are most responsive to inhibition.
Due to its large size, UFH only is partially absorbed from subcutaneous (SC) tissue, and it has a variable anticoagulant response due to interactions with plasma proteins, macrophages, and endothelial cells.8 However, in prophylactic SC doses (5,000 units two or three times daily), monitoring of the activated partial thromboplastin time (aPTT) is not required. In some cases, (e.g., frail or elderly patients), prophylactic SC doses may slightly prolong the aPTT.
UFH also binds to platelets and platelet factor 4 (PF4), and may precipitate heparin-induced thrombocytopenia (HIT). At least three clinical trials have compared the efficacy of SC UFH with a placebo and found prophylactic doses of UFH decrease the relative risk of DVT as detected by fibrinogen uptake test by about 70% without increasing the risk of bleeding.9-11
Low molecular weight heparins: LMWHs are derived from UFH through a chemical depolymerization, or fractionation, process. They are about one-third the size of UFH, with a molecular weight of approximately 5,000 Daltons.
These smaller molecules are readily absorbed from the SC tissue, eliciting a more predictable anticoagulant response than UFH. Unlike UFH, LMWHs have only minimal nonspecific binding to plasma proteins, endothelial cells, and monocytes, resulting in a predictable dose response. This obviates the need for lab monitoring, even when used in full, therapeutic dosing.
Compared with UFH, these agents have a longer plasma half-life, allowing them to be dosed SC once or twice daily. Also, they don’t bind platelets as readily as UFH resulting in a lower risk of HIT. Because they’re smaller, LMWHs tend to preferentially inhibit factor Xa, whereas UFH tends to inhibit factors Xa and IIa equally.
LMWHs have been evaluated in two large, placebo-controlled clinical trials for the prevention of VTE in medical inpatients.
In the first trial, MEDENOX, almost half the patients were older than 75 (mean age approximately 73). Inclusion criteria were NYHA class 3 or 4 heart failure, acute respiratory failure without mechanical ventilation, acute infection without septic shock, acute rheumatic disease, or inflammatory bowel disease. The primary outcome was assessed in 866 patients. Enoxaparin 40 mg SC once daily decreased the rate of VTE by two-thirds, from 15% to 5% (p=0.0002), without increased bleeding or thrombocytopenia compared with placebo.12 Enoxaparin 40 mg SC once daily is approved by the Food and Drug Administration (FDA) for VTE prophylaxis in medically ill patients.
PREVENT was an international, multicenter, randomized, double-blind, placebo-controlled trial evaluating dalteparin’s efficacy and safety. The inclusion criteria in this trial were acute congestive heart failure, non-ventilator-requiring acute respiratory failure, infection without septic shock, acute rheumatologic disorders, or inflammatory bowel disease. It studied 2,991 patients, and the primary outcome was VTE incidence and sudden death at day 21.
Dalteparin at 5,000 units decreased the rate of VTE, as detected by compression ultrasound, from 5% in the placebo group to 2.8%, a relative risk reduction of 45% (p=0.0015). The authors concluded the use of dalteparin reduced the incidence of VTE without increased risk of bleeding.13 Dalteparin is FDA approved for VTE prophylaxis in medical inpatients.
At least two meta-analyses have evaluated LMWHs compared with UFH. In the first, nine trials comparing LMWH to UFH (4,669 patients) were included. No significant effect was observed on DVT, clinical PE, or mortality. However, LMWH reduced the risk of major hemorrhage by 52% (p=0.049).14
In a more recent meta-analysis, 36 studies were included comparing placebos with UFH and LMWH. Both agents were associated with a reduced risk of VTE. A UFH dosage of 5,000 units three times daily was more effective in preventing DVT than a dosage of 5,000 units twice daily when compared with the control (risk ratio [RR], 0.27; 95% confidence interval [CI], 0.20-0.36; vs. RR, 0.52; 95% CI, 0.28-0.96). Neither UFH nor LMWH reduced mortality. When directly compared with UFH, LMWH was associated with a lower risk of DVT (RR, 0.68; 95% CI, 0.52-0.88) and injection-site hematoma (RR, 0.47; 95% CI, 0.36-0.62), but no difference was seen between the two agents in the risk of bleeding or thrombocytopenia.
This contemporary meta-analysis clearly illustrates that UFH and LMWH reduce VTE risk in hospitalized medical patients, but neither agent alters mortality. When directly compared, LMWH is more effective in preventing DVT.15
Despite the higher drug acquisition costs, LMWHs are more cost-effective than UFH for prophylaxis in medical patients because of their lower complication rates of HIT. LMWH reduces incremental costs by $13.88 per day compared with UFH.16, 17
Synthetic pentasaccharide: Fondaparinux is a synthetic analogue of the unique pentasaccharide sequence that mediates the interaction of heparin with antithrombin. It inhibits both free and platelet-bound factor Xa. It binds antithrombin with high affinity, has close to 100% bioavailability, and has a plasma half-life of 17 hours that permits once-daily administration.
The drug is excreted unchanged in the urine and therefore contraindicated in patients with severe renal impairment (e.g., creatinine clearance less than 30 mL/min). It does not bind PF4 in vitro and thus should not cause HIT.
Fondaparinux has been evaluated in medical inpatients in a randomized placebo controlled trial, ARTEMIS. Fondaparinux 2.5 mg SC once daily decreased the rate of venographically-confirmed DVT from 10.5% to 5.6% (p=0.029); there was also a decrease in fatal PE from 1.7% to 0.7% (p=0.029). A reduction in overall mortality from 6% to 3.3% (P=NS) was observed. Major bleeding occurred in 0.2% of patients in both groups. The drug is not FDA approved to prevent VTE in medical inpatients.18
Duration of therapy: Most clinical trials have used prophylaxis for seven to 14 days. The Extended Clinical Prophylaxis in Acutely Ill Medical Patients (EXCLAIM) trial evaluated duration of therapy, the results of which were presented recently at the 21st Congress of the International Society on Thrombosis and Haemostasis (ISTH).
Of the 5,105 patients who met inclusion criteria, 5,049, or 99%, received open-label prophylaxis with enoxaparin (10 ± four days); 2,013 patients subsequently received extended-duration enoxaparin; and 2,027 received placebo (each for 28 ± four days). Subjects were at least 40 years old, had been recently immobilized (for at least 3 days) and had a predefined acute medical illness. Mobility was defined as level 1 (total bed rest or sedentary) or level 2 (bathroom privileges). After a planned blinded interim analysis, the trial’s data safety monitoring board recommended an amendment to the inclusion criteria, changing level 2 mobility to include age >75 years, and/or prior VTE, and/or diagnosed cancer.
When compared with placebo, extended-duration enoxaparin following the open-label, standard-duration enoxaparin reduced the relative risk of VTE by 44% (2.8% vs. 4.9%; p=0.0011). There was major bleeding in 12 subjects who received extended-duration enoxaparin and three subjects receiving placebo (0.6% vs. 0.1%; p=0.0192).
There was no difference in all-cause mortality between the extended-duration enoxaparin and placebo groups at six months (10.1% vs. 8.9%, p=0.179). The authors concluded 38 days of enoxaparin 40 mg SC once daily significantly reduced the overall incidence of VTE compared with a 10-day regimen in acutely ill medical patients with reduced mobility. This reduction in overall risk for VTE was consistent with a reduction in risk for asymptomatic proximal DVT and symptomatic VTE.
Based on this trial, we would recommend five weeks of prophylaxis for those older than 75 years with prior history of VTE or with active cancer. In the absence of these criteria, we recommend up to 14 days of therapy.
For many patients, this will mean prophylaxis after discharge from the hospital. While this represents a change in practice for many and may significantly complicate some discharge care plans we believe the significant burden of post-hospital VTE mandates a more aggressive approach to peri-hospitalization prophylaxis.
Back to the Case
Our patient has acute decompensated heart failure and likely will be limited in his ability to ambulate. All the clinical trials discussed above included similar patients and support the use of pharmacological prophylaxis. All hospitalized medical patients should undergo VTE risk assessment and implementation of pharmacologic prophylaxis in the absence of contraindications. TH
Dr. Lenchus is an assistant professor of medicine at the University of Miami School of Medicine. Dr. Jaffer is an associate professor of medicine at the University of Miami School of Medicine, where he serves as the chief of the division of hospital medicine.
References
- Hirsh J, Hoak J. Management of deep vein thrombosis and pulmonary embolism. A statement for healthcare professionals. Council on Thrombosis (in consultation with the Council on Cardiovascular Radiology), American Heart Association. Circulation. 1996 Jun 15;93(12):2212-2245.
- Spencer FA, Lessard D, Emery C, Reed G, Goldberg RJ. Venous thromboembolism in the outpatient setting. Arch Intern Med. 2007 Jul 23;167(14):1471-1475.
- Goldhaber SZ, Tapson VF. A prospective registry of 5,451 patients with ultrasound-confirmed deep vein thrombosis. Am J Cardiol. 2004 Jan 15;93(2):259-262.
- Tapson VF, Decousus H, Pini M, et al. Venous thromboembolism prophylaxis in acutely ill hospitalized medical patients: findings from the International Medical Prevention Registry on Venous Thromboembolism. Chest. Sep 2007;132(3):936-945.
- Anderson FA, Jr., Spencer FA. Risk factors for venous thromboembolism. Circulation. 2003 Jun 17;107(23 Suppl 1):I9-16.
- Dentali F, Douketis JD, Gianni M, Lim W, Crowther MA. Meta-analysis: anticoagulant prophylaxis to prevent symptomatic venous thromboembolism in hospitalized medical patients. Ann Intern Med. 2007 Feb 20;146(4):278-288.
- Geerts WH, Pineo GF, Heit JA, et al. Prevention of venous thromboembolism: the Seventh ACCP Conference on Antithrombotic and Thrombolytic Therapy. Chest. 2004 Sep;126(3 Suppl):338S-400S.
- Hirsh J, Raschke R. Heparin and low-molecular-weight heparin: the Seventh ACCP Conference on Antithrombotic and Thrombolytic Therapy. Chest. 2004 Sep;126(3 Suppl):188S-203S.
- Cade JF, Andrews JT, Stubbs AE. Comparison of sodium and calcium heparin in prevention of venous thromboembolism. Aust N Z J Med. 1982 Oct;12(5):501-504.
- Gallus AS, Hirsh J, Tutle RJ, et al. Small subcutaneous doses of heparin in prevention of venous thrombosis. N Engl J Med. 1973 Mar 15;288(11):545-551.
- Belch JJ, Lowe GD, Ward AG, Forbes CD, Prentice CR. Prevention of deep vein thrombosis in medical patients by low-dose heparin. Scott Med J. 1981 Apr;26(2):115-117.
- Samama MM, Cohen AT, Darmon JY, et al. A comparison of enoxaparin with placebo for the prevention of venous thromboembolism in acutely ill medical patients. Prophylaxis in Medical Patients with Enoxaparin Study Group. N Engl J Med. 1999 Sep 9;341(11):793-800.
- Leizorovicz A, Cohen AT, Turpie AG, Olsson CG, Vaitkus PT, Goldhaber SZ. Randomized, placebo-controlled trial of dalteparin for the prevention of venous thromboembolism in acutely ill medical patients. Circulation. 2004 Aug 17;110(7):874-879.
- Mismetti P, Laporte-Simitsidis S, Tardy B, et al. Prevention of venous thromboembolism in internal medicine with unfractionated or low-molecular-weight heparins: a meta-analysis of randomised clinical trials. Thromb Haemost. Jan 2000;83(1):14-19.
- Wein L, Wein S, Haas SJ, Shaw J, Krum H. Pharmacological venous thromboembolism prophylaxis in hospitalized medical patients: a meta-analysis of randomized controlled trials. Arch Intern Med. 2007 Jul 23;167(14):1476-1486.
- McGarry LJ, Thompson D, Weinstein MC, Goldhaber SZ. Cost effectiveness of thromboprophylaxis with a low-molecular-weight heparin versus unfractionated heparin in acutely ill medical inpatients. Am J Manag Care. 2004 Sep;10(9):632-642.
- Creekmore FM, Oderda GM, Pendleton RC, Brixner DI. Incidence and economic implications of heparin-induced thrombocytopenia in medical patients receiving prophylaxis for venous thromboembolism. Pharmacotherapy. 2006 Oct;26(10):1438-1445.
- Cohen AT, Davidson BL, Gallus AS, et al. Efficacy and safety of fondaparinux for the prevention of venous thromboembolism in older acute medical patients: randomised placebo controlled trial. BMJ. 2006 Feb 11;332(7537):325-329.
Case
A 76-year-old gentleman is admitted for progressively worsening dyspnea, cough, and bilateral leg edema. Upon admission, his blood pressure is 150/90 mm/Hg, pulse 90 beats per minute, and respiration is 24 per minute.
Pertinent physical findings include jugular venous distension, bilateral crackles, S3 gallop, and 2+ bilateral lower extremity edema. The chest radiograph shows cardiomegaly and pulmonary edema. He is admitted to the hospital with a diagnosis of acute decompensated heart failure and starts aggressive medical therapy.
Overview
Approximately 2 million cases of deep-vein thrombosis (DVT) occur annually in the United States. Based on studies utilizing ventilation-perfusion scanning, half these patients likely have a silent pulmonary embolism (PE); of these, approximately 250,000 die.
The spectrum of venous thromboembolism (VTE), which includes DVT and PE, can vary from being asymptomatic to sudden death. Autopsy studies suggest a leading cause of sudden death in hospitalized medical patients is often a PE. There also are sequelae, such as chronic pulmonary hypertension, occurring in approximately 5% of PE cases, and post-thrombotic syndrome, occurring in approximately 40% of patients with DVT at two years.1
A recent study suggests DVT occurs three times more commonly in the outpatient setting. However, more than half of these patients were hospitalized in the three months prior.2 This is likely due to inadequate in-hospital prevention because of absence of prophylaxis, use of an unsuitable modality, insufficient dose of the drug, or ineffective duration of therapy. Inadequate and omitted VTE prophylaxis for medical patients was clearly demonstrated in the DVT Free Registry. This registry was created by 183 U.S. hospitals and included 5,451 patients, inpatients, and outpatients with ultrasound-confirmed DVT.
The number of medical inpatients who received prophylaxis in the 30 days prior to diagnosis was 28%—lower than the 48% of surgical patients.3 In a recent international registry, IMPROVE, only approximately 50% of hospitalized patients received prophylaxis.4
Virchow’s triad describes three underlying etiologic factors for thrombosis: stasis of blood flow, endothelial injury, and hypercoagulability. Established VTE risk factors reflect these underlying pathophysiologic processes. Important risk factors for VTE include increasing age, prolonged immobility, malignancy, major surgery, multiple trauma, prior VTE, and chronic heart failure.5
However, the magnitude of risk conferred by these and other risk factors varies (see Table 1, p. 35). It is not known how these factors interact to determine a patient’s individual VTE risk, but there is evidence it increases in proportion to the number of predisposing factors present.
In a recent systematic review of nine studies, including approximately 20,000 patients, prophylaxis reduced the rate of symptomatic VTE in at-risk hospitalized medical patients without increasing major bleeding.6
Multiple healthcare organizations, such as the National Quality Forum (NQF), Joint Commission on Accreditation of Healthcare Organizations (JCAHO), and Agency for Healthcare Research and Quality (AHRQ) have identified VTE as a preventable condition in hospitalized patients. Formal risk assessment must be conducted as a first step, followed by the initiation of timely prophylaxis to improve patient safety.
Review of the Data
Mechanical forms of prophylaxis, such as graduated compression stockings, have been evaluated in patients with stroke and myocardial infarction. Intermittent pneumatic compression stockings and venous foot pumps have not been studied in randomized controlled trials (RCTs) in general medical patients.
Although there is data supporting the efficacy of these devices in surgical patients, the American College of Chest Physicians’ (ACCP) guidelines recommend against the use of mechanical forms of prophylaxis in medical patients unless there is a contraindication to pharmacologic prophylaxis.7
The ideal prophylactic agent is cost-effective and has no side effects. Available pharmacologic options for prevention of VTE in medical patients include unfractionated heparin (UFH), low molecular weight heparins (LMWHs), and the synthetic pentasaccharide, fondaparinux. Oral anticoagulants, (e.g., vitamin K antagonists [VKA]), have not been adequately studied in medical inpatients. Since VKA take several days to achieve therapeutic anticoagulation, we do not recommend using them de novo as VTE prophylaxis.
However, patients taking an oral VKA in the outpatient setting who have a therapeutic international normalized ratio (INR) during hospitalization probably are adequately protected from VTE and do not need additional pharmacologic prophylaxis. Newer anticoagulants in phase III testing for prevention of VTE in medically ill patients include oral direct thrombin inhibitors and anti-Xa inhibitors. ACCP guidelines recommend either low-dose UFH or LMWH as first-line agents for VTE prevention in medical inpatients.
Unfractionated heparin: UFH is a heterogeneous mixture of repeating polysaccharide chains of varying sizes, averaging about 15,000 Daltons. It binds anti-thrombin III (AT-III) and facilitates AT-III-mediated inactivation of factors IIa, IXa, Xa, and XIIa; of these, IIa and Xa are most responsive to inhibition.
Due to its large size, UFH only is partially absorbed from subcutaneous (SC) tissue, and it has a variable anticoagulant response due to interactions with plasma proteins, macrophages, and endothelial cells.8 However, in prophylactic SC doses (5,000 units two or three times daily), monitoring of the activated partial thromboplastin time (aPTT) is not required. In some cases, (e.g., frail or elderly patients), prophylactic SC doses may slightly prolong the aPTT.
UFH also binds to platelets and platelet factor 4 (PF4), and may precipitate heparin-induced thrombocytopenia (HIT). At least three clinical trials have compared the efficacy of SC UFH with a placebo and found prophylactic doses of UFH decrease the relative risk of DVT as detected by fibrinogen uptake test by about 70% without increasing the risk of bleeding.9-11
Low molecular weight heparins: LMWHs are derived from UFH through a chemical depolymerization, or fractionation, process. They are about one-third the size of UFH, with a molecular weight of approximately 5,000 Daltons.
These smaller molecules are readily absorbed from the SC tissue, eliciting a more predictable anticoagulant response than UFH. Unlike UFH, LMWHs have only minimal nonspecific binding to plasma proteins, endothelial cells, and monocytes, resulting in a predictable dose response. This obviates the need for lab monitoring, even when used in full, therapeutic dosing.
Compared with UFH, these agents have a longer plasma half-life, allowing them to be dosed SC once or twice daily. Also, they don’t bind platelets as readily as UFH resulting in a lower risk of HIT. Because they’re smaller, LMWHs tend to preferentially inhibit factor Xa, whereas UFH tends to inhibit factors Xa and IIa equally.
LMWHs have been evaluated in two large, placebo-controlled clinical trials for the prevention of VTE in medical inpatients.
In the first trial, MEDENOX, almost half the patients were older than 75 (mean age approximately 73). Inclusion criteria were NYHA class 3 or 4 heart failure, acute respiratory failure without mechanical ventilation, acute infection without septic shock, acute rheumatic disease, or inflammatory bowel disease. The primary outcome was assessed in 866 patients. Enoxaparin 40 mg SC once daily decreased the rate of VTE by two-thirds, from 15% to 5% (p=0.0002), without increased bleeding or thrombocytopenia compared with placebo.12 Enoxaparin 40 mg SC once daily is approved by the Food and Drug Administration (FDA) for VTE prophylaxis in medically ill patients.
PREVENT was an international, multicenter, randomized, double-blind, placebo-controlled trial evaluating dalteparin’s efficacy and safety. The inclusion criteria in this trial were acute congestive heart failure, non-ventilator-requiring acute respiratory failure, infection without septic shock, acute rheumatologic disorders, or inflammatory bowel disease. It studied 2,991 patients, and the primary outcome was VTE incidence and sudden death at day 21.
Dalteparin at 5,000 units decreased the rate of VTE, as detected by compression ultrasound, from 5% in the placebo group to 2.8%, a relative risk reduction of 45% (p=0.0015). The authors concluded the use of dalteparin reduced the incidence of VTE without increased risk of bleeding.13 Dalteparin is FDA approved for VTE prophylaxis in medical inpatients.
At least two meta-analyses have evaluated LMWHs compared with UFH. In the first, nine trials comparing LMWH to UFH (4,669 patients) were included. No significant effect was observed on DVT, clinical PE, or mortality. However, LMWH reduced the risk of major hemorrhage by 52% (p=0.049).14
In a more recent meta-analysis, 36 studies were included comparing placebos with UFH and LMWH. Both agents were associated with a reduced risk of VTE. A UFH dosage of 5,000 units three times daily was more effective in preventing DVT than a dosage of 5,000 units twice daily when compared with the control (risk ratio [RR], 0.27; 95% confidence interval [CI], 0.20-0.36; vs. RR, 0.52; 95% CI, 0.28-0.96). Neither UFH nor LMWH reduced mortality. When directly compared with UFH, LMWH was associated with a lower risk of DVT (RR, 0.68; 95% CI, 0.52-0.88) and injection-site hematoma (RR, 0.47; 95% CI, 0.36-0.62), but no difference was seen between the two agents in the risk of bleeding or thrombocytopenia.
This contemporary meta-analysis clearly illustrates that UFH and LMWH reduce VTE risk in hospitalized medical patients, but neither agent alters mortality. When directly compared, LMWH is more effective in preventing DVT.15
Despite the higher drug acquisition costs, LMWHs are more cost-effective than UFH for prophylaxis in medical patients because of their lower complication rates of HIT. LMWH reduces incremental costs by $13.88 per day compared with UFH.16, 17
Synthetic pentasaccharide: Fondaparinux is a synthetic analogue of the unique pentasaccharide sequence that mediates the interaction of heparin with antithrombin. It inhibits both free and platelet-bound factor Xa. It binds antithrombin with high affinity, has close to 100% bioavailability, and has a plasma half-life of 17 hours that permits once-daily administration.
The drug is excreted unchanged in the urine and therefore contraindicated in patients with severe renal impairment (e.g., creatinine clearance less than 30 mL/min). It does not bind PF4 in vitro and thus should not cause HIT.
Fondaparinux has been evaluated in medical inpatients in a randomized placebo controlled trial, ARTEMIS. Fondaparinux 2.5 mg SC once daily decreased the rate of venographically-confirmed DVT from 10.5% to 5.6% (p=0.029); there was also a decrease in fatal PE from 1.7% to 0.7% (p=0.029). A reduction in overall mortality from 6% to 3.3% (P=NS) was observed. Major bleeding occurred in 0.2% of patients in both groups. The drug is not FDA approved to prevent VTE in medical inpatients.18
Duration of therapy: Most clinical trials have used prophylaxis for seven to 14 days. The Extended Clinical Prophylaxis in Acutely Ill Medical Patients (EXCLAIM) trial evaluated duration of therapy, the results of which were presented recently at the 21st Congress of the International Society on Thrombosis and Haemostasis (ISTH).
Of the 5,105 patients who met inclusion criteria, 5,049, or 99%, received open-label prophylaxis with enoxaparin (10 ± four days); 2,013 patients subsequently received extended-duration enoxaparin; and 2,027 received placebo (each for 28 ± four days). Subjects were at least 40 years old, had been recently immobilized (for at least 3 days) and had a predefined acute medical illness. Mobility was defined as level 1 (total bed rest or sedentary) or level 2 (bathroom privileges). After a planned blinded interim analysis, the trial’s data safety monitoring board recommended an amendment to the inclusion criteria, changing level 2 mobility to include age >75 years, and/or prior VTE, and/or diagnosed cancer.
When compared with placebo, extended-duration enoxaparin following the open-label, standard-duration enoxaparin reduced the relative risk of VTE by 44% (2.8% vs. 4.9%; p=0.0011). There was major bleeding in 12 subjects who received extended-duration enoxaparin and three subjects receiving placebo (0.6% vs. 0.1%; p=0.0192).
There was no difference in all-cause mortality between the extended-duration enoxaparin and placebo groups at six months (10.1% vs. 8.9%, p=0.179). The authors concluded 38 days of enoxaparin 40 mg SC once daily significantly reduced the overall incidence of VTE compared with a 10-day regimen in acutely ill medical patients with reduced mobility. This reduction in overall risk for VTE was consistent with a reduction in risk for asymptomatic proximal DVT and symptomatic VTE.
Based on this trial, we would recommend five weeks of prophylaxis for those older than 75 years with prior history of VTE or with active cancer. In the absence of these criteria, we recommend up to 14 days of therapy.
For many patients, this will mean prophylaxis after discharge from the hospital. While this represents a change in practice for many and may significantly complicate some discharge care plans we believe the significant burden of post-hospital VTE mandates a more aggressive approach to peri-hospitalization prophylaxis.
Back to the Case
Our patient has acute decompensated heart failure and likely will be limited in his ability to ambulate. All the clinical trials discussed above included similar patients and support the use of pharmacological prophylaxis. All hospitalized medical patients should undergo VTE risk assessment and implementation of pharmacologic prophylaxis in the absence of contraindications. TH
Dr. Lenchus is an assistant professor of medicine at the University of Miami School of Medicine. Dr. Jaffer is an associate professor of medicine at the University of Miami School of Medicine, where he serves as the chief of the division of hospital medicine.
References
- Hirsh J, Hoak J. Management of deep vein thrombosis and pulmonary embolism. A statement for healthcare professionals. Council on Thrombosis (in consultation with the Council on Cardiovascular Radiology), American Heart Association. Circulation. 1996 Jun 15;93(12):2212-2245.
- Spencer FA, Lessard D, Emery C, Reed G, Goldberg RJ. Venous thromboembolism in the outpatient setting. Arch Intern Med. 2007 Jul 23;167(14):1471-1475.
- Goldhaber SZ, Tapson VF. A prospective registry of 5,451 patients with ultrasound-confirmed deep vein thrombosis. Am J Cardiol. 2004 Jan 15;93(2):259-262.
- Tapson VF, Decousus H, Pini M, et al. Venous thromboembolism prophylaxis in acutely ill hospitalized medical patients: findings from the International Medical Prevention Registry on Venous Thromboembolism. Chest. Sep 2007;132(3):936-945.
- Anderson FA, Jr., Spencer FA. Risk factors for venous thromboembolism. Circulation. 2003 Jun 17;107(23 Suppl 1):I9-16.
- Dentali F, Douketis JD, Gianni M, Lim W, Crowther MA. Meta-analysis: anticoagulant prophylaxis to prevent symptomatic venous thromboembolism in hospitalized medical patients. Ann Intern Med. 2007 Feb 20;146(4):278-288.
- Geerts WH, Pineo GF, Heit JA, et al. Prevention of venous thromboembolism: the Seventh ACCP Conference on Antithrombotic and Thrombolytic Therapy. Chest. 2004 Sep;126(3 Suppl):338S-400S.
- Hirsh J, Raschke R. Heparin and low-molecular-weight heparin: the Seventh ACCP Conference on Antithrombotic and Thrombolytic Therapy. Chest. 2004 Sep;126(3 Suppl):188S-203S.
- Cade JF, Andrews JT, Stubbs AE. Comparison of sodium and calcium heparin in prevention of venous thromboembolism. Aust N Z J Med. 1982 Oct;12(5):501-504.
- Gallus AS, Hirsh J, Tutle RJ, et al. Small subcutaneous doses of heparin in prevention of venous thrombosis. N Engl J Med. 1973 Mar 15;288(11):545-551.
- Belch JJ, Lowe GD, Ward AG, Forbes CD, Prentice CR. Prevention of deep vein thrombosis in medical patients by low-dose heparin. Scott Med J. 1981 Apr;26(2):115-117.
- Samama MM, Cohen AT, Darmon JY, et al. A comparison of enoxaparin with placebo for the prevention of venous thromboembolism in acutely ill medical patients. Prophylaxis in Medical Patients with Enoxaparin Study Group. N Engl J Med. 1999 Sep 9;341(11):793-800.
- Leizorovicz A, Cohen AT, Turpie AG, Olsson CG, Vaitkus PT, Goldhaber SZ. Randomized, placebo-controlled trial of dalteparin for the prevention of venous thromboembolism in acutely ill medical patients. Circulation. 2004 Aug 17;110(7):874-879.
- Mismetti P, Laporte-Simitsidis S, Tardy B, et al. Prevention of venous thromboembolism in internal medicine with unfractionated or low-molecular-weight heparins: a meta-analysis of randomised clinical trials. Thromb Haemost. Jan 2000;83(1):14-19.
- Wein L, Wein S, Haas SJ, Shaw J, Krum H. Pharmacological venous thromboembolism prophylaxis in hospitalized medical patients: a meta-analysis of randomized controlled trials. Arch Intern Med. 2007 Jul 23;167(14):1476-1486.
- McGarry LJ, Thompson D, Weinstein MC, Goldhaber SZ. Cost effectiveness of thromboprophylaxis with a low-molecular-weight heparin versus unfractionated heparin in acutely ill medical inpatients. Am J Manag Care. 2004 Sep;10(9):632-642.
- Creekmore FM, Oderda GM, Pendleton RC, Brixner DI. Incidence and economic implications of heparin-induced thrombocytopenia in medical patients receiving prophylaxis for venous thromboembolism. Pharmacotherapy. 2006 Oct;26(10):1438-1445.
- Cohen AT, Davidson BL, Gallus AS, et al. Efficacy and safety of fondaparinux for the prevention of venous thromboembolism in older acute medical patients: randomised placebo controlled trial. BMJ. 2006 Feb 11;332(7537):325-329.
Generalist
Medical generalists tell a sad story. Their steadily declining numbers reflect a compensation system that still rewards specialists handsomely at generalists’ expense.
Even though the venerable relative value unit (RVU)-based reimbursement system was intended to equalize pay between primary care’s cognitive work and specialists’ procedure-driven high pay, it hasn’t. Since 1992, when Medicare started paying physicians using RVUs based on the resources used, the specialist-generalist gap remains. RVUs comprise three factors:
- Work (55%);
- Practice expense (42%); and
- Malpractice insurance (3%).
Arguably, generalist RVUs have risen and proceduralist RVUs have decreased. However, generalists argue this skewed pay scale still causes residents to shun internal medicine, hospital medicine, family practice, general pediatrics, and general surgery. Is that true?
Hospitalists and RVUs
Although RVUs don’t always figure into hospitalist compensation, they can have an effect. Vibhu Sharma, MD, of SUNY Downstate Medical Center’s section director, hospital medicine program, heads a 13-hospitalist group employed by the medical center and carries extensive teaching responsibilities.
RVUs don’t currently factor into his hospitalists’ pay but that’s becoming troublesome to Dr. Sharma. “We’d make a lot more money if RVUs were factored in, but they aren’t because we’re a teaching hospital,” he says. “Our group is only four years old, and we aren’t ready to push for it.”
Without the RVU productivity component, Dr. Sharma says he’s at a disadvantage when recruiting. Internal medicine, family practice, and other generalists “stuck with the perception that specialization is a better career option,” he says. “If payers paid us the same as non-invasive cardiologists there’d be a lot more hospitalists.”
Boosts in compensation will be slow in coming, says Dr. Sharma, because hospitalists have demonstrated only modest cost savings and LOS decreases. He adds: “Today nobody wants to be a hospitalist for the rest of their career. We perceive that the patient care we deliver isn’t well compensated, and that the RVU gap between generalists and sub-specialists can never be closed.” As for RVUs, he sees the hospital eventually adding an RVU bonus component. For now, it bumps up hospitalist salaries when the group complains.
The three-member pediatric hospitalist group at Kentucky Children’s Hospital also doesn’t use RVUs, either for compensation or as a productivity proxy. Jeff Bennett, MD, its lead hospitalist, says pediatric outcomes data aren’t robust enough to establish proper RVU benchmarks. He adds that adult RVUs are “denser” than pediatric RVUs because of lower acuity and fewer procedures with children’s illnesses. Additionally, productivity measures don’t affect pediatrics significantly because children’s hospitals “are at the bottom of the funnel,” he says. “We have to take every kid who comes our way. Pediatric hospitals tend not to be competitive. There are four hospitals in town competing for adult patients, while we’re the only tertiary care hospital for 300 miles.”
Compounding the problem is that determining pediatric hospitalist compensation is problematic. With only 2,200 pediatric hospitalists versus 20,000 who work with adults, compensation packages tend to idiosyncratic. “Compensation is important, but RVUs won’t figure into pediatrics for a while,” says Dr. Bennett. “People chose hospital medicine from residency because they’re itching for inpatient work, with its complexity and sharp edges. The shine dims quickly, though, because they are protected during residency and then have full responsibility as hospitalists.”
David Dale, MD, director of the University of Washington’s internal medicine residency program, and American College of Physicians’ president, says hospitalist careers loom large for his annual crop of 35 to 40 residents—but RVUs don’t. “For them it’s an easy transition, a guaranteed salary versus establishing a small business,” he says. “The office practice is where the RVUs really impact generalists. We have a hard job preparing residents for those reimbursement issues.”
Dr. Dale says between two-thirds and three-quarters of his residents become hospitalists, although that’s often not their final career destination. “Some don’t treat hospitalist medicine as a long-term career because the work is hard and the hours are stressful. Many are waiting for a fellowship track to specialization.”
The General Surgeon
A 2007 article by Josef Fischer, MD, in the Journal of the American Medical Association raises questions about the dwindling general surgeon cadre.1 Dr. Fischer posits that RVUs can’t boost surgeons’ incomes because surgeons can’t increase utilization when reimbursement decreases.
For example, since patients have only one gallbladder and indications for removal are constant, there’s no way to increase surgical RVUs. He says this unattractive RVU scheme dissuades residents from general surgery careers.
Dr. Fischer’s concerns don’t faze David Joyce, CEO of Morrisville, N.C.-based Delphi Healthcare Partners, which has three surgicalist programs nationally. Each employs two general surgeons working two weeks on, two weeks off, covering indigent and unassigned patients.
On average, each sees eight patients daily, two requiring surgery. The surgicalists all are either age 50 to 55 or under 35 and reject the hassles of office-based practices at both ends of the career ladder. They earn fixed salaries; Delphi uses RVUs for reimbursement but not for productivity bonuses.
“RVUs aren’t very important in our surgicalist equation, which is a winning situation for everyone involved,” Joyce says. “Private-practice surgeons are thrilled because they don’t cover call and can build their practices. The hospitals do well and don’t mind kicking in several hundred thousand dollars to cover surgicalist compensation.
“In our Charleston, W. Va., program the hospital derived $1.6 million above our program’s cost because the private docs did more surgeries, our surgicalists do what they were trained to do and are well compensated. It’s great,” he says.
Delphi surgicalist Richard Fogle, MD, works at Thomas Memorial Hospital in South Charleston, W. Va., and doesn’t think about RVUs. “The problem with surgeons is lifestyle,” he asserts. “If you have 10 surgeons, you cover call once every 10 days. With three surgeons it’s once every three days.”
Delphi solved his hospital’s problem by recruiting him and another surgicalist. “Before we came most general surgeons had left,” Dr. Fogle says. “Now, two have come back, and four more have settled here. We’re not competing with them for business, and they can build their office practices — particularly with outpatient procedures.”
As a surgicalist, Dr. Fogle, doesn’t miss spending 50% of revenues on office overhead, or leaving 20 patients sitting in his office while answering a hospital page. “I keep waiting for the other shoe to drop, but it hasn’t,” he says of his freedom to practice surgery unfettered by office busyness. He’s happy with the compensation but has a bone to pick with the RVU system. “RVUs are too low for general surgery, and anyone who discounts the cognitive part of surgery procedures is seriously mistaken,” he says.
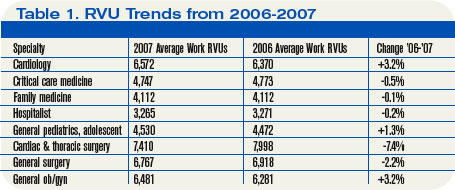
Different Strokes
John Marcelis, MD, an Erickson Retirement Communities regional medical director of 19 providers in four communities, gives the RVU discussion another twist. He practices at Ann’s Choice in Warminster, Pa., with four other physicians, each of whom acts as the group’s hospitalist once every five weeks.
Previously he spent 10 years at the University of Pennsylvania hospital system, where RVUs figured in significantly and volume was highly rewarded. Taking a huge pay cut to practice at Erickson, he happily left the RVU treadmill. “I didn’t like seeing patients at RVU factories,” he recalls. “At Erickson, we have half-hour office visits and see our hospitalized patients as needed. An RVU system doesn’t compute with us.”
Dr. Marcelis, who lost sleep when he was part of an RVU system, sees a bimodal curve of doctors—some thrive on RVUs, others don’t. “There are some doctors who want to see 50 MIs in a day,” he says. “They relish the high-volume intensity. ‘Bring ’em on,’ they say. RVU systems work well for them. For doctors who value longitudinal relationships with patients, RVUs don’t work well.”
He doesn’t see the cognitive vs. procedure gap leading to RVUs ever closing: “There’s a pool of dollars, and shifting 5% from procedures to cognitive work can’t change things. If payers lower RVUs for procedures, specialists will just do more procedures.” TH
Marlene Piturro is a medical writer based in New York.
Reference
- Fischer J. The impending disappearance of the general surgeon. JAMA. 2007;298:2191-2193.
Medical generalists tell a sad story. Their steadily declining numbers reflect a compensation system that still rewards specialists handsomely at generalists’ expense.
Even though the venerable relative value unit (RVU)-based reimbursement system was intended to equalize pay between primary care’s cognitive work and specialists’ procedure-driven high pay, it hasn’t. Since 1992, when Medicare started paying physicians using RVUs based on the resources used, the specialist-generalist gap remains. RVUs comprise three factors:
- Work (55%);
- Practice expense (42%); and
- Malpractice insurance (3%).
Arguably, generalist RVUs have risen and proceduralist RVUs have decreased. However, generalists argue this skewed pay scale still causes residents to shun internal medicine, hospital medicine, family practice, general pediatrics, and general surgery. Is that true?
Hospitalists and RVUs
Although RVUs don’t always figure into hospitalist compensation, they can have an effect. Vibhu Sharma, MD, of SUNY Downstate Medical Center’s section director, hospital medicine program, heads a 13-hospitalist group employed by the medical center and carries extensive teaching responsibilities.
RVUs don’t currently factor into his hospitalists’ pay but that’s becoming troublesome to Dr. Sharma. “We’d make a lot more money if RVUs were factored in, but they aren’t because we’re a teaching hospital,” he says. “Our group is only four years old, and we aren’t ready to push for it.”
Without the RVU productivity component, Dr. Sharma says he’s at a disadvantage when recruiting. Internal medicine, family practice, and other generalists “stuck with the perception that specialization is a better career option,” he says. “If payers paid us the same as non-invasive cardiologists there’d be a lot more hospitalists.”
Boosts in compensation will be slow in coming, says Dr. Sharma, because hospitalists have demonstrated only modest cost savings and LOS decreases. He adds: “Today nobody wants to be a hospitalist for the rest of their career. We perceive that the patient care we deliver isn’t well compensated, and that the RVU gap between generalists and sub-specialists can never be closed.” As for RVUs, he sees the hospital eventually adding an RVU bonus component. For now, it bumps up hospitalist salaries when the group complains.
The three-member pediatric hospitalist group at Kentucky Children’s Hospital also doesn’t use RVUs, either for compensation or as a productivity proxy. Jeff Bennett, MD, its lead hospitalist, says pediatric outcomes data aren’t robust enough to establish proper RVU benchmarks. He adds that adult RVUs are “denser” than pediatric RVUs because of lower acuity and fewer procedures with children’s illnesses. Additionally, productivity measures don’t affect pediatrics significantly because children’s hospitals “are at the bottom of the funnel,” he says. “We have to take every kid who comes our way. Pediatric hospitals tend not to be competitive. There are four hospitals in town competing for adult patients, while we’re the only tertiary care hospital for 300 miles.”
Compounding the problem is that determining pediatric hospitalist compensation is problematic. With only 2,200 pediatric hospitalists versus 20,000 who work with adults, compensation packages tend to idiosyncratic. “Compensation is important, but RVUs won’t figure into pediatrics for a while,” says Dr. Bennett. “People chose hospital medicine from residency because they’re itching for inpatient work, with its complexity and sharp edges. The shine dims quickly, though, because they are protected during residency and then have full responsibility as hospitalists.”
David Dale, MD, director of the University of Washington’s internal medicine residency program, and American College of Physicians’ president, says hospitalist careers loom large for his annual crop of 35 to 40 residents—but RVUs don’t. “For them it’s an easy transition, a guaranteed salary versus establishing a small business,” he says. “The office practice is where the RVUs really impact generalists. We have a hard job preparing residents for those reimbursement issues.”
Dr. Dale says between two-thirds and three-quarters of his residents become hospitalists, although that’s often not their final career destination. “Some don’t treat hospitalist medicine as a long-term career because the work is hard and the hours are stressful. Many are waiting for a fellowship track to specialization.”
The General Surgeon
A 2007 article by Josef Fischer, MD, in the Journal of the American Medical Association raises questions about the dwindling general surgeon cadre.1 Dr. Fischer posits that RVUs can’t boost surgeons’ incomes because surgeons can’t increase utilization when reimbursement decreases.
For example, since patients have only one gallbladder and indications for removal are constant, there’s no way to increase surgical RVUs. He says this unattractive RVU scheme dissuades residents from general surgery careers.
Dr. Fischer’s concerns don’t faze David Joyce, CEO of Morrisville, N.C.-based Delphi Healthcare Partners, which has three surgicalist programs nationally. Each employs two general surgeons working two weeks on, two weeks off, covering indigent and unassigned patients.
On average, each sees eight patients daily, two requiring surgery. The surgicalists all are either age 50 to 55 or under 35 and reject the hassles of office-based practices at both ends of the career ladder. They earn fixed salaries; Delphi uses RVUs for reimbursement but not for productivity bonuses.
“RVUs aren’t very important in our surgicalist equation, which is a winning situation for everyone involved,” Joyce says. “Private-practice surgeons are thrilled because they don’t cover call and can build their practices. The hospitals do well and don’t mind kicking in several hundred thousand dollars to cover surgicalist compensation.
“In our Charleston, W. Va., program the hospital derived $1.6 million above our program’s cost because the private docs did more surgeries, our surgicalists do what they were trained to do and are well compensated. It’s great,” he says.
Delphi surgicalist Richard Fogle, MD, works at Thomas Memorial Hospital in South Charleston, W. Va., and doesn’t think about RVUs. “The problem with surgeons is lifestyle,” he asserts. “If you have 10 surgeons, you cover call once every 10 days. With three surgeons it’s once every three days.”
Delphi solved his hospital’s problem by recruiting him and another surgicalist. “Before we came most general surgeons had left,” Dr. Fogle says. “Now, two have come back, and four more have settled here. We’re not competing with them for business, and they can build their office practices — particularly with outpatient procedures.”
As a surgicalist, Dr. Fogle, doesn’t miss spending 50% of revenues on office overhead, or leaving 20 patients sitting in his office while answering a hospital page. “I keep waiting for the other shoe to drop, but it hasn’t,” he says of his freedom to practice surgery unfettered by office busyness. He’s happy with the compensation but has a bone to pick with the RVU system. “RVUs are too low for general surgery, and anyone who discounts the cognitive part of surgery procedures is seriously mistaken,” he says.
Different Strokes
John Marcelis, MD, an Erickson Retirement Communities regional medical director of 19 providers in four communities, gives the RVU discussion another twist. He practices at Ann’s Choice in Warminster, Pa., with four other physicians, each of whom acts as the group’s hospitalist once every five weeks.
Previously he spent 10 years at the University of Pennsylvania hospital system, where RVUs figured in significantly and volume was highly rewarded. Taking a huge pay cut to practice at Erickson, he happily left the RVU treadmill. “I didn’t like seeing patients at RVU factories,” he recalls. “At Erickson, we have half-hour office visits and see our hospitalized patients as needed. An RVU system doesn’t compute with us.”
Dr. Marcelis, who lost sleep when he was part of an RVU system, sees a bimodal curve of doctors—some thrive on RVUs, others don’t. “There are some doctors who want to see 50 MIs in a day,” he says. “They relish the high-volume intensity. ‘Bring ’em on,’ they say. RVU systems work well for them. For doctors who value longitudinal relationships with patients, RVUs don’t work well.”
He doesn’t see the cognitive vs. procedure gap leading to RVUs ever closing: “There’s a pool of dollars, and shifting 5% from procedures to cognitive work can’t change things. If payers lower RVUs for procedures, specialists will just do more procedures.” TH
Marlene Piturro is a medical writer based in New York.
Reference
- Fischer J. The impending disappearance of the general surgeon. JAMA. 2007;298:2191-2193.
Medical generalists tell a sad story. Their steadily declining numbers reflect a compensation system that still rewards specialists handsomely at generalists’ expense.
Even though the venerable relative value unit (RVU)-based reimbursement system was intended to equalize pay between primary care’s cognitive work and specialists’ procedure-driven high pay, it hasn’t. Since 1992, when Medicare started paying physicians using RVUs based on the resources used, the specialist-generalist gap remains. RVUs comprise three factors:
- Work (55%);
- Practice expense (42%); and
- Malpractice insurance (3%).
Arguably, generalist RVUs have risen and proceduralist RVUs have decreased. However, generalists argue this skewed pay scale still causes residents to shun internal medicine, hospital medicine, family practice, general pediatrics, and general surgery. Is that true?
Hospitalists and RVUs
Although RVUs don’t always figure into hospitalist compensation, they can have an effect. Vibhu Sharma, MD, of SUNY Downstate Medical Center’s section director, hospital medicine program, heads a 13-hospitalist group employed by the medical center and carries extensive teaching responsibilities.
RVUs don’t currently factor into his hospitalists’ pay but that’s becoming troublesome to Dr. Sharma. “We’d make a lot more money if RVUs were factored in, but they aren’t because we’re a teaching hospital,” he says. “Our group is only four years old, and we aren’t ready to push for it.”
Without the RVU productivity component, Dr. Sharma says he’s at a disadvantage when recruiting. Internal medicine, family practice, and other generalists “stuck with the perception that specialization is a better career option,” he says. “If payers paid us the same as non-invasive cardiologists there’d be a lot more hospitalists.”
Boosts in compensation will be slow in coming, says Dr. Sharma, because hospitalists have demonstrated only modest cost savings and LOS decreases. He adds: “Today nobody wants to be a hospitalist for the rest of their career. We perceive that the patient care we deliver isn’t well compensated, and that the RVU gap between generalists and sub-specialists can never be closed.” As for RVUs, he sees the hospital eventually adding an RVU bonus component. For now, it bumps up hospitalist salaries when the group complains.
The three-member pediatric hospitalist group at Kentucky Children’s Hospital also doesn’t use RVUs, either for compensation or as a productivity proxy. Jeff Bennett, MD, its lead hospitalist, says pediatric outcomes data aren’t robust enough to establish proper RVU benchmarks. He adds that adult RVUs are “denser” than pediatric RVUs because of lower acuity and fewer procedures with children’s illnesses. Additionally, productivity measures don’t affect pediatrics significantly because children’s hospitals “are at the bottom of the funnel,” he says. “We have to take every kid who comes our way. Pediatric hospitals tend not to be competitive. There are four hospitals in town competing for adult patients, while we’re the only tertiary care hospital for 300 miles.”
Compounding the problem is that determining pediatric hospitalist compensation is problematic. With only 2,200 pediatric hospitalists versus 20,000 who work with adults, compensation packages tend to idiosyncratic. “Compensation is important, but RVUs won’t figure into pediatrics for a while,” says Dr. Bennett. “People chose hospital medicine from residency because they’re itching for inpatient work, with its complexity and sharp edges. The shine dims quickly, though, because they are protected during residency and then have full responsibility as hospitalists.”
David Dale, MD, director of the University of Washington’s internal medicine residency program, and American College of Physicians’ president, says hospitalist careers loom large for his annual crop of 35 to 40 residents—but RVUs don’t. “For them it’s an easy transition, a guaranteed salary versus establishing a small business,” he says. “The office practice is where the RVUs really impact generalists. We have a hard job preparing residents for those reimbursement issues.”
Dr. Dale says between two-thirds and three-quarters of his residents become hospitalists, although that’s often not their final career destination. “Some don’t treat hospitalist medicine as a long-term career because the work is hard and the hours are stressful. Many are waiting for a fellowship track to specialization.”
The General Surgeon
A 2007 article by Josef Fischer, MD, in the Journal of the American Medical Association raises questions about the dwindling general surgeon cadre.1 Dr. Fischer posits that RVUs can’t boost surgeons’ incomes because surgeons can’t increase utilization when reimbursement decreases.
For example, since patients have only one gallbladder and indications for removal are constant, there’s no way to increase surgical RVUs. He says this unattractive RVU scheme dissuades residents from general surgery careers.
Dr. Fischer’s concerns don’t faze David Joyce, CEO of Morrisville, N.C.-based Delphi Healthcare Partners, which has three surgicalist programs nationally. Each employs two general surgeons working two weeks on, two weeks off, covering indigent and unassigned patients.
On average, each sees eight patients daily, two requiring surgery. The surgicalists all are either age 50 to 55 or under 35 and reject the hassles of office-based practices at both ends of the career ladder. They earn fixed salaries; Delphi uses RVUs for reimbursement but not for productivity bonuses.
“RVUs aren’t very important in our surgicalist equation, which is a winning situation for everyone involved,” Joyce says. “Private-practice surgeons are thrilled because they don’t cover call and can build their practices. The hospitals do well and don’t mind kicking in several hundred thousand dollars to cover surgicalist compensation.
“In our Charleston, W. Va., program the hospital derived $1.6 million above our program’s cost because the private docs did more surgeries, our surgicalists do what they were trained to do and are well compensated. It’s great,” he says.
Delphi surgicalist Richard Fogle, MD, works at Thomas Memorial Hospital in South Charleston, W. Va., and doesn’t think about RVUs. “The problem with surgeons is lifestyle,” he asserts. “If you have 10 surgeons, you cover call once every 10 days. With three surgeons it’s once every three days.”
Delphi solved his hospital’s problem by recruiting him and another surgicalist. “Before we came most general surgeons had left,” Dr. Fogle says. “Now, two have come back, and four more have settled here. We’re not competing with them for business, and they can build their office practices — particularly with outpatient procedures.”
As a surgicalist, Dr. Fogle, doesn’t miss spending 50% of revenues on office overhead, or leaving 20 patients sitting in his office while answering a hospital page. “I keep waiting for the other shoe to drop, but it hasn’t,” he says of his freedom to practice surgery unfettered by office busyness. He’s happy with the compensation but has a bone to pick with the RVU system. “RVUs are too low for general surgery, and anyone who discounts the cognitive part of surgery procedures is seriously mistaken,” he says.
Different Strokes
John Marcelis, MD, an Erickson Retirement Communities regional medical director of 19 providers in four communities, gives the RVU discussion another twist. He practices at Ann’s Choice in Warminster, Pa., with four other physicians, each of whom acts as the group’s hospitalist once every five weeks.
Previously he spent 10 years at the University of Pennsylvania hospital system, where RVUs figured in significantly and volume was highly rewarded. Taking a huge pay cut to practice at Erickson, he happily left the RVU treadmill. “I didn’t like seeing patients at RVU factories,” he recalls. “At Erickson, we have half-hour office visits and see our hospitalized patients as needed. An RVU system doesn’t compute with us.”
Dr. Marcelis, who lost sleep when he was part of an RVU system, sees a bimodal curve of doctors—some thrive on RVUs, others don’t. “There are some doctors who want to see 50 MIs in a day,” he says. “They relish the high-volume intensity. ‘Bring ’em on,’ they say. RVU systems work well for them. For doctors who value longitudinal relationships with patients, RVUs don’t work well.”
He doesn’t see the cognitive vs. procedure gap leading to RVUs ever closing: “There’s a pool of dollars, and shifting 5% from procedures to cognitive work can’t change things. If payers lower RVUs for procedures, specialists will just do more procedures.” TH
Marlene Piturro is a medical writer based in New York.
Reference
- Fischer J. The impending disappearance of the general surgeon. JAMA. 2007;298:2191-2193.
Choose Your Exam Rules
Physicians only should perform patient examinations based upon the presenting problem and the standard of care. As mentioned in my previous column (April 2008, p. 21), the Centers for Medicare and Medicaid Services (CMS) and the American Medical Association (AMA) set forth two sets of documentation guidelines. The biggest difference between them is the exam component.
1995 Guidelines
The 1995 guidelines distinguish 10 body areas (head and face; neck; chest, breast, and axillae; abdomen; genitalia, groin, and buttocks; back and spine; right upper extremity; left upper extremity; right lower extremity; and left lower extremity) from 12 organ systems (constitutional; eyes; ears, nose, mouth, and throat; cardiovascular; respiratory; gastrointestinal; genitourinary; musculoskeletal; integumentary; neurological; psychiatric; hematologic, lymphatic, and immunologic).
Further, these guidelines let physicians document their findings in any manner while adhering to some simple rules:
- Document relevant negative findings. Commenting that a system or area is “negative” or “normal” is acceptable when referring to unaffected areas or asymptomatic organ systems; and
- Elaborate on abnormal findings. Commenting that a system or area is “abnormal” is not sufficient unless additional comments describing the abnormality are documented.
1997 Guidelines
The 1997 guidelines comprise bulleted items—referred to as elements—that correspond to each organ system. Some elements specify numeric criterion that must be met to credit the physician for documentation of that element.
For example, the physician only receives credit for documentation of vital signs (an element of the constitutional system) when three measurements are referenced (e.g., blood pressure, heart rate, and respiratory rate). Documentation that does not include three measurements or only contains a single generalized comment (e.g., vital signs stable) cannot be credited to the physician in the 1997 guidelines—even though these same comments are credited when applying the 1995 guidelines.
This logic also applies to the lymphatic system. The physician must identify findings associated with at least two lymphatic areas examined (e.g., “no lymphadenopathy of the neck or axillae”).
Elements that do not contain numeric criterion but identify multiple components require documentation of at least one component. For example, one psychiatric element involves the assessment of the patient’s “mood and affect.” If the physician comments that the patient appears depressed but does not comment on a flat (or normal) affect, the physician still receives credit for this exam element.
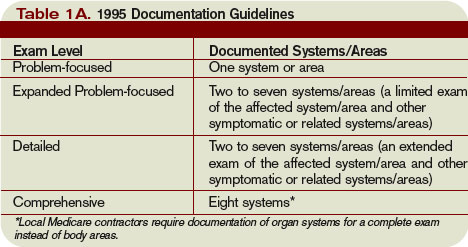
Levels of Exam
There are four levels of exam, determined by the number of elements documented in the progress note (see Tables 1A and 1B, p. below).
As with the history component, the physician must meet the requirements for a particular level of exam before assigning it. The most problematic feature of the 1995 guidelines involves the “detailed” exam. Both the expanded problem-focused and detailed exams involve two to seven systems/areas, but the detailed exam requires an “extended” exam of the affected system/area related to the presenting problem. Questions surround the number of elements needed to qualify as an “extended” exam of the affected system/area.
Does “regular rate and rhythm; normal S1, S2; no jugular venous distention; no murmur, gallop, or rub; peripheral pulses intact; no edema noted” constitute an “extended” exam of the cardiovascular system, or should there be an additional comment regarding the abdominal aorta? This decision is left to the discretion of the local Medicare contractor and/or the medical reviewer.
Since no other CMS directive has been provided, documentation of the detailed exam continues to be inconsistent. More importantly, review and audit of the detailed exam remains arbitrary. Some Medicare contractors suggest using the 1997 requirements for the detailed exam, while others create their own definition and corresponding number of exam elements needed for documentation of the detailed exam. This issue exemplifies the ambiguity for which the 1995 guidelines often are criticized.
Meanwhile, the 1997 guidelines often are criticized as too specific. While this may help the medical reviewer/auditor, it hinders the physician. Physicians are frequently frustrated trying to remember the explicit comments and number of elements associated with a particular level of exam.
One solution is documentation templates. Physicians can use paper or electronic templates that incorporate cues and prompts for normal exam findings, incorporating adequate space to elaborate abnormal findings.
Remember the physician has the option of utilizing either the 1995 or 1997 guidelines, depending upon which set he perceives as easier to implement.
Additionally, auditors must review physician documentation using both the 1995 and 1997 guidelines, and apply the most favorable result to the final audit score.
Each type of evaluation and management service identifies a specific level of exam that must be documented in the medical record before the associated CPT code is submitted on a claim.
The most common visit categories provided by hospitalists and corresponding exam levels are outlined in Table 2 (above). Similar to the history component, other visit categories, such as critical care and discharge day management, do not have specified levels of exam or associated documentation requirements for physical exam elements. TH
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center, Philadelphia. She also is on the faculty of SHM’s inpatient coding course.
Physicians only should perform patient examinations based upon the presenting problem and the standard of care. As mentioned in my previous column (April 2008, p. 21), the Centers for Medicare and Medicaid Services (CMS) and the American Medical Association (AMA) set forth two sets of documentation guidelines. The biggest difference between them is the exam component.
1995 Guidelines
The 1995 guidelines distinguish 10 body areas (head and face; neck; chest, breast, and axillae; abdomen; genitalia, groin, and buttocks; back and spine; right upper extremity; left upper extremity; right lower extremity; and left lower extremity) from 12 organ systems (constitutional; eyes; ears, nose, mouth, and throat; cardiovascular; respiratory; gastrointestinal; genitourinary; musculoskeletal; integumentary; neurological; psychiatric; hematologic, lymphatic, and immunologic).
Further, these guidelines let physicians document their findings in any manner while adhering to some simple rules:
- Document relevant negative findings. Commenting that a system or area is “negative” or “normal” is acceptable when referring to unaffected areas or asymptomatic organ systems; and
- Elaborate on abnormal findings. Commenting that a system or area is “abnormal” is not sufficient unless additional comments describing the abnormality are documented.
1997 Guidelines
The 1997 guidelines comprise bulleted items—referred to as elements—that correspond to each organ system. Some elements specify numeric criterion that must be met to credit the physician for documentation of that element.
For example, the physician only receives credit for documentation of vital signs (an element of the constitutional system) when three measurements are referenced (e.g., blood pressure, heart rate, and respiratory rate). Documentation that does not include three measurements or only contains a single generalized comment (e.g., vital signs stable) cannot be credited to the physician in the 1997 guidelines—even though these same comments are credited when applying the 1995 guidelines.
This logic also applies to the lymphatic system. The physician must identify findings associated with at least two lymphatic areas examined (e.g., “no lymphadenopathy of the neck or axillae”).
Elements that do not contain numeric criterion but identify multiple components require documentation of at least one component. For example, one psychiatric element involves the assessment of the patient’s “mood and affect.” If the physician comments that the patient appears depressed but does not comment on a flat (or normal) affect, the physician still receives credit for this exam element.
Levels of Exam
There are four levels of exam, determined by the number of elements documented in the progress note (see Tables 1A and 1B, p. below).
As with the history component, the physician must meet the requirements for a particular level of exam before assigning it. The most problematic feature of the 1995 guidelines involves the “detailed” exam. Both the expanded problem-focused and detailed exams involve two to seven systems/areas, but the detailed exam requires an “extended” exam of the affected system/area related to the presenting problem. Questions surround the number of elements needed to qualify as an “extended” exam of the affected system/area.
Does “regular rate and rhythm; normal S1, S2; no jugular venous distention; no murmur, gallop, or rub; peripheral pulses intact; no edema noted” constitute an “extended” exam of the cardiovascular system, or should there be an additional comment regarding the abdominal aorta? This decision is left to the discretion of the local Medicare contractor and/or the medical reviewer.
Since no other CMS directive has been provided, documentation of the detailed exam continues to be inconsistent. More importantly, review and audit of the detailed exam remains arbitrary. Some Medicare contractors suggest using the 1997 requirements for the detailed exam, while others create their own definition and corresponding number of exam elements needed for documentation of the detailed exam. This issue exemplifies the ambiguity for which the 1995 guidelines often are criticized.
Meanwhile, the 1997 guidelines often are criticized as too specific. While this may help the medical reviewer/auditor, it hinders the physician. Physicians are frequently frustrated trying to remember the explicit comments and number of elements associated with a particular level of exam.
One solution is documentation templates. Physicians can use paper or electronic templates that incorporate cues and prompts for normal exam findings, incorporating adequate space to elaborate abnormal findings.
Remember the physician has the option of utilizing either the 1995 or 1997 guidelines, depending upon which set he perceives as easier to implement.
Additionally, auditors must review physician documentation using both the 1995 and 1997 guidelines, and apply the most favorable result to the final audit score.
Each type of evaluation and management service identifies a specific level of exam that must be documented in the medical record before the associated CPT code is submitted on a claim.
The most common visit categories provided by hospitalists and corresponding exam levels are outlined in Table 2 (above). Similar to the history component, other visit categories, such as critical care and discharge day management, do not have specified levels of exam or associated documentation requirements for physical exam elements. TH
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center, Philadelphia. She also is on the faculty of SHM’s inpatient coding course.
Physicians only should perform patient examinations based upon the presenting problem and the standard of care. As mentioned in my previous column (April 2008, p. 21), the Centers for Medicare and Medicaid Services (CMS) and the American Medical Association (AMA) set forth two sets of documentation guidelines. The biggest difference between them is the exam component.
1995 Guidelines
The 1995 guidelines distinguish 10 body areas (head and face; neck; chest, breast, and axillae; abdomen; genitalia, groin, and buttocks; back and spine; right upper extremity; left upper extremity; right lower extremity; and left lower extremity) from 12 organ systems (constitutional; eyes; ears, nose, mouth, and throat; cardiovascular; respiratory; gastrointestinal; genitourinary; musculoskeletal; integumentary; neurological; psychiatric; hematologic, lymphatic, and immunologic).
Further, these guidelines let physicians document their findings in any manner while adhering to some simple rules:
- Document relevant negative findings. Commenting that a system or area is “negative” or “normal” is acceptable when referring to unaffected areas or asymptomatic organ systems; and
- Elaborate on abnormal findings. Commenting that a system or area is “abnormal” is not sufficient unless additional comments describing the abnormality are documented.
1997 Guidelines
The 1997 guidelines comprise bulleted items—referred to as elements—that correspond to each organ system. Some elements specify numeric criterion that must be met to credit the physician for documentation of that element.
For example, the physician only receives credit for documentation of vital signs (an element of the constitutional system) when three measurements are referenced (e.g., blood pressure, heart rate, and respiratory rate). Documentation that does not include three measurements or only contains a single generalized comment (e.g., vital signs stable) cannot be credited to the physician in the 1997 guidelines—even though these same comments are credited when applying the 1995 guidelines.
This logic also applies to the lymphatic system. The physician must identify findings associated with at least two lymphatic areas examined (e.g., “no lymphadenopathy of the neck or axillae”).
Elements that do not contain numeric criterion but identify multiple components require documentation of at least one component. For example, one psychiatric element involves the assessment of the patient’s “mood and affect.” If the physician comments that the patient appears depressed but does not comment on a flat (or normal) affect, the physician still receives credit for this exam element.
Levels of Exam
There are four levels of exam, determined by the number of elements documented in the progress note (see Tables 1A and 1B, p. below).
As with the history component, the physician must meet the requirements for a particular level of exam before assigning it. The most problematic feature of the 1995 guidelines involves the “detailed” exam. Both the expanded problem-focused and detailed exams involve two to seven systems/areas, but the detailed exam requires an “extended” exam of the affected system/area related to the presenting problem. Questions surround the number of elements needed to qualify as an “extended” exam of the affected system/area.
Does “regular rate and rhythm; normal S1, S2; no jugular venous distention; no murmur, gallop, or rub; peripheral pulses intact; no edema noted” constitute an “extended” exam of the cardiovascular system, or should there be an additional comment regarding the abdominal aorta? This decision is left to the discretion of the local Medicare contractor and/or the medical reviewer.
Since no other CMS directive has been provided, documentation of the detailed exam continues to be inconsistent. More importantly, review and audit of the detailed exam remains arbitrary. Some Medicare contractors suggest using the 1997 requirements for the detailed exam, while others create their own definition and corresponding number of exam elements needed for documentation of the detailed exam. This issue exemplifies the ambiguity for which the 1995 guidelines often are criticized.
Meanwhile, the 1997 guidelines often are criticized as too specific. While this may help the medical reviewer/auditor, it hinders the physician. Physicians are frequently frustrated trying to remember the explicit comments and number of elements associated with a particular level of exam.
One solution is documentation templates. Physicians can use paper or electronic templates that incorporate cues and prompts for normal exam findings, incorporating adequate space to elaborate abnormal findings.
Remember the physician has the option of utilizing either the 1995 or 1997 guidelines, depending upon which set he perceives as easier to implement.
Additionally, auditors must review physician documentation using both the 1995 and 1997 guidelines, and apply the most favorable result to the final audit score.
Each type of evaluation and management service identifies a specific level of exam that must be documented in the medical record before the associated CPT code is submitted on a claim.
The most common visit categories provided by hospitalists and corresponding exam levels are outlined in Table 2 (above). Similar to the history component, other visit categories, such as critical care and discharge day management, do not have specified levels of exam or associated documentation requirements for physical exam elements. TH
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center, Philadelphia. She also is on the faculty of SHM’s inpatient coding course.