User login
How best to address these common movement disorders
• Initiate neuroprotective therapy with a monoamine oxidase B inhibitor to slow the progression of Parkinson’s disease. With onset of functional impairment, give levodopa at the lowest effective dose. A
• Give propranolol for essential tremor causing a patient distress, starting at 20 to 40 mg twice daily and increasing the dose (to a maximum of 320 mg/d) until relief is achieved. B
• Consider giving a dopamine receptor blocker for Tourette syndrome or other tic disorder; alternative agents are clonidine or a newer agent, tetrabenazine. B
Strength of recommendation (SOR)
A Good-quality patient-oriented evidence
B Inconsistent or limited-quality patient-oriented evidence
C Consensus, usual practice, opinion, disease-oriented evidence, case series
Movement disorders often require consultation with a neurologist, and a working knowledge of established and novel treatments can set the stage for optimal long-term cooperative management.1 In this article, we review therapeutic options for common movement disorders, including hypokinetic, hyperkinetic, and dyskinetic disturbances.
Parkinson’s disease treatment: MAO-B inhibitor, levodopa are mainstays
Parkinson’s disease, the most common hypokinetic movement disorder, is a chronic, progressive, neurodegenerative disease. It affects 1% of individuals older than 65 years and 4% to 5% of individuals older than 85 years. Its cardinal symptoms are resting tremor, bradykinesia, rigidity, a flexed posture, and loss of postural reflexes. Resting tremor, referred to as “pill rolling” tremor, is 4 to 6 Hz and usually begins unilaterally.2,3 Associated symptoms can include dystonia, dementia, psychiatric disorders, sleep disorders, and autonomic symptoms.
Neuroprotective therapy is used to slow the progression of the disease, particularly in its early stage. The monoamine oxidase B (MAO-B) inhibitor selegiline has proven effective in this regard2 (strength of recommendation [SOR]: A). In randomized controlled studies, selegiline has delayed the need for levodopa for 9 to 12 months4 (SOR: A). Another MAO-B inhibitor, rasagiline, has demonstrated neuroprotective effects as well5 (SOR: B). These medications may also be used with levodopa for symptom control and as adjuvant therapy in patients with motor fluctuations.2 A conventional dose of selegiline is 10 mg/d (5 mg at breakfast; 5 mg at lunch). Rasagiline is given at 1 mg/d. Concomitant use of ciprofloxacin or other CYP1A2 inhibitors limits its effectiveness.6,7
Symptomatic therapy is indicated at the onset of functional impairment. The dopamine precursor levodopa is the most widely used and effective drug for Parkinson’s disease symptoms, especially bradykinesia and rigidity. Use the lowest possible dose to control symptoms (eg, 100 mg twice daily) and protect against motor complications of the drug7-9 (SOR: A). To prevent conversion of levodopa to dopamine outside the blood-brain barrier, combine it with the decarboxylase inhibitor carbidopa. Dietary restriction of proteins may be needed, because amino acids can interfere with the absorption of levodopa.
Especially with prolonged use, levodopa can cause disturbing adverse effects, such as nausea, vomiting, psychosis, cardiac arrhythmia, and orthostatic hypotension. Dyskinesias and motor fluctuations are complications of long-term treatment and are irreversible. Adding a cathecol-O-methyltransferase (COMT) inhibitor, such as entacapone, to increase levodopa’s effectiveness has been shown to reduce motor fluctuations2,3,10 (SOR: B). Dopamine agonists such as bromocriptine, ropinirole, and pramipexole used in early Parkinson’s disease can also reduce dyskinesias and motor fluctuations. Dopamine agonists may be preferred to levodopa in early Parkinson’s disease because they are better tolerated and cause fewer adverse effects. Or they may be used as adjuncts for patients whose response to levodopa is deteriorating or fluctuating3,7,8 (SOR: B). In advanced disease, motor complications can also be managed by augmenting levodopa therapy with a dopamine agonist, MAO-B inhibitor, or COMT inhibitor7,8 (SOR: A).
Anticholinergics, mainly benztropine and trihexyphenidyl, may be used as symptomatic treatment, especially in young people with early Parkinson’s disease and severe tremor. However, they are not the first drugs of choice due to limited efficacy and the potential for neuropsychiatric side effects8 (SOR: C). Amantadine can reduce dyskinesia in people with advanced Parkinson’s disease8 (SOR: C). For patients who have Parkinson’s disease with severe motor complications, intermittent apomorphine injections can help reduce “off time” periods in the daily treatment cycle when the efficacy of drugs wanes9 (SOR: B).
Deep brain stimulation of the subthalamic nucleus has only SOR C support for reducing dyskinesias and off time.9
Treating nonmotor symptoms of Parkinson’s disease can be challenging. For dementia in these patients, consider cholinesterase inhibitors6,8 (SOR: C). For depression, selective serotonin reuptake inhibitors are effective6,8,9 (SOR: C). For psychosis, preferred agents are low-dose clozapine or quetiapine6,8-10 (SOR: C). Plan for supportive and symptomatic management of constipation, dysphagia, sialorrhea, orthostatic hypotension, sleep disturbances, and urinary urgency.2,3
Tremor
Tremor is a common form of hyperkinesia, presenting either as a primary disorder or as a symptom of another condition.11 By definition, it is a rhythmical, involuntary, oscillatory movement of 1 or more body parts. Tremors are classified as rest or action tremors, with the latter being further categorized as postural (occurring while the patient maintains a position against gravity) or kinetic (occurring during voluntary movement).2,10
Physiologic tremor: Pharmacologic Tx is usually not needed
Physiologic tremor is benign, high frequency (8-12 Hz), low amplitude, and postural. An exaggerated form of this tremor may result from anxiety, hyperthyroidism, pheochromocytoma, hypoglycemia, excessive caffeine consumption, fever, withdrawal from opioids and sedatives, and some medications. No drug treatment is necessary unless symptoms become bothersome. Correct the underlying cause or have the patient avoid the triggering factor, and offer reassurance that the condition is not pathological or progressive.2,12 For anxiety, consider cognitive-behavioral/relaxation therapy or benzodiazepines (if tremor did not result from withdrawal of benzodiazepines) or beta-adrenergic antagonists (eg, propranolol).12,13
Essential tremor: Try propranolol or primidone first
Essential tremor (ET) is the most common movement disorder. It often results in functional disability and leads to many physical and emotional difficulties. ET is bilateral, usually symmetric (although mild asymmetry is possible), and postural or kinetic, typically affecting hands and forearms. The frequency of ET is 4 to 12 Hz. Cranial musculature may be involved in 30% of cases, affecting the head and voice.3 Prevalence ranges from 4 to 40 cases per 1000 people. The age-adjusted incidence is 17.5/100,000 per year; it peaks during the teen years and the fifth decade.2,3
Autosomal dominant type of inheritance is common, and a family history of ET is often present, particularly with younger patients. The differential diagnosis includes Parkinson’s disease tremor; dystonic, cerebellar, rubral, and psychogenic tremors; and asterixis.3 Unlike ET, many of these disorders have associated neurologic, psychiatric, or systemic signs.
Treatment with propranolol or primidone is indicated if ET causes functional impairment or social or emotional problems for the patient.2,3,10,13 Both propranolol and primidone reduce limb tremor2,10,13 (SOR: B), but only propranolol is approved by the US Food and Drug Administration (FDA) for treatment of ET. Propranolol is more effective for hand and forearm tremor than for head and voice tremor. Start propranolol at 20 to 40 mg twice a day and increase the dose as needed to achieve symptom relief.14
A maintenance dose of 240 to 320 mg/d may be needed. Major adverse effects are fatigue, sedation, depression, and erectile dysfunction. Contraindications to propranolol include asthma, second-degree atrioventricular block, and insulin-dependent diabetes.
If starting with primidone alone, prescribe at a dose <25 mg at bedtime and increase the dose slowly over several weeks to prevent onset of nausea, vomiting, sedation, confusion, or ataxia. The maximum allowable dose is 750 mg/d in 3 divided doses.10 Primidone and propranolol may be used in combination to treat limb tremor when monotherapy is insufficient (SOR: B).13
Thirty percent of patients with ET will not respond to propranolol or primidone. An alternative choice is the anticonvulsant gabapentin10,12-14 (SOR: C). However, clinical experience with it is limited. Lethargy, fatigue, decreased libido, dizziness, nervousness, and shortness of breath are adverse effects of gabapentin; they are usually mild and tolerable.13 Topiramate is another option that seems to be as effective as gabapentin10,13 (SOR: C), but studies of long-term outcomes are lacking. Topiramate’s side effects include weight loss and paresthesias. Additionally, alprazolam, clonazepam, clozapine, olanzapine, atenolol, sotalol, nadolol, and nimodipine may reduce limb tremor2 (SOR: C). Alcohol reduces tremor amplitude in 50% to 90% of patients, but tremor may worsen after the effect of alcohol has worn off.15
For patients with essential hand tremor that fails to respond to oral agents, consider botulinum toxin A16 (SOR: B). However, it is also associated with dose-dependent hand weakness16 (SOR: C). Botulinum toxin may reduce head and voice tremor16 (SOR: C), but hoarseness and swallowing difficulties may occur after use for voice tremor.16
Invasive therapies may benefit patients with refractory tremor. Deep brain stimulation and thalamotomy are highly effective in reducing limb tremor13 (SOR: C). Each carries a small risk of major complications. Some deep brain stimulation adverse events may resolve with time. Other adverse events may resolve with adjustment of stimulator settings. No evidence exists for surgical treatment for voice and head tremor or for gamma-knife thalamotomy.13
Drug-induced tremor
Drugs with the potential to cause postural tremor, intention tremor, or rest tremor include the following: 15
- alcohol (chronic)
- amiodarone
- amphetamines
- beta-adrenergic agonists
- caffeine
- calcitonin
- carbamazepine
- cocaine
- cyclosporine
- dopamine
- lithium
- metoclopramide
- neuroleptics
- procainamide
- steroids
- theophylline
- thyroid hormones
- tricyclic antidepressants
- trifluoperazine
- valproic acid
With drug-induced tremor, carefully evaluate a patient’s need for the drug. Discontinue the offending agent if possible, or try lowering the dose.
Psychogenic tremor: A history of somatization is a clue
Psychogenic tremor can occur at rest or during postural or kinetic movement. Clinical features include an abrupt onset, a static course, spontaneous remission, and unclassifiable tremors.17 Psychogenic tremor increases under direct observation and decreases with distraction. Patients with psychogenic tremor often have a history of somatization.18 Electrophysiologic testing can help confirm the diagnosis. If remission does not occur spontaneously, patients may find relief with psychotherapy or placebo.19
Tic disorders: Opt for dopamine receptor blockers
Tics are involuntary or semivoluntary movements or sounds that are sudden, brief, intermittent, repetitive, nonrhythmic, unpredictable, and purposeless. Tics can occur in any part of the body.20
The most common tic disorder is Tourette syndrome—a combination of motor and phonic tics with onset before age 21. It affects approximately 5 to 10 children out of 10,000. Boys are more commonly affected than girls. Attention deficit hyperactivity disorder frequently accompanies this syndrome.2
The goal of treatment with any tic disorder is to improve social functioning, self-esteem, and quality of life. Education and support of patients is important. Tic disorders, including Tourette, rarely require drugs. But if tics become too distressing, first-line treatment would be a dopamine modulator, tetrabenazine, or clonidine. Randomized controlled trials with various neuroleptics have revealed dramatic reductions in tic severity. However, many patients do not tolerate the acute adverse effects (most commonly sedation, weight gain, depression, lethargy, and akathisia), and prolonged treatment confers a small risk of tardive dyskinesia. Behavioral therapy is an important part of management.20
Dopamine-receptor blocking drugs such as haloperidol, pimozide, and fluphenazine are the most effective treatment for tics20 (SOR: B). Tetrabenazine is a promising new dopamine-depleting drug; controlled trials are ongoing2,20 (SOR: B). Clonidine, an alpha 2-adrenergic agonist, is useful in treating patients with Tourette syndrome, helping to improve sleep and attention2,21 (SOR: C). Medically refractory motor and disabling phonic tics such as coprolalia can be ameliorated by botulinum toxin injections21 (SOR: B). Deep brain stimulation is being used at an increasing rate for medically refractory tics in Tourette syndrome21 (SOR: B).
Restless legs syndrome: Dopamine agonists are preferred
Restless legs syndrome (RLS) is a disorder characterized by sensory symptoms and motor disturbances of the legs, mainly during rest. Treatment may not be necessary for patients with mild or sporadic symptoms. For moderate to severe RLS with significant impairment, dopamine agonists are the preferred agents22 (SOR: A). RLS can also occur secondary to such conditions as iron deficiency and uremia, and correction of the underlying disorder is the goal. Prescribe iron replacement for patients with a ferritin level <50 ng/mL22 (SOR: C). Medications known to cause or exacerbate the symptoms of RLS are anti-dopaminergic agents (such as neuroleptics), diphenhydramine, tricyclic antidepressants, alcohol, caffeine, lithium, and beta-blockers. If a patient is taking medications that exacerbate symptoms of RLS, discontinue them and use appropriate substitutes22 (SOR: C).
Myoclonus: Clonazepam for essential disorder
Myoclonus is a brief, sudden, shock-like movement caused by involuntary muscle contractions or lapse of muscle contraction (asterixis). Given the complex origins of myoclonus, multiple drugs may be needed. Essential myoclonus is disabling and can be treated with clonazepam. Start with 0.25 mg orally twice daily, and increase the dosage over 3 days to 1 mg/d23 (SOR: C). Most cases of myoclonus are secondary due to drugs such as lithium, toxins, advanced liver disease, infections including human immunodeficiency virus, dementia, and brain lesions. Treatment should also address the underlying disorder.2,23
Chorea
Chorea is an abnormal involuntary movement disorder described as “a state of excessive, spontaneous movements, irregularly timed, nonrepetitive, randomly distributed, and abrupt in character.”24
Treatment of chorea is symptomatic, aiming to reduce morbidity and prevent complications. Haloperidol and fluphenazine are effective but can impair voluntary movements2,10,25 (SOR: C). The dopamine-depleting drugs reserpine and tetrabenazine are also effective2,10,25 (SOR: C). GABAergic drugs, such as clonazepam, gabapentin, and valproate, can be used adjunctively.10,25
Dystonia
Dystonia is a syndrome involving sustained contractions of opposing muscles that cause twisting, repetitive movements and abnormal postures. Primary dystonia can be treated successfully with high doses of trihexyphenidyl alone, starting with 1 mg orally per day and increasing gradually to 6 to 80 mg/d until symptoms are controlled; or in combination with baclofen, starting with 10 mg orally once daily and increasing to a maximum dose of 30 to 120 mg/d1,2 (SOR: C).
Consider botulinum neurotoxin injection for focal upper extremity dystonia and adductor spasmodic dysphonia16 (SOR: B).
Ataxia
Ataxia is an unsteady gait associated with cerebellar dysfunction, proprioceptive defects, or both. Ataxia may be primary (Friedreich ataxia and spinocerebellar ataxia) or secondary to stroke, trauma, alcoholic degeneration, multiple sclerosis, vitamin B12 deficiency, and hydrocephalus. Treatment, when possible, should target the underlying cause.1,2
CORRESPONDENCE Hakan Yaman, MD, Akdeniz University, Department of Family Medicine, Antalya, Turkey 07058; [email protected]
1. Deuschl G, Bain P, Brin M. Consensus statement of the Movement Disorder Society on Tremor. Ad Hoc Scientific Committee. Mov Disord. 1998;13(suppl 3):2-23.
2. Yaman A, Yaman H, Rao G. Tremors and other movement disorders. In: Mengel MB, et al, eds. Family Medicine Ambulatory Care and Prevention. 5th ed. New York: McGraw-Hill; 2009:400–407.
3. Harris MK, Shneyder N, Borazanci A, et al. Movement disorders. Med Clin North Am. 2009;93:371-388.
4. Palhagen S, Heinonen E, Hagglund J, et al. Selegiline slows the progression of the symptoms of Parkinson disease. Neurology. 2006;66:1200-1206.
5. Olanow CW, Rascol O, Hauser R, et al. A double-blind, delayed-start trial of rasagiline in Parkinson’s disease. N Engl J Med. 2009;361:1268-1278.
6. Zesiewicz TA, Sullivan KL, Arnulf I, et al. Treatment of nonmotor symptoms of Parkinson disease. Neurology. 2010;74:924-931.
7. Suchowersky O, Reich S, Perlmutter J, et al. Practice parameter: diagnosis and prognosis of new onset Parkinson disease (an evidence-based review). Neurology. 2006;66:968-975.
8. Rao SS, Hofmann LA, Shakil A. Parkinson’s disease: diagnosis and treatment. Am Fam Physician. 2006;74:2046-2054.
9. The National Collaborating Centre for Chronic Conditions Parkinson’s Disease. National Clinical Guideline for Diagnosis and Management in Primary and Secondary Care. 2006. Available at: http://www.nice.org.uk/nicemedia/live/10984/30087/30087.pdf. Accessed May 12, 2010.
10. Jankovic J. Treatment of hyperkinetic movement disorders. Lancet Neurol. 2009;8:844-856.
11. Kerlsberg G, Rubenstein C, St Anna L, et al. Differential diagnosis of tremor. Am Fam Physician. 2008;77:1305-1306.
12. Burke DA, Hauser RA, McClain T. Essential tremor. Available at: http://emedicine.medscape.com/article/1150290-overview. Accessed May 12, 2010.
13. Zesiewicz TA, Elble R, Louis ED, et al. Practice parameter: therapies for essential tremor. Neurology. 2005;64:2008-2020.
14. Elble RJ. Tremor: clinical features, pathophysiology, and treatment. Neurol Clin. 2009;27:679-695.
15. Smaga S. Tremor. Am Fam Physician. 2003;68:1545-1552.
16. Use of botulinum neurotoxin for the treatment of movement disorders. AAN summary of evidence-based guidelines for clinicians. 2008. Available at: http://www.aan.com/practice/guideline/uploads/280.pdf. Accessed May 25, 2010.
17. Redondo L, Morgado Y, Durán E. Psychogenic tremor: a positive diagnosis [ in Spanish]. Neurología. 2010;25:51-57.
18. Schwingenschuh P, Katschnig P, Seiler S, et al. Moving toward ‘‘laboratory-supported’’ criteria for psychogenic tremor. Mov Disord. 2011;Sep 28. [Epub ahead of print].
19. McKeon A, Ahlskog JE, Bower JH, et al. Psychogenic tremor: long-term prognosis in patients with electrophysiologically confirmed disease. Mov Disord. 2009;24:72-76.
20. Shprecher D, Kurlan R. The management of tics. Mov Disord. 2009;24:15-24.
21. Kenney C, Kuo SH, Jimenez-Shahed J. Tourette’s syndrome. Am Fam Physician. 2008;77:651-658.
22. Bayard M, Avonda T, Wadzinsky J. Restless legs syndrome. Am Fam Physician. 2008;78:235-240.
23. Caviness JN. Pathophysiology and treatment of myoclonus. Neurol Clin. 2009;27:757-777.
24. Barbeau A, Duvoisin RC, Gerstenbrand F, et al. Classification of extrapyramidal disorders. J Neurol Sci. 1981;51:311-327.
25. Vertrees SM, Berman SA. Chorea in adults: treatment & management. Available at: http://emedicine.medscape.com/article/1149854-treatment. Accessed February 12, 2010.
• Initiate neuroprotective therapy with a monoamine oxidase B inhibitor to slow the progression of Parkinson’s disease. With onset of functional impairment, give levodopa at the lowest effective dose. A
• Give propranolol for essential tremor causing a patient distress, starting at 20 to 40 mg twice daily and increasing the dose (to a maximum of 320 mg/d) until relief is achieved. B
• Consider giving a dopamine receptor blocker for Tourette syndrome or other tic disorder; alternative agents are clonidine or a newer agent, tetrabenazine. B
Strength of recommendation (SOR)
A Good-quality patient-oriented evidence
B Inconsistent or limited-quality patient-oriented evidence
C Consensus, usual practice, opinion, disease-oriented evidence, case series
Movement disorders often require consultation with a neurologist, and a working knowledge of established and novel treatments can set the stage for optimal long-term cooperative management.1 In this article, we review therapeutic options for common movement disorders, including hypokinetic, hyperkinetic, and dyskinetic disturbances.
Parkinson’s disease treatment: MAO-B inhibitor, levodopa are mainstays
Parkinson’s disease, the most common hypokinetic movement disorder, is a chronic, progressive, neurodegenerative disease. It affects 1% of individuals older than 65 years and 4% to 5% of individuals older than 85 years. Its cardinal symptoms are resting tremor, bradykinesia, rigidity, a flexed posture, and loss of postural reflexes. Resting tremor, referred to as “pill rolling” tremor, is 4 to 6 Hz and usually begins unilaterally.2,3 Associated symptoms can include dystonia, dementia, psychiatric disorders, sleep disorders, and autonomic symptoms.
Neuroprotective therapy is used to slow the progression of the disease, particularly in its early stage. The monoamine oxidase B (MAO-B) inhibitor selegiline has proven effective in this regard2 (strength of recommendation [SOR]: A). In randomized controlled studies, selegiline has delayed the need for levodopa for 9 to 12 months4 (SOR: A). Another MAO-B inhibitor, rasagiline, has demonstrated neuroprotective effects as well5 (SOR: B). These medications may also be used with levodopa for symptom control and as adjuvant therapy in patients with motor fluctuations.2 A conventional dose of selegiline is 10 mg/d (5 mg at breakfast; 5 mg at lunch). Rasagiline is given at 1 mg/d. Concomitant use of ciprofloxacin or other CYP1A2 inhibitors limits its effectiveness.6,7
Symptomatic therapy is indicated at the onset of functional impairment. The dopamine precursor levodopa is the most widely used and effective drug for Parkinson’s disease symptoms, especially bradykinesia and rigidity. Use the lowest possible dose to control symptoms (eg, 100 mg twice daily) and protect against motor complications of the drug7-9 (SOR: A). To prevent conversion of levodopa to dopamine outside the blood-brain barrier, combine it with the decarboxylase inhibitor carbidopa. Dietary restriction of proteins may be needed, because amino acids can interfere with the absorption of levodopa.
Especially with prolonged use, levodopa can cause disturbing adverse effects, such as nausea, vomiting, psychosis, cardiac arrhythmia, and orthostatic hypotension. Dyskinesias and motor fluctuations are complications of long-term treatment and are irreversible. Adding a cathecol-O-methyltransferase (COMT) inhibitor, such as entacapone, to increase levodopa’s effectiveness has been shown to reduce motor fluctuations2,3,10 (SOR: B). Dopamine agonists such as bromocriptine, ropinirole, and pramipexole used in early Parkinson’s disease can also reduce dyskinesias and motor fluctuations. Dopamine agonists may be preferred to levodopa in early Parkinson’s disease because they are better tolerated and cause fewer adverse effects. Or they may be used as adjuncts for patients whose response to levodopa is deteriorating or fluctuating3,7,8 (SOR: B). In advanced disease, motor complications can also be managed by augmenting levodopa therapy with a dopamine agonist, MAO-B inhibitor, or COMT inhibitor7,8 (SOR: A).
Anticholinergics, mainly benztropine and trihexyphenidyl, may be used as symptomatic treatment, especially in young people with early Parkinson’s disease and severe tremor. However, they are not the first drugs of choice due to limited efficacy and the potential for neuropsychiatric side effects8 (SOR: C). Amantadine can reduce dyskinesia in people with advanced Parkinson’s disease8 (SOR: C). For patients who have Parkinson’s disease with severe motor complications, intermittent apomorphine injections can help reduce “off time” periods in the daily treatment cycle when the efficacy of drugs wanes9 (SOR: B).
Deep brain stimulation of the subthalamic nucleus has only SOR C support for reducing dyskinesias and off time.9
Treating nonmotor symptoms of Parkinson’s disease can be challenging. For dementia in these patients, consider cholinesterase inhibitors6,8 (SOR: C). For depression, selective serotonin reuptake inhibitors are effective6,8,9 (SOR: C). For psychosis, preferred agents are low-dose clozapine or quetiapine6,8-10 (SOR: C). Plan for supportive and symptomatic management of constipation, dysphagia, sialorrhea, orthostatic hypotension, sleep disturbances, and urinary urgency.2,3
Tremor
Tremor is a common form of hyperkinesia, presenting either as a primary disorder or as a symptom of another condition.11 By definition, it is a rhythmical, involuntary, oscillatory movement of 1 or more body parts. Tremors are classified as rest or action tremors, with the latter being further categorized as postural (occurring while the patient maintains a position against gravity) or kinetic (occurring during voluntary movement).2,10
Physiologic tremor: Pharmacologic Tx is usually not needed
Physiologic tremor is benign, high frequency (8-12 Hz), low amplitude, and postural. An exaggerated form of this tremor may result from anxiety, hyperthyroidism, pheochromocytoma, hypoglycemia, excessive caffeine consumption, fever, withdrawal from opioids and sedatives, and some medications. No drug treatment is necessary unless symptoms become bothersome. Correct the underlying cause or have the patient avoid the triggering factor, and offer reassurance that the condition is not pathological or progressive.2,12 For anxiety, consider cognitive-behavioral/relaxation therapy or benzodiazepines (if tremor did not result from withdrawal of benzodiazepines) or beta-adrenergic antagonists (eg, propranolol).12,13
Essential tremor: Try propranolol or primidone first
Essential tremor (ET) is the most common movement disorder. It often results in functional disability and leads to many physical and emotional difficulties. ET is bilateral, usually symmetric (although mild asymmetry is possible), and postural or kinetic, typically affecting hands and forearms. The frequency of ET is 4 to 12 Hz. Cranial musculature may be involved in 30% of cases, affecting the head and voice.3 Prevalence ranges from 4 to 40 cases per 1000 people. The age-adjusted incidence is 17.5/100,000 per year; it peaks during the teen years and the fifth decade.2,3
Autosomal dominant type of inheritance is common, and a family history of ET is often present, particularly with younger patients. The differential diagnosis includes Parkinson’s disease tremor; dystonic, cerebellar, rubral, and psychogenic tremors; and asterixis.3 Unlike ET, many of these disorders have associated neurologic, psychiatric, or systemic signs.
Treatment with propranolol or primidone is indicated if ET causes functional impairment or social or emotional problems for the patient.2,3,10,13 Both propranolol and primidone reduce limb tremor2,10,13 (SOR: B), but only propranolol is approved by the US Food and Drug Administration (FDA) for treatment of ET. Propranolol is more effective for hand and forearm tremor than for head and voice tremor. Start propranolol at 20 to 40 mg twice a day and increase the dose as needed to achieve symptom relief.14
A maintenance dose of 240 to 320 mg/d may be needed. Major adverse effects are fatigue, sedation, depression, and erectile dysfunction. Contraindications to propranolol include asthma, second-degree atrioventricular block, and insulin-dependent diabetes.
If starting with primidone alone, prescribe at a dose <25 mg at bedtime and increase the dose slowly over several weeks to prevent onset of nausea, vomiting, sedation, confusion, or ataxia. The maximum allowable dose is 750 mg/d in 3 divided doses.10 Primidone and propranolol may be used in combination to treat limb tremor when monotherapy is insufficient (SOR: B).13
Thirty percent of patients with ET will not respond to propranolol or primidone. An alternative choice is the anticonvulsant gabapentin10,12-14 (SOR: C). However, clinical experience with it is limited. Lethargy, fatigue, decreased libido, dizziness, nervousness, and shortness of breath are adverse effects of gabapentin; they are usually mild and tolerable.13 Topiramate is another option that seems to be as effective as gabapentin10,13 (SOR: C), but studies of long-term outcomes are lacking. Topiramate’s side effects include weight loss and paresthesias. Additionally, alprazolam, clonazepam, clozapine, olanzapine, atenolol, sotalol, nadolol, and nimodipine may reduce limb tremor2 (SOR: C). Alcohol reduces tremor amplitude in 50% to 90% of patients, but tremor may worsen after the effect of alcohol has worn off.15
For patients with essential hand tremor that fails to respond to oral agents, consider botulinum toxin A16 (SOR: B). However, it is also associated with dose-dependent hand weakness16 (SOR: C). Botulinum toxin may reduce head and voice tremor16 (SOR: C), but hoarseness and swallowing difficulties may occur after use for voice tremor.16
Invasive therapies may benefit patients with refractory tremor. Deep brain stimulation and thalamotomy are highly effective in reducing limb tremor13 (SOR: C). Each carries a small risk of major complications. Some deep brain stimulation adverse events may resolve with time. Other adverse events may resolve with adjustment of stimulator settings. No evidence exists for surgical treatment for voice and head tremor or for gamma-knife thalamotomy.13
Drug-induced tremor
Drugs with the potential to cause postural tremor, intention tremor, or rest tremor include the following: 15
- alcohol (chronic)
- amiodarone
- amphetamines
- beta-adrenergic agonists
- caffeine
- calcitonin
- carbamazepine
- cocaine
- cyclosporine
- dopamine
- lithium
- metoclopramide
- neuroleptics
- procainamide
- steroids
- theophylline
- thyroid hormones
- tricyclic antidepressants
- trifluoperazine
- valproic acid
With drug-induced tremor, carefully evaluate a patient’s need for the drug. Discontinue the offending agent if possible, or try lowering the dose.
Psychogenic tremor: A history of somatization is a clue
Psychogenic tremor can occur at rest or during postural or kinetic movement. Clinical features include an abrupt onset, a static course, spontaneous remission, and unclassifiable tremors.17 Psychogenic tremor increases under direct observation and decreases with distraction. Patients with psychogenic tremor often have a history of somatization.18 Electrophysiologic testing can help confirm the diagnosis. If remission does not occur spontaneously, patients may find relief with psychotherapy or placebo.19
Tic disorders: Opt for dopamine receptor blockers
Tics are involuntary or semivoluntary movements or sounds that are sudden, brief, intermittent, repetitive, nonrhythmic, unpredictable, and purposeless. Tics can occur in any part of the body.20
The most common tic disorder is Tourette syndrome—a combination of motor and phonic tics with onset before age 21. It affects approximately 5 to 10 children out of 10,000. Boys are more commonly affected than girls. Attention deficit hyperactivity disorder frequently accompanies this syndrome.2
The goal of treatment with any tic disorder is to improve social functioning, self-esteem, and quality of life. Education and support of patients is important. Tic disorders, including Tourette, rarely require drugs. But if tics become too distressing, first-line treatment would be a dopamine modulator, tetrabenazine, or clonidine. Randomized controlled trials with various neuroleptics have revealed dramatic reductions in tic severity. However, many patients do not tolerate the acute adverse effects (most commonly sedation, weight gain, depression, lethargy, and akathisia), and prolonged treatment confers a small risk of tardive dyskinesia. Behavioral therapy is an important part of management.20
Dopamine-receptor blocking drugs such as haloperidol, pimozide, and fluphenazine are the most effective treatment for tics20 (SOR: B). Tetrabenazine is a promising new dopamine-depleting drug; controlled trials are ongoing2,20 (SOR: B). Clonidine, an alpha 2-adrenergic agonist, is useful in treating patients with Tourette syndrome, helping to improve sleep and attention2,21 (SOR: C). Medically refractory motor and disabling phonic tics such as coprolalia can be ameliorated by botulinum toxin injections21 (SOR: B). Deep brain stimulation is being used at an increasing rate for medically refractory tics in Tourette syndrome21 (SOR: B).
Restless legs syndrome: Dopamine agonists are preferred
Restless legs syndrome (RLS) is a disorder characterized by sensory symptoms and motor disturbances of the legs, mainly during rest. Treatment may not be necessary for patients with mild or sporadic symptoms. For moderate to severe RLS with significant impairment, dopamine agonists are the preferred agents22 (SOR: A). RLS can also occur secondary to such conditions as iron deficiency and uremia, and correction of the underlying disorder is the goal. Prescribe iron replacement for patients with a ferritin level <50 ng/mL22 (SOR: C). Medications known to cause or exacerbate the symptoms of RLS are anti-dopaminergic agents (such as neuroleptics), diphenhydramine, tricyclic antidepressants, alcohol, caffeine, lithium, and beta-blockers. If a patient is taking medications that exacerbate symptoms of RLS, discontinue them and use appropriate substitutes22 (SOR: C).
Myoclonus: Clonazepam for essential disorder
Myoclonus is a brief, sudden, shock-like movement caused by involuntary muscle contractions or lapse of muscle contraction (asterixis). Given the complex origins of myoclonus, multiple drugs may be needed. Essential myoclonus is disabling and can be treated with clonazepam. Start with 0.25 mg orally twice daily, and increase the dosage over 3 days to 1 mg/d23 (SOR: C). Most cases of myoclonus are secondary due to drugs such as lithium, toxins, advanced liver disease, infections including human immunodeficiency virus, dementia, and brain lesions. Treatment should also address the underlying disorder.2,23
Chorea
Chorea is an abnormal involuntary movement disorder described as “a state of excessive, spontaneous movements, irregularly timed, nonrepetitive, randomly distributed, and abrupt in character.”24
Treatment of chorea is symptomatic, aiming to reduce morbidity and prevent complications. Haloperidol and fluphenazine are effective but can impair voluntary movements2,10,25 (SOR: C). The dopamine-depleting drugs reserpine and tetrabenazine are also effective2,10,25 (SOR: C). GABAergic drugs, such as clonazepam, gabapentin, and valproate, can be used adjunctively.10,25
Dystonia
Dystonia is a syndrome involving sustained contractions of opposing muscles that cause twisting, repetitive movements and abnormal postures. Primary dystonia can be treated successfully with high doses of trihexyphenidyl alone, starting with 1 mg orally per day and increasing gradually to 6 to 80 mg/d until symptoms are controlled; or in combination with baclofen, starting with 10 mg orally once daily and increasing to a maximum dose of 30 to 120 mg/d1,2 (SOR: C).
Consider botulinum neurotoxin injection for focal upper extremity dystonia and adductor spasmodic dysphonia16 (SOR: B).
Ataxia
Ataxia is an unsteady gait associated with cerebellar dysfunction, proprioceptive defects, or both. Ataxia may be primary (Friedreich ataxia and spinocerebellar ataxia) or secondary to stroke, trauma, alcoholic degeneration, multiple sclerosis, vitamin B12 deficiency, and hydrocephalus. Treatment, when possible, should target the underlying cause.1,2
CORRESPONDENCE Hakan Yaman, MD, Akdeniz University, Department of Family Medicine, Antalya, Turkey 07058; [email protected]
• Initiate neuroprotective therapy with a monoamine oxidase B inhibitor to slow the progression of Parkinson’s disease. With onset of functional impairment, give levodopa at the lowest effective dose. A
• Give propranolol for essential tremor causing a patient distress, starting at 20 to 40 mg twice daily and increasing the dose (to a maximum of 320 mg/d) until relief is achieved. B
• Consider giving a dopamine receptor blocker for Tourette syndrome or other tic disorder; alternative agents are clonidine or a newer agent, tetrabenazine. B
Strength of recommendation (SOR)
A Good-quality patient-oriented evidence
B Inconsistent or limited-quality patient-oriented evidence
C Consensus, usual practice, opinion, disease-oriented evidence, case series
Movement disorders often require consultation with a neurologist, and a working knowledge of established and novel treatments can set the stage for optimal long-term cooperative management.1 In this article, we review therapeutic options for common movement disorders, including hypokinetic, hyperkinetic, and dyskinetic disturbances.
Parkinson’s disease treatment: MAO-B inhibitor, levodopa are mainstays
Parkinson’s disease, the most common hypokinetic movement disorder, is a chronic, progressive, neurodegenerative disease. It affects 1% of individuals older than 65 years and 4% to 5% of individuals older than 85 years. Its cardinal symptoms are resting tremor, bradykinesia, rigidity, a flexed posture, and loss of postural reflexes. Resting tremor, referred to as “pill rolling” tremor, is 4 to 6 Hz and usually begins unilaterally.2,3 Associated symptoms can include dystonia, dementia, psychiatric disorders, sleep disorders, and autonomic symptoms.
Neuroprotective therapy is used to slow the progression of the disease, particularly in its early stage. The monoamine oxidase B (MAO-B) inhibitor selegiline has proven effective in this regard2 (strength of recommendation [SOR]: A). In randomized controlled studies, selegiline has delayed the need for levodopa for 9 to 12 months4 (SOR: A). Another MAO-B inhibitor, rasagiline, has demonstrated neuroprotective effects as well5 (SOR: B). These medications may also be used with levodopa for symptom control and as adjuvant therapy in patients with motor fluctuations.2 A conventional dose of selegiline is 10 mg/d (5 mg at breakfast; 5 mg at lunch). Rasagiline is given at 1 mg/d. Concomitant use of ciprofloxacin or other CYP1A2 inhibitors limits its effectiveness.6,7
Symptomatic therapy is indicated at the onset of functional impairment. The dopamine precursor levodopa is the most widely used and effective drug for Parkinson’s disease symptoms, especially bradykinesia and rigidity. Use the lowest possible dose to control symptoms (eg, 100 mg twice daily) and protect against motor complications of the drug7-9 (SOR: A). To prevent conversion of levodopa to dopamine outside the blood-brain barrier, combine it with the decarboxylase inhibitor carbidopa. Dietary restriction of proteins may be needed, because amino acids can interfere with the absorption of levodopa.
Especially with prolonged use, levodopa can cause disturbing adverse effects, such as nausea, vomiting, psychosis, cardiac arrhythmia, and orthostatic hypotension. Dyskinesias and motor fluctuations are complications of long-term treatment and are irreversible. Adding a cathecol-O-methyltransferase (COMT) inhibitor, such as entacapone, to increase levodopa’s effectiveness has been shown to reduce motor fluctuations2,3,10 (SOR: B). Dopamine agonists such as bromocriptine, ropinirole, and pramipexole used in early Parkinson’s disease can also reduce dyskinesias and motor fluctuations. Dopamine agonists may be preferred to levodopa in early Parkinson’s disease because they are better tolerated and cause fewer adverse effects. Or they may be used as adjuncts for patients whose response to levodopa is deteriorating or fluctuating3,7,8 (SOR: B). In advanced disease, motor complications can also be managed by augmenting levodopa therapy with a dopamine agonist, MAO-B inhibitor, or COMT inhibitor7,8 (SOR: A).
Anticholinergics, mainly benztropine and trihexyphenidyl, may be used as symptomatic treatment, especially in young people with early Parkinson’s disease and severe tremor. However, they are not the first drugs of choice due to limited efficacy and the potential for neuropsychiatric side effects8 (SOR: C). Amantadine can reduce dyskinesia in people with advanced Parkinson’s disease8 (SOR: C). For patients who have Parkinson’s disease with severe motor complications, intermittent apomorphine injections can help reduce “off time” periods in the daily treatment cycle when the efficacy of drugs wanes9 (SOR: B).
Deep brain stimulation of the subthalamic nucleus has only SOR C support for reducing dyskinesias and off time.9
Treating nonmotor symptoms of Parkinson’s disease can be challenging. For dementia in these patients, consider cholinesterase inhibitors6,8 (SOR: C). For depression, selective serotonin reuptake inhibitors are effective6,8,9 (SOR: C). For psychosis, preferred agents are low-dose clozapine or quetiapine6,8-10 (SOR: C). Plan for supportive and symptomatic management of constipation, dysphagia, sialorrhea, orthostatic hypotension, sleep disturbances, and urinary urgency.2,3
Tremor
Tremor is a common form of hyperkinesia, presenting either as a primary disorder or as a symptom of another condition.11 By definition, it is a rhythmical, involuntary, oscillatory movement of 1 or more body parts. Tremors are classified as rest or action tremors, with the latter being further categorized as postural (occurring while the patient maintains a position against gravity) or kinetic (occurring during voluntary movement).2,10
Physiologic tremor: Pharmacologic Tx is usually not needed
Physiologic tremor is benign, high frequency (8-12 Hz), low amplitude, and postural. An exaggerated form of this tremor may result from anxiety, hyperthyroidism, pheochromocytoma, hypoglycemia, excessive caffeine consumption, fever, withdrawal from opioids and sedatives, and some medications. No drug treatment is necessary unless symptoms become bothersome. Correct the underlying cause or have the patient avoid the triggering factor, and offer reassurance that the condition is not pathological or progressive.2,12 For anxiety, consider cognitive-behavioral/relaxation therapy or benzodiazepines (if tremor did not result from withdrawal of benzodiazepines) or beta-adrenergic antagonists (eg, propranolol).12,13
Essential tremor: Try propranolol or primidone first
Essential tremor (ET) is the most common movement disorder. It often results in functional disability and leads to many physical and emotional difficulties. ET is bilateral, usually symmetric (although mild asymmetry is possible), and postural or kinetic, typically affecting hands and forearms. The frequency of ET is 4 to 12 Hz. Cranial musculature may be involved in 30% of cases, affecting the head and voice.3 Prevalence ranges from 4 to 40 cases per 1000 people. The age-adjusted incidence is 17.5/100,000 per year; it peaks during the teen years and the fifth decade.2,3
Autosomal dominant type of inheritance is common, and a family history of ET is often present, particularly with younger patients. The differential diagnosis includes Parkinson’s disease tremor; dystonic, cerebellar, rubral, and psychogenic tremors; and asterixis.3 Unlike ET, many of these disorders have associated neurologic, psychiatric, or systemic signs.
Treatment with propranolol or primidone is indicated if ET causes functional impairment or social or emotional problems for the patient.2,3,10,13 Both propranolol and primidone reduce limb tremor2,10,13 (SOR: B), but only propranolol is approved by the US Food and Drug Administration (FDA) for treatment of ET. Propranolol is more effective for hand and forearm tremor than for head and voice tremor. Start propranolol at 20 to 40 mg twice a day and increase the dose as needed to achieve symptom relief.14
A maintenance dose of 240 to 320 mg/d may be needed. Major adverse effects are fatigue, sedation, depression, and erectile dysfunction. Contraindications to propranolol include asthma, second-degree atrioventricular block, and insulin-dependent diabetes.
If starting with primidone alone, prescribe at a dose <25 mg at bedtime and increase the dose slowly over several weeks to prevent onset of nausea, vomiting, sedation, confusion, or ataxia. The maximum allowable dose is 750 mg/d in 3 divided doses.10 Primidone and propranolol may be used in combination to treat limb tremor when monotherapy is insufficient (SOR: B).13
Thirty percent of patients with ET will not respond to propranolol or primidone. An alternative choice is the anticonvulsant gabapentin10,12-14 (SOR: C). However, clinical experience with it is limited. Lethargy, fatigue, decreased libido, dizziness, nervousness, and shortness of breath are adverse effects of gabapentin; they are usually mild and tolerable.13 Topiramate is another option that seems to be as effective as gabapentin10,13 (SOR: C), but studies of long-term outcomes are lacking. Topiramate’s side effects include weight loss and paresthesias. Additionally, alprazolam, clonazepam, clozapine, olanzapine, atenolol, sotalol, nadolol, and nimodipine may reduce limb tremor2 (SOR: C). Alcohol reduces tremor amplitude in 50% to 90% of patients, but tremor may worsen after the effect of alcohol has worn off.15
For patients with essential hand tremor that fails to respond to oral agents, consider botulinum toxin A16 (SOR: B). However, it is also associated with dose-dependent hand weakness16 (SOR: C). Botulinum toxin may reduce head and voice tremor16 (SOR: C), but hoarseness and swallowing difficulties may occur after use for voice tremor.16
Invasive therapies may benefit patients with refractory tremor. Deep brain stimulation and thalamotomy are highly effective in reducing limb tremor13 (SOR: C). Each carries a small risk of major complications. Some deep brain stimulation adverse events may resolve with time. Other adverse events may resolve with adjustment of stimulator settings. No evidence exists for surgical treatment for voice and head tremor or for gamma-knife thalamotomy.13
Drug-induced tremor
Drugs with the potential to cause postural tremor, intention tremor, or rest tremor include the following: 15
- alcohol (chronic)
- amiodarone
- amphetamines
- beta-adrenergic agonists
- caffeine
- calcitonin
- carbamazepine
- cocaine
- cyclosporine
- dopamine
- lithium
- metoclopramide
- neuroleptics
- procainamide
- steroids
- theophylline
- thyroid hormones
- tricyclic antidepressants
- trifluoperazine
- valproic acid
With drug-induced tremor, carefully evaluate a patient’s need for the drug. Discontinue the offending agent if possible, or try lowering the dose.
Psychogenic tremor: A history of somatization is a clue
Psychogenic tremor can occur at rest or during postural or kinetic movement. Clinical features include an abrupt onset, a static course, spontaneous remission, and unclassifiable tremors.17 Psychogenic tremor increases under direct observation and decreases with distraction. Patients with psychogenic tremor often have a history of somatization.18 Electrophysiologic testing can help confirm the diagnosis. If remission does not occur spontaneously, patients may find relief with psychotherapy or placebo.19
Tic disorders: Opt for dopamine receptor blockers
Tics are involuntary or semivoluntary movements or sounds that are sudden, brief, intermittent, repetitive, nonrhythmic, unpredictable, and purposeless. Tics can occur in any part of the body.20
The most common tic disorder is Tourette syndrome—a combination of motor and phonic tics with onset before age 21. It affects approximately 5 to 10 children out of 10,000. Boys are more commonly affected than girls. Attention deficit hyperactivity disorder frequently accompanies this syndrome.2
The goal of treatment with any tic disorder is to improve social functioning, self-esteem, and quality of life. Education and support of patients is important. Tic disorders, including Tourette, rarely require drugs. But if tics become too distressing, first-line treatment would be a dopamine modulator, tetrabenazine, or clonidine. Randomized controlled trials with various neuroleptics have revealed dramatic reductions in tic severity. However, many patients do not tolerate the acute adverse effects (most commonly sedation, weight gain, depression, lethargy, and akathisia), and prolonged treatment confers a small risk of tardive dyskinesia. Behavioral therapy is an important part of management.20
Dopamine-receptor blocking drugs such as haloperidol, pimozide, and fluphenazine are the most effective treatment for tics20 (SOR: B). Tetrabenazine is a promising new dopamine-depleting drug; controlled trials are ongoing2,20 (SOR: B). Clonidine, an alpha 2-adrenergic agonist, is useful in treating patients with Tourette syndrome, helping to improve sleep and attention2,21 (SOR: C). Medically refractory motor and disabling phonic tics such as coprolalia can be ameliorated by botulinum toxin injections21 (SOR: B). Deep brain stimulation is being used at an increasing rate for medically refractory tics in Tourette syndrome21 (SOR: B).
Restless legs syndrome: Dopamine agonists are preferred
Restless legs syndrome (RLS) is a disorder characterized by sensory symptoms and motor disturbances of the legs, mainly during rest. Treatment may not be necessary for patients with mild or sporadic symptoms. For moderate to severe RLS with significant impairment, dopamine agonists are the preferred agents22 (SOR: A). RLS can also occur secondary to such conditions as iron deficiency and uremia, and correction of the underlying disorder is the goal. Prescribe iron replacement for patients with a ferritin level <50 ng/mL22 (SOR: C). Medications known to cause or exacerbate the symptoms of RLS are anti-dopaminergic agents (such as neuroleptics), diphenhydramine, tricyclic antidepressants, alcohol, caffeine, lithium, and beta-blockers. If a patient is taking medications that exacerbate symptoms of RLS, discontinue them and use appropriate substitutes22 (SOR: C).
Myoclonus: Clonazepam for essential disorder
Myoclonus is a brief, sudden, shock-like movement caused by involuntary muscle contractions or lapse of muscle contraction (asterixis). Given the complex origins of myoclonus, multiple drugs may be needed. Essential myoclonus is disabling and can be treated with clonazepam. Start with 0.25 mg orally twice daily, and increase the dosage over 3 days to 1 mg/d23 (SOR: C). Most cases of myoclonus are secondary due to drugs such as lithium, toxins, advanced liver disease, infections including human immunodeficiency virus, dementia, and brain lesions. Treatment should also address the underlying disorder.2,23
Chorea
Chorea is an abnormal involuntary movement disorder described as “a state of excessive, spontaneous movements, irregularly timed, nonrepetitive, randomly distributed, and abrupt in character.”24
Treatment of chorea is symptomatic, aiming to reduce morbidity and prevent complications. Haloperidol and fluphenazine are effective but can impair voluntary movements2,10,25 (SOR: C). The dopamine-depleting drugs reserpine and tetrabenazine are also effective2,10,25 (SOR: C). GABAergic drugs, such as clonazepam, gabapentin, and valproate, can be used adjunctively.10,25
Dystonia
Dystonia is a syndrome involving sustained contractions of opposing muscles that cause twisting, repetitive movements and abnormal postures. Primary dystonia can be treated successfully with high doses of trihexyphenidyl alone, starting with 1 mg orally per day and increasing gradually to 6 to 80 mg/d until symptoms are controlled; or in combination with baclofen, starting with 10 mg orally once daily and increasing to a maximum dose of 30 to 120 mg/d1,2 (SOR: C).
Consider botulinum neurotoxin injection for focal upper extremity dystonia and adductor spasmodic dysphonia16 (SOR: B).
Ataxia
Ataxia is an unsteady gait associated with cerebellar dysfunction, proprioceptive defects, or both. Ataxia may be primary (Friedreich ataxia and spinocerebellar ataxia) or secondary to stroke, trauma, alcoholic degeneration, multiple sclerosis, vitamin B12 deficiency, and hydrocephalus. Treatment, when possible, should target the underlying cause.1,2
CORRESPONDENCE Hakan Yaman, MD, Akdeniz University, Department of Family Medicine, Antalya, Turkey 07058; [email protected]
1. Deuschl G, Bain P, Brin M. Consensus statement of the Movement Disorder Society on Tremor. Ad Hoc Scientific Committee. Mov Disord. 1998;13(suppl 3):2-23.
2. Yaman A, Yaman H, Rao G. Tremors and other movement disorders. In: Mengel MB, et al, eds. Family Medicine Ambulatory Care and Prevention. 5th ed. New York: McGraw-Hill; 2009:400–407.
3. Harris MK, Shneyder N, Borazanci A, et al. Movement disorders. Med Clin North Am. 2009;93:371-388.
4. Palhagen S, Heinonen E, Hagglund J, et al. Selegiline slows the progression of the symptoms of Parkinson disease. Neurology. 2006;66:1200-1206.
5. Olanow CW, Rascol O, Hauser R, et al. A double-blind, delayed-start trial of rasagiline in Parkinson’s disease. N Engl J Med. 2009;361:1268-1278.
6. Zesiewicz TA, Sullivan KL, Arnulf I, et al. Treatment of nonmotor symptoms of Parkinson disease. Neurology. 2010;74:924-931.
7. Suchowersky O, Reich S, Perlmutter J, et al. Practice parameter: diagnosis and prognosis of new onset Parkinson disease (an evidence-based review). Neurology. 2006;66:968-975.
8. Rao SS, Hofmann LA, Shakil A. Parkinson’s disease: diagnosis and treatment. Am Fam Physician. 2006;74:2046-2054.
9. The National Collaborating Centre for Chronic Conditions Parkinson’s Disease. National Clinical Guideline for Diagnosis and Management in Primary and Secondary Care. 2006. Available at: http://www.nice.org.uk/nicemedia/live/10984/30087/30087.pdf. Accessed May 12, 2010.
10. Jankovic J. Treatment of hyperkinetic movement disorders. Lancet Neurol. 2009;8:844-856.
11. Kerlsberg G, Rubenstein C, St Anna L, et al. Differential diagnosis of tremor. Am Fam Physician. 2008;77:1305-1306.
12. Burke DA, Hauser RA, McClain T. Essential tremor. Available at: http://emedicine.medscape.com/article/1150290-overview. Accessed May 12, 2010.
13. Zesiewicz TA, Elble R, Louis ED, et al. Practice parameter: therapies for essential tremor. Neurology. 2005;64:2008-2020.
14. Elble RJ. Tremor: clinical features, pathophysiology, and treatment. Neurol Clin. 2009;27:679-695.
15. Smaga S. Tremor. Am Fam Physician. 2003;68:1545-1552.
16. Use of botulinum neurotoxin for the treatment of movement disorders. AAN summary of evidence-based guidelines for clinicians. 2008. Available at: http://www.aan.com/practice/guideline/uploads/280.pdf. Accessed May 25, 2010.
17. Redondo L, Morgado Y, Durán E. Psychogenic tremor: a positive diagnosis [ in Spanish]. Neurología. 2010;25:51-57.
18. Schwingenschuh P, Katschnig P, Seiler S, et al. Moving toward ‘‘laboratory-supported’’ criteria for psychogenic tremor. Mov Disord. 2011;Sep 28. [Epub ahead of print].
19. McKeon A, Ahlskog JE, Bower JH, et al. Psychogenic tremor: long-term prognosis in patients with electrophysiologically confirmed disease. Mov Disord. 2009;24:72-76.
20. Shprecher D, Kurlan R. The management of tics. Mov Disord. 2009;24:15-24.
21. Kenney C, Kuo SH, Jimenez-Shahed J. Tourette’s syndrome. Am Fam Physician. 2008;77:651-658.
22. Bayard M, Avonda T, Wadzinsky J. Restless legs syndrome. Am Fam Physician. 2008;78:235-240.
23. Caviness JN. Pathophysiology and treatment of myoclonus. Neurol Clin. 2009;27:757-777.
24. Barbeau A, Duvoisin RC, Gerstenbrand F, et al. Classification of extrapyramidal disorders. J Neurol Sci. 1981;51:311-327.
25. Vertrees SM, Berman SA. Chorea in adults: treatment & management. Available at: http://emedicine.medscape.com/article/1149854-treatment. Accessed February 12, 2010.
1. Deuschl G, Bain P, Brin M. Consensus statement of the Movement Disorder Society on Tremor. Ad Hoc Scientific Committee. Mov Disord. 1998;13(suppl 3):2-23.
2. Yaman A, Yaman H, Rao G. Tremors and other movement disorders. In: Mengel MB, et al, eds. Family Medicine Ambulatory Care and Prevention. 5th ed. New York: McGraw-Hill; 2009:400–407.
3. Harris MK, Shneyder N, Borazanci A, et al. Movement disorders. Med Clin North Am. 2009;93:371-388.
4. Palhagen S, Heinonen E, Hagglund J, et al. Selegiline slows the progression of the symptoms of Parkinson disease. Neurology. 2006;66:1200-1206.
5. Olanow CW, Rascol O, Hauser R, et al. A double-blind, delayed-start trial of rasagiline in Parkinson’s disease. N Engl J Med. 2009;361:1268-1278.
6. Zesiewicz TA, Sullivan KL, Arnulf I, et al. Treatment of nonmotor symptoms of Parkinson disease. Neurology. 2010;74:924-931.
7. Suchowersky O, Reich S, Perlmutter J, et al. Practice parameter: diagnosis and prognosis of new onset Parkinson disease (an evidence-based review). Neurology. 2006;66:968-975.
8. Rao SS, Hofmann LA, Shakil A. Parkinson’s disease: diagnosis and treatment. Am Fam Physician. 2006;74:2046-2054.
9. The National Collaborating Centre for Chronic Conditions Parkinson’s Disease. National Clinical Guideline for Diagnosis and Management in Primary and Secondary Care. 2006. Available at: http://www.nice.org.uk/nicemedia/live/10984/30087/30087.pdf. Accessed May 12, 2010.
10. Jankovic J. Treatment of hyperkinetic movement disorders. Lancet Neurol. 2009;8:844-856.
11. Kerlsberg G, Rubenstein C, St Anna L, et al. Differential diagnosis of tremor. Am Fam Physician. 2008;77:1305-1306.
12. Burke DA, Hauser RA, McClain T. Essential tremor. Available at: http://emedicine.medscape.com/article/1150290-overview. Accessed May 12, 2010.
13. Zesiewicz TA, Elble R, Louis ED, et al. Practice parameter: therapies for essential tremor. Neurology. 2005;64:2008-2020.
14. Elble RJ. Tremor: clinical features, pathophysiology, and treatment. Neurol Clin. 2009;27:679-695.
15. Smaga S. Tremor. Am Fam Physician. 2003;68:1545-1552.
16. Use of botulinum neurotoxin for the treatment of movement disorders. AAN summary of evidence-based guidelines for clinicians. 2008. Available at: http://www.aan.com/practice/guideline/uploads/280.pdf. Accessed May 25, 2010.
17. Redondo L, Morgado Y, Durán E. Psychogenic tremor: a positive diagnosis [ in Spanish]. Neurología. 2010;25:51-57.
18. Schwingenschuh P, Katschnig P, Seiler S, et al. Moving toward ‘‘laboratory-supported’’ criteria for psychogenic tremor. Mov Disord. 2011;Sep 28. [Epub ahead of print].
19. McKeon A, Ahlskog JE, Bower JH, et al. Psychogenic tremor: long-term prognosis in patients with electrophysiologically confirmed disease. Mov Disord. 2009;24:72-76.
20. Shprecher D, Kurlan R. The management of tics. Mov Disord. 2009;24:15-24.
21. Kenney C, Kuo SH, Jimenez-Shahed J. Tourette’s syndrome. Am Fam Physician. 2008;77:651-658.
22. Bayard M, Avonda T, Wadzinsky J. Restless legs syndrome. Am Fam Physician. 2008;78:235-240.
23. Caviness JN. Pathophysiology and treatment of myoclonus. Neurol Clin. 2009;27:757-777.
24. Barbeau A, Duvoisin RC, Gerstenbrand F, et al. Classification of extrapyramidal disorders. J Neurol Sci. 1981;51:311-327.
25. Vertrees SM, Berman SA. Chorea in adults: treatment & management. Available at: http://emedicine.medscape.com/article/1149854-treatment. Accessed February 12, 2010.
Inhalation therapy: Help patients avoid these mistakes
• Stress the importance of exhaling gently for a few seconds before inhaling (deeply and slowly for a metered dose inhaler, and deeply and rapidly for most dry powder inhalers). C
• Observe the inhaler technique of every patient receiving inhalation therapy on more than one occasion. C
• Don’t rely on self-reports regarding inhaler technique; despite claims of proficiency, most patients make at least one mistake. C
Strength of recommendation (SOR)
A Good-quality patient-oriented evidence
B Inconsistent or limited-quality patient-oriented evidence
C Consensus, usual practice, opinion, disease-oriented evidence, case series
For patients with asthma or chronic obstructive pulmonary disease (COPD), inhalation therapy is the foundation of treatment. Yet all too often, patients don’t get the full value of their inhaled medications because they use their inhaler incorrectly. When technique is markedly flawed, suboptimal outcomes typically result.
Given the number of Americans with asthma (at least 22 million)1 and COPD (more than 13 million adults),2 faulty inhaler technique is a major public health problem. In fact, the number of people suffering from COPD may be even larger: Close to 24 million US adults are believed to have impaired lung function.3,4 For patients with asthma or COPD—many of whom are treated by family physicians—comprehensive education with a focus on correct use of an inhaler is essential.
In this review, we present evidence of frequent inhaler errors (from clinical studies) and highlight some of the more common mistakes (based on our clinical experience [TABLE]5). Finally, we offer ‘‘time-efficient’’ solutions to inhaler problems—steps that physicians in busy primary care practices can take to ensure that patients with asthma or COPD get the maximum benefit from inhalation therapy.
TABLE
Caution patients about these device-specific mistakes*
| Metered dose inhaler |
|---|
|
| Metered dose inhaler plus spacer/VHC |
|
| Dry powder inhaler |
|
| *These are examples based on the experience of the authors; other errors are possible. †Timing is not as crucial as it is for an MDI without a spacer, but the drug is still lost if inhalation is delayed. ‡Correct use varies by type of product (see product literature for specifics). DPI, dry powder inhaler; MDI, metered dose inhaler; VHC, valved holding chamber. Source: Adapted with permission from Self TH, et al. Consultant. 2003.5 |
Inhaler error is well documented
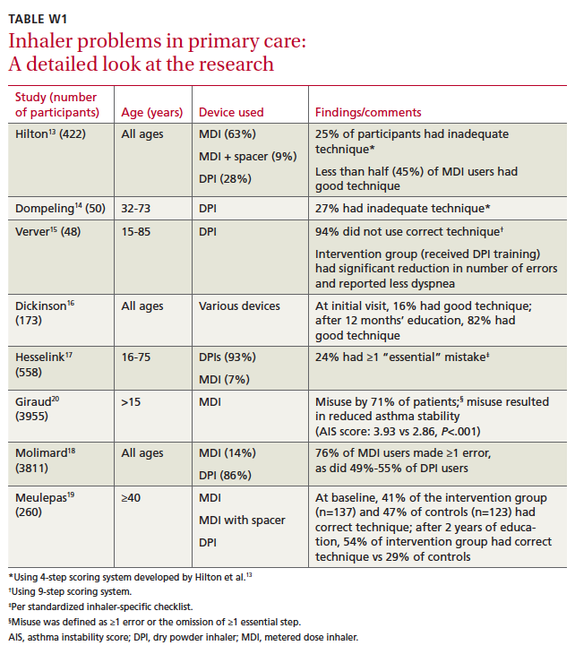
Since 1965, when it was first reported that many patients used metered dose inhalers (MDIs) incorrectly,6 evidence has accumulated supporting the magnitude of the problem.7-12 (Studies conducted in family practice settings are described in “Researchers look at inhaler problems in primary care” and in TABLE W1.13-20)
A number of studies of various sizes (from 41 to 3955 patients) have assessed inhaler technique in patients being treated by clinicians in primary care. The researchers used a variety of scoring methods, as well. Among them were a simple 4-step (0-4) rating system, a 9-step system, a standardized inhaler-specific checklist, and a system that tracked the number of omissions patients made.13-20 All found significant problems with inhaler technique. (You’ll find a detailed look at the studies in TABLE W1 at jfponline.com.)
In one study of 422 patients,13 including young children, adolescents, and adults, participants received one point for correctly performing each of the following steps:
- Adequate preparation (shaking well for those using a metered dose inhaler [MDI]; loading correctly for patients using a dry powder inhaler [DPI])
- Adequate expiration, correct head position
- Adequate inspiratory technique
- Holding breath afterwards.
The researchers found that 25% of the patients had inadequate technique (≤2 on a 0-4 point scale). In this study, as in others that included patients using various types of devices, use of an MDI was associated with a higher rate of incorrect technique.
Another much-smaller study14 used the same 4-step system to assess the technique of 50 patients, all of whom had the same type of DPI and had received extensive training in the correct use of the device. Despite the training, 27% of the patients received scores of ≤2 (inadequate technique). Sixty-eight percent received a score of 3 (adequate); only 5% received a score of 4 (good).
The 2 largest studies—one including 3955 patients using MDIs20 and the other looking at 3811 patients using various kinds of devices18—found high levels of errors, as well. In the latter study, 76% of patients with MDIs made at least one error vs 49% to 55% of patients using DPIs.18 The results convinced a large majority of the physicians caring for these patients of the need to check inhaler technique more frequently. In the study of MDI users alone, 71% of the patients made at least one mistake.20 inhaler misuse was associated with higher asthma instability scores, this study showed.
More recently, a researcher assessed the effects of an integrated primary care model on the management of asthma and/or COPD in middle-aged and elderly patients, in a study of 260 patients in 44 family practices.19 The study included an evaluation of inhaler technique.
Participants were divided into an intervention group—137 patients who received education regarding inhaler use from a nurse—and a usual care group (123 patients). After 2 years, correct inhaler technique among those in the intervention group went from 41% at baseline to 54%. At the same time, the proportion of those in the usual care group with correct technique fell from 47% to 29%.19
Error rates vary widely from one clinical trial to another, depending on study criteria, type of device, and extent of patient education, among other factors. Nonetheless, several studies (spanning 3 decades) found the error rate to be close to, or greater than, 90%.7,10,21
The most recent of these, published in 2009,21 was based on observation of the inhaler technique used by patients with asthma or COPD directly following appointments in an outpatient clinic. The authors found that, although >98% of the study participants claimed to know how to use their inhalers, 94% committed at least one error. In this study and a number of others, user error was more likely in patients using MDIs.13,18,21,22
Adding a spacer (eg, a valved holding chamber such as the AeroChamber) can be helpful, as the spacer affords the patient more time to inhale the medication. But patients who use an MDI with a spacer often make mistakes, too, and patient education is essential.23-26
Breath-activated dry powder inhalers (DPIs)—such as the Flexhaler, HandiHaler, Aerolizer, and Diskus—also reduce the likelihood of error. DPIs eliminate a step that MDI users often struggle with: the need to simultaneously press down on the canister and begin a slow, deep inhalation.
What’s more, DPIs do not have to be shaken before use. Nonetheless, using a DPI still involves a series of actions. For the HandiHaler and Aerolizer, patients must load the dose, and some patients fail to read the directions and swallow the capsule instead of loading it into the device. Patients must remember to exhale away from the device (ie, not into the dry powder) before inhaling, then hold their breath for approximately 10 seconds. There is potential for error at each step.
Stress the need to exhale before using the inhaler
Forgetting to exhale before inhaling is a common, and significant, mistake regardless of the type of device. It is paramount to stress the need to exhale gently for a few seconds before inhaling (slowly and deeply for patients using an MDI, rapidly and deeply with most DPIs). For MDI users, poor timing, described earlier, is another common and serious mistake. Patients using an MDI with a valved holding chamber sometimes inhale for too long before pressing down on the inhaler, then are unable to continue inhaling although the aerosol is still in the chamber. A common error made by patients using multidose DPIs is simply to forget to load the dose.
Physicians need to brush up on their skills, too
It’s not just patients who lack proficiency in inhaler technique. Numerous studies have demonstrated poor skill among physicians and other health care professionals.27-34 Evidence also shows that targeted education results in substantial improvement.32,35
In one study undertaken to evaluate family medicine residents’ proficiency in using asthma inhalers, participants (an intervention group at one clinic and a control group at another) all were given a pretest. The intervention group then received educational materials and a tutorial, as well as the opportunity for hands-on practice, after which both groups were given a post-test. The residents who received the training had a 170% jump, on average, in proficiency score, vs a 55% increase for the control group (P<.001).35
Inhaled Medication Instructional Videos
Courtesy of: National Jewish Health
Go to http://www.nationaljewish.org/healthinfo/medications/lung-diseases/devices/instructional-videos
Another study—this one involving first-year interns—looked at level of improvement based on the type of education provided. Initially, only 5% of the interns could use an MDI without error. After a lecture and demonstration, 13% had an error-free technique. But when each intern participated in an intensive one-on-one session, the error-free rate reached 73%. The researchers’ conclusion: Lectures are relatively ineffective in teaching interns inhaler technique compared with a one-on-one approach.32
The Chicago Breathe Project,36 a new program aimed at improving education in the use of asthma inhalers for physicians and minority patients, provides further evidence of the value of clinician education. After a series of workshops for residents at 5 academic institutions, the physicians’ knowledge of proper use of inhalers rose dramatically—from just 5% preprogram to 91% postprogram (P<.001). Six months after the educational activity, the residents (n=161) were more likely (44% vs 11% preprogram) to assess patients’ inhaler technique.36
Teaching patients when time is tight
National and international guidelines stress the need to teach patients correct use of asthma and COPD inhalers.1,37,38 Providing the requisite education includes observation of each patient’s inhaler technique with proper use demonstrated, as needed.
The problem, of course, is how to provide that level of patient education within the time constraints of a busy family practice. We recommend these time-efficient solutions:
Enlist the help of other clinicians. While it is important that someone in your office be well trained and able to instruct patients in the proper use of inhalers, that individual need not be you. The National Institutes of Health recommends that the “principal clinician” introduce key educational messages, which can be reinforced and expanded on by other members of the health care team.1
After you advise patients that it is crucial for them to be trained in and adhere to proper inhaler technique, another health care professional—often a clinic nurse or pharmacist who has had special training—can provide the hands-on education. Studies have shown that when pharmacists who are competent in asthma management, including inhaler technique, work with physicians to optimize the education and overall management of patients with asthma, better outcomes often result, including a reduction in both emergency department visits and hospitalizations.1,39,40
Use videos to demonstrate correct technique. Videos are an effective teaching tool,9 and many of them are device-specific. National Jewish Health, which is world renowned for its asthma care, has a set of instructional videos posted on You-Tube and accessible from its Web site (http://www.nationaljewish.org/healthinfo/medications/lung-diseases/devices/instructional-videos). In addition to videos that demonstrate the use of an MDI alone and an MDI plus a valved holding chamber, the site has links to 6 DPI videos, each covering a different device.
Use intermittent observation. After the patient views the appropriate video, you or a member of your staff will still need to observe the patient’s inhaler technique to ensure correct use. Ideally, this should occur at every visit.1,37 When that’s not possible, use intermittent observation, starting with the first 2 or 3 visits after the introduction of inhalation therapy and then switching to periodic observation to ensure that the patient is maintaining good technique.
In determining how often observation is necessary, keep in mind that simply asking patients whether they are having inhaler problems is not sufficient.1 Patients tend to say they have little or no trouble when, in fact, most struggle, at times, with the devices. What’s more, good technique tends to decrease over time, and repetitive education is important.
To motivate patients, try this communication technique
Motivational interviewing, a technique that has been used to help patients battle obesity, quit smoking, and control hypertension,41-43 among other health problems, can help you identify inhaler problems that need to be addressed. It involves the use of open-ended questions (eg, “What worries you most about your asthma?”), affirmations (“You’ve done a great job testing your peak flow level every morning”), reflective listening (“You’re tired of taking medicine every day”), and summary statements (“You know you should take your medicine every day but you’re having trouble remembering it. Is that right?”).
A pilot study44 showed that when this technique was incorporated into an asthma education session, patient motivation increased. The ratio of perceived advantages vs disadvantages of taking asthma medication correctly improved, as well. Another study45 found that when motivational interviewing was used during home visits to inner-city African American adolescents for asthma care, the patients’ motivation, readiness to adhere to treatment, and asthma-related quality of life improved, although self-reported adherence to asthma medication did not. Further studies involving patients with asthma are under way (www.clinicaltrials.gov/ct2/results?term=asthma).
It is important to note that the use of motivational interviewing does not require a lengthy visit. One study found that on average, visits in which primary care physicians used this communication technique lasted less than 10 minutes.46
CORRESPONDENCE Timothy H. Self, PharmD, University of Tennessee Health Science Center, 881 Madison Avenue, Room 235, Memphis, TN 38163; [email protected]
1. National Heart, Lung, and Blood Institute; National Asthma Education and Prevention Program Expert Panel Report 3: Guidelines for the Diagnosis and Management of Asthma. Bethesda, MD: National Institutes of Health; 2007.
2. Centers for Disease Control and Prevention. National Center for Health Statistics: National health interview survey raw data, 2008. Analysis performed by American Lung Association Research and Program Services.
3. American Lung Association. COPD—Helping the missing millions. February 24, 2010. Available at: http://www.lungusa.org/about-us/our-impact/top-stories/copd-helping-the-missing.html. Accessed November 9, 2011.
4. Centers for Disease Control and Prevention. Chronic obstructive pulmonary disease surveillance—United States, 1971-2000. MMWR Surveill Summ. 2002;51(6):1-16.
5. Self TH, Kilgore KE, Shelton V. MDIs, spacers, and dry powder inhalers: what patients are likely to do wrong. Consultant. 2003;49:702-705.
6. Saunders KB. Misuse of inhaled bronchodilator agents. Br Med J. 1965;1:1037-1038.
7. Epstein SW, Manning CPR, Ashley MJ, et al. Survey of the clinical uses of pressurized aerosol inhalers. Can Med Assoc J. 1979;120:813-816.
8. Shim C, Williams MH. The adequacy of inhalation of aerosol from canister nebulizers. Am J Med. 1980;69:891-894.
9. Self TH, Brooks JB, Lieberman P, et al. The value of demonstration and role of the pharmacist in teaching the correct use of pressurized bronchodilators. Can Med Assoc J. 1983;128:129-131.
10. Hartert TV, Windom HH, Peeples RS, et al. Inadequate outpatient medical therapy for patients with asthma admitted to two urban hospitals. Am J Med. 1996;100:386-394.
11. Goodman DE, Israel E, Rosenberg M, et al. The influence of age, diagnosis, and gender on proper use of metered-dose inhalers. Am J Respir Crit Care Med. 1994;150:1256-1261.
12. Newman SP, Pavia D, Clarke SW. How should a pressurized beta-adrenergic bronchodilator be inhaled? Eur J Respir Dis. 1981;62:3-21.
13. Hilton S. An audit of inhaler technique among asthma patients of 34 general practitioners. Br J Gen Pract. 1990;40:505-506.
14. Dompeling E, Van Grunsven PM, Van Schayck GP, et al. Treatment with inhaled steroids in asthma and chronic bronchitis: long-term compliance and inhaler technique. Fam Pract. 1992;9:161-166.
15. Verver S, Poelman M, Bogels A, et al. Effects of instruction by practice assistants on inhaler technique and respiratory symptoms of patients. A controlled randomized videotaped intervention study. Fam Pract. 1996;13:35-40.
16. Dickinson J, Hutton S, Atkin A, et al. Reducing asthma morbidity in the community: the effect of a targeted nurse-run asthma clinic in an English general practice. Respir Med. 1997;91:634-640.
17. Hesselink AE, Penninx BW, Wijnhoven HA, et al. Determinants of an incorrect inhalation technique in patients with asthma or COPD. Scand J Prim Health Care. 2001;19:255-260.
18. Molimard M, Raherison C, Lignot S, et al. Assessment of handling of inhaler devices in real life: An observational study in 3811 patients in primary care. J Aerosol Med. 2003;16:249-254.
19. Meulepas MA, Jacobs JE, Smeenk FW, et al. Effect of an integrated primary care model on the management of middle-aged and old patients with obstructive lung diseases. Scand J Prim Health Care. 2007;25:186-192.
20. Giraud V, Roche N. Misuse of corticosteroid metered-dose inhaler is associated with decreased asthma stability. Eur Respir J. 2002;19:246-251.
21. Souza ML, Meneghini AC, Ferraz E, et al. Knowledge of and technique for using inhalation devices among asthma patients and COPD patients. J Bras Pneumol. 2009;35:824-831.
22. Rootmensen GN, van Keimpema AR, Jansen HM, et al. Predictors of incorrect inhalation technique in patients with asthma or COPD: a study using a validated videotaped scoring method. J Aerosol Med Pulm Drug Deliv. 2010;23:323-328.
23. Rachelefsky GS, Rohr AS, Wo J, et al. Use of a tube spacer to improve the efficacy of a metered dose inhaler in asthmatic children. Am J Dis Child. 1986;140:1191-1193.
24. Demirkan K, Tolley E, Mastin T, et al. Salmeterol administration by metered-dose inhaler alone vs metered-dose inhaler plus valved holding chamber. Chest. 2000;117:1314-1318.
25. Pedersen S, Ostergaard PA. Nasal inhalation as a cause of inefficient pulmonal aerosol inhalation technique in children. Allergy. 1983;38:191-194.
26. Dolovich MD, Ahrens RS, Hess DR, et al. Device selection an outcomes of aerosol therapy: evidence-based guidelines: American College of Chest Physicians/American College of Asthma, Allergy, and Immunology. Chest. 2005;127:335-371.
27. Interiano B, Guntupalli KK. Metered-dose inhalers: do health care providers know what to teach? Arch Intern Med. 1993;153:81-85.
28. Hanania NA, Wittman R, Kesten S, et al. Medical personnel’s knowledge of and ability to use inhaling devices. Metered-dose inhalers, spacing chambers, and breath-actuated dry powder inhalers. Chest. 1994;105:111-116.
29. Amirav I, Goren A, Pawlowski NA. What do pediatricians in training know about the correct use of inhalers and spacer devices? J Allergy Clin Immunol. 1994;94:669-675.
30. Chopra N, Oprescu N, Fask A, et al. Does introduction of new “easy to use” inhalational devices improve medical personnel’s knowledge of their proper use? Ann Allergy Asthma Immunol. 2002;88:395-400.
31. Self TH, Arnold LB, Czosnowski LM, et al. Inadequate skill of healthcare professionals in using asthma inhalation devices. J Asthma. 2007;44:593-598.
32. Lee-Wong M, Mayo PH. Results of a programme to improve house staff use of metered dose inhalers and spacers. Postgrad Med J. 2003;79:221-225.
33. Muchao FP, Pern SL, Rodriques JC, et al. Evaluation of the knowledge of health professionals at a pediatric hospital regarding the use of metered dose inhalers. J Bras Pneumol. 2008;34:4-12.
34. Kim SH, Kwak HJ, Kim TB, et al. Inappropriate techniques used by internal medicine residents with three kinds of inhalers (a metered dose inhaler, Diskus, and Turbuhaler): changes after a single teaching session. J Asthma. 2009;46:944-950.
35. Kelcher S, Brownoff R. Teaching residents to use asthma devices. Assessing family residents’ skill and a brief intervention. Can Fam Physician. 1994;40:2090-2095.
36. Press VG, Pincayage AT, Pappalardo AA, et al. The Chicago Breathe Project: a regional approach to improving education on asthma inhalers for resident physicians and minority patients. J Natl Med Assoc. 2010;102:548-555.
37. Global Initiative for Asthma (GINA). Global strategy for asthma management and prevention. 2010. Available at: www.ginasthma.org. Accessed November 9, 2011.
38. Executive Summary: global strategy on the diagnosis and management and prevention of chronic obstructive pulmonary disease. NHLBI/WHO Workshop Report, 2009. Available at: www.goldcopd.com. Accessed November 9, 2011.
39. Self TH, Chrisman CR, Mason DL, et al. Reducing emergency department visits and hospitalizations in African American and Hispanic patients: a 15-year review. J Asthma. 2005;42:807-812.
40. Armour C, Bosnic-Anticevich S, Brillant M, et al. Pharmacy asthma care program (PACP) improves outcomes for patients in the community. Thorax. 2007;62:496-502.
41. DiLillo V, Nicole J, West DS. Incorporating motivational interviewing into behavioral obesity treatment. Cogn Behav Pract. 2003;10:120-130.
42. Borrelli B, Novak S, Hecht J, et al. Home health care nurses as a new channel for smoking cessation treatment: outcomes from project CARES (Community-nurse Assisted Research and Education on Smoking). Prev Med. 2005;41:815-821.
43. Woollard L, Beilin L, Lord T, et al. A controlled trial of nurse counselling on lifestyle change for hypertensives treated in general practice: preliminary results. Clin Exp Pharmacol Physiol. 1995;22:466-468.
44. Schmaling K, Blume A, Afari N. A randomized controlled pilot study of motivational interviewing to change attitudes about adherence to medications for asthma. J Clin Psych Med Settings. 2001;8:167-172.
45. Riekert KA, Borrelli B, Bilderback A, et al. The development of a motivational interviewing intervention to promote medication adherence among inner-city, African-American adolescents with asthma. Patient Educ Couns. 2011;82:117-122.
46. Butler C, Rollnick S, Cohen D, et al. Motivational consulting versus brief advice for smokers in general practice: a randomized trial. Br J Gen Pract. 1999;49:611-616.
• Stress the importance of exhaling gently for a few seconds before inhaling (deeply and slowly for a metered dose inhaler, and deeply and rapidly for most dry powder inhalers). C
• Observe the inhaler technique of every patient receiving inhalation therapy on more than one occasion. C
• Don’t rely on self-reports regarding inhaler technique; despite claims of proficiency, most patients make at least one mistake. C
Strength of recommendation (SOR)
A Good-quality patient-oriented evidence
B Inconsistent or limited-quality patient-oriented evidence
C Consensus, usual practice, opinion, disease-oriented evidence, case series
For patients with asthma or chronic obstructive pulmonary disease (COPD), inhalation therapy is the foundation of treatment. Yet all too often, patients don’t get the full value of their inhaled medications because they use their inhaler incorrectly. When technique is markedly flawed, suboptimal outcomes typically result.
Given the number of Americans with asthma (at least 22 million)1 and COPD (more than 13 million adults),2 faulty inhaler technique is a major public health problem. In fact, the number of people suffering from COPD may be even larger: Close to 24 million US adults are believed to have impaired lung function.3,4 For patients with asthma or COPD—many of whom are treated by family physicians—comprehensive education with a focus on correct use of an inhaler is essential.
In this review, we present evidence of frequent inhaler errors (from clinical studies) and highlight some of the more common mistakes (based on our clinical experience [TABLE]5). Finally, we offer ‘‘time-efficient’’ solutions to inhaler problems—steps that physicians in busy primary care practices can take to ensure that patients with asthma or COPD get the maximum benefit from inhalation therapy.
TABLE
Caution patients about these device-specific mistakes*
| Metered dose inhaler |
|---|
|
| Metered dose inhaler plus spacer/VHC |
|
| Dry powder inhaler |
|
| *These are examples based on the experience of the authors; other errors are possible. †Timing is not as crucial as it is for an MDI without a spacer, but the drug is still lost if inhalation is delayed. ‡Correct use varies by type of product (see product literature for specifics). DPI, dry powder inhaler; MDI, metered dose inhaler; VHC, valved holding chamber. Source: Adapted with permission from Self TH, et al. Consultant. 2003.5 |
Inhaler error is well documented
Since 1965, when it was first reported that many patients used metered dose inhalers (MDIs) incorrectly,6 evidence has accumulated supporting the magnitude of the problem.7-12 (Studies conducted in family practice settings are described in “Researchers look at inhaler problems in primary care” and in TABLE W1.13-20)
A number of studies of various sizes (from 41 to 3955 patients) have assessed inhaler technique in patients being treated by clinicians in primary care. The researchers used a variety of scoring methods, as well. Among them were a simple 4-step (0-4) rating system, a 9-step system, a standardized inhaler-specific checklist, and a system that tracked the number of omissions patients made.13-20 All found significant problems with inhaler technique. (You’ll find a detailed look at the studies in TABLE W1 at jfponline.com.)
In one study of 422 patients,13 including young children, adolescents, and adults, participants received one point for correctly performing each of the following steps:
- Adequate preparation (shaking well for those using a metered dose inhaler [MDI]; loading correctly for patients using a dry powder inhaler [DPI])
- Adequate expiration, correct head position
- Adequate inspiratory technique
- Holding breath afterwards.
The researchers found that 25% of the patients had inadequate technique (≤2 on a 0-4 point scale). In this study, as in others that included patients using various types of devices, use of an MDI was associated with a higher rate of incorrect technique.
Another much-smaller study14 used the same 4-step system to assess the technique of 50 patients, all of whom had the same type of DPI and had received extensive training in the correct use of the device. Despite the training, 27% of the patients received scores of ≤2 (inadequate technique). Sixty-eight percent received a score of 3 (adequate); only 5% received a score of 4 (good).
The 2 largest studies—one including 3955 patients using MDIs20 and the other looking at 3811 patients using various kinds of devices18—found high levels of errors, as well. In the latter study, 76% of patients with MDIs made at least one error vs 49% to 55% of patients using DPIs.18 The results convinced a large majority of the physicians caring for these patients of the need to check inhaler technique more frequently. In the study of MDI users alone, 71% of the patients made at least one mistake.20 inhaler misuse was associated with higher asthma instability scores, this study showed.
More recently, a researcher assessed the effects of an integrated primary care model on the management of asthma and/or COPD in middle-aged and elderly patients, in a study of 260 patients in 44 family practices.19 The study included an evaluation of inhaler technique.
Participants were divided into an intervention group—137 patients who received education regarding inhaler use from a nurse—and a usual care group (123 patients). After 2 years, correct inhaler technique among those in the intervention group went from 41% at baseline to 54%. At the same time, the proportion of those in the usual care group with correct technique fell from 47% to 29%.19
Error rates vary widely from one clinical trial to another, depending on study criteria, type of device, and extent of patient education, among other factors. Nonetheless, several studies (spanning 3 decades) found the error rate to be close to, or greater than, 90%.7,10,21
The most recent of these, published in 2009,21 was based on observation of the inhaler technique used by patients with asthma or COPD directly following appointments in an outpatient clinic. The authors found that, although >98% of the study participants claimed to know how to use their inhalers, 94% committed at least one error. In this study and a number of others, user error was more likely in patients using MDIs.13,18,21,22
Adding a spacer (eg, a valved holding chamber such as the AeroChamber) can be helpful, as the spacer affords the patient more time to inhale the medication. But patients who use an MDI with a spacer often make mistakes, too, and patient education is essential.23-26
Breath-activated dry powder inhalers (DPIs)—such as the Flexhaler, HandiHaler, Aerolizer, and Diskus—also reduce the likelihood of error. DPIs eliminate a step that MDI users often struggle with: the need to simultaneously press down on the canister and begin a slow, deep inhalation.
What’s more, DPIs do not have to be shaken before use. Nonetheless, using a DPI still involves a series of actions. For the HandiHaler and Aerolizer, patients must load the dose, and some patients fail to read the directions and swallow the capsule instead of loading it into the device. Patients must remember to exhale away from the device (ie, not into the dry powder) before inhaling, then hold their breath for approximately 10 seconds. There is potential for error at each step.
Stress the need to exhale before using the inhaler
Forgetting to exhale before inhaling is a common, and significant, mistake regardless of the type of device. It is paramount to stress the need to exhale gently for a few seconds before inhaling (slowly and deeply for patients using an MDI, rapidly and deeply with most DPIs). For MDI users, poor timing, described earlier, is another common and serious mistake. Patients using an MDI with a valved holding chamber sometimes inhale for too long before pressing down on the inhaler, then are unable to continue inhaling although the aerosol is still in the chamber. A common error made by patients using multidose DPIs is simply to forget to load the dose.
Physicians need to brush up on their skills, too
It’s not just patients who lack proficiency in inhaler technique. Numerous studies have demonstrated poor skill among physicians and other health care professionals.27-34 Evidence also shows that targeted education results in substantial improvement.32,35
In one study undertaken to evaluate family medicine residents’ proficiency in using asthma inhalers, participants (an intervention group at one clinic and a control group at another) all were given a pretest. The intervention group then received educational materials and a tutorial, as well as the opportunity for hands-on practice, after which both groups were given a post-test. The residents who received the training had a 170% jump, on average, in proficiency score, vs a 55% increase for the control group (P<.001).35
Inhaled Medication Instructional Videos
Courtesy of: National Jewish Health
Go to http://www.nationaljewish.org/healthinfo/medications/lung-diseases/devices/instructional-videos
Another study—this one involving first-year interns—looked at level of improvement based on the type of education provided. Initially, only 5% of the interns could use an MDI without error. After a lecture and demonstration, 13% had an error-free technique. But when each intern participated in an intensive one-on-one session, the error-free rate reached 73%. The researchers’ conclusion: Lectures are relatively ineffective in teaching interns inhaler technique compared with a one-on-one approach.32
The Chicago Breathe Project,36 a new program aimed at improving education in the use of asthma inhalers for physicians and minority patients, provides further evidence of the value of clinician education. After a series of workshops for residents at 5 academic institutions, the physicians’ knowledge of proper use of inhalers rose dramatically—from just 5% preprogram to 91% postprogram (P<.001). Six months after the educational activity, the residents (n=161) were more likely (44% vs 11% preprogram) to assess patients’ inhaler technique.36
Teaching patients when time is tight
National and international guidelines stress the need to teach patients correct use of asthma and COPD inhalers.1,37,38 Providing the requisite education includes observation of each patient’s inhaler technique with proper use demonstrated, as needed.
The problem, of course, is how to provide that level of patient education within the time constraints of a busy family practice. We recommend these time-efficient solutions:
Enlist the help of other clinicians. While it is important that someone in your office be well trained and able to instruct patients in the proper use of inhalers, that individual need not be you. The National Institutes of Health recommends that the “principal clinician” introduce key educational messages, which can be reinforced and expanded on by other members of the health care team.1
After you advise patients that it is crucial for them to be trained in and adhere to proper inhaler technique, another health care professional—often a clinic nurse or pharmacist who has had special training—can provide the hands-on education. Studies have shown that when pharmacists who are competent in asthma management, including inhaler technique, work with physicians to optimize the education and overall management of patients with asthma, better outcomes often result, including a reduction in both emergency department visits and hospitalizations.1,39,40
Use videos to demonstrate correct technique. Videos are an effective teaching tool,9 and many of them are device-specific. National Jewish Health, which is world renowned for its asthma care, has a set of instructional videos posted on You-Tube and accessible from its Web site (http://www.nationaljewish.org/healthinfo/medications/lung-diseases/devices/instructional-videos). In addition to videos that demonstrate the use of an MDI alone and an MDI plus a valved holding chamber, the site has links to 6 DPI videos, each covering a different device.
Use intermittent observation. After the patient views the appropriate video, you or a member of your staff will still need to observe the patient’s inhaler technique to ensure correct use. Ideally, this should occur at every visit.1,37 When that’s not possible, use intermittent observation, starting with the first 2 or 3 visits after the introduction of inhalation therapy and then switching to periodic observation to ensure that the patient is maintaining good technique.
In determining how often observation is necessary, keep in mind that simply asking patients whether they are having inhaler problems is not sufficient.1 Patients tend to say they have little or no trouble when, in fact, most struggle, at times, with the devices. What’s more, good technique tends to decrease over time, and repetitive education is important.
To motivate patients, try this communication technique
Motivational interviewing, a technique that has been used to help patients battle obesity, quit smoking, and control hypertension,41-43 among other health problems, can help you identify inhaler problems that need to be addressed. It involves the use of open-ended questions (eg, “What worries you most about your asthma?”), affirmations (“You’ve done a great job testing your peak flow level every morning”), reflective listening (“You’re tired of taking medicine every day”), and summary statements (“You know you should take your medicine every day but you’re having trouble remembering it. Is that right?”).
A pilot study44 showed that when this technique was incorporated into an asthma education session, patient motivation increased. The ratio of perceived advantages vs disadvantages of taking asthma medication correctly improved, as well. Another study45 found that when motivational interviewing was used during home visits to inner-city African American adolescents for asthma care, the patients’ motivation, readiness to adhere to treatment, and asthma-related quality of life improved, although self-reported adherence to asthma medication did not. Further studies involving patients with asthma are under way (www.clinicaltrials.gov/ct2/results?term=asthma).
It is important to note that the use of motivational interviewing does not require a lengthy visit. One study found that on average, visits in which primary care physicians used this communication technique lasted less than 10 minutes.46
CORRESPONDENCE Timothy H. Self, PharmD, University of Tennessee Health Science Center, 881 Madison Avenue, Room 235, Memphis, TN 38163; [email protected]
• Stress the importance of exhaling gently for a few seconds before inhaling (deeply and slowly for a metered dose inhaler, and deeply and rapidly for most dry powder inhalers). C
• Observe the inhaler technique of every patient receiving inhalation therapy on more than one occasion. C
• Don’t rely on self-reports regarding inhaler technique; despite claims of proficiency, most patients make at least one mistake. C
Strength of recommendation (SOR)
A Good-quality patient-oriented evidence
B Inconsistent or limited-quality patient-oriented evidence
C Consensus, usual practice, opinion, disease-oriented evidence, case series
For patients with asthma or chronic obstructive pulmonary disease (COPD), inhalation therapy is the foundation of treatment. Yet all too often, patients don’t get the full value of their inhaled medications because they use their inhaler incorrectly. When technique is markedly flawed, suboptimal outcomes typically result.
Given the number of Americans with asthma (at least 22 million)1 and COPD (more than 13 million adults),2 faulty inhaler technique is a major public health problem. In fact, the number of people suffering from COPD may be even larger: Close to 24 million US adults are believed to have impaired lung function.3,4 For patients with asthma or COPD—many of whom are treated by family physicians—comprehensive education with a focus on correct use of an inhaler is essential.
In this review, we present evidence of frequent inhaler errors (from clinical studies) and highlight some of the more common mistakes (based on our clinical experience [TABLE]5). Finally, we offer ‘‘time-efficient’’ solutions to inhaler problems—steps that physicians in busy primary care practices can take to ensure that patients with asthma or COPD get the maximum benefit from inhalation therapy.
TABLE
Caution patients about these device-specific mistakes*
| Metered dose inhaler |
|---|
|
| Metered dose inhaler plus spacer/VHC |
|
| Dry powder inhaler |
|
| *These are examples based on the experience of the authors; other errors are possible. †Timing is not as crucial as it is for an MDI without a spacer, but the drug is still lost if inhalation is delayed. ‡Correct use varies by type of product (see product literature for specifics). DPI, dry powder inhaler; MDI, metered dose inhaler; VHC, valved holding chamber. Source: Adapted with permission from Self TH, et al. Consultant. 2003.5 |
Inhaler error is well documented
Since 1965, when it was first reported that many patients used metered dose inhalers (MDIs) incorrectly,6 evidence has accumulated supporting the magnitude of the problem.7-12 (Studies conducted in family practice settings are described in “Researchers look at inhaler problems in primary care” and in TABLE W1.13-20)
A number of studies of various sizes (from 41 to 3955 patients) have assessed inhaler technique in patients being treated by clinicians in primary care. The researchers used a variety of scoring methods, as well. Among them were a simple 4-step (0-4) rating system, a 9-step system, a standardized inhaler-specific checklist, and a system that tracked the number of omissions patients made.13-20 All found significant problems with inhaler technique. (You’ll find a detailed look at the studies in TABLE W1 at jfponline.com.)
In one study of 422 patients,13 including young children, adolescents, and adults, participants received one point for correctly performing each of the following steps:
- Adequate preparation (shaking well for those using a metered dose inhaler [MDI]; loading correctly for patients using a dry powder inhaler [DPI])
- Adequate expiration, correct head position
- Adequate inspiratory technique
- Holding breath afterwards.
The researchers found that 25% of the patients had inadequate technique (≤2 on a 0-4 point scale). In this study, as in others that included patients using various types of devices, use of an MDI was associated with a higher rate of incorrect technique.
Another much-smaller study14 used the same 4-step system to assess the technique of 50 patients, all of whom had the same type of DPI and had received extensive training in the correct use of the device. Despite the training, 27% of the patients received scores of ≤2 (inadequate technique). Sixty-eight percent received a score of 3 (adequate); only 5% received a score of 4 (good).
The 2 largest studies—one including 3955 patients using MDIs20 and the other looking at 3811 patients using various kinds of devices18—found high levels of errors, as well. In the latter study, 76% of patients with MDIs made at least one error vs 49% to 55% of patients using DPIs.18 The results convinced a large majority of the physicians caring for these patients of the need to check inhaler technique more frequently. In the study of MDI users alone, 71% of the patients made at least one mistake.20 inhaler misuse was associated with higher asthma instability scores, this study showed.
More recently, a researcher assessed the effects of an integrated primary care model on the management of asthma and/or COPD in middle-aged and elderly patients, in a study of 260 patients in 44 family practices.19 The study included an evaluation of inhaler technique.
Participants were divided into an intervention group—137 patients who received education regarding inhaler use from a nurse—and a usual care group (123 patients). After 2 years, correct inhaler technique among those in the intervention group went from 41% at baseline to 54%. At the same time, the proportion of those in the usual care group with correct technique fell from 47% to 29%.19
Error rates vary widely from one clinical trial to another, depending on study criteria, type of device, and extent of patient education, among other factors. Nonetheless, several studies (spanning 3 decades) found the error rate to be close to, or greater than, 90%.7,10,21
The most recent of these, published in 2009,21 was based on observation of the inhaler technique used by patients with asthma or COPD directly following appointments in an outpatient clinic. The authors found that, although >98% of the study participants claimed to know how to use their inhalers, 94% committed at least one error. In this study and a number of others, user error was more likely in patients using MDIs.13,18,21,22
Adding a spacer (eg, a valved holding chamber such as the AeroChamber) can be helpful, as the spacer affords the patient more time to inhale the medication. But patients who use an MDI with a spacer often make mistakes, too, and patient education is essential.23-26
Breath-activated dry powder inhalers (DPIs)—such as the Flexhaler, HandiHaler, Aerolizer, and Diskus—also reduce the likelihood of error. DPIs eliminate a step that MDI users often struggle with: the need to simultaneously press down on the canister and begin a slow, deep inhalation.
What’s more, DPIs do not have to be shaken before use. Nonetheless, using a DPI still involves a series of actions. For the HandiHaler and Aerolizer, patients must load the dose, and some patients fail to read the directions and swallow the capsule instead of loading it into the device. Patients must remember to exhale away from the device (ie, not into the dry powder) before inhaling, then hold their breath for approximately 10 seconds. There is potential for error at each step.
Stress the need to exhale before using the inhaler
Forgetting to exhale before inhaling is a common, and significant, mistake regardless of the type of device. It is paramount to stress the need to exhale gently for a few seconds before inhaling (slowly and deeply for patients using an MDI, rapidly and deeply with most DPIs). For MDI users, poor timing, described earlier, is another common and serious mistake. Patients using an MDI with a valved holding chamber sometimes inhale for too long before pressing down on the inhaler, then are unable to continue inhaling although the aerosol is still in the chamber. A common error made by patients using multidose DPIs is simply to forget to load the dose.
Physicians need to brush up on their skills, too
It’s not just patients who lack proficiency in inhaler technique. Numerous studies have demonstrated poor skill among physicians and other health care professionals.27-34 Evidence also shows that targeted education results in substantial improvement.32,35
In one study undertaken to evaluate family medicine residents’ proficiency in using asthma inhalers, participants (an intervention group at one clinic and a control group at another) all were given a pretest. The intervention group then received educational materials and a tutorial, as well as the opportunity for hands-on practice, after which both groups were given a post-test. The residents who received the training had a 170% jump, on average, in proficiency score, vs a 55% increase for the control group (P<.001).35
Inhaled Medication Instructional Videos
Courtesy of: National Jewish Health
Go to http://www.nationaljewish.org/healthinfo/medications/lung-diseases/devices/instructional-videos
Another study—this one involving first-year interns—looked at level of improvement based on the type of education provided. Initially, only 5% of the interns could use an MDI without error. After a lecture and demonstration, 13% had an error-free technique. But when each intern participated in an intensive one-on-one session, the error-free rate reached 73%. The researchers’ conclusion: Lectures are relatively ineffective in teaching interns inhaler technique compared with a one-on-one approach.32
The Chicago Breathe Project,36 a new program aimed at improving education in the use of asthma inhalers for physicians and minority patients, provides further evidence of the value of clinician education. After a series of workshops for residents at 5 academic institutions, the physicians’ knowledge of proper use of inhalers rose dramatically—from just 5% preprogram to 91% postprogram (P<.001). Six months after the educational activity, the residents (n=161) were more likely (44% vs 11% preprogram) to assess patients’ inhaler technique.36
Teaching patients when time is tight
National and international guidelines stress the need to teach patients correct use of asthma and COPD inhalers.1,37,38 Providing the requisite education includes observation of each patient’s inhaler technique with proper use demonstrated, as needed.
The problem, of course, is how to provide that level of patient education within the time constraints of a busy family practice. We recommend these time-efficient solutions:
Enlist the help of other clinicians. While it is important that someone in your office be well trained and able to instruct patients in the proper use of inhalers, that individual need not be you. The National Institutes of Health recommends that the “principal clinician” introduce key educational messages, which can be reinforced and expanded on by other members of the health care team.1
After you advise patients that it is crucial for them to be trained in and adhere to proper inhaler technique, another health care professional—often a clinic nurse or pharmacist who has had special training—can provide the hands-on education. Studies have shown that when pharmacists who are competent in asthma management, including inhaler technique, work with physicians to optimize the education and overall management of patients with asthma, better outcomes often result, including a reduction in both emergency department visits and hospitalizations.1,39,40
Use videos to demonstrate correct technique. Videos are an effective teaching tool,9 and many of them are device-specific. National Jewish Health, which is world renowned for its asthma care, has a set of instructional videos posted on You-Tube and accessible from its Web site (http://www.nationaljewish.org/healthinfo/medications/lung-diseases/devices/instructional-videos). In addition to videos that demonstrate the use of an MDI alone and an MDI plus a valved holding chamber, the site has links to 6 DPI videos, each covering a different device.
Use intermittent observation. After the patient views the appropriate video, you or a member of your staff will still need to observe the patient’s inhaler technique to ensure correct use. Ideally, this should occur at every visit.1,37 When that’s not possible, use intermittent observation, starting with the first 2 or 3 visits after the introduction of inhalation therapy and then switching to periodic observation to ensure that the patient is maintaining good technique.
In determining how often observation is necessary, keep in mind that simply asking patients whether they are having inhaler problems is not sufficient.1 Patients tend to say they have little or no trouble when, in fact, most struggle, at times, with the devices. What’s more, good technique tends to decrease over time, and repetitive education is important.
To motivate patients, try this communication technique
Motivational interviewing, a technique that has been used to help patients battle obesity, quit smoking, and control hypertension,41-43 among other health problems, can help you identify inhaler problems that need to be addressed. It involves the use of open-ended questions (eg, “What worries you most about your asthma?”), affirmations (“You’ve done a great job testing your peak flow level every morning”), reflective listening (“You’re tired of taking medicine every day”), and summary statements (“You know you should take your medicine every day but you’re having trouble remembering it. Is that right?”).
A pilot study44 showed that when this technique was incorporated into an asthma education session, patient motivation increased. The ratio of perceived advantages vs disadvantages of taking asthma medication correctly improved, as well. Another study45 found that when motivational interviewing was used during home visits to inner-city African American adolescents for asthma care, the patients’ motivation, readiness to adhere to treatment, and asthma-related quality of life improved, although self-reported adherence to asthma medication did not. Further studies involving patients with asthma are under way (www.clinicaltrials.gov/ct2/results?term=asthma).
It is important to note that the use of motivational interviewing does not require a lengthy visit. One study found that on average, visits in which primary care physicians used this communication technique lasted less than 10 minutes.46
CORRESPONDENCE Timothy H. Self, PharmD, University of Tennessee Health Science Center, 881 Madison Avenue, Room 235, Memphis, TN 38163; [email protected]
1. National Heart, Lung, and Blood Institute; National Asthma Education and Prevention Program Expert Panel Report 3: Guidelines for the Diagnosis and Management of Asthma. Bethesda, MD: National Institutes of Health; 2007.
2. Centers for Disease Control and Prevention. National Center for Health Statistics: National health interview survey raw data, 2008. Analysis performed by American Lung Association Research and Program Services.
3. American Lung Association. COPD—Helping the missing millions. February 24, 2010. Available at: http://www.lungusa.org/about-us/our-impact/top-stories/copd-helping-the-missing.html. Accessed November 9, 2011.
4. Centers for Disease Control and Prevention. Chronic obstructive pulmonary disease surveillance—United States, 1971-2000. MMWR Surveill Summ. 2002;51(6):1-16.
5. Self TH, Kilgore KE, Shelton V. MDIs, spacers, and dry powder inhalers: what patients are likely to do wrong. Consultant. 2003;49:702-705.
6. Saunders KB. Misuse of inhaled bronchodilator agents. Br Med J. 1965;1:1037-1038.
7. Epstein SW, Manning CPR, Ashley MJ, et al. Survey of the clinical uses of pressurized aerosol inhalers. Can Med Assoc J. 1979;120:813-816.
8. Shim C, Williams MH. The adequacy of inhalation of aerosol from canister nebulizers. Am J Med. 1980;69:891-894.
9. Self TH, Brooks JB, Lieberman P, et al. The value of demonstration and role of the pharmacist in teaching the correct use of pressurized bronchodilators. Can Med Assoc J. 1983;128:129-131.
10. Hartert TV, Windom HH, Peeples RS, et al. Inadequate outpatient medical therapy for patients with asthma admitted to two urban hospitals. Am J Med. 1996;100:386-394.
11. Goodman DE, Israel E, Rosenberg M, et al. The influence of age, diagnosis, and gender on proper use of metered-dose inhalers. Am J Respir Crit Care Med. 1994;150:1256-1261.
12. Newman SP, Pavia D, Clarke SW. How should a pressurized beta-adrenergic bronchodilator be inhaled? Eur J Respir Dis. 1981;62:3-21.
13. Hilton S. An audit of inhaler technique among asthma patients of 34 general practitioners. Br J Gen Pract. 1990;40:505-506.
14. Dompeling E, Van Grunsven PM, Van Schayck GP, et al. Treatment with inhaled steroids in asthma and chronic bronchitis: long-term compliance and inhaler technique. Fam Pract. 1992;9:161-166.
15. Verver S, Poelman M, Bogels A, et al. Effects of instruction by practice assistants on inhaler technique and respiratory symptoms of patients. A controlled randomized videotaped intervention study. Fam Pract. 1996;13:35-40.
16. Dickinson J, Hutton S, Atkin A, et al. Reducing asthma morbidity in the community: the effect of a targeted nurse-run asthma clinic in an English general practice. Respir Med. 1997;91:634-640.
17. Hesselink AE, Penninx BW, Wijnhoven HA, et al. Determinants of an incorrect inhalation technique in patients with asthma or COPD. Scand J Prim Health Care. 2001;19:255-260.
18. Molimard M, Raherison C, Lignot S, et al. Assessment of handling of inhaler devices in real life: An observational study in 3811 patients in primary care. J Aerosol Med. 2003;16:249-254.
19. Meulepas MA, Jacobs JE, Smeenk FW, et al. Effect of an integrated primary care model on the management of middle-aged and old patients with obstructive lung diseases. Scand J Prim Health Care. 2007;25:186-192.
20. Giraud V, Roche N. Misuse of corticosteroid metered-dose inhaler is associated with decreased asthma stability. Eur Respir J. 2002;19:246-251.
21. Souza ML, Meneghini AC, Ferraz E, et al. Knowledge of and technique for using inhalation devices among asthma patients and COPD patients. J Bras Pneumol. 2009;35:824-831.
22. Rootmensen GN, van Keimpema AR, Jansen HM, et al. Predictors of incorrect inhalation technique in patients with asthma or COPD: a study using a validated videotaped scoring method. J Aerosol Med Pulm Drug Deliv. 2010;23:323-328.
23. Rachelefsky GS, Rohr AS, Wo J, et al. Use of a tube spacer to improve the efficacy of a metered dose inhaler in asthmatic children. Am J Dis Child. 1986;140:1191-1193.
24. Demirkan K, Tolley E, Mastin T, et al. Salmeterol administration by metered-dose inhaler alone vs metered-dose inhaler plus valved holding chamber. Chest. 2000;117:1314-1318.
25. Pedersen S, Ostergaard PA. Nasal inhalation as a cause of inefficient pulmonal aerosol inhalation technique in children. Allergy. 1983;38:191-194.
26. Dolovich MD, Ahrens RS, Hess DR, et al. Device selection an outcomes of aerosol therapy: evidence-based guidelines: American College of Chest Physicians/American College of Asthma, Allergy, and Immunology. Chest. 2005;127:335-371.
27. Interiano B, Guntupalli KK. Metered-dose inhalers: do health care providers know what to teach? Arch Intern Med. 1993;153:81-85.
28. Hanania NA, Wittman R, Kesten S, et al. Medical personnel’s knowledge of and ability to use inhaling devices. Metered-dose inhalers, spacing chambers, and breath-actuated dry powder inhalers. Chest. 1994;105:111-116.
29. Amirav I, Goren A, Pawlowski NA. What do pediatricians in training know about the correct use of inhalers and spacer devices? J Allergy Clin Immunol. 1994;94:669-675.
30. Chopra N, Oprescu N, Fask A, et al. Does introduction of new “easy to use” inhalational devices improve medical personnel’s knowledge of their proper use? Ann Allergy Asthma Immunol. 2002;88:395-400.
31. Self TH, Arnold LB, Czosnowski LM, et al. Inadequate skill of healthcare professionals in using asthma inhalation devices. J Asthma. 2007;44:593-598.
32. Lee-Wong M, Mayo PH. Results of a programme to improve house staff use of metered dose inhalers and spacers. Postgrad Med J. 2003;79:221-225.
33. Muchao FP, Pern SL, Rodriques JC, et al. Evaluation of the knowledge of health professionals at a pediatric hospital regarding the use of metered dose inhalers. J Bras Pneumol. 2008;34:4-12.
34. Kim SH, Kwak HJ, Kim TB, et al. Inappropriate techniques used by internal medicine residents with three kinds of inhalers (a metered dose inhaler, Diskus, and Turbuhaler): changes after a single teaching session. J Asthma. 2009;46:944-950.
35. Kelcher S, Brownoff R. Teaching residents to use asthma devices. Assessing family residents’ skill and a brief intervention. Can Fam Physician. 1994;40:2090-2095.
36. Press VG, Pincayage AT, Pappalardo AA, et al. The Chicago Breathe Project: a regional approach to improving education on asthma inhalers for resident physicians and minority patients. J Natl Med Assoc. 2010;102:548-555.
37. Global Initiative for Asthma (GINA). Global strategy for asthma management and prevention. 2010. Available at: www.ginasthma.org. Accessed November 9, 2011.
38. Executive Summary: global strategy on the diagnosis and management and prevention of chronic obstructive pulmonary disease. NHLBI/WHO Workshop Report, 2009. Available at: www.goldcopd.com. Accessed November 9, 2011.
39. Self TH, Chrisman CR, Mason DL, et al. Reducing emergency department visits and hospitalizations in African American and Hispanic patients: a 15-year review. J Asthma. 2005;42:807-812.
40. Armour C, Bosnic-Anticevich S, Brillant M, et al. Pharmacy asthma care program (PACP) improves outcomes for patients in the community. Thorax. 2007;62:496-502.
41. DiLillo V, Nicole J, West DS. Incorporating motivational interviewing into behavioral obesity treatment. Cogn Behav Pract. 2003;10:120-130.
42. Borrelli B, Novak S, Hecht J, et al. Home health care nurses as a new channel for smoking cessation treatment: outcomes from project CARES (Community-nurse Assisted Research and Education on Smoking). Prev Med. 2005;41:815-821.
43. Woollard L, Beilin L, Lord T, et al. A controlled trial of nurse counselling on lifestyle change for hypertensives treated in general practice: preliminary results. Clin Exp Pharmacol Physiol. 1995;22:466-468.
44. Schmaling K, Blume A, Afari N. A randomized controlled pilot study of motivational interviewing to change attitudes about adherence to medications for asthma. J Clin Psych Med Settings. 2001;8:167-172.
45. Riekert KA, Borrelli B, Bilderback A, et al. The development of a motivational interviewing intervention to promote medication adherence among inner-city, African-American adolescents with asthma. Patient Educ Couns. 2011;82:117-122.
46. Butler C, Rollnick S, Cohen D, et al. Motivational consulting versus brief advice for smokers in general practice: a randomized trial. Br J Gen Pract. 1999;49:611-616.
1. National Heart, Lung, and Blood Institute; National Asthma Education and Prevention Program Expert Panel Report 3: Guidelines for the Diagnosis and Management of Asthma. Bethesda, MD: National Institutes of Health; 2007.
2. Centers for Disease Control and Prevention. National Center for Health Statistics: National health interview survey raw data, 2008. Analysis performed by American Lung Association Research and Program Services.
3. American Lung Association. COPD—Helping the missing millions. February 24, 2010. Available at: http://www.lungusa.org/about-us/our-impact/top-stories/copd-helping-the-missing.html. Accessed November 9, 2011.
4. Centers for Disease Control and Prevention. Chronic obstructive pulmonary disease surveillance—United States, 1971-2000. MMWR Surveill Summ. 2002;51(6):1-16.
5. Self TH, Kilgore KE, Shelton V. MDIs, spacers, and dry powder inhalers: what patients are likely to do wrong. Consultant. 2003;49:702-705.
6. Saunders KB. Misuse of inhaled bronchodilator agents. Br Med J. 1965;1:1037-1038.
7. Epstein SW, Manning CPR, Ashley MJ, et al. Survey of the clinical uses of pressurized aerosol inhalers. Can Med Assoc J. 1979;120:813-816.
8. Shim C, Williams MH. The adequacy of inhalation of aerosol from canister nebulizers. Am J Med. 1980;69:891-894.
9. Self TH, Brooks JB, Lieberman P, et al. The value of demonstration and role of the pharmacist in teaching the correct use of pressurized bronchodilators. Can Med Assoc J. 1983;128:129-131.
10. Hartert TV, Windom HH, Peeples RS, et al. Inadequate outpatient medical therapy for patients with asthma admitted to two urban hospitals. Am J Med. 1996;100:386-394.
11. Goodman DE, Israel E, Rosenberg M, et al. The influence of age, diagnosis, and gender on proper use of metered-dose inhalers. Am J Respir Crit Care Med. 1994;150:1256-1261.
12. Newman SP, Pavia D, Clarke SW. How should a pressurized beta-adrenergic bronchodilator be inhaled? Eur J Respir Dis. 1981;62:3-21.
13. Hilton S. An audit of inhaler technique among asthma patients of 34 general practitioners. Br J Gen Pract. 1990;40:505-506.
14. Dompeling E, Van Grunsven PM, Van Schayck GP, et al. Treatment with inhaled steroids in asthma and chronic bronchitis: long-term compliance and inhaler technique. Fam Pract. 1992;9:161-166.
15. Verver S, Poelman M, Bogels A, et al. Effects of instruction by practice assistants on inhaler technique and respiratory symptoms of patients. A controlled randomized videotaped intervention study. Fam Pract. 1996;13:35-40.
16. Dickinson J, Hutton S, Atkin A, et al. Reducing asthma morbidity in the community: the effect of a targeted nurse-run asthma clinic in an English general practice. Respir Med. 1997;91:634-640.
17. Hesselink AE, Penninx BW, Wijnhoven HA, et al. Determinants of an incorrect inhalation technique in patients with asthma or COPD. Scand J Prim Health Care. 2001;19:255-260.
18. Molimard M, Raherison C, Lignot S, et al. Assessment of handling of inhaler devices in real life: An observational study in 3811 patients in primary care. J Aerosol Med. 2003;16:249-254.
19. Meulepas MA, Jacobs JE, Smeenk FW, et al. Effect of an integrated primary care model on the management of middle-aged and old patients with obstructive lung diseases. Scand J Prim Health Care. 2007;25:186-192.
20. Giraud V, Roche N. Misuse of corticosteroid metered-dose inhaler is associated with decreased asthma stability. Eur Respir J. 2002;19:246-251.
21. Souza ML, Meneghini AC, Ferraz E, et al. Knowledge of and technique for using inhalation devices among asthma patients and COPD patients. J Bras Pneumol. 2009;35:824-831.
22. Rootmensen GN, van Keimpema AR, Jansen HM, et al. Predictors of incorrect inhalation technique in patients with asthma or COPD: a study using a validated videotaped scoring method. J Aerosol Med Pulm Drug Deliv. 2010;23:323-328.
23. Rachelefsky GS, Rohr AS, Wo J, et al. Use of a tube spacer to improve the efficacy of a metered dose inhaler in asthmatic children. Am J Dis Child. 1986;140:1191-1193.
24. Demirkan K, Tolley E, Mastin T, et al. Salmeterol administration by metered-dose inhaler alone vs metered-dose inhaler plus valved holding chamber. Chest. 2000;117:1314-1318.
25. Pedersen S, Ostergaard PA. Nasal inhalation as a cause of inefficient pulmonal aerosol inhalation technique in children. Allergy. 1983;38:191-194.
26. Dolovich MD, Ahrens RS, Hess DR, et al. Device selection an outcomes of aerosol therapy: evidence-based guidelines: American College of Chest Physicians/American College of Asthma, Allergy, and Immunology. Chest. 2005;127:335-371.
27. Interiano B, Guntupalli KK. Metered-dose inhalers: do health care providers know what to teach? Arch Intern Med. 1993;153:81-85.
28. Hanania NA, Wittman R, Kesten S, et al. Medical personnel’s knowledge of and ability to use inhaling devices. Metered-dose inhalers, spacing chambers, and breath-actuated dry powder inhalers. Chest. 1994;105:111-116.
29. Amirav I, Goren A, Pawlowski NA. What do pediatricians in training know about the correct use of inhalers and spacer devices? J Allergy Clin Immunol. 1994;94:669-675.
30. Chopra N, Oprescu N, Fask A, et al. Does introduction of new “easy to use” inhalational devices improve medical personnel’s knowledge of their proper use? Ann Allergy Asthma Immunol. 2002;88:395-400.
31. Self TH, Arnold LB, Czosnowski LM, et al. Inadequate skill of healthcare professionals in using asthma inhalation devices. J Asthma. 2007;44:593-598.
32. Lee-Wong M, Mayo PH. Results of a programme to improve house staff use of metered dose inhalers and spacers. Postgrad Med J. 2003;79:221-225.
33. Muchao FP, Pern SL, Rodriques JC, et al. Evaluation of the knowledge of health professionals at a pediatric hospital regarding the use of metered dose inhalers. J Bras Pneumol. 2008;34:4-12.
34. Kim SH, Kwak HJ, Kim TB, et al. Inappropriate techniques used by internal medicine residents with three kinds of inhalers (a metered dose inhaler, Diskus, and Turbuhaler): changes after a single teaching session. J Asthma. 2009;46:944-950.
35. Kelcher S, Brownoff R. Teaching residents to use asthma devices. Assessing family residents’ skill and a brief intervention. Can Fam Physician. 1994;40:2090-2095.
36. Press VG, Pincayage AT, Pappalardo AA, et al. The Chicago Breathe Project: a regional approach to improving education on asthma inhalers for resident physicians and minority patients. J Natl Med Assoc. 2010;102:548-555.
37. Global Initiative for Asthma (GINA). Global strategy for asthma management and prevention. 2010. Available at: www.ginasthma.org. Accessed November 9, 2011.
38. Executive Summary: global strategy on the diagnosis and management and prevention of chronic obstructive pulmonary disease. NHLBI/WHO Workshop Report, 2009. Available at: www.goldcopd.com. Accessed November 9, 2011.
39. Self TH, Chrisman CR, Mason DL, et al. Reducing emergency department visits and hospitalizations in African American and Hispanic patients: a 15-year review. J Asthma. 2005;42:807-812.
40. Armour C, Bosnic-Anticevich S, Brillant M, et al. Pharmacy asthma care program (PACP) improves outcomes for patients in the community. Thorax. 2007;62:496-502.
41. DiLillo V, Nicole J, West DS. Incorporating motivational interviewing into behavioral obesity treatment. Cogn Behav Pract. 2003;10:120-130.
42. Borrelli B, Novak S, Hecht J, et al. Home health care nurses as a new channel for smoking cessation treatment: outcomes from project CARES (Community-nurse Assisted Research and Education on Smoking). Prev Med. 2005;41:815-821.
43. Woollard L, Beilin L, Lord T, et al. A controlled trial of nurse counselling on lifestyle change for hypertensives treated in general practice: preliminary results. Clin Exp Pharmacol Physiol. 1995;22:466-468.
44. Schmaling K, Blume A, Afari N. A randomized controlled pilot study of motivational interviewing to change attitudes about adherence to medications for asthma. J Clin Psych Med Settings. 2001;8:167-172.
45. Riekert KA, Borrelli B, Bilderback A, et al. The development of a motivational interviewing intervention to promote medication adherence among inner-city, African-American adolescents with asthma. Patient Educ Couns. 2011;82:117-122.
46. Butler C, Rollnick S, Cohen D, et al. Motivational consulting versus brief advice for smokers in general practice: a randomized trial. Br J Gen Pract. 1999;49:611-616.
Bromocriptine: Its place in type 2 diabetes Tx
• Reserve bromocriptine for cases in which only a modest reduction in A1c is needed. A
• Advise patients to take bromocriptine in the morning with food to maximize its bioavailability. A
Strength of recommendation (SOR)
A Good-quality patient-oriented evidence
B Inconsistent or limited-quality patient-oriented evidence
C Consensus, usual practice, opinion, disease-oriented evidence, case series
For obese patients with type 2 diabetes (T2D) who do not tolerate other diabetes medications or for patients who need only a minimal reduction in glycosylated hemoglobin (A1c) to reach goal, bromocriptine may be a therapeutic agent to consider. Approved by the US Food and Drug Administration (FDA) in 2009, Cycloset is a quick-release formulation of bromocriptine mesylate, an ergot alkaloid dopamine D2 receptor agonist that has a faster onset of action than the customary formulation, Parlodel, which has been used to treat Parkinson’s disease, acromegaly, and hyperprolactinemia.1 In addition to its modest benefit in improving glycemic control, Cyclocet avoids undesirable side effects such as hypoglycemia and weight gain.
VeroScience, LLC holds the new drug application and related technologies for Cycloset and partnered with Santarus, Inc. and S2 Therapeutics to market it in September 2010.2
Bromocriptine’s likely mechanism of action
Although its exact mechanism of action is unclear, bromocriptine does not stimulate insulin release, reduce hepatic glucose production, increase glucose transporter production, or increase or mimic glucagon-like peptide-1 activity as other T2D agents do.3 Its contribution to glycemic control in T2D has been hypothesized to be due to adjustments in the neural control of seasonal and diurnal patterns of food intake and nutrient storage.4
Early hunter-gatherers and farmers are thought to have benefited from a “thrifty genotype” that favored fat deposition when food was seasonally abundant. With food in western society available year-round and often energy dense in both fat and carbohydrates, this same gene may lead to obesity and noninsulin-dependent diabetes mellitus.5
The hypothesis assumes that circadian rhythm, photo- periodism, and seasonal factors play a role in insulin resistance, hepatic gluconeogenesis, and weight gain. In vertebrates, the neuroendocrine system plays an important role in synchronizing the animal with cyclic environmental changes. The hypothalamic suprachiasmatic nucleus (SCN) is known as the circadian pacemaker that maintains this rhythm. Oscillations in the SCN occur due to external cues such as changes in light or temperature. Circadian dopaminergic and serotonergic activities are likely responsible for modifying such oscillations, and neurotransmitters have been shown to regulate the dramatic seasonal alterations in body weight and body composition of all vertebrate classes.6 Bromocriptine can reverse metabolic alterations associated with insulin resistance and obesity by resetting central (hypothalamic) circadian organization of monoamine neuronal activities.7
Proven anti-T2D effects. When administered systemically or into the cerebral ventricle at first light, bromocriptine prevents or reverses seasonal fattening, insulin resistance, and hyperinsulinemia, and it decreases endogenous (hepatic) glucose production in mammals.8-11 Bromocriptine also decreases both fasting and postprandial triglyceride and free fatty acid levels.1
Clinical trials show modest benefit
Although bromocriptine has been studied since 1980 for its effects on hyperglycemia in T2D,12 trials leading to the approval of the drug for clinical use with T2D have only been completed within the last 15 years. Randomized controlled trials of varying sizes and lasting from 6 to 52 weeks have shown absolute A1c reductions from 0.1% to 0.6%.1,12-16 Compared with placebo, A1c reductions have ranged from 0.4% to 1.2% with monotherapy and in combination with other antidiabetes medications.1,13-16
The manufacturer assessed bromocriptine in 4 studies involving patients with T2D. In all 4 studies, the bromocriptine dose was titrated to a maximum of 4.8 mg/d.16
One study involved 159 overweight subjects who were not meeting glycemic goals.16 Patients received either placebo or bromocriptine for 24 weeks in addition to diet and exercise. Mean baseline A1c was 9.0% in the bromocriptine group and 8.8% in the placebo group. After 24 weeks, A1c was reduced by 0.1% in the treatment group and increased by 0.3% in the placebo group. Mean fasting glucose was 215 mg/dL at baseline in the treatment group and was unchanged after 24 weeks. In the placebo group, fasting glucose increased from 205 to 228 mg/dL during the study. Weight increased by 0.2 kg in the treatment group and by 0.5 kg in the placebo group.
The next two 24-week manufacturer studies used similar designs to compare the addition of either bromocriptine or placebo to existing sulfonylurea therapy in patients with uncontrolled T2D.16 One study assigned 122 patients to bromocriptine and 127 to placebo. The bromocriptine group demonstrated mean reductions of 0.4% in A1c and 3 mg/dL in fasting glucose. In the placebo group, A1c increased by 0.3% and fasting glucose rose by 23 mg/dL.
The other study assigned 122 patients to bromocriptine and 123 to placebo. Adding bromocriptine reduced A1c, on average, by 0.1% and fasting glucose by 10 mg/dL. In the placebo group, A1c increased by 0.4% and fasting glucose increased by 28 mg/dL. All of these results were statistically significant.
The last manufacturer-reported study evaluated the addition of bromocriptine to other diabetes treatments (diet or up to 2 anti-diabetes medications).13 While the primary intent of this study was to evaluate safety, it also assessed efficacy. This was a 52-week, randomized placebo-controlled trial involving 3095 patients.
Overall, after 24 weeks there was no change in A1c levels after adding bromocriptine. However, most patients in this study were already at goal (A1c <7.0%). A subgroup analysis of those with an A1c level <7.5% while taking other agents did show some improvement with the addition of bromocriptine. Adding bromocriptine to metformin and a sulfonylurea significantly reduced A1c by 0.5%, on average. Similar results were seen in those who received other combinations of diabetes medications. After 52 weeks, 25% of those receiving bromocriptine who originally had an A1c level >7.5% achieved an A1c level <7.0%. Of the patients who received placebo, 9% obtained an A1c level <7%.
In a 24-week study, bromocriptine titrated up to 4.8 mg/d was given to patients either on no other diabetes medication or on a sulfonylurea.1 In individuals not on any current treatment, A1c decreased by 0.2% in those who received bromocriptine. In patients already on a sulfonylurea, A1c declined by 0.1%. A1c increased by 0.3% in those receiving placebo.
Bromocriptine most effective when taken with food
When bromocriptine is taken orally, 65% to 95% of the dose is absorbed; however, only 7% reaches systemic circulation due to extensive hepatic extraction and first-pass metabolism.17 Bioavailability increases by 55% to 65% when the drug is taken with food, which is how it should be administered. The time to maximum plasma concentration is within an hour. With a high-fat meal, however, the time increases to 90 to 120 minutes. Bromocriptine is highly protein bound (90%-96%) and is metabolized extensively in the gastrointestinal (GI) tract and liver.17 CYP3A4 is the major metabolic pathway.1,18 Most excretion of bromocriptine is through bile, with approximately 2% to 6% of an oral dose eliminated via urine. The elimination half-life is approximately 6 hours.17,18
Dosing is once a day in the morning
Clinical trials investigating the use of bromocriptine in diabetes used doses ranging from 1.6 to 4.8 mg/d.13-16,19 The FDA-approved dose range is 1.6 to 4.8 mg administered once daily with food, within 2 hours of waking in the morning.16 In healthy individuals, central nervous system (CNS) dopaminergic activity peaks in the early morning. Thus, morning dosing attempts to mimic dopaminergic activity and circadian rhythms in healthy lean individuals.6
Titrate to maximum dose. The product is available in a 0.8-mg tablet (TABLE). Titration to the maximum dose is recommended to reduce GI adverse effects, particularly nausea. Start treatment with 1 tablet (0.8 mg) and increase the dose by 1 tablet per week until the patient reaches a maximum tolerated dose or the maximum allowable daily dose of 4.8 mg (6 tablets).
Precautions with renal or hepatic impairment. No pharmacokinetic studies of bromocriptine have been conducted with patients who have renal impairment, and the kidney is a minor elimination pathway for bromocriptine. The package insert offers no specific dose recommendations for such patients, although it does recommend caution when using this product in patients with renal impairment. Studies of bromocriptine in patients with liver dysfunction are also lacking. However, as bromocriptine is predominately metabolized in the liver, use caution in patients with hepatic impairment.16
TABLE
Key prescribing information for bromocriptine16
| How supplied | 0.8-mg tablets |
| Indication | Adjunct to diet and exercise in type 2 diabetes mellitus |
| Dosing | Initial: 0.8 mg once daily with food, in the morning within 2 hours of waking Titration: increase by 1 tablet (0.8 mg) per week until maximum dose or maximum tolerance is reached |
| Maximum dose | 4.8 mg daily |
| Renal/hepatic impairment | Use with caution in patients with renal or hepatic impairment |
| Pregnancy; lactation | Pregnancy, category B; contraindicated for nursing women |
| Effectiveness | A1c reduced 0.1%-0.6% vs 0.3%-1.1% increase with placebo Fasting glucose reduced 0-10 mg/dl vs 23-28 mg/dl increase with placebo |
| Common adverse effects | Nausea, fatigue, headache, dizziness, vomiting |
| Adverse drug interactions | Highly protein-bound drugs Dopamine antagonists Drugs metabolized via cyp3a4 pathway Ergot-related migraine therapies 5-HT1B agonists (eg, sumatriptan) |
| Cost | $155.97 (90 tablets)* |
| *pricing from www.drugstore.com. | |
Adverse effects are mostly GI related
In phase 3 clinical trials (bromocriptine n=2298; placebo n=1266), adverse events leading to drug discontinuation occurred in 539 (24%) of bromocriptine-treated patients and 118 (9%) placebo-treated patients.16 This difference was mostly driven by an increase in GI adverse events with bromocriptine, particularly nausea. The most commonly reported adverse events from bromocriptine (nausea, fatigue, vomiting, headache, and dizziness) lasted a median of 14 days and were more likely to occur during the initial titration period. None of the reports of nausea or vomiting was considered serious.
There were no differences in the pattern of common adverse events across races or age groups (<65 vs >65 years old). Hypoglycemia occurred infrequently during the 52-week safety trial, with 6.9% of the bromocriptine patients and 5.3% of the placebo patients reporting an event.13 In this same safety trial, 1.6% of bromocriptine patients experienced syncope vs 0.7% of placebo-treated patients. CNS effects (somnolence and hypoesthesia) were minimal. Serious adverse events affected 8.5% of bromocriptine patients and 9.6% of placebo-treated patients (hazard ratio=1.02; 96% one-sided confidence interval, 1.27). Fewer people in the bromocriptine group reported a cardiovascular disease endpoint (composite of myocardial infarction, stroke, coronary revascularization, hospitalization for angina, and hospitalization for congestive heart failure) than did those in the placebo group (1.8% vs 3.2%, respectively).13,16
Postmarketing data link bromocriptine with hallucinations, fibrotic complications, and psychotic disorders. However, these adverse reactions were found with the use of much higher doses (30-140 mg/d) and with other indications for bromocriptine. These reactions have not been reported in clinical trials of bromocriptine used to treat T2D.16
Drugs to avoid (or use cautiously) with bromocriptine
Because bromocriptine is highly bound to serum proteins, it may increase the unbound fraction of other highly protein-bound drugs (eg, salicylates, sulfonamides, chloramphenicol, probenecid), which could alter their effectiveness or risk for adverse effects. Because bromocriptine is a dopamine receptor agonist, concomitant use of dopamine antagonists such as neuroleptic agents (clozapine, olanzapine) or metoclopramide is not recommended.16
Combining bromocriptine with ergot-related drugs (eg, migraine therapies) may increase the occurrence of ergot-related adverse effects such as nausea, vomiting, and fatigue, and may diminish effectiveness of migraine therapies. Dosing of the 2 therapies should occur at least 6 hours apart.16
Bromocriptine is extensively metabolized via CYP3A4. Potent inhibitors of this enzyme (eg, azole antimycotics, HIV protease inhibitors) or inducers (eg, rifampin, carbamazepine, phenytoin, phenobarbital) should be used with caution. Clinical trial data are limited regarding the safety of sumatriptan (5-HT1B agonist) used concurrently with bromocriptine, so it is prudent to avoid using them together.16
Not for breastfeeding moms, migraine sufferers
Bromocriptine is contraindicated for patients with syncopal migraine due to an increase in the likelihood of a hypotensive episode. It is also contraindicated for women who are breastfeeding due to its ability to inhibit lactation and to postmarketing reports of stroke in this population. Bromocriptine can lead to hypotension; monitor blood pressure during dose escalation and when a patient is taking antihypertensives.
Bromocriptine should not be used in patients with severe psychiatric disorders, as it may exacerbate their conditions or diminish the effectiveness of their treatment. Warn patients that somnolence can occur with bromocriptine, particularly during titration. No clinical studies have shown conclusive evidence of macrovascular risk reduction with bromocriptine or any other antidiabetic drug.16 But neither has bromocriptine increased risk for cardiovascular events.13
Putting bromocriptine’s usefulness into perspective
The larger studies of bromocriptine have shown absolute mean reductions in A1c of 0.1% to 0.6% and in fasting glucose of 0 to 10 mg/dL. When compared with placebo, mean A1c and fasting glucose differences were 0.4% to 1.2% and 23 to 38 mg/dL, respectively. While these findings were statistically significant when compared with placebo, they are clinically modest.
Although bromocriptine offers a few advantages, such as no weight gain, low risk of hypoglycemia, and possible beneficial effects on insulin resistance and triglyceride levels, its use should be limited at this time because it is less efficacious than other agents and long-term trials are lacking. Bromocriptine is not currently included in any treatment guidelines for the management of T2D. Cost is also a concern (TABLE). Because the medication is supplied only as 0.8-mg tablets, patients on the maximum dose would need to take 6 tablets once daily.
CORRESPONDENCE
Karen R. Sando, PharmD, CDE, University of Florida, College of Pharmacy, Department of Pharmacotherapy and Translational Research, 101 S. Newell Drive, HPNP Building, Room 3306, Gainesville, FL 32610; [email protected]
1. Cincotta AH, Meier AH, Cincotta JM. Bromocriptine improves glycaemic control and serum lipid profile in obese type 2 diabetic subjects: a new approach in the treatment of diabetes. Expert Opin Investig Drugs. 1999;8:1683-1707.
2. Santarus, Inc. Santarus Licenses Novel Type 2 Diabetes Drug CYCLOSET [press release]. Available at: http://ir.santarus.com/releasedetail.cfm?ReleaseID=505694. Accessed May 9, 2011.
3. Cornell S, Lullo A. Getting to goal for patients with type 2 diabetes: mission possible. Diabetes Trends. 2009;21:2-10.
4. Holt RIG, Barnett AH, Bailey CJ. Bromocriptine: old drug, new formulation, and new indication. Diabet Obes Metab. 2010;12:1048-1057.
5. Dowse G, Zimmet P. The thrifty genotype in non-insulin dependent diabetes. BMJ. 1993;306:532-533.
6. Meier AH, Cincotta A. Circadian rhythms regulate the expression of the thrifty genotype/phenotype. Diabetes Rev. 1996;4:464-487.
7. Luo S, Luo J, Cincotta AH. Association of the antidiabetic effects of bromocriptine with a shift in the daily rhythm of monoamine metabolism within the suprachiasmatic nuclei of the Syrian hamster. Chronobiol Int. 2000;17:155-172.
8. Cincotta AH, Schiller BC, Meier AH. Bromocriptine inhibits the seasonally occurring obesity, hyperinsulinemia, insulin resistance, and impaired glucose tolerance in the Syrian hamster, Mesocricterus auratus. Metabolism. 1991;40:639-644.
9. Cincotta AH, Meier AH, Southern LL. Bromocriptine alters hormone rhythms and lipid metabolism in swine. Ann Nutr Metab. 1989;33:305-314.
10. Cincotta AH, MacEachern TA, Meier AH. Bromocriptine redirects metabolism and prevents seasonal onset of obese hyperinsulinemic state in Syrian hamsters. Am J Physiol. 1993;254:E285-E293.
11. Luo S, Liang Y, Cincotta AH. Intracerebroventricular administration of bromocriptine ameliorates the insulin-resistant/ glucose-intolerant state in hamsters. Neuroendocrinology. 1999;69:160-166.
12. Barnett AH, Chapman C, Gailer K, et al. Effect of bromocriptine on maturity onset diabetes. Postgrad Med J. 1980;56:11-14.
13. Gaziano JM, Cincotta AH, O’Connor CM, et al. Randomized clinical trial of quick-release bromocriptine among patients with type 2 diabetes on overall safety and cardiovascular outcomes. Diabetes Care. 2010;33:1503-1508.
14. Aminorroaya A, Janghorbani M, Ramezani M, et al. Does bromocriptine improve glycemic control of obese type-2 diabetics? Horm Res. 2004;62:55-59.
15. Pijl H, Ohashi S, Matsuda M, et al. Bromocriptine: a novel approach to the treatment of type 2 diabetes. Diabetes Care. 2000;23:1154-1161.
16. Cycloset (bromocriptine mesylate) [prescribing information]. Tiverton, RI: VeroScience LLC; September 2010.
17. Scranton R, Cincotta A. Bromocriptine-unique formulation of a dopamine agonist for the treatment of type 2 diabetes. Expert Opin Pharmacother. 2010;11:269-279.
18. Maurer G, Schreier E, Delaborde S, et al. Fate and disposition of bromocriptine in animals and man. II: Absorption, elimination, and metabolism. Eur J Drug Metab Pharmacokinet. 1983;8:51-62.
19. Cincotta A, Meier AH. Bromocriptine (Ergoset) reduces body weight and improves glucose tolerance in obese subjects. Diabetes Care. 1996;19:667-670.
• Reserve bromocriptine for cases in which only a modest reduction in A1c is needed. A
• Advise patients to take bromocriptine in the morning with food to maximize its bioavailability. A
Strength of recommendation (SOR)
A Good-quality patient-oriented evidence
B Inconsistent or limited-quality patient-oriented evidence
C Consensus, usual practice, opinion, disease-oriented evidence, case series
For obese patients with type 2 diabetes (T2D) who do not tolerate other diabetes medications or for patients who need only a minimal reduction in glycosylated hemoglobin (A1c) to reach goal, bromocriptine may be a therapeutic agent to consider. Approved by the US Food and Drug Administration (FDA) in 2009, Cycloset is a quick-release formulation of bromocriptine mesylate, an ergot alkaloid dopamine D2 receptor agonist that has a faster onset of action than the customary formulation, Parlodel, which has been used to treat Parkinson’s disease, acromegaly, and hyperprolactinemia.1 In addition to its modest benefit in improving glycemic control, Cyclocet avoids undesirable side effects such as hypoglycemia and weight gain.
VeroScience, LLC holds the new drug application and related technologies for Cycloset and partnered with Santarus, Inc. and S2 Therapeutics to market it in September 2010.2
Bromocriptine’s likely mechanism of action
Although its exact mechanism of action is unclear, bromocriptine does not stimulate insulin release, reduce hepatic glucose production, increase glucose transporter production, or increase or mimic glucagon-like peptide-1 activity as other T2D agents do.3 Its contribution to glycemic control in T2D has been hypothesized to be due to adjustments in the neural control of seasonal and diurnal patterns of food intake and nutrient storage.4
Early hunter-gatherers and farmers are thought to have benefited from a “thrifty genotype” that favored fat deposition when food was seasonally abundant. With food in western society available year-round and often energy dense in both fat and carbohydrates, this same gene may lead to obesity and noninsulin-dependent diabetes mellitus.5
The hypothesis assumes that circadian rhythm, photo- periodism, and seasonal factors play a role in insulin resistance, hepatic gluconeogenesis, and weight gain. In vertebrates, the neuroendocrine system plays an important role in synchronizing the animal with cyclic environmental changes. The hypothalamic suprachiasmatic nucleus (SCN) is known as the circadian pacemaker that maintains this rhythm. Oscillations in the SCN occur due to external cues such as changes in light or temperature. Circadian dopaminergic and serotonergic activities are likely responsible for modifying such oscillations, and neurotransmitters have been shown to regulate the dramatic seasonal alterations in body weight and body composition of all vertebrate classes.6 Bromocriptine can reverse metabolic alterations associated with insulin resistance and obesity by resetting central (hypothalamic) circadian organization of monoamine neuronal activities.7
Proven anti-T2D effects. When administered systemically or into the cerebral ventricle at first light, bromocriptine prevents or reverses seasonal fattening, insulin resistance, and hyperinsulinemia, and it decreases endogenous (hepatic) glucose production in mammals.8-11 Bromocriptine also decreases both fasting and postprandial triglyceride and free fatty acid levels.1
Clinical trials show modest benefit
Although bromocriptine has been studied since 1980 for its effects on hyperglycemia in T2D,12 trials leading to the approval of the drug for clinical use with T2D have only been completed within the last 15 years. Randomized controlled trials of varying sizes and lasting from 6 to 52 weeks have shown absolute A1c reductions from 0.1% to 0.6%.1,12-16 Compared with placebo, A1c reductions have ranged from 0.4% to 1.2% with monotherapy and in combination with other antidiabetes medications.1,13-16
The manufacturer assessed bromocriptine in 4 studies involving patients with T2D. In all 4 studies, the bromocriptine dose was titrated to a maximum of 4.8 mg/d.16
One study involved 159 overweight subjects who were not meeting glycemic goals.16 Patients received either placebo or bromocriptine for 24 weeks in addition to diet and exercise. Mean baseline A1c was 9.0% in the bromocriptine group and 8.8% in the placebo group. After 24 weeks, A1c was reduced by 0.1% in the treatment group and increased by 0.3% in the placebo group. Mean fasting glucose was 215 mg/dL at baseline in the treatment group and was unchanged after 24 weeks. In the placebo group, fasting glucose increased from 205 to 228 mg/dL during the study. Weight increased by 0.2 kg in the treatment group and by 0.5 kg in the placebo group.
The next two 24-week manufacturer studies used similar designs to compare the addition of either bromocriptine or placebo to existing sulfonylurea therapy in patients with uncontrolled T2D.16 One study assigned 122 patients to bromocriptine and 127 to placebo. The bromocriptine group demonstrated mean reductions of 0.4% in A1c and 3 mg/dL in fasting glucose. In the placebo group, A1c increased by 0.3% and fasting glucose rose by 23 mg/dL.
The other study assigned 122 patients to bromocriptine and 123 to placebo. Adding bromocriptine reduced A1c, on average, by 0.1% and fasting glucose by 10 mg/dL. In the placebo group, A1c increased by 0.4% and fasting glucose increased by 28 mg/dL. All of these results were statistically significant.
The last manufacturer-reported study evaluated the addition of bromocriptine to other diabetes treatments (diet or up to 2 anti-diabetes medications).13 While the primary intent of this study was to evaluate safety, it also assessed efficacy. This was a 52-week, randomized placebo-controlled trial involving 3095 patients.
Overall, after 24 weeks there was no change in A1c levels after adding bromocriptine. However, most patients in this study were already at goal (A1c <7.0%). A subgroup analysis of those with an A1c level <7.5% while taking other agents did show some improvement with the addition of bromocriptine. Adding bromocriptine to metformin and a sulfonylurea significantly reduced A1c by 0.5%, on average. Similar results were seen in those who received other combinations of diabetes medications. After 52 weeks, 25% of those receiving bromocriptine who originally had an A1c level >7.5% achieved an A1c level <7.0%. Of the patients who received placebo, 9% obtained an A1c level <7%.
In a 24-week study, bromocriptine titrated up to 4.8 mg/d was given to patients either on no other diabetes medication or on a sulfonylurea.1 In individuals not on any current treatment, A1c decreased by 0.2% in those who received bromocriptine. In patients already on a sulfonylurea, A1c declined by 0.1%. A1c increased by 0.3% in those receiving placebo.
Bromocriptine most effective when taken with food
When bromocriptine is taken orally, 65% to 95% of the dose is absorbed; however, only 7% reaches systemic circulation due to extensive hepatic extraction and first-pass metabolism.17 Bioavailability increases by 55% to 65% when the drug is taken with food, which is how it should be administered. The time to maximum plasma concentration is within an hour. With a high-fat meal, however, the time increases to 90 to 120 minutes. Bromocriptine is highly protein bound (90%-96%) and is metabolized extensively in the gastrointestinal (GI) tract and liver.17 CYP3A4 is the major metabolic pathway.1,18 Most excretion of bromocriptine is through bile, with approximately 2% to 6% of an oral dose eliminated via urine. The elimination half-life is approximately 6 hours.17,18
Dosing is once a day in the morning
Clinical trials investigating the use of bromocriptine in diabetes used doses ranging from 1.6 to 4.8 mg/d.13-16,19 The FDA-approved dose range is 1.6 to 4.8 mg administered once daily with food, within 2 hours of waking in the morning.16 In healthy individuals, central nervous system (CNS) dopaminergic activity peaks in the early morning. Thus, morning dosing attempts to mimic dopaminergic activity and circadian rhythms in healthy lean individuals.6
Titrate to maximum dose. The product is available in a 0.8-mg tablet (TABLE). Titration to the maximum dose is recommended to reduce GI adverse effects, particularly nausea. Start treatment with 1 tablet (0.8 mg) and increase the dose by 1 tablet per week until the patient reaches a maximum tolerated dose or the maximum allowable daily dose of 4.8 mg (6 tablets).
Precautions with renal or hepatic impairment. No pharmacokinetic studies of bromocriptine have been conducted with patients who have renal impairment, and the kidney is a minor elimination pathway for bromocriptine. The package insert offers no specific dose recommendations for such patients, although it does recommend caution when using this product in patients with renal impairment. Studies of bromocriptine in patients with liver dysfunction are also lacking. However, as bromocriptine is predominately metabolized in the liver, use caution in patients with hepatic impairment.16
TABLE
Key prescribing information for bromocriptine16
| How supplied | 0.8-mg tablets |
| Indication | Adjunct to diet and exercise in type 2 diabetes mellitus |
| Dosing | Initial: 0.8 mg once daily with food, in the morning within 2 hours of waking Titration: increase by 1 tablet (0.8 mg) per week until maximum dose or maximum tolerance is reached |
| Maximum dose | 4.8 mg daily |
| Renal/hepatic impairment | Use with caution in patients with renal or hepatic impairment |
| Pregnancy; lactation | Pregnancy, category B; contraindicated for nursing women |
| Effectiveness | A1c reduced 0.1%-0.6% vs 0.3%-1.1% increase with placebo Fasting glucose reduced 0-10 mg/dl vs 23-28 mg/dl increase with placebo |
| Common adverse effects | Nausea, fatigue, headache, dizziness, vomiting |
| Adverse drug interactions | Highly protein-bound drugs Dopamine antagonists Drugs metabolized via cyp3a4 pathway Ergot-related migraine therapies 5-HT1B agonists (eg, sumatriptan) |
| Cost | $155.97 (90 tablets)* |
| *pricing from www.drugstore.com. | |
Adverse effects are mostly GI related
In phase 3 clinical trials (bromocriptine n=2298; placebo n=1266), adverse events leading to drug discontinuation occurred in 539 (24%) of bromocriptine-treated patients and 118 (9%) placebo-treated patients.16 This difference was mostly driven by an increase in GI adverse events with bromocriptine, particularly nausea. The most commonly reported adverse events from bromocriptine (nausea, fatigue, vomiting, headache, and dizziness) lasted a median of 14 days and were more likely to occur during the initial titration period. None of the reports of nausea or vomiting was considered serious.
There were no differences in the pattern of common adverse events across races or age groups (<65 vs >65 years old). Hypoglycemia occurred infrequently during the 52-week safety trial, with 6.9% of the bromocriptine patients and 5.3% of the placebo patients reporting an event.13 In this same safety trial, 1.6% of bromocriptine patients experienced syncope vs 0.7% of placebo-treated patients. CNS effects (somnolence and hypoesthesia) were minimal. Serious adverse events affected 8.5% of bromocriptine patients and 9.6% of placebo-treated patients (hazard ratio=1.02; 96% one-sided confidence interval, 1.27). Fewer people in the bromocriptine group reported a cardiovascular disease endpoint (composite of myocardial infarction, stroke, coronary revascularization, hospitalization for angina, and hospitalization for congestive heart failure) than did those in the placebo group (1.8% vs 3.2%, respectively).13,16
Postmarketing data link bromocriptine with hallucinations, fibrotic complications, and psychotic disorders. However, these adverse reactions were found with the use of much higher doses (30-140 mg/d) and with other indications for bromocriptine. These reactions have not been reported in clinical trials of bromocriptine used to treat T2D.16
Drugs to avoid (or use cautiously) with bromocriptine
Because bromocriptine is highly bound to serum proteins, it may increase the unbound fraction of other highly protein-bound drugs (eg, salicylates, sulfonamides, chloramphenicol, probenecid), which could alter their effectiveness or risk for adverse effects. Because bromocriptine is a dopamine receptor agonist, concomitant use of dopamine antagonists such as neuroleptic agents (clozapine, olanzapine) or metoclopramide is not recommended.16
Combining bromocriptine with ergot-related drugs (eg, migraine therapies) may increase the occurrence of ergot-related adverse effects such as nausea, vomiting, and fatigue, and may diminish effectiveness of migraine therapies. Dosing of the 2 therapies should occur at least 6 hours apart.16
Bromocriptine is extensively metabolized via CYP3A4. Potent inhibitors of this enzyme (eg, azole antimycotics, HIV protease inhibitors) or inducers (eg, rifampin, carbamazepine, phenytoin, phenobarbital) should be used with caution. Clinical trial data are limited regarding the safety of sumatriptan (5-HT1B agonist) used concurrently with bromocriptine, so it is prudent to avoid using them together.16
Not for breastfeeding moms, migraine sufferers
Bromocriptine is contraindicated for patients with syncopal migraine due to an increase in the likelihood of a hypotensive episode. It is also contraindicated for women who are breastfeeding due to its ability to inhibit lactation and to postmarketing reports of stroke in this population. Bromocriptine can lead to hypotension; monitor blood pressure during dose escalation and when a patient is taking antihypertensives.
Bromocriptine should not be used in patients with severe psychiatric disorders, as it may exacerbate their conditions or diminish the effectiveness of their treatment. Warn patients that somnolence can occur with bromocriptine, particularly during titration. No clinical studies have shown conclusive evidence of macrovascular risk reduction with bromocriptine or any other antidiabetic drug.16 But neither has bromocriptine increased risk for cardiovascular events.13
Putting bromocriptine’s usefulness into perspective
The larger studies of bromocriptine have shown absolute mean reductions in A1c of 0.1% to 0.6% and in fasting glucose of 0 to 10 mg/dL. When compared with placebo, mean A1c and fasting glucose differences were 0.4% to 1.2% and 23 to 38 mg/dL, respectively. While these findings were statistically significant when compared with placebo, they are clinically modest.
Although bromocriptine offers a few advantages, such as no weight gain, low risk of hypoglycemia, and possible beneficial effects on insulin resistance and triglyceride levels, its use should be limited at this time because it is less efficacious than other agents and long-term trials are lacking. Bromocriptine is not currently included in any treatment guidelines for the management of T2D. Cost is also a concern (TABLE). Because the medication is supplied only as 0.8-mg tablets, patients on the maximum dose would need to take 6 tablets once daily.
CORRESPONDENCE
Karen R. Sando, PharmD, CDE, University of Florida, College of Pharmacy, Department of Pharmacotherapy and Translational Research, 101 S. Newell Drive, HPNP Building, Room 3306, Gainesville, FL 32610; [email protected]
• Reserve bromocriptine for cases in which only a modest reduction in A1c is needed. A
• Advise patients to take bromocriptine in the morning with food to maximize its bioavailability. A
Strength of recommendation (SOR)
A Good-quality patient-oriented evidence
B Inconsistent or limited-quality patient-oriented evidence
C Consensus, usual practice, opinion, disease-oriented evidence, case series
For obese patients with type 2 diabetes (T2D) who do not tolerate other diabetes medications or for patients who need only a minimal reduction in glycosylated hemoglobin (A1c) to reach goal, bromocriptine may be a therapeutic agent to consider. Approved by the US Food and Drug Administration (FDA) in 2009, Cycloset is a quick-release formulation of bromocriptine mesylate, an ergot alkaloid dopamine D2 receptor agonist that has a faster onset of action than the customary formulation, Parlodel, which has been used to treat Parkinson’s disease, acromegaly, and hyperprolactinemia.1 In addition to its modest benefit in improving glycemic control, Cyclocet avoids undesirable side effects such as hypoglycemia and weight gain.
VeroScience, LLC holds the new drug application and related technologies for Cycloset and partnered with Santarus, Inc. and S2 Therapeutics to market it in September 2010.2
Bromocriptine’s likely mechanism of action
Although its exact mechanism of action is unclear, bromocriptine does not stimulate insulin release, reduce hepatic glucose production, increase glucose transporter production, or increase or mimic glucagon-like peptide-1 activity as other T2D agents do.3 Its contribution to glycemic control in T2D has been hypothesized to be due to adjustments in the neural control of seasonal and diurnal patterns of food intake and nutrient storage.4
Early hunter-gatherers and farmers are thought to have benefited from a “thrifty genotype” that favored fat deposition when food was seasonally abundant. With food in western society available year-round and often energy dense in both fat and carbohydrates, this same gene may lead to obesity and noninsulin-dependent diabetes mellitus.5
The hypothesis assumes that circadian rhythm, photo- periodism, and seasonal factors play a role in insulin resistance, hepatic gluconeogenesis, and weight gain. In vertebrates, the neuroendocrine system plays an important role in synchronizing the animal with cyclic environmental changes. The hypothalamic suprachiasmatic nucleus (SCN) is known as the circadian pacemaker that maintains this rhythm. Oscillations in the SCN occur due to external cues such as changes in light or temperature. Circadian dopaminergic and serotonergic activities are likely responsible for modifying such oscillations, and neurotransmitters have been shown to regulate the dramatic seasonal alterations in body weight and body composition of all vertebrate classes.6 Bromocriptine can reverse metabolic alterations associated with insulin resistance and obesity by resetting central (hypothalamic) circadian organization of monoamine neuronal activities.7
Proven anti-T2D effects. When administered systemically or into the cerebral ventricle at first light, bromocriptine prevents or reverses seasonal fattening, insulin resistance, and hyperinsulinemia, and it decreases endogenous (hepatic) glucose production in mammals.8-11 Bromocriptine also decreases both fasting and postprandial triglyceride and free fatty acid levels.1
Clinical trials show modest benefit
Although bromocriptine has been studied since 1980 for its effects on hyperglycemia in T2D,12 trials leading to the approval of the drug for clinical use with T2D have only been completed within the last 15 years. Randomized controlled trials of varying sizes and lasting from 6 to 52 weeks have shown absolute A1c reductions from 0.1% to 0.6%.1,12-16 Compared with placebo, A1c reductions have ranged from 0.4% to 1.2% with monotherapy and in combination with other antidiabetes medications.1,13-16
The manufacturer assessed bromocriptine in 4 studies involving patients with T2D. In all 4 studies, the bromocriptine dose was titrated to a maximum of 4.8 mg/d.16
One study involved 159 overweight subjects who were not meeting glycemic goals.16 Patients received either placebo or bromocriptine for 24 weeks in addition to diet and exercise. Mean baseline A1c was 9.0% in the bromocriptine group and 8.8% in the placebo group. After 24 weeks, A1c was reduced by 0.1% in the treatment group and increased by 0.3% in the placebo group. Mean fasting glucose was 215 mg/dL at baseline in the treatment group and was unchanged after 24 weeks. In the placebo group, fasting glucose increased from 205 to 228 mg/dL during the study. Weight increased by 0.2 kg in the treatment group and by 0.5 kg in the placebo group.
The next two 24-week manufacturer studies used similar designs to compare the addition of either bromocriptine or placebo to existing sulfonylurea therapy in patients with uncontrolled T2D.16 One study assigned 122 patients to bromocriptine and 127 to placebo. The bromocriptine group demonstrated mean reductions of 0.4% in A1c and 3 mg/dL in fasting glucose. In the placebo group, A1c increased by 0.3% and fasting glucose rose by 23 mg/dL.
The other study assigned 122 patients to bromocriptine and 123 to placebo. Adding bromocriptine reduced A1c, on average, by 0.1% and fasting glucose by 10 mg/dL. In the placebo group, A1c increased by 0.4% and fasting glucose increased by 28 mg/dL. All of these results were statistically significant.
The last manufacturer-reported study evaluated the addition of bromocriptine to other diabetes treatments (diet or up to 2 anti-diabetes medications).13 While the primary intent of this study was to evaluate safety, it also assessed efficacy. This was a 52-week, randomized placebo-controlled trial involving 3095 patients.
Overall, after 24 weeks there was no change in A1c levels after adding bromocriptine. However, most patients in this study were already at goal (A1c <7.0%). A subgroup analysis of those with an A1c level <7.5% while taking other agents did show some improvement with the addition of bromocriptine. Adding bromocriptine to metformin and a sulfonylurea significantly reduced A1c by 0.5%, on average. Similar results were seen in those who received other combinations of diabetes medications. After 52 weeks, 25% of those receiving bromocriptine who originally had an A1c level >7.5% achieved an A1c level <7.0%. Of the patients who received placebo, 9% obtained an A1c level <7%.
In a 24-week study, bromocriptine titrated up to 4.8 mg/d was given to patients either on no other diabetes medication or on a sulfonylurea.1 In individuals not on any current treatment, A1c decreased by 0.2% in those who received bromocriptine. In patients already on a sulfonylurea, A1c declined by 0.1%. A1c increased by 0.3% in those receiving placebo.
Bromocriptine most effective when taken with food
When bromocriptine is taken orally, 65% to 95% of the dose is absorbed; however, only 7% reaches systemic circulation due to extensive hepatic extraction and first-pass metabolism.17 Bioavailability increases by 55% to 65% when the drug is taken with food, which is how it should be administered. The time to maximum plasma concentration is within an hour. With a high-fat meal, however, the time increases to 90 to 120 minutes. Bromocriptine is highly protein bound (90%-96%) and is metabolized extensively in the gastrointestinal (GI) tract and liver.17 CYP3A4 is the major metabolic pathway.1,18 Most excretion of bromocriptine is through bile, with approximately 2% to 6% of an oral dose eliminated via urine. The elimination half-life is approximately 6 hours.17,18
Dosing is once a day in the morning
Clinical trials investigating the use of bromocriptine in diabetes used doses ranging from 1.6 to 4.8 mg/d.13-16,19 The FDA-approved dose range is 1.6 to 4.8 mg administered once daily with food, within 2 hours of waking in the morning.16 In healthy individuals, central nervous system (CNS) dopaminergic activity peaks in the early morning. Thus, morning dosing attempts to mimic dopaminergic activity and circadian rhythms in healthy lean individuals.6
Titrate to maximum dose. The product is available in a 0.8-mg tablet (TABLE). Titration to the maximum dose is recommended to reduce GI adverse effects, particularly nausea. Start treatment with 1 tablet (0.8 mg) and increase the dose by 1 tablet per week until the patient reaches a maximum tolerated dose or the maximum allowable daily dose of 4.8 mg (6 tablets).
Precautions with renal or hepatic impairment. No pharmacokinetic studies of bromocriptine have been conducted with patients who have renal impairment, and the kidney is a minor elimination pathway for bromocriptine. The package insert offers no specific dose recommendations for such patients, although it does recommend caution when using this product in patients with renal impairment. Studies of bromocriptine in patients with liver dysfunction are also lacking. However, as bromocriptine is predominately metabolized in the liver, use caution in patients with hepatic impairment.16
TABLE
Key prescribing information for bromocriptine16
| How supplied | 0.8-mg tablets |
| Indication | Adjunct to diet and exercise in type 2 diabetes mellitus |
| Dosing | Initial: 0.8 mg once daily with food, in the morning within 2 hours of waking Titration: increase by 1 tablet (0.8 mg) per week until maximum dose or maximum tolerance is reached |
| Maximum dose | 4.8 mg daily |
| Renal/hepatic impairment | Use with caution in patients with renal or hepatic impairment |
| Pregnancy; lactation | Pregnancy, category B; contraindicated for nursing women |
| Effectiveness | A1c reduced 0.1%-0.6% vs 0.3%-1.1% increase with placebo Fasting glucose reduced 0-10 mg/dl vs 23-28 mg/dl increase with placebo |
| Common adverse effects | Nausea, fatigue, headache, dizziness, vomiting |
| Adverse drug interactions | Highly protein-bound drugs Dopamine antagonists Drugs metabolized via cyp3a4 pathway Ergot-related migraine therapies 5-HT1B agonists (eg, sumatriptan) |
| Cost | $155.97 (90 tablets)* |
| *pricing from www.drugstore.com. | |
Adverse effects are mostly GI related
In phase 3 clinical trials (bromocriptine n=2298; placebo n=1266), adverse events leading to drug discontinuation occurred in 539 (24%) of bromocriptine-treated patients and 118 (9%) placebo-treated patients.16 This difference was mostly driven by an increase in GI adverse events with bromocriptine, particularly nausea. The most commonly reported adverse events from bromocriptine (nausea, fatigue, vomiting, headache, and dizziness) lasted a median of 14 days and were more likely to occur during the initial titration period. None of the reports of nausea or vomiting was considered serious.
There were no differences in the pattern of common adverse events across races or age groups (<65 vs >65 years old). Hypoglycemia occurred infrequently during the 52-week safety trial, with 6.9% of the bromocriptine patients and 5.3% of the placebo patients reporting an event.13 In this same safety trial, 1.6% of bromocriptine patients experienced syncope vs 0.7% of placebo-treated patients. CNS effects (somnolence and hypoesthesia) were minimal. Serious adverse events affected 8.5% of bromocriptine patients and 9.6% of placebo-treated patients (hazard ratio=1.02; 96% one-sided confidence interval, 1.27). Fewer people in the bromocriptine group reported a cardiovascular disease endpoint (composite of myocardial infarction, stroke, coronary revascularization, hospitalization for angina, and hospitalization for congestive heart failure) than did those in the placebo group (1.8% vs 3.2%, respectively).13,16
Postmarketing data link bromocriptine with hallucinations, fibrotic complications, and psychotic disorders. However, these adverse reactions were found with the use of much higher doses (30-140 mg/d) and with other indications for bromocriptine. These reactions have not been reported in clinical trials of bromocriptine used to treat T2D.16
Drugs to avoid (or use cautiously) with bromocriptine
Because bromocriptine is highly bound to serum proteins, it may increase the unbound fraction of other highly protein-bound drugs (eg, salicylates, sulfonamides, chloramphenicol, probenecid), which could alter their effectiveness or risk for adverse effects. Because bromocriptine is a dopamine receptor agonist, concomitant use of dopamine antagonists such as neuroleptic agents (clozapine, olanzapine) or metoclopramide is not recommended.16
Combining bromocriptine with ergot-related drugs (eg, migraine therapies) may increase the occurrence of ergot-related adverse effects such as nausea, vomiting, and fatigue, and may diminish effectiveness of migraine therapies. Dosing of the 2 therapies should occur at least 6 hours apart.16
Bromocriptine is extensively metabolized via CYP3A4. Potent inhibitors of this enzyme (eg, azole antimycotics, HIV protease inhibitors) or inducers (eg, rifampin, carbamazepine, phenytoin, phenobarbital) should be used with caution. Clinical trial data are limited regarding the safety of sumatriptan (5-HT1B agonist) used concurrently with bromocriptine, so it is prudent to avoid using them together.16
Not for breastfeeding moms, migraine sufferers
Bromocriptine is contraindicated for patients with syncopal migraine due to an increase in the likelihood of a hypotensive episode. It is also contraindicated for women who are breastfeeding due to its ability to inhibit lactation and to postmarketing reports of stroke in this population. Bromocriptine can lead to hypotension; monitor blood pressure during dose escalation and when a patient is taking antihypertensives.
Bromocriptine should not be used in patients with severe psychiatric disorders, as it may exacerbate their conditions or diminish the effectiveness of their treatment. Warn patients that somnolence can occur with bromocriptine, particularly during titration. No clinical studies have shown conclusive evidence of macrovascular risk reduction with bromocriptine or any other antidiabetic drug.16 But neither has bromocriptine increased risk for cardiovascular events.13
Putting bromocriptine’s usefulness into perspective
The larger studies of bromocriptine have shown absolute mean reductions in A1c of 0.1% to 0.6% and in fasting glucose of 0 to 10 mg/dL. When compared with placebo, mean A1c and fasting glucose differences were 0.4% to 1.2% and 23 to 38 mg/dL, respectively. While these findings were statistically significant when compared with placebo, they are clinically modest.
Although bromocriptine offers a few advantages, such as no weight gain, low risk of hypoglycemia, and possible beneficial effects on insulin resistance and triglyceride levels, its use should be limited at this time because it is less efficacious than other agents and long-term trials are lacking. Bromocriptine is not currently included in any treatment guidelines for the management of T2D. Cost is also a concern (TABLE). Because the medication is supplied only as 0.8-mg tablets, patients on the maximum dose would need to take 6 tablets once daily.
CORRESPONDENCE
Karen R. Sando, PharmD, CDE, University of Florida, College of Pharmacy, Department of Pharmacotherapy and Translational Research, 101 S. Newell Drive, HPNP Building, Room 3306, Gainesville, FL 32610; [email protected]
1. Cincotta AH, Meier AH, Cincotta JM. Bromocriptine improves glycaemic control and serum lipid profile in obese type 2 diabetic subjects: a new approach in the treatment of diabetes. Expert Opin Investig Drugs. 1999;8:1683-1707.
2. Santarus, Inc. Santarus Licenses Novel Type 2 Diabetes Drug CYCLOSET [press release]. Available at: http://ir.santarus.com/releasedetail.cfm?ReleaseID=505694. Accessed May 9, 2011.
3. Cornell S, Lullo A. Getting to goal for patients with type 2 diabetes: mission possible. Diabetes Trends. 2009;21:2-10.
4. Holt RIG, Barnett AH, Bailey CJ. Bromocriptine: old drug, new formulation, and new indication. Diabet Obes Metab. 2010;12:1048-1057.
5. Dowse G, Zimmet P. The thrifty genotype in non-insulin dependent diabetes. BMJ. 1993;306:532-533.
6. Meier AH, Cincotta A. Circadian rhythms regulate the expression of the thrifty genotype/phenotype. Diabetes Rev. 1996;4:464-487.
7. Luo S, Luo J, Cincotta AH. Association of the antidiabetic effects of bromocriptine with a shift in the daily rhythm of monoamine metabolism within the suprachiasmatic nuclei of the Syrian hamster. Chronobiol Int. 2000;17:155-172.
8. Cincotta AH, Schiller BC, Meier AH. Bromocriptine inhibits the seasonally occurring obesity, hyperinsulinemia, insulin resistance, and impaired glucose tolerance in the Syrian hamster, Mesocricterus auratus. Metabolism. 1991;40:639-644.
9. Cincotta AH, Meier AH, Southern LL. Bromocriptine alters hormone rhythms and lipid metabolism in swine. Ann Nutr Metab. 1989;33:305-314.
10. Cincotta AH, MacEachern TA, Meier AH. Bromocriptine redirects metabolism and prevents seasonal onset of obese hyperinsulinemic state in Syrian hamsters. Am J Physiol. 1993;254:E285-E293.
11. Luo S, Liang Y, Cincotta AH. Intracerebroventricular administration of bromocriptine ameliorates the insulin-resistant/ glucose-intolerant state in hamsters. Neuroendocrinology. 1999;69:160-166.
12. Barnett AH, Chapman C, Gailer K, et al. Effect of bromocriptine on maturity onset diabetes. Postgrad Med J. 1980;56:11-14.
13. Gaziano JM, Cincotta AH, O’Connor CM, et al. Randomized clinical trial of quick-release bromocriptine among patients with type 2 diabetes on overall safety and cardiovascular outcomes. Diabetes Care. 2010;33:1503-1508.
14. Aminorroaya A, Janghorbani M, Ramezani M, et al. Does bromocriptine improve glycemic control of obese type-2 diabetics? Horm Res. 2004;62:55-59.
15. Pijl H, Ohashi S, Matsuda M, et al. Bromocriptine: a novel approach to the treatment of type 2 diabetes. Diabetes Care. 2000;23:1154-1161.
16. Cycloset (bromocriptine mesylate) [prescribing information]. Tiverton, RI: VeroScience LLC; September 2010.
17. Scranton R, Cincotta A. Bromocriptine-unique formulation of a dopamine agonist for the treatment of type 2 diabetes. Expert Opin Pharmacother. 2010;11:269-279.
18. Maurer G, Schreier E, Delaborde S, et al. Fate and disposition of bromocriptine in animals and man. II: Absorption, elimination, and metabolism. Eur J Drug Metab Pharmacokinet. 1983;8:51-62.
19. Cincotta A, Meier AH. Bromocriptine (Ergoset) reduces body weight and improves glucose tolerance in obese subjects. Diabetes Care. 1996;19:667-670.
1. Cincotta AH, Meier AH, Cincotta JM. Bromocriptine improves glycaemic control and serum lipid profile in obese type 2 diabetic subjects: a new approach in the treatment of diabetes. Expert Opin Investig Drugs. 1999;8:1683-1707.
2. Santarus, Inc. Santarus Licenses Novel Type 2 Diabetes Drug CYCLOSET [press release]. Available at: http://ir.santarus.com/releasedetail.cfm?ReleaseID=505694. Accessed May 9, 2011.
3. Cornell S, Lullo A. Getting to goal for patients with type 2 diabetes: mission possible. Diabetes Trends. 2009;21:2-10.
4. Holt RIG, Barnett AH, Bailey CJ. Bromocriptine: old drug, new formulation, and new indication. Diabet Obes Metab. 2010;12:1048-1057.
5. Dowse G, Zimmet P. The thrifty genotype in non-insulin dependent diabetes. BMJ. 1993;306:532-533.
6. Meier AH, Cincotta A. Circadian rhythms regulate the expression of the thrifty genotype/phenotype. Diabetes Rev. 1996;4:464-487.
7. Luo S, Luo J, Cincotta AH. Association of the antidiabetic effects of bromocriptine with a shift in the daily rhythm of monoamine metabolism within the suprachiasmatic nuclei of the Syrian hamster. Chronobiol Int. 2000;17:155-172.
8. Cincotta AH, Schiller BC, Meier AH. Bromocriptine inhibits the seasonally occurring obesity, hyperinsulinemia, insulin resistance, and impaired glucose tolerance in the Syrian hamster, Mesocricterus auratus. Metabolism. 1991;40:639-644.
9. Cincotta AH, Meier AH, Southern LL. Bromocriptine alters hormone rhythms and lipid metabolism in swine. Ann Nutr Metab. 1989;33:305-314.
10. Cincotta AH, MacEachern TA, Meier AH. Bromocriptine redirects metabolism and prevents seasonal onset of obese hyperinsulinemic state in Syrian hamsters. Am J Physiol. 1993;254:E285-E293.
11. Luo S, Liang Y, Cincotta AH. Intracerebroventricular administration of bromocriptine ameliorates the insulin-resistant/ glucose-intolerant state in hamsters. Neuroendocrinology. 1999;69:160-166.
12. Barnett AH, Chapman C, Gailer K, et al. Effect of bromocriptine on maturity onset diabetes. Postgrad Med J. 1980;56:11-14.
13. Gaziano JM, Cincotta AH, O’Connor CM, et al. Randomized clinical trial of quick-release bromocriptine among patients with type 2 diabetes on overall safety and cardiovascular outcomes. Diabetes Care. 2010;33:1503-1508.
14. Aminorroaya A, Janghorbani M, Ramezani M, et al. Does bromocriptine improve glycemic control of obese type-2 diabetics? Horm Res. 2004;62:55-59.
15. Pijl H, Ohashi S, Matsuda M, et al. Bromocriptine: a novel approach to the treatment of type 2 diabetes. Diabetes Care. 2000;23:1154-1161.
16. Cycloset (bromocriptine mesylate) [prescribing information]. Tiverton, RI: VeroScience LLC; September 2010.
17. Scranton R, Cincotta A. Bromocriptine-unique formulation of a dopamine agonist for the treatment of type 2 diabetes. Expert Opin Pharmacother. 2010;11:269-279.
18. Maurer G, Schreier E, Delaborde S, et al. Fate and disposition of bromocriptine in animals and man. II: Absorption, elimination, and metabolism. Eur J Drug Metab Pharmacokinet. 1983;8:51-62.
19. Cincotta A, Meier AH. Bromocriptine (Ergoset) reduces body weight and improves glucose tolerance in obese subjects. Diabetes Care. 1996;19:667-670.
Managing eczema in children—a treatment update
• Emollients should be used during acute flares as well as regularly for maintenance therapy in children with atopic dermatitis (AD). A
• Topical corticosteroids are the first-line therapy for acute AD flares. A
• There is no evidence to support the use of antihistamines for treatment of AD. A
• Exclusion of cow’s milk and eggs is not recommended except in proven cases of milk or egg allergy with sensitivity testing and food challenge. B
Strength of recommendation (SOR)
A Good-quality patient-oriented evidence
B Inconsistent or limited-quality patient-oriented evidence
C Consensus, usual practice, opinion, disease-oriented evidence, case series
CASE 1 Dylan, an 8-month-old boy whom you had seen for a routine check-up a little over a month ago, is in your office today because of a rash on his face and elbows. The rash began about 2 weeks ago, his mother reports—shortly after she had weaned him from the breast milk to formula. Certain that Dylan has a milk allergy, his mother tells you she plans to switch to a soy-based formula—and wants you to give her something to put on the rash to help clear it up.
CASE 2 Eighteen-month-old Angela had a mild case of atopic dermatitis when you saw her about 3 months ago. The reason for today’s visit is that “her eczema is getting worse,” according to her mother, and the moisturizing cream that you recommended at her last visit “stopped working.” The rash, which had been confined to the patient’s forearms and knees (FIGURE 1), now covers much of her face, forearms, knees, and trunk. Angela’s mother says that the rash appears to be very itchy and that her daughter has been crying and scratching at night.
If Dylan and Angela were your patients, what would you advise their parents to do, and how would you treat them?
FIGURE 1
An 18-month-old girl with an acute flare
This child has moderate atopic dermatitis, with erythema and localized thickened skin at the medial knee—a typical site for atopic dermatitis.
Atopic dermatitis (AD), or eczema, is a chronic inflammatory skin condition that affects up to 20% of children.1 The incidence of pediatric AD has increased 2- to 3-fold in the last 30 years (it’s not clear why), and the condition is a common reason for pediatric visits to family physicians.1,2
AD is marked by phases of pruritus and rash and, depending on the severity, can significantly affect the quality of life of young patients and their families.1-4 The pathophysiology involves structural abnormalities of the epidermis—leading to dry and sensitive skin—combined with immune dysregulation.

Topical corticosteroids to decrease the inflammation and emollients to repair and hydrate the skin are the mainstay of treatment.3,5,6 But numerous considerations, including what triggers patients should avoid; how potent a steroid to prescribe; how long to continue treatment; and when, or whether, to initiate systemic treatment, remain. The evidence-based review of traditional and alternative treatments (TABLE)1-3,7-19 and practical step-wise approach (FIGURE 2)1-3,5,6,9,19-22 that follow can help ensure that you give children with AD the best possible care.
FIGURE 2
A stepped approach to atopic dermatitis1-3,5,6,9,19-22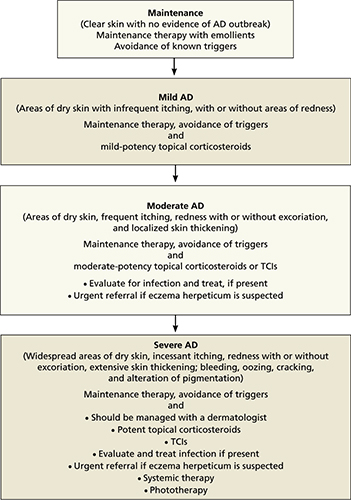
AD, atopic dermatitis; TCIs, topical calcineurin inhibitors.
TABLE
Treating atopic dermatitis: What the evidence shows
| Intervention (SOR) | Comments |
|---|---|
| Maintenance | |
| Emollients (A)1,2,7,8 | Mainstay of maintenance therapy |
| Treatment | |
| Corticosteroids9-15 – Topical (A) – Oral (B) | First-line treatment No proven benefit |
| TCIs:3,16,17 – Pimecrolimus (A) – Tacrolimus (A) | Second-line treatment |
| Symptom relief | |
| Antihistamines (A)11,14 | No proven benefit in the treatment of AD; sedating antihistamines may improve sleep |
| Tar (C)14 | |
| Wet wrap dressings (C )18 | |
| Infection1,11 | |
| Antibiotics – Topical (A) – Oral (A) | |
| Antifungals – Topical (A) – Oral (A) | |
| Alternative/preventive measures11,19 | |
| Breastfeeding (B) | May reduce risk of developing AD (poor quality study) |
| Essential fatty acids* | No proven benefit |
| Exclusion of eggs or cow’s milk (B) | Only in proven cases of allergy |
| Multivitamins, B6, zinc supplements (C) | No proven benefit |
| Probiotics (B) | No proven benefit |
| Vitamin D supplementation (C) | More studies needed |
| *Black currant seed oil, evening primrose oil, fish oil. AD, atopic dermatitis; TCIs, topical calcineurin inhibitors. | |
The patient has a rash, but what’s the trigger?
Epidemiologic studies have identified numerous AD triggers, including sweating, stress, dust, hard water, food allergies, and seasonality.23 Environmental or situational triggers should be avoided whenever possible,20 of course, but first, they must be identified—an often-difficult task. Establishing the role of any exacerbating factor in AD involves documentation of a temporal relationship between exposure and the development or worsening of symptoms; a dose-response effect; and remission after withdrawal of the trigger.
What’s more, avoidance does not always have the desired result. There is a well-demonstrated correlation between house dust mite sensitization and AD, especially in children of preschool age and older.7,21 Studies performed to determine whether decreasing house dust mite antigen would have a positive effect on disease severity, however, have had conflicting results.23
Food allergies are more likely in the youngest patients
For about a third (35%) of children with AD, the trigger is a food allergy.22 This is most common in infants, with one study showing a peak at 18 months.20,24 The most common food allergens are milk and egg, but wheat, soy, and peanuts are potential allergens, as well.22,25 Food allergies, which are difficult to identify, should be suspected in patients with a poor response to first-line treatment. Sensitivity testing with food challenge may be worthwhile only in severe cases that are refractory to routine care.20
We caution parents not to attempt to withhold a suspected food allergen on their own. To avoid the risk of malnutrition, young children should be placed on elimination diet trials only if the allergen has first been identified by sensitivity testing and food challenge tests, because the allergen may not be clinically significant.21,22 Neither skin prick tests nor serum tests for allergies have been found to be accurate, and parents themselves are often mistaken. Several studies have found a discrepancy between the foods parents think their child is allergic to and the substances that are later found to be clinically significant allergens.21
CASE 1 You advise Dylan’s mother not to switch formulas because answers to further questions about other symptoms were unremarkable (eg, diarrhea). Dylan is treated with a low-potency (class VII) topical steroid (1% hydrocortisone cream) with instructions for the parents to maintain hydration and call you in 5 to 7 days.
Topical corticosteroids are first-line treatment
Two major classes of pharmacologic agents are used for the treatment of AD: topical corticosteroids and topical calcineurin inhibitors (TCIs). Corticosteroids are first-line treatment, as their clinical effectiveness has been well established; TCIs are indicated only as second-line therapy.26,27
Which dosing regimen is best?
The potency of corticosteroids is expressed by a numerical scale, ranging from class I (the most potent) to class VII (the least potent). Class I steroids are about 1800 times more potent than class VII preparations.8
A decision about which strength to use is based on several factors, including the severity of the child’s AD, his or her age, and the affected body site. For infants ≤12 months old, the lowest potency preparations (such as 1% hydrocortisone) are preferable, but should be used in the diaper area for no more than 3 to 7 days at a time.8 In general, potent topical corticosteroids should not be used for children <12 months of age without a dermatology consult.8,9
For children ages 1 through 5 years, intermittent (1- to 2-week) bursts of mild to moderate potency corticosteroids (class VI and VII) are suitable; for older children, a 7- to 10-day course of more potent preparations (class II-V) can be used for nonflexural and nonfacial skin.
While clinical trials have addressed the issues of quantity, duration, potency, and frequency (one large systematic review found twice-daily application of topical corticosteroids to be no more effective than once-daily applications10), an optimal approach to their use in the long-term management of pediatric AD is largely undefined. Various approaches include:
- starting with a more potent preparation to induce remission, followed by a less potent corticosteroid as the AD improves
- using short bursts (5-7 days) of a potent topical corticosteroid, followed by emollient use until a flare-up occurs
- relying on prolonged, or continuous, treatment with less potent preparations.11,23
Long-term use of topical corticosteroids of any potency should be avoided in areas of high risk for cutaneous side effects, such as the face and intertriginous areas.
Emollients are also an important part of therapy for all pediatric patients. Emollients help restore the integrity of the skin barrier and inhibit water loss,1,2,12,20 and should be used not only during an acute flare, but also for maintenance therapy. Tell parents to look for emollients that are unscented and contain fewer additives, and to apply the emollient at least twice daily, and after bathing or swimming.5,20
CASE 2 You prescribe a class V steroid (triamcinolone ointment 0.025%) for Angela, to be applied once a day for 5 to 7 days. You instruct her mother in basic skin care and stress the importance of using an emollient regularly, not just during a flare-up.
What to tell parents about side effects
Discuss the benefits and potential harms of topical corticosteroids with parents (and youngsters who are old enough to understand), emphasizing that when used correctly, the benefits outweigh the risks.
Potential side effects include skin atrophy, striae, telangiectasia, hypopigmentation, rosacea, glaucoma, and cataracts, with studies suggesting that local adverse effects are related to the potency.13 Because there are few prospective controlled trials of sufficient duration, however, the incidence of local reactions to topical corticosteroids in patients with AD is uncertain.
The potential for topical corticosteroids to suppress the hypothalamic-pituitary-adrenal (HPA) axis has been investigated in a small number of studies, with inconclusive results. Effects on the HPA axis appear to be associated with percutaneous absorption in patients who either have a more severe case of AD or are <2 years old.14 A recent systematic review confirmed that the degree of systemic absorption is based on the severity and extent of the disease as well as the formulation and potency of the topical agent.14,15
When to consider TCIs
Pimecrolimus and tacrolimus, the 2 TCIs on the market, are second-line agents for AD. Both have US Food and Drug Administration (FDA) approval for short-term treatment of moderate to severe AD in immunocompetent patients who have failed to respond to topical corticosteroids and children >2 years.26,27 Both TCIs provide targeted anti-inflammatory activity without the local and systemic side effects of topical corticosteroids.
Pimecrolimus cream 1% is approved for treatment in children >2 years.27 Tacrolimus ointment 0.03% is approved for children ages 2 to 15 years with moderate to severe AD, and tacrolimus ointment 0.1% is approved for children older than 16 years with moderate to severe AD.26 Data from clinical trials have shown that pimecrolimus reduces the number and severity of flares, extends the time between flares, and decreases pruritus and other cutaneous signs associated with AD.3 Common side effects, which are usually mild and resolve within days, include pruritus, burning, and stinging at the application site.
In 2006 the FDA added a black-box warning stating that their long-term safety has not been established—a response to widespread off-label use of TCIs in children <2 years and concerns about a theoretical cancer risk based on their mechanism of action—and concluded in 2010 that the labeling adequately warns providers of the potential safety risks.28 Recent reviews have concluded that systemic exposure to topical TCIs is minimal and that there is no evidence linking TCIs to an increased risk of lymphoproliferative disease.16,17,29
Combining corticosteroids and TCIs
In clinical practice, both topical corticosteroids and TCIs are often used for long-term management of moderate to severe AD. TCIs are valuable alternatives to continuous use of corticosteroids for patients with persistent AD and recurrent flares. They’re also beneficial for patients with outbreaks in sensitive areas, such as the face and genitals.
Adjunctive therapies—what’s best for pruritus?
Pruritus is a major feature of AD, and a source of considerable distress. Here are some treatment options that often come up, and what we know about their usefulness.
Antihistamines. There is no evidence to support the use of nonsedating antihistamines in the treatment of AD. Sedating systemic antihistamines such as hydroxyzine and diphenhydramine don’t have a direct effect on the pruritus either, but they can be used to help patients with acute flare-ups improve their sleep.9,14
CASE 2 Antihistamines would not be recommended for Angela at this time; instead, you wait to see whether the topical corticosteroid you have just prescribed is effective. If the patient is still having trouble sleeping after she completes the corticosteroid trial, you can recommend the use of a sedating antihistamine at night as a sleeping aid.
Wet wraps. Wet wrap treatments using occlusive dressings were first recommended as a safe and effective treatment more than 20 years ago.18 Their application may be indicated for children with severe or refractory AD, provided there are no signs or symptoms of infection.
No large prospective studies have evaluated the safety and efficacy of wet wrap treatment or compared it with more conventional modalities. In a recent review, temporary systemic bioactivity of the corticosteroid was the only reported adverse effect.18
There are numerous wet wrap techniques. One effective short-term intervention is to use cream or ointment and a double layer of cotton bandages, with a moist first layer and a dry second layer. Wet wrap dressings with once-daily diluted topical corticosteroids can be used for up to 14 days.18
Coal tar. Although coal tar and coal tar derivatives have been used for many years in the treatment of AD, a lack of data on the clinical efficacy of their application, along with the cosmetic disadvantage, makes compliance with this treatment challenging.
Alternative treatments. A number of alternative measures purport to reduce a child’s risk of developing AD and/or reduce its severity (TABLE), but in most cases, evidence is lacking.
Consider systemic treatment for refractory AD
In a subgroup of patients with moderate to severe AD, the condition is refractory to standard topical therapy and systemic treatment is required. Systemic treatments—including oral corticosteroids, cyclosporine, mycophenolate mofetil, azathioprine, methotrexate, and interferon—should be undertaken only under supervision of a dermatologist.
Oral corticosteroids (typically, prednisone) are sometimes used for short-term treatment of severe AD, although rarely for young children. Evidence of their efficacy is insufficient, and their use is controversial. Patients may have severe symptom flares when an oral corticosteroid is tapered or discontinued. And no randomized controlled trials of prednisone therapy for AD were found in the peer-reviewed medical literature, despite the drug’s long-standing use in AD treatment.30
Systemic immunomodulatory therapies such as cyclosporine, azathioprine, interferon gamma, intravenous immune globulin, mycophenolate, and infliximab have been used for recalcitrant AD. Cyclosporine, an immunosuppressant that acts directly on the cells of the immune system and has an inhibitory effect on T cells, decreases AD severity in the short term. Cyclosporine has been found to be safe, effective, and well tolerated in children with AD, but the potential for hypertension and renal toxicity limits its usefulness for long-term therapy.30
Other systemic immunomodulatory therapies, including those listed above, should be considered when cyclosporine is contraindicated or does not produce a suitable response. Prospective controlled trials in a pediatric population are needed to evaluate the long-term effectiveness and safety of other agents.
Phototherapy is another option
Phototherapy has evolved as a treatment for recalcitrant AD, based on the observation that the condition often improves during the summer months with increased exposure to natural light. Adverse effects of phototherapy can include erythema, pruritus, and pigment changes. Ultraviolet light is also known to cause premature aging of the skin, as well as cutaneous malignancies.4,10,14 Therefore, phototherapy, like systemic treatment, should be undertaken only with the supervision of a dermatologist.
When infection complicates care
Colonization with Staphylococcus aureus is common in patients with AD. In addition to contributing to pruritus and chronic inflammation, S aureus is a risk factor for infection.
Treatment with topical or systemic antibiotics has no clear benefit for patients with AD, except when skin infection is present, When there is evidence of infection, however, methicillin-resistant S aureus must be considered, and any abscess incised and drained.1
Herpes simplex virus infection, another possibility in patients with AD, should be treated immediately with antiviral therapy. If the lesions are widely distributed or the patient has a toxic appearance, hospitalization and IV therapy is warranted—as is an ophthalmology consult when eye or periocular involvement is suspected.1,9
Dermatophyte infections are also more common in patients with AD and can be treated with standard regimens of topical or oral antifungals. Fungi may play a role in chronic inflammation; if there is no infection, however, patients respond better to anti-inflammatory agents than to antifungals.1
Time for a referral
As already noted, a dermatology consult is indicated for refractory AD and when systemic treatment and/or phototherapy is being considered. The suspicion of eczema herpeticum indicates a need for an immediate dermatology referral. An urgent referral is needed for patients with severe AD that has not responded to a week of optimum topical therapy—or whose treatment of bacterial infection has failed. Consider a dermatology consult, as well, when the diagnosis is uncertain or the patient’s symptoms have been poorly controlled. If you (or the child’s parents) suspect that a food allergy is the cause of a severe case of AD, a referral to an allergist is recommended.6,19,21,22
CASE 1 Dylan’s mother calls to tell you that, to her surprise, his eczema has completely cleared up, even though she did not change his formula. You advise her to continue to use the emollient at least twice a day and to bring him in if he develops another flare.
CASE 2 Two weeks after Angela’s office visit, her mother calls to report that her daughter has responded well to triamcinolone ointment 0.025%, the topical steroid you prescribed. When Angela comes in for a well-child visit at age 2, however, she has a mild flare. You prescribe a brief course of triamcinolone ointment and remind her mother to be diligent about skin care.
CORRESPONDENCE Joanne Dempster, MD, New York Presbyterian Hospital, Family & Community Medicine, 610 West 158th Street, New York, NY 10032; [email protected]
1. Boguniewicz M, Leung D. Recent insights into atopic dermatitis and implications for management of infectious complications. J Allergy Clin Immunol. 2010;125:4-13.
2. Lucinda BM. Treatment options for atopic dermatitis. Am Fam Physician. 2007;75:523-530.
3. Levy ML. Atopic dermatitis: understanding the disease and its management. Curr Med Res Opin. 2007;23:3091-3103.
4. Brown S, Reynolds NJ. Atopic and non-atopic eczema. BMJ. 2006;332:584-588.
5. Carbone A, Siu A, Patel R, et al. Pediatric atopic dermatitis: a review of the medical management. Ann Pharmacother. 2010;44:1448-1458.
6. Akadis CA, Akadis M, Beiber T, et al. Diagnosis and treatment of atopic dermatitis in children and adults: European Academy of Allergy and Clinical Immunology/American Academy of Allergy, Asthma and Immunology/PRACTALL consensus report. Allergy. 2006;61:969-987.
7. Schafer T. The impact of allergy on atopic eczema from data from epidemiological studies. Curr Opin Allergy Clin Immunol. 2008;8:418-422.
8. Charman C, Williams H. The use of corticosteroids and corticosteroid phobia in atopic dermatitis. Clin Dermatol. 2003;21:193-200.
9. National Collaborating Centre for Women’s and Children’s Health. Atopic eczema in children. Management of atopic eczema in children from birth up to age of 12 years. Clinical guideline no. 57. London, UK: National Institute for Health and Clinical Excellence (NICE); 2007.
10. Hoare C, Li Wan Po A, Williams H. Systematic review of treatments of atopic eczema. Health Technol Assess. 2000;4:1-191.
11. Simpson E, Hanifin J. Atopic dermatitis. J Am Acad Dermatol. 2005;53:115-128.
12. Grimalt R, Mengeaud V, Cambazard F, et al. The steroid-sparing effect of an emollient therapy in infants with atopic dermatitis: a randomized controlled study. Dermatology. 2007;214:61-67.
13. Callen J, Chamlin S, Eichenfield LF, et al. A systematic review of the safety of topical therapies for atopic dermatitis. Br J Dermatol. 2007;156:203-221.
14. Hanifin JM, Cooper KD, Ho VC, et al. Guidelines for the care of atopic dermatitis developed in accordance with the American Academy of Dermatology (AAD)/American Academy of Dermatology Association. “Administrative regulations for evidence-based clinical practice guidelines”. J Am Acad Dermatol. 2004;50:391-404.
15. Simpson E. Atopic dermatitis: a review of topical treatment options. Curr Med Res Opin. 2010;26:633-640.
16. Munzenberger PJ, Monejo JM. Safety of topical calcineurin inhibitors for the treatment of atopic dermatitis. Pharmacotherapy. 2007;27:1020-1028.
17. Kang S, Lucky AW, Pariser D, et al. Long-term safety and efficacy of tacrolimus ointment for the treatment of atopic dermatitis in children. J Am Acad Dermatol. 2001;44(suppl):S58-S64.
18. Devillers ACA, Oranje AP. Efficacy and safety of ‘wet wrap’ dressings as an intervention treatment in children with severe and/or refractory atopic dermatitis: a critical review of the literature. Br J Dermatol. 2006;154:579-585.
19. Boyl RJ, Bath-Hextall FJ, Leonardi-Bee J, et al. Probiotics for treating eczema. Cochrane Database Syst Rev. 2008;(4):CD006135.-
20. Ellis C, Luger T. International Consensus Conference of Atopic Dermatitis (ICCAD II*): clinical update and current treatment strategies. Br J Dermatol. 2003;148(suppl 63):S3-S10.
21. Han KL, Leung TF, Ching G, et al. Patterns of food and aeroallergen sensitization in childhood eczema. Acta Pediatrica. 2008;97:1734-1737.
22. Greenhawt M. The role of food allergy in atopic dermatitis. Allergy Asthma Proc. 2010;31:392-397.
23. Langan SM, Williams HC. What causes worsening of eczema? A systemic review. Br J Dermatol. 2006;155:505-514.
24. Eller E, Kjaer HF, et al. Food allergy and food sensitization in early childhood: results from the DARC cohort. Allergy. 2009;63:1023-1029.
25. Leung DY, Bieber T. Atopic dermatitis. Lancet. 2003;361:151-160.
26. Protopic [prescribing information]. Deerfield, IL: Astellas Pharma US, Inc; 2006.
27. Elidel [prescribing information]. East Hanover, NJ: Novartis Pharmaceuticals Corp; 2006.
28. US Food and Drug Administration. Topical calcineurin inhibitors. Pediatric safety update: regulatory background. FDA Pediatric Advisory Committee Meeting; March 22, 2010; Bethesda, Md.
29. Kalavala M, Dohil MA. Calcineurin inhibitors in pediatric atopic dermatitis: a review of current evidence. Am J Clin Dermatol. 2011;12:15-24.
30. Ricci G, Dondi A, Patrizi A, et al. Systemic therapy of atopic dermatitis in children. Drugs. 2009;69:297-306.
• Emollients should be used during acute flares as well as regularly for maintenance therapy in children with atopic dermatitis (AD). A
• Topical corticosteroids are the first-line therapy for acute AD flares. A
• There is no evidence to support the use of antihistamines for treatment of AD. A
• Exclusion of cow’s milk and eggs is not recommended except in proven cases of milk or egg allergy with sensitivity testing and food challenge. B
Strength of recommendation (SOR)
A Good-quality patient-oriented evidence
B Inconsistent or limited-quality patient-oriented evidence
C Consensus, usual practice, opinion, disease-oriented evidence, case series
CASE 1 Dylan, an 8-month-old boy whom you had seen for a routine check-up a little over a month ago, is in your office today because of a rash on his face and elbows. The rash began about 2 weeks ago, his mother reports—shortly after she had weaned him from the breast milk to formula. Certain that Dylan has a milk allergy, his mother tells you she plans to switch to a soy-based formula—and wants you to give her something to put on the rash to help clear it up.
CASE 2 Eighteen-month-old Angela had a mild case of atopic dermatitis when you saw her about 3 months ago. The reason for today’s visit is that “her eczema is getting worse,” according to her mother, and the moisturizing cream that you recommended at her last visit “stopped working.” The rash, which had been confined to the patient’s forearms and knees (FIGURE 1), now covers much of her face, forearms, knees, and trunk. Angela’s mother says that the rash appears to be very itchy and that her daughter has been crying and scratching at night.
If Dylan and Angela were your patients, what would you advise their parents to do, and how would you treat them?
FIGURE 1
An 18-month-old girl with an acute flare
This child has moderate atopic dermatitis, with erythema and localized thickened skin at the medial knee—a typical site for atopic dermatitis.
Atopic dermatitis (AD), or eczema, is a chronic inflammatory skin condition that affects up to 20% of children.1 The incidence of pediatric AD has increased 2- to 3-fold in the last 30 years (it’s not clear why), and the condition is a common reason for pediatric visits to family physicians.1,2
AD is marked by phases of pruritus and rash and, depending on the severity, can significantly affect the quality of life of young patients and their families.1-4 The pathophysiology involves structural abnormalities of the epidermis—leading to dry and sensitive skin—combined with immune dysregulation.
Topical corticosteroids to decrease the inflammation and emollients to repair and hydrate the skin are the mainstay of treatment.3,5,6 But numerous considerations, including what triggers patients should avoid; how potent a steroid to prescribe; how long to continue treatment; and when, or whether, to initiate systemic treatment, remain. The evidence-based review of traditional and alternative treatments (TABLE)1-3,7-19 and practical step-wise approach (FIGURE 2)1-3,5,6,9,19-22 that follow can help ensure that you give children with AD the best possible care.
FIGURE 2
A stepped approach to atopic dermatitis1-3,5,6,9,19-22
AD, atopic dermatitis; TCIs, topical calcineurin inhibitors.
TABLE
Treating atopic dermatitis: What the evidence shows
| Intervention (SOR) | Comments |
|---|---|
| Maintenance | |
| Emollients (A)1,2,7,8 | Mainstay of maintenance therapy |
| Treatment | |
| Corticosteroids9-15 – Topical (A) – Oral (B) | First-line treatment No proven benefit |
| TCIs:3,16,17 – Pimecrolimus (A) – Tacrolimus (A) | Second-line treatment |
| Symptom relief | |
| Antihistamines (A)11,14 | No proven benefit in the treatment of AD; sedating antihistamines may improve sleep |
| Tar (C)14 | |
| Wet wrap dressings (C )18 | |
| Infection1,11 | |
| Antibiotics – Topical (A) – Oral (A) | |
| Antifungals – Topical (A) – Oral (A) | |
| Alternative/preventive measures11,19 | |
| Breastfeeding (B) | May reduce risk of developing AD (poor quality study) |
| Essential fatty acids* | No proven benefit |
| Exclusion of eggs or cow’s milk (B) | Only in proven cases of allergy |
| Multivitamins, B6, zinc supplements (C) | No proven benefit |
| Probiotics (B) | No proven benefit |
| Vitamin D supplementation (C) | More studies needed |
| *Black currant seed oil, evening primrose oil, fish oil. AD, atopic dermatitis; TCIs, topical calcineurin inhibitors. | |
The patient has a rash, but what’s the trigger?
Epidemiologic studies have identified numerous AD triggers, including sweating, stress, dust, hard water, food allergies, and seasonality.23 Environmental or situational triggers should be avoided whenever possible,20 of course, but first, they must be identified—an often-difficult task. Establishing the role of any exacerbating factor in AD involves documentation of a temporal relationship between exposure and the development or worsening of symptoms; a dose-response effect; and remission after withdrawal of the trigger.
What’s more, avoidance does not always have the desired result. There is a well-demonstrated correlation between house dust mite sensitization and AD, especially in children of preschool age and older.7,21 Studies performed to determine whether decreasing house dust mite antigen would have a positive effect on disease severity, however, have had conflicting results.23
Food allergies are more likely in the youngest patients
For about a third (35%) of children with AD, the trigger is a food allergy.22 This is most common in infants, with one study showing a peak at 18 months.20,24 The most common food allergens are milk and egg, but wheat, soy, and peanuts are potential allergens, as well.22,25 Food allergies, which are difficult to identify, should be suspected in patients with a poor response to first-line treatment. Sensitivity testing with food challenge may be worthwhile only in severe cases that are refractory to routine care.20
We caution parents not to attempt to withhold a suspected food allergen on their own. To avoid the risk of malnutrition, young children should be placed on elimination diet trials only if the allergen has first been identified by sensitivity testing and food challenge tests, because the allergen may not be clinically significant.21,22 Neither skin prick tests nor serum tests for allergies have been found to be accurate, and parents themselves are often mistaken. Several studies have found a discrepancy between the foods parents think their child is allergic to and the substances that are later found to be clinically significant allergens.21
CASE 1 You advise Dylan’s mother not to switch formulas because answers to further questions about other symptoms were unremarkable (eg, diarrhea). Dylan is treated with a low-potency (class VII) topical steroid (1% hydrocortisone cream) with instructions for the parents to maintain hydration and call you in 5 to 7 days.
Topical corticosteroids are first-line treatment
Two major classes of pharmacologic agents are used for the treatment of AD: topical corticosteroids and topical calcineurin inhibitors (TCIs). Corticosteroids are first-line treatment, as their clinical effectiveness has been well established; TCIs are indicated only as second-line therapy.26,27
Which dosing regimen is best?
The potency of corticosteroids is expressed by a numerical scale, ranging from class I (the most potent) to class VII (the least potent). Class I steroids are about 1800 times more potent than class VII preparations.8
A decision about which strength to use is based on several factors, including the severity of the child’s AD, his or her age, and the affected body site. For infants ≤12 months old, the lowest potency preparations (such as 1% hydrocortisone) are preferable, but should be used in the diaper area for no more than 3 to 7 days at a time.8 In general, potent topical corticosteroids should not be used for children <12 months of age without a dermatology consult.8,9
For children ages 1 through 5 years, intermittent (1- to 2-week) bursts of mild to moderate potency corticosteroids (class VI and VII) are suitable; for older children, a 7- to 10-day course of more potent preparations (class II-V) can be used for nonflexural and nonfacial skin.
While clinical trials have addressed the issues of quantity, duration, potency, and frequency (one large systematic review found twice-daily application of topical corticosteroids to be no more effective than once-daily applications10), an optimal approach to their use in the long-term management of pediatric AD is largely undefined. Various approaches include:
- starting with a more potent preparation to induce remission, followed by a less potent corticosteroid as the AD improves
- using short bursts (5-7 days) of a potent topical corticosteroid, followed by emollient use until a flare-up occurs
- relying on prolonged, or continuous, treatment with less potent preparations.11,23
Long-term use of topical corticosteroids of any potency should be avoided in areas of high risk for cutaneous side effects, such as the face and intertriginous areas.
Emollients are also an important part of therapy for all pediatric patients. Emollients help restore the integrity of the skin barrier and inhibit water loss,1,2,12,20 and should be used not only during an acute flare, but also for maintenance therapy. Tell parents to look for emollients that are unscented and contain fewer additives, and to apply the emollient at least twice daily, and after bathing or swimming.5,20
CASE 2 You prescribe a class V steroid (triamcinolone ointment 0.025%) for Angela, to be applied once a day for 5 to 7 days. You instruct her mother in basic skin care and stress the importance of using an emollient regularly, not just during a flare-up.
What to tell parents about side effects
Discuss the benefits and potential harms of topical corticosteroids with parents (and youngsters who are old enough to understand), emphasizing that when used correctly, the benefits outweigh the risks.
Potential side effects include skin atrophy, striae, telangiectasia, hypopigmentation, rosacea, glaucoma, and cataracts, with studies suggesting that local adverse effects are related to the potency.13 Because there are few prospective controlled trials of sufficient duration, however, the incidence of local reactions to topical corticosteroids in patients with AD is uncertain.
The potential for topical corticosteroids to suppress the hypothalamic-pituitary-adrenal (HPA) axis has been investigated in a small number of studies, with inconclusive results. Effects on the HPA axis appear to be associated with percutaneous absorption in patients who either have a more severe case of AD or are <2 years old.14 A recent systematic review confirmed that the degree of systemic absorption is based on the severity and extent of the disease as well as the formulation and potency of the topical agent.14,15
When to consider TCIs
Pimecrolimus and tacrolimus, the 2 TCIs on the market, are second-line agents for AD. Both have US Food and Drug Administration (FDA) approval for short-term treatment of moderate to severe AD in immunocompetent patients who have failed to respond to topical corticosteroids and children >2 years.26,27 Both TCIs provide targeted anti-inflammatory activity without the local and systemic side effects of topical corticosteroids.
Pimecrolimus cream 1% is approved for treatment in children >2 years.27 Tacrolimus ointment 0.03% is approved for children ages 2 to 15 years with moderate to severe AD, and tacrolimus ointment 0.1% is approved for children older than 16 years with moderate to severe AD.26 Data from clinical trials have shown that pimecrolimus reduces the number and severity of flares, extends the time between flares, and decreases pruritus and other cutaneous signs associated with AD.3 Common side effects, which are usually mild and resolve within days, include pruritus, burning, and stinging at the application site.
In 2006 the FDA added a black-box warning stating that their long-term safety has not been established—a response to widespread off-label use of TCIs in children <2 years and concerns about a theoretical cancer risk based on their mechanism of action—and concluded in 2010 that the labeling adequately warns providers of the potential safety risks.28 Recent reviews have concluded that systemic exposure to topical TCIs is minimal and that there is no evidence linking TCIs to an increased risk of lymphoproliferative disease.16,17,29
Combining corticosteroids and TCIs
In clinical practice, both topical corticosteroids and TCIs are often used for long-term management of moderate to severe AD. TCIs are valuable alternatives to continuous use of corticosteroids for patients with persistent AD and recurrent flares. They’re also beneficial for patients with outbreaks in sensitive areas, such as the face and genitals.
Adjunctive therapies—what’s best for pruritus?
Pruritus is a major feature of AD, and a source of considerable distress. Here are some treatment options that often come up, and what we know about their usefulness.
Antihistamines. There is no evidence to support the use of nonsedating antihistamines in the treatment of AD. Sedating systemic antihistamines such as hydroxyzine and diphenhydramine don’t have a direct effect on the pruritus either, but they can be used to help patients with acute flare-ups improve their sleep.9,14
CASE 2 Antihistamines would not be recommended for Angela at this time; instead, you wait to see whether the topical corticosteroid you have just prescribed is effective. If the patient is still having trouble sleeping after she completes the corticosteroid trial, you can recommend the use of a sedating antihistamine at night as a sleeping aid.
Wet wraps. Wet wrap treatments using occlusive dressings were first recommended as a safe and effective treatment more than 20 years ago.18 Their application may be indicated for children with severe or refractory AD, provided there are no signs or symptoms of infection.
No large prospective studies have evaluated the safety and efficacy of wet wrap treatment or compared it with more conventional modalities. In a recent review, temporary systemic bioactivity of the corticosteroid was the only reported adverse effect.18
There are numerous wet wrap techniques. One effective short-term intervention is to use cream or ointment and a double layer of cotton bandages, with a moist first layer and a dry second layer. Wet wrap dressings with once-daily diluted topical corticosteroids can be used for up to 14 days.18
Coal tar. Although coal tar and coal tar derivatives have been used for many years in the treatment of AD, a lack of data on the clinical efficacy of their application, along with the cosmetic disadvantage, makes compliance with this treatment challenging.
Alternative treatments. A number of alternative measures purport to reduce a child’s risk of developing AD and/or reduce its severity (TABLE), but in most cases, evidence is lacking.
Consider systemic treatment for refractory AD
In a subgroup of patients with moderate to severe AD, the condition is refractory to standard topical therapy and systemic treatment is required. Systemic treatments—including oral corticosteroids, cyclosporine, mycophenolate mofetil, azathioprine, methotrexate, and interferon—should be undertaken only under supervision of a dermatologist.
Oral corticosteroids (typically, prednisone) are sometimes used for short-term treatment of severe AD, although rarely for young children. Evidence of their efficacy is insufficient, and their use is controversial. Patients may have severe symptom flares when an oral corticosteroid is tapered or discontinued. And no randomized controlled trials of prednisone therapy for AD were found in the peer-reviewed medical literature, despite the drug’s long-standing use in AD treatment.30
Systemic immunomodulatory therapies such as cyclosporine, azathioprine, interferon gamma, intravenous immune globulin, mycophenolate, and infliximab have been used for recalcitrant AD. Cyclosporine, an immunosuppressant that acts directly on the cells of the immune system and has an inhibitory effect on T cells, decreases AD severity in the short term. Cyclosporine has been found to be safe, effective, and well tolerated in children with AD, but the potential for hypertension and renal toxicity limits its usefulness for long-term therapy.30
Other systemic immunomodulatory therapies, including those listed above, should be considered when cyclosporine is contraindicated or does not produce a suitable response. Prospective controlled trials in a pediatric population are needed to evaluate the long-term effectiveness and safety of other agents.
Phototherapy is another option
Phototherapy has evolved as a treatment for recalcitrant AD, based on the observation that the condition often improves during the summer months with increased exposure to natural light. Adverse effects of phototherapy can include erythema, pruritus, and pigment changes. Ultraviolet light is also known to cause premature aging of the skin, as well as cutaneous malignancies.4,10,14 Therefore, phototherapy, like systemic treatment, should be undertaken only with the supervision of a dermatologist.
When infection complicates care
Colonization with Staphylococcus aureus is common in patients with AD. In addition to contributing to pruritus and chronic inflammation, S aureus is a risk factor for infection.
Treatment with topical or systemic antibiotics has no clear benefit for patients with AD, except when skin infection is present, When there is evidence of infection, however, methicillin-resistant S aureus must be considered, and any abscess incised and drained.1
Herpes simplex virus infection, another possibility in patients with AD, should be treated immediately with antiviral therapy. If the lesions are widely distributed or the patient has a toxic appearance, hospitalization and IV therapy is warranted—as is an ophthalmology consult when eye or periocular involvement is suspected.1,9
Dermatophyte infections are also more common in patients with AD and can be treated with standard regimens of topical or oral antifungals. Fungi may play a role in chronic inflammation; if there is no infection, however, patients respond better to anti-inflammatory agents than to antifungals.1
Time for a referral
As already noted, a dermatology consult is indicated for refractory AD and when systemic treatment and/or phototherapy is being considered. The suspicion of eczema herpeticum indicates a need for an immediate dermatology referral. An urgent referral is needed for patients with severe AD that has not responded to a week of optimum topical therapy—or whose treatment of bacterial infection has failed. Consider a dermatology consult, as well, when the diagnosis is uncertain or the patient’s symptoms have been poorly controlled. If you (or the child’s parents) suspect that a food allergy is the cause of a severe case of AD, a referral to an allergist is recommended.6,19,21,22
CASE 1 Dylan’s mother calls to tell you that, to her surprise, his eczema has completely cleared up, even though she did not change his formula. You advise her to continue to use the emollient at least twice a day and to bring him in if he develops another flare.
CASE 2 Two weeks after Angela’s office visit, her mother calls to report that her daughter has responded well to triamcinolone ointment 0.025%, the topical steroid you prescribed. When Angela comes in for a well-child visit at age 2, however, she has a mild flare. You prescribe a brief course of triamcinolone ointment and remind her mother to be diligent about skin care.
CORRESPONDENCE Joanne Dempster, MD, New York Presbyterian Hospital, Family & Community Medicine, 610 West 158th Street, New York, NY 10032; [email protected]
• Emollients should be used during acute flares as well as regularly for maintenance therapy in children with atopic dermatitis (AD). A
• Topical corticosteroids are the first-line therapy for acute AD flares. A
• There is no evidence to support the use of antihistamines for treatment of AD. A
• Exclusion of cow’s milk and eggs is not recommended except in proven cases of milk or egg allergy with sensitivity testing and food challenge. B
Strength of recommendation (SOR)
A Good-quality patient-oriented evidence
B Inconsistent or limited-quality patient-oriented evidence
C Consensus, usual practice, opinion, disease-oriented evidence, case series
CASE 1 Dylan, an 8-month-old boy whom you had seen for a routine check-up a little over a month ago, is in your office today because of a rash on his face and elbows. The rash began about 2 weeks ago, his mother reports—shortly after she had weaned him from the breast milk to formula. Certain that Dylan has a milk allergy, his mother tells you she plans to switch to a soy-based formula—and wants you to give her something to put on the rash to help clear it up.
CASE 2 Eighteen-month-old Angela had a mild case of atopic dermatitis when you saw her about 3 months ago. The reason for today’s visit is that “her eczema is getting worse,” according to her mother, and the moisturizing cream that you recommended at her last visit “stopped working.” The rash, which had been confined to the patient’s forearms and knees (FIGURE 1), now covers much of her face, forearms, knees, and trunk. Angela’s mother says that the rash appears to be very itchy and that her daughter has been crying and scratching at night.
If Dylan and Angela were your patients, what would you advise their parents to do, and how would you treat them?
FIGURE 1
An 18-month-old girl with an acute flare
This child has moderate atopic dermatitis, with erythema and localized thickened skin at the medial knee—a typical site for atopic dermatitis.
Atopic dermatitis (AD), or eczema, is a chronic inflammatory skin condition that affects up to 20% of children.1 The incidence of pediatric AD has increased 2- to 3-fold in the last 30 years (it’s not clear why), and the condition is a common reason for pediatric visits to family physicians.1,2
AD is marked by phases of pruritus and rash and, depending on the severity, can significantly affect the quality of life of young patients and their families.1-4 The pathophysiology involves structural abnormalities of the epidermis—leading to dry and sensitive skin—combined with immune dysregulation.
Topical corticosteroids to decrease the inflammation and emollients to repair and hydrate the skin are the mainstay of treatment.3,5,6 But numerous considerations, including what triggers patients should avoid; how potent a steroid to prescribe; how long to continue treatment; and when, or whether, to initiate systemic treatment, remain. The evidence-based review of traditional and alternative treatments (TABLE)1-3,7-19 and practical step-wise approach (FIGURE 2)1-3,5,6,9,19-22 that follow can help ensure that you give children with AD the best possible care.
FIGURE 2
A stepped approach to atopic dermatitis1-3,5,6,9,19-22
AD, atopic dermatitis; TCIs, topical calcineurin inhibitors.
TABLE
Treating atopic dermatitis: What the evidence shows
| Intervention (SOR) | Comments |
|---|---|
| Maintenance | |
| Emollients (A)1,2,7,8 | Mainstay of maintenance therapy |
| Treatment | |
| Corticosteroids9-15 – Topical (A) – Oral (B) | First-line treatment No proven benefit |
| TCIs:3,16,17 – Pimecrolimus (A) – Tacrolimus (A) | Second-line treatment |
| Symptom relief | |
| Antihistamines (A)11,14 | No proven benefit in the treatment of AD; sedating antihistamines may improve sleep |
| Tar (C)14 | |
| Wet wrap dressings (C )18 | |
| Infection1,11 | |
| Antibiotics – Topical (A) – Oral (A) | |
| Antifungals – Topical (A) – Oral (A) | |
| Alternative/preventive measures11,19 | |
| Breastfeeding (B) | May reduce risk of developing AD (poor quality study) |
| Essential fatty acids* | No proven benefit |
| Exclusion of eggs or cow’s milk (B) | Only in proven cases of allergy |
| Multivitamins, B6, zinc supplements (C) | No proven benefit |
| Probiotics (B) | No proven benefit |
| Vitamin D supplementation (C) | More studies needed |
| *Black currant seed oil, evening primrose oil, fish oil. AD, atopic dermatitis; TCIs, topical calcineurin inhibitors. | |
The patient has a rash, but what’s the trigger?
Epidemiologic studies have identified numerous AD triggers, including sweating, stress, dust, hard water, food allergies, and seasonality.23 Environmental or situational triggers should be avoided whenever possible,20 of course, but first, they must be identified—an often-difficult task. Establishing the role of any exacerbating factor in AD involves documentation of a temporal relationship between exposure and the development or worsening of symptoms; a dose-response effect; and remission after withdrawal of the trigger.
What’s more, avoidance does not always have the desired result. There is a well-demonstrated correlation between house dust mite sensitization and AD, especially in children of preschool age and older.7,21 Studies performed to determine whether decreasing house dust mite antigen would have a positive effect on disease severity, however, have had conflicting results.23
Food allergies are more likely in the youngest patients
For about a third (35%) of children with AD, the trigger is a food allergy.22 This is most common in infants, with one study showing a peak at 18 months.20,24 The most common food allergens are milk and egg, but wheat, soy, and peanuts are potential allergens, as well.22,25 Food allergies, which are difficult to identify, should be suspected in patients with a poor response to first-line treatment. Sensitivity testing with food challenge may be worthwhile only in severe cases that are refractory to routine care.20
We caution parents not to attempt to withhold a suspected food allergen on their own. To avoid the risk of malnutrition, young children should be placed on elimination diet trials only if the allergen has first been identified by sensitivity testing and food challenge tests, because the allergen may not be clinically significant.21,22 Neither skin prick tests nor serum tests for allergies have been found to be accurate, and parents themselves are often mistaken. Several studies have found a discrepancy between the foods parents think their child is allergic to and the substances that are later found to be clinically significant allergens.21
CASE 1 You advise Dylan’s mother not to switch formulas because answers to further questions about other symptoms were unremarkable (eg, diarrhea). Dylan is treated with a low-potency (class VII) topical steroid (1% hydrocortisone cream) with instructions for the parents to maintain hydration and call you in 5 to 7 days.
Topical corticosteroids are first-line treatment
Two major classes of pharmacologic agents are used for the treatment of AD: topical corticosteroids and topical calcineurin inhibitors (TCIs). Corticosteroids are first-line treatment, as their clinical effectiveness has been well established; TCIs are indicated only as second-line therapy.26,27
Which dosing regimen is best?
The potency of corticosteroids is expressed by a numerical scale, ranging from class I (the most potent) to class VII (the least potent). Class I steroids are about 1800 times more potent than class VII preparations.8
A decision about which strength to use is based on several factors, including the severity of the child’s AD, his or her age, and the affected body site. For infants ≤12 months old, the lowest potency preparations (such as 1% hydrocortisone) are preferable, but should be used in the diaper area for no more than 3 to 7 days at a time.8 In general, potent topical corticosteroids should not be used for children <12 months of age without a dermatology consult.8,9
For children ages 1 through 5 years, intermittent (1- to 2-week) bursts of mild to moderate potency corticosteroids (class VI and VII) are suitable; for older children, a 7- to 10-day course of more potent preparations (class II-V) can be used for nonflexural and nonfacial skin.
While clinical trials have addressed the issues of quantity, duration, potency, and frequency (one large systematic review found twice-daily application of topical corticosteroids to be no more effective than once-daily applications10), an optimal approach to their use in the long-term management of pediatric AD is largely undefined. Various approaches include:
- starting with a more potent preparation to induce remission, followed by a less potent corticosteroid as the AD improves
- using short bursts (5-7 days) of a potent topical corticosteroid, followed by emollient use until a flare-up occurs
- relying on prolonged, or continuous, treatment with less potent preparations.11,23
Long-term use of topical corticosteroids of any potency should be avoided in areas of high risk for cutaneous side effects, such as the face and intertriginous areas.
Emollients are also an important part of therapy for all pediatric patients. Emollients help restore the integrity of the skin barrier and inhibit water loss,1,2,12,20 and should be used not only during an acute flare, but also for maintenance therapy. Tell parents to look for emollients that are unscented and contain fewer additives, and to apply the emollient at least twice daily, and after bathing or swimming.5,20
CASE 2 You prescribe a class V steroid (triamcinolone ointment 0.025%) for Angela, to be applied once a day for 5 to 7 days. You instruct her mother in basic skin care and stress the importance of using an emollient regularly, not just during a flare-up.
What to tell parents about side effects
Discuss the benefits and potential harms of topical corticosteroids with parents (and youngsters who are old enough to understand), emphasizing that when used correctly, the benefits outweigh the risks.
Potential side effects include skin atrophy, striae, telangiectasia, hypopigmentation, rosacea, glaucoma, and cataracts, with studies suggesting that local adverse effects are related to the potency.13 Because there are few prospective controlled trials of sufficient duration, however, the incidence of local reactions to topical corticosteroids in patients with AD is uncertain.
The potential for topical corticosteroids to suppress the hypothalamic-pituitary-adrenal (HPA) axis has been investigated in a small number of studies, with inconclusive results. Effects on the HPA axis appear to be associated with percutaneous absorption in patients who either have a more severe case of AD or are <2 years old.14 A recent systematic review confirmed that the degree of systemic absorption is based on the severity and extent of the disease as well as the formulation and potency of the topical agent.14,15
When to consider TCIs
Pimecrolimus and tacrolimus, the 2 TCIs on the market, are second-line agents for AD. Both have US Food and Drug Administration (FDA) approval for short-term treatment of moderate to severe AD in immunocompetent patients who have failed to respond to topical corticosteroids and children >2 years.26,27 Both TCIs provide targeted anti-inflammatory activity without the local and systemic side effects of topical corticosteroids.
Pimecrolimus cream 1% is approved for treatment in children >2 years.27 Tacrolimus ointment 0.03% is approved for children ages 2 to 15 years with moderate to severe AD, and tacrolimus ointment 0.1% is approved for children older than 16 years with moderate to severe AD.26 Data from clinical trials have shown that pimecrolimus reduces the number and severity of flares, extends the time between flares, and decreases pruritus and other cutaneous signs associated with AD.3 Common side effects, which are usually mild and resolve within days, include pruritus, burning, and stinging at the application site.
In 2006 the FDA added a black-box warning stating that their long-term safety has not been established—a response to widespread off-label use of TCIs in children <2 years and concerns about a theoretical cancer risk based on their mechanism of action—and concluded in 2010 that the labeling adequately warns providers of the potential safety risks.28 Recent reviews have concluded that systemic exposure to topical TCIs is minimal and that there is no evidence linking TCIs to an increased risk of lymphoproliferative disease.16,17,29
Combining corticosteroids and TCIs
In clinical practice, both topical corticosteroids and TCIs are often used for long-term management of moderate to severe AD. TCIs are valuable alternatives to continuous use of corticosteroids for patients with persistent AD and recurrent flares. They’re also beneficial for patients with outbreaks in sensitive areas, such as the face and genitals.
Adjunctive therapies—what’s best for pruritus?
Pruritus is a major feature of AD, and a source of considerable distress. Here are some treatment options that often come up, and what we know about their usefulness.
Antihistamines. There is no evidence to support the use of nonsedating antihistamines in the treatment of AD. Sedating systemic antihistamines such as hydroxyzine and diphenhydramine don’t have a direct effect on the pruritus either, but they can be used to help patients with acute flare-ups improve their sleep.9,14
CASE 2 Antihistamines would not be recommended for Angela at this time; instead, you wait to see whether the topical corticosteroid you have just prescribed is effective. If the patient is still having trouble sleeping after she completes the corticosteroid trial, you can recommend the use of a sedating antihistamine at night as a sleeping aid.
Wet wraps. Wet wrap treatments using occlusive dressings were first recommended as a safe and effective treatment more than 20 years ago.18 Their application may be indicated for children with severe or refractory AD, provided there are no signs or symptoms of infection.
No large prospective studies have evaluated the safety and efficacy of wet wrap treatment or compared it with more conventional modalities. In a recent review, temporary systemic bioactivity of the corticosteroid was the only reported adverse effect.18
There are numerous wet wrap techniques. One effective short-term intervention is to use cream or ointment and a double layer of cotton bandages, with a moist first layer and a dry second layer. Wet wrap dressings with once-daily diluted topical corticosteroids can be used for up to 14 days.18
Coal tar. Although coal tar and coal tar derivatives have been used for many years in the treatment of AD, a lack of data on the clinical efficacy of their application, along with the cosmetic disadvantage, makes compliance with this treatment challenging.
Alternative treatments. A number of alternative measures purport to reduce a child’s risk of developing AD and/or reduce its severity (TABLE), but in most cases, evidence is lacking.
Consider systemic treatment for refractory AD
In a subgroup of patients with moderate to severe AD, the condition is refractory to standard topical therapy and systemic treatment is required. Systemic treatments—including oral corticosteroids, cyclosporine, mycophenolate mofetil, azathioprine, methotrexate, and interferon—should be undertaken only under supervision of a dermatologist.
Oral corticosteroids (typically, prednisone) are sometimes used for short-term treatment of severe AD, although rarely for young children. Evidence of their efficacy is insufficient, and their use is controversial. Patients may have severe symptom flares when an oral corticosteroid is tapered or discontinued. And no randomized controlled trials of prednisone therapy for AD were found in the peer-reviewed medical literature, despite the drug’s long-standing use in AD treatment.30
Systemic immunomodulatory therapies such as cyclosporine, azathioprine, interferon gamma, intravenous immune globulin, mycophenolate, and infliximab have been used for recalcitrant AD. Cyclosporine, an immunosuppressant that acts directly on the cells of the immune system and has an inhibitory effect on T cells, decreases AD severity in the short term. Cyclosporine has been found to be safe, effective, and well tolerated in children with AD, but the potential for hypertension and renal toxicity limits its usefulness for long-term therapy.30
Other systemic immunomodulatory therapies, including those listed above, should be considered when cyclosporine is contraindicated or does not produce a suitable response. Prospective controlled trials in a pediatric population are needed to evaluate the long-term effectiveness and safety of other agents.
Phototherapy is another option
Phototherapy has evolved as a treatment for recalcitrant AD, based on the observation that the condition often improves during the summer months with increased exposure to natural light. Adverse effects of phototherapy can include erythema, pruritus, and pigment changes. Ultraviolet light is also known to cause premature aging of the skin, as well as cutaneous malignancies.4,10,14 Therefore, phototherapy, like systemic treatment, should be undertaken only with the supervision of a dermatologist.
When infection complicates care
Colonization with Staphylococcus aureus is common in patients with AD. In addition to contributing to pruritus and chronic inflammation, S aureus is a risk factor for infection.
Treatment with topical or systemic antibiotics has no clear benefit for patients with AD, except when skin infection is present, When there is evidence of infection, however, methicillin-resistant S aureus must be considered, and any abscess incised and drained.1
Herpes simplex virus infection, another possibility in patients with AD, should be treated immediately with antiviral therapy. If the lesions are widely distributed or the patient has a toxic appearance, hospitalization and IV therapy is warranted—as is an ophthalmology consult when eye or periocular involvement is suspected.1,9
Dermatophyte infections are also more common in patients with AD and can be treated with standard regimens of topical or oral antifungals. Fungi may play a role in chronic inflammation; if there is no infection, however, patients respond better to anti-inflammatory agents than to antifungals.1
Time for a referral
As already noted, a dermatology consult is indicated for refractory AD and when systemic treatment and/or phototherapy is being considered. The suspicion of eczema herpeticum indicates a need for an immediate dermatology referral. An urgent referral is needed for patients with severe AD that has not responded to a week of optimum topical therapy—or whose treatment of bacterial infection has failed. Consider a dermatology consult, as well, when the diagnosis is uncertain or the patient’s symptoms have been poorly controlled. If you (or the child’s parents) suspect that a food allergy is the cause of a severe case of AD, a referral to an allergist is recommended.6,19,21,22
CASE 1 Dylan’s mother calls to tell you that, to her surprise, his eczema has completely cleared up, even though she did not change his formula. You advise her to continue to use the emollient at least twice a day and to bring him in if he develops another flare.
CASE 2 Two weeks after Angela’s office visit, her mother calls to report that her daughter has responded well to triamcinolone ointment 0.025%, the topical steroid you prescribed. When Angela comes in for a well-child visit at age 2, however, she has a mild flare. You prescribe a brief course of triamcinolone ointment and remind her mother to be diligent about skin care.
CORRESPONDENCE Joanne Dempster, MD, New York Presbyterian Hospital, Family & Community Medicine, 610 West 158th Street, New York, NY 10032; [email protected]
1. Boguniewicz M, Leung D. Recent insights into atopic dermatitis and implications for management of infectious complications. J Allergy Clin Immunol. 2010;125:4-13.
2. Lucinda BM. Treatment options for atopic dermatitis. Am Fam Physician. 2007;75:523-530.
3. Levy ML. Atopic dermatitis: understanding the disease and its management. Curr Med Res Opin. 2007;23:3091-3103.
4. Brown S, Reynolds NJ. Atopic and non-atopic eczema. BMJ. 2006;332:584-588.
5. Carbone A, Siu A, Patel R, et al. Pediatric atopic dermatitis: a review of the medical management. Ann Pharmacother. 2010;44:1448-1458.
6. Akadis CA, Akadis M, Beiber T, et al. Diagnosis and treatment of atopic dermatitis in children and adults: European Academy of Allergy and Clinical Immunology/American Academy of Allergy, Asthma and Immunology/PRACTALL consensus report. Allergy. 2006;61:969-987.
7. Schafer T. The impact of allergy on atopic eczema from data from epidemiological studies. Curr Opin Allergy Clin Immunol. 2008;8:418-422.
8. Charman C, Williams H. The use of corticosteroids and corticosteroid phobia in atopic dermatitis. Clin Dermatol. 2003;21:193-200.
9. National Collaborating Centre for Women’s and Children’s Health. Atopic eczema in children. Management of atopic eczema in children from birth up to age of 12 years. Clinical guideline no. 57. London, UK: National Institute for Health and Clinical Excellence (NICE); 2007.
10. Hoare C, Li Wan Po A, Williams H. Systematic review of treatments of atopic eczema. Health Technol Assess. 2000;4:1-191.
11. Simpson E, Hanifin J. Atopic dermatitis. J Am Acad Dermatol. 2005;53:115-128.
12. Grimalt R, Mengeaud V, Cambazard F, et al. The steroid-sparing effect of an emollient therapy in infants with atopic dermatitis: a randomized controlled study. Dermatology. 2007;214:61-67.
13. Callen J, Chamlin S, Eichenfield LF, et al. A systematic review of the safety of topical therapies for atopic dermatitis. Br J Dermatol. 2007;156:203-221.
14. Hanifin JM, Cooper KD, Ho VC, et al. Guidelines for the care of atopic dermatitis developed in accordance with the American Academy of Dermatology (AAD)/American Academy of Dermatology Association. “Administrative regulations for evidence-based clinical practice guidelines”. J Am Acad Dermatol. 2004;50:391-404.
15. Simpson E. Atopic dermatitis: a review of topical treatment options. Curr Med Res Opin. 2010;26:633-640.
16. Munzenberger PJ, Monejo JM. Safety of topical calcineurin inhibitors for the treatment of atopic dermatitis. Pharmacotherapy. 2007;27:1020-1028.
17. Kang S, Lucky AW, Pariser D, et al. Long-term safety and efficacy of tacrolimus ointment for the treatment of atopic dermatitis in children. J Am Acad Dermatol. 2001;44(suppl):S58-S64.
18. Devillers ACA, Oranje AP. Efficacy and safety of ‘wet wrap’ dressings as an intervention treatment in children with severe and/or refractory atopic dermatitis: a critical review of the literature. Br J Dermatol. 2006;154:579-585.
19. Boyl RJ, Bath-Hextall FJ, Leonardi-Bee J, et al. Probiotics for treating eczema. Cochrane Database Syst Rev. 2008;(4):CD006135.-
20. Ellis C, Luger T. International Consensus Conference of Atopic Dermatitis (ICCAD II*): clinical update and current treatment strategies. Br J Dermatol. 2003;148(suppl 63):S3-S10.
21. Han KL, Leung TF, Ching G, et al. Patterns of food and aeroallergen sensitization in childhood eczema. Acta Pediatrica. 2008;97:1734-1737.
22. Greenhawt M. The role of food allergy in atopic dermatitis. Allergy Asthma Proc. 2010;31:392-397.
23. Langan SM, Williams HC. What causes worsening of eczema? A systemic review. Br J Dermatol. 2006;155:505-514.
24. Eller E, Kjaer HF, et al. Food allergy and food sensitization in early childhood: results from the DARC cohort. Allergy. 2009;63:1023-1029.
25. Leung DY, Bieber T. Atopic dermatitis. Lancet. 2003;361:151-160.
26. Protopic [prescribing information]. Deerfield, IL: Astellas Pharma US, Inc; 2006.
27. Elidel [prescribing information]. East Hanover, NJ: Novartis Pharmaceuticals Corp; 2006.
28. US Food and Drug Administration. Topical calcineurin inhibitors. Pediatric safety update: regulatory background. FDA Pediatric Advisory Committee Meeting; March 22, 2010; Bethesda, Md.
29. Kalavala M, Dohil MA. Calcineurin inhibitors in pediatric atopic dermatitis: a review of current evidence. Am J Clin Dermatol. 2011;12:15-24.
30. Ricci G, Dondi A, Patrizi A, et al. Systemic therapy of atopic dermatitis in children. Drugs. 2009;69:297-306.
1. Boguniewicz M, Leung D. Recent insights into atopic dermatitis and implications for management of infectious complications. J Allergy Clin Immunol. 2010;125:4-13.
2. Lucinda BM. Treatment options for atopic dermatitis. Am Fam Physician. 2007;75:523-530.
3. Levy ML. Atopic dermatitis: understanding the disease and its management. Curr Med Res Opin. 2007;23:3091-3103.
4. Brown S, Reynolds NJ. Atopic and non-atopic eczema. BMJ. 2006;332:584-588.
5. Carbone A, Siu A, Patel R, et al. Pediatric atopic dermatitis: a review of the medical management. Ann Pharmacother. 2010;44:1448-1458.
6. Akadis CA, Akadis M, Beiber T, et al. Diagnosis and treatment of atopic dermatitis in children and adults: European Academy of Allergy and Clinical Immunology/American Academy of Allergy, Asthma and Immunology/PRACTALL consensus report. Allergy. 2006;61:969-987.
7. Schafer T. The impact of allergy on atopic eczema from data from epidemiological studies. Curr Opin Allergy Clin Immunol. 2008;8:418-422.
8. Charman C, Williams H. The use of corticosteroids and corticosteroid phobia in atopic dermatitis. Clin Dermatol. 2003;21:193-200.
9. National Collaborating Centre for Women’s and Children’s Health. Atopic eczema in children. Management of atopic eczema in children from birth up to age of 12 years. Clinical guideline no. 57. London, UK: National Institute for Health and Clinical Excellence (NICE); 2007.
10. Hoare C, Li Wan Po A, Williams H. Systematic review of treatments of atopic eczema. Health Technol Assess. 2000;4:1-191.
11. Simpson E, Hanifin J. Atopic dermatitis. J Am Acad Dermatol. 2005;53:115-128.
12. Grimalt R, Mengeaud V, Cambazard F, et al. The steroid-sparing effect of an emollient therapy in infants with atopic dermatitis: a randomized controlled study. Dermatology. 2007;214:61-67.
13. Callen J, Chamlin S, Eichenfield LF, et al. A systematic review of the safety of topical therapies for atopic dermatitis. Br J Dermatol. 2007;156:203-221.
14. Hanifin JM, Cooper KD, Ho VC, et al. Guidelines for the care of atopic dermatitis developed in accordance with the American Academy of Dermatology (AAD)/American Academy of Dermatology Association. “Administrative regulations for evidence-based clinical practice guidelines”. J Am Acad Dermatol. 2004;50:391-404.
15. Simpson E. Atopic dermatitis: a review of topical treatment options. Curr Med Res Opin. 2010;26:633-640.
16. Munzenberger PJ, Monejo JM. Safety of topical calcineurin inhibitors for the treatment of atopic dermatitis. Pharmacotherapy. 2007;27:1020-1028.
17. Kang S, Lucky AW, Pariser D, et al. Long-term safety and efficacy of tacrolimus ointment for the treatment of atopic dermatitis in children. J Am Acad Dermatol. 2001;44(suppl):S58-S64.
18. Devillers ACA, Oranje AP. Efficacy and safety of ‘wet wrap’ dressings as an intervention treatment in children with severe and/or refractory atopic dermatitis: a critical review of the literature. Br J Dermatol. 2006;154:579-585.
19. Boyl RJ, Bath-Hextall FJ, Leonardi-Bee J, et al. Probiotics for treating eczema. Cochrane Database Syst Rev. 2008;(4):CD006135.-
20. Ellis C, Luger T. International Consensus Conference of Atopic Dermatitis (ICCAD II*): clinical update and current treatment strategies. Br J Dermatol. 2003;148(suppl 63):S3-S10.
21. Han KL, Leung TF, Ching G, et al. Patterns of food and aeroallergen sensitization in childhood eczema. Acta Pediatrica. 2008;97:1734-1737.
22. Greenhawt M. The role of food allergy in atopic dermatitis. Allergy Asthma Proc. 2010;31:392-397.
23. Langan SM, Williams HC. What causes worsening of eczema? A systemic review. Br J Dermatol. 2006;155:505-514.
24. Eller E, Kjaer HF, et al. Food allergy and food sensitization in early childhood: results from the DARC cohort. Allergy. 2009;63:1023-1029.
25. Leung DY, Bieber T. Atopic dermatitis. Lancet. 2003;361:151-160.
26. Protopic [prescribing information]. Deerfield, IL: Astellas Pharma US, Inc; 2006.
27. Elidel [prescribing information]. East Hanover, NJ: Novartis Pharmaceuticals Corp; 2006.
28. US Food and Drug Administration. Topical calcineurin inhibitors. Pediatric safety update: regulatory background. FDA Pediatric Advisory Committee Meeting; March 22, 2010; Bethesda, Md.
29. Kalavala M, Dohil MA. Calcineurin inhibitors in pediatric atopic dermatitis: a review of current evidence. Am J Clin Dermatol. 2011;12:15-24.
30. Ricci G, Dondi A, Patrizi A, et al. Systemic therapy of atopic dermatitis in children. Drugs. 2009;69:297-306.
Getting injured runners back on track
• Advise patients with metatarsalgia to use metatarsal pads, consider orthotics, use contrast baths, and avoid high heels and pointy-toed shoes. C
• Recommend that runners with stress fractures of the foot have at least 4 weeks of rest before a gradual return to activity. C
• Consider short-term physical therapy for patients with plantar fasciitis to enable them to learn proper stretching and strengthening techniques. C
Strength of recommendation (SOR)
A Good-quality patient-oriented evidence
B Inconsistent or limited-quality patient-oriented evidence
C Consensus, usual practice, opinion, disease-oriented evidence, case series
CASE Jim F, 40 years old and overweight (BMI=28 kg/m2), has come to see you because of foot pain that began shortly after he took up running. Jim tells you that turning 40 was “an eye opener” that prompted him to “get healthy.” He says that while he was a competitive athlete in high school, he never ran regularly—until he embarked on a running program 3 months ago.
Jim denies acute injury, bruising, swelling, redness, fever, or chills, but states that the pain, which he describes as dull and achy, is gradually getting worse. It hurts the most when he stands for long periods of time. He says that he occasionally takes ibuprofen for the foot pain, but has not tried icing or stretching. When you ask him what kind of sneakers he wears during his runs, Jim reports that his running shoes—purchased at a discount store—are about 5 years old.
Participation in running has grown by more than 40% in the United States in the past decade.1 As a result, patients like Jim are bound to have their share of aches, pains, and injuries that prompt them to visit their family physician. And that’s where this review can help. This rundown of the most common foot pain diagnoses, as well as the at-a-glance summaries of the differential diagnosis (TABLE 1)2-5 and treatment options (TABLE 2),3,6-25 can help you quickly get patients the relief they need to return to running.
TABLE 1
Differential diagnosis for runners’ foot pain2-5
| Symptom | Differential diagnosis |
|---|---|
| Foot pain |
|
| Heel pain |
|
| *Represents a more common diagnosis. | |
TABLE 2
Diagnosing and treating common runners’ injuries
| Diagnosis | History | Physical exam | Interventions |
|---|---|---|---|
| Metatarsalgia | Plantar foot pain, insidious onset; occasional swelling, bruising, or deformity | Tenderness of MT heads; possible edema or hyperkeratosis; negative tuning fork test | Footwear: cushioning, wide toe box, MT pads; consider orthotics. Contrast baths; NSAIDs6-9 |
| Stress fracture | Pain, insidious onset, increasing in intensity and duration | Localized TTP; possible swelling or bruising; positive tuning fork test; X-rays/MRI may be helpful | Boot for minimum of 3-4 weeks, followed by PT for foot/ankle ROM, strength, proprioception Ice, acetaminophen (NSAIDs controversial)10-12 Progressive return to running* |
| Plantar fasciitis | Plantar foot/heel pain, worse with first steps in AM and after prolonged weight-bearing | TTP at medial calcaneal tubercle | Relative rest, NSAIDs, PT for HEP, Graston technique, taping; possible night splinting13-15 Consider ESWT, corticosteroid injection for refractory cases16-18 |
| MAT | Posterior heel/Achilles pain in midportion; insidious onset, increasing in intensity, worse with activity | Tenderness midportion Achilles; possible tendon thickening; warmth, crepitus, nodules | Relative rest; PT for eccentric exercises; heel lift, with or without orthotics19-22 Consider PRP, prolotherapy, ESWT, or ultrasound in refractory cases†23,24 Surgical intervention rarely indicated3 |
| IAT | Posterior heel/Achilles pain in insertion of Achilles; insidious onset, increasing in intensity; swelling possible; worse with activity | Tenderness with or without swelling; deformity at Achilles insertion | Relative rest; footwear modification (heel lift, possibly with orthotics); PT for eccentric exercises, though less valuable than for MAT†25 |
| *Starting with cross-training exercise, progressing to running on a treadmill, then to running outdoors. †Corticosteroid injection contraindicated. ESWT, extracorporeal shock wave therapy; HEP, home exercise program; IAT, insertional Achilles tendinopathy; MAT, midportion Achilles tendinopathy; MRI, magnetic resonance imaging; MT, metatarsal; NSAIDs, nonsteroidal anti-inflammatory drugs; PRP, plasma-rich protein; PT, physical therapy; ROM, range of motion; TTP, tenderness to palpation. | |||
Metatarsalgia: Pain on the plantar surface
Typically associated with a recent increase in activity or change in footwear, metatarsalgia is defined by pain on the plantar surface of the forefoot in the area of the metatarsal heads. The second, third, and fourth metatarsals are the most common offenders, and the pain may or may not be accompanied by swelling, bruising, or deformity.
Mechanical irregularities in the foot are thought to contribute to the development of metatarsalgia, which is typically inflammatory in nature. Physical exam often reveals tenderness at the affected metatarsal heads, with or without pain in the corresponding metatarsophalangeal joint, and occasionally, with overlying edema or hyperkeratosis.
Tuning fork test. Commonly used but weakly supported, this diagnostic test is performed by applying a vibrating tuning fork to a site of possible fracture. If the maneuver produces focal pain, the test is positive and may be helpful in ruling in metatarsal stress fractures.26
Treatment: Change shoes, consider NSAIDs. Treatment for metatarsalgia begins conservatively, with a change in footwear. High heels or pointy-toed shoes should be avoided, and metatarsal pads (FIGURE 1) can be placed inside the shoes to help off-load the metatarsal head.6 The pads come prefabricated or can be custom made, and are typically placed by physical therapists to ensure proper placement. Orthotics should also be considered, as they can help normalize abnormal foot mechanics that may contribute to metatarsalgia.7,8 (See “A word about runners’ footwear”.9,27-31)
Metatarsalgia is believed to be an inflammatory process, and NSAIDs may be helpful. Contrast baths—alternately submerging the affected foot in a basin of hot (but not scalding) water for 1 to 2 minutes, then immersing it in cold water for 30 to 60 seconds and repeating the process for about 20 minutes once or twice daily—may be helpful. Magnetic insoles are not recommended, as they have been found to be no better than sham insoles.32 Rarely, surgical repair of underlying mechanical abnormalities is indicated for treatment of refractory metatarsalgia.
CASE On examination, Jim F has no swelling, but some hyperkeratosis overlying the second and third metatarsal heads. He has tenderness to palpation at these heads as well as the corresponding metatarsophalangeal joints, and a negative tuning fork test.
You advise Jim that he has metatarsalgia, educate him about the pathophysiology of this condition, and give him a prescription for a nonsteroidal anti-inflammatory drug. You suggest he use contrast baths—and explain how this is done—once or twice a day and refer him to physical therapy for proper placement of metatarsal pads in his shoes, and schedule an appointment for a 6-week follow-up.
Return to running. There is no firm recommendation regarding abstaining from running with metatarsalgia. Advise patients to use pain as a guide in determining the intensity and duration of activity.
FIGURE 1
Treatment for metatarsalgia is conservative
In addition to changing to more comfortable footwear, patients with metatarsalgia can place metatarsal pads like the one shown here in their shoes to ease the metatarsal load.
The proper footwear for runners is subject to considerable debate, with arguments supported by contradictory evidence. What is known, however, is that running shoes should:
- be a comfortable fit with cushioning chosen to accommodate arch type
- be replaced after running 300 to 500 miles or every 12 months, whichever comes first27,28
- be purchased from a sporting goods or running store, rather than at a discount retailer. That’s because the shoes sold at discount stores are often older, and breakdown of the protective cushioning is more likely to have occurred prior to purchase.28
The most expensive shoe is not automatically the best choice for the runner, however. Some studies have found no benefit in foot strike pressures with expensive cushioned running shoes compared with low- or medium-cost brands.29 Shoes should be selected based on comfort, although the patient’s arch type should also be considered when selecting running footwear.30
Barefoot running shoes, designed to simulate barefoot running, are also an option. As with cushioned running shoes, evidence regarding barefoot running is contradictory. Some studies suggest that running mechanics are improved with barefoot running or barefoot running shoes; others have had unfavorable or inconsistent results, indicating a need for further research.9,31
Stress fracture: Tenderness and pain of insidious onset
Stress fractures of the foot (SFF)—overuse injuries also known as fatigue fractures—are common in recreational runners. They are thought to result from microtraumas, which alone are not sufficient to break bone but together overwhelm the bone’s natural ability to remodel and recover over time. SFF are characterized by tenderness and pain of insidious onset, and typically occur when more than one training variable (eg, frequency, duration, and intensity) is changed simultaneously. SFF can also result from a change in exercise mechanics, such as foot strike.
Stress fractures can occur in any bone in the foot, but are most common in the metatarsal bones, specifically the mid or distal portion of the second or third metatarsal, or the tarsal navicular.2,33 On examination, the patient will have tenderness to palpation, often well localized. A positive tuning fork test (see page 647) is highly suggestive of a stress fracture.
![]()
Some studies suggest that barefoot running or barefoot running shoes improve running mechanics; other studies have had unfavorable or inconsistent results.
In female runners, stress fractures may be associated with the female athlete triad—osteoporosis or osteopenia, disordered eating (specifically caloric deficiency and low BMI), and amenorrhea. In addition to the major long-term health problems that may result from even one component of the triad, SFF may be a short-term consequence.34
Although SFF is a clinical diagnosis, x-rays—including 3-view plain films of the foot, with the area of concern clearly noted on the order—are recommended. Magnetic resonance imaging may be used for secondary imaging if doubt about the source of the pain remains.35
Of note: Occasionally, a metatarsal stress fracture progresses to a frank fracture, specifically of the metaphyseal-diaphyseal junction of the fifth metatarsal—known as a Jones fracture. This type of fracture has a high rate of malunion or nonunion.36 If there is any suspicion of a fracture in this area, consider a referral to a sports medicine specialist or orthopedic surgeon.
Treatment: Icing, analgesics, and a boot. Standard treatment for SFF includes icing for 15 to 20 minutes up to 3 times a day for a minimum of 72 hours after injury, but may be continued throughout the healing period. Analgesics such as acetaminophen and a walking boot for 3 to 4 weeks, with follow-up at 3 weeks, should also be implemented. Recent evidence suggests that NSAIDs may hinder the bone healing process, and their use in treating SFF is controversial.10-12
Weaning from the boot can begin when the patient is pain free with the boot on, usually by 3 to 4 weeks. Patients often progress quickly from wearing the boot at all times to wearing it only outside of the house, to not wearing it at all. Advise patients who need to walk long distances for a good portion of the day to keep the boot nearby and to put it on if the pain returns.
Once weaning from the boot begins, physical therapy (PT) should be considered to help the patient regain foot and ankle range of motion (ROM), proprioception, and strength. Once he or she learns the exercises, rehabilitation can be accomplished with a home exercise program. Foot deformities, such as pes planus or pes cavus, may indicate a need for orthotics. A well-structured athletic shoe may help to prevent future injury.7,8
Return to running. Once adequate ROM and strength in the foot and ankle are recovered, the patient can begin to resume activity, starting with a low-impact cross-training exercise, such as a stationary bike or elliptical, for a week or 2. A patient who remains pain free can progress from cross-training to running on a treadmill for another week or 2, then gradually switch to outdoor running.
Plantar fasciitis: Heel pain with an insidious onset
Plantar fasciitis is one of the most common causes of heel pain in athletes (primarily runners) and nonathletes alike. Plantar fasciitis may be associated with acute trauma, but is more commonly insidious in onset. The diagnosis is clinical and rarely requires imaging.
Pain associated with plantar fasciitis may be described as sharp and stabbing or dull and aching. It is on the plantar surface of the heel, sometimes radiating to the arch, and may localize to the insertion of the plantar fascia on the medial calcaneal tubercle (FIGURE 2). The pain is typically most severe with the first few steps in the morning or after other periods of prolonged rest. It usually improves after a few steps, but may return later in the day. Plantar fasciitis does not cause paresthesias or other neurologic symptoms, so their presence is suggestive of a different diagnosis, such as nerve entrapment, compartment syndrome, or tarsal tunnel syndrome.3,5
Treatment: It’s multifactorial. NSAIDs are commonly used. Relative rest is recommended, but cross training may be considered to maintain fitness.37 Short-term PT is also recommended to teach the patient proper stretching and strengthening techniques in the form of a home exercise plan. Modalities such as iontophoresis (a system of transdermal delivery of medication with the use of electrical currents), Graston (a form of instrument-assisted soft tissue mobilization), and taping may be incorporated into PT, as well.13
Night splinting may also be used to keep the foot in a dorsiflexed position. A splint can be purchased without a prescription and prevents the plantar fascia from shortening overnight by providing a continuous passive stretch, thus reducing pain with first steps.14
Orthotics may also help to reduce symptom severity and duration, and studies have found no difference in outcomes with prefabricated vs custom-made devices.15 Another treatment to consider, particularly for recalcitrant cases of plantar fasciitis, is extracorporeal shock wave therapy, which has been studied for more than a decade with conflicting results.16 Corticosteroid injection may also be used for treatment-refractory plantar fasciitis, but caution is required, as the injection may increase the risk of rupture of the plantar fascia.17,18
Return to running. There are no set guidelines for when an athlete with plantar fasciitis can return to running. Typically, after 2 to 4 weeks of relative rest and other treatments, the runner can begin to transition from cross-training to treadmill running.
FIGURE 2
Severe pain with first steps of the day
The pain of plantar fasciitis—often most severe first thing in the morning—may localize to the insertion of the plantar fascia on the medial calcaneal tubercle, as shown above.
Achilles tendinopathy: An overuse injury
Achilles tendinopathy (AT) is typically an overuse injury incurred by athletes, although it is sometimes seen in patients who are sedentary and overweight. With a prevalence among runners of approximately 11%, AT is sometimes called the “runners’ disease.”4
Tendinopathy is a more accurate description than tendonitis, as histologic studies of affected Achilles tendons suggest that AT is a degenerative, rather than an inflammatory, condition.38 A diagnosis of AT can be further classified as midportion or insertional.
Midportion Achilles tendinopathy (MAT), characterized by pain that occurs in the body of the Achilles tendon and worsens with activity, is often a clinical diagnosis. Physical findings suggestive of MAT are tenderness to palpation of the midportion of the Achilles tendon, with thickening of the tendon, warmth, crepitus, or palpable nodules in the tendon body. Onset is insidious and is commonly associated with an increase in activity.
Treatment: Orthotics or a heel lift. Like that of plantar fasciitis, treatment of midportion Achilles tendinopathy is primarily conservative. The use of orthotics, or a heel lift, is one of the most cost-effective interventions, and they are widely used, despite limited evidence of efficacy.39 Custom orthotics are costly, and patients often benefit from trying prefabricated orthotics first to determine whether they will help.
Eccentric exercises. One of the most studied interventions for MAT is eccentric exercise training. Studies of eccentric exercises have been very favorable, and the exercises can be taught during routine PT sessions.19-22 Modalities such as ultrasound therapy and extracorporeal shock wave therapy (ESWT) have also been studied. But because results have been inconsistent, they are generally reserved for treatment-refractory cases.23
In patients with no contraindications, NSAIDs may be a good choice for pain management with relatively favorable results in the literature.24 Corticosteroid injections should not be used, as they have been directly linked to rupture of the Achilles tendon.23
Other interventions, such as plasma-rich protein injections and prolotherapy—a technique in which an irritant is injected into the tendon in an attempt to create an inflammatory reaction, thus increasing local blood flow and healing—are being studied for the treatment of AT, but are not routinely used or covered by insurance for this purpose. Surgical intervention may be considered for patients whose symptoms last for more than 3 to 6 months despite conservative treatment.
Insertional Achilles tendinopathy (IAT) can be clinically differentiated from MAT by the location of symptoms and tenderness to palpation at the insertion site of the Achilles into the calcaneous. Like MAT, IAT is exacerbated by activity. Other conditions that may contribute to, or be mistaken for, IAT are a Haglund deformity and retrocalcaneal bursitis.
Treatment: Footwear modification. Treatment of IAT, like that of MAT, is primarily conservative. Orthotics or heel lifts are commonly used. However, there is greater emphasis on footwear modification due to the mechanical irritation and resultant posterior heel swelling often associated with IAT. While eccentric exercises play a role in IAT treatment, the benefits are limited.25
As with MAT, corticosteroid injections are contraindicated due to the risk of tendon rupture. Modalities such as ultrasound, ESWT, plasma-rich protein, and prolotherapy lack sufficient evidence to be widely recommended.
For refractory cases of IAT, surgical intervention often relieves the pain.
Return to running. After an initial rest of 2 to 4 weeks, patients may return to running while completing therapy. It’s not necessary to wait until the patient is completely pain free, but pain should be used to guide decisions about intensity and duration of activity.
CASE When Jim returns 6 weeks later, he reports that he took 3 weeks off from running because of the pain. Initially, he used contrast baths daily, Jim says, but now he uses them only when he is symptomatic, and he discontinued the NSAID a few weeks ago. Jim tells you he went to the local running store for a new pair of running shoes and that he is now able to run at his previous pace while remaining relatively pain free.
CORRESPONDENCE Jessica Favero Butts, MD, One American Square, Suite 185, Indianapolis, IN 46282; [email protected]
1. Sporting Goods Manufacturers Association (SGMA) 2010 Sports & Fitness Participation Report. Silver Spring, Md: SGMA; 2011.
2. Tuan K, Wu S, Sennett B. Stress fractures in athletes: risk fractures, diagnosis, and management. Orthopedics. 2004;27:583-593.
3. Wapner KL, Parekh SG. Heel pain. In: DeLee J, Drez D, Miller M, eds. DeLee and Drez’s Orthopaedic Sports Medicine. 3rd ed. Philadelphia, Pa: Saunders; 2010:2030–2056.
4. Lysholm J, Wiklander J. Injuries in runners. Am J Sports Med. 1987;15:168-171.
5. Guyton G, Gomez L, Mann R. Entrapment neuropathies of the foot. In: DeLee J, Drez D, Miller M, eds. DeLee and Drez’s Orthopaedic Sports Medicine. 3rd ed. Philadelphia, Pa: Saunders; 2010:2057–2063.
6. Kang JH, Chen MD, Chen SC, et al. Correlations between subjective treatment responses and plantar pressure parameters of metatarsal pad treatment in metatarsalgia patients: a prospective study. BMC Musculoskelet Disord. 2006;7:95.-
7. MacLean CL, van Emmerik R, Hamill J. Influence of custom foot orthotic intervention on lower extremity intralimb coupling during a 30-minute run. J Appl Biomech. 2010;26:390-399.
8. MacLean CL, Davis IS, Hamill J. Short- and long-term influences of a custom foot orthotic intervention on lower extremity dynamics. Clin J Sport Med. 2008;18:338-343.
9. Bishop M, Fiolkowski P, Conrad B, et al. Athletic footwear, leg stiffness, and running kinematics. J Athl Train. 2006;41:387-392.
10. Burd TA, Hughes MS, Anglen JO. Heterotopic ossification prophylaxis with indomethacin increases the risk of long-bone nonunion. J Bone Joint Surg Br. 2003;85:700-705.
11. Butcher CK, Marsh DR. Nonsteroidal anti-inflammatory drugs delay tibial fracture union. Injury. 1996;27:375.-
12. Yates JE, Shah SH. Do NSAIDS impede fracture healing? J Fam Pract. 2011;60:41-42.
13. Hyland M, Webber-Gaffney A, Cohen L. Randomized controlled trial of calcaneal taping, sham taping, and plantar fascia stretching for the short-term management of plantar heel pain. J Orthop Sports Phys Ther. 2006;36:364-371.
14. Powell M, Post WR, Keener J, et al. Effective treatment of chronic plantar fasciitis with dorsiflexion night splints: a crossover prospective randomized outcome study. Foot Ankle Int. 1998;19:10-18.
15. Baldassin V, Gomes CR, Beraldo PS. Effectiveness of prefabricated and customized foot orthoses made from low-cost foam for noncomplicated plantar fasciitis: a randomized controlled trial. Arch Phys Med Rehabil. 2009;90:701-706.
16. Rompe JD, Furia J, Weil L, et al. Shock wave therapy for chronic plantar fasciopathy. Br Med Bull. 2007;81-82:183-208.
17. Kleinman M, Gross AF. Achilles tendon rupture following steroid injection. Report of three cases. J Bone Joint Surg Am. 1983;65:1345-1347.
18. Hamilton B, Remedios D, Loosemore M, et al. Achilles tendon rupture in an elite athlete following multiple injection therapies. J Sci Med Sport. 2008;11:566-568.
19. Wasielewski NJ, Kotsko KM. Does eccentric exercise reduce pain and improve strength in physically active adults with symptomatic lower extremity tendinosis? A systematic review. J Athl Train. 2007;42:409-421.
20. Kingma JJ, de Knikker R, Wittink HM, et al. Eccentric overload training in patients with chronic Achilles tendinopathy: a systematic review. Br J Sports Med. 2007;41:e3.-
21. Norregaard J, Larsen CC, Bieler T, et al. Eccentric exercise in treatment of Achilles tendinopathy. Scand J Med Sci Sports. 2007;17:133-138.
22. Roos EM, Engstrom M, Lagerquist A, et al. Clinical improvement after 6 weeks of eccentric exercise in patients with mid-portion Achilles tendinopathy – a randomized trial with 1-year follow-up. Scand J Med Sci Sports. 2004;14:286-295.
23. Magnusse RA, Dunn WR, Thompson AB. Nonoperative treatment of midportion Achilles tendinopathy: a systematic review. Clin J Sports Med. 2009;19:54-64.
24. McShane JM, Ostick B, McCabe F. Noninsertional Achilles tendinopathy: pathology and management. Curr Sports Med Rep. 2007;6:288-292.
25. Fahlstrom M, Jonsson P, Lorentzon R, et al. Chronic Achilles tendon pain treated with eccentric calf-muscle training. Knee Surg Sports Traumatol Arthrosc. 2003;11:327-333.
26. Lesho EP. Can tuning forks replace bone scans for identification of tibial stress fractures? Mil Med. 1997;162:802-803.
27. Clinghan R, Arnold GP, Drew TS, et al. Do you get value for money when you buy an expensive pair of running shoes? Br J Sports Med. 2008;42:189-193.
28. Butler RJ, Davis IS, Hamill J. Interaction of arch type and footwear on running mechanics. Am J Sports Med. 2006;34:1998-2005.
29. Divert C, Mornieux G, Freychat P, et al. Barefoot-shot running differences: shoe or mass effect? Int J Sports Med. 2008;29:512-518.
30. Taunton JE, Ryan MB, Clement DB, et al. A prospective study of running injuries: the Vancouver Sun Run “In Training” clinics. Br J Sports Med. 2003;37:239-244.
31. Verdejo R, Mills NJ. Heel-shoe interactions and the durability of EVA foam running-shoe midsoles. J Biomech. 2004;37:1379-1386.
32. Winemiller MH, Billow RG, Laskowski ER, et al. Effect of magnetic vs sham-magnetic insoles on nonspecific foot pain in the workplace: a randomized, double-blind, placebo-controlled trial. Mayo Clin Proc. 2005;80:1138-1145.
33. Logan K. Stress fractures in the adolescent athlete. Pediatr Ann. 2007;36:738-745.
34. Thein-Nissenbaum JM, Carr KE. Female athlete triad syndrome in the high school athlete. Phys Ther Sport. 2011;12:108-116.
35. Umans H. Imaging sports medicine injuries of the foot and toes. Clin Sports Med. 2006;25:763-780.
36. Vorlat P, Achtergael W, Haentjens P. Predictors of outcome of non-displaced fractures of the base of the fifth metatarsal. Int Orthop. 2007;31:5-10.
37. Dyck D, Boyajian-O’Neill L. Plantar fasciitis. Clin J Sports Med. 2004;14:305-309.
38. Alfredson H, Thorsen K, Lorentzon R. In situ microdialysis in tendon tissue: high levels of glutamate, but not prostaglandin E2 in chronic Achilles tendon pain. Knee Surg Sports Traumatol Arthrosc. 1999;7:378-381.
39. Seligman DA, Dawson DR. Customized heel pads and soft orthotics to treat heel pain and plantar fasciitis. Arch Phys Med Rehab. 2003;84:1564-1567.
• Advise patients with metatarsalgia to use metatarsal pads, consider orthotics, use contrast baths, and avoid high heels and pointy-toed shoes. C
• Recommend that runners with stress fractures of the foot have at least 4 weeks of rest before a gradual return to activity. C
• Consider short-term physical therapy for patients with plantar fasciitis to enable them to learn proper stretching and strengthening techniques. C
Strength of recommendation (SOR)
A Good-quality patient-oriented evidence
B Inconsistent or limited-quality patient-oriented evidence
C Consensus, usual practice, opinion, disease-oriented evidence, case series
CASE Jim F, 40 years old and overweight (BMI=28 kg/m2), has come to see you because of foot pain that began shortly after he took up running. Jim tells you that turning 40 was “an eye opener” that prompted him to “get healthy.” He says that while he was a competitive athlete in high school, he never ran regularly—until he embarked on a running program 3 months ago.
Jim denies acute injury, bruising, swelling, redness, fever, or chills, but states that the pain, which he describes as dull and achy, is gradually getting worse. It hurts the most when he stands for long periods of time. He says that he occasionally takes ibuprofen for the foot pain, but has not tried icing or stretching. When you ask him what kind of sneakers he wears during his runs, Jim reports that his running shoes—purchased at a discount store—are about 5 years old.
Participation in running has grown by more than 40% in the United States in the past decade.1 As a result, patients like Jim are bound to have their share of aches, pains, and injuries that prompt them to visit their family physician. And that’s where this review can help. This rundown of the most common foot pain diagnoses, as well as the at-a-glance summaries of the differential diagnosis (TABLE 1)2-5 and treatment options (TABLE 2),3,6-25 can help you quickly get patients the relief they need to return to running.
TABLE 1
Differential diagnosis for runners’ foot pain2-5
| Symptom | Differential diagnosis |
|---|---|
| Foot pain |
|
| Heel pain |
|
| *Represents a more common diagnosis. | |
TABLE 2
Diagnosing and treating common runners’ injuries
| Diagnosis | History | Physical exam | Interventions |
|---|---|---|---|
| Metatarsalgia | Plantar foot pain, insidious onset; occasional swelling, bruising, or deformity | Tenderness of MT heads; possible edema or hyperkeratosis; negative tuning fork test | Footwear: cushioning, wide toe box, MT pads; consider orthotics. Contrast baths; NSAIDs6-9 |
| Stress fracture | Pain, insidious onset, increasing in intensity and duration | Localized TTP; possible swelling or bruising; positive tuning fork test; X-rays/MRI may be helpful | Boot for minimum of 3-4 weeks, followed by PT for foot/ankle ROM, strength, proprioception Ice, acetaminophen (NSAIDs controversial)10-12 Progressive return to running* |
| Plantar fasciitis | Plantar foot/heel pain, worse with first steps in AM and after prolonged weight-bearing | TTP at medial calcaneal tubercle | Relative rest, NSAIDs, PT for HEP, Graston technique, taping; possible night splinting13-15 Consider ESWT, corticosteroid injection for refractory cases16-18 |
| MAT | Posterior heel/Achilles pain in midportion; insidious onset, increasing in intensity, worse with activity | Tenderness midportion Achilles; possible tendon thickening; warmth, crepitus, nodules | Relative rest; PT for eccentric exercises; heel lift, with or without orthotics19-22 Consider PRP, prolotherapy, ESWT, or ultrasound in refractory cases†23,24 Surgical intervention rarely indicated3 |
| IAT | Posterior heel/Achilles pain in insertion of Achilles; insidious onset, increasing in intensity; swelling possible; worse with activity | Tenderness with or without swelling; deformity at Achilles insertion | Relative rest; footwear modification (heel lift, possibly with orthotics); PT for eccentric exercises, though less valuable than for MAT†25 |
| *Starting with cross-training exercise, progressing to running on a treadmill, then to running outdoors. †Corticosteroid injection contraindicated. ESWT, extracorporeal shock wave therapy; HEP, home exercise program; IAT, insertional Achilles tendinopathy; MAT, midportion Achilles tendinopathy; MRI, magnetic resonance imaging; MT, metatarsal; NSAIDs, nonsteroidal anti-inflammatory drugs; PRP, plasma-rich protein; PT, physical therapy; ROM, range of motion; TTP, tenderness to palpation. | |||
Metatarsalgia: Pain on the plantar surface
Typically associated with a recent increase in activity or change in footwear, metatarsalgia is defined by pain on the plantar surface of the forefoot in the area of the metatarsal heads. The second, third, and fourth metatarsals are the most common offenders, and the pain may or may not be accompanied by swelling, bruising, or deformity.
Mechanical irregularities in the foot are thought to contribute to the development of metatarsalgia, which is typically inflammatory in nature. Physical exam often reveals tenderness at the affected metatarsal heads, with or without pain in the corresponding metatarsophalangeal joint, and occasionally, with overlying edema or hyperkeratosis.
Tuning fork test. Commonly used but weakly supported, this diagnostic test is performed by applying a vibrating tuning fork to a site of possible fracture. If the maneuver produces focal pain, the test is positive and may be helpful in ruling in metatarsal stress fractures.26
Treatment: Change shoes, consider NSAIDs. Treatment for metatarsalgia begins conservatively, with a change in footwear. High heels or pointy-toed shoes should be avoided, and metatarsal pads (FIGURE 1) can be placed inside the shoes to help off-load the metatarsal head.6 The pads come prefabricated or can be custom made, and are typically placed by physical therapists to ensure proper placement. Orthotics should also be considered, as they can help normalize abnormal foot mechanics that may contribute to metatarsalgia.7,8 (See “A word about runners’ footwear”.9,27-31)
Metatarsalgia is believed to be an inflammatory process, and NSAIDs may be helpful. Contrast baths—alternately submerging the affected foot in a basin of hot (but not scalding) water for 1 to 2 minutes, then immersing it in cold water for 30 to 60 seconds and repeating the process for about 20 minutes once or twice daily—may be helpful. Magnetic insoles are not recommended, as they have been found to be no better than sham insoles.32 Rarely, surgical repair of underlying mechanical abnormalities is indicated for treatment of refractory metatarsalgia.
CASE On examination, Jim F has no swelling, but some hyperkeratosis overlying the second and third metatarsal heads. He has tenderness to palpation at these heads as well as the corresponding metatarsophalangeal joints, and a negative tuning fork test.
You advise Jim that he has metatarsalgia, educate him about the pathophysiology of this condition, and give him a prescription for a nonsteroidal anti-inflammatory drug. You suggest he use contrast baths—and explain how this is done—once or twice a day and refer him to physical therapy for proper placement of metatarsal pads in his shoes, and schedule an appointment for a 6-week follow-up.
Return to running. There is no firm recommendation regarding abstaining from running with metatarsalgia. Advise patients to use pain as a guide in determining the intensity and duration of activity.
FIGURE 1
Treatment for metatarsalgia is conservative
In addition to changing to more comfortable footwear, patients with metatarsalgia can place metatarsal pads like the one shown here in their shoes to ease the metatarsal load.
The proper footwear for runners is subject to considerable debate, with arguments supported by contradictory evidence. What is known, however, is that running shoes should:
- be a comfortable fit with cushioning chosen to accommodate arch type
- be replaced after running 300 to 500 miles or every 12 months, whichever comes first27,28
- be purchased from a sporting goods or running store, rather than at a discount retailer. That’s because the shoes sold at discount stores are often older, and breakdown of the protective cushioning is more likely to have occurred prior to purchase.28
The most expensive shoe is not automatically the best choice for the runner, however. Some studies have found no benefit in foot strike pressures with expensive cushioned running shoes compared with low- or medium-cost brands.29 Shoes should be selected based on comfort, although the patient’s arch type should also be considered when selecting running footwear.30
Barefoot running shoes, designed to simulate barefoot running, are also an option. As with cushioned running shoes, evidence regarding barefoot running is contradictory. Some studies suggest that running mechanics are improved with barefoot running or barefoot running shoes; others have had unfavorable or inconsistent results, indicating a need for further research.9,31
Stress fracture: Tenderness and pain of insidious onset
Stress fractures of the foot (SFF)—overuse injuries also known as fatigue fractures—are common in recreational runners. They are thought to result from microtraumas, which alone are not sufficient to break bone but together overwhelm the bone’s natural ability to remodel and recover over time. SFF are characterized by tenderness and pain of insidious onset, and typically occur when more than one training variable (eg, frequency, duration, and intensity) is changed simultaneously. SFF can also result from a change in exercise mechanics, such as foot strike.
Stress fractures can occur in any bone in the foot, but are most common in the metatarsal bones, specifically the mid or distal portion of the second or third metatarsal, or the tarsal navicular.2,33 On examination, the patient will have tenderness to palpation, often well localized. A positive tuning fork test (see page 647) is highly suggestive of a stress fracture.
![]()
Some studies suggest that barefoot running or barefoot running shoes improve running mechanics; other studies have had unfavorable or inconsistent results.
In female runners, stress fractures may be associated with the female athlete triad—osteoporosis or osteopenia, disordered eating (specifically caloric deficiency and low BMI), and amenorrhea. In addition to the major long-term health problems that may result from even one component of the triad, SFF may be a short-term consequence.34
Although SFF is a clinical diagnosis, x-rays—including 3-view plain films of the foot, with the area of concern clearly noted on the order—are recommended. Magnetic resonance imaging may be used for secondary imaging if doubt about the source of the pain remains.35
Of note: Occasionally, a metatarsal stress fracture progresses to a frank fracture, specifically of the metaphyseal-diaphyseal junction of the fifth metatarsal—known as a Jones fracture. This type of fracture has a high rate of malunion or nonunion.36 If there is any suspicion of a fracture in this area, consider a referral to a sports medicine specialist or orthopedic surgeon.
Treatment: Icing, analgesics, and a boot. Standard treatment for SFF includes icing for 15 to 20 minutes up to 3 times a day for a minimum of 72 hours after injury, but may be continued throughout the healing period. Analgesics such as acetaminophen and a walking boot for 3 to 4 weeks, with follow-up at 3 weeks, should also be implemented. Recent evidence suggests that NSAIDs may hinder the bone healing process, and their use in treating SFF is controversial.10-12
Weaning from the boot can begin when the patient is pain free with the boot on, usually by 3 to 4 weeks. Patients often progress quickly from wearing the boot at all times to wearing it only outside of the house, to not wearing it at all. Advise patients who need to walk long distances for a good portion of the day to keep the boot nearby and to put it on if the pain returns.
Once weaning from the boot begins, physical therapy (PT) should be considered to help the patient regain foot and ankle range of motion (ROM), proprioception, and strength. Once he or she learns the exercises, rehabilitation can be accomplished with a home exercise program. Foot deformities, such as pes planus or pes cavus, may indicate a need for orthotics. A well-structured athletic shoe may help to prevent future injury.7,8
Return to running. Once adequate ROM and strength in the foot and ankle are recovered, the patient can begin to resume activity, starting with a low-impact cross-training exercise, such as a stationary bike or elliptical, for a week or 2. A patient who remains pain free can progress from cross-training to running on a treadmill for another week or 2, then gradually switch to outdoor running.
Plantar fasciitis: Heel pain with an insidious onset
Plantar fasciitis is one of the most common causes of heel pain in athletes (primarily runners) and nonathletes alike. Plantar fasciitis may be associated with acute trauma, but is more commonly insidious in onset. The diagnosis is clinical and rarely requires imaging.
Pain associated with plantar fasciitis may be described as sharp and stabbing or dull and aching. It is on the plantar surface of the heel, sometimes radiating to the arch, and may localize to the insertion of the plantar fascia on the medial calcaneal tubercle (FIGURE 2). The pain is typically most severe with the first few steps in the morning or after other periods of prolonged rest. It usually improves after a few steps, but may return later in the day. Plantar fasciitis does not cause paresthesias or other neurologic symptoms, so their presence is suggestive of a different diagnosis, such as nerve entrapment, compartment syndrome, or tarsal tunnel syndrome.3,5
Treatment: It’s multifactorial. NSAIDs are commonly used. Relative rest is recommended, but cross training may be considered to maintain fitness.37 Short-term PT is also recommended to teach the patient proper stretching and strengthening techniques in the form of a home exercise plan. Modalities such as iontophoresis (a system of transdermal delivery of medication with the use of electrical currents), Graston (a form of instrument-assisted soft tissue mobilization), and taping may be incorporated into PT, as well.13
Night splinting may also be used to keep the foot in a dorsiflexed position. A splint can be purchased without a prescription and prevents the plantar fascia from shortening overnight by providing a continuous passive stretch, thus reducing pain with first steps.14
Orthotics may also help to reduce symptom severity and duration, and studies have found no difference in outcomes with prefabricated vs custom-made devices.15 Another treatment to consider, particularly for recalcitrant cases of plantar fasciitis, is extracorporeal shock wave therapy, which has been studied for more than a decade with conflicting results.16 Corticosteroid injection may also be used for treatment-refractory plantar fasciitis, but caution is required, as the injection may increase the risk of rupture of the plantar fascia.17,18
Return to running. There are no set guidelines for when an athlete with plantar fasciitis can return to running. Typically, after 2 to 4 weeks of relative rest and other treatments, the runner can begin to transition from cross-training to treadmill running.
FIGURE 2
Severe pain with first steps of the day
The pain of plantar fasciitis—often most severe first thing in the morning—may localize to the insertion of the plantar fascia on the medial calcaneal tubercle, as shown above.
Achilles tendinopathy: An overuse injury
Achilles tendinopathy (AT) is typically an overuse injury incurred by athletes, although it is sometimes seen in patients who are sedentary and overweight. With a prevalence among runners of approximately 11%, AT is sometimes called the “runners’ disease.”4
Tendinopathy is a more accurate description than tendonitis, as histologic studies of affected Achilles tendons suggest that AT is a degenerative, rather than an inflammatory, condition.38 A diagnosis of AT can be further classified as midportion or insertional.
Midportion Achilles tendinopathy (MAT), characterized by pain that occurs in the body of the Achilles tendon and worsens with activity, is often a clinical diagnosis. Physical findings suggestive of MAT are tenderness to palpation of the midportion of the Achilles tendon, with thickening of the tendon, warmth, crepitus, or palpable nodules in the tendon body. Onset is insidious and is commonly associated with an increase in activity.
Treatment: Orthotics or a heel lift. Like that of plantar fasciitis, treatment of midportion Achilles tendinopathy is primarily conservative. The use of orthotics, or a heel lift, is one of the most cost-effective interventions, and they are widely used, despite limited evidence of efficacy.39 Custom orthotics are costly, and patients often benefit from trying prefabricated orthotics first to determine whether they will help.
Eccentric exercises. One of the most studied interventions for MAT is eccentric exercise training. Studies of eccentric exercises have been very favorable, and the exercises can be taught during routine PT sessions.19-22 Modalities such as ultrasound therapy and extracorporeal shock wave therapy (ESWT) have also been studied. But because results have been inconsistent, they are generally reserved for treatment-refractory cases.23
In patients with no contraindications, NSAIDs may be a good choice for pain management with relatively favorable results in the literature.24 Corticosteroid injections should not be used, as they have been directly linked to rupture of the Achilles tendon.23
Other interventions, such as plasma-rich protein injections and prolotherapy—a technique in which an irritant is injected into the tendon in an attempt to create an inflammatory reaction, thus increasing local blood flow and healing—are being studied for the treatment of AT, but are not routinely used or covered by insurance for this purpose. Surgical intervention may be considered for patients whose symptoms last for more than 3 to 6 months despite conservative treatment.
Insertional Achilles tendinopathy (IAT) can be clinically differentiated from MAT by the location of symptoms and tenderness to palpation at the insertion site of the Achilles into the calcaneous. Like MAT, IAT is exacerbated by activity. Other conditions that may contribute to, or be mistaken for, IAT are a Haglund deformity and retrocalcaneal bursitis.
Treatment: Footwear modification. Treatment of IAT, like that of MAT, is primarily conservative. Orthotics or heel lifts are commonly used. However, there is greater emphasis on footwear modification due to the mechanical irritation and resultant posterior heel swelling often associated with IAT. While eccentric exercises play a role in IAT treatment, the benefits are limited.25
As with MAT, corticosteroid injections are contraindicated due to the risk of tendon rupture. Modalities such as ultrasound, ESWT, plasma-rich protein, and prolotherapy lack sufficient evidence to be widely recommended.
For refractory cases of IAT, surgical intervention often relieves the pain.
Return to running. After an initial rest of 2 to 4 weeks, patients may return to running while completing therapy. It’s not necessary to wait until the patient is completely pain free, but pain should be used to guide decisions about intensity and duration of activity.
CASE When Jim returns 6 weeks later, he reports that he took 3 weeks off from running because of the pain. Initially, he used contrast baths daily, Jim says, but now he uses them only when he is symptomatic, and he discontinued the NSAID a few weeks ago. Jim tells you he went to the local running store for a new pair of running shoes and that he is now able to run at his previous pace while remaining relatively pain free.
CORRESPONDENCE Jessica Favero Butts, MD, One American Square, Suite 185, Indianapolis, IN 46282; [email protected]
• Advise patients with metatarsalgia to use metatarsal pads, consider orthotics, use contrast baths, and avoid high heels and pointy-toed shoes. C
• Recommend that runners with stress fractures of the foot have at least 4 weeks of rest before a gradual return to activity. C
• Consider short-term physical therapy for patients with plantar fasciitis to enable them to learn proper stretching and strengthening techniques. C
Strength of recommendation (SOR)
A Good-quality patient-oriented evidence
B Inconsistent or limited-quality patient-oriented evidence
C Consensus, usual practice, opinion, disease-oriented evidence, case series
CASE Jim F, 40 years old and overweight (BMI=28 kg/m2), has come to see you because of foot pain that began shortly after he took up running. Jim tells you that turning 40 was “an eye opener” that prompted him to “get healthy.” He says that while he was a competitive athlete in high school, he never ran regularly—until he embarked on a running program 3 months ago.
Jim denies acute injury, bruising, swelling, redness, fever, or chills, but states that the pain, which he describes as dull and achy, is gradually getting worse. It hurts the most when he stands for long periods of time. He says that he occasionally takes ibuprofen for the foot pain, but has not tried icing or stretching. When you ask him what kind of sneakers he wears during his runs, Jim reports that his running shoes—purchased at a discount store—are about 5 years old.
Participation in running has grown by more than 40% in the United States in the past decade.1 As a result, patients like Jim are bound to have their share of aches, pains, and injuries that prompt them to visit their family physician. And that’s where this review can help. This rundown of the most common foot pain diagnoses, as well as the at-a-glance summaries of the differential diagnosis (TABLE 1)2-5 and treatment options (TABLE 2),3,6-25 can help you quickly get patients the relief they need to return to running.
TABLE 1
Differential diagnosis for runners’ foot pain2-5
| Symptom | Differential diagnosis |
|---|---|
| Foot pain |
|
| Heel pain |
|
| *Represents a more common diagnosis. | |
TABLE 2
Diagnosing and treating common runners’ injuries
| Diagnosis | History | Physical exam | Interventions |
|---|---|---|---|
| Metatarsalgia | Plantar foot pain, insidious onset; occasional swelling, bruising, or deformity | Tenderness of MT heads; possible edema or hyperkeratosis; negative tuning fork test | Footwear: cushioning, wide toe box, MT pads; consider orthotics. Contrast baths; NSAIDs6-9 |
| Stress fracture | Pain, insidious onset, increasing in intensity and duration | Localized TTP; possible swelling or bruising; positive tuning fork test; X-rays/MRI may be helpful | Boot for minimum of 3-4 weeks, followed by PT for foot/ankle ROM, strength, proprioception Ice, acetaminophen (NSAIDs controversial)10-12 Progressive return to running* |
| Plantar fasciitis | Plantar foot/heel pain, worse with first steps in AM and after prolonged weight-bearing | TTP at medial calcaneal tubercle | Relative rest, NSAIDs, PT for HEP, Graston technique, taping; possible night splinting13-15 Consider ESWT, corticosteroid injection for refractory cases16-18 |
| MAT | Posterior heel/Achilles pain in midportion; insidious onset, increasing in intensity, worse with activity | Tenderness midportion Achilles; possible tendon thickening; warmth, crepitus, nodules | Relative rest; PT for eccentric exercises; heel lift, with or without orthotics19-22 Consider PRP, prolotherapy, ESWT, or ultrasound in refractory cases†23,24 Surgical intervention rarely indicated3 |
| IAT | Posterior heel/Achilles pain in insertion of Achilles; insidious onset, increasing in intensity; swelling possible; worse with activity | Tenderness with or without swelling; deformity at Achilles insertion | Relative rest; footwear modification (heel lift, possibly with orthotics); PT for eccentric exercises, though less valuable than for MAT†25 |
| *Starting with cross-training exercise, progressing to running on a treadmill, then to running outdoors. †Corticosteroid injection contraindicated. ESWT, extracorporeal shock wave therapy; HEP, home exercise program; IAT, insertional Achilles tendinopathy; MAT, midportion Achilles tendinopathy; MRI, magnetic resonance imaging; MT, metatarsal; NSAIDs, nonsteroidal anti-inflammatory drugs; PRP, plasma-rich protein; PT, physical therapy; ROM, range of motion; TTP, tenderness to palpation. | |||
Metatarsalgia: Pain on the plantar surface
Typically associated with a recent increase in activity or change in footwear, metatarsalgia is defined by pain on the plantar surface of the forefoot in the area of the metatarsal heads. The second, third, and fourth metatarsals are the most common offenders, and the pain may or may not be accompanied by swelling, bruising, or deformity.
Mechanical irregularities in the foot are thought to contribute to the development of metatarsalgia, which is typically inflammatory in nature. Physical exam often reveals tenderness at the affected metatarsal heads, with or without pain in the corresponding metatarsophalangeal joint, and occasionally, with overlying edema or hyperkeratosis.
Tuning fork test. Commonly used but weakly supported, this diagnostic test is performed by applying a vibrating tuning fork to a site of possible fracture. If the maneuver produces focal pain, the test is positive and may be helpful in ruling in metatarsal stress fractures.26
Treatment: Change shoes, consider NSAIDs. Treatment for metatarsalgia begins conservatively, with a change in footwear. High heels or pointy-toed shoes should be avoided, and metatarsal pads (FIGURE 1) can be placed inside the shoes to help off-load the metatarsal head.6 The pads come prefabricated or can be custom made, and are typically placed by physical therapists to ensure proper placement. Orthotics should also be considered, as they can help normalize abnormal foot mechanics that may contribute to metatarsalgia.7,8 (See “A word about runners’ footwear”.9,27-31)
Metatarsalgia is believed to be an inflammatory process, and NSAIDs may be helpful. Contrast baths—alternately submerging the affected foot in a basin of hot (but not scalding) water for 1 to 2 minutes, then immersing it in cold water for 30 to 60 seconds and repeating the process for about 20 minutes once or twice daily—may be helpful. Magnetic insoles are not recommended, as they have been found to be no better than sham insoles.32 Rarely, surgical repair of underlying mechanical abnormalities is indicated for treatment of refractory metatarsalgia.
CASE On examination, Jim F has no swelling, but some hyperkeratosis overlying the second and third metatarsal heads. He has tenderness to palpation at these heads as well as the corresponding metatarsophalangeal joints, and a negative tuning fork test.
You advise Jim that he has metatarsalgia, educate him about the pathophysiology of this condition, and give him a prescription for a nonsteroidal anti-inflammatory drug. You suggest he use contrast baths—and explain how this is done—once or twice a day and refer him to physical therapy for proper placement of metatarsal pads in his shoes, and schedule an appointment for a 6-week follow-up.
Return to running. There is no firm recommendation regarding abstaining from running with metatarsalgia. Advise patients to use pain as a guide in determining the intensity and duration of activity.
FIGURE 1
Treatment for metatarsalgia is conservative
In addition to changing to more comfortable footwear, patients with metatarsalgia can place metatarsal pads like the one shown here in their shoes to ease the metatarsal load.
The proper footwear for runners is subject to considerable debate, with arguments supported by contradictory evidence. What is known, however, is that running shoes should:
- be a comfortable fit with cushioning chosen to accommodate arch type
- be replaced after running 300 to 500 miles or every 12 months, whichever comes first27,28
- be purchased from a sporting goods or running store, rather than at a discount retailer. That’s because the shoes sold at discount stores are often older, and breakdown of the protective cushioning is more likely to have occurred prior to purchase.28
The most expensive shoe is not automatically the best choice for the runner, however. Some studies have found no benefit in foot strike pressures with expensive cushioned running shoes compared with low- or medium-cost brands.29 Shoes should be selected based on comfort, although the patient’s arch type should also be considered when selecting running footwear.30
Barefoot running shoes, designed to simulate barefoot running, are also an option. As with cushioned running shoes, evidence regarding barefoot running is contradictory. Some studies suggest that running mechanics are improved with barefoot running or barefoot running shoes; others have had unfavorable or inconsistent results, indicating a need for further research.9,31
Stress fracture: Tenderness and pain of insidious onset
Stress fractures of the foot (SFF)—overuse injuries also known as fatigue fractures—are common in recreational runners. They are thought to result from microtraumas, which alone are not sufficient to break bone but together overwhelm the bone’s natural ability to remodel and recover over time. SFF are characterized by tenderness and pain of insidious onset, and typically occur when more than one training variable (eg, frequency, duration, and intensity) is changed simultaneously. SFF can also result from a change in exercise mechanics, such as foot strike.
Stress fractures can occur in any bone in the foot, but are most common in the metatarsal bones, specifically the mid or distal portion of the second or third metatarsal, or the tarsal navicular.2,33 On examination, the patient will have tenderness to palpation, often well localized. A positive tuning fork test (see page 647) is highly suggestive of a stress fracture.
![]()
Some studies suggest that barefoot running or barefoot running shoes improve running mechanics; other studies have had unfavorable or inconsistent results.
In female runners, stress fractures may be associated with the female athlete triad—osteoporosis or osteopenia, disordered eating (specifically caloric deficiency and low BMI), and amenorrhea. In addition to the major long-term health problems that may result from even one component of the triad, SFF may be a short-term consequence.34
Although SFF is a clinical diagnosis, x-rays—including 3-view plain films of the foot, with the area of concern clearly noted on the order—are recommended. Magnetic resonance imaging may be used for secondary imaging if doubt about the source of the pain remains.35
Of note: Occasionally, a metatarsal stress fracture progresses to a frank fracture, specifically of the metaphyseal-diaphyseal junction of the fifth metatarsal—known as a Jones fracture. This type of fracture has a high rate of malunion or nonunion.36 If there is any suspicion of a fracture in this area, consider a referral to a sports medicine specialist or orthopedic surgeon.
Treatment: Icing, analgesics, and a boot. Standard treatment for SFF includes icing for 15 to 20 minutes up to 3 times a day for a minimum of 72 hours after injury, but may be continued throughout the healing period. Analgesics such as acetaminophen and a walking boot for 3 to 4 weeks, with follow-up at 3 weeks, should also be implemented. Recent evidence suggests that NSAIDs may hinder the bone healing process, and their use in treating SFF is controversial.10-12
Weaning from the boot can begin when the patient is pain free with the boot on, usually by 3 to 4 weeks. Patients often progress quickly from wearing the boot at all times to wearing it only outside of the house, to not wearing it at all. Advise patients who need to walk long distances for a good portion of the day to keep the boot nearby and to put it on if the pain returns.
Once weaning from the boot begins, physical therapy (PT) should be considered to help the patient regain foot and ankle range of motion (ROM), proprioception, and strength. Once he or she learns the exercises, rehabilitation can be accomplished with a home exercise program. Foot deformities, such as pes planus or pes cavus, may indicate a need for orthotics. A well-structured athletic shoe may help to prevent future injury.7,8
Return to running. Once adequate ROM and strength in the foot and ankle are recovered, the patient can begin to resume activity, starting with a low-impact cross-training exercise, such as a stationary bike or elliptical, for a week or 2. A patient who remains pain free can progress from cross-training to running on a treadmill for another week or 2, then gradually switch to outdoor running.
Plantar fasciitis: Heel pain with an insidious onset
Plantar fasciitis is one of the most common causes of heel pain in athletes (primarily runners) and nonathletes alike. Plantar fasciitis may be associated with acute trauma, but is more commonly insidious in onset. The diagnosis is clinical and rarely requires imaging.
Pain associated with plantar fasciitis may be described as sharp and stabbing or dull and aching. It is on the plantar surface of the heel, sometimes radiating to the arch, and may localize to the insertion of the plantar fascia on the medial calcaneal tubercle (FIGURE 2). The pain is typically most severe with the first few steps in the morning or after other periods of prolonged rest. It usually improves after a few steps, but may return later in the day. Plantar fasciitis does not cause paresthesias or other neurologic symptoms, so their presence is suggestive of a different diagnosis, such as nerve entrapment, compartment syndrome, or tarsal tunnel syndrome.3,5
Treatment: It’s multifactorial. NSAIDs are commonly used. Relative rest is recommended, but cross training may be considered to maintain fitness.37 Short-term PT is also recommended to teach the patient proper stretching and strengthening techniques in the form of a home exercise plan. Modalities such as iontophoresis (a system of transdermal delivery of medication with the use of electrical currents), Graston (a form of instrument-assisted soft tissue mobilization), and taping may be incorporated into PT, as well.13
Night splinting may also be used to keep the foot in a dorsiflexed position. A splint can be purchased without a prescription and prevents the plantar fascia from shortening overnight by providing a continuous passive stretch, thus reducing pain with first steps.14
Orthotics may also help to reduce symptom severity and duration, and studies have found no difference in outcomes with prefabricated vs custom-made devices.15 Another treatment to consider, particularly for recalcitrant cases of plantar fasciitis, is extracorporeal shock wave therapy, which has been studied for more than a decade with conflicting results.16 Corticosteroid injection may also be used for treatment-refractory plantar fasciitis, but caution is required, as the injection may increase the risk of rupture of the plantar fascia.17,18
Return to running. There are no set guidelines for when an athlete with plantar fasciitis can return to running. Typically, after 2 to 4 weeks of relative rest and other treatments, the runner can begin to transition from cross-training to treadmill running.
FIGURE 2
Severe pain with first steps of the day
The pain of plantar fasciitis—often most severe first thing in the morning—may localize to the insertion of the plantar fascia on the medial calcaneal tubercle, as shown above.
Achilles tendinopathy: An overuse injury
Achilles tendinopathy (AT) is typically an overuse injury incurred by athletes, although it is sometimes seen in patients who are sedentary and overweight. With a prevalence among runners of approximately 11%, AT is sometimes called the “runners’ disease.”4
Tendinopathy is a more accurate description than tendonitis, as histologic studies of affected Achilles tendons suggest that AT is a degenerative, rather than an inflammatory, condition.38 A diagnosis of AT can be further classified as midportion or insertional.
Midportion Achilles tendinopathy (MAT), characterized by pain that occurs in the body of the Achilles tendon and worsens with activity, is often a clinical diagnosis. Physical findings suggestive of MAT are tenderness to palpation of the midportion of the Achilles tendon, with thickening of the tendon, warmth, crepitus, or palpable nodules in the tendon body. Onset is insidious and is commonly associated with an increase in activity.
Treatment: Orthotics or a heel lift. Like that of plantar fasciitis, treatment of midportion Achilles tendinopathy is primarily conservative. The use of orthotics, or a heel lift, is one of the most cost-effective interventions, and they are widely used, despite limited evidence of efficacy.39 Custom orthotics are costly, and patients often benefit from trying prefabricated orthotics first to determine whether they will help.
Eccentric exercises. One of the most studied interventions for MAT is eccentric exercise training. Studies of eccentric exercises have been very favorable, and the exercises can be taught during routine PT sessions.19-22 Modalities such as ultrasound therapy and extracorporeal shock wave therapy (ESWT) have also been studied. But because results have been inconsistent, they are generally reserved for treatment-refractory cases.23
In patients with no contraindications, NSAIDs may be a good choice for pain management with relatively favorable results in the literature.24 Corticosteroid injections should not be used, as they have been directly linked to rupture of the Achilles tendon.23
Other interventions, such as plasma-rich protein injections and prolotherapy—a technique in which an irritant is injected into the tendon in an attempt to create an inflammatory reaction, thus increasing local blood flow and healing—are being studied for the treatment of AT, but are not routinely used or covered by insurance for this purpose. Surgical intervention may be considered for patients whose symptoms last for more than 3 to 6 months despite conservative treatment.
Insertional Achilles tendinopathy (IAT) can be clinically differentiated from MAT by the location of symptoms and tenderness to palpation at the insertion site of the Achilles into the calcaneous. Like MAT, IAT is exacerbated by activity. Other conditions that may contribute to, or be mistaken for, IAT are a Haglund deformity and retrocalcaneal bursitis.
Treatment: Footwear modification. Treatment of IAT, like that of MAT, is primarily conservative. Orthotics or heel lifts are commonly used. However, there is greater emphasis on footwear modification due to the mechanical irritation and resultant posterior heel swelling often associated with IAT. While eccentric exercises play a role in IAT treatment, the benefits are limited.25
As with MAT, corticosteroid injections are contraindicated due to the risk of tendon rupture. Modalities such as ultrasound, ESWT, plasma-rich protein, and prolotherapy lack sufficient evidence to be widely recommended.
For refractory cases of IAT, surgical intervention often relieves the pain.
Return to running. After an initial rest of 2 to 4 weeks, patients may return to running while completing therapy. It’s not necessary to wait until the patient is completely pain free, but pain should be used to guide decisions about intensity and duration of activity.
CASE When Jim returns 6 weeks later, he reports that he took 3 weeks off from running because of the pain. Initially, he used contrast baths daily, Jim says, but now he uses them only when he is symptomatic, and he discontinued the NSAID a few weeks ago. Jim tells you he went to the local running store for a new pair of running shoes and that he is now able to run at his previous pace while remaining relatively pain free.
CORRESPONDENCE Jessica Favero Butts, MD, One American Square, Suite 185, Indianapolis, IN 46282; [email protected]
1. Sporting Goods Manufacturers Association (SGMA) 2010 Sports & Fitness Participation Report. Silver Spring, Md: SGMA; 2011.
2. Tuan K, Wu S, Sennett B. Stress fractures in athletes: risk fractures, diagnosis, and management. Orthopedics. 2004;27:583-593.
3. Wapner KL, Parekh SG. Heel pain. In: DeLee J, Drez D, Miller M, eds. DeLee and Drez’s Orthopaedic Sports Medicine. 3rd ed. Philadelphia, Pa: Saunders; 2010:2030–2056.
4. Lysholm J, Wiklander J. Injuries in runners. Am J Sports Med. 1987;15:168-171.
5. Guyton G, Gomez L, Mann R. Entrapment neuropathies of the foot. In: DeLee J, Drez D, Miller M, eds. DeLee and Drez’s Orthopaedic Sports Medicine. 3rd ed. Philadelphia, Pa: Saunders; 2010:2057–2063.
6. Kang JH, Chen MD, Chen SC, et al. Correlations between subjective treatment responses and plantar pressure parameters of metatarsal pad treatment in metatarsalgia patients: a prospective study. BMC Musculoskelet Disord. 2006;7:95.-
7. MacLean CL, van Emmerik R, Hamill J. Influence of custom foot orthotic intervention on lower extremity intralimb coupling during a 30-minute run. J Appl Biomech. 2010;26:390-399.
8. MacLean CL, Davis IS, Hamill J. Short- and long-term influences of a custom foot orthotic intervention on lower extremity dynamics. Clin J Sport Med. 2008;18:338-343.
9. Bishop M, Fiolkowski P, Conrad B, et al. Athletic footwear, leg stiffness, and running kinematics. J Athl Train. 2006;41:387-392.
10. Burd TA, Hughes MS, Anglen JO. Heterotopic ossification prophylaxis with indomethacin increases the risk of long-bone nonunion. J Bone Joint Surg Br. 2003;85:700-705.
11. Butcher CK, Marsh DR. Nonsteroidal anti-inflammatory drugs delay tibial fracture union. Injury. 1996;27:375.-
12. Yates JE, Shah SH. Do NSAIDS impede fracture healing? J Fam Pract. 2011;60:41-42.
13. Hyland M, Webber-Gaffney A, Cohen L. Randomized controlled trial of calcaneal taping, sham taping, and plantar fascia stretching for the short-term management of plantar heel pain. J Orthop Sports Phys Ther. 2006;36:364-371.
14. Powell M, Post WR, Keener J, et al. Effective treatment of chronic plantar fasciitis with dorsiflexion night splints: a crossover prospective randomized outcome study. Foot Ankle Int. 1998;19:10-18.
15. Baldassin V, Gomes CR, Beraldo PS. Effectiveness of prefabricated and customized foot orthoses made from low-cost foam for noncomplicated plantar fasciitis: a randomized controlled trial. Arch Phys Med Rehabil. 2009;90:701-706.
16. Rompe JD, Furia J, Weil L, et al. Shock wave therapy for chronic plantar fasciopathy. Br Med Bull. 2007;81-82:183-208.
17. Kleinman M, Gross AF. Achilles tendon rupture following steroid injection. Report of three cases. J Bone Joint Surg Am. 1983;65:1345-1347.
18. Hamilton B, Remedios D, Loosemore M, et al. Achilles tendon rupture in an elite athlete following multiple injection therapies. J Sci Med Sport. 2008;11:566-568.
19. Wasielewski NJ, Kotsko KM. Does eccentric exercise reduce pain and improve strength in physically active adults with symptomatic lower extremity tendinosis? A systematic review. J Athl Train. 2007;42:409-421.
20. Kingma JJ, de Knikker R, Wittink HM, et al. Eccentric overload training in patients with chronic Achilles tendinopathy: a systematic review. Br J Sports Med. 2007;41:e3.-
21. Norregaard J, Larsen CC, Bieler T, et al. Eccentric exercise in treatment of Achilles tendinopathy. Scand J Med Sci Sports. 2007;17:133-138.
22. Roos EM, Engstrom M, Lagerquist A, et al. Clinical improvement after 6 weeks of eccentric exercise in patients with mid-portion Achilles tendinopathy – a randomized trial with 1-year follow-up. Scand J Med Sci Sports. 2004;14:286-295.
23. Magnusse RA, Dunn WR, Thompson AB. Nonoperative treatment of midportion Achilles tendinopathy: a systematic review. Clin J Sports Med. 2009;19:54-64.
24. McShane JM, Ostick B, McCabe F. Noninsertional Achilles tendinopathy: pathology and management. Curr Sports Med Rep. 2007;6:288-292.
25. Fahlstrom M, Jonsson P, Lorentzon R, et al. Chronic Achilles tendon pain treated with eccentric calf-muscle training. Knee Surg Sports Traumatol Arthrosc. 2003;11:327-333.
26. Lesho EP. Can tuning forks replace bone scans for identification of tibial stress fractures? Mil Med. 1997;162:802-803.
27. Clinghan R, Arnold GP, Drew TS, et al. Do you get value for money when you buy an expensive pair of running shoes? Br J Sports Med. 2008;42:189-193.
28. Butler RJ, Davis IS, Hamill J. Interaction of arch type and footwear on running mechanics. Am J Sports Med. 2006;34:1998-2005.
29. Divert C, Mornieux G, Freychat P, et al. Barefoot-shot running differences: shoe or mass effect? Int J Sports Med. 2008;29:512-518.
30. Taunton JE, Ryan MB, Clement DB, et al. A prospective study of running injuries: the Vancouver Sun Run “In Training” clinics. Br J Sports Med. 2003;37:239-244.
31. Verdejo R, Mills NJ. Heel-shoe interactions and the durability of EVA foam running-shoe midsoles. J Biomech. 2004;37:1379-1386.
32. Winemiller MH, Billow RG, Laskowski ER, et al. Effect of magnetic vs sham-magnetic insoles on nonspecific foot pain in the workplace: a randomized, double-blind, placebo-controlled trial. Mayo Clin Proc. 2005;80:1138-1145.
33. Logan K. Stress fractures in the adolescent athlete. Pediatr Ann. 2007;36:738-745.
34. Thein-Nissenbaum JM, Carr KE. Female athlete triad syndrome in the high school athlete. Phys Ther Sport. 2011;12:108-116.
35. Umans H. Imaging sports medicine injuries of the foot and toes. Clin Sports Med. 2006;25:763-780.
36. Vorlat P, Achtergael W, Haentjens P. Predictors of outcome of non-displaced fractures of the base of the fifth metatarsal. Int Orthop. 2007;31:5-10.
37. Dyck D, Boyajian-O’Neill L. Plantar fasciitis. Clin J Sports Med. 2004;14:305-309.
38. Alfredson H, Thorsen K, Lorentzon R. In situ microdialysis in tendon tissue: high levels of glutamate, but not prostaglandin E2 in chronic Achilles tendon pain. Knee Surg Sports Traumatol Arthrosc. 1999;7:378-381.
39. Seligman DA, Dawson DR. Customized heel pads and soft orthotics to treat heel pain and plantar fasciitis. Arch Phys Med Rehab. 2003;84:1564-1567.
1. Sporting Goods Manufacturers Association (SGMA) 2010 Sports & Fitness Participation Report. Silver Spring, Md: SGMA; 2011.
2. Tuan K, Wu S, Sennett B. Stress fractures in athletes: risk fractures, diagnosis, and management. Orthopedics. 2004;27:583-593.
3. Wapner KL, Parekh SG. Heel pain. In: DeLee J, Drez D, Miller M, eds. DeLee and Drez’s Orthopaedic Sports Medicine. 3rd ed. Philadelphia, Pa: Saunders; 2010:2030–2056.
4. Lysholm J, Wiklander J. Injuries in runners. Am J Sports Med. 1987;15:168-171.
5. Guyton G, Gomez L, Mann R. Entrapment neuropathies of the foot. In: DeLee J, Drez D, Miller M, eds. DeLee and Drez’s Orthopaedic Sports Medicine. 3rd ed. Philadelphia, Pa: Saunders; 2010:2057–2063.
6. Kang JH, Chen MD, Chen SC, et al. Correlations between subjective treatment responses and plantar pressure parameters of metatarsal pad treatment in metatarsalgia patients: a prospective study. BMC Musculoskelet Disord. 2006;7:95.-
7. MacLean CL, van Emmerik R, Hamill J. Influence of custom foot orthotic intervention on lower extremity intralimb coupling during a 30-minute run. J Appl Biomech. 2010;26:390-399.
8. MacLean CL, Davis IS, Hamill J. Short- and long-term influences of a custom foot orthotic intervention on lower extremity dynamics. Clin J Sport Med. 2008;18:338-343.
9. Bishop M, Fiolkowski P, Conrad B, et al. Athletic footwear, leg stiffness, and running kinematics. J Athl Train. 2006;41:387-392.
10. Burd TA, Hughes MS, Anglen JO. Heterotopic ossification prophylaxis with indomethacin increases the risk of long-bone nonunion. J Bone Joint Surg Br. 2003;85:700-705.
11. Butcher CK, Marsh DR. Nonsteroidal anti-inflammatory drugs delay tibial fracture union. Injury. 1996;27:375.-
12. Yates JE, Shah SH. Do NSAIDS impede fracture healing? J Fam Pract. 2011;60:41-42.
13. Hyland M, Webber-Gaffney A, Cohen L. Randomized controlled trial of calcaneal taping, sham taping, and plantar fascia stretching for the short-term management of plantar heel pain. J Orthop Sports Phys Ther. 2006;36:364-371.
14. Powell M, Post WR, Keener J, et al. Effective treatment of chronic plantar fasciitis with dorsiflexion night splints: a crossover prospective randomized outcome study. Foot Ankle Int. 1998;19:10-18.
15. Baldassin V, Gomes CR, Beraldo PS. Effectiveness of prefabricated and customized foot orthoses made from low-cost foam for noncomplicated plantar fasciitis: a randomized controlled trial. Arch Phys Med Rehabil. 2009;90:701-706.
16. Rompe JD, Furia J, Weil L, et al. Shock wave therapy for chronic plantar fasciopathy. Br Med Bull. 2007;81-82:183-208.
17. Kleinman M, Gross AF. Achilles tendon rupture following steroid injection. Report of three cases. J Bone Joint Surg Am. 1983;65:1345-1347.
18. Hamilton B, Remedios D, Loosemore M, et al. Achilles tendon rupture in an elite athlete following multiple injection therapies. J Sci Med Sport. 2008;11:566-568.
19. Wasielewski NJ, Kotsko KM. Does eccentric exercise reduce pain and improve strength in physically active adults with symptomatic lower extremity tendinosis? A systematic review. J Athl Train. 2007;42:409-421.
20. Kingma JJ, de Knikker R, Wittink HM, et al. Eccentric overload training in patients with chronic Achilles tendinopathy: a systematic review. Br J Sports Med. 2007;41:e3.-
21. Norregaard J, Larsen CC, Bieler T, et al. Eccentric exercise in treatment of Achilles tendinopathy. Scand J Med Sci Sports. 2007;17:133-138.
22. Roos EM, Engstrom M, Lagerquist A, et al. Clinical improvement after 6 weeks of eccentric exercise in patients with mid-portion Achilles tendinopathy – a randomized trial with 1-year follow-up. Scand J Med Sci Sports. 2004;14:286-295.
23. Magnusse RA, Dunn WR, Thompson AB. Nonoperative treatment of midportion Achilles tendinopathy: a systematic review. Clin J Sports Med. 2009;19:54-64.
24. McShane JM, Ostick B, McCabe F. Noninsertional Achilles tendinopathy: pathology and management. Curr Sports Med Rep. 2007;6:288-292.
25. Fahlstrom M, Jonsson P, Lorentzon R, et al. Chronic Achilles tendon pain treated with eccentric calf-muscle training. Knee Surg Sports Traumatol Arthrosc. 2003;11:327-333.
26. Lesho EP. Can tuning forks replace bone scans for identification of tibial stress fractures? Mil Med. 1997;162:802-803.
27. Clinghan R, Arnold GP, Drew TS, et al. Do you get value for money when you buy an expensive pair of running shoes? Br J Sports Med. 2008;42:189-193.
28. Butler RJ, Davis IS, Hamill J. Interaction of arch type and footwear on running mechanics. Am J Sports Med. 2006;34:1998-2005.
29. Divert C, Mornieux G, Freychat P, et al. Barefoot-shot running differences: shoe or mass effect? Int J Sports Med. 2008;29:512-518.
30. Taunton JE, Ryan MB, Clement DB, et al. A prospective study of running injuries: the Vancouver Sun Run “In Training” clinics. Br J Sports Med. 2003;37:239-244.
31. Verdejo R, Mills NJ. Heel-shoe interactions and the durability of EVA foam running-shoe midsoles. J Biomech. 2004;37:1379-1386.
32. Winemiller MH, Billow RG, Laskowski ER, et al. Effect of magnetic vs sham-magnetic insoles on nonspecific foot pain in the workplace: a randomized, double-blind, placebo-controlled trial. Mayo Clin Proc. 2005;80:1138-1145.
33. Logan K. Stress fractures in the adolescent athlete. Pediatr Ann. 2007;36:738-745.
34. Thein-Nissenbaum JM, Carr KE. Female athlete triad syndrome in the high school athlete. Phys Ther Sport. 2011;12:108-116.
35. Umans H. Imaging sports medicine injuries of the foot and toes. Clin Sports Med. 2006;25:763-780.
36. Vorlat P, Achtergael W, Haentjens P. Predictors of outcome of non-displaced fractures of the base of the fifth metatarsal. Int Orthop. 2007;31:5-10.
37. Dyck D, Boyajian-O’Neill L. Plantar fasciitis. Clin J Sports Med. 2004;14:305-309.
38. Alfredson H, Thorsen K, Lorentzon R. In situ microdialysis in tendon tissue: high levels of glutamate, but not prostaglandin E2 in chronic Achilles tendon pain. Knee Surg Sports Traumatol Arthrosc. 1999;7:378-381.
39. Seligman DA, Dawson DR. Customized heel pads and soft orthotics to treat heel pain and plantar fasciitis. Arch Phys Med Rehab. 2003;84:1564-1567.
Intra-Articular Injections of the Knee: A Step-by-Step Guide
Although some training is required, intra-articular injections are no longer considered an orthopedic subspecialty procedure, and there are a number of benefits to incorporating these injections into your practice. Many patients appreciate their primary care clinician making available services that traditionally required a referral to a specialist. Patients also avoid treatment delays.
Here is a step-by-step guide to familiarize you with the technique.
STEP 1: Selecting an injection approach
Common approaches for injecting the knee include the following1 :
- Anterolateral (flexed knee)
- Anteromedial (flexed knee)
- Superolateral/lateral suprapatellar (straight knee)
- Superomedial/medial suprapatellar (straight knee)
- Lateral mid-patellar
- Medial mid-patellar.
One study found that the accuracy of the first attempt at needle placement was highest for lateral mid-patellar (93%) compared with anteromedial (75%) and anterolateral (71%) approaches (superolateral approach not done).
STEP 2: Identify and mark the injection site2
For superolateral approach:
- Palpate superolateral and lateral edges of patella with patient supine and leg straight
- Mark where lines intersect as in diagram.
If the patient cannot completely extend the knee, placement of a rolled towel to support the knee will help provide the patient comfort and minimize muscle spasm, improving the likelihood of a successful and comfortable injection.
STEP 3: Preparing the injection site2
- Aseptic technique
- – Swab area 3 times with a povidone iodine preparation (Beta-dine) and let dry.
- Local anesthetic options
- – Lidocaine
- – Vapocoolant spray
STEP 4: Aspiration (skip to Step 5 if no effusion is present)
If effusion is present, aspiration of the effusion can relieve patient discomfort, be of diagnostic benefit, and avoid dilution of a visco-supplement to be injected.2
- Insert 1 ½” 18-gauge needle for aspiration3
- If needle is accurately placed, the syringe should fill with fluid1
- Compression of the opposite side of the joint or the patella may aid in arthrocentesis.3
STEP 5: Injection
If aspiration was required, the same needle can be used for aspiration and injection by changing the syringe.
- Insert needle (1 ½”, 21-gauge for corticosteroids; 1 ½”, 20- or 22-gauge for viscosupplementation) ¾” to 1 ¼” for injection
- Remove needle, wipe off povidone iodine solution, and apply bandage.
Post-injection care: Setting patient expectations and managing adverse effects
- Patient should avoid strenuous activity for 1 to 2 days after injection and apply ice to injection site
- Mild pain or swelling at the injection site can occur, but is rare
- – If mild pain or swelling occurs, recommend ice, nonsteroidal anti-inflammatory drug (NSAID), rest, and elevation
- – If significant pain or swelling occurs:
- Joint aspiration
- Send aspirate to lab to rule out joint infection
- Crystal analysis
- May provide intra-articular corticosteroid to decrease pain and inflammation after viscosupplementation if infection has been excluded.
1. Jackson DW, Evans NA, Thomas BM. Accuracy of needle placement into the intra-articular space of the knee. J Bone Joint Surg Am. 2002;84-A(9):1522-1527.
2. Waddell DD. The tolerability of viscosupplementation: low incidence and clinical management of local adverse events. Curr Med Res Opin. 2003;19(7):575-580.
3. Wen DY. Intra-articular hyaluronic acid injections for knee osteoarthritis. Am Fam Physician. 2000;62(3):565-570, 572.
Although some training is required, intra-articular injections are no longer considered an orthopedic subspecialty procedure, and there are a number of benefits to incorporating these injections into your practice. Many patients appreciate their primary care clinician making available services that traditionally required a referral to a specialist. Patients also avoid treatment delays.
Here is a step-by-step guide to familiarize you with the technique.
STEP 1: Selecting an injection approach
Common approaches for injecting the knee include the following1 :
- Anterolateral (flexed knee)
- Anteromedial (flexed knee)
- Superolateral/lateral suprapatellar (straight knee)
- Superomedial/medial suprapatellar (straight knee)
- Lateral mid-patellar
- Medial mid-patellar.
One study found that the accuracy of the first attempt at needle placement was highest for lateral mid-patellar (93%) compared with anteromedial (75%) and anterolateral (71%) approaches (superolateral approach not done).
STEP 2: Identify and mark the injection site2
For superolateral approach:
- Palpate superolateral and lateral edges of patella with patient supine and leg straight
- Mark where lines intersect as in diagram.
If the patient cannot completely extend the knee, placement of a rolled towel to support the knee will help provide the patient comfort and minimize muscle spasm, improving the likelihood of a successful and comfortable injection.
STEP 3: Preparing the injection site2
- Aseptic technique
- – Swab area 3 times with a povidone iodine preparation (Beta-dine) and let dry.
- Local anesthetic options
- – Lidocaine
- – Vapocoolant spray
STEP 4: Aspiration (skip to Step 5 if no effusion is present)
If effusion is present, aspiration of the effusion can relieve patient discomfort, be of diagnostic benefit, and avoid dilution of a visco-supplement to be injected.2
- Insert 1 ½” 18-gauge needle for aspiration3
- If needle is accurately placed, the syringe should fill with fluid1
- Compression of the opposite side of the joint or the patella may aid in arthrocentesis.3
STEP 5: Injection
If aspiration was required, the same needle can be used for aspiration and injection by changing the syringe.
- Insert needle (1 ½”, 21-gauge for corticosteroids; 1 ½”, 20- or 22-gauge for viscosupplementation) ¾” to 1 ¼” for injection
- Remove needle, wipe off povidone iodine solution, and apply bandage.
Post-injection care: Setting patient expectations and managing adverse effects
- Patient should avoid strenuous activity for 1 to 2 days after injection and apply ice to injection site
- Mild pain or swelling at the injection site can occur, but is rare
- – If mild pain or swelling occurs, recommend ice, nonsteroidal anti-inflammatory drug (NSAID), rest, and elevation
- – If significant pain or swelling occurs:
- Joint aspiration
- Send aspirate to lab to rule out joint infection
- Crystal analysis
- May provide intra-articular corticosteroid to decrease pain and inflammation after viscosupplementation if infection has been excluded.
Although some training is required, intra-articular injections are no longer considered an orthopedic subspecialty procedure, and there are a number of benefits to incorporating these injections into your practice. Many patients appreciate their primary care clinician making available services that traditionally required a referral to a specialist. Patients also avoid treatment delays.
Here is a step-by-step guide to familiarize you with the technique.
STEP 1: Selecting an injection approach
Common approaches for injecting the knee include the following1 :
- Anterolateral (flexed knee)
- Anteromedial (flexed knee)
- Superolateral/lateral suprapatellar (straight knee)
- Superomedial/medial suprapatellar (straight knee)
- Lateral mid-patellar
- Medial mid-patellar.
One study found that the accuracy of the first attempt at needle placement was highest for lateral mid-patellar (93%) compared with anteromedial (75%) and anterolateral (71%) approaches (superolateral approach not done).
STEP 2: Identify and mark the injection site2
For superolateral approach:
- Palpate superolateral and lateral edges of patella with patient supine and leg straight
- Mark where lines intersect as in diagram.
If the patient cannot completely extend the knee, placement of a rolled towel to support the knee will help provide the patient comfort and minimize muscle spasm, improving the likelihood of a successful and comfortable injection.
STEP 3: Preparing the injection site2
- Aseptic technique
- – Swab area 3 times with a povidone iodine preparation (Beta-dine) and let dry.
- Local anesthetic options
- – Lidocaine
- – Vapocoolant spray
STEP 4: Aspiration (skip to Step 5 if no effusion is present)
If effusion is present, aspiration of the effusion can relieve patient discomfort, be of diagnostic benefit, and avoid dilution of a visco-supplement to be injected.2
- Insert 1 ½” 18-gauge needle for aspiration3
- If needle is accurately placed, the syringe should fill with fluid1
- Compression of the opposite side of the joint or the patella may aid in arthrocentesis.3
STEP 5: Injection
If aspiration was required, the same needle can be used for aspiration and injection by changing the syringe.
- Insert needle (1 ½”, 21-gauge for corticosteroids; 1 ½”, 20- or 22-gauge for viscosupplementation) ¾” to 1 ¼” for injection
- Remove needle, wipe off povidone iodine solution, and apply bandage.
Post-injection care: Setting patient expectations and managing adverse effects
- Patient should avoid strenuous activity for 1 to 2 days after injection and apply ice to injection site
- Mild pain or swelling at the injection site can occur, but is rare
- – If mild pain or swelling occurs, recommend ice, nonsteroidal anti-inflammatory drug (NSAID), rest, and elevation
- – If significant pain or swelling occurs:
- Joint aspiration
- Send aspirate to lab to rule out joint infection
- Crystal analysis
- May provide intra-articular corticosteroid to decrease pain and inflammation after viscosupplementation if infection has been excluded.
1. Jackson DW, Evans NA, Thomas BM. Accuracy of needle placement into the intra-articular space of the knee. J Bone Joint Surg Am. 2002;84-A(9):1522-1527.
2. Waddell DD. The tolerability of viscosupplementation: low incidence and clinical management of local adverse events. Curr Med Res Opin. 2003;19(7):575-580.
3. Wen DY. Intra-articular hyaluronic acid injections for knee osteoarthritis. Am Fam Physician. 2000;62(3):565-570, 572.
1. Jackson DW, Evans NA, Thomas BM. Accuracy of needle placement into the intra-articular space of the knee. J Bone Joint Surg Am. 2002;84-A(9):1522-1527.
2. Waddell DD. The tolerability of viscosupplementation: low incidence and clinical management of local adverse events. Curr Med Res Opin. 2003;19(7):575-580.
3. Wen DY. Intra-articular hyaluronic acid injections for knee osteoarthritis. Am Fam Physician. 2000;62(3):565-570, 572.
Supine infant positioning—Yes, but there’s more to it
• Continue to advise parents to place their infants on their backs for sleeping, to prevent sudden infant death. A
• Educate parents about the value of supervised prone positioning (“tummy time”) during waking hours, which helps infants learn to raise their head, push up on their arms, and attain on-time milestones such as rolling over and unsupported sitting. A
• Tell parents that supervised abdominal positioning aids in preventing plagiocephaly and torticollis. B
Strength of recommendation (SOR)
A Good-quality patient-oriented evidence
B Inconsistent or limited-quality patient-oriented evidence
C Consensus, usual practice, opinion, disease-oriented evidence, case series
As happens with many interventions, the Back-to-Sleep campaign1 to prevent sudden infant death syndrome (SIDS) has led to unintended consequences. The campaign’s primary recommendation—that infants be placed on their backs for sleeping instead of on their stomachs—has of course yielded tremendous benefits. The prevalence of SIDS among healthy infants has dropped to 0.57 children per 1000 live births, totaling 2200 deaths per year, compared with 1.2 children per 1000 births in 1997.2-4 However, as the incidence of SIDS began to decline, it became apparent that children were experiencing delayed gross motor movement coincident with placement in the supine sleeping position5-7—or, more accurately, because parents following the Back-to-Sleep recommendation also generally avoided placing their infants in the prone position when they were awake.7
These delays become apparent as early as 2 to 3 months of age and manifest as the inability of an infant to raise his or her head when placed in the prone position.8 Because of this finding, the American Academy of Pediatrics modified its original recommendation for healthy infants, in part stating, “A certain amount of tummy time while the infant is awake and observed is recommended for developmental reasons….”9
In this article, I address the 3 most common unintended consequences for infants perpetually placed in the supine position: developmental motor delays, plagiocephaly (flattening of the occiput) and brachycephaly (widening of the skull), and congenital muscular torticollis (CMT) (a head tilt to one side). Each of these outcomes is preventable with vigilance in the care of newborns.
Prevent developmental motor delays with “tummy time”
The need for prone positioning, or “tummy time,” while an infant is awake cannot be overestimated. Particularly for preterm infants, a delayed acquisition of the ability to lift and turn the head could result in upper airway compromise or rebreathing and, thus, asphyxia.10 Infants who sleep in the supine position and exhibit delayed motor development by age 6 months very often are also found to have had their awake prone positioning restricted.11 In one study, delays in gross motor skills persisted in some cases to 15 months of age, and fine motor skills were delayed in 6-month-old infants who had little prone positioning.11 Infants who sleep in the side or supine position roll over later than those who sleep in the prone position.5 The TABLE compares mean age differences for milestone achievements with varying sleep positions.
On multiple regression analyses, awake prone positioning has consistently emerged as the most significant predictor of early motor development.11 For babies regularly placed in the prone position, the average Peabody Development Motor Scales-2 locomotion score has been significantly higher than that of babies not placed in the prone position when tested at 6 and 18 months.12 For infants routinely sleeping supine, supervised “prone to play” during waking hours enables them to practice prone-related motor skills such as head control.13
Infants with prone experience have attained the milestone of crawling on the abdomen significantly earlier than those without prone experience, leading to a higher 6-month gross motor development quotient.14 For children with just over an hour of daily prone positioning, an advantage in motor skill development has revealed itself as early as 4 months of age.15,16 Somewhat reassuring is evidence from one study that all infants, whether sleeping prone or supine, achieve all milestones within the accepted normal age range as long as prone positioning is initiated.7
What you’ll need to do. Stress to parents the importance of tummy time, or prone to play, in enabling normal developmental progression. Encourage this practice even if parents report that their infant cries or otherwise appears not to tolerate the prone position.15 In general, sleeping in the supine position does not negatively impact motor development as long as there is awake time with supervised prone positioning.17
TABLE
Mean age (months) for milestone acquisition
| Milestone | Prone sleepers | Mixed/side sleepers | Supine sleepers | P value* (linear regression)† |
|---|---|---|---|---|
| Rolls prone to supine | 3.93 ± 1.2 | 4.48 ± 1.8 | 4.87 ± 1.33 | .002 (.02) |
| Rolls supine to prone | 4.9 ± 1.3 | 4.97 ± 1.9 | 5.0 ± 1.6 | .95 |
| Sits supported | 4.7 ± 1.3 | 5.02 ± 1.4 | 5.13 ± 0.9 | .003 (.03) |
| Sits unsupported | 5.13 ± 1.1 | 5.17 ± 1.2 | 5.17 ± 1.0 | .80 |
| Transfers object | 5.87 ± 1.2 | 5.99 ± 6.5 | 6.23 ± 1.1 | .11 |
| Creeps | 6.07 ± 1.9 | 6.49 ± 1.9 | 7.23 ± 1.6 | .0002 (.001) |
| Crawls | 7.83 ± 2.0 | 8.47 ± 2.1 | 8.6 ± 1.7 | .003 (.05) |
| Pulls to stand | 8.1 ± 1.6 | 8.7 ± 1.5 | 8.77 ± 1.6 | .01 (.04) |
| Walks alone | 12.1 ± 2.0 | 12.2 ± 2.0 | 12.2 ± 1.7 | .4 |
| *Represents P value for prone sleepers vs supine sleepers. †Multivariate regression analysis controlling for infant size, gender, ethnicity, presence of siblings, and maternal education. Source: Davis BE, Moon RY, Sachs HC, et al. Pediatrics. 1998.7 Reproduced with permission of American Academy of Pediatrics. | ||||
Plagiocephaly and brachycephaly: Vary position for feeding, sleeping
Plagiocephaly and brachycephaly may occur as a consequence of prolonged supine positioning. Indeed, the incidence of plagiocephaly has increased since 1992, due largely to widespread adoption of the supine sleeping position.18 Plagiocephaly and/or brachycephaly is also more likely to occur in the first 4 months of life in infants who are male, firstborn, or who exhibit limited head rotation or low activity levels.19 Feeding with a bottle only and with the child’s head persistently placed to one side can lead to plagiocephaly.20
Delayed achievement of motor milestones is also associated with plagiocephaly, and tummy time to facilitate motor skill development helps protect against the deformity.20 Varying the head position when laying the infant down for sleep is also protective.21 One systematic review has shown considerable evidence that molding therapy with a helmet may reduce skull asymmetry more effectively than repositioning therapy.22
What you’ll need to do. Ask parents about their infant’s activity level, and encourage tummy time to protect against plagiocephaly. Also advise parents who bottle feed to alternate the feeding position between left and right arms.
Torticollis: Assess neck function in weeks after birth
Not only do infants with CMT display a head tilt to one side, but they also often have rotation of the head to the opposite side with the chin appearing to jut out.23 This postural deformity—primarily resulting from unilateral shortening and fibrosis of the sternocleidomastoid muscle24—is detectable at birth or shortly thereafter. CMT occurs in 1 of every 300 live births.25 Torticollis discovered at birth is likely related to a constrained intrauterine position. In one study, 1 in 6 newborns were born with torticollis, and mothers reported that the infants had felt “stuck” in the same position for several weeks before birth.26 The consequent restricted neck range of motion puts infants at risk of developing cranial deformations that may be prevented by changing their sleeping positions.26
What you’ll need to do. Check for limited neck function in the early weeks after birth and recommend neck motion exercises, if necessary, to encourage full head turning to both sides.19 Both torticollis and plagiocephaly due to static supine positioning can be largely eliminated with early written instructions about the value of tummy time when a baby is awake and supervised and the value of changing sleep positions.12 If repositioning or other forms of physical therapy fail to resolve the condition, surgical correction may be necessary.27
- Newer evidence indicates that the rebreathing of exhaled gases in the face-down position and the inability of the infant to reflexively lift his or her head may play a role in sudden infant death syndrome.28
- Nearly 13% of infants are still placed prone for sleep, according to an estimate from the National Infant Sleep Survey.29
- Resources are available from Pathways Awareness (www.pathwaysawareness.org), a not-for-profit foundation, to educate parents (and healthcare professionals) about early detection and intervention of motor delays in children. (The author is a member of the foundation’s Physicians’ Roundtable.)
Acknowledgement
I would like to acknowledge the review and comments of John F. Sarwark, MD.
CORRESPONDENCE
Russell Robertson, MD, Rosalind Franklin University of Medicine and Science, 3333 Green Bay Road North, Chicago, IL 60064; [email protected]
1. Willinger M, Hoffman HJ, Hartford RB. Infant sleep position and risk for sudden infant death syndrome: report of a meeting held January 13 and 14, 1994, National Institutes of Health, Bethesda, MD. Pediatrics. 1994;93:814-819.
2. Hauck FR, Tanabe KO. International trends in sudden infant death syndrome: stabilization of rates requires further action. Pediatrics. 2008;122:660-666.
3. Willinger M, James LS, Catz C. Defining the sudden infant death syndrome (SIDS): deliberations of an expert panel convened by the National Institute of Child Health and Human Development. Pediatr Pathol. 1991;11:677-684.
4. Moon RY, Horne RS, Hauck FR. Sudden infant death syndrome. Lancet. 2007;370:1578-1587.
5. Jantz JW, Blosser CD, Fruechting LA. A motor milestone change noted with a change in sleep position. Arch Pediatr Adolesc Med. 1997;151:565-568.
6. Dwyer T, Ponsonby AL. Sudden infant death syndrome and prone sleeping position. Ann Epidemiol. 2009;19:245-249.
7. Davis BE, Moon RY, Sachs HC, et al. Effects of sleep position on infant motor development. Pediatrics. 1998;102:1135-1140.
8. Perniciaro J. Development, behavior, and mental health. In: Tschudy MM, Arcara KM, eds. The Harriet Lane Handbook. 19th ed. Philadelphia, PA: Mosby; 2011;228:229.-
9. Changing concepts on sudden infant death syndrome: implications for infant sleeping environment and sleep position. American Academy of Pediatrics. Task Force on Infant Sleep Position and Sudden Infant Death Syndrome. Pediatrics. 2000;105:650-656.
10. Lijowska AS, Reed NW, Chiodini BA, et al. Sequential arousal behaviour in infants in asphyxial sleep environments. J Appl Physiol. 1997;83:219-228.
11. Majnemer A, Barr RG. Influence of supine sleep positioning on early motor milestone acquisition. Dev Med Child Neurol. 2005;47:370-376.
12. Jennings JT, Sarbaugh BG, Payne NS. Conveying the message about optimal infant positions. Phys Occup Ther Pediatr. 2005;25:3-18.
13. Ratliff-Schaub K, Hunt CE, Crowell D, et al. Relationship between infant sleep position and motor development in preterm infants. J Dev Behav Pediatr. 2001;22:293-299.
14. Kuo YL, Liao HF, Chen PC, et al. The influence of wakeful prone positioning on motor development during the early life. J Dev Behav Pediatr. 2008;295:367-376.
15. Dudek-Shriber L, Zelazny S. The effects of prone positioning on the quality and acquisition of developmental milestones in four-month-old infants. Pediatr Phys Ther. 2007;19:48-55.
16. Salls JS, Silverman LN, Gatty CM. The relationship of infant sleep and play positioning to motor milestone achievement. Am J Occup Ther. 2002;56:577-580.
17. Fetters L, Huang HH. Motor development and sleep, play, and feeding positions in very-low-birthweight infants with and without white matter disease. Dev Med Child Neurol. 2007;49:807-813.
18. Persing J, James H, Swanson J, et al. Prevention and management of positional skull deformities in infants—American Academy of Pediatrics clinical report. Pediatrics. 2003;112:199-202.
19. Hutchison BL, Hutchison LA, Thompson JM, et al. Plagiocephaly and brachycephaly in the first two years of life: a prospective cohort study. Pediatrics. 2004;114:970-980.
20. van Vlimmeren LA, van der Graaf Y, Boere-Boonekamp MM, et al. Risk factors for deformational plagiocephaly at birth and at 7 weeks of age: a prospective cohort study. Pediatrics. 2007;119:e408-e418.
21. Hutchison BL, Thompson JM, Mitchell EA. Determinants of nonsynostotic plagiocephaly: a case-control study. Pediatrics. 2003;112:e316.-
22. Xia JJ, Kennedy KA, Teichgraeber JF, et al. Nonsurgical treatment of deformational plagiocephaly: a systematic review. Arch Pediatr Adolesc Med. 2008;162:719-727.
23. Cheng JCY. Clinical determinants of the outcome of manual stretching in the treatment of congenital muscular torticollis in infants. A prospective study of eight hundred and twenty one cases. J Bone Joint Surg. 2001;83:679-687.
24. Cheng JCY, Tang SP, Chen TMK. The clinical presentation and outcome of treatment of congenital muscular torticollis in infants. A study of 1086 cases. J Pediatr Surg. 2000;35:1091-1096.
25. Clarren SK, Smith DW, Hanson JW. Helmet treatment for plagiocephaly and congenital muscular torticollis. J Pediatr. 1979;94:43-46.
26. Stellwagen L, Hubbard E, Chambers C, et al. Torticollis, facial asymmetry and plagiocephaly in normal newborns. Arch Dis Child. 2008;93:827-831.
27. de Chalain TM, Park S. Torticollis associated with positional plagiocephaly: a growing epidemic. J Craniofac Surg. 2005;16:411-418.
28. Kinney HC, Thach BT. The sudden infant death syndrome. N Engl J Med. 2009;361:795-805.
29. National Infant Sleep Position. Available at: http://dccwww.bumc.bu.edu/ChimeNisp/Main_Nisp.asp. Accessed February 8, 2010.
• Continue to advise parents to place their infants on their backs for sleeping, to prevent sudden infant death. A
• Educate parents about the value of supervised prone positioning (“tummy time”) during waking hours, which helps infants learn to raise their head, push up on their arms, and attain on-time milestones such as rolling over and unsupported sitting. A
• Tell parents that supervised abdominal positioning aids in preventing plagiocephaly and torticollis. B
Strength of recommendation (SOR)
A Good-quality patient-oriented evidence
B Inconsistent or limited-quality patient-oriented evidence
C Consensus, usual practice, opinion, disease-oriented evidence, case series
As happens with many interventions, the Back-to-Sleep campaign1 to prevent sudden infant death syndrome (SIDS) has led to unintended consequences. The campaign’s primary recommendation—that infants be placed on their backs for sleeping instead of on their stomachs—has of course yielded tremendous benefits. The prevalence of SIDS among healthy infants has dropped to 0.57 children per 1000 live births, totaling 2200 deaths per year, compared with 1.2 children per 1000 births in 1997.2-4 However, as the incidence of SIDS began to decline, it became apparent that children were experiencing delayed gross motor movement coincident with placement in the supine sleeping position5-7—or, more accurately, because parents following the Back-to-Sleep recommendation also generally avoided placing their infants in the prone position when they were awake.7
These delays become apparent as early as 2 to 3 months of age and manifest as the inability of an infant to raise his or her head when placed in the prone position.8 Because of this finding, the American Academy of Pediatrics modified its original recommendation for healthy infants, in part stating, “A certain amount of tummy time while the infant is awake and observed is recommended for developmental reasons….”9
In this article, I address the 3 most common unintended consequences for infants perpetually placed in the supine position: developmental motor delays, plagiocephaly (flattening of the occiput) and brachycephaly (widening of the skull), and congenital muscular torticollis (CMT) (a head tilt to one side). Each of these outcomes is preventable with vigilance in the care of newborns.
Prevent developmental motor delays with “tummy time”
The need for prone positioning, or “tummy time,” while an infant is awake cannot be overestimated. Particularly for preterm infants, a delayed acquisition of the ability to lift and turn the head could result in upper airway compromise or rebreathing and, thus, asphyxia.10 Infants who sleep in the supine position and exhibit delayed motor development by age 6 months very often are also found to have had their awake prone positioning restricted.11 In one study, delays in gross motor skills persisted in some cases to 15 months of age, and fine motor skills were delayed in 6-month-old infants who had little prone positioning.11 Infants who sleep in the side or supine position roll over later than those who sleep in the prone position.5 The TABLE compares mean age differences for milestone achievements with varying sleep positions.
On multiple regression analyses, awake prone positioning has consistently emerged as the most significant predictor of early motor development.11 For babies regularly placed in the prone position, the average Peabody Development Motor Scales-2 locomotion score has been significantly higher than that of babies not placed in the prone position when tested at 6 and 18 months.12 For infants routinely sleeping supine, supervised “prone to play” during waking hours enables them to practice prone-related motor skills such as head control.13
Infants with prone experience have attained the milestone of crawling on the abdomen significantly earlier than those without prone experience, leading to a higher 6-month gross motor development quotient.14 For children with just over an hour of daily prone positioning, an advantage in motor skill development has revealed itself as early as 4 months of age.15,16 Somewhat reassuring is evidence from one study that all infants, whether sleeping prone or supine, achieve all milestones within the accepted normal age range as long as prone positioning is initiated.7
What you’ll need to do. Stress to parents the importance of tummy time, or prone to play, in enabling normal developmental progression. Encourage this practice even if parents report that their infant cries or otherwise appears not to tolerate the prone position.15 In general, sleeping in the supine position does not negatively impact motor development as long as there is awake time with supervised prone positioning.17
TABLE
Mean age (months) for milestone acquisition
| Milestone | Prone sleepers | Mixed/side sleepers | Supine sleepers | P value* (linear regression)† |
|---|---|---|---|---|
| Rolls prone to supine | 3.93 ± 1.2 | 4.48 ± 1.8 | 4.87 ± 1.33 | .002 (.02) |
| Rolls supine to prone | 4.9 ± 1.3 | 4.97 ± 1.9 | 5.0 ± 1.6 | .95 |
| Sits supported | 4.7 ± 1.3 | 5.02 ± 1.4 | 5.13 ± 0.9 | .003 (.03) |
| Sits unsupported | 5.13 ± 1.1 | 5.17 ± 1.2 | 5.17 ± 1.0 | .80 |
| Transfers object | 5.87 ± 1.2 | 5.99 ± 6.5 | 6.23 ± 1.1 | .11 |
| Creeps | 6.07 ± 1.9 | 6.49 ± 1.9 | 7.23 ± 1.6 | .0002 (.001) |
| Crawls | 7.83 ± 2.0 | 8.47 ± 2.1 | 8.6 ± 1.7 | .003 (.05) |
| Pulls to stand | 8.1 ± 1.6 | 8.7 ± 1.5 | 8.77 ± 1.6 | .01 (.04) |
| Walks alone | 12.1 ± 2.0 | 12.2 ± 2.0 | 12.2 ± 1.7 | .4 |
| *Represents P value for prone sleepers vs supine sleepers. †Multivariate regression analysis controlling for infant size, gender, ethnicity, presence of siblings, and maternal education. Source: Davis BE, Moon RY, Sachs HC, et al. Pediatrics. 1998.7 Reproduced with permission of American Academy of Pediatrics. | ||||
Plagiocephaly and brachycephaly: Vary position for feeding, sleeping
Plagiocephaly and brachycephaly may occur as a consequence of prolonged supine positioning. Indeed, the incidence of plagiocephaly has increased since 1992, due largely to widespread adoption of the supine sleeping position.18 Plagiocephaly and/or brachycephaly is also more likely to occur in the first 4 months of life in infants who are male, firstborn, or who exhibit limited head rotation or low activity levels.19 Feeding with a bottle only and with the child’s head persistently placed to one side can lead to plagiocephaly.20
Delayed achievement of motor milestones is also associated with plagiocephaly, and tummy time to facilitate motor skill development helps protect against the deformity.20 Varying the head position when laying the infant down for sleep is also protective.21 One systematic review has shown considerable evidence that molding therapy with a helmet may reduce skull asymmetry more effectively than repositioning therapy.22
What you’ll need to do. Ask parents about their infant’s activity level, and encourage tummy time to protect against plagiocephaly. Also advise parents who bottle feed to alternate the feeding position between left and right arms.
Torticollis: Assess neck function in weeks after birth
Not only do infants with CMT display a head tilt to one side, but they also often have rotation of the head to the opposite side with the chin appearing to jut out.23 This postural deformity—primarily resulting from unilateral shortening and fibrosis of the sternocleidomastoid muscle24—is detectable at birth or shortly thereafter. CMT occurs in 1 of every 300 live births.25 Torticollis discovered at birth is likely related to a constrained intrauterine position. In one study, 1 in 6 newborns were born with torticollis, and mothers reported that the infants had felt “stuck” in the same position for several weeks before birth.26 The consequent restricted neck range of motion puts infants at risk of developing cranial deformations that may be prevented by changing their sleeping positions.26
What you’ll need to do. Check for limited neck function in the early weeks after birth and recommend neck motion exercises, if necessary, to encourage full head turning to both sides.19 Both torticollis and plagiocephaly due to static supine positioning can be largely eliminated with early written instructions about the value of tummy time when a baby is awake and supervised and the value of changing sleep positions.12 If repositioning or other forms of physical therapy fail to resolve the condition, surgical correction may be necessary.27
- Newer evidence indicates that the rebreathing of exhaled gases in the face-down position and the inability of the infant to reflexively lift his or her head may play a role in sudden infant death syndrome.28
- Nearly 13% of infants are still placed prone for sleep, according to an estimate from the National Infant Sleep Survey.29
- Resources are available from Pathways Awareness (www.pathwaysawareness.org), a not-for-profit foundation, to educate parents (and healthcare professionals) about early detection and intervention of motor delays in children. (The author is a member of the foundation’s Physicians’ Roundtable.)
Acknowledgement
I would like to acknowledge the review and comments of John F. Sarwark, MD.
CORRESPONDENCE
Russell Robertson, MD, Rosalind Franklin University of Medicine and Science, 3333 Green Bay Road North, Chicago, IL 60064; [email protected]
• Continue to advise parents to place their infants on their backs for sleeping, to prevent sudden infant death. A
• Educate parents about the value of supervised prone positioning (“tummy time”) during waking hours, which helps infants learn to raise their head, push up on their arms, and attain on-time milestones such as rolling over and unsupported sitting. A
• Tell parents that supervised abdominal positioning aids in preventing plagiocephaly and torticollis. B
Strength of recommendation (SOR)
A Good-quality patient-oriented evidence
B Inconsistent or limited-quality patient-oriented evidence
C Consensus, usual practice, opinion, disease-oriented evidence, case series
As happens with many interventions, the Back-to-Sleep campaign1 to prevent sudden infant death syndrome (SIDS) has led to unintended consequences. The campaign’s primary recommendation—that infants be placed on their backs for sleeping instead of on their stomachs—has of course yielded tremendous benefits. The prevalence of SIDS among healthy infants has dropped to 0.57 children per 1000 live births, totaling 2200 deaths per year, compared with 1.2 children per 1000 births in 1997.2-4 However, as the incidence of SIDS began to decline, it became apparent that children were experiencing delayed gross motor movement coincident with placement in the supine sleeping position5-7—or, more accurately, because parents following the Back-to-Sleep recommendation also generally avoided placing their infants in the prone position when they were awake.7
These delays become apparent as early as 2 to 3 months of age and manifest as the inability of an infant to raise his or her head when placed in the prone position.8 Because of this finding, the American Academy of Pediatrics modified its original recommendation for healthy infants, in part stating, “A certain amount of tummy time while the infant is awake and observed is recommended for developmental reasons….”9
In this article, I address the 3 most common unintended consequences for infants perpetually placed in the supine position: developmental motor delays, plagiocephaly (flattening of the occiput) and brachycephaly (widening of the skull), and congenital muscular torticollis (CMT) (a head tilt to one side). Each of these outcomes is preventable with vigilance in the care of newborns.
Prevent developmental motor delays with “tummy time”
The need for prone positioning, or “tummy time,” while an infant is awake cannot be overestimated. Particularly for preterm infants, a delayed acquisition of the ability to lift and turn the head could result in upper airway compromise or rebreathing and, thus, asphyxia.10 Infants who sleep in the supine position and exhibit delayed motor development by age 6 months very often are also found to have had their awake prone positioning restricted.11 In one study, delays in gross motor skills persisted in some cases to 15 months of age, and fine motor skills were delayed in 6-month-old infants who had little prone positioning.11 Infants who sleep in the side or supine position roll over later than those who sleep in the prone position.5 The TABLE compares mean age differences for milestone achievements with varying sleep positions.
On multiple regression analyses, awake prone positioning has consistently emerged as the most significant predictor of early motor development.11 For babies regularly placed in the prone position, the average Peabody Development Motor Scales-2 locomotion score has been significantly higher than that of babies not placed in the prone position when tested at 6 and 18 months.12 For infants routinely sleeping supine, supervised “prone to play” during waking hours enables them to practice prone-related motor skills such as head control.13
Infants with prone experience have attained the milestone of crawling on the abdomen significantly earlier than those without prone experience, leading to a higher 6-month gross motor development quotient.14 For children with just over an hour of daily prone positioning, an advantage in motor skill development has revealed itself as early as 4 months of age.15,16 Somewhat reassuring is evidence from one study that all infants, whether sleeping prone or supine, achieve all milestones within the accepted normal age range as long as prone positioning is initiated.7
What you’ll need to do. Stress to parents the importance of tummy time, or prone to play, in enabling normal developmental progression. Encourage this practice even if parents report that their infant cries or otherwise appears not to tolerate the prone position.15 In general, sleeping in the supine position does not negatively impact motor development as long as there is awake time with supervised prone positioning.17
TABLE
Mean age (months) for milestone acquisition
| Milestone | Prone sleepers | Mixed/side sleepers | Supine sleepers | P value* (linear regression)† |
|---|---|---|---|---|
| Rolls prone to supine | 3.93 ± 1.2 | 4.48 ± 1.8 | 4.87 ± 1.33 | .002 (.02) |
| Rolls supine to prone | 4.9 ± 1.3 | 4.97 ± 1.9 | 5.0 ± 1.6 | .95 |
| Sits supported | 4.7 ± 1.3 | 5.02 ± 1.4 | 5.13 ± 0.9 | .003 (.03) |
| Sits unsupported | 5.13 ± 1.1 | 5.17 ± 1.2 | 5.17 ± 1.0 | .80 |
| Transfers object | 5.87 ± 1.2 | 5.99 ± 6.5 | 6.23 ± 1.1 | .11 |
| Creeps | 6.07 ± 1.9 | 6.49 ± 1.9 | 7.23 ± 1.6 | .0002 (.001) |
| Crawls | 7.83 ± 2.0 | 8.47 ± 2.1 | 8.6 ± 1.7 | .003 (.05) |
| Pulls to stand | 8.1 ± 1.6 | 8.7 ± 1.5 | 8.77 ± 1.6 | .01 (.04) |
| Walks alone | 12.1 ± 2.0 | 12.2 ± 2.0 | 12.2 ± 1.7 | .4 |
| *Represents P value for prone sleepers vs supine sleepers. †Multivariate regression analysis controlling for infant size, gender, ethnicity, presence of siblings, and maternal education. Source: Davis BE, Moon RY, Sachs HC, et al. Pediatrics. 1998.7 Reproduced with permission of American Academy of Pediatrics. | ||||
Plagiocephaly and brachycephaly: Vary position for feeding, sleeping
Plagiocephaly and brachycephaly may occur as a consequence of prolonged supine positioning. Indeed, the incidence of plagiocephaly has increased since 1992, due largely to widespread adoption of the supine sleeping position.18 Plagiocephaly and/or brachycephaly is also more likely to occur in the first 4 months of life in infants who are male, firstborn, or who exhibit limited head rotation or low activity levels.19 Feeding with a bottle only and with the child’s head persistently placed to one side can lead to plagiocephaly.20
Delayed achievement of motor milestones is also associated with plagiocephaly, and tummy time to facilitate motor skill development helps protect against the deformity.20 Varying the head position when laying the infant down for sleep is also protective.21 One systematic review has shown considerable evidence that molding therapy with a helmet may reduce skull asymmetry more effectively than repositioning therapy.22
What you’ll need to do. Ask parents about their infant’s activity level, and encourage tummy time to protect against plagiocephaly. Also advise parents who bottle feed to alternate the feeding position between left and right arms.
Torticollis: Assess neck function in weeks after birth
Not only do infants with CMT display a head tilt to one side, but they also often have rotation of the head to the opposite side with the chin appearing to jut out.23 This postural deformity—primarily resulting from unilateral shortening and fibrosis of the sternocleidomastoid muscle24—is detectable at birth or shortly thereafter. CMT occurs in 1 of every 300 live births.25 Torticollis discovered at birth is likely related to a constrained intrauterine position. In one study, 1 in 6 newborns were born with torticollis, and mothers reported that the infants had felt “stuck” in the same position for several weeks before birth.26 The consequent restricted neck range of motion puts infants at risk of developing cranial deformations that may be prevented by changing their sleeping positions.26
What you’ll need to do. Check for limited neck function in the early weeks after birth and recommend neck motion exercises, if necessary, to encourage full head turning to both sides.19 Both torticollis and plagiocephaly due to static supine positioning can be largely eliminated with early written instructions about the value of tummy time when a baby is awake and supervised and the value of changing sleep positions.12 If repositioning or other forms of physical therapy fail to resolve the condition, surgical correction may be necessary.27
- Newer evidence indicates that the rebreathing of exhaled gases in the face-down position and the inability of the infant to reflexively lift his or her head may play a role in sudden infant death syndrome.28
- Nearly 13% of infants are still placed prone for sleep, according to an estimate from the National Infant Sleep Survey.29
- Resources are available from Pathways Awareness (www.pathwaysawareness.org), a not-for-profit foundation, to educate parents (and healthcare professionals) about early detection and intervention of motor delays in children. (The author is a member of the foundation’s Physicians’ Roundtable.)
Acknowledgement
I would like to acknowledge the review and comments of John F. Sarwark, MD.
CORRESPONDENCE
Russell Robertson, MD, Rosalind Franklin University of Medicine and Science, 3333 Green Bay Road North, Chicago, IL 60064; [email protected]
1. Willinger M, Hoffman HJ, Hartford RB. Infant sleep position and risk for sudden infant death syndrome: report of a meeting held January 13 and 14, 1994, National Institutes of Health, Bethesda, MD. Pediatrics. 1994;93:814-819.
2. Hauck FR, Tanabe KO. International trends in sudden infant death syndrome: stabilization of rates requires further action. Pediatrics. 2008;122:660-666.
3. Willinger M, James LS, Catz C. Defining the sudden infant death syndrome (SIDS): deliberations of an expert panel convened by the National Institute of Child Health and Human Development. Pediatr Pathol. 1991;11:677-684.
4. Moon RY, Horne RS, Hauck FR. Sudden infant death syndrome. Lancet. 2007;370:1578-1587.
5. Jantz JW, Blosser CD, Fruechting LA. A motor milestone change noted with a change in sleep position. Arch Pediatr Adolesc Med. 1997;151:565-568.
6. Dwyer T, Ponsonby AL. Sudden infant death syndrome and prone sleeping position. Ann Epidemiol. 2009;19:245-249.
7. Davis BE, Moon RY, Sachs HC, et al. Effects of sleep position on infant motor development. Pediatrics. 1998;102:1135-1140.
8. Perniciaro J. Development, behavior, and mental health. In: Tschudy MM, Arcara KM, eds. The Harriet Lane Handbook. 19th ed. Philadelphia, PA: Mosby; 2011;228:229.-
9. Changing concepts on sudden infant death syndrome: implications for infant sleeping environment and sleep position. American Academy of Pediatrics. Task Force on Infant Sleep Position and Sudden Infant Death Syndrome. Pediatrics. 2000;105:650-656.
10. Lijowska AS, Reed NW, Chiodini BA, et al. Sequential arousal behaviour in infants in asphyxial sleep environments. J Appl Physiol. 1997;83:219-228.
11. Majnemer A, Barr RG. Influence of supine sleep positioning on early motor milestone acquisition. Dev Med Child Neurol. 2005;47:370-376.
12. Jennings JT, Sarbaugh BG, Payne NS. Conveying the message about optimal infant positions. Phys Occup Ther Pediatr. 2005;25:3-18.
13. Ratliff-Schaub K, Hunt CE, Crowell D, et al. Relationship between infant sleep position and motor development in preterm infants. J Dev Behav Pediatr. 2001;22:293-299.
14. Kuo YL, Liao HF, Chen PC, et al. The influence of wakeful prone positioning on motor development during the early life. J Dev Behav Pediatr. 2008;295:367-376.
15. Dudek-Shriber L, Zelazny S. The effects of prone positioning on the quality and acquisition of developmental milestones in four-month-old infants. Pediatr Phys Ther. 2007;19:48-55.
16. Salls JS, Silverman LN, Gatty CM. The relationship of infant sleep and play positioning to motor milestone achievement. Am J Occup Ther. 2002;56:577-580.
17. Fetters L, Huang HH. Motor development and sleep, play, and feeding positions in very-low-birthweight infants with and without white matter disease. Dev Med Child Neurol. 2007;49:807-813.
18. Persing J, James H, Swanson J, et al. Prevention and management of positional skull deformities in infants—American Academy of Pediatrics clinical report. Pediatrics. 2003;112:199-202.
19. Hutchison BL, Hutchison LA, Thompson JM, et al. Plagiocephaly and brachycephaly in the first two years of life: a prospective cohort study. Pediatrics. 2004;114:970-980.
20. van Vlimmeren LA, van der Graaf Y, Boere-Boonekamp MM, et al. Risk factors for deformational plagiocephaly at birth and at 7 weeks of age: a prospective cohort study. Pediatrics. 2007;119:e408-e418.
21. Hutchison BL, Thompson JM, Mitchell EA. Determinants of nonsynostotic plagiocephaly: a case-control study. Pediatrics. 2003;112:e316.-
22. Xia JJ, Kennedy KA, Teichgraeber JF, et al. Nonsurgical treatment of deformational plagiocephaly: a systematic review. Arch Pediatr Adolesc Med. 2008;162:719-727.
23. Cheng JCY. Clinical determinants of the outcome of manual stretching in the treatment of congenital muscular torticollis in infants. A prospective study of eight hundred and twenty one cases. J Bone Joint Surg. 2001;83:679-687.
24. Cheng JCY, Tang SP, Chen TMK. The clinical presentation and outcome of treatment of congenital muscular torticollis in infants. A study of 1086 cases. J Pediatr Surg. 2000;35:1091-1096.
25. Clarren SK, Smith DW, Hanson JW. Helmet treatment for plagiocephaly and congenital muscular torticollis. J Pediatr. 1979;94:43-46.
26. Stellwagen L, Hubbard E, Chambers C, et al. Torticollis, facial asymmetry and plagiocephaly in normal newborns. Arch Dis Child. 2008;93:827-831.
27. de Chalain TM, Park S. Torticollis associated with positional plagiocephaly: a growing epidemic. J Craniofac Surg. 2005;16:411-418.
28. Kinney HC, Thach BT. The sudden infant death syndrome. N Engl J Med. 2009;361:795-805.
29. National Infant Sleep Position. Available at: http://dccwww.bumc.bu.edu/ChimeNisp/Main_Nisp.asp. Accessed February 8, 2010.
1. Willinger M, Hoffman HJ, Hartford RB. Infant sleep position and risk for sudden infant death syndrome: report of a meeting held January 13 and 14, 1994, National Institutes of Health, Bethesda, MD. Pediatrics. 1994;93:814-819.
2. Hauck FR, Tanabe KO. International trends in sudden infant death syndrome: stabilization of rates requires further action. Pediatrics. 2008;122:660-666.
3. Willinger M, James LS, Catz C. Defining the sudden infant death syndrome (SIDS): deliberations of an expert panel convened by the National Institute of Child Health and Human Development. Pediatr Pathol. 1991;11:677-684.
4. Moon RY, Horne RS, Hauck FR. Sudden infant death syndrome. Lancet. 2007;370:1578-1587.
5. Jantz JW, Blosser CD, Fruechting LA. A motor milestone change noted with a change in sleep position. Arch Pediatr Adolesc Med. 1997;151:565-568.
6. Dwyer T, Ponsonby AL. Sudden infant death syndrome and prone sleeping position. Ann Epidemiol. 2009;19:245-249.
7. Davis BE, Moon RY, Sachs HC, et al. Effects of sleep position on infant motor development. Pediatrics. 1998;102:1135-1140.
8. Perniciaro J. Development, behavior, and mental health. In: Tschudy MM, Arcara KM, eds. The Harriet Lane Handbook. 19th ed. Philadelphia, PA: Mosby; 2011;228:229.-
9. Changing concepts on sudden infant death syndrome: implications for infant sleeping environment and sleep position. American Academy of Pediatrics. Task Force on Infant Sleep Position and Sudden Infant Death Syndrome. Pediatrics. 2000;105:650-656.
10. Lijowska AS, Reed NW, Chiodini BA, et al. Sequential arousal behaviour in infants in asphyxial sleep environments. J Appl Physiol. 1997;83:219-228.
11. Majnemer A, Barr RG. Influence of supine sleep positioning on early motor milestone acquisition. Dev Med Child Neurol. 2005;47:370-376.
12. Jennings JT, Sarbaugh BG, Payne NS. Conveying the message about optimal infant positions. Phys Occup Ther Pediatr. 2005;25:3-18.
13. Ratliff-Schaub K, Hunt CE, Crowell D, et al. Relationship between infant sleep position and motor development in preterm infants. J Dev Behav Pediatr. 2001;22:293-299.
14. Kuo YL, Liao HF, Chen PC, et al. The influence of wakeful prone positioning on motor development during the early life. J Dev Behav Pediatr. 2008;295:367-376.
15. Dudek-Shriber L, Zelazny S. The effects of prone positioning on the quality and acquisition of developmental milestones in four-month-old infants. Pediatr Phys Ther. 2007;19:48-55.
16. Salls JS, Silverman LN, Gatty CM. The relationship of infant sleep and play positioning to motor milestone achievement. Am J Occup Ther. 2002;56:577-580.
17. Fetters L, Huang HH. Motor development and sleep, play, and feeding positions in very-low-birthweight infants with and without white matter disease. Dev Med Child Neurol. 2007;49:807-813.
18. Persing J, James H, Swanson J, et al. Prevention and management of positional skull deformities in infants—American Academy of Pediatrics clinical report. Pediatrics. 2003;112:199-202.
19. Hutchison BL, Hutchison LA, Thompson JM, et al. Plagiocephaly and brachycephaly in the first two years of life: a prospective cohort study. Pediatrics. 2004;114:970-980.
20. van Vlimmeren LA, van der Graaf Y, Boere-Boonekamp MM, et al. Risk factors for deformational plagiocephaly at birth and at 7 weeks of age: a prospective cohort study. Pediatrics. 2007;119:e408-e418.
21. Hutchison BL, Thompson JM, Mitchell EA. Determinants of nonsynostotic plagiocephaly: a case-control study. Pediatrics. 2003;112:e316.-
22. Xia JJ, Kennedy KA, Teichgraeber JF, et al. Nonsurgical treatment of deformational plagiocephaly: a systematic review. Arch Pediatr Adolesc Med. 2008;162:719-727.
23. Cheng JCY. Clinical determinants of the outcome of manual stretching in the treatment of congenital muscular torticollis in infants. A prospective study of eight hundred and twenty one cases. J Bone Joint Surg. 2001;83:679-687.
24. Cheng JCY, Tang SP, Chen TMK. The clinical presentation and outcome of treatment of congenital muscular torticollis in infants. A study of 1086 cases. J Pediatr Surg. 2000;35:1091-1096.
25. Clarren SK, Smith DW, Hanson JW. Helmet treatment for plagiocephaly and congenital muscular torticollis. J Pediatr. 1979;94:43-46.
26. Stellwagen L, Hubbard E, Chambers C, et al. Torticollis, facial asymmetry and plagiocephaly in normal newborns. Arch Dis Child. 2008;93:827-831.
27. de Chalain TM, Park S. Torticollis associated with positional plagiocephaly: a growing epidemic. J Craniofac Surg. 2005;16:411-418.
28. Kinney HC, Thach BT. The sudden infant death syndrome. N Engl J Med. 2009;361:795-805.
29. National Infant Sleep Position. Available at: http://dccwww.bumc.bu.edu/ChimeNisp/Main_Nisp.asp. Accessed February 8, 2010.
Elbow injuries: Getting kids back in the game
• Administer the valgus stress test, the “milking maneuver,” and the moving valgus stress test to athletes suspected of having ulnar collateral ligament injury. C
• Treat Little League elbow with nonsteroidal anti-inflammatory drugs, ice, brief immobilization, and a 4- to 6-week “break” from throwing. A
• Advise young baseball players (and their parents) to avoid pitching year-round, and to get 3 months of rest per year. A
Strength of recommendation (SOR)
A Good-quality patient-oriented evidence
B Inconsistent or limited-quality patient-oriented evidence
C Consensus, usual practice, opinion, disease-oriented evidence, case series
The growing popularity of club teams and year-round participation in sports has spawned an epidemic of elbow injuries in primary and secondary school students and young adults alike. The incidence of elbow pain in children engaged in sports that require overhead throwing, such as baseball, football, volleyball, tennis, and javelin, ranges from 45% to 78%.1
Fortunately, acute traumatic elbow injury, with pain severe enough to force the athlete to cease participation entirely, is relatively rare, accounting for only 1% to 5% of cases.1,2 Far more often, elbow pain is associated with overuse, resulting in a gradual onset of medial elbow soreness that does not prevent the athlete from playing.
When an athlete seeks care for elbow pain, there are a number of things to consider, including the patient’s age, skeletal maturity, and type and frequency of throwing. Younger “throwers” typically incur injuries related to the physes, while adolescents and adults are more likely to sustain injuries to the ligaments and tendons.3 In both cases, repetitive valgus stress is the mechanism of injury. This review—of elbow anatomy (see the box),4-6 injury, differential diagnosis, and treatment—will make it easier for you to get injured athletes back in the game.

The elbow has 3 articulations—ulnohumeral, radiocapitellar, and proximal radioulnar—that provide primary stability to valgus stress. The elbow’s soft tissue restraints include 2 ligament complexes (medial and lateral collateral), 4 muscle groups (flexors, extensors, pronators, supinators), and 3 major nerves (radial, median, ulnar) and their branches.
The ulnar collateral ligament (UCL) complex—which consists of the anterior and posterior bundles and the transverse ligament—is the main source of medial elbow stability. 4 Mechanical stability for overhead throwing is provided by both bony and soft tissue restraints. During the pitching motion, the forces generated exceed the UCL’s tensile strength, and protective flexor muscles are activated.5,6
And the pitch…There are 6 stages of throwing: windup, early cocking, late cocking, acceleration, deceleration, and follow-through. Elbow pain is most likely during the late-cocking or early acceleration phase of a throw, the point of ball/javelin release, or the moment the racquet hits the ball.4
Is it Little League elbow? Start with a targeted history
In skeletally immature athletes, open physes result in the epicondylar apophysis being the weakest structure on the medial aspect of the elbow. Thus, repetitive valgus stress and tension overload often lead to “Little League elbow”—an umbrella term with a differential diagnosis that encompasses medial epicondylar fragmentation, delayed or accelerated growth of the medial epicondyle, and delayed closure of its growth plate, among other conditions (TABLE 1).3,7,8
In more mature athletes, repetitive microtrauma to the ulnar collateral ligament (UCL) leads to its gradual attenuation or complete failure.7 This increases the stress on the radiocapitellar joint and olecranon, and can lead to edema, scarring, calcification, osteophyte formation, medial epicondylitis, ulnar nerve neurapraxia, or radiocapitellar chondral damage.9 Extended practices and tournaments, with no substantial rest period throughout the year, put adolescents at increased risk for UCL injuries.10
Regardless of age, the medical history of an athlete with elbow pain should elicit information about the mechanism of injury; the location, duration, and quality of the pain; factors that alleviate or exacerbate the pain; the presence of weakness or paresthesias; and the extent to which the pain has affected the patient’s ability to throw. Patients with chronic UCL injuries, for example, often report a loss of arm control and decrease in throwing speed. It is also important to address hand dominance, level of participation, the position played, changes in technique or training regimen, prior injuries, and the effects of any previous treatment.11
TABLE 1
Differential diagnosis of elbow injuries
| Location | Differential diagnosis |
|---|---|
| Medial | Little League elbow
|
| Anterior | Anterior capsule strain Biceps tendon rupture Biceps tendonitis Dislocation Median nerve compression (pronator) syndrome |
| Posterior | Olecranon bursitis Olecranon process or tip stress fracture Triceps rupture/olecranon avulsion Triceps tendonitis Trochlear rupture Valgus overload syndrome (posterior olecranon impingement syndrome) |
| Lateral | Capitellum fracture Lateral epicondylitis Lateral ulnar collateral ligament injury Osteochondritis dissecans Posterior interosseous nerve syndrome Posterolateral rotary instability Radial head fracture Radiocapitellar chondromalacia |
| Adapted from: McKeag DB, Moeller JL. ACSM’s Primary Care Sports Medicine. 2nd ed.3 | |
Compare the affected and uninjured extremities
Inspect, palpate, and assess the active and passive range of motion, strength, and neurovascular status of both arms, with the uninjured side serving as a comparison. The scapula, shoulder, and wrist are also involved in throwing, so these joints should be examined along with the elbow.
Measure range of motion. Normal ranges for the flexion-extension arc are 0 to 140°, with 75° of pronation and 82° of supination.12 Use a goniometer, if available, to ensure accuracy and reproducibility,1 and pay close attention to the position that elicits pain.
In medial epicondylitis, the full range of motion should be preserved. Patients experience pain at the medial epicondyle and overlying flexor-pronator mass proximately, and pain or weakness with resisted wrist flexion, and resisted pronation, at full extension.4,11 Flexor-pronator strain will produce similar findings, but edema or ecchymosis may be present and there may be pain immediately distal to the medial epicondyle.11
Pain associated with injury to the UCL—which courses distal and slightly posterior to the medial epicondyle—typically occurs 2 cm distal to the medial epicondyle over the anterior bundle. Tenderness over the UCL has a sensitivity of 81% to 94% for UCL tears, but a specificity of only 22%.13
Physical maneuvers can help identify source of elbow pain
A complete UCL tear can cause valgus gapping as small as 3 mm, which makes it difficult to detect on physical exam alone.4 Orthopedic and sports medicine literature recommend that 3 maneuvers be used to identify UCL pathology:4,14,15
The valgus stress test (FIGURE 1) assesses the effects of valgus stress on the UCL. Gapping >3 mm signifies UCL instability. The test has a sensitivity of 66% and a specificity of 60% for detecting a UCL strain or tear.13,16
The milking maneuver (FIGURE 2), performed by the patient (or by a clinician if the patient lacks flexibility), reproduces a common pitching exercise. Medial elbow pain or apprehension indicates UCL injury.13,16
The moving valgus stress test (FIGURE 3A-C) is done in an effort to recreate the flexion angles of the elbow during the late cocking and early acceleration phases of throwing. Pain anywhere in the arc of motion suggests a UCL injury; pain elicited at 45° of flexion suggests osteochondrosis of the humeral capitellum, while pain closer to full extension suggests osteochondrosis of the trochlea.13,16
FIGURE 1
Valgus stress test
With the injured elbow at 30° of flexion, the shoulder abducted and fully externally rotated, and the patient’s wrist under your arm, place one hand laterally over the elbow. Place the other hand under the ulna and the thumb over the ulnar collateral ligament and apply valgus stress. Gapping >3 mm is abnormal.
FIGURE 2
Milking maneuver
The patient grasps the thumb of the affected arm and pulls downward, with the affected elbow positioned as shown, stressing the ulnar collateral ligament (UCL). Elbow pain or apprehension is positive for UCL injury.
FIGURE 3
Moving valgus stress test
With the shoulder in abduction and maximum external rotation (A), place the elbow in maximum flexion and apply valgus force (B), and extend the elbow from full flexion to full extension (C) in an attempt to reproduce the medial pain.
Does your patient have 2 positive valgus tests and posterior pain?
Valgus extension overload syndrome, which is caused by repetitive stress and results in osteophytes, chondromalacia of the medial olecranon fossa, tension in the UCL, and compression of the radiocapitellar joint, will also produce positive valgus stress and positive moving valgus stress tests. Keep in mind, however, that patients with valgus extension overload often have loss of full extension and posterior elbow pain with forced elbow hyperextension.17
Look for ulnar nerve injury
The physical examination should also be used to test for ulnar nerve injury. The elbow flexion test—a provocative maneuver in which the patient flexes the elbow as far as possible and reports any tingling or numbness of the hand—should be included in the work-up. Symptoms that develop in <60 seconds indicate a positive test for ulnar nerve compression, with the pinky and ulnar half of the ring finger most likely to have loss of vibration and light touch perception. A positive Tinel’s sign over the cubital tunnel is an indication of ulnar neuritis.18
If the ulnar nerve moves out of the ulnar groove when the groove is palpated as the elbow is flexed and extended, subluxating ulnar nerve is the likely diagnosis. If 2 structures displace over the medial epicondyle with elbow flexion, the first will be the ulnar nerve and the second will be the medial head of the triceps—an indication of a snapping medial head of triceps.18
Imaging studies may require a second look
Imaging studies are sometimes used to further aid in diagnosis of elbow injury. However, standard elbow x-rays, including an anteroposterior view in full extension, an oblique view, and a lateral view at 90° flexion, can be deceiving, as they often appear normal in conditions causing medial elbow pain associated with overhead throwing.
Careful review of the images may be needed to rule out fracture and other conditions, keeping the following factors in mind:
- A supracondylar fracture is likely if the anterior humeral line that is drawn along the anterior surface of the humeral cortex (on a lateral view) does not transect the middle third of the midcapitellum.3,11,18
- Dislocation of the radial head is suggested if the radiocapitellar line (drawn through the center of the radial head and neck) does not transect the midcapitellum on a lateral view.3,11,18
- Intra-articular injury with a joint effusion is indicated when an enlarged anterior fat pad, which is slightly anterior to the distal humeral diaphysis, is visible (the “sail sign”) on a normal elbow radiograph.3,11,18
- A fracture is likely if a posterior fat pad (which lies in the olecranon fossa and is not usually visible unless an effusion elevates the fat pad away from the cortex) is visible on an elbow x-ray. 3,11,18
- A chronic UCL tear is suggested by heterotropic calcification of the UCL.19
It is useful to x-ray both the injured and the unaffected elbows in skeletally immature athletes to compare secondary ossification centers. Little League elbow demonstrates a widening of the medial epicondyle physis, for example, when the x-rays are compared.3 Secondary ossification centers of the elbow appear first at the capitellum (age 2), followed by the radial head (age 5), medial epicondyle (age 7), trochlea (age 9), and lateral epicondyle (age 11). Most ossification centers fuse between 14 and 17 years of age.3
Computed tomography arthrograms, magnetic resonance imaging (MRI), and ultrasonography are also used to identify UCL tears. MRI, which can reveal injuries to cartilage and tendons as well, is the most commonly used imaging technique for musculoskeletal diagnosis of the elbow.16,20
Treatment gets most athletes back on track
Most medial elbow injuries respond to conservative treatment—typically, with some combination of activity modification, nonsteroidal anti-inflammatory drugs (NSAIDs), icing, physical therapy aimed at flexor-pronator strengthening, and counterforce bracing.11 Medial epicondylosis and flexor-pronator strain injuries have an excellent prognosis, with more than 90% of patients back to their previous level of activity at 1 year. Initial treatment consists of a 2- to 3-week rest period, followed by a 6- to 12-week rehabilitation protocol.11
Randomized controlled trials have found limited evidence of short-term improvement in symptoms with corticosteroid injections compared with placebo or no treatment, local anesthetic, orthosis, physical therapy, and NSAIDs. However, corticosteroids were less effective than physiotherapy or oral NSAIDs in improving long-term outcomes.21 Despite a paucity of well-designed studies to prove their use, autologous blood, platelet-rich plasma, and botulinum toxin are sometimes used for refractory elbow pain.21
Treatment of Little League elbow consists of cessation of throwing for at least 4 to 6 weeks, with a gradual return to throwing and emphasis on proper throwing mechanics after the pain resolves. Most throwers are out of competition for 2 to 3 months, but fully recover with nonoperative management.21
UCL injuries, too, are initially treated with rest, NSAIDs, icing, bracing, and physical therapy, typically with 2 to 3 months of no throwing. Some patients also use a splint at 90° flexion at night and as needed for pain during the day. Patients whose symptoms last more than a year despite treatment may be candidates for arthroscopic debridement.11
Consider reconstruction when nonsurgical management fails
UCL reconstruction was introduced in 1974, when reconstruction was performed on professional pitcher Tommy John, who went on to win 164 games.4,9 The procedure has since undergone numerous modifications. Surgery is indicated for acute rupture, significant chronic instability, insufficient UCL tissue after debridement, or recurrent pain and valgus instability with throwing after rehabilitation.2,4,6,9
Reconstruction generally entails fixing a tendon graft through bone tunnels in the medial epicondyle of the humerus and sublime tubercle of the ulna to reestablish valgus stability. A recent systematic review of reconstruction methods found a 76% to 95% rate of excellent results, with patients returned to their prior level of activity at a mean follow-up of 1 year.22 Rehabilitation typically begins 7 days postop; throwing (without windup) may begin in 4 to 5 months, with a gradual increase in speed and force and a return to the game at 12 months.
A stepped-up focus on prevention
The increase in UCL injuries in adolescents highlights the need for greater emphasis on prevention.10 Several governing bodies, including USA Baseball and the American Academy of Pediatrics, have developed research-based guidelines for young athletes (TABLE 2).1,10,23-25
One of the easiest to follow is to limit an athlete’s weekly pitch count to 10 times his age. Thus, a 10 year old should pitch no more than 100 pitches in a given 7-day period. Another important measure—in addition to ensuring that young athletes receive instruction in proper pitching mechanics (see http://www.littleleague.org/Little_League_Online.htm)—is to urge coaches and parents to require players to get at least 3 months of rest after each season and to stop throwing if they have pain or fatigue.24
TABLE 2
Keeping young pitchers injury-free1,10,23-25
| Recommendations for coaches and parents |
|---|
| Record the number of pitches thrown at each outing/sports event for all young pitchers |
| Avoid allowing young athletes to pitch competitively >8 months per year |
| Limit the number of pitches to ≤2500 per year and 10 × the pitcher’s age per week, or 90 per outing |
| Ensure that young pitchers are instructed in proper pitching mechanics |
| Restrict throwing breaking ball pitches* prior to puberty |
| Ensure that young pitchers get 3 months of rest per year. |
| *A pitch that changes direction either sideways or downwards as it approaches the batter, eg, a slider or curve ball. |
CORRESPONDENCE
Jennifer A. Southard, MD, MSc, Saint Alphonsus Medical Group, 6533 Emerald Street, Boise, ID 83704; [email protected]
1. American Academy of Pediatrics Committee on Sports Medicine and Fitness. Risk of injury from baseball and softball in children. Pediatrics. 2001;107:782-784.
2. Maloney MD, Morhr KJ, el Attrache NS, et al. Elbow injuries in the throwing athlete. Clin Sports Med. 1999;18:795-809.
3. McKeag DB, Moeller JL. ACSM’s Primary Care Sports Medicine. 2nd ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2007:387–402.
4. Hariri S, Safran MR. Ulnar collateral ligament injury in the overhead athlete. Clin Sports Med. 2010;29:619-644.
5. Park MJ, Kim HG, Lee JY. Surgical treatment of post-traumatic stiffness of the elbow. J Bone Joint Surg Br. 2004;86:1158-1162.
6. Lin F, Kohli N, Perlmutter S, et al. Muscle contribution to elbow joint valgus stability. J Shoulder Elbow Surg. 2007;16:795-802.
7. Fleisig GS, Andrews JR, Dillman CJ, et al. Kinetics of baseball pitching with implications about injury mechanisms. Am J Sports Med. 1995;23:233-239.
8. Baker CL, Romero AA. Osteochondritis dissecans of the capitellum. Am J Sports Med. 2010;38:1917-1928.
9. Cain EL, Andrews JR, Dugas JR, et al. Outcome of ulnar collateral ligament reconstruction of the elbow in 1281 athletes: results in 743 athletes with minimum 2-year follow-up. Am J Sports Med. 2010;38:2426-2434.
10. Fleisig GS, Andrews JR, Cutter GR, et al. Prevention of elbow injuries in youth baseball pitchers. Curr Sports Med Rep. 2009;8:250-254.
11. Madden CC, Putukian M, McCarty E, et al. Netter’s Sports Medicine. Philadelphia, PA: Saunders Elsevier; 2010:360–367.
12. Boone DC, Azen SP. Normal range of motion of joints in male subjects. J Bone Joint Surg Am. 1979;61:756-759.
13. Timmerman LA, Schwartz ML, Andrews JR. Preoperative evaluation of the ulnar collateral ligament by magnetic resonance imaging and computed tomography arthrography. Evaluation in 25 baseball players with surgical confirmation. Am J Sports Med. 1994;22:26-31.
14. Mehlhoff TL, Bennet JB. Elbow injuries. In: Mellion MB, Walsh WM, Shelton GI, eds. The Team Physician’s Handbook. 2nd ed. Philadelphia, PA: Hanley & Belfus; 1997:461–473.
15. O’Connor FG, Ollivierre CO, Nirschl RP. Elbow and forearm injuries. In: Lillegard WA, Butcher KS, eds. Handbook of Sports Medicine: A Symptom-Oriented Approach. 2nd ed. Boston, MA: Butterworth-Heinemann; 1999:141–157.
16. Safran MR, Greene H, Lee TQ. Comparison of elbow valgus laxity using radiographic and non-radiographic objective measurement. 73rd Annual Meeting of the American Academy of Orthopaedic Surgeons; May 22, 2006; Chicago, IL.
17. Ahmad CS, El Attrache NS. Valgus extension overload syndrome and stress injury of the olecranon. Clin Sports Med. 2004;23:665-676.
18. Sarwart JF. Essentials of Musculoskeletal Care. 4th ed. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2010:384–387.
19. Mulligan SA, Schwartz ML, Broussard MF, et al. Heterotopic calcification and tears of the ulnar collateral ligament: radiographic and MR imaging findings. AJR Am J Roentgenol. 2000;175:1099-1102.
20. Tuite MJ, Kijowski R. Sports related injures of the elbow: an approach to MRI interpretation. Clin Sports Med. 2006;25:387-408.
21. Rineer CA, Ruch DS. Elbow tendinopathy and tendon ruptures: epicondylitis, biceps and triceps ruptures. J Hand Surg Am. 2009;34:566-576.
22. Vitale MA, Ahmad CS. The outcome of elbow ulnar collateral ligament reconstruction in overhead athletes: a systematic review. Am J Sports Med. 2008;36:1993-205.
23. Olsen SJ, Fleisig GS, Dun S, et al. Risk factors for shoulder and elbow injuries in adolescent baseball pitchers. Am J Sports Med. 2006;34:905-912.
24. Lyman S, Fleisig GS, Andrews JR, et al. Effect of pitch type, pitch count, and pitching mechanics on risk of elbow and shoulder pain in youth baseball pitchers. Am J Sports Med. 2002;30:463-468.
25. Fleisig GS, Andrews JR, Cutter GR, et al. Risk of serious injury for young baseball pitchers: a 10-year prospective study. Am J Sports Med. 2011;39:253-257.
• Administer the valgus stress test, the “milking maneuver,” and the moving valgus stress test to athletes suspected of having ulnar collateral ligament injury. C
• Treat Little League elbow with nonsteroidal anti-inflammatory drugs, ice, brief immobilization, and a 4- to 6-week “break” from throwing. A
• Advise young baseball players (and their parents) to avoid pitching year-round, and to get 3 months of rest per year. A
Strength of recommendation (SOR)
A Good-quality patient-oriented evidence
B Inconsistent or limited-quality patient-oriented evidence
C Consensus, usual practice, opinion, disease-oriented evidence, case series
The growing popularity of club teams and year-round participation in sports has spawned an epidemic of elbow injuries in primary and secondary school students and young adults alike. The incidence of elbow pain in children engaged in sports that require overhead throwing, such as baseball, football, volleyball, tennis, and javelin, ranges from 45% to 78%.1
Fortunately, acute traumatic elbow injury, with pain severe enough to force the athlete to cease participation entirely, is relatively rare, accounting for only 1% to 5% of cases.1,2 Far more often, elbow pain is associated with overuse, resulting in a gradual onset of medial elbow soreness that does not prevent the athlete from playing.
When an athlete seeks care for elbow pain, there are a number of things to consider, including the patient’s age, skeletal maturity, and type and frequency of throwing. Younger “throwers” typically incur injuries related to the physes, while adolescents and adults are more likely to sustain injuries to the ligaments and tendons.3 In both cases, repetitive valgus stress is the mechanism of injury. This review—of elbow anatomy (see the box),4-6 injury, differential diagnosis, and treatment—will make it easier for you to get injured athletes back in the game.
The elbow has 3 articulations—ulnohumeral, radiocapitellar, and proximal radioulnar—that provide primary stability to valgus stress. The elbow’s soft tissue restraints include 2 ligament complexes (medial and lateral collateral), 4 muscle groups (flexors, extensors, pronators, supinators), and 3 major nerves (radial, median, ulnar) and their branches.
The ulnar collateral ligament (UCL) complex—which consists of the anterior and posterior bundles and the transverse ligament—is the main source of medial elbow stability. 4 Mechanical stability for overhead throwing is provided by both bony and soft tissue restraints. During the pitching motion, the forces generated exceed the UCL’s tensile strength, and protective flexor muscles are activated.5,6
And the pitch…There are 6 stages of throwing: windup, early cocking, late cocking, acceleration, deceleration, and follow-through. Elbow pain is most likely during the late-cocking or early acceleration phase of a throw, the point of ball/javelin release, or the moment the racquet hits the ball.4
Is it Little League elbow? Start with a targeted history
In skeletally immature athletes, open physes result in the epicondylar apophysis being the weakest structure on the medial aspect of the elbow. Thus, repetitive valgus stress and tension overload often lead to “Little League elbow”—an umbrella term with a differential diagnosis that encompasses medial epicondylar fragmentation, delayed or accelerated growth of the medial epicondyle, and delayed closure of its growth plate, among other conditions (TABLE 1).3,7,8
In more mature athletes, repetitive microtrauma to the ulnar collateral ligament (UCL) leads to its gradual attenuation or complete failure.7 This increases the stress on the radiocapitellar joint and olecranon, and can lead to edema, scarring, calcification, osteophyte formation, medial epicondylitis, ulnar nerve neurapraxia, or radiocapitellar chondral damage.9 Extended practices and tournaments, with no substantial rest period throughout the year, put adolescents at increased risk for UCL injuries.10
Regardless of age, the medical history of an athlete with elbow pain should elicit information about the mechanism of injury; the location, duration, and quality of the pain; factors that alleviate or exacerbate the pain; the presence of weakness or paresthesias; and the extent to which the pain has affected the patient’s ability to throw. Patients with chronic UCL injuries, for example, often report a loss of arm control and decrease in throwing speed. It is also important to address hand dominance, level of participation, the position played, changes in technique or training regimen, prior injuries, and the effects of any previous treatment.11
TABLE 1
Differential diagnosis of elbow injuries
| Location | Differential diagnosis |
|---|---|
| Medial | Little League elbow
|
| Anterior | Anterior capsule strain Biceps tendon rupture Biceps tendonitis Dislocation Median nerve compression (pronator) syndrome |
| Posterior | Olecranon bursitis Olecranon process or tip stress fracture Triceps rupture/olecranon avulsion Triceps tendonitis Trochlear rupture Valgus overload syndrome (posterior olecranon impingement syndrome) |
| Lateral | Capitellum fracture Lateral epicondylitis Lateral ulnar collateral ligament injury Osteochondritis dissecans Posterior interosseous nerve syndrome Posterolateral rotary instability Radial head fracture Radiocapitellar chondromalacia |
| Adapted from: McKeag DB, Moeller JL. ACSM’s Primary Care Sports Medicine. 2nd ed.3 | |
Compare the affected and uninjured extremities
Inspect, palpate, and assess the active and passive range of motion, strength, and neurovascular status of both arms, with the uninjured side serving as a comparison. The scapula, shoulder, and wrist are also involved in throwing, so these joints should be examined along with the elbow.
Measure range of motion. Normal ranges for the flexion-extension arc are 0 to 140°, with 75° of pronation and 82° of supination.12 Use a goniometer, if available, to ensure accuracy and reproducibility,1 and pay close attention to the position that elicits pain.
In medial epicondylitis, the full range of motion should be preserved. Patients experience pain at the medial epicondyle and overlying flexor-pronator mass proximately, and pain or weakness with resisted wrist flexion, and resisted pronation, at full extension.4,11 Flexor-pronator strain will produce similar findings, but edema or ecchymosis may be present and there may be pain immediately distal to the medial epicondyle.11
Pain associated with injury to the UCL—which courses distal and slightly posterior to the medial epicondyle—typically occurs 2 cm distal to the medial epicondyle over the anterior bundle. Tenderness over the UCL has a sensitivity of 81% to 94% for UCL tears, but a specificity of only 22%.13
Physical maneuvers can help identify source of elbow pain
A complete UCL tear can cause valgus gapping as small as 3 mm, which makes it difficult to detect on physical exam alone.4 Orthopedic and sports medicine literature recommend that 3 maneuvers be used to identify UCL pathology:4,14,15
The valgus stress test (FIGURE 1) assesses the effects of valgus stress on the UCL. Gapping >3 mm signifies UCL instability. The test has a sensitivity of 66% and a specificity of 60% for detecting a UCL strain or tear.13,16
The milking maneuver (FIGURE 2), performed by the patient (or by a clinician if the patient lacks flexibility), reproduces a common pitching exercise. Medial elbow pain or apprehension indicates UCL injury.13,16
The moving valgus stress test (FIGURE 3A-C) is done in an effort to recreate the flexion angles of the elbow during the late cocking and early acceleration phases of throwing. Pain anywhere in the arc of motion suggests a UCL injury; pain elicited at 45° of flexion suggests osteochondrosis of the humeral capitellum, while pain closer to full extension suggests osteochondrosis of the trochlea.13,16
FIGURE 1
Valgus stress test
With the injured elbow at 30° of flexion, the shoulder abducted and fully externally rotated, and the patient’s wrist under your arm, place one hand laterally over the elbow. Place the other hand under the ulna and the thumb over the ulnar collateral ligament and apply valgus stress. Gapping >3 mm is abnormal.
FIGURE 2
Milking maneuver
The patient grasps the thumb of the affected arm and pulls downward, with the affected elbow positioned as shown, stressing the ulnar collateral ligament (UCL). Elbow pain or apprehension is positive for UCL injury.
FIGURE 3
Moving valgus stress test
With the shoulder in abduction and maximum external rotation (A), place the elbow in maximum flexion and apply valgus force (B), and extend the elbow from full flexion to full extension (C) in an attempt to reproduce the medial pain.
Does your patient have 2 positive valgus tests and posterior pain?
Valgus extension overload syndrome, which is caused by repetitive stress and results in osteophytes, chondromalacia of the medial olecranon fossa, tension in the UCL, and compression of the radiocapitellar joint, will also produce positive valgus stress and positive moving valgus stress tests. Keep in mind, however, that patients with valgus extension overload often have loss of full extension and posterior elbow pain with forced elbow hyperextension.17
Look for ulnar nerve injury
The physical examination should also be used to test for ulnar nerve injury. The elbow flexion test—a provocative maneuver in which the patient flexes the elbow as far as possible and reports any tingling or numbness of the hand—should be included in the work-up. Symptoms that develop in <60 seconds indicate a positive test for ulnar nerve compression, with the pinky and ulnar half of the ring finger most likely to have loss of vibration and light touch perception. A positive Tinel’s sign over the cubital tunnel is an indication of ulnar neuritis.18
If the ulnar nerve moves out of the ulnar groove when the groove is palpated as the elbow is flexed and extended, subluxating ulnar nerve is the likely diagnosis. If 2 structures displace over the medial epicondyle with elbow flexion, the first will be the ulnar nerve and the second will be the medial head of the triceps—an indication of a snapping medial head of triceps.18
Imaging studies may require a second look
Imaging studies are sometimes used to further aid in diagnosis of elbow injury. However, standard elbow x-rays, including an anteroposterior view in full extension, an oblique view, and a lateral view at 90° flexion, can be deceiving, as they often appear normal in conditions causing medial elbow pain associated with overhead throwing.
Careful review of the images may be needed to rule out fracture and other conditions, keeping the following factors in mind:
- A supracondylar fracture is likely if the anterior humeral line that is drawn along the anterior surface of the humeral cortex (on a lateral view) does not transect the middle third of the midcapitellum.3,11,18
- Dislocation of the radial head is suggested if the radiocapitellar line (drawn through the center of the radial head and neck) does not transect the midcapitellum on a lateral view.3,11,18
- Intra-articular injury with a joint effusion is indicated when an enlarged anterior fat pad, which is slightly anterior to the distal humeral diaphysis, is visible (the “sail sign”) on a normal elbow radiograph.3,11,18
- A fracture is likely if a posterior fat pad (which lies in the olecranon fossa and is not usually visible unless an effusion elevates the fat pad away from the cortex) is visible on an elbow x-ray. 3,11,18
- A chronic UCL tear is suggested by heterotropic calcification of the UCL.19
It is useful to x-ray both the injured and the unaffected elbows in skeletally immature athletes to compare secondary ossification centers. Little League elbow demonstrates a widening of the medial epicondyle physis, for example, when the x-rays are compared.3 Secondary ossification centers of the elbow appear first at the capitellum (age 2), followed by the radial head (age 5), medial epicondyle (age 7), trochlea (age 9), and lateral epicondyle (age 11). Most ossification centers fuse between 14 and 17 years of age.3
Computed tomography arthrograms, magnetic resonance imaging (MRI), and ultrasonography are also used to identify UCL tears. MRI, which can reveal injuries to cartilage and tendons as well, is the most commonly used imaging technique for musculoskeletal diagnosis of the elbow.16,20
Treatment gets most athletes back on track
Most medial elbow injuries respond to conservative treatment—typically, with some combination of activity modification, nonsteroidal anti-inflammatory drugs (NSAIDs), icing, physical therapy aimed at flexor-pronator strengthening, and counterforce bracing.11 Medial epicondylosis and flexor-pronator strain injuries have an excellent prognosis, with more than 90% of patients back to their previous level of activity at 1 year. Initial treatment consists of a 2- to 3-week rest period, followed by a 6- to 12-week rehabilitation protocol.11
Randomized controlled trials have found limited evidence of short-term improvement in symptoms with corticosteroid injections compared with placebo or no treatment, local anesthetic, orthosis, physical therapy, and NSAIDs. However, corticosteroids were less effective than physiotherapy or oral NSAIDs in improving long-term outcomes.21 Despite a paucity of well-designed studies to prove their use, autologous blood, platelet-rich plasma, and botulinum toxin are sometimes used for refractory elbow pain.21
Treatment of Little League elbow consists of cessation of throwing for at least 4 to 6 weeks, with a gradual return to throwing and emphasis on proper throwing mechanics after the pain resolves. Most throwers are out of competition for 2 to 3 months, but fully recover with nonoperative management.21
UCL injuries, too, are initially treated with rest, NSAIDs, icing, bracing, and physical therapy, typically with 2 to 3 months of no throwing. Some patients also use a splint at 90° flexion at night and as needed for pain during the day. Patients whose symptoms last more than a year despite treatment may be candidates for arthroscopic debridement.11
Consider reconstruction when nonsurgical management fails
UCL reconstruction was introduced in 1974, when reconstruction was performed on professional pitcher Tommy John, who went on to win 164 games.4,9 The procedure has since undergone numerous modifications. Surgery is indicated for acute rupture, significant chronic instability, insufficient UCL tissue after debridement, or recurrent pain and valgus instability with throwing after rehabilitation.2,4,6,9
Reconstruction generally entails fixing a tendon graft through bone tunnels in the medial epicondyle of the humerus and sublime tubercle of the ulna to reestablish valgus stability. A recent systematic review of reconstruction methods found a 76% to 95% rate of excellent results, with patients returned to their prior level of activity at a mean follow-up of 1 year.22 Rehabilitation typically begins 7 days postop; throwing (without windup) may begin in 4 to 5 months, with a gradual increase in speed and force and a return to the game at 12 months.
A stepped-up focus on prevention
The increase in UCL injuries in adolescents highlights the need for greater emphasis on prevention.10 Several governing bodies, including USA Baseball and the American Academy of Pediatrics, have developed research-based guidelines for young athletes (TABLE 2).1,10,23-25
One of the easiest to follow is to limit an athlete’s weekly pitch count to 10 times his age. Thus, a 10 year old should pitch no more than 100 pitches in a given 7-day period. Another important measure—in addition to ensuring that young athletes receive instruction in proper pitching mechanics (see http://www.littleleague.org/Little_League_Online.htm)—is to urge coaches and parents to require players to get at least 3 months of rest after each season and to stop throwing if they have pain or fatigue.24
TABLE 2
Keeping young pitchers injury-free1,10,23-25
| Recommendations for coaches and parents |
|---|
| Record the number of pitches thrown at each outing/sports event for all young pitchers |
| Avoid allowing young athletes to pitch competitively >8 months per year |
| Limit the number of pitches to ≤2500 per year and 10 × the pitcher’s age per week, or 90 per outing |
| Ensure that young pitchers are instructed in proper pitching mechanics |
| Restrict throwing breaking ball pitches* prior to puberty |
| Ensure that young pitchers get 3 months of rest per year. |
| *A pitch that changes direction either sideways or downwards as it approaches the batter, eg, a slider or curve ball. |
CORRESPONDENCE
Jennifer A. Southard, MD, MSc, Saint Alphonsus Medical Group, 6533 Emerald Street, Boise, ID 83704; [email protected]
• Administer the valgus stress test, the “milking maneuver,” and the moving valgus stress test to athletes suspected of having ulnar collateral ligament injury. C
• Treat Little League elbow with nonsteroidal anti-inflammatory drugs, ice, brief immobilization, and a 4- to 6-week “break” from throwing. A
• Advise young baseball players (and their parents) to avoid pitching year-round, and to get 3 months of rest per year. A
Strength of recommendation (SOR)
A Good-quality patient-oriented evidence
B Inconsistent or limited-quality patient-oriented evidence
C Consensus, usual practice, opinion, disease-oriented evidence, case series
The growing popularity of club teams and year-round participation in sports has spawned an epidemic of elbow injuries in primary and secondary school students and young adults alike. The incidence of elbow pain in children engaged in sports that require overhead throwing, such as baseball, football, volleyball, tennis, and javelin, ranges from 45% to 78%.1
Fortunately, acute traumatic elbow injury, with pain severe enough to force the athlete to cease participation entirely, is relatively rare, accounting for only 1% to 5% of cases.1,2 Far more often, elbow pain is associated with overuse, resulting in a gradual onset of medial elbow soreness that does not prevent the athlete from playing.
When an athlete seeks care for elbow pain, there are a number of things to consider, including the patient’s age, skeletal maturity, and type and frequency of throwing. Younger “throwers” typically incur injuries related to the physes, while adolescents and adults are more likely to sustain injuries to the ligaments and tendons.3 In both cases, repetitive valgus stress is the mechanism of injury. This review—of elbow anatomy (see the box),4-6 injury, differential diagnosis, and treatment—will make it easier for you to get injured athletes back in the game.
The elbow has 3 articulations—ulnohumeral, radiocapitellar, and proximal radioulnar—that provide primary stability to valgus stress. The elbow’s soft tissue restraints include 2 ligament complexes (medial and lateral collateral), 4 muscle groups (flexors, extensors, pronators, supinators), and 3 major nerves (radial, median, ulnar) and their branches.
The ulnar collateral ligament (UCL) complex—which consists of the anterior and posterior bundles and the transverse ligament—is the main source of medial elbow stability. 4 Mechanical stability for overhead throwing is provided by both bony and soft tissue restraints. During the pitching motion, the forces generated exceed the UCL’s tensile strength, and protective flexor muscles are activated.5,6
And the pitch…There are 6 stages of throwing: windup, early cocking, late cocking, acceleration, deceleration, and follow-through. Elbow pain is most likely during the late-cocking or early acceleration phase of a throw, the point of ball/javelin release, or the moment the racquet hits the ball.4
Is it Little League elbow? Start with a targeted history
In skeletally immature athletes, open physes result in the epicondylar apophysis being the weakest structure on the medial aspect of the elbow. Thus, repetitive valgus stress and tension overload often lead to “Little League elbow”—an umbrella term with a differential diagnosis that encompasses medial epicondylar fragmentation, delayed or accelerated growth of the medial epicondyle, and delayed closure of its growth plate, among other conditions (TABLE 1).3,7,8
In more mature athletes, repetitive microtrauma to the ulnar collateral ligament (UCL) leads to its gradual attenuation or complete failure.7 This increases the stress on the radiocapitellar joint and olecranon, and can lead to edema, scarring, calcification, osteophyte formation, medial epicondylitis, ulnar nerve neurapraxia, or radiocapitellar chondral damage.9 Extended practices and tournaments, with no substantial rest period throughout the year, put adolescents at increased risk for UCL injuries.10
Regardless of age, the medical history of an athlete with elbow pain should elicit information about the mechanism of injury; the location, duration, and quality of the pain; factors that alleviate or exacerbate the pain; the presence of weakness or paresthesias; and the extent to which the pain has affected the patient’s ability to throw. Patients with chronic UCL injuries, for example, often report a loss of arm control and decrease in throwing speed. It is also important to address hand dominance, level of participation, the position played, changes in technique or training regimen, prior injuries, and the effects of any previous treatment.11
TABLE 1
Differential diagnosis of elbow injuries
| Location | Differential diagnosis |
|---|---|
| Medial | Little League elbow
|
| Anterior | Anterior capsule strain Biceps tendon rupture Biceps tendonitis Dislocation Median nerve compression (pronator) syndrome |
| Posterior | Olecranon bursitis Olecranon process or tip stress fracture Triceps rupture/olecranon avulsion Triceps tendonitis Trochlear rupture Valgus overload syndrome (posterior olecranon impingement syndrome) |
| Lateral | Capitellum fracture Lateral epicondylitis Lateral ulnar collateral ligament injury Osteochondritis dissecans Posterior interosseous nerve syndrome Posterolateral rotary instability Radial head fracture Radiocapitellar chondromalacia |
| Adapted from: McKeag DB, Moeller JL. ACSM’s Primary Care Sports Medicine. 2nd ed.3 | |
Compare the affected and uninjured extremities
Inspect, palpate, and assess the active and passive range of motion, strength, and neurovascular status of both arms, with the uninjured side serving as a comparison. The scapula, shoulder, and wrist are also involved in throwing, so these joints should be examined along with the elbow.
Measure range of motion. Normal ranges for the flexion-extension arc are 0 to 140°, with 75° of pronation and 82° of supination.12 Use a goniometer, if available, to ensure accuracy and reproducibility,1 and pay close attention to the position that elicits pain.
In medial epicondylitis, the full range of motion should be preserved. Patients experience pain at the medial epicondyle and overlying flexor-pronator mass proximately, and pain or weakness with resisted wrist flexion, and resisted pronation, at full extension.4,11 Flexor-pronator strain will produce similar findings, but edema or ecchymosis may be present and there may be pain immediately distal to the medial epicondyle.11
Pain associated with injury to the UCL—which courses distal and slightly posterior to the medial epicondyle—typically occurs 2 cm distal to the medial epicondyle over the anterior bundle. Tenderness over the UCL has a sensitivity of 81% to 94% for UCL tears, but a specificity of only 22%.13
Physical maneuvers can help identify source of elbow pain
A complete UCL tear can cause valgus gapping as small as 3 mm, which makes it difficult to detect on physical exam alone.4 Orthopedic and sports medicine literature recommend that 3 maneuvers be used to identify UCL pathology:4,14,15
The valgus stress test (FIGURE 1) assesses the effects of valgus stress on the UCL. Gapping >3 mm signifies UCL instability. The test has a sensitivity of 66% and a specificity of 60% for detecting a UCL strain or tear.13,16
The milking maneuver (FIGURE 2), performed by the patient (or by a clinician if the patient lacks flexibility), reproduces a common pitching exercise. Medial elbow pain or apprehension indicates UCL injury.13,16
The moving valgus stress test (FIGURE 3A-C) is done in an effort to recreate the flexion angles of the elbow during the late cocking and early acceleration phases of throwing. Pain anywhere in the arc of motion suggests a UCL injury; pain elicited at 45° of flexion suggests osteochondrosis of the humeral capitellum, while pain closer to full extension suggests osteochondrosis of the trochlea.13,16
FIGURE 1
Valgus stress test
With the injured elbow at 30° of flexion, the shoulder abducted and fully externally rotated, and the patient’s wrist under your arm, place one hand laterally over the elbow. Place the other hand under the ulna and the thumb over the ulnar collateral ligament and apply valgus stress. Gapping >3 mm is abnormal.
FIGURE 2
Milking maneuver
The patient grasps the thumb of the affected arm and pulls downward, with the affected elbow positioned as shown, stressing the ulnar collateral ligament (UCL). Elbow pain or apprehension is positive for UCL injury.
FIGURE 3
Moving valgus stress test
With the shoulder in abduction and maximum external rotation (A), place the elbow in maximum flexion and apply valgus force (B), and extend the elbow from full flexion to full extension (C) in an attempt to reproduce the medial pain.
Does your patient have 2 positive valgus tests and posterior pain?
Valgus extension overload syndrome, which is caused by repetitive stress and results in osteophytes, chondromalacia of the medial olecranon fossa, tension in the UCL, and compression of the radiocapitellar joint, will also produce positive valgus stress and positive moving valgus stress tests. Keep in mind, however, that patients with valgus extension overload often have loss of full extension and posterior elbow pain with forced elbow hyperextension.17
Look for ulnar nerve injury
The physical examination should also be used to test for ulnar nerve injury. The elbow flexion test—a provocative maneuver in which the patient flexes the elbow as far as possible and reports any tingling or numbness of the hand—should be included in the work-up. Symptoms that develop in <60 seconds indicate a positive test for ulnar nerve compression, with the pinky and ulnar half of the ring finger most likely to have loss of vibration and light touch perception. A positive Tinel’s sign over the cubital tunnel is an indication of ulnar neuritis.18
If the ulnar nerve moves out of the ulnar groove when the groove is palpated as the elbow is flexed and extended, subluxating ulnar nerve is the likely diagnosis. If 2 structures displace over the medial epicondyle with elbow flexion, the first will be the ulnar nerve and the second will be the medial head of the triceps—an indication of a snapping medial head of triceps.18
Imaging studies may require a second look
Imaging studies are sometimes used to further aid in diagnosis of elbow injury. However, standard elbow x-rays, including an anteroposterior view in full extension, an oblique view, and a lateral view at 90° flexion, can be deceiving, as they often appear normal in conditions causing medial elbow pain associated with overhead throwing.
Careful review of the images may be needed to rule out fracture and other conditions, keeping the following factors in mind:
- A supracondylar fracture is likely if the anterior humeral line that is drawn along the anterior surface of the humeral cortex (on a lateral view) does not transect the middle third of the midcapitellum.3,11,18
- Dislocation of the radial head is suggested if the radiocapitellar line (drawn through the center of the radial head and neck) does not transect the midcapitellum on a lateral view.3,11,18
- Intra-articular injury with a joint effusion is indicated when an enlarged anterior fat pad, which is slightly anterior to the distal humeral diaphysis, is visible (the “sail sign”) on a normal elbow radiograph.3,11,18
- A fracture is likely if a posterior fat pad (which lies in the olecranon fossa and is not usually visible unless an effusion elevates the fat pad away from the cortex) is visible on an elbow x-ray. 3,11,18
- A chronic UCL tear is suggested by heterotropic calcification of the UCL.19
It is useful to x-ray both the injured and the unaffected elbows in skeletally immature athletes to compare secondary ossification centers. Little League elbow demonstrates a widening of the medial epicondyle physis, for example, when the x-rays are compared.3 Secondary ossification centers of the elbow appear first at the capitellum (age 2), followed by the radial head (age 5), medial epicondyle (age 7), trochlea (age 9), and lateral epicondyle (age 11). Most ossification centers fuse between 14 and 17 years of age.3
Computed tomography arthrograms, magnetic resonance imaging (MRI), and ultrasonography are also used to identify UCL tears. MRI, which can reveal injuries to cartilage and tendons as well, is the most commonly used imaging technique for musculoskeletal diagnosis of the elbow.16,20
Treatment gets most athletes back on track
Most medial elbow injuries respond to conservative treatment—typically, with some combination of activity modification, nonsteroidal anti-inflammatory drugs (NSAIDs), icing, physical therapy aimed at flexor-pronator strengthening, and counterforce bracing.11 Medial epicondylosis and flexor-pronator strain injuries have an excellent prognosis, with more than 90% of patients back to their previous level of activity at 1 year. Initial treatment consists of a 2- to 3-week rest period, followed by a 6- to 12-week rehabilitation protocol.11
Randomized controlled trials have found limited evidence of short-term improvement in symptoms with corticosteroid injections compared with placebo or no treatment, local anesthetic, orthosis, physical therapy, and NSAIDs. However, corticosteroids were less effective than physiotherapy or oral NSAIDs in improving long-term outcomes.21 Despite a paucity of well-designed studies to prove their use, autologous blood, platelet-rich plasma, and botulinum toxin are sometimes used for refractory elbow pain.21
Treatment of Little League elbow consists of cessation of throwing for at least 4 to 6 weeks, with a gradual return to throwing and emphasis on proper throwing mechanics after the pain resolves. Most throwers are out of competition for 2 to 3 months, but fully recover with nonoperative management.21
UCL injuries, too, are initially treated with rest, NSAIDs, icing, bracing, and physical therapy, typically with 2 to 3 months of no throwing. Some patients also use a splint at 90° flexion at night and as needed for pain during the day. Patients whose symptoms last more than a year despite treatment may be candidates for arthroscopic debridement.11
Consider reconstruction when nonsurgical management fails
UCL reconstruction was introduced in 1974, when reconstruction was performed on professional pitcher Tommy John, who went on to win 164 games.4,9 The procedure has since undergone numerous modifications. Surgery is indicated for acute rupture, significant chronic instability, insufficient UCL tissue after debridement, or recurrent pain and valgus instability with throwing after rehabilitation.2,4,6,9
Reconstruction generally entails fixing a tendon graft through bone tunnels in the medial epicondyle of the humerus and sublime tubercle of the ulna to reestablish valgus stability. A recent systematic review of reconstruction methods found a 76% to 95% rate of excellent results, with patients returned to their prior level of activity at a mean follow-up of 1 year.22 Rehabilitation typically begins 7 days postop; throwing (without windup) may begin in 4 to 5 months, with a gradual increase in speed and force and a return to the game at 12 months.
A stepped-up focus on prevention
The increase in UCL injuries in adolescents highlights the need for greater emphasis on prevention.10 Several governing bodies, including USA Baseball and the American Academy of Pediatrics, have developed research-based guidelines for young athletes (TABLE 2).1,10,23-25
One of the easiest to follow is to limit an athlete’s weekly pitch count to 10 times his age. Thus, a 10 year old should pitch no more than 100 pitches in a given 7-day period. Another important measure—in addition to ensuring that young athletes receive instruction in proper pitching mechanics (see http://www.littleleague.org/Little_League_Online.htm)—is to urge coaches and parents to require players to get at least 3 months of rest after each season and to stop throwing if they have pain or fatigue.24
TABLE 2
Keeping young pitchers injury-free1,10,23-25
| Recommendations for coaches and parents |
|---|
| Record the number of pitches thrown at each outing/sports event for all young pitchers |
| Avoid allowing young athletes to pitch competitively >8 months per year |
| Limit the number of pitches to ≤2500 per year and 10 × the pitcher’s age per week, or 90 per outing |
| Ensure that young pitchers are instructed in proper pitching mechanics |
| Restrict throwing breaking ball pitches* prior to puberty |
| Ensure that young pitchers get 3 months of rest per year. |
| *A pitch that changes direction either sideways or downwards as it approaches the batter, eg, a slider or curve ball. |
CORRESPONDENCE
Jennifer A. Southard, MD, MSc, Saint Alphonsus Medical Group, 6533 Emerald Street, Boise, ID 83704; [email protected]
1. American Academy of Pediatrics Committee on Sports Medicine and Fitness. Risk of injury from baseball and softball in children. Pediatrics. 2001;107:782-784.
2. Maloney MD, Morhr KJ, el Attrache NS, et al. Elbow injuries in the throwing athlete. Clin Sports Med. 1999;18:795-809.
3. McKeag DB, Moeller JL. ACSM’s Primary Care Sports Medicine. 2nd ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2007:387–402.
4. Hariri S, Safran MR. Ulnar collateral ligament injury in the overhead athlete. Clin Sports Med. 2010;29:619-644.
5. Park MJ, Kim HG, Lee JY. Surgical treatment of post-traumatic stiffness of the elbow. J Bone Joint Surg Br. 2004;86:1158-1162.
6. Lin F, Kohli N, Perlmutter S, et al. Muscle contribution to elbow joint valgus stability. J Shoulder Elbow Surg. 2007;16:795-802.
7. Fleisig GS, Andrews JR, Dillman CJ, et al. Kinetics of baseball pitching with implications about injury mechanisms. Am J Sports Med. 1995;23:233-239.
8. Baker CL, Romero AA. Osteochondritis dissecans of the capitellum. Am J Sports Med. 2010;38:1917-1928.
9. Cain EL, Andrews JR, Dugas JR, et al. Outcome of ulnar collateral ligament reconstruction of the elbow in 1281 athletes: results in 743 athletes with minimum 2-year follow-up. Am J Sports Med. 2010;38:2426-2434.
10. Fleisig GS, Andrews JR, Cutter GR, et al. Prevention of elbow injuries in youth baseball pitchers. Curr Sports Med Rep. 2009;8:250-254.
11. Madden CC, Putukian M, McCarty E, et al. Netter’s Sports Medicine. Philadelphia, PA: Saunders Elsevier; 2010:360–367.
12. Boone DC, Azen SP. Normal range of motion of joints in male subjects. J Bone Joint Surg Am. 1979;61:756-759.
13. Timmerman LA, Schwartz ML, Andrews JR. Preoperative evaluation of the ulnar collateral ligament by magnetic resonance imaging and computed tomography arthrography. Evaluation in 25 baseball players with surgical confirmation. Am J Sports Med. 1994;22:26-31.
14. Mehlhoff TL, Bennet JB. Elbow injuries. In: Mellion MB, Walsh WM, Shelton GI, eds. The Team Physician’s Handbook. 2nd ed. Philadelphia, PA: Hanley & Belfus; 1997:461–473.
15. O’Connor FG, Ollivierre CO, Nirschl RP. Elbow and forearm injuries. In: Lillegard WA, Butcher KS, eds. Handbook of Sports Medicine: A Symptom-Oriented Approach. 2nd ed. Boston, MA: Butterworth-Heinemann; 1999:141–157.
16. Safran MR, Greene H, Lee TQ. Comparison of elbow valgus laxity using radiographic and non-radiographic objective measurement. 73rd Annual Meeting of the American Academy of Orthopaedic Surgeons; May 22, 2006; Chicago, IL.
17. Ahmad CS, El Attrache NS. Valgus extension overload syndrome and stress injury of the olecranon. Clin Sports Med. 2004;23:665-676.
18. Sarwart JF. Essentials of Musculoskeletal Care. 4th ed. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2010:384–387.
19. Mulligan SA, Schwartz ML, Broussard MF, et al. Heterotopic calcification and tears of the ulnar collateral ligament: radiographic and MR imaging findings. AJR Am J Roentgenol. 2000;175:1099-1102.
20. Tuite MJ, Kijowski R. Sports related injures of the elbow: an approach to MRI interpretation. Clin Sports Med. 2006;25:387-408.
21. Rineer CA, Ruch DS. Elbow tendinopathy and tendon ruptures: epicondylitis, biceps and triceps ruptures. J Hand Surg Am. 2009;34:566-576.
22. Vitale MA, Ahmad CS. The outcome of elbow ulnar collateral ligament reconstruction in overhead athletes: a systematic review. Am J Sports Med. 2008;36:1993-205.
23. Olsen SJ, Fleisig GS, Dun S, et al. Risk factors for shoulder and elbow injuries in adolescent baseball pitchers. Am J Sports Med. 2006;34:905-912.
24. Lyman S, Fleisig GS, Andrews JR, et al. Effect of pitch type, pitch count, and pitching mechanics on risk of elbow and shoulder pain in youth baseball pitchers. Am J Sports Med. 2002;30:463-468.
25. Fleisig GS, Andrews JR, Cutter GR, et al. Risk of serious injury for young baseball pitchers: a 10-year prospective study. Am J Sports Med. 2011;39:253-257.
1. American Academy of Pediatrics Committee on Sports Medicine and Fitness. Risk of injury from baseball and softball in children. Pediatrics. 2001;107:782-784.
2. Maloney MD, Morhr KJ, el Attrache NS, et al. Elbow injuries in the throwing athlete. Clin Sports Med. 1999;18:795-809.
3. McKeag DB, Moeller JL. ACSM’s Primary Care Sports Medicine. 2nd ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2007:387–402.
4. Hariri S, Safran MR. Ulnar collateral ligament injury in the overhead athlete. Clin Sports Med. 2010;29:619-644.
5. Park MJ, Kim HG, Lee JY. Surgical treatment of post-traumatic stiffness of the elbow. J Bone Joint Surg Br. 2004;86:1158-1162.
6. Lin F, Kohli N, Perlmutter S, et al. Muscle contribution to elbow joint valgus stability. J Shoulder Elbow Surg. 2007;16:795-802.
7. Fleisig GS, Andrews JR, Dillman CJ, et al. Kinetics of baseball pitching with implications about injury mechanisms. Am J Sports Med. 1995;23:233-239.
8. Baker CL, Romero AA. Osteochondritis dissecans of the capitellum. Am J Sports Med. 2010;38:1917-1928.
9. Cain EL, Andrews JR, Dugas JR, et al. Outcome of ulnar collateral ligament reconstruction of the elbow in 1281 athletes: results in 743 athletes with minimum 2-year follow-up. Am J Sports Med. 2010;38:2426-2434.
10. Fleisig GS, Andrews JR, Cutter GR, et al. Prevention of elbow injuries in youth baseball pitchers. Curr Sports Med Rep. 2009;8:250-254.
11. Madden CC, Putukian M, McCarty E, et al. Netter’s Sports Medicine. Philadelphia, PA: Saunders Elsevier; 2010:360–367.
12. Boone DC, Azen SP. Normal range of motion of joints in male subjects. J Bone Joint Surg Am. 1979;61:756-759.
13. Timmerman LA, Schwartz ML, Andrews JR. Preoperative evaluation of the ulnar collateral ligament by magnetic resonance imaging and computed tomography arthrography. Evaluation in 25 baseball players with surgical confirmation. Am J Sports Med. 1994;22:26-31.
14. Mehlhoff TL, Bennet JB. Elbow injuries. In: Mellion MB, Walsh WM, Shelton GI, eds. The Team Physician’s Handbook. 2nd ed. Philadelphia, PA: Hanley & Belfus; 1997:461–473.
15. O’Connor FG, Ollivierre CO, Nirschl RP. Elbow and forearm injuries. In: Lillegard WA, Butcher KS, eds. Handbook of Sports Medicine: A Symptom-Oriented Approach. 2nd ed. Boston, MA: Butterworth-Heinemann; 1999:141–157.
16. Safran MR, Greene H, Lee TQ. Comparison of elbow valgus laxity using radiographic and non-radiographic objective measurement. 73rd Annual Meeting of the American Academy of Orthopaedic Surgeons; May 22, 2006; Chicago, IL.
17. Ahmad CS, El Attrache NS. Valgus extension overload syndrome and stress injury of the olecranon. Clin Sports Med. 2004;23:665-676.
18. Sarwart JF. Essentials of Musculoskeletal Care. 4th ed. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2010:384–387.
19. Mulligan SA, Schwartz ML, Broussard MF, et al. Heterotopic calcification and tears of the ulnar collateral ligament: radiographic and MR imaging findings. AJR Am J Roentgenol. 2000;175:1099-1102.
20. Tuite MJ, Kijowski R. Sports related injures of the elbow: an approach to MRI interpretation. Clin Sports Med. 2006;25:387-408.
21. Rineer CA, Ruch DS. Elbow tendinopathy and tendon ruptures: epicondylitis, biceps and triceps ruptures. J Hand Surg Am. 2009;34:566-576.
22. Vitale MA, Ahmad CS. The outcome of elbow ulnar collateral ligament reconstruction in overhead athletes: a systematic review. Am J Sports Med. 2008;36:1993-205.
23. Olsen SJ, Fleisig GS, Dun S, et al. Risk factors for shoulder and elbow injuries in adolescent baseball pitchers. Am J Sports Med. 2006;34:905-912.
24. Lyman S, Fleisig GS, Andrews JR, et al. Effect of pitch type, pitch count, and pitching mechanics on risk of elbow and shoulder pain in youth baseball pitchers. Am J Sports Med. 2002;30:463-468.
25. Fleisig GS, Andrews JR, Cutter GR, et al. Risk of serious injury for young baseball pitchers: a 10-year prospective study. Am J Sports Med. 2011;39:253-257.
Removing barriers to insulin use
• Reassure patients who fear stigmatization that the small needles and devices available today make it easy to discreetly incorporate insulin therapy into everyday life. C
• Consider making a referral to a diabetes support group or a mental health counselor when a patient is reluctant to pursue insulin therapy, despite the benefits to his or her health. C
Strength of recommendation (SOR)
A Good-quality patient-oriented evidence
B Inconsistent or limited-quality patient-oriented evidence
C Consensus, usual practice, opinion, disease-oriented evidence, case series
PATIENT HANDOUT
Is it time for insulin? (PDF)
For patients with type 2 diabetes, control of hyperglycemia through diet, exercise, and pharmacologic therapy reduces the risk of microvascular complications and may have long-term cardiovascular benefits.1,2 But when the disease progresses and oral medication and lifestyle changes are no longer sufficient, many patients experience long periods of elevated glucose concentrations before insulin is added to (or replaces) a failing oral regimen.3
Both the American Diabetes Association and the American Association of Clinical Endocrinologists recommend early initiation of insulin therapy4,5 for patients with significantly elevated HbA1c, and a stepwise treatment approach, beginning with oral medications, for more modest elevations. Overall, insulin therapy offers the greatest potential for improved glycemic control.4,6,7 Yet patients, as well as their physicians, are often reluctant to initiate it. In the review that follows, we identify common barriers to insulin therapy and provide practical tips on how best to overcome them.
Why patients are “insulin resistant”
Patient barriers to insulin therapy can be divided into 3 general categories (TABLE 1)—psychological resistance, harmful effects (whether real or perceived), and financial barriers. Understanding what’s behind their hesitancy (as well as your own) makes it easier to overcome these barriers and properly integrate insulin into their health care regimen.
TABLE 1
Patient barriers to insulin8-11
| Psychological |
Belief that insulin represents failure of self-care Lack of perceived benefit Pain/fear of injections Belief that insulin use is complicated Loss of independence/change in lifestyle Stigma related to needle use |
| Harmful effects |
Hypoglycemia Weight gain Perceived adverse effects |
| Financial |
| Cost of insulin and supplies |
Most barriers are psychological
Because insulin therapy is typically introduced some time after diagnosis (and conservative management), patients often view the need for insulin as an indication that they have failed to manage their type 2 disease effectively. What’s more, many patients are convinced that insulin will provide few, if any, benefits.8
The Diabetes Attitudes, Wishes, and Needs (DAWN) study, a large international trial, found that only 27% of noninsulin-dependent patients believed that insulin could help manage their disease.8 Patients’ lack of belief in insulin’s efficacy can be attributed to negative experiences with insulin therapy, which may have been related by family or friends or simply reflect societal views. The complex nature of insulin therapy is another problem, as patients often feel overwhelmed by the prospect of having to adhere to what they consider to be a stringent daily regimen.
And for many, resistance to insulin therapy is triggered by fear of:
- needles and subcutaneous injections9-11
- loss of independence and lifestyle changes (eg, having to sacrifice pleasurable activities, such as eating out and traveling)9
- adverse effects, most notably hypoglycemia and weight gain.9-11
Other psychological barriers can be attributed to perceived societal norms, including the stigma associated with the use of needles and illicit drug use and the potential embarrassment of self-injection.9
Harmful effects. Concern about insulin’s negative effects may be exacerbated by the fact that symptoms or complications of diabetes itself, which often develop as the disease progresses, are often mistakenly attributed to insulin therapy.
Financial concerns, too, are often associated with resistance to insulin therapy, relating to the costs of newer insulin analogs and insulin administration devices.
Replace misconceptions with facts
Patients respond in different ways to a discussion of insulin initiation, and it is important to identify barriers and help resolve them. Yet there are few validated measurement tools designed for this purpose. We’ve created a patient handout, “Is it time for insulin?”, which addresses a number of common concerns. The tips that follow here should also help.
“It won’t help me”
If a patient tells you that insulin therapy will be of little or no benefit, explain that type 2 diabetes is largely due to a lack of insulin activity and that the newer insulin analogs mimic the normal physiologic response. Make it clear that insulin use is not a punishment or evidence of personal failure, but a therapeutic option that most patients need as their diabetes progresses.9,10,12
“My friend takes insulin, and her diabetes still isn’t under control”
Tell a patient who is convinced that insulin provides few benefits or has heard about people whose diabetes was not controlled by insulin that the dosing may not have been appropriate,9 and that it is important for you to work together to make any necessary adjustments.
Fear of hypoglycemia can be addressed through patient education about how to recognize signs and symptoms of low blood sugar and what actions to take to resolve it.13 Explain that frequent blood glucose monitoring; regularly scheduled, balanced meals; increased physical activity; and referral to a dietitian, when needed, will go a long way toward preventing swings in blood sugar as well as weight gain.9,14 Emphasize that exercise will improve insulin sensitivity, helping to control weight and ensure better glucose uptake, as well.
“I hate needles!”
Address needle phobia and fear of social stigma with reassurance and a demonstration of the small, thin needles on the market and the devices designed to conceal them. Point out that such devices promote privacy and make it easy for patients to discreetly incorporate insulin therapy into everyday life.
“It will be too expensive”
Patient assistance programs are available for eligible patients, with online resources such as www.Rxassist.org and www.xubex.com. You can also remind patients that health insurers, including Medicare and Medicaid plans, contribute to the cost of glucometers, test strips, and lancets, as well as the insulin itself. Diabetes supplies are often available from medical supply companies that bill health insurers directly but mail the supplies to the patients.
Are you putting up some barriers of your own?
Reluctance to introduce insulin therapy or negative feelings about it (TABLE 2)9,14,15 on the part of clinicians creates, or contributes to, “clinical inertia”—defined as awareness of a problem but a lack of action to resolve it. What’s more, any hesitancy you have about insulin therapy is likely to influence the perception of your patients.10,14
In general, physician barriers center on the fact that managing insulin therapy can be a cumbersome task for which they may not have the time or the resources. A study of clinician encounters with patients with type 2 diabetes in primary care clinics supports that belief. Each additional concern raised by a patient during the course of a visit was associated with a 49% reduction in the likelihood of a change in medication.15
TABLE 2
Provider barriers to insulin10,14,15
| Negative attitude |
| Time constraints |
| Lack of health care system support/resources |
| Concern about adverse effects |
| Fear of patient response/lack of adherence |
Hypoglycemia is a particular concern for clinicians because of its close association with tight glucose control—which relates to another barrier: the problem of patient adherence. Evidence-based findings, algorithms, and guidelines for insulin therapy can help you handle these and other clinical issues with confidence. (See “Removing physician barriers with education and evidence”.)
Learning more about insulin administration, including which formulations to use and how to ensure proper dosing, will go a long way toward eliminating clinician barriers to insulin initiation. These online resources can help.
The Treat-to-Target Trial (http://care.diabetesjournals.org/content/26/11/3080.short), for example, demonstrated that patients using long-acting insulin had lower rates of nocturnal and symptomatic hypoglycemia and were more likely to reach their target HbA1c than those on intermediate-acting insulin.16 The researchers also found that weight gain was more significant in patients with prescriptions for multiple doses of insulin each day vs those on a once-daily regimen, and that when metformin was used in conjunction with insulin therapy, weight gain was avoided.
Continuing education courses and treatment algorithms published by the American Diabetes Association (http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2606813/pdf/193.pdf) and the American Association of Clinical Endocrinologists (https://www.aace.com/sites/default/files/GlycemicControlAlgorithmPPT.pdf) can provide additional guidance.
Don’t go it alone—draw on other resources
Patient education regarding insulin therapy can also be time consuming and cumbersome, and difficult to manage in a busy primary care practice. Certified diabetes educators can help reduce your burden and address patient concerns, as can nurses, pharmacists, case managers, and behavioral therapists, as needed. For patients who need insulin but continue to resist or reject it based on overwhelming or unfounded fears, a referral to a diabetes support group, mental health provider, or behavioral counselor may be in order.
Why do I need insulin?
Oftentimes, insulin is unavoidable. Diabetes is a progressive illness, and patients often find that it gets harder and harder to keep their blood sugar at a healthy level. Over time, high blood sugar (hyperglycemia) can lead to many serious complications, such as heart disease, nerve damage, kidney disease, and damage to your eyes (retinas). Taking insulin is the best way to control your blood sugar when other steps like changes in your diet and exercise are no longer working. This does not mean that you failed in your efforts to control your diabetes—it simply means that your disease has progressed.

What can I do about low blood sugar?
Consider these steps to reduce your risk of hypoglycemia (low blood sugar) and to deal with it if it happens.
To avoid low blood sugar, take insulin exactly as prescribed; check your glucose levels often; and eat regularly scheduled, balanced meals.
If your blood sugar does get low and you start to feel very tired, begin yawning a lot, start to sweat, or feel light-headed, eat some hard candies or a handful of raisins, or drink some fruit juice.
Your doctor will work with you to adjust the amount of insulin you take to keep your blood sugar levels from getting too high or too low.
Will insulin make me gain weight?
It may. When you start taking insulin and your high blood sugar is corrected, your body will begin using glucose properly. This means that part of the food you eat, and the energy it provides, will no longer be wasted. Regular exercise will be more important than ever, both to prevent weight gain and to improve your body’s ability to use the insulin you are taking. If you are still concerned about diet and weight gain, ask your doctor to refer you to a dietitian.
Will insulin interfere with my life?
It doesn’t have to. The very small needles and devices that are now being used make it easy to incorporate insulin into your lifestyle and, if necessary, to administer it without being noticed. You will, of course, have to plan your meals and mealtimes carefully to avoid blood sugar peaks and dips, as you’re probably doing already.
Where can I go for more information?
There are 2 resources that you may find especially helpful. The American Diabetes Association Web site (www.diabetes.org)—particularly its “Living with diabetes” page—is an excellent resource. In addition, the National Institutes of Health provides many helpful facts and figures in its PubMed Health patient resource (http://www.ncbi.nlm.nih.gov/pubmedhealth/PMH0002194/).
CORRESPONDENCE
Molly G. Minze, PharmD, Department of Pharmacy Practice, School of Pharmacy, Texas Tech University Health Sciences Center,1718 Pine Street, Abilene, TX 79601; [email protected]
1. United Kingdom Prospective Diabetes Study Group. Intensive blood-glucose control with sulphonylureas or insulin compared with conventional treatment and risk of complications in patients with type 2 diabetes (UKPDS 33). Lancet. 1998;352:837-853.
2. Holman R, Paul S, Bethel M, et al. 10-year follow-up of intensive glucose control in type 2 diabetes. N Engl J Med. 2008;359:1577-1589.
3. Brown J, Nichols G, Perry A. The burden of treatment failure in type 2 diabetes. Diabetes Care. 2004;27:1535-1540.
4. Nathan D, Buse J, Davidson M, et al. Medical management of hyperglycemia in type 2 diabetes: a consensus algorithm for the initiation and adjustment of therapy. Diabetes Care. 2009;32:193-203.
5. Rodbard H, Jellinger P, Davidson J, et al. Statement by an American Association of Clinical Endocrinologists/American College of Endocrinology consensus panel on type 2 diabetes mellitus: an algorithm for glycemic control. Endocr Pract. 2009;15:540-559.
6. DeFronzo R, Stonehouse A, Han J, et al. Relationship of baseline HbA1c and efficacy of current glucose-lowering therapies: a meta-analysis of randomized clinical trials. Diabet Med. 2010;27:309-317.
7. Gerstein H, Yale J, Harris S, et al. A randomized trial of adding insulin glargine vs. avoidance of insulin in people with type 2 diabetes on either no oral glucose-lowering agents or submaximal doses of metformin and/or sulphonylureas. The Canadian INSIGHT (Implementing New Strategies with Insulin Glargine for Hyperglycaemia Treatment) Study. Diabet Med. 2006;23:736-742.
8. Skovlund SE, Peyrot M, et al. The Diabetes Attitudes, Wishes, and Needs (DAWN) program: a new approach to improving outcomes of diabetes care. Diabetes Spectrum. 2005;18:136-142.
9. Funnell MM. Overcoming barriers to the initiation of insulin therapy. Clin Diabetes. 2007;25:36-38.
10. Polonsky WH, Jackson RA. What’s so tough about taking Insulin? Addressing the problem of psychological insulin resistance in type 2 diabetes. Clin Diabetes. 2004;22:147-150.
11. Zambanini A, Newson RB, Maisey M, et al. Injection related anxiety in insulin-treated diabetes. Diabetes Res Clin Pract. 1999;46:239-246.
12. Brunton SA, Renda SM, Davis SN. Overcoming psychological barriers to insulin use in type 2 diabetes. Clin Cornerstone. 2006;8(suppl 2):S19-S26.
13. Peragallo-Dittko V. Removing barriers to insulin therapy. Diabetes Educ. 2007;33(suppl 3):60S-65S.
14. Korytkowski M. When oral agents fail: practical barriers to starting insulin. Int J Obes Relat Metab Disord. 2002;26(suppl 3):S18-S24.
15. Parchman ML, Pugh JA, Romero RL, et al. Competing demands or clinical inertia: the case of elevated glycosylated hemoglobin. Ann Fam Med. 2007;5:196-201.
16. Riddle MC, Rosenstock J, Gerich J. Insulin Glargine 4002 Study Investigators. The Treat-to-Target Trial: randomized addition of glargine or human NPH insulin to oral therapy of type 2 diabetic patients. Diabetes Care. 2003;26:3080-3086
• Reassure patients who fear stigmatization that the small needles and devices available today make it easy to discreetly incorporate insulin therapy into everyday life. C
• Consider making a referral to a diabetes support group or a mental health counselor when a patient is reluctant to pursue insulin therapy, despite the benefits to his or her health. C
Strength of recommendation (SOR)
A Good-quality patient-oriented evidence
B Inconsistent or limited-quality patient-oriented evidence
C Consensus, usual practice, opinion, disease-oriented evidence, case series
PATIENT HANDOUT
Is it time for insulin? (PDF)
For patients with type 2 diabetes, control of hyperglycemia through diet, exercise, and pharmacologic therapy reduces the risk of microvascular complications and may have long-term cardiovascular benefits.1,2 But when the disease progresses and oral medication and lifestyle changes are no longer sufficient, many patients experience long periods of elevated glucose concentrations before insulin is added to (or replaces) a failing oral regimen.3
Both the American Diabetes Association and the American Association of Clinical Endocrinologists recommend early initiation of insulin therapy4,5 for patients with significantly elevated HbA1c, and a stepwise treatment approach, beginning with oral medications, for more modest elevations. Overall, insulin therapy offers the greatest potential for improved glycemic control.4,6,7 Yet patients, as well as their physicians, are often reluctant to initiate it. In the review that follows, we identify common barriers to insulin therapy and provide practical tips on how best to overcome them.
Why patients are “insulin resistant”
Patient barriers to insulin therapy can be divided into 3 general categories (TABLE 1)—psychological resistance, harmful effects (whether real or perceived), and financial barriers. Understanding what’s behind their hesitancy (as well as your own) makes it easier to overcome these barriers and properly integrate insulin into their health care regimen.
TABLE 1
Patient barriers to insulin8-11
| Psychological |
Belief that insulin represents failure of self-care Lack of perceived benefit Pain/fear of injections Belief that insulin use is complicated Loss of independence/change in lifestyle Stigma related to needle use |
| Harmful effects |
Hypoglycemia Weight gain Perceived adverse effects |
| Financial |
| Cost of insulin and supplies |
Most barriers are psychological
Because insulin therapy is typically introduced some time after diagnosis (and conservative management), patients often view the need for insulin as an indication that they have failed to manage their type 2 disease effectively. What’s more, many patients are convinced that insulin will provide few, if any, benefits.8
The Diabetes Attitudes, Wishes, and Needs (DAWN) study, a large international trial, found that only 27% of noninsulin-dependent patients believed that insulin could help manage their disease.8 Patients’ lack of belief in insulin’s efficacy can be attributed to negative experiences with insulin therapy, which may have been related by family or friends or simply reflect societal views. The complex nature of insulin therapy is another problem, as patients often feel overwhelmed by the prospect of having to adhere to what they consider to be a stringent daily regimen.
And for many, resistance to insulin therapy is triggered by fear of:
- needles and subcutaneous injections9-11
- loss of independence and lifestyle changes (eg, having to sacrifice pleasurable activities, such as eating out and traveling)9
- adverse effects, most notably hypoglycemia and weight gain.9-11
Other psychological barriers can be attributed to perceived societal norms, including the stigma associated with the use of needles and illicit drug use and the potential embarrassment of self-injection.9
Harmful effects. Concern about insulin’s negative effects may be exacerbated by the fact that symptoms or complications of diabetes itself, which often develop as the disease progresses, are often mistakenly attributed to insulin therapy.
Financial concerns, too, are often associated with resistance to insulin therapy, relating to the costs of newer insulin analogs and insulin administration devices.
Replace misconceptions with facts
Patients respond in different ways to a discussion of insulin initiation, and it is important to identify barriers and help resolve them. Yet there are few validated measurement tools designed for this purpose. We’ve created a patient handout, “Is it time for insulin?”, which addresses a number of common concerns. The tips that follow here should also help.
“It won’t help me”
If a patient tells you that insulin therapy will be of little or no benefit, explain that type 2 diabetes is largely due to a lack of insulin activity and that the newer insulin analogs mimic the normal physiologic response. Make it clear that insulin use is not a punishment or evidence of personal failure, but a therapeutic option that most patients need as their diabetes progresses.9,10,12
“My friend takes insulin, and her diabetes still isn’t under control”
Tell a patient who is convinced that insulin provides few benefits or has heard about people whose diabetes was not controlled by insulin that the dosing may not have been appropriate,9 and that it is important for you to work together to make any necessary adjustments.
Fear of hypoglycemia can be addressed through patient education about how to recognize signs and symptoms of low blood sugar and what actions to take to resolve it.13 Explain that frequent blood glucose monitoring; regularly scheduled, balanced meals; increased physical activity; and referral to a dietitian, when needed, will go a long way toward preventing swings in blood sugar as well as weight gain.9,14 Emphasize that exercise will improve insulin sensitivity, helping to control weight and ensure better glucose uptake, as well.
“I hate needles!”
Address needle phobia and fear of social stigma with reassurance and a demonstration of the small, thin needles on the market and the devices designed to conceal them. Point out that such devices promote privacy and make it easy for patients to discreetly incorporate insulin therapy into everyday life.
“It will be too expensive”
Patient assistance programs are available for eligible patients, with online resources such as www.Rxassist.org and www.xubex.com. You can also remind patients that health insurers, including Medicare and Medicaid plans, contribute to the cost of glucometers, test strips, and lancets, as well as the insulin itself. Diabetes supplies are often available from medical supply companies that bill health insurers directly but mail the supplies to the patients.
Are you putting up some barriers of your own?
Reluctance to introduce insulin therapy or negative feelings about it (TABLE 2)9,14,15 on the part of clinicians creates, or contributes to, “clinical inertia”—defined as awareness of a problem but a lack of action to resolve it. What’s more, any hesitancy you have about insulin therapy is likely to influence the perception of your patients.10,14
In general, physician barriers center on the fact that managing insulin therapy can be a cumbersome task for which they may not have the time or the resources. A study of clinician encounters with patients with type 2 diabetes in primary care clinics supports that belief. Each additional concern raised by a patient during the course of a visit was associated with a 49% reduction in the likelihood of a change in medication.15
TABLE 2
Provider barriers to insulin10,14,15
| Negative attitude |
| Time constraints |
| Lack of health care system support/resources |
| Concern about adverse effects |
| Fear of patient response/lack of adherence |
Hypoglycemia is a particular concern for clinicians because of its close association with tight glucose control—which relates to another barrier: the problem of patient adherence. Evidence-based findings, algorithms, and guidelines for insulin therapy can help you handle these and other clinical issues with confidence. (See “Removing physician barriers with education and evidence”.)
Learning more about insulin administration, including which formulations to use and how to ensure proper dosing, will go a long way toward eliminating clinician barriers to insulin initiation. These online resources can help.
The Treat-to-Target Trial (http://care.diabetesjournals.org/content/26/11/3080.short), for example, demonstrated that patients using long-acting insulin had lower rates of nocturnal and symptomatic hypoglycemia and were more likely to reach their target HbA1c than those on intermediate-acting insulin.16 The researchers also found that weight gain was more significant in patients with prescriptions for multiple doses of insulin each day vs those on a once-daily regimen, and that when metformin was used in conjunction with insulin therapy, weight gain was avoided.
Continuing education courses and treatment algorithms published by the American Diabetes Association (http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2606813/pdf/193.pdf) and the American Association of Clinical Endocrinologists (https://www.aace.com/sites/default/files/GlycemicControlAlgorithmPPT.pdf) can provide additional guidance.
Don’t go it alone—draw on other resources
Patient education regarding insulin therapy can also be time consuming and cumbersome, and difficult to manage in a busy primary care practice. Certified diabetes educators can help reduce your burden and address patient concerns, as can nurses, pharmacists, case managers, and behavioral therapists, as needed. For patients who need insulin but continue to resist or reject it based on overwhelming or unfounded fears, a referral to a diabetes support group, mental health provider, or behavioral counselor may be in order.
Why do I need insulin?
Oftentimes, insulin is unavoidable. Diabetes is a progressive illness, and patients often find that it gets harder and harder to keep their blood sugar at a healthy level. Over time, high blood sugar (hyperglycemia) can lead to many serious complications, such as heart disease, nerve damage, kidney disease, and damage to your eyes (retinas). Taking insulin is the best way to control your blood sugar when other steps like changes in your diet and exercise are no longer working. This does not mean that you failed in your efforts to control your diabetes—it simply means that your disease has progressed.
What can I do about low blood sugar?
Consider these steps to reduce your risk of hypoglycemia (low blood sugar) and to deal with it if it happens.
To avoid low blood sugar, take insulin exactly as prescribed; check your glucose levels often; and eat regularly scheduled, balanced meals.
If your blood sugar does get low and you start to feel very tired, begin yawning a lot, start to sweat, or feel light-headed, eat some hard candies or a handful of raisins, or drink some fruit juice.
Your doctor will work with you to adjust the amount of insulin you take to keep your blood sugar levels from getting too high or too low.
Will insulin make me gain weight?
It may. When you start taking insulin and your high blood sugar is corrected, your body will begin using glucose properly. This means that part of the food you eat, and the energy it provides, will no longer be wasted. Regular exercise will be more important than ever, both to prevent weight gain and to improve your body’s ability to use the insulin you are taking. If you are still concerned about diet and weight gain, ask your doctor to refer you to a dietitian.
Will insulin interfere with my life?
It doesn’t have to. The very small needles and devices that are now being used make it easy to incorporate insulin into your lifestyle and, if necessary, to administer it without being noticed. You will, of course, have to plan your meals and mealtimes carefully to avoid blood sugar peaks and dips, as you’re probably doing already.
Where can I go for more information?
There are 2 resources that you may find especially helpful. The American Diabetes Association Web site (www.diabetes.org)—particularly its “Living with diabetes” page—is an excellent resource. In addition, the National Institutes of Health provides many helpful facts and figures in its PubMed Health patient resource (http://www.ncbi.nlm.nih.gov/pubmedhealth/PMH0002194/).
CORRESPONDENCE
Molly G. Minze, PharmD, Department of Pharmacy Practice, School of Pharmacy, Texas Tech University Health Sciences Center,1718 Pine Street, Abilene, TX 79601; [email protected]
• Reassure patients who fear stigmatization that the small needles and devices available today make it easy to discreetly incorporate insulin therapy into everyday life. C
• Consider making a referral to a diabetes support group or a mental health counselor when a patient is reluctant to pursue insulin therapy, despite the benefits to his or her health. C
Strength of recommendation (SOR)
A Good-quality patient-oriented evidence
B Inconsistent or limited-quality patient-oriented evidence
C Consensus, usual practice, opinion, disease-oriented evidence, case series
PATIENT HANDOUT
Is it time for insulin? (PDF)
For patients with type 2 diabetes, control of hyperglycemia through diet, exercise, and pharmacologic therapy reduces the risk of microvascular complications and may have long-term cardiovascular benefits.1,2 But when the disease progresses and oral medication and lifestyle changes are no longer sufficient, many patients experience long periods of elevated glucose concentrations before insulin is added to (or replaces) a failing oral regimen.3
Both the American Diabetes Association and the American Association of Clinical Endocrinologists recommend early initiation of insulin therapy4,5 for patients with significantly elevated HbA1c, and a stepwise treatment approach, beginning with oral medications, for more modest elevations. Overall, insulin therapy offers the greatest potential for improved glycemic control.4,6,7 Yet patients, as well as their physicians, are often reluctant to initiate it. In the review that follows, we identify common barriers to insulin therapy and provide practical tips on how best to overcome them.
Why patients are “insulin resistant”
Patient barriers to insulin therapy can be divided into 3 general categories (TABLE 1)—psychological resistance, harmful effects (whether real or perceived), and financial barriers. Understanding what’s behind their hesitancy (as well as your own) makes it easier to overcome these barriers and properly integrate insulin into their health care regimen.
TABLE 1
Patient barriers to insulin8-11
| Psychological |
Belief that insulin represents failure of self-care Lack of perceived benefit Pain/fear of injections Belief that insulin use is complicated Loss of independence/change in lifestyle Stigma related to needle use |
| Harmful effects |
Hypoglycemia Weight gain Perceived adverse effects |
| Financial |
| Cost of insulin and supplies |
Most barriers are psychological
Because insulin therapy is typically introduced some time after diagnosis (and conservative management), patients often view the need for insulin as an indication that they have failed to manage their type 2 disease effectively. What’s more, many patients are convinced that insulin will provide few, if any, benefits.8
The Diabetes Attitudes, Wishes, and Needs (DAWN) study, a large international trial, found that only 27% of noninsulin-dependent patients believed that insulin could help manage their disease.8 Patients’ lack of belief in insulin’s efficacy can be attributed to negative experiences with insulin therapy, which may have been related by family or friends or simply reflect societal views. The complex nature of insulin therapy is another problem, as patients often feel overwhelmed by the prospect of having to adhere to what they consider to be a stringent daily regimen.
And for many, resistance to insulin therapy is triggered by fear of:
- needles and subcutaneous injections9-11
- loss of independence and lifestyle changes (eg, having to sacrifice pleasurable activities, such as eating out and traveling)9
- adverse effects, most notably hypoglycemia and weight gain.9-11
Other psychological barriers can be attributed to perceived societal norms, including the stigma associated with the use of needles and illicit drug use and the potential embarrassment of self-injection.9
Harmful effects. Concern about insulin’s negative effects may be exacerbated by the fact that symptoms or complications of diabetes itself, which often develop as the disease progresses, are often mistakenly attributed to insulin therapy.
Financial concerns, too, are often associated with resistance to insulin therapy, relating to the costs of newer insulin analogs and insulin administration devices.
Replace misconceptions with facts
Patients respond in different ways to a discussion of insulin initiation, and it is important to identify barriers and help resolve them. Yet there are few validated measurement tools designed for this purpose. We’ve created a patient handout, “Is it time for insulin?”, which addresses a number of common concerns. The tips that follow here should also help.
“It won’t help me”
If a patient tells you that insulin therapy will be of little or no benefit, explain that type 2 diabetes is largely due to a lack of insulin activity and that the newer insulin analogs mimic the normal physiologic response. Make it clear that insulin use is not a punishment or evidence of personal failure, but a therapeutic option that most patients need as their diabetes progresses.9,10,12
“My friend takes insulin, and her diabetes still isn’t under control”
Tell a patient who is convinced that insulin provides few benefits or has heard about people whose diabetes was not controlled by insulin that the dosing may not have been appropriate,9 and that it is important for you to work together to make any necessary adjustments.
Fear of hypoglycemia can be addressed through patient education about how to recognize signs and symptoms of low blood sugar and what actions to take to resolve it.13 Explain that frequent blood glucose monitoring; regularly scheduled, balanced meals; increased physical activity; and referral to a dietitian, when needed, will go a long way toward preventing swings in blood sugar as well as weight gain.9,14 Emphasize that exercise will improve insulin sensitivity, helping to control weight and ensure better glucose uptake, as well.
“I hate needles!”
Address needle phobia and fear of social stigma with reassurance and a demonstration of the small, thin needles on the market and the devices designed to conceal them. Point out that such devices promote privacy and make it easy for patients to discreetly incorporate insulin therapy into everyday life.
“It will be too expensive”
Patient assistance programs are available for eligible patients, with online resources such as www.Rxassist.org and www.xubex.com. You can also remind patients that health insurers, including Medicare and Medicaid plans, contribute to the cost of glucometers, test strips, and lancets, as well as the insulin itself. Diabetes supplies are often available from medical supply companies that bill health insurers directly but mail the supplies to the patients.
Are you putting up some barriers of your own?
Reluctance to introduce insulin therapy or negative feelings about it (TABLE 2)9,14,15 on the part of clinicians creates, or contributes to, “clinical inertia”—defined as awareness of a problem but a lack of action to resolve it. What’s more, any hesitancy you have about insulin therapy is likely to influence the perception of your patients.10,14
In general, physician barriers center on the fact that managing insulin therapy can be a cumbersome task for which they may not have the time or the resources. A study of clinician encounters with patients with type 2 diabetes in primary care clinics supports that belief. Each additional concern raised by a patient during the course of a visit was associated with a 49% reduction in the likelihood of a change in medication.15
TABLE 2
Provider barriers to insulin10,14,15
| Negative attitude |
| Time constraints |
| Lack of health care system support/resources |
| Concern about adverse effects |
| Fear of patient response/lack of adherence |
Hypoglycemia is a particular concern for clinicians because of its close association with tight glucose control—which relates to another barrier: the problem of patient adherence. Evidence-based findings, algorithms, and guidelines for insulin therapy can help you handle these and other clinical issues with confidence. (See “Removing physician barriers with education and evidence”.)
Learning more about insulin administration, including which formulations to use and how to ensure proper dosing, will go a long way toward eliminating clinician barriers to insulin initiation. These online resources can help.
The Treat-to-Target Trial (http://care.diabetesjournals.org/content/26/11/3080.short), for example, demonstrated that patients using long-acting insulin had lower rates of nocturnal and symptomatic hypoglycemia and were more likely to reach their target HbA1c than those on intermediate-acting insulin.16 The researchers also found that weight gain was more significant in patients with prescriptions for multiple doses of insulin each day vs those on a once-daily regimen, and that when metformin was used in conjunction with insulin therapy, weight gain was avoided.
Continuing education courses and treatment algorithms published by the American Diabetes Association (http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2606813/pdf/193.pdf) and the American Association of Clinical Endocrinologists (https://www.aace.com/sites/default/files/GlycemicControlAlgorithmPPT.pdf) can provide additional guidance.
Don’t go it alone—draw on other resources
Patient education regarding insulin therapy can also be time consuming and cumbersome, and difficult to manage in a busy primary care practice. Certified diabetes educators can help reduce your burden and address patient concerns, as can nurses, pharmacists, case managers, and behavioral therapists, as needed. For patients who need insulin but continue to resist or reject it based on overwhelming or unfounded fears, a referral to a diabetes support group, mental health provider, or behavioral counselor may be in order.
Why do I need insulin?
Oftentimes, insulin is unavoidable. Diabetes is a progressive illness, and patients often find that it gets harder and harder to keep their blood sugar at a healthy level. Over time, high blood sugar (hyperglycemia) can lead to many serious complications, such as heart disease, nerve damage, kidney disease, and damage to your eyes (retinas). Taking insulin is the best way to control your blood sugar when other steps like changes in your diet and exercise are no longer working. This does not mean that you failed in your efforts to control your diabetes—it simply means that your disease has progressed.
What can I do about low blood sugar?
Consider these steps to reduce your risk of hypoglycemia (low blood sugar) and to deal with it if it happens.
To avoid low blood sugar, take insulin exactly as prescribed; check your glucose levels often; and eat regularly scheduled, balanced meals.
If your blood sugar does get low and you start to feel very tired, begin yawning a lot, start to sweat, or feel light-headed, eat some hard candies or a handful of raisins, or drink some fruit juice.
Your doctor will work with you to adjust the amount of insulin you take to keep your blood sugar levels from getting too high or too low.
Will insulin make me gain weight?
It may. When you start taking insulin and your high blood sugar is corrected, your body will begin using glucose properly. This means that part of the food you eat, and the energy it provides, will no longer be wasted. Regular exercise will be more important than ever, both to prevent weight gain and to improve your body’s ability to use the insulin you are taking. If you are still concerned about diet and weight gain, ask your doctor to refer you to a dietitian.
Will insulin interfere with my life?
It doesn’t have to. The very small needles and devices that are now being used make it easy to incorporate insulin into your lifestyle and, if necessary, to administer it without being noticed. You will, of course, have to plan your meals and mealtimes carefully to avoid blood sugar peaks and dips, as you’re probably doing already.
Where can I go for more information?
There are 2 resources that you may find especially helpful. The American Diabetes Association Web site (www.diabetes.org)—particularly its “Living with diabetes” page—is an excellent resource. In addition, the National Institutes of Health provides many helpful facts and figures in its PubMed Health patient resource (http://www.ncbi.nlm.nih.gov/pubmedhealth/PMH0002194/).
CORRESPONDENCE
Molly G. Minze, PharmD, Department of Pharmacy Practice, School of Pharmacy, Texas Tech University Health Sciences Center,1718 Pine Street, Abilene, TX 79601; [email protected]
1. United Kingdom Prospective Diabetes Study Group. Intensive blood-glucose control with sulphonylureas or insulin compared with conventional treatment and risk of complications in patients with type 2 diabetes (UKPDS 33). Lancet. 1998;352:837-853.
2. Holman R, Paul S, Bethel M, et al. 10-year follow-up of intensive glucose control in type 2 diabetes. N Engl J Med. 2008;359:1577-1589.
3. Brown J, Nichols G, Perry A. The burden of treatment failure in type 2 diabetes. Diabetes Care. 2004;27:1535-1540.
4. Nathan D, Buse J, Davidson M, et al. Medical management of hyperglycemia in type 2 diabetes: a consensus algorithm for the initiation and adjustment of therapy. Diabetes Care. 2009;32:193-203.
5. Rodbard H, Jellinger P, Davidson J, et al. Statement by an American Association of Clinical Endocrinologists/American College of Endocrinology consensus panel on type 2 diabetes mellitus: an algorithm for glycemic control. Endocr Pract. 2009;15:540-559.
6. DeFronzo R, Stonehouse A, Han J, et al. Relationship of baseline HbA1c and efficacy of current glucose-lowering therapies: a meta-analysis of randomized clinical trials. Diabet Med. 2010;27:309-317.
7. Gerstein H, Yale J, Harris S, et al. A randomized trial of adding insulin glargine vs. avoidance of insulin in people with type 2 diabetes on either no oral glucose-lowering agents or submaximal doses of metformin and/or sulphonylureas. The Canadian INSIGHT (Implementing New Strategies with Insulin Glargine for Hyperglycaemia Treatment) Study. Diabet Med. 2006;23:736-742.
8. Skovlund SE, Peyrot M, et al. The Diabetes Attitudes, Wishes, and Needs (DAWN) program: a new approach to improving outcomes of diabetes care. Diabetes Spectrum. 2005;18:136-142.
9. Funnell MM. Overcoming barriers to the initiation of insulin therapy. Clin Diabetes. 2007;25:36-38.
10. Polonsky WH, Jackson RA. What’s so tough about taking Insulin? Addressing the problem of psychological insulin resistance in type 2 diabetes. Clin Diabetes. 2004;22:147-150.
11. Zambanini A, Newson RB, Maisey M, et al. Injection related anxiety in insulin-treated diabetes. Diabetes Res Clin Pract. 1999;46:239-246.
12. Brunton SA, Renda SM, Davis SN. Overcoming psychological barriers to insulin use in type 2 diabetes. Clin Cornerstone. 2006;8(suppl 2):S19-S26.
13. Peragallo-Dittko V. Removing barriers to insulin therapy. Diabetes Educ. 2007;33(suppl 3):60S-65S.
14. Korytkowski M. When oral agents fail: practical barriers to starting insulin. Int J Obes Relat Metab Disord. 2002;26(suppl 3):S18-S24.
15. Parchman ML, Pugh JA, Romero RL, et al. Competing demands or clinical inertia: the case of elevated glycosylated hemoglobin. Ann Fam Med. 2007;5:196-201.
16. Riddle MC, Rosenstock J, Gerich J. Insulin Glargine 4002 Study Investigators. The Treat-to-Target Trial: randomized addition of glargine or human NPH insulin to oral therapy of type 2 diabetic patients. Diabetes Care. 2003;26:3080-3086
1. United Kingdom Prospective Diabetes Study Group. Intensive blood-glucose control with sulphonylureas or insulin compared with conventional treatment and risk of complications in patients with type 2 diabetes (UKPDS 33). Lancet. 1998;352:837-853.
2. Holman R, Paul S, Bethel M, et al. 10-year follow-up of intensive glucose control in type 2 diabetes. N Engl J Med. 2008;359:1577-1589.
3. Brown J, Nichols G, Perry A. The burden of treatment failure in type 2 diabetes. Diabetes Care. 2004;27:1535-1540.
4. Nathan D, Buse J, Davidson M, et al. Medical management of hyperglycemia in type 2 diabetes: a consensus algorithm for the initiation and adjustment of therapy. Diabetes Care. 2009;32:193-203.
5. Rodbard H, Jellinger P, Davidson J, et al. Statement by an American Association of Clinical Endocrinologists/American College of Endocrinology consensus panel on type 2 diabetes mellitus: an algorithm for glycemic control. Endocr Pract. 2009;15:540-559.
6. DeFronzo R, Stonehouse A, Han J, et al. Relationship of baseline HbA1c and efficacy of current glucose-lowering therapies: a meta-analysis of randomized clinical trials. Diabet Med. 2010;27:309-317.
7. Gerstein H, Yale J, Harris S, et al. A randomized trial of adding insulin glargine vs. avoidance of insulin in people with type 2 diabetes on either no oral glucose-lowering agents or submaximal doses of metformin and/or sulphonylureas. The Canadian INSIGHT (Implementing New Strategies with Insulin Glargine for Hyperglycaemia Treatment) Study. Diabet Med. 2006;23:736-742.
8. Skovlund SE, Peyrot M, et al. The Diabetes Attitudes, Wishes, and Needs (DAWN) program: a new approach to improving outcomes of diabetes care. Diabetes Spectrum. 2005;18:136-142.
9. Funnell MM. Overcoming barriers to the initiation of insulin therapy. Clin Diabetes. 2007;25:36-38.
10. Polonsky WH, Jackson RA. What’s so tough about taking Insulin? Addressing the problem of psychological insulin resistance in type 2 diabetes. Clin Diabetes. 2004;22:147-150.
11. Zambanini A, Newson RB, Maisey M, et al. Injection related anxiety in insulin-treated diabetes. Diabetes Res Clin Pract. 1999;46:239-246.
12. Brunton SA, Renda SM, Davis SN. Overcoming psychological barriers to insulin use in type 2 diabetes. Clin Cornerstone. 2006;8(suppl 2):S19-S26.
13. Peragallo-Dittko V. Removing barriers to insulin therapy. Diabetes Educ. 2007;33(suppl 3):60S-65S.
14. Korytkowski M. When oral agents fail: practical barriers to starting insulin. Int J Obes Relat Metab Disord. 2002;26(suppl 3):S18-S24.
15. Parchman ML, Pugh JA, Romero RL, et al. Competing demands or clinical inertia: the case of elevated glycosylated hemoglobin. Ann Fam Med. 2007;5:196-201.
16. Riddle MC, Rosenstock J, Gerich J. Insulin Glargine 4002 Study Investigators. The Treat-to-Target Trial: randomized addition of glargine or human NPH insulin to oral therapy of type 2 diabetic patients. Diabetes Care. 2003;26:3080-3086
Chronic hepatitis B infection: A workshop consensus statement and algorithm
• Screen patients at risk of contracting hepatits B virus (HBV), especially those from HBV-endemic regions of the world, by testing for hepatitis B surface antigen and antibody (HBsAg and anti-HBs). A
• Vaccinate all infants, children, and adolescents following guidelines of the Centers for Disease Control and Prevention and American Academy of Pediatrics, as well as at-risk adults whose screening results are negative for both HBsAg and anti-HBs. A
• Provide periodic monitoring for patients who are HBsAg-positive. While these patients may appear asymptomatic, they are infected with HBV and require further evaluation. A
• Consult a specialist experienced in treating hepatitis if active liver disease is suspected in patients with chronic HBV infection who present with elevated alanine aminotransferase and HBV DNA >2,000 IU/mL. B
Screening for hepatitis B virus (HBV) infection is simple and relatively inexpensive. Yet it is underused in everyday practice, leaving some HBV-positive patients unaware and at risk for serious health consequences, including cirrhosis, liver failure, and hepatocellular carcinoma (HCC).1 In addition, many primary care providers do not follow existing guidelines for HBV screening and management.2 Yet they are often the first, and sometimes the only, clinicians that infected individuals will see.
Why chronic HBV is still a problem. Although the incidence of acute HBV infection has declined significantly as a result of universal infant vaccination in the United States, chronic infections are still prevalent in this country due to such factors as immigration from areas where HBV is endemic, perinatal transmission, transmission among household contacts, and risky behaviors. In most adolescents and adults, HBV infection leads to acute hepatitis from which they fully recover; chronic infection ensues in only 5% to 10% of cases. However, 90% of infants and 25% to 50% of children younger than 5 years who become infected with HBV go on to develop lifelong infection. Most people with chronic HBV infection do not exhibit any signs of clinical illness, which makes screening all the more important—particularly since effective antiviral treatments are available.1,3
To help primary care providers address the issues of screening for HBV, the Hepatitis B Foundation convened a workshop of prominent primary care practitioners and specialists in hepatitis and liver diseases. The workshop panel reviewed evidence-based guidelines and reports from the American Association for the Study of Liver Diseases (AASLD), the Centers for Disease Control and Prevention (CDC), the National Institutes of Health (NIH), and the Institute of Medicine (IOM), as well as a recent Hepatitis B Foundation publication on HBV screening and management in children and other relevant publications.1-5 The resultant algorithm and consensus recommendations presented here can assist primary care providers in applying evidence-based guidelines for HBV infection to everyday practice.
3 phases of HBV infection: What screening results mean
Hepatitis B surface antigen (HBsAg) that is persistently detectable in a patient’s serum for more than 6 months signifies chronic HBV infection.1,3,4 The 3 immunologic phases of chronic HBV infection—immune tolerant, immune active, and inactive carrier—are determined by serum levels of alanine aminotransferase (ALT) and HBV DNA, and the presence or absence of hepatitis B e antigen (HBeAg) (TABLE 1).6
All individuals with chronic HBV infection are initially HBeAg positive. Those in the immune tolerant phase also have high levels of circulating virus, indicated by HBV DNA levels. However, the body does not mount an immune response to the virus; there is no active liver disease, and the serum ALT level is normal.
When the immune system recognizes HBV as foreign, the patient enters the immune active phase, wherein liver inflammation and fibrosis can develop and ALT is correspondingly elevated. HBV antibody (anti-HBe) may be present.
In nearly all patients, HBeAg seroconversion to HBeAg-negative/anti-HBe-positive status occurs spontaneously or as a result of antiviral treatment. After seroconversion, most patients enter the HBsAg inactive carrier phase, in which a strong cellular immune response is able to suppress, but not eliminate, the virus. This phase typically features low or undetectable serum levels of HBV DNA and normal ALT levels. Over time, liver inflammation and fibrosis improve, and the risk of cirrhosis and HCC declines.7
However, some patients do not enter the inactive phase after HBeAg seroconversion. They instead continue to exhibit active viral replication and liver disease due to the emergence of one or more HBeAg-negative viral mutants. Moreover, in as many as 20% of those who enter the inactive HBsAg carrier state, infection will reactivate and possibly return the patient to HBeAg-positive status. HBV infection is a dynamic condition: Individuals can go from active disease to the inactive phase and then have reactivation of liver disease at any point during their lifetime. Thus, patients require lifelong monitoring of their chronic infection.8 .
Since chronic HBV infection cannot be cured, the desired clinical outcome is for patients to enter and remain in the inactive HBsAg carrier phase. Evidence suggests that, in this phase, the risk of decompensated cirrhosis may also significantly decrease.9 A few inactive HBsAg carriers (0.5%/year) will clear the surface antigen and may develop protective antibodies (anti-HBs). Development of cirrhosis after loss of HBsAg is extremely rare; however, the risk of HCC, although reduced, is not eliminated.10
If a patient is unable to suppress the virus, or if infection reactivates after the patient achieves inactive carrier status, antiviral therapy may still decrease the risk of cirrhosis and HCC through durable suppression of HBV DNA to low or undetectable levels and normalization of ALT. Seven drugs are approved by the U.S. Food and Drug Administration (FDA) for treatment of chronic hepatitis B infection (TABLE 2).3 The decision to treat must take into account multiple factors, including phase of disease, age of the patient, extent of liver involvement on biopsy, potential efficacy of and adverse events associated with available therapies, cost of long-term medication, and, importantly, the high risk of development of nucleos(t)ide analog-resistant viral strains. Many studies have demonstrated the benefit of treating patients with advanced fibrosis or cirrhosis.9,11–13 However, no study has shown a benefit of treating those in the immune tolerant or inactive carrier phases.
TABLE 1
Phases of chronic HBV infection (HBsAg+ >6 mos)6
| Phase | Labs and histology |
|---|---|
| immune tolerant | HBV DNA >20,000 IU/mL* ALT normal HBeAg detectable No or minimal liver inflammation and fibrosis |
| Immune active | HBV DNA usually >20,000 IU/mL* ALT elevated HBeAg may be detectable or not; anti-HBe may be present Liver inflammation and fibrosis can develop |
| Inactive HBsAg carrier | HBV DNA <2000 IU/mL or undetectable* ALT normal HBeAg undetectable; anti-HBe present Minimal to no liver inflammation; fibrosis may regress |
| Reactivation | HBV DNA levels increase ALT normal or elevated HBeAg undetectable. |
| ALT, alanine aminotransferase; anti-HBe, antibody to HBeAg; HBsAg, hepatitis B surface antigen; HBeAg, hepatitis B e-antigen; HBV, hepatitis B virus. *For HBV DNA: 2000 IU/ml=104 copies/ml; 20,000 IU/mL=105 copies/mL | |
TABLE 2
FDA-approved drugs for the treatment of chronic HBV infection3
| Drug | labeled for use in: |
|---|---|
| Interferons | |
| Interferon alfa-2b (Intron A) | Adults; children >12 months |
| Peginterferon alfa-2a (Pegasys) | Adults |
| Nucleos(t)ide analogs | |
| Lamivudine (Epivir-HBV) | Adults; children >3 years |
| Adefovir dipivoxil (Hepsera) | Adults; children >12 years |
| Entecavir (Baraclude) | Adults; children >16 years |
| Telbivudine (Tyzeka) | Adults |
| Tenofovir disoproxil fumarate (Viread) | Adults |
| HBV, hepatitis B virus. | |
Key opportunities to make a difference
Primary care providers can form an effective first-line of defense against morbidity and mortality associated with chronic HBV infection by:
- immunizing all infants, children, and adolescents, as well as adults at risk to acquire HBV, following guidelines from the CDC and American Academy of Pediatrics;
- screening those at high risk, as per CDC guidelines;
- performing clinical and laboratory evaluation of patients who have chronic HBV infection, to determine current phase of disease;
- monitoring patients in the immune tolerant or inactive phases every 6 to 12 months for disease progression; and
- consulting with a liver specialist or HBV-experienced provider for patients in the immune active phase, to determine treatment strategies.
Our panel has developed an algorithm (FIGURE) that addresses the screening of individuals at risk of contracting HBV and the evaluation and monitoring of those who are identified as HBsAg-positive. Although the algorithm cannot anticipate all possible clinical circumstances, it offers a general path forward based on the results of routine laboratory tests. Ideally, an office system—whether using electronic medical records or not—would incorporate guideline-based prompts for screening and management.
FIGURE
Suspect HBV infection? Use this algorithm to screen and intervene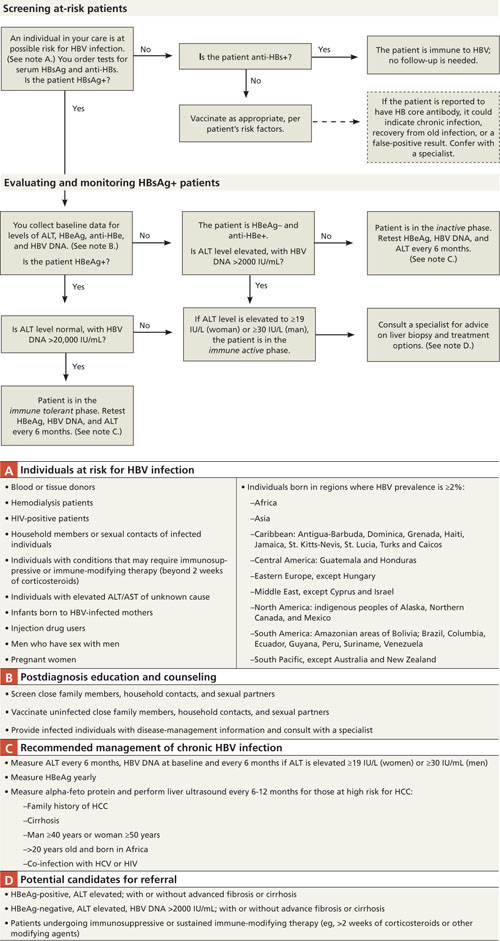
ALT, alanine aminotransferase; anti-HBe, antibody to HBeAg; anti-HBs, antibody to HBsAg; AST, aspartate aminotransferase; DNA, deoxyribose nucleic acid; HBeAg, hepatitis B e-antigen (protein produced by HBV, indicating heightened viral activity); HBsAg, hepatitis B surface antigen; HBV, hepatitis B virus; HIV, human immunodeficiency virus; HCC, hepatocellular carcinoma.
Source: Primary Care Provider Workshop on Hepatitis B, sponsored by the Hepatitis B Foundation in Doylestown, Pa (March 10-11, 2010).
Underuse of screening means many infected individuals are missed
The CDC has identified high-risk groups for HBV screening, including all individuals born in geographic regions where HBsAg prevalence is ≥2% (FIGURE, NOTE A).4 Screening is simple and relatively inexpensive (commercial diagnostic laboratories currently charge $150-$250 to screen for HBsAg and anti-HBs). Despite these recommendations, the recent IOM report confirms that screening is under-used or is not being done appropriately.2
Screening is also recommended for individuals about to undergo immunosuppressive or immune-modifying therapy (eg, for treatment of cancer, rheumatoid arthritis, or inflammatory bowel disease, or in preparation for bone marrow or other transplant). For these patients who are also asymptomatic inactive carriers of HBV, the risk of reactivation can be as high as 50%, especially in patients receiving chemotherapy for lymphoma. Deaths from fulminant hepatitis have also been reported; however, preemptive HBV antiviral treatment can reduce this risk to about 10% or less.14,15 The workshop panel recommends that providers screen for HBV under these circumstances, and that HBsAg-positive patients should start preemptive oral HBV antiviral therapy before receiving immunosuppressive or immune-modifying therapy (including systemic corticosteroids >2 weeks) to prevent a flare of hepatitis.2
Differentiate those who are chronically infected, immune, or susceptible
The CDC recommends screening for both HBsAg and anti-HBs. Taken together, the results of these tests can help you discern if the patient is actively infected (HBsAg-positive); immune (HBsAg-negative and anti-HBs-positive); or susceptible (negative for both seromarkers).
Testing for the antibody to HBV core antigen (anti-HBc) is occasionally included in screening panels. Its presence cannot distinguish between current and previous infection. False-positive test results also occur.
Vaccinate seronegative individuals who are at risk for HBV
Although the CDC recommends vaccination of all HBsAg-negative individuals at risk for acquiring HBV, vaccine coverage of adults in the United States remains low.2,16 The workshop panel recommends that all primary care offices treating adults stock HBV vaccine. Of course, routinely stocking vaccine may present financial challenges, including purchase cost, storage, unused expired product, and reimbursement. Your practice may want to coordinate coverage with the local department of health, area hospitals, or large practices that stock vaccine, to ensure timely vaccination of patients.
No further follow-up is needed for patients immune to HBV
If the screening result for HBsAg is negative but anti-HBs is positive, the patient is immune to HBV. If the screening panel also included testing for anti-HBc and it is positive, the patient has natural immunity. A positive result for anti-HBs alone indicates prior vaccination or prior infection and seroconversion.
A positive HBsAg screening test calls for further patient work-up
If a patient tests positive for HBsAg, collect baseline data for ALT, HBeAg, anti-HBe, and HBV DNA levels.
In addition, encourage screening and vaccination of sexual partners and close household contacts of infected individuals. Patient education and counseling are important to dispel myths about HBV transmission (eg, HBV is not spread through casual contact such as handshakes or food sharing) and to reinforce the importance of regular care to prevent disease progression.
Evaluating and monitoring the chronic HBV patient
Use serum ALT levels, HBeAg and anti-HBe serology, and HBV DNA levels to identify the phase of HBV infection and guide patient management (FIGURE).
Interpreting viral DNA levels: Knowing when not to treat
The presence of HBeAg in serum indicates viral replication. Although HBeAg-positive patients in the immune tolerant or immune active phases generally have high levels of circulating HBV DNA (>20,000 IU/mL), these DNA levels do not necessarily correlate with active liver disease. In the immune tolerant phase, there is no clearly established benefit of antiviral treatment regardless of HBV DNA levels, and the risk of development of viral resistance to oral antiviral drugs is a serious concern. There is also no indication for treatment in the inactive carrier phase.
Discuss with patients why treatment is inappropriate in these phases and how the development of resistance to antiviral therapies can have serious negative consequences for their future treatment needs. Also explain that, because chronic HBV infection is dynamic, they will require lifetime follow-up care, even if they are currently in the immune tolerant or inactive phase.1,3
Surveillance for HCC in patients with chronic HBV infection
The most common adverse outcome of chronic HBV infection is HCC, occurring in up to 25% of men and 15% of women over their lifetimes.17 Because early detection and effective treatment for HCC can prolong life in HBsAg-positive individuals who have HCC or are at risk for acquiring it, the workshop panel recommends that primary care providers perform periodic screening for HCC according to the current AASLD guidelines.3,17 Candidates for HCC screening are those with family histories of HCC; those with cirrhosis or co-infection with HCV or HIV; and men >40 years and women >50 years. HBV-infected men born in Africa may acquire HCC at a younger age due to possible environmental exposure to aflatoxin, a carcinogenic mold. The AASLD guideline suggests screening this group with liver ultrasound every 6 months, starting at age 20. Although the AASLD guideline does not specifically recommend measuring serum alpha-fetoprotein (AFP), many practitioners monitor AFP, which improves sensitivity but has low specificity.17
Rising ALT suggests active liver disease
Serum ALT is a surrogate indicator of possible liver damage or disease. Generally, when an HBsAg-positive patient’s ALT rises above normal (≥19 IU/L for women and ≥30 IU/L for men, when standard reference ranges are 0-40), they have moved into the immune active phase, where liver inflammation and fibrosis can develop.
Also consider other potential causes of ALT elevation, especially when it occurs in association with low or undetectable levels of HBV DNA. Alternative causes include hepatitis C, heavy alcohol use, medications, and nonalcoholic fatty liver disease. Consultation with a liver specialist may be helpful to rule out or confirm these comorbidities.
Seeking out expertise in HBV patient management
When a patient with chronic HBV infection has moved into the immune active phase, consult with a provider who has expertise in HBV—whether you choose to refer or to co-manage the patient with the specialist—to obtain advice on further work-up and development of a long-term management and treatment strategy. Individuals with small liver tumors identified on ultrasound or an elevated AFP level require immediate referral to a clinician who treats HCC, such as a transplant hepatologist.
Ensuring the health of pregnant women
The CDC recommends that all pregnant women be tested for HBsAg at an early prenatal visit. Counsel women who are HBsAg-positive on what this status means for their own health, in addition to that of their newborn. If you are providing prenatal care, collect baseline data for ALT, HBe serology, and HBV DNA levels. Promptly refer any patient with an elevated ALT level to a specialist for care during pregnancy.
Acknowledgement
Medical writing services were provided by Theresa M. Wizemann, PhD, of Wizemann Scientific Communications, LLC, under contract with the Hepatitis B Foundation.
CORRESPONDENCE
Joan M. Block, RN, BSN, executive director, Hepatitis B Foundation, 3805 Old Easton Road, Doylestown, PA 18902; [email protected]
1. Sorrell MF, Belongia EA, Costa J, et al. National Institutes of Health Consensus Development Conference statement: management of Hepatitis B. Ann Intern Med. 2009;150:104-110.
2. Institute of Medicine Hepatitis and Liver Cancer: A National Strategy for Prevention and Control of Hepatitis B and C. Washington, DC: National Academies Press; 2010.
3. Lok AS, McMahon BJ. Chronic hepatitis B: update 2009. AASLD practice guideline. Hepatology. 2009;50:661-662.
4. Weinbaum CM, Williams I, Mast EE, et al. Recommendations for identification and public health management of persons with chronic hepatitis B virus infection. MMWR Recomm Rep. 2008;57(RR08):1-20.
5. Haber BA, Block JM, Jonas MM, et al. Recommendations for screening, monitoring, and referral of pediatric chronic hepatitis B. Pediatrics. 2009;124:e1007-e1113.
6. Hoofnagle JH, Doo E, Liang TJ, et al. Management of hepatitis B: summary of a clinical research workshop. Hepatology. 2007;45:1056-1075.
7. Yang HI, Lu SN, Liaw YF, et al. Hepatitis B e antigen and the risk of hepatocellular carcinoma. N Engl J Med. 2002;347:168-174.
8. McMahon BJ. The natural history of chronic hepatitis B virus infection. Hepatology. 2009;49:S45-S55.
9. Liaw YF, Sung JJ, Chow WC, et al. Lamivudine for patients with chronic hepatitis B and advanced liver disease. N Engl J Med. 2004;351:1521-1531.
10. Simonetti J, Bulkow L, McMahon BJ, et al. Clearance of hepatitis B surface antigen and risk of hepatocellular carcinoma in a cohort chronically infected with hepatitis B virus. Hepatology. 2010;51:1531-1537.
11. Perrillo RP, Wright T, Rakela J, et al. A multicenter United States-Canadian trial to assess lamivudine monotherapy before and after liver transplantation for chronic hepatitis B. Hepatology. 2001;33:424-432.
12. Villeneuve JP, Condreay LD, Willems B, et al. Lamivudine treatment for decompensated cirrhosis resulting from chronic hepatitis B. Hepatology. 2000;31:207-210.
13. Fontana RJ, Hann HW, Perrillo RP, et al. Determinants of early mortality in patients with decompensated chronic hepatitis B treated with antiviral therapy. Gastroenterology. 2002;123:719-727.
14. Yeo W, Chan PK, Zhong S, et al. Frequency of hepatitis B virus reactivation in cancer patients undergoing cytotoxic chemotherapy: a prospective study of 626 patients with identification of risk factors. J Med Virol. 2000;62:299-307.
15. Loomba R, Rowley A, Wesley R, et al. Systematic review: the effect of preventive lamivudine on hepatitis B reactivation during chemotherapy. Ann Intern Med. 2008;148:519-528.
16. Mast EE, Weinbaum CM, Fiore AE, et al. A comprehensive immunization strategy to eliminate transmission of hepatitis B virus infection in the United States. recommendations of the Advisory Committee on Immunization Practices (ACIP) part II: immunization of adults. MMWR Recomm Rep. 2006;55(RR-16):1-33.
17. Bruix J, Sherman M. Management of hepatocellular carcinoma: an update. AASLD Practice Guideline. 2010. Available at: http://www.aasld.org/practiceguidelines/Documents/Bookmarked%20Practice%20Guidelines/HCCUpdate2010.pdf. Accessed November 8, 2010.
• Screen patients at risk of contracting hepatits B virus (HBV), especially those from HBV-endemic regions of the world, by testing for hepatitis B surface antigen and antibody (HBsAg and anti-HBs). A
• Vaccinate all infants, children, and adolescents following guidelines of the Centers for Disease Control and Prevention and American Academy of Pediatrics, as well as at-risk adults whose screening results are negative for both HBsAg and anti-HBs. A
• Provide periodic monitoring for patients who are HBsAg-positive. While these patients may appear asymptomatic, they are infected with HBV and require further evaluation. A
• Consult a specialist experienced in treating hepatitis if active liver disease is suspected in patients with chronic HBV infection who present with elevated alanine aminotransferase and HBV DNA >2,000 IU/mL. B
Screening for hepatitis B virus (HBV) infection is simple and relatively inexpensive. Yet it is underused in everyday practice, leaving some HBV-positive patients unaware and at risk for serious health consequences, including cirrhosis, liver failure, and hepatocellular carcinoma (HCC).1 In addition, many primary care providers do not follow existing guidelines for HBV screening and management.2 Yet they are often the first, and sometimes the only, clinicians that infected individuals will see.
Why chronic HBV is still a problem. Although the incidence of acute HBV infection has declined significantly as a result of universal infant vaccination in the United States, chronic infections are still prevalent in this country due to such factors as immigration from areas where HBV is endemic, perinatal transmission, transmission among household contacts, and risky behaviors. In most adolescents and adults, HBV infection leads to acute hepatitis from which they fully recover; chronic infection ensues in only 5% to 10% of cases. However, 90% of infants and 25% to 50% of children younger than 5 years who become infected with HBV go on to develop lifelong infection. Most people with chronic HBV infection do not exhibit any signs of clinical illness, which makes screening all the more important—particularly since effective antiviral treatments are available.1,3
To help primary care providers address the issues of screening for HBV, the Hepatitis B Foundation convened a workshop of prominent primary care practitioners and specialists in hepatitis and liver diseases. The workshop panel reviewed evidence-based guidelines and reports from the American Association for the Study of Liver Diseases (AASLD), the Centers for Disease Control and Prevention (CDC), the National Institutes of Health (NIH), and the Institute of Medicine (IOM), as well as a recent Hepatitis B Foundation publication on HBV screening and management in children and other relevant publications.1-5 The resultant algorithm and consensus recommendations presented here can assist primary care providers in applying evidence-based guidelines for HBV infection to everyday practice.
3 phases of HBV infection: What screening results mean
Hepatitis B surface antigen (HBsAg) that is persistently detectable in a patient’s serum for more than 6 months signifies chronic HBV infection.1,3,4 The 3 immunologic phases of chronic HBV infection—immune tolerant, immune active, and inactive carrier—are determined by serum levels of alanine aminotransferase (ALT) and HBV DNA, and the presence or absence of hepatitis B e antigen (HBeAg) (TABLE 1).6
All individuals with chronic HBV infection are initially HBeAg positive. Those in the immune tolerant phase also have high levels of circulating virus, indicated by HBV DNA levels. However, the body does not mount an immune response to the virus; there is no active liver disease, and the serum ALT level is normal.
When the immune system recognizes HBV as foreign, the patient enters the immune active phase, wherein liver inflammation and fibrosis can develop and ALT is correspondingly elevated. HBV antibody (anti-HBe) may be present.
In nearly all patients, HBeAg seroconversion to HBeAg-negative/anti-HBe-positive status occurs spontaneously or as a result of antiviral treatment. After seroconversion, most patients enter the HBsAg inactive carrier phase, in which a strong cellular immune response is able to suppress, but not eliminate, the virus. This phase typically features low or undetectable serum levels of HBV DNA and normal ALT levels. Over time, liver inflammation and fibrosis improve, and the risk of cirrhosis and HCC declines.7
However, some patients do not enter the inactive phase after HBeAg seroconversion. They instead continue to exhibit active viral replication and liver disease due to the emergence of one or more HBeAg-negative viral mutants. Moreover, in as many as 20% of those who enter the inactive HBsAg carrier state, infection will reactivate and possibly return the patient to HBeAg-positive status. HBV infection is a dynamic condition: Individuals can go from active disease to the inactive phase and then have reactivation of liver disease at any point during their lifetime. Thus, patients require lifelong monitoring of their chronic infection.8 .
Since chronic HBV infection cannot be cured, the desired clinical outcome is for patients to enter and remain in the inactive HBsAg carrier phase. Evidence suggests that, in this phase, the risk of decompensated cirrhosis may also significantly decrease.9 A few inactive HBsAg carriers (0.5%/year) will clear the surface antigen and may develop protective antibodies (anti-HBs). Development of cirrhosis after loss of HBsAg is extremely rare; however, the risk of HCC, although reduced, is not eliminated.10
If a patient is unable to suppress the virus, or if infection reactivates after the patient achieves inactive carrier status, antiviral therapy may still decrease the risk of cirrhosis and HCC through durable suppression of HBV DNA to low or undetectable levels and normalization of ALT. Seven drugs are approved by the U.S. Food and Drug Administration (FDA) for treatment of chronic hepatitis B infection (TABLE 2).3 The decision to treat must take into account multiple factors, including phase of disease, age of the patient, extent of liver involvement on biopsy, potential efficacy of and adverse events associated with available therapies, cost of long-term medication, and, importantly, the high risk of development of nucleos(t)ide analog-resistant viral strains. Many studies have demonstrated the benefit of treating patients with advanced fibrosis or cirrhosis.9,11–13 However, no study has shown a benefit of treating those in the immune tolerant or inactive carrier phases.
TABLE 1
Phases of chronic HBV infection (HBsAg+ >6 mos)6
| Phase | Labs and histology |
|---|---|
| immune tolerant | HBV DNA >20,000 IU/mL* ALT normal HBeAg detectable No or minimal liver inflammation and fibrosis |
| Immune active | HBV DNA usually >20,000 IU/mL* ALT elevated HBeAg may be detectable or not; anti-HBe may be present Liver inflammation and fibrosis can develop |
| Inactive HBsAg carrier | HBV DNA <2000 IU/mL or undetectable* ALT normal HBeAg undetectable; anti-HBe present Minimal to no liver inflammation; fibrosis may regress |
| Reactivation | HBV DNA levels increase ALT normal or elevated HBeAg undetectable. |
| ALT, alanine aminotransferase; anti-HBe, antibody to HBeAg; HBsAg, hepatitis B surface antigen; HBeAg, hepatitis B e-antigen; HBV, hepatitis B virus. *For HBV DNA: 2000 IU/ml=104 copies/ml; 20,000 IU/mL=105 copies/mL | |
TABLE 2
FDA-approved drugs for the treatment of chronic HBV infection3
| Drug | labeled for use in: |
|---|---|
| Interferons | |
| Interferon alfa-2b (Intron A) | Adults; children >12 months |
| Peginterferon alfa-2a (Pegasys) | Adults |
| Nucleos(t)ide analogs | |
| Lamivudine (Epivir-HBV) | Adults; children >3 years |
| Adefovir dipivoxil (Hepsera) | Adults; children >12 years |
| Entecavir (Baraclude) | Adults; children >16 years |
| Telbivudine (Tyzeka) | Adults |
| Tenofovir disoproxil fumarate (Viread) | Adults |
| HBV, hepatitis B virus. | |
Key opportunities to make a difference
Primary care providers can form an effective first-line of defense against morbidity and mortality associated with chronic HBV infection by:
- immunizing all infants, children, and adolescents, as well as adults at risk to acquire HBV, following guidelines from the CDC and American Academy of Pediatrics;
- screening those at high risk, as per CDC guidelines;
- performing clinical and laboratory evaluation of patients who have chronic HBV infection, to determine current phase of disease;
- monitoring patients in the immune tolerant or inactive phases every 6 to 12 months for disease progression; and
- consulting with a liver specialist or HBV-experienced provider for patients in the immune active phase, to determine treatment strategies.
Our panel has developed an algorithm (FIGURE) that addresses the screening of individuals at risk of contracting HBV and the evaluation and monitoring of those who are identified as HBsAg-positive. Although the algorithm cannot anticipate all possible clinical circumstances, it offers a general path forward based on the results of routine laboratory tests. Ideally, an office system—whether using electronic medical records or not—would incorporate guideline-based prompts for screening and management.
FIGURE
Suspect HBV infection? Use this algorithm to screen and intervene
ALT, alanine aminotransferase; anti-HBe, antibody to HBeAg; anti-HBs, antibody to HBsAg; AST, aspartate aminotransferase; DNA, deoxyribose nucleic acid; HBeAg, hepatitis B e-antigen (protein produced by HBV, indicating heightened viral activity); HBsAg, hepatitis B surface antigen; HBV, hepatitis B virus; HIV, human immunodeficiency virus; HCC, hepatocellular carcinoma.
Source: Primary Care Provider Workshop on Hepatitis B, sponsored by the Hepatitis B Foundation in Doylestown, Pa (March 10-11, 2010).
Underuse of screening means many infected individuals are missed
The CDC has identified high-risk groups for HBV screening, including all individuals born in geographic regions where HBsAg prevalence is ≥2% (FIGURE, NOTE A).4 Screening is simple and relatively inexpensive (commercial diagnostic laboratories currently charge $150-$250 to screen for HBsAg and anti-HBs). Despite these recommendations, the recent IOM report confirms that screening is under-used or is not being done appropriately.2
Screening is also recommended for individuals about to undergo immunosuppressive or immune-modifying therapy (eg, for treatment of cancer, rheumatoid arthritis, or inflammatory bowel disease, or in preparation for bone marrow or other transplant). For these patients who are also asymptomatic inactive carriers of HBV, the risk of reactivation can be as high as 50%, especially in patients receiving chemotherapy for lymphoma. Deaths from fulminant hepatitis have also been reported; however, preemptive HBV antiviral treatment can reduce this risk to about 10% or less.14,15 The workshop panel recommends that providers screen for HBV under these circumstances, and that HBsAg-positive patients should start preemptive oral HBV antiviral therapy before receiving immunosuppressive or immune-modifying therapy (including systemic corticosteroids >2 weeks) to prevent a flare of hepatitis.2
Differentiate those who are chronically infected, immune, or susceptible
The CDC recommends screening for both HBsAg and anti-HBs. Taken together, the results of these tests can help you discern if the patient is actively infected (HBsAg-positive); immune (HBsAg-negative and anti-HBs-positive); or susceptible (negative for both seromarkers).
Testing for the antibody to HBV core antigen (anti-HBc) is occasionally included in screening panels. Its presence cannot distinguish between current and previous infection. False-positive test results also occur.
Vaccinate seronegative individuals who are at risk for HBV
Although the CDC recommends vaccination of all HBsAg-negative individuals at risk for acquiring HBV, vaccine coverage of adults in the United States remains low.2,16 The workshop panel recommends that all primary care offices treating adults stock HBV vaccine. Of course, routinely stocking vaccine may present financial challenges, including purchase cost, storage, unused expired product, and reimbursement. Your practice may want to coordinate coverage with the local department of health, area hospitals, or large practices that stock vaccine, to ensure timely vaccination of patients.
No further follow-up is needed for patients immune to HBV
If the screening result for HBsAg is negative but anti-HBs is positive, the patient is immune to HBV. If the screening panel also included testing for anti-HBc and it is positive, the patient has natural immunity. A positive result for anti-HBs alone indicates prior vaccination or prior infection and seroconversion.
A positive HBsAg screening test calls for further patient work-up
If a patient tests positive for HBsAg, collect baseline data for ALT, HBeAg, anti-HBe, and HBV DNA levels.
In addition, encourage screening and vaccination of sexual partners and close household contacts of infected individuals. Patient education and counseling are important to dispel myths about HBV transmission (eg, HBV is not spread through casual contact such as handshakes or food sharing) and to reinforce the importance of regular care to prevent disease progression.
Evaluating and monitoring the chronic HBV patient
Use serum ALT levels, HBeAg and anti-HBe serology, and HBV DNA levels to identify the phase of HBV infection and guide patient management (FIGURE).
Interpreting viral DNA levels: Knowing when not to treat
The presence of HBeAg in serum indicates viral replication. Although HBeAg-positive patients in the immune tolerant or immune active phases generally have high levels of circulating HBV DNA (>20,000 IU/mL), these DNA levels do not necessarily correlate with active liver disease. In the immune tolerant phase, there is no clearly established benefit of antiviral treatment regardless of HBV DNA levels, and the risk of development of viral resistance to oral antiviral drugs is a serious concern. There is also no indication for treatment in the inactive carrier phase.
Discuss with patients why treatment is inappropriate in these phases and how the development of resistance to antiviral therapies can have serious negative consequences for their future treatment needs. Also explain that, because chronic HBV infection is dynamic, they will require lifetime follow-up care, even if they are currently in the immune tolerant or inactive phase.1,3
Surveillance for HCC in patients with chronic HBV infection
The most common adverse outcome of chronic HBV infection is HCC, occurring in up to 25% of men and 15% of women over their lifetimes.17 Because early detection and effective treatment for HCC can prolong life in HBsAg-positive individuals who have HCC or are at risk for acquiring it, the workshop panel recommends that primary care providers perform periodic screening for HCC according to the current AASLD guidelines.3,17 Candidates for HCC screening are those with family histories of HCC; those with cirrhosis or co-infection with HCV or HIV; and men >40 years and women >50 years. HBV-infected men born in Africa may acquire HCC at a younger age due to possible environmental exposure to aflatoxin, a carcinogenic mold. The AASLD guideline suggests screening this group with liver ultrasound every 6 months, starting at age 20. Although the AASLD guideline does not specifically recommend measuring serum alpha-fetoprotein (AFP), many practitioners monitor AFP, which improves sensitivity but has low specificity.17
Rising ALT suggests active liver disease
Serum ALT is a surrogate indicator of possible liver damage or disease. Generally, when an HBsAg-positive patient’s ALT rises above normal (≥19 IU/L for women and ≥30 IU/L for men, when standard reference ranges are 0-40), they have moved into the immune active phase, where liver inflammation and fibrosis can develop.
Also consider other potential causes of ALT elevation, especially when it occurs in association with low or undetectable levels of HBV DNA. Alternative causes include hepatitis C, heavy alcohol use, medications, and nonalcoholic fatty liver disease. Consultation with a liver specialist may be helpful to rule out or confirm these comorbidities.
Seeking out expertise in HBV patient management
When a patient with chronic HBV infection has moved into the immune active phase, consult with a provider who has expertise in HBV—whether you choose to refer or to co-manage the patient with the specialist—to obtain advice on further work-up and development of a long-term management and treatment strategy. Individuals with small liver tumors identified on ultrasound or an elevated AFP level require immediate referral to a clinician who treats HCC, such as a transplant hepatologist.
Ensuring the health of pregnant women
The CDC recommends that all pregnant women be tested for HBsAg at an early prenatal visit. Counsel women who are HBsAg-positive on what this status means for their own health, in addition to that of their newborn. If you are providing prenatal care, collect baseline data for ALT, HBe serology, and HBV DNA levels. Promptly refer any patient with an elevated ALT level to a specialist for care during pregnancy.
Acknowledgement
Medical writing services were provided by Theresa M. Wizemann, PhD, of Wizemann Scientific Communications, LLC, under contract with the Hepatitis B Foundation.
CORRESPONDENCE
Joan M. Block, RN, BSN, executive director, Hepatitis B Foundation, 3805 Old Easton Road, Doylestown, PA 18902; [email protected]
• Screen patients at risk of contracting hepatits B virus (HBV), especially those from HBV-endemic regions of the world, by testing for hepatitis B surface antigen and antibody (HBsAg and anti-HBs). A
• Vaccinate all infants, children, and adolescents following guidelines of the Centers for Disease Control and Prevention and American Academy of Pediatrics, as well as at-risk adults whose screening results are negative for both HBsAg and anti-HBs. A
• Provide periodic monitoring for patients who are HBsAg-positive. While these patients may appear asymptomatic, they are infected with HBV and require further evaluation. A
• Consult a specialist experienced in treating hepatitis if active liver disease is suspected in patients with chronic HBV infection who present with elevated alanine aminotransferase and HBV DNA >2,000 IU/mL. B
Screening for hepatitis B virus (HBV) infection is simple and relatively inexpensive. Yet it is underused in everyday practice, leaving some HBV-positive patients unaware and at risk for serious health consequences, including cirrhosis, liver failure, and hepatocellular carcinoma (HCC).1 In addition, many primary care providers do not follow existing guidelines for HBV screening and management.2 Yet they are often the first, and sometimes the only, clinicians that infected individuals will see.
Why chronic HBV is still a problem. Although the incidence of acute HBV infection has declined significantly as a result of universal infant vaccination in the United States, chronic infections are still prevalent in this country due to such factors as immigration from areas where HBV is endemic, perinatal transmission, transmission among household contacts, and risky behaviors. In most adolescents and adults, HBV infection leads to acute hepatitis from which they fully recover; chronic infection ensues in only 5% to 10% of cases. However, 90% of infants and 25% to 50% of children younger than 5 years who become infected with HBV go on to develop lifelong infection. Most people with chronic HBV infection do not exhibit any signs of clinical illness, which makes screening all the more important—particularly since effective antiviral treatments are available.1,3
To help primary care providers address the issues of screening for HBV, the Hepatitis B Foundation convened a workshop of prominent primary care practitioners and specialists in hepatitis and liver diseases. The workshop panel reviewed evidence-based guidelines and reports from the American Association for the Study of Liver Diseases (AASLD), the Centers for Disease Control and Prevention (CDC), the National Institutes of Health (NIH), and the Institute of Medicine (IOM), as well as a recent Hepatitis B Foundation publication on HBV screening and management in children and other relevant publications.1-5 The resultant algorithm and consensus recommendations presented here can assist primary care providers in applying evidence-based guidelines for HBV infection to everyday practice.
3 phases of HBV infection: What screening results mean
Hepatitis B surface antigen (HBsAg) that is persistently detectable in a patient’s serum for more than 6 months signifies chronic HBV infection.1,3,4 The 3 immunologic phases of chronic HBV infection—immune tolerant, immune active, and inactive carrier—are determined by serum levels of alanine aminotransferase (ALT) and HBV DNA, and the presence or absence of hepatitis B e antigen (HBeAg) (TABLE 1).6
All individuals with chronic HBV infection are initially HBeAg positive. Those in the immune tolerant phase also have high levels of circulating virus, indicated by HBV DNA levels. However, the body does not mount an immune response to the virus; there is no active liver disease, and the serum ALT level is normal.
When the immune system recognizes HBV as foreign, the patient enters the immune active phase, wherein liver inflammation and fibrosis can develop and ALT is correspondingly elevated. HBV antibody (anti-HBe) may be present.
In nearly all patients, HBeAg seroconversion to HBeAg-negative/anti-HBe-positive status occurs spontaneously or as a result of antiviral treatment. After seroconversion, most patients enter the HBsAg inactive carrier phase, in which a strong cellular immune response is able to suppress, but not eliminate, the virus. This phase typically features low or undetectable serum levels of HBV DNA and normal ALT levels. Over time, liver inflammation and fibrosis improve, and the risk of cirrhosis and HCC declines.7
However, some patients do not enter the inactive phase after HBeAg seroconversion. They instead continue to exhibit active viral replication and liver disease due to the emergence of one or more HBeAg-negative viral mutants. Moreover, in as many as 20% of those who enter the inactive HBsAg carrier state, infection will reactivate and possibly return the patient to HBeAg-positive status. HBV infection is a dynamic condition: Individuals can go from active disease to the inactive phase and then have reactivation of liver disease at any point during their lifetime. Thus, patients require lifelong monitoring of their chronic infection.8 .
Since chronic HBV infection cannot be cured, the desired clinical outcome is for patients to enter and remain in the inactive HBsAg carrier phase. Evidence suggests that, in this phase, the risk of decompensated cirrhosis may also significantly decrease.9 A few inactive HBsAg carriers (0.5%/year) will clear the surface antigen and may develop protective antibodies (anti-HBs). Development of cirrhosis after loss of HBsAg is extremely rare; however, the risk of HCC, although reduced, is not eliminated.10
If a patient is unable to suppress the virus, or if infection reactivates after the patient achieves inactive carrier status, antiviral therapy may still decrease the risk of cirrhosis and HCC through durable suppression of HBV DNA to low or undetectable levels and normalization of ALT. Seven drugs are approved by the U.S. Food and Drug Administration (FDA) for treatment of chronic hepatitis B infection (TABLE 2).3 The decision to treat must take into account multiple factors, including phase of disease, age of the patient, extent of liver involvement on biopsy, potential efficacy of and adverse events associated with available therapies, cost of long-term medication, and, importantly, the high risk of development of nucleos(t)ide analog-resistant viral strains. Many studies have demonstrated the benefit of treating patients with advanced fibrosis or cirrhosis.9,11–13 However, no study has shown a benefit of treating those in the immune tolerant or inactive carrier phases.
TABLE 1
Phases of chronic HBV infection (HBsAg+ >6 mos)6
| Phase | Labs and histology |
|---|---|
| immune tolerant | HBV DNA >20,000 IU/mL* ALT normal HBeAg detectable No or minimal liver inflammation and fibrosis |
| Immune active | HBV DNA usually >20,000 IU/mL* ALT elevated HBeAg may be detectable or not; anti-HBe may be present Liver inflammation and fibrosis can develop |
| Inactive HBsAg carrier | HBV DNA <2000 IU/mL or undetectable* ALT normal HBeAg undetectable; anti-HBe present Minimal to no liver inflammation; fibrosis may regress |
| Reactivation | HBV DNA levels increase ALT normal or elevated HBeAg undetectable. |
| ALT, alanine aminotransferase; anti-HBe, antibody to HBeAg; HBsAg, hepatitis B surface antigen; HBeAg, hepatitis B e-antigen; HBV, hepatitis B virus. *For HBV DNA: 2000 IU/ml=104 copies/ml; 20,000 IU/mL=105 copies/mL | |
TABLE 2
FDA-approved drugs for the treatment of chronic HBV infection3
| Drug | labeled for use in: |
|---|---|
| Interferons | |
| Interferon alfa-2b (Intron A) | Adults; children >12 months |
| Peginterferon alfa-2a (Pegasys) | Adults |
| Nucleos(t)ide analogs | |
| Lamivudine (Epivir-HBV) | Adults; children >3 years |
| Adefovir dipivoxil (Hepsera) | Adults; children >12 years |
| Entecavir (Baraclude) | Adults; children >16 years |
| Telbivudine (Tyzeka) | Adults |
| Tenofovir disoproxil fumarate (Viread) | Adults |
| HBV, hepatitis B virus. | |
Key opportunities to make a difference
Primary care providers can form an effective first-line of defense against morbidity and mortality associated with chronic HBV infection by:
- immunizing all infants, children, and adolescents, as well as adults at risk to acquire HBV, following guidelines from the CDC and American Academy of Pediatrics;
- screening those at high risk, as per CDC guidelines;
- performing clinical and laboratory evaluation of patients who have chronic HBV infection, to determine current phase of disease;
- monitoring patients in the immune tolerant or inactive phases every 6 to 12 months for disease progression; and
- consulting with a liver specialist or HBV-experienced provider for patients in the immune active phase, to determine treatment strategies.
Our panel has developed an algorithm (FIGURE) that addresses the screening of individuals at risk of contracting HBV and the evaluation and monitoring of those who are identified as HBsAg-positive. Although the algorithm cannot anticipate all possible clinical circumstances, it offers a general path forward based on the results of routine laboratory tests. Ideally, an office system—whether using electronic medical records or not—would incorporate guideline-based prompts for screening and management.
FIGURE
Suspect HBV infection? Use this algorithm to screen and intervene
ALT, alanine aminotransferase; anti-HBe, antibody to HBeAg; anti-HBs, antibody to HBsAg; AST, aspartate aminotransferase; DNA, deoxyribose nucleic acid; HBeAg, hepatitis B e-antigen (protein produced by HBV, indicating heightened viral activity); HBsAg, hepatitis B surface antigen; HBV, hepatitis B virus; HIV, human immunodeficiency virus; HCC, hepatocellular carcinoma.
Source: Primary Care Provider Workshop on Hepatitis B, sponsored by the Hepatitis B Foundation in Doylestown, Pa (March 10-11, 2010).
Underuse of screening means many infected individuals are missed
The CDC has identified high-risk groups for HBV screening, including all individuals born in geographic regions where HBsAg prevalence is ≥2% (FIGURE, NOTE A).4 Screening is simple and relatively inexpensive (commercial diagnostic laboratories currently charge $150-$250 to screen for HBsAg and anti-HBs). Despite these recommendations, the recent IOM report confirms that screening is under-used or is not being done appropriately.2
Screening is also recommended for individuals about to undergo immunosuppressive or immune-modifying therapy (eg, for treatment of cancer, rheumatoid arthritis, or inflammatory bowel disease, or in preparation for bone marrow or other transplant). For these patients who are also asymptomatic inactive carriers of HBV, the risk of reactivation can be as high as 50%, especially in patients receiving chemotherapy for lymphoma. Deaths from fulminant hepatitis have also been reported; however, preemptive HBV antiviral treatment can reduce this risk to about 10% or less.14,15 The workshop panel recommends that providers screen for HBV under these circumstances, and that HBsAg-positive patients should start preemptive oral HBV antiviral therapy before receiving immunosuppressive or immune-modifying therapy (including systemic corticosteroids >2 weeks) to prevent a flare of hepatitis.2
Differentiate those who are chronically infected, immune, or susceptible
The CDC recommends screening for both HBsAg and anti-HBs. Taken together, the results of these tests can help you discern if the patient is actively infected (HBsAg-positive); immune (HBsAg-negative and anti-HBs-positive); or susceptible (negative for both seromarkers).
Testing for the antibody to HBV core antigen (anti-HBc) is occasionally included in screening panels. Its presence cannot distinguish between current and previous infection. False-positive test results also occur.
Vaccinate seronegative individuals who are at risk for HBV
Although the CDC recommends vaccination of all HBsAg-negative individuals at risk for acquiring HBV, vaccine coverage of adults in the United States remains low.2,16 The workshop panel recommends that all primary care offices treating adults stock HBV vaccine. Of course, routinely stocking vaccine may present financial challenges, including purchase cost, storage, unused expired product, and reimbursement. Your practice may want to coordinate coverage with the local department of health, area hospitals, or large practices that stock vaccine, to ensure timely vaccination of patients.
No further follow-up is needed for patients immune to HBV
If the screening result for HBsAg is negative but anti-HBs is positive, the patient is immune to HBV. If the screening panel also included testing for anti-HBc and it is positive, the patient has natural immunity. A positive result for anti-HBs alone indicates prior vaccination or prior infection and seroconversion.
A positive HBsAg screening test calls for further patient work-up
If a patient tests positive for HBsAg, collect baseline data for ALT, HBeAg, anti-HBe, and HBV DNA levels.
In addition, encourage screening and vaccination of sexual partners and close household contacts of infected individuals. Patient education and counseling are important to dispel myths about HBV transmission (eg, HBV is not spread through casual contact such as handshakes or food sharing) and to reinforce the importance of regular care to prevent disease progression.
Evaluating and monitoring the chronic HBV patient
Use serum ALT levels, HBeAg and anti-HBe serology, and HBV DNA levels to identify the phase of HBV infection and guide patient management (FIGURE).
Interpreting viral DNA levels: Knowing when not to treat
The presence of HBeAg in serum indicates viral replication. Although HBeAg-positive patients in the immune tolerant or immune active phases generally have high levels of circulating HBV DNA (>20,000 IU/mL), these DNA levels do not necessarily correlate with active liver disease. In the immune tolerant phase, there is no clearly established benefit of antiviral treatment regardless of HBV DNA levels, and the risk of development of viral resistance to oral antiviral drugs is a serious concern. There is also no indication for treatment in the inactive carrier phase.
Discuss with patients why treatment is inappropriate in these phases and how the development of resistance to antiviral therapies can have serious negative consequences for their future treatment needs. Also explain that, because chronic HBV infection is dynamic, they will require lifetime follow-up care, even if they are currently in the immune tolerant or inactive phase.1,3
Surveillance for HCC in patients with chronic HBV infection
The most common adverse outcome of chronic HBV infection is HCC, occurring in up to 25% of men and 15% of women over their lifetimes.17 Because early detection and effective treatment for HCC can prolong life in HBsAg-positive individuals who have HCC or are at risk for acquiring it, the workshop panel recommends that primary care providers perform periodic screening for HCC according to the current AASLD guidelines.3,17 Candidates for HCC screening are those with family histories of HCC; those with cirrhosis or co-infection with HCV or HIV; and men >40 years and women >50 years. HBV-infected men born in Africa may acquire HCC at a younger age due to possible environmental exposure to aflatoxin, a carcinogenic mold. The AASLD guideline suggests screening this group with liver ultrasound every 6 months, starting at age 20. Although the AASLD guideline does not specifically recommend measuring serum alpha-fetoprotein (AFP), many practitioners monitor AFP, which improves sensitivity but has low specificity.17
Rising ALT suggests active liver disease
Serum ALT is a surrogate indicator of possible liver damage or disease. Generally, when an HBsAg-positive patient’s ALT rises above normal (≥19 IU/L for women and ≥30 IU/L for men, when standard reference ranges are 0-40), they have moved into the immune active phase, where liver inflammation and fibrosis can develop.
Also consider other potential causes of ALT elevation, especially when it occurs in association with low or undetectable levels of HBV DNA. Alternative causes include hepatitis C, heavy alcohol use, medications, and nonalcoholic fatty liver disease. Consultation with a liver specialist may be helpful to rule out or confirm these comorbidities.
Seeking out expertise in HBV patient management
When a patient with chronic HBV infection has moved into the immune active phase, consult with a provider who has expertise in HBV—whether you choose to refer or to co-manage the patient with the specialist—to obtain advice on further work-up and development of a long-term management and treatment strategy. Individuals with small liver tumors identified on ultrasound or an elevated AFP level require immediate referral to a clinician who treats HCC, such as a transplant hepatologist.
Ensuring the health of pregnant women
The CDC recommends that all pregnant women be tested for HBsAg at an early prenatal visit. Counsel women who are HBsAg-positive on what this status means for their own health, in addition to that of their newborn. If you are providing prenatal care, collect baseline data for ALT, HBe serology, and HBV DNA levels. Promptly refer any patient with an elevated ALT level to a specialist for care during pregnancy.
Acknowledgement
Medical writing services were provided by Theresa M. Wizemann, PhD, of Wizemann Scientific Communications, LLC, under contract with the Hepatitis B Foundation.
CORRESPONDENCE
Joan M. Block, RN, BSN, executive director, Hepatitis B Foundation, 3805 Old Easton Road, Doylestown, PA 18902; [email protected]
1. Sorrell MF, Belongia EA, Costa J, et al. National Institutes of Health Consensus Development Conference statement: management of Hepatitis B. Ann Intern Med. 2009;150:104-110.
2. Institute of Medicine Hepatitis and Liver Cancer: A National Strategy for Prevention and Control of Hepatitis B and C. Washington, DC: National Academies Press; 2010.
3. Lok AS, McMahon BJ. Chronic hepatitis B: update 2009. AASLD practice guideline. Hepatology. 2009;50:661-662.
4. Weinbaum CM, Williams I, Mast EE, et al. Recommendations for identification and public health management of persons with chronic hepatitis B virus infection. MMWR Recomm Rep. 2008;57(RR08):1-20.
5. Haber BA, Block JM, Jonas MM, et al. Recommendations for screening, monitoring, and referral of pediatric chronic hepatitis B. Pediatrics. 2009;124:e1007-e1113.
6. Hoofnagle JH, Doo E, Liang TJ, et al. Management of hepatitis B: summary of a clinical research workshop. Hepatology. 2007;45:1056-1075.
7. Yang HI, Lu SN, Liaw YF, et al. Hepatitis B e antigen and the risk of hepatocellular carcinoma. N Engl J Med. 2002;347:168-174.
8. McMahon BJ. The natural history of chronic hepatitis B virus infection. Hepatology. 2009;49:S45-S55.
9. Liaw YF, Sung JJ, Chow WC, et al. Lamivudine for patients with chronic hepatitis B and advanced liver disease. N Engl J Med. 2004;351:1521-1531.
10. Simonetti J, Bulkow L, McMahon BJ, et al. Clearance of hepatitis B surface antigen and risk of hepatocellular carcinoma in a cohort chronically infected with hepatitis B virus. Hepatology. 2010;51:1531-1537.
11. Perrillo RP, Wright T, Rakela J, et al. A multicenter United States-Canadian trial to assess lamivudine monotherapy before and after liver transplantation for chronic hepatitis B. Hepatology. 2001;33:424-432.
12. Villeneuve JP, Condreay LD, Willems B, et al. Lamivudine treatment for decompensated cirrhosis resulting from chronic hepatitis B. Hepatology. 2000;31:207-210.
13. Fontana RJ, Hann HW, Perrillo RP, et al. Determinants of early mortality in patients with decompensated chronic hepatitis B treated with antiviral therapy. Gastroenterology. 2002;123:719-727.
14. Yeo W, Chan PK, Zhong S, et al. Frequency of hepatitis B virus reactivation in cancer patients undergoing cytotoxic chemotherapy: a prospective study of 626 patients with identification of risk factors. J Med Virol. 2000;62:299-307.
15. Loomba R, Rowley A, Wesley R, et al. Systematic review: the effect of preventive lamivudine on hepatitis B reactivation during chemotherapy. Ann Intern Med. 2008;148:519-528.
16. Mast EE, Weinbaum CM, Fiore AE, et al. A comprehensive immunization strategy to eliminate transmission of hepatitis B virus infection in the United States. recommendations of the Advisory Committee on Immunization Practices (ACIP) part II: immunization of adults. MMWR Recomm Rep. 2006;55(RR-16):1-33.
17. Bruix J, Sherman M. Management of hepatocellular carcinoma: an update. AASLD Practice Guideline. 2010. Available at: http://www.aasld.org/practiceguidelines/Documents/Bookmarked%20Practice%20Guidelines/HCCUpdate2010.pdf. Accessed November 8, 2010.
1. Sorrell MF, Belongia EA, Costa J, et al. National Institutes of Health Consensus Development Conference statement: management of Hepatitis B. Ann Intern Med. 2009;150:104-110.
2. Institute of Medicine Hepatitis and Liver Cancer: A National Strategy for Prevention and Control of Hepatitis B and C. Washington, DC: National Academies Press; 2010.
3. Lok AS, McMahon BJ. Chronic hepatitis B: update 2009. AASLD practice guideline. Hepatology. 2009;50:661-662.
4. Weinbaum CM, Williams I, Mast EE, et al. Recommendations for identification and public health management of persons with chronic hepatitis B virus infection. MMWR Recomm Rep. 2008;57(RR08):1-20.
5. Haber BA, Block JM, Jonas MM, et al. Recommendations for screening, monitoring, and referral of pediatric chronic hepatitis B. Pediatrics. 2009;124:e1007-e1113.
6. Hoofnagle JH, Doo E, Liang TJ, et al. Management of hepatitis B: summary of a clinical research workshop. Hepatology. 2007;45:1056-1075.
7. Yang HI, Lu SN, Liaw YF, et al. Hepatitis B e antigen and the risk of hepatocellular carcinoma. N Engl J Med. 2002;347:168-174.
8. McMahon BJ. The natural history of chronic hepatitis B virus infection. Hepatology. 2009;49:S45-S55.
9. Liaw YF, Sung JJ, Chow WC, et al. Lamivudine for patients with chronic hepatitis B and advanced liver disease. N Engl J Med. 2004;351:1521-1531.
10. Simonetti J, Bulkow L, McMahon BJ, et al. Clearance of hepatitis B surface antigen and risk of hepatocellular carcinoma in a cohort chronically infected with hepatitis B virus. Hepatology. 2010;51:1531-1537.
11. Perrillo RP, Wright T, Rakela J, et al. A multicenter United States-Canadian trial to assess lamivudine monotherapy before and after liver transplantation for chronic hepatitis B. Hepatology. 2001;33:424-432.
12. Villeneuve JP, Condreay LD, Willems B, et al. Lamivudine treatment for decompensated cirrhosis resulting from chronic hepatitis B. Hepatology. 2000;31:207-210.
13. Fontana RJ, Hann HW, Perrillo RP, et al. Determinants of early mortality in patients with decompensated chronic hepatitis B treated with antiviral therapy. Gastroenterology. 2002;123:719-727.
14. Yeo W, Chan PK, Zhong S, et al. Frequency of hepatitis B virus reactivation in cancer patients undergoing cytotoxic chemotherapy: a prospective study of 626 patients with identification of risk factors. J Med Virol. 2000;62:299-307.
15. Loomba R, Rowley A, Wesley R, et al. Systematic review: the effect of preventive lamivudine on hepatitis B reactivation during chemotherapy. Ann Intern Med. 2008;148:519-528.
16. Mast EE, Weinbaum CM, Fiore AE, et al. A comprehensive immunization strategy to eliminate transmission of hepatitis B virus infection in the United States. recommendations of the Advisory Committee on Immunization Practices (ACIP) part II: immunization of adults. MMWR Recomm Rep. 2006;55(RR-16):1-33.
17. Bruix J, Sherman M. Management of hepatocellular carcinoma: an update. AASLD Practice Guideline. 2010. Available at: http://www.aasld.org/practiceguidelines/Documents/Bookmarked%20Practice%20Guidelines/HCCUpdate2010.pdf. Accessed November 8, 2010.