User login
Bringing you the latest news, research and reviews, exclusive interviews, podcasts, quizzes, and more.
div[contains(@class, 'read-next-article')]
div[contains(@class, 'nav-primary')]
nav[contains(@class, 'nav-primary')]
section[contains(@class, 'footer-nav-section-wrapper')]
nav[contains(@class, 'nav-ce-stack nav-ce-stack__large-screen')]
header[@id='header']
div[contains(@class, 'header__large-screen')]
div[contains(@class, 'main-prefix')]
footer[@id='footer']
section[contains(@class, 'nav-hidden')]
div[contains(@class, 'ce-card-content')]
nav[contains(@class, 'nav-ce-stack')]
div[contains(@class, 'view-medstat-quiz-listing-panes')]
Moral distress: COVID-19 shortages prompt tough decisions at bedside
Choosing which hospitalized COVID-19 patients receive potentially lifesaving care, making urgent calls for ventilators and other equipment, and triaging care based on patient age and comorbidities were among the challenges revealed in new feedback from health care leaders and frontline workers.
Even though many hospitals have contingency plans for how to allocate resources and triage patient care during crisis capacity, for many providers during the real-world COVID-19 trial of these protocols, they fell short.
Many hospital crisis capacity plans, for example, were too general to address all the specific challenges arising during the pandemic, investigators report in a study published online Nov. 6 in JAMA Network Open.
“Our research shows that the types of challenges and approach to resource limitation in real-world clinical settings during the pandemic differed in practice from how we had prepared in theory,” lead author Catherine Butler, MD, told Medscape Medical News. Insufficient dialysis treatment time, staff shortages, and routine supply scarcity are examples “for which there was not an established plan or approach for appropriate allocation.”
“This left frontline clinicians to determine what constituted an acceptable standard of care and to make difficult allocation decisions at the bedside,” added Butler, acting instructor in the Division of Nephrology at the University of Washington in Seattle and a research fellow at the VA Health Services Research and Development Seattle-Denver Center of Innovation.
The investigators conducted semistructured interviews in April and May with 61 clinicians and health leaders. Mean age was 46 years, 63% were women, and participants practiced in 15 states. Most participants hailed from locations hard-hit by the pandemic at the time, including Seattle, New York City, and New Orleans.
Triage tribulations
The qualitative study included comments from respondents on three major themes that emerged: planning for crisis capacity, adapting to resource limitation, and the multiple unprecedented barriers to care delivery.
Overall, planning and support from institutional leaders varied. One provider said, “Talking to administration, and they just seemed really disengaged with the problem. We asked multiple times if there was a triage command center or a plan for what would occur if we got to the point where we had to triage resources. They said there was, but they wouldn’t provide it to us.”
Another had a more positive experience. “The biggest deal in the ethics world in the last 2 months has been preparing in case we need to triage. So, we have a very detailed, elaborate, well thought-out triage policy … that was done at the highest levels of the system.”
Clinicians said they participate on triage teams – despite the moral weight and likely emotional burden – out of a sense of duty.
Interestingly, some providers on these teams also reported a reluctance to reveal their participation to colleagues. “I didn’t feel like I should tell anybody … even some of my close friends who are physicians and nurses here … that I’ve been asked to be on this [triage team],” one respondent said. “I didn’t feel like I should make it known.”
Adapting to scarce resources
Multiple providers said they faced difficult care decisions because of limited dialysis or supply shortages. “They felt that this patient had the greatest likelihood of benefiting from most aggressive therapy. … I think there was probably like 5 or 6 patients in the ICU … and then you had this 35-year-old with no comorbidities,” one respondent said. “That’s who the ICU dialyzed, and I couldn’t really disagree.”
“I emailed all of [my colleagues], and I said ‘Help! We need X, we need CRRT [continuous renal replacement therapy] machines, we need dialysates,’ “ another responded.
“One of the attendings had a tweet when we were running out of CRRT. He had a tweet about, ‘Can anybody give us supplies for CRRT?’ So, it got to that. You do anything. You get really desperate,” the clinician said.
Other providers reported getting innovative under the circumstances. “My partner’s son, he actually borrowed a couple of 3D printers. He printed some of these face shields, and then they got the formula, or the specifics as to how to make this particular connection to connect to a dialysis machine to generate dialysate. So, he also printed some of those from the 3D printer.”
Dire situations with dialysis
Another respondent understood the focus on ventilators and ICU beds throughout the crisis, but said “no one has acknowledged that dialysis has been one of the most, if not the most, limited resources.”
Another clinician expressed surprise at a decision made in the face of limited availability of traditional dialysis. “A month ago, people said we were going to do acute peritoneal dialysis [PD]. And I said, ‘No, we’re not going to do acute PD. PD, it’s not that great for acute patients, sick people in the ICUs. I don’t think we’re going to do PD.’
“Three days later we were doing acute PD. I mean, that was unbelievable!”
Some institutions rationed dialysis therapy. “We went through the entire list at the beginning of the week and [said], this person has to dialyze these days, this person would probably benefit from a dialysis session, a third group person we could probably just string along and medically manage if we needed to,” one provider said.
Another respondent reported a different strategy. “No one was not getting dialysis, but there were a lot of people getting minimal dialysis. Even though people were getting treated, resources were very stretched.”
Changing family dynamics
COVID-19 has naturally changed how clinicians speak with families. One respondent recalled looking at the ICU physician and being like, ‘Have you talked to the son this week?’ And she’s like, ‘Oh my God, no. … Did you talk to the son?’ I’m like, ‘Oh my God, no.’ “
They realized, the respondent added, “that none of us had called the family because it’s just not in your workflow. You’re so used to the family being there.”
Multiple providers also feared a conversation with family regarding necessary changes to care given the limitation of resources during the pandemic.
“Most families have been actually very understanding. This is a crisis, and we’re in a pandemic, and we’re all doing things we wouldn’t normally do.”
Another respondent said, “We were pretty honest about how resources were limited and how we were doing with this COVID-19 surge. And I think we talked about how the usual ability to provide aggressive dialysis was not the case with COVID-19. There was a lot of understanding, sometimes to my surprise. I would think people would be more upset when hearing something like that.”
Many clinicians facing these challenges experience moral distress, the researchers noted.
“Early in the pandemic, it became quickly apparent that possible resource limitation, such as scarce ventilators, was a major ethical concern. There was robust debate and discussion published in medical journals and the popular press about how to appropriately allocate health care resources,” the University of Washington’s Butler said.
“Transparency, accountability, and standardized processes for rationing these resources in ‘crisis capacity’ settings were seen as key to avoiding the impact of implicit bias and moral distress for clinicians,” she added.
Lessons learned
In terms of potential solutions that could mitigate these challenges in the future, health care leaders “could develop standardized protocols or guidelines for allocating a broader range of potentially scarce health care resources even before ‘crisis capacity’ is declared,” Butler said.
Furthermore, no frontline worker should have to go it alone. “Medical ethicists and/or other clinicians familiar with ethical considerations in settings of scarce health care resources might provide bedside consultation and collaborate with frontline providers who must grapple with the impact of more subtle forms of resource limitation on clinical decision-making.”
The study was partially funded by grants from the National Institute of Diabetes and Digestive and Kidney Diseases and a COVID-19 Research Award from the University of Washington Institute of Translational Health Sciences given to Butler.
This article first appeared on Medscape.com.
Choosing which hospitalized COVID-19 patients receive potentially lifesaving care, making urgent calls for ventilators and other equipment, and triaging care based on patient age and comorbidities were among the challenges revealed in new feedback from health care leaders and frontline workers.
Even though many hospitals have contingency plans for how to allocate resources and triage patient care during crisis capacity, for many providers during the real-world COVID-19 trial of these protocols, they fell short.
Many hospital crisis capacity plans, for example, were too general to address all the specific challenges arising during the pandemic, investigators report in a study published online Nov. 6 in JAMA Network Open.
“Our research shows that the types of challenges and approach to resource limitation in real-world clinical settings during the pandemic differed in practice from how we had prepared in theory,” lead author Catherine Butler, MD, told Medscape Medical News. Insufficient dialysis treatment time, staff shortages, and routine supply scarcity are examples “for which there was not an established plan or approach for appropriate allocation.”
“This left frontline clinicians to determine what constituted an acceptable standard of care and to make difficult allocation decisions at the bedside,” added Butler, acting instructor in the Division of Nephrology at the University of Washington in Seattle and a research fellow at the VA Health Services Research and Development Seattle-Denver Center of Innovation.
The investigators conducted semistructured interviews in April and May with 61 clinicians and health leaders. Mean age was 46 years, 63% were women, and participants practiced in 15 states. Most participants hailed from locations hard-hit by the pandemic at the time, including Seattle, New York City, and New Orleans.
Triage tribulations
The qualitative study included comments from respondents on three major themes that emerged: planning for crisis capacity, adapting to resource limitation, and the multiple unprecedented barriers to care delivery.
Overall, planning and support from institutional leaders varied. One provider said, “Talking to administration, and they just seemed really disengaged with the problem. We asked multiple times if there was a triage command center or a plan for what would occur if we got to the point where we had to triage resources. They said there was, but they wouldn’t provide it to us.”
Another had a more positive experience. “The biggest deal in the ethics world in the last 2 months has been preparing in case we need to triage. So, we have a very detailed, elaborate, well thought-out triage policy … that was done at the highest levels of the system.”
Clinicians said they participate on triage teams – despite the moral weight and likely emotional burden – out of a sense of duty.
Interestingly, some providers on these teams also reported a reluctance to reveal their participation to colleagues. “I didn’t feel like I should tell anybody … even some of my close friends who are physicians and nurses here … that I’ve been asked to be on this [triage team],” one respondent said. “I didn’t feel like I should make it known.”
Adapting to scarce resources
Multiple providers said they faced difficult care decisions because of limited dialysis or supply shortages. “They felt that this patient had the greatest likelihood of benefiting from most aggressive therapy. … I think there was probably like 5 or 6 patients in the ICU … and then you had this 35-year-old with no comorbidities,” one respondent said. “That’s who the ICU dialyzed, and I couldn’t really disagree.”
“I emailed all of [my colleagues], and I said ‘Help! We need X, we need CRRT [continuous renal replacement therapy] machines, we need dialysates,’ “ another responded.
“One of the attendings had a tweet when we were running out of CRRT. He had a tweet about, ‘Can anybody give us supplies for CRRT?’ So, it got to that. You do anything. You get really desperate,” the clinician said.
Other providers reported getting innovative under the circumstances. “My partner’s son, he actually borrowed a couple of 3D printers. He printed some of these face shields, and then they got the formula, or the specifics as to how to make this particular connection to connect to a dialysis machine to generate dialysate. So, he also printed some of those from the 3D printer.”
Dire situations with dialysis
Another respondent understood the focus on ventilators and ICU beds throughout the crisis, but said “no one has acknowledged that dialysis has been one of the most, if not the most, limited resources.”
Another clinician expressed surprise at a decision made in the face of limited availability of traditional dialysis. “A month ago, people said we were going to do acute peritoneal dialysis [PD]. And I said, ‘No, we’re not going to do acute PD. PD, it’s not that great for acute patients, sick people in the ICUs. I don’t think we’re going to do PD.’
“Three days later we were doing acute PD. I mean, that was unbelievable!”
Some institutions rationed dialysis therapy. “We went through the entire list at the beginning of the week and [said], this person has to dialyze these days, this person would probably benefit from a dialysis session, a third group person we could probably just string along and medically manage if we needed to,” one provider said.
Another respondent reported a different strategy. “No one was not getting dialysis, but there were a lot of people getting minimal dialysis. Even though people were getting treated, resources were very stretched.”
Changing family dynamics
COVID-19 has naturally changed how clinicians speak with families. One respondent recalled looking at the ICU physician and being like, ‘Have you talked to the son this week?’ And she’s like, ‘Oh my God, no. … Did you talk to the son?’ I’m like, ‘Oh my God, no.’ “
They realized, the respondent added, “that none of us had called the family because it’s just not in your workflow. You’re so used to the family being there.”
Multiple providers also feared a conversation with family regarding necessary changes to care given the limitation of resources during the pandemic.
“Most families have been actually very understanding. This is a crisis, and we’re in a pandemic, and we’re all doing things we wouldn’t normally do.”
Another respondent said, “We were pretty honest about how resources were limited and how we were doing with this COVID-19 surge. And I think we talked about how the usual ability to provide aggressive dialysis was not the case with COVID-19. There was a lot of understanding, sometimes to my surprise. I would think people would be more upset when hearing something like that.”
Many clinicians facing these challenges experience moral distress, the researchers noted.
“Early in the pandemic, it became quickly apparent that possible resource limitation, such as scarce ventilators, was a major ethical concern. There was robust debate and discussion published in medical journals and the popular press about how to appropriately allocate health care resources,” the University of Washington’s Butler said.
“Transparency, accountability, and standardized processes for rationing these resources in ‘crisis capacity’ settings were seen as key to avoiding the impact of implicit bias and moral distress for clinicians,” she added.
Lessons learned
In terms of potential solutions that could mitigate these challenges in the future, health care leaders “could develop standardized protocols or guidelines for allocating a broader range of potentially scarce health care resources even before ‘crisis capacity’ is declared,” Butler said.
Furthermore, no frontline worker should have to go it alone. “Medical ethicists and/or other clinicians familiar with ethical considerations in settings of scarce health care resources might provide bedside consultation and collaborate with frontline providers who must grapple with the impact of more subtle forms of resource limitation on clinical decision-making.”
The study was partially funded by grants from the National Institute of Diabetes and Digestive and Kidney Diseases and a COVID-19 Research Award from the University of Washington Institute of Translational Health Sciences given to Butler.
This article first appeared on Medscape.com.
Choosing which hospitalized COVID-19 patients receive potentially lifesaving care, making urgent calls for ventilators and other equipment, and triaging care based on patient age and comorbidities were among the challenges revealed in new feedback from health care leaders and frontline workers.
Even though many hospitals have contingency plans for how to allocate resources and triage patient care during crisis capacity, for many providers during the real-world COVID-19 trial of these protocols, they fell short.
Many hospital crisis capacity plans, for example, were too general to address all the specific challenges arising during the pandemic, investigators report in a study published online Nov. 6 in JAMA Network Open.
“Our research shows that the types of challenges and approach to resource limitation in real-world clinical settings during the pandemic differed in practice from how we had prepared in theory,” lead author Catherine Butler, MD, told Medscape Medical News. Insufficient dialysis treatment time, staff shortages, and routine supply scarcity are examples “for which there was not an established plan or approach for appropriate allocation.”
“This left frontline clinicians to determine what constituted an acceptable standard of care and to make difficult allocation decisions at the bedside,” added Butler, acting instructor in the Division of Nephrology at the University of Washington in Seattle and a research fellow at the VA Health Services Research and Development Seattle-Denver Center of Innovation.
The investigators conducted semistructured interviews in April and May with 61 clinicians and health leaders. Mean age was 46 years, 63% were women, and participants practiced in 15 states. Most participants hailed from locations hard-hit by the pandemic at the time, including Seattle, New York City, and New Orleans.
Triage tribulations
The qualitative study included comments from respondents on three major themes that emerged: planning for crisis capacity, adapting to resource limitation, and the multiple unprecedented barriers to care delivery.
Overall, planning and support from institutional leaders varied. One provider said, “Talking to administration, and they just seemed really disengaged with the problem. We asked multiple times if there was a triage command center or a plan for what would occur if we got to the point where we had to triage resources. They said there was, but they wouldn’t provide it to us.”
Another had a more positive experience. “The biggest deal in the ethics world in the last 2 months has been preparing in case we need to triage. So, we have a very detailed, elaborate, well thought-out triage policy … that was done at the highest levels of the system.”
Clinicians said they participate on triage teams – despite the moral weight and likely emotional burden – out of a sense of duty.
Interestingly, some providers on these teams also reported a reluctance to reveal their participation to colleagues. “I didn’t feel like I should tell anybody … even some of my close friends who are physicians and nurses here … that I’ve been asked to be on this [triage team],” one respondent said. “I didn’t feel like I should make it known.”
Adapting to scarce resources
Multiple providers said they faced difficult care decisions because of limited dialysis or supply shortages. “They felt that this patient had the greatest likelihood of benefiting from most aggressive therapy. … I think there was probably like 5 or 6 patients in the ICU … and then you had this 35-year-old with no comorbidities,” one respondent said. “That’s who the ICU dialyzed, and I couldn’t really disagree.”
“I emailed all of [my colleagues], and I said ‘Help! We need X, we need CRRT [continuous renal replacement therapy] machines, we need dialysates,’ “ another responded.
“One of the attendings had a tweet when we were running out of CRRT. He had a tweet about, ‘Can anybody give us supplies for CRRT?’ So, it got to that. You do anything. You get really desperate,” the clinician said.
Other providers reported getting innovative under the circumstances. “My partner’s son, he actually borrowed a couple of 3D printers. He printed some of these face shields, and then they got the formula, or the specifics as to how to make this particular connection to connect to a dialysis machine to generate dialysate. So, he also printed some of those from the 3D printer.”
Dire situations with dialysis
Another respondent understood the focus on ventilators and ICU beds throughout the crisis, but said “no one has acknowledged that dialysis has been one of the most, if not the most, limited resources.”
Another clinician expressed surprise at a decision made in the face of limited availability of traditional dialysis. “A month ago, people said we were going to do acute peritoneal dialysis [PD]. And I said, ‘No, we’re not going to do acute PD. PD, it’s not that great for acute patients, sick people in the ICUs. I don’t think we’re going to do PD.’
“Three days later we were doing acute PD. I mean, that was unbelievable!”
Some institutions rationed dialysis therapy. “We went through the entire list at the beginning of the week and [said], this person has to dialyze these days, this person would probably benefit from a dialysis session, a third group person we could probably just string along and medically manage if we needed to,” one provider said.
Another respondent reported a different strategy. “No one was not getting dialysis, but there were a lot of people getting minimal dialysis. Even though people were getting treated, resources were very stretched.”
Changing family dynamics
COVID-19 has naturally changed how clinicians speak with families. One respondent recalled looking at the ICU physician and being like, ‘Have you talked to the son this week?’ And she’s like, ‘Oh my God, no. … Did you talk to the son?’ I’m like, ‘Oh my God, no.’ “
They realized, the respondent added, “that none of us had called the family because it’s just not in your workflow. You’re so used to the family being there.”
Multiple providers also feared a conversation with family regarding necessary changes to care given the limitation of resources during the pandemic.
“Most families have been actually very understanding. This is a crisis, and we’re in a pandemic, and we’re all doing things we wouldn’t normally do.”
Another respondent said, “We were pretty honest about how resources were limited and how we were doing with this COVID-19 surge. And I think we talked about how the usual ability to provide aggressive dialysis was not the case with COVID-19. There was a lot of understanding, sometimes to my surprise. I would think people would be more upset when hearing something like that.”
Many clinicians facing these challenges experience moral distress, the researchers noted.
“Early in the pandemic, it became quickly apparent that possible resource limitation, such as scarce ventilators, was a major ethical concern. There was robust debate and discussion published in medical journals and the popular press about how to appropriately allocate health care resources,” the University of Washington’s Butler said.
“Transparency, accountability, and standardized processes for rationing these resources in ‘crisis capacity’ settings were seen as key to avoiding the impact of implicit bias and moral distress for clinicians,” she added.
Lessons learned
In terms of potential solutions that could mitigate these challenges in the future, health care leaders “could develop standardized protocols or guidelines for allocating a broader range of potentially scarce health care resources even before ‘crisis capacity’ is declared,” Butler said.
Furthermore, no frontline worker should have to go it alone. “Medical ethicists and/or other clinicians familiar with ethical considerations in settings of scarce health care resources might provide bedside consultation and collaborate with frontline providers who must grapple with the impact of more subtle forms of resource limitation on clinical decision-making.”
The study was partially funded by grants from the National Institute of Diabetes and Digestive and Kidney Diseases and a COVID-19 Research Award from the University of Washington Institute of Translational Health Sciences given to Butler.
This article first appeared on Medscape.com.
What happened to melanoma care during COVID-19 sequestration
Initial evidence suggests that the , Rebecca I. Hartman, MD, MPH, said at a virtual forum on cutaneous malignancies jointly presented by Postgraduate Institute for Medicine and Global Academy for Medication Education.

This is not what National Comprehensive Cancer Network officials expected when they issued short-term recommendations on how to manage cutaneous melanoma during the first wave of the COVID-19 pandemic. Those recommendations for restriction of care, which Dr. Hartman characterized as “pretty significant changes from how we typically practice melanoma care in the U.S.,” came at a time when there was justifiable concern that the first COVID-19 surge would strain the U.S. health care system beyond the breaking point.
The rationale given for the NCCN recommendations was that most time-to-treat studies have shown no adverse patient outcomes for 90-day delays in treatment, even for thicker melanomas. But those studies, all retrospective, have been called into question. And the first real-world data on the impact of care restrictions during the lockdown, reported by Italian dermatologists, highlights adverse effects with potentially far-reaching consequences, noted Dr. Hartman, director of melanoma epidemiology at Brigham and Women’s Hospital and a dermatologist, Harvard University, Boston.
Analysis of the impact of lockdown-induced delays in melanoma care is not merely an academic exercise, she added. While everyone hopes that the spring 2020 COVID-19 shelter-in-place was a once-in-a-lifetime event, there’s no guarantee that will be the case. Moreover, the lockdown provides a natural experiment addressing the possible consequences of melanoma care delays on patient outcomes, a topic that for ethical reasons could never be addressed in a randomized trial.
The short-term NCCN recommendations included the use of excisional biopsies for melanoma diagnosis whenever possible; and delay of up to 3 months for wide local excision of in situ melanoma, any invasive melanoma with negative margins, and even T1 melanomas with positive margins provided the bulk of the lesion had been excised. The guidance also suggested delaying sentinel lymph node biopsy (SLNB), along with increased use of neoadjuvant therapy in patients with clinically palpable regional lymph nodes in order to delay surgery for up to 8 weeks. Single-agent systemic therapy at the least-frequent dosing was advised in order to minimize toxicity and reduce the need for additional health care resources: for example, nivolumab (Opdivo) at 480 mg every 4 weeks instead of every 2 weeks, and pembrolizumab (Keytruda) at 400 mg every 6 weeks, rather than every 3 weeks.
So, that’s what the NCCN recommended. Here’s what actually happened during shelter-in-place as captured in Dr. Hartman’s survey of 18 U.S. members of the Melanoma Prevention Working Group, all practicing dermatology in centers particularly hard-hit in the first wave of the pandemic: In-person new melanoma patient visits plunged from an average of 4.83 per week per provider to 0.83 per week. Telemedicine visits with new melanoma patients went from zero prepandemic to 0.67 visits per week per provider, which doesn’t come close to making up for the drop in in-person visits. Interestingly, two respondents reported turning to gene-expression profile testing for patient prognostication because of delays in SLNB.
Wide local excision was delayed by an average of 6 weeks in roughly one-third of melanoma patients with early tumor stage disease, regardless of margin status. For patients with stage T1b disease, wide local excision was typically performed on time during shelter-in-place; however, SLNB was delayed by an average of 5 weeks in 22% of patients with positive margins and 28% of those with negative margins. In contrast, 80% of patients with more advanced T2-T4 melanoma underwent on-schedule definitive management with wide local excision and SLNB, Dr. Hartman reported.
Critics have taken issue with the NCCN’s conclusion that most time-to-treatment studies show no harm arising from 90-day treatment delays. A review of the relevant published literature by Dr. Hartman’s Harvard colleagues, published in July, found that the evidence is mixed. “There is insufficient evidence to definitively conclude that delayed wide resection after gross removal of the primary melanoma is without harm,” they concluded in the review.
Spanish dermatologists performed a modeling study in order to estimate the potential impact of COVID-19 lockdowns on 5- and 10-year survival of melanoma patients. Using the growth rate of a random sample of 1,000 melanomas to model estimates of tumor thickness after various delays, coupled with American Joint Committee on Cancer survival data for different T stages, they estimated that 5-year survival would be reduced from 94.2% to 92.3% with a 90-day delay in diagnosis, and that 10-year survival would drop from 90.0% to 87.6%.
But that’s merely modeling. Francesco Ricci, MD, PhD, and colleagues from the melanoma unit at the Istituto Dermopatico dell’Immacolata, Rome, have provided a first look at the real-world impact of the lockdown. In the prelockdown period of January through March 9th, 2020, the referral center averaged 2.3 new melanoma diagnoses per day. During the Rome lockdown, from March 10th through May 3rd, this figure dropped to a mean of 0.6 melanoma diagnoses per day. Postlockdown, from May 4th to June 6th, the average climbed to 1.3 per day. The rate of newly diagnosed nodular melanoma was 5.5-fold greater postlockdown, compared with prelockdown; the rate of ulcerated melanoma was 4.9-fold greater.
“We can hypothesize that this may have been due to delays in diagnosis and care,” Dr. Hartman commented. “This is important because we know that nodular melanoma as well as ulceration tend to have a worse prognosis in terms of mortality.”
The mean Breslow thickness of newly diagnosed melanomas was 0.88 mm prelockdown, 0.66 mm during lockdown, and 1.96 mm postlockdown. The investigators speculated that the reduced Breslow thickness of melanomas diagnosed during lockdown might be explained by a greater willingness of more health-conscious people to defy the shelter-in-place instructions because of their concern about a suspicious skin lesion. “Though it is way too early to gauge the consequences of such diagnostic delay, should this issue be neglected, dermatologists and their patients may pay a higher price later with increased morbidity, mortality, and financial burden,” according to the investigators.
Dr. Hartman observed that it will be important to learn whether similar experiences occurred elsewhere during lockdown.

Another speaker, John M. Kirkwood, MD, said he has seen several melanoma patients referred from outside centers who had delays of up to 3 months in sentinel lymph node management of T2 and T3 tumors during lockdown who now have widespread metastatic disease.
“Now, is that anecdotal? I don’t know, it’s just worrisome to me,” commented Dr. Kirkwood, professor of medicine, dermatology, and translational science at the University of Pittsburgh.
Merrick Ross, MD, professor of surgical oncology at M.D. Anderson Cancer Center, Houston, recalled, “There was a period of time [during the lockdown] when we weren’t allowed to do certain elective procedures, if you want to call cancer surgery elective.”

“It’s too soon to talk about outcomes because a lot of patients are still in the process of being treated after what I would consider a significant delay in diagnosis,” the surgeon added.
An audience member asked if there will be an opportunity to see data on the damage done by delaying melanoma management as compared to lives saved through the lockdown for COVID-19. Dr. Ross replied that M.D. Anderson is in the midst of an institution-wide study analyzing the delay in diagnosis of a range of cancers.
“In our melanoma center it is absolutely clear, although we’re still collecting data, that the median tumor thickness is much higher since the lockdown,” Dr. Ross commented.
Dr. Hartman said she and her coinvestigators in the Melanoma Prevention Working Group are attempting to tally up the damage done via the lockdown by delaying melanoma diagnosis and treatment. But she agreed with the questioner that the most important thing is overall net lives saved through shelter-in-place.
“I’m sure that, separately, nondermatologists – perhaps infectious disease doctors and internists – are looking at how many lives were saved by the lockdown policy. So I do think all that data will come out,” Dr. Hartman predicted.
She reported having no financial conflicts regarding her presentation.
Global Academy for Medical Education and this news organization are owned by the same company.
SOURCE: Hartman, R. Cutaneous malignancies forum.
Initial evidence suggests that the , Rebecca I. Hartman, MD, MPH, said at a virtual forum on cutaneous malignancies jointly presented by Postgraduate Institute for Medicine and Global Academy for Medication Education.
This is not what National Comprehensive Cancer Network officials expected when they issued short-term recommendations on how to manage cutaneous melanoma during the first wave of the COVID-19 pandemic. Those recommendations for restriction of care, which Dr. Hartman characterized as “pretty significant changes from how we typically practice melanoma care in the U.S.,” came at a time when there was justifiable concern that the first COVID-19 surge would strain the U.S. health care system beyond the breaking point.
The rationale given for the NCCN recommendations was that most time-to-treat studies have shown no adverse patient outcomes for 90-day delays in treatment, even for thicker melanomas. But those studies, all retrospective, have been called into question. And the first real-world data on the impact of care restrictions during the lockdown, reported by Italian dermatologists, highlights adverse effects with potentially far-reaching consequences, noted Dr. Hartman, director of melanoma epidemiology at Brigham and Women’s Hospital and a dermatologist, Harvard University, Boston.
Analysis of the impact of lockdown-induced delays in melanoma care is not merely an academic exercise, she added. While everyone hopes that the spring 2020 COVID-19 shelter-in-place was a once-in-a-lifetime event, there’s no guarantee that will be the case. Moreover, the lockdown provides a natural experiment addressing the possible consequences of melanoma care delays on patient outcomes, a topic that for ethical reasons could never be addressed in a randomized trial.
The short-term NCCN recommendations included the use of excisional biopsies for melanoma diagnosis whenever possible; and delay of up to 3 months for wide local excision of in situ melanoma, any invasive melanoma with negative margins, and even T1 melanomas with positive margins provided the bulk of the lesion had been excised. The guidance also suggested delaying sentinel lymph node biopsy (SLNB), along with increased use of neoadjuvant therapy in patients with clinically palpable regional lymph nodes in order to delay surgery for up to 8 weeks. Single-agent systemic therapy at the least-frequent dosing was advised in order to minimize toxicity and reduce the need for additional health care resources: for example, nivolumab (Opdivo) at 480 mg every 4 weeks instead of every 2 weeks, and pembrolizumab (Keytruda) at 400 mg every 6 weeks, rather than every 3 weeks.
So, that’s what the NCCN recommended. Here’s what actually happened during shelter-in-place as captured in Dr. Hartman’s survey of 18 U.S. members of the Melanoma Prevention Working Group, all practicing dermatology in centers particularly hard-hit in the first wave of the pandemic: In-person new melanoma patient visits plunged from an average of 4.83 per week per provider to 0.83 per week. Telemedicine visits with new melanoma patients went from zero prepandemic to 0.67 visits per week per provider, which doesn’t come close to making up for the drop in in-person visits. Interestingly, two respondents reported turning to gene-expression profile testing for patient prognostication because of delays in SLNB.
Wide local excision was delayed by an average of 6 weeks in roughly one-third of melanoma patients with early tumor stage disease, regardless of margin status. For patients with stage T1b disease, wide local excision was typically performed on time during shelter-in-place; however, SLNB was delayed by an average of 5 weeks in 22% of patients with positive margins and 28% of those with negative margins. In contrast, 80% of patients with more advanced T2-T4 melanoma underwent on-schedule definitive management with wide local excision and SLNB, Dr. Hartman reported.
Critics have taken issue with the NCCN’s conclusion that most time-to-treatment studies show no harm arising from 90-day treatment delays. A review of the relevant published literature by Dr. Hartman’s Harvard colleagues, published in July, found that the evidence is mixed. “There is insufficient evidence to definitively conclude that delayed wide resection after gross removal of the primary melanoma is without harm,” they concluded in the review.
Spanish dermatologists performed a modeling study in order to estimate the potential impact of COVID-19 lockdowns on 5- and 10-year survival of melanoma patients. Using the growth rate of a random sample of 1,000 melanomas to model estimates of tumor thickness after various delays, coupled with American Joint Committee on Cancer survival data for different T stages, they estimated that 5-year survival would be reduced from 94.2% to 92.3% with a 90-day delay in diagnosis, and that 10-year survival would drop from 90.0% to 87.6%.
But that’s merely modeling. Francesco Ricci, MD, PhD, and colleagues from the melanoma unit at the Istituto Dermopatico dell’Immacolata, Rome, have provided a first look at the real-world impact of the lockdown. In the prelockdown period of January through March 9th, 2020, the referral center averaged 2.3 new melanoma diagnoses per day. During the Rome lockdown, from March 10th through May 3rd, this figure dropped to a mean of 0.6 melanoma diagnoses per day. Postlockdown, from May 4th to June 6th, the average climbed to 1.3 per day. The rate of newly diagnosed nodular melanoma was 5.5-fold greater postlockdown, compared with prelockdown; the rate of ulcerated melanoma was 4.9-fold greater.
“We can hypothesize that this may have been due to delays in diagnosis and care,” Dr. Hartman commented. “This is important because we know that nodular melanoma as well as ulceration tend to have a worse prognosis in terms of mortality.”
The mean Breslow thickness of newly diagnosed melanomas was 0.88 mm prelockdown, 0.66 mm during lockdown, and 1.96 mm postlockdown. The investigators speculated that the reduced Breslow thickness of melanomas diagnosed during lockdown might be explained by a greater willingness of more health-conscious people to defy the shelter-in-place instructions because of their concern about a suspicious skin lesion. “Though it is way too early to gauge the consequences of such diagnostic delay, should this issue be neglected, dermatologists and their patients may pay a higher price later with increased morbidity, mortality, and financial burden,” according to the investigators.
Dr. Hartman observed that it will be important to learn whether similar experiences occurred elsewhere during lockdown.
Another speaker, John M. Kirkwood, MD, said he has seen several melanoma patients referred from outside centers who had delays of up to 3 months in sentinel lymph node management of T2 and T3 tumors during lockdown who now have widespread metastatic disease.
“Now, is that anecdotal? I don’t know, it’s just worrisome to me,” commented Dr. Kirkwood, professor of medicine, dermatology, and translational science at the University of Pittsburgh.
Merrick Ross, MD, professor of surgical oncology at M.D. Anderson Cancer Center, Houston, recalled, “There was a period of time [during the lockdown] when we weren’t allowed to do certain elective procedures, if you want to call cancer surgery elective.”
“It’s too soon to talk about outcomes because a lot of patients are still in the process of being treated after what I would consider a significant delay in diagnosis,” the surgeon added.
An audience member asked if there will be an opportunity to see data on the damage done by delaying melanoma management as compared to lives saved through the lockdown for COVID-19. Dr. Ross replied that M.D. Anderson is in the midst of an institution-wide study analyzing the delay in diagnosis of a range of cancers.
“In our melanoma center it is absolutely clear, although we’re still collecting data, that the median tumor thickness is much higher since the lockdown,” Dr. Ross commented.
Dr. Hartman said she and her coinvestigators in the Melanoma Prevention Working Group are attempting to tally up the damage done via the lockdown by delaying melanoma diagnosis and treatment. But she agreed with the questioner that the most important thing is overall net lives saved through shelter-in-place.
“I’m sure that, separately, nondermatologists – perhaps infectious disease doctors and internists – are looking at how many lives were saved by the lockdown policy. So I do think all that data will come out,” Dr. Hartman predicted.
She reported having no financial conflicts regarding her presentation.
Global Academy for Medical Education and this news organization are owned by the same company.
SOURCE: Hartman, R. Cutaneous malignancies forum.
Initial evidence suggests that the , Rebecca I. Hartman, MD, MPH, said at a virtual forum on cutaneous malignancies jointly presented by Postgraduate Institute for Medicine and Global Academy for Medication Education.
This is not what National Comprehensive Cancer Network officials expected when they issued short-term recommendations on how to manage cutaneous melanoma during the first wave of the COVID-19 pandemic. Those recommendations for restriction of care, which Dr. Hartman characterized as “pretty significant changes from how we typically practice melanoma care in the U.S.,” came at a time when there was justifiable concern that the first COVID-19 surge would strain the U.S. health care system beyond the breaking point.
The rationale given for the NCCN recommendations was that most time-to-treat studies have shown no adverse patient outcomes for 90-day delays in treatment, even for thicker melanomas. But those studies, all retrospective, have been called into question. And the first real-world data on the impact of care restrictions during the lockdown, reported by Italian dermatologists, highlights adverse effects with potentially far-reaching consequences, noted Dr. Hartman, director of melanoma epidemiology at Brigham and Women’s Hospital and a dermatologist, Harvard University, Boston.
Analysis of the impact of lockdown-induced delays in melanoma care is not merely an academic exercise, she added. While everyone hopes that the spring 2020 COVID-19 shelter-in-place was a once-in-a-lifetime event, there’s no guarantee that will be the case. Moreover, the lockdown provides a natural experiment addressing the possible consequences of melanoma care delays on patient outcomes, a topic that for ethical reasons could never be addressed in a randomized trial.
The short-term NCCN recommendations included the use of excisional biopsies for melanoma diagnosis whenever possible; and delay of up to 3 months for wide local excision of in situ melanoma, any invasive melanoma with negative margins, and even T1 melanomas with positive margins provided the bulk of the lesion had been excised. The guidance also suggested delaying sentinel lymph node biopsy (SLNB), along with increased use of neoadjuvant therapy in patients with clinically palpable regional lymph nodes in order to delay surgery for up to 8 weeks. Single-agent systemic therapy at the least-frequent dosing was advised in order to minimize toxicity and reduce the need for additional health care resources: for example, nivolumab (Opdivo) at 480 mg every 4 weeks instead of every 2 weeks, and pembrolizumab (Keytruda) at 400 mg every 6 weeks, rather than every 3 weeks.
So, that’s what the NCCN recommended. Here’s what actually happened during shelter-in-place as captured in Dr. Hartman’s survey of 18 U.S. members of the Melanoma Prevention Working Group, all practicing dermatology in centers particularly hard-hit in the first wave of the pandemic: In-person new melanoma patient visits plunged from an average of 4.83 per week per provider to 0.83 per week. Telemedicine visits with new melanoma patients went from zero prepandemic to 0.67 visits per week per provider, which doesn’t come close to making up for the drop in in-person visits. Interestingly, two respondents reported turning to gene-expression profile testing for patient prognostication because of delays in SLNB.
Wide local excision was delayed by an average of 6 weeks in roughly one-third of melanoma patients with early tumor stage disease, regardless of margin status. For patients with stage T1b disease, wide local excision was typically performed on time during shelter-in-place; however, SLNB was delayed by an average of 5 weeks in 22% of patients with positive margins and 28% of those with negative margins. In contrast, 80% of patients with more advanced T2-T4 melanoma underwent on-schedule definitive management with wide local excision and SLNB, Dr. Hartman reported.
Critics have taken issue with the NCCN’s conclusion that most time-to-treatment studies show no harm arising from 90-day treatment delays. A review of the relevant published literature by Dr. Hartman’s Harvard colleagues, published in July, found that the evidence is mixed. “There is insufficient evidence to definitively conclude that delayed wide resection after gross removal of the primary melanoma is without harm,” they concluded in the review.
Spanish dermatologists performed a modeling study in order to estimate the potential impact of COVID-19 lockdowns on 5- and 10-year survival of melanoma patients. Using the growth rate of a random sample of 1,000 melanomas to model estimates of tumor thickness after various delays, coupled with American Joint Committee on Cancer survival data for different T stages, they estimated that 5-year survival would be reduced from 94.2% to 92.3% with a 90-day delay in diagnosis, and that 10-year survival would drop from 90.0% to 87.6%.
But that’s merely modeling. Francesco Ricci, MD, PhD, and colleagues from the melanoma unit at the Istituto Dermopatico dell’Immacolata, Rome, have provided a first look at the real-world impact of the lockdown. In the prelockdown period of January through March 9th, 2020, the referral center averaged 2.3 new melanoma diagnoses per day. During the Rome lockdown, from March 10th through May 3rd, this figure dropped to a mean of 0.6 melanoma diagnoses per day. Postlockdown, from May 4th to June 6th, the average climbed to 1.3 per day. The rate of newly diagnosed nodular melanoma was 5.5-fold greater postlockdown, compared with prelockdown; the rate of ulcerated melanoma was 4.9-fold greater.
“We can hypothesize that this may have been due to delays in diagnosis and care,” Dr. Hartman commented. “This is important because we know that nodular melanoma as well as ulceration tend to have a worse prognosis in terms of mortality.”
The mean Breslow thickness of newly diagnosed melanomas was 0.88 mm prelockdown, 0.66 mm during lockdown, and 1.96 mm postlockdown. The investigators speculated that the reduced Breslow thickness of melanomas diagnosed during lockdown might be explained by a greater willingness of more health-conscious people to defy the shelter-in-place instructions because of their concern about a suspicious skin lesion. “Though it is way too early to gauge the consequences of such diagnostic delay, should this issue be neglected, dermatologists and their patients may pay a higher price later with increased morbidity, mortality, and financial burden,” according to the investigators.
Dr. Hartman observed that it will be important to learn whether similar experiences occurred elsewhere during lockdown.
Another speaker, John M. Kirkwood, MD, said he has seen several melanoma patients referred from outside centers who had delays of up to 3 months in sentinel lymph node management of T2 and T3 tumors during lockdown who now have widespread metastatic disease.
“Now, is that anecdotal? I don’t know, it’s just worrisome to me,” commented Dr. Kirkwood, professor of medicine, dermatology, and translational science at the University of Pittsburgh.
Merrick Ross, MD, professor of surgical oncology at M.D. Anderson Cancer Center, Houston, recalled, “There was a period of time [during the lockdown] when we weren’t allowed to do certain elective procedures, if you want to call cancer surgery elective.”
“It’s too soon to talk about outcomes because a lot of patients are still in the process of being treated after what I would consider a significant delay in diagnosis,” the surgeon added.
An audience member asked if there will be an opportunity to see data on the damage done by delaying melanoma management as compared to lives saved through the lockdown for COVID-19. Dr. Ross replied that M.D. Anderson is in the midst of an institution-wide study analyzing the delay in diagnosis of a range of cancers.
“In our melanoma center it is absolutely clear, although we’re still collecting data, that the median tumor thickness is much higher since the lockdown,” Dr. Ross commented.
Dr. Hartman said she and her coinvestigators in the Melanoma Prevention Working Group are attempting to tally up the damage done via the lockdown by delaying melanoma diagnosis and treatment. But she agreed with the questioner that the most important thing is overall net lives saved through shelter-in-place.
“I’m sure that, separately, nondermatologists – perhaps infectious disease doctors and internists – are looking at how many lives were saved by the lockdown policy. So I do think all that data will come out,” Dr. Hartman predicted.
She reported having no financial conflicts regarding her presentation.
Global Academy for Medical Education and this news organization are owned by the same company.
SOURCE: Hartman, R. Cutaneous malignancies forum.
REPORTING FROM THE CUTANEOUS MALIGNANCIES FORUM
Use long-acting second-generation antipsychotics ‘as early as possible’ in psychosis
Don’t wait to give patients with first-episode psychosis long-acting injectable formulations of second-generation antipsychotics, according to Henry A. Nasrallah, MD.

Many clinicians wait to use long-acting injectables (LAIs) until the patient has experienced multiple relapses, but using them after the first discharge may help prevent future relapse, Dr. Nasrallah, professor of psychiatry, neurology, and neuroscience at the University of Cincinnati, said at the virtual Psychopharmacology Update presented by Current Psychiatry and Global Academy for Medical Education.
LAIs and clozapine are “vastly underutilized” after the first discharge, he noted. “I really encourage everybody to use them without hesitation as early as possible.”
In patients with first-episode psychosis, “the most important thing, in my opinion, is to start establishing a therapeutic alliance with the patient from day one,” Dr. Nasrallah said. “It’s always important in psychiatry, but it’s particularly important for first-episode psychosis.”
These patients respond to low doses of antipsychotics and should not be given first-generation antipsychotics because of a risk for acute extrapyramidal symptoms, tardive dyskinesia, and neurotoxicity.
“I usually select an antipsychotic that is extended release and also available as a long-acting injectable formulation,” Dr. Nasrallah said, noting that it helps when he gives a patient a long-acting injectable right after discharge. During hospitalization, Dr. Nasrallah said, he educates the patient and their family about psychosis, treatment, how psychosis affects the brain, and adherence to treatment.
“The primary goal, of course, is to achieve remission and very importantly, to prevent a second episode,” he said. “This is the golden opportunity for us psychiatrists to prevent the patient from relapsing again and again. That is the reason for disability and for brain damage, because every psychotic episode destroys brain tissue. That is why I am very eager to not only achieve a remission in the first episode but also to position the patient to be protected after discharge by giving them long-acting injectable.”
After a clinician performs a full workup to rule out substance use or a general medical condition inducing first-episode psychosis, Dr. Nasrallah recommends paliperidone extended-release (ER), given to patients in the morning because of its tolerability and the availability of an LAI version of the drug. “If the patient is very sick and agitated, I might go to 6 mg a day, which is actually a very good dose for first-episode patients, and it’s still quite well tolerated.”
Oral or injectable lorazepam taken as needed may be given to a patient with first-episode psychosis with agitation. For patients who manifest akathisia, twice or thrice daily propranolol at dose of 10-20 mg can be used off label, he said. Dr. Nasrallah also recommended twice-daily omega 3 at a dose of 1,000 mg or N-acetylcysteine at a dose of 600 mg per day as supplements.
“They’re not approved by the [Food and Drug Administration] for first-episode psychosis, but there are numerous publications in the literature by academic psychiatrists showing that they are quite beneficial, and they reduce the two destructive processes during psychosis, which are neuroinflammation and oxidative stress, or free radicals,” he said. “Those two supplements can help in the acute phase of the illness.”
Another option for clinicians is to begin a patient with first-episode psychosis on oral aripiprazole at a dose of 5 mg per day for 2 days, increasing the dose to 7.5 mg per day for 2 days, then increasing to 10 mg per day. “It is not extended-release, so you have to start with low doses to protect the patient from side effects,” Dr. Nasrallah explained. “Some patients may need 15 or 20 [mg], but most first-episode patients may do well on 10 [mg] without risking side effects.”
Planning for discharge
Patients who tolerate aripiprazole can start the long-acting aripiprazole lauroxil at discharge, and clinicians have two options to choose from. One formulation “requires 2 weeks of oral supplementation, which you can do in the hospital if you start the patient on oral aripiprazole, and then you can give that injection prior to discharge.” Another option involves giving the patient “any antipsychotic you like and then switch[ing] the patient to aripiprazole lauroxil. The full dose can be given without oral supplementation on the day of discharge.”
Dr. Nasrallah emphasized the use of LAIs in patients discharged for first-episode psychosis. In a study published in JAMA Psychiatry, researchers found use of LAI risperidone in patients with first-episode psychosis significantly reduced the risk of psychotic exacerbation and relapse compared with patients who were given oral risperidone (JAMA Psychiatry. 2015;72:822-9).
“This kind of well-done study shows you that you can do a great job protecting your patient from the very beginning by giving long-acting injectables,” Dr. Nasrallah explained. “That’s why you have to develop rapport with the patient. That’s why you have to convince the patient to take the injectable, and that’s why you have to educate the patient about the hazards of psychosis to the brain, and the fact that it’s very hard to remember to take the pills, because the illness itself can interfere with that due to cognitive impairment [and] negative symptoms.” Another reason for nonadherence is that the patients might not believe they are sick, he added.
After 2 or 3 weeks, if a patient with first-episode psychosis has a minimal response or does not response at all to an LAI, clozapine is an “aggressive” option that may help nonresponders. For patients with schizophrenia, “about 65%-70% would respond to a dopamine antagonist and the remaining 30% are going to need clozapine sooner or later,” Dr. Nasrallah said. “For clozapine after one or two failures [on LAIs] with an adequate dose and adequate duration, don’t wait. Give the patient clozapine, give them an opportunity to regain their life. I’ve seen some very gratifying results with clozapine in those who respond to it.
“The outcome of schizophrenia may be far less malignant than the perception out there if we actually ensure adherence very early and manage the first-episode aggressively, like cardiologists manage the first heart attack,” he said. “[Cardiologists] do everything in their power to protect the patient from a second heart attack, and I regard psychosis as a ‘brain attack.’ ”
Global Academy and this news organization are owned by the same parent company. Dr. Nasrallah reported that he has received research grants from Acadia; served as a consultant for Acadia, Alkermes, Allergan, Janssen, Otsuka, Indivior, Intracellular, Neurocrine, Sunovion, Teva, and Boehringer-Ingelheim; and is on the speakers bureau for Acadia, Alkermes, Allergan, Janssen, Otsuka, Indivior, Intracellular, Neurocrine, Noven, Sunovion, and Teva.
Don’t wait to give patients with first-episode psychosis long-acting injectable formulations of second-generation antipsychotics, according to Henry A. Nasrallah, MD.
Many clinicians wait to use long-acting injectables (LAIs) until the patient has experienced multiple relapses, but using them after the first discharge may help prevent future relapse, Dr. Nasrallah, professor of psychiatry, neurology, and neuroscience at the University of Cincinnati, said at the virtual Psychopharmacology Update presented by Current Psychiatry and Global Academy for Medical Education.
LAIs and clozapine are “vastly underutilized” after the first discharge, he noted. “I really encourage everybody to use them without hesitation as early as possible.”
In patients with first-episode psychosis, “the most important thing, in my opinion, is to start establishing a therapeutic alliance with the patient from day one,” Dr. Nasrallah said. “It’s always important in psychiatry, but it’s particularly important for first-episode psychosis.”
These patients respond to low doses of antipsychotics and should not be given first-generation antipsychotics because of a risk for acute extrapyramidal symptoms, tardive dyskinesia, and neurotoxicity.
“I usually select an antipsychotic that is extended release and also available as a long-acting injectable formulation,” Dr. Nasrallah said, noting that it helps when he gives a patient a long-acting injectable right after discharge. During hospitalization, Dr. Nasrallah said, he educates the patient and their family about psychosis, treatment, how psychosis affects the brain, and adherence to treatment.
“The primary goal, of course, is to achieve remission and very importantly, to prevent a second episode,” he said. “This is the golden opportunity for us psychiatrists to prevent the patient from relapsing again and again. That is the reason for disability and for brain damage, because every psychotic episode destroys brain tissue. That is why I am very eager to not only achieve a remission in the first episode but also to position the patient to be protected after discharge by giving them long-acting injectable.”
After a clinician performs a full workup to rule out substance use or a general medical condition inducing first-episode psychosis, Dr. Nasrallah recommends paliperidone extended-release (ER), given to patients in the morning because of its tolerability and the availability of an LAI version of the drug. “If the patient is very sick and agitated, I might go to 6 mg a day, which is actually a very good dose for first-episode patients, and it’s still quite well tolerated.”
Oral or injectable lorazepam taken as needed may be given to a patient with first-episode psychosis with agitation. For patients who manifest akathisia, twice or thrice daily propranolol at dose of 10-20 mg can be used off label, he said. Dr. Nasrallah also recommended twice-daily omega 3 at a dose of 1,000 mg or N-acetylcysteine at a dose of 600 mg per day as supplements.
“They’re not approved by the [Food and Drug Administration] for first-episode psychosis, but there are numerous publications in the literature by academic psychiatrists showing that they are quite beneficial, and they reduce the two destructive processes during psychosis, which are neuroinflammation and oxidative stress, or free radicals,” he said. “Those two supplements can help in the acute phase of the illness.”
Another option for clinicians is to begin a patient with first-episode psychosis on oral aripiprazole at a dose of 5 mg per day for 2 days, increasing the dose to 7.5 mg per day for 2 days, then increasing to 10 mg per day. “It is not extended-release, so you have to start with low doses to protect the patient from side effects,” Dr. Nasrallah explained. “Some patients may need 15 or 20 [mg], but most first-episode patients may do well on 10 [mg] without risking side effects.”
Planning for discharge
Patients who tolerate aripiprazole can start the long-acting aripiprazole lauroxil at discharge, and clinicians have two options to choose from. One formulation “requires 2 weeks of oral supplementation, which you can do in the hospital if you start the patient on oral aripiprazole, and then you can give that injection prior to discharge.” Another option involves giving the patient “any antipsychotic you like and then switch[ing] the patient to aripiprazole lauroxil. The full dose can be given without oral supplementation on the day of discharge.”
Dr. Nasrallah emphasized the use of LAIs in patients discharged for first-episode psychosis. In a study published in JAMA Psychiatry, researchers found use of LAI risperidone in patients with first-episode psychosis significantly reduced the risk of psychotic exacerbation and relapse compared with patients who were given oral risperidone (JAMA Psychiatry. 2015;72:822-9).
“This kind of well-done study shows you that you can do a great job protecting your patient from the very beginning by giving long-acting injectables,” Dr. Nasrallah explained. “That’s why you have to develop rapport with the patient. That’s why you have to convince the patient to take the injectable, and that’s why you have to educate the patient about the hazards of psychosis to the brain, and the fact that it’s very hard to remember to take the pills, because the illness itself can interfere with that due to cognitive impairment [and] negative symptoms.” Another reason for nonadherence is that the patients might not believe they are sick, he added.
After 2 or 3 weeks, if a patient with first-episode psychosis has a minimal response or does not response at all to an LAI, clozapine is an “aggressive” option that may help nonresponders. For patients with schizophrenia, “about 65%-70% would respond to a dopamine antagonist and the remaining 30% are going to need clozapine sooner or later,” Dr. Nasrallah said. “For clozapine after one or two failures [on LAIs] with an adequate dose and adequate duration, don’t wait. Give the patient clozapine, give them an opportunity to regain their life. I’ve seen some very gratifying results with clozapine in those who respond to it.
“The outcome of schizophrenia may be far less malignant than the perception out there if we actually ensure adherence very early and manage the first-episode aggressively, like cardiologists manage the first heart attack,” he said. “[Cardiologists] do everything in their power to protect the patient from a second heart attack, and I regard psychosis as a ‘brain attack.’ ”
Global Academy and this news organization are owned by the same parent company. Dr. Nasrallah reported that he has received research grants from Acadia; served as a consultant for Acadia, Alkermes, Allergan, Janssen, Otsuka, Indivior, Intracellular, Neurocrine, Sunovion, Teva, and Boehringer-Ingelheim; and is on the speakers bureau for Acadia, Alkermes, Allergan, Janssen, Otsuka, Indivior, Intracellular, Neurocrine, Noven, Sunovion, and Teva.
Don’t wait to give patients with first-episode psychosis long-acting injectable formulations of second-generation antipsychotics, according to Henry A. Nasrallah, MD.
Many clinicians wait to use long-acting injectables (LAIs) until the patient has experienced multiple relapses, but using them after the first discharge may help prevent future relapse, Dr. Nasrallah, professor of psychiatry, neurology, and neuroscience at the University of Cincinnati, said at the virtual Psychopharmacology Update presented by Current Psychiatry and Global Academy for Medical Education.
LAIs and clozapine are “vastly underutilized” after the first discharge, he noted. “I really encourage everybody to use them without hesitation as early as possible.”
In patients with first-episode psychosis, “the most important thing, in my opinion, is to start establishing a therapeutic alliance with the patient from day one,” Dr. Nasrallah said. “It’s always important in psychiatry, but it’s particularly important for first-episode psychosis.”
These patients respond to low doses of antipsychotics and should not be given first-generation antipsychotics because of a risk for acute extrapyramidal symptoms, tardive dyskinesia, and neurotoxicity.
“I usually select an antipsychotic that is extended release and also available as a long-acting injectable formulation,” Dr. Nasrallah said, noting that it helps when he gives a patient a long-acting injectable right after discharge. During hospitalization, Dr. Nasrallah said, he educates the patient and their family about psychosis, treatment, how psychosis affects the brain, and adherence to treatment.
“The primary goal, of course, is to achieve remission and very importantly, to prevent a second episode,” he said. “This is the golden opportunity for us psychiatrists to prevent the patient from relapsing again and again. That is the reason for disability and for brain damage, because every psychotic episode destroys brain tissue. That is why I am very eager to not only achieve a remission in the first episode but also to position the patient to be protected after discharge by giving them long-acting injectable.”
After a clinician performs a full workup to rule out substance use or a general medical condition inducing first-episode psychosis, Dr. Nasrallah recommends paliperidone extended-release (ER), given to patients in the morning because of its tolerability and the availability of an LAI version of the drug. “If the patient is very sick and agitated, I might go to 6 mg a day, which is actually a very good dose for first-episode patients, and it’s still quite well tolerated.”
Oral or injectable lorazepam taken as needed may be given to a patient with first-episode psychosis with agitation. For patients who manifest akathisia, twice or thrice daily propranolol at dose of 10-20 mg can be used off label, he said. Dr. Nasrallah also recommended twice-daily omega 3 at a dose of 1,000 mg or N-acetylcysteine at a dose of 600 mg per day as supplements.
“They’re not approved by the [Food and Drug Administration] for first-episode psychosis, but there are numerous publications in the literature by academic psychiatrists showing that they are quite beneficial, and they reduce the two destructive processes during psychosis, which are neuroinflammation and oxidative stress, or free radicals,” he said. “Those two supplements can help in the acute phase of the illness.”
Another option for clinicians is to begin a patient with first-episode psychosis on oral aripiprazole at a dose of 5 mg per day for 2 days, increasing the dose to 7.5 mg per day for 2 days, then increasing to 10 mg per day. “It is not extended-release, so you have to start with low doses to protect the patient from side effects,” Dr. Nasrallah explained. “Some patients may need 15 or 20 [mg], but most first-episode patients may do well on 10 [mg] without risking side effects.”
Planning for discharge
Patients who tolerate aripiprazole can start the long-acting aripiprazole lauroxil at discharge, and clinicians have two options to choose from. One formulation “requires 2 weeks of oral supplementation, which you can do in the hospital if you start the patient on oral aripiprazole, and then you can give that injection prior to discharge.” Another option involves giving the patient “any antipsychotic you like and then switch[ing] the patient to aripiprazole lauroxil. The full dose can be given without oral supplementation on the day of discharge.”
Dr. Nasrallah emphasized the use of LAIs in patients discharged for first-episode psychosis. In a study published in JAMA Psychiatry, researchers found use of LAI risperidone in patients with first-episode psychosis significantly reduced the risk of psychotic exacerbation and relapse compared with patients who were given oral risperidone (JAMA Psychiatry. 2015;72:822-9).
“This kind of well-done study shows you that you can do a great job protecting your patient from the very beginning by giving long-acting injectables,” Dr. Nasrallah explained. “That’s why you have to develop rapport with the patient. That’s why you have to convince the patient to take the injectable, and that’s why you have to educate the patient about the hazards of psychosis to the brain, and the fact that it’s very hard to remember to take the pills, because the illness itself can interfere with that due to cognitive impairment [and] negative symptoms.” Another reason for nonadherence is that the patients might not believe they are sick, he added.
After 2 or 3 weeks, if a patient with first-episode psychosis has a minimal response or does not response at all to an LAI, clozapine is an “aggressive” option that may help nonresponders. For patients with schizophrenia, “about 65%-70% would respond to a dopamine antagonist and the remaining 30% are going to need clozapine sooner or later,” Dr. Nasrallah said. “For clozapine after one or two failures [on LAIs] with an adequate dose and adequate duration, don’t wait. Give the patient clozapine, give them an opportunity to regain their life. I’ve seen some very gratifying results with clozapine in those who respond to it.
“The outcome of schizophrenia may be far less malignant than the perception out there if we actually ensure adherence very early and manage the first-episode aggressively, like cardiologists manage the first heart attack,” he said. “[Cardiologists] do everything in their power to protect the patient from a second heart attack, and I regard psychosis as a ‘brain attack.’ ”
Global Academy and this news organization are owned by the same parent company. Dr. Nasrallah reported that he has received research grants from Acadia; served as a consultant for Acadia, Alkermes, Allergan, Janssen, Otsuka, Indivior, Intracellular, Neurocrine, Sunovion, Teva, and Boehringer-Ingelheim; and is on the speakers bureau for Acadia, Alkermes, Allergan, Janssen, Otsuka, Indivior, Intracellular, Neurocrine, Noven, Sunovion, and Teva.
FROM PSYCHOPHARMACOLOGY UPDATE
Trump could clean house at health agencies
Others may soon depart voluntarily. Politico reported in late October that more than two dozen political appointees had already left the U.S. Department Health and Human Services (HHS) since the start of the COVID-19 pandemic in February and that potentially dozens of the more than 100 in the department would leave if Trump was not reelected.
Trump hasn’t conceded, he is challenging the election results, and he has already fired his Defense Secretary, Mark Esper.
Among those possibly in Trump’s sights: HHS Secretary Alex Azar, US Food and Drug Administration (FDA) Commissioner Stephen Hahn, MD, Centers for Disease Control and Prevention (CDC) Director Robert Redfield, MD, and White House Coronavirus Task Force member Anthony Fauci, MD, who is also the director of the National Institutes of Allergy and Infectious Diseases.
Seema Verma, the administrator of the Centers for Medicare & Medicaid Services (CMS), is likely safe. According to Politico, Verma is expected to leave on her own terms.
Azar has had a long run as a Trump appointee. He took office in January 2018 and has been a staunch loyalist. But he’s frequently been the butt of grousing by Trump for not doing enough to help lower drug prices and for his handling of the coronavirus pandemic. Azar was initially in charge of the Trump virus effort but was quickly replaced by Vice President Mike Pence.
It was widely reported in late April that Trump was considering firing Azar, but the president called that “fake news” in a tweet.
Azar has complained about Hahn, who was confirmed in December 2019. According to Politico, Azar was looking into how to remove Hahn as commissioner because of the FDA’s battle with the White House over standards for emergency use authorization of a coronavirus vaccine.
In addition, Trump was infuriated by the agency’s insistence that it stick to the highest bar for an emergency approval. “The deep state, or whoever, over at the FDA is making it very difficult for drug companies to get people in order to test the vaccines and therapeutics. Obviously, they are hoping to delay the answer until after November 3rd,” Trump tweeted at Hahn.
Fauci on the firing line?
Most of the president’s ire has been directed at Fauci. As far back as April, Trump retweeted a call for Fauci’s firing. Twitter removed the original tweet but kept Trump’s comments on the original tweet.
The president has frequently questioned Fauci’s advice, sidelined him from task force meetings, and infrequently met with him. Trump called Fauci a “disaster” during a call with supporters in October, and then, at a campaign rally in November, intimated that he would fire the scientist after the election, according to The Washington Post.
But such a firing cannot be easily done. Some have speculated that Trump could pressure Fauci’s boss, Francis Collins, MD, PhD — the director of the National Institutes of Health (NIH), who is a political appointee — to get rid of him. But Collins would have to come up with a reason to fire Fauci. Because he is not a political appointee, Fauci is afforded a raft of protections given to civil service employees of the federal government.
To demote or fire Fauci, Collins would have to give him 30 days’ notice unless there’s a belief that he committed a crime. Fauci would have at least a week to offer evidence and affidavits in support of his service.
He’d also be entitled to legal representation, a written decision, and the specific reasons for the action being taken quickly. He could also request a hearing, and he’d be able to appeal any action to the Merit Systems Protection Board. The process could take months, if not years.
In late October, Trump issued an executive order that would reclassify certain federal employees so that they wouldn’t have such protections. But agencies have until mid-January to come up with lists of such workers, according to Government Executive.
Collins has been with NIH since 1993, when he headed the Human Genome Project and the National Human Genome Research Institute. Politico has speculated that Collins, 70, might retire if Trump was reelected. It’s unclear what he’ll do now.
Redfield, who has taken heat for his leadership from many in public health — and was asked in October to stand up to Trump by former CDC Director William H. Foege, MD — has been openly contradicted by the president on more than one occasion, according to The New York Times.
In September, The Hill reported that Trump told reporters that he’d chastised Redfield by phone soon after Redfield had told a Senate committee that a coronavirus vaccine would not be available until mid-2021.
This article first appeared on Medscape.com.
Others may soon depart voluntarily. Politico reported in late October that more than two dozen political appointees had already left the U.S. Department Health and Human Services (HHS) since the start of the COVID-19 pandemic in February and that potentially dozens of the more than 100 in the department would leave if Trump was not reelected.
Trump hasn’t conceded, he is challenging the election results, and he has already fired his Defense Secretary, Mark Esper.
Among those possibly in Trump’s sights: HHS Secretary Alex Azar, US Food and Drug Administration (FDA) Commissioner Stephen Hahn, MD, Centers for Disease Control and Prevention (CDC) Director Robert Redfield, MD, and White House Coronavirus Task Force member Anthony Fauci, MD, who is also the director of the National Institutes of Allergy and Infectious Diseases.
Seema Verma, the administrator of the Centers for Medicare & Medicaid Services (CMS), is likely safe. According to Politico, Verma is expected to leave on her own terms.
Azar has had a long run as a Trump appointee. He took office in January 2018 and has been a staunch loyalist. But he’s frequently been the butt of grousing by Trump for not doing enough to help lower drug prices and for his handling of the coronavirus pandemic. Azar was initially in charge of the Trump virus effort but was quickly replaced by Vice President Mike Pence.
It was widely reported in late April that Trump was considering firing Azar, but the president called that “fake news” in a tweet.
Azar has complained about Hahn, who was confirmed in December 2019. According to Politico, Azar was looking into how to remove Hahn as commissioner because of the FDA’s battle with the White House over standards for emergency use authorization of a coronavirus vaccine.
In addition, Trump was infuriated by the agency’s insistence that it stick to the highest bar for an emergency approval. “The deep state, or whoever, over at the FDA is making it very difficult for drug companies to get people in order to test the vaccines and therapeutics. Obviously, they are hoping to delay the answer until after November 3rd,” Trump tweeted at Hahn.
Fauci on the firing line?
Most of the president’s ire has been directed at Fauci. As far back as April, Trump retweeted a call for Fauci’s firing. Twitter removed the original tweet but kept Trump’s comments on the original tweet.
The president has frequently questioned Fauci’s advice, sidelined him from task force meetings, and infrequently met with him. Trump called Fauci a “disaster” during a call with supporters in October, and then, at a campaign rally in November, intimated that he would fire the scientist after the election, according to The Washington Post.
But such a firing cannot be easily done. Some have speculated that Trump could pressure Fauci’s boss, Francis Collins, MD, PhD — the director of the National Institutes of Health (NIH), who is a political appointee — to get rid of him. But Collins would have to come up with a reason to fire Fauci. Because he is not a political appointee, Fauci is afforded a raft of protections given to civil service employees of the federal government.
To demote or fire Fauci, Collins would have to give him 30 days’ notice unless there’s a belief that he committed a crime. Fauci would have at least a week to offer evidence and affidavits in support of his service.
He’d also be entitled to legal representation, a written decision, and the specific reasons for the action being taken quickly. He could also request a hearing, and he’d be able to appeal any action to the Merit Systems Protection Board. The process could take months, if not years.
In late October, Trump issued an executive order that would reclassify certain federal employees so that they wouldn’t have such protections. But agencies have until mid-January to come up with lists of such workers, according to Government Executive.
Collins has been with NIH since 1993, when he headed the Human Genome Project and the National Human Genome Research Institute. Politico has speculated that Collins, 70, might retire if Trump was reelected. It’s unclear what he’ll do now.
Redfield, who has taken heat for his leadership from many in public health — and was asked in October to stand up to Trump by former CDC Director William H. Foege, MD — has been openly contradicted by the president on more than one occasion, according to The New York Times.
In September, The Hill reported that Trump told reporters that he’d chastised Redfield by phone soon after Redfield had told a Senate committee that a coronavirus vaccine would not be available until mid-2021.
This article first appeared on Medscape.com.
Others may soon depart voluntarily. Politico reported in late October that more than two dozen political appointees had already left the U.S. Department Health and Human Services (HHS) since the start of the COVID-19 pandemic in February and that potentially dozens of the more than 100 in the department would leave if Trump was not reelected.
Trump hasn’t conceded, he is challenging the election results, and he has already fired his Defense Secretary, Mark Esper.
Among those possibly in Trump’s sights: HHS Secretary Alex Azar, US Food and Drug Administration (FDA) Commissioner Stephen Hahn, MD, Centers for Disease Control and Prevention (CDC) Director Robert Redfield, MD, and White House Coronavirus Task Force member Anthony Fauci, MD, who is also the director of the National Institutes of Allergy and Infectious Diseases.
Seema Verma, the administrator of the Centers for Medicare & Medicaid Services (CMS), is likely safe. According to Politico, Verma is expected to leave on her own terms.
Azar has had a long run as a Trump appointee. He took office in January 2018 and has been a staunch loyalist. But he’s frequently been the butt of grousing by Trump for not doing enough to help lower drug prices and for his handling of the coronavirus pandemic. Azar was initially in charge of the Trump virus effort but was quickly replaced by Vice President Mike Pence.
It was widely reported in late April that Trump was considering firing Azar, but the president called that “fake news” in a tweet.
Azar has complained about Hahn, who was confirmed in December 2019. According to Politico, Azar was looking into how to remove Hahn as commissioner because of the FDA’s battle with the White House over standards for emergency use authorization of a coronavirus vaccine.
In addition, Trump was infuriated by the agency’s insistence that it stick to the highest bar for an emergency approval. “The deep state, or whoever, over at the FDA is making it very difficult for drug companies to get people in order to test the vaccines and therapeutics. Obviously, they are hoping to delay the answer until after November 3rd,” Trump tweeted at Hahn.
Fauci on the firing line?
Most of the president’s ire has been directed at Fauci. As far back as April, Trump retweeted a call for Fauci’s firing. Twitter removed the original tweet but kept Trump’s comments on the original tweet.
The president has frequently questioned Fauci’s advice, sidelined him from task force meetings, and infrequently met with him. Trump called Fauci a “disaster” during a call with supporters in October, and then, at a campaign rally in November, intimated that he would fire the scientist after the election, according to The Washington Post.
But such a firing cannot be easily done. Some have speculated that Trump could pressure Fauci’s boss, Francis Collins, MD, PhD — the director of the National Institutes of Health (NIH), who is a political appointee — to get rid of him. But Collins would have to come up with a reason to fire Fauci. Because he is not a political appointee, Fauci is afforded a raft of protections given to civil service employees of the federal government.
To demote or fire Fauci, Collins would have to give him 30 days’ notice unless there’s a belief that he committed a crime. Fauci would have at least a week to offer evidence and affidavits in support of his service.
He’d also be entitled to legal representation, a written decision, and the specific reasons for the action being taken quickly. He could also request a hearing, and he’d be able to appeal any action to the Merit Systems Protection Board. The process could take months, if not years.
In late October, Trump issued an executive order that would reclassify certain federal employees so that they wouldn’t have such protections. But agencies have until mid-January to come up with lists of such workers, according to Government Executive.
Collins has been with NIH since 1993, when he headed the Human Genome Project and the National Human Genome Research Institute. Politico has speculated that Collins, 70, might retire if Trump was reelected. It’s unclear what he’ll do now.
Redfield, who has taken heat for his leadership from many in public health — and was asked in October to stand up to Trump by former CDC Director William H. Foege, MD — has been openly contradicted by the president on more than one occasion, according to The New York Times.
In September, The Hill reported that Trump told reporters that he’d chastised Redfield by phone soon after Redfield had told a Senate committee that a coronavirus vaccine would not be available until mid-2021.
This article first appeared on Medscape.com.
Supreme Court Justices seem skeptical of case to overturn ACA
The Justices conducted arguments by telephone in the case, California v Texas (previously California v US), which was brought by 18 Republican state officials and two individual plaintiffs. The Trump administration joined the plaintiffs in June, arguing that the entire law should be overturned. The ACA is being defended by Democratic state officials from 16 states and Washington, D.C.
The Republican plaintiffs have essentially argued that the ACA cannot stand without the individual mandate requirement – that it is not possible to “sever” it from the rest of the Act. In 2017, Congress set the tax penalty to $0 if an individual did not buy insurance. The mandate to buy insurance was left in place, but there were no longer any consequences. The plaintiffs said that congressional act was equivalent to severing the mandate.
But many Justices appeared to take a dim view of that argument.
“It’s a very straightforward case for severability under our precedents,” said Justice Brett Kavanaugh. “Meaning that we would excise the mandate and leave the rest of the Act in play. Congress knows how to write an inseverability clause and that is not the language that they chose here,” he said.
Justice Elena Kagan also questioned how it would jibe with legal precedent to allow the severing of one part of a law when there was no clear instruction from Congress on the issue. She also raised the concern that it would open the door to all sorts of challenges.
“It would seem a big deal to say that, if you can point to injury with respect to one provision and you can concoct some kind of inseverability argument, that allows you to challenge anything else in the statute,” she said.
“Isn’t that something that really cuts against all of our doctrine?” asked Kagan.
“I think it’s hard for you to argue that Congress intended the entire Act to fall if the mandate was struck down when the same Congress that lowered the penalty to zero did not even try to repeal the rest of the act,” said Chief Justice John Roberts.
“I think, frankly, that they wanted the Court to do that but that’s not our job,” he added.
Proof of harm?
To have the standing to sue, the plaintiffs have to prove they have been harmed by the ACA. Texas Solicitor General Kyle Hawkins said that individuals feel compelled to buy insurance – even without a penalty hanging over their heads.
Justice Stephen Breyer argued that many laws include what he called “precatory” language – that is, they seek to compel citizens to do something. But most don’t penalize those who fail to act – just like the ACA currently.
If, as the Texas plaintiffs argued, it’s still unconstitutional to make such a request, “I think there will be an awful lot of language in an awful lot of statutes that will suddenly be the subject of court constitutional challenge,” he said.
Hawkins disagreed. He said the ACA’s mandate “is not some suggestion, not some hortatory statement. It is the law of the United States of America today that you have to purchase health insurance and not just any health insurance, but health insurance that the federal government has decided would be best for you.”
Hawkins said that, if just one additional person signed up for Medicaid, the state of Texas and the other plaintiff states would be harmed. He said people were continuing to enroll in the program because they believed the law required them to get health insurance.
Justice Sonia Sotomayor said that defied common sense. “The problem is that your theory assumes people that people are going to pay a tax and break the law by not buying insurance, but they wouldn’t do it when the tax is zero.”
What’s at stake
It’s unlikely the justices will issue a decision immediately. They have until the end of the term in June to rule.
Katie Keith, JD, MPH, a principal at Keith Policy Solutions, LLC, outlined the potential outcomes in Health Affairs .
“The most likely scenario is that the Court maintains the status quo,” she wrote. They could get there by deciding Texas et al. did not have standing to bring the case. Or they could decide that either the mandate is constitutional or that it is unconstitutional but can be severed from the rest of the ACA.
The Court could alternatively find that some or all of the law’s insurance provisions – such as protections for people with pre-existing conditions – can’t be severed from the mandate. Or the justices could strike down all of the insurance consumer protections, the health insurance marketplaces, premium tax credits, and other provisions, which would force states to come up with the money to help people buy insurance. And states are unlikely to be able to do so, especially with the pandemic stretching their budgets.
Finally, the Court could find that the mandate can’t be separated, which would essentially overturn the law.
If that happens, some 15 million people could lose Medicaid coverage, 11 million who buy on health insurance exchanges could lose coverage, and 2.3 million young adults would no longer be able to stay on parents’ policies, according to the Kaiser Family Foundation. Kaiser also estimates that 54 million people under age 65 who have pre-existing conditions would no longer be guaranteed coverage.
The Urban Institute estimates that 21 million people could lose insurance – 15 million through Medicaid and the Children’s Health Insurance Program (CHIP) and 7.6 million through private nongroup coverage.
Medical societies weigh in
Multiple physicians’ groups, patient advocates, and hospital organizations have filed briefs with the Court in favor of keeping the law intact.
Twenty patient groups representing millions with pre-existing conditions – including the American Cancer Society, American Diabetes Association, American Heart Association, National Alliance on Mental Illness, National Organization for Rare Disorders, and the Kennedy Forum – filed a court brief in May arguing that the law has expanded access to insurance and improved patient outcomes.
“The coronavirus pandemic has only served to underscore the necessity of meaningful coverage – especially for those who are at high risk of being severely affected by the virus – including countless Americans who have pre-existing, acute or chronic conditions like heart disease, cancer, diabetes, lung diseases and multiple sclerosis,” they said in a statement.
Jacqueline W. Fincher, MD, MACP, president of the American College of Physicians, which joined a court brief in support of the law with 19 other medical organizations, said the law has worked.
“The coverage, protections and benefits provided by the ACA are critical to the well-being of millions of Americans,” she said in a statement.
“If the ACA were to be thrown out at the same time that we face the pandemic, it would cause chaos for physicians and our patients, and for the entire health care system,” said Fincher, adding that millions of Americans who have been infected could lose insurance if protections for pre-existing conditions disappeared.
“The ACA has revolutionized access to care for tens of millions of women by helping them obtain meaningful health coverage, ensuring that essential care is covered by insurers, and protecting patients from unfair insurance practices,” said Maureen G. Phipps, MD, MPH, CEO of the American College of Obstetricians and Gynecologists (ACOG), in a statement.
Overturning the ACA “would be one of the most singularly disruptive acts to be committed during this public health crisis,” she said.
American Psychiatric Association President Jeffrey Geller, MD, MPH, also warned of disruptions to care, especially for those with mental health and substance use disorders. “We urge the Supreme Court to preserve the entire Act, including the individual mandate,” he said, in a statement.
“In the midst of COVID is no time to let down the millions who we serve as our patients,” said Chip Kahn, Federation of American Health Systems president and CEO, in a statement.
“As caregivers, the goal of hospitals for our patients is to see increased access to affordable coverage for all Americans – not new obstacles,” he said, adding that the ACA “can accomplish this goal. We hope the Supreme Court will see its way clear to allow it to go forward.”
For the defense
Many legal analysts on social media who listened in to today’s hearing agreed that the tenor of the proceedings seemed to lean toward survival of the ACA.
“At this point I would say it is *extremely* likely that the ACA will be upheld, but the mandate struck down and severed out,” tweeted Raffi Melkonian, an appellate lawyer in Houston, Texas. “A decision on standing (throwing out the case entirely) is also possible. The chance that the ACA is struck down v. low.”
“Both Kavanaugh and Roberts have suggested this morning that they may view the individual mandate as severable from the rest of the law. If those two justices join the court’s three liberals in finding that the mandate is severable, that would be five votes to save the ACA,” tweeted the analysts at SCOTUS Blog.
Sean Marotta, a lawyer with Hogan Lovells’ Supreme Court group, agreed. “Oral argument is always an imperfect measure, but the Act’s defenders should feel good today,” he tweeted.
This article first appeared on Medscape.com.
The Justices conducted arguments by telephone in the case, California v Texas (previously California v US), which was brought by 18 Republican state officials and two individual plaintiffs. The Trump administration joined the plaintiffs in June, arguing that the entire law should be overturned. The ACA is being defended by Democratic state officials from 16 states and Washington, D.C.
The Republican plaintiffs have essentially argued that the ACA cannot stand without the individual mandate requirement – that it is not possible to “sever” it from the rest of the Act. In 2017, Congress set the tax penalty to $0 if an individual did not buy insurance. The mandate to buy insurance was left in place, but there were no longer any consequences. The plaintiffs said that congressional act was equivalent to severing the mandate.
But many Justices appeared to take a dim view of that argument.
“It’s a very straightforward case for severability under our precedents,” said Justice Brett Kavanaugh. “Meaning that we would excise the mandate and leave the rest of the Act in play. Congress knows how to write an inseverability clause and that is not the language that they chose here,” he said.
Justice Elena Kagan also questioned how it would jibe with legal precedent to allow the severing of one part of a law when there was no clear instruction from Congress on the issue. She also raised the concern that it would open the door to all sorts of challenges.
“It would seem a big deal to say that, if you can point to injury with respect to one provision and you can concoct some kind of inseverability argument, that allows you to challenge anything else in the statute,” she said.
“Isn’t that something that really cuts against all of our doctrine?” asked Kagan.
“I think it’s hard for you to argue that Congress intended the entire Act to fall if the mandate was struck down when the same Congress that lowered the penalty to zero did not even try to repeal the rest of the act,” said Chief Justice John Roberts.
“I think, frankly, that they wanted the Court to do that but that’s not our job,” he added.
Proof of harm?
To have the standing to sue, the plaintiffs have to prove they have been harmed by the ACA. Texas Solicitor General Kyle Hawkins said that individuals feel compelled to buy insurance – even without a penalty hanging over their heads.
Justice Stephen Breyer argued that many laws include what he called “precatory” language – that is, they seek to compel citizens to do something. But most don’t penalize those who fail to act – just like the ACA currently.
If, as the Texas plaintiffs argued, it’s still unconstitutional to make such a request, “I think there will be an awful lot of language in an awful lot of statutes that will suddenly be the subject of court constitutional challenge,” he said.
Hawkins disagreed. He said the ACA’s mandate “is not some suggestion, not some hortatory statement. It is the law of the United States of America today that you have to purchase health insurance and not just any health insurance, but health insurance that the federal government has decided would be best for you.”
Hawkins said that, if just one additional person signed up for Medicaid, the state of Texas and the other plaintiff states would be harmed. He said people were continuing to enroll in the program because they believed the law required them to get health insurance.
Justice Sonia Sotomayor said that defied common sense. “The problem is that your theory assumes people that people are going to pay a tax and break the law by not buying insurance, but they wouldn’t do it when the tax is zero.”
What’s at stake
It’s unlikely the justices will issue a decision immediately. They have until the end of the term in June to rule.
Katie Keith, JD, MPH, a principal at Keith Policy Solutions, LLC, outlined the potential outcomes in Health Affairs .
“The most likely scenario is that the Court maintains the status quo,” she wrote. They could get there by deciding Texas et al. did not have standing to bring the case. Or they could decide that either the mandate is constitutional or that it is unconstitutional but can be severed from the rest of the ACA.
The Court could alternatively find that some or all of the law’s insurance provisions – such as protections for people with pre-existing conditions – can’t be severed from the mandate. Or the justices could strike down all of the insurance consumer protections, the health insurance marketplaces, premium tax credits, and other provisions, which would force states to come up with the money to help people buy insurance. And states are unlikely to be able to do so, especially with the pandemic stretching their budgets.
Finally, the Court could find that the mandate can’t be separated, which would essentially overturn the law.
If that happens, some 15 million people could lose Medicaid coverage, 11 million who buy on health insurance exchanges could lose coverage, and 2.3 million young adults would no longer be able to stay on parents’ policies, according to the Kaiser Family Foundation. Kaiser also estimates that 54 million people under age 65 who have pre-existing conditions would no longer be guaranteed coverage.
The Urban Institute estimates that 21 million people could lose insurance – 15 million through Medicaid and the Children’s Health Insurance Program (CHIP) and 7.6 million through private nongroup coverage.
Medical societies weigh in
Multiple physicians’ groups, patient advocates, and hospital organizations have filed briefs with the Court in favor of keeping the law intact.
Twenty patient groups representing millions with pre-existing conditions – including the American Cancer Society, American Diabetes Association, American Heart Association, National Alliance on Mental Illness, National Organization for Rare Disorders, and the Kennedy Forum – filed a court brief in May arguing that the law has expanded access to insurance and improved patient outcomes.
“The coronavirus pandemic has only served to underscore the necessity of meaningful coverage – especially for those who are at high risk of being severely affected by the virus – including countless Americans who have pre-existing, acute or chronic conditions like heart disease, cancer, diabetes, lung diseases and multiple sclerosis,” they said in a statement.
Jacqueline W. Fincher, MD, MACP, president of the American College of Physicians, which joined a court brief in support of the law with 19 other medical organizations, said the law has worked.
“The coverage, protections and benefits provided by the ACA are critical to the well-being of millions of Americans,” she said in a statement.
“If the ACA were to be thrown out at the same time that we face the pandemic, it would cause chaos for physicians and our patients, and for the entire health care system,” said Fincher, adding that millions of Americans who have been infected could lose insurance if protections for pre-existing conditions disappeared.
“The ACA has revolutionized access to care for tens of millions of women by helping them obtain meaningful health coverage, ensuring that essential care is covered by insurers, and protecting patients from unfair insurance practices,” said Maureen G. Phipps, MD, MPH, CEO of the American College of Obstetricians and Gynecologists (ACOG), in a statement.
Overturning the ACA “would be one of the most singularly disruptive acts to be committed during this public health crisis,” she said.
American Psychiatric Association President Jeffrey Geller, MD, MPH, also warned of disruptions to care, especially for those with mental health and substance use disorders. “We urge the Supreme Court to preserve the entire Act, including the individual mandate,” he said, in a statement.
“In the midst of COVID is no time to let down the millions who we serve as our patients,” said Chip Kahn, Federation of American Health Systems president and CEO, in a statement.
“As caregivers, the goal of hospitals for our patients is to see increased access to affordable coverage for all Americans – not new obstacles,” he said, adding that the ACA “can accomplish this goal. We hope the Supreme Court will see its way clear to allow it to go forward.”
For the defense
Many legal analysts on social media who listened in to today’s hearing agreed that the tenor of the proceedings seemed to lean toward survival of the ACA.
“At this point I would say it is *extremely* likely that the ACA will be upheld, but the mandate struck down and severed out,” tweeted Raffi Melkonian, an appellate lawyer in Houston, Texas. “A decision on standing (throwing out the case entirely) is also possible. The chance that the ACA is struck down v. low.”
“Both Kavanaugh and Roberts have suggested this morning that they may view the individual mandate as severable from the rest of the law. If those two justices join the court’s three liberals in finding that the mandate is severable, that would be five votes to save the ACA,” tweeted the analysts at SCOTUS Blog.
Sean Marotta, a lawyer with Hogan Lovells’ Supreme Court group, agreed. “Oral argument is always an imperfect measure, but the Act’s defenders should feel good today,” he tweeted.
This article first appeared on Medscape.com.
The Justices conducted arguments by telephone in the case, California v Texas (previously California v US), which was brought by 18 Republican state officials and two individual plaintiffs. The Trump administration joined the plaintiffs in June, arguing that the entire law should be overturned. The ACA is being defended by Democratic state officials from 16 states and Washington, D.C.
The Republican plaintiffs have essentially argued that the ACA cannot stand without the individual mandate requirement – that it is not possible to “sever” it from the rest of the Act. In 2017, Congress set the tax penalty to $0 if an individual did not buy insurance. The mandate to buy insurance was left in place, but there were no longer any consequences. The plaintiffs said that congressional act was equivalent to severing the mandate.
But many Justices appeared to take a dim view of that argument.
“It’s a very straightforward case for severability under our precedents,” said Justice Brett Kavanaugh. “Meaning that we would excise the mandate and leave the rest of the Act in play. Congress knows how to write an inseverability clause and that is not the language that they chose here,” he said.
Justice Elena Kagan also questioned how it would jibe with legal precedent to allow the severing of one part of a law when there was no clear instruction from Congress on the issue. She also raised the concern that it would open the door to all sorts of challenges.
“It would seem a big deal to say that, if you can point to injury with respect to one provision and you can concoct some kind of inseverability argument, that allows you to challenge anything else in the statute,” she said.
“Isn’t that something that really cuts against all of our doctrine?” asked Kagan.
“I think it’s hard for you to argue that Congress intended the entire Act to fall if the mandate was struck down when the same Congress that lowered the penalty to zero did not even try to repeal the rest of the act,” said Chief Justice John Roberts.
“I think, frankly, that they wanted the Court to do that but that’s not our job,” he added.
Proof of harm?
To have the standing to sue, the plaintiffs have to prove they have been harmed by the ACA. Texas Solicitor General Kyle Hawkins said that individuals feel compelled to buy insurance – even without a penalty hanging over their heads.
Justice Stephen Breyer argued that many laws include what he called “precatory” language – that is, they seek to compel citizens to do something. But most don’t penalize those who fail to act – just like the ACA currently.
If, as the Texas plaintiffs argued, it’s still unconstitutional to make such a request, “I think there will be an awful lot of language in an awful lot of statutes that will suddenly be the subject of court constitutional challenge,” he said.
Hawkins disagreed. He said the ACA’s mandate “is not some suggestion, not some hortatory statement. It is the law of the United States of America today that you have to purchase health insurance and not just any health insurance, but health insurance that the federal government has decided would be best for you.”
Hawkins said that, if just one additional person signed up for Medicaid, the state of Texas and the other plaintiff states would be harmed. He said people were continuing to enroll in the program because they believed the law required them to get health insurance.
Justice Sonia Sotomayor said that defied common sense. “The problem is that your theory assumes people that people are going to pay a tax and break the law by not buying insurance, but they wouldn’t do it when the tax is zero.”
What’s at stake
It’s unlikely the justices will issue a decision immediately. They have until the end of the term in June to rule.
Katie Keith, JD, MPH, a principal at Keith Policy Solutions, LLC, outlined the potential outcomes in Health Affairs .
“The most likely scenario is that the Court maintains the status quo,” she wrote. They could get there by deciding Texas et al. did not have standing to bring the case. Or they could decide that either the mandate is constitutional or that it is unconstitutional but can be severed from the rest of the ACA.
The Court could alternatively find that some or all of the law’s insurance provisions – such as protections for people with pre-existing conditions – can’t be severed from the mandate. Or the justices could strike down all of the insurance consumer protections, the health insurance marketplaces, premium tax credits, and other provisions, which would force states to come up with the money to help people buy insurance. And states are unlikely to be able to do so, especially with the pandemic stretching their budgets.
Finally, the Court could find that the mandate can’t be separated, which would essentially overturn the law.
If that happens, some 15 million people could lose Medicaid coverage, 11 million who buy on health insurance exchanges could lose coverage, and 2.3 million young adults would no longer be able to stay on parents’ policies, according to the Kaiser Family Foundation. Kaiser also estimates that 54 million people under age 65 who have pre-existing conditions would no longer be guaranteed coverage.
The Urban Institute estimates that 21 million people could lose insurance – 15 million through Medicaid and the Children’s Health Insurance Program (CHIP) and 7.6 million through private nongroup coverage.
Medical societies weigh in
Multiple physicians’ groups, patient advocates, and hospital organizations have filed briefs with the Court in favor of keeping the law intact.
Twenty patient groups representing millions with pre-existing conditions – including the American Cancer Society, American Diabetes Association, American Heart Association, National Alliance on Mental Illness, National Organization for Rare Disorders, and the Kennedy Forum – filed a court brief in May arguing that the law has expanded access to insurance and improved patient outcomes.
“The coronavirus pandemic has only served to underscore the necessity of meaningful coverage – especially for those who are at high risk of being severely affected by the virus – including countless Americans who have pre-existing, acute or chronic conditions like heart disease, cancer, diabetes, lung diseases and multiple sclerosis,” they said in a statement.
Jacqueline W. Fincher, MD, MACP, president of the American College of Physicians, which joined a court brief in support of the law with 19 other medical organizations, said the law has worked.
“The coverage, protections and benefits provided by the ACA are critical to the well-being of millions of Americans,” she said in a statement.
“If the ACA were to be thrown out at the same time that we face the pandemic, it would cause chaos for physicians and our patients, and for the entire health care system,” said Fincher, adding that millions of Americans who have been infected could lose insurance if protections for pre-existing conditions disappeared.
“The ACA has revolutionized access to care for tens of millions of women by helping them obtain meaningful health coverage, ensuring that essential care is covered by insurers, and protecting patients from unfair insurance practices,” said Maureen G. Phipps, MD, MPH, CEO of the American College of Obstetricians and Gynecologists (ACOG), in a statement.
Overturning the ACA “would be one of the most singularly disruptive acts to be committed during this public health crisis,” she said.
American Psychiatric Association President Jeffrey Geller, MD, MPH, also warned of disruptions to care, especially for those with mental health and substance use disorders. “We urge the Supreme Court to preserve the entire Act, including the individual mandate,” he said, in a statement.
“In the midst of COVID is no time to let down the millions who we serve as our patients,” said Chip Kahn, Federation of American Health Systems president and CEO, in a statement.
“As caregivers, the goal of hospitals for our patients is to see increased access to affordable coverage for all Americans – not new obstacles,” he said, adding that the ACA “can accomplish this goal. We hope the Supreme Court will see its way clear to allow it to go forward.”
For the defense
Many legal analysts on social media who listened in to today’s hearing agreed that the tenor of the proceedings seemed to lean toward survival of the ACA.
“At this point I would say it is *extremely* likely that the ACA will be upheld, but the mandate struck down and severed out,” tweeted Raffi Melkonian, an appellate lawyer in Houston, Texas. “A decision on standing (throwing out the case entirely) is also possible. The chance that the ACA is struck down v. low.”
“Both Kavanaugh and Roberts have suggested this morning that they may view the individual mandate as severable from the rest of the law. If those two justices join the court’s three liberals in finding that the mandate is severable, that would be five votes to save the ACA,” tweeted the analysts at SCOTUS Blog.
Sean Marotta, a lawyer with Hogan Lovells’ Supreme Court group, agreed. “Oral argument is always an imperfect measure, but the Act’s defenders should feel good today,” he tweeted.
This article first appeared on Medscape.com.
FDA grants emergency use authorization to Lilly’s antibody COVID-19 therapy

The monoclonal antibody therapy has emergency authorization for treating patients who have tested positive for SARS-CoV-2 infection and who are considered to be at high risk for progression to severe COVID-19 or hospitalization. To be eligible for treatment with bamlanivimab, patients must be at least 12 years of age and weigh at least 40 kg (approximately 88 lb). The agency notes that this includes patients aged 65 years and older or people with certain chronic conditions.
Bamlanivimab is not authorized for use in patients who are hospitalized or who require oxygen therapy because of COVID-19. The FDA’s action comes less than 2 weeks after Eli Lilly halted the ACTIV-3 study of the therapy for severe, hospitalized COVID-19 patients after evidence showed that adding the antibody therapy to standard care did not improve outcomes over standard care alone for patients with advanced COVID-19.
The government contract with Eli Lilly involves the purchase of 300,000 doses through December, with the option to procure another 650,000 doses through June 2021.
Because of Operation Warp Speed, “we have supplies to distribute now. Product distribution will begin this week,” US Health & Human Services (HHS) Secretary Alex Azar said at a news conference today.
“We talked about building the bridge to safe and effective vaccines” for COVID-19, Azar added. “With this therapeutic, the bridge is taking shape.”
Bamlanivimab 700 mg will be administered as a 1-hour infusion followed by a 1-hour observation period for detecting any infusion-related side effects. The authorized dose is 700 mg, which was on the lower end of the dose range evaluated in studies.
During the press conference, a reporter asked whether the lower dose was chosen in order that more doses of the antibody could be made available. “The lower dose is a rational choice in this situation because we don’t want to give more of a drug than you need,” said Janet Woodcock, MD, the therapeutics lead for Operation Warp Speed. “I think we could probably go lower.”
Bamlanivimab works by attaching to the virus and blocking its entry into the cells and possibly by helping the patients’ immune system clear the virus, said Woodcock, who is also director of the FDA’s Center for Drug Evaluation and Research.
“The goal is to treat high-risk people as soon as possible after they show symptoms and are diagnosed,” she added.
Infusions an initial challenge?
There could be some logistic challenges at first because the antibody is administered via infusion. “We expect there will initially be a challenge in administering ... these infusions and setting up infusion centers,” Woodcock said.
Outpatient intravenous infusions are normally performed at infusion centers for patients with cancer and immune disorders, she noted. “You really don’t want them mixing with people who have COVID-19 disease, so we will need to set up separate sites.”
Bamlanivimab will be provided free of cost to patients, Azar said. Patients should be aware that coinsurance may be required for the infusion.
“Fair and equitable” distribution planned
During phase 1 of distribution, the agent will first be allocated to hospitals and hospital-affiliated locations only, John Redd, MD, MPH, chief medical officer, Office of the Assistant Secretary for Preparedness and Response at HHS, said at the press conference.
During phase 2, “there will be expanded distribution to outpatient sites,” he said. In an effort to keep the process transparent, a new website features the latest updates on the distribution of bamlanivimab.
Allocation will be based on two factors: the number of new cases reported in a state or territory in the prior 7 days, and rates of COVID-19 hospitalization during the same period.
Asked why the government would determine distribution of the antibody on the basis of the number of hospitalized patients when the indication includes prevention of admission, Woodcock replied that hospitalization is a surrogate measure that can reflect risk factors in a particular state population, such as obesity, diabetes, or the proportion of older people.
Furthermore, the confirmed cases are a “leading indicator,” she said, that can help identify a steep rise in COVID-19 cases that could indicate more hospitalizations are likely soon. “We don’t want to miss that.”
Data underlying the EUA decision
A decrease in hospitalizations or emergency department visits within 28 days of treatment in preclinical studies was “the most important evidence that bamlanivimab may be effective,” the agency noted in the press release announcing the EUA. Among patients at high risk for progression, 3% required such interventions, compared with 10% of placebo-treated patients.
Potential side effects of bamlanivimab include anaphylaxis, infusion-related reactions, nausea, diarrhea, dizziness, headache, itching, and vomiting.
“As illustrated by today’s action, the FDA remains committed to expediting the development and availability of potential COVID-19 treatments and providing sick patients timely access to new therapies where appropriate,” FDA Commissioner Stephen M. Hahn, MD, said in the news release.
Healthcare providers can download a detailed FDA fact sheet on the EUA for bamlanivimab, which includes dosing instructions.
This article first appeared on Medscape.com.
The monoclonal antibody therapy has emergency authorization for treating patients who have tested positive for SARS-CoV-2 infection and who are considered to be at high risk for progression to severe COVID-19 or hospitalization. To be eligible for treatment with bamlanivimab, patients must be at least 12 years of age and weigh at least 40 kg (approximately 88 lb). The agency notes that this includes patients aged 65 years and older or people with certain chronic conditions.
Bamlanivimab is not authorized for use in patients who are hospitalized or who require oxygen therapy because of COVID-19. The FDA’s action comes less than 2 weeks after Eli Lilly halted the ACTIV-3 study of the therapy for severe, hospitalized COVID-19 patients after evidence showed that adding the antibody therapy to standard care did not improve outcomes over standard care alone for patients with advanced COVID-19.
The government contract with Eli Lilly involves the purchase of 300,000 doses through December, with the option to procure another 650,000 doses through June 2021.
Because of Operation Warp Speed, “we have supplies to distribute now. Product distribution will begin this week,” US Health & Human Services (HHS) Secretary Alex Azar said at a news conference today.
“We talked about building the bridge to safe and effective vaccines” for COVID-19, Azar added. “With this therapeutic, the bridge is taking shape.”
Bamlanivimab 700 mg will be administered as a 1-hour infusion followed by a 1-hour observation period for detecting any infusion-related side effects. The authorized dose is 700 mg, which was on the lower end of the dose range evaluated in studies.
During the press conference, a reporter asked whether the lower dose was chosen in order that more doses of the antibody could be made available. “The lower dose is a rational choice in this situation because we don’t want to give more of a drug than you need,” said Janet Woodcock, MD, the therapeutics lead for Operation Warp Speed. “I think we could probably go lower.”
Bamlanivimab works by attaching to the virus and blocking its entry into the cells and possibly by helping the patients’ immune system clear the virus, said Woodcock, who is also director of the FDA’s Center for Drug Evaluation and Research.
“The goal is to treat high-risk people as soon as possible after they show symptoms and are diagnosed,” she added.
Infusions an initial challenge?
There could be some logistic challenges at first because the antibody is administered via infusion. “We expect there will initially be a challenge in administering ... these infusions and setting up infusion centers,” Woodcock said.
Outpatient intravenous infusions are normally performed at infusion centers for patients with cancer and immune disorders, she noted. “You really don’t want them mixing with people who have COVID-19 disease, so we will need to set up separate sites.”
Bamlanivimab will be provided free of cost to patients, Azar said. Patients should be aware that coinsurance may be required for the infusion.
“Fair and equitable” distribution planned
During phase 1 of distribution, the agent will first be allocated to hospitals and hospital-affiliated locations only, John Redd, MD, MPH, chief medical officer, Office of the Assistant Secretary for Preparedness and Response at HHS, said at the press conference.
During phase 2, “there will be expanded distribution to outpatient sites,” he said. In an effort to keep the process transparent, a new website features the latest updates on the distribution of bamlanivimab.
Allocation will be based on two factors: the number of new cases reported in a state or territory in the prior 7 days, and rates of COVID-19 hospitalization during the same period.
Asked why the government would determine distribution of the antibody on the basis of the number of hospitalized patients when the indication includes prevention of admission, Woodcock replied that hospitalization is a surrogate measure that can reflect risk factors in a particular state population, such as obesity, diabetes, or the proportion of older people.
Furthermore, the confirmed cases are a “leading indicator,” she said, that can help identify a steep rise in COVID-19 cases that could indicate more hospitalizations are likely soon. “We don’t want to miss that.”
Data underlying the EUA decision
A decrease in hospitalizations or emergency department visits within 28 days of treatment in preclinical studies was “the most important evidence that bamlanivimab may be effective,” the agency noted in the press release announcing the EUA. Among patients at high risk for progression, 3% required such interventions, compared with 10% of placebo-treated patients.
Potential side effects of bamlanivimab include anaphylaxis, infusion-related reactions, nausea, diarrhea, dizziness, headache, itching, and vomiting.
“As illustrated by today’s action, the FDA remains committed to expediting the development and availability of potential COVID-19 treatments and providing sick patients timely access to new therapies where appropriate,” FDA Commissioner Stephen M. Hahn, MD, said in the news release.
Healthcare providers can download a detailed FDA fact sheet on the EUA for bamlanivimab, which includes dosing instructions.
This article first appeared on Medscape.com.
The monoclonal antibody therapy has emergency authorization for treating patients who have tested positive for SARS-CoV-2 infection and who are considered to be at high risk for progression to severe COVID-19 or hospitalization. To be eligible for treatment with bamlanivimab, patients must be at least 12 years of age and weigh at least 40 kg (approximately 88 lb). The agency notes that this includes patients aged 65 years and older or people with certain chronic conditions.
Bamlanivimab is not authorized for use in patients who are hospitalized or who require oxygen therapy because of COVID-19. The FDA’s action comes less than 2 weeks after Eli Lilly halted the ACTIV-3 study of the therapy for severe, hospitalized COVID-19 patients after evidence showed that adding the antibody therapy to standard care did not improve outcomes over standard care alone for patients with advanced COVID-19.
The government contract with Eli Lilly involves the purchase of 300,000 doses through December, with the option to procure another 650,000 doses through June 2021.
Because of Operation Warp Speed, “we have supplies to distribute now. Product distribution will begin this week,” US Health & Human Services (HHS) Secretary Alex Azar said at a news conference today.
“We talked about building the bridge to safe and effective vaccines” for COVID-19, Azar added. “With this therapeutic, the bridge is taking shape.”
Bamlanivimab 700 mg will be administered as a 1-hour infusion followed by a 1-hour observation period for detecting any infusion-related side effects. The authorized dose is 700 mg, which was on the lower end of the dose range evaluated in studies.
During the press conference, a reporter asked whether the lower dose was chosen in order that more doses of the antibody could be made available. “The lower dose is a rational choice in this situation because we don’t want to give more of a drug than you need,” said Janet Woodcock, MD, the therapeutics lead for Operation Warp Speed. “I think we could probably go lower.”
Bamlanivimab works by attaching to the virus and blocking its entry into the cells and possibly by helping the patients’ immune system clear the virus, said Woodcock, who is also director of the FDA’s Center for Drug Evaluation and Research.
“The goal is to treat high-risk people as soon as possible after they show symptoms and are diagnosed,” she added.
Infusions an initial challenge?
There could be some logistic challenges at first because the antibody is administered via infusion. “We expect there will initially be a challenge in administering ... these infusions and setting up infusion centers,” Woodcock said.
Outpatient intravenous infusions are normally performed at infusion centers for patients with cancer and immune disorders, she noted. “You really don’t want them mixing with people who have COVID-19 disease, so we will need to set up separate sites.”
Bamlanivimab will be provided free of cost to patients, Azar said. Patients should be aware that coinsurance may be required for the infusion.
“Fair and equitable” distribution planned
During phase 1 of distribution, the agent will first be allocated to hospitals and hospital-affiliated locations only, John Redd, MD, MPH, chief medical officer, Office of the Assistant Secretary for Preparedness and Response at HHS, said at the press conference.
During phase 2, “there will be expanded distribution to outpatient sites,” he said. In an effort to keep the process transparent, a new website features the latest updates on the distribution of bamlanivimab.
Allocation will be based on two factors: the number of new cases reported in a state or territory in the prior 7 days, and rates of COVID-19 hospitalization during the same period.
Asked why the government would determine distribution of the antibody on the basis of the number of hospitalized patients when the indication includes prevention of admission, Woodcock replied that hospitalization is a surrogate measure that can reflect risk factors in a particular state population, such as obesity, diabetes, or the proportion of older people.
Furthermore, the confirmed cases are a “leading indicator,” she said, that can help identify a steep rise in COVID-19 cases that could indicate more hospitalizations are likely soon. “We don’t want to miss that.”
Data underlying the EUA decision
A decrease in hospitalizations or emergency department visits within 28 days of treatment in preclinical studies was “the most important evidence that bamlanivimab may be effective,” the agency noted in the press release announcing the EUA. Among patients at high risk for progression, 3% required such interventions, compared with 10% of placebo-treated patients.
Potential side effects of bamlanivimab include anaphylaxis, infusion-related reactions, nausea, diarrhea, dizziness, headache, itching, and vomiting.
“As illustrated by today’s action, the FDA remains committed to expediting the development and availability of potential COVID-19 treatments and providing sick patients timely access to new therapies where appropriate,” FDA Commissioner Stephen M. Hahn, MD, said in the news release.
Healthcare providers can download a detailed FDA fact sheet on the EUA for bamlanivimab, which includes dosing instructions.
This article first appeared on Medscape.com.
FDA clears smartphone app to interrupt PTSD-related nightmares
The Food and Drug Administration has cleared for marketing a smartphone app that can detect and interrupt nightmares in adults with posttraumatic stress disorder (PTSD).
The NightWare app, from Minneapolis-based NightWare Inc., runs on the Apple Watch and Apple iPhone.
During sleep, Apple Watch sensors monitor heart rate and body movement. These data are used to create a unique sleep profile using a proprietary algorithm.
When the NightWare app detects that a patient is experiencing a nightmare based on changes in heart rate and movement, it provides slight vibrations through the Apple Watch to arouse the patient and interrupt the nightmare, without fully awakening the patient, the company notes.
NightWare is available by prescription only and is intended for use in adults aged 22 years and older with PTSD.
“Sleep is an essential part of a person’s daily routine. However, certain adults who have a nightmare disorder or who experience nightmares from PTSD are not able to get the rest they need,” Carlos Peña, PhD, director, Office of Neurological and Physical Medicine Devices, Center for Devices and Radiological Health at the FDA, said in a news release.
This authorization “offers a new, low-risk treatment option that uses digital technology in an effort to provide temporary relief from sleep disturbance related to nightmares,” said Dr. Peña.
NightWare was tested in a 30-day randomized, sham-controlled trial of 70 patients. Patients in the sham group wore the device, but no vibrations were provided.
Both the sham and active groups showed improvement in sleep on standard sleep scales, with the active group showing greater improvement than sham. “The evidence demonstrated the probable benefits outweighed the probable risks,” the FDA said in a statement.
and other recommended therapies for PTSD-associated nightmares and nightmare disorder, the agency said.
NightWare was granted breakthrough device designation for the treatment of nightmares in patients with PTSD. The device reviewed through the de novo premarket pathway, a regulatory pathway for some low- to moderate-risk devices of a new type.
Along with this marketing authorization, the FDA is establishing “special controls” designed to provide a “reasonable assurance of safety and effectiveness for tests of this type,” the agency said.
A version of this article originally appeared on Medscape.com.
The Food and Drug Administration has cleared for marketing a smartphone app that can detect and interrupt nightmares in adults with posttraumatic stress disorder (PTSD).
The NightWare app, from Minneapolis-based NightWare Inc., runs on the Apple Watch and Apple iPhone.
During sleep, Apple Watch sensors monitor heart rate and body movement. These data are used to create a unique sleep profile using a proprietary algorithm.
When the NightWare app detects that a patient is experiencing a nightmare based on changes in heart rate and movement, it provides slight vibrations through the Apple Watch to arouse the patient and interrupt the nightmare, without fully awakening the patient, the company notes.
NightWare is available by prescription only and is intended for use in adults aged 22 years and older with PTSD.
“Sleep is an essential part of a person’s daily routine. However, certain adults who have a nightmare disorder or who experience nightmares from PTSD are not able to get the rest they need,” Carlos Peña, PhD, director, Office of Neurological and Physical Medicine Devices, Center for Devices and Radiological Health at the FDA, said in a news release.
This authorization “offers a new, low-risk treatment option that uses digital technology in an effort to provide temporary relief from sleep disturbance related to nightmares,” said Dr. Peña.
NightWare was tested in a 30-day randomized, sham-controlled trial of 70 patients. Patients in the sham group wore the device, but no vibrations were provided.
Both the sham and active groups showed improvement in sleep on standard sleep scales, with the active group showing greater improvement than sham. “The evidence demonstrated the probable benefits outweighed the probable risks,” the FDA said in a statement.
and other recommended therapies for PTSD-associated nightmares and nightmare disorder, the agency said.
NightWare was granted breakthrough device designation for the treatment of nightmares in patients with PTSD. The device reviewed through the de novo premarket pathway, a regulatory pathway for some low- to moderate-risk devices of a new type.
Along with this marketing authorization, the FDA is establishing “special controls” designed to provide a “reasonable assurance of safety and effectiveness for tests of this type,” the agency said.
A version of this article originally appeared on Medscape.com.
The Food and Drug Administration has cleared for marketing a smartphone app that can detect and interrupt nightmares in adults with posttraumatic stress disorder (PTSD).
The NightWare app, from Minneapolis-based NightWare Inc., runs on the Apple Watch and Apple iPhone.
During sleep, Apple Watch sensors monitor heart rate and body movement. These data are used to create a unique sleep profile using a proprietary algorithm.
When the NightWare app detects that a patient is experiencing a nightmare based on changes in heart rate and movement, it provides slight vibrations through the Apple Watch to arouse the patient and interrupt the nightmare, without fully awakening the patient, the company notes.
NightWare is available by prescription only and is intended for use in adults aged 22 years and older with PTSD.
“Sleep is an essential part of a person’s daily routine. However, certain adults who have a nightmare disorder or who experience nightmares from PTSD are not able to get the rest they need,” Carlos Peña, PhD, director, Office of Neurological and Physical Medicine Devices, Center for Devices and Radiological Health at the FDA, said in a news release.
This authorization “offers a new, low-risk treatment option that uses digital technology in an effort to provide temporary relief from sleep disturbance related to nightmares,” said Dr. Peña.
NightWare was tested in a 30-day randomized, sham-controlled trial of 70 patients. Patients in the sham group wore the device, but no vibrations were provided.
Both the sham and active groups showed improvement in sleep on standard sleep scales, with the active group showing greater improvement than sham. “The evidence demonstrated the probable benefits outweighed the probable risks,” the FDA said in a statement.
and other recommended therapies for PTSD-associated nightmares and nightmare disorder, the agency said.
NightWare was granted breakthrough device designation for the treatment of nightmares in patients with PTSD. The device reviewed through the de novo premarket pathway, a regulatory pathway for some low- to moderate-risk devices of a new type.
Along with this marketing authorization, the FDA is establishing “special controls” designed to provide a “reasonable assurance of safety and effectiveness for tests of this type,” the agency said.
A version of this article originally appeared on Medscape.com.
Great Barrington coauthor backs off strict reliance on herd immunity
A coauthor of the Great Barrington Declaration says that he and colleagues have never argued against using mitigation strategies to keep COVID-19 from spreading, and that critics have mischaracterized the document as a “let it rip” strategy.
Jay Bhattacharya, MD, PhD, a professor and public health policy expert in infectious diseases at Stanford University in California, spoke on a JAMA Livestream debate on November 6. Marc Lipsitch, MD, an epidemiology professor at the Harvard T.H. Chan School of Public Health in Boston, Massachusetts, represented the 6900 signatories of the John Snow Memorandum, a rebuttal to the Great Barrington document.
The Great Barrington approach of “Focused Protection” advocates isolation and protection of people who are most vulnerable to COVID-19 while avoiding what they characterize as lockdowns. “The most compassionate approach that balances the risks and benefits of reaching herd immunity, is to allow those who are at minimal risk of death to live their lives normally to build up immunity to the virus through natural infection, while better protecting those who are at highest risk,” the document reads.
The Infectious Diseases Society of America (IDSA) and its HIV Medicine Association denounced the declaration, as reported by Medscape Medical News, and the World Health Organization (WHO) Director General Tedros Adhanom Ghebreyesus called the proposal “unethical.” But the idea has gained some traction at the White House, where Coronavirus Task Force Member and Stanford professor Scott Atlas, MD, has been advising President Donald J. Trump.
On the JAMA debate, Bhattacharya said, “I think all of the mitigation measures are really important,” listing social distancing, hand washing, and masks when distancing is not possible as chief among those strategies for the less vulnerable. “I don’t want to create infections intentionally, but I want us to allow people to go back to their lives as best they can, understanding of the risks they are taking when they do it,” he said, claiming that 99.95% of the population will survive infection.
“The harmful lockdowns are worse for many, many people,” Bhattacharya said.
“I think Jay is moving towards a middle ground which is not really what the Great Barrington Declaration seems to promote,” countered Lipsitch. The declaration does not say use masks or social distance, he said. “It just says we need to go back to a normal life.”
Bhattacharya’s statements to JAMA mean that “maybe we are approaching some common ground,” Lipsitch said.
Definition of a lockdown
Both men were asked to give their definition of a “lockdown.” To Lipsitch, it means people are not allowed out except for essential services and that most businesses are closed, with exceptions for those deemed essential.
Bhattacharya, however, said he views that as a quarantine. Lockdowns “are what we’re currently doing,” he said. Schools, churches, businesses, and arts and culture organizations are shuttered, and “almost every aspect of society is restricted in some way,” Bhattacharya said.
He blamed these lockdowns for most of the excess deaths over and above the COVID-19 deaths and said they had failed to control the pandemic.
Lipsitch said that “it feels to me that Jay is describing as lockdown everything that causes harm, even when it’s not locked down.” He noted that the country was truly closed down for 2 months or so in the spring.
“All of these harms I agree are real,” said Lipsitch. “But they are because the normal life of our society is being interfered with by viral transmission and by people’s inability to live their normal lives.”
Closures and lockdowns are essential to delaying cases and deaths, said Lipsitch. “A case today is worse than a case tomorrow and a lot worse than a case 6 months from now,” he said, noting that a vaccine or improved therapeutics could evolve.
“Delay is not nothing,” Lipsitch added. “It’s actually the goal as I see it, and as the John Snow memo says, we want to keep the virus under control in such a way as that the vulnerable people are not at risk.”
He predicted that cases will continue to grow exponentially because the nation is “not even close to herd immunity.” And, if intensive care units fill up, “there will be a responsive lockdown,” he said, adding that he did not endorse that as a general matter or favor it as a default position.
Bhattacharya claimed that Sweden has tallied only 1800 excess deaths since the pandemic began. “That’s lockdown harm avoided,” he said, advocating a similar strategy for the United States. But, infections have been on the rise in Sweden, and the nation has a higher COVID-19 death rate — with 6000 deaths — than other Nordic countries.
“If we keep this policy of lockdown we will have the same kind of outcomes we’ve already had — high excess deaths and sort of indifferent control of COVID,” Bhattacharya said.
“We’re still going to have misery and death going forward until we reach a point where there’s sufficient immunity either though a vaccine or through natural infection,” he said.
This article first appeared on Medscape.com.
A coauthor of the Great Barrington Declaration says that he and colleagues have never argued against using mitigation strategies to keep COVID-19 from spreading, and that critics have mischaracterized the document as a “let it rip” strategy.
Jay Bhattacharya, MD, PhD, a professor and public health policy expert in infectious diseases at Stanford University in California, spoke on a JAMA Livestream debate on November 6. Marc Lipsitch, MD, an epidemiology professor at the Harvard T.H. Chan School of Public Health in Boston, Massachusetts, represented the 6900 signatories of the John Snow Memorandum, a rebuttal to the Great Barrington document.
The Great Barrington approach of “Focused Protection” advocates isolation and protection of people who are most vulnerable to COVID-19 while avoiding what they characterize as lockdowns. “The most compassionate approach that balances the risks and benefits of reaching herd immunity, is to allow those who are at minimal risk of death to live their lives normally to build up immunity to the virus through natural infection, while better protecting those who are at highest risk,” the document reads.
The Infectious Diseases Society of America (IDSA) and its HIV Medicine Association denounced the declaration, as reported by Medscape Medical News, and the World Health Organization (WHO) Director General Tedros Adhanom Ghebreyesus called the proposal “unethical.” But the idea has gained some traction at the White House, where Coronavirus Task Force Member and Stanford professor Scott Atlas, MD, has been advising President Donald J. Trump.
On the JAMA debate, Bhattacharya said, “I think all of the mitigation measures are really important,” listing social distancing, hand washing, and masks when distancing is not possible as chief among those strategies for the less vulnerable. “I don’t want to create infections intentionally, but I want us to allow people to go back to their lives as best they can, understanding of the risks they are taking when they do it,” he said, claiming that 99.95% of the population will survive infection.
“The harmful lockdowns are worse for many, many people,” Bhattacharya said.
“I think Jay is moving towards a middle ground which is not really what the Great Barrington Declaration seems to promote,” countered Lipsitch. The declaration does not say use masks or social distance, he said. “It just says we need to go back to a normal life.”
Bhattacharya’s statements to JAMA mean that “maybe we are approaching some common ground,” Lipsitch said.
Definition of a lockdown
Both men were asked to give their definition of a “lockdown.” To Lipsitch, it means people are not allowed out except for essential services and that most businesses are closed, with exceptions for those deemed essential.
Bhattacharya, however, said he views that as a quarantine. Lockdowns “are what we’re currently doing,” he said. Schools, churches, businesses, and arts and culture organizations are shuttered, and “almost every aspect of society is restricted in some way,” Bhattacharya said.
He blamed these lockdowns for most of the excess deaths over and above the COVID-19 deaths and said they had failed to control the pandemic.
Lipsitch said that “it feels to me that Jay is describing as lockdown everything that causes harm, even when it’s not locked down.” He noted that the country was truly closed down for 2 months or so in the spring.
“All of these harms I agree are real,” said Lipsitch. “But they are because the normal life of our society is being interfered with by viral transmission and by people’s inability to live their normal lives.”
Closures and lockdowns are essential to delaying cases and deaths, said Lipsitch. “A case today is worse than a case tomorrow and a lot worse than a case 6 months from now,” he said, noting that a vaccine or improved therapeutics could evolve.
“Delay is not nothing,” Lipsitch added. “It’s actually the goal as I see it, and as the John Snow memo says, we want to keep the virus under control in such a way as that the vulnerable people are not at risk.”
He predicted that cases will continue to grow exponentially because the nation is “not even close to herd immunity.” And, if intensive care units fill up, “there will be a responsive lockdown,” he said, adding that he did not endorse that as a general matter or favor it as a default position.
Bhattacharya claimed that Sweden has tallied only 1800 excess deaths since the pandemic began. “That’s lockdown harm avoided,” he said, advocating a similar strategy for the United States. But, infections have been on the rise in Sweden, and the nation has a higher COVID-19 death rate — with 6000 deaths — than other Nordic countries.
“If we keep this policy of lockdown we will have the same kind of outcomes we’ve already had — high excess deaths and sort of indifferent control of COVID,” Bhattacharya said.
“We’re still going to have misery and death going forward until we reach a point where there’s sufficient immunity either though a vaccine or through natural infection,” he said.
This article first appeared on Medscape.com.
A coauthor of the Great Barrington Declaration says that he and colleagues have never argued against using mitigation strategies to keep COVID-19 from spreading, and that critics have mischaracterized the document as a “let it rip” strategy.
Jay Bhattacharya, MD, PhD, a professor and public health policy expert in infectious diseases at Stanford University in California, spoke on a JAMA Livestream debate on November 6. Marc Lipsitch, MD, an epidemiology professor at the Harvard T.H. Chan School of Public Health in Boston, Massachusetts, represented the 6900 signatories of the John Snow Memorandum, a rebuttal to the Great Barrington document.
The Great Barrington approach of “Focused Protection” advocates isolation and protection of people who are most vulnerable to COVID-19 while avoiding what they characterize as lockdowns. “The most compassionate approach that balances the risks and benefits of reaching herd immunity, is to allow those who are at minimal risk of death to live their lives normally to build up immunity to the virus through natural infection, while better protecting those who are at highest risk,” the document reads.
The Infectious Diseases Society of America (IDSA) and its HIV Medicine Association denounced the declaration, as reported by Medscape Medical News, and the World Health Organization (WHO) Director General Tedros Adhanom Ghebreyesus called the proposal “unethical.” But the idea has gained some traction at the White House, where Coronavirus Task Force Member and Stanford professor Scott Atlas, MD, has been advising President Donald J. Trump.
On the JAMA debate, Bhattacharya said, “I think all of the mitigation measures are really important,” listing social distancing, hand washing, and masks when distancing is not possible as chief among those strategies for the less vulnerable. “I don’t want to create infections intentionally, but I want us to allow people to go back to their lives as best they can, understanding of the risks they are taking when they do it,” he said, claiming that 99.95% of the population will survive infection.
“The harmful lockdowns are worse for many, many people,” Bhattacharya said.
“I think Jay is moving towards a middle ground which is not really what the Great Barrington Declaration seems to promote,” countered Lipsitch. The declaration does not say use masks or social distance, he said. “It just says we need to go back to a normal life.”
Bhattacharya’s statements to JAMA mean that “maybe we are approaching some common ground,” Lipsitch said.
Definition of a lockdown
Both men were asked to give their definition of a “lockdown.” To Lipsitch, it means people are not allowed out except for essential services and that most businesses are closed, with exceptions for those deemed essential.
Bhattacharya, however, said he views that as a quarantine. Lockdowns “are what we’re currently doing,” he said. Schools, churches, businesses, and arts and culture organizations are shuttered, and “almost every aspect of society is restricted in some way,” Bhattacharya said.
He blamed these lockdowns for most of the excess deaths over and above the COVID-19 deaths and said they had failed to control the pandemic.
Lipsitch said that “it feels to me that Jay is describing as lockdown everything that causes harm, even when it’s not locked down.” He noted that the country was truly closed down for 2 months or so in the spring.
“All of these harms I agree are real,” said Lipsitch. “But they are because the normal life of our society is being interfered with by viral transmission and by people’s inability to live their normal lives.”
Closures and lockdowns are essential to delaying cases and deaths, said Lipsitch. “A case today is worse than a case tomorrow and a lot worse than a case 6 months from now,” he said, noting that a vaccine or improved therapeutics could evolve.
“Delay is not nothing,” Lipsitch added. “It’s actually the goal as I see it, and as the John Snow memo says, we want to keep the virus under control in such a way as that the vulnerable people are not at risk.”
He predicted that cases will continue to grow exponentially because the nation is “not even close to herd immunity.” And, if intensive care units fill up, “there will be a responsive lockdown,” he said, adding that he did not endorse that as a general matter or favor it as a default position.
Bhattacharya claimed that Sweden has tallied only 1800 excess deaths since the pandemic began. “That’s lockdown harm avoided,” he said, advocating a similar strategy for the United States. But, infections have been on the rise in Sweden, and the nation has a higher COVID-19 death rate — with 6000 deaths — than other Nordic countries.
“If we keep this policy of lockdown we will have the same kind of outcomes we’ve already had — high excess deaths and sort of indifferent control of COVID,” Bhattacharya said.
“We’re still going to have misery and death going forward until we reach a point where there’s sufficient immunity either though a vaccine or through natural infection,” he said.
This article first appeared on Medscape.com.
Hospitals poised to launch first COVID-19 vaccines in clinicians
At first, when news spread of a 28-year-old doctor on the COVID-19 front lines in Brazil who died after receiving an experimental vaccine, doubts arose about the safety of one of the most promising coronavirus vaccine candidates. But then the story flipped. Although the vaccine maker wouldn’t confirm it, the doctor appeared to have been in the control group and had received a dose of an established meningitis vaccine. The danger came from exposure to the coronavirus itself.
That tragedy underscores the ongoing risk of COVID-19 to healthcare workers, who have been designated by US advisory panels as part of phase 1A – the first to receive doses of any approved vaccine. The Centers for Disease Control and Prevention (CDC) recently reported that 6% of adults hospitalized with COVID from March to May were healthcare workers. The report was based on surveillance data from 13 states. The average age of the patients was 49 years. The agency set a November 15 vaccination “readiness date” for jurisdictions, such as state health departments, even though a vaccine isn’t likely to be authorized by then.
As hospitals scramble to prepare, their watchword is flexibility. They don’t yet know how many initial doses they will get, of which vaccine, or in what time frame. They have a sophisticated infrastructure to deliver flu vaccines each fall, but that framework doesn’t align with the likely scenarios of limited supply, additional reporting requirements, two-dose regimens, and differing storage needs.
“Healthcare organizations have consistently risen to the challenge. I wholeheartedly believe in their potential to do this,” Anna Legreid Dopp, PharmD, senior director of quality improvement and guidelines for the American Society of Health-System Pharmacists, told Medscape Medical News.
Healthcare workers won’t face a vaccine mandate
Even after months of caring for COVID patients, most clinicians remain vulnerable to infection – at work and in their communities. That was what occupational medicine physician Kevin Smith, MD, realized when his health system, Toledo, Ohio–based ProMedica, offered antibody testing to all its 50,000 employees. About 2% of the 6933 tests given came back positive, he says.
Yet many physicians, nurses, and other healthcare workers share the public’s skepticism about the safety and effectiveness of a vaccine that receives swift US Food and Drug Administration (FDA) approval for emergency use. About half of nurses (47%) and almost 1 in 3 physicians (30%) say that they don’t want to get the vaccine when it first becomes available or that they’re unsure about vaccination, according to a Medscape survey.
Because vaccination of healthcare workers will set the stage for public acceptance of the vaccine, hospital epidemiologists are concerned. “We know that there will be some hesitancy in the healthcare workforce, just as there will be in the broader public,” said Marci Drees, MD, chief infection prevention officer and hospital epidemiologist for ChristianaCare in Newark, Delaware, and liaison from the Society for Healthcare Epidemiology of America to the CDC’s Advisory Committee on Immunization Practices.* “I do not think we can expect anyone to be vaccinated if we’re not willing to vaccinate ourselves.”
Healthcare workers are typically required to receive a range of vaccines, including measles, mumps, and rubella (MMR) and pertussis shots. Each year, close to half of US healthcare workers receive a flu vaccine under a workplace mandate. But COVID-19 will be different. The FDA requires anyone given products under an emergency use authorization (EUA) to receive information about risks and benefits and to have the option to decline. Hospitals instead will rely on education as they offer a novel vaccine (or more than one) that will have a minimum effectiveness of 50%.
ProMedica doesn’t require employees to be vaccinated against flu, but employees who decline must get a note from a doctor indicating that they have talked about the risks and benefits of the vaccine. A similar approach may be used with a COVID-19 vaccine, in which employees may be required to learn about the vaccine before they decline, Smith says. “I do believe some people will say they don’t want to get it,” he added.
Like colleagues across the country, Smith is identifying healthcare workers who are involved in direct care of COVID-19 patients and are at highest risk for exposure. Even within the top tier, those performing the riskiest tasks, such as respiratory therapists who provide breathing treatments that spread aerosols and droplets, will be tagged as a priority group, he says. Healthcare workers who spend the most time in proximity to COVID patients, such as nurses in a COVID unit, also are likely to get the first doses, he says.
Swirl, don’t shake, the vaccine
Hospitals are adept at ramping up vaccination campaigns. For example, last year, Vanderbilt University Medical Center, in Nashville, Tennessee, vaccinated nearly 16,000 employees against influenza in their 1-day “Flulapalooza” event. The medical center even earned a Guinness world record in 2011 at the first Flulapalooza for giving the most vaccinations ever within 8 hours.
The 10th anniversary of the event was canceled this year because of COVID restrictions. Instead, nurses, pharmacists, and other clinicians pitched in to vaccinate their coworkers against influenza. Now, plans for COVID-19 vaccination move forward amid uncertainty.
Instead of holding a mass event, “the delivery mechanisms will need to be more targeted and focused,” said Lori Rolando, MD, MPH, director of the Vanderbilt Occupational Health Clinic. In the CDC’s most recent version of its vaccination program “playbook,” the agency recommends giving the vaccines in an area that allows people to remain 6 feet apart and for them to wait for 15 minutes after receiving the shot to make sure they don’t faint, a potential risk common to almost all vaccines.
That’s the easy part. Planning becomes more complex, given the uncertainty as to which vaccines will receive approval and which one a hospital will receive.
If the Pfizer/BioNTech vaccine receives EUA in 2020, about 10 to 20 million doses could be available in November and 20 to 30 million doses in December. The ultracold containers used to ship the vaccines have to be replenished with dry ice within 24 hours of receipt and every 5 days thereafter. Hospitals will need temperature probes to monitor storage in the containers. The five-dose vials can be refrigerated before administering, but only for 5 days. The product must be diluted, and it then must be used within 6 hours.
The Moderna vaccine will be somewhat less plentiful at first. About 10 million doses are expected in November and 15 million doses by the end of December. The 10-dose vials are stored in a freezer. Once they are placed in a refrigerator to thaw, they have to be used within 7 days, and once they’re removed from the refrigerator, they have to be used within 12 hours. The pharmacist or other vaccinator must swirl – but not shake! – the vial before delivering a dose, according to the CDC playbook.
As more information emerges about the vaccines, instructions may change, and Smith is steeled for shifting scenarios. “These are all draft plans. We’re going to modify as we go along,” he says.
The Pfizer vaccine requires a second dose at 21 days, and the Moderna vaccine targets the second dose at 28 days. In addition to using information systems to track vaccinations and any adverse effects, hospitals will give employees a card indicating what vaccine they received, the date it was administered, and the date on which they need to return. (At this point, the time frame for the second dose doesn’t appear to be flexible.)
Regardless of the vaccine, one message stays the same: COVID precautions must continue. That means mask wearing, social distancing, and hand washing – practices that also must be followed by healthcare workers who test positive for naturally acquired antibodies.
“I don’t think anyone expects the COVID vaccine to be 100% effective at preventing COVID,” says Rolando. “So all of the other tools in our toolbox are going to need to be continued to be used as well.”
*Correction, 11/12/20: An earlier version of this article misstated the name of Dr. Drees' institution.
This article first appeared on Medscape.com.
At first, when news spread of a 28-year-old doctor on the COVID-19 front lines in Brazil who died after receiving an experimental vaccine, doubts arose about the safety of one of the most promising coronavirus vaccine candidates. But then the story flipped. Although the vaccine maker wouldn’t confirm it, the doctor appeared to have been in the control group and had received a dose of an established meningitis vaccine. The danger came from exposure to the coronavirus itself.
That tragedy underscores the ongoing risk of COVID-19 to healthcare workers, who have been designated by US advisory panels as part of phase 1A – the first to receive doses of any approved vaccine. The Centers for Disease Control and Prevention (CDC) recently reported that 6% of adults hospitalized with COVID from March to May were healthcare workers. The report was based on surveillance data from 13 states. The average age of the patients was 49 years. The agency set a November 15 vaccination “readiness date” for jurisdictions, such as state health departments, even though a vaccine isn’t likely to be authorized by then.
As hospitals scramble to prepare, their watchword is flexibility. They don’t yet know how many initial doses they will get, of which vaccine, or in what time frame. They have a sophisticated infrastructure to deliver flu vaccines each fall, but that framework doesn’t align with the likely scenarios of limited supply, additional reporting requirements, two-dose regimens, and differing storage needs.
“Healthcare organizations have consistently risen to the challenge. I wholeheartedly believe in their potential to do this,” Anna Legreid Dopp, PharmD, senior director of quality improvement and guidelines for the American Society of Health-System Pharmacists, told Medscape Medical News.
Healthcare workers won’t face a vaccine mandate
Even after months of caring for COVID patients, most clinicians remain vulnerable to infection – at work and in their communities. That was what occupational medicine physician Kevin Smith, MD, realized when his health system, Toledo, Ohio–based ProMedica, offered antibody testing to all its 50,000 employees. About 2% of the 6933 tests given came back positive, he says.
Yet many physicians, nurses, and other healthcare workers share the public’s skepticism about the safety and effectiveness of a vaccine that receives swift US Food and Drug Administration (FDA) approval for emergency use. About half of nurses (47%) and almost 1 in 3 physicians (30%) say that they don’t want to get the vaccine when it first becomes available or that they’re unsure about vaccination, according to a Medscape survey.
Because vaccination of healthcare workers will set the stage for public acceptance of the vaccine, hospital epidemiologists are concerned. “We know that there will be some hesitancy in the healthcare workforce, just as there will be in the broader public,” said Marci Drees, MD, chief infection prevention officer and hospital epidemiologist for ChristianaCare in Newark, Delaware, and liaison from the Society for Healthcare Epidemiology of America to the CDC’s Advisory Committee on Immunization Practices.* “I do not think we can expect anyone to be vaccinated if we’re not willing to vaccinate ourselves.”
Healthcare workers are typically required to receive a range of vaccines, including measles, mumps, and rubella (MMR) and pertussis shots. Each year, close to half of US healthcare workers receive a flu vaccine under a workplace mandate. But COVID-19 will be different. The FDA requires anyone given products under an emergency use authorization (EUA) to receive information about risks and benefits and to have the option to decline. Hospitals instead will rely on education as they offer a novel vaccine (or more than one) that will have a minimum effectiveness of 50%.
ProMedica doesn’t require employees to be vaccinated against flu, but employees who decline must get a note from a doctor indicating that they have talked about the risks and benefits of the vaccine. A similar approach may be used with a COVID-19 vaccine, in which employees may be required to learn about the vaccine before they decline, Smith says. “I do believe some people will say they don’t want to get it,” he added.
Like colleagues across the country, Smith is identifying healthcare workers who are involved in direct care of COVID-19 patients and are at highest risk for exposure. Even within the top tier, those performing the riskiest tasks, such as respiratory therapists who provide breathing treatments that spread aerosols and droplets, will be tagged as a priority group, he says. Healthcare workers who spend the most time in proximity to COVID patients, such as nurses in a COVID unit, also are likely to get the first doses, he says.
Swirl, don’t shake, the vaccine
Hospitals are adept at ramping up vaccination campaigns. For example, last year, Vanderbilt University Medical Center, in Nashville, Tennessee, vaccinated nearly 16,000 employees against influenza in their 1-day “Flulapalooza” event. The medical center even earned a Guinness world record in 2011 at the first Flulapalooza for giving the most vaccinations ever within 8 hours.
The 10th anniversary of the event was canceled this year because of COVID restrictions. Instead, nurses, pharmacists, and other clinicians pitched in to vaccinate their coworkers against influenza. Now, plans for COVID-19 vaccination move forward amid uncertainty.
Instead of holding a mass event, “the delivery mechanisms will need to be more targeted and focused,” said Lori Rolando, MD, MPH, director of the Vanderbilt Occupational Health Clinic. In the CDC’s most recent version of its vaccination program “playbook,” the agency recommends giving the vaccines in an area that allows people to remain 6 feet apart and for them to wait for 15 minutes after receiving the shot to make sure they don’t faint, a potential risk common to almost all vaccines.
That’s the easy part. Planning becomes more complex, given the uncertainty as to which vaccines will receive approval and which one a hospital will receive.
If the Pfizer/BioNTech vaccine receives EUA in 2020, about 10 to 20 million doses could be available in November and 20 to 30 million doses in December. The ultracold containers used to ship the vaccines have to be replenished with dry ice within 24 hours of receipt and every 5 days thereafter. Hospitals will need temperature probes to monitor storage in the containers. The five-dose vials can be refrigerated before administering, but only for 5 days. The product must be diluted, and it then must be used within 6 hours.
The Moderna vaccine will be somewhat less plentiful at first. About 10 million doses are expected in November and 15 million doses by the end of December. The 10-dose vials are stored in a freezer. Once they are placed in a refrigerator to thaw, they have to be used within 7 days, and once they’re removed from the refrigerator, they have to be used within 12 hours. The pharmacist or other vaccinator must swirl – but not shake! – the vial before delivering a dose, according to the CDC playbook.
As more information emerges about the vaccines, instructions may change, and Smith is steeled for shifting scenarios. “These are all draft plans. We’re going to modify as we go along,” he says.
The Pfizer vaccine requires a second dose at 21 days, and the Moderna vaccine targets the second dose at 28 days. In addition to using information systems to track vaccinations and any adverse effects, hospitals will give employees a card indicating what vaccine they received, the date it was administered, and the date on which they need to return. (At this point, the time frame for the second dose doesn’t appear to be flexible.)
Regardless of the vaccine, one message stays the same: COVID precautions must continue. That means mask wearing, social distancing, and hand washing – practices that also must be followed by healthcare workers who test positive for naturally acquired antibodies.
“I don’t think anyone expects the COVID vaccine to be 100% effective at preventing COVID,” says Rolando. “So all of the other tools in our toolbox are going to need to be continued to be used as well.”
*Correction, 11/12/20: An earlier version of this article misstated the name of Dr. Drees' institution.
This article first appeared on Medscape.com.
At first, when news spread of a 28-year-old doctor on the COVID-19 front lines in Brazil who died after receiving an experimental vaccine, doubts arose about the safety of one of the most promising coronavirus vaccine candidates. But then the story flipped. Although the vaccine maker wouldn’t confirm it, the doctor appeared to have been in the control group and had received a dose of an established meningitis vaccine. The danger came from exposure to the coronavirus itself.
That tragedy underscores the ongoing risk of COVID-19 to healthcare workers, who have been designated by US advisory panels as part of phase 1A – the first to receive doses of any approved vaccine. The Centers for Disease Control and Prevention (CDC) recently reported that 6% of adults hospitalized with COVID from March to May were healthcare workers. The report was based on surveillance data from 13 states. The average age of the patients was 49 years. The agency set a November 15 vaccination “readiness date” for jurisdictions, such as state health departments, even though a vaccine isn’t likely to be authorized by then.
As hospitals scramble to prepare, their watchword is flexibility. They don’t yet know how many initial doses they will get, of which vaccine, or in what time frame. They have a sophisticated infrastructure to deliver flu vaccines each fall, but that framework doesn’t align with the likely scenarios of limited supply, additional reporting requirements, two-dose regimens, and differing storage needs.
“Healthcare organizations have consistently risen to the challenge. I wholeheartedly believe in their potential to do this,” Anna Legreid Dopp, PharmD, senior director of quality improvement and guidelines for the American Society of Health-System Pharmacists, told Medscape Medical News.
Healthcare workers won’t face a vaccine mandate
Even after months of caring for COVID patients, most clinicians remain vulnerable to infection – at work and in their communities. That was what occupational medicine physician Kevin Smith, MD, realized when his health system, Toledo, Ohio–based ProMedica, offered antibody testing to all its 50,000 employees. About 2% of the 6933 tests given came back positive, he says.
Yet many physicians, nurses, and other healthcare workers share the public’s skepticism about the safety and effectiveness of a vaccine that receives swift US Food and Drug Administration (FDA) approval for emergency use. About half of nurses (47%) and almost 1 in 3 physicians (30%) say that they don’t want to get the vaccine when it first becomes available or that they’re unsure about vaccination, according to a Medscape survey.
Because vaccination of healthcare workers will set the stage for public acceptance of the vaccine, hospital epidemiologists are concerned. “We know that there will be some hesitancy in the healthcare workforce, just as there will be in the broader public,” said Marci Drees, MD, chief infection prevention officer and hospital epidemiologist for ChristianaCare in Newark, Delaware, and liaison from the Society for Healthcare Epidemiology of America to the CDC’s Advisory Committee on Immunization Practices.* “I do not think we can expect anyone to be vaccinated if we’re not willing to vaccinate ourselves.”
Healthcare workers are typically required to receive a range of vaccines, including measles, mumps, and rubella (MMR) and pertussis shots. Each year, close to half of US healthcare workers receive a flu vaccine under a workplace mandate. But COVID-19 will be different. The FDA requires anyone given products under an emergency use authorization (EUA) to receive information about risks and benefits and to have the option to decline. Hospitals instead will rely on education as they offer a novel vaccine (or more than one) that will have a minimum effectiveness of 50%.
ProMedica doesn’t require employees to be vaccinated against flu, but employees who decline must get a note from a doctor indicating that they have talked about the risks and benefits of the vaccine. A similar approach may be used with a COVID-19 vaccine, in which employees may be required to learn about the vaccine before they decline, Smith says. “I do believe some people will say they don’t want to get it,” he added.
Like colleagues across the country, Smith is identifying healthcare workers who are involved in direct care of COVID-19 patients and are at highest risk for exposure. Even within the top tier, those performing the riskiest tasks, such as respiratory therapists who provide breathing treatments that spread aerosols and droplets, will be tagged as a priority group, he says. Healthcare workers who spend the most time in proximity to COVID patients, such as nurses in a COVID unit, also are likely to get the first doses, he says.
Swirl, don’t shake, the vaccine
Hospitals are adept at ramping up vaccination campaigns. For example, last year, Vanderbilt University Medical Center, in Nashville, Tennessee, vaccinated nearly 16,000 employees against influenza in their 1-day “Flulapalooza” event. The medical center even earned a Guinness world record in 2011 at the first Flulapalooza for giving the most vaccinations ever within 8 hours.
The 10th anniversary of the event was canceled this year because of COVID restrictions. Instead, nurses, pharmacists, and other clinicians pitched in to vaccinate their coworkers against influenza. Now, plans for COVID-19 vaccination move forward amid uncertainty.
Instead of holding a mass event, “the delivery mechanisms will need to be more targeted and focused,” said Lori Rolando, MD, MPH, director of the Vanderbilt Occupational Health Clinic. In the CDC’s most recent version of its vaccination program “playbook,” the agency recommends giving the vaccines in an area that allows people to remain 6 feet apart and for them to wait for 15 minutes after receiving the shot to make sure they don’t faint, a potential risk common to almost all vaccines.
That’s the easy part. Planning becomes more complex, given the uncertainty as to which vaccines will receive approval and which one a hospital will receive.
If the Pfizer/BioNTech vaccine receives EUA in 2020, about 10 to 20 million doses could be available in November and 20 to 30 million doses in December. The ultracold containers used to ship the vaccines have to be replenished with dry ice within 24 hours of receipt and every 5 days thereafter. Hospitals will need temperature probes to monitor storage in the containers. The five-dose vials can be refrigerated before administering, but only for 5 days. The product must be diluted, and it then must be used within 6 hours.
The Moderna vaccine will be somewhat less plentiful at first. About 10 million doses are expected in November and 15 million doses by the end of December. The 10-dose vials are stored in a freezer. Once they are placed in a refrigerator to thaw, they have to be used within 7 days, and once they’re removed from the refrigerator, they have to be used within 12 hours. The pharmacist or other vaccinator must swirl – but not shake! – the vial before delivering a dose, according to the CDC playbook.
As more information emerges about the vaccines, instructions may change, and Smith is steeled for shifting scenarios. “These are all draft plans. We’re going to modify as we go along,” he says.
The Pfizer vaccine requires a second dose at 21 days, and the Moderna vaccine targets the second dose at 28 days. In addition to using information systems to track vaccinations and any adverse effects, hospitals will give employees a card indicating what vaccine they received, the date it was administered, and the date on which they need to return. (At this point, the time frame for the second dose doesn’t appear to be flexible.)
Regardless of the vaccine, one message stays the same: COVID precautions must continue. That means mask wearing, social distancing, and hand washing – practices that also must be followed by healthcare workers who test positive for naturally acquired antibodies.
“I don’t think anyone expects the COVID vaccine to be 100% effective at preventing COVID,” says Rolando. “So all of the other tools in our toolbox are going to need to be continued to be used as well.”
*Correction, 11/12/20: An earlier version of this article misstated the name of Dr. Drees' institution.
This article first appeared on Medscape.com.
United States adds nearly 74,000 more children with COVID-19
The new weekly high for COVID-19 cases in children announced last week has been surpassed already, as the United States experienced almost 74,000 new pediatric cases for the week ending Nov. 5, according to the American Academy of Pediatrics and the Children’s Hospital Association.
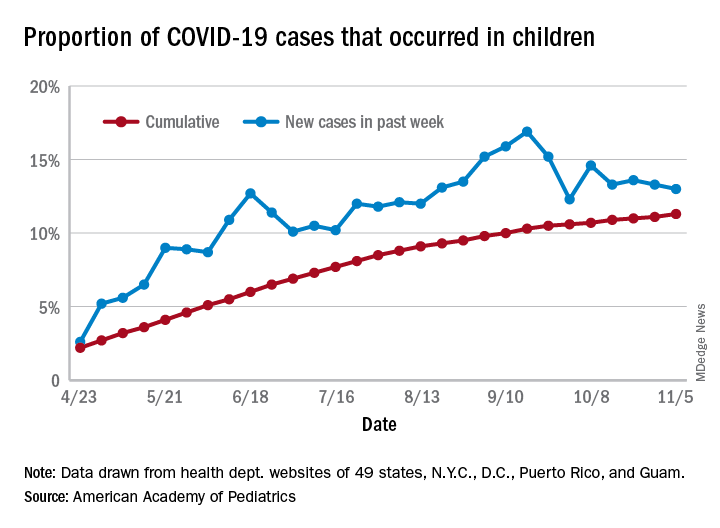
The total number of COVID-19 cases in children is now 927,518 in 49 states, the District of Columbia, New York City, Puerto Rico, and Guam, the AAP and CHA said in their weekly report.
Cumulatively, children represent 11.3% of all COVID-19 cases in those jurisdictions, up from 11.1% a week ago. For just the past week, those 73,883 children represent 13.0% of the 567,672 new cases reported among all ages. That proportion peaked at 16.9% in mid-September, the AAP/CHA data show.
Dropping down to the state level, cumulative proportions as of Nov. 5 range from 5.2% in New Jersey to 23.3% in Wyoming, with 11 other states over 15%. California has had more cases, 100,856, than any other state, and Vermont the fewest at 329, the AAP and CHA said.
The national rate per 100,000 children is now 1,232, up from 1,134 the previous week and more than doubled since mid-August (582.2 per 100,000 on Aug. 20). North Dakota’s rate of 3,990 per 100,000 children is the highest of any state (South Dakota is next at 2,779), while Vermont is again the lowest at 245 per 100,000, based on data collected from state health department websites.
Two COVID-19–related deaths in children were reported during the week ending Nov. 5, bringing the total to 123 but leaving the overall proportion of deaths in children unchanged at 0.06% of all deaths. Texas has reported the most COVID-19 deaths in children with 29, while 15 states have recorded no deaths so far (mortality data in children reported by 42 states and New York City), the AAP and CHA said.
The new weekly high for COVID-19 cases in children announced last week has been surpassed already, as the United States experienced almost 74,000 new pediatric cases for the week ending Nov. 5, according to the American Academy of Pediatrics and the Children’s Hospital Association.
The total number of COVID-19 cases in children is now 927,518 in 49 states, the District of Columbia, New York City, Puerto Rico, and Guam, the AAP and CHA said in their weekly report.
Cumulatively, children represent 11.3% of all COVID-19 cases in those jurisdictions, up from 11.1% a week ago. For just the past week, those 73,883 children represent 13.0% of the 567,672 new cases reported among all ages. That proportion peaked at 16.9% in mid-September, the AAP/CHA data show.
Dropping down to the state level, cumulative proportions as of Nov. 5 range from 5.2% in New Jersey to 23.3% in Wyoming, with 11 other states over 15%. California has had more cases, 100,856, than any other state, and Vermont the fewest at 329, the AAP and CHA said.
The national rate per 100,000 children is now 1,232, up from 1,134 the previous week and more than doubled since mid-August (582.2 per 100,000 on Aug. 20). North Dakota’s rate of 3,990 per 100,000 children is the highest of any state (South Dakota is next at 2,779), while Vermont is again the lowest at 245 per 100,000, based on data collected from state health department websites.
Two COVID-19–related deaths in children were reported during the week ending Nov. 5, bringing the total to 123 but leaving the overall proportion of deaths in children unchanged at 0.06% of all deaths. Texas has reported the most COVID-19 deaths in children with 29, while 15 states have recorded no deaths so far (mortality data in children reported by 42 states and New York City), the AAP and CHA said.
The new weekly high for COVID-19 cases in children announced last week has been surpassed already, as the United States experienced almost 74,000 new pediatric cases for the week ending Nov. 5, according to the American Academy of Pediatrics and the Children’s Hospital Association.
The total number of COVID-19 cases in children is now 927,518 in 49 states, the District of Columbia, New York City, Puerto Rico, and Guam, the AAP and CHA said in their weekly report.
Cumulatively, children represent 11.3% of all COVID-19 cases in those jurisdictions, up from 11.1% a week ago. For just the past week, those 73,883 children represent 13.0% of the 567,672 new cases reported among all ages. That proportion peaked at 16.9% in mid-September, the AAP/CHA data show.
Dropping down to the state level, cumulative proportions as of Nov. 5 range from 5.2% in New Jersey to 23.3% in Wyoming, with 11 other states over 15%. California has had more cases, 100,856, than any other state, and Vermont the fewest at 329, the AAP and CHA said.
The national rate per 100,000 children is now 1,232, up from 1,134 the previous week and more than doubled since mid-August (582.2 per 100,000 on Aug. 20). North Dakota’s rate of 3,990 per 100,000 children is the highest of any state (South Dakota is next at 2,779), while Vermont is again the lowest at 245 per 100,000, based on data collected from state health department websites.
Two COVID-19–related deaths in children were reported during the week ending Nov. 5, bringing the total to 123 but leaving the overall proportion of deaths in children unchanged at 0.06% of all deaths. Texas has reported the most COVID-19 deaths in children with 29, while 15 states have recorded no deaths so far (mortality data in children reported by 42 states and New York City), the AAP and CHA said.