User login
Alternative Bearings in Total Knee Arthroplasty
UPDATE: INFECTIOUS DISEASE
- 10 practical, evidence-based recommendations for perioperative antibiotic prophylaxis
Meghan O. Schimpf (June 2012) - Gaps in Chlamydia testing threaten reproductive health, CDC warns
Janelle Yates, Senior Editor (Web exclusive, May 2012)
Dr. Duff reports no financial relationships relevant to this article.
In this Update, I’ve highlighted four interesting articles about infectious disease management in obstetric and gyn practice that appeared in the medical literature over the past 12 months:
- One describes a study that reminds physicians of the importance of an unusual manifestation of gonococcal infection
- A second article demonstrates the importance of making a change in the prophylactic antibiotic regimen provided to morbidly obese patients who are having a cesarean delivery
- A third describes an exciting development in the treatment of chronic hepatitis C virus infection
- The final article makes interesting observations about the proper duration of treatment for patients who have chorioamnionitis.
N gonorrhoeae causes illness beyond the urogenital tract
Bleich AT, Sheffield JS, Wendel GD, Sigman A, Cunningham FG. Disseminated gonococcal infection in women. Obstet Gynecol. 2012;119(3):597–602.
This article describes a retrospective review of 112 women who were admitted to Parkland Memorial Hospital in Dallas, Texas, from January 1975 through December 2008 and given a diagnosis of disseminated infection with Neisseria gonorrhoeae. Eighty (71%) of these women were not pregnant and were cared for on the internal medicine service; 32 (29%) were pregnant and were treated by faculty members and residents on the ObGyn service.
Over the course of the study, the frequency of disseminated gonococcal infection decreased significantly. Among pregnant women, the rate of infection was 11 for every 100,000 deliveries before 1980 and, after 1985, five for every 100,000 deliveries.
The most common clinical manifestation of disseminated gonococcal infection was arthritis. The most commonly affected joints were the knee, wrist, elbow, and ankle.
Other common clinical manifestations included dermatitis, fever, chills, and a purulent cervical discharge. Notably, the frequency of a purulent joint effusion was 50% in pregnant women and 70% in nonpregnant women—reflecting the fact that the duration of symptoms was approximately 3 days shorter in pregnant women than in nonpregnant women. Otherwise, the clinical presentation in pregnant women did not differ significantly from that of nonpregnant women.
In addition, the clinical course and the response to intravenous (IV) antibiotic therapy did not differ significantly between pregnant and nonpregnant women.
The authors were unable to document that disseminated gonococcal infection had any deleterious effect on the outcome of pregnancy among the patients studied. Although four of the 32 women delivered preterm, in only one instance was delivery related temporally to the disseminated gonococcal infection.
Commentary
Because of their experience treating women who have gonorrhea, I would say that most ObGyns think of N gonorrhoeae as causing localized infection in the lower genital tract (urethritis, endocervicitis, inflammatory proctitis) or upper genital tract (pelvic inflammatory disease). We should recognize, however, that gonorrhea also can cause prominent extra-pelvic findings, such as severe pharyngitis (in patients who practice orogenital intercourse) and perihepatitis (Fitz-Hugh-Curtis syndrome).
In addition, always bear in mind that, in rare instances, gonorrhea can become disseminated, causing quite serious illness. The most common extra-pelvic manifestation of disseminated gonococcal infection is arthritis. As noted in this study of a series of patients, the arthritis is usually polyarticular and affects medium or small joints.
The second most common manifestation of disseminated gonococcal infection is dermatitis. Characteristic lesions are raised, red or purple papules. These lesions are not a simple vasculitis; rather, they contain a high concentration of microorganisms.
Other possible manifestations of disseminated infection include pericarditis, endocarditis, and meningitis.
The diagnosis of disseminated gonococcal infection is usually made by clinical examination and culture of specimens from the genital tract, blood, or joint effusion.
Disseminated gonococcal infection usually responds promptly to intravenous antibiotic therapy.
Recommended therapy is ceftriaxone:
• 25 to 50 mg/kg/d IV for 7 days
or
• a single, daily, 25 to 50 mg/kg intramuscular dose, also for 7 days.
Continue therapy for 10 to 14 days if the patient has meningitis.
An alternative regimen is cefotaxime:
• 25 mg/kg/d IV for 7 days
or
• 25 mg/kg IM every 12 hours, also for 7 days.
Extend treatment for 10 to 14 days if meningitis is present.1
Obesity curtails effectiveness of antibiotic prophylaxis in cesarean delivery
Pevzner L, Swank M, Krepel C, Wing DA, Chan K, Edmiston CE Jr. Effects of maternal obesity on tissue concentrations of prophylactic cefazolin during cesarean delivery. Obstet Gynecol. 2011;117(4):877–882.
In this prospective study of the influence of an obese habitus on antibiotic prophylaxis during cesarean delivery, researchers divided 29 patients who were scheduled for cesarean into three groups, by body mass index (BMI):
- lean (BMI, <30; n = 10)
- obese (30–39.9; n = 10)
- extremely obese (>40; n = 9).
All patients were given a 2-g dose of IV cefazolin 30 to 60 minutes before surgery.
During delivery, the team took two specimens of adipose tissue: one immediately after the skin incision and one later, after fascia was closed. They also obtained a specimen of myometrial tissue after delivery and a blood specimen after surgery was completed.
The concentration of cefazolin was then measured in adipose and myometrial tissue and in serum.
Findings. The researchers demonstrated that the mean concentration of cefazolin in the initial specimen of adipose tissue was significantly higher in lean patients than in obese and extremely obese patients. All 10 women who had a BMI less than 30 had a serum cefazolin concentration greater than 4 μg/g—the theoretical break-point for defining resistance to cefazolin. The initial adipose tissue specimen from two of the 10 obese patients and three of the nine extremely obese patients showed cefazolin concentrations less than 4 μg/g.
Of particular interest, two women—both of whom had a BMI greater than 40—developed a wound infection that required antibiotic therapy. Their initial and subsequent adipose tissue concentrations of cefazolin were less than the 4 μg/g break-point for resistance.
The concentration of cefazolin in the patients’ myometrial and serum specimens demonstrated a pattern similar to what the researchers observed in adipose tissue, but these results were not statistically significant across BMI groups. In fact, the cefazolin concentration in all groups’ myometrial and serum specimens exceeded the minimum inhibitory concentration for most potential pathogens in the setting of cesarean delivery.
Commentary
Clearly, prophylactic antibiotics are indicated for all women who are having a cesarean delivery. Antibiotics have their greatest impact when administered before the surgical incision is made; to exert their full protective effect against endometritis and wound infection, however, antibiotics should reach a recognized therapeutic concentration—not only in serum and myometrium but in the subcutaneous tissue.
The customary dosage of cefazolin for cesarean delivery prophylaxis has been 1 g. This study demonstrated that, although a 2-g dose of cefazolin reached a therapeutic concentration in myometrial tissue and serum, it did not consistently do so in the adipose tissue of obese and extremely obese patients.
Pending further investigation, I strongly recommend that all women who have a BMI greater than 30 receive a 2-g dose of cefazolin 30 to 60 minutes before cesarean delivery. Future research is needed to determine whether an even higher dosage is necessary to achieve a therapeutic concentration in the subcutaneous tissue of morbidly obese patients.
New therapies promise a better outcome in hepatitis C
Jacobson IM, McHutchison JG, Dusheiko G, et al; ADVANCE Study Team. Telaprevir for previously untreated hepatitis C virus infection. N Engl J Med. 2011;364(25):2405–2416.
The authors conducted an international Phase-3, randomized, double-blind, placebo-controlled trial of two different treatment modalities for chronic hepatitis C virus (HCV) infection. The authors assigned 1,088 patients who had HCV genotype-1 infection and who had not received prior therapy to one of three treatment groups:
- telaprevir (Incivek, Vertex Pharmaceuticals), an HCV genotype-1 protease inhibitor, combined with peginterferon alfa-2a (Pegasys, Genetech) plus ribavirin (Copegus, Genetech; Rebetol, Merck; etc.) for 12 weeks; patients then were given peginterferon alfa-2a plus ribavirin only for 12 additional weeks if HCV RNA was undetectable at weeks 4 and 12 or peginterferon alfa-2a plus ribavirin only for 36 weeks if HCV RNA was detectable at either time point (Group 1)
- telaprevir with peginterferon alfa-2a plus ribavirin for 8 weeks, then placebo with peginterferon alfa-2a plus ribavirin for 4 weeks, followed by 12 to 36 weeks of peginterferon alfa-2a plus ribavirin using the HCV RNA criteria applied to Group 1 (Group 2)
- placebo with peginterferon alfa-2a plus ribavirin for 12 weeks, followed by 36 weeks of peginterferon alfa-2a plus ribavirin (Group 3).
The primary endpoint of the trial was the percentage of patients who had undetectable plasma HCV RNA at 24 weeks after the last planned dose of the study drugs. The investigators considered that this endpoint represented a sustained virologic response.
Findings. Seventy-five percent of patients in Group 1 and 69% of those in Group 2 had a sustained virologic response. By comparison, only 44% of patients in Group 3 had a sustained response. The differences in outcome between Group 1 and Group 3, and between Group 2 and Group 3, were highly significant (P<.001). Virologic failure was more common among patients who had HCV genotype-1a infection than among those who had HCV genotype-1b infection.
The most common side effects noted by patients who received telaprevir were gastrointestinal irritation, rash, and anemia. Ten percent of patients in the telaprevir group discontinued therapy, compared with 7% in the peginterferon-ribavirin-alone group.
Commentary
Worldwide, approximately 170 million people have chronic hepatitis C, which is the most common indication for liver transplantation. Until recently, the principal treatments for hepatitis C were pegylated interferon alfa with ribavirin and without ribavirin; the response rate with these regimens was in the range of 55%. This study shows that adding telaprevir to regimens for HCV infection significantly improves prospects for long-term resolution of infection.
In some obstetric and gynecologic populations, HCV is more common than hepatitis B virus. Risk factors for hepatitis C include hepatitis B, intravenous drug abuse, and human immunodeficiency virus infection. HCV-infected women pose a risk to their sex partners; infected pregnant women can transmit the virus to their baby.
Unlike hepatitis A and hepatitis B, immunoprophylaxis is not available for hepatitis C. That reality is what makes the study by Jacobsen and colleagues so compelling: They have clearly demonstrated that multi-agent antiviral therapy might be able to truly cure this infection.
The lesson here for ObGyns? Screen at-risk patients and then refer the hepatitis C-seropositive ones to a specialist in gastroenterology, who can determine candidacy for one of the new treatment regimens.
Clearly, the prognosis for people who have hepatitis C is much better today than it was 20 years ago.
For how long should chorioamnionitis be treated?
Black LP, Hinson L, Duff P. Limited course of antibiotic treatment for chorioamnionitis. Obstet Gynecol. 2012;119(6):1102-1105.
The authors conducted a retrospective review of 423 women who had been treated for chorioamnionitis at the University of Florida from 2005 to 2009.
Patients had been given IV ampicillin (2 g every 6 h) plus IV gentamicin (1.5 mg/kg every 8 h) as soon as the diagnosis of chorioamnionitis was established; postpartum, they were given only the one next scheduled dose of each antibiotic. Patients who had a cesarean received either metronidazole (500 mg) or clindamycin (900 mg) immediately after cord clamping to enhance coverage of anaerobic organisms.
The primary outcome was treatment failure, defined as persistent fever requiring continued antibiotics, surgical intervention, or administration of heparin for septic pelvic-vein thrombophlebitis.
Findings. Here is a breakdown of what the investigators found regarding the 282 women who delivered vaginally and the 141 who underwent cesarean delivery:
- Overall, 399 of the patients (94%; 95% confidence interval [CI], 92% and 96%) were treated successfully; 24 (6%; 95% CI, 3.7% and 8.3%) failed short-course treatment
- Of the 282 patients who delivered vaginally, 279 (99%; 95% CI, 98% and 100%) were cured with short-term therapy
- Of the 141 who delivered by cesarean, 120 (85%; 95% CI, 79% and 91%) were cured (P<.001).
- Seventeen of the total treatment failures had endometritis and responded quickly to continuation of antibiotics. Of the 17 patients with endometritis, 14 had a cesarean delivery.
- Seven patients had more serious complications: four, wound infection; three, septic pelvic-vein thrombophlebitis. All serious complications occurred after cesarean delivery.
- Of the four patients who had a wound infection, three had labor induced by misoprostol; their BMI was 44.8, 31.1, and 48.5, respectively. The fourth had a cesarean delivery at 29 weeks for preterm premature rupture of membranes (PPROM), chorioamnionitis, and malpresentation.
- Of the three patients who had septic pelvic-vein thrombophlebitis, two had labor induced by misoprostol. One had a BMI of 29.2; the other, 31.1. The third patient was delivered secondary to PPROM; her BMI was 40.3.
In addition, of the 21 treatment failures in the cesarean delivery group, 6 had prolonged rupture of membranes (ROM) and 10 had a BMI greater than 30. Six patients had both prolonged ROM and were obese or morbidly obese.
Of the 120 women who had a cesarean delivery and were treated successfully, 3 had prolonged ROM and 39 had a BMI greater than 30. None had both prolonged ROM and a BMI greater than 30.
Last, the difference between treatment failures and treatment successes in regard to the frequency of prolonged ROM or a BMI greater than 30 was highly significant (P<.01).
Commentary
In most published reports of patients who have chorioamnionitis, antibiotic treatment continues until the patient is afebrile and asymptomatic for 24 to 48 hours. This treatment approach has been based largely on expert opinion, however, not on Level-1 or Level-2 evidence.
In 2003, Edwards and Duff published a study of chorioamnionitis antibiotic regimens that compared single-dose postpartum treatment to extended treatment.2 This randomized controlled trial demonstrated that there was no statistically significant difference between patients who had only a single dose of postpartum antibiotics and those who received an extended course of medication (i.e., who were treated until they had been afebrile and asymptomatic for a minimum of 24 hours) in regard to adverse outcomes (2.9% and 4.3%, respectively). The study discussed here extends and refines the observations made in the 2003 Edwards and Duff randomized controlled trial.
The new study shows that a limited course of antibiotics was, overall, effective in treating 94% of patients with chorioamnionitis (95% CI, 92% and 96%). Only 1% of patients who delivered vaginally failed therapy, compared with 15% of patients who delivered by cesarean (P<.001). In the cesarean group, women who failed therapy were likely to 1) be obese or 2) have a relatively long duration of labor or ruptured membranes, or both. These patients may have benefitted from a more extended course of antibiotic therapy.
Based on this investigation, I strongly recommend a limited course of antibiotic therapy (ampicillin plus gentamicin) for women with chorioamnionitis who deliver vaginally. Patients who have had a cesarean delivery—particularly those who are obese or have had an extended duration of labor, or both—should be treated with antibiotics until they have been afebrile and asymptomatic for 24 hours.
We want to hear from you! Tell us what you think.
1. Workowski KA, Berman S. Centers for Disease Control and Prevention (CDC). Sexually transmitted diseases treatment guidelines, 2010. MMWR Recomm Rep. 2010;59(RR-12):1-110.
2. Edwards RK, Duff P. Single dose postpartum therapy for women with chorioamnionitis. Obstet Gynecol. 2003;102(5 Pt 1):957-961.

Patrick Duff, MD
Dr. Duff is Professor, Division of Maternal Fetal Medicine, Department of Obstetrics and Gynecology, at the University of Florida College of Medicine, Gainesville.
Patrick Duff, MD
Dr. Duff is Professor, Division of Maternal Fetal Medicine, Department of Obstetrics and Gynecology, at the University of Florida College of Medicine, Gainesville.
Patrick Duff, MD
Dr. Duff is Professor, Division of Maternal Fetal Medicine, Department of Obstetrics and Gynecology, at the University of Florida College of Medicine, Gainesville.
- 10 practical, evidence-based recommendations for perioperative antibiotic prophylaxis
Meghan O. Schimpf (June 2012) - Gaps in Chlamydia testing threaten reproductive health, CDC warns
Janelle Yates, Senior Editor (Web exclusive, May 2012)
Dr. Duff reports no financial relationships relevant to this article.
In this Update, I’ve highlighted four interesting articles about infectious disease management in obstetric and gyn practice that appeared in the medical literature over the past 12 months:
- One describes a study that reminds physicians of the importance of an unusual manifestation of gonococcal infection
- A second article demonstrates the importance of making a change in the prophylactic antibiotic regimen provided to morbidly obese patients who are having a cesarean delivery
- A third describes an exciting development in the treatment of chronic hepatitis C virus infection
- The final article makes interesting observations about the proper duration of treatment for patients who have chorioamnionitis.
N gonorrhoeae causes illness beyond the urogenital tract
Bleich AT, Sheffield JS, Wendel GD, Sigman A, Cunningham FG. Disseminated gonococcal infection in women. Obstet Gynecol. 2012;119(3):597–602.
This article describes a retrospective review of 112 women who were admitted to Parkland Memorial Hospital in Dallas, Texas, from January 1975 through December 2008 and given a diagnosis of disseminated infection with Neisseria gonorrhoeae. Eighty (71%) of these women were not pregnant and were cared for on the internal medicine service; 32 (29%) were pregnant and were treated by faculty members and residents on the ObGyn service.
Over the course of the study, the frequency of disseminated gonococcal infection decreased significantly. Among pregnant women, the rate of infection was 11 for every 100,000 deliveries before 1980 and, after 1985, five for every 100,000 deliveries.
The most common clinical manifestation of disseminated gonococcal infection was arthritis. The most commonly affected joints were the knee, wrist, elbow, and ankle.
Other common clinical manifestations included dermatitis, fever, chills, and a purulent cervical discharge. Notably, the frequency of a purulent joint effusion was 50% in pregnant women and 70% in nonpregnant women—reflecting the fact that the duration of symptoms was approximately 3 days shorter in pregnant women than in nonpregnant women. Otherwise, the clinical presentation in pregnant women did not differ significantly from that of nonpregnant women.
In addition, the clinical course and the response to intravenous (IV) antibiotic therapy did not differ significantly between pregnant and nonpregnant women.
The authors were unable to document that disseminated gonococcal infection had any deleterious effect on the outcome of pregnancy among the patients studied. Although four of the 32 women delivered preterm, in only one instance was delivery related temporally to the disseminated gonococcal infection.
Commentary
Because of their experience treating women who have gonorrhea, I would say that most ObGyns think of N gonorrhoeae as causing localized infection in the lower genital tract (urethritis, endocervicitis, inflammatory proctitis) or upper genital tract (pelvic inflammatory disease). We should recognize, however, that gonorrhea also can cause prominent extra-pelvic findings, such as severe pharyngitis (in patients who practice orogenital intercourse) and perihepatitis (Fitz-Hugh-Curtis syndrome).
In addition, always bear in mind that, in rare instances, gonorrhea can become disseminated, causing quite serious illness. The most common extra-pelvic manifestation of disseminated gonococcal infection is arthritis. As noted in this study of a series of patients, the arthritis is usually polyarticular and affects medium or small joints.
The second most common manifestation of disseminated gonococcal infection is dermatitis. Characteristic lesions are raised, red or purple papules. These lesions are not a simple vasculitis; rather, they contain a high concentration of microorganisms.
Other possible manifestations of disseminated infection include pericarditis, endocarditis, and meningitis.
The diagnosis of disseminated gonococcal infection is usually made by clinical examination and culture of specimens from the genital tract, blood, or joint effusion.
Disseminated gonococcal infection usually responds promptly to intravenous antibiotic therapy.
Recommended therapy is ceftriaxone:
• 25 to 50 mg/kg/d IV for 7 days
or
• a single, daily, 25 to 50 mg/kg intramuscular dose, also for 7 days.
Continue therapy for 10 to 14 days if the patient has meningitis.
An alternative regimen is cefotaxime:
• 25 mg/kg/d IV for 7 days
or
• 25 mg/kg IM every 12 hours, also for 7 days.
Extend treatment for 10 to 14 days if meningitis is present.1
Obesity curtails effectiveness of antibiotic prophylaxis in cesarean delivery
Pevzner L, Swank M, Krepel C, Wing DA, Chan K, Edmiston CE Jr. Effects of maternal obesity on tissue concentrations of prophylactic cefazolin during cesarean delivery. Obstet Gynecol. 2011;117(4):877–882.
In this prospective study of the influence of an obese habitus on antibiotic prophylaxis during cesarean delivery, researchers divided 29 patients who were scheduled for cesarean into three groups, by body mass index (BMI):
- lean (BMI, <30; n = 10)
- obese (30–39.9; n = 10)
- extremely obese (>40; n = 9).
All patients were given a 2-g dose of IV cefazolin 30 to 60 minutes before surgery.
During delivery, the team took two specimens of adipose tissue: one immediately after the skin incision and one later, after fascia was closed. They also obtained a specimen of myometrial tissue after delivery and a blood specimen after surgery was completed.
The concentration of cefazolin was then measured in adipose and myometrial tissue and in serum.
Findings. The researchers demonstrated that the mean concentration of cefazolin in the initial specimen of adipose tissue was significantly higher in lean patients than in obese and extremely obese patients. All 10 women who had a BMI less than 30 had a serum cefazolin concentration greater than 4 μg/g—the theoretical break-point for defining resistance to cefazolin. The initial adipose tissue specimen from two of the 10 obese patients and three of the nine extremely obese patients showed cefazolin concentrations less than 4 μg/g.
Of particular interest, two women—both of whom had a BMI greater than 40—developed a wound infection that required antibiotic therapy. Their initial and subsequent adipose tissue concentrations of cefazolin were less than the 4 μg/g break-point for resistance.
The concentration of cefazolin in the patients’ myometrial and serum specimens demonstrated a pattern similar to what the researchers observed in adipose tissue, but these results were not statistically significant across BMI groups. In fact, the cefazolin concentration in all groups’ myometrial and serum specimens exceeded the minimum inhibitory concentration for most potential pathogens in the setting of cesarean delivery.
Commentary
Clearly, prophylactic antibiotics are indicated for all women who are having a cesarean delivery. Antibiotics have their greatest impact when administered before the surgical incision is made; to exert their full protective effect against endometritis and wound infection, however, antibiotics should reach a recognized therapeutic concentration—not only in serum and myometrium but in the subcutaneous tissue.
The customary dosage of cefazolin for cesarean delivery prophylaxis has been 1 g. This study demonstrated that, although a 2-g dose of cefazolin reached a therapeutic concentration in myometrial tissue and serum, it did not consistently do so in the adipose tissue of obese and extremely obese patients.
Pending further investigation, I strongly recommend that all women who have a BMI greater than 30 receive a 2-g dose of cefazolin 30 to 60 minutes before cesarean delivery. Future research is needed to determine whether an even higher dosage is necessary to achieve a therapeutic concentration in the subcutaneous tissue of morbidly obese patients.
New therapies promise a better outcome in hepatitis C
Jacobson IM, McHutchison JG, Dusheiko G, et al; ADVANCE Study Team. Telaprevir for previously untreated hepatitis C virus infection. N Engl J Med. 2011;364(25):2405–2416.
The authors conducted an international Phase-3, randomized, double-blind, placebo-controlled trial of two different treatment modalities for chronic hepatitis C virus (HCV) infection. The authors assigned 1,088 patients who had HCV genotype-1 infection and who had not received prior therapy to one of three treatment groups:
- telaprevir (Incivek, Vertex Pharmaceuticals), an HCV genotype-1 protease inhibitor, combined with peginterferon alfa-2a (Pegasys, Genetech) plus ribavirin (Copegus, Genetech; Rebetol, Merck; etc.) for 12 weeks; patients then were given peginterferon alfa-2a plus ribavirin only for 12 additional weeks if HCV RNA was undetectable at weeks 4 and 12 or peginterferon alfa-2a plus ribavirin only for 36 weeks if HCV RNA was detectable at either time point (Group 1)
- telaprevir with peginterferon alfa-2a plus ribavirin for 8 weeks, then placebo with peginterferon alfa-2a plus ribavirin for 4 weeks, followed by 12 to 36 weeks of peginterferon alfa-2a plus ribavirin using the HCV RNA criteria applied to Group 1 (Group 2)
- placebo with peginterferon alfa-2a plus ribavirin for 12 weeks, followed by 36 weeks of peginterferon alfa-2a plus ribavirin (Group 3).
The primary endpoint of the trial was the percentage of patients who had undetectable plasma HCV RNA at 24 weeks after the last planned dose of the study drugs. The investigators considered that this endpoint represented a sustained virologic response.
Findings. Seventy-five percent of patients in Group 1 and 69% of those in Group 2 had a sustained virologic response. By comparison, only 44% of patients in Group 3 had a sustained response. The differences in outcome between Group 1 and Group 3, and between Group 2 and Group 3, were highly significant (P<.001). Virologic failure was more common among patients who had HCV genotype-1a infection than among those who had HCV genotype-1b infection.
The most common side effects noted by patients who received telaprevir were gastrointestinal irritation, rash, and anemia. Ten percent of patients in the telaprevir group discontinued therapy, compared with 7% in the peginterferon-ribavirin-alone group.
Commentary
Worldwide, approximately 170 million people have chronic hepatitis C, which is the most common indication for liver transplantation. Until recently, the principal treatments for hepatitis C were pegylated interferon alfa with ribavirin and without ribavirin; the response rate with these regimens was in the range of 55%. This study shows that adding telaprevir to regimens for HCV infection significantly improves prospects for long-term resolution of infection.
In some obstetric and gynecologic populations, HCV is more common than hepatitis B virus. Risk factors for hepatitis C include hepatitis B, intravenous drug abuse, and human immunodeficiency virus infection. HCV-infected women pose a risk to their sex partners; infected pregnant women can transmit the virus to their baby.
Unlike hepatitis A and hepatitis B, immunoprophylaxis is not available for hepatitis C. That reality is what makes the study by Jacobsen and colleagues so compelling: They have clearly demonstrated that multi-agent antiviral therapy might be able to truly cure this infection.
The lesson here for ObGyns? Screen at-risk patients and then refer the hepatitis C-seropositive ones to a specialist in gastroenterology, who can determine candidacy for one of the new treatment regimens.
Clearly, the prognosis for people who have hepatitis C is much better today than it was 20 years ago.
For how long should chorioamnionitis be treated?
Black LP, Hinson L, Duff P. Limited course of antibiotic treatment for chorioamnionitis. Obstet Gynecol. 2012;119(6):1102-1105.
The authors conducted a retrospective review of 423 women who had been treated for chorioamnionitis at the University of Florida from 2005 to 2009.
Patients had been given IV ampicillin (2 g every 6 h) plus IV gentamicin (1.5 mg/kg every 8 h) as soon as the diagnosis of chorioamnionitis was established; postpartum, they were given only the one next scheduled dose of each antibiotic. Patients who had a cesarean received either metronidazole (500 mg) or clindamycin (900 mg) immediately after cord clamping to enhance coverage of anaerobic organisms.
The primary outcome was treatment failure, defined as persistent fever requiring continued antibiotics, surgical intervention, or administration of heparin for septic pelvic-vein thrombophlebitis.
Findings. Here is a breakdown of what the investigators found regarding the 282 women who delivered vaginally and the 141 who underwent cesarean delivery:
- Overall, 399 of the patients (94%; 95% confidence interval [CI], 92% and 96%) were treated successfully; 24 (6%; 95% CI, 3.7% and 8.3%) failed short-course treatment
- Of the 282 patients who delivered vaginally, 279 (99%; 95% CI, 98% and 100%) were cured with short-term therapy
- Of the 141 who delivered by cesarean, 120 (85%; 95% CI, 79% and 91%) were cured (P<.001).
- Seventeen of the total treatment failures had endometritis and responded quickly to continuation of antibiotics. Of the 17 patients with endometritis, 14 had a cesarean delivery.
- Seven patients had more serious complications: four, wound infection; three, septic pelvic-vein thrombophlebitis. All serious complications occurred after cesarean delivery.
- Of the four patients who had a wound infection, three had labor induced by misoprostol; their BMI was 44.8, 31.1, and 48.5, respectively. The fourth had a cesarean delivery at 29 weeks for preterm premature rupture of membranes (PPROM), chorioamnionitis, and malpresentation.
- Of the three patients who had septic pelvic-vein thrombophlebitis, two had labor induced by misoprostol. One had a BMI of 29.2; the other, 31.1. The third patient was delivered secondary to PPROM; her BMI was 40.3.
In addition, of the 21 treatment failures in the cesarean delivery group, 6 had prolonged rupture of membranes (ROM) and 10 had a BMI greater than 30. Six patients had both prolonged ROM and were obese or morbidly obese.
Of the 120 women who had a cesarean delivery and were treated successfully, 3 had prolonged ROM and 39 had a BMI greater than 30. None had both prolonged ROM and a BMI greater than 30.
Last, the difference between treatment failures and treatment successes in regard to the frequency of prolonged ROM or a BMI greater than 30 was highly significant (P<.01).
Commentary
In most published reports of patients who have chorioamnionitis, antibiotic treatment continues until the patient is afebrile and asymptomatic for 24 to 48 hours. This treatment approach has been based largely on expert opinion, however, not on Level-1 or Level-2 evidence.
In 2003, Edwards and Duff published a study of chorioamnionitis antibiotic regimens that compared single-dose postpartum treatment to extended treatment.2 This randomized controlled trial demonstrated that there was no statistically significant difference between patients who had only a single dose of postpartum antibiotics and those who received an extended course of medication (i.e., who were treated until they had been afebrile and asymptomatic for a minimum of 24 hours) in regard to adverse outcomes (2.9% and 4.3%, respectively). The study discussed here extends and refines the observations made in the 2003 Edwards and Duff randomized controlled trial.
The new study shows that a limited course of antibiotics was, overall, effective in treating 94% of patients with chorioamnionitis (95% CI, 92% and 96%). Only 1% of patients who delivered vaginally failed therapy, compared with 15% of patients who delivered by cesarean (P<.001). In the cesarean group, women who failed therapy were likely to 1) be obese or 2) have a relatively long duration of labor or ruptured membranes, or both. These patients may have benefitted from a more extended course of antibiotic therapy.
Based on this investigation, I strongly recommend a limited course of antibiotic therapy (ampicillin plus gentamicin) for women with chorioamnionitis who deliver vaginally. Patients who have had a cesarean delivery—particularly those who are obese or have had an extended duration of labor, or both—should be treated with antibiotics until they have been afebrile and asymptomatic for 24 hours.
We want to hear from you! Tell us what you think.
- 10 practical, evidence-based recommendations for perioperative antibiotic prophylaxis
Meghan O. Schimpf (June 2012) - Gaps in Chlamydia testing threaten reproductive health, CDC warns
Janelle Yates, Senior Editor (Web exclusive, May 2012)
Dr. Duff reports no financial relationships relevant to this article.
In this Update, I’ve highlighted four interesting articles about infectious disease management in obstetric and gyn practice that appeared in the medical literature over the past 12 months:
- One describes a study that reminds physicians of the importance of an unusual manifestation of gonococcal infection
- A second article demonstrates the importance of making a change in the prophylactic antibiotic regimen provided to morbidly obese patients who are having a cesarean delivery
- A third describes an exciting development in the treatment of chronic hepatitis C virus infection
- The final article makes interesting observations about the proper duration of treatment for patients who have chorioamnionitis.
N gonorrhoeae causes illness beyond the urogenital tract
Bleich AT, Sheffield JS, Wendel GD, Sigman A, Cunningham FG. Disseminated gonococcal infection in women. Obstet Gynecol. 2012;119(3):597–602.
This article describes a retrospective review of 112 women who were admitted to Parkland Memorial Hospital in Dallas, Texas, from January 1975 through December 2008 and given a diagnosis of disseminated infection with Neisseria gonorrhoeae. Eighty (71%) of these women were not pregnant and were cared for on the internal medicine service; 32 (29%) were pregnant and were treated by faculty members and residents on the ObGyn service.
Over the course of the study, the frequency of disseminated gonococcal infection decreased significantly. Among pregnant women, the rate of infection was 11 for every 100,000 deliveries before 1980 and, after 1985, five for every 100,000 deliveries.
The most common clinical manifestation of disseminated gonococcal infection was arthritis. The most commonly affected joints were the knee, wrist, elbow, and ankle.
Other common clinical manifestations included dermatitis, fever, chills, and a purulent cervical discharge. Notably, the frequency of a purulent joint effusion was 50% in pregnant women and 70% in nonpregnant women—reflecting the fact that the duration of symptoms was approximately 3 days shorter in pregnant women than in nonpregnant women. Otherwise, the clinical presentation in pregnant women did not differ significantly from that of nonpregnant women.
In addition, the clinical course and the response to intravenous (IV) antibiotic therapy did not differ significantly between pregnant and nonpregnant women.
The authors were unable to document that disseminated gonococcal infection had any deleterious effect on the outcome of pregnancy among the patients studied. Although four of the 32 women delivered preterm, in only one instance was delivery related temporally to the disseminated gonococcal infection.
Commentary
Because of their experience treating women who have gonorrhea, I would say that most ObGyns think of N gonorrhoeae as causing localized infection in the lower genital tract (urethritis, endocervicitis, inflammatory proctitis) or upper genital tract (pelvic inflammatory disease). We should recognize, however, that gonorrhea also can cause prominent extra-pelvic findings, such as severe pharyngitis (in patients who practice orogenital intercourse) and perihepatitis (Fitz-Hugh-Curtis syndrome).
In addition, always bear in mind that, in rare instances, gonorrhea can become disseminated, causing quite serious illness. The most common extra-pelvic manifestation of disseminated gonococcal infection is arthritis. As noted in this study of a series of patients, the arthritis is usually polyarticular and affects medium or small joints.
The second most common manifestation of disseminated gonococcal infection is dermatitis. Characteristic lesions are raised, red or purple papules. These lesions are not a simple vasculitis; rather, they contain a high concentration of microorganisms.
Other possible manifestations of disseminated infection include pericarditis, endocarditis, and meningitis.
The diagnosis of disseminated gonococcal infection is usually made by clinical examination and culture of specimens from the genital tract, blood, or joint effusion.
Disseminated gonococcal infection usually responds promptly to intravenous antibiotic therapy.
Recommended therapy is ceftriaxone:
• 25 to 50 mg/kg/d IV for 7 days
or
• a single, daily, 25 to 50 mg/kg intramuscular dose, also for 7 days.
Continue therapy for 10 to 14 days if the patient has meningitis.
An alternative regimen is cefotaxime:
• 25 mg/kg/d IV for 7 days
or
• 25 mg/kg IM every 12 hours, also for 7 days.
Extend treatment for 10 to 14 days if meningitis is present.1
Obesity curtails effectiveness of antibiotic prophylaxis in cesarean delivery
Pevzner L, Swank M, Krepel C, Wing DA, Chan K, Edmiston CE Jr. Effects of maternal obesity on tissue concentrations of prophylactic cefazolin during cesarean delivery. Obstet Gynecol. 2011;117(4):877–882.
In this prospective study of the influence of an obese habitus on antibiotic prophylaxis during cesarean delivery, researchers divided 29 patients who were scheduled for cesarean into three groups, by body mass index (BMI):
- lean (BMI, <30; n = 10)
- obese (30–39.9; n = 10)
- extremely obese (>40; n = 9).
All patients were given a 2-g dose of IV cefazolin 30 to 60 minutes before surgery.
During delivery, the team took two specimens of adipose tissue: one immediately after the skin incision and one later, after fascia was closed. They also obtained a specimen of myometrial tissue after delivery and a blood specimen after surgery was completed.
The concentration of cefazolin was then measured in adipose and myometrial tissue and in serum.
Findings. The researchers demonstrated that the mean concentration of cefazolin in the initial specimen of adipose tissue was significantly higher in lean patients than in obese and extremely obese patients. All 10 women who had a BMI less than 30 had a serum cefazolin concentration greater than 4 μg/g—the theoretical break-point for defining resistance to cefazolin. The initial adipose tissue specimen from two of the 10 obese patients and three of the nine extremely obese patients showed cefazolin concentrations less than 4 μg/g.
Of particular interest, two women—both of whom had a BMI greater than 40—developed a wound infection that required antibiotic therapy. Their initial and subsequent adipose tissue concentrations of cefazolin were less than the 4 μg/g break-point for resistance.
The concentration of cefazolin in the patients’ myometrial and serum specimens demonstrated a pattern similar to what the researchers observed in adipose tissue, but these results were not statistically significant across BMI groups. In fact, the cefazolin concentration in all groups’ myometrial and serum specimens exceeded the minimum inhibitory concentration for most potential pathogens in the setting of cesarean delivery.
Commentary
Clearly, prophylactic antibiotics are indicated for all women who are having a cesarean delivery. Antibiotics have their greatest impact when administered before the surgical incision is made; to exert their full protective effect against endometritis and wound infection, however, antibiotics should reach a recognized therapeutic concentration—not only in serum and myometrium but in the subcutaneous tissue.
The customary dosage of cefazolin for cesarean delivery prophylaxis has been 1 g. This study demonstrated that, although a 2-g dose of cefazolin reached a therapeutic concentration in myometrial tissue and serum, it did not consistently do so in the adipose tissue of obese and extremely obese patients.
Pending further investigation, I strongly recommend that all women who have a BMI greater than 30 receive a 2-g dose of cefazolin 30 to 60 minutes before cesarean delivery. Future research is needed to determine whether an even higher dosage is necessary to achieve a therapeutic concentration in the subcutaneous tissue of morbidly obese patients.
New therapies promise a better outcome in hepatitis C
Jacobson IM, McHutchison JG, Dusheiko G, et al; ADVANCE Study Team. Telaprevir for previously untreated hepatitis C virus infection. N Engl J Med. 2011;364(25):2405–2416.
The authors conducted an international Phase-3, randomized, double-blind, placebo-controlled trial of two different treatment modalities for chronic hepatitis C virus (HCV) infection. The authors assigned 1,088 patients who had HCV genotype-1 infection and who had not received prior therapy to one of three treatment groups:
- telaprevir (Incivek, Vertex Pharmaceuticals), an HCV genotype-1 protease inhibitor, combined with peginterferon alfa-2a (Pegasys, Genetech) plus ribavirin (Copegus, Genetech; Rebetol, Merck; etc.) for 12 weeks; patients then were given peginterferon alfa-2a plus ribavirin only for 12 additional weeks if HCV RNA was undetectable at weeks 4 and 12 or peginterferon alfa-2a plus ribavirin only for 36 weeks if HCV RNA was detectable at either time point (Group 1)
- telaprevir with peginterferon alfa-2a plus ribavirin for 8 weeks, then placebo with peginterferon alfa-2a plus ribavirin for 4 weeks, followed by 12 to 36 weeks of peginterferon alfa-2a plus ribavirin using the HCV RNA criteria applied to Group 1 (Group 2)
- placebo with peginterferon alfa-2a plus ribavirin for 12 weeks, followed by 36 weeks of peginterferon alfa-2a plus ribavirin (Group 3).
The primary endpoint of the trial was the percentage of patients who had undetectable plasma HCV RNA at 24 weeks after the last planned dose of the study drugs. The investigators considered that this endpoint represented a sustained virologic response.
Findings. Seventy-five percent of patients in Group 1 and 69% of those in Group 2 had a sustained virologic response. By comparison, only 44% of patients in Group 3 had a sustained response. The differences in outcome between Group 1 and Group 3, and between Group 2 and Group 3, were highly significant (P<.001). Virologic failure was more common among patients who had HCV genotype-1a infection than among those who had HCV genotype-1b infection.
The most common side effects noted by patients who received telaprevir were gastrointestinal irritation, rash, and anemia. Ten percent of patients in the telaprevir group discontinued therapy, compared with 7% in the peginterferon-ribavirin-alone group.
Commentary
Worldwide, approximately 170 million people have chronic hepatitis C, which is the most common indication for liver transplantation. Until recently, the principal treatments for hepatitis C were pegylated interferon alfa with ribavirin and without ribavirin; the response rate with these regimens was in the range of 55%. This study shows that adding telaprevir to regimens for HCV infection significantly improves prospects for long-term resolution of infection.
In some obstetric and gynecologic populations, HCV is more common than hepatitis B virus. Risk factors for hepatitis C include hepatitis B, intravenous drug abuse, and human immunodeficiency virus infection. HCV-infected women pose a risk to their sex partners; infected pregnant women can transmit the virus to their baby.
Unlike hepatitis A and hepatitis B, immunoprophylaxis is not available for hepatitis C. That reality is what makes the study by Jacobsen and colleagues so compelling: They have clearly demonstrated that multi-agent antiviral therapy might be able to truly cure this infection.
The lesson here for ObGyns? Screen at-risk patients and then refer the hepatitis C-seropositive ones to a specialist in gastroenterology, who can determine candidacy for one of the new treatment regimens.
Clearly, the prognosis for people who have hepatitis C is much better today than it was 20 years ago.
For how long should chorioamnionitis be treated?
Black LP, Hinson L, Duff P. Limited course of antibiotic treatment for chorioamnionitis. Obstet Gynecol. 2012;119(6):1102-1105.
The authors conducted a retrospective review of 423 women who had been treated for chorioamnionitis at the University of Florida from 2005 to 2009.
Patients had been given IV ampicillin (2 g every 6 h) plus IV gentamicin (1.5 mg/kg every 8 h) as soon as the diagnosis of chorioamnionitis was established; postpartum, they were given only the one next scheduled dose of each antibiotic. Patients who had a cesarean received either metronidazole (500 mg) or clindamycin (900 mg) immediately after cord clamping to enhance coverage of anaerobic organisms.
The primary outcome was treatment failure, defined as persistent fever requiring continued antibiotics, surgical intervention, or administration of heparin for septic pelvic-vein thrombophlebitis.
Findings. Here is a breakdown of what the investigators found regarding the 282 women who delivered vaginally and the 141 who underwent cesarean delivery:
- Overall, 399 of the patients (94%; 95% confidence interval [CI], 92% and 96%) were treated successfully; 24 (6%; 95% CI, 3.7% and 8.3%) failed short-course treatment
- Of the 282 patients who delivered vaginally, 279 (99%; 95% CI, 98% and 100%) were cured with short-term therapy
- Of the 141 who delivered by cesarean, 120 (85%; 95% CI, 79% and 91%) were cured (P<.001).
- Seventeen of the total treatment failures had endometritis and responded quickly to continuation of antibiotics. Of the 17 patients with endometritis, 14 had a cesarean delivery.
- Seven patients had more serious complications: four, wound infection; three, septic pelvic-vein thrombophlebitis. All serious complications occurred after cesarean delivery.
- Of the four patients who had a wound infection, three had labor induced by misoprostol; their BMI was 44.8, 31.1, and 48.5, respectively. The fourth had a cesarean delivery at 29 weeks for preterm premature rupture of membranes (PPROM), chorioamnionitis, and malpresentation.
- Of the three patients who had septic pelvic-vein thrombophlebitis, two had labor induced by misoprostol. One had a BMI of 29.2; the other, 31.1. The third patient was delivered secondary to PPROM; her BMI was 40.3.
In addition, of the 21 treatment failures in the cesarean delivery group, 6 had prolonged rupture of membranes (ROM) and 10 had a BMI greater than 30. Six patients had both prolonged ROM and were obese or morbidly obese.
Of the 120 women who had a cesarean delivery and were treated successfully, 3 had prolonged ROM and 39 had a BMI greater than 30. None had both prolonged ROM and a BMI greater than 30.
Last, the difference between treatment failures and treatment successes in regard to the frequency of prolonged ROM or a BMI greater than 30 was highly significant (P<.01).
Commentary
In most published reports of patients who have chorioamnionitis, antibiotic treatment continues until the patient is afebrile and asymptomatic for 24 to 48 hours. This treatment approach has been based largely on expert opinion, however, not on Level-1 or Level-2 evidence.
In 2003, Edwards and Duff published a study of chorioamnionitis antibiotic regimens that compared single-dose postpartum treatment to extended treatment.2 This randomized controlled trial demonstrated that there was no statistically significant difference between patients who had only a single dose of postpartum antibiotics and those who received an extended course of medication (i.e., who were treated until they had been afebrile and asymptomatic for a minimum of 24 hours) in regard to adverse outcomes (2.9% and 4.3%, respectively). The study discussed here extends and refines the observations made in the 2003 Edwards and Duff randomized controlled trial.
The new study shows that a limited course of antibiotics was, overall, effective in treating 94% of patients with chorioamnionitis (95% CI, 92% and 96%). Only 1% of patients who delivered vaginally failed therapy, compared with 15% of patients who delivered by cesarean (P<.001). In the cesarean group, women who failed therapy were likely to 1) be obese or 2) have a relatively long duration of labor or ruptured membranes, or both. These patients may have benefitted from a more extended course of antibiotic therapy.
Based on this investigation, I strongly recommend a limited course of antibiotic therapy (ampicillin plus gentamicin) for women with chorioamnionitis who deliver vaginally. Patients who have had a cesarean delivery—particularly those who are obese or have had an extended duration of labor, or both—should be treated with antibiotics until they have been afebrile and asymptomatic for 24 hours.
We want to hear from you! Tell us what you think.
1. Workowski KA, Berman S. Centers for Disease Control and Prevention (CDC). Sexually transmitted diseases treatment guidelines, 2010. MMWR Recomm Rep. 2010;59(RR-12):1-110.
2. Edwards RK, Duff P. Single dose postpartum therapy for women with chorioamnionitis. Obstet Gynecol. 2003;102(5 Pt 1):957-961.
1. Workowski KA, Berman S. Centers for Disease Control and Prevention (CDC). Sexually transmitted diseases treatment guidelines, 2010. MMWR Recomm Rep. 2010;59(RR-12):1-110.
2. Edwards RK, Duff P. Single dose postpartum therapy for women with chorioamnionitis. Obstet Gynecol. 2003;102(5 Pt 1):957-961.
Pregnancy-Induced Hypertension
Hypertensive disorders represent one of the most common medical complications of pregnancy.1,2 Based on a nationwide inpatient sample examining more than 36 million deliveries in the United States, the prevalence of associated hypertensive disorders increased from 67.2 per 1,000 deliveries in 1998 to 83.4 per 1,000 deliveries in 2006.3Pregnancy-induced hypertension (also referred to as gestational hypertension or hypertensive disorder of pregnancy)4-6 is estimated to affect 6% to 8% of US pregnancies.1,2
Women who develop severe hypertension during pregnancy may experience adverse effects similar to those associated with mild preeclampsia.2,7,8 In the mother, these may range from elevated liver enzymes to renal dysfunction; and in the fetus, from preterm delivery to intrauterine restriction of fetal growth.7,8
This article will review the risk factors, clinical presentation, diagnosis, and management of pregnancy-induced hypertension. A brief discussion of preeclampsia as it relates to gestational hypertension will be included (see Table 12,6,9).

Classification, Definitions
Pregnancy-induced hypertension (PIH) is classified as mild or severe. Mild PIH is defined as new-onset hypertension (systolic blood pressure ≥ 140 mm Hg and/or diastolic blood pressure ≥ 90 mm Hg), occurring after 20 weeks’ gestation. The majority of cases of mild PIH develop beyond 37 weeks’ gestation, and in these cases, pregnancy outcomes are comparable to those of normotensive pregnancies.2,7,8
Severe PIH is defined as sustained elevated blood pressures of ≥ 160 mm Hg systolic and ≥ 110 mm Hg diastolic. In prospective cohort studies in which calcium supplementation and low-dose aspirin use were being investigated for prevention of preeclampsia in healthy pregnant women, those who were severely hypertensive were found to be at increased risk for certain maternal comorbidities (eg, cesarean delivery, renal dysfunction, elevated liver enzymes, placental abruption) and perinatal morbidities (delivery before 37 weeks’ gestation, low birth weight, fetal growth restriction, and neonatal ICU admission), compared with patients who were normotensive or mildly hypertensive.7,8
The diagnosis of PIH may later be amended or replaced by one of the following diagnoses: preeclampsia, if proteinuria (to be defined and discussed later) develops; chronic hypertension, if blood pressure remains elevated past 12 weeks postpartum; or transient hypertension of pregnancy, if blood pressure normalizes by 12 weeks postpartum.5,6,10
Pathophysiology and Risk Factors
Although the pathophysiology of PIH is not well understood, the pathogenesis of preeclampsia likely involves abnormalities in the development, implantation, or perfusion of the placenta, and often leads to impaired maternal organ function.6,11 It is not clear whether PIH and preeclampsia are two different diseases that share a manifestation of elevated blood pressure or whether PIH represents an early stage of preeclampsia.4,12 However, women with preexisting hypertension, especially severe hypertension, are at increased risk for preeclampsia, placental abruption, and fetal growth restriction.2
There are some similarities and some distinct differences among the clinical features and risk factors associated with PIH, compared with those of preeclampsia. Risk factors for PIH include a pre-pregnancy BMI of 25 or greater, PIH and/or preeclampsia in previous pregnancies, and history of renal disease, cardiac disease, or diabetes. The most important risk factors for preeclampsia include preexisting diabetes or nephropathy, chronic hypertension, PIH or preeclampsia in a previous pregnancy, maternal age younger than 18 or older than 34, African-American ethnicity, first pregnancy, multiple pregnancy, history of preeclampsia in the patient’s mother or sister, obesity, autoimmune disease, and an interval between pregnancies longer than 10 years.4-6,13-15
The risk for preeclampsia in patients with PIH is approximately 15% to 25%12,16; according to Magee et al,6 35% of women with PIH onset before 37 weeks’ gestation develop preeclampsia.6,12,17 The risk for recurrence of PIH in subsequent pregnancies is about 26%, whereas women who experience preeclampsia in one pregnancy have a comparable risk for PIH or preeclampsia (about 14% each) in subsequent pregnancies.18
Clinical Presentation and Diagnostic Evaluation
Blood pressure should be measured and recorded at every prenatal visit, using the correct-sized cuff, with the patient in a seated position.5 Gestational hypertension is a clinical diagnosis confirmed by at least two accurate blood pressure measurements in the same arm in women without proteinuria, with readings of ≥ 140 mm Hg systolic and/or ≥ 90 mm Hg diastolic. It should then be determined whether the patient’s hypertension is mild or severe (ie, blood pressure > 160/110 mm Hg). The patient with severe PIH should be evaluated for signs of preeclampsia, as discussed below.
Patients with mild PIH are often asymptomatic, and the diagnosis is made at a prenatal visit as a result of routine blood pressure monitoring; this is one of many reasons to encourage early and regular prenatal care. Blood pressure may be higher at night in hypertensive disorders of pregnancy.10
In contrast to patients with mild PIH, the clinical presentation of those with severe PIH or preeclampsia (and the potential for impending eclampsia) may include the following symptoms and signs:
- Generalized edema, including that of the face and hands
- Rapid weight gain
- Blurred vision or scotomata (ie, areas of diminished vision in the visual field)
- Severe, throbbing or pounding headaches
- Epigastric or right upper quadrant pain
- Oliguria (urinary output < 500 mL/d)
- Nausea, with or without vomiting
- Hyperactive reflexes
- Chest pain or tightness
- Shortness of breath.2,6,14
Medical History
Important questions to address in the patient’s medical history relate to risk factors for PIH, such as a history of renal disease, cardiac disease, or diabetes, previous history of PIH and/or preeclampsia, and abuse of cocaine or amphetamines—in addition to the specific aforementioned symptoms and signs of severe preeclampsia.5,6
Physical Examination
The clinician performing the physical exam should be attentive to accurate blood pressure measurements and any signs that suggest preeclampsia. Weight should be measured and BMI calculated at each prenatal visit.
If the patient’s blood pressure is markedly elevated, the focused physical examination should include an ophthalmologic examination for jaundice and for evidence of hypertensive retinopathy or papilledema; pulmonary and cardiac examination; abdominal examination, including palpation of the liver; examination of the face and extremities for edema; and a complete neurologic examination, including assessment of deep tendon reflexes and examination for clonus.
Laboratory Testing
In patients with PIH, laboratory evaluation should be focused to rule out preeclampsia. The potential for proteinuria (defined as ≥ 0.3 g/d in a 24-hour urine sample1,14) must be investigated at diagnosis and at regular visits during the pregnancy.1 At least two random urine samples, collected at least 6 hours apart, should be evaluated for protein. A spot (random) urine sample with a result of 2+ protein or greater is highly suggestive of proteinuria; a 24-hour urine collection is the gold standard by which such findings should be confirmed and protein levels in the urine quantified.1,14
Elevated blood pressure and proteinuria are the hallmarks of preeclampsia.6 Patients affected by these developments must be evaluated for signs and symptoms of severe preeclampsia. However, those with only mild elevations in blood pressure and little or no proteinuria may complain of sudden-onset throbbing or pounding headache, blurry vision, and severe epigastric pain—possibly indicating severe preeclampsia.5,10
In addition to laboratory evaluation for urinary protein excretion, the following tests are recommended by the American College of Obstetricians and Gynecologists (ACOG)14 to assess for end organ involvement, which is consistent with severe preeclampsia:
- Hematocrit, which may be either high, to suggest hemoconcentration; or low, indicating hemolysis
- Platelet count, which is normal in women with PIH and low in those with severe preeclampsia; if results are abnormal, this test should be followed by coagulation testing (international normalized ratio, activated partial thromboplastin time, fibrinogen)
- Renal function testing (blood urea nitrogen and creatinine may be elevated in severe preeclampsia), and random urine testing for proteinuria, as explained earlier
- Liver enzymes (which are elevated in severe preeclampsia), and
- Lactate dehydrogenase (which is elevated in severe preeclampsia).1,14
Additionally, researchers conducting a small cohort study (n = 163) reported in 2009 that in women with PIH, serum uric acid levels exceeding 309 µmol/L were predictive of preeclampsia, with 87.7% sensitivity and 93.3% specificity.19 An increase from first-trimester serum uric acid levels was also a strong prognostic factor for preeclampsia. Earlier this year, a Canadian investigative team reported an increased risk for premature birth (odds ratio, 3.2) and small infant size for gestational age (odds ratio, 2.5) in women with PIH and hyperuricemia.20 While the predictive value of uric acid has been debated to some extent,14 measurement is often included in the workup of patients with hypertensive pregnancies.5,6
The frequency of prenatal visits, laboratory testing, and fetal monitoring should be adjusted according to the severity of PIH. In mildly hypertensive patients, the general recommendation is urine and blood testing at weekly prenatal visits.14 Fetal well-being must be monitored regularly, although neither the type nor frequency of such testing has been well established. Generally, patients should be advised to count daily fetal movements, and they should be scheduled for either a nonstress test (NST) or a biophysical profile as soon as a diagnosis of PIH is made.1,2,6,14
According to a 2010 guidance from the United Kingdom’s National Institute for Health and Clinical Excellence (NICE),13,21 pregnant women with mild to moderate hypertension should undergo an initial ultrasonographic assessment of fetal growth and amniotic fluid volume at the time of diagnosis, then serially every 3 to 4 weeks. If results from initial fetal testing are normal, patients with mild PIH do not require repeat testing after 34 weeks’ gestation, unless conditions change (eg, preeclampsia, worsening hypertension, and/or change in fetal movements).1,2,14 The NICE guidelines also recommend umbilical artery Doppler velocimetry.13,21
In patients with severe PIH, an NST ultrasound assessment of fetal growth and amniotic fluid volume and umbilical artery Doppler velocimetry should be performed at diagnosis to evaluate for placental dysfunction.6,21 If all test results are normal, the ultrasound and umbilical artery Doppler velocimetry need not be repeated more frequently than every two weeks, and the NST no more than once per week.13
Treatment/Management and Follow-Up
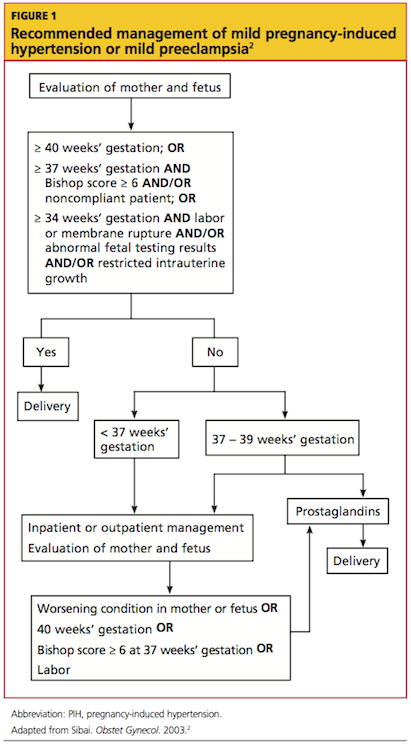
Regular prenatal monitoring to assess for worsening of PIH and/or development of preeclampsia is key to management. Figure 12 outlines an algorithm for managing PIH, which is guided by the severity of the condition. Patients with mild PIH can be managed with weekly outpatient visits and assessed for signs and symptoms of preeclampsia, monitoring of fetal movements, weight, blood pressure measurements, and urine and blood tests.2
At each visit, it is important to instruct patients to report immediately any of the following symptoms: new-onset severe headache, visual changes, epigastric or right upper quadrant pain, nausea or vomiting, difficulty breathing or chest tightness, as well as vaginal bleeding, decreased fetal movements, or uterine contractions.6,14
Generally, expectant management with delivery at term is recommended for women with mild PIH.2 Vaginal delivery (or cesarean delivery, if indicated) is recommended at 37 weeks or when fetal maturity is confirmed; and at 34 weeks if fetal or maternal distress is evident.2,6
Findings from the Hypertension and Preeclampsia Intervention Trial At Term (HYPITAT),22 an open-label, randomized clinical trial in women with PIH or mild preeclampsia, suggested an association between induction of labor between 36 and 41 weeks’ gestation and improved maternal outcomes (specifically, reduced risk for severe hypertension), compared with expectant management. Similarly, in a literature review by Caughey et al,23 results from nine randomized controlled trials indicated a reduced risk for cesarean delivery in women who underwent induction of labor, compared with expectant management. Rates of “successful” induction of labor (ie, procedures resulting in vaginal rather than cesarean delivery) were greater in women with higher parity, a favorable cervix, and earlier gestational age.
Based on data from the HYPITAT trial,22 a cost-effectiveness analysis of induction of labor compared with expectant management revealed an 11% reduction in the average cost in delivery that followed induction of labor, compared with expectant management, in women with PIH or mild preeclampsia.24 Caughey et al23 reported similar savings, particularly when induction of labor was performed at 41 weeks’ gestation.
If induction of labor is being considered in a woman with an unfavorable cervix, administration of prostaglandins is recommended to enhance cervical ripening.6
Medication
Pregnant women should be advised to discontinue previously prescribed ACE inhibitors, angiotensin receptor blockers, or thiazide diuretics, which are associated with congenital abnormalities, intrauterine growth restriction, and/or neonatal nephropathy.5,6,13,21
Antihypertensive medication is not recommended for women with mild to moderate PIH, as it does not appear to improve outcomes. Evidence was found insufficient in a 2007 Cochrane review to determine the potential impact of antihypertensive medications for treatment of mild to moderate PIH on clinical outcomes such as preterm birth, infant mortality, and infant size relative to gestational age.25 A similar review conducted in 2011, with primary outcomes that included severe preeclampsia, eclampsia, and maternal death or perinatal death, concluded only that further study was needed to determine how tightly blood pressure must be controlled to improve maternal and fetal outcomes in patients with PIH.26
ACOG14 recommends antihypertensive therapy (eg, hydralazine, labetalol) only for women with diastolic blood pressure of 105 to 110 mm Hg or higher.1,2 There are several recommendations from different organizations regarding the choice of antihypertensive medications for PIH. In the UK’s NICE guidance,21 it is recommended that patients with moderate to severe PIH take oral labetalol as first-line treatment to keep systolic blood pressure below 150 mm Hg and diastolic blood pressure between 80 and 100 mm Hg.
Like severe preeclampsia, severe PIH should be managed in an inpatient setting.6,14 IV labetalol or hydralazine is recommended to lower the blood pressure to less than 160/110 mm Hg, although current evidence is insufficient to identify a target blood pressure.6,26 A 2002 ACOG practice bulletin recommends one of the following:
- Hydralazine 5 to 10 mg IV every 15 to 20 minutes until the desired response is achieved; or
- Labetalol 20 mg IV bolus, followed by 40 mg if not effective within 10 minutes, then 80 mg every 10 minutes with maximum total dose of 220 mg.1,14
In women who have severe PIH or who develop severe preeclampsia or eclampsia, magnesium sulfate is administered to prevent or treat seizures.14 This agent should be used during labor and for at least 24 hours postpartum.2 Dosing of magnesium sulfate for this indication is 4 g IV bolus, followed by infusion of 1 g/h. It is important to monitor treated patients for signs of toxicity, including muscle weakness, loss of patellar reflexes, hypoventilation, pulmonary edema, hypotension, and bradycardia. IV calcium gluconate should be readily available for use as an antidote to life-threatening hypermagnesemia.27,28
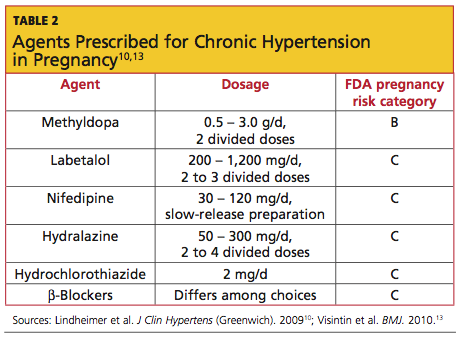
For chronic hypertension in pregnancy, the American Society of Hypertension10 has recommended several agents. There is no consensus on which medication is most appropriate (see Table 210,13).
Patient Education
Patient education is an important aspect of caring for women with PIH. The American Academy of Family Physicians29,30 provides a comprehensive patient education resource that defines the hypertensive disorders in pregnancy, explains the symptoms and signs of severe hypertension or preeclampsia, and describes appropriate diagnostic tests, monitoring, and treatment options. (See http://familydoctor.org/familydoctor/en/diseases-conditions/pregnancy-induced-hypertension.printerview.all.html.)
Patients who are considering pregnancy should be counseled to maintain a healthy weight prior to and during pregnancy. Adequate dietary calcium can reduce the risk for PIH, and calcium supplementation has been shown to reduce the risk for preeclampsia, especially in women at high risk.31 The Society of Obstetricians and Gynaecologists of Canada recommends low-dose aspirin (75 mg/d) at bedtime for high-risk women, starting before pregnancy, or upon diagnosis of pregnancy to prevent preeclampsia.6 Although there is insufficient evidence to recommend dietary salt restriction, excess salt can increase fluid retention and possibly blood pressure. Patients should be urged to attend all scheduled prenatal visits and to review the warning signs and symptoms of severe hypertension and preeclampsia at each visit.
Mode of delivery may be discussed and will depend on the severity of hypertension, presence of preeclampsia, and fetal well-being. Vaginal delivery at term is considered optimal unless there are indications for cesarean delivery. Induction of labor may be considered at term in patients with PIH. Those with severe preeclampsia who may require preterm delivery must be prepared for potential issues associated with prematurity.
Follow-Up and Prognosis
Patients with PIH should be evaluated postpartum for persistent hypertension. Blood pressure in patients with PIH usually normalizes by day 7 postpartum.32 If blood pressure elevation persists past 12 weeks postpartum, the patient’s diagnosis is revised to chronic hypertension and managed accordingly.
In the patient with persistent hypertension who chooses breastfeeding, it is important to select an antihypertensive medication with low transfer into breast milk. Many β-adrenergic antagonists and calcium channel antagonists are considered “compatible” with breastfeeding by the American Academy of Pediatrics.33
In addition to the potential for recurrent PIH in subsequent pregnancies, women with PIH are at increased risk for hypertension later in life, and findings from several large cohort studies suggest increased cardiovascular risk in patients with hypertensive pregnancies.16,34 Magnussen et al,9 who followed more than 15,000 mothers of singleton infants for several years postpartum, found that those who experienced hypertensive disorders (particularly recurrent hypertensive disorders) during pregnancy were more likely than normotensive women to subsequently develop diabetes, dyslipidemia, and hypertension. Women who remained normotensive while pregnant generally had lower BMI measurements than those who experienced PIH or preeclampsia.
Conclusion
Hypertensive disorders commonly develop during pregnancy. It is important to diagnose and classify PIH during routine prenatal visits. Once the diagnosis is made, patients must be monitored closely for increasing blood pressure or development of preeclampsia. Urine protein testing is a key clinical test to detect preeclampsia, and positive findings on a random urine protein dipstick should be confirmed and quantified with a 24-hour urine collection.
In addition to undergoing frequent blood pressure measurements and urine protein tests, patients should be asked about signs and symptoms that suggest preeclampsia. Women with mild PIH can be managed as outpatients with prenatal visits at least weekly, followed by delivery at term. Severely hypertensive patients are managed in the hospital with antihypertensive medications and prompt delivery at 34 weeks’ gestation or beyond, should maternal or fetal distress become evident.
1. Report of the National High Blood Pressure Education Program Working Group on high blood pressure in pregnancy. Am J Obstet Gynecol. 2000;183(1):S1-S22.
2. Sibai BM. Diagnosis and management of gestational hypertension and preeclampsia. Obstet Gynecol. 2003;102(1):181-192.
3. Kuklina EV, Ayala C, Callaghan WM. Hypertensive disorders and severe obstetric morbidity in the United States. Obstet Gynecol. 2009; 113(6):1299-1306.
4. Villar J, Carroli, G, Wojdyla D, et al; World Health Organization Antenatal Care Trial Research Group. Preeclampsia, gestational hypertension and intrauterine growth restriction, related or independent conditions. Am J Obstet Gynecol. 2006;194(4):921-931.
5. Leeman L, Fontaine P. Hypertensive disorders of pregnancy. Am Fam Physician. 2008;78(1):
93-100.
6. Magee LA, Helewa M, Moutquin JM, von Dadelszen P; Hypertension Guideline Committee; Strategic Training Initiative in Research in the Reproductive Health Sciences (STIRRHS) Scholars. Diagnosis, evaluation, and management of the hypertensive disorders of pregnancy. J Obstet Gynaecol Can. 2008;30(3 suppl):S1-S48.
7. Buchbinder A, Sibai BM, Caritis S, et al. Adverse perinatal outcomes are significantly higher in severe gestational hypertension than in mild preeclampsia. Am J Obstet Gynecol. 2002;186(1):66-71.
8. Hauth JC, Ewell MG, Levine RJ, et al; Calcium for Preeclampsia Prevention Study Group. Pregnancy outcomes in healthy nulliparas who developed hypertension. Obstet Gynecol. 2000;95(1):24-28.
9. Magnussen EB, Vatten LJ, Smith GD, Romundstad PR. Hypertensive disorders in pregnancy and subsequently measured cardiovascular risk factors. Obstet Gynecol. 2009; 114(5):961-970.
10. Lindheimer MD, Taler SJ, Cunningham FG; American Society of Hypertension (ASH). ASH position paper: hypertension in pregnancy. J Clin Hypertens (Greenwich). 2009;11(4):214-225.
11. Roberts JM, Gammill HS. Preeclampsia: recent insights. Hypertension. 2005;46(6):
1243-1249.
12. Saudan P, Brown MA, Buddle ML, Jones M. Does gestational hypertension become pre-eclampsia? Br J Obstet Gynaecol. 1998;105 (11):1177-1184.
13. Visintin C, Mugglestone MA, Almerie MQ, et al; Guideline Development Group. Management of hypertensive disorders during pregnancy: summary of NICE guidance. BMJ. 2010;341:c2207.
14. ACOG Committee on Practice Bulletins—Obstetrics. Clinical Management Guidelines for Obstetrician–Gynecologists. Diagnosis and management of preeclampsia and eclampsia: ACOG practice bulletin No. 33. Obstet Gynecol. 2002;99:159-167.
15. Parazzini F, Bortolus R, Chatenoud L, et al; Italian Study of Aspirin in Pregnancy Group. Risk factors for pregnancy-induced hypertension in women at high risk for the condition. Epidemiology. 1996;7(3):306-308.
16. Hjartardottir S, Leifsson BG, Geirsson RT, Steinthorsdottir V. Recurrence of hypertensive disorder in second pregnancy. Am J Obstet Gynecol. 2006;194(4):916-920.
17. Barton JR, O’Brien JM, Bergauer NK, et al. Mild gestational hypertension remote from term: progression and outcome. Am J Obstet Gynecol. 2001;184(5):979-983.
18. Brown MA, Mackenzie C, Dunsmuir W, et al. Can we predict recurrence of pre-eclampsia or gestational hypertension? BJOG. 2007; 114(8):984-993.
19. Bellomo G, Venanzi S, Saronio P, et al. Prognostic significance of serum uric acid in women with gestational hypertension. Hypertension. 2011;58(4):704-708.
20. Hawkins TL, Roberts JM, Mangos GJ, et al. Plasma uric acid remains a marker of poor outcome in hypertensive pregnancy: a retrospective cohort study. BJOG. 2012;119(4):484-492.
21. National Institute for Health and Clinical Excellence. Hypertension in pregnancy: the management of hypertensive disorders during pregnancy. www.nice.org.uk/nicemedia/live/13098/50418/50418.pdf. Accessed April 16, 2012.
22. Koopmans CM, Bijlenga D, Groen H, et al. Induction of labour versus expectant monitoring for gestational hypertension or mild pre-eclampsia after 36 weeks’ gestation (HYPITAT): a multicentre, open-label randomised controlled trial. Lancet. 2009;374(9694):979-988.
23. Caughey AB, Sundaram V, Kaimal AJ, et al. Maternal and neonatal outcomes of elective induction of labor. Evid Rep Technol Assess (Full Rep). 2009;(176):1-257.
24. Shennan A, Hezelgrave N. An economic analysis of induction of labour and expectant monitoring in women with gestational hypertension or pre-eclampsia at term (HYPITAT trial). BJOG. 2010;117(13):1575-1576.
25. Abalos E, Duley L, Steyn DW, Henderson-Smart DJ. Antihypertensive drug therapy for mild to moderate hypertension during pregnancy. Cochrane Database Syst Rev. 2007 Jan 24;(1):CD002252.
26. Nabhan AF, Elsedawy MM. Tight control of mild-moderate pre-existing or non-proteinuric gestational hypertension. Cochrane Database Syst Rev. 2011 Jul 6;(7):CD006907.
27. Duley L, Gülmezoglu AM, Henderson-Smart DJ. Magnesium sulphate and other anticonvulsants for women with preeclampsia. Cochrane Database Syst Rev. 2003;(2):CD000025.
28. Kraft MD, Btaiche IF, Sacks GS, Kudsk KA. Treatment of electrolyte disorders in adult patients in the intensive care unit. Am J Health Syst Pharm. 2005;62(16):1663-1682.
29. FamilyDoctor.org. Pregnancy-induced hypertension (updated 2010). http://familydoctor.org/familydoctor/en/diseases-conditions/pregnancy-induced-hypertension.printerview
.all.html. Accessed April 16, 2012.
30. Zamorski MA, Green LA. NHBPEP report on high blood pressure in pregnancy: a summary for family physicians. Am Fam Physician. 2001; 64(2):263-270.
31. Hofmeyr GJ, Duley L, Atallah A. Dietary calcium supplementation for prevention of pre-eclampsia and related problems: a systematic review and commentary. BJOG. 2007;114(8): 933-943.
32. Ferrazzani S, De Carolis S, Pomini F, et al. The duration of hypertension in the puerperium of preeclamptic women: relationship with renal impairment and week of delivery. Am J Obstet Gynecol. 1994;171(2):506-512.
33. Beardmore KS, Morris JM, Gallery ED. Excretion of antihypertensive medication into human breast milk: a systematic review. Hypertens Pregnancy. 2002;21(1):85-95.
34. Wilson BJ, Watson MS, Prescott GJ, et al. Hypertensive diseases of pregnancy and risk of hypertension and stroke in later life: results from cohort study. BMJ. 2003;326(7394):845.
Hypertensive disorders represent one of the most common medical complications of pregnancy.1,2 Based on a nationwide inpatient sample examining more than 36 million deliveries in the United States, the prevalence of associated hypertensive disorders increased from 67.2 per 1,000 deliveries in 1998 to 83.4 per 1,000 deliveries in 2006.3Pregnancy-induced hypertension (also referred to as gestational hypertension or hypertensive disorder of pregnancy)4-6 is estimated to affect 6% to 8% of US pregnancies.1,2
Women who develop severe hypertension during pregnancy may experience adverse effects similar to those associated with mild preeclampsia.2,7,8 In the mother, these may range from elevated liver enzymes to renal dysfunction; and in the fetus, from preterm delivery to intrauterine restriction of fetal growth.7,8
This article will review the risk factors, clinical presentation, diagnosis, and management of pregnancy-induced hypertension. A brief discussion of preeclampsia as it relates to gestational hypertension will be included (see Table 12,6,9).
Classification, Definitions
Pregnancy-induced hypertension (PIH) is classified as mild or severe. Mild PIH is defined as new-onset hypertension (systolic blood pressure ≥ 140 mm Hg and/or diastolic blood pressure ≥ 90 mm Hg), occurring after 20 weeks’ gestation. The majority of cases of mild PIH develop beyond 37 weeks’ gestation, and in these cases, pregnancy outcomes are comparable to those of normotensive pregnancies.2,7,8
Severe PIH is defined as sustained elevated blood pressures of ≥ 160 mm Hg systolic and ≥ 110 mm Hg diastolic. In prospective cohort studies in which calcium supplementation and low-dose aspirin use were being investigated for prevention of preeclampsia in healthy pregnant women, those who were severely hypertensive were found to be at increased risk for certain maternal comorbidities (eg, cesarean delivery, renal dysfunction, elevated liver enzymes, placental abruption) and perinatal morbidities (delivery before 37 weeks’ gestation, low birth weight, fetal growth restriction, and neonatal ICU admission), compared with patients who were normotensive or mildly hypertensive.7,8
The diagnosis of PIH may later be amended or replaced by one of the following diagnoses: preeclampsia, if proteinuria (to be defined and discussed later) develops; chronic hypertension, if blood pressure remains elevated past 12 weeks postpartum; or transient hypertension of pregnancy, if blood pressure normalizes by 12 weeks postpartum.5,6,10
Pathophysiology and Risk Factors
Although the pathophysiology of PIH is not well understood, the pathogenesis of preeclampsia likely involves abnormalities in the development, implantation, or perfusion of the placenta, and often leads to impaired maternal organ function.6,11 It is not clear whether PIH and preeclampsia are two different diseases that share a manifestation of elevated blood pressure or whether PIH represents an early stage of preeclampsia.4,12 However, women with preexisting hypertension, especially severe hypertension, are at increased risk for preeclampsia, placental abruption, and fetal growth restriction.2
There are some similarities and some distinct differences among the clinical features and risk factors associated with PIH, compared with those of preeclampsia. Risk factors for PIH include a pre-pregnancy BMI of 25 or greater, PIH and/or preeclampsia in previous pregnancies, and history of renal disease, cardiac disease, or diabetes. The most important risk factors for preeclampsia include preexisting diabetes or nephropathy, chronic hypertension, PIH or preeclampsia in a previous pregnancy, maternal age younger than 18 or older than 34, African-American ethnicity, first pregnancy, multiple pregnancy, history of preeclampsia in the patient’s mother or sister, obesity, autoimmune disease, and an interval between pregnancies longer than 10 years.4-6,13-15
The risk for preeclampsia in patients with PIH is approximately 15% to 25%12,16; according to Magee et al,6 35% of women with PIH onset before 37 weeks’ gestation develop preeclampsia.6,12,17 The risk for recurrence of PIH in subsequent pregnancies is about 26%, whereas women who experience preeclampsia in one pregnancy have a comparable risk for PIH or preeclampsia (about 14% each) in subsequent pregnancies.18
Clinical Presentation and Diagnostic Evaluation
Blood pressure should be measured and recorded at every prenatal visit, using the correct-sized cuff, with the patient in a seated position.5 Gestational hypertension is a clinical diagnosis confirmed by at least two accurate blood pressure measurements in the same arm in women without proteinuria, with readings of ≥ 140 mm Hg systolic and/or ≥ 90 mm Hg diastolic. It should then be determined whether the patient’s hypertension is mild or severe (ie, blood pressure > 160/110 mm Hg). The patient with severe PIH should be evaluated for signs of preeclampsia, as discussed below.
Patients with mild PIH are often asymptomatic, and the diagnosis is made at a prenatal visit as a result of routine blood pressure monitoring; this is one of many reasons to encourage early and regular prenatal care. Blood pressure may be higher at night in hypertensive disorders of pregnancy.10
In contrast to patients with mild PIH, the clinical presentation of those with severe PIH or preeclampsia (and the potential for impending eclampsia) may include the following symptoms and signs:
- Generalized edema, including that of the face and hands
- Rapid weight gain
- Blurred vision or scotomata (ie, areas of diminished vision in the visual field)
- Severe, throbbing or pounding headaches
- Epigastric or right upper quadrant pain
- Oliguria (urinary output < 500 mL/d)
- Nausea, with or without vomiting
- Hyperactive reflexes
- Chest pain or tightness
- Shortness of breath.2,6,14
Medical History
Important questions to address in the patient’s medical history relate to risk factors for PIH, such as a history of renal disease, cardiac disease, or diabetes, previous history of PIH and/or preeclampsia, and abuse of cocaine or amphetamines—in addition to the specific aforementioned symptoms and signs of severe preeclampsia.5,6
Physical Examination
The clinician performing the physical exam should be attentive to accurate blood pressure measurements and any signs that suggest preeclampsia. Weight should be measured and BMI calculated at each prenatal visit.
If the patient’s blood pressure is markedly elevated, the focused physical examination should include an ophthalmologic examination for jaundice and for evidence of hypertensive retinopathy or papilledema; pulmonary and cardiac examination; abdominal examination, including palpation of the liver; examination of the face and extremities for edema; and a complete neurologic examination, including assessment of deep tendon reflexes and examination for clonus.
Laboratory Testing
In patients with PIH, laboratory evaluation should be focused to rule out preeclampsia. The potential for proteinuria (defined as ≥ 0.3 g/d in a 24-hour urine sample1,14) must be investigated at diagnosis and at regular visits during the pregnancy.1 At least two random urine samples, collected at least 6 hours apart, should be evaluated for protein. A spot (random) urine sample with a result of 2+ protein or greater is highly suggestive of proteinuria; a 24-hour urine collection is the gold standard by which such findings should be confirmed and protein levels in the urine quantified.1,14
Elevated blood pressure and proteinuria are the hallmarks of preeclampsia.6 Patients affected by these developments must be evaluated for signs and symptoms of severe preeclampsia. However, those with only mild elevations in blood pressure and little or no proteinuria may complain of sudden-onset throbbing or pounding headache, blurry vision, and severe epigastric pain—possibly indicating severe preeclampsia.5,10
In addition to laboratory evaluation for urinary protein excretion, the following tests are recommended by the American College of Obstetricians and Gynecologists (ACOG)14 to assess for end organ involvement, which is consistent with severe preeclampsia:
- Hematocrit, which may be either high, to suggest hemoconcentration; or low, indicating hemolysis
- Platelet count, which is normal in women with PIH and low in those with severe preeclampsia; if results are abnormal, this test should be followed by coagulation testing (international normalized ratio, activated partial thromboplastin time, fibrinogen)
- Renal function testing (blood urea nitrogen and creatinine may be elevated in severe preeclampsia), and random urine testing for proteinuria, as explained earlier
- Liver enzymes (which are elevated in severe preeclampsia), and
- Lactate dehydrogenase (which is elevated in severe preeclampsia).1,14
Additionally, researchers conducting a small cohort study (n = 163) reported in 2009 that in women with PIH, serum uric acid levels exceeding 309 µmol/L were predictive of preeclampsia, with 87.7% sensitivity and 93.3% specificity.19 An increase from first-trimester serum uric acid levels was also a strong prognostic factor for preeclampsia. Earlier this year, a Canadian investigative team reported an increased risk for premature birth (odds ratio, 3.2) and small infant size for gestational age (odds ratio, 2.5) in women with PIH and hyperuricemia.20 While the predictive value of uric acid has been debated to some extent,14 measurement is often included in the workup of patients with hypertensive pregnancies.5,6
The frequency of prenatal visits, laboratory testing, and fetal monitoring should be adjusted according to the severity of PIH. In mildly hypertensive patients, the general recommendation is urine and blood testing at weekly prenatal visits.14 Fetal well-being must be monitored regularly, although neither the type nor frequency of such testing has been well established. Generally, patients should be advised to count daily fetal movements, and they should be scheduled for either a nonstress test (NST) or a biophysical profile as soon as a diagnosis of PIH is made.1,2,6,14
According to a 2010 guidance from the United Kingdom’s National Institute for Health and Clinical Excellence (NICE),13,21 pregnant women with mild to moderate hypertension should undergo an initial ultrasonographic assessment of fetal growth and amniotic fluid volume at the time of diagnosis, then serially every 3 to 4 weeks. If results from initial fetal testing are normal, patients with mild PIH do not require repeat testing after 34 weeks’ gestation, unless conditions change (eg, preeclampsia, worsening hypertension, and/or change in fetal movements).1,2,14 The NICE guidelines also recommend umbilical artery Doppler velocimetry.13,21
In patients with severe PIH, an NST ultrasound assessment of fetal growth and amniotic fluid volume and umbilical artery Doppler velocimetry should be performed at diagnosis to evaluate for placental dysfunction.6,21 If all test results are normal, the ultrasound and umbilical artery Doppler velocimetry need not be repeated more frequently than every two weeks, and the NST no more than once per week.13
Treatment/Management and Follow-Up
Regular prenatal monitoring to assess for worsening of PIH and/or development of preeclampsia is key to management. Figure 12 outlines an algorithm for managing PIH, which is guided by the severity of the condition. Patients with mild PIH can be managed with weekly outpatient visits and assessed for signs and symptoms of preeclampsia, monitoring of fetal movements, weight, blood pressure measurements, and urine and blood tests.2
At each visit, it is important to instruct patients to report immediately any of the following symptoms: new-onset severe headache, visual changes, epigastric or right upper quadrant pain, nausea or vomiting, difficulty breathing or chest tightness, as well as vaginal bleeding, decreased fetal movements, or uterine contractions.6,14
Generally, expectant management with delivery at term is recommended for women with mild PIH.2 Vaginal delivery (or cesarean delivery, if indicated) is recommended at 37 weeks or when fetal maturity is confirmed; and at 34 weeks if fetal or maternal distress is evident.2,6
Findings from the Hypertension and Preeclampsia Intervention Trial At Term (HYPITAT),22 an open-label, randomized clinical trial in women with PIH or mild preeclampsia, suggested an association between induction of labor between 36 and 41 weeks’ gestation and improved maternal outcomes (specifically, reduced risk for severe hypertension), compared with expectant management. Similarly, in a literature review by Caughey et al,23 results from nine randomized controlled trials indicated a reduced risk for cesarean delivery in women who underwent induction of labor, compared with expectant management. Rates of “successful” induction of labor (ie, procedures resulting in vaginal rather than cesarean delivery) were greater in women with higher parity, a favorable cervix, and earlier gestational age.
Based on data from the HYPITAT trial,22 a cost-effectiveness analysis of induction of labor compared with expectant management revealed an 11% reduction in the average cost in delivery that followed induction of labor, compared with expectant management, in women with PIH or mild preeclampsia.24 Caughey et al23 reported similar savings, particularly when induction of labor was performed at 41 weeks’ gestation.
If induction of labor is being considered in a woman with an unfavorable cervix, administration of prostaglandins is recommended to enhance cervical ripening.6
Medication
Pregnant women should be advised to discontinue previously prescribed ACE inhibitors, angiotensin receptor blockers, or thiazide diuretics, which are associated with congenital abnormalities, intrauterine growth restriction, and/or neonatal nephropathy.5,6,13,21
Antihypertensive medication is not recommended for women with mild to moderate PIH, as it does not appear to improve outcomes. Evidence was found insufficient in a 2007 Cochrane review to determine the potential impact of antihypertensive medications for treatment of mild to moderate PIH on clinical outcomes such as preterm birth, infant mortality, and infant size relative to gestational age.25 A similar review conducted in 2011, with primary outcomes that included severe preeclampsia, eclampsia, and maternal death or perinatal death, concluded only that further study was needed to determine how tightly blood pressure must be controlled to improve maternal and fetal outcomes in patients with PIH.26
ACOG14 recommends antihypertensive therapy (eg, hydralazine, labetalol) only for women with diastolic blood pressure of 105 to 110 mm Hg or higher.1,2 There are several recommendations from different organizations regarding the choice of antihypertensive medications for PIH. In the UK’s NICE guidance,21 it is recommended that patients with moderate to severe PIH take oral labetalol as first-line treatment to keep systolic blood pressure below 150 mm Hg and diastolic blood pressure between 80 and 100 mm Hg.
Like severe preeclampsia, severe PIH should be managed in an inpatient setting.6,14 IV labetalol or hydralazine is recommended to lower the blood pressure to less than 160/110 mm Hg, although current evidence is insufficient to identify a target blood pressure.6,26 A 2002 ACOG practice bulletin recommends one of the following:
- Hydralazine 5 to 10 mg IV every 15 to 20 minutes until the desired response is achieved; or
- Labetalol 20 mg IV bolus, followed by 40 mg if not effective within 10 minutes, then 80 mg every 10 minutes with maximum total dose of 220 mg.1,14
In women who have severe PIH or who develop severe preeclampsia or eclampsia, magnesium sulfate is administered to prevent or treat seizures.14 This agent should be used during labor and for at least 24 hours postpartum.2 Dosing of magnesium sulfate for this indication is 4 g IV bolus, followed by infusion of 1 g/h. It is important to monitor treated patients for signs of toxicity, including muscle weakness, loss of patellar reflexes, hypoventilation, pulmonary edema, hypotension, and bradycardia. IV calcium gluconate should be readily available for use as an antidote to life-threatening hypermagnesemia.27,28
For chronic hypertension in pregnancy, the American Society of Hypertension10 has recommended several agents. There is no consensus on which medication is most appropriate (see Table 210,13).
Patient Education
Patient education is an important aspect of caring for women with PIH. The American Academy of Family Physicians29,30 provides a comprehensive patient education resource that defines the hypertensive disorders in pregnancy, explains the symptoms and signs of severe hypertension or preeclampsia, and describes appropriate diagnostic tests, monitoring, and treatment options. (See http://familydoctor.org/familydoctor/en/diseases-conditions/pregnancy-induced-hypertension.printerview.all.html.)
Patients who are considering pregnancy should be counseled to maintain a healthy weight prior to and during pregnancy. Adequate dietary calcium can reduce the risk for PIH, and calcium supplementation has been shown to reduce the risk for preeclampsia, especially in women at high risk.31 The Society of Obstetricians and Gynaecologists of Canada recommends low-dose aspirin (75 mg/d) at bedtime for high-risk women, starting before pregnancy, or upon diagnosis of pregnancy to prevent preeclampsia.6 Although there is insufficient evidence to recommend dietary salt restriction, excess salt can increase fluid retention and possibly blood pressure. Patients should be urged to attend all scheduled prenatal visits and to review the warning signs and symptoms of severe hypertension and preeclampsia at each visit.
Mode of delivery may be discussed and will depend on the severity of hypertension, presence of preeclampsia, and fetal well-being. Vaginal delivery at term is considered optimal unless there are indications for cesarean delivery. Induction of labor may be considered at term in patients with PIH. Those with severe preeclampsia who may require preterm delivery must be prepared for potential issues associated with prematurity.
Follow-Up and Prognosis
Patients with PIH should be evaluated postpartum for persistent hypertension. Blood pressure in patients with PIH usually normalizes by day 7 postpartum.32 If blood pressure elevation persists past 12 weeks postpartum, the patient’s diagnosis is revised to chronic hypertension and managed accordingly.
In the patient with persistent hypertension who chooses breastfeeding, it is important to select an antihypertensive medication with low transfer into breast milk. Many β-adrenergic antagonists and calcium channel antagonists are considered “compatible” with breastfeeding by the American Academy of Pediatrics.33
In addition to the potential for recurrent PIH in subsequent pregnancies, women with PIH are at increased risk for hypertension later in life, and findings from several large cohort studies suggest increased cardiovascular risk in patients with hypertensive pregnancies.16,34 Magnussen et al,9 who followed more than 15,000 mothers of singleton infants for several years postpartum, found that those who experienced hypertensive disorders (particularly recurrent hypertensive disorders) during pregnancy were more likely than normotensive women to subsequently develop diabetes, dyslipidemia, and hypertension. Women who remained normotensive while pregnant generally had lower BMI measurements than those who experienced PIH or preeclampsia.
Conclusion
Hypertensive disorders commonly develop during pregnancy. It is important to diagnose and classify PIH during routine prenatal visits. Once the diagnosis is made, patients must be monitored closely for increasing blood pressure or development of preeclampsia. Urine protein testing is a key clinical test to detect preeclampsia, and positive findings on a random urine protein dipstick should be confirmed and quantified with a 24-hour urine collection.
In addition to undergoing frequent blood pressure measurements and urine protein tests, patients should be asked about signs and symptoms that suggest preeclampsia. Women with mild PIH can be managed as outpatients with prenatal visits at least weekly, followed by delivery at term. Severely hypertensive patients are managed in the hospital with antihypertensive medications and prompt delivery at 34 weeks’ gestation or beyond, should maternal or fetal distress become evident.
Hypertensive disorders represent one of the most common medical complications of pregnancy.1,2 Based on a nationwide inpatient sample examining more than 36 million deliveries in the United States, the prevalence of associated hypertensive disorders increased from 67.2 per 1,000 deliveries in 1998 to 83.4 per 1,000 deliveries in 2006.3Pregnancy-induced hypertension (also referred to as gestational hypertension or hypertensive disorder of pregnancy)4-6 is estimated to affect 6% to 8% of US pregnancies.1,2
Women who develop severe hypertension during pregnancy may experience adverse effects similar to those associated with mild preeclampsia.2,7,8 In the mother, these may range from elevated liver enzymes to renal dysfunction; and in the fetus, from preterm delivery to intrauterine restriction of fetal growth.7,8
This article will review the risk factors, clinical presentation, diagnosis, and management of pregnancy-induced hypertension. A brief discussion of preeclampsia as it relates to gestational hypertension will be included (see Table 12,6,9).
Classification, Definitions
Pregnancy-induced hypertension (PIH) is classified as mild or severe. Mild PIH is defined as new-onset hypertension (systolic blood pressure ≥ 140 mm Hg and/or diastolic blood pressure ≥ 90 mm Hg), occurring after 20 weeks’ gestation. The majority of cases of mild PIH develop beyond 37 weeks’ gestation, and in these cases, pregnancy outcomes are comparable to those of normotensive pregnancies.2,7,8
Severe PIH is defined as sustained elevated blood pressures of ≥ 160 mm Hg systolic and ≥ 110 mm Hg diastolic. In prospective cohort studies in which calcium supplementation and low-dose aspirin use were being investigated for prevention of preeclampsia in healthy pregnant women, those who were severely hypertensive were found to be at increased risk for certain maternal comorbidities (eg, cesarean delivery, renal dysfunction, elevated liver enzymes, placental abruption) and perinatal morbidities (delivery before 37 weeks’ gestation, low birth weight, fetal growth restriction, and neonatal ICU admission), compared with patients who were normotensive or mildly hypertensive.7,8
The diagnosis of PIH may later be amended or replaced by one of the following diagnoses: preeclampsia, if proteinuria (to be defined and discussed later) develops; chronic hypertension, if blood pressure remains elevated past 12 weeks postpartum; or transient hypertension of pregnancy, if blood pressure normalizes by 12 weeks postpartum.5,6,10
Pathophysiology and Risk Factors
Although the pathophysiology of PIH is not well understood, the pathogenesis of preeclampsia likely involves abnormalities in the development, implantation, or perfusion of the placenta, and often leads to impaired maternal organ function.6,11 It is not clear whether PIH and preeclampsia are two different diseases that share a manifestation of elevated blood pressure or whether PIH represents an early stage of preeclampsia.4,12 However, women with preexisting hypertension, especially severe hypertension, are at increased risk for preeclampsia, placental abruption, and fetal growth restriction.2
There are some similarities and some distinct differences among the clinical features and risk factors associated with PIH, compared with those of preeclampsia. Risk factors for PIH include a pre-pregnancy BMI of 25 or greater, PIH and/or preeclampsia in previous pregnancies, and history of renal disease, cardiac disease, or diabetes. The most important risk factors for preeclampsia include preexisting diabetes or nephropathy, chronic hypertension, PIH or preeclampsia in a previous pregnancy, maternal age younger than 18 or older than 34, African-American ethnicity, first pregnancy, multiple pregnancy, history of preeclampsia in the patient’s mother or sister, obesity, autoimmune disease, and an interval between pregnancies longer than 10 years.4-6,13-15
The risk for preeclampsia in patients with PIH is approximately 15% to 25%12,16; according to Magee et al,6 35% of women with PIH onset before 37 weeks’ gestation develop preeclampsia.6,12,17 The risk for recurrence of PIH in subsequent pregnancies is about 26%, whereas women who experience preeclampsia in one pregnancy have a comparable risk for PIH or preeclampsia (about 14% each) in subsequent pregnancies.18
Clinical Presentation and Diagnostic Evaluation
Blood pressure should be measured and recorded at every prenatal visit, using the correct-sized cuff, with the patient in a seated position.5 Gestational hypertension is a clinical diagnosis confirmed by at least two accurate blood pressure measurements in the same arm in women without proteinuria, with readings of ≥ 140 mm Hg systolic and/or ≥ 90 mm Hg diastolic. It should then be determined whether the patient’s hypertension is mild or severe (ie, blood pressure > 160/110 mm Hg). The patient with severe PIH should be evaluated for signs of preeclampsia, as discussed below.
Patients with mild PIH are often asymptomatic, and the diagnosis is made at a prenatal visit as a result of routine blood pressure monitoring; this is one of many reasons to encourage early and regular prenatal care. Blood pressure may be higher at night in hypertensive disorders of pregnancy.10
In contrast to patients with mild PIH, the clinical presentation of those with severe PIH or preeclampsia (and the potential for impending eclampsia) may include the following symptoms and signs:
- Generalized edema, including that of the face and hands
- Rapid weight gain
- Blurred vision or scotomata (ie, areas of diminished vision in the visual field)
- Severe, throbbing or pounding headaches
- Epigastric or right upper quadrant pain
- Oliguria (urinary output < 500 mL/d)
- Nausea, with or without vomiting
- Hyperactive reflexes
- Chest pain or tightness
- Shortness of breath.2,6,14
Medical History
Important questions to address in the patient’s medical history relate to risk factors for PIH, such as a history of renal disease, cardiac disease, or diabetes, previous history of PIH and/or preeclampsia, and abuse of cocaine or amphetamines—in addition to the specific aforementioned symptoms and signs of severe preeclampsia.5,6
Physical Examination
The clinician performing the physical exam should be attentive to accurate blood pressure measurements and any signs that suggest preeclampsia. Weight should be measured and BMI calculated at each prenatal visit.
If the patient’s blood pressure is markedly elevated, the focused physical examination should include an ophthalmologic examination for jaundice and for evidence of hypertensive retinopathy or papilledema; pulmonary and cardiac examination; abdominal examination, including palpation of the liver; examination of the face and extremities for edema; and a complete neurologic examination, including assessment of deep tendon reflexes and examination for clonus.
Laboratory Testing
In patients with PIH, laboratory evaluation should be focused to rule out preeclampsia. The potential for proteinuria (defined as ≥ 0.3 g/d in a 24-hour urine sample1,14) must be investigated at diagnosis and at regular visits during the pregnancy.1 At least two random urine samples, collected at least 6 hours apart, should be evaluated for protein. A spot (random) urine sample with a result of 2+ protein or greater is highly suggestive of proteinuria; a 24-hour urine collection is the gold standard by which such findings should be confirmed and protein levels in the urine quantified.1,14
Elevated blood pressure and proteinuria are the hallmarks of preeclampsia.6 Patients affected by these developments must be evaluated for signs and symptoms of severe preeclampsia. However, those with only mild elevations in blood pressure and little or no proteinuria may complain of sudden-onset throbbing or pounding headache, blurry vision, and severe epigastric pain—possibly indicating severe preeclampsia.5,10
In addition to laboratory evaluation for urinary protein excretion, the following tests are recommended by the American College of Obstetricians and Gynecologists (ACOG)14 to assess for end organ involvement, which is consistent with severe preeclampsia:
- Hematocrit, which may be either high, to suggest hemoconcentration; or low, indicating hemolysis
- Platelet count, which is normal in women with PIH and low in those with severe preeclampsia; if results are abnormal, this test should be followed by coagulation testing (international normalized ratio, activated partial thromboplastin time, fibrinogen)
- Renal function testing (blood urea nitrogen and creatinine may be elevated in severe preeclampsia), and random urine testing for proteinuria, as explained earlier
- Liver enzymes (which are elevated in severe preeclampsia), and
- Lactate dehydrogenase (which is elevated in severe preeclampsia).1,14
Additionally, researchers conducting a small cohort study (n = 163) reported in 2009 that in women with PIH, serum uric acid levels exceeding 309 µmol/L were predictive of preeclampsia, with 87.7% sensitivity and 93.3% specificity.19 An increase from first-trimester serum uric acid levels was also a strong prognostic factor for preeclampsia. Earlier this year, a Canadian investigative team reported an increased risk for premature birth (odds ratio, 3.2) and small infant size for gestational age (odds ratio, 2.5) in women with PIH and hyperuricemia.20 While the predictive value of uric acid has been debated to some extent,14 measurement is often included in the workup of patients with hypertensive pregnancies.5,6
The frequency of prenatal visits, laboratory testing, and fetal monitoring should be adjusted according to the severity of PIH. In mildly hypertensive patients, the general recommendation is urine and blood testing at weekly prenatal visits.14 Fetal well-being must be monitored regularly, although neither the type nor frequency of such testing has been well established. Generally, patients should be advised to count daily fetal movements, and they should be scheduled for either a nonstress test (NST) or a biophysical profile as soon as a diagnosis of PIH is made.1,2,6,14
According to a 2010 guidance from the United Kingdom’s National Institute for Health and Clinical Excellence (NICE),13,21 pregnant women with mild to moderate hypertension should undergo an initial ultrasonographic assessment of fetal growth and amniotic fluid volume at the time of diagnosis, then serially every 3 to 4 weeks. If results from initial fetal testing are normal, patients with mild PIH do not require repeat testing after 34 weeks’ gestation, unless conditions change (eg, preeclampsia, worsening hypertension, and/or change in fetal movements).1,2,14 The NICE guidelines also recommend umbilical artery Doppler velocimetry.13,21
In patients with severe PIH, an NST ultrasound assessment of fetal growth and amniotic fluid volume and umbilical artery Doppler velocimetry should be performed at diagnosis to evaluate for placental dysfunction.6,21 If all test results are normal, the ultrasound and umbilical artery Doppler velocimetry need not be repeated more frequently than every two weeks, and the NST no more than once per week.13
Treatment/Management and Follow-Up
Regular prenatal monitoring to assess for worsening of PIH and/or development of preeclampsia is key to management. Figure 12 outlines an algorithm for managing PIH, which is guided by the severity of the condition. Patients with mild PIH can be managed with weekly outpatient visits and assessed for signs and symptoms of preeclampsia, monitoring of fetal movements, weight, blood pressure measurements, and urine and blood tests.2
At each visit, it is important to instruct patients to report immediately any of the following symptoms: new-onset severe headache, visual changes, epigastric or right upper quadrant pain, nausea or vomiting, difficulty breathing or chest tightness, as well as vaginal bleeding, decreased fetal movements, or uterine contractions.6,14
Generally, expectant management with delivery at term is recommended for women with mild PIH.2 Vaginal delivery (or cesarean delivery, if indicated) is recommended at 37 weeks or when fetal maturity is confirmed; and at 34 weeks if fetal or maternal distress is evident.2,6
Findings from the Hypertension and Preeclampsia Intervention Trial At Term (HYPITAT),22 an open-label, randomized clinical trial in women with PIH or mild preeclampsia, suggested an association between induction of labor between 36 and 41 weeks’ gestation and improved maternal outcomes (specifically, reduced risk for severe hypertension), compared with expectant management. Similarly, in a literature review by Caughey et al,23 results from nine randomized controlled trials indicated a reduced risk for cesarean delivery in women who underwent induction of labor, compared with expectant management. Rates of “successful” induction of labor (ie, procedures resulting in vaginal rather than cesarean delivery) were greater in women with higher parity, a favorable cervix, and earlier gestational age.
Based on data from the HYPITAT trial,22 a cost-effectiveness analysis of induction of labor compared with expectant management revealed an 11% reduction in the average cost in delivery that followed induction of labor, compared with expectant management, in women with PIH or mild preeclampsia.24 Caughey et al23 reported similar savings, particularly when induction of labor was performed at 41 weeks’ gestation.
If induction of labor is being considered in a woman with an unfavorable cervix, administration of prostaglandins is recommended to enhance cervical ripening.6
Medication
Pregnant women should be advised to discontinue previously prescribed ACE inhibitors, angiotensin receptor blockers, or thiazide diuretics, which are associated with congenital abnormalities, intrauterine growth restriction, and/or neonatal nephropathy.5,6,13,21
Antihypertensive medication is not recommended for women with mild to moderate PIH, as it does not appear to improve outcomes. Evidence was found insufficient in a 2007 Cochrane review to determine the potential impact of antihypertensive medications for treatment of mild to moderate PIH on clinical outcomes such as preterm birth, infant mortality, and infant size relative to gestational age.25 A similar review conducted in 2011, with primary outcomes that included severe preeclampsia, eclampsia, and maternal death or perinatal death, concluded only that further study was needed to determine how tightly blood pressure must be controlled to improve maternal and fetal outcomes in patients with PIH.26
ACOG14 recommends antihypertensive therapy (eg, hydralazine, labetalol) only for women with diastolic blood pressure of 105 to 110 mm Hg or higher.1,2 There are several recommendations from different organizations regarding the choice of antihypertensive medications for PIH. In the UK’s NICE guidance,21 it is recommended that patients with moderate to severe PIH take oral labetalol as first-line treatment to keep systolic blood pressure below 150 mm Hg and diastolic blood pressure between 80 and 100 mm Hg.
Like severe preeclampsia, severe PIH should be managed in an inpatient setting.6,14 IV labetalol or hydralazine is recommended to lower the blood pressure to less than 160/110 mm Hg, although current evidence is insufficient to identify a target blood pressure.6,26 A 2002 ACOG practice bulletin recommends one of the following:
- Hydralazine 5 to 10 mg IV every 15 to 20 minutes until the desired response is achieved; or
- Labetalol 20 mg IV bolus, followed by 40 mg if not effective within 10 minutes, then 80 mg every 10 minutes with maximum total dose of 220 mg.1,14
In women who have severe PIH or who develop severe preeclampsia or eclampsia, magnesium sulfate is administered to prevent or treat seizures.14 This agent should be used during labor and for at least 24 hours postpartum.2 Dosing of magnesium sulfate for this indication is 4 g IV bolus, followed by infusion of 1 g/h. It is important to monitor treated patients for signs of toxicity, including muscle weakness, loss of patellar reflexes, hypoventilation, pulmonary edema, hypotension, and bradycardia. IV calcium gluconate should be readily available for use as an antidote to life-threatening hypermagnesemia.27,28
For chronic hypertension in pregnancy, the American Society of Hypertension10 has recommended several agents. There is no consensus on which medication is most appropriate (see Table 210,13).
Patient Education
Patient education is an important aspect of caring for women with PIH. The American Academy of Family Physicians29,30 provides a comprehensive patient education resource that defines the hypertensive disorders in pregnancy, explains the symptoms and signs of severe hypertension or preeclampsia, and describes appropriate diagnostic tests, monitoring, and treatment options. (See http://familydoctor.org/familydoctor/en/diseases-conditions/pregnancy-induced-hypertension.printerview.all.html.)
Patients who are considering pregnancy should be counseled to maintain a healthy weight prior to and during pregnancy. Adequate dietary calcium can reduce the risk for PIH, and calcium supplementation has been shown to reduce the risk for preeclampsia, especially in women at high risk.31 The Society of Obstetricians and Gynaecologists of Canada recommends low-dose aspirin (75 mg/d) at bedtime for high-risk women, starting before pregnancy, or upon diagnosis of pregnancy to prevent preeclampsia.6 Although there is insufficient evidence to recommend dietary salt restriction, excess salt can increase fluid retention and possibly blood pressure. Patients should be urged to attend all scheduled prenatal visits and to review the warning signs and symptoms of severe hypertension and preeclampsia at each visit.
Mode of delivery may be discussed and will depend on the severity of hypertension, presence of preeclampsia, and fetal well-being. Vaginal delivery at term is considered optimal unless there are indications for cesarean delivery. Induction of labor may be considered at term in patients with PIH. Those with severe preeclampsia who may require preterm delivery must be prepared for potential issues associated with prematurity.
Follow-Up and Prognosis
Patients with PIH should be evaluated postpartum for persistent hypertension. Blood pressure in patients with PIH usually normalizes by day 7 postpartum.32 If blood pressure elevation persists past 12 weeks postpartum, the patient’s diagnosis is revised to chronic hypertension and managed accordingly.
In the patient with persistent hypertension who chooses breastfeeding, it is important to select an antihypertensive medication with low transfer into breast milk. Many β-adrenergic antagonists and calcium channel antagonists are considered “compatible” with breastfeeding by the American Academy of Pediatrics.33
In addition to the potential for recurrent PIH in subsequent pregnancies, women with PIH are at increased risk for hypertension later in life, and findings from several large cohort studies suggest increased cardiovascular risk in patients with hypertensive pregnancies.16,34 Magnussen et al,9 who followed more than 15,000 mothers of singleton infants for several years postpartum, found that those who experienced hypertensive disorders (particularly recurrent hypertensive disorders) during pregnancy were more likely than normotensive women to subsequently develop diabetes, dyslipidemia, and hypertension. Women who remained normotensive while pregnant generally had lower BMI measurements than those who experienced PIH or preeclampsia.
Conclusion
Hypertensive disorders commonly develop during pregnancy. It is important to diagnose and classify PIH during routine prenatal visits. Once the diagnosis is made, patients must be monitored closely for increasing blood pressure or development of preeclampsia. Urine protein testing is a key clinical test to detect preeclampsia, and positive findings on a random urine protein dipstick should be confirmed and quantified with a 24-hour urine collection.
In addition to undergoing frequent blood pressure measurements and urine protein tests, patients should be asked about signs and symptoms that suggest preeclampsia. Women with mild PIH can be managed as outpatients with prenatal visits at least weekly, followed by delivery at term. Severely hypertensive patients are managed in the hospital with antihypertensive medications and prompt delivery at 34 weeks’ gestation or beyond, should maternal or fetal distress become evident.
1. Report of the National High Blood Pressure Education Program Working Group on high blood pressure in pregnancy. Am J Obstet Gynecol. 2000;183(1):S1-S22.
2. Sibai BM. Diagnosis and management of gestational hypertension and preeclampsia. Obstet Gynecol. 2003;102(1):181-192.
3. Kuklina EV, Ayala C, Callaghan WM. Hypertensive disorders and severe obstetric morbidity in the United States. Obstet Gynecol. 2009; 113(6):1299-1306.
4. Villar J, Carroli, G, Wojdyla D, et al; World Health Organization Antenatal Care Trial Research Group. Preeclampsia, gestational hypertension and intrauterine growth restriction, related or independent conditions. Am J Obstet Gynecol. 2006;194(4):921-931.
5. Leeman L, Fontaine P. Hypertensive disorders of pregnancy. Am Fam Physician. 2008;78(1):
93-100.
6. Magee LA, Helewa M, Moutquin JM, von Dadelszen P; Hypertension Guideline Committee; Strategic Training Initiative in Research in the Reproductive Health Sciences (STIRRHS) Scholars. Diagnosis, evaluation, and management of the hypertensive disorders of pregnancy. J Obstet Gynaecol Can. 2008;30(3 suppl):S1-S48.
7. Buchbinder A, Sibai BM, Caritis S, et al. Adverse perinatal outcomes are significantly higher in severe gestational hypertension than in mild preeclampsia. Am J Obstet Gynecol. 2002;186(1):66-71.
8. Hauth JC, Ewell MG, Levine RJ, et al; Calcium for Preeclampsia Prevention Study Group. Pregnancy outcomes in healthy nulliparas who developed hypertension. Obstet Gynecol. 2000;95(1):24-28.
9. Magnussen EB, Vatten LJ, Smith GD, Romundstad PR. Hypertensive disorders in pregnancy and subsequently measured cardiovascular risk factors. Obstet Gynecol. 2009; 114(5):961-970.
10. Lindheimer MD, Taler SJ, Cunningham FG; American Society of Hypertension (ASH). ASH position paper: hypertension in pregnancy. J Clin Hypertens (Greenwich). 2009;11(4):214-225.
11. Roberts JM, Gammill HS. Preeclampsia: recent insights. Hypertension. 2005;46(6):
1243-1249.
12. Saudan P, Brown MA, Buddle ML, Jones M. Does gestational hypertension become pre-eclampsia? Br J Obstet Gynaecol. 1998;105 (11):1177-1184.
13. Visintin C, Mugglestone MA, Almerie MQ, et al; Guideline Development Group. Management of hypertensive disorders during pregnancy: summary of NICE guidance. BMJ. 2010;341:c2207.
14. ACOG Committee on Practice Bulletins—Obstetrics. Clinical Management Guidelines for Obstetrician–Gynecologists. Diagnosis and management of preeclampsia and eclampsia: ACOG practice bulletin No. 33. Obstet Gynecol. 2002;99:159-167.
15. Parazzini F, Bortolus R, Chatenoud L, et al; Italian Study of Aspirin in Pregnancy Group. Risk factors for pregnancy-induced hypertension in women at high risk for the condition. Epidemiology. 1996;7(3):306-308.
16. Hjartardottir S, Leifsson BG, Geirsson RT, Steinthorsdottir V. Recurrence of hypertensive disorder in second pregnancy. Am J Obstet Gynecol. 2006;194(4):916-920.
17. Barton JR, O’Brien JM, Bergauer NK, et al. Mild gestational hypertension remote from term: progression and outcome. Am J Obstet Gynecol. 2001;184(5):979-983.
18. Brown MA, Mackenzie C, Dunsmuir W, et al. Can we predict recurrence of pre-eclampsia or gestational hypertension? BJOG. 2007; 114(8):984-993.
19. Bellomo G, Venanzi S, Saronio P, et al. Prognostic significance of serum uric acid in women with gestational hypertension. Hypertension. 2011;58(4):704-708.
20. Hawkins TL, Roberts JM, Mangos GJ, et al. Plasma uric acid remains a marker of poor outcome in hypertensive pregnancy: a retrospective cohort study. BJOG. 2012;119(4):484-492.
21. National Institute for Health and Clinical Excellence. Hypertension in pregnancy: the management of hypertensive disorders during pregnancy. www.nice.org.uk/nicemedia/live/13098/50418/50418.pdf. Accessed April 16, 2012.
22. Koopmans CM, Bijlenga D, Groen H, et al. Induction of labour versus expectant monitoring for gestational hypertension or mild pre-eclampsia after 36 weeks’ gestation (HYPITAT): a multicentre, open-label randomised controlled trial. Lancet. 2009;374(9694):979-988.
23. Caughey AB, Sundaram V, Kaimal AJ, et al. Maternal and neonatal outcomes of elective induction of labor. Evid Rep Technol Assess (Full Rep). 2009;(176):1-257.
24. Shennan A, Hezelgrave N. An economic analysis of induction of labour and expectant monitoring in women with gestational hypertension or pre-eclampsia at term (HYPITAT trial). BJOG. 2010;117(13):1575-1576.
25. Abalos E, Duley L, Steyn DW, Henderson-Smart DJ. Antihypertensive drug therapy for mild to moderate hypertension during pregnancy. Cochrane Database Syst Rev. 2007 Jan 24;(1):CD002252.
26. Nabhan AF, Elsedawy MM. Tight control of mild-moderate pre-existing or non-proteinuric gestational hypertension. Cochrane Database Syst Rev. 2011 Jul 6;(7):CD006907.
27. Duley L, Gülmezoglu AM, Henderson-Smart DJ. Magnesium sulphate and other anticonvulsants for women with preeclampsia. Cochrane Database Syst Rev. 2003;(2):CD000025.
28. Kraft MD, Btaiche IF, Sacks GS, Kudsk KA. Treatment of electrolyte disorders in adult patients in the intensive care unit. Am J Health Syst Pharm. 2005;62(16):1663-1682.
29. FamilyDoctor.org. Pregnancy-induced hypertension (updated 2010). http://familydoctor.org/familydoctor/en/diseases-conditions/pregnancy-induced-hypertension.printerview
.all.html. Accessed April 16, 2012.
30. Zamorski MA, Green LA. NHBPEP report on high blood pressure in pregnancy: a summary for family physicians. Am Fam Physician. 2001; 64(2):263-270.
31. Hofmeyr GJ, Duley L, Atallah A. Dietary calcium supplementation for prevention of pre-eclampsia and related problems: a systematic review and commentary. BJOG. 2007;114(8): 933-943.
32. Ferrazzani S, De Carolis S, Pomini F, et al. The duration of hypertension in the puerperium of preeclamptic women: relationship with renal impairment and week of delivery. Am J Obstet Gynecol. 1994;171(2):506-512.
33. Beardmore KS, Morris JM, Gallery ED. Excretion of antihypertensive medication into human breast milk: a systematic review. Hypertens Pregnancy. 2002;21(1):85-95.
34. Wilson BJ, Watson MS, Prescott GJ, et al. Hypertensive diseases of pregnancy and risk of hypertension and stroke in later life: results from cohort study. BMJ. 2003;326(7394):845.
1. Report of the National High Blood Pressure Education Program Working Group on high blood pressure in pregnancy. Am J Obstet Gynecol. 2000;183(1):S1-S22.
2. Sibai BM. Diagnosis and management of gestational hypertension and preeclampsia. Obstet Gynecol. 2003;102(1):181-192.
3. Kuklina EV, Ayala C, Callaghan WM. Hypertensive disorders and severe obstetric morbidity in the United States. Obstet Gynecol. 2009; 113(6):1299-1306.
4. Villar J, Carroli, G, Wojdyla D, et al; World Health Organization Antenatal Care Trial Research Group. Preeclampsia, gestational hypertension and intrauterine growth restriction, related or independent conditions. Am J Obstet Gynecol. 2006;194(4):921-931.
5. Leeman L, Fontaine P. Hypertensive disorders of pregnancy. Am Fam Physician. 2008;78(1):
93-100.
6. Magee LA, Helewa M, Moutquin JM, von Dadelszen P; Hypertension Guideline Committee; Strategic Training Initiative in Research in the Reproductive Health Sciences (STIRRHS) Scholars. Diagnosis, evaluation, and management of the hypertensive disorders of pregnancy. J Obstet Gynaecol Can. 2008;30(3 suppl):S1-S48.
7. Buchbinder A, Sibai BM, Caritis S, et al. Adverse perinatal outcomes are significantly higher in severe gestational hypertension than in mild preeclampsia. Am J Obstet Gynecol. 2002;186(1):66-71.
8. Hauth JC, Ewell MG, Levine RJ, et al; Calcium for Preeclampsia Prevention Study Group. Pregnancy outcomes in healthy nulliparas who developed hypertension. Obstet Gynecol. 2000;95(1):24-28.
9. Magnussen EB, Vatten LJ, Smith GD, Romundstad PR. Hypertensive disorders in pregnancy and subsequently measured cardiovascular risk factors. Obstet Gynecol. 2009; 114(5):961-970.
10. Lindheimer MD, Taler SJ, Cunningham FG; American Society of Hypertension (ASH). ASH position paper: hypertension in pregnancy. J Clin Hypertens (Greenwich). 2009;11(4):214-225.
11. Roberts JM, Gammill HS. Preeclampsia: recent insights. Hypertension. 2005;46(6):
1243-1249.
12. Saudan P, Brown MA, Buddle ML, Jones M. Does gestational hypertension become pre-eclampsia? Br J Obstet Gynaecol. 1998;105 (11):1177-1184.
13. Visintin C, Mugglestone MA, Almerie MQ, et al; Guideline Development Group. Management of hypertensive disorders during pregnancy: summary of NICE guidance. BMJ. 2010;341:c2207.
14. ACOG Committee on Practice Bulletins—Obstetrics. Clinical Management Guidelines for Obstetrician–Gynecologists. Diagnosis and management of preeclampsia and eclampsia: ACOG practice bulletin No. 33. Obstet Gynecol. 2002;99:159-167.
15. Parazzini F, Bortolus R, Chatenoud L, et al; Italian Study of Aspirin in Pregnancy Group. Risk factors for pregnancy-induced hypertension in women at high risk for the condition. Epidemiology. 1996;7(3):306-308.
16. Hjartardottir S, Leifsson BG, Geirsson RT, Steinthorsdottir V. Recurrence of hypertensive disorder in second pregnancy. Am J Obstet Gynecol. 2006;194(4):916-920.
17. Barton JR, O’Brien JM, Bergauer NK, et al. Mild gestational hypertension remote from term: progression and outcome. Am J Obstet Gynecol. 2001;184(5):979-983.
18. Brown MA, Mackenzie C, Dunsmuir W, et al. Can we predict recurrence of pre-eclampsia or gestational hypertension? BJOG. 2007; 114(8):984-993.
19. Bellomo G, Venanzi S, Saronio P, et al. Prognostic significance of serum uric acid in women with gestational hypertension. Hypertension. 2011;58(4):704-708.
20. Hawkins TL, Roberts JM, Mangos GJ, et al. Plasma uric acid remains a marker of poor outcome in hypertensive pregnancy: a retrospective cohort study. BJOG. 2012;119(4):484-492.
21. National Institute for Health and Clinical Excellence. Hypertension in pregnancy: the management of hypertensive disorders during pregnancy. www.nice.org.uk/nicemedia/live/13098/50418/50418.pdf. Accessed April 16, 2012.
22. Koopmans CM, Bijlenga D, Groen H, et al. Induction of labour versus expectant monitoring for gestational hypertension or mild pre-eclampsia after 36 weeks’ gestation (HYPITAT): a multicentre, open-label randomised controlled trial. Lancet. 2009;374(9694):979-988.
23. Caughey AB, Sundaram V, Kaimal AJ, et al. Maternal and neonatal outcomes of elective induction of labor. Evid Rep Technol Assess (Full Rep). 2009;(176):1-257.
24. Shennan A, Hezelgrave N. An economic analysis of induction of labour and expectant monitoring in women with gestational hypertension or pre-eclampsia at term (HYPITAT trial). BJOG. 2010;117(13):1575-1576.
25. Abalos E, Duley L, Steyn DW, Henderson-Smart DJ. Antihypertensive drug therapy for mild to moderate hypertension during pregnancy. Cochrane Database Syst Rev. 2007 Jan 24;(1):CD002252.
26. Nabhan AF, Elsedawy MM. Tight control of mild-moderate pre-existing or non-proteinuric gestational hypertension. Cochrane Database Syst Rev. 2011 Jul 6;(7):CD006907.
27. Duley L, Gülmezoglu AM, Henderson-Smart DJ. Magnesium sulphate and other anticonvulsants for women with preeclampsia. Cochrane Database Syst Rev. 2003;(2):CD000025.
28. Kraft MD, Btaiche IF, Sacks GS, Kudsk KA. Treatment of electrolyte disorders in adult patients in the intensive care unit. Am J Health Syst Pharm. 2005;62(16):1663-1682.
29. FamilyDoctor.org. Pregnancy-induced hypertension (updated 2010). http://familydoctor.org/familydoctor/en/diseases-conditions/pregnancy-induced-hypertension.printerview
.all.html. Accessed April 16, 2012.
30. Zamorski MA, Green LA. NHBPEP report on high blood pressure in pregnancy: a summary for family physicians. Am Fam Physician. 2001; 64(2):263-270.
31. Hofmeyr GJ, Duley L, Atallah A. Dietary calcium supplementation for prevention of pre-eclampsia and related problems: a systematic review and commentary. BJOG. 2007;114(8): 933-943.
32. Ferrazzani S, De Carolis S, Pomini F, et al. The duration of hypertension in the puerperium of preeclamptic women: relationship with renal impairment and week of delivery. Am J Obstet Gynecol. 1994;171(2):506-512.
33. Beardmore KS, Morris JM, Gallery ED. Excretion of antihypertensive medication into human breast milk: a systematic review. Hypertens Pregnancy. 2002;21(1):85-95.
34. Wilson BJ, Watson MS, Prescott GJ, et al. Hypertensive diseases of pregnancy and risk of hypertension and stroke in later life: results from cohort study. BMJ. 2003;326(7394):845.
Chronic Lymphocytic Leukemia
Series Editor: Eric D. Jacobsen, MD
Chronic lymphocytic leukemia (CLL) is the most common hematologic malignancy in the Western world, representing 30% of leukemias. The median age at diagnosis is 72 years, and fewer than 10% of patients are under 60. CLL occurs more frequently in Caucasians than in other ethnic groups and more often in men than in women. The age-adjusted incidence rate is 4.2 per 100,000 population. Although CLL is generally considered indolent, it is a heterogeneous disease, and while many patients have slowly progressive disease, a proportion of patients have disease that will have a more aggressive course, requiring treatment soon after diagnosis. Over the past 3 decades, increasing knowledge about the mechanism of CLL and the introduction of new chemotherapeutic and biologic agents has led to better treatments, improved risk stratification, and more durable remissions. Despite these advances in treatment, CLL remains incurable outside the setting of hematopoietic stem cell transplant.
To read the full article in PDF:
Series Editor: Eric D. Jacobsen, MD
Chronic lymphocytic leukemia (CLL) is the most common hematologic malignancy in the Western world, representing 30% of leukemias. The median age at diagnosis is 72 years, and fewer than 10% of patients are under 60. CLL occurs more frequently in Caucasians than in other ethnic groups and more often in men than in women. The age-adjusted incidence rate is 4.2 per 100,000 population. Although CLL is generally considered indolent, it is a heterogeneous disease, and while many patients have slowly progressive disease, a proportion of patients have disease that will have a more aggressive course, requiring treatment soon after diagnosis. Over the past 3 decades, increasing knowledge about the mechanism of CLL and the introduction of new chemotherapeutic and biologic agents has led to better treatments, improved risk stratification, and more durable remissions. Despite these advances in treatment, CLL remains incurable outside the setting of hematopoietic stem cell transplant.
To read the full article in PDF:
Series Editor: Eric D. Jacobsen, MD
Chronic lymphocytic leukemia (CLL) is the most common hematologic malignancy in the Western world, representing 30% of leukemias. The median age at diagnosis is 72 years, and fewer than 10% of patients are under 60. CLL occurs more frequently in Caucasians than in other ethnic groups and more often in men than in women. The age-adjusted incidence rate is 4.2 per 100,000 population. Although CLL is generally considered indolent, it is a heterogeneous disease, and while many patients have slowly progressive disease, a proportion of patients have disease that will have a more aggressive course, requiring treatment soon after diagnosis. Over the past 3 decades, increasing knowledge about the mechanism of CLL and the introduction of new chemotherapeutic and biologic agents has led to better treatments, improved risk stratification, and more durable remissions. Despite these advances in treatment, CLL remains incurable outside the setting of hematopoietic stem cell transplant.
To read the full article in PDF:
Nutritional Support Benefits Elderly Outpatients
The Effect of Colestipol on Glycemic Control in Patients With Type 2 Diabetes
Optimizing Office Blood Pressure Measurement at a VAMC
High-Speed Hyponatremia: Exercise-Associated Hyponatremia in a Young Male Soldier
Grand Rounds: Man, 62, With New-Onset Atrial Fibrillation
A 62-year-old black nursing home resident was transported to the hospital emergency department with fever of 102°F, new-onset atrial fibrillation (A-fib), and dementia. His medical history was significant for hypertension and multiple strokes.
His inpatient work-up for A-fib and dementia revealed a thyroid-stimulating hormone (TSH) level below 0.005 µIU/mL (normal range, 0.3 to 3.0 µIU/mL). Results of thyroid function testing (TFT) revealed a triiodothyronine (T3) level within normal range but a free thyroxine (T4) level of 2.9 ng/dL (normal range, 0.7 to 1.5 ng/dL) and a total T4 of 17.8 µg/dL (normal, 4.5 to 12.0 µg/dL). The abnormal TSH and T4 levels were considered suggestive of a thyrotoxic state, warranting an endocrinology consult. Cardiology was consulted regarding new-onset A-fib.
During history taking, the patient denied any shortness of breath, cough, palpitations, heat intolerance, anxiety, tremors, insomnia, dysphagia, diarrhea, dysuria, weight loss, or recent ingestion of iodine-containing medications or supplements.
On examination, the patient was febrile, with a blood pressure of 106/71 mm Hg; pulse, 74 beats/min; respiratory rate, 20 breaths/min; and O2 saturation, 98% to 99% on room air. ECG showed a normal sinus rhythm and a ventricular rate of 64 beats/min.
The patient's weight was 58.9 kg, and his height, 63" (BMI, 22.8). The patient had no skin changes, and his mucous membranes were slightly moist. The patient's head was atraumatic and normocephalic. His extraocular movements were intact, and his pupils were equal, round, and reactive to light, with nonicteric sclera. There was no proptosis or ophthalmoplegia. The patient's neck was supple, with no jugular venous distension, tracheal deviation, or thyromegaly.
The cardiovascular exam revealed an irregular heartbeat, and repeat ECG showed A-fib with a ventricular rate of 151 beats/min (see Figure 1). The patient's chest was clear, with no wheezing or rhonchi. The abdomen was soft and slightly obese, and bowel sounds were present. The neurologic examination revealed no hyperreflexia. The patient's mental status was altered at times and he was alert, awake, and oriented to others. His speech was slightly slow, and some left-sided weakness was noted.
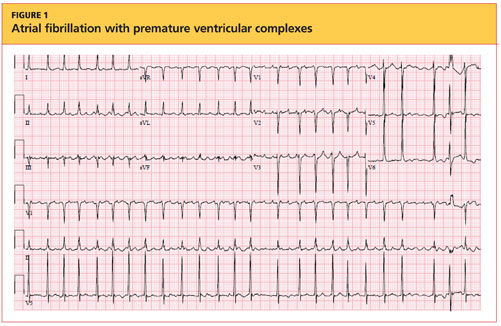
As recommended during the endocrinology consult, the patient underwent an I-123 sodium iodide thyroid scan, which showed faint uptake at the base of the neck, slightly to the left of midline; and a 24-hour radioactive iodide uptake (RAIU), which measured 2.8% (normal range, 8% to 35%).
The patient's chest X-ray showed a right tracheal deviation not previously noted on physical examination (see Figure 2); the possible cause of a thyroid mass was considered. Subsequent ultrasonography of the thyroid revealed generally normal dimensions and parenchymal echogenicity. However, a large complex mass was detected, arising from the inferior pole of the thyroid and displacing the trachea toward the right (see Figure 3). According to the radiologist's notes, the mass contained both solid and cystic elements, scattered calcifications, and foci of flow on color Doppler. It measured about 6 cm in the largest (transverse) dimension. A 2.0-mm nodule was noted in the isthmus, slightly to the right of midline, consistent with multinodular goiter.
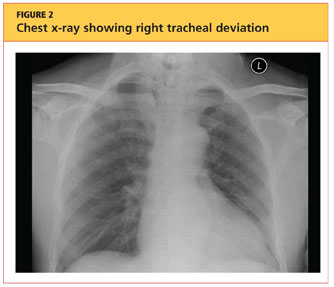
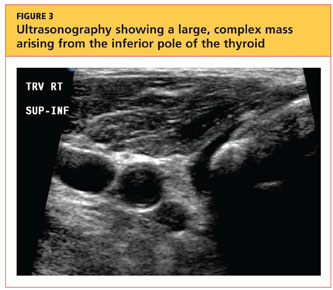
Following the cardiology consult, a diltiazem drip was initiated, but the patient was later optimized on flecainide for rhythm control and metoprolol for rate control. He was also initially anticoagulated using a heparin drip and bridged to warfarin, with target international normalized ratio (INR) between 2.0 and 3.0. Echocardiography revealed normal systolic function with ejection fraction of 55%, left ventricular hypertrophy, pulmonary artery systolic pressure of 35 mm Hg, and no pericardial effusions or valvular disease.
Regarding the patient's unexplained fever, results of chest imaging were negative for signs of pneumonia or atelectasis, which might have suggested a pulmonary cause. Urinalysis results were normal. Complete blood count showed no leukocytosis. The patient's fever subsided within 48 hours.
The differential diagnosis included Graves' disease, toxic multinodular goiter, Jod-Basedow syndrome, and subacute thyroiditis.
Graves' disease, an autoimmune disease with an unknown trigger, is the most common cause of hyperthyroidism. In affected patients, the thyroid gland overproduces thyroid hormones, leading to thyrotoxicosis. Thyrotoxicosis can result in multiple clinical signs and symptoms, including Graves' ophthalmopathy, pretibial myxedema, and goiter; TFT results typically include elevated T3 and T4 and low TSH.1-5 In the case patient (who had no history of thyroid disease, nor clinical signs or symptoms of Graves' disease), low uptake of iodine on thyroid scan precluded this diagnosis.
Toxic multinodular goiter, the second most common cause of hyperthyroidism, can be responsible for A-fib, tachycardia, and congestive heart failure.6,7 Iodine deficiency causes enlargement of the thyroid gland, where numerous nodules can develop, as seen in the case patient. These nodules can function independently, sometimes producing excess thyroid hormone; this leads to hyperplasia of the thyroid gland, resulting in a nontoxic multinodular goiter. From this goiter, a toxic multinodular goiter can emerge insidiously. However, in this condition, RAIU typically exceeds 30%; in the case patient, low 24-hour RAIU (2.8%) and the absence of functioning nodules on scanning made it possible to rule out this diagnosis.
Jod-Basedow syndrome refers to hyperthyroidism that develops as a result of administration of iodide, either as a dietary supplement or as IV contrast medium, or as an adverse effect of the antiarrhythmic drug amiodarone. This phenomenon is usually seen in a patient with endemic goiter.8-11 The relatively limited nature of the case patient's goiter and absence of a precipitating exposure to iodine made this diagnosis highly unlikely.
Subacute thyroiditis is a condition to which the patient's abnormal TFT results could reasonably be attributed. The patient had a substernal multinodular goiter that could not be palpated on physical examination, but it was visualized in the extended lower neck during thyroid scintigraphy.3 RAIU was minimal—a typical finding in this disorder,6 as TSH is suppressed by leakage of the excessive amounts of thyroid hormone. A tentative diagnosis of subacute thyroiditis was made.
As subacute thyroiditis is a self-limiting disorder, the patient was not started on any medications for hyperthyroidism but was advised to follow up with his primary care provider or an endocrinologist for repeat TFT and for fine-needle aspiration biopsy of the large thyroid nodule (a complex mass, containing cystic elements and calcifications, with a potential for malignancy) to rule out thyroid cancer.
Repeat ECG before discharge showed normal sinus rhythm with a ventricular rate of 74 beats/min. The patient was alert, awake, and oriented at discharge. He was continued on flecainide, metoprolol, and warfarin and advised to follow up with his primary care provider regarding his target INR.
DISCUSSION
The incidence of subacute thyroiditis, according to findings reported in 2003 from the Rochester Epidemiology Project in Olmsted County, Minnesota,12 is 12.1 cases per 100,000/year, with a higher incidence in women than men. It is most common in young adults and decreases with advancing age. Coxsackie virus, adenovirus, mumps, echovirus, influenza, and Epstein-Barr virus have been implicated in the disorder.12,13
Subacute thyroiditis is associated with a triphasic clinical course of hyperthyroidism, then hypothyroidism, then a return to normal thyroid function—as was seen in the case patient. Onset of subacute thyroiditis has been associated with recent viral infection, which may serve as a precipitant. The cause of this patient's high fever was never identified; thus, the etiology may have been viral.
The initial high thyroid hormone levels result from inflammation of thyroid tissue and release of preformed thyroid hormone into the circulation.6 At this point, TSH is suppressed and patients have very low RAIU, as was true in the case patient.
The condition is self-limiting and does not require treatment in the majority of patients, as TFT results return to normal levels within about two months.6 Patients can appear extremely ill due to thyrotoxicosis from subacute thyroiditis, but this usually lasts no longer than six to eight weeks.3 Subacute thyroiditis can be associated with atrial arrhythmia or heart failure.14,15
PATIENT OUTCOME
New-onset A-fib was attributed to the patient's thyrotoxicosis, which in turn was caused by subacute thyroiditis. He had a multinodular goiter, although he had not received any iodine supplements or IV contrast. As in most cases of subacute thyroiditis, no precipitating event was identified. However, given this patient's residence in a nursing facility and presentation with a high fever with no identifiable cause, a viral etiology for his subacute thyroiditis is possible.6
The patient's dementia may have been secondary to acute thyrotoxicosis, as his mental state improved during the hospital stay. His vitamin B12, folate, and A1C levels were within normal range. CT of the head showed multiple chronic infarcts and cerebral atrophy, and MRI of the brain indicated microvascular ischemic disease.
The patient was readmitted one month later for an episode of near-syncope (which, it was concluded, was a vasovagal episode). At that time, his TSH was found normal at 1.350 µIU/mL. Flecainide and metoprolol were discontinued; he was started on diltiazem for continued rate and rhythm control (as recommended by cardiology) and continued on warfarin.
CONCLUSION
In this case, subacute thyroiditis was most likely caused by a viral infection that led to destruction of the normal thyroid follicles and release of their preformed thyroid hormone into the circulation; this in turn led to sudden-onset A-fib. The diagnosis of subacute thyroiditis was suggested based on the abnormalities seen in this patient's TFT results, coupled with the suppressed RAIU—a typical finding in this disease.
Because subacute thyroiditis is a self-limiting condition, there is no role for antithyroid medication. Instead, treatment should be focused on relieving the patient's symptoms, such as ß-blockade or calcium channel blockers for tachycardia and corticosteroids or NSAIDs for neck pain.
REFERENCES
1. Weetman AP. Graves' disease. N Engl J Med. 2000;343(17):1236-1248.
2. Delgado Hurtado JJ, Pineda M. Images in medicine: Graves' disease. N Engl J Med. 2011; 364(20):1955.
3. Al-Sharif AA, Abujbara MA, Chiacchio S, et al. Contribution of radioiodine uptake measurement and thyroid scintigraphy to the differential diagnosis of thyrotoxicosis. Hell J Nucl Med. 2010;13(2):132-137.
4. Buccelletti F, Carroccia A, Marsiliani D, et al. Utility of routine thyroid-stimulating hormone determination in new-onset atrial fibrillation in the ED. Am J Emerg Med. 2011;29(9):1158-1162.
5. Ross DS. Radioiodine therapy for hyperthyroidism. N Engl J Med. 2011;364(6):542-550.
6. Bahn RS, Burch HB, Cooper DS, et al. Hyperthyroidism and other causes of thyrotoxicosis: management guidelines of the American Thyroid Association and American Association of Clinical Endocrinologists. Endocr Pract. 2011;17(3):456-520.
7. Erickson D, Gharib H, Li H, van Heerden JA. Treatment of patients with toxic multinodular goiter. Thyroid. 1998;8(4):277-282.
8. Basaria S, Cooper DS. Amiodarone and the thyroid. Am J Med. 2005;118(7):706-714.
9. Bogazzi F, Bartalena L, Martino E. Approach to the patient with amiodarone-induced thyrotoxicosis. J Clin Endocrinol Metab. 2010;95(6):2529-2535.
10. El-Shirbiny AM, Stavrou SS, Dnistrian A, et al. Jod-Basedow syndrome following oral iodine and radioiodinated-antibody administration. J Nucl Med. 1997;38(11):1816-1817.
11. Stanbury JB, Ermans AE, Bourdoux P, et al. Iodine-induced hyperthyroidism: occurrence and epidemiology. Thyroid. 1998;8(1):83-100.
12. Fatourechi V, Aniszewski JP, Fatourechi GZ, et al. Clinical features and outcome of subacute thyroiditis in an incidence cohort: Olmsted County, Minnesota, study. J Clin Endocrinol Metab. 2003;88(5):2100-2105.
13. Golden SH, Robinson KA, Saldanha I, et al. Clinical review: prevalence and incidence of endocrine and metabolic disorders in the United States: a comprehensive review. J Clin Endocrinol Metab. 2009;94(6):1853-1878.
14. Volpé R. The management of subacute (DeQuervain's) thyroiditis. Thyroid. 1993;3(3):253-255.
15. Lee SL. Subacute thyroiditis (2009). http://emedicine.medscape.com/article/125648-overview. Accessed April 17, 2012.
A 62-year-old black nursing home resident was transported to the hospital emergency department with fever of 102°F, new-onset atrial fibrillation (A-fib), and dementia. His medical history was significant for hypertension and multiple strokes.
His inpatient work-up for A-fib and dementia revealed a thyroid-stimulating hormone (TSH) level below 0.005 µIU/mL (normal range, 0.3 to 3.0 µIU/mL). Results of thyroid function testing (TFT) revealed a triiodothyronine (T3) level within normal range but a free thyroxine (T4) level of 2.9 ng/dL (normal range, 0.7 to 1.5 ng/dL) and a total T4 of 17.8 µg/dL (normal, 4.5 to 12.0 µg/dL). The abnormal TSH and T4 levels were considered suggestive of a thyrotoxic state, warranting an endocrinology consult. Cardiology was consulted regarding new-onset A-fib.
During history taking, the patient denied any shortness of breath, cough, palpitations, heat intolerance, anxiety, tremors, insomnia, dysphagia, diarrhea, dysuria, weight loss, or recent ingestion of iodine-containing medications or supplements.
On examination, the patient was febrile, with a blood pressure of 106/71 mm Hg; pulse, 74 beats/min; respiratory rate, 20 breaths/min; and O2 saturation, 98% to 99% on room air. ECG showed a normal sinus rhythm and a ventricular rate of 64 beats/min.
The patient's weight was 58.9 kg, and his height, 63" (BMI, 22.8). The patient had no skin changes, and his mucous membranes were slightly moist. The patient's head was atraumatic and normocephalic. His extraocular movements were intact, and his pupils were equal, round, and reactive to light, with nonicteric sclera. There was no proptosis or ophthalmoplegia. The patient's neck was supple, with no jugular venous distension, tracheal deviation, or thyromegaly.
The cardiovascular exam revealed an irregular heartbeat, and repeat ECG showed A-fib with a ventricular rate of 151 beats/min (see Figure 1). The patient's chest was clear, with no wheezing or rhonchi. The abdomen was soft and slightly obese, and bowel sounds were present. The neurologic examination revealed no hyperreflexia. The patient's mental status was altered at times and he was alert, awake, and oriented to others. His speech was slightly slow, and some left-sided weakness was noted.
As recommended during the endocrinology consult, the patient underwent an I-123 sodium iodide thyroid scan, which showed faint uptake at the base of the neck, slightly to the left of midline; and a 24-hour radioactive iodide uptake (RAIU), which measured 2.8% (normal range, 8% to 35%).
The patient's chest X-ray showed a right tracheal deviation not previously noted on physical examination (see Figure 2); the possible cause of a thyroid mass was considered. Subsequent ultrasonography of the thyroid revealed generally normal dimensions and parenchymal echogenicity. However, a large complex mass was detected, arising from the inferior pole of the thyroid and displacing the trachea toward the right (see Figure 3). According to the radiologist's notes, the mass contained both solid and cystic elements, scattered calcifications, and foci of flow on color Doppler. It measured about 6 cm in the largest (transverse) dimension. A 2.0-mm nodule was noted in the isthmus, slightly to the right of midline, consistent with multinodular goiter.
Following the cardiology consult, a diltiazem drip was initiated, but the patient was later optimized on flecainide for rhythm control and metoprolol for rate control. He was also initially anticoagulated using a heparin drip and bridged to warfarin, with target international normalized ratio (INR) between 2.0 and 3.0. Echocardiography revealed normal systolic function with ejection fraction of 55%, left ventricular hypertrophy, pulmonary artery systolic pressure of 35 mm Hg, and no pericardial effusions or valvular disease.
Regarding the patient's unexplained fever, results of chest imaging were negative for signs of pneumonia or atelectasis, which might have suggested a pulmonary cause. Urinalysis results were normal. Complete blood count showed no leukocytosis. The patient's fever subsided within 48 hours.
The differential diagnosis included Graves' disease, toxic multinodular goiter, Jod-Basedow syndrome, and subacute thyroiditis.
Graves' disease, an autoimmune disease with an unknown trigger, is the most common cause of hyperthyroidism. In affected patients, the thyroid gland overproduces thyroid hormones, leading to thyrotoxicosis. Thyrotoxicosis can result in multiple clinical signs and symptoms, including Graves' ophthalmopathy, pretibial myxedema, and goiter; TFT results typically include elevated T3 and T4 and low TSH.1-5 In the case patient (who had no history of thyroid disease, nor clinical signs or symptoms of Graves' disease), low uptake of iodine on thyroid scan precluded this diagnosis.
Toxic multinodular goiter, the second most common cause of hyperthyroidism, can be responsible for A-fib, tachycardia, and congestive heart failure.6,7 Iodine deficiency causes enlargement of the thyroid gland, where numerous nodules can develop, as seen in the case patient. These nodules can function independently, sometimes producing excess thyroid hormone; this leads to hyperplasia of the thyroid gland, resulting in a nontoxic multinodular goiter. From this goiter, a toxic multinodular goiter can emerge insidiously. However, in this condition, RAIU typically exceeds 30%; in the case patient, low 24-hour RAIU (2.8%) and the absence of functioning nodules on scanning made it possible to rule out this diagnosis.
Jod-Basedow syndrome refers to hyperthyroidism that develops as a result of administration of iodide, either as a dietary supplement or as IV contrast medium, or as an adverse effect of the antiarrhythmic drug amiodarone. This phenomenon is usually seen in a patient with endemic goiter.8-11 The relatively limited nature of the case patient's goiter and absence of a precipitating exposure to iodine made this diagnosis highly unlikely.
Subacute thyroiditis is a condition to which the patient's abnormal TFT results could reasonably be attributed. The patient had a substernal multinodular goiter that could not be palpated on physical examination, but it was visualized in the extended lower neck during thyroid scintigraphy.3 RAIU was minimal—a typical finding in this disorder,6 as TSH is suppressed by leakage of the excessive amounts of thyroid hormone. A tentative diagnosis of subacute thyroiditis was made.
As subacute thyroiditis is a self-limiting disorder, the patient was not started on any medications for hyperthyroidism but was advised to follow up with his primary care provider or an endocrinologist for repeat TFT and for fine-needle aspiration biopsy of the large thyroid nodule (a complex mass, containing cystic elements and calcifications, with a potential for malignancy) to rule out thyroid cancer.
Repeat ECG before discharge showed normal sinus rhythm with a ventricular rate of 74 beats/min. The patient was alert, awake, and oriented at discharge. He was continued on flecainide, metoprolol, and warfarin and advised to follow up with his primary care provider regarding his target INR.
DISCUSSION
The incidence of subacute thyroiditis, according to findings reported in 2003 from the Rochester Epidemiology Project in Olmsted County, Minnesota,12 is 12.1 cases per 100,000/year, with a higher incidence in women than men. It is most common in young adults and decreases with advancing age. Coxsackie virus, adenovirus, mumps, echovirus, influenza, and Epstein-Barr virus have been implicated in the disorder.12,13
Subacute thyroiditis is associated with a triphasic clinical course of hyperthyroidism, then hypothyroidism, then a return to normal thyroid function—as was seen in the case patient. Onset of subacute thyroiditis has been associated with recent viral infection, which may serve as a precipitant. The cause of this patient's high fever was never identified; thus, the etiology may have been viral.
The initial high thyroid hormone levels result from inflammation of thyroid tissue and release of preformed thyroid hormone into the circulation.6 At this point, TSH is suppressed and patients have very low RAIU, as was true in the case patient.
The condition is self-limiting and does not require treatment in the majority of patients, as TFT results return to normal levels within about two months.6 Patients can appear extremely ill due to thyrotoxicosis from subacute thyroiditis, but this usually lasts no longer than six to eight weeks.3 Subacute thyroiditis can be associated with atrial arrhythmia or heart failure.14,15
PATIENT OUTCOME
New-onset A-fib was attributed to the patient's thyrotoxicosis, which in turn was caused by subacute thyroiditis. He had a multinodular goiter, although he had not received any iodine supplements or IV contrast. As in most cases of subacute thyroiditis, no precipitating event was identified. However, given this patient's residence in a nursing facility and presentation with a high fever with no identifiable cause, a viral etiology for his subacute thyroiditis is possible.6
The patient's dementia may have been secondary to acute thyrotoxicosis, as his mental state improved during the hospital stay. His vitamin B12, folate, and A1C levels were within normal range. CT of the head showed multiple chronic infarcts and cerebral atrophy, and MRI of the brain indicated microvascular ischemic disease.
The patient was readmitted one month later for an episode of near-syncope (which, it was concluded, was a vasovagal episode). At that time, his TSH was found normal at 1.350 µIU/mL. Flecainide and metoprolol were discontinued; he was started on diltiazem for continued rate and rhythm control (as recommended by cardiology) and continued on warfarin.
CONCLUSION
In this case, subacute thyroiditis was most likely caused by a viral infection that led to destruction of the normal thyroid follicles and release of their preformed thyroid hormone into the circulation; this in turn led to sudden-onset A-fib. The diagnosis of subacute thyroiditis was suggested based on the abnormalities seen in this patient's TFT results, coupled with the suppressed RAIU—a typical finding in this disease.
Because subacute thyroiditis is a self-limiting condition, there is no role for antithyroid medication. Instead, treatment should be focused on relieving the patient's symptoms, such as ß-blockade or calcium channel blockers for tachycardia and corticosteroids or NSAIDs for neck pain.
REFERENCES
1. Weetman AP. Graves' disease. N Engl J Med. 2000;343(17):1236-1248.
2. Delgado Hurtado JJ, Pineda M. Images in medicine: Graves' disease. N Engl J Med. 2011; 364(20):1955.
3. Al-Sharif AA, Abujbara MA, Chiacchio S, et al. Contribution of radioiodine uptake measurement and thyroid scintigraphy to the differential diagnosis of thyrotoxicosis. Hell J Nucl Med. 2010;13(2):132-137.
4. Buccelletti F, Carroccia A, Marsiliani D, et al. Utility of routine thyroid-stimulating hormone determination in new-onset atrial fibrillation in the ED. Am J Emerg Med. 2011;29(9):1158-1162.
5. Ross DS. Radioiodine therapy for hyperthyroidism. N Engl J Med. 2011;364(6):542-550.
6. Bahn RS, Burch HB, Cooper DS, et al. Hyperthyroidism and other causes of thyrotoxicosis: management guidelines of the American Thyroid Association and American Association of Clinical Endocrinologists. Endocr Pract. 2011;17(3):456-520.
7. Erickson D, Gharib H, Li H, van Heerden JA. Treatment of patients with toxic multinodular goiter. Thyroid. 1998;8(4):277-282.
8. Basaria S, Cooper DS. Amiodarone and the thyroid. Am J Med. 2005;118(7):706-714.
9. Bogazzi F, Bartalena L, Martino E. Approach to the patient with amiodarone-induced thyrotoxicosis. J Clin Endocrinol Metab. 2010;95(6):2529-2535.
10. El-Shirbiny AM, Stavrou SS, Dnistrian A, et al. Jod-Basedow syndrome following oral iodine and radioiodinated-antibody administration. J Nucl Med. 1997;38(11):1816-1817.
11. Stanbury JB, Ermans AE, Bourdoux P, et al. Iodine-induced hyperthyroidism: occurrence and epidemiology. Thyroid. 1998;8(1):83-100.
12. Fatourechi V, Aniszewski JP, Fatourechi GZ, et al. Clinical features and outcome of subacute thyroiditis in an incidence cohort: Olmsted County, Minnesota, study. J Clin Endocrinol Metab. 2003;88(5):2100-2105.
13. Golden SH, Robinson KA, Saldanha I, et al. Clinical review: prevalence and incidence of endocrine and metabolic disorders in the United States: a comprehensive review. J Clin Endocrinol Metab. 2009;94(6):1853-1878.
14. Volpé R. The management of subacute (DeQuervain's) thyroiditis. Thyroid. 1993;3(3):253-255.
15. Lee SL. Subacute thyroiditis (2009). http://emedicine.medscape.com/article/125648-overview. Accessed April 17, 2012.
A 62-year-old black nursing home resident was transported to the hospital emergency department with fever of 102°F, new-onset atrial fibrillation (A-fib), and dementia. His medical history was significant for hypertension and multiple strokes.
His inpatient work-up for A-fib and dementia revealed a thyroid-stimulating hormone (TSH) level below 0.005 µIU/mL (normal range, 0.3 to 3.0 µIU/mL). Results of thyroid function testing (TFT) revealed a triiodothyronine (T3) level within normal range but a free thyroxine (T4) level of 2.9 ng/dL (normal range, 0.7 to 1.5 ng/dL) and a total T4 of 17.8 µg/dL (normal, 4.5 to 12.0 µg/dL). The abnormal TSH and T4 levels were considered suggestive of a thyrotoxic state, warranting an endocrinology consult. Cardiology was consulted regarding new-onset A-fib.
During history taking, the patient denied any shortness of breath, cough, palpitations, heat intolerance, anxiety, tremors, insomnia, dysphagia, diarrhea, dysuria, weight loss, or recent ingestion of iodine-containing medications or supplements.
On examination, the patient was febrile, with a blood pressure of 106/71 mm Hg; pulse, 74 beats/min; respiratory rate, 20 breaths/min; and O2 saturation, 98% to 99% on room air. ECG showed a normal sinus rhythm and a ventricular rate of 64 beats/min.
The patient's weight was 58.9 kg, and his height, 63" (BMI, 22.8). The patient had no skin changes, and his mucous membranes were slightly moist. The patient's head was atraumatic and normocephalic. His extraocular movements were intact, and his pupils were equal, round, and reactive to light, with nonicteric sclera. There was no proptosis or ophthalmoplegia. The patient's neck was supple, with no jugular venous distension, tracheal deviation, or thyromegaly.
The cardiovascular exam revealed an irregular heartbeat, and repeat ECG showed A-fib with a ventricular rate of 151 beats/min (see Figure 1). The patient's chest was clear, with no wheezing or rhonchi. The abdomen was soft and slightly obese, and bowel sounds were present. The neurologic examination revealed no hyperreflexia. The patient's mental status was altered at times and he was alert, awake, and oriented to others. His speech was slightly slow, and some left-sided weakness was noted.
As recommended during the endocrinology consult, the patient underwent an I-123 sodium iodide thyroid scan, which showed faint uptake at the base of the neck, slightly to the left of midline; and a 24-hour radioactive iodide uptake (RAIU), which measured 2.8% (normal range, 8% to 35%).
The patient's chest X-ray showed a right tracheal deviation not previously noted on physical examination (see Figure 2); the possible cause of a thyroid mass was considered. Subsequent ultrasonography of the thyroid revealed generally normal dimensions and parenchymal echogenicity. However, a large complex mass was detected, arising from the inferior pole of the thyroid and displacing the trachea toward the right (see Figure 3). According to the radiologist's notes, the mass contained both solid and cystic elements, scattered calcifications, and foci of flow on color Doppler. It measured about 6 cm in the largest (transverse) dimension. A 2.0-mm nodule was noted in the isthmus, slightly to the right of midline, consistent with multinodular goiter.
Following the cardiology consult, a diltiazem drip was initiated, but the patient was later optimized on flecainide for rhythm control and metoprolol for rate control. He was also initially anticoagulated using a heparin drip and bridged to warfarin, with target international normalized ratio (INR) between 2.0 and 3.0. Echocardiography revealed normal systolic function with ejection fraction of 55%, left ventricular hypertrophy, pulmonary artery systolic pressure of 35 mm Hg, and no pericardial effusions or valvular disease.
Regarding the patient's unexplained fever, results of chest imaging were negative for signs of pneumonia or atelectasis, which might have suggested a pulmonary cause. Urinalysis results were normal. Complete blood count showed no leukocytosis. The patient's fever subsided within 48 hours.
The differential diagnosis included Graves' disease, toxic multinodular goiter, Jod-Basedow syndrome, and subacute thyroiditis.
Graves' disease, an autoimmune disease with an unknown trigger, is the most common cause of hyperthyroidism. In affected patients, the thyroid gland overproduces thyroid hormones, leading to thyrotoxicosis. Thyrotoxicosis can result in multiple clinical signs and symptoms, including Graves' ophthalmopathy, pretibial myxedema, and goiter; TFT results typically include elevated T3 and T4 and low TSH.1-5 In the case patient (who had no history of thyroid disease, nor clinical signs or symptoms of Graves' disease), low uptake of iodine on thyroid scan precluded this diagnosis.
Toxic multinodular goiter, the second most common cause of hyperthyroidism, can be responsible for A-fib, tachycardia, and congestive heart failure.6,7 Iodine deficiency causes enlargement of the thyroid gland, where numerous nodules can develop, as seen in the case patient. These nodules can function independently, sometimes producing excess thyroid hormone; this leads to hyperplasia of the thyroid gland, resulting in a nontoxic multinodular goiter. From this goiter, a toxic multinodular goiter can emerge insidiously. However, in this condition, RAIU typically exceeds 30%; in the case patient, low 24-hour RAIU (2.8%) and the absence of functioning nodules on scanning made it possible to rule out this diagnosis.
Jod-Basedow syndrome refers to hyperthyroidism that develops as a result of administration of iodide, either as a dietary supplement or as IV contrast medium, or as an adverse effect of the antiarrhythmic drug amiodarone. This phenomenon is usually seen in a patient with endemic goiter.8-11 The relatively limited nature of the case patient's goiter and absence of a precipitating exposure to iodine made this diagnosis highly unlikely.
Subacute thyroiditis is a condition to which the patient's abnormal TFT results could reasonably be attributed. The patient had a substernal multinodular goiter that could not be palpated on physical examination, but it was visualized in the extended lower neck during thyroid scintigraphy.3 RAIU was minimal—a typical finding in this disorder,6 as TSH is suppressed by leakage of the excessive amounts of thyroid hormone. A tentative diagnosis of subacute thyroiditis was made.
As subacute thyroiditis is a self-limiting disorder, the patient was not started on any medications for hyperthyroidism but was advised to follow up with his primary care provider or an endocrinologist for repeat TFT and for fine-needle aspiration biopsy of the large thyroid nodule (a complex mass, containing cystic elements and calcifications, with a potential for malignancy) to rule out thyroid cancer.
Repeat ECG before discharge showed normal sinus rhythm with a ventricular rate of 74 beats/min. The patient was alert, awake, and oriented at discharge. He was continued on flecainide, metoprolol, and warfarin and advised to follow up with his primary care provider regarding his target INR.
DISCUSSION
The incidence of subacute thyroiditis, according to findings reported in 2003 from the Rochester Epidemiology Project in Olmsted County, Minnesota,12 is 12.1 cases per 100,000/year, with a higher incidence in women than men. It is most common in young adults and decreases with advancing age. Coxsackie virus, adenovirus, mumps, echovirus, influenza, and Epstein-Barr virus have been implicated in the disorder.12,13
Subacute thyroiditis is associated with a triphasic clinical course of hyperthyroidism, then hypothyroidism, then a return to normal thyroid function—as was seen in the case patient. Onset of subacute thyroiditis has been associated with recent viral infection, which may serve as a precipitant. The cause of this patient's high fever was never identified; thus, the etiology may have been viral.
The initial high thyroid hormone levels result from inflammation of thyroid tissue and release of preformed thyroid hormone into the circulation.6 At this point, TSH is suppressed and patients have very low RAIU, as was true in the case patient.
The condition is self-limiting and does not require treatment in the majority of patients, as TFT results return to normal levels within about two months.6 Patients can appear extremely ill due to thyrotoxicosis from subacute thyroiditis, but this usually lasts no longer than six to eight weeks.3 Subacute thyroiditis can be associated with atrial arrhythmia or heart failure.14,15
PATIENT OUTCOME
New-onset A-fib was attributed to the patient's thyrotoxicosis, which in turn was caused by subacute thyroiditis. He had a multinodular goiter, although he had not received any iodine supplements or IV contrast. As in most cases of subacute thyroiditis, no precipitating event was identified. However, given this patient's residence in a nursing facility and presentation with a high fever with no identifiable cause, a viral etiology for his subacute thyroiditis is possible.6
The patient's dementia may have been secondary to acute thyrotoxicosis, as his mental state improved during the hospital stay. His vitamin B12, folate, and A1C levels were within normal range. CT of the head showed multiple chronic infarcts and cerebral atrophy, and MRI of the brain indicated microvascular ischemic disease.
The patient was readmitted one month later for an episode of near-syncope (which, it was concluded, was a vasovagal episode). At that time, his TSH was found normal at 1.350 µIU/mL. Flecainide and metoprolol were discontinued; he was started on diltiazem for continued rate and rhythm control (as recommended by cardiology) and continued on warfarin.
CONCLUSION
In this case, subacute thyroiditis was most likely caused by a viral infection that led to destruction of the normal thyroid follicles and release of their preformed thyroid hormone into the circulation; this in turn led to sudden-onset A-fib. The diagnosis of subacute thyroiditis was suggested based on the abnormalities seen in this patient's TFT results, coupled with the suppressed RAIU—a typical finding in this disease.
Because subacute thyroiditis is a self-limiting condition, there is no role for antithyroid medication. Instead, treatment should be focused on relieving the patient's symptoms, such as ß-blockade or calcium channel blockers for tachycardia and corticosteroids or NSAIDs for neck pain.
REFERENCES
1. Weetman AP. Graves' disease. N Engl J Med. 2000;343(17):1236-1248.
2. Delgado Hurtado JJ, Pineda M. Images in medicine: Graves' disease. N Engl J Med. 2011; 364(20):1955.
3. Al-Sharif AA, Abujbara MA, Chiacchio S, et al. Contribution of radioiodine uptake measurement and thyroid scintigraphy to the differential diagnosis of thyrotoxicosis. Hell J Nucl Med. 2010;13(2):132-137.
4. Buccelletti F, Carroccia A, Marsiliani D, et al. Utility of routine thyroid-stimulating hormone determination in new-onset atrial fibrillation in the ED. Am J Emerg Med. 2011;29(9):1158-1162.
5. Ross DS. Radioiodine therapy for hyperthyroidism. N Engl J Med. 2011;364(6):542-550.
6. Bahn RS, Burch HB, Cooper DS, et al. Hyperthyroidism and other causes of thyrotoxicosis: management guidelines of the American Thyroid Association and American Association of Clinical Endocrinologists. Endocr Pract. 2011;17(3):456-520.
7. Erickson D, Gharib H, Li H, van Heerden JA. Treatment of patients with toxic multinodular goiter. Thyroid. 1998;8(4):277-282.
8. Basaria S, Cooper DS. Amiodarone and the thyroid. Am J Med. 2005;118(7):706-714.
9. Bogazzi F, Bartalena L, Martino E. Approach to the patient with amiodarone-induced thyrotoxicosis. J Clin Endocrinol Metab. 2010;95(6):2529-2535.
10. El-Shirbiny AM, Stavrou SS, Dnistrian A, et al. Jod-Basedow syndrome following oral iodine and radioiodinated-antibody administration. J Nucl Med. 1997;38(11):1816-1817.
11. Stanbury JB, Ermans AE, Bourdoux P, et al. Iodine-induced hyperthyroidism: occurrence and epidemiology. Thyroid. 1998;8(1):83-100.
12. Fatourechi V, Aniszewski JP, Fatourechi GZ, et al. Clinical features and outcome of subacute thyroiditis in an incidence cohort: Olmsted County, Minnesota, study. J Clin Endocrinol Metab. 2003;88(5):2100-2105.
13. Golden SH, Robinson KA, Saldanha I, et al. Clinical review: prevalence and incidence of endocrine and metabolic disorders in the United States: a comprehensive review. J Clin Endocrinol Metab. 2009;94(6):1853-1878.
14. Volpé R. The management of subacute (DeQuervain's) thyroiditis. Thyroid. 1993;3(3):253-255.
15. Lee SL. Subacute thyroiditis (2009). http://emedicine.medscape.com/article/125648-overview. Accessed April 17, 2012.