User login
Infusing Gerontologic Practice Into PACT
The older adult population in the VA is growing. Adults aged > 85 years are the fastest growing segment of the older veteran population and many are afflicted with multiple medical problems and functional impairments.1,2 The majority of older veterans (94.6%, or about 1.9 million veterans) who seek care at the VA obtain care through primary care providers (PCPs) who are often not formally trained in geriatrics.1,3 With the increasing number of older patients, new models of care are needed to provide coordinated, comprehensive, efficient, and patient-centered care.4,5
Common themes found in successful models of care for older patients include a team approach, care management (comprehensive and coordinated), and patients who are active partners.4 These themes are reflected in the VA Patient Aligned Care Team (PACT) primary care program. PACT, a model of care that was initiated in 2010 and is built on a foundation of patient-centered care, encompasses a team approach to provide comprehensive, coordinated, and personalized care.6-8 The challenge for the VA is to integrate gerontologic principles and tools into the daily practice of all PACTs in order to improve care provided for older veterans.9
This article discusses current challenges in caring for older veterans in the VA system and recommends tools that can be used to infuse geriatric care principles into VA primary care by the PACT, to improve the quality of care provided to older veterans. In addition, the article also describes VA geriatric programs that PACT clinicians can access to supplement older veterans’ care.
Challenges of Caring for Older Veterans
One concern when caring for older veterans arises when the veteran accesses both VA and non-VA health care services to offset medication costs and obtain services not covered by Medicare or other insurance companies.2,3 This “dual care” can exacerbate polypharmacy issues and increase confusion regarding plans of care. Problems may arise when multiple providers from different systems of care prescribe medications available only within their own formulary and/or order diagnostic and laboratory tests with results available only within their own health care system.
The VA is also challenged by health care delivery for rural veterans. Thirty-six percent of all veterans live in rural areas, and they often depend on non-VA services to meet their health care needs due to difficulty traveling to the nearest VA facility.10 Seasonal residency also presents challenges. An increasing number of older veterans are seen at different VA facilities when they “winter” in a different section of the country.
Fortunately, a VA provider in one facility can access a patient’s electronic medical records in another facility, using the VA Computerized Patient Record System (CPRS). However, it is unclear to what extent busy VA PCPs use this function when seeing patients. Although individual pilot programs have shown promise, integrated electronic health records between VA and non-VA health care have not advanced to the point of sharing data or reconciling care plans (R. Rupper, personal communication, March 1, 2013).
Many PCPs and other PACT staff are not formally trained in geriatrics and may have had limited exposure to geriatric principles.3 Clinic time pressures, multiple clinical reminders (eg, vaccinations), and panel management of specific diseases make it challenging to find time to focus on complex geriatric syndromes. Current PACT performance measures also do not routinely include geriatric-specific quality of care criteria or focus on patient function (K. Shay, personal communication, February 12, 2013), a hallmark of geriatric care.8 Furthermore, with increasing complexity of the health care system and limited availability of resources, it is often time consuming to identify and collaborate with non-VA resources to ensure patients’ needs are met in their communities.
Opportunities for Improvement in Care
The VA transformation to PACTs has led to process changes in clinic workflow that may aid in addressing the aforementioned challenges in caring for older veterans. Each patient is assigned to a PCP-led team that includes a registered nurse care manager, a clinical associate, and an administrative associate. The PACT model of care has increased access to care by redesigning face-to-face visits, increasingly moving toward open access, and through the increased use of virtual access via secured e-mail, telephone visits, and telehealth.8
In addition to process changes, the VA has created new tools to assist teams in patient management. One of these is the Care Assessment Need (CAN) score, a risk stratification tool available for use by PACTs to identify patients at highest risk for hospital admission and/or death for focused care management.11 It is based on statistical prediction models of veterans enrolled in primary care, using patient characteristics and health care use information.11 Although the CAN score looks promising, more research is needed to evaluate its effectiveness in improving care for older veterans and its association with better patient functioning—an important focus in quality geriatric care.
A tool that takes into account daily function is the Vulnerable Elders Survey-13 (VES-13). As measured by the VES-13, functional ability has been shown to be a strong predictor of decline and death in older adults independent of gender or comorbidities.12 Integration of the VES-13 into the evaluation of older veterans could assist PACTs in considering patients’ current function and life expectancy in their care plans along with patient and family goals.
Another potentially useful tool for the PACT team is the SPICES mnemonic (Sleeping, Problems with feeding/eating, Incontinence or urinary problems, Confusion, Evidence of falls, and Skin breakdown).13 Although SPICES is not comprehensive, this mnemonic highlights potential problems facing older patients that may not be brought up routinely. It provides a concise, formalized format that can be used by clerks or patient support assistants as part of the check-in process.
This tool has been used successfully by the Geriatric Evaluation and Management Clinic of the South Texas Veterans Health Care System (STVHCS) to improve communication between the PCP and nurse so that pertinent patient information is relayed concisely. SPICES was helpful in identifying patients needing interventions for fall risk. In a retrospective chart review of 100 randomly selected patients aged 75 to 90 years enrolled in the clinic, a 75% reduction in falls was noted during the first year of implementation (STVHCS unpublished data, 2012).
Additional tools that focus on identifying specific geriatric syndromes are available online from the Hartford Institute for Geriatric Nursing, which provides evidence-based information and training on how to assess, evaluate, and manage common geriatric syndromes such as depression, dementia, and delirium.14 The site also includes videos on how to use common brief geriatric assessment tools that can be performed by nurses and health care associates while the patient is in the waiting room. Though promising, further research is needed to study the effects of these tools on patient, provider, and system outcomes.
Infusing quality of care indicators (QI) can play an integral role in achieving PACT goals while improving the older veterans’ quality of life. For example, polypharmacy and medication-related injuries in older adults continue to pose both a safety and economic challenge to patients and the health care system.15-17 The 2012 Beers criteria for Potentially Inappropriate Medications in Older Adults lists 53 medication classes that have been identified as potentially inappropriate medications for use in older adults.17 Use of this tool by PACTs in the development of patient care plans has the potential to reduce medication-related adverse reactions and improper prescribing.18,19
Assessing Care of Vulnerable Elders (ACOVE ) also provides QIs that are specific to vulnerable older persons.20-24 The most recent version, ACOVE-3, includes 392 QIs for 26 conditions and 14 types of care processes and covers all domains of care.20 Findings from a study applying QIs involving vulnerable elderly patients in 2 managed care programs revealed that recipients of better-quality care had a 10% higher survival rate over 3 years.25
The VA currently monitors 6 frail elderly QIs based on ACOVE criteria via reviews of medical records in veterans aged > 75 years. These QIs cover falls, incontinence, functional assessment, and the presence of a surrogate decision maker. PACT staff, unfortunately, do not receive feedback on these, because they are still QIs and not part of the performance measures (K. Shay, personal communication, February 12, 2013). Though some VA sites have adopted these QIs to some extent, until these frail elderly QIs become performance measures throughout VA, other competing priorities may be more at the forefront of quality improvement projects done by PACT teams.5
The American Geriatrics Society recently published recommendations on the care of older adults with multiple chronic conditions, to aid PCPs in practicing a more individualized, patient-centered care in complex cases.26 In addition to focusing on a patient’s primary concern during a clinic visit and eliciting preferences, considering prognosis in deciding on treatment options allows patients to better weigh the potential benefits and burdens in their daily living.26 A discussion on how aggressive potential treatments are and what the patient is willing to undertake is an important component of patient-centered care and should be incorporated during routine PACT clinic visits.
VA Geriatric Programs
It is important for PACT clinicians to be familiar with the geriatric programs and resources available within the VA medical home “neighborhood,” which can supplement care. One such resource is the Geriatric Research Education and Clinical Centers (GRECCs). There are currently 19 GRECCs throughout the nation that serve as Centers of Excellence in the care of older veterans.27 The GRECCs provide training for clinicians, test innovative ways to care for older veterans, and collaborate with other staff to improve the care provided. Some have also developed Geriatric Primary Care Clinics (or Geri PACTs) to provide team care to very frail and high-risk older veterans. Since not all VA facilities have access to Geri PACTs, the GRECCs play an important role in making geriatric expertise and training available to the PACTs.3
To address this limitation in access, VA programs have begun using telehealth technology to increase competencies of PCPs in caring for older veterans. For example, the VA Geriatric Scholars Program is a national educational program with different avenues to “geriatricize” VA primary care services and improve knowledge and care provided to older veterans.28 It consists of several subprograms: Geriatric Scholars Program for Rural Community Based Outpatient Clinics; Geriatric Scholars Program for Primary Care Providers; Rural Interdisciplinary Team Training; and the Geriatric Assessment Pocket Guide.29 These components may include didactics both face-to-face and online, clinical experience with performing common geriatric screening tools, and a quality improvement project.
Some local VAMCs have also developed programs to address this need to improve care provided to older veterans in PACT. The VA Greater Los Angeles Healthcare System (GLA) GRECC, for example, has started several programs to infuse geriatrics into PACTs, including the Geri Specialty Care Access Network-Extension for Community Healthcare Outcomes (SCAN-ECHO). VA SCAN-ECHO was developed to increase access to specialty care in rural/underserved areas. The PCP presents a case and a specialty provider gives guidance in the assessment and/or management of a specific clinical problem.30 Unlike many other SCAN-ECHO programs, the GLA Geri SCAN-ECHO program encourages not only PCPs, but also nurses and social workers to submit consults for discussion and encourages team management (a hallmark of quality geriatric care). Another important GLA GRECC project is the Veterans Cognitive Assessment and Management Program (V-CAMP), which uses videoconferencing to assess and manage veterans with cognitive impairment/dementia who reside in underserved areas in the GLA region. The program provides dementia care management and access to neuropsychological examinations—services that are often not available in rural areas.31
Various VA program offices have also published useful resources to help PACT clinicians infuse gerontologic principles into their practice. The VA Office of Nursing Services has a Geriatrics and Extended Care Field Advisory Committee, which recently produced on-demand lectures in the virtual VA eHealth University (also known as myVeHU campus) on improving the PACT’s management of progressive chronic diseases and dementia recognition and initial evaluation. They also produced a resource guide for VA clinicians (nursing and non-nursing), based on a team consensus of what the workgroup thinks a clinician would find helpful in clinical practice to improve care of older veterans. The VA Office of Geriatrics and Extended Care Service also identified a list of clinical and educational resources to help PACT clinicians. These include the Geriatrics Evaluation and management (GEM) Tools Booklet (http://geriatricscareonline.org) and a SharePoint site to improve dementia care in all settings.
The VA Office of Geriatrics and Extended Care provides additional geriatric-specific programs (http://va.gov/geriatrics). These programs may be useful for consultation and collaboration for patients whom the PACT teams have found to be more challenging and require more assistance to meet performance measures and patient needs. A recent evidence synthesis notes that direct involvement of geriatricians (as opposed to indirect care with limited contact) is more likely to result in positive patient outcomes and should be considered for those patients who are the most frail and/or high utilizers of services.32
Conclusion
The PACT initiative in the VA health care system may prove to be an important vehicle for improving and standardizing the care provided to older veterans. Use of reliable and valid tools in the identification and assessment of geriatric syndromes, provision of quality standards, and use of innovative telehealth practices are promising enhancements for the primary care of older veterans.
Acknowledgements
We would like to thank the following contributors for their thoughtful review of the initial drafts of this article: Dr. Balmatee Bidassie; Dr. Kathryn Corrigan; Dr. Gail McNut; Dr. Linda Kinsinger, chief consultant for preventive medicine in the Office of Patient Care Services; Dr. Theodore Hahn, GRECC deputy director from VA Greater Los Angeles Healthcare System; Dr. James Hallenbeck, associate chief of staff, Extended Care at VA Palo Alto Health Care System; Ms. Storm Morgan, VA Office of Nursing Services PACT program manager; and Dr. Kenneth Shay, director of Geriatric Programs for the VA Office of Geriatrics and Extended Care.
The authors also would like to express their gratitude to the VA Office of Nursing Services, Clinical Practice Program, Geriatrics and Extended Care Field Advisory Committee for the opportunity to work on this manuscript.
Author disclosures
The authors report no actual or potential conflicts of interest with regard to this article.
Disclaimer
The opinions expressed herein are those of the authors and do not necessarily reflect those of Federal Practitioner, Frontline Medical Communications Inc., the U.S. Government, or any of its agencies. This article may discuss unlabeled or investigational use of certain drugs. Please review the complete prescribing information for specific drugs or drug combinations—including indications, contraindications, warnings, and adverse effects—before administering pharmacologic therapy to patients.
1. U.S. Department of Veterans Affairs. Geriatric Ambulatory Care. VHA Handbook 1140.10. U.S. Department of Veterans Affairs Website. http://www.va.gov/vhapublications/ViewPublication.asp?pub_ID=2202. Published April 26, 2010. Accessed September 29, 2014.
2. Federal Interagency Forum on Aging-Related Statistics. Older Americans 2012: Key indicators of well-being. AgingStats.gov Website. http://www.agingstats.gov/agingstatsdotnet/main_site/default.aspx. Accessed September 29, 2014.
3. Shay K, Schectman G. Primary care for older veterans. Generations. 2010;34(2):35-42.
4. Institute of Medicine. Retooling for an Aging America: Building the Health Care Workforce. Washington, DC: The National Academies Press; 2008.
5. Shay K, Hyduke B, Burris JF. Strategic plan for geriatrics and extended care in the veterans health administration: Background, plan, and progress to date. J Am Geriatr Soc. 2013;61(4):632-638.
6. Berenson RA, Devers KJ, Burton RA. Will the patient-centered medical home transform the delivery of health care? Timely analysis of immediate health policy issues. Urban Institute Website. http://www.urban.org/uploadedpdf/412373-will-patient-centered-medical-home-transform-delivery-health-care.pdf. Published August 2011. Accessed September 29, 2014.
7. U.S. Department of Veterans Affairs. VA Primary Care Services. Patient-centered medical home model concept paper. U.S. Department of Veterans Affairs Website. http://www.va.gov/health/services/PrimaryCare/docs/pcmh_ConceptPaper.doc. Accessed October 7, 2014.
8. VA Undersecretary for Health. What is PACT? U.S. Department of Veterans Affairs Website http://www.va.gov/health/services/primarycare/pact/index.asp. Updated February 18, 2014. Accessed October 7, 2014.
9. Askari M, Wierenga PC, Eslami S, Medlock S, de Rooij SE, Abu-Hanna A. Assessing quality of care of elderly patients using the ACOVE quality indicator set: A systematic review. PLoS ONE. 2011;6(12):e28631.
10. U.S. Department of Veterans Affairs. Office of Rural Health. About the office of rural health. U.S. Department of Veterans Affairs Website. http://www.ruralhealth.va.gov/about/index.asp. Update June 12, 2014. Accessed October 10, 2014.
11. Schectman G, Stark R, Fihn S, VanEe H, Box T. Care assessment need score: A tool for care management. Presented on March 29, 2012. http://www.myvehucampus.com/#loc=auditoriumRoom. Accessed October 14, 2014.
12. Min L, Yoon W, Mariano J, et al. The vulnerable elders-13 survey predicts 5-year functional decline and mortality outcomes in older ambulatory care patients. J Am Geriatr Soc. 2009;57(11):2070-2076.
13. Fulmer T, Wallace M. Fulmer SPICES: An overall assessment tool for older adults. http://consultgerirn.org/uploads/File/trythis/try_this_1.pdf. Revised 2012. Accessed October 1, 2014.
14. Hartford Institute for Geriatric Nursing. ConsultGeriRN.org Website. http://consultgerirn.org. Accessed September 30, 2014.
15. Opondo D, Eslami S, Visscher S, et al. Inappropriateness of medication prescriptions to elderly patients in the primary care setting: A systemic Review. PLoS One. 2012;7(8):e43617.
16. Fick DM, Cooper JW, Wade WE, Waller JL, Maclean JR, Beers MH. Updating the Beers criteria for potentially inappropriate medication use in older adults: Results of a US consensus panel of experts. Arch Intern Med. 2003;163(22):2716-2724.
17. The American Geriatrics Society 2012 Beers Criteria Update Expert Panel. American Geriatrics Society updated Beers criteria for potentially inappropriate medication use in older adults. J Am Geriatr Soc. 2012;60(4):616-631.
18. Higashi T, Shekelle PG, Solomon DH, et al. The quality of pharmacologic care for vulnerable older patients. Ann Intern Med. 2004;140(9):714-720.
19. Lund BC, Steinman MA, Chrischilles EA, Kaboli PJ. Beers criteria as a proxy for inappropriate prescribing of other medications among older adults. Ann Pharmacother. 2011;45(11):1363-1370.
20. RAND. Assessing care of vulnerable elders. Quality indicators- ACOVE 3. RAND Website. http://www.rand.org/health/projects/acove/acove3.html. Accessed October 7, 2014.
21. Wenger NS, Shekelle PG. Assessing care of vulnerable elders: ACOVE project overview. Ann Intern Med. 2001;135(8, pt 2):642-646.
22. Shekelle PG, MacLean CH, Morton SC, Wenger NS. Assessing care of vulnerable elders: Methods for developing quality indicators. Ann Intern Med. 2001;135(8, pt 2):647-652.
23. Reuben DB, Roth C, Kamberg C, Wenger NS. Restructuring primary care practices to manage geriatric syndromes: The ACOVE-2 intervention. J Am Geriatr Soc. 2003;51(12):1787-1793.
24. Wenger NS, Roth CP, Shekelle P; ACOVE Investigators. Introduction to the assessing care of vulnerable elders-3 quality indicator measurement set. J Am Geriatr Soc. 2007;55(suppl 2):S247-S252.
25. Higashi T, Shekelle PG, Solomon DH, et al. The quality of pharmacologic care for vulnerable older patients. Ann Intern Med. 2004;140(9):714-720.
26. American Geriatrics Society Expert Panel on the Care of Older Adults with Multimorbidity. Patient-centered care for older adults with multiple chronic conditions: A stepwise approach from the American Geriatrics Society. J Am Geriatr Soc. 2012;60(10):1957-1968.
27. U.S. Department of Veterans Affairs. Geriatric Research Education and Clinical Centers. GRECC. U.S. Department of Veterans Affairs Website. http://www.va.gov/GRECC/index.asp . Updated August 17, 2012. Accessed October 10, 2014.
28. Tumosa N, Horvath KJ, Huh T, et al. Health care workforce development in rural America: When geriatrics expertise is 100 miles away. Gerontol Geriatr Educ. 2012;33(2):133-151.
29. U.S. Department of Veterans Affairs. Geriatric Research Education and Clinical Centers. The VA Geriatrics Scholars Program. U.S. Department of Veterans Affairs Website. http://www.va.gov/GRECC/GRECC_Educational_Events_and_Products.asp. Updated February 21, 2013. Accessed October 1, 2014.
30. U.S. Department of Veterans Affairs. Office of Public and Intergovernmental Affairs. VA uses technology to provide rural veterans greater access to specialty care services. U.S. Department of Veterans Affairs Website. http://www.va.gov/opa/pressrel/pressrelease.cfm?id=2353. Updated July 10, 2012. Accessed October 1, 2014.
31. Harrell KM, Wilkins SS, Connor MK, Chodosh J. Telemedicine and the evaluation of cognitive impairment: The additive value of neuropsychological assessment. J Am Med Dir Assoc. 2014;15(8):600-606.
32. Totten A, Carson S, Peterson K, Low A, Christense V, Tiwari A. Evidence brief: Effect of geriatricians on outcomes of inpatient and outpatient care, VA-ESP Project #09-199. U.S. Department of Veterans Affairs Website. http://www.hsrd.research.va.gov/publications/esp/Geriatricians.pdf. Accessed October 1, 2014.
The older adult population in the VA is growing. Adults aged > 85 years are the fastest growing segment of the older veteran population and many are afflicted with multiple medical problems and functional impairments.1,2 The majority of older veterans (94.6%, or about 1.9 million veterans) who seek care at the VA obtain care through primary care providers (PCPs) who are often not formally trained in geriatrics.1,3 With the increasing number of older patients, new models of care are needed to provide coordinated, comprehensive, efficient, and patient-centered care.4,5
Common themes found in successful models of care for older patients include a team approach, care management (comprehensive and coordinated), and patients who are active partners.4 These themes are reflected in the VA Patient Aligned Care Team (PACT) primary care program. PACT, a model of care that was initiated in 2010 and is built on a foundation of patient-centered care, encompasses a team approach to provide comprehensive, coordinated, and personalized care.6-8 The challenge for the VA is to integrate gerontologic principles and tools into the daily practice of all PACTs in order to improve care provided for older veterans.9
This article discusses current challenges in caring for older veterans in the VA system and recommends tools that can be used to infuse geriatric care principles into VA primary care by the PACT, to improve the quality of care provided to older veterans. In addition, the article also describes VA geriatric programs that PACT clinicians can access to supplement older veterans’ care.
Challenges of Caring for Older Veterans
One concern when caring for older veterans arises when the veteran accesses both VA and non-VA health care services to offset medication costs and obtain services not covered by Medicare or other insurance companies.2,3 This “dual care” can exacerbate polypharmacy issues and increase confusion regarding plans of care. Problems may arise when multiple providers from different systems of care prescribe medications available only within their own formulary and/or order diagnostic and laboratory tests with results available only within their own health care system.
The VA is also challenged by health care delivery for rural veterans. Thirty-six percent of all veterans live in rural areas, and they often depend on non-VA services to meet their health care needs due to difficulty traveling to the nearest VA facility.10 Seasonal residency also presents challenges. An increasing number of older veterans are seen at different VA facilities when they “winter” in a different section of the country.
Fortunately, a VA provider in one facility can access a patient’s electronic medical records in another facility, using the VA Computerized Patient Record System (CPRS). However, it is unclear to what extent busy VA PCPs use this function when seeing patients. Although individual pilot programs have shown promise, integrated electronic health records between VA and non-VA health care have not advanced to the point of sharing data or reconciling care plans (R. Rupper, personal communication, March 1, 2013).
Many PCPs and other PACT staff are not formally trained in geriatrics and may have had limited exposure to geriatric principles.3 Clinic time pressures, multiple clinical reminders (eg, vaccinations), and panel management of specific diseases make it challenging to find time to focus on complex geriatric syndromes. Current PACT performance measures also do not routinely include geriatric-specific quality of care criteria or focus on patient function (K. Shay, personal communication, February 12, 2013), a hallmark of geriatric care.8 Furthermore, with increasing complexity of the health care system and limited availability of resources, it is often time consuming to identify and collaborate with non-VA resources to ensure patients’ needs are met in their communities.
Opportunities for Improvement in Care
The VA transformation to PACTs has led to process changes in clinic workflow that may aid in addressing the aforementioned challenges in caring for older veterans. Each patient is assigned to a PCP-led team that includes a registered nurse care manager, a clinical associate, and an administrative associate. The PACT model of care has increased access to care by redesigning face-to-face visits, increasingly moving toward open access, and through the increased use of virtual access via secured e-mail, telephone visits, and telehealth.8
In addition to process changes, the VA has created new tools to assist teams in patient management. One of these is the Care Assessment Need (CAN) score, a risk stratification tool available for use by PACTs to identify patients at highest risk for hospital admission and/or death for focused care management.11 It is based on statistical prediction models of veterans enrolled in primary care, using patient characteristics and health care use information.11 Although the CAN score looks promising, more research is needed to evaluate its effectiveness in improving care for older veterans and its association with better patient functioning—an important focus in quality geriatric care.
A tool that takes into account daily function is the Vulnerable Elders Survey-13 (VES-13). As measured by the VES-13, functional ability has been shown to be a strong predictor of decline and death in older adults independent of gender or comorbidities.12 Integration of the VES-13 into the evaluation of older veterans could assist PACTs in considering patients’ current function and life expectancy in their care plans along with patient and family goals.
Another potentially useful tool for the PACT team is the SPICES mnemonic (Sleeping, Problems with feeding/eating, Incontinence or urinary problems, Confusion, Evidence of falls, and Skin breakdown).13 Although SPICES is not comprehensive, this mnemonic highlights potential problems facing older patients that may not be brought up routinely. It provides a concise, formalized format that can be used by clerks or patient support assistants as part of the check-in process.
This tool has been used successfully by the Geriatric Evaluation and Management Clinic of the South Texas Veterans Health Care System (STVHCS) to improve communication between the PCP and nurse so that pertinent patient information is relayed concisely. SPICES was helpful in identifying patients needing interventions for fall risk. In a retrospective chart review of 100 randomly selected patients aged 75 to 90 years enrolled in the clinic, a 75% reduction in falls was noted during the first year of implementation (STVHCS unpublished data, 2012).
Additional tools that focus on identifying specific geriatric syndromes are available online from the Hartford Institute for Geriatric Nursing, which provides evidence-based information and training on how to assess, evaluate, and manage common geriatric syndromes such as depression, dementia, and delirium.14 The site also includes videos on how to use common brief geriatric assessment tools that can be performed by nurses and health care associates while the patient is in the waiting room. Though promising, further research is needed to study the effects of these tools on patient, provider, and system outcomes.
Infusing quality of care indicators (QI) can play an integral role in achieving PACT goals while improving the older veterans’ quality of life. For example, polypharmacy and medication-related injuries in older adults continue to pose both a safety and economic challenge to patients and the health care system.15-17 The 2012 Beers criteria for Potentially Inappropriate Medications in Older Adults lists 53 medication classes that have been identified as potentially inappropriate medications for use in older adults.17 Use of this tool by PACTs in the development of patient care plans has the potential to reduce medication-related adverse reactions and improper prescribing.18,19
Assessing Care of Vulnerable Elders (ACOVE ) also provides QIs that are specific to vulnerable older persons.20-24 The most recent version, ACOVE-3, includes 392 QIs for 26 conditions and 14 types of care processes and covers all domains of care.20 Findings from a study applying QIs involving vulnerable elderly patients in 2 managed care programs revealed that recipients of better-quality care had a 10% higher survival rate over 3 years.25
The VA currently monitors 6 frail elderly QIs based on ACOVE criteria via reviews of medical records in veterans aged > 75 years. These QIs cover falls, incontinence, functional assessment, and the presence of a surrogate decision maker. PACT staff, unfortunately, do not receive feedback on these, because they are still QIs and not part of the performance measures (K. Shay, personal communication, February 12, 2013). Though some VA sites have adopted these QIs to some extent, until these frail elderly QIs become performance measures throughout VA, other competing priorities may be more at the forefront of quality improvement projects done by PACT teams.5
The American Geriatrics Society recently published recommendations on the care of older adults with multiple chronic conditions, to aid PCPs in practicing a more individualized, patient-centered care in complex cases.26 In addition to focusing on a patient’s primary concern during a clinic visit and eliciting preferences, considering prognosis in deciding on treatment options allows patients to better weigh the potential benefits and burdens in their daily living.26 A discussion on how aggressive potential treatments are and what the patient is willing to undertake is an important component of patient-centered care and should be incorporated during routine PACT clinic visits.
VA Geriatric Programs
It is important for PACT clinicians to be familiar with the geriatric programs and resources available within the VA medical home “neighborhood,” which can supplement care. One such resource is the Geriatric Research Education and Clinical Centers (GRECCs). There are currently 19 GRECCs throughout the nation that serve as Centers of Excellence in the care of older veterans.27 The GRECCs provide training for clinicians, test innovative ways to care for older veterans, and collaborate with other staff to improve the care provided. Some have also developed Geriatric Primary Care Clinics (or Geri PACTs) to provide team care to very frail and high-risk older veterans. Since not all VA facilities have access to Geri PACTs, the GRECCs play an important role in making geriatric expertise and training available to the PACTs.3
To address this limitation in access, VA programs have begun using telehealth technology to increase competencies of PCPs in caring for older veterans. For example, the VA Geriatric Scholars Program is a national educational program with different avenues to “geriatricize” VA primary care services and improve knowledge and care provided to older veterans.28 It consists of several subprograms: Geriatric Scholars Program for Rural Community Based Outpatient Clinics; Geriatric Scholars Program for Primary Care Providers; Rural Interdisciplinary Team Training; and the Geriatric Assessment Pocket Guide.29 These components may include didactics both face-to-face and online, clinical experience with performing common geriatric screening tools, and a quality improvement project.
Some local VAMCs have also developed programs to address this need to improve care provided to older veterans in PACT. The VA Greater Los Angeles Healthcare System (GLA) GRECC, for example, has started several programs to infuse geriatrics into PACTs, including the Geri Specialty Care Access Network-Extension for Community Healthcare Outcomes (SCAN-ECHO). VA SCAN-ECHO was developed to increase access to specialty care in rural/underserved areas. The PCP presents a case and a specialty provider gives guidance in the assessment and/or management of a specific clinical problem.30 Unlike many other SCAN-ECHO programs, the GLA Geri SCAN-ECHO program encourages not only PCPs, but also nurses and social workers to submit consults for discussion and encourages team management (a hallmark of quality geriatric care). Another important GLA GRECC project is the Veterans Cognitive Assessment and Management Program (V-CAMP), which uses videoconferencing to assess and manage veterans with cognitive impairment/dementia who reside in underserved areas in the GLA region. The program provides dementia care management and access to neuropsychological examinations—services that are often not available in rural areas.31
Various VA program offices have also published useful resources to help PACT clinicians infuse gerontologic principles into their practice. The VA Office of Nursing Services has a Geriatrics and Extended Care Field Advisory Committee, which recently produced on-demand lectures in the virtual VA eHealth University (also known as myVeHU campus) on improving the PACT’s management of progressive chronic diseases and dementia recognition and initial evaluation. They also produced a resource guide for VA clinicians (nursing and non-nursing), based on a team consensus of what the workgroup thinks a clinician would find helpful in clinical practice to improve care of older veterans. The VA Office of Geriatrics and Extended Care Service also identified a list of clinical and educational resources to help PACT clinicians. These include the Geriatrics Evaluation and management (GEM) Tools Booklet (http://geriatricscareonline.org) and a SharePoint site to improve dementia care in all settings.
The VA Office of Geriatrics and Extended Care provides additional geriatric-specific programs (http://va.gov/geriatrics). These programs may be useful for consultation and collaboration for patients whom the PACT teams have found to be more challenging and require more assistance to meet performance measures and patient needs. A recent evidence synthesis notes that direct involvement of geriatricians (as opposed to indirect care with limited contact) is more likely to result in positive patient outcomes and should be considered for those patients who are the most frail and/or high utilizers of services.32
Conclusion
The PACT initiative in the VA health care system may prove to be an important vehicle for improving and standardizing the care provided to older veterans. Use of reliable and valid tools in the identification and assessment of geriatric syndromes, provision of quality standards, and use of innovative telehealth practices are promising enhancements for the primary care of older veterans.
Acknowledgements
We would like to thank the following contributors for their thoughtful review of the initial drafts of this article: Dr. Balmatee Bidassie; Dr. Kathryn Corrigan; Dr. Gail McNut; Dr. Linda Kinsinger, chief consultant for preventive medicine in the Office of Patient Care Services; Dr. Theodore Hahn, GRECC deputy director from VA Greater Los Angeles Healthcare System; Dr. James Hallenbeck, associate chief of staff, Extended Care at VA Palo Alto Health Care System; Ms. Storm Morgan, VA Office of Nursing Services PACT program manager; and Dr. Kenneth Shay, director of Geriatric Programs for the VA Office of Geriatrics and Extended Care.
The authors also would like to express their gratitude to the VA Office of Nursing Services, Clinical Practice Program, Geriatrics and Extended Care Field Advisory Committee for the opportunity to work on this manuscript.
Author disclosures
The authors report no actual or potential conflicts of interest with regard to this article.
Disclaimer
The opinions expressed herein are those of the authors and do not necessarily reflect those of Federal Practitioner, Frontline Medical Communications Inc., the U.S. Government, or any of its agencies. This article may discuss unlabeled or investigational use of certain drugs. Please review the complete prescribing information for specific drugs or drug combinations—including indications, contraindications, warnings, and adverse effects—before administering pharmacologic therapy to patients.
The older adult population in the VA is growing. Adults aged > 85 years are the fastest growing segment of the older veteran population and many are afflicted with multiple medical problems and functional impairments.1,2 The majority of older veterans (94.6%, or about 1.9 million veterans) who seek care at the VA obtain care through primary care providers (PCPs) who are often not formally trained in geriatrics.1,3 With the increasing number of older patients, new models of care are needed to provide coordinated, comprehensive, efficient, and patient-centered care.4,5
Common themes found in successful models of care for older patients include a team approach, care management (comprehensive and coordinated), and patients who are active partners.4 These themes are reflected in the VA Patient Aligned Care Team (PACT) primary care program. PACT, a model of care that was initiated in 2010 and is built on a foundation of patient-centered care, encompasses a team approach to provide comprehensive, coordinated, and personalized care.6-8 The challenge for the VA is to integrate gerontologic principles and tools into the daily practice of all PACTs in order to improve care provided for older veterans.9
This article discusses current challenges in caring for older veterans in the VA system and recommends tools that can be used to infuse geriatric care principles into VA primary care by the PACT, to improve the quality of care provided to older veterans. In addition, the article also describes VA geriatric programs that PACT clinicians can access to supplement older veterans’ care.
Challenges of Caring for Older Veterans
One concern when caring for older veterans arises when the veteran accesses both VA and non-VA health care services to offset medication costs and obtain services not covered by Medicare or other insurance companies.2,3 This “dual care” can exacerbate polypharmacy issues and increase confusion regarding plans of care. Problems may arise when multiple providers from different systems of care prescribe medications available only within their own formulary and/or order diagnostic and laboratory tests with results available only within their own health care system.
The VA is also challenged by health care delivery for rural veterans. Thirty-six percent of all veterans live in rural areas, and they often depend on non-VA services to meet their health care needs due to difficulty traveling to the nearest VA facility.10 Seasonal residency also presents challenges. An increasing number of older veterans are seen at different VA facilities when they “winter” in a different section of the country.
Fortunately, a VA provider in one facility can access a patient’s electronic medical records in another facility, using the VA Computerized Patient Record System (CPRS). However, it is unclear to what extent busy VA PCPs use this function when seeing patients. Although individual pilot programs have shown promise, integrated electronic health records between VA and non-VA health care have not advanced to the point of sharing data or reconciling care plans (R. Rupper, personal communication, March 1, 2013).
Many PCPs and other PACT staff are not formally trained in geriatrics and may have had limited exposure to geriatric principles.3 Clinic time pressures, multiple clinical reminders (eg, vaccinations), and panel management of specific diseases make it challenging to find time to focus on complex geriatric syndromes. Current PACT performance measures also do not routinely include geriatric-specific quality of care criteria or focus on patient function (K. Shay, personal communication, February 12, 2013), a hallmark of geriatric care.8 Furthermore, with increasing complexity of the health care system and limited availability of resources, it is often time consuming to identify and collaborate with non-VA resources to ensure patients’ needs are met in their communities.
Opportunities for Improvement in Care
The VA transformation to PACTs has led to process changes in clinic workflow that may aid in addressing the aforementioned challenges in caring for older veterans. Each patient is assigned to a PCP-led team that includes a registered nurse care manager, a clinical associate, and an administrative associate. The PACT model of care has increased access to care by redesigning face-to-face visits, increasingly moving toward open access, and through the increased use of virtual access via secured e-mail, telephone visits, and telehealth.8
In addition to process changes, the VA has created new tools to assist teams in patient management. One of these is the Care Assessment Need (CAN) score, a risk stratification tool available for use by PACTs to identify patients at highest risk for hospital admission and/or death for focused care management.11 It is based on statistical prediction models of veterans enrolled in primary care, using patient characteristics and health care use information.11 Although the CAN score looks promising, more research is needed to evaluate its effectiveness in improving care for older veterans and its association with better patient functioning—an important focus in quality geriatric care.
A tool that takes into account daily function is the Vulnerable Elders Survey-13 (VES-13). As measured by the VES-13, functional ability has been shown to be a strong predictor of decline and death in older adults independent of gender or comorbidities.12 Integration of the VES-13 into the evaluation of older veterans could assist PACTs in considering patients’ current function and life expectancy in their care plans along with patient and family goals.
Another potentially useful tool for the PACT team is the SPICES mnemonic (Sleeping, Problems with feeding/eating, Incontinence or urinary problems, Confusion, Evidence of falls, and Skin breakdown).13 Although SPICES is not comprehensive, this mnemonic highlights potential problems facing older patients that may not be brought up routinely. It provides a concise, formalized format that can be used by clerks or patient support assistants as part of the check-in process.
This tool has been used successfully by the Geriatric Evaluation and Management Clinic of the South Texas Veterans Health Care System (STVHCS) to improve communication between the PCP and nurse so that pertinent patient information is relayed concisely. SPICES was helpful in identifying patients needing interventions for fall risk. In a retrospective chart review of 100 randomly selected patients aged 75 to 90 years enrolled in the clinic, a 75% reduction in falls was noted during the first year of implementation (STVHCS unpublished data, 2012).
Additional tools that focus on identifying specific geriatric syndromes are available online from the Hartford Institute for Geriatric Nursing, which provides evidence-based information and training on how to assess, evaluate, and manage common geriatric syndromes such as depression, dementia, and delirium.14 The site also includes videos on how to use common brief geriatric assessment tools that can be performed by nurses and health care associates while the patient is in the waiting room. Though promising, further research is needed to study the effects of these tools on patient, provider, and system outcomes.
Infusing quality of care indicators (QI) can play an integral role in achieving PACT goals while improving the older veterans’ quality of life. For example, polypharmacy and medication-related injuries in older adults continue to pose both a safety and economic challenge to patients and the health care system.15-17 The 2012 Beers criteria for Potentially Inappropriate Medications in Older Adults lists 53 medication classes that have been identified as potentially inappropriate medications for use in older adults.17 Use of this tool by PACTs in the development of patient care plans has the potential to reduce medication-related adverse reactions and improper prescribing.18,19
Assessing Care of Vulnerable Elders (ACOVE ) also provides QIs that are specific to vulnerable older persons.20-24 The most recent version, ACOVE-3, includes 392 QIs for 26 conditions and 14 types of care processes and covers all domains of care.20 Findings from a study applying QIs involving vulnerable elderly patients in 2 managed care programs revealed that recipients of better-quality care had a 10% higher survival rate over 3 years.25
The VA currently monitors 6 frail elderly QIs based on ACOVE criteria via reviews of medical records in veterans aged > 75 years. These QIs cover falls, incontinence, functional assessment, and the presence of a surrogate decision maker. PACT staff, unfortunately, do not receive feedback on these, because they are still QIs and not part of the performance measures (K. Shay, personal communication, February 12, 2013). Though some VA sites have adopted these QIs to some extent, until these frail elderly QIs become performance measures throughout VA, other competing priorities may be more at the forefront of quality improvement projects done by PACT teams.5
The American Geriatrics Society recently published recommendations on the care of older adults with multiple chronic conditions, to aid PCPs in practicing a more individualized, patient-centered care in complex cases.26 In addition to focusing on a patient’s primary concern during a clinic visit and eliciting preferences, considering prognosis in deciding on treatment options allows patients to better weigh the potential benefits and burdens in their daily living.26 A discussion on how aggressive potential treatments are and what the patient is willing to undertake is an important component of patient-centered care and should be incorporated during routine PACT clinic visits.
VA Geriatric Programs
It is important for PACT clinicians to be familiar with the geriatric programs and resources available within the VA medical home “neighborhood,” which can supplement care. One such resource is the Geriatric Research Education and Clinical Centers (GRECCs). There are currently 19 GRECCs throughout the nation that serve as Centers of Excellence in the care of older veterans.27 The GRECCs provide training for clinicians, test innovative ways to care for older veterans, and collaborate with other staff to improve the care provided. Some have also developed Geriatric Primary Care Clinics (or Geri PACTs) to provide team care to very frail and high-risk older veterans. Since not all VA facilities have access to Geri PACTs, the GRECCs play an important role in making geriatric expertise and training available to the PACTs.3
To address this limitation in access, VA programs have begun using telehealth technology to increase competencies of PCPs in caring for older veterans. For example, the VA Geriatric Scholars Program is a national educational program with different avenues to “geriatricize” VA primary care services and improve knowledge and care provided to older veterans.28 It consists of several subprograms: Geriatric Scholars Program for Rural Community Based Outpatient Clinics; Geriatric Scholars Program for Primary Care Providers; Rural Interdisciplinary Team Training; and the Geriatric Assessment Pocket Guide.29 These components may include didactics both face-to-face and online, clinical experience with performing common geriatric screening tools, and a quality improvement project.
Some local VAMCs have also developed programs to address this need to improve care provided to older veterans in PACT. The VA Greater Los Angeles Healthcare System (GLA) GRECC, for example, has started several programs to infuse geriatrics into PACTs, including the Geri Specialty Care Access Network-Extension for Community Healthcare Outcomes (SCAN-ECHO). VA SCAN-ECHO was developed to increase access to specialty care in rural/underserved areas. The PCP presents a case and a specialty provider gives guidance in the assessment and/or management of a specific clinical problem.30 Unlike many other SCAN-ECHO programs, the GLA Geri SCAN-ECHO program encourages not only PCPs, but also nurses and social workers to submit consults for discussion and encourages team management (a hallmark of quality geriatric care). Another important GLA GRECC project is the Veterans Cognitive Assessment and Management Program (V-CAMP), which uses videoconferencing to assess and manage veterans with cognitive impairment/dementia who reside in underserved areas in the GLA region. The program provides dementia care management and access to neuropsychological examinations—services that are often not available in rural areas.31
Various VA program offices have also published useful resources to help PACT clinicians infuse gerontologic principles into their practice. The VA Office of Nursing Services has a Geriatrics and Extended Care Field Advisory Committee, which recently produced on-demand lectures in the virtual VA eHealth University (also known as myVeHU campus) on improving the PACT’s management of progressive chronic diseases and dementia recognition and initial evaluation. They also produced a resource guide for VA clinicians (nursing and non-nursing), based on a team consensus of what the workgroup thinks a clinician would find helpful in clinical practice to improve care of older veterans. The VA Office of Geriatrics and Extended Care Service also identified a list of clinical and educational resources to help PACT clinicians. These include the Geriatrics Evaluation and management (GEM) Tools Booklet (http://geriatricscareonline.org) and a SharePoint site to improve dementia care in all settings.
The VA Office of Geriatrics and Extended Care provides additional geriatric-specific programs (http://va.gov/geriatrics). These programs may be useful for consultation and collaboration for patients whom the PACT teams have found to be more challenging and require more assistance to meet performance measures and patient needs. A recent evidence synthesis notes that direct involvement of geriatricians (as opposed to indirect care with limited contact) is more likely to result in positive patient outcomes and should be considered for those patients who are the most frail and/or high utilizers of services.32
Conclusion
The PACT initiative in the VA health care system may prove to be an important vehicle for improving and standardizing the care provided to older veterans. Use of reliable and valid tools in the identification and assessment of geriatric syndromes, provision of quality standards, and use of innovative telehealth practices are promising enhancements for the primary care of older veterans.
Acknowledgements
We would like to thank the following contributors for their thoughtful review of the initial drafts of this article: Dr. Balmatee Bidassie; Dr. Kathryn Corrigan; Dr. Gail McNut; Dr. Linda Kinsinger, chief consultant for preventive medicine in the Office of Patient Care Services; Dr. Theodore Hahn, GRECC deputy director from VA Greater Los Angeles Healthcare System; Dr. James Hallenbeck, associate chief of staff, Extended Care at VA Palo Alto Health Care System; Ms. Storm Morgan, VA Office of Nursing Services PACT program manager; and Dr. Kenneth Shay, director of Geriatric Programs for the VA Office of Geriatrics and Extended Care.
The authors also would like to express their gratitude to the VA Office of Nursing Services, Clinical Practice Program, Geriatrics and Extended Care Field Advisory Committee for the opportunity to work on this manuscript.
Author disclosures
The authors report no actual or potential conflicts of interest with regard to this article.
Disclaimer
The opinions expressed herein are those of the authors and do not necessarily reflect those of Federal Practitioner, Frontline Medical Communications Inc., the U.S. Government, or any of its agencies. This article may discuss unlabeled or investigational use of certain drugs. Please review the complete prescribing information for specific drugs or drug combinations—including indications, contraindications, warnings, and adverse effects—before administering pharmacologic therapy to patients.
1. U.S. Department of Veterans Affairs. Geriatric Ambulatory Care. VHA Handbook 1140.10. U.S. Department of Veterans Affairs Website. http://www.va.gov/vhapublications/ViewPublication.asp?pub_ID=2202. Published April 26, 2010. Accessed September 29, 2014.
2. Federal Interagency Forum on Aging-Related Statistics. Older Americans 2012: Key indicators of well-being. AgingStats.gov Website. http://www.agingstats.gov/agingstatsdotnet/main_site/default.aspx. Accessed September 29, 2014.
3. Shay K, Schectman G. Primary care for older veterans. Generations. 2010;34(2):35-42.
4. Institute of Medicine. Retooling for an Aging America: Building the Health Care Workforce. Washington, DC: The National Academies Press; 2008.
5. Shay K, Hyduke B, Burris JF. Strategic plan for geriatrics and extended care in the veterans health administration: Background, plan, and progress to date. J Am Geriatr Soc. 2013;61(4):632-638.
6. Berenson RA, Devers KJ, Burton RA. Will the patient-centered medical home transform the delivery of health care? Timely analysis of immediate health policy issues. Urban Institute Website. http://www.urban.org/uploadedpdf/412373-will-patient-centered-medical-home-transform-delivery-health-care.pdf. Published August 2011. Accessed September 29, 2014.
7. U.S. Department of Veterans Affairs. VA Primary Care Services. Patient-centered medical home model concept paper. U.S. Department of Veterans Affairs Website. http://www.va.gov/health/services/PrimaryCare/docs/pcmh_ConceptPaper.doc. Accessed October 7, 2014.
8. VA Undersecretary for Health. What is PACT? U.S. Department of Veterans Affairs Website http://www.va.gov/health/services/primarycare/pact/index.asp. Updated February 18, 2014. Accessed October 7, 2014.
9. Askari M, Wierenga PC, Eslami S, Medlock S, de Rooij SE, Abu-Hanna A. Assessing quality of care of elderly patients using the ACOVE quality indicator set: A systematic review. PLoS ONE. 2011;6(12):e28631.
10. U.S. Department of Veterans Affairs. Office of Rural Health. About the office of rural health. U.S. Department of Veterans Affairs Website. http://www.ruralhealth.va.gov/about/index.asp. Update June 12, 2014. Accessed October 10, 2014.
11. Schectman G, Stark R, Fihn S, VanEe H, Box T. Care assessment need score: A tool for care management. Presented on March 29, 2012. http://www.myvehucampus.com/#loc=auditoriumRoom. Accessed October 14, 2014.
12. Min L, Yoon W, Mariano J, et al. The vulnerable elders-13 survey predicts 5-year functional decline and mortality outcomes in older ambulatory care patients. J Am Geriatr Soc. 2009;57(11):2070-2076.
13. Fulmer T, Wallace M. Fulmer SPICES: An overall assessment tool for older adults. http://consultgerirn.org/uploads/File/trythis/try_this_1.pdf. Revised 2012. Accessed October 1, 2014.
14. Hartford Institute for Geriatric Nursing. ConsultGeriRN.org Website. http://consultgerirn.org. Accessed September 30, 2014.
15. Opondo D, Eslami S, Visscher S, et al. Inappropriateness of medication prescriptions to elderly patients in the primary care setting: A systemic Review. PLoS One. 2012;7(8):e43617.
16. Fick DM, Cooper JW, Wade WE, Waller JL, Maclean JR, Beers MH. Updating the Beers criteria for potentially inappropriate medication use in older adults: Results of a US consensus panel of experts. Arch Intern Med. 2003;163(22):2716-2724.
17. The American Geriatrics Society 2012 Beers Criteria Update Expert Panel. American Geriatrics Society updated Beers criteria for potentially inappropriate medication use in older adults. J Am Geriatr Soc. 2012;60(4):616-631.
18. Higashi T, Shekelle PG, Solomon DH, et al. The quality of pharmacologic care for vulnerable older patients. Ann Intern Med. 2004;140(9):714-720.
19. Lund BC, Steinman MA, Chrischilles EA, Kaboli PJ. Beers criteria as a proxy for inappropriate prescribing of other medications among older adults. Ann Pharmacother. 2011;45(11):1363-1370.
20. RAND. Assessing care of vulnerable elders. Quality indicators- ACOVE 3. RAND Website. http://www.rand.org/health/projects/acove/acove3.html. Accessed October 7, 2014.
21. Wenger NS, Shekelle PG. Assessing care of vulnerable elders: ACOVE project overview. Ann Intern Med. 2001;135(8, pt 2):642-646.
22. Shekelle PG, MacLean CH, Morton SC, Wenger NS. Assessing care of vulnerable elders: Methods for developing quality indicators. Ann Intern Med. 2001;135(8, pt 2):647-652.
23. Reuben DB, Roth C, Kamberg C, Wenger NS. Restructuring primary care practices to manage geriatric syndromes: The ACOVE-2 intervention. J Am Geriatr Soc. 2003;51(12):1787-1793.
24. Wenger NS, Roth CP, Shekelle P; ACOVE Investigators. Introduction to the assessing care of vulnerable elders-3 quality indicator measurement set. J Am Geriatr Soc. 2007;55(suppl 2):S247-S252.
25. Higashi T, Shekelle PG, Solomon DH, et al. The quality of pharmacologic care for vulnerable older patients. Ann Intern Med. 2004;140(9):714-720.
26. American Geriatrics Society Expert Panel on the Care of Older Adults with Multimorbidity. Patient-centered care for older adults with multiple chronic conditions: A stepwise approach from the American Geriatrics Society. J Am Geriatr Soc. 2012;60(10):1957-1968.
27. U.S. Department of Veterans Affairs. Geriatric Research Education and Clinical Centers. GRECC. U.S. Department of Veterans Affairs Website. http://www.va.gov/GRECC/index.asp . Updated August 17, 2012. Accessed October 10, 2014.
28. Tumosa N, Horvath KJ, Huh T, et al. Health care workforce development in rural America: When geriatrics expertise is 100 miles away. Gerontol Geriatr Educ. 2012;33(2):133-151.
29. U.S. Department of Veterans Affairs. Geriatric Research Education and Clinical Centers. The VA Geriatrics Scholars Program. U.S. Department of Veterans Affairs Website. http://www.va.gov/GRECC/GRECC_Educational_Events_and_Products.asp. Updated February 21, 2013. Accessed October 1, 2014.
30. U.S. Department of Veterans Affairs. Office of Public and Intergovernmental Affairs. VA uses technology to provide rural veterans greater access to specialty care services. U.S. Department of Veterans Affairs Website. http://www.va.gov/opa/pressrel/pressrelease.cfm?id=2353. Updated July 10, 2012. Accessed October 1, 2014.
31. Harrell KM, Wilkins SS, Connor MK, Chodosh J. Telemedicine and the evaluation of cognitive impairment: The additive value of neuropsychological assessment. J Am Med Dir Assoc. 2014;15(8):600-606.
32. Totten A, Carson S, Peterson K, Low A, Christense V, Tiwari A. Evidence brief: Effect of geriatricians on outcomes of inpatient and outpatient care, VA-ESP Project #09-199. U.S. Department of Veterans Affairs Website. http://www.hsrd.research.va.gov/publications/esp/Geriatricians.pdf. Accessed October 1, 2014.
1. U.S. Department of Veterans Affairs. Geriatric Ambulatory Care. VHA Handbook 1140.10. U.S. Department of Veterans Affairs Website. http://www.va.gov/vhapublications/ViewPublication.asp?pub_ID=2202. Published April 26, 2010. Accessed September 29, 2014.
2. Federal Interagency Forum on Aging-Related Statistics. Older Americans 2012: Key indicators of well-being. AgingStats.gov Website. http://www.agingstats.gov/agingstatsdotnet/main_site/default.aspx. Accessed September 29, 2014.
3. Shay K, Schectman G. Primary care for older veterans. Generations. 2010;34(2):35-42.
4. Institute of Medicine. Retooling for an Aging America: Building the Health Care Workforce. Washington, DC: The National Academies Press; 2008.
5. Shay K, Hyduke B, Burris JF. Strategic plan for geriatrics and extended care in the veterans health administration: Background, plan, and progress to date. J Am Geriatr Soc. 2013;61(4):632-638.
6. Berenson RA, Devers KJ, Burton RA. Will the patient-centered medical home transform the delivery of health care? Timely analysis of immediate health policy issues. Urban Institute Website. http://www.urban.org/uploadedpdf/412373-will-patient-centered-medical-home-transform-delivery-health-care.pdf. Published August 2011. Accessed September 29, 2014.
7. U.S. Department of Veterans Affairs. VA Primary Care Services. Patient-centered medical home model concept paper. U.S. Department of Veterans Affairs Website. http://www.va.gov/health/services/PrimaryCare/docs/pcmh_ConceptPaper.doc. Accessed October 7, 2014.
8. VA Undersecretary for Health. What is PACT? U.S. Department of Veterans Affairs Website http://www.va.gov/health/services/primarycare/pact/index.asp. Updated February 18, 2014. Accessed October 7, 2014.
9. Askari M, Wierenga PC, Eslami S, Medlock S, de Rooij SE, Abu-Hanna A. Assessing quality of care of elderly patients using the ACOVE quality indicator set: A systematic review. PLoS ONE. 2011;6(12):e28631.
10. U.S. Department of Veterans Affairs. Office of Rural Health. About the office of rural health. U.S. Department of Veterans Affairs Website. http://www.ruralhealth.va.gov/about/index.asp. Update June 12, 2014. Accessed October 10, 2014.
11. Schectman G, Stark R, Fihn S, VanEe H, Box T. Care assessment need score: A tool for care management. Presented on March 29, 2012. http://www.myvehucampus.com/#loc=auditoriumRoom. Accessed October 14, 2014.
12. Min L, Yoon W, Mariano J, et al. The vulnerable elders-13 survey predicts 5-year functional decline and mortality outcomes in older ambulatory care patients. J Am Geriatr Soc. 2009;57(11):2070-2076.
13. Fulmer T, Wallace M. Fulmer SPICES: An overall assessment tool for older adults. http://consultgerirn.org/uploads/File/trythis/try_this_1.pdf. Revised 2012. Accessed October 1, 2014.
14. Hartford Institute for Geriatric Nursing. ConsultGeriRN.org Website. http://consultgerirn.org. Accessed September 30, 2014.
15. Opondo D, Eslami S, Visscher S, et al. Inappropriateness of medication prescriptions to elderly patients in the primary care setting: A systemic Review. PLoS One. 2012;7(8):e43617.
16. Fick DM, Cooper JW, Wade WE, Waller JL, Maclean JR, Beers MH. Updating the Beers criteria for potentially inappropriate medication use in older adults: Results of a US consensus panel of experts. Arch Intern Med. 2003;163(22):2716-2724.
17. The American Geriatrics Society 2012 Beers Criteria Update Expert Panel. American Geriatrics Society updated Beers criteria for potentially inappropriate medication use in older adults. J Am Geriatr Soc. 2012;60(4):616-631.
18. Higashi T, Shekelle PG, Solomon DH, et al. The quality of pharmacologic care for vulnerable older patients. Ann Intern Med. 2004;140(9):714-720.
19. Lund BC, Steinman MA, Chrischilles EA, Kaboli PJ. Beers criteria as a proxy for inappropriate prescribing of other medications among older adults. Ann Pharmacother. 2011;45(11):1363-1370.
20. RAND. Assessing care of vulnerable elders. Quality indicators- ACOVE 3. RAND Website. http://www.rand.org/health/projects/acove/acove3.html. Accessed October 7, 2014.
21. Wenger NS, Shekelle PG. Assessing care of vulnerable elders: ACOVE project overview. Ann Intern Med. 2001;135(8, pt 2):642-646.
22. Shekelle PG, MacLean CH, Morton SC, Wenger NS. Assessing care of vulnerable elders: Methods for developing quality indicators. Ann Intern Med. 2001;135(8, pt 2):647-652.
23. Reuben DB, Roth C, Kamberg C, Wenger NS. Restructuring primary care practices to manage geriatric syndromes: The ACOVE-2 intervention. J Am Geriatr Soc. 2003;51(12):1787-1793.
24. Wenger NS, Roth CP, Shekelle P; ACOVE Investigators. Introduction to the assessing care of vulnerable elders-3 quality indicator measurement set. J Am Geriatr Soc. 2007;55(suppl 2):S247-S252.
25. Higashi T, Shekelle PG, Solomon DH, et al. The quality of pharmacologic care for vulnerable older patients. Ann Intern Med. 2004;140(9):714-720.
26. American Geriatrics Society Expert Panel on the Care of Older Adults with Multimorbidity. Patient-centered care for older adults with multiple chronic conditions: A stepwise approach from the American Geriatrics Society. J Am Geriatr Soc. 2012;60(10):1957-1968.
27. U.S. Department of Veterans Affairs. Geriatric Research Education and Clinical Centers. GRECC. U.S. Department of Veterans Affairs Website. http://www.va.gov/GRECC/index.asp . Updated August 17, 2012. Accessed October 10, 2014.
28. Tumosa N, Horvath KJ, Huh T, et al. Health care workforce development in rural America: When geriatrics expertise is 100 miles away. Gerontol Geriatr Educ. 2012;33(2):133-151.
29. U.S. Department of Veterans Affairs. Geriatric Research Education and Clinical Centers. The VA Geriatrics Scholars Program. U.S. Department of Veterans Affairs Website. http://www.va.gov/GRECC/GRECC_Educational_Events_and_Products.asp. Updated February 21, 2013. Accessed October 1, 2014.
30. U.S. Department of Veterans Affairs. Office of Public and Intergovernmental Affairs. VA uses technology to provide rural veterans greater access to specialty care services. U.S. Department of Veterans Affairs Website. http://www.va.gov/opa/pressrel/pressrelease.cfm?id=2353. Updated July 10, 2012. Accessed October 1, 2014.
31. Harrell KM, Wilkins SS, Connor MK, Chodosh J. Telemedicine and the evaluation of cognitive impairment: The additive value of neuropsychological assessment. J Am Med Dir Assoc. 2014;15(8):600-606.
32. Totten A, Carson S, Peterson K, Low A, Christense V, Tiwari A. Evidence brief: Effect of geriatricians on outcomes of inpatient and outpatient care, VA-ESP Project #09-199. U.S. Department of Veterans Affairs Website. http://www.hsrd.research.va.gov/publications/esp/Geriatricians.pdf. Accessed October 1, 2014.
E-Consults in Gastroenterology: A Quality Improvement Project
Although the VA has the largest health care system in the U.S., not every VA facility offers medical subspecialty care. As a result, patients are often separated by long distances from services they need.
At the VA Pittsburgh Healthcare System (VAPHS) in Pennsylvania, about 15,700 veterans received care in 2011. The Gastroenterology Department (GD) served many of these patients: 5,800 patients were seen in clinic appointments, 2,500 underwent colonoscopy, and 1,700 underwent esophagogastroduodenoscopy (EGD). Patients traveled up to 150 miles from 3 states for appointments and procedures. Prior to each procedure, a face-to-face appointment was standard practice for most patients to plan procedures and ensure medical stability. Patients expressed dissatisfaction with transportation, cost, time, and inconvenience, particularly when they were required to attend both the preprocedure and procedure appointments.
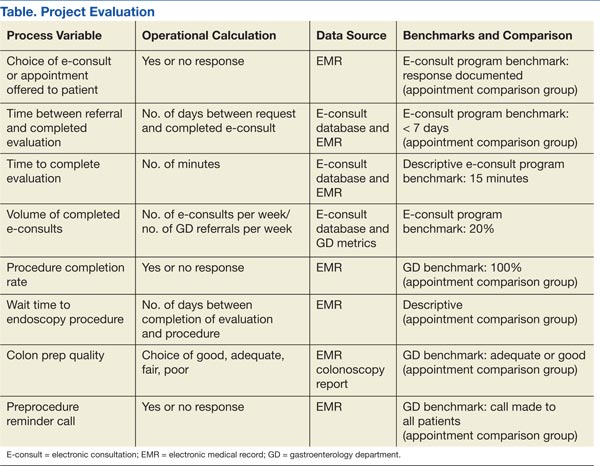
Patient satisfaction, timely care, and appropriate use of resources are important VA goals of care, so the VAPHS developed an electronic consultation (e-consult) program as a component of its long-term strategic plan. The goal was to increase access to care through the use of an e-consult in lieu of a face-to-face appointment for select patients. The e-consult program established guidelines and benchmark goals (Table). The program also established a database to track the benchmarks.
The purpose of this quality improvement (QI) project was to evaluate e-consults in the GD over a 6-month period from January 2012, when e-consults were implemented in the GD, to July 2012. Based on the outcomes, recommendations for program continuation, change, and sustainability were made.
Background
Telemedicine using information technologies has been reported as a viable solution to support health care delivery when distance limits patients’ access to care.1,2 Telemedicine has also been shown to improve efficacy in clinical decision making and reduce costs. It also can increase patient satisfaction by reducing travel and time, minimize duplication of diagnostic testing, and integrate services effectively across multiple sites when an electronic medical record (EMR) is in place.1-5
A randomized controlled trial in 2004 compared a standard outpatient referral appointment with a joint teleconsultation between provider, specialist, and patient.3 In the teleconsultation arm, there was higher patient satisfaction, fewer diagnostic tests (particularly in gastroenterology), and lower patient costs.
A study published in 2009 examined the impact of cardiac, dermatologic, and diabetes teleconsultations on organization and patient outcomes in 950 patients in 30 rural communities.2 Rapid access to care was provided for 85% of the patients. Organizational benefits included resource savings and efficacy improvement measured by a provider opinion Likert scale. Patient benefits included reductions in wait times, transportation savings, avoidance of unnecessary office visits, and ease of use.
A large systematic review of telemedicine services across all medical specialties in 2006 included 106 published studies.4 Clinical outcomes (decision making, diagnosis, and management) were similar between conventional care and telemedicine in specialty care, particularly in neurology and psychiatry. Virtual consults provided equal care to traditional specialty visits.6
Communication and coordination of care via an e-consult instead of a face-to-face clinic visit was evaluated by Horner and colleagues.5 The authors identified e-consult benefits for patients and specialists and that e-consults can reduce unnecessary referrals and appointments by 30%. They concluded that reserved time to complete e-consults must be built into workflow systems and that an advanced EMR was necessary for successful use of e-consults.
Two studies have evaluated satisfaction with e-consults. A preliminary analysis of satisfaction with e-consults was conducted in 2009 by K. L. Rodriguez, PhD, and colleagues (unpublished data). Patients, primary care providers (PCPs), and medical specialists reported overall satisfaction in 8 satisfaction domains. A pilot study of 34 patients in 2011 with inflammatory bowel disease compared a standard patient-GD physician encounter with a video encounter.7 The authors reported patient satisfaction, appointment time, wait times, and quality of care were similar for the 2 groups.
Methods
The GD where this QI project was completed consisted of a clinic staffed by nurse practitioners (NPs) and a procedure lab staffed by gastroenterology physicians. Before e-consult implementation, a NP reviewed and triaged new referrals daily. During the project period, an average of 25 to 35 new referrals were received daily via the EMR. Referrals came mostly from PCPs requesting an evaluation of their patients’ gastroenterology problem. Patients were triaged either to an appointment for evaluation or directly to the GD procedure lab for EGD or colonoscopy.
When e-consults were implemented, several changes occurred. Two providers were assigned to new referral triage, and they were expected to process 20% as e-consults. In the EMR, e-consult note titles, templates, and an e-consult encounter form were created, and staff was given access to the e-consult tracking database. The EMR referral template was amended so the entering provider could say whether a face-to-face appointment was desired or whether an e-consult was acceptable. The patient was to be included in decision making about this choice. Department staff had permission to triage according to judgment and expertise; thus, appointment requests could be triaged to e-consults, and e-consult requests could be triaged to appointments.
To complete an e-consult, the EMR was reviewed for medical diagnoses, medications, diagnostics, and recent physical exam. A summary note outlining an impression, treatment recommendations, and follow-up was entered in the EMR and communicated to the PCP. In most cases, no discussion with the patient occurred. The encounter form was completed, and information was entered into the tracking database. The database was installed on each provider’s computer who processed e-consults. If EGD or colonoscopy was indicated, the scheduler was notified to call the patient. Once a procedure date was established, procedure orders were completed in the EMR, and instructions were mailed to the patient.
Project Description and Evaluation
The project was reviewed by the Institutional Review Board and determined to be a QI project. VA organizational policies were followed for data collection and security. Benchmarks were identified from the e-consult program and from the GD, where available. Process variables were determined to measure benchmark outcomes. (Table)
To identify participants, a retrospective chart review was performed. A total of 203 potential patients were identified from the e-consult program database for the 6-month period between January and July 2012. For comparison, 50 patients who attended an appointment during the same time frame were systematically identified in the EMR. Although this comparison group was eligible for e-consults, they were triaged to in-person appointments and subsequently had colonoscopies completed.
Outcome data were extracted from the e-consult program database and the EMR. The data analysis was descriptive. Summary aggregate data were compared with the benchmarks and comparison patient outcomes. The Table summarizes the process variables, how they were measured, where they came from, and what the comparisons were.
Discussion
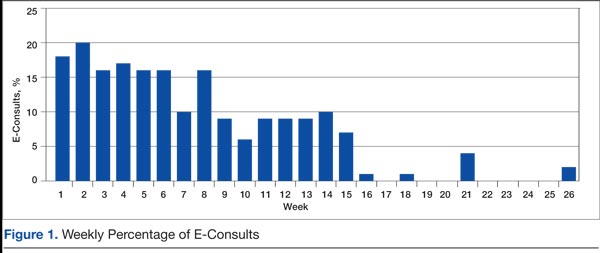
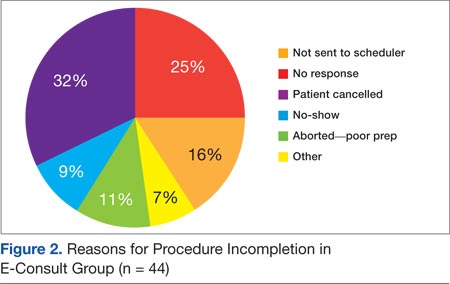
Figure 1 illustrates the volume of completed e-consults from January to July 2012. A gastroenterology procedure was not indicated in 43 patients. A procedure was indicated for 160 patients and completed in 116 patients (72%). One hundred procedures were colonoscopies, and 16 were EGDs. Figure 2 provides reasons why procedures were not completed in 44 patients (27%). Group comparisons of colon prep quality and preprocedure reminder calls are displayed in Figures 3 and 4, respectively.
This project sought to evaluate VAPHS GD e-consults beginning in January 2012. Process variables were established to measure benchmarks in the e-consult program and in the GD. Some benchmarks were met with outcomes that were comparable between the groups, while others were not. To our knowledge, this project is the first to evaluate e-consults in the subspecialty of gastroenterology.
Volume of Completed E-Consults
The benchmark for 20% e-consults was not met (Figure 1). For weeks 1 through 8, the volume was between 10% and 20%. Lower volume in weeks 9 through 15 (late March and April) may have been due to staff vacations. Not only do the outcomes show a downward trend in e-consult volume, they also show a precipitous fall in volume at week 15 to almost no e-consults for the remainder of the project. To explore reasons for this outcome, the workflow process of new referral triage and e-consults was reviewed.
Two providers (1 NP, 1 physician) were assigned to new referral triage and e-consults from weeks 1 through 14. At week 15, the physician was reassigned to perform procedures. From this point, only 1 NP worked on e-consults and referral triage. Competing time demands included an e-consult encounter form, tracking database entry, procedure orders, patient instructions, appointment changes, phone calls, and resolution of medications issues for procedures. The triage NP was also required to see patients in the clinic. Each day, only a half-day was allotted to complete e-consults, new referral triage (25-35/day), and the aforementioned tasks.
Therefore, it became clear that a half-day was not sufficient to meet the 20% benchmark for e-consults. Horner and colleagues also found that dedicated time in workflow processes was necessary to allow for e-consult completion.5
E-Consults vs Appointment Groups
All patients in both groups were offered the choice of e-consult or appointment; this benchmark was met. Of the 203 e-consult patients, 70% requested an appointment, but their evaluation was completed as an e-consult. By design, the appointment group patients chose e-consult but were triaged to appointment due to time constraints and the high volume of new referrals.
Evaluations via e-consult were completed within 2 to 3 days, whereas the mean for appointments was 19 days, with the longest time frame of 44 days. Thus, e-consult evaluations were completed sooner. Rapid access to care was also found by Zanaboni and colleagues.2
When appointments are delayed, patient complaints or status may change, which in turn may affect treatment plans. In addition, the reason for referral may have already resolved by the actual appointment, rendering the appointment unnecessary. This can be viewed as a missed opportunity for another patient to be seen. Ideally, it is best for a patient to be evaluated soon after a new referral is made.
The VA encounter form for an e-consult had only one 5-digit code, which allotted only 15 minutes of work credit. Encounter form codes were established by the Center for Medicare and Medicaid Services (CMS) for billing purposes in the private sector, with coding levels based on information documented in a chart note: review of systems, physical exam, and diagnoses decision making. Because all criteria could not be met in an e-consult, only 1 code was assigned for VAPHS e-consults. The CMS has specific telemedicine codes; it was unknown why they were not used for e-consults.
E-consults took an average of 19 minutes to complete, with 91 completed in ≤ 15 minutes and over half (112) having taken > 15 minutes. Therefore, the actual workload was not captured, and more work was done than was credited. To speculate, e-consults were in their infancy; a learning curve may have existed as staff became accustomed to this new process.
The EMRs were reviewed for the 7 e-consults that took > 30 minutes to complete. Two were in the early stage of e-consult implementation, but the remainder were scattered throughout. Patients in these e-consults had complicated medical histories and perhaps should not have been triaged to e-consult. Theoretically, only uncomplicated patients with simple reasons for gastroenterology referral should be triaged to e-consult, allowing for a shorter time frame and higher volume.
The wait times to procedure were 58 days for the e-consult group and 39 days in the appointment group. Although wait time was originally identified as an outcome, its relevance is questionable after looking at the outcome data. The procedure appointment date was a subjective decision by the patient; many factors affected what date the patient established, including weekday preference, time off from work, caretaker availability, season, and staffing. Many patients rescheduled their initial procedure dates, often several times. These factors are reflected in the variable ranges of wait times.
Colon Prep Quality
Colon prep refers to patient instructions on the day before the procedure and includes a clear liquid diet, drinking a liquid solution to empty bowel contents, and no food or liquid after midnight. Prep quality is stated in the colonoscopy report. During the procedure, the physician makes a visual decision based on presence or absence of stool inside the colon. Prep quality is important, because retained stool can preclude thorough visualization of the colon wall for polyps or abnormalities. In the event of fair and poor preps, the colonoscopy might be aborted and rescheduled or completed, but with the recommendation for another colonoscopy in a short time frame, such as 1 to 3 years.
Forty-four percent of the e-consult group and 62% of the appointment group had good or adequate preps. Thus, more patients in the appointment group achieved good and adequate preps, and far fewer achieved fair or poor preps. One important point was that almost half (47%) of the e-consult group had only a fair prep (Figure 3).
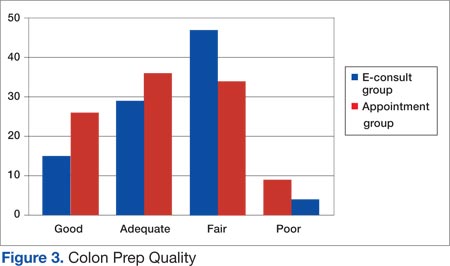
A number of reasons have been identified in the literature, which might help us understand these findings. First, patients may not fully understand or adhere to prep instructions.8-10 Furthermore, certain medical diagnoses are known to affect prep quality (ie, diabetes, thyroid disease, constipation).11,12 Another potential factor is the manner in which prep quality is determined.13,14 However, due to the focus of this QI study, the influential drivers of prep quality can only be inferred from the literature; thus, a future research or QI study is warranted to ascertain the underlying mechanism of colon prep quality in our specific veteran population.
Preprocedure Reminder Calls
Outcomes were essentially reversed between the 2 groups (Figure 4). Between 50% and 60% of the e-consult group received a call, while the same percentage of appointment patients did not. All patients did attend their procedure appointment. A GD goal was to call every patient before their procedure, but the ability to make the calls was staffing-dependent, which may explain these findings.
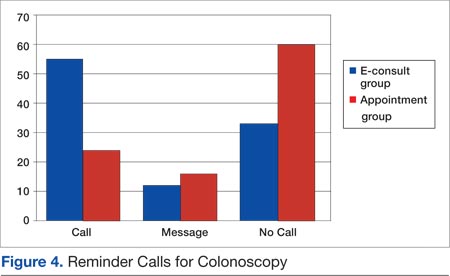
Most Relevant Findings
Although this project provides a thorough analysis of various benchmarks within this recently implemented e-consult gastroenterology program, 3 findings emerged that were identified as most relevant. First, the benchmark of 20% volume of completed e-consults was not met. A review of the workflow processes revealed that a daily allotment of only a half-day was not sufficient to complete e-consults, referral triage, and related tasks.
Second, outcomes for colon prep quality and preprocedure reminder calls were also relevant. Although beyond the scope of this project, the question arose of a relationship between prep quality and the reminder call: Does the reminder call affect prep quality? The goal of colon prep is to achieve a good or adequate prep. The purpose of the reminder call was to confirm the appointment and to review the colon prep. Among patients in both groups who achieved only a fair prep, 62% in the e-consult group did receive the reminder call; thus, the call seemed to have failed in helping these patients achieve an adequate or good prep. The actual content of colon prep review during the call was unknown, but certainly bears improvement.
Another speculation concerned the prep instruction sheet. Although all patients received the same sheet, e-consult patients received it in the mail and read it themselves, while it was directly reviewed face-to-face with the appointment patients. Questions remain whether a face-to-face review increases the likelihood for a better prep and how to help e-consult patients achieve optimal prep, since they are not seen face-to-face.
Practice Implications and Sustaining Measures
Theoretically, e-consults are a viable alternative to face-to-face appointments. Potential advantages include efficient use of an EMR, avoidance of unnecessary appointments, and improved access to care for patients who require an appointment. Although patient satisfaction was not measured in this project, the literature review revealed that satisfaction was increased through use of various virtual health care modalities, including a preliminary analysis in this facility by the aforementioned 2009 study by K. L. Rodriguez (unpublished data). Based on findings in this project, the following 4 recommendations were made to improve benchmark outcomes and quality of care.
- Provide dedicated time to complete e-consults and related tasks. In this setting, a full day was recommended. An alternative was to hire a NP whose sole responsibility was e-consults.
- Develop a selection process to determine which new referrals are best suited for e-consult. This process will increase e-consult efficiency and decrease the time to complete an e-consult. Recommended selection criteria were (A) gastroenterology referrals only for simple symptoms or issues; (B) referrals only for a procedure; and (C) stable patients with uncomplicated medical histories.
- Sustain the preprocedure reminder phone call. The reminder call helps patients keep appointments and thus reduces a missed opportunity for care.
- Plan a future QI project or research study on patient colon prep quality for colonoscopy. Such a project might evaluate types of colon prep, how prep quality is measured, patient instructions, and the timing/content of pre-procedure reminder phone calls, particularly for e-consult patients.
Conclusion
This QI project provided outcomes for e-consults in the subspecialty of gastroenterology at the VAPHS. Although some benchmark outcomes were met and favorable, others were less favorable. By conducting this benchmark analysis, the areas of needed improvement are now clear. This analysis provides information so recommendations for process improvements can be made.
Quality of care improvement is an ongoing process at VAPHS. Since completion of this project, several processes have been adjusted so that outcomes will be improved. For example, corrective actions were taken for patients who did not complete their gastroenterology procedure. The process for scheduling gastroenterology procedures was adjusted for appointments and cancellations. Ongoing efforts to sustain the reminder phone call were put in place. Changes in NP staffing and time assigned for both clinical and nonclinical work were proposed and are currently under review.
It is the mission of the VA to provide access to care, patient satisfaction, timely care, and appropriate use of resources. Having the ability to highlight our strengths, as well as the willingness to recognize weaknesses, allows us to create new improved processes to provide the best care possible for our veterans.
Acknowledgments
This project was Elena Swann’s capstone for the Doctor of Nursing Practice Program, University of Pittsburgh School of Nursing in Pennsylvania. Rich Laufer, Larry Priscella, and Janie Fleming assisted with the VA Gastroenterology Clinic and procedure metrics. Dr. Melissa Taylor, VA associate chief nurse for research provided project guidance and manuscript revisions. Dr. Sandra Engberg, University of Pittsburgh School of Nursing faculty, assisted with project and manuscript development.
Author disclosures
The author reports no actual or potential conflicts of interest with regard to this article.
Disclaimer
The opinions expressed herein are those of the author and do not necessarily reflect those of Federal Practitioner, Frontline Medical Communications Inc., the U.S. Government, or any of its agencies. This article may discuss unlabeled or investigational use of certain drugs. Please review complete prescribing information for specific drugs or drug combinations—including indications, contraindications, warnings, and adverse effects—before administering pharmacologic therapy to patients.
1. Bashshur RL, Shannon GW, Krupinski EA, et al. National telemedicine initiatives: Essential to healthcare reform. Telemed J E Health. 2009;15(6):600-610.
2. Zanaboni P, Scalvini S, Bernocchi P, Borghi G, Tridico C, Masella C. Teleconsultation service to improve healthcare in rural areas: Acceptance, organizational impact and appropriateness. BMC Health Serv Res. 2009;9:238.
3. Wallace P, Barber J, Clayton W, et al. Virtual outreach: A randomised controlled trial and economic evaluation of joint teleconferenced medical consultations. Health Technol Assess. 2004;8(50):1-106, iii-iv.
4. Hersh WR, Hickam DH, Severance SM, Dana TL, Pyle Krages K, Helfand M. Diagnosis, access and outcomes: Update of a systematic review of telemedicine services. J Telemed Telecare. 2006;12(suppl 2):S3-S31.
5. Horner K, Wagner E, Tufano J. Electronic consultations between primary and specialty care clinicians: Early insights. Issue Brief (Commonw Fund). 2011;23:1-14.
6. Angstman KB, Adamson SC, Furst JW, Houston MS, Rohrer JE. Provider satisfaction with virtual specialist consultations in a family medicine department. Health Care Manag (Frederick). 2009;28(1):14-18.
7. Krier M, Kaltenbach T, McQuaid K, Soetikno R. Potential use of telemedicine to provide outpatient care for inflammatory bowel disease. Am J Gastroenterol. 2011;106(12):2063-2067.
8. Calderwood AH, Lai EJ, Fix OK, Jacobson BC. An endoscopist-blinded, randomized, controlled trial of a simple visual aid to improve bowel preparation for screening colonoscopy. Gastrointest Endosc. 2011;73(2):307-314.
9. Hillyer GC, Basch CH, Basch CE, et al. Gastroenterologists’ perceived barriers to optimal pre-colonoscopy bowel preparation: Results of a national survey. J Cancer Educ. 2012;27(3):526-532.
10. Smith SG, von Wagner C, McGregor LM, et al. The influence of health literacy on comprehension of a colonoscopy preparation information leaflet. Dis Colon Rectum. 2012;55(10):1074-1080.
11. Mittal S, Lin YL, Tan A, Kuo YF, El-Serag HB, Goodwin JS. Limited life expectancy among a subgroup of Medicare beneficiaries receiving screening colonoscopies. Clin Gastroenterol Hepatol. 2014;12(3):443-450.e1.
12. Ko CW, Sonnenberg A. Comparing risks and benefits of colorectal cancer screening in elderly patients. Gastroenterology. 2005;129(4):1163-1170.
13. Ell C, Fischbach W, Keller R, et al; Hintertux Study Group. A randomized, blinded, prospective trial to compare the safety and efficacy of three bowel-cleansing solutions for colonoscopy (HSG-01*). Endoscopy. 2003;35(4):300-304.
14. Jansen SV, Goedhard JG, Winkens B, van Deursen CT. Preparation before colonoscopy: A randomized controlled trial comparing different regimes. Eur J Gastroenterol Hepatol. 2011;23(10):897-902.
Although the VA has the largest health care system in the U.S., not every VA facility offers medical subspecialty care. As a result, patients are often separated by long distances from services they need.
At the VA Pittsburgh Healthcare System (VAPHS) in Pennsylvania, about 15,700 veterans received care in 2011. The Gastroenterology Department (GD) served many of these patients: 5,800 patients were seen in clinic appointments, 2,500 underwent colonoscopy, and 1,700 underwent esophagogastroduodenoscopy (EGD). Patients traveled up to 150 miles from 3 states for appointments and procedures. Prior to each procedure, a face-to-face appointment was standard practice for most patients to plan procedures and ensure medical stability. Patients expressed dissatisfaction with transportation, cost, time, and inconvenience, particularly when they were required to attend both the preprocedure and procedure appointments.
Patient satisfaction, timely care, and appropriate use of resources are important VA goals of care, so the VAPHS developed an electronic consultation (e-consult) program as a component of its long-term strategic plan. The goal was to increase access to care through the use of an e-consult in lieu of a face-to-face appointment for select patients. The e-consult program established guidelines and benchmark goals (Table). The program also established a database to track the benchmarks.
The purpose of this quality improvement (QI) project was to evaluate e-consults in the GD over a 6-month period from January 2012, when e-consults were implemented in the GD, to July 2012. Based on the outcomes, recommendations for program continuation, change, and sustainability were made.
Background
Telemedicine using information technologies has been reported as a viable solution to support health care delivery when distance limits patients’ access to care.1,2 Telemedicine has also been shown to improve efficacy in clinical decision making and reduce costs. It also can increase patient satisfaction by reducing travel and time, minimize duplication of diagnostic testing, and integrate services effectively across multiple sites when an electronic medical record (EMR) is in place.1-5
A randomized controlled trial in 2004 compared a standard outpatient referral appointment with a joint teleconsultation between provider, specialist, and patient.3 In the teleconsultation arm, there was higher patient satisfaction, fewer diagnostic tests (particularly in gastroenterology), and lower patient costs.
A study published in 2009 examined the impact of cardiac, dermatologic, and diabetes teleconsultations on organization and patient outcomes in 950 patients in 30 rural communities.2 Rapid access to care was provided for 85% of the patients. Organizational benefits included resource savings and efficacy improvement measured by a provider opinion Likert scale. Patient benefits included reductions in wait times, transportation savings, avoidance of unnecessary office visits, and ease of use.
A large systematic review of telemedicine services across all medical specialties in 2006 included 106 published studies.4 Clinical outcomes (decision making, diagnosis, and management) were similar between conventional care and telemedicine in specialty care, particularly in neurology and psychiatry. Virtual consults provided equal care to traditional specialty visits.6
Communication and coordination of care via an e-consult instead of a face-to-face clinic visit was evaluated by Horner and colleagues.5 The authors identified e-consult benefits for patients and specialists and that e-consults can reduce unnecessary referrals and appointments by 30%. They concluded that reserved time to complete e-consults must be built into workflow systems and that an advanced EMR was necessary for successful use of e-consults.
Two studies have evaluated satisfaction with e-consults. A preliminary analysis of satisfaction with e-consults was conducted in 2009 by K. L. Rodriguez, PhD, and colleagues (unpublished data). Patients, primary care providers (PCPs), and medical specialists reported overall satisfaction in 8 satisfaction domains. A pilot study of 34 patients in 2011 with inflammatory bowel disease compared a standard patient-GD physician encounter with a video encounter.7 The authors reported patient satisfaction, appointment time, wait times, and quality of care were similar for the 2 groups.
Methods
The GD where this QI project was completed consisted of a clinic staffed by nurse practitioners (NPs) and a procedure lab staffed by gastroenterology physicians. Before e-consult implementation, a NP reviewed and triaged new referrals daily. During the project period, an average of 25 to 35 new referrals were received daily via the EMR. Referrals came mostly from PCPs requesting an evaluation of their patients’ gastroenterology problem. Patients were triaged either to an appointment for evaluation or directly to the GD procedure lab for EGD or colonoscopy.
When e-consults were implemented, several changes occurred. Two providers were assigned to new referral triage, and they were expected to process 20% as e-consults. In the EMR, e-consult note titles, templates, and an e-consult encounter form were created, and staff was given access to the e-consult tracking database. The EMR referral template was amended so the entering provider could say whether a face-to-face appointment was desired or whether an e-consult was acceptable. The patient was to be included in decision making about this choice. Department staff had permission to triage according to judgment and expertise; thus, appointment requests could be triaged to e-consults, and e-consult requests could be triaged to appointments.
To complete an e-consult, the EMR was reviewed for medical diagnoses, medications, diagnostics, and recent physical exam. A summary note outlining an impression, treatment recommendations, and follow-up was entered in the EMR and communicated to the PCP. In most cases, no discussion with the patient occurred. The encounter form was completed, and information was entered into the tracking database. The database was installed on each provider’s computer who processed e-consults. If EGD or colonoscopy was indicated, the scheduler was notified to call the patient. Once a procedure date was established, procedure orders were completed in the EMR, and instructions were mailed to the patient.
Project Description and Evaluation
The project was reviewed by the Institutional Review Board and determined to be a QI project. VA organizational policies were followed for data collection and security. Benchmarks were identified from the e-consult program and from the GD, where available. Process variables were determined to measure benchmark outcomes. (Table)
To identify participants, a retrospective chart review was performed. A total of 203 potential patients were identified from the e-consult program database for the 6-month period between January and July 2012. For comparison, 50 patients who attended an appointment during the same time frame were systematically identified in the EMR. Although this comparison group was eligible for e-consults, they were triaged to in-person appointments and subsequently had colonoscopies completed.
Outcome data were extracted from the e-consult program database and the EMR. The data analysis was descriptive. Summary aggregate data were compared with the benchmarks and comparison patient outcomes. The Table summarizes the process variables, how they were measured, where they came from, and what the comparisons were.
Discussion
Figure 1 illustrates the volume of completed e-consults from January to July 2012. A gastroenterology procedure was not indicated in 43 patients. A procedure was indicated for 160 patients and completed in 116 patients (72%). One hundred procedures were colonoscopies, and 16 were EGDs. Figure 2 provides reasons why procedures were not completed in 44 patients (27%). Group comparisons of colon prep quality and preprocedure reminder calls are displayed in Figures 3 and 4, respectively.
This project sought to evaluate VAPHS GD e-consults beginning in January 2012. Process variables were established to measure benchmarks in the e-consult program and in the GD. Some benchmarks were met with outcomes that were comparable between the groups, while others were not. To our knowledge, this project is the first to evaluate e-consults in the subspecialty of gastroenterology.
Volume of Completed E-Consults
The benchmark for 20% e-consults was not met (Figure 1). For weeks 1 through 8, the volume was between 10% and 20%. Lower volume in weeks 9 through 15 (late March and April) may have been due to staff vacations. Not only do the outcomes show a downward trend in e-consult volume, they also show a precipitous fall in volume at week 15 to almost no e-consults for the remainder of the project. To explore reasons for this outcome, the workflow process of new referral triage and e-consults was reviewed.
Two providers (1 NP, 1 physician) were assigned to new referral triage and e-consults from weeks 1 through 14. At week 15, the physician was reassigned to perform procedures. From this point, only 1 NP worked on e-consults and referral triage. Competing time demands included an e-consult encounter form, tracking database entry, procedure orders, patient instructions, appointment changes, phone calls, and resolution of medications issues for procedures. The triage NP was also required to see patients in the clinic. Each day, only a half-day was allotted to complete e-consults, new referral triage (25-35/day), and the aforementioned tasks.
Therefore, it became clear that a half-day was not sufficient to meet the 20% benchmark for e-consults. Horner and colleagues also found that dedicated time in workflow processes was necessary to allow for e-consult completion.5
E-Consults vs Appointment Groups
All patients in both groups were offered the choice of e-consult or appointment; this benchmark was met. Of the 203 e-consult patients, 70% requested an appointment, but their evaluation was completed as an e-consult. By design, the appointment group patients chose e-consult but were triaged to appointment due to time constraints and the high volume of new referrals.
Evaluations via e-consult were completed within 2 to 3 days, whereas the mean for appointments was 19 days, with the longest time frame of 44 days. Thus, e-consult evaluations were completed sooner. Rapid access to care was also found by Zanaboni and colleagues.2
When appointments are delayed, patient complaints or status may change, which in turn may affect treatment plans. In addition, the reason for referral may have already resolved by the actual appointment, rendering the appointment unnecessary. This can be viewed as a missed opportunity for another patient to be seen. Ideally, it is best for a patient to be evaluated soon after a new referral is made.
The VA encounter form for an e-consult had only one 5-digit code, which allotted only 15 minutes of work credit. Encounter form codes were established by the Center for Medicare and Medicaid Services (CMS) for billing purposes in the private sector, with coding levels based on information documented in a chart note: review of systems, physical exam, and diagnoses decision making. Because all criteria could not be met in an e-consult, only 1 code was assigned for VAPHS e-consults. The CMS has specific telemedicine codes; it was unknown why they were not used for e-consults.
E-consults took an average of 19 minutes to complete, with 91 completed in ≤ 15 minutes and over half (112) having taken > 15 minutes. Therefore, the actual workload was not captured, and more work was done than was credited. To speculate, e-consults were in their infancy; a learning curve may have existed as staff became accustomed to this new process.
The EMRs were reviewed for the 7 e-consults that took > 30 minutes to complete. Two were in the early stage of e-consult implementation, but the remainder were scattered throughout. Patients in these e-consults had complicated medical histories and perhaps should not have been triaged to e-consult. Theoretically, only uncomplicated patients with simple reasons for gastroenterology referral should be triaged to e-consult, allowing for a shorter time frame and higher volume.
The wait times to procedure were 58 days for the e-consult group and 39 days in the appointment group. Although wait time was originally identified as an outcome, its relevance is questionable after looking at the outcome data. The procedure appointment date was a subjective decision by the patient; many factors affected what date the patient established, including weekday preference, time off from work, caretaker availability, season, and staffing. Many patients rescheduled their initial procedure dates, often several times. These factors are reflected in the variable ranges of wait times.
Colon Prep Quality
Colon prep refers to patient instructions on the day before the procedure and includes a clear liquid diet, drinking a liquid solution to empty bowel contents, and no food or liquid after midnight. Prep quality is stated in the colonoscopy report. During the procedure, the physician makes a visual decision based on presence or absence of stool inside the colon. Prep quality is important, because retained stool can preclude thorough visualization of the colon wall for polyps or abnormalities. In the event of fair and poor preps, the colonoscopy might be aborted and rescheduled or completed, but with the recommendation for another colonoscopy in a short time frame, such as 1 to 3 years.
Forty-four percent of the e-consult group and 62% of the appointment group had good or adequate preps. Thus, more patients in the appointment group achieved good and adequate preps, and far fewer achieved fair or poor preps. One important point was that almost half (47%) of the e-consult group had only a fair prep (Figure 3).
A number of reasons have been identified in the literature, which might help us understand these findings. First, patients may not fully understand or adhere to prep instructions.8-10 Furthermore, certain medical diagnoses are known to affect prep quality (ie, diabetes, thyroid disease, constipation).11,12 Another potential factor is the manner in which prep quality is determined.13,14 However, due to the focus of this QI study, the influential drivers of prep quality can only be inferred from the literature; thus, a future research or QI study is warranted to ascertain the underlying mechanism of colon prep quality in our specific veteran population.
Preprocedure Reminder Calls
Outcomes were essentially reversed between the 2 groups (Figure 4). Between 50% and 60% of the e-consult group received a call, while the same percentage of appointment patients did not. All patients did attend their procedure appointment. A GD goal was to call every patient before their procedure, but the ability to make the calls was staffing-dependent, which may explain these findings.
Most Relevant Findings
Although this project provides a thorough analysis of various benchmarks within this recently implemented e-consult gastroenterology program, 3 findings emerged that were identified as most relevant. First, the benchmark of 20% volume of completed e-consults was not met. A review of the workflow processes revealed that a daily allotment of only a half-day was not sufficient to complete e-consults, referral triage, and related tasks.
Second, outcomes for colon prep quality and preprocedure reminder calls were also relevant. Although beyond the scope of this project, the question arose of a relationship between prep quality and the reminder call: Does the reminder call affect prep quality? The goal of colon prep is to achieve a good or adequate prep. The purpose of the reminder call was to confirm the appointment and to review the colon prep. Among patients in both groups who achieved only a fair prep, 62% in the e-consult group did receive the reminder call; thus, the call seemed to have failed in helping these patients achieve an adequate or good prep. The actual content of colon prep review during the call was unknown, but certainly bears improvement.
Another speculation concerned the prep instruction sheet. Although all patients received the same sheet, e-consult patients received it in the mail and read it themselves, while it was directly reviewed face-to-face with the appointment patients. Questions remain whether a face-to-face review increases the likelihood for a better prep and how to help e-consult patients achieve optimal prep, since they are not seen face-to-face.
Practice Implications and Sustaining Measures
Theoretically, e-consults are a viable alternative to face-to-face appointments. Potential advantages include efficient use of an EMR, avoidance of unnecessary appointments, and improved access to care for patients who require an appointment. Although patient satisfaction was not measured in this project, the literature review revealed that satisfaction was increased through use of various virtual health care modalities, including a preliminary analysis in this facility by the aforementioned 2009 study by K. L. Rodriguez (unpublished data). Based on findings in this project, the following 4 recommendations were made to improve benchmark outcomes and quality of care.
- Provide dedicated time to complete e-consults and related tasks. In this setting, a full day was recommended. An alternative was to hire a NP whose sole responsibility was e-consults.
- Develop a selection process to determine which new referrals are best suited for e-consult. This process will increase e-consult efficiency and decrease the time to complete an e-consult. Recommended selection criteria were (A) gastroenterology referrals only for simple symptoms or issues; (B) referrals only for a procedure; and (C) stable patients with uncomplicated medical histories.
- Sustain the preprocedure reminder phone call. The reminder call helps patients keep appointments and thus reduces a missed opportunity for care.
- Plan a future QI project or research study on patient colon prep quality for colonoscopy. Such a project might evaluate types of colon prep, how prep quality is measured, patient instructions, and the timing/content of pre-procedure reminder phone calls, particularly for e-consult patients.
Conclusion
This QI project provided outcomes for e-consults in the subspecialty of gastroenterology at the VAPHS. Although some benchmark outcomes were met and favorable, others were less favorable. By conducting this benchmark analysis, the areas of needed improvement are now clear. This analysis provides information so recommendations for process improvements can be made.
Quality of care improvement is an ongoing process at VAPHS. Since completion of this project, several processes have been adjusted so that outcomes will be improved. For example, corrective actions were taken for patients who did not complete their gastroenterology procedure. The process for scheduling gastroenterology procedures was adjusted for appointments and cancellations. Ongoing efforts to sustain the reminder phone call were put in place. Changes in NP staffing and time assigned for both clinical and nonclinical work were proposed and are currently under review.
It is the mission of the VA to provide access to care, patient satisfaction, timely care, and appropriate use of resources. Having the ability to highlight our strengths, as well as the willingness to recognize weaknesses, allows us to create new improved processes to provide the best care possible for our veterans.
Acknowledgments
This project was Elena Swann’s capstone for the Doctor of Nursing Practice Program, University of Pittsburgh School of Nursing in Pennsylvania. Rich Laufer, Larry Priscella, and Janie Fleming assisted with the VA Gastroenterology Clinic and procedure metrics. Dr. Melissa Taylor, VA associate chief nurse for research provided project guidance and manuscript revisions. Dr. Sandra Engberg, University of Pittsburgh School of Nursing faculty, assisted with project and manuscript development.
Author disclosures
The author reports no actual or potential conflicts of interest with regard to this article.
Disclaimer
The opinions expressed herein are those of the author and do not necessarily reflect those of Federal Practitioner, Frontline Medical Communications Inc., the U.S. Government, or any of its agencies. This article may discuss unlabeled or investigational use of certain drugs. Please review complete prescribing information for specific drugs or drug combinations—including indications, contraindications, warnings, and adverse effects—before administering pharmacologic therapy to patients.
Although the VA has the largest health care system in the U.S., not every VA facility offers medical subspecialty care. As a result, patients are often separated by long distances from services they need.
At the VA Pittsburgh Healthcare System (VAPHS) in Pennsylvania, about 15,700 veterans received care in 2011. The Gastroenterology Department (GD) served many of these patients: 5,800 patients were seen in clinic appointments, 2,500 underwent colonoscopy, and 1,700 underwent esophagogastroduodenoscopy (EGD). Patients traveled up to 150 miles from 3 states for appointments and procedures. Prior to each procedure, a face-to-face appointment was standard practice for most patients to plan procedures and ensure medical stability. Patients expressed dissatisfaction with transportation, cost, time, and inconvenience, particularly when they were required to attend both the preprocedure and procedure appointments.
Patient satisfaction, timely care, and appropriate use of resources are important VA goals of care, so the VAPHS developed an electronic consultation (e-consult) program as a component of its long-term strategic plan. The goal was to increase access to care through the use of an e-consult in lieu of a face-to-face appointment for select patients. The e-consult program established guidelines and benchmark goals (Table). The program also established a database to track the benchmarks.
The purpose of this quality improvement (QI) project was to evaluate e-consults in the GD over a 6-month period from January 2012, when e-consults were implemented in the GD, to July 2012. Based on the outcomes, recommendations for program continuation, change, and sustainability were made.
Background
Telemedicine using information technologies has been reported as a viable solution to support health care delivery when distance limits patients’ access to care.1,2 Telemedicine has also been shown to improve efficacy in clinical decision making and reduce costs. It also can increase patient satisfaction by reducing travel and time, minimize duplication of diagnostic testing, and integrate services effectively across multiple sites when an electronic medical record (EMR) is in place.1-5
A randomized controlled trial in 2004 compared a standard outpatient referral appointment with a joint teleconsultation between provider, specialist, and patient.3 In the teleconsultation arm, there was higher patient satisfaction, fewer diagnostic tests (particularly in gastroenterology), and lower patient costs.
A study published in 2009 examined the impact of cardiac, dermatologic, and diabetes teleconsultations on organization and patient outcomes in 950 patients in 30 rural communities.2 Rapid access to care was provided for 85% of the patients. Organizational benefits included resource savings and efficacy improvement measured by a provider opinion Likert scale. Patient benefits included reductions in wait times, transportation savings, avoidance of unnecessary office visits, and ease of use.
A large systematic review of telemedicine services across all medical specialties in 2006 included 106 published studies.4 Clinical outcomes (decision making, diagnosis, and management) were similar between conventional care and telemedicine in specialty care, particularly in neurology and psychiatry. Virtual consults provided equal care to traditional specialty visits.6
Communication and coordination of care via an e-consult instead of a face-to-face clinic visit was evaluated by Horner and colleagues.5 The authors identified e-consult benefits for patients and specialists and that e-consults can reduce unnecessary referrals and appointments by 30%. They concluded that reserved time to complete e-consults must be built into workflow systems and that an advanced EMR was necessary for successful use of e-consults.
Two studies have evaluated satisfaction with e-consults. A preliminary analysis of satisfaction with e-consults was conducted in 2009 by K. L. Rodriguez, PhD, and colleagues (unpublished data). Patients, primary care providers (PCPs), and medical specialists reported overall satisfaction in 8 satisfaction domains. A pilot study of 34 patients in 2011 with inflammatory bowel disease compared a standard patient-GD physician encounter with a video encounter.7 The authors reported patient satisfaction, appointment time, wait times, and quality of care were similar for the 2 groups.
Methods
The GD where this QI project was completed consisted of a clinic staffed by nurse practitioners (NPs) and a procedure lab staffed by gastroenterology physicians. Before e-consult implementation, a NP reviewed and triaged new referrals daily. During the project period, an average of 25 to 35 new referrals were received daily via the EMR. Referrals came mostly from PCPs requesting an evaluation of their patients’ gastroenterology problem. Patients were triaged either to an appointment for evaluation or directly to the GD procedure lab for EGD or colonoscopy.
When e-consults were implemented, several changes occurred. Two providers were assigned to new referral triage, and they were expected to process 20% as e-consults. In the EMR, e-consult note titles, templates, and an e-consult encounter form were created, and staff was given access to the e-consult tracking database. The EMR referral template was amended so the entering provider could say whether a face-to-face appointment was desired or whether an e-consult was acceptable. The patient was to be included in decision making about this choice. Department staff had permission to triage according to judgment and expertise; thus, appointment requests could be triaged to e-consults, and e-consult requests could be triaged to appointments.
To complete an e-consult, the EMR was reviewed for medical diagnoses, medications, diagnostics, and recent physical exam. A summary note outlining an impression, treatment recommendations, and follow-up was entered in the EMR and communicated to the PCP. In most cases, no discussion with the patient occurred. The encounter form was completed, and information was entered into the tracking database. The database was installed on each provider’s computer who processed e-consults. If EGD or colonoscopy was indicated, the scheduler was notified to call the patient. Once a procedure date was established, procedure orders were completed in the EMR, and instructions were mailed to the patient.
Project Description and Evaluation
The project was reviewed by the Institutional Review Board and determined to be a QI project. VA organizational policies were followed for data collection and security. Benchmarks were identified from the e-consult program and from the GD, where available. Process variables were determined to measure benchmark outcomes. (Table)
To identify participants, a retrospective chart review was performed. A total of 203 potential patients were identified from the e-consult program database for the 6-month period between January and July 2012. For comparison, 50 patients who attended an appointment during the same time frame were systematically identified in the EMR. Although this comparison group was eligible for e-consults, they were triaged to in-person appointments and subsequently had colonoscopies completed.
Outcome data were extracted from the e-consult program database and the EMR. The data analysis was descriptive. Summary aggregate data were compared with the benchmarks and comparison patient outcomes. The Table summarizes the process variables, how they were measured, where they came from, and what the comparisons were.
Discussion
Figure 1 illustrates the volume of completed e-consults from January to July 2012. A gastroenterology procedure was not indicated in 43 patients. A procedure was indicated for 160 patients and completed in 116 patients (72%). One hundred procedures were colonoscopies, and 16 were EGDs. Figure 2 provides reasons why procedures were not completed in 44 patients (27%). Group comparisons of colon prep quality and preprocedure reminder calls are displayed in Figures 3 and 4, respectively.
This project sought to evaluate VAPHS GD e-consults beginning in January 2012. Process variables were established to measure benchmarks in the e-consult program and in the GD. Some benchmarks were met with outcomes that were comparable between the groups, while others were not. To our knowledge, this project is the first to evaluate e-consults in the subspecialty of gastroenterology.
Volume of Completed E-Consults
The benchmark for 20% e-consults was not met (Figure 1). For weeks 1 through 8, the volume was between 10% and 20%. Lower volume in weeks 9 through 15 (late March and April) may have been due to staff vacations. Not only do the outcomes show a downward trend in e-consult volume, they also show a precipitous fall in volume at week 15 to almost no e-consults for the remainder of the project. To explore reasons for this outcome, the workflow process of new referral triage and e-consults was reviewed.
Two providers (1 NP, 1 physician) were assigned to new referral triage and e-consults from weeks 1 through 14. At week 15, the physician was reassigned to perform procedures. From this point, only 1 NP worked on e-consults and referral triage. Competing time demands included an e-consult encounter form, tracking database entry, procedure orders, patient instructions, appointment changes, phone calls, and resolution of medications issues for procedures. The triage NP was also required to see patients in the clinic. Each day, only a half-day was allotted to complete e-consults, new referral triage (25-35/day), and the aforementioned tasks.
Therefore, it became clear that a half-day was not sufficient to meet the 20% benchmark for e-consults. Horner and colleagues also found that dedicated time in workflow processes was necessary to allow for e-consult completion.5
E-Consults vs Appointment Groups
All patients in both groups were offered the choice of e-consult or appointment; this benchmark was met. Of the 203 e-consult patients, 70% requested an appointment, but their evaluation was completed as an e-consult. By design, the appointment group patients chose e-consult but were triaged to appointment due to time constraints and the high volume of new referrals.
Evaluations via e-consult were completed within 2 to 3 days, whereas the mean for appointments was 19 days, with the longest time frame of 44 days. Thus, e-consult evaluations were completed sooner. Rapid access to care was also found by Zanaboni and colleagues.2
When appointments are delayed, patient complaints or status may change, which in turn may affect treatment plans. In addition, the reason for referral may have already resolved by the actual appointment, rendering the appointment unnecessary. This can be viewed as a missed opportunity for another patient to be seen. Ideally, it is best for a patient to be evaluated soon after a new referral is made.
The VA encounter form for an e-consult had only one 5-digit code, which allotted only 15 minutes of work credit. Encounter form codes were established by the Center for Medicare and Medicaid Services (CMS) for billing purposes in the private sector, with coding levels based on information documented in a chart note: review of systems, physical exam, and diagnoses decision making. Because all criteria could not be met in an e-consult, only 1 code was assigned for VAPHS e-consults. The CMS has specific telemedicine codes; it was unknown why they were not used for e-consults.
E-consults took an average of 19 minutes to complete, with 91 completed in ≤ 15 minutes and over half (112) having taken > 15 minutes. Therefore, the actual workload was not captured, and more work was done than was credited. To speculate, e-consults were in their infancy; a learning curve may have existed as staff became accustomed to this new process.
The EMRs were reviewed for the 7 e-consults that took > 30 minutes to complete. Two were in the early stage of e-consult implementation, but the remainder were scattered throughout. Patients in these e-consults had complicated medical histories and perhaps should not have been triaged to e-consult. Theoretically, only uncomplicated patients with simple reasons for gastroenterology referral should be triaged to e-consult, allowing for a shorter time frame and higher volume.
The wait times to procedure were 58 days for the e-consult group and 39 days in the appointment group. Although wait time was originally identified as an outcome, its relevance is questionable after looking at the outcome data. The procedure appointment date was a subjective decision by the patient; many factors affected what date the patient established, including weekday preference, time off from work, caretaker availability, season, and staffing. Many patients rescheduled their initial procedure dates, often several times. These factors are reflected in the variable ranges of wait times.
Colon Prep Quality
Colon prep refers to patient instructions on the day before the procedure and includes a clear liquid diet, drinking a liquid solution to empty bowel contents, and no food or liquid after midnight. Prep quality is stated in the colonoscopy report. During the procedure, the physician makes a visual decision based on presence or absence of stool inside the colon. Prep quality is important, because retained stool can preclude thorough visualization of the colon wall for polyps or abnormalities. In the event of fair and poor preps, the colonoscopy might be aborted and rescheduled or completed, but with the recommendation for another colonoscopy in a short time frame, such as 1 to 3 years.
Forty-four percent of the e-consult group and 62% of the appointment group had good or adequate preps. Thus, more patients in the appointment group achieved good and adequate preps, and far fewer achieved fair or poor preps. One important point was that almost half (47%) of the e-consult group had only a fair prep (Figure 3).
A number of reasons have been identified in the literature, which might help us understand these findings. First, patients may not fully understand or adhere to prep instructions.8-10 Furthermore, certain medical diagnoses are known to affect prep quality (ie, diabetes, thyroid disease, constipation).11,12 Another potential factor is the manner in which prep quality is determined.13,14 However, due to the focus of this QI study, the influential drivers of prep quality can only be inferred from the literature; thus, a future research or QI study is warranted to ascertain the underlying mechanism of colon prep quality in our specific veteran population.
Preprocedure Reminder Calls
Outcomes were essentially reversed between the 2 groups (Figure 4). Between 50% and 60% of the e-consult group received a call, while the same percentage of appointment patients did not. All patients did attend their procedure appointment. A GD goal was to call every patient before their procedure, but the ability to make the calls was staffing-dependent, which may explain these findings.
Most Relevant Findings
Although this project provides a thorough analysis of various benchmarks within this recently implemented e-consult gastroenterology program, 3 findings emerged that were identified as most relevant. First, the benchmark of 20% volume of completed e-consults was not met. A review of the workflow processes revealed that a daily allotment of only a half-day was not sufficient to complete e-consults, referral triage, and related tasks.
Second, outcomes for colon prep quality and preprocedure reminder calls were also relevant. Although beyond the scope of this project, the question arose of a relationship between prep quality and the reminder call: Does the reminder call affect prep quality? The goal of colon prep is to achieve a good or adequate prep. The purpose of the reminder call was to confirm the appointment and to review the colon prep. Among patients in both groups who achieved only a fair prep, 62% in the e-consult group did receive the reminder call; thus, the call seemed to have failed in helping these patients achieve an adequate or good prep. The actual content of colon prep review during the call was unknown, but certainly bears improvement.
Another speculation concerned the prep instruction sheet. Although all patients received the same sheet, e-consult patients received it in the mail and read it themselves, while it was directly reviewed face-to-face with the appointment patients. Questions remain whether a face-to-face review increases the likelihood for a better prep and how to help e-consult patients achieve optimal prep, since they are not seen face-to-face.
Practice Implications and Sustaining Measures
Theoretically, e-consults are a viable alternative to face-to-face appointments. Potential advantages include efficient use of an EMR, avoidance of unnecessary appointments, and improved access to care for patients who require an appointment. Although patient satisfaction was not measured in this project, the literature review revealed that satisfaction was increased through use of various virtual health care modalities, including a preliminary analysis in this facility by the aforementioned 2009 study by K. L. Rodriguez (unpublished data). Based on findings in this project, the following 4 recommendations were made to improve benchmark outcomes and quality of care.
- Provide dedicated time to complete e-consults and related tasks. In this setting, a full day was recommended. An alternative was to hire a NP whose sole responsibility was e-consults.
- Develop a selection process to determine which new referrals are best suited for e-consult. This process will increase e-consult efficiency and decrease the time to complete an e-consult. Recommended selection criteria were (A) gastroenterology referrals only for simple symptoms or issues; (B) referrals only for a procedure; and (C) stable patients with uncomplicated medical histories.
- Sustain the preprocedure reminder phone call. The reminder call helps patients keep appointments and thus reduces a missed opportunity for care.
- Plan a future QI project or research study on patient colon prep quality for colonoscopy. Such a project might evaluate types of colon prep, how prep quality is measured, patient instructions, and the timing/content of pre-procedure reminder phone calls, particularly for e-consult patients.
Conclusion
This QI project provided outcomes for e-consults in the subspecialty of gastroenterology at the VAPHS. Although some benchmark outcomes were met and favorable, others were less favorable. By conducting this benchmark analysis, the areas of needed improvement are now clear. This analysis provides information so recommendations for process improvements can be made.
Quality of care improvement is an ongoing process at VAPHS. Since completion of this project, several processes have been adjusted so that outcomes will be improved. For example, corrective actions were taken for patients who did not complete their gastroenterology procedure. The process for scheduling gastroenterology procedures was adjusted for appointments and cancellations. Ongoing efforts to sustain the reminder phone call were put in place. Changes in NP staffing and time assigned for both clinical and nonclinical work were proposed and are currently under review.
It is the mission of the VA to provide access to care, patient satisfaction, timely care, and appropriate use of resources. Having the ability to highlight our strengths, as well as the willingness to recognize weaknesses, allows us to create new improved processes to provide the best care possible for our veterans.
Acknowledgments
This project was Elena Swann’s capstone for the Doctor of Nursing Practice Program, University of Pittsburgh School of Nursing in Pennsylvania. Rich Laufer, Larry Priscella, and Janie Fleming assisted with the VA Gastroenterology Clinic and procedure metrics. Dr. Melissa Taylor, VA associate chief nurse for research provided project guidance and manuscript revisions. Dr. Sandra Engberg, University of Pittsburgh School of Nursing faculty, assisted with project and manuscript development.
Author disclosures
The author reports no actual or potential conflicts of interest with regard to this article.
Disclaimer
The opinions expressed herein are those of the author and do not necessarily reflect those of Federal Practitioner, Frontline Medical Communications Inc., the U.S. Government, or any of its agencies. This article may discuss unlabeled or investigational use of certain drugs. Please review complete prescribing information for specific drugs or drug combinations—including indications, contraindications, warnings, and adverse effects—before administering pharmacologic therapy to patients.
1. Bashshur RL, Shannon GW, Krupinski EA, et al. National telemedicine initiatives: Essential to healthcare reform. Telemed J E Health. 2009;15(6):600-610.
2. Zanaboni P, Scalvini S, Bernocchi P, Borghi G, Tridico C, Masella C. Teleconsultation service to improve healthcare in rural areas: Acceptance, organizational impact and appropriateness. BMC Health Serv Res. 2009;9:238.
3. Wallace P, Barber J, Clayton W, et al. Virtual outreach: A randomised controlled trial and economic evaluation of joint teleconferenced medical consultations. Health Technol Assess. 2004;8(50):1-106, iii-iv.
4. Hersh WR, Hickam DH, Severance SM, Dana TL, Pyle Krages K, Helfand M. Diagnosis, access and outcomes: Update of a systematic review of telemedicine services. J Telemed Telecare. 2006;12(suppl 2):S3-S31.
5. Horner K, Wagner E, Tufano J. Electronic consultations between primary and specialty care clinicians: Early insights. Issue Brief (Commonw Fund). 2011;23:1-14.
6. Angstman KB, Adamson SC, Furst JW, Houston MS, Rohrer JE. Provider satisfaction with virtual specialist consultations in a family medicine department. Health Care Manag (Frederick). 2009;28(1):14-18.
7. Krier M, Kaltenbach T, McQuaid K, Soetikno R. Potential use of telemedicine to provide outpatient care for inflammatory bowel disease. Am J Gastroenterol. 2011;106(12):2063-2067.
8. Calderwood AH, Lai EJ, Fix OK, Jacobson BC. An endoscopist-blinded, randomized, controlled trial of a simple visual aid to improve bowel preparation for screening colonoscopy. Gastrointest Endosc. 2011;73(2):307-314.
9. Hillyer GC, Basch CH, Basch CE, et al. Gastroenterologists’ perceived barriers to optimal pre-colonoscopy bowel preparation: Results of a national survey. J Cancer Educ. 2012;27(3):526-532.
10. Smith SG, von Wagner C, McGregor LM, et al. The influence of health literacy on comprehension of a colonoscopy preparation information leaflet. Dis Colon Rectum. 2012;55(10):1074-1080.
11. Mittal S, Lin YL, Tan A, Kuo YF, El-Serag HB, Goodwin JS. Limited life expectancy among a subgroup of Medicare beneficiaries receiving screening colonoscopies. Clin Gastroenterol Hepatol. 2014;12(3):443-450.e1.
12. Ko CW, Sonnenberg A. Comparing risks and benefits of colorectal cancer screening in elderly patients. Gastroenterology. 2005;129(4):1163-1170.
13. Ell C, Fischbach W, Keller R, et al; Hintertux Study Group. A randomized, blinded, prospective trial to compare the safety and efficacy of three bowel-cleansing solutions for colonoscopy (HSG-01*). Endoscopy. 2003;35(4):300-304.
14. Jansen SV, Goedhard JG, Winkens B, van Deursen CT. Preparation before colonoscopy: A randomized controlled trial comparing different regimes. Eur J Gastroenterol Hepatol. 2011;23(10):897-902.
1. Bashshur RL, Shannon GW, Krupinski EA, et al. National telemedicine initiatives: Essential to healthcare reform. Telemed J E Health. 2009;15(6):600-610.
2. Zanaboni P, Scalvini S, Bernocchi P, Borghi G, Tridico C, Masella C. Teleconsultation service to improve healthcare in rural areas: Acceptance, organizational impact and appropriateness. BMC Health Serv Res. 2009;9:238.
3. Wallace P, Barber J, Clayton W, et al. Virtual outreach: A randomised controlled trial and economic evaluation of joint teleconferenced medical consultations. Health Technol Assess. 2004;8(50):1-106, iii-iv.
4. Hersh WR, Hickam DH, Severance SM, Dana TL, Pyle Krages K, Helfand M. Diagnosis, access and outcomes: Update of a systematic review of telemedicine services. J Telemed Telecare. 2006;12(suppl 2):S3-S31.
5. Horner K, Wagner E, Tufano J. Electronic consultations between primary and specialty care clinicians: Early insights. Issue Brief (Commonw Fund). 2011;23:1-14.
6. Angstman KB, Adamson SC, Furst JW, Houston MS, Rohrer JE. Provider satisfaction with virtual specialist consultations in a family medicine department. Health Care Manag (Frederick). 2009;28(1):14-18.
7. Krier M, Kaltenbach T, McQuaid K, Soetikno R. Potential use of telemedicine to provide outpatient care for inflammatory bowel disease. Am J Gastroenterol. 2011;106(12):2063-2067.
8. Calderwood AH, Lai EJ, Fix OK, Jacobson BC. An endoscopist-blinded, randomized, controlled trial of a simple visual aid to improve bowel preparation for screening colonoscopy. Gastrointest Endosc. 2011;73(2):307-314.
9. Hillyer GC, Basch CH, Basch CE, et al. Gastroenterologists’ perceived barriers to optimal pre-colonoscopy bowel preparation: Results of a national survey. J Cancer Educ. 2012;27(3):526-532.
10. Smith SG, von Wagner C, McGregor LM, et al. The influence of health literacy on comprehension of a colonoscopy preparation information leaflet. Dis Colon Rectum. 2012;55(10):1074-1080.
11. Mittal S, Lin YL, Tan A, Kuo YF, El-Serag HB, Goodwin JS. Limited life expectancy among a subgroup of Medicare beneficiaries receiving screening colonoscopies. Clin Gastroenterol Hepatol. 2014;12(3):443-450.e1.
12. Ko CW, Sonnenberg A. Comparing risks and benefits of colorectal cancer screening in elderly patients. Gastroenterology. 2005;129(4):1163-1170.
13. Ell C, Fischbach W, Keller R, et al; Hintertux Study Group. A randomized, blinded, prospective trial to compare the safety and efficacy of three bowel-cleansing solutions for colonoscopy (HSG-01*). Endoscopy. 2003;35(4):300-304.
14. Jansen SV, Goedhard JG, Winkens B, van Deursen CT. Preparation before colonoscopy: A randomized controlled trial comparing different regimes. Eur J Gastroenterol Hepatol. 2011;23(10):897-902.
Improving Functional Outcomes in Patients with Intermittent Claudication
From the University of York, York, UK, and the University Hospital of Angers, Angers, France.
Abstract
- Objective: To provide an overview of therapies for improving functional outcomes in individuals with intermittent claudication due to lower-limb peripheral arterial disease (PAD).
- Methods: Literature review.
- Results: Treatment approaches that aim to improve functional outcomes (and walking performance specifically) in individuals with intermittent claudication include exercise training, lower-limb revascularization, and prescription of various drugs, including peripheral vasodilators. Supervised exercise training, particularly that which involves walking as the main exercise modality, is an effective treatment for improving walking performance in individuals with intermittent claudication; however, few supervised exercise programs exist specifically for these patients, limiting access to this therapy. Consequently, most patients with intermittent claudication do not participate in supervised exercise. The evidence for the effectiveness of unsupervised exercise programs is currently weak and mixed, and lack of motivation and pain have been cited as major barriers to participation in self-managed exercise. Lower-limb revascularization procedures (angioplasty or bypass surgery) can improve walking performance; however, such procedures are not feasible for some patients (eg, in the case of extensive multi-segmental disease) and are invasive and expensive. Medications used to treat PAD-related functional impairment (eg, cilostazol, pentoxifylline, inositol nicotinate, and naftidrofuryl oxalate [not approved in the US]) all have limited efficacy.
- Conclusion: Supervised walking exercise is a cheap and effective approach for improving walking performance in individuals with intermittent claudication. Therefore, efforts should be made to provide patients with access to a supervised exercise program, or to promote self-managed walking when supervised exercise is not available or practical.
Peripheral arterial disease (PAD) is a chronic cardiovascular disease characterised by atherosclerotic narrowing or occlusion of the arteries supplying the legs. It is highly prevalent in older adults, affecting around 20% of adults aged > 70 years [1,2]. Around 10% to 35% of patients report the typical symptoms of intermittent claudication, which is specifically defined as lower-limb discomfort or pain on exertion that is relieved within 10 minutes of rest; however, a further 30% to 40% report other, atypical lower-limb symptoms [3]. Intermittent claudication impairs quality of life by limiting ambulation and activities of daily living [4] and is associated with a several-fold increased risk of cardiovascular and all-cause mortality compared with age-matched healthy controls [5,6]. The treatment of individuals with intermittent claudication has 2 main objectives: secondary prevention of cardiovascular disease and improvement of functional status (and, in turn, quality of life) [3,7,8]. The former objective is usually pursued through prescribing various medications to help manage cardiovascular risk factors (eg, antiplatelets, HMG-CoA reductase inhibitors, antihypertensive and antidiabetic medication) and promoting lifestyle changes such as smoking cessation, increased physical activity, and consumption of a healthy diet. This review focuses on the latter objective by providing an overview of the evidence for different treatments to improve functional outcomes in individuals with intermittent claudication. Patients with PAD often present with multiple comorbidities that may have independent adverse effects on functional capacity (eg, osteoarthritis, chronic heart failure, chronic obstructive pulmonary disease) [9]; therefore, concomitant treatment of comorbidities should be considered when attempting to optimize the functional status of patients.
Assessing Function Outcomes
Functional capacity is a multidimensional construct that represents the highest level of activity that a person may reach at a given moment in a standardized environment [10]. It can encompass one’s ability to perform work-related activities (eg, lifting, static work), activities of daily living (eg, walking, climbing stairs, standing up from a chair), and other exercise-related activities (eg, walking, cycling, weight lifting). Given that the primary functional limitation in intermittent claudication is walking impairment, most functional capacity evaluations in this population focus on walking capacity as the outcome of interest. In terms of walking impairment, individuals with intermittent claudication have poorer walking endurance and slower walking velocity compared to individuals without PAD [4]. People with intermittent claudication may reduce their walking activity to avoid leg symptoms. Thus, clinicians should not equate stabilization or improvement in intermittent claudication with stabilization or improvement in walking performance [11].
There are several methods for assessing walking capacity in individuals with intermittent claudication. Treadmill walking tests are commonly used. Following a transatlantic conference on clinical trials guidelines in PAD [12], two internationally accepted treadmill protocols were recommended: (1) constant-pace treadmill protocol (constant walking speed of 3.2 km·h–1 at 10%–12% gradient), and (2) incremental treadmill protocol (starting horizontally at a constant speed of 3.2 km·h–1, but with the gradient increasing in pre-defined steps (eg, 2%) at pre-defined time intervals (eg, every 2 minutes). The main variables measured during treadmill testing are (1) time to the onset of claudication pain (ie, claudication onset time), and (2) peak walking time, at which point patients request to stop, usually because of intolerable claudication pain [13]. The latter measure is used most frequently in clinical trials as the primary outcome. Previous terms for these variables include pain-free walking distance/time and maximum walking distance/time, respectively.
The 6-minute walk test is an alternative to treadmill testing that is highly reproducible, valid, and sensitive to change in patients with claudication [14,15]. Advantages of this test include the lack of need for special equipment and that it provides a better approximation of community walking compared to treadmill walking in older patients [16,17]. More recently, global positioning system technology has been used to provide an objective assessment of walking capacity under free-living conditions in patients with intermittent claudication [17,18]. This may provide a useful method for physicians who do not have a treadmill and have trouble performing a 6-minute walk test (eg, due to space limitations); however, the validity and reliability of this method is dependent on patients adhering to standardized instructions for conducting a self-managed walking assessment in the community.
Self-reported walking capacity, assessed using standardized questionnaires, can provide a convenient alternative to objective measurement procedures. Various questionnaires have been proposed, of which the Walking Impairment Questionnaire (WIQ) is the most widely used. The WIQ, which was proposed over 20 years ago to standardize the estimation of walking limitation by patient interview [19], involves 14 items with 5 possible items for each item. The 14 items are divided into 3 sub-scales: a distance sub-scale (7 items), a speed sub-scale (4 items), and a stair-climbing sub-scale (3 items). It has been translated into several languages [20–22] and has been shown to be responsive to various treatment modalities [23,24]. Recently, a new shorter questionnaire has been proposed for estimating walking capacity in intermittent claudication, the Walking Estimated Limitation Calculated by History (WELCH) questionnaire [25,26]. Patients are required to report the maximum duration (8 possible responses ranging from “impossible” to “3 hours or more”) they can walk at 3 different speeds (ranging “slow” to “fast”), as well as what their normal walking speed is in comparison to their friends, relatives, and people of a similar age. Compared to the WIQ, the WELCH is shorter, suffers fewer errors when self-completed, provides comparable correlation with treadmill walking capacity data, and can be easily scored without a calculator or computer spreadsheet [25,27,28]. Further research is needed to assess its responsiveness to various interventions. Many other generic and disease-specific questionnaires have been proposed for assessing functional status and quality of life in claudication patients; an extensive review of these questionnaires can be found elsewhere [29]. In our opinion, very few questionnaires besides the WIQ and WELCH are useful for the routine assessment of patients’ walking limitation.
Several tests have been used to assess other aspects of functional capacity in patients with PAD, such as 4-meter walking speed, time to rise from a seated position 5 times, and standing balance (23). Although the inclusion of such measures may provide a more complete picture of a patient’s functional status than by assessing walking capacity alone, given the important of walking impairment in these patients and the predominant focus on this in the literature, the following sections on different treatments will focus solely on walking outcomes.
Treatments
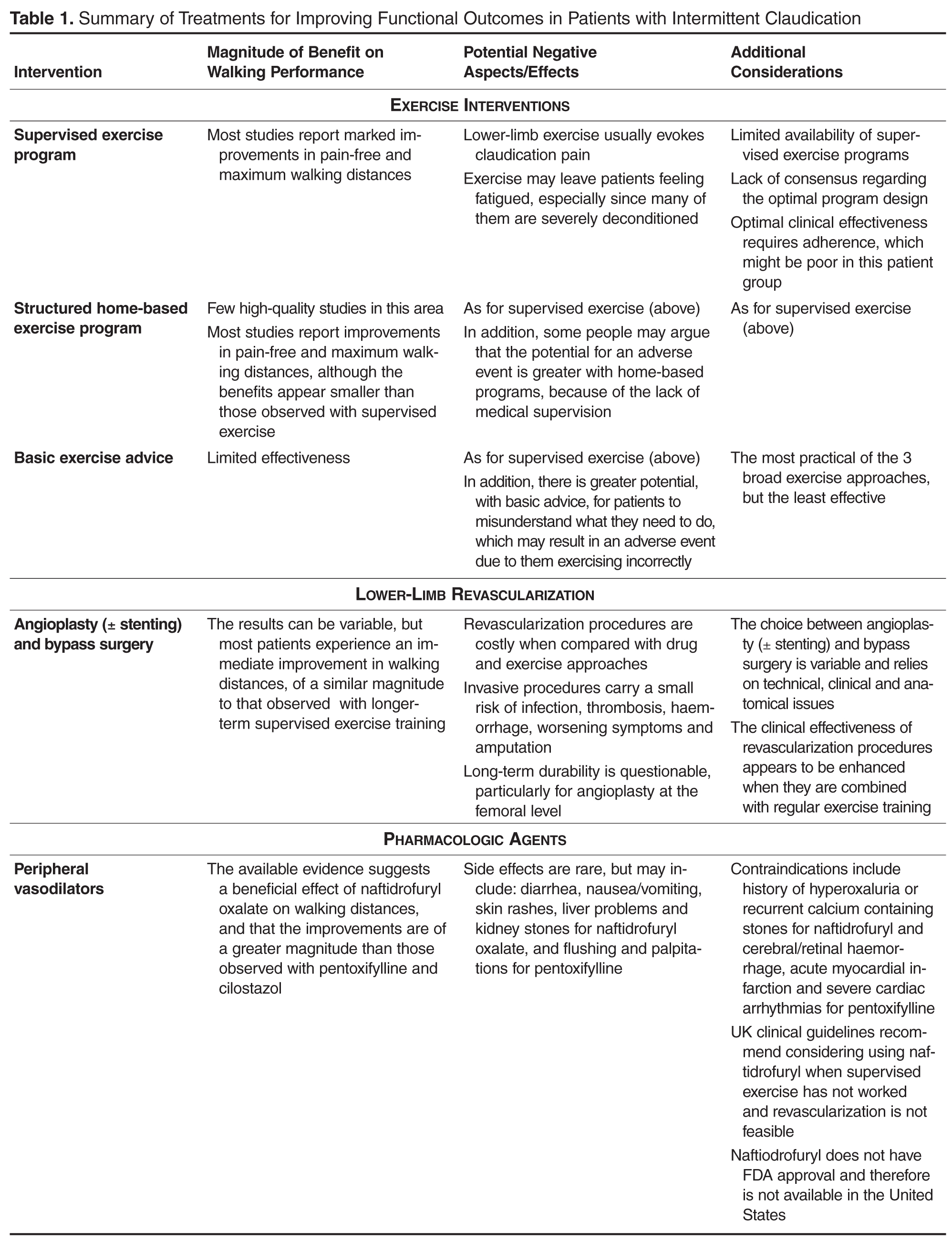
Supervised Exercise Training
There is a considerable body of evidence to support a beneficial effect of supervised exercise training on walking performance in individuals with intermittent claudication. As such, supervised exercise training is recommended as a first-line therapy in clinical guidelines throughout the world [3,7,8]. Several systematic reviews and meta-analyses have attempted to quantify the effects of supervised exercise programs on walking performance [30–34]. For example, Fakhry et al [31] conducted a meta-analysis of 25 randomized controlled trials from 1966 to 2012, 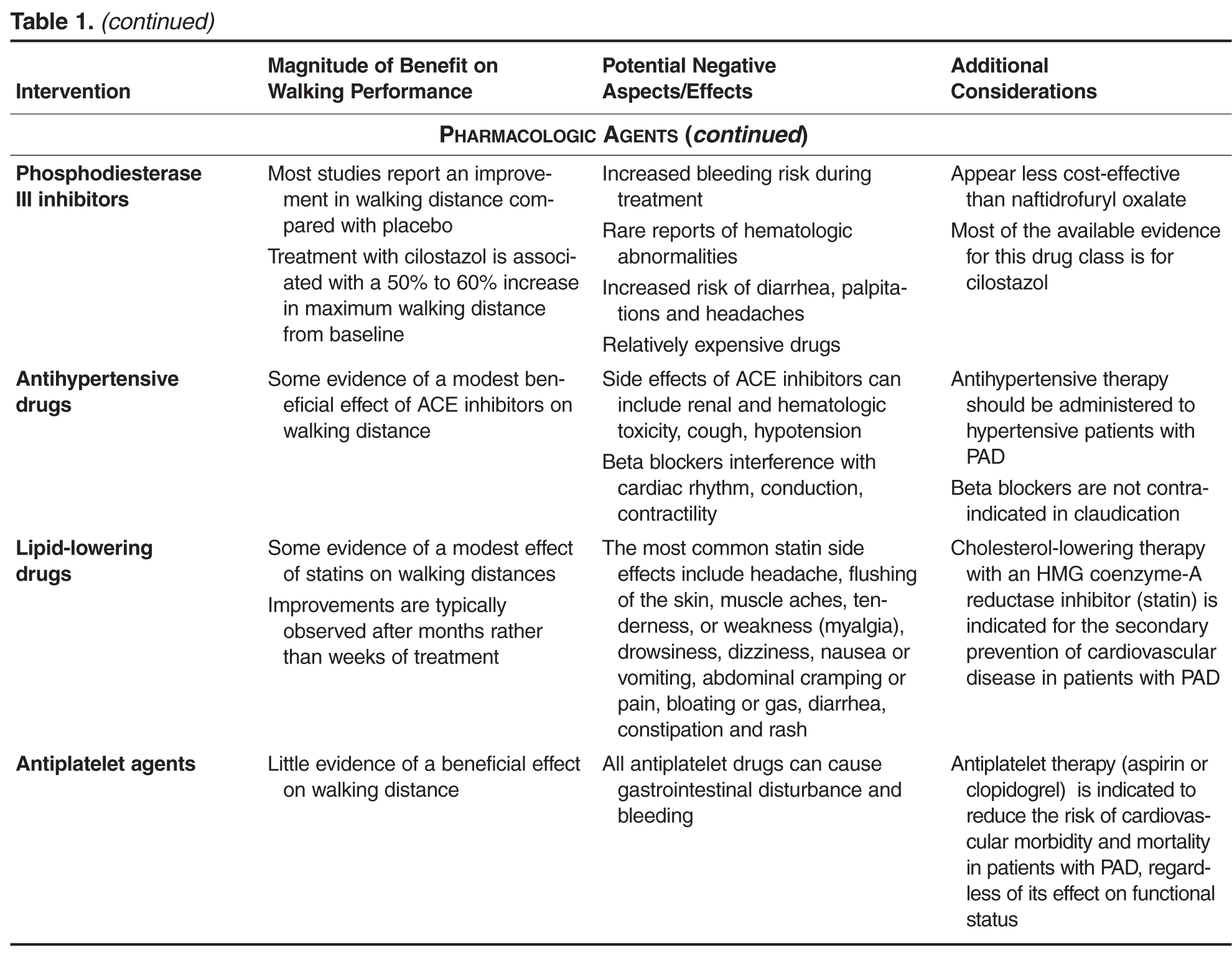
Exercise programs comprise several components, including the mode and intensity of exercise, the duration and frequency of exercise sessions, the length of the program, and the level of supervision. Although few studies have directly compared different exercise regimes, some meta-analyses and systematic reviews have been conducted in an attempt to identify the program components that are the best predictors of improvement in walking distances [31,34,36–39]. For example, the meta-analysis of Gardner and Poehlman [36], which synthesized data from 21 randomized and nonrandomized exercise studies conducted between 1966 and 1993, indicated that claudication pain endpoint, program length, and mode of exercise explained 87% of the variance in improvements in maximum walking distance. Specifically, walking exercise appeared about twice as effective compared with other exercise modalities, walking to near-maximal leg pain was about 3 times more effective than walking to the point of claudication onset, and programs of at least 6 months' duration were about twice as effective as shorter programs. In contrast, the more contemporary synthesis of Fakhry et al [31] found that none of their predefined exercise components were independently associated with improvements in walking distances. Although walking programs are beneficial and frequently recommended 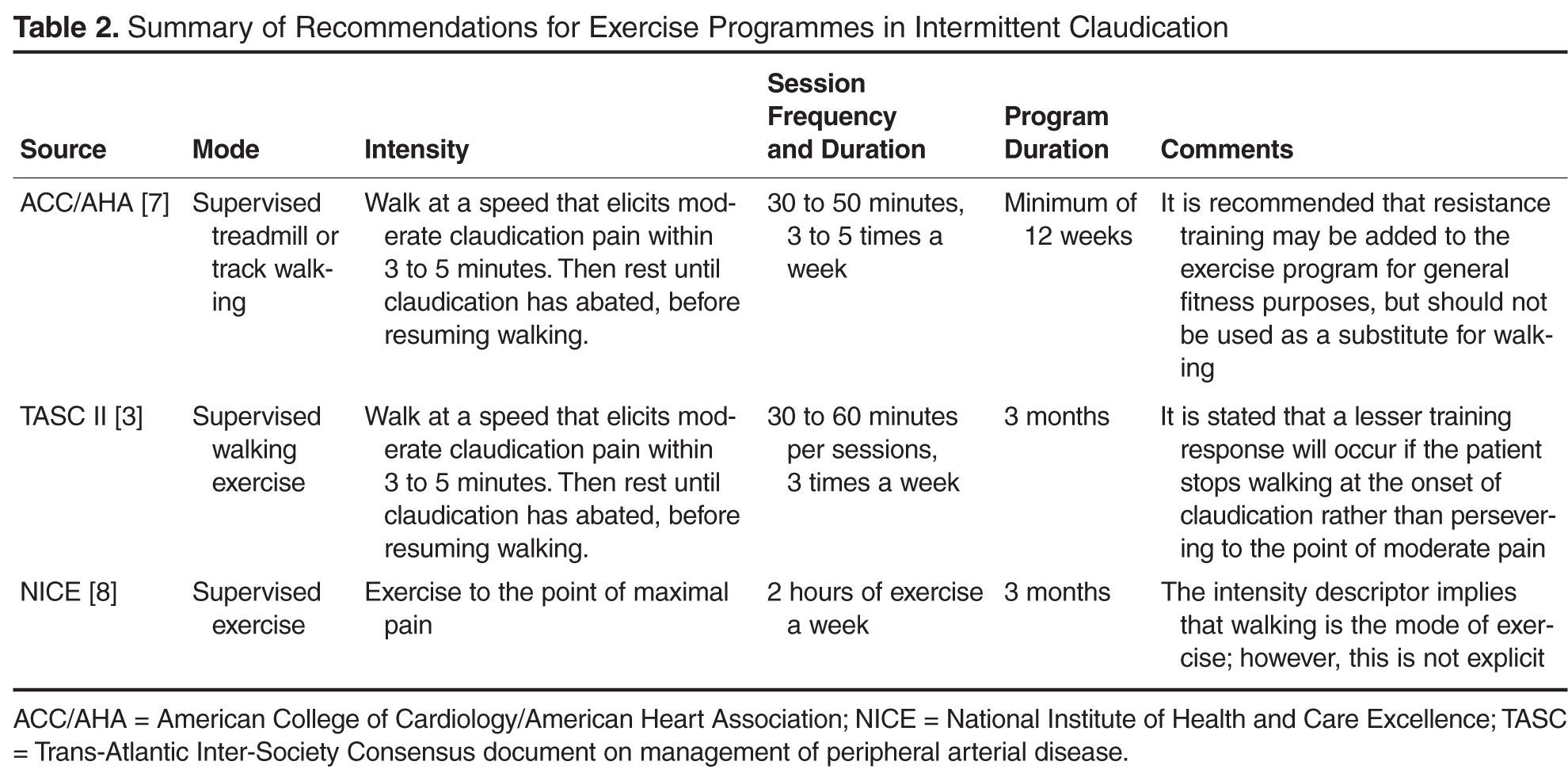
The role of supervision has attracted much interest in recent years. Currently, clinical guidelines recommend supervised exercise as a primary therapy for people with PAD, but not unsupervised exercise because of insufficient supporting evidence [3,7,8]. Unfortunately, most patients with intermittent claudication do not participate in supervised exercise training because of issues such as limited provision and patients being unable or unwilling to travel regularly to an exercise center [42–44]. Therefore, exercise is usually promoted in the form of “go home and walk” advice, but several studies have demonstrated this to have limited efficacy [41,45]. This has prompted researchers to develop and evaluate home-based exercise programs (HEPs), which are structured interventions that include at least one recognized behavior change technique [46] to promote self-managed walking. Recent reviews suggest that HEPs have superior effects on walking distance compared with basic advice to walk more, but inferior effects when compared with supervised exercise training [34,47]. However, most of the HEPs included in those reviews were poorly defined and failed to address patients’ knowledge gaps and uncertainty around the disease process and the role of walking, which is likely critical for providing impetus to behaviour change [48]. Recent trials that have included HEPs that have a clear theoretical underpinning and evidence-based behavior change techniques such as goal-setting, self-monitoring, and barrier identification and problem-solving have shown promising results and therefore may offer a pragmatic approach to promoting self-managed exercise in patients who are unwilling or unable to engage in supervised exercise training [45,49,50].
Safety Considerations
The risk of adverse cardiovascular and physiologic responses during exercise training is higher in patients with cardiovascular disease; therefore, to minimize the risk of exercise-related adverse events, patients with intermittent claudication should be evaluated clinically before initiating an exercise program. Patients should ideally perform a standard treadmill exercise test, with 12-lead electro-cardiographic monitoring if available, before a therapeutic exercise program is initiated [7], to determine that there are no untoward cardiovascular responses during exercise. It will also provide information about claudication thresholds and heart rate and blood pressure responses for establishing an exercise prescription. In best practice it is generally recommended that heart rate, exertion and ischemic symptoms are always monitored, given that an improvement in exercise tolerance might unmask myocardial ischemia. Patients should be counselled that although walking with claudication pain can improve walking distances and will not cause lasting harm, exercising with cardiac ischemia is not desirable and that if they experience chest pain they should stop exercising and, if it persists, contact a doctor or paramedic immediately. Proper foot care is also important, especially in those with diabetes mellitus, to prevent blisters and possible infections, which might in some cases develop into arterial ulcers. Daily inspection of the toes and plantar surfaces of the feet is therefore essential for early detection of any abnormality. Patients should be advised to return to their physician/general practitioner immediately if any changes occur in their feet.
Pharmacologic Therapies
In the UK, 4 drugs are licensed for the symptomatic relief of intermittent claudication: pentoxifylline, inositol nicotinate, cilostazol, and naftidrofuryl oxalate (in the US, naftidrofuryl oxalate is not FDA approved, and inositol is labeled GRAS [generally regarded as safe]). Pentoxifylline (Trental 400, Sanofi-Aventis) is an oral peripheral vasodilator derived from methylxanthine. To date, most studies have found no significant difference in walking distances between pentoxifylline and placebo groups, and a recent meta-analysis suggested that pentoxifylline only increased maximum walking distance by 11% (95% credible interval, –1 to 24%) relative to placebo [51]. Inositol nicotinate (Hexopal, Genus Pharmaceuticals) is an oral peripheral vasodilator that slows the release of nicotinic acid. A recent Health Technology Assessment highlighted that there have only been a few trials of this drug in claudication patients, and that the available data show limited efficacy [52]. It is also relatively expensive and has potential side effects of nausea/vomiting, skin rashes, and headache. Cilostazol (Pletal, Otsuka Pharmaceuticals) is an oral phosphodiesterase type 3 inhibitor, which is reported to have both antiplatelet and vasodilator effects [53]. In a systematic review and meta-analysis of drug therapies for intermittent claudication, Momsen et al reported a dose-dependent positive effect of cilostazol, with mean differences for maximum walking distance of 36 m (95% CI, 30 to 41 m) and 70 m (95% CI, 47 to 93), respectively, for 50 and 100 mg doses taken twice daily [50]. In a separate review, cilostazol was shown to increase maximum walking distance by 25% relative to placebo (95% credible interval, 20 to 114%), and pain-free walking distance by 13% [52]. Naftidrofuryl oxalate (Praxilene, Merck Serono) is an oral peripheral vasodilator that selectively blocks vascular and platelet 5-hydroxytryptamine 2 (5-HT2) receptors. The meta-analysis of Stevens et al, which included 2 trials of naftidrofuryl oxalate for claudication, indicated that this drug increased maximum walking distance by 60% (95% credible interval, 20 to 114%) and pain-free walking distance by 49% (95% credible interval, 23 to 81%) relative to placebo [51]. Comparative analyses indicated that the improvements were of a greater magnitude than those observed with pentoxifylline and cilostazol. An economic evaluation also suggested that naftidrofuryl oxalate “dominated” cilostazol and pentoxifylline, and has an incremental cost per QALY (quality-adjusted life-years) gained of around $9720 compared with no vasoactive drug [52]. However, Hong and Mackey recently concluded that the clinical data for both naftidrofuryl and cilostazol are plagued by flaws related to lack of protocol standardization, objective endpoints, and strict eligibility criteria in study subjects, making identification of a true treatment effect difficult [54].
Other studies have investigated the functional effects of drugs that are commonly used to reduce the risk of cardiovascular events in patients with PAD, including antiplatelet, antihypertensive and lipid-lowering agents. The meta-analysis of Momsen et al assessed the effects of antiplatelet agents on walking distances in intermittent claudication [55]. The included studies involved 5 different drugs (ticlopidine, cloricromene, mesoglycan, indobufen and defibrotide), and while some studies did not show a statistically significant benefit of antiplatelet therapy, the pooled estimate showed a modest increase in maximum walking distance favoring treatment of 59 m (95% CI, 37 to 81 m). The same paper also assessed the effects of 4 lipid-lowering drugs: atorvastatin, simvastatin, policosanol, and avasimibe [55]. Despite variable results according to the specific drug used, the effect estimates favored lipid-lowering agents in all studies and was statistically significant in all but one study. The pooled effect estimate was in favor of intervention, with a clinically relevant increase in maximum walking distance of 163 m (95% CI, 83 to 242 m). Two recent meta-analyses have also reviewed the functional effects of ACE inhibitors in patients with intermittent claudication [56,57], and although data are conflicting, a recent large trial of 212 patients reported that ramipril increased claudication onset time by 75 seconds (95% CI, 60 to 89 seconds) and peak walking time by 255 seconds (215 to 295 seconds) [58]. These changes were independent of the small change in blood pressure that occurred with ramipril treatment.
In summary, while some drugs have been shown to improve walking performance in patients with intermittent claudication, the effect has tended to be modest at best and smaller than that observed with supervised exercise training. Momsen et al concluded that statins probably have the greatest functional benefits [55], and clinical guidelines recommend that all patients with PAD should receive statin therapy [3,7,8], irrespective of its effect on functional status. The UK clinical guidelines recommend considering using naftidrofuryl oxalate for the treatment of claudication, but only when supervised exercise has not worked and revascularization is not feasible or declined by the patient [8]. The ACC/AHA guidelines state that a therapeutic trial of cilostazol should be considered in all patients with lifestyle-limiting claudication in the absence of heart failure [7].
Lower-Limb Revascularization
Intermittent claudication can also be treated using endovascular procedures (angioplasty ± stent placement) or bypass surgery, both of which constitute a relatively more direct means of addressing the problem since they target the arterial lesions causing claudication. Trials of revascularization in PAD have typically focused on vessel/graft patency as the primary outcome, with less emphasis placed on functional endpoints [59]. Despite this, it is clear that successful revascularization rapidly improves walking performance [60,61], whereas noticeable improvements with supervised exercise training can take several weeks to occur (assuming good adherence) [62]. Long-term comparisons of lower-limb revascularization with alternative treatment modalities for people with intermittent claudication are scarce. Recently, Fakhry et al [63] reported the long-term clinical effectiveness of supervised exercise therapy and endovascular revascularization from a randomized trial of 151 patients. After 7 years, the treatment strategies were similarly effective in improving functional performance and quality of life; however, the total number of endovascular and surgical interventions (primary and secondary) was substantially higher in the revascularization group, which will have resulted in significantly higher health care costs in this group. Furthermore, given that supervised exercise training costs substantially less than any revascularization procedure, it is not surprising that economic analyses indicate supervised exercise training as being more cost-effective [64,65]. This is reflected in clinical guidelines, which promote supervised exercise training as the first-line therapy [3,7,8]. In the UK, NICE recommends that clinicians should only offer angioplasty for treating people with intermittent claudication when advice on the benefits of modifying risk factors has been reinforced, a supervised exercise program has not led to a satisfactory improvement in symptoms, and imaging has confirmed that angioplasty is suitable for the person [8]. Bypass surgery for treating people with severe lifestyle-limiting intermittent claudication is only recommended when angioplasty has been unsuccessful or is unsuitable, and imaging has confirmed that bypass surgery is appropriate for the person. Overall, from a technical point of view during revascularization, there is no strong evidence to support that differences in clinical outcomes are observed as a function of technical choices of anastomoses in aortobifemoral bypasses [66] or kind of angioplasty in femoropopliteal lesions [67].
Potential Alternative Therapeutic Approaches
Several non-drug, non-exercise, and non-revascularization approaches have been investigated for their impact on claudication-related functional impairment, including (but not limited to) acupuncture, biofeedback, chelation therapy, CO2-applications, and the dietary supplements Allium sativum (garlic), Ginkgo biloba, omega-3 fatty acids, Padma 28, Vitamin E, and carnitine supplementation. In a recent systematic review, Delaney et al highlighted that most of the 8 parallel-group randomized controlled trials of propionyl-L-carnitine supplementation (600 to 3000 mg administered orally) demonstrated improvements in walking performance between 31 and 54 m greater than placebo for pain-free walking distance and between 9 and 86 m greater than placebo for maximum walking distance [68]. Propionyl-L-carnitine has been postulated to improve walking distance by improving endothelial function, and increasing total carnitine content in the ischemic muscle, which improves muscle metabolism and stimulates oxidative phosphorylation resulting in a decrease in plasma lactate concentration on exercise [68]. In a systematic review of these complementary therapies for PAD from 2005 [69], Pittler and Ernst concluded that there was some evidence for a beneficial effect of Ginkgo biloba and Padma 28 in claudication patients; however, recent meta-analyses have concluded that there is no evidence that Ginkgo biloba produces clinically meaningful improvements in walking distances [70], and that further well-designed research is required to determine the true effects of Padma 28 [71]. None of the other complementary treatment options have sufficient supporting evidence for them to be proposed as a routine approach [72–75]. Last, a few small studies have indicated that intermittent pneumatic compression (IPC) interventions can improve walking distances in people with intermittent claudication [76–78]. To date, IPC has received limited use in the clinical setting due to issues of cost and constraint; however, modern technology has permitted the development of portable systems to be made readily available for affordable at-home use. Adequately powered randomized controlled trials and economic evaluations are required to clarify the role of IPC for improving functional outcomes in intermittent claudication.
Conclusion
Intermittent claudication, the main symptom of mild-to-moderate PAD, is common in older adults. Individuals with intermittent claudication have reduced walking endurance and slower walking speed compared to individuals without PAD, and impairments in walking can reduce patients’ quality of life. There are several therapeutic options for improving walking performance in intermittent claudication, none of which are without limitations. Lower-limb revascularization procedures (angioplasty, bypass surgery) are invasive and have limited durability, and the medications approved for claudication-related functional impairment have limited efficacy. Supervised walking exercise can substantially improve walking performance; however, most patients do not participate in a supervised program due to issues of availability, awareness and access. Therefore, efforts should be made to provide patients with access to a supervised exercise program and encouragement to attend, or to promote self-managed walking when supervised exercise is not available or practical.
Corresponding author: Dr Garry A. Tew, York Trials Unit, Dept. of Health Sciences, University of York, York, YO10 5DD, UK, [email protected].
Financial disclosures: None.
Author contributions: conception and design, GAT, PA; drafting of article, GAT, PA; critical revision of the article, GAT, PA.
1. Fowkes FG, Housley E, Cawood EH, et al. Edinburgh Artery Study: prevalence of asymptomatic and symptomatic peripheral arterial disease in the general population. Int J Epidemiol 1991;20:384–92.
2. Criqui MH, Fronek A, Barrett-Connor E, et al. The prevalence of peripheral arterial disease in a defined population. Circulation 1985;71;510–5.
3. Norgren L, Hiatt WR, Dormandy JA, et al. Inter-Society Consensus for the Management of Peripheral Arterial Disease (TASC II). Eur J Vasc Endovasc Surg. 2007;33 Suppl 1:S1–75.
4. Nehler MR, McDermott MM, Treat-Jacobson D, et al. Functional outcomes and quality of life in peripheral arterial disease: current status. Vasc Med 2003;8:115–26.
5. Caro J, Migliaccio-Walle K, Ishak KJ, Proskorovsky I. The morbidity and mortality following a diagnosis of peripheral arterial disease: long-term follow-up of a large database. BMC Cardiovasc Disord 2005;5:14.
6. Criqui MH, Langer RD, Fronek A, et al. Mortality over a period of 10 years in patients with peripheral arterial disease. N Engl J Med 1992;326:381–6.
7. Hirsch AT, Haskal ZJ, Hertzer NR, et al. ACC/AHA 2005 Practice Guidelines for the management of patients with peripheral arterial disease (lower extremity, renal, mesenteric, and abdominal aortic): a collaborative report from the American Association for Vascular Surgery/Society for Vascular Surgery, Society for Cardiovascular Angiography and Interventions, Society for Vascular Medicine and Biology, Society of Interventional Radiology, and the ACC/AHA Task Force on Practice Guidelines (Writing Committee to Develop Guidelines for the Management of Patients With Peripheral Arterial Disease): endorsed by the American Association of Cardiovascular and Pulmonary Rehabilitation; National Heart, Lung, and Blood Institute; Society for Vascular Nursing; TransAtlantic Inter-Society Consensus; and Vascular Disease Foundation. Circulation 2006;113:e463–654.
8. Layden J, Michaels J, Bermingham S, et al. Diagnosis and management of lower limb peripheral arterial disease: summary of NICE guidance. BMJ 2012;345:e4947.
9. Diehm C, Schuster A, Allenberg JR, et al. High prevalence of peripheral arterial disease and co-morbidity in 6880 primary care patients: cross-sectional study. Atherosclerosis 2004;172:95–105.
10. Soer R, van der Schans CP, Groothoff JW, et al. Towards consensus in operational definitions in functional capacity evaluation: a Delphi Survey. J Occup Rehabil 2008;18:389–400.
11. McDermott MM. Functional impairment in peripheral artery disease and how to improve it in 2013. Curr Cardiol Rep 2013;15:347.
12. Labs KH, Dormandy JA, Jaeger KA, et al. Transatlantic Conference on Clinical Trial Guidelines in Peripheral Arterial Disease: clinical trial methodology. Basel PAD Clinical Trial Methodology Group. Circulation 1999;100:e75–81.
13. Hiatt WR, Goldstone J, Smith SC, et al. Atherosclerotic Peripheral Vascular Disease Symposium II: nomenclature for vascular diseases. Circulation 2008;118:2826–9.
14. Montgomery PS, Gardner AW. The clinical utility of a six-minute walk test in peripheral arterial occlusive disease patients. J Am Geriatr Soc 1998;46:706–11.
15. McDermott MM, Guralnik JM, Criqui MH, et al. Six-minute walk is a better outcome measure than treadmill walking tests in therapeutic trials of patients with peripheral artery disease. Circulation 2014;130:61–8.
16. McDermott MM, Ades PA, Dyer A, et al. Corridor-based functional performance measures correlate better with physical activity during daily life than treadmill measures in persons with peripheral arterial disease. J Vasc Surg 2008;48:1231–7, 7.e1.
17. Tew G, Copeland R, Le Faucheur A, et al. Feasibility and validity of self-reported walking capacity in patients with intermittent claudication. J Vasc Surg 2013;57:1227–34.
18. Le Faucheur A, Abraham P, Jaquinandi V, et al. Measurement of walking distance and speed in patients with peripheral arterial disease: a novel method using a global positioning system. Circulation 2008;117:897–904.
19. Regensteiner JG, Steiner JF, Panzer RJ, Hiatt WR. Evaluation of walking impairment by questionnaire in patients with peripheral arterial disease. J Vasc Med Biol 1990;2:142–52.
20. Verspaget M, Nicolaï SP, Kruidenier LM, et al. Validation of the Dutch version of the Walking Impairment Questionnaire. Eur J Vasc Endovasc Surg 2009;37:56–61.
21. Yan BP, Lau JY, Yu CM, et al. Chinese translation and validation of the Walking Impairment Questionnaire in patients with peripheral artery disease. Vasc Med 2011;16:167–72.
22. Collins TC, Suarez-Almazor M, Petersen NJ, O'Malley KJ. A Spanish translation of the Walking Impairment Questionnaire was validated for patients with peripheral arterial disease. J Clin Epidemiol 2004;57:1305–15.
23. McDermott MM, Ades P, Guralnik JM, et al. Treadmill exercise and resistance training in patients with peripheral arterial disease with and without intermittent claudication: a randomized controlled trial. JAMA 2009;301:165–74.
24. Murphy TP, Cutlip DE, Regensteiner JG, et al. Supervised exercise versus primary stenting for claudication resulting from aortoiliac peripheral artery disease: six-month outcomes from the claudication: exercise versus endoluminal revascularization (CLEVER) study. Circulation 2012;125:130–9.
25. Ouedraogo N, Chanut M, Aubourg M, et al. Development and evaluation of the Walking Estimated-Limitation Calculated by History questionnaire in patients with claudication. J Vasc Surg 2013;58:981–8.
26. Tew GA, Nawaz S, Humphreys L, et al. Validation of the English version of the Walking Estimated-Limitation Calculated by History (WELCH) questionnaire in patients with intermittent claudication. Vasc Med 2014;19:27–32.
27. Mahe G, Ouedraogo N, Vasseur M, et al. Limitations of self-reported estimates of functional capacity using the Walking Impairment Questionnaire. Eur J Vasc Endovasc Surg 2011;41:104–9.
28. Ouedraogo N, Mahe G, Marchand J, et al. Validation of a new simple questionnaire to "estimate ambulation capacity by history" (EACH) in patients with claudication. J Vasc Surg 2011;54:133–8.
29. Mays RJ, Casserly IP, Kohrt WM, et al. Assessment of functional status and quality of life in claudication. J Vasc Surg 2011;53:1410–21.
30. Wind J, Koelemay MJ. Exercise therapy and the additional effect of supervision on exercise therapy in patients with intermittent claudication. Systematic review of randomised controlled trials. Eur J Vasc Endovasc Surg 2007;34:1–9.
31. Fakhry F, van de Luijtgaarden KM, Bax L, et al. Supervised walking therapy in patients with intermittent claudication. J Vasc Surg 2012;56:1132–42.
32. Fokkenrood HJ, Bendermacher BL, Lauret GJ, et al. Supervised exercise therapy versus non-supervised exercise therapy for intermittent claudication. Cochrane Database Syst Rev 2013;8:CD005263.
33. Lane R, Ellis B, Watson L, Leng GC. Exercise for intermittent claudication. Cochrane Database Syst Rev 2014;7:CD000990.
34. Gommans LN, Saarloos R, Schelting MR, et al. Editor's choice--The effect of supervision on walking distance in patients with intermittent claudication: a meta-analysis. Eur J Vasc Endovasc Surg 2014;48:169–84.
35. Hamburg NM, Balady GJ. Exercise rehabilitation in peripheral artery disease: functional impact and mechanisms of benefits. Circulation 2011;123:87–97.
36. Gardner AW, Poehlman ET. Exercise rehabilitation programs for the treatment of claudication pain. A meta-analysis. JAMA 1995;274:975–80.
37. Bulmer AC, Coombes JS. Optimising exercise training in peripheral arterial disease. Sports Med 2004;34:983–1003.
38. Parmenter BJ, Raymond J, Dinnen P, Singh MA. A systematic review of randomized controlled trials: Walking versus alternative exercise prescription as treatment for intermittent claudication. Atherosclerosis 2011;218:1–12.
39. Lauret GJ, Fakhry F, Fokkenrood HJ, et al. Modes of exercise training for intermittent claudication. Cochrane Database Syst Rev 2014;7:CD009638.
40. Zwierska I, Walker RD, Choksy SA, et al. Upper- vs lower-limb aerobic exercise rehabilitation in patients with symptomatic peripheral arterial disease: a randomized controlled trial. J Vasc Surg 2005;42:1122–30.
41. Tew G, Nawaz S, Zwierska I, Saxton JM. Limb-specific and cross-transfer effects of arm-crank exercise training in patients with symptomatic peripheral arterial disease. Clin Sci (Lond) 2009;117:405–13.
42. Regensteiner JG. Exercise rehabilitation for the patient with intermittent claudication: a highly effective yet underutilized treatment. Curr Drug Targets Cardiovasc Haematol Disord 2004;4:233–9.
43. Makris GC, Lattimer CR, Lavida A, Geroulakos G. Availability of supervised exercise programs and the role of structured home-based exercise in peripheral arterial disease. Eur J Vasc Endovasc Surg 2012;44:569–75.
44. Popplewell MA, Bradbury AW. Why do health systems not fund supervised exercise programmes for intermittent claudication? Eur J Vasc Endovasc Surg. 2014 Aug 28. [Epub ahead of print]
45. Cunningham MA, Swanson V, O'Carroll RE, et al. Randomized clinical trial of a brief psychological intervention to increase walking in patients with intermittent claudication. Br J Surg 2012;99:49–56.
46. Michie S, Ashford S, Sniehotta FF, et al. A refined taxonomy of behaviour change techniques to help people change their physical activity and healthy eating behaviours: the CALO-RE taxonomy. Psychol Health 2011;26:1479–98.
47. Al-Jundi W, Madbak K, Beard JD, et al. Systematic review of home-based exercise programmes for individuals with intermittent claudication. Eur J Vasc Endovasc Surg 2013;46:690–706.
48. Egberg L, Andreassen S, Mattiasson AC. Experiences of living with intermittent claudication. J Vasc Nurs 2012;30:5–10.
49. McDermott MM, Liu K, Guralnik JM, et al. Home-based walking exercise intervention in peripheral artery disease: a randomized clinical trial. JAMA 2013;310:57–65.
50. Gardner AW, Parker DE, Montgomery PS, Scott KJ, Blevins SM. Efficacy of quantified home-based exercise and supervised exercise in patients with intermittent claudication: a randomized controlled trial. Circulation 2011;123:491–8.
51. Stevens JW, Simpson E, Harnan S, et al. Systematic review of the efficacy of cilostazol, naftidrofuryl oxalate and pentoxifylline for the treatment of intermittent claudication. Br J Surg 2012;99:1630–8.
52. Squires H, Simpson E, Meng Y, et al. A systematic review and economic evaluation of cilostazol, naftidrofuryl oxalate, pentoxifylline and inositol nicotinate for the treatment of intermittent claudication in people with peripheral arterial disease. Health Technol Assess 2011;15:1–210.
53. Takahashi S, Oida K, Fujiwara R, et al. Effect of cilostazol, a cyclic AMP phosphodiesterase inhibitor, on the proliferation of rat aortic smooth muscle cells in culture. J Cardiovasc Pharmacol 1992;20:900–6.
54. Hong H, Mackey WC. The limits of evidence in drug approval and availability: a case study of cilostazol and naftidrofuryl for the treatment of intermittent claudication. Clin Ther 2014;36:1290–301.
55. Momsen AH, Jensen MB, Norager CB, et al. Drug therapy for improving walking distance in intermittent claudication: a systematic review and meta-analysis of robust randomised controlled studies. Eur J Vasc Endovasc Surg 2009;38:463–74.
56. Shahin Y, Mazari F, Chetter I. Do angiotensin converting enzyme inhibitors improve walking distance in patients with symptomatic lower limb arterial disease? A systematic review and meta-analysis of randomised controlled trials. Int J Surg 2011;9:209–13.
57. Hunter MR, Cahoon WD, Lowe DK. Angiotensin-converting enzyme inhibitors for intermittent claudication associated with peripheral arterial disease. Ann Pharmacother 2013;47:1552–7.
58. Ahimastos AA, Walker PJ, Askew C, et al. Effect of ramipril on walking times and quality of life among patients with peripheral artery disease and intermittent claudication: a randomized controlled trial. JAMA 2013;309:453–60.
59. Kinlay S. Outcomes for clinical studies assessing drug and revascularization therapies for claudication and critical limb ischemia in peripheral artery disease. Circulation 2013;127:1241–50.
60. Ahimastos AA, Pappas EP, Buttner PG, et al. A meta-analysis of the outcome of endovascular and noninvasive therapies in the treatment of intermittent claudication. J Vasc Surg 2011;54:1511–21.
61. Nordanstig J, Taft C, Hensäter M, et al. Improved quality of life after one year with an invasive versus a non-invasive treatment strategy in claudicants: one year results of the IRONIC Trial. Circulation 2014 Aug. [Epub ahead of print]
62. Gardner AW, Montgomery PS, Parker DE. Optimal exercise program length for patients with claudication. J Vasc Surg 2012;55:1346–54.
63. Fakhry F, Rouwet EV, den Hoed PT, et al. Long-term clinical effectiveness of supervised exercise therapy versus endovascular revascularization for intermittent claudication from a randomized clinical trial. Br J Surg 2013;100:1164–71.
64. Fokkenrood HJ, Scheltinga MR, Koelemay MJ, et al. Significant savings with a stepped care model for treatment of patients with intermittent claudication. Eur J Vasc Endovasc Surg 2014;48:423–9.
65. Spronk S, Bosch JL, den Hoed PT, et al. Cost-effectiveness of endovascular revascularization compared to supervised hospital-based exercise training in patients with intermittent claudication: a randomized controlled trial. J Vasc Surg 2008;48:1472–80.
66. Ameli FM, Stein M, Aro L, et al. End-to-end versus end-to-side proximal anastomosis in aortobifemoral bypass surgery: does it matter? Can J Surg 1991;34:243–6.
67. Cejna M, Thurnher S, Illiasch H, et al. PTA versus Palmaz stent placement in femoropopliteal artery obstructions: a multicenter prospective randomized study. J Vasc Interv Radiol 2001;12:23–31.
68. Delaney CL, Spark JI, Thomas J, et al. A systematic review to evaluate the effectiveness of carnitine supplementation in improving walking performance among individuals with intermittent claudication. Atherosclerosis 2013;229:1–9.
69. Pittler MH, Ernst E. Complementary therapies for peripheral arterial disease: systematic review. Atherosclerosis 2005;181:1–7.
70. Nicolaï SP, Kruidenier LM, Bendermacher BL, et al. Ginkgo biloba for intermittent claudication. Cochrane Database Syst Rev 2009 (2):CD006888.
71. Morling JR, Maxwell H, Stewart M. Padma 28 for intermittent claudication. Cochrane Database Syst Rev 2013;7:CD007371.
72. Campbell A, Price J, Hiatt WR. Omega-3 fatty acids for intermittent claudication. Cochrane Database Syst Rev 2013;7:CD003833.
73. Kleijnen J, Mackerras D. Vitamin E for intermittent claudication. Cochrane Database Syst Rev 2000;2:CD000987.
74. Jepson RG, Kleijnen J, Leng GC. Garlic for peripheral arterial occlusive disease. Cochrane Database Syst Rev 2013;4:CD000095.
75. Villarruz MV, Dans A, Tan F. Chelation therapy for atherosclerotic cardiovascular disease. Cochrane Database Syst Rev 2002;4:CD002785.
76. Kakkos SK, Geroulakos G, Nicolaides AN. Improvement of the walking ability in intermittent claudication due to superficial femoral artery occlusion with supervised exercise and pneumatic foot and calf compression: a randomised controlled trial. Eur J Vasc Endovasc Surg 2005;30:164–75.
77. Delis KT, Nicolaides AN. Effect of intermittent pneumatic compression of foot and calf on walking distance, hemodynamics, and quality of life in patients with arterial claudication: a prospective randomized controlled study with 1-year follow-up. Ann Surg 2005;241:431–41.
78. de Haro J, Acin F, Florez A, et al. A prospective randomized controlled study with intermittent mechanical compression of the calf in patients with claudication. J Vasc Surg 2010;51:857–62.
From the University of York, York, UK, and the University Hospital of Angers, Angers, France.
Abstract
- Objective: To provide an overview of therapies for improving functional outcomes in individuals with intermittent claudication due to lower-limb peripheral arterial disease (PAD).
- Methods: Literature review.
- Results: Treatment approaches that aim to improve functional outcomes (and walking performance specifically) in individuals with intermittent claudication include exercise training, lower-limb revascularization, and prescription of various drugs, including peripheral vasodilators. Supervised exercise training, particularly that which involves walking as the main exercise modality, is an effective treatment for improving walking performance in individuals with intermittent claudication; however, few supervised exercise programs exist specifically for these patients, limiting access to this therapy. Consequently, most patients with intermittent claudication do not participate in supervised exercise. The evidence for the effectiveness of unsupervised exercise programs is currently weak and mixed, and lack of motivation and pain have been cited as major barriers to participation in self-managed exercise. Lower-limb revascularization procedures (angioplasty or bypass surgery) can improve walking performance; however, such procedures are not feasible for some patients (eg, in the case of extensive multi-segmental disease) and are invasive and expensive. Medications used to treat PAD-related functional impairment (eg, cilostazol, pentoxifylline, inositol nicotinate, and naftidrofuryl oxalate [not approved in the US]) all have limited efficacy.
- Conclusion: Supervised walking exercise is a cheap and effective approach for improving walking performance in individuals with intermittent claudication. Therefore, efforts should be made to provide patients with access to a supervised exercise program, or to promote self-managed walking when supervised exercise is not available or practical.
Peripheral arterial disease (PAD) is a chronic cardiovascular disease characterised by atherosclerotic narrowing or occlusion of the arteries supplying the legs. It is highly prevalent in older adults, affecting around 20% of adults aged > 70 years [1,2]. Around 10% to 35% of patients report the typical symptoms of intermittent claudication, which is specifically defined as lower-limb discomfort or pain on exertion that is relieved within 10 minutes of rest; however, a further 30% to 40% report other, atypical lower-limb symptoms [3]. Intermittent claudication impairs quality of life by limiting ambulation and activities of daily living [4] and is associated with a several-fold increased risk of cardiovascular and all-cause mortality compared with age-matched healthy controls [5,6]. The treatment of individuals with intermittent claudication has 2 main objectives: secondary prevention of cardiovascular disease and improvement of functional status (and, in turn, quality of life) [3,7,8]. The former objective is usually pursued through prescribing various medications to help manage cardiovascular risk factors (eg, antiplatelets, HMG-CoA reductase inhibitors, antihypertensive and antidiabetic medication) and promoting lifestyle changes such as smoking cessation, increased physical activity, and consumption of a healthy diet. This review focuses on the latter objective by providing an overview of the evidence for different treatments to improve functional outcomes in individuals with intermittent claudication. Patients with PAD often present with multiple comorbidities that may have independent adverse effects on functional capacity (eg, osteoarthritis, chronic heart failure, chronic obstructive pulmonary disease) [9]; therefore, concomitant treatment of comorbidities should be considered when attempting to optimize the functional status of patients.
Assessing Function Outcomes
Functional capacity is a multidimensional construct that represents the highest level of activity that a person may reach at a given moment in a standardized environment [10]. It can encompass one’s ability to perform work-related activities (eg, lifting, static work), activities of daily living (eg, walking, climbing stairs, standing up from a chair), and other exercise-related activities (eg, walking, cycling, weight lifting). Given that the primary functional limitation in intermittent claudication is walking impairment, most functional capacity evaluations in this population focus on walking capacity as the outcome of interest. In terms of walking impairment, individuals with intermittent claudication have poorer walking endurance and slower walking velocity compared to individuals without PAD [4]. People with intermittent claudication may reduce their walking activity to avoid leg symptoms. Thus, clinicians should not equate stabilization or improvement in intermittent claudication with stabilization or improvement in walking performance [11].
There are several methods for assessing walking capacity in individuals with intermittent claudication. Treadmill walking tests are commonly used. Following a transatlantic conference on clinical trials guidelines in PAD [12], two internationally accepted treadmill protocols were recommended: (1) constant-pace treadmill protocol (constant walking speed of 3.2 km·h–1 at 10%–12% gradient), and (2) incremental treadmill protocol (starting horizontally at a constant speed of 3.2 km·h–1, but with the gradient increasing in pre-defined steps (eg, 2%) at pre-defined time intervals (eg, every 2 minutes). The main variables measured during treadmill testing are (1) time to the onset of claudication pain (ie, claudication onset time), and (2) peak walking time, at which point patients request to stop, usually because of intolerable claudication pain [13]. The latter measure is used most frequently in clinical trials as the primary outcome. Previous terms for these variables include pain-free walking distance/time and maximum walking distance/time, respectively.
The 6-minute walk test is an alternative to treadmill testing that is highly reproducible, valid, and sensitive to change in patients with claudication [14,15]. Advantages of this test include the lack of need for special equipment and that it provides a better approximation of community walking compared to treadmill walking in older patients [16,17]. More recently, global positioning system technology has been used to provide an objective assessment of walking capacity under free-living conditions in patients with intermittent claudication [17,18]. This may provide a useful method for physicians who do not have a treadmill and have trouble performing a 6-minute walk test (eg, due to space limitations); however, the validity and reliability of this method is dependent on patients adhering to standardized instructions for conducting a self-managed walking assessment in the community.
Self-reported walking capacity, assessed using standardized questionnaires, can provide a convenient alternative to objective measurement procedures. Various questionnaires have been proposed, of which the Walking Impairment Questionnaire (WIQ) is the most widely used. The WIQ, which was proposed over 20 years ago to standardize the estimation of walking limitation by patient interview [19], involves 14 items with 5 possible items for each item. The 14 items are divided into 3 sub-scales: a distance sub-scale (7 items), a speed sub-scale (4 items), and a stair-climbing sub-scale (3 items). It has been translated into several languages [20–22] and has been shown to be responsive to various treatment modalities [23,24]. Recently, a new shorter questionnaire has been proposed for estimating walking capacity in intermittent claudication, the Walking Estimated Limitation Calculated by History (WELCH) questionnaire [25,26]. Patients are required to report the maximum duration (8 possible responses ranging from “impossible” to “3 hours or more”) they can walk at 3 different speeds (ranging “slow” to “fast”), as well as what their normal walking speed is in comparison to their friends, relatives, and people of a similar age. Compared to the WIQ, the WELCH is shorter, suffers fewer errors when self-completed, provides comparable correlation with treadmill walking capacity data, and can be easily scored without a calculator or computer spreadsheet [25,27,28]. Further research is needed to assess its responsiveness to various interventions. Many other generic and disease-specific questionnaires have been proposed for assessing functional status and quality of life in claudication patients; an extensive review of these questionnaires can be found elsewhere [29]. In our opinion, very few questionnaires besides the WIQ and WELCH are useful for the routine assessment of patients’ walking limitation.
Several tests have been used to assess other aspects of functional capacity in patients with PAD, such as 4-meter walking speed, time to rise from a seated position 5 times, and standing balance (23). Although the inclusion of such measures may provide a more complete picture of a patient’s functional status than by assessing walking capacity alone, given the important of walking impairment in these patients and the predominant focus on this in the literature, the following sections on different treatments will focus solely on walking outcomes.
Treatments
Supervised Exercise Training
There is a considerable body of evidence to support a beneficial effect of supervised exercise training on walking performance in individuals with intermittent claudication. As such, supervised exercise training is recommended as a first-line therapy in clinical guidelines throughout the world [3,7,8]. Several systematic reviews and meta-analyses have attempted to quantify the effects of supervised exercise programs on walking performance [30–34]. For example, Fakhry et al [31] conducted a meta-analysis of 25 randomized controlled trials from 1966 to 2012,
Exercise programs comprise several components, including the mode and intensity of exercise, the duration and frequency of exercise sessions, the length of the program, and the level of supervision. Although few studies have directly compared different exercise regimes, some meta-analyses and systematic reviews have been conducted in an attempt to identify the program components that are the best predictors of improvement in walking distances [31,34,36–39]. For example, the meta-analysis of Gardner and Poehlman [36], which synthesized data from 21 randomized and nonrandomized exercise studies conducted between 1966 and 1993, indicated that claudication pain endpoint, program length, and mode of exercise explained 87% of the variance in improvements in maximum walking distance. Specifically, walking exercise appeared about twice as effective compared with other exercise modalities, walking to near-maximal leg pain was about 3 times more effective than walking to the point of claudication onset, and programs of at least 6 months' duration were about twice as effective as shorter programs. In contrast, the more contemporary synthesis of Fakhry et al [31] found that none of their predefined exercise components were independently associated with improvements in walking distances. Although walking programs are beneficial and frequently recommended
The role of supervision has attracted much interest in recent years. Currently, clinical guidelines recommend supervised exercise as a primary therapy for people with PAD, but not unsupervised exercise because of insufficient supporting evidence [3,7,8]. Unfortunately, most patients with intermittent claudication do not participate in supervised exercise training because of issues such as limited provision and patients being unable or unwilling to travel regularly to an exercise center [42–44]. Therefore, exercise is usually promoted in the form of “go home and walk” advice, but several studies have demonstrated this to have limited efficacy [41,45]. This has prompted researchers to develop and evaluate home-based exercise programs (HEPs), which are structured interventions that include at least one recognized behavior change technique [46] to promote self-managed walking. Recent reviews suggest that HEPs have superior effects on walking distance compared with basic advice to walk more, but inferior effects when compared with supervised exercise training [34,47]. However, most of the HEPs included in those reviews were poorly defined and failed to address patients’ knowledge gaps and uncertainty around the disease process and the role of walking, which is likely critical for providing impetus to behaviour change [48]. Recent trials that have included HEPs that have a clear theoretical underpinning and evidence-based behavior change techniques such as goal-setting, self-monitoring, and barrier identification and problem-solving have shown promising results and therefore may offer a pragmatic approach to promoting self-managed exercise in patients who are unwilling or unable to engage in supervised exercise training [45,49,50].
Safety Considerations
The risk of adverse cardiovascular and physiologic responses during exercise training is higher in patients with cardiovascular disease; therefore, to minimize the risk of exercise-related adverse events, patients with intermittent claudication should be evaluated clinically before initiating an exercise program. Patients should ideally perform a standard treadmill exercise test, with 12-lead electro-cardiographic monitoring if available, before a therapeutic exercise program is initiated [7], to determine that there are no untoward cardiovascular responses during exercise. It will also provide information about claudication thresholds and heart rate and blood pressure responses for establishing an exercise prescription. In best practice it is generally recommended that heart rate, exertion and ischemic symptoms are always monitored, given that an improvement in exercise tolerance might unmask myocardial ischemia. Patients should be counselled that although walking with claudication pain can improve walking distances and will not cause lasting harm, exercising with cardiac ischemia is not desirable and that if they experience chest pain they should stop exercising and, if it persists, contact a doctor or paramedic immediately. Proper foot care is also important, especially in those with diabetes mellitus, to prevent blisters and possible infections, which might in some cases develop into arterial ulcers. Daily inspection of the toes and plantar surfaces of the feet is therefore essential for early detection of any abnormality. Patients should be advised to return to their physician/general practitioner immediately if any changes occur in their feet.
Pharmacologic Therapies
In the UK, 4 drugs are licensed for the symptomatic relief of intermittent claudication: pentoxifylline, inositol nicotinate, cilostazol, and naftidrofuryl oxalate (in the US, naftidrofuryl oxalate is not FDA approved, and inositol is labeled GRAS [generally regarded as safe]). Pentoxifylline (Trental 400, Sanofi-Aventis) is an oral peripheral vasodilator derived from methylxanthine. To date, most studies have found no significant difference in walking distances between pentoxifylline and placebo groups, and a recent meta-analysis suggested that pentoxifylline only increased maximum walking distance by 11% (95% credible interval, –1 to 24%) relative to placebo [51]. Inositol nicotinate (Hexopal, Genus Pharmaceuticals) is an oral peripheral vasodilator that slows the release of nicotinic acid. A recent Health Technology Assessment highlighted that there have only been a few trials of this drug in claudication patients, and that the available data show limited efficacy [52]. It is also relatively expensive and has potential side effects of nausea/vomiting, skin rashes, and headache. Cilostazol (Pletal, Otsuka Pharmaceuticals) is an oral phosphodiesterase type 3 inhibitor, which is reported to have both antiplatelet and vasodilator effects [53]. In a systematic review and meta-analysis of drug therapies for intermittent claudication, Momsen et al reported a dose-dependent positive effect of cilostazol, with mean differences for maximum walking distance of 36 m (95% CI, 30 to 41 m) and 70 m (95% CI, 47 to 93), respectively, for 50 and 100 mg doses taken twice daily [50]. In a separate review, cilostazol was shown to increase maximum walking distance by 25% relative to placebo (95% credible interval, 20 to 114%), and pain-free walking distance by 13% [52]. Naftidrofuryl oxalate (Praxilene, Merck Serono) is an oral peripheral vasodilator that selectively blocks vascular and platelet 5-hydroxytryptamine 2 (5-HT2) receptors. The meta-analysis of Stevens et al, which included 2 trials of naftidrofuryl oxalate for claudication, indicated that this drug increased maximum walking distance by 60% (95% credible interval, 20 to 114%) and pain-free walking distance by 49% (95% credible interval, 23 to 81%) relative to placebo [51]. Comparative analyses indicated that the improvements were of a greater magnitude than those observed with pentoxifylline and cilostazol. An economic evaluation also suggested that naftidrofuryl oxalate “dominated” cilostazol and pentoxifylline, and has an incremental cost per QALY (quality-adjusted life-years) gained of around $9720 compared with no vasoactive drug [52]. However, Hong and Mackey recently concluded that the clinical data for both naftidrofuryl and cilostazol are plagued by flaws related to lack of protocol standardization, objective endpoints, and strict eligibility criteria in study subjects, making identification of a true treatment effect difficult [54].
Other studies have investigated the functional effects of drugs that are commonly used to reduce the risk of cardiovascular events in patients with PAD, including antiplatelet, antihypertensive and lipid-lowering agents. The meta-analysis of Momsen et al assessed the effects of antiplatelet agents on walking distances in intermittent claudication [55]. The included studies involved 5 different drugs (ticlopidine, cloricromene, mesoglycan, indobufen and defibrotide), and while some studies did not show a statistically significant benefit of antiplatelet therapy, the pooled estimate showed a modest increase in maximum walking distance favoring treatment of 59 m (95% CI, 37 to 81 m). The same paper also assessed the effects of 4 lipid-lowering drugs: atorvastatin, simvastatin, policosanol, and avasimibe [55]. Despite variable results according to the specific drug used, the effect estimates favored lipid-lowering agents in all studies and was statistically significant in all but one study. The pooled effect estimate was in favor of intervention, with a clinically relevant increase in maximum walking distance of 163 m (95% CI, 83 to 242 m). Two recent meta-analyses have also reviewed the functional effects of ACE inhibitors in patients with intermittent claudication [56,57], and although data are conflicting, a recent large trial of 212 patients reported that ramipril increased claudication onset time by 75 seconds (95% CI, 60 to 89 seconds) and peak walking time by 255 seconds (215 to 295 seconds) [58]. These changes were independent of the small change in blood pressure that occurred with ramipril treatment.
In summary, while some drugs have been shown to improve walking performance in patients with intermittent claudication, the effect has tended to be modest at best and smaller than that observed with supervised exercise training. Momsen et al concluded that statins probably have the greatest functional benefits [55], and clinical guidelines recommend that all patients with PAD should receive statin therapy [3,7,8], irrespective of its effect on functional status. The UK clinical guidelines recommend considering using naftidrofuryl oxalate for the treatment of claudication, but only when supervised exercise has not worked and revascularization is not feasible or declined by the patient [8]. The ACC/AHA guidelines state that a therapeutic trial of cilostazol should be considered in all patients with lifestyle-limiting claudication in the absence of heart failure [7].
Lower-Limb Revascularization
Intermittent claudication can also be treated using endovascular procedures (angioplasty ± stent placement) or bypass surgery, both of which constitute a relatively more direct means of addressing the problem since they target the arterial lesions causing claudication. Trials of revascularization in PAD have typically focused on vessel/graft patency as the primary outcome, with less emphasis placed on functional endpoints [59]. Despite this, it is clear that successful revascularization rapidly improves walking performance [60,61], whereas noticeable improvements with supervised exercise training can take several weeks to occur (assuming good adherence) [62]. Long-term comparisons of lower-limb revascularization with alternative treatment modalities for people with intermittent claudication are scarce. Recently, Fakhry et al [63] reported the long-term clinical effectiveness of supervised exercise therapy and endovascular revascularization from a randomized trial of 151 patients. After 7 years, the treatment strategies were similarly effective in improving functional performance and quality of life; however, the total number of endovascular and surgical interventions (primary and secondary) was substantially higher in the revascularization group, which will have resulted in significantly higher health care costs in this group. Furthermore, given that supervised exercise training costs substantially less than any revascularization procedure, it is not surprising that economic analyses indicate supervised exercise training as being more cost-effective [64,65]. This is reflected in clinical guidelines, which promote supervised exercise training as the first-line therapy [3,7,8]. In the UK, NICE recommends that clinicians should only offer angioplasty for treating people with intermittent claudication when advice on the benefits of modifying risk factors has been reinforced, a supervised exercise program has not led to a satisfactory improvement in symptoms, and imaging has confirmed that angioplasty is suitable for the person [8]. Bypass surgery for treating people with severe lifestyle-limiting intermittent claudication is only recommended when angioplasty has been unsuccessful or is unsuitable, and imaging has confirmed that bypass surgery is appropriate for the person. Overall, from a technical point of view during revascularization, there is no strong evidence to support that differences in clinical outcomes are observed as a function of technical choices of anastomoses in aortobifemoral bypasses [66] or kind of angioplasty in femoropopliteal lesions [67].
Potential Alternative Therapeutic Approaches
Several non-drug, non-exercise, and non-revascularization approaches have been investigated for their impact on claudication-related functional impairment, including (but not limited to) acupuncture, biofeedback, chelation therapy, CO2-applications, and the dietary supplements Allium sativum (garlic), Ginkgo biloba, omega-3 fatty acids, Padma 28, Vitamin E, and carnitine supplementation. In a recent systematic review, Delaney et al highlighted that most of the 8 parallel-group randomized controlled trials of propionyl-L-carnitine supplementation (600 to 3000 mg administered orally) demonstrated improvements in walking performance between 31 and 54 m greater than placebo for pain-free walking distance and between 9 and 86 m greater than placebo for maximum walking distance [68]. Propionyl-L-carnitine has been postulated to improve walking distance by improving endothelial function, and increasing total carnitine content in the ischemic muscle, which improves muscle metabolism and stimulates oxidative phosphorylation resulting in a decrease in plasma lactate concentration on exercise [68]. In a systematic review of these complementary therapies for PAD from 2005 [69], Pittler and Ernst concluded that there was some evidence for a beneficial effect of Ginkgo biloba and Padma 28 in claudication patients; however, recent meta-analyses have concluded that there is no evidence that Ginkgo biloba produces clinically meaningful improvements in walking distances [70], and that further well-designed research is required to determine the true effects of Padma 28 [71]. None of the other complementary treatment options have sufficient supporting evidence for them to be proposed as a routine approach [72–75]. Last, a few small studies have indicated that intermittent pneumatic compression (IPC) interventions can improve walking distances in people with intermittent claudication [76–78]. To date, IPC has received limited use in the clinical setting due to issues of cost and constraint; however, modern technology has permitted the development of portable systems to be made readily available for affordable at-home use. Adequately powered randomized controlled trials and economic evaluations are required to clarify the role of IPC for improving functional outcomes in intermittent claudication.
Conclusion
Intermittent claudication, the main symptom of mild-to-moderate PAD, is common in older adults. Individuals with intermittent claudication have reduced walking endurance and slower walking speed compared to individuals without PAD, and impairments in walking can reduce patients’ quality of life. There are several therapeutic options for improving walking performance in intermittent claudication, none of which are without limitations. Lower-limb revascularization procedures (angioplasty, bypass surgery) are invasive and have limited durability, and the medications approved for claudication-related functional impairment have limited efficacy. Supervised walking exercise can substantially improve walking performance; however, most patients do not participate in a supervised program due to issues of availability, awareness and access. Therefore, efforts should be made to provide patients with access to a supervised exercise program and encouragement to attend, or to promote self-managed walking when supervised exercise is not available or practical.
Corresponding author: Dr Garry A. Tew, York Trials Unit, Dept. of Health Sciences, University of York, York, YO10 5DD, UK, [email protected].
Financial disclosures: None.
Author contributions: conception and design, GAT, PA; drafting of article, GAT, PA; critical revision of the article, GAT, PA.
From the University of York, York, UK, and the University Hospital of Angers, Angers, France.
Abstract
- Objective: To provide an overview of therapies for improving functional outcomes in individuals with intermittent claudication due to lower-limb peripheral arterial disease (PAD).
- Methods: Literature review.
- Results: Treatment approaches that aim to improve functional outcomes (and walking performance specifically) in individuals with intermittent claudication include exercise training, lower-limb revascularization, and prescription of various drugs, including peripheral vasodilators. Supervised exercise training, particularly that which involves walking as the main exercise modality, is an effective treatment for improving walking performance in individuals with intermittent claudication; however, few supervised exercise programs exist specifically for these patients, limiting access to this therapy. Consequently, most patients with intermittent claudication do not participate in supervised exercise. The evidence for the effectiveness of unsupervised exercise programs is currently weak and mixed, and lack of motivation and pain have been cited as major barriers to participation in self-managed exercise. Lower-limb revascularization procedures (angioplasty or bypass surgery) can improve walking performance; however, such procedures are not feasible for some patients (eg, in the case of extensive multi-segmental disease) and are invasive and expensive. Medications used to treat PAD-related functional impairment (eg, cilostazol, pentoxifylline, inositol nicotinate, and naftidrofuryl oxalate [not approved in the US]) all have limited efficacy.
- Conclusion: Supervised walking exercise is a cheap and effective approach for improving walking performance in individuals with intermittent claudication. Therefore, efforts should be made to provide patients with access to a supervised exercise program, or to promote self-managed walking when supervised exercise is not available or practical.
Peripheral arterial disease (PAD) is a chronic cardiovascular disease characterised by atherosclerotic narrowing or occlusion of the arteries supplying the legs. It is highly prevalent in older adults, affecting around 20% of adults aged > 70 years [1,2]. Around 10% to 35% of patients report the typical symptoms of intermittent claudication, which is specifically defined as lower-limb discomfort or pain on exertion that is relieved within 10 minutes of rest; however, a further 30% to 40% report other, atypical lower-limb symptoms [3]. Intermittent claudication impairs quality of life by limiting ambulation and activities of daily living [4] and is associated with a several-fold increased risk of cardiovascular and all-cause mortality compared with age-matched healthy controls [5,6]. The treatment of individuals with intermittent claudication has 2 main objectives: secondary prevention of cardiovascular disease and improvement of functional status (and, in turn, quality of life) [3,7,8]. The former objective is usually pursued through prescribing various medications to help manage cardiovascular risk factors (eg, antiplatelets, HMG-CoA reductase inhibitors, antihypertensive and antidiabetic medication) and promoting lifestyle changes such as smoking cessation, increased physical activity, and consumption of a healthy diet. This review focuses on the latter objective by providing an overview of the evidence for different treatments to improve functional outcomes in individuals with intermittent claudication. Patients with PAD often present with multiple comorbidities that may have independent adverse effects on functional capacity (eg, osteoarthritis, chronic heart failure, chronic obstructive pulmonary disease) [9]; therefore, concomitant treatment of comorbidities should be considered when attempting to optimize the functional status of patients.
Assessing Function Outcomes
Functional capacity is a multidimensional construct that represents the highest level of activity that a person may reach at a given moment in a standardized environment [10]. It can encompass one’s ability to perform work-related activities (eg, lifting, static work), activities of daily living (eg, walking, climbing stairs, standing up from a chair), and other exercise-related activities (eg, walking, cycling, weight lifting). Given that the primary functional limitation in intermittent claudication is walking impairment, most functional capacity evaluations in this population focus on walking capacity as the outcome of interest. In terms of walking impairment, individuals with intermittent claudication have poorer walking endurance and slower walking velocity compared to individuals without PAD [4]. People with intermittent claudication may reduce their walking activity to avoid leg symptoms. Thus, clinicians should not equate stabilization or improvement in intermittent claudication with stabilization or improvement in walking performance [11].
There are several methods for assessing walking capacity in individuals with intermittent claudication. Treadmill walking tests are commonly used. Following a transatlantic conference on clinical trials guidelines in PAD [12], two internationally accepted treadmill protocols were recommended: (1) constant-pace treadmill protocol (constant walking speed of 3.2 km·h–1 at 10%–12% gradient), and (2) incremental treadmill protocol (starting horizontally at a constant speed of 3.2 km·h–1, but with the gradient increasing in pre-defined steps (eg, 2%) at pre-defined time intervals (eg, every 2 minutes). The main variables measured during treadmill testing are (1) time to the onset of claudication pain (ie, claudication onset time), and (2) peak walking time, at which point patients request to stop, usually because of intolerable claudication pain [13]. The latter measure is used most frequently in clinical trials as the primary outcome. Previous terms for these variables include pain-free walking distance/time and maximum walking distance/time, respectively.
The 6-minute walk test is an alternative to treadmill testing that is highly reproducible, valid, and sensitive to change in patients with claudication [14,15]. Advantages of this test include the lack of need for special equipment and that it provides a better approximation of community walking compared to treadmill walking in older patients [16,17]. More recently, global positioning system technology has been used to provide an objective assessment of walking capacity under free-living conditions in patients with intermittent claudication [17,18]. This may provide a useful method for physicians who do not have a treadmill and have trouble performing a 6-minute walk test (eg, due to space limitations); however, the validity and reliability of this method is dependent on patients adhering to standardized instructions for conducting a self-managed walking assessment in the community.
Self-reported walking capacity, assessed using standardized questionnaires, can provide a convenient alternative to objective measurement procedures. Various questionnaires have been proposed, of which the Walking Impairment Questionnaire (WIQ) is the most widely used. The WIQ, which was proposed over 20 years ago to standardize the estimation of walking limitation by patient interview [19], involves 14 items with 5 possible items for each item. The 14 items are divided into 3 sub-scales: a distance sub-scale (7 items), a speed sub-scale (4 items), and a stair-climbing sub-scale (3 items). It has been translated into several languages [20–22] and has been shown to be responsive to various treatment modalities [23,24]. Recently, a new shorter questionnaire has been proposed for estimating walking capacity in intermittent claudication, the Walking Estimated Limitation Calculated by History (WELCH) questionnaire [25,26]. Patients are required to report the maximum duration (8 possible responses ranging from “impossible” to “3 hours or more”) they can walk at 3 different speeds (ranging “slow” to “fast”), as well as what their normal walking speed is in comparison to their friends, relatives, and people of a similar age. Compared to the WIQ, the WELCH is shorter, suffers fewer errors when self-completed, provides comparable correlation with treadmill walking capacity data, and can be easily scored without a calculator or computer spreadsheet [25,27,28]. Further research is needed to assess its responsiveness to various interventions. Many other generic and disease-specific questionnaires have been proposed for assessing functional status and quality of life in claudication patients; an extensive review of these questionnaires can be found elsewhere [29]. In our opinion, very few questionnaires besides the WIQ and WELCH are useful for the routine assessment of patients’ walking limitation.
Several tests have been used to assess other aspects of functional capacity in patients with PAD, such as 4-meter walking speed, time to rise from a seated position 5 times, and standing balance (23). Although the inclusion of such measures may provide a more complete picture of a patient’s functional status than by assessing walking capacity alone, given the important of walking impairment in these patients and the predominant focus on this in the literature, the following sections on different treatments will focus solely on walking outcomes.
Treatments
Supervised Exercise Training
There is a considerable body of evidence to support a beneficial effect of supervised exercise training on walking performance in individuals with intermittent claudication. As such, supervised exercise training is recommended as a first-line therapy in clinical guidelines throughout the world [3,7,8]. Several systematic reviews and meta-analyses have attempted to quantify the effects of supervised exercise programs on walking performance [30–34]. For example, Fakhry et al [31] conducted a meta-analysis of 25 randomized controlled trials from 1966 to 2012,
Exercise programs comprise several components, including the mode and intensity of exercise, the duration and frequency of exercise sessions, the length of the program, and the level of supervision. Although few studies have directly compared different exercise regimes, some meta-analyses and systematic reviews have been conducted in an attempt to identify the program components that are the best predictors of improvement in walking distances [31,34,36–39]. For example, the meta-analysis of Gardner and Poehlman [36], which synthesized data from 21 randomized and nonrandomized exercise studies conducted between 1966 and 1993, indicated that claudication pain endpoint, program length, and mode of exercise explained 87% of the variance in improvements in maximum walking distance. Specifically, walking exercise appeared about twice as effective compared with other exercise modalities, walking to near-maximal leg pain was about 3 times more effective than walking to the point of claudication onset, and programs of at least 6 months' duration were about twice as effective as shorter programs. In contrast, the more contemporary synthesis of Fakhry et al [31] found that none of their predefined exercise components were independently associated with improvements in walking distances. Although walking programs are beneficial and frequently recommended
The role of supervision has attracted much interest in recent years. Currently, clinical guidelines recommend supervised exercise as a primary therapy for people with PAD, but not unsupervised exercise because of insufficient supporting evidence [3,7,8]. Unfortunately, most patients with intermittent claudication do not participate in supervised exercise training because of issues such as limited provision and patients being unable or unwilling to travel regularly to an exercise center [42–44]. Therefore, exercise is usually promoted in the form of “go home and walk” advice, but several studies have demonstrated this to have limited efficacy [41,45]. This has prompted researchers to develop and evaluate home-based exercise programs (HEPs), which are structured interventions that include at least one recognized behavior change technique [46] to promote self-managed walking. Recent reviews suggest that HEPs have superior effects on walking distance compared with basic advice to walk more, but inferior effects when compared with supervised exercise training [34,47]. However, most of the HEPs included in those reviews were poorly defined and failed to address patients’ knowledge gaps and uncertainty around the disease process and the role of walking, which is likely critical for providing impetus to behaviour change [48]. Recent trials that have included HEPs that have a clear theoretical underpinning and evidence-based behavior change techniques such as goal-setting, self-monitoring, and barrier identification and problem-solving have shown promising results and therefore may offer a pragmatic approach to promoting self-managed exercise in patients who are unwilling or unable to engage in supervised exercise training [45,49,50].
Safety Considerations
The risk of adverse cardiovascular and physiologic responses during exercise training is higher in patients with cardiovascular disease; therefore, to minimize the risk of exercise-related adverse events, patients with intermittent claudication should be evaluated clinically before initiating an exercise program. Patients should ideally perform a standard treadmill exercise test, with 12-lead electro-cardiographic monitoring if available, before a therapeutic exercise program is initiated [7], to determine that there are no untoward cardiovascular responses during exercise. It will also provide information about claudication thresholds and heart rate and blood pressure responses for establishing an exercise prescription. In best practice it is generally recommended that heart rate, exertion and ischemic symptoms are always monitored, given that an improvement in exercise tolerance might unmask myocardial ischemia. Patients should be counselled that although walking with claudication pain can improve walking distances and will not cause lasting harm, exercising with cardiac ischemia is not desirable and that if they experience chest pain they should stop exercising and, if it persists, contact a doctor or paramedic immediately. Proper foot care is also important, especially in those with diabetes mellitus, to prevent blisters and possible infections, which might in some cases develop into arterial ulcers. Daily inspection of the toes and plantar surfaces of the feet is therefore essential for early detection of any abnormality. Patients should be advised to return to their physician/general practitioner immediately if any changes occur in their feet.
Pharmacologic Therapies
In the UK, 4 drugs are licensed for the symptomatic relief of intermittent claudication: pentoxifylline, inositol nicotinate, cilostazol, and naftidrofuryl oxalate (in the US, naftidrofuryl oxalate is not FDA approved, and inositol is labeled GRAS [generally regarded as safe]). Pentoxifylline (Trental 400, Sanofi-Aventis) is an oral peripheral vasodilator derived from methylxanthine. To date, most studies have found no significant difference in walking distances between pentoxifylline and placebo groups, and a recent meta-analysis suggested that pentoxifylline only increased maximum walking distance by 11% (95% credible interval, –1 to 24%) relative to placebo [51]. Inositol nicotinate (Hexopal, Genus Pharmaceuticals) is an oral peripheral vasodilator that slows the release of nicotinic acid. A recent Health Technology Assessment highlighted that there have only been a few trials of this drug in claudication patients, and that the available data show limited efficacy [52]. It is also relatively expensive and has potential side effects of nausea/vomiting, skin rashes, and headache. Cilostazol (Pletal, Otsuka Pharmaceuticals) is an oral phosphodiesterase type 3 inhibitor, which is reported to have both antiplatelet and vasodilator effects [53]. In a systematic review and meta-analysis of drug therapies for intermittent claudication, Momsen et al reported a dose-dependent positive effect of cilostazol, with mean differences for maximum walking distance of 36 m (95% CI, 30 to 41 m) and 70 m (95% CI, 47 to 93), respectively, for 50 and 100 mg doses taken twice daily [50]. In a separate review, cilostazol was shown to increase maximum walking distance by 25% relative to placebo (95% credible interval, 20 to 114%), and pain-free walking distance by 13% [52]. Naftidrofuryl oxalate (Praxilene, Merck Serono) is an oral peripheral vasodilator that selectively blocks vascular and platelet 5-hydroxytryptamine 2 (5-HT2) receptors. The meta-analysis of Stevens et al, which included 2 trials of naftidrofuryl oxalate for claudication, indicated that this drug increased maximum walking distance by 60% (95% credible interval, 20 to 114%) and pain-free walking distance by 49% (95% credible interval, 23 to 81%) relative to placebo [51]. Comparative analyses indicated that the improvements were of a greater magnitude than those observed with pentoxifylline and cilostazol. An economic evaluation also suggested that naftidrofuryl oxalate “dominated” cilostazol and pentoxifylline, and has an incremental cost per QALY (quality-adjusted life-years) gained of around $9720 compared with no vasoactive drug [52]. However, Hong and Mackey recently concluded that the clinical data for both naftidrofuryl and cilostazol are plagued by flaws related to lack of protocol standardization, objective endpoints, and strict eligibility criteria in study subjects, making identification of a true treatment effect difficult [54].
Other studies have investigated the functional effects of drugs that are commonly used to reduce the risk of cardiovascular events in patients with PAD, including antiplatelet, antihypertensive and lipid-lowering agents. The meta-analysis of Momsen et al assessed the effects of antiplatelet agents on walking distances in intermittent claudication [55]. The included studies involved 5 different drugs (ticlopidine, cloricromene, mesoglycan, indobufen and defibrotide), and while some studies did not show a statistically significant benefit of antiplatelet therapy, the pooled estimate showed a modest increase in maximum walking distance favoring treatment of 59 m (95% CI, 37 to 81 m). The same paper also assessed the effects of 4 lipid-lowering drugs: atorvastatin, simvastatin, policosanol, and avasimibe [55]. Despite variable results according to the specific drug used, the effect estimates favored lipid-lowering agents in all studies and was statistically significant in all but one study. The pooled effect estimate was in favor of intervention, with a clinically relevant increase in maximum walking distance of 163 m (95% CI, 83 to 242 m). Two recent meta-analyses have also reviewed the functional effects of ACE inhibitors in patients with intermittent claudication [56,57], and although data are conflicting, a recent large trial of 212 patients reported that ramipril increased claudication onset time by 75 seconds (95% CI, 60 to 89 seconds) and peak walking time by 255 seconds (215 to 295 seconds) [58]. These changes were independent of the small change in blood pressure that occurred with ramipril treatment.
In summary, while some drugs have been shown to improve walking performance in patients with intermittent claudication, the effect has tended to be modest at best and smaller than that observed with supervised exercise training. Momsen et al concluded that statins probably have the greatest functional benefits [55], and clinical guidelines recommend that all patients with PAD should receive statin therapy [3,7,8], irrespective of its effect on functional status. The UK clinical guidelines recommend considering using naftidrofuryl oxalate for the treatment of claudication, but only when supervised exercise has not worked and revascularization is not feasible or declined by the patient [8]. The ACC/AHA guidelines state that a therapeutic trial of cilostazol should be considered in all patients with lifestyle-limiting claudication in the absence of heart failure [7].
Lower-Limb Revascularization
Intermittent claudication can also be treated using endovascular procedures (angioplasty ± stent placement) or bypass surgery, both of which constitute a relatively more direct means of addressing the problem since they target the arterial lesions causing claudication. Trials of revascularization in PAD have typically focused on vessel/graft patency as the primary outcome, with less emphasis placed on functional endpoints [59]. Despite this, it is clear that successful revascularization rapidly improves walking performance [60,61], whereas noticeable improvements with supervised exercise training can take several weeks to occur (assuming good adherence) [62]. Long-term comparisons of lower-limb revascularization with alternative treatment modalities for people with intermittent claudication are scarce. Recently, Fakhry et al [63] reported the long-term clinical effectiveness of supervised exercise therapy and endovascular revascularization from a randomized trial of 151 patients. After 7 years, the treatment strategies were similarly effective in improving functional performance and quality of life; however, the total number of endovascular and surgical interventions (primary and secondary) was substantially higher in the revascularization group, which will have resulted in significantly higher health care costs in this group. Furthermore, given that supervised exercise training costs substantially less than any revascularization procedure, it is not surprising that economic analyses indicate supervised exercise training as being more cost-effective [64,65]. This is reflected in clinical guidelines, which promote supervised exercise training as the first-line therapy [3,7,8]. In the UK, NICE recommends that clinicians should only offer angioplasty for treating people with intermittent claudication when advice on the benefits of modifying risk factors has been reinforced, a supervised exercise program has not led to a satisfactory improvement in symptoms, and imaging has confirmed that angioplasty is suitable for the person [8]. Bypass surgery for treating people with severe lifestyle-limiting intermittent claudication is only recommended when angioplasty has been unsuccessful or is unsuitable, and imaging has confirmed that bypass surgery is appropriate for the person. Overall, from a technical point of view during revascularization, there is no strong evidence to support that differences in clinical outcomes are observed as a function of technical choices of anastomoses in aortobifemoral bypasses [66] or kind of angioplasty in femoropopliteal lesions [67].
Potential Alternative Therapeutic Approaches
Several non-drug, non-exercise, and non-revascularization approaches have been investigated for their impact on claudication-related functional impairment, including (but not limited to) acupuncture, biofeedback, chelation therapy, CO2-applications, and the dietary supplements Allium sativum (garlic), Ginkgo biloba, omega-3 fatty acids, Padma 28, Vitamin E, and carnitine supplementation. In a recent systematic review, Delaney et al highlighted that most of the 8 parallel-group randomized controlled trials of propionyl-L-carnitine supplementation (600 to 3000 mg administered orally) demonstrated improvements in walking performance between 31 and 54 m greater than placebo for pain-free walking distance and between 9 and 86 m greater than placebo for maximum walking distance [68]. Propionyl-L-carnitine has been postulated to improve walking distance by improving endothelial function, and increasing total carnitine content in the ischemic muscle, which improves muscle metabolism and stimulates oxidative phosphorylation resulting in a decrease in plasma lactate concentration on exercise [68]. In a systematic review of these complementary therapies for PAD from 2005 [69], Pittler and Ernst concluded that there was some evidence for a beneficial effect of Ginkgo biloba and Padma 28 in claudication patients; however, recent meta-analyses have concluded that there is no evidence that Ginkgo biloba produces clinically meaningful improvements in walking distances [70], and that further well-designed research is required to determine the true effects of Padma 28 [71]. None of the other complementary treatment options have sufficient supporting evidence for them to be proposed as a routine approach [72–75]. Last, a few small studies have indicated that intermittent pneumatic compression (IPC) interventions can improve walking distances in people with intermittent claudication [76–78]. To date, IPC has received limited use in the clinical setting due to issues of cost and constraint; however, modern technology has permitted the development of portable systems to be made readily available for affordable at-home use. Adequately powered randomized controlled trials and economic evaluations are required to clarify the role of IPC for improving functional outcomes in intermittent claudication.
Conclusion
Intermittent claudication, the main symptom of mild-to-moderate PAD, is common in older adults. Individuals with intermittent claudication have reduced walking endurance and slower walking speed compared to individuals without PAD, and impairments in walking can reduce patients’ quality of life. There are several therapeutic options for improving walking performance in intermittent claudication, none of which are without limitations. Lower-limb revascularization procedures (angioplasty, bypass surgery) are invasive and have limited durability, and the medications approved for claudication-related functional impairment have limited efficacy. Supervised walking exercise can substantially improve walking performance; however, most patients do not participate in a supervised program due to issues of availability, awareness and access. Therefore, efforts should be made to provide patients with access to a supervised exercise program and encouragement to attend, or to promote self-managed walking when supervised exercise is not available or practical.
Corresponding author: Dr Garry A. Tew, York Trials Unit, Dept. of Health Sciences, University of York, York, YO10 5DD, UK, [email protected].
Financial disclosures: None.
Author contributions: conception and design, GAT, PA; drafting of article, GAT, PA; critical revision of the article, GAT, PA.
1. Fowkes FG, Housley E, Cawood EH, et al. Edinburgh Artery Study: prevalence of asymptomatic and symptomatic peripheral arterial disease in the general population. Int J Epidemiol 1991;20:384–92.
2. Criqui MH, Fronek A, Barrett-Connor E, et al. The prevalence of peripheral arterial disease in a defined population. Circulation 1985;71;510–5.
3. Norgren L, Hiatt WR, Dormandy JA, et al. Inter-Society Consensus for the Management of Peripheral Arterial Disease (TASC II). Eur J Vasc Endovasc Surg. 2007;33 Suppl 1:S1–75.
4. Nehler MR, McDermott MM, Treat-Jacobson D, et al. Functional outcomes and quality of life in peripheral arterial disease: current status. Vasc Med 2003;8:115–26.
5. Caro J, Migliaccio-Walle K, Ishak KJ, Proskorovsky I. The morbidity and mortality following a diagnosis of peripheral arterial disease: long-term follow-up of a large database. BMC Cardiovasc Disord 2005;5:14.
6. Criqui MH, Langer RD, Fronek A, et al. Mortality over a period of 10 years in patients with peripheral arterial disease. N Engl J Med 1992;326:381–6.
7. Hirsch AT, Haskal ZJ, Hertzer NR, et al. ACC/AHA 2005 Practice Guidelines for the management of patients with peripheral arterial disease (lower extremity, renal, mesenteric, and abdominal aortic): a collaborative report from the American Association for Vascular Surgery/Society for Vascular Surgery, Society for Cardiovascular Angiography and Interventions, Society for Vascular Medicine and Biology, Society of Interventional Radiology, and the ACC/AHA Task Force on Practice Guidelines (Writing Committee to Develop Guidelines for the Management of Patients With Peripheral Arterial Disease): endorsed by the American Association of Cardiovascular and Pulmonary Rehabilitation; National Heart, Lung, and Blood Institute; Society for Vascular Nursing; TransAtlantic Inter-Society Consensus; and Vascular Disease Foundation. Circulation 2006;113:e463–654.
8. Layden J, Michaels J, Bermingham S, et al. Diagnosis and management of lower limb peripheral arterial disease: summary of NICE guidance. BMJ 2012;345:e4947.
9. Diehm C, Schuster A, Allenberg JR, et al. High prevalence of peripheral arterial disease and co-morbidity in 6880 primary care patients: cross-sectional study. Atherosclerosis 2004;172:95–105.
10. Soer R, van der Schans CP, Groothoff JW, et al. Towards consensus in operational definitions in functional capacity evaluation: a Delphi Survey. J Occup Rehabil 2008;18:389–400.
11. McDermott MM. Functional impairment in peripheral artery disease and how to improve it in 2013. Curr Cardiol Rep 2013;15:347.
12. Labs KH, Dormandy JA, Jaeger KA, et al. Transatlantic Conference on Clinical Trial Guidelines in Peripheral Arterial Disease: clinical trial methodology. Basel PAD Clinical Trial Methodology Group. Circulation 1999;100:e75–81.
13. Hiatt WR, Goldstone J, Smith SC, et al. Atherosclerotic Peripheral Vascular Disease Symposium II: nomenclature for vascular diseases. Circulation 2008;118:2826–9.
14. Montgomery PS, Gardner AW. The clinical utility of a six-minute walk test in peripheral arterial occlusive disease patients. J Am Geriatr Soc 1998;46:706–11.
15. McDermott MM, Guralnik JM, Criqui MH, et al. Six-minute walk is a better outcome measure than treadmill walking tests in therapeutic trials of patients with peripheral artery disease. Circulation 2014;130:61–8.
16. McDermott MM, Ades PA, Dyer A, et al. Corridor-based functional performance measures correlate better with physical activity during daily life than treadmill measures in persons with peripheral arterial disease. J Vasc Surg 2008;48:1231–7, 7.e1.
17. Tew G, Copeland R, Le Faucheur A, et al. Feasibility and validity of self-reported walking capacity in patients with intermittent claudication. J Vasc Surg 2013;57:1227–34.
18. Le Faucheur A, Abraham P, Jaquinandi V, et al. Measurement of walking distance and speed in patients with peripheral arterial disease: a novel method using a global positioning system. Circulation 2008;117:897–904.
19. Regensteiner JG, Steiner JF, Panzer RJ, Hiatt WR. Evaluation of walking impairment by questionnaire in patients with peripheral arterial disease. J Vasc Med Biol 1990;2:142–52.
20. Verspaget M, Nicolaï SP, Kruidenier LM, et al. Validation of the Dutch version of the Walking Impairment Questionnaire. Eur J Vasc Endovasc Surg 2009;37:56–61.
21. Yan BP, Lau JY, Yu CM, et al. Chinese translation and validation of the Walking Impairment Questionnaire in patients with peripheral artery disease. Vasc Med 2011;16:167–72.
22. Collins TC, Suarez-Almazor M, Petersen NJ, O'Malley KJ. A Spanish translation of the Walking Impairment Questionnaire was validated for patients with peripheral arterial disease. J Clin Epidemiol 2004;57:1305–15.
23. McDermott MM, Ades P, Guralnik JM, et al. Treadmill exercise and resistance training in patients with peripheral arterial disease with and without intermittent claudication: a randomized controlled trial. JAMA 2009;301:165–74.
24. Murphy TP, Cutlip DE, Regensteiner JG, et al. Supervised exercise versus primary stenting for claudication resulting from aortoiliac peripheral artery disease: six-month outcomes from the claudication: exercise versus endoluminal revascularization (CLEVER) study. Circulation 2012;125:130–9.
25. Ouedraogo N, Chanut M, Aubourg M, et al. Development and evaluation of the Walking Estimated-Limitation Calculated by History questionnaire in patients with claudication. J Vasc Surg 2013;58:981–8.
26. Tew GA, Nawaz S, Humphreys L, et al. Validation of the English version of the Walking Estimated-Limitation Calculated by History (WELCH) questionnaire in patients with intermittent claudication. Vasc Med 2014;19:27–32.
27. Mahe G, Ouedraogo N, Vasseur M, et al. Limitations of self-reported estimates of functional capacity using the Walking Impairment Questionnaire. Eur J Vasc Endovasc Surg 2011;41:104–9.
28. Ouedraogo N, Mahe G, Marchand J, et al. Validation of a new simple questionnaire to "estimate ambulation capacity by history" (EACH) in patients with claudication. J Vasc Surg 2011;54:133–8.
29. Mays RJ, Casserly IP, Kohrt WM, et al. Assessment of functional status and quality of life in claudication. J Vasc Surg 2011;53:1410–21.
30. Wind J, Koelemay MJ. Exercise therapy and the additional effect of supervision on exercise therapy in patients with intermittent claudication. Systematic review of randomised controlled trials. Eur J Vasc Endovasc Surg 2007;34:1–9.
31. Fakhry F, van de Luijtgaarden KM, Bax L, et al. Supervised walking therapy in patients with intermittent claudication. J Vasc Surg 2012;56:1132–42.
32. Fokkenrood HJ, Bendermacher BL, Lauret GJ, et al. Supervised exercise therapy versus non-supervised exercise therapy for intermittent claudication. Cochrane Database Syst Rev 2013;8:CD005263.
33. Lane R, Ellis B, Watson L, Leng GC. Exercise for intermittent claudication. Cochrane Database Syst Rev 2014;7:CD000990.
34. Gommans LN, Saarloos R, Schelting MR, et al. Editor's choice--The effect of supervision on walking distance in patients with intermittent claudication: a meta-analysis. Eur J Vasc Endovasc Surg 2014;48:169–84.
35. Hamburg NM, Balady GJ. Exercise rehabilitation in peripheral artery disease: functional impact and mechanisms of benefits. Circulation 2011;123:87–97.
36. Gardner AW, Poehlman ET. Exercise rehabilitation programs for the treatment of claudication pain. A meta-analysis. JAMA 1995;274:975–80.
37. Bulmer AC, Coombes JS. Optimising exercise training in peripheral arterial disease. Sports Med 2004;34:983–1003.
38. Parmenter BJ, Raymond J, Dinnen P, Singh MA. A systematic review of randomized controlled trials: Walking versus alternative exercise prescription as treatment for intermittent claudication. Atherosclerosis 2011;218:1–12.
39. Lauret GJ, Fakhry F, Fokkenrood HJ, et al. Modes of exercise training for intermittent claudication. Cochrane Database Syst Rev 2014;7:CD009638.
40. Zwierska I, Walker RD, Choksy SA, et al. Upper- vs lower-limb aerobic exercise rehabilitation in patients with symptomatic peripheral arterial disease: a randomized controlled trial. J Vasc Surg 2005;42:1122–30.
41. Tew G, Nawaz S, Zwierska I, Saxton JM. Limb-specific and cross-transfer effects of arm-crank exercise training in patients with symptomatic peripheral arterial disease. Clin Sci (Lond) 2009;117:405–13.
42. Regensteiner JG. Exercise rehabilitation for the patient with intermittent claudication: a highly effective yet underutilized treatment. Curr Drug Targets Cardiovasc Haematol Disord 2004;4:233–9.
43. Makris GC, Lattimer CR, Lavida A, Geroulakos G. Availability of supervised exercise programs and the role of structured home-based exercise in peripheral arterial disease. Eur J Vasc Endovasc Surg 2012;44:569–75.
44. Popplewell MA, Bradbury AW. Why do health systems not fund supervised exercise programmes for intermittent claudication? Eur J Vasc Endovasc Surg. 2014 Aug 28. [Epub ahead of print]
45. Cunningham MA, Swanson V, O'Carroll RE, et al. Randomized clinical trial of a brief psychological intervention to increase walking in patients with intermittent claudication. Br J Surg 2012;99:49–56.
46. Michie S, Ashford S, Sniehotta FF, et al. A refined taxonomy of behaviour change techniques to help people change their physical activity and healthy eating behaviours: the CALO-RE taxonomy. Psychol Health 2011;26:1479–98.
47. Al-Jundi W, Madbak K, Beard JD, et al. Systematic review of home-based exercise programmes for individuals with intermittent claudication. Eur J Vasc Endovasc Surg 2013;46:690–706.
48. Egberg L, Andreassen S, Mattiasson AC. Experiences of living with intermittent claudication. J Vasc Nurs 2012;30:5–10.
49. McDermott MM, Liu K, Guralnik JM, et al. Home-based walking exercise intervention in peripheral artery disease: a randomized clinical trial. JAMA 2013;310:57–65.
50. Gardner AW, Parker DE, Montgomery PS, Scott KJ, Blevins SM. Efficacy of quantified home-based exercise and supervised exercise in patients with intermittent claudication: a randomized controlled trial. Circulation 2011;123:491–8.
51. Stevens JW, Simpson E, Harnan S, et al. Systematic review of the efficacy of cilostazol, naftidrofuryl oxalate and pentoxifylline for the treatment of intermittent claudication. Br J Surg 2012;99:1630–8.
52. Squires H, Simpson E, Meng Y, et al. A systematic review and economic evaluation of cilostazol, naftidrofuryl oxalate, pentoxifylline and inositol nicotinate for the treatment of intermittent claudication in people with peripheral arterial disease. Health Technol Assess 2011;15:1–210.
53. Takahashi S, Oida K, Fujiwara R, et al. Effect of cilostazol, a cyclic AMP phosphodiesterase inhibitor, on the proliferation of rat aortic smooth muscle cells in culture. J Cardiovasc Pharmacol 1992;20:900–6.
54. Hong H, Mackey WC. The limits of evidence in drug approval and availability: a case study of cilostazol and naftidrofuryl for the treatment of intermittent claudication. Clin Ther 2014;36:1290–301.
55. Momsen AH, Jensen MB, Norager CB, et al. Drug therapy for improving walking distance in intermittent claudication: a systematic review and meta-analysis of robust randomised controlled studies. Eur J Vasc Endovasc Surg 2009;38:463–74.
56. Shahin Y, Mazari F, Chetter I. Do angiotensin converting enzyme inhibitors improve walking distance in patients with symptomatic lower limb arterial disease? A systematic review and meta-analysis of randomised controlled trials. Int J Surg 2011;9:209–13.
57. Hunter MR, Cahoon WD, Lowe DK. Angiotensin-converting enzyme inhibitors for intermittent claudication associated with peripheral arterial disease. Ann Pharmacother 2013;47:1552–7.
58. Ahimastos AA, Walker PJ, Askew C, et al. Effect of ramipril on walking times and quality of life among patients with peripheral artery disease and intermittent claudication: a randomized controlled trial. JAMA 2013;309:453–60.
59. Kinlay S. Outcomes for clinical studies assessing drug and revascularization therapies for claudication and critical limb ischemia in peripheral artery disease. Circulation 2013;127:1241–50.
60. Ahimastos AA, Pappas EP, Buttner PG, et al. A meta-analysis of the outcome of endovascular and noninvasive therapies in the treatment of intermittent claudication. J Vasc Surg 2011;54:1511–21.
61. Nordanstig J, Taft C, Hensäter M, et al. Improved quality of life after one year with an invasive versus a non-invasive treatment strategy in claudicants: one year results of the IRONIC Trial. Circulation 2014 Aug. [Epub ahead of print]
62. Gardner AW, Montgomery PS, Parker DE. Optimal exercise program length for patients with claudication. J Vasc Surg 2012;55:1346–54.
63. Fakhry F, Rouwet EV, den Hoed PT, et al. Long-term clinical effectiveness of supervised exercise therapy versus endovascular revascularization for intermittent claudication from a randomized clinical trial. Br J Surg 2013;100:1164–71.
64. Fokkenrood HJ, Scheltinga MR, Koelemay MJ, et al. Significant savings with a stepped care model for treatment of patients with intermittent claudication. Eur J Vasc Endovasc Surg 2014;48:423–9.
65. Spronk S, Bosch JL, den Hoed PT, et al. Cost-effectiveness of endovascular revascularization compared to supervised hospital-based exercise training in patients with intermittent claudication: a randomized controlled trial. J Vasc Surg 2008;48:1472–80.
66. Ameli FM, Stein M, Aro L, et al. End-to-end versus end-to-side proximal anastomosis in aortobifemoral bypass surgery: does it matter? Can J Surg 1991;34:243–6.
67. Cejna M, Thurnher S, Illiasch H, et al. PTA versus Palmaz stent placement in femoropopliteal artery obstructions: a multicenter prospective randomized study. J Vasc Interv Radiol 2001;12:23–31.
68. Delaney CL, Spark JI, Thomas J, et al. A systematic review to evaluate the effectiveness of carnitine supplementation in improving walking performance among individuals with intermittent claudication. Atherosclerosis 2013;229:1–9.
69. Pittler MH, Ernst E. Complementary therapies for peripheral arterial disease: systematic review. Atherosclerosis 2005;181:1–7.
70. Nicolaï SP, Kruidenier LM, Bendermacher BL, et al. Ginkgo biloba for intermittent claudication. Cochrane Database Syst Rev 2009 (2):CD006888.
71. Morling JR, Maxwell H, Stewart M. Padma 28 for intermittent claudication. Cochrane Database Syst Rev 2013;7:CD007371.
72. Campbell A, Price J, Hiatt WR. Omega-3 fatty acids for intermittent claudication. Cochrane Database Syst Rev 2013;7:CD003833.
73. Kleijnen J, Mackerras D. Vitamin E for intermittent claudication. Cochrane Database Syst Rev 2000;2:CD000987.
74. Jepson RG, Kleijnen J, Leng GC. Garlic for peripheral arterial occlusive disease. Cochrane Database Syst Rev 2013;4:CD000095.
75. Villarruz MV, Dans A, Tan F. Chelation therapy for atherosclerotic cardiovascular disease. Cochrane Database Syst Rev 2002;4:CD002785.
76. Kakkos SK, Geroulakos G, Nicolaides AN. Improvement of the walking ability in intermittent claudication due to superficial femoral artery occlusion with supervised exercise and pneumatic foot and calf compression: a randomised controlled trial. Eur J Vasc Endovasc Surg 2005;30:164–75.
77. Delis KT, Nicolaides AN. Effect of intermittent pneumatic compression of foot and calf on walking distance, hemodynamics, and quality of life in patients with arterial claudication: a prospective randomized controlled study with 1-year follow-up. Ann Surg 2005;241:431–41.
78. de Haro J, Acin F, Florez A, et al. A prospective randomized controlled study with intermittent mechanical compression of the calf in patients with claudication. J Vasc Surg 2010;51:857–62.
1. Fowkes FG, Housley E, Cawood EH, et al. Edinburgh Artery Study: prevalence of asymptomatic and symptomatic peripheral arterial disease in the general population. Int J Epidemiol 1991;20:384–92.
2. Criqui MH, Fronek A, Barrett-Connor E, et al. The prevalence of peripheral arterial disease in a defined population. Circulation 1985;71;510–5.
3. Norgren L, Hiatt WR, Dormandy JA, et al. Inter-Society Consensus for the Management of Peripheral Arterial Disease (TASC II). Eur J Vasc Endovasc Surg. 2007;33 Suppl 1:S1–75.
4. Nehler MR, McDermott MM, Treat-Jacobson D, et al. Functional outcomes and quality of life in peripheral arterial disease: current status. Vasc Med 2003;8:115–26.
5. Caro J, Migliaccio-Walle K, Ishak KJ, Proskorovsky I. The morbidity and mortality following a diagnosis of peripheral arterial disease: long-term follow-up of a large database. BMC Cardiovasc Disord 2005;5:14.
6. Criqui MH, Langer RD, Fronek A, et al. Mortality over a period of 10 years in patients with peripheral arterial disease. N Engl J Med 1992;326:381–6.
7. Hirsch AT, Haskal ZJ, Hertzer NR, et al. ACC/AHA 2005 Practice Guidelines for the management of patients with peripheral arterial disease (lower extremity, renal, mesenteric, and abdominal aortic): a collaborative report from the American Association for Vascular Surgery/Society for Vascular Surgery, Society for Cardiovascular Angiography and Interventions, Society for Vascular Medicine and Biology, Society of Interventional Radiology, and the ACC/AHA Task Force on Practice Guidelines (Writing Committee to Develop Guidelines for the Management of Patients With Peripheral Arterial Disease): endorsed by the American Association of Cardiovascular and Pulmonary Rehabilitation; National Heart, Lung, and Blood Institute; Society for Vascular Nursing; TransAtlantic Inter-Society Consensus; and Vascular Disease Foundation. Circulation 2006;113:e463–654.
8. Layden J, Michaels J, Bermingham S, et al. Diagnosis and management of lower limb peripheral arterial disease: summary of NICE guidance. BMJ 2012;345:e4947.
9. Diehm C, Schuster A, Allenberg JR, et al. High prevalence of peripheral arterial disease and co-morbidity in 6880 primary care patients: cross-sectional study. Atherosclerosis 2004;172:95–105.
10. Soer R, van der Schans CP, Groothoff JW, et al. Towards consensus in operational definitions in functional capacity evaluation: a Delphi Survey. J Occup Rehabil 2008;18:389–400.
11. McDermott MM. Functional impairment in peripheral artery disease and how to improve it in 2013. Curr Cardiol Rep 2013;15:347.
12. Labs KH, Dormandy JA, Jaeger KA, et al. Transatlantic Conference on Clinical Trial Guidelines in Peripheral Arterial Disease: clinical trial methodology. Basel PAD Clinical Trial Methodology Group. Circulation 1999;100:e75–81.
13. Hiatt WR, Goldstone J, Smith SC, et al. Atherosclerotic Peripheral Vascular Disease Symposium II: nomenclature for vascular diseases. Circulation 2008;118:2826–9.
14. Montgomery PS, Gardner AW. The clinical utility of a six-minute walk test in peripheral arterial occlusive disease patients. J Am Geriatr Soc 1998;46:706–11.
15. McDermott MM, Guralnik JM, Criqui MH, et al. Six-minute walk is a better outcome measure than treadmill walking tests in therapeutic trials of patients with peripheral artery disease. Circulation 2014;130:61–8.
16. McDermott MM, Ades PA, Dyer A, et al. Corridor-based functional performance measures correlate better with physical activity during daily life than treadmill measures in persons with peripheral arterial disease. J Vasc Surg 2008;48:1231–7, 7.e1.
17. Tew G, Copeland R, Le Faucheur A, et al. Feasibility and validity of self-reported walking capacity in patients with intermittent claudication. J Vasc Surg 2013;57:1227–34.
18. Le Faucheur A, Abraham P, Jaquinandi V, et al. Measurement of walking distance and speed in patients with peripheral arterial disease: a novel method using a global positioning system. Circulation 2008;117:897–904.
19. Regensteiner JG, Steiner JF, Panzer RJ, Hiatt WR. Evaluation of walking impairment by questionnaire in patients with peripheral arterial disease. J Vasc Med Biol 1990;2:142–52.
20. Verspaget M, Nicolaï SP, Kruidenier LM, et al. Validation of the Dutch version of the Walking Impairment Questionnaire. Eur J Vasc Endovasc Surg 2009;37:56–61.
21. Yan BP, Lau JY, Yu CM, et al. Chinese translation and validation of the Walking Impairment Questionnaire in patients with peripheral artery disease. Vasc Med 2011;16:167–72.
22. Collins TC, Suarez-Almazor M, Petersen NJ, O'Malley KJ. A Spanish translation of the Walking Impairment Questionnaire was validated for patients with peripheral arterial disease. J Clin Epidemiol 2004;57:1305–15.
23. McDermott MM, Ades P, Guralnik JM, et al. Treadmill exercise and resistance training in patients with peripheral arterial disease with and without intermittent claudication: a randomized controlled trial. JAMA 2009;301:165–74.
24. Murphy TP, Cutlip DE, Regensteiner JG, et al. Supervised exercise versus primary stenting for claudication resulting from aortoiliac peripheral artery disease: six-month outcomes from the claudication: exercise versus endoluminal revascularization (CLEVER) study. Circulation 2012;125:130–9.
25. Ouedraogo N, Chanut M, Aubourg M, et al. Development and evaluation of the Walking Estimated-Limitation Calculated by History questionnaire in patients with claudication. J Vasc Surg 2013;58:981–8.
26. Tew GA, Nawaz S, Humphreys L, et al. Validation of the English version of the Walking Estimated-Limitation Calculated by History (WELCH) questionnaire in patients with intermittent claudication. Vasc Med 2014;19:27–32.
27. Mahe G, Ouedraogo N, Vasseur M, et al. Limitations of self-reported estimates of functional capacity using the Walking Impairment Questionnaire. Eur J Vasc Endovasc Surg 2011;41:104–9.
28. Ouedraogo N, Mahe G, Marchand J, et al. Validation of a new simple questionnaire to "estimate ambulation capacity by history" (EACH) in patients with claudication. J Vasc Surg 2011;54:133–8.
29. Mays RJ, Casserly IP, Kohrt WM, et al. Assessment of functional status and quality of life in claudication. J Vasc Surg 2011;53:1410–21.
30. Wind J, Koelemay MJ. Exercise therapy and the additional effect of supervision on exercise therapy in patients with intermittent claudication. Systematic review of randomised controlled trials. Eur J Vasc Endovasc Surg 2007;34:1–9.
31. Fakhry F, van de Luijtgaarden KM, Bax L, et al. Supervised walking therapy in patients with intermittent claudication. J Vasc Surg 2012;56:1132–42.
32. Fokkenrood HJ, Bendermacher BL, Lauret GJ, et al. Supervised exercise therapy versus non-supervised exercise therapy for intermittent claudication. Cochrane Database Syst Rev 2013;8:CD005263.
33. Lane R, Ellis B, Watson L, Leng GC. Exercise for intermittent claudication. Cochrane Database Syst Rev 2014;7:CD000990.
34. Gommans LN, Saarloos R, Schelting MR, et al. Editor's choice--The effect of supervision on walking distance in patients with intermittent claudication: a meta-analysis. Eur J Vasc Endovasc Surg 2014;48:169–84.
35. Hamburg NM, Balady GJ. Exercise rehabilitation in peripheral artery disease: functional impact and mechanisms of benefits. Circulation 2011;123:87–97.
36. Gardner AW, Poehlman ET. Exercise rehabilitation programs for the treatment of claudication pain. A meta-analysis. JAMA 1995;274:975–80.
37. Bulmer AC, Coombes JS. Optimising exercise training in peripheral arterial disease. Sports Med 2004;34:983–1003.
38. Parmenter BJ, Raymond J, Dinnen P, Singh MA. A systematic review of randomized controlled trials: Walking versus alternative exercise prescription as treatment for intermittent claudication. Atherosclerosis 2011;218:1–12.
39. Lauret GJ, Fakhry F, Fokkenrood HJ, et al. Modes of exercise training for intermittent claudication. Cochrane Database Syst Rev 2014;7:CD009638.
40. Zwierska I, Walker RD, Choksy SA, et al. Upper- vs lower-limb aerobic exercise rehabilitation in patients with symptomatic peripheral arterial disease: a randomized controlled trial. J Vasc Surg 2005;42:1122–30.
41. Tew G, Nawaz S, Zwierska I, Saxton JM. Limb-specific and cross-transfer effects of arm-crank exercise training in patients with symptomatic peripheral arterial disease. Clin Sci (Lond) 2009;117:405–13.
42. Regensteiner JG. Exercise rehabilitation for the patient with intermittent claudication: a highly effective yet underutilized treatment. Curr Drug Targets Cardiovasc Haematol Disord 2004;4:233–9.
43. Makris GC, Lattimer CR, Lavida A, Geroulakos G. Availability of supervised exercise programs and the role of structured home-based exercise in peripheral arterial disease. Eur J Vasc Endovasc Surg 2012;44:569–75.
44. Popplewell MA, Bradbury AW. Why do health systems not fund supervised exercise programmes for intermittent claudication? Eur J Vasc Endovasc Surg. 2014 Aug 28. [Epub ahead of print]
45. Cunningham MA, Swanson V, O'Carroll RE, et al. Randomized clinical trial of a brief psychological intervention to increase walking in patients with intermittent claudication. Br J Surg 2012;99:49–56.
46. Michie S, Ashford S, Sniehotta FF, et al. A refined taxonomy of behaviour change techniques to help people change their physical activity and healthy eating behaviours: the CALO-RE taxonomy. Psychol Health 2011;26:1479–98.
47. Al-Jundi W, Madbak K, Beard JD, et al. Systematic review of home-based exercise programmes for individuals with intermittent claudication. Eur J Vasc Endovasc Surg 2013;46:690–706.
48. Egberg L, Andreassen S, Mattiasson AC. Experiences of living with intermittent claudication. J Vasc Nurs 2012;30:5–10.
49. McDermott MM, Liu K, Guralnik JM, et al. Home-based walking exercise intervention in peripheral artery disease: a randomized clinical trial. JAMA 2013;310:57–65.
50. Gardner AW, Parker DE, Montgomery PS, Scott KJ, Blevins SM. Efficacy of quantified home-based exercise and supervised exercise in patients with intermittent claudication: a randomized controlled trial. Circulation 2011;123:491–8.
51. Stevens JW, Simpson E, Harnan S, et al. Systematic review of the efficacy of cilostazol, naftidrofuryl oxalate and pentoxifylline for the treatment of intermittent claudication. Br J Surg 2012;99:1630–8.
52. Squires H, Simpson E, Meng Y, et al. A systematic review and economic evaluation of cilostazol, naftidrofuryl oxalate, pentoxifylline and inositol nicotinate for the treatment of intermittent claudication in people with peripheral arterial disease. Health Technol Assess 2011;15:1–210.
53. Takahashi S, Oida K, Fujiwara R, et al. Effect of cilostazol, a cyclic AMP phosphodiesterase inhibitor, on the proliferation of rat aortic smooth muscle cells in culture. J Cardiovasc Pharmacol 1992;20:900–6.
54. Hong H, Mackey WC. The limits of evidence in drug approval and availability: a case study of cilostazol and naftidrofuryl for the treatment of intermittent claudication. Clin Ther 2014;36:1290–301.
55. Momsen AH, Jensen MB, Norager CB, et al. Drug therapy for improving walking distance in intermittent claudication: a systematic review and meta-analysis of robust randomised controlled studies. Eur J Vasc Endovasc Surg 2009;38:463–74.
56. Shahin Y, Mazari F, Chetter I. Do angiotensin converting enzyme inhibitors improve walking distance in patients with symptomatic lower limb arterial disease? A systematic review and meta-analysis of randomised controlled trials. Int J Surg 2011;9:209–13.
57. Hunter MR, Cahoon WD, Lowe DK. Angiotensin-converting enzyme inhibitors for intermittent claudication associated with peripheral arterial disease. Ann Pharmacother 2013;47:1552–7.
58. Ahimastos AA, Walker PJ, Askew C, et al. Effect of ramipril on walking times and quality of life among patients with peripheral artery disease and intermittent claudication: a randomized controlled trial. JAMA 2013;309:453–60.
59. Kinlay S. Outcomes for clinical studies assessing drug and revascularization therapies for claudication and critical limb ischemia in peripheral artery disease. Circulation 2013;127:1241–50.
60. Ahimastos AA, Pappas EP, Buttner PG, et al. A meta-analysis of the outcome of endovascular and noninvasive therapies in the treatment of intermittent claudication. J Vasc Surg 2011;54:1511–21.
61. Nordanstig J, Taft C, Hensäter M, et al. Improved quality of life after one year with an invasive versus a non-invasive treatment strategy in claudicants: one year results of the IRONIC Trial. Circulation 2014 Aug. [Epub ahead of print]
62. Gardner AW, Montgomery PS, Parker DE. Optimal exercise program length for patients with claudication. J Vasc Surg 2012;55:1346–54.
63. Fakhry F, Rouwet EV, den Hoed PT, et al. Long-term clinical effectiveness of supervised exercise therapy versus endovascular revascularization for intermittent claudication from a randomized clinical trial. Br J Surg 2013;100:1164–71.
64. Fokkenrood HJ, Scheltinga MR, Koelemay MJ, et al. Significant savings with a stepped care model for treatment of patients with intermittent claudication. Eur J Vasc Endovasc Surg 2014;48:423–9.
65. Spronk S, Bosch JL, den Hoed PT, et al. Cost-effectiveness of endovascular revascularization compared to supervised hospital-based exercise training in patients with intermittent claudication: a randomized controlled trial. J Vasc Surg 2008;48:1472–80.
66. Ameli FM, Stein M, Aro L, et al. End-to-end versus end-to-side proximal anastomosis in aortobifemoral bypass surgery: does it matter? Can J Surg 1991;34:243–6.
67. Cejna M, Thurnher S, Illiasch H, et al. PTA versus Palmaz stent placement in femoropopliteal artery obstructions: a multicenter prospective randomized study. J Vasc Interv Radiol 2001;12:23–31.
68. Delaney CL, Spark JI, Thomas J, et al. A systematic review to evaluate the effectiveness of carnitine supplementation in improving walking performance among individuals with intermittent claudication. Atherosclerosis 2013;229:1–9.
69. Pittler MH, Ernst E. Complementary therapies for peripheral arterial disease: systematic review. Atherosclerosis 2005;181:1–7.
70. Nicolaï SP, Kruidenier LM, Bendermacher BL, et al. Ginkgo biloba for intermittent claudication. Cochrane Database Syst Rev 2009 (2):CD006888.
71. Morling JR, Maxwell H, Stewart M. Padma 28 for intermittent claudication. Cochrane Database Syst Rev 2013;7:CD007371.
72. Campbell A, Price J, Hiatt WR. Omega-3 fatty acids for intermittent claudication. Cochrane Database Syst Rev 2013;7:CD003833.
73. Kleijnen J, Mackerras D. Vitamin E for intermittent claudication. Cochrane Database Syst Rev 2000;2:CD000987.
74. Jepson RG, Kleijnen J, Leng GC. Garlic for peripheral arterial occlusive disease. Cochrane Database Syst Rev 2013;4:CD000095.
75. Villarruz MV, Dans A, Tan F. Chelation therapy for atherosclerotic cardiovascular disease. Cochrane Database Syst Rev 2002;4:CD002785.
76. Kakkos SK, Geroulakos G, Nicolaides AN. Improvement of the walking ability in intermittent claudication due to superficial femoral artery occlusion with supervised exercise and pneumatic foot and calf compression: a randomised controlled trial. Eur J Vasc Endovasc Surg 2005;30:164–75.
77. Delis KT, Nicolaides AN. Effect of intermittent pneumatic compression of foot and calf on walking distance, hemodynamics, and quality of life in patients with arterial claudication: a prospective randomized controlled study with 1-year follow-up. Ann Surg 2005;241:431–41.
78. de Haro J, Acin F, Florez A, et al. A prospective randomized controlled study with intermittent mechanical compression of the calf in patients with claudication. J Vasc Surg 2010;51:857–62.
Is Age-Based HCV Screening a Benefit?
Using age as the determining factor when screening for hepatitis is more useful than is measuring for elevated levels of alanine aminotransferase (ALT), an enzyme produced by the liver, say researchers from the CDC in Atlanta, Georgia.
Most people with hepatitis C virus (HCV) infection are aged in their late 40s to late 60s and were likely infected 25 to 45 years ago, the researchers say. Most were infected by tainted blood transfusions or IV drug use, kidney dialysis, or use of blood-clotting products.
Both the CDC and the American Association for the Study of Liver Disease recommend HCV testing for people with elevated ALT levels. The authors of the CDC study say that previous studies suggest that providers are more likely to test patients for HCV based on elevated ALT than on assessment of exposure risk factors. In fact, risk-based testing can identify most HCV infection, but only 58% to 63% of primary care providers ask about patients’ risk factors. And about 20% to 30% of HCV-infected people do not report risk factors, or they do not remember having been exposed to a risk.
However, only about 46% of patients are evaluated for liver function, and the ALT test has drawbacks, the researchers say. These include lack of a standard definition for the upper limit of normal and the need for multiple tests over time.
In 2012, the CDC recommended a onetime HCV test for people born between 1945 and 1965. According to the researchers, patients born during that time belong to a “high-prevalence cohort” of nearly 200 million people who could account for 67% to 76% of adult HCV infections.
Which approach is best able to diagnose the most HCV-infected individuals?
The researchers say targeting via the birth cohort has the potential to identify about 1 million more anti-HCV positive people, compared with the strategy based on an elevated ALT result. The prevalence of anti-HCV within the birth cohort was about 4 times that in the adult population born before 1945 or after 1965. Using the birth year cohort as the basis of anti-HCV testing would identify nearly 77% of anti-HCV cases in the U.S. adult population, compared with 50% identification using the ALT strategy.
In 2007, according to study researchers, HCV infection surpassed HIV as an underlying or contributing cause of mortality and accounted for > 15,000 deaths in the U.S. More than 1 million more are projected to die of complications of untreated HCV, they add. Without testing and treatment, the CDC estimates that 60% of people with HCV infection will develop cirrhosis, or the scarring of the liver found in advanced liver disease. Testing ALT would screen about 60 million fewer people than the birth cohort strategy and could fail to identify about 700,000 to 900,000 individual cases of current HCV infection, the researchers say. Implementing both strategies concurrently, however, would identify 87% of anti-HCV cases.
Source
Smith BD, Yartel AK. Am J Prev Med. 2014;47(3):233-241.
doi: 10.1016/j.amepre.2014.05.011.
Using age as the determining factor when screening for hepatitis is more useful than is measuring for elevated levels of alanine aminotransferase (ALT), an enzyme produced by the liver, say researchers from the CDC in Atlanta, Georgia.
Most people with hepatitis C virus (HCV) infection are aged in their late 40s to late 60s and were likely infected 25 to 45 years ago, the researchers say. Most were infected by tainted blood transfusions or IV drug use, kidney dialysis, or use of blood-clotting products.
Both the CDC and the American Association for the Study of Liver Disease recommend HCV testing for people with elevated ALT levels. The authors of the CDC study say that previous studies suggest that providers are more likely to test patients for HCV based on elevated ALT than on assessment of exposure risk factors. In fact, risk-based testing can identify most HCV infection, but only 58% to 63% of primary care providers ask about patients’ risk factors. And about 20% to 30% of HCV-infected people do not report risk factors, or they do not remember having been exposed to a risk.
However, only about 46% of patients are evaluated for liver function, and the ALT test has drawbacks, the researchers say. These include lack of a standard definition for the upper limit of normal and the need for multiple tests over time.
In 2012, the CDC recommended a onetime HCV test for people born between 1945 and 1965. According to the researchers, patients born during that time belong to a “high-prevalence cohort” of nearly 200 million people who could account for 67% to 76% of adult HCV infections.
Which approach is best able to diagnose the most HCV-infected individuals?
The researchers say targeting via the birth cohort has the potential to identify about 1 million more anti-HCV positive people, compared with the strategy based on an elevated ALT result. The prevalence of anti-HCV within the birth cohort was about 4 times that in the adult population born before 1945 or after 1965. Using the birth year cohort as the basis of anti-HCV testing would identify nearly 77% of anti-HCV cases in the U.S. adult population, compared with 50% identification using the ALT strategy.
In 2007, according to study researchers, HCV infection surpassed HIV as an underlying or contributing cause of mortality and accounted for > 15,000 deaths in the U.S. More than 1 million more are projected to die of complications of untreated HCV, they add. Without testing and treatment, the CDC estimates that 60% of people with HCV infection will develop cirrhosis, or the scarring of the liver found in advanced liver disease. Testing ALT would screen about 60 million fewer people than the birth cohort strategy and could fail to identify about 700,000 to 900,000 individual cases of current HCV infection, the researchers say. Implementing both strategies concurrently, however, would identify 87% of anti-HCV cases.
Source
Smith BD, Yartel AK. Am J Prev Med. 2014;47(3):233-241.
doi: 10.1016/j.amepre.2014.05.011.
Using age as the determining factor when screening for hepatitis is more useful than is measuring for elevated levels of alanine aminotransferase (ALT), an enzyme produced by the liver, say researchers from the CDC in Atlanta, Georgia.
Most people with hepatitis C virus (HCV) infection are aged in their late 40s to late 60s and were likely infected 25 to 45 years ago, the researchers say. Most were infected by tainted blood transfusions or IV drug use, kidney dialysis, or use of blood-clotting products.
Both the CDC and the American Association for the Study of Liver Disease recommend HCV testing for people with elevated ALT levels. The authors of the CDC study say that previous studies suggest that providers are more likely to test patients for HCV based on elevated ALT than on assessment of exposure risk factors. In fact, risk-based testing can identify most HCV infection, but only 58% to 63% of primary care providers ask about patients’ risk factors. And about 20% to 30% of HCV-infected people do not report risk factors, or they do not remember having been exposed to a risk.
However, only about 46% of patients are evaluated for liver function, and the ALT test has drawbacks, the researchers say. These include lack of a standard definition for the upper limit of normal and the need for multiple tests over time.
In 2012, the CDC recommended a onetime HCV test for people born between 1945 and 1965. According to the researchers, patients born during that time belong to a “high-prevalence cohort” of nearly 200 million people who could account for 67% to 76% of adult HCV infections.
Which approach is best able to diagnose the most HCV-infected individuals?
The researchers say targeting via the birth cohort has the potential to identify about 1 million more anti-HCV positive people, compared with the strategy based on an elevated ALT result. The prevalence of anti-HCV within the birth cohort was about 4 times that in the adult population born before 1945 or after 1965. Using the birth year cohort as the basis of anti-HCV testing would identify nearly 77% of anti-HCV cases in the U.S. adult population, compared with 50% identification using the ALT strategy.
In 2007, according to study researchers, HCV infection surpassed HIV as an underlying or contributing cause of mortality and accounted for > 15,000 deaths in the U.S. More than 1 million more are projected to die of complications of untreated HCV, they add. Without testing and treatment, the CDC estimates that 60% of people with HCV infection will develop cirrhosis, or the scarring of the liver found in advanced liver disease. Testing ALT would screen about 60 million fewer people than the birth cohort strategy and could fail to identify about 700,000 to 900,000 individual cases of current HCV infection, the researchers say. Implementing both strategies concurrently, however, would identify 87% of anti-HCV cases.
Source
Smith BD, Yartel AK. Am J Prev Med. 2014;47(3):233-241.
doi: 10.1016/j.amepre.2014.05.011.
Optimal obstetric care for women aged 40 and older
CASE: Preterm labor in an older woman
G.S. is a 41-year-old G1P0 with a several-year history of infertility and a medical history of chronic hypertension. She undergoes in vitro fertilization (IVF) using her own oocytes, with transfer of two embryos. Early ultrasonography (US) confirms a diamniotic/dichorionic twin gestation. She undergoes chorionic villus sampling (CVS) during the first trimester, with normal fetal karyotypes noted.
For her chronic hypertension, the patient is treated with oral labetalol 200 mg twice daily, beginning in the first trimester. Results of a baseline comprehensive metabolic profile and complete blood count, and electrocardiogram are normal. Baseline 24-hour urine study results reveal no significant proteinuria and a normal creatinine clearance.
At 18 weeks’ gestation, US results show normal growth and amniotic fluid volume for each fetus, with no anomalies detected. Because of a gradual increase in the patient’s blood pressure, her labetalol dose is increased to 400 mg orally thrice daily. Her urine protein output remains negative on dipstick, and US every 4 weeks until 28 weeks’ gestation continues to show normal fetal growth and amniotic fluid volume.
At 33 weeks’ gestation, the patient presents with regular uterine activity. Nonstress tests for both fetuses are reactive. She is given a 1-L intravenous (IV) fluid bolus of lactated Ringers solution, as well as subcutaneous terbutaline sulfate every 15 minutes for four doses, without resolution of the uterine contractions. Her pulse has increased to 120 bpm.
How do you manage this patient’s care?
Nine times as many women aged 35 and older gave birth to their first child in 2012 than did women of the same age 40 years ago, according to the most recent data from the National Center for Health Statistics.1 The rate of first births for women aged 40 to 44 remained essentially stable during the 1970s and early 1980s but increased more than fourfold from 1985 through 2012—from 0.5 to 2.3 per 1,000 women.1 Clearly, more women are delaying childbearing to a later age by personal choice for reasons such as completion of education and career advancement.2
The path to late motherhood is not without thorns, however. Heightened risks associated with increasing maternal age include:
- fetal aneuploidy
- fetal malformation
- gestational diabetes
- chronic and gestational hypertension
- antepartum hemorrhage
- placenta previa
- prelabor rupture of membranes
- preterm labor.3,4
Women with advanced age at conception also are more likely to have a multifetal gestation because of the need for assisted reproduction and are more likely to require cesarean delivery5 as a result of abnormal placentation, fetal malpresentation, an abnormal pattern of labor, or increased use of oxytocin in labor. In addition, they are more likely to experience rupture of the sphincter, postpartum hemorrhage, and thromboembolism.3 Advanced maternal age also is associated with a higher risk of stillbirth throughout gestation, with the peak risk period reported to occur at 37 to 41 weeks.6
Maternal age-related risks of autosomal trisomies (especially Down syndrome) are well understood and have been quantified for singleton and twin gestations. TABLE 1 shows the risks at term for singleton and twin gestations for at least one chromosomally abnormal fetus by maternal age (40–46 years) and race.7
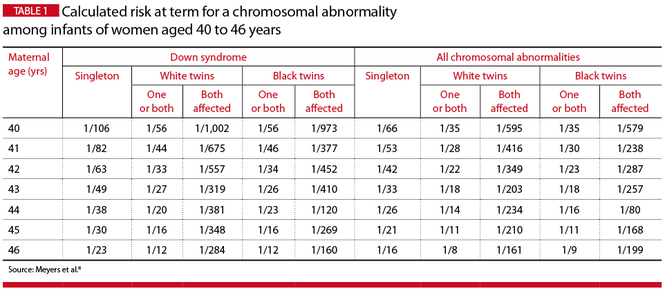
Preconception considerations
Aging and fertility
These combined result of aging of the ovary and uterus and an escalating risk of underlying medical comorbidities has a detrimental effect on fertility.8 Although assisted reproductive technologies are helpful, they cannot guarantee a live birth or completely compensate for an age-related decline in fertility.9
Many IVF programs refuse infertility treatment to women over age 43 or 44 who want to use their own oocytes. The reason: low pregnancy rates. The use of donor oocytes, however, increases the risks of gestational hypertension and preeclampsia. And if assisted reproductive technologies are needed, the risk for multifetal pregnancy increases.
Women of advanced maternal age are likely to have an older spouse or partner. There is no clearly accepted definition of advanced paternal age, but it is most often defined as an age of 40 years or older at the time of conception. Advanced paternal age has been associated with a higher risk for autism spectrum disorder and schizophrenia, as well as mutations in the FGFR2 and FGFR3 genes that result in skeletal dysplasias and craniosynostosis syndromes.10
Medical conditions are more common
Women of advanced maternal age have an increased rate of such prepregnancy chronic medical complications as diabetes, chronic hypertension, obesity, and renal and cardiac disease. Therefore, it is best to optimize control of these chronic illnesses prior to conception to minimize the risks of miscarriage, fetal anomalies, and gestational hypertension and preeclampsia.
Preeclampsia. Although daily low-dose (60–81 mg) aspirin has been used to reduce the risk of preeclampsia, current recommendations from the American College of Obstetricians and Gynecologists (ACOG) suggest that this therapy be reserved for women with a medical history of early-onset preeclampsia or those who have had preeclampsia in more than one pregnancy.11
Impact of obesity. We recently examined the influence of age and obesity on pregnancy outcomes of nulliparous women aged 40 or older at delivery.12 The study included women aged 20 to 29 years (n = 52,249) and 40 or older (n = 1,231) who delivered singleton infants. Women who reported medical disorders, tobacco use, or conception with assisted reproductive technology were excluded.
In the older age group (≥40 years), obese women had significantly higher rates of cesarean delivery, gestational hypertension, preeclampsia, gestational diabetes, preterm delivery before 37 weeks’ gestation, and preterm delivery before 28 weeks, and their infants had higher rates of admission to the neonatal intensive care unit (NICU), compared with nonobese women (FIGURE).
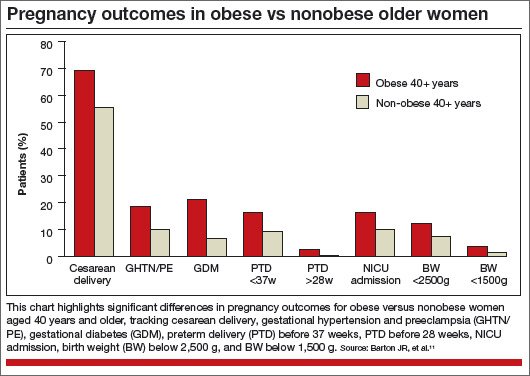
It would appear, however, that healthy, obese women who delay pregnancy until the age of 40 or later may modify their risk for cesarean delivery, gestational diabetes mellitus, and gestational hypertension and preeclampsia by reducing their body mass index to nonobese levels prior to conception.
In addition to maternal risks for women of advanced maternal age, there are risks to the fetus and neonate, as well as a risk of placental abnormalities. These risks are summarized in TABLE 2.
Placental
- Molar or partial molar pregnancy
- Fetus or twins with a complete mole
- Placenta previa, vasa previa
Fetal/neonatal
- Aneuploidy
- Selective fetal growth restriction in twin gestation
- Twin-twin transfusion syndrome
- Preterm birth
- Perinatal death
Antepartum
- Gestational diabetes
- Insulin-dependent diabetes
- Gestational hypertension and preeclampsia
- Cholestasis of pregnancy
- Acute fatty liver of pregnancy
- Venous thromboembolism
- Preterm labor, preterm premature rupture
of membranes
Intrapartum
- Dysfunctional labor
- Malpresentation
- Cesarean delivery
Postpartum
- Venous thromboembolism
- Postpartum hemorrhage
Folic acid supplementation can reduce some risks
The potential benefit of folic acid supplementation to reduce the risk of fetal open neural tube defects is well documented. More recent data suggest that folic acid also is associated with a reduction in the risks of congenital heart defects, abdominal wall defects, cleft lip and palate, and spontaneous abortion. Supplementation should be initiated at least 3 months prior to conception and continued through the first trimester.
The first trimester
Early pregnancy loss is a risk
Women of advanced maternal age are more likely than younger women to experience early pregnancy loss. This risk is due to higher rates of fetal aneuploidy as well as declining ovarian and uterine function and a higher rate of ectopic pregnancy.
In the First and Second Trimester Evaluation of Risk (FASTER) trial, in which investigators reported pregnancy outcomes by maternal age for 36,056 pregnancies, the rate of spontaneous abortion after 10 weeks of gestation was 0.8% among women younger than 35 years, compared with 2.2% for women aged 40 or older.4
The likelihood of multiple gestation increases
The background risk of multiple births is higher in women of advanced maternal age, compared with younger women. This risk increases further with fertility treatment.
Multiple gestations at any age are associated with increased risks for preterm birth and very-low–birthweight infants. Potential maternal risks are listed in TABLE 3.
- Hypertension (2.5 times the risk of a singleton gestation)
- Abruption (3.0 times the risk)
- Anemia (2.5 times the risk)
- Urinary tract infection (1.5 times the risk)
- Preeclampsia (risk of 26%–75%) (occurs at earlier gestation) — HELLP syndrome (risk of 9%)
- Abruption (20%) (10 times the risk of a singleton gestation)
- Anemia (24%)
- Preterm premature rupture of membranes (24%)
- Gestational diabetes (14%)
- Acute fatty liver (4%) (1 in 10,000 singletons)
- Postpartum hemorrhage (9%)
To reduce the number of multiple gestations with assisted reproduction, consider elective single embryo transfer, especially if the mother has significant underlying medical complications.
Multiple gestations present difficult management issues in older women. Strategies shown to prevent preterm delivery in singleton gestations, including weekly 17-hydroxyprogesterone injections and cervical cerclage, are not effective in multiple gestations. Moreover, many of these therapies—including bed rest—increase the risk of thromboembolic events in multiple gestations, particularly when the mother is of advanced age.
Maternal adaptations in multiple gestations also may be poorly tolerated by older patients, particularly cardiac changes that markedly increase stroke volume, heart rate, cardiac output, and plasma volume.
The range of genetic screening and testing options has broadened
Options include first-trimester CVS, which provides information about the fetal chromosomal complement but not the presence of a fetal open neural tube defect. The procedure-related rate of fetal loss with CVS is quoted as 1%.
Options for genetic testing in the second trimester include transabdominal amniocentesis. A procedure-related fetal loss rate of 1 in 500 to 1 in 1,600 is quoted for midtrimester amniocentesis.
A relatively new screening option is analysis of cell-free fetal DNA in maternal blood, which can be performed after 10 weeks’ gestation in singleton and multiple gestations. This directed analysis measures the relative proportions of chromosomes. The detection rate for fetal Down syndrome using cell-free fetal DNA is greater than 98%, with a false-positive rate of less than 0.5%. However, this screening is unreliable in triplet gestations.
Other screening options include US and biochemical screening to detect fetal aneuploidy and open neural tube defects during the second trimester. These options should be included in counseling of the patient.
Second and third trimesters
Gestational hypertension and preeclampsia are significant risks
Older pregnant women have an incidence of gestational hypertension and preeclampsia 2 to 4 times as high as that of patients younger than 30 years.13 The underlying risk for preeclampsia is further increased if coexisting medical disorders such as diabetes or chronic hypertension are present. Moreover, the risk for preeclampsia increases to 10% to 20% in twin gestations and 25% to 60% in triplet gestations. Le Ray and colleagues reported that, if oocyte donation is used with IVF in women older than age 43, the risk for preeclampsia triples.14
We previously studied 379 women aged 35 and older who had mild gestational hypertension remote from term, comparing them with their younger adult counterparts in a matched cohort design.15 Outpatient management produced similar maternal outcomes in both groups, but older women had a statistically insignificant increase in the rate of stillbirth (5 vs 0; P = .063).15
Gestational diabetes risk doubles
The rates of both diabetes mellitus and gestational diabetes increase with advanced maternal age. Data from the FASTER consortium included an adjusted odds ratio of 2.4 for gestational diabetes in women aged 40 or older, compared with a younger control group.4 This increased risk may be a consequence of greater maternal habitus as well as declining insulin sensitivity.
Diabetes increases the risks of macrosomia, cesarean birth, and gestational hypertension. Among women with pregestational diabetes, the risks of congenital heart disease and fetal neural tube defects increase threefold. Because of this increased risk, perinatal screening is indicated for both anomalies in older women.
Pulmonary complications increase
Another risk facing women of advanced maternal age—particularly those carrying a multiple gestation—is pulmonary edema, owing to the increased cardiac output, heart rate, and blood volume, the decreased systemic vascular resistance, and the physiologic anemia of pregnancy. These risks rise further in women who develop preterm labor that requires therapy and in those who develop gestational hypertension and/or preeclampsia. Judicious use of IV fluids, particularly those with lower sodium concentrations, can reduce the risk of pulmonary complications.
Women who develop pulmonary edema have an increased risk of peripartum cardiomyopathy.16
Preterm delivery is more common
Cleary-Goodman and colleagues noted an increased incidence of preterm delivery in women aged 40 and older, compared with women younger than age 35, but no increase in spontaneous preterm labor.4 Advanced maternal age appears to be associated with an increased risk of preterm birth largely as a consequence of underlying complications of fetal growth restriction and maternal disease, including hypertension. Because preterm birth is an important contributor to perinatal morbidity and mortality, steroids should be administered for fetal lung maturity whenever preterm labor is diagnosed before 34 weeks’ gestation.
Risk of placenta previa is 1.1%
Joseph and colleagues found the risk of placenta previa to be 1.1% in women aged 40 and older, compared with 0.3% in women aged 25 to 29 years.17 This increased risk likely is a consequence not only of maternal age but increased parity and a history of prior uterine surgery. If transabdominal US results are suspicious for placenta previa, transvaginal US is indicated for confirmation. Additional US assessment of the cord insertion site to the placenta also should be performed to rule out vasa previa.
Look for neonatal complications
Ziadeh and colleagues found that, although maternal morbidity was increased in older women, the overall neonatal outcome did not appear to be affected.18 However, we noted a higher rate of neonatal complications in women aged 40 or older, including higher NICU admission rates and more low-birth–weight infants.11
In addition, Odibo and colleagues found advanced maternal age to be an independent risk factor for intrauterine growth restriction (IUGR).19 In that study, the odds ratio for IUGR was 3.2 (95% confidence interval [CI], 1.9–5.4) for a maternal age of 40 years or older, compared with a control group. For that reason, they recommend routine screening for IUGR in all pregnant women of advanced age.
Stillbirth risk peaks at 37 to 41 weeks
In a review of more than 5.4 million singleton pregnancies without reported congenital anomalies, Reddy and colleagues found an association between advanced maternal age and stillbirth, with a higher risk of stillbirth at 37 to 41 weeks’ gestation.6 This effect of maternal age persisted despite adjusting for medical disease, parity, and race/ethnicity.
Many women older than age 40 have independent medical or fetal indications for antenatal testing. Some experts have suggested antepartum surveillance starting at 37 weeks for women of advanced maternal age; they argue that the risk of stillbirth at this gestational age is similar in frequency to other high-risk conditions for which testing is performed routinely. However, the National Institute of Child Health and Human Development (NICHD) workshop on antepartum fetal monitoring found insufficient evidence that antenatal testing for the sole indication of advanced maternal age reduces stillbirth or improves perinatal outcomes.20
If increased antenatal testing is indicated for a high-risk condition or electively chosen given advanced age, it should include electronic fetal monitoring as well as amniotic fluid volume assessment. Because the risk of fetal loss sharply increased at 40 weeks’ gestation in the study by Reddy and colleagues,6 women older than age 40 should be considered for delivery by 40 weeks’ gestation in the presence of good dating criteria.
Some clinicians also would consider delivery by 39 weeks’ gestation with good dating criteria if the Bishop score is favorable.
Risks of labor and delivery
Multiple variables contribute to a higher cesarean delivery rate
The risk of cesarean delivery increases with advancing maternal age.5,11 This increased risk is a consequence of multiple variables, including the rate of previous cesarean delivery, malpresentation, underlying complications such as preeclampsia and diabetes, and a higher prevalence of dysfunctional labor.21 Further, Vaughn and colleagues noted that the cesarean delivery rate increases in direct proportion to age, with a rate of 54.4% in women older than age 40.5
As Cohen pointed out in a commentary accompanying a study of dysfunctional labor in women of advancing age, “the notion of a premium baby (ie, that the fetus of a woman with a reduced likelihood of having another pregnancy is somehow more deserving of being spared the rigours of labour than the fetus of a young woman) may play a role” in the high rate of cesarean delivery.21,22
Postpartum hemorrhage risk may be lower in older women
Advanced maternal age is assumed to be a risk factor for postpartum hemorrhage.23 The increased risk was thought to be related to the increased incidence of multiple underlying factors, such as cesarean delivery, multiple gestation, and hypertensive disorders of pregnancy.
However, in a retrospective cohort study, Lao and colleagues found that advanced maternal age (≥35 years) served only as a surrogate factor for postpartum hemorrhage due to associated risk factors, obstetric complications, and interventions.24 After multivariate analysis, aging was associated with a decreased rate of postpartum hemorrhage, which declined progressively from ages 25 to 40 years and older, compared with women aged 20 to 24.24
Nevertheless, medical interventions should be readily available at the time of delivery for treatment of uterine atony, especially with multiple gestation and grand multiparity.
Case: Resolved
The patient is admitted to the hospital, where she is given IV magnesium sulfate (6-g load followed by an infusion of 3 g/hr) and betamethasone for fetal lung maturity enhancement. She continues to receive IV fluids as well (125 mL/hr lactated Ringers solution). Uterine activity abates.
IV magnesium sulfate is continued for 36 hours, but urine protein output is not monitored. Her heart rate ranges from 105 to 115 bpm, and blood pressure from 130/80 mm Hg to 138/88 mm Hg. Forty-eight hours after admission, she reports a gradual onset of tightness of the chest and breathlessness. She is agitated, with a pulse of 130 bpm, 30 respirations/min, and room air pulse oximetry of 90%. Rales are noted upon auscultation of both lungs. A radiograph of the chest demonstrates bilateral air-space disease consistent with pulmonary edema. IV furosemide and oxygen (by mask) are provided, with some respiratory improvement.
The patient then reports leakage of amniotic fluid, and preterm rupture of membranes is confirmed on examination. Because steroids for fetal lung maturity have been administered, and given improvement in her pulmonary edema and a footling breech presentation for Twin A, cesarean delivery is performed.
The patient’s immediate postoperative course is uncomplicated. On postoperative day 2, however, she develops recurrent pulmonary edema, as confirmed by physical examination and chest radiograph. She also reports headache, and her blood pressure rises to 164/114 mm Hg—findings consistent with postpartum preeclampsia. Magnesium sulfate and antihypertensive therapy are initiated, along with IV furosemide and oxygen, which improves her respiratory status.
An echocardiogram to rule out peripartum dilated cardiomyopathy finds no evidence of a dilated left ventricle, and the calculated left ventricular ejection fraction (55%) is normal.
After diuresis and improvement in her blood pressure, she is discharged home. By the time of her follow-up office visit 7 days later, her blood pressure has normalized on labetalol therapy.
For an overview of evaluation and management of pregnant women aged 40 or older, see TABLE 4.
Preconception
- Identify risk factors (ie, diabetes, obesity, hypertension, cardiac dysfunction, family history
- Review outcome of previous pregnancy, if applicable
- Review risks (multiple gestation, birth defects) associated with assisted reproductive technologies if they were needed to achieve pregnancy
- Optimize maternal health
- Begin folic acid supplementation
- Encourage smoking cessation
- If the patient is ≥45 years old:
– Electrocardiogram
– Glucose screening (fasting plasma glucose or hemoglobin A1c)
– Echocardiogram for patients with chronic hypertension
First trimester
- Ultrasonography for dating and to assess fetal number and chorionicity
- Baseline metabolic profile and complete blood count
- Baseline urinalysis
- Continue folic acid supplementation
- Offer first-trimester genetic testing or other genetic screening
Second trimester
- If first-trimester genetic testing is declined, offer second-trimester testing or screening
- Detailed fetal anomaly evaluation by ultrasound
- Fetal echocardiogram if pregnancy was achieved by in vitro fertilization or if it is a monochorionic twin gestation
- Screen for gestational diabetes
Third trimester
- Increased antenatal testing for routine indications, including hypertension, diabetes, and lupus
- Ultrasonography for growth and later ultrasonographic findings of fetal aneuploidy
- Consider delivery
Share your thoughts on this article! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.
1. Mathews TJ, Hamilton BE. First births to older women continue to rise. National Center for Health Statistics. NCHS Data Brief No. 152. May 2014. http://www.cdc.gov/nchs/data/databriefs/db152.pdf. Accessed October 3, 2014.
2. Mills M, Rindfuss RR, McDonald P, te Velde E. Why do people postpone parenthood? Reasons and social policy incentives. Hum Reprod Update. 2011;17(6):848–860.
3. Ziadeh SM. Maternal and perinatal outcome in nulliparous women aged 35 and older. Gynecol Obstet Invest. 2002;54(1):6–10.
4. Cleary-Goldman J, Malone FD, Vidaver J, et al; FASTER Consortium. Impact of maternal age on obstetric outcome. Obstet Gynecol. 2005;105(5 pt 1):983–990.
5. Vaughn DA, Cleary BJ, Murphy DJ. Delivery outcomes for nulliparous women at the extremes of maternal age—a cohort study. BJOG. 2014;121(3):261–268.
6. Reddy UM, Ko CW, Willinger M. Maternal age and the risk of stillbirth through pregnancy in the United States. Am J Obstet Gynecol. 2006;195(3):764–770.
7. Meyers C, Adam R, Dungan J, Prenger V. Aneuploidy in twin gestations: when is maternal age advanced? Obstet Gynecol. 1997;89(2):248–251.
8. Nelson SM, Telfer EE, Anderson RA. The ageing ovary and uterus: new biological insights. Hum Reprod Update. 2013;19(1):67–83.
9. Johnson JA, Tough S. Delayed child-bearing. J Obstet Gynaecol Can. 2012;34(1):80–93.
10. Goriely A, Wilkie AO. Paternal age effect mutations and selfish spermatogonial selection: causes and consequences for human disease. Am J Hum Genet. 2012;90(2):175–200.
11. Barton JR, Sibai AJ, Istwan NB, Rhea DJ, Desch CN, Sibai BM. Spontaneously conceived pregnancy after 40: influence of age and obesity on outcome. Am J Perinatol. 2014;31(9):795–798.
12. Roberts JM, August PA, Bakris JR, et al. Hypertension in pregnancy. Report of the American College of Obstetricians and Gynecologists Task Force on Hypertension in Pregnancy. Obstet Gynecol. 2013;122(5):1122–1131.
13. Jahromi BN, Husseini Z. Pregnancy outcome at maternal age 40 and older. Taiwan J Obstet Gynecol. 2008;47(3):318–321.
14. Le Ray C, Scherier S, Anselem O, et al. Association between oocyte donation and maternal and perinatal outcomes in women aged 43 years or older. Hum Reprod. 2012;27(3):896–901.
15. Barton JR, Bergauer NK, Jacques DL, Coleman SK, Stanziano GJ, Sibai BM. Does advanced maternal age affect pregnancy outcome in women with mild hypertension remote from term? Am J Obstet Gynecol. 1997;176(6):1236–1243.
16. Habli M, O’Brien T, Nowack E, et al. Peripartum cardiomyopathy: prognostic factors for long-term maternal outcome. Am J Obstet Gynecol. 2008;199(4):415.e1–e5.
17. Joseph KS, Allen AC, Dodds L, Turner LA, Scott H, Liston R. The perinatal effects of delayed childbearing. Obstet Gynecol. 2005;105(6):1410–1418.
18. Ziadeh S, Yahaya A. Pregnancy outcome at age 40 and older. Arch Gynecol Obstet. 2001;265(1):30–33.
19. Odibo AO, Nelson D, Stamilio DM, Sehdev HM, Macones GA. Advanced maternal age is an independent risk factor for intrauterine growth restriction. Am J Perinatol. 2006;23(5):325–328.
20. Signore C, Freeman RK, Spong CY. Antenatal testing—a reevaluation: executive summary of a Eunice Kennedy Shriver National Institute of Child Health and Human Development workshop. Obstet Gynecol. 2009;113(3):687–701.
21. Cohen WR, Newman L, Friedman EA. Risk of labor abnormalities with advancing maternal age. Obstet Gynecol. 1980;55(4):414–416.
22. Cohen WR. Does maternal age affect pregnancy outcome? BJOG. 2014;121(3):252–254.
23. Bateman BT, Berman MF, Riley LE, Leffert LR. The epidemiology of postpartum hemorrhage in a large, nationwide sample of deliveries. Anesth Analg. 2010;110(5):1368–1373.
24. Lao TT, Sahota DS, Cheng YK, Law LW, Leung TY. Advanced maternal age and postpartum hemorrhage—risk factor or red herring? J Matern Fetal Neonatal Med. 2014;27(3):243–246.
John R. Barton, MD, and Baha M. Sibai, MD

Dr. Barton is Director of Maternal-Fetal Medicine at Baptist Health Lexington in Lexington, Kentucky.

Dr. Sibai is Professor of Maternal-Fetal Medicine (MFM) and Director of the MFM Fellowship Program, Department of Obstetrics, Gynecology, and Reproductive Sciences, at the University of Texas Medical School at Houston, Texas.
Dr. Barton reports that he receives grant or research support from Alere, and that he is on the clinical advisory board of NX PharmaGen Inc.
Dr. Sibai reports no financial relationships relevant to this article.
John R. Barton, MD, and Baha M. Sibai, MD
Dr. Barton is Director of Maternal-Fetal Medicine at Baptist Health Lexington in Lexington, Kentucky.
Dr. Sibai is Professor of Maternal-Fetal Medicine (MFM) and Director of the MFM Fellowship Program, Department of Obstetrics, Gynecology, and Reproductive Sciences, at the University of Texas Medical School at Houston, Texas.
Dr. Barton reports that he receives grant or research support from Alere, and that he is on the clinical advisory board of NX PharmaGen Inc.
Dr. Sibai reports no financial relationships relevant to this article.
John R. Barton, MD, and Baha M. Sibai, MD
Dr. Barton is Director of Maternal-Fetal Medicine at Baptist Health Lexington in Lexington, Kentucky.
Dr. Sibai is Professor of Maternal-Fetal Medicine (MFM) and Director of the MFM Fellowship Program, Department of Obstetrics, Gynecology, and Reproductive Sciences, at the University of Texas Medical School at Houston, Texas.
Dr. Barton reports that he receives grant or research support from Alere, and that he is on the clinical advisory board of NX PharmaGen Inc.
Dr. Sibai reports no financial relationships relevant to this article.
CASE: Preterm labor in an older woman
G.S. is a 41-year-old G1P0 with a several-year history of infertility and a medical history of chronic hypertension. She undergoes in vitro fertilization (IVF) using her own oocytes, with transfer of two embryos. Early ultrasonography (US) confirms a diamniotic/dichorionic twin gestation. She undergoes chorionic villus sampling (CVS) during the first trimester, with normal fetal karyotypes noted.
For her chronic hypertension, the patient is treated with oral labetalol 200 mg twice daily, beginning in the first trimester. Results of a baseline comprehensive metabolic profile and complete blood count, and electrocardiogram are normal. Baseline 24-hour urine study results reveal no significant proteinuria and a normal creatinine clearance.
At 18 weeks’ gestation, US results show normal growth and amniotic fluid volume for each fetus, with no anomalies detected. Because of a gradual increase in the patient’s blood pressure, her labetalol dose is increased to 400 mg orally thrice daily. Her urine protein output remains negative on dipstick, and US every 4 weeks until 28 weeks’ gestation continues to show normal fetal growth and amniotic fluid volume.
At 33 weeks’ gestation, the patient presents with regular uterine activity. Nonstress tests for both fetuses are reactive. She is given a 1-L intravenous (IV) fluid bolus of lactated Ringers solution, as well as subcutaneous terbutaline sulfate every 15 minutes for four doses, without resolution of the uterine contractions. Her pulse has increased to 120 bpm.
How do you manage this patient’s care?
Nine times as many women aged 35 and older gave birth to their first child in 2012 than did women of the same age 40 years ago, according to the most recent data from the National Center for Health Statistics.1 The rate of first births for women aged 40 to 44 remained essentially stable during the 1970s and early 1980s but increased more than fourfold from 1985 through 2012—from 0.5 to 2.3 per 1,000 women.1 Clearly, more women are delaying childbearing to a later age by personal choice for reasons such as completion of education and career advancement.2
The path to late motherhood is not without thorns, however. Heightened risks associated with increasing maternal age include:
- fetal aneuploidy
- fetal malformation
- gestational diabetes
- chronic and gestational hypertension
- antepartum hemorrhage
- placenta previa
- prelabor rupture of membranes
- preterm labor.3,4
Women with advanced age at conception also are more likely to have a multifetal gestation because of the need for assisted reproduction and are more likely to require cesarean delivery5 as a result of abnormal placentation, fetal malpresentation, an abnormal pattern of labor, or increased use of oxytocin in labor. In addition, they are more likely to experience rupture of the sphincter, postpartum hemorrhage, and thromboembolism.3 Advanced maternal age also is associated with a higher risk of stillbirth throughout gestation, with the peak risk period reported to occur at 37 to 41 weeks.6
Maternal age-related risks of autosomal trisomies (especially Down syndrome) are well understood and have been quantified for singleton and twin gestations. TABLE 1 shows the risks at term for singleton and twin gestations for at least one chromosomally abnormal fetus by maternal age (40–46 years) and race.7
Preconception considerations
Aging and fertility
These combined result of aging of the ovary and uterus and an escalating risk of underlying medical comorbidities has a detrimental effect on fertility.8 Although assisted reproductive technologies are helpful, they cannot guarantee a live birth or completely compensate for an age-related decline in fertility.9
Many IVF programs refuse infertility treatment to women over age 43 or 44 who want to use their own oocytes. The reason: low pregnancy rates. The use of donor oocytes, however, increases the risks of gestational hypertension and preeclampsia. And if assisted reproductive technologies are needed, the risk for multifetal pregnancy increases.
Women of advanced maternal age are likely to have an older spouse or partner. There is no clearly accepted definition of advanced paternal age, but it is most often defined as an age of 40 years or older at the time of conception. Advanced paternal age has been associated with a higher risk for autism spectrum disorder and schizophrenia, as well as mutations in the FGFR2 and FGFR3 genes that result in skeletal dysplasias and craniosynostosis syndromes.10
Medical conditions are more common
Women of advanced maternal age have an increased rate of such prepregnancy chronic medical complications as diabetes, chronic hypertension, obesity, and renal and cardiac disease. Therefore, it is best to optimize control of these chronic illnesses prior to conception to minimize the risks of miscarriage, fetal anomalies, and gestational hypertension and preeclampsia.
Preeclampsia. Although daily low-dose (60–81 mg) aspirin has been used to reduce the risk of preeclampsia, current recommendations from the American College of Obstetricians and Gynecologists (ACOG) suggest that this therapy be reserved for women with a medical history of early-onset preeclampsia or those who have had preeclampsia in more than one pregnancy.11
Impact of obesity. We recently examined the influence of age and obesity on pregnancy outcomes of nulliparous women aged 40 or older at delivery.12 The study included women aged 20 to 29 years (n = 52,249) and 40 or older (n = 1,231) who delivered singleton infants. Women who reported medical disorders, tobacco use, or conception with assisted reproductive technology were excluded.
In the older age group (≥40 years), obese women had significantly higher rates of cesarean delivery, gestational hypertension, preeclampsia, gestational diabetes, preterm delivery before 37 weeks’ gestation, and preterm delivery before 28 weeks, and their infants had higher rates of admission to the neonatal intensive care unit (NICU), compared with nonobese women (FIGURE).
It would appear, however, that healthy, obese women who delay pregnancy until the age of 40 or later may modify their risk for cesarean delivery, gestational diabetes mellitus, and gestational hypertension and preeclampsia by reducing their body mass index to nonobese levels prior to conception.
In addition to maternal risks for women of advanced maternal age, there are risks to the fetus and neonate, as well as a risk of placental abnormalities. These risks are summarized in TABLE 2.
Placental
- Molar or partial molar pregnancy
- Fetus or twins with a complete mole
- Placenta previa, vasa previa
Fetal/neonatal
- Aneuploidy
- Selective fetal growth restriction in twin gestation
- Twin-twin transfusion syndrome
- Preterm birth
- Perinatal death
Antepartum
- Gestational diabetes
- Insulin-dependent diabetes
- Gestational hypertension and preeclampsia
- Cholestasis of pregnancy
- Acute fatty liver of pregnancy
- Venous thromboembolism
- Preterm labor, preterm premature rupture
of membranes
Intrapartum
- Dysfunctional labor
- Malpresentation
- Cesarean delivery
Postpartum
- Venous thromboembolism
- Postpartum hemorrhage
Folic acid supplementation can reduce some risks
The potential benefit of folic acid supplementation to reduce the risk of fetal open neural tube defects is well documented. More recent data suggest that folic acid also is associated with a reduction in the risks of congenital heart defects, abdominal wall defects, cleft lip and palate, and spontaneous abortion. Supplementation should be initiated at least 3 months prior to conception and continued through the first trimester.
The first trimester
Early pregnancy loss is a risk
Women of advanced maternal age are more likely than younger women to experience early pregnancy loss. This risk is due to higher rates of fetal aneuploidy as well as declining ovarian and uterine function and a higher rate of ectopic pregnancy.
In the First and Second Trimester Evaluation of Risk (FASTER) trial, in which investigators reported pregnancy outcomes by maternal age for 36,056 pregnancies, the rate of spontaneous abortion after 10 weeks of gestation was 0.8% among women younger than 35 years, compared with 2.2% for women aged 40 or older.4
The likelihood of multiple gestation increases
The background risk of multiple births is higher in women of advanced maternal age, compared with younger women. This risk increases further with fertility treatment.
Multiple gestations at any age are associated with increased risks for preterm birth and very-low–birthweight infants. Potential maternal risks are listed in TABLE 3.
- Hypertension (2.5 times the risk of a singleton gestation)
- Abruption (3.0 times the risk)
- Anemia (2.5 times the risk)
- Urinary tract infection (1.5 times the risk)
- Preeclampsia (risk of 26%–75%) (occurs at earlier gestation) — HELLP syndrome (risk of 9%)
- Abruption (20%) (10 times the risk of a singleton gestation)
- Anemia (24%)
- Preterm premature rupture of membranes (24%)
- Gestational diabetes (14%)
- Acute fatty liver (4%) (1 in 10,000 singletons)
- Postpartum hemorrhage (9%)
To reduce the number of multiple gestations with assisted reproduction, consider elective single embryo transfer, especially if the mother has significant underlying medical complications.
Multiple gestations present difficult management issues in older women. Strategies shown to prevent preterm delivery in singleton gestations, including weekly 17-hydroxyprogesterone injections and cervical cerclage, are not effective in multiple gestations. Moreover, many of these therapies—including bed rest—increase the risk of thromboembolic events in multiple gestations, particularly when the mother is of advanced age.
Maternal adaptations in multiple gestations also may be poorly tolerated by older patients, particularly cardiac changes that markedly increase stroke volume, heart rate, cardiac output, and plasma volume.
The range of genetic screening and testing options has broadened
Options include first-trimester CVS, which provides information about the fetal chromosomal complement but not the presence of a fetal open neural tube defect. The procedure-related rate of fetal loss with CVS is quoted as 1%.
Options for genetic testing in the second trimester include transabdominal amniocentesis. A procedure-related fetal loss rate of 1 in 500 to 1 in 1,600 is quoted for midtrimester amniocentesis.
A relatively new screening option is analysis of cell-free fetal DNA in maternal blood, which can be performed after 10 weeks’ gestation in singleton and multiple gestations. This directed analysis measures the relative proportions of chromosomes. The detection rate for fetal Down syndrome using cell-free fetal DNA is greater than 98%, with a false-positive rate of less than 0.5%. However, this screening is unreliable in triplet gestations.
Other screening options include US and biochemical screening to detect fetal aneuploidy and open neural tube defects during the second trimester. These options should be included in counseling of the patient.
Second and third trimesters
Gestational hypertension and preeclampsia are significant risks
Older pregnant women have an incidence of gestational hypertension and preeclampsia 2 to 4 times as high as that of patients younger than 30 years.13 The underlying risk for preeclampsia is further increased if coexisting medical disorders such as diabetes or chronic hypertension are present. Moreover, the risk for preeclampsia increases to 10% to 20% in twin gestations and 25% to 60% in triplet gestations. Le Ray and colleagues reported that, if oocyte donation is used with IVF in women older than age 43, the risk for preeclampsia triples.14
We previously studied 379 women aged 35 and older who had mild gestational hypertension remote from term, comparing them with their younger adult counterparts in a matched cohort design.15 Outpatient management produced similar maternal outcomes in both groups, but older women had a statistically insignificant increase in the rate of stillbirth (5 vs 0; P = .063).15
Gestational diabetes risk doubles
The rates of both diabetes mellitus and gestational diabetes increase with advanced maternal age. Data from the FASTER consortium included an adjusted odds ratio of 2.4 for gestational diabetes in women aged 40 or older, compared with a younger control group.4 This increased risk may be a consequence of greater maternal habitus as well as declining insulin sensitivity.
Diabetes increases the risks of macrosomia, cesarean birth, and gestational hypertension. Among women with pregestational diabetes, the risks of congenital heart disease and fetal neural tube defects increase threefold. Because of this increased risk, perinatal screening is indicated for both anomalies in older women.
Pulmonary complications increase
Another risk facing women of advanced maternal age—particularly those carrying a multiple gestation—is pulmonary edema, owing to the increased cardiac output, heart rate, and blood volume, the decreased systemic vascular resistance, and the physiologic anemia of pregnancy. These risks rise further in women who develop preterm labor that requires therapy and in those who develop gestational hypertension and/or preeclampsia. Judicious use of IV fluids, particularly those with lower sodium concentrations, can reduce the risk of pulmonary complications.
Women who develop pulmonary edema have an increased risk of peripartum cardiomyopathy.16
Preterm delivery is more common
Cleary-Goodman and colleagues noted an increased incidence of preterm delivery in women aged 40 and older, compared with women younger than age 35, but no increase in spontaneous preterm labor.4 Advanced maternal age appears to be associated with an increased risk of preterm birth largely as a consequence of underlying complications of fetal growth restriction and maternal disease, including hypertension. Because preterm birth is an important contributor to perinatal morbidity and mortality, steroids should be administered for fetal lung maturity whenever preterm labor is diagnosed before 34 weeks’ gestation.
Risk of placenta previa is 1.1%
Joseph and colleagues found the risk of placenta previa to be 1.1% in women aged 40 and older, compared with 0.3% in women aged 25 to 29 years.17 This increased risk likely is a consequence not only of maternal age but increased parity and a history of prior uterine surgery. If transabdominal US results are suspicious for placenta previa, transvaginal US is indicated for confirmation. Additional US assessment of the cord insertion site to the placenta also should be performed to rule out vasa previa.
Look for neonatal complications
Ziadeh and colleagues found that, although maternal morbidity was increased in older women, the overall neonatal outcome did not appear to be affected.18 However, we noted a higher rate of neonatal complications in women aged 40 or older, including higher NICU admission rates and more low-birth–weight infants.11
In addition, Odibo and colleagues found advanced maternal age to be an independent risk factor for intrauterine growth restriction (IUGR).19 In that study, the odds ratio for IUGR was 3.2 (95% confidence interval [CI], 1.9–5.4) for a maternal age of 40 years or older, compared with a control group. For that reason, they recommend routine screening for IUGR in all pregnant women of advanced age.
Stillbirth risk peaks at 37 to 41 weeks
In a review of more than 5.4 million singleton pregnancies without reported congenital anomalies, Reddy and colleagues found an association between advanced maternal age and stillbirth, with a higher risk of stillbirth at 37 to 41 weeks’ gestation.6 This effect of maternal age persisted despite adjusting for medical disease, parity, and race/ethnicity.
Many women older than age 40 have independent medical or fetal indications for antenatal testing. Some experts have suggested antepartum surveillance starting at 37 weeks for women of advanced maternal age; they argue that the risk of stillbirth at this gestational age is similar in frequency to other high-risk conditions for which testing is performed routinely. However, the National Institute of Child Health and Human Development (NICHD) workshop on antepartum fetal monitoring found insufficient evidence that antenatal testing for the sole indication of advanced maternal age reduces stillbirth or improves perinatal outcomes.20
If increased antenatal testing is indicated for a high-risk condition or electively chosen given advanced age, it should include electronic fetal monitoring as well as amniotic fluid volume assessment. Because the risk of fetal loss sharply increased at 40 weeks’ gestation in the study by Reddy and colleagues,6 women older than age 40 should be considered for delivery by 40 weeks’ gestation in the presence of good dating criteria.
Some clinicians also would consider delivery by 39 weeks’ gestation with good dating criteria if the Bishop score is favorable.
Risks of labor and delivery
Multiple variables contribute to a higher cesarean delivery rate
The risk of cesarean delivery increases with advancing maternal age.5,11 This increased risk is a consequence of multiple variables, including the rate of previous cesarean delivery, malpresentation, underlying complications such as preeclampsia and diabetes, and a higher prevalence of dysfunctional labor.21 Further, Vaughn and colleagues noted that the cesarean delivery rate increases in direct proportion to age, with a rate of 54.4% in women older than age 40.5
As Cohen pointed out in a commentary accompanying a study of dysfunctional labor in women of advancing age, “the notion of a premium baby (ie, that the fetus of a woman with a reduced likelihood of having another pregnancy is somehow more deserving of being spared the rigours of labour than the fetus of a young woman) may play a role” in the high rate of cesarean delivery.21,22
Postpartum hemorrhage risk may be lower in older women
Advanced maternal age is assumed to be a risk factor for postpartum hemorrhage.23 The increased risk was thought to be related to the increased incidence of multiple underlying factors, such as cesarean delivery, multiple gestation, and hypertensive disorders of pregnancy.
However, in a retrospective cohort study, Lao and colleagues found that advanced maternal age (≥35 years) served only as a surrogate factor for postpartum hemorrhage due to associated risk factors, obstetric complications, and interventions.24 After multivariate analysis, aging was associated with a decreased rate of postpartum hemorrhage, which declined progressively from ages 25 to 40 years and older, compared with women aged 20 to 24.24
Nevertheless, medical interventions should be readily available at the time of delivery for treatment of uterine atony, especially with multiple gestation and grand multiparity.
Case: Resolved
The patient is admitted to the hospital, where she is given IV magnesium sulfate (6-g load followed by an infusion of 3 g/hr) and betamethasone for fetal lung maturity enhancement. She continues to receive IV fluids as well (125 mL/hr lactated Ringers solution). Uterine activity abates.
IV magnesium sulfate is continued for 36 hours, but urine protein output is not monitored. Her heart rate ranges from 105 to 115 bpm, and blood pressure from 130/80 mm Hg to 138/88 mm Hg. Forty-eight hours after admission, she reports a gradual onset of tightness of the chest and breathlessness. She is agitated, with a pulse of 130 bpm, 30 respirations/min, and room air pulse oximetry of 90%. Rales are noted upon auscultation of both lungs. A radiograph of the chest demonstrates bilateral air-space disease consistent with pulmonary edema. IV furosemide and oxygen (by mask) are provided, with some respiratory improvement.
The patient then reports leakage of amniotic fluid, and preterm rupture of membranes is confirmed on examination. Because steroids for fetal lung maturity have been administered, and given improvement in her pulmonary edema and a footling breech presentation for Twin A, cesarean delivery is performed.
The patient’s immediate postoperative course is uncomplicated. On postoperative day 2, however, she develops recurrent pulmonary edema, as confirmed by physical examination and chest radiograph. She also reports headache, and her blood pressure rises to 164/114 mm Hg—findings consistent with postpartum preeclampsia. Magnesium sulfate and antihypertensive therapy are initiated, along with IV furosemide and oxygen, which improves her respiratory status.
An echocardiogram to rule out peripartum dilated cardiomyopathy finds no evidence of a dilated left ventricle, and the calculated left ventricular ejection fraction (55%) is normal.
After diuresis and improvement in her blood pressure, she is discharged home. By the time of her follow-up office visit 7 days later, her blood pressure has normalized on labetalol therapy.
For an overview of evaluation and management of pregnant women aged 40 or older, see TABLE 4.
Preconception
- Identify risk factors (ie, diabetes, obesity, hypertension, cardiac dysfunction, family history
- Review outcome of previous pregnancy, if applicable
- Review risks (multiple gestation, birth defects) associated with assisted reproductive technologies if they were needed to achieve pregnancy
- Optimize maternal health
- Begin folic acid supplementation
- Encourage smoking cessation
- If the patient is ≥45 years old:
– Electrocardiogram
– Glucose screening (fasting plasma glucose or hemoglobin A1c)
– Echocardiogram for patients with chronic hypertension
First trimester
- Ultrasonography for dating and to assess fetal number and chorionicity
- Baseline metabolic profile and complete blood count
- Baseline urinalysis
- Continue folic acid supplementation
- Offer first-trimester genetic testing or other genetic screening
Second trimester
- If first-trimester genetic testing is declined, offer second-trimester testing or screening
- Detailed fetal anomaly evaluation by ultrasound
- Fetal echocardiogram if pregnancy was achieved by in vitro fertilization or if it is a monochorionic twin gestation
- Screen for gestational diabetes
Third trimester
- Increased antenatal testing for routine indications, including hypertension, diabetes, and lupus
- Ultrasonography for growth and later ultrasonographic findings of fetal aneuploidy
- Consider delivery
Share your thoughts on this article! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.
CASE: Preterm labor in an older woman
G.S. is a 41-year-old G1P0 with a several-year history of infertility and a medical history of chronic hypertension. She undergoes in vitro fertilization (IVF) using her own oocytes, with transfer of two embryos. Early ultrasonography (US) confirms a diamniotic/dichorionic twin gestation. She undergoes chorionic villus sampling (CVS) during the first trimester, with normal fetal karyotypes noted.
For her chronic hypertension, the patient is treated with oral labetalol 200 mg twice daily, beginning in the first trimester. Results of a baseline comprehensive metabolic profile and complete blood count, and electrocardiogram are normal. Baseline 24-hour urine study results reveal no significant proteinuria and a normal creatinine clearance.
At 18 weeks’ gestation, US results show normal growth and amniotic fluid volume for each fetus, with no anomalies detected. Because of a gradual increase in the patient’s blood pressure, her labetalol dose is increased to 400 mg orally thrice daily. Her urine protein output remains negative on dipstick, and US every 4 weeks until 28 weeks’ gestation continues to show normal fetal growth and amniotic fluid volume.
At 33 weeks’ gestation, the patient presents with regular uterine activity. Nonstress tests for both fetuses are reactive. She is given a 1-L intravenous (IV) fluid bolus of lactated Ringers solution, as well as subcutaneous terbutaline sulfate every 15 minutes for four doses, without resolution of the uterine contractions. Her pulse has increased to 120 bpm.
How do you manage this patient’s care?
Nine times as many women aged 35 and older gave birth to their first child in 2012 than did women of the same age 40 years ago, according to the most recent data from the National Center for Health Statistics.1 The rate of first births for women aged 40 to 44 remained essentially stable during the 1970s and early 1980s but increased more than fourfold from 1985 through 2012—from 0.5 to 2.3 per 1,000 women.1 Clearly, more women are delaying childbearing to a later age by personal choice for reasons such as completion of education and career advancement.2
The path to late motherhood is not without thorns, however. Heightened risks associated with increasing maternal age include:
- fetal aneuploidy
- fetal malformation
- gestational diabetes
- chronic and gestational hypertension
- antepartum hemorrhage
- placenta previa
- prelabor rupture of membranes
- preterm labor.3,4
Women with advanced age at conception also are more likely to have a multifetal gestation because of the need for assisted reproduction and are more likely to require cesarean delivery5 as a result of abnormal placentation, fetal malpresentation, an abnormal pattern of labor, or increased use of oxytocin in labor. In addition, they are more likely to experience rupture of the sphincter, postpartum hemorrhage, and thromboembolism.3 Advanced maternal age also is associated with a higher risk of stillbirth throughout gestation, with the peak risk period reported to occur at 37 to 41 weeks.6
Maternal age-related risks of autosomal trisomies (especially Down syndrome) are well understood and have been quantified for singleton and twin gestations. TABLE 1 shows the risks at term for singleton and twin gestations for at least one chromosomally abnormal fetus by maternal age (40–46 years) and race.7
Preconception considerations
Aging and fertility
These combined result of aging of the ovary and uterus and an escalating risk of underlying medical comorbidities has a detrimental effect on fertility.8 Although assisted reproductive technologies are helpful, they cannot guarantee a live birth or completely compensate for an age-related decline in fertility.9
Many IVF programs refuse infertility treatment to women over age 43 or 44 who want to use their own oocytes. The reason: low pregnancy rates. The use of donor oocytes, however, increases the risks of gestational hypertension and preeclampsia. And if assisted reproductive technologies are needed, the risk for multifetal pregnancy increases.
Women of advanced maternal age are likely to have an older spouse or partner. There is no clearly accepted definition of advanced paternal age, but it is most often defined as an age of 40 years or older at the time of conception. Advanced paternal age has been associated with a higher risk for autism spectrum disorder and schizophrenia, as well as mutations in the FGFR2 and FGFR3 genes that result in skeletal dysplasias and craniosynostosis syndromes.10
Medical conditions are more common
Women of advanced maternal age have an increased rate of such prepregnancy chronic medical complications as diabetes, chronic hypertension, obesity, and renal and cardiac disease. Therefore, it is best to optimize control of these chronic illnesses prior to conception to minimize the risks of miscarriage, fetal anomalies, and gestational hypertension and preeclampsia.
Preeclampsia. Although daily low-dose (60–81 mg) aspirin has been used to reduce the risk of preeclampsia, current recommendations from the American College of Obstetricians and Gynecologists (ACOG) suggest that this therapy be reserved for women with a medical history of early-onset preeclampsia or those who have had preeclampsia in more than one pregnancy.11
Impact of obesity. We recently examined the influence of age and obesity on pregnancy outcomes of nulliparous women aged 40 or older at delivery.12 The study included women aged 20 to 29 years (n = 52,249) and 40 or older (n = 1,231) who delivered singleton infants. Women who reported medical disorders, tobacco use, or conception with assisted reproductive technology were excluded.
In the older age group (≥40 years), obese women had significantly higher rates of cesarean delivery, gestational hypertension, preeclampsia, gestational diabetes, preterm delivery before 37 weeks’ gestation, and preterm delivery before 28 weeks, and their infants had higher rates of admission to the neonatal intensive care unit (NICU), compared with nonobese women (FIGURE).
It would appear, however, that healthy, obese women who delay pregnancy until the age of 40 or later may modify their risk for cesarean delivery, gestational diabetes mellitus, and gestational hypertension and preeclampsia by reducing their body mass index to nonobese levels prior to conception.
In addition to maternal risks for women of advanced maternal age, there are risks to the fetus and neonate, as well as a risk of placental abnormalities. These risks are summarized in TABLE 2.
Placental
- Molar or partial molar pregnancy
- Fetus or twins with a complete mole
- Placenta previa, vasa previa
Fetal/neonatal
- Aneuploidy
- Selective fetal growth restriction in twin gestation
- Twin-twin transfusion syndrome
- Preterm birth
- Perinatal death
Antepartum
- Gestational diabetes
- Insulin-dependent diabetes
- Gestational hypertension and preeclampsia
- Cholestasis of pregnancy
- Acute fatty liver of pregnancy
- Venous thromboembolism
- Preterm labor, preterm premature rupture
of membranes
Intrapartum
- Dysfunctional labor
- Malpresentation
- Cesarean delivery
Postpartum
- Venous thromboembolism
- Postpartum hemorrhage
Folic acid supplementation can reduce some risks
The potential benefit of folic acid supplementation to reduce the risk of fetal open neural tube defects is well documented. More recent data suggest that folic acid also is associated with a reduction in the risks of congenital heart defects, abdominal wall defects, cleft lip and palate, and spontaneous abortion. Supplementation should be initiated at least 3 months prior to conception and continued through the first trimester.
The first trimester
Early pregnancy loss is a risk
Women of advanced maternal age are more likely than younger women to experience early pregnancy loss. This risk is due to higher rates of fetal aneuploidy as well as declining ovarian and uterine function and a higher rate of ectopic pregnancy.
In the First and Second Trimester Evaluation of Risk (FASTER) trial, in which investigators reported pregnancy outcomes by maternal age for 36,056 pregnancies, the rate of spontaneous abortion after 10 weeks of gestation was 0.8% among women younger than 35 years, compared with 2.2% for women aged 40 or older.4
The likelihood of multiple gestation increases
The background risk of multiple births is higher in women of advanced maternal age, compared with younger women. This risk increases further with fertility treatment.
Multiple gestations at any age are associated with increased risks for preterm birth and very-low–birthweight infants. Potential maternal risks are listed in TABLE 3.
- Hypertension (2.5 times the risk of a singleton gestation)
- Abruption (3.0 times the risk)
- Anemia (2.5 times the risk)
- Urinary tract infection (1.5 times the risk)
- Preeclampsia (risk of 26%–75%) (occurs at earlier gestation) — HELLP syndrome (risk of 9%)
- Abruption (20%) (10 times the risk of a singleton gestation)
- Anemia (24%)
- Preterm premature rupture of membranes (24%)
- Gestational diabetes (14%)
- Acute fatty liver (4%) (1 in 10,000 singletons)
- Postpartum hemorrhage (9%)
To reduce the number of multiple gestations with assisted reproduction, consider elective single embryo transfer, especially if the mother has significant underlying medical complications.
Multiple gestations present difficult management issues in older women. Strategies shown to prevent preterm delivery in singleton gestations, including weekly 17-hydroxyprogesterone injections and cervical cerclage, are not effective in multiple gestations. Moreover, many of these therapies—including bed rest—increase the risk of thromboembolic events in multiple gestations, particularly when the mother is of advanced age.
Maternal adaptations in multiple gestations also may be poorly tolerated by older patients, particularly cardiac changes that markedly increase stroke volume, heart rate, cardiac output, and plasma volume.
The range of genetic screening and testing options has broadened
Options include first-trimester CVS, which provides information about the fetal chromosomal complement but not the presence of a fetal open neural tube defect. The procedure-related rate of fetal loss with CVS is quoted as 1%.
Options for genetic testing in the second trimester include transabdominal amniocentesis. A procedure-related fetal loss rate of 1 in 500 to 1 in 1,600 is quoted for midtrimester amniocentesis.
A relatively new screening option is analysis of cell-free fetal DNA in maternal blood, which can be performed after 10 weeks’ gestation in singleton and multiple gestations. This directed analysis measures the relative proportions of chromosomes. The detection rate for fetal Down syndrome using cell-free fetal DNA is greater than 98%, with a false-positive rate of less than 0.5%. However, this screening is unreliable in triplet gestations.
Other screening options include US and biochemical screening to detect fetal aneuploidy and open neural tube defects during the second trimester. These options should be included in counseling of the patient.
Second and third trimesters
Gestational hypertension and preeclampsia are significant risks
Older pregnant women have an incidence of gestational hypertension and preeclampsia 2 to 4 times as high as that of patients younger than 30 years.13 The underlying risk for preeclampsia is further increased if coexisting medical disorders such as diabetes or chronic hypertension are present. Moreover, the risk for preeclampsia increases to 10% to 20% in twin gestations and 25% to 60% in triplet gestations. Le Ray and colleagues reported that, if oocyte donation is used with IVF in women older than age 43, the risk for preeclampsia triples.14
We previously studied 379 women aged 35 and older who had mild gestational hypertension remote from term, comparing them with their younger adult counterparts in a matched cohort design.15 Outpatient management produced similar maternal outcomes in both groups, but older women had a statistically insignificant increase in the rate of stillbirth (5 vs 0; P = .063).15
Gestational diabetes risk doubles
The rates of both diabetes mellitus and gestational diabetes increase with advanced maternal age. Data from the FASTER consortium included an adjusted odds ratio of 2.4 for gestational diabetes in women aged 40 or older, compared with a younger control group.4 This increased risk may be a consequence of greater maternal habitus as well as declining insulin sensitivity.
Diabetes increases the risks of macrosomia, cesarean birth, and gestational hypertension. Among women with pregestational diabetes, the risks of congenital heart disease and fetal neural tube defects increase threefold. Because of this increased risk, perinatal screening is indicated for both anomalies in older women.
Pulmonary complications increase
Another risk facing women of advanced maternal age—particularly those carrying a multiple gestation—is pulmonary edema, owing to the increased cardiac output, heart rate, and blood volume, the decreased systemic vascular resistance, and the physiologic anemia of pregnancy. These risks rise further in women who develop preterm labor that requires therapy and in those who develop gestational hypertension and/or preeclampsia. Judicious use of IV fluids, particularly those with lower sodium concentrations, can reduce the risk of pulmonary complications.
Women who develop pulmonary edema have an increased risk of peripartum cardiomyopathy.16
Preterm delivery is more common
Cleary-Goodman and colleagues noted an increased incidence of preterm delivery in women aged 40 and older, compared with women younger than age 35, but no increase in spontaneous preterm labor.4 Advanced maternal age appears to be associated with an increased risk of preterm birth largely as a consequence of underlying complications of fetal growth restriction and maternal disease, including hypertension. Because preterm birth is an important contributor to perinatal morbidity and mortality, steroids should be administered for fetal lung maturity whenever preterm labor is diagnosed before 34 weeks’ gestation.
Risk of placenta previa is 1.1%
Joseph and colleagues found the risk of placenta previa to be 1.1% in women aged 40 and older, compared with 0.3% in women aged 25 to 29 years.17 This increased risk likely is a consequence not only of maternal age but increased parity and a history of prior uterine surgery. If transabdominal US results are suspicious for placenta previa, transvaginal US is indicated for confirmation. Additional US assessment of the cord insertion site to the placenta also should be performed to rule out vasa previa.
Look for neonatal complications
Ziadeh and colleagues found that, although maternal morbidity was increased in older women, the overall neonatal outcome did not appear to be affected.18 However, we noted a higher rate of neonatal complications in women aged 40 or older, including higher NICU admission rates and more low-birth–weight infants.11
In addition, Odibo and colleagues found advanced maternal age to be an independent risk factor for intrauterine growth restriction (IUGR).19 In that study, the odds ratio for IUGR was 3.2 (95% confidence interval [CI], 1.9–5.4) for a maternal age of 40 years or older, compared with a control group. For that reason, they recommend routine screening for IUGR in all pregnant women of advanced age.
Stillbirth risk peaks at 37 to 41 weeks
In a review of more than 5.4 million singleton pregnancies without reported congenital anomalies, Reddy and colleagues found an association between advanced maternal age and stillbirth, with a higher risk of stillbirth at 37 to 41 weeks’ gestation.6 This effect of maternal age persisted despite adjusting for medical disease, parity, and race/ethnicity.
Many women older than age 40 have independent medical or fetal indications for antenatal testing. Some experts have suggested antepartum surveillance starting at 37 weeks for women of advanced maternal age; they argue that the risk of stillbirth at this gestational age is similar in frequency to other high-risk conditions for which testing is performed routinely. However, the National Institute of Child Health and Human Development (NICHD) workshop on antepartum fetal monitoring found insufficient evidence that antenatal testing for the sole indication of advanced maternal age reduces stillbirth or improves perinatal outcomes.20
If increased antenatal testing is indicated for a high-risk condition or electively chosen given advanced age, it should include electronic fetal monitoring as well as amniotic fluid volume assessment. Because the risk of fetal loss sharply increased at 40 weeks’ gestation in the study by Reddy and colleagues,6 women older than age 40 should be considered for delivery by 40 weeks’ gestation in the presence of good dating criteria.
Some clinicians also would consider delivery by 39 weeks’ gestation with good dating criteria if the Bishop score is favorable.
Risks of labor and delivery
Multiple variables contribute to a higher cesarean delivery rate
The risk of cesarean delivery increases with advancing maternal age.5,11 This increased risk is a consequence of multiple variables, including the rate of previous cesarean delivery, malpresentation, underlying complications such as preeclampsia and diabetes, and a higher prevalence of dysfunctional labor.21 Further, Vaughn and colleagues noted that the cesarean delivery rate increases in direct proportion to age, with a rate of 54.4% in women older than age 40.5
As Cohen pointed out in a commentary accompanying a study of dysfunctional labor in women of advancing age, “the notion of a premium baby (ie, that the fetus of a woman with a reduced likelihood of having another pregnancy is somehow more deserving of being spared the rigours of labour than the fetus of a young woman) may play a role” in the high rate of cesarean delivery.21,22
Postpartum hemorrhage risk may be lower in older women
Advanced maternal age is assumed to be a risk factor for postpartum hemorrhage.23 The increased risk was thought to be related to the increased incidence of multiple underlying factors, such as cesarean delivery, multiple gestation, and hypertensive disorders of pregnancy.
However, in a retrospective cohort study, Lao and colleagues found that advanced maternal age (≥35 years) served only as a surrogate factor for postpartum hemorrhage due to associated risk factors, obstetric complications, and interventions.24 After multivariate analysis, aging was associated with a decreased rate of postpartum hemorrhage, which declined progressively from ages 25 to 40 years and older, compared with women aged 20 to 24.24
Nevertheless, medical interventions should be readily available at the time of delivery for treatment of uterine atony, especially with multiple gestation and grand multiparity.
Case: Resolved
The patient is admitted to the hospital, where she is given IV magnesium sulfate (6-g load followed by an infusion of 3 g/hr) and betamethasone for fetal lung maturity enhancement. She continues to receive IV fluids as well (125 mL/hr lactated Ringers solution). Uterine activity abates.
IV magnesium sulfate is continued for 36 hours, but urine protein output is not monitored. Her heart rate ranges from 105 to 115 bpm, and blood pressure from 130/80 mm Hg to 138/88 mm Hg. Forty-eight hours after admission, she reports a gradual onset of tightness of the chest and breathlessness. She is agitated, with a pulse of 130 bpm, 30 respirations/min, and room air pulse oximetry of 90%. Rales are noted upon auscultation of both lungs. A radiograph of the chest demonstrates bilateral air-space disease consistent with pulmonary edema. IV furosemide and oxygen (by mask) are provided, with some respiratory improvement.
The patient then reports leakage of amniotic fluid, and preterm rupture of membranes is confirmed on examination. Because steroids for fetal lung maturity have been administered, and given improvement in her pulmonary edema and a footling breech presentation for Twin A, cesarean delivery is performed.
The patient’s immediate postoperative course is uncomplicated. On postoperative day 2, however, she develops recurrent pulmonary edema, as confirmed by physical examination and chest radiograph. She also reports headache, and her blood pressure rises to 164/114 mm Hg—findings consistent with postpartum preeclampsia. Magnesium sulfate and antihypertensive therapy are initiated, along with IV furosemide and oxygen, which improves her respiratory status.
An echocardiogram to rule out peripartum dilated cardiomyopathy finds no evidence of a dilated left ventricle, and the calculated left ventricular ejection fraction (55%) is normal.
After diuresis and improvement in her blood pressure, she is discharged home. By the time of her follow-up office visit 7 days later, her blood pressure has normalized on labetalol therapy.
For an overview of evaluation and management of pregnant women aged 40 or older, see TABLE 4.
Preconception
- Identify risk factors (ie, diabetes, obesity, hypertension, cardiac dysfunction, family history
- Review outcome of previous pregnancy, if applicable
- Review risks (multiple gestation, birth defects) associated with assisted reproductive technologies if they were needed to achieve pregnancy
- Optimize maternal health
- Begin folic acid supplementation
- Encourage smoking cessation
- If the patient is ≥45 years old:
– Electrocardiogram
– Glucose screening (fasting plasma glucose or hemoglobin A1c)
– Echocardiogram for patients with chronic hypertension
First trimester
- Ultrasonography for dating and to assess fetal number and chorionicity
- Baseline metabolic profile and complete blood count
- Baseline urinalysis
- Continue folic acid supplementation
- Offer first-trimester genetic testing or other genetic screening
Second trimester
- If first-trimester genetic testing is declined, offer second-trimester testing or screening
- Detailed fetal anomaly evaluation by ultrasound
- Fetal echocardiogram if pregnancy was achieved by in vitro fertilization or if it is a monochorionic twin gestation
- Screen for gestational diabetes
Third trimester
- Increased antenatal testing for routine indications, including hypertension, diabetes, and lupus
- Ultrasonography for growth and later ultrasonographic findings of fetal aneuploidy
- Consider delivery
Share your thoughts on this article! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.
1. Mathews TJ, Hamilton BE. First births to older women continue to rise. National Center for Health Statistics. NCHS Data Brief No. 152. May 2014. http://www.cdc.gov/nchs/data/databriefs/db152.pdf. Accessed October 3, 2014.
2. Mills M, Rindfuss RR, McDonald P, te Velde E. Why do people postpone parenthood? Reasons and social policy incentives. Hum Reprod Update. 2011;17(6):848–860.
3. Ziadeh SM. Maternal and perinatal outcome in nulliparous women aged 35 and older. Gynecol Obstet Invest. 2002;54(1):6–10.
4. Cleary-Goldman J, Malone FD, Vidaver J, et al; FASTER Consortium. Impact of maternal age on obstetric outcome. Obstet Gynecol. 2005;105(5 pt 1):983–990.
5. Vaughn DA, Cleary BJ, Murphy DJ. Delivery outcomes for nulliparous women at the extremes of maternal age—a cohort study. BJOG. 2014;121(3):261–268.
6. Reddy UM, Ko CW, Willinger M. Maternal age and the risk of stillbirth through pregnancy in the United States. Am J Obstet Gynecol. 2006;195(3):764–770.
7. Meyers C, Adam R, Dungan J, Prenger V. Aneuploidy in twin gestations: when is maternal age advanced? Obstet Gynecol. 1997;89(2):248–251.
8. Nelson SM, Telfer EE, Anderson RA. The ageing ovary and uterus: new biological insights. Hum Reprod Update. 2013;19(1):67–83.
9. Johnson JA, Tough S. Delayed child-bearing. J Obstet Gynaecol Can. 2012;34(1):80–93.
10. Goriely A, Wilkie AO. Paternal age effect mutations and selfish spermatogonial selection: causes and consequences for human disease. Am J Hum Genet. 2012;90(2):175–200.
11. Barton JR, Sibai AJ, Istwan NB, Rhea DJ, Desch CN, Sibai BM. Spontaneously conceived pregnancy after 40: influence of age and obesity on outcome. Am J Perinatol. 2014;31(9):795–798.
12. Roberts JM, August PA, Bakris JR, et al. Hypertension in pregnancy. Report of the American College of Obstetricians and Gynecologists Task Force on Hypertension in Pregnancy. Obstet Gynecol. 2013;122(5):1122–1131.
13. Jahromi BN, Husseini Z. Pregnancy outcome at maternal age 40 and older. Taiwan J Obstet Gynecol. 2008;47(3):318–321.
14. Le Ray C, Scherier S, Anselem O, et al. Association between oocyte donation and maternal and perinatal outcomes in women aged 43 years or older. Hum Reprod. 2012;27(3):896–901.
15. Barton JR, Bergauer NK, Jacques DL, Coleman SK, Stanziano GJ, Sibai BM. Does advanced maternal age affect pregnancy outcome in women with mild hypertension remote from term? Am J Obstet Gynecol. 1997;176(6):1236–1243.
16. Habli M, O’Brien T, Nowack E, et al. Peripartum cardiomyopathy: prognostic factors for long-term maternal outcome. Am J Obstet Gynecol. 2008;199(4):415.e1–e5.
17. Joseph KS, Allen AC, Dodds L, Turner LA, Scott H, Liston R. The perinatal effects of delayed childbearing. Obstet Gynecol. 2005;105(6):1410–1418.
18. Ziadeh S, Yahaya A. Pregnancy outcome at age 40 and older. Arch Gynecol Obstet. 2001;265(1):30–33.
19. Odibo AO, Nelson D, Stamilio DM, Sehdev HM, Macones GA. Advanced maternal age is an independent risk factor for intrauterine growth restriction. Am J Perinatol. 2006;23(5):325–328.
20. Signore C, Freeman RK, Spong CY. Antenatal testing—a reevaluation: executive summary of a Eunice Kennedy Shriver National Institute of Child Health and Human Development workshop. Obstet Gynecol. 2009;113(3):687–701.
21. Cohen WR, Newman L, Friedman EA. Risk of labor abnormalities with advancing maternal age. Obstet Gynecol. 1980;55(4):414–416.
22. Cohen WR. Does maternal age affect pregnancy outcome? BJOG. 2014;121(3):252–254.
23. Bateman BT, Berman MF, Riley LE, Leffert LR. The epidemiology of postpartum hemorrhage in a large, nationwide sample of deliveries. Anesth Analg. 2010;110(5):1368–1373.
24. Lao TT, Sahota DS, Cheng YK, Law LW, Leung TY. Advanced maternal age and postpartum hemorrhage—risk factor or red herring? J Matern Fetal Neonatal Med. 2014;27(3):243–246.
1. Mathews TJ, Hamilton BE. First births to older women continue to rise. National Center for Health Statistics. NCHS Data Brief No. 152. May 2014. http://www.cdc.gov/nchs/data/databriefs/db152.pdf. Accessed October 3, 2014.
2. Mills M, Rindfuss RR, McDonald P, te Velde E. Why do people postpone parenthood? Reasons and social policy incentives. Hum Reprod Update. 2011;17(6):848–860.
3. Ziadeh SM. Maternal and perinatal outcome in nulliparous women aged 35 and older. Gynecol Obstet Invest. 2002;54(1):6–10.
4. Cleary-Goldman J, Malone FD, Vidaver J, et al; FASTER Consortium. Impact of maternal age on obstetric outcome. Obstet Gynecol. 2005;105(5 pt 1):983–990.
5. Vaughn DA, Cleary BJ, Murphy DJ. Delivery outcomes for nulliparous women at the extremes of maternal age—a cohort study. BJOG. 2014;121(3):261–268.
6. Reddy UM, Ko CW, Willinger M. Maternal age and the risk of stillbirth through pregnancy in the United States. Am J Obstet Gynecol. 2006;195(3):764–770.
7. Meyers C, Adam R, Dungan J, Prenger V. Aneuploidy in twin gestations: when is maternal age advanced? Obstet Gynecol. 1997;89(2):248–251.
8. Nelson SM, Telfer EE, Anderson RA. The ageing ovary and uterus: new biological insights. Hum Reprod Update. 2013;19(1):67–83.
9. Johnson JA, Tough S. Delayed child-bearing. J Obstet Gynaecol Can. 2012;34(1):80–93.
10. Goriely A, Wilkie AO. Paternal age effect mutations and selfish spermatogonial selection: causes and consequences for human disease. Am J Hum Genet. 2012;90(2):175–200.
11. Barton JR, Sibai AJ, Istwan NB, Rhea DJ, Desch CN, Sibai BM. Spontaneously conceived pregnancy after 40: influence of age and obesity on outcome. Am J Perinatol. 2014;31(9):795–798.
12. Roberts JM, August PA, Bakris JR, et al. Hypertension in pregnancy. Report of the American College of Obstetricians and Gynecologists Task Force on Hypertension in Pregnancy. Obstet Gynecol. 2013;122(5):1122–1131.
13. Jahromi BN, Husseini Z. Pregnancy outcome at maternal age 40 and older. Taiwan J Obstet Gynecol. 2008;47(3):318–321.
14. Le Ray C, Scherier S, Anselem O, et al. Association between oocyte donation and maternal and perinatal outcomes in women aged 43 years or older. Hum Reprod. 2012;27(3):896–901.
15. Barton JR, Bergauer NK, Jacques DL, Coleman SK, Stanziano GJ, Sibai BM. Does advanced maternal age affect pregnancy outcome in women with mild hypertension remote from term? Am J Obstet Gynecol. 1997;176(6):1236–1243.
16. Habli M, O’Brien T, Nowack E, et al. Peripartum cardiomyopathy: prognostic factors for long-term maternal outcome. Am J Obstet Gynecol. 2008;199(4):415.e1–e5.
17. Joseph KS, Allen AC, Dodds L, Turner LA, Scott H, Liston R. The perinatal effects of delayed childbearing. Obstet Gynecol. 2005;105(6):1410–1418.
18. Ziadeh S, Yahaya A. Pregnancy outcome at age 40 and older. Arch Gynecol Obstet. 2001;265(1):30–33.
19. Odibo AO, Nelson D, Stamilio DM, Sehdev HM, Macones GA. Advanced maternal age is an independent risk factor for intrauterine growth restriction. Am J Perinatol. 2006;23(5):325–328.
20. Signore C, Freeman RK, Spong CY. Antenatal testing—a reevaluation: executive summary of a Eunice Kennedy Shriver National Institute of Child Health and Human Development workshop. Obstet Gynecol. 2009;113(3):687–701.
21. Cohen WR, Newman L, Friedman EA. Risk of labor abnormalities with advancing maternal age. Obstet Gynecol. 1980;55(4):414–416.
22. Cohen WR. Does maternal age affect pregnancy outcome? BJOG. 2014;121(3):252–254.
23. Bateman BT, Berman MF, Riley LE, Leffert LR. The epidemiology of postpartum hemorrhage in a large, nationwide sample of deliveries. Anesth Analg. 2010;110(5):1368–1373.
24. Lao TT, Sahota DS, Cheng YK, Law LW, Leung TY. Advanced maternal age and postpartum hemorrhage—risk factor or red herring? J Matern Fetal Neonatal Med. 2014;27(3):243–246.
2014 Update on pelvic floor dysfunction
Constipation is estimated to affect up to 27% of the general population and is more common in women, with a 2:1 female-to-male ratio.1 Because gynecologists are frequently the main care provider for many women, understanding the diagnosis and treatment options for constipation is important. Additionally, gynecologists must manage bowel function during the perioperative period.
The diagnosis of constipation is based on the Rome III criteria.2 Besides frequency of bowel movements (BMs), these criteria include evacuation symptoms and the presence of hard stools (TABLE 1). These symptoms can result from delay in colonic transit or outlet dysfunction. Constipation may be secondary to medical illness, such as central or peripheral neurologic disease, diabetes mellitus, hypothyroidism, or medications. Evaluation begins with a careful history and vaginal and perianal/anal examination.3 Initially, a trial of fiber supplementation with or without over-the-counter (OTC) laxatives may be tried (TABLE 2). If patients have an inadequate response to this therapy, further evaluation may be pursued (ALGORITHM).
------
| TABLE1 Rome III criteria for functional constipation in adults* |
1. Must include ≥2 of the following signs
2. Loose stools are rarely present without the use of laxatives 3. Insufficient criteria for irritable bowel syndrome |
| *At least 3 months, with symptoms beginning ≥6 months before diagnosis. |
--------
| TABLE 2 Common treatments for constipation |
Bulk-forming laxatives absorb water, increasing fecal mass
Surfactant agents lower the surface tension of stool, allowing water to enter the stool
Osmotic laxatives contain poorly/nonabsorbed substances, leading to intestinal water secretion
Stimulant laxatives increase colonic transit and alter electrolyte transport across the colonic mucosa
|
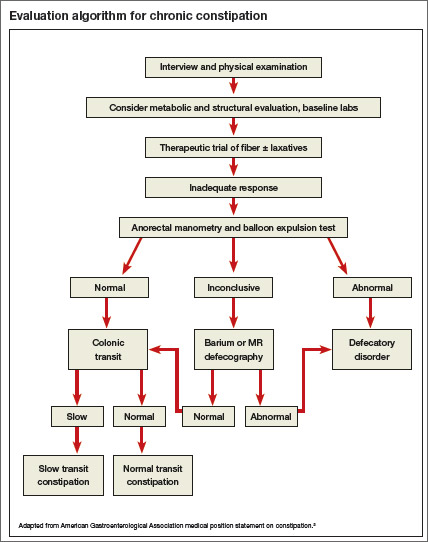
In this article, we review the results of randomized trials comparing the efficacy of OTC medical treatments for constipation, including daily, low-dose polyethylene glycol (PEG) and probiotics. Additionally, we review key trials evaluating perioperative bowel management prior to laparoscopic gynecologic and vaginal surgery.
LONG-TERM PEG USAGE SAFE AND EFFECTIVE?
Corazziari E, Badiali D, Bazzocchi G, et al. Long-term efficacy, safety, and tolerability of low daily doses of isosmotic polyethylene glycol electrolyte balanced solution (PMF-100) in the treatment of functional chronic constipation. Gut. 2000;46(4):522–526.
In this multicenter, randomized, double-blind, placebo-controlled, parallel trial, investigators evaluated the safety, efficacy, and tolerability of a daily low-dose PEG-based osmotic diuretic.
Details of the study
Seventy-eight patients (80% of them female) aged 18 to 75 years with chronic constipation, defined by Rome III diagnostic criteria, underwent a 4-week “run-in” period, with a standardized daily diet of fiber 15 g, water 1500 mL, and twice-daily PMF-100 (PEG/osmotic solution). Patients were randomized if they responded to the regimen, with response defined as having at least two BMs per week and no defecatory disturbance or at least three BMs per week with or without defecatory disturbance. Eight patients were not randomized, one due to nonresponsiveness. Study patients completed 20 weeks of either twice-daily PMF-100 or placebo. Patients, at their own discretion, decreased the frequency of the study drug based on the frequency of their BMs. Use of another laxative was not allowed unless a BM had not occurred over a 5-day period.
The combined primary outcome was at least three BMs per week, no defecatory disturbances, and no additional laxative use. Secondary outcomes (frequency of BMs and defecatory disturbances) were assessed using a bowel diary.
No differences were noted in baseline measurements between the two groups. Of the PMF-100 group, 70% completed the study, compared with 30% of the placebo group (P<.01). Nonresponse to treatment was the reason for dropout in 7% and 46% of patients, respectively (P<.005). Other causes of withdrawal did not differ between the groups.
At the end of the 20 weeks, 77% of patients in the PMF-100 group reported remission, compared with 20% in the placebo group (P<.001). During the study, the PMF-100 group reported more BMs per week (7.4 vs 4.3; P<.001). Furthermore, the treatment group was less likely to report straining at defecation, hard/pellet stools, and need for use of additional laxatives. Adverse events (nausea, anal pain/itching, hematochezia, epigastric pain, and fecal incontinence) were similar between groups. There were no differences in laboratory values.
Study strengths
This was a well-designed trial showing the safety, efficacy, and tolerability of a daily low-dose PEG-based osmotic diuretic. The population was mainly women with functional chronic constipation, similar to a gynecologic population. The results of this trial are consistent with what has been shown for other trials various PEG preparations.4,5
WHAT THIS EVIDENCE MEANS FOR PRACTICE
Women who fail initial fiber therapy may respond to daily low-dose PEG on a continuous basis. Resolution of constipation and defecatory symptoms is likely and should be seen within 1 month. Therapy can be continued safely for at least 6 months.
--------------
NEW AND TRENDY OTC TREATMENT OPTION
Del Piano M, Carmagnola S, Anderloni A, et al. The use of probiotics in healthy volunteers with evacuation disorders and hard stools: a double-blind, randomized, placebo-controlled study. J Clin Gastroenterol. 2010;44(suppl 1):S30–S34.
Factors such as age, unhealthy diet, and use of prescription drugs alter the intestinal bacterial flora. As patients strive for a more holistic approach to their health, interest is growing in the benefit of probiotics for treating chronic constipation. To explore the value of such probiotics, Del Piano and colleagues conducted a three-armed, randomized, double-blind placebo-controlled trial of two different probiotic preparations and a placebo among patients aged 24 to 71 years with evacuation disorders and constipation.
Details of the study
One probiotic preparation (A) was composed of Lactobacillus plantarum and Bifidobacterium breve at a concentration of 2.5×109 cfu per day; the other (B) was composed of Bifidobacterium animalis subspecies lactis at a concentration of 5×109 cfu per day. Patients took their preparation for 30 days and recorded data on weekly defecations (primary outcome), along with feces consistency, ease of expulsion, sensation emptying, anal itching/burning/pain with defecation, and abdominal bloating (secondary outcomes).
A total of 300 patients were enrolled in the study; 50% were female. No difference was noted in baseline symptoms among the three groups. No change from baseline was noted in BMs per week within the placebo group during the 30 days (5.6 vs 5.8, respectively). However, both probiotic preparations resulted in increased bowel frequency by day 30 (5.3 vs 7.3 BMs per week for probiotic A [P<.001] and 5.8 vs 6.9 BMs per week for probiotic B [P<.001]).
When comparing each probiotic with the placebo at days 15 and 30, a statistically significant increase in bowel frequency was found with each probiotic preparation. Furthermore, all secondary outcomes improved during the 30 days with the probiotic preparations but not the placebo. There was a statistically significant improvement in these variables when either probiotic was compared with placebo. No adverse events were reported.
Strengths and limitations
This randomized, double-blind, placebo-controlled trial showed improvement in bowel frequency, based on a bowel diary, with two different probiotic preparations when compared with placebo. The study population did not have to meet Rome III criteria for constipation, and baseline frequency of BMs was high. Patients did report subjective improvement in their defecatory symptoms with both probiotic preparations, but use of validated questionnaires would have strengthened this finding.
WHAT THIS EVIDENCE MEANS FOR PRACTICE
Patients with mild constipation and defecatory complaints may benefit from the addition of a probiotic preparation. However, more thorough studies need to be performed to characterize the true extent of probiotics’ benefits.
--------------
BOWEL PREP BEFORE LAPAROSCOPIC GYNECOLOGIC SURGERY
Siedhoff MT, Clark LH, Hobbs KA, Findley AD, Moulder JK, Garrett JM. Mechanic bowel preparation before laparoscopic hysterectomy: a randomized controlled trial. Obstet Gynecol. 2014;123(3):562–567.
Over the past decade, extrapolation of data from colorectal surgery literature, showing no benefit from preoperative mechanical bowel preparation,6 has led to less frequent use of mechanical bowel preparations for open benign gynecologic surgery. Nevertheless, there has been slower adoption of this practice with laparoscopic and vaginal surgery. In a recent study, Siedhoff and colleagues explored surgeons’ assessments of surgical field exposure in patients who did and did not complete preoperative mechanical bowel preparation.
Details of the study
This was a single-masked, randomized, controlled trial involving women undergoing laparoscopic hysterectomy for benign indications. Patients were randomly assigned to either a sodium phosphate enema the night before surgery and, if their stool was not clear, another enema on the morning of surgery versus no preparation. All patients had clear liquids the day prior to surgery, then fasted beginning at midnight. The surgeon was blinded to the randomization.
The primary outcome was a questionnaire completed by the surgeon that assessed surgical field exposure. Secondarily, patients completed a questionnaire addressing symptoms (cramps, hunger, bloating, embarrassment, insomnia, weakness, dizziness, thirst, nausea, and incontinence).
Baseline characteristics of the 160 randomized patients did not differ between the two groups. Analysis was on an intent-to-treat basis, but only two patients did not complete the bowel preparation. Overall, the study population had a mean age of 41 and body mass index of 33.5 kg/m2. No differences were noted in surgical characteristics between the two groups, including complication rate. The mean surgery time was 139 minutes with a mean estimated blood loss of 61 mL and a mean uterine weight of 385 g.
The surgeon’s assessment of the surgical field did not differ between the two groups. This finding also held true when subgroup analysis was performed for obesity, endometriosis, irritable bowel syndrome or inflammatory bowel disease, and chronic constipation. Interestingly, the odds of the surgeon guessing whether a patient had had a preparation were 50:50. The only difference in patient symptoms was an increase in insomnia in the no-preparation group.
Minor drawback
This well-performed trial demonstrated no significant value for mechanical bowel preparation before benign laparoscopic hysterectomy in a young population. How these results might extrapolate to an older population who may have a higher rate of prior pelvic surgery or diverticular disease is uncertain.
WHAT THIS EVIDENCE MEANS FOR PRACTICE
Women undergoing laparoscopic hysterectomy for a benign indication may forego a mechanical bowel preparation as such preparation did not improve the surgical field.
--------------
BOWEL PREP BEFORE VAGINAL SURGERY
Ballard AC, Parker-Autry CY, Markland AD, Varner RE, Huisingh C, Richter HE. Bowel preparation before vaginal prolapse surgery: a randomized controlled trial. Obstet Gynecol. 2014;123(2 pt 1):232–238.
In this single-masked, randomized controlled trial in women undergoing reconstructive vaginal prolapse surgery, Ballard and colleagues randomly assigned patients to either a clear liquid diet with two saline enemas the day before surgery or a regular diet the day before surgery.
Details of the study
All 150 patients were instructed to fast beginning at midnight the night before surgery, and the surgeon was blinded to randomization. The study’s primary outcome was the surgeon’s perception of the operative field assessed by a questionnaire. The secondary outcome was the patient’s satisfaction with their preoperative regimen as reported on validated questionnaires.
An intent-to-treat analysis was performed (mean age, 60 years); 84% of patients assigned to bowel preparation completed more than 50% of the enemas. Baseline characteristics and surgical procedures were similar between groups. Approximately 33% of patients underwent hysterectomy concomitantly with the prolapse repair. Operative time, estimated blood loss, and bowel injury were similar between the two groups.
No difference between groups was noted in the surgeons’ assessment of the surgical field—which was rated as excellent or good in 85% of patients who underwent the bowel preparation compared with 90% in the no-preparation group (P = .3). Additionally, no difference was noted in the presence of rectal stool or gas by inspection and palpation. Patient satisfaction was significantly lower among those who underwent bowel preparation compared with patients who did not. Patients undergoing bowel preparation were more likely to have abdominal fullness or bloating (P = .004), abdominal cramps or pain (P<.001), anal irritation (P<.001), and hunger pains (P<.001).
Prep group saw no benefit and decreased satisfaction
This well-performed clinical trial showed that the use of mechanical bowel preparation did not significantly improve surgeons’ intraoperative acceptability of the operative field during vaginal prolapse surgery. However, approximately 25% of patients underwent sacrospinous suspensions; therefore, intraperitoneal access was not necessary in these patients. The study results demonstrated decreased patient satisfaction and more distressing bowel symptoms in patients who underwent a mechanical bowel preparation with an enema.
WHAT THIS EVIDENCE MEANS FOR PRACTICE
Use of a mechanical bowel preparation is not necessary to improve the surgical field in vaginal prolapse surgery. Not having patients undergo a bowel preparation will improve patients’ assessment of their preparation for surgery.
--------------
Share your thoughts on this article! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.
- Higgins PD, Johanson JF. Epidemiology of constipation in North America: a systematic review. Am J Gastroenterol. 2004;99(4):750–759.
- Longstreth GF, Thompson WG, Chey WD, Houghton LA, Mearin F, Spiller RC. Functional bowel disorders. Gastroenterology. 2006;130(5):1480–1491.
- Bharucha AE, Dorn SD, Lembo A, Pressman A. American Gastroenterological Association medical position statement on constipation. Gastroenterology. 2013;144(1):211–217.
- American College of Gastroenterology Chronic Constipation Task Force. An evidence-based approach to the management of chronic constipation in North America. Am J Gastroenterol. 2005;100(suppl 1):S1–S22.
- Ramkumar D, Rao SS. Efficacy and safety of traditional medical therapies for chronic constipation: systematic review. Am J Gastroenterol. 2005;100(4):936–971.
- Guenaga KF, Matos D, Wille-Jørgensen P. Mechanical bowel preparation for elective colorectal surgery. Cochrane Database Syst Rev. 2011;(9):CD001544.

Dr. Polin is Fellow, Female Pelvic Medicine and Reconstructive Surgery, and Clinical Instructor, Obstetrics and Gynecology, Department of Obstetrics and Gynecology, at Duke University in Durham, North Carolina.

Dr. Amundsen is Professor and Female Pelvic Medicine and Reconstructive Surgery Fellowship Director, Department of Obstetrics and Gynecology, at Duke University.
Dr. Polin reports no financial relationships relevant to this article. Dr. Amundsen reports that she receives grant or research support from the National Institutes of Health.
Dr. Polin is Fellow, Female Pelvic Medicine and Reconstructive Surgery, and Clinical Instructor, Obstetrics and Gynecology, Department of Obstetrics and Gynecology, at Duke University in Durham, North Carolina.
Dr. Amundsen is Professor and Female Pelvic Medicine and Reconstructive Surgery Fellowship Director, Department of Obstetrics and Gynecology, at Duke University.
Dr. Polin reports no financial relationships relevant to this article. Dr. Amundsen reports that she receives grant or research support from the National Institutes of Health.
Dr. Polin is Fellow, Female Pelvic Medicine and Reconstructive Surgery, and Clinical Instructor, Obstetrics and Gynecology, Department of Obstetrics and Gynecology, at Duke University in Durham, North Carolina.
Dr. Amundsen is Professor and Female Pelvic Medicine and Reconstructive Surgery Fellowship Director, Department of Obstetrics and Gynecology, at Duke University.
Dr. Polin reports no financial relationships relevant to this article. Dr. Amundsen reports that she receives grant or research support from the National Institutes of Health.
Constipation is estimated to affect up to 27% of the general population and is more common in women, with a 2:1 female-to-male ratio.1 Because gynecologists are frequently the main care provider for many women, understanding the diagnosis and treatment options for constipation is important. Additionally, gynecologists must manage bowel function during the perioperative period.
The diagnosis of constipation is based on the Rome III criteria.2 Besides frequency of bowel movements (BMs), these criteria include evacuation symptoms and the presence of hard stools (TABLE 1). These symptoms can result from delay in colonic transit or outlet dysfunction. Constipation may be secondary to medical illness, such as central or peripheral neurologic disease, diabetes mellitus, hypothyroidism, or medications. Evaluation begins with a careful history and vaginal and perianal/anal examination.3 Initially, a trial of fiber supplementation with or without over-the-counter (OTC) laxatives may be tried (TABLE 2). If patients have an inadequate response to this therapy, further evaluation may be pursued (ALGORITHM).
------
| TABLE1 Rome III criteria for functional constipation in adults* |
1. Must include ≥2 of the following signs
2. Loose stools are rarely present without the use of laxatives 3. Insufficient criteria for irritable bowel syndrome |
| *At least 3 months, with symptoms beginning ≥6 months before diagnosis. |
--------
| TABLE 2 Common treatments for constipation |
Bulk-forming laxatives absorb water, increasing fecal mass
Surfactant agents lower the surface tension of stool, allowing water to enter the stool
Osmotic laxatives contain poorly/nonabsorbed substances, leading to intestinal water secretion
Stimulant laxatives increase colonic transit and alter electrolyte transport across the colonic mucosa
|
In this article, we review the results of randomized trials comparing the efficacy of OTC medical treatments for constipation, including daily, low-dose polyethylene glycol (PEG) and probiotics. Additionally, we review key trials evaluating perioperative bowel management prior to laparoscopic gynecologic and vaginal surgery.
LONG-TERM PEG USAGE SAFE AND EFFECTIVE?
Corazziari E, Badiali D, Bazzocchi G, et al. Long-term efficacy, safety, and tolerability of low daily doses of isosmotic polyethylene glycol electrolyte balanced solution (PMF-100) in the treatment of functional chronic constipation. Gut. 2000;46(4):522–526.
In this multicenter, randomized, double-blind, placebo-controlled, parallel trial, investigators evaluated the safety, efficacy, and tolerability of a daily low-dose PEG-based osmotic diuretic.
Details of the study
Seventy-eight patients (80% of them female) aged 18 to 75 years with chronic constipation, defined by Rome III diagnostic criteria, underwent a 4-week “run-in” period, with a standardized daily diet of fiber 15 g, water 1500 mL, and twice-daily PMF-100 (PEG/osmotic solution). Patients were randomized if they responded to the regimen, with response defined as having at least two BMs per week and no defecatory disturbance or at least three BMs per week with or without defecatory disturbance. Eight patients were not randomized, one due to nonresponsiveness. Study patients completed 20 weeks of either twice-daily PMF-100 or placebo. Patients, at their own discretion, decreased the frequency of the study drug based on the frequency of their BMs. Use of another laxative was not allowed unless a BM had not occurred over a 5-day period.
The combined primary outcome was at least three BMs per week, no defecatory disturbances, and no additional laxative use. Secondary outcomes (frequency of BMs and defecatory disturbances) were assessed using a bowel diary.
No differences were noted in baseline measurements between the two groups. Of the PMF-100 group, 70% completed the study, compared with 30% of the placebo group (P<.01). Nonresponse to treatment was the reason for dropout in 7% and 46% of patients, respectively (P<.005). Other causes of withdrawal did not differ between the groups.
At the end of the 20 weeks, 77% of patients in the PMF-100 group reported remission, compared with 20% in the placebo group (P<.001). During the study, the PMF-100 group reported more BMs per week (7.4 vs 4.3; P<.001). Furthermore, the treatment group was less likely to report straining at defecation, hard/pellet stools, and need for use of additional laxatives. Adverse events (nausea, anal pain/itching, hematochezia, epigastric pain, and fecal incontinence) were similar between groups. There were no differences in laboratory values.
Study strengths
This was a well-designed trial showing the safety, efficacy, and tolerability of a daily low-dose PEG-based osmotic diuretic. The population was mainly women with functional chronic constipation, similar to a gynecologic population. The results of this trial are consistent with what has been shown for other trials various PEG preparations.4,5
WHAT THIS EVIDENCE MEANS FOR PRACTICE
Women who fail initial fiber therapy may respond to daily low-dose PEG on a continuous basis. Resolution of constipation and defecatory symptoms is likely and should be seen within 1 month. Therapy can be continued safely for at least 6 months.
--------------
NEW AND TRENDY OTC TREATMENT OPTION
Del Piano M, Carmagnola S, Anderloni A, et al. The use of probiotics in healthy volunteers with evacuation disorders and hard stools: a double-blind, randomized, placebo-controlled study. J Clin Gastroenterol. 2010;44(suppl 1):S30–S34.
Factors such as age, unhealthy diet, and use of prescription drugs alter the intestinal bacterial flora. As patients strive for a more holistic approach to their health, interest is growing in the benefit of probiotics for treating chronic constipation. To explore the value of such probiotics, Del Piano and colleagues conducted a three-armed, randomized, double-blind placebo-controlled trial of two different probiotic preparations and a placebo among patients aged 24 to 71 years with evacuation disorders and constipation.
Details of the study
One probiotic preparation (A) was composed of Lactobacillus plantarum and Bifidobacterium breve at a concentration of 2.5×109 cfu per day; the other (B) was composed of Bifidobacterium animalis subspecies lactis at a concentration of 5×109 cfu per day. Patients took their preparation for 30 days and recorded data on weekly defecations (primary outcome), along with feces consistency, ease of expulsion, sensation emptying, anal itching/burning/pain with defecation, and abdominal bloating (secondary outcomes).
A total of 300 patients were enrolled in the study; 50% were female. No difference was noted in baseline symptoms among the three groups. No change from baseline was noted in BMs per week within the placebo group during the 30 days (5.6 vs 5.8, respectively). However, both probiotic preparations resulted in increased bowel frequency by day 30 (5.3 vs 7.3 BMs per week for probiotic A [P<.001] and 5.8 vs 6.9 BMs per week for probiotic B [P<.001]).
When comparing each probiotic with the placebo at days 15 and 30, a statistically significant increase in bowel frequency was found with each probiotic preparation. Furthermore, all secondary outcomes improved during the 30 days with the probiotic preparations but not the placebo. There was a statistically significant improvement in these variables when either probiotic was compared with placebo. No adverse events were reported.
Strengths and limitations
This randomized, double-blind, placebo-controlled trial showed improvement in bowel frequency, based on a bowel diary, with two different probiotic preparations when compared with placebo. The study population did not have to meet Rome III criteria for constipation, and baseline frequency of BMs was high. Patients did report subjective improvement in their defecatory symptoms with both probiotic preparations, but use of validated questionnaires would have strengthened this finding.
WHAT THIS EVIDENCE MEANS FOR PRACTICE
Patients with mild constipation and defecatory complaints may benefit from the addition of a probiotic preparation. However, more thorough studies need to be performed to characterize the true extent of probiotics’ benefits.
--------------
BOWEL PREP BEFORE LAPAROSCOPIC GYNECOLOGIC SURGERY
Siedhoff MT, Clark LH, Hobbs KA, Findley AD, Moulder JK, Garrett JM. Mechanic bowel preparation before laparoscopic hysterectomy: a randomized controlled trial. Obstet Gynecol. 2014;123(3):562–567.
Over the past decade, extrapolation of data from colorectal surgery literature, showing no benefit from preoperative mechanical bowel preparation,6 has led to less frequent use of mechanical bowel preparations for open benign gynecologic surgery. Nevertheless, there has been slower adoption of this practice with laparoscopic and vaginal surgery. In a recent study, Siedhoff and colleagues explored surgeons’ assessments of surgical field exposure in patients who did and did not complete preoperative mechanical bowel preparation.
Details of the study
This was a single-masked, randomized, controlled trial involving women undergoing laparoscopic hysterectomy for benign indications. Patients were randomly assigned to either a sodium phosphate enema the night before surgery and, if their stool was not clear, another enema on the morning of surgery versus no preparation. All patients had clear liquids the day prior to surgery, then fasted beginning at midnight. The surgeon was blinded to the randomization.
The primary outcome was a questionnaire completed by the surgeon that assessed surgical field exposure. Secondarily, patients completed a questionnaire addressing symptoms (cramps, hunger, bloating, embarrassment, insomnia, weakness, dizziness, thirst, nausea, and incontinence).
Baseline characteristics of the 160 randomized patients did not differ between the two groups. Analysis was on an intent-to-treat basis, but only two patients did not complete the bowel preparation. Overall, the study population had a mean age of 41 and body mass index of 33.5 kg/m2. No differences were noted in surgical characteristics between the two groups, including complication rate. The mean surgery time was 139 minutes with a mean estimated blood loss of 61 mL and a mean uterine weight of 385 g.
The surgeon’s assessment of the surgical field did not differ between the two groups. This finding also held true when subgroup analysis was performed for obesity, endometriosis, irritable bowel syndrome or inflammatory bowel disease, and chronic constipation. Interestingly, the odds of the surgeon guessing whether a patient had had a preparation were 50:50. The only difference in patient symptoms was an increase in insomnia in the no-preparation group.
Minor drawback
This well-performed trial demonstrated no significant value for mechanical bowel preparation before benign laparoscopic hysterectomy in a young population. How these results might extrapolate to an older population who may have a higher rate of prior pelvic surgery or diverticular disease is uncertain.
WHAT THIS EVIDENCE MEANS FOR PRACTICE
Women undergoing laparoscopic hysterectomy for a benign indication may forego a mechanical bowel preparation as such preparation did not improve the surgical field.
--------------
BOWEL PREP BEFORE VAGINAL SURGERY
Ballard AC, Parker-Autry CY, Markland AD, Varner RE, Huisingh C, Richter HE. Bowel preparation before vaginal prolapse surgery: a randomized controlled trial. Obstet Gynecol. 2014;123(2 pt 1):232–238.
In this single-masked, randomized controlled trial in women undergoing reconstructive vaginal prolapse surgery, Ballard and colleagues randomly assigned patients to either a clear liquid diet with two saline enemas the day before surgery or a regular diet the day before surgery.
Details of the study
All 150 patients were instructed to fast beginning at midnight the night before surgery, and the surgeon was blinded to randomization. The study’s primary outcome was the surgeon’s perception of the operative field assessed by a questionnaire. The secondary outcome was the patient’s satisfaction with their preoperative regimen as reported on validated questionnaires.
An intent-to-treat analysis was performed (mean age, 60 years); 84% of patients assigned to bowel preparation completed more than 50% of the enemas. Baseline characteristics and surgical procedures were similar between groups. Approximately 33% of patients underwent hysterectomy concomitantly with the prolapse repair. Operative time, estimated blood loss, and bowel injury were similar between the two groups.
No difference between groups was noted in the surgeons’ assessment of the surgical field—which was rated as excellent or good in 85% of patients who underwent the bowel preparation compared with 90% in the no-preparation group (P = .3). Additionally, no difference was noted in the presence of rectal stool or gas by inspection and palpation. Patient satisfaction was significantly lower among those who underwent bowel preparation compared with patients who did not. Patients undergoing bowel preparation were more likely to have abdominal fullness or bloating (P = .004), abdominal cramps or pain (P<.001), anal irritation (P<.001), and hunger pains (P<.001).
Prep group saw no benefit and decreased satisfaction
This well-performed clinical trial showed that the use of mechanical bowel preparation did not significantly improve surgeons’ intraoperative acceptability of the operative field during vaginal prolapse surgery. However, approximately 25% of patients underwent sacrospinous suspensions; therefore, intraperitoneal access was not necessary in these patients. The study results demonstrated decreased patient satisfaction and more distressing bowel symptoms in patients who underwent a mechanical bowel preparation with an enema.
WHAT THIS EVIDENCE MEANS FOR PRACTICE
Use of a mechanical bowel preparation is not necessary to improve the surgical field in vaginal prolapse surgery. Not having patients undergo a bowel preparation will improve patients’ assessment of their preparation for surgery.
--------------
Share your thoughts on this article! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.
Constipation is estimated to affect up to 27% of the general population and is more common in women, with a 2:1 female-to-male ratio.1 Because gynecologists are frequently the main care provider for many women, understanding the diagnosis and treatment options for constipation is important. Additionally, gynecologists must manage bowel function during the perioperative period.
The diagnosis of constipation is based on the Rome III criteria.2 Besides frequency of bowel movements (BMs), these criteria include evacuation symptoms and the presence of hard stools (TABLE 1). These symptoms can result from delay in colonic transit or outlet dysfunction. Constipation may be secondary to medical illness, such as central or peripheral neurologic disease, diabetes mellitus, hypothyroidism, or medications. Evaluation begins with a careful history and vaginal and perianal/anal examination.3 Initially, a trial of fiber supplementation with or without over-the-counter (OTC) laxatives may be tried (TABLE 2). If patients have an inadequate response to this therapy, further evaluation may be pursued (ALGORITHM).
------
| TABLE1 Rome III criteria for functional constipation in adults* |
1. Must include ≥2 of the following signs
2. Loose stools are rarely present without the use of laxatives 3. Insufficient criteria for irritable bowel syndrome |
| *At least 3 months, with symptoms beginning ≥6 months before diagnosis. |
--------
| TABLE 2 Common treatments for constipation |
Bulk-forming laxatives absorb water, increasing fecal mass
Surfactant agents lower the surface tension of stool, allowing water to enter the stool
Osmotic laxatives contain poorly/nonabsorbed substances, leading to intestinal water secretion
Stimulant laxatives increase colonic transit and alter electrolyte transport across the colonic mucosa
|
In this article, we review the results of randomized trials comparing the efficacy of OTC medical treatments for constipation, including daily, low-dose polyethylene glycol (PEG) and probiotics. Additionally, we review key trials evaluating perioperative bowel management prior to laparoscopic gynecologic and vaginal surgery.
LONG-TERM PEG USAGE SAFE AND EFFECTIVE?
Corazziari E, Badiali D, Bazzocchi G, et al. Long-term efficacy, safety, and tolerability of low daily doses of isosmotic polyethylene glycol electrolyte balanced solution (PMF-100) in the treatment of functional chronic constipation. Gut. 2000;46(4):522–526.
In this multicenter, randomized, double-blind, placebo-controlled, parallel trial, investigators evaluated the safety, efficacy, and tolerability of a daily low-dose PEG-based osmotic diuretic.
Details of the study
Seventy-eight patients (80% of them female) aged 18 to 75 years with chronic constipation, defined by Rome III diagnostic criteria, underwent a 4-week “run-in” period, with a standardized daily diet of fiber 15 g, water 1500 mL, and twice-daily PMF-100 (PEG/osmotic solution). Patients were randomized if they responded to the regimen, with response defined as having at least two BMs per week and no defecatory disturbance or at least three BMs per week with or without defecatory disturbance. Eight patients were not randomized, one due to nonresponsiveness. Study patients completed 20 weeks of either twice-daily PMF-100 or placebo. Patients, at their own discretion, decreased the frequency of the study drug based on the frequency of their BMs. Use of another laxative was not allowed unless a BM had not occurred over a 5-day period.
The combined primary outcome was at least three BMs per week, no defecatory disturbances, and no additional laxative use. Secondary outcomes (frequency of BMs and defecatory disturbances) were assessed using a bowel diary.
No differences were noted in baseline measurements between the two groups. Of the PMF-100 group, 70% completed the study, compared with 30% of the placebo group (P<.01). Nonresponse to treatment was the reason for dropout in 7% and 46% of patients, respectively (P<.005). Other causes of withdrawal did not differ between the groups.
At the end of the 20 weeks, 77% of patients in the PMF-100 group reported remission, compared with 20% in the placebo group (P<.001). During the study, the PMF-100 group reported more BMs per week (7.4 vs 4.3; P<.001). Furthermore, the treatment group was less likely to report straining at defecation, hard/pellet stools, and need for use of additional laxatives. Adverse events (nausea, anal pain/itching, hematochezia, epigastric pain, and fecal incontinence) were similar between groups. There were no differences in laboratory values.
Study strengths
This was a well-designed trial showing the safety, efficacy, and tolerability of a daily low-dose PEG-based osmotic diuretic. The population was mainly women with functional chronic constipation, similar to a gynecologic population. The results of this trial are consistent with what has been shown for other trials various PEG preparations.4,5
WHAT THIS EVIDENCE MEANS FOR PRACTICE
Women who fail initial fiber therapy may respond to daily low-dose PEG on a continuous basis. Resolution of constipation and defecatory symptoms is likely and should be seen within 1 month. Therapy can be continued safely for at least 6 months.
--------------
NEW AND TRENDY OTC TREATMENT OPTION
Del Piano M, Carmagnola S, Anderloni A, et al. The use of probiotics in healthy volunteers with evacuation disorders and hard stools: a double-blind, randomized, placebo-controlled study. J Clin Gastroenterol. 2010;44(suppl 1):S30–S34.
Factors such as age, unhealthy diet, and use of prescription drugs alter the intestinal bacterial flora. As patients strive for a more holistic approach to their health, interest is growing in the benefit of probiotics for treating chronic constipation. To explore the value of such probiotics, Del Piano and colleagues conducted a three-armed, randomized, double-blind placebo-controlled trial of two different probiotic preparations and a placebo among patients aged 24 to 71 years with evacuation disorders and constipation.
Details of the study
One probiotic preparation (A) was composed of Lactobacillus plantarum and Bifidobacterium breve at a concentration of 2.5×109 cfu per day; the other (B) was composed of Bifidobacterium animalis subspecies lactis at a concentration of 5×109 cfu per day. Patients took their preparation for 30 days and recorded data on weekly defecations (primary outcome), along with feces consistency, ease of expulsion, sensation emptying, anal itching/burning/pain with defecation, and abdominal bloating (secondary outcomes).
A total of 300 patients were enrolled in the study; 50% were female. No difference was noted in baseline symptoms among the three groups. No change from baseline was noted in BMs per week within the placebo group during the 30 days (5.6 vs 5.8, respectively). However, both probiotic preparations resulted in increased bowel frequency by day 30 (5.3 vs 7.3 BMs per week for probiotic A [P<.001] and 5.8 vs 6.9 BMs per week for probiotic B [P<.001]).
When comparing each probiotic with the placebo at days 15 and 30, a statistically significant increase in bowel frequency was found with each probiotic preparation. Furthermore, all secondary outcomes improved during the 30 days with the probiotic preparations but not the placebo. There was a statistically significant improvement in these variables when either probiotic was compared with placebo. No adverse events were reported.
Strengths and limitations
This randomized, double-blind, placebo-controlled trial showed improvement in bowel frequency, based on a bowel diary, with two different probiotic preparations when compared with placebo. The study population did not have to meet Rome III criteria for constipation, and baseline frequency of BMs was high. Patients did report subjective improvement in their defecatory symptoms with both probiotic preparations, but use of validated questionnaires would have strengthened this finding.
WHAT THIS EVIDENCE MEANS FOR PRACTICE
Patients with mild constipation and defecatory complaints may benefit from the addition of a probiotic preparation. However, more thorough studies need to be performed to characterize the true extent of probiotics’ benefits.
--------------
BOWEL PREP BEFORE LAPAROSCOPIC GYNECOLOGIC SURGERY
Siedhoff MT, Clark LH, Hobbs KA, Findley AD, Moulder JK, Garrett JM. Mechanic bowel preparation before laparoscopic hysterectomy: a randomized controlled trial. Obstet Gynecol. 2014;123(3):562–567.
Over the past decade, extrapolation of data from colorectal surgery literature, showing no benefit from preoperative mechanical bowel preparation,6 has led to less frequent use of mechanical bowel preparations for open benign gynecologic surgery. Nevertheless, there has been slower adoption of this practice with laparoscopic and vaginal surgery. In a recent study, Siedhoff and colleagues explored surgeons’ assessments of surgical field exposure in patients who did and did not complete preoperative mechanical bowel preparation.
Details of the study
This was a single-masked, randomized, controlled trial involving women undergoing laparoscopic hysterectomy for benign indications. Patients were randomly assigned to either a sodium phosphate enema the night before surgery and, if their stool was not clear, another enema on the morning of surgery versus no preparation. All patients had clear liquids the day prior to surgery, then fasted beginning at midnight. The surgeon was blinded to the randomization.
The primary outcome was a questionnaire completed by the surgeon that assessed surgical field exposure. Secondarily, patients completed a questionnaire addressing symptoms (cramps, hunger, bloating, embarrassment, insomnia, weakness, dizziness, thirst, nausea, and incontinence).
Baseline characteristics of the 160 randomized patients did not differ between the two groups. Analysis was on an intent-to-treat basis, but only two patients did not complete the bowel preparation. Overall, the study population had a mean age of 41 and body mass index of 33.5 kg/m2. No differences were noted in surgical characteristics between the two groups, including complication rate. The mean surgery time was 139 minutes with a mean estimated blood loss of 61 mL and a mean uterine weight of 385 g.
The surgeon’s assessment of the surgical field did not differ between the two groups. This finding also held true when subgroup analysis was performed for obesity, endometriosis, irritable bowel syndrome or inflammatory bowel disease, and chronic constipation. Interestingly, the odds of the surgeon guessing whether a patient had had a preparation were 50:50. The only difference in patient symptoms was an increase in insomnia in the no-preparation group.
Minor drawback
This well-performed trial demonstrated no significant value for mechanical bowel preparation before benign laparoscopic hysterectomy in a young population. How these results might extrapolate to an older population who may have a higher rate of prior pelvic surgery or diverticular disease is uncertain.
WHAT THIS EVIDENCE MEANS FOR PRACTICE
Women undergoing laparoscopic hysterectomy for a benign indication may forego a mechanical bowel preparation as such preparation did not improve the surgical field.
--------------
BOWEL PREP BEFORE VAGINAL SURGERY
Ballard AC, Parker-Autry CY, Markland AD, Varner RE, Huisingh C, Richter HE. Bowel preparation before vaginal prolapse surgery: a randomized controlled trial. Obstet Gynecol. 2014;123(2 pt 1):232–238.
In this single-masked, randomized controlled trial in women undergoing reconstructive vaginal prolapse surgery, Ballard and colleagues randomly assigned patients to either a clear liquid diet with two saline enemas the day before surgery or a regular diet the day before surgery.
Details of the study
All 150 patients were instructed to fast beginning at midnight the night before surgery, and the surgeon was blinded to randomization. The study’s primary outcome was the surgeon’s perception of the operative field assessed by a questionnaire. The secondary outcome was the patient’s satisfaction with their preoperative regimen as reported on validated questionnaires.
An intent-to-treat analysis was performed (mean age, 60 years); 84% of patients assigned to bowel preparation completed more than 50% of the enemas. Baseline characteristics and surgical procedures were similar between groups. Approximately 33% of patients underwent hysterectomy concomitantly with the prolapse repair. Operative time, estimated blood loss, and bowel injury were similar between the two groups.
No difference between groups was noted in the surgeons’ assessment of the surgical field—which was rated as excellent or good in 85% of patients who underwent the bowel preparation compared with 90% in the no-preparation group (P = .3). Additionally, no difference was noted in the presence of rectal stool or gas by inspection and palpation. Patient satisfaction was significantly lower among those who underwent bowel preparation compared with patients who did not. Patients undergoing bowel preparation were more likely to have abdominal fullness or bloating (P = .004), abdominal cramps or pain (P<.001), anal irritation (P<.001), and hunger pains (P<.001).
Prep group saw no benefit and decreased satisfaction
This well-performed clinical trial showed that the use of mechanical bowel preparation did not significantly improve surgeons’ intraoperative acceptability of the operative field during vaginal prolapse surgery. However, approximately 25% of patients underwent sacrospinous suspensions; therefore, intraperitoneal access was not necessary in these patients. The study results demonstrated decreased patient satisfaction and more distressing bowel symptoms in patients who underwent a mechanical bowel preparation with an enema.
WHAT THIS EVIDENCE MEANS FOR PRACTICE
Use of a mechanical bowel preparation is not necessary to improve the surgical field in vaginal prolapse surgery. Not having patients undergo a bowel preparation will improve patients’ assessment of their preparation for surgery.
--------------
Share your thoughts on this article! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.
- Higgins PD, Johanson JF. Epidemiology of constipation in North America: a systematic review. Am J Gastroenterol. 2004;99(4):750–759.
- Longstreth GF, Thompson WG, Chey WD, Houghton LA, Mearin F, Spiller RC. Functional bowel disorders. Gastroenterology. 2006;130(5):1480–1491.
- Bharucha AE, Dorn SD, Lembo A, Pressman A. American Gastroenterological Association medical position statement on constipation. Gastroenterology. 2013;144(1):211–217.
- American College of Gastroenterology Chronic Constipation Task Force. An evidence-based approach to the management of chronic constipation in North America. Am J Gastroenterol. 2005;100(suppl 1):S1–S22.
- Ramkumar D, Rao SS. Efficacy and safety of traditional medical therapies for chronic constipation: systematic review. Am J Gastroenterol. 2005;100(4):936–971.
- Guenaga KF, Matos D, Wille-Jørgensen P. Mechanical bowel preparation for elective colorectal surgery. Cochrane Database Syst Rev. 2011;(9):CD001544.
- Higgins PD, Johanson JF. Epidemiology of constipation in North America: a systematic review. Am J Gastroenterol. 2004;99(4):750–759.
- Longstreth GF, Thompson WG, Chey WD, Houghton LA, Mearin F, Spiller RC. Functional bowel disorders. Gastroenterology. 2006;130(5):1480–1491.
- Bharucha AE, Dorn SD, Lembo A, Pressman A. American Gastroenterological Association medical position statement on constipation. Gastroenterology. 2013;144(1):211–217.
- American College of Gastroenterology Chronic Constipation Task Force. An evidence-based approach to the management of chronic constipation in North America. Am J Gastroenterol. 2005;100(suppl 1):S1–S22.
- Ramkumar D, Rao SS. Efficacy and safety of traditional medical therapies for chronic constipation: systematic review. Am J Gastroenterol. 2005;100(4):936–971.
- Guenaga KF, Matos D, Wille-Jørgensen P. Mechanical bowel preparation for elective colorectal surgery. Cochrane Database Syst Rev. 2011;(9):CD001544.
IN THIS ARTICLE
- Long-term PEG usage safe and effective?
- New and trendy OTC treatment option
- Bowel prep before laparoscopic gynecologic surgery
- Bowel prep before vaginal surgery

Can Neighborhoods Make People Gain Weight?
Can a neighborhood be “obesogenic”? Yes, suggest researchers from the University of Washington in Seattle. According to their study, living in neighborhoods with lower property values may impact whether or not residents are likely to be overweight and obese.
For their study, the researchers used data from the Seattle Obesity Study of 2,001 adults in King County, Washington. The survey asked people 11 questions about their neighborhood, including whether they felt safe, whether the neighborhood was clean and well lit, whether traffic was a problem, and whether neighbors knew and trusted one another.
Having a fast-food restaurant within a 10-minute walk lowered property values by $50,000. Being within 10 minutes of a park boosted property values by an average $30,000. Neighborhoods with higher property values (P < .001) were perceived as safe, quiet, clean, and attractive, with parks, playing fields, and full-service restaurants within walking distance. Seven of the perceived environmental measures were significantly associated with body mass index (BMI), especially for women, the researchers found. These included feeling safe, trusting neighbors, and lower neighborhood diversity, but not traffic or perceiving the neighborhood as clean and attractive.
Neighborhoods with lower property values were also often obesogenic communities: Residents who reported living with crime, heavy traffic, bars, liquor stores, and fast food, had BMIs of about 27 on average, compared with 23.9 for women and 26.4 for men in the highest-valued neighborhoods.
But the amenities people value in their neighborhoods can vary. In New York, New York, and Seattle, Washington, for instance, having a park nearby was associated with higher property values. In Detroit, Michigan, having a supermarket nearby was more valued. Those kinds of independent variables can help explain inconsistent associations between environmental measures and BMI, the researchers say. Sometimes having fast food nearby is linked to obesity, sometimes not. Parks are not always linked to lower BMIs, either.
Establishing links between multiple measures of the environment, activity levels, and obesity rates is a “continuing challenge,” the researchers acknowledge. But they feel using property values as a marker is a new “wealth metric” that may offer a way to resolve the complexity. Because real estate stays put and people do not, the researchers suggest that property value is an effective way to sort the population by material resources and socioeconomic status.
Source
Drewnowski A, Aggarwal A, Rehm CD, Cohen-Cline H, Hurvitz PM, Moudon AV. Am J Prev Med. 2014;47(3):260-274.
doi: 10.1016/j.amepre.2014.05.006.
Can a neighborhood be “obesogenic”? Yes, suggest researchers from the University of Washington in Seattle. According to their study, living in neighborhoods with lower property values may impact whether or not residents are likely to be overweight and obese.
For their study, the researchers used data from the Seattle Obesity Study of 2,001 adults in King County, Washington. The survey asked people 11 questions about their neighborhood, including whether they felt safe, whether the neighborhood was clean and well lit, whether traffic was a problem, and whether neighbors knew and trusted one another.
Having a fast-food restaurant within a 10-minute walk lowered property values by $50,000. Being within 10 minutes of a park boosted property values by an average $30,000. Neighborhoods with higher property values (P < .001) were perceived as safe, quiet, clean, and attractive, with parks, playing fields, and full-service restaurants within walking distance. Seven of the perceived environmental measures were significantly associated with body mass index (BMI), especially for women, the researchers found. These included feeling safe, trusting neighbors, and lower neighborhood diversity, but not traffic or perceiving the neighborhood as clean and attractive.
Neighborhoods with lower property values were also often obesogenic communities: Residents who reported living with crime, heavy traffic, bars, liquor stores, and fast food, had BMIs of about 27 on average, compared with 23.9 for women and 26.4 for men in the highest-valued neighborhoods.
But the amenities people value in their neighborhoods can vary. In New York, New York, and Seattle, Washington, for instance, having a park nearby was associated with higher property values. In Detroit, Michigan, having a supermarket nearby was more valued. Those kinds of independent variables can help explain inconsistent associations between environmental measures and BMI, the researchers say. Sometimes having fast food nearby is linked to obesity, sometimes not. Parks are not always linked to lower BMIs, either.
Establishing links between multiple measures of the environment, activity levels, and obesity rates is a “continuing challenge,” the researchers acknowledge. But they feel using property values as a marker is a new “wealth metric” that may offer a way to resolve the complexity. Because real estate stays put and people do not, the researchers suggest that property value is an effective way to sort the population by material resources and socioeconomic status.
Source
Drewnowski A, Aggarwal A, Rehm CD, Cohen-Cline H, Hurvitz PM, Moudon AV. Am J Prev Med. 2014;47(3):260-274.
doi: 10.1016/j.amepre.2014.05.006.
Can a neighborhood be “obesogenic”? Yes, suggest researchers from the University of Washington in Seattle. According to their study, living in neighborhoods with lower property values may impact whether or not residents are likely to be overweight and obese.
For their study, the researchers used data from the Seattle Obesity Study of 2,001 adults in King County, Washington. The survey asked people 11 questions about their neighborhood, including whether they felt safe, whether the neighborhood was clean and well lit, whether traffic was a problem, and whether neighbors knew and trusted one another.
Having a fast-food restaurant within a 10-minute walk lowered property values by $50,000. Being within 10 minutes of a park boosted property values by an average $30,000. Neighborhoods with higher property values (P < .001) were perceived as safe, quiet, clean, and attractive, with parks, playing fields, and full-service restaurants within walking distance. Seven of the perceived environmental measures were significantly associated with body mass index (BMI), especially for women, the researchers found. These included feeling safe, trusting neighbors, and lower neighborhood diversity, but not traffic or perceiving the neighborhood as clean and attractive.
Neighborhoods with lower property values were also often obesogenic communities: Residents who reported living with crime, heavy traffic, bars, liquor stores, and fast food, had BMIs of about 27 on average, compared with 23.9 for women and 26.4 for men in the highest-valued neighborhoods.
But the amenities people value in their neighborhoods can vary. In New York, New York, and Seattle, Washington, for instance, having a park nearby was associated with higher property values. In Detroit, Michigan, having a supermarket nearby was more valued. Those kinds of independent variables can help explain inconsistent associations between environmental measures and BMI, the researchers say. Sometimes having fast food nearby is linked to obesity, sometimes not. Parks are not always linked to lower BMIs, either.
Establishing links between multiple measures of the environment, activity levels, and obesity rates is a “continuing challenge,” the researchers acknowledge. But they feel using property values as a marker is a new “wealth metric” that may offer a way to resolve the complexity. Because real estate stays put and people do not, the researchers suggest that property value is an effective way to sort the population by material resources and socioeconomic status.
Source
Drewnowski A, Aggarwal A, Rehm CD, Cohen-Cline H, Hurvitz PM, Moudon AV. Am J Prev Med. 2014;47(3):260-274.
doi: 10.1016/j.amepre.2014.05.006.
Radiating Low Back Pain • History of Urinary Symptoms • Past Surgery for Scoliosis • Dx?
THE CASE
A 23-year-old immunocompetent woman was referred to our spinal clinic with a 6-month history of low back pain that radiated to her right flank, buttock, and groin. She’d had intermittent urinary problems, including mild dysuria and frequency, and had been treated with antibiotics for a presumed urinary tract infection on 3 previous occasions, but her pain gradually increased and eventually became constant.
The patient had no history of fever, malaise, or weight loss. She denied consuming unpasteurized milk or undercooked poultry, and hadn’t recently experienced diarrhea or vomiting.
Eight years earlier, she had undergone anterior fusion of her spine for idiopathic scoliosis. At that time, she was at Risser grade 1, and her Cobb angle was 50°; metallic instrumentation was implanted at T10 to L3 to prevent progression of the scoliosis. Her recovery had been uneventful.
During examination, her temperature, pulse, respiratory rate, blood pressure, and nervous system were all normal. Her hips appeared normal, as well, and a straight leg raise was negative bilaterally. The patient had mild midline lumbar tenderness. Spinal range of movement revealed decreased flexion and mild pain.
X-rays (FIGURE 1) showed no changes in the previous metalwork in her spine. There was decreased disk height at the L3/4 level, but no significant bony erosion or soft-tissue shadows. Laboratory testing revealed a C-reactive protein (CRP) level of 240 mg/dL (normal, <1 mg/dL) and her erythrocyte sedimentation rate (ESR) was 102 mm/h—more than 5 times higher than it should have been.1 The patient had a normal peripheral white cell count (WCC). Midstream urine cultures were negative.


The patient was admitted to the hospital for further work-up. Magnetic resonance imaging (MRI) of the lumbar spine showed gross abnormality at the L3-L4 disk level with erosion of the end plates, fluid in the disk space, marked enhancing edema, and mild surrounding soft-tissue edematous changes, but no evidence of any epidural abscess (FIGURE 2). The patient had a fluoroscopy-guided needle biopsy of the disk on the same day and received intravenous (IV) ceftriaxone 2 g twice a day. Blood and urine cultures were negative.
THE DIAGNOSIS
We suspected our patient had spondylodiscitis, an infection of the spine that includes spondylitis (inflammation of the vertebrae) and discitis (inflammation of the vertebral disk space). After 48 hours, the biopsy sample grew Salmonella typhimurium and confirmed the diagnosis. The organism was sensitive to ceftriaxone and ciprofloxacin; parenteral ceftriaxone was continued and the patient wore a thoracolumbar brace for immobilization. For 3 days, her inflammatory marker levels were checked daily, then every other day for the rest of that first week, and then 2 more times in the following week.
DISCUSSION
Thoracic and lumbar vertebrae are the most common sites of spondylodiscitis.2 Spondylodiscitis accounts for 3% to 5% of pyogenic osteomyelitis in patients in developed countries.3 The incidence of pyogenic spondylodiscitis may be rising due to an increase in the number of elderly and immunocompromised patients, as well as a rise in invasive medical procedures.4-6
If left untreated, spondylodiscitis can spread longitudinally (involving the adjacent levels), posteriorly (causing bacterial meningitis, abscess formation, and cord compromise), or anteriorly (causing paravertebral abscess). Untreated spondylodiscitis can also send distant infective emboli and cause endocarditis7-9 or mycotic abdominal aneurysm.10
Historically, mortality in patients with vertebral osteomyelitis has been as high as 25%.11 The combination of earlier diagnosis, antibiotics, and surgical debridement and stabilization has decreased mortality to less than 15%.12-14
Risk factors for spondylodiscitis include male sex, IV drug abuse, diabetes, morbid obesity, having had a genitourinary or spinal procedure, and being immunocompromised (eg, from alcohol abuse, malignancy, organ transplantation, chemotherapy, or corticosteroid use).12,15,16
Gram-positive organisms cause most spine infections in both adults and children, with 40% to 90% caused by Staphylococcus aureus.17 Gram-negative organisms (Escherichia coli, Pseudomonas, and Proteus), which can also cause spondylodiscitis, typically occur after genitourinary infections or procedures. IV drug abusers are prone to Pseudomonas infections.18 Anaerobic infections may be seen in patients with diabetes or after penetrating trauma.15 Salmonella species can cause spondylodiscitis, especially in patients with sickle cell disease from an intestinal source.19
Mycobacterium tuberculosis is the most common nonpyogenic infecting agent that also can cause spondylodiscitis. Infection caused by tuberculosis (TB) has had a recent resurgence with resistant strains, especially in patients with human immunodeficiency virus.15 Although less than 10% of patients with TB have skeletal involvement, 50% of the skeletal involvement occurs in the spine.15
The clinical presentation of spondylodiscitis depends on the location of the infection, the virulence of the organism, and the immune status of the patient. Discitis can present as pain in the back, hip, abdomen (especially in children20) and, occasionally, with meningeal involvement.11 Patients with discitis often have a normal temperature.15,21 In patients with discitis, the patient’s WCC will be normal, but the ESR is almost always elevated.15,22 Suspect spondylodiscitis in patients who present with persistent or increasing pain 3 to 4 weeks after back surgery. For such patients, measure inflammatory markers and order imaging of the spine.
X-ray findings for patients with spondylodiscitis will include osteolysis and end plate erosions (early) and narrowing and collapse of the disk space (late). (In TB, relative preservation of the disk spaces is seen, with significant vertebral destruction.)
MRI is the modality of choice for diagnosis and assessment of suspected spondylodiscitis because it can provide imaging of the soft tissue, neural elements, and bony changes with a high sensitivity and specificity.23 Once infection is suspected, the diagnosis should be confirmed by fluoroscopic- or computed tomography-guided biopsy before starting antibiotic treatment.
Long-term antibiotics are required to prevent recurrence
IV antibiotics are the mainstay of treatment for spondylodiscitis;24 the specific drug used will depend upon the organism identified. Patients typically receive 2 to 6 weeks of IV therapy. Then, once the patient improves and inflammatory markers return to normal levels, the patient receives a course of oral antibiotics for 2 to 6 more weeks. Grados et al19 found recurrence rates of 10% to 15% for patients who were treated 4 to 8 weeks compared to 3.9% in those treated for 12 weeks or longer; therefore, a total duration of 12 weeks is commonly chosen.25-28
To minimize the risk of spondylolisthesis, kyphosis, and fractures of the infected bone, patients are advised to rest and the spine is often immobilized with a spinal brace. Surgery may be needed if antibiotics are not effective, or for patients who develop complications such as fluid collection, neurologic deficits, or deformity.
Our patient’s pain improved after 2 weeks and she became more comfortable wearing the thoracolumbar brace. Her CRP and ESR also improved and there was no radiologic evidence of fluid collection. The patient was discharged with a peripherally inserted central catheter in place and received IV ceftriaxone for 6 more weeks at home. This was followed by 4 weeks of oral ciprofloxacin 750 mg twice daily, thereby completing a 12-week course of antibiotics.
Our patient’s response to treatment was monitored clinically and the inflammatory markers were checked weekly after discharge until the end of treatment and at 6 and 12 months after start of treatment. At 12 months, our patient’s CRP was <1 mg/dL and ESR was 22 mm/h. One year later, our patient remained asymptomatic with normal inflammatory marker levels and no evidence of recurrence.
THE TAKEAWAY
Spondylodiscitis is an important differential diagnosis of lower back, flank, groin, and buttock pain. It’s important to be aware of this diagnosis, especially in patients who have risk factors such as IV drug abuse, diabetes, and morbid obesity. Although previous spinal surgery is a risk factor, spondylodiscitis should be considered in patients with persistent back pain even if they haven’t had spinal surgery. It can be present even when there is no tenderness over the spinous process or any fever.
Checking inflammatory markers is a reasonable next step if a patient’s pain does not resolve after at least 4 weeks. If levels of inflammatory markers such as CRP and ESR are elevated and symptoms continue, MRI can confirm or rule out the presence of spondylodiscitis. Treatments include orthotic support, antibiotics, and surgical intervention when complications arise.
REFERENCES
1. Miller A, Green M, Robinson D. Simple rule for calculating normal erythrocyte sedimentation rate. Br Med J. 1983;286:266.
2. Calhoun JH, Manring MM. Adult osteomyelitis. Infect Dis Clin North Am. 2005;19:765-786.
3. Sobottke R, Seifert H, Fätkenheuer G, et al. Current diagnosis and treatment of spondylodiscitis. Dtsch Arztebl Int. 2008;105:181-187.
4. Beronius M, Bergman B, Andersson R. Vertebral osteomyelitis in Göteborg, Sweden: a retrospective study of patients during 1990-95. Scand J Infect Dis. 2001;33:527-532.
5. Digby JM, Kersley JB. Pyogenic non-tuberculous spinal infection: an analysis of thirty cases. J Bone Joint Surg Br. 1979;61: 47-55.
6. Gouliouris T, Aliyu SH, Brown NM. Spondylodiscitis: update on diagnosis and management. J Antimicrob Chemother. 2010;65 suppl 3:iii11-iii24.
7. Aoki K, Watanabe M, Ohzeki H. Successful surgical treatment of tricuspid valve endocarditis associated with vertebral osteomyelitis. Ann Thorac Cardiovasc Surg. 2010;16:207-209.
8. Gonzalez-Juanatey C, Testa-Fernandez A, Gonzalez-Gay MA. Septic discitis as initial manifestation of streptococcus bovis endocarditis. Int J Cardiol. 2006;108:128-129.
9. Morelli S, Carmenini E, Caporossi AP, et al. Spondylodiscitis and infective endocarditis: case studies and review of the literature. Spine (Phila Pa 1976). 2001;26:499-500.
10. Learch TJ, Sakamoto B, Ling AC, et al. Salmonella spondylodiscitis associated with a mycotic abdominal aortic aneurysm and paravertebral abscess. Emerg Radiol. 2009;16:147-150.
11. Guri JP. Pyogenic osteomyelitis of the spine. J Bone Joint Surg Am. 1946;28:29-39.
12. Carragee EJ. Pyogenic vertebral osteomyelitis. J Bone Joint Surg Am. 1997;79:874-880.
13. Garcia A Jr, Grantham SA. Hematogenous pyogenic vertebral osteomyelitis. J Bone Joint Surg Am. 1960;42-A:429-436.
14. Eismont FJ, Bohlman HH, Soni PL, et al. Pyogenic and fungal vertebral osteomyelitis with paralysis. J Bone Joint Surg Am. 1983;65:19-29.
15. Tay BK, Deckey J, Hu SS. Spinal infections. J Am Acad Orthop Surg. 2002;10:188-197.
16. Krogsgaard MR, Wagn P, Bengtsson J. Epidemiology of acute vertebral osteomyelitis in Denmark: 137 cases in Denmark 1978-1982, compared to cases reported to the National Patient Register 1991-1993. Acta Orthop Scand. 1998;69:513-517.
17. Francis X. Infections of spine. In: Canale ST, Beaty JH, eds. Campbell’s Operative Orthopaedics. 11th ed. New York, NY: Mosby; 2007:2241.
18. Roca RP, Yoshikawa TT. Primary skeletal infections in heroin users: a clinical characterization, diagnosis and therapy. Clin Orthop Relat Res. 1979;(144):238-248.
19. Grados F, Lescure FX, Senneville E, et al. Suggestions for managing pyogenic (non-tuberculous) discitis in adults. Joint Bone Spine. 2007;74:133-139.
20. Cheyne G, Runau F, Lloyd DM. Right upper quadrant pain and raised alkaline phosphatase is not always a hepatobiliary problem. Ann R Coll Surg Engl. 2014;96:118E-120E.
21. Varma R, Lander P, Assaf A. Imaging of pyogenic infectious spondylodiskitis. Radiol Clin North Am. 2001;39: 203-213.
22. Lehovsky J. Pyogenic vertebral osteomyelitis/disc infection. Baillieres Best Pract Res Clin Rheumatol. 1999;13:59-75.
23. Modic MT, Feiglin DH, Piraino DW, et al. Vertebral osteomyelitis: assessment using MR. Radiology. 1985;157:157-166.
24. Amritanand R, Venkatesh K, Sundararaj GD. Salmonella spondylodiscitis in the immunocompetent: our experience with eleven patients. Spine (Phila Pa 1976). 2010;35:E1317-E1321.
25. Govender S. Spinal infections. J Bone Joint Surg Br. 2005;87:1454-1458.
26. Lam KS, Webb JK. Discitis. Hosp Med. 2004;65:280-286.
27. Gasbarrini AL, Bertoldi E, Mazzetti M, et al. Clinical features, diagnostic and therapeutic approaches to haematogenous vertebral osteomyelitis. Eur Rev Med Pharmacol Sci. 2005;9: 53-66.
28. Cottle L, Riordan T. Infectious spondylodiscitis. J Infect. 2008;56:401-412.
THE CASE
A 23-year-old immunocompetent woman was referred to our spinal clinic with a 6-month history of low back pain that radiated to her right flank, buttock, and groin. She’d had intermittent urinary problems, including mild dysuria and frequency, and had been treated with antibiotics for a presumed urinary tract infection on 3 previous occasions, but her pain gradually increased and eventually became constant.
The patient had no history of fever, malaise, or weight loss. She denied consuming unpasteurized milk or undercooked poultry, and hadn’t recently experienced diarrhea or vomiting.
Eight years earlier, she had undergone anterior fusion of her spine for idiopathic scoliosis. At that time, she was at Risser grade 1, and her Cobb angle was 50°; metallic instrumentation was implanted at T10 to L3 to prevent progression of the scoliosis. Her recovery had been uneventful.
During examination, her temperature, pulse, respiratory rate, blood pressure, and nervous system were all normal. Her hips appeared normal, as well, and a straight leg raise was negative bilaterally. The patient had mild midline lumbar tenderness. Spinal range of movement revealed decreased flexion and mild pain.
X-rays (FIGURE 1) showed no changes in the previous metalwork in her spine. There was decreased disk height at the L3/4 level, but no significant bony erosion or soft-tissue shadows. Laboratory testing revealed a C-reactive protein (CRP) level of 240 mg/dL (normal, <1 mg/dL) and her erythrocyte sedimentation rate (ESR) was 102 mm/h—more than 5 times higher than it should have been.1 The patient had a normal peripheral white cell count (WCC). Midstream urine cultures were negative.
The patient was admitted to the hospital for further work-up. Magnetic resonance imaging (MRI) of the lumbar spine showed gross abnormality at the L3-L4 disk level with erosion of the end plates, fluid in the disk space, marked enhancing edema, and mild surrounding soft-tissue edematous changes, but no evidence of any epidural abscess (FIGURE 2). The patient had a fluoroscopy-guided needle biopsy of the disk on the same day and received intravenous (IV) ceftriaxone 2 g twice a day. Blood and urine cultures were negative.
THE DIAGNOSIS
We suspected our patient had spondylodiscitis, an infection of the spine that includes spondylitis (inflammation of the vertebrae) and discitis (inflammation of the vertebral disk space). After 48 hours, the biopsy sample grew Salmonella typhimurium and confirmed the diagnosis. The organism was sensitive to ceftriaxone and ciprofloxacin; parenteral ceftriaxone was continued and the patient wore a thoracolumbar brace for immobilization. For 3 days, her inflammatory marker levels were checked daily, then every other day for the rest of that first week, and then 2 more times in the following week.
DISCUSSION
Thoracic and lumbar vertebrae are the most common sites of spondylodiscitis.2 Spondylodiscitis accounts for 3% to 5% of pyogenic osteomyelitis in patients in developed countries.3 The incidence of pyogenic spondylodiscitis may be rising due to an increase in the number of elderly and immunocompromised patients, as well as a rise in invasive medical procedures.4-6
If left untreated, spondylodiscitis can spread longitudinally (involving the adjacent levels), posteriorly (causing bacterial meningitis, abscess formation, and cord compromise), or anteriorly (causing paravertebral abscess). Untreated spondylodiscitis can also send distant infective emboli and cause endocarditis7-9 or mycotic abdominal aneurysm.10
Historically, mortality in patients with vertebral osteomyelitis has been as high as 25%.11 The combination of earlier diagnosis, antibiotics, and surgical debridement and stabilization has decreased mortality to less than 15%.12-14
Risk factors for spondylodiscitis include male sex, IV drug abuse, diabetes, morbid obesity, having had a genitourinary or spinal procedure, and being immunocompromised (eg, from alcohol abuse, malignancy, organ transplantation, chemotherapy, or corticosteroid use).12,15,16
Gram-positive organisms cause most spine infections in both adults and children, with 40% to 90% caused by Staphylococcus aureus.17 Gram-negative organisms (Escherichia coli, Pseudomonas, and Proteus), which can also cause spondylodiscitis, typically occur after genitourinary infections or procedures. IV drug abusers are prone to Pseudomonas infections.18 Anaerobic infections may be seen in patients with diabetes or after penetrating trauma.15 Salmonella species can cause spondylodiscitis, especially in patients with sickle cell disease from an intestinal source.19
Mycobacterium tuberculosis is the most common nonpyogenic infecting agent that also can cause spondylodiscitis. Infection caused by tuberculosis (TB) has had a recent resurgence with resistant strains, especially in patients with human immunodeficiency virus.15 Although less than 10% of patients with TB have skeletal involvement, 50% of the skeletal involvement occurs in the spine.15
The clinical presentation of spondylodiscitis depends on the location of the infection, the virulence of the organism, and the immune status of the patient. Discitis can present as pain in the back, hip, abdomen (especially in children20) and, occasionally, with meningeal involvement.11 Patients with discitis often have a normal temperature.15,21 In patients with discitis, the patient’s WCC will be normal, but the ESR is almost always elevated.15,22 Suspect spondylodiscitis in patients who present with persistent or increasing pain 3 to 4 weeks after back surgery. For such patients, measure inflammatory markers and order imaging of the spine.
X-ray findings for patients with spondylodiscitis will include osteolysis and end plate erosions (early) and narrowing and collapse of the disk space (late). (In TB, relative preservation of the disk spaces is seen, with significant vertebral destruction.)
MRI is the modality of choice for diagnosis and assessment of suspected spondylodiscitis because it can provide imaging of the soft tissue, neural elements, and bony changes with a high sensitivity and specificity.23 Once infection is suspected, the diagnosis should be confirmed by fluoroscopic- or computed tomography-guided biopsy before starting antibiotic treatment.
Long-term antibiotics are required to prevent recurrence
IV antibiotics are the mainstay of treatment for spondylodiscitis;24 the specific drug used will depend upon the organism identified. Patients typically receive 2 to 6 weeks of IV therapy. Then, once the patient improves and inflammatory markers return to normal levels, the patient receives a course of oral antibiotics for 2 to 6 more weeks. Grados et al19 found recurrence rates of 10% to 15% for patients who were treated 4 to 8 weeks compared to 3.9% in those treated for 12 weeks or longer; therefore, a total duration of 12 weeks is commonly chosen.25-28
To minimize the risk of spondylolisthesis, kyphosis, and fractures of the infected bone, patients are advised to rest and the spine is often immobilized with a spinal brace. Surgery may be needed if antibiotics are not effective, or for patients who develop complications such as fluid collection, neurologic deficits, or deformity.
Our patient’s pain improved after 2 weeks and she became more comfortable wearing the thoracolumbar brace. Her CRP and ESR also improved and there was no radiologic evidence of fluid collection. The patient was discharged with a peripherally inserted central catheter in place and received IV ceftriaxone for 6 more weeks at home. This was followed by 4 weeks of oral ciprofloxacin 750 mg twice daily, thereby completing a 12-week course of antibiotics.
Our patient’s response to treatment was monitored clinically and the inflammatory markers were checked weekly after discharge until the end of treatment and at 6 and 12 months after start of treatment. At 12 months, our patient’s CRP was <1 mg/dL and ESR was 22 mm/h. One year later, our patient remained asymptomatic with normal inflammatory marker levels and no evidence of recurrence.
THE TAKEAWAY
Spondylodiscitis is an important differential diagnosis of lower back, flank, groin, and buttock pain. It’s important to be aware of this diagnosis, especially in patients who have risk factors such as IV drug abuse, diabetes, and morbid obesity. Although previous spinal surgery is a risk factor, spondylodiscitis should be considered in patients with persistent back pain even if they haven’t had spinal surgery. It can be present even when there is no tenderness over the spinous process or any fever.
Checking inflammatory markers is a reasonable next step if a patient’s pain does not resolve after at least 4 weeks. If levels of inflammatory markers such as CRP and ESR are elevated and symptoms continue, MRI can confirm or rule out the presence of spondylodiscitis. Treatments include orthotic support, antibiotics, and surgical intervention when complications arise.
REFERENCES
1. Miller A, Green M, Robinson D. Simple rule for calculating normal erythrocyte sedimentation rate. Br Med J. 1983;286:266.
2. Calhoun JH, Manring MM. Adult osteomyelitis. Infect Dis Clin North Am. 2005;19:765-786.
3. Sobottke R, Seifert H, Fätkenheuer G, et al. Current diagnosis and treatment of spondylodiscitis. Dtsch Arztebl Int. 2008;105:181-187.
4. Beronius M, Bergman B, Andersson R. Vertebral osteomyelitis in Göteborg, Sweden: a retrospective study of patients during 1990-95. Scand J Infect Dis. 2001;33:527-532.
5. Digby JM, Kersley JB. Pyogenic non-tuberculous spinal infection: an analysis of thirty cases. J Bone Joint Surg Br. 1979;61: 47-55.
6. Gouliouris T, Aliyu SH, Brown NM. Spondylodiscitis: update on diagnosis and management. J Antimicrob Chemother. 2010;65 suppl 3:iii11-iii24.
7. Aoki K, Watanabe M, Ohzeki H. Successful surgical treatment of tricuspid valve endocarditis associated with vertebral osteomyelitis. Ann Thorac Cardiovasc Surg. 2010;16:207-209.
8. Gonzalez-Juanatey C, Testa-Fernandez A, Gonzalez-Gay MA. Septic discitis as initial manifestation of streptococcus bovis endocarditis. Int J Cardiol. 2006;108:128-129.
9. Morelli S, Carmenini E, Caporossi AP, et al. Spondylodiscitis and infective endocarditis: case studies and review of the literature. Spine (Phila Pa 1976). 2001;26:499-500.
10. Learch TJ, Sakamoto B, Ling AC, et al. Salmonella spondylodiscitis associated with a mycotic abdominal aortic aneurysm and paravertebral abscess. Emerg Radiol. 2009;16:147-150.
11. Guri JP. Pyogenic osteomyelitis of the spine. J Bone Joint Surg Am. 1946;28:29-39.
12. Carragee EJ. Pyogenic vertebral osteomyelitis. J Bone Joint Surg Am. 1997;79:874-880.
13. Garcia A Jr, Grantham SA. Hematogenous pyogenic vertebral osteomyelitis. J Bone Joint Surg Am. 1960;42-A:429-436.
14. Eismont FJ, Bohlman HH, Soni PL, et al. Pyogenic and fungal vertebral osteomyelitis with paralysis. J Bone Joint Surg Am. 1983;65:19-29.
15. Tay BK, Deckey J, Hu SS. Spinal infections. J Am Acad Orthop Surg. 2002;10:188-197.
16. Krogsgaard MR, Wagn P, Bengtsson J. Epidemiology of acute vertebral osteomyelitis in Denmark: 137 cases in Denmark 1978-1982, compared to cases reported to the National Patient Register 1991-1993. Acta Orthop Scand. 1998;69:513-517.
17. Francis X. Infections of spine. In: Canale ST, Beaty JH, eds. Campbell’s Operative Orthopaedics. 11th ed. New York, NY: Mosby; 2007:2241.
18. Roca RP, Yoshikawa TT. Primary skeletal infections in heroin users: a clinical characterization, diagnosis and therapy. Clin Orthop Relat Res. 1979;(144):238-248.
19. Grados F, Lescure FX, Senneville E, et al. Suggestions for managing pyogenic (non-tuberculous) discitis in adults. Joint Bone Spine. 2007;74:133-139.
20. Cheyne G, Runau F, Lloyd DM. Right upper quadrant pain and raised alkaline phosphatase is not always a hepatobiliary problem. Ann R Coll Surg Engl. 2014;96:118E-120E.
21. Varma R, Lander P, Assaf A. Imaging of pyogenic infectious spondylodiskitis. Radiol Clin North Am. 2001;39: 203-213.
22. Lehovsky J. Pyogenic vertebral osteomyelitis/disc infection. Baillieres Best Pract Res Clin Rheumatol. 1999;13:59-75.
23. Modic MT, Feiglin DH, Piraino DW, et al. Vertebral osteomyelitis: assessment using MR. Radiology. 1985;157:157-166.
24. Amritanand R, Venkatesh K, Sundararaj GD. Salmonella spondylodiscitis in the immunocompetent: our experience with eleven patients. Spine (Phila Pa 1976). 2010;35:E1317-E1321.
25. Govender S. Spinal infections. J Bone Joint Surg Br. 2005;87:1454-1458.
26. Lam KS, Webb JK. Discitis. Hosp Med. 2004;65:280-286.
27. Gasbarrini AL, Bertoldi E, Mazzetti M, et al. Clinical features, diagnostic and therapeutic approaches to haematogenous vertebral osteomyelitis. Eur Rev Med Pharmacol Sci. 2005;9: 53-66.
28. Cottle L, Riordan T. Infectious spondylodiscitis. J Infect. 2008;56:401-412.
THE CASE
A 23-year-old immunocompetent woman was referred to our spinal clinic with a 6-month history of low back pain that radiated to her right flank, buttock, and groin. She’d had intermittent urinary problems, including mild dysuria and frequency, and had been treated with antibiotics for a presumed urinary tract infection on 3 previous occasions, but her pain gradually increased and eventually became constant.
The patient had no history of fever, malaise, or weight loss. She denied consuming unpasteurized milk or undercooked poultry, and hadn’t recently experienced diarrhea or vomiting.
Eight years earlier, she had undergone anterior fusion of her spine for idiopathic scoliosis. At that time, she was at Risser grade 1, and her Cobb angle was 50°; metallic instrumentation was implanted at T10 to L3 to prevent progression of the scoliosis. Her recovery had been uneventful.
During examination, her temperature, pulse, respiratory rate, blood pressure, and nervous system were all normal. Her hips appeared normal, as well, and a straight leg raise was negative bilaterally. The patient had mild midline lumbar tenderness. Spinal range of movement revealed decreased flexion and mild pain.
X-rays (FIGURE 1) showed no changes in the previous metalwork in her spine. There was decreased disk height at the L3/4 level, but no significant bony erosion or soft-tissue shadows. Laboratory testing revealed a C-reactive protein (CRP) level of 240 mg/dL (normal, <1 mg/dL) and her erythrocyte sedimentation rate (ESR) was 102 mm/h—more than 5 times higher than it should have been.1 The patient had a normal peripheral white cell count (WCC). Midstream urine cultures were negative.
The patient was admitted to the hospital for further work-up. Magnetic resonance imaging (MRI) of the lumbar spine showed gross abnormality at the L3-L4 disk level with erosion of the end plates, fluid in the disk space, marked enhancing edema, and mild surrounding soft-tissue edematous changes, but no evidence of any epidural abscess (FIGURE 2). The patient had a fluoroscopy-guided needle biopsy of the disk on the same day and received intravenous (IV) ceftriaxone 2 g twice a day. Blood and urine cultures were negative.
THE DIAGNOSIS
We suspected our patient had spondylodiscitis, an infection of the spine that includes spondylitis (inflammation of the vertebrae) and discitis (inflammation of the vertebral disk space). After 48 hours, the biopsy sample grew Salmonella typhimurium and confirmed the diagnosis. The organism was sensitive to ceftriaxone and ciprofloxacin; parenteral ceftriaxone was continued and the patient wore a thoracolumbar brace for immobilization. For 3 days, her inflammatory marker levels were checked daily, then every other day for the rest of that first week, and then 2 more times in the following week.
DISCUSSION
Thoracic and lumbar vertebrae are the most common sites of spondylodiscitis.2 Spondylodiscitis accounts for 3% to 5% of pyogenic osteomyelitis in patients in developed countries.3 The incidence of pyogenic spondylodiscitis may be rising due to an increase in the number of elderly and immunocompromised patients, as well as a rise in invasive medical procedures.4-6
If left untreated, spondylodiscitis can spread longitudinally (involving the adjacent levels), posteriorly (causing bacterial meningitis, abscess formation, and cord compromise), or anteriorly (causing paravertebral abscess). Untreated spondylodiscitis can also send distant infective emboli and cause endocarditis7-9 or mycotic abdominal aneurysm.10
Historically, mortality in patients with vertebral osteomyelitis has been as high as 25%.11 The combination of earlier diagnosis, antibiotics, and surgical debridement and stabilization has decreased mortality to less than 15%.12-14
Risk factors for spondylodiscitis include male sex, IV drug abuse, diabetes, morbid obesity, having had a genitourinary or spinal procedure, and being immunocompromised (eg, from alcohol abuse, malignancy, organ transplantation, chemotherapy, or corticosteroid use).12,15,16
Gram-positive organisms cause most spine infections in both adults and children, with 40% to 90% caused by Staphylococcus aureus.17 Gram-negative organisms (Escherichia coli, Pseudomonas, and Proteus), which can also cause spondylodiscitis, typically occur after genitourinary infections or procedures. IV drug abusers are prone to Pseudomonas infections.18 Anaerobic infections may be seen in patients with diabetes or after penetrating trauma.15 Salmonella species can cause spondylodiscitis, especially in patients with sickle cell disease from an intestinal source.19
Mycobacterium tuberculosis is the most common nonpyogenic infecting agent that also can cause spondylodiscitis. Infection caused by tuberculosis (TB) has had a recent resurgence with resistant strains, especially in patients with human immunodeficiency virus.15 Although less than 10% of patients with TB have skeletal involvement, 50% of the skeletal involvement occurs in the spine.15
The clinical presentation of spondylodiscitis depends on the location of the infection, the virulence of the organism, and the immune status of the patient. Discitis can present as pain in the back, hip, abdomen (especially in children20) and, occasionally, with meningeal involvement.11 Patients with discitis often have a normal temperature.15,21 In patients with discitis, the patient’s WCC will be normal, but the ESR is almost always elevated.15,22 Suspect spondylodiscitis in patients who present with persistent or increasing pain 3 to 4 weeks after back surgery. For such patients, measure inflammatory markers and order imaging of the spine.
X-ray findings for patients with spondylodiscitis will include osteolysis and end plate erosions (early) and narrowing and collapse of the disk space (late). (In TB, relative preservation of the disk spaces is seen, with significant vertebral destruction.)
MRI is the modality of choice for diagnosis and assessment of suspected spondylodiscitis because it can provide imaging of the soft tissue, neural elements, and bony changes with a high sensitivity and specificity.23 Once infection is suspected, the diagnosis should be confirmed by fluoroscopic- or computed tomography-guided biopsy before starting antibiotic treatment.
Long-term antibiotics are required to prevent recurrence
IV antibiotics are the mainstay of treatment for spondylodiscitis;24 the specific drug used will depend upon the organism identified. Patients typically receive 2 to 6 weeks of IV therapy. Then, once the patient improves and inflammatory markers return to normal levels, the patient receives a course of oral antibiotics for 2 to 6 more weeks. Grados et al19 found recurrence rates of 10% to 15% for patients who were treated 4 to 8 weeks compared to 3.9% in those treated for 12 weeks or longer; therefore, a total duration of 12 weeks is commonly chosen.25-28
To minimize the risk of spondylolisthesis, kyphosis, and fractures of the infected bone, patients are advised to rest and the spine is often immobilized with a spinal brace. Surgery may be needed if antibiotics are not effective, or for patients who develop complications such as fluid collection, neurologic deficits, or deformity.
Our patient’s pain improved after 2 weeks and she became more comfortable wearing the thoracolumbar brace. Her CRP and ESR also improved and there was no radiologic evidence of fluid collection. The patient was discharged with a peripherally inserted central catheter in place and received IV ceftriaxone for 6 more weeks at home. This was followed by 4 weeks of oral ciprofloxacin 750 mg twice daily, thereby completing a 12-week course of antibiotics.
Our patient’s response to treatment was monitored clinically and the inflammatory markers were checked weekly after discharge until the end of treatment and at 6 and 12 months after start of treatment. At 12 months, our patient’s CRP was <1 mg/dL and ESR was 22 mm/h. One year later, our patient remained asymptomatic with normal inflammatory marker levels and no evidence of recurrence.
THE TAKEAWAY
Spondylodiscitis is an important differential diagnosis of lower back, flank, groin, and buttock pain. It’s important to be aware of this diagnosis, especially in patients who have risk factors such as IV drug abuse, diabetes, and morbid obesity. Although previous spinal surgery is a risk factor, spondylodiscitis should be considered in patients with persistent back pain even if they haven’t had spinal surgery. It can be present even when there is no tenderness over the spinous process or any fever.
Checking inflammatory markers is a reasonable next step if a patient’s pain does not resolve after at least 4 weeks. If levels of inflammatory markers such as CRP and ESR are elevated and symptoms continue, MRI can confirm or rule out the presence of spondylodiscitis. Treatments include orthotic support, antibiotics, and surgical intervention when complications arise.
REFERENCES
1. Miller A, Green M, Robinson D. Simple rule for calculating normal erythrocyte sedimentation rate. Br Med J. 1983;286:266.
2. Calhoun JH, Manring MM. Adult osteomyelitis. Infect Dis Clin North Am. 2005;19:765-786.
3. Sobottke R, Seifert H, Fätkenheuer G, et al. Current diagnosis and treatment of spondylodiscitis. Dtsch Arztebl Int. 2008;105:181-187.
4. Beronius M, Bergman B, Andersson R. Vertebral osteomyelitis in Göteborg, Sweden: a retrospective study of patients during 1990-95. Scand J Infect Dis. 2001;33:527-532.
5. Digby JM, Kersley JB. Pyogenic non-tuberculous spinal infection: an analysis of thirty cases. J Bone Joint Surg Br. 1979;61: 47-55.
6. Gouliouris T, Aliyu SH, Brown NM. Spondylodiscitis: update on diagnosis and management. J Antimicrob Chemother. 2010;65 suppl 3:iii11-iii24.
7. Aoki K, Watanabe M, Ohzeki H. Successful surgical treatment of tricuspid valve endocarditis associated with vertebral osteomyelitis. Ann Thorac Cardiovasc Surg. 2010;16:207-209.
8. Gonzalez-Juanatey C, Testa-Fernandez A, Gonzalez-Gay MA. Septic discitis as initial manifestation of streptococcus bovis endocarditis. Int J Cardiol. 2006;108:128-129.
9. Morelli S, Carmenini E, Caporossi AP, et al. Spondylodiscitis and infective endocarditis: case studies and review of the literature. Spine (Phila Pa 1976). 2001;26:499-500.
10. Learch TJ, Sakamoto B, Ling AC, et al. Salmonella spondylodiscitis associated with a mycotic abdominal aortic aneurysm and paravertebral abscess. Emerg Radiol. 2009;16:147-150.
11. Guri JP. Pyogenic osteomyelitis of the spine. J Bone Joint Surg Am. 1946;28:29-39.
12. Carragee EJ. Pyogenic vertebral osteomyelitis. J Bone Joint Surg Am. 1997;79:874-880.
13. Garcia A Jr, Grantham SA. Hematogenous pyogenic vertebral osteomyelitis. J Bone Joint Surg Am. 1960;42-A:429-436.
14. Eismont FJ, Bohlman HH, Soni PL, et al. Pyogenic and fungal vertebral osteomyelitis with paralysis. J Bone Joint Surg Am. 1983;65:19-29.
15. Tay BK, Deckey J, Hu SS. Spinal infections. J Am Acad Orthop Surg. 2002;10:188-197.
16. Krogsgaard MR, Wagn P, Bengtsson J. Epidemiology of acute vertebral osteomyelitis in Denmark: 137 cases in Denmark 1978-1982, compared to cases reported to the National Patient Register 1991-1993. Acta Orthop Scand. 1998;69:513-517.
17. Francis X. Infections of spine. In: Canale ST, Beaty JH, eds. Campbell’s Operative Orthopaedics. 11th ed. New York, NY: Mosby; 2007:2241.
18. Roca RP, Yoshikawa TT. Primary skeletal infections in heroin users: a clinical characterization, diagnosis and therapy. Clin Orthop Relat Res. 1979;(144):238-248.
19. Grados F, Lescure FX, Senneville E, et al. Suggestions for managing pyogenic (non-tuberculous) discitis in adults. Joint Bone Spine. 2007;74:133-139.
20. Cheyne G, Runau F, Lloyd DM. Right upper quadrant pain and raised alkaline phosphatase is not always a hepatobiliary problem. Ann R Coll Surg Engl. 2014;96:118E-120E.
21. Varma R, Lander P, Assaf A. Imaging of pyogenic infectious spondylodiskitis. Radiol Clin North Am. 2001;39: 203-213.
22. Lehovsky J. Pyogenic vertebral osteomyelitis/disc infection. Baillieres Best Pract Res Clin Rheumatol. 1999;13:59-75.
23. Modic MT, Feiglin DH, Piraino DW, et al. Vertebral osteomyelitis: assessment using MR. Radiology. 1985;157:157-166.
24. Amritanand R, Venkatesh K, Sundararaj GD. Salmonella spondylodiscitis in the immunocompetent: our experience with eleven patients. Spine (Phila Pa 1976). 2010;35:E1317-E1321.
25. Govender S. Spinal infections. J Bone Joint Surg Br. 2005;87:1454-1458.
26. Lam KS, Webb JK. Discitis. Hosp Med. 2004;65:280-286.
27. Gasbarrini AL, Bertoldi E, Mazzetti M, et al. Clinical features, diagnostic and therapeutic approaches to haematogenous vertebral osteomyelitis. Eur Rev Med Pharmacol Sci. 2005;9: 53-66.
28. Cottle L, Riordan T. Infectious spondylodiscitis. J Infect. 2008;56:401-412.
Stage III Non–Small Cell Lung Cancer
Series Editor: Arthur T. Skarin, MD, FACP, FCCP
Each year approximately 228,000 Americans will be diagnosed with lung cancer, and 159,000 will die of this disease. An estimated 85% of lung cancer cases are non–small cell lung cancer (NSCLC), more than 50% of NSCLC is comprised of adenocarcinoma, the median age at diagnosis is 71 years, and 25% of patients with this diagnosis present with stage III disease. In 2010 the seventh edition of the American Joint Committee on Cancer (AJCC) TNM staging system for lung cancer was released, and several changes were made which affect the patient population designated as having stage III disease.
To read the full article in PDF:
Series Editor: Arthur T. Skarin, MD, FACP, FCCP
Each year approximately 228,000 Americans will be diagnosed with lung cancer, and 159,000 will die of this disease. An estimated 85% of lung cancer cases are non–small cell lung cancer (NSCLC), more than 50% of NSCLC is comprised of adenocarcinoma, the median age at diagnosis is 71 years, and 25% of patients with this diagnosis present with stage III disease. In 2010 the seventh edition of the American Joint Committee on Cancer (AJCC) TNM staging system for lung cancer was released, and several changes were made which affect the patient population designated as having stage III disease.
To read the full article in PDF:
Series Editor: Arthur T. Skarin, MD, FACP, FCCP
Each year approximately 228,000 Americans will be diagnosed with lung cancer, and 159,000 will die of this disease. An estimated 85% of lung cancer cases are non–small cell lung cancer (NSCLC), more than 50% of NSCLC is comprised of adenocarcinoma, the median age at diagnosis is 71 years, and 25% of patients with this diagnosis present with stage III disease. In 2010 the seventh edition of the American Joint Committee on Cancer (AJCC) TNM staging system for lung cancer was released, and several changes were made which affect the patient population designated as having stage III disease.
To read the full article in PDF:
Large-Diameter Femoral Heads in Total Hip Arthroplasty: An Evidence-Based Review
A common cause for total hip arthroplasty (THA) revision is joint instability.1,2 The reported incidence of dislocation in primary THA ranges from 0.4% to 5.8%,3-5 but this rate increases after revision surgery.1,3-8 Use of large-diameter femoral heads has been proposed to decrease the risks for instability and to improve impingement-free range of motion (ROM).
The biomechanical rationale for using large-diameter femoral heads is that they must travel farther before subluxation or dislocation occurs (jump distance). Despite these benefits, there were initial concerns that catastrophic failure and high levels of volumetric wear would occur if these heads were used with conventional polyethylene liners. These concerns led to the development of alternative bearing surfaces, particularly metal-on-metal bearings, which offered theoretical benefits of large-diameter articulations that improved stability while purportedly being highly wear-resistant.9-11 However, concerns about adverse local soft-tissue reactions and high blood concentrations of metal ions tempered the initial enthusiasm for metal bearings.12-16 Fortunately, highly cross-linked polyethylene and fourth-generation ceramic bearing surfaces, with improved toughness and better wear properties, may allow use of large-diameter heads without the need for metal-on-metal bearings.17,18
In this article, we review the concepts and principles behind use of large-diameter ceramic or cobalt-chromium femoral heads on polyethylene-bearing surfaces in THA with particular attention to biomechanics, early concerns about polyethylene wear and rim fractures, recent improvements in material properties of polyethylene and ceramic bearings, dislocation rates, and clinical and functional outcomes.
Definitions
For this review, we define large-diameter femoral heads as having diameters of 36 mm or more and conventional or small-diameter femoral heads as having diameters between 22 and 32 mm.
Biomechanics
Head–Neck Ratio, Impingement-Free ROM, and Jump Distance
Several implant design principles have been proposed to reduce the risks for impingement and dislocation. Of these, large femoral head diameters have been extensively studied.19,20 It is well known that impingement of the femoral neck on the cup edge promotes edge loading and higher wear rates. In addition, impingement increases the tendency of the head to sublux from the acetabulum. One strategy for avoiding this component-to-component impingement is to increase the head–neck ratio (HNR), the ratio of the femoral head to the neck diameter. Biomechanically, increased HNRs lead to delayed contact between the femoral neck and the acetabular liner.21,22 Therefore, with large femoral heads, which have large HNRs, impingement occurs later and at larger ROMs—compared with small-diameter femoral heads, which have lower HNRs and are more prone to early impingement and subluxation (Figure 1).23-26
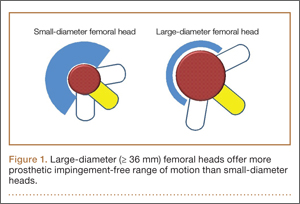
In a cadaveric study of 6 hips, Bartz and colleagues23 reported a significantly higher preimpingement ROM when the prosthetic head size increased from 22 mm to 28 mm (P < .05). They found a change from prosthetic to osseous impingement when the head size increased from 22 mm to 32 mm. Similar results were observed in a computer simulation model by Cinotti and colleagues,27 who demonstrated that increasing the femoral head size from 28 mm to 38 mm resulted in a 5° improvement in ROM. However, the largest gains were observed when the heads with the smallest diameters were upsized; ROM improved only marginally when femoral head size was further increased from 32 mm to 38 mm. The primary reason for the lack of expected improvement in ROM with head sizes of more than 32 mm is often bone-on-bone impingement. Burroughs and colleagues28 demonstrated that the 38-mm and 44-mm heads virtually eliminated component-to-component impingement except in extremes of external rotation. However, there were no differences in ROM between 38-mm and 44-mm heads because of osseous impingement. In addition, large heads are less likely to sublux or dislocate, as they need to travel farther before reaching the edge of the acetabular cup before dislocation. This is known as the jump distance, and it corresponds to the depth of the acetabular shell, which in turn equates with the radius of the femoral head (Figures 2A, 2B). For this reason, the larger the femoral head diameter, the farther the jump distance and, correspondingly, the lower the risk for dislocation.29
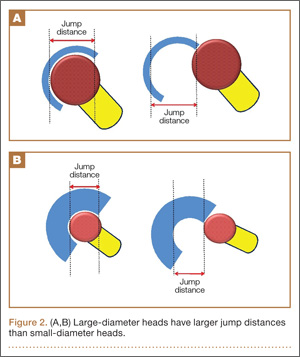
Elevated liners historically were used to increase the jump distance for dislocation.30 These liners, however, can increase impingement at the extremes of motion.31 Some of these problems can be avoided with use of larger heads, which have increased jump distances without additional risks for impingement. Moreover, large heads create a suction effect that provides passive resistance to dislocation.32 With head diameters beyond 38 mm, impingement-free ROM often plateaus. However, the jump distance required for dislocations to occur continues to increase as femoral head diameters increase in size. Thus, patients may experience fewer motion benefits but continue to benefit from overall stability with femoral head sizes increasing beyond 38 mm.
Current evidence suggests there may be substantial benefits toward improved stability from increasing head diameters from 22 mm to 38 mm because of the increase in jump distances and improvements in prosthetic impingement-free ROM. However, there may be little gain in ROM from increasing the head diameters beyond these dimensions because of the potential risks of bony impingement. Nevertheless, there may be some additional benefits toward stability from improvement in jump distances with incremental head sizes
beyond 38 mm.29,33,34
Finite Element Analysis Studies
Finite element analysis of large-diameter heads in THA has shown that, at optimal cup inclination (45°), most stresses occur on the articular surface of the liner. However, these stresses remain well below the yield strength of the polyethylene liners.29 With increasing abduction angles, the stress concentration increases substantially because of the decreased contact surface area. At these angles, the point of maximum contact moves toward the rim of the polyethylene liner, which can lead to rim fractures or failure of locking mechanisms.29,35,36
Early Concerns With Large-Diameter Femoral Heads: Wear, Liner Failure, and Fracture of Ceramic Components
Use of small-diameter femoral heads started with the first report by Charnley37 of “low frictional torque arthroplasty.” Charnley initially considered a 41.5-mm femoral head, but he thought it would increase risks for acetabular loosening from high frictional torque generated by the large head, and he switched to a small-diameter (22.5 mm) design. One of the tradeoffs with smaller diameter heads was decreased jump height in addition to increased linear wear.
Large femoral heads used with cemented polyethylene acetabular components historically have been associated with increased rates of volumetric wear but low rates of linear wear, which potentially may increase the risk for osteolysis.38-40 However, newer highly cross-linked polyethylene liners have shown improved in vitro and in vivo volumetric wear characteristics and potentially lower linear wear rates compared with earlier designs (Table 1).28,41-43
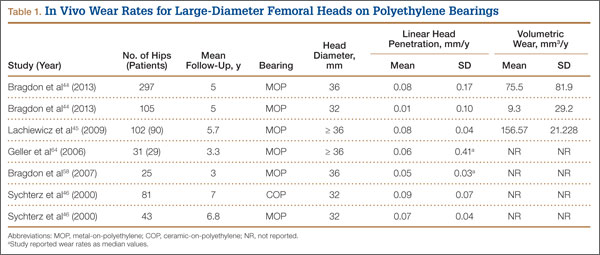
Another concern about earlier generations of large femoral heads was the risk for catastrophic liner failure on conventional polyethylene. This was originally reported by Berry and colleagues,47 who described wear-through and failure in patients with thin (< 5 mm) acetabular cups. However, these concerns have been largely addressed by the development of highly cross-linked polyethylene, which has improved wear characteristics and fatigue resistance.48
Recent Improvements in Material Properties of Polyethylene and Ceramic Bearings
The development of highly cross-linked polyethylene and fourth-generation ceramics has renewed interest in large-diameter bearings in THA. These bearing surfaces improve wear, enhance material properties, and have superior oxidation resistance.42,48-53
We now briefly describe the methods used to improve the material properties of polyethylene and ceramics. Studies have shown that increasing the radiation dose (up to 200 kGy) increases cross-linking and causes an inverse exponential decrease in polyethylene wear.28,41,48-51 However, increasing radiation doses also increases production of free radicals, which diminish the material strength of these polyethylenes. The current generation of highly cross-linked polyethylene liners is produced through a variety of manufacturing strategies to improve cross-linking and reduce wear. These strategies include differential radiation doses (50-100 kGy), techniques (electron beam, radiation), and thermal treatments (melting, annealing). Moreover, to enhance the material properties and reduce the incidence of rim cracking and delamination, authors have proposed using vitamin E supplementation to minimize the amount of subsurface oxidation that occurs as an inevitable consequence of free radical formation during fabrication.54,55 A terminal sterilization process (eg, gas plasma, ethylene oxide, or gamma sterilization in nitrogen) is needed to make commercial, highly cross-linked polyethylene.52,53
Fourth-generation ceramics manufactured with nano-sized yttria-stabilized tetragonal zirconia particles in a stable alumina matrix have more fracture toughness and improved wear characteristics.54,55 In addition, oxide additives (eg, chromium oxide, strontium oxide) improve hardness and dissipate energy by deflecting cracks to prevent their propagation.56 Moreover, the smaller grain sizes of fourth-generation ceramic bearings compared with third-generation designs (0.8 µm vs 1-5 µm) cause less disruption of the fluid film layer, which ultimately results in improved wear performance.57
Multiple studies have found reduced wear rates with metal and ceramic large heads coupled with highly cross-linked polyethylene-bearings (Table 2).17,41,50,58 Bragdon and colleagues,58 using radiostereometric analysis in 25 patients, found no significant differences in mean head penetration rates between 36-mm and 28-mm cobalt-chromium (Co-Cr) heads articulating with highly cross-linked polyethylene cups at a mean follow-up of 3 years (0.035 mm/y vs 0.046 mm/y; P = .11). Geller and colleagues,64 in their study of 42 patients with large-diameter (> 32 mm) Co-Cr femoral heads, found low mean (SD) linear wear rates of 0.06 (0.41) mm/y at a mean follow-up of 3 years. D’Antonio and colleagues,65 in a multicenter study, reported low average linear wear (0.015 mm/y) and volumetric wear (12.1 mm3/y) over 5 years using sequentially annealed cross-linked polyethylene. In vitro reports suggest that large-diameter ceramic heads may have lower wear properties than Co-Cr heads do. Galvin and colleagues,66 in an in vitro hip simulator study, found that large-diameter ceramic heads on highly cross-linked ultrahigh-molecular-weight polyethylene had 40% reductions in steady-state wear rates compared with Co-Cr heads on highly cross-linked bearings (4.7 vs 8.1 mm3/million cycles; P < 0.01).
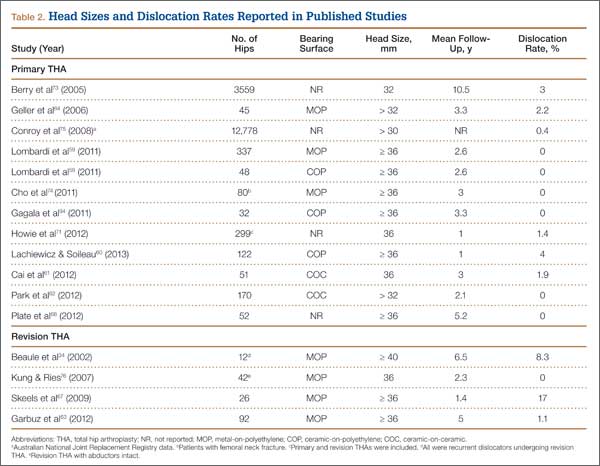
Dislocation Rates
Several patient, surgeon, and implant factors affect the rate of dislocations after THA. Multiple implant options utilize the biomechanical advantage that large-diameter heads have in improving stability. Various alternatives include use of constrained tripolar heads, dual-mobility bearings, and conventional large-diameter heads with standard liners.67-69
Large-Diameter Heads
Despite the biomechanical advantages of large-diameter metal-on-polyethylene bearings, prior studies have questioned use of these bearings because of risks for increased wear and rim failures. However, the improved wear properties of highly cross-linked polyethylene, elaborated earlier, have led to a reappraisal of this option (Table 2).4,70 Howie and colleagues,71 in a randomized control trial of 644 patients, also found significantly lower rates of dislocation after primary THA with 36-mm heads compared with 28-mm heads (1.3% vs 5.4%; P = .012); in addition, fewer dislocations occurred with 36-mm heads than with 28-mm heads (4.9% vs 12.2%; P = .27) in a series of 44 patients in revision settings. Similarly, in a study conducted with 39,271 Medicare patients between 1998 and 2007, Malkani and colleagues72 found a decrease in the dislocation rate, from 4.21% to 2.14%, with use of large-diameter femoral heads. These results have been confirmed by several other authors.34,66,73,74 Similar results were observed in 65,992 patients in the Australian National Joint Replacement Registry by Conroy and colleagues,75 who reported a significant decrease in the risk for dislocation with large heads (≥ 30 mm) compared with 22-mm heads (relative risk, 1.0 vs 3.1; P ≤ .001).
Few studies have analyzed the role of large-diameter femoral heads in the presence of compromised soft tissues around the hip. Kung and Ries,76 evaluating the influence of large-diameter heads in the presence and absence of a deficient abductor mechanism, demonstrated statistically significant reductions in rates of dislocation after 230 revision THAs when the abductor mechanism was intact with use of 36-mm heads compared with 28-mm heads (12.7% vs 0%; P = .015). With abductor deficiency, though, the positive effect of large heads in reducing dislocation rates was substantially reduced and was similar to that of small heads (P = .74).76
Large heads considerably improve overall stability and lower dislocation rates in THA. With the development of newer ceramics and highly cross-linked polyethylenes, the wear rates reported in multiple studies appear to be less concerning.
Constrained Tripolar Heads
Tripolar heads have been proposed as treatment options for improving stability in patients with chronic and recurrent instability after THA. The tripolar implant consists of a metal head that snap-fits into a polyethylene liner with a polished Co-Cr backing. This bipolar head articulates with a polyethylene bearing that is press-fitted onto a metal acetabular shell and constrained by a metal ring snapped to the outer polyethylene bearing. The bipolar component behaves as a large-diameter femoral head, and the metal ring provides additional restraint, further improving stability.
Williams and colleagues77 performed a systematic review and reported on the outcomes of constrained tripolar liners in 1199 hips at a mean follow-up of 4 years (range, 2-10 years). The mean dislocation rate was 10%, and the mean rate of revision surgery unrelated to instability was 4%. In a study of 43 hips at a mean follow-up of 4 years (range, 2-9 years), Zywiel and colleagues78 reported on the clinical and radiographic outcomes of tripolar constrained liners. Their study group had a mean Harris Hip Score (HHS) of 82 points (range, 38-100 points) and overall survival of 91%, with no evidence of radiographic loosening during follow-up. Despite the improvements in stability with constrained tripolar liners, some authors have reported multiple mechanisms of failure with these devices.79-81 In a study of 43 failed constrained tripolar liners with a mean time to failure of about 2 years, Guyen and colleagues79 identified 5 different failure modes (types 1-5) involving all 4 interfaces in these components.
Encouraging outcomes have been reported at midterm follow-up with tripolar constrained liners. However, concerns about failure at the interfaces suggest that use of these components should be restricted to patients with deficient abductor mechanisms or neuromuscular compromise, low-demand elderly patients, and salvage cases of recurrent dislocations.79
Dual-Mobility Bearings
For more than 20 years, different dual-mobility bearings have been used for difficult acetabular reconstructive scenarios and prevention of instability.82,83 Dual-mobility cups provide constructs that snap-fit a small-diameter femoral head within a large polyethylene insert that articulates with a fixed metal shell. This effectively increases the functional head diameter.
Various authors have reported excellent survivorship rates (92%-99%) and low dislocation rates for these bearings at 5- to 10-year follow-up.82,84-90 Philippot and colleagues,86 in a recent study of 438 hips with dual-mobility cups, reported excellent survivorship (96%) and no early or late instability within a 15-year follow-up. Bouchet and colleagues69 compared dual-mobility bearings (105 hips) with conventional metal-on-polythene bearings (108 hips) and found significantly (P < .05) lower dislocation rates for the dual-mobility implants at a minimum 1-year follow-up. The French Society of Orthopaedics and Traumatology performed a multicenter analysis of 3473 hips with dual-mobility cups implanted in France between January 1998 and December 2003.87 During a mean follow-up of 7 years (range, 5-11 years), there were 15 dislocations (0.43%), 14 of which occurred early, within 3 months of implantation (0.4%). Aseptic implant survivorship was 95% at 10-year follow-up.
Use of these bearings has recently increased in the United States. Short-term and midterm follow-up data show low rates of dislocation and wear. Long-term data are to come.
Clinical and Functional Outcomes of Large-Diameter Femoral Heads
There is a paucity of long-term outcomes data on use of large-diameter heads with highly cross-linked polyethylene bearings. Short-term and midterm clinical results appear to be excellent, with low rates of wear, osteolysis, and aseptic loosening.28,41,73,89-92
Plate and colleagues91 compared the effects of large-diameter (≥ 36 mm) and small-diameter (26 mm, 28 mm) metal heads on highly cross-linked polyethylene bearings. At a mean follow-up of 5 years (range, 4-8.4 years), the large-head cohort had a mean HHS of 90 points (range, 50-100 points) and no dislocations or radiographic evidence of stem or cup loosening. Similarly, Meftah and colleagues93 reported 100% stem survivorship and excellent clinical outcomes—a mean Western Ontario and McMaster Universities Arthritis Index (WOMAC) score of 30 points—for 72 hips with use of large ceramic heads (≥ 32 mm) on highly cross-linked polyethylene at a mean follow-up of 3 years. Gagala and colleagues94 reported excellent clinical and radiographic outcomes in 50 hips (18 ceramic on ceramic, 32 ceramic on polyethylene; 36-mm heads) at a mean follow-up of 3.5 years. Mean HHS was 94 points, and there was no evidence of liner fractures, aseptic loosening, or osteolysis.
In summary, large-diameter femoral heads in THA have become increasingly popular because of improvements in the material properties and wear characteristics of highly cross-linked polyethylene and fourth-generation ceramics. Despite the potential advantages of large heads in preventing dislocations, the basic surgical tenets of placing the acetabular component in appropriate alignment remain firmly established. Implants with functionally large heads (eg, dual-mobility bearings, constrained tripolar liners) may play an important role in patients at high risk for dislocation—particularly elderly patients with poor neuromuscular muscle coordination or deficient abductors, trauma patients, and patients with prior dislocations. Short-term and midterm results are excellent; rates of wear, aseptic loosening, and osteolysis are low. However, long-term outcomes data are needed to support widespread use of large heads in younger and more active patients.
1. Dorr LD, Wolf AW, Chandler R, Conaty JP. Classification and treatment of dislocations of total hip arthroplasty. Clin Orthop. 1983;(173):151-158.
2. Dorr LD, Wan Z. Causes of and treatment protocol for instability of total hip replacement. Clin Orthop. 1998;(355):144-151.
3. Turner RS. Postoperative total hip prosthetic femoral head dislocations. Incidence, etiologic factors, and management. Clin Orthop. 1994;(301):196-204.
4. Woo RY, Morrey BF. Dislocations after total hip arthroplasty. J Bone Joint Surg Am. 1982;64(9):1295-1306.
5. Etienne A, Cupic Z, Charnley J. Postoperative dislocation after Charnley low-friction arthroplasty. Clin Orthop. 1978;(132):19-23.
6. Fackler CD, Poss R. Dislocation in total hip arthroplasties. Clin Orthop. 1980;(151):169-178.
7. Joshi A, Lee CM, Markovic L, Vlatis G, Murphy JC. Prognosis of dislocation after total hip arthroplasty. J Arthroplasty. 1998;13(1):17-21.
8. Lindberg HO, Carlsson AS, Gentz CF, Pettersson H. Recurrent and non-recurrent dislocation following total hip arthroplasty. Acta Orthop Scand. 1982;53(6):947-952.
9. Eswaramoorthy V, Moonot P, Kalairajah Y, Biant LC, Field RE. The Metasul metal-on-metal articulation in primary total hip replacement: clinical and radiological results at ten years. J Bone Joint Surg Br. 2008;90(10):1278-1283.
10. Grubl A, Marker M, Brodner W, et al. Long-term follow-up of metal-on-metal total hip replacement. J Orthop Res. 2007;25(7):841-848.
11. Leslie I, Williams S, Brown C, et al. Effect of bearing size on the long-term wear, wear debris, and ion levels of large diameter metal-on-metal hip replacements—an in vitro study. J Biomed Mater Res B Appl Biomater. 2008;87(1):163-172.
12. Verhaar JA. The hard lesson of metal-on-metal hip implants [in Dutch]. Ned Tijdschr Geneeskd. 2012;156(42):A5564.
13. Fabi D, Levine B, Paprosky W, et al. Metal-on-metal total hip arthroplasty: causes and high incidence of early failure. Orthopedics. 2012;35(7):e1009-e1016.
14. Heneghan C, Langton D, Thompson M. Ongoing problems with metal-on-metal hip implants. BMJ. 2012;344:e1349.
15. Lee RK, Nevelos J, Vigdorchik J, Markel DC. Bearing surfaces for hip arthroplasty—is metal-on-metal a passing fancy? Surg Technol Int. 2012;22:243-249.
16. Voleti PB, Baldwin KD, Lee GC. Metal-on-metal vs conventional total hip arthroplasty: a systematic review and meta-analysis of randomized controlled trials. J Arthroplasty. 2012;27(10):1844-1849.
17. Urban JA, Garvin KL, Boese CK, et al. Ceramic-on-polyethylene bearing surfaces in total hip arthroplasty. Seventeen to twenty-one-year results.
J Bone Joint Surg Am. 2001;83(11):1688-1694.
18. Callaghan JJ, Liu SS. Ceramic on crosslinked polyethylene in total hip replacement: any better than metal on crosslinked polyethylene? Iowa Orthop J. 2009;29:1-4.
19. Barrack RL. Dislocation after total hip arthroplasty: implant design and orientation. J Am Acad Orthop Surg. 2003;11(2):89-99.
20. Krushell RJ, Burke DW, Harris WH. Elevated-rim acetabular components. Effect on range of motion and stability in total hip arthroplasty. J Arthroplasty. 1991;6(suppl):S53-S58.
21. Morrey BF. Instability after total hip arthroplasty. Orthop Clin North Am. 1992;23(2):237-248.
22. Morrey BF. Dislocation. In: Morrey BF, ed. Joint Replacement Arthroplasty. New York, NY: Churchill Livingstone; 1991:851-865.
23. Bartz RL, Nobel PC, Kadakia NR, Tullos HS. The effect of femoral component head size on posterior dislocation of the artificial hip joint. J Bone Joint Surg Am. 2000;82(9):1300-1307.
24. Nicholas RM, Orr JF, Mollan RA, Calderwood JW, Nixon JR, Watson P. Dislocation of total hip replacements. A comparative study of standard, long posterior wall and augmented acetabular components. J Bone Joint Surg Br. 1990;72(3):418-422.
25. McCollum DE, Gray WJ. Dislocation after total hip arthroplasty. Causes and prevention. Clin Orthop. 1990;(261):159-170.
26. Herrlin K, Selvik G, Pettersson H, Kesek P, Onnerfalt R, Ohlin A. Position, orientation and component interaction in dislocation of the total hip prosthesis. Acta Radiol. 1988;29(4):441-444.
27. Cinotti G, Lucioli N, Malagoli A, Calderoli C, Cassese F. Do large femoral heads reduce the risks of impingement in total hip arthroplasty with optimal and non-optimal cup positioning? Int Orthop. 2011;35(3):317-323.
28. Burroughs BR, Rubash HE, Harris WH. Femoral head sizes larger than 32 mm against highly cross-linked polyethylene. Clin Orthop. 2002;(405):150-157.
29. Crowninshield RD, Maloney WJ, Wentz DH, Humphrey SM, Blanchard CR. Biomechanics of large femoral heads: what they do and don‘t do. Clin Orthop. 2004;(429):102-107.
30. Charnley J. Low Friction Arthroplasty of the Hip: Theory and Practice. New York, NY: Springer; 1979.
31. Yamaguchi M, Akisue T, Bauer TW, Hashimoto Y. The spatial location of impingement in total hip arthroplasty. J Arthroplasty. 2000;15(3):305-313.
32. Peters CL, McPherson E, Jackson JD, Erickson JA. Reduction in early dislocation rate with large-diameter femoral heads in primary total hip arthroplasty. J Arthroplasty. 2007;22(6 suppl 2):140-144.
33. Masonis JL, Bourne RB. Surgical approach, abductor function, and total hip arthroplasty dislocation. Clin Orthop. 2002;(405):46-53.
34. Beaule PE, Schmalzried TP, Udomkiat P, Amstutz HC. Jumbo femoral head for the treatment of recurrent dislocation following total hip replacement. J Bone Joint Surg Am. 2002;84(2):256-263.
35. Oral E, Malhi AS, Muratoglu OK. Mechanisms of decrease in fatigue crack propagation resistance in irradiated and melted UHMWPE. Biomaterials. 2006;27(6):917-925.
36. Baker DA, Bellare A, Pruitt L. The effects of degree of crosslinking on the fatigue crack initiation and propagation resistance of orthopedic-grade polyethylene. J Biomed Mater Res A. 2003;66(1):146-154.
37. Charnley J. Total hip replacement by low-friction arthroplasty. Clin Orthop. 1970;(72):7-21.
38. Kabo JM, Gebhard JS, Loren G, Amstutz HC. In vivo wear of polyethylene acetabular components. J Bone Joint Surg Br. 1993;75(2):254-258.
39. Livermore J, Ilstrup D, Morrey B. Effect of femoral head size on wear of the polyethylene acetabular component. J Bone Joint Surg Am. 1990;72(4):518-528.
40. Ma SM, Kabo JM, Amstutz HC. Frictional torque in surface and conventional hip replacement. J Bone Joint Surg Am. 1983;65(3):366-370.
41. Muratoglu OK, Bragdon CR, O‘Connor D, et al. Larger diameter femoral heads used in conjunction with a highly cross-linked ultra-high molecular weight polyethylene: a new concept. J Arthroplasty. 2001;16(8 suppl 1):24-30.
42. Thomas GER, Simpson DJ, Mehmood S, et al. The seven-year wear of highly cross-linked polyethylene in total hip arthroplasty: a double-blind, randomized controlled trial using radiostereometric analysis. J Bone Joint Surg Am. 2011;93(8):716-722.
43. Mutimer J, Devane PA, Adams K, Horne JG. Highly crosslinked polyethylene reduces wear in total hip arthroplasty at 5 years. Clin Orthop. 2010;468(12):3228-3233.
44. Bragdon CR, Doerner M, Martell J, Jarrett B, Palm H, Malchau H. The 2012 John Charnley Award: clinical multicenter studies of the wear performance of highly crosslinked remelted polyethylene in THA. Clin Orthop. 2013;471(2):393-402.
45. Lachiewicz PF, Heckman DS, Soileau ES, Mangla J, Martell JM. Femoral head size and wear of highly cross-linked polyethylene at 5 to 8 years. Clin Orthop. 2009;467(12):3290-3296.
46. Sychterz CJ, Engh CA Jr, Young AM, Hopper RH Jr, Engh CA. Comparison of in vivo wear between polyethylene liners articulating with ceramic and cobalt-chrome femoral heads. J Bone Joint Surg Br. 2000;82(7):948-951.
47. Berry DJ, Barnes CL, Scott RD, Cabanela ME, Poss R. Catastrophic failure of the polyethylene liner of uncemented acetabular components.
J Bone Joint Surg Br. 1994;76(4):575-578.
48. McKellop H, Shen FW, Lu B, Campbell P, Salovey R. Development of an extremely wear-resistant ultra high molecular weight polyethylene for total hip replacements. J Orthop Res. 1999;17(2):157-167.
49. Wang A, Essner A, Polineni VK, Stark C, Dumbleton JH. Lubrication and wear of ultra-high molecular weight polyethylene in total joint replacements. Tribol Int. 1998;31(1-3):17-33.
50. Estok DM 2nd, Burroughs BR, Muratoglu OK, Harris WH. Comparison of hip simulator wear of 2 different highly cross-linked ultra high molecular weight polyethylene acetabular components using both 32- and 38-mm femoral heads. J Arthroplasty. 2007;22(4):581-589.
51. Muratoglu OK, Bragdon CR, O‘Connor DO, et al. Unified wear model for highly crosslinked ultra-high molecular weight polyethylenes (UHMWPE). Biomaterials. 1999;20(16):1463-1470.
52. Harris WH, Muratoglu OK. A review of current cross-linked polyethylenes used in total joint arthroplasty. Clin Orthop. 2005;(430):46-52.
53. Muratoglu OK, Bragdon CR, O‘Connor DO, Jasty M, Harris WH. A novel method of cross-linking ultra-high-molecular-weight polyethylene to improve wear, reduce oxidation, and retain mechanical properties. Recipient of the 1999 HAP Paul Award. J Arthroplasty. 2001;16(2):149-160.
54. Bal BS, Garino J, Ries M, Rahaman MN. A review of ceramic bearing materials in total joint arthroplasty. Hip Int. 2007;17(1):21-30.
55. Traina F, De Fine M, Di Martino A, Faldini C. Fracture of ceramic bearing surfaces following total hip replacement: a systematic review. Biomed Res Int. 2013;2013:157247.
56. Cai YZ, Yan SG. Development of ceramic-on-ceramic implants for total hip arthroplasty. Orthop Surg. 2010;2(3):175-181.
57. Stewart TD, Tipper JL, Insley G, Streicher RM, Ingham E, Fisher J. Long-term wear of ceramic matrix composite materials for hip prostheses under severe swing phase microseparation. J Biomed Mater Res B Appl Biomater. 2003;66(2):567-573.
58. Bragdon CR, Greene ME, Freiberg AA, Harris WH, Malchau H. Radiostereometric analysis comparison of wear of highly cross-linked polyethylene against 36- vs 28-mm femoral heads. J Arthroplasty. 2007;22(6 suppl 2):125-129.
59. Lombardi AV Jr, Skeels MD, Berend KR, Adams JB, Franchi OJ. Do large heads enhance stability and restore native anatomy in primary total hip arthroplasty? Clin Orthop. 2011;469(6):1547-1553.
60. Lachiewicz PF, Soileau ES. Low early and late dislocation rates with 36- and 40-mm heads in patients at high risk for dislocation. Clin Orthop. 2013;471(2):439-443.
61. Cai P, Hu Y, Xie J. Large-diameter Delta ceramic-on-ceramic versus common-sized ceramic-on-polyethylene bearings in THA. Orthopedics. 2012;35(9):e1307-e1313.
62. Park KS, Yoon TR, Hwang SY, Lee KB. Modified minimally invasive two-incision total hip arthroplasty using large diameter femoral head. Indian
J Orthop. 2012;46(1):29-35.
63. Garbuz DS, Masri BA, Duncan CP, et al. The Frank Stinchfield Award: dislocation in revision THA: do large heads (36 and 40 mm) result in reduced dislocation rates in a randomized clinical trial? Clin Orthop. 2012;470(2):351-356.
64. Geller JA, Malchau H, Bragdon C, Greene M, Harris WH, Freiberg AA. Large diameter femoral heads on highly cross-linked polyethylene: minimum 3-year results. Clin Orthop. 2006;(447):53-59.
65. D’Antonio JA, Capello WN, Ramakrishnan R. Second-generation annealed highly cross-linked polyethylene exhibits low wear. Clin Orthop. 2012;470(6):1696-1704.
66. Galvin AL, Jennings LM, Tipper JL, Ingham E, Fisher J. Wear and creep of highly crosslinked polyethylene against cobalt chrome and ceramic femoral heads. Proc Inst Mech Eng H. 2010;224(10):1175-1183.
67. Skeels MD, Berend KR, Lombardi AV Jr. The dislocator, early and late: the role of large heads. Orthopedics. 2009;32(9).
68. Plate JF, Seyler TM, Stroh DA, Issa K, Akbar M, Mont MA. Risk of dislocation using large- vs. small-diameter femoral heads in total hip arthroplasty. BMC Res Notes. 2012;5(1):553.
69. Bouchet R, Mercier N, Saragaglia D. Posterior approach and dislocation rate: a 213 total hip replacements case–control study comparing the dual mobility cup with a conventional 28-mm metal head/polyethylene prosthesis. Orthop Traumatol Surg Res. 2011;97(1):2-7.
70. Ali Khan MA, Brakenbury PH, Reynolds IS. Dislocation following total hip replacement. J Bone Joint Surg Br. 1981;63(2):214-218.
71. Howie DW, Holubowycz OT, Middleton R. Large femoral heads decrease the incidence of dislocation after total hip arthroplasty: a randomized controlled trial. J Bone Joint Surg Am. 2012;94(12):1095-1102.
72. Malkani AL, Ong KL, Lau E, Kurtz SM, Justice BJ, Manley MT. Early- and late-term dislocation risk after primary hip arthroplasty in the Medicare population. J Arthroplasty. 2010;25(6 suppl):21-25.
73. Berry DJ, von Knoch M, Schleck CD, Harmsen WS. Effect of femoral head diameter and operative approach on risk of dislocation after primary total hip arthroplasty. J Bone Joint Surg Am. 2005;87(11):2456-2463.
74. Cho MR, Lee HS, Lee SW, Choi CH, Kim SK, Ko SB. Results after total hip arthroplasty with a large head and bipolar arthroplasty in patients with displaced femoral neck fractures. J Arthroplasty. 2011;26(6):893-896.
75. Conroy JL, Whitehouse SL, Graves SE, Pratt NL, Ryan P, Crawford RW. Risk factors for revision for early dislocation in total hip arthroplasty.
J Arthroplasty. 2008;23(6):867-872.
76. Kung PL, Ries MD. Effect of femoral head size and abductors on dislocation after revision THA. Clin Orthop. 2007;(465):170-174.
77. Williams JT Jr, Ragland PS, Clarke S. Constrained components for the unstable hip following total hip arthroplasty: a literature review. Int Orthop. 2007;31(3):273-277.
78. Zywiel MG, Mustafa LH, Bonutti PM, Mont MA. Are abductor muscle quality and previous revision surgery predictors of constrained liner failure in hip arthroplasty? Int Orthop. 2011;35(6):797-802.
79. Guyen O, Lewallen DG, Cabanela ME. Modes of failure of Osteonics constrained tripolar implants: a retrospective analysis of forty-three failed implants. J Bone Joint Surg Am. 2008;90(7):1553-1560.
80. Banks LN, McElwain JP. An unusual mode of failure of a tripolar constrained acetabular liner: a case report. Arch Orthop Trauma Surg. 2010;130(4):503-505.
81. Robertson WJ, Mattern CJ, Hur J, Su EP, Pellicci PM. Failure mechanisms and closed reduction of a constrained tripolar acetabular liner.
J Arthroplasty. 2009;24(2):322.e5-e11.
82. Aubriot JH, Lesimple P, Leclercq S. Study of Bousquet‘s non-cemented acetabular implant in 100 hybrid total hip prostheses (Charnley type cemented femoral component). Average 5-year follow-up [in French]. Acta Orthop Belg. 1993;59(suppl 1):267-271.
83. Farizon F, de Lavison R, Azoulai JJ, Bousquet G. Results with a cementless alumina-coated cup with dual mobility. A twelve-year follow-up study. Int Orthop. 1998;22(4):219-224.
84. Mertl P, Combes A, Leiber-Wackenheim F, Fessy MH, Girard J, Migaud H. Recurrence of dislocation following total hip arthroplasty revision using dual mobility cups was rare in 180 hips followed over 7 years. HSS J. 2012;8(3):251-256.
85. Langlais FL, Ropars M, Gaucher F, Musset T, Chaix O. Dual mobility cemented cups have low dislocation rates in THA revisions. Clin Orthop. 2008;466(2):389-395.
86. Philippot R, Farizon F, Camilleri JP, et al. Survival of dual mobility socket with a mean 17 years follow-up [in French]. Rev Chir Orthop Reparatrice Appar Mot. 2008;94(1):43-48.
87. Adam P, Philippe R, Ehlinger M, et al. Dual mobility cups hip arthroplasty as a treatment for displaced fracture of the femoral neck in the elderly.
A prospective, systematic, multicenter study with specific focus on postoperative dislocation. Orthop Traumatol Surg Res. 2012;98(3):296-300.
88. Fessy MH. La double mobilité [Dual mobility]. Revue de Chirurgie Orthopédique et Traumatologique. 2010;96(7):891-898.
89. Mont MA, Issa K, Naziri Q, Harwin SF, Delanois RE, Johnson AJ. The use of dual-mobility bearings in difficult hip arthroplasty reconstructive cases. Surg Technol Int. 2011;21:234-240.
90. Sayeed SA, Mont MA, Costa CR, et al. Early outcomes of sequentially cross-linked thin polyethylene liners with large diameter femoral heads in total hip arthroplasty. Bull NYU Hosp Jt Dis. 2011;69(suppl 1):S90-S94.
91. Plate JF, Seyler TM, Stroh DA, Issa K, Akbar M, Mont MA. Risk of dislocation using large- vs. small-diameter femoral heads in total hip arthroplasty. BMC Res Notes. 2012;5(1):553.
92. Sato T, Nakashima Y, Akiyama M, et al. Wear resistant performance of highly cross-linked and annealed ultra-high molecular weight polyethylene against ceramic heads in total hip arthroplasty. J Orthop Res. 2012;30(12):2031-2037.
93. Meftah M, Ebrahimpour PB, He C, Ranawat AS, Ranawat CS. Preliminary clinical and radiographic results of large ceramic heads on highly cross-linked polyethylene. Orthopedics. 2011;34(6):133.
94. Gagala J, Mazurkiewicz T, Dajewski Z. Large diameter femoral heads in primary alumina/alumina and XSPE/alumina total hip arthroplasty.
A follow-up study of 50 hips after average 40 months and review of literature [in Polish]. Chir Narzadow Ruchu Ortop Pol. 2011;76(1):14-20.
A common cause for total hip arthroplasty (THA) revision is joint instability.1,2 The reported incidence of dislocation in primary THA ranges from 0.4% to 5.8%,3-5 but this rate increases after revision surgery.1,3-8 Use of large-diameter femoral heads has been proposed to decrease the risks for instability and to improve impingement-free range of motion (ROM).
The biomechanical rationale for using large-diameter femoral heads is that they must travel farther before subluxation or dislocation occurs (jump distance). Despite these benefits, there were initial concerns that catastrophic failure and high levels of volumetric wear would occur if these heads were used with conventional polyethylene liners. These concerns led to the development of alternative bearing surfaces, particularly metal-on-metal bearings, which offered theoretical benefits of large-diameter articulations that improved stability while purportedly being highly wear-resistant.9-11 However, concerns about adverse local soft-tissue reactions and high blood concentrations of metal ions tempered the initial enthusiasm for metal bearings.12-16 Fortunately, highly cross-linked polyethylene and fourth-generation ceramic bearing surfaces, with improved toughness and better wear properties, may allow use of large-diameter heads without the need for metal-on-metal bearings.17,18
In this article, we review the concepts and principles behind use of large-diameter ceramic or cobalt-chromium femoral heads on polyethylene-bearing surfaces in THA with particular attention to biomechanics, early concerns about polyethylene wear and rim fractures, recent improvements in material properties of polyethylene and ceramic bearings, dislocation rates, and clinical and functional outcomes.
Definitions
For this review, we define large-diameter femoral heads as having diameters of 36 mm or more and conventional or small-diameter femoral heads as having diameters between 22 and 32 mm.
Biomechanics
Head–Neck Ratio, Impingement-Free ROM, and Jump Distance
Several implant design principles have been proposed to reduce the risks for impingement and dislocation. Of these, large femoral head diameters have been extensively studied.19,20 It is well known that impingement of the femoral neck on the cup edge promotes edge loading and higher wear rates. In addition, impingement increases the tendency of the head to sublux from the acetabulum. One strategy for avoiding this component-to-component impingement is to increase the head–neck ratio (HNR), the ratio of the femoral head to the neck diameter. Biomechanically, increased HNRs lead to delayed contact between the femoral neck and the acetabular liner.21,22 Therefore, with large femoral heads, which have large HNRs, impingement occurs later and at larger ROMs—compared with small-diameter femoral heads, which have lower HNRs and are more prone to early impingement and subluxation (Figure 1).23-26
In a cadaveric study of 6 hips, Bartz and colleagues23 reported a significantly higher preimpingement ROM when the prosthetic head size increased from 22 mm to 28 mm (P < .05). They found a change from prosthetic to osseous impingement when the head size increased from 22 mm to 32 mm. Similar results were observed in a computer simulation model by Cinotti and colleagues,27 who demonstrated that increasing the femoral head size from 28 mm to 38 mm resulted in a 5° improvement in ROM. However, the largest gains were observed when the heads with the smallest diameters were upsized; ROM improved only marginally when femoral head size was further increased from 32 mm to 38 mm. The primary reason for the lack of expected improvement in ROM with head sizes of more than 32 mm is often bone-on-bone impingement. Burroughs and colleagues28 demonstrated that the 38-mm and 44-mm heads virtually eliminated component-to-component impingement except in extremes of external rotation. However, there were no differences in ROM between 38-mm and 44-mm heads because of osseous impingement. In addition, large heads are less likely to sublux or dislocate, as they need to travel farther before reaching the edge of the acetabular cup before dislocation. This is known as the jump distance, and it corresponds to the depth of the acetabular shell, which in turn equates with the radius of the femoral head (Figures 2A, 2B). For this reason, the larger the femoral head diameter, the farther the jump distance and, correspondingly, the lower the risk for dislocation.29
Elevated liners historically were used to increase the jump distance for dislocation.30 These liners, however, can increase impingement at the extremes of motion.31 Some of these problems can be avoided with use of larger heads, which have increased jump distances without additional risks for impingement. Moreover, large heads create a suction effect that provides passive resistance to dislocation.32 With head diameters beyond 38 mm, impingement-free ROM often plateaus. However, the jump distance required for dislocations to occur continues to increase as femoral head diameters increase in size. Thus, patients may experience fewer motion benefits but continue to benefit from overall stability with femoral head sizes increasing beyond 38 mm.
Current evidence suggests there may be substantial benefits toward improved stability from increasing head diameters from 22 mm to 38 mm because of the increase in jump distances and improvements in prosthetic impingement-free ROM. However, there may be little gain in ROM from increasing the head diameters beyond these dimensions because of the potential risks of bony impingement. Nevertheless, there may be some additional benefits toward stability from improvement in jump distances with incremental head sizes
beyond 38 mm.29,33,34
Finite Element Analysis Studies
Finite element analysis of large-diameter heads in THA has shown that, at optimal cup inclination (45°), most stresses occur on the articular surface of the liner. However, these stresses remain well below the yield strength of the polyethylene liners.29 With increasing abduction angles, the stress concentration increases substantially because of the decreased contact surface area. At these angles, the point of maximum contact moves toward the rim of the polyethylene liner, which can lead to rim fractures or failure of locking mechanisms.29,35,36
Early Concerns With Large-Diameter Femoral Heads: Wear, Liner Failure, and Fracture of Ceramic Components
Use of small-diameter femoral heads started with the first report by Charnley37 of “low frictional torque arthroplasty.” Charnley initially considered a 41.5-mm femoral head, but he thought it would increase risks for acetabular loosening from high frictional torque generated by the large head, and he switched to a small-diameter (22.5 mm) design. One of the tradeoffs with smaller diameter heads was decreased jump height in addition to increased linear wear.
Large femoral heads used with cemented polyethylene acetabular components historically have been associated with increased rates of volumetric wear but low rates of linear wear, which potentially may increase the risk for osteolysis.38-40 However, newer highly cross-linked polyethylene liners have shown improved in vitro and in vivo volumetric wear characteristics and potentially lower linear wear rates compared with earlier designs (Table 1).28,41-43
Another concern about earlier generations of large femoral heads was the risk for catastrophic liner failure on conventional polyethylene. This was originally reported by Berry and colleagues,47 who described wear-through and failure in patients with thin (< 5 mm) acetabular cups. However, these concerns have been largely addressed by the development of highly cross-linked polyethylene, which has improved wear characteristics and fatigue resistance.48
Recent Improvements in Material Properties of Polyethylene and Ceramic Bearings
The development of highly cross-linked polyethylene and fourth-generation ceramics has renewed interest in large-diameter bearings in THA. These bearing surfaces improve wear, enhance material properties, and have superior oxidation resistance.42,48-53
We now briefly describe the methods used to improve the material properties of polyethylene and ceramics. Studies have shown that increasing the radiation dose (up to 200 kGy) increases cross-linking and causes an inverse exponential decrease in polyethylene wear.28,41,48-51 However, increasing radiation doses also increases production of free radicals, which diminish the material strength of these polyethylenes. The current generation of highly cross-linked polyethylene liners is produced through a variety of manufacturing strategies to improve cross-linking and reduce wear. These strategies include differential radiation doses (50-100 kGy), techniques (electron beam, radiation), and thermal treatments (melting, annealing). Moreover, to enhance the material properties and reduce the incidence of rim cracking and delamination, authors have proposed using vitamin E supplementation to minimize the amount of subsurface oxidation that occurs as an inevitable consequence of free radical formation during fabrication.54,55 A terminal sterilization process (eg, gas plasma, ethylene oxide, or gamma sterilization in nitrogen) is needed to make commercial, highly cross-linked polyethylene.52,53
Fourth-generation ceramics manufactured with nano-sized yttria-stabilized tetragonal zirconia particles in a stable alumina matrix have more fracture toughness and improved wear characteristics.54,55 In addition, oxide additives (eg, chromium oxide, strontium oxide) improve hardness and dissipate energy by deflecting cracks to prevent their propagation.56 Moreover, the smaller grain sizes of fourth-generation ceramic bearings compared with third-generation designs (0.8 µm vs 1-5 µm) cause less disruption of the fluid film layer, which ultimately results in improved wear performance.57
Multiple studies have found reduced wear rates with metal and ceramic large heads coupled with highly cross-linked polyethylene-bearings (Table 2).17,41,50,58 Bragdon and colleagues,58 using radiostereometric analysis in 25 patients, found no significant differences in mean head penetration rates between 36-mm and 28-mm cobalt-chromium (Co-Cr) heads articulating with highly cross-linked polyethylene cups at a mean follow-up of 3 years (0.035 mm/y vs 0.046 mm/y; P = .11). Geller and colleagues,64 in their study of 42 patients with large-diameter (> 32 mm) Co-Cr femoral heads, found low mean (SD) linear wear rates of 0.06 (0.41) mm/y at a mean follow-up of 3 years. D’Antonio and colleagues,65 in a multicenter study, reported low average linear wear (0.015 mm/y) and volumetric wear (12.1 mm3/y) over 5 years using sequentially annealed cross-linked polyethylene. In vitro reports suggest that large-diameter ceramic heads may have lower wear properties than Co-Cr heads do. Galvin and colleagues,66 in an in vitro hip simulator study, found that large-diameter ceramic heads on highly cross-linked ultrahigh-molecular-weight polyethylene had 40% reductions in steady-state wear rates compared with Co-Cr heads on highly cross-linked bearings (4.7 vs 8.1 mm3/million cycles; P < 0.01).
Dislocation Rates
Several patient, surgeon, and implant factors affect the rate of dislocations after THA. Multiple implant options utilize the biomechanical advantage that large-diameter heads have in improving stability. Various alternatives include use of constrained tripolar heads, dual-mobility bearings, and conventional large-diameter heads with standard liners.67-69
Large-Diameter Heads
Despite the biomechanical advantages of large-diameter metal-on-polyethylene bearings, prior studies have questioned use of these bearings because of risks for increased wear and rim failures. However, the improved wear properties of highly cross-linked polyethylene, elaborated earlier, have led to a reappraisal of this option (Table 2).4,70 Howie and colleagues,71 in a randomized control trial of 644 patients, also found significantly lower rates of dislocation after primary THA with 36-mm heads compared with 28-mm heads (1.3% vs 5.4%; P = .012); in addition, fewer dislocations occurred with 36-mm heads than with 28-mm heads (4.9% vs 12.2%; P = .27) in a series of 44 patients in revision settings. Similarly, in a study conducted with 39,271 Medicare patients between 1998 and 2007, Malkani and colleagues72 found a decrease in the dislocation rate, from 4.21% to 2.14%, with use of large-diameter femoral heads. These results have been confirmed by several other authors.34,66,73,74 Similar results were observed in 65,992 patients in the Australian National Joint Replacement Registry by Conroy and colleagues,75 who reported a significant decrease in the risk for dislocation with large heads (≥ 30 mm) compared with 22-mm heads (relative risk, 1.0 vs 3.1; P ≤ .001).
Few studies have analyzed the role of large-diameter femoral heads in the presence of compromised soft tissues around the hip. Kung and Ries,76 evaluating the influence of large-diameter heads in the presence and absence of a deficient abductor mechanism, demonstrated statistically significant reductions in rates of dislocation after 230 revision THAs when the abductor mechanism was intact with use of 36-mm heads compared with 28-mm heads (12.7% vs 0%; P = .015). With abductor deficiency, though, the positive effect of large heads in reducing dislocation rates was substantially reduced and was similar to that of small heads (P = .74).76
Large heads considerably improve overall stability and lower dislocation rates in THA. With the development of newer ceramics and highly cross-linked polyethylenes, the wear rates reported in multiple studies appear to be less concerning.
Constrained Tripolar Heads
Tripolar heads have been proposed as treatment options for improving stability in patients with chronic and recurrent instability after THA. The tripolar implant consists of a metal head that snap-fits into a polyethylene liner with a polished Co-Cr backing. This bipolar head articulates with a polyethylene bearing that is press-fitted onto a metal acetabular shell and constrained by a metal ring snapped to the outer polyethylene bearing. The bipolar component behaves as a large-diameter femoral head, and the metal ring provides additional restraint, further improving stability.
Williams and colleagues77 performed a systematic review and reported on the outcomes of constrained tripolar liners in 1199 hips at a mean follow-up of 4 years (range, 2-10 years). The mean dislocation rate was 10%, and the mean rate of revision surgery unrelated to instability was 4%. In a study of 43 hips at a mean follow-up of 4 years (range, 2-9 years), Zywiel and colleagues78 reported on the clinical and radiographic outcomes of tripolar constrained liners. Their study group had a mean Harris Hip Score (HHS) of 82 points (range, 38-100 points) and overall survival of 91%, with no evidence of radiographic loosening during follow-up. Despite the improvements in stability with constrained tripolar liners, some authors have reported multiple mechanisms of failure with these devices.79-81 In a study of 43 failed constrained tripolar liners with a mean time to failure of about 2 years, Guyen and colleagues79 identified 5 different failure modes (types 1-5) involving all 4 interfaces in these components.
Encouraging outcomes have been reported at midterm follow-up with tripolar constrained liners. However, concerns about failure at the interfaces suggest that use of these components should be restricted to patients with deficient abductor mechanisms or neuromuscular compromise, low-demand elderly patients, and salvage cases of recurrent dislocations.79
Dual-Mobility Bearings
For more than 20 years, different dual-mobility bearings have been used for difficult acetabular reconstructive scenarios and prevention of instability.82,83 Dual-mobility cups provide constructs that snap-fit a small-diameter femoral head within a large polyethylene insert that articulates with a fixed metal shell. This effectively increases the functional head diameter.
Various authors have reported excellent survivorship rates (92%-99%) and low dislocation rates for these bearings at 5- to 10-year follow-up.82,84-90 Philippot and colleagues,86 in a recent study of 438 hips with dual-mobility cups, reported excellent survivorship (96%) and no early or late instability within a 15-year follow-up. Bouchet and colleagues69 compared dual-mobility bearings (105 hips) with conventional metal-on-polythene bearings (108 hips) and found significantly (P < .05) lower dislocation rates for the dual-mobility implants at a minimum 1-year follow-up. The French Society of Orthopaedics and Traumatology performed a multicenter analysis of 3473 hips with dual-mobility cups implanted in France between January 1998 and December 2003.87 During a mean follow-up of 7 years (range, 5-11 years), there were 15 dislocations (0.43%), 14 of which occurred early, within 3 months of implantation (0.4%). Aseptic implant survivorship was 95% at 10-year follow-up.
Use of these bearings has recently increased in the United States. Short-term and midterm follow-up data show low rates of dislocation and wear. Long-term data are to come.
Clinical and Functional Outcomes of Large-Diameter Femoral Heads
There is a paucity of long-term outcomes data on use of large-diameter heads with highly cross-linked polyethylene bearings. Short-term and midterm clinical results appear to be excellent, with low rates of wear, osteolysis, and aseptic loosening.28,41,73,89-92
Plate and colleagues91 compared the effects of large-diameter (≥ 36 mm) and small-diameter (26 mm, 28 mm) metal heads on highly cross-linked polyethylene bearings. At a mean follow-up of 5 years (range, 4-8.4 years), the large-head cohort had a mean HHS of 90 points (range, 50-100 points) and no dislocations or radiographic evidence of stem or cup loosening. Similarly, Meftah and colleagues93 reported 100% stem survivorship and excellent clinical outcomes—a mean Western Ontario and McMaster Universities Arthritis Index (WOMAC) score of 30 points—for 72 hips with use of large ceramic heads (≥ 32 mm) on highly cross-linked polyethylene at a mean follow-up of 3 years. Gagala and colleagues94 reported excellent clinical and radiographic outcomes in 50 hips (18 ceramic on ceramic, 32 ceramic on polyethylene; 36-mm heads) at a mean follow-up of 3.5 years. Mean HHS was 94 points, and there was no evidence of liner fractures, aseptic loosening, or osteolysis.
In summary, large-diameter femoral heads in THA have become increasingly popular because of improvements in the material properties and wear characteristics of highly cross-linked polyethylene and fourth-generation ceramics. Despite the potential advantages of large heads in preventing dislocations, the basic surgical tenets of placing the acetabular component in appropriate alignment remain firmly established. Implants with functionally large heads (eg, dual-mobility bearings, constrained tripolar liners) may play an important role in patients at high risk for dislocation—particularly elderly patients with poor neuromuscular muscle coordination or deficient abductors, trauma patients, and patients with prior dislocations. Short-term and midterm results are excellent; rates of wear, aseptic loosening, and osteolysis are low. However, long-term outcomes data are needed to support widespread use of large heads in younger and more active patients.
A common cause for total hip arthroplasty (THA) revision is joint instability.1,2 The reported incidence of dislocation in primary THA ranges from 0.4% to 5.8%,3-5 but this rate increases after revision surgery.1,3-8 Use of large-diameter femoral heads has been proposed to decrease the risks for instability and to improve impingement-free range of motion (ROM).
The biomechanical rationale for using large-diameter femoral heads is that they must travel farther before subluxation or dislocation occurs (jump distance). Despite these benefits, there were initial concerns that catastrophic failure and high levels of volumetric wear would occur if these heads were used with conventional polyethylene liners. These concerns led to the development of alternative bearing surfaces, particularly metal-on-metal bearings, which offered theoretical benefits of large-diameter articulations that improved stability while purportedly being highly wear-resistant.9-11 However, concerns about adverse local soft-tissue reactions and high blood concentrations of metal ions tempered the initial enthusiasm for metal bearings.12-16 Fortunately, highly cross-linked polyethylene and fourth-generation ceramic bearing surfaces, with improved toughness and better wear properties, may allow use of large-diameter heads without the need for metal-on-metal bearings.17,18
In this article, we review the concepts and principles behind use of large-diameter ceramic or cobalt-chromium femoral heads on polyethylene-bearing surfaces in THA with particular attention to biomechanics, early concerns about polyethylene wear and rim fractures, recent improvements in material properties of polyethylene and ceramic bearings, dislocation rates, and clinical and functional outcomes.
Definitions
For this review, we define large-diameter femoral heads as having diameters of 36 mm or more and conventional or small-diameter femoral heads as having diameters between 22 and 32 mm.
Biomechanics
Head–Neck Ratio, Impingement-Free ROM, and Jump Distance
Several implant design principles have been proposed to reduce the risks for impingement and dislocation. Of these, large femoral head diameters have been extensively studied.19,20 It is well known that impingement of the femoral neck on the cup edge promotes edge loading and higher wear rates. In addition, impingement increases the tendency of the head to sublux from the acetabulum. One strategy for avoiding this component-to-component impingement is to increase the head–neck ratio (HNR), the ratio of the femoral head to the neck diameter. Biomechanically, increased HNRs lead to delayed contact between the femoral neck and the acetabular liner.21,22 Therefore, with large femoral heads, which have large HNRs, impingement occurs later and at larger ROMs—compared with small-diameter femoral heads, which have lower HNRs and are more prone to early impingement and subluxation (Figure 1).23-26
In a cadaveric study of 6 hips, Bartz and colleagues23 reported a significantly higher preimpingement ROM when the prosthetic head size increased from 22 mm to 28 mm (P < .05). They found a change from prosthetic to osseous impingement when the head size increased from 22 mm to 32 mm. Similar results were observed in a computer simulation model by Cinotti and colleagues,27 who demonstrated that increasing the femoral head size from 28 mm to 38 mm resulted in a 5° improvement in ROM. However, the largest gains were observed when the heads with the smallest diameters were upsized; ROM improved only marginally when femoral head size was further increased from 32 mm to 38 mm. The primary reason for the lack of expected improvement in ROM with head sizes of more than 32 mm is often bone-on-bone impingement. Burroughs and colleagues28 demonstrated that the 38-mm and 44-mm heads virtually eliminated component-to-component impingement except in extremes of external rotation. However, there were no differences in ROM between 38-mm and 44-mm heads because of osseous impingement. In addition, large heads are less likely to sublux or dislocate, as they need to travel farther before reaching the edge of the acetabular cup before dislocation. This is known as the jump distance, and it corresponds to the depth of the acetabular shell, which in turn equates with the radius of the femoral head (Figures 2A, 2B). For this reason, the larger the femoral head diameter, the farther the jump distance and, correspondingly, the lower the risk for dislocation.29
Elevated liners historically were used to increase the jump distance for dislocation.30 These liners, however, can increase impingement at the extremes of motion.31 Some of these problems can be avoided with use of larger heads, which have increased jump distances without additional risks for impingement. Moreover, large heads create a suction effect that provides passive resistance to dislocation.32 With head diameters beyond 38 mm, impingement-free ROM often plateaus. However, the jump distance required for dislocations to occur continues to increase as femoral head diameters increase in size. Thus, patients may experience fewer motion benefits but continue to benefit from overall stability with femoral head sizes increasing beyond 38 mm.
Current evidence suggests there may be substantial benefits toward improved stability from increasing head diameters from 22 mm to 38 mm because of the increase in jump distances and improvements in prosthetic impingement-free ROM. However, there may be little gain in ROM from increasing the head diameters beyond these dimensions because of the potential risks of bony impingement. Nevertheless, there may be some additional benefits toward stability from improvement in jump distances with incremental head sizes
beyond 38 mm.29,33,34
Finite Element Analysis Studies
Finite element analysis of large-diameter heads in THA has shown that, at optimal cup inclination (45°), most stresses occur on the articular surface of the liner. However, these stresses remain well below the yield strength of the polyethylene liners.29 With increasing abduction angles, the stress concentration increases substantially because of the decreased contact surface area. At these angles, the point of maximum contact moves toward the rim of the polyethylene liner, which can lead to rim fractures or failure of locking mechanisms.29,35,36
Early Concerns With Large-Diameter Femoral Heads: Wear, Liner Failure, and Fracture of Ceramic Components
Use of small-diameter femoral heads started with the first report by Charnley37 of “low frictional torque arthroplasty.” Charnley initially considered a 41.5-mm femoral head, but he thought it would increase risks for acetabular loosening from high frictional torque generated by the large head, and he switched to a small-diameter (22.5 mm) design. One of the tradeoffs with smaller diameter heads was decreased jump height in addition to increased linear wear.
Large femoral heads used with cemented polyethylene acetabular components historically have been associated with increased rates of volumetric wear but low rates of linear wear, which potentially may increase the risk for osteolysis.38-40 However, newer highly cross-linked polyethylene liners have shown improved in vitro and in vivo volumetric wear characteristics and potentially lower linear wear rates compared with earlier designs (Table 1).28,41-43
Another concern about earlier generations of large femoral heads was the risk for catastrophic liner failure on conventional polyethylene. This was originally reported by Berry and colleagues,47 who described wear-through and failure in patients with thin (< 5 mm) acetabular cups. However, these concerns have been largely addressed by the development of highly cross-linked polyethylene, which has improved wear characteristics and fatigue resistance.48
Recent Improvements in Material Properties of Polyethylene and Ceramic Bearings
The development of highly cross-linked polyethylene and fourth-generation ceramics has renewed interest in large-diameter bearings in THA. These bearing surfaces improve wear, enhance material properties, and have superior oxidation resistance.42,48-53
We now briefly describe the methods used to improve the material properties of polyethylene and ceramics. Studies have shown that increasing the radiation dose (up to 200 kGy) increases cross-linking and causes an inverse exponential decrease in polyethylene wear.28,41,48-51 However, increasing radiation doses also increases production of free radicals, which diminish the material strength of these polyethylenes. The current generation of highly cross-linked polyethylene liners is produced through a variety of manufacturing strategies to improve cross-linking and reduce wear. These strategies include differential radiation doses (50-100 kGy), techniques (electron beam, radiation), and thermal treatments (melting, annealing). Moreover, to enhance the material properties and reduce the incidence of rim cracking and delamination, authors have proposed using vitamin E supplementation to minimize the amount of subsurface oxidation that occurs as an inevitable consequence of free radical formation during fabrication.54,55 A terminal sterilization process (eg, gas plasma, ethylene oxide, or gamma sterilization in nitrogen) is needed to make commercial, highly cross-linked polyethylene.52,53
Fourth-generation ceramics manufactured with nano-sized yttria-stabilized tetragonal zirconia particles in a stable alumina matrix have more fracture toughness and improved wear characteristics.54,55 In addition, oxide additives (eg, chromium oxide, strontium oxide) improve hardness and dissipate energy by deflecting cracks to prevent their propagation.56 Moreover, the smaller grain sizes of fourth-generation ceramic bearings compared with third-generation designs (0.8 µm vs 1-5 µm) cause less disruption of the fluid film layer, which ultimately results in improved wear performance.57
Multiple studies have found reduced wear rates with metal and ceramic large heads coupled with highly cross-linked polyethylene-bearings (Table 2).17,41,50,58 Bragdon and colleagues,58 using radiostereometric analysis in 25 patients, found no significant differences in mean head penetration rates between 36-mm and 28-mm cobalt-chromium (Co-Cr) heads articulating with highly cross-linked polyethylene cups at a mean follow-up of 3 years (0.035 mm/y vs 0.046 mm/y; P = .11). Geller and colleagues,64 in their study of 42 patients with large-diameter (> 32 mm) Co-Cr femoral heads, found low mean (SD) linear wear rates of 0.06 (0.41) mm/y at a mean follow-up of 3 years. D’Antonio and colleagues,65 in a multicenter study, reported low average linear wear (0.015 mm/y) and volumetric wear (12.1 mm3/y) over 5 years using sequentially annealed cross-linked polyethylene. In vitro reports suggest that large-diameter ceramic heads may have lower wear properties than Co-Cr heads do. Galvin and colleagues,66 in an in vitro hip simulator study, found that large-diameter ceramic heads on highly cross-linked ultrahigh-molecular-weight polyethylene had 40% reductions in steady-state wear rates compared with Co-Cr heads on highly cross-linked bearings (4.7 vs 8.1 mm3/million cycles; P < 0.01).
Dislocation Rates
Several patient, surgeon, and implant factors affect the rate of dislocations after THA. Multiple implant options utilize the biomechanical advantage that large-diameter heads have in improving stability. Various alternatives include use of constrained tripolar heads, dual-mobility bearings, and conventional large-diameter heads with standard liners.67-69
Large-Diameter Heads
Despite the biomechanical advantages of large-diameter metal-on-polyethylene bearings, prior studies have questioned use of these bearings because of risks for increased wear and rim failures. However, the improved wear properties of highly cross-linked polyethylene, elaborated earlier, have led to a reappraisal of this option (Table 2).4,70 Howie and colleagues,71 in a randomized control trial of 644 patients, also found significantly lower rates of dislocation after primary THA with 36-mm heads compared with 28-mm heads (1.3% vs 5.4%; P = .012); in addition, fewer dislocations occurred with 36-mm heads than with 28-mm heads (4.9% vs 12.2%; P = .27) in a series of 44 patients in revision settings. Similarly, in a study conducted with 39,271 Medicare patients between 1998 and 2007, Malkani and colleagues72 found a decrease in the dislocation rate, from 4.21% to 2.14%, with use of large-diameter femoral heads. These results have been confirmed by several other authors.34,66,73,74 Similar results were observed in 65,992 patients in the Australian National Joint Replacement Registry by Conroy and colleagues,75 who reported a significant decrease in the risk for dislocation with large heads (≥ 30 mm) compared with 22-mm heads (relative risk, 1.0 vs 3.1; P ≤ .001).
Few studies have analyzed the role of large-diameter femoral heads in the presence of compromised soft tissues around the hip. Kung and Ries,76 evaluating the influence of large-diameter heads in the presence and absence of a deficient abductor mechanism, demonstrated statistically significant reductions in rates of dislocation after 230 revision THAs when the abductor mechanism was intact with use of 36-mm heads compared with 28-mm heads (12.7% vs 0%; P = .015). With abductor deficiency, though, the positive effect of large heads in reducing dislocation rates was substantially reduced and was similar to that of small heads (P = .74).76
Large heads considerably improve overall stability and lower dislocation rates in THA. With the development of newer ceramics and highly cross-linked polyethylenes, the wear rates reported in multiple studies appear to be less concerning.
Constrained Tripolar Heads
Tripolar heads have been proposed as treatment options for improving stability in patients with chronic and recurrent instability after THA. The tripolar implant consists of a metal head that snap-fits into a polyethylene liner with a polished Co-Cr backing. This bipolar head articulates with a polyethylene bearing that is press-fitted onto a metal acetabular shell and constrained by a metal ring snapped to the outer polyethylene bearing. The bipolar component behaves as a large-diameter femoral head, and the metal ring provides additional restraint, further improving stability.
Williams and colleagues77 performed a systematic review and reported on the outcomes of constrained tripolar liners in 1199 hips at a mean follow-up of 4 years (range, 2-10 years). The mean dislocation rate was 10%, and the mean rate of revision surgery unrelated to instability was 4%. In a study of 43 hips at a mean follow-up of 4 years (range, 2-9 years), Zywiel and colleagues78 reported on the clinical and radiographic outcomes of tripolar constrained liners. Their study group had a mean Harris Hip Score (HHS) of 82 points (range, 38-100 points) and overall survival of 91%, with no evidence of radiographic loosening during follow-up. Despite the improvements in stability with constrained tripolar liners, some authors have reported multiple mechanisms of failure with these devices.79-81 In a study of 43 failed constrained tripolar liners with a mean time to failure of about 2 years, Guyen and colleagues79 identified 5 different failure modes (types 1-5) involving all 4 interfaces in these components.
Encouraging outcomes have been reported at midterm follow-up with tripolar constrained liners. However, concerns about failure at the interfaces suggest that use of these components should be restricted to patients with deficient abductor mechanisms or neuromuscular compromise, low-demand elderly patients, and salvage cases of recurrent dislocations.79
Dual-Mobility Bearings
For more than 20 years, different dual-mobility bearings have been used for difficult acetabular reconstructive scenarios and prevention of instability.82,83 Dual-mobility cups provide constructs that snap-fit a small-diameter femoral head within a large polyethylene insert that articulates with a fixed metal shell. This effectively increases the functional head diameter.
Various authors have reported excellent survivorship rates (92%-99%) and low dislocation rates for these bearings at 5- to 10-year follow-up.82,84-90 Philippot and colleagues,86 in a recent study of 438 hips with dual-mobility cups, reported excellent survivorship (96%) and no early or late instability within a 15-year follow-up. Bouchet and colleagues69 compared dual-mobility bearings (105 hips) with conventional metal-on-polythene bearings (108 hips) and found significantly (P < .05) lower dislocation rates for the dual-mobility implants at a minimum 1-year follow-up. The French Society of Orthopaedics and Traumatology performed a multicenter analysis of 3473 hips with dual-mobility cups implanted in France between January 1998 and December 2003.87 During a mean follow-up of 7 years (range, 5-11 years), there were 15 dislocations (0.43%), 14 of which occurred early, within 3 months of implantation (0.4%). Aseptic implant survivorship was 95% at 10-year follow-up.
Use of these bearings has recently increased in the United States. Short-term and midterm follow-up data show low rates of dislocation and wear. Long-term data are to come.
Clinical and Functional Outcomes of Large-Diameter Femoral Heads
There is a paucity of long-term outcomes data on use of large-diameter heads with highly cross-linked polyethylene bearings. Short-term and midterm clinical results appear to be excellent, with low rates of wear, osteolysis, and aseptic loosening.28,41,73,89-92
Plate and colleagues91 compared the effects of large-diameter (≥ 36 mm) and small-diameter (26 mm, 28 mm) metal heads on highly cross-linked polyethylene bearings. At a mean follow-up of 5 years (range, 4-8.4 years), the large-head cohort had a mean HHS of 90 points (range, 50-100 points) and no dislocations or radiographic evidence of stem or cup loosening. Similarly, Meftah and colleagues93 reported 100% stem survivorship and excellent clinical outcomes—a mean Western Ontario and McMaster Universities Arthritis Index (WOMAC) score of 30 points—for 72 hips with use of large ceramic heads (≥ 32 mm) on highly cross-linked polyethylene at a mean follow-up of 3 years. Gagala and colleagues94 reported excellent clinical and radiographic outcomes in 50 hips (18 ceramic on ceramic, 32 ceramic on polyethylene; 36-mm heads) at a mean follow-up of 3.5 years. Mean HHS was 94 points, and there was no evidence of liner fractures, aseptic loosening, or osteolysis.
In summary, large-diameter femoral heads in THA have become increasingly popular because of improvements in the material properties and wear characteristics of highly cross-linked polyethylene and fourth-generation ceramics. Despite the potential advantages of large heads in preventing dislocations, the basic surgical tenets of placing the acetabular component in appropriate alignment remain firmly established. Implants with functionally large heads (eg, dual-mobility bearings, constrained tripolar liners) may play an important role in patients at high risk for dislocation—particularly elderly patients with poor neuromuscular muscle coordination or deficient abductors, trauma patients, and patients with prior dislocations. Short-term and midterm results are excellent; rates of wear, aseptic loosening, and osteolysis are low. However, long-term outcomes data are needed to support widespread use of large heads in younger and more active patients.
1. Dorr LD, Wolf AW, Chandler R, Conaty JP. Classification and treatment of dislocations of total hip arthroplasty. Clin Orthop. 1983;(173):151-158.
2. Dorr LD, Wan Z. Causes of and treatment protocol for instability of total hip replacement. Clin Orthop. 1998;(355):144-151.
3. Turner RS. Postoperative total hip prosthetic femoral head dislocations. Incidence, etiologic factors, and management. Clin Orthop. 1994;(301):196-204.
4. Woo RY, Morrey BF. Dislocations after total hip arthroplasty. J Bone Joint Surg Am. 1982;64(9):1295-1306.
5. Etienne A, Cupic Z, Charnley J. Postoperative dislocation after Charnley low-friction arthroplasty. Clin Orthop. 1978;(132):19-23.
6. Fackler CD, Poss R. Dislocation in total hip arthroplasties. Clin Orthop. 1980;(151):169-178.
7. Joshi A, Lee CM, Markovic L, Vlatis G, Murphy JC. Prognosis of dislocation after total hip arthroplasty. J Arthroplasty. 1998;13(1):17-21.
8. Lindberg HO, Carlsson AS, Gentz CF, Pettersson H. Recurrent and non-recurrent dislocation following total hip arthroplasty. Acta Orthop Scand. 1982;53(6):947-952.
9. Eswaramoorthy V, Moonot P, Kalairajah Y, Biant LC, Field RE. The Metasul metal-on-metal articulation in primary total hip replacement: clinical and radiological results at ten years. J Bone Joint Surg Br. 2008;90(10):1278-1283.
10. Grubl A, Marker M, Brodner W, et al. Long-term follow-up of metal-on-metal total hip replacement. J Orthop Res. 2007;25(7):841-848.
11. Leslie I, Williams S, Brown C, et al. Effect of bearing size on the long-term wear, wear debris, and ion levels of large diameter metal-on-metal hip replacements—an in vitro study. J Biomed Mater Res B Appl Biomater. 2008;87(1):163-172.
12. Verhaar JA. The hard lesson of metal-on-metal hip implants [in Dutch]. Ned Tijdschr Geneeskd. 2012;156(42):A5564.
13. Fabi D, Levine B, Paprosky W, et al. Metal-on-metal total hip arthroplasty: causes and high incidence of early failure. Orthopedics. 2012;35(7):e1009-e1016.
14. Heneghan C, Langton D, Thompson M. Ongoing problems with metal-on-metal hip implants. BMJ. 2012;344:e1349.
15. Lee RK, Nevelos J, Vigdorchik J, Markel DC. Bearing surfaces for hip arthroplasty—is metal-on-metal a passing fancy? Surg Technol Int. 2012;22:243-249.
16. Voleti PB, Baldwin KD, Lee GC. Metal-on-metal vs conventional total hip arthroplasty: a systematic review and meta-analysis of randomized controlled trials. J Arthroplasty. 2012;27(10):1844-1849.
17. Urban JA, Garvin KL, Boese CK, et al. Ceramic-on-polyethylene bearing surfaces in total hip arthroplasty. Seventeen to twenty-one-year results.
J Bone Joint Surg Am. 2001;83(11):1688-1694.
18. Callaghan JJ, Liu SS. Ceramic on crosslinked polyethylene in total hip replacement: any better than metal on crosslinked polyethylene? Iowa Orthop J. 2009;29:1-4.
19. Barrack RL. Dislocation after total hip arthroplasty: implant design and orientation. J Am Acad Orthop Surg. 2003;11(2):89-99.
20. Krushell RJ, Burke DW, Harris WH. Elevated-rim acetabular components. Effect on range of motion and stability in total hip arthroplasty. J Arthroplasty. 1991;6(suppl):S53-S58.
21. Morrey BF. Instability after total hip arthroplasty. Orthop Clin North Am. 1992;23(2):237-248.
22. Morrey BF. Dislocation. In: Morrey BF, ed. Joint Replacement Arthroplasty. New York, NY: Churchill Livingstone; 1991:851-865.
23. Bartz RL, Nobel PC, Kadakia NR, Tullos HS. The effect of femoral component head size on posterior dislocation of the artificial hip joint. J Bone Joint Surg Am. 2000;82(9):1300-1307.
24. Nicholas RM, Orr JF, Mollan RA, Calderwood JW, Nixon JR, Watson P. Dislocation of total hip replacements. A comparative study of standard, long posterior wall and augmented acetabular components. J Bone Joint Surg Br. 1990;72(3):418-422.
25. McCollum DE, Gray WJ. Dislocation after total hip arthroplasty. Causes and prevention. Clin Orthop. 1990;(261):159-170.
26. Herrlin K, Selvik G, Pettersson H, Kesek P, Onnerfalt R, Ohlin A. Position, orientation and component interaction in dislocation of the total hip prosthesis. Acta Radiol. 1988;29(4):441-444.
27. Cinotti G, Lucioli N, Malagoli A, Calderoli C, Cassese F. Do large femoral heads reduce the risks of impingement in total hip arthroplasty with optimal and non-optimal cup positioning? Int Orthop. 2011;35(3):317-323.
28. Burroughs BR, Rubash HE, Harris WH. Femoral head sizes larger than 32 mm against highly cross-linked polyethylene. Clin Orthop. 2002;(405):150-157.
29. Crowninshield RD, Maloney WJ, Wentz DH, Humphrey SM, Blanchard CR. Biomechanics of large femoral heads: what they do and don‘t do. Clin Orthop. 2004;(429):102-107.
30. Charnley J. Low Friction Arthroplasty of the Hip: Theory and Practice. New York, NY: Springer; 1979.
31. Yamaguchi M, Akisue T, Bauer TW, Hashimoto Y. The spatial location of impingement in total hip arthroplasty. J Arthroplasty. 2000;15(3):305-313.
32. Peters CL, McPherson E, Jackson JD, Erickson JA. Reduction in early dislocation rate with large-diameter femoral heads in primary total hip arthroplasty. J Arthroplasty. 2007;22(6 suppl 2):140-144.
33. Masonis JL, Bourne RB. Surgical approach, abductor function, and total hip arthroplasty dislocation. Clin Orthop. 2002;(405):46-53.
34. Beaule PE, Schmalzried TP, Udomkiat P, Amstutz HC. Jumbo femoral head for the treatment of recurrent dislocation following total hip replacement. J Bone Joint Surg Am. 2002;84(2):256-263.
35. Oral E, Malhi AS, Muratoglu OK. Mechanisms of decrease in fatigue crack propagation resistance in irradiated and melted UHMWPE. Biomaterials. 2006;27(6):917-925.
36. Baker DA, Bellare A, Pruitt L. The effects of degree of crosslinking on the fatigue crack initiation and propagation resistance of orthopedic-grade polyethylene. J Biomed Mater Res A. 2003;66(1):146-154.
37. Charnley J. Total hip replacement by low-friction arthroplasty. Clin Orthop. 1970;(72):7-21.
38. Kabo JM, Gebhard JS, Loren G, Amstutz HC. In vivo wear of polyethylene acetabular components. J Bone Joint Surg Br. 1993;75(2):254-258.
39. Livermore J, Ilstrup D, Morrey B. Effect of femoral head size on wear of the polyethylene acetabular component. J Bone Joint Surg Am. 1990;72(4):518-528.
40. Ma SM, Kabo JM, Amstutz HC. Frictional torque in surface and conventional hip replacement. J Bone Joint Surg Am. 1983;65(3):366-370.
41. Muratoglu OK, Bragdon CR, O‘Connor D, et al. Larger diameter femoral heads used in conjunction with a highly cross-linked ultra-high molecular weight polyethylene: a new concept. J Arthroplasty. 2001;16(8 suppl 1):24-30.
42. Thomas GER, Simpson DJ, Mehmood S, et al. The seven-year wear of highly cross-linked polyethylene in total hip arthroplasty: a double-blind, randomized controlled trial using radiostereometric analysis. J Bone Joint Surg Am. 2011;93(8):716-722.
43. Mutimer J, Devane PA, Adams K, Horne JG. Highly crosslinked polyethylene reduces wear in total hip arthroplasty at 5 years. Clin Orthop. 2010;468(12):3228-3233.
44. Bragdon CR, Doerner M, Martell J, Jarrett B, Palm H, Malchau H. The 2012 John Charnley Award: clinical multicenter studies of the wear performance of highly crosslinked remelted polyethylene in THA. Clin Orthop. 2013;471(2):393-402.
45. Lachiewicz PF, Heckman DS, Soileau ES, Mangla J, Martell JM. Femoral head size and wear of highly cross-linked polyethylene at 5 to 8 years. Clin Orthop. 2009;467(12):3290-3296.
46. Sychterz CJ, Engh CA Jr, Young AM, Hopper RH Jr, Engh CA. Comparison of in vivo wear between polyethylene liners articulating with ceramic and cobalt-chrome femoral heads. J Bone Joint Surg Br. 2000;82(7):948-951.
47. Berry DJ, Barnes CL, Scott RD, Cabanela ME, Poss R. Catastrophic failure of the polyethylene liner of uncemented acetabular components.
J Bone Joint Surg Br. 1994;76(4):575-578.
48. McKellop H, Shen FW, Lu B, Campbell P, Salovey R. Development of an extremely wear-resistant ultra high molecular weight polyethylene for total hip replacements. J Orthop Res. 1999;17(2):157-167.
49. Wang A, Essner A, Polineni VK, Stark C, Dumbleton JH. Lubrication and wear of ultra-high molecular weight polyethylene in total joint replacements. Tribol Int. 1998;31(1-3):17-33.
50. Estok DM 2nd, Burroughs BR, Muratoglu OK, Harris WH. Comparison of hip simulator wear of 2 different highly cross-linked ultra high molecular weight polyethylene acetabular components using both 32- and 38-mm femoral heads. J Arthroplasty. 2007;22(4):581-589.
51. Muratoglu OK, Bragdon CR, O‘Connor DO, et al. Unified wear model for highly crosslinked ultra-high molecular weight polyethylenes (UHMWPE). Biomaterials. 1999;20(16):1463-1470.
52. Harris WH, Muratoglu OK. A review of current cross-linked polyethylenes used in total joint arthroplasty. Clin Orthop. 2005;(430):46-52.
53. Muratoglu OK, Bragdon CR, O‘Connor DO, Jasty M, Harris WH. A novel method of cross-linking ultra-high-molecular-weight polyethylene to improve wear, reduce oxidation, and retain mechanical properties. Recipient of the 1999 HAP Paul Award. J Arthroplasty. 2001;16(2):149-160.
54. Bal BS, Garino J, Ries M, Rahaman MN. A review of ceramic bearing materials in total joint arthroplasty. Hip Int. 2007;17(1):21-30.
55. Traina F, De Fine M, Di Martino A, Faldini C. Fracture of ceramic bearing surfaces following total hip replacement: a systematic review. Biomed Res Int. 2013;2013:157247.
56. Cai YZ, Yan SG. Development of ceramic-on-ceramic implants for total hip arthroplasty. Orthop Surg. 2010;2(3):175-181.
57. Stewart TD, Tipper JL, Insley G, Streicher RM, Ingham E, Fisher J. Long-term wear of ceramic matrix composite materials for hip prostheses under severe swing phase microseparation. J Biomed Mater Res B Appl Biomater. 2003;66(2):567-573.
58. Bragdon CR, Greene ME, Freiberg AA, Harris WH, Malchau H. Radiostereometric analysis comparison of wear of highly cross-linked polyethylene against 36- vs 28-mm femoral heads. J Arthroplasty. 2007;22(6 suppl 2):125-129.
59. Lombardi AV Jr, Skeels MD, Berend KR, Adams JB, Franchi OJ. Do large heads enhance stability and restore native anatomy in primary total hip arthroplasty? Clin Orthop. 2011;469(6):1547-1553.
60. Lachiewicz PF, Soileau ES. Low early and late dislocation rates with 36- and 40-mm heads in patients at high risk for dislocation. Clin Orthop. 2013;471(2):439-443.
61. Cai P, Hu Y, Xie J. Large-diameter Delta ceramic-on-ceramic versus common-sized ceramic-on-polyethylene bearings in THA. Orthopedics. 2012;35(9):e1307-e1313.
62. Park KS, Yoon TR, Hwang SY, Lee KB. Modified minimally invasive two-incision total hip arthroplasty using large diameter femoral head. Indian
J Orthop. 2012;46(1):29-35.
63. Garbuz DS, Masri BA, Duncan CP, et al. The Frank Stinchfield Award: dislocation in revision THA: do large heads (36 and 40 mm) result in reduced dislocation rates in a randomized clinical trial? Clin Orthop. 2012;470(2):351-356.
64. Geller JA, Malchau H, Bragdon C, Greene M, Harris WH, Freiberg AA. Large diameter femoral heads on highly cross-linked polyethylene: minimum 3-year results. Clin Orthop. 2006;(447):53-59.
65. D’Antonio JA, Capello WN, Ramakrishnan R. Second-generation annealed highly cross-linked polyethylene exhibits low wear. Clin Orthop. 2012;470(6):1696-1704.
66. Galvin AL, Jennings LM, Tipper JL, Ingham E, Fisher J. Wear and creep of highly crosslinked polyethylene against cobalt chrome and ceramic femoral heads. Proc Inst Mech Eng H. 2010;224(10):1175-1183.
67. Skeels MD, Berend KR, Lombardi AV Jr. The dislocator, early and late: the role of large heads. Orthopedics. 2009;32(9).
68. Plate JF, Seyler TM, Stroh DA, Issa K, Akbar M, Mont MA. Risk of dislocation using large- vs. small-diameter femoral heads in total hip arthroplasty. BMC Res Notes. 2012;5(1):553.
69. Bouchet R, Mercier N, Saragaglia D. Posterior approach and dislocation rate: a 213 total hip replacements case–control study comparing the dual mobility cup with a conventional 28-mm metal head/polyethylene prosthesis. Orthop Traumatol Surg Res. 2011;97(1):2-7.
70. Ali Khan MA, Brakenbury PH, Reynolds IS. Dislocation following total hip replacement. J Bone Joint Surg Br. 1981;63(2):214-218.
71. Howie DW, Holubowycz OT, Middleton R. Large femoral heads decrease the incidence of dislocation after total hip arthroplasty: a randomized controlled trial. J Bone Joint Surg Am. 2012;94(12):1095-1102.
72. Malkani AL, Ong KL, Lau E, Kurtz SM, Justice BJ, Manley MT. Early- and late-term dislocation risk after primary hip arthroplasty in the Medicare population. J Arthroplasty. 2010;25(6 suppl):21-25.
73. Berry DJ, von Knoch M, Schleck CD, Harmsen WS. Effect of femoral head diameter and operative approach on risk of dislocation after primary total hip arthroplasty. J Bone Joint Surg Am. 2005;87(11):2456-2463.
74. Cho MR, Lee HS, Lee SW, Choi CH, Kim SK, Ko SB. Results after total hip arthroplasty with a large head and bipolar arthroplasty in patients with displaced femoral neck fractures. J Arthroplasty. 2011;26(6):893-896.
75. Conroy JL, Whitehouse SL, Graves SE, Pratt NL, Ryan P, Crawford RW. Risk factors for revision for early dislocation in total hip arthroplasty.
J Arthroplasty. 2008;23(6):867-872.
76. Kung PL, Ries MD. Effect of femoral head size and abductors on dislocation after revision THA. Clin Orthop. 2007;(465):170-174.
77. Williams JT Jr, Ragland PS, Clarke S. Constrained components for the unstable hip following total hip arthroplasty: a literature review. Int Orthop. 2007;31(3):273-277.
78. Zywiel MG, Mustafa LH, Bonutti PM, Mont MA. Are abductor muscle quality and previous revision surgery predictors of constrained liner failure in hip arthroplasty? Int Orthop. 2011;35(6):797-802.
79. Guyen O, Lewallen DG, Cabanela ME. Modes of failure of Osteonics constrained tripolar implants: a retrospective analysis of forty-three failed implants. J Bone Joint Surg Am. 2008;90(7):1553-1560.
80. Banks LN, McElwain JP. An unusual mode of failure of a tripolar constrained acetabular liner: a case report. Arch Orthop Trauma Surg. 2010;130(4):503-505.
81. Robertson WJ, Mattern CJ, Hur J, Su EP, Pellicci PM. Failure mechanisms and closed reduction of a constrained tripolar acetabular liner.
J Arthroplasty. 2009;24(2):322.e5-e11.
82. Aubriot JH, Lesimple P, Leclercq S. Study of Bousquet‘s non-cemented acetabular implant in 100 hybrid total hip prostheses (Charnley type cemented femoral component). Average 5-year follow-up [in French]. Acta Orthop Belg. 1993;59(suppl 1):267-271.
83. Farizon F, de Lavison R, Azoulai JJ, Bousquet G. Results with a cementless alumina-coated cup with dual mobility. A twelve-year follow-up study. Int Orthop. 1998;22(4):219-224.
84. Mertl P, Combes A, Leiber-Wackenheim F, Fessy MH, Girard J, Migaud H. Recurrence of dislocation following total hip arthroplasty revision using dual mobility cups was rare in 180 hips followed over 7 years. HSS J. 2012;8(3):251-256.
85. Langlais FL, Ropars M, Gaucher F, Musset T, Chaix O. Dual mobility cemented cups have low dislocation rates in THA revisions. Clin Orthop. 2008;466(2):389-395.
86. Philippot R, Farizon F, Camilleri JP, et al. Survival of dual mobility socket with a mean 17 years follow-up [in French]. Rev Chir Orthop Reparatrice Appar Mot. 2008;94(1):43-48.
87. Adam P, Philippe R, Ehlinger M, et al. Dual mobility cups hip arthroplasty as a treatment for displaced fracture of the femoral neck in the elderly.
A prospective, systematic, multicenter study with specific focus on postoperative dislocation. Orthop Traumatol Surg Res. 2012;98(3):296-300.
88. Fessy MH. La double mobilité [Dual mobility]. Revue de Chirurgie Orthopédique et Traumatologique. 2010;96(7):891-898.
89. Mont MA, Issa K, Naziri Q, Harwin SF, Delanois RE, Johnson AJ. The use of dual-mobility bearings in difficult hip arthroplasty reconstructive cases. Surg Technol Int. 2011;21:234-240.
90. Sayeed SA, Mont MA, Costa CR, et al. Early outcomes of sequentially cross-linked thin polyethylene liners with large diameter femoral heads in total hip arthroplasty. Bull NYU Hosp Jt Dis. 2011;69(suppl 1):S90-S94.
91. Plate JF, Seyler TM, Stroh DA, Issa K, Akbar M, Mont MA. Risk of dislocation using large- vs. small-diameter femoral heads in total hip arthroplasty. BMC Res Notes. 2012;5(1):553.
92. Sato T, Nakashima Y, Akiyama M, et al. Wear resistant performance of highly cross-linked and annealed ultra-high molecular weight polyethylene against ceramic heads in total hip arthroplasty. J Orthop Res. 2012;30(12):2031-2037.
93. Meftah M, Ebrahimpour PB, He C, Ranawat AS, Ranawat CS. Preliminary clinical and radiographic results of large ceramic heads on highly cross-linked polyethylene. Orthopedics. 2011;34(6):133.
94. Gagala J, Mazurkiewicz T, Dajewski Z. Large diameter femoral heads in primary alumina/alumina and XSPE/alumina total hip arthroplasty.
A follow-up study of 50 hips after average 40 months and review of literature [in Polish]. Chir Narzadow Ruchu Ortop Pol. 2011;76(1):14-20.
1. Dorr LD, Wolf AW, Chandler R, Conaty JP. Classification and treatment of dislocations of total hip arthroplasty. Clin Orthop. 1983;(173):151-158.
2. Dorr LD, Wan Z. Causes of and treatment protocol for instability of total hip replacement. Clin Orthop. 1998;(355):144-151.
3. Turner RS. Postoperative total hip prosthetic femoral head dislocations. Incidence, etiologic factors, and management. Clin Orthop. 1994;(301):196-204.
4. Woo RY, Morrey BF. Dislocations after total hip arthroplasty. J Bone Joint Surg Am. 1982;64(9):1295-1306.
5. Etienne A, Cupic Z, Charnley J. Postoperative dislocation after Charnley low-friction arthroplasty. Clin Orthop. 1978;(132):19-23.
6. Fackler CD, Poss R. Dislocation in total hip arthroplasties. Clin Orthop. 1980;(151):169-178.
7. Joshi A, Lee CM, Markovic L, Vlatis G, Murphy JC. Prognosis of dislocation after total hip arthroplasty. J Arthroplasty. 1998;13(1):17-21.
8. Lindberg HO, Carlsson AS, Gentz CF, Pettersson H. Recurrent and non-recurrent dislocation following total hip arthroplasty. Acta Orthop Scand. 1982;53(6):947-952.
9. Eswaramoorthy V, Moonot P, Kalairajah Y, Biant LC, Field RE. The Metasul metal-on-metal articulation in primary total hip replacement: clinical and radiological results at ten years. J Bone Joint Surg Br. 2008;90(10):1278-1283.
10. Grubl A, Marker M, Brodner W, et al. Long-term follow-up of metal-on-metal total hip replacement. J Orthop Res. 2007;25(7):841-848.
11. Leslie I, Williams S, Brown C, et al. Effect of bearing size on the long-term wear, wear debris, and ion levels of large diameter metal-on-metal hip replacements—an in vitro study. J Biomed Mater Res B Appl Biomater. 2008;87(1):163-172.
12. Verhaar JA. The hard lesson of metal-on-metal hip implants [in Dutch]. Ned Tijdschr Geneeskd. 2012;156(42):A5564.
13. Fabi D, Levine B, Paprosky W, et al. Metal-on-metal total hip arthroplasty: causes and high incidence of early failure. Orthopedics. 2012;35(7):e1009-e1016.
14. Heneghan C, Langton D, Thompson M. Ongoing problems with metal-on-metal hip implants. BMJ. 2012;344:e1349.
15. Lee RK, Nevelos J, Vigdorchik J, Markel DC. Bearing surfaces for hip arthroplasty—is metal-on-metal a passing fancy? Surg Technol Int. 2012;22:243-249.
16. Voleti PB, Baldwin KD, Lee GC. Metal-on-metal vs conventional total hip arthroplasty: a systematic review and meta-analysis of randomized controlled trials. J Arthroplasty. 2012;27(10):1844-1849.
17. Urban JA, Garvin KL, Boese CK, et al. Ceramic-on-polyethylene bearing surfaces in total hip arthroplasty. Seventeen to twenty-one-year results.
J Bone Joint Surg Am. 2001;83(11):1688-1694.
18. Callaghan JJ, Liu SS. Ceramic on crosslinked polyethylene in total hip replacement: any better than metal on crosslinked polyethylene? Iowa Orthop J. 2009;29:1-4.
19. Barrack RL. Dislocation after total hip arthroplasty: implant design and orientation. J Am Acad Orthop Surg. 2003;11(2):89-99.
20. Krushell RJ, Burke DW, Harris WH. Elevated-rim acetabular components. Effect on range of motion and stability in total hip arthroplasty. J Arthroplasty. 1991;6(suppl):S53-S58.
21. Morrey BF. Instability after total hip arthroplasty. Orthop Clin North Am. 1992;23(2):237-248.
22. Morrey BF. Dislocation. In: Morrey BF, ed. Joint Replacement Arthroplasty. New York, NY: Churchill Livingstone; 1991:851-865.
23. Bartz RL, Nobel PC, Kadakia NR, Tullos HS. The effect of femoral component head size on posterior dislocation of the artificial hip joint. J Bone Joint Surg Am. 2000;82(9):1300-1307.
24. Nicholas RM, Orr JF, Mollan RA, Calderwood JW, Nixon JR, Watson P. Dislocation of total hip replacements. A comparative study of standard, long posterior wall and augmented acetabular components. J Bone Joint Surg Br. 1990;72(3):418-422.
25. McCollum DE, Gray WJ. Dislocation after total hip arthroplasty. Causes and prevention. Clin Orthop. 1990;(261):159-170.
26. Herrlin K, Selvik G, Pettersson H, Kesek P, Onnerfalt R, Ohlin A. Position, orientation and component interaction in dislocation of the total hip prosthesis. Acta Radiol. 1988;29(4):441-444.
27. Cinotti G, Lucioli N, Malagoli A, Calderoli C, Cassese F. Do large femoral heads reduce the risks of impingement in total hip arthroplasty with optimal and non-optimal cup positioning? Int Orthop. 2011;35(3):317-323.
28. Burroughs BR, Rubash HE, Harris WH. Femoral head sizes larger than 32 mm against highly cross-linked polyethylene. Clin Orthop. 2002;(405):150-157.
29. Crowninshield RD, Maloney WJ, Wentz DH, Humphrey SM, Blanchard CR. Biomechanics of large femoral heads: what they do and don‘t do. Clin Orthop. 2004;(429):102-107.
30. Charnley J. Low Friction Arthroplasty of the Hip: Theory and Practice. New York, NY: Springer; 1979.
31. Yamaguchi M, Akisue T, Bauer TW, Hashimoto Y. The spatial location of impingement in total hip arthroplasty. J Arthroplasty. 2000;15(3):305-313.
32. Peters CL, McPherson E, Jackson JD, Erickson JA. Reduction in early dislocation rate with large-diameter femoral heads in primary total hip arthroplasty. J Arthroplasty. 2007;22(6 suppl 2):140-144.
33. Masonis JL, Bourne RB. Surgical approach, abductor function, and total hip arthroplasty dislocation. Clin Orthop. 2002;(405):46-53.
34. Beaule PE, Schmalzried TP, Udomkiat P, Amstutz HC. Jumbo femoral head for the treatment of recurrent dislocation following total hip replacement. J Bone Joint Surg Am. 2002;84(2):256-263.
35. Oral E, Malhi AS, Muratoglu OK. Mechanisms of decrease in fatigue crack propagation resistance in irradiated and melted UHMWPE. Biomaterials. 2006;27(6):917-925.
36. Baker DA, Bellare A, Pruitt L. The effects of degree of crosslinking on the fatigue crack initiation and propagation resistance of orthopedic-grade polyethylene. J Biomed Mater Res A. 2003;66(1):146-154.
37. Charnley J. Total hip replacement by low-friction arthroplasty. Clin Orthop. 1970;(72):7-21.
38. Kabo JM, Gebhard JS, Loren G, Amstutz HC. In vivo wear of polyethylene acetabular components. J Bone Joint Surg Br. 1993;75(2):254-258.
39. Livermore J, Ilstrup D, Morrey B. Effect of femoral head size on wear of the polyethylene acetabular component. J Bone Joint Surg Am. 1990;72(4):518-528.
40. Ma SM, Kabo JM, Amstutz HC. Frictional torque in surface and conventional hip replacement. J Bone Joint Surg Am. 1983;65(3):366-370.
41. Muratoglu OK, Bragdon CR, O‘Connor D, et al. Larger diameter femoral heads used in conjunction with a highly cross-linked ultra-high molecular weight polyethylene: a new concept. J Arthroplasty. 2001;16(8 suppl 1):24-30.
42. Thomas GER, Simpson DJ, Mehmood S, et al. The seven-year wear of highly cross-linked polyethylene in total hip arthroplasty: a double-blind, randomized controlled trial using radiostereometric analysis. J Bone Joint Surg Am. 2011;93(8):716-722.
43. Mutimer J, Devane PA, Adams K, Horne JG. Highly crosslinked polyethylene reduces wear in total hip arthroplasty at 5 years. Clin Orthop. 2010;468(12):3228-3233.
44. Bragdon CR, Doerner M, Martell J, Jarrett B, Palm H, Malchau H. The 2012 John Charnley Award: clinical multicenter studies of the wear performance of highly crosslinked remelted polyethylene in THA. Clin Orthop. 2013;471(2):393-402.
45. Lachiewicz PF, Heckman DS, Soileau ES, Mangla J, Martell JM. Femoral head size and wear of highly cross-linked polyethylene at 5 to 8 years. Clin Orthop. 2009;467(12):3290-3296.
46. Sychterz CJ, Engh CA Jr, Young AM, Hopper RH Jr, Engh CA. Comparison of in vivo wear between polyethylene liners articulating with ceramic and cobalt-chrome femoral heads. J Bone Joint Surg Br. 2000;82(7):948-951.
47. Berry DJ, Barnes CL, Scott RD, Cabanela ME, Poss R. Catastrophic failure of the polyethylene liner of uncemented acetabular components.
J Bone Joint Surg Br. 1994;76(4):575-578.
48. McKellop H, Shen FW, Lu B, Campbell P, Salovey R. Development of an extremely wear-resistant ultra high molecular weight polyethylene for total hip replacements. J Orthop Res. 1999;17(2):157-167.
49. Wang A, Essner A, Polineni VK, Stark C, Dumbleton JH. Lubrication and wear of ultra-high molecular weight polyethylene in total joint replacements. Tribol Int. 1998;31(1-3):17-33.
50. Estok DM 2nd, Burroughs BR, Muratoglu OK, Harris WH. Comparison of hip simulator wear of 2 different highly cross-linked ultra high molecular weight polyethylene acetabular components using both 32- and 38-mm femoral heads. J Arthroplasty. 2007;22(4):581-589.
51. Muratoglu OK, Bragdon CR, O‘Connor DO, et al. Unified wear model for highly crosslinked ultra-high molecular weight polyethylenes (UHMWPE). Biomaterials. 1999;20(16):1463-1470.
52. Harris WH, Muratoglu OK. A review of current cross-linked polyethylenes used in total joint arthroplasty. Clin Orthop. 2005;(430):46-52.
53. Muratoglu OK, Bragdon CR, O‘Connor DO, Jasty M, Harris WH. A novel method of cross-linking ultra-high-molecular-weight polyethylene to improve wear, reduce oxidation, and retain mechanical properties. Recipient of the 1999 HAP Paul Award. J Arthroplasty. 2001;16(2):149-160.
54. Bal BS, Garino J, Ries M, Rahaman MN. A review of ceramic bearing materials in total joint arthroplasty. Hip Int. 2007;17(1):21-30.
55. Traina F, De Fine M, Di Martino A, Faldini C. Fracture of ceramic bearing surfaces following total hip replacement: a systematic review. Biomed Res Int. 2013;2013:157247.
56. Cai YZ, Yan SG. Development of ceramic-on-ceramic implants for total hip arthroplasty. Orthop Surg. 2010;2(3):175-181.
57. Stewart TD, Tipper JL, Insley G, Streicher RM, Ingham E, Fisher J. Long-term wear of ceramic matrix composite materials for hip prostheses under severe swing phase microseparation. J Biomed Mater Res B Appl Biomater. 2003;66(2):567-573.
58. Bragdon CR, Greene ME, Freiberg AA, Harris WH, Malchau H. Radiostereometric analysis comparison of wear of highly cross-linked polyethylene against 36- vs 28-mm femoral heads. J Arthroplasty. 2007;22(6 suppl 2):125-129.
59. Lombardi AV Jr, Skeels MD, Berend KR, Adams JB, Franchi OJ. Do large heads enhance stability and restore native anatomy in primary total hip arthroplasty? Clin Orthop. 2011;469(6):1547-1553.
60. Lachiewicz PF, Soileau ES. Low early and late dislocation rates with 36- and 40-mm heads in patients at high risk for dislocation. Clin Orthop. 2013;471(2):439-443.
61. Cai P, Hu Y, Xie J. Large-diameter Delta ceramic-on-ceramic versus common-sized ceramic-on-polyethylene bearings in THA. Orthopedics. 2012;35(9):e1307-e1313.
62. Park KS, Yoon TR, Hwang SY, Lee KB. Modified minimally invasive two-incision total hip arthroplasty using large diameter femoral head. Indian
J Orthop. 2012;46(1):29-35.
63. Garbuz DS, Masri BA, Duncan CP, et al. The Frank Stinchfield Award: dislocation in revision THA: do large heads (36 and 40 mm) result in reduced dislocation rates in a randomized clinical trial? Clin Orthop. 2012;470(2):351-356.
64. Geller JA, Malchau H, Bragdon C, Greene M, Harris WH, Freiberg AA. Large diameter femoral heads on highly cross-linked polyethylene: minimum 3-year results. Clin Orthop. 2006;(447):53-59.
65. D’Antonio JA, Capello WN, Ramakrishnan R. Second-generation annealed highly cross-linked polyethylene exhibits low wear. Clin Orthop. 2012;470(6):1696-1704.
66. Galvin AL, Jennings LM, Tipper JL, Ingham E, Fisher J. Wear and creep of highly crosslinked polyethylene against cobalt chrome and ceramic femoral heads. Proc Inst Mech Eng H. 2010;224(10):1175-1183.
67. Skeels MD, Berend KR, Lombardi AV Jr. The dislocator, early and late: the role of large heads. Orthopedics. 2009;32(9).
68. Plate JF, Seyler TM, Stroh DA, Issa K, Akbar M, Mont MA. Risk of dislocation using large- vs. small-diameter femoral heads in total hip arthroplasty. BMC Res Notes. 2012;5(1):553.
69. Bouchet R, Mercier N, Saragaglia D. Posterior approach and dislocation rate: a 213 total hip replacements case–control study comparing the dual mobility cup with a conventional 28-mm metal head/polyethylene prosthesis. Orthop Traumatol Surg Res. 2011;97(1):2-7.
70. Ali Khan MA, Brakenbury PH, Reynolds IS. Dislocation following total hip replacement. J Bone Joint Surg Br. 1981;63(2):214-218.
71. Howie DW, Holubowycz OT, Middleton R. Large femoral heads decrease the incidence of dislocation after total hip arthroplasty: a randomized controlled trial. J Bone Joint Surg Am. 2012;94(12):1095-1102.
72. Malkani AL, Ong KL, Lau E, Kurtz SM, Justice BJ, Manley MT. Early- and late-term dislocation risk after primary hip arthroplasty in the Medicare population. J Arthroplasty. 2010;25(6 suppl):21-25.
73. Berry DJ, von Knoch M, Schleck CD, Harmsen WS. Effect of femoral head diameter and operative approach on risk of dislocation after primary total hip arthroplasty. J Bone Joint Surg Am. 2005;87(11):2456-2463.
74. Cho MR, Lee HS, Lee SW, Choi CH, Kim SK, Ko SB. Results after total hip arthroplasty with a large head and bipolar arthroplasty in patients with displaced femoral neck fractures. J Arthroplasty. 2011;26(6):893-896.
75. Conroy JL, Whitehouse SL, Graves SE, Pratt NL, Ryan P, Crawford RW. Risk factors for revision for early dislocation in total hip arthroplasty.
J Arthroplasty. 2008;23(6):867-872.
76. Kung PL, Ries MD. Effect of femoral head size and abductors on dislocation after revision THA. Clin Orthop. 2007;(465):170-174.
77. Williams JT Jr, Ragland PS, Clarke S. Constrained components for the unstable hip following total hip arthroplasty: a literature review. Int Orthop. 2007;31(3):273-277.
78. Zywiel MG, Mustafa LH, Bonutti PM, Mont MA. Are abductor muscle quality and previous revision surgery predictors of constrained liner failure in hip arthroplasty? Int Orthop. 2011;35(6):797-802.
79. Guyen O, Lewallen DG, Cabanela ME. Modes of failure of Osteonics constrained tripolar implants: a retrospective analysis of forty-three failed implants. J Bone Joint Surg Am. 2008;90(7):1553-1560.
80. Banks LN, McElwain JP. An unusual mode of failure of a tripolar constrained acetabular liner: a case report. Arch Orthop Trauma Surg. 2010;130(4):503-505.
81. Robertson WJ, Mattern CJ, Hur J, Su EP, Pellicci PM. Failure mechanisms and closed reduction of a constrained tripolar acetabular liner.
J Arthroplasty. 2009;24(2):322.e5-e11.
82. Aubriot JH, Lesimple P, Leclercq S. Study of Bousquet‘s non-cemented acetabular implant in 100 hybrid total hip prostheses (Charnley type cemented femoral component). Average 5-year follow-up [in French]. Acta Orthop Belg. 1993;59(suppl 1):267-271.
83. Farizon F, de Lavison R, Azoulai JJ, Bousquet G. Results with a cementless alumina-coated cup with dual mobility. A twelve-year follow-up study. Int Orthop. 1998;22(4):219-224.
84. Mertl P, Combes A, Leiber-Wackenheim F, Fessy MH, Girard J, Migaud H. Recurrence of dislocation following total hip arthroplasty revision using dual mobility cups was rare in 180 hips followed over 7 years. HSS J. 2012;8(3):251-256.
85. Langlais FL, Ropars M, Gaucher F, Musset T, Chaix O. Dual mobility cemented cups have low dislocation rates in THA revisions. Clin Orthop. 2008;466(2):389-395.
86. Philippot R, Farizon F, Camilleri JP, et al. Survival of dual mobility socket with a mean 17 years follow-up [in French]. Rev Chir Orthop Reparatrice Appar Mot. 2008;94(1):43-48.
87. Adam P, Philippe R, Ehlinger M, et al. Dual mobility cups hip arthroplasty as a treatment for displaced fracture of the femoral neck in the elderly.
A prospective, systematic, multicenter study with specific focus on postoperative dislocation. Orthop Traumatol Surg Res. 2012;98(3):296-300.
88. Fessy MH. La double mobilité [Dual mobility]. Revue de Chirurgie Orthopédique et Traumatologique. 2010;96(7):891-898.
89. Mont MA, Issa K, Naziri Q, Harwin SF, Delanois RE, Johnson AJ. The use of dual-mobility bearings in difficult hip arthroplasty reconstructive cases. Surg Technol Int. 2011;21:234-240.
90. Sayeed SA, Mont MA, Costa CR, et al. Early outcomes of sequentially cross-linked thin polyethylene liners with large diameter femoral heads in total hip arthroplasty. Bull NYU Hosp Jt Dis. 2011;69(suppl 1):S90-S94.
91. Plate JF, Seyler TM, Stroh DA, Issa K, Akbar M, Mont MA. Risk of dislocation using large- vs. small-diameter femoral heads in total hip arthroplasty. BMC Res Notes. 2012;5(1):553.
92. Sato T, Nakashima Y, Akiyama M, et al. Wear resistant performance of highly cross-linked and annealed ultra-high molecular weight polyethylene against ceramic heads in total hip arthroplasty. J Orthop Res. 2012;30(12):2031-2037.
93. Meftah M, Ebrahimpour PB, He C, Ranawat AS, Ranawat CS. Preliminary clinical and radiographic results of large ceramic heads on highly cross-linked polyethylene. Orthopedics. 2011;34(6):133.
94. Gagala J, Mazurkiewicz T, Dajewski Z. Large diameter femoral heads in primary alumina/alumina and XSPE/alumina total hip arthroplasty.
A follow-up study of 50 hips after average 40 months and review of literature [in Polish]. Chir Narzadow Ruchu Ortop Pol. 2011;76(1):14-20.
