User login
Somatization: Diagnosing it sooner through emotion-focused interviewing
- Obvious anxiety in a patient with physical complaints should prompt an evaluation for somatization.
- Become familiar with the 4 patterns of somatization and their manifestations.
- Learn how to conduct an emotion-focused interview, which, when applied appropriately, will help rule somatization in or out.
A 42-year-old man has chronic fatigue and fibromyalgia that has led to a 13-month disability leave from work. The reason for his current office visit is longstanding pain in his shoulders. As you take his history, he is sitting with hands clenched and he generally appears tense.
A 38-year-old woman with severe incapacitating gastroesophageal reflux disease, irritable bowel syndrome, and depression has been too disabled to work for 2 years. At the time of your interview, her posture is relaxed and she shows no signs of anxiety.
These 2 very different patients (whose cases I will review in detail) share a common problem: somatization, the translation of emotions into somatic problems or complaints. It is well documented—though still largely unrecognized in practice—that somatization accounts for a large proportion of office visits to primary care physicians as well as specialists,1,2 leading to unnecessary testing, treatment, and hospitalization, disability and corporate financial loss,3 likely earlier mortality,4 and frustration for patients and physicians.5
No longer a diagnosis of exclusion
Despite the burden somatization places on the medical system, the diagnosis is often made by indirect methods such as checklist, speculation, or exclusion when other problems are ruled out.6 The common position, even in recent reviews, is that somatization should be treated by nonspecific measures, such as frequent office visits to increase the patient’s and physician’s ability to cope with what is often seen to be a chronic and incurable disorder.7-11 Such a position is no longer warranted.
Based on recent quantitative and extensive case-based research, specific emotion-focused brief therapies and videotape-based research have clarified how emotions are experienced in the body and how somatization of emotions occurs (see The physiology of emotions). These methods, including short-term dynamic psychotherapy (STDP) have been used to diagnose and treat somatization effectively since the 1980s. Somatization, with its morbidity and chronicity, need no longer be diagnosed by exclusion nor treated palliatively without specific diagnostic testing.
To diagnose and manage somatization we must know how emotions are experienced and how they may become somatized. Davanloo discovered through studying several hundred case videotapes that specific emotions manifest in specific ways regardless of gender, age, or ethnicity.12 This emotion physiology constitutes a norm to compare with a patient who somatizes emotions.
For example, rage is experienced as an internal energy sensation, heat, or “volcano” that rises from the lower abdomen to the chest, neck, and finally to the hands with an urge to grab and do some form of violence. Guilt about rage is experienced with upper chest constriction or even pain, intense painful feeling with waves of tears and with thoughts of remorse about experiencing the rage.13 When feelings are experienced consciously, by definition they are not being somatized at that moment.
Why somatization occurs
When feelings are intense, frightening, or conflicted, they create anxiety and defense mechanisms to cover the anxiety (see the Figure ). If these feelings are unconscious to the patient, the subsequent anxiety and defenses may also be outside of awareness.
This is the finding common in people who have been traumatized by someone close to them: feelings of rage toward a loved one are unacceptable, frightening, and avoided through somatization and other defenses.14 Diverse research has found that patients with hypertension, migraine, irritable bowel syndrome, and other conditions internalize anger and thus increase their somatic problems.15-17 Blocking and inhibiting of emotions, including anger, is a common finding in somatizing patients.
FIGURE
The 4 patterns of somatization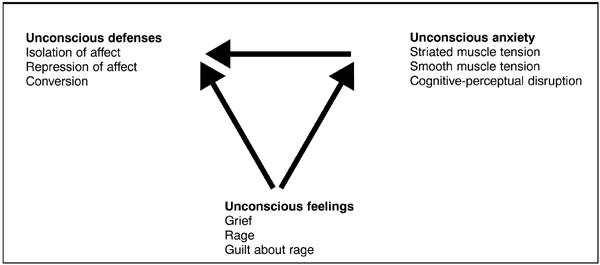
Videotaped case-series research shows 4 main patterns of somatization: 1) striated muscle unconscious anxiety, 2) smooth muscle tension 3) cognitive-perceptual disruption, and 4) conversion.18
Striated muscle tension due to unconscious anxiety manifests through hand clenching, sighing, and even hyperventilation that the patient is not aware of. These patients may report panic attacks, chest pain, headache, fibromyalgia, and other musculoskeletal complaints. These conditions are often frustrating to family, employers, and physicians since conditions like chronic pain respond to treatment slowly or not at all.
Smooth muscle tension due to unconscious anxiety causes acute or chronic spasm of blood vessels, GI tract, airways, and the bladder. Patients exhibiting smooth muscle tension may present with GI symptoms, migraine, hypertension, urinary frequency, and upper airway constriction mimicking asthma. They often report histories of depression, panic, substance abuse, personality disorders, and past sexual or physical abuse.
Cognitive perceptual disruption due to unconscious anxiety typically involves visual blurring, tunnel vision, loss of train of thought, and “drifting,” wherein the patient is temporarily mentally absent from the room. These patients have chronically poor memories and concentration. They are commonly victims or perpetrators of partner abuse, have frequent accidents, and have transient paranoia. They often end up seeing neurologists and undergoing expensive testing. Most have histories of dissociative disorders, personality disorders, or childhood abuse. In the family doctor’s office they frequently forget what was said and call back after the appointment. They appear confused and easily flustered and either avoid physical examinations entirely or endure them with great anxiety.
Conversion manifests as muscle weakness or paralysis in any voluntary muscle. Patients with acute conversion describe dropping items or even dropping to the floor as muscles give way without explanation. They will often report histories of witnessing or experiencing violent abuse.
One pattern usually predominates
The total amount of somatized emotion is distributed over the 4 pathways ( Table 1 ). One pathway generally prevails at any given time, though different pathways may come into play as anxiety waxes or wanes. When anxiety is expressed primarily through smooth muscle tension, cognitive perceptual disruption, or conversion, the striated muscles are relatively relaxed.
This finding of apparent calm while somatizing has been noted elsewhere in research of patients with hypertension. This is the “belle indifference” a patient expresses as they are temporarily relieved of muscle tension through somatization elsewhere.19
TABLE 1
Examples of diagnosable somatization patterns
| Somatization format | Observations during emotion-focused diagnostic assessment | Examples of related health complaints or health problems |
|---|---|---|
| Striated muscle tension | Progression from hand clenching, arm tension, neck tension, sighing respirations to whole-body tension | Fibromyalgia, headache, muscle spasm, backache, chest pain, shortness of breath, abdominal (wall) pain, fatigue |
| Smooth muscle tension | Relative absence of striated muscle tension. Instead activation of smooth muscles causes, for example, cramps in the abdomen or heartburn. | Irritable bowel symptoms, abdominal pain, nausea, bladder spasm, bronchospasm, coronary artery spasm, hypertension, migraine |
| Cognitive-perceptual disruption | Relative absence of striated muscle tension. Instead patient loses track of thoughts, becomes confused, gets blurry vision | Visual blurring, blindness, mental confusion, memory loss, dizziness, weakness, pseudo-seizures, paresthesias, fainting, conversion |
| Conversion | Relative absence of striated muscle tension. Instead patient goes weak in some or all voluntary muscle | Falling, aphonia, paralysis, weakness |
Major types of defense
Two important categories of defense include isolation of affect and repression.
Isolation of affect is awareness of emotions in one’s head without experiencing them in the body. Intellectualization is a form of isolation of affect.
Repression is the unconscious process by which emotions are shunted into the body rather than reaching consciousness at all. For example, strong emotions, including rage, may directly cause sighing and a panic attack without the person being aware of either the emotion or the sighing.20
Experiencing the emotions overcomes somatization
Videotaped research also shows that if a person can experience true feelings in the moment, somatization of these feelings is weakened and overcome. The feelings being experienced push out the anxiety and somatization ( Figure ). Thus, somatization can be reduced or removed by helping a patient feel emotions being stirred by recent events or from past events. Through this process one may diagnose somatization and also produce a therapeutic effect for a patient.
Direct diagnosis of somatization
An objective assessment
Because the process of somatization is unconscious to the patient, diagnosis is based on objective findings during examination rather than on a patient’s report. This is similar to evaluating a patient with abdominal pathology: we would not expect the patient to report an abdominal mass, even though we could detect it and train the patient to palpate it. The somatizing patient believes the problem is physical, so the history reported is more likely to lead to physical testing and medical treatments than to a direct examination of the emotional system. Although clues in the history may suggest a patient is somatizing,20 the definitive test, like that of an abdominal examination, is “hands on,” observing the patient’s direct response to an emotion-focused interview.
Actively exploring emotions
Examination of the emotional system is analogous to a physical examination of other systems, and progresses from observation to “palpation” or “percussion” ( Table 2 ).
Observe the patient for visible unconscious anxiety. Then, in the context of a supportive patient-doctor relationship, explore emotionally charged situations that generate symptoms.
Alternatively, one may ask in what way strong emotions like anger affect the patient’s physical problems. Asking about specific recent events and feelings that were triggered usually mobilizes emotions, giving you and the patient a direct look at how emotions affect them physically.
If a patient is anxious in the office, it will be most meaningful to examine the feelings they experience during the interview.
TABLE 2
Exploring emotions in a patient-centered interview
| Action | Example |
|---|---|
| Observation | Note any signs of unconscious tension, somatic distress, or defensiveness from the start of the interview |
| Ask about emotions | Can you describe a situation when the symptoms get worse? |
| What feelings do you have when you talk about that? | |
| How do you experience the feeling of anger in your body when it is there? | |
| Distinguish feelings from anxiety or defenses | The tension you had was anxiety, but how did the anger feel? |
| Becoming quiet was what you did but how did you feel inside? | |
| Observe physical responses | Observe the physical and behavioral responses in the patient when the emotional system is activated |
| Give feedback and plan | Review all findings with the patient. Verify the patient agrees with what you have observed. Plan any further treatments or referra |
Managing defenses
At times, the defenses used to avoid feelings must be pointed out before the patient can see and interrupt these behaviors. If the process is too detached or intellectual, then feelings will not be activated and the system cannot be assessed. The physician’s rapport allows him or her to clarify the process and the need for the patient to try to approach and experience feelings when speaking about them. This is analogous to the process of examining a sore abdomen when a patient is guarding: the patient must relax for examination to take place, and we help them do this by explaining the process.
Patients who are defensive and insist the problem is not related to emotions are managed differently. These patients usually are quite tense and already emotionally activated. An open examination of feelings the patient has about coming to see you that day is a good way to begin. Through this focus one can see the patient’s somatizing patterns directly as well as develop a working rapport.
Managing anxiety
If the patient becomes anxious when asked about emotions, introduce a calming step by asking the patient to intellectualize about the specific bodily anxiety symptoms. This reduces the anxiety by using the defense of intellectualization.
Recap and planning
The interview is concluded by reviewing the findings with the patient in the same way one would share findings of a blood test. Management options would depend on the findings and may include another interview, further medical investigations, referral for treatment, or follow-up to gauge the patient’s response to the interview itself.
Interpreting the patient’s responses
With the focused assessment, the somatic symptoms will transiently increase or decrease, disappear, or not change at all ( Table 3 ).
An increase in symptoms with emotional focus suggests that emotions aggravate or directly cause the problems. A decrease in symptoms during the test also suggests a linkage to emotions. Disappearance of the symptoms by bringing emotional experiences to awareness is the best direct evidence that somatization of these emotions was causing the patient’s symptoms.
No change in a patient’s symptoms or signs—provided there was adequate emotional activation—suggests no somatization of emotions. In these cases, other physical factors must be sought. For example, a woman with chronic left leg weakness and numbness had no shift in symptoms with this test: she was found to have neuropathy due to multiple sclerosis. We have found that 5% to 10% of patients referred to our diagnostic clinic have physical problems that were mistaken for somatization.
TABLE 3
Interpretation of responses to emotionally focused assessment
| Response | Interpretation and action | Beware of |
|---|---|---|
| Response 1: Symptoms go up with emotional focus then down after focusing away from emotions | The diagnosis is likely somatization. Prescribe emotion-focused psychotherapy and monitor for gradual symptom removal | False positives due to coincidental symptom changes in interview |
| Health problems unrelated to the somatization could always be present | ||
| Response 2: Symptoms are improved or removed by emotional focus or emotional experience in the office | The diagnosis is (was) somatization of those emotions. Follow-up to see if gains are maintained | |
| Response 3: No change in symptoms | Somatization is unlikely to be the cause of the symptoms. Look for physical causes. | False negatives due to high defenses, sedation, lack of cooperation, inadequate focus by physician |
| Response 4: Unclear response | May or may not be an emotionbased component in the symptoms. Repeat test, consider other diagnostic tests or referral for emotion-focused diagnostic testing |
False negatives
False negatives occur when the test does not detect the process of somatization when it is present. This will occur if the level of emotion mobilized was too low, if the patient is too sedated, if the defenses the patient used were not sufficiently interrupted, or when the patient is not working collaboratively with the doctor during the test. In each case the patient must allow emotions to be mobilized and the doctor must focus adequately on the emotional experiences to yield an interpretable response.
False positives
False positives occur when the patient has a rise or fall in symptoms during the test for other reasons—eg, coincidental shifts in episodic conditions like muscle spasm or symptom reduction due to distraction during the test itself. It is important in these cases to repeat the test more than once and see if the results are reproducible.
Treatment: short-term dynamic psychotherapy
STDP is clinically effective for patients with somatization
Short-term dynamic psychotherapy (STDP) formats specifically help a patient to examine trauma and loss-related emotions that result in somatization, depression, anxiety, and self-defeating behaviors. Case-series videotaped research over the past 30 years has established the effectiveness of the methods in both short and long term follow-up.21
STDP is efficacious in controlled trials and meta-analyses
In 1995, Anderson and Lambert22 conducted a meta-analysis of 26 controlled studies and found STDP to be superior to minimal treatment controls and wait lists including in samples with somatization. It was found to be as effective in removing anxiety and depressive symptoms as cognitive behavioral therapy. A recent meta-analysis,23 using more strict inclusion criteria, yielded the same findings. In a recent randomized controlled trial of symptomatic patients with personality disorders, STDP brought significant symptom reduction while cognitive therapy did not, suggesting that STDP may have added benefits in more resistant and complex symptomatic patients.24
In our current Cochrane review search,25 we have found 40 published randomized controlled trials supporting its efficacy with a range of disorders including ulcer disease, irritable bowel syndrome, dyspepsia, and urethral syndrome.26-29 Our review has likewise found STDP to be superior to minimal treatment or waitlist controls and that the gains are maintained in follow-up averaging over 1 year.
STDP is cost-effective and reduces health care utilization
STDP has been shown to reduce healthcare utilization and to be cost-effective in treating patients with dyspepsia, irritable bowel syndrome, depression, and self-harm and treatment-resistant conditions.30 Of specific cost figures cited in reviewed papers, 27 out of 34 showed cost savings with STDP including reduction in total costs, medication costs, disability, hospital, and physician use.
Case Illustrations
Case 1: Striated muscle anxiety
This 42-year-old man had chronic fatigue and fibromyalgia which lead to a 13 month disability up to the time of consultation. He came to the office with longstanding pain in his shoulders. His hands were clenched during the interview, and he appeared tense while giving his history.
- DOCTOR: Can you tell about a specific time when you had an emotional upset so we can understand how exactly it affects you?
- PATIENT: Yeah, problems at home with my wife…. Saturday she wanted me to do some work on the garage. She started to yell. Every day it’s the same thing and I’m getting tired of it.… DOCTOR: So how do you feel toward her?
- PATIENT: [Takes a deep sigh, hands become clenched] Mad.
- DOCTOR: You mean mad … angry?
- PATIENT: Yeah.
- DOCTOR: How do you experience the anger inside physically?
- PATIENT: Very, very… tense
- DOCTOR: That is tension…anxiety?
- PATIENT: Yeah.
- DOCTOR: How did you experience the anger?
- PATIENT: I start to ignore her.
- DOCTOR: Is that a mechanism to deal with anger?
- PATIENT: It’s really hard to put a word on it…. I get really mad…it’s like a rage.
- DOCTOR: So how do you experience the rage?
- PATIENT: [Patient takes a big sigh and clenches his hands tightly]
- DOCTOR: Do you notice you sigh and become tense when you talk about the rage.
- PATIENT: No, I didn’t. I don’t feel anxious.
- DOCTOR: But, do you notice the sigh and your hands?
- PATIENT: I do now, but didn’t see it before.
- DOCTOR: Is this what is happening to you … that you are getting all tensed up about these feelings?
- PATIENT: Yeah, it must be.
At a later point in the 1-hour session, the patient was able to feel the visceral emotions of rage, guilt about the rage, and sadness over several years of conflict. When the feelings were experienced in the office, he had an abrupt drop in muscle tension and bodily pain: this was further evidence he had been somatizing, or as he said, “bottling up” these complex feelings.
As is typical of patients with primarily striated muscle anxiety, he denies being nervous despite showing obvious anxiety in the interview. He denies anxiety because it has been unconscious to him, thus free to create fibromyalgia pain. Through this single interview a link is made for both patient and doctor between blocked feelings and body pain. With 10 treatment sessions focused on this process, his fibromyalgia resolved; he returned to work and no longer needed antidepressants.
Case 2: Smooth muscle anxiety
This patient is a 38 year-old woman with severe incapacitating GERD, irritable bowel syndrome, and depression who was disabled from work for 2 years at the time of consultation. This woman had a very relaxed posture with relaxed hands and an absence of obvious anxiety. After 10 minutes of exploring situations and events that make her stomach worse, we arrive at the following point.
- DOCTOR: Can you tell me about another time when your stomach felt worse?
- PATIENT: Yes. There was once when my sister-inlaw did something and it made me angry. Yeah, when people make me angry I don’t tell them, I just avoid them.
- DOCTOR: Can you describe one of those times, so we can see how that affects you.
- PATIENT: Once she was arguing with my brother, like they usually do….
- DOCTOR: How did you feel then?
- PATIENT: … Now I just got that again [pointing to her stomach and chest with upward motion and burps]
- DOCTOR: Heartburn? Just came on?
- PATIENT: Yeah, heartburn, just came on.
- DOCTOR: Is there anything else you notice? Like in your stomach?
- PATIENT: No, just that … but I can hear my stomach churning.
- DOCTOR: So is it when you have anger your stomach churns and you get this acid?
- PATIENT: Must be….
- DOCTOR: …because in your approach to talk about anger you got cramps and acid. So is that one way the anger goes?
- PATIENT: Yes it must be, but I never thought of that part. [Stomach stops churning and heartburn stops as we talk about it for few minutes.] You know, this all started to get worse when my fiancé dumped me. [She goes onto describe a story of being not only rejected but also feeling humiliated by how it was done. She never felt emotional about it but just got severe diarrhea and was confined to her room for 3 weeks.]
- DOCTOR: How did you feel toward your fiancé when he dumped you that way?
- PATIENT: I was just so sick and depressed. I didn’t feel any anger. [Patient burps again this time rubs abdomen due to some discomfort.]
- DOCTOR: Did you get the stomach upset just now again?
- PATIENT: My stomach is upset again. Just the noise and acid again.
- DOCTOR: So again, when we focus on the feelings, the cramps and acid come back.
- PATIENT: For sure. What can we do about that?
- DOCTOR: Can we try to help you identify these feelings before they go to your stomach, to try to interrupt that process. Can you tell me about another incident like that?
The patient required 3 one-hour sessions to improve her tolerance of anxiety, so she could intellectualize about feelings rather than have them directly affect her stomach. The feelings of rejection had triggered rage and guilt about rage associated with sexual abuse by her brother and the abandonment she felt from her mother when she told her mother about it. With 12 sessions of therapy, she was able to stop her IBS medication, anxiolytic, and antidepressant.
This vignette is typical for patients with primarily smooth muscle unconscious anxiety. The patient had no visible anxiety but had GI symptoms when focusing on emotions about recent trauma. The symptoms were mobilized and reduced repeatedly, confirming a link with emotions. Note that outwardly she looked calm, but the emotions mobilized were being shunted to her GI tract.
Incorporating emotion diagnostics into practice
To perform these interview procedures, the physician must understand emotion physiology and the patterns of somatization as outlined above. This is entirely intuitive to many physicians the first time seeing this material: they can readily employ that which they already know. In general, though, physicians reading this will want to ponder it and see how it may apply case by case as they develop skills with it over time. Senior clinicians have usually done these assessments by default, by pressure from patients, or because they learned elements of this over time from various experiences.
Helpful short-cuts
Family physicians trained in emotion assessment note that abbreviated elements can easily be incorporated into a patient-centered assessment process. For example, one may ask how “stress,” “emotions,” or “anger” affects the person and their body or ask how the person handles anger in specific incidents.
In an initial patient questionnaire, one can include a few questions that encourage the patient to think about how stress affects them and to describe their body’s tendency to experience anxiety. When they later present with symptoms, one can use these baseline data to aid in the new assessment. Thus, a culture of considering emotional factors can be woven into practice, weakening any resistance to the idea that emotions and health, mind and body, are tightly bound.
Time factors
Based on our experience, family physicians can perform two thirds of these diagnostic assessments during 15 minutes of focused interviewing. More complex cases, such as patients with cognitive disruption or multiple manifestations of anxiety, may take longer to diagnose and generally need more specialized care or referral. If required, a patient could be asked back for a 1 half-hour session later in the day or week.
Taking care of ourselves
Despite the importance of the emotional system in medicine, medical curricula generally fail to provide sufficient education in this area. At the same time, up to half of our own ranks report emotional burnout.31 Even with the lack of mainstream medical teaching about emotions and health, it behooves us to learn what we can about the emotional system as it applies to the patient and to ourselves in relation to these most challenging problems. Focused seminars, peer case review, select reading, and videotape training can all help in this educational process.32
Acknowledgments
The author wishes to thank the many colleagues who reviewed and commented on this manuscript. This work is supported by Dalhousie University, Capital Health and the Nova Scotia Department of Health.
Correspondence
Allan Abbass, MD, FRCPC, Associate Professor and Director of Education, Psychiatry, Director, Center for Emotions and Health, 8th Floor, Abbie J. Lane Memorial Building, Halifax, NS B3H 2E2, Canada. E-mail: [email protected].
1. Fink P, Sorensen L, Engberg M, Holm M, Munk-Jorgensen P. Somatization in primary care. Prevalence, health care utilization, and general practitioner recognition. Psychosomatics 1999;40:330-338.
2. Kroenke K, Mangelsdorff AD. Common symptoms in ambulatory care: incidence, evaluation, therapy, and outcome. Am J Med 1989;86:262-266.
3. Barsky AJ, Ettner SL, Horsky J, Bates DW. Resource utilization of patients with hypochondriacal health anxiety and somatization. Medical Care 2001;39:705-715.
4. Engel CC, Jr, Liu X, Hoge C, Smith S. Multiple idiopathic physical symptoms in the ECA study: competing-risks analysis of 1-year incidence, mortality, and resolution. Am J Psychiatry 2002;159:998-1004.
5. Bellon JA, Fernandez-Asensio ME. Emotional profile of physicians who interview frequent attenders. Patient Education & Counseling 2002;48:33-41.
6. De Gucht V, Fischler B. Somatization: A critical review of conceptual and methodological issues. Psychosomatics 2002;43:1-9.
7. Righter EL, Sansone RA. Managing somatic preoccupation. Am Fam Physician 1999;59:3113-20.
8. Holloway KL, Zerbe KJ. Simplified approach to somatization disorder. When less may prove to be more. Postgrad Med 2000;108:89-9295.
9. Servan-Schreiber D, Tabas G, Kolb NR. Somatizing patients: part II. Practical management. Am Fam Physician 2000;61:1423-1428,1431-1432.
10. Servan-Schreiber D, Kolb R, Tabas G. The somatizing patient. Prim Care 1999;26:225-242.
11. Noyes R, Jr, Holt CS, Kathol RG. Somatization. Diagnosis and management. Arch Fam Med 1995;4:790-795.
12. Davanloo H. Intensive short-term dynamic psychotherapy with highly resistant patients. I. Handling resistance. International Journal of Short-Term Psychotherapy 1986;1:107-133.
13. Davanloo H. The technique of unlocking the unconscious in patients suffering from functional disorders. Part I. Restructuring ego’s defenses. In: Davanloo H. Unlocking the Unconscious. Chichester, England: John Wiley & Sons; 1990;283-306.
14. Katon W, Sullivan M, Walker E. Medical symptoms without identified pathology: relationship to psychiatric disorders and adult trauma, and personality traits. Ann Intern Med 2001;1:917-925.
15. Roter D, Ewart CK. Emotional inhibition in essential hypertension: Obstacle to communication during medical visits? Health Psychology 1992;11:163-169.
16. Venable VL, Carlson CR, Wilson J. The role of anger and depression in recurrent headache. Headache 2001;41:21-30.
17. Whorwell PJ, Houghton LA, Taylor EE, Maxton DG. Physiological effects of emotion: assessment via hypnosis. Lancet 1992;340:434.-
18. Davanloo H. Intensive short term dynamic psychotherapy: Spectrum of psychoneurotic disorders. In Davanloo H. Intensive Short-Term Dynamic Psychotherapy. Chichester, England: John Wiley and Sons; 2001
19. Servan-Schreiber D, Tabas G. Somatizing patients part I: practical diagnosis. Am Fam Physician 2000;61:1073-1078.
20. Abelson JL, W. J., Neese RM, Curtis GC. Persistent respiratory irregularity in patients with panic disorder. Biological Psychiatry 2001;49:588-595.
21. Davanloo H. Short-Term Dynamic Psychotherapy New York: Jason Aronson; 1980
22. Anderson E, Lambert M. Short-term dynamically oriented psychotherapy: A review and meta-analysis. Clinical Psychology Review 1995;15:503-514.
23. Leichsenring F, Rabung S, Leibing E. The efficacy of short-term psychodynamic psychotherapy in specific psychiatric disorders: a meta-analysis. Arch Gen Psychiatry 2004;61:1208-1216.
24. Svartberg M, Stiles TC, Seltzer MH. Randomized controlled trial of the effectiveness of short-term dynamic psychotherapy and cognitive therapy for cluster C personality disorders. Am J Psychiatry 2004;161:810-817.
25. Abbass AA, Hancock JT, Henderson J, Kisely S. Shortterm psychodynamic psychotherapies for common mental disorders (Protocol for a Cochrane Review). 2004 In: The Cochrane Library Chichester, UK: John Wiley and Sons.
26. Sjodin I, Svedlund J, Ottoson J, Dotevall G. Controlled study of psychotherapy in chronic peptic ulcer disease. Psychosomatics 1986;27:187-200.
27. Creed FLF, Guthrie E, Palmer S, et al. The cost-effectiveness of psychotherapy and paroxetine for severe irritable bowel syndrome. Gastroenterology 2003;124:303-317.
28. Hamilton J, Guthrie E, Creed F. A randomized controlled trial of psychotherapy in patients with chronic functional dyspepsia. Gastroenterology 2000;119:661-669.
29. Baldoni F, Baldaro B, Trombini G. Psychotherapeutic perspectives in urethral syndrome. Stress Medicine 1995;11:79-84.
30. Abbass A. The cost-effectiveness of short-term dynamic psychotherapy. Journal of Pharmacoeconomics and Outcomes Research 2003;3:535-539.
31. CMA Guide to Physician Health and Well-being 2003. Canadian Medical Association.
32. Coombs RH, Perrell K, Ruckh JM. Primary prevention of emotional impairment among medical trainees. Acad Med 1990;65:576-581.
- Obvious anxiety in a patient with physical complaints should prompt an evaluation for somatization.
- Become familiar with the 4 patterns of somatization and their manifestations.
- Learn how to conduct an emotion-focused interview, which, when applied appropriately, will help rule somatization in or out.
A 42-year-old man has chronic fatigue and fibromyalgia that has led to a 13-month disability leave from work. The reason for his current office visit is longstanding pain in his shoulders. As you take his history, he is sitting with hands clenched and he generally appears tense.
A 38-year-old woman with severe incapacitating gastroesophageal reflux disease, irritable bowel syndrome, and depression has been too disabled to work for 2 years. At the time of your interview, her posture is relaxed and she shows no signs of anxiety.
These 2 very different patients (whose cases I will review in detail) share a common problem: somatization, the translation of emotions into somatic problems or complaints. It is well documented—though still largely unrecognized in practice—that somatization accounts for a large proportion of office visits to primary care physicians as well as specialists,1,2 leading to unnecessary testing, treatment, and hospitalization, disability and corporate financial loss,3 likely earlier mortality,4 and frustration for patients and physicians.5
No longer a diagnosis of exclusion
Despite the burden somatization places on the medical system, the diagnosis is often made by indirect methods such as checklist, speculation, or exclusion when other problems are ruled out.6 The common position, even in recent reviews, is that somatization should be treated by nonspecific measures, such as frequent office visits to increase the patient’s and physician’s ability to cope with what is often seen to be a chronic and incurable disorder.7-11 Such a position is no longer warranted.
Based on recent quantitative and extensive case-based research, specific emotion-focused brief therapies and videotape-based research have clarified how emotions are experienced in the body and how somatization of emotions occurs (see The physiology of emotions). These methods, including short-term dynamic psychotherapy (STDP) have been used to diagnose and treat somatization effectively since the 1980s. Somatization, with its morbidity and chronicity, need no longer be diagnosed by exclusion nor treated palliatively without specific diagnostic testing.
To diagnose and manage somatization we must know how emotions are experienced and how they may become somatized. Davanloo discovered through studying several hundred case videotapes that specific emotions manifest in specific ways regardless of gender, age, or ethnicity.12 This emotion physiology constitutes a norm to compare with a patient who somatizes emotions.
For example, rage is experienced as an internal energy sensation, heat, or “volcano” that rises from the lower abdomen to the chest, neck, and finally to the hands with an urge to grab and do some form of violence. Guilt about rage is experienced with upper chest constriction or even pain, intense painful feeling with waves of tears and with thoughts of remorse about experiencing the rage.13 When feelings are experienced consciously, by definition they are not being somatized at that moment.
Why somatization occurs
When feelings are intense, frightening, or conflicted, they create anxiety and defense mechanisms to cover the anxiety (see the Figure ). If these feelings are unconscious to the patient, the subsequent anxiety and defenses may also be outside of awareness.
This is the finding common in people who have been traumatized by someone close to them: feelings of rage toward a loved one are unacceptable, frightening, and avoided through somatization and other defenses.14 Diverse research has found that patients with hypertension, migraine, irritable bowel syndrome, and other conditions internalize anger and thus increase their somatic problems.15-17 Blocking and inhibiting of emotions, including anger, is a common finding in somatizing patients.
FIGURE
The 4 patterns of somatization
Videotaped case-series research shows 4 main patterns of somatization: 1) striated muscle unconscious anxiety, 2) smooth muscle tension 3) cognitive-perceptual disruption, and 4) conversion.18
Striated muscle tension due to unconscious anxiety manifests through hand clenching, sighing, and even hyperventilation that the patient is not aware of. These patients may report panic attacks, chest pain, headache, fibromyalgia, and other musculoskeletal complaints. These conditions are often frustrating to family, employers, and physicians since conditions like chronic pain respond to treatment slowly or not at all.
Smooth muscle tension due to unconscious anxiety causes acute or chronic spasm of blood vessels, GI tract, airways, and the bladder. Patients exhibiting smooth muscle tension may present with GI symptoms, migraine, hypertension, urinary frequency, and upper airway constriction mimicking asthma. They often report histories of depression, panic, substance abuse, personality disorders, and past sexual or physical abuse.
Cognitive perceptual disruption due to unconscious anxiety typically involves visual blurring, tunnel vision, loss of train of thought, and “drifting,” wherein the patient is temporarily mentally absent from the room. These patients have chronically poor memories and concentration. They are commonly victims or perpetrators of partner abuse, have frequent accidents, and have transient paranoia. They often end up seeing neurologists and undergoing expensive testing. Most have histories of dissociative disorders, personality disorders, or childhood abuse. In the family doctor’s office they frequently forget what was said and call back after the appointment. They appear confused and easily flustered and either avoid physical examinations entirely or endure them with great anxiety.
Conversion manifests as muscle weakness or paralysis in any voluntary muscle. Patients with acute conversion describe dropping items or even dropping to the floor as muscles give way without explanation. They will often report histories of witnessing or experiencing violent abuse.
One pattern usually predominates
The total amount of somatized emotion is distributed over the 4 pathways ( Table 1 ). One pathway generally prevails at any given time, though different pathways may come into play as anxiety waxes or wanes. When anxiety is expressed primarily through smooth muscle tension, cognitive perceptual disruption, or conversion, the striated muscles are relatively relaxed.
This finding of apparent calm while somatizing has been noted elsewhere in research of patients with hypertension. This is the “belle indifference” a patient expresses as they are temporarily relieved of muscle tension through somatization elsewhere.19
TABLE 1
Examples of diagnosable somatization patterns
| Somatization format | Observations during emotion-focused diagnostic assessment | Examples of related health complaints or health problems |
|---|---|---|
| Striated muscle tension | Progression from hand clenching, arm tension, neck tension, sighing respirations to whole-body tension | Fibromyalgia, headache, muscle spasm, backache, chest pain, shortness of breath, abdominal (wall) pain, fatigue |
| Smooth muscle tension | Relative absence of striated muscle tension. Instead activation of smooth muscles causes, for example, cramps in the abdomen or heartburn. | Irritable bowel symptoms, abdominal pain, nausea, bladder spasm, bronchospasm, coronary artery spasm, hypertension, migraine |
| Cognitive-perceptual disruption | Relative absence of striated muscle tension. Instead patient loses track of thoughts, becomes confused, gets blurry vision | Visual blurring, blindness, mental confusion, memory loss, dizziness, weakness, pseudo-seizures, paresthesias, fainting, conversion |
| Conversion | Relative absence of striated muscle tension. Instead patient goes weak in some or all voluntary muscle | Falling, aphonia, paralysis, weakness |
Major types of defense
Two important categories of defense include isolation of affect and repression.
Isolation of affect is awareness of emotions in one’s head without experiencing them in the body. Intellectualization is a form of isolation of affect.
Repression is the unconscious process by which emotions are shunted into the body rather than reaching consciousness at all. For example, strong emotions, including rage, may directly cause sighing and a panic attack without the person being aware of either the emotion or the sighing.20
Experiencing the emotions overcomes somatization
Videotaped research also shows that if a person can experience true feelings in the moment, somatization of these feelings is weakened and overcome. The feelings being experienced push out the anxiety and somatization ( Figure ). Thus, somatization can be reduced or removed by helping a patient feel emotions being stirred by recent events or from past events. Through this process one may diagnose somatization and also produce a therapeutic effect for a patient.
Direct diagnosis of somatization
An objective assessment
Because the process of somatization is unconscious to the patient, diagnosis is based on objective findings during examination rather than on a patient’s report. This is similar to evaluating a patient with abdominal pathology: we would not expect the patient to report an abdominal mass, even though we could detect it and train the patient to palpate it. The somatizing patient believes the problem is physical, so the history reported is more likely to lead to physical testing and medical treatments than to a direct examination of the emotional system. Although clues in the history may suggest a patient is somatizing,20 the definitive test, like that of an abdominal examination, is “hands on,” observing the patient’s direct response to an emotion-focused interview.
Actively exploring emotions
Examination of the emotional system is analogous to a physical examination of other systems, and progresses from observation to “palpation” or “percussion” ( Table 2 ).
Observe the patient for visible unconscious anxiety. Then, in the context of a supportive patient-doctor relationship, explore emotionally charged situations that generate symptoms.
Alternatively, one may ask in what way strong emotions like anger affect the patient’s physical problems. Asking about specific recent events and feelings that were triggered usually mobilizes emotions, giving you and the patient a direct look at how emotions affect them physically.
If a patient is anxious in the office, it will be most meaningful to examine the feelings they experience during the interview.
TABLE 2
Exploring emotions in a patient-centered interview
| Action | Example |
|---|---|
| Observation | Note any signs of unconscious tension, somatic distress, or defensiveness from the start of the interview |
| Ask about emotions | Can you describe a situation when the symptoms get worse? |
| What feelings do you have when you talk about that? | |
| How do you experience the feeling of anger in your body when it is there? | |
| Distinguish feelings from anxiety or defenses | The tension you had was anxiety, but how did the anger feel? |
| Becoming quiet was what you did but how did you feel inside? | |
| Observe physical responses | Observe the physical and behavioral responses in the patient when the emotional system is activated |
| Give feedback and plan | Review all findings with the patient. Verify the patient agrees with what you have observed. Plan any further treatments or referra |
Managing defenses
At times, the defenses used to avoid feelings must be pointed out before the patient can see and interrupt these behaviors. If the process is too detached or intellectual, then feelings will not be activated and the system cannot be assessed. The physician’s rapport allows him or her to clarify the process and the need for the patient to try to approach and experience feelings when speaking about them. This is analogous to the process of examining a sore abdomen when a patient is guarding: the patient must relax for examination to take place, and we help them do this by explaining the process.
Patients who are defensive and insist the problem is not related to emotions are managed differently. These patients usually are quite tense and already emotionally activated. An open examination of feelings the patient has about coming to see you that day is a good way to begin. Through this focus one can see the patient’s somatizing patterns directly as well as develop a working rapport.
Managing anxiety
If the patient becomes anxious when asked about emotions, introduce a calming step by asking the patient to intellectualize about the specific bodily anxiety symptoms. This reduces the anxiety by using the defense of intellectualization.
Recap and planning
The interview is concluded by reviewing the findings with the patient in the same way one would share findings of a blood test. Management options would depend on the findings and may include another interview, further medical investigations, referral for treatment, or follow-up to gauge the patient’s response to the interview itself.
Interpreting the patient’s responses
With the focused assessment, the somatic symptoms will transiently increase or decrease, disappear, or not change at all ( Table 3 ).
An increase in symptoms with emotional focus suggests that emotions aggravate or directly cause the problems. A decrease in symptoms during the test also suggests a linkage to emotions. Disappearance of the symptoms by bringing emotional experiences to awareness is the best direct evidence that somatization of these emotions was causing the patient’s symptoms.
No change in a patient’s symptoms or signs—provided there was adequate emotional activation—suggests no somatization of emotions. In these cases, other physical factors must be sought. For example, a woman with chronic left leg weakness and numbness had no shift in symptoms with this test: she was found to have neuropathy due to multiple sclerosis. We have found that 5% to 10% of patients referred to our diagnostic clinic have physical problems that were mistaken for somatization.
TABLE 3
Interpretation of responses to emotionally focused assessment
| Response | Interpretation and action | Beware of |
|---|---|---|
| Response 1: Symptoms go up with emotional focus then down after focusing away from emotions | The diagnosis is likely somatization. Prescribe emotion-focused psychotherapy and monitor for gradual symptom removal | False positives due to coincidental symptom changes in interview |
| Health problems unrelated to the somatization could always be present | ||
| Response 2: Symptoms are improved or removed by emotional focus or emotional experience in the office | The diagnosis is (was) somatization of those emotions. Follow-up to see if gains are maintained | |
| Response 3: No change in symptoms | Somatization is unlikely to be the cause of the symptoms. Look for physical causes. | False negatives due to high defenses, sedation, lack of cooperation, inadequate focus by physician |
| Response 4: Unclear response | May or may not be an emotionbased component in the symptoms. Repeat test, consider other diagnostic tests or referral for emotion-focused diagnostic testing |
False negatives
False negatives occur when the test does not detect the process of somatization when it is present. This will occur if the level of emotion mobilized was too low, if the patient is too sedated, if the defenses the patient used were not sufficiently interrupted, or when the patient is not working collaboratively with the doctor during the test. In each case the patient must allow emotions to be mobilized and the doctor must focus adequately on the emotional experiences to yield an interpretable response.
False positives
False positives occur when the patient has a rise or fall in symptoms during the test for other reasons—eg, coincidental shifts in episodic conditions like muscle spasm or symptom reduction due to distraction during the test itself. It is important in these cases to repeat the test more than once and see if the results are reproducible.
Treatment: short-term dynamic psychotherapy
STDP is clinically effective for patients with somatization
Short-term dynamic psychotherapy (STDP) formats specifically help a patient to examine trauma and loss-related emotions that result in somatization, depression, anxiety, and self-defeating behaviors. Case-series videotaped research over the past 30 years has established the effectiveness of the methods in both short and long term follow-up.21
STDP is efficacious in controlled trials and meta-analyses
In 1995, Anderson and Lambert22 conducted a meta-analysis of 26 controlled studies and found STDP to be superior to minimal treatment controls and wait lists including in samples with somatization. It was found to be as effective in removing anxiety and depressive symptoms as cognitive behavioral therapy. A recent meta-analysis,23 using more strict inclusion criteria, yielded the same findings. In a recent randomized controlled trial of symptomatic patients with personality disorders, STDP brought significant symptom reduction while cognitive therapy did not, suggesting that STDP may have added benefits in more resistant and complex symptomatic patients.24
In our current Cochrane review search,25 we have found 40 published randomized controlled trials supporting its efficacy with a range of disorders including ulcer disease, irritable bowel syndrome, dyspepsia, and urethral syndrome.26-29 Our review has likewise found STDP to be superior to minimal treatment or waitlist controls and that the gains are maintained in follow-up averaging over 1 year.
STDP is cost-effective and reduces health care utilization
STDP has been shown to reduce healthcare utilization and to be cost-effective in treating patients with dyspepsia, irritable bowel syndrome, depression, and self-harm and treatment-resistant conditions.30 Of specific cost figures cited in reviewed papers, 27 out of 34 showed cost savings with STDP including reduction in total costs, medication costs, disability, hospital, and physician use.
Case Illustrations
Case 1: Striated muscle anxiety
This 42-year-old man had chronic fatigue and fibromyalgia which lead to a 13 month disability up to the time of consultation. He came to the office with longstanding pain in his shoulders. His hands were clenched during the interview, and he appeared tense while giving his history.
- DOCTOR: Can you tell about a specific time when you had an emotional upset so we can understand how exactly it affects you?
- PATIENT: Yeah, problems at home with my wife…. Saturday she wanted me to do some work on the garage. She started to yell. Every day it’s the same thing and I’m getting tired of it.… DOCTOR: So how do you feel toward her?
- PATIENT: [Takes a deep sigh, hands become clenched] Mad.
- DOCTOR: You mean mad … angry?
- PATIENT: Yeah.
- DOCTOR: How do you experience the anger inside physically?
- PATIENT: Very, very… tense
- DOCTOR: That is tension…anxiety?
- PATIENT: Yeah.
- DOCTOR: How did you experience the anger?
- PATIENT: I start to ignore her.
- DOCTOR: Is that a mechanism to deal with anger?
- PATIENT: It’s really hard to put a word on it…. I get really mad…it’s like a rage.
- DOCTOR: So how do you experience the rage?
- PATIENT: [Patient takes a big sigh and clenches his hands tightly]
- DOCTOR: Do you notice you sigh and become tense when you talk about the rage.
- PATIENT: No, I didn’t. I don’t feel anxious.
- DOCTOR: But, do you notice the sigh and your hands?
- PATIENT: I do now, but didn’t see it before.
- DOCTOR: Is this what is happening to you … that you are getting all tensed up about these feelings?
- PATIENT: Yeah, it must be.
At a later point in the 1-hour session, the patient was able to feel the visceral emotions of rage, guilt about the rage, and sadness over several years of conflict. When the feelings were experienced in the office, he had an abrupt drop in muscle tension and bodily pain: this was further evidence he had been somatizing, or as he said, “bottling up” these complex feelings.
As is typical of patients with primarily striated muscle anxiety, he denies being nervous despite showing obvious anxiety in the interview. He denies anxiety because it has been unconscious to him, thus free to create fibromyalgia pain. Through this single interview a link is made for both patient and doctor between blocked feelings and body pain. With 10 treatment sessions focused on this process, his fibromyalgia resolved; he returned to work and no longer needed antidepressants.
Case 2: Smooth muscle anxiety
This patient is a 38 year-old woman with severe incapacitating GERD, irritable bowel syndrome, and depression who was disabled from work for 2 years at the time of consultation. This woman had a very relaxed posture with relaxed hands and an absence of obvious anxiety. After 10 minutes of exploring situations and events that make her stomach worse, we arrive at the following point.
- DOCTOR: Can you tell me about another time when your stomach felt worse?
- PATIENT: Yes. There was once when my sister-inlaw did something and it made me angry. Yeah, when people make me angry I don’t tell them, I just avoid them.
- DOCTOR: Can you describe one of those times, so we can see how that affects you.
- PATIENT: Once she was arguing with my brother, like they usually do….
- DOCTOR: How did you feel then?
- PATIENT: … Now I just got that again [pointing to her stomach and chest with upward motion and burps]
- DOCTOR: Heartburn? Just came on?
- PATIENT: Yeah, heartburn, just came on.
- DOCTOR: Is there anything else you notice? Like in your stomach?
- PATIENT: No, just that … but I can hear my stomach churning.
- DOCTOR: So is it when you have anger your stomach churns and you get this acid?
- PATIENT: Must be….
- DOCTOR: …because in your approach to talk about anger you got cramps and acid. So is that one way the anger goes?
- PATIENT: Yes it must be, but I never thought of that part. [Stomach stops churning and heartburn stops as we talk about it for few minutes.] You know, this all started to get worse when my fiancé dumped me. [She goes onto describe a story of being not only rejected but also feeling humiliated by how it was done. She never felt emotional about it but just got severe diarrhea and was confined to her room for 3 weeks.]
- DOCTOR: How did you feel toward your fiancé when he dumped you that way?
- PATIENT: I was just so sick and depressed. I didn’t feel any anger. [Patient burps again this time rubs abdomen due to some discomfort.]
- DOCTOR: Did you get the stomach upset just now again?
- PATIENT: My stomach is upset again. Just the noise and acid again.
- DOCTOR: So again, when we focus on the feelings, the cramps and acid come back.
- PATIENT: For sure. What can we do about that?
- DOCTOR: Can we try to help you identify these feelings before they go to your stomach, to try to interrupt that process. Can you tell me about another incident like that?
The patient required 3 one-hour sessions to improve her tolerance of anxiety, so she could intellectualize about feelings rather than have them directly affect her stomach. The feelings of rejection had triggered rage and guilt about rage associated with sexual abuse by her brother and the abandonment she felt from her mother when she told her mother about it. With 12 sessions of therapy, she was able to stop her IBS medication, anxiolytic, and antidepressant.
This vignette is typical for patients with primarily smooth muscle unconscious anxiety. The patient had no visible anxiety but had GI symptoms when focusing on emotions about recent trauma. The symptoms were mobilized and reduced repeatedly, confirming a link with emotions. Note that outwardly she looked calm, but the emotions mobilized were being shunted to her GI tract.
Incorporating emotion diagnostics into practice
To perform these interview procedures, the physician must understand emotion physiology and the patterns of somatization as outlined above. This is entirely intuitive to many physicians the first time seeing this material: they can readily employ that which they already know. In general, though, physicians reading this will want to ponder it and see how it may apply case by case as they develop skills with it over time. Senior clinicians have usually done these assessments by default, by pressure from patients, or because they learned elements of this over time from various experiences.
Helpful short-cuts
Family physicians trained in emotion assessment note that abbreviated elements can easily be incorporated into a patient-centered assessment process. For example, one may ask how “stress,” “emotions,” or “anger” affects the person and their body or ask how the person handles anger in specific incidents.
In an initial patient questionnaire, one can include a few questions that encourage the patient to think about how stress affects them and to describe their body’s tendency to experience anxiety. When they later present with symptoms, one can use these baseline data to aid in the new assessment. Thus, a culture of considering emotional factors can be woven into practice, weakening any resistance to the idea that emotions and health, mind and body, are tightly bound.
Time factors
Based on our experience, family physicians can perform two thirds of these diagnostic assessments during 15 minutes of focused interviewing. More complex cases, such as patients with cognitive disruption or multiple manifestations of anxiety, may take longer to diagnose and generally need more specialized care or referral. If required, a patient could be asked back for a 1 half-hour session later in the day or week.
Taking care of ourselves
Despite the importance of the emotional system in medicine, medical curricula generally fail to provide sufficient education in this area. At the same time, up to half of our own ranks report emotional burnout.31 Even with the lack of mainstream medical teaching about emotions and health, it behooves us to learn what we can about the emotional system as it applies to the patient and to ourselves in relation to these most challenging problems. Focused seminars, peer case review, select reading, and videotape training can all help in this educational process.32
Acknowledgments
The author wishes to thank the many colleagues who reviewed and commented on this manuscript. This work is supported by Dalhousie University, Capital Health and the Nova Scotia Department of Health.
Correspondence
Allan Abbass, MD, FRCPC, Associate Professor and Director of Education, Psychiatry, Director, Center for Emotions and Health, 8th Floor, Abbie J. Lane Memorial Building, Halifax, NS B3H 2E2, Canada. E-mail: [email protected].
- Obvious anxiety in a patient with physical complaints should prompt an evaluation for somatization.
- Become familiar with the 4 patterns of somatization and their manifestations.
- Learn how to conduct an emotion-focused interview, which, when applied appropriately, will help rule somatization in or out.
A 42-year-old man has chronic fatigue and fibromyalgia that has led to a 13-month disability leave from work. The reason for his current office visit is longstanding pain in his shoulders. As you take his history, he is sitting with hands clenched and he generally appears tense.
A 38-year-old woman with severe incapacitating gastroesophageal reflux disease, irritable bowel syndrome, and depression has been too disabled to work for 2 years. At the time of your interview, her posture is relaxed and she shows no signs of anxiety.
These 2 very different patients (whose cases I will review in detail) share a common problem: somatization, the translation of emotions into somatic problems or complaints. It is well documented—though still largely unrecognized in practice—that somatization accounts for a large proportion of office visits to primary care physicians as well as specialists,1,2 leading to unnecessary testing, treatment, and hospitalization, disability and corporate financial loss,3 likely earlier mortality,4 and frustration for patients and physicians.5
No longer a diagnosis of exclusion
Despite the burden somatization places on the medical system, the diagnosis is often made by indirect methods such as checklist, speculation, or exclusion when other problems are ruled out.6 The common position, even in recent reviews, is that somatization should be treated by nonspecific measures, such as frequent office visits to increase the patient’s and physician’s ability to cope with what is often seen to be a chronic and incurable disorder.7-11 Such a position is no longer warranted.
Based on recent quantitative and extensive case-based research, specific emotion-focused brief therapies and videotape-based research have clarified how emotions are experienced in the body and how somatization of emotions occurs (see The physiology of emotions). These methods, including short-term dynamic psychotherapy (STDP) have been used to diagnose and treat somatization effectively since the 1980s. Somatization, with its morbidity and chronicity, need no longer be diagnosed by exclusion nor treated palliatively without specific diagnostic testing.
To diagnose and manage somatization we must know how emotions are experienced and how they may become somatized. Davanloo discovered through studying several hundred case videotapes that specific emotions manifest in specific ways regardless of gender, age, or ethnicity.12 This emotion physiology constitutes a norm to compare with a patient who somatizes emotions.
For example, rage is experienced as an internal energy sensation, heat, or “volcano” that rises from the lower abdomen to the chest, neck, and finally to the hands with an urge to grab and do some form of violence. Guilt about rage is experienced with upper chest constriction or even pain, intense painful feeling with waves of tears and with thoughts of remorse about experiencing the rage.13 When feelings are experienced consciously, by definition they are not being somatized at that moment.
Why somatization occurs
When feelings are intense, frightening, or conflicted, they create anxiety and defense mechanisms to cover the anxiety (see the Figure ). If these feelings are unconscious to the patient, the subsequent anxiety and defenses may also be outside of awareness.
This is the finding common in people who have been traumatized by someone close to them: feelings of rage toward a loved one are unacceptable, frightening, and avoided through somatization and other defenses.14 Diverse research has found that patients with hypertension, migraine, irritable bowel syndrome, and other conditions internalize anger and thus increase their somatic problems.15-17 Blocking and inhibiting of emotions, including anger, is a common finding in somatizing patients.
FIGURE
The 4 patterns of somatization
Videotaped case-series research shows 4 main patterns of somatization: 1) striated muscle unconscious anxiety, 2) smooth muscle tension 3) cognitive-perceptual disruption, and 4) conversion.18
Striated muscle tension due to unconscious anxiety manifests through hand clenching, sighing, and even hyperventilation that the patient is not aware of. These patients may report panic attacks, chest pain, headache, fibromyalgia, and other musculoskeletal complaints. These conditions are often frustrating to family, employers, and physicians since conditions like chronic pain respond to treatment slowly or not at all.
Smooth muscle tension due to unconscious anxiety causes acute or chronic spasm of blood vessels, GI tract, airways, and the bladder. Patients exhibiting smooth muscle tension may present with GI symptoms, migraine, hypertension, urinary frequency, and upper airway constriction mimicking asthma. They often report histories of depression, panic, substance abuse, personality disorders, and past sexual or physical abuse.
Cognitive perceptual disruption due to unconscious anxiety typically involves visual blurring, tunnel vision, loss of train of thought, and “drifting,” wherein the patient is temporarily mentally absent from the room. These patients have chronically poor memories and concentration. They are commonly victims or perpetrators of partner abuse, have frequent accidents, and have transient paranoia. They often end up seeing neurologists and undergoing expensive testing. Most have histories of dissociative disorders, personality disorders, or childhood abuse. In the family doctor’s office they frequently forget what was said and call back after the appointment. They appear confused and easily flustered and either avoid physical examinations entirely or endure them with great anxiety.
Conversion manifests as muscle weakness or paralysis in any voluntary muscle. Patients with acute conversion describe dropping items or even dropping to the floor as muscles give way without explanation. They will often report histories of witnessing or experiencing violent abuse.
One pattern usually predominates
The total amount of somatized emotion is distributed over the 4 pathways ( Table 1 ). One pathway generally prevails at any given time, though different pathways may come into play as anxiety waxes or wanes. When anxiety is expressed primarily through smooth muscle tension, cognitive perceptual disruption, or conversion, the striated muscles are relatively relaxed.
This finding of apparent calm while somatizing has been noted elsewhere in research of patients with hypertension. This is the “belle indifference” a patient expresses as they are temporarily relieved of muscle tension through somatization elsewhere.19
TABLE 1
Examples of diagnosable somatization patterns
| Somatization format | Observations during emotion-focused diagnostic assessment | Examples of related health complaints or health problems |
|---|---|---|
| Striated muscle tension | Progression from hand clenching, arm tension, neck tension, sighing respirations to whole-body tension | Fibromyalgia, headache, muscle spasm, backache, chest pain, shortness of breath, abdominal (wall) pain, fatigue |
| Smooth muscle tension | Relative absence of striated muscle tension. Instead activation of smooth muscles causes, for example, cramps in the abdomen or heartburn. | Irritable bowel symptoms, abdominal pain, nausea, bladder spasm, bronchospasm, coronary artery spasm, hypertension, migraine |
| Cognitive-perceptual disruption | Relative absence of striated muscle tension. Instead patient loses track of thoughts, becomes confused, gets blurry vision | Visual blurring, blindness, mental confusion, memory loss, dizziness, weakness, pseudo-seizures, paresthesias, fainting, conversion |
| Conversion | Relative absence of striated muscle tension. Instead patient goes weak in some or all voluntary muscle | Falling, aphonia, paralysis, weakness |
Major types of defense
Two important categories of defense include isolation of affect and repression.
Isolation of affect is awareness of emotions in one’s head without experiencing them in the body. Intellectualization is a form of isolation of affect.
Repression is the unconscious process by which emotions are shunted into the body rather than reaching consciousness at all. For example, strong emotions, including rage, may directly cause sighing and a panic attack without the person being aware of either the emotion or the sighing.20
Experiencing the emotions overcomes somatization
Videotaped research also shows that if a person can experience true feelings in the moment, somatization of these feelings is weakened and overcome. The feelings being experienced push out the anxiety and somatization ( Figure ). Thus, somatization can be reduced or removed by helping a patient feel emotions being stirred by recent events or from past events. Through this process one may diagnose somatization and also produce a therapeutic effect for a patient.
Direct diagnosis of somatization
An objective assessment
Because the process of somatization is unconscious to the patient, diagnosis is based on objective findings during examination rather than on a patient’s report. This is similar to evaluating a patient with abdominal pathology: we would not expect the patient to report an abdominal mass, even though we could detect it and train the patient to palpate it. The somatizing patient believes the problem is physical, so the history reported is more likely to lead to physical testing and medical treatments than to a direct examination of the emotional system. Although clues in the history may suggest a patient is somatizing,20 the definitive test, like that of an abdominal examination, is “hands on,” observing the patient’s direct response to an emotion-focused interview.
Actively exploring emotions
Examination of the emotional system is analogous to a physical examination of other systems, and progresses from observation to “palpation” or “percussion” ( Table 2 ).
Observe the patient for visible unconscious anxiety. Then, in the context of a supportive patient-doctor relationship, explore emotionally charged situations that generate symptoms.
Alternatively, one may ask in what way strong emotions like anger affect the patient’s physical problems. Asking about specific recent events and feelings that were triggered usually mobilizes emotions, giving you and the patient a direct look at how emotions affect them physically.
If a patient is anxious in the office, it will be most meaningful to examine the feelings they experience during the interview.
TABLE 2
Exploring emotions in a patient-centered interview
| Action | Example |
|---|---|
| Observation | Note any signs of unconscious tension, somatic distress, or defensiveness from the start of the interview |
| Ask about emotions | Can you describe a situation when the symptoms get worse? |
| What feelings do you have when you talk about that? | |
| How do you experience the feeling of anger in your body when it is there? | |
| Distinguish feelings from anxiety or defenses | The tension you had was anxiety, but how did the anger feel? |
| Becoming quiet was what you did but how did you feel inside? | |
| Observe physical responses | Observe the physical and behavioral responses in the patient when the emotional system is activated |
| Give feedback and plan | Review all findings with the patient. Verify the patient agrees with what you have observed. Plan any further treatments or referra |
Managing defenses
At times, the defenses used to avoid feelings must be pointed out before the patient can see and interrupt these behaviors. If the process is too detached or intellectual, then feelings will not be activated and the system cannot be assessed. The physician’s rapport allows him or her to clarify the process and the need for the patient to try to approach and experience feelings when speaking about them. This is analogous to the process of examining a sore abdomen when a patient is guarding: the patient must relax for examination to take place, and we help them do this by explaining the process.
Patients who are defensive and insist the problem is not related to emotions are managed differently. These patients usually are quite tense and already emotionally activated. An open examination of feelings the patient has about coming to see you that day is a good way to begin. Through this focus one can see the patient’s somatizing patterns directly as well as develop a working rapport.
Managing anxiety
If the patient becomes anxious when asked about emotions, introduce a calming step by asking the patient to intellectualize about the specific bodily anxiety symptoms. This reduces the anxiety by using the defense of intellectualization.
Recap and planning
The interview is concluded by reviewing the findings with the patient in the same way one would share findings of a blood test. Management options would depend on the findings and may include another interview, further medical investigations, referral for treatment, or follow-up to gauge the patient’s response to the interview itself.
Interpreting the patient’s responses
With the focused assessment, the somatic symptoms will transiently increase or decrease, disappear, or not change at all ( Table 3 ).
An increase in symptoms with emotional focus suggests that emotions aggravate or directly cause the problems. A decrease in symptoms during the test also suggests a linkage to emotions. Disappearance of the symptoms by bringing emotional experiences to awareness is the best direct evidence that somatization of these emotions was causing the patient’s symptoms.
No change in a patient’s symptoms or signs—provided there was adequate emotional activation—suggests no somatization of emotions. In these cases, other physical factors must be sought. For example, a woman with chronic left leg weakness and numbness had no shift in symptoms with this test: she was found to have neuropathy due to multiple sclerosis. We have found that 5% to 10% of patients referred to our diagnostic clinic have physical problems that were mistaken for somatization.
TABLE 3
Interpretation of responses to emotionally focused assessment
| Response | Interpretation and action | Beware of |
|---|---|---|
| Response 1: Symptoms go up with emotional focus then down after focusing away from emotions | The diagnosis is likely somatization. Prescribe emotion-focused psychotherapy and monitor for gradual symptom removal | False positives due to coincidental symptom changes in interview |
| Health problems unrelated to the somatization could always be present | ||
| Response 2: Symptoms are improved or removed by emotional focus or emotional experience in the office | The diagnosis is (was) somatization of those emotions. Follow-up to see if gains are maintained | |
| Response 3: No change in symptoms | Somatization is unlikely to be the cause of the symptoms. Look for physical causes. | False negatives due to high defenses, sedation, lack of cooperation, inadequate focus by physician |
| Response 4: Unclear response | May or may not be an emotionbased component in the symptoms. Repeat test, consider other diagnostic tests or referral for emotion-focused diagnostic testing |
False negatives
False negatives occur when the test does not detect the process of somatization when it is present. This will occur if the level of emotion mobilized was too low, if the patient is too sedated, if the defenses the patient used were not sufficiently interrupted, or when the patient is not working collaboratively with the doctor during the test. In each case the patient must allow emotions to be mobilized and the doctor must focus adequately on the emotional experiences to yield an interpretable response.
False positives
False positives occur when the patient has a rise or fall in symptoms during the test for other reasons—eg, coincidental shifts in episodic conditions like muscle spasm or symptom reduction due to distraction during the test itself. It is important in these cases to repeat the test more than once and see if the results are reproducible.
Treatment: short-term dynamic psychotherapy
STDP is clinically effective for patients with somatization
Short-term dynamic psychotherapy (STDP) formats specifically help a patient to examine trauma and loss-related emotions that result in somatization, depression, anxiety, and self-defeating behaviors. Case-series videotaped research over the past 30 years has established the effectiveness of the methods in both short and long term follow-up.21
STDP is efficacious in controlled trials and meta-analyses
In 1995, Anderson and Lambert22 conducted a meta-analysis of 26 controlled studies and found STDP to be superior to minimal treatment controls and wait lists including in samples with somatization. It was found to be as effective in removing anxiety and depressive symptoms as cognitive behavioral therapy. A recent meta-analysis,23 using more strict inclusion criteria, yielded the same findings. In a recent randomized controlled trial of symptomatic patients with personality disorders, STDP brought significant symptom reduction while cognitive therapy did not, suggesting that STDP may have added benefits in more resistant and complex symptomatic patients.24
In our current Cochrane review search,25 we have found 40 published randomized controlled trials supporting its efficacy with a range of disorders including ulcer disease, irritable bowel syndrome, dyspepsia, and urethral syndrome.26-29 Our review has likewise found STDP to be superior to minimal treatment or waitlist controls and that the gains are maintained in follow-up averaging over 1 year.
STDP is cost-effective and reduces health care utilization
STDP has been shown to reduce healthcare utilization and to be cost-effective in treating patients with dyspepsia, irritable bowel syndrome, depression, and self-harm and treatment-resistant conditions.30 Of specific cost figures cited in reviewed papers, 27 out of 34 showed cost savings with STDP including reduction in total costs, medication costs, disability, hospital, and physician use.
Case Illustrations
Case 1: Striated muscle anxiety
This 42-year-old man had chronic fatigue and fibromyalgia which lead to a 13 month disability up to the time of consultation. He came to the office with longstanding pain in his shoulders. His hands were clenched during the interview, and he appeared tense while giving his history.
- DOCTOR: Can you tell about a specific time when you had an emotional upset so we can understand how exactly it affects you?
- PATIENT: Yeah, problems at home with my wife…. Saturday she wanted me to do some work on the garage. She started to yell. Every day it’s the same thing and I’m getting tired of it.… DOCTOR: So how do you feel toward her?
- PATIENT: [Takes a deep sigh, hands become clenched] Mad.
- DOCTOR: You mean mad … angry?
- PATIENT: Yeah.
- DOCTOR: How do you experience the anger inside physically?
- PATIENT: Very, very… tense
- DOCTOR: That is tension…anxiety?
- PATIENT: Yeah.
- DOCTOR: How did you experience the anger?
- PATIENT: I start to ignore her.
- DOCTOR: Is that a mechanism to deal with anger?
- PATIENT: It’s really hard to put a word on it…. I get really mad…it’s like a rage.
- DOCTOR: So how do you experience the rage?
- PATIENT: [Patient takes a big sigh and clenches his hands tightly]
- DOCTOR: Do you notice you sigh and become tense when you talk about the rage.
- PATIENT: No, I didn’t. I don’t feel anxious.
- DOCTOR: But, do you notice the sigh and your hands?
- PATIENT: I do now, but didn’t see it before.
- DOCTOR: Is this what is happening to you … that you are getting all tensed up about these feelings?
- PATIENT: Yeah, it must be.
At a later point in the 1-hour session, the patient was able to feel the visceral emotions of rage, guilt about the rage, and sadness over several years of conflict. When the feelings were experienced in the office, he had an abrupt drop in muscle tension and bodily pain: this was further evidence he had been somatizing, or as he said, “bottling up” these complex feelings.
As is typical of patients with primarily striated muscle anxiety, he denies being nervous despite showing obvious anxiety in the interview. He denies anxiety because it has been unconscious to him, thus free to create fibromyalgia pain. Through this single interview a link is made for both patient and doctor between blocked feelings and body pain. With 10 treatment sessions focused on this process, his fibromyalgia resolved; he returned to work and no longer needed antidepressants.
Case 2: Smooth muscle anxiety
This patient is a 38 year-old woman with severe incapacitating GERD, irritable bowel syndrome, and depression who was disabled from work for 2 years at the time of consultation. This woman had a very relaxed posture with relaxed hands and an absence of obvious anxiety. After 10 minutes of exploring situations and events that make her stomach worse, we arrive at the following point.
- DOCTOR: Can you tell me about another time when your stomach felt worse?
- PATIENT: Yes. There was once when my sister-inlaw did something and it made me angry. Yeah, when people make me angry I don’t tell them, I just avoid them.
- DOCTOR: Can you describe one of those times, so we can see how that affects you.
- PATIENT: Once she was arguing with my brother, like they usually do….
- DOCTOR: How did you feel then?
- PATIENT: … Now I just got that again [pointing to her stomach and chest with upward motion and burps]
- DOCTOR: Heartburn? Just came on?
- PATIENT: Yeah, heartburn, just came on.
- DOCTOR: Is there anything else you notice? Like in your stomach?
- PATIENT: No, just that … but I can hear my stomach churning.
- DOCTOR: So is it when you have anger your stomach churns and you get this acid?
- PATIENT: Must be….
- DOCTOR: …because in your approach to talk about anger you got cramps and acid. So is that one way the anger goes?
- PATIENT: Yes it must be, but I never thought of that part. [Stomach stops churning and heartburn stops as we talk about it for few minutes.] You know, this all started to get worse when my fiancé dumped me. [She goes onto describe a story of being not only rejected but also feeling humiliated by how it was done. She never felt emotional about it but just got severe diarrhea and was confined to her room for 3 weeks.]
- DOCTOR: How did you feel toward your fiancé when he dumped you that way?
- PATIENT: I was just so sick and depressed. I didn’t feel any anger. [Patient burps again this time rubs abdomen due to some discomfort.]
- DOCTOR: Did you get the stomach upset just now again?
- PATIENT: My stomach is upset again. Just the noise and acid again.
- DOCTOR: So again, when we focus on the feelings, the cramps and acid come back.
- PATIENT: For sure. What can we do about that?
- DOCTOR: Can we try to help you identify these feelings before they go to your stomach, to try to interrupt that process. Can you tell me about another incident like that?
The patient required 3 one-hour sessions to improve her tolerance of anxiety, so she could intellectualize about feelings rather than have them directly affect her stomach. The feelings of rejection had triggered rage and guilt about rage associated with sexual abuse by her brother and the abandonment she felt from her mother when she told her mother about it. With 12 sessions of therapy, she was able to stop her IBS medication, anxiolytic, and antidepressant.
This vignette is typical for patients with primarily smooth muscle unconscious anxiety. The patient had no visible anxiety but had GI symptoms when focusing on emotions about recent trauma. The symptoms were mobilized and reduced repeatedly, confirming a link with emotions. Note that outwardly she looked calm, but the emotions mobilized were being shunted to her GI tract.
Incorporating emotion diagnostics into practice
To perform these interview procedures, the physician must understand emotion physiology and the patterns of somatization as outlined above. This is entirely intuitive to many physicians the first time seeing this material: they can readily employ that which they already know. In general, though, physicians reading this will want to ponder it and see how it may apply case by case as they develop skills with it over time. Senior clinicians have usually done these assessments by default, by pressure from patients, or because they learned elements of this over time from various experiences.
Helpful short-cuts
Family physicians trained in emotion assessment note that abbreviated elements can easily be incorporated into a patient-centered assessment process. For example, one may ask how “stress,” “emotions,” or “anger” affects the person and their body or ask how the person handles anger in specific incidents.
In an initial patient questionnaire, one can include a few questions that encourage the patient to think about how stress affects them and to describe their body’s tendency to experience anxiety. When they later present with symptoms, one can use these baseline data to aid in the new assessment. Thus, a culture of considering emotional factors can be woven into practice, weakening any resistance to the idea that emotions and health, mind and body, are tightly bound.
Time factors
Based on our experience, family physicians can perform two thirds of these diagnostic assessments during 15 minutes of focused interviewing. More complex cases, such as patients with cognitive disruption or multiple manifestations of anxiety, may take longer to diagnose and generally need more specialized care or referral. If required, a patient could be asked back for a 1 half-hour session later in the day or week.
Taking care of ourselves
Despite the importance of the emotional system in medicine, medical curricula generally fail to provide sufficient education in this area. At the same time, up to half of our own ranks report emotional burnout.31 Even with the lack of mainstream medical teaching about emotions and health, it behooves us to learn what we can about the emotional system as it applies to the patient and to ourselves in relation to these most challenging problems. Focused seminars, peer case review, select reading, and videotape training can all help in this educational process.32
Acknowledgments
The author wishes to thank the many colleagues who reviewed and commented on this manuscript. This work is supported by Dalhousie University, Capital Health and the Nova Scotia Department of Health.
Correspondence
Allan Abbass, MD, FRCPC, Associate Professor and Director of Education, Psychiatry, Director, Center for Emotions and Health, 8th Floor, Abbie J. Lane Memorial Building, Halifax, NS B3H 2E2, Canada. E-mail: [email protected].
1. Fink P, Sorensen L, Engberg M, Holm M, Munk-Jorgensen P. Somatization in primary care. Prevalence, health care utilization, and general practitioner recognition. Psychosomatics 1999;40:330-338.
2. Kroenke K, Mangelsdorff AD. Common symptoms in ambulatory care: incidence, evaluation, therapy, and outcome. Am J Med 1989;86:262-266.
3. Barsky AJ, Ettner SL, Horsky J, Bates DW. Resource utilization of patients with hypochondriacal health anxiety and somatization. Medical Care 2001;39:705-715.
4. Engel CC, Jr, Liu X, Hoge C, Smith S. Multiple idiopathic physical symptoms in the ECA study: competing-risks analysis of 1-year incidence, mortality, and resolution. Am J Psychiatry 2002;159:998-1004.
5. Bellon JA, Fernandez-Asensio ME. Emotional profile of physicians who interview frequent attenders. Patient Education & Counseling 2002;48:33-41.
6. De Gucht V, Fischler B. Somatization: A critical review of conceptual and methodological issues. Psychosomatics 2002;43:1-9.
7. Righter EL, Sansone RA. Managing somatic preoccupation. Am Fam Physician 1999;59:3113-20.
8. Holloway KL, Zerbe KJ. Simplified approach to somatization disorder. When less may prove to be more. Postgrad Med 2000;108:89-9295.
9. Servan-Schreiber D, Tabas G, Kolb NR. Somatizing patients: part II. Practical management. Am Fam Physician 2000;61:1423-1428,1431-1432.
10. Servan-Schreiber D, Kolb R, Tabas G. The somatizing patient. Prim Care 1999;26:225-242.
11. Noyes R, Jr, Holt CS, Kathol RG. Somatization. Diagnosis and management. Arch Fam Med 1995;4:790-795.
12. Davanloo H. Intensive short-term dynamic psychotherapy with highly resistant patients. I. Handling resistance. International Journal of Short-Term Psychotherapy 1986;1:107-133.
13. Davanloo H. The technique of unlocking the unconscious in patients suffering from functional disorders. Part I. Restructuring ego’s defenses. In: Davanloo H. Unlocking the Unconscious. Chichester, England: John Wiley & Sons; 1990;283-306.
14. Katon W, Sullivan M, Walker E. Medical symptoms without identified pathology: relationship to psychiatric disorders and adult trauma, and personality traits. Ann Intern Med 2001;1:917-925.
15. Roter D, Ewart CK. Emotional inhibition in essential hypertension: Obstacle to communication during medical visits? Health Psychology 1992;11:163-169.
16. Venable VL, Carlson CR, Wilson J. The role of anger and depression in recurrent headache. Headache 2001;41:21-30.
17. Whorwell PJ, Houghton LA, Taylor EE, Maxton DG. Physiological effects of emotion: assessment via hypnosis. Lancet 1992;340:434.-
18. Davanloo H. Intensive short term dynamic psychotherapy: Spectrum of psychoneurotic disorders. In Davanloo H. Intensive Short-Term Dynamic Psychotherapy. Chichester, England: John Wiley and Sons; 2001
19. Servan-Schreiber D, Tabas G. Somatizing patients part I: practical diagnosis. Am Fam Physician 2000;61:1073-1078.
20. Abelson JL, W. J., Neese RM, Curtis GC. Persistent respiratory irregularity in patients with panic disorder. Biological Psychiatry 2001;49:588-595.
21. Davanloo H. Short-Term Dynamic Psychotherapy New York: Jason Aronson; 1980
22. Anderson E, Lambert M. Short-term dynamically oriented psychotherapy: A review and meta-analysis. Clinical Psychology Review 1995;15:503-514.
23. Leichsenring F, Rabung S, Leibing E. The efficacy of short-term psychodynamic psychotherapy in specific psychiatric disorders: a meta-analysis. Arch Gen Psychiatry 2004;61:1208-1216.
24. Svartberg M, Stiles TC, Seltzer MH. Randomized controlled trial of the effectiveness of short-term dynamic psychotherapy and cognitive therapy for cluster C personality disorders. Am J Psychiatry 2004;161:810-817.
25. Abbass AA, Hancock JT, Henderson J, Kisely S. Shortterm psychodynamic psychotherapies for common mental disorders (Protocol for a Cochrane Review). 2004 In: The Cochrane Library Chichester, UK: John Wiley and Sons.
26. Sjodin I, Svedlund J, Ottoson J, Dotevall G. Controlled study of psychotherapy in chronic peptic ulcer disease. Psychosomatics 1986;27:187-200.
27. Creed FLF, Guthrie E, Palmer S, et al. The cost-effectiveness of psychotherapy and paroxetine for severe irritable bowel syndrome. Gastroenterology 2003;124:303-317.
28. Hamilton J, Guthrie E, Creed F. A randomized controlled trial of psychotherapy in patients with chronic functional dyspepsia. Gastroenterology 2000;119:661-669.
29. Baldoni F, Baldaro B, Trombini G. Psychotherapeutic perspectives in urethral syndrome. Stress Medicine 1995;11:79-84.
30. Abbass A. The cost-effectiveness of short-term dynamic psychotherapy. Journal of Pharmacoeconomics and Outcomes Research 2003;3:535-539.
31. CMA Guide to Physician Health and Well-being 2003. Canadian Medical Association.
32. Coombs RH, Perrell K, Ruckh JM. Primary prevention of emotional impairment among medical trainees. Acad Med 1990;65:576-581.
1. Fink P, Sorensen L, Engberg M, Holm M, Munk-Jorgensen P. Somatization in primary care. Prevalence, health care utilization, and general practitioner recognition. Psychosomatics 1999;40:330-338.
2. Kroenke K, Mangelsdorff AD. Common symptoms in ambulatory care: incidence, evaluation, therapy, and outcome. Am J Med 1989;86:262-266.
3. Barsky AJ, Ettner SL, Horsky J, Bates DW. Resource utilization of patients with hypochondriacal health anxiety and somatization. Medical Care 2001;39:705-715.
4. Engel CC, Jr, Liu X, Hoge C, Smith S. Multiple idiopathic physical symptoms in the ECA study: competing-risks analysis of 1-year incidence, mortality, and resolution. Am J Psychiatry 2002;159:998-1004.
5. Bellon JA, Fernandez-Asensio ME. Emotional profile of physicians who interview frequent attenders. Patient Education & Counseling 2002;48:33-41.
6. De Gucht V, Fischler B. Somatization: A critical review of conceptual and methodological issues. Psychosomatics 2002;43:1-9.
7. Righter EL, Sansone RA. Managing somatic preoccupation. Am Fam Physician 1999;59:3113-20.
8. Holloway KL, Zerbe KJ. Simplified approach to somatization disorder. When less may prove to be more. Postgrad Med 2000;108:89-9295.
9. Servan-Schreiber D, Tabas G, Kolb NR. Somatizing patients: part II. Practical management. Am Fam Physician 2000;61:1423-1428,1431-1432.
10. Servan-Schreiber D, Kolb R, Tabas G. The somatizing patient. Prim Care 1999;26:225-242.
11. Noyes R, Jr, Holt CS, Kathol RG. Somatization. Diagnosis and management. Arch Fam Med 1995;4:790-795.
12. Davanloo H. Intensive short-term dynamic psychotherapy with highly resistant patients. I. Handling resistance. International Journal of Short-Term Psychotherapy 1986;1:107-133.
13. Davanloo H. The technique of unlocking the unconscious in patients suffering from functional disorders. Part I. Restructuring ego’s defenses. In: Davanloo H. Unlocking the Unconscious. Chichester, England: John Wiley & Sons; 1990;283-306.
14. Katon W, Sullivan M, Walker E. Medical symptoms without identified pathology: relationship to psychiatric disorders and adult trauma, and personality traits. Ann Intern Med 2001;1:917-925.
15. Roter D, Ewart CK. Emotional inhibition in essential hypertension: Obstacle to communication during medical visits? Health Psychology 1992;11:163-169.
16. Venable VL, Carlson CR, Wilson J. The role of anger and depression in recurrent headache. Headache 2001;41:21-30.
17. Whorwell PJ, Houghton LA, Taylor EE, Maxton DG. Physiological effects of emotion: assessment via hypnosis. Lancet 1992;340:434.-
18. Davanloo H. Intensive short term dynamic psychotherapy: Spectrum of psychoneurotic disorders. In Davanloo H. Intensive Short-Term Dynamic Psychotherapy. Chichester, England: John Wiley and Sons; 2001
19. Servan-Schreiber D, Tabas G. Somatizing patients part I: practical diagnosis. Am Fam Physician 2000;61:1073-1078.
20. Abelson JL, W. J., Neese RM, Curtis GC. Persistent respiratory irregularity in patients with panic disorder. Biological Psychiatry 2001;49:588-595.
21. Davanloo H. Short-Term Dynamic Psychotherapy New York: Jason Aronson; 1980
22. Anderson E, Lambert M. Short-term dynamically oriented psychotherapy: A review and meta-analysis. Clinical Psychology Review 1995;15:503-514.
23. Leichsenring F, Rabung S, Leibing E. The efficacy of short-term psychodynamic psychotherapy in specific psychiatric disorders: a meta-analysis. Arch Gen Psychiatry 2004;61:1208-1216.
24. Svartberg M, Stiles TC, Seltzer MH. Randomized controlled trial of the effectiveness of short-term dynamic psychotherapy and cognitive therapy for cluster C personality disorders. Am J Psychiatry 2004;161:810-817.
25. Abbass AA, Hancock JT, Henderson J, Kisely S. Shortterm psychodynamic psychotherapies for common mental disorders (Protocol for a Cochrane Review). 2004 In: The Cochrane Library Chichester, UK: John Wiley and Sons.
26. Sjodin I, Svedlund J, Ottoson J, Dotevall G. Controlled study of psychotherapy in chronic peptic ulcer disease. Psychosomatics 1986;27:187-200.
27. Creed FLF, Guthrie E, Palmer S, et al. The cost-effectiveness of psychotherapy and paroxetine for severe irritable bowel syndrome. Gastroenterology 2003;124:303-317.
28. Hamilton J, Guthrie E, Creed F. A randomized controlled trial of psychotherapy in patients with chronic functional dyspepsia. Gastroenterology 2000;119:661-669.
29. Baldoni F, Baldaro B, Trombini G. Psychotherapeutic perspectives in urethral syndrome. Stress Medicine 1995;11:79-84.
30. Abbass A. The cost-effectiveness of short-term dynamic psychotherapy. Journal of Pharmacoeconomics and Outcomes Research 2003;3:535-539.
31. CMA Guide to Physician Health and Well-being 2003. Canadian Medical Association.
32. Coombs RH, Perrell K, Ruckh JM. Primary prevention of emotional impairment among medical trainees. Acad Med 1990;65:576-581.
What can we expect from nonoperative treatment options for shoulder pain?
- First-line treatment for shoulder pain and stage 1 impingement may include nonsteroidal anti-inflammatory drugs (NSAIDs) (B) or corticosteroid injection (A).
- Stage II or III Impingement (rotator cuff tears) are best treated initially with physical therapy (supervised or home exercise program) or corticosteroid injection.
- Steroid injections added to NSAID treatment probably confer no extra benefit.
- High pain levels during the day and associated neck pain may predict a longer recovery period.
Most shoulder pain responds best to NSAIDs or subacromial corticosteroid injections followed by a home exercise program or formal physical therapy exercises. Accumulating evidence is making it clearer what works and what doesn’t for specific diagnoses.
Time to healing varies greatly among persons with shoulder pain, and specific prognostic indicators may help you and your patients know what to expect.
Quick diagnostic review
Consider the patient’s age, history of trauma, details of injury, and previous shoulder problems. Observe the patient’s general movements, assess range of motion, and use provocative testing to form a differential diagnosis ( Figure 1 ).
If the diagnosis is unclear, arrange for imaging studies ( Table 1 ). A more thorough review for diagnosing shoulder pain may be found in the article “Approach to the patient with shoulder pain” (J Fam Pract 2002; 7:605–611). The conditions causing shoulder pain (in order of frequency, as seen by primary care physicians) are subacromial impingement syndrome (SIS), adhesive capsulitis, acute bursitis, calcific tendinitis, glenohumeral arthrosis, biceps tendinitis, and labral tear.1,2
TABLE 1
Value of imaging tests for shoulder injuries
| Test | LOE | Sn | Sp | LR+ | LR− | PV+ | PV− |
|---|---|---|---|---|---|---|---|
| MRI | |||||||
| Rotator cuff tears | |||||||
| Partial41 | 2b | 82 | 85 | 5.5 | 0.21 | 82 | 85 |
| Complete41 | 1a | 81 | 78 | 3.7 | 0.24 | — | — |
| Overall42-44 | 2b | 89–96 | 49–100 | 1.9–>25 | 0.08 | 58 | 94 |
| Impingement 42 | 2b | 93 | 87 | 7.2 | 0.08 | 93 | 87 |
| Labral tears* 45,46 | 1b | 75–89 | 97–100 | >25 | 0.11–0.25 | 100 | 41 |
| Plain arthrogram | |||||||
| Rotator cuff tears | |||||||
| Partial47 | 1b | 70 | — | — | — | — | — |
| Complete41 | 1b | 50 | 96 | 13 | 0.52 | — | — |
| CT arthrogram | |||||||
| Rotator cuff tears | |||||||
| Partial47 | 1b | 70 | — | — | — | — | — |
| Complete47 | 1b | 95 | — | — | — | — | — |
| Overall47 | 1b | 86 | 98 | >25 | 0.14 | 96 | 93 |
| Ultrasound | |||||||
| Rotator cuff tears | |||||||
| Partial47 | 1b | 80 | — | — | — | — | — |
| Complete47,4848 | 1b | 90–100 | 85 | 6.7 | >25 | — | — |
| Overall47 | 1b | 86 | 91–98 | 9.6–>25 | 0.14–0.15 | 96 | 73–93 |
| *MRI arthrography. | |||||||
| LOE, level of evidence (SORT); Sn, sensitivity; Sp, specificity; LR, likelihood ratio; PV, predictive value; MRI, magnetic resonance imaging; CT, computed tomography. | |||||||
FIGURE 1
Evaluating shoulder pain for possible rotator cuff tear
Subacromial impingement syndrome
This condition was first described by Neer, who estimated it leads to 95% of rotator cuff tears.3
Impingement occurs from repetitive overhead activities, acute trauma, or instability of the glenohumeral joint (subtle or overt). Current theory holds that degeneration of the rotator cuff tendons or inflammation of the subacromial bursa—caused by irritation against the coracoacromial arch—can progress to degeneration and a complete rotator cuff tear. So-called rotator cuff tendinitis is better described as a tendinopathy with mucoid degeneration of the tendon. SIS stage I involves edema and hemorrhage, as would be seen with rotator cuff tendinopathy or bursitis.
Progressive feedback loop of subacromial impingement syndrome. Acute bursitis involves the subacromial bursa and typically is secondary to subacromial impingement. As underlying tendinopathy, instability, or heterotrophic bone irritates the bursa, it will become inflamed and irritated. Inflammation exacerbates the impingement and that in turn causes worsening of the bursitis.
Stage II and III impingement syndrome. SIS stage II is a progression to fibrosis and partial tear of the rotator cuff. Stage III is a full-thickness tear of the rotator cuff. These stages of SIS are seen predominantly in patients over the age of 40 years, and they become more common with increasing age. The tear—partial or complete— usually occurs in the supraspinatus tendon. Tears of other rotator cuff muscles are less common.
Magnetic resonance imaging (MRI), with or without arthrography, is used in clinical practice and in research to diagnose rotator cuff tears. Growing evidence indicates that ultrasound is a less expensive and equally effective way to diagnose stage II or III impingement. In the United States, however, the option of ultrasound is limited by scarce availability and inadequate operator skill.
The subacromial injection test is useful in clinical practice. Local anesthetic is injected into the subacromial space. Persisting loss of strength despite pain relief is a positive sign of impairment of the rotator cuff.
MRI or ultrasound must be done in conjunction with history taking and physical examination. As the age of a person increases, the amount of asymptomatic rotator cuff tendon injury will also increase. The incidence of rotator cuff tears has been found to be between 50% to 60% in cadavers of deceased elderly. Thirty percent were found to be stage III impingement; 20% to 30% were partial stage II impingement.4
Adhesive capsulitis
Also known as frozen shoulder, adhesive capsulitis may begin with any inflammatory condition, but it is most commonly idiopathic. It characteristically progresses through 3 stages.
The hallmark of adhesive capsulitis is a progressive lack of range of motion with both passive and active movement.
The first stage involves progressive pain and decreased range of motion as the capsule scars.
The second stage involves maturation of capsule scaring, resulting in decreased pain and increased restriction of movement.
The third stage is resolution of the condition, leading to a gradual increase in range of motion.
Full range of motion may or may not return, and the time to resolution is typically 1 to 2 years. Adhesive capsulitis is most common in older persons, especially women in the fourth and fifth decades.5
Comparing nonoperative treatments
Nonoperative treatment modalities include protection, relative rest, and ice (PRI); anti-inflammatory medications; physical therapy (supervised or home exercise program); acupuncture; and steroid injection.
Operative treatments, depending on the particular disorder, include rotator cuff repair, subacromial decompression, capsular tightening, or manipulation under anesthesia.
The efficacy of nonoperative treatments for shoulder pain is not well known. Studies of treatment modalities have been numerous but generally of poor quality due to a lack of uniformity in how shoulder disorders are defined and in the variability of outcome measures used. Several recent systematic reviews have tried to identify which interventions are efficacious ( Table 2 ).6-11
Overall, NSAIDs and subacromial steroid injections are effective in the short-term treatment of shoulder pain.26-28 However, only nonselective NSAIDs have been studied. Evidence is insufficient to recommend use of cyclooxygenase-2 (COX-2) medications for shoulder pain.
Steroid injections may not confer extra benefit when added to NSAIDs, but they appear superior to NSAIDs in improving shoulder abduction. This is particularly true for the painful stiff shoulder, as seen with impingement or rotator cuff disease.26,28
Two recent randomized control trials showed corticosteroid injections to be superior to physical therapy for treatment of shoulder complaints.12,13
Shoulder instability may be treated nonoperatively at first with PRI, NSAIDs, and strengthening and proprioceptive exercises for the rotator cuff. If 3 to 6 months of nonoperative treatment fails, the patient should be referred for surgical evaluation, especially in cases of full-thickness rotator cuff tears.14
TABLE 2
Nonoperative treatment options for shoulder pain
| Treatment | Comment | SOR |
|---|---|---|
| NSAIDs |
| C |
| Physical therapy |
| B |
| Ultrasound |
| A |
| Steroid injection |
| B |
| Acupuncture |
| C |
| SOR, strength of recommendation (SORT); NSAIDs, nonsteroidal anti-inflammatory drugs. | ||
Treatment of specific shoulder disorders
Subacromial impingement syndrome stage I
A recommendation (SOR: B) can be made for the use of NSAIDs in the treatment of stage I impingement ( Table 3 ). This is based on level 2 evidence that NSAIDs are beneficial for rotator cuff tendinopathy and bicipital tendinitis, compared with placebo in a 1 to 2 week follow-up.15,17 No specific NSAID has proved better than another.18,19
Steroid injection ( Figure 2 ) is beneficial for the acute treatment of SIS I reflected by improvement in pain (SOR: A).20-23 This is particularly evident during the first 1 to 2 weeks following injections.38 At 4 to 6 weeks, there appears to be no difference in the efficacy of steroid injection compared with NSAIDs,24,25 but they are both better than placebo.43
Physical therapy, specifically rotator cuff strengthening and range of motion, is as beneficial as surgery for SIS I at 6 month and 21/2-year follow-up, and both were better than placebo (SOR: B).26,27
TABLE 3
Treatments for SIS I impingement (rotator cuff tendinitis/tendinosis)
| Treatment | Comment | LOE |
|---|---|---|
| NSAIDs |
| 1c |
| NSAIDs vs steroid injection |
| 1a |
| Subacromial steroid injection |
| 1b |
| Surgery |
| 2a |
FIGURE 2
Steroid injection in the subacromial space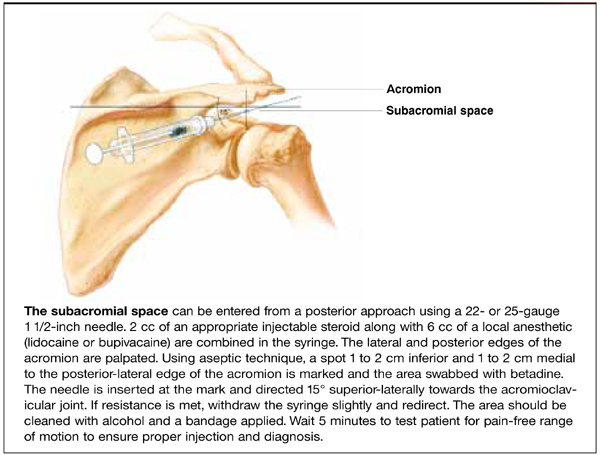
SIS stages II and III
There is very good evidence (SOR: B) regarding the efficacy of nonoperative treatment of SIS II and III, based on level 2 cohort studies that suggest nonoperative care leads to improvements in patient satisfaction, pain, and daily activities.28,29 Similar outcomes are reported for patients undergoing physical therapy alone.30,31 Weiss reported that corticosteroid injections for stage III/full-thickness rotator cuff tears resulted in an 86% improvement as measured by return to previous activities and less or no pain with motion ( Table 4 ).32
The most constant outcome measure was report of a reduction in pain. Younger patients or those with higher functional demands will likely consider surgical repair if nonoperative measures fail, particularly for full-thickness tears.
TABLE 4
Nonoperative treatments for SIS III (full-thickness rotator cuff tears)
| Treatment | Comment | SOR |
|---|---|---|
| Physical therapy |
| B |
| Subacromial injection |
| B |
| Multiple nonoperativetherapies |
| B |
Adhesive capsulitis
There is no consistent evidence that treatment of any one form reduces the pain or improves range of motion in frozen shoulders. Various treatments that have been tried include, though are not limited to, steroid injection, NSAIDs, and physical therapy.33-37 Studies on treatment efficacy are complicated by inherent discrepancy between patient and observer opinions of limitations in this condition, with objective range of motion findings often not being consistent with patient reported limitations.38
Indicators of quicker or slower recovery
Studies of prognosis following treatment have been difficult to assess due the heterogeneity of the underlying conditions and variability of treatments. A follow-up questionnaire in one instance found no difference between treatment groups. Complaints of pain or impaired mobility 2 to 3 years after treatment were similar among patients treated with steroid injection and physical therapy and with physical therapy alone.30 Overall, 76% of respondents were symptom free at 2 to 3 years.
Two prospective studies confirm that speed of recovery is slow, with complete recovery 23% at 1 month, 21% to 51% at 6 months, 59% at 1 year, and 69% at 18 months.39,40
Prognostic indicators of quicker recovery were preceding overuse or slight trauma and early presentation to the physician.58 Protracted recovery occurred more often with high pain levels during the day or associated neck pain.58 These results suggest that patients with subacromial impingement stage I respond better to nonoperative treatment than those patients with underlying degenerative changes or referred pain from the neck.
Finally, specialty surgical referral may be necessary in cases of failed nonoperative therapy or persistent diagnostic and therapeutic challenges.
Corresponding author
Thomas H. Trojian, MD, 99 Woodland Street, Hartford, CT 06105. E-mail: [email protected].
1. Van der Windt DA, Koes BW, De Jong BA, Bouter LM. Shoulder disorders in general practice: incidence, patient characteristics, and management. Ann Rheum Dis 1995;54:959-964.
2. Blanchard TK, Bearcroft PW, Constant CR, Griffin DR, Dixon AK. Diagnostic and therapeutic impact of MRI and arthrography in the investigation of full-thickness rotator cuff tears. Eur Radiol 1999;9:638-642.
3. Neer CS. Anterior acromioplasty for chronic impingement syndrome of shoulder. J Bone Joint Surg 1972;54A:41-50.
4. Dalton SE. The conservative management of rotator cuff disorders. Br J Rheumatol 1994;33:663-667.
5. Matsen FA, Lippitt SB, Sidles JA, Harryman DT. Practical Evaluation and Management of the Shoulder. Philadelphia, Pa: W.B. Saunders; 1994.
6. Green S, Buchbinder R, Glazier R, Forbes A. Interventions for shoulder pain (Cochrane Review). In: The Cochrane Library, Issue 1, 2001. Oxdord: Update Software.
7. Van der Hiejden GJ, Van der Windt DA, Kleijnen J, et al. Steroid injections for shoulder disorders: a systematic review of randomized clinical trials. Br J Gen Pract 1996;46:309-316.
8. Van der Windt DA, Van der Heijden GJ, Scholten RJ, et al. The efficacy of non-steroidal anti-inflammatory drugs (NSAIDs) for shoulder complaints. A systematic review. J Clin Epidemiol 1995;48:691-704.
9. Van der Heijden GJ, Van der Windt DA, De Winter AF. Physiotherapy for patients with soft tissue shoulder disorders: a systematic review of randomized clinical trials. BMJ 1997;15:25-30.
10. Van der Windt DA, Van der Heijden GJ, Van den Berg GJ, et al. Ultrasound therapy for musculoskeletal disorders: a systematic review. Pain 1999;81:257-271.
11. Smith LA, Oldman AD, McQuay HJ, Moore RA. Teasing apart quality and validity in systematic reviews: an example from acupuncture trials in chronic neck and back pain. Pain 2000;86:119-132.
12. Winters JC, Sobel JS, Groenier KH, et al. Comparison of physiotherapy, manipulation, and corticosteroid injection for treating shoulder complaints in general practice: randomized, single blind study. BMJ 1997;314:1320-1325.
13. Van der Windt DA, Koes BW, Deville W, et al. Effectiveness of corticosteroid injections versus physiotherapy for treatment of painful stiff shoulder in primary care: randomized trial. BMJ 1998;317:1292-1296.
14. Mantone JK, Burkhead WZ, Noonan J. Nonoperative treatment of rotator cuff tears. Orthop Clin North Am 2000;31:295-311.
15. Lopez JM. Treatment of acute tendinitis and bursitis with fentiazac. A double blind comparison with placebo. Clin Ther 1982;5:79-84.
16. Zuinen C. Diclofenac/misprostol vs diclofenac/placebo in treating acute episodes of tendinitis/bursitis of the shoulder. Drugs 1993;45 Suppl 1:17-23.
17. Ginsberg F, Famaey JP. A double-blind comparison of slow-release and standard tablet formulations of fentiazac in the treatment of patients with tendinitis and bursitis. Curr Med Res Opin 1985;9:42-448.
18. Wober W. Comparative efficacy and safety of nimesulide and diclofenac in patients with acute shoulder, and a meta-analysis of controlled studies with nimesulide. Rheum 1999;38(Suppl 1):33-38.
19. Wober W, Rahlfs VW, Buchl N, et al. Comparative efficacy and safety of the non-steroidal anti-inflammatory drugs nimesulide and diclofenac in patients with acute subdeltoid bursitis and bicipital tendinitis. Int J Clin Pract 1998;52:169-175.
20. Valtonen E. Double acting betamethasone (celestone chronodose) in the treatment of supraspinatus tendinitis: A comparison of subacromial and gluteal single injections with placebo. J Int Men Res 1978;6:463-467.
21. Blair B, Rokito A, Cuomo F, Jarolem K, Zuckerman J. Efficacy of corticosteroids for subacromial impingement syndrome. J Bone Joint Surg Am 1996;78:1685-1689.
22. Withrington R, Girgis F, Seifert M. A placebo-controlled trial of steroid injections in the treatment of supraspinatus tendinitis. Scand J Rheumatol 1985M;14:76-78.
23. Vecchio PC, Hazleman BL, King RH. A double-blind trial comparing subacromial methylprednisolone and ligno-caine in acute rotator cuff tendinitis. Br J Rheumatol 1993;32:743-745.
24. White R, Paull D, Fleming K. Rotator cuff tendinitis: comparison of subacromial injection of a long acting corticosteroid vs oral indomethacin therapy. J Rheumatol 1986;13:608-613.
25. Adebajo A, Nash P, Hazleman B. A Prospective double blind dummy placebo controlled study comparing triamcinolone hexacetonide injection with oral diclofenac 50mg TDS in patients with rotator cuff tendinitis. J Rheumatol 1990;17:1207-1210.
26. Brox JI, Staff PH, Ljunggren AE, Revik JI. Arthroscopic Surgery compared with supervised exercises in patients with rotator cuff disease (stage II impingement syndrome). BMJ 1993;307:899-903
27. Brox JI, Gjengedal E, Uppheim G, et al. Arthroscopic surgery versus supervised exercises in patients with rotator cuff disease (stage II impingement syndrome): a prosprective, randomized, controlled study in 125 patients with a 2 1/2 year follow up. J Shoulder Elbow Surg 1999;8:102-111.
28. Bokor DJ, Hawkins RJ, Huckell GH, Angelo RL, Schickendantz MS. Results of nonoperative management of full-thickness tears of the rotator cuff. Clin Orthop 1993;294:103-110.
29. Itoi E, Tabata S. Conservative treatment of rotator cuff tears. Clin Orthop 1992;275:165-173.
30. Hawkins RH, Dunlop R. Nonoperative treatment of rotator cuff tears. Clin Orthop 1995;321:178-188.
31. Goldberg BA, Nowinski RJ, Matsen FA. Outcome of non-operative management of full thickness rotator cuff tears. Clin Orthop 2001;382:99-107.
32. Weiss JJ. Intra-articular steroids in the treatment of rota-tor cuff tear: reappraisal by arthrography. Arch Phys Med Rehabil 1981;62:555-557.
33. De Jong BA, Dahmen R, Hogeweg JA, Marti RK. Intra-articular triamcinolone acetonide injection in patients with capsulitis of the shoulder: a comparative study of two dose regimens. Clin Rehab 1998;12:211-215.
34. Bulgen DY, Binder AI, Hazleman BL, Dutton J, Roberts S. Frozen shoulder: prospective clonical study with an evaluation of three treatment regimens. Ann Rheum Dis 1984;43:353-360.
35. Thumb N, Kolarz G, Scherak O, Mayrhofer F. The efficacy and safety of Fentiazac and Diclofenac sodium in peri-arthritis of the shoulder: a multi-center, double-blind comparison. J Int Med Res 1987;15:327-334.
36. Rhind V, Downie WW, Bird HA, Wright V, Engler C. Naproxen and indomethacin in periarthritis of the shoulder. Rheumatol Rehabil 1982;21:51-53.
37. Lee PN, Lee M, Haq AM, Longton EB, Wright V. Periarthritis of the shoulder. Ann Rheum Dis 1974;33:116-119.
38. Hazleman BL. The painful stiff shoulder. Rheumatol Rehabil 1972;11:413-421.
39. Croft P, Pope D, Silman A. The clinical course of shoulder pain: prospective cohort study in primary care. BMJ 1996;313:601-602.
40. Van der Windt DA, Koes BW, Boeke AJ, Deville W, De Jong BA, Bouter LM. Shoulder disorders in general practice: prognostic indicators of outcome. Br J Gen Pract 1996;46:519-523.
41. Iannotti JP, Zlatkin MB, Esterhai JL, Kressel HY, Dalinka MK, Spindler KP. Magnetic resonance imaging of the shoulder. Sensitivity, specificity, and predictive value. J Bone Joint Surg 1991;73:17-29.
42. Burk DL, Karasick D, Kurtz AB, et al. Rotator cuff tears: prospective comparison of MR imaging with arthrography, sonography, and surgery. Am J Roentgenol 1989;153:87-92.
43. Torstensen ET, Hollinshead RM. Comparison of magnetic resonance imaging and arthroscopy in the evaluation of shoulder pathology. J Shoulder Elbow Surg 1999;8:42-45.
44. Yeu K, Jiang CC, Shih TT. Correlation between MRI and operative findings of the rotator cuff tear. J Formos Med Assoc 1994;93:134-139.
45. Green MR, Christensen KP. Magnetic resonance imaging of the glenoid labrum in anterior shoulder instability. Am J Sports Med 1994;22:493-498.
46. Gusmer PB, Potter HG, Schaltz JA, et al. Labral injuries: accuracy of detection with en-enhanced MR imaging of the shoulder. Radiology 1996;200:519-524.
47. Farin PU, Kaukanen E, Jaroma H, Vaatainen U, Miettinen H, Soimakallio S. Site and size of rotator cuff tear. Findings at ultrasound, double contrast arthrography, and computed tomography arthrography with surgical correlation. Invest Radiol 1996;31:387-394.
48. Teefey SA, Hasan SA, Middleton WD, Patel M, Wright RW, Yamaguchi K. Ultrasonography of the rotator cuff. A comparison of ultrasonographic and arthroscopic findings in one hundred consecutive cases. J Bone Joint Surg Am 2000;82:498-504.
49. Van Moppes FI, Veldkam O, Roorda J. Role of shoulder ultrasonography in the evaluation of the painful shoulder. Eur J Radiol 1995;19:142-146.
- First-line treatment for shoulder pain and stage 1 impingement may include nonsteroidal anti-inflammatory drugs (NSAIDs) (B) or corticosteroid injection (A).
- Stage II or III Impingement (rotator cuff tears) are best treated initially with physical therapy (supervised or home exercise program) or corticosteroid injection.
- Steroid injections added to NSAID treatment probably confer no extra benefit.
- High pain levels during the day and associated neck pain may predict a longer recovery period.
Most shoulder pain responds best to NSAIDs or subacromial corticosteroid injections followed by a home exercise program or formal physical therapy exercises. Accumulating evidence is making it clearer what works and what doesn’t for specific diagnoses.
Time to healing varies greatly among persons with shoulder pain, and specific prognostic indicators may help you and your patients know what to expect.
Quick diagnostic review
Consider the patient’s age, history of trauma, details of injury, and previous shoulder problems. Observe the patient’s general movements, assess range of motion, and use provocative testing to form a differential diagnosis ( Figure 1 ).
If the diagnosis is unclear, arrange for imaging studies ( Table 1 ). A more thorough review for diagnosing shoulder pain may be found in the article “Approach to the patient with shoulder pain” (J Fam Pract 2002; 7:605–611). The conditions causing shoulder pain (in order of frequency, as seen by primary care physicians) are subacromial impingement syndrome (SIS), adhesive capsulitis, acute bursitis, calcific tendinitis, glenohumeral arthrosis, biceps tendinitis, and labral tear.1,2
TABLE 1
Value of imaging tests for shoulder injuries
| Test | LOE | Sn | Sp | LR+ | LR− | PV+ | PV− |
|---|---|---|---|---|---|---|---|
| MRI | |||||||
| Rotator cuff tears | |||||||
| Partial41 | 2b | 82 | 85 | 5.5 | 0.21 | 82 | 85 |
| Complete41 | 1a | 81 | 78 | 3.7 | 0.24 | — | — |
| Overall42-44 | 2b | 89–96 | 49–100 | 1.9–>25 | 0.08 | 58 | 94 |
| Impingement 42 | 2b | 93 | 87 | 7.2 | 0.08 | 93 | 87 |
| Labral tears* 45,46 | 1b | 75–89 | 97–100 | >25 | 0.11–0.25 | 100 | 41 |
| Plain arthrogram | |||||||
| Rotator cuff tears | |||||||
| Partial47 | 1b | 70 | — | — | — | — | — |
| Complete41 | 1b | 50 | 96 | 13 | 0.52 | — | — |
| CT arthrogram | |||||||
| Rotator cuff tears | |||||||
| Partial47 | 1b | 70 | — | — | — | — | — |
| Complete47 | 1b | 95 | — | — | — | — | — |
| Overall47 | 1b | 86 | 98 | >25 | 0.14 | 96 | 93 |
| Ultrasound | |||||||
| Rotator cuff tears | |||||||
| Partial47 | 1b | 80 | — | — | — | — | — |
| Complete47,4848 | 1b | 90–100 | 85 | 6.7 | >25 | — | — |
| Overall47 | 1b | 86 | 91–98 | 9.6–>25 | 0.14–0.15 | 96 | 73–93 |
| *MRI arthrography. | |||||||
| LOE, level of evidence (SORT); Sn, sensitivity; Sp, specificity; LR, likelihood ratio; PV, predictive value; MRI, magnetic resonance imaging; CT, computed tomography. | |||||||
FIGURE 1
Evaluating shoulder pain for possible rotator cuff tear
Subacromial impingement syndrome
This condition was first described by Neer, who estimated it leads to 95% of rotator cuff tears.3
Impingement occurs from repetitive overhead activities, acute trauma, or instability of the glenohumeral joint (subtle or overt). Current theory holds that degeneration of the rotator cuff tendons or inflammation of the subacromial bursa—caused by irritation against the coracoacromial arch—can progress to degeneration and a complete rotator cuff tear. So-called rotator cuff tendinitis is better described as a tendinopathy with mucoid degeneration of the tendon. SIS stage I involves edema and hemorrhage, as would be seen with rotator cuff tendinopathy or bursitis.
Progressive feedback loop of subacromial impingement syndrome. Acute bursitis involves the subacromial bursa and typically is secondary to subacromial impingement. As underlying tendinopathy, instability, or heterotrophic bone irritates the bursa, it will become inflamed and irritated. Inflammation exacerbates the impingement and that in turn causes worsening of the bursitis.
Stage II and III impingement syndrome. SIS stage II is a progression to fibrosis and partial tear of the rotator cuff. Stage III is a full-thickness tear of the rotator cuff. These stages of SIS are seen predominantly in patients over the age of 40 years, and they become more common with increasing age. The tear—partial or complete— usually occurs in the supraspinatus tendon. Tears of other rotator cuff muscles are less common.
Magnetic resonance imaging (MRI), with or without arthrography, is used in clinical practice and in research to diagnose rotator cuff tears. Growing evidence indicates that ultrasound is a less expensive and equally effective way to diagnose stage II or III impingement. In the United States, however, the option of ultrasound is limited by scarce availability and inadequate operator skill.
The subacromial injection test is useful in clinical practice. Local anesthetic is injected into the subacromial space. Persisting loss of strength despite pain relief is a positive sign of impairment of the rotator cuff.
MRI or ultrasound must be done in conjunction with history taking and physical examination. As the age of a person increases, the amount of asymptomatic rotator cuff tendon injury will also increase. The incidence of rotator cuff tears has been found to be between 50% to 60% in cadavers of deceased elderly. Thirty percent were found to be stage III impingement; 20% to 30% were partial stage II impingement.4
Adhesive capsulitis
Also known as frozen shoulder, adhesive capsulitis may begin with any inflammatory condition, but it is most commonly idiopathic. It characteristically progresses through 3 stages.
The hallmark of adhesive capsulitis is a progressive lack of range of motion with both passive and active movement.
The first stage involves progressive pain and decreased range of motion as the capsule scars.
The second stage involves maturation of capsule scaring, resulting in decreased pain and increased restriction of movement.
The third stage is resolution of the condition, leading to a gradual increase in range of motion.
Full range of motion may or may not return, and the time to resolution is typically 1 to 2 years. Adhesive capsulitis is most common in older persons, especially women in the fourth and fifth decades.5
Comparing nonoperative treatments
Nonoperative treatment modalities include protection, relative rest, and ice (PRI); anti-inflammatory medications; physical therapy (supervised or home exercise program); acupuncture; and steroid injection.
Operative treatments, depending on the particular disorder, include rotator cuff repair, subacromial decompression, capsular tightening, or manipulation under anesthesia.
The efficacy of nonoperative treatments for shoulder pain is not well known. Studies of treatment modalities have been numerous but generally of poor quality due to a lack of uniformity in how shoulder disorders are defined and in the variability of outcome measures used. Several recent systematic reviews have tried to identify which interventions are efficacious ( Table 2 ).6-11
Overall, NSAIDs and subacromial steroid injections are effective in the short-term treatment of shoulder pain.26-28 However, only nonselective NSAIDs have been studied. Evidence is insufficient to recommend use of cyclooxygenase-2 (COX-2) medications for shoulder pain.
Steroid injections may not confer extra benefit when added to NSAIDs, but they appear superior to NSAIDs in improving shoulder abduction. This is particularly true for the painful stiff shoulder, as seen with impingement or rotator cuff disease.26,28
Two recent randomized control trials showed corticosteroid injections to be superior to physical therapy for treatment of shoulder complaints.12,13
Shoulder instability may be treated nonoperatively at first with PRI, NSAIDs, and strengthening and proprioceptive exercises for the rotator cuff. If 3 to 6 months of nonoperative treatment fails, the patient should be referred for surgical evaluation, especially in cases of full-thickness rotator cuff tears.14
TABLE 2
Nonoperative treatment options for shoulder pain
| Treatment | Comment | SOR |
|---|---|---|
| NSAIDs |
| C |
| Physical therapy |
| B |
| Ultrasound |
| A |
| Steroid injection |
| B |
| Acupuncture |
| C |
| SOR, strength of recommendation (SORT); NSAIDs, nonsteroidal anti-inflammatory drugs. | ||
Treatment of specific shoulder disorders
Subacromial impingement syndrome stage I
A recommendation (SOR: B) can be made for the use of NSAIDs in the treatment of stage I impingement ( Table 3 ). This is based on level 2 evidence that NSAIDs are beneficial for rotator cuff tendinopathy and bicipital tendinitis, compared with placebo in a 1 to 2 week follow-up.15,17 No specific NSAID has proved better than another.18,19
Steroid injection ( Figure 2 ) is beneficial for the acute treatment of SIS I reflected by improvement in pain (SOR: A).20-23 This is particularly evident during the first 1 to 2 weeks following injections.38 At 4 to 6 weeks, there appears to be no difference in the efficacy of steroid injection compared with NSAIDs,24,25 but they are both better than placebo.43
Physical therapy, specifically rotator cuff strengthening and range of motion, is as beneficial as surgery for SIS I at 6 month and 21/2-year follow-up, and both were better than placebo (SOR: B).26,27
TABLE 3
Treatments for SIS I impingement (rotator cuff tendinitis/tendinosis)
| Treatment | Comment | LOE |
|---|---|---|
| NSAIDs |
| 1c |
| NSAIDs vs steroid injection |
| 1a |
| Subacromial steroid injection |
| 1b |
| Surgery |
| 2a |
FIGURE 2
Steroid injection in the subacromial space
SIS stages II and III
There is very good evidence (SOR: B) regarding the efficacy of nonoperative treatment of SIS II and III, based on level 2 cohort studies that suggest nonoperative care leads to improvements in patient satisfaction, pain, and daily activities.28,29 Similar outcomes are reported for patients undergoing physical therapy alone.30,31 Weiss reported that corticosteroid injections for stage III/full-thickness rotator cuff tears resulted in an 86% improvement as measured by return to previous activities and less or no pain with motion ( Table 4 ).32
The most constant outcome measure was report of a reduction in pain. Younger patients or those with higher functional demands will likely consider surgical repair if nonoperative measures fail, particularly for full-thickness tears.
TABLE 4
Nonoperative treatments for SIS III (full-thickness rotator cuff tears)
| Treatment | Comment | SOR |
|---|---|---|
| Physical therapy |
| B |
| Subacromial injection |
| B |
| Multiple nonoperativetherapies |
| B |
Adhesive capsulitis
There is no consistent evidence that treatment of any one form reduces the pain or improves range of motion in frozen shoulders. Various treatments that have been tried include, though are not limited to, steroid injection, NSAIDs, and physical therapy.33-37 Studies on treatment efficacy are complicated by inherent discrepancy between patient and observer opinions of limitations in this condition, with objective range of motion findings often not being consistent with patient reported limitations.38
Indicators of quicker or slower recovery
Studies of prognosis following treatment have been difficult to assess due the heterogeneity of the underlying conditions and variability of treatments. A follow-up questionnaire in one instance found no difference between treatment groups. Complaints of pain or impaired mobility 2 to 3 years after treatment were similar among patients treated with steroid injection and physical therapy and with physical therapy alone.30 Overall, 76% of respondents were symptom free at 2 to 3 years.
Two prospective studies confirm that speed of recovery is slow, with complete recovery 23% at 1 month, 21% to 51% at 6 months, 59% at 1 year, and 69% at 18 months.39,40
Prognostic indicators of quicker recovery were preceding overuse or slight trauma and early presentation to the physician.58 Protracted recovery occurred more often with high pain levels during the day or associated neck pain.58 These results suggest that patients with subacromial impingement stage I respond better to nonoperative treatment than those patients with underlying degenerative changes or referred pain from the neck.
Finally, specialty surgical referral may be necessary in cases of failed nonoperative therapy or persistent diagnostic and therapeutic challenges.
Corresponding author
Thomas H. Trojian, MD, 99 Woodland Street, Hartford, CT 06105. E-mail: [email protected].
- First-line treatment for shoulder pain and stage 1 impingement may include nonsteroidal anti-inflammatory drugs (NSAIDs) (B) or corticosteroid injection (A).
- Stage II or III Impingement (rotator cuff tears) are best treated initially with physical therapy (supervised or home exercise program) or corticosteroid injection.
- Steroid injections added to NSAID treatment probably confer no extra benefit.
- High pain levels during the day and associated neck pain may predict a longer recovery period.
Most shoulder pain responds best to NSAIDs or subacromial corticosteroid injections followed by a home exercise program or formal physical therapy exercises. Accumulating evidence is making it clearer what works and what doesn’t for specific diagnoses.
Time to healing varies greatly among persons with shoulder pain, and specific prognostic indicators may help you and your patients know what to expect.
Quick diagnostic review
Consider the patient’s age, history of trauma, details of injury, and previous shoulder problems. Observe the patient’s general movements, assess range of motion, and use provocative testing to form a differential diagnosis ( Figure 1 ).
If the diagnosis is unclear, arrange for imaging studies ( Table 1 ). A more thorough review for diagnosing shoulder pain may be found in the article “Approach to the patient with shoulder pain” (J Fam Pract 2002; 7:605–611). The conditions causing shoulder pain (in order of frequency, as seen by primary care physicians) are subacromial impingement syndrome (SIS), adhesive capsulitis, acute bursitis, calcific tendinitis, glenohumeral arthrosis, biceps tendinitis, and labral tear.1,2
TABLE 1
Value of imaging tests for shoulder injuries
| Test | LOE | Sn | Sp | LR+ | LR− | PV+ | PV− |
|---|---|---|---|---|---|---|---|
| MRI | |||||||
| Rotator cuff tears | |||||||
| Partial41 | 2b | 82 | 85 | 5.5 | 0.21 | 82 | 85 |
| Complete41 | 1a | 81 | 78 | 3.7 | 0.24 | — | — |
| Overall42-44 | 2b | 89–96 | 49–100 | 1.9–>25 | 0.08 | 58 | 94 |
| Impingement 42 | 2b | 93 | 87 | 7.2 | 0.08 | 93 | 87 |
| Labral tears* 45,46 | 1b | 75–89 | 97–100 | >25 | 0.11–0.25 | 100 | 41 |
| Plain arthrogram | |||||||
| Rotator cuff tears | |||||||
| Partial47 | 1b | 70 | — | — | — | — | — |
| Complete41 | 1b | 50 | 96 | 13 | 0.52 | — | — |
| CT arthrogram | |||||||
| Rotator cuff tears | |||||||
| Partial47 | 1b | 70 | — | — | — | — | — |
| Complete47 | 1b | 95 | — | — | — | — | — |
| Overall47 | 1b | 86 | 98 | >25 | 0.14 | 96 | 93 |
| Ultrasound | |||||||
| Rotator cuff tears | |||||||
| Partial47 | 1b | 80 | — | — | — | — | — |
| Complete47,4848 | 1b | 90–100 | 85 | 6.7 | >25 | — | — |
| Overall47 | 1b | 86 | 91–98 | 9.6–>25 | 0.14–0.15 | 96 | 73–93 |
| *MRI arthrography. | |||||||
| LOE, level of evidence (SORT); Sn, sensitivity; Sp, specificity; LR, likelihood ratio; PV, predictive value; MRI, magnetic resonance imaging; CT, computed tomography. | |||||||
FIGURE 1
Evaluating shoulder pain for possible rotator cuff tear
Subacromial impingement syndrome
This condition was first described by Neer, who estimated it leads to 95% of rotator cuff tears.3
Impingement occurs from repetitive overhead activities, acute trauma, or instability of the glenohumeral joint (subtle or overt). Current theory holds that degeneration of the rotator cuff tendons or inflammation of the subacromial bursa—caused by irritation against the coracoacromial arch—can progress to degeneration and a complete rotator cuff tear. So-called rotator cuff tendinitis is better described as a tendinopathy with mucoid degeneration of the tendon. SIS stage I involves edema and hemorrhage, as would be seen with rotator cuff tendinopathy or bursitis.
Progressive feedback loop of subacromial impingement syndrome. Acute bursitis involves the subacromial bursa and typically is secondary to subacromial impingement. As underlying tendinopathy, instability, or heterotrophic bone irritates the bursa, it will become inflamed and irritated. Inflammation exacerbates the impingement and that in turn causes worsening of the bursitis.
Stage II and III impingement syndrome. SIS stage II is a progression to fibrosis and partial tear of the rotator cuff. Stage III is a full-thickness tear of the rotator cuff. These stages of SIS are seen predominantly in patients over the age of 40 years, and they become more common with increasing age. The tear—partial or complete— usually occurs in the supraspinatus tendon. Tears of other rotator cuff muscles are less common.
Magnetic resonance imaging (MRI), with or without arthrography, is used in clinical practice and in research to diagnose rotator cuff tears. Growing evidence indicates that ultrasound is a less expensive and equally effective way to diagnose stage II or III impingement. In the United States, however, the option of ultrasound is limited by scarce availability and inadequate operator skill.
The subacromial injection test is useful in clinical practice. Local anesthetic is injected into the subacromial space. Persisting loss of strength despite pain relief is a positive sign of impairment of the rotator cuff.
MRI or ultrasound must be done in conjunction with history taking and physical examination. As the age of a person increases, the amount of asymptomatic rotator cuff tendon injury will also increase. The incidence of rotator cuff tears has been found to be between 50% to 60% in cadavers of deceased elderly. Thirty percent were found to be stage III impingement; 20% to 30% were partial stage II impingement.4
Adhesive capsulitis
Also known as frozen shoulder, adhesive capsulitis may begin with any inflammatory condition, but it is most commonly idiopathic. It characteristically progresses through 3 stages.
The hallmark of adhesive capsulitis is a progressive lack of range of motion with both passive and active movement.
The first stage involves progressive pain and decreased range of motion as the capsule scars.
The second stage involves maturation of capsule scaring, resulting in decreased pain and increased restriction of movement.
The third stage is resolution of the condition, leading to a gradual increase in range of motion.
Full range of motion may or may not return, and the time to resolution is typically 1 to 2 years. Adhesive capsulitis is most common in older persons, especially women in the fourth and fifth decades.5
Comparing nonoperative treatments
Nonoperative treatment modalities include protection, relative rest, and ice (PRI); anti-inflammatory medications; physical therapy (supervised or home exercise program); acupuncture; and steroid injection.
Operative treatments, depending on the particular disorder, include rotator cuff repair, subacromial decompression, capsular tightening, or manipulation under anesthesia.
The efficacy of nonoperative treatments for shoulder pain is not well known. Studies of treatment modalities have been numerous but generally of poor quality due to a lack of uniformity in how shoulder disorders are defined and in the variability of outcome measures used. Several recent systematic reviews have tried to identify which interventions are efficacious ( Table 2 ).6-11
Overall, NSAIDs and subacromial steroid injections are effective in the short-term treatment of shoulder pain.26-28 However, only nonselective NSAIDs have been studied. Evidence is insufficient to recommend use of cyclooxygenase-2 (COX-2) medications for shoulder pain.
Steroid injections may not confer extra benefit when added to NSAIDs, but they appear superior to NSAIDs in improving shoulder abduction. This is particularly true for the painful stiff shoulder, as seen with impingement or rotator cuff disease.26,28
Two recent randomized control trials showed corticosteroid injections to be superior to physical therapy for treatment of shoulder complaints.12,13
Shoulder instability may be treated nonoperatively at first with PRI, NSAIDs, and strengthening and proprioceptive exercises for the rotator cuff. If 3 to 6 months of nonoperative treatment fails, the patient should be referred for surgical evaluation, especially in cases of full-thickness rotator cuff tears.14
TABLE 2
Nonoperative treatment options for shoulder pain
| Treatment | Comment | SOR |
|---|---|---|
| NSAIDs |
| C |
| Physical therapy |
| B |
| Ultrasound |
| A |
| Steroid injection |
| B |
| Acupuncture |
| C |
| SOR, strength of recommendation (SORT); NSAIDs, nonsteroidal anti-inflammatory drugs. | ||
Treatment of specific shoulder disorders
Subacromial impingement syndrome stage I
A recommendation (SOR: B) can be made for the use of NSAIDs in the treatment of stage I impingement ( Table 3 ). This is based on level 2 evidence that NSAIDs are beneficial for rotator cuff tendinopathy and bicipital tendinitis, compared with placebo in a 1 to 2 week follow-up.15,17 No specific NSAID has proved better than another.18,19
Steroid injection ( Figure 2 ) is beneficial for the acute treatment of SIS I reflected by improvement in pain (SOR: A).20-23 This is particularly evident during the first 1 to 2 weeks following injections.38 At 4 to 6 weeks, there appears to be no difference in the efficacy of steroid injection compared with NSAIDs,24,25 but they are both better than placebo.43
Physical therapy, specifically rotator cuff strengthening and range of motion, is as beneficial as surgery for SIS I at 6 month and 21/2-year follow-up, and both were better than placebo (SOR: B).26,27
TABLE 3
Treatments for SIS I impingement (rotator cuff tendinitis/tendinosis)
| Treatment | Comment | LOE |
|---|---|---|
| NSAIDs |
| 1c |
| NSAIDs vs steroid injection |
| 1a |
| Subacromial steroid injection |
| 1b |
| Surgery |
| 2a |
FIGURE 2
Steroid injection in the subacromial space
SIS stages II and III
There is very good evidence (SOR: B) regarding the efficacy of nonoperative treatment of SIS II and III, based on level 2 cohort studies that suggest nonoperative care leads to improvements in patient satisfaction, pain, and daily activities.28,29 Similar outcomes are reported for patients undergoing physical therapy alone.30,31 Weiss reported that corticosteroid injections for stage III/full-thickness rotator cuff tears resulted in an 86% improvement as measured by return to previous activities and less or no pain with motion ( Table 4 ).32
The most constant outcome measure was report of a reduction in pain. Younger patients or those with higher functional demands will likely consider surgical repair if nonoperative measures fail, particularly for full-thickness tears.
TABLE 4
Nonoperative treatments for SIS III (full-thickness rotator cuff tears)
| Treatment | Comment | SOR |
|---|---|---|
| Physical therapy |
| B |
| Subacromial injection |
| B |
| Multiple nonoperativetherapies |
| B |
Adhesive capsulitis
There is no consistent evidence that treatment of any one form reduces the pain or improves range of motion in frozen shoulders. Various treatments that have been tried include, though are not limited to, steroid injection, NSAIDs, and physical therapy.33-37 Studies on treatment efficacy are complicated by inherent discrepancy between patient and observer opinions of limitations in this condition, with objective range of motion findings often not being consistent with patient reported limitations.38
Indicators of quicker or slower recovery
Studies of prognosis following treatment have been difficult to assess due the heterogeneity of the underlying conditions and variability of treatments. A follow-up questionnaire in one instance found no difference between treatment groups. Complaints of pain or impaired mobility 2 to 3 years after treatment were similar among patients treated with steroid injection and physical therapy and with physical therapy alone.30 Overall, 76% of respondents were symptom free at 2 to 3 years.
Two prospective studies confirm that speed of recovery is slow, with complete recovery 23% at 1 month, 21% to 51% at 6 months, 59% at 1 year, and 69% at 18 months.39,40
Prognostic indicators of quicker recovery were preceding overuse or slight trauma and early presentation to the physician.58 Protracted recovery occurred more often with high pain levels during the day or associated neck pain.58 These results suggest that patients with subacromial impingement stage I respond better to nonoperative treatment than those patients with underlying degenerative changes or referred pain from the neck.
Finally, specialty surgical referral may be necessary in cases of failed nonoperative therapy or persistent diagnostic and therapeutic challenges.
Corresponding author
Thomas H. Trojian, MD, 99 Woodland Street, Hartford, CT 06105. E-mail: [email protected].
1. Van der Windt DA, Koes BW, De Jong BA, Bouter LM. Shoulder disorders in general practice: incidence, patient characteristics, and management. Ann Rheum Dis 1995;54:959-964.
2. Blanchard TK, Bearcroft PW, Constant CR, Griffin DR, Dixon AK. Diagnostic and therapeutic impact of MRI and arthrography in the investigation of full-thickness rotator cuff tears. Eur Radiol 1999;9:638-642.
3. Neer CS. Anterior acromioplasty for chronic impingement syndrome of shoulder. J Bone Joint Surg 1972;54A:41-50.
4. Dalton SE. The conservative management of rotator cuff disorders. Br J Rheumatol 1994;33:663-667.
5. Matsen FA, Lippitt SB, Sidles JA, Harryman DT. Practical Evaluation and Management of the Shoulder. Philadelphia, Pa: W.B. Saunders; 1994.
6. Green S, Buchbinder R, Glazier R, Forbes A. Interventions for shoulder pain (Cochrane Review). In: The Cochrane Library, Issue 1, 2001. Oxdord: Update Software.
7. Van der Hiejden GJ, Van der Windt DA, Kleijnen J, et al. Steroid injections for shoulder disorders: a systematic review of randomized clinical trials. Br J Gen Pract 1996;46:309-316.
8. Van der Windt DA, Van der Heijden GJ, Scholten RJ, et al. The efficacy of non-steroidal anti-inflammatory drugs (NSAIDs) for shoulder complaints. A systematic review. J Clin Epidemiol 1995;48:691-704.
9. Van der Heijden GJ, Van der Windt DA, De Winter AF. Physiotherapy for patients with soft tissue shoulder disorders: a systematic review of randomized clinical trials. BMJ 1997;15:25-30.
10. Van der Windt DA, Van der Heijden GJ, Van den Berg GJ, et al. Ultrasound therapy for musculoskeletal disorders: a systematic review. Pain 1999;81:257-271.
11. Smith LA, Oldman AD, McQuay HJ, Moore RA. Teasing apart quality and validity in systematic reviews: an example from acupuncture trials in chronic neck and back pain. Pain 2000;86:119-132.
12. Winters JC, Sobel JS, Groenier KH, et al. Comparison of physiotherapy, manipulation, and corticosteroid injection for treating shoulder complaints in general practice: randomized, single blind study. BMJ 1997;314:1320-1325.
13. Van der Windt DA, Koes BW, Deville W, et al. Effectiveness of corticosteroid injections versus physiotherapy for treatment of painful stiff shoulder in primary care: randomized trial. BMJ 1998;317:1292-1296.
14. Mantone JK, Burkhead WZ, Noonan J. Nonoperative treatment of rotator cuff tears. Orthop Clin North Am 2000;31:295-311.
15. Lopez JM. Treatment of acute tendinitis and bursitis with fentiazac. A double blind comparison with placebo. Clin Ther 1982;5:79-84.
16. Zuinen C. Diclofenac/misprostol vs diclofenac/placebo in treating acute episodes of tendinitis/bursitis of the shoulder. Drugs 1993;45 Suppl 1:17-23.
17. Ginsberg F, Famaey JP. A double-blind comparison of slow-release and standard tablet formulations of fentiazac in the treatment of patients with tendinitis and bursitis. Curr Med Res Opin 1985;9:42-448.
18. Wober W. Comparative efficacy and safety of nimesulide and diclofenac in patients with acute shoulder, and a meta-analysis of controlled studies with nimesulide. Rheum 1999;38(Suppl 1):33-38.
19. Wober W, Rahlfs VW, Buchl N, et al. Comparative efficacy and safety of the non-steroidal anti-inflammatory drugs nimesulide and diclofenac in patients with acute subdeltoid bursitis and bicipital tendinitis. Int J Clin Pract 1998;52:169-175.
20. Valtonen E. Double acting betamethasone (celestone chronodose) in the treatment of supraspinatus tendinitis: A comparison of subacromial and gluteal single injections with placebo. J Int Men Res 1978;6:463-467.
21. Blair B, Rokito A, Cuomo F, Jarolem K, Zuckerman J. Efficacy of corticosteroids for subacromial impingement syndrome. J Bone Joint Surg Am 1996;78:1685-1689.
22. Withrington R, Girgis F, Seifert M. A placebo-controlled trial of steroid injections in the treatment of supraspinatus tendinitis. Scand J Rheumatol 1985M;14:76-78.
23. Vecchio PC, Hazleman BL, King RH. A double-blind trial comparing subacromial methylprednisolone and ligno-caine in acute rotator cuff tendinitis. Br J Rheumatol 1993;32:743-745.
24. White R, Paull D, Fleming K. Rotator cuff tendinitis: comparison of subacromial injection of a long acting corticosteroid vs oral indomethacin therapy. J Rheumatol 1986;13:608-613.
25. Adebajo A, Nash P, Hazleman B. A Prospective double blind dummy placebo controlled study comparing triamcinolone hexacetonide injection with oral diclofenac 50mg TDS in patients with rotator cuff tendinitis. J Rheumatol 1990;17:1207-1210.
26. Brox JI, Staff PH, Ljunggren AE, Revik JI. Arthroscopic Surgery compared with supervised exercises in patients with rotator cuff disease (stage II impingement syndrome). BMJ 1993;307:899-903
27. Brox JI, Gjengedal E, Uppheim G, et al. Arthroscopic surgery versus supervised exercises in patients with rotator cuff disease (stage II impingement syndrome): a prosprective, randomized, controlled study in 125 patients with a 2 1/2 year follow up. J Shoulder Elbow Surg 1999;8:102-111.
28. Bokor DJ, Hawkins RJ, Huckell GH, Angelo RL, Schickendantz MS. Results of nonoperative management of full-thickness tears of the rotator cuff. Clin Orthop 1993;294:103-110.
29. Itoi E, Tabata S. Conservative treatment of rotator cuff tears. Clin Orthop 1992;275:165-173.
30. Hawkins RH, Dunlop R. Nonoperative treatment of rotator cuff tears. Clin Orthop 1995;321:178-188.
31. Goldberg BA, Nowinski RJ, Matsen FA. Outcome of non-operative management of full thickness rotator cuff tears. Clin Orthop 2001;382:99-107.
32. Weiss JJ. Intra-articular steroids in the treatment of rota-tor cuff tear: reappraisal by arthrography. Arch Phys Med Rehabil 1981;62:555-557.
33. De Jong BA, Dahmen R, Hogeweg JA, Marti RK. Intra-articular triamcinolone acetonide injection in patients with capsulitis of the shoulder: a comparative study of two dose regimens. Clin Rehab 1998;12:211-215.
34. Bulgen DY, Binder AI, Hazleman BL, Dutton J, Roberts S. Frozen shoulder: prospective clonical study with an evaluation of three treatment regimens. Ann Rheum Dis 1984;43:353-360.
35. Thumb N, Kolarz G, Scherak O, Mayrhofer F. The efficacy and safety of Fentiazac and Diclofenac sodium in peri-arthritis of the shoulder: a multi-center, double-blind comparison. J Int Med Res 1987;15:327-334.
36. Rhind V, Downie WW, Bird HA, Wright V, Engler C. Naproxen and indomethacin in periarthritis of the shoulder. Rheumatol Rehabil 1982;21:51-53.
37. Lee PN, Lee M, Haq AM, Longton EB, Wright V. Periarthritis of the shoulder. Ann Rheum Dis 1974;33:116-119.
38. Hazleman BL. The painful stiff shoulder. Rheumatol Rehabil 1972;11:413-421.
39. Croft P, Pope D, Silman A. The clinical course of shoulder pain: prospective cohort study in primary care. BMJ 1996;313:601-602.
40. Van der Windt DA, Koes BW, Boeke AJ, Deville W, De Jong BA, Bouter LM. Shoulder disorders in general practice: prognostic indicators of outcome. Br J Gen Pract 1996;46:519-523.
41. Iannotti JP, Zlatkin MB, Esterhai JL, Kressel HY, Dalinka MK, Spindler KP. Magnetic resonance imaging of the shoulder. Sensitivity, specificity, and predictive value. J Bone Joint Surg 1991;73:17-29.
42. Burk DL, Karasick D, Kurtz AB, et al. Rotator cuff tears: prospective comparison of MR imaging with arthrography, sonography, and surgery. Am J Roentgenol 1989;153:87-92.
43. Torstensen ET, Hollinshead RM. Comparison of magnetic resonance imaging and arthroscopy in the evaluation of shoulder pathology. J Shoulder Elbow Surg 1999;8:42-45.
44. Yeu K, Jiang CC, Shih TT. Correlation between MRI and operative findings of the rotator cuff tear. J Formos Med Assoc 1994;93:134-139.
45. Green MR, Christensen KP. Magnetic resonance imaging of the glenoid labrum in anterior shoulder instability. Am J Sports Med 1994;22:493-498.
46. Gusmer PB, Potter HG, Schaltz JA, et al. Labral injuries: accuracy of detection with en-enhanced MR imaging of the shoulder. Radiology 1996;200:519-524.
47. Farin PU, Kaukanen E, Jaroma H, Vaatainen U, Miettinen H, Soimakallio S. Site and size of rotator cuff tear. Findings at ultrasound, double contrast arthrography, and computed tomography arthrography with surgical correlation. Invest Radiol 1996;31:387-394.
48. Teefey SA, Hasan SA, Middleton WD, Patel M, Wright RW, Yamaguchi K. Ultrasonography of the rotator cuff. A comparison of ultrasonographic and arthroscopic findings in one hundred consecutive cases. J Bone Joint Surg Am 2000;82:498-504.
49. Van Moppes FI, Veldkam O, Roorda J. Role of shoulder ultrasonography in the evaluation of the painful shoulder. Eur J Radiol 1995;19:142-146.
1. Van der Windt DA, Koes BW, De Jong BA, Bouter LM. Shoulder disorders in general practice: incidence, patient characteristics, and management. Ann Rheum Dis 1995;54:959-964.
2. Blanchard TK, Bearcroft PW, Constant CR, Griffin DR, Dixon AK. Diagnostic and therapeutic impact of MRI and arthrography in the investigation of full-thickness rotator cuff tears. Eur Radiol 1999;9:638-642.
3. Neer CS. Anterior acromioplasty for chronic impingement syndrome of shoulder. J Bone Joint Surg 1972;54A:41-50.
4. Dalton SE. The conservative management of rotator cuff disorders. Br J Rheumatol 1994;33:663-667.
5. Matsen FA, Lippitt SB, Sidles JA, Harryman DT. Practical Evaluation and Management of the Shoulder. Philadelphia, Pa: W.B. Saunders; 1994.
6. Green S, Buchbinder R, Glazier R, Forbes A. Interventions for shoulder pain (Cochrane Review). In: The Cochrane Library, Issue 1, 2001. Oxdord: Update Software.
7. Van der Hiejden GJ, Van der Windt DA, Kleijnen J, et al. Steroid injections for shoulder disorders: a systematic review of randomized clinical trials. Br J Gen Pract 1996;46:309-316.
8. Van der Windt DA, Van der Heijden GJ, Scholten RJ, et al. The efficacy of non-steroidal anti-inflammatory drugs (NSAIDs) for shoulder complaints. A systematic review. J Clin Epidemiol 1995;48:691-704.
9. Van der Heijden GJ, Van der Windt DA, De Winter AF. Physiotherapy for patients with soft tissue shoulder disorders: a systematic review of randomized clinical trials. BMJ 1997;15:25-30.
10. Van der Windt DA, Van der Heijden GJ, Van den Berg GJ, et al. Ultrasound therapy for musculoskeletal disorders: a systematic review. Pain 1999;81:257-271.
11. Smith LA, Oldman AD, McQuay HJ, Moore RA. Teasing apart quality and validity in systematic reviews: an example from acupuncture trials in chronic neck and back pain. Pain 2000;86:119-132.
12. Winters JC, Sobel JS, Groenier KH, et al. Comparison of physiotherapy, manipulation, and corticosteroid injection for treating shoulder complaints in general practice: randomized, single blind study. BMJ 1997;314:1320-1325.
13. Van der Windt DA, Koes BW, Deville W, et al. Effectiveness of corticosteroid injections versus physiotherapy for treatment of painful stiff shoulder in primary care: randomized trial. BMJ 1998;317:1292-1296.
14. Mantone JK, Burkhead WZ, Noonan J. Nonoperative treatment of rotator cuff tears. Orthop Clin North Am 2000;31:295-311.
15. Lopez JM. Treatment of acute tendinitis and bursitis with fentiazac. A double blind comparison with placebo. Clin Ther 1982;5:79-84.
16. Zuinen C. Diclofenac/misprostol vs diclofenac/placebo in treating acute episodes of tendinitis/bursitis of the shoulder. Drugs 1993;45 Suppl 1:17-23.
17. Ginsberg F, Famaey JP. A double-blind comparison of slow-release and standard tablet formulations of fentiazac in the treatment of patients with tendinitis and bursitis. Curr Med Res Opin 1985;9:42-448.
18. Wober W. Comparative efficacy and safety of nimesulide and diclofenac in patients with acute shoulder, and a meta-analysis of controlled studies with nimesulide. Rheum 1999;38(Suppl 1):33-38.
19. Wober W, Rahlfs VW, Buchl N, et al. Comparative efficacy and safety of the non-steroidal anti-inflammatory drugs nimesulide and diclofenac in patients with acute subdeltoid bursitis and bicipital tendinitis. Int J Clin Pract 1998;52:169-175.
20. Valtonen E. Double acting betamethasone (celestone chronodose) in the treatment of supraspinatus tendinitis: A comparison of subacromial and gluteal single injections with placebo. J Int Men Res 1978;6:463-467.
21. Blair B, Rokito A, Cuomo F, Jarolem K, Zuckerman J. Efficacy of corticosteroids for subacromial impingement syndrome. J Bone Joint Surg Am 1996;78:1685-1689.
22. Withrington R, Girgis F, Seifert M. A placebo-controlled trial of steroid injections in the treatment of supraspinatus tendinitis. Scand J Rheumatol 1985M;14:76-78.
23. Vecchio PC, Hazleman BL, King RH. A double-blind trial comparing subacromial methylprednisolone and ligno-caine in acute rotator cuff tendinitis. Br J Rheumatol 1993;32:743-745.
24. White R, Paull D, Fleming K. Rotator cuff tendinitis: comparison of subacromial injection of a long acting corticosteroid vs oral indomethacin therapy. J Rheumatol 1986;13:608-613.
25. Adebajo A, Nash P, Hazleman B. A Prospective double blind dummy placebo controlled study comparing triamcinolone hexacetonide injection with oral diclofenac 50mg TDS in patients with rotator cuff tendinitis. J Rheumatol 1990;17:1207-1210.
26. Brox JI, Staff PH, Ljunggren AE, Revik JI. Arthroscopic Surgery compared with supervised exercises in patients with rotator cuff disease (stage II impingement syndrome). BMJ 1993;307:899-903
27. Brox JI, Gjengedal E, Uppheim G, et al. Arthroscopic surgery versus supervised exercises in patients with rotator cuff disease (stage II impingement syndrome): a prosprective, randomized, controlled study in 125 patients with a 2 1/2 year follow up. J Shoulder Elbow Surg 1999;8:102-111.
28. Bokor DJ, Hawkins RJ, Huckell GH, Angelo RL, Schickendantz MS. Results of nonoperative management of full-thickness tears of the rotator cuff. Clin Orthop 1993;294:103-110.
29. Itoi E, Tabata S. Conservative treatment of rotator cuff tears. Clin Orthop 1992;275:165-173.
30. Hawkins RH, Dunlop R. Nonoperative treatment of rotator cuff tears. Clin Orthop 1995;321:178-188.
31. Goldberg BA, Nowinski RJ, Matsen FA. Outcome of non-operative management of full thickness rotator cuff tears. Clin Orthop 2001;382:99-107.
32. Weiss JJ. Intra-articular steroids in the treatment of rota-tor cuff tear: reappraisal by arthrography. Arch Phys Med Rehabil 1981;62:555-557.
33. De Jong BA, Dahmen R, Hogeweg JA, Marti RK. Intra-articular triamcinolone acetonide injection in patients with capsulitis of the shoulder: a comparative study of two dose regimens. Clin Rehab 1998;12:211-215.
34. Bulgen DY, Binder AI, Hazleman BL, Dutton J, Roberts S. Frozen shoulder: prospective clonical study with an evaluation of three treatment regimens. Ann Rheum Dis 1984;43:353-360.
35. Thumb N, Kolarz G, Scherak O, Mayrhofer F. The efficacy and safety of Fentiazac and Diclofenac sodium in peri-arthritis of the shoulder: a multi-center, double-blind comparison. J Int Med Res 1987;15:327-334.
36. Rhind V, Downie WW, Bird HA, Wright V, Engler C. Naproxen and indomethacin in periarthritis of the shoulder. Rheumatol Rehabil 1982;21:51-53.
37. Lee PN, Lee M, Haq AM, Longton EB, Wright V. Periarthritis of the shoulder. Ann Rheum Dis 1974;33:116-119.
38. Hazleman BL. The painful stiff shoulder. Rheumatol Rehabil 1972;11:413-421.
39. Croft P, Pope D, Silman A. The clinical course of shoulder pain: prospective cohort study in primary care. BMJ 1996;313:601-602.
40. Van der Windt DA, Koes BW, Boeke AJ, Deville W, De Jong BA, Bouter LM. Shoulder disorders in general practice: prognostic indicators of outcome. Br J Gen Pract 1996;46:519-523.
41. Iannotti JP, Zlatkin MB, Esterhai JL, Kressel HY, Dalinka MK, Spindler KP. Magnetic resonance imaging of the shoulder. Sensitivity, specificity, and predictive value. J Bone Joint Surg 1991;73:17-29.
42. Burk DL, Karasick D, Kurtz AB, et al. Rotator cuff tears: prospective comparison of MR imaging with arthrography, sonography, and surgery. Am J Roentgenol 1989;153:87-92.
43. Torstensen ET, Hollinshead RM. Comparison of magnetic resonance imaging and arthroscopy in the evaluation of shoulder pathology. J Shoulder Elbow Surg 1999;8:42-45.
44. Yeu K, Jiang CC, Shih TT. Correlation between MRI and operative findings of the rotator cuff tear. J Formos Med Assoc 1994;93:134-139.
45. Green MR, Christensen KP. Magnetic resonance imaging of the glenoid labrum in anterior shoulder instability. Am J Sports Med 1994;22:493-498.
46. Gusmer PB, Potter HG, Schaltz JA, et al. Labral injuries: accuracy of detection with en-enhanced MR imaging of the shoulder. Radiology 1996;200:519-524.
47. Farin PU, Kaukanen E, Jaroma H, Vaatainen U, Miettinen H, Soimakallio S. Site and size of rotator cuff tear. Findings at ultrasound, double contrast arthrography, and computed tomography arthrography with surgical correlation. Invest Radiol 1996;31:387-394.
48. Teefey SA, Hasan SA, Middleton WD, Patel M, Wright RW, Yamaguchi K. Ultrasonography of the rotator cuff. A comparison of ultrasonographic and arthroscopic findings in one hundred consecutive cases. J Bone Joint Surg Am 2000;82:498-504.
49. Van Moppes FI, Veldkam O, Roorda J. Role of shoulder ultrasonography in the evaluation of the painful shoulder. Eur J Radiol 1995;19:142-146.
Open-angle glaucoma: Tips for earlier detection and treatment selection
- Screen persons older than 60 years, African Americans of any age, and those with a family history of open-angle glaucoma (C). Further evaluation by an ophthalmologist is warranted if optic nerve damage is suspected or if a patient reports decreasing vision.
- Elevated intraocular pressure (IOP) is not necessary for open-angle glaucoma to occur. Assess optic nerve status and visual field in those at risk. (C)
- Inquire about topical ocular drops recommended by an ophthalmologist, to be certain they are not contraindicated for other conditions the patient might have, and to be alert to the potential for adverse effects. (C)
Evaluate for open-angle glaucoma (OAG) when a patient reports decreased vision, or when a patient even with good eyesight is found to be at high risk for the disease. Most patients with early glaucoma are unaware of the initial decrease in peripheral vision.1
A relatively new diagnostic technique can detect even moderate damage to the optic nerve, and the procedure is brief. Ophthalmologists can choose from among several topical medications to reduce intraocular pressure. Your knowledge of the patient’s medical history is critical to avoiding potential drug-drug interactions.
Laser surgery and trabeculectomy may be indicated as first-line therapy for select patients.
Whom to screen
Persons aged older than 60 years, African Americans of any age, and those with a family history of OAG are at particularly high risk, and all risk factors should be fully assessed (SOR: B).2 (See Open-angle glaucoma: The scope of the problem.)
In the Caucasian population aged 40 to 49 years with no family history of OAG, disease prevalence is just 0.18%. Prevalence is 4 times greater in African Americans of the same age range. Caucasians aged 60 to 69 years have a prevalence of OAG 4 times greater than patients aged 40 to 49. For African Americans older than 80 years, prevalence exceeds 11%.3
For persons with a first-degree relative with OAG, risk was found to be 9.2 times greater than for those without such a history.8
Ask specifically about decreased vision, loss of peripheral vision, difficulty seeing in the dark, and difficulty reading (SOR: B).
Before referring high-risk patients for a full ophthalmologic examination, examine the optic nerve with direct ophthalmoscopy (SOR: B).
Open-angle glaucoma (OAG) is defined as an optic neuropathy in which there is damage to the optic nerve with a loss of retinal ganglion cells that carry visual impulses from the eye to the brain. It is the second most common cause of legal blindness in the United States and the leading cause of blindness among African Americans.2 A population-based evaluation of glaucoma screening, the Baltimore Eye Survey, estimates about 2.5 million Americans as having OAG with as many as half of them unaware that they have the disease.3,4
More than 8 million office visits to office-based clinicians occur per year by patients with a primary diagnosis of glaucoma.5 The National Eye Institute, a division of the NIH, reports that as many as 120,000 Americans are currently blind as a result of glaucoma, costing the US government over $1.5 billion annually in Social Security benefits, lost income tax revenues, and health care expenditures.
An asymptomatic disease in its early stages,1 glaucoma progresses to cause permanent blindness in the absence of treatment. This article addresses the features, diagnostic methods, and treatment modalities of glaucoma as well as the role of the family physician in its management.
What causes OAG?
The pathogenesis of glaucoma is multifactorial and is thought, in most cases, to be caused by an abnormally high intraocular pressure (IOP), which mechanically compresses and causes subsequent atrophy of optic nerve fibers. The increased pressure is due to impaired drainage of aqueous humor out of the eye. Aqueous humor, produced by the ciliary body, normally provides nutrients to the iris, lens, and cornea before being drained through the trabecular meshwork.
It should be noted, however, that an elevated IOP is not necessary in glaucoma; optic nerve atrophy can occur in the absence of high IOP. The mechanism for optic nerve damage in this form of glaucoma is unknown.6
In angle-closure glaucoma, the angle between the iris and the trabecular meshwork is occluded, preventing normal drainage of aqueous humor. In open-angle glaucoma, the angle appears open but does not function properly in draining aqueous humor out of the eye.6 It is open-angle glaucoma that will be discussed here as it accounts for 75% to 95% of all glaucoma cases.7
Determining optic nerve status
Examination of the optic nerve head provides clues as to whether structural damage has occurred. Cup-disc ratio is used to assess risk of glaucoma development. The probability of abnormality increases dramatically for values above 0.5.9
The standard clinical technique used by primary care clinicians is with the direct ophthalmoscope. Sensitivity and specificity for a cup-disc ratio greater than 0.6 have been reported to be 64% and 96%, respectively, using direct ophthalmoscopy.10
Ophthalmologists use stereoscopic fundus photography to visualize the optic nerve. With this technique, sensitivity and specificity for a cup-disc ratio greater than 0.5 have been found to be 48% and 89%, respectively.11 Studies, however, have reported a high interobserver variation in measurement of the cup-disc ratio even among experts in the field.12
What to look for. Characteristic changes include narrowing or notching of the neuroretinal rim, or characteristic visual field loss, such as arcuate defects and nasal loss.13 Describe an abnormal optic disc in terms of its cup-disc ratio, and report visual loss to the ophthalmologist as a defect in a respective field quadrant as detected on confrontational visual field testing or as an afferent pupillary defect in a given eye.
Referral. A final diagnosis of open-angle glaucoma can be made only after characteristic damage to the optic nerve has been confirmed by an ophthalmologist (SOR: B). Therefore, patients at high risk of developing OAG (age >60 years, African American race, positive family history) should be referred for an eye examination.
Other key diagnostic tests include measurement of intraocular pressure and visual field testing.2 The accuracy of these tests is outlined in Table 1.
TABLE 1
Characteristics of diagnostic tests for open-angle glaucoma
| Test | Study quality | Sn% | Sp% | LR+ | LR– | PV+ | PV– |
|---|---|---|---|---|---|---|---|
| Tonometry14 | 2 | ||||||
| IOP >21 mm Hg | 47.1 | 92.4 | 6.20 | 24.6 | |||
| IOP <21 mm Hg | .57 | 97 | |||||
| Cup-disc ratio, stereoscopic photography14 | 2 | ||||||
| Cup-disc ratio >.5 | 48 | 89 | 4.36 | .187 | |||
| Cup-disc ratio <.5 | .58 | 97 | |||||
| Cup-disc ratio, direct ophthalmoscopy10 | 1 | ||||||
| Cup-disc ratio >.6 | 64 | 96 | 16 | 46 | |||
| Cup-disc ratio <.6 | .375 | 98 | |||||
| Visual field15 | 2 | ||||||
| Abnormal | 97 | 84 | 6.06 | 24.2 | |||
| Normal | .036 | 99.8 | |||||
| LR+ = positive likelihood ratio; the likelihood that a person with OAG will have a positive test result (eg, a person with OAG is 16 times more likely to exhibit a cup-disc ratio >.6 than a person without the disease). See “Using the likelihood ratio,” page 127 of this issue. | |||||||
| LR– = negative likelihood ratio; the likelihood that a person with OAG will have a negative test result (eg, a person with OAG is only .375 times as likely to exhibit a cup-disc ratio <.6 as a person without the disease) | |||||||
| PV+ = positive predictive value; the probability that a positive test result indicates disease | |||||||
| PV– = negative predictive value; the probability that a negative test result indicates absence of disease | |||||||
| PV+ and PV- assume a baseline likelihood of disease of 5% (prevalence among African Americans aged 60–69 years)3 | |||||||
Intraocular pressure: Caveats
Intraocular pressure (IOP) is measured by a tonometer. The eye is subjected to a force that flattens the cornea. This force is then related to the pressure in the eye, or IOP. The standard instrument for measuring IOP is the Goldman applanation tonometer. Handheld versions (tonopen) are useful for screening by the primary care clinician.11 Studies of IOP distribution show the normal range of IOP values to be less than 21 mm Hg with a slight skew towards higher values.16
The altering effect of corneal thickness. IOP measurement may vary with the thickness of one’s cornea. A corneal thickness greater than 555 μm can produce falsely high readings, and a corneal thickness less than 540 μm can produce falsely low readings.2,17,18 Thus, central corneal thickness (CCT) is a factor that may affect the accuracy of an IOP reading. Central corneal thickness is measured with a pachymeter, and an ophthalmologist must take this measurement into account when assessing a patient’s IOP.
Pressure may not be elevated in OAG. A number of population-based studies have documented an increase in the prevalence of OAG with an increase in IOP.7,19,20 However, these same studies have also concluded that many patients with OAG have IOP levels in the normal range. These patients are deemed to have normal pressure glaucoma (NPG), a subtype of OAG.21
Likewise, many patients with elevated IOP have no demonstrable optic nerve damage;19,20 this condition has been termed ocular hypertension (OHT).
A proper perspective. So, although an elevated IOP is associated with glaucoma, it is important to note that OAG is not defined by the presence of an elevated IOP. Optic nerve atrophy can occur in the absence of an increased IOP. 21 These findings, taken together with the variance of IOP with CCT, are reflected in the modest sensitivity and specificity for IOP readings greater than 21 mm Hg—47.1% and 92.4%, respectively. 14 Patients with a high IOP (>21 mm Hg) are at higher risk for developing OAG, but further ancillary studies and tests are necessary to confirm the diagnosis. 13
Evaluating the visual field
Visual field deterioration is the final manifestation of glaucoma. Vision is first lost peripherally. Central vision loss occurs at the end stage of the disease.
An ophthalmologist will use automated static threshold perimetry to evaluate the visual field. With this technique, the patient must identify white target lights of variable brightness in different locations of a dim 1-m bowl. Various data algorithms are then employed to compare any abnormality in the visual field with patterns that are characteristic of glaucoma.9 One study reported a 97% sensitivity and 84% specificity using a certain algorithm to recognize field abnormalities due to glaucoma.15 However, automated perimetry requires 10 to 20 minutes per eye, and patient fatigue often reduces reliability of the test. Also, an optic nerve head has typically undergone considerable damage before visual field changes are detected.2
An improved test. Frequency doubling technology promises to detect glaucomatous visual defects when there has been only moderate damage to the optic nerve. With frequency doubling technology, patients must recognize patterns of alternating light and dark bars. An abnormality in recognition is thought to be indicative of the pattern of field loss in glaucoma. One study found a sensitivity and specificity each greater than 90% for identifying patients thought to have glaucoma. Another benefit is that the exam takes an average of only 6 minutes to complete in both eyes. 22
No single test result is enough
Successful screening for glaucoma should not rely solely on measuring IOP, assessment of the optic nerve, or visual field testing. These diagnostic clues are complementary and must be taken together to evaluate high-risk populations, including African Americans, those with a family history of glaucoma, and the elderly (SOR: C).
Regular follow-up
Regardless of findings, patients aged 40 to 60 years should be encouraged to have eye exams every other year, and those over age 60 should have annual eye exams (SOR: B).13 Regular ocular exams including vision check, extraocular muscle exam, papillary exam, and confrontational visual fields should be performed in these patients as well (SOR: C).
Treatment
IOP is the only risk factor for glaucoma that can be treated. Lowering IOP in randomized control trials has reduced the progression of visual field loss in OAG patients with abnormally high pressures23 as well as in NPG patients with pressures in the normal range.24
In the Early Manifest Glaucoma Trial, a 30% reduction in IOP reduced the rate of progression in the treatment group (45%) compared with the control group (62%; P=.007).25 Progression risk decreased by approximately 10% per mm Hg of IOP reduction.
Setting a target pressure. Before beginning therapy, an ophthalmologist sets a target pressure that should halt further optic nerve damage. The initial target pressure is usually 20% to 30% lower than the pretreatment pressure. If damage to the optic nerve is already substantial, the target pressure may be set even lower.2
Stepwise therapy. Topical medications are usually given first, as eye drops. A comparison of these medications is outlined in Table 2. If IOP cannot be lowered pharmacologically, argon laser trabeculoplasty (ALT) is the next step. If the pressure still cannot be lowered, filtering surgery is the final alternative (SOR: C).2
TABLE 2
Pharmacologic options for patients with open-angle glaucoma
| Medication(SOR) | % IOP reduction | % RR* | NNT to prevent visualfield loss* | Side effects | Comments |
|---|---|---|---|---|---|
| Beta-blockers (A), non-selective (timolol, carteolol, levobunolol, metipranolol) and selective (betaxolol) | 31 | 74 | 2.17 | Bradycardia, hypotension, bronchospasm (timolol, carteolol, levobunolol, metipranolol) | Cochrane review with clear recommendation as first-line treatment21 |
| Prostaglandin analogues (A) (latanoprost, travoprost, unoprostone) | 40 | 96 | 1.68 | Increased eyelash growth, iris pigmentation, muscle and joint pain | Multiple RCTs and systematic review show show clinical and statistical superiorityover beta-blockers26,27 |
| Alpha adrenergic drugs (A) (apraclonidine, brimonidine) | 23 | 55 | 2.93 | Dry nose, dry mouth, follicular conjunctivitis, hypotension (brimonidine) | Multiple RCTs support effectiveness 28-30 |
| Topical carbonic anhydrase inhibitors (A) (brinzolamide, dorzolamide) | 26 | 62 | 2.6 | GI disturbances, headache, local irritation, redness, sulfa allergies | RCT,31 Cochranereview with clear recommendation26 |
| Cholinergic agonists (A) (pilocarpine, carbachol) | 29 | 69 | 2.32 | Small, fixed pupils, induced myopia, cataracts | Consistently recommended assecond-or third-line drugs in systematic reviews and RCTs27,32 |
| *Percent decrease in risk of visual field loss and NNT to prevent visual field loss were calculated for a patient with a baseline IOP of 24 mm Hg. | |||||
| SOR, strength of recommendation; IOP, intraocular pressure; RR, relative risk; NNT, number needed to treat; RCT, randomized controlled trial. | |||||
Pharmacologic options
Medical agents work in 1 of 2 ways to lower IOP: by decreasing production of aqueous humor, or by increasing drainage of aqueous humor out of the eye. Though most glaucoma medications are given topically, severe systemic side effects can occur.2 Because the consulting ophthalmologist may not be aware of a patient’s other medical conditions, inquire about the topical ocular drops being recommended to make certain they are not contraindicated and to be alert to the potential for adverse effects (SOR: C).13
Beta-adrenergic antagonists can lower IOP by up to 31% 25 and are often used as first-line treatment (SOR: A).21 However, nonselective beta-blockers (timolol, carteolol, levobunolol, metipranolol) are associated with a number of adverse effects including bronchospasm,33 bradycardia, and hypotension. 34
Betaxolol is a selective beta-blocker with less tendency to cause pulmonary side effects,34 but it may still do so in patients with severe pulmonary disease.35 Selective beta-blockers lower IOP to a lesser degree than nonselective drugs36 and can cause the same cardiac effects of bradycardia and hypotension.38
Prostaglandin analogs (latanoprost, travoprost, unoprostone) increase drainage of the aqueous humor. Prostaglandins are clinically and statistically superior to beta-blockers, having lowered IOP by up to 40% in randomized controlled trials.37 Side effects include increased eyelash growth and iris pigmentation,26 and muscle and joint pain.38
Alpha-adrenergic drugs (apraclonidine, brimonidine) lower aqueous humor production. Apraclonidine administered topically does not cross the blood-brain barrier, effectively lowering IOP without causing cardiovascular side effects.28 The most common side effects are dry nose, dry mouth,28 and follicular conjunctivitis.29 Unlike apraclonidine, brimonidine crosses the blood-brain barrier and can cause mild hypotension.30 One randomized controlled trial found no statistical difference in efficacy between brimonidine and apraclonidine, both lowering IOP by up to 23%.39
Carbonic anhydrase inhibitors block water flow into the eye, preventing aqueous humor formation. Until recently, carbonic anhydrase inhibitors such as acetazolamide were administered only orally and adverse effects were therefore common.27 Topical carbonic anhydrase inhibitors (brinzolamide, dorzolamide), recently introduced, lower IOP by up to 26% and with few side effects.31
Cholinergic agonists (pilocarpine, carbachol) increase aqueous outflow from the eye by stimulating contraction of the ciliary body, which opens the trabecular meshwork to allow further drainage.40 Because of its ocular side effects including small, fixed pupils, induced myopia, and cataracts, pilocarpine is reserved for second-or third-line therapy (SOR: A). 9,27,32
Medicinal marijuana used to lower IOP in glaucoma patients is controversial. The primary active ingredient in marijuana, tetrahydrocannabinol (THC), lowers IOP when inhaled. However, it lowers IOP for only 3 hours, and glaucoma management requires a constant reduction in IOP. Due to its intense side effects of altered mental status, tachycardia, and systemic hypotension, medicinal marijuana is not desirable for the treatment of glaucoma.41
Benefit in combining regimens. Using different classes of drugs produces an additive effect in lowering IOP, so the ophthalmologist may use up to 3 drugs simultaneously. When therapy is begun, a topical drug is often applied to only 1 eye, letting the opposite eye serve as a control. If IOP is not lowered in the treated eye when compared with the control eye, the drug is discontinued (SOR: A).27
Dealing with noncompliance. More than one third of patients exhibit poor compliance with therapy,9 and strict adherence to the regimen is necessary to lower IOP. Instruct patients in proper techniques for taking and using medications, and record dosage and frequency at each physician visit.
Advise patients that glaucoma can progress, but that blindness is not inevitable. Stress the importance of adhering to the prescribed treatment regimen (SOR: C). 13 If poor compliance remains an issue, let the patient know that therapeutic alternatives may be possible (SOR: C). 2
Argon laser trabeculoplasty
Argon laser trabeculoplasty (ALT) is an outpatient procedure. Laser energy is directed at the trabecular meshwork to facilitate aqueous humor outflow. In a large clinical trial with long-term follow-up, initial ALT therapy was found to be at least as effective as initial pharmacological treatment.42
Medical treatment is often continued after ALT.43 In the Early Manifest Glaucoma Trial,25 glaucoma patients randomized to receive ALT therapy plus a topical beta-blocker (betaxolol) had a 30% reduction in IOP. Compared with the control group, patients treated with ALT and beta-blocker exhibited half the risk of visual field deterioration, with a number needed to treat of 2.24 to prevent field loss in a patient with a baseline IOP of 24 mm Hg.
Surgery
Although surgical treatment is generally considered a final alternative in management, it may be an appropriate first-line therapy for patients with cardiovascular or pulmonary conditions contraindicating use of medical therapy. 13
Filtering surgery (trabeculectomy) (Figure) is an outpatient procedure wherein IOP is lowered by creating a fistula in the globe of the eye to drain aqueous humor into the sub-conjunctival space.21 In a randomized controlled trial, trabeculectomy used alone or with medical therapy in a previously unoperated eye successfully lowered IOP by a rate of 85% to 95% at 2 years.44 At 5 years, the success rate in Caucasians is 90%; in African Americans, 80%.44 However, a recent meta-analysis suggests that glaucoma surgery is associated with accelerated progression of cataract.45 The Collaborative Initial Glaucoma Treatment Study (CIGTS) found 3 times the incidence of cataract surgery among subjects randomized to initial filtration surgery as opposed to medical management (P=.0001).46
FIGURE
Filtering surgery for glaucoma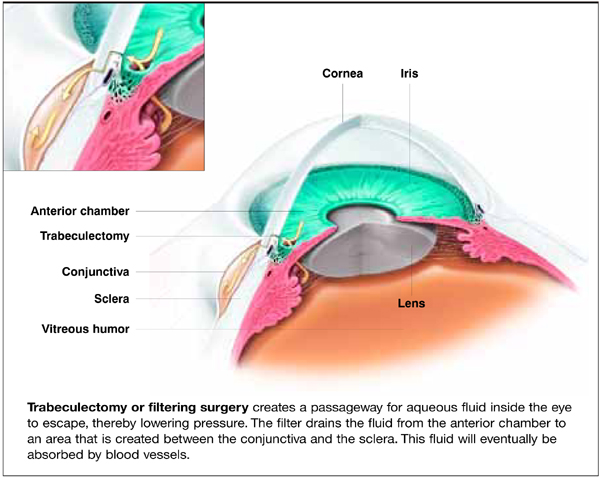
Prognosis
Glaucoma progresses insidiously. Peripheral vision is lost first in early stages of the disease and may not even be noticed by the patient. Central vision is spared until late stages of the disease.
Blindness can usually be prevented if glaucoma is detected early and IOP is lowered sufficiently.47 Unfortunately a small number of patients may suffer irreversible vision loss even with adequate treatment; they should be referred for low-vision rehabilitation and social services (SOR: C).2 In May 2002, the Centers for Medicare and Medicaid Services approved Medicare coverage for these services.48 Services offering rehabilitation for those with low-vision: Prevent Blindness America (preventblindness.org), National Federation of the Blind (www.nfb.org), National Library Service for the Blind and Physically Handicapped (www.loc.gov/nls), and the Foundation Fighting Blindness (www.blindness.org).
- Amlodipine • Norvasc
- Acetazolamide • AK Zol; Diamox
- Apraclonidine • Iopidine
- Betaxolol • Betoptic
- Brimonodine • Alphagan
- Brinzolamide • Azopt
- Carbachol • Carbastat, Carboptic, Isopto Carbachol, Miostat
- Carteolol • Ocupress
- Dorzolamide • Trusopt
- Latanoprost • Xalatan
- Levobunolol • AKBeta, Betagan
- Metipranolol • OptiPranolol
- Timolol • Timoptic
- Travoprost • Travatan
- Unoprostone • Rescula
Corresponding author
Ahmad A. Aref, BS, 401 East Ontario St, Suite 710, Chicago, IL 60611. E-mail:[email protected].
1. Zeyen TG, Caprioli J. Progression of disc and field damage in early glaucoma. Arch Ophthalmol 1993;111:62-65.
2. American Academy of Ophthalmology Glaucoma Panel Primary openangle glaucoma, Limited Revision. Preferred practice pattern. San Francisco: American Academy of Ophthalmology, 2003;1-37.
3. Tielsch JM, Sommer A, Katz J, et al. Racial variations in the prevalence of primary open-angle glaucoma. The Baltimore Eye Survey. JAMA 1991;266:369-374.
4. Quigley HA, Vitale S. Models of glaucoma prevalence and incidence in the United States. Invest Ophthalmol Vis Sci 1997;38:83-91.
5. Schappert SM. Office visits for glaucoma: United States, 1991–92. Adv Data 1995;262:1-14.
6. Albert DM, Dryja TP. The eye. In: Cotran RS, Kumar V, Collins T. Robbins Pathologic Basis of Disease. 6th ed. Philadelphia, Pa: W.B. Saunders Company, 1999;1374-1375.
7. Congdon N, Wang F, Tielsch JM. Issues in epidemiology and population based screening of primary angle-closure glaucoma. Surv Ophthalmol 1992;36:411-423.
8. Wolfs RC, Klaver CC, Ramrattan RS, et al. Genetic risk of primary open angle glaucoma. Population-based familial aggregation study. Arch Ophthalmol 1998;116:1640-1645.
9. Quigley HA. Open-angle glaucoma. N Eng J Med 1993;328:1097-1106.
10. Harper R, Reeves B. The sensitivity and specificity of direct ophthalmoscopic optic disc assessment in screening for glaucoma: a multivariate analysis. Graefes Arch Clin Exp Ophthalmol 2000;238:949-955.
11. Schottenstein EM. Intraocular pressure and tonometry. In: Ritch R, Shields BM, Krupin T. The Glaucomas. 2nd ed. St. Louis, Mo: Mosby Yearbook, 1996;411.-
12. Lichter PR. Variability of expert observers in evaluating the optic disc. Trans Am Ophthalmol Soc 1976;74:532-572.
13. Smith OU, Seligsohn AL, Khan SJ, Spaeth GL. Primary Open Angle Glaucoma. American College of Physicians PIER Guideline. 2004.
14. Tielsch JM, Katz J, Singh K, et al. A population based evaluation of glaucoma screening: The Baltimore Eye Survey. Am J Epidemiol 1991;134:1102-1110.
15. Katz J, Sommer A, Gaasterland DE, Anderson DR. Comparison of analytic algorithms for detecting glaucomatous visual field loss. Arch Ophthalmol 1991;109:1684-1689.
16. Colton T, Ederer F. The distribution of intraocular pressures in the general population. Surv Ophthalmol 1980;25:123.-
17. Brandt JD, Beiser JA, Kass MA, et al. Central corneal thickness in the Ocular Hypertension Treatment Study. Opthalmology 2001;108:1779-1788.
18. Herndon LW, Weizer JS, Stinnett SS. Central corneal thickness as a risk factor for advanced glaucoma damage. Arch Opthalmol 2004;122:17-21.
19. Klein BE, Klein R, Sponsel WE, Franke T, Cantor LB, Martone J. Prevalence of glaucoma. The Beaver Dam Eye Study. Ophthalmology 1992;99:1499-1504.
20. Mitchell P, Smith W, Attebo K, Healey PR. Prevalence of open angle glaucoma in Australia. The Blue Mountains Study. Ophthalmology 1996;103:1661-1669.
21. Burr J, Azuara-Blanco A, Avenell A. Medical versus surgical interventions for open angle glaucoma. The Cochrane Library, Volume 1, 2004.
22. Quigley HA. Identification of glaucoma-related visual field abnormality with the screening protocol of frequency doubling technology. Am J Ophthalmol 1998;125:819-829.
23. The AGIS investigators. The Advanced Glaucoma Intervention Study (AGIS). The relationship between control of intraocular pressure and visual field deterioration. Am J Ophthalmol 2000;130:4:429-440.
24. Collaborative Normal Tension Glaucoma Study Group. Comparison of glaucomatous progression between untreated patients with normaltension glaucoma and patients with therapeutically reduced intraocular pressures. Am J Ophthalmol 1998;126:4:487-497.
25. Leske MC, Heijl A, Hussein M, Bengtsson B, Hyman L, Kornakoff E. Factors for glaucoma progression and the effect of treatment: the early manifest glaucoma trial. Early Manifest Glaucoma Trial Group. Arch Ophthalmol 2003;121:48-56.
26. Johnstone MA. Hypertrichosis and increased pigmentation of eyelashes and adjacent hair in the region of the ipsilateral eyelids of patients treated with unilateral topical latanoprost. Am J Ophthalmol 1997;124:544-547.
27. Alward WL. Medical management of glaucoma. N Eng J Med 1998;339:1298-1307.
28. Coleman AL, Robin AL, Pollack IP, Rudikoff MT, Enger C, Mayer PR. Cardiovascular and intraocular pressure effects and plasma concentrations of apraclonidine. Arch Ophthalmol 1990;108:1264-1267.
29. Butler P, Mannschreck M, Lin S, Hwang I, Alvarado J. Clinical experience with the long term use of 1% apraclonidine: incidence of allergic reactions. Arch Ophthalmol 1995;113:293-296.
30. Nordlund JR, Pasquale LR, Robin AL, et al. The cardiovascular, pulmonary, and ocular hypotensive effects of 2% brimonidine. Arch Ophthalmol 1995;113:77-83.
31. Lippa EA, Schuman JS, Higginbotham EJ, et al. MK507 versus sezolamide: comparative efficacy of two topically active carbonic anhydrase inhibitors. Ophthalmology 1991;98:308-312.
32. Hyong PF, van Beek LM. Pharmacological therapy for glaucoma: a review. Drugs 2000;59:411-434.
33. Avorn J, Glynn RJ, Gurwitz JH, et al. Adverse pulmonary effects of topical beta blockers used in the treatment of glaucoma. J Glaucoma 1993;2:158-165.
34. Leier CV, Baker ND, Weber PA. Cardiovascular effects of ophthalmic timolol. Ann Intern Med 1986;104:197-199.
35. Nelson WL, Kuritsky JN. Early postmarketing surveillance of betaxolol hydrochloride, September 1985 September 1986. Am J Ophthalmol 1987;103:512.-
36. Yogel R, Tipping R, Kudaga SF, Clineschmidt CM. Timolol-Betaxolol Study Group. Changing therapy from timolol to betaxolol: effect on intraocular pressure in selected patients with glaucoma. Arch Ophthalmol 1989;107:1303-1307.
37. Walters TR, DuBiner HB, Carpenter SP, Khan B, VanDenburgh AM. Bimatoprost Circadian IOP Study Group. 24-Hour IOP control with once-daily bimatoprost, timolol gel-forming solution, or latanoprost: a 1-month, randomized, comparative clinical trial. Surv Ophthalmol 2004;49 Suppl 1:S26-S35.
38. Higginbotham EJ, Schuman JS, Goldberg I, et al. One-year randomized study comparing bimatoprost and timolol in glaucoma and ocular hypertension. Arch Ophthalmol 2002;120:1286-1293.
39. Schadlu R, Maus TL, Nau CB, Brubaker RF. Comparison of the efficacy of apraclonidine and brimonidine as aqueous suppressants in humans. Arch Ophthalmol 1998;116:1441-1444.
40. Pappano AJ. Cholinoreceptor activating and cholinesterase inhibiting drugs. In: Katzung BG. Basic and Clinical Pharmacology. 8th ed. New York, NY: Lange Medical Books/McGraw Hill, 2001;102:103.-
41. Green K. Marijuana smoking vs cannabinoids for glaucoma therapy. Arch Ophthalmol 1998;116:1433-1437.
42. The Glaucoma Laser Trial (GLT) and glaucoma laser trial followup study: 7. Results. Am J Ophthalmol 1995;120:718-731.
43. The AGIS Investigators. The Advanced Glaucoma Intervention Study (AGIS): 4. Comparison of treatment outcomes within race. Seven year results. Ophthalmology 1998;105:146-164.
44. Roth SM, Spaeth GL, Starita RJ, et al. The effects of postoperative corticosteroids on trabeculolectomy and the clinical course of glaucoma: five-year follow-up study. Ophthalmic Surg. 1991;22:924-929.
45. Hylton C, Congdon N, Friedman D, et al. Cataract after glaucoma filtration surgery. Am J Ophthalmol 2003;135:231-232.
46. Lichter PR, Musch DC, Gillespie BW, et al. CIGTS Study Group. Interim clinical outcomes in the Collaborative Initial Glaucoma Treatment Study comparing initial treatment randomized to medications or surgery. Ophthalmology 2001;108:1943-1953.
47. Bradford CA. Basic Ophthalmology. 7th ed. San Francisco, Calif: American Academy of Ophthalmology, 1999.
48. Gieser JP. When treatment fails, caring for patients with visual disability. Arch Ophthalmol 2004;122:1208-1209.
- Screen persons older than 60 years, African Americans of any age, and those with a family history of open-angle glaucoma (C). Further evaluation by an ophthalmologist is warranted if optic nerve damage is suspected or if a patient reports decreasing vision.
- Elevated intraocular pressure (IOP) is not necessary for open-angle glaucoma to occur. Assess optic nerve status and visual field in those at risk. (C)
- Inquire about topical ocular drops recommended by an ophthalmologist, to be certain they are not contraindicated for other conditions the patient might have, and to be alert to the potential for adverse effects. (C)
Evaluate for open-angle glaucoma (OAG) when a patient reports decreased vision, or when a patient even with good eyesight is found to be at high risk for the disease. Most patients with early glaucoma are unaware of the initial decrease in peripheral vision.1
A relatively new diagnostic technique can detect even moderate damage to the optic nerve, and the procedure is brief. Ophthalmologists can choose from among several topical medications to reduce intraocular pressure. Your knowledge of the patient’s medical history is critical to avoiding potential drug-drug interactions.
Laser surgery and trabeculectomy may be indicated as first-line therapy for select patients.
Whom to screen
Persons aged older than 60 years, African Americans of any age, and those with a family history of OAG are at particularly high risk, and all risk factors should be fully assessed (SOR: B).2 (See Open-angle glaucoma: The scope of the problem.)
In the Caucasian population aged 40 to 49 years with no family history of OAG, disease prevalence is just 0.18%. Prevalence is 4 times greater in African Americans of the same age range. Caucasians aged 60 to 69 years have a prevalence of OAG 4 times greater than patients aged 40 to 49. For African Americans older than 80 years, prevalence exceeds 11%.3
For persons with a first-degree relative with OAG, risk was found to be 9.2 times greater than for those without such a history.8
Ask specifically about decreased vision, loss of peripheral vision, difficulty seeing in the dark, and difficulty reading (SOR: B).
Before referring high-risk patients for a full ophthalmologic examination, examine the optic nerve with direct ophthalmoscopy (SOR: B).
Open-angle glaucoma (OAG) is defined as an optic neuropathy in which there is damage to the optic nerve with a loss of retinal ganglion cells that carry visual impulses from the eye to the brain. It is the second most common cause of legal blindness in the United States and the leading cause of blindness among African Americans.2 A population-based evaluation of glaucoma screening, the Baltimore Eye Survey, estimates about 2.5 million Americans as having OAG with as many as half of them unaware that they have the disease.3,4
More than 8 million office visits to office-based clinicians occur per year by patients with a primary diagnosis of glaucoma.5 The National Eye Institute, a division of the NIH, reports that as many as 120,000 Americans are currently blind as a result of glaucoma, costing the US government over $1.5 billion annually in Social Security benefits, lost income tax revenues, and health care expenditures.
An asymptomatic disease in its early stages,1 glaucoma progresses to cause permanent blindness in the absence of treatment. This article addresses the features, diagnostic methods, and treatment modalities of glaucoma as well as the role of the family physician in its management.
What causes OAG?
The pathogenesis of glaucoma is multifactorial and is thought, in most cases, to be caused by an abnormally high intraocular pressure (IOP), which mechanically compresses and causes subsequent atrophy of optic nerve fibers. The increased pressure is due to impaired drainage of aqueous humor out of the eye. Aqueous humor, produced by the ciliary body, normally provides nutrients to the iris, lens, and cornea before being drained through the trabecular meshwork.
It should be noted, however, that an elevated IOP is not necessary in glaucoma; optic nerve atrophy can occur in the absence of high IOP. The mechanism for optic nerve damage in this form of glaucoma is unknown.6
In angle-closure glaucoma, the angle between the iris and the trabecular meshwork is occluded, preventing normal drainage of aqueous humor. In open-angle glaucoma, the angle appears open but does not function properly in draining aqueous humor out of the eye.6 It is open-angle glaucoma that will be discussed here as it accounts for 75% to 95% of all glaucoma cases.7
Determining optic nerve status
Examination of the optic nerve head provides clues as to whether structural damage has occurred. Cup-disc ratio is used to assess risk of glaucoma development. The probability of abnormality increases dramatically for values above 0.5.9
The standard clinical technique used by primary care clinicians is with the direct ophthalmoscope. Sensitivity and specificity for a cup-disc ratio greater than 0.6 have been reported to be 64% and 96%, respectively, using direct ophthalmoscopy.10
Ophthalmologists use stereoscopic fundus photography to visualize the optic nerve. With this technique, sensitivity and specificity for a cup-disc ratio greater than 0.5 have been found to be 48% and 89%, respectively.11 Studies, however, have reported a high interobserver variation in measurement of the cup-disc ratio even among experts in the field.12
What to look for. Characteristic changes include narrowing or notching of the neuroretinal rim, or characteristic visual field loss, such as arcuate defects and nasal loss.13 Describe an abnormal optic disc in terms of its cup-disc ratio, and report visual loss to the ophthalmologist as a defect in a respective field quadrant as detected on confrontational visual field testing or as an afferent pupillary defect in a given eye.
Referral. A final diagnosis of open-angle glaucoma can be made only after characteristic damage to the optic nerve has been confirmed by an ophthalmologist (SOR: B). Therefore, patients at high risk of developing OAG (age >60 years, African American race, positive family history) should be referred for an eye examination.
Other key diagnostic tests include measurement of intraocular pressure and visual field testing.2 The accuracy of these tests is outlined in Table 1.
TABLE 1
Characteristics of diagnostic tests for open-angle glaucoma
| Test | Study quality | Sn% | Sp% | LR+ | LR– | PV+ | PV– |
|---|---|---|---|---|---|---|---|
| Tonometry14 | 2 | ||||||
| IOP >21 mm Hg | 47.1 | 92.4 | 6.20 | 24.6 | |||
| IOP <21 mm Hg | .57 | 97 | |||||
| Cup-disc ratio, stereoscopic photography14 | 2 | ||||||
| Cup-disc ratio >.5 | 48 | 89 | 4.36 | .187 | |||
| Cup-disc ratio <.5 | .58 | 97 | |||||
| Cup-disc ratio, direct ophthalmoscopy10 | 1 | ||||||
| Cup-disc ratio >.6 | 64 | 96 | 16 | 46 | |||
| Cup-disc ratio <.6 | .375 | 98 | |||||
| Visual field15 | 2 | ||||||
| Abnormal | 97 | 84 | 6.06 | 24.2 | |||
| Normal | .036 | 99.8 | |||||
| LR+ = positive likelihood ratio; the likelihood that a person with OAG will have a positive test result (eg, a person with OAG is 16 times more likely to exhibit a cup-disc ratio >.6 than a person without the disease). See “Using the likelihood ratio,” page 127 of this issue. | |||||||
| LR– = negative likelihood ratio; the likelihood that a person with OAG will have a negative test result (eg, a person with OAG is only .375 times as likely to exhibit a cup-disc ratio <.6 as a person without the disease) | |||||||
| PV+ = positive predictive value; the probability that a positive test result indicates disease | |||||||
| PV– = negative predictive value; the probability that a negative test result indicates absence of disease | |||||||
| PV+ and PV- assume a baseline likelihood of disease of 5% (prevalence among African Americans aged 60–69 years)3 | |||||||
Intraocular pressure: Caveats
Intraocular pressure (IOP) is measured by a tonometer. The eye is subjected to a force that flattens the cornea. This force is then related to the pressure in the eye, or IOP. The standard instrument for measuring IOP is the Goldman applanation tonometer. Handheld versions (tonopen) are useful for screening by the primary care clinician.11 Studies of IOP distribution show the normal range of IOP values to be less than 21 mm Hg with a slight skew towards higher values.16
The altering effect of corneal thickness. IOP measurement may vary with the thickness of one’s cornea. A corneal thickness greater than 555 μm can produce falsely high readings, and a corneal thickness less than 540 μm can produce falsely low readings.2,17,18 Thus, central corneal thickness (CCT) is a factor that may affect the accuracy of an IOP reading. Central corneal thickness is measured with a pachymeter, and an ophthalmologist must take this measurement into account when assessing a patient’s IOP.
Pressure may not be elevated in OAG. A number of population-based studies have documented an increase in the prevalence of OAG with an increase in IOP.7,19,20 However, these same studies have also concluded that many patients with OAG have IOP levels in the normal range. These patients are deemed to have normal pressure glaucoma (NPG), a subtype of OAG.21
Likewise, many patients with elevated IOP have no demonstrable optic nerve damage;19,20 this condition has been termed ocular hypertension (OHT).
A proper perspective. So, although an elevated IOP is associated with glaucoma, it is important to note that OAG is not defined by the presence of an elevated IOP. Optic nerve atrophy can occur in the absence of an increased IOP. 21 These findings, taken together with the variance of IOP with CCT, are reflected in the modest sensitivity and specificity for IOP readings greater than 21 mm Hg—47.1% and 92.4%, respectively. 14 Patients with a high IOP (>21 mm Hg) are at higher risk for developing OAG, but further ancillary studies and tests are necessary to confirm the diagnosis. 13
Evaluating the visual field
Visual field deterioration is the final manifestation of glaucoma. Vision is first lost peripherally. Central vision loss occurs at the end stage of the disease.
An ophthalmologist will use automated static threshold perimetry to evaluate the visual field. With this technique, the patient must identify white target lights of variable brightness in different locations of a dim 1-m bowl. Various data algorithms are then employed to compare any abnormality in the visual field with patterns that are characteristic of glaucoma.9 One study reported a 97% sensitivity and 84% specificity using a certain algorithm to recognize field abnormalities due to glaucoma.15 However, automated perimetry requires 10 to 20 minutes per eye, and patient fatigue often reduces reliability of the test. Also, an optic nerve head has typically undergone considerable damage before visual field changes are detected.2
An improved test. Frequency doubling technology promises to detect glaucomatous visual defects when there has been only moderate damage to the optic nerve. With frequency doubling technology, patients must recognize patterns of alternating light and dark bars. An abnormality in recognition is thought to be indicative of the pattern of field loss in glaucoma. One study found a sensitivity and specificity each greater than 90% for identifying patients thought to have glaucoma. Another benefit is that the exam takes an average of only 6 minutes to complete in both eyes. 22
No single test result is enough
Successful screening for glaucoma should not rely solely on measuring IOP, assessment of the optic nerve, or visual field testing. These diagnostic clues are complementary and must be taken together to evaluate high-risk populations, including African Americans, those with a family history of glaucoma, and the elderly (SOR: C).
Regular follow-up
Regardless of findings, patients aged 40 to 60 years should be encouraged to have eye exams every other year, and those over age 60 should have annual eye exams (SOR: B).13 Regular ocular exams including vision check, extraocular muscle exam, papillary exam, and confrontational visual fields should be performed in these patients as well (SOR: C).
Treatment
IOP is the only risk factor for glaucoma that can be treated. Lowering IOP in randomized control trials has reduced the progression of visual field loss in OAG patients with abnormally high pressures23 as well as in NPG patients with pressures in the normal range.24
In the Early Manifest Glaucoma Trial, a 30% reduction in IOP reduced the rate of progression in the treatment group (45%) compared with the control group (62%; P=.007).25 Progression risk decreased by approximately 10% per mm Hg of IOP reduction.
Setting a target pressure. Before beginning therapy, an ophthalmologist sets a target pressure that should halt further optic nerve damage. The initial target pressure is usually 20% to 30% lower than the pretreatment pressure. If damage to the optic nerve is already substantial, the target pressure may be set even lower.2
Stepwise therapy. Topical medications are usually given first, as eye drops. A comparison of these medications is outlined in Table 2. If IOP cannot be lowered pharmacologically, argon laser trabeculoplasty (ALT) is the next step. If the pressure still cannot be lowered, filtering surgery is the final alternative (SOR: C).2
TABLE 2
Pharmacologic options for patients with open-angle glaucoma
| Medication(SOR) | % IOP reduction | % RR* | NNT to prevent visualfield loss* | Side effects | Comments |
|---|---|---|---|---|---|
| Beta-blockers (A), non-selective (timolol, carteolol, levobunolol, metipranolol) and selective (betaxolol) | 31 | 74 | 2.17 | Bradycardia, hypotension, bronchospasm (timolol, carteolol, levobunolol, metipranolol) | Cochrane review with clear recommendation as first-line treatment21 |
| Prostaglandin analogues (A) (latanoprost, travoprost, unoprostone) | 40 | 96 | 1.68 | Increased eyelash growth, iris pigmentation, muscle and joint pain | Multiple RCTs and systematic review show show clinical and statistical superiorityover beta-blockers26,27 |
| Alpha adrenergic drugs (A) (apraclonidine, brimonidine) | 23 | 55 | 2.93 | Dry nose, dry mouth, follicular conjunctivitis, hypotension (brimonidine) | Multiple RCTs support effectiveness 28-30 |
| Topical carbonic anhydrase inhibitors (A) (brinzolamide, dorzolamide) | 26 | 62 | 2.6 | GI disturbances, headache, local irritation, redness, sulfa allergies | RCT,31 Cochranereview with clear recommendation26 |
| Cholinergic agonists (A) (pilocarpine, carbachol) | 29 | 69 | 2.32 | Small, fixed pupils, induced myopia, cataracts | Consistently recommended assecond-or third-line drugs in systematic reviews and RCTs27,32 |
| *Percent decrease in risk of visual field loss and NNT to prevent visual field loss were calculated for a patient with a baseline IOP of 24 mm Hg. | |||||
| SOR, strength of recommendation; IOP, intraocular pressure; RR, relative risk; NNT, number needed to treat; RCT, randomized controlled trial. | |||||
Pharmacologic options
Medical agents work in 1 of 2 ways to lower IOP: by decreasing production of aqueous humor, or by increasing drainage of aqueous humor out of the eye. Though most glaucoma medications are given topically, severe systemic side effects can occur.2 Because the consulting ophthalmologist may not be aware of a patient’s other medical conditions, inquire about the topical ocular drops being recommended to make certain they are not contraindicated and to be alert to the potential for adverse effects (SOR: C).13
Beta-adrenergic antagonists can lower IOP by up to 31% 25 and are often used as first-line treatment (SOR: A).21 However, nonselective beta-blockers (timolol, carteolol, levobunolol, metipranolol) are associated with a number of adverse effects including bronchospasm,33 bradycardia, and hypotension. 34
Betaxolol is a selective beta-blocker with less tendency to cause pulmonary side effects,34 but it may still do so in patients with severe pulmonary disease.35 Selective beta-blockers lower IOP to a lesser degree than nonselective drugs36 and can cause the same cardiac effects of bradycardia and hypotension.38
Prostaglandin analogs (latanoprost, travoprost, unoprostone) increase drainage of the aqueous humor. Prostaglandins are clinically and statistically superior to beta-blockers, having lowered IOP by up to 40% in randomized controlled trials.37 Side effects include increased eyelash growth and iris pigmentation,26 and muscle and joint pain.38
Alpha-adrenergic drugs (apraclonidine, brimonidine) lower aqueous humor production. Apraclonidine administered topically does not cross the blood-brain barrier, effectively lowering IOP without causing cardiovascular side effects.28 The most common side effects are dry nose, dry mouth,28 and follicular conjunctivitis.29 Unlike apraclonidine, brimonidine crosses the blood-brain barrier and can cause mild hypotension.30 One randomized controlled trial found no statistical difference in efficacy between brimonidine and apraclonidine, both lowering IOP by up to 23%.39
Carbonic anhydrase inhibitors block water flow into the eye, preventing aqueous humor formation. Until recently, carbonic anhydrase inhibitors such as acetazolamide were administered only orally and adverse effects were therefore common.27 Topical carbonic anhydrase inhibitors (brinzolamide, dorzolamide), recently introduced, lower IOP by up to 26% and with few side effects.31
Cholinergic agonists (pilocarpine, carbachol) increase aqueous outflow from the eye by stimulating contraction of the ciliary body, which opens the trabecular meshwork to allow further drainage.40 Because of its ocular side effects including small, fixed pupils, induced myopia, and cataracts, pilocarpine is reserved for second-or third-line therapy (SOR: A). 9,27,32
Medicinal marijuana used to lower IOP in glaucoma patients is controversial. The primary active ingredient in marijuana, tetrahydrocannabinol (THC), lowers IOP when inhaled. However, it lowers IOP for only 3 hours, and glaucoma management requires a constant reduction in IOP. Due to its intense side effects of altered mental status, tachycardia, and systemic hypotension, medicinal marijuana is not desirable for the treatment of glaucoma.41
Benefit in combining regimens. Using different classes of drugs produces an additive effect in lowering IOP, so the ophthalmologist may use up to 3 drugs simultaneously. When therapy is begun, a topical drug is often applied to only 1 eye, letting the opposite eye serve as a control. If IOP is not lowered in the treated eye when compared with the control eye, the drug is discontinued (SOR: A).27
Dealing with noncompliance. More than one third of patients exhibit poor compliance with therapy,9 and strict adherence to the regimen is necessary to lower IOP. Instruct patients in proper techniques for taking and using medications, and record dosage and frequency at each physician visit.
Advise patients that glaucoma can progress, but that blindness is not inevitable. Stress the importance of adhering to the prescribed treatment regimen (SOR: C). 13 If poor compliance remains an issue, let the patient know that therapeutic alternatives may be possible (SOR: C). 2
Argon laser trabeculoplasty
Argon laser trabeculoplasty (ALT) is an outpatient procedure. Laser energy is directed at the trabecular meshwork to facilitate aqueous humor outflow. In a large clinical trial with long-term follow-up, initial ALT therapy was found to be at least as effective as initial pharmacological treatment.42
Medical treatment is often continued after ALT.43 In the Early Manifest Glaucoma Trial,25 glaucoma patients randomized to receive ALT therapy plus a topical beta-blocker (betaxolol) had a 30% reduction in IOP. Compared with the control group, patients treated with ALT and beta-blocker exhibited half the risk of visual field deterioration, with a number needed to treat of 2.24 to prevent field loss in a patient with a baseline IOP of 24 mm Hg.
Surgery
Although surgical treatment is generally considered a final alternative in management, it may be an appropriate first-line therapy for patients with cardiovascular or pulmonary conditions contraindicating use of medical therapy. 13
Filtering surgery (trabeculectomy) (Figure) is an outpatient procedure wherein IOP is lowered by creating a fistula in the globe of the eye to drain aqueous humor into the sub-conjunctival space.21 In a randomized controlled trial, trabeculectomy used alone or with medical therapy in a previously unoperated eye successfully lowered IOP by a rate of 85% to 95% at 2 years.44 At 5 years, the success rate in Caucasians is 90%; in African Americans, 80%.44 However, a recent meta-analysis suggests that glaucoma surgery is associated with accelerated progression of cataract.45 The Collaborative Initial Glaucoma Treatment Study (CIGTS) found 3 times the incidence of cataract surgery among subjects randomized to initial filtration surgery as opposed to medical management (P=.0001).46
FIGURE
Filtering surgery for glaucoma
Prognosis
Glaucoma progresses insidiously. Peripheral vision is lost first in early stages of the disease and may not even be noticed by the patient. Central vision is spared until late stages of the disease.
Blindness can usually be prevented if glaucoma is detected early and IOP is lowered sufficiently.47 Unfortunately a small number of patients may suffer irreversible vision loss even with adequate treatment; they should be referred for low-vision rehabilitation and social services (SOR: C).2 In May 2002, the Centers for Medicare and Medicaid Services approved Medicare coverage for these services.48 Services offering rehabilitation for those with low-vision: Prevent Blindness America (preventblindness.org), National Federation of the Blind (www.nfb.org), National Library Service for the Blind and Physically Handicapped (www.loc.gov/nls), and the Foundation Fighting Blindness (www.blindness.org).
- Amlodipine • Norvasc
- Acetazolamide • AK Zol; Diamox
- Apraclonidine • Iopidine
- Betaxolol • Betoptic
- Brimonodine • Alphagan
- Brinzolamide • Azopt
- Carbachol • Carbastat, Carboptic, Isopto Carbachol, Miostat
- Carteolol • Ocupress
- Dorzolamide • Trusopt
- Latanoprost • Xalatan
- Levobunolol • AKBeta, Betagan
- Metipranolol • OptiPranolol
- Timolol • Timoptic
- Travoprost • Travatan
- Unoprostone • Rescula
Corresponding author
Ahmad A. Aref, BS, 401 East Ontario St, Suite 710, Chicago, IL 60611. E-mail:[email protected].
- Screen persons older than 60 years, African Americans of any age, and those with a family history of open-angle glaucoma (C). Further evaluation by an ophthalmologist is warranted if optic nerve damage is suspected or if a patient reports decreasing vision.
- Elevated intraocular pressure (IOP) is not necessary for open-angle glaucoma to occur. Assess optic nerve status and visual field in those at risk. (C)
- Inquire about topical ocular drops recommended by an ophthalmologist, to be certain they are not contraindicated for other conditions the patient might have, and to be alert to the potential for adverse effects. (C)
Evaluate for open-angle glaucoma (OAG) when a patient reports decreased vision, or when a patient even with good eyesight is found to be at high risk for the disease. Most patients with early glaucoma are unaware of the initial decrease in peripheral vision.1
A relatively new diagnostic technique can detect even moderate damage to the optic nerve, and the procedure is brief. Ophthalmologists can choose from among several topical medications to reduce intraocular pressure. Your knowledge of the patient’s medical history is critical to avoiding potential drug-drug interactions.
Laser surgery and trabeculectomy may be indicated as first-line therapy for select patients.
Whom to screen
Persons aged older than 60 years, African Americans of any age, and those with a family history of OAG are at particularly high risk, and all risk factors should be fully assessed (SOR: B).2 (See Open-angle glaucoma: The scope of the problem.)
In the Caucasian population aged 40 to 49 years with no family history of OAG, disease prevalence is just 0.18%. Prevalence is 4 times greater in African Americans of the same age range. Caucasians aged 60 to 69 years have a prevalence of OAG 4 times greater than patients aged 40 to 49. For African Americans older than 80 years, prevalence exceeds 11%.3
For persons with a first-degree relative with OAG, risk was found to be 9.2 times greater than for those without such a history.8
Ask specifically about decreased vision, loss of peripheral vision, difficulty seeing in the dark, and difficulty reading (SOR: B).
Before referring high-risk patients for a full ophthalmologic examination, examine the optic nerve with direct ophthalmoscopy (SOR: B).
Open-angle glaucoma (OAG) is defined as an optic neuropathy in which there is damage to the optic nerve with a loss of retinal ganglion cells that carry visual impulses from the eye to the brain. It is the second most common cause of legal blindness in the United States and the leading cause of blindness among African Americans.2 A population-based evaluation of glaucoma screening, the Baltimore Eye Survey, estimates about 2.5 million Americans as having OAG with as many as half of them unaware that they have the disease.3,4
More than 8 million office visits to office-based clinicians occur per year by patients with a primary diagnosis of glaucoma.5 The National Eye Institute, a division of the NIH, reports that as many as 120,000 Americans are currently blind as a result of glaucoma, costing the US government over $1.5 billion annually in Social Security benefits, lost income tax revenues, and health care expenditures.
An asymptomatic disease in its early stages,1 glaucoma progresses to cause permanent blindness in the absence of treatment. This article addresses the features, diagnostic methods, and treatment modalities of glaucoma as well as the role of the family physician in its management.
What causes OAG?
The pathogenesis of glaucoma is multifactorial and is thought, in most cases, to be caused by an abnormally high intraocular pressure (IOP), which mechanically compresses and causes subsequent atrophy of optic nerve fibers. The increased pressure is due to impaired drainage of aqueous humor out of the eye. Aqueous humor, produced by the ciliary body, normally provides nutrients to the iris, lens, and cornea before being drained through the trabecular meshwork.
It should be noted, however, that an elevated IOP is not necessary in glaucoma; optic nerve atrophy can occur in the absence of high IOP. The mechanism for optic nerve damage in this form of glaucoma is unknown.6
In angle-closure glaucoma, the angle between the iris and the trabecular meshwork is occluded, preventing normal drainage of aqueous humor. In open-angle glaucoma, the angle appears open but does not function properly in draining aqueous humor out of the eye.6 It is open-angle glaucoma that will be discussed here as it accounts for 75% to 95% of all glaucoma cases.7
Determining optic nerve status
Examination of the optic nerve head provides clues as to whether structural damage has occurred. Cup-disc ratio is used to assess risk of glaucoma development. The probability of abnormality increases dramatically for values above 0.5.9
The standard clinical technique used by primary care clinicians is with the direct ophthalmoscope. Sensitivity and specificity for a cup-disc ratio greater than 0.6 have been reported to be 64% and 96%, respectively, using direct ophthalmoscopy.10
Ophthalmologists use stereoscopic fundus photography to visualize the optic nerve. With this technique, sensitivity and specificity for a cup-disc ratio greater than 0.5 have been found to be 48% and 89%, respectively.11 Studies, however, have reported a high interobserver variation in measurement of the cup-disc ratio even among experts in the field.12
What to look for. Characteristic changes include narrowing or notching of the neuroretinal rim, or characteristic visual field loss, such as arcuate defects and nasal loss.13 Describe an abnormal optic disc in terms of its cup-disc ratio, and report visual loss to the ophthalmologist as a defect in a respective field quadrant as detected on confrontational visual field testing or as an afferent pupillary defect in a given eye.
Referral. A final diagnosis of open-angle glaucoma can be made only after characteristic damage to the optic nerve has been confirmed by an ophthalmologist (SOR: B). Therefore, patients at high risk of developing OAG (age >60 years, African American race, positive family history) should be referred for an eye examination.
Other key diagnostic tests include measurement of intraocular pressure and visual field testing.2 The accuracy of these tests is outlined in Table 1.
TABLE 1
Characteristics of diagnostic tests for open-angle glaucoma
| Test | Study quality | Sn% | Sp% | LR+ | LR– | PV+ | PV– |
|---|---|---|---|---|---|---|---|
| Tonometry14 | 2 | ||||||
| IOP >21 mm Hg | 47.1 | 92.4 | 6.20 | 24.6 | |||
| IOP <21 mm Hg | .57 | 97 | |||||
| Cup-disc ratio, stereoscopic photography14 | 2 | ||||||
| Cup-disc ratio >.5 | 48 | 89 | 4.36 | .187 | |||
| Cup-disc ratio <.5 | .58 | 97 | |||||
| Cup-disc ratio, direct ophthalmoscopy10 | 1 | ||||||
| Cup-disc ratio >.6 | 64 | 96 | 16 | 46 | |||
| Cup-disc ratio <.6 | .375 | 98 | |||||
| Visual field15 | 2 | ||||||
| Abnormal | 97 | 84 | 6.06 | 24.2 | |||
| Normal | .036 | 99.8 | |||||
| LR+ = positive likelihood ratio; the likelihood that a person with OAG will have a positive test result (eg, a person with OAG is 16 times more likely to exhibit a cup-disc ratio >.6 than a person without the disease). See “Using the likelihood ratio,” page 127 of this issue. | |||||||
| LR– = negative likelihood ratio; the likelihood that a person with OAG will have a negative test result (eg, a person with OAG is only .375 times as likely to exhibit a cup-disc ratio <.6 as a person without the disease) | |||||||
| PV+ = positive predictive value; the probability that a positive test result indicates disease | |||||||
| PV– = negative predictive value; the probability that a negative test result indicates absence of disease | |||||||
| PV+ and PV- assume a baseline likelihood of disease of 5% (prevalence among African Americans aged 60–69 years)3 | |||||||
Intraocular pressure: Caveats
Intraocular pressure (IOP) is measured by a tonometer. The eye is subjected to a force that flattens the cornea. This force is then related to the pressure in the eye, or IOP. The standard instrument for measuring IOP is the Goldman applanation tonometer. Handheld versions (tonopen) are useful for screening by the primary care clinician.11 Studies of IOP distribution show the normal range of IOP values to be less than 21 mm Hg with a slight skew towards higher values.16
The altering effect of corneal thickness. IOP measurement may vary with the thickness of one’s cornea. A corneal thickness greater than 555 μm can produce falsely high readings, and a corneal thickness less than 540 μm can produce falsely low readings.2,17,18 Thus, central corneal thickness (CCT) is a factor that may affect the accuracy of an IOP reading. Central corneal thickness is measured with a pachymeter, and an ophthalmologist must take this measurement into account when assessing a patient’s IOP.
Pressure may not be elevated in OAG. A number of population-based studies have documented an increase in the prevalence of OAG with an increase in IOP.7,19,20 However, these same studies have also concluded that many patients with OAG have IOP levels in the normal range. These patients are deemed to have normal pressure glaucoma (NPG), a subtype of OAG.21
Likewise, many patients with elevated IOP have no demonstrable optic nerve damage;19,20 this condition has been termed ocular hypertension (OHT).
A proper perspective. So, although an elevated IOP is associated with glaucoma, it is important to note that OAG is not defined by the presence of an elevated IOP. Optic nerve atrophy can occur in the absence of an increased IOP. 21 These findings, taken together with the variance of IOP with CCT, are reflected in the modest sensitivity and specificity for IOP readings greater than 21 mm Hg—47.1% and 92.4%, respectively. 14 Patients with a high IOP (>21 mm Hg) are at higher risk for developing OAG, but further ancillary studies and tests are necessary to confirm the diagnosis. 13
Evaluating the visual field
Visual field deterioration is the final manifestation of glaucoma. Vision is first lost peripherally. Central vision loss occurs at the end stage of the disease.
An ophthalmologist will use automated static threshold perimetry to evaluate the visual field. With this technique, the patient must identify white target lights of variable brightness in different locations of a dim 1-m bowl. Various data algorithms are then employed to compare any abnormality in the visual field with patterns that are characteristic of glaucoma.9 One study reported a 97% sensitivity and 84% specificity using a certain algorithm to recognize field abnormalities due to glaucoma.15 However, automated perimetry requires 10 to 20 minutes per eye, and patient fatigue often reduces reliability of the test. Also, an optic nerve head has typically undergone considerable damage before visual field changes are detected.2
An improved test. Frequency doubling technology promises to detect glaucomatous visual defects when there has been only moderate damage to the optic nerve. With frequency doubling technology, patients must recognize patterns of alternating light and dark bars. An abnormality in recognition is thought to be indicative of the pattern of field loss in glaucoma. One study found a sensitivity and specificity each greater than 90% for identifying patients thought to have glaucoma. Another benefit is that the exam takes an average of only 6 minutes to complete in both eyes. 22
No single test result is enough
Successful screening for glaucoma should not rely solely on measuring IOP, assessment of the optic nerve, or visual field testing. These diagnostic clues are complementary and must be taken together to evaluate high-risk populations, including African Americans, those with a family history of glaucoma, and the elderly (SOR: C).
Regular follow-up
Regardless of findings, patients aged 40 to 60 years should be encouraged to have eye exams every other year, and those over age 60 should have annual eye exams (SOR: B).13 Regular ocular exams including vision check, extraocular muscle exam, papillary exam, and confrontational visual fields should be performed in these patients as well (SOR: C).
Treatment
IOP is the only risk factor for glaucoma that can be treated. Lowering IOP in randomized control trials has reduced the progression of visual field loss in OAG patients with abnormally high pressures23 as well as in NPG patients with pressures in the normal range.24
In the Early Manifest Glaucoma Trial, a 30% reduction in IOP reduced the rate of progression in the treatment group (45%) compared with the control group (62%; P=.007).25 Progression risk decreased by approximately 10% per mm Hg of IOP reduction.
Setting a target pressure. Before beginning therapy, an ophthalmologist sets a target pressure that should halt further optic nerve damage. The initial target pressure is usually 20% to 30% lower than the pretreatment pressure. If damage to the optic nerve is already substantial, the target pressure may be set even lower.2
Stepwise therapy. Topical medications are usually given first, as eye drops. A comparison of these medications is outlined in Table 2. If IOP cannot be lowered pharmacologically, argon laser trabeculoplasty (ALT) is the next step. If the pressure still cannot be lowered, filtering surgery is the final alternative (SOR: C).2
TABLE 2
Pharmacologic options for patients with open-angle glaucoma
| Medication(SOR) | % IOP reduction | % RR* | NNT to prevent visualfield loss* | Side effects | Comments |
|---|---|---|---|---|---|
| Beta-blockers (A), non-selective (timolol, carteolol, levobunolol, metipranolol) and selective (betaxolol) | 31 | 74 | 2.17 | Bradycardia, hypotension, bronchospasm (timolol, carteolol, levobunolol, metipranolol) | Cochrane review with clear recommendation as first-line treatment21 |
| Prostaglandin analogues (A) (latanoprost, travoprost, unoprostone) | 40 | 96 | 1.68 | Increased eyelash growth, iris pigmentation, muscle and joint pain | Multiple RCTs and systematic review show show clinical and statistical superiorityover beta-blockers26,27 |
| Alpha adrenergic drugs (A) (apraclonidine, brimonidine) | 23 | 55 | 2.93 | Dry nose, dry mouth, follicular conjunctivitis, hypotension (brimonidine) | Multiple RCTs support effectiveness 28-30 |
| Topical carbonic anhydrase inhibitors (A) (brinzolamide, dorzolamide) | 26 | 62 | 2.6 | GI disturbances, headache, local irritation, redness, sulfa allergies | RCT,31 Cochranereview with clear recommendation26 |
| Cholinergic agonists (A) (pilocarpine, carbachol) | 29 | 69 | 2.32 | Small, fixed pupils, induced myopia, cataracts | Consistently recommended assecond-or third-line drugs in systematic reviews and RCTs27,32 |
| *Percent decrease in risk of visual field loss and NNT to prevent visual field loss were calculated for a patient with a baseline IOP of 24 mm Hg. | |||||
| SOR, strength of recommendation; IOP, intraocular pressure; RR, relative risk; NNT, number needed to treat; RCT, randomized controlled trial. | |||||
Pharmacologic options
Medical agents work in 1 of 2 ways to lower IOP: by decreasing production of aqueous humor, or by increasing drainage of aqueous humor out of the eye. Though most glaucoma medications are given topically, severe systemic side effects can occur.2 Because the consulting ophthalmologist may not be aware of a patient’s other medical conditions, inquire about the topical ocular drops being recommended to make certain they are not contraindicated and to be alert to the potential for adverse effects (SOR: C).13
Beta-adrenergic antagonists can lower IOP by up to 31% 25 and are often used as first-line treatment (SOR: A).21 However, nonselective beta-blockers (timolol, carteolol, levobunolol, metipranolol) are associated with a number of adverse effects including bronchospasm,33 bradycardia, and hypotension. 34
Betaxolol is a selective beta-blocker with less tendency to cause pulmonary side effects,34 but it may still do so in patients with severe pulmonary disease.35 Selective beta-blockers lower IOP to a lesser degree than nonselective drugs36 and can cause the same cardiac effects of bradycardia and hypotension.38
Prostaglandin analogs (latanoprost, travoprost, unoprostone) increase drainage of the aqueous humor. Prostaglandins are clinically and statistically superior to beta-blockers, having lowered IOP by up to 40% in randomized controlled trials.37 Side effects include increased eyelash growth and iris pigmentation,26 and muscle and joint pain.38
Alpha-adrenergic drugs (apraclonidine, brimonidine) lower aqueous humor production. Apraclonidine administered topically does not cross the blood-brain barrier, effectively lowering IOP without causing cardiovascular side effects.28 The most common side effects are dry nose, dry mouth,28 and follicular conjunctivitis.29 Unlike apraclonidine, brimonidine crosses the blood-brain barrier and can cause mild hypotension.30 One randomized controlled trial found no statistical difference in efficacy between brimonidine and apraclonidine, both lowering IOP by up to 23%.39
Carbonic anhydrase inhibitors block water flow into the eye, preventing aqueous humor formation. Until recently, carbonic anhydrase inhibitors such as acetazolamide were administered only orally and adverse effects were therefore common.27 Topical carbonic anhydrase inhibitors (brinzolamide, dorzolamide), recently introduced, lower IOP by up to 26% and with few side effects.31
Cholinergic agonists (pilocarpine, carbachol) increase aqueous outflow from the eye by stimulating contraction of the ciliary body, which opens the trabecular meshwork to allow further drainage.40 Because of its ocular side effects including small, fixed pupils, induced myopia, and cataracts, pilocarpine is reserved for second-or third-line therapy (SOR: A). 9,27,32
Medicinal marijuana used to lower IOP in glaucoma patients is controversial. The primary active ingredient in marijuana, tetrahydrocannabinol (THC), lowers IOP when inhaled. However, it lowers IOP for only 3 hours, and glaucoma management requires a constant reduction in IOP. Due to its intense side effects of altered mental status, tachycardia, and systemic hypotension, medicinal marijuana is not desirable for the treatment of glaucoma.41
Benefit in combining regimens. Using different classes of drugs produces an additive effect in lowering IOP, so the ophthalmologist may use up to 3 drugs simultaneously. When therapy is begun, a topical drug is often applied to only 1 eye, letting the opposite eye serve as a control. If IOP is not lowered in the treated eye when compared with the control eye, the drug is discontinued (SOR: A).27
Dealing with noncompliance. More than one third of patients exhibit poor compliance with therapy,9 and strict adherence to the regimen is necessary to lower IOP. Instruct patients in proper techniques for taking and using medications, and record dosage and frequency at each physician visit.
Advise patients that glaucoma can progress, but that blindness is not inevitable. Stress the importance of adhering to the prescribed treatment regimen (SOR: C). 13 If poor compliance remains an issue, let the patient know that therapeutic alternatives may be possible (SOR: C). 2
Argon laser trabeculoplasty
Argon laser trabeculoplasty (ALT) is an outpatient procedure. Laser energy is directed at the trabecular meshwork to facilitate aqueous humor outflow. In a large clinical trial with long-term follow-up, initial ALT therapy was found to be at least as effective as initial pharmacological treatment.42
Medical treatment is often continued after ALT.43 In the Early Manifest Glaucoma Trial,25 glaucoma patients randomized to receive ALT therapy plus a topical beta-blocker (betaxolol) had a 30% reduction in IOP. Compared with the control group, patients treated with ALT and beta-blocker exhibited half the risk of visual field deterioration, with a number needed to treat of 2.24 to prevent field loss in a patient with a baseline IOP of 24 mm Hg.
Surgery
Although surgical treatment is generally considered a final alternative in management, it may be an appropriate first-line therapy for patients with cardiovascular or pulmonary conditions contraindicating use of medical therapy. 13
Filtering surgery (trabeculectomy) (Figure) is an outpatient procedure wherein IOP is lowered by creating a fistula in the globe of the eye to drain aqueous humor into the sub-conjunctival space.21 In a randomized controlled trial, trabeculectomy used alone or with medical therapy in a previously unoperated eye successfully lowered IOP by a rate of 85% to 95% at 2 years.44 At 5 years, the success rate in Caucasians is 90%; in African Americans, 80%.44 However, a recent meta-analysis suggests that glaucoma surgery is associated with accelerated progression of cataract.45 The Collaborative Initial Glaucoma Treatment Study (CIGTS) found 3 times the incidence of cataract surgery among subjects randomized to initial filtration surgery as opposed to medical management (P=.0001).46
FIGURE
Filtering surgery for glaucoma
Prognosis
Glaucoma progresses insidiously. Peripheral vision is lost first in early stages of the disease and may not even be noticed by the patient. Central vision is spared until late stages of the disease.
Blindness can usually be prevented if glaucoma is detected early and IOP is lowered sufficiently.47 Unfortunately a small number of patients may suffer irreversible vision loss even with adequate treatment; they should be referred for low-vision rehabilitation and social services (SOR: C).2 In May 2002, the Centers for Medicare and Medicaid Services approved Medicare coverage for these services.48 Services offering rehabilitation for those with low-vision: Prevent Blindness America (preventblindness.org), National Federation of the Blind (www.nfb.org), National Library Service for the Blind and Physically Handicapped (www.loc.gov/nls), and the Foundation Fighting Blindness (www.blindness.org).
- Amlodipine • Norvasc
- Acetazolamide • AK Zol; Diamox
- Apraclonidine • Iopidine
- Betaxolol • Betoptic
- Brimonodine • Alphagan
- Brinzolamide • Azopt
- Carbachol • Carbastat, Carboptic, Isopto Carbachol, Miostat
- Carteolol • Ocupress
- Dorzolamide • Trusopt
- Latanoprost • Xalatan
- Levobunolol • AKBeta, Betagan
- Metipranolol • OptiPranolol
- Timolol • Timoptic
- Travoprost • Travatan
- Unoprostone • Rescula
Corresponding author
Ahmad A. Aref, BS, 401 East Ontario St, Suite 710, Chicago, IL 60611. E-mail:[email protected].
1. Zeyen TG, Caprioli J. Progression of disc and field damage in early glaucoma. Arch Ophthalmol 1993;111:62-65.
2. American Academy of Ophthalmology Glaucoma Panel Primary openangle glaucoma, Limited Revision. Preferred practice pattern. San Francisco: American Academy of Ophthalmology, 2003;1-37.
3. Tielsch JM, Sommer A, Katz J, et al. Racial variations in the prevalence of primary open-angle glaucoma. The Baltimore Eye Survey. JAMA 1991;266:369-374.
4. Quigley HA, Vitale S. Models of glaucoma prevalence and incidence in the United States. Invest Ophthalmol Vis Sci 1997;38:83-91.
5. Schappert SM. Office visits for glaucoma: United States, 1991–92. Adv Data 1995;262:1-14.
6. Albert DM, Dryja TP. The eye. In: Cotran RS, Kumar V, Collins T. Robbins Pathologic Basis of Disease. 6th ed. Philadelphia, Pa: W.B. Saunders Company, 1999;1374-1375.
7. Congdon N, Wang F, Tielsch JM. Issues in epidemiology and population based screening of primary angle-closure glaucoma. Surv Ophthalmol 1992;36:411-423.
8. Wolfs RC, Klaver CC, Ramrattan RS, et al. Genetic risk of primary open angle glaucoma. Population-based familial aggregation study. Arch Ophthalmol 1998;116:1640-1645.
9. Quigley HA. Open-angle glaucoma. N Eng J Med 1993;328:1097-1106.
10. Harper R, Reeves B. The sensitivity and specificity of direct ophthalmoscopic optic disc assessment in screening for glaucoma: a multivariate analysis. Graefes Arch Clin Exp Ophthalmol 2000;238:949-955.
11. Schottenstein EM. Intraocular pressure and tonometry. In: Ritch R, Shields BM, Krupin T. The Glaucomas. 2nd ed. St. Louis, Mo: Mosby Yearbook, 1996;411.-
12. Lichter PR. Variability of expert observers in evaluating the optic disc. Trans Am Ophthalmol Soc 1976;74:532-572.
13. Smith OU, Seligsohn AL, Khan SJ, Spaeth GL. Primary Open Angle Glaucoma. American College of Physicians PIER Guideline. 2004.
14. Tielsch JM, Katz J, Singh K, et al. A population based evaluation of glaucoma screening: The Baltimore Eye Survey. Am J Epidemiol 1991;134:1102-1110.
15. Katz J, Sommer A, Gaasterland DE, Anderson DR. Comparison of analytic algorithms for detecting glaucomatous visual field loss. Arch Ophthalmol 1991;109:1684-1689.
16. Colton T, Ederer F. The distribution of intraocular pressures in the general population. Surv Ophthalmol 1980;25:123.-
17. Brandt JD, Beiser JA, Kass MA, et al. Central corneal thickness in the Ocular Hypertension Treatment Study. Opthalmology 2001;108:1779-1788.
18. Herndon LW, Weizer JS, Stinnett SS. Central corneal thickness as a risk factor for advanced glaucoma damage. Arch Opthalmol 2004;122:17-21.
19. Klein BE, Klein R, Sponsel WE, Franke T, Cantor LB, Martone J. Prevalence of glaucoma. The Beaver Dam Eye Study. Ophthalmology 1992;99:1499-1504.
20. Mitchell P, Smith W, Attebo K, Healey PR. Prevalence of open angle glaucoma in Australia. The Blue Mountains Study. Ophthalmology 1996;103:1661-1669.
21. Burr J, Azuara-Blanco A, Avenell A. Medical versus surgical interventions for open angle glaucoma. The Cochrane Library, Volume 1, 2004.
22. Quigley HA. Identification of glaucoma-related visual field abnormality with the screening protocol of frequency doubling technology. Am J Ophthalmol 1998;125:819-829.
23. The AGIS investigators. The Advanced Glaucoma Intervention Study (AGIS). The relationship between control of intraocular pressure and visual field deterioration. Am J Ophthalmol 2000;130:4:429-440.
24. Collaborative Normal Tension Glaucoma Study Group. Comparison of glaucomatous progression between untreated patients with normaltension glaucoma and patients with therapeutically reduced intraocular pressures. Am J Ophthalmol 1998;126:4:487-497.
25. Leske MC, Heijl A, Hussein M, Bengtsson B, Hyman L, Kornakoff E. Factors for glaucoma progression and the effect of treatment: the early manifest glaucoma trial. Early Manifest Glaucoma Trial Group. Arch Ophthalmol 2003;121:48-56.
26. Johnstone MA. Hypertrichosis and increased pigmentation of eyelashes and adjacent hair in the region of the ipsilateral eyelids of patients treated with unilateral topical latanoprost. Am J Ophthalmol 1997;124:544-547.
27. Alward WL. Medical management of glaucoma. N Eng J Med 1998;339:1298-1307.
28. Coleman AL, Robin AL, Pollack IP, Rudikoff MT, Enger C, Mayer PR. Cardiovascular and intraocular pressure effects and plasma concentrations of apraclonidine. Arch Ophthalmol 1990;108:1264-1267.
29. Butler P, Mannschreck M, Lin S, Hwang I, Alvarado J. Clinical experience with the long term use of 1% apraclonidine: incidence of allergic reactions. Arch Ophthalmol 1995;113:293-296.
30. Nordlund JR, Pasquale LR, Robin AL, et al. The cardiovascular, pulmonary, and ocular hypotensive effects of 2% brimonidine. Arch Ophthalmol 1995;113:77-83.
31. Lippa EA, Schuman JS, Higginbotham EJ, et al. MK507 versus sezolamide: comparative efficacy of two topically active carbonic anhydrase inhibitors. Ophthalmology 1991;98:308-312.
32. Hyong PF, van Beek LM. Pharmacological therapy for glaucoma: a review. Drugs 2000;59:411-434.
33. Avorn J, Glynn RJ, Gurwitz JH, et al. Adverse pulmonary effects of topical beta blockers used in the treatment of glaucoma. J Glaucoma 1993;2:158-165.
34. Leier CV, Baker ND, Weber PA. Cardiovascular effects of ophthalmic timolol. Ann Intern Med 1986;104:197-199.
35. Nelson WL, Kuritsky JN. Early postmarketing surveillance of betaxolol hydrochloride, September 1985 September 1986. Am J Ophthalmol 1987;103:512.-
36. Yogel R, Tipping R, Kudaga SF, Clineschmidt CM. Timolol-Betaxolol Study Group. Changing therapy from timolol to betaxolol: effect on intraocular pressure in selected patients with glaucoma. Arch Ophthalmol 1989;107:1303-1307.
37. Walters TR, DuBiner HB, Carpenter SP, Khan B, VanDenburgh AM. Bimatoprost Circadian IOP Study Group. 24-Hour IOP control with once-daily bimatoprost, timolol gel-forming solution, or latanoprost: a 1-month, randomized, comparative clinical trial. Surv Ophthalmol 2004;49 Suppl 1:S26-S35.
38. Higginbotham EJ, Schuman JS, Goldberg I, et al. One-year randomized study comparing bimatoprost and timolol in glaucoma and ocular hypertension. Arch Ophthalmol 2002;120:1286-1293.
39. Schadlu R, Maus TL, Nau CB, Brubaker RF. Comparison of the efficacy of apraclonidine and brimonidine as aqueous suppressants in humans. Arch Ophthalmol 1998;116:1441-1444.
40. Pappano AJ. Cholinoreceptor activating and cholinesterase inhibiting drugs. In: Katzung BG. Basic and Clinical Pharmacology. 8th ed. New York, NY: Lange Medical Books/McGraw Hill, 2001;102:103.-
41. Green K. Marijuana smoking vs cannabinoids for glaucoma therapy. Arch Ophthalmol 1998;116:1433-1437.
42. The Glaucoma Laser Trial (GLT) and glaucoma laser trial followup study: 7. Results. Am J Ophthalmol 1995;120:718-731.
43. The AGIS Investigators. The Advanced Glaucoma Intervention Study (AGIS): 4. Comparison of treatment outcomes within race. Seven year results. Ophthalmology 1998;105:146-164.
44. Roth SM, Spaeth GL, Starita RJ, et al. The effects of postoperative corticosteroids on trabeculolectomy and the clinical course of glaucoma: five-year follow-up study. Ophthalmic Surg. 1991;22:924-929.
45. Hylton C, Congdon N, Friedman D, et al. Cataract after glaucoma filtration surgery. Am J Ophthalmol 2003;135:231-232.
46. Lichter PR, Musch DC, Gillespie BW, et al. CIGTS Study Group. Interim clinical outcomes in the Collaborative Initial Glaucoma Treatment Study comparing initial treatment randomized to medications or surgery. Ophthalmology 2001;108:1943-1953.
47. Bradford CA. Basic Ophthalmology. 7th ed. San Francisco, Calif: American Academy of Ophthalmology, 1999.
48. Gieser JP. When treatment fails, caring for patients with visual disability. Arch Ophthalmol 2004;122:1208-1209.
1. Zeyen TG, Caprioli J. Progression of disc and field damage in early glaucoma. Arch Ophthalmol 1993;111:62-65.
2. American Academy of Ophthalmology Glaucoma Panel Primary openangle glaucoma, Limited Revision. Preferred practice pattern. San Francisco: American Academy of Ophthalmology, 2003;1-37.
3. Tielsch JM, Sommer A, Katz J, et al. Racial variations in the prevalence of primary open-angle glaucoma. The Baltimore Eye Survey. JAMA 1991;266:369-374.
4. Quigley HA, Vitale S. Models of glaucoma prevalence and incidence in the United States. Invest Ophthalmol Vis Sci 1997;38:83-91.
5. Schappert SM. Office visits for glaucoma: United States, 1991–92. Adv Data 1995;262:1-14.
6. Albert DM, Dryja TP. The eye. In: Cotran RS, Kumar V, Collins T. Robbins Pathologic Basis of Disease. 6th ed. Philadelphia, Pa: W.B. Saunders Company, 1999;1374-1375.
7. Congdon N, Wang F, Tielsch JM. Issues in epidemiology and population based screening of primary angle-closure glaucoma. Surv Ophthalmol 1992;36:411-423.
8. Wolfs RC, Klaver CC, Ramrattan RS, et al. Genetic risk of primary open angle glaucoma. Population-based familial aggregation study. Arch Ophthalmol 1998;116:1640-1645.
9. Quigley HA. Open-angle glaucoma. N Eng J Med 1993;328:1097-1106.
10. Harper R, Reeves B. The sensitivity and specificity of direct ophthalmoscopic optic disc assessment in screening for glaucoma: a multivariate analysis. Graefes Arch Clin Exp Ophthalmol 2000;238:949-955.
11. Schottenstein EM. Intraocular pressure and tonometry. In: Ritch R, Shields BM, Krupin T. The Glaucomas. 2nd ed. St. Louis, Mo: Mosby Yearbook, 1996;411.-
12. Lichter PR. Variability of expert observers in evaluating the optic disc. Trans Am Ophthalmol Soc 1976;74:532-572.
13. Smith OU, Seligsohn AL, Khan SJ, Spaeth GL. Primary Open Angle Glaucoma. American College of Physicians PIER Guideline. 2004.
14. Tielsch JM, Katz J, Singh K, et al. A population based evaluation of glaucoma screening: The Baltimore Eye Survey. Am J Epidemiol 1991;134:1102-1110.
15. Katz J, Sommer A, Gaasterland DE, Anderson DR. Comparison of analytic algorithms for detecting glaucomatous visual field loss. Arch Ophthalmol 1991;109:1684-1689.
16. Colton T, Ederer F. The distribution of intraocular pressures in the general population. Surv Ophthalmol 1980;25:123.-
17. Brandt JD, Beiser JA, Kass MA, et al. Central corneal thickness in the Ocular Hypertension Treatment Study. Opthalmology 2001;108:1779-1788.
18. Herndon LW, Weizer JS, Stinnett SS. Central corneal thickness as a risk factor for advanced glaucoma damage. Arch Opthalmol 2004;122:17-21.
19. Klein BE, Klein R, Sponsel WE, Franke T, Cantor LB, Martone J. Prevalence of glaucoma. The Beaver Dam Eye Study. Ophthalmology 1992;99:1499-1504.
20. Mitchell P, Smith W, Attebo K, Healey PR. Prevalence of open angle glaucoma in Australia. The Blue Mountains Study. Ophthalmology 1996;103:1661-1669.
21. Burr J, Azuara-Blanco A, Avenell A. Medical versus surgical interventions for open angle glaucoma. The Cochrane Library, Volume 1, 2004.
22. Quigley HA. Identification of glaucoma-related visual field abnormality with the screening protocol of frequency doubling technology. Am J Ophthalmol 1998;125:819-829.
23. The AGIS investigators. The Advanced Glaucoma Intervention Study (AGIS). The relationship between control of intraocular pressure and visual field deterioration. Am J Ophthalmol 2000;130:4:429-440.
24. Collaborative Normal Tension Glaucoma Study Group. Comparison of glaucomatous progression between untreated patients with normaltension glaucoma and patients with therapeutically reduced intraocular pressures. Am J Ophthalmol 1998;126:4:487-497.
25. Leske MC, Heijl A, Hussein M, Bengtsson B, Hyman L, Kornakoff E. Factors for glaucoma progression and the effect of treatment: the early manifest glaucoma trial. Early Manifest Glaucoma Trial Group. Arch Ophthalmol 2003;121:48-56.
26. Johnstone MA. Hypertrichosis and increased pigmentation of eyelashes and adjacent hair in the region of the ipsilateral eyelids of patients treated with unilateral topical latanoprost. Am J Ophthalmol 1997;124:544-547.
27. Alward WL. Medical management of glaucoma. N Eng J Med 1998;339:1298-1307.
28. Coleman AL, Robin AL, Pollack IP, Rudikoff MT, Enger C, Mayer PR. Cardiovascular and intraocular pressure effects and plasma concentrations of apraclonidine. Arch Ophthalmol 1990;108:1264-1267.
29. Butler P, Mannschreck M, Lin S, Hwang I, Alvarado J. Clinical experience with the long term use of 1% apraclonidine: incidence of allergic reactions. Arch Ophthalmol 1995;113:293-296.
30. Nordlund JR, Pasquale LR, Robin AL, et al. The cardiovascular, pulmonary, and ocular hypotensive effects of 2% brimonidine. Arch Ophthalmol 1995;113:77-83.
31. Lippa EA, Schuman JS, Higginbotham EJ, et al. MK507 versus sezolamide: comparative efficacy of two topically active carbonic anhydrase inhibitors. Ophthalmology 1991;98:308-312.
32. Hyong PF, van Beek LM. Pharmacological therapy for glaucoma: a review. Drugs 2000;59:411-434.
33. Avorn J, Glynn RJ, Gurwitz JH, et al. Adverse pulmonary effects of topical beta blockers used in the treatment of glaucoma. J Glaucoma 1993;2:158-165.
34. Leier CV, Baker ND, Weber PA. Cardiovascular effects of ophthalmic timolol. Ann Intern Med 1986;104:197-199.
35. Nelson WL, Kuritsky JN. Early postmarketing surveillance of betaxolol hydrochloride, September 1985 September 1986. Am J Ophthalmol 1987;103:512.-
36. Yogel R, Tipping R, Kudaga SF, Clineschmidt CM. Timolol-Betaxolol Study Group. Changing therapy from timolol to betaxolol: effect on intraocular pressure in selected patients with glaucoma. Arch Ophthalmol 1989;107:1303-1307.
37. Walters TR, DuBiner HB, Carpenter SP, Khan B, VanDenburgh AM. Bimatoprost Circadian IOP Study Group. 24-Hour IOP control with once-daily bimatoprost, timolol gel-forming solution, or latanoprost: a 1-month, randomized, comparative clinical trial. Surv Ophthalmol 2004;49 Suppl 1:S26-S35.
38. Higginbotham EJ, Schuman JS, Goldberg I, et al. One-year randomized study comparing bimatoprost and timolol in glaucoma and ocular hypertension. Arch Ophthalmol 2002;120:1286-1293.
39. Schadlu R, Maus TL, Nau CB, Brubaker RF. Comparison of the efficacy of apraclonidine and brimonidine as aqueous suppressants in humans. Arch Ophthalmol 1998;116:1441-1444.
40. Pappano AJ. Cholinoreceptor activating and cholinesterase inhibiting drugs. In: Katzung BG. Basic and Clinical Pharmacology. 8th ed. New York, NY: Lange Medical Books/McGraw Hill, 2001;102:103.-
41. Green K. Marijuana smoking vs cannabinoids for glaucoma therapy. Arch Ophthalmol 1998;116:1433-1437.
42. The Glaucoma Laser Trial (GLT) and glaucoma laser trial followup study: 7. Results. Am J Ophthalmol 1995;120:718-731.
43. The AGIS Investigators. The Advanced Glaucoma Intervention Study (AGIS): 4. Comparison of treatment outcomes within race. Seven year results. Ophthalmology 1998;105:146-164.
44. Roth SM, Spaeth GL, Starita RJ, et al. The effects of postoperative corticosteroids on trabeculolectomy and the clinical course of glaucoma: five-year follow-up study. Ophthalmic Surg. 1991;22:924-929.
45. Hylton C, Congdon N, Friedman D, et al. Cataract after glaucoma filtration surgery. Am J Ophthalmol 2003;135:231-232.
46. Lichter PR, Musch DC, Gillespie BW, et al. CIGTS Study Group. Interim clinical outcomes in the Collaborative Initial Glaucoma Treatment Study comparing initial treatment randomized to medications or surgery. Ophthalmology 2001;108:1943-1953.
47. Bradford CA. Basic Ophthalmology. 7th ed. San Francisco, Calif: American Academy of Ophthalmology, 1999.
48. Gieser JP. When treatment fails, caring for patients with visual disability. Arch Ophthalmol 2004;122:1208-1209.
Isolated oligohydramnios at term: Is induction indicated?
- Isolated term oligohydramnios, as defined by an amniotic fluid index (AFI) of less than 5 cm, has not been shown to be associated with poor maternal or fetal outcomes. Management may be individualized based on factors such as parity, cervical ripeness, and patient preference (SOR: B).
- Maternal hydration with oral water has been shown to increase AFI in a few hours, likely due to improved uteroplacental perfusion. This is a reasonable alternative to immediate labor induction in women with isolated term oligohydramnios (SOR: B).
- An isolated finding of a so-called “border-line” AFI (5–8 cm) is not an indication for labor induction (SOR: B).
Family physicians providing maternity care often face a scenario in which an otherwise low-risk, term patient is incidentally noted to have a low amniotic fluid index (AFI). Common reasons for obtaining an AFI in a woman with a low-risk pregnancy include evaluation of decreased fetal movement, spontaneous variable decelerations during monitoring to evaluate for labor, or an ultrasound evaluation for fundal height measurements discordant with gestational age. How should “isolated” oligohydramnios—an AFI <5 cm—be interpreted, and should immediate induction be recommended for such patients?
Oligohydramnios occurs in about 1% to 5% of pregnancies at term.1,2 Because adverse outcomes occur in high-risk pregnancies complicated by low amniotic fluid volume, oligohydramnios commonly prompts labor induction.1,3,4 At one university center, oligohydramnios is now the leading indication for labor induction.5 Many centers may even induce labor when the AFI is between 5 cm and 8 cm, the so-called borderline AFI.3
Labor induction increases the use of cesarean delivery, particularly for the primiparous woman with an unripe cervix.6 Recent studies questioning the safety of labor induction in women who have had a cesarean may increase the number of elective repeat cesarean procedures when delivery is believed indicated for oligohydramnios.7 (See Underlying causes of oligohydramnios.)
By the second trimester, amniotic fluid is being produced primarily through fetal urine production and is primarily resorbed through fetal swallowing. Significant amounts of amniotic fluid are also produced and resorbed by the fetal lung and directly resorbed from the amniotic cavity by the placenta.8,9 Amniotic fluid volume is affected by the status of maternal hydration and maternal plasma osmolality.10-13
Acute oligohydramnios may occur from ruptured membranes, usually diagnosed by clinical signs and vaginal fluid with altered pH and a ferning pattern on microscopic exam.
Chronic oligohydramnios arises from prerenal, renal, and postrenal causes. The latter 2 groups reflect fetal kidney and urogenital abnormalities, which directly decrease fetal amniotic fluid production. Uteroplacental insufficiency is the most common cause of prerenal oligohydramnios, and the decreased amniotic fluid is a direct result of decreased fetal renal perfusion.14 Uteroplacental insufficiency may result in intrauterine growth restriction as the fetus shunts blood away from the growing torso and limbs and to vital organs such as the brain. Preeclampsia and postdate pregnancies both involve pathologic changes in the placenta that may result in uteroplacental insufficiency and oligohydramnios.
Oligohydramnios is difficult to assess
True oligohydramnios can be difficult to confirm due to the questionable accuracy of amniotic fluid measurement by ultrasound. There is controversy, for example, about whether (and how) to include pockets of amniotic fluid containing umbilical cord.15 The AFI was introduced in 19872 to replace the 2 cm “pocket technique” of fluid assessment, and studies continue to question to what extent the AFI reflects actual amniotic fluid volume.
AFI measurements may vary with the amount of pressure applied to the abdomen and with fetal position or movement.16
Serial measurements taken by the same ultrasound operator have been shown to differ from the true volume by 1 cm, or 10.8%; serial measurements taken by multiple operators have differed by as much as 2 cm, or 15.4%.17,18
O’Reilly-Green compared the diagnosis of oligohydramnios in 449 post-term patients with actual amniotic fluid volume measured at rupture of membranes.19 They found a positive predictive value of 50% for oligohydramnios at an AFI of 5 cm as the lower limit of normal. A study of 144 third trimester patients using the dye-dilution technique found that, to achieve 95% confidence for ruling out oligohydramnios, a cutoff AFI of 30 cm would need to be used, a value consistent with polyhydramnios.20
What is the association between oligohydramnios and poor fetal outcomes?
A number of studies over the past 15 years have shown an association between oligohydramnios and poor fetal outcomes. These were predominantly retrospective studies, which failed to control for the presence of factors known to be associated with oligohydramnios such as intrauterine growth restriction (IUGR) and urogenital malformations.
No studies have directly addressed whether labor induction improves outcomes. A meta-analysis of 18 studies examining outcomes of pregnancies with AFI <5 cm found an increased risk of cesarean delivery for fetal distress and low Apgar scores at 5 minutes. Most of these studies, however, had high-risk patients including IUGR (level of evidence [LOE]: 2).21
A recent study of high-risk patients failed to detect a difference in the incidence of nonreactive nonstress tests, meconium-stained amniotic fluid cesarean delivery for fetal distress, low Apgar scores, or infants with a cord pH of <7.10 when oligohydramnios (AFI <5.0 cm) was present (LOE: 1).2 The patients with oligohydramnios were all induced, while many of the other high-risk patients were expectantly managed. The study therefore provides no guidance on the safety of expectant management for patients with oligohydramnios. To eliminate the potential effect of induction versus expectant management the same authors performed a case-control study of 79 high-risk women with AFI <5 cm matched to 79 women with the same high-risk pregnancy complication who had an AFI >5 cm at the time of induction (LOE: 2).23 They failed to detect any significant differences in neonatal outcomes between the groups.
Studies of the “borderline” AFI (between 5 cm and 8 cm) may also demonstrate an association with adverse neonatal outcomes if researchers include fetuses with IUGR or malformations. In one retrospective case review of 214 women with AFI of 5 cm to 10 cm, the only statistically significant finding was an association with IUGR.3 The authors recommended antepartum surveillance twice a week for mothers with borderline AFI, but they did not comment on induction (LOE: 2). Correspondence regarding this study argued that this recommendation was not supported by the evidence and would lead to unnecessary antenatal testing.24
Studies of isolated oligohydramnios
Investigators have conducted studies (Table 1) excluding fetuses with intrauterine growth restriction or anomalies to try to determine if isolated oligohydramnios is associated with poorer outcomes.25-30
Rainford’s study of outcomes in exclusively term, low-risk patients failed to show significant outcome differences in Apgar scores, NICU admissions, or rates of cesarean delivery for non-reassuring fetal heart rate monitoring (LOE: 2).29 This study was limited due to its retrospective design. The authors comment that the relatively good outcomes in the oligohydramnios group may be due to the widespread practice of inducing such patients.
In a case-control study by Conway, 183 low-risk, term parturients with oligohydramnios were matched to 183 women of similar gestational age and parity who presented in spontaneous labor. The patients with isolated oligohydramnios were induced and showed an increased cesarean delivery rate. The increased rate of cesarean delivery was not due to nonreassuring fetal surveillance and was attributed to the induction process (LOE: 2).25
An analysis of woman diagnosed with isolated oligohydramnios (AFI <5) at any gestational age in the multicenter prospective RADIUS trial demonstrated similar perinatal outcomes and fetal growth compared with pregnancies with a normal amniotic fluid (LOE: 2).30
The only randomized clinical trial of labor induction vs expectant management for term isolated oligohydramnios showed similar outcomes in each group. But this study was small (n=61) and has only been published as an abstract.31
TABLE 1
Isolated oligohydramnios and perinatal outcomes
| Study | Design | Study number n vs controls | Patient-oriented outcomes | Comment | LOE | |
|---|---|---|---|---|---|---|
| Population | Significant findings | Non-significant findings | ||||
| Garmel19 | Prospective cohort | N=187 | Increased preterm birth (OR=3.23; 95% CI, 1.4–7.3) in oligohydramnios group | IUGR, asphyxia, death, NICU admit | Delivery recommended at 37 weeks | 2 |
| 17–37 week with subnormal EFW (>10%) | 65 AFI <8 cm vs 122 AFI >8 cm | |||||
| Conway18 | Prospective cohort | N=366 | Increased CS rate (OR=2.7 95% CI, 1.3–5.4) in oligohydramnios group | CS for fetal distress; all neonatal outcomes | Treatment group induced, controls spontaneous | 2 |
| Term, isolated oligohydramnios undergoing induction | 183 AFI <5 cm vs 183 AFI >5 cm | |||||
| Roberts21 | Prospective cohort | N=206 | Increased IUGR (OR=5.2; 95% CI, 1.6–22), induction (OR=34.4, 95% CI, 4–1425.5), NICU admit (OR=9.8; 95% CI, 1.3–432) | Fetal distress requiring CS | Used >5%ile to exclude IUGR. Included some high-risk pts (diabetes or hypertension) | 2 |
| 3rd trimester, isolated oligohydramnios | 103 AFI 3%ile (N=103) vs matched control | |||||
| Rainford22 | Retrospective cohort | N=232 | Induction rate for AFI <5 = 98% vs 51% AFI >5 P<.001; increased meconium staining in controls without oligohydramnios | NICU 2 admissions, 5-minute Apgar scores | 2 | |
| 37–41 week, low-risk. AFI within 4 days of delivery | AFI <5 (n=44) vs >5 (n=188) | |||||
| Zhang23 | Retrospective nested cohort | N=6657 | Malpresentation (RR=3.5, 95% CI 1.8–6.60) | Fetal growth, CS, low Apgar, overall neonatal morbidity | Benefit of routine ultrasound was the primary study outcome study endpoint | 2 |
| Term or near-term, low-risk | AFI <5 (n=86) vs >5 (n=6571) | |||||
| AFI, amniotic fluid index; CI, confidence interval; CS, cesarean section; EFW, estimated fetal weight; IUGR, intrauterine growth restriction; LOE, level of evidence; NICU, neonatal intensive care unit; OR, odds ratio; RR, relative risk. | ||||||
Effect of maternal hydration
Maternal hydration status and plasma osmolality have an affect on amniotic fluid volume (Table 2). Maternal hydration with oral water or intravenous hypotonic solutions has been shown to increase amniotic fluid volume.8,11-13 Oral hydration with hypotonic fluid has been demonstrated to increase fetal urine production in one observational study.32 Another observational study demonstrated increased amniotic fluid volume and uteroplacental perfusion without alteration of fetal urine production suggesting the possibility that transmembranous fluid shifts from the placenta to the amniotic cavity may be involved.12
Two small, randomized controlled trials (RCTs) demonstrated an increase in amniotic fluid volume in women with oligohydramnios after oral hydration.11,13 Doi demonstrated significant increases in AFI in women with oligohydramnios beyond 35 weeks when given oral hydration with free water (increase of 3.8 cm ± 1.9; P<. 001) or hypotonic intravenous solution (increase of 2.8 cm ± 1.9; P<.001) (LOE: 3).11 Interestingly, this study did not demonstrate an increase in amniotic fluid volume with intravenous hydration with isotonic fluid.
Kirkpatrick demonstrated a 30% increase in amniotic fluid compared with controls in women of unspecified gestational age with oligohydramnios given 2 liters of oral water 2 to 5 hours before repeat amniotic fluid index (LOE: 3).13
A randomized trial in women with normal amniotic fluid demonstrated a 16% increase in amniotic fluid index 4 to 6 hours after hydration with 2 liters of oral water, compared with an 8% decrease after fluid restriction during the same period.8
A recent study of daily oral hydration in women with amniotic fluid volume <10% percentile showed increased amniotic fluid volume at 1 week, suggesting long-term benefit, although the study lacked an appropriate control group (LOE: 3).33
There are no studies of clinical outcomes such as fetal heart rate decelerations during labor, or neonatal outcomes. A Cochrane systematic review concluded that maternal hydration appears to increase amniotic fluid and may be beneficial in management of oligohydramnios; however, it recommended controlled trials to assess clinical outcome benefits (LOE: 3).34
TABLE 2
Effect of hydration on amniotic fluid index
| Study | Design | Population | Intervention | Outcome | Comment | LOE |
|---|---|---|---|---|---|---|
| Kilpatrick32 | RCT | N=40, AFI 2.1–6.0; population of patients referred for antenatal testing | Treatment group drank 2 L water and repeat AFI same or next day | Increase of 1.5 ± 1.4 cm (P<.01) in treatment group | Gestational ages of subjects not stated | 3 |
| Kilpatrick37 | RCT | N=40, AFI 7–24 cm, gestational 28 weeks | Treatment group instructed to drink 2 L and restricted group 0.1 L water. AFI repeated in 4–6 h | Increase of 3.0 ± 2.4 cm (P<.0001) in treatment group; decrease of 1.5 ± 2.7cm in controls (P <.02) | Subjects had normal AFI at entry | 3 |
| Flack36 | Prospective cohort | N=20, 10 w/AFI <5 cm, 10 controls AFI >7, 3rd trimester | 2 L oral water over 2 h for treatment and control groups, repeat AFI at 2 h | Increase in 3.2 cm in AFI (95% CI, 1.1–5.3) in oligohydramnios group but not in normal AFI group | Improved uterine perfusion shown by increased uterine artery velocity only in oligohydramnios group | 3 |
| Doi35 | RCT | N=84, AFI <5, at least 35 wks; randomized three maternal hydration methods (2 L oral water, hypotonic saline IV, or isotonic saline IV) | Hydration with 2 L fluid and AFI repeated in 1 h compared with controls | Significant increases in AFI in oral water and hypotonic IV groups by 3.8 cm and 2.8 cm (P<.001) respectively | IV isotonic solutions did not increase amniotic fluid volume in study population | 3 |
| RCT, randomized controlled trial; AFI, amniotic fluid index; CI, confidence interval. | ||||||
Management recommendations
The AFI has low specificity and positive predictive value for oligohydramnios, and there is scant evidence that isolated term oligohydramnios causes adverse fetal outcomes. We recommend that an AFI under 5 cm should prompt additional antenatal testing rather than immediate induction in low-risk term pregnancies (SOR: B).
Though we acknowledge the lack of high-quality studies with patient-oriented outcomes to support observation and maternal hydration, we have developed a management strategy that does not require immediate induction of labor in women with uncomplicated term pregnancies.
The following recommendations apply to women having oligohydramnios as defined by amniotic fluid volume of less than 5 cm and gestational age between 37 and 41 weeks.
Initial assessment
- Assess for premature rupture of membranes with a thorough history and a sterile speculum exam
- Reassess dating as oligohydramnios in post-dates pregnancy (>41 weeks) is an indication for induction (SOR: C)35
- Perform a nonstress test to assess fetal wellbeing
- Assess for IUGR with an ultrasound for estimated fetal weight and for the ratio of head circumference (HC) to abdominal circumference (AC). A comparison with prior ultrasounds can aid in assessing interval growth. An estimated fetal weight below the 10%, an elevated HC/AC ratio, or poor interval growth would suggest IUGR
- Arrange for an ultrasound anatomic survey for fetal anomalies, if not done previously
- Determine if preeclampsia, chronic hypertension, diabetes, or other maternal conditions associated with uteroplacental insufficiency are present.
Action steps
With any positive findings in the initial evaluation, proceed to labor induction, as the patient does not have isolated, term oligohydramnios (SOR: C). If the initial assessment is unremarkable and the AFI is less than 5, consider hydration with oral water and repeating the AFI 2 to 6 hours later (SOR: B).
Persistent oligohydramnios at term, particularly with a ripe cervix, may lead you to consider labor induction. Continued expectant management of isolated term oligohydramnios with twice weekly fetal surveillance may also be a reasonable option due to the paucity of evidence that oligohydramnios is associated with an adverse outcome in this scenario (SOR: C). Normal results with umbilical artery Doppler flow studies have been used to decrease the need for induction in high-risk pregnancies with oligohydramnios, and this technique may eventually have a role in isolated term oligohydramnios.36
It is essential that patients receive counseling and give informed consent regarding the risks and benefits of observation or induction for isolated term oligohydramnios. The ease of induction based on parity and cervical ripeness should be considered.
A primiparous woman with an unfavorable cervix who strongly desires a spontaneous, vaginal birth could be told that, although there may be a small risk for her baby, no study has demonstrated any increased long-term morbidity or mortality associated with low fluid in her situation and that labor induction may double her chance of cesarean delivery.37,38 In such a situation, an acceptable approach for mother and clinician may be rehydration followed by a repeat AFI and close follow-up with testing for fetal well-being according to the algorithm (Figure). In a practical sense, rehydration with 2 liters of oral water for oligohydramnios may be done whether or not immediate induction is chosen, as this is a safe measure that has been shown to significantly increase AFI. Alternatively, the preferred approach for a multiparous woman with a ripe cervix by Bishop score may be labor induction.
As adverse fetal outcomes have not been demonstrated in women with isolated term oligohydramnios, there is no rationale for routinely inducing labor based on an isolated finding of a so called “borderline” amniotic fluid index in the 5-to-8 range. In this situation it is appropriate to perform the initial assessment described above and may be reasonable to repeat the amniotic fluid index in 3 to 4 days to determine if true oligohydramnios has developed.
FIGURE
Assessment of the pregnant woman with oligohydramnios at term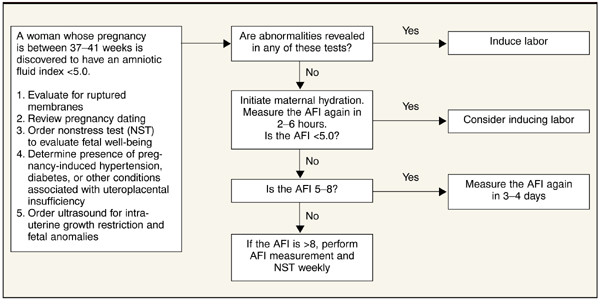
Acknowledgments
We appreciate the assistance of George Gilson MD, Lauren Plante MD, and William Rayburn MD in manuscript review.
Corresponding author
Lawrence Leeman, MD, MPH, University of New Mexico Depts of Family and Community Medicine, Obstetrics and Gynecology, 2400 Tucker NE, 3rd floor, Albuquerque, NM 87131. E-mail: [email protected].
1. Moore TR. Clinical assessment of amniotic fluid. Clin Obstet Gynecol 1997;40:303-313.
2. Phelan JP, Smith CV, Broussard P, Small M. Amniotic fluid volume assessment with the four-quadrant technique at 36–42weeks’ gestation. J Reprod Med 1987;32:540-542.
3. Banks EH. Perinatal risks associated with borderline amniotic fluid index. Am J Obstet Gynecol 1999;180:1461-1463.
4. Casey BM. Pregnancy outcomes after antepartum diagnosis of oligohydramnios at or beyond 34 weeks gestation. Am J Obstet Gynecol 2000;182:909-912.
5. Hobbins JC. Oligohydramnios and post-term pregnancy. Ob/Gyn Clinical Alert December 2002;59-60.
6. Johnson DP, Davis NR, Brown AJ. Risk of cesarean delivery after induction at term in nulliparous women with an unfavorable cervix. Am J Obstet Gynecol 2003;188:1565-1572.
7. Lydon-Rochelle M, Holt VL, Easterling TR, Martin DP. Risk of uterine rupture during labor among women with a prior cesarean delivery. N Engl J Med 2001;345:3-8.
8. Kilpatrick SJ, Safford KL. Maternal hydration increases amniotic fluid index in women with normal amniotic fluid. Obstet Gynecol 1993;81:49-52.
9. Gilbert WM, Brace RA. Amniotic fluid volume and normal flows to and from the amniotic cavity. Seminars in Perinatology 1993;17:150-157.
10. Chandra PC, Schiavello HJ, Lewandowski MA. Effect of oral and intravenous hydration on oligohydramnios. J Reprod Med 2000;45:337-340.
11. Doi S, Osada H, Seki K, Sekiya S. Effect of maternal hydration on oligohydramnios: a comparison of three volume expansion methods. Obstet Gynecol 1998;92:525-529.
12. Flack NJ, Sepulveda W, Bower S, Fisk NM. Acute maternal hydration in third-trimester oligohydramnios: effects on amniotic fluid volume, uteroplacental perfusion, and fetal blood flow and urine output. Am J Obstet Gynecol 1995;173:1186-1191.
13. Kilpatrick SJ, Safford KL, Pomeroy T, Hoedt L, Scheerer L, Laros RK. Maternal hydration increases amniotic fluid index. Obstet Gynecol 1991;78:1098-1102.
14. Larmon JE, Ross BS. Clinical utility of amniotic fluid volume assessment. Obstet Gynecol Clin North Am 1998;25:639-661.
15. Hill LM. Oligohydramnios: sonographic diagnosis and clinical implications. Clin Obstet Gynecol 1997;40:314-327.
16. Flack NJ, Dore C, Southwell D, Kourtis P, Sepulveda W, Fisk NM. The influence of operator transducer pressure on ultrasonographic measurements of amniotic fluid volume. Am J Obstet Gynecol 1994;171:218-222.
17. Rutherford SE, Smith CV, Phelan JP, Kawakami K, Ahn MO. Four-quadrant assessment of amniotic fluid volume: interobserver and intraobserver variation. J Reprod Med 1987;32:587-589.
18. Bruner JP, Reed GW, Sarno AP, Harrington RA, Goodman MA. Intraobserver and interobserver variability of the amniotic fluid index. Am J Obstet Gynecol 1993;168:1309-1313.
19. O’Reilly-Green CP, Divon MY. Predictive value of amniotic fluid index for oligohydramnios in patients with prolonged pregnancies. J Matern Fetal Med 1996;5:218-226.
20. Chauhan SP, Magann EF, Morrison JC, Whitworth NS, Hendrix NW, Devoe LD. Ultrasonographic assessment of amniotic fluid does not reflect actual amniotic fluid volume. Am J Obstet Gynecol 1997;177:291-297.
21. Chauhan SP, Sanderson M, Hendrix NW, Magann EF, Devoe LD. Perinatal outcome and amniotic fluid index in the antepartum and intrapartum periods: a meta-analysis. Am J Obstet Gynecol 1999;181:1473-1478.
22. Magann EF. Antenatal testing among 1001 patients at high risk: the role of ultrasonographic estimate of amniotic fluid volume. Am J Obstet Gynecol 1999;180:1330-1336.
23. Magann EF. Does an amniotic fluid index of 5 cm necessitate delivery in high-risk pregnancies? A case-control study. Am J Obstet Gynecol 1999;180:1354-1359.
24. Nisell H, Ek S. Perinatal risks associated with borderline amniotic fluid index. Am J Obstet Gynecol. 2000;182:750-751.
25. Conway DL, et al. Isolated oligohydramnios in the term pregnancy: Is it a clinical entity. J Matern Fetal Med 1998;7:197-200.
26. Garmel SH, Chelmow D, Sha SJ, Roan JT, D’Alton ME. Oligohydramnios and the appropriately grown fetus. Am J Perinatol 1997;14:359-363.
27. Kreiser D, el-Sayed YY, Sorem KA, Chitkara U, Holbrook RH, Jr, Druzin ML. Decreased amniotic fluid index in low-risk pregnancy. J Reprod Med 2001;46:743-746.
28. Roberts D, Nwosu EC, Walkinshaw SA. The fetal outcome in pregnancies with isolated reduced amniotic fluid volume in the third trimester. J Perinat Med 1998;26:390-395.
29. Rainford M, Adair R, Scialli AR, Ghidini A, Spong CY. Amniotic fluid index in the uncomplicated term pregnancy. Prediction of outcome. J Reprod Med 2001;46:589-592.
30. Zhang J, Troendle J, Meikle S, Klebanoff MA, Rayburn WF. Isolated oligohydramnios is not associated with adverse perinatal outcomes. BJOG 2004;111:220-225.
31. Conway DL, Groth S, Adkins WB, Langer O. Management of isolated oligohyramnios in the term pregnancy: a randomized clinical trial. Am J Obstet Gynecol 2000;182:S21.-
32. Oosterhof H, Haak MC, Aarnoudse JG. Acute maternal rehydration increases the urine production rate in the near-term human fetus. Am J Obstet Gynecol 2000;183:226-229.
33. Fait G, Pauzner D, Gull I, Lessing JB, Jaffa AJ, Wolman I. Effect of 1 week or oral hydration on the amniotic fluid index. J Reprod Med 2003;48:187-190.
34. Hofmeyr GJ, Gulmezoglu AM. Maternal hydration for increasing amniotic fluid volume in oligohydramnios and normal amniotic fluid volute (Cochrane Review). In: The Cochrane Library. Issue 4, 2002. Oxford: Update Software.
35. Sherer DM, Langer O. Oligohydramnios: use and misuse in clinical management. Ultrasound Obstet Gynecol 2001;18:411-419.
36. Carroll BC, Bruner JP. Umbilical artery Doppler velocimetry in pregnancies complicated by oligohydramnios. J Reprod Med 2000;45:562-566.
37. Seyb ST, Berka RJ, Socol ML, Dooley SL. Risk of cesarean delivery with elective induction of labor at term in nulliparous women. Obstet Gynecol 1999;94:600-607.
38. Yeast JD, Jones A, Poskin M. Induction of labor and the relationship to cesarean delivery: A review of 7001 consecutive inductions. Am J Obstet Gynecol 1999;180:628-633.
- Isolated term oligohydramnios, as defined by an amniotic fluid index (AFI) of less than 5 cm, has not been shown to be associated with poor maternal or fetal outcomes. Management may be individualized based on factors such as parity, cervical ripeness, and patient preference (SOR: B).
- Maternal hydration with oral water has been shown to increase AFI in a few hours, likely due to improved uteroplacental perfusion. This is a reasonable alternative to immediate labor induction in women with isolated term oligohydramnios (SOR: B).
- An isolated finding of a so-called “border-line” AFI (5–8 cm) is not an indication for labor induction (SOR: B).
Family physicians providing maternity care often face a scenario in which an otherwise low-risk, term patient is incidentally noted to have a low amniotic fluid index (AFI). Common reasons for obtaining an AFI in a woman with a low-risk pregnancy include evaluation of decreased fetal movement, spontaneous variable decelerations during monitoring to evaluate for labor, or an ultrasound evaluation for fundal height measurements discordant with gestational age. How should “isolated” oligohydramnios—an AFI <5 cm—be interpreted, and should immediate induction be recommended for such patients?
Oligohydramnios occurs in about 1% to 5% of pregnancies at term.1,2 Because adverse outcomes occur in high-risk pregnancies complicated by low amniotic fluid volume, oligohydramnios commonly prompts labor induction.1,3,4 At one university center, oligohydramnios is now the leading indication for labor induction.5 Many centers may even induce labor when the AFI is between 5 cm and 8 cm, the so-called borderline AFI.3
Labor induction increases the use of cesarean delivery, particularly for the primiparous woman with an unripe cervix.6 Recent studies questioning the safety of labor induction in women who have had a cesarean may increase the number of elective repeat cesarean procedures when delivery is believed indicated for oligohydramnios.7 (See Underlying causes of oligohydramnios.)
By the second trimester, amniotic fluid is being produced primarily through fetal urine production and is primarily resorbed through fetal swallowing. Significant amounts of amniotic fluid are also produced and resorbed by the fetal lung and directly resorbed from the amniotic cavity by the placenta.8,9 Amniotic fluid volume is affected by the status of maternal hydration and maternal plasma osmolality.10-13
Acute oligohydramnios may occur from ruptured membranes, usually diagnosed by clinical signs and vaginal fluid with altered pH and a ferning pattern on microscopic exam.
Chronic oligohydramnios arises from prerenal, renal, and postrenal causes. The latter 2 groups reflect fetal kidney and urogenital abnormalities, which directly decrease fetal amniotic fluid production. Uteroplacental insufficiency is the most common cause of prerenal oligohydramnios, and the decreased amniotic fluid is a direct result of decreased fetal renal perfusion.14 Uteroplacental insufficiency may result in intrauterine growth restriction as the fetus shunts blood away from the growing torso and limbs and to vital organs such as the brain. Preeclampsia and postdate pregnancies both involve pathologic changes in the placenta that may result in uteroplacental insufficiency and oligohydramnios.
Oligohydramnios is difficult to assess
True oligohydramnios can be difficult to confirm due to the questionable accuracy of amniotic fluid measurement by ultrasound. There is controversy, for example, about whether (and how) to include pockets of amniotic fluid containing umbilical cord.15 The AFI was introduced in 19872 to replace the 2 cm “pocket technique” of fluid assessment, and studies continue to question to what extent the AFI reflects actual amniotic fluid volume.
AFI measurements may vary with the amount of pressure applied to the abdomen and with fetal position or movement.16
Serial measurements taken by the same ultrasound operator have been shown to differ from the true volume by 1 cm, or 10.8%; serial measurements taken by multiple operators have differed by as much as 2 cm, or 15.4%.17,18
O’Reilly-Green compared the diagnosis of oligohydramnios in 449 post-term patients with actual amniotic fluid volume measured at rupture of membranes.19 They found a positive predictive value of 50% for oligohydramnios at an AFI of 5 cm as the lower limit of normal. A study of 144 third trimester patients using the dye-dilution technique found that, to achieve 95% confidence for ruling out oligohydramnios, a cutoff AFI of 30 cm would need to be used, a value consistent with polyhydramnios.20
What is the association between oligohydramnios and poor fetal outcomes?
A number of studies over the past 15 years have shown an association between oligohydramnios and poor fetal outcomes. These were predominantly retrospective studies, which failed to control for the presence of factors known to be associated with oligohydramnios such as intrauterine growth restriction (IUGR) and urogenital malformations.
No studies have directly addressed whether labor induction improves outcomes. A meta-analysis of 18 studies examining outcomes of pregnancies with AFI <5 cm found an increased risk of cesarean delivery for fetal distress and low Apgar scores at 5 minutes. Most of these studies, however, had high-risk patients including IUGR (level of evidence [LOE]: 2).21
A recent study of high-risk patients failed to detect a difference in the incidence of nonreactive nonstress tests, meconium-stained amniotic fluid cesarean delivery for fetal distress, low Apgar scores, or infants with a cord pH of <7.10 when oligohydramnios (AFI <5.0 cm) was present (LOE: 1).2 The patients with oligohydramnios were all induced, while many of the other high-risk patients were expectantly managed. The study therefore provides no guidance on the safety of expectant management for patients with oligohydramnios. To eliminate the potential effect of induction versus expectant management the same authors performed a case-control study of 79 high-risk women with AFI <5 cm matched to 79 women with the same high-risk pregnancy complication who had an AFI >5 cm at the time of induction (LOE: 2).23 They failed to detect any significant differences in neonatal outcomes between the groups.
Studies of the “borderline” AFI (between 5 cm and 8 cm) may also demonstrate an association with adverse neonatal outcomes if researchers include fetuses with IUGR or malformations. In one retrospective case review of 214 women with AFI of 5 cm to 10 cm, the only statistically significant finding was an association with IUGR.3 The authors recommended antepartum surveillance twice a week for mothers with borderline AFI, but they did not comment on induction (LOE: 2). Correspondence regarding this study argued that this recommendation was not supported by the evidence and would lead to unnecessary antenatal testing.24
Studies of isolated oligohydramnios
Investigators have conducted studies (Table 1) excluding fetuses with intrauterine growth restriction or anomalies to try to determine if isolated oligohydramnios is associated with poorer outcomes.25-30
Rainford’s study of outcomes in exclusively term, low-risk patients failed to show significant outcome differences in Apgar scores, NICU admissions, or rates of cesarean delivery for non-reassuring fetal heart rate monitoring (LOE: 2).29 This study was limited due to its retrospective design. The authors comment that the relatively good outcomes in the oligohydramnios group may be due to the widespread practice of inducing such patients.
In a case-control study by Conway, 183 low-risk, term parturients with oligohydramnios were matched to 183 women of similar gestational age and parity who presented in spontaneous labor. The patients with isolated oligohydramnios were induced and showed an increased cesarean delivery rate. The increased rate of cesarean delivery was not due to nonreassuring fetal surveillance and was attributed to the induction process (LOE: 2).25
An analysis of woman diagnosed with isolated oligohydramnios (AFI <5) at any gestational age in the multicenter prospective RADIUS trial demonstrated similar perinatal outcomes and fetal growth compared with pregnancies with a normal amniotic fluid (LOE: 2).30
The only randomized clinical trial of labor induction vs expectant management for term isolated oligohydramnios showed similar outcomes in each group. But this study was small (n=61) and has only been published as an abstract.31
TABLE 1
Isolated oligohydramnios and perinatal outcomes
| Study | Design | Study number n vs controls | Patient-oriented outcomes | Comment | LOE | |
|---|---|---|---|---|---|---|
| Population | Significant findings | Non-significant findings | ||||
| Garmel19 | Prospective cohort | N=187 | Increased preterm birth (OR=3.23; 95% CI, 1.4–7.3) in oligohydramnios group | IUGR, asphyxia, death, NICU admit | Delivery recommended at 37 weeks | 2 |
| 17–37 week with subnormal EFW (>10%) | 65 AFI <8 cm vs 122 AFI >8 cm | |||||
| Conway18 | Prospective cohort | N=366 | Increased CS rate (OR=2.7 95% CI, 1.3–5.4) in oligohydramnios group | CS for fetal distress; all neonatal outcomes | Treatment group induced, controls spontaneous | 2 |
| Term, isolated oligohydramnios undergoing induction | 183 AFI <5 cm vs 183 AFI >5 cm | |||||
| Roberts21 | Prospective cohort | N=206 | Increased IUGR (OR=5.2; 95% CI, 1.6–22), induction (OR=34.4, 95% CI, 4–1425.5), NICU admit (OR=9.8; 95% CI, 1.3–432) | Fetal distress requiring CS | Used >5%ile to exclude IUGR. Included some high-risk pts (diabetes or hypertension) | 2 |
| 3rd trimester, isolated oligohydramnios | 103 AFI 3%ile (N=103) vs matched control | |||||
| Rainford22 | Retrospective cohort | N=232 | Induction rate for AFI <5 = 98% vs 51% AFI >5 P<.001; increased meconium staining in controls without oligohydramnios | NICU 2 admissions, 5-minute Apgar scores | 2 | |
| 37–41 week, low-risk. AFI within 4 days of delivery | AFI <5 (n=44) vs >5 (n=188) | |||||
| Zhang23 | Retrospective nested cohort | N=6657 | Malpresentation (RR=3.5, 95% CI 1.8–6.60) | Fetal growth, CS, low Apgar, overall neonatal morbidity | Benefit of routine ultrasound was the primary study outcome study endpoint | 2 |
| Term or near-term, low-risk | AFI <5 (n=86) vs >5 (n=6571) | |||||
| AFI, amniotic fluid index; CI, confidence interval; CS, cesarean section; EFW, estimated fetal weight; IUGR, intrauterine growth restriction; LOE, level of evidence; NICU, neonatal intensive care unit; OR, odds ratio; RR, relative risk. | ||||||
Effect of maternal hydration
Maternal hydration status and plasma osmolality have an affect on amniotic fluid volume (Table 2). Maternal hydration with oral water or intravenous hypotonic solutions has been shown to increase amniotic fluid volume.8,11-13 Oral hydration with hypotonic fluid has been demonstrated to increase fetal urine production in one observational study.32 Another observational study demonstrated increased amniotic fluid volume and uteroplacental perfusion without alteration of fetal urine production suggesting the possibility that transmembranous fluid shifts from the placenta to the amniotic cavity may be involved.12
Two small, randomized controlled trials (RCTs) demonstrated an increase in amniotic fluid volume in women with oligohydramnios after oral hydration.11,13 Doi demonstrated significant increases in AFI in women with oligohydramnios beyond 35 weeks when given oral hydration with free water (increase of 3.8 cm ± 1.9; P<. 001) or hypotonic intravenous solution (increase of 2.8 cm ± 1.9; P<.001) (LOE: 3).11 Interestingly, this study did not demonstrate an increase in amniotic fluid volume with intravenous hydration with isotonic fluid.
Kirkpatrick demonstrated a 30% increase in amniotic fluid compared with controls in women of unspecified gestational age with oligohydramnios given 2 liters of oral water 2 to 5 hours before repeat amniotic fluid index (LOE: 3).13
A randomized trial in women with normal amniotic fluid demonstrated a 16% increase in amniotic fluid index 4 to 6 hours after hydration with 2 liters of oral water, compared with an 8% decrease after fluid restriction during the same period.8
A recent study of daily oral hydration in women with amniotic fluid volume <10% percentile showed increased amniotic fluid volume at 1 week, suggesting long-term benefit, although the study lacked an appropriate control group (LOE: 3).33
There are no studies of clinical outcomes such as fetal heart rate decelerations during labor, or neonatal outcomes. A Cochrane systematic review concluded that maternal hydration appears to increase amniotic fluid and may be beneficial in management of oligohydramnios; however, it recommended controlled trials to assess clinical outcome benefits (LOE: 3).34
TABLE 2
Effect of hydration on amniotic fluid index
| Study | Design | Population | Intervention | Outcome | Comment | LOE |
|---|---|---|---|---|---|---|
| Kilpatrick32 | RCT | N=40, AFI 2.1–6.0; population of patients referred for antenatal testing | Treatment group drank 2 L water and repeat AFI same or next day | Increase of 1.5 ± 1.4 cm (P<.01) in treatment group | Gestational ages of subjects not stated | 3 |
| Kilpatrick37 | RCT | N=40, AFI 7–24 cm, gestational 28 weeks | Treatment group instructed to drink 2 L and restricted group 0.1 L water. AFI repeated in 4–6 h | Increase of 3.0 ± 2.4 cm (P<.0001) in treatment group; decrease of 1.5 ± 2.7cm in controls (P <.02) | Subjects had normal AFI at entry | 3 |
| Flack36 | Prospective cohort | N=20, 10 w/AFI <5 cm, 10 controls AFI >7, 3rd trimester | 2 L oral water over 2 h for treatment and control groups, repeat AFI at 2 h | Increase in 3.2 cm in AFI (95% CI, 1.1–5.3) in oligohydramnios group but not in normal AFI group | Improved uterine perfusion shown by increased uterine artery velocity only in oligohydramnios group | 3 |
| Doi35 | RCT | N=84, AFI <5, at least 35 wks; randomized three maternal hydration methods (2 L oral water, hypotonic saline IV, or isotonic saline IV) | Hydration with 2 L fluid and AFI repeated in 1 h compared with controls | Significant increases in AFI in oral water and hypotonic IV groups by 3.8 cm and 2.8 cm (P<.001) respectively | IV isotonic solutions did not increase amniotic fluid volume in study population | 3 |
| RCT, randomized controlled trial; AFI, amniotic fluid index; CI, confidence interval. | ||||||
Management recommendations
The AFI has low specificity and positive predictive value for oligohydramnios, and there is scant evidence that isolated term oligohydramnios causes adverse fetal outcomes. We recommend that an AFI under 5 cm should prompt additional antenatal testing rather than immediate induction in low-risk term pregnancies (SOR: B).
Though we acknowledge the lack of high-quality studies with patient-oriented outcomes to support observation and maternal hydration, we have developed a management strategy that does not require immediate induction of labor in women with uncomplicated term pregnancies.
The following recommendations apply to women having oligohydramnios as defined by amniotic fluid volume of less than 5 cm and gestational age between 37 and 41 weeks.
Initial assessment
- Assess for premature rupture of membranes with a thorough history and a sterile speculum exam
- Reassess dating as oligohydramnios in post-dates pregnancy (>41 weeks) is an indication for induction (SOR: C)35
- Perform a nonstress test to assess fetal wellbeing
- Assess for IUGR with an ultrasound for estimated fetal weight and for the ratio of head circumference (HC) to abdominal circumference (AC). A comparison with prior ultrasounds can aid in assessing interval growth. An estimated fetal weight below the 10%, an elevated HC/AC ratio, or poor interval growth would suggest IUGR
- Arrange for an ultrasound anatomic survey for fetal anomalies, if not done previously
- Determine if preeclampsia, chronic hypertension, diabetes, or other maternal conditions associated with uteroplacental insufficiency are present.
Action steps
With any positive findings in the initial evaluation, proceed to labor induction, as the patient does not have isolated, term oligohydramnios (SOR: C). If the initial assessment is unremarkable and the AFI is less than 5, consider hydration with oral water and repeating the AFI 2 to 6 hours later (SOR: B).
Persistent oligohydramnios at term, particularly with a ripe cervix, may lead you to consider labor induction. Continued expectant management of isolated term oligohydramnios with twice weekly fetal surveillance may also be a reasonable option due to the paucity of evidence that oligohydramnios is associated with an adverse outcome in this scenario (SOR: C). Normal results with umbilical artery Doppler flow studies have been used to decrease the need for induction in high-risk pregnancies with oligohydramnios, and this technique may eventually have a role in isolated term oligohydramnios.36
It is essential that patients receive counseling and give informed consent regarding the risks and benefits of observation or induction for isolated term oligohydramnios. The ease of induction based on parity and cervical ripeness should be considered.
A primiparous woman with an unfavorable cervix who strongly desires a spontaneous, vaginal birth could be told that, although there may be a small risk for her baby, no study has demonstrated any increased long-term morbidity or mortality associated with low fluid in her situation and that labor induction may double her chance of cesarean delivery.37,38 In such a situation, an acceptable approach for mother and clinician may be rehydration followed by a repeat AFI and close follow-up with testing for fetal well-being according to the algorithm (Figure). In a practical sense, rehydration with 2 liters of oral water for oligohydramnios may be done whether or not immediate induction is chosen, as this is a safe measure that has been shown to significantly increase AFI. Alternatively, the preferred approach for a multiparous woman with a ripe cervix by Bishop score may be labor induction.
As adverse fetal outcomes have not been demonstrated in women with isolated term oligohydramnios, there is no rationale for routinely inducing labor based on an isolated finding of a so called “borderline” amniotic fluid index in the 5-to-8 range. In this situation it is appropriate to perform the initial assessment described above and may be reasonable to repeat the amniotic fluid index in 3 to 4 days to determine if true oligohydramnios has developed.
FIGURE
Assessment of the pregnant woman with oligohydramnios at term
Acknowledgments
We appreciate the assistance of George Gilson MD, Lauren Plante MD, and William Rayburn MD in manuscript review.
Corresponding author
Lawrence Leeman, MD, MPH, University of New Mexico Depts of Family and Community Medicine, Obstetrics and Gynecology, 2400 Tucker NE, 3rd floor, Albuquerque, NM 87131. E-mail: [email protected].
- Isolated term oligohydramnios, as defined by an amniotic fluid index (AFI) of less than 5 cm, has not been shown to be associated with poor maternal or fetal outcomes. Management may be individualized based on factors such as parity, cervical ripeness, and patient preference (SOR: B).
- Maternal hydration with oral water has been shown to increase AFI in a few hours, likely due to improved uteroplacental perfusion. This is a reasonable alternative to immediate labor induction in women with isolated term oligohydramnios (SOR: B).
- An isolated finding of a so-called “border-line” AFI (5–8 cm) is not an indication for labor induction (SOR: B).
Family physicians providing maternity care often face a scenario in which an otherwise low-risk, term patient is incidentally noted to have a low amniotic fluid index (AFI). Common reasons for obtaining an AFI in a woman with a low-risk pregnancy include evaluation of decreased fetal movement, spontaneous variable decelerations during monitoring to evaluate for labor, or an ultrasound evaluation for fundal height measurements discordant with gestational age. How should “isolated” oligohydramnios—an AFI <5 cm—be interpreted, and should immediate induction be recommended for such patients?
Oligohydramnios occurs in about 1% to 5% of pregnancies at term.1,2 Because adverse outcomes occur in high-risk pregnancies complicated by low amniotic fluid volume, oligohydramnios commonly prompts labor induction.1,3,4 At one university center, oligohydramnios is now the leading indication for labor induction.5 Many centers may even induce labor when the AFI is between 5 cm and 8 cm, the so-called borderline AFI.3
Labor induction increases the use of cesarean delivery, particularly for the primiparous woman with an unripe cervix.6 Recent studies questioning the safety of labor induction in women who have had a cesarean may increase the number of elective repeat cesarean procedures when delivery is believed indicated for oligohydramnios.7 (See Underlying causes of oligohydramnios.)
By the second trimester, amniotic fluid is being produced primarily through fetal urine production and is primarily resorbed through fetal swallowing. Significant amounts of amniotic fluid are also produced and resorbed by the fetal lung and directly resorbed from the amniotic cavity by the placenta.8,9 Amniotic fluid volume is affected by the status of maternal hydration and maternal plasma osmolality.10-13
Acute oligohydramnios may occur from ruptured membranes, usually diagnosed by clinical signs and vaginal fluid with altered pH and a ferning pattern on microscopic exam.
Chronic oligohydramnios arises from prerenal, renal, and postrenal causes. The latter 2 groups reflect fetal kidney and urogenital abnormalities, which directly decrease fetal amniotic fluid production. Uteroplacental insufficiency is the most common cause of prerenal oligohydramnios, and the decreased amniotic fluid is a direct result of decreased fetal renal perfusion.14 Uteroplacental insufficiency may result in intrauterine growth restriction as the fetus shunts blood away from the growing torso and limbs and to vital organs such as the brain. Preeclampsia and postdate pregnancies both involve pathologic changes in the placenta that may result in uteroplacental insufficiency and oligohydramnios.
Oligohydramnios is difficult to assess
True oligohydramnios can be difficult to confirm due to the questionable accuracy of amniotic fluid measurement by ultrasound. There is controversy, for example, about whether (and how) to include pockets of amniotic fluid containing umbilical cord.15 The AFI was introduced in 19872 to replace the 2 cm “pocket technique” of fluid assessment, and studies continue to question to what extent the AFI reflects actual amniotic fluid volume.
AFI measurements may vary with the amount of pressure applied to the abdomen and with fetal position or movement.16
Serial measurements taken by the same ultrasound operator have been shown to differ from the true volume by 1 cm, or 10.8%; serial measurements taken by multiple operators have differed by as much as 2 cm, or 15.4%.17,18
O’Reilly-Green compared the diagnosis of oligohydramnios in 449 post-term patients with actual amniotic fluid volume measured at rupture of membranes.19 They found a positive predictive value of 50% for oligohydramnios at an AFI of 5 cm as the lower limit of normal. A study of 144 third trimester patients using the dye-dilution technique found that, to achieve 95% confidence for ruling out oligohydramnios, a cutoff AFI of 30 cm would need to be used, a value consistent with polyhydramnios.20
What is the association between oligohydramnios and poor fetal outcomes?
A number of studies over the past 15 years have shown an association between oligohydramnios and poor fetal outcomes. These were predominantly retrospective studies, which failed to control for the presence of factors known to be associated with oligohydramnios such as intrauterine growth restriction (IUGR) and urogenital malformations.
No studies have directly addressed whether labor induction improves outcomes. A meta-analysis of 18 studies examining outcomes of pregnancies with AFI <5 cm found an increased risk of cesarean delivery for fetal distress and low Apgar scores at 5 minutes. Most of these studies, however, had high-risk patients including IUGR (level of evidence [LOE]: 2).21
A recent study of high-risk patients failed to detect a difference in the incidence of nonreactive nonstress tests, meconium-stained amniotic fluid cesarean delivery for fetal distress, low Apgar scores, or infants with a cord pH of <7.10 when oligohydramnios (AFI <5.0 cm) was present (LOE: 1).2 The patients with oligohydramnios were all induced, while many of the other high-risk patients were expectantly managed. The study therefore provides no guidance on the safety of expectant management for patients with oligohydramnios. To eliminate the potential effect of induction versus expectant management the same authors performed a case-control study of 79 high-risk women with AFI <5 cm matched to 79 women with the same high-risk pregnancy complication who had an AFI >5 cm at the time of induction (LOE: 2).23 They failed to detect any significant differences in neonatal outcomes between the groups.
Studies of the “borderline” AFI (between 5 cm and 8 cm) may also demonstrate an association with adverse neonatal outcomes if researchers include fetuses with IUGR or malformations. In one retrospective case review of 214 women with AFI of 5 cm to 10 cm, the only statistically significant finding was an association with IUGR.3 The authors recommended antepartum surveillance twice a week for mothers with borderline AFI, but they did not comment on induction (LOE: 2). Correspondence regarding this study argued that this recommendation was not supported by the evidence and would lead to unnecessary antenatal testing.24
Studies of isolated oligohydramnios
Investigators have conducted studies (Table 1) excluding fetuses with intrauterine growth restriction or anomalies to try to determine if isolated oligohydramnios is associated with poorer outcomes.25-30
Rainford’s study of outcomes in exclusively term, low-risk patients failed to show significant outcome differences in Apgar scores, NICU admissions, or rates of cesarean delivery for non-reassuring fetal heart rate monitoring (LOE: 2).29 This study was limited due to its retrospective design. The authors comment that the relatively good outcomes in the oligohydramnios group may be due to the widespread practice of inducing such patients.
In a case-control study by Conway, 183 low-risk, term parturients with oligohydramnios were matched to 183 women of similar gestational age and parity who presented in spontaneous labor. The patients with isolated oligohydramnios were induced and showed an increased cesarean delivery rate. The increased rate of cesarean delivery was not due to nonreassuring fetal surveillance and was attributed to the induction process (LOE: 2).25
An analysis of woman diagnosed with isolated oligohydramnios (AFI <5) at any gestational age in the multicenter prospective RADIUS trial demonstrated similar perinatal outcomes and fetal growth compared with pregnancies with a normal amniotic fluid (LOE: 2).30
The only randomized clinical trial of labor induction vs expectant management for term isolated oligohydramnios showed similar outcomes in each group. But this study was small (n=61) and has only been published as an abstract.31
TABLE 1
Isolated oligohydramnios and perinatal outcomes
| Study | Design | Study number n vs controls | Patient-oriented outcomes | Comment | LOE | |
|---|---|---|---|---|---|---|
| Population | Significant findings | Non-significant findings | ||||
| Garmel19 | Prospective cohort | N=187 | Increased preterm birth (OR=3.23; 95% CI, 1.4–7.3) in oligohydramnios group | IUGR, asphyxia, death, NICU admit | Delivery recommended at 37 weeks | 2 |
| 17–37 week with subnormal EFW (>10%) | 65 AFI <8 cm vs 122 AFI >8 cm | |||||
| Conway18 | Prospective cohort | N=366 | Increased CS rate (OR=2.7 95% CI, 1.3–5.4) in oligohydramnios group | CS for fetal distress; all neonatal outcomes | Treatment group induced, controls spontaneous | 2 |
| Term, isolated oligohydramnios undergoing induction | 183 AFI <5 cm vs 183 AFI >5 cm | |||||
| Roberts21 | Prospective cohort | N=206 | Increased IUGR (OR=5.2; 95% CI, 1.6–22), induction (OR=34.4, 95% CI, 4–1425.5), NICU admit (OR=9.8; 95% CI, 1.3–432) | Fetal distress requiring CS | Used >5%ile to exclude IUGR. Included some high-risk pts (diabetes or hypertension) | 2 |
| 3rd trimester, isolated oligohydramnios | 103 AFI 3%ile (N=103) vs matched control | |||||
| Rainford22 | Retrospective cohort | N=232 | Induction rate for AFI <5 = 98% vs 51% AFI >5 P<.001; increased meconium staining in controls without oligohydramnios | NICU 2 admissions, 5-minute Apgar scores | 2 | |
| 37–41 week, low-risk. AFI within 4 days of delivery | AFI <5 (n=44) vs >5 (n=188) | |||||
| Zhang23 | Retrospective nested cohort | N=6657 | Malpresentation (RR=3.5, 95% CI 1.8–6.60) | Fetal growth, CS, low Apgar, overall neonatal morbidity | Benefit of routine ultrasound was the primary study outcome study endpoint | 2 |
| Term or near-term, low-risk | AFI <5 (n=86) vs >5 (n=6571) | |||||
| AFI, amniotic fluid index; CI, confidence interval; CS, cesarean section; EFW, estimated fetal weight; IUGR, intrauterine growth restriction; LOE, level of evidence; NICU, neonatal intensive care unit; OR, odds ratio; RR, relative risk. | ||||||
Effect of maternal hydration
Maternal hydration status and plasma osmolality have an affect on amniotic fluid volume (Table 2). Maternal hydration with oral water or intravenous hypotonic solutions has been shown to increase amniotic fluid volume.8,11-13 Oral hydration with hypotonic fluid has been demonstrated to increase fetal urine production in one observational study.32 Another observational study demonstrated increased amniotic fluid volume and uteroplacental perfusion without alteration of fetal urine production suggesting the possibility that transmembranous fluid shifts from the placenta to the amniotic cavity may be involved.12
Two small, randomized controlled trials (RCTs) demonstrated an increase in amniotic fluid volume in women with oligohydramnios after oral hydration.11,13 Doi demonstrated significant increases in AFI in women with oligohydramnios beyond 35 weeks when given oral hydration with free water (increase of 3.8 cm ± 1.9; P<. 001) or hypotonic intravenous solution (increase of 2.8 cm ± 1.9; P<.001) (LOE: 3).11 Interestingly, this study did not demonstrate an increase in amniotic fluid volume with intravenous hydration with isotonic fluid.
Kirkpatrick demonstrated a 30% increase in amniotic fluid compared with controls in women of unspecified gestational age with oligohydramnios given 2 liters of oral water 2 to 5 hours before repeat amniotic fluid index (LOE: 3).13
A randomized trial in women with normal amniotic fluid demonstrated a 16% increase in amniotic fluid index 4 to 6 hours after hydration with 2 liters of oral water, compared with an 8% decrease after fluid restriction during the same period.8
A recent study of daily oral hydration in women with amniotic fluid volume <10% percentile showed increased amniotic fluid volume at 1 week, suggesting long-term benefit, although the study lacked an appropriate control group (LOE: 3).33
There are no studies of clinical outcomes such as fetal heart rate decelerations during labor, or neonatal outcomes. A Cochrane systematic review concluded that maternal hydration appears to increase amniotic fluid and may be beneficial in management of oligohydramnios; however, it recommended controlled trials to assess clinical outcome benefits (LOE: 3).34
TABLE 2
Effect of hydration on amniotic fluid index
| Study | Design | Population | Intervention | Outcome | Comment | LOE |
|---|---|---|---|---|---|---|
| Kilpatrick32 | RCT | N=40, AFI 2.1–6.0; population of patients referred for antenatal testing | Treatment group drank 2 L water and repeat AFI same or next day | Increase of 1.5 ± 1.4 cm (P<.01) in treatment group | Gestational ages of subjects not stated | 3 |
| Kilpatrick37 | RCT | N=40, AFI 7–24 cm, gestational 28 weeks | Treatment group instructed to drink 2 L and restricted group 0.1 L water. AFI repeated in 4–6 h | Increase of 3.0 ± 2.4 cm (P<.0001) in treatment group; decrease of 1.5 ± 2.7cm in controls (P <.02) | Subjects had normal AFI at entry | 3 |
| Flack36 | Prospective cohort | N=20, 10 w/AFI <5 cm, 10 controls AFI >7, 3rd trimester | 2 L oral water over 2 h for treatment and control groups, repeat AFI at 2 h | Increase in 3.2 cm in AFI (95% CI, 1.1–5.3) in oligohydramnios group but not in normal AFI group | Improved uterine perfusion shown by increased uterine artery velocity only in oligohydramnios group | 3 |
| Doi35 | RCT | N=84, AFI <5, at least 35 wks; randomized three maternal hydration methods (2 L oral water, hypotonic saline IV, or isotonic saline IV) | Hydration with 2 L fluid and AFI repeated in 1 h compared with controls | Significant increases in AFI in oral water and hypotonic IV groups by 3.8 cm and 2.8 cm (P<.001) respectively | IV isotonic solutions did not increase amniotic fluid volume in study population | 3 |
| RCT, randomized controlled trial; AFI, amniotic fluid index; CI, confidence interval. | ||||||
Management recommendations
The AFI has low specificity and positive predictive value for oligohydramnios, and there is scant evidence that isolated term oligohydramnios causes adverse fetal outcomes. We recommend that an AFI under 5 cm should prompt additional antenatal testing rather than immediate induction in low-risk term pregnancies (SOR: B).
Though we acknowledge the lack of high-quality studies with patient-oriented outcomes to support observation and maternal hydration, we have developed a management strategy that does not require immediate induction of labor in women with uncomplicated term pregnancies.
The following recommendations apply to women having oligohydramnios as defined by amniotic fluid volume of less than 5 cm and gestational age between 37 and 41 weeks.
Initial assessment
- Assess for premature rupture of membranes with a thorough history and a sterile speculum exam
- Reassess dating as oligohydramnios in post-dates pregnancy (>41 weeks) is an indication for induction (SOR: C)35
- Perform a nonstress test to assess fetal wellbeing
- Assess for IUGR with an ultrasound for estimated fetal weight and for the ratio of head circumference (HC) to abdominal circumference (AC). A comparison with prior ultrasounds can aid in assessing interval growth. An estimated fetal weight below the 10%, an elevated HC/AC ratio, or poor interval growth would suggest IUGR
- Arrange for an ultrasound anatomic survey for fetal anomalies, if not done previously
- Determine if preeclampsia, chronic hypertension, diabetes, or other maternal conditions associated with uteroplacental insufficiency are present.
Action steps
With any positive findings in the initial evaluation, proceed to labor induction, as the patient does not have isolated, term oligohydramnios (SOR: C). If the initial assessment is unremarkable and the AFI is less than 5, consider hydration with oral water and repeating the AFI 2 to 6 hours later (SOR: B).
Persistent oligohydramnios at term, particularly with a ripe cervix, may lead you to consider labor induction. Continued expectant management of isolated term oligohydramnios with twice weekly fetal surveillance may also be a reasonable option due to the paucity of evidence that oligohydramnios is associated with an adverse outcome in this scenario (SOR: C). Normal results with umbilical artery Doppler flow studies have been used to decrease the need for induction in high-risk pregnancies with oligohydramnios, and this technique may eventually have a role in isolated term oligohydramnios.36
It is essential that patients receive counseling and give informed consent regarding the risks and benefits of observation or induction for isolated term oligohydramnios. The ease of induction based on parity and cervical ripeness should be considered.
A primiparous woman with an unfavorable cervix who strongly desires a spontaneous, vaginal birth could be told that, although there may be a small risk for her baby, no study has demonstrated any increased long-term morbidity or mortality associated with low fluid in her situation and that labor induction may double her chance of cesarean delivery.37,38 In such a situation, an acceptable approach for mother and clinician may be rehydration followed by a repeat AFI and close follow-up with testing for fetal well-being according to the algorithm (Figure). In a practical sense, rehydration with 2 liters of oral water for oligohydramnios may be done whether or not immediate induction is chosen, as this is a safe measure that has been shown to significantly increase AFI. Alternatively, the preferred approach for a multiparous woman with a ripe cervix by Bishop score may be labor induction.
As adverse fetal outcomes have not been demonstrated in women with isolated term oligohydramnios, there is no rationale for routinely inducing labor based on an isolated finding of a so called “borderline” amniotic fluid index in the 5-to-8 range. In this situation it is appropriate to perform the initial assessment described above and may be reasonable to repeat the amniotic fluid index in 3 to 4 days to determine if true oligohydramnios has developed.
FIGURE
Assessment of the pregnant woman with oligohydramnios at term
Acknowledgments
We appreciate the assistance of George Gilson MD, Lauren Plante MD, and William Rayburn MD in manuscript review.
Corresponding author
Lawrence Leeman, MD, MPH, University of New Mexico Depts of Family and Community Medicine, Obstetrics and Gynecology, 2400 Tucker NE, 3rd floor, Albuquerque, NM 87131. E-mail: [email protected].
1. Moore TR. Clinical assessment of amniotic fluid. Clin Obstet Gynecol 1997;40:303-313.
2. Phelan JP, Smith CV, Broussard P, Small M. Amniotic fluid volume assessment with the four-quadrant technique at 36–42weeks’ gestation. J Reprod Med 1987;32:540-542.
3. Banks EH. Perinatal risks associated with borderline amniotic fluid index. Am J Obstet Gynecol 1999;180:1461-1463.
4. Casey BM. Pregnancy outcomes after antepartum diagnosis of oligohydramnios at or beyond 34 weeks gestation. Am J Obstet Gynecol 2000;182:909-912.
5. Hobbins JC. Oligohydramnios and post-term pregnancy. Ob/Gyn Clinical Alert December 2002;59-60.
6. Johnson DP, Davis NR, Brown AJ. Risk of cesarean delivery after induction at term in nulliparous women with an unfavorable cervix. Am J Obstet Gynecol 2003;188:1565-1572.
7. Lydon-Rochelle M, Holt VL, Easterling TR, Martin DP. Risk of uterine rupture during labor among women with a prior cesarean delivery. N Engl J Med 2001;345:3-8.
8. Kilpatrick SJ, Safford KL. Maternal hydration increases amniotic fluid index in women with normal amniotic fluid. Obstet Gynecol 1993;81:49-52.
9. Gilbert WM, Brace RA. Amniotic fluid volume and normal flows to and from the amniotic cavity. Seminars in Perinatology 1993;17:150-157.
10. Chandra PC, Schiavello HJ, Lewandowski MA. Effect of oral and intravenous hydration on oligohydramnios. J Reprod Med 2000;45:337-340.
11. Doi S, Osada H, Seki K, Sekiya S. Effect of maternal hydration on oligohydramnios: a comparison of three volume expansion methods. Obstet Gynecol 1998;92:525-529.
12. Flack NJ, Sepulveda W, Bower S, Fisk NM. Acute maternal hydration in third-trimester oligohydramnios: effects on amniotic fluid volume, uteroplacental perfusion, and fetal blood flow and urine output. Am J Obstet Gynecol 1995;173:1186-1191.
13. Kilpatrick SJ, Safford KL, Pomeroy T, Hoedt L, Scheerer L, Laros RK. Maternal hydration increases amniotic fluid index. Obstet Gynecol 1991;78:1098-1102.
14. Larmon JE, Ross BS. Clinical utility of amniotic fluid volume assessment. Obstet Gynecol Clin North Am 1998;25:639-661.
15. Hill LM. Oligohydramnios: sonographic diagnosis and clinical implications. Clin Obstet Gynecol 1997;40:314-327.
16. Flack NJ, Dore C, Southwell D, Kourtis P, Sepulveda W, Fisk NM. The influence of operator transducer pressure on ultrasonographic measurements of amniotic fluid volume. Am J Obstet Gynecol 1994;171:218-222.
17. Rutherford SE, Smith CV, Phelan JP, Kawakami K, Ahn MO. Four-quadrant assessment of amniotic fluid volume: interobserver and intraobserver variation. J Reprod Med 1987;32:587-589.
18. Bruner JP, Reed GW, Sarno AP, Harrington RA, Goodman MA. Intraobserver and interobserver variability of the amniotic fluid index. Am J Obstet Gynecol 1993;168:1309-1313.
19. O’Reilly-Green CP, Divon MY. Predictive value of amniotic fluid index for oligohydramnios in patients with prolonged pregnancies. J Matern Fetal Med 1996;5:218-226.
20. Chauhan SP, Magann EF, Morrison JC, Whitworth NS, Hendrix NW, Devoe LD. Ultrasonographic assessment of amniotic fluid does not reflect actual amniotic fluid volume. Am J Obstet Gynecol 1997;177:291-297.
21. Chauhan SP, Sanderson M, Hendrix NW, Magann EF, Devoe LD. Perinatal outcome and amniotic fluid index in the antepartum and intrapartum periods: a meta-analysis. Am J Obstet Gynecol 1999;181:1473-1478.
22. Magann EF. Antenatal testing among 1001 patients at high risk: the role of ultrasonographic estimate of amniotic fluid volume. Am J Obstet Gynecol 1999;180:1330-1336.
23. Magann EF. Does an amniotic fluid index of 5 cm necessitate delivery in high-risk pregnancies? A case-control study. Am J Obstet Gynecol 1999;180:1354-1359.
24. Nisell H, Ek S. Perinatal risks associated with borderline amniotic fluid index. Am J Obstet Gynecol. 2000;182:750-751.
25. Conway DL, et al. Isolated oligohydramnios in the term pregnancy: Is it a clinical entity. J Matern Fetal Med 1998;7:197-200.
26. Garmel SH, Chelmow D, Sha SJ, Roan JT, D’Alton ME. Oligohydramnios and the appropriately grown fetus. Am J Perinatol 1997;14:359-363.
27. Kreiser D, el-Sayed YY, Sorem KA, Chitkara U, Holbrook RH, Jr, Druzin ML. Decreased amniotic fluid index in low-risk pregnancy. J Reprod Med 2001;46:743-746.
28. Roberts D, Nwosu EC, Walkinshaw SA. The fetal outcome in pregnancies with isolated reduced amniotic fluid volume in the third trimester. J Perinat Med 1998;26:390-395.
29. Rainford M, Adair R, Scialli AR, Ghidini A, Spong CY. Amniotic fluid index in the uncomplicated term pregnancy. Prediction of outcome. J Reprod Med 2001;46:589-592.
30. Zhang J, Troendle J, Meikle S, Klebanoff MA, Rayburn WF. Isolated oligohydramnios is not associated with adverse perinatal outcomes. BJOG 2004;111:220-225.
31. Conway DL, Groth S, Adkins WB, Langer O. Management of isolated oligohyramnios in the term pregnancy: a randomized clinical trial. Am J Obstet Gynecol 2000;182:S21.-
32. Oosterhof H, Haak MC, Aarnoudse JG. Acute maternal rehydration increases the urine production rate in the near-term human fetus. Am J Obstet Gynecol 2000;183:226-229.
33. Fait G, Pauzner D, Gull I, Lessing JB, Jaffa AJ, Wolman I. Effect of 1 week or oral hydration on the amniotic fluid index. J Reprod Med 2003;48:187-190.
34. Hofmeyr GJ, Gulmezoglu AM. Maternal hydration for increasing amniotic fluid volume in oligohydramnios and normal amniotic fluid volute (Cochrane Review). In: The Cochrane Library. Issue 4, 2002. Oxford: Update Software.
35. Sherer DM, Langer O. Oligohydramnios: use and misuse in clinical management. Ultrasound Obstet Gynecol 2001;18:411-419.
36. Carroll BC, Bruner JP. Umbilical artery Doppler velocimetry in pregnancies complicated by oligohydramnios. J Reprod Med 2000;45:562-566.
37. Seyb ST, Berka RJ, Socol ML, Dooley SL. Risk of cesarean delivery with elective induction of labor at term in nulliparous women. Obstet Gynecol 1999;94:600-607.
38. Yeast JD, Jones A, Poskin M. Induction of labor and the relationship to cesarean delivery: A review of 7001 consecutive inductions. Am J Obstet Gynecol 1999;180:628-633.
1. Moore TR. Clinical assessment of amniotic fluid. Clin Obstet Gynecol 1997;40:303-313.
2. Phelan JP, Smith CV, Broussard P, Small M. Amniotic fluid volume assessment with the four-quadrant technique at 36–42weeks’ gestation. J Reprod Med 1987;32:540-542.
3. Banks EH. Perinatal risks associated with borderline amniotic fluid index. Am J Obstet Gynecol 1999;180:1461-1463.
4. Casey BM. Pregnancy outcomes after antepartum diagnosis of oligohydramnios at or beyond 34 weeks gestation. Am J Obstet Gynecol 2000;182:909-912.
5. Hobbins JC. Oligohydramnios and post-term pregnancy. Ob/Gyn Clinical Alert December 2002;59-60.
6. Johnson DP, Davis NR, Brown AJ. Risk of cesarean delivery after induction at term in nulliparous women with an unfavorable cervix. Am J Obstet Gynecol 2003;188:1565-1572.
7. Lydon-Rochelle M, Holt VL, Easterling TR, Martin DP. Risk of uterine rupture during labor among women with a prior cesarean delivery. N Engl J Med 2001;345:3-8.
8. Kilpatrick SJ, Safford KL. Maternal hydration increases amniotic fluid index in women with normal amniotic fluid. Obstet Gynecol 1993;81:49-52.
9. Gilbert WM, Brace RA. Amniotic fluid volume and normal flows to and from the amniotic cavity. Seminars in Perinatology 1993;17:150-157.
10. Chandra PC, Schiavello HJ, Lewandowski MA. Effect of oral and intravenous hydration on oligohydramnios. J Reprod Med 2000;45:337-340.
11. Doi S, Osada H, Seki K, Sekiya S. Effect of maternal hydration on oligohydramnios: a comparison of three volume expansion methods. Obstet Gynecol 1998;92:525-529.
12. Flack NJ, Sepulveda W, Bower S, Fisk NM. Acute maternal hydration in third-trimester oligohydramnios: effects on amniotic fluid volume, uteroplacental perfusion, and fetal blood flow and urine output. Am J Obstet Gynecol 1995;173:1186-1191.
13. Kilpatrick SJ, Safford KL, Pomeroy T, Hoedt L, Scheerer L, Laros RK. Maternal hydration increases amniotic fluid index. Obstet Gynecol 1991;78:1098-1102.
14. Larmon JE, Ross BS. Clinical utility of amniotic fluid volume assessment. Obstet Gynecol Clin North Am 1998;25:639-661.
15. Hill LM. Oligohydramnios: sonographic diagnosis and clinical implications. Clin Obstet Gynecol 1997;40:314-327.
16. Flack NJ, Dore C, Southwell D, Kourtis P, Sepulveda W, Fisk NM. The influence of operator transducer pressure on ultrasonographic measurements of amniotic fluid volume. Am J Obstet Gynecol 1994;171:218-222.
17. Rutherford SE, Smith CV, Phelan JP, Kawakami K, Ahn MO. Four-quadrant assessment of amniotic fluid volume: interobserver and intraobserver variation. J Reprod Med 1987;32:587-589.
18. Bruner JP, Reed GW, Sarno AP, Harrington RA, Goodman MA. Intraobserver and interobserver variability of the amniotic fluid index. Am J Obstet Gynecol 1993;168:1309-1313.
19. O’Reilly-Green CP, Divon MY. Predictive value of amniotic fluid index for oligohydramnios in patients with prolonged pregnancies. J Matern Fetal Med 1996;5:218-226.
20. Chauhan SP, Magann EF, Morrison JC, Whitworth NS, Hendrix NW, Devoe LD. Ultrasonographic assessment of amniotic fluid does not reflect actual amniotic fluid volume. Am J Obstet Gynecol 1997;177:291-297.
21. Chauhan SP, Sanderson M, Hendrix NW, Magann EF, Devoe LD. Perinatal outcome and amniotic fluid index in the antepartum and intrapartum periods: a meta-analysis. Am J Obstet Gynecol 1999;181:1473-1478.
22. Magann EF. Antenatal testing among 1001 patients at high risk: the role of ultrasonographic estimate of amniotic fluid volume. Am J Obstet Gynecol 1999;180:1330-1336.
23. Magann EF. Does an amniotic fluid index of 5 cm necessitate delivery in high-risk pregnancies? A case-control study. Am J Obstet Gynecol 1999;180:1354-1359.
24. Nisell H, Ek S. Perinatal risks associated with borderline amniotic fluid index. Am J Obstet Gynecol. 2000;182:750-751.
25. Conway DL, et al. Isolated oligohydramnios in the term pregnancy: Is it a clinical entity. J Matern Fetal Med 1998;7:197-200.
26. Garmel SH, Chelmow D, Sha SJ, Roan JT, D’Alton ME. Oligohydramnios and the appropriately grown fetus. Am J Perinatol 1997;14:359-363.
27. Kreiser D, el-Sayed YY, Sorem KA, Chitkara U, Holbrook RH, Jr, Druzin ML. Decreased amniotic fluid index in low-risk pregnancy. J Reprod Med 2001;46:743-746.
28. Roberts D, Nwosu EC, Walkinshaw SA. The fetal outcome in pregnancies with isolated reduced amniotic fluid volume in the third trimester. J Perinat Med 1998;26:390-395.
29. Rainford M, Adair R, Scialli AR, Ghidini A, Spong CY. Amniotic fluid index in the uncomplicated term pregnancy. Prediction of outcome. J Reprod Med 2001;46:589-592.
30. Zhang J, Troendle J, Meikle S, Klebanoff MA, Rayburn WF. Isolated oligohydramnios is not associated with adverse perinatal outcomes. BJOG 2004;111:220-225.
31. Conway DL, Groth S, Adkins WB, Langer O. Management of isolated oligohyramnios in the term pregnancy: a randomized clinical trial. Am J Obstet Gynecol 2000;182:S21.-
32. Oosterhof H, Haak MC, Aarnoudse JG. Acute maternal rehydration increases the urine production rate in the near-term human fetus. Am J Obstet Gynecol 2000;183:226-229.
33. Fait G, Pauzner D, Gull I, Lessing JB, Jaffa AJ, Wolman I. Effect of 1 week or oral hydration on the amniotic fluid index. J Reprod Med 2003;48:187-190.
34. Hofmeyr GJ, Gulmezoglu AM. Maternal hydration for increasing amniotic fluid volume in oligohydramnios and normal amniotic fluid volute (Cochrane Review). In: The Cochrane Library. Issue 4, 2002. Oxford: Update Software.
35. Sherer DM, Langer O. Oligohydramnios: use and misuse in clinical management. Ultrasound Obstet Gynecol 2001;18:411-419.
36. Carroll BC, Bruner JP. Umbilical artery Doppler velocimetry in pregnancies complicated by oligohydramnios. J Reprod Med 2000;45:562-566.
37. Seyb ST, Berka RJ, Socol ML, Dooley SL. Risk of cesarean delivery with elective induction of labor at term in nulliparous women. Obstet Gynecol 1999;94:600-607.
38. Yeast JD, Jones A, Poskin M. Induction of labor and the relationship to cesarean delivery: A review of 7001 consecutive inductions. Am J Obstet Gynecol 1999;180:628-633.
Does continuity of care improve patient outcomes?
- Sustained continuity of care (SCOC) improves quality of care, by decreasing hospitalizations, decreasing emergency department use, and improving receipt of preventive services (SOR: B, based primarily on cohort studies).
- SCOC has been consistently documented to improve quality of care for patients with chronic conditions such as asthma and diabetes (SOR: B, primarily on cohort studies).
Objective Continuity of care is a cornerstone of primary care that has been promoted by recent trends in medical education and in the way health care delivery is organized. We sought to determine the effect of sustained continuity of care (SCOC) on the quality of patient care.
Data sources We conducted a systematic review of all articles in Medline (January, 1966 to January, 2002), Educational Resources Information Center (ERIC), and PSYCH INFO using the terms “continuity of care” or “continuity of patient care.” We identified additional titles of candidate articles by reviewing the bibliographies of articles from our original MEDLINE search, contacting experts in primary care, health care management, and health services research, and by reviewing bibliographies of textbooks of primary care and public health.
Study selection and data extraction Two investigators (MDC, SHJ) independently reviewed the full text to exclude articles that did not fulfill search criteria. Articles excluded were those that focused on physicians-in-training, on SCOC in a non–primary care setting, such as an inpatient ward, or on transitions from inpatient to the outpatient setting. We also excluded articles that did not correlate SCOC to a quality of care measure.
Data synthesis From 5070 candidate titles, we examined the full text of 260 articles and found 18 (12 cross-sectional studies, 5 cohort studies and 1 randomized controlled trial) that fulfilled our criteria. Five studies focused on patients with chronic illness (eg, asthma, diabetes).
Results No studies documented negative effects of increased SCOC on quality of care. SCOC is associated with patient satisfaction (4 studies), decreased hospitalizations and emergency department visits (7 studies), and improved receipt of preventive services (5 studies).
Conclusions SCOC improves quality of care, and this association is consistently documented for patients with chronic conditions. Programs to promote SCOC may best maximize impact by focusing on populations with chronic conditions.
Continuity of care (COC) has been promoted recently by such trends as the concept of the “medical home” for patients, use of gatekeepers in managed care organizations (MCOs), and “continuity clinics” for residency training.1-4 In assessing quality of care provided by MCOs, COC is indirectly measured through physician turnover rate.5 In addition, many states have enacted laws to guarantee patients’ rights to continue seeing their physician, when a physician’s contract with a MCO has been terminated.6
Continuity refers to “care over time by a single individual or team of health care professionals and to effective and timely communication of health information.”7 Previous work distinguishes continuity from longitudinality. Continuity refers to whether a patient sees the same clinician from one visit to the next. Longitudinality refers to whether the patient has an established, long-term relationship with a clinician.8 The term continuity is often used when actually describing longitudinality.
In this analysis, we distinguish between the 2 concepts and focus on the sustained continuity of care between a patient and a health care provider through a relationship over time. Since this focus most closely resembles the concept of longitudinality, we will distinguish this from COC as sustained continuity of care (SCOC).
SCOC may encourage communication between physician and patient throughout the course of a long-term relationship. As health care providers gain familiarity with a patient’s history, they may more effectively manage chronic conditions or monitor long-term development.
The advantage of SCOC lessens, however, as electronic medical information becomes more prevalent, allowing different providers to stay up to date on long-term issues. There are tradeoffs, too, with SCOC, such as not being able to see the next available provider in an urgent situation.9 Also, one provider voices one perspective or opinion; access to multiple perspectives can serve as a “check” for avoiding incorrect or delayed diagnoses.10 Providers with different expertise11 may be able to complement others’ skills and thus provide better services overall.12 Furthermore, SCOC could decrease communication if physicians or patients assume they know (or are known by) the other so well that new issues are not introduced or discussed.
Given these tradeoffs, it is not surprising that different studies suggest conflicting results regarding SCOC and quality.13, 15 Although Dietrich et al previously reviewed this topic, the following analysis incorporates new studies published since the previous analysis.16
Methods
Data sources
We conducted a systematic review to identify studies examining the relationship between SCOC and quality of care. We searched articles limited to the English language and human subjects, published from January 1, 1966, to January 1, 2002, using Medline, the Educational Resources Information Center (ERIC) and PSYCH INFO. Candidate articles were those with titles containing the medical subject heading (MeSH) descriptors “continuity of patient care” or “continuity of care.”
Additional titles were found in the bibliographies of articles accepted in our original search, through experts in primary care, health care management, and research, and in the bibliographies of relevant textbooks.
Data selection
Two investigators (MDC, SHJ) screened titles and full bibliographic citations to identify candidate articles. We excluded letters, editorials, and practice guidelines. We accepted randomized controlled trials (RCT), cross-sectional, case-control, and cohort studies.
We excluded articles in which a significant percentage of providers were physicians in training. Our focus was SCOC in the outpatient setting; we excluded articles that analyzed inpatient or chronic care facility settings, or transitions to or from an outpatient setting (eg, post-hospitalization discharge care).
In many RCTs, implementation of SCOC was part of a multifaceted intervention (eg, multidisciplinary clinic and home care).17, 18 Although these studies examined quality of care, the effect of SCOC was indistinguishable from that of broader intervention. If the effect of SCOC could not be distinguished, we excluded the study. Finally, we excluded articles that did not measure SCOC in relation to a quality of care endpoint or a cost of care endpoint, defined below.
Quality-of-care and cost endpoints for analysis
The definition of quality of care was based on a framework described by Donabedian.19Structure is part of this framework for quality and includes resources (such as buildings, equipment, staff) available to provide health care that may or not promote SCOC. Since SCOC itself is a product of structure, we did not include structure in our analysis.
We defined 4 possible endpoints: process of care, outcomes, satisfaction, and cost of care. Process of care refers to differences in the delivery of care or differences in the receipt of care by patients. Outcome is any change in the health status of a patient. Satisfaction is an individual’s (eg, patient, caregiver, or provider) emotional or cognitive evaluation of the structure, process, or outcome of health care.20Cost of care encompasses direct and indirect costs to patient, payer, and society.
Determination of SCOC
Though there is no standard method to determine SCOC, we accepted only studies that fulfilled the criteria below.
The method had to (i) measure SCOC at the provider-level. We did not use a site-based measure, since it is possible for a patient to visit the same clinic multiple times and see different providers.
The method had to (ii) determine SCOC over a time frame longer than one visit. We did not include studies that used “did you see the physician at the last visit?” as a method for determining SCOC. Although this fulfills definition for continuity used in other studies,8 the purpose of the current analysis was to examine the effect of SCOC (ie, longitudinality) on quality.
The method had to (iii) be applied consistently to all patients. We did not accept studies that used “number of physicians seen” if the study did not standardize the observation period. Patients observed for longer periods would likely have seen more physicians in general, and have been at greater risk for lower SCOC, than would patients observed for shorter periods. Since it is not clear if the SCOC measure would be consistently applied, a study using this type of measure was excluded.
Finally, the method had to (iv) account for the possibility of more than one provider during the observed time period. We did not include studies that used “duration of time that the patient has seen the provider” as a measure of SCOC. Theoretically, any number of other providers could have seen the patient during this time and affected the SCOC.
Two investigators (MDC, SHJ) independentlyreviewed the full text to exclude articles not fulfilling criteria. Differences were resolved by informal consensus. We calculated a kappa score to measure the degree of agreement in the selection process.
Data extraction and analysis
We abstracted study design, location, population, method to calculate SCOC, and the association of SCOC with a study endpoint. We grouped articles in relation to endpoint measured. Simple counts and descriptive statistics of the articles were calculated. If 2 articles used data from the same study, we used the more recent article.
Results
Search yield
We found 5087 candidate titles in our original search. We excluded 4891 titles after examination of the bibliographic citation, which left 196 articles. After examining the full text of these remaining articles, 18 fulfilled our criteria (Table 1). The kappa to measure the preconsensus inter-rater reliability for article selection was 0.93.
Study designs
Of the 18 articles in the final analysis, 12 (67%) were cross-sectional studies,21-32 five (28%) were cohort studies,33- 37 and one (6%) was an RCT.38 In the RCT, subjects were elderly men enrolled in a Veteran’s Administration outpatient clinic. Subjects randomized to the “discontinuity” group had a 33% chance of being scheduled with a different provider at each visit and were also scheduled with a different provider if they had seen the same provider for the previous 2 visits. Subjects in the “continuity” group were scheduled to see the same provider routinely.38
Study populations, providers, and settings
Fifteen of the 18 studies (83%) were conducted in the United States. Ten studies (56%) focused on specific groups of patients: those insured by Medicaid (n=4), adults with diabetes (n=2), multiethnic women, elderly men, adults with seizure disorder, children with chronic diseases, and children and adults with asthma (n=1 each).
Health care providers in these studies included different primary care specialties, such as family medicine (n=4), pediatrics (n=4), general practice (n=2), internal medicine (n=1), and mixed primary care physicians (n=5). One study included pediatric subspecialists. In 5, the SCOC was described for the patient’s “regular physician.”
Methods used to measure SCOC
Table 2 displays the different methods and data sources used to determine SCOC. Data sources included medical records (n=3), medical claims data (n=5), and surveys (n=10). One study calculated SCOC separately using both medical records and a patient survey.22
Six of the methods used formulas to account for different combinations of factors, such as number of visits, dispersion of providers, and number of visits to a particular provider (see Appendix). There were 8 different methods to determine SCOC based on survey responses, ranging from single item questions24, 32 to a 23-item perception of continuity scale.22
Associations between SCOC and quality or cost of care
Overall, we found no studies documenting any negative effects of increased SCOC on quality or care. Due to the heterogeneity of methods to calculate SCOC and endpoints, we were unable to combine results.
Costs. Two cross-sectional studies examined factors associated with cost of care (Table 1). Increased SCOC measured by the usual provider continuity (UPC) index correlated with increased provider or MCO cost of care (P<.05); however, the results were not significant when SCOC was measured using other indicies.22 Another study found that increased SCOC was associated with decreased total annual health care expenditures.23
Satisfaction. Although we could not pool results of studies due to heterogeneity, there is a consistent association between SCOC and patient satisfaction, based on the results of 4 studies (Table 1).
Three cross-sectional studies in different settings21, 22, 31 found a positive association between increased SCOC and patient satisfaction. However, all 3 studies used subjective methods to determine SCOC. One study that used quantitative methods to measure SCOC (ie, COC index, UPC scale) did not find a statistically significant association with patient satisfaction.22 One RCT found no effect on satisfaction with patient-provider interaction overall (P>.05).38
Patient outcomes. The effect of SCOC seems consistent across studies for patients with chronic conditions who were hospitalized or visited emergency departments (Table 1).
In one RCT, the continuity group had fewer hospital days (5.7 vs. 9.1, P=.02); fewer intensive care days (0.4 vs. 1.4, P=.01); shorter hospital length of stay (15.5 vs. 25.5, P=.008); and lower percentages of emergent hospitalization (20% vs 39%, P=.002) compared with the discontinuity group. Of note, the subjects were all elderly men, of whom 47% had cardiovascular disease and 18% had respiratory disease.38
In 2 cross-sectional and 4 cohort studies, SCOC led to decreased hospitalizations and emergency department use, and to some improvements in preventive health behavior. Half of the studies focused on patients with chronic conditions (asthma or diabetes).33, 34, 37 Medicaid claims data analyses suggest that higher SCOC is associated with decreased likelihood of making single and multiple emergency department visits, hospitalizations overall, and hospitalizations for chronic conditions.26, 36 However, higher SCOC did not decrease the risk of hospitalization for acute ambulatory care sensitive conditions (eg, gastroenteritis).36
Process of care. For preventive services, 5 cross-sectional studies found that increased SCOC improved receipt of preventive services (Table 1).24, 28-30, 32, 33, 35
Two cross-sectional studies examined the association between SCOC and patient-provider communication.35 One study found that increased SCOC improved communication and patient perception regarding the ability to influence treatment.27 One study on epilepsy care found greater patient ease in talking to the physician.25
One RCT found no differences in scheduled or unscheduled clinic visits, specialty referrals, or receipt of preventive care procedures such as blood pressure measurement, weight assessment, or assessment of smoking status (P>.05).38
Discussion
Increased SCOC has not had any negative effects on quality of care. Indeed, in many cases, increased SCOC heightens patient satisfaction, decreases hospitalizations and emergency department visits, and improves receipt of preventive services. The positive effect of SCOC on health care use has been well documented for patients with chronic conditions. Although our search strategy and exclusion criteria differed from a previous review by Dietrich et al, we report similar conclusions regarding SCOC and patient satisfaction.16
We observed that the association between SCOC and quality of care appears most consistent for patients with chronic conditions, and we think there are several reasons for this relationship. Improved care should evolve throughout the course of a long-term relationship. The time frame of most studies in our analysis was limited, with the longest being only 2 years. It is possible that the benefits of SCOC do not become manifest until a much longer time period or after many visits with the same primary care provider.
However, patients with chronic disease are more likely to use outpatient, emergency department, and hospital services than are otherwise healthy persons. The increased number of outpatient visits by a patient with chronic disease may establish SCOC more quickly in a relationship, compared with patients who have fewer outpatient visits in general. The increased frequency of emergency department use and hospitalizations for patients with chronic disease may also magnify the effects and benefits of SCOC. As a result, it may be easier to detect the positive effects of SCOC for patients with chronic disease.
Finally, low SCOC may simply be a marker for other factors (associated with the patient or health care system) that are linked to decreased quality of care or increased costs.
Limitations
Because this review included only published articles, it is susceptible to publication bias.40 We included only studies that looked at the effect of SCOC on quality of care, and excluded studies that considered SCOC as part of a larger intervention. It is not clear if this under- or overestimates the effect of SCOC. However, by including only such studies, we are underreporting the overall evidence base of the effect of SCOC on quality of care.
Benefits of SCOC may occur if a patient develops a consistent relationship with a specific clinic or practice site. Since we limited our analysis to the provider-level, our results might not reflect the benefits of SCOC in broader contexts.
Although SCOC has many positive effects on quality of care, absolute or complete SCOC may not necessarily be ideal. There may be tradeoffs between SCOC and patient access to care. One study suggested that in certain scenarios (ie, “minor problems”), convenience was more important than SCOC; however for chronic issues, SCOC was more valued.39 Although this analysis suggests that SCOC is associated with improved quality of care, it is beyond the scope of this study to suggest the ideal level of SCOC in relation to other factors such as access. The published studies in this analysis were not designed to address these issues.
Finally, patient satisfaction may not be an appropriate measure for quality in this particular analysis. Patients who are dissatisfied with care may be more likely to change physicians and thus have less continuity. However, in this analysis we examined quality-of-care endpoints separately from other endpoints.
Implications and future research
Based on our study criteria, our analysis suggests an association between SCOC and patient satisfaction, as well as improved process of care and patient outcomes.
Other areas remain to be investigated. We found few studies, for example, that examined the impact of SCOC on cost of care. Programs that attempt to maximize SCOC may require significant administrative resources and costs (ie, to improve scheduling or provider availability). In an era of limited resources, promoting increased investment in this area may necessitate a demonstration of the long-term financial effects of SCOC and the absence of any unintended consequences (eg, delays in diagnosis). Although there are specific expenditures associated with promoting SCOC, such changes should theoretically lower health care costs overall by decreasing avoidable hospitalizations or emergency department visits.
Future research should investigate which populations benefit most from SCOC. A significant portion of the evidence for the positive effects of SCOC on quality of care includes patients with chronic disease, such as asthma and diabetes. Programs or clinics with limited resources to promote SCOC may be able to maximize impact by focusing on such populations.
Acknowledgements
Presented in part at the Pediatric Academic Societies Annual Meeting, Seattle, Wash. May 6, 2003. Support (SHJ) provided by the National Institute of Child Health and Human Development T32 HD07534-03. The authors would like to thank Ms. Lucy M. Schiller and Ms. Kathryn L. Wheeler for their assistance in data collection, as well Ms. Kathryn Slish for her editorial assistance.
Corresponding author
Michael D. Cabana, MD, MPH, 6-D-19 NIB, Box 0456, 300 North Ingalls Street, Ann Arbor, MI 48109-0456. E-mail: [email protected]
1. Starfield B. Primary Care: Concept Evaluation and Policy New York, NY: Oxford University Press 1998.;
2. American Academy of Pediatrics The Medical Home: Organizational Principles to Guide and Define the Child Health Care System and/or Improve the Health of All Children Pediatrics 2002;110:184-186.
3. Hunt CE, Kallenberg GA, Whitcomb ME. Trends in clinical education of medical students Arch Pediatr Adol Med 1999;153:297-302.
4. Halm EA, Causino N, Blumenthal D. Is gatekeeping better than traditional care? A survey of physicians’ attitudes JAMA 1997;278:1677-1681.
5. National Committee for Quality Assurance HEDIS 2003 Volume 2. Washington, DC: National Committee for Quality Assurance, 2003: Health Plan Stability pp. 151-158.
6. Guglielmo WJ. Mandated continuity of care: a solution in search of a problem? Med Econ December 1999;pp. 45-52.
7. Institute of Medicine Primary Care: America’s Health in a New Era Washington, DC: National Academy Press 1996.;
8. Starfield B. Continuous confusions? Am J Pub Health 1980;70-120.
9. Love MM, Mainous AG. Commitment to a regular physician: how long will patients wait to see their own physician for acute illness? J Fam Pract 1999;48:202-207.
10. Freeman G, Hjortdahl P. What future for continuity of care in general practice? BMJ 1997;314:1870.
11. Schroeder SA. Primary care at the crossroads Acad Med 2002;77:767-773.
12. Gallagher TC, Geling O, Comite F. Use of multiple providers for regular care and women’s receipt of hormone replacement therapy counseling Med Care 2001;39:1086-1096.
13. Christakis D. Consistent contact with a physician improves outcomes West J Med 2001;175:4.
14. Wachter RM. Discontinuity can improve patient care West J Med 2001;175:5.
15. Freeman G. What is the future for continuity of care in general practice? BMJ 1997;314:1870.
16. Dietrich AJ, Marton KI. Does continuous care from a physician make a difference? J Fam Pract 1982;15:929-937.
17. Becker MH, Drachman RH, Kirscht JP. A field experiment to evaluate various outcomes of continuity of physician care Am J Pub Health 1974;64:1062-1070.
18. Katz S, Vignos PJ, Moskowitz RW, Thompson HM, Svec KH. Comprehensive outpatient care in rheumatoid arthritis JAMA 1968;206:1249-1254.
19. Donabedian A. Evaluating the quality of medical care Milbank Quarterly 1966;44:166.
20. Campbell SM, Roland MO, Buetow S. Defining quality of care Soc Sci Med 2000;51:1611-1625.
21. Breslau N, Mortimer EA. Seeing the same doctor: determinants of satisfaction with specialty care for disabled children Med Care 1981;19:741-758.
22. Chao J. Continuity of care: incorporating patient perceptions Fam Med 1988;20:333-337.
23. Connelius LJ. The degree of usual provider continuity for African and Latino Americans J Health Care Poor Underserved 1997;8:170-185.
24. Ettner SL. The relationship between continuity of care and the health behaviors of patients: does having a usual physician make a difference? Med Care 1999;37:547-555.
25. Freeman GK, Richards SC. Personal continuity and the care of patients with epilepsy in general practice Brit J Gen Pract 1994;44:395-399.
26. Gill JM, Mainous AG, Nsereko M. The effect of continuity of care on emergency department use Arch Fam Med 2000;9:333-338.
27. Love MM, Mainous AG, Talbert JC, Hager GL. Continuity of care and the physician-patient relationship J Fam Pract 2000;49:998-1004.
28. O’Malley AS, Forrest CB. Continuity of care and delivery of ambulatory services to children in community health clinics J Comm Health 1996;21:159-173.
29. O’Malley AS, Mandelblatt J, Gold K, Cagney KA, Kerner J. Continuity of care and the use of breast and cervical cancer screening services in a multiethnic community Arch Intern Med 1997;157:1462-1470.
30. Strumberg JP, Schattner P. Personal doctoring: its impact on continuity of care as measured by the comprehensiveness of care score Austral Fam Physician 2001;30:513-518.
31. Weiss GL, Ramsey CA. Regular source of primary medical care and patient satisfaction QRB 1989;180-184.
32. Lambrew JM, DeFriese GH, Carey TS, Ricketts TC, Biddle AK. The effects of having a regular doctor on access to primary care Med Care 1996;34:138-151.
33. Christakis DA, Feudtner C, Pihoker C, Connell FA. Continuity and quality of care for children with diabetes who are covered by Medicaid Amb Peds 2001;1:99-103.
34. Christakis DA, Mell L, Koepsell TD, Zimmerman FJ, Connell FA. Association of lower continuity of care with greater risk of emergency department use and hospitalization in children Peds 2001;103:524-529.
35. Christakis DA, Mell L, Wright JA, Davis R, Connell FA. The association between greater continuity of care and timely measure-mumps-rubella vaccination Am J Pub Health 2000;90:962-965.
36. Gill JM, Mainous AG. The role of provider continuity in preventing hospitalizations Arch Fam Med 1998;7:352-357.
37. Parchman ML, Pugh JA, Noel PH, Larme AC. Continuity of care self managementbehaviors and glucose control in patients with type 2 diabetes Med Care 2002;40:137-144.
38. Wasson JH, Sauvigne AE, Mogielnicki P, et al. Continuity of outpatient medical care in elderly men. JAMA 1984;252:2413-2417.
39. Kearley KE, Freeman GK, Health A. An exploration of the value of the personal doctor patient relationship in general practice Brit J Gen Prac 2001;51:712-718.
40. Begg CB, Berlin JA. Publication bias: a problem in interpreting medical data J R Stat Soc 1988;151:419-463.
- Sustained continuity of care (SCOC) improves quality of care, by decreasing hospitalizations, decreasing emergency department use, and improving receipt of preventive services (SOR: B, based primarily on cohort studies).
- SCOC has been consistently documented to improve quality of care for patients with chronic conditions such as asthma and diabetes (SOR: B, primarily on cohort studies).
Objective Continuity of care is a cornerstone of primary care that has been promoted by recent trends in medical education and in the way health care delivery is organized. We sought to determine the effect of sustained continuity of care (SCOC) on the quality of patient care.
Data sources We conducted a systematic review of all articles in Medline (January, 1966 to January, 2002), Educational Resources Information Center (ERIC), and PSYCH INFO using the terms “continuity of care” or “continuity of patient care.” We identified additional titles of candidate articles by reviewing the bibliographies of articles from our original MEDLINE search, contacting experts in primary care, health care management, and health services research, and by reviewing bibliographies of textbooks of primary care and public health.
Study selection and data extraction Two investigators (MDC, SHJ) independently reviewed the full text to exclude articles that did not fulfill search criteria. Articles excluded were those that focused on physicians-in-training, on SCOC in a non–primary care setting, such as an inpatient ward, or on transitions from inpatient to the outpatient setting. We also excluded articles that did not correlate SCOC to a quality of care measure.
Data synthesis From 5070 candidate titles, we examined the full text of 260 articles and found 18 (12 cross-sectional studies, 5 cohort studies and 1 randomized controlled trial) that fulfilled our criteria. Five studies focused on patients with chronic illness (eg, asthma, diabetes).
Results No studies documented negative effects of increased SCOC on quality of care. SCOC is associated with patient satisfaction (4 studies), decreased hospitalizations and emergency department visits (7 studies), and improved receipt of preventive services (5 studies).
Conclusions SCOC improves quality of care, and this association is consistently documented for patients with chronic conditions. Programs to promote SCOC may best maximize impact by focusing on populations with chronic conditions.
Continuity of care (COC) has been promoted recently by such trends as the concept of the “medical home” for patients, use of gatekeepers in managed care organizations (MCOs), and “continuity clinics” for residency training.1-4 In assessing quality of care provided by MCOs, COC is indirectly measured through physician turnover rate.5 In addition, many states have enacted laws to guarantee patients’ rights to continue seeing their physician, when a physician’s contract with a MCO has been terminated.6
Continuity refers to “care over time by a single individual or team of health care professionals and to effective and timely communication of health information.”7 Previous work distinguishes continuity from longitudinality. Continuity refers to whether a patient sees the same clinician from one visit to the next. Longitudinality refers to whether the patient has an established, long-term relationship with a clinician.8 The term continuity is often used when actually describing longitudinality.
In this analysis, we distinguish between the 2 concepts and focus on the sustained continuity of care between a patient and a health care provider through a relationship over time. Since this focus most closely resembles the concept of longitudinality, we will distinguish this from COC as sustained continuity of care (SCOC).
SCOC may encourage communication between physician and patient throughout the course of a long-term relationship. As health care providers gain familiarity with a patient’s history, they may more effectively manage chronic conditions or monitor long-term development.
The advantage of SCOC lessens, however, as electronic medical information becomes more prevalent, allowing different providers to stay up to date on long-term issues. There are tradeoffs, too, with SCOC, such as not being able to see the next available provider in an urgent situation.9 Also, one provider voices one perspective or opinion; access to multiple perspectives can serve as a “check” for avoiding incorrect or delayed diagnoses.10 Providers with different expertise11 may be able to complement others’ skills and thus provide better services overall.12 Furthermore, SCOC could decrease communication if physicians or patients assume they know (or are known by) the other so well that new issues are not introduced or discussed.
Given these tradeoffs, it is not surprising that different studies suggest conflicting results regarding SCOC and quality.13, 15 Although Dietrich et al previously reviewed this topic, the following analysis incorporates new studies published since the previous analysis.16
Methods
Data sources
We conducted a systematic review to identify studies examining the relationship between SCOC and quality of care. We searched articles limited to the English language and human subjects, published from January 1, 1966, to January 1, 2002, using Medline, the Educational Resources Information Center (ERIC) and PSYCH INFO. Candidate articles were those with titles containing the medical subject heading (MeSH) descriptors “continuity of patient care” or “continuity of care.”
Additional titles were found in the bibliographies of articles accepted in our original search, through experts in primary care, health care management, and research, and in the bibliographies of relevant textbooks.
Data selection
Two investigators (MDC, SHJ) screened titles and full bibliographic citations to identify candidate articles. We excluded letters, editorials, and practice guidelines. We accepted randomized controlled trials (RCT), cross-sectional, case-control, and cohort studies.
We excluded articles in which a significant percentage of providers were physicians in training. Our focus was SCOC in the outpatient setting; we excluded articles that analyzed inpatient or chronic care facility settings, or transitions to or from an outpatient setting (eg, post-hospitalization discharge care).
In many RCTs, implementation of SCOC was part of a multifaceted intervention (eg, multidisciplinary clinic and home care).17, 18 Although these studies examined quality of care, the effect of SCOC was indistinguishable from that of broader intervention. If the effect of SCOC could not be distinguished, we excluded the study. Finally, we excluded articles that did not measure SCOC in relation to a quality of care endpoint or a cost of care endpoint, defined below.
Quality-of-care and cost endpoints for analysis
The definition of quality of care was based on a framework described by Donabedian.19Structure is part of this framework for quality and includes resources (such as buildings, equipment, staff) available to provide health care that may or not promote SCOC. Since SCOC itself is a product of structure, we did not include structure in our analysis.
We defined 4 possible endpoints: process of care, outcomes, satisfaction, and cost of care. Process of care refers to differences in the delivery of care or differences in the receipt of care by patients. Outcome is any change in the health status of a patient. Satisfaction is an individual’s (eg, patient, caregiver, or provider) emotional or cognitive evaluation of the structure, process, or outcome of health care.20Cost of care encompasses direct and indirect costs to patient, payer, and society.
Determination of SCOC
Though there is no standard method to determine SCOC, we accepted only studies that fulfilled the criteria below.
The method had to (i) measure SCOC at the provider-level. We did not use a site-based measure, since it is possible for a patient to visit the same clinic multiple times and see different providers.
The method had to (ii) determine SCOC over a time frame longer than one visit. We did not include studies that used “did you see the physician at the last visit?” as a method for determining SCOC. Although this fulfills definition for continuity used in other studies,8 the purpose of the current analysis was to examine the effect of SCOC (ie, longitudinality) on quality.
The method had to (iii) be applied consistently to all patients. We did not accept studies that used “number of physicians seen” if the study did not standardize the observation period. Patients observed for longer periods would likely have seen more physicians in general, and have been at greater risk for lower SCOC, than would patients observed for shorter periods. Since it is not clear if the SCOC measure would be consistently applied, a study using this type of measure was excluded.
Finally, the method had to (iv) account for the possibility of more than one provider during the observed time period. We did not include studies that used “duration of time that the patient has seen the provider” as a measure of SCOC. Theoretically, any number of other providers could have seen the patient during this time and affected the SCOC.
Two investigators (MDC, SHJ) independentlyreviewed the full text to exclude articles not fulfilling criteria. Differences were resolved by informal consensus. We calculated a kappa score to measure the degree of agreement in the selection process.
Data extraction and analysis
We abstracted study design, location, population, method to calculate SCOC, and the association of SCOC with a study endpoint. We grouped articles in relation to endpoint measured. Simple counts and descriptive statistics of the articles were calculated. If 2 articles used data from the same study, we used the more recent article.
Results
Search yield
We found 5087 candidate titles in our original search. We excluded 4891 titles after examination of the bibliographic citation, which left 196 articles. After examining the full text of these remaining articles, 18 fulfilled our criteria (Table 1). The kappa to measure the preconsensus inter-rater reliability for article selection was 0.93.
Study designs
Of the 18 articles in the final analysis, 12 (67%) were cross-sectional studies,21-32 five (28%) were cohort studies,33- 37 and one (6%) was an RCT.38 In the RCT, subjects were elderly men enrolled in a Veteran’s Administration outpatient clinic. Subjects randomized to the “discontinuity” group had a 33% chance of being scheduled with a different provider at each visit and were also scheduled with a different provider if they had seen the same provider for the previous 2 visits. Subjects in the “continuity” group were scheduled to see the same provider routinely.38
Study populations, providers, and settings
Fifteen of the 18 studies (83%) were conducted in the United States. Ten studies (56%) focused on specific groups of patients: those insured by Medicaid (n=4), adults with diabetes (n=2), multiethnic women, elderly men, adults with seizure disorder, children with chronic diseases, and children and adults with asthma (n=1 each).
Health care providers in these studies included different primary care specialties, such as family medicine (n=4), pediatrics (n=4), general practice (n=2), internal medicine (n=1), and mixed primary care physicians (n=5). One study included pediatric subspecialists. In 5, the SCOC was described for the patient’s “regular physician.”
Methods used to measure SCOC
Table 2 displays the different methods and data sources used to determine SCOC. Data sources included medical records (n=3), medical claims data (n=5), and surveys (n=10). One study calculated SCOC separately using both medical records and a patient survey.22
Six of the methods used formulas to account for different combinations of factors, such as number of visits, dispersion of providers, and number of visits to a particular provider (see Appendix). There were 8 different methods to determine SCOC based on survey responses, ranging from single item questions24, 32 to a 23-item perception of continuity scale.22
Associations between SCOC and quality or cost of care
Overall, we found no studies documenting any negative effects of increased SCOC on quality or care. Due to the heterogeneity of methods to calculate SCOC and endpoints, we were unable to combine results.
Costs. Two cross-sectional studies examined factors associated with cost of care (Table 1). Increased SCOC measured by the usual provider continuity (UPC) index correlated with increased provider or MCO cost of care (P<.05); however, the results were not significant when SCOC was measured using other indicies.22 Another study found that increased SCOC was associated with decreased total annual health care expenditures.23
Satisfaction. Although we could not pool results of studies due to heterogeneity, there is a consistent association between SCOC and patient satisfaction, based on the results of 4 studies (Table 1).
Three cross-sectional studies in different settings21, 22, 31 found a positive association between increased SCOC and patient satisfaction. However, all 3 studies used subjective methods to determine SCOC. One study that used quantitative methods to measure SCOC (ie, COC index, UPC scale) did not find a statistically significant association with patient satisfaction.22 One RCT found no effect on satisfaction with patient-provider interaction overall (P>.05).38
Patient outcomes. The effect of SCOC seems consistent across studies for patients with chronic conditions who were hospitalized or visited emergency departments (Table 1).
In one RCT, the continuity group had fewer hospital days (5.7 vs. 9.1, P=.02); fewer intensive care days (0.4 vs. 1.4, P=.01); shorter hospital length of stay (15.5 vs. 25.5, P=.008); and lower percentages of emergent hospitalization (20% vs 39%, P=.002) compared with the discontinuity group. Of note, the subjects were all elderly men, of whom 47% had cardiovascular disease and 18% had respiratory disease.38
In 2 cross-sectional and 4 cohort studies, SCOC led to decreased hospitalizations and emergency department use, and to some improvements in preventive health behavior. Half of the studies focused on patients with chronic conditions (asthma or diabetes).33, 34, 37 Medicaid claims data analyses suggest that higher SCOC is associated with decreased likelihood of making single and multiple emergency department visits, hospitalizations overall, and hospitalizations for chronic conditions.26, 36 However, higher SCOC did not decrease the risk of hospitalization for acute ambulatory care sensitive conditions (eg, gastroenteritis).36
Process of care. For preventive services, 5 cross-sectional studies found that increased SCOC improved receipt of preventive services (Table 1).24, 28-30, 32, 33, 35
Two cross-sectional studies examined the association between SCOC and patient-provider communication.35 One study found that increased SCOC improved communication and patient perception regarding the ability to influence treatment.27 One study on epilepsy care found greater patient ease in talking to the physician.25
One RCT found no differences in scheduled or unscheduled clinic visits, specialty referrals, or receipt of preventive care procedures such as blood pressure measurement, weight assessment, or assessment of smoking status (P>.05).38
Discussion
Increased SCOC has not had any negative effects on quality of care. Indeed, in many cases, increased SCOC heightens patient satisfaction, decreases hospitalizations and emergency department visits, and improves receipt of preventive services. The positive effect of SCOC on health care use has been well documented for patients with chronic conditions. Although our search strategy and exclusion criteria differed from a previous review by Dietrich et al, we report similar conclusions regarding SCOC and patient satisfaction.16
We observed that the association between SCOC and quality of care appears most consistent for patients with chronic conditions, and we think there are several reasons for this relationship. Improved care should evolve throughout the course of a long-term relationship. The time frame of most studies in our analysis was limited, with the longest being only 2 years. It is possible that the benefits of SCOC do not become manifest until a much longer time period or after many visits with the same primary care provider.
However, patients with chronic disease are more likely to use outpatient, emergency department, and hospital services than are otherwise healthy persons. The increased number of outpatient visits by a patient with chronic disease may establish SCOC more quickly in a relationship, compared with patients who have fewer outpatient visits in general. The increased frequency of emergency department use and hospitalizations for patients with chronic disease may also magnify the effects and benefits of SCOC. As a result, it may be easier to detect the positive effects of SCOC for patients with chronic disease.
Finally, low SCOC may simply be a marker for other factors (associated with the patient or health care system) that are linked to decreased quality of care or increased costs.
Limitations
Because this review included only published articles, it is susceptible to publication bias.40 We included only studies that looked at the effect of SCOC on quality of care, and excluded studies that considered SCOC as part of a larger intervention. It is not clear if this under- or overestimates the effect of SCOC. However, by including only such studies, we are underreporting the overall evidence base of the effect of SCOC on quality of care.
Benefits of SCOC may occur if a patient develops a consistent relationship with a specific clinic or practice site. Since we limited our analysis to the provider-level, our results might not reflect the benefits of SCOC in broader contexts.
Although SCOC has many positive effects on quality of care, absolute or complete SCOC may not necessarily be ideal. There may be tradeoffs between SCOC and patient access to care. One study suggested that in certain scenarios (ie, “minor problems”), convenience was more important than SCOC; however for chronic issues, SCOC was more valued.39 Although this analysis suggests that SCOC is associated with improved quality of care, it is beyond the scope of this study to suggest the ideal level of SCOC in relation to other factors such as access. The published studies in this analysis were not designed to address these issues.
Finally, patient satisfaction may not be an appropriate measure for quality in this particular analysis. Patients who are dissatisfied with care may be more likely to change physicians and thus have less continuity. However, in this analysis we examined quality-of-care endpoints separately from other endpoints.
Implications and future research
Based on our study criteria, our analysis suggests an association between SCOC and patient satisfaction, as well as improved process of care and patient outcomes.
Other areas remain to be investigated. We found few studies, for example, that examined the impact of SCOC on cost of care. Programs that attempt to maximize SCOC may require significant administrative resources and costs (ie, to improve scheduling or provider availability). In an era of limited resources, promoting increased investment in this area may necessitate a demonstration of the long-term financial effects of SCOC and the absence of any unintended consequences (eg, delays in diagnosis). Although there are specific expenditures associated with promoting SCOC, such changes should theoretically lower health care costs overall by decreasing avoidable hospitalizations or emergency department visits.
Future research should investigate which populations benefit most from SCOC. A significant portion of the evidence for the positive effects of SCOC on quality of care includes patients with chronic disease, such as asthma and diabetes. Programs or clinics with limited resources to promote SCOC may be able to maximize impact by focusing on such populations.
Acknowledgements
Presented in part at the Pediatric Academic Societies Annual Meeting, Seattle, Wash. May 6, 2003. Support (SHJ) provided by the National Institute of Child Health and Human Development T32 HD07534-03. The authors would like to thank Ms. Lucy M. Schiller and Ms. Kathryn L. Wheeler for their assistance in data collection, as well Ms. Kathryn Slish for her editorial assistance.
Corresponding author
Michael D. Cabana, MD, MPH, 6-D-19 NIB, Box 0456, 300 North Ingalls Street, Ann Arbor, MI 48109-0456. E-mail: [email protected]
- Sustained continuity of care (SCOC) improves quality of care, by decreasing hospitalizations, decreasing emergency department use, and improving receipt of preventive services (SOR: B, based primarily on cohort studies).
- SCOC has been consistently documented to improve quality of care for patients with chronic conditions such as asthma and diabetes (SOR: B, primarily on cohort studies).
Objective Continuity of care is a cornerstone of primary care that has been promoted by recent trends in medical education and in the way health care delivery is organized. We sought to determine the effect of sustained continuity of care (SCOC) on the quality of patient care.
Data sources We conducted a systematic review of all articles in Medline (January, 1966 to January, 2002), Educational Resources Information Center (ERIC), and PSYCH INFO using the terms “continuity of care” or “continuity of patient care.” We identified additional titles of candidate articles by reviewing the bibliographies of articles from our original MEDLINE search, contacting experts in primary care, health care management, and health services research, and by reviewing bibliographies of textbooks of primary care and public health.
Study selection and data extraction Two investigators (MDC, SHJ) independently reviewed the full text to exclude articles that did not fulfill search criteria. Articles excluded were those that focused on physicians-in-training, on SCOC in a non–primary care setting, such as an inpatient ward, or on transitions from inpatient to the outpatient setting. We also excluded articles that did not correlate SCOC to a quality of care measure.
Data synthesis From 5070 candidate titles, we examined the full text of 260 articles and found 18 (12 cross-sectional studies, 5 cohort studies and 1 randomized controlled trial) that fulfilled our criteria. Five studies focused on patients with chronic illness (eg, asthma, diabetes).
Results No studies documented negative effects of increased SCOC on quality of care. SCOC is associated with patient satisfaction (4 studies), decreased hospitalizations and emergency department visits (7 studies), and improved receipt of preventive services (5 studies).
Conclusions SCOC improves quality of care, and this association is consistently documented for patients with chronic conditions. Programs to promote SCOC may best maximize impact by focusing on populations with chronic conditions.
Continuity of care (COC) has been promoted recently by such trends as the concept of the “medical home” for patients, use of gatekeepers in managed care organizations (MCOs), and “continuity clinics” for residency training.1-4 In assessing quality of care provided by MCOs, COC is indirectly measured through physician turnover rate.5 In addition, many states have enacted laws to guarantee patients’ rights to continue seeing their physician, when a physician’s contract with a MCO has been terminated.6
Continuity refers to “care over time by a single individual or team of health care professionals and to effective and timely communication of health information.”7 Previous work distinguishes continuity from longitudinality. Continuity refers to whether a patient sees the same clinician from one visit to the next. Longitudinality refers to whether the patient has an established, long-term relationship with a clinician.8 The term continuity is often used when actually describing longitudinality.
In this analysis, we distinguish between the 2 concepts and focus on the sustained continuity of care between a patient and a health care provider through a relationship over time. Since this focus most closely resembles the concept of longitudinality, we will distinguish this from COC as sustained continuity of care (SCOC).
SCOC may encourage communication between physician and patient throughout the course of a long-term relationship. As health care providers gain familiarity with a patient’s history, they may more effectively manage chronic conditions or monitor long-term development.
The advantage of SCOC lessens, however, as electronic medical information becomes more prevalent, allowing different providers to stay up to date on long-term issues. There are tradeoffs, too, with SCOC, such as not being able to see the next available provider in an urgent situation.9 Also, one provider voices one perspective or opinion; access to multiple perspectives can serve as a “check” for avoiding incorrect or delayed diagnoses.10 Providers with different expertise11 may be able to complement others’ skills and thus provide better services overall.12 Furthermore, SCOC could decrease communication if physicians or patients assume they know (or are known by) the other so well that new issues are not introduced or discussed.
Given these tradeoffs, it is not surprising that different studies suggest conflicting results regarding SCOC and quality.13, 15 Although Dietrich et al previously reviewed this topic, the following analysis incorporates new studies published since the previous analysis.16
Methods
Data sources
We conducted a systematic review to identify studies examining the relationship between SCOC and quality of care. We searched articles limited to the English language and human subjects, published from January 1, 1966, to January 1, 2002, using Medline, the Educational Resources Information Center (ERIC) and PSYCH INFO. Candidate articles were those with titles containing the medical subject heading (MeSH) descriptors “continuity of patient care” or “continuity of care.”
Additional titles were found in the bibliographies of articles accepted in our original search, through experts in primary care, health care management, and research, and in the bibliographies of relevant textbooks.
Data selection
Two investigators (MDC, SHJ) screened titles and full bibliographic citations to identify candidate articles. We excluded letters, editorials, and practice guidelines. We accepted randomized controlled trials (RCT), cross-sectional, case-control, and cohort studies.
We excluded articles in which a significant percentage of providers were physicians in training. Our focus was SCOC in the outpatient setting; we excluded articles that analyzed inpatient or chronic care facility settings, or transitions to or from an outpatient setting (eg, post-hospitalization discharge care).
In many RCTs, implementation of SCOC was part of a multifaceted intervention (eg, multidisciplinary clinic and home care).17, 18 Although these studies examined quality of care, the effect of SCOC was indistinguishable from that of broader intervention. If the effect of SCOC could not be distinguished, we excluded the study. Finally, we excluded articles that did not measure SCOC in relation to a quality of care endpoint or a cost of care endpoint, defined below.
Quality-of-care and cost endpoints for analysis
The definition of quality of care was based on a framework described by Donabedian.19Structure is part of this framework for quality and includes resources (such as buildings, equipment, staff) available to provide health care that may or not promote SCOC. Since SCOC itself is a product of structure, we did not include structure in our analysis.
We defined 4 possible endpoints: process of care, outcomes, satisfaction, and cost of care. Process of care refers to differences in the delivery of care or differences in the receipt of care by patients. Outcome is any change in the health status of a patient. Satisfaction is an individual’s (eg, patient, caregiver, or provider) emotional or cognitive evaluation of the structure, process, or outcome of health care.20Cost of care encompasses direct and indirect costs to patient, payer, and society.
Determination of SCOC
Though there is no standard method to determine SCOC, we accepted only studies that fulfilled the criteria below.
The method had to (i) measure SCOC at the provider-level. We did not use a site-based measure, since it is possible for a patient to visit the same clinic multiple times and see different providers.
The method had to (ii) determine SCOC over a time frame longer than one visit. We did not include studies that used “did you see the physician at the last visit?” as a method for determining SCOC. Although this fulfills definition for continuity used in other studies,8 the purpose of the current analysis was to examine the effect of SCOC (ie, longitudinality) on quality.
The method had to (iii) be applied consistently to all patients. We did not accept studies that used “number of physicians seen” if the study did not standardize the observation period. Patients observed for longer periods would likely have seen more physicians in general, and have been at greater risk for lower SCOC, than would patients observed for shorter periods. Since it is not clear if the SCOC measure would be consistently applied, a study using this type of measure was excluded.
Finally, the method had to (iv) account for the possibility of more than one provider during the observed time period. We did not include studies that used “duration of time that the patient has seen the provider” as a measure of SCOC. Theoretically, any number of other providers could have seen the patient during this time and affected the SCOC.
Two investigators (MDC, SHJ) independentlyreviewed the full text to exclude articles not fulfilling criteria. Differences were resolved by informal consensus. We calculated a kappa score to measure the degree of agreement in the selection process.
Data extraction and analysis
We abstracted study design, location, population, method to calculate SCOC, and the association of SCOC with a study endpoint. We grouped articles in relation to endpoint measured. Simple counts and descriptive statistics of the articles were calculated. If 2 articles used data from the same study, we used the more recent article.
Results
Search yield
We found 5087 candidate titles in our original search. We excluded 4891 titles after examination of the bibliographic citation, which left 196 articles. After examining the full text of these remaining articles, 18 fulfilled our criteria (Table 1). The kappa to measure the preconsensus inter-rater reliability for article selection was 0.93.
Study designs
Of the 18 articles in the final analysis, 12 (67%) were cross-sectional studies,21-32 five (28%) were cohort studies,33- 37 and one (6%) was an RCT.38 In the RCT, subjects were elderly men enrolled in a Veteran’s Administration outpatient clinic. Subjects randomized to the “discontinuity” group had a 33% chance of being scheduled with a different provider at each visit and were also scheduled with a different provider if they had seen the same provider for the previous 2 visits. Subjects in the “continuity” group were scheduled to see the same provider routinely.38
Study populations, providers, and settings
Fifteen of the 18 studies (83%) were conducted in the United States. Ten studies (56%) focused on specific groups of patients: those insured by Medicaid (n=4), adults with diabetes (n=2), multiethnic women, elderly men, adults with seizure disorder, children with chronic diseases, and children and adults with asthma (n=1 each).
Health care providers in these studies included different primary care specialties, such as family medicine (n=4), pediatrics (n=4), general practice (n=2), internal medicine (n=1), and mixed primary care physicians (n=5). One study included pediatric subspecialists. In 5, the SCOC was described for the patient’s “regular physician.”
Methods used to measure SCOC
Table 2 displays the different methods and data sources used to determine SCOC. Data sources included medical records (n=3), medical claims data (n=5), and surveys (n=10). One study calculated SCOC separately using both medical records and a patient survey.22
Six of the methods used formulas to account for different combinations of factors, such as number of visits, dispersion of providers, and number of visits to a particular provider (see Appendix). There were 8 different methods to determine SCOC based on survey responses, ranging from single item questions24, 32 to a 23-item perception of continuity scale.22
Associations between SCOC and quality or cost of care
Overall, we found no studies documenting any negative effects of increased SCOC on quality or care. Due to the heterogeneity of methods to calculate SCOC and endpoints, we were unable to combine results.
Costs. Two cross-sectional studies examined factors associated with cost of care (Table 1). Increased SCOC measured by the usual provider continuity (UPC) index correlated with increased provider or MCO cost of care (P<.05); however, the results were not significant when SCOC was measured using other indicies.22 Another study found that increased SCOC was associated with decreased total annual health care expenditures.23
Satisfaction. Although we could not pool results of studies due to heterogeneity, there is a consistent association between SCOC and patient satisfaction, based on the results of 4 studies (Table 1).
Three cross-sectional studies in different settings21, 22, 31 found a positive association between increased SCOC and patient satisfaction. However, all 3 studies used subjective methods to determine SCOC. One study that used quantitative methods to measure SCOC (ie, COC index, UPC scale) did not find a statistically significant association with patient satisfaction.22 One RCT found no effect on satisfaction with patient-provider interaction overall (P>.05).38
Patient outcomes. The effect of SCOC seems consistent across studies for patients with chronic conditions who were hospitalized or visited emergency departments (Table 1).
In one RCT, the continuity group had fewer hospital days (5.7 vs. 9.1, P=.02); fewer intensive care days (0.4 vs. 1.4, P=.01); shorter hospital length of stay (15.5 vs. 25.5, P=.008); and lower percentages of emergent hospitalization (20% vs 39%, P=.002) compared with the discontinuity group. Of note, the subjects were all elderly men, of whom 47% had cardiovascular disease and 18% had respiratory disease.38
In 2 cross-sectional and 4 cohort studies, SCOC led to decreased hospitalizations and emergency department use, and to some improvements in preventive health behavior. Half of the studies focused on patients with chronic conditions (asthma or diabetes).33, 34, 37 Medicaid claims data analyses suggest that higher SCOC is associated with decreased likelihood of making single and multiple emergency department visits, hospitalizations overall, and hospitalizations for chronic conditions.26, 36 However, higher SCOC did not decrease the risk of hospitalization for acute ambulatory care sensitive conditions (eg, gastroenteritis).36
Process of care. For preventive services, 5 cross-sectional studies found that increased SCOC improved receipt of preventive services (Table 1).24, 28-30, 32, 33, 35
Two cross-sectional studies examined the association between SCOC and patient-provider communication.35 One study found that increased SCOC improved communication and patient perception regarding the ability to influence treatment.27 One study on epilepsy care found greater patient ease in talking to the physician.25
One RCT found no differences in scheduled or unscheduled clinic visits, specialty referrals, or receipt of preventive care procedures such as blood pressure measurement, weight assessment, or assessment of smoking status (P>.05).38
Discussion
Increased SCOC has not had any negative effects on quality of care. Indeed, in many cases, increased SCOC heightens patient satisfaction, decreases hospitalizations and emergency department visits, and improves receipt of preventive services. The positive effect of SCOC on health care use has been well documented for patients with chronic conditions. Although our search strategy and exclusion criteria differed from a previous review by Dietrich et al, we report similar conclusions regarding SCOC and patient satisfaction.16
We observed that the association between SCOC and quality of care appears most consistent for patients with chronic conditions, and we think there are several reasons for this relationship. Improved care should evolve throughout the course of a long-term relationship. The time frame of most studies in our analysis was limited, with the longest being only 2 years. It is possible that the benefits of SCOC do not become manifest until a much longer time period or after many visits with the same primary care provider.
However, patients with chronic disease are more likely to use outpatient, emergency department, and hospital services than are otherwise healthy persons. The increased number of outpatient visits by a patient with chronic disease may establish SCOC more quickly in a relationship, compared with patients who have fewer outpatient visits in general. The increased frequency of emergency department use and hospitalizations for patients with chronic disease may also magnify the effects and benefits of SCOC. As a result, it may be easier to detect the positive effects of SCOC for patients with chronic disease.
Finally, low SCOC may simply be a marker for other factors (associated with the patient or health care system) that are linked to decreased quality of care or increased costs.
Limitations
Because this review included only published articles, it is susceptible to publication bias.40 We included only studies that looked at the effect of SCOC on quality of care, and excluded studies that considered SCOC as part of a larger intervention. It is not clear if this under- or overestimates the effect of SCOC. However, by including only such studies, we are underreporting the overall evidence base of the effect of SCOC on quality of care.
Benefits of SCOC may occur if a patient develops a consistent relationship with a specific clinic or practice site. Since we limited our analysis to the provider-level, our results might not reflect the benefits of SCOC in broader contexts.
Although SCOC has many positive effects on quality of care, absolute or complete SCOC may not necessarily be ideal. There may be tradeoffs between SCOC and patient access to care. One study suggested that in certain scenarios (ie, “minor problems”), convenience was more important than SCOC; however for chronic issues, SCOC was more valued.39 Although this analysis suggests that SCOC is associated with improved quality of care, it is beyond the scope of this study to suggest the ideal level of SCOC in relation to other factors such as access. The published studies in this analysis were not designed to address these issues.
Finally, patient satisfaction may not be an appropriate measure for quality in this particular analysis. Patients who are dissatisfied with care may be more likely to change physicians and thus have less continuity. However, in this analysis we examined quality-of-care endpoints separately from other endpoints.
Implications and future research
Based on our study criteria, our analysis suggests an association between SCOC and patient satisfaction, as well as improved process of care and patient outcomes.
Other areas remain to be investigated. We found few studies, for example, that examined the impact of SCOC on cost of care. Programs that attempt to maximize SCOC may require significant administrative resources and costs (ie, to improve scheduling or provider availability). In an era of limited resources, promoting increased investment in this area may necessitate a demonstration of the long-term financial effects of SCOC and the absence of any unintended consequences (eg, delays in diagnosis). Although there are specific expenditures associated with promoting SCOC, such changes should theoretically lower health care costs overall by decreasing avoidable hospitalizations or emergency department visits.
Future research should investigate which populations benefit most from SCOC. A significant portion of the evidence for the positive effects of SCOC on quality of care includes patients with chronic disease, such as asthma and diabetes. Programs or clinics with limited resources to promote SCOC may be able to maximize impact by focusing on such populations.
Acknowledgements
Presented in part at the Pediatric Academic Societies Annual Meeting, Seattle, Wash. May 6, 2003. Support (SHJ) provided by the National Institute of Child Health and Human Development T32 HD07534-03. The authors would like to thank Ms. Lucy M. Schiller and Ms. Kathryn L. Wheeler for their assistance in data collection, as well Ms. Kathryn Slish for her editorial assistance.
Corresponding author
Michael D. Cabana, MD, MPH, 6-D-19 NIB, Box 0456, 300 North Ingalls Street, Ann Arbor, MI 48109-0456. E-mail: [email protected]
1. Starfield B. Primary Care: Concept Evaluation and Policy New York, NY: Oxford University Press 1998.;
2. American Academy of Pediatrics The Medical Home: Organizational Principles to Guide and Define the Child Health Care System and/or Improve the Health of All Children Pediatrics 2002;110:184-186.
3. Hunt CE, Kallenberg GA, Whitcomb ME. Trends in clinical education of medical students Arch Pediatr Adol Med 1999;153:297-302.
4. Halm EA, Causino N, Blumenthal D. Is gatekeeping better than traditional care? A survey of physicians’ attitudes JAMA 1997;278:1677-1681.
5. National Committee for Quality Assurance HEDIS 2003 Volume 2. Washington, DC: National Committee for Quality Assurance, 2003: Health Plan Stability pp. 151-158.
6. Guglielmo WJ. Mandated continuity of care: a solution in search of a problem? Med Econ December 1999;pp. 45-52.
7. Institute of Medicine Primary Care: America’s Health in a New Era Washington, DC: National Academy Press 1996.;
8. Starfield B. Continuous confusions? Am J Pub Health 1980;70-120.
9. Love MM, Mainous AG. Commitment to a regular physician: how long will patients wait to see their own physician for acute illness? J Fam Pract 1999;48:202-207.
10. Freeman G, Hjortdahl P. What future for continuity of care in general practice? BMJ 1997;314:1870.
11. Schroeder SA. Primary care at the crossroads Acad Med 2002;77:767-773.
12. Gallagher TC, Geling O, Comite F. Use of multiple providers for regular care and women’s receipt of hormone replacement therapy counseling Med Care 2001;39:1086-1096.
13. Christakis D. Consistent contact with a physician improves outcomes West J Med 2001;175:4.
14. Wachter RM. Discontinuity can improve patient care West J Med 2001;175:5.
15. Freeman G. What is the future for continuity of care in general practice? BMJ 1997;314:1870.
16. Dietrich AJ, Marton KI. Does continuous care from a physician make a difference? J Fam Pract 1982;15:929-937.
17. Becker MH, Drachman RH, Kirscht JP. A field experiment to evaluate various outcomes of continuity of physician care Am J Pub Health 1974;64:1062-1070.
18. Katz S, Vignos PJ, Moskowitz RW, Thompson HM, Svec KH. Comprehensive outpatient care in rheumatoid arthritis JAMA 1968;206:1249-1254.
19. Donabedian A. Evaluating the quality of medical care Milbank Quarterly 1966;44:166.
20. Campbell SM, Roland MO, Buetow S. Defining quality of care Soc Sci Med 2000;51:1611-1625.
21. Breslau N, Mortimer EA. Seeing the same doctor: determinants of satisfaction with specialty care for disabled children Med Care 1981;19:741-758.
22. Chao J. Continuity of care: incorporating patient perceptions Fam Med 1988;20:333-337.
23. Connelius LJ. The degree of usual provider continuity for African and Latino Americans J Health Care Poor Underserved 1997;8:170-185.
24. Ettner SL. The relationship between continuity of care and the health behaviors of patients: does having a usual physician make a difference? Med Care 1999;37:547-555.
25. Freeman GK, Richards SC. Personal continuity and the care of patients with epilepsy in general practice Brit J Gen Pract 1994;44:395-399.
26. Gill JM, Mainous AG, Nsereko M. The effect of continuity of care on emergency department use Arch Fam Med 2000;9:333-338.
27. Love MM, Mainous AG, Talbert JC, Hager GL. Continuity of care and the physician-patient relationship J Fam Pract 2000;49:998-1004.
28. O’Malley AS, Forrest CB. Continuity of care and delivery of ambulatory services to children in community health clinics J Comm Health 1996;21:159-173.
29. O’Malley AS, Mandelblatt J, Gold K, Cagney KA, Kerner J. Continuity of care and the use of breast and cervical cancer screening services in a multiethnic community Arch Intern Med 1997;157:1462-1470.
30. Strumberg JP, Schattner P. Personal doctoring: its impact on continuity of care as measured by the comprehensiveness of care score Austral Fam Physician 2001;30:513-518.
31. Weiss GL, Ramsey CA. Regular source of primary medical care and patient satisfaction QRB 1989;180-184.
32. Lambrew JM, DeFriese GH, Carey TS, Ricketts TC, Biddle AK. The effects of having a regular doctor on access to primary care Med Care 1996;34:138-151.
33. Christakis DA, Feudtner C, Pihoker C, Connell FA. Continuity and quality of care for children with diabetes who are covered by Medicaid Amb Peds 2001;1:99-103.
34. Christakis DA, Mell L, Koepsell TD, Zimmerman FJ, Connell FA. Association of lower continuity of care with greater risk of emergency department use and hospitalization in children Peds 2001;103:524-529.
35. Christakis DA, Mell L, Wright JA, Davis R, Connell FA. The association between greater continuity of care and timely measure-mumps-rubella vaccination Am J Pub Health 2000;90:962-965.
36. Gill JM, Mainous AG. The role of provider continuity in preventing hospitalizations Arch Fam Med 1998;7:352-357.
37. Parchman ML, Pugh JA, Noel PH, Larme AC. Continuity of care self managementbehaviors and glucose control in patients with type 2 diabetes Med Care 2002;40:137-144.
38. Wasson JH, Sauvigne AE, Mogielnicki P, et al. Continuity of outpatient medical care in elderly men. JAMA 1984;252:2413-2417.
39. Kearley KE, Freeman GK, Health A. An exploration of the value of the personal doctor patient relationship in general practice Brit J Gen Prac 2001;51:712-718.
40. Begg CB, Berlin JA. Publication bias: a problem in interpreting medical data J R Stat Soc 1988;151:419-463.
1. Starfield B. Primary Care: Concept Evaluation and Policy New York, NY: Oxford University Press 1998.;
2. American Academy of Pediatrics The Medical Home: Organizational Principles to Guide and Define the Child Health Care System and/or Improve the Health of All Children Pediatrics 2002;110:184-186.
3. Hunt CE, Kallenberg GA, Whitcomb ME. Trends in clinical education of medical students Arch Pediatr Adol Med 1999;153:297-302.
4. Halm EA, Causino N, Blumenthal D. Is gatekeeping better than traditional care? A survey of physicians’ attitudes JAMA 1997;278:1677-1681.
5. National Committee for Quality Assurance HEDIS 2003 Volume 2. Washington, DC: National Committee for Quality Assurance, 2003: Health Plan Stability pp. 151-158.
6. Guglielmo WJ. Mandated continuity of care: a solution in search of a problem? Med Econ December 1999;pp. 45-52.
7. Institute of Medicine Primary Care: America’s Health in a New Era Washington, DC: National Academy Press 1996.;
8. Starfield B. Continuous confusions? Am J Pub Health 1980;70-120.
9. Love MM, Mainous AG. Commitment to a regular physician: how long will patients wait to see their own physician for acute illness? J Fam Pract 1999;48:202-207.
10. Freeman G, Hjortdahl P. What future for continuity of care in general practice? BMJ 1997;314:1870.
11. Schroeder SA. Primary care at the crossroads Acad Med 2002;77:767-773.
12. Gallagher TC, Geling O, Comite F. Use of multiple providers for regular care and women’s receipt of hormone replacement therapy counseling Med Care 2001;39:1086-1096.
13. Christakis D. Consistent contact with a physician improves outcomes West J Med 2001;175:4.
14. Wachter RM. Discontinuity can improve patient care West J Med 2001;175:5.
15. Freeman G. What is the future for continuity of care in general practice? BMJ 1997;314:1870.
16. Dietrich AJ, Marton KI. Does continuous care from a physician make a difference? J Fam Pract 1982;15:929-937.
17. Becker MH, Drachman RH, Kirscht JP. A field experiment to evaluate various outcomes of continuity of physician care Am J Pub Health 1974;64:1062-1070.
18. Katz S, Vignos PJ, Moskowitz RW, Thompson HM, Svec KH. Comprehensive outpatient care in rheumatoid arthritis JAMA 1968;206:1249-1254.
19. Donabedian A. Evaluating the quality of medical care Milbank Quarterly 1966;44:166.
20. Campbell SM, Roland MO, Buetow S. Defining quality of care Soc Sci Med 2000;51:1611-1625.
21. Breslau N, Mortimer EA. Seeing the same doctor: determinants of satisfaction with specialty care for disabled children Med Care 1981;19:741-758.
22. Chao J. Continuity of care: incorporating patient perceptions Fam Med 1988;20:333-337.
23. Connelius LJ. The degree of usual provider continuity for African and Latino Americans J Health Care Poor Underserved 1997;8:170-185.
24. Ettner SL. The relationship between continuity of care and the health behaviors of patients: does having a usual physician make a difference? Med Care 1999;37:547-555.
25. Freeman GK, Richards SC. Personal continuity and the care of patients with epilepsy in general practice Brit J Gen Pract 1994;44:395-399.
26. Gill JM, Mainous AG, Nsereko M. The effect of continuity of care on emergency department use Arch Fam Med 2000;9:333-338.
27. Love MM, Mainous AG, Talbert JC, Hager GL. Continuity of care and the physician-patient relationship J Fam Pract 2000;49:998-1004.
28. O’Malley AS, Forrest CB. Continuity of care and delivery of ambulatory services to children in community health clinics J Comm Health 1996;21:159-173.
29. O’Malley AS, Mandelblatt J, Gold K, Cagney KA, Kerner J. Continuity of care and the use of breast and cervical cancer screening services in a multiethnic community Arch Intern Med 1997;157:1462-1470.
30. Strumberg JP, Schattner P. Personal doctoring: its impact on continuity of care as measured by the comprehensiveness of care score Austral Fam Physician 2001;30:513-518.
31. Weiss GL, Ramsey CA. Regular source of primary medical care and patient satisfaction QRB 1989;180-184.
32. Lambrew JM, DeFriese GH, Carey TS, Ricketts TC, Biddle AK. The effects of having a regular doctor on access to primary care Med Care 1996;34:138-151.
33. Christakis DA, Feudtner C, Pihoker C, Connell FA. Continuity and quality of care for children with diabetes who are covered by Medicaid Amb Peds 2001;1:99-103.
34. Christakis DA, Mell L, Koepsell TD, Zimmerman FJ, Connell FA. Association of lower continuity of care with greater risk of emergency department use and hospitalization in children Peds 2001;103:524-529.
35. Christakis DA, Mell L, Wright JA, Davis R, Connell FA. The association between greater continuity of care and timely measure-mumps-rubella vaccination Am J Pub Health 2000;90:962-965.
36. Gill JM, Mainous AG. The role of provider continuity in preventing hospitalizations Arch Fam Med 1998;7:352-357.
37. Parchman ML, Pugh JA, Noel PH, Larme AC. Continuity of care self managementbehaviors and glucose control in patients with type 2 diabetes Med Care 2002;40:137-144.
38. Wasson JH, Sauvigne AE, Mogielnicki P, et al. Continuity of outpatient medical care in elderly men. JAMA 1984;252:2413-2417.
39. Kearley KE, Freeman GK, Health A. An exploration of the value of the personal doctor patient relationship in general practice Brit J Gen Prac 2001;51:712-718.
40. Begg CB, Berlin JA. Publication bias: a problem in interpreting medical data J R Stat Soc 1988;151:419-463.
Pulmonary arterial hypertension: Newer treatments are improving outcomes
- Echocardiography is useful for screening high-risk patients (SOR: A).
- The New York Heart Association classification of dyspnea has been modified by the World Health Organization to categorize pulmonary hypertension by the severity of symptoms, which, unlike pulmonary arterial pressure, correlates well with survival (SOR: A).
- Calcium channel blockers are useful only for patients who respond to vasodilator testing in a cardiac catheterization laboratory (SOR: A).
- Therapeutic modalities now include parenteral prostanoids, oral endothelin receptor antagonists, PDE5 inhibitors, and lung transplantation (SOR:A; for PDE5 inhibitors, SOR: B)
- Early referral to expert centers is crucial to patient survival (SOR: B).
Recent progress in understanding the pathobiology of pulmonary arterial hypertension (PAH) has been tremendous, and treatment options have multiplied to include prostanoids, endothelin antagonists, phosphodiesterase-5 inhibitors, anticoagulants, and surgical options such as lung transplantation and atrial septostomy.
Although idiopathic pulmonary arterial hypertension, formerly called “primary,” is rare, other forms of PAH and associated cor pulmonale are more prevalent than conventionally believed. It is a life-threatening disease best managed within a diagnostic framework such as the one reviewed here with a treatment algorithm and recommendations from evidence-based guidelines.
Patients most likely to experience pulmonary arterial hypertension
Pulmonary arterial hypertension may be idiopathic and sporadic (IPAH), familial (FPAH), or associated with (APAH) connective tissue diseases, congenital systemic to pulmonary shunts, portal hypertension, HIV, drugs including anorexigens or cocaine, and other disorders ( Table 1 ).1
Annually, 1 to 2 cases of IPAH occur per million population.2 The mean age at diagnosis is 36 years, and women are affected more often than men by a ratio of 1.7–3.5:1. This female predominance has also been noted in PAH associated with scleroderma,3 congenital heart disease,4 and anorexigen-induced PAH.5 The incidence among users of anorexigens such as fenfluramine, dexfenfluramine, and aminorex is estimated to be 25 to 50 per million per year.2
The prevalence of portopulmonary hypertension is about 0.73% in cirrhosis.6 In scleroderma, the incidence is between 6% to 60%,7,8 while in systemic lupus erythematosus (SLE) it is reported to be 4% to 14%.9,10 In one study, 21% of rheumatoid arthritis patients without underlying cardiopulmonary disease had mild pulmonary hypertension (PH).11 PAH occurs in about 0.5% of patients with HIV infection.12
Included in the “others” group are hemoglobinopathies such as sickle cell anemia. This classification does not include PH due to end-stage renal disease, a recently described entity in patients with arteriovenous fistulae that portends a poorer prognosis.13 PH was present in a surprising 40% of hemodialysis patients.
TABLE 1
The 2003 Venice clinical classification of pulmonary hypertension*
|
| *Classification does not include pulmonary hypertension due to end-stage renal disease.13 |
Ortner’s syndrome was first described in 1897. The commonest cause has been thought to be mitral valve stenosis or prolapse leading to left atrial dilatation that compresses the recurrent laryngeal nerve as it hooks around the aorta next to the ligamentum arteriosum and courses up in the groove between the trachea and esophagus. However, other vascular structures can also compress this nerve, including a thoracic aortic aneurysm, or a dilated pulmonary artery from pulmonary arterial hypertension.
Clinical presentation
Pulmonary arterial hypertension manifests the following symptoms and signs:
Symptoms
- Progressive onset of exertional dyspnea (60%)14
- Chest pain or discomfort (17%)
- Palpitations (5%)
- Dizziness and light-headedness. There may be a history of near-syncope or syncope (13%)
- Fatigue (19%)
- Ortner’s syndrome: hoarseness from compression of left recurrent laryngeal nerve by enlarged pulmonary artery (<1%) (See Ortner’s syndrome)
- Raynaud’s phenomenon (10%)
Signs
- Loud P2 (93%)
- Tricuspid regurgitation murmur (40%)
- Right ventricular heave
- Jugular venous distention with a prominent “a” wave
- Graham Steell’s murmur: diastolic pulmonary regurgitation murmur best heard at upper left sternal border (13%)
- Signs of right heart failure including S3 gallop, “v” wave in central venous pressure tracing, hepatojugular reflux, peripheral edema, and ascites
- Cutaneous telangiectasia.
An efficient diagnostic framework
Proceed with a stepwise assessment ( Figure 1 ) of any patient exhibiting signs or symptoms suggestive of PH, particularly if there is an associated underlying condition or suggestive imaging study. Echocardiography (ECG) is usually the first test ordered, to detect thickening of the right ventricle or regurgitation of blood into the right atrium. ECG is neither sensitive nor specific for PAH. Not every patient will require the full work-up outlined in Figure 1 . The sequence and extent of testing depend on the clinical scenario. Cardiac catheterization is sometimes the last procedure, given its risks of invasiveness. A surface echocardiogram has a sensitivity of 79% to 100% and specificity of 60% to 98% for detecting PAH.15
FIGURE 1
Conceptual diagnostic framework for pulmonary hypertension
Functional assessment most important
Mean blood pressure above 25 mm Hg at rest or systolic pressure over 40 mm Hg in the pulmonary circulation constitutes pulmonary hypertension (see Pulmonary hypertension criteria ). However, the correlation of mean pulmonary arterial pressure to disease severity is not straightforward.16 Higher pulmonary artery pressure may portend better survival. The severity of pulmonary arterial hypertension is better determined by functional assessment. The New York Heart Association (NYHA) classification of dyspnea has been modified by the World Health Organization (WHO) to categorize PH by the severity of symptoms, which, unlike pulmonary arterial pressure, correlates well with survival. Even with epoprostenol treatment, functional class III patients have a survival of 60% at 7 years compared with less than 20% for class IV.17
Class I: Patients with pulmonary hypertension but without limitation of physical activity. Ordinary physical activity does not cause undue dyspnea or fatigue, chest pain, or near syncope.
Class II: Patients with pulmonary hypertension resulting in slight limitation of physical activity. They are comfortable at rest. Ordinary physical activity causes undue dyspnea or fatigue, chest pain, or near syncope.
Class III: Patients with pulmonary hypertension resulting in marked limitation of physical activity. They are comfortable at rest. Less than ordinary activity causes undue dyspnea or fatigue, chest pain, or near syncope.
Class IV: Patients with pulmonary hypertension with inability to carry out any physical activity without symptoms. These patients manifest signs of right heart failure. Dyspnea or fatigue may be present even at rest. Discomfort increases with any physical activity.
Pulmonary hypertension (PH) refers to elevated blood pressure within the pulmonary circulation. The term pulmonary arterial hypertension (PAH) encompasses a spectrum of disorders that cause PH with a common histopathology and pathobiology.56 The hallmark histopathologic lesion is plexogenic pulmonary arteriopathy.57
Normal mean pulmonary artery (PA) pressure is 12 to 16 mm Hg. PH is defined as a mean PA pressure greater than 25 mm Hg at rest, or greater than 30 mm Hg on exertion. Alternatively, systolic PA pressure greater than 40 mm Hg is also considered to be PH.58 Pulmonary arterial hypertension (PAH) is defined as a mean PA pressure greater than 25 mm Hg at rest (or 30 mm Hg with exercise), with a concomitant pulmonary capillary wedge pressure less than 15 mm Hg and a pulmonary vascular resistance (PVR) greater than 3 Woods units14 or 240 dyn•sec•cm-5.
Choosing from among improved therapeutic options
Main therapeutic goals are to prevent or reverse vasoconstriction, inhibit smooth muscle proliferation, impede thrombosis, and thereby reduce right ventricular failure. Newer pharmacologic agents have improved outcomes for patients and may even obviate the need for surgery. Treating the underlying cause of PH may be helpful, such as immunosuppression for SLE18 or positive pressure in sleep-disordered breathing.19 Table 2 outlines therapeutic options, and Figure 2 presents a strategy for applying these options.
FIGURE 2
Treatment algorithm for pulmonary arterial hypertension
TABLE 2
Treatment options for pulmonary arterial hypertension
| Medication | SOR* | Route | Adverse effects | Cost † | |
|---|---|---|---|---|---|
| Prostanoids | Epoprostenol | A | Intravenous | Line-related sepsis and thrombosis, jaw pain, fatal arrhythmia with sudden interruption | $$$$ |
| Treprostinil | B | Subcutaneous | Site pain (85%), jaw pain | $$$$ | |
| Iloprost | B | Inhaled | Short half-life with intermittent benefit | ||
| Endothelin antagonists | Bosentan | A | Oral | Hepatotoxicity, teratogenicity, fluid retention | $$$ |
| Sitaxsentan | B | ||||
| Ambrisentan | C | ||||
| PDE5 inhibitors | Sildenafil | B | Oral | Short half-life, retinopathy | $$ |
| Vardenafil | I | Short half-life | |||
| Tadalafil | I | ||||
| Surgical options | Lung transplant | C | Complicated procedure, lifelong immunosuppression | $$$$ | |
| Atrial septostomy | C | Invasive procedure, hypoxemia | $$ | ||
| Conventional therapy | Diuretics | C | Electrolyte imbalance, dehydration, etc | $ | |
| Digoxin | C | Higher mortality with high serum level | $ | ||
| Warfarin | C | Bleeding diathesis, dosing difficult in liver disease | $ | ||
| Calcium channel blockers | C | Harmful in vasodilator nonresponders | $ | ||
| Note: The level of evidence implied by the strength of recommendation must not be confused with level of efficacy. Medications not currently approved by the FDA for any indication are listed in italics. Only epoprostenol, bosentan, and trepros-tinil are approved specifically for pulmonary arterial hypertension. | |||||
| *SOR = strength of recommendation. A = Data derived from multiple randomized clinical trials or meta-analyses; B = Data derived from single randomized clinical trials or from multiple randomized clinical trials with heterogeneous results; C = Data derived from small randomized studies or consensus opinion of experts;59 I = indeterminate, no data available, theoretical basis only. See “Evidence-based medicine terms” on page 995. | |||||
Conventional therapies
Calcium channel blockers. Calcium channel block-ers (CCBs) are useful only for PAH patients who respond to vasodilator testing in a cardiac catheter-ization laboratory (SOR: B). Criteria for vasore-sponsiveness have changed and it is now generally agreed that the mean PA pressure must fall by at least 10 mm Hg to 40 mm Hg with increased or unchanged cardiac output. CCB use for nonrespon-ders leads to higher morbidity and mortality.20
Digoxin. In left ventricular failure, digoxin relieves symptoms, but without mortality benefit (SOR: A).21 Only 1 study has shown a hemodynamic benefit in PAH in the intensive-care setting.22 Therefore, experts do not agree that digoxin is useful in right ventricular failure from PAH. Digoxin may be warranted in the presence of concomitant left ventricular dysfunction or digoxin-responsive arrhythmias.
Warfarin. Two retrospective studies have shown a decrease in mortality with warfarin in PAH.23,24 There is no consensus, though, on the degree of anticoagulation, with recommendations of INR ranging from 1.5 to 4.0.
Diuretics. Judicious use of diuretics is recommended in PAH. Loop diuretics, thiazides, and spironolactone are commonly titrated to achieve symptomatic relief.
Ambulatory oxygen therapy. This option is indicated for resting and exercise-induced hypoxia. Experts usually recommend titration to achieve a PO2 >60 mm Hg.
Prostanoids: Epoprostenol, treprostinil, iloprost
Prostanoids cause vasodilation, inhibit platelet aggregation, prevent smooth muscle proliferation, decrease inflammation, and increase cardiac output.25 Epoprostenol improves exercise tolerance, hemodynamics and quality of life in patients with IPAH and PAH secondary to scleroderma (SOR: A).3,26 Treprostinil and iloprost show similar benefits. A survival advantage has only been shown for epoprostenol and treprostinil.27 Epoprostenol is useful in both vasodilator “responders” and “nonresponders.”28
Administration. Epoprostenol is administered with a central venous catheter. Usual starting dose is 2 ng/kg/min or higher with increase by 1 ng/kg/min every 1 to 2 weeks until the desired clinical improvement is manifested, or side effects preclude dose escalation.29
Treprostinil is given subcutaneously and is under investigation as an intravenous agent. The optimal dose for treprostinil is 13.8 ng/kg/min and above.30
Iloprost is delivered via inhalation, although it has also been used intravenously. Iloprost is not approved by the Food and Drug Administration but is available in clinical trials. Inhaled iloprost is short-lived and only provides intermittent hemodynamic benefit.31
Side effects. Side effects include jaw pain, nausea, anorexia, diarrhea, flushing, and headache. With the exception of jaw pain, these side effects are dose-related. The risk of catheter sepsis with epoprostenol is 0.1% to 0.4% per patient-year. More serious side effects include arrhythmia with sudden interruption of drug delivery. Treprostinil causes infusion site pain (85%), necessitating discontinuation in 8% of the patients.
Endothelin receptor antagonists: Bosentan, sitaxsentan, ambrisentan
In the lung parenchyma of patients with PH, expression of endothelin-1, a 21-amino-acid peptide, increases.32 Higher levels of serum endothelin-1 correlate directly with severity of PH and poorer outcomes.33 Endothelin-1 mediates vasoconstriction and smooth muscle proliferation primarily through endothelin type A (ETA) receptors and vasodilatation mostly through endothelin type B (ETB) receptors, although a dynamic relationship exists between the two.34
Oral formulation a plus. Bosentan is the only endothelin antagonist currently approved by the FDA. It is a low-molecular-weight, nonpeptide, competitive, dual receptor antagonist. Sitaxsentan and ambrisentan are available in clinical trials only. They are ETA-selective with the premise that sparing the ETB receptor, which is responsible for pulmonary vasodilation, will lead to better clinical outcomes. All these compounds can be given orally, a major advantage over prostanoids.
Bosentan improves exercise capacity, hemodynamics, symptoms, and time to clinical worsening.35,36 Patients studied in bosentan trials had NYHA class III or IV dyspnea due to IPAH, APAH due to scleroderma, and others. Bosentan is not approved by the FDA for functional class II patients, but has been used for such patients.
Indicated for milder PAH. Bosentan outcome data were presented at the American Thoracic Society Meeting (2003) but have not been published so far. At 3 years, 86% of patients were still alive when only 48% were expected based on historical data from the NIH registry.37 Epoprostenol survival at 3 years is about 63%.16,17 However, only patients with milder PAH receive bosentan, while the more seriously ill ones require prostanoids. This selection may explain the survival difference.
Administration. Recommended starting dose of bosentan is 62.5 mg twice daily for 4 weeks. It is then increased to 125 mg twice daily if there is no elevation of aminotransferases. Bosentan is now known to be safe in children.38 Ambrisentan and sitaxsentan should to be available in 2005 or later.
Side effects. The most common side effect of bosentan is hepatic aminotransferase elevation (9% of patients), usually occurring within 16 weeks (90%). All elevations have resolved upon drug withdrawal (97% within 8 weeks). The FDA mandates monthly monitoring of aminotransferase for bosentan. Furthermore, bosentan is teratogenic39 and absolutely contraindicated in pregnancy. There may be significant fluid retention. Sitaxsentan and ambrisentan have similar side effects and their eventual clinical use is expected to require similar monitoring.
Phosphodiesterase-5 inhibitors: Sildenafil, vardenafil, tadalafil
Phosphodiesterases (PDEs) are a group of isoenzymes widely distributed in various organs. PDE5 is found in the corpus cavernosum, pulmonary vasculature, muscle, and platelets.
Use for PAH off-label. Sildenafil, vardenafil, and tadalafil are cyclic guanosine monophosphate-specific PDE5 inhibitors with potent, selective pulmonary vasodilatory and antiplatelet effects. Sildenafil and vardenafil have relatively short half-lives (4–6 hours). Tadalafil has a longer half-life (17.5 hours) with potential for once-daily administration. All these compounds are only available orally. The FDA has approved these for erectile dysfunction only, but they have been used off-label.
A phase III study of sildenafil in PAH has been completed, but has not been published. One randomized study has shown clinical efficacy.40 Small series have also shown clinical improvement.41,42
Due to their short half-lives, sildenafil and vardenafil require multidose regimens, with potential for noncompliance leading to rebound pulmonary vasoconstriction. Retinopathy at high dose, from inhibition of PDE6, remains a concern for sildenafil.43 Priapism has not been reported in the PAH population so far, but may be a relevant consideration in sickle cell anemia.
Lung transplantation
Lung transplantation should be considered if functional class II is not achieved despite optimal medical therapy.44 Improved medical therapy has decreased the need for this surgical option, lengthened the time to transplantation, or even eliminated the requirement altogether.45 The 5-year survival of patients on epoprostenol is comparable with, or better than, that with lung transplant.46 Patient selection and early referral for transplantation are crucial to success in this process. Published international guidelines help guide this process.47 In general, PAH patients in WHO functional class II, III, or IV should be medically treated. Concurrently, referral for transplantation should be considered, even before there are signs that functional class I or II cannot be achieved. This is because transplant evaluation is a fairly lengthy process and it is not unusual for patients to die while on the long waiting list. If medical therapy is successful, the patient can be inactivated. In case medical therapy begins to fail subsequently, listing can be reactivated.
Lung transplantation remains the surgical treatment of choice for refractory PAH. Heart-lung transplants tend to be reserved for patients with structural cardiac abnormalities. Single lung transplantation has the advantages of less complex surgery and more efficient use of harvested organs to benefit more patients, thereby leading to shorter waiting periods. However, most transplant centers in the US prefer double lung transplantation, mainly because there is greater pulmonary reserve should the patient sustain rejection or infection.48
The operative mortality range is between 16% to 29%.48 The 1-year survival rate after lung transplantation (single as well as double) is approximately 70% to 75%, 2-year survival is 50% to 60%, and 5-year survival is 40% to 45%.49 The International Society of Heart and Lung Transplantation database shows that overall survival for both single and double lung transplantation is nearly equal up to 3 years postsurgery. After that, there is a significant survival advantage for double lung transplant.50 Although several studies have documented a significant improvement in the quality of life after transplantation for PH, cost-effectiveness has not yet been addressed.
Balloon atrial septostomy
Balloon atrial septostomy reduces strain on the right ventricle and improves cardiac output. Its use is limited by systemic hypoxemia caused by the right-to-left shunt and perioperative morbidity. It may be used as a bridge procedure while awaiting lung transplantation.51 Functional improvement has been demonstrated in a small series.52 Patient selection, improvement in hemodynamics, and clinical outcomes vary from center to center.53,54 It is likely that patient selection, technique, and experience influence the outcome considerably. This procedure should only be performed in experienced centers on carefully selected patients.
Combination therapy increasingly used
There are no prospective data on combination therapy for PAH. Whether combination therapy has an additive, synergistic, or even antagonistic effect is uncertain. However, there is pathophysiologic rationale for this approach, especially in therapeutic failure following monotherapy. Addition of sildenafil to epoprostenol reduces PA pressure and PVR without hypotension or desaturation.42 When iloprost failed as monotherapy for 14 patients with PAH, addition of sildenafil reversed clinical deterioration, increased functional capacity, and yielded favorable hemodynamics at 3 months, with sustained efficacy up to 12 months.55 There are no data showing whether sildenafil will have synergistic benefits with bosentan. Despite lack of evidence, combination therapy has been used increasingly in clinical practice.
- Amlodipine • Norvasc
- Bosentan • Tracleer
- Digoxin • Lanoxin
- Epoprostenol • Flolan
- Iloprost • Ventavis
- Nifedipine • Adalat, Procardia
- Sildenafil • Viagra
- Sitaxsentan • Thelin
- Spironolactone • Aldactone
- Tadalafil • Cialis
- Treprostinil • Remodulin
- Vardenafil • Levitra
- Warfarin • Coumadin
Corresponding author
Kamal K. Mubarak, MD, Wayne State University, 3990 John R, 3937 Hudson, Detroit, MI 48201. E-mail: [email protected].
1. Simonneau G, Galie N, Rubin LJ, et al. Clinical classification of pulmonary hypertension. J Am Coll Cardiol 2004;43:5S-12S.
2. Gaine SP, Rubin LJ. Primary pulmonary hypertension. Lancet 1998;352:719-725.
3. Badesch DB, Tapson VF, McGoon MD, et al. Continuous intravenous epoprostenol for pulmonary hypertension due to the scleroderma spectrum of disease. A randomized, controlled trial. Ann Intern Med 2000;132:425-434.
4. Rosenzweig EB, Kerstein D, Barst RJ. Long-term prostacyclin for pulmonary hypertension with associated congenital heart defects. Circulation 1999;99:1858-1865.
5. Fishman AP. Aminorex to fen/phen: an epidemic foretold. Circulation 1999;99:156-161.
6. McDonnell PJ, Toye PA, Hutchins GM. Primary pulmonary hypertension and cirrhosis: are they related? Am Rev Respir Dis 1983;127:437-441.
7. Battle RW, Davitt MA, Cooper SM, et al. Prevalence of pulmonary hypertension in limited and diffuse scleroderma. Chest 1996;110:1515-1519.
8. Stupi AM, Steen VD, Owens GR, et al. Pulmonary hypertension in the CREST syndrome variant of systemic sclerosis. Arthritis Rheum 1986;29:515-524.
9. Asherson RA, Higenbottam TW, Dinh Xuan AT, et al. Pulmonary hypertension in a lupus clinic: experience with twenty-four patients. J Rheumatol 1990;17:1292-1298.
10. Shen JY, Chen SL, Wu YX, et al. Pulmonary hypertension in systemic lupus erythematosus. Rheumatol Int 1999;18:147-151.
11. Dawson JK, Goodson NG, Graham DR, et al. Raised pulmonary artery pressures measured with Doppler echocardiography in rheumatoid arthritis patients. Rheumatology (Oxford) 2000;39:1320-1325.
12. Mehta NJ, Khan IA, Mehta RN, et al. HIV-Related pulmonary hypertension: analytic review of 131 cases. Chest 2000;118:1133-1141.
13. Yigla M, Nakhoul F, Sabag A, et al. Pulmonary hypertension in patients with end-stage renal disease. Chest 2003;123:1577-1582.
14. Rich S, Dantzker DR, Ayres SM, et al. Primary pulmonary hypertension. A national prospective study. Ann Intern Med 1987;107:216-223.
15. Denton CP, Cailes JB, Phillips GD, et al. Comparison of Doppler echocardiography and right heart catheterization to assess pulmonary hypertension in systemic sclerosis. Br J Rheumatol 1997;36:239-243.
16. Sitbon O, Humbert M, Nunes H, et al. Long-term intravenous epoprostenol infusion in primary pulmonary hypertension: prognostic factors and survival. J Am Coll Cardiol 2002;40:780-788.
17. McLaughlin VV, Shillington A, Rich S. Survival in primary pulmonary hypertension: the impact of epoprostenol therapy. Circulation 2002;106:1477-1482.
18. Groen H, Bootsma H, Postma DS, et al. Primary pulmonary hypertension in a patient with systemic lupus erythematosus: partial improvement with cyclophosphamide. J Rheumatol 1993;20:1055-1057.
19. Thalhofer S, Dorow P. [Effect of n-BiPAP therapy on the hemodynamics in patients with central sleep apnea]. Pneumologie 1995;49 Suppl 1:165-166.
20. Farber HW, Karlinsky JB, Faling LJ. Fatal outcome following nifedipine for pulmonary hypertension. Chest 1983;83:708-709.
21. The effect of digoxin on mortality and morbidity in patients with heart failure. The Digitalis Investigation Group. N Engl J Med 1997;336:525-533.
22. Rich S, Seidlitz M, Dodin E, et al. The short-term effects of digoxin in patients with right ventricular dysfunction from pulmonary hypertension. Chest 1998;114:787-792.
23. Frank H, Mlczoch J, Huber K, et al. The effect of anticoagulant therapy in primary and anorectic drug-induced pulmonary hypertension. Chest 1997;112:714-721.
24. Rich S, Kaufmann E, Levy PS. The effect of high doses of calcium-channel blockers on survival in primary pulmonary hypertension. N Engl J Med 1992;327:76-81.
25. Rich S, McLaughlin VV. The effects of chronic prostacyclin therapy on cardiac output and symptoms in primary pulmonary hypertension. J Am Coll Cardiol 1999;34:1184-1187.
26. Barst RJ, Rubin LJ, Long WA, et al. A comparison of continuous intravenous epoprostenol (prostacyclin) with conventional therapy for primary pulmonary hypertension. The Primary Pulmonary Hypertension Study Group. N Engl J Med 1996;334:296-302.
27. Gibbs J, Arneson C, Mottola D. Chronic infusion of Treprostinil is safe, and appears to prolong survival over a three-year period in patients with Pulmonary Arterial Hypertension. Abstract presented at American Thoracic Society Meeting, 2003.
28. McLaughlin VV, Genthner DE, Panella MM, et al. Reduction in pulmonary vascular resistance with long-term epoprostenol (prostacyclin) therapy in primary pulmonary hypertension. N Engl J Med 1998;338:273-277.
29. Hoeper MM, Galie N, Simonneau G, et al. New treatments for pulmonary arterial hypertension. Am J Respir Crit Care Med 2002;165:1209-1216.
30. Simonneau G, Barst RJ, Galie N, et al. Continuous subcutaneous infusion of treprostinil, a prostacyclin analogue, in patients with pulmonary arterial hypertension: a double-blind, randomized, placebo-controlled trial. Am J Respir Crit Care Med 2002;165:800-804.
31. Fruhwald FM, Kjellstrom B, Perthold W, et al. Continuous hemodynamic monitoring in pulmonary hypertensive patients treated with inhaled iloprost. Chest 2003;124:351-359.
32. Giaid A, Yanagisawa M, Langleben D, et al. Expression of endothelin-1 in the lungs of patients with pulmonary hypertension. N Engl J Med 1993;328:1732-1739.
33. Rubens C, Ewert R, Halank M, et al. Big endothelin-1 and endothelin-1 plasma levels are correlated with the severity of primary pulmonary hypertension. Chest 2001;120:1562-1569.
34. Zuccarello M, Boccaletti R, Rapoport RM. Does blockade of endothelinB1-receptor activation increase endothelinB2/endothelinA receptor-mediated constriction in the rabbit basilar artery? J Cardiovasc Pharmacol 1999;33:679-684.
35. Channick RN, Simonneau G, Sitbon O, et al. Effects of the dual endothelin-receptor antagonist bosentan in patients with pulmonary hypertension: a randomised placebo-controlled study. Lancet 2001;358:1119-1123.
36. Rubin LJ, Badesch DB, Barst RJ, et al. Bosentan therapy for pulmonary arterial hypertension. N Engl J Med 2002;346:896-903.
37. D’Alonzo GE, Barst RJ, Ayres SM, et al. Survival in patients with primary pulmonary hypertension. Results from a national prospective registry. Ann Intern Med 1991;115:343-349.
38. Barst RJ, Ivy D, Dingemanse J, et al. Pharmacokinetics, safety, and efficacy of bosentan in pediatric patients with pulmonary arterial hypertension. Clin Pharmacol Ther 2003;73:372-382.
39. Actelion Pharmaceuticals. Package insert. Tracleer (bosentan). Physician’s Desk Reference (www.pdr.net). South San Francisco, Calif, 2002.
40. Sastry BK, Narasimhan C, Reddy NK, et al. Clinical efficacy of sildenafil in primary pulmonary hypertension: a randomized, placebo-controlled, double-blind, crossover study. J Am Coll Cardiol 2004;43:1149-1153.
41. Prasad S, Wilkinson J, Gatzoulis MA. Sildenafil in primary pulmonary hypertension. N Engl J Med 2000;343:1342.-
42. Stiebellehner L, Petkov V, Vonbank K, et al. Long-term treatment with oral sildenafil in addition to continuous IV epoprostenol in patients with pulmonary arterial hypertension. Chest 2003;123:1293-1295.
43. Behn D, Potter MJ. Sildenafil-mediated reduction in retinal function in heterozygous mice lacking the gamma-subunit of phosphodiesterase. Invest Ophthalmol Vis Sci 2001;42:523-527.
44. Rubin LJ. Primary pulmonary hypertension. N Engl J Med 1997;336:111-117.
45. Conte JV, Gaine SP, Orens JB, et al. The influence of continuous intravenous prostacyclin therapy for primary pulmonary hypertension on the timing and outcome of transplantation. J Heart Lung Transplant 1998;17:679-685.
46. Rich S, McLaughlin VV. Lung transplantation for pulmonary hypertension: patient selection and maintenance therapy while awaiting transplantation. Semin Thorac Cardiovasc Surg 1998;10:135-138.
47. Maurer JR, Frost AE, Estenne M, et al. International guidelines for the selection of lung transplant candidates. The International Society for Heart and Lung Transplantation, the American Thoracic Society, the American Society of Transplant Physicians, the European Respiratory Society. J Heart Lung Transplant 1998;17:703-709.
48. McLaughlin VV, Rich S. Severe pulmonary hypertension: critical care clinics. Crit Care Clin 2001;17:453-467.
49. Hosenpud JD, Bennett LE, Keck BM, et al. The Registry of the International Society for Heart and Lung Transplantation: sixteenth official report—1999. J Heart Lung Transplant 1999;18:611-626.
50. Hertz MI, Mohacsi PJ, Taylor DO, et al. The registry of the International Society for Heart and Lung Transplantation: introduction to the Twentieth Annual Reports—2003. J Heart Lung Transplant 2003;22:610-615.
51. Rich S. Primary Pulmonary Hypertension. Curr Treat Options Cardiovasc Med 2000;2:135-140.
52. Sandoval J, Gaspar J, Pulido T, et al. Graded balloon dilation atrial septostomy in severe primary pulmonary hypertension. A therapeutic alternative for patients nonresponsive to vasodilator treatment. J Am Coll Cardiol 1998;32:297-304.
53. Reichenberger F, Pepke-Zaba J, McNeil K, et al. Atrial septostomy in the treatment of severe pulmonary arterial hypertension. Thorax 2003;58:797-800.
54. Nihill MR, O’Laughlin MP, Mullins CE. Effects of atrial septostomy in patients with terminal cor pulmonale due to pulmonary vascular disease. Cathet Cardiovasc Diagn 1991;24:166-172.
55. Ghofrani HA, Rose F, Schermuly RT, et al. Oral sildenafil as long-term adjunct therapy to inhaled iloprost in severe pulmonary arterial hypertension. J Am Coll Cardiol 2003;42:158-164.
56. Chatterjee K, De Marco T, Alpert JS. Pulmonary hypertension: hemodynamic diagnosis and management. Arch Intern Med 2002;162:1925-1933.
57. Tuder RM, Groves B, Badesch DB, et al. Exuberant endothelial cell growth and elements of inflammation are present in plexiform lesions of pulmonary hypertension. Am J Pathol 1994;144:275-285.
58. Maloney JP. Advances in the treatment of secondary pulmonary hypertension. Curr Opin Pulm Med 2003;9:139-143.
59. Galie N, Seeger W, Naeije R, et al. Comparative analysis of clinical trials and evidence-based treatment algorithm in pulmonary arterial hypertension. J Am Coll Cardiol 2004;43:81S-88S.
- Echocardiography is useful for screening high-risk patients (SOR: A).
- The New York Heart Association classification of dyspnea has been modified by the World Health Organization to categorize pulmonary hypertension by the severity of symptoms, which, unlike pulmonary arterial pressure, correlates well with survival (SOR: A).
- Calcium channel blockers are useful only for patients who respond to vasodilator testing in a cardiac catheterization laboratory (SOR: A).
- Therapeutic modalities now include parenteral prostanoids, oral endothelin receptor antagonists, PDE5 inhibitors, and lung transplantation (SOR:A; for PDE5 inhibitors, SOR: B)
- Early referral to expert centers is crucial to patient survival (SOR: B).
Recent progress in understanding the pathobiology of pulmonary arterial hypertension (PAH) has been tremendous, and treatment options have multiplied to include prostanoids, endothelin antagonists, phosphodiesterase-5 inhibitors, anticoagulants, and surgical options such as lung transplantation and atrial septostomy.
Although idiopathic pulmonary arterial hypertension, formerly called “primary,” is rare, other forms of PAH and associated cor pulmonale are more prevalent than conventionally believed. It is a life-threatening disease best managed within a diagnostic framework such as the one reviewed here with a treatment algorithm and recommendations from evidence-based guidelines.
Patients most likely to experience pulmonary arterial hypertension
Pulmonary arterial hypertension may be idiopathic and sporadic (IPAH), familial (FPAH), or associated with (APAH) connective tissue diseases, congenital systemic to pulmonary shunts, portal hypertension, HIV, drugs including anorexigens or cocaine, and other disorders ( Table 1 ).1
Annually, 1 to 2 cases of IPAH occur per million population.2 The mean age at diagnosis is 36 years, and women are affected more often than men by a ratio of 1.7–3.5:1. This female predominance has also been noted in PAH associated with scleroderma,3 congenital heart disease,4 and anorexigen-induced PAH.5 The incidence among users of anorexigens such as fenfluramine, dexfenfluramine, and aminorex is estimated to be 25 to 50 per million per year.2
The prevalence of portopulmonary hypertension is about 0.73% in cirrhosis.6 In scleroderma, the incidence is between 6% to 60%,7,8 while in systemic lupus erythematosus (SLE) it is reported to be 4% to 14%.9,10 In one study, 21% of rheumatoid arthritis patients without underlying cardiopulmonary disease had mild pulmonary hypertension (PH).11 PAH occurs in about 0.5% of patients with HIV infection.12
Included in the “others” group are hemoglobinopathies such as sickle cell anemia. This classification does not include PH due to end-stage renal disease, a recently described entity in patients with arteriovenous fistulae that portends a poorer prognosis.13 PH was present in a surprising 40% of hemodialysis patients.
TABLE 1
The 2003 Venice clinical classification of pulmonary hypertension*
|
| *Classification does not include pulmonary hypertension due to end-stage renal disease.13 |
Ortner’s syndrome was first described in 1897. The commonest cause has been thought to be mitral valve stenosis or prolapse leading to left atrial dilatation that compresses the recurrent laryngeal nerve as it hooks around the aorta next to the ligamentum arteriosum and courses up in the groove between the trachea and esophagus. However, other vascular structures can also compress this nerve, including a thoracic aortic aneurysm, or a dilated pulmonary artery from pulmonary arterial hypertension.
Clinical presentation
Pulmonary arterial hypertension manifests the following symptoms and signs:
Symptoms
- Progressive onset of exertional dyspnea (60%)14
- Chest pain or discomfort (17%)
- Palpitations (5%)
- Dizziness and light-headedness. There may be a history of near-syncope or syncope (13%)
- Fatigue (19%)
- Ortner’s syndrome: hoarseness from compression of left recurrent laryngeal nerve by enlarged pulmonary artery (<1%) (See Ortner’s syndrome)
- Raynaud’s phenomenon (10%)
Signs
- Loud P2 (93%)
- Tricuspid regurgitation murmur (40%)
- Right ventricular heave
- Jugular venous distention with a prominent “a” wave
- Graham Steell’s murmur: diastolic pulmonary regurgitation murmur best heard at upper left sternal border (13%)
- Signs of right heart failure including S3 gallop, “v” wave in central venous pressure tracing, hepatojugular reflux, peripheral edema, and ascites
- Cutaneous telangiectasia.
An efficient diagnostic framework
Proceed with a stepwise assessment ( Figure 1 ) of any patient exhibiting signs or symptoms suggestive of PH, particularly if there is an associated underlying condition or suggestive imaging study. Echocardiography (ECG) is usually the first test ordered, to detect thickening of the right ventricle or regurgitation of blood into the right atrium. ECG is neither sensitive nor specific for PAH. Not every patient will require the full work-up outlined in Figure 1 . The sequence and extent of testing depend on the clinical scenario. Cardiac catheterization is sometimes the last procedure, given its risks of invasiveness. A surface echocardiogram has a sensitivity of 79% to 100% and specificity of 60% to 98% for detecting PAH.15
FIGURE 1
Conceptual diagnostic framework for pulmonary hypertension
Functional assessment most important
Mean blood pressure above 25 mm Hg at rest or systolic pressure over 40 mm Hg in the pulmonary circulation constitutes pulmonary hypertension (see Pulmonary hypertension criteria ). However, the correlation of mean pulmonary arterial pressure to disease severity is not straightforward.16 Higher pulmonary artery pressure may portend better survival. The severity of pulmonary arterial hypertension is better determined by functional assessment. The New York Heart Association (NYHA) classification of dyspnea has been modified by the World Health Organization (WHO) to categorize PH by the severity of symptoms, which, unlike pulmonary arterial pressure, correlates well with survival. Even with epoprostenol treatment, functional class III patients have a survival of 60% at 7 years compared with less than 20% for class IV.17
Class I: Patients with pulmonary hypertension but without limitation of physical activity. Ordinary physical activity does not cause undue dyspnea or fatigue, chest pain, or near syncope.
Class II: Patients with pulmonary hypertension resulting in slight limitation of physical activity. They are comfortable at rest. Ordinary physical activity causes undue dyspnea or fatigue, chest pain, or near syncope.
Class III: Patients with pulmonary hypertension resulting in marked limitation of physical activity. They are comfortable at rest. Less than ordinary activity causes undue dyspnea or fatigue, chest pain, or near syncope.
Class IV: Patients with pulmonary hypertension with inability to carry out any physical activity without symptoms. These patients manifest signs of right heart failure. Dyspnea or fatigue may be present even at rest. Discomfort increases with any physical activity.
Pulmonary hypertension (PH) refers to elevated blood pressure within the pulmonary circulation. The term pulmonary arterial hypertension (PAH) encompasses a spectrum of disorders that cause PH with a common histopathology and pathobiology.56 The hallmark histopathologic lesion is plexogenic pulmonary arteriopathy.57
Normal mean pulmonary artery (PA) pressure is 12 to 16 mm Hg. PH is defined as a mean PA pressure greater than 25 mm Hg at rest, or greater than 30 mm Hg on exertion. Alternatively, systolic PA pressure greater than 40 mm Hg is also considered to be PH.58 Pulmonary arterial hypertension (PAH) is defined as a mean PA pressure greater than 25 mm Hg at rest (or 30 mm Hg with exercise), with a concomitant pulmonary capillary wedge pressure less than 15 mm Hg and a pulmonary vascular resistance (PVR) greater than 3 Woods units14 or 240 dyn•sec•cm-5.
Choosing from among improved therapeutic options
Main therapeutic goals are to prevent or reverse vasoconstriction, inhibit smooth muscle proliferation, impede thrombosis, and thereby reduce right ventricular failure. Newer pharmacologic agents have improved outcomes for patients and may even obviate the need for surgery. Treating the underlying cause of PH may be helpful, such as immunosuppression for SLE18 or positive pressure in sleep-disordered breathing.19 Table 2 outlines therapeutic options, and Figure 2 presents a strategy for applying these options.
FIGURE 2
Treatment algorithm for pulmonary arterial hypertension
TABLE 2
Treatment options for pulmonary arterial hypertension
| Medication | SOR* | Route | Adverse effects | Cost † | |
|---|---|---|---|---|---|
| Prostanoids | Epoprostenol | A | Intravenous | Line-related sepsis and thrombosis, jaw pain, fatal arrhythmia with sudden interruption | $$$$ |
| Treprostinil | B | Subcutaneous | Site pain (85%), jaw pain | $$$$ | |
| Iloprost | B | Inhaled | Short half-life with intermittent benefit | ||
| Endothelin antagonists | Bosentan | A | Oral | Hepatotoxicity, teratogenicity, fluid retention | $$$ |
| Sitaxsentan | B | ||||
| Ambrisentan | C | ||||
| PDE5 inhibitors | Sildenafil | B | Oral | Short half-life, retinopathy | $$ |
| Vardenafil | I | Short half-life | |||
| Tadalafil | I | ||||
| Surgical options | Lung transplant | C | Complicated procedure, lifelong immunosuppression | $$$$ | |
| Atrial septostomy | C | Invasive procedure, hypoxemia | $$ | ||
| Conventional therapy | Diuretics | C | Electrolyte imbalance, dehydration, etc | $ | |
| Digoxin | C | Higher mortality with high serum level | $ | ||
| Warfarin | C | Bleeding diathesis, dosing difficult in liver disease | $ | ||
| Calcium channel blockers | C | Harmful in vasodilator nonresponders | $ | ||
| Note: The level of evidence implied by the strength of recommendation must not be confused with level of efficacy. Medications not currently approved by the FDA for any indication are listed in italics. Only epoprostenol, bosentan, and trepros-tinil are approved specifically for pulmonary arterial hypertension. | |||||
| *SOR = strength of recommendation. A = Data derived from multiple randomized clinical trials or meta-analyses; B = Data derived from single randomized clinical trials or from multiple randomized clinical trials with heterogeneous results; C = Data derived from small randomized studies or consensus opinion of experts;59 I = indeterminate, no data available, theoretical basis only. See “Evidence-based medicine terms” on page 995. | |||||
Conventional therapies
Calcium channel blockers. Calcium channel block-ers (CCBs) are useful only for PAH patients who respond to vasodilator testing in a cardiac catheter-ization laboratory (SOR: B). Criteria for vasore-sponsiveness have changed and it is now generally agreed that the mean PA pressure must fall by at least 10 mm Hg to 40 mm Hg with increased or unchanged cardiac output. CCB use for nonrespon-ders leads to higher morbidity and mortality.20
Digoxin. In left ventricular failure, digoxin relieves symptoms, but without mortality benefit (SOR: A).21 Only 1 study has shown a hemodynamic benefit in PAH in the intensive-care setting.22 Therefore, experts do not agree that digoxin is useful in right ventricular failure from PAH. Digoxin may be warranted in the presence of concomitant left ventricular dysfunction or digoxin-responsive arrhythmias.
Warfarin. Two retrospective studies have shown a decrease in mortality with warfarin in PAH.23,24 There is no consensus, though, on the degree of anticoagulation, with recommendations of INR ranging from 1.5 to 4.0.
Diuretics. Judicious use of diuretics is recommended in PAH. Loop diuretics, thiazides, and spironolactone are commonly titrated to achieve symptomatic relief.
Ambulatory oxygen therapy. This option is indicated for resting and exercise-induced hypoxia. Experts usually recommend titration to achieve a PO2 >60 mm Hg.
Prostanoids: Epoprostenol, treprostinil, iloprost
Prostanoids cause vasodilation, inhibit platelet aggregation, prevent smooth muscle proliferation, decrease inflammation, and increase cardiac output.25 Epoprostenol improves exercise tolerance, hemodynamics and quality of life in patients with IPAH and PAH secondary to scleroderma (SOR: A).3,26 Treprostinil and iloprost show similar benefits. A survival advantage has only been shown for epoprostenol and treprostinil.27 Epoprostenol is useful in both vasodilator “responders” and “nonresponders.”28
Administration. Epoprostenol is administered with a central venous catheter. Usual starting dose is 2 ng/kg/min or higher with increase by 1 ng/kg/min every 1 to 2 weeks until the desired clinical improvement is manifested, or side effects preclude dose escalation.29
Treprostinil is given subcutaneously and is under investigation as an intravenous agent. The optimal dose for treprostinil is 13.8 ng/kg/min and above.30
Iloprost is delivered via inhalation, although it has also been used intravenously. Iloprost is not approved by the Food and Drug Administration but is available in clinical trials. Inhaled iloprost is short-lived and only provides intermittent hemodynamic benefit.31
Side effects. Side effects include jaw pain, nausea, anorexia, diarrhea, flushing, and headache. With the exception of jaw pain, these side effects are dose-related. The risk of catheter sepsis with epoprostenol is 0.1% to 0.4% per patient-year. More serious side effects include arrhythmia with sudden interruption of drug delivery. Treprostinil causes infusion site pain (85%), necessitating discontinuation in 8% of the patients.
Endothelin receptor antagonists: Bosentan, sitaxsentan, ambrisentan
In the lung parenchyma of patients with PH, expression of endothelin-1, a 21-amino-acid peptide, increases.32 Higher levels of serum endothelin-1 correlate directly with severity of PH and poorer outcomes.33 Endothelin-1 mediates vasoconstriction and smooth muscle proliferation primarily through endothelin type A (ETA) receptors and vasodilatation mostly through endothelin type B (ETB) receptors, although a dynamic relationship exists between the two.34
Oral formulation a plus. Bosentan is the only endothelin antagonist currently approved by the FDA. It is a low-molecular-weight, nonpeptide, competitive, dual receptor antagonist. Sitaxsentan and ambrisentan are available in clinical trials only. They are ETA-selective with the premise that sparing the ETB receptor, which is responsible for pulmonary vasodilation, will lead to better clinical outcomes. All these compounds can be given orally, a major advantage over prostanoids.
Bosentan improves exercise capacity, hemodynamics, symptoms, and time to clinical worsening.35,36 Patients studied in bosentan trials had NYHA class III or IV dyspnea due to IPAH, APAH due to scleroderma, and others. Bosentan is not approved by the FDA for functional class II patients, but has been used for such patients.
Indicated for milder PAH. Bosentan outcome data were presented at the American Thoracic Society Meeting (2003) but have not been published so far. At 3 years, 86% of patients were still alive when only 48% were expected based on historical data from the NIH registry.37 Epoprostenol survival at 3 years is about 63%.16,17 However, only patients with milder PAH receive bosentan, while the more seriously ill ones require prostanoids. This selection may explain the survival difference.
Administration. Recommended starting dose of bosentan is 62.5 mg twice daily for 4 weeks. It is then increased to 125 mg twice daily if there is no elevation of aminotransferases. Bosentan is now known to be safe in children.38 Ambrisentan and sitaxsentan should to be available in 2005 or later.
Side effects. The most common side effect of bosentan is hepatic aminotransferase elevation (9% of patients), usually occurring within 16 weeks (90%). All elevations have resolved upon drug withdrawal (97% within 8 weeks). The FDA mandates monthly monitoring of aminotransferase for bosentan. Furthermore, bosentan is teratogenic39 and absolutely contraindicated in pregnancy. There may be significant fluid retention. Sitaxsentan and ambrisentan have similar side effects and their eventual clinical use is expected to require similar monitoring.
Phosphodiesterase-5 inhibitors: Sildenafil, vardenafil, tadalafil
Phosphodiesterases (PDEs) are a group of isoenzymes widely distributed in various organs. PDE5 is found in the corpus cavernosum, pulmonary vasculature, muscle, and platelets.
Use for PAH off-label. Sildenafil, vardenafil, and tadalafil are cyclic guanosine monophosphate-specific PDE5 inhibitors with potent, selective pulmonary vasodilatory and antiplatelet effects. Sildenafil and vardenafil have relatively short half-lives (4–6 hours). Tadalafil has a longer half-life (17.5 hours) with potential for once-daily administration. All these compounds are only available orally. The FDA has approved these for erectile dysfunction only, but they have been used off-label.
A phase III study of sildenafil in PAH has been completed, but has not been published. One randomized study has shown clinical efficacy.40 Small series have also shown clinical improvement.41,42
Due to their short half-lives, sildenafil and vardenafil require multidose regimens, with potential for noncompliance leading to rebound pulmonary vasoconstriction. Retinopathy at high dose, from inhibition of PDE6, remains a concern for sildenafil.43 Priapism has not been reported in the PAH population so far, but may be a relevant consideration in sickle cell anemia.
Lung transplantation
Lung transplantation should be considered if functional class II is not achieved despite optimal medical therapy.44 Improved medical therapy has decreased the need for this surgical option, lengthened the time to transplantation, or even eliminated the requirement altogether.45 The 5-year survival of patients on epoprostenol is comparable with, or better than, that with lung transplant.46 Patient selection and early referral for transplantation are crucial to success in this process. Published international guidelines help guide this process.47 In general, PAH patients in WHO functional class II, III, or IV should be medically treated. Concurrently, referral for transplantation should be considered, even before there are signs that functional class I or II cannot be achieved. This is because transplant evaluation is a fairly lengthy process and it is not unusual for patients to die while on the long waiting list. If medical therapy is successful, the patient can be inactivated. In case medical therapy begins to fail subsequently, listing can be reactivated.
Lung transplantation remains the surgical treatment of choice for refractory PAH. Heart-lung transplants tend to be reserved for patients with structural cardiac abnormalities. Single lung transplantation has the advantages of less complex surgery and more efficient use of harvested organs to benefit more patients, thereby leading to shorter waiting periods. However, most transplant centers in the US prefer double lung transplantation, mainly because there is greater pulmonary reserve should the patient sustain rejection or infection.48
The operative mortality range is between 16% to 29%.48 The 1-year survival rate after lung transplantation (single as well as double) is approximately 70% to 75%, 2-year survival is 50% to 60%, and 5-year survival is 40% to 45%.49 The International Society of Heart and Lung Transplantation database shows that overall survival for both single and double lung transplantation is nearly equal up to 3 years postsurgery. After that, there is a significant survival advantage for double lung transplant.50 Although several studies have documented a significant improvement in the quality of life after transplantation for PH, cost-effectiveness has not yet been addressed.
Balloon atrial septostomy
Balloon atrial septostomy reduces strain on the right ventricle and improves cardiac output. Its use is limited by systemic hypoxemia caused by the right-to-left shunt and perioperative morbidity. It may be used as a bridge procedure while awaiting lung transplantation.51 Functional improvement has been demonstrated in a small series.52 Patient selection, improvement in hemodynamics, and clinical outcomes vary from center to center.53,54 It is likely that patient selection, technique, and experience influence the outcome considerably. This procedure should only be performed in experienced centers on carefully selected patients.
Combination therapy increasingly used
There are no prospective data on combination therapy for PAH. Whether combination therapy has an additive, synergistic, or even antagonistic effect is uncertain. However, there is pathophysiologic rationale for this approach, especially in therapeutic failure following monotherapy. Addition of sildenafil to epoprostenol reduces PA pressure and PVR without hypotension or desaturation.42 When iloprost failed as monotherapy for 14 patients with PAH, addition of sildenafil reversed clinical deterioration, increased functional capacity, and yielded favorable hemodynamics at 3 months, with sustained efficacy up to 12 months.55 There are no data showing whether sildenafil will have synergistic benefits with bosentan. Despite lack of evidence, combination therapy has been used increasingly in clinical practice.
- Amlodipine • Norvasc
- Bosentan • Tracleer
- Digoxin • Lanoxin
- Epoprostenol • Flolan
- Iloprost • Ventavis
- Nifedipine • Adalat, Procardia
- Sildenafil • Viagra
- Sitaxsentan • Thelin
- Spironolactone • Aldactone
- Tadalafil • Cialis
- Treprostinil • Remodulin
- Vardenafil • Levitra
- Warfarin • Coumadin
Corresponding author
Kamal K. Mubarak, MD, Wayne State University, 3990 John R, 3937 Hudson, Detroit, MI 48201. E-mail: [email protected].
- Echocardiography is useful for screening high-risk patients (SOR: A).
- The New York Heart Association classification of dyspnea has been modified by the World Health Organization to categorize pulmonary hypertension by the severity of symptoms, which, unlike pulmonary arterial pressure, correlates well with survival (SOR: A).
- Calcium channel blockers are useful only for patients who respond to vasodilator testing in a cardiac catheterization laboratory (SOR: A).
- Therapeutic modalities now include parenteral prostanoids, oral endothelin receptor antagonists, PDE5 inhibitors, and lung transplantation (SOR:A; for PDE5 inhibitors, SOR: B)
- Early referral to expert centers is crucial to patient survival (SOR: B).
Recent progress in understanding the pathobiology of pulmonary arterial hypertension (PAH) has been tremendous, and treatment options have multiplied to include prostanoids, endothelin antagonists, phosphodiesterase-5 inhibitors, anticoagulants, and surgical options such as lung transplantation and atrial septostomy.
Although idiopathic pulmonary arterial hypertension, formerly called “primary,” is rare, other forms of PAH and associated cor pulmonale are more prevalent than conventionally believed. It is a life-threatening disease best managed within a diagnostic framework such as the one reviewed here with a treatment algorithm and recommendations from evidence-based guidelines.
Patients most likely to experience pulmonary arterial hypertension
Pulmonary arterial hypertension may be idiopathic and sporadic (IPAH), familial (FPAH), or associated with (APAH) connective tissue diseases, congenital systemic to pulmonary shunts, portal hypertension, HIV, drugs including anorexigens or cocaine, and other disorders ( Table 1 ).1
Annually, 1 to 2 cases of IPAH occur per million population.2 The mean age at diagnosis is 36 years, and women are affected more often than men by a ratio of 1.7–3.5:1. This female predominance has also been noted in PAH associated with scleroderma,3 congenital heart disease,4 and anorexigen-induced PAH.5 The incidence among users of anorexigens such as fenfluramine, dexfenfluramine, and aminorex is estimated to be 25 to 50 per million per year.2
The prevalence of portopulmonary hypertension is about 0.73% in cirrhosis.6 In scleroderma, the incidence is between 6% to 60%,7,8 while in systemic lupus erythematosus (SLE) it is reported to be 4% to 14%.9,10 In one study, 21% of rheumatoid arthritis patients without underlying cardiopulmonary disease had mild pulmonary hypertension (PH).11 PAH occurs in about 0.5% of patients with HIV infection.12
Included in the “others” group are hemoglobinopathies such as sickle cell anemia. This classification does not include PH due to end-stage renal disease, a recently described entity in patients with arteriovenous fistulae that portends a poorer prognosis.13 PH was present in a surprising 40% of hemodialysis patients.
TABLE 1
The 2003 Venice clinical classification of pulmonary hypertension*
|
| *Classification does not include pulmonary hypertension due to end-stage renal disease.13 |
Ortner’s syndrome was first described in 1897. The commonest cause has been thought to be mitral valve stenosis or prolapse leading to left atrial dilatation that compresses the recurrent laryngeal nerve as it hooks around the aorta next to the ligamentum arteriosum and courses up in the groove between the trachea and esophagus. However, other vascular structures can also compress this nerve, including a thoracic aortic aneurysm, or a dilated pulmonary artery from pulmonary arterial hypertension.
Clinical presentation
Pulmonary arterial hypertension manifests the following symptoms and signs:
Symptoms
- Progressive onset of exertional dyspnea (60%)14
- Chest pain or discomfort (17%)
- Palpitations (5%)
- Dizziness and light-headedness. There may be a history of near-syncope or syncope (13%)
- Fatigue (19%)
- Ortner’s syndrome: hoarseness from compression of left recurrent laryngeal nerve by enlarged pulmonary artery (<1%) (See Ortner’s syndrome)
- Raynaud’s phenomenon (10%)
Signs
- Loud P2 (93%)
- Tricuspid regurgitation murmur (40%)
- Right ventricular heave
- Jugular venous distention with a prominent “a” wave
- Graham Steell’s murmur: diastolic pulmonary regurgitation murmur best heard at upper left sternal border (13%)
- Signs of right heart failure including S3 gallop, “v” wave in central venous pressure tracing, hepatojugular reflux, peripheral edema, and ascites
- Cutaneous telangiectasia.
An efficient diagnostic framework
Proceed with a stepwise assessment ( Figure 1 ) of any patient exhibiting signs or symptoms suggestive of PH, particularly if there is an associated underlying condition or suggestive imaging study. Echocardiography (ECG) is usually the first test ordered, to detect thickening of the right ventricle or regurgitation of blood into the right atrium. ECG is neither sensitive nor specific for PAH. Not every patient will require the full work-up outlined in Figure 1 . The sequence and extent of testing depend on the clinical scenario. Cardiac catheterization is sometimes the last procedure, given its risks of invasiveness. A surface echocardiogram has a sensitivity of 79% to 100% and specificity of 60% to 98% for detecting PAH.15
FIGURE 1
Conceptual diagnostic framework for pulmonary hypertension
Functional assessment most important
Mean blood pressure above 25 mm Hg at rest or systolic pressure over 40 mm Hg in the pulmonary circulation constitutes pulmonary hypertension (see Pulmonary hypertension criteria ). However, the correlation of mean pulmonary arterial pressure to disease severity is not straightforward.16 Higher pulmonary artery pressure may portend better survival. The severity of pulmonary arterial hypertension is better determined by functional assessment. The New York Heart Association (NYHA) classification of dyspnea has been modified by the World Health Organization (WHO) to categorize PH by the severity of symptoms, which, unlike pulmonary arterial pressure, correlates well with survival. Even with epoprostenol treatment, functional class III patients have a survival of 60% at 7 years compared with less than 20% for class IV.17
Class I: Patients with pulmonary hypertension but without limitation of physical activity. Ordinary physical activity does not cause undue dyspnea or fatigue, chest pain, or near syncope.
Class II: Patients with pulmonary hypertension resulting in slight limitation of physical activity. They are comfortable at rest. Ordinary physical activity causes undue dyspnea or fatigue, chest pain, or near syncope.
Class III: Patients with pulmonary hypertension resulting in marked limitation of physical activity. They are comfortable at rest. Less than ordinary activity causes undue dyspnea or fatigue, chest pain, or near syncope.
Class IV: Patients with pulmonary hypertension with inability to carry out any physical activity without symptoms. These patients manifest signs of right heart failure. Dyspnea or fatigue may be present even at rest. Discomfort increases with any physical activity.
Pulmonary hypertension (PH) refers to elevated blood pressure within the pulmonary circulation. The term pulmonary arterial hypertension (PAH) encompasses a spectrum of disorders that cause PH with a common histopathology and pathobiology.56 The hallmark histopathologic lesion is plexogenic pulmonary arteriopathy.57
Normal mean pulmonary artery (PA) pressure is 12 to 16 mm Hg. PH is defined as a mean PA pressure greater than 25 mm Hg at rest, or greater than 30 mm Hg on exertion. Alternatively, systolic PA pressure greater than 40 mm Hg is also considered to be PH.58 Pulmonary arterial hypertension (PAH) is defined as a mean PA pressure greater than 25 mm Hg at rest (or 30 mm Hg with exercise), with a concomitant pulmonary capillary wedge pressure less than 15 mm Hg and a pulmonary vascular resistance (PVR) greater than 3 Woods units14 or 240 dyn•sec•cm-5.
Choosing from among improved therapeutic options
Main therapeutic goals are to prevent or reverse vasoconstriction, inhibit smooth muscle proliferation, impede thrombosis, and thereby reduce right ventricular failure. Newer pharmacologic agents have improved outcomes for patients and may even obviate the need for surgery. Treating the underlying cause of PH may be helpful, such as immunosuppression for SLE18 or positive pressure in sleep-disordered breathing.19 Table 2 outlines therapeutic options, and Figure 2 presents a strategy for applying these options.
FIGURE 2
Treatment algorithm for pulmonary arterial hypertension
TABLE 2
Treatment options for pulmonary arterial hypertension
| Medication | SOR* | Route | Adverse effects | Cost † | |
|---|---|---|---|---|---|
| Prostanoids | Epoprostenol | A | Intravenous | Line-related sepsis and thrombosis, jaw pain, fatal arrhythmia with sudden interruption | $$$$ |
| Treprostinil | B | Subcutaneous | Site pain (85%), jaw pain | $$$$ | |
| Iloprost | B | Inhaled | Short half-life with intermittent benefit | ||
| Endothelin antagonists | Bosentan | A | Oral | Hepatotoxicity, teratogenicity, fluid retention | $$$ |
| Sitaxsentan | B | ||||
| Ambrisentan | C | ||||
| PDE5 inhibitors | Sildenafil | B | Oral | Short half-life, retinopathy | $$ |
| Vardenafil | I | Short half-life | |||
| Tadalafil | I | ||||
| Surgical options | Lung transplant | C | Complicated procedure, lifelong immunosuppression | $$$$ | |
| Atrial septostomy | C | Invasive procedure, hypoxemia | $$ | ||
| Conventional therapy | Diuretics | C | Electrolyte imbalance, dehydration, etc | $ | |
| Digoxin | C | Higher mortality with high serum level | $ | ||
| Warfarin | C | Bleeding diathesis, dosing difficult in liver disease | $ | ||
| Calcium channel blockers | C | Harmful in vasodilator nonresponders | $ | ||
| Note: The level of evidence implied by the strength of recommendation must not be confused with level of efficacy. Medications not currently approved by the FDA for any indication are listed in italics. Only epoprostenol, bosentan, and trepros-tinil are approved specifically for pulmonary arterial hypertension. | |||||
| *SOR = strength of recommendation. A = Data derived from multiple randomized clinical trials or meta-analyses; B = Data derived from single randomized clinical trials or from multiple randomized clinical trials with heterogeneous results; C = Data derived from small randomized studies or consensus opinion of experts;59 I = indeterminate, no data available, theoretical basis only. See “Evidence-based medicine terms” on page 995. | |||||
Conventional therapies
Calcium channel blockers. Calcium channel block-ers (CCBs) are useful only for PAH patients who respond to vasodilator testing in a cardiac catheter-ization laboratory (SOR: B). Criteria for vasore-sponsiveness have changed and it is now generally agreed that the mean PA pressure must fall by at least 10 mm Hg to 40 mm Hg with increased or unchanged cardiac output. CCB use for nonrespon-ders leads to higher morbidity and mortality.20
Digoxin. In left ventricular failure, digoxin relieves symptoms, but without mortality benefit (SOR: A).21 Only 1 study has shown a hemodynamic benefit in PAH in the intensive-care setting.22 Therefore, experts do not agree that digoxin is useful in right ventricular failure from PAH. Digoxin may be warranted in the presence of concomitant left ventricular dysfunction or digoxin-responsive arrhythmias.
Warfarin. Two retrospective studies have shown a decrease in mortality with warfarin in PAH.23,24 There is no consensus, though, on the degree of anticoagulation, with recommendations of INR ranging from 1.5 to 4.0.
Diuretics. Judicious use of diuretics is recommended in PAH. Loop diuretics, thiazides, and spironolactone are commonly titrated to achieve symptomatic relief.
Ambulatory oxygen therapy. This option is indicated for resting and exercise-induced hypoxia. Experts usually recommend titration to achieve a PO2 >60 mm Hg.
Prostanoids: Epoprostenol, treprostinil, iloprost
Prostanoids cause vasodilation, inhibit platelet aggregation, prevent smooth muscle proliferation, decrease inflammation, and increase cardiac output.25 Epoprostenol improves exercise tolerance, hemodynamics and quality of life in patients with IPAH and PAH secondary to scleroderma (SOR: A).3,26 Treprostinil and iloprost show similar benefits. A survival advantage has only been shown for epoprostenol and treprostinil.27 Epoprostenol is useful in both vasodilator “responders” and “nonresponders.”28
Administration. Epoprostenol is administered with a central venous catheter. Usual starting dose is 2 ng/kg/min or higher with increase by 1 ng/kg/min every 1 to 2 weeks until the desired clinical improvement is manifested, or side effects preclude dose escalation.29
Treprostinil is given subcutaneously and is under investigation as an intravenous agent. The optimal dose for treprostinil is 13.8 ng/kg/min and above.30
Iloprost is delivered via inhalation, although it has also been used intravenously. Iloprost is not approved by the Food and Drug Administration but is available in clinical trials. Inhaled iloprost is short-lived and only provides intermittent hemodynamic benefit.31
Side effects. Side effects include jaw pain, nausea, anorexia, diarrhea, flushing, and headache. With the exception of jaw pain, these side effects are dose-related. The risk of catheter sepsis with epoprostenol is 0.1% to 0.4% per patient-year. More serious side effects include arrhythmia with sudden interruption of drug delivery. Treprostinil causes infusion site pain (85%), necessitating discontinuation in 8% of the patients.
Endothelin receptor antagonists: Bosentan, sitaxsentan, ambrisentan
In the lung parenchyma of patients with PH, expression of endothelin-1, a 21-amino-acid peptide, increases.32 Higher levels of serum endothelin-1 correlate directly with severity of PH and poorer outcomes.33 Endothelin-1 mediates vasoconstriction and smooth muscle proliferation primarily through endothelin type A (ETA) receptors and vasodilatation mostly through endothelin type B (ETB) receptors, although a dynamic relationship exists between the two.34
Oral formulation a plus. Bosentan is the only endothelin antagonist currently approved by the FDA. It is a low-molecular-weight, nonpeptide, competitive, dual receptor antagonist. Sitaxsentan and ambrisentan are available in clinical trials only. They are ETA-selective with the premise that sparing the ETB receptor, which is responsible for pulmonary vasodilation, will lead to better clinical outcomes. All these compounds can be given orally, a major advantage over prostanoids.
Bosentan improves exercise capacity, hemodynamics, symptoms, and time to clinical worsening.35,36 Patients studied in bosentan trials had NYHA class III or IV dyspnea due to IPAH, APAH due to scleroderma, and others. Bosentan is not approved by the FDA for functional class II patients, but has been used for such patients.
Indicated for milder PAH. Bosentan outcome data were presented at the American Thoracic Society Meeting (2003) but have not been published so far. At 3 years, 86% of patients were still alive when only 48% were expected based on historical data from the NIH registry.37 Epoprostenol survival at 3 years is about 63%.16,17 However, only patients with milder PAH receive bosentan, while the more seriously ill ones require prostanoids. This selection may explain the survival difference.
Administration. Recommended starting dose of bosentan is 62.5 mg twice daily for 4 weeks. It is then increased to 125 mg twice daily if there is no elevation of aminotransferases. Bosentan is now known to be safe in children.38 Ambrisentan and sitaxsentan should to be available in 2005 or later.
Side effects. The most common side effect of bosentan is hepatic aminotransferase elevation (9% of patients), usually occurring within 16 weeks (90%). All elevations have resolved upon drug withdrawal (97% within 8 weeks). The FDA mandates monthly monitoring of aminotransferase for bosentan. Furthermore, bosentan is teratogenic39 and absolutely contraindicated in pregnancy. There may be significant fluid retention. Sitaxsentan and ambrisentan have similar side effects and their eventual clinical use is expected to require similar monitoring.
Phosphodiesterase-5 inhibitors: Sildenafil, vardenafil, tadalafil
Phosphodiesterases (PDEs) are a group of isoenzymes widely distributed in various organs. PDE5 is found in the corpus cavernosum, pulmonary vasculature, muscle, and platelets.
Use for PAH off-label. Sildenafil, vardenafil, and tadalafil are cyclic guanosine monophosphate-specific PDE5 inhibitors with potent, selective pulmonary vasodilatory and antiplatelet effects. Sildenafil and vardenafil have relatively short half-lives (4–6 hours). Tadalafil has a longer half-life (17.5 hours) with potential for once-daily administration. All these compounds are only available orally. The FDA has approved these for erectile dysfunction only, but they have been used off-label.
A phase III study of sildenafil in PAH has been completed, but has not been published. One randomized study has shown clinical efficacy.40 Small series have also shown clinical improvement.41,42
Due to their short half-lives, sildenafil and vardenafil require multidose regimens, with potential for noncompliance leading to rebound pulmonary vasoconstriction. Retinopathy at high dose, from inhibition of PDE6, remains a concern for sildenafil.43 Priapism has not been reported in the PAH population so far, but may be a relevant consideration in sickle cell anemia.
Lung transplantation
Lung transplantation should be considered if functional class II is not achieved despite optimal medical therapy.44 Improved medical therapy has decreased the need for this surgical option, lengthened the time to transplantation, or even eliminated the requirement altogether.45 The 5-year survival of patients on epoprostenol is comparable with, or better than, that with lung transplant.46 Patient selection and early referral for transplantation are crucial to success in this process. Published international guidelines help guide this process.47 In general, PAH patients in WHO functional class II, III, or IV should be medically treated. Concurrently, referral for transplantation should be considered, even before there are signs that functional class I or II cannot be achieved. This is because transplant evaluation is a fairly lengthy process and it is not unusual for patients to die while on the long waiting list. If medical therapy is successful, the patient can be inactivated. In case medical therapy begins to fail subsequently, listing can be reactivated.
Lung transplantation remains the surgical treatment of choice for refractory PAH. Heart-lung transplants tend to be reserved for patients with structural cardiac abnormalities. Single lung transplantation has the advantages of less complex surgery and more efficient use of harvested organs to benefit more patients, thereby leading to shorter waiting periods. However, most transplant centers in the US prefer double lung transplantation, mainly because there is greater pulmonary reserve should the patient sustain rejection or infection.48
The operative mortality range is between 16% to 29%.48 The 1-year survival rate after lung transplantation (single as well as double) is approximately 70% to 75%, 2-year survival is 50% to 60%, and 5-year survival is 40% to 45%.49 The International Society of Heart and Lung Transplantation database shows that overall survival for both single and double lung transplantation is nearly equal up to 3 years postsurgery. After that, there is a significant survival advantage for double lung transplant.50 Although several studies have documented a significant improvement in the quality of life after transplantation for PH, cost-effectiveness has not yet been addressed.
Balloon atrial septostomy
Balloon atrial septostomy reduces strain on the right ventricle and improves cardiac output. Its use is limited by systemic hypoxemia caused by the right-to-left shunt and perioperative morbidity. It may be used as a bridge procedure while awaiting lung transplantation.51 Functional improvement has been demonstrated in a small series.52 Patient selection, improvement in hemodynamics, and clinical outcomes vary from center to center.53,54 It is likely that patient selection, technique, and experience influence the outcome considerably. This procedure should only be performed in experienced centers on carefully selected patients.
Combination therapy increasingly used
There are no prospective data on combination therapy for PAH. Whether combination therapy has an additive, synergistic, or even antagonistic effect is uncertain. However, there is pathophysiologic rationale for this approach, especially in therapeutic failure following monotherapy. Addition of sildenafil to epoprostenol reduces PA pressure and PVR without hypotension or desaturation.42 When iloprost failed as monotherapy for 14 patients with PAH, addition of sildenafil reversed clinical deterioration, increased functional capacity, and yielded favorable hemodynamics at 3 months, with sustained efficacy up to 12 months.55 There are no data showing whether sildenafil will have synergistic benefits with bosentan. Despite lack of evidence, combination therapy has been used increasingly in clinical practice.
- Amlodipine • Norvasc
- Bosentan • Tracleer
- Digoxin • Lanoxin
- Epoprostenol • Flolan
- Iloprost • Ventavis
- Nifedipine • Adalat, Procardia
- Sildenafil • Viagra
- Sitaxsentan • Thelin
- Spironolactone • Aldactone
- Tadalafil • Cialis
- Treprostinil • Remodulin
- Vardenafil • Levitra
- Warfarin • Coumadin
Corresponding author
Kamal K. Mubarak, MD, Wayne State University, 3990 John R, 3937 Hudson, Detroit, MI 48201. E-mail: [email protected].
1. Simonneau G, Galie N, Rubin LJ, et al. Clinical classification of pulmonary hypertension. J Am Coll Cardiol 2004;43:5S-12S.
2. Gaine SP, Rubin LJ. Primary pulmonary hypertension. Lancet 1998;352:719-725.
3. Badesch DB, Tapson VF, McGoon MD, et al. Continuous intravenous epoprostenol for pulmonary hypertension due to the scleroderma spectrum of disease. A randomized, controlled trial. Ann Intern Med 2000;132:425-434.
4. Rosenzweig EB, Kerstein D, Barst RJ. Long-term prostacyclin for pulmonary hypertension with associated congenital heart defects. Circulation 1999;99:1858-1865.
5. Fishman AP. Aminorex to fen/phen: an epidemic foretold. Circulation 1999;99:156-161.
6. McDonnell PJ, Toye PA, Hutchins GM. Primary pulmonary hypertension and cirrhosis: are they related? Am Rev Respir Dis 1983;127:437-441.
7. Battle RW, Davitt MA, Cooper SM, et al. Prevalence of pulmonary hypertension in limited and diffuse scleroderma. Chest 1996;110:1515-1519.
8. Stupi AM, Steen VD, Owens GR, et al. Pulmonary hypertension in the CREST syndrome variant of systemic sclerosis. Arthritis Rheum 1986;29:515-524.
9. Asherson RA, Higenbottam TW, Dinh Xuan AT, et al. Pulmonary hypertension in a lupus clinic: experience with twenty-four patients. J Rheumatol 1990;17:1292-1298.
10. Shen JY, Chen SL, Wu YX, et al. Pulmonary hypertension in systemic lupus erythematosus. Rheumatol Int 1999;18:147-151.
11. Dawson JK, Goodson NG, Graham DR, et al. Raised pulmonary artery pressures measured with Doppler echocardiography in rheumatoid arthritis patients. Rheumatology (Oxford) 2000;39:1320-1325.
12. Mehta NJ, Khan IA, Mehta RN, et al. HIV-Related pulmonary hypertension: analytic review of 131 cases. Chest 2000;118:1133-1141.
13. Yigla M, Nakhoul F, Sabag A, et al. Pulmonary hypertension in patients with end-stage renal disease. Chest 2003;123:1577-1582.
14. Rich S, Dantzker DR, Ayres SM, et al. Primary pulmonary hypertension. A national prospective study. Ann Intern Med 1987;107:216-223.
15. Denton CP, Cailes JB, Phillips GD, et al. Comparison of Doppler echocardiography and right heart catheterization to assess pulmonary hypertension in systemic sclerosis. Br J Rheumatol 1997;36:239-243.
16. Sitbon O, Humbert M, Nunes H, et al. Long-term intravenous epoprostenol infusion in primary pulmonary hypertension: prognostic factors and survival. J Am Coll Cardiol 2002;40:780-788.
17. McLaughlin VV, Shillington A, Rich S. Survival in primary pulmonary hypertension: the impact of epoprostenol therapy. Circulation 2002;106:1477-1482.
18. Groen H, Bootsma H, Postma DS, et al. Primary pulmonary hypertension in a patient with systemic lupus erythematosus: partial improvement with cyclophosphamide. J Rheumatol 1993;20:1055-1057.
19. Thalhofer S, Dorow P. [Effect of n-BiPAP therapy on the hemodynamics in patients with central sleep apnea]. Pneumologie 1995;49 Suppl 1:165-166.
20. Farber HW, Karlinsky JB, Faling LJ. Fatal outcome following nifedipine for pulmonary hypertension. Chest 1983;83:708-709.
21. The effect of digoxin on mortality and morbidity in patients with heart failure. The Digitalis Investigation Group. N Engl J Med 1997;336:525-533.
22. Rich S, Seidlitz M, Dodin E, et al. The short-term effects of digoxin in patients with right ventricular dysfunction from pulmonary hypertension. Chest 1998;114:787-792.
23. Frank H, Mlczoch J, Huber K, et al. The effect of anticoagulant therapy in primary and anorectic drug-induced pulmonary hypertension. Chest 1997;112:714-721.
24. Rich S, Kaufmann E, Levy PS. The effect of high doses of calcium-channel blockers on survival in primary pulmonary hypertension. N Engl J Med 1992;327:76-81.
25. Rich S, McLaughlin VV. The effects of chronic prostacyclin therapy on cardiac output and symptoms in primary pulmonary hypertension. J Am Coll Cardiol 1999;34:1184-1187.
26. Barst RJ, Rubin LJ, Long WA, et al. A comparison of continuous intravenous epoprostenol (prostacyclin) with conventional therapy for primary pulmonary hypertension. The Primary Pulmonary Hypertension Study Group. N Engl J Med 1996;334:296-302.
27. Gibbs J, Arneson C, Mottola D. Chronic infusion of Treprostinil is safe, and appears to prolong survival over a three-year period in patients with Pulmonary Arterial Hypertension. Abstract presented at American Thoracic Society Meeting, 2003.
28. McLaughlin VV, Genthner DE, Panella MM, et al. Reduction in pulmonary vascular resistance with long-term epoprostenol (prostacyclin) therapy in primary pulmonary hypertension. N Engl J Med 1998;338:273-277.
29. Hoeper MM, Galie N, Simonneau G, et al. New treatments for pulmonary arterial hypertension. Am J Respir Crit Care Med 2002;165:1209-1216.
30. Simonneau G, Barst RJ, Galie N, et al. Continuous subcutaneous infusion of treprostinil, a prostacyclin analogue, in patients with pulmonary arterial hypertension: a double-blind, randomized, placebo-controlled trial. Am J Respir Crit Care Med 2002;165:800-804.
31. Fruhwald FM, Kjellstrom B, Perthold W, et al. Continuous hemodynamic monitoring in pulmonary hypertensive patients treated with inhaled iloprost. Chest 2003;124:351-359.
32. Giaid A, Yanagisawa M, Langleben D, et al. Expression of endothelin-1 in the lungs of patients with pulmonary hypertension. N Engl J Med 1993;328:1732-1739.
33. Rubens C, Ewert R, Halank M, et al. Big endothelin-1 and endothelin-1 plasma levels are correlated with the severity of primary pulmonary hypertension. Chest 2001;120:1562-1569.
34. Zuccarello M, Boccaletti R, Rapoport RM. Does blockade of endothelinB1-receptor activation increase endothelinB2/endothelinA receptor-mediated constriction in the rabbit basilar artery? J Cardiovasc Pharmacol 1999;33:679-684.
35. Channick RN, Simonneau G, Sitbon O, et al. Effects of the dual endothelin-receptor antagonist bosentan in patients with pulmonary hypertension: a randomised placebo-controlled study. Lancet 2001;358:1119-1123.
36. Rubin LJ, Badesch DB, Barst RJ, et al. Bosentan therapy for pulmonary arterial hypertension. N Engl J Med 2002;346:896-903.
37. D’Alonzo GE, Barst RJ, Ayres SM, et al. Survival in patients with primary pulmonary hypertension. Results from a national prospective registry. Ann Intern Med 1991;115:343-349.
38. Barst RJ, Ivy D, Dingemanse J, et al. Pharmacokinetics, safety, and efficacy of bosentan in pediatric patients with pulmonary arterial hypertension. Clin Pharmacol Ther 2003;73:372-382.
39. Actelion Pharmaceuticals. Package insert. Tracleer (bosentan). Physician’s Desk Reference (www.pdr.net). South San Francisco, Calif, 2002.
40. Sastry BK, Narasimhan C, Reddy NK, et al. Clinical efficacy of sildenafil in primary pulmonary hypertension: a randomized, placebo-controlled, double-blind, crossover study. J Am Coll Cardiol 2004;43:1149-1153.
41. Prasad S, Wilkinson J, Gatzoulis MA. Sildenafil in primary pulmonary hypertension. N Engl J Med 2000;343:1342.-
42. Stiebellehner L, Petkov V, Vonbank K, et al. Long-term treatment with oral sildenafil in addition to continuous IV epoprostenol in patients with pulmonary arterial hypertension. Chest 2003;123:1293-1295.
43. Behn D, Potter MJ. Sildenafil-mediated reduction in retinal function in heterozygous mice lacking the gamma-subunit of phosphodiesterase. Invest Ophthalmol Vis Sci 2001;42:523-527.
44. Rubin LJ. Primary pulmonary hypertension. N Engl J Med 1997;336:111-117.
45. Conte JV, Gaine SP, Orens JB, et al. The influence of continuous intravenous prostacyclin therapy for primary pulmonary hypertension on the timing and outcome of transplantation. J Heart Lung Transplant 1998;17:679-685.
46. Rich S, McLaughlin VV. Lung transplantation for pulmonary hypertension: patient selection and maintenance therapy while awaiting transplantation. Semin Thorac Cardiovasc Surg 1998;10:135-138.
47. Maurer JR, Frost AE, Estenne M, et al. International guidelines for the selection of lung transplant candidates. The International Society for Heart and Lung Transplantation, the American Thoracic Society, the American Society of Transplant Physicians, the European Respiratory Society. J Heart Lung Transplant 1998;17:703-709.
48. McLaughlin VV, Rich S. Severe pulmonary hypertension: critical care clinics. Crit Care Clin 2001;17:453-467.
49. Hosenpud JD, Bennett LE, Keck BM, et al. The Registry of the International Society for Heart and Lung Transplantation: sixteenth official report—1999. J Heart Lung Transplant 1999;18:611-626.
50. Hertz MI, Mohacsi PJ, Taylor DO, et al. The registry of the International Society for Heart and Lung Transplantation: introduction to the Twentieth Annual Reports—2003. J Heart Lung Transplant 2003;22:610-615.
51. Rich S. Primary Pulmonary Hypertension. Curr Treat Options Cardiovasc Med 2000;2:135-140.
52. Sandoval J, Gaspar J, Pulido T, et al. Graded balloon dilation atrial septostomy in severe primary pulmonary hypertension. A therapeutic alternative for patients nonresponsive to vasodilator treatment. J Am Coll Cardiol 1998;32:297-304.
53. Reichenberger F, Pepke-Zaba J, McNeil K, et al. Atrial septostomy in the treatment of severe pulmonary arterial hypertension. Thorax 2003;58:797-800.
54. Nihill MR, O’Laughlin MP, Mullins CE. Effects of atrial septostomy in patients with terminal cor pulmonale due to pulmonary vascular disease. Cathet Cardiovasc Diagn 1991;24:166-172.
55. Ghofrani HA, Rose F, Schermuly RT, et al. Oral sildenafil as long-term adjunct therapy to inhaled iloprost in severe pulmonary arterial hypertension. J Am Coll Cardiol 2003;42:158-164.
56. Chatterjee K, De Marco T, Alpert JS. Pulmonary hypertension: hemodynamic diagnosis and management. Arch Intern Med 2002;162:1925-1933.
57. Tuder RM, Groves B, Badesch DB, et al. Exuberant endothelial cell growth and elements of inflammation are present in plexiform lesions of pulmonary hypertension. Am J Pathol 1994;144:275-285.
58. Maloney JP. Advances in the treatment of secondary pulmonary hypertension. Curr Opin Pulm Med 2003;9:139-143.
59. Galie N, Seeger W, Naeije R, et al. Comparative analysis of clinical trials and evidence-based treatment algorithm in pulmonary arterial hypertension. J Am Coll Cardiol 2004;43:81S-88S.
1. Simonneau G, Galie N, Rubin LJ, et al. Clinical classification of pulmonary hypertension. J Am Coll Cardiol 2004;43:5S-12S.
2. Gaine SP, Rubin LJ. Primary pulmonary hypertension. Lancet 1998;352:719-725.
3. Badesch DB, Tapson VF, McGoon MD, et al. Continuous intravenous epoprostenol for pulmonary hypertension due to the scleroderma spectrum of disease. A randomized, controlled trial. Ann Intern Med 2000;132:425-434.
4. Rosenzweig EB, Kerstein D, Barst RJ. Long-term prostacyclin for pulmonary hypertension with associated congenital heart defects. Circulation 1999;99:1858-1865.
5. Fishman AP. Aminorex to fen/phen: an epidemic foretold. Circulation 1999;99:156-161.
6. McDonnell PJ, Toye PA, Hutchins GM. Primary pulmonary hypertension and cirrhosis: are they related? Am Rev Respir Dis 1983;127:437-441.
7. Battle RW, Davitt MA, Cooper SM, et al. Prevalence of pulmonary hypertension in limited and diffuse scleroderma. Chest 1996;110:1515-1519.
8. Stupi AM, Steen VD, Owens GR, et al. Pulmonary hypertension in the CREST syndrome variant of systemic sclerosis. Arthritis Rheum 1986;29:515-524.
9. Asherson RA, Higenbottam TW, Dinh Xuan AT, et al. Pulmonary hypertension in a lupus clinic: experience with twenty-four patients. J Rheumatol 1990;17:1292-1298.
10. Shen JY, Chen SL, Wu YX, et al. Pulmonary hypertension in systemic lupus erythematosus. Rheumatol Int 1999;18:147-151.
11. Dawson JK, Goodson NG, Graham DR, et al. Raised pulmonary artery pressures measured with Doppler echocardiography in rheumatoid arthritis patients. Rheumatology (Oxford) 2000;39:1320-1325.
12. Mehta NJ, Khan IA, Mehta RN, et al. HIV-Related pulmonary hypertension: analytic review of 131 cases. Chest 2000;118:1133-1141.
13. Yigla M, Nakhoul F, Sabag A, et al. Pulmonary hypertension in patients with end-stage renal disease. Chest 2003;123:1577-1582.
14. Rich S, Dantzker DR, Ayres SM, et al. Primary pulmonary hypertension. A national prospective study. Ann Intern Med 1987;107:216-223.
15. Denton CP, Cailes JB, Phillips GD, et al. Comparison of Doppler echocardiography and right heart catheterization to assess pulmonary hypertension in systemic sclerosis. Br J Rheumatol 1997;36:239-243.
16. Sitbon O, Humbert M, Nunes H, et al. Long-term intravenous epoprostenol infusion in primary pulmonary hypertension: prognostic factors and survival. J Am Coll Cardiol 2002;40:780-788.
17. McLaughlin VV, Shillington A, Rich S. Survival in primary pulmonary hypertension: the impact of epoprostenol therapy. Circulation 2002;106:1477-1482.
18. Groen H, Bootsma H, Postma DS, et al. Primary pulmonary hypertension in a patient with systemic lupus erythematosus: partial improvement with cyclophosphamide. J Rheumatol 1993;20:1055-1057.
19. Thalhofer S, Dorow P. [Effect of n-BiPAP therapy on the hemodynamics in patients with central sleep apnea]. Pneumologie 1995;49 Suppl 1:165-166.
20. Farber HW, Karlinsky JB, Faling LJ. Fatal outcome following nifedipine for pulmonary hypertension. Chest 1983;83:708-709.
21. The effect of digoxin on mortality and morbidity in patients with heart failure. The Digitalis Investigation Group. N Engl J Med 1997;336:525-533.
22. Rich S, Seidlitz M, Dodin E, et al. The short-term effects of digoxin in patients with right ventricular dysfunction from pulmonary hypertension. Chest 1998;114:787-792.
23. Frank H, Mlczoch J, Huber K, et al. The effect of anticoagulant therapy in primary and anorectic drug-induced pulmonary hypertension. Chest 1997;112:714-721.
24. Rich S, Kaufmann E, Levy PS. The effect of high doses of calcium-channel blockers on survival in primary pulmonary hypertension. N Engl J Med 1992;327:76-81.
25. Rich S, McLaughlin VV. The effects of chronic prostacyclin therapy on cardiac output and symptoms in primary pulmonary hypertension. J Am Coll Cardiol 1999;34:1184-1187.
26. Barst RJ, Rubin LJ, Long WA, et al. A comparison of continuous intravenous epoprostenol (prostacyclin) with conventional therapy for primary pulmonary hypertension. The Primary Pulmonary Hypertension Study Group. N Engl J Med 1996;334:296-302.
27. Gibbs J, Arneson C, Mottola D. Chronic infusion of Treprostinil is safe, and appears to prolong survival over a three-year period in patients with Pulmonary Arterial Hypertension. Abstract presented at American Thoracic Society Meeting, 2003.
28. McLaughlin VV, Genthner DE, Panella MM, et al. Reduction in pulmonary vascular resistance with long-term epoprostenol (prostacyclin) therapy in primary pulmonary hypertension. N Engl J Med 1998;338:273-277.
29. Hoeper MM, Galie N, Simonneau G, et al. New treatments for pulmonary arterial hypertension. Am J Respir Crit Care Med 2002;165:1209-1216.
30. Simonneau G, Barst RJ, Galie N, et al. Continuous subcutaneous infusion of treprostinil, a prostacyclin analogue, in patients with pulmonary arterial hypertension: a double-blind, randomized, placebo-controlled trial. Am J Respir Crit Care Med 2002;165:800-804.
31. Fruhwald FM, Kjellstrom B, Perthold W, et al. Continuous hemodynamic monitoring in pulmonary hypertensive patients treated with inhaled iloprost. Chest 2003;124:351-359.
32. Giaid A, Yanagisawa M, Langleben D, et al. Expression of endothelin-1 in the lungs of patients with pulmonary hypertension. N Engl J Med 1993;328:1732-1739.
33. Rubens C, Ewert R, Halank M, et al. Big endothelin-1 and endothelin-1 plasma levels are correlated with the severity of primary pulmonary hypertension. Chest 2001;120:1562-1569.
34. Zuccarello M, Boccaletti R, Rapoport RM. Does blockade of endothelinB1-receptor activation increase endothelinB2/endothelinA receptor-mediated constriction in the rabbit basilar artery? J Cardiovasc Pharmacol 1999;33:679-684.
35. Channick RN, Simonneau G, Sitbon O, et al. Effects of the dual endothelin-receptor antagonist bosentan in patients with pulmonary hypertension: a randomised placebo-controlled study. Lancet 2001;358:1119-1123.
36. Rubin LJ, Badesch DB, Barst RJ, et al. Bosentan therapy for pulmonary arterial hypertension. N Engl J Med 2002;346:896-903.
37. D’Alonzo GE, Barst RJ, Ayres SM, et al. Survival in patients with primary pulmonary hypertension. Results from a national prospective registry. Ann Intern Med 1991;115:343-349.
38. Barst RJ, Ivy D, Dingemanse J, et al. Pharmacokinetics, safety, and efficacy of bosentan in pediatric patients with pulmonary arterial hypertension. Clin Pharmacol Ther 2003;73:372-382.
39. Actelion Pharmaceuticals. Package insert. Tracleer (bosentan). Physician’s Desk Reference (www.pdr.net). South San Francisco, Calif, 2002.
40. Sastry BK, Narasimhan C, Reddy NK, et al. Clinical efficacy of sildenafil in primary pulmonary hypertension: a randomized, placebo-controlled, double-blind, crossover study. J Am Coll Cardiol 2004;43:1149-1153.
41. Prasad S, Wilkinson J, Gatzoulis MA. Sildenafil in primary pulmonary hypertension. N Engl J Med 2000;343:1342.-
42. Stiebellehner L, Petkov V, Vonbank K, et al. Long-term treatment with oral sildenafil in addition to continuous IV epoprostenol in patients with pulmonary arterial hypertension. Chest 2003;123:1293-1295.
43. Behn D, Potter MJ. Sildenafil-mediated reduction in retinal function in heterozygous mice lacking the gamma-subunit of phosphodiesterase. Invest Ophthalmol Vis Sci 2001;42:523-527.
44. Rubin LJ. Primary pulmonary hypertension. N Engl J Med 1997;336:111-117.
45. Conte JV, Gaine SP, Orens JB, et al. The influence of continuous intravenous prostacyclin therapy for primary pulmonary hypertension on the timing and outcome of transplantation. J Heart Lung Transplant 1998;17:679-685.
46. Rich S, McLaughlin VV. Lung transplantation for pulmonary hypertension: patient selection and maintenance therapy while awaiting transplantation. Semin Thorac Cardiovasc Surg 1998;10:135-138.
47. Maurer JR, Frost AE, Estenne M, et al. International guidelines for the selection of lung transplant candidates. The International Society for Heart and Lung Transplantation, the American Thoracic Society, the American Society of Transplant Physicians, the European Respiratory Society. J Heart Lung Transplant 1998;17:703-709.
48. McLaughlin VV, Rich S. Severe pulmonary hypertension: critical care clinics. Crit Care Clin 2001;17:453-467.
49. Hosenpud JD, Bennett LE, Keck BM, et al. The Registry of the International Society for Heart and Lung Transplantation: sixteenth official report—1999. J Heart Lung Transplant 1999;18:611-626.
50. Hertz MI, Mohacsi PJ, Taylor DO, et al. The registry of the International Society for Heart and Lung Transplantation: introduction to the Twentieth Annual Reports—2003. J Heart Lung Transplant 2003;22:610-615.
51. Rich S. Primary Pulmonary Hypertension. Curr Treat Options Cardiovasc Med 2000;2:135-140.
52. Sandoval J, Gaspar J, Pulido T, et al. Graded balloon dilation atrial septostomy in severe primary pulmonary hypertension. A therapeutic alternative for patients nonresponsive to vasodilator treatment. J Am Coll Cardiol 1998;32:297-304.
53. Reichenberger F, Pepke-Zaba J, McNeil K, et al. Atrial septostomy in the treatment of severe pulmonary arterial hypertension. Thorax 2003;58:797-800.
54. Nihill MR, O’Laughlin MP, Mullins CE. Effects of atrial septostomy in patients with terminal cor pulmonale due to pulmonary vascular disease. Cathet Cardiovasc Diagn 1991;24:166-172.
55. Ghofrani HA, Rose F, Schermuly RT, et al. Oral sildenafil as long-term adjunct therapy to inhaled iloprost in severe pulmonary arterial hypertension. J Am Coll Cardiol 2003;42:158-164.
56. Chatterjee K, De Marco T, Alpert JS. Pulmonary hypertension: hemodynamic diagnosis and management. Arch Intern Med 2002;162:1925-1933.
57. Tuder RM, Groves B, Badesch DB, et al. Exuberant endothelial cell growth and elements of inflammation are present in plexiform lesions of pulmonary hypertension. Am J Pathol 1994;144:275-285.
58. Maloney JP. Advances in the treatment of secondary pulmonary hypertension. Curr Opin Pulm Med 2003;9:139-143.
59. Galie N, Seeger W, Naeije R, et al. Comparative analysis of clinical trials and evidence-based treatment algorithm in pulmonary arterial hypertension. J Am Coll Cardiol 2004;43:81S-88S.
How should we diagnose and treat obstructive sleep apnea?
- What are the risk factors for obstructive sleep apnea (OSA)?
- What is the standard for diagnostic testing?
- How does management of mild OSA differ from severe OSA?
- Can other illnesses complicate OSA?
Obstructive sleep apnea is underdiagnosed.1 These recommendations (from the Institute for Clinical Systems Improvement’s Respiratory Steering Committee) can help providers more accurately identify adults who have OSA through a sleep study evaluation, prescribe appropriate treatment, document cases for appropriate follow-up, and increase patient understanding of related health risks. The target audience is physicians, nurses, advanced practice nurses, and physician assistants. The target population is adults.
The evidence categories for this guideline are diagnosis, evaluation, management, risk assessment, and treatment. Outcomes considered are signs and symptoms of OSA; patient risk factors, including comorbidities; accuracy of diagnostic tests; effects of treatment on apneahypopnea index and other measures; patient compliance and satisfaction with treatment; and complications of treatment. Their rating scheme has been updated to comply with the SORT taxonomy.2
Relevance and limitations
OSA affects more than 12 million people in the US, 2% of women and 4% of men aged >35 years. The patient with OSA commonly consults a physician after a sleep partner reports loud snoring and irregular breathing. The methods used to collect and select evidence is not stated.
Development and review
This guideline was accessed through the National Guideline Clearinghouse (www.ngc.gov). The Institute for Clinical Systems Improvement is an independent, nonprofit organization sponsored by 6 Minnesota health plans.
The authors completed an electronic search of databases. Data were analyzed by systematic review with evidence table and were validated by clinical validation-pilot testing and internal peer review. The methods used to make the recommendations were not discussed. Quality and strength of evidence were weighted according to a rating scheme furnished in the guideline. Two excellent algorithms are attached to this guideline: diagnosis and treatment. There are 92 references.
Guideline source
Institute for Clinical Systems Improvement. Diagnosis and Treatment of Obstructive Sleep Apnea. Bloomington, Minn: Institute for Clinical Systems Improvement; 2003. 53 pages.
Other guidelines on osa
- Practice parameters for the use of autotitrating continuous positive airway pressure devices for titrating pressures and treating adult patients with obstructive sleep apnea syndrome. Standards of Practice Committee. Sleep 2002; 25:143–147 [29 references]. Web access at: www.aasmnet.org/PDF/autotitratingreview.pdf.
- Practice parameters for the use of portable monitoring devices in the investigation of suspected obstructive sleep apnea in adults. Chesson AL Jr, Berry RB, Pack A. Practice parameters for the use of portable monitoring devices in the investigation of suspected obstructive sleep apnea in adults. Sleep2003; 26:907–913 [11 references]. Web access at: www.aasmnet.org/PDF/260719.pdf.
- Clinical practice guideline: diagnosis and management of childhood obstructive sleep apnea syndrome. Pediatrics 2002; 109:704–712 [63 references]. Web access at: www.aappolicy. aappublications.org/cgi/content/full/pediatrics; 109/4/704.
Grade A Recommendations
- Large neck circumference, obesity, and hypertension are risk factors for OSA.
- OSA occurs frequently in patients with cardiovascular disease, coronary artery disease, and hypertension.
- Additional signs and symptoms of OSA include reports of choking by sleep partner, awakening with choking, intense snoring, severe daytime sleepiness (with driving impairment), and male gender.
- Polysomography should be performed to determine the diagnosis and is the standard for diagnosis. Unattended portable monitoring is a reasonable alternative when the patient has severe symptoms requiring prompt evaluation/treatment or for follow-up studies.
- Lifestyle modification, including weight loss, reduced alcohol consumption, and lateral sleep positioning are recommended for treatment.
- Severity of OSA is based on magnitude of sleepiness, hypoxia, and the Apnea-Hypopnea Index (AHI).
- Mild OSA can be treated with oral appliances, positive airway pressure devices, or surgical procedures.
- Moderate to severe obstructive sleep apnea should always be treated with positive airway pressure devices, continuous positive airway pressure (CPAP) most commonly.
Grade B Recommendations
- Unattended portable monitoring may be acceptable for rural areas where polysomography is unavailable.
- Surgical procedures (septoplasty, nasal polypectomy, tonsillectomy, turbinoplasty, and uvulopalatopharyngoplasty) to correct anatomical obstructions might be necessary for treatment of mild OSA prior to a positive pressure device.
- After initiating treatment patients should be seen in follow-up in 1 month to assess snoring and sleepiness.
1. Strollo PJ, Jr, Rogers RM. Obstructive sleep apnea. N Engl J Med 1996;334:99-104.
2. Ebell M, Siwek J, Weiss BD, et al. Strength of recommendation taxonomy (SORT): A patient-centered approach to grading evidence in the medical literature. Am Fam Physician 2004;69:548-556.
Correspondence: Keith B. Holten, MD, Clinton Memorial Hospital/University of Cincinnati Family Practice Residency, 825 W. Locust St., Wilmington, OH, 45177. E-mail: [email protected].
- What are the risk factors for obstructive sleep apnea (OSA)?
- What is the standard for diagnostic testing?
- How does management of mild OSA differ from severe OSA?
- Can other illnesses complicate OSA?
Obstructive sleep apnea is underdiagnosed.1 These recommendations (from the Institute for Clinical Systems Improvement’s Respiratory Steering Committee) can help providers more accurately identify adults who have OSA through a sleep study evaluation, prescribe appropriate treatment, document cases for appropriate follow-up, and increase patient understanding of related health risks. The target audience is physicians, nurses, advanced practice nurses, and physician assistants. The target population is adults.
The evidence categories for this guideline are diagnosis, evaluation, management, risk assessment, and treatment. Outcomes considered are signs and symptoms of OSA; patient risk factors, including comorbidities; accuracy of diagnostic tests; effects of treatment on apneahypopnea index and other measures; patient compliance and satisfaction with treatment; and complications of treatment. Their rating scheme has been updated to comply with the SORT taxonomy.2
Relevance and limitations
OSA affects more than 12 million people in the US, 2% of women and 4% of men aged >35 years. The patient with OSA commonly consults a physician after a sleep partner reports loud snoring and irregular breathing. The methods used to collect and select evidence is not stated.
Development and review
This guideline was accessed through the National Guideline Clearinghouse (www.ngc.gov). The Institute for Clinical Systems Improvement is an independent, nonprofit organization sponsored by 6 Minnesota health plans.
The authors completed an electronic search of databases. Data were analyzed by systematic review with evidence table and were validated by clinical validation-pilot testing and internal peer review. The methods used to make the recommendations were not discussed. Quality and strength of evidence were weighted according to a rating scheme furnished in the guideline. Two excellent algorithms are attached to this guideline: diagnosis and treatment. There are 92 references.
Guideline source
Institute for Clinical Systems Improvement. Diagnosis and Treatment of Obstructive Sleep Apnea. Bloomington, Minn: Institute for Clinical Systems Improvement; 2003. 53 pages.
Other guidelines on osa
- Practice parameters for the use of autotitrating continuous positive airway pressure devices for titrating pressures and treating adult patients with obstructive sleep apnea syndrome. Standards of Practice Committee. Sleep 2002; 25:143–147 [29 references]. Web access at: www.aasmnet.org/PDF/autotitratingreview.pdf.
- Practice parameters for the use of portable monitoring devices in the investigation of suspected obstructive sleep apnea in adults. Chesson AL Jr, Berry RB, Pack A. Practice parameters for the use of portable monitoring devices in the investigation of suspected obstructive sleep apnea in adults. Sleep2003; 26:907–913 [11 references]. Web access at: www.aasmnet.org/PDF/260719.pdf.
- Clinical practice guideline: diagnosis and management of childhood obstructive sleep apnea syndrome. Pediatrics 2002; 109:704–712 [63 references]. Web access at: www.aappolicy. aappublications.org/cgi/content/full/pediatrics; 109/4/704.
Grade A Recommendations
- Large neck circumference, obesity, and hypertension are risk factors for OSA.
- OSA occurs frequently in patients with cardiovascular disease, coronary artery disease, and hypertension.
- Additional signs and symptoms of OSA include reports of choking by sleep partner, awakening with choking, intense snoring, severe daytime sleepiness (with driving impairment), and male gender.
- Polysomography should be performed to determine the diagnosis and is the standard for diagnosis. Unattended portable monitoring is a reasonable alternative when the patient has severe symptoms requiring prompt evaluation/treatment or for follow-up studies.
- Lifestyle modification, including weight loss, reduced alcohol consumption, and lateral sleep positioning are recommended for treatment.
- Severity of OSA is based on magnitude of sleepiness, hypoxia, and the Apnea-Hypopnea Index (AHI).
- Mild OSA can be treated with oral appliances, positive airway pressure devices, or surgical procedures.
- Moderate to severe obstructive sleep apnea should always be treated with positive airway pressure devices, continuous positive airway pressure (CPAP) most commonly.
Grade B Recommendations
- Unattended portable monitoring may be acceptable for rural areas where polysomography is unavailable.
- Surgical procedures (septoplasty, nasal polypectomy, tonsillectomy, turbinoplasty, and uvulopalatopharyngoplasty) to correct anatomical obstructions might be necessary for treatment of mild OSA prior to a positive pressure device.
- After initiating treatment patients should be seen in follow-up in 1 month to assess snoring and sleepiness.
- What are the risk factors for obstructive sleep apnea (OSA)?
- What is the standard for diagnostic testing?
- How does management of mild OSA differ from severe OSA?
- Can other illnesses complicate OSA?
Obstructive sleep apnea is underdiagnosed.1 These recommendations (from the Institute for Clinical Systems Improvement’s Respiratory Steering Committee) can help providers more accurately identify adults who have OSA through a sleep study evaluation, prescribe appropriate treatment, document cases for appropriate follow-up, and increase patient understanding of related health risks. The target audience is physicians, nurses, advanced practice nurses, and physician assistants. The target population is adults.
The evidence categories for this guideline are diagnosis, evaluation, management, risk assessment, and treatment. Outcomes considered are signs and symptoms of OSA; patient risk factors, including comorbidities; accuracy of diagnostic tests; effects of treatment on apneahypopnea index and other measures; patient compliance and satisfaction with treatment; and complications of treatment. Their rating scheme has been updated to comply with the SORT taxonomy.2
Relevance and limitations
OSA affects more than 12 million people in the US, 2% of women and 4% of men aged >35 years. The patient with OSA commonly consults a physician after a sleep partner reports loud snoring and irregular breathing. The methods used to collect and select evidence is not stated.
Development and review
This guideline was accessed through the National Guideline Clearinghouse (www.ngc.gov). The Institute for Clinical Systems Improvement is an independent, nonprofit organization sponsored by 6 Minnesota health plans.
The authors completed an electronic search of databases. Data were analyzed by systematic review with evidence table and were validated by clinical validation-pilot testing and internal peer review. The methods used to make the recommendations were not discussed. Quality and strength of evidence were weighted according to a rating scheme furnished in the guideline. Two excellent algorithms are attached to this guideline: diagnosis and treatment. There are 92 references.
Guideline source
Institute for Clinical Systems Improvement. Diagnosis and Treatment of Obstructive Sleep Apnea. Bloomington, Minn: Institute for Clinical Systems Improvement; 2003. 53 pages.
Other guidelines on osa
- Practice parameters for the use of autotitrating continuous positive airway pressure devices for titrating pressures and treating adult patients with obstructive sleep apnea syndrome. Standards of Practice Committee. Sleep 2002; 25:143–147 [29 references]. Web access at: www.aasmnet.org/PDF/autotitratingreview.pdf.
- Practice parameters for the use of portable monitoring devices in the investigation of suspected obstructive sleep apnea in adults. Chesson AL Jr, Berry RB, Pack A. Practice parameters for the use of portable monitoring devices in the investigation of suspected obstructive sleep apnea in adults. Sleep2003; 26:907–913 [11 references]. Web access at: www.aasmnet.org/PDF/260719.pdf.
- Clinical practice guideline: diagnosis and management of childhood obstructive sleep apnea syndrome. Pediatrics 2002; 109:704–712 [63 references]. Web access at: www.aappolicy. aappublications.org/cgi/content/full/pediatrics; 109/4/704.
Grade A Recommendations
- Large neck circumference, obesity, and hypertension are risk factors for OSA.
- OSA occurs frequently in patients with cardiovascular disease, coronary artery disease, and hypertension.
- Additional signs and symptoms of OSA include reports of choking by sleep partner, awakening with choking, intense snoring, severe daytime sleepiness (with driving impairment), and male gender.
- Polysomography should be performed to determine the diagnosis and is the standard for diagnosis. Unattended portable monitoring is a reasonable alternative when the patient has severe symptoms requiring prompt evaluation/treatment or for follow-up studies.
- Lifestyle modification, including weight loss, reduced alcohol consumption, and lateral sleep positioning are recommended for treatment.
- Severity of OSA is based on magnitude of sleepiness, hypoxia, and the Apnea-Hypopnea Index (AHI).
- Mild OSA can be treated with oral appliances, positive airway pressure devices, or surgical procedures.
- Moderate to severe obstructive sleep apnea should always be treated with positive airway pressure devices, continuous positive airway pressure (CPAP) most commonly.
Grade B Recommendations
- Unattended portable monitoring may be acceptable for rural areas where polysomography is unavailable.
- Surgical procedures (septoplasty, nasal polypectomy, tonsillectomy, turbinoplasty, and uvulopalatopharyngoplasty) to correct anatomical obstructions might be necessary for treatment of mild OSA prior to a positive pressure device.
- After initiating treatment patients should be seen in follow-up in 1 month to assess snoring and sleepiness.
1. Strollo PJ, Jr, Rogers RM. Obstructive sleep apnea. N Engl J Med 1996;334:99-104.
2. Ebell M, Siwek J, Weiss BD, et al. Strength of recommendation taxonomy (SORT): A patient-centered approach to grading evidence in the medical literature. Am Fam Physician 2004;69:548-556.
Correspondence: Keith B. Holten, MD, Clinton Memorial Hospital/University of Cincinnati Family Practice Residency, 825 W. Locust St., Wilmington, OH, 45177. E-mail: [email protected].
1. Strollo PJ, Jr, Rogers RM. Obstructive sleep apnea. N Engl J Med 1996;334:99-104.
2. Ebell M, Siwek J, Weiss BD, et al. Strength of recommendation taxonomy (SORT): A patient-centered approach to grading evidence in the medical literature. Am Fam Physician 2004;69:548-556.
Correspondence: Keith B. Holten, MD, Clinton Memorial Hospital/University of Cincinnati Family Practice Residency, 825 W. Locust St., Wilmington, OH, 45177. E-mail: [email protected].
Nondaily hormonal contraceptives: Establishing a fit between product characteristics and patient preferences
- Consider progestin-only DMPA-IM or L-IUS methods for women who want highly effective, nondaily, reversible contraception, and who regard amenorrhea as a desirable side effect; also suitable when estrogen therapy is contraindicated (SOR: C).
- Consider the NE-patch or EE-ring, both containing estrogen and progestin, for women who are candidates for combined oral contraceptives, including those desiring shorter-term contraception and regular bleeding cycles (SOR:C).
- To help women select the most appropriate and acceptable nondaily contraceptive option, review with patients each method’s route and schedule of administration, perfect vs typical use efficacy, potential noncontraceptive health benefits, reversibility, side effects, and long-term safety profile (SOR:C).
Oral contraceptives have made a major contribution to both women and society by substantially reducing the rate of unintended pregnancies. However, in actual clinical practice, contraceptive failures remain a problem. For example, the first-year pregnancy rate with oral contraceptives can be as high as 5% to 8%.1 Experts agree that a leading reason for unintended pregnancy among oral contraceptive users is incorrect and inconsistent use. Women who do not use oral contraceptives consistently are nearly 3 times as likely to become pregnant as those who use them consistently.2
Today, women have alternatives to the daily regimen of oral contraceptives. Highly effective, convenient, nondaily contraceptive choices are available in injectable, intrauterine, intravaginal, and transdermal delivery systems, which may be administered weekly, monthly, every 3 months, or every 5 years, depending on a woman’s family planning needs and preferences.
This article compares the efficacy, non-contraceptive health benefits, side-effect profiles, and long-term safety of the available nondaily hormonal contraceptive options. It also reviews other factors to consider when selecting the most appropriate and acceptable option for women who are seeking nondaily contraception.
Options for nondaily contraception
The first available nondaily contraceptive, depot-medroxyprogesterone acetate (DMPA-IM; Depo-Provera), is a progestin-only injectable introduced in 1963 that has been used by more than 30 million women worldwide.3 Its efficacy, safety, and health benefits have been established through large-scale epidemiologic investigations, and it was approved for use in the United States in 1992.
In the past 2 years, other nondaily hormonal contraceptives with a variety of delivery systems have been introduced to the US market. The levonorgestrel-releasing intrauterine system (L-IUS; Mirena) is also a progestin-only method that has been in use worldwide for 10 years. Its health benefits and hormone-associated side-effect profile are similar to DMPA-IM (particularly bleeding patterns).
The etonogestrel/ethinyl estradiol vaginal ring (EE-ring; NuvaRing), and the norelgestromin/ethinyl estradiol transdermal system (NE-patch; Ortho Evra) will likely offer improved efficacy to oral contraceptives with a similar long-term safety profile.
Nondaily contraception potentially more convenient and effective
Unlike oral contraceptives, which must be taken every day, nondaily contraceptives offer dosing options ranging from weekly to every 5 years ( Table 1 ). These extended dosing intervals reduce the likelihood of missed doses and are more convenient for many women than daily dosing. These methods also provide greater privacy because there is no visible evidence of their use, with the exception of the patch, which can be worn on discreet locations under clothing.
Improved adherence associated with less frequent dosing of nondaily hormonal contraceptives appears to enhance contraceptive efficacy, an example of which is the similarity between first-year pregnancy rates during perfect and typical use of DMPA-IM ( Table 2 ). The antiovulatory concentrations of medroxyprogesterone acetate achieved within 24 hours of injection provide almost immediate protection against pregnancy and likely contribute to the high contraceptive efficacy seen with DMPA-IM.4 The lowest reported pregnancy rates with perfect and typical use of L-IUS are comparable, and there is no need for backup contraception following insertion.5 Furthermore, even with typical use, reported pregnancy rates for DMPA-IM and L-IUS (0.3% and 0.1%, respectively) are comparable to sterilization (0.5%).1,5
Pregnancy rates during perfect use of the NE-patch and EE-ring also are low, but it is not yet possible to accurately estimate the failure rates of these methods during typical use due to limited US postmarketing experience.6,7 A backup method is recommended for the first 7 days of EE-ring use if the patient has not previously taken hormonal contraception or is switching from a progestin-only method,7 and for the first 7 days of NE-patch use if the first patch is applied after Day 1 of menses.6
TABLE 1
Nondaily hormonal contraceptives (currently available in the US), compared with oral contraceptives
| Method, Administration | Mechanism of action | Dosing schedule | Pregnancy first year (%) | |
|---|---|---|---|---|
| Perfect use | Typical use | |||
| DMPA-IM 1 (Medroxyprogesterone acetate; Depo-Provera) Intramuscular injection, given by health provider | Inhibits secretion of gonadotropins, which prevents follicular maturation and ovulation and results in endometrial thinning | Every 3 mo | 0.3 | 0.3 |
| L-IUS 5 (Levonorgestrel; Mirena) Intrauterine system, placed by health provider | Effects morphological changes in the endometrium, including stromal pseudodecidualization, glandular atrophy, and leukocytic infiltration; inhibition of ovulation is observed in some women | Every 5 y | 0.1 | 0.1 |
| EE-Ring 7 (Etonogestrel/ethinyl estradiol; NuvaRing) Intravaginal ring, self-applied | Suppression of gonadotropins inhibits ovulation; other alterations include changes in cervical mucus and endometrium | Monthly (1 ring-free wk/mo) | 1.0–2.0 | Unknown* |
| NE-Patch 6 (Norelgestromin/ethinyl estradiol; Ortho Evra) Transdermal patch, self-applied | Suppression of gonadotropins inhibits ovulation; other alterations include changes in cervical mucus and endometrium | Weekly (1 patch-free wk/mo) | 1.0 | Unknown* |
| Oral contraceptives 1 Combined or progestin-only Oral pills, self-administered | Suppression of gonadotropins inhibits ovulation; other alterations include changes in cervical mucus and endometrium | Daily (1 hormone-free wk/mo) | Combined: 0.1 Progestin: 0.5 | Combined: 5.0 Progestin: 5.0 |
| *Due to limited US postmarketing experience, a precise estimate of failure rate during typical use is not yet available. | ||||
TABLE 2
Nondaily hormonal contraceptive side effects and long-term safety
| Side effect | Combined oral contraceptives | Depo-Provera | Mirena | NuvaRing | Ortho Evra |
|---|---|---|---|---|---|
| Bleeding patterns | |||||
| Regular cycles | Yes | No | Variable | Yes | Yes |
| Intermenstrual bleeding/spotting | 7.6%–27% at 1 year17,18 | 16% at 1 year20 | 3.8% at 1 year32 | <10% at 1 year22,38 | |
| Menorrhagia | 6.7% at 9 mo16 | Rare20 | None reported32 | None reported22 | |
| Amenorrhea | 70%–73% at 1 year17,18 | 20%–50% at 1 year5,20 | None reported32 | 0.1%22 | |
| Discontinuation due to bleeding changes | 20% at 1 year16 | 10.6% at 1 year57 | <1% at 1 year32 | <1% at 1 year22 | |
| Weight gain | Mean 1.3 kg at 1 year29 | Mean 2.5–3.0 kg at 1 year13,29 | <1.0 kg at 1 year33 | <1.0 kg at 1 year32 | <1.0 kg at 1 year22 |
| Mood | Depression, 4.8%40 | Depression, <2%19 | Depression 5%5 | Emotional lability 2.8%32 | Emotional lability 1.5%38 |
| Hormone delivery system–related side effects | Allergies to dyes in pills; efficacy may be compromised by gastrointestinal or hepatic metabolism | Minor injection sitepain (<1%)13 | Expulsion (6.6%)20 Sepsis, PID, embedment/perforation5 | Vaginitis (5.6%) leukorrhea (4.8%) device-related events (4.4%)32 | Patch application site reactions (20%)22 |
| Breast and gynecologic cancers* | |||||
| Breast | 1.24 (1.15–1.33)39†§ | 1.5 (1–2.2)40†§ | No studies | No studies | No studies |
| 1.01 (0.96–1.05)58‡ | 1.1 (0.97–1.4)40‡ | ||||
| Endometrial | 0.55 (0.26–1.17)41 | 0.21 (0.06–0.79)8 | |||
| Ovarian | 0.5 (0.3–0.6)42 | 1.07 (0.6–1.8)43 | |||
| Cervical | 1.30 (0.5–3.3)45 | 1.11 (0.96–1.29)46 | |||
| 1.53 (0.99–2.36)44 | |||||
| Relative risk of cardiovascular disease | |||||
| All stroke | 1.41 (0.90–2.20)49 | 0.89 (0.53–1.49)50 | No studies | No studies | No studies |
| Acute MI | 4.69 (2.02–10.9)48§ | 0.66 (0.07–6.0)50 | |||
| Smokers <35 y | 34.947 | ||||
| Smokers 35 y | 396.247§ | ||||
| VTE | 4.32 (2.88–6.49)47§ | 2.19 (0.66–7.26)50 | |||
| Effects on bone mineral density | Variable, but usually positive | Reversible reduction | No studies | No studies | No studies |
| *Relative risk (95% CI). †Current use; ‡Any use; §Likelihood was significantly different relative to control; §Confidence intervals not reported. | |||||
| PID, pelvic inflammatory disease; CI, confidence interval; MI, myocardial infarction; VTE, venous thromboembolism. | |||||
Noncontraceptive health benefits
Nondaily hormonal contraceptive options have documented non-contraceptive health benefits.
DMPA-IM. This drug reduces the risk of endometrial cancer by 80% after 1 year, a protective effect that appears to extend for at least 8 years after cessation of use.8 DMPA-IM also decreases risk of iron deficiency anemia, pelvic inflammatory disease9 and uterine leiomyomas,10 and reduces pain crises among users with sickle cell disease.11
Clinical experience has shown that DMPA-IM may be an effective treatment option for a number of gynecologic conditions, including (though these are unapproved off-label uses) menorrhagia and dysmenorrhea, pain associated with endometriosis, ovulatory pain, and menopause-related vasomotor symptoms.9,12 Many of the menstrual-cycle related benefits of DMPA-IM result from the high incidence of amenorrhea, which may be particularly appealing to women who have menstrual-cycle related disorders, such as mittelschmerz, and for women who have problems with menstrual hygiene.
Additional advantages of progestin-only DMPA-IM compared with estrogen-containing contraceptive options include efficacy that is not compromised by concomitant anticonvulsive therapy.9 It also has no adverse effect on lactation, allowing use as early as the sixth week postpartum in breast-feeding women.13
L-IUS. This agent may also have several non-contraceptive benefits related primarily to the oligoamenorrhea experienced by many users. These include increased hemoglobin concentrations (thus possibly preventing iron deficiency anemia), off-label use as a treatment for menorrhagia or dysmenorrhea, an alternative to hysterectomy for heavy menstrual bleeding, and for progestin opposition in post-menopausal women on estrogen replacement therapy.14 Small case-series reports also suggest that L-IUS may have a modulatory effect on endometrial hyperplasia associated with tamoxifen exposure in women with breast cancer.15
EE-ring, NE-patch. Due to the limited experience with these products, it is not known whether users will enjoy noncontraceptive health benefits, although it is reasonable to assume that since they are derived from combinations of well-studied estrogens and progestins, their benefits may be similar to those of combined oral contraceptives.
Side-effect profiles
Hormone-related side effects—including changes in bleeding pattern, weight gain, mood changes, headaches, breast tenderness, and nausea—can be problematic for many women using hormonal contraceptives (both oral contraceptives and nondaily methods) and are common reasons for discontinuation.2,16 Therefore, it is important to consider differences in side-effect profiles when helping women to select an appropriate method, and to adequately counsel women regarding the expected effects prior to starting therapy.
Bleeding patterns
Nondaily hormonal contraceptives differ considerably in their effects on bleeding patterns ( Table 2 ).
DMPA-IM is characterized by amenorrhea, which develops in 70% to 73% of users after 1 year.17,18 Intermenstrual bleeding and spotting has been reported in 7.6% to 27% of DMPA-IM users at 12 months.17,18 However, among those who experience irregular bleeding, it generally consists of spotting or light bleeding rather than heavy intermenstrual flow.19
Amenorrhea has been reported in 20% to 50% of L-IUS users after 1 year.5,20 Among L-IUS users who do not experience amenorrhea, cycles are variable,5 with spotting observed in 25% of women at 6 months, decreasing to 11% at 2 years.20
Amenorrhea is rarely seen among women using the EE-ring or NE-patch; rather, similar to oral contraceptives, regular menstrual cycles are established within the first few cycles of use.21,22 Rates of intermenstrual bleeding/spotting at 1 year are less than 10% for each of these methods, with bleeding changes rarely cited as a reason for drug discontinuation.21,22
Counseling before treatment improves adherence. Counseling about menstrual changes, especially the absence of menses associated with DMPA-IM and L-IUS, can significantly increase user satisfaction and continuation rates.23,24 In a prospective study of new users of DMPA-IM, women who were told about the possibility of amenorrhea were 2.5 times more likely to continue use at 1 year than those who were not given this information.23 In fact, surveys of women’s preferences indicate that most women prefer the convenience, comfort, and freedom of less frequent or absent menses.25 Because the decision whether or not to menstruate is a personal one, this is an important issue to discuss with a patient selecting a contraceptive method.
Weight gain
Concern about weight gain can be significant enough for some women to pose a barrier to hormonal contraceptive selection and compliance. Variable effects of DMPA-IM on body weight have been reported, ranging from nonsignificant changes26,27 to gains of approximately 3 kg to 4 kg at 1 year.28,29 However, the most pronounced weight changes occurred in women who were overweight at the initiation of use or who may have been inherently predisposed to gain weight.28,29
In a long-term study of Thai women using either DMPA-IM or a nonhormonal intrauterine device, weight gain in both groups was comparable after 10 years of use (10.9 and 11.2 kg, respectively).30 Furthermore, in the only randomized, placebo-controlled trial to assess weight gain, normal-weight women observed during the first 2 menstrual cycles following the initial injection of DMPA-IM did not experience weight gain.31
Data from 1-year multicenter clinical trials with the NE-patch, EE-ring, and L-IUS indicate that users of these methods experience minimal (<1 kg) or no weight gain. ,32,33 However, long-term follow-up of women using L-IUS for 12 years found an increase in body weight of 0.49 kg/year during the study period and a mean overall increase of 5.7 kg.34
Mood changes
Although mood changes are often cited by women as a reason for discontinuing hormonal contraception,2 data from clinical trials indicate that DMPA-IM does not cause mood changes or worsen existing depressive symptoms. Fewer than 2% of 3857 US women who used DMPA-IM in a 1-year multicenter trial reported depression.19 Other studies specifically assessing mood changes in an adolescent health clinic35 and inner-city family planning clinics36 failed to find any adverse impact of DMPA-IM on mood. Only 1 study of women enrolled in a health maintenance organization found an association between DMPA-IM and symptoms of depression, but a causal relationship could not be established.37
To date, no studies have specifically examined the effects of the other nondaily hormonal contraceptive options on mood. L-IUS product labeling states that depression has been reported in more than 5% of patients,5 while 1-year clinical trials report emotional lability in 1.5% of NE-patch users and 2.8% of EE-ring users.32,38 However, in a small comparative trial, there were no reports of depression among 121 EE-ring users, whereas it was reported by 4.8% of 126 women using a combined oral contraceptive containing 30 μg ethinyl estradiol and 150 μg levonorgestrel.21
Delivery system–related side effects
All nondaily options have specific side effects related to local effects or the delivery system. DMPA-IM may cause pain on injection, but this is reported as an adverse event by fewer than 1% of subjects.13
In a US clinical trial of the NE-patch, application-site reactions were reported by 20% of participants, leading to discontinuation by 2.6% of women in the patch group; 4.6% of patches were replaced for either complete (1.8%) or partial detachment (2.8%).22
In a 1-year multicenter study of the EE-ring in 2322 women, common complaints were vaginitis (5.6%), leukorrhea (4.8%), and device-related events (4.4%) consisting of foreign body sensation, coital problems, and expulsion. The latter problem can occur during removal of a tampon or during bowel or bladder emptying, necessitating immediate reinsertion of the ring or replacement with a new ring.7,32
Expulsion is also a problem with L-IUS and can result in unintended pregnancy. During the first 2 years following insertion, L-IUS was discontinued by 6.6% of 256 women as the result of expulsion, which occurred significantly more frequently among women with heavy menstrual bleeding than those with normal bleeding (13% vs 5%, P=.01).20 Other potential device-related effects of L-IUS include pelvic inflammatory disease, embedment or perforation, and sepsis.5
Long-term safety profiles
Cancer risks
To date, cancer risks associated with long-term use have been investigated only for DMPA-IM and combined oral contraceptives in large epidemiological studies ( Table 2 ). Because women’s concerns regarding the risk of breast cancer may make them reluctant to use a hormonal method of contraception, it is particularly important for clinicians to emphasize the evidence showing that use of hormonal contraceptives is not associated with an increase in the overall risk of breast cancer. Though a large-scale reanalysis of 54 studies found a slight increase in breast cancer risk among current combined oral contraceptive users (relative risk [RR]=1.24; 95% confidence interval [CI], 1.15–1.33), this risk decreased over time and was the same as that of combined oral contraceptive never-users 10 or more years after cessation of use (RR=1.01; 95% CI, 0.96–1.05).39 Similarly, a pooled analysis of DMPA-IM data from the World Health Organization (WHO) and New Zealand trials, which were completed in the early 1990s, also found a slight increase in breast cancer risk among current users (RR=1.50; 95% CI, 1.0–2.2), but showed no increase in the overall risk of breast cancer among ever-users.40
Women can also be advised that neither DMPA-IM nor combined oral contraceptives appear to significantly increase their risk of gynecologic cancers ( Table 2 ). In fact, as previously discussed, these contraceptives decrease the risk of endometrial cancer,8,41 an effect that is particularly strong for DMPA-IM (an 80% reduction in risk for ever-users, which appeared to last for at least 8 years following cessation of use).8 Combined oral contraceptives are also associated with an approximately 50% reduction in risk of ovarian cancer.42 While there is no evidence that DMPA-IM reduces the risk of ovarian cancers, it does not appear to be associated with a significant increase in risk (RR=1.07; 95% CI, 0.6–1.8).43
Because of confounding factors such as smoking, risk factors for sexually transmitted disease, and screening detection bias, it has been difficult to firmly establish the relationship between contraceptive use and cervical cancer. However, several studies suggest the use of combined oral contraceptives, particularly for longer durations, slightly increases the risk of invasive cervical cancer.44,45 In contrast, the risk of invasive cervical cancer does not appear to increase in users of DMPA-IM, and no consistent pattern of risk with either duration of use or other time-related factors has been observed.46
Cardiovascular risks
DMPA-IM. Only DMPA-IM and combined oral contraceptives have been the subject of large-scale epidemiological investigations to assess the risk of cardiovascular disease, also summarized in Table 2 . Increased risk for venous thromboembolism (VTE) is related to the dose of estrogen in combined oral contraceptives. While currently available low-dose combined oral contraceptives (<50 μg estrogen) confer less risk than the higher-dose preparations of the past, they still confer a 3- to 4-fold higher risk of VTE than that experienced by nonusers.47 The risk of VTE conferred by DMPA-IM is less than half that of combined oral contraceptives.
Users of low-dose combined oral contraceptives are also at increased risk of acute myocardial infarction compared with nonusers, though this risk reflects the frequent coexistence of other cardiovascular risk factors.48 In fact, acute myocardial infarction is very rare among younger women (<35 years) who use combined oral contraceptives but who do not smoke, with an estimated attributable risk of approximately 3 per million woman-years. However, this attributable risk rises steeply to nearly 400 per million woman-years in older women (≥35 years) who smoke.48
Risk of stroke is slightly increased among users of low-dose combined oral contraceptives, again primarily among women aged ≥35 years. Overall, the excess attributable risk estimate is approximately 2 per 100,000 woman-years, which decreases to 1 per 200,000 woman-years in women <35 years who use low-dose combined oral contraceptives.49
In light of these risks, combined oral contraceptives are contraindicated for smokers ≥35 years, women with an increased risk or history of thromboembolism, and women with cerebrovascular or coronary artery disease.
Epidemiologic data from the WHO found no association between DMPA-IM use and an increased risk of any type of stroke or myocardial infarction (MI) ( Table 2 ).50 Although there was a slight increase in the risk of VTE compared with nonusers, this was not considered statistically significant (odds ratio [OR]=2.19; 95% CI, 0.66–7.26).50 In addition, compared with nonusers, DMPA-IM users did not exhibit increased combined cardiovascular disease risk (eg, stroke, VTE, myocardial infarction) (OR=1.02; 95% CI, 0.68–1.54).50
L-IUS, NE-patch, and EE-ring. Long-term epidemiologic data for these products are unavailable due to the relatively short postmarket experience, which precludes assumptions of long-term cardiovascular safety. Likewise, no evidence is available regarding whether the safety profile for transdermal or vaginal administration differs from oral administration. Therefore, it is not known whether NE-patch or EE-ring confer different risks for venous thromboembolism than combined oral contraceptives. Warnings about thromboembolic disorders are similarly listed in the package inserts of these options.6,7
Norelgestromin has been reported to have minimal androgenic activity, suggesting a possible lower risk of myocardial infarction than reported for more androgenically active progestin formulation.6 In contrast, etonogestrel, the biologically active metabolite of desogestrel, has been associated with a higher risk of venous thromboembolism than some second-generation combined oral contraceptives.7 For women with these risk factors, progestin-only methods, such as DMPA-IM or L-IUS, should be considered.
Bone mineral density
Historically, data have shown that oral contraceptives most often effect bone mineral density (BMD) positively in premenopausal women; retrospective studies of menopausal cohorts have shown positive effects from oral contraceptive use on BMD.51 However, a recent study of 524 pre-menopausal women found that women who used oral contraceptives, compared with those that did not, had significantly lower BMD values (adjusted differences of 2.4% at the femoral neck to 4.3% at the trochanter).51
Use of progestin-only DMPA-IM particularly raises concern regarding effects on BMD. However, no increased incidence of fractures has been noted in more than 30 years of DMPA-IM use worldwide.
In a recent meta-analysis that compared data from 10 cross-sectional and 7 longitudinal studies of BMD in 1039 women exposed to DMPA-IM with that of 2086 controls,52 average BMD was decreased in current users of DMPA-IM compared with nonusers, but was within 1 standard deviation of the mean in nonusers.52 Reductions in BMD tended to be greater as the duration of use of DMPA-IM increased, but stabilized after 3 to 5 years of use.52,53 Notably, the loss of BMD seen among current users of DMPA-IM is reversible following cessation of use.
Cross-sectional studies in both postmenopausal women52,54 and reproductive-age women,52,55 showed that BMD in former users of DMPA-IM was not significantly different from that of never-users at any site, and a recent prospective study also confirmed the reversibility of bone loss after cessation of DMPA-IM use.56
Establishing a good contraceptive fit
Overall, clinicians can prescribe nondaily hormonal contraceptives with confidence. Primary considerations in selecting a contraceptive method are its efficacy during typical use and its suitability for the medical needs and lifestyle preferences of the individual.
DMPA-IM and L-IUS. Consider the progestin-only nondaily methods DMPA-IM and L-IUS for women who want highly effective, nondaily, reversible contraception and who regard amenorrhea is a desirable side effect. These methods are also suitable when estrogen therapy is contraindicated.
L-IUS, unlike DMPA-IM, is not recommended for teens, nulliparous women, or those who are not in a stable, mutually monogamous relationship. L-IUS should also be avoided when there is a history of pelvic inflammatory disease or ectopic pregnancy.5
Because of its 5-year efficacy, L-IUS should be offered only to those desiring contraception for several years. Likewise, DMPA-IM is not recommended for those who wish to become pregnant within 1 to 2 years, because suppression of ovulation may persist beyond the 3-month dosing interval.
NE-patch and EE-ring. These products containing both estrogen and progestin are effective alternatives for women who would be candidates for combined oral contraceptives, including those desiring shorter-term or more rapidly reversible contraception and regular bleeding cycles.
When discussing contraceptive choices with a patient, review each method’s route and schedule of administration, efficacy in typical and nontypical use, potential noncontraceptive health benefits, reversibility, side effects, and long-term safety profile. The availability of a broader array of contraceptive choices should help women and their clinicians find a method that will fit individual medical needs as well as lifestyle preferences.
Correspondence
Jeffrey P. Levine, MD, MPH, Associate Professor, Departments of Family Medicine and Obstetrics, Gynecology & Reproductive Sciences, UMDNJ–Robert Wood Johnson Medical School, 1 RWJ Place, CN19, New Brunswick, NJ 08903-0019. E-mail: [email protected].
1. Hatcher RA, Trussell J, Stewart F, Cates W, Jr, Stewart GK, Guest F, Kowal D. The essentials of contraception efficacy, safety, and personal considerations. In Contraceptive Technology New York: Ardent Media, Inc., 1998;211-247.
2. Rosenberg MJ, Waugh MS, Meehan TE. Use and misuse of oral contraceptives: risk indicators for poor pill taking and discontinuation. Contraception 1995;51:283-288.
3. Bigrigg A, Evans M, Gbolade B, et al. Depo Provera. Position paper on clinical use, effectiveness and side effects. Br J Fam Plann 1999;25:69-76.
4. Mishell DR, Jr. Pharmacokinetics of depot medroxyprogesterone acetate contraception. J Reprod Med 1996;41:381-390.
5. Mirena US Prescribing Information. Berlex Laboratories, Inc. 2000.
6. Full US Prescribing Information for Ortho Evra (norelge-stromin/ethinyl estradiol transdermal system). Ortho-McNeil Pharmaceutical, Inc. 2001.
7. Full US Prescribing Information for NuvaRing (etonogestrel/ethinyl estradiol vaginal ring). 2003.
8. Depot-medroxyprogesterone acetate (DMPA) and risk of endometrial cancer. The WHO Collaborative Study of Neoplasia and Steroid Contraceptives. Int J Cancer 1991;49:186-190.
9. Cullins VE. Noncontraceptive benefits and therapeutic uses of depot medroxyprogesterone acetate. J Reprod Med 1996;41:428-433.
10. Lumbiganon P, Rugpao S, Phandhu-fung S, Laopaiboon M, Vudhikamraksa N, Werawatakul Y. Protective effect of depot-medroxyprogesterone acetate on surgically treated uterine leiomyomas: a multicentre case—control study. Br J Obstet Gynaecol 1996;103:909-914.
11. de Abood M, de Castillo Z, Guerrero F, Espino M, Austin KL. Effect of Depo-Provera or Microgynon on the painful crises of sickle cell anemia patients. Contraception 1997;56:313-316.
12. Vercellini P, De Giorgi O, Oldani S, Cortesi I, Panazza S, Crosignani PG. Depot medroxyprogesterone acetate versus an oral contraceptive combined with very-low-dose danazol for long-term treatment of pelvic pain associated with endometriosis. Am J Obstet Gynecol 1996;175:396-401.
13. US Approved Prescribing Information for Depo-Provera Contraceptive Injection. Pfizer, Inc. 2003.
14. Hubacher D, Grimes DA. Noncontraceptive health benefits of intrauterine devices: a systematic review. Obstet Gynecol Surv 2002;57:120-128.
15. Gardner FJ, Konje JC, Abrams KR, et al. Endometrial protection from tamoxifen-stimulated changes by a levonorgestrel-releasing intrauterine system: a randomised controlled trial. Lancet 2000;356:1711-1717.
16. Sangi-haghpeykar H, Poindexter A, III, Bateman L, Ditmore JR. Experiences of injectable contraceptive users in an urban setting. Obstet Gynecol 1996;88:227-233.
17. Canto De Cetina TE, Canto P, Ordonez LM. Effect of counseling to improve compliance in Mexican women receiving depot-medroxyprogesterone acetate. Contraception 2001;63:143-146.
18. Mainwaring R, Hales HA, Stevenson K, et al. Metabolic parameter, bleeding, and weight changes in U.S. women using progestin only contraceptives. Contraception 1995;51:149-153.
19. Schwallie PC, Assenzo JR. Contraceptive use—efficacy study utilizing medroxyprogesterone acetate administered as an intramuscular injection once every 90 days. Fertil Steril 1973;24:331-339.
20. Hidalgo M, Bahamondes L, Perrotti M, Diaz J, Dantas-Monteiro C, Petta C. Bleeding patterns and clinical performance of the levonorgestrel-releasing intrauterine system (Mirena) up to two years. Contraception 2002;65:129-132.
21. Bjarnadottir RI, Tuppurainen M, Killick SR. Comparison of cycle control with a combined contraceptive vaginal ring and oral levonorgestrel/ethinyl estradiol. Am J Obstet Gynecol 2002;186:389-395.
22. Audet MC, Moreau M, Koltun WD, et al. Evaluation of contraceptive efficacy and cycle control of a transdermal contraceptive patch vs an oral contraceptive: a randomized controlled trial. JAMA 2001;285:2347-2354.
23. Hubacher D, Goco N, Gonzalez B, Taylor D. Factors affecting continuation rates of DMPA. Contraception 1999;60:345-351.
24. Backman T, Huhtala S, Luoto R, Tuominen J, Rauramo I, Koskenvuo M. Advance information improves user satisfaction with the levonorgestrel intrauterine system. Obstet Gynecol 2002;99:608-613.
25. den Tonkelaar I, Oddens BJ. Preferred frequency and characteristics of menstrual bleeding in relation to reproductive status, oral contraceptive use, and hormone replacement therapy use. Contraception 1999;59:357-362.
26. Danli S, Qingxiang S, Guowei S. A multicentered clinical trial of the long-acting injectable contraceptive Depo Provera in Chinese women. Contraception 2000;62:15-18.
27. Moore LL, Valuck R, McDougall C, Fink W. A comparative study of one-year weight gain among users of medroxyprogesterone acetate, levonorgestrel implants, and oral contraceptives. Contraception 1995;52:215-219.
28. Espey E, Steinhart J, Ogburn T, Qualls C. Depo-provera associated with weight gain in Navajo women. Contraception 2000;62:55-58.
29. Risser WL, Gefter LR, Barratt MS, Risser JM. Weight change in adolescents who used hormonal contraception. J Adolesc Health 1999;24:433-436.
30. Taneepanichskul S, Reinprayoon D, Khaosadad P. Comparative study of weight change between long-term DMPA and IUD acceptors. Contraception 1998;58:149-151.
31. Pelkman CL, Chow M, Heinbach RA, Rolls BJ. Short-term effects of a progestational contraceptive drug on food intake, resting energy expenditure, and body weight in young women. Am J Clin Nutr 2001;73:19-26.
32. Dieben TO, Roumen FJ, Apter D. Efficacy, cycle control, and user acceptability of a novel combined contraceptive vaginal ring. Obstet Gynecol 2002;100:585-593.
33. Dubuisson JB, Mugnier E. Acceptability of the levonorgestrel-releasing intrauterine system after discontinuation of previous contraception: results of a French clinical study in women aged 35 to 45 years. Contraception 2002;66:121-128.
34. Ronnerdag M, Odlind V. Health effects of long-term use of the intrauterine levonorgestrel-releasing system. A follow-up study over 12 years of continuous use. Acta Obstet Gynecol Scand 1999;78:716-721.
35. Gupta N, O’Brien R, Jacobsen LJ, et al. Mood changes in adolescents using depot-medroxyprogesterone acetate for contraception: a prospective study. J Pediatr Adolesc Gynecol 2001;14:71-6.
36. Westhoff C, Truman C, Kalmuss D, et al. Depressive symptoms and Depo-Provera. Contraception 1998;57:237-240.
37. Civic D, Scholes D, Ichikawa L, et al. Depressive symptoms in users and non-users of depot medroxyproges-terone acetate. Contraception 2000;61:385-390.
38. Smallwood GH, Meador ML, Lenihan JP, Shangold GA, Fisher AC, Creasy GW. Efficacy and safety of a transder-mal contraceptive system. Obstet Gynecol 2001;98:799-805.
39. Collaborative Group on Hormonal Factors in Breast Cancer. Breast cancer and hormonal contraceptives: collaborative reanalysis of individual data on 53 297 women with breast cancer and 100 239 women without breast cancer from 54 epidemiological studies. Collaborative Group on Hormonal Factors in Breast Cancer. Lancet 1996;347:1713-1727.
40. Skegg DC, Noonan EA, Paul C, Spears GF, Meirik O, Thomas DB. Depot medroxyprogesterone acetate and breast cancer. A pooled analysis of the World Health Organization and New Zealand studies. JAMA 1995;273:799-804.
41. The Who Collaborative Study of Neoplasia and Steroid Contraceptives. Endometrial cancer and combined oral contraceptives. Int J Epidemiol 1988;17:263-269.
42. Ness RB, Grisso JA, Klapper J, et al. Risk of ovarian cancer in relation to estrogen and progestin dose and use characteristics of oral contraceptives. SHARE Study Group. Steroid Hormones and Reproductions. Am J Epidemiol 2000;152:233-241.
43. Stanford JL, Thomas DB. Depot-medroxyprogesterone acetate (DMPA) and risk of epithelial ovarian cancer. The WHO Collaborative Study of Neoplasia and Steroid Contraceptives. Int J Cancer 1991;49:191-195.
44. Parazzini F, La Vecchia C, Negri E, Maggi R. Oral contraceptive use and invasive cervical cancer. Int J Epidemiol 1990;19:259-263.
45. Kjaer SK, Engholm G, Dahl C, Bock JE, Lynge E, Jensen OM. Case-control study of risk factors for cervical squamous cell neoplasia in Denmark. Role of oral contraceptive use. Cancer Causes Control 1993;4:513-519.
46. WHO Collaborative Study of Neoplasia and Steroid Contraceptives. Depot-medroxyprogesterone acetate and risk of invasive squamous cell cervical cancer.The WHO Collaborative Study of Neoplasia and Steroid Contraceptives. Contraception 1992;45:299-312.
47. WHO Collaborative Study of Cardiovascular Disease and Steroid Hormone Contraception. Venous thromboembolic disease and combined oral contraceptives: results of international multicentre case-control study. World Health Organization Collaborative Study of Cardiovascular Disease and Steroid Hormone Contraception. Lancet 1995;346:1575-1582.
48. WHO Collaborative Study of Cardiovascular Disease and Steroid Hormone Contraception. Acute myocardial infarction and combined oral contraceptives: results of an international multicentre case-control study. WHO Collaborative Study of Cardiovascular Disease and Steroid Hormone Contraception. Lancet 1997;349:1202-1209.
49. WHO Collaborative Study of Cardiovascular Disease and Steroid Hormone Contraception. Haemorrhagic stroke, overall stroke risk, and combined oral contraceptives: results of an international, multicentre, case-control study. WHO Collaborative Study of Cardiovascular Disease and Steroid Hormone Contraception. Lancet 1996;348:505-510.
50. WHO Collaborative Study of Cardiovascular Disease and Steroid Hormone Contraception. Cardiovascular disease and use of oral and injectable progestogen-only contraceptives and combined injectable contraceptives. Results of an international, multicenter, case-control study. World Health Organization Collaborative Study of Cardiovascular Disease and Steroid Hormone Contraception. Contraception 1998;57:315-324.
51. Prior JC, Kirkland SA, Joseph L, et al. Oral contraceptive use and bone mineral density in premenopausal women: cross-sectional, population-based data from the Canadian Multicentre Osteoporosis Study. CMAJ 2001;165:1023-1029.
52. Banks E, Berrington A, Casabonne D. Overview of the relationship between use of progestogen-only contraceptives and bone mineral density. BJOG 2001;108:1214-21.
53. Tang OS, Tang G, Yip PS, Li B. Further evaluation on long-term depot-medroxyprogesterone acetate use and bone mineral density: a longitudinal cohort study. Contraception 2000;62:161-164.
54. Orr-Walker BJ, Evans MC, Ames RW, Clearwater JM, Cundy T, Reid IR. The effect of past use of the injectable contraceptive depot medroxyprogesterone acetate on bone mineral density in normal post-menopausal women. Clin Endocrinol (Oxf) 1998;49:615-618.
55. Petitti DB, Piaggio G, Mehta S, Cravioto MC, Meirik O. Steroid hormone contraception and bone mineral density: a cross-sectional study in an international population. Obstet Gynecol 2000;95:736-744.
56. Scholes D, Lacroix AZ, Ichikawa LE, Barlow WE, Ott SM. Injectable hormone contraception and bone density: results from a prospective study. Epidemiology 2002;13:581-587.
57. Sivin I, el Mahgoub S, McCarthy T, et al. Long-term contraception with the levonorgestrel 20 mcg/day (LNg 20) and the copper T 380Ag intrauterine devices: a five-year randomized study. Contraception 1990;42:361-378.
58. Marchbanks PA, McDonald JA, Wilson HG, et al. Oral contraceptives and the risk of breast cancer. N Engl J Med 2002;346:2025-2032.
- Consider progestin-only DMPA-IM or L-IUS methods for women who want highly effective, nondaily, reversible contraception, and who regard amenorrhea as a desirable side effect; also suitable when estrogen therapy is contraindicated (SOR: C).
- Consider the NE-patch or EE-ring, both containing estrogen and progestin, for women who are candidates for combined oral contraceptives, including those desiring shorter-term contraception and regular bleeding cycles (SOR:C).
- To help women select the most appropriate and acceptable nondaily contraceptive option, review with patients each method’s route and schedule of administration, perfect vs typical use efficacy, potential noncontraceptive health benefits, reversibility, side effects, and long-term safety profile (SOR:C).
Oral contraceptives have made a major contribution to both women and society by substantially reducing the rate of unintended pregnancies. However, in actual clinical practice, contraceptive failures remain a problem. For example, the first-year pregnancy rate with oral contraceptives can be as high as 5% to 8%.1 Experts agree that a leading reason for unintended pregnancy among oral contraceptive users is incorrect and inconsistent use. Women who do not use oral contraceptives consistently are nearly 3 times as likely to become pregnant as those who use them consistently.2
Today, women have alternatives to the daily regimen of oral contraceptives. Highly effective, convenient, nondaily contraceptive choices are available in injectable, intrauterine, intravaginal, and transdermal delivery systems, which may be administered weekly, monthly, every 3 months, or every 5 years, depending on a woman’s family planning needs and preferences.
This article compares the efficacy, non-contraceptive health benefits, side-effect profiles, and long-term safety of the available nondaily hormonal contraceptive options. It also reviews other factors to consider when selecting the most appropriate and acceptable option for women who are seeking nondaily contraception.
Options for nondaily contraception
The first available nondaily contraceptive, depot-medroxyprogesterone acetate (DMPA-IM; Depo-Provera), is a progestin-only injectable introduced in 1963 that has been used by more than 30 million women worldwide.3 Its efficacy, safety, and health benefits have been established through large-scale epidemiologic investigations, and it was approved for use in the United States in 1992.
In the past 2 years, other nondaily hormonal contraceptives with a variety of delivery systems have been introduced to the US market. The levonorgestrel-releasing intrauterine system (L-IUS; Mirena) is also a progestin-only method that has been in use worldwide for 10 years. Its health benefits and hormone-associated side-effect profile are similar to DMPA-IM (particularly bleeding patterns).
The etonogestrel/ethinyl estradiol vaginal ring (EE-ring; NuvaRing), and the norelgestromin/ethinyl estradiol transdermal system (NE-patch; Ortho Evra) will likely offer improved efficacy to oral contraceptives with a similar long-term safety profile.
Nondaily contraception potentially more convenient and effective
Unlike oral contraceptives, which must be taken every day, nondaily contraceptives offer dosing options ranging from weekly to every 5 years ( Table 1 ). These extended dosing intervals reduce the likelihood of missed doses and are more convenient for many women than daily dosing. These methods also provide greater privacy because there is no visible evidence of their use, with the exception of the patch, which can be worn on discreet locations under clothing.
Improved adherence associated with less frequent dosing of nondaily hormonal contraceptives appears to enhance contraceptive efficacy, an example of which is the similarity between first-year pregnancy rates during perfect and typical use of DMPA-IM ( Table 2 ). The antiovulatory concentrations of medroxyprogesterone acetate achieved within 24 hours of injection provide almost immediate protection against pregnancy and likely contribute to the high contraceptive efficacy seen with DMPA-IM.4 The lowest reported pregnancy rates with perfect and typical use of L-IUS are comparable, and there is no need for backup contraception following insertion.5 Furthermore, even with typical use, reported pregnancy rates for DMPA-IM and L-IUS (0.3% and 0.1%, respectively) are comparable to sterilization (0.5%).1,5
Pregnancy rates during perfect use of the NE-patch and EE-ring also are low, but it is not yet possible to accurately estimate the failure rates of these methods during typical use due to limited US postmarketing experience.6,7 A backup method is recommended for the first 7 days of EE-ring use if the patient has not previously taken hormonal contraception or is switching from a progestin-only method,7 and for the first 7 days of NE-patch use if the first patch is applied after Day 1 of menses.6
TABLE 1
Nondaily hormonal contraceptives (currently available in the US), compared with oral contraceptives
| Method, Administration | Mechanism of action | Dosing schedule | Pregnancy first year (%) | |
|---|---|---|---|---|
| Perfect use | Typical use | |||
| DMPA-IM 1 (Medroxyprogesterone acetate; Depo-Provera) Intramuscular injection, given by health provider | Inhibits secretion of gonadotropins, which prevents follicular maturation and ovulation and results in endometrial thinning | Every 3 mo | 0.3 | 0.3 |
| L-IUS 5 (Levonorgestrel; Mirena) Intrauterine system, placed by health provider | Effects morphological changes in the endometrium, including stromal pseudodecidualization, glandular atrophy, and leukocytic infiltration; inhibition of ovulation is observed in some women | Every 5 y | 0.1 | 0.1 |
| EE-Ring 7 (Etonogestrel/ethinyl estradiol; NuvaRing) Intravaginal ring, self-applied | Suppression of gonadotropins inhibits ovulation; other alterations include changes in cervical mucus and endometrium | Monthly (1 ring-free wk/mo) | 1.0–2.0 | Unknown* |
| NE-Patch 6 (Norelgestromin/ethinyl estradiol; Ortho Evra) Transdermal patch, self-applied | Suppression of gonadotropins inhibits ovulation; other alterations include changes in cervical mucus and endometrium | Weekly (1 patch-free wk/mo) | 1.0 | Unknown* |
| Oral contraceptives 1 Combined or progestin-only Oral pills, self-administered | Suppression of gonadotropins inhibits ovulation; other alterations include changes in cervical mucus and endometrium | Daily (1 hormone-free wk/mo) | Combined: 0.1 Progestin: 0.5 | Combined: 5.0 Progestin: 5.0 |
| *Due to limited US postmarketing experience, a precise estimate of failure rate during typical use is not yet available. | ||||
TABLE 2
Nondaily hormonal contraceptive side effects and long-term safety
| Side effect | Combined oral contraceptives | Depo-Provera | Mirena | NuvaRing | Ortho Evra |
|---|---|---|---|---|---|
| Bleeding patterns | |||||
| Regular cycles | Yes | No | Variable | Yes | Yes |
| Intermenstrual bleeding/spotting | 7.6%–27% at 1 year17,18 | 16% at 1 year20 | 3.8% at 1 year32 | <10% at 1 year22,38 | |
| Menorrhagia | 6.7% at 9 mo16 | Rare20 | None reported32 | None reported22 | |
| Amenorrhea | 70%–73% at 1 year17,18 | 20%–50% at 1 year5,20 | None reported32 | 0.1%22 | |
| Discontinuation due to bleeding changes | 20% at 1 year16 | 10.6% at 1 year57 | <1% at 1 year32 | <1% at 1 year22 | |
| Weight gain | Mean 1.3 kg at 1 year29 | Mean 2.5–3.0 kg at 1 year13,29 | <1.0 kg at 1 year33 | <1.0 kg at 1 year32 | <1.0 kg at 1 year22 |
| Mood | Depression, 4.8%40 | Depression, <2%19 | Depression 5%5 | Emotional lability 2.8%32 | Emotional lability 1.5%38 |
| Hormone delivery system–related side effects | Allergies to dyes in pills; efficacy may be compromised by gastrointestinal or hepatic metabolism | Minor injection sitepain (<1%)13 | Expulsion (6.6%)20 Sepsis, PID, embedment/perforation5 | Vaginitis (5.6%) leukorrhea (4.8%) device-related events (4.4%)32 | Patch application site reactions (20%)22 |
| Breast and gynecologic cancers* | |||||
| Breast | 1.24 (1.15–1.33)39†§ | 1.5 (1–2.2)40†§ | No studies | No studies | No studies |
| 1.01 (0.96–1.05)58‡ | 1.1 (0.97–1.4)40‡ | ||||
| Endometrial | 0.55 (0.26–1.17)41 | 0.21 (0.06–0.79)8 | |||
| Ovarian | 0.5 (0.3–0.6)42 | 1.07 (0.6–1.8)43 | |||
| Cervical | 1.30 (0.5–3.3)45 | 1.11 (0.96–1.29)46 | |||
| 1.53 (0.99–2.36)44 | |||||
| Relative risk of cardiovascular disease | |||||
| All stroke | 1.41 (0.90–2.20)49 | 0.89 (0.53–1.49)50 | No studies | No studies | No studies |
| Acute MI | 4.69 (2.02–10.9)48§ | 0.66 (0.07–6.0)50 | |||
| Smokers <35 y | 34.947 | ||||
| Smokers 35 y | 396.247§ | ||||
| VTE | 4.32 (2.88–6.49)47§ | 2.19 (0.66–7.26)50 | |||
| Effects on bone mineral density | Variable, but usually positive | Reversible reduction | No studies | No studies | No studies |
| *Relative risk (95% CI). †Current use; ‡Any use; §Likelihood was significantly different relative to control; §Confidence intervals not reported. | |||||
| PID, pelvic inflammatory disease; CI, confidence interval; MI, myocardial infarction; VTE, venous thromboembolism. | |||||
Noncontraceptive health benefits
Nondaily hormonal contraceptive options have documented non-contraceptive health benefits.
DMPA-IM. This drug reduces the risk of endometrial cancer by 80% after 1 year, a protective effect that appears to extend for at least 8 years after cessation of use.8 DMPA-IM also decreases risk of iron deficiency anemia, pelvic inflammatory disease9 and uterine leiomyomas,10 and reduces pain crises among users with sickle cell disease.11
Clinical experience has shown that DMPA-IM may be an effective treatment option for a number of gynecologic conditions, including (though these are unapproved off-label uses) menorrhagia and dysmenorrhea, pain associated with endometriosis, ovulatory pain, and menopause-related vasomotor symptoms.9,12 Many of the menstrual-cycle related benefits of DMPA-IM result from the high incidence of amenorrhea, which may be particularly appealing to women who have menstrual-cycle related disorders, such as mittelschmerz, and for women who have problems with menstrual hygiene.
Additional advantages of progestin-only DMPA-IM compared with estrogen-containing contraceptive options include efficacy that is not compromised by concomitant anticonvulsive therapy.9 It also has no adverse effect on lactation, allowing use as early as the sixth week postpartum in breast-feeding women.13
L-IUS. This agent may also have several non-contraceptive benefits related primarily to the oligoamenorrhea experienced by many users. These include increased hemoglobin concentrations (thus possibly preventing iron deficiency anemia), off-label use as a treatment for menorrhagia or dysmenorrhea, an alternative to hysterectomy for heavy menstrual bleeding, and for progestin opposition in post-menopausal women on estrogen replacement therapy.14 Small case-series reports also suggest that L-IUS may have a modulatory effect on endometrial hyperplasia associated with tamoxifen exposure in women with breast cancer.15
EE-ring, NE-patch. Due to the limited experience with these products, it is not known whether users will enjoy noncontraceptive health benefits, although it is reasonable to assume that since they are derived from combinations of well-studied estrogens and progestins, their benefits may be similar to those of combined oral contraceptives.
Side-effect profiles
Hormone-related side effects—including changes in bleeding pattern, weight gain, mood changes, headaches, breast tenderness, and nausea—can be problematic for many women using hormonal contraceptives (both oral contraceptives and nondaily methods) and are common reasons for discontinuation.2,16 Therefore, it is important to consider differences in side-effect profiles when helping women to select an appropriate method, and to adequately counsel women regarding the expected effects prior to starting therapy.
Bleeding patterns
Nondaily hormonal contraceptives differ considerably in their effects on bleeding patterns ( Table 2 ).
DMPA-IM is characterized by amenorrhea, which develops in 70% to 73% of users after 1 year.17,18 Intermenstrual bleeding and spotting has been reported in 7.6% to 27% of DMPA-IM users at 12 months.17,18 However, among those who experience irregular bleeding, it generally consists of spotting or light bleeding rather than heavy intermenstrual flow.19
Amenorrhea has been reported in 20% to 50% of L-IUS users after 1 year.5,20 Among L-IUS users who do not experience amenorrhea, cycles are variable,5 with spotting observed in 25% of women at 6 months, decreasing to 11% at 2 years.20
Amenorrhea is rarely seen among women using the EE-ring or NE-patch; rather, similar to oral contraceptives, regular menstrual cycles are established within the first few cycles of use.21,22 Rates of intermenstrual bleeding/spotting at 1 year are less than 10% for each of these methods, with bleeding changes rarely cited as a reason for drug discontinuation.21,22
Counseling before treatment improves adherence. Counseling about menstrual changes, especially the absence of menses associated with DMPA-IM and L-IUS, can significantly increase user satisfaction and continuation rates.23,24 In a prospective study of new users of DMPA-IM, women who were told about the possibility of amenorrhea were 2.5 times more likely to continue use at 1 year than those who were not given this information.23 In fact, surveys of women’s preferences indicate that most women prefer the convenience, comfort, and freedom of less frequent or absent menses.25 Because the decision whether or not to menstruate is a personal one, this is an important issue to discuss with a patient selecting a contraceptive method.
Weight gain
Concern about weight gain can be significant enough for some women to pose a barrier to hormonal contraceptive selection and compliance. Variable effects of DMPA-IM on body weight have been reported, ranging from nonsignificant changes26,27 to gains of approximately 3 kg to 4 kg at 1 year.28,29 However, the most pronounced weight changes occurred in women who were overweight at the initiation of use or who may have been inherently predisposed to gain weight.28,29
In a long-term study of Thai women using either DMPA-IM or a nonhormonal intrauterine device, weight gain in both groups was comparable after 10 years of use (10.9 and 11.2 kg, respectively).30 Furthermore, in the only randomized, placebo-controlled trial to assess weight gain, normal-weight women observed during the first 2 menstrual cycles following the initial injection of DMPA-IM did not experience weight gain.31
Data from 1-year multicenter clinical trials with the NE-patch, EE-ring, and L-IUS indicate that users of these methods experience minimal (<1 kg) or no weight gain. ,32,33 However, long-term follow-up of women using L-IUS for 12 years found an increase in body weight of 0.49 kg/year during the study period and a mean overall increase of 5.7 kg.34
Mood changes
Although mood changes are often cited by women as a reason for discontinuing hormonal contraception,2 data from clinical trials indicate that DMPA-IM does not cause mood changes or worsen existing depressive symptoms. Fewer than 2% of 3857 US women who used DMPA-IM in a 1-year multicenter trial reported depression.19 Other studies specifically assessing mood changes in an adolescent health clinic35 and inner-city family planning clinics36 failed to find any adverse impact of DMPA-IM on mood. Only 1 study of women enrolled in a health maintenance organization found an association between DMPA-IM and symptoms of depression, but a causal relationship could not be established.37
To date, no studies have specifically examined the effects of the other nondaily hormonal contraceptive options on mood. L-IUS product labeling states that depression has been reported in more than 5% of patients,5 while 1-year clinical trials report emotional lability in 1.5% of NE-patch users and 2.8% of EE-ring users.32,38 However, in a small comparative trial, there were no reports of depression among 121 EE-ring users, whereas it was reported by 4.8% of 126 women using a combined oral contraceptive containing 30 μg ethinyl estradiol and 150 μg levonorgestrel.21
Delivery system–related side effects
All nondaily options have specific side effects related to local effects or the delivery system. DMPA-IM may cause pain on injection, but this is reported as an adverse event by fewer than 1% of subjects.13
In a US clinical trial of the NE-patch, application-site reactions were reported by 20% of participants, leading to discontinuation by 2.6% of women in the patch group; 4.6% of patches were replaced for either complete (1.8%) or partial detachment (2.8%).22
In a 1-year multicenter study of the EE-ring in 2322 women, common complaints were vaginitis (5.6%), leukorrhea (4.8%), and device-related events (4.4%) consisting of foreign body sensation, coital problems, and expulsion. The latter problem can occur during removal of a tampon or during bowel or bladder emptying, necessitating immediate reinsertion of the ring or replacement with a new ring.7,32
Expulsion is also a problem with L-IUS and can result in unintended pregnancy. During the first 2 years following insertion, L-IUS was discontinued by 6.6% of 256 women as the result of expulsion, which occurred significantly more frequently among women with heavy menstrual bleeding than those with normal bleeding (13% vs 5%, P=.01).20 Other potential device-related effects of L-IUS include pelvic inflammatory disease, embedment or perforation, and sepsis.5
Long-term safety profiles
Cancer risks
To date, cancer risks associated with long-term use have been investigated only for DMPA-IM and combined oral contraceptives in large epidemiological studies ( Table 2 ). Because women’s concerns regarding the risk of breast cancer may make them reluctant to use a hormonal method of contraception, it is particularly important for clinicians to emphasize the evidence showing that use of hormonal contraceptives is not associated with an increase in the overall risk of breast cancer. Though a large-scale reanalysis of 54 studies found a slight increase in breast cancer risk among current combined oral contraceptive users (relative risk [RR]=1.24; 95% confidence interval [CI], 1.15–1.33), this risk decreased over time and was the same as that of combined oral contraceptive never-users 10 or more years after cessation of use (RR=1.01; 95% CI, 0.96–1.05).39 Similarly, a pooled analysis of DMPA-IM data from the World Health Organization (WHO) and New Zealand trials, which were completed in the early 1990s, also found a slight increase in breast cancer risk among current users (RR=1.50; 95% CI, 1.0–2.2), but showed no increase in the overall risk of breast cancer among ever-users.40
Women can also be advised that neither DMPA-IM nor combined oral contraceptives appear to significantly increase their risk of gynecologic cancers ( Table 2 ). In fact, as previously discussed, these contraceptives decrease the risk of endometrial cancer,8,41 an effect that is particularly strong for DMPA-IM (an 80% reduction in risk for ever-users, which appeared to last for at least 8 years following cessation of use).8 Combined oral contraceptives are also associated with an approximately 50% reduction in risk of ovarian cancer.42 While there is no evidence that DMPA-IM reduces the risk of ovarian cancers, it does not appear to be associated with a significant increase in risk (RR=1.07; 95% CI, 0.6–1.8).43
Because of confounding factors such as smoking, risk factors for sexually transmitted disease, and screening detection bias, it has been difficult to firmly establish the relationship between contraceptive use and cervical cancer. However, several studies suggest the use of combined oral contraceptives, particularly for longer durations, slightly increases the risk of invasive cervical cancer.44,45 In contrast, the risk of invasive cervical cancer does not appear to increase in users of DMPA-IM, and no consistent pattern of risk with either duration of use or other time-related factors has been observed.46
Cardiovascular risks
DMPA-IM. Only DMPA-IM and combined oral contraceptives have been the subject of large-scale epidemiological investigations to assess the risk of cardiovascular disease, also summarized in Table 2 . Increased risk for venous thromboembolism (VTE) is related to the dose of estrogen in combined oral contraceptives. While currently available low-dose combined oral contraceptives (<50 μg estrogen) confer less risk than the higher-dose preparations of the past, they still confer a 3- to 4-fold higher risk of VTE than that experienced by nonusers.47 The risk of VTE conferred by DMPA-IM is less than half that of combined oral contraceptives.
Users of low-dose combined oral contraceptives are also at increased risk of acute myocardial infarction compared with nonusers, though this risk reflects the frequent coexistence of other cardiovascular risk factors.48 In fact, acute myocardial infarction is very rare among younger women (<35 years) who use combined oral contraceptives but who do not smoke, with an estimated attributable risk of approximately 3 per million woman-years. However, this attributable risk rises steeply to nearly 400 per million woman-years in older women (≥35 years) who smoke.48
Risk of stroke is slightly increased among users of low-dose combined oral contraceptives, again primarily among women aged ≥35 years. Overall, the excess attributable risk estimate is approximately 2 per 100,000 woman-years, which decreases to 1 per 200,000 woman-years in women <35 years who use low-dose combined oral contraceptives.49
In light of these risks, combined oral contraceptives are contraindicated for smokers ≥35 years, women with an increased risk or history of thromboembolism, and women with cerebrovascular or coronary artery disease.
Epidemiologic data from the WHO found no association between DMPA-IM use and an increased risk of any type of stroke or myocardial infarction (MI) ( Table 2 ).50 Although there was a slight increase in the risk of VTE compared with nonusers, this was not considered statistically significant (odds ratio [OR]=2.19; 95% CI, 0.66–7.26).50 In addition, compared with nonusers, DMPA-IM users did not exhibit increased combined cardiovascular disease risk (eg, stroke, VTE, myocardial infarction) (OR=1.02; 95% CI, 0.68–1.54).50
L-IUS, NE-patch, and EE-ring. Long-term epidemiologic data for these products are unavailable due to the relatively short postmarket experience, which precludes assumptions of long-term cardiovascular safety. Likewise, no evidence is available regarding whether the safety profile for transdermal or vaginal administration differs from oral administration. Therefore, it is not known whether NE-patch or EE-ring confer different risks for venous thromboembolism than combined oral contraceptives. Warnings about thromboembolic disorders are similarly listed in the package inserts of these options.6,7
Norelgestromin has been reported to have minimal androgenic activity, suggesting a possible lower risk of myocardial infarction than reported for more androgenically active progestin formulation.6 In contrast, etonogestrel, the biologically active metabolite of desogestrel, has been associated with a higher risk of venous thromboembolism than some second-generation combined oral contraceptives.7 For women with these risk factors, progestin-only methods, such as DMPA-IM or L-IUS, should be considered.
Bone mineral density
Historically, data have shown that oral contraceptives most often effect bone mineral density (BMD) positively in premenopausal women; retrospective studies of menopausal cohorts have shown positive effects from oral contraceptive use on BMD.51 However, a recent study of 524 pre-menopausal women found that women who used oral contraceptives, compared with those that did not, had significantly lower BMD values (adjusted differences of 2.4% at the femoral neck to 4.3% at the trochanter).51
Use of progestin-only DMPA-IM particularly raises concern regarding effects on BMD. However, no increased incidence of fractures has been noted in more than 30 years of DMPA-IM use worldwide.
In a recent meta-analysis that compared data from 10 cross-sectional and 7 longitudinal studies of BMD in 1039 women exposed to DMPA-IM with that of 2086 controls,52 average BMD was decreased in current users of DMPA-IM compared with nonusers, but was within 1 standard deviation of the mean in nonusers.52 Reductions in BMD tended to be greater as the duration of use of DMPA-IM increased, but stabilized after 3 to 5 years of use.52,53 Notably, the loss of BMD seen among current users of DMPA-IM is reversible following cessation of use.
Cross-sectional studies in both postmenopausal women52,54 and reproductive-age women,52,55 showed that BMD in former users of DMPA-IM was not significantly different from that of never-users at any site, and a recent prospective study also confirmed the reversibility of bone loss after cessation of DMPA-IM use.56
Establishing a good contraceptive fit
Overall, clinicians can prescribe nondaily hormonal contraceptives with confidence. Primary considerations in selecting a contraceptive method are its efficacy during typical use and its suitability for the medical needs and lifestyle preferences of the individual.
DMPA-IM and L-IUS. Consider the progestin-only nondaily methods DMPA-IM and L-IUS for women who want highly effective, nondaily, reversible contraception and who regard amenorrhea is a desirable side effect. These methods are also suitable when estrogen therapy is contraindicated.
L-IUS, unlike DMPA-IM, is not recommended for teens, nulliparous women, or those who are not in a stable, mutually monogamous relationship. L-IUS should also be avoided when there is a history of pelvic inflammatory disease or ectopic pregnancy.5
Because of its 5-year efficacy, L-IUS should be offered only to those desiring contraception for several years. Likewise, DMPA-IM is not recommended for those who wish to become pregnant within 1 to 2 years, because suppression of ovulation may persist beyond the 3-month dosing interval.
NE-patch and EE-ring. These products containing both estrogen and progestin are effective alternatives for women who would be candidates for combined oral contraceptives, including those desiring shorter-term or more rapidly reversible contraception and regular bleeding cycles.
When discussing contraceptive choices with a patient, review each method’s route and schedule of administration, efficacy in typical and nontypical use, potential noncontraceptive health benefits, reversibility, side effects, and long-term safety profile. The availability of a broader array of contraceptive choices should help women and their clinicians find a method that will fit individual medical needs as well as lifestyle preferences.
Correspondence
Jeffrey P. Levine, MD, MPH, Associate Professor, Departments of Family Medicine and Obstetrics, Gynecology & Reproductive Sciences, UMDNJ–Robert Wood Johnson Medical School, 1 RWJ Place, CN19, New Brunswick, NJ 08903-0019. E-mail: [email protected].
- Consider progestin-only DMPA-IM or L-IUS methods for women who want highly effective, nondaily, reversible contraception, and who regard amenorrhea as a desirable side effect; also suitable when estrogen therapy is contraindicated (SOR: C).
- Consider the NE-patch or EE-ring, both containing estrogen and progestin, for women who are candidates for combined oral contraceptives, including those desiring shorter-term contraception and regular bleeding cycles (SOR:C).
- To help women select the most appropriate and acceptable nondaily contraceptive option, review with patients each method’s route and schedule of administration, perfect vs typical use efficacy, potential noncontraceptive health benefits, reversibility, side effects, and long-term safety profile (SOR:C).
Oral contraceptives have made a major contribution to both women and society by substantially reducing the rate of unintended pregnancies. However, in actual clinical practice, contraceptive failures remain a problem. For example, the first-year pregnancy rate with oral contraceptives can be as high as 5% to 8%.1 Experts agree that a leading reason for unintended pregnancy among oral contraceptive users is incorrect and inconsistent use. Women who do not use oral contraceptives consistently are nearly 3 times as likely to become pregnant as those who use them consistently.2
Today, women have alternatives to the daily regimen of oral contraceptives. Highly effective, convenient, nondaily contraceptive choices are available in injectable, intrauterine, intravaginal, and transdermal delivery systems, which may be administered weekly, monthly, every 3 months, or every 5 years, depending on a woman’s family planning needs and preferences.
This article compares the efficacy, non-contraceptive health benefits, side-effect profiles, and long-term safety of the available nondaily hormonal contraceptive options. It also reviews other factors to consider when selecting the most appropriate and acceptable option for women who are seeking nondaily contraception.
Options for nondaily contraception
The first available nondaily contraceptive, depot-medroxyprogesterone acetate (DMPA-IM; Depo-Provera), is a progestin-only injectable introduced in 1963 that has been used by more than 30 million women worldwide.3 Its efficacy, safety, and health benefits have been established through large-scale epidemiologic investigations, and it was approved for use in the United States in 1992.
In the past 2 years, other nondaily hormonal contraceptives with a variety of delivery systems have been introduced to the US market. The levonorgestrel-releasing intrauterine system (L-IUS; Mirena) is also a progestin-only method that has been in use worldwide for 10 years. Its health benefits and hormone-associated side-effect profile are similar to DMPA-IM (particularly bleeding patterns).
The etonogestrel/ethinyl estradiol vaginal ring (EE-ring; NuvaRing), and the norelgestromin/ethinyl estradiol transdermal system (NE-patch; Ortho Evra) will likely offer improved efficacy to oral contraceptives with a similar long-term safety profile.
Nondaily contraception potentially more convenient and effective
Unlike oral contraceptives, which must be taken every day, nondaily contraceptives offer dosing options ranging from weekly to every 5 years ( Table 1 ). These extended dosing intervals reduce the likelihood of missed doses and are more convenient for many women than daily dosing. These methods also provide greater privacy because there is no visible evidence of their use, with the exception of the patch, which can be worn on discreet locations under clothing.
Improved adherence associated with less frequent dosing of nondaily hormonal contraceptives appears to enhance contraceptive efficacy, an example of which is the similarity between first-year pregnancy rates during perfect and typical use of DMPA-IM ( Table 2 ). The antiovulatory concentrations of medroxyprogesterone acetate achieved within 24 hours of injection provide almost immediate protection against pregnancy and likely contribute to the high contraceptive efficacy seen with DMPA-IM.4 The lowest reported pregnancy rates with perfect and typical use of L-IUS are comparable, and there is no need for backup contraception following insertion.5 Furthermore, even with typical use, reported pregnancy rates for DMPA-IM and L-IUS (0.3% and 0.1%, respectively) are comparable to sterilization (0.5%).1,5
Pregnancy rates during perfect use of the NE-patch and EE-ring also are low, but it is not yet possible to accurately estimate the failure rates of these methods during typical use due to limited US postmarketing experience.6,7 A backup method is recommended for the first 7 days of EE-ring use if the patient has not previously taken hormonal contraception or is switching from a progestin-only method,7 and for the first 7 days of NE-patch use if the first patch is applied after Day 1 of menses.6
TABLE 1
Nondaily hormonal contraceptives (currently available in the US), compared with oral contraceptives
| Method, Administration | Mechanism of action | Dosing schedule | Pregnancy first year (%) | |
|---|---|---|---|---|
| Perfect use | Typical use | |||
| DMPA-IM 1 (Medroxyprogesterone acetate; Depo-Provera) Intramuscular injection, given by health provider | Inhibits secretion of gonadotropins, which prevents follicular maturation and ovulation and results in endometrial thinning | Every 3 mo | 0.3 | 0.3 |
| L-IUS 5 (Levonorgestrel; Mirena) Intrauterine system, placed by health provider | Effects morphological changes in the endometrium, including stromal pseudodecidualization, glandular atrophy, and leukocytic infiltration; inhibition of ovulation is observed in some women | Every 5 y | 0.1 | 0.1 |
| EE-Ring 7 (Etonogestrel/ethinyl estradiol; NuvaRing) Intravaginal ring, self-applied | Suppression of gonadotropins inhibits ovulation; other alterations include changes in cervical mucus and endometrium | Monthly (1 ring-free wk/mo) | 1.0–2.0 | Unknown* |
| NE-Patch 6 (Norelgestromin/ethinyl estradiol; Ortho Evra) Transdermal patch, self-applied | Suppression of gonadotropins inhibits ovulation; other alterations include changes in cervical mucus and endometrium | Weekly (1 patch-free wk/mo) | 1.0 | Unknown* |
| Oral contraceptives 1 Combined or progestin-only Oral pills, self-administered | Suppression of gonadotropins inhibits ovulation; other alterations include changes in cervical mucus and endometrium | Daily (1 hormone-free wk/mo) | Combined: 0.1 Progestin: 0.5 | Combined: 5.0 Progestin: 5.0 |
| *Due to limited US postmarketing experience, a precise estimate of failure rate during typical use is not yet available. | ||||
TABLE 2
Nondaily hormonal contraceptive side effects and long-term safety
| Side effect | Combined oral contraceptives | Depo-Provera | Mirena | NuvaRing | Ortho Evra |
|---|---|---|---|---|---|
| Bleeding patterns | |||||
| Regular cycles | Yes | No | Variable | Yes | Yes |
| Intermenstrual bleeding/spotting | 7.6%–27% at 1 year17,18 | 16% at 1 year20 | 3.8% at 1 year32 | <10% at 1 year22,38 | |
| Menorrhagia | 6.7% at 9 mo16 | Rare20 | None reported32 | None reported22 | |
| Amenorrhea | 70%–73% at 1 year17,18 | 20%–50% at 1 year5,20 | None reported32 | 0.1%22 | |
| Discontinuation due to bleeding changes | 20% at 1 year16 | 10.6% at 1 year57 | <1% at 1 year32 | <1% at 1 year22 | |
| Weight gain | Mean 1.3 kg at 1 year29 | Mean 2.5–3.0 kg at 1 year13,29 | <1.0 kg at 1 year33 | <1.0 kg at 1 year32 | <1.0 kg at 1 year22 |
| Mood | Depression, 4.8%40 | Depression, <2%19 | Depression 5%5 | Emotional lability 2.8%32 | Emotional lability 1.5%38 |
| Hormone delivery system–related side effects | Allergies to dyes in pills; efficacy may be compromised by gastrointestinal or hepatic metabolism | Minor injection sitepain (<1%)13 | Expulsion (6.6%)20 Sepsis, PID, embedment/perforation5 | Vaginitis (5.6%) leukorrhea (4.8%) device-related events (4.4%)32 | Patch application site reactions (20%)22 |
| Breast and gynecologic cancers* | |||||
| Breast | 1.24 (1.15–1.33)39†§ | 1.5 (1–2.2)40†§ | No studies | No studies | No studies |
| 1.01 (0.96–1.05)58‡ | 1.1 (0.97–1.4)40‡ | ||||
| Endometrial | 0.55 (0.26–1.17)41 | 0.21 (0.06–0.79)8 | |||
| Ovarian | 0.5 (0.3–0.6)42 | 1.07 (0.6–1.8)43 | |||
| Cervical | 1.30 (0.5–3.3)45 | 1.11 (0.96–1.29)46 | |||
| 1.53 (0.99–2.36)44 | |||||
| Relative risk of cardiovascular disease | |||||
| All stroke | 1.41 (0.90–2.20)49 | 0.89 (0.53–1.49)50 | No studies | No studies | No studies |
| Acute MI | 4.69 (2.02–10.9)48§ | 0.66 (0.07–6.0)50 | |||
| Smokers <35 y | 34.947 | ||||
| Smokers 35 y | 396.247§ | ||||
| VTE | 4.32 (2.88–6.49)47§ | 2.19 (0.66–7.26)50 | |||
| Effects on bone mineral density | Variable, but usually positive | Reversible reduction | No studies | No studies | No studies |
| *Relative risk (95% CI). †Current use; ‡Any use; §Likelihood was significantly different relative to control; §Confidence intervals not reported. | |||||
| PID, pelvic inflammatory disease; CI, confidence interval; MI, myocardial infarction; VTE, venous thromboembolism. | |||||
Noncontraceptive health benefits
Nondaily hormonal contraceptive options have documented non-contraceptive health benefits.
DMPA-IM. This drug reduces the risk of endometrial cancer by 80% after 1 year, a protective effect that appears to extend for at least 8 years after cessation of use.8 DMPA-IM also decreases risk of iron deficiency anemia, pelvic inflammatory disease9 and uterine leiomyomas,10 and reduces pain crises among users with sickle cell disease.11
Clinical experience has shown that DMPA-IM may be an effective treatment option for a number of gynecologic conditions, including (though these are unapproved off-label uses) menorrhagia and dysmenorrhea, pain associated with endometriosis, ovulatory pain, and menopause-related vasomotor symptoms.9,12 Many of the menstrual-cycle related benefits of DMPA-IM result from the high incidence of amenorrhea, which may be particularly appealing to women who have menstrual-cycle related disorders, such as mittelschmerz, and for women who have problems with menstrual hygiene.
Additional advantages of progestin-only DMPA-IM compared with estrogen-containing contraceptive options include efficacy that is not compromised by concomitant anticonvulsive therapy.9 It also has no adverse effect on lactation, allowing use as early as the sixth week postpartum in breast-feeding women.13
L-IUS. This agent may also have several non-contraceptive benefits related primarily to the oligoamenorrhea experienced by many users. These include increased hemoglobin concentrations (thus possibly preventing iron deficiency anemia), off-label use as a treatment for menorrhagia or dysmenorrhea, an alternative to hysterectomy for heavy menstrual bleeding, and for progestin opposition in post-menopausal women on estrogen replacement therapy.14 Small case-series reports also suggest that L-IUS may have a modulatory effect on endometrial hyperplasia associated with tamoxifen exposure in women with breast cancer.15
EE-ring, NE-patch. Due to the limited experience with these products, it is not known whether users will enjoy noncontraceptive health benefits, although it is reasonable to assume that since they are derived from combinations of well-studied estrogens and progestins, their benefits may be similar to those of combined oral contraceptives.
Side-effect profiles
Hormone-related side effects—including changes in bleeding pattern, weight gain, mood changes, headaches, breast tenderness, and nausea—can be problematic for many women using hormonal contraceptives (both oral contraceptives and nondaily methods) and are common reasons for discontinuation.2,16 Therefore, it is important to consider differences in side-effect profiles when helping women to select an appropriate method, and to adequately counsel women regarding the expected effects prior to starting therapy.
Bleeding patterns
Nondaily hormonal contraceptives differ considerably in their effects on bleeding patterns ( Table 2 ).
DMPA-IM is characterized by amenorrhea, which develops in 70% to 73% of users after 1 year.17,18 Intermenstrual bleeding and spotting has been reported in 7.6% to 27% of DMPA-IM users at 12 months.17,18 However, among those who experience irregular bleeding, it generally consists of spotting or light bleeding rather than heavy intermenstrual flow.19
Amenorrhea has been reported in 20% to 50% of L-IUS users after 1 year.5,20 Among L-IUS users who do not experience amenorrhea, cycles are variable,5 with spotting observed in 25% of women at 6 months, decreasing to 11% at 2 years.20
Amenorrhea is rarely seen among women using the EE-ring or NE-patch; rather, similar to oral contraceptives, regular menstrual cycles are established within the first few cycles of use.21,22 Rates of intermenstrual bleeding/spotting at 1 year are less than 10% for each of these methods, with bleeding changes rarely cited as a reason for drug discontinuation.21,22
Counseling before treatment improves adherence. Counseling about menstrual changes, especially the absence of menses associated with DMPA-IM and L-IUS, can significantly increase user satisfaction and continuation rates.23,24 In a prospective study of new users of DMPA-IM, women who were told about the possibility of amenorrhea were 2.5 times more likely to continue use at 1 year than those who were not given this information.23 In fact, surveys of women’s preferences indicate that most women prefer the convenience, comfort, and freedom of less frequent or absent menses.25 Because the decision whether or not to menstruate is a personal one, this is an important issue to discuss with a patient selecting a contraceptive method.
Weight gain
Concern about weight gain can be significant enough for some women to pose a barrier to hormonal contraceptive selection and compliance. Variable effects of DMPA-IM on body weight have been reported, ranging from nonsignificant changes26,27 to gains of approximately 3 kg to 4 kg at 1 year.28,29 However, the most pronounced weight changes occurred in women who were overweight at the initiation of use or who may have been inherently predisposed to gain weight.28,29
In a long-term study of Thai women using either DMPA-IM or a nonhormonal intrauterine device, weight gain in both groups was comparable after 10 years of use (10.9 and 11.2 kg, respectively).30 Furthermore, in the only randomized, placebo-controlled trial to assess weight gain, normal-weight women observed during the first 2 menstrual cycles following the initial injection of DMPA-IM did not experience weight gain.31
Data from 1-year multicenter clinical trials with the NE-patch, EE-ring, and L-IUS indicate that users of these methods experience minimal (<1 kg) or no weight gain. ,32,33 However, long-term follow-up of women using L-IUS for 12 years found an increase in body weight of 0.49 kg/year during the study period and a mean overall increase of 5.7 kg.34
Mood changes
Although mood changes are often cited by women as a reason for discontinuing hormonal contraception,2 data from clinical trials indicate that DMPA-IM does not cause mood changes or worsen existing depressive symptoms. Fewer than 2% of 3857 US women who used DMPA-IM in a 1-year multicenter trial reported depression.19 Other studies specifically assessing mood changes in an adolescent health clinic35 and inner-city family planning clinics36 failed to find any adverse impact of DMPA-IM on mood. Only 1 study of women enrolled in a health maintenance organization found an association between DMPA-IM and symptoms of depression, but a causal relationship could not be established.37
To date, no studies have specifically examined the effects of the other nondaily hormonal contraceptive options on mood. L-IUS product labeling states that depression has been reported in more than 5% of patients,5 while 1-year clinical trials report emotional lability in 1.5% of NE-patch users and 2.8% of EE-ring users.32,38 However, in a small comparative trial, there were no reports of depression among 121 EE-ring users, whereas it was reported by 4.8% of 126 women using a combined oral contraceptive containing 30 μg ethinyl estradiol and 150 μg levonorgestrel.21
Delivery system–related side effects
All nondaily options have specific side effects related to local effects or the delivery system. DMPA-IM may cause pain on injection, but this is reported as an adverse event by fewer than 1% of subjects.13
In a US clinical trial of the NE-patch, application-site reactions were reported by 20% of participants, leading to discontinuation by 2.6% of women in the patch group; 4.6% of patches were replaced for either complete (1.8%) or partial detachment (2.8%).22
In a 1-year multicenter study of the EE-ring in 2322 women, common complaints were vaginitis (5.6%), leukorrhea (4.8%), and device-related events (4.4%) consisting of foreign body sensation, coital problems, and expulsion. The latter problem can occur during removal of a tampon or during bowel or bladder emptying, necessitating immediate reinsertion of the ring or replacement with a new ring.7,32
Expulsion is also a problem with L-IUS and can result in unintended pregnancy. During the first 2 years following insertion, L-IUS was discontinued by 6.6% of 256 women as the result of expulsion, which occurred significantly more frequently among women with heavy menstrual bleeding than those with normal bleeding (13% vs 5%, P=.01).20 Other potential device-related effects of L-IUS include pelvic inflammatory disease, embedment or perforation, and sepsis.5
Long-term safety profiles
Cancer risks
To date, cancer risks associated with long-term use have been investigated only for DMPA-IM and combined oral contraceptives in large epidemiological studies ( Table 2 ). Because women’s concerns regarding the risk of breast cancer may make them reluctant to use a hormonal method of contraception, it is particularly important for clinicians to emphasize the evidence showing that use of hormonal contraceptives is not associated with an increase in the overall risk of breast cancer. Though a large-scale reanalysis of 54 studies found a slight increase in breast cancer risk among current combined oral contraceptive users (relative risk [RR]=1.24; 95% confidence interval [CI], 1.15–1.33), this risk decreased over time and was the same as that of combined oral contraceptive never-users 10 or more years after cessation of use (RR=1.01; 95% CI, 0.96–1.05).39 Similarly, a pooled analysis of DMPA-IM data from the World Health Organization (WHO) and New Zealand trials, which were completed in the early 1990s, also found a slight increase in breast cancer risk among current users (RR=1.50; 95% CI, 1.0–2.2), but showed no increase in the overall risk of breast cancer among ever-users.40
Women can also be advised that neither DMPA-IM nor combined oral contraceptives appear to significantly increase their risk of gynecologic cancers ( Table 2 ). In fact, as previously discussed, these contraceptives decrease the risk of endometrial cancer,8,41 an effect that is particularly strong for DMPA-IM (an 80% reduction in risk for ever-users, which appeared to last for at least 8 years following cessation of use).8 Combined oral contraceptives are also associated with an approximately 50% reduction in risk of ovarian cancer.42 While there is no evidence that DMPA-IM reduces the risk of ovarian cancers, it does not appear to be associated with a significant increase in risk (RR=1.07; 95% CI, 0.6–1.8).43
Because of confounding factors such as smoking, risk factors for sexually transmitted disease, and screening detection bias, it has been difficult to firmly establish the relationship between contraceptive use and cervical cancer. However, several studies suggest the use of combined oral contraceptives, particularly for longer durations, slightly increases the risk of invasive cervical cancer.44,45 In contrast, the risk of invasive cervical cancer does not appear to increase in users of DMPA-IM, and no consistent pattern of risk with either duration of use or other time-related factors has been observed.46
Cardiovascular risks
DMPA-IM. Only DMPA-IM and combined oral contraceptives have been the subject of large-scale epidemiological investigations to assess the risk of cardiovascular disease, also summarized in Table 2 . Increased risk for venous thromboembolism (VTE) is related to the dose of estrogen in combined oral contraceptives. While currently available low-dose combined oral contraceptives (<50 μg estrogen) confer less risk than the higher-dose preparations of the past, they still confer a 3- to 4-fold higher risk of VTE than that experienced by nonusers.47 The risk of VTE conferred by DMPA-IM is less than half that of combined oral contraceptives.
Users of low-dose combined oral contraceptives are also at increased risk of acute myocardial infarction compared with nonusers, though this risk reflects the frequent coexistence of other cardiovascular risk factors.48 In fact, acute myocardial infarction is very rare among younger women (<35 years) who use combined oral contraceptives but who do not smoke, with an estimated attributable risk of approximately 3 per million woman-years. However, this attributable risk rises steeply to nearly 400 per million woman-years in older women (≥35 years) who smoke.48
Risk of stroke is slightly increased among users of low-dose combined oral contraceptives, again primarily among women aged ≥35 years. Overall, the excess attributable risk estimate is approximately 2 per 100,000 woman-years, which decreases to 1 per 200,000 woman-years in women <35 years who use low-dose combined oral contraceptives.49
In light of these risks, combined oral contraceptives are contraindicated for smokers ≥35 years, women with an increased risk or history of thromboembolism, and women with cerebrovascular or coronary artery disease.
Epidemiologic data from the WHO found no association between DMPA-IM use and an increased risk of any type of stroke or myocardial infarction (MI) ( Table 2 ).50 Although there was a slight increase in the risk of VTE compared with nonusers, this was not considered statistically significant (odds ratio [OR]=2.19; 95% CI, 0.66–7.26).50 In addition, compared with nonusers, DMPA-IM users did not exhibit increased combined cardiovascular disease risk (eg, stroke, VTE, myocardial infarction) (OR=1.02; 95% CI, 0.68–1.54).50
L-IUS, NE-patch, and EE-ring. Long-term epidemiologic data for these products are unavailable due to the relatively short postmarket experience, which precludes assumptions of long-term cardiovascular safety. Likewise, no evidence is available regarding whether the safety profile for transdermal or vaginal administration differs from oral administration. Therefore, it is not known whether NE-patch or EE-ring confer different risks for venous thromboembolism than combined oral contraceptives. Warnings about thromboembolic disorders are similarly listed in the package inserts of these options.6,7
Norelgestromin has been reported to have minimal androgenic activity, suggesting a possible lower risk of myocardial infarction than reported for more androgenically active progestin formulation.6 In contrast, etonogestrel, the biologically active metabolite of desogestrel, has been associated with a higher risk of venous thromboembolism than some second-generation combined oral contraceptives.7 For women with these risk factors, progestin-only methods, such as DMPA-IM or L-IUS, should be considered.
Bone mineral density
Historically, data have shown that oral contraceptives most often effect bone mineral density (BMD) positively in premenopausal women; retrospective studies of menopausal cohorts have shown positive effects from oral contraceptive use on BMD.51 However, a recent study of 524 pre-menopausal women found that women who used oral contraceptives, compared with those that did not, had significantly lower BMD values (adjusted differences of 2.4% at the femoral neck to 4.3% at the trochanter).51
Use of progestin-only DMPA-IM particularly raises concern regarding effects on BMD. However, no increased incidence of fractures has been noted in more than 30 years of DMPA-IM use worldwide.
In a recent meta-analysis that compared data from 10 cross-sectional and 7 longitudinal studies of BMD in 1039 women exposed to DMPA-IM with that of 2086 controls,52 average BMD was decreased in current users of DMPA-IM compared with nonusers, but was within 1 standard deviation of the mean in nonusers.52 Reductions in BMD tended to be greater as the duration of use of DMPA-IM increased, but stabilized after 3 to 5 years of use.52,53 Notably, the loss of BMD seen among current users of DMPA-IM is reversible following cessation of use.
Cross-sectional studies in both postmenopausal women52,54 and reproductive-age women,52,55 showed that BMD in former users of DMPA-IM was not significantly different from that of never-users at any site, and a recent prospective study also confirmed the reversibility of bone loss after cessation of DMPA-IM use.56
Establishing a good contraceptive fit
Overall, clinicians can prescribe nondaily hormonal contraceptives with confidence. Primary considerations in selecting a contraceptive method are its efficacy during typical use and its suitability for the medical needs and lifestyle preferences of the individual.
DMPA-IM and L-IUS. Consider the progestin-only nondaily methods DMPA-IM and L-IUS for women who want highly effective, nondaily, reversible contraception and who regard amenorrhea is a desirable side effect. These methods are also suitable when estrogen therapy is contraindicated.
L-IUS, unlike DMPA-IM, is not recommended for teens, nulliparous women, or those who are not in a stable, mutually monogamous relationship. L-IUS should also be avoided when there is a history of pelvic inflammatory disease or ectopic pregnancy.5
Because of its 5-year efficacy, L-IUS should be offered only to those desiring contraception for several years. Likewise, DMPA-IM is not recommended for those who wish to become pregnant within 1 to 2 years, because suppression of ovulation may persist beyond the 3-month dosing interval.
NE-patch and EE-ring. These products containing both estrogen and progestin are effective alternatives for women who would be candidates for combined oral contraceptives, including those desiring shorter-term or more rapidly reversible contraception and regular bleeding cycles.
When discussing contraceptive choices with a patient, review each method’s route and schedule of administration, efficacy in typical and nontypical use, potential noncontraceptive health benefits, reversibility, side effects, and long-term safety profile. The availability of a broader array of contraceptive choices should help women and their clinicians find a method that will fit individual medical needs as well as lifestyle preferences.
Correspondence
Jeffrey P. Levine, MD, MPH, Associate Professor, Departments of Family Medicine and Obstetrics, Gynecology & Reproductive Sciences, UMDNJ–Robert Wood Johnson Medical School, 1 RWJ Place, CN19, New Brunswick, NJ 08903-0019. E-mail: [email protected].
1. Hatcher RA, Trussell J, Stewart F, Cates W, Jr, Stewart GK, Guest F, Kowal D. The essentials of contraception efficacy, safety, and personal considerations. In Contraceptive Technology New York: Ardent Media, Inc., 1998;211-247.
2. Rosenberg MJ, Waugh MS, Meehan TE. Use and misuse of oral contraceptives: risk indicators for poor pill taking and discontinuation. Contraception 1995;51:283-288.
3. Bigrigg A, Evans M, Gbolade B, et al. Depo Provera. Position paper on clinical use, effectiveness and side effects. Br J Fam Plann 1999;25:69-76.
4. Mishell DR, Jr. Pharmacokinetics of depot medroxyprogesterone acetate contraception. J Reprod Med 1996;41:381-390.
5. Mirena US Prescribing Information. Berlex Laboratories, Inc. 2000.
6. Full US Prescribing Information for Ortho Evra (norelge-stromin/ethinyl estradiol transdermal system). Ortho-McNeil Pharmaceutical, Inc. 2001.
7. Full US Prescribing Information for NuvaRing (etonogestrel/ethinyl estradiol vaginal ring). 2003.
8. Depot-medroxyprogesterone acetate (DMPA) and risk of endometrial cancer. The WHO Collaborative Study of Neoplasia and Steroid Contraceptives. Int J Cancer 1991;49:186-190.
9. Cullins VE. Noncontraceptive benefits and therapeutic uses of depot medroxyprogesterone acetate. J Reprod Med 1996;41:428-433.
10. Lumbiganon P, Rugpao S, Phandhu-fung S, Laopaiboon M, Vudhikamraksa N, Werawatakul Y. Protective effect of depot-medroxyprogesterone acetate on surgically treated uterine leiomyomas: a multicentre case—control study. Br J Obstet Gynaecol 1996;103:909-914.
11. de Abood M, de Castillo Z, Guerrero F, Espino M, Austin KL. Effect of Depo-Provera or Microgynon on the painful crises of sickle cell anemia patients. Contraception 1997;56:313-316.
12. Vercellini P, De Giorgi O, Oldani S, Cortesi I, Panazza S, Crosignani PG. Depot medroxyprogesterone acetate versus an oral contraceptive combined with very-low-dose danazol for long-term treatment of pelvic pain associated with endometriosis. Am J Obstet Gynecol 1996;175:396-401.
13. US Approved Prescribing Information for Depo-Provera Contraceptive Injection. Pfizer, Inc. 2003.
14. Hubacher D, Grimes DA. Noncontraceptive health benefits of intrauterine devices: a systematic review. Obstet Gynecol Surv 2002;57:120-128.
15. Gardner FJ, Konje JC, Abrams KR, et al. Endometrial protection from tamoxifen-stimulated changes by a levonorgestrel-releasing intrauterine system: a randomised controlled trial. Lancet 2000;356:1711-1717.
16. Sangi-haghpeykar H, Poindexter A, III, Bateman L, Ditmore JR. Experiences of injectable contraceptive users in an urban setting. Obstet Gynecol 1996;88:227-233.
17. Canto De Cetina TE, Canto P, Ordonez LM. Effect of counseling to improve compliance in Mexican women receiving depot-medroxyprogesterone acetate. Contraception 2001;63:143-146.
18. Mainwaring R, Hales HA, Stevenson K, et al. Metabolic parameter, bleeding, and weight changes in U.S. women using progestin only contraceptives. Contraception 1995;51:149-153.
19. Schwallie PC, Assenzo JR. Contraceptive use—efficacy study utilizing medroxyprogesterone acetate administered as an intramuscular injection once every 90 days. Fertil Steril 1973;24:331-339.
20. Hidalgo M, Bahamondes L, Perrotti M, Diaz J, Dantas-Monteiro C, Petta C. Bleeding patterns and clinical performance of the levonorgestrel-releasing intrauterine system (Mirena) up to two years. Contraception 2002;65:129-132.
21. Bjarnadottir RI, Tuppurainen M, Killick SR. Comparison of cycle control with a combined contraceptive vaginal ring and oral levonorgestrel/ethinyl estradiol. Am J Obstet Gynecol 2002;186:389-395.
22. Audet MC, Moreau M, Koltun WD, et al. Evaluation of contraceptive efficacy and cycle control of a transdermal contraceptive patch vs an oral contraceptive: a randomized controlled trial. JAMA 2001;285:2347-2354.
23. Hubacher D, Goco N, Gonzalez B, Taylor D. Factors affecting continuation rates of DMPA. Contraception 1999;60:345-351.
24. Backman T, Huhtala S, Luoto R, Tuominen J, Rauramo I, Koskenvuo M. Advance information improves user satisfaction with the levonorgestrel intrauterine system. Obstet Gynecol 2002;99:608-613.
25. den Tonkelaar I, Oddens BJ. Preferred frequency and characteristics of menstrual bleeding in relation to reproductive status, oral contraceptive use, and hormone replacement therapy use. Contraception 1999;59:357-362.
26. Danli S, Qingxiang S, Guowei S. A multicentered clinical trial of the long-acting injectable contraceptive Depo Provera in Chinese women. Contraception 2000;62:15-18.
27. Moore LL, Valuck R, McDougall C, Fink W. A comparative study of one-year weight gain among users of medroxyprogesterone acetate, levonorgestrel implants, and oral contraceptives. Contraception 1995;52:215-219.
28. Espey E, Steinhart J, Ogburn T, Qualls C. Depo-provera associated with weight gain in Navajo women. Contraception 2000;62:55-58.
29. Risser WL, Gefter LR, Barratt MS, Risser JM. Weight change in adolescents who used hormonal contraception. J Adolesc Health 1999;24:433-436.
30. Taneepanichskul S, Reinprayoon D, Khaosadad P. Comparative study of weight change between long-term DMPA and IUD acceptors. Contraception 1998;58:149-151.
31. Pelkman CL, Chow M, Heinbach RA, Rolls BJ. Short-term effects of a progestational contraceptive drug on food intake, resting energy expenditure, and body weight in young women. Am J Clin Nutr 2001;73:19-26.
32. Dieben TO, Roumen FJ, Apter D. Efficacy, cycle control, and user acceptability of a novel combined contraceptive vaginal ring. Obstet Gynecol 2002;100:585-593.
33. Dubuisson JB, Mugnier E. Acceptability of the levonorgestrel-releasing intrauterine system after discontinuation of previous contraception: results of a French clinical study in women aged 35 to 45 years. Contraception 2002;66:121-128.
34. Ronnerdag M, Odlind V. Health effects of long-term use of the intrauterine levonorgestrel-releasing system. A follow-up study over 12 years of continuous use. Acta Obstet Gynecol Scand 1999;78:716-721.
35. Gupta N, O’Brien R, Jacobsen LJ, et al. Mood changes in adolescents using depot-medroxyprogesterone acetate for contraception: a prospective study. J Pediatr Adolesc Gynecol 2001;14:71-6.
36. Westhoff C, Truman C, Kalmuss D, et al. Depressive symptoms and Depo-Provera. Contraception 1998;57:237-240.
37. Civic D, Scholes D, Ichikawa L, et al. Depressive symptoms in users and non-users of depot medroxyproges-terone acetate. Contraception 2000;61:385-390.
38. Smallwood GH, Meador ML, Lenihan JP, Shangold GA, Fisher AC, Creasy GW. Efficacy and safety of a transder-mal contraceptive system. Obstet Gynecol 2001;98:799-805.
39. Collaborative Group on Hormonal Factors in Breast Cancer. Breast cancer and hormonal contraceptives: collaborative reanalysis of individual data on 53 297 women with breast cancer and 100 239 women without breast cancer from 54 epidemiological studies. Collaborative Group on Hormonal Factors in Breast Cancer. Lancet 1996;347:1713-1727.
40. Skegg DC, Noonan EA, Paul C, Spears GF, Meirik O, Thomas DB. Depot medroxyprogesterone acetate and breast cancer. A pooled analysis of the World Health Organization and New Zealand studies. JAMA 1995;273:799-804.
41. The Who Collaborative Study of Neoplasia and Steroid Contraceptives. Endometrial cancer and combined oral contraceptives. Int J Epidemiol 1988;17:263-269.
42. Ness RB, Grisso JA, Klapper J, et al. Risk of ovarian cancer in relation to estrogen and progestin dose and use characteristics of oral contraceptives. SHARE Study Group. Steroid Hormones and Reproductions. Am J Epidemiol 2000;152:233-241.
43. Stanford JL, Thomas DB. Depot-medroxyprogesterone acetate (DMPA) and risk of epithelial ovarian cancer. The WHO Collaborative Study of Neoplasia and Steroid Contraceptives. Int J Cancer 1991;49:191-195.
44. Parazzini F, La Vecchia C, Negri E, Maggi R. Oral contraceptive use and invasive cervical cancer. Int J Epidemiol 1990;19:259-263.
45. Kjaer SK, Engholm G, Dahl C, Bock JE, Lynge E, Jensen OM. Case-control study of risk factors for cervical squamous cell neoplasia in Denmark. Role of oral contraceptive use. Cancer Causes Control 1993;4:513-519.
46. WHO Collaborative Study of Neoplasia and Steroid Contraceptives. Depot-medroxyprogesterone acetate and risk of invasive squamous cell cervical cancer.The WHO Collaborative Study of Neoplasia and Steroid Contraceptives. Contraception 1992;45:299-312.
47. WHO Collaborative Study of Cardiovascular Disease and Steroid Hormone Contraception. Venous thromboembolic disease and combined oral contraceptives: results of international multicentre case-control study. World Health Organization Collaborative Study of Cardiovascular Disease and Steroid Hormone Contraception. Lancet 1995;346:1575-1582.
48. WHO Collaborative Study of Cardiovascular Disease and Steroid Hormone Contraception. Acute myocardial infarction and combined oral contraceptives: results of an international multicentre case-control study. WHO Collaborative Study of Cardiovascular Disease and Steroid Hormone Contraception. Lancet 1997;349:1202-1209.
49. WHO Collaborative Study of Cardiovascular Disease and Steroid Hormone Contraception. Haemorrhagic stroke, overall stroke risk, and combined oral contraceptives: results of an international, multicentre, case-control study. WHO Collaborative Study of Cardiovascular Disease and Steroid Hormone Contraception. Lancet 1996;348:505-510.
50. WHO Collaborative Study of Cardiovascular Disease and Steroid Hormone Contraception. Cardiovascular disease and use of oral and injectable progestogen-only contraceptives and combined injectable contraceptives. Results of an international, multicenter, case-control study. World Health Organization Collaborative Study of Cardiovascular Disease and Steroid Hormone Contraception. Contraception 1998;57:315-324.
51. Prior JC, Kirkland SA, Joseph L, et al. Oral contraceptive use and bone mineral density in premenopausal women: cross-sectional, population-based data from the Canadian Multicentre Osteoporosis Study. CMAJ 2001;165:1023-1029.
52. Banks E, Berrington A, Casabonne D. Overview of the relationship between use of progestogen-only contraceptives and bone mineral density. BJOG 2001;108:1214-21.
53. Tang OS, Tang G, Yip PS, Li B. Further evaluation on long-term depot-medroxyprogesterone acetate use and bone mineral density: a longitudinal cohort study. Contraception 2000;62:161-164.
54. Orr-Walker BJ, Evans MC, Ames RW, Clearwater JM, Cundy T, Reid IR. The effect of past use of the injectable contraceptive depot medroxyprogesterone acetate on bone mineral density in normal post-menopausal women. Clin Endocrinol (Oxf) 1998;49:615-618.
55. Petitti DB, Piaggio G, Mehta S, Cravioto MC, Meirik O. Steroid hormone contraception and bone mineral density: a cross-sectional study in an international population. Obstet Gynecol 2000;95:736-744.
56. Scholes D, Lacroix AZ, Ichikawa LE, Barlow WE, Ott SM. Injectable hormone contraception and bone density: results from a prospective study. Epidemiology 2002;13:581-587.
57. Sivin I, el Mahgoub S, McCarthy T, et al. Long-term contraception with the levonorgestrel 20 mcg/day (LNg 20) and the copper T 380Ag intrauterine devices: a five-year randomized study. Contraception 1990;42:361-378.
58. Marchbanks PA, McDonald JA, Wilson HG, et al. Oral contraceptives and the risk of breast cancer. N Engl J Med 2002;346:2025-2032.
1. Hatcher RA, Trussell J, Stewart F, Cates W, Jr, Stewart GK, Guest F, Kowal D. The essentials of contraception efficacy, safety, and personal considerations. In Contraceptive Technology New York: Ardent Media, Inc., 1998;211-247.
2. Rosenberg MJ, Waugh MS, Meehan TE. Use and misuse of oral contraceptives: risk indicators for poor pill taking and discontinuation. Contraception 1995;51:283-288.
3. Bigrigg A, Evans M, Gbolade B, et al. Depo Provera. Position paper on clinical use, effectiveness and side effects. Br J Fam Plann 1999;25:69-76.
4. Mishell DR, Jr. Pharmacokinetics of depot medroxyprogesterone acetate contraception. J Reprod Med 1996;41:381-390.
5. Mirena US Prescribing Information. Berlex Laboratories, Inc. 2000.
6. Full US Prescribing Information for Ortho Evra (norelge-stromin/ethinyl estradiol transdermal system). Ortho-McNeil Pharmaceutical, Inc. 2001.
7. Full US Prescribing Information for NuvaRing (etonogestrel/ethinyl estradiol vaginal ring). 2003.
8. Depot-medroxyprogesterone acetate (DMPA) and risk of endometrial cancer. The WHO Collaborative Study of Neoplasia and Steroid Contraceptives. Int J Cancer 1991;49:186-190.
9. Cullins VE. Noncontraceptive benefits and therapeutic uses of depot medroxyprogesterone acetate. J Reprod Med 1996;41:428-433.
10. Lumbiganon P, Rugpao S, Phandhu-fung S, Laopaiboon M, Vudhikamraksa N, Werawatakul Y. Protective effect of depot-medroxyprogesterone acetate on surgically treated uterine leiomyomas: a multicentre case—control study. Br J Obstet Gynaecol 1996;103:909-914.
11. de Abood M, de Castillo Z, Guerrero F, Espino M, Austin KL. Effect of Depo-Provera or Microgynon on the painful crises of sickle cell anemia patients. Contraception 1997;56:313-316.
12. Vercellini P, De Giorgi O, Oldani S, Cortesi I, Panazza S, Crosignani PG. Depot medroxyprogesterone acetate versus an oral contraceptive combined with very-low-dose danazol for long-term treatment of pelvic pain associated with endometriosis. Am J Obstet Gynecol 1996;175:396-401.
13. US Approved Prescribing Information for Depo-Provera Contraceptive Injection. Pfizer, Inc. 2003.
14. Hubacher D, Grimes DA. Noncontraceptive health benefits of intrauterine devices: a systematic review. Obstet Gynecol Surv 2002;57:120-128.
15. Gardner FJ, Konje JC, Abrams KR, et al. Endometrial protection from tamoxifen-stimulated changes by a levonorgestrel-releasing intrauterine system: a randomised controlled trial. Lancet 2000;356:1711-1717.
16. Sangi-haghpeykar H, Poindexter A, III, Bateman L, Ditmore JR. Experiences of injectable contraceptive users in an urban setting. Obstet Gynecol 1996;88:227-233.
17. Canto De Cetina TE, Canto P, Ordonez LM. Effect of counseling to improve compliance in Mexican women receiving depot-medroxyprogesterone acetate. Contraception 2001;63:143-146.
18. Mainwaring R, Hales HA, Stevenson K, et al. Metabolic parameter, bleeding, and weight changes in U.S. women using progestin only contraceptives. Contraception 1995;51:149-153.
19. Schwallie PC, Assenzo JR. Contraceptive use—efficacy study utilizing medroxyprogesterone acetate administered as an intramuscular injection once every 90 days. Fertil Steril 1973;24:331-339.
20. Hidalgo M, Bahamondes L, Perrotti M, Diaz J, Dantas-Monteiro C, Petta C. Bleeding patterns and clinical performance of the levonorgestrel-releasing intrauterine system (Mirena) up to two years. Contraception 2002;65:129-132.
21. Bjarnadottir RI, Tuppurainen M, Killick SR. Comparison of cycle control with a combined contraceptive vaginal ring and oral levonorgestrel/ethinyl estradiol. Am J Obstet Gynecol 2002;186:389-395.
22. Audet MC, Moreau M, Koltun WD, et al. Evaluation of contraceptive efficacy and cycle control of a transdermal contraceptive patch vs an oral contraceptive: a randomized controlled trial. JAMA 2001;285:2347-2354.
23. Hubacher D, Goco N, Gonzalez B, Taylor D. Factors affecting continuation rates of DMPA. Contraception 1999;60:345-351.
24. Backman T, Huhtala S, Luoto R, Tuominen J, Rauramo I, Koskenvuo M. Advance information improves user satisfaction with the levonorgestrel intrauterine system. Obstet Gynecol 2002;99:608-613.
25. den Tonkelaar I, Oddens BJ. Preferred frequency and characteristics of menstrual bleeding in relation to reproductive status, oral contraceptive use, and hormone replacement therapy use. Contraception 1999;59:357-362.
26. Danli S, Qingxiang S, Guowei S. A multicentered clinical trial of the long-acting injectable contraceptive Depo Provera in Chinese women. Contraception 2000;62:15-18.
27. Moore LL, Valuck R, McDougall C, Fink W. A comparative study of one-year weight gain among users of medroxyprogesterone acetate, levonorgestrel implants, and oral contraceptives. Contraception 1995;52:215-219.
28. Espey E, Steinhart J, Ogburn T, Qualls C. Depo-provera associated with weight gain in Navajo women. Contraception 2000;62:55-58.
29. Risser WL, Gefter LR, Barratt MS, Risser JM. Weight change in adolescents who used hormonal contraception. J Adolesc Health 1999;24:433-436.
30. Taneepanichskul S, Reinprayoon D, Khaosadad P. Comparative study of weight change between long-term DMPA and IUD acceptors. Contraception 1998;58:149-151.
31. Pelkman CL, Chow M, Heinbach RA, Rolls BJ. Short-term effects of a progestational contraceptive drug on food intake, resting energy expenditure, and body weight in young women. Am J Clin Nutr 2001;73:19-26.
32. Dieben TO, Roumen FJ, Apter D. Efficacy, cycle control, and user acceptability of a novel combined contraceptive vaginal ring. Obstet Gynecol 2002;100:585-593.
33. Dubuisson JB, Mugnier E. Acceptability of the levonorgestrel-releasing intrauterine system after discontinuation of previous contraception: results of a French clinical study in women aged 35 to 45 years. Contraception 2002;66:121-128.
34. Ronnerdag M, Odlind V. Health effects of long-term use of the intrauterine levonorgestrel-releasing system. A follow-up study over 12 years of continuous use. Acta Obstet Gynecol Scand 1999;78:716-721.
35. Gupta N, O’Brien R, Jacobsen LJ, et al. Mood changes in adolescents using depot-medroxyprogesterone acetate for contraception: a prospective study. J Pediatr Adolesc Gynecol 2001;14:71-6.
36. Westhoff C, Truman C, Kalmuss D, et al. Depressive symptoms and Depo-Provera. Contraception 1998;57:237-240.
37. Civic D, Scholes D, Ichikawa L, et al. Depressive symptoms in users and non-users of depot medroxyproges-terone acetate. Contraception 2000;61:385-390.
38. Smallwood GH, Meador ML, Lenihan JP, Shangold GA, Fisher AC, Creasy GW. Efficacy and safety of a transder-mal contraceptive system. Obstet Gynecol 2001;98:799-805.
39. Collaborative Group on Hormonal Factors in Breast Cancer. Breast cancer and hormonal contraceptives: collaborative reanalysis of individual data on 53 297 women with breast cancer and 100 239 women without breast cancer from 54 epidemiological studies. Collaborative Group on Hormonal Factors in Breast Cancer. Lancet 1996;347:1713-1727.
40. Skegg DC, Noonan EA, Paul C, Spears GF, Meirik O, Thomas DB. Depot medroxyprogesterone acetate and breast cancer. A pooled analysis of the World Health Organization and New Zealand studies. JAMA 1995;273:799-804.
41. The Who Collaborative Study of Neoplasia and Steroid Contraceptives. Endometrial cancer and combined oral contraceptives. Int J Epidemiol 1988;17:263-269.
42. Ness RB, Grisso JA, Klapper J, et al. Risk of ovarian cancer in relation to estrogen and progestin dose and use characteristics of oral contraceptives. SHARE Study Group. Steroid Hormones and Reproductions. Am J Epidemiol 2000;152:233-241.
43. Stanford JL, Thomas DB. Depot-medroxyprogesterone acetate (DMPA) and risk of epithelial ovarian cancer. The WHO Collaborative Study of Neoplasia and Steroid Contraceptives. Int J Cancer 1991;49:191-195.
44. Parazzini F, La Vecchia C, Negri E, Maggi R. Oral contraceptive use and invasive cervical cancer. Int J Epidemiol 1990;19:259-263.
45. Kjaer SK, Engholm G, Dahl C, Bock JE, Lynge E, Jensen OM. Case-control study of risk factors for cervical squamous cell neoplasia in Denmark. Role of oral contraceptive use. Cancer Causes Control 1993;4:513-519.
46. WHO Collaborative Study of Neoplasia and Steroid Contraceptives. Depot-medroxyprogesterone acetate and risk of invasive squamous cell cervical cancer.The WHO Collaborative Study of Neoplasia and Steroid Contraceptives. Contraception 1992;45:299-312.
47. WHO Collaborative Study of Cardiovascular Disease and Steroid Hormone Contraception. Venous thromboembolic disease and combined oral contraceptives: results of international multicentre case-control study. World Health Organization Collaborative Study of Cardiovascular Disease and Steroid Hormone Contraception. Lancet 1995;346:1575-1582.
48. WHO Collaborative Study of Cardiovascular Disease and Steroid Hormone Contraception. Acute myocardial infarction and combined oral contraceptives: results of an international multicentre case-control study. WHO Collaborative Study of Cardiovascular Disease and Steroid Hormone Contraception. Lancet 1997;349:1202-1209.
49. WHO Collaborative Study of Cardiovascular Disease and Steroid Hormone Contraception. Haemorrhagic stroke, overall stroke risk, and combined oral contraceptives: results of an international, multicentre, case-control study. WHO Collaborative Study of Cardiovascular Disease and Steroid Hormone Contraception. Lancet 1996;348:505-510.
50. WHO Collaborative Study of Cardiovascular Disease and Steroid Hormone Contraception. Cardiovascular disease and use of oral and injectable progestogen-only contraceptives and combined injectable contraceptives. Results of an international, multicenter, case-control study. World Health Organization Collaborative Study of Cardiovascular Disease and Steroid Hormone Contraception. Contraception 1998;57:315-324.
51. Prior JC, Kirkland SA, Joseph L, et al. Oral contraceptive use and bone mineral density in premenopausal women: cross-sectional, population-based data from the Canadian Multicentre Osteoporosis Study. CMAJ 2001;165:1023-1029.
52. Banks E, Berrington A, Casabonne D. Overview of the relationship between use of progestogen-only contraceptives and bone mineral density. BJOG 2001;108:1214-21.
53. Tang OS, Tang G, Yip PS, Li B. Further evaluation on long-term depot-medroxyprogesterone acetate use and bone mineral density: a longitudinal cohort study. Contraception 2000;62:161-164.
54. Orr-Walker BJ, Evans MC, Ames RW, Clearwater JM, Cundy T, Reid IR. The effect of past use of the injectable contraceptive depot medroxyprogesterone acetate on bone mineral density in normal post-menopausal women. Clin Endocrinol (Oxf) 1998;49:615-618.
55. Petitti DB, Piaggio G, Mehta S, Cravioto MC, Meirik O. Steroid hormone contraception and bone mineral density: a cross-sectional study in an international population. Obstet Gynecol 2000;95:736-744.
56. Scholes D, Lacroix AZ, Ichikawa LE, Barlow WE, Ott SM. Injectable hormone contraception and bone density: results from a prospective study. Epidemiology 2002;13:581-587.
57. Sivin I, el Mahgoub S, McCarthy T, et al. Long-term contraception with the levonorgestrel 20 mcg/day (LNg 20) and the copper T 380Ag intrauterine devices: a five-year randomized study. Contraception 1990;42:361-378.
58. Marchbanks PA, McDonald JA, Wilson HG, et al. Oral contraceptives and the risk of breast cancer. N Engl J Med 2002;346:2025-2032.
Abnormal vaginal discharge: What does and does not work in treating underlying causes
- Treat bacterial vaginosis with oral or intravaginal metronidazole or with clindamycin (SOR: A);recurrences are common (SOR:C).
- Oral and intravaginal imidazoles are equally effective in the treatment of candidiasis (SOR:A); alternate therapies for resistant cases have been little studied. Oral metronidazole is the standard therapy for trichomoniasis (SOR: A).
- Oral tinidazole, newly available in the US in 2004, should be used in resistant cases (SOR: B).
Antifungal medications for intravaginal use have been available in the United States for more than a decade. Women may be inclined to self-diagnose yeast infections with any vaginal discharge or other vulvovaginal symptoms that they deem abnormal. As we saw in the first part of this article, “Abnormal vaginal discharge: Using office diagnostic testing more effectively” (JFP2004; 53[10]:805–814), abnormal discharge is more likely to be bacterial vaginosis or no pathogen at all. Potential delay in diagnosis and treatment of a sexually transmitted disease is also a concern. Increasing resistance of Candida sp. to imidazoles is associated with indiscriminate use of over-the-counter products.
Bacterial vaginosis
The standard treatment for bacterial vaginosis (BV) has been oral metronidazole (Flagyl) 500 mg twice daily for 5 to 7 days. Intravaginal 0.75% metronidazole gel (MetroGel) has been shown to be as effective as oral metronidazole (SOR: A).1,2
Oral metronidazole can cause nausea and abdominal pain in some patients; vaginal treatment may be preferable for them. A meta-analysis of 52 studies of regimens of oral metronidazole at a dose of 2 g daily of varying duration showed similar initial cure rates of 85%, 87%, 86%, and 87% for 1, 2, 5, and 7 days, respectively (strength of recommendation [SOR]: A).3 Single-dose therapy may improve adherence (SOR: C).
Clindamycin (Cleocin), orally or in vaginal cream, for 5 days is also effective for BV (SOR: A).4-8 Clindamycin cream is used at a dose of 5 g daily and a concentration of 2%. Lower concentration (1%) has been less effective.6 Oral regimens range from 300 mg twice daily to 450 mg 3 times daily. Oral and vaginal preparations have shown equal efficacy in direct comparisons (SOR: A).8 A 3-day course of vaginal clindamycin is as effective as a 5-day course (SOR: B).9
Several studies have compared clindamycin and metronidazole head to head. They have shown similar cure rates that were not statistically different in the 75% to 90% range (SOR: A).4,5,10,11 Other antibiotics that have shown in vitro efficacy for treating the spectrum of microbes associated with BV are amoxicillin-clavulanate (Augmentin), imipenem (Primaxin), and cefmetazole (Zefazone) (SOR: C).8,12 Some Mobiluncus strains show resistance to metronidazole (SOR: C).12
Recurrences of BV are common. The initial regimen or an alternative regimen may be used. A longer, 10- to 14-day, course of antibiotic therapy has been recommended by one expert for treating relapses (SOR: C).13 Recolonizing the vagina with lactobacilli by eating yogurt or using bacteria-containing suppositories is an approach that deserves further study (SOR: C).14 Suppressive therapy such as intravaginal metronidazole twice weekly may also be considered as maintenance therapy to prevent recurrences (SOR: C).
BV and pregnancy
A number of studies have been published on screening for BV in pregnancy using Gram stain and on treating positive cases with antibiotics. While studies that used metronidazole for treatment have not shown consistently good results, more recent studies using clindamycin orally or intravaginally have been promising (SOR: B).7,15 Oral dosing at 300 mg twice daily, at 12 to 22 weeks gestation, has reduced preterm delivery for pregnant women with BV diagnosed by Nugent’s criteria (number needed to treat [NNT]=10).7 Likewise, for women with BV treated at 13 to 20 weeks gestation, intravaginal clindamycin therapy for 3 days has reduced the incidence of preterm births (NNT=17).15
Clindamycin appears to be the treatment of choice for BV in pregnancy (SOR: C) since it is considered safe (category B) throughout pregnancy, and because use of metronidazole in the first trimester is controversial.
Candidiasis
Treating vulvovaginal candidiasis (VVC) with intravaginal imidazoles reduces symptoms with NNT=3 after 1 month (SOR: A) ( Table ).16 No difference has been seen in outcomes with the various imidazoles or with treatment durations of 1 to 14 days. Intravaginal nystatin also decreases symptoms of VVC, with a NNT of 3 after 1 week compared with placebo (SOR: B).
Data showing that imidazoles are more effective than nystatin are not strong (SOR: B). A Clinical Evidencereview16 identified 1 trial comparing intravaginal miconazole, clotrimazole, econazole, and nystatin; symptomatic relapse was lower with intravaginal imidazoles than with nystatin. Another trial comparing clotrimazole and nystatin showed no difference in the proportion of women with persistent symptoms after 4 weeks. An open label study17 comparing econazole, miconazole, and nystatin showed that the imidazoles had more antifungal activity, but there was no difference in clinical outcome assessment.
Oral treatments are popular, most commonly a single dose of fluconazole. Oral itraconazole and ketoconazole have also been used successfully (SOR: A).18-21 A systematic review of oral vs vaginal azoles showed similar efficacy, but more side effects occurred with oral therapy (SOR: A).22 Gastrointestinal side effects occur in up to 15% of women.23
TABLE
Antifungal medications used to treat vulvovaginal candidiasis
| Generic name | Trade name | Dose | Duration | Cost per course of treatment* |
|---|---|---|---|---|
| Over the counter | ||||
| Butoconazole 2% cream | Femstat-3 Mycelex-3 generic | 5 g every night | 3 days | $5–$34 |
| Clotrimazole 1% cream | Mycelex-7 generic | 5 g every night | 7–10 days | $2–$7 |
| Clotrimazole 200 mg suppository | Gyne-Lotrimin generic | 1 every night | 3 days | $2–$9 |
| Miconazole 100 mg suppository | Monistat generic | 1 every night | 7 days | $2–$14 |
| Miconazole 2% cream | Monistat generic | 5 g every night | 7–10 days | $2–$11 |
| Miconazole 200 mg suppository | Monistat-3 | 1 every night | 3 days | $3–$22 |
| Miconazole 100 mg suppository plus 2% external cream | Gyne-Lotrimin generic | 1 every night | 5 days | $5–$12 |
| Tioconazole 6.5% ointment | Vagistat-1 generic | 4.6 g | 1 day | $2–$19 |
| Prescription | ||||
| Econazole 1% cream | Spectazole | 5 g | 3–6 days | $18 for 15 g $31 for 30 g |
| Terconazole 0.4% cream | Terazol-7 | 5 g | 7 days | $41 |
| Terconazole 0.8% cream | Terazol-3 | 5 g | 3 days | $41 |
| Terconazole 80 mg suppository | Terazol-3 | 1 every night | 3 days | $41 |
| Nystatin 100,000 U vaginal tablets | Generic | 1 every night | 7–14 days | $14–$35 |
| Fluconazole 150 mg tablet | Diflucan | 1 orally daily | 1 day | $14 |
| Itraconazole 100 mg tablet | Sporonox | 2 orally daily 4 orally | 3 days 1 day | $56 $37 ($281 for 30 tablets) |
| Ketoconazole 200 mg tablet | Nizoral generic | 2 orally daily | 5 days | $32–$43 ($95 for 30 generic tablets) |
| *Average wholesale price for entire regimen in US dollars. | ||||
Treating complicated VVC
About 5% of women diagnosed with VVC will have frequent recurrences, 4 or more per year.24 Current therapies are fungistatic rather than fungicidal, so the yeast are reduced but not eradicated. Hypersensitivity and allergic reactions to topical preparations may be confused with recurrences. Experts recommend that, if wet mount or culture results confirm recurrent vaginitis, topical therapy should be increased from 5 to 7 days up to 10 to 14 days, or that a second oral fluconazole tablet be given 3 days after the first (SOR: C).24 Women with severe cases of VVC also benefit from 2 sequential doses of fluconazole given 3 days apart (SOR: B).25
Suppressive therapy may be used after initial treatment for 6 months or more (SOR: B). Suppressive therapy options include oral fluconazole 150 mg or vaginal clotrimazole 500 mg once a week, oral or intravaginal nystatin twice weekly, and oral itraconazole 200 mg monthly.24,26
Non-albicans species tend to be more resistant to oral and topical azoles (SOR: B).27-29 If this species is detected on culture, a long course of suppressive therapy should be attempted (SOR: C).24 If imidazole therapy fails to control symptoms, suspect resistance.
Resistance to azoles may be demonstrated by in vitro susceptibility testing. Cross-resistance to topical and oral (fluconazole) azoles has been documented.30 There have been few studies of alternatives to azoles for treatment of resistant yeast vaginitis. One little-studied alternative is intravaginal boric acid, which may be used as a 14-day course of 600 mg daily in gelatin capsules (SOR: C).31 Nystatin and flucytosine (Ancoban) for 7 to 14 days are other alternatives (SOR: C).24
Candida in pregnancy
Commonly used topical imidazoles are classified as category C in pregnancy and have not been associated with increased risk of birth defects.
Trichomoniasis
Current treatment for trichomoniasis is oral metronidazole, given as a 2-g single dose, 250 mg 3 times daily for 7 days or 500 mg twice a day for 7 days. Treatment should also be given to the woman’s partner (SOR: A).32 Intravaginal therapy is not effective, probably due to the parasite’s presence in inaccessible areas such as the vaginal glands and urethra.33,34 Short-term treatment is comparable with long-term treatment, with similar rates of nausea and vomiting (SOR: A).32 A 1.5-g single-dose treatment has been shown to be equivalent to 2 g (SOR: B).35
The incidence metronidazole-resistant trichomoniasis has been estimated at 5%.36 In such cases, higher-dose therapy may be still be effective. For low to moderate resistance, 2 too 2.5 g daily for 3 to 10 days has been recommended (SOR: B).37 Intravenous high-dose metronidazole, 2 g every 8 hours for 3 days, has been reported to successfully treat highly resistant trichomonas (SOR: C).38 Another case report of 2 women with presumed allergy to metronidazole were successfully treated with incremental dosing of IV metronidazole (SOR: C).39 A small case series of women with metronidazole allergy or resistance treated with paromomycin cream intravaginally showed cure in 6 of 9 cases (SOR: C).40 Oral tinidazole has been approved in 2004 for use in the treatment of metronidazole-resistant trichomoniasis (SOR: B).41
Corresponding author
Linda French, MD, Associate Professor, Department of Family Practice, College of Human Medicine, Michigan State University, B101 Clinical Center, East Lansing, MI 48824. E-mail: [email protected].
1. Hillier SL, Lipinski C, Briselden AM, Eschenbach DA. Efficacy of intravaginal 0.75% metronidazole gel for the treatment of bacterial vaginosis. Obstet Gynecol 1993;81:963-967.
2. Hanson JM, McGregor JA, Hillier SL, et al. Metronidazole for bacterial vaginosis. A comparison of vaginal gel vs. oral therapy. J Reprod Med 2000;45:889-896.
3. Lugo-Miro VI, Green M, Mazur L. Comparison of different metronidazole therapeutic regimens for bacterial vaginosis. A meta-analysis. JAMA 1992;268:92-95.
4. Ferris DG, Litaker MS, Woodward L, Mathis D, Hendrich J. Treatment of bacterial vaginosis: a comparison of oral metronidazole, metronidazole vaginal gel, and clindamycin vaginal cream. J Fam Pract 1995;41:443-449.
5. Fischbach F, Petersen EE, Weissenbacher ER, Martius J, Hosmann J, Mayer H. Efficacy of clindamycin vaginal cream versus oral metronidazole in the treatment of bacterial vaginosis. Obstet Gynecol 1993;82:405-410.
6. Hillier S, Krohn MA, Watts DH, Wolner-Hanssen P, Eschenbach D. Microbiologic efficacy of intravaginal clindamycin cream for the treatment of bacterial vaginosis. Obstet Gynecol 1990;76:407-413.
7. Ugwumadu A, Manyonda I, Reid F, Hay P. Effect of early oral clindamycin on late miscarriage and preterm delivery in asymptomatic women with abnormal vaginal flora and bacterial vaginosis: a randomised controlled trial. Lancet 2003;361:983-988.
8. Mikamo H, Kawazoe K, Izumi K, Watanabe K, Ueno K, Tamaya T. Comparative study on vaginal or oral treatment of bacterial vaginosis. Chemotherapy 1997;43:60-68.
9. Ahmed-Jushuf IH, Shahmanesh M, Arya OP. The treatment of bacterial vaginosis with a 3 day course of 2% clindamycin cream: results of a multicentre, double blind, placebo controlled trial. B V Investigators Group. Genitourin Med 1995;71:254-256.
10. Schmitt C, Sobel JD, Meriwether C. Bacterial vaginosis: treatment with clindamycin cream versus oral metronidazole. Obstet Gynecol 1992;79:1020-1023.
11. Paavonen J, Mangioni C, Martin MA, Wajszczuk CP. Vaginal clindamycin and oral metronidazole for bacterial vaginosis: a randomized trial. Obstet Gynecol 2000;96:256-260.
12. Puapermpoonsiri S, Watanabe K, Kato N, Ueno K. In vitro activities of 10 antimicrobial agents against bacterial vaginosis-associated anaerobic isolates from pregnant Japanese and Thai women. Antimicrob Agents Chemother 1997;41:2297-2299.
13. Sobel JD. Vaginitis. N Engl J Med 1997;337:1896-1903.
14. Shalev E, Battino S, Weiner E, Colodner R, Keness Y. Ingestion of yogurt containing Lactobacillus acidophilus compared with pasteurized yogurt as prophylaxis for recurrent candidal vaginitis and bacterial vaginosis. Arch Fam Med 1996;5:593-596.
15. Lamont RF, Jones BM, Mandal D, Hay PE, Sheehan M. The efficacy of vaginal clindamycin for the treatment of abnormal genital tract flora in pregnancy. Infect Dis Obstet Gynecol 2003;11:181-189.
16. Marrazzo J. Vulvovaginal candidiasis. BMJ 2002;325:586.
17. Emele FE, Fadahunsi AA, Anyiwo CE, Ogunleye O. A comparative clinical evaluation of econazole nitrate, miconazole, and nystatin in the treatment of vaginal candidiasis. West Afr J Med 2000;19:12-15.
18. Stein GE, Mummaw N. Placebo controlled trial of itraconazole for treatment of acute vaginal candidiasis. Antimicrob Agents Chemother 1993;37:89-92.
19. Van der Pas H, Peeters F, Janssens D, Snauwaert E, Van Cutsem J. Treatment of vaginal candidosis with oral ketoconazole. Eur J Obstet Gynecol Reprod Biol 1983;14:399-404.
20. Sanz Sanz F, del Palacio Hernanz A. Randomized comparative trial of three regimens of itraconazole for treatment of vaginal mycoses. Rev Infect Dis 1987;9 Suppl 1:S139-S142.
21. Silva-Cruz A, Andrade L, Sobral L, Francisca A. Itraconazole versus placebo in the management of vaginal candidiasis. Int J Gynaecol Obstet 1991;36:229-232.
22. Watson MC, Grimshaw JM, Bond CM, Mollison J, Ludbrook A. Oral versus intravaginal imidazole and triazole anti-fungal agents for the treatment of uncomplicated vulvovaginal candidiasis (thrush): a systematic review. BJOG 2002;109:85-95.
23. van Heusden AM, Merkus HM, Corbeij RS, et al. Single-dose oral fluconazole versus single-dose topical miconazole for the treatment of acute vulvovaginal candidosis. Acta Obstet Gynecol Scand 1990;69:417-422.
24. Sobel JD. Vulvovaginitis. When Candida becomes a problem. Dermatol Clin 1998;16:763-768,xii.-
25. Sobel JD, Kapernick PS, Zervos M, et al. Treatment of complicated Candida vaginitis: comparison of single and sequential doses of fluconazole. Am J Obstet Gynecol 2001;185:363-369.
26. Creatsas GC, Charalambidis VM, Zagotzidou EH, Anthopoulou HN, Michailidis DC, Aravantinos DI. Chronic or recurrent vaginal candidosis: short-term treatment and prophylaxis with itraconazole. Clin Ther 1993;15:662-671.
27. Horowitz BJ, Giaquinta D, Ito S. Evolving pathogens in vulvovaginal candidiasis: implications for patient care. J Clin Pharmacol 1992;32:248-255.
28. del Palacio A, Sanz F, Sanchez-Alor G, et al. Double-blind randomized dose-finding study in acute vulvovaginal can-didosis. Comparison of flutrimazole site-release cream (1, 2 and 4%) with placebo site-release vaginal cream. Mycoses 2000;43:355-365.
29. Singh S, Sobel JD, Bhargava P, Boikov D, Vazquez JA. Vaginitis due to Candida krusei: epidemiology, clinical aspects, and therapy. Clin Infect Dis 2002;35:1066-1070.
30. Cross EW, Park S, Perlin DS. Cross-Resistance of clinical isolates of Candida albicans and Candida glabrata to over-the-counter azoles used in the treatment of vaginitis. Microb Drug Resist 2000;6:155-161.
31. Sobel JD, Chaim W. Treatment of Torulopsis glabrata vaginitis: retrospective review of boric acid therapy. Clin Infect Dis 1997;24:649-652.
32. Forna F, Gulmezoglu AM. Interventions for treating trichomoniasis in women. Cochrane Database Syst Rev 2003(2);CD000218.
33. duBouchet L, McGregor JA, Ismail M, McCormack WM. A pilot study of metronidazole vaginal gel versus oral metronidazole for the treatment of Trichomonas vaginalis vaginitis. Sex Transm Dis 1998;25:176-179.
34. Tidwell BH, Lushbaugh WB, Laughlin MD, Cleary JD, Finley RW. A double-blind placebo-controlled trial of single-dose intravaginal versus single-dose oral metronidazole in the treatment of trichomonal vaginitis. J Infect Dis 1994;170:242-246.
35. Spence MR, Harwell TS, Davies MC, Smith JL. The minimum single oral metronidazole dose for treating trichomoniasis: a randomized, blinded study. Obstet Gynecol 1997;89:699-703.
36. Petrin D, Delgaty K, Bhatt R, Garber G. Clinical and microbiological aspects of Trichomonas vaginalis. Clin Microbiol Rev 1998;11:300-317.
37. Lossick JG, Kent HL. Trichomoniasis: trends in diagnosis and management. Am J Obstet Gynecol 1991;165:1217-1222.
38. Dombrowski MP, Sokol RJ, Brown WJ, Bronsteen RA. Intravenous therapy of metronidazole-resistant Trichomonas vaginalis. Obstet Gynecol 1987;69:524-525.
39. Pearlman MD, Yashar C, Ernst S, Solomon W. An incremental dosing protocol for women with severe vaginal trichomoniasis and adverse reaction to metronidazole. Am J Obstet Gynecol 1996;174:934-936.
40. Nyirjesy P, Sobel JD, Weitz MV, Leaman DJ, Gelone SP. Difficult-to-treat trichomoniasis: results with paromomycin cream. Clin Infect Dis. 1998;26:986-988.
41. Sobel JD, Nyirjesy P, Brown W. Tinidazole therapy for metronidazole resistant vaginal trichomoniasis. Clin Infect Dis 2001;33:1341-1346.
- Treat bacterial vaginosis with oral or intravaginal metronidazole or with clindamycin (SOR: A);recurrences are common (SOR:C).
- Oral and intravaginal imidazoles are equally effective in the treatment of candidiasis (SOR:A); alternate therapies for resistant cases have been little studied. Oral metronidazole is the standard therapy for trichomoniasis (SOR: A).
- Oral tinidazole, newly available in the US in 2004, should be used in resistant cases (SOR: B).
Antifungal medications for intravaginal use have been available in the United States for more than a decade. Women may be inclined to self-diagnose yeast infections with any vaginal discharge or other vulvovaginal symptoms that they deem abnormal. As we saw in the first part of this article, “Abnormal vaginal discharge: Using office diagnostic testing more effectively” (JFP2004; 53[10]:805–814), abnormal discharge is more likely to be bacterial vaginosis or no pathogen at all. Potential delay in diagnosis and treatment of a sexually transmitted disease is also a concern. Increasing resistance of Candida sp. to imidazoles is associated with indiscriminate use of over-the-counter products.
Bacterial vaginosis
The standard treatment for bacterial vaginosis (BV) has been oral metronidazole (Flagyl) 500 mg twice daily for 5 to 7 days. Intravaginal 0.75% metronidazole gel (MetroGel) has been shown to be as effective as oral metronidazole (SOR: A).1,2
Oral metronidazole can cause nausea and abdominal pain in some patients; vaginal treatment may be preferable for them. A meta-analysis of 52 studies of regimens of oral metronidazole at a dose of 2 g daily of varying duration showed similar initial cure rates of 85%, 87%, 86%, and 87% for 1, 2, 5, and 7 days, respectively (strength of recommendation [SOR]: A).3 Single-dose therapy may improve adherence (SOR: C).
Clindamycin (Cleocin), orally or in vaginal cream, for 5 days is also effective for BV (SOR: A).4-8 Clindamycin cream is used at a dose of 5 g daily and a concentration of 2%. Lower concentration (1%) has been less effective.6 Oral regimens range from 300 mg twice daily to 450 mg 3 times daily. Oral and vaginal preparations have shown equal efficacy in direct comparisons (SOR: A).8 A 3-day course of vaginal clindamycin is as effective as a 5-day course (SOR: B).9
Several studies have compared clindamycin and metronidazole head to head. They have shown similar cure rates that were not statistically different in the 75% to 90% range (SOR: A).4,5,10,11 Other antibiotics that have shown in vitro efficacy for treating the spectrum of microbes associated with BV are amoxicillin-clavulanate (Augmentin), imipenem (Primaxin), and cefmetazole (Zefazone) (SOR: C).8,12 Some Mobiluncus strains show resistance to metronidazole (SOR: C).12
Recurrences of BV are common. The initial regimen or an alternative regimen may be used. A longer, 10- to 14-day, course of antibiotic therapy has been recommended by one expert for treating relapses (SOR: C).13 Recolonizing the vagina with lactobacilli by eating yogurt or using bacteria-containing suppositories is an approach that deserves further study (SOR: C).14 Suppressive therapy such as intravaginal metronidazole twice weekly may also be considered as maintenance therapy to prevent recurrences (SOR: C).
BV and pregnancy
A number of studies have been published on screening for BV in pregnancy using Gram stain and on treating positive cases with antibiotics. While studies that used metronidazole for treatment have not shown consistently good results, more recent studies using clindamycin orally or intravaginally have been promising (SOR: B).7,15 Oral dosing at 300 mg twice daily, at 12 to 22 weeks gestation, has reduced preterm delivery for pregnant women with BV diagnosed by Nugent’s criteria (number needed to treat [NNT]=10).7 Likewise, for women with BV treated at 13 to 20 weeks gestation, intravaginal clindamycin therapy for 3 days has reduced the incidence of preterm births (NNT=17).15
Clindamycin appears to be the treatment of choice for BV in pregnancy (SOR: C) since it is considered safe (category B) throughout pregnancy, and because use of metronidazole in the first trimester is controversial.
Candidiasis
Treating vulvovaginal candidiasis (VVC) with intravaginal imidazoles reduces symptoms with NNT=3 after 1 month (SOR: A) ( Table ).16 No difference has been seen in outcomes with the various imidazoles or with treatment durations of 1 to 14 days. Intravaginal nystatin also decreases symptoms of VVC, with a NNT of 3 after 1 week compared with placebo (SOR: B).
Data showing that imidazoles are more effective than nystatin are not strong (SOR: B). A Clinical Evidencereview16 identified 1 trial comparing intravaginal miconazole, clotrimazole, econazole, and nystatin; symptomatic relapse was lower with intravaginal imidazoles than with nystatin. Another trial comparing clotrimazole and nystatin showed no difference in the proportion of women with persistent symptoms after 4 weeks. An open label study17 comparing econazole, miconazole, and nystatin showed that the imidazoles had more antifungal activity, but there was no difference in clinical outcome assessment.
Oral treatments are popular, most commonly a single dose of fluconazole. Oral itraconazole and ketoconazole have also been used successfully (SOR: A).18-21 A systematic review of oral vs vaginal azoles showed similar efficacy, but more side effects occurred with oral therapy (SOR: A).22 Gastrointestinal side effects occur in up to 15% of women.23
TABLE
Antifungal medications used to treat vulvovaginal candidiasis
| Generic name | Trade name | Dose | Duration | Cost per course of treatment* |
|---|---|---|---|---|
| Over the counter | ||||
| Butoconazole 2% cream | Femstat-3 Mycelex-3 generic | 5 g every night | 3 days | $5–$34 |
| Clotrimazole 1% cream | Mycelex-7 generic | 5 g every night | 7–10 days | $2–$7 |
| Clotrimazole 200 mg suppository | Gyne-Lotrimin generic | 1 every night | 3 days | $2–$9 |
| Miconazole 100 mg suppository | Monistat generic | 1 every night | 7 days | $2–$14 |
| Miconazole 2% cream | Monistat generic | 5 g every night | 7–10 days | $2–$11 |
| Miconazole 200 mg suppository | Monistat-3 | 1 every night | 3 days | $3–$22 |
| Miconazole 100 mg suppository plus 2% external cream | Gyne-Lotrimin generic | 1 every night | 5 days | $5–$12 |
| Tioconazole 6.5% ointment | Vagistat-1 generic | 4.6 g | 1 day | $2–$19 |
| Prescription | ||||
| Econazole 1% cream | Spectazole | 5 g | 3–6 days | $18 for 15 g $31 for 30 g |
| Terconazole 0.4% cream | Terazol-7 | 5 g | 7 days | $41 |
| Terconazole 0.8% cream | Terazol-3 | 5 g | 3 days | $41 |
| Terconazole 80 mg suppository | Terazol-3 | 1 every night | 3 days | $41 |
| Nystatin 100,000 U vaginal tablets | Generic | 1 every night | 7–14 days | $14–$35 |
| Fluconazole 150 mg tablet | Diflucan | 1 orally daily | 1 day | $14 |
| Itraconazole 100 mg tablet | Sporonox | 2 orally daily 4 orally | 3 days 1 day | $56 $37 ($281 for 30 tablets) |
| Ketoconazole 200 mg tablet | Nizoral generic | 2 orally daily | 5 days | $32–$43 ($95 for 30 generic tablets) |
| *Average wholesale price for entire regimen in US dollars. | ||||
Treating complicated VVC
About 5% of women diagnosed with VVC will have frequent recurrences, 4 or more per year.24 Current therapies are fungistatic rather than fungicidal, so the yeast are reduced but not eradicated. Hypersensitivity and allergic reactions to topical preparations may be confused with recurrences. Experts recommend that, if wet mount or culture results confirm recurrent vaginitis, topical therapy should be increased from 5 to 7 days up to 10 to 14 days, or that a second oral fluconazole tablet be given 3 days after the first (SOR: C).24 Women with severe cases of VVC also benefit from 2 sequential doses of fluconazole given 3 days apart (SOR: B).25
Suppressive therapy may be used after initial treatment for 6 months or more (SOR: B). Suppressive therapy options include oral fluconazole 150 mg or vaginal clotrimazole 500 mg once a week, oral or intravaginal nystatin twice weekly, and oral itraconazole 200 mg monthly.24,26
Non-albicans species tend to be more resistant to oral and topical azoles (SOR: B).27-29 If this species is detected on culture, a long course of suppressive therapy should be attempted (SOR: C).24 If imidazole therapy fails to control symptoms, suspect resistance.
Resistance to azoles may be demonstrated by in vitro susceptibility testing. Cross-resistance to topical and oral (fluconazole) azoles has been documented.30 There have been few studies of alternatives to azoles for treatment of resistant yeast vaginitis. One little-studied alternative is intravaginal boric acid, which may be used as a 14-day course of 600 mg daily in gelatin capsules (SOR: C).31 Nystatin and flucytosine (Ancoban) for 7 to 14 days are other alternatives (SOR: C).24
Candida in pregnancy
Commonly used topical imidazoles are classified as category C in pregnancy and have not been associated with increased risk of birth defects.
Trichomoniasis
Current treatment for trichomoniasis is oral metronidazole, given as a 2-g single dose, 250 mg 3 times daily for 7 days or 500 mg twice a day for 7 days. Treatment should also be given to the woman’s partner (SOR: A).32 Intravaginal therapy is not effective, probably due to the parasite’s presence in inaccessible areas such as the vaginal glands and urethra.33,34 Short-term treatment is comparable with long-term treatment, with similar rates of nausea and vomiting (SOR: A).32 A 1.5-g single-dose treatment has been shown to be equivalent to 2 g (SOR: B).35
The incidence metronidazole-resistant trichomoniasis has been estimated at 5%.36 In such cases, higher-dose therapy may be still be effective. For low to moderate resistance, 2 too 2.5 g daily for 3 to 10 days has been recommended (SOR: B).37 Intravenous high-dose metronidazole, 2 g every 8 hours for 3 days, has been reported to successfully treat highly resistant trichomonas (SOR: C).38 Another case report of 2 women with presumed allergy to metronidazole were successfully treated with incremental dosing of IV metronidazole (SOR: C).39 A small case series of women with metronidazole allergy or resistance treated with paromomycin cream intravaginally showed cure in 6 of 9 cases (SOR: C).40 Oral tinidazole has been approved in 2004 for use in the treatment of metronidazole-resistant trichomoniasis (SOR: B).41
Corresponding author
Linda French, MD, Associate Professor, Department of Family Practice, College of Human Medicine, Michigan State University, B101 Clinical Center, East Lansing, MI 48824. E-mail: [email protected].
- Treat bacterial vaginosis with oral or intravaginal metronidazole or with clindamycin (SOR: A);recurrences are common (SOR:C).
- Oral and intravaginal imidazoles are equally effective in the treatment of candidiasis (SOR:A); alternate therapies for resistant cases have been little studied. Oral metronidazole is the standard therapy for trichomoniasis (SOR: A).
- Oral tinidazole, newly available in the US in 2004, should be used in resistant cases (SOR: B).
Antifungal medications for intravaginal use have been available in the United States for more than a decade. Women may be inclined to self-diagnose yeast infections with any vaginal discharge or other vulvovaginal symptoms that they deem abnormal. As we saw in the first part of this article, “Abnormal vaginal discharge: Using office diagnostic testing more effectively” (JFP2004; 53[10]:805–814), abnormal discharge is more likely to be bacterial vaginosis or no pathogen at all. Potential delay in diagnosis and treatment of a sexually transmitted disease is also a concern. Increasing resistance of Candida sp. to imidazoles is associated with indiscriminate use of over-the-counter products.
Bacterial vaginosis
The standard treatment for bacterial vaginosis (BV) has been oral metronidazole (Flagyl) 500 mg twice daily for 5 to 7 days. Intravaginal 0.75% metronidazole gel (MetroGel) has been shown to be as effective as oral metronidazole (SOR: A).1,2
Oral metronidazole can cause nausea and abdominal pain in some patients; vaginal treatment may be preferable for them. A meta-analysis of 52 studies of regimens of oral metronidazole at a dose of 2 g daily of varying duration showed similar initial cure rates of 85%, 87%, 86%, and 87% for 1, 2, 5, and 7 days, respectively (strength of recommendation [SOR]: A).3 Single-dose therapy may improve adherence (SOR: C).
Clindamycin (Cleocin), orally or in vaginal cream, for 5 days is also effective for BV (SOR: A).4-8 Clindamycin cream is used at a dose of 5 g daily and a concentration of 2%. Lower concentration (1%) has been less effective.6 Oral regimens range from 300 mg twice daily to 450 mg 3 times daily. Oral and vaginal preparations have shown equal efficacy in direct comparisons (SOR: A).8 A 3-day course of vaginal clindamycin is as effective as a 5-day course (SOR: B).9
Several studies have compared clindamycin and metronidazole head to head. They have shown similar cure rates that were not statistically different in the 75% to 90% range (SOR: A).4,5,10,11 Other antibiotics that have shown in vitro efficacy for treating the spectrum of microbes associated with BV are amoxicillin-clavulanate (Augmentin), imipenem (Primaxin), and cefmetazole (Zefazone) (SOR: C).8,12 Some Mobiluncus strains show resistance to metronidazole (SOR: C).12
Recurrences of BV are common. The initial regimen or an alternative regimen may be used. A longer, 10- to 14-day, course of antibiotic therapy has been recommended by one expert for treating relapses (SOR: C).13 Recolonizing the vagina with lactobacilli by eating yogurt or using bacteria-containing suppositories is an approach that deserves further study (SOR: C).14 Suppressive therapy such as intravaginal metronidazole twice weekly may also be considered as maintenance therapy to prevent recurrences (SOR: C).
BV and pregnancy
A number of studies have been published on screening for BV in pregnancy using Gram stain and on treating positive cases with antibiotics. While studies that used metronidazole for treatment have not shown consistently good results, more recent studies using clindamycin orally or intravaginally have been promising (SOR: B).7,15 Oral dosing at 300 mg twice daily, at 12 to 22 weeks gestation, has reduced preterm delivery for pregnant women with BV diagnosed by Nugent’s criteria (number needed to treat [NNT]=10).7 Likewise, for women with BV treated at 13 to 20 weeks gestation, intravaginal clindamycin therapy for 3 days has reduced the incidence of preterm births (NNT=17).15
Clindamycin appears to be the treatment of choice for BV in pregnancy (SOR: C) since it is considered safe (category B) throughout pregnancy, and because use of metronidazole in the first trimester is controversial.
Candidiasis
Treating vulvovaginal candidiasis (VVC) with intravaginal imidazoles reduces symptoms with NNT=3 after 1 month (SOR: A) ( Table ).16 No difference has been seen in outcomes with the various imidazoles or with treatment durations of 1 to 14 days. Intravaginal nystatin also decreases symptoms of VVC, with a NNT of 3 after 1 week compared with placebo (SOR: B).
Data showing that imidazoles are more effective than nystatin are not strong (SOR: B). A Clinical Evidencereview16 identified 1 trial comparing intravaginal miconazole, clotrimazole, econazole, and nystatin; symptomatic relapse was lower with intravaginal imidazoles than with nystatin. Another trial comparing clotrimazole and nystatin showed no difference in the proportion of women with persistent symptoms after 4 weeks. An open label study17 comparing econazole, miconazole, and nystatin showed that the imidazoles had more antifungal activity, but there was no difference in clinical outcome assessment.
Oral treatments are popular, most commonly a single dose of fluconazole. Oral itraconazole and ketoconazole have also been used successfully (SOR: A).18-21 A systematic review of oral vs vaginal azoles showed similar efficacy, but more side effects occurred with oral therapy (SOR: A).22 Gastrointestinal side effects occur in up to 15% of women.23
TABLE
Antifungal medications used to treat vulvovaginal candidiasis
| Generic name | Trade name | Dose | Duration | Cost per course of treatment* |
|---|---|---|---|---|
| Over the counter | ||||
| Butoconazole 2% cream | Femstat-3 Mycelex-3 generic | 5 g every night | 3 days | $5–$34 |
| Clotrimazole 1% cream | Mycelex-7 generic | 5 g every night | 7–10 days | $2–$7 |
| Clotrimazole 200 mg suppository | Gyne-Lotrimin generic | 1 every night | 3 days | $2–$9 |
| Miconazole 100 mg suppository | Monistat generic | 1 every night | 7 days | $2–$14 |
| Miconazole 2% cream | Monistat generic | 5 g every night | 7–10 days | $2–$11 |
| Miconazole 200 mg suppository | Monistat-3 | 1 every night | 3 days | $3–$22 |
| Miconazole 100 mg suppository plus 2% external cream | Gyne-Lotrimin generic | 1 every night | 5 days | $5–$12 |
| Tioconazole 6.5% ointment | Vagistat-1 generic | 4.6 g | 1 day | $2–$19 |
| Prescription | ||||
| Econazole 1% cream | Spectazole | 5 g | 3–6 days | $18 for 15 g $31 for 30 g |
| Terconazole 0.4% cream | Terazol-7 | 5 g | 7 days | $41 |
| Terconazole 0.8% cream | Terazol-3 | 5 g | 3 days | $41 |
| Terconazole 80 mg suppository | Terazol-3 | 1 every night | 3 days | $41 |
| Nystatin 100,000 U vaginal tablets | Generic | 1 every night | 7–14 days | $14–$35 |
| Fluconazole 150 mg tablet | Diflucan | 1 orally daily | 1 day | $14 |
| Itraconazole 100 mg tablet | Sporonox | 2 orally daily 4 orally | 3 days 1 day | $56 $37 ($281 for 30 tablets) |
| Ketoconazole 200 mg tablet | Nizoral generic | 2 orally daily | 5 days | $32–$43 ($95 for 30 generic tablets) |
| *Average wholesale price for entire regimen in US dollars. | ||||
Treating complicated VVC
About 5% of women diagnosed with VVC will have frequent recurrences, 4 or more per year.24 Current therapies are fungistatic rather than fungicidal, so the yeast are reduced but not eradicated. Hypersensitivity and allergic reactions to topical preparations may be confused with recurrences. Experts recommend that, if wet mount or culture results confirm recurrent vaginitis, topical therapy should be increased from 5 to 7 days up to 10 to 14 days, or that a second oral fluconazole tablet be given 3 days after the first (SOR: C).24 Women with severe cases of VVC also benefit from 2 sequential doses of fluconazole given 3 days apart (SOR: B).25
Suppressive therapy may be used after initial treatment for 6 months or more (SOR: B). Suppressive therapy options include oral fluconazole 150 mg or vaginal clotrimazole 500 mg once a week, oral or intravaginal nystatin twice weekly, and oral itraconazole 200 mg monthly.24,26
Non-albicans species tend to be more resistant to oral and topical azoles (SOR: B).27-29 If this species is detected on culture, a long course of suppressive therapy should be attempted (SOR: C).24 If imidazole therapy fails to control symptoms, suspect resistance.
Resistance to azoles may be demonstrated by in vitro susceptibility testing. Cross-resistance to topical and oral (fluconazole) azoles has been documented.30 There have been few studies of alternatives to azoles for treatment of resistant yeast vaginitis. One little-studied alternative is intravaginal boric acid, which may be used as a 14-day course of 600 mg daily in gelatin capsules (SOR: C).31 Nystatin and flucytosine (Ancoban) for 7 to 14 days are other alternatives (SOR: C).24
Candida in pregnancy
Commonly used topical imidazoles are classified as category C in pregnancy and have not been associated with increased risk of birth defects.
Trichomoniasis
Current treatment for trichomoniasis is oral metronidazole, given as a 2-g single dose, 250 mg 3 times daily for 7 days or 500 mg twice a day for 7 days. Treatment should also be given to the woman’s partner (SOR: A).32 Intravaginal therapy is not effective, probably due to the parasite’s presence in inaccessible areas such as the vaginal glands and urethra.33,34 Short-term treatment is comparable with long-term treatment, with similar rates of nausea and vomiting (SOR: A).32 A 1.5-g single-dose treatment has been shown to be equivalent to 2 g (SOR: B).35
The incidence metronidazole-resistant trichomoniasis has been estimated at 5%.36 In such cases, higher-dose therapy may be still be effective. For low to moderate resistance, 2 too 2.5 g daily for 3 to 10 days has been recommended (SOR: B).37 Intravenous high-dose metronidazole, 2 g every 8 hours for 3 days, has been reported to successfully treat highly resistant trichomonas (SOR: C).38 Another case report of 2 women with presumed allergy to metronidazole were successfully treated with incremental dosing of IV metronidazole (SOR: C).39 A small case series of women with metronidazole allergy or resistance treated with paromomycin cream intravaginally showed cure in 6 of 9 cases (SOR: C).40 Oral tinidazole has been approved in 2004 for use in the treatment of metronidazole-resistant trichomoniasis (SOR: B).41
Corresponding author
Linda French, MD, Associate Professor, Department of Family Practice, College of Human Medicine, Michigan State University, B101 Clinical Center, East Lansing, MI 48824. E-mail: [email protected].
1. Hillier SL, Lipinski C, Briselden AM, Eschenbach DA. Efficacy of intravaginal 0.75% metronidazole gel for the treatment of bacterial vaginosis. Obstet Gynecol 1993;81:963-967.
2. Hanson JM, McGregor JA, Hillier SL, et al. Metronidazole for bacterial vaginosis. A comparison of vaginal gel vs. oral therapy. J Reprod Med 2000;45:889-896.
3. Lugo-Miro VI, Green M, Mazur L. Comparison of different metronidazole therapeutic regimens for bacterial vaginosis. A meta-analysis. JAMA 1992;268:92-95.
4. Ferris DG, Litaker MS, Woodward L, Mathis D, Hendrich J. Treatment of bacterial vaginosis: a comparison of oral metronidazole, metronidazole vaginal gel, and clindamycin vaginal cream. J Fam Pract 1995;41:443-449.
5. Fischbach F, Petersen EE, Weissenbacher ER, Martius J, Hosmann J, Mayer H. Efficacy of clindamycin vaginal cream versus oral metronidazole in the treatment of bacterial vaginosis. Obstet Gynecol 1993;82:405-410.
6. Hillier S, Krohn MA, Watts DH, Wolner-Hanssen P, Eschenbach D. Microbiologic efficacy of intravaginal clindamycin cream for the treatment of bacterial vaginosis. Obstet Gynecol 1990;76:407-413.
7. Ugwumadu A, Manyonda I, Reid F, Hay P. Effect of early oral clindamycin on late miscarriage and preterm delivery in asymptomatic women with abnormal vaginal flora and bacterial vaginosis: a randomised controlled trial. Lancet 2003;361:983-988.
8. Mikamo H, Kawazoe K, Izumi K, Watanabe K, Ueno K, Tamaya T. Comparative study on vaginal or oral treatment of bacterial vaginosis. Chemotherapy 1997;43:60-68.
9. Ahmed-Jushuf IH, Shahmanesh M, Arya OP. The treatment of bacterial vaginosis with a 3 day course of 2% clindamycin cream: results of a multicentre, double blind, placebo controlled trial. B V Investigators Group. Genitourin Med 1995;71:254-256.
10. Schmitt C, Sobel JD, Meriwether C. Bacterial vaginosis: treatment with clindamycin cream versus oral metronidazole. Obstet Gynecol 1992;79:1020-1023.
11. Paavonen J, Mangioni C, Martin MA, Wajszczuk CP. Vaginal clindamycin and oral metronidazole for bacterial vaginosis: a randomized trial. Obstet Gynecol 2000;96:256-260.
12. Puapermpoonsiri S, Watanabe K, Kato N, Ueno K. In vitro activities of 10 antimicrobial agents against bacterial vaginosis-associated anaerobic isolates from pregnant Japanese and Thai women. Antimicrob Agents Chemother 1997;41:2297-2299.
13. Sobel JD. Vaginitis. N Engl J Med 1997;337:1896-1903.
14. Shalev E, Battino S, Weiner E, Colodner R, Keness Y. Ingestion of yogurt containing Lactobacillus acidophilus compared with pasteurized yogurt as prophylaxis for recurrent candidal vaginitis and bacterial vaginosis. Arch Fam Med 1996;5:593-596.
15. Lamont RF, Jones BM, Mandal D, Hay PE, Sheehan M. The efficacy of vaginal clindamycin for the treatment of abnormal genital tract flora in pregnancy. Infect Dis Obstet Gynecol 2003;11:181-189.
16. Marrazzo J. Vulvovaginal candidiasis. BMJ 2002;325:586.
17. Emele FE, Fadahunsi AA, Anyiwo CE, Ogunleye O. A comparative clinical evaluation of econazole nitrate, miconazole, and nystatin in the treatment of vaginal candidiasis. West Afr J Med 2000;19:12-15.
18. Stein GE, Mummaw N. Placebo controlled trial of itraconazole for treatment of acute vaginal candidiasis. Antimicrob Agents Chemother 1993;37:89-92.
19. Van der Pas H, Peeters F, Janssens D, Snauwaert E, Van Cutsem J. Treatment of vaginal candidosis with oral ketoconazole. Eur J Obstet Gynecol Reprod Biol 1983;14:399-404.
20. Sanz Sanz F, del Palacio Hernanz A. Randomized comparative trial of three regimens of itraconazole for treatment of vaginal mycoses. Rev Infect Dis 1987;9 Suppl 1:S139-S142.
21. Silva-Cruz A, Andrade L, Sobral L, Francisca A. Itraconazole versus placebo in the management of vaginal candidiasis. Int J Gynaecol Obstet 1991;36:229-232.
22. Watson MC, Grimshaw JM, Bond CM, Mollison J, Ludbrook A. Oral versus intravaginal imidazole and triazole anti-fungal agents for the treatment of uncomplicated vulvovaginal candidiasis (thrush): a systematic review. BJOG 2002;109:85-95.
23. van Heusden AM, Merkus HM, Corbeij RS, et al. Single-dose oral fluconazole versus single-dose topical miconazole for the treatment of acute vulvovaginal candidosis. Acta Obstet Gynecol Scand 1990;69:417-422.
24. Sobel JD. Vulvovaginitis. When Candida becomes a problem. Dermatol Clin 1998;16:763-768,xii.-
25. Sobel JD, Kapernick PS, Zervos M, et al. Treatment of complicated Candida vaginitis: comparison of single and sequential doses of fluconazole. Am J Obstet Gynecol 2001;185:363-369.
26. Creatsas GC, Charalambidis VM, Zagotzidou EH, Anthopoulou HN, Michailidis DC, Aravantinos DI. Chronic or recurrent vaginal candidosis: short-term treatment and prophylaxis with itraconazole. Clin Ther 1993;15:662-671.
27. Horowitz BJ, Giaquinta D, Ito S. Evolving pathogens in vulvovaginal candidiasis: implications for patient care. J Clin Pharmacol 1992;32:248-255.
28. del Palacio A, Sanz F, Sanchez-Alor G, et al. Double-blind randomized dose-finding study in acute vulvovaginal can-didosis. Comparison of flutrimazole site-release cream (1, 2 and 4%) with placebo site-release vaginal cream. Mycoses 2000;43:355-365.
29. Singh S, Sobel JD, Bhargava P, Boikov D, Vazquez JA. Vaginitis due to Candida krusei: epidemiology, clinical aspects, and therapy. Clin Infect Dis 2002;35:1066-1070.
30. Cross EW, Park S, Perlin DS. Cross-Resistance of clinical isolates of Candida albicans and Candida glabrata to over-the-counter azoles used in the treatment of vaginitis. Microb Drug Resist 2000;6:155-161.
31. Sobel JD, Chaim W. Treatment of Torulopsis glabrata vaginitis: retrospective review of boric acid therapy. Clin Infect Dis 1997;24:649-652.
32. Forna F, Gulmezoglu AM. Interventions for treating trichomoniasis in women. Cochrane Database Syst Rev 2003(2);CD000218.
33. duBouchet L, McGregor JA, Ismail M, McCormack WM. A pilot study of metronidazole vaginal gel versus oral metronidazole for the treatment of Trichomonas vaginalis vaginitis. Sex Transm Dis 1998;25:176-179.
34. Tidwell BH, Lushbaugh WB, Laughlin MD, Cleary JD, Finley RW. A double-blind placebo-controlled trial of single-dose intravaginal versus single-dose oral metronidazole in the treatment of trichomonal vaginitis. J Infect Dis 1994;170:242-246.
35. Spence MR, Harwell TS, Davies MC, Smith JL. The minimum single oral metronidazole dose for treating trichomoniasis: a randomized, blinded study. Obstet Gynecol 1997;89:699-703.
36. Petrin D, Delgaty K, Bhatt R, Garber G. Clinical and microbiological aspects of Trichomonas vaginalis. Clin Microbiol Rev 1998;11:300-317.
37. Lossick JG, Kent HL. Trichomoniasis: trends in diagnosis and management. Am J Obstet Gynecol 1991;165:1217-1222.
38. Dombrowski MP, Sokol RJ, Brown WJ, Bronsteen RA. Intravenous therapy of metronidazole-resistant Trichomonas vaginalis. Obstet Gynecol 1987;69:524-525.
39. Pearlman MD, Yashar C, Ernst S, Solomon W. An incremental dosing protocol for women with severe vaginal trichomoniasis and adverse reaction to metronidazole. Am J Obstet Gynecol 1996;174:934-936.
40. Nyirjesy P, Sobel JD, Weitz MV, Leaman DJ, Gelone SP. Difficult-to-treat trichomoniasis: results with paromomycin cream. Clin Infect Dis. 1998;26:986-988.
41. Sobel JD, Nyirjesy P, Brown W. Tinidazole therapy for metronidazole resistant vaginal trichomoniasis. Clin Infect Dis 2001;33:1341-1346.
1. Hillier SL, Lipinski C, Briselden AM, Eschenbach DA. Efficacy of intravaginal 0.75% metronidazole gel for the treatment of bacterial vaginosis. Obstet Gynecol 1993;81:963-967.
2. Hanson JM, McGregor JA, Hillier SL, et al. Metronidazole for bacterial vaginosis. A comparison of vaginal gel vs. oral therapy. J Reprod Med 2000;45:889-896.
3. Lugo-Miro VI, Green M, Mazur L. Comparison of different metronidazole therapeutic regimens for bacterial vaginosis. A meta-analysis. JAMA 1992;268:92-95.
4. Ferris DG, Litaker MS, Woodward L, Mathis D, Hendrich J. Treatment of bacterial vaginosis: a comparison of oral metronidazole, metronidazole vaginal gel, and clindamycin vaginal cream. J Fam Pract 1995;41:443-449.
5. Fischbach F, Petersen EE, Weissenbacher ER, Martius J, Hosmann J, Mayer H. Efficacy of clindamycin vaginal cream versus oral metronidazole in the treatment of bacterial vaginosis. Obstet Gynecol 1993;82:405-410.
6. Hillier S, Krohn MA, Watts DH, Wolner-Hanssen P, Eschenbach D. Microbiologic efficacy of intravaginal clindamycin cream for the treatment of bacterial vaginosis. Obstet Gynecol 1990;76:407-413.
7. Ugwumadu A, Manyonda I, Reid F, Hay P. Effect of early oral clindamycin on late miscarriage and preterm delivery in asymptomatic women with abnormal vaginal flora and bacterial vaginosis: a randomised controlled trial. Lancet 2003;361:983-988.
8. Mikamo H, Kawazoe K, Izumi K, Watanabe K, Ueno K, Tamaya T. Comparative study on vaginal or oral treatment of bacterial vaginosis. Chemotherapy 1997;43:60-68.
9. Ahmed-Jushuf IH, Shahmanesh M, Arya OP. The treatment of bacterial vaginosis with a 3 day course of 2% clindamycin cream: results of a multicentre, double blind, placebo controlled trial. B V Investigators Group. Genitourin Med 1995;71:254-256.
10. Schmitt C, Sobel JD, Meriwether C. Bacterial vaginosis: treatment with clindamycin cream versus oral metronidazole. Obstet Gynecol 1992;79:1020-1023.
11. Paavonen J, Mangioni C, Martin MA, Wajszczuk CP. Vaginal clindamycin and oral metronidazole for bacterial vaginosis: a randomized trial. Obstet Gynecol 2000;96:256-260.
12. Puapermpoonsiri S, Watanabe K, Kato N, Ueno K. In vitro activities of 10 antimicrobial agents against bacterial vaginosis-associated anaerobic isolates from pregnant Japanese and Thai women. Antimicrob Agents Chemother 1997;41:2297-2299.
13. Sobel JD. Vaginitis. N Engl J Med 1997;337:1896-1903.
14. Shalev E, Battino S, Weiner E, Colodner R, Keness Y. Ingestion of yogurt containing Lactobacillus acidophilus compared with pasteurized yogurt as prophylaxis for recurrent candidal vaginitis and bacterial vaginosis. Arch Fam Med 1996;5:593-596.
15. Lamont RF, Jones BM, Mandal D, Hay PE, Sheehan M. The efficacy of vaginal clindamycin for the treatment of abnormal genital tract flora in pregnancy. Infect Dis Obstet Gynecol 2003;11:181-189.
16. Marrazzo J. Vulvovaginal candidiasis. BMJ 2002;325:586.
17. Emele FE, Fadahunsi AA, Anyiwo CE, Ogunleye O. A comparative clinical evaluation of econazole nitrate, miconazole, and nystatin in the treatment of vaginal candidiasis. West Afr J Med 2000;19:12-15.
18. Stein GE, Mummaw N. Placebo controlled trial of itraconazole for treatment of acute vaginal candidiasis. Antimicrob Agents Chemother 1993;37:89-92.
19. Van der Pas H, Peeters F, Janssens D, Snauwaert E, Van Cutsem J. Treatment of vaginal candidosis with oral ketoconazole. Eur J Obstet Gynecol Reprod Biol 1983;14:399-404.
20. Sanz Sanz F, del Palacio Hernanz A. Randomized comparative trial of three regimens of itraconazole for treatment of vaginal mycoses. Rev Infect Dis 1987;9 Suppl 1:S139-S142.
21. Silva-Cruz A, Andrade L, Sobral L, Francisca A. Itraconazole versus placebo in the management of vaginal candidiasis. Int J Gynaecol Obstet 1991;36:229-232.
22. Watson MC, Grimshaw JM, Bond CM, Mollison J, Ludbrook A. Oral versus intravaginal imidazole and triazole anti-fungal agents for the treatment of uncomplicated vulvovaginal candidiasis (thrush): a systematic review. BJOG 2002;109:85-95.
23. van Heusden AM, Merkus HM, Corbeij RS, et al. Single-dose oral fluconazole versus single-dose topical miconazole for the treatment of acute vulvovaginal candidosis. Acta Obstet Gynecol Scand 1990;69:417-422.
24. Sobel JD. Vulvovaginitis. When Candida becomes a problem. Dermatol Clin 1998;16:763-768,xii.-
25. Sobel JD, Kapernick PS, Zervos M, et al. Treatment of complicated Candida vaginitis: comparison of single and sequential doses of fluconazole. Am J Obstet Gynecol 2001;185:363-369.
26. Creatsas GC, Charalambidis VM, Zagotzidou EH, Anthopoulou HN, Michailidis DC, Aravantinos DI. Chronic or recurrent vaginal candidosis: short-term treatment and prophylaxis with itraconazole. Clin Ther 1993;15:662-671.
27. Horowitz BJ, Giaquinta D, Ito S. Evolving pathogens in vulvovaginal candidiasis: implications for patient care. J Clin Pharmacol 1992;32:248-255.
28. del Palacio A, Sanz F, Sanchez-Alor G, et al. Double-blind randomized dose-finding study in acute vulvovaginal can-didosis. Comparison of flutrimazole site-release cream (1, 2 and 4%) with placebo site-release vaginal cream. Mycoses 2000;43:355-365.
29. Singh S, Sobel JD, Bhargava P, Boikov D, Vazquez JA. Vaginitis due to Candida krusei: epidemiology, clinical aspects, and therapy. Clin Infect Dis 2002;35:1066-1070.
30. Cross EW, Park S, Perlin DS. Cross-Resistance of clinical isolates of Candida albicans and Candida glabrata to over-the-counter azoles used in the treatment of vaginitis. Microb Drug Resist 2000;6:155-161.
31. Sobel JD, Chaim W. Treatment of Torulopsis glabrata vaginitis: retrospective review of boric acid therapy. Clin Infect Dis 1997;24:649-652.
32. Forna F, Gulmezoglu AM. Interventions for treating trichomoniasis in women. Cochrane Database Syst Rev 2003(2);CD000218.
33. duBouchet L, McGregor JA, Ismail M, McCormack WM. A pilot study of metronidazole vaginal gel versus oral metronidazole for the treatment of Trichomonas vaginalis vaginitis. Sex Transm Dis 1998;25:176-179.
34. Tidwell BH, Lushbaugh WB, Laughlin MD, Cleary JD, Finley RW. A double-blind placebo-controlled trial of single-dose intravaginal versus single-dose oral metronidazole in the treatment of trichomonal vaginitis. J Infect Dis 1994;170:242-246.
35. Spence MR, Harwell TS, Davies MC, Smith JL. The minimum single oral metronidazole dose for treating trichomoniasis: a randomized, blinded study. Obstet Gynecol 1997;89:699-703.
36. Petrin D, Delgaty K, Bhatt R, Garber G. Clinical and microbiological aspects of Trichomonas vaginalis. Clin Microbiol Rev 1998;11:300-317.
37. Lossick JG, Kent HL. Trichomoniasis: trends in diagnosis and management. Am J Obstet Gynecol 1991;165:1217-1222.
38. Dombrowski MP, Sokol RJ, Brown WJ, Bronsteen RA. Intravenous therapy of metronidazole-resistant Trichomonas vaginalis. Obstet Gynecol 1987;69:524-525.
39. Pearlman MD, Yashar C, Ernst S, Solomon W. An incremental dosing protocol for women with severe vaginal trichomoniasis and adverse reaction to metronidazole. Am J Obstet Gynecol 1996;174:934-936.
40. Nyirjesy P, Sobel JD, Weitz MV, Leaman DJ, Gelone SP. Difficult-to-treat trichomoniasis: results with paromomycin cream. Clin Infect Dis. 1998;26:986-988.
41. Sobel JD, Nyirjesy P, Brown W. Tinidazole therapy for metronidazole resistant vaginal trichomoniasis. Clin Infect Dis 2001;33:1341-1346.
A new treatment option for grades III and IV hemorrhoids
Although effective for grades III and IV hemorrhoids, conventional hemorrhoidectomy is known to entail a significant recovery period and postoperative pain (strength of recommendation [SOR]: B).
The newest treatment option for grades III and IV hemorrhoids, the procedure for prolapse and hemorrhoids, is an effective technique with the potential to incur less pain and a quicker return to work and daily activities (SOR: B).
For patients with severe hemorrhoidal symptoms who do not want, or are unable, to undergo any type of surgical procedure, rubber band ligation is a viable option (SOR: B).
Hemorrhoids represent one of the most common colorectal complaints heard by family physicians. Each year approximately 10.5 million Americans experience hemorrhoidal symptoms; one fourth of those patients consult a physician.1
The most common symptom of internal hemorrhoids is bright red blood that covers the stool or appears on toilet paper or in the toilet bowl. Other symptoms include irritation of the skin around the anus; pain, swelling, or a hard lump around the anus; hemorrhoidal protrusion; and mucous discharge. Excessive rubbing or cleaning around the anus may exacerbate symptoms and even cause a vicious cycle of irritation, bleeding, and itching termed pruritus ani. Hemorrhoids also may thrombose, causing severe pain.
More than half of men and women aged 50 years and older will develop hemorrhoidal symptoms throughout their lifetime.2 Hemorrhoidal symptoms also tend to flare up during pregnancy, when hormonal changes and the pressure of the fetus cause the hemorrhoidal vessels to enlarge.
The likelihood of hemorrhoidal disease increases with age. By age 30, the anal support structure diminishes in function.3 This microscopic evidence, along with increased sphincter tone, may contribute to the progression of hemorrhoids.4
Although hemorrhoidal symptoms may subside after several days, they most often return, causing long-lasting discomfort and pain. Many affected persons—particularly those with severe hemorrhoids—suffer in silence for years before seeking treatment.5 Fortunately, only about 10% of patients have symptoms severe enough to require surgery.6
Differential diagnosis
Many anorectal problems, including fissures, fistulae, abscesses, or irritation and itching, have symptoms similar to those of hemorrhoids and must be ruled out prior to recommending appropriate treatment. In addition, the correlation of rectal bleeding with colorectal cancer becomes stronger with age, as demonstrated in a retrospective study of the diagnostic value of rectal bleeding in relation to a subsequent diagnosis of colorectal cancer.7 Therefore, further evaluation with colonoscopy should be made in patients who are older than 50 years of age, have a family history of colon cancer, and experience fatigue or weight loss or have a palpable mass.8
Classification of hemorrhoids
External hemorrhoids originate below the dentate line (FIGURE 1). Internal hemorrhoids are above the line and are classified according to their degree of prolapse:
- Grade I hemorrhoids protrude into the lumen of the anal canal but do not prolapse.
- Grade II hemorrhoids protrude with a bowel movement but spontaneously return when straining stops.
- Grade III hemorrhoids protrude either spontaneously or with a bowel movement, and can be manually reduced.
- Grade IV hemorrhoids have an irreducible prolapse.
This article focuses on a new treatment option for grades III and IV.
FIGURE 1 Mucosal Prolapse and Hemorrhoids
Methods of treating grades III and IV hemorrhoids
Until recently, the recommended treatments for grades III and IV hemorrhoids were limited to rubber band ligation (RBL) and conventional hemorrhoidectomy.
An office procedure not requiring anesthesia, RBL is the use of a latex band to cut off blood flow to the symptomatic hemorrhoid. The procedure is not without complications; there have been several reports of fatal and nonfatal retroperitoneal sepsis after RBL.9,10
Most conventional hemorrhoidectomies are performed in 1 of 2 ways. Outside the United States, the Milligan-Morgan technique, which excises the 3 major hemorrhoidal vessels, is considered the gold standard hemorrhoidectomy. Developed in 1937 in the United Kingdom, the surgery is also known as “open” hemorrhoidectomy because the incisions, which are separated by bridges of skin and mucosa, are left open to avoid stenosis. The Ferguson technique, developed in the United States in 1952, differs from the Milligan-Morgan procedure in that the incisions are sutured shut. Accordingly, it is commonly known as “closed” hemorrhoidectomy.
Regardless of technique, conventional hemorrhoidectomy is known to involve significant postoperative pain and an extended recovery time that precludes a fast return to work and daily activities.
A new stapling technique, the procedure for prolapse and hemorrhoids (PPH), was introduced in the mid-1990s and has been used extensively since then. Also known as stapled hemorrhoidopexy, stapled hemorrhoidectomy, or Longo stapled circumferential mucosectomy, PPH involves the use of a specially designed circular stapler that is inserted through the anus (FIGURE 2). The procedure reduces the prolapse of hemorrhoidal tissue by excising a band of the prolapsed rectal mucosa/internal hemorrhoid. The remaining hemorrhoidal tissue is drawn back into the correct anatomic position within the anal canal.
The stapling technique markedly reduces swelling by disrupting the hemorrhoidal artery blood flow, thereby reducing inflow to the hemorrhoids themselves. In addition, restoring the internal hemorrhoids to their normal anatomic position prevents prolapse and alleviates patients’ symptoms.11 The staples are placed well above the dentate line, and the majority of PPH is performed where there are autonomic nerve fibers, as opposed to somatic innervation. Thus, patients who undergo PPH tend to experience less postoperative pain than do those who undergo conventional hemorrhoidectomy, which involves the cutting of innervated perianal skin. Notably, the function and morphology of the internal anal sphincter, which have a direct bearing on anal continence, are not typically affected by PPH.12 Moreover, in patients with preoperative sensory impairment, the procedure improves anal-canal sensitivity—that is, the ability to distinguish between air and warm water in the anal canal.12 In contrast, research has shown that only about half of the patients who undergo conventional hemorrhoidectomy are able to detect water in the anal canal after surgery, and an additional 25% lose this ability within 6 months of the operation.13 Loss of anal-canal sensitivity affects internal-anal-sphincter function and morphology, which in turn affects anal continence.
Since 2000, several studies have been published confirming that PPH is associated with a low rate of compli-cations.14-16 Rare instances of sepsis following PPH have been reported. Some clinicians recommend administration of prophylactic antibiotics prior to the procedure. Guy and Seow-Choen suggest that the potential for sepsis is high only in cases where an excess amount of muscle is incorporated into the stapler housing. Thus, in recent years, the surgical technique has been refined so as to reduce the potential for postoperative infection.17,18
Randomized controlled trials
PPH versus other methods
Many individuals with extensive hemorrhoidal prolapse may not want to undergo, or will not be candidates for, any type of surgical intervention. For such patients, RBL is a viable option. Indeed, a number of studies endorse RBL as a first-line option for grade III hemorrhoids. However, one should note that RBL carries a high potential for symptomatic recurrence, which often results in the need for multiple bandings.19,20
Peng and colleagues conducted a study in which 55 patients with grade III or small grade IV hemorrhoids were randomized to either RBL or PPH.19 There was a higher incidence of pain at discharge and at 2-week follow-up in the PPH group (P<.001). Six patients in the PPH group experienced procedure-related complications, as opposed to none in the RBL group (P=.027). Despite these results, the authors recommended PPH for patients who did not want to run the risk of requiring further interventions. Notably, the group that underwent RBL had a significantly higher incidence of recurrent bleeding at 2 weeks’ follow-up (68% vs 27%, P=.002). More important, 5 patients in the RBL group needed to undergo excisional hemorrhoidectomy to resolve persistent bleeding or prolapse, whereas none of the PPH patients required further intervention (P<.05).
The earliest randomized controlled clinical trials directly comparing PPH with conventional hemorrhoidectomy reported excellent results21,22; however, patient numbers were small, and, of course, no long-term data were available. Now, reports are in from larger trials and studies with longer-term follow-up.
Shalaby and Desoky conducted a trial in which 200 patients were randomized to either Milligan-Morgan hemorrhoidectomy or PPH. Compared with hemorrhoidectomy, PPH required less operating time (9.0 vs 19.7 minutes, P<.001) and a shorter hospital stay (1.1 vs 2.2 days, P<.001), and provided a faster return to full activity (8.2 vs 53.9 days, P<.001).23 In addition, pain scores were significantly lower in the stapled group after the first 24 hours, at the time of first bowel movement, and at 1 week postoperatively (TABLE 1).
In a 100-patient, prospective, randomized trial, Ganio and colleagues compared PPH with open hemorrhoidectomy and found PPH to be as effective as conventional surgery.24 Postoperative bleeding occurred in 3 patients in each group. However, reduced postoperative pain, a shorter hospital stay, and a trend toward a quicker return to work were reported for the group of patients who underwent PPH. Moderate pain for hemorrhoidectomy patients occurred for a median of 5.3 days (range, 0–19 days) compared with only 3.1 days (range, 0–10 days) in the PPH group. Hemorrhoidectomy patients complained of severe pain for 2.3 days (range, 0–24 days), whereas the PPH patients had only 1 day (range, 0–14 days) of severe pain (P=.01). Functionally, the investigators found no difference between the 2 groups with respect to postoperative fecal incontinence. But, at 1 month, patients in the hemorrhoidectomy group were significantly less continent to flatus.25 The patients who underwent PPH also showed a statistically significant improvement in constipation scores, unlike the group who underwent conventional surgery.
In another study, Palimento and colleagues used several methods to evaluate postoperative pain in a group of 74 patients randomized either to PPH or open hemorrhoidectomy.26 Patients were encouraged to ask freely for pain relief, and the amounts of analgesic consumed were recorded. A visual analogue scale (VAS) from 0 (no pain) to 10 (worst pain imaginable) was completed by each patient at 4 and 24 hours following surgery. The researchers also requested a VAS score to evaluate pain at first defecation. In addition, patients were asked to record when they were able to have completely pain-free bowel movements and when there was pain-free return to normal activities and work. Analgesia requirements were similar between the 2 groups. Median VAS scores in the PPH group were significantly lower than in the open-hemorrhoidectomy group at 4 and 24 hours postoperatively and after first defecation (TABLE 2).
No statistically significant difference between the groups was found for incidence of postoperative bleeding. Nor did the groups differ regarding return to normal activities or return to work. However, the investigators noted that many factors affect the latter 2 outcome measures, including a patient’s motivation and his/her insurance coverage for disability, making comparisons somewhat unreliable. Hence, time to resumption of pain-free defecation was evaluated as a more objective measure and was found to be significantly less in the stapled group (10 vs 12 days, P=.001). At long-term follow-up (median, 17.5 months; range, 10–27 months), occasional pain was reported by 6 (16.2%) of the 37 patients in the PPH group and by 7 (18.9%) of the 37 patients in the open-hemorrhoidectomy group (P=1.000).
Racalbuto and colleagues performed a long-term randomized trial comparing results for 50 patients who underwent PPH with another 50 who underwent Milligan-Morgan hemorrhoidectomy.27 Patients were followed over a period of 48 months. Once again, patients who underwent PPH experienced significantly less pain and therefore were able to return to activities much more quickly than those who underwent conventional hemorrhoidectomy (8.04 ± 1.37 days vs 16.9 ± 2.50 days, P<.0001). In the long-term follow-up evaluation, none of the patients in either treatment group experienced stenosis. In addition, when comparing the 2 groups with respect to anal incontinence and recurrence of prolapse, the investigators did not find any significant differences.
TABLE 1
Mean Pain Scores for PPH vs Milligan-Morgan Hemorrhoidectomy
| PPH Mean (SD) | Milligan-Morgan Mean (SD) | P Value | |
|---|---|---|---|
| First 24 hours | 2.5 (1.3) | 7.6 (0.7) | <.001 |
| First bowel movement | 1.1 (0.3) | 6.6 (1.2) | <.001 |
| 1 week after operation | 0.4 (0.7) | 2.6 (0.6) | <.001 |
| PPH = procedure for prolapse and hemorrhoids; SD = standard deviation. | |||
| Adapted from Shalaby and Desoky.23 | |||
TABLE 2
Median Pain Scores for PPH vs Open Hemorrhoidectomy
| PPH Median (range) | Open Hemorrhoidectomy Median (range) | P Value | |
|---|---|---|---|
| 4 hours after operation | 4 (2–6) | 5 (2–8) | .001 |
| 24 hours after operation | 3 (1–6) | 5 (3–7) | .000 |
| First defecation | 5 (3–8) | 7 (3–9) | .000 |
| PPH = procedure for prolapse and hemorrhoids. | |||
| Data from Palimento et al.26 | |||
Contraindications to PPH
Contraindications to PPH include anal stenosis, that is, an anal canal that does not allow the stapler to be inserted. The PPH procedure also should be avoided in patients with an anorectal abscess, a complex fistula in ano, and perianal Crohn’s disease. As with any other type of surgery, patients undergoing anticoagulation therapy must be carefully evaluated.
Conclusion
The stapling technique is the newest treatment option for grades III and IV hemorrhoids. Although more randomized trials are needed, it appears from the research thus far that PPH is effective, with the potential to involve less pain and a shorter recovery time than conventional hemorrhoidectomy.
Disclosures
Dr Parker serves as a consultant to Ethicon Endo-Surgery. This supplement is supported by a grant from Ethicon Endo-Surgery.
1. Helton WS. for The SSAT, AGA, ASGE Consensus Panel 2001 consensus statement on benign anorectal disease. J Gastrointestinal Surg. 2002;6:302-303.
2. Bailey HR. Innovations for age-old problem: hemorrhoids in the female patient. Female Patient. 2004;29:17-23.
3. Haas PA, Fox TA, Jr, Haas GP. The pathogenesis of hemorrhoids. Dis Colon Rectum. 1984;27:442-450.
4. Hancock BD. Internal sphincter and the nature of haemorrhoids. Gut. 1977;18:651-655.
5. Pfenninger J, Zainea G. Common anorectal conditions: Part I. Symptoms and complaints. Am Fam Physician. 2001;63:2391-2398.
6. Bleday R, Pena JP, Rothenberger DA, et al. Symptomatic hemorrhoids: current incidence and complications of operative therapy. Dis Colon Rectum. 1992;35:477-481.
7. Wauters H, Van Casteren V, Buntinx F. Rectal bleeding and colorectal cancer in general practice: diagnostic study. BMJ. 2000;321:998-999.
8. Smith RA, Cokkinides V, Eyre HJ. American Cancer Society guidelines for the early detection of cancer, 2004. CA Cancer J Clin. 2004;54:41-52.
9. Quevedo-Bonilla G, Farkas AM, Abcarian H, et al. Septic complications of haemorrhoidal banding. Arch Surg. 1988;123:650-651.
10. Scarpa FJ, Hillis W, Sabetta JR. Pelvic cellulitis: a life-threatening complication of hemorrhoidal banding. Surgery. 1988;103:383-385.
11. Hetzer FH, Demartines N, Handschin AE, Clavien PA. Stapled vs excision hemorrhoidectomy: long-term results of a prospective randomized trial. Arch Surg. 2002;137:337-340.
12. Altomare DF, Rinaldi M, Sallustio PL, et al. Long-term effects of stapled haemorrhoidectomy on internal anal function and sensitivity. Br J Surg. 2001;88:1487-1491.
13. Read MG, Read NW, Haynes WG, et al. A prospective study of the effect of haemorrhoidectomy on sphincter function and faecal continence. Br J Surg. 1982;69:396-398.
14. Singer MA, Cintron JR, Fleshman JW, et al. Early experience with stapled hemorrhoidectomy in the United States. Dis Colon Rectum. 2002;45:360-367.
15. Dixon MR, Stamos MJ, Grant SR, et al. Stapled hemorrhoidectomy: a review of our early experience. Am Surg. 2003;69:862-865.
16. Hoffman GH, Firoozmand E. Hemorrhoids—To staple or not to staple: that is the question. Surg Rounds. 2004;27:213-224.
17. Guy RJ, Seow-Choen F. Septic complications after treatment of haemorrhoids. Br J Surg. 2003;90:147-156.
18. Molloy RG, Kingsmore D. Life threatening pelvic sepsis after stapled haemorrhoidectomy [letter]. Lancet. 2000;355:810.-
19. Peng BC, Jayne DG, Ho YH. Randomized trial of rubber band ligation vs. stapled hemorrhoidectomy for prolapsed piles. Dis Colon Rectum. 2003;46:291-297.
20. Komborozos VA, Skrekas GJ, Pissiotis CA. Rubber band ligation of symptomatic internal hemorrhoids: results of 500 cases. Dig Surg. 2000;17:71-76.
21. Mehigan BJ, Monson JRT, Hartley JE. Stapling procedure for haemorrhoids versus Milligan-Morgan haemorrhoidectomy: randomized controlled trial. Lancet. 2000;355:782-785.
22. Rowsell M, Bello M, Hemingway DM. Circumferential mucosectomy (stapled haemorrhoidectomy) versus conventional haemorrhoidectomy: randomized controlled trial. Lancet. 2000;355:779-781.
23. Shalaby R, Desoky A. Randomized clinical trial of stapled versus Milligan-Morgan haemorrhoidectomy. Br J Surg. 2001;88:1049-1053.
24. Ganio E, Altomare DF, Gabrielli F, et al. Prospective randomized multicentre trial comparing stapled with open haemorrhoidectomy. Br J Surg. 2001;88:669-674.
25. Williams NS, Patel J, George BD, et al. Development of an electrically stimulated neoanal sphincter. Lancet. 1991;338:1166-1169.
26. Palimento D, Picchio M, Attanasio U, et al. Stapled and open hemorrhoidectomy: randomized controlled trial of early results. World J Surg. 2003;27:203-207.
27. Racalbuto A, Aliotta I, Corsaro G, et al. Hemorrhoidal stapler prolapsectomy vs. Milligan-Morgan hemorrhoidectomy: a long-term randomized trial. Int J Colorectal Dis. 2004;19:239-244.
Although effective for grades III and IV hemorrhoids, conventional hemorrhoidectomy is known to entail a significant recovery period and postoperative pain (strength of recommendation [SOR]: B).
The newest treatment option for grades III and IV hemorrhoids, the procedure for prolapse and hemorrhoids, is an effective technique with the potential to incur less pain and a quicker return to work and daily activities (SOR: B).
For patients with severe hemorrhoidal symptoms who do not want, or are unable, to undergo any type of surgical procedure, rubber band ligation is a viable option (SOR: B).
Hemorrhoids represent one of the most common colorectal complaints heard by family physicians. Each year approximately 10.5 million Americans experience hemorrhoidal symptoms; one fourth of those patients consult a physician.1
The most common symptom of internal hemorrhoids is bright red blood that covers the stool or appears on toilet paper or in the toilet bowl. Other symptoms include irritation of the skin around the anus; pain, swelling, or a hard lump around the anus; hemorrhoidal protrusion; and mucous discharge. Excessive rubbing or cleaning around the anus may exacerbate symptoms and even cause a vicious cycle of irritation, bleeding, and itching termed pruritus ani. Hemorrhoids also may thrombose, causing severe pain.
More than half of men and women aged 50 years and older will develop hemorrhoidal symptoms throughout their lifetime.2 Hemorrhoidal symptoms also tend to flare up during pregnancy, when hormonal changes and the pressure of the fetus cause the hemorrhoidal vessels to enlarge.
The likelihood of hemorrhoidal disease increases with age. By age 30, the anal support structure diminishes in function.3 This microscopic evidence, along with increased sphincter tone, may contribute to the progression of hemorrhoids.4
Although hemorrhoidal symptoms may subside after several days, they most often return, causing long-lasting discomfort and pain. Many affected persons—particularly those with severe hemorrhoids—suffer in silence for years before seeking treatment.5 Fortunately, only about 10% of patients have symptoms severe enough to require surgery.6
Differential diagnosis
Many anorectal problems, including fissures, fistulae, abscesses, or irritation and itching, have symptoms similar to those of hemorrhoids and must be ruled out prior to recommending appropriate treatment. In addition, the correlation of rectal bleeding with colorectal cancer becomes stronger with age, as demonstrated in a retrospective study of the diagnostic value of rectal bleeding in relation to a subsequent diagnosis of colorectal cancer.7 Therefore, further evaluation with colonoscopy should be made in patients who are older than 50 years of age, have a family history of colon cancer, and experience fatigue or weight loss or have a palpable mass.8
Classification of hemorrhoids
External hemorrhoids originate below the dentate line (FIGURE 1). Internal hemorrhoids are above the line and are classified according to their degree of prolapse:
- Grade I hemorrhoids protrude into the lumen of the anal canal but do not prolapse.
- Grade II hemorrhoids protrude with a bowel movement but spontaneously return when straining stops.
- Grade III hemorrhoids protrude either spontaneously or with a bowel movement, and can be manually reduced.
- Grade IV hemorrhoids have an irreducible prolapse.
This article focuses on a new treatment option for grades III and IV.
FIGURE 1 Mucosal Prolapse and Hemorrhoids
Methods of treating grades III and IV hemorrhoids
Until recently, the recommended treatments for grades III and IV hemorrhoids were limited to rubber band ligation (RBL) and conventional hemorrhoidectomy.
An office procedure not requiring anesthesia, RBL is the use of a latex band to cut off blood flow to the symptomatic hemorrhoid. The procedure is not without complications; there have been several reports of fatal and nonfatal retroperitoneal sepsis after RBL.9,10
Most conventional hemorrhoidectomies are performed in 1 of 2 ways. Outside the United States, the Milligan-Morgan technique, which excises the 3 major hemorrhoidal vessels, is considered the gold standard hemorrhoidectomy. Developed in 1937 in the United Kingdom, the surgery is also known as “open” hemorrhoidectomy because the incisions, which are separated by bridges of skin and mucosa, are left open to avoid stenosis. The Ferguson technique, developed in the United States in 1952, differs from the Milligan-Morgan procedure in that the incisions are sutured shut. Accordingly, it is commonly known as “closed” hemorrhoidectomy.
Regardless of technique, conventional hemorrhoidectomy is known to involve significant postoperative pain and an extended recovery time that precludes a fast return to work and daily activities.
A new stapling technique, the procedure for prolapse and hemorrhoids (PPH), was introduced in the mid-1990s and has been used extensively since then. Also known as stapled hemorrhoidopexy, stapled hemorrhoidectomy, or Longo stapled circumferential mucosectomy, PPH involves the use of a specially designed circular stapler that is inserted through the anus (FIGURE 2). The procedure reduces the prolapse of hemorrhoidal tissue by excising a band of the prolapsed rectal mucosa/internal hemorrhoid. The remaining hemorrhoidal tissue is drawn back into the correct anatomic position within the anal canal.
The stapling technique markedly reduces swelling by disrupting the hemorrhoidal artery blood flow, thereby reducing inflow to the hemorrhoids themselves. In addition, restoring the internal hemorrhoids to their normal anatomic position prevents prolapse and alleviates patients’ symptoms.11 The staples are placed well above the dentate line, and the majority of PPH is performed where there are autonomic nerve fibers, as opposed to somatic innervation. Thus, patients who undergo PPH tend to experience less postoperative pain than do those who undergo conventional hemorrhoidectomy, which involves the cutting of innervated perianal skin. Notably, the function and morphology of the internal anal sphincter, which have a direct bearing on anal continence, are not typically affected by PPH.12 Moreover, in patients with preoperative sensory impairment, the procedure improves anal-canal sensitivity—that is, the ability to distinguish between air and warm water in the anal canal.12 In contrast, research has shown that only about half of the patients who undergo conventional hemorrhoidectomy are able to detect water in the anal canal after surgery, and an additional 25% lose this ability within 6 months of the operation.13 Loss of anal-canal sensitivity affects internal-anal-sphincter function and morphology, which in turn affects anal continence.
Since 2000, several studies have been published confirming that PPH is associated with a low rate of compli-cations.14-16 Rare instances of sepsis following PPH have been reported. Some clinicians recommend administration of prophylactic antibiotics prior to the procedure. Guy and Seow-Choen suggest that the potential for sepsis is high only in cases where an excess amount of muscle is incorporated into the stapler housing. Thus, in recent years, the surgical technique has been refined so as to reduce the potential for postoperative infection.17,18
Randomized controlled trials
PPH versus other methods
Many individuals with extensive hemorrhoidal prolapse may not want to undergo, or will not be candidates for, any type of surgical intervention. For such patients, RBL is a viable option. Indeed, a number of studies endorse RBL as a first-line option for grade III hemorrhoids. However, one should note that RBL carries a high potential for symptomatic recurrence, which often results in the need for multiple bandings.19,20
Peng and colleagues conducted a study in which 55 patients with grade III or small grade IV hemorrhoids were randomized to either RBL or PPH.19 There was a higher incidence of pain at discharge and at 2-week follow-up in the PPH group (P<.001). Six patients in the PPH group experienced procedure-related complications, as opposed to none in the RBL group (P=.027). Despite these results, the authors recommended PPH for patients who did not want to run the risk of requiring further interventions. Notably, the group that underwent RBL had a significantly higher incidence of recurrent bleeding at 2 weeks’ follow-up (68% vs 27%, P=.002). More important, 5 patients in the RBL group needed to undergo excisional hemorrhoidectomy to resolve persistent bleeding or prolapse, whereas none of the PPH patients required further intervention (P<.05).
The earliest randomized controlled clinical trials directly comparing PPH with conventional hemorrhoidectomy reported excellent results21,22; however, patient numbers were small, and, of course, no long-term data were available. Now, reports are in from larger trials and studies with longer-term follow-up.
Shalaby and Desoky conducted a trial in which 200 patients were randomized to either Milligan-Morgan hemorrhoidectomy or PPH. Compared with hemorrhoidectomy, PPH required less operating time (9.0 vs 19.7 minutes, P<.001) and a shorter hospital stay (1.1 vs 2.2 days, P<.001), and provided a faster return to full activity (8.2 vs 53.9 days, P<.001).23 In addition, pain scores were significantly lower in the stapled group after the first 24 hours, at the time of first bowel movement, and at 1 week postoperatively (TABLE 1).
In a 100-patient, prospective, randomized trial, Ganio and colleagues compared PPH with open hemorrhoidectomy and found PPH to be as effective as conventional surgery.24 Postoperative bleeding occurred in 3 patients in each group. However, reduced postoperative pain, a shorter hospital stay, and a trend toward a quicker return to work were reported for the group of patients who underwent PPH. Moderate pain for hemorrhoidectomy patients occurred for a median of 5.3 days (range, 0–19 days) compared with only 3.1 days (range, 0–10 days) in the PPH group. Hemorrhoidectomy patients complained of severe pain for 2.3 days (range, 0–24 days), whereas the PPH patients had only 1 day (range, 0–14 days) of severe pain (P=.01). Functionally, the investigators found no difference between the 2 groups with respect to postoperative fecal incontinence. But, at 1 month, patients in the hemorrhoidectomy group were significantly less continent to flatus.25 The patients who underwent PPH also showed a statistically significant improvement in constipation scores, unlike the group who underwent conventional surgery.
In another study, Palimento and colleagues used several methods to evaluate postoperative pain in a group of 74 patients randomized either to PPH or open hemorrhoidectomy.26 Patients were encouraged to ask freely for pain relief, and the amounts of analgesic consumed were recorded. A visual analogue scale (VAS) from 0 (no pain) to 10 (worst pain imaginable) was completed by each patient at 4 and 24 hours following surgery. The researchers also requested a VAS score to evaluate pain at first defecation. In addition, patients were asked to record when they were able to have completely pain-free bowel movements and when there was pain-free return to normal activities and work. Analgesia requirements were similar between the 2 groups. Median VAS scores in the PPH group were significantly lower than in the open-hemorrhoidectomy group at 4 and 24 hours postoperatively and after first defecation (TABLE 2).
No statistically significant difference between the groups was found for incidence of postoperative bleeding. Nor did the groups differ regarding return to normal activities or return to work. However, the investigators noted that many factors affect the latter 2 outcome measures, including a patient’s motivation and his/her insurance coverage for disability, making comparisons somewhat unreliable. Hence, time to resumption of pain-free defecation was evaluated as a more objective measure and was found to be significantly less in the stapled group (10 vs 12 days, P=.001). At long-term follow-up (median, 17.5 months; range, 10–27 months), occasional pain was reported by 6 (16.2%) of the 37 patients in the PPH group and by 7 (18.9%) of the 37 patients in the open-hemorrhoidectomy group (P=1.000).
Racalbuto and colleagues performed a long-term randomized trial comparing results for 50 patients who underwent PPH with another 50 who underwent Milligan-Morgan hemorrhoidectomy.27 Patients were followed over a period of 48 months. Once again, patients who underwent PPH experienced significantly less pain and therefore were able to return to activities much more quickly than those who underwent conventional hemorrhoidectomy (8.04 ± 1.37 days vs 16.9 ± 2.50 days, P<.0001). In the long-term follow-up evaluation, none of the patients in either treatment group experienced stenosis. In addition, when comparing the 2 groups with respect to anal incontinence and recurrence of prolapse, the investigators did not find any significant differences.
TABLE 1
Mean Pain Scores for PPH vs Milligan-Morgan Hemorrhoidectomy
| PPH Mean (SD) | Milligan-Morgan Mean (SD) | P Value | |
|---|---|---|---|
| First 24 hours | 2.5 (1.3) | 7.6 (0.7) | <.001 |
| First bowel movement | 1.1 (0.3) | 6.6 (1.2) | <.001 |
| 1 week after operation | 0.4 (0.7) | 2.6 (0.6) | <.001 |
| PPH = procedure for prolapse and hemorrhoids; SD = standard deviation. | |||
| Adapted from Shalaby and Desoky.23 | |||
TABLE 2
Median Pain Scores for PPH vs Open Hemorrhoidectomy
| PPH Median (range) | Open Hemorrhoidectomy Median (range) | P Value | |
|---|---|---|---|
| 4 hours after operation | 4 (2–6) | 5 (2–8) | .001 |
| 24 hours after operation | 3 (1–6) | 5 (3–7) | .000 |
| First defecation | 5 (3–8) | 7 (3–9) | .000 |
| PPH = procedure for prolapse and hemorrhoids. | |||
| Data from Palimento et al.26 | |||
Contraindications to PPH
Contraindications to PPH include anal stenosis, that is, an anal canal that does not allow the stapler to be inserted. The PPH procedure also should be avoided in patients with an anorectal abscess, a complex fistula in ano, and perianal Crohn’s disease. As with any other type of surgery, patients undergoing anticoagulation therapy must be carefully evaluated.
Conclusion
The stapling technique is the newest treatment option for grades III and IV hemorrhoids. Although more randomized trials are needed, it appears from the research thus far that PPH is effective, with the potential to involve less pain and a shorter recovery time than conventional hemorrhoidectomy.
Disclosures
Dr Parker serves as a consultant to Ethicon Endo-Surgery. This supplement is supported by a grant from Ethicon Endo-Surgery.
Although effective for grades III and IV hemorrhoids, conventional hemorrhoidectomy is known to entail a significant recovery period and postoperative pain (strength of recommendation [SOR]: B).
The newest treatment option for grades III and IV hemorrhoids, the procedure for prolapse and hemorrhoids, is an effective technique with the potential to incur less pain and a quicker return to work and daily activities (SOR: B).
For patients with severe hemorrhoidal symptoms who do not want, or are unable, to undergo any type of surgical procedure, rubber band ligation is a viable option (SOR: B).
Hemorrhoids represent one of the most common colorectal complaints heard by family physicians. Each year approximately 10.5 million Americans experience hemorrhoidal symptoms; one fourth of those patients consult a physician.1
The most common symptom of internal hemorrhoids is bright red blood that covers the stool or appears on toilet paper or in the toilet bowl. Other symptoms include irritation of the skin around the anus; pain, swelling, or a hard lump around the anus; hemorrhoidal protrusion; and mucous discharge. Excessive rubbing or cleaning around the anus may exacerbate symptoms and even cause a vicious cycle of irritation, bleeding, and itching termed pruritus ani. Hemorrhoids also may thrombose, causing severe pain.
More than half of men and women aged 50 years and older will develop hemorrhoidal symptoms throughout their lifetime.2 Hemorrhoidal symptoms also tend to flare up during pregnancy, when hormonal changes and the pressure of the fetus cause the hemorrhoidal vessels to enlarge.
The likelihood of hemorrhoidal disease increases with age. By age 30, the anal support structure diminishes in function.3 This microscopic evidence, along with increased sphincter tone, may contribute to the progression of hemorrhoids.4
Although hemorrhoidal symptoms may subside after several days, they most often return, causing long-lasting discomfort and pain. Many affected persons—particularly those with severe hemorrhoids—suffer in silence for years before seeking treatment.5 Fortunately, only about 10% of patients have symptoms severe enough to require surgery.6
Differential diagnosis
Many anorectal problems, including fissures, fistulae, abscesses, or irritation and itching, have symptoms similar to those of hemorrhoids and must be ruled out prior to recommending appropriate treatment. In addition, the correlation of rectal bleeding with colorectal cancer becomes stronger with age, as demonstrated in a retrospective study of the diagnostic value of rectal bleeding in relation to a subsequent diagnosis of colorectal cancer.7 Therefore, further evaluation with colonoscopy should be made in patients who are older than 50 years of age, have a family history of colon cancer, and experience fatigue or weight loss or have a palpable mass.8
Classification of hemorrhoids
External hemorrhoids originate below the dentate line (FIGURE 1). Internal hemorrhoids are above the line and are classified according to their degree of prolapse:
- Grade I hemorrhoids protrude into the lumen of the anal canal but do not prolapse.
- Grade II hemorrhoids protrude with a bowel movement but spontaneously return when straining stops.
- Grade III hemorrhoids protrude either spontaneously or with a bowel movement, and can be manually reduced.
- Grade IV hemorrhoids have an irreducible prolapse.
This article focuses on a new treatment option for grades III and IV.
FIGURE 1 Mucosal Prolapse and Hemorrhoids
Methods of treating grades III and IV hemorrhoids
Until recently, the recommended treatments for grades III and IV hemorrhoids were limited to rubber band ligation (RBL) and conventional hemorrhoidectomy.
An office procedure not requiring anesthesia, RBL is the use of a latex band to cut off blood flow to the symptomatic hemorrhoid. The procedure is not without complications; there have been several reports of fatal and nonfatal retroperitoneal sepsis after RBL.9,10
Most conventional hemorrhoidectomies are performed in 1 of 2 ways. Outside the United States, the Milligan-Morgan technique, which excises the 3 major hemorrhoidal vessels, is considered the gold standard hemorrhoidectomy. Developed in 1937 in the United Kingdom, the surgery is also known as “open” hemorrhoidectomy because the incisions, which are separated by bridges of skin and mucosa, are left open to avoid stenosis. The Ferguson technique, developed in the United States in 1952, differs from the Milligan-Morgan procedure in that the incisions are sutured shut. Accordingly, it is commonly known as “closed” hemorrhoidectomy.
Regardless of technique, conventional hemorrhoidectomy is known to involve significant postoperative pain and an extended recovery time that precludes a fast return to work and daily activities.
A new stapling technique, the procedure for prolapse and hemorrhoids (PPH), was introduced in the mid-1990s and has been used extensively since then. Also known as stapled hemorrhoidopexy, stapled hemorrhoidectomy, or Longo stapled circumferential mucosectomy, PPH involves the use of a specially designed circular stapler that is inserted through the anus (FIGURE 2). The procedure reduces the prolapse of hemorrhoidal tissue by excising a band of the prolapsed rectal mucosa/internal hemorrhoid. The remaining hemorrhoidal tissue is drawn back into the correct anatomic position within the anal canal.
The stapling technique markedly reduces swelling by disrupting the hemorrhoidal artery blood flow, thereby reducing inflow to the hemorrhoids themselves. In addition, restoring the internal hemorrhoids to their normal anatomic position prevents prolapse and alleviates patients’ symptoms.11 The staples are placed well above the dentate line, and the majority of PPH is performed where there are autonomic nerve fibers, as opposed to somatic innervation. Thus, patients who undergo PPH tend to experience less postoperative pain than do those who undergo conventional hemorrhoidectomy, which involves the cutting of innervated perianal skin. Notably, the function and morphology of the internal anal sphincter, which have a direct bearing on anal continence, are not typically affected by PPH.12 Moreover, in patients with preoperative sensory impairment, the procedure improves anal-canal sensitivity—that is, the ability to distinguish between air and warm water in the anal canal.12 In contrast, research has shown that only about half of the patients who undergo conventional hemorrhoidectomy are able to detect water in the anal canal after surgery, and an additional 25% lose this ability within 6 months of the operation.13 Loss of anal-canal sensitivity affects internal-anal-sphincter function and morphology, which in turn affects anal continence.
Since 2000, several studies have been published confirming that PPH is associated with a low rate of compli-cations.14-16 Rare instances of sepsis following PPH have been reported. Some clinicians recommend administration of prophylactic antibiotics prior to the procedure. Guy and Seow-Choen suggest that the potential for sepsis is high only in cases where an excess amount of muscle is incorporated into the stapler housing. Thus, in recent years, the surgical technique has been refined so as to reduce the potential for postoperative infection.17,18
Randomized controlled trials
PPH versus other methods
Many individuals with extensive hemorrhoidal prolapse may not want to undergo, or will not be candidates for, any type of surgical intervention. For such patients, RBL is a viable option. Indeed, a number of studies endorse RBL as a first-line option for grade III hemorrhoids. However, one should note that RBL carries a high potential for symptomatic recurrence, which often results in the need for multiple bandings.19,20
Peng and colleagues conducted a study in which 55 patients with grade III or small grade IV hemorrhoids were randomized to either RBL or PPH.19 There was a higher incidence of pain at discharge and at 2-week follow-up in the PPH group (P<.001). Six patients in the PPH group experienced procedure-related complications, as opposed to none in the RBL group (P=.027). Despite these results, the authors recommended PPH for patients who did not want to run the risk of requiring further interventions. Notably, the group that underwent RBL had a significantly higher incidence of recurrent bleeding at 2 weeks’ follow-up (68% vs 27%, P=.002). More important, 5 patients in the RBL group needed to undergo excisional hemorrhoidectomy to resolve persistent bleeding or prolapse, whereas none of the PPH patients required further intervention (P<.05).
The earliest randomized controlled clinical trials directly comparing PPH with conventional hemorrhoidectomy reported excellent results21,22; however, patient numbers were small, and, of course, no long-term data were available. Now, reports are in from larger trials and studies with longer-term follow-up.
Shalaby and Desoky conducted a trial in which 200 patients were randomized to either Milligan-Morgan hemorrhoidectomy or PPH. Compared with hemorrhoidectomy, PPH required less operating time (9.0 vs 19.7 minutes, P<.001) and a shorter hospital stay (1.1 vs 2.2 days, P<.001), and provided a faster return to full activity (8.2 vs 53.9 days, P<.001).23 In addition, pain scores were significantly lower in the stapled group after the first 24 hours, at the time of first bowel movement, and at 1 week postoperatively (TABLE 1).
In a 100-patient, prospective, randomized trial, Ganio and colleagues compared PPH with open hemorrhoidectomy and found PPH to be as effective as conventional surgery.24 Postoperative bleeding occurred in 3 patients in each group. However, reduced postoperative pain, a shorter hospital stay, and a trend toward a quicker return to work were reported for the group of patients who underwent PPH. Moderate pain for hemorrhoidectomy patients occurred for a median of 5.3 days (range, 0–19 days) compared with only 3.1 days (range, 0–10 days) in the PPH group. Hemorrhoidectomy patients complained of severe pain for 2.3 days (range, 0–24 days), whereas the PPH patients had only 1 day (range, 0–14 days) of severe pain (P=.01). Functionally, the investigators found no difference between the 2 groups with respect to postoperative fecal incontinence. But, at 1 month, patients in the hemorrhoidectomy group were significantly less continent to flatus.25 The patients who underwent PPH also showed a statistically significant improvement in constipation scores, unlike the group who underwent conventional surgery.
In another study, Palimento and colleagues used several methods to evaluate postoperative pain in a group of 74 patients randomized either to PPH or open hemorrhoidectomy.26 Patients were encouraged to ask freely for pain relief, and the amounts of analgesic consumed were recorded. A visual analogue scale (VAS) from 0 (no pain) to 10 (worst pain imaginable) was completed by each patient at 4 and 24 hours following surgery. The researchers also requested a VAS score to evaluate pain at first defecation. In addition, patients were asked to record when they were able to have completely pain-free bowel movements and when there was pain-free return to normal activities and work. Analgesia requirements were similar between the 2 groups. Median VAS scores in the PPH group were significantly lower than in the open-hemorrhoidectomy group at 4 and 24 hours postoperatively and after first defecation (TABLE 2).
No statistically significant difference between the groups was found for incidence of postoperative bleeding. Nor did the groups differ regarding return to normal activities or return to work. However, the investigators noted that many factors affect the latter 2 outcome measures, including a patient’s motivation and his/her insurance coverage for disability, making comparisons somewhat unreliable. Hence, time to resumption of pain-free defecation was evaluated as a more objective measure and was found to be significantly less in the stapled group (10 vs 12 days, P=.001). At long-term follow-up (median, 17.5 months; range, 10–27 months), occasional pain was reported by 6 (16.2%) of the 37 patients in the PPH group and by 7 (18.9%) of the 37 patients in the open-hemorrhoidectomy group (P=1.000).
Racalbuto and colleagues performed a long-term randomized trial comparing results for 50 patients who underwent PPH with another 50 who underwent Milligan-Morgan hemorrhoidectomy.27 Patients were followed over a period of 48 months. Once again, patients who underwent PPH experienced significantly less pain and therefore were able to return to activities much more quickly than those who underwent conventional hemorrhoidectomy (8.04 ± 1.37 days vs 16.9 ± 2.50 days, P<.0001). In the long-term follow-up evaluation, none of the patients in either treatment group experienced stenosis. In addition, when comparing the 2 groups with respect to anal incontinence and recurrence of prolapse, the investigators did not find any significant differences.
TABLE 1
Mean Pain Scores for PPH vs Milligan-Morgan Hemorrhoidectomy
| PPH Mean (SD) | Milligan-Morgan Mean (SD) | P Value | |
|---|---|---|---|
| First 24 hours | 2.5 (1.3) | 7.6 (0.7) | <.001 |
| First bowel movement | 1.1 (0.3) | 6.6 (1.2) | <.001 |
| 1 week after operation | 0.4 (0.7) | 2.6 (0.6) | <.001 |
| PPH = procedure for prolapse and hemorrhoids; SD = standard deviation. | |||
| Adapted from Shalaby and Desoky.23 | |||
TABLE 2
Median Pain Scores for PPH vs Open Hemorrhoidectomy
| PPH Median (range) | Open Hemorrhoidectomy Median (range) | P Value | |
|---|---|---|---|
| 4 hours after operation | 4 (2–6) | 5 (2–8) | .001 |
| 24 hours after operation | 3 (1–6) | 5 (3–7) | .000 |
| First defecation | 5 (3–8) | 7 (3–9) | .000 |
| PPH = procedure for prolapse and hemorrhoids. | |||
| Data from Palimento et al.26 | |||
Contraindications to PPH
Contraindications to PPH include anal stenosis, that is, an anal canal that does not allow the stapler to be inserted. The PPH procedure also should be avoided in patients with an anorectal abscess, a complex fistula in ano, and perianal Crohn’s disease. As with any other type of surgery, patients undergoing anticoagulation therapy must be carefully evaluated.
Conclusion
The stapling technique is the newest treatment option for grades III and IV hemorrhoids. Although more randomized trials are needed, it appears from the research thus far that PPH is effective, with the potential to involve less pain and a shorter recovery time than conventional hemorrhoidectomy.
Disclosures
Dr Parker serves as a consultant to Ethicon Endo-Surgery. This supplement is supported by a grant from Ethicon Endo-Surgery.
1. Helton WS. for The SSAT, AGA, ASGE Consensus Panel 2001 consensus statement on benign anorectal disease. J Gastrointestinal Surg. 2002;6:302-303.
2. Bailey HR. Innovations for age-old problem: hemorrhoids in the female patient. Female Patient. 2004;29:17-23.
3. Haas PA, Fox TA, Jr, Haas GP. The pathogenesis of hemorrhoids. Dis Colon Rectum. 1984;27:442-450.
4. Hancock BD. Internal sphincter and the nature of haemorrhoids. Gut. 1977;18:651-655.
5. Pfenninger J, Zainea G. Common anorectal conditions: Part I. Symptoms and complaints. Am Fam Physician. 2001;63:2391-2398.
6. Bleday R, Pena JP, Rothenberger DA, et al. Symptomatic hemorrhoids: current incidence and complications of operative therapy. Dis Colon Rectum. 1992;35:477-481.
7. Wauters H, Van Casteren V, Buntinx F. Rectal bleeding and colorectal cancer in general practice: diagnostic study. BMJ. 2000;321:998-999.
8. Smith RA, Cokkinides V, Eyre HJ. American Cancer Society guidelines for the early detection of cancer, 2004. CA Cancer J Clin. 2004;54:41-52.
9. Quevedo-Bonilla G, Farkas AM, Abcarian H, et al. Septic complications of haemorrhoidal banding. Arch Surg. 1988;123:650-651.
10. Scarpa FJ, Hillis W, Sabetta JR. Pelvic cellulitis: a life-threatening complication of hemorrhoidal banding. Surgery. 1988;103:383-385.
11. Hetzer FH, Demartines N, Handschin AE, Clavien PA. Stapled vs excision hemorrhoidectomy: long-term results of a prospective randomized trial. Arch Surg. 2002;137:337-340.
12. Altomare DF, Rinaldi M, Sallustio PL, et al. Long-term effects of stapled haemorrhoidectomy on internal anal function and sensitivity. Br J Surg. 2001;88:1487-1491.
13. Read MG, Read NW, Haynes WG, et al. A prospective study of the effect of haemorrhoidectomy on sphincter function and faecal continence. Br J Surg. 1982;69:396-398.
14. Singer MA, Cintron JR, Fleshman JW, et al. Early experience with stapled hemorrhoidectomy in the United States. Dis Colon Rectum. 2002;45:360-367.
15. Dixon MR, Stamos MJ, Grant SR, et al. Stapled hemorrhoidectomy: a review of our early experience. Am Surg. 2003;69:862-865.
16. Hoffman GH, Firoozmand E. Hemorrhoids—To staple or not to staple: that is the question. Surg Rounds. 2004;27:213-224.
17. Guy RJ, Seow-Choen F. Septic complications after treatment of haemorrhoids. Br J Surg. 2003;90:147-156.
18. Molloy RG, Kingsmore D. Life threatening pelvic sepsis after stapled haemorrhoidectomy [letter]. Lancet. 2000;355:810.-
19. Peng BC, Jayne DG, Ho YH. Randomized trial of rubber band ligation vs. stapled hemorrhoidectomy for prolapsed piles. Dis Colon Rectum. 2003;46:291-297.
20. Komborozos VA, Skrekas GJ, Pissiotis CA. Rubber band ligation of symptomatic internal hemorrhoids: results of 500 cases. Dig Surg. 2000;17:71-76.
21. Mehigan BJ, Monson JRT, Hartley JE. Stapling procedure for haemorrhoids versus Milligan-Morgan haemorrhoidectomy: randomized controlled trial. Lancet. 2000;355:782-785.
22. Rowsell M, Bello M, Hemingway DM. Circumferential mucosectomy (stapled haemorrhoidectomy) versus conventional haemorrhoidectomy: randomized controlled trial. Lancet. 2000;355:779-781.
23. Shalaby R, Desoky A. Randomized clinical trial of stapled versus Milligan-Morgan haemorrhoidectomy. Br J Surg. 2001;88:1049-1053.
24. Ganio E, Altomare DF, Gabrielli F, et al. Prospective randomized multicentre trial comparing stapled with open haemorrhoidectomy. Br J Surg. 2001;88:669-674.
25. Williams NS, Patel J, George BD, et al. Development of an electrically stimulated neoanal sphincter. Lancet. 1991;338:1166-1169.
26. Palimento D, Picchio M, Attanasio U, et al. Stapled and open hemorrhoidectomy: randomized controlled trial of early results. World J Surg. 2003;27:203-207.
27. Racalbuto A, Aliotta I, Corsaro G, et al. Hemorrhoidal stapler prolapsectomy vs. Milligan-Morgan hemorrhoidectomy: a long-term randomized trial. Int J Colorectal Dis. 2004;19:239-244.
1. Helton WS. for The SSAT, AGA, ASGE Consensus Panel 2001 consensus statement on benign anorectal disease. J Gastrointestinal Surg. 2002;6:302-303.
2. Bailey HR. Innovations for age-old problem: hemorrhoids in the female patient. Female Patient. 2004;29:17-23.
3. Haas PA, Fox TA, Jr, Haas GP. The pathogenesis of hemorrhoids. Dis Colon Rectum. 1984;27:442-450.
4. Hancock BD. Internal sphincter and the nature of haemorrhoids. Gut. 1977;18:651-655.
5. Pfenninger J, Zainea G. Common anorectal conditions: Part I. Symptoms and complaints. Am Fam Physician. 2001;63:2391-2398.
6. Bleday R, Pena JP, Rothenberger DA, et al. Symptomatic hemorrhoids: current incidence and complications of operative therapy. Dis Colon Rectum. 1992;35:477-481.
7. Wauters H, Van Casteren V, Buntinx F. Rectal bleeding and colorectal cancer in general practice: diagnostic study. BMJ. 2000;321:998-999.
8. Smith RA, Cokkinides V, Eyre HJ. American Cancer Society guidelines for the early detection of cancer, 2004. CA Cancer J Clin. 2004;54:41-52.
9. Quevedo-Bonilla G, Farkas AM, Abcarian H, et al. Septic complications of haemorrhoidal banding. Arch Surg. 1988;123:650-651.
10. Scarpa FJ, Hillis W, Sabetta JR. Pelvic cellulitis: a life-threatening complication of hemorrhoidal banding. Surgery. 1988;103:383-385.
11. Hetzer FH, Demartines N, Handschin AE, Clavien PA. Stapled vs excision hemorrhoidectomy: long-term results of a prospective randomized trial. Arch Surg. 2002;137:337-340.
12. Altomare DF, Rinaldi M, Sallustio PL, et al. Long-term effects of stapled haemorrhoidectomy on internal anal function and sensitivity. Br J Surg. 2001;88:1487-1491.
13. Read MG, Read NW, Haynes WG, et al. A prospective study of the effect of haemorrhoidectomy on sphincter function and faecal continence. Br J Surg. 1982;69:396-398.
14. Singer MA, Cintron JR, Fleshman JW, et al. Early experience with stapled hemorrhoidectomy in the United States. Dis Colon Rectum. 2002;45:360-367.
15. Dixon MR, Stamos MJ, Grant SR, et al. Stapled hemorrhoidectomy: a review of our early experience. Am Surg. 2003;69:862-865.
16. Hoffman GH, Firoozmand E. Hemorrhoids—To staple or not to staple: that is the question. Surg Rounds. 2004;27:213-224.
17. Guy RJ, Seow-Choen F. Septic complications after treatment of haemorrhoids. Br J Surg. 2003;90:147-156.
18. Molloy RG, Kingsmore D. Life threatening pelvic sepsis after stapled haemorrhoidectomy [letter]. Lancet. 2000;355:810.-
19. Peng BC, Jayne DG, Ho YH. Randomized trial of rubber band ligation vs. stapled hemorrhoidectomy for prolapsed piles. Dis Colon Rectum. 2003;46:291-297.
20. Komborozos VA, Skrekas GJ, Pissiotis CA. Rubber band ligation of symptomatic internal hemorrhoids: results of 500 cases. Dig Surg. 2000;17:71-76.
21. Mehigan BJ, Monson JRT, Hartley JE. Stapling procedure for haemorrhoids versus Milligan-Morgan haemorrhoidectomy: randomized controlled trial. Lancet. 2000;355:782-785.
22. Rowsell M, Bello M, Hemingway DM. Circumferential mucosectomy (stapled haemorrhoidectomy) versus conventional haemorrhoidectomy: randomized controlled trial. Lancet. 2000;355:779-781.
23. Shalaby R, Desoky A. Randomized clinical trial of stapled versus Milligan-Morgan haemorrhoidectomy. Br J Surg. 2001;88:1049-1053.
24. Ganio E, Altomare DF, Gabrielli F, et al. Prospective randomized multicentre trial comparing stapled with open haemorrhoidectomy. Br J Surg. 2001;88:669-674.
25. Williams NS, Patel J, George BD, et al. Development of an electrically stimulated neoanal sphincter. Lancet. 1991;338:1166-1169.
26. Palimento D, Picchio M, Attanasio U, et al. Stapled and open hemorrhoidectomy: randomized controlled trial of early results. World J Surg. 2003;27:203-207.
27. Racalbuto A, Aliotta I, Corsaro G, et al. Hemorrhoidal stapler prolapsectomy vs. Milligan-Morgan hemorrhoidectomy: a long-term randomized trial. Int J Colorectal Dis. 2004;19:239-244.