User login
Bringing you the latest news, research and reviews, exclusive interviews, podcasts, quizzes, and more.
div[contains(@class, 'header__large-screen')]
div[contains(@class, 'read-next-article')]
div[contains(@class, 'nav-primary')]
nav[contains(@class, 'nav-primary')]
section[contains(@class, 'footer-nav-section-wrapper')]
footer[@id='footer']
div[contains(@class, 'main-prefix')]
section[contains(@class, 'nav-hidden')]
div[contains(@class, 'ce-card-content')]
nav[contains(@class, 'nav-ce-stack')]
Low HPV Vaccination in the United States Is a Public Health ‘Failure’
This transcript has been edited for clarity.
I would like to briefly discuss what I consider to be a very discouraging report and one that I believe we as an oncology society and, quite frankly, as a medical community need to deal with.
The manuscript I’m referring to is from the United States Department of Health and Human Services, titled, “Human Papillomavirus Vaccination Coverage in Children Ages 9-17 Years: United States, 2022.” This particular analysis looked at the coverage of both men and women — young boys and young girls, I would say — receiving at least one dose of the recommended human papillomavirus (HPV) vaccination.
Since 2006, girls have been recommended to receive HPV vaccination; for boys, it’s been since 2011. Certainly, the time period that we’re considering falls within the recommendations based on overwhelmingly positive data. Now, today, still, the recommendation is for more than one vaccine. Obviously, there may be evidence in the future that a single vaccination may be acceptable or appropriate. But today, it’s more than one.
In this particular analysis, they were looking at just a single vaccination. The vaccines have targeted young individuals, both male and female children aged 11-12 years, but it’s certainly acceptable to look starting at age 9.
What is the bottom line? At least one dose of the HPV vaccination was given to 38.6% of children aged 9-17 years in 2022. We are talking about a cancer-preventive vaccine, which on the basis of population-based data in the United States, but also in other countries, is incredibly effective in preventing HPV-associated cancers. This not only includes cervical cancer, but also a large percentage of head and neck cancers.
For this vaccine, which is incredibly safe and incredibly effective, in this country, only 38.6% have received even a single dose. It is noted that the individuals with private insurance had a higher rate, at 41.5%, than individuals with no insurance, at only 20.7%.
In my opinion, this is clearly a failure of our public health establishment at all levels. My own focus has been in gynecologic cancers. I’ve seen young women with advanced cervical cancer, and this is a disease we can prevent. Yet, this is where we are.
For those of you who are interested in cancer prevention or public health, I think this is a very sobering statistic. It’s my plea and my hope that we can, as a society, somehow do something about it.
I thank you for listening. I would encourage you to think about this question if you’re in this area.
Dr. Markman, professor, Department of Medical Oncology and Therapeutics Research, City of Hope, Duarte, California, and president of Medicine & Science, City of Hope Atlanta, Chicago, and Phoenix, disclosed ties with GlaxoSmithKline and AstraZeneca.
A version of this article appeared on Medscape.com.
This transcript has been edited for clarity.
I would like to briefly discuss what I consider to be a very discouraging report and one that I believe we as an oncology society and, quite frankly, as a medical community need to deal with.
The manuscript I’m referring to is from the United States Department of Health and Human Services, titled, “Human Papillomavirus Vaccination Coverage in Children Ages 9-17 Years: United States, 2022.” This particular analysis looked at the coverage of both men and women — young boys and young girls, I would say — receiving at least one dose of the recommended human papillomavirus (HPV) vaccination.
Since 2006, girls have been recommended to receive HPV vaccination; for boys, it’s been since 2011. Certainly, the time period that we’re considering falls within the recommendations based on overwhelmingly positive data. Now, today, still, the recommendation is for more than one vaccine. Obviously, there may be evidence in the future that a single vaccination may be acceptable or appropriate. But today, it’s more than one.
In this particular analysis, they were looking at just a single vaccination. The vaccines have targeted young individuals, both male and female children aged 11-12 years, but it’s certainly acceptable to look starting at age 9.
What is the bottom line? At least one dose of the HPV vaccination was given to 38.6% of children aged 9-17 years in 2022. We are talking about a cancer-preventive vaccine, which on the basis of population-based data in the United States, but also in other countries, is incredibly effective in preventing HPV-associated cancers. This not only includes cervical cancer, but also a large percentage of head and neck cancers.
For this vaccine, which is incredibly safe and incredibly effective, in this country, only 38.6% have received even a single dose. It is noted that the individuals with private insurance had a higher rate, at 41.5%, than individuals with no insurance, at only 20.7%.
In my opinion, this is clearly a failure of our public health establishment at all levels. My own focus has been in gynecologic cancers. I’ve seen young women with advanced cervical cancer, and this is a disease we can prevent. Yet, this is where we are.
For those of you who are interested in cancer prevention or public health, I think this is a very sobering statistic. It’s my plea and my hope that we can, as a society, somehow do something about it.
I thank you for listening. I would encourage you to think about this question if you’re in this area.
Dr. Markman, professor, Department of Medical Oncology and Therapeutics Research, City of Hope, Duarte, California, and president of Medicine & Science, City of Hope Atlanta, Chicago, and Phoenix, disclosed ties with GlaxoSmithKline and AstraZeneca.
A version of this article appeared on Medscape.com.
This transcript has been edited for clarity.
I would like to briefly discuss what I consider to be a very discouraging report and one that I believe we as an oncology society and, quite frankly, as a medical community need to deal with.
The manuscript I’m referring to is from the United States Department of Health and Human Services, titled, “Human Papillomavirus Vaccination Coverage in Children Ages 9-17 Years: United States, 2022.” This particular analysis looked at the coverage of both men and women — young boys and young girls, I would say — receiving at least one dose of the recommended human papillomavirus (HPV) vaccination.
Since 2006, girls have been recommended to receive HPV vaccination; for boys, it’s been since 2011. Certainly, the time period that we’re considering falls within the recommendations based on overwhelmingly positive data. Now, today, still, the recommendation is for more than one vaccine. Obviously, there may be evidence in the future that a single vaccination may be acceptable or appropriate. But today, it’s more than one.
In this particular analysis, they were looking at just a single vaccination. The vaccines have targeted young individuals, both male and female children aged 11-12 years, but it’s certainly acceptable to look starting at age 9.
What is the bottom line? At least one dose of the HPV vaccination was given to 38.6% of children aged 9-17 years in 2022. We are talking about a cancer-preventive vaccine, which on the basis of population-based data in the United States, but also in other countries, is incredibly effective in preventing HPV-associated cancers. This not only includes cervical cancer, but also a large percentage of head and neck cancers.
For this vaccine, which is incredibly safe and incredibly effective, in this country, only 38.6% have received even a single dose. It is noted that the individuals with private insurance had a higher rate, at 41.5%, than individuals with no insurance, at only 20.7%.
In my opinion, this is clearly a failure of our public health establishment at all levels. My own focus has been in gynecologic cancers. I’ve seen young women with advanced cervical cancer, and this is a disease we can prevent. Yet, this is where we are.
For those of you who are interested in cancer prevention or public health, I think this is a very sobering statistic. It’s my plea and my hope that we can, as a society, somehow do something about it.
I thank you for listening. I would encourage you to think about this question if you’re in this area.
Dr. Markman, professor, Department of Medical Oncology and Therapeutics Research, City of Hope, Duarte, California, and president of Medicine & Science, City of Hope Atlanta, Chicago, and Phoenix, disclosed ties with GlaxoSmithKline and AstraZeneca.
A version of this article appeared on Medscape.com.
Gender and Sports: Can Science Enable Fair Competition?
The allegations against Algerian boxer Imane Khelif at the Paris Olympics raised the questions of intersexuality and its implications in competitive sports. This news organization has decided to delve into the topic to assist doctors who suspect a similar condition in their patients. No certain clinical data about Ms. Khelif have been made public, so this article does not concern the boxer but rather takes inspiration from the media controversy.
What Is Intersexuality?
Intersexuality encompasses a spectrum of variations in sexual development that lead to the simultaneous presence of typical male and female characteristics. As reiterated by the United Nations Office of the High Commissioner for Human Rights, the medical definition does not affect the patient’s self-identification of gender or sexual orientation.
“The percentage of people who fall within the intersexuality spectrum is less than 0.5 per thousand of the general population, but there are no precise statistics, given the difficulty of definition,” said Roberto Lala, MD, pediatric endocrinologist and president of the Federation of Rare Childhood Diseases.
Indeed, there is not only a strict definition of intersexuality that involves a significant presence of these mixed physical characteristics in a way that conditions the self-image of the subject but also a broad definition, said Dr. Lala. “For example, clitoral hypertrophy in a female otherwise conforming to the female gender, which does not raise doubts about identity,” he said.
Chromosomes, Genes, and Hormones
“The human body is, so to speak, programmed to take on female appearances in development and shifts toward male ones only if exposed to testosterone and other factors. For this to happen, testosterone must be produced during embryonic development, and it must function properly,” said Paolo Moghetti, full professor of endocrinology at the University of Verona, Italy.
The protein encoded by SRY, which is located on the Y chromosome, determines the development of the testicles from undifferentiated tissue of the embryonic gonads. The testicles of the embryo then produce testosterone. The absence of the Y chromosome is a common characteristic of most female individuals. However, there are individuals with a female phenotype who have X and Y chromosomes but lack SRY or have a variant of it that is not entirely functional.
Numerous other chromosomal or genetic variations can lead to alterations in sexual differentiation. “In phenotypically male adult subjects (with a chromosomal makeup of 46XY) with complete androgen insensitivity (so-called Morris syndrome), testosterone levels in the blood are elevated, above normal even for a male, but the hormone is totally ineffective, and the phenotype is totally female at birth, with completely female development of secondary sexual characteristics at puberty,” said Dr. Moghetti.
This means that affected individuals have well-developed breasts and a complete lack or extremely reduced presence of hair, including underarm and pubic hair. Menstruation is also completely absent because there is no uterus, and there are testes, not visible because they are considered in the abdomen.
“There are syndromes that are currently considered congenital but not genetic, of which a genetic origin will probably be identified in the future,” said Dr. Lala.
Some variations in sexual development can be diagnosed prenatally, such as an alteration of the number of sex chromosomes or a discordance between the morphologic characteristics highlighted by ultrasound and the genotype detected by amniocentesis. Some variations are evident at birth because of atypical anatomical characteristics. Others are diagnosed during puberty or later in adulthood, in the presence of infertility. The Italian National Institute of Health details these variations on its website, describing the characteristics that determine diagnosis and treatment.
Pathologies or Variations?
Some anomalies in sexual development negatively affect the patient’s physical health. One example is congenital adrenal hyperplasia. “It results from an inherited defect of the adrenal glands, which reduces cortisol production while increasing testosterone production,” said Dr. Lala. “In addition to the appearance of male characteristics in females, in more severe forms, it carries the risk of collapse and shock and requires pharmacological treatment.” It is undoubtedly a pathology.
Other variations in sexual characteristics do not affect the patient’s physical health negatively. They may, however, have a psychologic effect, sometimes a significant one, because of the lack of social acceptance of a person who cannot be classified within the binary classification of sexes.
“Conditions in which mixed male and female aspects are clearly evident have been and are still pathologized by the family, the treating physician, and society,” said Dr. Lala. “In the late 1970s, when a child was born with intersexual anatomical characteristics, it was common practice to surgically intervene, making them female, because it was technically easier.”
Over the years, patients who, as they grew up, were dissatisfied with the solution adopted at birth began to make their voices heard, Dr. Lala added. Scientific societies and international organizations have spoken out against subjecting intersexual newborns to surgical interventions that are not medically necessary. “Nowadays, decisions are made on a case-by-case basis, taking into account the families’ wishes. Interventions are justified with medical reasons, which are often very nuanced,” Dr. Lala concluded.
Implications for Sports
Traditionally, athletes participating in competitions in certain sports have been divided into male and female categories to ensure a certain equity and uniformity in performance. Over the years, the emergence of new information about sexual development has made it necessary to update the criteria used in this division.
The main factor responsible for the performance diversity between males and females is the action of testosterone on the male and female organism. “Testosterone has important effects on muscle mass and enhances training results,” said Dr. Moghetti. “As a demonstration of this fact, before puberty, the best performances in athletics or swimming by males and females are similar, then males gain a significant advantage of around 10%-20%.”
A few years ago, the World Athletics Federation conducted widespread screening of athletes participating in its world championships. “It identified a small group of individuals with potentially abnormal testosterone levels for the female sex,” said Dr. Moghetti. “Some were found to be doping, others had genetic defects, and for some, an interpretation was not even possible.”
Some of the individuals had a male genotype but a defect in 5-alpha-reductase, an enzyme essential for the formation of male genitals and hair growth. An athlete with these characteristics, assigned female sex at birth, has a male level of testosterone that stimulates the accumulation of muscle mass, Dr. Moghetti explained. Therefore, the individual has a considerable advantage in performances influenced by this hormone.
“In the end, the Federation decided to set limits on the testosterone levels of athletes participating in certain types of races, especially those in middle distance, that appeared to be more sensitive to differences in hormone levels,” said Dr. Moghetti. “The limitation does not apply to athletes with Morris syndrome, ie, with a male genotype and complete resistance to testosterone, for whom the high level of this hormone does not provide any advantage.” Given the complexity of the problem, he hopes for a case-by-case policy that considers the needs of patients with genetic alterations and those of athletes who have to compete with them.
Not the First Time
A recent incident underscored the difficulty of regulating such complex issues. The World Athletics Federation excluded South African middle-distance runner Caster Semenya from competitions years ago because of excessively high testosterone levels.
“The Federation’s regulations recommend that athletes in these cases reduce hormone levels to values below the threshold of 5 nmol/L of blood for a period of at least 6 months before the race by using hormonal contraceptives. The use of such drugs does not pose a health risk, as they are substances normally taken by women for contraception purposes,” said Amelia Filippelli, a pharmacologist at the University of Salerno in Italy. The South African middle-distance runner refused the drug and appealed to the Court of Arbitration for Sport and later to the Swiss Federal Court. Both rejected her appeal. Finally, Ms. Semenya appealed to the European Court of Human Rights, which in 2023 recognized a violation of her rights but does not have the authority to order a change in the Federation’s regulations.
Beyond the ideologic positions of nonexperts, therefore, the issue is still the subject of debate in the scientific community, which is evaluating not only its medical aspects but also its ethical implications.
This story was translated from Univadis Italy, which is part of the Medscape professional network, using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article appeared on Medscape.com.
The allegations against Algerian boxer Imane Khelif at the Paris Olympics raised the questions of intersexuality and its implications in competitive sports. This news organization has decided to delve into the topic to assist doctors who suspect a similar condition in their patients. No certain clinical data about Ms. Khelif have been made public, so this article does not concern the boxer but rather takes inspiration from the media controversy.
What Is Intersexuality?
Intersexuality encompasses a spectrum of variations in sexual development that lead to the simultaneous presence of typical male and female characteristics. As reiterated by the United Nations Office of the High Commissioner for Human Rights, the medical definition does not affect the patient’s self-identification of gender or sexual orientation.
“The percentage of people who fall within the intersexuality spectrum is less than 0.5 per thousand of the general population, but there are no precise statistics, given the difficulty of definition,” said Roberto Lala, MD, pediatric endocrinologist and president of the Federation of Rare Childhood Diseases.
Indeed, there is not only a strict definition of intersexuality that involves a significant presence of these mixed physical characteristics in a way that conditions the self-image of the subject but also a broad definition, said Dr. Lala. “For example, clitoral hypertrophy in a female otherwise conforming to the female gender, which does not raise doubts about identity,” he said.
Chromosomes, Genes, and Hormones
“The human body is, so to speak, programmed to take on female appearances in development and shifts toward male ones only if exposed to testosterone and other factors. For this to happen, testosterone must be produced during embryonic development, and it must function properly,” said Paolo Moghetti, full professor of endocrinology at the University of Verona, Italy.
The protein encoded by SRY, which is located on the Y chromosome, determines the development of the testicles from undifferentiated tissue of the embryonic gonads. The testicles of the embryo then produce testosterone. The absence of the Y chromosome is a common characteristic of most female individuals. However, there are individuals with a female phenotype who have X and Y chromosomes but lack SRY or have a variant of it that is not entirely functional.
Numerous other chromosomal or genetic variations can lead to alterations in sexual differentiation. “In phenotypically male adult subjects (with a chromosomal makeup of 46XY) with complete androgen insensitivity (so-called Morris syndrome), testosterone levels in the blood are elevated, above normal even for a male, but the hormone is totally ineffective, and the phenotype is totally female at birth, with completely female development of secondary sexual characteristics at puberty,” said Dr. Moghetti.
This means that affected individuals have well-developed breasts and a complete lack or extremely reduced presence of hair, including underarm and pubic hair. Menstruation is also completely absent because there is no uterus, and there are testes, not visible because they are considered in the abdomen.
“There are syndromes that are currently considered congenital but not genetic, of which a genetic origin will probably be identified in the future,” said Dr. Lala.
Some variations in sexual development can be diagnosed prenatally, such as an alteration of the number of sex chromosomes or a discordance between the morphologic characteristics highlighted by ultrasound and the genotype detected by amniocentesis. Some variations are evident at birth because of atypical anatomical characteristics. Others are diagnosed during puberty or later in adulthood, in the presence of infertility. The Italian National Institute of Health details these variations on its website, describing the characteristics that determine diagnosis and treatment.
Pathologies or Variations?
Some anomalies in sexual development negatively affect the patient’s physical health. One example is congenital adrenal hyperplasia. “It results from an inherited defect of the adrenal glands, which reduces cortisol production while increasing testosterone production,” said Dr. Lala. “In addition to the appearance of male characteristics in females, in more severe forms, it carries the risk of collapse and shock and requires pharmacological treatment.” It is undoubtedly a pathology.
Other variations in sexual characteristics do not affect the patient’s physical health negatively. They may, however, have a psychologic effect, sometimes a significant one, because of the lack of social acceptance of a person who cannot be classified within the binary classification of sexes.
“Conditions in which mixed male and female aspects are clearly evident have been and are still pathologized by the family, the treating physician, and society,” said Dr. Lala. “In the late 1970s, when a child was born with intersexual anatomical characteristics, it was common practice to surgically intervene, making them female, because it was technically easier.”
Over the years, patients who, as they grew up, were dissatisfied with the solution adopted at birth began to make their voices heard, Dr. Lala added. Scientific societies and international organizations have spoken out against subjecting intersexual newborns to surgical interventions that are not medically necessary. “Nowadays, decisions are made on a case-by-case basis, taking into account the families’ wishes. Interventions are justified with medical reasons, which are often very nuanced,” Dr. Lala concluded.
Implications for Sports
Traditionally, athletes participating in competitions in certain sports have been divided into male and female categories to ensure a certain equity and uniformity in performance. Over the years, the emergence of new information about sexual development has made it necessary to update the criteria used in this division.
The main factor responsible for the performance diversity between males and females is the action of testosterone on the male and female organism. “Testosterone has important effects on muscle mass and enhances training results,” said Dr. Moghetti. “As a demonstration of this fact, before puberty, the best performances in athletics or swimming by males and females are similar, then males gain a significant advantage of around 10%-20%.”
A few years ago, the World Athletics Federation conducted widespread screening of athletes participating in its world championships. “It identified a small group of individuals with potentially abnormal testosterone levels for the female sex,” said Dr. Moghetti. “Some were found to be doping, others had genetic defects, and for some, an interpretation was not even possible.”
Some of the individuals had a male genotype but a defect in 5-alpha-reductase, an enzyme essential for the formation of male genitals and hair growth. An athlete with these characteristics, assigned female sex at birth, has a male level of testosterone that stimulates the accumulation of muscle mass, Dr. Moghetti explained. Therefore, the individual has a considerable advantage in performances influenced by this hormone.
“In the end, the Federation decided to set limits on the testosterone levels of athletes participating in certain types of races, especially those in middle distance, that appeared to be more sensitive to differences in hormone levels,” said Dr. Moghetti. “The limitation does not apply to athletes with Morris syndrome, ie, with a male genotype and complete resistance to testosterone, for whom the high level of this hormone does not provide any advantage.” Given the complexity of the problem, he hopes for a case-by-case policy that considers the needs of patients with genetic alterations and those of athletes who have to compete with them.
Not the First Time
A recent incident underscored the difficulty of regulating such complex issues. The World Athletics Federation excluded South African middle-distance runner Caster Semenya from competitions years ago because of excessively high testosterone levels.
“The Federation’s regulations recommend that athletes in these cases reduce hormone levels to values below the threshold of 5 nmol/L of blood for a period of at least 6 months before the race by using hormonal contraceptives. The use of such drugs does not pose a health risk, as they are substances normally taken by women for contraception purposes,” said Amelia Filippelli, a pharmacologist at the University of Salerno in Italy. The South African middle-distance runner refused the drug and appealed to the Court of Arbitration for Sport and later to the Swiss Federal Court. Both rejected her appeal. Finally, Ms. Semenya appealed to the European Court of Human Rights, which in 2023 recognized a violation of her rights but does not have the authority to order a change in the Federation’s regulations.
Beyond the ideologic positions of nonexperts, therefore, the issue is still the subject of debate in the scientific community, which is evaluating not only its medical aspects but also its ethical implications.
This story was translated from Univadis Italy, which is part of the Medscape professional network, using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article appeared on Medscape.com.
The allegations against Algerian boxer Imane Khelif at the Paris Olympics raised the questions of intersexuality and its implications in competitive sports. This news organization has decided to delve into the topic to assist doctors who suspect a similar condition in their patients. No certain clinical data about Ms. Khelif have been made public, so this article does not concern the boxer but rather takes inspiration from the media controversy.
What Is Intersexuality?
Intersexuality encompasses a spectrum of variations in sexual development that lead to the simultaneous presence of typical male and female characteristics. As reiterated by the United Nations Office of the High Commissioner for Human Rights, the medical definition does not affect the patient’s self-identification of gender or sexual orientation.
“The percentage of people who fall within the intersexuality spectrum is less than 0.5 per thousand of the general population, but there are no precise statistics, given the difficulty of definition,” said Roberto Lala, MD, pediatric endocrinologist and president of the Federation of Rare Childhood Diseases.
Indeed, there is not only a strict definition of intersexuality that involves a significant presence of these mixed physical characteristics in a way that conditions the self-image of the subject but also a broad definition, said Dr. Lala. “For example, clitoral hypertrophy in a female otherwise conforming to the female gender, which does not raise doubts about identity,” he said.
Chromosomes, Genes, and Hormones
“The human body is, so to speak, programmed to take on female appearances in development and shifts toward male ones only if exposed to testosterone and other factors. For this to happen, testosterone must be produced during embryonic development, and it must function properly,” said Paolo Moghetti, full professor of endocrinology at the University of Verona, Italy.
The protein encoded by SRY, which is located on the Y chromosome, determines the development of the testicles from undifferentiated tissue of the embryonic gonads. The testicles of the embryo then produce testosterone. The absence of the Y chromosome is a common characteristic of most female individuals. However, there are individuals with a female phenotype who have X and Y chromosomes but lack SRY or have a variant of it that is not entirely functional.
Numerous other chromosomal or genetic variations can lead to alterations in sexual differentiation. “In phenotypically male adult subjects (with a chromosomal makeup of 46XY) with complete androgen insensitivity (so-called Morris syndrome), testosterone levels in the blood are elevated, above normal even for a male, but the hormone is totally ineffective, and the phenotype is totally female at birth, with completely female development of secondary sexual characteristics at puberty,” said Dr. Moghetti.
This means that affected individuals have well-developed breasts and a complete lack or extremely reduced presence of hair, including underarm and pubic hair. Menstruation is also completely absent because there is no uterus, and there are testes, not visible because they are considered in the abdomen.
“There are syndromes that are currently considered congenital but not genetic, of which a genetic origin will probably be identified in the future,” said Dr. Lala.
Some variations in sexual development can be diagnosed prenatally, such as an alteration of the number of sex chromosomes or a discordance between the morphologic characteristics highlighted by ultrasound and the genotype detected by amniocentesis. Some variations are evident at birth because of atypical anatomical characteristics. Others are diagnosed during puberty or later in adulthood, in the presence of infertility. The Italian National Institute of Health details these variations on its website, describing the characteristics that determine diagnosis and treatment.
Pathologies or Variations?
Some anomalies in sexual development negatively affect the patient’s physical health. One example is congenital adrenal hyperplasia. “It results from an inherited defect of the adrenal glands, which reduces cortisol production while increasing testosterone production,” said Dr. Lala. “In addition to the appearance of male characteristics in females, in more severe forms, it carries the risk of collapse and shock and requires pharmacological treatment.” It is undoubtedly a pathology.
Other variations in sexual characteristics do not affect the patient’s physical health negatively. They may, however, have a psychologic effect, sometimes a significant one, because of the lack of social acceptance of a person who cannot be classified within the binary classification of sexes.
“Conditions in which mixed male and female aspects are clearly evident have been and are still pathologized by the family, the treating physician, and society,” said Dr. Lala. “In the late 1970s, when a child was born with intersexual anatomical characteristics, it was common practice to surgically intervene, making them female, because it was technically easier.”
Over the years, patients who, as they grew up, were dissatisfied with the solution adopted at birth began to make their voices heard, Dr. Lala added. Scientific societies and international organizations have spoken out against subjecting intersexual newborns to surgical interventions that are not medically necessary. “Nowadays, decisions are made on a case-by-case basis, taking into account the families’ wishes. Interventions are justified with medical reasons, which are often very nuanced,” Dr. Lala concluded.
Implications for Sports
Traditionally, athletes participating in competitions in certain sports have been divided into male and female categories to ensure a certain equity and uniformity in performance. Over the years, the emergence of new information about sexual development has made it necessary to update the criteria used in this division.
The main factor responsible for the performance diversity between males and females is the action of testosterone on the male and female organism. “Testosterone has important effects on muscle mass and enhances training results,” said Dr. Moghetti. “As a demonstration of this fact, before puberty, the best performances in athletics or swimming by males and females are similar, then males gain a significant advantage of around 10%-20%.”
A few years ago, the World Athletics Federation conducted widespread screening of athletes participating in its world championships. “It identified a small group of individuals with potentially abnormal testosterone levels for the female sex,” said Dr. Moghetti. “Some were found to be doping, others had genetic defects, and for some, an interpretation was not even possible.”
Some of the individuals had a male genotype but a defect in 5-alpha-reductase, an enzyme essential for the formation of male genitals and hair growth. An athlete with these characteristics, assigned female sex at birth, has a male level of testosterone that stimulates the accumulation of muscle mass, Dr. Moghetti explained. Therefore, the individual has a considerable advantage in performances influenced by this hormone.
“In the end, the Federation decided to set limits on the testosterone levels of athletes participating in certain types of races, especially those in middle distance, that appeared to be more sensitive to differences in hormone levels,” said Dr. Moghetti. “The limitation does not apply to athletes with Morris syndrome, ie, with a male genotype and complete resistance to testosterone, for whom the high level of this hormone does not provide any advantage.” Given the complexity of the problem, he hopes for a case-by-case policy that considers the needs of patients with genetic alterations and those of athletes who have to compete with them.
Not the First Time
A recent incident underscored the difficulty of regulating such complex issues. The World Athletics Federation excluded South African middle-distance runner Caster Semenya from competitions years ago because of excessively high testosterone levels.
“The Federation’s regulations recommend that athletes in these cases reduce hormone levels to values below the threshold of 5 nmol/L of blood for a period of at least 6 months before the race by using hormonal contraceptives. The use of such drugs does not pose a health risk, as they are substances normally taken by women for contraception purposes,” said Amelia Filippelli, a pharmacologist at the University of Salerno in Italy. The South African middle-distance runner refused the drug and appealed to the Court of Arbitration for Sport and later to the Swiss Federal Court. Both rejected her appeal. Finally, Ms. Semenya appealed to the European Court of Human Rights, which in 2023 recognized a violation of her rights but does not have the authority to order a change in the Federation’s regulations.
Beyond the ideologic positions of nonexperts, therefore, the issue is still the subject of debate in the scientific community, which is evaluating not only its medical aspects but also its ethical implications.
This story was translated from Univadis Italy, which is part of the Medscape professional network, using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article appeared on Medscape.com.
Storybooks Can Help Children Deal with Skin Conditions
TORONTO —
So far, “the study demonstrates that these books have value to patients and families,” one of the study authors, Sonia Havele, MD, a pediatrician and dermatology resident at Children’s Mercy Hospital Kansas City, Kansas City, Missouri, said in an interview.
“There are tools to help kids cope with their skin conditions, but we’re underutilizing them,” she added. “And part of the reason we’re underutilizing storybooks is that we just don’t know what’s out there.” For the study, the researchers received funding to purchase 18 “creative and thoughtful” storybooks related to pediatric skin conditions, reviewed by at least two pediatric dermatologists before being selected, which are just a sample of related books that are available.
The study results were presented as a poster at the annual meeting of the Society for Pediatric Dermatology.
Children with visible skin conditions, which can include port-wine stains, capillary malformations, and congenital moles, may be subjected to teasing or bullying at school, and the conditions can also affect their quality of life.
Beauty and the Birthmark
The books include one titled “Beauty with a Birthmark” and another, “My Hair Went on Vacation.” An illustrated book, “Just Ask: Be Different, Be Brave, Be You,” by US Supreme Court Justice Sonia Sotomayor, offers tips on how to answer common questions about someone’s appearance.
Dr. Havele said that Justice Sotomayor’s book “empowers kids, their siblings, their classmates ... to ask questions, and it teaches patients not to be afraid of those questions, and to really lean into educating their peers, and their family members.”
“Kids are really just curious,” she added. “They’ll make comments like: ‘Hey, what’s that spot on your face?’ Or, they’ll ask about vitiligo because they’ve never seen somebody with it before.”
To evaluate the psychosocial impact of these types of books for children with visible skin conditions, Dr. Havele and colleagues designed a study that includes patients aged 2-12 years dealing with issues related to self-esteem, acceptance, coping, or bullying. Parents are provided with a relevant storybook to read at home with their child in a “safe and comfortable space” and “at their own pace and their own time,” said Dr. Havele.
Inside the book is a QR code to access the validated Children’s Dermatology Life Quality Index (CDLQI). Families complete the survey at baseline and provide feedback after reading the book. Researchers collect information about demographics, age, gender, and skin conditions, which included atopic dermatitis, alopecia areata, vitiligo, hemangioma, and port-wine stain.
The response rate so far is 34%, and close to 80 parents have completed the survey with their child, Dr. Havele said.
At baseline, many of the children were either moderately or severely affected in terms of their quality of life (45% scored ≥ 6 on the CDLQI).
After reading the book, about 80% of parents reported it had a positive impact, and about 20% said it had a somewhat positive impact on their child’s self-image or confidence. Almost 80% agreed, and the remainder somewhat agreed it encouraged their child to embrace differences.
Most respondents also said the book helped the parent and child cope with the child’s condition. “So really, it was overall a positive response,” said Dr. Havele. “We are able to demonstrate that these books have value in a more scientific or objective way.”
This may not be surprising. Dr. Havele referred to more formal bibliotherapy (book therapy), which has been studied in other pediatric populations, including patients with cancer and those who have experienced trauma.
Awesome Space
Pediatric dermatologists are perfectly positioned to play a role in improving the lives of their patients with skin issues. “We see the impact of visible skin disease on children all the time,” said Dr. Havele. “The dermatology visit is an awesome space and opportunity to introduce these books to families and potentially help them talk about the skin condition with their child.”
In addition to prescribing therapies, “we’re also with these kids through an emotional journey, and I think giving them tools for that emotional journey is very helpful,” she added.
Such books would have been a great help to Dr. Havele herself. Growing up, she had severe atopic dermatitis covering much of her body. “Having such a resource would have helped me better cope with my reality of being different than everyone else.”
She hopes a database will be established to house these resources so other providers can refer patients to the list of books. Other books include “The Itchy-saurus: The Dino with an itch that can’t be scratched,” “Hair in My Brush,” and “I am Unique!”
Dr. Havele had no relevant disclosures.
A version of this article first appeared on Medscape.com.
TORONTO —
So far, “the study demonstrates that these books have value to patients and families,” one of the study authors, Sonia Havele, MD, a pediatrician and dermatology resident at Children’s Mercy Hospital Kansas City, Kansas City, Missouri, said in an interview.
“There are tools to help kids cope with their skin conditions, but we’re underutilizing them,” she added. “And part of the reason we’re underutilizing storybooks is that we just don’t know what’s out there.” For the study, the researchers received funding to purchase 18 “creative and thoughtful” storybooks related to pediatric skin conditions, reviewed by at least two pediatric dermatologists before being selected, which are just a sample of related books that are available.
The study results were presented as a poster at the annual meeting of the Society for Pediatric Dermatology.
Children with visible skin conditions, which can include port-wine stains, capillary malformations, and congenital moles, may be subjected to teasing or bullying at school, and the conditions can also affect their quality of life.
Beauty and the Birthmark
The books include one titled “Beauty with a Birthmark” and another, “My Hair Went on Vacation.” An illustrated book, “Just Ask: Be Different, Be Brave, Be You,” by US Supreme Court Justice Sonia Sotomayor, offers tips on how to answer common questions about someone’s appearance.
Dr. Havele said that Justice Sotomayor’s book “empowers kids, their siblings, their classmates ... to ask questions, and it teaches patients not to be afraid of those questions, and to really lean into educating their peers, and their family members.”
“Kids are really just curious,” she added. “They’ll make comments like: ‘Hey, what’s that spot on your face?’ Or, they’ll ask about vitiligo because they’ve never seen somebody with it before.”
To evaluate the psychosocial impact of these types of books for children with visible skin conditions, Dr. Havele and colleagues designed a study that includes patients aged 2-12 years dealing with issues related to self-esteem, acceptance, coping, or bullying. Parents are provided with a relevant storybook to read at home with their child in a “safe and comfortable space” and “at their own pace and their own time,” said Dr. Havele.
Inside the book is a QR code to access the validated Children’s Dermatology Life Quality Index (CDLQI). Families complete the survey at baseline and provide feedback after reading the book. Researchers collect information about demographics, age, gender, and skin conditions, which included atopic dermatitis, alopecia areata, vitiligo, hemangioma, and port-wine stain.
The response rate so far is 34%, and close to 80 parents have completed the survey with their child, Dr. Havele said.
At baseline, many of the children were either moderately or severely affected in terms of their quality of life (45% scored ≥ 6 on the CDLQI).
After reading the book, about 80% of parents reported it had a positive impact, and about 20% said it had a somewhat positive impact on their child’s self-image or confidence. Almost 80% agreed, and the remainder somewhat agreed it encouraged their child to embrace differences.
Most respondents also said the book helped the parent and child cope with the child’s condition. “So really, it was overall a positive response,” said Dr. Havele. “We are able to demonstrate that these books have value in a more scientific or objective way.”
This may not be surprising. Dr. Havele referred to more formal bibliotherapy (book therapy), which has been studied in other pediatric populations, including patients with cancer and those who have experienced trauma.
Awesome Space
Pediatric dermatologists are perfectly positioned to play a role in improving the lives of their patients with skin issues. “We see the impact of visible skin disease on children all the time,” said Dr. Havele. “The dermatology visit is an awesome space and opportunity to introduce these books to families and potentially help them talk about the skin condition with their child.”
In addition to prescribing therapies, “we’re also with these kids through an emotional journey, and I think giving them tools for that emotional journey is very helpful,” she added.
Such books would have been a great help to Dr. Havele herself. Growing up, she had severe atopic dermatitis covering much of her body. “Having such a resource would have helped me better cope with my reality of being different than everyone else.”
She hopes a database will be established to house these resources so other providers can refer patients to the list of books. Other books include “The Itchy-saurus: The Dino with an itch that can’t be scratched,” “Hair in My Brush,” and “I am Unique!”
Dr. Havele had no relevant disclosures.
A version of this article first appeared on Medscape.com.
TORONTO —
So far, “the study demonstrates that these books have value to patients and families,” one of the study authors, Sonia Havele, MD, a pediatrician and dermatology resident at Children’s Mercy Hospital Kansas City, Kansas City, Missouri, said in an interview.
“There are tools to help kids cope with their skin conditions, but we’re underutilizing them,” she added. “And part of the reason we’re underutilizing storybooks is that we just don’t know what’s out there.” For the study, the researchers received funding to purchase 18 “creative and thoughtful” storybooks related to pediatric skin conditions, reviewed by at least two pediatric dermatologists before being selected, which are just a sample of related books that are available.
The study results were presented as a poster at the annual meeting of the Society for Pediatric Dermatology.
Children with visible skin conditions, which can include port-wine stains, capillary malformations, and congenital moles, may be subjected to teasing or bullying at school, and the conditions can also affect their quality of life.
Beauty and the Birthmark
The books include one titled “Beauty with a Birthmark” and another, “My Hair Went on Vacation.” An illustrated book, “Just Ask: Be Different, Be Brave, Be You,” by US Supreme Court Justice Sonia Sotomayor, offers tips on how to answer common questions about someone’s appearance.
Dr. Havele said that Justice Sotomayor’s book “empowers kids, their siblings, their classmates ... to ask questions, and it teaches patients not to be afraid of those questions, and to really lean into educating their peers, and their family members.”
“Kids are really just curious,” she added. “They’ll make comments like: ‘Hey, what’s that spot on your face?’ Or, they’ll ask about vitiligo because they’ve never seen somebody with it before.”
To evaluate the psychosocial impact of these types of books for children with visible skin conditions, Dr. Havele and colleagues designed a study that includes patients aged 2-12 years dealing with issues related to self-esteem, acceptance, coping, or bullying. Parents are provided with a relevant storybook to read at home with their child in a “safe and comfortable space” and “at their own pace and their own time,” said Dr. Havele.
Inside the book is a QR code to access the validated Children’s Dermatology Life Quality Index (CDLQI). Families complete the survey at baseline and provide feedback after reading the book. Researchers collect information about demographics, age, gender, and skin conditions, which included atopic dermatitis, alopecia areata, vitiligo, hemangioma, and port-wine stain.
The response rate so far is 34%, and close to 80 parents have completed the survey with their child, Dr. Havele said.
At baseline, many of the children were either moderately or severely affected in terms of their quality of life (45% scored ≥ 6 on the CDLQI).
After reading the book, about 80% of parents reported it had a positive impact, and about 20% said it had a somewhat positive impact on their child’s self-image or confidence. Almost 80% agreed, and the remainder somewhat agreed it encouraged their child to embrace differences.
Most respondents also said the book helped the parent and child cope with the child’s condition. “So really, it was overall a positive response,” said Dr. Havele. “We are able to demonstrate that these books have value in a more scientific or objective way.”
This may not be surprising. Dr. Havele referred to more formal bibliotherapy (book therapy), which has been studied in other pediatric populations, including patients with cancer and those who have experienced trauma.
Awesome Space
Pediatric dermatologists are perfectly positioned to play a role in improving the lives of their patients with skin issues. “We see the impact of visible skin disease on children all the time,” said Dr. Havele. “The dermatology visit is an awesome space and opportunity to introduce these books to families and potentially help them talk about the skin condition with their child.”
In addition to prescribing therapies, “we’re also with these kids through an emotional journey, and I think giving them tools for that emotional journey is very helpful,” she added.
Such books would have been a great help to Dr. Havele herself. Growing up, she had severe atopic dermatitis covering much of her body. “Having such a resource would have helped me better cope with my reality of being different than everyone else.”
She hopes a database will be established to house these resources so other providers can refer patients to the list of books. Other books include “The Itchy-saurus: The Dino with an itch that can’t be scratched,” “Hair in My Brush,” and “I am Unique!”
Dr. Havele had no relevant disclosures.
A version of this article first appeared on Medscape.com.
FROM SPD 2024
Predicting RSV’s Role in the Upcoming Winter Respiratory Season
For children younger than 5 years old, RSV is the main drive — approximately 2,000,000 outpatient/ED visits and about 75,000 hospitalizations annually. RSV disease ranges from upper respiratory tract infections, eg, in older children and healthy adults, to more severe lower tract disease in young children and the elderly. Premature infants and high-risk groups are particularly prone to severe disease.1 Up to 300 pediatric RSV deaths occur yearly. “Normal” RSV seasons start in mid-November, peak in late December-January, and end after April. Note: More drawn out seasons occur in southern latitudes, eg Texas or Florida. But lately RSV seasons have been anything but normal.
2015-2016 to 2022-2023
RSV data from the Pediatric Health Information System (PHIS), collected at over 49 US children’s hospitals during 2015 to early 2023, show how crazy RSV seasons have been lately.2 The involved months, intensity, and duration of four prepandemic seasons were pretty “normal” (Figure 1). The 2019-2020 season started normally, peaked in January 2020, and was slowing as expected by February. But when SARS-Cov-2 restrictions kicked in during mid-March, RSV detections tanked to almost nothing (ditto other respiratory viruses). A near 14-month RSV hiatus meant that the 2020-2021 RSV season never materialized. However, RSV was not done with us in 2021. It rebounded in May with weekly hospitalizations peaking in late July; this “rebound season” lasted 9 months, not dropping to baseline until February 2022 (Figure 1).
I guess we should have expected a post-pandemic “disturbance in the Force,” as Yoda once said; but I sure didn’t see a prolonged summer/fall/early winter RSV season coming. It was like two “normal” seasons mashed up into one late-but-long season. Not to be outdone, the 2022-2023 RSV season started early (September) and hospitalizations skyrocketed to peak in November at over twice the peak number from any year since 2015, overloading hospitals (influenza and SARS-Cov-2 seasons were co-circulating). The season terminated early though (March 2023).
Okay, so RSV seasonality/intensity were weird post pandemic, but was anything else different? Some 2021-2023 data suggest more RSV disease in older children, rather than the usual younger than 18 month-olds going through their first winter.3 More medically attended RSV in older ages (2-4 years of life) may have been due to the pandemic year without RSV circulation distorting herd immunity, ie older children remained RSV naive. Other data suggest the apparent increase was really just more frequent multiplex viral testing in older children triggered by SARS-CoV-2 co-circulation.4 More data are needed to decide.
CDC 2023-2024 RESP-NET data
The 2023-2024 winter surge (Figure 2), as measured by RESP-NET’s cumulative RSV, influenza and SARS-CoV-2 hospitalization rates for 0- to 5-year-olds,5 shows that all three viruses’ seasonal months were normal-ish: late October 2023 start, late December-early January peak, and mid-May 2024 return to baseline. RSV season was approximately 22% less severe by area-under-the-curve calculations compared with 2022-2023, but still worse than prepandemic years.6 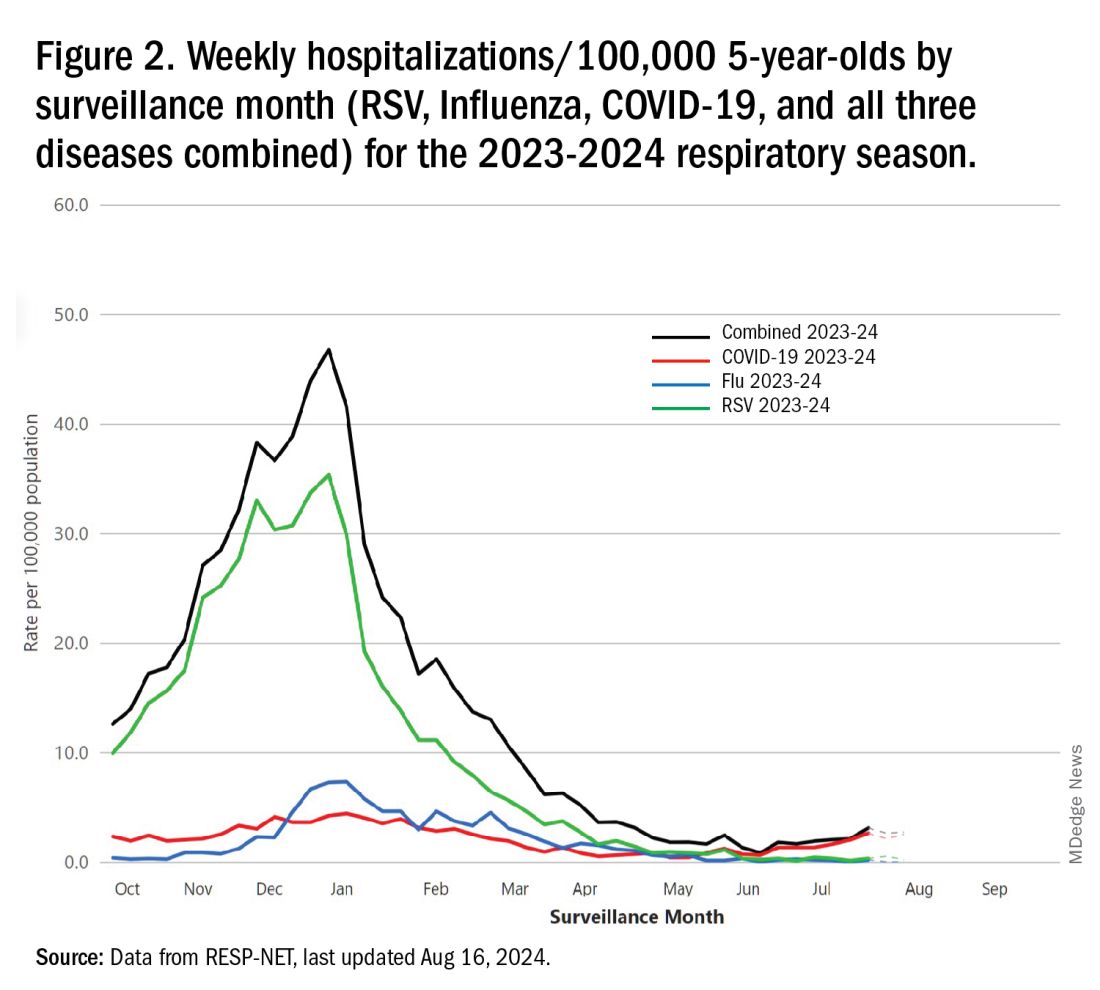
One wonders if the 2022-2023 RSV season might have been worse but for use of the limited supply of nirsevimab.7
Viral Parade
Now we ready ourselves for the 2024-2025 respiratory surge, wondering what nature has in store for us. Will the usual “respiratory virus parade” occur? Will rhinovirus and parainfluenza prevalence bump after a few weeks of schools being in session, adding to the now-usual summer/fall SARS-CoV-2 surge? Note: Twenty-seven states as of Aug. 16 had high SARS-CoV-2 detection in wastewater. Will RSV and influenza start sometime in October/November, peak in January (along with rising SARS-CoV2 activity), followed by a second parainfluenza bump as SARS-CoV-2, influenza, and RSV drop off in April/May? Further, will RSV and influenza seasons be more or less severe than the last 2 years?
Prediction
The overall 2024-2025 respiratory season will be less severe than the past 2 years and hopefully than recent prepandemic years. What is the blueprint for a milder season? First, herd immunity to non-RSV and non-influenza viruses (parainfluenza, rhinovirus, metapneumovirus, adenovirus) in older children should be normalized after 2 years back to usual social activity. So, I expect no mega-seasons from them. The emerging SARS-CoV-2 virus (LB.1) is immunologically close to its recent still-circulating ancestors (KP.2, KP.2.3, KP.3 and KP.3.1.1), so existing SARS-CoV2 herd immunity along with recommended booster vaccine uptake should keep the lid on SARS-CoV2.

Influenza Could Be the Bad News
Which type will dominate? Will a drift/shift occur or vaccine-mismatch reduce vaccine effectiveness? Can we get at least half the population influenza vaccinated, given the vaccine fatigue permeating the US population? The influenza season now underway in the Southern Hemisphere usually helps us predict our season. The Australian May-August 2024 experience (still on an upward trajectory for severity in mid-August) saw no drift/shift or vaccine mismatch. However, this 2024 season has been as severe as 2022 (their worst in a decade). That said, more than 95% has been type A (mostly H1N1 but H3N2 increased in July). So, if our overall 2024-2025 respiratory season is not milder, influenza is the most likely culprit. To reduce chances of influenza being the fly-in-the-ointment, we need to be particularly proactive with seasonal influenza vaccine which is back to the traditional trivalent formulation (one H1N1, one H3N2, and one B type).8 All of this could go out the window if avian influenza becomes more transmissible, but that seems unlikely at present.
Mild RSV Season?
RSV season should be blunted because of the increased use of both the remarkably effective CDC-recommended maternal RSV vaccine9 (one dose during pregnancy weeks 32 through 36, administered September through January) and of nirsevimab (up to 90% reduction in hospitalizations and ED visits).10 (See Figure 3.) 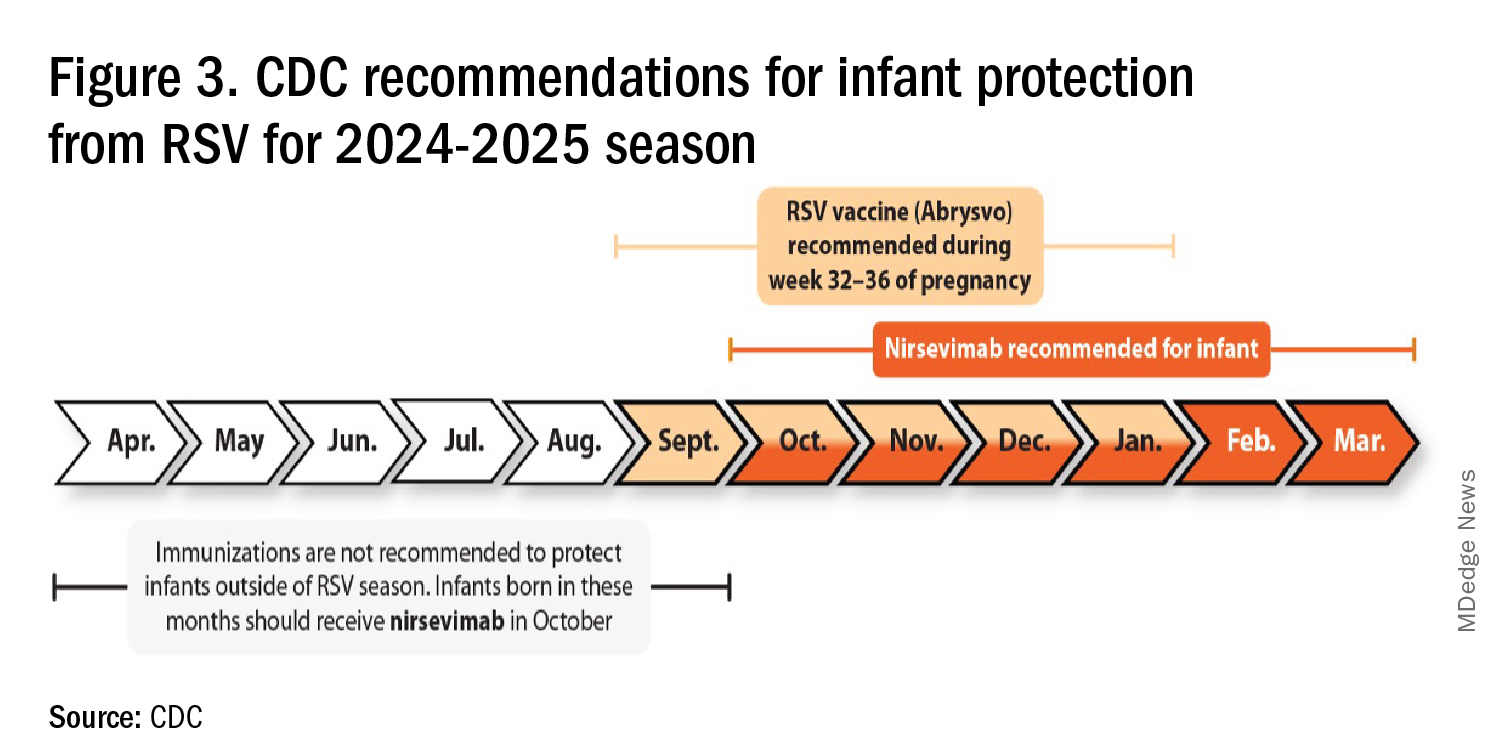
I also expect residual disease to occur mostly in younger than 18 month-olds (the “normal” aged population experiencing their first winter), who received no passive immunity (mother RSV unvaccinated and child did not receive nirsevimab). Some disease will still occur in high-risk infants/children. However, unlike active vaccination strategies, a competent immune system is not required to benefit from passive antibody, whether transplacental or directly administered.
Deep Thought
What if the traditional RSV seasonal hospitalization surge fails to materialize this season? It could happen. If we could get high acceptance/uptake of maternal vaccine and infant nirsevimab, RSV season could resemble the dramatic drop in rotavirus disease the second year after rotavirus vaccine introduction. We could be asking ourselves — “What happened to RSV?”
Dr. Harrison is professor of pediatrics and pediatric infectious diseases at Children’s Mercy Hospitals and Clinics, Kansas City, Missouri. He said he had no relevant financial disclosures. Email him at [email protected].
References
1. CDC. RSV in Infants and Young Children. Respiratory Syncytial Virus Infection (RSV). June 18, 2024. https://www.cdc.gov/rsv/infants-young-children/index.html.
2. Suss RJ and Simões EAF. Respiratory Syncytial Virus Hospital-Based Burden of Disease in Children Younger Than 5 Respiratory Syncytial Virus Hospital-Based Burden of Disease in Children Younger Than 5 Years, 2015-2022. JAMA Netw Open. 2024;7(4):e247125. doi:10.1001/jamanetworkopen.2024.7125.
3. Winthrop ZA et al. Pediatric Respiratory Syncytial Virus Hospitalizations and Respiratory Support After the COVID-19 Pandemic. JAMA Netw Open. 2024;7(6):e2416852. doi:10.1001/jamanetworkopen.2024.16852.
4. Petros BA et al. Increased Pediatric RSV Case Counts Following the Emergence of SARS-CoV-2 Are Attributable to Increased Testing. medRxiv [Preprint]. 2024 Feb 12:2024.02.06.24302387. doi: 10.1101/2024.02.06.24302387.
5. Rates of Laboratory-Confirmed RSV, COVID-19, and Flu Hospitalizations from the RESP-NET Surveillance Systems. Centers for Disease Control and Prevention. https://data.cdc.gov/Public-Health-Surveillance/Rates-of-Laboratory-Confirmed-RSV-COVID-19-and-Flu/kvib-3txy/about_data.
6. CDC. Evaluating the 2023-2024 Respiratory Disease Season Outlook. CFA: Qualitative Assessments. August 14, 2024. https://www.cdc.gov/cfa-qualitative-assessments/php/data-research/2023-2024-season-outlook-retro.html.
7. Health Alert Network (HAN). Limited Availability of Nirsevimab in the United States—Interim CDC Recommendations to Protect Infants from Respiratory Syncytial Virus (RSV) during the 2023–2024 Respiratory Virus Season. October 23, 2023. https://emergency.cdc.gov/han/2023/han00499.asp.
8. CDC. Information for the 2024-2025 Flu Season. Centers for Disease Control and Prevention. March 14, 2024. https://www.cdc.gov/flu/season/faq-flu-season-2024-2025.htm.
9. Kampmann B et al. Bivalent Prefusion F Vaccine in Pregnancy to Prevent RSV Illness in Infants. N Engl J Med. 2023 Apr 20;388(16):1451-1464. doi: 10.1056/NEJMoa2216480.
10. Moline HL. Early Estimate of Nirsevimab Effectiveness for Prevention of Respiratory Syncytial Virus–Associated Hospitalization Among Infants Entering Their First Respiratory Syncytial Virus Season — New Vaccine Surveillance Network, October 2023–February 2024. MMWR Morb Mortal Wkly Rep. 2024;73. doi: 10.15585/mmwr.mm7309a4.
For children younger than 5 years old, RSV is the main drive — approximately 2,000,000 outpatient/ED visits and about 75,000 hospitalizations annually. RSV disease ranges from upper respiratory tract infections, eg, in older children and healthy adults, to more severe lower tract disease in young children and the elderly. Premature infants and high-risk groups are particularly prone to severe disease.1 Up to 300 pediatric RSV deaths occur yearly. “Normal” RSV seasons start in mid-November, peak in late December-January, and end after April. Note: More drawn out seasons occur in southern latitudes, eg Texas or Florida. But lately RSV seasons have been anything but normal.
2015-2016 to 2022-2023
RSV data from the Pediatric Health Information System (PHIS), collected at over 49 US children’s hospitals during 2015 to early 2023, show how crazy RSV seasons have been lately.2 The involved months, intensity, and duration of four prepandemic seasons were pretty “normal” (Figure 1). The 2019-2020 season started normally, peaked in January 2020, and was slowing as expected by February. But when SARS-Cov-2 restrictions kicked in during mid-March, RSV detections tanked to almost nothing (ditto other respiratory viruses). A near 14-month RSV hiatus meant that the 2020-2021 RSV season never materialized. However, RSV was not done with us in 2021. It rebounded in May with weekly hospitalizations peaking in late July; this “rebound season” lasted 9 months, not dropping to baseline until February 2022 (Figure 1).
I guess we should have expected a post-pandemic “disturbance in the Force,” as Yoda once said; but I sure didn’t see a prolonged summer/fall/early winter RSV season coming. It was like two “normal” seasons mashed up into one late-but-long season. Not to be outdone, the 2022-2023 RSV season started early (September) and hospitalizations skyrocketed to peak in November at over twice the peak number from any year since 2015, overloading hospitals (influenza and SARS-Cov-2 seasons were co-circulating). The season terminated early though (March 2023).
Okay, so RSV seasonality/intensity were weird post pandemic, but was anything else different? Some 2021-2023 data suggest more RSV disease in older children, rather than the usual younger than 18 month-olds going through their first winter.3 More medically attended RSV in older ages (2-4 years of life) may have been due to the pandemic year without RSV circulation distorting herd immunity, ie older children remained RSV naive. Other data suggest the apparent increase was really just more frequent multiplex viral testing in older children triggered by SARS-CoV-2 co-circulation.4 More data are needed to decide.
CDC 2023-2024 RESP-NET data
The 2023-2024 winter surge (Figure 2), as measured by RESP-NET’s cumulative RSV, influenza and SARS-CoV-2 hospitalization rates for 0- to 5-year-olds,5 shows that all three viruses’ seasonal months were normal-ish: late October 2023 start, late December-early January peak, and mid-May 2024 return to baseline. RSV season was approximately 22% less severe by area-under-the-curve calculations compared with 2022-2023, but still worse than prepandemic years.6
One wonders if the 2022-2023 RSV season might have been worse but for use of the limited supply of nirsevimab.7
Viral Parade
Now we ready ourselves for the 2024-2025 respiratory surge, wondering what nature has in store for us. Will the usual “respiratory virus parade” occur? Will rhinovirus and parainfluenza prevalence bump after a few weeks of schools being in session, adding to the now-usual summer/fall SARS-CoV-2 surge? Note: Twenty-seven states as of Aug. 16 had high SARS-CoV-2 detection in wastewater. Will RSV and influenza start sometime in October/November, peak in January (along with rising SARS-CoV2 activity), followed by a second parainfluenza bump as SARS-CoV-2, influenza, and RSV drop off in April/May? Further, will RSV and influenza seasons be more or less severe than the last 2 years?
Prediction
The overall 2024-2025 respiratory season will be less severe than the past 2 years and hopefully than recent prepandemic years. What is the blueprint for a milder season? First, herd immunity to non-RSV and non-influenza viruses (parainfluenza, rhinovirus, metapneumovirus, adenovirus) in older children should be normalized after 2 years back to usual social activity. So, I expect no mega-seasons from them. The emerging SARS-CoV-2 virus (LB.1) is immunologically close to its recent still-circulating ancestors (KP.2, KP.2.3, KP.3 and KP.3.1.1), so existing SARS-CoV2 herd immunity along with recommended booster vaccine uptake should keep the lid on SARS-CoV2.
Influenza Could Be the Bad News
Which type will dominate? Will a drift/shift occur or vaccine-mismatch reduce vaccine effectiveness? Can we get at least half the population influenza vaccinated, given the vaccine fatigue permeating the US population? The influenza season now underway in the Southern Hemisphere usually helps us predict our season. The Australian May-August 2024 experience (still on an upward trajectory for severity in mid-August) saw no drift/shift or vaccine mismatch. However, this 2024 season has been as severe as 2022 (their worst in a decade). That said, more than 95% has been type A (mostly H1N1 but H3N2 increased in July). So, if our overall 2024-2025 respiratory season is not milder, influenza is the most likely culprit. To reduce chances of influenza being the fly-in-the-ointment, we need to be particularly proactive with seasonal influenza vaccine which is back to the traditional trivalent formulation (one H1N1, one H3N2, and one B type).8 All of this could go out the window if avian influenza becomes more transmissible, but that seems unlikely at present.
Mild RSV Season?
RSV season should be blunted because of the increased use of both the remarkably effective CDC-recommended maternal RSV vaccine9 (one dose during pregnancy weeks 32 through 36, administered September through January) and of nirsevimab (up to 90% reduction in hospitalizations and ED visits).10 (See Figure 3.)
I also expect residual disease to occur mostly in younger than 18 month-olds (the “normal” aged population experiencing their first winter), who received no passive immunity (mother RSV unvaccinated and child did not receive nirsevimab). Some disease will still occur in high-risk infants/children. However, unlike active vaccination strategies, a competent immune system is not required to benefit from passive antibody, whether transplacental or directly administered.
Deep Thought
What if the traditional RSV seasonal hospitalization surge fails to materialize this season? It could happen. If we could get high acceptance/uptake of maternal vaccine and infant nirsevimab, RSV season could resemble the dramatic drop in rotavirus disease the second year after rotavirus vaccine introduction. We could be asking ourselves — “What happened to RSV?”
Dr. Harrison is professor of pediatrics and pediatric infectious diseases at Children’s Mercy Hospitals and Clinics, Kansas City, Missouri. He said he had no relevant financial disclosures. Email him at [email protected].
References
1. CDC. RSV in Infants and Young Children. Respiratory Syncytial Virus Infection (RSV). June 18, 2024. https://www.cdc.gov/rsv/infants-young-children/index.html.
2. Suss RJ and Simões EAF. Respiratory Syncytial Virus Hospital-Based Burden of Disease in Children Younger Than 5 Respiratory Syncytial Virus Hospital-Based Burden of Disease in Children Younger Than 5 Years, 2015-2022. JAMA Netw Open. 2024;7(4):e247125. doi:10.1001/jamanetworkopen.2024.7125.
3. Winthrop ZA et al. Pediatric Respiratory Syncytial Virus Hospitalizations and Respiratory Support After the COVID-19 Pandemic. JAMA Netw Open. 2024;7(6):e2416852. doi:10.1001/jamanetworkopen.2024.16852.
4. Petros BA et al. Increased Pediatric RSV Case Counts Following the Emergence of SARS-CoV-2 Are Attributable to Increased Testing. medRxiv [Preprint]. 2024 Feb 12:2024.02.06.24302387. doi: 10.1101/2024.02.06.24302387.
5. Rates of Laboratory-Confirmed RSV, COVID-19, and Flu Hospitalizations from the RESP-NET Surveillance Systems. Centers for Disease Control and Prevention. https://data.cdc.gov/Public-Health-Surveillance/Rates-of-Laboratory-Confirmed-RSV-COVID-19-and-Flu/kvib-3txy/about_data.
6. CDC. Evaluating the 2023-2024 Respiratory Disease Season Outlook. CFA: Qualitative Assessments. August 14, 2024. https://www.cdc.gov/cfa-qualitative-assessments/php/data-research/2023-2024-season-outlook-retro.html.
7. Health Alert Network (HAN). Limited Availability of Nirsevimab in the United States—Interim CDC Recommendations to Protect Infants from Respiratory Syncytial Virus (RSV) during the 2023–2024 Respiratory Virus Season. October 23, 2023. https://emergency.cdc.gov/han/2023/han00499.asp.
8. CDC. Information for the 2024-2025 Flu Season. Centers for Disease Control and Prevention. March 14, 2024. https://www.cdc.gov/flu/season/faq-flu-season-2024-2025.htm.
9. Kampmann B et al. Bivalent Prefusion F Vaccine in Pregnancy to Prevent RSV Illness in Infants. N Engl J Med. 2023 Apr 20;388(16):1451-1464. doi: 10.1056/NEJMoa2216480.
10. Moline HL. Early Estimate of Nirsevimab Effectiveness for Prevention of Respiratory Syncytial Virus–Associated Hospitalization Among Infants Entering Their First Respiratory Syncytial Virus Season — New Vaccine Surveillance Network, October 2023–February 2024. MMWR Morb Mortal Wkly Rep. 2024;73. doi: 10.15585/mmwr.mm7309a4.
For children younger than 5 years old, RSV is the main drive — approximately 2,000,000 outpatient/ED visits and about 75,000 hospitalizations annually. RSV disease ranges from upper respiratory tract infections, eg, in older children and healthy adults, to more severe lower tract disease in young children and the elderly. Premature infants and high-risk groups are particularly prone to severe disease.1 Up to 300 pediatric RSV deaths occur yearly. “Normal” RSV seasons start in mid-November, peak in late December-January, and end after April. Note: More drawn out seasons occur in southern latitudes, eg Texas or Florida. But lately RSV seasons have been anything but normal.
2015-2016 to 2022-2023
RSV data from the Pediatric Health Information System (PHIS), collected at over 49 US children’s hospitals during 2015 to early 2023, show how crazy RSV seasons have been lately.2 The involved months, intensity, and duration of four prepandemic seasons were pretty “normal” (Figure 1). The 2019-2020 season started normally, peaked in January 2020, and was slowing as expected by February. But when SARS-Cov-2 restrictions kicked in during mid-March, RSV detections tanked to almost nothing (ditto other respiratory viruses). A near 14-month RSV hiatus meant that the 2020-2021 RSV season never materialized. However, RSV was not done with us in 2021. It rebounded in May with weekly hospitalizations peaking in late July; this “rebound season” lasted 9 months, not dropping to baseline until February 2022 (Figure 1).
I guess we should have expected a post-pandemic “disturbance in the Force,” as Yoda once said; but I sure didn’t see a prolonged summer/fall/early winter RSV season coming. It was like two “normal” seasons mashed up into one late-but-long season. Not to be outdone, the 2022-2023 RSV season started early (September) and hospitalizations skyrocketed to peak in November at over twice the peak number from any year since 2015, overloading hospitals (influenza and SARS-Cov-2 seasons were co-circulating). The season terminated early though (March 2023).
Okay, so RSV seasonality/intensity were weird post pandemic, but was anything else different? Some 2021-2023 data suggest more RSV disease in older children, rather than the usual younger than 18 month-olds going through their first winter.3 More medically attended RSV in older ages (2-4 years of life) may have been due to the pandemic year without RSV circulation distorting herd immunity, ie older children remained RSV naive. Other data suggest the apparent increase was really just more frequent multiplex viral testing in older children triggered by SARS-CoV-2 co-circulation.4 More data are needed to decide.
CDC 2023-2024 RESP-NET data
The 2023-2024 winter surge (Figure 2), as measured by RESP-NET’s cumulative RSV, influenza and SARS-CoV-2 hospitalization rates for 0- to 5-year-olds,5 shows that all three viruses’ seasonal months were normal-ish: late October 2023 start, late December-early January peak, and mid-May 2024 return to baseline. RSV season was approximately 22% less severe by area-under-the-curve calculations compared with 2022-2023, but still worse than prepandemic years.6
One wonders if the 2022-2023 RSV season might have been worse but for use of the limited supply of nirsevimab.7
Viral Parade
Now we ready ourselves for the 2024-2025 respiratory surge, wondering what nature has in store for us. Will the usual “respiratory virus parade” occur? Will rhinovirus and parainfluenza prevalence bump after a few weeks of schools being in session, adding to the now-usual summer/fall SARS-CoV-2 surge? Note: Twenty-seven states as of Aug. 16 had high SARS-CoV-2 detection in wastewater. Will RSV and influenza start sometime in October/November, peak in January (along with rising SARS-CoV2 activity), followed by a second parainfluenza bump as SARS-CoV-2, influenza, and RSV drop off in April/May? Further, will RSV and influenza seasons be more or less severe than the last 2 years?
Prediction
The overall 2024-2025 respiratory season will be less severe than the past 2 years and hopefully than recent prepandemic years. What is the blueprint for a milder season? First, herd immunity to non-RSV and non-influenza viruses (parainfluenza, rhinovirus, metapneumovirus, adenovirus) in older children should be normalized after 2 years back to usual social activity. So, I expect no mega-seasons from them. The emerging SARS-CoV-2 virus (LB.1) is immunologically close to its recent still-circulating ancestors (KP.2, KP.2.3, KP.3 and KP.3.1.1), so existing SARS-CoV2 herd immunity along with recommended booster vaccine uptake should keep the lid on SARS-CoV2.
Influenza Could Be the Bad News
Which type will dominate? Will a drift/shift occur or vaccine-mismatch reduce vaccine effectiveness? Can we get at least half the population influenza vaccinated, given the vaccine fatigue permeating the US population? The influenza season now underway in the Southern Hemisphere usually helps us predict our season. The Australian May-August 2024 experience (still on an upward trajectory for severity in mid-August) saw no drift/shift or vaccine mismatch. However, this 2024 season has been as severe as 2022 (their worst in a decade). That said, more than 95% has been type A (mostly H1N1 but H3N2 increased in July). So, if our overall 2024-2025 respiratory season is not milder, influenza is the most likely culprit. To reduce chances of influenza being the fly-in-the-ointment, we need to be particularly proactive with seasonal influenza vaccine which is back to the traditional trivalent formulation (one H1N1, one H3N2, and one B type).8 All of this could go out the window if avian influenza becomes more transmissible, but that seems unlikely at present.
Mild RSV Season?
RSV season should be blunted because of the increased use of both the remarkably effective CDC-recommended maternal RSV vaccine9 (one dose during pregnancy weeks 32 through 36, administered September through January) and of nirsevimab (up to 90% reduction in hospitalizations and ED visits).10 (See Figure 3.)
I also expect residual disease to occur mostly in younger than 18 month-olds (the “normal” aged population experiencing their first winter), who received no passive immunity (mother RSV unvaccinated and child did not receive nirsevimab). Some disease will still occur in high-risk infants/children. However, unlike active vaccination strategies, a competent immune system is not required to benefit from passive antibody, whether transplacental or directly administered.
Deep Thought
What if the traditional RSV seasonal hospitalization surge fails to materialize this season? It could happen. If we could get high acceptance/uptake of maternal vaccine and infant nirsevimab, RSV season could resemble the dramatic drop in rotavirus disease the second year after rotavirus vaccine introduction. We could be asking ourselves — “What happened to RSV?”
Dr. Harrison is professor of pediatrics and pediatric infectious diseases at Children’s Mercy Hospitals and Clinics, Kansas City, Missouri. He said he had no relevant financial disclosures. Email him at [email protected].
References
1. CDC. RSV in Infants and Young Children. Respiratory Syncytial Virus Infection (RSV). June 18, 2024. https://www.cdc.gov/rsv/infants-young-children/index.html.
2. Suss RJ and Simões EAF. Respiratory Syncytial Virus Hospital-Based Burden of Disease in Children Younger Than 5 Respiratory Syncytial Virus Hospital-Based Burden of Disease in Children Younger Than 5 Years, 2015-2022. JAMA Netw Open. 2024;7(4):e247125. doi:10.1001/jamanetworkopen.2024.7125.
3. Winthrop ZA et al. Pediatric Respiratory Syncytial Virus Hospitalizations and Respiratory Support After the COVID-19 Pandemic. JAMA Netw Open. 2024;7(6):e2416852. doi:10.1001/jamanetworkopen.2024.16852.
4. Petros BA et al. Increased Pediatric RSV Case Counts Following the Emergence of SARS-CoV-2 Are Attributable to Increased Testing. medRxiv [Preprint]. 2024 Feb 12:2024.02.06.24302387. doi: 10.1101/2024.02.06.24302387.
5. Rates of Laboratory-Confirmed RSV, COVID-19, and Flu Hospitalizations from the RESP-NET Surveillance Systems. Centers for Disease Control and Prevention. https://data.cdc.gov/Public-Health-Surveillance/Rates-of-Laboratory-Confirmed-RSV-COVID-19-and-Flu/kvib-3txy/about_data.
6. CDC. Evaluating the 2023-2024 Respiratory Disease Season Outlook. CFA: Qualitative Assessments. August 14, 2024. https://www.cdc.gov/cfa-qualitative-assessments/php/data-research/2023-2024-season-outlook-retro.html.
7. Health Alert Network (HAN). Limited Availability of Nirsevimab in the United States—Interim CDC Recommendations to Protect Infants from Respiratory Syncytial Virus (RSV) during the 2023–2024 Respiratory Virus Season. October 23, 2023. https://emergency.cdc.gov/han/2023/han00499.asp.
8. CDC. Information for the 2024-2025 Flu Season. Centers for Disease Control and Prevention. March 14, 2024. https://www.cdc.gov/flu/season/faq-flu-season-2024-2025.htm.
9. Kampmann B et al. Bivalent Prefusion F Vaccine in Pregnancy to Prevent RSV Illness in Infants. N Engl J Med. 2023 Apr 20;388(16):1451-1464. doi: 10.1056/NEJMoa2216480.
10. Moline HL. Early Estimate of Nirsevimab Effectiveness for Prevention of Respiratory Syncytial Virus–Associated Hospitalization Among Infants Entering Their First Respiratory Syncytial Virus Season — New Vaccine Surveillance Network, October 2023–February 2024. MMWR Morb Mortal Wkly Rep. 2024;73. doi: 10.15585/mmwr.mm7309a4.
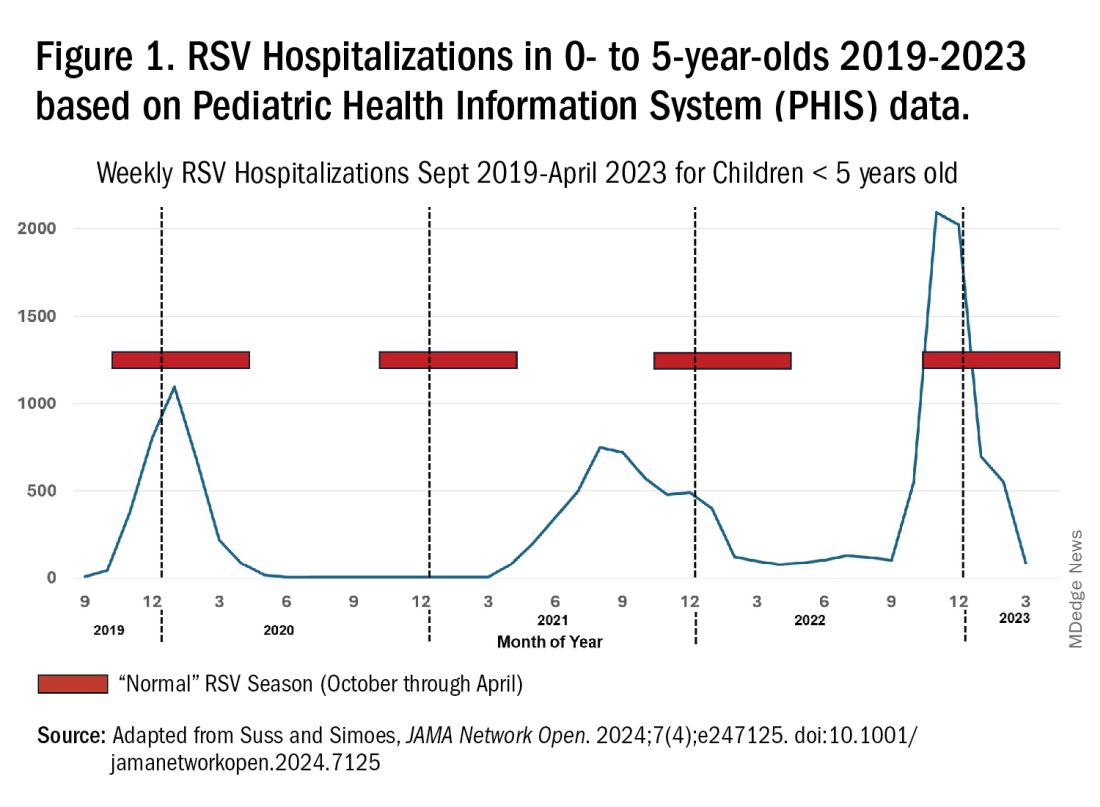
Primary Care: Re Carpe Your Diem
William Fox, MD, a self-described “dinosaur,” works in an independent internal medicine practice with two other physicians in Charlottesville, Virginia. He is rarely able to accept new patients, and when he does see one, they often have to wait months for the appointment. He accepts the burden of many pent-up needs, along with the huge administrative chore of coordinating their care with subspecialists.
“I will probably have to make multiple visits in a quick succession in order to make sure that I stabilize all the various issues,” Dr. Fox said. Doing so for a complicated new patient is nearly impossible because of time pressures, especially as it has become increasingly difficult for his patients to access subspecialists.
Dr. Fox traced the roots of the problem to a shortage of primary care physicians.
“Primary care is a vital part of healthcare and infrastructure in the United States, and it is being eroded unfortunately, as fewer and fewer medical students and residents choose to go into the primary care field,” Fox said. “And the reason it’s being eroded partly is because it is undervalued” and under-reimbursed, he added.
A study published 2 years ago in the Journal of General Internal Medicine proved what every primary care clinician already knows: The 24-hour day simply isn’t long enough.
Assuming an average panel of 2500 patients, the authors estimated the average time needed to provide currently recommended preventive care services and vaccines, chronic disease care, and management of acute illnesses. The answer: 26.7 hours a day.
However, using a team-based approach in which the necessary care was divided between physicians, advanced practice providers, and medical assistants, the physician component could be whittled down to 9 hours.
As chair of the Board of Regents of the American College of Physicians (ACP), Dr. Fox champions the ACP’s endorsement of physician-led team-based care, which improves patient outcomes and increases well-being among health professionals. But practices like his rarely have the necessary resources to support advanced practice clinicians or social workers. “Team-based care can be achieved in larger healthcare systems that have the resources to do it,” said Dr. Fox. “We need to find a way for smaller independent practices to also participate in team-based care.”
The solution? Major reform in the current fee-for-service payment structure, which incentivizes patient volume over patient outcomes. Dr. Fox co-authored a 2022 position statement from ACP outlining strategies such as prospective payment models that could achieve high-quality care and address social inequities. “We need to evolve our payment system from a fee-for-service system into a blended system where you have some population-based payments along with fee-for-service, or a fully capitated system,” he said.
Advantages of Team-Based Care
When a patient wrote on a satisfaction survey “the doctor spent more time examining the computer than examining me,” Kevin Hopkins, MD, decided he needed to change some things. Now the vice chief of Cleveland Clinic’s Primary Care Institute in Cleveland, in 2010, he developed a rudimentary team-based care model consisting of himself and two medical assistants at Cleveland Clinic.
The assistants did much of the patient intake, served as scribes while Dr. Hopkins saw his patients, and completed most of the required documentation. “I was able to see 30% more patients in a day and still take great care of them,” Dr. Hopkins said.
The concept of team-based care has evolved since then, often including some combination of advanced practice providers such as physician assistants (PAs) or nurse practitioners (NPs), nurses or medical assistants, and social workers or case managers working under the leadership of a physician. According to Dr. Hopkins, the basic strategy should be that “the physician does what only the physician is uniquely trained and qualified to do.” All other tasks, such as data entry, handling refill requests and messages from the patient portal, scheduling, or patient education, can — and should — be done by someone else.
Dr. Hopkins also serves as a senior physician advisor to the American Medical Association (AMA) and an instructor for workshops like “Saving Time: Practice Innovation Boot Camp.” His advice for clinicians who would like to streamline their workflow is to start with small steps.
“You’re not going to be able to hire all the people that you’d like to have,” he said. “I encourage physicians to look around at the people that they have and what they are currently doing as a part of their roles and responsibilities.”
The AMA Team-Based Care and Workflow website provides brief continuing medical education activities on topics such as implementing lab testing prior to office visits or advanced protocols for rooming and discharge; adopting any of these strategies can help save steps during office visits.
Dr. Hopkins said the AMA is committed to reducing the regulatory burden on clinicians. Clinical compliance officers may misinterpret regulatory requirements, putting into place overly conservative internal policies and procedures. The AMA’s “Reducing Regulatory Burden Playbook” offers advice on practices that could be stopped, such as two-factor authentication for approving or signing orders unless they are for controlled substances, or started, such as writing prescriptions for chronic daily medications for the maximum allowed length. Reducing a few clicks with each log-on to the electronic health record or reducing the number of tasks physicians must complete to log on can dramatically reduce hours spent on the computer.
Telehealth Changes Everything
But it might be even more efficient to keep patients out of the office.
Initially piloted in Palo Alto, California, from 2018 to 2022, the Tera Practice adopted team-based care strategies in a practice that conducts most of its work virtually. Sutter Health has since expanded the concept to three “Connected Care Clinics” in the San Francisco area, which provide 80% of their care via secure messaging, telephone, or video visit. Staff work primarily from home, and patients do not need to take off work or spend time driving to in-person visits to access care.
Matthew Sakumoto, MD, is a virtualist primary care physician at Sutter Health’s San Francisco clinic and an adjunct assistant clinical professor at the University of California, San Francisco. He leads a three-person team, which typically has included either an NP or a PA, along with a licensed vocational nurse or medical assistant.
“I go into clinic once a week, but a lot of the visits are video visits, so I don’t feel the pressure to address everything all in one visit,” Dr. Sakumoto said. “It is really freeing for both me and the patient.”
For more complex patients, for example, he prioritizes one problem at a visit because his team will follow up virtually for administrative issues like refills or specialty referrals. He can easily find time to schedule a patient for a follow-up virtual visit in the next week or 2 weeks to address additional needs. And on days he and his staff work from home, patients who message with an urgent concern can often be seen by video that same day.
Dr. Sakumoto and his team have a traditional huddle in the office the morning of their clinic day to plan for the scheduled visits, but most of their days are less structured. On non-clinic days, their morning Zoom huddle has a much different focus.
“We’re saying, ‘Okay, who are our high-risk patients? Who haven’t we seen in a while?’ ” Dr. Sakumoto said. They group patients into tiers based on factors such as age, number of complex medical needs, and frequency of emergency visits or hospitalizations. They also check in with higher-risk patients who haven’t contacted the office or been seen recently.
Dr. Sakumoto noticed in medical school doctors take excellent care of the patients who show up to the clinic. “We don’t do quite as well for those that don’t show up,” he said. The hybrid-virtual model gives him time to think in a more population-based way about engaging his entire panel of patients. The majority have capitated or value-based insurance plans, providing a dedicated monthly revenue stream that funds his virtual practice.
More clinicians may be able to hire staff and adopt some of these innovative approaches if Congress approves proposed changes to Medicare and Medicaid increasing the use of value-based payment systems. Although these changes may not provide all the funding needed to reinvigorate the field of primary care medicine, Dr. Fox said, “at least some people in positions of power and responsibility are beginning to think more seriously about these issues.”
Dr. Sakumoto reported personal fees from the following companies within the past 24 months: Clearstep Health, Carbon Health, Matter Health, CareAlign, PlushCare, Teladoc, and Nabla Health. Dr. Fox and Dr. Hopkins reported no financial conflicts of interest.
A former pediatrician and disease detective, Ann Thomas, MD, MPH, is a freelance science writer living in Portland, Oregon.
A version of this article first appeared on Medscape.com.
William Fox, MD, a self-described “dinosaur,” works in an independent internal medicine practice with two other physicians in Charlottesville, Virginia. He is rarely able to accept new patients, and when he does see one, they often have to wait months for the appointment. He accepts the burden of many pent-up needs, along with the huge administrative chore of coordinating their care with subspecialists.
“I will probably have to make multiple visits in a quick succession in order to make sure that I stabilize all the various issues,” Dr. Fox said. Doing so for a complicated new patient is nearly impossible because of time pressures, especially as it has become increasingly difficult for his patients to access subspecialists.
Dr. Fox traced the roots of the problem to a shortage of primary care physicians.
“Primary care is a vital part of healthcare and infrastructure in the United States, and it is being eroded unfortunately, as fewer and fewer medical students and residents choose to go into the primary care field,” Fox said. “And the reason it’s being eroded partly is because it is undervalued” and under-reimbursed, he added.
A study published 2 years ago in the Journal of General Internal Medicine proved what every primary care clinician already knows: The 24-hour day simply isn’t long enough.
Assuming an average panel of 2500 patients, the authors estimated the average time needed to provide currently recommended preventive care services and vaccines, chronic disease care, and management of acute illnesses. The answer: 26.7 hours a day.
However, using a team-based approach in which the necessary care was divided between physicians, advanced practice providers, and medical assistants, the physician component could be whittled down to 9 hours.
As chair of the Board of Regents of the American College of Physicians (ACP), Dr. Fox champions the ACP’s endorsement of physician-led team-based care, which improves patient outcomes and increases well-being among health professionals. But practices like his rarely have the necessary resources to support advanced practice clinicians or social workers. “Team-based care can be achieved in larger healthcare systems that have the resources to do it,” said Dr. Fox. “We need to find a way for smaller independent practices to also participate in team-based care.”
The solution? Major reform in the current fee-for-service payment structure, which incentivizes patient volume over patient outcomes. Dr. Fox co-authored a 2022 position statement from ACP outlining strategies such as prospective payment models that could achieve high-quality care and address social inequities. “We need to evolve our payment system from a fee-for-service system into a blended system where you have some population-based payments along with fee-for-service, or a fully capitated system,” he said.
Advantages of Team-Based Care
When a patient wrote on a satisfaction survey “the doctor spent more time examining the computer than examining me,” Kevin Hopkins, MD, decided he needed to change some things. Now the vice chief of Cleveland Clinic’s Primary Care Institute in Cleveland, in 2010, he developed a rudimentary team-based care model consisting of himself and two medical assistants at Cleveland Clinic.
The assistants did much of the patient intake, served as scribes while Dr. Hopkins saw his patients, and completed most of the required documentation. “I was able to see 30% more patients in a day and still take great care of them,” Dr. Hopkins said.
The concept of team-based care has evolved since then, often including some combination of advanced practice providers such as physician assistants (PAs) or nurse practitioners (NPs), nurses or medical assistants, and social workers or case managers working under the leadership of a physician. According to Dr. Hopkins, the basic strategy should be that “the physician does what only the physician is uniquely trained and qualified to do.” All other tasks, such as data entry, handling refill requests and messages from the patient portal, scheduling, or patient education, can — and should — be done by someone else.
Dr. Hopkins also serves as a senior physician advisor to the American Medical Association (AMA) and an instructor for workshops like “Saving Time: Practice Innovation Boot Camp.” His advice for clinicians who would like to streamline their workflow is to start with small steps.
“You’re not going to be able to hire all the people that you’d like to have,” he said. “I encourage physicians to look around at the people that they have and what they are currently doing as a part of their roles and responsibilities.”
The AMA Team-Based Care and Workflow website provides brief continuing medical education activities on topics such as implementing lab testing prior to office visits or advanced protocols for rooming and discharge; adopting any of these strategies can help save steps during office visits.
Dr. Hopkins said the AMA is committed to reducing the regulatory burden on clinicians. Clinical compliance officers may misinterpret regulatory requirements, putting into place overly conservative internal policies and procedures. The AMA’s “Reducing Regulatory Burden Playbook” offers advice on practices that could be stopped, such as two-factor authentication for approving or signing orders unless they are for controlled substances, or started, such as writing prescriptions for chronic daily medications for the maximum allowed length. Reducing a few clicks with each log-on to the electronic health record or reducing the number of tasks physicians must complete to log on can dramatically reduce hours spent on the computer.
Telehealth Changes Everything
But it might be even more efficient to keep patients out of the office.
Initially piloted in Palo Alto, California, from 2018 to 2022, the Tera Practice adopted team-based care strategies in a practice that conducts most of its work virtually. Sutter Health has since expanded the concept to three “Connected Care Clinics” in the San Francisco area, which provide 80% of their care via secure messaging, telephone, or video visit. Staff work primarily from home, and patients do not need to take off work or spend time driving to in-person visits to access care.
Matthew Sakumoto, MD, is a virtualist primary care physician at Sutter Health’s San Francisco clinic and an adjunct assistant clinical professor at the University of California, San Francisco. He leads a three-person team, which typically has included either an NP or a PA, along with a licensed vocational nurse or medical assistant.
“I go into clinic once a week, but a lot of the visits are video visits, so I don’t feel the pressure to address everything all in one visit,” Dr. Sakumoto said. “It is really freeing for both me and the patient.”
For more complex patients, for example, he prioritizes one problem at a visit because his team will follow up virtually for administrative issues like refills or specialty referrals. He can easily find time to schedule a patient for a follow-up virtual visit in the next week or 2 weeks to address additional needs. And on days he and his staff work from home, patients who message with an urgent concern can often be seen by video that same day.
Dr. Sakumoto and his team have a traditional huddle in the office the morning of their clinic day to plan for the scheduled visits, but most of their days are less structured. On non-clinic days, their morning Zoom huddle has a much different focus.
“We’re saying, ‘Okay, who are our high-risk patients? Who haven’t we seen in a while?’ ” Dr. Sakumoto said. They group patients into tiers based on factors such as age, number of complex medical needs, and frequency of emergency visits or hospitalizations. They also check in with higher-risk patients who haven’t contacted the office or been seen recently.
Dr. Sakumoto noticed in medical school doctors take excellent care of the patients who show up to the clinic. “We don’t do quite as well for those that don’t show up,” he said. The hybrid-virtual model gives him time to think in a more population-based way about engaging his entire panel of patients. The majority have capitated or value-based insurance plans, providing a dedicated monthly revenue stream that funds his virtual practice.
More clinicians may be able to hire staff and adopt some of these innovative approaches if Congress approves proposed changes to Medicare and Medicaid increasing the use of value-based payment systems. Although these changes may not provide all the funding needed to reinvigorate the field of primary care medicine, Dr. Fox said, “at least some people in positions of power and responsibility are beginning to think more seriously about these issues.”
Dr. Sakumoto reported personal fees from the following companies within the past 24 months: Clearstep Health, Carbon Health, Matter Health, CareAlign, PlushCare, Teladoc, and Nabla Health. Dr. Fox and Dr. Hopkins reported no financial conflicts of interest.
A former pediatrician and disease detective, Ann Thomas, MD, MPH, is a freelance science writer living in Portland, Oregon.
A version of this article first appeared on Medscape.com.
William Fox, MD, a self-described “dinosaur,” works in an independent internal medicine practice with two other physicians in Charlottesville, Virginia. He is rarely able to accept new patients, and when he does see one, they often have to wait months for the appointment. He accepts the burden of many pent-up needs, along with the huge administrative chore of coordinating their care with subspecialists.
“I will probably have to make multiple visits in a quick succession in order to make sure that I stabilize all the various issues,” Dr. Fox said. Doing so for a complicated new patient is nearly impossible because of time pressures, especially as it has become increasingly difficult for his patients to access subspecialists.
Dr. Fox traced the roots of the problem to a shortage of primary care physicians.
“Primary care is a vital part of healthcare and infrastructure in the United States, and it is being eroded unfortunately, as fewer and fewer medical students and residents choose to go into the primary care field,” Fox said. “And the reason it’s being eroded partly is because it is undervalued” and under-reimbursed, he added.
A study published 2 years ago in the Journal of General Internal Medicine proved what every primary care clinician already knows: The 24-hour day simply isn’t long enough.
Assuming an average panel of 2500 patients, the authors estimated the average time needed to provide currently recommended preventive care services and vaccines, chronic disease care, and management of acute illnesses. The answer: 26.7 hours a day.
However, using a team-based approach in which the necessary care was divided between physicians, advanced practice providers, and medical assistants, the physician component could be whittled down to 9 hours.
As chair of the Board of Regents of the American College of Physicians (ACP), Dr. Fox champions the ACP’s endorsement of physician-led team-based care, which improves patient outcomes and increases well-being among health professionals. But practices like his rarely have the necessary resources to support advanced practice clinicians or social workers. “Team-based care can be achieved in larger healthcare systems that have the resources to do it,” said Dr. Fox. “We need to find a way for smaller independent practices to also participate in team-based care.”
The solution? Major reform in the current fee-for-service payment structure, which incentivizes patient volume over patient outcomes. Dr. Fox co-authored a 2022 position statement from ACP outlining strategies such as prospective payment models that could achieve high-quality care and address social inequities. “We need to evolve our payment system from a fee-for-service system into a blended system where you have some population-based payments along with fee-for-service, or a fully capitated system,” he said.
Advantages of Team-Based Care
When a patient wrote on a satisfaction survey “the doctor spent more time examining the computer than examining me,” Kevin Hopkins, MD, decided he needed to change some things. Now the vice chief of Cleveland Clinic’s Primary Care Institute in Cleveland, in 2010, he developed a rudimentary team-based care model consisting of himself and two medical assistants at Cleveland Clinic.
The assistants did much of the patient intake, served as scribes while Dr. Hopkins saw his patients, and completed most of the required documentation. “I was able to see 30% more patients in a day and still take great care of them,” Dr. Hopkins said.
The concept of team-based care has evolved since then, often including some combination of advanced practice providers such as physician assistants (PAs) or nurse practitioners (NPs), nurses or medical assistants, and social workers or case managers working under the leadership of a physician. According to Dr. Hopkins, the basic strategy should be that “the physician does what only the physician is uniquely trained and qualified to do.” All other tasks, such as data entry, handling refill requests and messages from the patient portal, scheduling, or patient education, can — and should — be done by someone else.
Dr. Hopkins also serves as a senior physician advisor to the American Medical Association (AMA) and an instructor for workshops like “Saving Time: Practice Innovation Boot Camp.” His advice for clinicians who would like to streamline their workflow is to start with small steps.
“You’re not going to be able to hire all the people that you’d like to have,” he said. “I encourage physicians to look around at the people that they have and what they are currently doing as a part of their roles and responsibilities.”
The AMA Team-Based Care and Workflow website provides brief continuing medical education activities on topics such as implementing lab testing prior to office visits or advanced protocols for rooming and discharge; adopting any of these strategies can help save steps during office visits.
Dr. Hopkins said the AMA is committed to reducing the regulatory burden on clinicians. Clinical compliance officers may misinterpret regulatory requirements, putting into place overly conservative internal policies and procedures. The AMA’s “Reducing Regulatory Burden Playbook” offers advice on practices that could be stopped, such as two-factor authentication for approving or signing orders unless they are for controlled substances, or started, such as writing prescriptions for chronic daily medications for the maximum allowed length. Reducing a few clicks with each log-on to the electronic health record or reducing the number of tasks physicians must complete to log on can dramatically reduce hours spent on the computer.
Telehealth Changes Everything
But it might be even more efficient to keep patients out of the office.
Initially piloted in Palo Alto, California, from 2018 to 2022, the Tera Practice adopted team-based care strategies in a practice that conducts most of its work virtually. Sutter Health has since expanded the concept to three “Connected Care Clinics” in the San Francisco area, which provide 80% of their care via secure messaging, telephone, or video visit. Staff work primarily from home, and patients do not need to take off work or spend time driving to in-person visits to access care.
Matthew Sakumoto, MD, is a virtualist primary care physician at Sutter Health’s San Francisco clinic and an adjunct assistant clinical professor at the University of California, San Francisco. He leads a three-person team, which typically has included either an NP or a PA, along with a licensed vocational nurse or medical assistant.
“I go into clinic once a week, but a lot of the visits are video visits, so I don’t feel the pressure to address everything all in one visit,” Dr. Sakumoto said. “It is really freeing for both me and the patient.”
For more complex patients, for example, he prioritizes one problem at a visit because his team will follow up virtually for administrative issues like refills or specialty referrals. He can easily find time to schedule a patient for a follow-up virtual visit in the next week or 2 weeks to address additional needs. And on days he and his staff work from home, patients who message with an urgent concern can often be seen by video that same day.
Dr. Sakumoto and his team have a traditional huddle in the office the morning of their clinic day to plan for the scheduled visits, but most of their days are less structured. On non-clinic days, their morning Zoom huddle has a much different focus.
“We’re saying, ‘Okay, who are our high-risk patients? Who haven’t we seen in a while?’ ” Dr. Sakumoto said. They group patients into tiers based on factors such as age, number of complex medical needs, and frequency of emergency visits or hospitalizations. They also check in with higher-risk patients who haven’t contacted the office or been seen recently.
Dr. Sakumoto noticed in medical school doctors take excellent care of the patients who show up to the clinic. “We don’t do quite as well for those that don’t show up,” he said. The hybrid-virtual model gives him time to think in a more population-based way about engaging his entire panel of patients. The majority have capitated or value-based insurance plans, providing a dedicated monthly revenue stream that funds his virtual practice.
More clinicians may be able to hire staff and adopt some of these innovative approaches if Congress approves proposed changes to Medicare and Medicaid increasing the use of value-based payment systems. Although these changes may not provide all the funding needed to reinvigorate the field of primary care medicine, Dr. Fox said, “at least some people in positions of power and responsibility are beginning to think more seriously about these issues.”
Dr. Sakumoto reported personal fees from the following companies within the past 24 months: Clearstep Health, Carbon Health, Matter Health, CareAlign, PlushCare, Teladoc, and Nabla Health. Dr. Fox and Dr. Hopkins reported no financial conflicts of interest.
A former pediatrician and disease detective, Ann Thomas, MD, MPH, is a freelance science writer living in Portland, Oregon.
A version of this article first appeared on Medscape.com.
Doctors Are Seeking Professional Coaches More Often. Here’s Why
When Andrea Austin, MD, an emergency medicine specialist, left the military in 2020, she knew the adjustment to civilian life and practice might be difficult. To help smooth the transition, she reached out to a physician mentor who also had a professional coaching certificate. After a conversation, Dr. Austin signed up for 6 months of career coaching.
It was time well spent, according to Dr. Austin, who today is a coach herself. “It was really the first time I had the ability to choose what I wanted to do, and that required a mindset shift,” she explains. “A big part of coaching is helping physicians discover their agency so that they can make the best career choices.”

Physicians have long lacked the coaching resources typically made available to corporate executives. But that’s changing. In today’s high-pressure environment, where doctors are burning out at a rapid pace, coaching can sometimes be an avenue to staying in the field, especially if that coach is a fellow physician who understands what you’re facing.
With a physician shortage that the Association of American Medical Colleges expects to hit 86,000 in the next decade or so, coaching could be a stone worth turning over. A 2024 report in JAMA Network Open found that coaching provided by physician peers led to a significant reduction in interpersonal disengagement and burnout.
“What I think is exciting about coaching is that it allows you to better understand yourself and know your strengths and weaknesses,” said Dr. Austin. “It might seem simple, but many ‘soft skills’ aren’t considered mainstream in medicine. Coaching allows us to understand them and ourselves better.”
Why Are Doctors Using Coaches?
Although it’s hard to put a number on how many physicians are turning to coaches, the number of coaches available for doctors is growing rapidly. The American Medical Women’s Association maintains a database of physician coaches. According to deputy director Jodi Godfrey, MS, RDN, the number of members who have added coaching to their skill set has tripled in the past 4 years. “Many cite burnout as the reason they sought coaching support, and then they decided to go on to get certified in coaching.”

The pandemic is one reason physician coaching has grown, said Elizabeth Esparaz, MD, an ophthalmologist and physician coach. “Since the pandemic, the word ‘burnout’ is thrown around a good deal.” And the causes are clear. “Doctors are facing longer hours, they must make split-second decisions, they’re multitasking, and they have less support staff.”
Among her coaching clients, Dr. Austin has noticed other common struggles: fears of litigation, time scarcity with patients, declining reimbursement that hasn’t kept up with inflation, and loss of autonomy because of the corporatization of healthcare.
Coaching, Dr. Esparaz believes, can be an antidote to many of these issues. “Coaches help doctors see their strengths and find better ways of applying them,” she said. “We help them move forward, and also see their blind spots.”
Clarity, Goals, and Making the Right Choices
Physician coaching comes in a variety of flavors — some one on one, and others in the form of group sessions. All, however, serve the purpose of helping physicians gain career clarity. “Sometimes clients realize their job may not be working for them, but that there are things they can do to change that without having to leave the field,” said Jattu Senesie, MD, a former ob.gyn. who is now a physician coach.
Dr. Esparaz works with doctors to establish SMART goals: specific, measurable, attainable, realistic, and time based. She gave the example of learning how to set boundaries. “If a physician is asked to create a presentation for work, I encourage them to ask for compensation or administrative time before committing to unpaid tasks.”
Another big issue: charting. It’s increasingly burdensome, and many doctors find it encroaching on their home lives. “If we can identify a problem like that, we can come up with a strategy for mitigating it,” Dr. Esparaz said. This might include setting a goal of getting 80% of charting completed immediately after the patient encounter on the busiest clinic day of the week. The client tests the experiment and then revisits it with the coach to discuss what worked and what didn’t, refining the process until it has freed up the physician’s home life.

The younger generation of doctors often struggles with career choices, too, because it’s the first time they are without structure, said Dr. Senesie. There’s med school and residency, which puts a framework around every move a doctor makes. But once they become attending physicians, the choices are endless. “Coaching can help them find a new structure and systems that will allow them to thrive.”
Although mentoring has been a well-embraced concept for decades, it “hits a wall,” at some point in terms of what it can offer, Dr. Austin said. That’s where coaching can take over. “There’s a point where a mentor cannot help someone self-actualize. As a coach, you don’t need to know everything about a doctor’s life, but you can help them learn to ask themselves the right questions to solve problems.”
Should You Stay or Should You Go?
Dr. Austin’s approach begins with the premise that healthcare today is challenging and dysfunctional — but doctors still have agency. She has worked with clients on the verge of leaving the field and helped them find their way back.
“They have a light bulb moment and open up to the idea that they have much to give still,” she said. “We take an inventory to help them better communicate their needs and make changes, and I help them connect to their values. Sometimes that exercise allows them to reframe their current work environment.”
Not every doctor who goes through coaching remains in the field. But “that’s the exception, not the rule,” Dr. Austin said. And that’s okay. “If that’s the outcome, coaching probably helped them get to that point faster, and with an informed decision.”
Dr. Senesie has been coaching for about a decade, and in that time, she’s seen a shift that goes beyond figuring out career goals. “Doctors are more aware of the need for well-being today. The pandemic made it impossible to ignore what doesn’t work for us. When I work with clients, we look for ways to make the job more tenable.”
According to Dr. Senesie, younger doctors are looking for that balance at the outset. “They want to be physicians, but they also want a life,” she said. “It’s a challenge for them because in addition to that mindset, they’re also coming out with more debt than older generations. They want out from underneath that.”
When It’s Time to Find a Physician Coach
Wondering whether coaching is right for you? Consider these symptoms:
- You need help setting boundaries at work.
- You feel like you’re sacrificing your own well-being for your job.
- You’re using maladaptive strategies to cope with the stress at work.
- You’ve reached a point where you are considering leaving the field.
If you’re interested in finding a physician coach, there are several places to begin your search, word of mouth being one of them. “Conferences and social media can also expose you to coaches,” suggested Dr. Esparaz. There are different methods and approaches to coaching. So, as you research, “make sure the coach you choose has techniques and a framework that fit what you’re after.”
Dr. Austin warned that it is an unregulated industry, so buyer beware. To ensure you’re getting an accredited physician coach, look for people who have obtained an International Coach Federation (ICF) accreditation. These coaches will hold an associate certified coach credential, which requires at least 60 hours of coaching-specific training approved by the ICF, in addition to other assessments and education.
Ensure that the coach you choose is within your budget. “There are some people charging astronomical rates out there,” Dr. Austin said. “If you’re burned out or struggling, it can be easy to reach for your credit card.”
Dr. Austin also cautioned doctors seeking a coach to avoid promises that sound too good to be true. Some coaching can have a gaslighting quality to it, she warned, “suggesting it can allow you to endure any environment.” But positive self-talk alone won’t cure an abusive or discriminatory situation. “If a client describes a toxic work environment,” the coach has an “ethical imperative” to help that person protect themselves.
A Side Gig or a New Career Path
After Dr. Austin’s experience with her coach, she made the choice to continue as an emergency physician part-time while starting her own coaching business. “It’s important for me personally to keep in touch with what’s happening on the ground, but I have no judgment for anyone who chooses to leave clinical practice to become a coach.”
When Dr. Senesie looks back on her own struggles as a clinician, she recognizes the state of burnout she was in 10 years ago. “I knew there was an issue, but I didn’t have the mindset to find a way to make it work,” she said. “I left the field when I was at my depths of burnout, which is generally not the best way to go about it.”
Guidance might have allowed her to take into account other avenues and helped her remain in the field, said Dr. Senesie. She has since learned that “there are many ways to practice medicine, and the way we’ve gone about it traditionally has worked for some, but not necessarily for everyone.”
There may be more possibilities than you think. By helping you assess your path and make meaningful changes, a physician coach might be the key to remaining in the field you love.
A version of this article first appeared on Medscape.com.
When Andrea Austin, MD, an emergency medicine specialist, left the military in 2020, she knew the adjustment to civilian life and practice might be difficult. To help smooth the transition, she reached out to a physician mentor who also had a professional coaching certificate. After a conversation, Dr. Austin signed up for 6 months of career coaching.
It was time well spent, according to Dr. Austin, who today is a coach herself. “It was really the first time I had the ability to choose what I wanted to do, and that required a mindset shift,” she explains. “A big part of coaching is helping physicians discover their agency so that they can make the best career choices.”
Physicians have long lacked the coaching resources typically made available to corporate executives. But that’s changing. In today’s high-pressure environment, where doctors are burning out at a rapid pace, coaching can sometimes be an avenue to staying in the field, especially if that coach is a fellow physician who understands what you’re facing.
With a physician shortage that the Association of American Medical Colleges expects to hit 86,000 in the next decade or so, coaching could be a stone worth turning over. A 2024 report in JAMA Network Open found that coaching provided by physician peers led to a significant reduction in interpersonal disengagement and burnout.
“What I think is exciting about coaching is that it allows you to better understand yourself and know your strengths and weaknesses,” said Dr. Austin. “It might seem simple, but many ‘soft skills’ aren’t considered mainstream in medicine. Coaching allows us to understand them and ourselves better.”
Why Are Doctors Using Coaches?
Although it’s hard to put a number on how many physicians are turning to coaches, the number of coaches available for doctors is growing rapidly. The American Medical Women’s Association maintains a database of physician coaches. According to deputy director Jodi Godfrey, MS, RDN, the number of members who have added coaching to their skill set has tripled in the past 4 years. “Many cite burnout as the reason they sought coaching support, and then they decided to go on to get certified in coaching.”
The pandemic is one reason physician coaching has grown, said Elizabeth Esparaz, MD, an ophthalmologist and physician coach. “Since the pandemic, the word ‘burnout’ is thrown around a good deal.” And the causes are clear. “Doctors are facing longer hours, they must make split-second decisions, they’re multitasking, and they have less support staff.”
Among her coaching clients, Dr. Austin has noticed other common struggles: fears of litigation, time scarcity with patients, declining reimbursement that hasn’t kept up with inflation, and loss of autonomy because of the corporatization of healthcare.
Coaching, Dr. Esparaz believes, can be an antidote to many of these issues. “Coaches help doctors see their strengths and find better ways of applying them,” she said. “We help them move forward, and also see their blind spots.”
Clarity, Goals, and Making the Right Choices
Physician coaching comes in a variety of flavors — some one on one, and others in the form of group sessions. All, however, serve the purpose of helping physicians gain career clarity. “Sometimes clients realize their job may not be working for them, but that there are things they can do to change that without having to leave the field,” said Jattu Senesie, MD, a former ob.gyn. who is now a physician coach.
Dr. Esparaz works with doctors to establish SMART goals: specific, measurable, attainable, realistic, and time based. She gave the example of learning how to set boundaries. “If a physician is asked to create a presentation for work, I encourage them to ask for compensation or administrative time before committing to unpaid tasks.”
Another big issue: charting. It’s increasingly burdensome, and many doctors find it encroaching on their home lives. “If we can identify a problem like that, we can come up with a strategy for mitigating it,” Dr. Esparaz said. This might include setting a goal of getting 80% of charting completed immediately after the patient encounter on the busiest clinic day of the week. The client tests the experiment and then revisits it with the coach to discuss what worked and what didn’t, refining the process until it has freed up the physician’s home life.
The younger generation of doctors often struggles with career choices, too, because it’s the first time they are without structure, said Dr. Senesie. There’s med school and residency, which puts a framework around every move a doctor makes. But once they become attending physicians, the choices are endless. “Coaching can help them find a new structure and systems that will allow them to thrive.”
Although mentoring has been a well-embraced concept for decades, it “hits a wall,” at some point in terms of what it can offer, Dr. Austin said. That’s where coaching can take over. “There’s a point where a mentor cannot help someone self-actualize. As a coach, you don’t need to know everything about a doctor’s life, but you can help them learn to ask themselves the right questions to solve problems.”
Should You Stay or Should You Go?
Dr. Austin’s approach begins with the premise that healthcare today is challenging and dysfunctional — but doctors still have agency. She has worked with clients on the verge of leaving the field and helped them find their way back.
“They have a light bulb moment and open up to the idea that they have much to give still,” she said. “We take an inventory to help them better communicate their needs and make changes, and I help them connect to their values. Sometimes that exercise allows them to reframe their current work environment.”
Not every doctor who goes through coaching remains in the field. But “that’s the exception, not the rule,” Dr. Austin said. And that’s okay. “If that’s the outcome, coaching probably helped them get to that point faster, and with an informed decision.”
Dr. Senesie has been coaching for about a decade, and in that time, she’s seen a shift that goes beyond figuring out career goals. “Doctors are more aware of the need for well-being today. The pandemic made it impossible to ignore what doesn’t work for us. When I work with clients, we look for ways to make the job more tenable.”
According to Dr. Senesie, younger doctors are looking for that balance at the outset. “They want to be physicians, but they also want a life,” she said. “It’s a challenge for them because in addition to that mindset, they’re also coming out with more debt than older generations. They want out from underneath that.”
When It’s Time to Find a Physician Coach
Wondering whether coaching is right for you? Consider these symptoms:
- You need help setting boundaries at work.
- You feel like you’re sacrificing your own well-being for your job.
- You’re using maladaptive strategies to cope with the stress at work.
- You’ve reached a point where you are considering leaving the field.
If you’re interested in finding a physician coach, there are several places to begin your search, word of mouth being one of them. “Conferences and social media can also expose you to coaches,” suggested Dr. Esparaz. There are different methods and approaches to coaching. So, as you research, “make sure the coach you choose has techniques and a framework that fit what you’re after.”
Dr. Austin warned that it is an unregulated industry, so buyer beware. To ensure you’re getting an accredited physician coach, look for people who have obtained an International Coach Federation (ICF) accreditation. These coaches will hold an associate certified coach credential, which requires at least 60 hours of coaching-specific training approved by the ICF, in addition to other assessments and education.
Ensure that the coach you choose is within your budget. “There are some people charging astronomical rates out there,” Dr. Austin said. “If you’re burned out or struggling, it can be easy to reach for your credit card.”
Dr. Austin also cautioned doctors seeking a coach to avoid promises that sound too good to be true. Some coaching can have a gaslighting quality to it, she warned, “suggesting it can allow you to endure any environment.” But positive self-talk alone won’t cure an abusive or discriminatory situation. “If a client describes a toxic work environment,” the coach has an “ethical imperative” to help that person protect themselves.
A Side Gig or a New Career Path
After Dr. Austin’s experience with her coach, she made the choice to continue as an emergency physician part-time while starting her own coaching business. “It’s important for me personally to keep in touch with what’s happening on the ground, but I have no judgment for anyone who chooses to leave clinical practice to become a coach.”
When Dr. Senesie looks back on her own struggles as a clinician, she recognizes the state of burnout she was in 10 years ago. “I knew there was an issue, but I didn’t have the mindset to find a way to make it work,” she said. “I left the field when I was at my depths of burnout, which is generally not the best way to go about it.”
Guidance might have allowed her to take into account other avenues and helped her remain in the field, said Dr. Senesie. She has since learned that “there are many ways to practice medicine, and the way we’ve gone about it traditionally has worked for some, but not necessarily for everyone.”
There may be more possibilities than you think. By helping you assess your path and make meaningful changes, a physician coach might be the key to remaining in the field you love.
A version of this article first appeared on Medscape.com.
When Andrea Austin, MD, an emergency medicine specialist, left the military in 2020, she knew the adjustment to civilian life and practice might be difficult. To help smooth the transition, she reached out to a physician mentor who also had a professional coaching certificate. After a conversation, Dr. Austin signed up for 6 months of career coaching.
It was time well spent, according to Dr. Austin, who today is a coach herself. “It was really the first time I had the ability to choose what I wanted to do, and that required a mindset shift,” she explains. “A big part of coaching is helping physicians discover their agency so that they can make the best career choices.”
Physicians have long lacked the coaching resources typically made available to corporate executives. But that’s changing. In today’s high-pressure environment, where doctors are burning out at a rapid pace, coaching can sometimes be an avenue to staying in the field, especially if that coach is a fellow physician who understands what you’re facing.
With a physician shortage that the Association of American Medical Colleges expects to hit 86,000 in the next decade or so, coaching could be a stone worth turning over. A 2024 report in JAMA Network Open found that coaching provided by physician peers led to a significant reduction in interpersonal disengagement and burnout.
“What I think is exciting about coaching is that it allows you to better understand yourself and know your strengths and weaknesses,” said Dr. Austin. “It might seem simple, but many ‘soft skills’ aren’t considered mainstream in medicine. Coaching allows us to understand them and ourselves better.”
Why Are Doctors Using Coaches?
Although it’s hard to put a number on how many physicians are turning to coaches, the number of coaches available for doctors is growing rapidly. The American Medical Women’s Association maintains a database of physician coaches. According to deputy director Jodi Godfrey, MS, RDN, the number of members who have added coaching to their skill set has tripled in the past 4 years. “Many cite burnout as the reason they sought coaching support, and then they decided to go on to get certified in coaching.”
The pandemic is one reason physician coaching has grown, said Elizabeth Esparaz, MD, an ophthalmologist and physician coach. “Since the pandemic, the word ‘burnout’ is thrown around a good deal.” And the causes are clear. “Doctors are facing longer hours, they must make split-second decisions, they’re multitasking, and they have less support staff.”
Among her coaching clients, Dr. Austin has noticed other common struggles: fears of litigation, time scarcity with patients, declining reimbursement that hasn’t kept up with inflation, and loss of autonomy because of the corporatization of healthcare.
Coaching, Dr. Esparaz believes, can be an antidote to many of these issues. “Coaches help doctors see their strengths and find better ways of applying them,” she said. “We help them move forward, and also see their blind spots.”
Clarity, Goals, and Making the Right Choices
Physician coaching comes in a variety of flavors — some one on one, and others in the form of group sessions. All, however, serve the purpose of helping physicians gain career clarity. “Sometimes clients realize their job may not be working for them, but that there are things they can do to change that without having to leave the field,” said Jattu Senesie, MD, a former ob.gyn. who is now a physician coach.
Dr. Esparaz works with doctors to establish SMART goals: specific, measurable, attainable, realistic, and time based. She gave the example of learning how to set boundaries. “If a physician is asked to create a presentation for work, I encourage them to ask for compensation or administrative time before committing to unpaid tasks.”
Another big issue: charting. It’s increasingly burdensome, and many doctors find it encroaching on their home lives. “If we can identify a problem like that, we can come up with a strategy for mitigating it,” Dr. Esparaz said. This might include setting a goal of getting 80% of charting completed immediately after the patient encounter on the busiest clinic day of the week. The client tests the experiment and then revisits it with the coach to discuss what worked and what didn’t, refining the process until it has freed up the physician’s home life.
The younger generation of doctors often struggles with career choices, too, because it’s the first time they are without structure, said Dr. Senesie. There’s med school and residency, which puts a framework around every move a doctor makes. But once they become attending physicians, the choices are endless. “Coaching can help them find a new structure and systems that will allow them to thrive.”
Although mentoring has been a well-embraced concept for decades, it “hits a wall,” at some point in terms of what it can offer, Dr. Austin said. That’s where coaching can take over. “There’s a point where a mentor cannot help someone self-actualize. As a coach, you don’t need to know everything about a doctor’s life, but you can help them learn to ask themselves the right questions to solve problems.”
Should You Stay or Should You Go?
Dr. Austin’s approach begins with the premise that healthcare today is challenging and dysfunctional — but doctors still have agency. She has worked with clients on the verge of leaving the field and helped them find their way back.
“They have a light bulb moment and open up to the idea that they have much to give still,” she said. “We take an inventory to help them better communicate their needs and make changes, and I help them connect to their values. Sometimes that exercise allows them to reframe their current work environment.”
Not every doctor who goes through coaching remains in the field. But “that’s the exception, not the rule,” Dr. Austin said. And that’s okay. “If that’s the outcome, coaching probably helped them get to that point faster, and with an informed decision.”
Dr. Senesie has been coaching for about a decade, and in that time, she’s seen a shift that goes beyond figuring out career goals. “Doctors are more aware of the need for well-being today. The pandemic made it impossible to ignore what doesn’t work for us. When I work with clients, we look for ways to make the job more tenable.”
According to Dr. Senesie, younger doctors are looking for that balance at the outset. “They want to be physicians, but they also want a life,” she said. “It’s a challenge for them because in addition to that mindset, they’re also coming out with more debt than older generations. They want out from underneath that.”
When It’s Time to Find a Physician Coach
Wondering whether coaching is right for you? Consider these symptoms:
- You need help setting boundaries at work.
- You feel like you’re sacrificing your own well-being for your job.
- You’re using maladaptive strategies to cope with the stress at work.
- You’ve reached a point where you are considering leaving the field.
If you’re interested in finding a physician coach, there are several places to begin your search, word of mouth being one of them. “Conferences and social media can also expose you to coaches,” suggested Dr. Esparaz. There are different methods and approaches to coaching. So, as you research, “make sure the coach you choose has techniques and a framework that fit what you’re after.”
Dr. Austin warned that it is an unregulated industry, so buyer beware. To ensure you’re getting an accredited physician coach, look for people who have obtained an International Coach Federation (ICF) accreditation. These coaches will hold an associate certified coach credential, which requires at least 60 hours of coaching-specific training approved by the ICF, in addition to other assessments and education.
Ensure that the coach you choose is within your budget. “There are some people charging astronomical rates out there,” Dr. Austin said. “If you’re burned out or struggling, it can be easy to reach for your credit card.”
Dr. Austin also cautioned doctors seeking a coach to avoid promises that sound too good to be true. Some coaching can have a gaslighting quality to it, she warned, “suggesting it can allow you to endure any environment.” But positive self-talk alone won’t cure an abusive or discriminatory situation. “If a client describes a toxic work environment,” the coach has an “ethical imperative” to help that person protect themselves.
A Side Gig or a New Career Path
After Dr. Austin’s experience with her coach, she made the choice to continue as an emergency physician part-time while starting her own coaching business. “It’s important for me personally to keep in touch with what’s happening on the ground, but I have no judgment for anyone who chooses to leave clinical practice to become a coach.”
When Dr. Senesie looks back on her own struggles as a clinician, she recognizes the state of burnout she was in 10 years ago. “I knew there was an issue, but I didn’t have the mindset to find a way to make it work,” she said. “I left the field when I was at my depths of burnout, which is generally not the best way to go about it.”
Guidance might have allowed her to take into account other avenues and helped her remain in the field, said Dr. Senesie. She has since learned that “there are many ways to practice medicine, and the way we’ve gone about it traditionally has worked for some, but not necessarily for everyone.”
There may be more possibilities than you think. By helping you assess your path and make meaningful changes, a physician coach might be the key to remaining in the field you love.
A version of this article first appeared on Medscape.com.
Whooping Cough Likely on Pace for a 5-Year High
Like many diseases, whooping cough reached record low levels during the early days of the COVID pandemic.
More than 10,000 cases of whooping cough have been reported in the United States so far this year, and weekly reports say cases have more than tripled 2023 levels as of June, according to the Centers for Disease Control and Prevention (CDC). In 2023, there were 2815 cases reported during the entire year.
“The number of reported cases this year is close to what was seen at the same time in 2019, prior to the pandemic,” the CDC reported. There were 18,617 cases of whooping cough in 2019.
There were 259 cases reported nationwide for the week ending Aug. 3, with nearly half occurring in the mid-Atlantic region. Public health officials believe the resurgence of whooping cough is likely due to declining vaccination rates, mainly due to the missed vaccines during the height of the COVID pandemic. The diphtheria, tetanus, and pertussis vaccines (DTaP) have been given together since the 1940s, typically during infancy and again during early childhood. In 1941, there were more than 220,000 cases of whooping cough.
Whooping cough is caused by the bacteria Bordetella pertussis. The bacteria attach to tiny, hair-like extensions in the upper respiratory system called cilia, and toxins released by them damage the cilia and cause airways to swell. Early symptoms are similar to the common cold, but the condition eventually leads to coughing fits and a high-pitched “whoop” sound made when inhaling after a fit subsides. Coughing fits can be so severe that people can fracture a rib.
Vaccinated people may get a less severe illness, compared to unvaccinated people, the CDC says. Babies and children are particularly at risk for severe and even potentially deadly complications. About one in three babies under age 1 who get whooping cough will need to be hospitalized, and among those hospitalized babies, 1 in 100 die from complications.
A version of this article appeared on WebMD.com.
Like many diseases, whooping cough reached record low levels during the early days of the COVID pandemic.
More than 10,000 cases of whooping cough have been reported in the United States so far this year, and weekly reports say cases have more than tripled 2023 levels as of June, according to the Centers for Disease Control and Prevention (CDC). In 2023, there were 2815 cases reported during the entire year.
“The number of reported cases this year is close to what was seen at the same time in 2019, prior to the pandemic,” the CDC reported. There were 18,617 cases of whooping cough in 2019.
There were 259 cases reported nationwide for the week ending Aug. 3, with nearly half occurring in the mid-Atlantic region. Public health officials believe the resurgence of whooping cough is likely due to declining vaccination rates, mainly due to the missed vaccines during the height of the COVID pandemic. The diphtheria, tetanus, and pertussis vaccines (DTaP) have been given together since the 1940s, typically during infancy and again during early childhood. In 1941, there were more than 220,000 cases of whooping cough.
Whooping cough is caused by the bacteria Bordetella pertussis. The bacteria attach to tiny, hair-like extensions in the upper respiratory system called cilia, and toxins released by them damage the cilia and cause airways to swell. Early symptoms are similar to the common cold, but the condition eventually leads to coughing fits and a high-pitched “whoop” sound made when inhaling after a fit subsides. Coughing fits can be so severe that people can fracture a rib.
Vaccinated people may get a less severe illness, compared to unvaccinated people, the CDC says. Babies and children are particularly at risk for severe and even potentially deadly complications. About one in three babies under age 1 who get whooping cough will need to be hospitalized, and among those hospitalized babies, 1 in 100 die from complications.
A version of this article appeared on WebMD.com.
Like many diseases, whooping cough reached record low levels during the early days of the COVID pandemic.
More than 10,000 cases of whooping cough have been reported in the United States so far this year, and weekly reports say cases have more than tripled 2023 levels as of June, according to the Centers for Disease Control and Prevention (CDC). In 2023, there were 2815 cases reported during the entire year.
“The number of reported cases this year is close to what was seen at the same time in 2019, prior to the pandemic,” the CDC reported. There were 18,617 cases of whooping cough in 2019.
There were 259 cases reported nationwide for the week ending Aug. 3, with nearly half occurring in the mid-Atlantic region. Public health officials believe the resurgence of whooping cough is likely due to declining vaccination rates, mainly due to the missed vaccines during the height of the COVID pandemic. The diphtheria, tetanus, and pertussis vaccines (DTaP) have been given together since the 1940s, typically during infancy and again during early childhood. In 1941, there were more than 220,000 cases of whooping cough.
Whooping cough is caused by the bacteria Bordetella pertussis. The bacteria attach to tiny, hair-like extensions in the upper respiratory system called cilia, and toxins released by them damage the cilia and cause airways to swell. Early symptoms are similar to the common cold, but the condition eventually leads to coughing fits and a high-pitched “whoop” sound made when inhaling after a fit subsides. Coughing fits can be so severe that people can fracture a rib.
Vaccinated people may get a less severe illness, compared to unvaccinated people, the CDC says. Babies and children are particularly at risk for severe and even potentially deadly complications. About one in three babies under age 1 who get whooping cough will need to be hospitalized, and among those hospitalized babies, 1 in 100 die from complications.
A version of this article appeared on WebMD.com.
A 7-Month-Old Female Presented With Nail Changes
Given the clinical presentation and the absence of other systemic or dermatological findings, the diagnosis of chevron nails was made.
Discussion
The condition is characterized by transverse ridges on the nails that converge towards the center, forming a V or chevron shape. This condition was first described by Perry et al. and later by Shuster et al., who explained that the condition might result from axial growth of the nail with synchronous growth occurring from a chevron-shaped growing edge of the nail root. Alternatively, Shuster suggested that sequential growth, with localized variation in the nail production rate, could propagate a wave from the center of the nail to the edge.
The etiology of chevron nails is not well understood, but it is believed to result from temporary disruptions in the nail matrix, possibly related to minor illness or physiological stress during infancy.
In the case of our 7-month-old patient, the history of mild upper respiratory infections might have contributed to the development of chevron nails. However, the lack of other significant illness, skin involvement, or systemic findings supports the benign and self-limiting nature of this condition. Parents were reassured that chevron nails typically resolve on their own as the child grows and that no specific treatment is necessary.
Differential Diagnosis
The differential diagnosis of transverse nail changes in children includes other conditions such as trachyonychia, lichen planus, Darier disease, and pachyonychia congenita.
Trachyonychia, also known as “sandpaper nails,” trachyonychia is characterized by the roughening of the nail surface, giving it a dull and ridged appearance. The condition may affect all 20 nails and is often associated with underlying dermatological conditions such as lichen planus or alopecia areata. Unlike chevron nails, trachyonychia presents with more diffuse nail changes and does not typically feature the distinct V-shaped ridging seen in this patient.
Lichen planus is an inflammatory condition that can affect the skin, mucous membranes, and nails. Nail involvement in lichen planus can lead to longitudinal ridging, thinning, and sometimes even complete nail loss. The absence of other characteristic features of lichen planus, such as violaceous papules on the skin or white lacy patterns on mucous membranes (Wickham striae), makes this diagnosis less likely in our patient.
Darier disease, also known as keratosis follicularis, is a genetic disorder characterized by greasy, warty papules primarily on seborrheic areas of the skin, nail abnormalities, and sometimes mucosal involvement. Nail changes in Darier disease include longitudinal red and white streaks, V-shaped notching at the free edge of the nails, and subungual hyperkeratosis. These nail changes are more severe and distinct than the simple transverse ridging seen in chevron nails. The absence of other clinical signs of Darier disease, such as skin papules or characteristic nail notching, makes this diagnosis unlikely in our patient.
Pachyonychia congenita is a rare genetic disorder characterized by thickened nails (pachyonychia), painful plantar keratoderma, and sometimes oral leukokeratosis. The condition typically presents with significant nail thickening and other systemic findings, which were absent in our patient. The distinct pattern of V-shaped ridging observed in chevron nails does not align with the typical presentation of pachyonychia congenita.
Next Steps
No specific treatment is required for chevron nails. The condition is typically self-resolving, and the nails usually return to a normal appearance as the child continues to grow. Parents were advised to monitor the nails for any changes or new symptoms and were reassured about the benign nature of the findings. Follow-up was scheduled to ensure the resolution of the condition as the child develops.

Conclusion
Chevron nails are an important consideration in the differential diagnosis of transverse nail ridging in infants and young children. While the condition is benign and self-limiting, it is crucial to differentiate it from other nail dystrophies, such as trachyonychia, lichen planus, Darier disease, and pachyonychia congenita, which may require further investigation or intervention. Awareness of chevron nails can help prevent unnecessary worry and provide reassurance to parents and caregivers.
Dr. Matiz is a pediatric dermatologist at Southern California Permanente Medical Group, San Diego.
Suggested Reading
Delano S, Belazarian L. Chevron nails: A normal variant in the pediatric population. Pediatr Dermatol. 2014 Jan-Feb;31(1):e24-5. doi: 10.1111/pde.12193.
John JM et al. Chevron nail — An under-recognised normal variant of nail development. Arch Dis Child. 2024 Jul 18;109(8):648. doi: 10.1136/archdischild-2024-326975.
Shuster S. The significance of chevron nails. Br J Dermatol. 1996;135:151–152. doi: 10.1046/j.1365-2133.1996.d01-961.x.
Starace M et al. Nail disorders in children. Skin Appendage Disord. 2018 Oct;4(4):217-229. doi: 10.1159/000486020.
Given the clinical presentation and the absence of other systemic or dermatological findings, the diagnosis of chevron nails was made.
Discussion
The condition is characterized by transverse ridges on the nails that converge towards the center, forming a V or chevron shape. This condition was first described by Perry et al. and later by Shuster et al., who explained that the condition might result from axial growth of the nail with synchronous growth occurring from a chevron-shaped growing edge of the nail root. Alternatively, Shuster suggested that sequential growth, with localized variation in the nail production rate, could propagate a wave from the center of the nail to the edge.
The etiology of chevron nails is not well understood, but it is believed to result from temporary disruptions in the nail matrix, possibly related to minor illness or physiological stress during infancy.
In the case of our 7-month-old patient, the history of mild upper respiratory infections might have contributed to the development of chevron nails. However, the lack of other significant illness, skin involvement, or systemic findings supports the benign and self-limiting nature of this condition. Parents were reassured that chevron nails typically resolve on their own as the child grows and that no specific treatment is necessary.
Differential Diagnosis
The differential diagnosis of transverse nail changes in children includes other conditions such as trachyonychia, lichen planus, Darier disease, and pachyonychia congenita.
Trachyonychia, also known as “sandpaper nails,” trachyonychia is characterized by the roughening of the nail surface, giving it a dull and ridged appearance. The condition may affect all 20 nails and is often associated with underlying dermatological conditions such as lichen planus or alopecia areata. Unlike chevron nails, trachyonychia presents with more diffuse nail changes and does not typically feature the distinct V-shaped ridging seen in this patient.
Lichen planus is an inflammatory condition that can affect the skin, mucous membranes, and nails. Nail involvement in lichen planus can lead to longitudinal ridging, thinning, and sometimes even complete nail loss. The absence of other characteristic features of lichen planus, such as violaceous papules on the skin or white lacy patterns on mucous membranes (Wickham striae), makes this diagnosis less likely in our patient.
Darier disease, also known as keratosis follicularis, is a genetic disorder characterized by greasy, warty papules primarily on seborrheic areas of the skin, nail abnormalities, and sometimes mucosal involvement. Nail changes in Darier disease include longitudinal red and white streaks, V-shaped notching at the free edge of the nails, and subungual hyperkeratosis. These nail changes are more severe and distinct than the simple transverse ridging seen in chevron nails. The absence of other clinical signs of Darier disease, such as skin papules or characteristic nail notching, makes this diagnosis unlikely in our patient.
Pachyonychia congenita is a rare genetic disorder characterized by thickened nails (pachyonychia), painful plantar keratoderma, and sometimes oral leukokeratosis. The condition typically presents with significant nail thickening and other systemic findings, which were absent in our patient. The distinct pattern of V-shaped ridging observed in chevron nails does not align with the typical presentation of pachyonychia congenita.
Next Steps
No specific treatment is required for chevron nails. The condition is typically self-resolving, and the nails usually return to a normal appearance as the child continues to grow. Parents were advised to monitor the nails for any changes or new symptoms and were reassured about the benign nature of the findings. Follow-up was scheduled to ensure the resolution of the condition as the child develops.
Conclusion
Chevron nails are an important consideration in the differential diagnosis of transverse nail ridging in infants and young children. While the condition is benign and self-limiting, it is crucial to differentiate it from other nail dystrophies, such as trachyonychia, lichen planus, Darier disease, and pachyonychia congenita, which may require further investigation or intervention. Awareness of chevron nails can help prevent unnecessary worry and provide reassurance to parents and caregivers.
Dr. Matiz is a pediatric dermatologist at Southern California Permanente Medical Group, San Diego.
Suggested Reading
Delano S, Belazarian L. Chevron nails: A normal variant in the pediatric population. Pediatr Dermatol. 2014 Jan-Feb;31(1):e24-5. doi: 10.1111/pde.12193.
John JM et al. Chevron nail — An under-recognised normal variant of nail development. Arch Dis Child. 2024 Jul 18;109(8):648. doi: 10.1136/archdischild-2024-326975.
Shuster S. The significance of chevron nails. Br J Dermatol. 1996;135:151–152. doi: 10.1046/j.1365-2133.1996.d01-961.x.
Starace M et al. Nail disorders in children. Skin Appendage Disord. 2018 Oct;4(4):217-229. doi: 10.1159/000486020.
Given the clinical presentation and the absence of other systemic or dermatological findings, the diagnosis of chevron nails was made.
Discussion
The condition is characterized by transverse ridges on the nails that converge towards the center, forming a V or chevron shape. This condition was first described by Perry et al. and later by Shuster et al., who explained that the condition might result from axial growth of the nail with synchronous growth occurring from a chevron-shaped growing edge of the nail root. Alternatively, Shuster suggested that sequential growth, with localized variation in the nail production rate, could propagate a wave from the center of the nail to the edge.
The etiology of chevron nails is not well understood, but it is believed to result from temporary disruptions in the nail matrix, possibly related to minor illness or physiological stress during infancy.
In the case of our 7-month-old patient, the history of mild upper respiratory infections might have contributed to the development of chevron nails. However, the lack of other significant illness, skin involvement, or systemic findings supports the benign and self-limiting nature of this condition. Parents were reassured that chevron nails typically resolve on their own as the child grows and that no specific treatment is necessary.
Differential Diagnosis
The differential diagnosis of transverse nail changes in children includes other conditions such as trachyonychia, lichen planus, Darier disease, and pachyonychia congenita.
Trachyonychia, also known as “sandpaper nails,” trachyonychia is characterized by the roughening of the nail surface, giving it a dull and ridged appearance. The condition may affect all 20 nails and is often associated with underlying dermatological conditions such as lichen planus or alopecia areata. Unlike chevron nails, trachyonychia presents with more diffuse nail changes and does not typically feature the distinct V-shaped ridging seen in this patient.
Lichen planus is an inflammatory condition that can affect the skin, mucous membranes, and nails. Nail involvement in lichen planus can lead to longitudinal ridging, thinning, and sometimes even complete nail loss. The absence of other characteristic features of lichen planus, such as violaceous papules on the skin or white lacy patterns on mucous membranes (Wickham striae), makes this diagnosis less likely in our patient.
Darier disease, also known as keratosis follicularis, is a genetic disorder characterized by greasy, warty papules primarily on seborrheic areas of the skin, nail abnormalities, and sometimes mucosal involvement. Nail changes in Darier disease include longitudinal red and white streaks, V-shaped notching at the free edge of the nails, and subungual hyperkeratosis. These nail changes are more severe and distinct than the simple transverse ridging seen in chevron nails. The absence of other clinical signs of Darier disease, such as skin papules or characteristic nail notching, makes this diagnosis unlikely in our patient.
Pachyonychia congenita is a rare genetic disorder characterized by thickened nails (pachyonychia), painful plantar keratoderma, and sometimes oral leukokeratosis. The condition typically presents with significant nail thickening and other systemic findings, which were absent in our patient. The distinct pattern of V-shaped ridging observed in chevron nails does not align with the typical presentation of pachyonychia congenita.
Next Steps
No specific treatment is required for chevron nails. The condition is typically self-resolving, and the nails usually return to a normal appearance as the child continues to grow. Parents were advised to monitor the nails for any changes or new symptoms and were reassured about the benign nature of the findings. Follow-up was scheduled to ensure the resolution of the condition as the child develops.
Conclusion
Chevron nails are an important consideration in the differential diagnosis of transverse nail ridging in infants and young children. While the condition is benign and self-limiting, it is crucial to differentiate it from other nail dystrophies, such as trachyonychia, lichen planus, Darier disease, and pachyonychia congenita, which may require further investigation or intervention. Awareness of chevron nails can help prevent unnecessary worry and provide reassurance to parents and caregivers.
Dr. Matiz is a pediatric dermatologist at Southern California Permanente Medical Group, San Diego.
Suggested Reading
Delano S, Belazarian L. Chevron nails: A normal variant in the pediatric population. Pediatr Dermatol. 2014 Jan-Feb;31(1):e24-5. doi: 10.1111/pde.12193.
John JM et al. Chevron nail — An under-recognised normal variant of nail development. Arch Dis Child. 2024 Jul 18;109(8):648. doi: 10.1136/archdischild-2024-326975.
Shuster S. The significance of chevron nails. Br J Dermatol. 1996;135:151–152. doi: 10.1046/j.1365-2133.1996.d01-961.x.
Starace M et al. Nail disorders in children. Skin Appendage Disord. 2018 Oct;4(4):217-229. doi: 10.1159/000486020.

There was no family history of similar nail findings and no relatives had a history of chronic skin conditions or congenital nail disorders.
On physical examination, several of the child’s fingernails exhibited distinct longitudinal ridges, with a characteristic pattern where the ridges converged at the center of the nail, forming a V-shape. There were no other concerning dermatologic findings, such as rashes, plaques, or erosions, and the skin and hair appeared otherwise normal. The rest of the physical exam was unremarkable.
FTC Interim Report on Pharmacy Middlemen Is First Step of Many Needed in Addressing Drug Costs, Access
Rising consolidation among pharmacy benefit managers (PBMs) allows the companies to profit at the expense of patients and independent pharmacists. That’s the conclusion of a recent Federal Trade Commission (FTC) report on interim findings from the agency’s ongoing investigation of PBMs.
Lawmakers are increasingly scrutinizing the industry amid growing concern among physicians and consumers about how PBMs exploit their market dominance. The top six PBMs managed 94% of US drug claims in 2023, with the majority handled by the industry’s three giants: CVS Caremark, Cigna’s Express Scripts, and United Healthcare’s OptumRx.
PBMs manage prescription drug benefits for health insurers, Medicare Part D drug plans, and large employers. They act as middlemen between health insurers and pharmacies, developing formularies of covered drugs and promising savings from the discounts and rebates they negotiate with drugmakers.
The FTC’s interim report found that the giant PBMs often exercise significant control over what drugs are available and at what price and which pharmacies patients can use to access their prescribed medications. Consumers suffer as a result, the report concluded.
Madelaine A. Feldman, MD, vice president for advocacy and government affairs for the Coalition of State Rheumatology Organizations, shared her perspective on the FTC report in an email Q&A with this news organization. She is affiliated with The Rheumatology Group, based in Metairie, Louisiana.

Dr. Feldman has long tracked the PBM industry and appeared as a witness before influential government panels, including the House Energy and Commerce Committee. She has highlighted for lawmakers the challenges physicians face in helping patients get needed medicines.
For example, she shared cases of PBMs steering patients toward the more expensive of three widely used rheumatoid arthritis medicines that have a similar mechanism of action, the Janus kinase (JAK) inhibitors, Dr. Feldman said.
One of the drugs cost roughly half of the other two — about $30,000 per year vs $65,000-$70,000. Yet only the two expensive drugs were included in the PBM formulary. As a result, the cheapest drug holds only a sliver of market share; the remainder is dominated by the two expensive products, she told the House Oversight and Accountability Committee in 2021.
This Q&A has been edited for length and clarity.
What would you want federal and state policymakers to do in response to the FTC’s report?
I think Congress needs to clearly delineate the differences between anticompetitive pharmacy issues, drug pricing issues, and their effect on formulary construction issues.
Lawmakers should demand more transparency and consider legislation that would remove perverse incentives that prompt PBMs to choose higher priced drugs for their formularies.
That may require other regulatory or legislative actions to ensure lower prices (not higher kickbacks) are incentivized. Ultimately, in order to gain true competition within the health insurance business, these oligopolies of multiple businesses need to be broken up. Anything less seems to be nibbling around the edges and allows the Big Three to continue their “whack-a mole” in circumventing piecemeal regulatory and legislative policies.
You’ve followed PBM practices closely for many years. Was there anything in this interim FTC report that surprised you?
Though not surprised, I am glad that it was released because it had been a year in investigation and there were many requests for some type of substantive report.
Two things that are missing that I feel are paramount are investigating how the three big PBMs are causing physical harm to patients as a result of the profit component in formulary construction and the profound financial impact of hidden PBM profit centers in self-insured employer health plans.
What we have seen over the years is the result of the perverse incentives for the PBMs to prefer the most profitable medications on their formularies.
They use utilization management tools such as step therapy, nonmedical switching, and exclusions to maintain their formularies’ profitability. These tools have been shown to delay and deny the proper care of patients, resulting in not just monetary but physical harm as well.
I would think the physical harm done to patients in manipulating the formularies should be addressed in this report as well and, in fact, may be the most important aspect of consumer protection of this issue.
In terms of the FTC’s mission to not “unduly burden” legitimate business, I would like to see the sector of self-insured employers addressed.
The report details how PBMs steer prescriptions to their affiliated pharmacies. The FTC says that can push smaller pharmacies out of the market, ultimately leading to higher costs and lower quality services for people. What’s your perspective?
Having more community pharmacies is better than having less. We are seeing more “pharmacy deserts” in rural areas as a result of many community pharmacies having to close.
The FTC voted 4-1 to allow staff to issue the interim report, with Commissioner Melissa Holyoak voting no. And some FTC commissioners seem divided on the usefulness of the report. Why?
Commissioner Holyoak states the “the Report leaves us without a better understanding of the competition concerns surrounding PBMs or how consumers are impacted by PBM practices.”
I do agree with her that the harm to patients’ medical status was not even addressed as far as I could tell in this report. There are multiple news articles and reports on the harms inflicted upon patients by the UM tools that drive the construction of ever changing formularies, all based on contracting with manufacturers that result in the highest profit for the PBM.
Holyoak also states, “Among other critical conclusions, the Report does not address the seemingly contradictory conclusions in the 2005 Report that PBMs, including vertically owned PBMs, generated cost savings for consumers.”
That may be true, but in 2005, the rise of PBMs was just beginning and the huge vertical and horizontal integration had yet to begin. Also, 2005 was still in the beginning of the biologic drug deluge, which did create competition to get on the formulary. Since then, PBMs have done nothing to control the rise in prices but instead, apparently have used the competition to get higher price concessions from manufacturers based on a percentage of the list price to line their pockets.
Commissioner Ferguson agreed with releasing the report but he had many issues with this report including the lack of PBM response.
I do agree with him that the FTC should have used some type of “force” to get the information they needed from the PBMs. The Big Three are known for obfuscation and delaying providing information to legislative and regulatory agencies.
A version of this article appeared on Medscape.com.
Rising consolidation among pharmacy benefit managers (PBMs) allows the companies to profit at the expense of patients and independent pharmacists. That’s the conclusion of a recent Federal Trade Commission (FTC) report on interim findings from the agency’s ongoing investigation of PBMs.
Lawmakers are increasingly scrutinizing the industry amid growing concern among physicians and consumers about how PBMs exploit their market dominance. The top six PBMs managed 94% of US drug claims in 2023, with the majority handled by the industry’s three giants: CVS Caremark, Cigna’s Express Scripts, and United Healthcare’s OptumRx.
PBMs manage prescription drug benefits for health insurers, Medicare Part D drug plans, and large employers. They act as middlemen between health insurers and pharmacies, developing formularies of covered drugs and promising savings from the discounts and rebates they negotiate with drugmakers.
The FTC’s interim report found that the giant PBMs often exercise significant control over what drugs are available and at what price and which pharmacies patients can use to access their prescribed medications. Consumers suffer as a result, the report concluded.
Madelaine A. Feldman, MD, vice president for advocacy and government affairs for the Coalition of State Rheumatology Organizations, shared her perspective on the FTC report in an email Q&A with this news organization. She is affiliated with The Rheumatology Group, based in Metairie, Louisiana.
Dr. Feldman has long tracked the PBM industry and appeared as a witness before influential government panels, including the House Energy and Commerce Committee. She has highlighted for lawmakers the challenges physicians face in helping patients get needed medicines.
For example, she shared cases of PBMs steering patients toward the more expensive of three widely used rheumatoid arthritis medicines that have a similar mechanism of action, the Janus kinase (JAK) inhibitors, Dr. Feldman said.
One of the drugs cost roughly half of the other two — about $30,000 per year vs $65,000-$70,000. Yet only the two expensive drugs were included in the PBM formulary. As a result, the cheapest drug holds only a sliver of market share; the remainder is dominated by the two expensive products, she told the House Oversight and Accountability Committee in 2021.
This Q&A has been edited for length and clarity.
What would you want federal and state policymakers to do in response to the FTC’s report?
I think Congress needs to clearly delineate the differences between anticompetitive pharmacy issues, drug pricing issues, and their effect on formulary construction issues.
Lawmakers should demand more transparency and consider legislation that would remove perverse incentives that prompt PBMs to choose higher priced drugs for their formularies.
That may require other regulatory or legislative actions to ensure lower prices (not higher kickbacks) are incentivized. Ultimately, in order to gain true competition within the health insurance business, these oligopolies of multiple businesses need to be broken up. Anything less seems to be nibbling around the edges and allows the Big Three to continue their “whack-a mole” in circumventing piecemeal regulatory and legislative policies.
You’ve followed PBM practices closely for many years. Was there anything in this interim FTC report that surprised you?
Though not surprised, I am glad that it was released because it had been a year in investigation and there were many requests for some type of substantive report.
Two things that are missing that I feel are paramount are investigating how the three big PBMs are causing physical harm to patients as a result of the profit component in formulary construction and the profound financial impact of hidden PBM profit centers in self-insured employer health plans.
What we have seen over the years is the result of the perverse incentives for the PBMs to prefer the most profitable medications on their formularies.
They use utilization management tools such as step therapy, nonmedical switching, and exclusions to maintain their formularies’ profitability. These tools have been shown to delay and deny the proper care of patients, resulting in not just monetary but physical harm as well.
I would think the physical harm done to patients in manipulating the formularies should be addressed in this report as well and, in fact, may be the most important aspect of consumer protection of this issue.
In terms of the FTC’s mission to not “unduly burden” legitimate business, I would like to see the sector of self-insured employers addressed.
The report details how PBMs steer prescriptions to their affiliated pharmacies. The FTC says that can push smaller pharmacies out of the market, ultimately leading to higher costs and lower quality services for people. What’s your perspective?
Having more community pharmacies is better than having less. We are seeing more “pharmacy deserts” in rural areas as a result of many community pharmacies having to close.
The FTC voted 4-1 to allow staff to issue the interim report, with Commissioner Melissa Holyoak voting no. And some FTC commissioners seem divided on the usefulness of the report. Why?
Commissioner Holyoak states the “the Report leaves us without a better understanding of the competition concerns surrounding PBMs or how consumers are impacted by PBM practices.”
I do agree with her that the harm to patients’ medical status was not even addressed as far as I could tell in this report. There are multiple news articles and reports on the harms inflicted upon patients by the UM tools that drive the construction of ever changing formularies, all based on contracting with manufacturers that result in the highest profit for the PBM.
Holyoak also states, “Among other critical conclusions, the Report does not address the seemingly contradictory conclusions in the 2005 Report that PBMs, including vertically owned PBMs, generated cost savings for consumers.”
That may be true, but in 2005, the rise of PBMs was just beginning and the huge vertical and horizontal integration had yet to begin. Also, 2005 was still in the beginning of the biologic drug deluge, which did create competition to get on the formulary. Since then, PBMs have done nothing to control the rise in prices but instead, apparently have used the competition to get higher price concessions from manufacturers based on a percentage of the list price to line their pockets.
Commissioner Ferguson agreed with releasing the report but he had many issues with this report including the lack of PBM response.
I do agree with him that the FTC should have used some type of “force” to get the information they needed from the PBMs. The Big Three are known for obfuscation and delaying providing information to legislative and regulatory agencies.
A version of this article appeared on Medscape.com.
Rising consolidation among pharmacy benefit managers (PBMs) allows the companies to profit at the expense of patients and independent pharmacists. That’s the conclusion of a recent Federal Trade Commission (FTC) report on interim findings from the agency’s ongoing investigation of PBMs.
Lawmakers are increasingly scrutinizing the industry amid growing concern among physicians and consumers about how PBMs exploit their market dominance. The top six PBMs managed 94% of US drug claims in 2023, with the majority handled by the industry’s three giants: CVS Caremark, Cigna’s Express Scripts, and United Healthcare’s OptumRx.
PBMs manage prescription drug benefits for health insurers, Medicare Part D drug plans, and large employers. They act as middlemen between health insurers and pharmacies, developing formularies of covered drugs and promising savings from the discounts and rebates they negotiate with drugmakers.
The FTC’s interim report found that the giant PBMs often exercise significant control over what drugs are available and at what price and which pharmacies patients can use to access their prescribed medications. Consumers suffer as a result, the report concluded.
Madelaine A. Feldman, MD, vice president for advocacy and government affairs for the Coalition of State Rheumatology Organizations, shared her perspective on the FTC report in an email Q&A with this news organization. She is affiliated with The Rheumatology Group, based in Metairie, Louisiana.
Dr. Feldman has long tracked the PBM industry and appeared as a witness before influential government panels, including the House Energy and Commerce Committee. She has highlighted for lawmakers the challenges physicians face in helping patients get needed medicines.
For example, she shared cases of PBMs steering patients toward the more expensive of three widely used rheumatoid arthritis medicines that have a similar mechanism of action, the Janus kinase (JAK) inhibitors, Dr. Feldman said.
One of the drugs cost roughly half of the other two — about $30,000 per year vs $65,000-$70,000. Yet only the two expensive drugs were included in the PBM formulary. As a result, the cheapest drug holds only a sliver of market share; the remainder is dominated by the two expensive products, she told the House Oversight and Accountability Committee in 2021.
This Q&A has been edited for length and clarity.
What would you want federal and state policymakers to do in response to the FTC’s report?
I think Congress needs to clearly delineate the differences between anticompetitive pharmacy issues, drug pricing issues, and their effect on formulary construction issues.
Lawmakers should demand more transparency and consider legislation that would remove perverse incentives that prompt PBMs to choose higher priced drugs for their formularies.
That may require other regulatory or legislative actions to ensure lower prices (not higher kickbacks) are incentivized. Ultimately, in order to gain true competition within the health insurance business, these oligopolies of multiple businesses need to be broken up. Anything less seems to be nibbling around the edges and allows the Big Three to continue their “whack-a mole” in circumventing piecemeal regulatory and legislative policies.
You’ve followed PBM practices closely for many years. Was there anything in this interim FTC report that surprised you?
Though not surprised, I am glad that it was released because it had been a year in investigation and there were many requests for some type of substantive report.
Two things that are missing that I feel are paramount are investigating how the three big PBMs are causing physical harm to patients as a result of the profit component in formulary construction and the profound financial impact of hidden PBM profit centers in self-insured employer health plans.
What we have seen over the years is the result of the perverse incentives for the PBMs to prefer the most profitable medications on their formularies.
They use utilization management tools such as step therapy, nonmedical switching, and exclusions to maintain their formularies’ profitability. These tools have been shown to delay and deny the proper care of patients, resulting in not just monetary but physical harm as well.
I would think the physical harm done to patients in manipulating the formularies should be addressed in this report as well and, in fact, may be the most important aspect of consumer protection of this issue.
In terms of the FTC’s mission to not “unduly burden” legitimate business, I would like to see the sector of self-insured employers addressed.
The report details how PBMs steer prescriptions to their affiliated pharmacies. The FTC says that can push smaller pharmacies out of the market, ultimately leading to higher costs and lower quality services for people. What’s your perspective?
Having more community pharmacies is better than having less. We are seeing more “pharmacy deserts” in rural areas as a result of many community pharmacies having to close.
The FTC voted 4-1 to allow staff to issue the interim report, with Commissioner Melissa Holyoak voting no. And some FTC commissioners seem divided on the usefulness of the report. Why?
Commissioner Holyoak states the “the Report leaves us without a better understanding of the competition concerns surrounding PBMs or how consumers are impacted by PBM practices.”
I do agree with her that the harm to patients’ medical status was not even addressed as far as I could tell in this report. There are multiple news articles and reports on the harms inflicted upon patients by the UM tools that drive the construction of ever changing formularies, all based on contracting with manufacturers that result in the highest profit for the PBM.
Holyoak also states, “Among other critical conclusions, the Report does not address the seemingly contradictory conclusions in the 2005 Report that PBMs, including vertically owned PBMs, generated cost savings for consumers.”
That may be true, but in 2005, the rise of PBMs was just beginning and the huge vertical and horizontal integration had yet to begin. Also, 2005 was still in the beginning of the biologic drug deluge, which did create competition to get on the formulary. Since then, PBMs have done nothing to control the rise in prices but instead, apparently have used the competition to get higher price concessions from manufacturers based on a percentage of the list price to line their pockets.
Commissioner Ferguson agreed with releasing the report but he had many issues with this report including the lack of PBM response.
I do agree with him that the FTC should have used some type of “force” to get the information they needed from the PBMs. The Big Three are known for obfuscation and delaying providing information to legislative and regulatory agencies.
A version of this article appeared on Medscape.com.
Family Not Flourishing? The Hidden Issue of Food Insecurity and How We Can Help
As pediatric providers we are dedicated to helping children have optimal health. And what could be more basic to health than having enough food? Yet, even in one of the richest countries on the planet, as much as 25% of US families are reported to have “food insecurity.”
What does this mean? The US Department of Agriculture (USDA), the agency tracking and addressing food issues, defines food security as “marginal” when there are one or two indications, typically anxiety over food sufficiency or shortage of food even with little or no alteration of diet or intake. “Low” includes reduced quality, variety, or desirability of the diet but little or no reduced intake. When eating patterns are disrupted and intake is reduced, this is considered “very low food security.” “Hunger” refers to an individual’s physiological state when prolonged, involuntary lack of food results in discomfort, illness, weakness, or pain beyond the usual uneasy sensation. Pediatric researchers include in the definition lack of access to enough food for an active and healthy life. I will use the common term “food insecurity” here.
Children under 3 years old in homes with food insecurity have been found to be sick more often, recover more slowly from illness, and be hospitalized more frequently. Deficiencies in nutrition vary by age, with children under 6 having low vegetable intake and low iron, ages 6-11 excess sugary food intake and lower bone density in boys, and adolescents, although harder to measure, had low iron.
Physical and Mental Effects of Food Insecurity
Associated with food insecurity in the home are more developmental delays in children 4-36 months old. Beyond that, children of all ages have lower cognitive indicators, dysregulated behavior, and emotional distress than those in homes with secure food access. These are persisting deficits: kindergarten children with food insecurity have lower math and reading abilities over at least 4 years.

Mental health is also affected by food insecurity. Reviews of multiple studies of children from preschool through adolescence show more child hyperactivity, emotional dysregulation, anxiety, depression, and stress beyond those attributable to their mother’s depression and anxiety. Food insecurity in the early years is associated with mental health issues even into adolescence. School aged children and youth are well aware of the family’s struggle with food access, even when their parents do not realize this. In addition to the anxiety and depression, they may feel shame or be socially ostracized. They may eat less, or choose low-quality foods to cope. Adolescents experiencing food insecurity report greater dysthymia and suicidal ideation. It is unknown whether these mental health difficulties are due to the stress, shame, or decreased intake of macronutrients important to emotional regulation or all of these. One implication is that pediatric providers should also screen for food insecurity as well as other social drivers of health (SDOH) when addressing developmental, behavioral, or mental health issues, not just at well visits.
While we worry about effects for the child, impact of food insecurity on caregivers is significant for parenting as well as adult well-being beginning prenatally. First trimester food insecurity is associated with increased maternal stress at 2 months postpartum and lower bonding scores at 6 months, although this is moderated by social support. The stress of food insecurity and other SDoH present are associated with parental depression, anxiety, and toxic stress, making optimal parenting difficult. Caregivers experiencing insecure food access worry most about their children and may reduce their own eating and food quality to spare the child. More than 30% of families indicated that they had to choose between paying for food and paying for medicine or medical care, jeopardizing their health, making this an important point of discussion for us as well.
Quality Versus Quantity
The total amount of food is not the only factor in adequate child nutrition. Healthy foods usually cost more and also may not be conveniently available. There are so called “food deserts,” areas with few/no full-service grocery stores, and also “food swamps” where unhealthy foods (eg fast food) are more available than healthy options. Life stress, higher in low-income populations, increases the impulse to consume sweet or high-fat “comfort foods” (we all know this!) due to the rush of calories and quick satiety. Children may be influenced in their food choices by media messages about non-nutritious foods. All of these may explain the association of food insecurity with obesity in both children and adults. It also sets them up for lifetime health problems of diabetes, hyperlipidemia, and cardiovascular conditions, especially in racial and ethnic minority groups and the poor.
The Larger Picture
Obvious to us all, low income is the main reason for inadequate access to enough or good quality food. Over 60% of families with food insecurity had incomes below the poverty threshold in 2013. Households without children are half as likely to be food insecure. But as 30% of food-insecure households have incomes above the eligibility cut offs for food programs — typically 130% of poverty for Special Supplemental Nutrition Program for Women, Infants, and Children (WIC) or 185% for Supplemental Nutrition Assistance Program (SNAP) — it is clear the problem is not related solely to poverty. Even small changes in income or expenses, such as a car breaking down, or heating or medical bills, can quickly result in inability to afford food, especially in areas of high food costs. This is particularly true for immigrant, large, and single-parent families and those with less education. Federal food programs do not cover all food needs for every family.
But we can’t tell if a child lives in a family with food insecurity by whether the child is thin, dropping growth percentiles, or receiving Medicaid insurance. Parents, and even youth, may be reluctant to tell us that they do not have enough to eat out of pride, fear, of prejudice, being reported to a contentious ex, being detected as an illegal immigrant, or even reported for neglect and having their child removed. Because of the suffering and impacts of food insecurity on child well-being, the American Academy of Pediatrics (AAP) published a Policy Statement in 2015, reaffirmed in 2021, recommending screening for food insecurity at all well visits and a toolkit to help. The USDA 18-item Household Food Security Scale (HFSS) has been the gold-standard screen, but affirmative answers to either of the 2-item Hunger Vital Sign (HVS) questionnaire identifies food insecurity with a sensitivity of 97% and a specificity of 83% compared with the HFSS. The questions ask how often the following were true in the past year: 1) “We worried whether our food would run out before we got money to buy more” and 2) “The food we bought just didn’t last and we didn’t have money to buy more.” This brief screen is now recommended and practical.
Screening for Food Insecurity
All set to manage food insecurity in your practice, then? Not exactly. Screening is only useful if it results in access to food. A study in a majority low-income clinic found that parents reported food insecurity 7% of the time when the clinician asked the HVS questions versus 45% when they self-reported on paper. Parent focus groups revealed reasons for the discrepant underreporting to the clinician: shame, concerns about stigma, and fear of the child being taken away. They felt more comfortable reporting about their child than about their own family situation. When asked what the clinician did that helped them disclose food insecurity, the caregivers cited strong interpersonal skills, open body language, and empathy. They also requested being given resources for other social issues, not just food insecurity. Clinic staff found paper screening inconvenient and recommended using tablet devices (such as with CHADIS that also scores and provides interviewing help, education, and local resource listings). Clinicians found the need for a follow-up conversation time consuming. Clinic staff thought screening could be facilitated by clinician’s initiating conversations, taking care about children present, and normalizing the screen as applying to all. Caregivers wanted know the use and privacy of the information. This same clinic referred the caregivers to a Benefits Data Trust with a goal of enrolling them in food programs. Of the food insecure, 55% were referred but only one third could be reached by phone with three attempts by the benefits group. Subsequent enrollment of those reached had barriers of verification requirements, wait times, and perceived mistreatment. The program concluded that this difficult two-step process of screening and referral would be improved by an integrated system of screening and enrollment in public benefits. Provision of information about free local food resources is also important, as 84% of those already receiving SNAP benefits remained food insecure.
Offering Assistance
To assist families where food insecurity is found, we need to understand the options of services both for referrals and advocacy. The AAP toolkit is designed to help. For pregnant and postpartum women and children 0-5 years in families with income less than 130% of the poverty level, the WIC program provides electronic cards to purchase approved categories of healthy food from participating vendors. For families with incomes less than 185% of the poverty level, the SNAP program, formerly called food stamps, provides benefits. There are other programs including free and reduced cost National School Breakfast and/or Lunch programs (best when open to all), Child and Adult Care Food Program for institutions (which may include medical offices), and Summer Food Service Programs providing lunch at community sites. Since not all food-insecure families are eligible for the above services, it is important that we are ready to provide information about local food banks, pantries, and low- or no-cost produce programs (see Healthy Food Bank Hub, Feeding America, 2-1-1, or FindHelp.org).
As pediatric providers we have a special opportunity and responsibility to expand our capabilities for sensitively addressing and advocating for help for food insecurity to improve the outlook for the families under our care.
Dr. Howard is assistant professor of pediatrics at The Johns Hopkins University School of Medicine, Baltimore, and creator of CHADIS. She had no other relevant disclosures. Dr. Howard’s contribution to this publication was as a paid expert to MDedge News. E-mail her at [email protected].
As pediatric providers we are dedicated to helping children have optimal health. And what could be more basic to health than having enough food? Yet, even in one of the richest countries on the planet, as much as 25% of US families are reported to have “food insecurity.”
What does this mean? The US Department of Agriculture (USDA), the agency tracking and addressing food issues, defines food security as “marginal” when there are one or two indications, typically anxiety over food sufficiency or shortage of food even with little or no alteration of diet or intake. “Low” includes reduced quality, variety, or desirability of the diet but little or no reduced intake. When eating patterns are disrupted and intake is reduced, this is considered “very low food security.” “Hunger” refers to an individual’s physiological state when prolonged, involuntary lack of food results in discomfort, illness, weakness, or pain beyond the usual uneasy sensation. Pediatric researchers include in the definition lack of access to enough food for an active and healthy life. I will use the common term “food insecurity” here.
Children under 3 years old in homes with food insecurity have been found to be sick more often, recover more slowly from illness, and be hospitalized more frequently. Deficiencies in nutrition vary by age, with children under 6 having low vegetable intake and low iron, ages 6-11 excess sugary food intake and lower bone density in boys, and adolescents, although harder to measure, had low iron.
Physical and Mental Effects of Food Insecurity
Associated with food insecurity in the home are more developmental delays in children 4-36 months old. Beyond that, children of all ages have lower cognitive indicators, dysregulated behavior, and emotional distress than those in homes with secure food access. These are persisting deficits: kindergarten children with food insecurity have lower math and reading abilities over at least 4 years.
Mental health is also affected by food insecurity. Reviews of multiple studies of children from preschool through adolescence show more child hyperactivity, emotional dysregulation, anxiety, depression, and stress beyond those attributable to their mother’s depression and anxiety. Food insecurity in the early years is associated with mental health issues even into adolescence. School aged children and youth are well aware of the family’s struggle with food access, even when their parents do not realize this. In addition to the anxiety and depression, they may feel shame or be socially ostracized. They may eat less, or choose low-quality foods to cope. Adolescents experiencing food insecurity report greater dysthymia and suicidal ideation. It is unknown whether these mental health difficulties are due to the stress, shame, or decreased intake of macronutrients important to emotional regulation or all of these. One implication is that pediatric providers should also screen for food insecurity as well as other social drivers of health (SDOH) when addressing developmental, behavioral, or mental health issues, not just at well visits.
While we worry about effects for the child, impact of food insecurity on caregivers is significant for parenting as well as adult well-being beginning prenatally. First trimester food insecurity is associated with increased maternal stress at 2 months postpartum and lower bonding scores at 6 months, although this is moderated by social support. The stress of food insecurity and other SDoH present are associated with parental depression, anxiety, and toxic stress, making optimal parenting difficult. Caregivers experiencing insecure food access worry most about their children and may reduce their own eating and food quality to spare the child. More than 30% of families indicated that they had to choose between paying for food and paying for medicine or medical care, jeopardizing their health, making this an important point of discussion for us as well.
Quality Versus Quantity
The total amount of food is not the only factor in adequate child nutrition. Healthy foods usually cost more and also may not be conveniently available. There are so called “food deserts,” areas with few/no full-service grocery stores, and also “food swamps” where unhealthy foods (eg fast food) are more available than healthy options. Life stress, higher in low-income populations, increases the impulse to consume sweet or high-fat “comfort foods” (we all know this!) due to the rush of calories and quick satiety. Children may be influenced in their food choices by media messages about non-nutritious foods. All of these may explain the association of food insecurity with obesity in both children and adults. It also sets them up for lifetime health problems of diabetes, hyperlipidemia, and cardiovascular conditions, especially in racial and ethnic minority groups and the poor.
The Larger Picture
Obvious to us all, low income is the main reason for inadequate access to enough or good quality food. Over 60% of families with food insecurity had incomes below the poverty threshold in 2013. Households without children are half as likely to be food insecure. But as 30% of food-insecure households have incomes above the eligibility cut offs for food programs — typically 130% of poverty for Special Supplemental Nutrition Program for Women, Infants, and Children (WIC) or 185% for Supplemental Nutrition Assistance Program (SNAP) — it is clear the problem is not related solely to poverty. Even small changes in income or expenses, such as a car breaking down, or heating or medical bills, can quickly result in inability to afford food, especially in areas of high food costs. This is particularly true for immigrant, large, and single-parent families and those with less education. Federal food programs do not cover all food needs for every family.
But we can’t tell if a child lives in a family with food insecurity by whether the child is thin, dropping growth percentiles, or receiving Medicaid insurance. Parents, and even youth, may be reluctant to tell us that they do not have enough to eat out of pride, fear, of prejudice, being reported to a contentious ex, being detected as an illegal immigrant, or even reported for neglect and having their child removed. Because of the suffering and impacts of food insecurity on child well-being, the American Academy of Pediatrics (AAP) published a Policy Statement in 2015, reaffirmed in 2021, recommending screening for food insecurity at all well visits and a toolkit to help. The USDA 18-item Household Food Security Scale (HFSS) has been the gold-standard screen, but affirmative answers to either of the 2-item Hunger Vital Sign (HVS) questionnaire identifies food insecurity with a sensitivity of 97% and a specificity of 83% compared with the HFSS. The questions ask how often the following were true in the past year: 1) “We worried whether our food would run out before we got money to buy more” and 2) “The food we bought just didn’t last and we didn’t have money to buy more.” This brief screen is now recommended and practical.
Screening for Food Insecurity
All set to manage food insecurity in your practice, then? Not exactly. Screening is only useful if it results in access to food. A study in a majority low-income clinic found that parents reported food insecurity 7% of the time when the clinician asked the HVS questions versus 45% when they self-reported on paper. Parent focus groups revealed reasons for the discrepant underreporting to the clinician: shame, concerns about stigma, and fear of the child being taken away. They felt more comfortable reporting about their child than about their own family situation. When asked what the clinician did that helped them disclose food insecurity, the caregivers cited strong interpersonal skills, open body language, and empathy. They also requested being given resources for other social issues, not just food insecurity. Clinic staff found paper screening inconvenient and recommended using tablet devices (such as with CHADIS that also scores and provides interviewing help, education, and local resource listings). Clinicians found the need for a follow-up conversation time consuming. Clinic staff thought screening could be facilitated by clinician’s initiating conversations, taking care about children present, and normalizing the screen as applying to all. Caregivers wanted know the use and privacy of the information. This same clinic referred the caregivers to a Benefits Data Trust with a goal of enrolling them in food programs. Of the food insecure, 55% were referred but only one third could be reached by phone with three attempts by the benefits group. Subsequent enrollment of those reached had barriers of verification requirements, wait times, and perceived mistreatment. The program concluded that this difficult two-step process of screening and referral would be improved by an integrated system of screening and enrollment in public benefits. Provision of information about free local food resources is also important, as 84% of those already receiving SNAP benefits remained food insecure.
Offering Assistance
To assist families where food insecurity is found, we need to understand the options of services both for referrals and advocacy. The AAP toolkit is designed to help. For pregnant and postpartum women and children 0-5 years in families with income less than 130% of the poverty level, the WIC program provides electronic cards to purchase approved categories of healthy food from participating vendors. For families with incomes less than 185% of the poverty level, the SNAP program, formerly called food stamps, provides benefits. There are other programs including free and reduced cost National School Breakfast and/or Lunch programs (best when open to all), Child and Adult Care Food Program for institutions (which may include medical offices), and Summer Food Service Programs providing lunch at community sites. Since not all food-insecure families are eligible for the above services, it is important that we are ready to provide information about local food banks, pantries, and low- or no-cost produce programs (see Healthy Food Bank Hub, Feeding America, 2-1-1, or FindHelp.org).
As pediatric providers we have a special opportunity and responsibility to expand our capabilities for sensitively addressing and advocating for help for food insecurity to improve the outlook for the families under our care.
Dr. Howard is assistant professor of pediatrics at The Johns Hopkins University School of Medicine, Baltimore, and creator of CHADIS. She had no other relevant disclosures. Dr. Howard’s contribution to this publication was as a paid expert to MDedge News. E-mail her at [email protected].
As pediatric providers we are dedicated to helping children have optimal health. And what could be more basic to health than having enough food? Yet, even in one of the richest countries on the planet, as much as 25% of US families are reported to have “food insecurity.”
What does this mean? The US Department of Agriculture (USDA), the agency tracking and addressing food issues, defines food security as “marginal” when there are one or two indications, typically anxiety over food sufficiency or shortage of food even with little or no alteration of diet or intake. “Low” includes reduced quality, variety, or desirability of the diet but little or no reduced intake. When eating patterns are disrupted and intake is reduced, this is considered “very low food security.” “Hunger” refers to an individual’s physiological state when prolonged, involuntary lack of food results in discomfort, illness, weakness, or pain beyond the usual uneasy sensation. Pediatric researchers include in the definition lack of access to enough food for an active and healthy life. I will use the common term “food insecurity” here.
Children under 3 years old in homes with food insecurity have been found to be sick more often, recover more slowly from illness, and be hospitalized more frequently. Deficiencies in nutrition vary by age, with children under 6 having low vegetable intake and low iron, ages 6-11 excess sugary food intake and lower bone density in boys, and adolescents, although harder to measure, had low iron.
Physical and Mental Effects of Food Insecurity
Associated with food insecurity in the home are more developmental delays in children 4-36 months old. Beyond that, children of all ages have lower cognitive indicators, dysregulated behavior, and emotional distress than those in homes with secure food access. These are persisting deficits: kindergarten children with food insecurity have lower math and reading abilities over at least 4 years.
Mental health is also affected by food insecurity. Reviews of multiple studies of children from preschool through adolescence show more child hyperactivity, emotional dysregulation, anxiety, depression, and stress beyond those attributable to their mother’s depression and anxiety. Food insecurity in the early years is associated with mental health issues even into adolescence. School aged children and youth are well aware of the family’s struggle with food access, even when their parents do not realize this. In addition to the anxiety and depression, they may feel shame or be socially ostracized. They may eat less, or choose low-quality foods to cope. Adolescents experiencing food insecurity report greater dysthymia and suicidal ideation. It is unknown whether these mental health difficulties are due to the stress, shame, or decreased intake of macronutrients important to emotional regulation or all of these. One implication is that pediatric providers should also screen for food insecurity as well as other social drivers of health (SDOH) when addressing developmental, behavioral, or mental health issues, not just at well visits.
While we worry about effects for the child, impact of food insecurity on caregivers is significant for parenting as well as adult well-being beginning prenatally. First trimester food insecurity is associated with increased maternal stress at 2 months postpartum and lower bonding scores at 6 months, although this is moderated by social support. The stress of food insecurity and other SDoH present are associated with parental depression, anxiety, and toxic stress, making optimal parenting difficult. Caregivers experiencing insecure food access worry most about their children and may reduce their own eating and food quality to spare the child. More than 30% of families indicated that they had to choose between paying for food and paying for medicine or medical care, jeopardizing their health, making this an important point of discussion for us as well.
Quality Versus Quantity
The total amount of food is not the only factor in adequate child nutrition. Healthy foods usually cost more and also may not be conveniently available. There are so called “food deserts,” areas with few/no full-service grocery stores, and also “food swamps” where unhealthy foods (eg fast food) are more available than healthy options. Life stress, higher in low-income populations, increases the impulse to consume sweet or high-fat “comfort foods” (we all know this!) due to the rush of calories and quick satiety. Children may be influenced in their food choices by media messages about non-nutritious foods. All of these may explain the association of food insecurity with obesity in both children and adults. It also sets them up for lifetime health problems of diabetes, hyperlipidemia, and cardiovascular conditions, especially in racial and ethnic minority groups and the poor.
The Larger Picture
Obvious to us all, low income is the main reason for inadequate access to enough or good quality food. Over 60% of families with food insecurity had incomes below the poverty threshold in 2013. Households without children are half as likely to be food insecure. But as 30% of food-insecure households have incomes above the eligibility cut offs for food programs — typically 130% of poverty for Special Supplemental Nutrition Program for Women, Infants, and Children (WIC) or 185% for Supplemental Nutrition Assistance Program (SNAP) — it is clear the problem is not related solely to poverty. Even small changes in income or expenses, such as a car breaking down, or heating or medical bills, can quickly result in inability to afford food, especially in areas of high food costs. This is particularly true for immigrant, large, and single-parent families and those with less education. Federal food programs do not cover all food needs for every family.
But we can’t tell if a child lives in a family with food insecurity by whether the child is thin, dropping growth percentiles, or receiving Medicaid insurance. Parents, and even youth, may be reluctant to tell us that they do not have enough to eat out of pride, fear, of prejudice, being reported to a contentious ex, being detected as an illegal immigrant, or even reported for neglect and having their child removed. Because of the suffering and impacts of food insecurity on child well-being, the American Academy of Pediatrics (AAP) published a Policy Statement in 2015, reaffirmed in 2021, recommending screening for food insecurity at all well visits and a toolkit to help. The USDA 18-item Household Food Security Scale (HFSS) has been the gold-standard screen, but affirmative answers to either of the 2-item Hunger Vital Sign (HVS) questionnaire identifies food insecurity with a sensitivity of 97% and a specificity of 83% compared with the HFSS. The questions ask how often the following were true in the past year: 1) “We worried whether our food would run out before we got money to buy more” and 2) “The food we bought just didn’t last and we didn’t have money to buy more.” This brief screen is now recommended and practical.
Screening for Food Insecurity
All set to manage food insecurity in your practice, then? Not exactly. Screening is only useful if it results in access to food. A study in a majority low-income clinic found that parents reported food insecurity 7% of the time when the clinician asked the HVS questions versus 45% when they self-reported on paper. Parent focus groups revealed reasons for the discrepant underreporting to the clinician: shame, concerns about stigma, and fear of the child being taken away. They felt more comfortable reporting about their child than about their own family situation. When asked what the clinician did that helped them disclose food insecurity, the caregivers cited strong interpersonal skills, open body language, and empathy. They also requested being given resources for other social issues, not just food insecurity. Clinic staff found paper screening inconvenient and recommended using tablet devices (such as with CHADIS that also scores and provides interviewing help, education, and local resource listings). Clinicians found the need for a follow-up conversation time consuming. Clinic staff thought screening could be facilitated by clinician’s initiating conversations, taking care about children present, and normalizing the screen as applying to all. Caregivers wanted know the use and privacy of the information. This same clinic referred the caregivers to a Benefits Data Trust with a goal of enrolling them in food programs. Of the food insecure, 55% were referred but only one third could be reached by phone with three attempts by the benefits group. Subsequent enrollment of those reached had barriers of verification requirements, wait times, and perceived mistreatment. The program concluded that this difficult two-step process of screening and referral would be improved by an integrated system of screening and enrollment in public benefits. Provision of information about free local food resources is also important, as 84% of those already receiving SNAP benefits remained food insecure.
Offering Assistance
To assist families where food insecurity is found, we need to understand the options of services both for referrals and advocacy. The AAP toolkit is designed to help. For pregnant and postpartum women and children 0-5 years in families with income less than 130% of the poverty level, the WIC program provides electronic cards to purchase approved categories of healthy food from participating vendors. For families with incomes less than 185% of the poverty level, the SNAP program, formerly called food stamps, provides benefits. There are other programs including free and reduced cost National School Breakfast and/or Lunch programs (best when open to all), Child and Adult Care Food Program for institutions (which may include medical offices), and Summer Food Service Programs providing lunch at community sites. Since not all food-insecure families are eligible for the above services, it is important that we are ready to provide information about local food banks, pantries, and low- or no-cost produce programs (see Healthy Food Bank Hub, Feeding America, 2-1-1, or FindHelp.org).
As pediatric providers we have a special opportunity and responsibility to expand our capabilities for sensitively addressing and advocating for help for food insecurity to improve the outlook for the families under our care.
Dr. Howard is assistant professor of pediatrics at The Johns Hopkins University School of Medicine, Baltimore, and creator of CHADIS. She had no other relevant disclosures. Dr. Howard’s contribution to this publication was as a paid expert to MDedge News. E-mail her at [email protected].