User login
Liver Transplant and HCV: The New Horizon
The question of when to treat liver transplant patients with chronic hepatitis C virus (HCV) infection is vital. HCV is the diagnosis most commonly leading to liver transplantation, and recurrence of HCV after transplant is nearly universal. An estimated 30% of HCV liver transplant recipients experience recurrence within five years of transplantation, resulting in death or loss of the allograft because of cirrhosis or graft failure.1 Thus, if we knew when and how to treat HCV in this population, we could envision a world in which liver transplants would not be required—and certainly one in which retransplant because of HCV would never be needed.
In planning to treat HCV-positive patients who need a liver transplant, the question arises: Do we treat them preoperatively, perioperatively, or postoperatively? And if we select postoperative treatment, do we wait until the graft shows HCV recurrence, or do we treat prophylactically—knowing that recurrence is likely?
Results from multiple small studies of interferon-free treatment of HCV, both prior to and following recurrence of HCV posttransplant, have been reported. The SOLAR trial, which used ribavirin plus sofosbuvir, demonstrated a sustained viral response (SVR) rate of 70%.2 The SOLAR-1 trial of ledipasvir/sofosbuvir (Harvoni®) plus ribavirin in patients with genotype 1 or 4 who were treated following posttransplant recurrence showed an average SVR rate of 96%.3 Duration of treatment varied, depending on genotype and presence of cirrhosis, and there was differing dosing and addition of ribavirin at multiple doses. A 10% mortality rate was reported, but deaths occurred mainly in patients with severe cirrhosis.
A small trial was also conducted of genotype 3 patients treated with ledipasvir/sofosbuvir, with or without ribavirin.4 The addition of ribavirin appeared to shorten treatment, but patients in both treatment groups had excellent rates of SVR. However, further study is needed before this combination of medications can be recommended and/or FDA approved. Full details are available at http://hcvguidelines.org.
Ombitasvir/paritaprevir/ ritonavir with dasabuvir (Viekira Pak™) plus ribavirin for 24 weeks was evaluated in patients with HCV recurrence following liver transplant.5 This group of patients had very minimal fibrosis and essentially normal liver function. In this study group, an SVR rate exceeding 95% was achieved.
Continue for data on treatment of patients >>
The data on treatment of patients who need a transplant or who experience HCV recurrence posttransplant are very encouraging. If the SVR rates are maintained over time, it may be possible to significantly decrease the requirement for retransplantation—or even transplant in the first place. As transplant is not without significant morbidity and mortality, especially in the recurrence group, avoiding it would allow patients to live longer and healthier lives. More work is needed to understand the optimal time to treat and the best and safest regimens. Numerous trials evaluating these important management questions are ongoing.6-9
In the not-too-distant future, the requirement for liver transplantation in patients with chronic HCV infection is likely to decrease substantially. A recent New England Journal of Medicine editorial discussing liver allocation concluded that transplant centers now treating significant numbers of patients with HCV cirrhosis may soon be idle.10
If only we could be so lucky ...
REFERENCES
1. Watt K, Veldt B, Charlton M. A practical guide to the management of HCV infection following liver transplantation. Am J Transplant. 2009;9(8):1707-1713.
2. Charlton M, Gane E, Manns MP, et al. Sofosbuvir and ribavirin for treatment of compensated recurrent hepatitis C virus infection after liver transplantation. Gastroenterology. 2015;148(1):108-117.
3. Reddy KR, Everson GT, Flamm SL, et al. Ledipasvir/sofosbuvir with ribavirin for the treatment of HCV in patients with post transplant recurrence: preliminary results of a prospective, multicenter study. Presented at: 65th Annual Meeting of the American Association for the Study of Liver Diseases; November 7-11, 2014; Boston, MA. Abstract 8.
4. Kohler JJ, Nettles JH, Amblard F, et al. Approaches to hepatitis C treatment and cure using NS5A inhibitors. Infect Drug Resist. 2014;7:41-56.
5. Curry MP, Forns X, Chung RT, et al. Sofosbuvir and ribavirin prevent recurrence of HCV infection after liver transplantation: an open-label study. Gastroenterology. 2015;148(1):100-107.
6. A Phase 2 open-label study in patients with recurrent genotype 1 hepatitis C post–orthotopic liver transplant to explore the safety and efficacy of simeprevir and sofosbuvir with and without ribavirin. https://clinicaltrials.gov/ct2/show/NCT02165189?term=%22olysio%22&rank=1. Accessed February 15, 2015.
7. Phase 2, open-label study to investigate the pharmacokinetics, efficacy, safety, and tolerability of the combination of simeprevir (TMC435), daclatasvir (BMS-790052) and ribavirin (RBV) in subjects with recurrent chronic hepatitis C genotype 1b infection after orthotopic liver transplantation. https://clinicaltrials.gov/ct2/show/NCT01938625?term=%22olysio%22&rank=4. Accessed February 15, 2015.
8. A Phase 3, multicenter, open-label, single-arm study to investigate the efficacy and safety of a 12-week regimen of simeprevir in combination with sofosbuvir in treatment-naïve or -experienced subjects with chronic genotype 4 hepatitis C virus infection. https://clinicaltrials.gov/ct2/show/NCT02250807?term=%22olysio%22&rank=7. Accessed February 15, 2015.
9. A Phase 2 open-label study in patients with recurrent genotype 1 hepatitis C post–orthotopic liver transplant to explore the safety and efficacy of simeprevir and sofosbuvir with and without ribavirin. https://clinicaltrials.gov/ct2/show/NCT02165189?term=%22sovaldi%22&rank=6. Accessed February 15, 2015.
10. Lamas D, Rosenbaum L. Very complicated math: reconfiguring organ allocation. N Engl J Med. 2014;371(26):2447-2450.
The question of when to treat liver transplant patients with chronic hepatitis C virus (HCV) infection is vital. HCV is the diagnosis most commonly leading to liver transplantation, and recurrence of HCV after transplant is nearly universal. An estimated 30% of HCV liver transplant recipients experience recurrence within five years of transplantation, resulting in death or loss of the allograft because of cirrhosis or graft failure.1 Thus, if we knew when and how to treat HCV in this population, we could envision a world in which liver transplants would not be required—and certainly one in which retransplant because of HCV would never be needed.
In planning to treat HCV-positive patients who need a liver transplant, the question arises: Do we treat them preoperatively, perioperatively, or postoperatively? And if we select postoperative treatment, do we wait until the graft shows HCV recurrence, or do we treat prophylactically—knowing that recurrence is likely?
Results from multiple small studies of interferon-free treatment of HCV, both prior to and following recurrence of HCV posttransplant, have been reported. The SOLAR trial, which used ribavirin plus sofosbuvir, demonstrated a sustained viral response (SVR) rate of 70%.2 The SOLAR-1 trial of ledipasvir/sofosbuvir (Harvoni®) plus ribavirin in patients with genotype 1 or 4 who were treated following posttransplant recurrence showed an average SVR rate of 96%.3 Duration of treatment varied, depending on genotype and presence of cirrhosis, and there was differing dosing and addition of ribavirin at multiple doses. A 10% mortality rate was reported, but deaths occurred mainly in patients with severe cirrhosis.
A small trial was also conducted of genotype 3 patients treated with ledipasvir/sofosbuvir, with or without ribavirin.4 The addition of ribavirin appeared to shorten treatment, but patients in both treatment groups had excellent rates of SVR. However, further study is needed before this combination of medications can be recommended and/or FDA approved. Full details are available at http://hcvguidelines.org.
Ombitasvir/paritaprevir/ ritonavir with dasabuvir (Viekira Pak™) plus ribavirin for 24 weeks was evaluated in patients with HCV recurrence following liver transplant.5 This group of patients had very minimal fibrosis and essentially normal liver function. In this study group, an SVR rate exceeding 95% was achieved.
Continue for data on treatment of patients >>
The data on treatment of patients who need a transplant or who experience HCV recurrence posttransplant are very encouraging. If the SVR rates are maintained over time, it may be possible to significantly decrease the requirement for retransplantation—or even transplant in the first place. As transplant is not without significant morbidity and mortality, especially in the recurrence group, avoiding it would allow patients to live longer and healthier lives. More work is needed to understand the optimal time to treat and the best and safest regimens. Numerous trials evaluating these important management questions are ongoing.6-9
In the not-too-distant future, the requirement for liver transplantation in patients with chronic HCV infection is likely to decrease substantially. A recent New England Journal of Medicine editorial discussing liver allocation concluded that transplant centers now treating significant numbers of patients with HCV cirrhosis may soon be idle.10
If only we could be so lucky ...
REFERENCES
1. Watt K, Veldt B, Charlton M. A practical guide to the management of HCV infection following liver transplantation. Am J Transplant. 2009;9(8):1707-1713.
2. Charlton M, Gane E, Manns MP, et al. Sofosbuvir and ribavirin for treatment of compensated recurrent hepatitis C virus infection after liver transplantation. Gastroenterology. 2015;148(1):108-117.
3. Reddy KR, Everson GT, Flamm SL, et al. Ledipasvir/sofosbuvir with ribavirin for the treatment of HCV in patients with post transplant recurrence: preliminary results of a prospective, multicenter study. Presented at: 65th Annual Meeting of the American Association for the Study of Liver Diseases; November 7-11, 2014; Boston, MA. Abstract 8.
4. Kohler JJ, Nettles JH, Amblard F, et al. Approaches to hepatitis C treatment and cure using NS5A inhibitors. Infect Drug Resist. 2014;7:41-56.
5. Curry MP, Forns X, Chung RT, et al. Sofosbuvir and ribavirin prevent recurrence of HCV infection after liver transplantation: an open-label study. Gastroenterology. 2015;148(1):100-107.
6. A Phase 2 open-label study in patients with recurrent genotype 1 hepatitis C post–orthotopic liver transplant to explore the safety and efficacy of simeprevir and sofosbuvir with and without ribavirin. https://clinicaltrials.gov/ct2/show/NCT02165189?term=%22olysio%22&rank=1. Accessed February 15, 2015.
7. Phase 2, open-label study to investigate the pharmacokinetics, efficacy, safety, and tolerability of the combination of simeprevir (TMC435), daclatasvir (BMS-790052) and ribavirin (RBV) in subjects with recurrent chronic hepatitis C genotype 1b infection after orthotopic liver transplantation. https://clinicaltrials.gov/ct2/show/NCT01938625?term=%22olysio%22&rank=4. Accessed February 15, 2015.
8. A Phase 3, multicenter, open-label, single-arm study to investigate the efficacy and safety of a 12-week regimen of simeprevir in combination with sofosbuvir in treatment-naïve or -experienced subjects with chronic genotype 4 hepatitis C virus infection. https://clinicaltrials.gov/ct2/show/NCT02250807?term=%22olysio%22&rank=7. Accessed February 15, 2015.
9. A Phase 2 open-label study in patients with recurrent genotype 1 hepatitis C post–orthotopic liver transplant to explore the safety and efficacy of simeprevir and sofosbuvir with and without ribavirin. https://clinicaltrials.gov/ct2/show/NCT02165189?term=%22sovaldi%22&rank=6. Accessed February 15, 2015.
10. Lamas D, Rosenbaum L. Very complicated math: reconfiguring organ allocation. N Engl J Med. 2014;371(26):2447-2450.
The question of when to treat liver transplant patients with chronic hepatitis C virus (HCV) infection is vital. HCV is the diagnosis most commonly leading to liver transplantation, and recurrence of HCV after transplant is nearly universal. An estimated 30% of HCV liver transplant recipients experience recurrence within five years of transplantation, resulting in death or loss of the allograft because of cirrhosis or graft failure.1 Thus, if we knew when and how to treat HCV in this population, we could envision a world in which liver transplants would not be required—and certainly one in which retransplant because of HCV would never be needed.
In planning to treat HCV-positive patients who need a liver transplant, the question arises: Do we treat them preoperatively, perioperatively, or postoperatively? And if we select postoperative treatment, do we wait until the graft shows HCV recurrence, or do we treat prophylactically—knowing that recurrence is likely?
Results from multiple small studies of interferon-free treatment of HCV, both prior to and following recurrence of HCV posttransplant, have been reported. The SOLAR trial, which used ribavirin plus sofosbuvir, demonstrated a sustained viral response (SVR) rate of 70%.2 The SOLAR-1 trial of ledipasvir/sofosbuvir (Harvoni®) plus ribavirin in patients with genotype 1 or 4 who were treated following posttransplant recurrence showed an average SVR rate of 96%.3 Duration of treatment varied, depending on genotype and presence of cirrhosis, and there was differing dosing and addition of ribavirin at multiple doses. A 10% mortality rate was reported, but deaths occurred mainly in patients with severe cirrhosis.
A small trial was also conducted of genotype 3 patients treated with ledipasvir/sofosbuvir, with or without ribavirin.4 The addition of ribavirin appeared to shorten treatment, but patients in both treatment groups had excellent rates of SVR. However, further study is needed before this combination of medications can be recommended and/or FDA approved. Full details are available at http://hcvguidelines.org.
Ombitasvir/paritaprevir/ ritonavir with dasabuvir (Viekira Pak™) plus ribavirin for 24 weeks was evaluated in patients with HCV recurrence following liver transplant.5 This group of patients had very minimal fibrosis and essentially normal liver function. In this study group, an SVR rate exceeding 95% was achieved.
Continue for data on treatment of patients >>
The data on treatment of patients who need a transplant or who experience HCV recurrence posttransplant are very encouraging. If the SVR rates are maintained over time, it may be possible to significantly decrease the requirement for retransplantation—or even transplant in the first place. As transplant is not without significant morbidity and mortality, especially in the recurrence group, avoiding it would allow patients to live longer and healthier lives. More work is needed to understand the optimal time to treat and the best and safest regimens. Numerous trials evaluating these important management questions are ongoing.6-9
In the not-too-distant future, the requirement for liver transplantation in patients with chronic HCV infection is likely to decrease substantially. A recent New England Journal of Medicine editorial discussing liver allocation concluded that transplant centers now treating significant numbers of patients with HCV cirrhosis may soon be idle.10
If only we could be so lucky ...
REFERENCES
1. Watt K, Veldt B, Charlton M. A practical guide to the management of HCV infection following liver transplantation. Am J Transplant. 2009;9(8):1707-1713.
2. Charlton M, Gane E, Manns MP, et al. Sofosbuvir and ribavirin for treatment of compensated recurrent hepatitis C virus infection after liver transplantation. Gastroenterology. 2015;148(1):108-117.
3. Reddy KR, Everson GT, Flamm SL, et al. Ledipasvir/sofosbuvir with ribavirin for the treatment of HCV in patients with post transplant recurrence: preliminary results of a prospective, multicenter study. Presented at: 65th Annual Meeting of the American Association for the Study of Liver Diseases; November 7-11, 2014; Boston, MA. Abstract 8.
4. Kohler JJ, Nettles JH, Amblard F, et al. Approaches to hepatitis C treatment and cure using NS5A inhibitors. Infect Drug Resist. 2014;7:41-56.
5. Curry MP, Forns X, Chung RT, et al. Sofosbuvir and ribavirin prevent recurrence of HCV infection after liver transplantation: an open-label study. Gastroenterology. 2015;148(1):100-107.
6. A Phase 2 open-label study in patients with recurrent genotype 1 hepatitis C post–orthotopic liver transplant to explore the safety and efficacy of simeprevir and sofosbuvir with and without ribavirin. https://clinicaltrials.gov/ct2/show/NCT02165189?term=%22olysio%22&rank=1. Accessed February 15, 2015.
7. Phase 2, open-label study to investigate the pharmacokinetics, efficacy, safety, and tolerability of the combination of simeprevir (TMC435), daclatasvir (BMS-790052) and ribavirin (RBV) in subjects with recurrent chronic hepatitis C genotype 1b infection after orthotopic liver transplantation. https://clinicaltrials.gov/ct2/show/NCT01938625?term=%22olysio%22&rank=4. Accessed February 15, 2015.
8. A Phase 3, multicenter, open-label, single-arm study to investigate the efficacy and safety of a 12-week regimen of simeprevir in combination with sofosbuvir in treatment-naïve or -experienced subjects with chronic genotype 4 hepatitis C virus infection. https://clinicaltrials.gov/ct2/show/NCT02250807?term=%22olysio%22&rank=7. Accessed February 15, 2015.
9. A Phase 2 open-label study in patients with recurrent genotype 1 hepatitis C post–orthotopic liver transplant to explore the safety and efficacy of simeprevir and sofosbuvir with and without ribavirin. https://clinicaltrials.gov/ct2/show/NCT02165189?term=%22sovaldi%22&rank=6. Accessed February 15, 2015.
10. Lamas D, Rosenbaum L. Very complicated math: reconfiguring organ allocation. N Engl J Med. 2014;371(26):2447-2450.
Identification and Management of Middle East Respiratory Syndrome
Human coronaviruses (CoVs) were first identified in the mid-1960s. Coronaviruses are a large family of viruses that cause a range of illnesses in humans, from the common cold to severe acute respiratory syndrome (SARS).1
In 2003, SARS caused one of the most devastating global epidemics known to the developed world. The important lesson learned from the SARS epidemic was that CoVs can cause severe and rapidly spreading infection. Since then, 2 human CoVs, HCoV-HKU1 and HCoV-NL63, have been identified as common causes of human respiratory tract infections.2,3 In September 2012, a novel CoV was recognized to cause a fatal human infection. This virus has become known as the Middle East respiratory syndrome CoV (MERS-CoV).4
Related: Health Care Use Among Iraq and Afghanistan Veterans With Infectious Diseases
Similar to SARS-CoV, MERS-CoV human infection has a high fatality rate and the ability to spread from person to person.5,6 Person-to-person transmission has resulted in secondary cases among close contacts, including health care providers (HCPs) who should, therefore, be cognizant of this infection. Federal HCPs in particular may be more likely to become involved in the care of patients with this disease, because many military personnel are returning from deployment in the Middle East.
History of MERS-CoV
MERS-CoV was first identified as an infectious disease in humans in Saudi Arabia. In June 2012, the index case was hospitalized with pneumonia and acute renal injury.7 Since then, MERS-CoV human infections and clusters of infection have been identified in multiple countries in the Arabian Peninsula (Table 1).8 There have also been cases of MERS-CoV infection in other countries involving travelers who had visited the Arabian Peninsula and, in some instances, after returning home, their close contacts (Table 1).8

On May 2, 2014, the first confirmed U.S. case was reported in Indiana in a HCP who had recently been to Saudi Arabia.9 A second case of a HCP traveling from Saudi Arabia was identified on May 13, 2014, in Orlando, Florida.9 As of June 11, 2014, 699 laboratory‐confirmed cases of MERS-CoV infection had been reported to the World Health Organization in 20 countries, resulting in 209 deaths. All cases to date have originated in 6 countries of the Arabian Peninsula.5,8
The Organism
Coronaviruses are enveloped RNA viruses named for the crownlike spikes on their surface. They are common viruses known to cause respiratory infections in humans.1 It is thought that most people are infected with these viruses during their lifetime. These viruses generally cause mild-to-moderate upper respiratory tract illnesses, otherwise known as the common cold. On occasion, CoVs can cause lower respiratory tract infections in elderly patients, neonates, and immune-compromised individuals.1
Related: Special Operations Training: An Atypical Presentation of Aspiration Pneumonia
Coronaviruses are also known to infect animals. Most known CoVs cause disease in only 1 animal species or, at most, in a small number of closely related species. However, SARS-CoV was noted to infect people and various animals, including monkeys, civets, raccoon dogs, cats, dogs, and rodents. The origin and natural reservoir of SARS-CoV was ultimately determined to be bats.10
Genetic sequencing has determined that the MERS-CoV is different from any other known human CoV. MERS-CoV is a beta-CoV and, like the SARS-CoV, is closely related to bat CoVs.11-15 The origin of the MERS-CoV is not known, but an animal reservoir is suspected. Because MERS-CoV is similar to SARS-CoV, bats are considered a possible animal reservoir. Dromedary camels may act as intermediate hosts by spreading the virus to humans.16-18 However, there is no consensus on the animal reservoir for MERS-CoV. It is also not known how the virus has spread from animals to humans.
Case Definition
In order to aid in the rapid recognition of MERS, the CDC has established case definitions.8
A patient under investigation is an individual with fever (> 38oC, > 100.4oF) and pneumonia or acute respiratory distress syndrome (ARDS); and either:
- history of travel from countries in or near the Arabian Peninsula within 14 days before the onset of symptoms; or
- close contact with a symptomatic traveler who developed fever and ARDS within 14 days after traveling from countries in or near the Arabian Peninsula; or
- is a member of a cluster of patients with severe acute respiratory illness of unknown etiology in which MERS-CoV is being evaluated, in consultation with state and local health departments.
A confirmed case is a patient with laboratory confirmation of MERS-CoV infection. A probable case is a patient under investigation with absent or inconclusive laboratory results for MERS-CoV infection who is a close contact of a laboratory- confirmed MERS-CoV case.
Transmission
MERS-CoV is thought to be of animal origin, but the mode of transmission from the animal reservoir is not known. It seems likely that some of the infections have occurred via intermittent zoonotic transmission, possibly by an environmental source.19 The presence of case clusters, however, suggests that human-to-human transmission also can occur. Human-to-human transmission has occurred in individuals living with an infected person and in HCPs caring for infected patients.20-24 The human-to-human transmission through close contact so far has been nonsustained.
It has been estimated that 75% of the reported cases are secondary, meaning that the patient acquired the MERS-CoV infection from another infected person. There is no evidence of sustained spread of MERS-CoV in community settings. The mode of human-to-human transmission has not been determined. Possible modes of transmission include droplet and contact transmission. The number of contacts infected by individuals with confirmed infections seems limited; the transmissibility, therefore, currently seems to be low.25,26 The results of a study of the transmissibility and epidemic potential for MERS-CoV suggest that it does not yet have pandemic potential.27
Bats may serve as a reservoir for MERS-CoV. However, because human contact with bats is uncommon, they are viewed as unlikely candidates for an immediate source of infection in most humans. It is possible that another animal or vector serves as an intermediate host. Camels have been proposed as a possible intermediate host, but this remains unproven. Interestingly, the MERS-CoV index patient had been caring for several ill camels in his herd; the camels had signs of respiratory illness, including nasal discharge.11,28 MERS-CoV sequences were subsequently isolated from a juvenile camel belonging to the index patient.
Symptoms
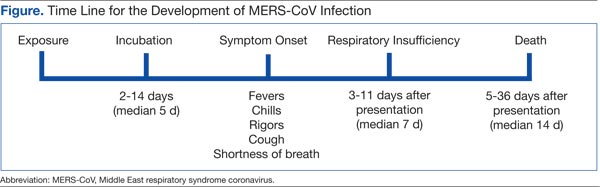
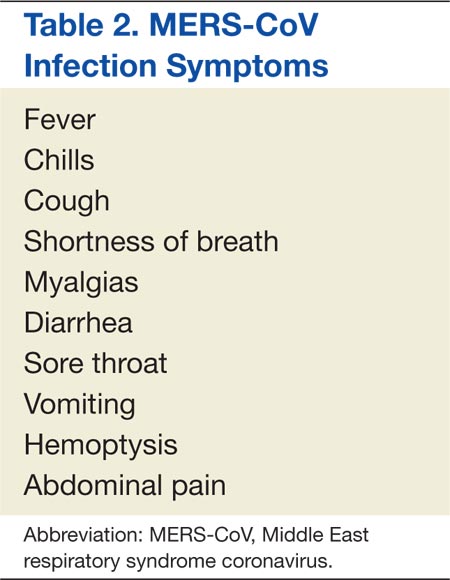
The incubation time after exposure to symptom onset ranges from 1.9 to 14.7 days (Figure). The median incubation period is 5.2 days.21 Patients are not believed to be contagious during the incubation period. Early symptoms of human infection with MERS-CoV include fever, chills or rigors, cough, and shortness of breath. Less frequently encountered symptoms include hemoptysis, sore throat, myalgias, diarrhea, vomiting, and abdominal pain (Table 2).20,21,23,26,27,29 Many patients infected with MERS-CoV develop a severe lower respiratory tract illness. The patient may progress to ARDS and require intubation and mechanical ventilator support. Mechanical ventilation has been required in 72% of patients.29 The median time from presentation for medical care to respiratory failure is 7 days, ranging from 3 to 11 days (Figure).
Physical Examination
The patients with MERS-CoV infection have been predominantly male and middle aged with an average age of 52 years. The clinical features depend on the severity of the illness. Some infected individuals have remained asymptomatic.27 Other patients have experienced mild lower respiratory illness and have not required hospitalization. However, about 40% of patients have experienced severe illness with pneumonia, respiratory insufficiency, multi-organ failure, and death. The percentage of severe illness is likely an overestimation, because patients with less severe symptoms probably are not tested for MERS-CoV. Most of the patients who have experienced a severe illness and/or death also had underlying comorbid conditions, such as diabetes mellitus, hypertension, chronic heart disease, and chronic renal disease.23,29
Laboratory Data
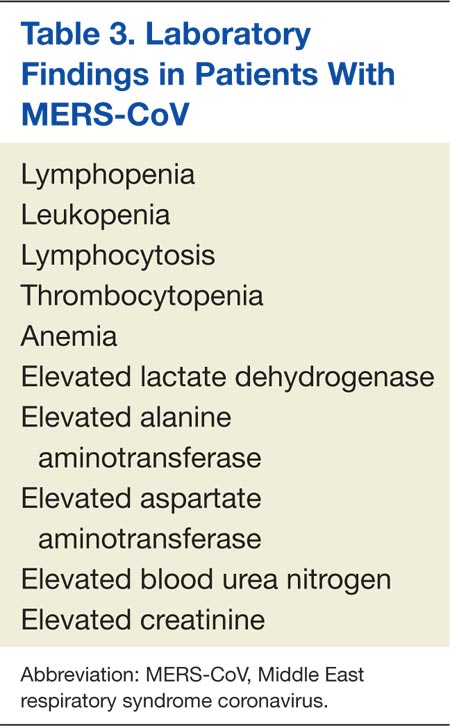
As with SARS-CoV, lymphopenia has been reported in patients infected with MERS-CoV.29 Other complete blood cell count abnormalities include leukopenia, lymphocytosis, thrombocytopenia, and anemia (Table 3).23,24,26,30 Blood chemistry profiles have identified elevated aspartate aminotransferase, alanine aminotransferase, and lactate dehydrogenase levels.29 Some patients have experienced progressive renal failure signaled by rising serum creatinine and blood urea nitrogen levels.11,23,24,26 Testing for disseminated intravascular coagulation and hemolysis has been positive in some patients.20,30 Oxyhemoglobin desaturation develops in patients with severe pneumonia.
Radiographic Imaging
Chest radiographs have been abnormal in the majority of patients with MERS-CoV. The radiographic findings may be minimal to extensive, depending on the severity of illness. The reported radiographic abnormalities include increased bronchovesicular markings, airspace opacities, patchy infiltrates, interstitial changes, confluent consolidations, nodular opacities, reticular infiltrate, pleural effusion, and total opacification of lung segments and lobes. These radiographic findings may be unilateral or bilateral.29
Specific Testing for MERS-CoV
The CDC recommends that lower respiratory tract specimens be collected for testing with real-time reverse-transcriptase polymerase chain reaction (rRT-PCR). The FDA has issued an emergency use authorization of the rRT-PCR assay developed by the CDC. The CDC recommends that multiple specimens from different sites in the lower respiratory system be collected at different times to increase the likelihood of detecting MERS-CoV. Acute and convalescent serum samples also should be obtained for serologic testing. Lower respiratory specimens (sputum, tracheal aspirates, and bronchoalveolar lavage fluid) are more sensitive than are upper respiratory tract samples (nasopharyngeal throat swabs and nasopharyngeal aspirates). Respiratory specimens should be collected as soon as possible after symptom onset. If negative testing is obtained from a patient with a high index of suspicion for MERS-CoV infection, then repeat testing should be performed.
Related: Another Reason Not to Smoke: Acute Eosinophilic Pneumonia
Several serology assays have been developed for the detection of MERS-CoV. An immunofluorescence assay should be confirmed with a neutralization test. In certain cases, the diagnosis should be confirmed by nucleic acid sequencing. The CDC has developed MERS-CoV testing kits, which have been provided to state health departments. Any case of suspected or proven MERS-CoV in the U.S. should be reported to the state and local health departments. Visit the CDC website for more information about collecting, handling, and testing clinical specimens from patients under investigation for MERS: http://www.cdc.gov/coronavirus/mers/guidelines -clinical-specimens.html.
Prognosis
Complications from the MERS- CoV infection include severe pneumonia and ARDS requiring mechanical ventilation, multi-organ failure, renal failure requiring dialysis, consumptive coagulopathy, and pericarditis.20,21,23,26,27,29 About 30% of people with MERS-CoV have died. SARS-CoV was the first CoV to cause severe lower respiratory disease and death in otherwise healthy humans; MERS-CoV is now the second.6 Death occurs a median of 14 days after presentation with a range of 5 to 36 days.20,21,23,26,27,29
Treatment
There is no available specific therapy recommended for MERS-CoV infection; therefore, the management of patients is supportive. As with other CoVs, there is no antiviral agent treatment for MERS-CoV. In experimental settings, combination therapy with interferon-alpha-2b and ribavirin seems promising.31 However, critically ill patients with MERS-CoV did not seem to respond favorably when treated with this regimen.32
Vaccine
There is no licensed vaccine for MERS-CoV, although experimental vaccines are being developed. Vaccines have successfully prevented CoV infection in animal models. The development of an effective vaccine for humans against MERS-CoV may, therefore, be a realistic possibility. Unfortunately, a vaccine is likely years away from approval.
Infection Control Measures
Careful attention to infection control precautions is critical to the containment of MERS-CoV. Patients should be encouraged to inform HCPs about symptoms and potential exposure risks, in particular travel to and/or exposure to travelers from the Arabian Peninsula. This practice should help to limit the transmission of MERS-CoV to HCPs. Standard contact and airborne precautions should be followed in patients with suspected or proven MERS-CoV infection.
Infection control measures should include hand hygiene; avoiding close contact with people who are sick; avoiding touching the eyes, nose, and/or mouth with unwashed hands; and disinfecting frequently touched surfaces. Patients with suspected or proven MERS-CoV should be admitted to single occupancy rooms to diminish the possibility of viral transmission to other patients. All persons entering the room of a patient with suspected or proven MERS-CoV should wear fitted N-95 filtering respirators. Until the mode of transmission is better defined, protective eyewear should be worn during all patient contacts. With implementation of these measures, there has been no institution that has experienced an outbreak of MERS-CoV infection. Unfortunately, the duration of viral shedding is not yet known.
Travel Restrictions
At this time the CDC has not recommended MERS-related travel restrictions. Because the spread of MERS-CoV has occurred in health care institutions, the CDC advises HCPs traveling to the Arabian Peninsula to follow recommendations for infection control of confirmed or suspected cases of MERS-CoV and to monitor their own health closely. Travelers who are going to the Arabian Peninsula for other reasons are advised to follow standard infection control precautions, such as hand washing and avoiding contact with ill people. Visit the CDC website for updated information of travel restrictions: http://www.cdc.gov/coronavirus/mers/travel.html.
Author disclosures
The authors report no actual or potential conflicts of interest with regard to this article.
Disclaimer
The opinions expressed herein are those of the authors and do not necessarily reflect those of Federal Practitioner, Frontline Medical Communications Inc., the U.S. Government, or any of its agencies. This article may discuss unlabeled or investigational use of certain drugs. Please review complete prescribing information for specific drugs or drug combinations—including indications, contraindications, warnings, and adverse effects—before administering pharmacologic therapy to patients.
1. To KK, Hung IF, Chan JF, Yuen KY. From SARS coronavirus to novel animal and human coronaviruses. J Thorac Dis. 2013;5(suppl 2):S103-S108.
2. Woo PC, Lau SK, Chu CM, et al. Characteristics and complete genome sequence of a novel coronavirus, coronavirus HKU1, from patients with pneumonia. J Virol. 2005;79(2):884-895.
3. van der Hoek L, Pyrc K, Jebbink MF, et al. Identification of a new human coronavirus. Nat Med. 2004;10(4):368-373.
4. de Groot RJ, Baker SC, Baric RS, et al. Middle East respiratory syndrome coronavirus (MERS-CoV): Announcement of the Coronavirus Study Group. J Virol. 2013;87(14):7790-7792.
5. World Health Organization. Middle East respiratory syndrome coronavirus (MERS-CoV) summary and literature update–as of 11 June 2014. http://www.who.int/csr/disease/coronavirus_infections/MERS-CoV_summary_update_20140611.pdf. Accessed February 3, 2015.
6. Byrd RP Jr, Roy TM. Severe acute respiratory syndrome. Fed Pract. 2003;20(9):62-71.
7. International Society for Infectious Diseases. Novel coronavirus–Saudi Arabia: Human isolate; Archive number: 20120920.1302733. ProMED-mail Website. http://www.promedmail.org/direct .php?id=20120920.1302733. Published September 20, 2012. Accessed January 23, 2015.
8. Centers for Disease Control and Prevention. Middle East respiratory syndrome (MERS). Centers for Disease Control and Prevention Website. http://www.cdc.gov/coronavirus/mers. Updated July 31, 2014. Accessed January 23, 2015.
9. Centers for Disease Control and Prevention. MERS in the U.S. Centers for Disease Control and Prevention Website. http://www.cdc.gov/coronavirus/mers/US.html. Updated December 9, 2014. Accessed January 23, 2015.
10. Lau SK, Li KS, Huang Y, et al. Ecoepidemiology and complete genome comparison of different strains of severe acute respiratory syndrome-related Rhinolophus bat coronavirus in China reveal bats as a reservoir for acute, self-limiting infection that allows recombination events. J Virol. 2010;84(6): 2808-2819.
11. Zaki AM, van Boheemen S, Bestebroer TM, Osterhaus AD, Fouchier RA. Isolation of a novel coronavirus from a man with pneumonia in Saudi Arabia. N Engl J Med. 2012;367(19):1814-1820.
12. Cotten M, Lam TT, Watson SJ, et al. Full-genome deep sequencing and phylogenetic analysis of novel human betacoronavirus. Emerg Infect Dis. 2013;19(5):736-742B.
13. Annan A, Baldwin HJ, Corman VM, et al. Human betacoronavirus 2c EMC/2012-related viruses in bats, Ghana and Europe. Emerg Infect Dis. 2013;19(3):456-459.
14. Ithete NL, Stoffberg S, Corman VM, et al. Close relative of human Middle East respiratory syndrome coronavirus in bat, South Africa. Emerg Infect Dis. 2013;19(10):1697-1699.
15. Memish ZA, Mishra N, Olival KJ, et al. Middle East respiratory syndrome coronavirus in bats, Saudi Arabia. Emerg Infect Dis. 2013;19(11):1819-1823.
16. Chu DK, Poon LL, Gomaa MM, et al. MERS coronavirus in dromedary camels, Egypt. Emerg Infect Dis. 2014;20(6):1049-1053.
17. Reusken CB, Haagmans BL, Müller MA, et al. Middle East respiratory syndrome coronavirus neutralising serum antibodies in dromedary camels: A comparative serological study. Lancet Infect Dis. 2013;13(10):859-866.
18. Haagmans BL, Al Dhahiry SH, Reusken CB, et al. Middle East respiratory syndrome coronavirus in dromedary camels: An outbreak investigation. Lancet Infect Dis. 2014;14(2):140-145.
19. Abdel-Moneim AS. Middle East respiratory syndrome coronavirus (MERS-CoV): Evidence and speculations. Arch Virol. 2014;159(7):1575-1584.
20. World Health Organization. Global Alert and Response. MERS-CoV summary and literature update—as of 31 May 2013. http://www.who.int/csr/disease/coronavirus_infections/update_20130531 /en. Accessed January 23, 2015.
21. Assiri A, McGeer A, Perl TM, et al; KSA MERS-CoV Investigation Team. Hospital outbreak of Middle East respiratory syndrome coronavirus. N Engl J Med. 2013;369(5):407-416.
22. Gulland A. Two cases of novel coronavirus are confirmed in France. BMJ. 2013;346:f3114.
23. Guery B, Poissy J, el Mansouf L, et al; MERS-CoV study group. Clinical features and viral diagnosis of two cases of infection with Middle East Respiratory Syndrome coronavirus: A report of nosocomial transmission. Lancet. 2013;381(9885):2265-2272.
24. Memish ZA, Zumla AI, Al-Hakeem RF, Al-Rabeeah AA, Stephens GM. Family cluster of Middle East respiratory syndrome coronavirus infections. N Engl J Med. 2013;368(26):2487-2494.
25. Reuss A, Litterst A, Drosten C, et al. Contact investigation for imported case of Middle East respiratory syndrome, Germany. Emerg Infect Dis. 2014;20(4):620-625.
26. Arabi YM, Arifi AA, Balkhy HH, et al. Clinical course and outcomes of critically ill patients with Middle East respiratory syndrome coronavirus infection. Ann Intern Med. 2014;160(6):389-397.
27. Memish ZA, Zumla AI, Assiri A. Middle East respiratory syndrome coronavirus infections in health care workers. N Engl J Med. 2013;369(9):884-886.
28. Memish ZA, Cotten M, Meyer B, et al. Human infection with MERS coronavirus after exposure to infected camels, Saudi Arabia, 2013. Emerg Infect Dis. 2014;20(6):1012-1015.
29. Assiri A, Al-Tawfiq JA, Al-Rabeeah AA, et al. Epidemiological, demographic, and clinical characteristics of 47 cases of Middle East respiratory syndrome coronavirus disease from Saudi Arabia: A descriptive study. Lancet Infect Dis. 2013;13(9):752-761.
30. Drosten C, Seilmaier M, Corman VM, et al. Clinical features and virological analysis of a case of Middle East respiratory syndrome coronavirus infection. Lancet Infect Dis. 2013;13(9):745-751.
31. Falzarano D, de Wit E, Rasmussen AL, et al. Treatment with interferon-α2b and ribavirin improves outcome in MERS-CoV-infected rhesus macaques. Nat Med. 2013;19(10):1313-1317.
32. Al-Tawfiq JA, Momattin H, Dib J, Memish ZA. Ribavirin and interferon therapy in patients infected with the Middle East respiratory syndrome coronavirus: An observational study. Int J Infect Dis. 2014;20:42-46.
Human coronaviruses (CoVs) were first identified in the mid-1960s. Coronaviruses are a large family of viruses that cause a range of illnesses in humans, from the common cold to severe acute respiratory syndrome (SARS).1
In 2003, SARS caused one of the most devastating global epidemics known to the developed world. The important lesson learned from the SARS epidemic was that CoVs can cause severe and rapidly spreading infection. Since then, 2 human CoVs, HCoV-HKU1 and HCoV-NL63, have been identified as common causes of human respiratory tract infections.2,3 In September 2012, a novel CoV was recognized to cause a fatal human infection. This virus has become known as the Middle East respiratory syndrome CoV (MERS-CoV).4
Related: Health Care Use Among Iraq and Afghanistan Veterans With Infectious Diseases
Similar to SARS-CoV, MERS-CoV human infection has a high fatality rate and the ability to spread from person to person.5,6 Person-to-person transmission has resulted in secondary cases among close contacts, including health care providers (HCPs) who should, therefore, be cognizant of this infection. Federal HCPs in particular may be more likely to become involved in the care of patients with this disease, because many military personnel are returning from deployment in the Middle East.
History of MERS-CoV
MERS-CoV was first identified as an infectious disease in humans in Saudi Arabia. In June 2012, the index case was hospitalized with pneumonia and acute renal injury.7 Since then, MERS-CoV human infections and clusters of infection have been identified in multiple countries in the Arabian Peninsula (Table 1).8 There have also been cases of MERS-CoV infection in other countries involving travelers who had visited the Arabian Peninsula and, in some instances, after returning home, their close contacts (Table 1).8
On May 2, 2014, the first confirmed U.S. case was reported in Indiana in a HCP who had recently been to Saudi Arabia.9 A second case of a HCP traveling from Saudi Arabia was identified on May 13, 2014, in Orlando, Florida.9 As of June 11, 2014, 699 laboratory‐confirmed cases of MERS-CoV infection had been reported to the World Health Organization in 20 countries, resulting in 209 deaths. All cases to date have originated in 6 countries of the Arabian Peninsula.5,8
The Organism
Coronaviruses are enveloped RNA viruses named for the crownlike spikes on their surface. They are common viruses known to cause respiratory infections in humans.1 It is thought that most people are infected with these viruses during their lifetime. These viruses generally cause mild-to-moderate upper respiratory tract illnesses, otherwise known as the common cold. On occasion, CoVs can cause lower respiratory tract infections in elderly patients, neonates, and immune-compromised individuals.1
Related: Special Operations Training: An Atypical Presentation of Aspiration Pneumonia
Coronaviruses are also known to infect animals. Most known CoVs cause disease in only 1 animal species or, at most, in a small number of closely related species. However, SARS-CoV was noted to infect people and various animals, including monkeys, civets, raccoon dogs, cats, dogs, and rodents. The origin and natural reservoir of SARS-CoV was ultimately determined to be bats.10
Genetic sequencing has determined that the MERS-CoV is different from any other known human CoV. MERS-CoV is a beta-CoV and, like the SARS-CoV, is closely related to bat CoVs.11-15 The origin of the MERS-CoV is not known, but an animal reservoir is suspected. Because MERS-CoV is similar to SARS-CoV, bats are considered a possible animal reservoir. Dromedary camels may act as intermediate hosts by spreading the virus to humans.16-18 However, there is no consensus on the animal reservoir for MERS-CoV. It is also not known how the virus has spread from animals to humans.
Case Definition
In order to aid in the rapid recognition of MERS, the CDC has established case definitions.8
A patient under investigation is an individual with fever (> 38oC, > 100.4oF) and pneumonia or acute respiratory distress syndrome (ARDS); and either:
- history of travel from countries in or near the Arabian Peninsula within 14 days before the onset of symptoms; or
- close contact with a symptomatic traveler who developed fever and ARDS within 14 days after traveling from countries in or near the Arabian Peninsula; or
- is a member of a cluster of patients with severe acute respiratory illness of unknown etiology in which MERS-CoV is being evaluated, in consultation with state and local health departments.
A confirmed case is a patient with laboratory confirmation of MERS-CoV infection. A probable case is a patient under investigation with absent or inconclusive laboratory results for MERS-CoV infection who is a close contact of a laboratory- confirmed MERS-CoV case.
Transmission
MERS-CoV is thought to be of animal origin, but the mode of transmission from the animal reservoir is not known. It seems likely that some of the infections have occurred via intermittent zoonotic transmission, possibly by an environmental source.19 The presence of case clusters, however, suggests that human-to-human transmission also can occur. Human-to-human transmission has occurred in individuals living with an infected person and in HCPs caring for infected patients.20-24 The human-to-human transmission through close contact so far has been nonsustained.
It has been estimated that 75% of the reported cases are secondary, meaning that the patient acquired the MERS-CoV infection from another infected person. There is no evidence of sustained spread of MERS-CoV in community settings. The mode of human-to-human transmission has not been determined. Possible modes of transmission include droplet and contact transmission. The number of contacts infected by individuals with confirmed infections seems limited; the transmissibility, therefore, currently seems to be low.25,26 The results of a study of the transmissibility and epidemic potential for MERS-CoV suggest that it does not yet have pandemic potential.27
Bats may serve as a reservoir for MERS-CoV. However, because human contact with bats is uncommon, they are viewed as unlikely candidates for an immediate source of infection in most humans. It is possible that another animal or vector serves as an intermediate host. Camels have been proposed as a possible intermediate host, but this remains unproven. Interestingly, the MERS-CoV index patient had been caring for several ill camels in his herd; the camels had signs of respiratory illness, including nasal discharge.11,28 MERS-CoV sequences were subsequently isolated from a juvenile camel belonging to the index patient.
Symptoms
The incubation time after exposure to symptom onset ranges from 1.9 to 14.7 days (Figure). The median incubation period is 5.2 days.21 Patients are not believed to be contagious during the incubation period. Early symptoms of human infection with MERS-CoV include fever, chills or rigors, cough, and shortness of breath. Less frequently encountered symptoms include hemoptysis, sore throat, myalgias, diarrhea, vomiting, and abdominal pain (Table 2).20,21,23,26,27,29 Many patients infected with MERS-CoV develop a severe lower respiratory tract illness. The patient may progress to ARDS and require intubation and mechanical ventilator support. Mechanical ventilation has been required in 72% of patients.29 The median time from presentation for medical care to respiratory failure is 7 days, ranging from 3 to 11 days (Figure).
Physical Examination
The patients with MERS-CoV infection have been predominantly male and middle aged with an average age of 52 years. The clinical features depend on the severity of the illness. Some infected individuals have remained asymptomatic.27 Other patients have experienced mild lower respiratory illness and have not required hospitalization. However, about 40% of patients have experienced severe illness with pneumonia, respiratory insufficiency, multi-organ failure, and death. The percentage of severe illness is likely an overestimation, because patients with less severe symptoms probably are not tested for MERS-CoV. Most of the patients who have experienced a severe illness and/or death also had underlying comorbid conditions, such as diabetes mellitus, hypertension, chronic heart disease, and chronic renal disease.23,29
Laboratory Data
As with SARS-CoV, lymphopenia has been reported in patients infected with MERS-CoV.29 Other complete blood cell count abnormalities include leukopenia, lymphocytosis, thrombocytopenia, and anemia (Table 3).23,24,26,30 Blood chemistry profiles have identified elevated aspartate aminotransferase, alanine aminotransferase, and lactate dehydrogenase levels.29 Some patients have experienced progressive renal failure signaled by rising serum creatinine and blood urea nitrogen levels.11,23,24,26 Testing for disseminated intravascular coagulation and hemolysis has been positive in some patients.20,30 Oxyhemoglobin desaturation develops in patients with severe pneumonia.
Radiographic Imaging
Chest radiographs have been abnormal in the majority of patients with MERS-CoV. The radiographic findings may be minimal to extensive, depending on the severity of illness. The reported radiographic abnormalities include increased bronchovesicular markings, airspace opacities, patchy infiltrates, interstitial changes, confluent consolidations, nodular opacities, reticular infiltrate, pleural effusion, and total opacification of lung segments and lobes. These radiographic findings may be unilateral or bilateral.29
Specific Testing for MERS-CoV
The CDC recommends that lower respiratory tract specimens be collected for testing with real-time reverse-transcriptase polymerase chain reaction (rRT-PCR). The FDA has issued an emergency use authorization of the rRT-PCR assay developed by the CDC. The CDC recommends that multiple specimens from different sites in the lower respiratory system be collected at different times to increase the likelihood of detecting MERS-CoV. Acute and convalescent serum samples also should be obtained for serologic testing. Lower respiratory specimens (sputum, tracheal aspirates, and bronchoalveolar lavage fluid) are more sensitive than are upper respiratory tract samples (nasopharyngeal throat swabs and nasopharyngeal aspirates). Respiratory specimens should be collected as soon as possible after symptom onset. If negative testing is obtained from a patient with a high index of suspicion for MERS-CoV infection, then repeat testing should be performed.
Related: Another Reason Not to Smoke: Acute Eosinophilic Pneumonia
Several serology assays have been developed for the detection of MERS-CoV. An immunofluorescence assay should be confirmed with a neutralization test. In certain cases, the diagnosis should be confirmed by nucleic acid sequencing. The CDC has developed MERS-CoV testing kits, which have been provided to state health departments. Any case of suspected or proven MERS-CoV in the U.S. should be reported to the state and local health departments. Visit the CDC website for more information about collecting, handling, and testing clinical specimens from patients under investigation for MERS: http://www.cdc.gov/coronavirus/mers/guidelines -clinical-specimens.html.
Prognosis
Complications from the MERS- CoV infection include severe pneumonia and ARDS requiring mechanical ventilation, multi-organ failure, renal failure requiring dialysis, consumptive coagulopathy, and pericarditis.20,21,23,26,27,29 About 30% of people with MERS-CoV have died. SARS-CoV was the first CoV to cause severe lower respiratory disease and death in otherwise healthy humans; MERS-CoV is now the second.6 Death occurs a median of 14 days after presentation with a range of 5 to 36 days.20,21,23,26,27,29
Treatment
There is no available specific therapy recommended for MERS-CoV infection; therefore, the management of patients is supportive. As with other CoVs, there is no antiviral agent treatment for MERS-CoV. In experimental settings, combination therapy with interferon-alpha-2b and ribavirin seems promising.31 However, critically ill patients with MERS-CoV did not seem to respond favorably when treated with this regimen.32
Vaccine
There is no licensed vaccine for MERS-CoV, although experimental vaccines are being developed. Vaccines have successfully prevented CoV infection in animal models. The development of an effective vaccine for humans against MERS-CoV may, therefore, be a realistic possibility. Unfortunately, a vaccine is likely years away from approval.
Infection Control Measures
Careful attention to infection control precautions is critical to the containment of MERS-CoV. Patients should be encouraged to inform HCPs about symptoms and potential exposure risks, in particular travel to and/or exposure to travelers from the Arabian Peninsula. This practice should help to limit the transmission of MERS-CoV to HCPs. Standard contact and airborne precautions should be followed in patients with suspected or proven MERS-CoV infection.
Infection control measures should include hand hygiene; avoiding close contact with people who are sick; avoiding touching the eyes, nose, and/or mouth with unwashed hands; and disinfecting frequently touched surfaces. Patients with suspected or proven MERS-CoV should be admitted to single occupancy rooms to diminish the possibility of viral transmission to other patients. All persons entering the room of a patient with suspected or proven MERS-CoV should wear fitted N-95 filtering respirators. Until the mode of transmission is better defined, protective eyewear should be worn during all patient contacts. With implementation of these measures, there has been no institution that has experienced an outbreak of MERS-CoV infection. Unfortunately, the duration of viral shedding is not yet known.
Travel Restrictions
At this time the CDC has not recommended MERS-related travel restrictions. Because the spread of MERS-CoV has occurred in health care institutions, the CDC advises HCPs traveling to the Arabian Peninsula to follow recommendations for infection control of confirmed or suspected cases of MERS-CoV and to monitor their own health closely. Travelers who are going to the Arabian Peninsula for other reasons are advised to follow standard infection control precautions, such as hand washing and avoiding contact with ill people. Visit the CDC website for updated information of travel restrictions: http://www.cdc.gov/coronavirus/mers/travel.html.
Author disclosures
The authors report no actual or potential conflicts of interest with regard to this article.
Disclaimer
The opinions expressed herein are those of the authors and do not necessarily reflect those of Federal Practitioner, Frontline Medical Communications Inc., the U.S. Government, or any of its agencies. This article may discuss unlabeled or investigational use of certain drugs. Please review complete prescribing information for specific drugs or drug combinations—including indications, contraindications, warnings, and adverse effects—before administering pharmacologic therapy to patients.
Human coronaviruses (CoVs) were first identified in the mid-1960s. Coronaviruses are a large family of viruses that cause a range of illnesses in humans, from the common cold to severe acute respiratory syndrome (SARS).1
In 2003, SARS caused one of the most devastating global epidemics known to the developed world. The important lesson learned from the SARS epidemic was that CoVs can cause severe and rapidly spreading infection. Since then, 2 human CoVs, HCoV-HKU1 and HCoV-NL63, have been identified as common causes of human respiratory tract infections.2,3 In September 2012, a novel CoV was recognized to cause a fatal human infection. This virus has become known as the Middle East respiratory syndrome CoV (MERS-CoV).4
Related: Health Care Use Among Iraq and Afghanistan Veterans With Infectious Diseases
Similar to SARS-CoV, MERS-CoV human infection has a high fatality rate and the ability to spread from person to person.5,6 Person-to-person transmission has resulted in secondary cases among close contacts, including health care providers (HCPs) who should, therefore, be cognizant of this infection. Federal HCPs in particular may be more likely to become involved in the care of patients with this disease, because many military personnel are returning from deployment in the Middle East.
History of MERS-CoV
MERS-CoV was first identified as an infectious disease in humans in Saudi Arabia. In June 2012, the index case was hospitalized with pneumonia and acute renal injury.7 Since then, MERS-CoV human infections and clusters of infection have been identified in multiple countries in the Arabian Peninsula (Table 1).8 There have also been cases of MERS-CoV infection in other countries involving travelers who had visited the Arabian Peninsula and, in some instances, after returning home, their close contacts (Table 1).8
On May 2, 2014, the first confirmed U.S. case was reported in Indiana in a HCP who had recently been to Saudi Arabia.9 A second case of a HCP traveling from Saudi Arabia was identified on May 13, 2014, in Orlando, Florida.9 As of June 11, 2014, 699 laboratory‐confirmed cases of MERS-CoV infection had been reported to the World Health Organization in 20 countries, resulting in 209 deaths. All cases to date have originated in 6 countries of the Arabian Peninsula.5,8
The Organism
Coronaviruses are enveloped RNA viruses named for the crownlike spikes on their surface. They are common viruses known to cause respiratory infections in humans.1 It is thought that most people are infected with these viruses during their lifetime. These viruses generally cause mild-to-moderate upper respiratory tract illnesses, otherwise known as the common cold. On occasion, CoVs can cause lower respiratory tract infections in elderly patients, neonates, and immune-compromised individuals.1
Related: Special Operations Training: An Atypical Presentation of Aspiration Pneumonia
Coronaviruses are also known to infect animals. Most known CoVs cause disease in only 1 animal species or, at most, in a small number of closely related species. However, SARS-CoV was noted to infect people and various animals, including monkeys, civets, raccoon dogs, cats, dogs, and rodents. The origin and natural reservoir of SARS-CoV was ultimately determined to be bats.10
Genetic sequencing has determined that the MERS-CoV is different from any other known human CoV. MERS-CoV is a beta-CoV and, like the SARS-CoV, is closely related to bat CoVs.11-15 The origin of the MERS-CoV is not known, but an animal reservoir is suspected. Because MERS-CoV is similar to SARS-CoV, bats are considered a possible animal reservoir. Dromedary camels may act as intermediate hosts by spreading the virus to humans.16-18 However, there is no consensus on the animal reservoir for MERS-CoV. It is also not known how the virus has spread from animals to humans.
Case Definition
In order to aid in the rapid recognition of MERS, the CDC has established case definitions.8
A patient under investigation is an individual with fever (> 38oC, > 100.4oF) and pneumonia or acute respiratory distress syndrome (ARDS); and either:
- history of travel from countries in or near the Arabian Peninsula within 14 days before the onset of symptoms; or
- close contact with a symptomatic traveler who developed fever and ARDS within 14 days after traveling from countries in or near the Arabian Peninsula; or
- is a member of a cluster of patients with severe acute respiratory illness of unknown etiology in which MERS-CoV is being evaluated, in consultation with state and local health departments.
A confirmed case is a patient with laboratory confirmation of MERS-CoV infection. A probable case is a patient under investigation with absent or inconclusive laboratory results for MERS-CoV infection who is a close contact of a laboratory- confirmed MERS-CoV case.
Transmission
MERS-CoV is thought to be of animal origin, but the mode of transmission from the animal reservoir is not known. It seems likely that some of the infections have occurred via intermittent zoonotic transmission, possibly by an environmental source.19 The presence of case clusters, however, suggests that human-to-human transmission also can occur. Human-to-human transmission has occurred in individuals living with an infected person and in HCPs caring for infected patients.20-24 The human-to-human transmission through close contact so far has been nonsustained.
It has been estimated that 75% of the reported cases are secondary, meaning that the patient acquired the MERS-CoV infection from another infected person. There is no evidence of sustained spread of MERS-CoV in community settings. The mode of human-to-human transmission has not been determined. Possible modes of transmission include droplet and contact transmission. The number of contacts infected by individuals with confirmed infections seems limited; the transmissibility, therefore, currently seems to be low.25,26 The results of a study of the transmissibility and epidemic potential for MERS-CoV suggest that it does not yet have pandemic potential.27
Bats may serve as a reservoir for MERS-CoV. However, because human contact with bats is uncommon, they are viewed as unlikely candidates for an immediate source of infection in most humans. It is possible that another animal or vector serves as an intermediate host. Camels have been proposed as a possible intermediate host, but this remains unproven. Interestingly, the MERS-CoV index patient had been caring for several ill camels in his herd; the camels had signs of respiratory illness, including nasal discharge.11,28 MERS-CoV sequences were subsequently isolated from a juvenile camel belonging to the index patient.
Symptoms
The incubation time after exposure to symptom onset ranges from 1.9 to 14.7 days (Figure). The median incubation period is 5.2 days.21 Patients are not believed to be contagious during the incubation period. Early symptoms of human infection with MERS-CoV include fever, chills or rigors, cough, and shortness of breath. Less frequently encountered symptoms include hemoptysis, sore throat, myalgias, diarrhea, vomiting, and abdominal pain (Table 2).20,21,23,26,27,29 Many patients infected with MERS-CoV develop a severe lower respiratory tract illness. The patient may progress to ARDS and require intubation and mechanical ventilator support. Mechanical ventilation has been required in 72% of patients.29 The median time from presentation for medical care to respiratory failure is 7 days, ranging from 3 to 11 days (Figure).
Physical Examination
The patients with MERS-CoV infection have been predominantly male and middle aged with an average age of 52 years. The clinical features depend on the severity of the illness. Some infected individuals have remained asymptomatic.27 Other patients have experienced mild lower respiratory illness and have not required hospitalization. However, about 40% of patients have experienced severe illness with pneumonia, respiratory insufficiency, multi-organ failure, and death. The percentage of severe illness is likely an overestimation, because patients with less severe symptoms probably are not tested for MERS-CoV. Most of the patients who have experienced a severe illness and/or death also had underlying comorbid conditions, such as diabetes mellitus, hypertension, chronic heart disease, and chronic renal disease.23,29
Laboratory Data
As with SARS-CoV, lymphopenia has been reported in patients infected with MERS-CoV.29 Other complete blood cell count abnormalities include leukopenia, lymphocytosis, thrombocytopenia, and anemia (Table 3).23,24,26,30 Blood chemistry profiles have identified elevated aspartate aminotransferase, alanine aminotransferase, and lactate dehydrogenase levels.29 Some patients have experienced progressive renal failure signaled by rising serum creatinine and blood urea nitrogen levels.11,23,24,26 Testing for disseminated intravascular coagulation and hemolysis has been positive in some patients.20,30 Oxyhemoglobin desaturation develops in patients with severe pneumonia.
Radiographic Imaging
Chest radiographs have been abnormal in the majority of patients with MERS-CoV. The radiographic findings may be minimal to extensive, depending on the severity of illness. The reported radiographic abnormalities include increased bronchovesicular markings, airspace opacities, patchy infiltrates, interstitial changes, confluent consolidations, nodular opacities, reticular infiltrate, pleural effusion, and total opacification of lung segments and lobes. These radiographic findings may be unilateral or bilateral.29
Specific Testing for MERS-CoV
The CDC recommends that lower respiratory tract specimens be collected for testing with real-time reverse-transcriptase polymerase chain reaction (rRT-PCR). The FDA has issued an emergency use authorization of the rRT-PCR assay developed by the CDC. The CDC recommends that multiple specimens from different sites in the lower respiratory system be collected at different times to increase the likelihood of detecting MERS-CoV. Acute and convalescent serum samples also should be obtained for serologic testing. Lower respiratory specimens (sputum, tracheal aspirates, and bronchoalveolar lavage fluid) are more sensitive than are upper respiratory tract samples (nasopharyngeal throat swabs and nasopharyngeal aspirates). Respiratory specimens should be collected as soon as possible after symptom onset. If negative testing is obtained from a patient with a high index of suspicion for MERS-CoV infection, then repeat testing should be performed.
Related: Another Reason Not to Smoke: Acute Eosinophilic Pneumonia
Several serology assays have been developed for the detection of MERS-CoV. An immunofluorescence assay should be confirmed with a neutralization test. In certain cases, the diagnosis should be confirmed by nucleic acid sequencing. The CDC has developed MERS-CoV testing kits, which have been provided to state health departments. Any case of suspected or proven MERS-CoV in the U.S. should be reported to the state and local health departments. Visit the CDC website for more information about collecting, handling, and testing clinical specimens from patients under investigation for MERS: http://www.cdc.gov/coronavirus/mers/guidelines -clinical-specimens.html.
Prognosis
Complications from the MERS- CoV infection include severe pneumonia and ARDS requiring mechanical ventilation, multi-organ failure, renal failure requiring dialysis, consumptive coagulopathy, and pericarditis.20,21,23,26,27,29 About 30% of people with MERS-CoV have died. SARS-CoV was the first CoV to cause severe lower respiratory disease and death in otherwise healthy humans; MERS-CoV is now the second.6 Death occurs a median of 14 days after presentation with a range of 5 to 36 days.20,21,23,26,27,29
Treatment
There is no available specific therapy recommended for MERS-CoV infection; therefore, the management of patients is supportive. As with other CoVs, there is no antiviral agent treatment for MERS-CoV. In experimental settings, combination therapy with interferon-alpha-2b and ribavirin seems promising.31 However, critically ill patients with MERS-CoV did not seem to respond favorably when treated with this regimen.32
Vaccine
There is no licensed vaccine for MERS-CoV, although experimental vaccines are being developed. Vaccines have successfully prevented CoV infection in animal models. The development of an effective vaccine for humans against MERS-CoV may, therefore, be a realistic possibility. Unfortunately, a vaccine is likely years away from approval.
Infection Control Measures
Careful attention to infection control precautions is critical to the containment of MERS-CoV. Patients should be encouraged to inform HCPs about symptoms and potential exposure risks, in particular travel to and/or exposure to travelers from the Arabian Peninsula. This practice should help to limit the transmission of MERS-CoV to HCPs. Standard contact and airborne precautions should be followed in patients with suspected or proven MERS-CoV infection.
Infection control measures should include hand hygiene; avoiding close contact with people who are sick; avoiding touching the eyes, nose, and/or mouth with unwashed hands; and disinfecting frequently touched surfaces. Patients with suspected or proven MERS-CoV should be admitted to single occupancy rooms to diminish the possibility of viral transmission to other patients. All persons entering the room of a patient with suspected or proven MERS-CoV should wear fitted N-95 filtering respirators. Until the mode of transmission is better defined, protective eyewear should be worn during all patient contacts. With implementation of these measures, there has been no institution that has experienced an outbreak of MERS-CoV infection. Unfortunately, the duration of viral shedding is not yet known.
Travel Restrictions
At this time the CDC has not recommended MERS-related travel restrictions. Because the spread of MERS-CoV has occurred in health care institutions, the CDC advises HCPs traveling to the Arabian Peninsula to follow recommendations for infection control of confirmed or suspected cases of MERS-CoV and to monitor their own health closely. Travelers who are going to the Arabian Peninsula for other reasons are advised to follow standard infection control precautions, such as hand washing and avoiding contact with ill people. Visit the CDC website for updated information of travel restrictions: http://www.cdc.gov/coronavirus/mers/travel.html.
Author disclosures
The authors report no actual or potential conflicts of interest with regard to this article.
Disclaimer
The opinions expressed herein are those of the authors and do not necessarily reflect those of Federal Practitioner, Frontline Medical Communications Inc., the U.S. Government, or any of its agencies. This article may discuss unlabeled or investigational use of certain drugs. Please review complete prescribing information for specific drugs or drug combinations—including indications, contraindications, warnings, and adverse effects—before administering pharmacologic therapy to patients.
1. To KK, Hung IF, Chan JF, Yuen KY. From SARS coronavirus to novel animal and human coronaviruses. J Thorac Dis. 2013;5(suppl 2):S103-S108.
2. Woo PC, Lau SK, Chu CM, et al. Characteristics and complete genome sequence of a novel coronavirus, coronavirus HKU1, from patients with pneumonia. J Virol. 2005;79(2):884-895.
3. van der Hoek L, Pyrc K, Jebbink MF, et al. Identification of a new human coronavirus. Nat Med. 2004;10(4):368-373.
4. de Groot RJ, Baker SC, Baric RS, et al. Middle East respiratory syndrome coronavirus (MERS-CoV): Announcement of the Coronavirus Study Group. J Virol. 2013;87(14):7790-7792.
5. World Health Organization. Middle East respiratory syndrome coronavirus (MERS-CoV) summary and literature update–as of 11 June 2014. http://www.who.int/csr/disease/coronavirus_infections/MERS-CoV_summary_update_20140611.pdf. Accessed February 3, 2015.
6. Byrd RP Jr, Roy TM. Severe acute respiratory syndrome. Fed Pract. 2003;20(9):62-71.
7. International Society for Infectious Diseases. Novel coronavirus–Saudi Arabia: Human isolate; Archive number: 20120920.1302733. ProMED-mail Website. http://www.promedmail.org/direct .php?id=20120920.1302733. Published September 20, 2012. Accessed January 23, 2015.
8. Centers for Disease Control and Prevention. Middle East respiratory syndrome (MERS). Centers for Disease Control and Prevention Website. http://www.cdc.gov/coronavirus/mers. Updated July 31, 2014. Accessed January 23, 2015.
9. Centers for Disease Control and Prevention. MERS in the U.S. Centers for Disease Control and Prevention Website. http://www.cdc.gov/coronavirus/mers/US.html. Updated December 9, 2014. Accessed January 23, 2015.
10. Lau SK, Li KS, Huang Y, et al. Ecoepidemiology and complete genome comparison of different strains of severe acute respiratory syndrome-related Rhinolophus bat coronavirus in China reveal bats as a reservoir for acute, self-limiting infection that allows recombination events. J Virol. 2010;84(6): 2808-2819.
11. Zaki AM, van Boheemen S, Bestebroer TM, Osterhaus AD, Fouchier RA. Isolation of a novel coronavirus from a man with pneumonia in Saudi Arabia. N Engl J Med. 2012;367(19):1814-1820.
12. Cotten M, Lam TT, Watson SJ, et al. Full-genome deep sequencing and phylogenetic analysis of novel human betacoronavirus. Emerg Infect Dis. 2013;19(5):736-742B.
13. Annan A, Baldwin HJ, Corman VM, et al. Human betacoronavirus 2c EMC/2012-related viruses in bats, Ghana and Europe. Emerg Infect Dis. 2013;19(3):456-459.
14. Ithete NL, Stoffberg S, Corman VM, et al. Close relative of human Middle East respiratory syndrome coronavirus in bat, South Africa. Emerg Infect Dis. 2013;19(10):1697-1699.
15. Memish ZA, Mishra N, Olival KJ, et al. Middle East respiratory syndrome coronavirus in bats, Saudi Arabia. Emerg Infect Dis. 2013;19(11):1819-1823.
16. Chu DK, Poon LL, Gomaa MM, et al. MERS coronavirus in dromedary camels, Egypt. Emerg Infect Dis. 2014;20(6):1049-1053.
17. Reusken CB, Haagmans BL, Müller MA, et al. Middle East respiratory syndrome coronavirus neutralising serum antibodies in dromedary camels: A comparative serological study. Lancet Infect Dis. 2013;13(10):859-866.
18. Haagmans BL, Al Dhahiry SH, Reusken CB, et al. Middle East respiratory syndrome coronavirus in dromedary camels: An outbreak investigation. Lancet Infect Dis. 2014;14(2):140-145.
19. Abdel-Moneim AS. Middle East respiratory syndrome coronavirus (MERS-CoV): Evidence and speculations. Arch Virol. 2014;159(7):1575-1584.
20. World Health Organization. Global Alert and Response. MERS-CoV summary and literature update—as of 31 May 2013. http://www.who.int/csr/disease/coronavirus_infections/update_20130531 /en. Accessed January 23, 2015.
21. Assiri A, McGeer A, Perl TM, et al; KSA MERS-CoV Investigation Team. Hospital outbreak of Middle East respiratory syndrome coronavirus. N Engl J Med. 2013;369(5):407-416.
22. Gulland A. Two cases of novel coronavirus are confirmed in France. BMJ. 2013;346:f3114.
23. Guery B, Poissy J, el Mansouf L, et al; MERS-CoV study group. Clinical features and viral diagnosis of two cases of infection with Middle East Respiratory Syndrome coronavirus: A report of nosocomial transmission. Lancet. 2013;381(9885):2265-2272.
24. Memish ZA, Zumla AI, Al-Hakeem RF, Al-Rabeeah AA, Stephens GM. Family cluster of Middle East respiratory syndrome coronavirus infections. N Engl J Med. 2013;368(26):2487-2494.
25. Reuss A, Litterst A, Drosten C, et al. Contact investigation for imported case of Middle East respiratory syndrome, Germany. Emerg Infect Dis. 2014;20(4):620-625.
26. Arabi YM, Arifi AA, Balkhy HH, et al. Clinical course and outcomes of critically ill patients with Middle East respiratory syndrome coronavirus infection. Ann Intern Med. 2014;160(6):389-397.
27. Memish ZA, Zumla AI, Assiri A. Middle East respiratory syndrome coronavirus infections in health care workers. N Engl J Med. 2013;369(9):884-886.
28. Memish ZA, Cotten M, Meyer B, et al. Human infection with MERS coronavirus after exposure to infected camels, Saudi Arabia, 2013. Emerg Infect Dis. 2014;20(6):1012-1015.
29. Assiri A, Al-Tawfiq JA, Al-Rabeeah AA, et al. Epidemiological, demographic, and clinical characteristics of 47 cases of Middle East respiratory syndrome coronavirus disease from Saudi Arabia: A descriptive study. Lancet Infect Dis. 2013;13(9):752-761.
30. Drosten C, Seilmaier M, Corman VM, et al. Clinical features and virological analysis of a case of Middle East respiratory syndrome coronavirus infection. Lancet Infect Dis. 2013;13(9):745-751.
31. Falzarano D, de Wit E, Rasmussen AL, et al. Treatment with interferon-α2b and ribavirin improves outcome in MERS-CoV-infected rhesus macaques. Nat Med. 2013;19(10):1313-1317.
32. Al-Tawfiq JA, Momattin H, Dib J, Memish ZA. Ribavirin and interferon therapy in patients infected with the Middle East respiratory syndrome coronavirus: An observational study. Int J Infect Dis. 2014;20:42-46.
1. To KK, Hung IF, Chan JF, Yuen KY. From SARS coronavirus to novel animal and human coronaviruses. J Thorac Dis. 2013;5(suppl 2):S103-S108.
2. Woo PC, Lau SK, Chu CM, et al. Characteristics and complete genome sequence of a novel coronavirus, coronavirus HKU1, from patients with pneumonia. J Virol. 2005;79(2):884-895.
3. van der Hoek L, Pyrc K, Jebbink MF, et al. Identification of a new human coronavirus. Nat Med. 2004;10(4):368-373.
4. de Groot RJ, Baker SC, Baric RS, et al. Middle East respiratory syndrome coronavirus (MERS-CoV): Announcement of the Coronavirus Study Group. J Virol. 2013;87(14):7790-7792.
5. World Health Organization. Middle East respiratory syndrome coronavirus (MERS-CoV) summary and literature update–as of 11 June 2014. http://www.who.int/csr/disease/coronavirus_infections/MERS-CoV_summary_update_20140611.pdf. Accessed February 3, 2015.
6. Byrd RP Jr, Roy TM. Severe acute respiratory syndrome. Fed Pract. 2003;20(9):62-71.
7. International Society for Infectious Diseases. Novel coronavirus–Saudi Arabia: Human isolate; Archive number: 20120920.1302733. ProMED-mail Website. http://www.promedmail.org/direct .php?id=20120920.1302733. Published September 20, 2012. Accessed January 23, 2015.
8. Centers for Disease Control and Prevention. Middle East respiratory syndrome (MERS). Centers for Disease Control and Prevention Website. http://www.cdc.gov/coronavirus/mers. Updated July 31, 2014. Accessed January 23, 2015.
9. Centers for Disease Control and Prevention. MERS in the U.S. Centers for Disease Control and Prevention Website. http://www.cdc.gov/coronavirus/mers/US.html. Updated December 9, 2014. Accessed January 23, 2015.
10. Lau SK, Li KS, Huang Y, et al. Ecoepidemiology and complete genome comparison of different strains of severe acute respiratory syndrome-related Rhinolophus bat coronavirus in China reveal bats as a reservoir for acute, self-limiting infection that allows recombination events. J Virol. 2010;84(6): 2808-2819.
11. Zaki AM, van Boheemen S, Bestebroer TM, Osterhaus AD, Fouchier RA. Isolation of a novel coronavirus from a man with pneumonia in Saudi Arabia. N Engl J Med. 2012;367(19):1814-1820.
12. Cotten M, Lam TT, Watson SJ, et al. Full-genome deep sequencing and phylogenetic analysis of novel human betacoronavirus. Emerg Infect Dis. 2013;19(5):736-742B.
13. Annan A, Baldwin HJ, Corman VM, et al. Human betacoronavirus 2c EMC/2012-related viruses in bats, Ghana and Europe. Emerg Infect Dis. 2013;19(3):456-459.
14. Ithete NL, Stoffberg S, Corman VM, et al. Close relative of human Middle East respiratory syndrome coronavirus in bat, South Africa. Emerg Infect Dis. 2013;19(10):1697-1699.
15. Memish ZA, Mishra N, Olival KJ, et al. Middle East respiratory syndrome coronavirus in bats, Saudi Arabia. Emerg Infect Dis. 2013;19(11):1819-1823.
16. Chu DK, Poon LL, Gomaa MM, et al. MERS coronavirus in dromedary camels, Egypt. Emerg Infect Dis. 2014;20(6):1049-1053.
17. Reusken CB, Haagmans BL, Müller MA, et al. Middle East respiratory syndrome coronavirus neutralising serum antibodies in dromedary camels: A comparative serological study. Lancet Infect Dis. 2013;13(10):859-866.
18. Haagmans BL, Al Dhahiry SH, Reusken CB, et al. Middle East respiratory syndrome coronavirus in dromedary camels: An outbreak investigation. Lancet Infect Dis. 2014;14(2):140-145.
19. Abdel-Moneim AS. Middle East respiratory syndrome coronavirus (MERS-CoV): Evidence and speculations. Arch Virol. 2014;159(7):1575-1584.
20. World Health Organization. Global Alert and Response. MERS-CoV summary and literature update—as of 31 May 2013. http://www.who.int/csr/disease/coronavirus_infections/update_20130531 /en. Accessed January 23, 2015.
21. Assiri A, McGeer A, Perl TM, et al; KSA MERS-CoV Investigation Team. Hospital outbreak of Middle East respiratory syndrome coronavirus. N Engl J Med. 2013;369(5):407-416.
22. Gulland A. Two cases of novel coronavirus are confirmed in France. BMJ. 2013;346:f3114.
23. Guery B, Poissy J, el Mansouf L, et al; MERS-CoV study group. Clinical features and viral diagnosis of two cases of infection with Middle East Respiratory Syndrome coronavirus: A report of nosocomial transmission. Lancet. 2013;381(9885):2265-2272.
24. Memish ZA, Zumla AI, Al-Hakeem RF, Al-Rabeeah AA, Stephens GM. Family cluster of Middle East respiratory syndrome coronavirus infections. N Engl J Med. 2013;368(26):2487-2494.
25. Reuss A, Litterst A, Drosten C, et al. Contact investigation for imported case of Middle East respiratory syndrome, Germany. Emerg Infect Dis. 2014;20(4):620-625.
26. Arabi YM, Arifi AA, Balkhy HH, et al. Clinical course and outcomes of critically ill patients with Middle East respiratory syndrome coronavirus infection. Ann Intern Med. 2014;160(6):389-397.
27. Memish ZA, Zumla AI, Assiri A. Middle East respiratory syndrome coronavirus infections in health care workers. N Engl J Med. 2013;369(9):884-886.
28. Memish ZA, Cotten M, Meyer B, et al. Human infection with MERS coronavirus after exposure to infected camels, Saudi Arabia, 2013. Emerg Infect Dis. 2014;20(6):1012-1015.
29. Assiri A, Al-Tawfiq JA, Al-Rabeeah AA, et al. Epidemiological, demographic, and clinical characteristics of 47 cases of Middle East respiratory syndrome coronavirus disease from Saudi Arabia: A descriptive study. Lancet Infect Dis. 2013;13(9):752-761.
30. Drosten C, Seilmaier M, Corman VM, et al. Clinical features and virological analysis of a case of Middle East respiratory syndrome coronavirus infection. Lancet Infect Dis. 2013;13(9):745-751.
31. Falzarano D, de Wit E, Rasmussen AL, et al. Treatment with interferon-α2b and ribavirin improves outcome in MERS-CoV-infected rhesus macaques. Nat Med. 2013;19(10):1313-1317.
32. Al-Tawfiq JA, Momattin H, Dib J, Memish ZA. Ribavirin and interferon therapy in patients infected with the Middle East respiratory syndrome coronavirus: An observational study. Int J Infect Dis. 2014;20:42-46.

Urologist Workforce Variation Across the VHA
The VHA is the nation’s largest integrated health care delivery system, providing comprehensive medical care to about 6 million patients annually. In addition to revolutionizing its primary care delivery through widespread implementation of patient-centered medical homes (Patient Aligned Care Teams), the VHA is also transforming its specialty care delivery through use of its specialist workforce and innovative technologies, such as telemedicine and electronic consultations (e-consults).1
VHA specialty care is currently distributed using a hub and spoke model within larger regional networks spanning the U.S. This approach helps overcome geographic variation in specialist workforce (eg, predilection for metropolitan areas) but limits specialty care access for patients and primary care providers (PCPs) due to distance barriers.2-4 With the VHA electronic medical record (EMR) system, it is now feasible to send expertise electronically across the system (eg, e-consult). Whether this should occur at the regional VISN or national level to smooth out variation in specialist workforce depends in part on current specialist distribution within and across regions.
Related: Recurrent Multidrug Resistant Urinary Tract Infections in Geriatric Patients
Hand in hand with an aging veteran population is a growing clinical demand for urologic specialty care to treat urinary incontinence, prostate enlargement, and prostate cancer. Unfortunately, over 60% of U.S. counties lack a urologist, creating troublesome workforce issues.3 For these reasons, this study analyzed existing administrative data to understand regional variations in the distribution of and demands for the VHA urologist workforce. This study tested whether workforce distribution is balanced or imbalanced across regional networks, in part to inform whether the VHA should offer electronic or other national access to its urologic specialty care.
Methods
Fiscal year (FY) 2011 Specialty Physician Workforce Annual Report data from the VHA Office of Productivity, Efficiency, and Staffing was used to characterize the distribution and concentration of urologists at 130 VHA facilities.5 The annual report provided a longitudinal management tool for reporting clinical productivity, efficiency, and staffing, and included benchmark data for each facility (eg, physician workforce, annual patient visits).
Demand for Urologic Specialty Care
The number of unique urology patients from the report was used as one approach to the demand for VHA urologic specialty care. This measure represented the number of unique patients evaluated in a urology clinic at least once over the FY. The number of newly diagnosed patients with prostate cancer in calendar year 2010 within each VISN was also used as a more discrete measure of regional urologic care demand. Whereas care for other common urologic conditions, such as incontinence or prostate enlargement, may or may not be referred (ie, latent demand), prostate cancer care consistently involves urologists and is more specific for caseload.
Related: Prostate Cancer Survivorship Care
Because each VISN covered a relatively large geographic area, most with roughly equivalent numbers of facilities, there was no a priori reason to expect a difference in urologic workload and consequently urologic workforce between networks. On the other hand, within networks one might expect that urologists would be concentrated in hospitals that have more complicated patient cases, because the hospitals serve a tertiary or referral role. Yet even within a network, significant imbalances in specialist supply might require creative solutions to maintain adequate access of patients and PCPs to specialists.
Urologist Workforce
The full-time equivalent employee (FTEE) variable for urologic specialty care from the 2011 annual report was used as the primary outcome measure for urology workforce.5 This facility-level measure represented the clinical time urologists spent in direct patient care at each facility. It included the clinical effort of full-time as well as contract physicians and was also reported as an aggregate measure at the regional VISN level. Urologist workforce at the VISN level was the sum of all urologist FTEEs within its facilities. Adjusted rates also were provided (eg, FTEE/10,000 urology patients).
Other Workforce Factors
Also examined as covariates in the analysis were other measures related to urologist workforce. As the nation’s largest provider of graduate medical education, urology residents rotate through many VHA facilities, contributing to the workforce totals. For this reason, resident FTEE was examined as an independent variable in this study.
Understanding facility complexity (ie, case mix) was also essential for rational allocation of specialty care resources, as demand generally increases with increasing case mix. Therefore, a medical center group (MCG) case mix measure of complexity and its relationship with urologist workforce was examined. It was expected that increasing specialty care volume, resident staff, and facility complexity would be associated with increasing urologist workforce.
Statistical Analysis
Descriptive statistics were used to characterize VHA urology patients and urologist workforce within each regional VISN and its facilities. To better understand the relationship between case mix and urologist workforce, facilities were sorted according to MCG and characterized the unique urology patients, urologists, and residents at each level. Analysis of variance was used to test whether increasing MCG was associated with a higher number of urology patient caseloads. Multivariable linear regression models were then used to determine whether complexity was associated with urologist workforce after adjusting for resident and patient volume.
Related: Antibiotic Therapy and Bacterial Resistance in Patients With Spinal Cord Injury
Multilevel regression modeling, an extension of linear regression modeling suitable for partitioning the variation in an outcome variable attributable to different levels (ie, facility and VISN), was used to examine whether variation in the urologist workforce was primarily based at the facility or regional VISN level.6 This approach accounted for the potentially correlated nature of the data (ie, multiple facilities within each VISN) by incorporating a VISN-level random effect in the model. A random intercept model with no explanatory variables, known as an empty model, was used as the primary model.6 The intraclass correlation coefficient (ICC) corresponding to the estimated variance components from the empty model was calculated to determine the portion of the total variation in unadjusted urologist workforce that occurs between VISNs.7 Prostate cancer caseload was then included to test whether allocation seemed to be driven by clinical need or other regional factors.
All analyses were performed using STATA, Version 12 (StataCorp LP, College Station, TX), and all testing was 2-sided. The probability of a type I error was set at .05. This study protocol was approved by the VA Ann Arbor Health Care System Research and Development Committee and Institutional Review Board.
Results
Nearly 1 in 20 VHA patients (n = 274,152) were evaluated in a urology clinic at least once in FY 2011. It was found that 252.7 FTEE and 193.1 residents comprised the VHA urologist workforce (Table 1). Marked regional variation was found in unadjusted urologist staffing at both the facility and VISN levels. The urologist workforce ranged from 0.17 to 5.91 FTEEs across the 130 VHA facilities. At the VISN level, staffing varied over 5-fold (5.8 FTEEs in VISN 2 to 27.6 FTEEs in VISN 8).
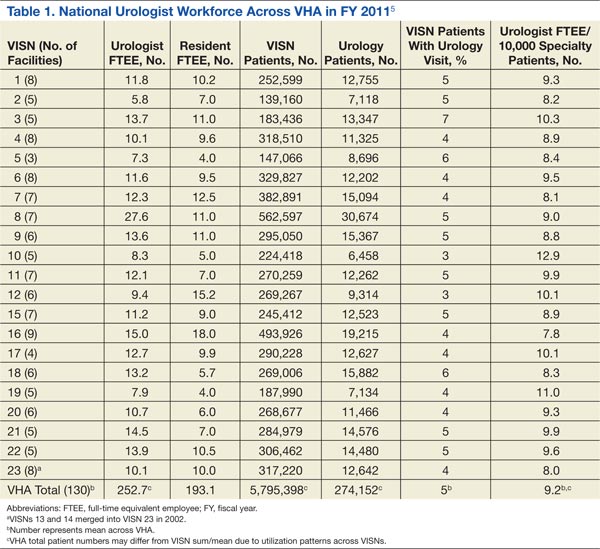
Variation in the VHA urologist workforce distribution persisted even after standardizing by patient volume. The urologist workforce continued to vary from 0.94 to 9.95 FTEEs per 100,000 facility patients. This was even more dramatic when adjusted for volume of unique urology patients, ranging from 2.2 to 24.2 FTEE urologists per 10,000 urology patients (Figure).5 From the specialist perspective, each might serve 18 to 64 newly diagnosed patients with prostate cancer annually, depending on the VISN.
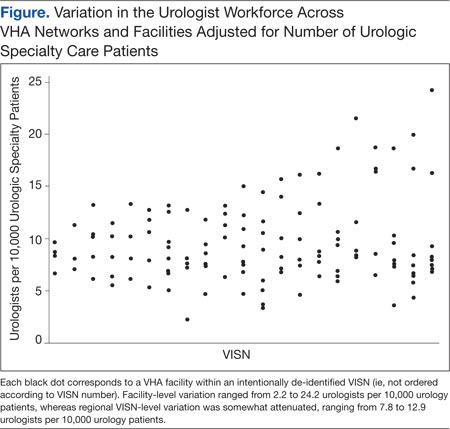
Forty percent of urologists were located in 34 of the most complex facilities (Table 2). Urology patient caseload was associated with facility complexity in univariate analysis (P < .001). In the adjusted multivariable model, increasing facility complexity was associated with increasing urologist workforce (P < .001) as well as resident staffing (P < .001), but not with urology patient caseload (P = .27). The empty multilevel model indicated that 27.3% of variation in unadjusted urologist workforce (ICC = 0.273, 95% confidence interval [CI], 0.098-0.448) was attributable to differences at the regional network level. After adjustment for VISN prostate cancer caseload, this decreased to 24.8% (ICC = 0.248; 95% CI, 0.076-0.419).
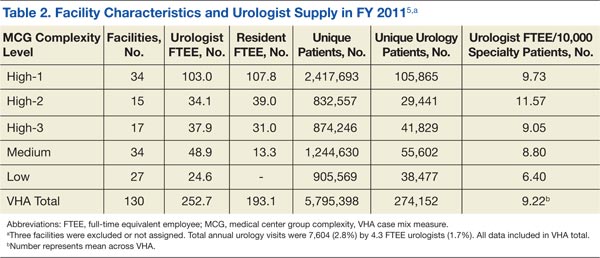
Discussion
The VHA urologist workforce served over 250,000 patients in FY 2011, and a substantial variation in workforce distribution at the facility and VISN levels was identified in this study. After adjusting for prostate cancer caseload as a proxy for clinical demand, there was some imbalance of urology specialists across regional networks, though most workforce variation occurred within networks in this integrated delivery system. Based on these findings, VHA specialty care initiatives should likely focus within regional networks rather than pursue electronic efforts nationally to improve specialty care access for patients and PCPs.
Regional variation in the VHA urologist workforce was expected, given a limited national supply of urologists and specialist preferences toward metropolitan areas.2-4 Overcoming this maldistribution has important implications for outcomes in many urologic disease processes.8-10 For example, counties with ≥ 1 urologist have up to a 20% reduction in bladder and prostate cancer-related mortality compared with those without a urologist.4 Moreover, the number of veterans with known urologic needs or currently receiving urologic specialty care likely significantly undercounts the total number who could benefit from this care. This is particularly true for facilities with fewer urology resources where patients may be less likely to get a referral, or if they are referred, it is likely outside VHA, creating fragmented care and potentially higher cost.
Understanding the urology workforce distribution, coupled with its sophisticated nationwide EMR, VHA has a unique opportunity to transform how urologic specialty care is delivered without moving around the current workforce. Based on these findings, the system could redistribute resources within each region to meet growing specialty care needs through telemedicine.
At least 2 innovative approaches are underway that might serve the system’s urology care needs: e-consults and the Specialty Care Access Network-Extension for Community Healthcare Outcomes (SCAN-ECHO) video teleconsulting and education project.11,12 The first allows PCPs to request specialist review of the EMR, interpretation of the specific problem, and recommendation for a plan of care, which may or may not include a specialist visit.1,13 The second involves video conferences, which allow multiple PCPs from less complex facilities or rural areas to present cases to specialists from tertiary medical centers for real-time consultation and case-based learning. These initiatives could take advantage of the facility-based variation in urologist workforce by linking facilities with relatively generous urology resources with those with fewer resources to meet the needs of each region’s population and their PCPs while minimizing travel and wait times.
Limitations
This study should be interpreted in the context of several limitations. First, FY 2011 data were used; notably, the VHA urologist workforce remained relatively stable from 2008 through 2011. Second, characteristics of individual VHA urologists, clinical productivity, and skill level were not examined. However, a 2008 study found that nearly all VHA urologists are board certified, mitigating skill level concerns.14 Third, it is possible that demand is partially driven by existence of resources, and there may be patients who might benefit from urologic care but who are not yet diagnosed. The analysis is conservative in this regard, in that demand may be greater than what was detected using the selected study methods. Last, this study examined specialist workforce within a single system. However, ensuring specialist resources are well distributed is a concern for most health systems, particularly in light of recent policy efforts, including accountable care organizations.15
Conclusion
Much of the variation in the VHA urologist workforce exists at the facility rather than the regional level. Optimizing the distribution of these specialty care resources could be achieved through novel care delivery models within each regional network that are well-aligned with current VHA initiatives. Successfully utilizing this workforce distribution has the potential to improve urologic care for veterans across the country and could be applied to improve access to all types of specialists in underserved and understaffed areas.
Acknowledgments
Dr. Skolarus is supported by a VA HSR&D Career Development Award (CDA 12-171).
Author disclosures
The authors report no actual or potential conflicts of interest with regard to this article.
Disclaimer
The opinions expressed herein are those of the authors and do not necessarily reflect those of Federal Practitioner, Frontline Medical Communications Inc., the U.S. Government, or any of its agencies. This article may discuss unlabeled or investigational use of certain drugs. Please review complete prescribing information for specific drugs or drug combinations—including indications, contraindications, warnings, and adverse effects—before administering pharmacologic therapy to patients.
1. Graham GD; Office of Specialty Care Transformation, Department of Veterans Affairs Patient Care Services. Specialty care transformation initiatives. http://www.pva.org/atf/cf/%7BCA2A0FFB-6859 -4BC1-BC96-6B57F57F0391%7D/Friday_Graham_Specialty%20Care%20Transformation%20Initiatives.pdf. Published December 2011. Accessed February 3, 2015.
2. Neuwahl S, Thompson K, Fraher E, Ricketts T. HPRI data tracks. Urology workforce trends. Bull Am Coll Surg. 2012;97(1):46-49.
3. Odisho AY, Fradet V, Cooperberg MR, Ahmad AE, Carroll PR. Geographic distribution of urologists throughout the United States using a county level approach. J Urol. 2009;181(2):760-765; discussion 765-766.
4. Odisho AY, Cooperberg MR, Fradet V, Ahmad AE, Carroll PR. Urologist density and county-level urologic cancer mortality. J Clin Oncol. 2010;28(15):2499-2504.
5. Fiscal Year 2011 VHA Physician Workforce & Support Staff Data. VHA Office of Productivity, Efficiency, & Staffing Website. https://opes.vscc.med.va.gov. Published December 2011.
6. Snijders TAB, Bosker RJ. Multilevel Analysis: An Introduction to Basic and Advanced Multilevel Modeling. Thousand Oaks, CA: Sage Publications Inc;1999.
7. Krein SL, Hofer TP, Kerr EA, Hayward RA. Whom should we profile? Examining diabetes care practice variation among primary care providers, provider groups, and health care facilities. Health Serv Res. 2002;37(5):1159-1180.
8. Weiner DM, McDaniel R, Lowe FC. Urologic manpower issues for the 21st century: Assessing the impact of changing population demographics. Urology. 1997;49(3):335-342.
9. Gee WF, Holtgrewe HL, Albertsen PC, et al. Subspecialization, recruitment and retirement trends of American urologists. J Urol. 1998;159(2): 509-511.
10. McCullough DL. Manpower needs in urology in the twenty-first century. Urol Clin North Am. 1998;25(1):15-22.
11. Saifu HN, Asch SM, Goetz MB, et al. Evaluation of human immunodeficiency virus and hepatitis C telemedicine clinics. Am J Manag Care. 2012;18(4):207-212.
12. Arora S, Geppert CM, Kalishman S, et al. Academic health center management of chronic diseases through knowledge networks: Project ECHO. Acad Med. 2007;82(2):154-160.
13. Hysong SJ, Esquivel A, Sittig DF, et al. Towards successful coordination of electronic health record based-referrals: A qualitative analysis. Implement Sci. 2011;6:84.
14. Tyson MD, Lerner LB. Profile of the veterans affairs urologist: Results from a national survey. J Urol. 2008;180(4):1460-1462.
15. Landon BE, Roberts DH. Reenvisioning specialty care and payment under global payment systems. JAMA. 2013;310(4):371-372.
The VHA is the nation’s largest integrated health care delivery system, providing comprehensive medical care to about 6 million patients annually. In addition to revolutionizing its primary care delivery through widespread implementation of patient-centered medical homes (Patient Aligned Care Teams), the VHA is also transforming its specialty care delivery through use of its specialist workforce and innovative technologies, such as telemedicine and electronic consultations (e-consults).1
VHA specialty care is currently distributed using a hub and spoke model within larger regional networks spanning the U.S. This approach helps overcome geographic variation in specialist workforce (eg, predilection for metropolitan areas) but limits specialty care access for patients and primary care providers (PCPs) due to distance barriers.2-4 With the VHA electronic medical record (EMR) system, it is now feasible to send expertise electronically across the system (eg, e-consult). Whether this should occur at the regional VISN or national level to smooth out variation in specialist workforce depends in part on current specialist distribution within and across regions.
Related: Recurrent Multidrug Resistant Urinary Tract Infections in Geriatric Patients
Hand in hand with an aging veteran population is a growing clinical demand for urologic specialty care to treat urinary incontinence, prostate enlargement, and prostate cancer. Unfortunately, over 60% of U.S. counties lack a urologist, creating troublesome workforce issues.3 For these reasons, this study analyzed existing administrative data to understand regional variations in the distribution of and demands for the VHA urologist workforce. This study tested whether workforce distribution is balanced or imbalanced across regional networks, in part to inform whether the VHA should offer electronic or other national access to its urologic specialty care.
Methods
Fiscal year (FY) 2011 Specialty Physician Workforce Annual Report data from the VHA Office of Productivity, Efficiency, and Staffing was used to characterize the distribution and concentration of urologists at 130 VHA facilities.5 The annual report provided a longitudinal management tool for reporting clinical productivity, efficiency, and staffing, and included benchmark data for each facility (eg, physician workforce, annual patient visits).
Demand for Urologic Specialty Care
The number of unique urology patients from the report was used as one approach to the demand for VHA urologic specialty care. This measure represented the number of unique patients evaluated in a urology clinic at least once over the FY. The number of newly diagnosed patients with prostate cancer in calendar year 2010 within each VISN was also used as a more discrete measure of regional urologic care demand. Whereas care for other common urologic conditions, such as incontinence or prostate enlargement, may or may not be referred (ie, latent demand), prostate cancer care consistently involves urologists and is more specific for caseload.
Related: Prostate Cancer Survivorship Care
Because each VISN covered a relatively large geographic area, most with roughly equivalent numbers of facilities, there was no a priori reason to expect a difference in urologic workload and consequently urologic workforce between networks. On the other hand, within networks one might expect that urologists would be concentrated in hospitals that have more complicated patient cases, because the hospitals serve a tertiary or referral role. Yet even within a network, significant imbalances in specialist supply might require creative solutions to maintain adequate access of patients and PCPs to specialists.
Urologist Workforce
The full-time equivalent employee (FTEE) variable for urologic specialty care from the 2011 annual report was used as the primary outcome measure for urology workforce.5 This facility-level measure represented the clinical time urologists spent in direct patient care at each facility. It included the clinical effort of full-time as well as contract physicians and was also reported as an aggregate measure at the regional VISN level. Urologist workforce at the VISN level was the sum of all urologist FTEEs within its facilities. Adjusted rates also were provided (eg, FTEE/10,000 urology patients).
Other Workforce Factors
Also examined as covariates in the analysis were other measures related to urologist workforce. As the nation’s largest provider of graduate medical education, urology residents rotate through many VHA facilities, contributing to the workforce totals. For this reason, resident FTEE was examined as an independent variable in this study.
Understanding facility complexity (ie, case mix) was also essential for rational allocation of specialty care resources, as demand generally increases with increasing case mix. Therefore, a medical center group (MCG) case mix measure of complexity and its relationship with urologist workforce was examined. It was expected that increasing specialty care volume, resident staff, and facility complexity would be associated with increasing urologist workforce.
Statistical Analysis
Descriptive statistics were used to characterize VHA urology patients and urologist workforce within each regional VISN and its facilities. To better understand the relationship between case mix and urologist workforce, facilities were sorted according to MCG and characterized the unique urology patients, urologists, and residents at each level. Analysis of variance was used to test whether increasing MCG was associated with a higher number of urology patient caseloads. Multivariable linear regression models were then used to determine whether complexity was associated with urologist workforce after adjusting for resident and patient volume.
Related: Antibiotic Therapy and Bacterial Resistance in Patients With Spinal Cord Injury
Multilevel regression modeling, an extension of linear regression modeling suitable for partitioning the variation in an outcome variable attributable to different levels (ie, facility and VISN), was used to examine whether variation in the urologist workforce was primarily based at the facility or regional VISN level.6 This approach accounted for the potentially correlated nature of the data (ie, multiple facilities within each VISN) by incorporating a VISN-level random effect in the model. A random intercept model with no explanatory variables, known as an empty model, was used as the primary model.6 The intraclass correlation coefficient (ICC) corresponding to the estimated variance components from the empty model was calculated to determine the portion of the total variation in unadjusted urologist workforce that occurs between VISNs.7 Prostate cancer caseload was then included to test whether allocation seemed to be driven by clinical need or other regional factors.
All analyses were performed using STATA, Version 12 (StataCorp LP, College Station, TX), and all testing was 2-sided. The probability of a type I error was set at .05. This study protocol was approved by the VA Ann Arbor Health Care System Research and Development Committee and Institutional Review Board.
Results
Nearly 1 in 20 VHA patients (n = 274,152) were evaluated in a urology clinic at least once in FY 2011. It was found that 252.7 FTEE and 193.1 residents comprised the VHA urologist workforce (Table 1). Marked regional variation was found in unadjusted urologist staffing at both the facility and VISN levels. The urologist workforce ranged from 0.17 to 5.91 FTEEs across the 130 VHA facilities. At the VISN level, staffing varied over 5-fold (5.8 FTEEs in VISN 2 to 27.6 FTEEs in VISN 8).
Variation in the VHA urologist workforce distribution persisted even after standardizing by patient volume. The urologist workforce continued to vary from 0.94 to 9.95 FTEEs per 100,000 facility patients. This was even more dramatic when adjusted for volume of unique urology patients, ranging from 2.2 to 24.2 FTEE urologists per 10,000 urology patients (Figure).5 From the specialist perspective, each might serve 18 to 64 newly diagnosed patients with prostate cancer annually, depending on the VISN.
Forty percent of urologists were located in 34 of the most complex facilities (Table 2). Urology patient caseload was associated with facility complexity in univariate analysis (P < .001). In the adjusted multivariable model, increasing facility complexity was associated with increasing urologist workforce (P < .001) as well as resident staffing (P < .001), but not with urology patient caseload (P = .27). The empty multilevel model indicated that 27.3% of variation in unadjusted urologist workforce (ICC = 0.273, 95% confidence interval [CI], 0.098-0.448) was attributable to differences at the regional network level. After adjustment for VISN prostate cancer caseload, this decreased to 24.8% (ICC = 0.248; 95% CI, 0.076-0.419).
Discussion
The VHA urologist workforce served over 250,000 patients in FY 2011, and a substantial variation in workforce distribution at the facility and VISN levels was identified in this study. After adjusting for prostate cancer caseload as a proxy for clinical demand, there was some imbalance of urology specialists across regional networks, though most workforce variation occurred within networks in this integrated delivery system. Based on these findings, VHA specialty care initiatives should likely focus within regional networks rather than pursue electronic efforts nationally to improve specialty care access for patients and PCPs.
Regional variation in the VHA urologist workforce was expected, given a limited national supply of urologists and specialist preferences toward metropolitan areas.2-4 Overcoming this maldistribution has important implications for outcomes in many urologic disease processes.8-10 For example, counties with ≥ 1 urologist have up to a 20% reduction in bladder and prostate cancer-related mortality compared with those without a urologist.4 Moreover, the number of veterans with known urologic needs or currently receiving urologic specialty care likely significantly undercounts the total number who could benefit from this care. This is particularly true for facilities with fewer urology resources where patients may be less likely to get a referral, or if they are referred, it is likely outside VHA, creating fragmented care and potentially higher cost.
Understanding the urology workforce distribution, coupled with its sophisticated nationwide EMR, VHA has a unique opportunity to transform how urologic specialty care is delivered without moving around the current workforce. Based on these findings, the system could redistribute resources within each region to meet growing specialty care needs through telemedicine.
At least 2 innovative approaches are underway that might serve the system’s urology care needs: e-consults and the Specialty Care Access Network-Extension for Community Healthcare Outcomes (SCAN-ECHO) video teleconsulting and education project.11,12 The first allows PCPs to request specialist review of the EMR, interpretation of the specific problem, and recommendation for a plan of care, which may or may not include a specialist visit.1,13 The second involves video conferences, which allow multiple PCPs from less complex facilities or rural areas to present cases to specialists from tertiary medical centers for real-time consultation and case-based learning. These initiatives could take advantage of the facility-based variation in urologist workforce by linking facilities with relatively generous urology resources with those with fewer resources to meet the needs of each region’s population and their PCPs while minimizing travel and wait times.
Limitations
This study should be interpreted in the context of several limitations. First, FY 2011 data were used; notably, the VHA urologist workforce remained relatively stable from 2008 through 2011. Second, characteristics of individual VHA urologists, clinical productivity, and skill level were not examined. However, a 2008 study found that nearly all VHA urologists are board certified, mitigating skill level concerns.14 Third, it is possible that demand is partially driven by existence of resources, and there may be patients who might benefit from urologic care but who are not yet diagnosed. The analysis is conservative in this regard, in that demand may be greater than what was detected using the selected study methods. Last, this study examined specialist workforce within a single system. However, ensuring specialist resources are well distributed is a concern for most health systems, particularly in light of recent policy efforts, including accountable care organizations.15
Conclusion
Much of the variation in the VHA urologist workforce exists at the facility rather than the regional level. Optimizing the distribution of these specialty care resources could be achieved through novel care delivery models within each regional network that are well-aligned with current VHA initiatives. Successfully utilizing this workforce distribution has the potential to improve urologic care for veterans across the country and could be applied to improve access to all types of specialists in underserved and understaffed areas.
Acknowledgments
Dr. Skolarus is supported by a VA HSR&D Career Development Award (CDA 12-171).
Author disclosures
The authors report no actual or potential conflicts of interest with regard to this article.
Disclaimer
The opinions expressed herein are those of the authors and do not necessarily reflect those of Federal Practitioner, Frontline Medical Communications Inc., the U.S. Government, or any of its agencies. This article may discuss unlabeled or investigational use of certain drugs. Please review complete prescribing information for specific drugs or drug combinations—including indications, contraindications, warnings, and adverse effects—before administering pharmacologic therapy to patients.
The VHA is the nation’s largest integrated health care delivery system, providing comprehensive medical care to about 6 million patients annually. In addition to revolutionizing its primary care delivery through widespread implementation of patient-centered medical homes (Patient Aligned Care Teams), the VHA is also transforming its specialty care delivery through use of its specialist workforce and innovative technologies, such as telemedicine and electronic consultations (e-consults).1
VHA specialty care is currently distributed using a hub and spoke model within larger regional networks spanning the U.S. This approach helps overcome geographic variation in specialist workforce (eg, predilection for metropolitan areas) but limits specialty care access for patients and primary care providers (PCPs) due to distance barriers.2-4 With the VHA electronic medical record (EMR) system, it is now feasible to send expertise electronically across the system (eg, e-consult). Whether this should occur at the regional VISN or national level to smooth out variation in specialist workforce depends in part on current specialist distribution within and across regions.
Related: Recurrent Multidrug Resistant Urinary Tract Infections in Geriatric Patients
Hand in hand with an aging veteran population is a growing clinical demand for urologic specialty care to treat urinary incontinence, prostate enlargement, and prostate cancer. Unfortunately, over 60% of U.S. counties lack a urologist, creating troublesome workforce issues.3 For these reasons, this study analyzed existing administrative data to understand regional variations in the distribution of and demands for the VHA urologist workforce. This study tested whether workforce distribution is balanced or imbalanced across regional networks, in part to inform whether the VHA should offer electronic or other national access to its urologic specialty care.
Methods
Fiscal year (FY) 2011 Specialty Physician Workforce Annual Report data from the VHA Office of Productivity, Efficiency, and Staffing was used to characterize the distribution and concentration of urologists at 130 VHA facilities.5 The annual report provided a longitudinal management tool for reporting clinical productivity, efficiency, and staffing, and included benchmark data for each facility (eg, physician workforce, annual patient visits).
Demand for Urologic Specialty Care
The number of unique urology patients from the report was used as one approach to the demand for VHA urologic specialty care. This measure represented the number of unique patients evaluated in a urology clinic at least once over the FY. The number of newly diagnosed patients with prostate cancer in calendar year 2010 within each VISN was also used as a more discrete measure of regional urologic care demand. Whereas care for other common urologic conditions, such as incontinence or prostate enlargement, may or may not be referred (ie, latent demand), prostate cancer care consistently involves urologists and is more specific for caseload.
Related: Prostate Cancer Survivorship Care
Because each VISN covered a relatively large geographic area, most with roughly equivalent numbers of facilities, there was no a priori reason to expect a difference in urologic workload and consequently urologic workforce between networks. On the other hand, within networks one might expect that urologists would be concentrated in hospitals that have more complicated patient cases, because the hospitals serve a tertiary or referral role. Yet even within a network, significant imbalances in specialist supply might require creative solutions to maintain adequate access of patients and PCPs to specialists.
Urologist Workforce
The full-time equivalent employee (FTEE) variable for urologic specialty care from the 2011 annual report was used as the primary outcome measure for urology workforce.5 This facility-level measure represented the clinical time urologists spent in direct patient care at each facility. It included the clinical effort of full-time as well as contract physicians and was also reported as an aggregate measure at the regional VISN level. Urologist workforce at the VISN level was the sum of all urologist FTEEs within its facilities. Adjusted rates also were provided (eg, FTEE/10,000 urology patients).
Other Workforce Factors
Also examined as covariates in the analysis were other measures related to urologist workforce. As the nation’s largest provider of graduate medical education, urology residents rotate through many VHA facilities, contributing to the workforce totals. For this reason, resident FTEE was examined as an independent variable in this study.
Understanding facility complexity (ie, case mix) was also essential for rational allocation of specialty care resources, as demand generally increases with increasing case mix. Therefore, a medical center group (MCG) case mix measure of complexity and its relationship with urologist workforce was examined. It was expected that increasing specialty care volume, resident staff, and facility complexity would be associated with increasing urologist workforce.
Statistical Analysis
Descriptive statistics were used to characterize VHA urology patients and urologist workforce within each regional VISN and its facilities. To better understand the relationship between case mix and urologist workforce, facilities were sorted according to MCG and characterized the unique urology patients, urologists, and residents at each level. Analysis of variance was used to test whether increasing MCG was associated with a higher number of urology patient caseloads. Multivariable linear regression models were then used to determine whether complexity was associated with urologist workforce after adjusting for resident and patient volume.
Related: Antibiotic Therapy and Bacterial Resistance in Patients With Spinal Cord Injury
Multilevel regression modeling, an extension of linear regression modeling suitable for partitioning the variation in an outcome variable attributable to different levels (ie, facility and VISN), was used to examine whether variation in the urologist workforce was primarily based at the facility or regional VISN level.6 This approach accounted for the potentially correlated nature of the data (ie, multiple facilities within each VISN) by incorporating a VISN-level random effect in the model. A random intercept model with no explanatory variables, known as an empty model, was used as the primary model.6 The intraclass correlation coefficient (ICC) corresponding to the estimated variance components from the empty model was calculated to determine the portion of the total variation in unadjusted urologist workforce that occurs between VISNs.7 Prostate cancer caseload was then included to test whether allocation seemed to be driven by clinical need or other regional factors.
All analyses were performed using STATA, Version 12 (StataCorp LP, College Station, TX), and all testing was 2-sided. The probability of a type I error was set at .05. This study protocol was approved by the VA Ann Arbor Health Care System Research and Development Committee and Institutional Review Board.
Results
Nearly 1 in 20 VHA patients (n = 274,152) were evaluated in a urology clinic at least once in FY 2011. It was found that 252.7 FTEE and 193.1 residents comprised the VHA urologist workforce (Table 1). Marked regional variation was found in unadjusted urologist staffing at both the facility and VISN levels. The urologist workforce ranged from 0.17 to 5.91 FTEEs across the 130 VHA facilities. At the VISN level, staffing varied over 5-fold (5.8 FTEEs in VISN 2 to 27.6 FTEEs in VISN 8).
Variation in the VHA urologist workforce distribution persisted even after standardizing by patient volume. The urologist workforce continued to vary from 0.94 to 9.95 FTEEs per 100,000 facility patients. This was even more dramatic when adjusted for volume of unique urology patients, ranging from 2.2 to 24.2 FTEE urologists per 10,000 urology patients (Figure).5 From the specialist perspective, each might serve 18 to 64 newly diagnosed patients with prostate cancer annually, depending on the VISN.
Forty percent of urologists were located in 34 of the most complex facilities (Table 2). Urology patient caseload was associated with facility complexity in univariate analysis (P < .001). In the adjusted multivariable model, increasing facility complexity was associated with increasing urologist workforce (P < .001) as well as resident staffing (P < .001), but not with urology patient caseload (P = .27). The empty multilevel model indicated that 27.3% of variation in unadjusted urologist workforce (ICC = 0.273, 95% confidence interval [CI], 0.098-0.448) was attributable to differences at the regional network level. After adjustment for VISN prostate cancer caseload, this decreased to 24.8% (ICC = 0.248; 95% CI, 0.076-0.419).
Discussion
The VHA urologist workforce served over 250,000 patients in FY 2011, and a substantial variation in workforce distribution at the facility and VISN levels was identified in this study. After adjusting for prostate cancer caseload as a proxy for clinical demand, there was some imbalance of urology specialists across regional networks, though most workforce variation occurred within networks in this integrated delivery system. Based on these findings, VHA specialty care initiatives should likely focus within regional networks rather than pursue electronic efforts nationally to improve specialty care access for patients and PCPs.
Regional variation in the VHA urologist workforce was expected, given a limited national supply of urologists and specialist preferences toward metropolitan areas.2-4 Overcoming this maldistribution has important implications for outcomes in many urologic disease processes.8-10 For example, counties with ≥ 1 urologist have up to a 20% reduction in bladder and prostate cancer-related mortality compared with those without a urologist.4 Moreover, the number of veterans with known urologic needs or currently receiving urologic specialty care likely significantly undercounts the total number who could benefit from this care. This is particularly true for facilities with fewer urology resources where patients may be less likely to get a referral, or if they are referred, it is likely outside VHA, creating fragmented care and potentially higher cost.
Understanding the urology workforce distribution, coupled with its sophisticated nationwide EMR, VHA has a unique opportunity to transform how urologic specialty care is delivered without moving around the current workforce. Based on these findings, the system could redistribute resources within each region to meet growing specialty care needs through telemedicine.
At least 2 innovative approaches are underway that might serve the system’s urology care needs: e-consults and the Specialty Care Access Network-Extension for Community Healthcare Outcomes (SCAN-ECHO) video teleconsulting and education project.11,12 The first allows PCPs to request specialist review of the EMR, interpretation of the specific problem, and recommendation for a plan of care, which may or may not include a specialist visit.1,13 The second involves video conferences, which allow multiple PCPs from less complex facilities or rural areas to present cases to specialists from tertiary medical centers for real-time consultation and case-based learning. These initiatives could take advantage of the facility-based variation in urologist workforce by linking facilities with relatively generous urology resources with those with fewer resources to meet the needs of each region’s population and their PCPs while minimizing travel and wait times.
Limitations
This study should be interpreted in the context of several limitations. First, FY 2011 data were used; notably, the VHA urologist workforce remained relatively stable from 2008 through 2011. Second, characteristics of individual VHA urologists, clinical productivity, and skill level were not examined. However, a 2008 study found that nearly all VHA urologists are board certified, mitigating skill level concerns.14 Third, it is possible that demand is partially driven by existence of resources, and there may be patients who might benefit from urologic care but who are not yet diagnosed. The analysis is conservative in this regard, in that demand may be greater than what was detected using the selected study methods. Last, this study examined specialist workforce within a single system. However, ensuring specialist resources are well distributed is a concern for most health systems, particularly in light of recent policy efforts, including accountable care organizations.15
Conclusion
Much of the variation in the VHA urologist workforce exists at the facility rather than the regional level. Optimizing the distribution of these specialty care resources could be achieved through novel care delivery models within each regional network that are well-aligned with current VHA initiatives. Successfully utilizing this workforce distribution has the potential to improve urologic care for veterans across the country and could be applied to improve access to all types of specialists in underserved and understaffed areas.
Acknowledgments
Dr. Skolarus is supported by a VA HSR&D Career Development Award (CDA 12-171).
Author disclosures
The authors report no actual or potential conflicts of interest with regard to this article.
Disclaimer
The opinions expressed herein are those of the authors and do not necessarily reflect those of Federal Practitioner, Frontline Medical Communications Inc., the U.S. Government, or any of its agencies. This article may discuss unlabeled or investigational use of certain drugs. Please review complete prescribing information for specific drugs or drug combinations—including indications, contraindications, warnings, and adverse effects—before administering pharmacologic therapy to patients.
1. Graham GD; Office of Specialty Care Transformation, Department of Veterans Affairs Patient Care Services. Specialty care transformation initiatives. http://www.pva.org/atf/cf/%7BCA2A0FFB-6859 -4BC1-BC96-6B57F57F0391%7D/Friday_Graham_Specialty%20Care%20Transformation%20Initiatives.pdf. Published December 2011. Accessed February 3, 2015.
2. Neuwahl S, Thompson K, Fraher E, Ricketts T. HPRI data tracks. Urology workforce trends. Bull Am Coll Surg. 2012;97(1):46-49.
3. Odisho AY, Fradet V, Cooperberg MR, Ahmad AE, Carroll PR. Geographic distribution of urologists throughout the United States using a county level approach. J Urol. 2009;181(2):760-765; discussion 765-766.
4. Odisho AY, Cooperberg MR, Fradet V, Ahmad AE, Carroll PR. Urologist density and county-level urologic cancer mortality. J Clin Oncol. 2010;28(15):2499-2504.
5. Fiscal Year 2011 VHA Physician Workforce & Support Staff Data. VHA Office of Productivity, Efficiency, & Staffing Website. https://opes.vscc.med.va.gov. Published December 2011.
6. Snijders TAB, Bosker RJ. Multilevel Analysis: An Introduction to Basic and Advanced Multilevel Modeling. Thousand Oaks, CA: Sage Publications Inc;1999.
7. Krein SL, Hofer TP, Kerr EA, Hayward RA. Whom should we profile? Examining diabetes care practice variation among primary care providers, provider groups, and health care facilities. Health Serv Res. 2002;37(5):1159-1180.
8. Weiner DM, McDaniel R, Lowe FC. Urologic manpower issues for the 21st century: Assessing the impact of changing population demographics. Urology. 1997;49(3):335-342.
9. Gee WF, Holtgrewe HL, Albertsen PC, et al. Subspecialization, recruitment and retirement trends of American urologists. J Urol. 1998;159(2): 509-511.
10. McCullough DL. Manpower needs in urology in the twenty-first century. Urol Clin North Am. 1998;25(1):15-22.
11. Saifu HN, Asch SM, Goetz MB, et al. Evaluation of human immunodeficiency virus and hepatitis C telemedicine clinics. Am J Manag Care. 2012;18(4):207-212.
12. Arora S, Geppert CM, Kalishman S, et al. Academic health center management of chronic diseases through knowledge networks: Project ECHO. Acad Med. 2007;82(2):154-160.
13. Hysong SJ, Esquivel A, Sittig DF, et al. Towards successful coordination of electronic health record based-referrals: A qualitative analysis. Implement Sci. 2011;6:84.
14. Tyson MD, Lerner LB. Profile of the veterans affairs urologist: Results from a national survey. J Urol. 2008;180(4):1460-1462.
15. Landon BE, Roberts DH. Reenvisioning specialty care and payment under global payment systems. JAMA. 2013;310(4):371-372.
1. Graham GD; Office of Specialty Care Transformation, Department of Veterans Affairs Patient Care Services. Specialty care transformation initiatives. http://www.pva.org/atf/cf/%7BCA2A0FFB-6859 -4BC1-BC96-6B57F57F0391%7D/Friday_Graham_Specialty%20Care%20Transformation%20Initiatives.pdf. Published December 2011. Accessed February 3, 2015.
2. Neuwahl S, Thompson K, Fraher E, Ricketts T. HPRI data tracks. Urology workforce trends. Bull Am Coll Surg. 2012;97(1):46-49.
3. Odisho AY, Fradet V, Cooperberg MR, Ahmad AE, Carroll PR. Geographic distribution of urologists throughout the United States using a county level approach. J Urol. 2009;181(2):760-765; discussion 765-766.
4. Odisho AY, Cooperberg MR, Fradet V, Ahmad AE, Carroll PR. Urologist density and county-level urologic cancer mortality. J Clin Oncol. 2010;28(15):2499-2504.
5. Fiscal Year 2011 VHA Physician Workforce & Support Staff Data. VHA Office of Productivity, Efficiency, & Staffing Website. https://opes.vscc.med.va.gov. Published December 2011.
6. Snijders TAB, Bosker RJ. Multilevel Analysis: An Introduction to Basic and Advanced Multilevel Modeling. Thousand Oaks, CA: Sage Publications Inc;1999.
7. Krein SL, Hofer TP, Kerr EA, Hayward RA. Whom should we profile? Examining diabetes care practice variation among primary care providers, provider groups, and health care facilities. Health Serv Res. 2002;37(5):1159-1180.
8. Weiner DM, McDaniel R, Lowe FC. Urologic manpower issues for the 21st century: Assessing the impact of changing population demographics. Urology. 1997;49(3):335-342.
9. Gee WF, Holtgrewe HL, Albertsen PC, et al. Subspecialization, recruitment and retirement trends of American urologists. J Urol. 1998;159(2): 509-511.
10. McCullough DL. Manpower needs in urology in the twenty-first century. Urol Clin North Am. 1998;25(1):15-22.
11. Saifu HN, Asch SM, Goetz MB, et al. Evaluation of human immunodeficiency virus and hepatitis C telemedicine clinics. Am J Manag Care. 2012;18(4):207-212.
12. Arora S, Geppert CM, Kalishman S, et al. Academic health center management of chronic diseases through knowledge networks: Project ECHO. Acad Med. 2007;82(2):154-160.
13. Hysong SJ, Esquivel A, Sittig DF, et al. Towards successful coordination of electronic health record based-referrals: A qualitative analysis. Implement Sci. 2011;6:84.
14. Tyson MD, Lerner LB. Profile of the veterans affairs urologist: Results from a national survey. J Urol. 2008;180(4):1460-1462.
15. Landon BE, Roberts DH. Reenvisioning specialty care and payment under global payment systems. JAMA. 2013;310(4):371-372.
Coaching Supports Patient Aligned Care Teams
In 2010, the VHA implemented the patient-centered medical home model of primary care health care as part of its transformational T-21 Initiatives.1 Now known as Patient Aligned Care Teams (PACTs), the key pillars of the model include the expanded roles and responsibilities of multidisciplinary care teams who provide enhanced access and coordinated care. This model is based on a foundation of adequate resources, patient centeredness, and process improvement (Figure 1).
The national implementation strategy consisted of an initial educational conference with 3,600 attendees. The conference included a series of PACT learning collaboratives that engaged > 300 primary care teams, 5 demonstration laboratories, and educational outreach through learning centers and on-site consultations. Despite an aggressive national implementation plan, many frontline primary care teams struggled to translate the medical home theory into process.
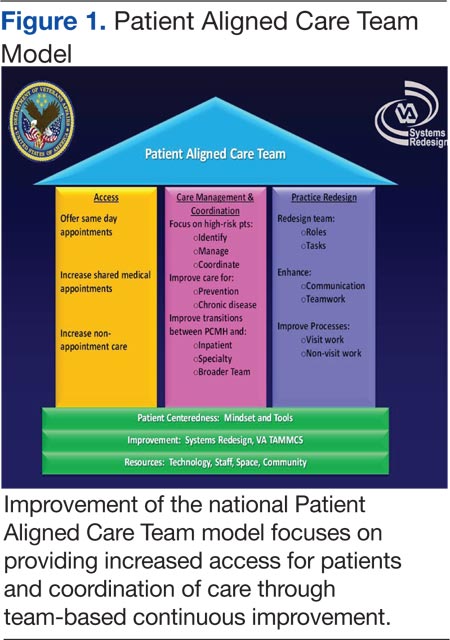
Background
The Richard L. Roudebush VAMC (RLRVAMC) is a large tertiary medical center providing care to > 44,000 primary care patients. This care is delivered by 58 primary care physicians (PCPs) in 5 hospital-based outpatient clinics, including 1 large teaching clinic, 3 community-based outpatient clinics (CBOCs), and a clinic that serves recently returned active-duty veterans. Administrative nursing and clerical associates report to the Office of Ambulatory Care, and physicians and nurse practitioners report to the Medicine Service. Before the implementation of the PACT model, the functional unit of primary care was an entire clinic, typically consisting of 4 to 10 PCPs, nurses, and clerical associates.
Discussions about process change had previously occurred through monthly service or clinic meetings in which administrative leaders provided direction to frontline staff. This culture of top-down leadership drove process change but was not always effective and empowering for practice change. With the implementation of PACT, the functional unit of primary care shifted from the larger clinic to a team composed of a PCP, a nurse, a licensed nurse practitioner or health technician, and a clerical associate.
The care delivery system fundamentally changed from the traditional model to a medical home model (Figure 2). This group now represented the fundamental clinical microsystem for the delivery of primary care within the VA medical home model.2 The experience of Batalden and colleagues at the Dartmouth Hitchcock Medical Center suggests that such microsystems are very effective units of change.3 The key challenge presented to the primary care leadership was how to link these clinical PACT microsystems with an effective process that would guide practice redesign.
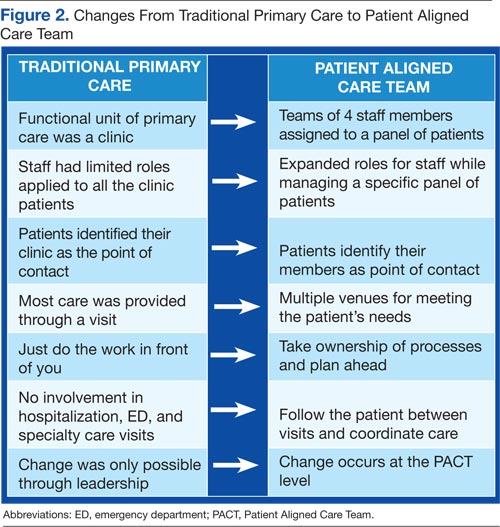
The concept of practice coaching or facilitation as a mechanism for physician offices to adopt evidence-based medicine and quality improvement dates to the early 1980s in England. This model spread to the U.S. in the 1990s and has continued to be used as a mechanism for leading clinical practice redesign.4 In traditional practice facilitation, a trained individual is brought in from outside the practice to help adopt evidence-based medicine guidelines.5 This individual works with the practice to implement changes that translate into patient outcome improvements.
Unlike consultation, this facilitator maintains a long-term relationship with the team as they work together to achieve goals. More important, the facilitator assists the team in developing improvement processes that are sustainable as they become incorporated within the fabric of the team culture and remain after the coach is gone. There are several reviews of clinical practice coaching that support its effectiveness in implementing evidence-based primary care guidelines.6,7 The Affordable Care Act contains provisions for the use of this model in promoting best practices and quality care.8 Manuals developed by the Agency for Healthcare Research and Quality outline how to develop a practice facilitation program.9,10
Related: Infusing Gerontologic Practice Into PACT
Essential to all practice facilitation models is the effective use of quality improvement tools. The RLRVAMC adopted the VHA Lean Healthcare Improvement Framework, which includes an approach for rapid cycle change.
The RLRVAMC adopted the facilitative coaching model in November 2011, using internal coaches who were assigned to the fundamental microsystem of its medical home.
Coach Selection
Many facilitative coaching models described in the literature use external coaches. Frequently cited advantages of external coaches include having dedicated time, receiving standardized training in facilitation, and being regarded as neutral to internal conflicts. The RLRVAMC staff elected to identify internal coaches. Advantages of this approach include the use of existing resources, the ability to develop long-term continuous relationships with PACTs, and the ability to access key internal resources to assist the team. Also, using internal individuals holding primary care leadership positions was critical to the coaching model.
Thirty-eight PACTs were initially created, and 15 internal coaches were identified. These individuals included the associate chief of staff of Ambulatory Care, chief nurse for Clinic Operations, business administrators in primary care, and all frontline unit managers and supervisors. This level of management involvement provided content expertise about primary care operations and equally important, carried the authority to implement change.
Related: Using H-PACT to Overcome Treatment Obstacles for Homeless Veterans
In addition, this approach provided considerable leadership credibility among frontline PACT staff. Given the large number of PACTs requiring coaching, coach recruitment was expanded to include other primary care administrative staff, such as the leads for the CBOCs, Prevention and Behavioral Health programs, System Redesign, and Telehealth Services. The most recent phase has included registered nurses, licensed practical nurses, health technicians, and physicians from high- functioning PACT teams who have experienced the process and who can now devote time to being coaches.
Qulifications and Training
Although the literature suggests multiple qualifications for practice coaches, there is a general agreement regarding core skills for strong facilitation, which includes interpersonal skills, knowledge of process improvement techniques, and an understanding of data acquisition and analysis.10 Strong interpersonal skills are often inherent but are a critical factor in motivating team members and managing conflicts that arise. Potential coaches were not selected if these skills were poorly developed.
The authors’ experiences have shown that although content knowledge about primary care operations is very helpful, it is not essential to being an effective coach. The facilitation model that was adopted for the program, as described by Bens, focuses predominately on process and not content expertise.11 The facilitator’s role is to apply a structural framework; ie, methods and tools that capitalize on content knowledge of frontline staff in identifying changes needed to implement the medical home.
Related: Updates in Specialty Care
Also, although knowledge of primary care operations was not required, formal training in understanding the goals of the medical home and the metrics related to PACT was essential for successful coaching. All coaches were required to attend PACT training sessions. Coaches were also expected to have basic training or experience in system redesign with the majority of the coaches completing Yellow Belt training, which is an introduction to the methods of process improvement through the lean thinking business model. A coaching manual was developed that contained information related to meeting structures, data definitions, extraction, and interpretation. A coaching website was developed that provided links to data sources and definitions. PACT-related tools, such as instructions on conducting group visits, phone visits, and use of population management were disseminated.
Coach-Team Meeting Structure
Coaches were assigned to teams by matching the skills of the coach with the team needs. Initially, sessions were held weekly for 1 hour, though this typically evolved into biweekly meetings. Clinic schedules were blocked, allowing PACTs the time to meet with their coaches. A ratio of 1 coach to 2 PACTs was considered optimal for individualized team meetings. The exceptions were the CBOCs, where several teams met together due to the need for coaches to travel. Meetings were held away from clinical areas to avoid distractions. Plan-Do-Study-Act (PDSA) cycles were used to plan and implement process improvements. The average time commitment for a coach assigned to 2 teams was between 2 to 4 hours a week.
The initial coaching sessions tended to be more structured, clearly defining the coach role, developing team building, identifying the goals, and outlining process improvement tools. Common challenges for the coaches were keeping teams focused and optimally managing time by preventing prolonged conversations unrelated to process improvement. Many frontline staff had never been empowered to change their practices, so their initial reaction was to focus on problems and not solutions. Once team relationships were established, the strong influence of nursing or clerical associates exerted on the PCP’ s willingness to change became evident and a key factor for success. Often the leaders of change are not the physicians, highlighting the influence of team building and the willingness of individuals to change practice due to team relationships and not by authority.12
Data Use
Before the implementation of this model, PACT data and metrics were posted in the clinics and briefly discussed at service-level meetings. However, this data-sharing approach rarely generated team members’ interest. By using coaching, personalized data reports that displayed team-specific information in comparison to the overall service and national VA goals were found to be a more effective technique for sharing data and performance metrics. National VA PACT core metrics tracked the following: (1) percentage of same-day appointments with PCP ratio—target 70%; (2) ratio of nontraditional encounters—target 20%; (3) percentage of continuity with PCP—target 77%; and (4) percentage of 2-day contact postdischarge ratio—target 75%. Figure 3 shows the improvements made as a facility from March 2011 (pre-PACT implementation) to March 2012 (post-PACT implementation).
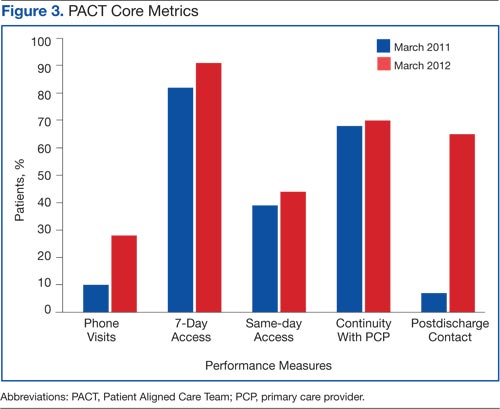
A graphic display of the team’s data, including metrics related to access, continuity, and postdischarge follow-up was reviewed monthly, and the coach provided detailed explanations (Figure 4). Of particular importance to the teams was the ability to individually identify those patients who failed the metric. Review of these “fallouts” at a coaching session often resulted in reliable, consistent process improvements that addressed the failed process.
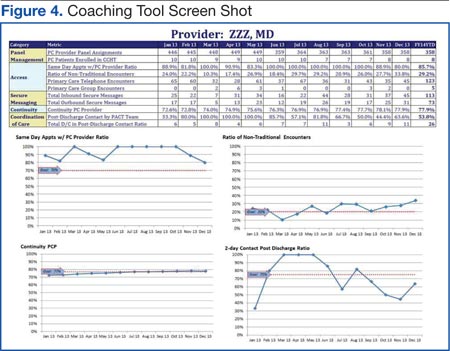
Coach-to-Coach Meetings
Critical to the RLRVAMC coaching model were the weekly 1-hour coach-to-coach meetings. Most of the coach training occurred during these sessions, either formally or via feedback and discussion. Coaches discussed their teams’ progress, brought back questions from the teams, and sought guidance from one another. Executive leaders, who were also coaches, were present at these meetings and provided the opportunity to implement broader operational changes quickly. Coaches also served as a communication venue for frontline staff to express their concerns to primary care leaders during these meetings.
Limitations
Practice facilitation that uses internal coaches for a clinical PACT microsystem may present several potential challenges. Large primary care practices require a pool of coaches who are willing to commit the necessary time required for successful implementation of this model. Although the coaches dedicate this time as collateral duty, many express that the time spent with their teams is a rewarding experience outside of their administrative roles. The coaches express satisfaction when teams meet their goals and PDSA cycles are successful.
Coaches require significant amounts of training to reach the level of effectiveness required. Teams must realize and appreciate the importance of dedicating time away from the competing priority of patient care.
Implementation of the coaching model for physician trainees in the teaching clinic has not been successful due to the teaching clinic schedule and other issues. Also related to the complexity of the teaching clinic schedule, the coaching model did not significantly improve continuity. Coaches have recently been assigned to the teaching clinic, and each team will be identifying PDSA cycles to approach the implementation of PACT principles.
Conclusion
Despite the aforementioned challenges, the outcomes are clear. The implementation of the coaching model, using internal coaches, resulted in a significant improvement of the ability of the staff to achieve the national PACT metrics (Figure 3). More important, the model created a new structural organization for change within primary care that reversed a culture of top-down leadership to that of team empowerment.
Teams that experienced practice facilitation developed ownership in their processes, data, and performance improvement and now have a more direct mechanism of communicating with primary care leadership. The coaching model moved the teams forward from having received PACT education to having the confidence and tools to implement PACTs. Staff progressed from looking at the data given to them to collecting and interpreting the data themselves. The teams are able to articulate how they fit in to the PACT model and enthusiastically monitor their progress. As primary care moves forward with the medical home, the facilitative coaching model offers a promising option for successful implementation.
Author disclosures
The authors report no actual or potential conflicts of interest with regard to this article.
Disclaimer
The opinions expressed herein are those of the authors and do not necessarily reflect those of Federal Practitioner, Frontline Medical Communications Inc., the U.S. Government, or any of its agencies. This article may discuss unlabeled or investigational use of certain drugs. Please review complete prescribing information for specific drugs or drug combinations—including indications, contraindications, warnings, and adverse effects— before administering pharmacologic therapy to patients.
1. Klein S. The Veterans Health Administration: Implementing patient-centered medical homes in the nation’s largest integrated delivery system. Issue Brief (Commonw Fund). 2011;16:1537.
2. Godfrey MM, ed. Clinical Microsystem Action Guide: Improving Health Care by Improving Your Microsystem. Version 2.1. The Dartmouth Institute Website. http://clinicalmicrosys.dartmouth.edu/wp -content/uploads/2014/07/CMAG040104.pdf. Published 2004. Accessed January 23, 2015.
3. Batalden PB, Nelson EC, Edwards WH, Godfrey MM, Mohr JJ. Microsystems in health care: Part 9. Developing a small clinical unit to attain peak performance. Jt Comm J Qual Saf. 2003;29(11):575-585.
4. Nutting PA, Crabtree BF, Stewart EE, et al. Effect of facilitation on practice outcomes in the National Demonstration Project model of the patient-centered medical home. Ann Fam Med. 2010;8(suppl 1):S33-S34, S92.
5. Nagykaldi Z, Mold JW, Robinson A, Niebauer L, Ford A. Practice facilitators and practice-based research networks. J Am Board Fam Med. 2006;19(5):506-510.
6. Baskerville NB, Liddy C, Hogg W. Systematic review and meta-analysis of practice facilitation within primary care settings. Ann Fam Med. 2012;10(1):63-74.
7. Nagykaldi Z, Mold JW, Aspy CB. Practice facilitators: A review of the literature. Fam Med. 2005;37(8):581-588.
8. Grumbach K, Bainbridge E, Bodenheimer T. Facilitating improvement in primary care: The promise of practice coaching. Issue Brief (Commonw Fund). 2012;15:1-14.
9. Knox L, Taylor EF, Geonnotti K, et al. Developing and Running a Primary Care Practice Facilitation Program: A How-To Guide. Rockville, MD: Agency for Healthcare Research and Quality. U.S. Department of Health and Human Services; 2011. AHRQ Publication No. 12-0011.
10. Agency for Healthcare Research and Quality. Integrating Chronic Care and Business Strategies in the Safety Net: A Practice Coaching Manual. Agency for Healthcare Research and Quality Website. http://www.ahrq.gov/professionals/systems/primary-care /coachmnl/index.html. Published December 2012. Accessed February 26, 2015.
11. Bens I. Facilitation With Ease! Core Skills for Facilitators, Team Leaders and Members, Managers, Consultants and Trainers. 2nd ed. San Francisco, CA: Jossey-Bass; 2005.
12. Bodenheimer T. Building Teams in Primary Care: Lessons Learned: Part 1 and 2. Oakland, CA: California Health Care Foundation; July 2007.
In 2010, the VHA implemented the patient-centered medical home model of primary care health care as part of its transformational T-21 Initiatives.1 Now known as Patient Aligned Care Teams (PACTs), the key pillars of the model include the expanded roles and responsibilities of multidisciplinary care teams who provide enhanced access and coordinated care. This model is based on a foundation of adequate resources, patient centeredness, and process improvement (Figure 1).
The national implementation strategy consisted of an initial educational conference with 3,600 attendees. The conference included a series of PACT learning collaboratives that engaged > 300 primary care teams, 5 demonstration laboratories, and educational outreach through learning centers and on-site consultations. Despite an aggressive national implementation plan, many frontline primary care teams struggled to translate the medical home theory into process.
Background
The Richard L. Roudebush VAMC (RLRVAMC) is a large tertiary medical center providing care to > 44,000 primary care patients. This care is delivered by 58 primary care physicians (PCPs) in 5 hospital-based outpatient clinics, including 1 large teaching clinic, 3 community-based outpatient clinics (CBOCs), and a clinic that serves recently returned active-duty veterans. Administrative nursing and clerical associates report to the Office of Ambulatory Care, and physicians and nurse practitioners report to the Medicine Service. Before the implementation of the PACT model, the functional unit of primary care was an entire clinic, typically consisting of 4 to 10 PCPs, nurses, and clerical associates.
Discussions about process change had previously occurred through monthly service or clinic meetings in which administrative leaders provided direction to frontline staff. This culture of top-down leadership drove process change but was not always effective and empowering for practice change. With the implementation of PACT, the functional unit of primary care shifted from the larger clinic to a team composed of a PCP, a nurse, a licensed nurse practitioner or health technician, and a clerical associate.
The care delivery system fundamentally changed from the traditional model to a medical home model (Figure 2). This group now represented the fundamental clinical microsystem for the delivery of primary care within the VA medical home model.2 The experience of Batalden and colleagues at the Dartmouth Hitchcock Medical Center suggests that such microsystems are very effective units of change.3 The key challenge presented to the primary care leadership was how to link these clinical PACT microsystems with an effective process that would guide practice redesign.
The concept of practice coaching or facilitation as a mechanism for physician offices to adopt evidence-based medicine and quality improvement dates to the early 1980s in England. This model spread to the U.S. in the 1990s and has continued to be used as a mechanism for leading clinical practice redesign.4 In traditional practice facilitation, a trained individual is brought in from outside the practice to help adopt evidence-based medicine guidelines.5 This individual works with the practice to implement changes that translate into patient outcome improvements.
Unlike consultation, this facilitator maintains a long-term relationship with the team as they work together to achieve goals. More important, the facilitator assists the team in developing improvement processes that are sustainable as they become incorporated within the fabric of the team culture and remain after the coach is gone. There are several reviews of clinical practice coaching that support its effectiveness in implementing evidence-based primary care guidelines.6,7 The Affordable Care Act contains provisions for the use of this model in promoting best practices and quality care.8 Manuals developed by the Agency for Healthcare Research and Quality outline how to develop a practice facilitation program.9,10
Related: Infusing Gerontologic Practice Into PACT
Essential to all practice facilitation models is the effective use of quality improvement tools. The RLRVAMC adopted the VHA Lean Healthcare Improvement Framework, which includes an approach for rapid cycle change.
The RLRVAMC adopted the facilitative coaching model in November 2011, using internal coaches who were assigned to the fundamental microsystem of its medical home.
Coach Selection
Many facilitative coaching models described in the literature use external coaches. Frequently cited advantages of external coaches include having dedicated time, receiving standardized training in facilitation, and being regarded as neutral to internal conflicts. The RLRVAMC staff elected to identify internal coaches. Advantages of this approach include the use of existing resources, the ability to develop long-term continuous relationships with PACTs, and the ability to access key internal resources to assist the team. Also, using internal individuals holding primary care leadership positions was critical to the coaching model.
Thirty-eight PACTs were initially created, and 15 internal coaches were identified. These individuals included the associate chief of staff of Ambulatory Care, chief nurse for Clinic Operations, business administrators in primary care, and all frontline unit managers and supervisors. This level of management involvement provided content expertise about primary care operations and equally important, carried the authority to implement change.
Related: Using H-PACT to Overcome Treatment Obstacles for Homeless Veterans
In addition, this approach provided considerable leadership credibility among frontline PACT staff. Given the large number of PACTs requiring coaching, coach recruitment was expanded to include other primary care administrative staff, such as the leads for the CBOCs, Prevention and Behavioral Health programs, System Redesign, and Telehealth Services. The most recent phase has included registered nurses, licensed practical nurses, health technicians, and physicians from high- functioning PACT teams who have experienced the process and who can now devote time to being coaches.
Qulifications and Training
Although the literature suggests multiple qualifications for practice coaches, there is a general agreement regarding core skills for strong facilitation, which includes interpersonal skills, knowledge of process improvement techniques, and an understanding of data acquisition and analysis.10 Strong interpersonal skills are often inherent but are a critical factor in motivating team members and managing conflicts that arise. Potential coaches were not selected if these skills were poorly developed.
The authors’ experiences have shown that although content knowledge about primary care operations is very helpful, it is not essential to being an effective coach. The facilitation model that was adopted for the program, as described by Bens, focuses predominately on process and not content expertise.11 The facilitator’s role is to apply a structural framework; ie, methods and tools that capitalize on content knowledge of frontline staff in identifying changes needed to implement the medical home.
Related: Updates in Specialty Care
Also, although knowledge of primary care operations was not required, formal training in understanding the goals of the medical home and the metrics related to PACT was essential for successful coaching. All coaches were required to attend PACT training sessions. Coaches were also expected to have basic training or experience in system redesign with the majority of the coaches completing Yellow Belt training, which is an introduction to the methods of process improvement through the lean thinking business model. A coaching manual was developed that contained information related to meeting structures, data definitions, extraction, and interpretation. A coaching website was developed that provided links to data sources and definitions. PACT-related tools, such as instructions on conducting group visits, phone visits, and use of population management were disseminated.
Coach-Team Meeting Structure
Coaches were assigned to teams by matching the skills of the coach with the team needs. Initially, sessions were held weekly for 1 hour, though this typically evolved into biweekly meetings. Clinic schedules were blocked, allowing PACTs the time to meet with their coaches. A ratio of 1 coach to 2 PACTs was considered optimal for individualized team meetings. The exceptions were the CBOCs, where several teams met together due to the need for coaches to travel. Meetings were held away from clinical areas to avoid distractions. Plan-Do-Study-Act (PDSA) cycles were used to plan and implement process improvements. The average time commitment for a coach assigned to 2 teams was between 2 to 4 hours a week.
The initial coaching sessions tended to be more structured, clearly defining the coach role, developing team building, identifying the goals, and outlining process improvement tools. Common challenges for the coaches were keeping teams focused and optimally managing time by preventing prolonged conversations unrelated to process improvement. Many frontline staff had never been empowered to change their practices, so their initial reaction was to focus on problems and not solutions. Once team relationships were established, the strong influence of nursing or clerical associates exerted on the PCP’ s willingness to change became evident and a key factor for success. Often the leaders of change are not the physicians, highlighting the influence of team building and the willingness of individuals to change practice due to team relationships and not by authority.12
Data Use
Before the implementation of this model, PACT data and metrics were posted in the clinics and briefly discussed at service-level meetings. However, this data-sharing approach rarely generated team members’ interest. By using coaching, personalized data reports that displayed team-specific information in comparison to the overall service and national VA goals were found to be a more effective technique for sharing data and performance metrics. National VA PACT core metrics tracked the following: (1) percentage of same-day appointments with PCP ratio—target 70%; (2) ratio of nontraditional encounters—target 20%; (3) percentage of continuity with PCP—target 77%; and (4) percentage of 2-day contact postdischarge ratio—target 75%. Figure 3 shows the improvements made as a facility from March 2011 (pre-PACT implementation) to March 2012 (post-PACT implementation).
A graphic display of the team’s data, including metrics related to access, continuity, and postdischarge follow-up was reviewed monthly, and the coach provided detailed explanations (Figure 4). Of particular importance to the teams was the ability to individually identify those patients who failed the metric. Review of these “fallouts” at a coaching session often resulted in reliable, consistent process improvements that addressed the failed process.
Coach-to-Coach Meetings
Critical to the RLRVAMC coaching model were the weekly 1-hour coach-to-coach meetings. Most of the coach training occurred during these sessions, either formally or via feedback and discussion. Coaches discussed their teams’ progress, brought back questions from the teams, and sought guidance from one another. Executive leaders, who were also coaches, were present at these meetings and provided the opportunity to implement broader operational changes quickly. Coaches also served as a communication venue for frontline staff to express their concerns to primary care leaders during these meetings.
Limitations
Practice facilitation that uses internal coaches for a clinical PACT microsystem may present several potential challenges. Large primary care practices require a pool of coaches who are willing to commit the necessary time required for successful implementation of this model. Although the coaches dedicate this time as collateral duty, many express that the time spent with their teams is a rewarding experience outside of their administrative roles. The coaches express satisfaction when teams meet their goals and PDSA cycles are successful.
Coaches require significant amounts of training to reach the level of effectiveness required. Teams must realize and appreciate the importance of dedicating time away from the competing priority of patient care.
Implementation of the coaching model for physician trainees in the teaching clinic has not been successful due to the teaching clinic schedule and other issues. Also related to the complexity of the teaching clinic schedule, the coaching model did not significantly improve continuity. Coaches have recently been assigned to the teaching clinic, and each team will be identifying PDSA cycles to approach the implementation of PACT principles.
Conclusion
Despite the aforementioned challenges, the outcomes are clear. The implementation of the coaching model, using internal coaches, resulted in a significant improvement of the ability of the staff to achieve the national PACT metrics (Figure 3). More important, the model created a new structural organization for change within primary care that reversed a culture of top-down leadership to that of team empowerment.
Teams that experienced practice facilitation developed ownership in their processes, data, and performance improvement and now have a more direct mechanism of communicating with primary care leadership. The coaching model moved the teams forward from having received PACT education to having the confidence and tools to implement PACTs. Staff progressed from looking at the data given to them to collecting and interpreting the data themselves. The teams are able to articulate how they fit in to the PACT model and enthusiastically monitor their progress. As primary care moves forward with the medical home, the facilitative coaching model offers a promising option for successful implementation.
Author disclosures
The authors report no actual or potential conflicts of interest with regard to this article.
Disclaimer
The opinions expressed herein are those of the authors and do not necessarily reflect those of Federal Practitioner, Frontline Medical Communications Inc., the U.S. Government, or any of its agencies. This article may discuss unlabeled or investigational use of certain drugs. Please review complete prescribing information for specific drugs or drug combinations—including indications, contraindications, warnings, and adverse effects— before administering pharmacologic therapy to patients.
In 2010, the VHA implemented the patient-centered medical home model of primary care health care as part of its transformational T-21 Initiatives.1 Now known as Patient Aligned Care Teams (PACTs), the key pillars of the model include the expanded roles and responsibilities of multidisciplinary care teams who provide enhanced access and coordinated care. This model is based on a foundation of adequate resources, patient centeredness, and process improvement (Figure 1).
The national implementation strategy consisted of an initial educational conference with 3,600 attendees. The conference included a series of PACT learning collaboratives that engaged > 300 primary care teams, 5 demonstration laboratories, and educational outreach through learning centers and on-site consultations. Despite an aggressive national implementation plan, many frontline primary care teams struggled to translate the medical home theory into process.
Background
The Richard L. Roudebush VAMC (RLRVAMC) is a large tertiary medical center providing care to > 44,000 primary care patients. This care is delivered by 58 primary care physicians (PCPs) in 5 hospital-based outpatient clinics, including 1 large teaching clinic, 3 community-based outpatient clinics (CBOCs), and a clinic that serves recently returned active-duty veterans. Administrative nursing and clerical associates report to the Office of Ambulatory Care, and physicians and nurse practitioners report to the Medicine Service. Before the implementation of the PACT model, the functional unit of primary care was an entire clinic, typically consisting of 4 to 10 PCPs, nurses, and clerical associates.
Discussions about process change had previously occurred through monthly service or clinic meetings in which administrative leaders provided direction to frontline staff. This culture of top-down leadership drove process change but was not always effective and empowering for practice change. With the implementation of PACT, the functional unit of primary care shifted from the larger clinic to a team composed of a PCP, a nurse, a licensed nurse practitioner or health technician, and a clerical associate.
The care delivery system fundamentally changed from the traditional model to a medical home model (Figure 2). This group now represented the fundamental clinical microsystem for the delivery of primary care within the VA medical home model.2 The experience of Batalden and colleagues at the Dartmouth Hitchcock Medical Center suggests that such microsystems are very effective units of change.3 The key challenge presented to the primary care leadership was how to link these clinical PACT microsystems with an effective process that would guide practice redesign.
The concept of practice coaching or facilitation as a mechanism for physician offices to adopt evidence-based medicine and quality improvement dates to the early 1980s in England. This model spread to the U.S. in the 1990s and has continued to be used as a mechanism for leading clinical practice redesign.4 In traditional practice facilitation, a trained individual is brought in from outside the practice to help adopt evidence-based medicine guidelines.5 This individual works with the practice to implement changes that translate into patient outcome improvements.
Unlike consultation, this facilitator maintains a long-term relationship with the team as they work together to achieve goals. More important, the facilitator assists the team in developing improvement processes that are sustainable as they become incorporated within the fabric of the team culture and remain after the coach is gone. There are several reviews of clinical practice coaching that support its effectiveness in implementing evidence-based primary care guidelines.6,7 The Affordable Care Act contains provisions for the use of this model in promoting best practices and quality care.8 Manuals developed by the Agency for Healthcare Research and Quality outline how to develop a practice facilitation program.9,10
Related: Infusing Gerontologic Practice Into PACT
Essential to all practice facilitation models is the effective use of quality improvement tools. The RLRVAMC adopted the VHA Lean Healthcare Improvement Framework, which includes an approach for rapid cycle change.
The RLRVAMC adopted the facilitative coaching model in November 2011, using internal coaches who were assigned to the fundamental microsystem of its medical home.
Coach Selection
Many facilitative coaching models described in the literature use external coaches. Frequently cited advantages of external coaches include having dedicated time, receiving standardized training in facilitation, and being regarded as neutral to internal conflicts. The RLRVAMC staff elected to identify internal coaches. Advantages of this approach include the use of existing resources, the ability to develop long-term continuous relationships with PACTs, and the ability to access key internal resources to assist the team. Also, using internal individuals holding primary care leadership positions was critical to the coaching model.
Thirty-eight PACTs were initially created, and 15 internal coaches were identified. These individuals included the associate chief of staff of Ambulatory Care, chief nurse for Clinic Operations, business administrators in primary care, and all frontline unit managers and supervisors. This level of management involvement provided content expertise about primary care operations and equally important, carried the authority to implement change.
Related: Using H-PACT to Overcome Treatment Obstacles for Homeless Veterans
In addition, this approach provided considerable leadership credibility among frontline PACT staff. Given the large number of PACTs requiring coaching, coach recruitment was expanded to include other primary care administrative staff, such as the leads for the CBOCs, Prevention and Behavioral Health programs, System Redesign, and Telehealth Services. The most recent phase has included registered nurses, licensed practical nurses, health technicians, and physicians from high- functioning PACT teams who have experienced the process and who can now devote time to being coaches.
Qulifications and Training
Although the literature suggests multiple qualifications for practice coaches, there is a general agreement regarding core skills for strong facilitation, which includes interpersonal skills, knowledge of process improvement techniques, and an understanding of data acquisition and analysis.10 Strong interpersonal skills are often inherent but are a critical factor in motivating team members and managing conflicts that arise. Potential coaches were not selected if these skills were poorly developed.
The authors’ experiences have shown that although content knowledge about primary care operations is very helpful, it is not essential to being an effective coach. The facilitation model that was adopted for the program, as described by Bens, focuses predominately on process and not content expertise.11 The facilitator’s role is to apply a structural framework; ie, methods and tools that capitalize on content knowledge of frontline staff in identifying changes needed to implement the medical home.
Related: Updates in Specialty Care
Also, although knowledge of primary care operations was not required, formal training in understanding the goals of the medical home and the metrics related to PACT was essential for successful coaching. All coaches were required to attend PACT training sessions. Coaches were also expected to have basic training or experience in system redesign with the majority of the coaches completing Yellow Belt training, which is an introduction to the methods of process improvement through the lean thinking business model. A coaching manual was developed that contained information related to meeting structures, data definitions, extraction, and interpretation. A coaching website was developed that provided links to data sources and definitions. PACT-related tools, such as instructions on conducting group visits, phone visits, and use of population management were disseminated.
Coach-Team Meeting Structure
Coaches were assigned to teams by matching the skills of the coach with the team needs. Initially, sessions were held weekly for 1 hour, though this typically evolved into biweekly meetings. Clinic schedules were blocked, allowing PACTs the time to meet with their coaches. A ratio of 1 coach to 2 PACTs was considered optimal for individualized team meetings. The exceptions were the CBOCs, where several teams met together due to the need for coaches to travel. Meetings were held away from clinical areas to avoid distractions. Plan-Do-Study-Act (PDSA) cycles were used to plan and implement process improvements. The average time commitment for a coach assigned to 2 teams was between 2 to 4 hours a week.
The initial coaching sessions tended to be more structured, clearly defining the coach role, developing team building, identifying the goals, and outlining process improvement tools. Common challenges for the coaches were keeping teams focused and optimally managing time by preventing prolonged conversations unrelated to process improvement. Many frontline staff had never been empowered to change their practices, so their initial reaction was to focus on problems and not solutions. Once team relationships were established, the strong influence of nursing or clerical associates exerted on the PCP’ s willingness to change became evident and a key factor for success. Often the leaders of change are not the physicians, highlighting the influence of team building and the willingness of individuals to change practice due to team relationships and not by authority.12
Data Use
Before the implementation of this model, PACT data and metrics were posted in the clinics and briefly discussed at service-level meetings. However, this data-sharing approach rarely generated team members’ interest. By using coaching, personalized data reports that displayed team-specific information in comparison to the overall service and national VA goals were found to be a more effective technique for sharing data and performance metrics. National VA PACT core metrics tracked the following: (1) percentage of same-day appointments with PCP ratio—target 70%; (2) ratio of nontraditional encounters—target 20%; (3) percentage of continuity with PCP—target 77%; and (4) percentage of 2-day contact postdischarge ratio—target 75%. Figure 3 shows the improvements made as a facility from March 2011 (pre-PACT implementation) to March 2012 (post-PACT implementation).
A graphic display of the team’s data, including metrics related to access, continuity, and postdischarge follow-up was reviewed monthly, and the coach provided detailed explanations (Figure 4). Of particular importance to the teams was the ability to individually identify those patients who failed the metric. Review of these “fallouts” at a coaching session often resulted in reliable, consistent process improvements that addressed the failed process.
Coach-to-Coach Meetings
Critical to the RLRVAMC coaching model were the weekly 1-hour coach-to-coach meetings. Most of the coach training occurred during these sessions, either formally or via feedback and discussion. Coaches discussed their teams’ progress, brought back questions from the teams, and sought guidance from one another. Executive leaders, who were also coaches, were present at these meetings and provided the opportunity to implement broader operational changes quickly. Coaches also served as a communication venue for frontline staff to express their concerns to primary care leaders during these meetings.
Limitations
Practice facilitation that uses internal coaches for a clinical PACT microsystem may present several potential challenges. Large primary care practices require a pool of coaches who are willing to commit the necessary time required for successful implementation of this model. Although the coaches dedicate this time as collateral duty, many express that the time spent with their teams is a rewarding experience outside of their administrative roles. The coaches express satisfaction when teams meet their goals and PDSA cycles are successful.
Coaches require significant amounts of training to reach the level of effectiveness required. Teams must realize and appreciate the importance of dedicating time away from the competing priority of patient care.
Implementation of the coaching model for physician trainees in the teaching clinic has not been successful due to the teaching clinic schedule and other issues. Also related to the complexity of the teaching clinic schedule, the coaching model did not significantly improve continuity. Coaches have recently been assigned to the teaching clinic, and each team will be identifying PDSA cycles to approach the implementation of PACT principles.
Conclusion
Despite the aforementioned challenges, the outcomes are clear. The implementation of the coaching model, using internal coaches, resulted in a significant improvement of the ability of the staff to achieve the national PACT metrics (Figure 3). More important, the model created a new structural organization for change within primary care that reversed a culture of top-down leadership to that of team empowerment.
Teams that experienced practice facilitation developed ownership in their processes, data, and performance improvement and now have a more direct mechanism of communicating with primary care leadership. The coaching model moved the teams forward from having received PACT education to having the confidence and tools to implement PACTs. Staff progressed from looking at the data given to them to collecting and interpreting the data themselves. The teams are able to articulate how they fit in to the PACT model and enthusiastically monitor their progress. As primary care moves forward with the medical home, the facilitative coaching model offers a promising option for successful implementation.
Author disclosures
The authors report no actual or potential conflicts of interest with regard to this article.
Disclaimer
The opinions expressed herein are those of the authors and do not necessarily reflect those of Federal Practitioner, Frontline Medical Communications Inc., the U.S. Government, or any of its agencies. This article may discuss unlabeled or investigational use of certain drugs. Please review complete prescribing information for specific drugs or drug combinations—including indications, contraindications, warnings, and adverse effects— before administering pharmacologic therapy to patients.
1. Klein S. The Veterans Health Administration: Implementing patient-centered medical homes in the nation’s largest integrated delivery system. Issue Brief (Commonw Fund). 2011;16:1537.
2. Godfrey MM, ed. Clinical Microsystem Action Guide: Improving Health Care by Improving Your Microsystem. Version 2.1. The Dartmouth Institute Website. http://clinicalmicrosys.dartmouth.edu/wp -content/uploads/2014/07/CMAG040104.pdf. Published 2004. Accessed January 23, 2015.
3. Batalden PB, Nelson EC, Edwards WH, Godfrey MM, Mohr JJ. Microsystems in health care: Part 9. Developing a small clinical unit to attain peak performance. Jt Comm J Qual Saf. 2003;29(11):575-585.
4. Nutting PA, Crabtree BF, Stewart EE, et al. Effect of facilitation on practice outcomes in the National Demonstration Project model of the patient-centered medical home. Ann Fam Med. 2010;8(suppl 1):S33-S34, S92.
5. Nagykaldi Z, Mold JW, Robinson A, Niebauer L, Ford A. Practice facilitators and practice-based research networks. J Am Board Fam Med. 2006;19(5):506-510.
6. Baskerville NB, Liddy C, Hogg W. Systematic review and meta-analysis of practice facilitation within primary care settings. Ann Fam Med. 2012;10(1):63-74.
7. Nagykaldi Z, Mold JW, Aspy CB. Practice facilitators: A review of the literature. Fam Med. 2005;37(8):581-588.
8. Grumbach K, Bainbridge E, Bodenheimer T. Facilitating improvement in primary care: The promise of practice coaching. Issue Brief (Commonw Fund). 2012;15:1-14.
9. Knox L, Taylor EF, Geonnotti K, et al. Developing and Running a Primary Care Practice Facilitation Program: A How-To Guide. Rockville, MD: Agency for Healthcare Research and Quality. U.S. Department of Health and Human Services; 2011. AHRQ Publication No. 12-0011.
10. Agency for Healthcare Research and Quality. Integrating Chronic Care and Business Strategies in the Safety Net: A Practice Coaching Manual. Agency for Healthcare Research and Quality Website. http://www.ahrq.gov/professionals/systems/primary-care /coachmnl/index.html. Published December 2012. Accessed February 26, 2015.
11. Bens I. Facilitation With Ease! Core Skills for Facilitators, Team Leaders and Members, Managers, Consultants and Trainers. 2nd ed. San Francisco, CA: Jossey-Bass; 2005.
12. Bodenheimer T. Building Teams in Primary Care: Lessons Learned: Part 1 and 2. Oakland, CA: California Health Care Foundation; July 2007.
1. Klein S. The Veterans Health Administration: Implementing patient-centered medical homes in the nation’s largest integrated delivery system. Issue Brief (Commonw Fund). 2011;16:1537.
2. Godfrey MM, ed. Clinical Microsystem Action Guide: Improving Health Care by Improving Your Microsystem. Version 2.1. The Dartmouth Institute Website. http://clinicalmicrosys.dartmouth.edu/wp -content/uploads/2014/07/CMAG040104.pdf. Published 2004. Accessed January 23, 2015.
3. Batalden PB, Nelson EC, Edwards WH, Godfrey MM, Mohr JJ. Microsystems in health care: Part 9. Developing a small clinical unit to attain peak performance. Jt Comm J Qual Saf. 2003;29(11):575-585.
4. Nutting PA, Crabtree BF, Stewart EE, et al. Effect of facilitation on practice outcomes in the National Demonstration Project model of the patient-centered medical home. Ann Fam Med. 2010;8(suppl 1):S33-S34, S92.
5. Nagykaldi Z, Mold JW, Robinson A, Niebauer L, Ford A. Practice facilitators and practice-based research networks. J Am Board Fam Med. 2006;19(5):506-510.
6. Baskerville NB, Liddy C, Hogg W. Systematic review and meta-analysis of practice facilitation within primary care settings. Ann Fam Med. 2012;10(1):63-74.
7. Nagykaldi Z, Mold JW, Aspy CB. Practice facilitators: A review of the literature. Fam Med. 2005;37(8):581-588.
8. Grumbach K, Bainbridge E, Bodenheimer T. Facilitating improvement in primary care: The promise of practice coaching. Issue Brief (Commonw Fund). 2012;15:1-14.
9. Knox L, Taylor EF, Geonnotti K, et al. Developing and Running a Primary Care Practice Facilitation Program: A How-To Guide. Rockville, MD: Agency for Healthcare Research and Quality. U.S. Department of Health and Human Services; 2011. AHRQ Publication No. 12-0011.
10. Agency for Healthcare Research and Quality. Integrating Chronic Care and Business Strategies in the Safety Net: A Practice Coaching Manual. Agency for Healthcare Research and Quality Website. http://www.ahrq.gov/professionals/systems/primary-care /coachmnl/index.html. Published December 2012. Accessed February 26, 2015.
11. Bens I. Facilitation With Ease! Core Skills for Facilitators, Team Leaders and Members, Managers, Consultants and Trainers. 2nd ed. San Francisco, CA: Jossey-Bass; 2005.
12. Bodenheimer T. Building Teams in Primary Care: Lessons Learned: Part 1 and 2. Oakland, CA: California Health Care Foundation; July 2007.
Importance of Early Initiation of Advance Care Planning
Every day, health care providers (HCPs) care for patients with advanced chronic illnesses. At times, HCPs make critical treatment decisions without input from the patient. As a result, patients are often confused about their disease trajectory, prognosis, benefits and burdens of treatments, and outcome preferences.1 Unfortunately, limited research has been conducted on patients who have chronic illnesses, such as congestive heart failure (CHF) and chronic obstructive pulmonary disease (COPD), regarding early discussion of advance care planning (ACP) and advance directives (ADs). This gap in the knowledge base has contributed to a delay in the initiation of ACP for patients with COPD or CHF, especially for those with end-stage illness.
Background
The Patient Self-Determination Act (PSDA) was passed in 1990 to inform patients of their rights about health care choices while in the hospital, but the completion rate for ADs remains poor.2 The 3 key elements include the right of patients to facilitate their own health care decisions, the right to refuse or accept treatment, and the right to make an AD.
One of the reasons for the poor AD completion rate may be increased confusion about the difference between ACP and an AD.3 Advance care planning is a discussion about overall goals of care related to health care and progression through the life cycle. Advance directives focus on more specific information, including who will be designated as health care proxy, which health care interventions would be requested and which would be declined, and decisions regarding code status and organ donation.
A case study was conducted at a long-term care facility to test beliefs that residents who made their wishes known through ACP would have a positive experience at the end of life (EOL).3 The study allowed the residents to provide direction on what are and are not acceptable treatments at EOL. Before this study, most residents did not have a health care proxy and had not discussed the topic of EOL care with their HCP. Treatment choices were also not designated.3 Results demonstrated that ACP had positive outcomes for residents and family members, including documentation of an AD, autonomy in decision making, person-centered approaches to care, and dying with dignity.
Related: Fiduciary Services for Veterans With Psychiatric Disabilities
Much of the research regarding ADs has been conducted with seniors, hospitalized patients, and those with critical or terminal illnesses. A study by Jackson and colleagues examined attitudes, experiences, and preferences about ADs among adults of all ages. The study used an age-stratified random sample of patients from a large managed care organization.4 Findings revealed that older subjects were likely to be comfortable with and complete an AD. The most valuable outcome was the discussion of personal wishes with family and loved ones. Overall, the findings of this study concurred with the findings of other studies demonstrating that patients wanted control over EOL care decisions or wanted family members or loved ones to make those decisions. Consequently, patients not only believe the decisions are their responsibility, but also feel comfortable if their HCP initiates this conversation.4
Open and direct discussion regarding care planning can ease many of the fears related to EOL care. Discussion of an AD is a way to prepare for death and dying, rather than just a preparation for being incapacitated in the future. The process allows improved communication between patients, surrogates, and HCPs.3
The importance of communication with the patient’s primary care provider (PCP) regarding discussion of ACP or an AD is demonstrated in a longitudinal study completed by Ramsaroop and colleagues from January 1991 through July 2005. This systematic review of studies was designed to increase the completion of an AD in primary care settings.5 The study reviewed interventions that were most successful in improving the AD completion rate. The investigators extracted physician and patient barriers to completion of an AD. Findings suggested that the most successful intervention for completion of an AD were conversations that took place between patients and HCPs about ACP and occurred over multiple visits. By contrast, passive education using written materials without any direct counseling was relatively ineffective.5 The study also demonstrated the importance of completion of an AD in the primary care setting, gauging patient readiness to complete an AD, and having the PCP initiate the AD conversation.5
Related: Personal Counseling Helps Prevent Cancer-Related Malnutrition
If communication does not occur between patients and HCPs, care preferences are often not documented. Without this documentation many patients do not receive appropriate palliative care services when needed. Palliative care is not available to and therefore often not used with patients with nononcologic diseases.6 A study by Mahtani-Chugani and colleagues evaluated barriers to providing palliative care to nononcologic patients and proposed strategies to overcome them. Findings suggested 4 barriers: (1) lack of clarity about illness and prognosis; (2) discussion limited exclusively to the curative approach; (3) avoiding terms such as “terminal illness”; and (4) cheating death, including linking nononcologic disease and death.6 A strategy to overcoming these barriers highlighted improved communication between HCP and patient and understanding that the communication process is as important as the content of the message. Therefore, equitable palliative care services should be offered to both nononcologic and oncologic patients.6
One life-limiting nononcologic disease is COPD. Chronic obstructive pulmonary disease remains a major public health problem. It is the fourth leading cause of chronic morbidity and mortality in the U.S. and is projected to rank fifth in 2020 in disease burden worldwide.7 Given its prevalence, COPD is found in all adult health care settings.
Among hospitalized veterans in the VHA in 2005, COPD was the fourth most common discharge diagnosis.8 In the veteran population, a high prevalence for developing COPD also exists due to high-risk factors including tobacco use in the military. According to a study conducted at the Cincinnati VAMC in Ohio, a 40% greater prevalence of COPD existed in this veteran population than in the general U.S. population.8
Related: Lifestyle Intervention for Veterans With Chronic Diseases
Another nononcologic, life-limiting disease is CHF. Both the prevalence and hospitalization rates for CHF show an upward trend since the 1970s, resulting in a continued increase in CHF death rates.9 According to 2008 estimates from the National Institutes of Health, there are 5 million CHF patients in the U.S. and hospitalization rates approach 1 million per year.9 Congestive heart failure affects 2.4% of the adult population and > 11% of the expanding population aged > 80 years. Existing care may slow the progression of the disease but can rarely reverse it, which usually results in a prolonged period of advanced illness. As a result of the increasing prevalence, there remains a high symptom burden for patients living with advanced CHF.10
In managing the high symptom burden of CHF and COPD, patient-centered care must be acknowledged and used. Patient-centered care mandates that beneficial therapies and recommended guidelines be offered and discussed with the patient, giving attention to patient preferences.10
Study Design
The theoretical framework for the development and implementation of this project is based on Ruland and Moore’s Peaceful End of Life Theory.11 This theory is based on 2 assumptions. The first is that each person’s approach to EOL is personal. The second is that nursing care plays a major role in making EOL a peaceful experience. The 5 outcome measures include: (1) not experiencing pain; (2) the experience of comfort; (3) the experience of dignity and respect; (4) being at peace; and (5) closeness to significant others or other caring persons.
The outcome indicator of the Peaceful End of Life Theory— experience of dignity/respect with its related criteria and prescriptors—provided structure for the development and implementation of this project. The prescriptors related to the experience of dignity/respect include involving the patient and significant others in decision making; treating the patient with dignity, empathy, and respect; and being attentive to the patient’s expressed needs, wishes, and preferences.11
Due to the increased prevalence of chronic illnesses in the VA system, veterans need encouragement to complete ADs. The VA instituted a national directive guiding education and implementation of an AD.12 These discussions occur at the first contact a veteran has with the system and at other times when appropriate. The purpose of the directive is to allow veterans to guide the course of their treatment and to assure that they are aware of the ability to refuse treatment at any time.12
Inconsistencies in Advance Directive Completion
Inconsistencies were noted with how ADs were completed at the VA Northern Indiana Health Care System in Muncie. For outpatients, the clinic nursing staff received an electronic medical record (EMR) reminder if the veteran did not have an AD. This reminder prompted the nurse to ask the veteran about completing an AD. If the veteran agreed, a social work consult was initiated by nursing. Of concern, the social worker is usually responsible for several clinics so it is unlikely the process of completing the AD would be accomplished on the day the veteran was already in the clinic.
Discussions in the inpatient setting included a physician, a nurse practitioner, or a social worker and were often disease specific and patient oriented. However, in an acute hospitalization, it was less likely that patients initiated ADs due to acute illness and rapid nature of treatment.
Another concern was related to the amount of clinical knowledge the social worker had about the specifics of each patient’s case. Without specifics, a social worker can make the AD discussion very broad. Patients want information regarding disease progression and prognosis specific to their own condition to be able to make an informed choice regarding ADs.13
A study population with the diagnoses of CHF and COPD was selected due to the prevalence in the facility and at the request of facility leadership.
Methods
The primary aim of this quality improvement (QI) project was to educate the PCP about the importance of allowing veterans to express their care goals in the form of ADs and to understand that veterans would prefer to discuss these goals with their PCP. A secondary aim was to improve goal-directed care for veterans with COPD or CHF by increasing the number of completed ADs.
By using a systems approach, ACP can be addressed in a uniform manner. This approach allows veterans to discuss their goals of care prior to the need for emergent interventions, avoiding burdensome and unwanted treatments. Through the completion of ADs, veterans are able to designate a surrogate decision maker and identify specific desired treatments and interventions as their illness advances.
Two physicians and 3 nurse practitioners volunteered to contribute to this study. In the participating clinics, veterans with a diagnosis of CHF or COPD were identified. Each veteran had 20 to 30 minutes per appointment to discuss concerns, be examined, have HCPs address concerns, and complete all clinical reminders.
The study design was a QI project focused on evaluating the following process: An EMR reminder alerted the clinic nurse who asked the veteran if he or she was interested in completing an AD. If the patient agreed, a consult was placed to the social worker for completion of the VA national form for AD. The completion rate for a sample of primary care clinics at the facility was 10% to 12%, with no participation from the PCP in the process.
The providers were educated in 5 areas: (1) the prevalence of CHF and COPD in the U.S.; (2) the difference between ACP and AD; (3) the percentage of ADs completed in the U.S. adult population and in the facility; (4) the importance of addressing ACP early in the disease trajectory of this population; and (5) the use of the EMR reminder and the template to guide discussion of ACP ( eAppendix A
The template was developed following the literature review and addressed the reoccurring themes that patients wanted to discuss concerning their specific diagnosis and treatment. The template was formatted to include 3 components: (1) health care surrogate; (2) code status; and (3) organ donation preference ( eAppendix B
The natural progression from discussion of goals of care led to the discussion regarding the initiation of an AD. When completed, the note automatically appeared in the Postings section of the EMR, making it easily accessible to all other providers in different care settings.
The project time was 3 months (December 2012 through February 2013). The education was completed and the EMR reminder was turned on at the beginning of the project for veterans with a diagnosis of CHF or COPD who had not completed an AD. At the conclusion of the project, the PCPs completed a post project survey to provide information regarding their opinions on facilitators and barriers in the AD completion process ( eAppendix C
Results
Five different primary care clinics in 4 different locations throughout the health care system provided a total of 294 veterans with diagnoses of CHF or COPD. On completion of the project, 35 veterans had completed ADs. These 35 veterans represent an additional 12% of patients who previously did not complete an AD despite being approached multiple times. The veterans completed an AD following PCP-initiated discussion due to this QI project.
All 5 providers completed the post project survey and agreed that it would be beneficial to have the information regarding ADs easily accessible in the EMR. Four out of 5 providers admitted to cutting corners by not opening a new note every time to complete the AD template. They reported completing the EMR reminder within the clinic note, making it difficult to locate the information. Providers also reported on the various facilitators and barriers to AD discussion with patients (Table).

Discussion
The completion of an AD remains an important part of health care that is often neglected. When patients receive care and treatments, they often do not desire an AD, because the goals of care have not been clearly communicated and clearly documented. This can lead to poor quality of care with increased dissatisfaction and burden on the patient and health care system.14 However, if goals of care are discussed and documented, the veteran may avoid these burdensome treatments, and health care will be congruent with patient wishes. Better communication and documentation promotes increased patient satisfaction and improved quality of health care.1
This project endorses findings from a previous case study that demonstrated better patient-centered, goal-directed care results when patients have the opportunity to complete an AD, thereby improving health care quality and patient/family satisfaction.3 Previous studies suggested one way to increase the AD completion rate involves the PCP initiating a discussion with the patient.5 This project supports that conclusion.
Limitations
All the project providers expressed support regarding the importance of discussing ACPs with their patients. The major limitation identified by the project providers was time constraints in a busy primary care clinic. One provider suggested initiation of an EMR reminder once per year to prompt discussion. The same provider also recommended rescheduling an additional clinic visit to have an in-depth discussion regarding ACP.
Another limitation to this project involved the EMR. Currently, there is no way to have information in the postings section without a separate note. The project providers all agreed that it was not always possible to open a new note to use the template due to limited clinic time. This allowed information regarding health care surrogates and discussions regarding code status and organ donation to be embedded in a clinic note, which can make it difficult for other providers at different levels of care to effectively locate. Incorporating a method to allow information from an EMR reminder to be automatically placed in the postings section would alleviate this limitation.
A further limitation involved the setting. The VA provides care only to veterans. The project can be generalized to other VA primary care clinics, but generalizability beyond the VA may be limited.
This QI project took place over 3 months, another potential limitation due to the limited study period. Also, due to the short time frame of the project, a small sample size was used. Further investigation of this topic by expanding the time frame and sample size would further develop this body of knowledge.
The VA uses an EMR that is accessible to all VA providers locally and nationwide. Due to the nationwide network, expansion of the project would be possible with the support of facility leadership and the EMR reminder staff. By using the education and the template for discussion, the project could be replicated throughout the system.
Conclusion
Advance care planning and ADs should be a regular part of the health care process, especially for veterans with noncancer diagnoses, such as CHF and COPD. Clear communication about disease trajectory and prognosis are an important part of this discussion. Primary care providers are in the optimal setting to initiate this discussion.
This project supports previous findings that a PCP initiating or participating in the ACP discussion would result in an improved completion rate for ADs.5 Theoretically, improved AD completions result in patient-centered care, leading to higher patient satisfaction.
Acknowledgements
The authors would like to acknowledge the VA Northern Indiana Health Care System for its support of this project.
Author disclosures
The authors report no actual or potential conflicts of interest with regard to this article.
Disclaimer
The opinions expressed herein are those of the authors and do not necessarily reflect those of Federal Practitioner, Frontline Medical Communications Inc., the U.S. Government, or any of its agencies. This article may discuss unlabeled or investigational use of certain drugs. Please review the complete prescribing information for specific drugs or drug combinations—including indications, contraindications, warnings, and adverse effects—before administering pharmacologic therapy to patients.



1. Pautex S, Herrmann FR, Zulian GB. Role of advance directives in palliative care units: A prospective study. Palliat Med. 2008;22(7):835-841.
2. Cohen MJ, McCannon JB, Edgman-Levitan S, Kormos WA. Exploring attitudes toward advance care directives in two diverse settings. J Palliat Med. 2010;13(12):1427-1432.
3. Jeong SY-S, Higgins I, McMillan M. The essentials of Advance Care Planning for end-of-life care for older people. J Clin Nurs. 2010;19(3-4):389-397.
4. Jackson JM, Rolnick SJ, Asche SE, Heinrich RL. Knowledge, attitudes, and p regarding advance directives among patients of a managed care organization. Am J Manag Care. 2009;15(3):177-186.
5. Ramsaroop SD, Reid MC, Adelman RD. Completing an advance directive in the primary care setting: What do we need for success? J Am Geriatr Soc. 2007;55(2):277-283.
6. Mahtani-Chugani V, González-Castro I, de Ormijana-Hernández AS, Martín-Fernández R, de la Vega EF. How to provide care for patients suffering from terminal non-oncological diseases: Barriers to a palliative care approach. Palliat Med. 2010;24(8):787-795.
7. Rabe KF, Hurd S, Anzueto A, et al; Global Initiative for Chronic Obstructive Lung Disease. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease: GOLD executive summary. Am J Respir Crit Care Med. 2007;176(6):532-555.
8. Murphy DE, Chaudhry Z, Almoosa KF, Panos RJ. High prevalence of chronic obstructive pulmonary disease among veterans in the urban midwest. Mil Med. 2011;176(5):552-560.
9. National Institutes of Health. Division of cardiovascular disease strategic plan. National Heart, Lung, and Blood Institute Website. http://www .nhlbi.nih.gov/about/org/dcvs/sp/goal-2.4b. 2012. Accessed January 29, 2015.
10. Allen LA, Stevenson LW, Grady KL; American Heart Association; Council on Quality of Care and Outcomes Research; Council on Cardiovascular Nursing; Council on Clinical Cardiology; Council on Cardiovascular Radiology and Intervention; Council on Cardiovascular Surgery and Anesthesia. Decision making in advanced heart failure: A scientific statement from the American Heart Association. Circulation. 2012;125(15):1928-1952.
11. Ruland CM, Moore SM. Theory construction based on standards of care: A proposed theory of the peaceful end of life. Nurs Outlook. 1998;46(4):169-175.
12. US Department of Veterans Affairs, Veterans Health Administration . VHA Handbook 1004.02 transmittal sheet. Published July 2, 2009. http://www.ethics.va.gov/docs/policy/ADTraining /vha_handbk_1004_02.pdf. Accessed January 29, 2015.
13. Gott M, Gardiner C, Small N, et al. Barriers to advance care planning in chronic obstructive pulmonary disease. Palliat Med. 2009;23(7): 642-648.
14. Teno JM, Gruneir A, Schwartz Z, Nanda A, Wetle T. Association between advance directives and quality end-of-life care: A national study. J Am Geriatr Soc. 2007;55(2):189-194.
Every day, health care providers (HCPs) care for patients with advanced chronic illnesses. At times, HCPs make critical treatment decisions without input from the patient. As a result, patients are often confused about their disease trajectory, prognosis, benefits and burdens of treatments, and outcome preferences.1 Unfortunately, limited research has been conducted on patients who have chronic illnesses, such as congestive heart failure (CHF) and chronic obstructive pulmonary disease (COPD), regarding early discussion of advance care planning (ACP) and advance directives (ADs). This gap in the knowledge base has contributed to a delay in the initiation of ACP for patients with COPD or CHF, especially for those with end-stage illness.
Background
The Patient Self-Determination Act (PSDA) was passed in 1990 to inform patients of their rights about health care choices while in the hospital, but the completion rate for ADs remains poor.2 The 3 key elements include the right of patients to facilitate their own health care decisions, the right to refuse or accept treatment, and the right to make an AD.
One of the reasons for the poor AD completion rate may be increased confusion about the difference between ACP and an AD.3 Advance care planning is a discussion about overall goals of care related to health care and progression through the life cycle. Advance directives focus on more specific information, including who will be designated as health care proxy, which health care interventions would be requested and which would be declined, and decisions regarding code status and organ donation.
A case study was conducted at a long-term care facility to test beliefs that residents who made their wishes known through ACP would have a positive experience at the end of life (EOL).3 The study allowed the residents to provide direction on what are and are not acceptable treatments at EOL. Before this study, most residents did not have a health care proxy and had not discussed the topic of EOL care with their HCP. Treatment choices were also not designated.3 Results demonstrated that ACP had positive outcomes for residents and family members, including documentation of an AD, autonomy in decision making, person-centered approaches to care, and dying with dignity.
Related: Fiduciary Services for Veterans With Psychiatric Disabilities
Much of the research regarding ADs has been conducted with seniors, hospitalized patients, and those with critical or terminal illnesses. A study by Jackson and colleagues examined attitudes, experiences, and preferences about ADs among adults of all ages. The study used an age-stratified random sample of patients from a large managed care organization.4 Findings revealed that older subjects were likely to be comfortable with and complete an AD. The most valuable outcome was the discussion of personal wishes with family and loved ones. Overall, the findings of this study concurred with the findings of other studies demonstrating that patients wanted control over EOL care decisions or wanted family members or loved ones to make those decisions. Consequently, patients not only believe the decisions are their responsibility, but also feel comfortable if their HCP initiates this conversation.4
Open and direct discussion regarding care planning can ease many of the fears related to EOL care. Discussion of an AD is a way to prepare for death and dying, rather than just a preparation for being incapacitated in the future. The process allows improved communication between patients, surrogates, and HCPs.3
The importance of communication with the patient’s primary care provider (PCP) regarding discussion of ACP or an AD is demonstrated in a longitudinal study completed by Ramsaroop and colleagues from January 1991 through July 2005. This systematic review of studies was designed to increase the completion of an AD in primary care settings.5 The study reviewed interventions that were most successful in improving the AD completion rate. The investigators extracted physician and patient barriers to completion of an AD. Findings suggested that the most successful intervention for completion of an AD were conversations that took place between patients and HCPs about ACP and occurred over multiple visits. By contrast, passive education using written materials without any direct counseling was relatively ineffective.5 The study also demonstrated the importance of completion of an AD in the primary care setting, gauging patient readiness to complete an AD, and having the PCP initiate the AD conversation.5
Related: Personal Counseling Helps Prevent Cancer-Related Malnutrition
If communication does not occur between patients and HCPs, care preferences are often not documented. Without this documentation many patients do not receive appropriate palliative care services when needed. Palliative care is not available to and therefore often not used with patients with nononcologic diseases.6 A study by Mahtani-Chugani and colleagues evaluated barriers to providing palliative care to nononcologic patients and proposed strategies to overcome them. Findings suggested 4 barriers: (1) lack of clarity about illness and prognosis; (2) discussion limited exclusively to the curative approach; (3) avoiding terms such as “terminal illness”; and (4) cheating death, including linking nononcologic disease and death.6 A strategy to overcoming these barriers highlighted improved communication between HCP and patient and understanding that the communication process is as important as the content of the message. Therefore, equitable palliative care services should be offered to both nononcologic and oncologic patients.6
One life-limiting nononcologic disease is COPD. Chronic obstructive pulmonary disease remains a major public health problem. It is the fourth leading cause of chronic morbidity and mortality in the U.S. and is projected to rank fifth in 2020 in disease burden worldwide.7 Given its prevalence, COPD is found in all adult health care settings.
Among hospitalized veterans in the VHA in 2005, COPD was the fourth most common discharge diagnosis.8 In the veteran population, a high prevalence for developing COPD also exists due to high-risk factors including tobacco use in the military. According to a study conducted at the Cincinnati VAMC in Ohio, a 40% greater prevalence of COPD existed in this veteran population than in the general U.S. population.8
Related: Lifestyle Intervention for Veterans With Chronic Diseases
Another nononcologic, life-limiting disease is CHF. Both the prevalence and hospitalization rates for CHF show an upward trend since the 1970s, resulting in a continued increase in CHF death rates.9 According to 2008 estimates from the National Institutes of Health, there are 5 million CHF patients in the U.S. and hospitalization rates approach 1 million per year.9 Congestive heart failure affects 2.4% of the adult population and > 11% of the expanding population aged > 80 years. Existing care may slow the progression of the disease but can rarely reverse it, which usually results in a prolonged period of advanced illness. As a result of the increasing prevalence, there remains a high symptom burden for patients living with advanced CHF.10
In managing the high symptom burden of CHF and COPD, patient-centered care must be acknowledged and used. Patient-centered care mandates that beneficial therapies and recommended guidelines be offered and discussed with the patient, giving attention to patient preferences.10
Study Design
The theoretical framework for the development and implementation of this project is based on Ruland and Moore’s Peaceful End of Life Theory.11 This theory is based on 2 assumptions. The first is that each person’s approach to EOL is personal. The second is that nursing care plays a major role in making EOL a peaceful experience. The 5 outcome measures include: (1) not experiencing pain; (2) the experience of comfort; (3) the experience of dignity and respect; (4) being at peace; and (5) closeness to significant others or other caring persons.
The outcome indicator of the Peaceful End of Life Theory— experience of dignity/respect with its related criteria and prescriptors—provided structure for the development and implementation of this project. The prescriptors related to the experience of dignity/respect include involving the patient and significant others in decision making; treating the patient with dignity, empathy, and respect; and being attentive to the patient’s expressed needs, wishes, and preferences.11
Due to the increased prevalence of chronic illnesses in the VA system, veterans need encouragement to complete ADs. The VA instituted a national directive guiding education and implementation of an AD.12 These discussions occur at the first contact a veteran has with the system and at other times when appropriate. The purpose of the directive is to allow veterans to guide the course of their treatment and to assure that they are aware of the ability to refuse treatment at any time.12
Inconsistencies in Advance Directive Completion
Inconsistencies were noted with how ADs were completed at the VA Northern Indiana Health Care System in Muncie. For outpatients, the clinic nursing staff received an electronic medical record (EMR) reminder if the veteran did not have an AD. This reminder prompted the nurse to ask the veteran about completing an AD. If the veteran agreed, a social work consult was initiated by nursing. Of concern, the social worker is usually responsible for several clinics so it is unlikely the process of completing the AD would be accomplished on the day the veteran was already in the clinic.
Discussions in the inpatient setting included a physician, a nurse practitioner, or a social worker and were often disease specific and patient oriented. However, in an acute hospitalization, it was less likely that patients initiated ADs due to acute illness and rapid nature of treatment.
Another concern was related to the amount of clinical knowledge the social worker had about the specifics of each patient’s case. Without specifics, a social worker can make the AD discussion very broad. Patients want information regarding disease progression and prognosis specific to their own condition to be able to make an informed choice regarding ADs.13
A study population with the diagnoses of CHF and COPD was selected due to the prevalence in the facility and at the request of facility leadership.
Methods
The primary aim of this quality improvement (QI) project was to educate the PCP about the importance of allowing veterans to express their care goals in the form of ADs and to understand that veterans would prefer to discuss these goals with their PCP. A secondary aim was to improve goal-directed care for veterans with COPD or CHF by increasing the number of completed ADs.
By using a systems approach, ACP can be addressed in a uniform manner. This approach allows veterans to discuss their goals of care prior to the need for emergent interventions, avoiding burdensome and unwanted treatments. Through the completion of ADs, veterans are able to designate a surrogate decision maker and identify specific desired treatments and interventions as their illness advances.
Two physicians and 3 nurse practitioners volunteered to contribute to this study. In the participating clinics, veterans with a diagnosis of CHF or COPD were identified. Each veteran had 20 to 30 minutes per appointment to discuss concerns, be examined, have HCPs address concerns, and complete all clinical reminders.
The study design was a QI project focused on evaluating the following process: An EMR reminder alerted the clinic nurse who asked the veteran if he or she was interested in completing an AD. If the patient agreed, a consult was placed to the social worker for completion of the VA national form for AD. The completion rate for a sample of primary care clinics at the facility was 10% to 12%, with no participation from the PCP in the process.
The providers were educated in 5 areas: (1) the prevalence of CHF and COPD in the U.S.; (2) the difference between ACP and AD; (3) the percentage of ADs completed in the U.S. adult population and in the facility; (4) the importance of addressing ACP early in the disease trajectory of this population; and (5) the use of the EMR reminder and the template to guide discussion of ACP ( eAppendix A
The template was developed following the literature review and addressed the reoccurring themes that patients wanted to discuss concerning their specific diagnosis and treatment. The template was formatted to include 3 components: (1) health care surrogate; (2) code status; and (3) organ donation preference ( eAppendix B
The natural progression from discussion of goals of care led to the discussion regarding the initiation of an AD. When completed, the note automatically appeared in the Postings section of the EMR, making it easily accessible to all other providers in different care settings.
The project time was 3 months (December 2012 through February 2013). The education was completed and the EMR reminder was turned on at the beginning of the project for veterans with a diagnosis of CHF or COPD who had not completed an AD. At the conclusion of the project, the PCPs completed a post project survey to provide information regarding their opinions on facilitators and barriers in the AD completion process ( eAppendix C
Results
Five different primary care clinics in 4 different locations throughout the health care system provided a total of 294 veterans with diagnoses of CHF or COPD. On completion of the project, 35 veterans had completed ADs. These 35 veterans represent an additional 12% of patients who previously did not complete an AD despite being approached multiple times. The veterans completed an AD following PCP-initiated discussion due to this QI project.
All 5 providers completed the post project survey and agreed that it would be beneficial to have the information regarding ADs easily accessible in the EMR. Four out of 5 providers admitted to cutting corners by not opening a new note every time to complete the AD template. They reported completing the EMR reminder within the clinic note, making it difficult to locate the information. Providers also reported on the various facilitators and barriers to AD discussion with patients (Table).
Discussion
The completion of an AD remains an important part of health care that is often neglected. When patients receive care and treatments, they often do not desire an AD, because the goals of care have not been clearly communicated and clearly documented. This can lead to poor quality of care with increased dissatisfaction and burden on the patient and health care system.14 However, if goals of care are discussed and documented, the veteran may avoid these burdensome treatments, and health care will be congruent with patient wishes. Better communication and documentation promotes increased patient satisfaction and improved quality of health care.1
This project endorses findings from a previous case study that demonstrated better patient-centered, goal-directed care results when patients have the opportunity to complete an AD, thereby improving health care quality and patient/family satisfaction.3 Previous studies suggested one way to increase the AD completion rate involves the PCP initiating a discussion with the patient.5 This project supports that conclusion.
Limitations
All the project providers expressed support regarding the importance of discussing ACPs with their patients. The major limitation identified by the project providers was time constraints in a busy primary care clinic. One provider suggested initiation of an EMR reminder once per year to prompt discussion. The same provider also recommended rescheduling an additional clinic visit to have an in-depth discussion regarding ACP.
Another limitation to this project involved the EMR. Currently, there is no way to have information in the postings section without a separate note. The project providers all agreed that it was not always possible to open a new note to use the template due to limited clinic time. This allowed information regarding health care surrogates and discussions regarding code status and organ donation to be embedded in a clinic note, which can make it difficult for other providers at different levels of care to effectively locate. Incorporating a method to allow information from an EMR reminder to be automatically placed in the postings section would alleviate this limitation.
A further limitation involved the setting. The VA provides care only to veterans. The project can be generalized to other VA primary care clinics, but generalizability beyond the VA may be limited.
This QI project took place over 3 months, another potential limitation due to the limited study period. Also, due to the short time frame of the project, a small sample size was used. Further investigation of this topic by expanding the time frame and sample size would further develop this body of knowledge.
The VA uses an EMR that is accessible to all VA providers locally and nationwide. Due to the nationwide network, expansion of the project would be possible with the support of facility leadership and the EMR reminder staff. By using the education and the template for discussion, the project could be replicated throughout the system.
Conclusion
Advance care planning and ADs should be a regular part of the health care process, especially for veterans with noncancer diagnoses, such as CHF and COPD. Clear communication about disease trajectory and prognosis are an important part of this discussion. Primary care providers are in the optimal setting to initiate this discussion.
This project supports previous findings that a PCP initiating or participating in the ACP discussion would result in an improved completion rate for ADs.5 Theoretically, improved AD completions result in patient-centered care, leading to higher patient satisfaction.
Acknowledgements
The authors would like to acknowledge the VA Northern Indiana Health Care System for its support of this project.
Author disclosures
The authors report no actual or potential conflicts of interest with regard to this article.
Disclaimer
The opinions expressed herein are those of the authors and do not necessarily reflect those of Federal Practitioner, Frontline Medical Communications Inc., the U.S. Government, or any of its agencies. This article may discuss unlabeled or investigational use of certain drugs. Please review the complete prescribing information for specific drugs or drug combinations—including indications, contraindications, warnings, and adverse effects—before administering pharmacologic therapy to patients.
Every day, health care providers (HCPs) care for patients with advanced chronic illnesses. At times, HCPs make critical treatment decisions without input from the patient. As a result, patients are often confused about their disease trajectory, prognosis, benefits and burdens of treatments, and outcome preferences.1 Unfortunately, limited research has been conducted on patients who have chronic illnesses, such as congestive heart failure (CHF) and chronic obstructive pulmonary disease (COPD), regarding early discussion of advance care planning (ACP) and advance directives (ADs). This gap in the knowledge base has contributed to a delay in the initiation of ACP for patients with COPD or CHF, especially for those with end-stage illness.
Background
The Patient Self-Determination Act (PSDA) was passed in 1990 to inform patients of their rights about health care choices while in the hospital, but the completion rate for ADs remains poor.2 The 3 key elements include the right of patients to facilitate their own health care decisions, the right to refuse or accept treatment, and the right to make an AD.
One of the reasons for the poor AD completion rate may be increased confusion about the difference between ACP and an AD.3 Advance care planning is a discussion about overall goals of care related to health care and progression through the life cycle. Advance directives focus on more specific information, including who will be designated as health care proxy, which health care interventions would be requested and which would be declined, and decisions regarding code status and organ donation.
A case study was conducted at a long-term care facility to test beliefs that residents who made their wishes known through ACP would have a positive experience at the end of life (EOL).3 The study allowed the residents to provide direction on what are and are not acceptable treatments at EOL. Before this study, most residents did not have a health care proxy and had not discussed the topic of EOL care with their HCP. Treatment choices were also not designated.3 Results demonstrated that ACP had positive outcomes for residents and family members, including documentation of an AD, autonomy in decision making, person-centered approaches to care, and dying with dignity.
Related: Fiduciary Services for Veterans With Psychiatric Disabilities
Much of the research regarding ADs has been conducted with seniors, hospitalized patients, and those with critical or terminal illnesses. A study by Jackson and colleagues examined attitudes, experiences, and preferences about ADs among adults of all ages. The study used an age-stratified random sample of patients from a large managed care organization.4 Findings revealed that older subjects were likely to be comfortable with and complete an AD. The most valuable outcome was the discussion of personal wishes with family and loved ones. Overall, the findings of this study concurred with the findings of other studies demonstrating that patients wanted control over EOL care decisions or wanted family members or loved ones to make those decisions. Consequently, patients not only believe the decisions are their responsibility, but also feel comfortable if their HCP initiates this conversation.4
Open and direct discussion regarding care planning can ease many of the fears related to EOL care. Discussion of an AD is a way to prepare for death and dying, rather than just a preparation for being incapacitated in the future. The process allows improved communication between patients, surrogates, and HCPs.3
The importance of communication with the patient’s primary care provider (PCP) regarding discussion of ACP or an AD is demonstrated in a longitudinal study completed by Ramsaroop and colleagues from January 1991 through July 2005. This systematic review of studies was designed to increase the completion of an AD in primary care settings.5 The study reviewed interventions that were most successful in improving the AD completion rate. The investigators extracted physician and patient barriers to completion of an AD. Findings suggested that the most successful intervention for completion of an AD were conversations that took place between patients and HCPs about ACP and occurred over multiple visits. By contrast, passive education using written materials without any direct counseling was relatively ineffective.5 The study also demonstrated the importance of completion of an AD in the primary care setting, gauging patient readiness to complete an AD, and having the PCP initiate the AD conversation.5
Related: Personal Counseling Helps Prevent Cancer-Related Malnutrition
If communication does not occur between patients and HCPs, care preferences are often not documented. Without this documentation many patients do not receive appropriate palliative care services when needed. Palliative care is not available to and therefore often not used with patients with nononcologic diseases.6 A study by Mahtani-Chugani and colleagues evaluated barriers to providing palliative care to nononcologic patients and proposed strategies to overcome them. Findings suggested 4 barriers: (1) lack of clarity about illness and prognosis; (2) discussion limited exclusively to the curative approach; (3) avoiding terms such as “terminal illness”; and (4) cheating death, including linking nononcologic disease and death.6 A strategy to overcoming these barriers highlighted improved communication between HCP and patient and understanding that the communication process is as important as the content of the message. Therefore, equitable palliative care services should be offered to both nononcologic and oncologic patients.6
One life-limiting nononcologic disease is COPD. Chronic obstructive pulmonary disease remains a major public health problem. It is the fourth leading cause of chronic morbidity and mortality in the U.S. and is projected to rank fifth in 2020 in disease burden worldwide.7 Given its prevalence, COPD is found in all adult health care settings.
Among hospitalized veterans in the VHA in 2005, COPD was the fourth most common discharge diagnosis.8 In the veteran population, a high prevalence for developing COPD also exists due to high-risk factors including tobacco use in the military. According to a study conducted at the Cincinnati VAMC in Ohio, a 40% greater prevalence of COPD existed in this veteran population than in the general U.S. population.8
Related: Lifestyle Intervention for Veterans With Chronic Diseases
Another nononcologic, life-limiting disease is CHF. Both the prevalence and hospitalization rates for CHF show an upward trend since the 1970s, resulting in a continued increase in CHF death rates.9 According to 2008 estimates from the National Institutes of Health, there are 5 million CHF patients in the U.S. and hospitalization rates approach 1 million per year.9 Congestive heart failure affects 2.4% of the adult population and > 11% of the expanding population aged > 80 years. Existing care may slow the progression of the disease but can rarely reverse it, which usually results in a prolonged period of advanced illness. As a result of the increasing prevalence, there remains a high symptom burden for patients living with advanced CHF.10
In managing the high symptom burden of CHF and COPD, patient-centered care must be acknowledged and used. Patient-centered care mandates that beneficial therapies and recommended guidelines be offered and discussed with the patient, giving attention to patient preferences.10
Study Design
The theoretical framework for the development and implementation of this project is based on Ruland and Moore’s Peaceful End of Life Theory.11 This theory is based on 2 assumptions. The first is that each person’s approach to EOL is personal. The second is that nursing care plays a major role in making EOL a peaceful experience. The 5 outcome measures include: (1) not experiencing pain; (2) the experience of comfort; (3) the experience of dignity and respect; (4) being at peace; and (5) closeness to significant others or other caring persons.
The outcome indicator of the Peaceful End of Life Theory— experience of dignity/respect with its related criteria and prescriptors—provided structure for the development and implementation of this project. The prescriptors related to the experience of dignity/respect include involving the patient and significant others in decision making; treating the patient with dignity, empathy, and respect; and being attentive to the patient’s expressed needs, wishes, and preferences.11
Due to the increased prevalence of chronic illnesses in the VA system, veterans need encouragement to complete ADs. The VA instituted a national directive guiding education and implementation of an AD.12 These discussions occur at the first contact a veteran has with the system and at other times when appropriate. The purpose of the directive is to allow veterans to guide the course of their treatment and to assure that they are aware of the ability to refuse treatment at any time.12
Inconsistencies in Advance Directive Completion
Inconsistencies were noted with how ADs were completed at the VA Northern Indiana Health Care System in Muncie. For outpatients, the clinic nursing staff received an electronic medical record (EMR) reminder if the veteran did not have an AD. This reminder prompted the nurse to ask the veteran about completing an AD. If the veteran agreed, a social work consult was initiated by nursing. Of concern, the social worker is usually responsible for several clinics so it is unlikely the process of completing the AD would be accomplished on the day the veteran was already in the clinic.
Discussions in the inpatient setting included a physician, a nurse practitioner, or a social worker and were often disease specific and patient oriented. However, in an acute hospitalization, it was less likely that patients initiated ADs due to acute illness and rapid nature of treatment.
Another concern was related to the amount of clinical knowledge the social worker had about the specifics of each patient’s case. Without specifics, a social worker can make the AD discussion very broad. Patients want information regarding disease progression and prognosis specific to their own condition to be able to make an informed choice regarding ADs.13
A study population with the diagnoses of CHF and COPD was selected due to the prevalence in the facility and at the request of facility leadership.
Methods
The primary aim of this quality improvement (QI) project was to educate the PCP about the importance of allowing veterans to express their care goals in the form of ADs and to understand that veterans would prefer to discuss these goals with their PCP. A secondary aim was to improve goal-directed care for veterans with COPD or CHF by increasing the number of completed ADs.
By using a systems approach, ACP can be addressed in a uniform manner. This approach allows veterans to discuss their goals of care prior to the need for emergent interventions, avoiding burdensome and unwanted treatments. Through the completion of ADs, veterans are able to designate a surrogate decision maker and identify specific desired treatments and interventions as their illness advances.
Two physicians and 3 nurse practitioners volunteered to contribute to this study. In the participating clinics, veterans with a diagnosis of CHF or COPD were identified. Each veteran had 20 to 30 minutes per appointment to discuss concerns, be examined, have HCPs address concerns, and complete all clinical reminders.
The study design was a QI project focused on evaluating the following process: An EMR reminder alerted the clinic nurse who asked the veteran if he or she was interested in completing an AD. If the patient agreed, a consult was placed to the social worker for completion of the VA national form for AD. The completion rate for a sample of primary care clinics at the facility was 10% to 12%, with no participation from the PCP in the process.
The providers were educated in 5 areas: (1) the prevalence of CHF and COPD in the U.S.; (2) the difference between ACP and AD; (3) the percentage of ADs completed in the U.S. adult population and in the facility; (4) the importance of addressing ACP early in the disease trajectory of this population; and (5) the use of the EMR reminder and the template to guide discussion of ACP ( eAppendix A
The template was developed following the literature review and addressed the reoccurring themes that patients wanted to discuss concerning their specific diagnosis and treatment. The template was formatted to include 3 components: (1) health care surrogate; (2) code status; and (3) organ donation preference ( eAppendix B
The natural progression from discussion of goals of care led to the discussion regarding the initiation of an AD. When completed, the note automatically appeared in the Postings section of the EMR, making it easily accessible to all other providers in different care settings.
The project time was 3 months (December 2012 through February 2013). The education was completed and the EMR reminder was turned on at the beginning of the project for veterans with a diagnosis of CHF or COPD who had not completed an AD. At the conclusion of the project, the PCPs completed a post project survey to provide information regarding their opinions on facilitators and barriers in the AD completion process ( eAppendix C
Results
Five different primary care clinics in 4 different locations throughout the health care system provided a total of 294 veterans with diagnoses of CHF or COPD. On completion of the project, 35 veterans had completed ADs. These 35 veterans represent an additional 12% of patients who previously did not complete an AD despite being approached multiple times. The veterans completed an AD following PCP-initiated discussion due to this QI project.
All 5 providers completed the post project survey and agreed that it would be beneficial to have the information regarding ADs easily accessible in the EMR. Four out of 5 providers admitted to cutting corners by not opening a new note every time to complete the AD template. They reported completing the EMR reminder within the clinic note, making it difficult to locate the information. Providers also reported on the various facilitators and barriers to AD discussion with patients (Table).
Discussion
The completion of an AD remains an important part of health care that is often neglected. When patients receive care and treatments, they often do not desire an AD, because the goals of care have not been clearly communicated and clearly documented. This can lead to poor quality of care with increased dissatisfaction and burden on the patient and health care system.14 However, if goals of care are discussed and documented, the veteran may avoid these burdensome treatments, and health care will be congruent with patient wishes. Better communication and documentation promotes increased patient satisfaction and improved quality of health care.1
This project endorses findings from a previous case study that demonstrated better patient-centered, goal-directed care results when patients have the opportunity to complete an AD, thereby improving health care quality and patient/family satisfaction.3 Previous studies suggested one way to increase the AD completion rate involves the PCP initiating a discussion with the patient.5 This project supports that conclusion.
Limitations
All the project providers expressed support regarding the importance of discussing ACPs with their patients. The major limitation identified by the project providers was time constraints in a busy primary care clinic. One provider suggested initiation of an EMR reminder once per year to prompt discussion. The same provider also recommended rescheduling an additional clinic visit to have an in-depth discussion regarding ACP.
Another limitation to this project involved the EMR. Currently, there is no way to have information in the postings section without a separate note. The project providers all agreed that it was not always possible to open a new note to use the template due to limited clinic time. This allowed information regarding health care surrogates and discussions regarding code status and organ donation to be embedded in a clinic note, which can make it difficult for other providers at different levels of care to effectively locate. Incorporating a method to allow information from an EMR reminder to be automatically placed in the postings section would alleviate this limitation.
A further limitation involved the setting. The VA provides care only to veterans. The project can be generalized to other VA primary care clinics, but generalizability beyond the VA may be limited.
This QI project took place over 3 months, another potential limitation due to the limited study period. Also, due to the short time frame of the project, a small sample size was used. Further investigation of this topic by expanding the time frame and sample size would further develop this body of knowledge.
The VA uses an EMR that is accessible to all VA providers locally and nationwide. Due to the nationwide network, expansion of the project would be possible with the support of facility leadership and the EMR reminder staff. By using the education and the template for discussion, the project could be replicated throughout the system.
Conclusion
Advance care planning and ADs should be a regular part of the health care process, especially for veterans with noncancer diagnoses, such as CHF and COPD. Clear communication about disease trajectory and prognosis are an important part of this discussion. Primary care providers are in the optimal setting to initiate this discussion.
This project supports previous findings that a PCP initiating or participating in the ACP discussion would result in an improved completion rate for ADs.5 Theoretically, improved AD completions result in patient-centered care, leading to higher patient satisfaction.
Acknowledgements
The authors would like to acknowledge the VA Northern Indiana Health Care System for its support of this project.
Author disclosures
The authors report no actual or potential conflicts of interest with regard to this article.
Disclaimer
The opinions expressed herein are those of the authors and do not necessarily reflect those of Federal Practitioner, Frontline Medical Communications Inc., the U.S. Government, or any of its agencies. This article may discuss unlabeled or investigational use of certain drugs. Please review the complete prescribing information for specific drugs or drug combinations—including indications, contraindications, warnings, and adverse effects—before administering pharmacologic therapy to patients.
1. Pautex S, Herrmann FR, Zulian GB. Role of advance directives in palliative care units: A prospective study. Palliat Med. 2008;22(7):835-841.
2. Cohen MJ, McCannon JB, Edgman-Levitan S, Kormos WA. Exploring attitudes toward advance care directives in two diverse settings. J Palliat Med. 2010;13(12):1427-1432.
3. Jeong SY-S, Higgins I, McMillan M. The essentials of Advance Care Planning for end-of-life care for older people. J Clin Nurs. 2010;19(3-4):389-397.
4. Jackson JM, Rolnick SJ, Asche SE, Heinrich RL. Knowledge, attitudes, and p regarding advance directives among patients of a managed care organization. Am J Manag Care. 2009;15(3):177-186.
5. Ramsaroop SD, Reid MC, Adelman RD. Completing an advance directive in the primary care setting: What do we need for success? J Am Geriatr Soc. 2007;55(2):277-283.
6. Mahtani-Chugani V, González-Castro I, de Ormijana-Hernández AS, Martín-Fernández R, de la Vega EF. How to provide care for patients suffering from terminal non-oncological diseases: Barriers to a palliative care approach. Palliat Med. 2010;24(8):787-795.
7. Rabe KF, Hurd S, Anzueto A, et al; Global Initiative for Chronic Obstructive Lung Disease. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease: GOLD executive summary. Am J Respir Crit Care Med. 2007;176(6):532-555.
8. Murphy DE, Chaudhry Z, Almoosa KF, Panos RJ. High prevalence of chronic obstructive pulmonary disease among veterans in the urban midwest. Mil Med. 2011;176(5):552-560.
9. National Institutes of Health. Division of cardiovascular disease strategic plan. National Heart, Lung, and Blood Institute Website. http://www .nhlbi.nih.gov/about/org/dcvs/sp/goal-2.4b. 2012. Accessed January 29, 2015.
10. Allen LA, Stevenson LW, Grady KL; American Heart Association; Council on Quality of Care and Outcomes Research; Council on Cardiovascular Nursing; Council on Clinical Cardiology; Council on Cardiovascular Radiology and Intervention; Council on Cardiovascular Surgery and Anesthesia. Decision making in advanced heart failure: A scientific statement from the American Heart Association. Circulation. 2012;125(15):1928-1952.
11. Ruland CM, Moore SM. Theory construction based on standards of care: A proposed theory of the peaceful end of life. Nurs Outlook. 1998;46(4):169-175.
12. US Department of Veterans Affairs, Veterans Health Administration . VHA Handbook 1004.02 transmittal sheet. Published July 2, 2009. http://www.ethics.va.gov/docs/policy/ADTraining /vha_handbk_1004_02.pdf. Accessed January 29, 2015.
13. Gott M, Gardiner C, Small N, et al. Barriers to advance care planning in chronic obstructive pulmonary disease. Palliat Med. 2009;23(7): 642-648.
14. Teno JM, Gruneir A, Schwartz Z, Nanda A, Wetle T. Association between advance directives and quality end-of-life care: A national study. J Am Geriatr Soc. 2007;55(2):189-194.
1. Pautex S, Herrmann FR, Zulian GB. Role of advance directives in palliative care units: A prospective study. Palliat Med. 2008;22(7):835-841.
2. Cohen MJ, McCannon JB, Edgman-Levitan S, Kormos WA. Exploring attitudes toward advance care directives in two diverse settings. J Palliat Med. 2010;13(12):1427-1432.
3. Jeong SY-S, Higgins I, McMillan M. The essentials of Advance Care Planning for end-of-life care for older people. J Clin Nurs. 2010;19(3-4):389-397.
4. Jackson JM, Rolnick SJ, Asche SE, Heinrich RL. Knowledge, attitudes, and p regarding advance directives among patients of a managed care organization. Am J Manag Care. 2009;15(3):177-186.
5. Ramsaroop SD, Reid MC, Adelman RD. Completing an advance directive in the primary care setting: What do we need for success? J Am Geriatr Soc. 2007;55(2):277-283.
6. Mahtani-Chugani V, González-Castro I, de Ormijana-Hernández AS, Martín-Fernández R, de la Vega EF. How to provide care for patients suffering from terminal non-oncological diseases: Barriers to a palliative care approach. Palliat Med. 2010;24(8):787-795.
7. Rabe KF, Hurd S, Anzueto A, et al; Global Initiative for Chronic Obstructive Lung Disease. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease: GOLD executive summary. Am J Respir Crit Care Med. 2007;176(6):532-555.
8. Murphy DE, Chaudhry Z, Almoosa KF, Panos RJ. High prevalence of chronic obstructive pulmonary disease among veterans in the urban midwest. Mil Med. 2011;176(5):552-560.
9. National Institutes of Health. Division of cardiovascular disease strategic plan. National Heart, Lung, and Blood Institute Website. http://www .nhlbi.nih.gov/about/org/dcvs/sp/goal-2.4b. 2012. Accessed January 29, 2015.
10. Allen LA, Stevenson LW, Grady KL; American Heart Association; Council on Quality of Care and Outcomes Research; Council on Cardiovascular Nursing; Council on Clinical Cardiology; Council on Cardiovascular Radiology and Intervention; Council on Cardiovascular Surgery and Anesthesia. Decision making in advanced heart failure: A scientific statement from the American Heart Association. Circulation. 2012;125(15):1928-1952.
11. Ruland CM, Moore SM. Theory construction based on standards of care: A proposed theory of the peaceful end of life. Nurs Outlook. 1998;46(4):169-175.
12. US Department of Veterans Affairs, Veterans Health Administration . VHA Handbook 1004.02 transmittal sheet. Published July 2, 2009. http://www.ethics.va.gov/docs/policy/ADTraining /vha_handbk_1004_02.pdf. Accessed January 29, 2015.
13. Gott M, Gardiner C, Small N, et al. Barriers to advance care planning in chronic obstructive pulmonary disease. Palliat Med. 2009;23(7): 642-648.
14. Teno JM, Gruneir A, Schwartz Z, Nanda A, Wetle T. Association between advance directives and quality end-of-life care: A national study. J Am Geriatr Soc. 2007;55(2):189-194.
Colonoscopy Bowel Preparation Instructions
According to the CDC, colorectal cancer (CRC) is largely preventable but remains the second leading cancer killer for men and women in the U.S. Screening for polyps (detection of abnormal growths) and surveillance (based on prior bowel preparation quality, findings, and personal and family histories) are key elements for CRC prevention and survival.1 However, inadequate bowel preparation greatly reduces accuracy of its intended purpose: finding and removing precancerous polyps or lesions before they develop into a cancer, typically within a 10-year window. If preparation quality is not satisfactory, the ability of the endoscopist to meet national polyp detection rates is limited. These rates are currently 25% for men and 15% for women.2 Compounding poor preparation, many veterans avoid CRC screening due to anxiety, shame, and fear of what could be found.
Related: Do I Need a Colonoscopy?
About 60% of veterans presenting for colonoscopy have inadequate bowel preparation.3 Colonoscopy remains the gold standard for detection of colorectal pathology and is available to veterans without insurance preauthorization, eliminating a significant barrier to screening.1 Inadequate bowel preparation can result in missed polyps, cancelled procedures, and increased procedure time. Nonadherence to the liquid diet and high-volume, bowel-cleansing solution can lead to a repeated colonoscopy.
Two nurse practitioners (NPs) at the Philadelphia VAMC (PVAMC) gastroenterology (GE) section recognized that many veterans had poor bowel preparation in spite of preprocedure visits, written instructions, and no financial limitations. Repeated colonoscopies were impacting patient satisfaction, facility costs, and endoscopy staff morale. The NPs developed a study to examine bowel preparation outcomes after a group preprocedure class that provided comprehensive and multimedia education in comparison to standard mailed instructions. The study was approved by the Institutional Review Board. The hypothesis was that group patient education would result in better adherence to bowel preparation instructions than did mailed instructions and that better adherence would result in significantly improved colonoscopy outcomes.
Methods
This was a descriptive pilot study with a convenience sample of 200 veterans randomly selected between 2009 and 2011. The study measured 2 groups. The control group received only the mailed standard bowel preparation instructions, whereas the intervention group received the standard bowel preparation instructions and participated in a group intervention class. Eligible participants were aged 45 to 79 years and were enrolled as patients in a single center (PVAMC GE clinic).
Related: E-Consults in Gastroenterology: A Quality Improvement Project
After referral consults were initially selected for appropriate colonoscopy screening or surveillance, potential patient subjects were randomized into either the control or intervention groups by the coin toss method, followed by mailed letters inviting them to participate in the study. If subjects expressed interest, then consent was obtained. The colonoscopy procedure note was updated to reflect bowel preparation quality. All subjects were de-identified. There were about 8 endoscopists; all were board-certified gastroenterologists plus GE fellows who performed procedures at the time of the study. (Fellows rotated every 2 to 4 weeks in the GE clinic and were always accompanied by an attending gastroenterologist.)
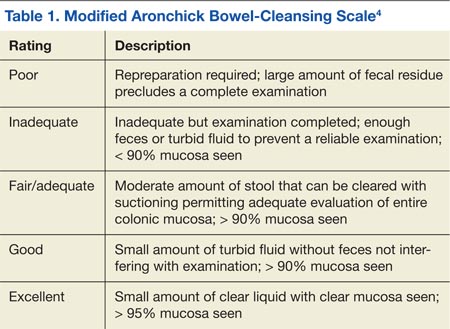
All the endoscopists were instructed in the grading system adapted from the modified Aronchick scale (Table 1).4 This scale measures the quality of bowel preparation for the entire colon: excellent (> 95% visualization of bowel mucosa); good (> 90% of mucosa was visible); fair (some semisolid stool could be suctioned out, but > 90% of mucosa was visible), and poor (semisolid stool cannot be suctioned out and < 90% of mucosa was seen). The modified Aronchick scale also has an inadequate rating, but this was not used in the study. For this study, bowel preparation that was excellent or good received a 1, a fair preparation received a 2, and poor preparation received a 3. The Pearson correlation for the modified Aronchick scale coefficients was 0.62 (P < .001). The value for the kappa statistic was 0.77 (P < .001).5
Results
There were 77 men and 5 women enrolled in the study. The control group had 43 subjects, and the intervention group had 39 subjects. Only 28 subjects each from the control and intervention groups had the quality of bowel preparation rated by the endoscopists. In the control group, 53.6% were rated excellent or good, 42.9% were fair, and 3.5% were poor. In the intervention group, 42.9 % of preparations were excellent or good, 42.8% were fair, and 14.3% were poor (Table 2).
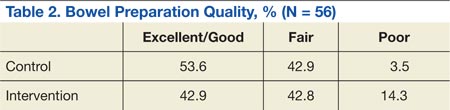
Preparation quality was not described in the procedure documentation for 34.9% and 28.2% of the subjects, respectively, for the control and intervention groups. There was no significant difference in no-show rates to procedures in either of the groups. Based on the data, a Fisher exact test for association was performed (P = .39), indicating there was no evidence of association between the intervention group and preparation quality.
The authors observed several recurrent themes during the group interventions. Fear of finding cancer and the perception of the procedure’s invasiveness were raised and addressed. Also misconceptions about CRC were debunked, such as the belief that a lack of bowel symptoms indicated no chance of having CRC or that only a family history indicated a risk factor. Patients discussed how much they learned about CRC, colon anatomy, and the importance of the bowel preparation. A multifaceted teaching approach was used to convey teaching points, such as flip charts, colonoscopy equipment, tours of procedure rooms, and visuals of various bowel preparation qualities. Throughout the educational intervention, humor, active listening, and reflection were woven into discussions to create a comfortable and relaxed learning environment.
Discussion and Limitations
The study results were unexpected. The authors had hypothesized that the group preprocedure educational intervention would have made a statistically significant difference in preparation quality, but it did not. In addition, the authors’ observations during the intervention led them to believe that the subjects had gained knowledge about how to correctly administer the bowel preparation.
Related: Do Age and Gender Matter in Colorectal Cancer?
A significant limitation of this pilot study was the difficulty in extrapolating meaningful data within the intervention group and between the intervention and control groups. After closely examining the raw data, the authors identified some key issues: There were only 28 subjects in each group who had bowel preparation quality described. This small sample size makes it difficult to draw meaningful conclusions. However, the education session in and of itself was clearly a positive experience for subjects, and the authors would recommend a future study with a larger sample size.
A prior power analysis would have helped this study determine a sufficient number of subjects that would be needed to determine whether the intervention had an effect. Furthermore, instead of tossing a coin to randomize the study groups, other types of randomization could have been used.
Other study limitations that came to light were:
- Variable preparation quality documentation by endoscopists;
- Limited availability of days to schedule group intervention classes;
- Some subjects did not attend the group session but still had the procedure done;
- The study invitation letter was long, and there were no financial incentives to participate;
- If pre- and postintervention testing had been conducted, effective and ineffective teaching strategies could have been identified; and
- The principal investigator also performed some of the procedures during the study, introducing potential bias.
Since the study, the authors have learned more about changes in national standards for bowel preparation administration and polyp surveillance. Preparation instructions need to be updated to reflect current recommendations for split-dose preparation administration in which the bowel preparation is taken in spaced doses, leading to better compliance and outcomes.6 Informally, patients and family have told staff that preparation instructions are difficult to understand. Following a Plan-Do-Study-Act cycle, feedback from patients should be obtained before revising and printing preparation instructions.7 This feedback could ensure that preparation instructions are written in patient-friendly, easily understood language.
Conclusion
Nursing professionals are likely to be effective in helping veterans achieve improved bowel preparation quality, because nurses have an established record as patient educators and advocates. Good bowel preparation quality is an important, achievable objective for veterans. As Mangnall reported, bowel preparation quality data are a strong nurse-sensitive quality measure that can be used to devise more effective interventions to obtain better bowel preparation results.8 As clinicians working on the frontline, nurses are well positioned to assess, intervene, and evaluate whether or not the modifications they have made to bowel preparation instructions are effective as they measure bowel preparation quality status post colonoscopy.
Author disclosures
The authors report no actual or potential conflicts of interest with regard to this article.
Disclaimer
The opinions expressed herein are those of the authors and do not necessarily reflect those of Federal Practitioner, Frontline Medical Communications Inc., the U.S. Government, or any of its agencies. This article may discuss unlabeled or investigational use of certain drugs. Please review complete prescribing information for specific drugs or drug combinations—including indications, contraindications, warnings, and adverse effects—before administering pharmacologic therapy to patients.
1. American Society of Gastrointestinal Endoscopy. Media backgrounder: Colorectal cancer screening. American Society of Gastrointestinal Endoscopy Website. http://www.asge.org/PressroomIndex .aspx?id=552. Updated August 2014. Accessed January 29, 2015.
2. Lee RH. Quality colonoscopy: A matter of time, technique or technology? World J Gastroenterol. 2013;19(10):1517-1522.
3. Health Services Research & Development. 1004—Impact of a novel patient educational booklet on colonoscopy preparation in veterans. US Department of Veterans Affairs Website. http://www.hsrd .research.va.gov/meetings/2009/print_abstract .cfm?recordid=541. Accessed January 29, 2015.
4. Gurudu SR, Ratuapli S, Heigh R, DiBaise J, Leighton J, Crowell M. Quality of bowel cleansing for afternoon colonoscopy is influenced by time of administration. Am J Gastroenterol. 2010;105(11):2318-2322.
5. Rostom A, Jolicoeur E. Validation of a new scale for the assessment of bowel preparation quality. Gastrointest Endosc. 2004;59(4):482-486.
6. Cohen, LB. Split dosing of bowel preparation for colonoscopy: An analysis of its efficacy, safety and tolerability. Gastrointest Endosc. 2010;72(2):406-412.
7. Institute for Healthcare Improvement. How to improve: Model for improvement. Institute for Healthcare improvement; 2015. Institute for Healthcare Improvement Website. http://www.ihi.org/resources/Pages/HowtoImprove/default.aspx. Accessed February 5, 2015.
8. Mangnall R. Good bowel cleaning vital for effective colonoscopy. Nurse N Z. 2012;18(16):17-19.
According to the CDC, colorectal cancer (CRC) is largely preventable but remains the second leading cancer killer for men and women in the U.S. Screening for polyps (detection of abnormal growths) and surveillance (based on prior bowel preparation quality, findings, and personal and family histories) are key elements for CRC prevention and survival.1 However, inadequate bowel preparation greatly reduces accuracy of its intended purpose: finding and removing precancerous polyps or lesions before they develop into a cancer, typically within a 10-year window. If preparation quality is not satisfactory, the ability of the endoscopist to meet national polyp detection rates is limited. These rates are currently 25% for men and 15% for women.2 Compounding poor preparation, many veterans avoid CRC screening due to anxiety, shame, and fear of what could be found.
Related: Do I Need a Colonoscopy?
About 60% of veterans presenting for colonoscopy have inadequate bowel preparation.3 Colonoscopy remains the gold standard for detection of colorectal pathology and is available to veterans without insurance preauthorization, eliminating a significant barrier to screening.1 Inadequate bowel preparation can result in missed polyps, cancelled procedures, and increased procedure time. Nonadherence to the liquid diet and high-volume, bowel-cleansing solution can lead to a repeated colonoscopy.
Two nurse practitioners (NPs) at the Philadelphia VAMC (PVAMC) gastroenterology (GE) section recognized that many veterans had poor bowel preparation in spite of preprocedure visits, written instructions, and no financial limitations. Repeated colonoscopies were impacting patient satisfaction, facility costs, and endoscopy staff morale. The NPs developed a study to examine bowel preparation outcomes after a group preprocedure class that provided comprehensive and multimedia education in comparison to standard mailed instructions. The study was approved by the Institutional Review Board. The hypothesis was that group patient education would result in better adherence to bowel preparation instructions than did mailed instructions and that better adherence would result in significantly improved colonoscopy outcomes.
Methods
This was a descriptive pilot study with a convenience sample of 200 veterans randomly selected between 2009 and 2011. The study measured 2 groups. The control group received only the mailed standard bowel preparation instructions, whereas the intervention group received the standard bowel preparation instructions and participated in a group intervention class. Eligible participants were aged 45 to 79 years and were enrolled as patients in a single center (PVAMC GE clinic).
Related: E-Consults in Gastroenterology: A Quality Improvement Project
After referral consults were initially selected for appropriate colonoscopy screening or surveillance, potential patient subjects were randomized into either the control or intervention groups by the coin toss method, followed by mailed letters inviting them to participate in the study. If subjects expressed interest, then consent was obtained. The colonoscopy procedure note was updated to reflect bowel preparation quality. All subjects were de-identified. There were about 8 endoscopists; all were board-certified gastroenterologists plus GE fellows who performed procedures at the time of the study. (Fellows rotated every 2 to 4 weeks in the GE clinic and were always accompanied by an attending gastroenterologist.)
All the endoscopists were instructed in the grading system adapted from the modified Aronchick scale (Table 1).4 This scale measures the quality of bowel preparation for the entire colon: excellent (> 95% visualization of bowel mucosa); good (> 90% of mucosa was visible); fair (some semisolid stool could be suctioned out, but > 90% of mucosa was visible), and poor (semisolid stool cannot be suctioned out and < 90% of mucosa was seen). The modified Aronchick scale also has an inadequate rating, but this was not used in the study. For this study, bowel preparation that was excellent or good received a 1, a fair preparation received a 2, and poor preparation received a 3. The Pearson correlation for the modified Aronchick scale coefficients was 0.62 (P < .001). The value for the kappa statistic was 0.77 (P < .001).5
Results
There were 77 men and 5 women enrolled in the study. The control group had 43 subjects, and the intervention group had 39 subjects. Only 28 subjects each from the control and intervention groups had the quality of bowel preparation rated by the endoscopists. In the control group, 53.6% were rated excellent or good, 42.9% were fair, and 3.5% were poor. In the intervention group, 42.9 % of preparations were excellent or good, 42.8% were fair, and 14.3% were poor (Table 2).
Preparation quality was not described in the procedure documentation for 34.9% and 28.2% of the subjects, respectively, for the control and intervention groups. There was no significant difference in no-show rates to procedures in either of the groups. Based on the data, a Fisher exact test for association was performed (P = .39), indicating there was no evidence of association between the intervention group and preparation quality.
The authors observed several recurrent themes during the group interventions. Fear of finding cancer and the perception of the procedure’s invasiveness were raised and addressed. Also misconceptions about CRC were debunked, such as the belief that a lack of bowel symptoms indicated no chance of having CRC or that only a family history indicated a risk factor. Patients discussed how much they learned about CRC, colon anatomy, and the importance of the bowel preparation. A multifaceted teaching approach was used to convey teaching points, such as flip charts, colonoscopy equipment, tours of procedure rooms, and visuals of various bowel preparation qualities. Throughout the educational intervention, humor, active listening, and reflection were woven into discussions to create a comfortable and relaxed learning environment.
Discussion and Limitations
The study results were unexpected. The authors had hypothesized that the group preprocedure educational intervention would have made a statistically significant difference in preparation quality, but it did not. In addition, the authors’ observations during the intervention led them to believe that the subjects had gained knowledge about how to correctly administer the bowel preparation.
Related: Do Age and Gender Matter in Colorectal Cancer?
A significant limitation of this pilot study was the difficulty in extrapolating meaningful data within the intervention group and between the intervention and control groups. After closely examining the raw data, the authors identified some key issues: There were only 28 subjects in each group who had bowel preparation quality described. This small sample size makes it difficult to draw meaningful conclusions. However, the education session in and of itself was clearly a positive experience for subjects, and the authors would recommend a future study with a larger sample size.
A prior power analysis would have helped this study determine a sufficient number of subjects that would be needed to determine whether the intervention had an effect. Furthermore, instead of tossing a coin to randomize the study groups, other types of randomization could have been used.
Other study limitations that came to light were:
- Variable preparation quality documentation by endoscopists;
- Limited availability of days to schedule group intervention classes;
- Some subjects did not attend the group session but still had the procedure done;
- The study invitation letter was long, and there were no financial incentives to participate;
- If pre- and postintervention testing had been conducted, effective and ineffective teaching strategies could have been identified; and
- The principal investigator also performed some of the procedures during the study, introducing potential bias.
Since the study, the authors have learned more about changes in national standards for bowel preparation administration and polyp surveillance. Preparation instructions need to be updated to reflect current recommendations for split-dose preparation administration in which the bowel preparation is taken in spaced doses, leading to better compliance and outcomes.6 Informally, patients and family have told staff that preparation instructions are difficult to understand. Following a Plan-Do-Study-Act cycle, feedback from patients should be obtained before revising and printing preparation instructions.7 This feedback could ensure that preparation instructions are written in patient-friendly, easily understood language.
Conclusion
Nursing professionals are likely to be effective in helping veterans achieve improved bowel preparation quality, because nurses have an established record as patient educators and advocates. Good bowel preparation quality is an important, achievable objective for veterans. As Mangnall reported, bowel preparation quality data are a strong nurse-sensitive quality measure that can be used to devise more effective interventions to obtain better bowel preparation results.8 As clinicians working on the frontline, nurses are well positioned to assess, intervene, and evaluate whether or not the modifications they have made to bowel preparation instructions are effective as they measure bowel preparation quality status post colonoscopy.
Author disclosures
The authors report no actual or potential conflicts of interest with regard to this article.
Disclaimer
The opinions expressed herein are those of the authors and do not necessarily reflect those of Federal Practitioner, Frontline Medical Communications Inc., the U.S. Government, or any of its agencies. This article may discuss unlabeled or investigational use of certain drugs. Please review complete prescribing information for specific drugs or drug combinations—including indications, contraindications, warnings, and adverse effects—before administering pharmacologic therapy to patients.
According to the CDC, colorectal cancer (CRC) is largely preventable but remains the second leading cancer killer for men and women in the U.S. Screening for polyps (detection of abnormal growths) and surveillance (based on prior bowel preparation quality, findings, and personal and family histories) are key elements for CRC prevention and survival.1 However, inadequate bowel preparation greatly reduces accuracy of its intended purpose: finding and removing precancerous polyps or lesions before they develop into a cancer, typically within a 10-year window. If preparation quality is not satisfactory, the ability of the endoscopist to meet national polyp detection rates is limited. These rates are currently 25% for men and 15% for women.2 Compounding poor preparation, many veterans avoid CRC screening due to anxiety, shame, and fear of what could be found.
Related: Do I Need a Colonoscopy?
About 60% of veterans presenting for colonoscopy have inadequate bowel preparation.3 Colonoscopy remains the gold standard for detection of colorectal pathology and is available to veterans without insurance preauthorization, eliminating a significant barrier to screening.1 Inadequate bowel preparation can result in missed polyps, cancelled procedures, and increased procedure time. Nonadherence to the liquid diet and high-volume, bowel-cleansing solution can lead to a repeated colonoscopy.
Two nurse practitioners (NPs) at the Philadelphia VAMC (PVAMC) gastroenterology (GE) section recognized that many veterans had poor bowel preparation in spite of preprocedure visits, written instructions, and no financial limitations. Repeated colonoscopies were impacting patient satisfaction, facility costs, and endoscopy staff morale. The NPs developed a study to examine bowel preparation outcomes after a group preprocedure class that provided comprehensive and multimedia education in comparison to standard mailed instructions. The study was approved by the Institutional Review Board. The hypothesis was that group patient education would result in better adherence to bowel preparation instructions than did mailed instructions and that better adherence would result in significantly improved colonoscopy outcomes.
Methods
This was a descriptive pilot study with a convenience sample of 200 veterans randomly selected between 2009 and 2011. The study measured 2 groups. The control group received only the mailed standard bowel preparation instructions, whereas the intervention group received the standard bowel preparation instructions and participated in a group intervention class. Eligible participants were aged 45 to 79 years and were enrolled as patients in a single center (PVAMC GE clinic).
Related: E-Consults in Gastroenterology: A Quality Improvement Project
After referral consults were initially selected for appropriate colonoscopy screening or surveillance, potential patient subjects were randomized into either the control or intervention groups by the coin toss method, followed by mailed letters inviting them to participate in the study. If subjects expressed interest, then consent was obtained. The colonoscopy procedure note was updated to reflect bowel preparation quality. All subjects were de-identified. There were about 8 endoscopists; all were board-certified gastroenterologists plus GE fellows who performed procedures at the time of the study. (Fellows rotated every 2 to 4 weeks in the GE clinic and were always accompanied by an attending gastroenterologist.)
All the endoscopists were instructed in the grading system adapted from the modified Aronchick scale (Table 1).4 This scale measures the quality of bowel preparation for the entire colon: excellent (> 95% visualization of bowel mucosa); good (> 90% of mucosa was visible); fair (some semisolid stool could be suctioned out, but > 90% of mucosa was visible), and poor (semisolid stool cannot be suctioned out and < 90% of mucosa was seen). The modified Aronchick scale also has an inadequate rating, but this was not used in the study. For this study, bowel preparation that was excellent or good received a 1, a fair preparation received a 2, and poor preparation received a 3. The Pearson correlation for the modified Aronchick scale coefficients was 0.62 (P < .001). The value for the kappa statistic was 0.77 (P < .001).5
Results
There were 77 men and 5 women enrolled in the study. The control group had 43 subjects, and the intervention group had 39 subjects. Only 28 subjects each from the control and intervention groups had the quality of bowel preparation rated by the endoscopists. In the control group, 53.6% were rated excellent or good, 42.9% were fair, and 3.5% were poor. In the intervention group, 42.9 % of preparations were excellent or good, 42.8% were fair, and 14.3% were poor (Table 2).
Preparation quality was not described in the procedure documentation for 34.9% and 28.2% of the subjects, respectively, for the control and intervention groups. There was no significant difference in no-show rates to procedures in either of the groups. Based on the data, a Fisher exact test for association was performed (P = .39), indicating there was no evidence of association between the intervention group and preparation quality.
The authors observed several recurrent themes during the group interventions. Fear of finding cancer and the perception of the procedure’s invasiveness were raised and addressed. Also misconceptions about CRC were debunked, such as the belief that a lack of bowel symptoms indicated no chance of having CRC or that only a family history indicated a risk factor. Patients discussed how much they learned about CRC, colon anatomy, and the importance of the bowel preparation. A multifaceted teaching approach was used to convey teaching points, such as flip charts, colonoscopy equipment, tours of procedure rooms, and visuals of various bowel preparation qualities. Throughout the educational intervention, humor, active listening, and reflection were woven into discussions to create a comfortable and relaxed learning environment.
Discussion and Limitations
The study results were unexpected. The authors had hypothesized that the group preprocedure educational intervention would have made a statistically significant difference in preparation quality, but it did not. In addition, the authors’ observations during the intervention led them to believe that the subjects had gained knowledge about how to correctly administer the bowel preparation.
Related: Do Age and Gender Matter in Colorectal Cancer?
A significant limitation of this pilot study was the difficulty in extrapolating meaningful data within the intervention group and between the intervention and control groups. After closely examining the raw data, the authors identified some key issues: There were only 28 subjects in each group who had bowel preparation quality described. This small sample size makes it difficult to draw meaningful conclusions. However, the education session in and of itself was clearly a positive experience for subjects, and the authors would recommend a future study with a larger sample size.
A prior power analysis would have helped this study determine a sufficient number of subjects that would be needed to determine whether the intervention had an effect. Furthermore, instead of tossing a coin to randomize the study groups, other types of randomization could have been used.
Other study limitations that came to light were:
- Variable preparation quality documentation by endoscopists;
- Limited availability of days to schedule group intervention classes;
- Some subjects did not attend the group session but still had the procedure done;
- The study invitation letter was long, and there were no financial incentives to participate;
- If pre- and postintervention testing had been conducted, effective and ineffective teaching strategies could have been identified; and
- The principal investigator also performed some of the procedures during the study, introducing potential bias.
Since the study, the authors have learned more about changes in national standards for bowel preparation administration and polyp surveillance. Preparation instructions need to be updated to reflect current recommendations for split-dose preparation administration in which the bowel preparation is taken in spaced doses, leading to better compliance and outcomes.6 Informally, patients and family have told staff that preparation instructions are difficult to understand. Following a Plan-Do-Study-Act cycle, feedback from patients should be obtained before revising and printing preparation instructions.7 This feedback could ensure that preparation instructions are written in patient-friendly, easily understood language.
Conclusion
Nursing professionals are likely to be effective in helping veterans achieve improved bowel preparation quality, because nurses have an established record as patient educators and advocates. Good bowel preparation quality is an important, achievable objective for veterans. As Mangnall reported, bowel preparation quality data are a strong nurse-sensitive quality measure that can be used to devise more effective interventions to obtain better bowel preparation results.8 As clinicians working on the frontline, nurses are well positioned to assess, intervene, and evaluate whether or not the modifications they have made to bowel preparation instructions are effective as they measure bowel preparation quality status post colonoscopy.
Author disclosures
The authors report no actual or potential conflicts of interest with regard to this article.
Disclaimer
The opinions expressed herein are those of the authors and do not necessarily reflect those of Federal Practitioner, Frontline Medical Communications Inc., the U.S. Government, or any of its agencies. This article may discuss unlabeled or investigational use of certain drugs. Please review complete prescribing information for specific drugs or drug combinations—including indications, contraindications, warnings, and adverse effects—before administering pharmacologic therapy to patients.
1. American Society of Gastrointestinal Endoscopy. Media backgrounder: Colorectal cancer screening. American Society of Gastrointestinal Endoscopy Website. http://www.asge.org/PressroomIndex .aspx?id=552. Updated August 2014. Accessed January 29, 2015.
2. Lee RH. Quality colonoscopy: A matter of time, technique or technology? World J Gastroenterol. 2013;19(10):1517-1522.
3. Health Services Research & Development. 1004—Impact of a novel patient educational booklet on colonoscopy preparation in veterans. US Department of Veterans Affairs Website. http://www.hsrd .research.va.gov/meetings/2009/print_abstract .cfm?recordid=541. Accessed January 29, 2015.
4. Gurudu SR, Ratuapli S, Heigh R, DiBaise J, Leighton J, Crowell M. Quality of bowel cleansing for afternoon colonoscopy is influenced by time of administration. Am J Gastroenterol. 2010;105(11):2318-2322.
5. Rostom A, Jolicoeur E. Validation of a new scale for the assessment of bowel preparation quality. Gastrointest Endosc. 2004;59(4):482-486.
6. Cohen, LB. Split dosing of bowel preparation for colonoscopy: An analysis of its efficacy, safety and tolerability. Gastrointest Endosc. 2010;72(2):406-412.
7. Institute for Healthcare Improvement. How to improve: Model for improvement. Institute for Healthcare improvement; 2015. Institute for Healthcare Improvement Website. http://www.ihi.org/resources/Pages/HowtoImprove/default.aspx. Accessed February 5, 2015.
8. Mangnall R. Good bowel cleaning vital for effective colonoscopy. Nurse N Z. 2012;18(16):17-19.
1. American Society of Gastrointestinal Endoscopy. Media backgrounder: Colorectal cancer screening. American Society of Gastrointestinal Endoscopy Website. http://www.asge.org/PressroomIndex .aspx?id=552. Updated August 2014. Accessed January 29, 2015.
2. Lee RH. Quality colonoscopy: A matter of time, technique or technology? World J Gastroenterol. 2013;19(10):1517-1522.
3. Health Services Research & Development. 1004—Impact of a novel patient educational booklet on colonoscopy preparation in veterans. US Department of Veterans Affairs Website. http://www.hsrd .research.va.gov/meetings/2009/print_abstract .cfm?recordid=541. Accessed January 29, 2015.
4. Gurudu SR, Ratuapli S, Heigh R, DiBaise J, Leighton J, Crowell M. Quality of bowel cleansing for afternoon colonoscopy is influenced by time of administration. Am J Gastroenterol. 2010;105(11):2318-2322.
5. Rostom A, Jolicoeur E. Validation of a new scale for the assessment of bowel preparation quality. Gastrointest Endosc. 2004;59(4):482-486.
6. Cohen, LB. Split dosing of bowel preparation for colonoscopy: An analysis of its efficacy, safety and tolerability. Gastrointest Endosc. 2010;72(2):406-412.
7. Institute for Healthcare Improvement. How to improve: Model for improvement. Institute for Healthcare improvement; 2015. Institute for Healthcare Improvement Website. http://www.ihi.org/resources/Pages/HowtoImprove/default.aspx. Accessed February 5, 2015.
8. Mangnall R. Good bowel cleaning vital for effective colonoscopy. Nurse N Z. 2012;18(16):17-19.
Novel Psoriasis Therapies and Patient Outcomes, Part 1: Topical Medications
Topical therapies are a mainstay in the management of patients with mild to moderate psoriasis (Figure). Presently, US Food and Drug Administration–approved topical medications that are commercially available for use in patients with psoriasis include corticosteroids, vitamin D3 analogues, calcineurin inhibitors, retinoids, anthralin, and tar-based formulations.1 In recent years, research has furthered our understanding of the molecular mechanisms underlying the pathogenesis of psoriasis and has afforded the development of more targeted therapies. Novel topical medications currently in phase 2 and phase 3 clinical trials are discussed in this article, and a summary is provided in the Table.

AN2728 (Phosphodiesterase 4 Inhibitor)
AN2728 (Anacor Pharmaceuticals, Inc) is a phosphodiesterase 4 inhibitor that blocks the inactivation of cyclic adenosine monophosphate, resulting in decreased production of inflammatory cytokines (eg, IL-6, IL-12, IL-23, tumor necrosis factor α [TNF-α]).2,3 In a randomized, double-blind, phase 2 clinical trial (N=35), 40% of patients treated with AN2728 ointment 5% reported improvement of more than 2 points in overall target plaque severity score versus 6% of patients treated with vehicle. In another randomized, double-blind, dose-response trial of 145 patients, those treated with AN2728 ointment 2% twice daily reported a 60% improvement versus 40% improvement in those treated with AN2728 ointment 0.5% once daily.3 In total, 3 phase 1 trials (registered at www.clinicaltrials.gov with the identifiers NCT01258088, NCT00762658, NCT00763204) and 4 phase 2 trials (NCT01029405, NCT00755196, NCT00759161, NCT01300052) have been completed; results were not available at the time of publication.
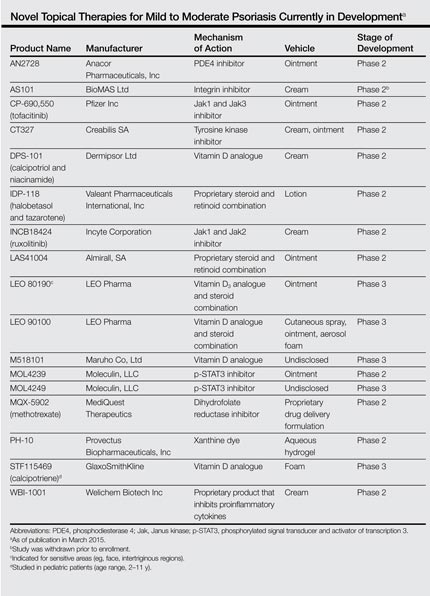
AS101 (Integrin Inhibitor)
AS101 (BioMAS Ltd), or ammonium trichloro (dioxoethylene-o,o') tellurate, acts as stimulator of regulatory T cells and a redox modulator inhibiting the leukocyte integrins α4β1 and α4β7 that enable CD4+ T-cell and macrophage extravasation; it also limits expression of the inflammatory cytokines IL-6 and IL-17.4 A randomized, placebo-controlled, double-blind, phase 2 study evaluating the efficacy of AS101 cream 4% twice daily for 12 weeks was withdrawn prior to enrollment (NCT00788424).
Tofacitinib (Janus Kinase 1 and 3 Inhibitor)
Tofacitinib (formerly known as CP-690,550)(Pfizer Inc) is a selective Janus kinase (Jak) 1 and Jak3 inhibitor that limits expression of cytokines that promote inflammation (eg, IFN-γ) and inhibits helper T cells (TH17) by downregulating expression of the IL-23 receptor. Epidermal keratinocyte proliferation in psoriasis is activated by TH17 cells that release IL-17 as well as TH1 cells that release IFN-γ and tumor necrosis factor. A phase 2a trial showed statistically significant improvement from baseline in the target plaque severity score for tofacitinib ointment 2% (least squares mean, −54.4%) versus vehicle (least squares mean, −41.5%).5 Two other phase 2 trials (NCT01246583, NCT00678561) assessing the efficacy, safety, tolerability, and pharmacokinetics of tofacitinib ointment in patients with mild to moderate psoriasis have been completed; results were not available at the time of publication. A phase 2b study that compared 2 dose strengths of tofacitinib ointment—10 mg/g and 20 mg/g—versus placebo over a 12-week period also was completed (NCT01831466); results were not available at the time of publication.
CT327 (Tyrosine Kinase Inhibitor)
CT327 (Creabilis SA) is a tyrosine kinase A (TrkA) inhibitor that affords a novel perspective in the treatment of pruritus by shifting the focus to sensory neurons. In a phase 2b study of 160 patients, a 60% change in the visual analog scale was noted at 8 weeks in the treatment group versus 21% in the placebo group.6 Two other phase 2 studies have been completed, one with a cream formulation of pegylated K252a (NCT00995969) and another with an ointment formulation (NCT01465282); results were not available at the time of publication.
DPS-101 (Vitamin D Analogue)
DPS-101 (Dermipsor Ltd) is a combination of calcipotriol and niacinamide. Calcipotriol is a vitamin D3 analogue that increases IL-10 expression while decreasing IL-8 expression.7 It curbs epidermal keratinocyte proliferation by limiting the expression of polo-like kinase 2 and early growth response-1.8 It also may induce keratinocyte apoptosis.9 Niacinamide is the amide of vitamin B3 and inhibits proinflammatory cytokines such as TNF-α, IL-1β, IL-6, and IL-8.10 In a dose-response phase 2b trial of 168 patients, DPS-101 demonstrated better results than either calcipotriol or niacinamide alone.11
IDP-118 (Proprietary Steroid and Retinoid Combination)
IDP-118 (Valeant Pharmaceuticals International, Inc) is a combination of halobetasol propionate (HP) 0.01% (a topical corticosteroid) and tazar-otene 0.045% (a selective topical retinoid) in a lotion formulation. In isolation, tazarotene is as effective as a mid to highly potent corticosteroid, but irritation may limit its tolerability. The use of combination treatments of mid to highly potent corticosteroids and tazarotene has shown enhanced tolerability and therapeutic efficacy.12 Ongoing studies include a phase 1 trial and a phase 2 trial to evaluate low- and high-strength preparations of IDP-118, respectively (NCT01670513). Another phase 2 trial evaluating the efficacy and safety of IDP-118 lotion (HP 0.01% and tazarotene 0.045%) versus IDP-118 monad HP 0.01% lotion, IDP-118 monad tazar-otene 0.045% lotion, and placebo has been completed (NCT02045277); results were not available at the time of publication.
Ruxolitinib (Jak1 and Jak2 Inhibitor)
Ruxolitinib (formerly known as INCB18424)(Incyte Corporation) is a selective Jak1 and Jak2 inhibitor. A phase 2 trial of ruxolitinib showed a 53% decline in the score for mean total lesions in patients treated with ruxolitinib phosphate cream 1% (P=.033) versus 54% in those treated with ruxolitinib phosphate cream 1.5% (P=.056) and 32% in those treated with placebo.13 Three other phase 2 studies (NCT00617994, NCT00820950, NCT00778700) have been completed; results were not available at the time of publication.
LAS41004 (Proprietary Steroid and Retinoid Combination)
LAS41004 (Almirall, SA) is an ointment containing the corticosteroid betamethasone dipropionate and the retinoid bexarotene that is being evaluated for treatment of mild to moderate psoriasis. Five phase 2 studies (NCT01119339, NCT01283698, NCT01360944, NCT02111499, NCT01462643) have been completed; results were not available at the time of publication. A randomized, double-blind, phase 2a study (NCT02180464) with a left-right design assessing clinical response to LAS41004 versus control in patients with mild to moderate psoriasis was actively recruiting at the time of publication.
LEO 80190 (Vitamin D3 Analogue and Steroid Combination)
LEO 80190 (LEO Pharma) is a combination of the vitamin D3 analogue calcipotriol and the corticosteroid hydrocortisone. It was developed as a treatment for sensitive areas such as the face and intertriginous regions. A randomized, investigator-blind, phase 3 trial (NCT00640822) of LEO 80190 ointment versus tacalcitol ointment and placebo once daily for 8 weeks demonstrated controlled disease of the face in 56.8% (183/322) of patients in the LEO 80190 group, 46.4% (147/317) in the tacalcitol group, and 36.3% (37/102) in the placebo group.14 Another phase 2 study (NCT00704262) and 2 phase 3 studies (NCT00691002, NCT01007591) have been completed; results were not available at the time of publication.
LEO 90100 (Vitamin D Analogue and Steroid Combination)
LEO 90100 (LEO Pharma) contains the vitamin D3 analogue calcipotriol and the corticosteroid betamethasone. Three phase 2 studies (NCT01347255, NCT01536886, NCT01536938) and a phase 3 study (NCT01866163) examining the efficacy and safety of various vehicles and formulations of LEO 90100 have been completed; results were not available at the time of publication. Another phase 3 study (NCT02132936) is ongoing but not recruiting participants. Other completed studies whose results were not yet available include a phase 1 pharmacodynamic study (NCT01946386), a phase 1 study that used patch testing to assess the degree of skin irritation and sensitization associated with LEO 90100 (NCT01935869), and a phase 2 study examining the impact of LEO 90100 on calcium metabolism and the hypothalamic-pituitary-adrenal axis (NCT01600222).
M518101 (Vitamin D Analogue)
M518101 (Maruho Co, Ltd) is a novel topical vitamin D3 analogue. Phase 1 (NCT01844973) and phase 2 (NCT01301157, NCT00884169) trials evaluating the safety, pharmacokinetics, and efficacy of M518101 have been completed; results were not available at the time of publication. A phase 3 study (NCT01989429) assessing the safety and therapeutic efficacy of M518101 according to changes in the modified psoriasis area and severity index over an 8-week treatment period also has been completed; results were not yet available. Three phase 3 studies assessing the safety and therapeutic efficacy of M518101 are ongoing: one is currently closed to recruitment (NCT01908595) and 2 are actively recruiting participants at the time of publication (NCT01878461, NCT01873677).
MOL4239 and MOL4249 (Phosphorylated Signal Transducer and Activator of Transcription 3 Inhibitors)
MOL4239 (Moleculin, LLC) is a novel topical agent for use in mild to moderate psoriasis that acts via phosphorylated signal transducer and activator of transcription 3 (p-STAT3) inhibition.15 The p-STAT3 protein has increased expression in psoriasis.16 A phase 2 trial of MOL4239 ointment (NCT01826201) has been completed, showing a greater mean (standard deviation) change in the psoriasis severity score in lesions treated at 28 days with MOL4239 ointment 10% (−1.9 [1.45]) versus lesions treated with placebo ointment (−1.5 [1.87]).17
MOL4249 (Moleculin, LLC) is more potent than MOL4239 with better lipid solubility. In the MOL4249 subset of a placebo-controlled, double-blind, phase 2a study of 16 patients with mild to moderate psoriasis, 10% (1/10) of patients experienced complete clearance of psoriatic plaques, 30% (3/10) of patients experienced 75% or greater improvement, and 50% (5/10) of patients experienced 50% or greater improvement compared to 17% (1/6) in the placebo group. Currently, a phase 2a contralateral study, a phase 2b psoriasis area and severity index trial, and a phase 3 pivotal trial are planned, according to the manufacturer.18
MQX-5902 (Dihydrofolate Reductase Inhibitor)
MQX-5902 (MediQuest Therapeutics) is a topical preparation of methotrexate for the treatment of fingernail psoriasis. Methotrexate is a dihydrofolate reductase inhibitor and antimetabolite that inhibits folic acid metabolism, thereby disrupting DNA synthesis.19 A phase 2b dose-ranging trial (NCT00666354) was designed to assess the therapeutic efficacy and safety of MQX-5902 delivered via a proprietary drug delivery formulation in fingernail psoriasis; the outcome of this trial was not available at the time of publication.
PH-10 (Xanthine Dye)
PH-10 (Provectus Biopharmaceuticals, Inc) is a topical aqueous hydrogel derived from rose bengal disodium that may be beneficial in treating skin conditions such as atopic dermatitis and mild to moderate psoriasis. Rose bengal disodium is a hydrophilic xanthine dye with diagnostic utility in ophthalmology and gastroenterology as well as projected use as a melanoma treatment as demonstrated in phase 1 and phase 2 clinical trials of PV-10 (Provectus Biopharmaceuticals, Inc).20 Two phase 2 studies assessing the safety and therapeutic efficacy of PH-10 in psoriasis (NCT01247818, NCT00941278) have been completed; results were not available at the time of publication.
STF115469 (Vitamin D Analogue)
STF115469 (GlaxoSmithKline) is a calcipotriene foam. At the time of publication, a randomized, placebo-controlled, double-blind, phase 3 trial (NCT01582932) of this vitamin D3 analogue with a projected enrollment of 180 participants was actively recruiting patients aged 2 to 11 years with mild to moderate plaque psoriasis to study the efficacy, safety, and tolerability of STF115469, as well as its pharmacokinetics and pharmacodynamics.
WBI-1001 (Proprietary Product)
WBI-1001 (Welichem Biotech Inc), or 2-isopropyl-5-[(E)-2-phenylethenyl] benzene-1, 3-diol, is a novel proprietary agent that inhibits proinflammatory cytokines (eg, IFN-γ, TNF-α). A randomized, placebo-controlled, double-blind, phase 1 trial (NCT00830817) assessing the efficacy, safety, tolerability, and pharmacokinetics of WBI-1001 has been completed; results were not available at the time of publication. Another randomized, placebo-controlled, double-blind, phase 2 trial (NCT01098721) evaluating its efficacy and safety according to the physician’s global assessment demonstrated a therapeutic benefit of 62.8% in patients treated with WBI-1001 cream 1% versus 13.0% in those treated with a placebo after a 12-week treatment period (P<.0001).21 WBI-1001 may offer a novel approach in the treatment of mild to moderate psoriasis.
Conclusion
Enhanced knowledge of the underlying pathogeneses of psoriasis and psoriatic arthritis has identified new therapeutic targets and enabled the development of exciting novel treatments for these conditions. The topical agents currently in phase 2 and phase 3 clinical trials show promise in enhancing the way physicians treat psoriasis. There is hope for more individualized treatment regimens with improved tolerability and better safety profiles with increased therapeutic efficacy. As our understanding of the molecular underpinnings of psoriasis continues to deepen, it will afford the development of even more innovative therapeutics for use in the management of psoriasis.
1. Mason A, Mason J, Cork M, et al. Topical treatments for chronic plaque psoriasis: an abridged Cochrane systematic review. J Am Acad Dermatol. 2013;69:799-807.
2. Nazarian R, Weinberg JM. AN-2728, a PDE4 inhibitor for the potential topical treatment of psoriasis and atopic dermatitis. Curr Opin Investig Drugs. 2009;10:1236-1242.
3. Moustafa F, Feldman SR. A review of phosphodiesterase-inhibition and the potential role for phosphodiesterase 4-inhibitors in clinical dermatology. Dermatol Online J. 2014;20:22608.
4. Halpert G, Sredni B. The effect of the novel tellurium compound AS101 on autoimmune diseases. Autoimmun Rev. 2014;13:1230-1235.
5. Ports WC, Khan S, Lan S, et al. A randomized phase 2a efficacy and safety trial of the topical Janus kinase inhibitor tofacitinib in the treatment of chronic plaque psoriasis. Br J Dermatol. 2013;169:137-145.
6. Yosipovitch G, Roblin D, Traversa S, et al. A novel topical targeted anti-pruritic treatment in phase 2b development for chronic pruritus. Paper presented at: 72nd Annual Meeting of the American Academy of Dermatology; March 21-25, 2014; Denver, CO.
7. Kang S, Yi S, Griffiths CE, et al. Calcipotriene-induced improvement in psoriasis is associated with reduced interleukin-8 and increased interleukin-10 levels within lesions. Br J Dermatol. 1998;138:77-83.
8. Kristl J, Slanc P, Krasna M, et al. Calcipotriol affects keratinocyte proliferation by decreasing expression of early growth response-1 and polo-like kinase-2. Pharm Res. 2008;25:521-529.
9. Tiberio R, Bozzo C, Pertusi G, et al. Calcipotriol induces apoptosis in psoriatic keratinocytes. Clin Exp Dermatol. 2009;34:e972-e974.
10. Luger T, Seite S, Humbert P, et al. Recommendations for adjunctive basic skin care in patients with psoriasis. Eur J Dermatol. 2014;24:194-200.
11. Dermipsor reports good results in DPS-101 Phase IIb study for plaque psoriasis [press release]. Evaluate Web site. http://www.evaluategroup.com/Universal/View.aspx?type=Story&id=250042. Published October 15, 2007. Accessed February 13, 2015.
12. Rivera AM, Hsu S. Topical halobetasol propionate in the treatment of plaque psoriasis: a review. Am J Clin Dermatol. 2005;6:311-316.
13. Punwani N, Scherle P, Flores R, et al. Preliminary clinical activity of a topical JAK1/2 inhibitor in the treatment of psoriasis. J Am Acad Dermatol. 2012;67:658-664.
14. Efficacy and safety of calcipotriol plus hydrocortisone ointment compared with tacalcitol ointment in patients with psoriasis on the face and skin folds (NCT00640822). https://clinicaltrials.gov/ct2/show/results/NCT00640822?term=NCT00640822&rank=1. Updated October 21, 2013. Accessed May 30, 2014.
15. Product candidates: targeting p-STAT3 for improved psoriasis treatment. Moleculin Web site. http://moleculin.com/product-candidates/mol4239. Accessed February 13, 2015.
16. Chowdhari S, Saini N. hsa-miR-4516 mediated downregulation of STAT3/CDK6/UBE2N plays a role in PUVA induced apoptosis in keratinocytes. J Cell Physiol. 2014;229:1630-1638.
17. Paired psoriasis lesion, comparative, study to evaluate MOL4239 in psoriasis (NCT01826201). https://clinicaltrials.gov/ct2/show/results/NCT01826201?term=NCT01826201&rank=1§=X01256#all. Updated December 22, 2014. Accessed February 25, 2015.
18. Clinical development pipeline. Moleculin Web site. http://moleculin.com/clinical-trials/psoriasis-trials. Accessed February 13, 2015.
19. de la Brassinne M, Nikkels A. Psoriasis: state of the art 2013. Acta Clin Belg. 2013;68:433-441.
20. Ross MI. Intralesional therapy with PV-10 (Rose Bengal) for in-transit melanoma. J Surg Oncol. 2014;109:314-319.
21. Bissonnette R, Bolduc C, Maari C, et al. Efficacy and safety of topical WBI-1001 in patients with mild to moderate psoriasis: results from a randomized, double-blind placebo-controlled, phase II trial. J Eur Acad Dermatol Venereol. 2012;26:1516-1521.
Topical therapies are a mainstay in the management of patients with mild to moderate psoriasis (Figure). Presently, US Food and Drug Administration–approved topical medications that are commercially available for use in patients with psoriasis include corticosteroids, vitamin D3 analogues, calcineurin inhibitors, retinoids, anthralin, and tar-based formulations.1 In recent years, research has furthered our understanding of the molecular mechanisms underlying the pathogenesis of psoriasis and has afforded the development of more targeted therapies. Novel topical medications currently in phase 2 and phase 3 clinical trials are discussed in this article, and a summary is provided in the Table.
AN2728 (Phosphodiesterase 4 Inhibitor)
AN2728 (Anacor Pharmaceuticals, Inc) is a phosphodiesterase 4 inhibitor that blocks the inactivation of cyclic adenosine monophosphate, resulting in decreased production of inflammatory cytokines (eg, IL-6, IL-12, IL-23, tumor necrosis factor α [TNF-α]).2,3 In a randomized, double-blind, phase 2 clinical trial (N=35), 40% of patients treated with AN2728 ointment 5% reported improvement of more than 2 points in overall target plaque severity score versus 6% of patients treated with vehicle. In another randomized, double-blind, dose-response trial of 145 patients, those treated with AN2728 ointment 2% twice daily reported a 60% improvement versus 40% improvement in those treated with AN2728 ointment 0.5% once daily.3 In total, 3 phase 1 trials (registered at www.clinicaltrials.gov with the identifiers NCT01258088, NCT00762658, NCT00763204) and 4 phase 2 trials (NCT01029405, NCT00755196, NCT00759161, NCT01300052) have been completed; results were not available at the time of publication.
AS101 (Integrin Inhibitor)
AS101 (BioMAS Ltd), or ammonium trichloro (dioxoethylene-o,o') tellurate, acts as stimulator of regulatory T cells and a redox modulator inhibiting the leukocyte integrins α4β1 and α4β7 that enable CD4+ T-cell and macrophage extravasation; it also limits expression of the inflammatory cytokines IL-6 and IL-17.4 A randomized, placebo-controlled, double-blind, phase 2 study evaluating the efficacy of AS101 cream 4% twice daily for 12 weeks was withdrawn prior to enrollment (NCT00788424).
Tofacitinib (Janus Kinase 1 and 3 Inhibitor)
Tofacitinib (formerly known as CP-690,550)(Pfizer Inc) is a selective Janus kinase (Jak) 1 and Jak3 inhibitor that limits expression of cytokines that promote inflammation (eg, IFN-γ) and inhibits helper T cells (TH17) by downregulating expression of the IL-23 receptor. Epidermal keratinocyte proliferation in psoriasis is activated by TH17 cells that release IL-17 as well as TH1 cells that release IFN-γ and tumor necrosis factor. A phase 2a trial showed statistically significant improvement from baseline in the target plaque severity score for tofacitinib ointment 2% (least squares mean, −54.4%) versus vehicle (least squares mean, −41.5%).5 Two other phase 2 trials (NCT01246583, NCT00678561) assessing the efficacy, safety, tolerability, and pharmacokinetics of tofacitinib ointment in patients with mild to moderate psoriasis have been completed; results were not available at the time of publication. A phase 2b study that compared 2 dose strengths of tofacitinib ointment—10 mg/g and 20 mg/g—versus placebo over a 12-week period also was completed (NCT01831466); results were not available at the time of publication.
CT327 (Tyrosine Kinase Inhibitor)
CT327 (Creabilis SA) is a tyrosine kinase A (TrkA) inhibitor that affords a novel perspective in the treatment of pruritus by shifting the focus to sensory neurons. In a phase 2b study of 160 patients, a 60% change in the visual analog scale was noted at 8 weeks in the treatment group versus 21% in the placebo group.6 Two other phase 2 studies have been completed, one with a cream formulation of pegylated K252a (NCT00995969) and another with an ointment formulation (NCT01465282); results were not available at the time of publication.
DPS-101 (Vitamin D Analogue)
DPS-101 (Dermipsor Ltd) is a combination of calcipotriol and niacinamide. Calcipotriol is a vitamin D3 analogue that increases IL-10 expression while decreasing IL-8 expression.7 It curbs epidermal keratinocyte proliferation by limiting the expression of polo-like kinase 2 and early growth response-1.8 It also may induce keratinocyte apoptosis.9 Niacinamide is the amide of vitamin B3 and inhibits proinflammatory cytokines such as TNF-α, IL-1β, IL-6, and IL-8.10 In a dose-response phase 2b trial of 168 patients, DPS-101 demonstrated better results than either calcipotriol or niacinamide alone.11
IDP-118 (Proprietary Steroid and Retinoid Combination)
IDP-118 (Valeant Pharmaceuticals International, Inc) is a combination of halobetasol propionate (HP) 0.01% (a topical corticosteroid) and tazar-otene 0.045% (a selective topical retinoid) in a lotion formulation. In isolation, tazarotene is as effective as a mid to highly potent corticosteroid, but irritation may limit its tolerability. The use of combination treatments of mid to highly potent corticosteroids and tazarotene has shown enhanced tolerability and therapeutic efficacy.12 Ongoing studies include a phase 1 trial and a phase 2 trial to evaluate low- and high-strength preparations of IDP-118, respectively (NCT01670513). Another phase 2 trial evaluating the efficacy and safety of IDP-118 lotion (HP 0.01% and tazarotene 0.045%) versus IDP-118 monad HP 0.01% lotion, IDP-118 monad tazar-otene 0.045% lotion, and placebo has been completed (NCT02045277); results were not available at the time of publication.
Ruxolitinib (Jak1 and Jak2 Inhibitor)
Ruxolitinib (formerly known as INCB18424)(Incyte Corporation) is a selective Jak1 and Jak2 inhibitor. A phase 2 trial of ruxolitinib showed a 53% decline in the score for mean total lesions in patients treated with ruxolitinib phosphate cream 1% (P=.033) versus 54% in those treated with ruxolitinib phosphate cream 1.5% (P=.056) and 32% in those treated with placebo.13 Three other phase 2 studies (NCT00617994, NCT00820950, NCT00778700) have been completed; results were not available at the time of publication.
LAS41004 (Proprietary Steroid and Retinoid Combination)
LAS41004 (Almirall, SA) is an ointment containing the corticosteroid betamethasone dipropionate and the retinoid bexarotene that is being evaluated for treatment of mild to moderate psoriasis. Five phase 2 studies (NCT01119339, NCT01283698, NCT01360944, NCT02111499, NCT01462643) have been completed; results were not available at the time of publication. A randomized, double-blind, phase 2a study (NCT02180464) with a left-right design assessing clinical response to LAS41004 versus control in patients with mild to moderate psoriasis was actively recruiting at the time of publication.
LEO 80190 (Vitamin D3 Analogue and Steroid Combination)
LEO 80190 (LEO Pharma) is a combination of the vitamin D3 analogue calcipotriol and the corticosteroid hydrocortisone. It was developed as a treatment for sensitive areas such as the face and intertriginous regions. A randomized, investigator-blind, phase 3 trial (NCT00640822) of LEO 80190 ointment versus tacalcitol ointment and placebo once daily for 8 weeks demonstrated controlled disease of the face in 56.8% (183/322) of patients in the LEO 80190 group, 46.4% (147/317) in the tacalcitol group, and 36.3% (37/102) in the placebo group.14 Another phase 2 study (NCT00704262) and 2 phase 3 studies (NCT00691002, NCT01007591) have been completed; results were not available at the time of publication.
LEO 90100 (Vitamin D Analogue and Steroid Combination)
LEO 90100 (LEO Pharma) contains the vitamin D3 analogue calcipotriol and the corticosteroid betamethasone. Three phase 2 studies (NCT01347255, NCT01536886, NCT01536938) and a phase 3 study (NCT01866163) examining the efficacy and safety of various vehicles and formulations of LEO 90100 have been completed; results were not available at the time of publication. Another phase 3 study (NCT02132936) is ongoing but not recruiting participants. Other completed studies whose results were not yet available include a phase 1 pharmacodynamic study (NCT01946386), a phase 1 study that used patch testing to assess the degree of skin irritation and sensitization associated with LEO 90100 (NCT01935869), and a phase 2 study examining the impact of LEO 90100 on calcium metabolism and the hypothalamic-pituitary-adrenal axis (NCT01600222).
M518101 (Vitamin D Analogue)
M518101 (Maruho Co, Ltd) is a novel topical vitamin D3 analogue. Phase 1 (NCT01844973) and phase 2 (NCT01301157, NCT00884169) trials evaluating the safety, pharmacokinetics, and efficacy of M518101 have been completed; results were not available at the time of publication. A phase 3 study (NCT01989429) assessing the safety and therapeutic efficacy of M518101 according to changes in the modified psoriasis area and severity index over an 8-week treatment period also has been completed; results were not yet available. Three phase 3 studies assessing the safety and therapeutic efficacy of M518101 are ongoing: one is currently closed to recruitment (NCT01908595) and 2 are actively recruiting participants at the time of publication (NCT01878461, NCT01873677).
MOL4239 and MOL4249 (Phosphorylated Signal Transducer and Activator of Transcription 3 Inhibitors)
MOL4239 (Moleculin, LLC) is a novel topical agent for use in mild to moderate psoriasis that acts via phosphorylated signal transducer and activator of transcription 3 (p-STAT3) inhibition.15 The p-STAT3 protein has increased expression in psoriasis.16 A phase 2 trial of MOL4239 ointment (NCT01826201) has been completed, showing a greater mean (standard deviation) change in the psoriasis severity score in lesions treated at 28 days with MOL4239 ointment 10% (−1.9 [1.45]) versus lesions treated with placebo ointment (−1.5 [1.87]).17
MOL4249 (Moleculin, LLC) is more potent than MOL4239 with better lipid solubility. In the MOL4249 subset of a placebo-controlled, double-blind, phase 2a study of 16 patients with mild to moderate psoriasis, 10% (1/10) of patients experienced complete clearance of psoriatic plaques, 30% (3/10) of patients experienced 75% or greater improvement, and 50% (5/10) of patients experienced 50% or greater improvement compared to 17% (1/6) in the placebo group. Currently, a phase 2a contralateral study, a phase 2b psoriasis area and severity index trial, and a phase 3 pivotal trial are planned, according to the manufacturer.18
MQX-5902 (Dihydrofolate Reductase Inhibitor)
MQX-5902 (MediQuest Therapeutics) is a topical preparation of methotrexate for the treatment of fingernail psoriasis. Methotrexate is a dihydrofolate reductase inhibitor and antimetabolite that inhibits folic acid metabolism, thereby disrupting DNA synthesis.19 A phase 2b dose-ranging trial (NCT00666354) was designed to assess the therapeutic efficacy and safety of MQX-5902 delivered via a proprietary drug delivery formulation in fingernail psoriasis; the outcome of this trial was not available at the time of publication.
PH-10 (Xanthine Dye)
PH-10 (Provectus Biopharmaceuticals, Inc) is a topical aqueous hydrogel derived from rose bengal disodium that may be beneficial in treating skin conditions such as atopic dermatitis and mild to moderate psoriasis. Rose bengal disodium is a hydrophilic xanthine dye with diagnostic utility in ophthalmology and gastroenterology as well as projected use as a melanoma treatment as demonstrated in phase 1 and phase 2 clinical trials of PV-10 (Provectus Biopharmaceuticals, Inc).20 Two phase 2 studies assessing the safety and therapeutic efficacy of PH-10 in psoriasis (NCT01247818, NCT00941278) have been completed; results were not available at the time of publication.
STF115469 (Vitamin D Analogue)
STF115469 (GlaxoSmithKline) is a calcipotriene foam. At the time of publication, a randomized, placebo-controlled, double-blind, phase 3 trial (NCT01582932) of this vitamin D3 analogue with a projected enrollment of 180 participants was actively recruiting patients aged 2 to 11 years with mild to moderate plaque psoriasis to study the efficacy, safety, and tolerability of STF115469, as well as its pharmacokinetics and pharmacodynamics.
WBI-1001 (Proprietary Product)
WBI-1001 (Welichem Biotech Inc), or 2-isopropyl-5-[(E)-2-phenylethenyl] benzene-1, 3-diol, is a novel proprietary agent that inhibits proinflammatory cytokines (eg, IFN-γ, TNF-α). A randomized, placebo-controlled, double-blind, phase 1 trial (NCT00830817) assessing the efficacy, safety, tolerability, and pharmacokinetics of WBI-1001 has been completed; results were not available at the time of publication. Another randomized, placebo-controlled, double-blind, phase 2 trial (NCT01098721) evaluating its efficacy and safety according to the physician’s global assessment demonstrated a therapeutic benefit of 62.8% in patients treated with WBI-1001 cream 1% versus 13.0% in those treated with a placebo after a 12-week treatment period (P<.0001).21 WBI-1001 may offer a novel approach in the treatment of mild to moderate psoriasis.
Conclusion
Enhanced knowledge of the underlying pathogeneses of psoriasis and psoriatic arthritis has identified new therapeutic targets and enabled the development of exciting novel treatments for these conditions. The topical agents currently in phase 2 and phase 3 clinical trials show promise in enhancing the way physicians treat psoriasis. There is hope for more individualized treatment regimens with improved tolerability and better safety profiles with increased therapeutic efficacy. As our understanding of the molecular underpinnings of psoriasis continues to deepen, it will afford the development of even more innovative therapeutics for use in the management of psoriasis.
Topical therapies are a mainstay in the management of patients with mild to moderate psoriasis (Figure). Presently, US Food and Drug Administration–approved topical medications that are commercially available for use in patients with psoriasis include corticosteroids, vitamin D3 analogues, calcineurin inhibitors, retinoids, anthralin, and tar-based formulations.1 In recent years, research has furthered our understanding of the molecular mechanisms underlying the pathogenesis of psoriasis and has afforded the development of more targeted therapies. Novel topical medications currently in phase 2 and phase 3 clinical trials are discussed in this article, and a summary is provided in the Table.
AN2728 (Phosphodiesterase 4 Inhibitor)
AN2728 (Anacor Pharmaceuticals, Inc) is a phosphodiesterase 4 inhibitor that blocks the inactivation of cyclic adenosine monophosphate, resulting in decreased production of inflammatory cytokines (eg, IL-6, IL-12, IL-23, tumor necrosis factor α [TNF-α]).2,3 In a randomized, double-blind, phase 2 clinical trial (N=35), 40% of patients treated with AN2728 ointment 5% reported improvement of more than 2 points in overall target plaque severity score versus 6% of patients treated with vehicle. In another randomized, double-blind, dose-response trial of 145 patients, those treated with AN2728 ointment 2% twice daily reported a 60% improvement versus 40% improvement in those treated with AN2728 ointment 0.5% once daily.3 In total, 3 phase 1 trials (registered at www.clinicaltrials.gov with the identifiers NCT01258088, NCT00762658, NCT00763204) and 4 phase 2 trials (NCT01029405, NCT00755196, NCT00759161, NCT01300052) have been completed; results were not available at the time of publication.
AS101 (Integrin Inhibitor)
AS101 (BioMAS Ltd), or ammonium trichloro (dioxoethylene-o,o') tellurate, acts as stimulator of regulatory T cells and a redox modulator inhibiting the leukocyte integrins α4β1 and α4β7 that enable CD4+ T-cell and macrophage extravasation; it also limits expression of the inflammatory cytokines IL-6 and IL-17.4 A randomized, placebo-controlled, double-blind, phase 2 study evaluating the efficacy of AS101 cream 4% twice daily for 12 weeks was withdrawn prior to enrollment (NCT00788424).
Tofacitinib (Janus Kinase 1 and 3 Inhibitor)
Tofacitinib (formerly known as CP-690,550)(Pfizer Inc) is a selective Janus kinase (Jak) 1 and Jak3 inhibitor that limits expression of cytokines that promote inflammation (eg, IFN-γ) and inhibits helper T cells (TH17) by downregulating expression of the IL-23 receptor. Epidermal keratinocyte proliferation in psoriasis is activated by TH17 cells that release IL-17 as well as TH1 cells that release IFN-γ and tumor necrosis factor. A phase 2a trial showed statistically significant improvement from baseline in the target plaque severity score for tofacitinib ointment 2% (least squares mean, −54.4%) versus vehicle (least squares mean, −41.5%).5 Two other phase 2 trials (NCT01246583, NCT00678561) assessing the efficacy, safety, tolerability, and pharmacokinetics of tofacitinib ointment in patients with mild to moderate psoriasis have been completed; results were not available at the time of publication. A phase 2b study that compared 2 dose strengths of tofacitinib ointment—10 mg/g and 20 mg/g—versus placebo over a 12-week period also was completed (NCT01831466); results were not available at the time of publication.
CT327 (Tyrosine Kinase Inhibitor)
CT327 (Creabilis SA) is a tyrosine kinase A (TrkA) inhibitor that affords a novel perspective in the treatment of pruritus by shifting the focus to sensory neurons. In a phase 2b study of 160 patients, a 60% change in the visual analog scale was noted at 8 weeks in the treatment group versus 21% in the placebo group.6 Two other phase 2 studies have been completed, one with a cream formulation of pegylated K252a (NCT00995969) and another with an ointment formulation (NCT01465282); results were not available at the time of publication.
DPS-101 (Vitamin D Analogue)
DPS-101 (Dermipsor Ltd) is a combination of calcipotriol and niacinamide. Calcipotriol is a vitamin D3 analogue that increases IL-10 expression while decreasing IL-8 expression.7 It curbs epidermal keratinocyte proliferation by limiting the expression of polo-like kinase 2 and early growth response-1.8 It also may induce keratinocyte apoptosis.9 Niacinamide is the amide of vitamin B3 and inhibits proinflammatory cytokines such as TNF-α, IL-1β, IL-6, and IL-8.10 In a dose-response phase 2b trial of 168 patients, DPS-101 demonstrated better results than either calcipotriol or niacinamide alone.11
IDP-118 (Proprietary Steroid and Retinoid Combination)
IDP-118 (Valeant Pharmaceuticals International, Inc) is a combination of halobetasol propionate (HP) 0.01% (a topical corticosteroid) and tazar-otene 0.045% (a selective topical retinoid) in a lotion formulation. In isolation, tazarotene is as effective as a mid to highly potent corticosteroid, but irritation may limit its tolerability. The use of combination treatments of mid to highly potent corticosteroids and tazarotene has shown enhanced tolerability and therapeutic efficacy.12 Ongoing studies include a phase 1 trial and a phase 2 trial to evaluate low- and high-strength preparations of IDP-118, respectively (NCT01670513). Another phase 2 trial evaluating the efficacy and safety of IDP-118 lotion (HP 0.01% and tazarotene 0.045%) versus IDP-118 monad HP 0.01% lotion, IDP-118 monad tazar-otene 0.045% lotion, and placebo has been completed (NCT02045277); results were not available at the time of publication.
Ruxolitinib (Jak1 and Jak2 Inhibitor)
Ruxolitinib (formerly known as INCB18424)(Incyte Corporation) is a selective Jak1 and Jak2 inhibitor. A phase 2 trial of ruxolitinib showed a 53% decline in the score for mean total lesions in patients treated with ruxolitinib phosphate cream 1% (P=.033) versus 54% in those treated with ruxolitinib phosphate cream 1.5% (P=.056) and 32% in those treated with placebo.13 Three other phase 2 studies (NCT00617994, NCT00820950, NCT00778700) have been completed; results were not available at the time of publication.
LAS41004 (Proprietary Steroid and Retinoid Combination)
LAS41004 (Almirall, SA) is an ointment containing the corticosteroid betamethasone dipropionate and the retinoid bexarotene that is being evaluated for treatment of mild to moderate psoriasis. Five phase 2 studies (NCT01119339, NCT01283698, NCT01360944, NCT02111499, NCT01462643) have been completed; results were not available at the time of publication. A randomized, double-blind, phase 2a study (NCT02180464) with a left-right design assessing clinical response to LAS41004 versus control in patients with mild to moderate psoriasis was actively recruiting at the time of publication.
LEO 80190 (Vitamin D3 Analogue and Steroid Combination)
LEO 80190 (LEO Pharma) is a combination of the vitamin D3 analogue calcipotriol and the corticosteroid hydrocortisone. It was developed as a treatment for sensitive areas such as the face and intertriginous regions. A randomized, investigator-blind, phase 3 trial (NCT00640822) of LEO 80190 ointment versus tacalcitol ointment and placebo once daily for 8 weeks demonstrated controlled disease of the face in 56.8% (183/322) of patients in the LEO 80190 group, 46.4% (147/317) in the tacalcitol group, and 36.3% (37/102) in the placebo group.14 Another phase 2 study (NCT00704262) and 2 phase 3 studies (NCT00691002, NCT01007591) have been completed; results were not available at the time of publication.
LEO 90100 (Vitamin D Analogue and Steroid Combination)
LEO 90100 (LEO Pharma) contains the vitamin D3 analogue calcipotriol and the corticosteroid betamethasone. Three phase 2 studies (NCT01347255, NCT01536886, NCT01536938) and a phase 3 study (NCT01866163) examining the efficacy and safety of various vehicles and formulations of LEO 90100 have been completed; results were not available at the time of publication. Another phase 3 study (NCT02132936) is ongoing but not recruiting participants. Other completed studies whose results were not yet available include a phase 1 pharmacodynamic study (NCT01946386), a phase 1 study that used patch testing to assess the degree of skin irritation and sensitization associated with LEO 90100 (NCT01935869), and a phase 2 study examining the impact of LEO 90100 on calcium metabolism and the hypothalamic-pituitary-adrenal axis (NCT01600222).
M518101 (Vitamin D Analogue)
M518101 (Maruho Co, Ltd) is a novel topical vitamin D3 analogue. Phase 1 (NCT01844973) and phase 2 (NCT01301157, NCT00884169) trials evaluating the safety, pharmacokinetics, and efficacy of M518101 have been completed; results were not available at the time of publication. A phase 3 study (NCT01989429) assessing the safety and therapeutic efficacy of M518101 according to changes in the modified psoriasis area and severity index over an 8-week treatment period also has been completed; results were not yet available. Three phase 3 studies assessing the safety and therapeutic efficacy of M518101 are ongoing: one is currently closed to recruitment (NCT01908595) and 2 are actively recruiting participants at the time of publication (NCT01878461, NCT01873677).
MOL4239 and MOL4249 (Phosphorylated Signal Transducer and Activator of Transcription 3 Inhibitors)
MOL4239 (Moleculin, LLC) is a novel topical agent for use in mild to moderate psoriasis that acts via phosphorylated signal transducer and activator of transcription 3 (p-STAT3) inhibition.15 The p-STAT3 protein has increased expression in psoriasis.16 A phase 2 trial of MOL4239 ointment (NCT01826201) has been completed, showing a greater mean (standard deviation) change in the psoriasis severity score in lesions treated at 28 days with MOL4239 ointment 10% (−1.9 [1.45]) versus lesions treated with placebo ointment (−1.5 [1.87]).17
MOL4249 (Moleculin, LLC) is more potent than MOL4239 with better lipid solubility. In the MOL4249 subset of a placebo-controlled, double-blind, phase 2a study of 16 patients with mild to moderate psoriasis, 10% (1/10) of patients experienced complete clearance of psoriatic plaques, 30% (3/10) of patients experienced 75% or greater improvement, and 50% (5/10) of patients experienced 50% or greater improvement compared to 17% (1/6) in the placebo group. Currently, a phase 2a contralateral study, a phase 2b psoriasis area and severity index trial, and a phase 3 pivotal trial are planned, according to the manufacturer.18
MQX-5902 (Dihydrofolate Reductase Inhibitor)
MQX-5902 (MediQuest Therapeutics) is a topical preparation of methotrexate for the treatment of fingernail psoriasis. Methotrexate is a dihydrofolate reductase inhibitor and antimetabolite that inhibits folic acid metabolism, thereby disrupting DNA synthesis.19 A phase 2b dose-ranging trial (NCT00666354) was designed to assess the therapeutic efficacy and safety of MQX-5902 delivered via a proprietary drug delivery formulation in fingernail psoriasis; the outcome of this trial was not available at the time of publication.
PH-10 (Xanthine Dye)
PH-10 (Provectus Biopharmaceuticals, Inc) is a topical aqueous hydrogel derived from rose bengal disodium that may be beneficial in treating skin conditions such as atopic dermatitis and mild to moderate psoriasis. Rose bengal disodium is a hydrophilic xanthine dye with diagnostic utility in ophthalmology and gastroenterology as well as projected use as a melanoma treatment as demonstrated in phase 1 and phase 2 clinical trials of PV-10 (Provectus Biopharmaceuticals, Inc).20 Two phase 2 studies assessing the safety and therapeutic efficacy of PH-10 in psoriasis (NCT01247818, NCT00941278) have been completed; results were not available at the time of publication.
STF115469 (Vitamin D Analogue)
STF115469 (GlaxoSmithKline) is a calcipotriene foam. At the time of publication, a randomized, placebo-controlled, double-blind, phase 3 trial (NCT01582932) of this vitamin D3 analogue with a projected enrollment of 180 participants was actively recruiting patients aged 2 to 11 years with mild to moderate plaque psoriasis to study the efficacy, safety, and tolerability of STF115469, as well as its pharmacokinetics and pharmacodynamics.
WBI-1001 (Proprietary Product)
WBI-1001 (Welichem Biotech Inc), or 2-isopropyl-5-[(E)-2-phenylethenyl] benzene-1, 3-diol, is a novel proprietary agent that inhibits proinflammatory cytokines (eg, IFN-γ, TNF-α). A randomized, placebo-controlled, double-blind, phase 1 trial (NCT00830817) assessing the efficacy, safety, tolerability, and pharmacokinetics of WBI-1001 has been completed; results were not available at the time of publication. Another randomized, placebo-controlled, double-blind, phase 2 trial (NCT01098721) evaluating its efficacy and safety according to the physician’s global assessment demonstrated a therapeutic benefit of 62.8% in patients treated with WBI-1001 cream 1% versus 13.0% in those treated with a placebo after a 12-week treatment period (P<.0001).21 WBI-1001 may offer a novel approach in the treatment of mild to moderate psoriasis.
Conclusion
Enhanced knowledge of the underlying pathogeneses of psoriasis and psoriatic arthritis has identified new therapeutic targets and enabled the development of exciting novel treatments for these conditions. The topical agents currently in phase 2 and phase 3 clinical trials show promise in enhancing the way physicians treat psoriasis. There is hope for more individualized treatment regimens with improved tolerability and better safety profiles with increased therapeutic efficacy. As our understanding of the molecular underpinnings of psoriasis continues to deepen, it will afford the development of even more innovative therapeutics for use in the management of psoriasis.
1. Mason A, Mason J, Cork M, et al. Topical treatments for chronic plaque psoriasis: an abridged Cochrane systematic review. J Am Acad Dermatol. 2013;69:799-807.
2. Nazarian R, Weinberg JM. AN-2728, a PDE4 inhibitor for the potential topical treatment of psoriasis and atopic dermatitis. Curr Opin Investig Drugs. 2009;10:1236-1242.
3. Moustafa F, Feldman SR. A review of phosphodiesterase-inhibition and the potential role for phosphodiesterase 4-inhibitors in clinical dermatology. Dermatol Online J. 2014;20:22608.
4. Halpert G, Sredni B. The effect of the novel tellurium compound AS101 on autoimmune diseases. Autoimmun Rev. 2014;13:1230-1235.
5. Ports WC, Khan S, Lan S, et al. A randomized phase 2a efficacy and safety trial of the topical Janus kinase inhibitor tofacitinib in the treatment of chronic plaque psoriasis. Br J Dermatol. 2013;169:137-145.
6. Yosipovitch G, Roblin D, Traversa S, et al. A novel topical targeted anti-pruritic treatment in phase 2b development for chronic pruritus. Paper presented at: 72nd Annual Meeting of the American Academy of Dermatology; March 21-25, 2014; Denver, CO.
7. Kang S, Yi S, Griffiths CE, et al. Calcipotriene-induced improvement in psoriasis is associated with reduced interleukin-8 and increased interleukin-10 levels within lesions. Br J Dermatol. 1998;138:77-83.
8. Kristl J, Slanc P, Krasna M, et al. Calcipotriol affects keratinocyte proliferation by decreasing expression of early growth response-1 and polo-like kinase-2. Pharm Res. 2008;25:521-529.
9. Tiberio R, Bozzo C, Pertusi G, et al. Calcipotriol induces apoptosis in psoriatic keratinocytes. Clin Exp Dermatol. 2009;34:e972-e974.
10. Luger T, Seite S, Humbert P, et al. Recommendations for adjunctive basic skin care in patients with psoriasis. Eur J Dermatol. 2014;24:194-200.
11. Dermipsor reports good results in DPS-101 Phase IIb study for plaque psoriasis [press release]. Evaluate Web site. http://www.evaluategroup.com/Universal/View.aspx?type=Story&id=250042. Published October 15, 2007. Accessed February 13, 2015.
12. Rivera AM, Hsu S. Topical halobetasol propionate in the treatment of plaque psoriasis: a review. Am J Clin Dermatol. 2005;6:311-316.
13. Punwani N, Scherle P, Flores R, et al. Preliminary clinical activity of a topical JAK1/2 inhibitor in the treatment of psoriasis. J Am Acad Dermatol. 2012;67:658-664.
14. Efficacy and safety of calcipotriol plus hydrocortisone ointment compared with tacalcitol ointment in patients with psoriasis on the face and skin folds (NCT00640822). https://clinicaltrials.gov/ct2/show/results/NCT00640822?term=NCT00640822&rank=1. Updated October 21, 2013. Accessed May 30, 2014.
15. Product candidates: targeting p-STAT3 for improved psoriasis treatment. Moleculin Web site. http://moleculin.com/product-candidates/mol4239. Accessed February 13, 2015.
16. Chowdhari S, Saini N. hsa-miR-4516 mediated downregulation of STAT3/CDK6/UBE2N plays a role in PUVA induced apoptosis in keratinocytes. J Cell Physiol. 2014;229:1630-1638.
17. Paired psoriasis lesion, comparative, study to evaluate MOL4239 in psoriasis (NCT01826201). https://clinicaltrials.gov/ct2/show/results/NCT01826201?term=NCT01826201&rank=1§=X01256#all. Updated December 22, 2014. Accessed February 25, 2015.
18. Clinical development pipeline. Moleculin Web site. http://moleculin.com/clinical-trials/psoriasis-trials. Accessed February 13, 2015.
19. de la Brassinne M, Nikkels A. Psoriasis: state of the art 2013. Acta Clin Belg. 2013;68:433-441.
20. Ross MI. Intralesional therapy with PV-10 (Rose Bengal) for in-transit melanoma. J Surg Oncol. 2014;109:314-319.
21. Bissonnette R, Bolduc C, Maari C, et al. Efficacy and safety of topical WBI-1001 in patients with mild to moderate psoriasis: results from a randomized, double-blind placebo-controlled, phase II trial. J Eur Acad Dermatol Venereol. 2012;26:1516-1521.
1. Mason A, Mason J, Cork M, et al. Topical treatments for chronic plaque psoriasis: an abridged Cochrane systematic review. J Am Acad Dermatol. 2013;69:799-807.
2. Nazarian R, Weinberg JM. AN-2728, a PDE4 inhibitor for the potential topical treatment of psoriasis and atopic dermatitis. Curr Opin Investig Drugs. 2009;10:1236-1242.
3. Moustafa F, Feldman SR. A review of phosphodiesterase-inhibition and the potential role for phosphodiesterase 4-inhibitors in clinical dermatology. Dermatol Online J. 2014;20:22608.
4. Halpert G, Sredni B. The effect of the novel tellurium compound AS101 on autoimmune diseases. Autoimmun Rev. 2014;13:1230-1235.
5. Ports WC, Khan S, Lan S, et al. A randomized phase 2a efficacy and safety trial of the topical Janus kinase inhibitor tofacitinib in the treatment of chronic plaque psoriasis. Br J Dermatol. 2013;169:137-145.
6. Yosipovitch G, Roblin D, Traversa S, et al. A novel topical targeted anti-pruritic treatment in phase 2b development for chronic pruritus. Paper presented at: 72nd Annual Meeting of the American Academy of Dermatology; March 21-25, 2014; Denver, CO.
7. Kang S, Yi S, Griffiths CE, et al. Calcipotriene-induced improvement in psoriasis is associated with reduced interleukin-8 and increased interleukin-10 levels within lesions. Br J Dermatol. 1998;138:77-83.
8. Kristl J, Slanc P, Krasna M, et al. Calcipotriol affects keratinocyte proliferation by decreasing expression of early growth response-1 and polo-like kinase-2. Pharm Res. 2008;25:521-529.
9. Tiberio R, Bozzo C, Pertusi G, et al. Calcipotriol induces apoptosis in psoriatic keratinocytes. Clin Exp Dermatol. 2009;34:e972-e974.
10. Luger T, Seite S, Humbert P, et al. Recommendations for adjunctive basic skin care in patients with psoriasis. Eur J Dermatol. 2014;24:194-200.
11. Dermipsor reports good results in DPS-101 Phase IIb study for plaque psoriasis [press release]. Evaluate Web site. http://www.evaluategroup.com/Universal/View.aspx?type=Story&id=250042. Published October 15, 2007. Accessed February 13, 2015.
12. Rivera AM, Hsu S. Topical halobetasol propionate in the treatment of plaque psoriasis: a review. Am J Clin Dermatol. 2005;6:311-316.
13. Punwani N, Scherle P, Flores R, et al. Preliminary clinical activity of a topical JAK1/2 inhibitor in the treatment of psoriasis. J Am Acad Dermatol. 2012;67:658-664.
14. Efficacy and safety of calcipotriol plus hydrocortisone ointment compared with tacalcitol ointment in patients with psoriasis on the face and skin folds (NCT00640822). https://clinicaltrials.gov/ct2/show/results/NCT00640822?term=NCT00640822&rank=1. Updated October 21, 2013. Accessed May 30, 2014.
15. Product candidates: targeting p-STAT3 for improved psoriasis treatment. Moleculin Web site. http://moleculin.com/product-candidates/mol4239. Accessed February 13, 2015.
16. Chowdhari S, Saini N. hsa-miR-4516 mediated downregulation of STAT3/CDK6/UBE2N plays a role in PUVA induced apoptosis in keratinocytes. J Cell Physiol. 2014;229:1630-1638.
17. Paired psoriasis lesion, comparative, study to evaluate MOL4239 in psoriasis (NCT01826201). https://clinicaltrials.gov/ct2/show/results/NCT01826201?term=NCT01826201&rank=1§=X01256#all. Updated December 22, 2014. Accessed February 25, 2015.
18. Clinical development pipeline. Moleculin Web site. http://moleculin.com/clinical-trials/psoriasis-trials. Accessed February 13, 2015.
19. de la Brassinne M, Nikkels A. Psoriasis: state of the art 2013. Acta Clin Belg. 2013;68:433-441.
20. Ross MI. Intralesional therapy with PV-10 (Rose Bengal) for in-transit melanoma. J Surg Oncol. 2014;109:314-319.
21. Bissonnette R, Bolduc C, Maari C, et al. Efficacy and safety of topical WBI-1001 in patients with mild to moderate psoriasis: results from a randomized, double-blind placebo-controlled, phase II trial. J Eur Acad Dermatol Venereol. 2012;26:1516-1521.
Practice Points
- Topical therapies are the cornerstone of treating patients with mild to moderate psoriasis. Commercially available medications approved by the US Food and Drug Administration for use in patients with psoriasis include corticosteroids, vitamin D3 analogues, calcineurin inhibitors, retinoids, anthralin, and tar-based formulations.
- Recent developments in our understanding of inflammatory mediators and the underlying pathogenesis of psoriasis have revealed new potential therapeutic targets, leading to the discovery of many promising treatments.
- Novel topical therapies currently in phase 2 and phase 3 clinical trials for patients with mild to moderate psoriasis may offer hope to patients who have reported a suboptimal therapeutic response to conventional treatments.

New Systemic Therapies for Psoriasis
Psoriasis is a common chronic inflammatory skin disease affecting 1% to 8% of the world population, depending on the country.1 Psoriasis can greatly impact quality of life in affected individuals, even in those with limited body surface involvement.2 Studies have demonstrated a high degree of psychological distress associated with psoriasis, leading to depression and poor self-esteem.3
Over the last decade, our improved understanding of the autoimmune inflammatory pathways and the associated changing concepts in psoriasis pathogenesis have led to the development of biological drugs targeting specific components of effector immune mechanisms, and these biological drugs have revolutionized the treatment of psoriasis.4 Although response rates of these biological agents are greater compared to those of conventional systemic drugs,5 current biological drugs fail to demonstrate efficacy in some patients or lose their efficacy over time. In addition to the high costs associated with these drugs, these limitations have driven a continued search for alternative therapies.
Helper T cells (TH17) and the proinflammatory cytokine IL-17 have been shown to play a key role in the pathophysiology of psoriasis, bridging innate and adaptive immune responses. IL-17 is involved in the modulation of proinflammatory cytokines, hematopoietic growth factors, antimicrobial peptides, and chemokines. Increased TH17 activity and high levels of IL-17 have been found in psoriatic plaques, and increased levels of TH17 are found in the plasma of psoriasis patients.6 Increased IL-17 induces neutrophilia, inflammation, and angiogenesis.7 Other cytokines that are highly upregulated in involved skin are tumor necrosis factor a (TNF-α), IL-23, IL-22, and IL-21.8 IL-23 is involved in regulating TH17 cells and is a potent activator of keratinocyte proliferation.9 Blockade of IL-12/23 causes downregulation of TH17 and TH22 cell responses.10 As IL-17 has a key role in protecting skin and mucous membranes from bacterial and fungal infections, IL-17 inhibition can potentially interfere with the inflammatory cascade. However, available data suggest that sufficient residual IL-17 activity remains to maintain immunity against infections.11
Currently approved biological agents for psoriasis target proinflammatory cytokines such as TNF-α, or the p40 subunit of IL-12 and IL-23. A number of novel targeted therapies including biologics as well as small molecule inhibitors targeting various cytokines and molecules involved in the pathogenesis of psoriasis are currently in different stages of development (Table). These drugs include 3 IL-17 inhibitors (secukinumab, ixekizumab, and brodalumab); 2 IL-23 blockers (tildrakizumab and guselkumab); and small molecule inhibitors that target the kinase pathway including apremilast (a phosphodiesterase 4 [PDE4] inhibitor), as well as tofacitinib, baricitinib, and ruxolitinib (Janus kinase [Jak] inhibitors). Small molecule inhibitors can be administered orally and are less expensive to produce than biological agents. This article reviews available data on these new systemic agents in the pipeline.
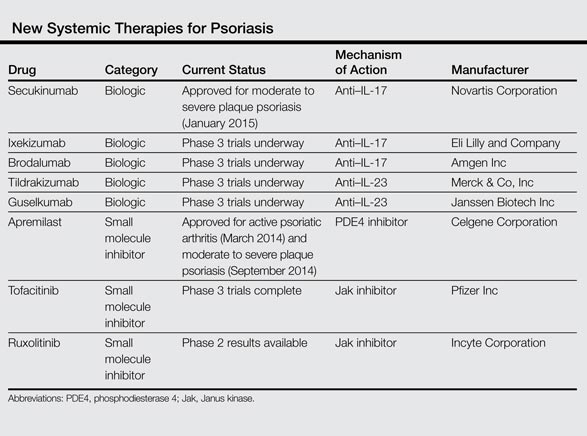
Novel Biologics
Secukinumab
Secukinumab is a fully human monoclonal IgG1k antibody that selectively binds and neutralizes IL-17A.12 It is the first of the IL-17 antibodies to receive approval for the treatment of moderate to severe psoriasis. In 2 phase 3, double-blind, 52-week trials—ERASURE (Efficacy of Response and Safety of Two Fixed Secukinumab Regimens in Psoriasis) and FIXTURE (Full Year Investigative Examination of Secukinumab vs Etanercept Using Two Dosing Regimens to Determine Efficacy in Psoriasis)—participants were randomly assigned to receive subcutaneous secukinumab at doses of 300 mg (n=245 and n=327, respectively) or 150 mg (n=245 and n=327, respectively) once weekly for 5 weeks then every 4 weeks, or placebo (n=248 and n=326, respectively); in the FIXTURE study only, an etanercept group (n=326) was given a 50-mg dose twice weekly for 12 weeks then once weekly.13
In the ERASURE study, the proportion of participants showing a reduction of 75% or more in psoriasis area and severity index (PASI) score from baseline to week 12 was 81.6% with secukinumab 300 mg, 71.6% with secukinumab 150 mg, and 4.5% with placebo.13 Secondary end point results demonstrated the proportion of participants showing a 90% reduction in PASI score was 59.2% with secukinumab 300 mg and 39.1% with secukinumab 150 mg, which were both superior to placebo (1.2%). The proportion of participants who met the criteria for 100% reduction in PASI score at week 12 also was greater with each secukinumab dose than with placebo.13
In the FIXTURE study, the proportion of participants showing a reduction of 75% or more from baseline in PASI score at week 12 was 77.1% with secukinumab 300 mg, 67.0% with secukinumab 150 mg, 44.0% with etanercept, and 4.9% with placebo.13 Secondary end point results demonstrated the proportion of participants showing a 90% reduction in PASI score was 54.2% with secukinumab 300 mg, 41.9% with secukinumab 150 mg, 20.7% with etanercept, and 1.5% with placebo. The speed of response, which was assessed as the median time to a 50% reduction in mean PASI score from baseline, was significantly shorter with both doses of secukinumab (3.0 weeks and 3.9 weeks, respectively) than with etanercept (7.0 weeks)(P<.001 for both).13
In the FIXTURE study, incidences of adverse events (AEs) were similar in the secukinumab and etanercept groups during both the induction period and the entire treatment period.13 The most common AEs in the secukinumab groups were nasopharyngitis, headache, and diarrhea. The rates of infections or infestations during the induction period were 26.7% with secukinumab 300 mg, 30.9% with secukinumab 150 mg, 24.5% with etanercept, and 19.3% with placebo. Candidal infections were more common with secukinumab than with etanercept during the entire treatment period (4.7% and 2.3% of participants in the secukinumab 300 mg and 150 mg groups, respectively, reported mild or moderate candidal infections). None of these infections resulted in chronic mucocutaneous candidiasis or discontinuation of the study drug and all resolved on their own or with standard therapy. Candidal infection was reported in 1.2% of participants in the etanercept group. Responses at week 12 were sustained in the majority of participants through week 52 with continued secukinumab therapy every 4 weeks. Grade 3 neutropenia occurred in 1.0% of secukinumab-treated participants and in none of the participants in the etanercept group. There were no apparent dose-related differences between the secukinumab groups with respect to AEs, with the exception of mild and moderate candidal infections.13
These efficacy data are impressive and no specific serious safety concerns have been identified to date. However, IL-17A plays a key role in host defense, particularly in mucocutaneous immunity against Candida albicans,14 as well as in hematopoiesis through stimulation of granulopoiesis and neutrophil trafficking,15 and thus we need to remain watchful with regards to Candida albicans infections and neutropenia.
Ixekizumab
Ixekizumab is a humanized IgG4 anti–IL-17A monoclonal antibody. In a phase 2, double-blind, placebo-controlled trial, 142 participants with chronic moderate to severe plaque psoriasis were randomly assigned to receive 150-mg (n=28), 75-mg (n=29), 25-mg (n=30), or 10-mg (n=28) subcutaneous injections of ixekizumab or placebo (n=27) at weeks 0, 2, 4, 8, 12, and 16.16 At 12 weeks, the percentage of participants who achieved a 75% reduction in PASI score from baseline was significantly greater with ixekizumab (82.1% with 150-mg dose, 82.8% with 75-mg dose, 76.7% with 25-mg dose) than with placebo (7.7%)(P<.001 for each comparison), except with the 10-mg dose. Similarly, a greater percentage of participants in the same ixekizumab groups achieved a 90% reduction (71.4% with 150-mg dose, 58.6% with 75-mg dose, 50.0% with 25-mg dose) and a 100% reduction (39.3% with 150-mg dose, 37.9% with 75-mg dose) in PASI score compared to placebo (0%)(P<.001 for each comparison). Significant reductions in PASI scores were evident as early as week 1 in the 150-mg and 75-mg groups, and these reductions were sustained for 20 weeks (P<.05).16 Phase 3 studies of ixekizumab currently are underway.
Brodalumab
The third IL-17 blocker in the pipeline is brodalumab, a human monoclonal antibody against IL-17RA, which blocks signaling of IL-17A and IL-17F as well as the IL-17A/F heterodimer, all of which are involved in the inflammatory process of psoriasis. Brodalumab was evaluated in a phase 2, double-blind, placebo-controlled, dose-ranging study of 198 participants who were randomized to receive 70 mg (n=39), 140 mg (n=39), 210 mg (n=40), or 280 mg (n=42) of brodalumab or placebo (n=38).17 At week 12, improvements of at least 75% and at least 90% in PASI score were achieved by 77% and 72%, respectively, in the 140-mg group, and 82% and 75%, respectively, in the 210-mg group compared to 0% of the placebo group (P<.001 for all comparisons). One hundred percent improvement in PASI was achieved by 38% of participants in the 140-mg group and 62% in the 210-mg group. No participants in the placebo group demonstrated improvement of 75% or higher. The most common AEs were nasopharyngitis, upper respiratory tract infection, arthralgia, and injection-site erythema. Serious AEs reported during the study included renal colic (1 participant), ec-topic pregnancy (1 participant), and grade 3 asymptomatic neutropenia (2 participants). Both cases of neutropenia were noted at the first assessment after brodalumab initiation (week 2) and resolved when the study drug was withheld.17
Results for this new IL-17 blocker are encouraging, but phase 3 data of brodalumab will need to be awaited.
Tildrakizumab
Tildrakizumab is a humanized IgG1 monoclonal antibody that blocks the p19 subunit of IL-23. In a randomized, double-blind, phase 2b trial, 355 adults with moderate to severe psoriasis were randomized to receive subcutaneous injections of tildrakizumab (5 mg, 25 mg, 100 mg, or 200 mg) or placebo.18 In part 1 of the study, injections were administered at weeks 0 and 4. Part 2 of the study started at week 16. In part 2, responders with a 75% improvement in PASI score in the 5- and 25-mg groups continued their dose, while responders in the 100- or 200-mg groups were randomized again to continue the same dose or a reduced dose (100 mg to 25 mg; 200 mg to 100 mg) every 12 weeks from weeks 16 to 52. Those in the placebo group received tildrakizumab 25 mg every 12 weeks in part 2. The primary end point was the mean change in PASI score from baseline to week 16, which was significantly greater in all tildrakizumab groups than in the placebo group (P<.001 for all comparisons). Improvements of 75% in PASI score were achieved by 74% in the 200-mg group, 66% in the 100-mg group, 64% in the 25-mg group, and 33% in the 5-mg group. In contrast, 4.9% in the placebo group achieved an improvement of 75%. At week 52, no loss of efficacy was seen in those participants who had achieved 75% improvement in PASI score at week 16 and had continued their prior doses. The rates of AEs seen in the tildrakizumab groups were 60% to 71% compared to 69% in the placebo group. The most common AE was nasopharyngitis, occurring in 12% to 20% of participants in each group. Serious AEs were uncommon.18 Phase 3 studies are currently underway.19
Guselkumab
Guselkumab is a human IgG1 monoclonal antibody in clinical development that specifically blocks the p19 subunit of IL-23. In a double-blind, placebo-controlled, phase 1 study, 24 participants with moderate to severe plaque psoriasis were randomized to receive a single 10-mg (n=5), 30-mg (n=5), 100-mg (n=5), or 300-mg (n=5) dose of guselkumab or placebo (n=4).20 At week 12, 50% in the 10-mg group, 60% in both the 30- and 100-mg groups, and 100% in the 300-mg group showed 75% improvement in PASI score versus 0% in the placebo group. Improvements in PASI scores were generally maintained through week 24. The rates of AEs were 65% (13/20) in the combined guselkumab group and 50% (2/4) in the placebo group.20
Small Molecule Inhibitors
In contrast to biologics, which mainly target soluble cytokine or cellular receptors, small molecule inhibitors target enzymes within signaling pathways. Small molecule inhibitors have some advantages over biologics in that they are relatively inexpensive to produce and can be administered orally; thus, they may be preferred by some patients over injectable drugs. There are several agents that are undergoing clinical trials in psoriasis, including PDE4 inhibitors and Jak inhibitors.
Apremilast
Apremilast is an oral small molecule PDE4 inhibitor that was approved by the US Food and Drug Administration in March 2014 for the treatment of adult patients with active psoriatic arthritis; an indication for moderate to severe plaque psoriasis was approved in September 2014.21 Phosphodiesterase 4 is a cyclic adenosine monophosphate–specific phosphodiesterase inhibitor, which is dominant in inflammatory cells. Inhibition of PDE4 increases intracellular cyclic adenosine monophosphate levels, thus downregulating proinflammatory cytokines such as TNF-α, IFN-γ, IL-2, IL-12, and IL-23, and increasing the production of anti-inflammatory cytokines such as IL-10.22
Phase 2 and phase 3 studies have demonstrated the clinical efficacy of apremilast in the treatment of patients with moderate to severe plaque psoriasis. In a 16-week randomized, placebo-controlled, phase 3 trial (ESTEEM 2), 408 participants were randomized to receive oral apremilast 30 mg twice daily (n=275) or placebo (n=138).23 Improvement of 75% in PASI score was achieved by 29% of participants in the apremilast group at week 16. The most common AEs were diarrhea (16%) and nausea (18%), which were predominantly mild, occurring most commonly in the first week and resolving within 1 month. No cases of severe diarrhea or severe nausea were reported. Apremilast had no apparent effect on the results of hematological or serum chemistry tests.23 Although the US Food and Drug Administration warns of a possible link between apremilast and depression,24 data are mostly related to roflumilast, another PDE4 inhibitor. Studies in patients with chronic obstructive pulmonary disease have noted increased cases of depression (1.21% vs 0.82%) and suicidal ideation/attempt (0.03% vs 0.02%) in patients treated with roflumilast versus placebo.25
Jak Inhibitors
Janus kinases are a family of intracellular tyrosine kinases that connect several cytokine receptors to the signal transducer and activator of transcription pathways.26 There are 4 Jak family members: Jak1, Jak2, Jak3, and tyrosine kinase 2. Janus kinases 1 and 2 have roles in interferon signaling, while Jak3 transduces signals from IL-2, IL-7, IL-15, and IL-21, which are T-cell growth and survival factors.
Tofacitinib is a novel oral signal transduction molecule that blocks the Jak3 pathway. A phase 2b, 12-week, dose-ranging study was conducted to assess the efficacy and safety of 3 twice-daily regimens of tofacitinib versus placebo in patients with moderate to severe chronic plaque psoriasis.27 One hundred and ninety-seven participants were randomized to receive oral tofacitinib (2 mg, 5 mg, or 15 mg; n=49 each) or placebo (n=50) twice daily for 12 weeks with a 4-week follow-up period. The primary end point was the proportion of participants achieving at least a 75% reduction in PASI score at week 12 (25.0% with 2 mg, 40.8% with 5 mg, 66.7% with 15 mg, 2.0% with placebo). Similarly, a higher proportion of participants achieving 90% reduction in PASI score was seen at weeks 8 and 12 in all tofacitinib-treated participants versus placebo. The most common AEs were upper respiratory tract infection, sinusitis, nasopharyngitis, and headache. A number of changes in laboratory parameters occurred in the tofacitinib groups. Mild dose-related decreases in hemoglobin were noted at week 12 for all tofacitinib groups, and a small increase (mean, 0.04 mg/dL) in serum creatinine levels was observed in the 15-mg group. Decreases in neutrophil counts were observed with higher doses of tofacitinib, with the maximum mean decrease of 0.9×103/mm3 from baseline observed in the 15-mg group at week 4. After weeks 4 through 8, mean neutrophil counts began to return to baseline levels. Dose-related increases in total cholesterol, high-density lipoprotein cholesterol, and low-density lipoprotein cholesterol were observed by week 2 and remained at this level through week 12; mean lipid levels decreased to baseline levels after cessation of active treatment. One participant in the 15-mg group developed an elevated alanine aminotransferase level that was more than 2.5 times the highest normal limit. Three participants experienced 5 serious AEs.27 These early results show that tofacitinib can be a safe and effective treatment in patients with psoriasis, but further data from phase 3 studies will need to be awaited.
Another Jak inhibitor under investigationfor the treatment of psoriasis is ruxolitinib, an inhibitor of Jak1 and Jak2, which has been primarily studied as a topical agent for milder cases of the disease.28
Conclusion
Many new drugs are currently on the horizon and will increase our armamentarium for treating psoriasis. Some of these agents promise greater levels of efficacy than currently used therapies. Although this review focuses on systemic agents, there also are a number of topical formulations in the pipeline. These new agents will certainly increase our options when choosing the most suitable treatment for a patient with psoriasis, but safety will remain a primary concern, and time and experience will tell whether efficacy outweighs any potential side effects.
1. Parisi R, Symmons DP, Griffiths CE, et al. Global epidemiology of psoriasis: a systematic review of incidence and prevalence. J Invest Dermatol. 2013;133:377-385.
2. Rapp SR, Feldman SR, Exum ML, et al. Psoriasis causes as much disability as other major medical diseases. J Am Acad Dermatol. 1999;41(3 pt 1):401-407.
3. Shah R, Bewley A. Psoriasis: ‘the badge of shame.’ a case report of a psychological intervention to reduce and potentially clear chronic skin disease. Clin Exp Dermatol. 2014;39:600-603.
4. Vincent FB, Morand EF, Murphy K, et al. Antidrug antibodies (ADAb) to tumour necrosis factor (TNF)-specific neutralising agents in chronic inflammatory diseases: a real issue, a clinical perspective. Ann Rheum Dis. 2013;72:165-178.
5. Chi CC, Wang SH. Efficacy and cost-efficacy of biologic therapies for moderate to severe psoriasis: a meta-analysis and cost-efficacy analysis using the intention-to-treat principle. Biomed Res Int. 2014;2014:862851.
6. Kagami S, Rizzo HL, Lee JJ, et al. Circulating Th17, Th22, and Th1 cells are increased in psoriasis. J Invest Dermatol. 2010;130:1373-1383.
7. Leonardi CL, Gordon KB. New and emerging therapies in psoriasis. Semin Cutan Med Surg. 2014;33(2, suppl 2):S37-S41.
8. Lowes MA, Kikuchi T, Fuentes-Duculan J, et al. Psoriasis vulgaris lesions contain discrete populations of Th1 and Th17 T cells. J Invest Dermatol. 2008;128:1207-1211.
9. Nickoloff BJ, Qin JZ, Nestle FO. Immunopathogenesis of psoriasis. Clin Rev Allergy Immunol. 2007;33:45-56.
10. Fitch E, Harper E, Skorcheva I, et al. Pathophysiology of psoriasis: recent advances on IL-23 and Th17 cytokines. Curr Rheumatol Rep. 2007;9:461-467.
11. Adami S, Cavani A, Rossi F, et al. The role of interleukin-17A in psoriatic disease. BioDrugs. 2014;28:487-497.
12. Hueber W, Patel DD, Dryja T, et al. Effects of AIN457, a fully human antibody to interleukin-17A, on psoriasis, rheumatoid arthritis, and uveitis. Sci Transl Med. 2010;2:52ra72.
13. Langley RG, Elewski BE, Lebwohl M, et al. Secukinumab in plaque psoriasis—results of two phase 3 trials. N Engl J Med. 2014;371:326-338.
14. Puel A, Cypowyj S, Bustamante J, et al. Chronic mucocutaneous candidiasis in humans with inborn errors of interleukin-17 immunity. Science. 2011;332:65-68.
15. Krstic A, Mojsilovic S, Jovcic G, et al. The potential of interleukin-17 to mediate hematopoietic response. Immunol Res. 2012;52:34-41.
16. Leonardi C, Matheson R, Zachariae C, et al. Anti-interleukin-17 monoclonal antibody ixekizumab in chronic plaque psoriasis. N Engl J Med. 2012;366:1190-1199.
17. Papp KA, Leonardi C, Menter A, et al. Brodalumab, an anti-interleukin-17-receptor antibody for psoriasis. N Engl J Med. 2012;366:1181-1189.
18. Langley RGB, Thaci D, Papp KA, et al. MK-3222, an anti–IL-23p19 humanized monoclonal antibody, provides significant improvement in psoriasis over 52 weeks of treatment that is maintained after discontinuation of dosing. Poster presented at: 73rd Annual Meeting of the American Academy of Dermatology; March 21-25, 2014; Denver, CO. Poster 8056.
19. Tausend W, Downing C, Tyring S. Systematic review of interleukin-12, interleukin-17, and interleukin-23 pathway inhibitors for the treatment of moderate-to-severe chronic plaque psoriasis: ustekinumab, briakinumab, tildrakizumab, guselkumab, secukinumab, ixekizumab, and brodalumab. J Cutan Med Surg. 2014;18:156-169.
20. Sofen H, Smith S, Matheson RT, et al. Guselkumab (an IL-23-specific mAb) demonstrates clinical and molecular response in patients with moderate-to-severe psoriasis. J Allergy Clin Immunol. 2014;133:1032-1040.
21. Schafer PH, Parton A, Capone L, et al. Apremilast is a selective PDE4 inhibitor with regulatory effects on innate immunity. Cell Signal. 2014;26:2016-2029.
22. van de Kerkhof PC. Apremilast: a step forward in the treatment of psoriasis? Lancet. 2012;380:708-709.
23. Paul C, Crowley J, Cather J, et al. Apremilast, an oral phosphodiesterase 4 inhibitor, in patients with moderate to severe psoriasis: 16-week results of a phase 3, randomized, controlled trial (ESTEEM 2). Poster presented at: 73rd Annual Meeting of the American Academy of Dermatology; March 21-25, 2014; Denver, CO. Poster 8412.
24. Otezla [product insert]. Summit, NJ: Celgene Corporation; 2014.
25. Rabe KF. Update on roflumilast, a phosphodiesterase 4 inhibitor for the treatment of chronic obstructive pulmonary disease. Br J Pharmacol. 2011;163:53-67.
26. Palanivel JA, Macbeth AE, Chetty NC, et al. An insight into JAK-STAT signalling in dermatology. Clin Exp Dermatol. 2014;39:513-518.
27. Papp KA, Menter A, Strober B, et al. Efficacy and safety of tofacitinib, an oral Janus kinase inhibitor, in the treatment of psoriasis: a phase 2b randomized placebo-controlled dose-ranging study. Br J Dermatol. 2012;167:668-677.
28. Hsu L, Armstrong AW. JAK inhibitors: treatment efficacy and safety profile in patients with psoriasis. J Immunol Res. 2014;2014:283617.
Psoriasis is a common chronic inflammatory skin disease affecting 1% to 8% of the world population, depending on the country.1 Psoriasis can greatly impact quality of life in affected individuals, even in those with limited body surface involvement.2 Studies have demonstrated a high degree of psychological distress associated with psoriasis, leading to depression and poor self-esteem.3
Over the last decade, our improved understanding of the autoimmune inflammatory pathways and the associated changing concepts in psoriasis pathogenesis have led to the development of biological drugs targeting specific components of effector immune mechanisms, and these biological drugs have revolutionized the treatment of psoriasis.4 Although response rates of these biological agents are greater compared to those of conventional systemic drugs,5 current biological drugs fail to demonstrate efficacy in some patients or lose their efficacy over time. In addition to the high costs associated with these drugs, these limitations have driven a continued search for alternative therapies.
Helper T cells (TH17) and the proinflammatory cytokine IL-17 have been shown to play a key role in the pathophysiology of psoriasis, bridging innate and adaptive immune responses. IL-17 is involved in the modulation of proinflammatory cytokines, hematopoietic growth factors, antimicrobial peptides, and chemokines. Increased TH17 activity and high levels of IL-17 have been found in psoriatic plaques, and increased levels of TH17 are found in the plasma of psoriasis patients.6 Increased IL-17 induces neutrophilia, inflammation, and angiogenesis.7 Other cytokines that are highly upregulated in involved skin are tumor necrosis factor a (TNF-α), IL-23, IL-22, and IL-21.8 IL-23 is involved in regulating TH17 cells and is a potent activator of keratinocyte proliferation.9 Blockade of IL-12/23 causes downregulation of TH17 and TH22 cell responses.10 As IL-17 has a key role in protecting skin and mucous membranes from bacterial and fungal infections, IL-17 inhibition can potentially interfere with the inflammatory cascade. However, available data suggest that sufficient residual IL-17 activity remains to maintain immunity against infections.11
Currently approved biological agents for psoriasis target proinflammatory cytokines such as TNF-α, or the p40 subunit of IL-12 and IL-23. A number of novel targeted therapies including biologics as well as small molecule inhibitors targeting various cytokines and molecules involved in the pathogenesis of psoriasis are currently in different stages of development (Table). These drugs include 3 IL-17 inhibitors (secukinumab, ixekizumab, and brodalumab); 2 IL-23 blockers (tildrakizumab and guselkumab); and small molecule inhibitors that target the kinase pathway including apremilast (a phosphodiesterase 4 [PDE4] inhibitor), as well as tofacitinib, baricitinib, and ruxolitinib (Janus kinase [Jak] inhibitors). Small molecule inhibitors can be administered orally and are less expensive to produce than biological agents. This article reviews available data on these new systemic agents in the pipeline.
Novel Biologics
Secukinumab
Secukinumab is a fully human monoclonal IgG1k antibody that selectively binds and neutralizes IL-17A.12 It is the first of the IL-17 antibodies to receive approval for the treatment of moderate to severe psoriasis. In 2 phase 3, double-blind, 52-week trials—ERASURE (Efficacy of Response and Safety of Two Fixed Secukinumab Regimens in Psoriasis) and FIXTURE (Full Year Investigative Examination of Secukinumab vs Etanercept Using Two Dosing Regimens to Determine Efficacy in Psoriasis)—participants were randomly assigned to receive subcutaneous secukinumab at doses of 300 mg (n=245 and n=327, respectively) or 150 mg (n=245 and n=327, respectively) once weekly for 5 weeks then every 4 weeks, or placebo (n=248 and n=326, respectively); in the FIXTURE study only, an etanercept group (n=326) was given a 50-mg dose twice weekly for 12 weeks then once weekly.13
In the ERASURE study, the proportion of participants showing a reduction of 75% or more in psoriasis area and severity index (PASI) score from baseline to week 12 was 81.6% with secukinumab 300 mg, 71.6% with secukinumab 150 mg, and 4.5% with placebo.13 Secondary end point results demonstrated the proportion of participants showing a 90% reduction in PASI score was 59.2% with secukinumab 300 mg and 39.1% with secukinumab 150 mg, which were both superior to placebo (1.2%). The proportion of participants who met the criteria for 100% reduction in PASI score at week 12 also was greater with each secukinumab dose than with placebo.13
In the FIXTURE study, the proportion of participants showing a reduction of 75% or more from baseline in PASI score at week 12 was 77.1% with secukinumab 300 mg, 67.0% with secukinumab 150 mg, 44.0% with etanercept, and 4.9% with placebo.13 Secondary end point results demonstrated the proportion of participants showing a 90% reduction in PASI score was 54.2% with secukinumab 300 mg, 41.9% with secukinumab 150 mg, 20.7% with etanercept, and 1.5% with placebo. The speed of response, which was assessed as the median time to a 50% reduction in mean PASI score from baseline, was significantly shorter with both doses of secukinumab (3.0 weeks and 3.9 weeks, respectively) than with etanercept (7.0 weeks)(P<.001 for both).13
In the FIXTURE study, incidences of adverse events (AEs) were similar in the secukinumab and etanercept groups during both the induction period and the entire treatment period.13 The most common AEs in the secukinumab groups were nasopharyngitis, headache, and diarrhea. The rates of infections or infestations during the induction period were 26.7% with secukinumab 300 mg, 30.9% with secukinumab 150 mg, 24.5% with etanercept, and 19.3% with placebo. Candidal infections were more common with secukinumab than with etanercept during the entire treatment period (4.7% and 2.3% of participants in the secukinumab 300 mg and 150 mg groups, respectively, reported mild or moderate candidal infections). None of these infections resulted in chronic mucocutaneous candidiasis or discontinuation of the study drug and all resolved on their own or with standard therapy. Candidal infection was reported in 1.2% of participants in the etanercept group. Responses at week 12 were sustained in the majority of participants through week 52 with continued secukinumab therapy every 4 weeks. Grade 3 neutropenia occurred in 1.0% of secukinumab-treated participants and in none of the participants in the etanercept group. There were no apparent dose-related differences between the secukinumab groups with respect to AEs, with the exception of mild and moderate candidal infections.13
These efficacy data are impressive and no specific serious safety concerns have been identified to date. However, IL-17A plays a key role in host defense, particularly in mucocutaneous immunity against Candida albicans,14 as well as in hematopoiesis through stimulation of granulopoiesis and neutrophil trafficking,15 and thus we need to remain watchful with regards to Candida albicans infections and neutropenia.
Ixekizumab
Ixekizumab is a humanized IgG4 anti–IL-17A monoclonal antibody. In a phase 2, double-blind, placebo-controlled trial, 142 participants with chronic moderate to severe plaque psoriasis were randomly assigned to receive 150-mg (n=28), 75-mg (n=29), 25-mg (n=30), or 10-mg (n=28) subcutaneous injections of ixekizumab or placebo (n=27) at weeks 0, 2, 4, 8, 12, and 16.16 At 12 weeks, the percentage of participants who achieved a 75% reduction in PASI score from baseline was significantly greater with ixekizumab (82.1% with 150-mg dose, 82.8% with 75-mg dose, 76.7% with 25-mg dose) than with placebo (7.7%)(P<.001 for each comparison), except with the 10-mg dose. Similarly, a greater percentage of participants in the same ixekizumab groups achieved a 90% reduction (71.4% with 150-mg dose, 58.6% with 75-mg dose, 50.0% with 25-mg dose) and a 100% reduction (39.3% with 150-mg dose, 37.9% with 75-mg dose) in PASI score compared to placebo (0%)(P<.001 for each comparison). Significant reductions in PASI scores were evident as early as week 1 in the 150-mg and 75-mg groups, and these reductions were sustained for 20 weeks (P<.05).16 Phase 3 studies of ixekizumab currently are underway.
Brodalumab
The third IL-17 blocker in the pipeline is brodalumab, a human monoclonal antibody against IL-17RA, which blocks signaling of IL-17A and IL-17F as well as the IL-17A/F heterodimer, all of which are involved in the inflammatory process of psoriasis. Brodalumab was evaluated in a phase 2, double-blind, placebo-controlled, dose-ranging study of 198 participants who were randomized to receive 70 mg (n=39), 140 mg (n=39), 210 mg (n=40), or 280 mg (n=42) of brodalumab or placebo (n=38).17 At week 12, improvements of at least 75% and at least 90% in PASI score were achieved by 77% and 72%, respectively, in the 140-mg group, and 82% and 75%, respectively, in the 210-mg group compared to 0% of the placebo group (P<.001 for all comparisons). One hundred percent improvement in PASI was achieved by 38% of participants in the 140-mg group and 62% in the 210-mg group. No participants in the placebo group demonstrated improvement of 75% or higher. The most common AEs were nasopharyngitis, upper respiratory tract infection, arthralgia, and injection-site erythema. Serious AEs reported during the study included renal colic (1 participant), ec-topic pregnancy (1 participant), and grade 3 asymptomatic neutropenia (2 participants). Both cases of neutropenia were noted at the first assessment after brodalumab initiation (week 2) and resolved when the study drug was withheld.17
Results for this new IL-17 blocker are encouraging, but phase 3 data of brodalumab will need to be awaited.
Tildrakizumab
Tildrakizumab is a humanized IgG1 monoclonal antibody that blocks the p19 subunit of IL-23. In a randomized, double-blind, phase 2b trial, 355 adults with moderate to severe psoriasis were randomized to receive subcutaneous injections of tildrakizumab (5 mg, 25 mg, 100 mg, or 200 mg) or placebo.18 In part 1 of the study, injections were administered at weeks 0 and 4. Part 2 of the study started at week 16. In part 2, responders with a 75% improvement in PASI score in the 5- and 25-mg groups continued their dose, while responders in the 100- or 200-mg groups were randomized again to continue the same dose or a reduced dose (100 mg to 25 mg; 200 mg to 100 mg) every 12 weeks from weeks 16 to 52. Those in the placebo group received tildrakizumab 25 mg every 12 weeks in part 2. The primary end point was the mean change in PASI score from baseline to week 16, which was significantly greater in all tildrakizumab groups than in the placebo group (P<.001 for all comparisons). Improvements of 75% in PASI score were achieved by 74% in the 200-mg group, 66% in the 100-mg group, 64% in the 25-mg group, and 33% in the 5-mg group. In contrast, 4.9% in the placebo group achieved an improvement of 75%. At week 52, no loss of efficacy was seen in those participants who had achieved 75% improvement in PASI score at week 16 and had continued their prior doses. The rates of AEs seen in the tildrakizumab groups were 60% to 71% compared to 69% in the placebo group. The most common AE was nasopharyngitis, occurring in 12% to 20% of participants in each group. Serious AEs were uncommon.18 Phase 3 studies are currently underway.19
Guselkumab
Guselkumab is a human IgG1 monoclonal antibody in clinical development that specifically blocks the p19 subunit of IL-23. In a double-blind, placebo-controlled, phase 1 study, 24 participants with moderate to severe plaque psoriasis were randomized to receive a single 10-mg (n=5), 30-mg (n=5), 100-mg (n=5), or 300-mg (n=5) dose of guselkumab or placebo (n=4).20 At week 12, 50% in the 10-mg group, 60% in both the 30- and 100-mg groups, and 100% in the 300-mg group showed 75% improvement in PASI score versus 0% in the placebo group. Improvements in PASI scores were generally maintained through week 24. The rates of AEs were 65% (13/20) in the combined guselkumab group and 50% (2/4) in the placebo group.20
Small Molecule Inhibitors
In contrast to biologics, which mainly target soluble cytokine or cellular receptors, small molecule inhibitors target enzymes within signaling pathways. Small molecule inhibitors have some advantages over biologics in that they are relatively inexpensive to produce and can be administered orally; thus, they may be preferred by some patients over injectable drugs. There are several agents that are undergoing clinical trials in psoriasis, including PDE4 inhibitors and Jak inhibitors.
Apremilast
Apremilast is an oral small molecule PDE4 inhibitor that was approved by the US Food and Drug Administration in March 2014 for the treatment of adult patients with active psoriatic arthritis; an indication for moderate to severe plaque psoriasis was approved in September 2014.21 Phosphodiesterase 4 is a cyclic adenosine monophosphate–specific phosphodiesterase inhibitor, which is dominant in inflammatory cells. Inhibition of PDE4 increases intracellular cyclic adenosine monophosphate levels, thus downregulating proinflammatory cytokines such as TNF-α, IFN-γ, IL-2, IL-12, and IL-23, and increasing the production of anti-inflammatory cytokines such as IL-10.22
Phase 2 and phase 3 studies have demonstrated the clinical efficacy of apremilast in the treatment of patients with moderate to severe plaque psoriasis. In a 16-week randomized, placebo-controlled, phase 3 trial (ESTEEM 2), 408 participants were randomized to receive oral apremilast 30 mg twice daily (n=275) or placebo (n=138).23 Improvement of 75% in PASI score was achieved by 29% of participants in the apremilast group at week 16. The most common AEs were diarrhea (16%) and nausea (18%), which were predominantly mild, occurring most commonly in the first week and resolving within 1 month. No cases of severe diarrhea or severe nausea were reported. Apremilast had no apparent effect on the results of hematological or serum chemistry tests.23 Although the US Food and Drug Administration warns of a possible link between apremilast and depression,24 data are mostly related to roflumilast, another PDE4 inhibitor. Studies in patients with chronic obstructive pulmonary disease have noted increased cases of depression (1.21% vs 0.82%) and suicidal ideation/attempt (0.03% vs 0.02%) in patients treated with roflumilast versus placebo.25
Jak Inhibitors
Janus kinases are a family of intracellular tyrosine kinases that connect several cytokine receptors to the signal transducer and activator of transcription pathways.26 There are 4 Jak family members: Jak1, Jak2, Jak3, and tyrosine kinase 2. Janus kinases 1 and 2 have roles in interferon signaling, while Jak3 transduces signals from IL-2, IL-7, IL-15, and IL-21, which are T-cell growth and survival factors.
Tofacitinib is a novel oral signal transduction molecule that blocks the Jak3 pathway. A phase 2b, 12-week, dose-ranging study was conducted to assess the efficacy and safety of 3 twice-daily regimens of tofacitinib versus placebo in patients with moderate to severe chronic plaque psoriasis.27 One hundred and ninety-seven participants were randomized to receive oral tofacitinib (2 mg, 5 mg, or 15 mg; n=49 each) or placebo (n=50) twice daily for 12 weeks with a 4-week follow-up period. The primary end point was the proportion of participants achieving at least a 75% reduction in PASI score at week 12 (25.0% with 2 mg, 40.8% with 5 mg, 66.7% with 15 mg, 2.0% with placebo). Similarly, a higher proportion of participants achieving 90% reduction in PASI score was seen at weeks 8 and 12 in all tofacitinib-treated participants versus placebo. The most common AEs were upper respiratory tract infection, sinusitis, nasopharyngitis, and headache. A number of changes in laboratory parameters occurred in the tofacitinib groups. Mild dose-related decreases in hemoglobin were noted at week 12 for all tofacitinib groups, and a small increase (mean, 0.04 mg/dL) in serum creatinine levels was observed in the 15-mg group. Decreases in neutrophil counts were observed with higher doses of tofacitinib, with the maximum mean decrease of 0.9×103/mm3 from baseline observed in the 15-mg group at week 4. After weeks 4 through 8, mean neutrophil counts began to return to baseline levels. Dose-related increases in total cholesterol, high-density lipoprotein cholesterol, and low-density lipoprotein cholesterol were observed by week 2 and remained at this level through week 12; mean lipid levels decreased to baseline levels after cessation of active treatment. One participant in the 15-mg group developed an elevated alanine aminotransferase level that was more than 2.5 times the highest normal limit. Three participants experienced 5 serious AEs.27 These early results show that tofacitinib can be a safe and effective treatment in patients with psoriasis, but further data from phase 3 studies will need to be awaited.
Another Jak inhibitor under investigationfor the treatment of psoriasis is ruxolitinib, an inhibitor of Jak1 and Jak2, which has been primarily studied as a topical agent for milder cases of the disease.28
Conclusion
Many new drugs are currently on the horizon and will increase our armamentarium for treating psoriasis. Some of these agents promise greater levels of efficacy than currently used therapies. Although this review focuses on systemic agents, there also are a number of topical formulations in the pipeline. These new agents will certainly increase our options when choosing the most suitable treatment for a patient with psoriasis, but safety will remain a primary concern, and time and experience will tell whether efficacy outweighs any potential side effects.
Psoriasis is a common chronic inflammatory skin disease affecting 1% to 8% of the world population, depending on the country.1 Psoriasis can greatly impact quality of life in affected individuals, even in those with limited body surface involvement.2 Studies have demonstrated a high degree of psychological distress associated with psoriasis, leading to depression and poor self-esteem.3
Over the last decade, our improved understanding of the autoimmune inflammatory pathways and the associated changing concepts in psoriasis pathogenesis have led to the development of biological drugs targeting specific components of effector immune mechanisms, and these biological drugs have revolutionized the treatment of psoriasis.4 Although response rates of these biological agents are greater compared to those of conventional systemic drugs,5 current biological drugs fail to demonstrate efficacy in some patients or lose their efficacy over time. In addition to the high costs associated with these drugs, these limitations have driven a continued search for alternative therapies.
Helper T cells (TH17) and the proinflammatory cytokine IL-17 have been shown to play a key role in the pathophysiology of psoriasis, bridging innate and adaptive immune responses. IL-17 is involved in the modulation of proinflammatory cytokines, hematopoietic growth factors, antimicrobial peptides, and chemokines. Increased TH17 activity and high levels of IL-17 have been found in psoriatic plaques, and increased levels of TH17 are found in the plasma of psoriasis patients.6 Increased IL-17 induces neutrophilia, inflammation, and angiogenesis.7 Other cytokines that are highly upregulated in involved skin are tumor necrosis factor a (TNF-α), IL-23, IL-22, and IL-21.8 IL-23 is involved in regulating TH17 cells and is a potent activator of keratinocyte proliferation.9 Blockade of IL-12/23 causes downregulation of TH17 and TH22 cell responses.10 As IL-17 has a key role in protecting skin and mucous membranes from bacterial and fungal infections, IL-17 inhibition can potentially interfere with the inflammatory cascade. However, available data suggest that sufficient residual IL-17 activity remains to maintain immunity against infections.11
Currently approved biological agents for psoriasis target proinflammatory cytokines such as TNF-α, or the p40 subunit of IL-12 and IL-23. A number of novel targeted therapies including biologics as well as small molecule inhibitors targeting various cytokines and molecules involved in the pathogenesis of psoriasis are currently in different stages of development (Table). These drugs include 3 IL-17 inhibitors (secukinumab, ixekizumab, and brodalumab); 2 IL-23 blockers (tildrakizumab and guselkumab); and small molecule inhibitors that target the kinase pathway including apremilast (a phosphodiesterase 4 [PDE4] inhibitor), as well as tofacitinib, baricitinib, and ruxolitinib (Janus kinase [Jak] inhibitors). Small molecule inhibitors can be administered orally and are less expensive to produce than biological agents. This article reviews available data on these new systemic agents in the pipeline.
Novel Biologics
Secukinumab
Secukinumab is a fully human monoclonal IgG1k antibody that selectively binds and neutralizes IL-17A.12 It is the first of the IL-17 antibodies to receive approval for the treatment of moderate to severe psoriasis. In 2 phase 3, double-blind, 52-week trials—ERASURE (Efficacy of Response and Safety of Two Fixed Secukinumab Regimens in Psoriasis) and FIXTURE (Full Year Investigative Examination of Secukinumab vs Etanercept Using Two Dosing Regimens to Determine Efficacy in Psoriasis)—participants were randomly assigned to receive subcutaneous secukinumab at doses of 300 mg (n=245 and n=327, respectively) or 150 mg (n=245 and n=327, respectively) once weekly for 5 weeks then every 4 weeks, or placebo (n=248 and n=326, respectively); in the FIXTURE study only, an etanercept group (n=326) was given a 50-mg dose twice weekly for 12 weeks then once weekly.13
In the ERASURE study, the proportion of participants showing a reduction of 75% or more in psoriasis area and severity index (PASI) score from baseline to week 12 was 81.6% with secukinumab 300 mg, 71.6% with secukinumab 150 mg, and 4.5% with placebo.13 Secondary end point results demonstrated the proportion of participants showing a 90% reduction in PASI score was 59.2% with secukinumab 300 mg and 39.1% with secukinumab 150 mg, which were both superior to placebo (1.2%). The proportion of participants who met the criteria for 100% reduction in PASI score at week 12 also was greater with each secukinumab dose than with placebo.13
In the FIXTURE study, the proportion of participants showing a reduction of 75% or more from baseline in PASI score at week 12 was 77.1% with secukinumab 300 mg, 67.0% with secukinumab 150 mg, 44.0% with etanercept, and 4.9% with placebo.13 Secondary end point results demonstrated the proportion of participants showing a 90% reduction in PASI score was 54.2% with secukinumab 300 mg, 41.9% with secukinumab 150 mg, 20.7% with etanercept, and 1.5% with placebo. The speed of response, which was assessed as the median time to a 50% reduction in mean PASI score from baseline, was significantly shorter with both doses of secukinumab (3.0 weeks and 3.9 weeks, respectively) than with etanercept (7.0 weeks)(P<.001 for both).13
In the FIXTURE study, incidences of adverse events (AEs) were similar in the secukinumab and etanercept groups during both the induction period and the entire treatment period.13 The most common AEs in the secukinumab groups were nasopharyngitis, headache, and diarrhea. The rates of infections or infestations during the induction period were 26.7% with secukinumab 300 mg, 30.9% with secukinumab 150 mg, 24.5% with etanercept, and 19.3% with placebo. Candidal infections were more common with secukinumab than with etanercept during the entire treatment period (4.7% and 2.3% of participants in the secukinumab 300 mg and 150 mg groups, respectively, reported mild or moderate candidal infections). None of these infections resulted in chronic mucocutaneous candidiasis or discontinuation of the study drug and all resolved on their own or with standard therapy. Candidal infection was reported in 1.2% of participants in the etanercept group. Responses at week 12 were sustained in the majority of participants through week 52 with continued secukinumab therapy every 4 weeks. Grade 3 neutropenia occurred in 1.0% of secukinumab-treated participants and in none of the participants in the etanercept group. There were no apparent dose-related differences between the secukinumab groups with respect to AEs, with the exception of mild and moderate candidal infections.13
These efficacy data are impressive and no specific serious safety concerns have been identified to date. However, IL-17A plays a key role in host defense, particularly in mucocutaneous immunity against Candida albicans,14 as well as in hematopoiesis through stimulation of granulopoiesis and neutrophil trafficking,15 and thus we need to remain watchful with regards to Candida albicans infections and neutropenia.
Ixekizumab
Ixekizumab is a humanized IgG4 anti–IL-17A monoclonal antibody. In a phase 2, double-blind, placebo-controlled trial, 142 participants with chronic moderate to severe plaque psoriasis were randomly assigned to receive 150-mg (n=28), 75-mg (n=29), 25-mg (n=30), or 10-mg (n=28) subcutaneous injections of ixekizumab or placebo (n=27) at weeks 0, 2, 4, 8, 12, and 16.16 At 12 weeks, the percentage of participants who achieved a 75% reduction in PASI score from baseline was significantly greater with ixekizumab (82.1% with 150-mg dose, 82.8% with 75-mg dose, 76.7% with 25-mg dose) than with placebo (7.7%)(P<.001 for each comparison), except with the 10-mg dose. Similarly, a greater percentage of participants in the same ixekizumab groups achieved a 90% reduction (71.4% with 150-mg dose, 58.6% with 75-mg dose, 50.0% with 25-mg dose) and a 100% reduction (39.3% with 150-mg dose, 37.9% with 75-mg dose) in PASI score compared to placebo (0%)(P<.001 for each comparison). Significant reductions in PASI scores were evident as early as week 1 in the 150-mg and 75-mg groups, and these reductions were sustained for 20 weeks (P<.05).16 Phase 3 studies of ixekizumab currently are underway.
Brodalumab
The third IL-17 blocker in the pipeline is brodalumab, a human monoclonal antibody against IL-17RA, which blocks signaling of IL-17A and IL-17F as well as the IL-17A/F heterodimer, all of which are involved in the inflammatory process of psoriasis. Brodalumab was evaluated in a phase 2, double-blind, placebo-controlled, dose-ranging study of 198 participants who were randomized to receive 70 mg (n=39), 140 mg (n=39), 210 mg (n=40), or 280 mg (n=42) of brodalumab or placebo (n=38).17 At week 12, improvements of at least 75% and at least 90% in PASI score were achieved by 77% and 72%, respectively, in the 140-mg group, and 82% and 75%, respectively, in the 210-mg group compared to 0% of the placebo group (P<.001 for all comparisons). One hundred percent improvement in PASI was achieved by 38% of participants in the 140-mg group and 62% in the 210-mg group. No participants in the placebo group demonstrated improvement of 75% or higher. The most common AEs were nasopharyngitis, upper respiratory tract infection, arthralgia, and injection-site erythema. Serious AEs reported during the study included renal colic (1 participant), ec-topic pregnancy (1 participant), and grade 3 asymptomatic neutropenia (2 participants). Both cases of neutropenia were noted at the first assessment after brodalumab initiation (week 2) and resolved when the study drug was withheld.17
Results for this new IL-17 blocker are encouraging, but phase 3 data of brodalumab will need to be awaited.
Tildrakizumab
Tildrakizumab is a humanized IgG1 monoclonal antibody that blocks the p19 subunit of IL-23. In a randomized, double-blind, phase 2b trial, 355 adults with moderate to severe psoriasis were randomized to receive subcutaneous injections of tildrakizumab (5 mg, 25 mg, 100 mg, or 200 mg) or placebo.18 In part 1 of the study, injections were administered at weeks 0 and 4. Part 2 of the study started at week 16. In part 2, responders with a 75% improvement in PASI score in the 5- and 25-mg groups continued their dose, while responders in the 100- or 200-mg groups were randomized again to continue the same dose or a reduced dose (100 mg to 25 mg; 200 mg to 100 mg) every 12 weeks from weeks 16 to 52. Those in the placebo group received tildrakizumab 25 mg every 12 weeks in part 2. The primary end point was the mean change in PASI score from baseline to week 16, which was significantly greater in all tildrakizumab groups than in the placebo group (P<.001 for all comparisons). Improvements of 75% in PASI score were achieved by 74% in the 200-mg group, 66% in the 100-mg group, 64% in the 25-mg group, and 33% in the 5-mg group. In contrast, 4.9% in the placebo group achieved an improvement of 75%. At week 52, no loss of efficacy was seen in those participants who had achieved 75% improvement in PASI score at week 16 and had continued their prior doses. The rates of AEs seen in the tildrakizumab groups were 60% to 71% compared to 69% in the placebo group. The most common AE was nasopharyngitis, occurring in 12% to 20% of participants in each group. Serious AEs were uncommon.18 Phase 3 studies are currently underway.19
Guselkumab
Guselkumab is a human IgG1 monoclonal antibody in clinical development that specifically blocks the p19 subunit of IL-23. In a double-blind, placebo-controlled, phase 1 study, 24 participants with moderate to severe plaque psoriasis were randomized to receive a single 10-mg (n=5), 30-mg (n=5), 100-mg (n=5), or 300-mg (n=5) dose of guselkumab or placebo (n=4).20 At week 12, 50% in the 10-mg group, 60% in both the 30- and 100-mg groups, and 100% in the 300-mg group showed 75% improvement in PASI score versus 0% in the placebo group. Improvements in PASI scores were generally maintained through week 24. The rates of AEs were 65% (13/20) in the combined guselkumab group and 50% (2/4) in the placebo group.20
Small Molecule Inhibitors
In contrast to biologics, which mainly target soluble cytokine or cellular receptors, small molecule inhibitors target enzymes within signaling pathways. Small molecule inhibitors have some advantages over biologics in that they are relatively inexpensive to produce and can be administered orally; thus, they may be preferred by some patients over injectable drugs. There are several agents that are undergoing clinical trials in psoriasis, including PDE4 inhibitors and Jak inhibitors.
Apremilast
Apremilast is an oral small molecule PDE4 inhibitor that was approved by the US Food and Drug Administration in March 2014 for the treatment of adult patients with active psoriatic arthritis; an indication for moderate to severe plaque psoriasis was approved in September 2014.21 Phosphodiesterase 4 is a cyclic adenosine monophosphate–specific phosphodiesterase inhibitor, which is dominant in inflammatory cells. Inhibition of PDE4 increases intracellular cyclic adenosine monophosphate levels, thus downregulating proinflammatory cytokines such as TNF-α, IFN-γ, IL-2, IL-12, and IL-23, and increasing the production of anti-inflammatory cytokines such as IL-10.22
Phase 2 and phase 3 studies have demonstrated the clinical efficacy of apremilast in the treatment of patients with moderate to severe plaque psoriasis. In a 16-week randomized, placebo-controlled, phase 3 trial (ESTEEM 2), 408 participants were randomized to receive oral apremilast 30 mg twice daily (n=275) or placebo (n=138).23 Improvement of 75% in PASI score was achieved by 29% of participants in the apremilast group at week 16. The most common AEs were diarrhea (16%) and nausea (18%), which were predominantly mild, occurring most commonly in the first week and resolving within 1 month. No cases of severe diarrhea or severe nausea were reported. Apremilast had no apparent effect on the results of hematological or serum chemistry tests.23 Although the US Food and Drug Administration warns of a possible link between apremilast and depression,24 data are mostly related to roflumilast, another PDE4 inhibitor. Studies in patients with chronic obstructive pulmonary disease have noted increased cases of depression (1.21% vs 0.82%) and suicidal ideation/attempt (0.03% vs 0.02%) in patients treated with roflumilast versus placebo.25
Jak Inhibitors
Janus kinases are a family of intracellular tyrosine kinases that connect several cytokine receptors to the signal transducer and activator of transcription pathways.26 There are 4 Jak family members: Jak1, Jak2, Jak3, and tyrosine kinase 2. Janus kinases 1 and 2 have roles in interferon signaling, while Jak3 transduces signals from IL-2, IL-7, IL-15, and IL-21, which are T-cell growth and survival factors.
Tofacitinib is a novel oral signal transduction molecule that blocks the Jak3 pathway. A phase 2b, 12-week, dose-ranging study was conducted to assess the efficacy and safety of 3 twice-daily regimens of tofacitinib versus placebo in patients with moderate to severe chronic plaque psoriasis.27 One hundred and ninety-seven participants were randomized to receive oral tofacitinib (2 mg, 5 mg, or 15 mg; n=49 each) or placebo (n=50) twice daily for 12 weeks with a 4-week follow-up period. The primary end point was the proportion of participants achieving at least a 75% reduction in PASI score at week 12 (25.0% with 2 mg, 40.8% with 5 mg, 66.7% with 15 mg, 2.0% with placebo). Similarly, a higher proportion of participants achieving 90% reduction in PASI score was seen at weeks 8 and 12 in all tofacitinib-treated participants versus placebo. The most common AEs were upper respiratory tract infection, sinusitis, nasopharyngitis, and headache. A number of changes in laboratory parameters occurred in the tofacitinib groups. Mild dose-related decreases in hemoglobin were noted at week 12 for all tofacitinib groups, and a small increase (mean, 0.04 mg/dL) in serum creatinine levels was observed in the 15-mg group. Decreases in neutrophil counts were observed with higher doses of tofacitinib, with the maximum mean decrease of 0.9×103/mm3 from baseline observed in the 15-mg group at week 4. After weeks 4 through 8, mean neutrophil counts began to return to baseline levels. Dose-related increases in total cholesterol, high-density lipoprotein cholesterol, and low-density lipoprotein cholesterol were observed by week 2 and remained at this level through week 12; mean lipid levels decreased to baseline levels after cessation of active treatment. One participant in the 15-mg group developed an elevated alanine aminotransferase level that was more than 2.5 times the highest normal limit. Three participants experienced 5 serious AEs.27 These early results show that tofacitinib can be a safe and effective treatment in patients with psoriasis, but further data from phase 3 studies will need to be awaited.
Another Jak inhibitor under investigationfor the treatment of psoriasis is ruxolitinib, an inhibitor of Jak1 and Jak2, which has been primarily studied as a topical agent for milder cases of the disease.28
Conclusion
Many new drugs are currently on the horizon and will increase our armamentarium for treating psoriasis. Some of these agents promise greater levels of efficacy than currently used therapies. Although this review focuses on systemic agents, there also are a number of topical formulations in the pipeline. These new agents will certainly increase our options when choosing the most suitable treatment for a patient with psoriasis, but safety will remain a primary concern, and time and experience will tell whether efficacy outweighs any potential side effects.
1. Parisi R, Symmons DP, Griffiths CE, et al. Global epidemiology of psoriasis: a systematic review of incidence and prevalence. J Invest Dermatol. 2013;133:377-385.
2. Rapp SR, Feldman SR, Exum ML, et al. Psoriasis causes as much disability as other major medical diseases. J Am Acad Dermatol. 1999;41(3 pt 1):401-407.
3. Shah R, Bewley A. Psoriasis: ‘the badge of shame.’ a case report of a psychological intervention to reduce and potentially clear chronic skin disease. Clin Exp Dermatol. 2014;39:600-603.
4. Vincent FB, Morand EF, Murphy K, et al. Antidrug antibodies (ADAb) to tumour necrosis factor (TNF)-specific neutralising agents in chronic inflammatory diseases: a real issue, a clinical perspective. Ann Rheum Dis. 2013;72:165-178.
5. Chi CC, Wang SH. Efficacy and cost-efficacy of biologic therapies for moderate to severe psoriasis: a meta-analysis and cost-efficacy analysis using the intention-to-treat principle. Biomed Res Int. 2014;2014:862851.
6. Kagami S, Rizzo HL, Lee JJ, et al. Circulating Th17, Th22, and Th1 cells are increased in psoriasis. J Invest Dermatol. 2010;130:1373-1383.
7. Leonardi CL, Gordon KB. New and emerging therapies in psoriasis. Semin Cutan Med Surg. 2014;33(2, suppl 2):S37-S41.
8. Lowes MA, Kikuchi T, Fuentes-Duculan J, et al. Psoriasis vulgaris lesions contain discrete populations of Th1 and Th17 T cells. J Invest Dermatol. 2008;128:1207-1211.
9. Nickoloff BJ, Qin JZ, Nestle FO. Immunopathogenesis of psoriasis. Clin Rev Allergy Immunol. 2007;33:45-56.
10. Fitch E, Harper E, Skorcheva I, et al. Pathophysiology of psoriasis: recent advances on IL-23 and Th17 cytokines. Curr Rheumatol Rep. 2007;9:461-467.
11. Adami S, Cavani A, Rossi F, et al. The role of interleukin-17A in psoriatic disease. BioDrugs. 2014;28:487-497.
12. Hueber W, Patel DD, Dryja T, et al. Effects of AIN457, a fully human antibody to interleukin-17A, on psoriasis, rheumatoid arthritis, and uveitis. Sci Transl Med. 2010;2:52ra72.
13. Langley RG, Elewski BE, Lebwohl M, et al. Secukinumab in plaque psoriasis—results of two phase 3 trials. N Engl J Med. 2014;371:326-338.
14. Puel A, Cypowyj S, Bustamante J, et al. Chronic mucocutaneous candidiasis in humans with inborn errors of interleukin-17 immunity. Science. 2011;332:65-68.
15. Krstic A, Mojsilovic S, Jovcic G, et al. The potential of interleukin-17 to mediate hematopoietic response. Immunol Res. 2012;52:34-41.
16. Leonardi C, Matheson R, Zachariae C, et al. Anti-interleukin-17 monoclonal antibody ixekizumab in chronic plaque psoriasis. N Engl J Med. 2012;366:1190-1199.
17. Papp KA, Leonardi C, Menter A, et al. Brodalumab, an anti-interleukin-17-receptor antibody for psoriasis. N Engl J Med. 2012;366:1181-1189.
18. Langley RGB, Thaci D, Papp KA, et al. MK-3222, an anti–IL-23p19 humanized monoclonal antibody, provides significant improvement in psoriasis over 52 weeks of treatment that is maintained after discontinuation of dosing. Poster presented at: 73rd Annual Meeting of the American Academy of Dermatology; March 21-25, 2014; Denver, CO. Poster 8056.
19. Tausend W, Downing C, Tyring S. Systematic review of interleukin-12, interleukin-17, and interleukin-23 pathway inhibitors for the treatment of moderate-to-severe chronic plaque psoriasis: ustekinumab, briakinumab, tildrakizumab, guselkumab, secukinumab, ixekizumab, and brodalumab. J Cutan Med Surg. 2014;18:156-169.
20. Sofen H, Smith S, Matheson RT, et al. Guselkumab (an IL-23-specific mAb) demonstrates clinical and molecular response in patients with moderate-to-severe psoriasis. J Allergy Clin Immunol. 2014;133:1032-1040.
21. Schafer PH, Parton A, Capone L, et al. Apremilast is a selective PDE4 inhibitor with regulatory effects on innate immunity. Cell Signal. 2014;26:2016-2029.
22. van de Kerkhof PC. Apremilast: a step forward in the treatment of psoriasis? Lancet. 2012;380:708-709.
23. Paul C, Crowley J, Cather J, et al. Apremilast, an oral phosphodiesterase 4 inhibitor, in patients with moderate to severe psoriasis: 16-week results of a phase 3, randomized, controlled trial (ESTEEM 2). Poster presented at: 73rd Annual Meeting of the American Academy of Dermatology; March 21-25, 2014; Denver, CO. Poster 8412.
24. Otezla [product insert]. Summit, NJ: Celgene Corporation; 2014.
25. Rabe KF. Update on roflumilast, a phosphodiesterase 4 inhibitor for the treatment of chronic obstructive pulmonary disease. Br J Pharmacol. 2011;163:53-67.
26. Palanivel JA, Macbeth AE, Chetty NC, et al. An insight into JAK-STAT signalling in dermatology. Clin Exp Dermatol. 2014;39:513-518.
27. Papp KA, Menter A, Strober B, et al. Efficacy and safety of tofacitinib, an oral Janus kinase inhibitor, in the treatment of psoriasis: a phase 2b randomized placebo-controlled dose-ranging study. Br J Dermatol. 2012;167:668-677.
28. Hsu L, Armstrong AW. JAK inhibitors: treatment efficacy and safety profile in patients with psoriasis. J Immunol Res. 2014;2014:283617.
1. Parisi R, Symmons DP, Griffiths CE, et al. Global epidemiology of psoriasis: a systematic review of incidence and prevalence. J Invest Dermatol. 2013;133:377-385.
2. Rapp SR, Feldman SR, Exum ML, et al. Psoriasis causes as much disability as other major medical diseases. J Am Acad Dermatol. 1999;41(3 pt 1):401-407.
3. Shah R, Bewley A. Psoriasis: ‘the badge of shame.’ a case report of a psychological intervention to reduce and potentially clear chronic skin disease. Clin Exp Dermatol. 2014;39:600-603.
4. Vincent FB, Morand EF, Murphy K, et al. Antidrug antibodies (ADAb) to tumour necrosis factor (TNF)-specific neutralising agents in chronic inflammatory diseases: a real issue, a clinical perspective. Ann Rheum Dis. 2013;72:165-178.
5. Chi CC, Wang SH. Efficacy and cost-efficacy of biologic therapies for moderate to severe psoriasis: a meta-analysis and cost-efficacy analysis using the intention-to-treat principle. Biomed Res Int. 2014;2014:862851.
6. Kagami S, Rizzo HL, Lee JJ, et al. Circulating Th17, Th22, and Th1 cells are increased in psoriasis. J Invest Dermatol. 2010;130:1373-1383.
7. Leonardi CL, Gordon KB. New and emerging therapies in psoriasis. Semin Cutan Med Surg. 2014;33(2, suppl 2):S37-S41.
8. Lowes MA, Kikuchi T, Fuentes-Duculan J, et al. Psoriasis vulgaris lesions contain discrete populations of Th1 and Th17 T cells. J Invest Dermatol. 2008;128:1207-1211.
9. Nickoloff BJ, Qin JZ, Nestle FO. Immunopathogenesis of psoriasis. Clin Rev Allergy Immunol. 2007;33:45-56.
10. Fitch E, Harper E, Skorcheva I, et al. Pathophysiology of psoriasis: recent advances on IL-23 and Th17 cytokines. Curr Rheumatol Rep. 2007;9:461-467.
11. Adami S, Cavani A, Rossi F, et al. The role of interleukin-17A in psoriatic disease. BioDrugs. 2014;28:487-497.
12. Hueber W, Patel DD, Dryja T, et al. Effects of AIN457, a fully human antibody to interleukin-17A, on psoriasis, rheumatoid arthritis, and uveitis. Sci Transl Med. 2010;2:52ra72.
13. Langley RG, Elewski BE, Lebwohl M, et al. Secukinumab in plaque psoriasis—results of two phase 3 trials. N Engl J Med. 2014;371:326-338.
14. Puel A, Cypowyj S, Bustamante J, et al. Chronic mucocutaneous candidiasis in humans with inborn errors of interleukin-17 immunity. Science. 2011;332:65-68.
15. Krstic A, Mojsilovic S, Jovcic G, et al. The potential of interleukin-17 to mediate hematopoietic response. Immunol Res. 2012;52:34-41.
16. Leonardi C, Matheson R, Zachariae C, et al. Anti-interleukin-17 monoclonal antibody ixekizumab in chronic plaque psoriasis. N Engl J Med. 2012;366:1190-1199.
17. Papp KA, Leonardi C, Menter A, et al. Brodalumab, an anti-interleukin-17-receptor antibody for psoriasis. N Engl J Med. 2012;366:1181-1189.
18. Langley RGB, Thaci D, Papp KA, et al. MK-3222, an anti–IL-23p19 humanized monoclonal antibody, provides significant improvement in psoriasis over 52 weeks of treatment that is maintained after discontinuation of dosing. Poster presented at: 73rd Annual Meeting of the American Academy of Dermatology; March 21-25, 2014; Denver, CO. Poster 8056.
19. Tausend W, Downing C, Tyring S. Systematic review of interleukin-12, interleukin-17, and interleukin-23 pathway inhibitors for the treatment of moderate-to-severe chronic plaque psoriasis: ustekinumab, briakinumab, tildrakizumab, guselkumab, secukinumab, ixekizumab, and brodalumab. J Cutan Med Surg. 2014;18:156-169.
20. Sofen H, Smith S, Matheson RT, et al. Guselkumab (an IL-23-specific mAb) demonstrates clinical and molecular response in patients with moderate-to-severe psoriasis. J Allergy Clin Immunol. 2014;133:1032-1040.
21. Schafer PH, Parton A, Capone L, et al. Apremilast is a selective PDE4 inhibitor with regulatory effects on innate immunity. Cell Signal. 2014;26:2016-2029.
22. van de Kerkhof PC. Apremilast: a step forward in the treatment of psoriasis? Lancet. 2012;380:708-709.
23. Paul C, Crowley J, Cather J, et al. Apremilast, an oral phosphodiesterase 4 inhibitor, in patients with moderate to severe psoriasis: 16-week results of a phase 3, randomized, controlled trial (ESTEEM 2). Poster presented at: 73rd Annual Meeting of the American Academy of Dermatology; March 21-25, 2014; Denver, CO. Poster 8412.
24. Otezla [product insert]. Summit, NJ: Celgene Corporation; 2014.
25. Rabe KF. Update on roflumilast, a phosphodiesterase 4 inhibitor for the treatment of chronic obstructive pulmonary disease. Br J Pharmacol. 2011;163:53-67.
26. Palanivel JA, Macbeth AE, Chetty NC, et al. An insight into JAK-STAT signalling in dermatology. Clin Exp Dermatol. 2014;39:513-518.
27. Papp KA, Menter A, Strober B, et al. Efficacy and safety of tofacitinib, an oral Janus kinase inhibitor, in the treatment of psoriasis: a phase 2b randomized placebo-controlled dose-ranging study. Br J Dermatol. 2012;167:668-677.
28. Hsu L, Armstrong AW. JAK inhibitors: treatment efficacy and safety profile in patients with psoriasis. J Immunol Res. 2014;2014:283617.
Practice Points
- Secukinumab is an anti–IL-17 antibody approved for the treatment of psoriasis. It is indicated for the treatment of moderate to severe plaque psoriasis in adult patients who are candidates for systemic therapy or phototherapy.
- The new biological agents have shown promising results with some patients achieving psoriasis area and severity index scores of 90 and 100.
- A number of small molecule inhibitors also are in the pipeline, with apremilast the first one to have reached approval for psoriasis.

Recovering From Cancer Through Dance
Belly dancing can help women rehabilitating from cancer, according to a yearlong study that compared 59 women receiving standard medical care with 55 women receiving standard care plus dancing at the National Institute of Oncology in Budapest, Hungary.
The voluntary program provided weekly 90-minute belly dancing sessions with an instructor, followed by 90 minutes of free interaction, during which participants could discuss body image, sexuality, social relationships, and other topics. The dancing and discussion were intended to help the women “reconstruct feminine sexual identity” and provide peer social support. The researchers chose 1 year as the time frame, because other studies have found that the first 6 to 12 months posttreatment are critical for providing supportive care.
Related: Early Cancer Detection Helps Underserved Women
As assessed by questionnaires, scores for quality of life, perceived social support, and overall life satisfaction improved in both groups, but the difference for the belly dancing group was significant (P = .000), with longer lasting effects.
Related: Timely Assessment of Cancer Symptoms
The researchers note that dance and movement therapy have been associated with improved vitality, greater self-esteem, less depression, and reduced levels of stress hormones. They also cite other research that has found that the positive effects of belly dancing include reinforcement of the sense of femininity, higher self-confidence, and promotion of a more positive body image.
Source
Szalai M, Lévay B, Szirmai A, Papp I, Prémusz V, Bódis J. Euro J Oncol Nurs. 2015;19(1):60-65.
doi: 10.1016/j.ejon.2014.07.009.
Belly dancing can help women rehabilitating from cancer, according to a yearlong study that compared 59 women receiving standard medical care with 55 women receiving standard care plus dancing at the National Institute of Oncology in Budapest, Hungary.
The voluntary program provided weekly 90-minute belly dancing sessions with an instructor, followed by 90 minutes of free interaction, during which participants could discuss body image, sexuality, social relationships, and other topics. The dancing and discussion were intended to help the women “reconstruct feminine sexual identity” and provide peer social support. The researchers chose 1 year as the time frame, because other studies have found that the first 6 to 12 months posttreatment are critical for providing supportive care.
Related: Early Cancer Detection Helps Underserved Women
As assessed by questionnaires, scores for quality of life, perceived social support, and overall life satisfaction improved in both groups, but the difference for the belly dancing group was significant (P = .000), with longer lasting effects.
Related: Timely Assessment of Cancer Symptoms
The researchers note that dance and movement therapy have been associated with improved vitality, greater self-esteem, less depression, and reduced levels of stress hormones. They also cite other research that has found that the positive effects of belly dancing include reinforcement of the sense of femininity, higher self-confidence, and promotion of a more positive body image.
Source
Szalai M, Lévay B, Szirmai A, Papp I, Prémusz V, Bódis J. Euro J Oncol Nurs. 2015;19(1):60-65.
doi: 10.1016/j.ejon.2014.07.009.
Belly dancing can help women rehabilitating from cancer, according to a yearlong study that compared 59 women receiving standard medical care with 55 women receiving standard care plus dancing at the National Institute of Oncology in Budapest, Hungary.
The voluntary program provided weekly 90-minute belly dancing sessions with an instructor, followed by 90 minutes of free interaction, during which participants could discuss body image, sexuality, social relationships, and other topics. The dancing and discussion were intended to help the women “reconstruct feminine sexual identity” and provide peer social support. The researchers chose 1 year as the time frame, because other studies have found that the first 6 to 12 months posttreatment are critical for providing supportive care.
Related: Early Cancer Detection Helps Underserved Women
As assessed by questionnaires, scores for quality of life, perceived social support, and overall life satisfaction improved in both groups, but the difference for the belly dancing group was significant (P = .000), with longer lasting effects.
Related: Timely Assessment of Cancer Symptoms
The researchers note that dance and movement therapy have been associated with improved vitality, greater self-esteem, less depression, and reduced levels of stress hormones. They also cite other research that has found that the positive effects of belly dancing include reinforcement of the sense of femininity, higher self-confidence, and promotion of a more positive body image.
Source
Szalai M, Lévay B, Szirmai A, Papp I, Prémusz V, Bódis J. Euro J Oncol Nurs. 2015;19(1):60-65.
doi: 10.1016/j.ejon.2014.07.009.
CKD and HCV: Do We Know What We’re Doing?
Oh what a tangled web it weaves, this virus called hepatitis C. HCV has evolved over several thousand years into seven genotypes and multiple subtypes, making identification and treatment extremely variable.1 The genotypes are usually geographically specific, with 70% to 75% of HCV patients in the United States classed as genotype 1.2 Genotypes 2 and 3 account for most of the rest.3
While genotype does not impact the course or severity of the disease, it does affect the response to treatment. With today’s newest treatments, success rates for sustained viral response (SVR) are as high as 90% in patients with genotype 1. However, the treatment is not without cost: About $100,000 for patients without cirrhosis and even more for those with it, due to the extended length of treatment.
Chronic kidney disease (CKD) and HCV overlap in 10% to nearly 59% of the population in some geographic areas.4 Those with CKD who have had a previous kidney transplant, been on dialysis, and/or been treated prior to the introduction of epoetin alfa (Epogen®, when blood transfusions were common) are more likely to be HCV-positive.
Unfortunately, patients often convert to HCV while on hemodialysis.4 This largely represents a nosocomial infection related to parenteral exposure. In the dialysis patient, the course of HCV is more aggressive than in others, with high morbidity—often resulting from cirrhosis and/or hepatocellular carcinoma.
With new HCV drugs available, CKD patients would appear to be a prime population to treat. In order to gain marketing approval, the FDA requires testing of new drugs in patients with varying degrees of renal impairment. However, the requirement is for “moderate” CKD, defined by the FDA as a glomerular filtration rate (GFR) of at least 30 mL/min/1.73m2. The FDA does not require testing for patients with a lower GFR, or what nephrology practices refer to as stage 4 or stage 5 CKD; thus, no data are available for this population. The available pharmacokinetic data for the recently approved regimens of sofosbuvir/ledipasvir (Harvoni®) and of ombitasvir/paritaprevir/ritonavir with dasabuvir (Viekira Pak™) suggest that no dosing modifications are necessary in the moderately impaired kidney population.
Continue for the newest HCV drugs >>
The recent approvals of Harvoni and Viekira Pak are considered game-changers in the treatment of chronic HCV infection: They demonstrate that interferon is no longer always necessary. Interferon, especially in combination with ribavirin, was especially toxic for patients in the kidney failure population, although the pegylated form of interferon was less problematic. FDA approvals for Harvoni and Viekira Pak were based on clinical data demonstrating SVR rates exceeding 90%, even in traditionally difficult-to-treat populations (ie, patients with genotype 1, African-Americans, those with high viral load levels), which include many CKD patients.
The lack of clinical data in the CKD stage 4/5 population at the time of drug approval raises significant management challenges for the HCV-positive CKD patient. It is encouraging, however, that the FDA is requiring that all new medications be tested in the renally impaired population, even if not in the severely impaired groups. In the interim, and based solely on renal impairment study results for patients with GFR at or exceeding 30 mL/min/1.73m2, HCV guidelines issued jointly by the American Association for the Study of Liver Diseases and the Infectious Diseases Society of America5 include the recommendation that these new HCV medications be considered for use in the CKD population. Furthermore, there are no dosing adjustments recommended for any of the new HCV medications in stage 4 or stage 5 CKD due to lack of data. However, until more data become available, CKD patients must be managed on a case-by-case basis after consultation with a renal expert, with close attention to changes in GFR and adverse events.
When these new HCV medications are used in the general population and those with significant CKD, postmarketing reports to the FDA will be vital. Practitioners are encouraged to report adverse outcomes to the FDA MedWatch system (https://www.accessdata.fda.gov/scripts/medwatch). As any nephrology practice will tell you, we are starting to get phone calls from our hepatology colleagues asking for guidance, and the next few years will be a fascinating time for all of us. The promise of virologic cure for our HCV-positive patients is tangible and on the horizon.
REFERENCES
1. Maeterns G, Stuyyver L. Genotypes and genetic variation of hepatitis C cirus. Hep C Review. Dec 1998;ed 23.
2. Spach DH, Kim HN. Treatment of HCV genotype 1 (2015). www.hepatitisc.uw.edu/go/treatment-infection/treatment-genotype-1/core-concept/all. Accessed February 15, 2015.
3. Hepatitis C Technical Advisory Group. Hepatitis C genotypes and quasispecies (2005). www.hepatitis.va.gov/provider/reviews/genotypes.asp. Accessed February 15, 2015.
4. Carvalho-Filho RJ, Feldner AC, Silva AE, Ferraz ML. Management of hepatitis C in patients with chronic kidney disease. World J Gastroenterol. 2015;21(2):408-422.
5. American Association for the Study of Liver Diseases, Infectious Diseases Society of America. Recommendations for testing, managing, and treating hepatitis C. http://hcvguidelines.org. Accessed February 15, 2015.
Oh what a tangled web it weaves, this virus called hepatitis C. HCV has evolved over several thousand years into seven genotypes and multiple subtypes, making identification and treatment extremely variable.1 The genotypes are usually geographically specific, with 70% to 75% of HCV patients in the United States classed as genotype 1.2 Genotypes 2 and 3 account for most of the rest.3
While genotype does not impact the course or severity of the disease, it does affect the response to treatment. With today’s newest treatments, success rates for sustained viral response (SVR) are as high as 90% in patients with genotype 1. However, the treatment is not without cost: About $100,000 for patients without cirrhosis and even more for those with it, due to the extended length of treatment.
Chronic kidney disease (CKD) and HCV overlap in 10% to nearly 59% of the population in some geographic areas.4 Those with CKD who have had a previous kidney transplant, been on dialysis, and/or been treated prior to the introduction of epoetin alfa (Epogen®, when blood transfusions were common) are more likely to be HCV-positive.
Unfortunately, patients often convert to HCV while on hemodialysis.4 This largely represents a nosocomial infection related to parenteral exposure. In the dialysis patient, the course of HCV is more aggressive than in others, with high morbidity—often resulting from cirrhosis and/or hepatocellular carcinoma.
With new HCV drugs available, CKD patients would appear to be a prime population to treat. In order to gain marketing approval, the FDA requires testing of new drugs in patients with varying degrees of renal impairment. However, the requirement is for “moderate” CKD, defined by the FDA as a glomerular filtration rate (GFR) of at least 30 mL/min/1.73m2. The FDA does not require testing for patients with a lower GFR, or what nephrology practices refer to as stage 4 or stage 5 CKD; thus, no data are available for this population. The available pharmacokinetic data for the recently approved regimens of sofosbuvir/ledipasvir (Harvoni®) and of ombitasvir/paritaprevir/ritonavir with dasabuvir (Viekira Pak™) suggest that no dosing modifications are necessary in the moderately impaired kidney population.
Continue for the newest HCV drugs >>
The recent approvals of Harvoni and Viekira Pak are considered game-changers in the treatment of chronic HCV infection: They demonstrate that interferon is no longer always necessary. Interferon, especially in combination with ribavirin, was especially toxic for patients in the kidney failure population, although the pegylated form of interferon was less problematic. FDA approvals for Harvoni and Viekira Pak were based on clinical data demonstrating SVR rates exceeding 90%, even in traditionally difficult-to-treat populations (ie, patients with genotype 1, African-Americans, those with high viral load levels), which include many CKD patients.
The lack of clinical data in the CKD stage 4/5 population at the time of drug approval raises significant management challenges for the HCV-positive CKD patient. It is encouraging, however, that the FDA is requiring that all new medications be tested in the renally impaired population, even if not in the severely impaired groups. In the interim, and based solely on renal impairment study results for patients with GFR at or exceeding 30 mL/min/1.73m2, HCV guidelines issued jointly by the American Association for the Study of Liver Diseases and the Infectious Diseases Society of America5 include the recommendation that these new HCV medications be considered for use in the CKD population. Furthermore, there are no dosing adjustments recommended for any of the new HCV medications in stage 4 or stage 5 CKD due to lack of data. However, until more data become available, CKD patients must be managed on a case-by-case basis after consultation with a renal expert, with close attention to changes in GFR and adverse events.
When these new HCV medications are used in the general population and those with significant CKD, postmarketing reports to the FDA will be vital. Practitioners are encouraged to report adverse outcomes to the FDA MedWatch system (https://www.accessdata.fda.gov/scripts/medwatch). As any nephrology practice will tell you, we are starting to get phone calls from our hepatology colleagues asking for guidance, and the next few years will be a fascinating time for all of us. The promise of virologic cure for our HCV-positive patients is tangible and on the horizon.
REFERENCES
1. Maeterns G, Stuyyver L. Genotypes and genetic variation of hepatitis C cirus. Hep C Review. Dec 1998;ed 23.
2. Spach DH, Kim HN. Treatment of HCV genotype 1 (2015). www.hepatitisc.uw.edu/go/treatment-infection/treatment-genotype-1/core-concept/all. Accessed February 15, 2015.
3. Hepatitis C Technical Advisory Group. Hepatitis C genotypes and quasispecies (2005). www.hepatitis.va.gov/provider/reviews/genotypes.asp. Accessed February 15, 2015.
4. Carvalho-Filho RJ, Feldner AC, Silva AE, Ferraz ML. Management of hepatitis C in patients with chronic kidney disease. World J Gastroenterol. 2015;21(2):408-422.
5. American Association for the Study of Liver Diseases, Infectious Diseases Society of America. Recommendations for testing, managing, and treating hepatitis C. http://hcvguidelines.org. Accessed February 15, 2015.
Oh what a tangled web it weaves, this virus called hepatitis C. HCV has evolved over several thousand years into seven genotypes and multiple subtypes, making identification and treatment extremely variable.1 The genotypes are usually geographically specific, with 70% to 75% of HCV patients in the United States classed as genotype 1.2 Genotypes 2 and 3 account for most of the rest.3
While genotype does not impact the course or severity of the disease, it does affect the response to treatment. With today’s newest treatments, success rates for sustained viral response (SVR) are as high as 90% in patients with genotype 1. However, the treatment is not without cost: About $100,000 for patients without cirrhosis and even more for those with it, due to the extended length of treatment.
Chronic kidney disease (CKD) and HCV overlap in 10% to nearly 59% of the population in some geographic areas.4 Those with CKD who have had a previous kidney transplant, been on dialysis, and/or been treated prior to the introduction of epoetin alfa (Epogen®, when blood transfusions were common) are more likely to be HCV-positive.
Unfortunately, patients often convert to HCV while on hemodialysis.4 This largely represents a nosocomial infection related to parenteral exposure. In the dialysis patient, the course of HCV is more aggressive than in others, with high morbidity—often resulting from cirrhosis and/or hepatocellular carcinoma.
With new HCV drugs available, CKD patients would appear to be a prime population to treat. In order to gain marketing approval, the FDA requires testing of new drugs in patients with varying degrees of renal impairment. However, the requirement is for “moderate” CKD, defined by the FDA as a glomerular filtration rate (GFR) of at least 30 mL/min/1.73m2. The FDA does not require testing for patients with a lower GFR, or what nephrology practices refer to as stage 4 or stage 5 CKD; thus, no data are available for this population. The available pharmacokinetic data for the recently approved regimens of sofosbuvir/ledipasvir (Harvoni®) and of ombitasvir/paritaprevir/ritonavir with dasabuvir (Viekira Pak™) suggest that no dosing modifications are necessary in the moderately impaired kidney population.
Continue for the newest HCV drugs >>
The recent approvals of Harvoni and Viekira Pak are considered game-changers in the treatment of chronic HCV infection: They demonstrate that interferon is no longer always necessary. Interferon, especially in combination with ribavirin, was especially toxic for patients in the kidney failure population, although the pegylated form of interferon was less problematic. FDA approvals for Harvoni and Viekira Pak were based on clinical data demonstrating SVR rates exceeding 90%, even in traditionally difficult-to-treat populations (ie, patients with genotype 1, African-Americans, those with high viral load levels), which include many CKD patients.
The lack of clinical data in the CKD stage 4/5 population at the time of drug approval raises significant management challenges for the HCV-positive CKD patient. It is encouraging, however, that the FDA is requiring that all new medications be tested in the renally impaired population, even if not in the severely impaired groups. In the interim, and based solely on renal impairment study results for patients with GFR at or exceeding 30 mL/min/1.73m2, HCV guidelines issued jointly by the American Association for the Study of Liver Diseases and the Infectious Diseases Society of America5 include the recommendation that these new HCV medications be considered for use in the CKD population. Furthermore, there are no dosing adjustments recommended for any of the new HCV medications in stage 4 or stage 5 CKD due to lack of data. However, until more data become available, CKD patients must be managed on a case-by-case basis after consultation with a renal expert, with close attention to changes in GFR and adverse events.
When these new HCV medications are used in the general population and those with significant CKD, postmarketing reports to the FDA will be vital. Practitioners are encouraged to report adverse outcomes to the FDA MedWatch system (https://www.accessdata.fda.gov/scripts/medwatch). As any nephrology practice will tell you, we are starting to get phone calls from our hepatology colleagues asking for guidance, and the next few years will be a fascinating time for all of us. The promise of virologic cure for our HCV-positive patients is tangible and on the horizon.
REFERENCES
1. Maeterns G, Stuyyver L. Genotypes and genetic variation of hepatitis C cirus. Hep C Review. Dec 1998;ed 23.
2. Spach DH, Kim HN. Treatment of HCV genotype 1 (2015). www.hepatitisc.uw.edu/go/treatment-infection/treatment-genotype-1/core-concept/all. Accessed February 15, 2015.
3. Hepatitis C Technical Advisory Group. Hepatitis C genotypes and quasispecies (2005). www.hepatitis.va.gov/provider/reviews/genotypes.asp. Accessed February 15, 2015.
4. Carvalho-Filho RJ, Feldner AC, Silva AE, Ferraz ML. Management of hepatitis C in patients with chronic kidney disease. World J Gastroenterol. 2015;21(2):408-422.
5. American Association for the Study of Liver Diseases, Infectious Diseases Society of America. Recommendations for testing, managing, and treating hepatitis C. http://hcvguidelines.org. Accessed February 15, 2015.