User login
Bringing you the latest news, research and reviews, exclusive interviews, podcasts, quizzes, and more.
div[contains(@class, 'read-next-article')]
div[contains(@class, 'nav-primary')]
nav[contains(@class, 'nav-primary')]
section[contains(@class, 'footer-nav-section-wrapper')]
nav[contains(@class, 'nav-ce-stack nav-ce-stack__large-screen')]
header[@id='header']
div[contains(@class, 'header__large-screen')]
div[contains(@class, 'main-prefix')]
footer[@id='footer']
section[contains(@class, 'nav-hidden')]
div[contains(@class, 'ce-card-content')]
nav[contains(@class, 'nav-ce-stack')]
div[contains(@class, 'view-medstat-quiz-listing-panes')]
Biden administration nixes buprenorphine waiver, docs disappointed
The Biden administration has halted a Trump administration initiative that would have allowed more physicians to prescribe buprenorphine for opioid use disorder (OUD).
Under the Trump administration’s plan, many doctors would be exempt from taking a day’s training before they could prescribe buprenorphine for OUD.
On Jan. 25, 2021, citing anonymous sources, the Washington Post reported that this action by the Biden administration was likely. At the time, there were concerns about whether the Department of Health & Human Services had the legal authority to make this policy change, the Post reported. The Substance Abuse and Mental Health Services Administration subsequently announced the derailment of the buprenorphine proposal on its website.
In SAMHSA’s view, the proposal was made “prematurely.” The SAMHSA statement did not detail the reasons for abandoning the Jan. 14 proposal. It had been scheduled to take effect upon publication in the Federal Register.
Instead of finalizing it in this way, the HHS said it would work with other federal agencies to “increase access to buprenorphine, reduce overdose rates and save lives.”
The HHS decision to scupper the proposal disappointed many physician groups. In a letter dated Jan. 27, several physician groups called on the Biden administration to proceed with the Trump proposal.
Under current federal law, physicians who wish to prescribe buprenorphine outside of opioid treatment programs must take an 8-hour course and receive a waiver from the Drug Enforcement Administration, the letter noted. It was signed by the American College of Emergency Physicians, the American Medical Association, and other organizations.
Treatment barrier
After taking the training course, it can take 60-90 days for physicians to receive the waiver. The license application can then be submitted. Physician groups argue that this so-called X-waiver requirement creates a barrier to providing medication-assisted treatment.
“Due to the stigma, some clinicians are not willing to pursue this DEA license or even engage in treatment of patients with [OUD],” the letter said.
The Trump administration’s proposal would have limited most physicians to treating no more than 30 patients with buprenorphine for OUD at any one time. This cap would not have applied to hospital-based physicians, such as those practicing emergency medicine, the HHS noted in a statement. The policy would have applied to only physicians who already have registered with the DEA.
Patrice A. Harris, MD, the immediate past president of the AMA and chair of the organization’s Opioid Task Force, was among the many physicians who supported the Trump administration proposal.
“It is estimated that more than 2 million Americans need treatment for opioid use disorder, but only a small percentage actually receive treatment,” Dr. Harris said in statement. Dr. Harris also noted that overdose deaths have reportedly accelerated during the COVID-19 pandemic.
Centers for Disease Control and Prevention data show there were more than 83,000 drug overdose deaths in the United States in the 12 months ending in June 2020. That is the highest number of overdose deaths ever recorded in a 12-month period and is an increase of more than 21%, compared with the previous year.
A ‘disappointment’
On Jan. 28, Dr. Harris said the decision to drop the plan was a disappointment.
“We encourage the current administration to quickly develop a path forward that removes the burdensome waiver requirement, thus allowing more physicians to prescribe this lifesaving medication,” she said in a statement sent to this news organization.
In a Jan. 26 statement, the American Society of Addiction Medicine urged Congress to eliminate the X-waiver and called for more education and training in the treatment of patients who struggle with opioids.
In the 116th session of Congress, which ended on Jan. 3, there was bipartisan support for proposed legislation to ease requirements for buprenorphine prescribing. A House bill had more than 90 Democratic and 21 Republican sponsors. A companion Senate bill had three Democratic and three Republican Sponsors, including Sen. Maggie Hassan (D-N.H.). On Jan. 25, Dr. Hassan tweeted that she would be seeking an explanation from the Biden administration if it halted the plan to ease the waiver restriction.
“Medication-assisted treatment can save lives, and the buprenorphine waiver requirement should be eliminated so that physicians can more easily prescribe it to those who need it,” she said.
Many clinicians and policy experts turned to Twitter to urge an easing of buprenorphine prescribing, using the hashtag “Xthexwaiver.”
Among them was the official who put forward the Jan. 14 proposal, Brett Giroir, MD. He served as assistant secretary for health during the Trump administration.
Objections
In its Jan. 25 article, the Washington Post referred to an article in Alcoholism and Drug Abuse Weekly in which a top federal official in the Trump administration objected to Dr. Giroir’s plan.
Elinore F. McCance-Katz, MD, PhD, who served as the assistant secretary of HHS for SAMHSA, had earlier proposed raising the cap for addiction experts. Alcoholism and Drug Abuse Weekly quotes Dr. McCance-Katz as saying the Trump buprenorphine proposal was “unfair to the incoming administration.”
“The Biden administration has so much work to do to get their programs and policies into place, and to do something like this at the 11th hour that could get doctors into trouble – it’s heinous,” she said in the article.
Dr. McCance-Katz had resigned before the Trump administration proposal was unveiled. On Jan. 7, she issued a public notice announcing she would resign, citing concerns about the previous day’s attack on the U.S. Capitol.
“It had been my plan to stay until the change in administration occurred, but my plans abruptly changed last evening when, on my way back from visiting an excellent residential treatment program in New York, I saw the violent takeover of the Capitol building,” she said.
On Twitter, Roland Flores, MD, an anesthesiologist and pain specialist, urged his colleagues to consider the need for more education among clinicians who treat OUD. He jousted a bit with those favoring a swift drive to “XtheXwaiver” and questioned their arguments about the burden of the current rules.
“I think ‘all this red tape’ is a little bit of an exaggeration – it’s an 8-hour online course, and an application,” Dr. Flores tweeted in one exchange. “But #XtheXwaiver is fine – it’s probably rooted in stigma. It’s unlikely to make much difference tho. The waiver wasn’t the thing keeping docs from prescribing.”
A version of this article first appeared on Medscape.com.
The Biden administration has halted a Trump administration initiative that would have allowed more physicians to prescribe buprenorphine for opioid use disorder (OUD).
Under the Trump administration’s plan, many doctors would be exempt from taking a day’s training before they could prescribe buprenorphine for OUD.
On Jan. 25, 2021, citing anonymous sources, the Washington Post reported that this action by the Biden administration was likely. At the time, there were concerns about whether the Department of Health & Human Services had the legal authority to make this policy change, the Post reported. The Substance Abuse and Mental Health Services Administration subsequently announced the derailment of the buprenorphine proposal on its website.
In SAMHSA’s view, the proposal was made “prematurely.” The SAMHSA statement did not detail the reasons for abandoning the Jan. 14 proposal. It had been scheduled to take effect upon publication in the Federal Register.
Instead of finalizing it in this way, the HHS said it would work with other federal agencies to “increase access to buprenorphine, reduce overdose rates and save lives.”
The HHS decision to scupper the proposal disappointed many physician groups. In a letter dated Jan. 27, several physician groups called on the Biden administration to proceed with the Trump proposal.
Under current federal law, physicians who wish to prescribe buprenorphine outside of opioid treatment programs must take an 8-hour course and receive a waiver from the Drug Enforcement Administration, the letter noted. It was signed by the American College of Emergency Physicians, the American Medical Association, and other organizations.
Treatment barrier
After taking the training course, it can take 60-90 days for physicians to receive the waiver. The license application can then be submitted. Physician groups argue that this so-called X-waiver requirement creates a barrier to providing medication-assisted treatment.
“Due to the stigma, some clinicians are not willing to pursue this DEA license or even engage in treatment of patients with [OUD],” the letter said.
The Trump administration’s proposal would have limited most physicians to treating no more than 30 patients with buprenorphine for OUD at any one time. This cap would not have applied to hospital-based physicians, such as those practicing emergency medicine, the HHS noted in a statement. The policy would have applied to only physicians who already have registered with the DEA.
Patrice A. Harris, MD, the immediate past president of the AMA and chair of the organization’s Opioid Task Force, was among the many physicians who supported the Trump administration proposal.
“It is estimated that more than 2 million Americans need treatment for opioid use disorder, but only a small percentage actually receive treatment,” Dr. Harris said in statement. Dr. Harris also noted that overdose deaths have reportedly accelerated during the COVID-19 pandemic.
Centers for Disease Control and Prevention data show there were more than 83,000 drug overdose deaths in the United States in the 12 months ending in June 2020. That is the highest number of overdose deaths ever recorded in a 12-month period and is an increase of more than 21%, compared with the previous year.
A ‘disappointment’
On Jan. 28, Dr. Harris said the decision to drop the plan was a disappointment.
“We encourage the current administration to quickly develop a path forward that removes the burdensome waiver requirement, thus allowing more physicians to prescribe this lifesaving medication,” she said in a statement sent to this news organization.
In a Jan. 26 statement, the American Society of Addiction Medicine urged Congress to eliminate the X-waiver and called for more education and training in the treatment of patients who struggle with opioids.
In the 116th session of Congress, which ended on Jan. 3, there was bipartisan support for proposed legislation to ease requirements for buprenorphine prescribing. A House bill had more than 90 Democratic and 21 Republican sponsors. A companion Senate bill had three Democratic and three Republican Sponsors, including Sen. Maggie Hassan (D-N.H.). On Jan. 25, Dr. Hassan tweeted that she would be seeking an explanation from the Biden administration if it halted the plan to ease the waiver restriction.
“Medication-assisted treatment can save lives, and the buprenorphine waiver requirement should be eliminated so that physicians can more easily prescribe it to those who need it,” she said.
Many clinicians and policy experts turned to Twitter to urge an easing of buprenorphine prescribing, using the hashtag “Xthexwaiver.”
Among them was the official who put forward the Jan. 14 proposal, Brett Giroir, MD. He served as assistant secretary for health during the Trump administration.
Objections
In its Jan. 25 article, the Washington Post referred to an article in Alcoholism and Drug Abuse Weekly in which a top federal official in the Trump administration objected to Dr. Giroir’s plan.
Elinore F. McCance-Katz, MD, PhD, who served as the assistant secretary of HHS for SAMHSA, had earlier proposed raising the cap for addiction experts. Alcoholism and Drug Abuse Weekly quotes Dr. McCance-Katz as saying the Trump buprenorphine proposal was “unfair to the incoming administration.”
“The Biden administration has so much work to do to get their programs and policies into place, and to do something like this at the 11th hour that could get doctors into trouble – it’s heinous,” she said in the article.
Dr. McCance-Katz had resigned before the Trump administration proposal was unveiled. On Jan. 7, she issued a public notice announcing she would resign, citing concerns about the previous day’s attack on the U.S. Capitol.
“It had been my plan to stay until the change in administration occurred, but my plans abruptly changed last evening when, on my way back from visiting an excellent residential treatment program in New York, I saw the violent takeover of the Capitol building,” she said.
On Twitter, Roland Flores, MD, an anesthesiologist and pain specialist, urged his colleagues to consider the need for more education among clinicians who treat OUD. He jousted a bit with those favoring a swift drive to “XtheXwaiver” and questioned their arguments about the burden of the current rules.
“I think ‘all this red tape’ is a little bit of an exaggeration – it’s an 8-hour online course, and an application,” Dr. Flores tweeted in one exchange. “But #XtheXwaiver is fine – it’s probably rooted in stigma. It’s unlikely to make much difference tho. The waiver wasn’t the thing keeping docs from prescribing.”
A version of this article first appeared on Medscape.com.
The Biden administration has halted a Trump administration initiative that would have allowed more physicians to prescribe buprenorphine for opioid use disorder (OUD).
Under the Trump administration’s plan, many doctors would be exempt from taking a day’s training before they could prescribe buprenorphine for OUD.
On Jan. 25, 2021, citing anonymous sources, the Washington Post reported that this action by the Biden administration was likely. At the time, there were concerns about whether the Department of Health & Human Services had the legal authority to make this policy change, the Post reported. The Substance Abuse and Mental Health Services Administration subsequently announced the derailment of the buprenorphine proposal on its website.
In SAMHSA’s view, the proposal was made “prematurely.” The SAMHSA statement did not detail the reasons for abandoning the Jan. 14 proposal. It had been scheduled to take effect upon publication in the Federal Register.
Instead of finalizing it in this way, the HHS said it would work with other federal agencies to “increase access to buprenorphine, reduce overdose rates and save lives.”
The HHS decision to scupper the proposal disappointed many physician groups. In a letter dated Jan. 27, several physician groups called on the Biden administration to proceed with the Trump proposal.
Under current federal law, physicians who wish to prescribe buprenorphine outside of opioid treatment programs must take an 8-hour course and receive a waiver from the Drug Enforcement Administration, the letter noted. It was signed by the American College of Emergency Physicians, the American Medical Association, and other organizations.
Treatment barrier
After taking the training course, it can take 60-90 days for physicians to receive the waiver. The license application can then be submitted. Physician groups argue that this so-called X-waiver requirement creates a barrier to providing medication-assisted treatment.
“Due to the stigma, some clinicians are not willing to pursue this DEA license or even engage in treatment of patients with [OUD],” the letter said.
The Trump administration’s proposal would have limited most physicians to treating no more than 30 patients with buprenorphine for OUD at any one time. This cap would not have applied to hospital-based physicians, such as those practicing emergency medicine, the HHS noted in a statement. The policy would have applied to only physicians who already have registered with the DEA.
Patrice A. Harris, MD, the immediate past president of the AMA and chair of the organization’s Opioid Task Force, was among the many physicians who supported the Trump administration proposal.
“It is estimated that more than 2 million Americans need treatment for opioid use disorder, but only a small percentage actually receive treatment,” Dr. Harris said in statement. Dr. Harris also noted that overdose deaths have reportedly accelerated during the COVID-19 pandemic.
Centers for Disease Control and Prevention data show there were more than 83,000 drug overdose deaths in the United States in the 12 months ending in June 2020. That is the highest number of overdose deaths ever recorded in a 12-month period and is an increase of more than 21%, compared with the previous year.
A ‘disappointment’
On Jan. 28, Dr. Harris said the decision to drop the plan was a disappointment.
“We encourage the current administration to quickly develop a path forward that removes the burdensome waiver requirement, thus allowing more physicians to prescribe this lifesaving medication,” she said in a statement sent to this news organization.
In a Jan. 26 statement, the American Society of Addiction Medicine urged Congress to eliminate the X-waiver and called for more education and training in the treatment of patients who struggle with opioids.
In the 116th session of Congress, which ended on Jan. 3, there was bipartisan support for proposed legislation to ease requirements for buprenorphine prescribing. A House bill had more than 90 Democratic and 21 Republican sponsors. A companion Senate bill had three Democratic and three Republican Sponsors, including Sen. Maggie Hassan (D-N.H.). On Jan. 25, Dr. Hassan tweeted that she would be seeking an explanation from the Biden administration if it halted the plan to ease the waiver restriction.
“Medication-assisted treatment can save lives, and the buprenorphine waiver requirement should be eliminated so that physicians can more easily prescribe it to those who need it,” she said.
Many clinicians and policy experts turned to Twitter to urge an easing of buprenorphine prescribing, using the hashtag “Xthexwaiver.”
Among them was the official who put forward the Jan. 14 proposal, Brett Giroir, MD. He served as assistant secretary for health during the Trump administration.
Objections
In its Jan. 25 article, the Washington Post referred to an article in Alcoholism and Drug Abuse Weekly in which a top federal official in the Trump administration objected to Dr. Giroir’s plan.
Elinore F. McCance-Katz, MD, PhD, who served as the assistant secretary of HHS for SAMHSA, had earlier proposed raising the cap for addiction experts. Alcoholism and Drug Abuse Weekly quotes Dr. McCance-Katz as saying the Trump buprenorphine proposal was “unfair to the incoming administration.”
“The Biden administration has so much work to do to get their programs and policies into place, and to do something like this at the 11th hour that could get doctors into trouble – it’s heinous,” she said in the article.
Dr. McCance-Katz had resigned before the Trump administration proposal was unveiled. On Jan. 7, she issued a public notice announcing she would resign, citing concerns about the previous day’s attack on the U.S. Capitol.
“It had been my plan to stay until the change in administration occurred, but my plans abruptly changed last evening when, on my way back from visiting an excellent residential treatment program in New York, I saw the violent takeover of the Capitol building,” she said.
On Twitter, Roland Flores, MD, an anesthesiologist and pain specialist, urged his colleagues to consider the need for more education among clinicians who treat OUD. He jousted a bit with those favoring a swift drive to “XtheXwaiver” and questioned their arguments about the burden of the current rules.
“I think ‘all this red tape’ is a little bit of an exaggeration – it’s an 8-hour online course, and an application,” Dr. Flores tweeted in one exchange. “But #XtheXwaiver is fine – it’s probably rooted in stigma. It’s unlikely to make much difference tho. The waiver wasn’t the thing keeping docs from prescribing.”
A version of this article first appeared on Medscape.com.
New NIH database will track neurologic effects of COVID-19
“We know COVID-19 can disrupt multiple body systems, but the effects of the virus and the body’s response to COVID-19 infection on the brain, spinal cord, nerves, and muscle can be particularly devastating and contribute to persistence of disability even after the virus is cleared,” said Barbara Karp, MD, program director at the National Institute of Neurological Disorders and Stroke.
“There is an urgent need to understand COVID-19–related neurological problems, which not uncommonly include headaches, fatigue, cognitive difficulties, stroke, pain, and sleep disorders as well as some very rare complications of serious infections,” said Dr. Karp.
The COVID-19 NeuroDatabank/BioBank (NeuroCOVID) is funded by the NINDS. It was created and will be maintained by researchers at NYU Langone Health in New York.
The project is led by Andrea Troxel, ScD, professor of population health, and Eva Petkova, PhD, professor of population health and child and adolescent psychiatry, both at New York University.
“We’ve built a pretty comprehensive database that will accept deidentified patient information about new neurological issues that coincide with their COVID disease or worsening of preexisting neurological problems,” said Dr. Troxel. “In addition, we have a bio repository that will accept almost any kind of biological sample, such as blood, plasma, cerebrospinal fluid, and tissue,” she said.
“Neuroimages are very difficult to store because the files are so enormous, but we’ve had some questions about that, and we’re looking into whether we can accommodate neuroimages,” Dr. Troxel noted.
Dr. Troxel said a “blast of information and invitations” has gone out in an effort to acquire data and biospecimens. “We’ve been really pleased with the amount of interest already, interest not only from large academic medical centers, as you might expect, but also from some smaller stand-alone clinics and even some individuals who have either experienced some of these neurological problems of COVID or know those who have and are really eager to try to provide information,” she added.
Researchers interested in using data and biosamples from the database may submit requests to the NeuroCOVID Steering Committee. More information is available online on the NeuroCOVID website.
A version of this article first appeared on Medscape.com.
“We know COVID-19 can disrupt multiple body systems, but the effects of the virus and the body’s response to COVID-19 infection on the brain, spinal cord, nerves, and muscle can be particularly devastating and contribute to persistence of disability even after the virus is cleared,” said Barbara Karp, MD, program director at the National Institute of Neurological Disorders and Stroke.
“There is an urgent need to understand COVID-19–related neurological problems, which not uncommonly include headaches, fatigue, cognitive difficulties, stroke, pain, and sleep disorders as well as some very rare complications of serious infections,” said Dr. Karp.
The COVID-19 NeuroDatabank/BioBank (NeuroCOVID) is funded by the NINDS. It was created and will be maintained by researchers at NYU Langone Health in New York.
The project is led by Andrea Troxel, ScD, professor of population health, and Eva Petkova, PhD, professor of population health and child and adolescent psychiatry, both at New York University.
“We’ve built a pretty comprehensive database that will accept deidentified patient information about new neurological issues that coincide with their COVID disease or worsening of preexisting neurological problems,” said Dr. Troxel. “In addition, we have a bio repository that will accept almost any kind of biological sample, such as blood, plasma, cerebrospinal fluid, and tissue,” she said.
“Neuroimages are very difficult to store because the files are so enormous, but we’ve had some questions about that, and we’re looking into whether we can accommodate neuroimages,” Dr. Troxel noted.
Dr. Troxel said a “blast of information and invitations” has gone out in an effort to acquire data and biospecimens. “We’ve been really pleased with the amount of interest already, interest not only from large academic medical centers, as you might expect, but also from some smaller stand-alone clinics and even some individuals who have either experienced some of these neurological problems of COVID or know those who have and are really eager to try to provide information,” she added.
Researchers interested in using data and biosamples from the database may submit requests to the NeuroCOVID Steering Committee. More information is available online on the NeuroCOVID website.
A version of this article first appeared on Medscape.com.
“We know COVID-19 can disrupt multiple body systems, but the effects of the virus and the body’s response to COVID-19 infection on the brain, spinal cord, nerves, and muscle can be particularly devastating and contribute to persistence of disability even after the virus is cleared,” said Barbara Karp, MD, program director at the National Institute of Neurological Disorders and Stroke.
“There is an urgent need to understand COVID-19–related neurological problems, which not uncommonly include headaches, fatigue, cognitive difficulties, stroke, pain, and sleep disorders as well as some very rare complications of serious infections,” said Dr. Karp.
The COVID-19 NeuroDatabank/BioBank (NeuroCOVID) is funded by the NINDS. It was created and will be maintained by researchers at NYU Langone Health in New York.
The project is led by Andrea Troxel, ScD, professor of population health, and Eva Petkova, PhD, professor of population health and child and adolescent psychiatry, both at New York University.
“We’ve built a pretty comprehensive database that will accept deidentified patient information about new neurological issues that coincide with their COVID disease or worsening of preexisting neurological problems,” said Dr. Troxel. “In addition, we have a bio repository that will accept almost any kind of biological sample, such as blood, plasma, cerebrospinal fluid, and tissue,” she said.
“Neuroimages are very difficult to store because the files are so enormous, but we’ve had some questions about that, and we’re looking into whether we can accommodate neuroimages,” Dr. Troxel noted.
Dr. Troxel said a “blast of information and invitations” has gone out in an effort to acquire data and biospecimens. “We’ve been really pleased with the amount of interest already, interest not only from large academic medical centers, as you might expect, but also from some smaller stand-alone clinics and even some individuals who have either experienced some of these neurological problems of COVID or know those who have and are really eager to try to provide information,” she added.
Researchers interested in using data and biosamples from the database may submit requests to the NeuroCOVID Steering Committee. More information is available online on the NeuroCOVID website.
A version of this article first appeared on Medscape.com.
Kids already coping with mental disorders spiral as pandemic topples vital support systems
A bag of Doritos, that’s all Princess wanted.

Her mom calls her Princess, but her real name is Lindsey. She’s 17 and lives with her mom, Sandra, a nurse, outside Atlanta. On May 17, 2020, a Sunday, Lindsey decided she didn’t want breakfast; she wanted Doritos. So she left home and walked to Family Dollar, taking her pants off on the way, while her mom followed on foot, talking to the police on her phone as they went.
Lindsey has autism. It can be hard for her to communicate and navigate social situations. She thrives on routine and gets special help at school. Or got help, before the coronavirus pandemic closed schools and forced tens of millions of children to stay home. Sandra said that’s when their living hell started.
“It’s like her brain was wired,” she said. “She’d just put on her jacket, and she’s out the door. And I’m chasing her.”
On May 17, Sandra chased her all the way to Family Dollar. Hours later, Lindsey was in jail, charged with assaulting her mom. (KHN and NPR are not using the family’s last name.)
Lindsey is 1 of almost 3 million children in the United States who have a serious emotional or behavioral health condition. When the pandemic forced schools and doctors’ offices to close last spring, it also cut children off from the trained teachers and therapists who understand their needs.
As a result, many, like Lindsey, spiraled into EDs and even police custody. Federal data shows a nationwide surge of children in mental health crisis during the pandemic – a surge that’s further taxing an already overstretched safety net.
‘Take her’
Even after schools closed, Lindsey continued to wake up early, get dressed and wait for the bus. When she realized it had stopped coming, Sandra said, her daughter just started walking out of the house, wandering, a few times a week.
In those situations, Sandra did what many families in crisis report they’ve had to do since the pandemic began: Race through the short list of places she could call for help.
First, her state’s mental health crisis hotline. But they often put Sandra on hold.
“This is ridiculous,” she said of the wait. “It’s supposed to be a crisis team. But I’m on hold for 40, 50 minutes. And by the time you get on the phone, [the crisis] is done!”
Then there’s the local hospital’s ED, but Sandra said she had taken Lindsey there for previous crises and been told there isn’t much they can do.
That’s why, on May 17, when Lindsey walked to Family Dollar in just a red T-shirt and underwear to get that bag of Doritos, Sandra called the last option on her list: the police.
Sandra arrived at the store before the police and paid for the chips. According to Sandra and police records, when an officer approached, Lindsey grew agitated and hit her mom on the back, hard.
Sandra said she explained to the officer: “‘She’s autistic. You know, I’m okay. I’m a nurse. I just need to take her home and give her her medication.’ ”
Lindsey takes a mood stabilizer, but because she left home before breakfast, she hadn’t taken it that morning. The officer asked if Sandra wanted to take her to the nearest hospital.
The hospital wouldn’t be able to help Lindsey, Sandra said. It hadn’t before. “They already told me: ‘Ma’am, there’s nothing we can do.’ They just check her labs, it’s fine, and they ship her back home. There’s nothing [the hospital] can do,” she recalled telling the officer.
Sandra asked if the police could drive her daughter home so the teen could take her medication, but the officer said no, they couldn’t. The only other thing they could do, the officer said, was take Lindsey to jail for hitting her mom.
“I’ve tried everything,” Sandra said, exasperated. She paced the parking lot, feeling hopeless, sad and out of options. Finally, in tears, she told the officers: “Take her.”
Lindsey does not like to be touched and fought back when authorities tried to handcuff her. Several officers wrestled her to the ground. At that point, Sandra protested and said an officer threatened to arrest her, too, if she didn’t back away. Lindsey was taken to jail, where she spent much of the night until Sandra was able to post bail.
Clayton County Solicitor-General Charles Brooks denied that Sandra was threatened with arrest and said that, while Lindsey’s case is still pending, his office “is working to ensure that the resolution in this matter involves a plan for medication compliance and not punitive action.”
Sandra isn’t alone in her experience. Multiple families interviewed for this story reported similar experiences of calling in the police when a child was in crisis because caretakers didn’t feel they had any other option.
‘The whole system is really grinding to a halt’
Roughly 6% of U.S. children ages 6-17 years are living with serious emotional or behavioral difficulties, including children with autism, severe anxiety, depression and trauma-related mental health conditions.
Many of these children depend on schools for access to vital therapies. When schools and doctors’ offices stopped providing in-person services last spring, kids were untethered from the people and supports they rely on.

“The lack of in-person services is really detrimental,” said Susan Duffy, MD,a pediatrician and professor of emergency medicine at Brown University, Providence, R.I.
Marjorie, a mother in Florida, said her 15-year-old son has suffered during these disruptions. He has ADHD and oppositional defiant disorder, a condition marked by frequent and persistent hostility. Little things – like being asked to do schoolwork – can send him into a rage, leading to holes punched in walls, broken doors and violent threats. (The family’s last name or her son’s first name are not used to protect her son’s privacy and future prospects.)
The pandemic has shifted both school and her son’s therapy sessions online. But Marjorie said virtual therapy isn’t working because her son doesn’t focus well during sessions and tries to watch television instead. Lately, she has simply been canceling them.
“I was paying for appointments and there was no therapeutic value,” Marjorie said.
The issues cut across socioeconomic lines – affecting families with private insurance, like Marjorie, as well as those who receive coverage through Medicaid, a federal-state program that provides health insurance to low-income people and those with disabilities.
In the first few months of the pandemic, between March and May, children on Medicaid received 44% fewer outpatient mental health services – including therapy and in-home support – compared with the same time period in 2019, according to the Centers for Medicare & Medicaid Services. That’s even after accounting for increased telehealth appointments.
And while the nation’s EDs have seen a decline in overall visits, there was a relative increase in mental health visits for kids in 2020, compared with 2019.
The Centers for Disease Control and Prevention found that, from April to October 2020, hospitals across the United States saw a 24% increase in the proportion of mental health emergency visits for children aged 5-11 years, and a 31% increase for children aged 12-17.
“Not only are we seeing more children, more children are being admitted” to inpatient care.
That’s because there are fewer outpatient services now available to children, she said, and because the conditions of the children showing up at EDs “are more serious.”
This crisis is not only making life harder for these kids and their families, but it’s also stressing the entire health care system.
Child and adolescent psychiatrists working in hospitals around the country said children are increasingly “boarding” in EDs for days, waiting for inpatient admission to a regular hospital or psychiatric hospital.

Before the pandemic, there was already a shortage of inpatient psychiatric beds for children, said Christopher Bellonci, MD, a child psychiatrist at Judge Baker Children’s Center in Boston. That shortage has only gotten worse as hospitals cut capacity to allow for more physical distancing within psychiatric units.
“The whole system is really grinding to a halt at a time when we have unprecedented need,” Dr. Bellonci said.
‘A signal that the rest of your system doesn’t work’
Psychiatrists on the front lines share the frustrations of parents struggling to find help for their children.
Part of the problem is there have never been enough psychiatrists and therapists trained to work with children, intervening in the early stages of their illness, said Jennifer Havens, MD, a child psychiatrist at New York University.
“Tons of people showing up in emergency rooms in bad shape is a signal that the rest of your system doesn’t work,” she said.
Too often, Dr. Havens said, services aren’t available until children are older – and in crisis. “Often for people who don’t have access to services, we wait until they’re too big to be managed.”
While the pandemic has made life harder for Marjorie and her son in Florida, she said it has always been difficult to find the support and care he needs. Last fall, he needed a psychiatric evaluation, but the nearest specialist who would accept her commercial insurance was 100 miles away, in Alabama.
“Even when you have the money or you have the insurance, it is still a travesty,” Marjorie said. “You cannot get help for these kids.”
Parents are frustrated, and so are psychiatrists on the front lines. C.J. Glawe, MD, who leads the psychiatric crisis department at Nationwide Children’s Hospital in Columbus, Ohio, said that once a child is stabilized after a crisis it can be hard to explain to parents that they may not be able to find follow-up care anywhere near their home.
“Especially when I can clearly tell you I know exactly what you need, I just can’t give it to you,” Dr. Glawe said. “It’s demoralizing.”
When states and communities fail to provide children the services they need to live at home, kids can deteriorate and even wind up in jail, like Lindsey. At that point, Dr. Glawe said, the cost and level of care required will be even higher, whether that’s hospitalization or long stays in residential treatment facilities.
That’s exactly the scenario Sandra, Lindsey’s mom, is hoping to avoid for her Princess.
“For me, as a nurse and as a provider, that will be the last thing for my daughter,” she said. “It’s like [state and local leaders] leave it to the school and the parent to deal with, and they don’t care. And that’s the problem. It’s sad because, if I’m not here...”
Her voice trailed off as tears welled.
“She didn’t ask to have autism.”
To help families like Sandra’s and Marjorie’s, advocates said, all levels of government need to invest in creating a mental health system that’s accessible to anyone who needs it.
But given that many states have seen their revenues drop because of the pandemic, there’s a concern services will instead be cut – at a time when the need has never been greater.
This story is part of a reporting partnership that includes NPR, Illinois Public Media and Kaiser Health News. Kaiser Health News is a nonprofit news service covering health issues. It is an editorially independent program of KFF (Kaiser Family Foundation), which is not affiliated with Kaiser Permanente.
A bag of Doritos, that’s all Princess wanted.
Her mom calls her Princess, but her real name is Lindsey. She’s 17 and lives with her mom, Sandra, a nurse, outside Atlanta. On May 17, 2020, a Sunday, Lindsey decided she didn’t want breakfast; she wanted Doritos. So she left home and walked to Family Dollar, taking her pants off on the way, while her mom followed on foot, talking to the police on her phone as they went.
Lindsey has autism. It can be hard for her to communicate and navigate social situations. She thrives on routine and gets special help at school. Or got help, before the coronavirus pandemic closed schools and forced tens of millions of children to stay home. Sandra said that’s when their living hell started.
“It’s like her brain was wired,” she said. “She’d just put on her jacket, and she’s out the door. And I’m chasing her.”
On May 17, Sandra chased her all the way to Family Dollar. Hours later, Lindsey was in jail, charged with assaulting her mom. (KHN and NPR are not using the family’s last name.)
Lindsey is 1 of almost 3 million children in the United States who have a serious emotional or behavioral health condition. When the pandemic forced schools and doctors’ offices to close last spring, it also cut children off from the trained teachers and therapists who understand their needs.
As a result, many, like Lindsey, spiraled into EDs and even police custody. Federal data shows a nationwide surge of children in mental health crisis during the pandemic – a surge that’s further taxing an already overstretched safety net.
‘Take her’
Even after schools closed, Lindsey continued to wake up early, get dressed and wait for the bus. When she realized it had stopped coming, Sandra said, her daughter just started walking out of the house, wandering, a few times a week.
In those situations, Sandra did what many families in crisis report they’ve had to do since the pandemic began: Race through the short list of places she could call for help.
First, her state’s mental health crisis hotline. But they often put Sandra on hold.
“This is ridiculous,” she said of the wait. “It’s supposed to be a crisis team. But I’m on hold for 40, 50 minutes. And by the time you get on the phone, [the crisis] is done!”
Then there’s the local hospital’s ED, but Sandra said she had taken Lindsey there for previous crises and been told there isn’t much they can do.
That’s why, on May 17, when Lindsey walked to Family Dollar in just a red T-shirt and underwear to get that bag of Doritos, Sandra called the last option on her list: the police.
Sandra arrived at the store before the police and paid for the chips. According to Sandra and police records, when an officer approached, Lindsey grew agitated and hit her mom on the back, hard.
Sandra said she explained to the officer: “‘She’s autistic. You know, I’m okay. I’m a nurse. I just need to take her home and give her her medication.’ ”
Lindsey takes a mood stabilizer, but because she left home before breakfast, she hadn’t taken it that morning. The officer asked if Sandra wanted to take her to the nearest hospital.
The hospital wouldn’t be able to help Lindsey, Sandra said. It hadn’t before. “They already told me: ‘Ma’am, there’s nothing we can do.’ They just check her labs, it’s fine, and they ship her back home. There’s nothing [the hospital] can do,” she recalled telling the officer.
Sandra asked if the police could drive her daughter home so the teen could take her medication, but the officer said no, they couldn’t. The only other thing they could do, the officer said, was take Lindsey to jail for hitting her mom.
“I’ve tried everything,” Sandra said, exasperated. She paced the parking lot, feeling hopeless, sad and out of options. Finally, in tears, she told the officers: “Take her.”
Lindsey does not like to be touched and fought back when authorities tried to handcuff her. Several officers wrestled her to the ground. At that point, Sandra protested and said an officer threatened to arrest her, too, if she didn’t back away. Lindsey was taken to jail, where she spent much of the night until Sandra was able to post bail.
Clayton County Solicitor-General Charles Brooks denied that Sandra was threatened with arrest and said that, while Lindsey’s case is still pending, his office “is working to ensure that the resolution in this matter involves a plan for medication compliance and not punitive action.”
Sandra isn’t alone in her experience. Multiple families interviewed for this story reported similar experiences of calling in the police when a child was in crisis because caretakers didn’t feel they had any other option.
‘The whole system is really grinding to a halt’
Roughly 6% of U.S. children ages 6-17 years are living with serious emotional or behavioral difficulties, including children with autism, severe anxiety, depression and trauma-related mental health conditions.
Many of these children depend on schools for access to vital therapies. When schools and doctors’ offices stopped providing in-person services last spring, kids were untethered from the people and supports they rely on.
“The lack of in-person services is really detrimental,” said Susan Duffy, MD,a pediatrician and professor of emergency medicine at Brown University, Providence, R.I.
Marjorie, a mother in Florida, said her 15-year-old son has suffered during these disruptions. He has ADHD and oppositional defiant disorder, a condition marked by frequent and persistent hostility. Little things – like being asked to do schoolwork – can send him into a rage, leading to holes punched in walls, broken doors and violent threats. (The family’s last name or her son’s first name are not used to protect her son’s privacy and future prospects.)
The pandemic has shifted both school and her son’s therapy sessions online. But Marjorie said virtual therapy isn’t working because her son doesn’t focus well during sessions and tries to watch television instead. Lately, she has simply been canceling them.
“I was paying for appointments and there was no therapeutic value,” Marjorie said.
The issues cut across socioeconomic lines – affecting families with private insurance, like Marjorie, as well as those who receive coverage through Medicaid, a federal-state program that provides health insurance to low-income people and those with disabilities.
In the first few months of the pandemic, between March and May, children on Medicaid received 44% fewer outpatient mental health services – including therapy and in-home support – compared with the same time period in 2019, according to the Centers for Medicare & Medicaid Services. That’s even after accounting for increased telehealth appointments.
And while the nation’s EDs have seen a decline in overall visits, there was a relative increase in mental health visits for kids in 2020, compared with 2019.
The Centers for Disease Control and Prevention found that, from April to October 2020, hospitals across the United States saw a 24% increase in the proportion of mental health emergency visits for children aged 5-11 years, and a 31% increase for children aged 12-17.
“Not only are we seeing more children, more children are being admitted” to inpatient care.
That’s because there are fewer outpatient services now available to children, she said, and because the conditions of the children showing up at EDs “are more serious.”
This crisis is not only making life harder for these kids and their families, but it’s also stressing the entire health care system.
Child and adolescent psychiatrists working in hospitals around the country said children are increasingly “boarding” in EDs for days, waiting for inpatient admission to a regular hospital or psychiatric hospital.
Before the pandemic, there was already a shortage of inpatient psychiatric beds for children, said Christopher Bellonci, MD, a child psychiatrist at Judge Baker Children’s Center in Boston. That shortage has only gotten worse as hospitals cut capacity to allow for more physical distancing within psychiatric units.
“The whole system is really grinding to a halt at a time when we have unprecedented need,” Dr. Bellonci said.
‘A signal that the rest of your system doesn’t work’
Psychiatrists on the front lines share the frustrations of parents struggling to find help for their children.
Part of the problem is there have never been enough psychiatrists and therapists trained to work with children, intervening in the early stages of their illness, said Jennifer Havens, MD, a child psychiatrist at New York University.
“Tons of people showing up in emergency rooms in bad shape is a signal that the rest of your system doesn’t work,” she said.
Too often, Dr. Havens said, services aren’t available until children are older – and in crisis. “Often for people who don’t have access to services, we wait until they’re too big to be managed.”
While the pandemic has made life harder for Marjorie and her son in Florida, she said it has always been difficult to find the support and care he needs. Last fall, he needed a psychiatric evaluation, but the nearest specialist who would accept her commercial insurance was 100 miles away, in Alabama.
“Even when you have the money or you have the insurance, it is still a travesty,” Marjorie said. “You cannot get help for these kids.”
Parents are frustrated, and so are psychiatrists on the front lines. C.J. Glawe, MD, who leads the psychiatric crisis department at Nationwide Children’s Hospital in Columbus, Ohio, said that once a child is stabilized after a crisis it can be hard to explain to parents that they may not be able to find follow-up care anywhere near their home.
“Especially when I can clearly tell you I know exactly what you need, I just can’t give it to you,” Dr. Glawe said. “It’s demoralizing.”
When states and communities fail to provide children the services they need to live at home, kids can deteriorate and even wind up in jail, like Lindsey. At that point, Dr. Glawe said, the cost and level of care required will be even higher, whether that’s hospitalization or long stays in residential treatment facilities.
That’s exactly the scenario Sandra, Lindsey’s mom, is hoping to avoid for her Princess.
“For me, as a nurse and as a provider, that will be the last thing for my daughter,” she said. “It’s like [state and local leaders] leave it to the school and the parent to deal with, and they don’t care. And that’s the problem. It’s sad because, if I’m not here...”
Her voice trailed off as tears welled.
“She didn’t ask to have autism.”
To help families like Sandra’s and Marjorie’s, advocates said, all levels of government need to invest in creating a mental health system that’s accessible to anyone who needs it.
But given that many states have seen their revenues drop because of the pandemic, there’s a concern services will instead be cut – at a time when the need has never been greater.
This story is part of a reporting partnership that includes NPR, Illinois Public Media and Kaiser Health News. Kaiser Health News is a nonprofit news service covering health issues. It is an editorially independent program of KFF (Kaiser Family Foundation), which is not affiliated with Kaiser Permanente.
A bag of Doritos, that’s all Princess wanted.
Her mom calls her Princess, but her real name is Lindsey. She’s 17 and lives with her mom, Sandra, a nurse, outside Atlanta. On May 17, 2020, a Sunday, Lindsey decided she didn’t want breakfast; she wanted Doritos. So she left home and walked to Family Dollar, taking her pants off on the way, while her mom followed on foot, talking to the police on her phone as they went.
Lindsey has autism. It can be hard for her to communicate and navigate social situations. She thrives on routine and gets special help at school. Or got help, before the coronavirus pandemic closed schools and forced tens of millions of children to stay home. Sandra said that’s when their living hell started.
“It’s like her brain was wired,” she said. “She’d just put on her jacket, and she’s out the door. And I’m chasing her.”
On May 17, Sandra chased her all the way to Family Dollar. Hours later, Lindsey was in jail, charged with assaulting her mom. (KHN and NPR are not using the family’s last name.)
Lindsey is 1 of almost 3 million children in the United States who have a serious emotional or behavioral health condition. When the pandemic forced schools and doctors’ offices to close last spring, it also cut children off from the trained teachers and therapists who understand their needs.
As a result, many, like Lindsey, spiraled into EDs and even police custody. Federal data shows a nationwide surge of children in mental health crisis during the pandemic – a surge that’s further taxing an already overstretched safety net.
‘Take her’
Even after schools closed, Lindsey continued to wake up early, get dressed and wait for the bus. When she realized it had stopped coming, Sandra said, her daughter just started walking out of the house, wandering, a few times a week.
In those situations, Sandra did what many families in crisis report they’ve had to do since the pandemic began: Race through the short list of places she could call for help.
First, her state’s mental health crisis hotline. But they often put Sandra on hold.
“This is ridiculous,” she said of the wait. “It’s supposed to be a crisis team. But I’m on hold for 40, 50 minutes. And by the time you get on the phone, [the crisis] is done!”
Then there’s the local hospital’s ED, but Sandra said she had taken Lindsey there for previous crises and been told there isn’t much they can do.
That’s why, on May 17, when Lindsey walked to Family Dollar in just a red T-shirt and underwear to get that bag of Doritos, Sandra called the last option on her list: the police.
Sandra arrived at the store before the police and paid for the chips. According to Sandra and police records, when an officer approached, Lindsey grew agitated and hit her mom on the back, hard.
Sandra said she explained to the officer: “‘She’s autistic. You know, I’m okay. I’m a nurse. I just need to take her home and give her her medication.’ ”
Lindsey takes a mood stabilizer, but because she left home before breakfast, she hadn’t taken it that morning. The officer asked if Sandra wanted to take her to the nearest hospital.
The hospital wouldn’t be able to help Lindsey, Sandra said. It hadn’t before. “They already told me: ‘Ma’am, there’s nothing we can do.’ They just check her labs, it’s fine, and they ship her back home. There’s nothing [the hospital] can do,” she recalled telling the officer.
Sandra asked if the police could drive her daughter home so the teen could take her medication, but the officer said no, they couldn’t. The only other thing they could do, the officer said, was take Lindsey to jail for hitting her mom.
“I’ve tried everything,” Sandra said, exasperated. She paced the parking lot, feeling hopeless, sad and out of options. Finally, in tears, she told the officers: “Take her.”
Lindsey does not like to be touched and fought back when authorities tried to handcuff her. Several officers wrestled her to the ground. At that point, Sandra protested and said an officer threatened to arrest her, too, if she didn’t back away. Lindsey was taken to jail, where she spent much of the night until Sandra was able to post bail.
Clayton County Solicitor-General Charles Brooks denied that Sandra was threatened with arrest and said that, while Lindsey’s case is still pending, his office “is working to ensure that the resolution in this matter involves a plan for medication compliance and not punitive action.”
Sandra isn’t alone in her experience. Multiple families interviewed for this story reported similar experiences of calling in the police when a child was in crisis because caretakers didn’t feel they had any other option.
‘The whole system is really grinding to a halt’
Roughly 6% of U.S. children ages 6-17 years are living with serious emotional or behavioral difficulties, including children with autism, severe anxiety, depression and trauma-related mental health conditions.
Many of these children depend on schools for access to vital therapies. When schools and doctors’ offices stopped providing in-person services last spring, kids were untethered from the people and supports they rely on.
“The lack of in-person services is really detrimental,” said Susan Duffy, MD,a pediatrician and professor of emergency medicine at Brown University, Providence, R.I.
Marjorie, a mother in Florida, said her 15-year-old son has suffered during these disruptions. He has ADHD and oppositional defiant disorder, a condition marked by frequent and persistent hostility. Little things – like being asked to do schoolwork – can send him into a rage, leading to holes punched in walls, broken doors and violent threats. (The family’s last name or her son’s first name are not used to protect her son’s privacy and future prospects.)
The pandemic has shifted both school and her son’s therapy sessions online. But Marjorie said virtual therapy isn’t working because her son doesn’t focus well during sessions and tries to watch television instead. Lately, she has simply been canceling them.
“I was paying for appointments and there was no therapeutic value,” Marjorie said.
The issues cut across socioeconomic lines – affecting families with private insurance, like Marjorie, as well as those who receive coverage through Medicaid, a federal-state program that provides health insurance to low-income people and those with disabilities.
In the first few months of the pandemic, between March and May, children on Medicaid received 44% fewer outpatient mental health services – including therapy and in-home support – compared with the same time period in 2019, according to the Centers for Medicare & Medicaid Services. That’s even after accounting for increased telehealth appointments.
And while the nation’s EDs have seen a decline in overall visits, there was a relative increase in mental health visits for kids in 2020, compared with 2019.
The Centers for Disease Control and Prevention found that, from April to October 2020, hospitals across the United States saw a 24% increase in the proportion of mental health emergency visits for children aged 5-11 years, and a 31% increase for children aged 12-17.
“Not only are we seeing more children, more children are being admitted” to inpatient care.
That’s because there are fewer outpatient services now available to children, she said, and because the conditions of the children showing up at EDs “are more serious.”
This crisis is not only making life harder for these kids and their families, but it’s also stressing the entire health care system.
Child and adolescent psychiatrists working in hospitals around the country said children are increasingly “boarding” in EDs for days, waiting for inpatient admission to a regular hospital or psychiatric hospital.
Before the pandemic, there was already a shortage of inpatient psychiatric beds for children, said Christopher Bellonci, MD, a child psychiatrist at Judge Baker Children’s Center in Boston. That shortage has only gotten worse as hospitals cut capacity to allow for more physical distancing within psychiatric units.
“The whole system is really grinding to a halt at a time when we have unprecedented need,” Dr. Bellonci said.
‘A signal that the rest of your system doesn’t work’
Psychiatrists on the front lines share the frustrations of parents struggling to find help for their children.
Part of the problem is there have never been enough psychiatrists and therapists trained to work with children, intervening in the early stages of their illness, said Jennifer Havens, MD, a child psychiatrist at New York University.
“Tons of people showing up in emergency rooms in bad shape is a signal that the rest of your system doesn’t work,” she said.
Too often, Dr. Havens said, services aren’t available until children are older – and in crisis. “Often for people who don’t have access to services, we wait until they’re too big to be managed.”
While the pandemic has made life harder for Marjorie and her son in Florida, she said it has always been difficult to find the support and care he needs. Last fall, he needed a psychiatric evaluation, but the nearest specialist who would accept her commercial insurance was 100 miles away, in Alabama.
“Even when you have the money or you have the insurance, it is still a travesty,” Marjorie said. “You cannot get help for these kids.”
Parents are frustrated, and so are psychiatrists on the front lines. C.J. Glawe, MD, who leads the psychiatric crisis department at Nationwide Children’s Hospital in Columbus, Ohio, said that once a child is stabilized after a crisis it can be hard to explain to parents that they may not be able to find follow-up care anywhere near their home.
“Especially when I can clearly tell you I know exactly what you need, I just can’t give it to you,” Dr. Glawe said. “It’s demoralizing.”
When states and communities fail to provide children the services they need to live at home, kids can deteriorate and even wind up in jail, like Lindsey. At that point, Dr. Glawe said, the cost and level of care required will be even higher, whether that’s hospitalization or long stays in residential treatment facilities.
That’s exactly the scenario Sandra, Lindsey’s mom, is hoping to avoid for her Princess.
“For me, as a nurse and as a provider, that will be the last thing for my daughter,” she said. “It’s like [state and local leaders] leave it to the school and the parent to deal with, and they don’t care. And that’s the problem. It’s sad because, if I’m not here...”
Her voice trailed off as tears welled.
“She didn’t ask to have autism.”
To help families like Sandra’s and Marjorie’s, advocates said, all levels of government need to invest in creating a mental health system that’s accessible to anyone who needs it.
But given that many states have seen their revenues drop because of the pandemic, there’s a concern services will instead be cut – at a time when the need has never been greater.
This story is part of a reporting partnership that includes NPR, Illinois Public Media and Kaiser Health News. Kaiser Health News is a nonprofit news service covering health issues. It is an editorially independent program of KFF (Kaiser Family Foundation), which is not affiliated with Kaiser Permanente.
‘Alarming finding’ in schizophrenia patients with COVID-19
Schizophrenia spectrum disorder is associated with a significantly increased risk of dying from COVID-19, new research shows.
After adjusting for demographic and medical risk factors, the investigators found that patients who had been diagnosed with schizophrenia were two to three times more likely to die of COVID-19 if they contracted the disease.
“ and efforts should be taken to reduce risk of infection [social distancing, masks, etc.], particularly in people with schizophrenia who live in congregate living situations [hospitals and group residences],” Donald Goff, MD, department of psychiatry, New York University Langone Medical Center, said in an interview.
The study was published online Jan. 27 in JAMA Psychiatry.

The study included 7,348 adults with laboratory-confirmed SARS-CoV-2 infection from the NYU Langone Health System; 75 (1.0%) had a history of schizophrenia spectrum disorder, 564 (7.7%) had a history of a mood disorder, and 360 (4.9%) had a history of an anxiety disorder.
Overall, 864 patients (11.8%) died or were discharged to hospice within 45 days of a positive SARS-CoV-2 test.
In the fully adjusted model, a premorbid diagnosis of schizophrenia spectrum disorder, but not mood or anxiety disorder, was significantly associated with an increased risk of dying from COVID-19 within 45 days.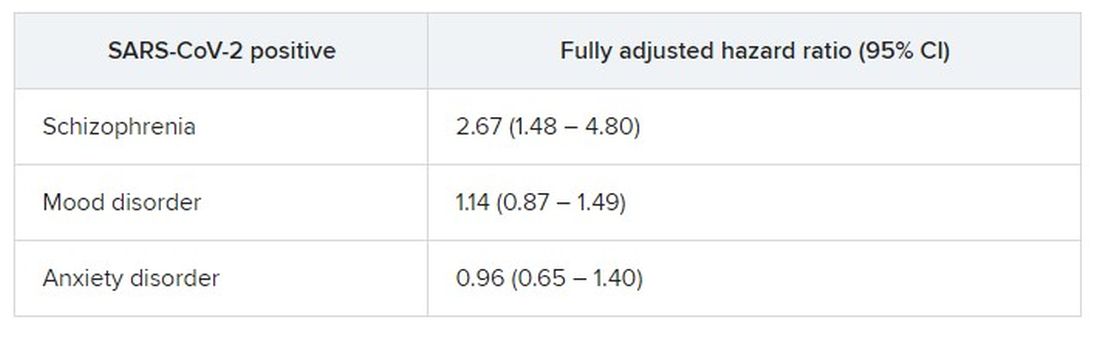
”A higher risk with schizophrenia spectrum diagnoses was expected based on previous studies of all-cause mortality, but the magnitude of the increase after adjusting for comorbid medical risk factors was unexpected,” the researchers wrote in the study, first authored by Katlyn Nemani, MD, research assistant professor of psychiatry at NYU Langone.
‘Alarming finding’
In an interview, Luming Li, MD, Yale New Haven (Conn.) Psychiatric Hospital, noted that, although the number patients with schizophrenia spectrum disorders in the sample is “fairly low,” she was not surprised by the increased risk for death from COVID-19.

“Schizophrenia falls into the serious mental illness category, and these patients are more often predisposed to homelessness, comorbid medical and substance use, living in congregate settings, lower socioeconomic status, etc,” Dr. Li noted.
Dr. Li’s advice for clinicians who treat patients who have schizophrenia during the COVID-19 pandemic is to minimize their risk in various care settings through the use of personal protective equipment and other infection prevention techniques.
“If a patient does contract COVID-19, make sure patient’s care is escalated appropriately, given the higher risk for mortality in patients with schizophrenia spectrum disorders,” she said.
Tom Pollak, PhD, MRCPsych, King’s College London, said that it has been known for some time that patients with serious mental illness have poorer physical health outcomes. More recently, it has been shown that those who have been diagnosed with psychiatric disorders appear to be at greater risk for poor COVID-19 outcomes.
“This study is the first to specifically highlight schizophrenia spectrum disorders as being particularly at risk. This is an alarming finding. These patients are already amongst the most vulnerable members of society and are probably underserved by most health care systems worldwide,” Dr. Pollak said in a statement.
“Although these findings need urgent replication in larger samples, there are clear reasons for policymakers to take notice now, including giving immediate consideration for prioritization of patients with serious mental illness in nationwide COVID-19 vaccination programs,” he added.
Matthew Hotopf, PhD, FRCPsych, FMedSci, also with King’s College London, said that the New York group has identified people with severe mental disorders as “a high-risk group, and this has immediate public health implications regarding vaccination – that’s the important message of the paper.
“Schizophrenia and other severe psychiatric disorders are risk factors for mortality in the general population before COVID. This is a group with a 10- to 20-year reduction in life expectancy – more than for many diseases we associated with early death,” said Dr. Hotopf.
“The reasons for this are multifactorial, including social deprivation, lifestyle factors (people with schizophrenia smoke more and have high rates of obesity), harms associated with some medications used to treat psychosis, and differential access to health care,” he noted.
“In COVID, we know that deprivation is associated with a much higher mortality, so we would therefore expect that people with severe mental illness will be particularly disadvantaged,” he said.
The study had no specific funding. Dr. Goff has received research support and travel reimbursement from Avanir Pharmaceuticals and Takeda. Dr. Nemani, Dr. Li, Dr. Pollak, and Dr. Hotopf disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Schizophrenia spectrum disorder is associated with a significantly increased risk of dying from COVID-19, new research shows.
After adjusting for demographic and medical risk factors, the investigators found that patients who had been diagnosed with schizophrenia were two to three times more likely to die of COVID-19 if they contracted the disease.
“ and efforts should be taken to reduce risk of infection [social distancing, masks, etc.], particularly in people with schizophrenia who live in congregate living situations [hospitals and group residences],” Donald Goff, MD, department of psychiatry, New York University Langone Medical Center, said in an interview.
The study was published online Jan. 27 in JAMA Psychiatry.
The study included 7,348 adults with laboratory-confirmed SARS-CoV-2 infection from the NYU Langone Health System; 75 (1.0%) had a history of schizophrenia spectrum disorder, 564 (7.7%) had a history of a mood disorder, and 360 (4.9%) had a history of an anxiety disorder.
Overall, 864 patients (11.8%) died or were discharged to hospice within 45 days of a positive SARS-CoV-2 test.
In the fully adjusted model, a premorbid diagnosis of schizophrenia spectrum disorder, but not mood or anxiety disorder, was significantly associated with an increased risk of dying from COVID-19 within 45 days.
”A higher risk with schizophrenia spectrum diagnoses was expected based on previous studies of all-cause mortality, but the magnitude of the increase after adjusting for comorbid medical risk factors was unexpected,” the researchers wrote in the study, first authored by Katlyn Nemani, MD, research assistant professor of psychiatry at NYU Langone.
‘Alarming finding’
In an interview, Luming Li, MD, Yale New Haven (Conn.) Psychiatric Hospital, noted that, although the number patients with schizophrenia spectrum disorders in the sample is “fairly low,” she was not surprised by the increased risk for death from COVID-19.
“Schizophrenia falls into the serious mental illness category, and these patients are more often predisposed to homelessness, comorbid medical and substance use, living in congregate settings, lower socioeconomic status, etc,” Dr. Li noted.
Dr. Li’s advice for clinicians who treat patients who have schizophrenia during the COVID-19 pandemic is to minimize their risk in various care settings through the use of personal protective equipment and other infection prevention techniques.
“If a patient does contract COVID-19, make sure patient’s care is escalated appropriately, given the higher risk for mortality in patients with schizophrenia spectrum disorders,” she said.
Tom Pollak, PhD, MRCPsych, King’s College London, said that it has been known for some time that patients with serious mental illness have poorer physical health outcomes. More recently, it has been shown that those who have been diagnosed with psychiatric disorders appear to be at greater risk for poor COVID-19 outcomes.
“This study is the first to specifically highlight schizophrenia spectrum disorders as being particularly at risk. This is an alarming finding. These patients are already amongst the most vulnerable members of society and are probably underserved by most health care systems worldwide,” Dr. Pollak said in a statement.
“Although these findings need urgent replication in larger samples, there are clear reasons for policymakers to take notice now, including giving immediate consideration for prioritization of patients with serious mental illness in nationwide COVID-19 vaccination programs,” he added.
Matthew Hotopf, PhD, FRCPsych, FMedSci, also with King’s College London, said that the New York group has identified people with severe mental disorders as “a high-risk group, and this has immediate public health implications regarding vaccination – that’s the important message of the paper.
“Schizophrenia and other severe psychiatric disorders are risk factors for mortality in the general population before COVID. This is a group with a 10- to 20-year reduction in life expectancy – more than for many diseases we associated with early death,” said Dr. Hotopf.
“The reasons for this are multifactorial, including social deprivation, lifestyle factors (people with schizophrenia smoke more and have high rates of obesity), harms associated with some medications used to treat psychosis, and differential access to health care,” he noted.
“In COVID, we know that deprivation is associated with a much higher mortality, so we would therefore expect that people with severe mental illness will be particularly disadvantaged,” he said.
The study had no specific funding. Dr. Goff has received research support and travel reimbursement from Avanir Pharmaceuticals and Takeda. Dr. Nemani, Dr. Li, Dr. Pollak, and Dr. Hotopf disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Schizophrenia spectrum disorder is associated with a significantly increased risk of dying from COVID-19, new research shows.
After adjusting for demographic and medical risk factors, the investigators found that patients who had been diagnosed with schizophrenia were two to three times more likely to die of COVID-19 if they contracted the disease.
“ and efforts should be taken to reduce risk of infection [social distancing, masks, etc.], particularly in people with schizophrenia who live in congregate living situations [hospitals and group residences],” Donald Goff, MD, department of psychiatry, New York University Langone Medical Center, said in an interview.
The study was published online Jan. 27 in JAMA Psychiatry.
The study included 7,348 adults with laboratory-confirmed SARS-CoV-2 infection from the NYU Langone Health System; 75 (1.0%) had a history of schizophrenia spectrum disorder, 564 (7.7%) had a history of a mood disorder, and 360 (4.9%) had a history of an anxiety disorder.
Overall, 864 patients (11.8%) died or were discharged to hospice within 45 days of a positive SARS-CoV-2 test.
In the fully adjusted model, a premorbid diagnosis of schizophrenia spectrum disorder, but not mood or anxiety disorder, was significantly associated with an increased risk of dying from COVID-19 within 45 days.
”A higher risk with schizophrenia spectrum diagnoses was expected based on previous studies of all-cause mortality, but the magnitude of the increase after adjusting for comorbid medical risk factors was unexpected,” the researchers wrote in the study, first authored by Katlyn Nemani, MD, research assistant professor of psychiatry at NYU Langone.
‘Alarming finding’
In an interview, Luming Li, MD, Yale New Haven (Conn.) Psychiatric Hospital, noted that, although the number patients with schizophrenia spectrum disorders in the sample is “fairly low,” she was not surprised by the increased risk for death from COVID-19.
“Schizophrenia falls into the serious mental illness category, and these patients are more often predisposed to homelessness, comorbid medical and substance use, living in congregate settings, lower socioeconomic status, etc,” Dr. Li noted.
Dr. Li’s advice for clinicians who treat patients who have schizophrenia during the COVID-19 pandemic is to minimize their risk in various care settings through the use of personal protective equipment and other infection prevention techniques.
“If a patient does contract COVID-19, make sure patient’s care is escalated appropriately, given the higher risk for mortality in patients with schizophrenia spectrum disorders,” she said.
Tom Pollak, PhD, MRCPsych, King’s College London, said that it has been known for some time that patients with serious mental illness have poorer physical health outcomes. More recently, it has been shown that those who have been diagnosed with psychiatric disorders appear to be at greater risk for poor COVID-19 outcomes.
“This study is the first to specifically highlight schizophrenia spectrum disorders as being particularly at risk. This is an alarming finding. These patients are already amongst the most vulnerable members of society and are probably underserved by most health care systems worldwide,” Dr. Pollak said in a statement.
“Although these findings need urgent replication in larger samples, there are clear reasons for policymakers to take notice now, including giving immediate consideration for prioritization of patients with serious mental illness in nationwide COVID-19 vaccination programs,” he added.
Matthew Hotopf, PhD, FRCPsych, FMedSci, also with King’s College London, said that the New York group has identified people with severe mental disorders as “a high-risk group, and this has immediate public health implications regarding vaccination – that’s the important message of the paper.
“Schizophrenia and other severe psychiatric disorders are risk factors for mortality in the general population before COVID. This is a group with a 10- to 20-year reduction in life expectancy – more than for many diseases we associated with early death,” said Dr. Hotopf.
“The reasons for this are multifactorial, including social deprivation, lifestyle factors (people with schizophrenia smoke more and have high rates of obesity), harms associated with some medications used to treat psychosis, and differential access to health care,” he noted.
“In COVID, we know that deprivation is associated with a much higher mortality, so we would therefore expect that people with severe mental illness will be particularly disadvantaged,” he said.
The study had no specific funding. Dr. Goff has received research support and travel reimbursement from Avanir Pharmaceuticals and Takeda. Dr. Nemani, Dr. Li, Dr. Pollak, and Dr. Hotopf disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.

J&J vaccine 85% efficacious against severe COVID globally
The Janssen/Johnson & Johnson single-dose adenovirus vaccine provides 85% efficacy globally against severe COVID-19 illness, according to the highly anticipated interim phase 3 results announced this morning.
The efficacy against severe disease provided by the Janssen/J&J vaccine held true regardless of age, race/ethnicity, absence or presence of comorbidities, and geography. The 44,000-participant ENSEMBLE study was conducted in the United States, South America, and South Africa.
“The team is very diligently monitoring all the variants that come up, and there are literally thousands of these. We are acting in anticipation of a variant being a potential problem. The South African variant we too acted on right away. So we too are preparing that antigen for testing.
“With data today, we do see that not a single South African, after 28 days post vaccination, ended up needing to go to the hospital, no South African died who was vaccinated.
“We do see that 85%-plus protection in South African against severe disease. That is one of the most exciting results in the dataset today,” said Mathai Mammen, MD, PhD, global head of Janssen Research & Development.
The overall efficacy was 66% globally, 72% in the United States, 66% in Latin America, and 57% in South Africa against moderate to severe SARS-CoV-2 28 days post vaccination, officials from the National Institutes of Health and Janssen reported during a media briefing.
But the J&J vaccine has potential advantages over the existing two-dose Pfizer/BioNTech and Moderna mRNA vaccines because it’s single dose and has less stringent storage requirements – only regular refrigeration is needed versus a need to freeze the two-dose Pfizer/BioNTech and Moderna COVID-19 vaccines. The J&J vaccine can be refrigerated for up to 3 months at 36°-46° F (2°-8° C).
But the difference between these just-released efficacy figures and the 94%-95% efficacy provided by the existing Pfizer/BioNTech and Moderna mRNA vaccines generated many questions during the briefing.
Anthony Fauci, MD, director of the National Institute of Allergy and Infectious Diseases, said the focus should not just be on the overall numbers. “The most important thing from a public health standpoint domestically is to keep people out of the hospital and prevent them from getting severe illness,” he said. “Many in the general public might look at a number and want to know if they get symptomatic disease or not.”
“More important than preventing someone from getting some aches and a sore throat is to prevent people – particularly people who have underlying conditions and the elderly, the ones most susceptible to a severe outcome – [from getting] severe disease,” Dr. Fauci added. Prevention of severe outcomes in a high percentage of individuals “will alleviate so much of the stress, human suffering, and death.”
Dr. Fauci acknowledged that many people will naturally focus on the distinction between 72% efficacy and 94%-95% efficacy. “This could be a messaging challenge [but] you have to make sure people understand the implications.”
It is more complex, he added, than just asking people: “If you go to the door on the left, you get 94% or 95%. If you go to the door to the right, you get 72%. What door do you want to go to?”
Instead, the messaging should be that “this and the other vaccines we have are actually preventing severe disease to a very substantial degree.”
Company defends numbers
Janssen defended their efficacy findings, pointing out that it is not a fair comparison.
“The vaccine programs that went a couple of months ago, they ran their studies during different times, when the pandemic was less complex. There were not these variants, and there was not the same level of incidence, which puts pressure on vaccine efficacy,” said Mathai Mammen, MD, PhD, global head of research and development for Janssen.
“So the numbers cannot really be compared, and that does pose a messaging challenge,” he said. “But the reality is, if one was to run the same studies [for the Pfizer and Moderna vaccines] today you would likely see different results.”
Asked if the efficacy figures could affect vaccine hesitancy, National Institutes of Health Director Francis Collins, MD, PhD, said at the announcement that most reluctance among people to get vaccinated against SARS-CoV-2 stems from concerns about safety. “The safety record is extremely good for this vaccine, as it is for the others that have received emergency use authorization.”
Janssen/J&J plans to submit for emergency use authorization from the U.S. Food and Drug Administration next week, at which point the company plans to release more information on side effects, deaths, and patient subpopulation efficacy, and more from the ENSEMBLE trial.
Janssen is aiming to provide 1 billion doses by the end of this year.
A version of this article first appeared on Medscape.com.
The Janssen/Johnson & Johnson single-dose adenovirus vaccine provides 85% efficacy globally against severe COVID-19 illness, according to the highly anticipated interim phase 3 results announced this morning.
The efficacy against severe disease provided by the Janssen/J&J vaccine held true regardless of age, race/ethnicity, absence or presence of comorbidities, and geography. The 44,000-participant ENSEMBLE study was conducted in the United States, South America, and South Africa.
“The team is very diligently monitoring all the variants that come up, and there are literally thousands of these. We are acting in anticipation of a variant being a potential problem. The South African variant we too acted on right away. So we too are preparing that antigen for testing.
“With data today, we do see that not a single South African, after 28 days post vaccination, ended up needing to go to the hospital, no South African died who was vaccinated.
“We do see that 85%-plus protection in South African against severe disease. That is one of the most exciting results in the dataset today,” said Mathai Mammen, MD, PhD, global head of Janssen Research & Development.
The overall efficacy was 66% globally, 72% in the United States, 66% in Latin America, and 57% in South Africa against moderate to severe SARS-CoV-2 28 days post vaccination, officials from the National Institutes of Health and Janssen reported during a media briefing.
But the J&J vaccine has potential advantages over the existing two-dose Pfizer/BioNTech and Moderna mRNA vaccines because it’s single dose and has less stringent storage requirements – only regular refrigeration is needed versus a need to freeze the two-dose Pfizer/BioNTech and Moderna COVID-19 vaccines. The J&J vaccine can be refrigerated for up to 3 months at 36°-46° F (2°-8° C).
But the difference between these just-released efficacy figures and the 94%-95% efficacy provided by the existing Pfizer/BioNTech and Moderna mRNA vaccines generated many questions during the briefing.
Anthony Fauci, MD, director of the National Institute of Allergy and Infectious Diseases, said the focus should not just be on the overall numbers. “The most important thing from a public health standpoint domestically is to keep people out of the hospital and prevent them from getting severe illness,” he said. “Many in the general public might look at a number and want to know if they get symptomatic disease or not.”
“More important than preventing someone from getting some aches and a sore throat is to prevent people – particularly people who have underlying conditions and the elderly, the ones most susceptible to a severe outcome – [from getting] severe disease,” Dr. Fauci added. Prevention of severe outcomes in a high percentage of individuals “will alleviate so much of the stress, human suffering, and death.”
Dr. Fauci acknowledged that many people will naturally focus on the distinction between 72% efficacy and 94%-95% efficacy. “This could be a messaging challenge [but] you have to make sure people understand the implications.”
It is more complex, he added, than just asking people: “If you go to the door on the left, you get 94% or 95%. If you go to the door to the right, you get 72%. What door do you want to go to?”
Instead, the messaging should be that “this and the other vaccines we have are actually preventing severe disease to a very substantial degree.”
Company defends numbers
Janssen defended their efficacy findings, pointing out that it is not a fair comparison.
“The vaccine programs that went a couple of months ago, they ran their studies during different times, when the pandemic was less complex. There were not these variants, and there was not the same level of incidence, which puts pressure on vaccine efficacy,” said Mathai Mammen, MD, PhD, global head of research and development for Janssen.
“So the numbers cannot really be compared, and that does pose a messaging challenge,” he said. “But the reality is, if one was to run the same studies [for the Pfizer and Moderna vaccines] today you would likely see different results.”
Asked if the efficacy figures could affect vaccine hesitancy, National Institutes of Health Director Francis Collins, MD, PhD, said at the announcement that most reluctance among people to get vaccinated against SARS-CoV-2 stems from concerns about safety. “The safety record is extremely good for this vaccine, as it is for the others that have received emergency use authorization.”
Janssen/J&J plans to submit for emergency use authorization from the U.S. Food and Drug Administration next week, at which point the company plans to release more information on side effects, deaths, and patient subpopulation efficacy, and more from the ENSEMBLE trial.
Janssen is aiming to provide 1 billion doses by the end of this year.
A version of this article first appeared on Medscape.com.
The Janssen/Johnson & Johnson single-dose adenovirus vaccine provides 85% efficacy globally against severe COVID-19 illness, according to the highly anticipated interim phase 3 results announced this morning.
The efficacy against severe disease provided by the Janssen/J&J vaccine held true regardless of age, race/ethnicity, absence or presence of comorbidities, and geography. The 44,000-participant ENSEMBLE study was conducted in the United States, South America, and South Africa.
“The team is very diligently monitoring all the variants that come up, and there are literally thousands of these. We are acting in anticipation of a variant being a potential problem. The South African variant we too acted on right away. So we too are preparing that antigen for testing.
“With data today, we do see that not a single South African, after 28 days post vaccination, ended up needing to go to the hospital, no South African died who was vaccinated.
“We do see that 85%-plus protection in South African against severe disease. That is one of the most exciting results in the dataset today,” said Mathai Mammen, MD, PhD, global head of Janssen Research & Development.
The overall efficacy was 66% globally, 72% in the United States, 66% in Latin America, and 57% in South Africa against moderate to severe SARS-CoV-2 28 days post vaccination, officials from the National Institutes of Health and Janssen reported during a media briefing.
But the J&J vaccine has potential advantages over the existing two-dose Pfizer/BioNTech and Moderna mRNA vaccines because it’s single dose and has less stringent storage requirements – only regular refrigeration is needed versus a need to freeze the two-dose Pfizer/BioNTech and Moderna COVID-19 vaccines. The J&J vaccine can be refrigerated for up to 3 months at 36°-46° F (2°-8° C).
But the difference between these just-released efficacy figures and the 94%-95% efficacy provided by the existing Pfizer/BioNTech and Moderna mRNA vaccines generated many questions during the briefing.
Anthony Fauci, MD, director of the National Institute of Allergy and Infectious Diseases, said the focus should not just be on the overall numbers. “The most important thing from a public health standpoint domestically is to keep people out of the hospital and prevent them from getting severe illness,” he said. “Many in the general public might look at a number and want to know if they get symptomatic disease or not.”
“More important than preventing someone from getting some aches and a sore throat is to prevent people – particularly people who have underlying conditions and the elderly, the ones most susceptible to a severe outcome – [from getting] severe disease,” Dr. Fauci added. Prevention of severe outcomes in a high percentage of individuals “will alleviate so much of the stress, human suffering, and death.”
Dr. Fauci acknowledged that many people will naturally focus on the distinction between 72% efficacy and 94%-95% efficacy. “This could be a messaging challenge [but] you have to make sure people understand the implications.”
It is more complex, he added, than just asking people: “If you go to the door on the left, you get 94% or 95%. If you go to the door to the right, you get 72%. What door do you want to go to?”
Instead, the messaging should be that “this and the other vaccines we have are actually preventing severe disease to a very substantial degree.”
Company defends numbers
Janssen defended their efficacy findings, pointing out that it is not a fair comparison.
“The vaccine programs that went a couple of months ago, they ran their studies during different times, when the pandemic was less complex. There were not these variants, and there was not the same level of incidence, which puts pressure on vaccine efficacy,” said Mathai Mammen, MD, PhD, global head of research and development for Janssen.
“So the numbers cannot really be compared, and that does pose a messaging challenge,” he said. “But the reality is, if one was to run the same studies [for the Pfizer and Moderna vaccines] today you would likely see different results.”
Asked if the efficacy figures could affect vaccine hesitancy, National Institutes of Health Director Francis Collins, MD, PhD, said at the announcement that most reluctance among people to get vaccinated against SARS-CoV-2 stems from concerns about safety. “The safety record is extremely good for this vaccine, as it is for the others that have received emergency use authorization.”
Janssen/J&J plans to submit for emergency use authorization from the U.S. Food and Drug Administration next week, at which point the company plans to release more information on side effects, deaths, and patient subpopulation efficacy, and more from the ENSEMBLE trial.
Janssen is aiming to provide 1 billion doses by the end of this year.
A version of this article first appeared on Medscape.com.
‘Category 5’ COVID hurricane approaches, expert says
The United States is facing a “Category 5” storm as coronavirus variants begin to spread across the country, one of the nation’s top infectious disease experts said Sunday.
“We are going to see something like we have not seen yet in this country,” Michael Osterholm, PhD, MPH, director of the Center for Infectious Disease Research and Policy at the University of Minnesota, Minneapolis, said on NBC’s Meet the Press.
The United States has reported 467 cases of the coronavirus variant first identified in the United Kingdom, across 32 states, according to the CDC variant tracker. The United States has also reported three cases of the variant first identified in South Africa in South Carolina and Maryland. One case of the variant first identified in Brazil has been found in Minnesota.
Although overall COVID-19 cases and hospitalizations have declined during the past few weeks, another storm is brewing on the horizon with the variants, Dr. Osterholm told host Chuck Todd. The U.K. variant will likely cause a surge in COVID-19 cases during the next 6-14 weeks, he said. “You and I are sitting on this beach where it’s 70 degrees, perfectly blue skies, gentle breeze. But I see that hurricane 5, Category 5 or higher, 450 miles offshore. And telling people to evacuate on that nice blue sky day is going to be hard. But I can also tell you that hurricane is coming.”
Dr. Osterholm urged federal and state officials to vaccinate as many people as possible to reduce the oncoming storm. The United States has distributed 49.9 million doses and administered 31.1 million doses, according to the latest CDC data updated Sunday, including 25.2 million first doses and 5.6 million second doses.
Doling out more doses to older Americans, rather than holding onto the second dose of the two-shot regimen, is an urgent decision, Dr. Osterholm said.
“I think right now, in advance of this surge, we need to get as many one doses in as many people over 65 as we possibly can to reduce serious illnesses and deaths that are going to occur over the weeks ahead,” he said.
The U.K. variant will likely become the dominant coronavirus strain in the United States in coming weeks, Dr. Osterholm said, adding that COVID-19 vaccines should be able to protect against it. In the meantime, however, he’s worried that the variant will cause more infections and deaths until more people get vaccinated.
“What we have to do now is also anticipate this and understand that we’re going to have change quickly,” he said. “As fast as we’re opening restaurants, we’re likely going to be closing them in the near term.”
A version of this article first appeared on WebMD.com.
The United States is facing a “Category 5” storm as coronavirus variants begin to spread across the country, one of the nation’s top infectious disease experts said Sunday.
“We are going to see something like we have not seen yet in this country,” Michael Osterholm, PhD, MPH, director of the Center for Infectious Disease Research and Policy at the University of Minnesota, Minneapolis, said on NBC’s Meet the Press.
The United States has reported 467 cases of the coronavirus variant first identified in the United Kingdom, across 32 states, according to the CDC variant tracker. The United States has also reported three cases of the variant first identified in South Africa in South Carolina and Maryland. One case of the variant first identified in Brazil has been found in Minnesota.
Although overall COVID-19 cases and hospitalizations have declined during the past few weeks, another storm is brewing on the horizon with the variants, Dr. Osterholm told host Chuck Todd. The U.K. variant will likely cause a surge in COVID-19 cases during the next 6-14 weeks, he said. “You and I are sitting on this beach where it’s 70 degrees, perfectly blue skies, gentle breeze. But I see that hurricane 5, Category 5 or higher, 450 miles offshore. And telling people to evacuate on that nice blue sky day is going to be hard. But I can also tell you that hurricane is coming.”
Dr. Osterholm urged federal and state officials to vaccinate as many people as possible to reduce the oncoming storm. The United States has distributed 49.9 million doses and administered 31.1 million doses, according to the latest CDC data updated Sunday, including 25.2 million first doses and 5.6 million second doses.
Doling out more doses to older Americans, rather than holding onto the second dose of the two-shot regimen, is an urgent decision, Dr. Osterholm said.
“I think right now, in advance of this surge, we need to get as many one doses in as many people over 65 as we possibly can to reduce serious illnesses and deaths that are going to occur over the weeks ahead,” he said.
The U.K. variant will likely become the dominant coronavirus strain in the United States in coming weeks, Dr. Osterholm said, adding that COVID-19 vaccines should be able to protect against it. In the meantime, however, he’s worried that the variant will cause more infections and deaths until more people get vaccinated.
“What we have to do now is also anticipate this and understand that we’re going to have change quickly,” he said. “As fast as we’re opening restaurants, we’re likely going to be closing them in the near term.”
A version of this article first appeared on WebMD.com.
The United States is facing a “Category 5” storm as coronavirus variants begin to spread across the country, one of the nation’s top infectious disease experts said Sunday.
“We are going to see something like we have not seen yet in this country,” Michael Osterholm, PhD, MPH, director of the Center for Infectious Disease Research and Policy at the University of Minnesota, Minneapolis, said on NBC’s Meet the Press.
The United States has reported 467 cases of the coronavirus variant first identified in the United Kingdom, across 32 states, according to the CDC variant tracker. The United States has also reported three cases of the variant first identified in South Africa in South Carolina and Maryland. One case of the variant first identified in Brazil has been found in Minnesota.
Although overall COVID-19 cases and hospitalizations have declined during the past few weeks, another storm is brewing on the horizon with the variants, Dr. Osterholm told host Chuck Todd. The U.K. variant will likely cause a surge in COVID-19 cases during the next 6-14 weeks, he said. “You and I are sitting on this beach where it’s 70 degrees, perfectly blue skies, gentle breeze. But I see that hurricane 5, Category 5 or higher, 450 miles offshore. And telling people to evacuate on that nice blue sky day is going to be hard. But I can also tell you that hurricane is coming.”
Dr. Osterholm urged federal and state officials to vaccinate as many people as possible to reduce the oncoming storm. The United States has distributed 49.9 million doses and administered 31.1 million doses, according to the latest CDC data updated Sunday, including 25.2 million first doses and 5.6 million second doses.
Doling out more doses to older Americans, rather than holding onto the second dose of the two-shot regimen, is an urgent decision, Dr. Osterholm said.
“I think right now, in advance of this surge, we need to get as many one doses in as many people over 65 as we possibly can to reduce serious illnesses and deaths that are going to occur over the weeks ahead,” he said.
The U.K. variant will likely become the dominant coronavirus strain in the United States in coming weeks, Dr. Osterholm said, adding that COVID-19 vaccines should be able to protect against it. In the meantime, however, he’s worried that the variant will cause more infections and deaths until more people get vaccinated.
“What we have to do now is also anticipate this and understand that we’re going to have change quickly,” he said. “As fast as we’re opening restaurants, we’re likely going to be closing them in the near term.”
A version of this article first appeared on WebMD.com.
School antibullying programs may have substantial population impact
School antibullying programs may have small effect sizes but a valuable population impact, according to research published in JAMA Pediatrics.
.
The investigators estimated population effect numbers for the interventions, such as the number of students needed to participate in an antibullying program to prevent one case of bullying.
Assuming a bullying prevalence of 15%, “an average antibullying intervention needs to include 207 people to prevent 1 case of bullying perpetration or 140 people to prevent 1 case of bullying exposure,” reported David Fraguas, MD, PhD, of the Institute of Psychiatry and Mental Health at Hospital Clínico San Carlos in Madrid, and colleagues. To improve mental health, the average antibullying program needs to include 107 people, the results indicate.
Few trials assessed the same antibullying program, so the researchers examined antibullying programs as a whole. Still, “not all antibullying programs are efficacious,” and “effectiveness may vary in different settings,” they noted.
Public health implications
Schools frequently implement programs to address bullying, which research suggests is a prevalent, modifiable risk factor for mental health disorders and therefore a “major public health concern,” the authors said. Studies have suggested that antibullying programs may be effective, though the evidence has been unclear.
“I see teens with mental health issues frequently in my practice, and often during their assessment, these patients and parents disclose a history of bullying at school or online,” said Kelly A. Curran, MD, associate professor of pediatrics at the University of Oklahoma, Oklahoma City. “The impact of bullying on these teens is obvious – from the mental health issues to school absenteeism and dropouts to long-term health consequences. Often, parents ask for guidance on how to ‘make it stop’ or for help working with the teen’s school. It’s hard in these cases as a clinician to know what to recommend – while it’s clear that the bullying is contributing to the teen’s health issues, giving evidenced-based guidance on bullying has been difficult.”

Dr. Curran had been “somewhat skeptical” of the effectiveness of antibullying curricula.
“I was pleasantly surprised to see that there is a significant population impact for interventions to prevent traditional bullying (207 people educated to prevent 1 case) and cyberbullying (167 people educated to prevent 1 case),” Dr. Curran said. “Additionally, these interventions do not have to be lengthy in duration – and may have long-term effectiveness. While there are limitations to this study, I feel more comfortable recommending and advocating for antibullying campaigns in schools.”
Relative to control groups
To assess the population impact of antibullying interventions, Dr. Fraguas and collaborators conducted random-effects meta-analyses. They identified 69 trials that included 56,511 participants in intervention groups and 55,148 in control groups. Five of the trials tested interventions targeting cyberbullying.
Participants ranged in age from 4 to 17 years, and the weighted average age was 11 years. The durations of the interventions ranged from 1 week to more than 2 years, with an average duration of 29.4 weeks.
“Antibullying interventions showed statistically significant effectiveness compared with control groups on all assessed bullying-related outcomes after the intervention,” the researchers reported. “The effect sizes were mostly statistically significant and small ... with high statistical heterogeneity and risk of publication bias. Antibullying interventions also showed statistically significant effectiveness in improving mental health problems (e.g., anxiety and depression) at study endpoint, with small effect size.”
Consistent with prior research, results varied by region. For example, interventions in Europe, where 31 of the trials were conducted, significantly decreased bullying exposure and attitudes that encourage bullying, whereas interventions in North America, where 19 of the trials were conducted, did not. In addition, European trials found greater effect sizes for the outcome measure of increasing attitudes that discourage bullying, compared with North American trials. The regional differences could reflect different programs or study designs, or differences in “social, educational, or cultural context,” the authors said.
‘Substantial’ impact
Together, the findings suggest that “universal antibullying interventions have a substantial population impact,” Dr. Fraguas and coauthors wrote. “To put these results into context, the [population impact number] is 35,450 for taking aspirin to avoid 1 death during the 6 months after a first nonhemorrhagic stroke, and the [population impact number] is 324 for human papillomavirus vaccination in girls to prevent cervical cancer.”
Furthermore, the interventions appear to be safe, they said. None of the trials in the meta-analysis reported an increase in bullying perpetration or bullying exposure at the end of the study or during follow-up, and mental health improved in all trials that assessed that outcome.
Pediatricians may be seen as resource
“From our survey work among parents all across Chicago, we know that almost one-half of all parents with children in school are concerned that their children get bullied,” said Matthew M. Davis, MD chair of the department of pediatrics at Ann & Robert H. Lurie Children’s Hospital of Chicago and professor of pediatrics, medicine, medical social sciences, and preventive medicine at Northwestern University in Chicago. “Among those parents, about one-half sought help from a teacher and about one-third asked a school administrator or school social worker for help. That means that schools are, by far, the go-to source for help when parents are worried about bullying.”

The survey of 1,642 parents in Chicago also found that 20% of parents with concerns sought help from mental health care providers, and 16% sought help from their pediatricians.
“Pediatricians can provide psychosocial support for their patients who are being bullied,” Dr. Davis said. “They can also talk with patients and their parents/guardians about how to team up with school personnel to address the bullying in the school environment.”
The meta-analysis was supported by grants from Instituto de Salud Carlos III (Spanish Ministry of Science and Innovation), cofinanced by the European Regional Development Fund from the European Commission. It also was supported by Madrid Regional Government, European Union programs, Fundación Familia Alonso, Fundación Alicia Koplowitz, and Fundación Mutua Madrileña.
Dr. Fraguas disclosed consulting for or receiving fees from Angelini, Eisai, IE4Lab, Janssen, Lundbeck, and Otsuka and grant support from Fundación Alicia Koplowitz and Instituto de Salud Carlos III. Coauthors disclosed financial ties to pharmaceutical companies, as well as government and foundation grants. Dr. Curran is a member of the Pediatric News editorial advisory board. Dr. Davis had no relevant disclosures.
School antibullying programs may have small effect sizes but a valuable population impact, according to research published in JAMA Pediatrics.
.
The investigators estimated population effect numbers for the interventions, such as the number of students needed to participate in an antibullying program to prevent one case of bullying.
Assuming a bullying prevalence of 15%, “an average antibullying intervention needs to include 207 people to prevent 1 case of bullying perpetration or 140 people to prevent 1 case of bullying exposure,” reported David Fraguas, MD, PhD, of the Institute of Psychiatry and Mental Health at Hospital Clínico San Carlos in Madrid, and colleagues. To improve mental health, the average antibullying program needs to include 107 people, the results indicate.
Few trials assessed the same antibullying program, so the researchers examined antibullying programs as a whole. Still, “not all antibullying programs are efficacious,” and “effectiveness may vary in different settings,” they noted.
Public health implications
Schools frequently implement programs to address bullying, which research suggests is a prevalent, modifiable risk factor for mental health disorders and therefore a “major public health concern,” the authors said. Studies have suggested that antibullying programs may be effective, though the evidence has been unclear.
“I see teens with mental health issues frequently in my practice, and often during their assessment, these patients and parents disclose a history of bullying at school or online,” said Kelly A. Curran, MD, associate professor of pediatrics at the University of Oklahoma, Oklahoma City. “The impact of bullying on these teens is obvious – from the mental health issues to school absenteeism and dropouts to long-term health consequences. Often, parents ask for guidance on how to ‘make it stop’ or for help working with the teen’s school. It’s hard in these cases as a clinician to know what to recommend – while it’s clear that the bullying is contributing to the teen’s health issues, giving evidenced-based guidance on bullying has been difficult.”
Dr. Curran had been “somewhat skeptical” of the effectiveness of antibullying curricula.
“I was pleasantly surprised to see that there is a significant population impact for interventions to prevent traditional bullying (207 people educated to prevent 1 case) and cyberbullying (167 people educated to prevent 1 case),” Dr. Curran said. “Additionally, these interventions do not have to be lengthy in duration – and may have long-term effectiveness. While there are limitations to this study, I feel more comfortable recommending and advocating for antibullying campaigns in schools.”
Relative to control groups
To assess the population impact of antibullying interventions, Dr. Fraguas and collaborators conducted random-effects meta-analyses. They identified 69 trials that included 56,511 participants in intervention groups and 55,148 in control groups. Five of the trials tested interventions targeting cyberbullying.
Participants ranged in age from 4 to 17 years, and the weighted average age was 11 years. The durations of the interventions ranged from 1 week to more than 2 years, with an average duration of 29.4 weeks.
“Antibullying interventions showed statistically significant effectiveness compared with control groups on all assessed bullying-related outcomes after the intervention,” the researchers reported. “The effect sizes were mostly statistically significant and small ... with high statistical heterogeneity and risk of publication bias. Antibullying interventions also showed statistically significant effectiveness in improving mental health problems (e.g., anxiety and depression) at study endpoint, with small effect size.”
Consistent with prior research, results varied by region. For example, interventions in Europe, where 31 of the trials were conducted, significantly decreased bullying exposure and attitudes that encourage bullying, whereas interventions in North America, where 19 of the trials were conducted, did not. In addition, European trials found greater effect sizes for the outcome measure of increasing attitudes that discourage bullying, compared with North American trials. The regional differences could reflect different programs or study designs, or differences in “social, educational, or cultural context,” the authors said.
‘Substantial’ impact
Together, the findings suggest that “universal antibullying interventions have a substantial population impact,” Dr. Fraguas and coauthors wrote. “To put these results into context, the [population impact number] is 35,450 for taking aspirin to avoid 1 death during the 6 months after a first nonhemorrhagic stroke, and the [population impact number] is 324 for human papillomavirus vaccination in girls to prevent cervical cancer.”
Furthermore, the interventions appear to be safe, they said. None of the trials in the meta-analysis reported an increase in bullying perpetration or bullying exposure at the end of the study or during follow-up, and mental health improved in all trials that assessed that outcome.
Pediatricians may be seen as resource
“From our survey work among parents all across Chicago, we know that almost one-half of all parents with children in school are concerned that their children get bullied,” said Matthew M. Davis, MD chair of the department of pediatrics at Ann & Robert H. Lurie Children’s Hospital of Chicago and professor of pediatrics, medicine, medical social sciences, and preventive medicine at Northwestern University in Chicago. “Among those parents, about one-half sought help from a teacher and about one-third asked a school administrator or school social worker for help. That means that schools are, by far, the go-to source for help when parents are worried about bullying.”
The survey of 1,642 parents in Chicago also found that 20% of parents with concerns sought help from mental health care providers, and 16% sought help from their pediatricians.
“Pediatricians can provide psychosocial support for their patients who are being bullied,” Dr. Davis said. “They can also talk with patients and their parents/guardians about how to team up with school personnel to address the bullying in the school environment.”
The meta-analysis was supported by grants from Instituto de Salud Carlos III (Spanish Ministry of Science and Innovation), cofinanced by the European Regional Development Fund from the European Commission. It also was supported by Madrid Regional Government, European Union programs, Fundación Familia Alonso, Fundación Alicia Koplowitz, and Fundación Mutua Madrileña.
Dr. Fraguas disclosed consulting for or receiving fees from Angelini, Eisai, IE4Lab, Janssen, Lundbeck, and Otsuka and grant support from Fundación Alicia Koplowitz and Instituto de Salud Carlos III. Coauthors disclosed financial ties to pharmaceutical companies, as well as government and foundation grants. Dr. Curran is a member of the Pediatric News editorial advisory board. Dr. Davis had no relevant disclosures.
School antibullying programs may have small effect sizes but a valuable population impact, according to research published in JAMA Pediatrics.
.
The investigators estimated population effect numbers for the interventions, such as the number of students needed to participate in an antibullying program to prevent one case of bullying.
Assuming a bullying prevalence of 15%, “an average antibullying intervention needs to include 207 people to prevent 1 case of bullying perpetration or 140 people to prevent 1 case of bullying exposure,” reported David Fraguas, MD, PhD, of the Institute of Psychiatry and Mental Health at Hospital Clínico San Carlos in Madrid, and colleagues. To improve mental health, the average antibullying program needs to include 107 people, the results indicate.
Few trials assessed the same antibullying program, so the researchers examined antibullying programs as a whole. Still, “not all antibullying programs are efficacious,” and “effectiveness may vary in different settings,” they noted.
Public health implications
Schools frequently implement programs to address bullying, which research suggests is a prevalent, modifiable risk factor for mental health disorders and therefore a “major public health concern,” the authors said. Studies have suggested that antibullying programs may be effective, though the evidence has been unclear.
“I see teens with mental health issues frequently in my practice, and often during their assessment, these patients and parents disclose a history of bullying at school or online,” said Kelly A. Curran, MD, associate professor of pediatrics at the University of Oklahoma, Oklahoma City. “The impact of bullying on these teens is obvious – from the mental health issues to school absenteeism and dropouts to long-term health consequences. Often, parents ask for guidance on how to ‘make it stop’ or for help working with the teen’s school. It’s hard in these cases as a clinician to know what to recommend – while it’s clear that the bullying is contributing to the teen’s health issues, giving evidenced-based guidance on bullying has been difficult.”
Dr. Curran had been “somewhat skeptical” of the effectiveness of antibullying curricula.
“I was pleasantly surprised to see that there is a significant population impact for interventions to prevent traditional bullying (207 people educated to prevent 1 case) and cyberbullying (167 people educated to prevent 1 case),” Dr. Curran said. “Additionally, these interventions do not have to be lengthy in duration – and may have long-term effectiveness. While there are limitations to this study, I feel more comfortable recommending and advocating for antibullying campaigns in schools.”
Relative to control groups
To assess the population impact of antibullying interventions, Dr. Fraguas and collaborators conducted random-effects meta-analyses. They identified 69 trials that included 56,511 participants in intervention groups and 55,148 in control groups. Five of the trials tested interventions targeting cyberbullying.
Participants ranged in age from 4 to 17 years, and the weighted average age was 11 years. The durations of the interventions ranged from 1 week to more than 2 years, with an average duration of 29.4 weeks.
“Antibullying interventions showed statistically significant effectiveness compared with control groups on all assessed bullying-related outcomes after the intervention,” the researchers reported. “The effect sizes were mostly statistically significant and small ... with high statistical heterogeneity and risk of publication bias. Antibullying interventions also showed statistically significant effectiveness in improving mental health problems (e.g., anxiety and depression) at study endpoint, with small effect size.”
Consistent with prior research, results varied by region. For example, interventions in Europe, where 31 of the trials were conducted, significantly decreased bullying exposure and attitudes that encourage bullying, whereas interventions in North America, where 19 of the trials were conducted, did not. In addition, European trials found greater effect sizes for the outcome measure of increasing attitudes that discourage bullying, compared with North American trials. The regional differences could reflect different programs or study designs, or differences in “social, educational, or cultural context,” the authors said.
‘Substantial’ impact
Together, the findings suggest that “universal antibullying interventions have a substantial population impact,” Dr. Fraguas and coauthors wrote. “To put these results into context, the [population impact number] is 35,450 for taking aspirin to avoid 1 death during the 6 months after a first nonhemorrhagic stroke, and the [population impact number] is 324 for human papillomavirus vaccination in girls to prevent cervical cancer.”
Furthermore, the interventions appear to be safe, they said. None of the trials in the meta-analysis reported an increase in bullying perpetration or bullying exposure at the end of the study or during follow-up, and mental health improved in all trials that assessed that outcome.
Pediatricians may be seen as resource
“From our survey work among parents all across Chicago, we know that almost one-half of all parents with children in school are concerned that their children get bullied,” said Matthew M. Davis, MD chair of the department of pediatrics at Ann & Robert H. Lurie Children’s Hospital of Chicago and professor of pediatrics, medicine, medical social sciences, and preventive medicine at Northwestern University in Chicago. “Among those parents, about one-half sought help from a teacher and about one-third asked a school administrator or school social worker for help. That means that schools are, by far, the go-to source for help when parents are worried about bullying.”
The survey of 1,642 parents in Chicago also found that 20% of parents with concerns sought help from mental health care providers, and 16% sought help from their pediatricians.
“Pediatricians can provide psychosocial support for their patients who are being bullied,” Dr. Davis said. “They can also talk with patients and their parents/guardians about how to team up with school personnel to address the bullying in the school environment.”
The meta-analysis was supported by grants from Instituto de Salud Carlos III (Spanish Ministry of Science and Innovation), cofinanced by the European Regional Development Fund from the European Commission. It also was supported by Madrid Regional Government, European Union programs, Fundación Familia Alonso, Fundación Alicia Koplowitz, and Fundación Mutua Madrileña.
Dr. Fraguas disclosed consulting for or receiving fees from Angelini, Eisai, IE4Lab, Janssen, Lundbeck, and Otsuka and grant support from Fundación Alicia Koplowitz and Instituto de Salud Carlos III. Coauthors disclosed financial ties to pharmaceutical companies, as well as government and foundation grants. Dr. Curran is a member of the Pediatric News editorial advisory board. Dr. Davis had no relevant disclosures.
FROM JAMA PEDIATRICS
Tough pain relief choices in the COVID-19 pandemic
More people with fever and body aches are turning to NSAIDs to ease symptoms, but the drugs have come under new scrutiny as investigators work to determine whether they are a safe way to relieve the pain of COVID-19 vaccination or symptoms of the disease.
Early on in the pandemic, French health officials warned that NSAIDs, such as ibuprofen, could worsen coronavirus disease, and they recommended switching to acetaminophen instead.
The National Health Service in the United Kingdom followed with a similar recommendation for acetaminophen.
But the European Medicines Agency took a different approach, reporting “no scientific evidence” that NSAIDs could worsen COVID-19. The U.S. Food and Drug Administration also opted not to take a stance.
The debate prompted discussion on social media, with various reactions from around the world. It also inspired Craig Wilen, MD, PhD, from Yale University, New Haven, Conn., and associates to examine the effect of NSAIDs on COVID-19 infection and immune response. Their findings were published online Jan.20 in the Journal of Virology.
“It really bothered me that non–evidence-based decisions were driving the conversation,” Dr. Wilen said. “Millions of people are taking NSAIDs every day and clinical decisions about their care shouldn’t be made on a hypothesis.”
One theory is that NSAIDs alter susceptibility to infection by modifying ACE2. The drugs might also change the cell entry receptor for SARS-CoV-2, alter virus replication, or even modify the immune response.
British researchers, also questioning the safety of NSAIDs in patients with COVID-19, delved into National Health Service records to study two large groups of patients, some of whom were taking the pain relievers.
“We were watching the controversy and the lack of evidence and wanted to contribute,” lead investigator Angel Wong, PhD, from the London School of Hygiene and Tropical Medicine, said in an interview.
And with nearly 11 million NSAID prescriptions dispensed in primary care in England alone in the past 12 months, the inconsistency was concerning.
The team compared COVID-19–related deaths in two groups: one group of more than 700,000 people taking NSAIDs, including patients with rheumatoid arthritis and osteoarthritis; and another of almost 3.5 million people not on the medication.
NSAIDs work by inhibiting cyclooxygenase-1 and COX-2 enzymes in the body, which are crucial for the generation of prostaglandins. These lipid molecules play a role in inflammation and are blocked by NSAIDs.
The investigators found no evidence of a harmful effect of NSAIDs on COVID-19-related deaths; their results were published online Jan. 21 in the Annals of the Rheumatic Diseases.
The results, they pointed out, are in line with a Danish study that also showed no evidence of a higher risk for severe COVID-19 outcomes with NSAID use.
“It’s reassuring,” Dr. Wong said, “that patients can safely continue treatment.”
More new evidence
Dr. Wilen’s team found that SARS-CoV-2 infection stimulated COX-2 expression in human and mice cells. However, suppression of COX-2 by two commonly used NSAIDs, ibuprofen and meloxicam, had no effect on ACE2 expression, viral entry, or viral replication.
In their mouse model of SARS-CoV-2 infection, the investigators saw that NSAIDs impaired the production of proinflammatory cytokines and neutralizing antibodies. The findings suggest that NSAIDs influence COVID-19 outcomes by dampening the inflammatory response and production of protective antibodies, rather than modifying susceptibility to infection or viral replication.
Understanding the effect of NSAIDs on cytokine production is critical, Dr. Wilen pointed out, because they might be protective early in COVID-19 but pathologic at later stages.
Timing is crucial in the case of other immunomodulatory drugs. For example, dexamethasone lowers mortality in COVID-19 patients on respiratory support but is potentially harmful for those with milder disease.
There still is a lot to learn, Dr. Wilen acknowledged. “We may be seeing something similar going on with NSAIDs, where the timing of treatment is important.”
A version of this article first appeared on Medscape.com.
More people with fever and body aches are turning to NSAIDs to ease symptoms, but the drugs have come under new scrutiny as investigators work to determine whether they are a safe way to relieve the pain of COVID-19 vaccination or symptoms of the disease.
Early on in the pandemic, French health officials warned that NSAIDs, such as ibuprofen, could worsen coronavirus disease, and they recommended switching to acetaminophen instead.
The National Health Service in the United Kingdom followed with a similar recommendation for acetaminophen.
But the European Medicines Agency took a different approach, reporting “no scientific evidence” that NSAIDs could worsen COVID-19. The U.S. Food and Drug Administration also opted not to take a stance.
The debate prompted discussion on social media, with various reactions from around the world. It also inspired Craig Wilen, MD, PhD, from Yale University, New Haven, Conn., and associates to examine the effect of NSAIDs on COVID-19 infection and immune response. Their findings were published online Jan.20 in the Journal of Virology.
“It really bothered me that non–evidence-based decisions were driving the conversation,” Dr. Wilen said. “Millions of people are taking NSAIDs every day and clinical decisions about their care shouldn’t be made on a hypothesis.”
One theory is that NSAIDs alter susceptibility to infection by modifying ACE2. The drugs might also change the cell entry receptor for SARS-CoV-2, alter virus replication, or even modify the immune response.
British researchers, also questioning the safety of NSAIDs in patients with COVID-19, delved into National Health Service records to study two large groups of patients, some of whom were taking the pain relievers.
“We were watching the controversy and the lack of evidence and wanted to contribute,” lead investigator Angel Wong, PhD, from the London School of Hygiene and Tropical Medicine, said in an interview.
And with nearly 11 million NSAID prescriptions dispensed in primary care in England alone in the past 12 months, the inconsistency was concerning.
The team compared COVID-19–related deaths in two groups: one group of more than 700,000 people taking NSAIDs, including patients with rheumatoid arthritis and osteoarthritis; and another of almost 3.5 million people not on the medication.
NSAIDs work by inhibiting cyclooxygenase-1 and COX-2 enzymes in the body, which are crucial for the generation of prostaglandins. These lipid molecules play a role in inflammation and are blocked by NSAIDs.
The investigators found no evidence of a harmful effect of NSAIDs on COVID-19-related deaths; their results were published online Jan. 21 in the Annals of the Rheumatic Diseases.
The results, they pointed out, are in line with a Danish study that also showed no evidence of a higher risk for severe COVID-19 outcomes with NSAID use.
“It’s reassuring,” Dr. Wong said, “that patients can safely continue treatment.”
More new evidence
Dr. Wilen’s team found that SARS-CoV-2 infection stimulated COX-2 expression in human and mice cells. However, suppression of COX-2 by two commonly used NSAIDs, ibuprofen and meloxicam, had no effect on ACE2 expression, viral entry, or viral replication.
In their mouse model of SARS-CoV-2 infection, the investigators saw that NSAIDs impaired the production of proinflammatory cytokines and neutralizing antibodies. The findings suggest that NSAIDs influence COVID-19 outcomes by dampening the inflammatory response and production of protective antibodies, rather than modifying susceptibility to infection or viral replication.
Understanding the effect of NSAIDs on cytokine production is critical, Dr. Wilen pointed out, because they might be protective early in COVID-19 but pathologic at later stages.
Timing is crucial in the case of other immunomodulatory drugs. For example, dexamethasone lowers mortality in COVID-19 patients on respiratory support but is potentially harmful for those with milder disease.
There still is a lot to learn, Dr. Wilen acknowledged. “We may be seeing something similar going on with NSAIDs, where the timing of treatment is important.”
A version of this article first appeared on Medscape.com.
More people with fever and body aches are turning to NSAIDs to ease symptoms, but the drugs have come under new scrutiny as investigators work to determine whether they are a safe way to relieve the pain of COVID-19 vaccination or symptoms of the disease.
Early on in the pandemic, French health officials warned that NSAIDs, such as ibuprofen, could worsen coronavirus disease, and they recommended switching to acetaminophen instead.
The National Health Service in the United Kingdom followed with a similar recommendation for acetaminophen.
But the European Medicines Agency took a different approach, reporting “no scientific evidence” that NSAIDs could worsen COVID-19. The U.S. Food and Drug Administration also opted not to take a stance.
The debate prompted discussion on social media, with various reactions from around the world. It also inspired Craig Wilen, MD, PhD, from Yale University, New Haven, Conn., and associates to examine the effect of NSAIDs on COVID-19 infection and immune response. Their findings were published online Jan.20 in the Journal of Virology.
“It really bothered me that non–evidence-based decisions were driving the conversation,” Dr. Wilen said. “Millions of people are taking NSAIDs every day and clinical decisions about their care shouldn’t be made on a hypothesis.”
One theory is that NSAIDs alter susceptibility to infection by modifying ACE2. The drugs might also change the cell entry receptor for SARS-CoV-2, alter virus replication, or even modify the immune response.
British researchers, also questioning the safety of NSAIDs in patients with COVID-19, delved into National Health Service records to study two large groups of patients, some of whom were taking the pain relievers.
“We were watching the controversy and the lack of evidence and wanted to contribute,” lead investigator Angel Wong, PhD, from the London School of Hygiene and Tropical Medicine, said in an interview.
And with nearly 11 million NSAID prescriptions dispensed in primary care in England alone in the past 12 months, the inconsistency was concerning.
The team compared COVID-19–related deaths in two groups: one group of more than 700,000 people taking NSAIDs, including patients with rheumatoid arthritis and osteoarthritis; and another of almost 3.5 million people not on the medication.
NSAIDs work by inhibiting cyclooxygenase-1 and COX-2 enzymes in the body, which are crucial for the generation of prostaglandins. These lipid molecules play a role in inflammation and are blocked by NSAIDs.
The investigators found no evidence of a harmful effect of NSAIDs on COVID-19-related deaths; their results were published online Jan. 21 in the Annals of the Rheumatic Diseases.
The results, they pointed out, are in line with a Danish study that also showed no evidence of a higher risk for severe COVID-19 outcomes with NSAID use.
“It’s reassuring,” Dr. Wong said, “that patients can safely continue treatment.”
More new evidence
Dr. Wilen’s team found that SARS-CoV-2 infection stimulated COX-2 expression in human and mice cells. However, suppression of COX-2 by two commonly used NSAIDs, ibuprofen and meloxicam, had no effect on ACE2 expression, viral entry, or viral replication.
In their mouse model of SARS-CoV-2 infection, the investigators saw that NSAIDs impaired the production of proinflammatory cytokines and neutralizing antibodies. The findings suggest that NSAIDs influence COVID-19 outcomes by dampening the inflammatory response and production of protective antibodies, rather than modifying susceptibility to infection or viral replication.
Understanding the effect of NSAIDs on cytokine production is critical, Dr. Wilen pointed out, because they might be protective early in COVID-19 but pathologic at later stages.
Timing is crucial in the case of other immunomodulatory drugs. For example, dexamethasone lowers mortality in COVID-19 patients on respiratory support but is potentially harmful for those with milder disease.
There still is a lot to learn, Dr. Wilen acknowledged. “We may be seeing something similar going on with NSAIDs, where the timing of treatment is important.”
A version of this article first appeared on Medscape.com.
The brother’s keeper: A psychiatrist writes about his career treating physicians and their families
I started reading “Becoming a Doctors’ Doctor: A Memoir” by Michael F. Myers, MD, with high expectations and enthusiasm. Dr. Myers is a Canadian psychiatrist who has devoted his career to caring for physicians in his half-time private practice; he turns all other comers away.
This career path began in 1962 during his first year in medical school when Dr. Myers returned to his apartment after Thanksgiving break to be greeted with tragic news: One of the young men he shared the apartment with had died of suicide. The tragedy marked him – along with the silence about what had transpired – and he would later look back to realize it was the beginning of his journey to becoming a psychiatrist, one who cares for other physicians.
The book is filled with patient vignettes, gentle musings that Dr. Myers recounts with warmth, adding what he has learned from them.

There is, for example, the heart-wrenching account of “DJ,” a lonely medical student who is emergently hospitalized for depression, after the worried author anxiously drove the patient from his office to the hospital. DJ is all alone, and he writes to a friend and offers to pay for her transportation if she will come visit him in the hospital, a fact Dr. Myers knows only because he was later shown a letter DJ had written to his friend.
“He has been diminished and altered by his disease and the requisite hospital treatment, factors that we as mental health caregivers must never forget – or minimize. Visits from friends become visits of the representatives from the outside world, the link to normality, sanity, and anticipated return. These encounters are precious,” Dr. Myers writes.
As the book progressed, I began to wonder more about the author as a person. It is a memoir, so stated on the cover, but very little about his life is revealed. There are résumé-style facts: where he studied, or worked, or went to conferences, what he learned and what he spoke about, but I wanted to know more about how his experiences intertwined with his life. In the foreword, he talks about having an alcoholic mother. He tells the reader that being a husband and father was important to him, and that his conversion to Judaism – his wife’s religion – was meaningful, but there is no backstory, and I was looking for more. A quick reference is made to visiting a therapist, but those few sentences are the total of what I knew about Michael Myers midway through his memoir.

I looked for a photo of the author. I found it at the back of the book with a brief biography beneath it, ending with the fact that he lives with his husband. I had gotten halfway through the memoir, including chapters about how Myers had treated gay physicians, gay couples, and physicians with AIDS, and yet there was no mention of his husband, and how his sexual orientation influenced these encounters. I didn’t quite know what to think.
And then, in a section called “Getting Personal,” suddenly the tone of the book changed. Dr. Myers talked about his own sexual confusion as a young man and about the decision to marry a woman, knowing he was bisexual. He wrote about the shame he felt concerning his sexual desires at a time when homosexuality was still classified as a psychiatric disorder, the fear of judgment, and the sense that this – his ninth book – was his first genuine book.
“And so, I come full circle. It is my otherness that fundamentally – but not with full awareness – attracted me to psychiatry, and ultimately to becoming a doctors’ doctor. I’ve been able to empathize with my doctor patients’ burden with the scourge of mental illness, coping with brokenness, and struggling for acceptance and belonging in a profession of perfection and stature. And I understand what it’s like to feel a bit of a misfit, less than, unclean and tattered. But as a wounded healer, I know the restorative value of listening, acceptance, caring, doggedness, and hope.” And so I found Dr. Myers.
These few pages in the middle of the book pulled everything else into focus. The writing opened and the rest of the book flowed. The author’s insights about physician-patients became even more insightful. It’s almost as though he was anxious about revealing himself, and his writing infused itself with this worry, so that once his secret was revealed, he was free to be genuine in a way that makes this book a gem of a read.
His insights about treating troubled physicians are invaluable. He talks of their struggles with loss, and of their flawed roles as patients.
“At the point that they become a patient these individuals may already be quite ill, and this needs to be recognized and accepted by the treating psychiatrist. Judging the doctor for so many self-defeating behaviors is unacceptable and unprofessional. I have found it best to simply accept the old adage ‘It is what it is.’ And I try my best to be patient and understanding with such difficult and interwoven issues, in that for physicians becoming a patient is a process not an event.”
Written with empathy, warmth, and vulnerability, “Becoming a Doctors’ Doctor” is a worthwhile read for any psychiatrist who treats other physicians.
Dr. Miller is coauthor of “Committed: The Battle over Involuntary Psychiatric Care” (Baltimore: Johns Hopkins University Press, 2016). She has a private practice and is assistant professor of psychiatry and behavioral sciences at Johns Hopkins, both in Baltimore. Dr. Miller has no conflicts of interest.
I started reading “Becoming a Doctors’ Doctor: A Memoir” by Michael F. Myers, MD, with high expectations and enthusiasm. Dr. Myers is a Canadian psychiatrist who has devoted his career to caring for physicians in his half-time private practice; he turns all other comers away.
This career path began in 1962 during his first year in medical school when Dr. Myers returned to his apartment after Thanksgiving break to be greeted with tragic news: One of the young men he shared the apartment with had died of suicide. The tragedy marked him – along with the silence about what had transpired – and he would later look back to realize it was the beginning of his journey to becoming a psychiatrist, one who cares for other physicians.
The book is filled with patient vignettes, gentle musings that Dr. Myers recounts with warmth, adding what he has learned from them.
There is, for example, the heart-wrenching account of “DJ,” a lonely medical student who is emergently hospitalized for depression, after the worried author anxiously drove the patient from his office to the hospital. DJ is all alone, and he writes to a friend and offers to pay for her transportation if she will come visit him in the hospital, a fact Dr. Myers knows only because he was later shown a letter DJ had written to his friend.
“He has been diminished and altered by his disease and the requisite hospital treatment, factors that we as mental health caregivers must never forget – or minimize. Visits from friends become visits of the representatives from the outside world, the link to normality, sanity, and anticipated return. These encounters are precious,” Dr. Myers writes.
As the book progressed, I began to wonder more about the author as a person. It is a memoir, so stated on the cover, but very little about his life is revealed. There are résumé-style facts: where he studied, or worked, or went to conferences, what he learned and what he spoke about, but I wanted to know more about how his experiences intertwined with his life. In the foreword, he talks about having an alcoholic mother. He tells the reader that being a husband and father was important to him, and that his conversion to Judaism – his wife’s religion – was meaningful, but there is no backstory, and I was looking for more. A quick reference is made to visiting a therapist, but those few sentences are the total of what I knew about Michael Myers midway through his memoir.
I looked for a photo of the author. I found it at the back of the book with a brief biography beneath it, ending with the fact that he lives with his husband. I had gotten halfway through the memoir, including chapters about how Myers had treated gay physicians, gay couples, and physicians with AIDS, and yet there was no mention of his husband, and how his sexual orientation influenced these encounters. I didn’t quite know what to think.
And then, in a section called “Getting Personal,” suddenly the tone of the book changed. Dr. Myers talked about his own sexual confusion as a young man and about the decision to marry a woman, knowing he was bisexual. He wrote about the shame he felt concerning his sexual desires at a time when homosexuality was still classified as a psychiatric disorder, the fear of judgment, and the sense that this – his ninth book – was his first genuine book.
“And so, I come full circle. It is my otherness that fundamentally – but not with full awareness – attracted me to psychiatry, and ultimately to becoming a doctors’ doctor. I’ve been able to empathize with my doctor patients’ burden with the scourge of mental illness, coping with brokenness, and struggling for acceptance and belonging in a profession of perfection and stature. And I understand what it’s like to feel a bit of a misfit, less than, unclean and tattered. But as a wounded healer, I know the restorative value of listening, acceptance, caring, doggedness, and hope.” And so I found Dr. Myers.
These few pages in the middle of the book pulled everything else into focus. The writing opened and the rest of the book flowed. The author’s insights about physician-patients became even more insightful. It’s almost as though he was anxious about revealing himself, and his writing infused itself with this worry, so that once his secret was revealed, he was free to be genuine in a way that makes this book a gem of a read.
His insights about treating troubled physicians are invaluable. He talks of their struggles with loss, and of their flawed roles as patients.
“At the point that they become a patient these individuals may already be quite ill, and this needs to be recognized and accepted by the treating psychiatrist. Judging the doctor for so many self-defeating behaviors is unacceptable and unprofessional. I have found it best to simply accept the old adage ‘It is what it is.’ And I try my best to be patient and understanding with such difficult and interwoven issues, in that for physicians becoming a patient is a process not an event.”
Written with empathy, warmth, and vulnerability, “Becoming a Doctors’ Doctor” is a worthwhile read for any psychiatrist who treats other physicians.
Dr. Miller is coauthor of “Committed: The Battle over Involuntary Psychiatric Care” (Baltimore: Johns Hopkins University Press, 2016). She has a private practice and is assistant professor of psychiatry and behavioral sciences at Johns Hopkins, both in Baltimore. Dr. Miller has no conflicts of interest.
I started reading “Becoming a Doctors’ Doctor: A Memoir” by Michael F. Myers, MD, with high expectations and enthusiasm. Dr. Myers is a Canadian psychiatrist who has devoted his career to caring for physicians in his half-time private practice; he turns all other comers away.
This career path began in 1962 during his first year in medical school when Dr. Myers returned to his apartment after Thanksgiving break to be greeted with tragic news: One of the young men he shared the apartment with had died of suicide. The tragedy marked him – along with the silence about what had transpired – and he would later look back to realize it was the beginning of his journey to becoming a psychiatrist, one who cares for other physicians.
The book is filled with patient vignettes, gentle musings that Dr. Myers recounts with warmth, adding what he has learned from them.
There is, for example, the heart-wrenching account of “DJ,” a lonely medical student who is emergently hospitalized for depression, after the worried author anxiously drove the patient from his office to the hospital. DJ is all alone, and he writes to a friend and offers to pay for her transportation if she will come visit him in the hospital, a fact Dr. Myers knows only because he was later shown a letter DJ had written to his friend.
“He has been diminished and altered by his disease and the requisite hospital treatment, factors that we as mental health caregivers must never forget – or minimize. Visits from friends become visits of the representatives from the outside world, the link to normality, sanity, and anticipated return. These encounters are precious,” Dr. Myers writes.
As the book progressed, I began to wonder more about the author as a person. It is a memoir, so stated on the cover, but very little about his life is revealed. There are résumé-style facts: where he studied, or worked, or went to conferences, what he learned and what he spoke about, but I wanted to know more about how his experiences intertwined with his life. In the foreword, he talks about having an alcoholic mother. He tells the reader that being a husband and father was important to him, and that his conversion to Judaism – his wife’s religion – was meaningful, but there is no backstory, and I was looking for more. A quick reference is made to visiting a therapist, but those few sentences are the total of what I knew about Michael Myers midway through his memoir.
I looked for a photo of the author. I found it at the back of the book with a brief biography beneath it, ending with the fact that he lives with his husband. I had gotten halfway through the memoir, including chapters about how Myers had treated gay physicians, gay couples, and physicians with AIDS, and yet there was no mention of his husband, and how his sexual orientation influenced these encounters. I didn’t quite know what to think.
And then, in a section called “Getting Personal,” suddenly the tone of the book changed. Dr. Myers talked about his own sexual confusion as a young man and about the decision to marry a woman, knowing he was bisexual. He wrote about the shame he felt concerning his sexual desires at a time when homosexuality was still classified as a psychiatric disorder, the fear of judgment, and the sense that this – his ninth book – was his first genuine book.
“And so, I come full circle. It is my otherness that fundamentally – but not with full awareness – attracted me to psychiatry, and ultimately to becoming a doctors’ doctor. I’ve been able to empathize with my doctor patients’ burden with the scourge of mental illness, coping with brokenness, and struggling for acceptance and belonging in a profession of perfection and stature. And I understand what it’s like to feel a bit of a misfit, less than, unclean and tattered. But as a wounded healer, I know the restorative value of listening, acceptance, caring, doggedness, and hope.” And so I found Dr. Myers.
These few pages in the middle of the book pulled everything else into focus. The writing opened and the rest of the book flowed. The author’s insights about physician-patients became even more insightful. It’s almost as though he was anxious about revealing himself, and his writing infused itself with this worry, so that once his secret was revealed, he was free to be genuine in a way that makes this book a gem of a read.
His insights about treating troubled physicians are invaluable. He talks of their struggles with loss, and of their flawed roles as patients.
“At the point that they become a patient these individuals may already be quite ill, and this needs to be recognized and accepted by the treating psychiatrist. Judging the doctor for so many self-defeating behaviors is unacceptable and unprofessional. I have found it best to simply accept the old adage ‘It is what it is.’ And I try my best to be patient and understanding with such difficult and interwoven issues, in that for physicians becoming a patient is a process not an event.”
Written with empathy, warmth, and vulnerability, “Becoming a Doctors’ Doctor” is a worthwhile read for any psychiatrist who treats other physicians.
Dr. Miller is coauthor of “Committed: The Battle over Involuntary Psychiatric Care” (Baltimore: Johns Hopkins University Press, 2016). She has a private practice and is assistant professor of psychiatry and behavioral sciences at Johns Hopkins, both in Baltimore. Dr. Miller has no conflicts of interest.
Mental health illness needs appropriate care
The January 2021 issue of JAMA Neurology had an article that stated that the current U.S. spending on emergency room (ER) and inpatient costs for patients with functional neurological disorders is $1.2 billion and climbing. That doesn’t include, obviously, the costs of treating functional disorders in other specialties.

Now, $1.2 billion is a pittance when you compare it with, say, the total costs of Alzheimer’s disease ($277 billion/year), but it’s still a lot of money. Especially when you consider that, unlike Alzheimer’s disease, a lot of the spending associated with functional disorders is avoidable.
The problem is that getting good psychiatric care isn’t easy, and that’s what many of these people really need. A lot of psychiatrists, including the excellent one my son sees, don’t take insurance. We’re fortunate to be able to pay for the visits, but most people aren’t. So the psychiatrists and mental health professionals who do accept insurance get rapidly overwhelmed and burned out, end up seeing their own psychiatrists, and then drop insurance plans, too.
Not only that, but insurers are willing to pay for these patients to go to ER and get labs and pricey imaging. At the same time mental health benefits are often limited or nonexistent, even when considerably less costly than the ER visits and imaging.
I don’t fault the ER doctors or hospitalists for ordering expensive tests on these patients. They often don’t know the patient and have to take them at face value. I’ve been there, too, when I’ve taken inpatient call. Someone comes in with a group of symptoms. You may be 99.999% sure they’re functional, but at the same time it’s not worth risking your medical license or malpractice premiums to just say that. Defensive medicine will always win that argument.
The trouble is that ER, and the inpatient setting, are often the worst possible places to be managing functional disorders. This is really a case where a stitch in time saves nine. The cost of their getting appropriate care to prevent underlying issues from driving them to ER is going to be less than the inevitable visit when they don’t.
That’s not to say these people might have a legitimate medical issue that should be evaluated – sometimes urgently. But once that’s off the table repeated ER visits and testing quickly become an exercise in futility and diminishing returns.
Many health care system payers need to recognize that, so these people can be treated appropriately from the beginning, and not end up shuttling between ERs, looking for an answer and help they aren’t equipped to provide at a cost that’s not sustainable.
Dr. Block has a solo neurology practice in Scottsdale, Ariz.
The January 2021 issue of JAMA Neurology had an article that stated that the current U.S. spending on emergency room (ER) and inpatient costs for patients with functional neurological disorders is $1.2 billion and climbing. That doesn’t include, obviously, the costs of treating functional disorders in other specialties.
Now, $1.2 billion is a pittance when you compare it with, say, the total costs of Alzheimer’s disease ($277 billion/year), but it’s still a lot of money. Especially when you consider that, unlike Alzheimer’s disease, a lot of the spending associated with functional disorders is avoidable.
The problem is that getting good psychiatric care isn’t easy, and that’s what many of these people really need. A lot of psychiatrists, including the excellent one my son sees, don’t take insurance. We’re fortunate to be able to pay for the visits, but most people aren’t. So the psychiatrists and mental health professionals who do accept insurance get rapidly overwhelmed and burned out, end up seeing their own psychiatrists, and then drop insurance plans, too.
Not only that, but insurers are willing to pay for these patients to go to ER and get labs and pricey imaging. At the same time mental health benefits are often limited or nonexistent, even when considerably less costly than the ER visits and imaging.
I don’t fault the ER doctors or hospitalists for ordering expensive tests on these patients. They often don’t know the patient and have to take them at face value. I’ve been there, too, when I’ve taken inpatient call. Someone comes in with a group of symptoms. You may be 99.999% sure they’re functional, but at the same time it’s not worth risking your medical license or malpractice premiums to just say that. Defensive medicine will always win that argument.
The trouble is that ER, and the inpatient setting, are often the worst possible places to be managing functional disorders. This is really a case where a stitch in time saves nine. The cost of their getting appropriate care to prevent underlying issues from driving them to ER is going to be less than the inevitable visit when they don’t.
That’s not to say these people might have a legitimate medical issue that should be evaluated – sometimes urgently. But once that’s off the table repeated ER visits and testing quickly become an exercise in futility and diminishing returns.
Many health care system payers need to recognize that, so these people can be treated appropriately from the beginning, and not end up shuttling between ERs, looking for an answer and help they aren’t equipped to provide at a cost that’s not sustainable.
Dr. Block has a solo neurology practice in Scottsdale, Ariz.
The January 2021 issue of JAMA Neurology had an article that stated that the current U.S. spending on emergency room (ER) and inpatient costs for patients with functional neurological disorders is $1.2 billion and climbing. That doesn’t include, obviously, the costs of treating functional disorders in other specialties.
Now, $1.2 billion is a pittance when you compare it with, say, the total costs of Alzheimer’s disease ($277 billion/year), but it’s still a lot of money. Especially when you consider that, unlike Alzheimer’s disease, a lot of the spending associated with functional disorders is avoidable.
The problem is that getting good psychiatric care isn’t easy, and that’s what many of these people really need. A lot of psychiatrists, including the excellent one my son sees, don’t take insurance. We’re fortunate to be able to pay for the visits, but most people aren’t. So the psychiatrists and mental health professionals who do accept insurance get rapidly overwhelmed and burned out, end up seeing their own psychiatrists, and then drop insurance plans, too.
Not only that, but insurers are willing to pay for these patients to go to ER and get labs and pricey imaging. At the same time mental health benefits are often limited or nonexistent, even when considerably less costly than the ER visits and imaging.
I don’t fault the ER doctors or hospitalists for ordering expensive tests on these patients. They often don’t know the patient and have to take them at face value. I’ve been there, too, when I’ve taken inpatient call. Someone comes in with a group of symptoms. You may be 99.999% sure they’re functional, but at the same time it’s not worth risking your medical license or malpractice premiums to just say that. Defensive medicine will always win that argument.
The trouble is that ER, and the inpatient setting, are often the worst possible places to be managing functional disorders. This is really a case where a stitch in time saves nine. The cost of their getting appropriate care to prevent underlying issues from driving them to ER is going to be less than the inevitable visit when they don’t.
That’s not to say these people might have a legitimate medical issue that should be evaluated – sometimes urgently. But once that’s off the table repeated ER visits and testing quickly become an exercise in futility and diminishing returns.
Many health care system payers need to recognize that, so these people can be treated appropriately from the beginning, and not end up shuttling between ERs, looking for an answer and help they aren’t equipped to provide at a cost that’s not sustainable.
Dr. Block has a solo neurology practice in Scottsdale, Ariz.