User login
Unhealthy Habits Make Diabetes Harder to Handle
VA Nurses' Opinions Regarding the Use of Evidence-Based Practice
Measuring Success Rates of Nonsurgical Treatment in Veterans With Chronic Low Back Pain and Posttraumatic Stress Disorder: A Pilot Study
Grand Rounds: Woman, 49, With Dyspnea and Chest Tightness
A 49-year-old woman presented to urgent care with complaints of worsening dyspnea for the previous two days. She reported that her symptoms had begun gradually; at the time of her presentation, however, she was also experiencing chest tightness, occasional wheezing, and a nonproductive cough. She had experienced similar symptoms in the past and obtained good results by using her albuterol inhaler. During the current episode, however, she had not had the usual response to inhaler treatment.
The patient’s medical history was positive for environmental allergies, asthma, and GERD. Two weeks earlier, she had undergone dilatation and curettage (D&C) for dysfunctional bleeding, with no associated complications.
In the social history, the patient reported drinking four to six caffeine beverages daily and consuming alcohol moderately (two to four glasses of wine per week). She was following no formal dietary regimen. The patient denied current or past history of tobacco use and had not traveled recently. She had no family history of coronary vascular disease.
Her medications included albuterol and desloratadine as needed, pantoprazole 40 mg/d, and drospirenone/ethinyl estradiol. The patient said she used her albuterol inhaler four to six times per month but more often in the summer and fall. Nighttime awakenings due to asthma symptoms occurred no more than twice per month. She denied prior history of acute asthma exacerbations requiring oral systemic corticosteroids. The patient stated that since her D&C, she had been using ibuprofen almost daily for mild abdominal cramping.
A review of systems was positive for mild fatigue since her D&C. The patient denied fever, chills, headache, sore throat, or cough. She did complain of daily nasal congestion but with no unusual drainage. The patient denied orthopnea, chest pain, palpitations, or peripheral edema, as well as nausea, vomiting, diarrhea, constipation, hematochezia, or melena. She admitted to daily heartburn for the previous two weeks that was relieved somewhat with pantoprazole. She had not experienced urinary frequency or urgency, dysuria, or hematuria. She also denied rash, pruritus, weakness, paresthesias, joint pain, or swelling.
Physical examination revealed an alert, oriented female who appeared slightly anxious but was in no acute distress. Specific findings were pulse, 110 beats/min; blood pressure, 138/88 mm Hg; respirations, 24 breaths/min; temperature, 97.7°F; O2 saturation, 92% on room air. Her height measured 5’2” and weight, 150 lb (BMI, 27.43).
Her conjunctiva were slightly injected, and the tympanic membranes were intact bilaterally with a light reflex; the septum was midline. The mucosa was pale, boggy, and moist with clear drainage and no inflammation. The nasopharynx had no erythema, and the tonsils appeared normal, although a cobblestone appearance was noted in the posterior pharynx. The neck was supple with no adenopathy.
The patient’s heart rate, 110 beats/min, was regular with no murmurs, rubs, or gallops. In the lungs, a prolonged expiratory phase was noted, with diffuse wheezing on chest auscultation bilaterally. Neither retractions nor use of accessory muscles with breathing was observed. The abdomen was soft, rounded, and nontender with no organomegaly. Bowel sounds were evident in all four quadrants. The patient’s skin was free of suspicious lesions or rashes. Her extremities were without edema, and no calf tenderness was noted; Homans’ sign was negative. Superficial varicosities were noted bilaterally.
The top differential diagnosis included:
• Acute asthma (risk factors: history of uncontrolled asthma, as evidenced by frequent use of albuterol)
• Acute anemia (risk factors: history of dysfunctional uterine bleeding, recent D&C)
• Pulmonary embolism (risk factors: recent surgery, recent start of oral contraceptive use).
Additional diagnoses to be considered less likely included:
• Acute coronary syndrome/MI (possible causes of chest tightness, dyspnea, dyspepsia; but no chest pain, diaphoresis, or nausea)
• Acute respiratory distress (history of tachycardia, possible dyspnea; but no diaphoresis, cyanosis, retractions, accessory muscle use, or lung crackles)
• Pneumonia (risk factors: recent surgery, possible cause of nonproductive cough; but no evidence of fever, chills, rales, or pleuritic chest pain).
Diagnostic testing included a 12-lead ECG to evaluate the patient for cardiac arrhythmia or injury; on it, tachycardia was noted, with a regular rate of 106 beats/min. The patient’s chest x-ray yielded normal results.
Laboratory testing included a complete blood count to screen for anemia and infection. Results included a white blood cell count of 8,200/mL (normal range, 4,500 to 11,000/mL); hematocrit, 38.2% (normal range for women, 36.1% to 44.3%); hemoglobin, 13.1 g/dL (normal for women, 12.1 to 15.1 g/dL). A comprehensive metabolic panel was performed to assess electrolyte levels and kidney and liver function; findings were normal. Results of a D-dimer assay, which was obtained to exclude pulmonary embolism,1 were normal at 0.5 mg/L (range, 0.4 to 1.4 mg/L).
In the case of heightened suspicion for MI, the patient would have been transferred to the emergency department (ED) for evaluation, including serial cardiac troponin levels; elevated troponin levels are deemed the standard criterion to define and diagnose MI in a consensus document from the European Society of Cardiology and the American College of Cardiology.2 (Troponin-T and troponin-I are more tissue-specific than the MB fraction of creatine kinase [CK-MB] in detecting MI; positive troponin levels are considered virtually diagnostic of MI.2 Typically, cardiac troponin levels are measured two to three times over a 12- to 16-hour period.)
Peak expiratory flow (PEF), which was measured to evaluate the patient’s respiratory status, was 150 L/min (compared with personal best for a patient of her height and age, approximately 460 L/min). She was given 2.5 mg/3 mL of inhaled albuterol over 15 minutes. Her PEF increased to 350 L/min. O2 saturation improved to 96% on room air, pulse to 104 beats/min, and respirations 20 breaths/min; her blood pressure reading was now 140/90 mm Hg. A prolonged expiratory phase persisted in the lungs, but diffuse wheezing decreased by 40% on chest auscultation.
A second albuterol treatment was administered 20 minutes later, and the patient’s PEF increased to 380 L/min and O2 saturation to 99%. The lungs presently cleared with no further wheezing noted.
In addition, the patient was given a GI cocktail (ie, liquid antacid combined with an anticholinergic agent and viscous lidocaine). Within 10 minutes, her chest tightness was relieved 100%. Her blood pressure was then measured at 135/84 mm Hg; respirations, 18 breaths/min; and pulse rate, 96 beats/min.
According to the National Asthma Education and Prevention Program (NAEPP) 2007 Guidelines for the Diagnosis and Management of Asthma, Expert Panel Report 3 (EPR-3),3 the patient was classified as having intermittent, not-well-controlled asthma with an acute exacerbation. In addition, she was given a diagnosis of uncontrolled GERD.
DISCUSSION
Asthma Incidence and Risk Factors
Asthma affects approximately 300 million people worldwide and remains a global respiratory concern.4 In the United States, this chronic health condition has a prevalence of 8% to 10%. It is estimated that 5% to 10% of asthmatic patients have severe disease that does not respond typically to therapeutic interventions.5
Asthma involves bronchial hyperresponsiveness, airflow obstruction, and underlying inflammation. Acute episodes of asthma, arising from bronchospasm, usually manifest with progressively worsening cough, shortness of breath, chest tightness and wheezing (asthma’s hallmark symptoms), or a combination of symptoms.3
Symptoms of asthma or exacerbations of reactive airway disease vary from patient to patient. In addition to the hallmark symptoms noted, subacute or acute episodes of asthma exacerbation are characterized by decreases in expiratory airflow that can be documented by objective measurements of lung function, such as PEF or spirometry; these measures of airflow indicate the severity of an exacerbation more reliably than does perceived symptom severity.3 The EPR-3 panelists recommend determining asthma severity using a combination of objective criteria and clinical symptoms,3 although few clinicians use the objective criteria.6
Estimates of the prevalence of GERD among patients with asthma have varied from 34% to 89%.7-9 Patients with GERD are 1.97 times more likely than patients without GERD to have asthma10; silent gastroesophageal reflux has been identified in 24% to 62% of patients with asthma, and early studies suggest that treatment for GERD may improve asthma control in patients with severe or difficult-to-control asthma.8,11,12
The exact link between the two conditions is unclear. However, possible explanations why GERD and asthma coincide are that acid flow causes injury to the lining of the throat, airways, and lungs, making inhalation difficult and often causing a persistent cough; or that when acid enters the esophagus, a nerve reflex is triggered that causes the airways to narrow in order to prevent the acid from entering; this can explain dyspnea.8,9
Economic Burden
Asthma is costly to treat, and because there is no cure, the expense is ongoing. According to a 2011 report,13 the average annual direct cost of care (eg, medications, hospital admissions, nonemergency office visits) for one asthma patient between 2002 and 2007 was $3,259. In 2007, the most current data available, the total cost of asthma in the US was $56 billion, with productivity losses due to mortality accounting for $2.1 billion and morbidity-related losses estimated at $3.8 billion.13 The economic consequences of asthma are substantial and can place a considerable burden on affected individuals, their families, the health care system, and society as a whole.3
Current Standard of Care
Based on the scientific literature and the opinions expressed by the NAEPP in the EPR-3,3 clinicians are advised to consider the following general principles and goals for managing asthma: early treatment, special attention to patients at high risk for asthma-related death, and special attention to infants.3 The guidelines emphasize the importance of a clinician/patient partnership to facilitate the asthma patient’s self-management.
Early treatment is a particularly important component for management of asthma exacerbations. Important elements of early treatment include a written asthma action plan, combined with enhanced awareness of the early indicators of an exacerbation (ie, worsening PEF).3,14 It is believed that if patients are able to monitor their respiratory condition and follow a plan of care based on their PEF and/or signs and symptoms of asthma, they are more likely to achieve optimal management of their disease.15
Written Asthma Action Plan. The EPR-33 recommends that health care providers supply all asthmatic patients with a written asthma action plan that will define and support the patient’s efforts at self-management. Written asthma action plans are particularly beneficial for patients with moderate to severe persistent asthma, poorly controlled asthma, or a history of severe exacerbations.3,14
The written asthma action plan should include instructions for daily management of asthma and ways to recognize and treat worsening asthma, including adjustments to medication dosing. Plans may be based on PEF and/or symptoms. Asthma action plans should be discussed and reevaluated at follow-up visits.3 A sample asthma action plan can be found at www.health.state.ny.us/diseases/asthma/pdf/4850.pdf.16
Peak Expiratory Flow (PEF). The EPR-33 recommends PEF monitoring in all asthma patients, regardless of the severity of their exacerbations.17 PEF-based plans are especially useful for the patient who has difficulty perceiving early signs and symptoms of worsening asthma.3,18 A PEF-based plan instructs the patient to use quick-relief medications if symptoms occur or if PEF drops below 80% of the patient’s personal or predicted best. (Measured personal best is the patient’s highest PEF in the previous two weeks of good asthma control,3,19 whereas predicted best is calculated based on findings from a 1983 study by Knudson et al.3,20)
A PEF between 50% and 79% requires the patient to carefully monitor his or her response to the quick-relief medication and, based on that response, consider whether to contact a health care provider. When PEF falls below 50%, a provider’s immediate intervention is usually recommended.3
In the urgent care or ED setting, according to EPR-3 recommendations,3 the PEF or forced expiratory volume in 1 second (FEV1) is used to indicate the following:
• ≥ 70% predicted PEF or FEV1: goal for discharge
• 40% to 69% predicted PEF or FEV1: incomplete response to treatment, frequent need for treatment in the ED
• 3
Treatment and Management
Asthma management interventions that target the treatment of active disease and predisposing triggers are designed to reduce the severity and/or duration of morbidity associated with asthma—principally, to prevent symptoms and exacerbations (see Table 13).
When patients are discharged following an asthma exacerbation, their medications should include an oral corticosteroid burst and a short-acting b2-agonist (SABA); the clinician should also consider prescribing an inhaled corticosteroid (ICS).3
It is no longer recommended that ICS dosing be doubled in place of an oral steroid burst.3,21 The addition of a leukotriene receptor antagonist (LTRA) may also be considered.3,22
Patients should be given an action plan, and follow-up with a primary care provider should be scheduled within a few days—or even the following day, depending on the severity of the patient’s condition. The importance of follow-up with a primary care provider, a pulmonologist, or an asthma/allergy specialist should be emphasized.3,23
For patients who have difficulty recognizing their symptoms, a peak flow meter may be useful. This device is also recommended for patients with moderate to severe asthma or a history of numerous severe exacerbations.3 Additionally, spacers should always be used with metered dose inhalers (MDIs), because they make it easier for medication to reach the lungs and reduce the amount deposited in the mouth and throat, where it can lead to irritation. At each office visit, use of the peak flow meter and inhaler technique should be observed, and the action plan reevaluated and changed if necessary.3,14
Additional components of patient education include instruction in controlling environmental factors: avoiding environmental tobacco smoke, exposure to insect allergens, and molds. It is also important to stress controlling comorbid conditions that influence asthma, such as allergies or GERD. Patients with symptoms of GERD should be advised to take the steps shown in Table 2.8,24
Clinical Implications
Assessment of the severity of an asthma exacerbation is an essential component of ambulatory asthma care. Underclassification of asthma severity has been associated with increased morbidity and mortality,6 and the NAEPP guidelines recommend that clinicians assess and document asthma severity at each clinic visit.3,25 Patients who receive care based on evidence-based practice guidelines have been shown to experience 28% better outcomes.26
PATIENT OUTCOME
The case patient was discharged on an oral corticosteroid burst and a low-dose ICS. She was instructed how and when to use her SABA and given a prescription for a spacer; use of a peak flow meter was initiated with an estimated personal best goal of 460 L/min. The patient was given a written asthma action plan to help her recognize early signs and symptoms of worsening asthma and was advised to use quick-relief medications if she experienced symptoms or if her PEF dropped below 80% of her predicted best.
The patient’s clinician emphasized the importance of controlling any asthma-triggering environmental factors and reviewed nonpharmacologic interventions to control GERD. The patient was advised to resume desloratadine 5 mg/d and pantoprazole 40 mg/d. She was also instructed to schedule an appointment with her primary care provider within 48 hours and to return to urgent care or the ED with any further exacerbation of respiratory symptoms not controlled by her SABA.
CONCLUSION
Asthma morbidity is a nationally recognized, major public health problem. Given the sharp rise in health care costs and limited resources, health care providers must factor in the comparative effectiveness, comparative cost, and cost-effectiveness of both new and existing health care interventions when making treatment decisions.
Many asthmatic patients face the challenges of health care access and quality. By promoting their self-care and awareness, clinicians can help asthmatic patients achieve better symptom management and use the health care system less often.
REFERENCES
1. Stein PD, Hull RD, Patel KC, et al. D-Dimer for the exclusion of acute venous thrombosis and pulmonary embolism. Ann Intern Med. 2004;140(8):589-602.
2. Alpert JS, Thygesen K, Antman E, Bassand JP. Myocardial infarction redefined: a consensus document of The Joint European Society of Cardiology/American College of Cardiology Committee for the redefinition of myocardial infarction. J Am Coll Cardiol. 2000;36(3):959-969.
3. National Asthma Education and Prevention Program, National Heart, Lung, and Blood Institute. Expert Panel Report 3: Guidelines for the Diagnosis and Management of Asthma. Bethesda, MD: National Heart, Lung, and Blood Institute; 2007. US Department of Health and Human Services publication NIH 07-4051.
4. Lougheed DM. Variability in asthma: symptom perception, care, and outcomes. Can J Physiol Pharmacol. 2007;85(1):149-154.
5. Higgins JC. The ‘crashing asthmatic.’ Am Fam Physician. 2003;67(5):997-1004.
6. Cowen MK, Wakefield DB, Cloutier MM. Classifying asthma severity: objective versus subjective measures. J Asthma. 2007;44(9):711-715.
7. Takenaka R, Matsuno O, Kitajima K, et al. The use of frequency scale for the symptoms of GERD in assessment of gastro-oesophageal reflux symptoms in asthma. Allergol Immunopathol (Madr). 2010;38(1):20-24.
8. Harding SM, Barnes PJ, Hollingsworth H. Gastroesophageal reflux and asthma (2010). www.uptodate.com/contents/gastroesophageal-reflux-and-asthma. Accessed April 5, 2011.
9. Havemann BD, Henderson CA, El-Serag HB. The association between gastro-oesophageal reflux disease and asthma: a systematic review. Gut. 2007;56(12):1654-1664.
10. Tsai MC, Lin HL, Lin CC, et al. Increased risk of concurrent asthma among patients with gastroesophageal reflux disease: a nationwide population-based study. Eur J Gastroenterol Hepatol. 2010;22(10):1169-1173.
11. Harding SM, Richter JE, Guzzo MR, et al. Asthma and gastroesophageal reflux: acid suppressive therapy improves asthma outcome. Am J Med. 1996;100(4):395-405.
12. Gibson PG, Henry RL, Coughlan JL. Gastro-oesophageal reflux treatment for asthma in adults and children. Cochrane Database Syst Rev. 2003;(2):CD001496.
13. Barnett SB, Nurmagambetov TA. Costs of asthma in the United States: 2002-2007. J Allergy Clin Immunol. 2011;127(1):145-152.
14. Walders N, Kercsmar C, Schluchter M, et al. An interdisciplinary intervention for undertreated pediatric asthma. Chest. 2006;129(2):292-299.
15. Morrow R, Fletcher J, Mulvihill M, Park H. The asthma dialogues: a model of interactive education for skills. J Contin Educ Health Prof. 2007;27(1): 49-58.
16. State of New York, Department of Health. Asthma action plan. www.health.state.ny.us/diseases/asthma/pdf/4850.pdf. Accessed April 11, 2011.
17. Picken HA, Greenfield S, Teres D, et al. Effects of local standards on the implementation of national guidelines for asthma: primary care agreement with national asthma guidelines. J Gen Intern Med. 1998;13(10):659-663.
18. Hardie GE, Gold WM, Janson S, et al. Understanding how asthmatics perceive symptom distress during a methacholine challenge. J Asthma. 2002;39(7):611-618.
19. Reddel HK, Marks GB, Jenkins CR. When can personal best peak flow be determined for asthma action plans? Thorax. 2004;59(11):922-924.
20. Knudson RJ, Lebowitz MD, Holberg CJ, Burrows B. Changes in the normal maximal expiratory flow-volume curve with growth and aging. Am Rev Respir Dis. 1983;127(6):725-734.
21. Ind PW, Dal Negro R, Colman NC, et al. Addition of salmeterol to fluticasone propionate treatment in moderate-to-severe asthma. Respir Med. 2003;97(5):555-562.
22. Price DB, Hernandez D, Magyar P, et al; Clinical Outcomes with Montelukast as a Partner Agent to Corticosteroid Therapy (COMPACT) International Study Group. Randomised controlled trial of montelukast plus inhaled budesonide versus double dose inhaled budesonide in adult patients with asthma. Thorax. 2003;58(3):211-216.
23. Schatz M, Zeiger RS, Mosen D, et al. Improved asthma outcomes from allergy specialist care: a population-based cross-sectional analysis. J Allergy Clin Immunol. 2005;116(6):1307-1313.
24. Hampel H, Abraham NS, El-Serag HB. Meta-analysis: obesity and the risk for gastroesophageal reflux disease and its complications. Ann Intern Med. 2005;143(3):199-211.
25. Cabana MD, Bruckman D, Meister K, et al. Documentation of asthma severity in pediatric outpatient clinics. Clin Pediatr (Phila). 2003;42(2):121-125.
26. Heater BS, Becker AM, Olson RK. Nursing interventions and patient outcomes: a meta-analysis of studies. Nurs Res. 1988;37(5):303-307.
A 49-year-old woman presented to urgent care with complaints of worsening dyspnea for the previous two days. She reported that her symptoms had begun gradually; at the time of her presentation, however, she was also experiencing chest tightness, occasional wheezing, and a nonproductive cough. She had experienced similar symptoms in the past and obtained good results by using her albuterol inhaler. During the current episode, however, she had not had the usual response to inhaler treatment.
The patient’s medical history was positive for environmental allergies, asthma, and GERD. Two weeks earlier, she had undergone dilatation and curettage (D&C) for dysfunctional bleeding, with no associated complications.
In the social history, the patient reported drinking four to six caffeine beverages daily and consuming alcohol moderately (two to four glasses of wine per week). She was following no formal dietary regimen. The patient denied current or past history of tobacco use and had not traveled recently. She had no family history of coronary vascular disease.
Her medications included albuterol and desloratadine as needed, pantoprazole 40 mg/d, and drospirenone/ethinyl estradiol. The patient said she used her albuterol inhaler four to six times per month but more often in the summer and fall. Nighttime awakenings due to asthma symptoms occurred no more than twice per month. She denied prior history of acute asthma exacerbations requiring oral systemic corticosteroids. The patient stated that since her D&C, she had been using ibuprofen almost daily for mild abdominal cramping.
A review of systems was positive for mild fatigue since her D&C. The patient denied fever, chills, headache, sore throat, or cough. She did complain of daily nasal congestion but with no unusual drainage. The patient denied orthopnea, chest pain, palpitations, or peripheral edema, as well as nausea, vomiting, diarrhea, constipation, hematochezia, or melena. She admitted to daily heartburn for the previous two weeks that was relieved somewhat with pantoprazole. She had not experienced urinary frequency or urgency, dysuria, or hematuria. She also denied rash, pruritus, weakness, paresthesias, joint pain, or swelling.
Physical examination revealed an alert, oriented female who appeared slightly anxious but was in no acute distress. Specific findings were pulse, 110 beats/min; blood pressure, 138/88 mm Hg; respirations, 24 breaths/min; temperature, 97.7°F; O2 saturation, 92% on room air. Her height measured 5’2” and weight, 150 lb (BMI, 27.43).
Her conjunctiva were slightly injected, and the tympanic membranes were intact bilaterally with a light reflex; the septum was midline. The mucosa was pale, boggy, and moist with clear drainage and no inflammation. The nasopharynx had no erythema, and the tonsils appeared normal, although a cobblestone appearance was noted in the posterior pharynx. The neck was supple with no adenopathy.
The patient’s heart rate, 110 beats/min, was regular with no murmurs, rubs, or gallops. In the lungs, a prolonged expiratory phase was noted, with diffuse wheezing on chest auscultation bilaterally. Neither retractions nor use of accessory muscles with breathing was observed. The abdomen was soft, rounded, and nontender with no organomegaly. Bowel sounds were evident in all four quadrants. The patient’s skin was free of suspicious lesions or rashes. Her extremities were without edema, and no calf tenderness was noted; Homans’ sign was negative. Superficial varicosities were noted bilaterally.
The top differential diagnosis included:
• Acute asthma (risk factors: history of uncontrolled asthma, as evidenced by frequent use of albuterol)
• Acute anemia (risk factors: history of dysfunctional uterine bleeding, recent D&C)
• Pulmonary embolism (risk factors: recent surgery, recent start of oral contraceptive use).
Additional diagnoses to be considered less likely included:
• Acute coronary syndrome/MI (possible causes of chest tightness, dyspnea, dyspepsia; but no chest pain, diaphoresis, or nausea)
• Acute respiratory distress (history of tachycardia, possible dyspnea; but no diaphoresis, cyanosis, retractions, accessory muscle use, or lung crackles)
• Pneumonia (risk factors: recent surgery, possible cause of nonproductive cough; but no evidence of fever, chills, rales, or pleuritic chest pain).
Diagnostic testing included a 12-lead ECG to evaluate the patient for cardiac arrhythmia or injury; on it, tachycardia was noted, with a regular rate of 106 beats/min. The patient’s chest x-ray yielded normal results.
Laboratory testing included a complete blood count to screen for anemia and infection. Results included a white blood cell count of 8,200/mL (normal range, 4,500 to 11,000/mL); hematocrit, 38.2% (normal range for women, 36.1% to 44.3%); hemoglobin, 13.1 g/dL (normal for women, 12.1 to 15.1 g/dL). A comprehensive metabolic panel was performed to assess electrolyte levels and kidney and liver function; findings were normal. Results of a D-dimer assay, which was obtained to exclude pulmonary embolism,1 were normal at 0.5 mg/L (range, 0.4 to 1.4 mg/L).
In the case of heightened suspicion for MI, the patient would have been transferred to the emergency department (ED) for evaluation, including serial cardiac troponin levels; elevated troponin levels are deemed the standard criterion to define and diagnose MI in a consensus document from the European Society of Cardiology and the American College of Cardiology.2 (Troponin-T and troponin-I are more tissue-specific than the MB fraction of creatine kinase [CK-MB] in detecting MI; positive troponin levels are considered virtually diagnostic of MI.2 Typically, cardiac troponin levels are measured two to three times over a 12- to 16-hour period.)
Peak expiratory flow (PEF), which was measured to evaluate the patient’s respiratory status, was 150 L/min (compared with personal best for a patient of her height and age, approximately 460 L/min). She was given 2.5 mg/3 mL of inhaled albuterol over 15 minutes. Her PEF increased to 350 L/min. O2 saturation improved to 96% on room air, pulse to 104 beats/min, and respirations 20 breaths/min; her blood pressure reading was now 140/90 mm Hg. A prolonged expiratory phase persisted in the lungs, but diffuse wheezing decreased by 40% on chest auscultation.
A second albuterol treatment was administered 20 minutes later, and the patient’s PEF increased to 380 L/min and O2 saturation to 99%. The lungs presently cleared with no further wheezing noted.
In addition, the patient was given a GI cocktail (ie, liquid antacid combined with an anticholinergic agent and viscous lidocaine). Within 10 minutes, her chest tightness was relieved 100%. Her blood pressure was then measured at 135/84 mm Hg; respirations, 18 breaths/min; and pulse rate, 96 beats/min.
According to the National Asthma Education and Prevention Program (NAEPP) 2007 Guidelines for the Diagnosis and Management of Asthma, Expert Panel Report 3 (EPR-3),3 the patient was classified as having intermittent, not-well-controlled asthma with an acute exacerbation. In addition, she was given a diagnosis of uncontrolled GERD.
DISCUSSION
Asthma Incidence and Risk Factors
Asthma affects approximately 300 million people worldwide and remains a global respiratory concern.4 In the United States, this chronic health condition has a prevalence of 8% to 10%. It is estimated that 5% to 10% of asthmatic patients have severe disease that does not respond typically to therapeutic interventions.5
Asthma involves bronchial hyperresponsiveness, airflow obstruction, and underlying inflammation. Acute episodes of asthma, arising from bronchospasm, usually manifest with progressively worsening cough, shortness of breath, chest tightness and wheezing (asthma’s hallmark symptoms), or a combination of symptoms.3
Symptoms of asthma or exacerbations of reactive airway disease vary from patient to patient. In addition to the hallmark symptoms noted, subacute or acute episodes of asthma exacerbation are characterized by decreases in expiratory airflow that can be documented by objective measurements of lung function, such as PEF or spirometry; these measures of airflow indicate the severity of an exacerbation more reliably than does perceived symptom severity.3 The EPR-3 panelists recommend determining asthma severity using a combination of objective criteria and clinical symptoms,3 although few clinicians use the objective criteria.6
Estimates of the prevalence of GERD among patients with asthma have varied from 34% to 89%.7-9 Patients with GERD are 1.97 times more likely than patients without GERD to have asthma10; silent gastroesophageal reflux has been identified in 24% to 62% of patients with asthma, and early studies suggest that treatment for GERD may improve asthma control in patients with severe or difficult-to-control asthma.8,11,12
The exact link between the two conditions is unclear. However, possible explanations why GERD and asthma coincide are that acid flow causes injury to the lining of the throat, airways, and lungs, making inhalation difficult and often causing a persistent cough; or that when acid enters the esophagus, a nerve reflex is triggered that causes the airways to narrow in order to prevent the acid from entering; this can explain dyspnea.8,9
Economic Burden
Asthma is costly to treat, and because there is no cure, the expense is ongoing. According to a 2011 report,13 the average annual direct cost of care (eg, medications, hospital admissions, nonemergency office visits) for one asthma patient between 2002 and 2007 was $3,259. In 2007, the most current data available, the total cost of asthma in the US was $56 billion, with productivity losses due to mortality accounting for $2.1 billion and morbidity-related losses estimated at $3.8 billion.13 The economic consequences of asthma are substantial and can place a considerable burden on affected individuals, their families, the health care system, and society as a whole.3
Current Standard of Care
Based on the scientific literature and the opinions expressed by the NAEPP in the EPR-3,3 clinicians are advised to consider the following general principles and goals for managing asthma: early treatment, special attention to patients at high risk for asthma-related death, and special attention to infants.3 The guidelines emphasize the importance of a clinician/patient partnership to facilitate the asthma patient’s self-management.
Early treatment is a particularly important component for management of asthma exacerbations. Important elements of early treatment include a written asthma action plan, combined with enhanced awareness of the early indicators of an exacerbation (ie, worsening PEF).3,14 It is believed that if patients are able to monitor their respiratory condition and follow a plan of care based on their PEF and/or signs and symptoms of asthma, they are more likely to achieve optimal management of their disease.15
Written Asthma Action Plan. The EPR-33 recommends that health care providers supply all asthmatic patients with a written asthma action plan that will define and support the patient’s efforts at self-management. Written asthma action plans are particularly beneficial for patients with moderate to severe persistent asthma, poorly controlled asthma, or a history of severe exacerbations.3,14
The written asthma action plan should include instructions for daily management of asthma and ways to recognize and treat worsening asthma, including adjustments to medication dosing. Plans may be based on PEF and/or symptoms. Asthma action plans should be discussed and reevaluated at follow-up visits.3 A sample asthma action plan can be found at www.health.state.ny.us/diseases/asthma/pdf/4850.pdf.16
Peak Expiratory Flow (PEF). The EPR-33 recommends PEF monitoring in all asthma patients, regardless of the severity of their exacerbations.17 PEF-based plans are especially useful for the patient who has difficulty perceiving early signs and symptoms of worsening asthma.3,18 A PEF-based plan instructs the patient to use quick-relief medications if symptoms occur or if PEF drops below 80% of the patient’s personal or predicted best. (Measured personal best is the patient’s highest PEF in the previous two weeks of good asthma control,3,19 whereas predicted best is calculated based on findings from a 1983 study by Knudson et al.3,20)
A PEF between 50% and 79% requires the patient to carefully monitor his or her response to the quick-relief medication and, based on that response, consider whether to contact a health care provider. When PEF falls below 50%, a provider’s immediate intervention is usually recommended.3
In the urgent care or ED setting, according to EPR-3 recommendations,3 the PEF or forced expiratory volume in 1 second (FEV1) is used to indicate the following:
• ≥ 70% predicted PEF or FEV1: goal for discharge
• 40% to 69% predicted PEF or FEV1: incomplete response to treatment, frequent need for treatment in the ED
• 3
Treatment and Management
Asthma management interventions that target the treatment of active disease and predisposing triggers are designed to reduce the severity and/or duration of morbidity associated with asthma—principally, to prevent symptoms and exacerbations (see Table 13).
When patients are discharged following an asthma exacerbation, their medications should include an oral corticosteroid burst and a short-acting b2-agonist (SABA); the clinician should also consider prescribing an inhaled corticosteroid (ICS).3
It is no longer recommended that ICS dosing be doubled in place of an oral steroid burst.3,21 The addition of a leukotriene receptor antagonist (LTRA) may also be considered.3,22
Patients should be given an action plan, and follow-up with a primary care provider should be scheduled within a few days—or even the following day, depending on the severity of the patient’s condition. The importance of follow-up with a primary care provider, a pulmonologist, or an asthma/allergy specialist should be emphasized.3,23
For patients who have difficulty recognizing their symptoms, a peak flow meter may be useful. This device is also recommended for patients with moderate to severe asthma or a history of numerous severe exacerbations.3 Additionally, spacers should always be used with metered dose inhalers (MDIs), because they make it easier for medication to reach the lungs and reduce the amount deposited in the mouth and throat, where it can lead to irritation. At each office visit, use of the peak flow meter and inhaler technique should be observed, and the action plan reevaluated and changed if necessary.3,14
Additional components of patient education include instruction in controlling environmental factors: avoiding environmental tobacco smoke, exposure to insect allergens, and molds. It is also important to stress controlling comorbid conditions that influence asthma, such as allergies or GERD. Patients with symptoms of GERD should be advised to take the steps shown in Table 2.8,24
Clinical Implications
Assessment of the severity of an asthma exacerbation is an essential component of ambulatory asthma care. Underclassification of asthma severity has been associated with increased morbidity and mortality,6 and the NAEPP guidelines recommend that clinicians assess and document asthma severity at each clinic visit.3,25 Patients who receive care based on evidence-based practice guidelines have been shown to experience 28% better outcomes.26
PATIENT OUTCOME
The case patient was discharged on an oral corticosteroid burst and a low-dose ICS. She was instructed how and when to use her SABA and given a prescription for a spacer; use of a peak flow meter was initiated with an estimated personal best goal of 460 L/min. The patient was given a written asthma action plan to help her recognize early signs and symptoms of worsening asthma and was advised to use quick-relief medications if she experienced symptoms or if her PEF dropped below 80% of her predicted best.
The patient’s clinician emphasized the importance of controlling any asthma-triggering environmental factors and reviewed nonpharmacologic interventions to control GERD. The patient was advised to resume desloratadine 5 mg/d and pantoprazole 40 mg/d. She was also instructed to schedule an appointment with her primary care provider within 48 hours and to return to urgent care or the ED with any further exacerbation of respiratory symptoms not controlled by her SABA.
CONCLUSION
Asthma morbidity is a nationally recognized, major public health problem. Given the sharp rise in health care costs and limited resources, health care providers must factor in the comparative effectiveness, comparative cost, and cost-effectiveness of both new and existing health care interventions when making treatment decisions.
Many asthmatic patients face the challenges of health care access and quality. By promoting their self-care and awareness, clinicians can help asthmatic patients achieve better symptom management and use the health care system less often.
REFERENCES
1. Stein PD, Hull RD, Patel KC, et al. D-Dimer for the exclusion of acute venous thrombosis and pulmonary embolism. Ann Intern Med. 2004;140(8):589-602.
2. Alpert JS, Thygesen K, Antman E, Bassand JP. Myocardial infarction redefined: a consensus document of The Joint European Society of Cardiology/American College of Cardiology Committee for the redefinition of myocardial infarction. J Am Coll Cardiol. 2000;36(3):959-969.
3. National Asthma Education and Prevention Program, National Heart, Lung, and Blood Institute. Expert Panel Report 3: Guidelines for the Diagnosis and Management of Asthma. Bethesda, MD: National Heart, Lung, and Blood Institute; 2007. US Department of Health and Human Services publication NIH 07-4051.
4. Lougheed DM. Variability in asthma: symptom perception, care, and outcomes. Can J Physiol Pharmacol. 2007;85(1):149-154.
5. Higgins JC. The ‘crashing asthmatic.’ Am Fam Physician. 2003;67(5):997-1004.
6. Cowen MK, Wakefield DB, Cloutier MM. Classifying asthma severity: objective versus subjective measures. J Asthma. 2007;44(9):711-715.
7. Takenaka R, Matsuno O, Kitajima K, et al. The use of frequency scale for the symptoms of GERD in assessment of gastro-oesophageal reflux symptoms in asthma. Allergol Immunopathol (Madr). 2010;38(1):20-24.
8. Harding SM, Barnes PJ, Hollingsworth H. Gastroesophageal reflux and asthma (2010). www.uptodate.com/contents/gastroesophageal-reflux-and-asthma. Accessed April 5, 2011.
9. Havemann BD, Henderson CA, El-Serag HB. The association between gastro-oesophageal reflux disease and asthma: a systematic review. Gut. 2007;56(12):1654-1664.
10. Tsai MC, Lin HL, Lin CC, et al. Increased risk of concurrent asthma among patients with gastroesophageal reflux disease: a nationwide population-based study. Eur J Gastroenterol Hepatol. 2010;22(10):1169-1173.
11. Harding SM, Richter JE, Guzzo MR, et al. Asthma and gastroesophageal reflux: acid suppressive therapy improves asthma outcome. Am J Med. 1996;100(4):395-405.
12. Gibson PG, Henry RL, Coughlan JL. Gastro-oesophageal reflux treatment for asthma in adults and children. Cochrane Database Syst Rev. 2003;(2):CD001496.
13. Barnett SB, Nurmagambetov TA. Costs of asthma in the United States: 2002-2007. J Allergy Clin Immunol. 2011;127(1):145-152.
14. Walders N, Kercsmar C, Schluchter M, et al. An interdisciplinary intervention for undertreated pediatric asthma. Chest. 2006;129(2):292-299.
15. Morrow R, Fletcher J, Mulvihill M, Park H. The asthma dialogues: a model of interactive education for skills. J Contin Educ Health Prof. 2007;27(1): 49-58.
16. State of New York, Department of Health. Asthma action plan. www.health.state.ny.us/diseases/asthma/pdf/4850.pdf. Accessed April 11, 2011.
17. Picken HA, Greenfield S, Teres D, et al. Effects of local standards on the implementation of national guidelines for asthma: primary care agreement with national asthma guidelines. J Gen Intern Med. 1998;13(10):659-663.
18. Hardie GE, Gold WM, Janson S, et al. Understanding how asthmatics perceive symptom distress during a methacholine challenge. J Asthma. 2002;39(7):611-618.
19. Reddel HK, Marks GB, Jenkins CR. When can personal best peak flow be determined for asthma action plans? Thorax. 2004;59(11):922-924.
20. Knudson RJ, Lebowitz MD, Holberg CJ, Burrows B. Changes in the normal maximal expiratory flow-volume curve with growth and aging. Am Rev Respir Dis. 1983;127(6):725-734.
21. Ind PW, Dal Negro R, Colman NC, et al. Addition of salmeterol to fluticasone propionate treatment in moderate-to-severe asthma. Respir Med. 2003;97(5):555-562.
22. Price DB, Hernandez D, Magyar P, et al; Clinical Outcomes with Montelukast as a Partner Agent to Corticosteroid Therapy (COMPACT) International Study Group. Randomised controlled trial of montelukast plus inhaled budesonide versus double dose inhaled budesonide in adult patients with asthma. Thorax. 2003;58(3):211-216.
23. Schatz M, Zeiger RS, Mosen D, et al. Improved asthma outcomes from allergy specialist care: a population-based cross-sectional analysis. J Allergy Clin Immunol. 2005;116(6):1307-1313.
24. Hampel H, Abraham NS, El-Serag HB. Meta-analysis: obesity and the risk for gastroesophageal reflux disease and its complications. Ann Intern Med. 2005;143(3):199-211.
25. Cabana MD, Bruckman D, Meister K, et al. Documentation of asthma severity in pediatric outpatient clinics. Clin Pediatr (Phila). 2003;42(2):121-125.
26. Heater BS, Becker AM, Olson RK. Nursing interventions and patient outcomes: a meta-analysis of studies. Nurs Res. 1988;37(5):303-307.
A 49-year-old woman presented to urgent care with complaints of worsening dyspnea for the previous two days. She reported that her symptoms had begun gradually; at the time of her presentation, however, she was also experiencing chest tightness, occasional wheezing, and a nonproductive cough. She had experienced similar symptoms in the past and obtained good results by using her albuterol inhaler. During the current episode, however, she had not had the usual response to inhaler treatment.
The patient’s medical history was positive for environmental allergies, asthma, and GERD. Two weeks earlier, she had undergone dilatation and curettage (D&C) for dysfunctional bleeding, with no associated complications.
In the social history, the patient reported drinking four to six caffeine beverages daily and consuming alcohol moderately (two to four glasses of wine per week). She was following no formal dietary regimen. The patient denied current or past history of tobacco use and had not traveled recently. She had no family history of coronary vascular disease.
Her medications included albuterol and desloratadine as needed, pantoprazole 40 mg/d, and drospirenone/ethinyl estradiol. The patient said she used her albuterol inhaler four to six times per month but more often in the summer and fall. Nighttime awakenings due to asthma symptoms occurred no more than twice per month. She denied prior history of acute asthma exacerbations requiring oral systemic corticosteroids. The patient stated that since her D&C, she had been using ibuprofen almost daily for mild abdominal cramping.
A review of systems was positive for mild fatigue since her D&C. The patient denied fever, chills, headache, sore throat, or cough. She did complain of daily nasal congestion but with no unusual drainage. The patient denied orthopnea, chest pain, palpitations, or peripheral edema, as well as nausea, vomiting, diarrhea, constipation, hematochezia, or melena. She admitted to daily heartburn for the previous two weeks that was relieved somewhat with pantoprazole. She had not experienced urinary frequency or urgency, dysuria, or hematuria. She also denied rash, pruritus, weakness, paresthesias, joint pain, or swelling.
Physical examination revealed an alert, oriented female who appeared slightly anxious but was in no acute distress. Specific findings were pulse, 110 beats/min; blood pressure, 138/88 mm Hg; respirations, 24 breaths/min; temperature, 97.7°F; O2 saturation, 92% on room air. Her height measured 5’2” and weight, 150 lb (BMI, 27.43).
Her conjunctiva were slightly injected, and the tympanic membranes were intact bilaterally with a light reflex; the septum was midline. The mucosa was pale, boggy, and moist with clear drainage and no inflammation. The nasopharynx had no erythema, and the tonsils appeared normal, although a cobblestone appearance was noted in the posterior pharynx. The neck was supple with no adenopathy.
The patient’s heart rate, 110 beats/min, was regular with no murmurs, rubs, or gallops. In the lungs, a prolonged expiratory phase was noted, with diffuse wheezing on chest auscultation bilaterally. Neither retractions nor use of accessory muscles with breathing was observed. The abdomen was soft, rounded, and nontender with no organomegaly. Bowel sounds were evident in all four quadrants. The patient’s skin was free of suspicious lesions or rashes. Her extremities were without edema, and no calf tenderness was noted; Homans’ sign was negative. Superficial varicosities were noted bilaterally.
The top differential diagnosis included:
• Acute asthma (risk factors: history of uncontrolled asthma, as evidenced by frequent use of albuterol)
• Acute anemia (risk factors: history of dysfunctional uterine bleeding, recent D&C)
• Pulmonary embolism (risk factors: recent surgery, recent start of oral contraceptive use).
Additional diagnoses to be considered less likely included:
• Acute coronary syndrome/MI (possible causes of chest tightness, dyspnea, dyspepsia; but no chest pain, diaphoresis, or nausea)
• Acute respiratory distress (history of tachycardia, possible dyspnea; but no diaphoresis, cyanosis, retractions, accessory muscle use, or lung crackles)
• Pneumonia (risk factors: recent surgery, possible cause of nonproductive cough; but no evidence of fever, chills, rales, or pleuritic chest pain).
Diagnostic testing included a 12-lead ECG to evaluate the patient for cardiac arrhythmia or injury; on it, tachycardia was noted, with a regular rate of 106 beats/min. The patient’s chest x-ray yielded normal results.
Laboratory testing included a complete blood count to screen for anemia and infection. Results included a white blood cell count of 8,200/mL (normal range, 4,500 to 11,000/mL); hematocrit, 38.2% (normal range for women, 36.1% to 44.3%); hemoglobin, 13.1 g/dL (normal for women, 12.1 to 15.1 g/dL). A comprehensive metabolic panel was performed to assess electrolyte levels and kidney and liver function; findings were normal. Results of a D-dimer assay, which was obtained to exclude pulmonary embolism,1 were normal at 0.5 mg/L (range, 0.4 to 1.4 mg/L).
In the case of heightened suspicion for MI, the patient would have been transferred to the emergency department (ED) for evaluation, including serial cardiac troponin levels; elevated troponin levels are deemed the standard criterion to define and diagnose MI in a consensus document from the European Society of Cardiology and the American College of Cardiology.2 (Troponin-T and troponin-I are more tissue-specific than the MB fraction of creatine kinase [CK-MB] in detecting MI; positive troponin levels are considered virtually diagnostic of MI.2 Typically, cardiac troponin levels are measured two to three times over a 12- to 16-hour period.)
Peak expiratory flow (PEF), which was measured to evaluate the patient’s respiratory status, was 150 L/min (compared with personal best for a patient of her height and age, approximately 460 L/min). She was given 2.5 mg/3 mL of inhaled albuterol over 15 minutes. Her PEF increased to 350 L/min. O2 saturation improved to 96% on room air, pulse to 104 beats/min, and respirations 20 breaths/min; her blood pressure reading was now 140/90 mm Hg. A prolonged expiratory phase persisted in the lungs, but diffuse wheezing decreased by 40% on chest auscultation.
A second albuterol treatment was administered 20 minutes later, and the patient’s PEF increased to 380 L/min and O2 saturation to 99%. The lungs presently cleared with no further wheezing noted.
In addition, the patient was given a GI cocktail (ie, liquid antacid combined with an anticholinergic agent and viscous lidocaine). Within 10 minutes, her chest tightness was relieved 100%. Her blood pressure was then measured at 135/84 mm Hg; respirations, 18 breaths/min; and pulse rate, 96 beats/min.
According to the National Asthma Education and Prevention Program (NAEPP) 2007 Guidelines for the Diagnosis and Management of Asthma, Expert Panel Report 3 (EPR-3),3 the patient was classified as having intermittent, not-well-controlled asthma with an acute exacerbation. In addition, she was given a diagnosis of uncontrolled GERD.
DISCUSSION
Asthma Incidence and Risk Factors
Asthma affects approximately 300 million people worldwide and remains a global respiratory concern.4 In the United States, this chronic health condition has a prevalence of 8% to 10%. It is estimated that 5% to 10% of asthmatic patients have severe disease that does not respond typically to therapeutic interventions.5
Asthma involves bronchial hyperresponsiveness, airflow obstruction, and underlying inflammation. Acute episodes of asthma, arising from bronchospasm, usually manifest with progressively worsening cough, shortness of breath, chest tightness and wheezing (asthma’s hallmark symptoms), or a combination of symptoms.3
Symptoms of asthma or exacerbations of reactive airway disease vary from patient to patient. In addition to the hallmark symptoms noted, subacute or acute episodes of asthma exacerbation are characterized by decreases in expiratory airflow that can be documented by objective measurements of lung function, such as PEF or spirometry; these measures of airflow indicate the severity of an exacerbation more reliably than does perceived symptom severity.3 The EPR-3 panelists recommend determining asthma severity using a combination of objective criteria and clinical symptoms,3 although few clinicians use the objective criteria.6
Estimates of the prevalence of GERD among patients with asthma have varied from 34% to 89%.7-9 Patients with GERD are 1.97 times more likely than patients without GERD to have asthma10; silent gastroesophageal reflux has been identified in 24% to 62% of patients with asthma, and early studies suggest that treatment for GERD may improve asthma control in patients with severe or difficult-to-control asthma.8,11,12
The exact link between the two conditions is unclear. However, possible explanations why GERD and asthma coincide are that acid flow causes injury to the lining of the throat, airways, and lungs, making inhalation difficult and often causing a persistent cough; or that when acid enters the esophagus, a nerve reflex is triggered that causes the airways to narrow in order to prevent the acid from entering; this can explain dyspnea.8,9
Economic Burden
Asthma is costly to treat, and because there is no cure, the expense is ongoing. According to a 2011 report,13 the average annual direct cost of care (eg, medications, hospital admissions, nonemergency office visits) for one asthma patient between 2002 and 2007 was $3,259. In 2007, the most current data available, the total cost of asthma in the US was $56 billion, with productivity losses due to mortality accounting for $2.1 billion and morbidity-related losses estimated at $3.8 billion.13 The economic consequences of asthma are substantial and can place a considerable burden on affected individuals, their families, the health care system, and society as a whole.3
Current Standard of Care
Based on the scientific literature and the opinions expressed by the NAEPP in the EPR-3,3 clinicians are advised to consider the following general principles and goals for managing asthma: early treatment, special attention to patients at high risk for asthma-related death, and special attention to infants.3 The guidelines emphasize the importance of a clinician/patient partnership to facilitate the asthma patient’s self-management.
Early treatment is a particularly important component for management of asthma exacerbations. Important elements of early treatment include a written asthma action plan, combined with enhanced awareness of the early indicators of an exacerbation (ie, worsening PEF).3,14 It is believed that if patients are able to monitor their respiratory condition and follow a plan of care based on their PEF and/or signs and symptoms of asthma, they are more likely to achieve optimal management of their disease.15
Written Asthma Action Plan. The EPR-33 recommends that health care providers supply all asthmatic patients with a written asthma action plan that will define and support the patient’s efforts at self-management. Written asthma action plans are particularly beneficial for patients with moderate to severe persistent asthma, poorly controlled asthma, or a history of severe exacerbations.3,14
The written asthma action plan should include instructions for daily management of asthma and ways to recognize and treat worsening asthma, including adjustments to medication dosing. Plans may be based on PEF and/or symptoms. Asthma action plans should be discussed and reevaluated at follow-up visits.3 A sample asthma action plan can be found at www.health.state.ny.us/diseases/asthma/pdf/4850.pdf.16
Peak Expiratory Flow (PEF). The EPR-33 recommends PEF monitoring in all asthma patients, regardless of the severity of their exacerbations.17 PEF-based plans are especially useful for the patient who has difficulty perceiving early signs and symptoms of worsening asthma.3,18 A PEF-based plan instructs the patient to use quick-relief medications if symptoms occur or if PEF drops below 80% of the patient’s personal or predicted best. (Measured personal best is the patient’s highest PEF in the previous two weeks of good asthma control,3,19 whereas predicted best is calculated based on findings from a 1983 study by Knudson et al.3,20)
A PEF between 50% and 79% requires the patient to carefully monitor his or her response to the quick-relief medication and, based on that response, consider whether to contact a health care provider. When PEF falls below 50%, a provider’s immediate intervention is usually recommended.3
In the urgent care or ED setting, according to EPR-3 recommendations,3 the PEF or forced expiratory volume in 1 second (FEV1) is used to indicate the following:
• ≥ 70% predicted PEF or FEV1: goal for discharge
• 40% to 69% predicted PEF or FEV1: incomplete response to treatment, frequent need for treatment in the ED
• 3
Treatment and Management
Asthma management interventions that target the treatment of active disease and predisposing triggers are designed to reduce the severity and/or duration of morbidity associated with asthma—principally, to prevent symptoms and exacerbations (see Table 13).
When patients are discharged following an asthma exacerbation, their medications should include an oral corticosteroid burst and a short-acting b2-agonist (SABA); the clinician should also consider prescribing an inhaled corticosteroid (ICS).3
It is no longer recommended that ICS dosing be doubled in place of an oral steroid burst.3,21 The addition of a leukotriene receptor antagonist (LTRA) may also be considered.3,22
Patients should be given an action plan, and follow-up with a primary care provider should be scheduled within a few days—or even the following day, depending on the severity of the patient’s condition. The importance of follow-up with a primary care provider, a pulmonologist, or an asthma/allergy specialist should be emphasized.3,23
For patients who have difficulty recognizing their symptoms, a peak flow meter may be useful. This device is also recommended for patients with moderate to severe asthma or a history of numerous severe exacerbations.3 Additionally, spacers should always be used with metered dose inhalers (MDIs), because they make it easier for medication to reach the lungs and reduce the amount deposited in the mouth and throat, where it can lead to irritation. At each office visit, use of the peak flow meter and inhaler technique should be observed, and the action plan reevaluated and changed if necessary.3,14
Additional components of patient education include instruction in controlling environmental factors: avoiding environmental tobacco smoke, exposure to insect allergens, and molds. It is also important to stress controlling comorbid conditions that influence asthma, such as allergies or GERD. Patients with symptoms of GERD should be advised to take the steps shown in Table 2.8,24
Clinical Implications
Assessment of the severity of an asthma exacerbation is an essential component of ambulatory asthma care. Underclassification of asthma severity has been associated with increased morbidity and mortality,6 and the NAEPP guidelines recommend that clinicians assess and document asthma severity at each clinic visit.3,25 Patients who receive care based on evidence-based practice guidelines have been shown to experience 28% better outcomes.26
PATIENT OUTCOME
The case patient was discharged on an oral corticosteroid burst and a low-dose ICS. She was instructed how and when to use her SABA and given a prescription for a spacer; use of a peak flow meter was initiated with an estimated personal best goal of 460 L/min. The patient was given a written asthma action plan to help her recognize early signs and symptoms of worsening asthma and was advised to use quick-relief medications if she experienced symptoms or if her PEF dropped below 80% of her predicted best.
The patient’s clinician emphasized the importance of controlling any asthma-triggering environmental factors and reviewed nonpharmacologic interventions to control GERD. The patient was advised to resume desloratadine 5 mg/d and pantoprazole 40 mg/d. She was also instructed to schedule an appointment with her primary care provider within 48 hours and to return to urgent care or the ED with any further exacerbation of respiratory symptoms not controlled by her SABA.
CONCLUSION
Asthma morbidity is a nationally recognized, major public health problem. Given the sharp rise in health care costs and limited resources, health care providers must factor in the comparative effectiveness, comparative cost, and cost-effectiveness of both new and existing health care interventions when making treatment decisions.
Many asthmatic patients face the challenges of health care access and quality. By promoting their self-care and awareness, clinicians can help asthmatic patients achieve better symptom management and use the health care system less often.
REFERENCES
1. Stein PD, Hull RD, Patel KC, et al. D-Dimer for the exclusion of acute venous thrombosis and pulmonary embolism. Ann Intern Med. 2004;140(8):589-602.
2. Alpert JS, Thygesen K, Antman E, Bassand JP. Myocardial infarction redefined: a consensus document of The Joint European Society of Cardiology/American College of Cardiology Committee for the redefinition of myocardial infarction. J Am Coll Cardiol. 2000;36(3):959-969.
3. National Asthma Education and Prevention Program, National Heart, Lung, and Blood Institute. Expert Panel Report 3: Guidelines for the Diagnosis and Management of Asthma. Bethesda, MD: National Heart, Lung, and Blood Institute; 2007. US Department of Health and Human Services publication NIH 07-4051.
4. Lougheed DM. Variability in asthma: symptom perception, care, and outcomes. Can J Physiol Pharmacol. 2007;85(1):149-154.
5. Higgins JC. The ‘crashing asthmatic.’ Am Fam Physician. 2003;67(5):997-1004.
6. Cowen MK, Wakefield DB, Cloutier MM. Classifying asthma severity: objective versus subjective measures. J Asthma. 2007;44(9):711-715.
7. Takenaka R, Matsuno O, Kitajima K, et al. The use of frequency scale for the symptoms of GERD in assessment of gastro-oesophageal reflux symptoms in asthma. Allergol Immunopathol (Madr). 2010;38(1):20-24.
8. Harding SM, Barnes PJ, Hollingsworth H. Gastroesophageal reflux and asthma (2010). www.uptodate.com/contents/gastroesophageal-reflux-and-asthma. Accessed April 5, 2011.
9. Havemann BD, Henderson CA, El-Serag HB. The association between gastro-oesophageal reflux disease and asthma: a systematic review. Gut. 2007;56(12):1654-1664.
10. Tsai MC, Lin HL, Lin CC, et al. Increased risk of concurrent asthma among patients with gastroesophageal reflux disease: a nationwide population-based study. Eur J Gastroenterol Hepatol. 2010;22(10):1169-1173.
11. Harding SM, Richter JE, Guzzo MR, et al. Asthma and gastroesophageal reflux: acid suppressive therapy improves asthma outcome. Am J Med. 1996;100(4):395-405.
12. Gibson PG, Henry RL, Coughlan JL. Gastro-oesophageal reflux treatment for asthma in adults and children. Cochrane Database Syst Rev. 2003;(2):CD001496.
13. Barnett SB, Nurmagambetov TA. Costs of asthma in the United States: 2002-2007. J Allergy Clin Immunol. 2011;127(1):145-152.
14. Walders N, Kercsmar C, Schluchter M, et al. An interdisciplinary intervention for undertreated pediatric asthma. Chest. 2006;129(2):292-299.
15. Morrow R, Fletcher J, Mulvihill M, Park H. The asthma dialogues: a model of interactive education for skills. J Contin Educ Health Prof. 2007;27(1): 49-58.
16. State of New York, Department of Health. Asthma action plan. www.health.state.ny.us/diseases/asthma/pdf/4850.pdf. Accessed April 11, 2011.
17. Picken HA, Greenfield S, Teres D, et al. Effects of local standards on the implementation of national guidelines for asthma: primary care agreement with national asthma guidelines. J Gen Intern Med. 1998;13(10):659-663.
18. Hardie GE, Gold WM, Janson S, et al. Understanding how asthmatics perceive symptom distress during a methacholine challenge. J Asthma. 2002;39(7):611-618.
19. Reddel HK, Marks GB, Jenkins CR. When can personal best peak flow be determined for asthma action plans? Thorax. 2004;59(11):922-924.
20. Knudson RJ, Lebowitz MD, Holberg CJ, Burrows B. Changes in the normal maximal expiratory flow-volume curve with growth and aging. Am Rev Respir Dis. 1983;127(6):725-734.
21. Ind PW, Dal Negro R, Colman NC, et al. Addition of salmeterol to fluticasone propionate treatment in moderate-to-severe asthma. Respir Med. 2003;97(5):555-562.
22. Price DB, Hernandez D, Magyar P, et al; Clinical Outcomes with Montelukast as a Partner Agent to Corticosteroid Therapy (COMPACT) International Study Group. Randomised controlled trial of montelukast plus inhaled budesonide versus double dose inhaled budesonide in adult patients with asthma. Thorax. 2003;58(3):211-216.
23. Schatz M, Zeiger RS, Mosen D, et al. Improved asthma outcomes from allergy specialist care: a population-based cross-sectional analysis. J Allergy Clin Immunol. 2005;116(6):1307-1313.
24. Hampel H, Abraham NS, El-Serag HB. Meta-analysis: obesity and the risk for gastroesophageal reflux disease and its complications. Ann Intern Med. 2005;143(3):199-211.
25. Cabana MD, Bruckman D, Meister K, et al. Documentation of asthma severity in pediatric outpatient clinics. Clin Pediatr (Phila). 2003;42(2):121-125.
26. Heater BS, Becker AM, Olson RK. Nursing interventions and patient outcomes: a meta-analysis of studies. Nurs Res. 1988;37(5):303-307.
Buyer Beware: Exotic Snakebite
Assessment and Management of Acute Hemoptysis
Ganglion Cysts of the Posterior Cruciate Ligament
UPDATE ON MENOPAUSE
- Is hormone therapy still a valid option? 12 ObGyns address this question
Members of the OBG MANAGEMENT Virtual Board of Editors and Janelle Yates, Senior Editor (May 2011)
Dr. Kaunitz receives grant or research support from Bayer, Agile, Noven, Teva, and Medical Diagnostic Laboratories, is a consultant to Bayer, Merck, and Teva, and owns stock in Becton Dickinson.
Among the developments of the past year in the care of menopausal women are:
- updated guidelines from the Institute of Medicine regarding vitamin D requirements—suggesting that fewer women are deficient in this nutrient than experts had believed
- new data from Europe on hormone therapy (HT) that highlight the safety of transdermal estrogen in comparison with oral administration
- a recent analysis from the Women’s Health Initiative (WHI), confirming a small elevated risk of breast cancer mortality with use of combination estrogen-progestin HT
- confirmation that age at initiation of HT determines its effect on cardiovascular health
- clarification of the association between HT and dementia
- new data demonstrating modest improvement in hot flushes when the serotonin reuptake inhibitor (SRI) escitalopram is used
- a brand new report from the WHI estrogen-alone arm that shows a protective effect against breast cancer.
The new data on HT suggest that we still have much to learn about its benefits and risks. We also are reaching an understanding that, for many young, symptomatic, menopausal patients, HT can represent a safe choice, with much depending on the timing and duration of therapy.
For more on how your colleagues are managing menopausal patients with and without hormone therapy, see “Is hormone therapy still a valid option? 12 ObGyns address this question,” on the facing page.
Menopausal women need less vitamin D than we thought
Institute of Medicine. Dietary reference intakes for calcium and vitamin D. Washington, DC: IOM; December 2010. http://www.iom.edu/~/media/Files/Report%20Files/2010/Dietary-Reference-Intakes-for-Calcium-and-Vitamin-D/Vitamin%20D%20and%20Calcium%202010%20Report%20Brief.pdf. Accessed March 24, 2011.
In the 2010 Update on Menopause, I summarized recent findings on vitamin D requirements, including recommendations that menopausal women should take at least 800 IU of vitamin D daily. I also described the prevailing expert opinion that many North American women are deficient in this nutrient.
What a difference a year can make! In late November, the Institute of Medicine (IOM) released a comprehensive report on vitamin D. Here are some of its conclusions:
- Vitamin D plays an important role in skeletal health but its role in other areas, including cardiovascular disease and cancer, is uncertain
- An intake of 600 IU of vitamin D daily is appropriate for girls and for women as old as 70 years; an in-take of 800 IU daily is appropriate for women older than 70 years
- A serum level of 25-hydroxy vitamin D of 20 ng/mL is consistent with adequate vitamin D status; this is lower than the threshold many have recommended
- With few exceptions, all people who live in North America—including those who have minimal or no exposure to sunlight—are receiving adequate calcium and vitamin D
- Ingestion of more than 4,000 IU of vitamin D daily can cause renal damage and injure other tissues.
The IOM report will likely prompt multivitamin manufacturers to increase the amount of vitamin D contained in their supplements to 600 IU daily. In addition, the report will probably discourage the common practice of checking serum 25-hydroxy vitamin D levels and prescribing a high dosage of vitamin D supplementation when the level is below 30 ng/mL.
I continue to recommend multivitamin supplements that include calcium and vitamin D (but no iron) to my menopausal patients. However, I no longer routinely recommend that they take additional calcium and vitamin D or undergo assessment of serum vitamin D levels.
Is transdermal estrogen safer than oral administration?
Canonico M, Fournier A, Carcaillon L, et al. Postmenopausal hormone therapy and risk of idiopathic venous thromboembolism: results from the E3N cohort study. Arterioscler Thromb Vasc Biol. 2010;30(2):340–345.
Renoux C, Dell’aniello S, Garbe E, Suissa S. Transdermal and oral hormone replacement therapy and the risk of stroke: a nested case-control study. BMJ. 2010;340:c2519. doi: 10.1136/bmj.c2519.
In the WHI, the combination of oral conjugated equine estrogen and medroxyprogesterone acetate more than doubled the risk of deep venous thrombosis and pulmonary embolism and modestly increased the risk of stroke, compared with nonuse.1
A year after publication of the initial findings of the WHI estrogen-progestin arm, the Estrogen and THromboEmbolism Risk Study Group (ESTHER) case-control study from France provided evidence that transdermal estrogen does not increase the risk of venous thrombosis.2 In France, many menopausal women use HT, and the transdermal route of administration is common.
In 2010, the E3N cohort study from France also assessed the risk of thrombosis associated with oral and transdermal HT. Investigators followed more than 80,000 postmenopausal women and found that, unlike oral HT, the transdermal route did not increase the risk of venous thrombosis.
More recent evidence also suggests a safety advantage for transdermal HT. The newest data come from the United Kingdom General Practice Research Database, which includes information on more than 870,000 women who were 50 to 70 years old from 1987 to 2006. Investigators identified more than 15,000 women who were given a diagnosis of stroke during this period and compared the use of HT in these women with that of almost 60,000 women in a control group. The risk of stroke associated with current use of transdermal HT was similar to the risk associated with nonuse of HT. Women who used a patch containing 0.05 mg of estradiol or less had a risk of stroke 19% lower than women who did not use HT.
In contrast, the risk of stroke in users of patches that contained a higher dosage of estradiol was almost twice the risk in nonusers of HT. Current users of oral HT had a risk of stroke 28% higher than that of nonusers of HT.
The WHI assessed the risks and benefits of oral HT only. Although no randomized, clinical trial has compared cardiovascular risks among users of oral and transdermal HT, I believe that a preponderance of evidence points to a superior safety profile for the transdermal route, particularly at a dosage of 0.05 mg of estradiol or less.
I encourage my patients who are initiating HT to consider the transdermal route—particularly women who have an elevated risk of cardiovascular disease, including those who are overweight, smoke cigarettes, or who have hypertension or diabetes. I suggest the transdermal route despite its higher cost (oral micronized estradiol can be purchased for as little as $4 for a month’s supply at a chain pharmacy).
When a patient prefers to avoid a patch (because of local irritation), I offer her estradiol gel or spray or the vaginal ring. (Femring is systemic estradiol, whereas Estring is local.) These formulations should provide the same safety benefits as the patch.
Estrogen-progestin HT raises the risk of death from breast cancer
Chlebowski RT, Anderson GL, Gass M, et al. Estrogen plus progestin and breast cancer incidence and mortality in postmenopausal women. JAMA. 2010;304(15):1684–1692.
Toh S, Hernandez-Diaz S, Logan R, Rossouw JE, Hernan MA. Coronary heart disease in postmenopausal recipients of estrogen plus progestin: does the increased risk ever disappear? Ann Intern Med. 2010;152(4):211–217.
In the estrogen-progestin arm of the WHI, initially published in 2002, the risk of invasive breast cancer was modestly elevated (hazard ratio [HR], 1.26) among women who had used HT longer than 5 years.3
In 2010, investigators reported on breast cancer mortality in WHI participants at a mean follow-up of 11 years. They found that combination HT users had breast cancer histology similar to that of nonusers. However, the tumors were more likely to be node-positive in combination HT users (23.7% vs 16.2%). In addition, breast cancer mortality was slightly higher among users of HT (2.6 vs 1.3 deaths in every 10,000 woman-years) (HR, 1.96; 95% confidence interval, 1.00–4.04).
Earlier observational studies had suggested that the death rate from breast cancer is lower in users of combination HT than in nonusers. Consistent with the UK Million Women Study, however, a 2010 report from the WHI found a higher mortality rate among women who have used HT.4
These new WHI findings reinforce the importance of assessing whether micronized progesterone combined with estrogen might lower the risk of death from breast cancer—a possibility suggested by findings of the French E3N cohort study.5
In addition, given the possibility that HT may be cardioprotective when it is initiated within 10 years after the onset of menopause, a WHI report that addresses long-term all-cause mortality would allow us to better counsel our menopausal patients who are trying to decide whether to start or continue HT. See, for example, the data from the California Teachers Study (below) and the estrogen-alone arm of the WHI (page 46).
The findings of this important WHI publication have strengthened the resolve of some clinicians to stop prescribing HT for menopausal women. I continue to prescribe HT to patients who have bothersome vasomotor and related symptoms, however. I also counsel women about the other benefits of HT, which include alleviation of genital atrophy and prevention of osteoporotic fractures. For patients considering or using estrogen-progestin HT, I include discussion of the small increase in their risk of developing, and dying from, breast cancer.
Age at initiation of HT determines its effect on CHD
Stram DO, Liu Y, Henderson KD, et al. Age-specific effects of hormone therapy use on overall mortality and ischemic heart disease mortality among women in the California Teachers Study. Menopause 2011;18(3):253-261.
Allison MA, Manson JE. Age, hormone therapy use, coronary heart disease, and mortality [editorial]. Menopause. 2011;18(3):243-245.
The initial findings of the WHI estrogen-progestin arm suggested that menopausal HT increases the risk of CHD. Since then, however, further analyses from the WHI and other HT trials, as well as reports from the observational Nurses’ Health Study, have suggested that the timing of initiation of HT determines its effect on cardiovascular health.
In this study from the California Teachers Study (CTS), investigators explored the effect of age at initiation of HT on cardiovascular and overall mortality. The CTS is a prospective study of more than 133,000 current and retired female teachers and administrators who returned an initial questionnaire in 1995 and 1996. Participants were then followed until late 2004, or death, whichever came first. More than 71,000 participants were eligible for analysis.
Current HT users were leaner, less likely to smoke, and more likely to exercise and consume alcohol than nonusers were. The analysis was adjusted for a variety of potential cardiovascular and other confounders.
Youngest HT users had the lowest risk of death
During follow-up, 18.3% of never-users of HT died, compared with 17.9% of former users. In contrast, 6.9% of women taking HT at the time of the baseline questionnaire died during follow-up.
Overall, current HT use was associated with a reduced risk of death from CHD (hazard ratio [HR], 0.84; 95% confidence interval, 0.74–0.95). This risk reduction was most notable (HR, 0.38) in the youngest HT users (36 to 59 years old). The risk of death from CHD gradually increased with the age of current HT users, reaching a hazard ratio of approximately 0.9 in current users who were 70 years and older. However, the CHD mortality hazard ratio did not reach or exceed the referent hazard ratio (1.0) assigned to never users of HT of any age.
The overall mortality rate was lowest for the youngest HT users (HR, 0.54) and approached 1.0 in the oldest current HT users.
The associations between overall and CHD mortality were similar among users of estrogen-only and estrogen-progestin HT.
As Allison and Manson point out in an editorial accompanying this study, the findings from the CTS are congruent with an extensive body of evidence from women and nonhuman primates. These data provide robust reassurance that HT does not increase the risk of death from CHD when it is used by recently menopausal women who have bothersome vasomotor symptoms.
Hormone therapy and dementia: Earlier use is better
Whitmer RA, Quesenberry CP, Zhou J, Yaffe K. Timing of hormone therapy and dementia: the critical window theory revisited. Ann Neurol. 2011;69(1):163–169.
Alzheimer’s disease is more common among women than men. In addition, caregivers to those who have dementia are more likely to be women. Therefore, it’s no surprise that women are especially concerned about their risk of dementia. Menopausal patients in my practice often ask whether use of HT might alter this risk.
Because vasomotor symptoms usually arise in late perimenopause or early menopause, women in observational studies (which reflect clinical practice) tend to begin HT when they are in their late 40s or early 50s. Overall, observational studies have suggested that HT is associated with a reduced risk of dementia. In contrast, the WHI clinical trial, in which the mean age of women who were randomized to HT or placebo was 63 years, found that the initiation of HT later in life increased the risk of dementia.
These observations led to the “critical window” theory regarding HT and dementia: Estrogen protects against dementia when it is taken by perimenopausal or early menopausal women, whereas it is not protective and may even accelerate cognitive decline when it is started many years after the onset of menopause.
In this recent study from the California Kaiser Permanente health maintenance organization, investigators assessed the long-term risk of dementia by timing of HT. From 1964 through 1973, menopausal “midlife” women who were 40 to 55 years old and free of dementia reported whether or not they used HT. Twenty-five to 30 years later, participants were reassessed for “late life” HT use.
Women who used HT in midlife only had the lowest prevalence of dementia, whereas those who used HT only in late life had the highest prevalence. Women who used HT at both time points had a prevalence of dementia similar to that of women who had never used HT.
Given these important findings, I believe it is now reasonable to counsel women in late perimenopause and early menopause that the use of HT may lower their risk of dementia. How long we should continue to prescribe HT depends on individual variables, including the presence of vasomotor symptoms, the risk of osteoporosis, and concerns about breast cancer.
I encourage women to taper their dosage of HT over time, aiming at complete discontinuation or a low maintenance dosage.
Are SRIs an effective alternative to HT for hot flushes?
Freeman EW, Guthrie K, Caan B, et al. Efficacy of escitalopram for hot flashes in healthy menopausal women: a randomized controlled trial. JAMA. 2011;305(3):267–274.
Interest in nonhormonal management of menopausal vasomotor symptoms continues to run high, although only hormonal therapy has FDA approval for this indication. Many trials of serotonin reuptake inhibitors (SRIs) for the treatment of vasomotor symptoms have focused on breast cancer survivors, many of whom use anti-estrogen agents that increase the prevalence of these symptoms. In contrast, this well-conducted multicenter trial, funded by the National Institutes of Health, enrolled healthy, symptomatic, menopausal women.
In the trial, 205 perimenopausal or postmenopausal women 40 to 62 years old who had at least 28 bothersome or severe episodes of hot flushes and night sweats a week were randomized to 10 mg daily of the SRI escitalopram (Lexapro) or placebo for 8 weeks. Women who did not report a reduction in hot flushes and night sweats of at least 50% at 4 weeks, or a decrease in the severity of these symptoms, were increased to a dosage of 20 mg daily of escitalopram or placebo. The mean baseline frequency of vasomotor symptoms was 9.79.
Within 1 week, women taking the SRI experienced significantly greater improvement than those taking placebo. By 8 weeks, the daily frequency of vasomotor symptoms had diminished by 4.6 hot flushes among women taking the SRI, compared with 3.20 among women taking placebo (P < .01).
Overall, adverse effects were reported by approximately 58% of participants. The pattern of these side effects was similar in the active and placebo treatment arms. No adverse events serious enough to require withdrawal from the study were reported in either arm.
Patient satisfaction with treatment was 70% in the SRI group, compared with 43% among women taking placebo (P < .001).
Although Freeman and colleagues convincingly demonstrate that escitalopram is more effective than placebo, the drug is less effective than HT. I agree with Nelson and coworkers, who, in a meta-analysis of nonhormonal treatments for vasomotor symptoms, concluded: “These therapies may be most useful for highly symptomatic women who cannot take estrogen but are not optimal choices for most women.”6
Unopposed estrogen appears to protect against breast cancer
LaCroix AZ, Chlebowski RT, Manson JE, et al; WHI Investigators. Health outcomes after stopping conjugated equine estrogens among postmenopausal women with prior hysterectomy. A randomized controlled trial. JAMA. 2011;305(13):1305–1314.
The WHI continues to surprise with its findings almost a decade after publication of initial data. In this brand new report from the estrogen-alone arm, postmenopausal, hysterectomized women who were followed for a mean of 10.7 years experienced a reduced risk of breast cancer after a mean of 5.9 years of use of conjugated equine estrogens (CEE).
They experienced no increased or diminished risk of coronary heart disease (CHD), deep venous thrombosis, stroke, hip fracture, colorectal cancer, or total mortality after post-intervention follow-up.
Keep in mind that the women in this arm were instructed to discontinue the study medication at the time the intervention phase was halted because of an increased risk of stroke among CEE users. The elevated risk of stroke attenuated with the longer follow-up.
All ages experienced a reduced risk of breast cancer
Some subgroup analyses from the WHI have found differential effects of HT by age of the user, with younger women experiencing fewer risks and more benefits than those who are more than 10 years past the menopausal transition. In this analysis, all three age groups (50–59 years, 60–69 years, and 70–79 years) of women who used CEE had a reduced risk of breast cancer, compared with placebo users.
Other risks did appear to differ by age. For example, the overall hazard ratio for CHD was 0.59 among CEE users 50 to 59 years old, but it approached unity among the older women.
As new and seemingly conflicting data are published, many clinicians and their menopausal patients may feel confused and frustrated. My perspective: It is becoming clear that age during HT use matters with respect to CHD and dementia, and that estrogen-only HT has a different impact on breast cancer risk than does combination estrogen-progestin HT. When this new information from the WHI is considered in aggregate with earlier WHI reports, as well as with data from the Nurses Health Study, the California Teachers Study, and Kaiser Permanente, we can, with growing confidence, advise our patients that menopausal HT does not increase the risk of fatal CHD and may reduce the risk of dementia when used by younger menopausal women with bothersome symptoms. I would define “younger” here as an age younger than 60 years or within 10 years of the onset of menopause.
In regard to breast cancer, it is now clear that, although estrogen-only HT lowers risk, use of combination estrogen-progestin therapy for more than approximately 5 years modestly elevates risk. Each menopausal woman may use this information to make an individual decision regarding use of HT.
In sum, current evidence allows me to feel comfortable counseling most young menopausal women who have bothersome symptoms that the initiation of HT for symptom relief is a safe and reasonable option.
We want to hear from you! Tell us what you think.
1. Rossouw JE, Anderson GL, Prentice RL, et al. Writing Group for the Women’s Health Initiative Investigators. Risks and benefits of estrogen plus progestin in healthy postmenopausal women. Principal results from the Women’s Health Initiative Randomized Controlled Trial. JAMA. 2002;288(3):321-333.
2. Scarabin PY, Oger E, Plu-Bureau G. Estrogen and THromboembolism Risk (ESTHER) Study Group. Differential association of oral and transdermal oestrogen-replacement therapy with venous thromboembolism risk. Lancet. 2003;362(9382):428-432.
3. Anderson GL, Chlebowski RT, Rossouw JE, et al. Prior hormone therapy and breast cancer risk in the Women’s Health Initiative randomized trial of estrogen and progestin. Maturitas. 2006;55(2):103-115.
4. Million Women Study Collaborators. Breast cancer and hormone-replacement therapy in the Million Women Study. Lancet. 2003;362(9382):419-427.
5. Fournier A, Fabre A, Misrine S, et al. Use of different postmenopausal hormone therapies and risk of histology- and hormone receptor-defined invasive breast cancer. J Clin Oncol. 2008;26(8):1260-1268.
6. Nelson HD, Vesco KK, Haney E, et al. Nonhormonal therapies for menopausal hot flashes: systematic review and meta-analysis. JAMA. 2006;295(17):2057-2071.
| Hear Dr. Kaunitz discuss the overall risks and benefits of hormone therapy |

Andrew M. Kaunitz, MD
Dr. Kaunitz is Professor and Associate Chairman, Department of Obstetrics and Gynecology, University of Florida College of Medicine–Jacksonville. He serves on the OBG MANAGEMENT Board of Editors.
| Hear Dr. Kaunitz discuss the overall risks and benefits of hormone therapy |
Andrew M. Kaunitz, MD
Dr. Kaunitz is Professor and Associate Chairman, Department of Obstetrics and Gynecology, University of Florida College of Medicine–Jacksonville. He serves on the OBG MANAGEMENT Board of Editors.
| Hear Dr. Kaunitz discuss the overall risks and benefits of hormone therapy |
Andrew M. Kaunitz, MD
Dr. Kaunitz is Professor and Associate Chairman, Department of Obstetrics and Gynecology, University of Florida College of Medicine–Jacksonville. He serves on the OBG MANAGEMENT Board of Editors.
- Is hormone therapy still a valid option? 12 ObGyns address this question
Members of the OBG MANAGEMENT Virtual Board of Editors and Janelle Yates, Senior Editor (May 2011)
Dr. Kaunitz receives grant or research support from Bayer, Agile, Noven, Teva, and Medical Diagnostic Laboratories, is a consultant to Bayer, Merck, and Teva, and owns stock in Becton Dickinson.
Among the developments of the past year in the care of menopausal women are:
- updated guidelines from the Institute of Medicine regarding vitamin D requirements—suggesting that fewer women are deficient in this nutrient than experts had believed
- new data from Europe on hormone therapy (HT) that highlight the safety of transdermal estrogen in comparison with oral administration
- a recent analysis from the Women’s Health Initiative (WHI), confirming a small elevated risk of breast cancer mortality with use of combination estrogen-progestin HT
- confirmation that age at initiation of HT determines its effect on cardiovascular health
- clarification of the association between HT and dementia
- new data demonstrating modest improvement in hot flushes when the serotonin reuptake inhibitor (SRI) escitalopram is used
- a brand new report from the WHI estrogen-alone arm that shows a protective effect against breast cancer.
The new data on HT suggest that we still have much to learn about its benefits and risks. We also are reaching an understanding that, for many young, symptomatic, menopausal patients, HT can represent a safe choice, with much depending on the timing and duration of therapy.
For more on how your colleagues are managing menopausal patients with and without hormone therapy, see “Is hormone therapy still a valid option? 12 ObGyns address this question,” on the facing page.
Menopausal women need less vitamin D than we thought
Institute of Medicine. Dietary reference intakes for calcium and vitamin D. Washington, DC: IOM; December 2010. http://www.iom.edu/~/media/Files/Report%20Files/2010/Dietary-Reference-Intakes-for-Calcium-and-Vitamin-D/Vitamin%20D%20and%20Calcium%202010%20Report%20Brief.pdf. Accessed March 24, 2011.
In the 2010 Update on Menopause, I summarized recent findings on vitamin D requirements, including recommendations that menopausal women should take at least 800 IU of vitamin D daily. I also described the prevailing expert opinion that many North American women are deficient in this nutrient.
What a difference a year can make! In late November, the Institute of Medicine (IOM) released a comprehensive report on vitamin D. Here are some of its conclusions:
- Vitamin D plays an important role in skeletal health but its role in other areas, including cardiovascular disease and cancer, is uncertain
- An intake of 600 IU of vitamin D daily is appropriate for girls and for women as old as 70 years; an in-take of 800 IU daily is appropriate for women older than 70 years
- A serum level of 25-hydroxy vitamin D of 20 ng/mL is consistent with adequate vitamin D status; this is lower than the threshold many have recommended
- With few exceptions, all people who live in North America—including those who have minimal or no exposure to sunlight—are receiving adequate calcium and vitamin D
- Ingestion of more than 4,000 IU of vitamin D daily can cause renal damage and injure other tissues.
The IOM report will likely prompt multivitamin manufacturers to increase the amount of vitamin D contained in their supplements to 600 IU daily. In addition, the report will probably discourage the common practice of checking serum 25-hydroxy vitamin D levels and prescribing a high dosage of vitamin D supplementation when the level is below 30 ng/mL.
I continue to recommend multivitamin supplements that include calcium and vitamin D (but no iron) to my menopausal patients. However, I no longer routinely recommend that they take additional calcium and vitamin D or undergo assessment of serum vitamin D levels.
Is transdermal estrogen safer than oral administration?
Canonico M, Fournier A, Carcaillon L, et al. Postmenopausal hormone therapy and risk of idiopathic venous thromboembolism: results from the E3N cohort study. Arterioscler Thromb Vasc Biol. 2010;30(2):340–345.
Renoux C, Dell’aniello S, Garbe E, Suissa S. Transdermal and oral hormone replacement therapy and the risk of stroke: a nested case-control study. BMJ. 2010;340:c2519. doi: 10.1136/bmj.c2519.
In the WHI, the combination of oral conjugated equine estrogen and medroxyprogesterone acetate more than doubled the risk of deep venous thrombosis and pulmonary embolism and modestly increased the risk of stroke, compared with nonuse.1
A year after publication of the initial findings of the WHI estrogen-progestin arm, the Estrogen and THromboEmbolism Risk Study Group (ESTHER) case-control study from France provided evidence that transdermal estrogen does not increase the risk of venous thrombosis.2 In France, many menopausal women use HT, and the transdermal route of administration is common.
In 2010, the E3N cohort study from France also assessed the risk of thrombosis associated with oral and transdermal HT. Investigators followed more than 80,000 postmenopausal women and found that, unlike oral HT, the transdermal route did not increase the risk of venous thrombosis.
More recent evidence also suggests a safety advantage for transdermal HT. The newest data come from the United Kingdom General Practice Research Database, which includes information on more than 870,000 women who were 50 to 70 years old from 1987 to 2006. Investigators identified more than 15,000 women who were given a diagnosis of stroke during this period and compared the use of HT in these women with that of almost 60,000 women in a control group. The risk of stroke associated with current use of transdermal HT was similar to the risk associated with nonuse of HT. Women who used a patch containing 0.05 mg of estradiol or less had a risk of stroke 19% lower than women who did not use HT.
In contrast, the risk of stroke in users of patches that contained a higher dosage of estradiol was almost twice the risk in nonusers of HT. Current users of oral HT had a risk of stroke 28% higher than that of nonusers of HT.
The WHI assessed the risks and benefits of oral HT only. Although no randomized, clinical trial has compared cardiovascular risks among users of oral and transdermal HT, I believe that a preponderance of evidence points to a superior safety profile for the transdermal route, particularly at a dosage of 0.05 mg of estradiol or less.
I encourage my patients who are initiating HT to consider the transdermal route—particularly women who have an elevated risk of cardiovascular disease, including those who are overweight, smoke cigarettes, or who have hypertension or diabetes. I suggest the transdermal route despite its higher cost (oral micronized estradiol can be purchased for as little as $4 for a month’s supply at a chain pharmacy).
When a patient prefers to avoid a patch (because of local irritation), I offer her estradiol gel or spray or the vaginal ring. (Femring is systemic estradiol, whereas Estring is local.) These formulations should provide the same safety benefits as the patch.
Estrogen-progestin HT raises the risk of death from breast cancer
Chlebowski RT, Anderson GL, Gass M, et al. Estrogen plus progestin and breast cancer incidence and mortality in postmenopausal women. JAMA. 2010;304(15):1684–1692.
Toh S, Hernandez-Diaz S, Logan R, Rossouw JE, Hernan MA. Coronary heart disease in postmenopausal recipients of estrogen plus progestin: does the increased risk ever disappear? Ann Intern Med. 2010;152(4):211–217.
In the estrogen-progestin arm of the WHI, initially published in 2002, the risk of invasive breast cancer was modestly elevated (hazard ratio [HR], 1.26) among women who had used HT longer than 5 years.3
In 2010, investigators reported on breast cancer mortality in WHI participants at a mean follow-up of 11 years. They found that combination HT users had breast cancer histology similar to that of nonusers. However, the tumors were more likely to be node-positive in combination HT users (23.7% vs 16.2%). In addition, breast cancer mortality was slightly higher among users of HT (2.6 vs 1.3 deaths in every 10,000 woman-years) (HR, 1.96; 95% confidence interval, 1.00–4.04).
Earlier observational studies had suggested that the death rate from breast cancer is lower in users of combination HT than in nonusers. Consistent with the UK Million Women Study, however, a 2010 report from the WHI found a higher mortality rate among women who have used HT.4
These new WHI findings reinforce the importance of assessing whether micronized progesterone combined with estrogen might lower the risk of death from breast cancer—a possibility suggested by findings of the French E3N cohort study.5
In addition, given the possibility that HT may be cardioprotective when it is initiated within 10 years after the onset of menopause, a WHI report that addresses long-term all-cause mortality would allow us to better counsel our menopausal patients who are trying to decide whether to start or continue HT. See, for example, the data from the California Teachers Study (below) and the estrogen-alone arm of the WHI (page 46).
The findings of this important WHI publication have strengthened the resolve of some clinicians to stop prescribing HT for menopausal women. I continue to prescribe HT to patients who have bothersome vasomotor and related symptoms, however. I also counsel women about the other benefits of HT, which include alleviation of genital atrophy and prevention of osteoporotic fractures. For patients considering or using estrogen-progestin HT, I include discussion of the small increase in their risk of developing, and dying from, breast cancer.
Age at initiation of HT determines its effect on CHD
Stram DO, Liu Y, Henderson KD, et al. Age-specific effects of hormone therapy use on overall mortality and ischemic heart disease mortality among women in the California Teachers Study. Menopause 2011;18(3):253-261.
Allison MA, Manson JE. Age, hormone therapy use, coronary heart disease, and mortality [editorial]. Menopause. 2011;18(3):243-245.
The initial findings of the WHI estrogen-progestin arm suggested that menopausal HT increases the risk of CHD. Since then, however, further analyses from the WHI and other HT trials, as well as reports from the observational Nurses’ Health Study, have suggested that the timing of initiation of HT determines its effect on cardiovascular health.
In this study from the California Teachers Study (CTS), investigators explored the effect of age at initiation of HT on cardiovascular and overall mortality. The CTS is a prospective study of more than 133,000 current and retired female teachers and administrators who returned an initial questionnaire in 1995 and 1996. Participants were then followed until late 2004, or death, whichever came first. More than 71,000 participants were eligible for analysis.
Current HT users were leaner, less likely to smoke, and more likely to exercise and consume alcohol than nonusers were. The analysis was adjusted for a variety of potential cardiovascular and other confounders.
Youngest HT users had the lowest risk of death
During follow-up, 18.3% of never-users of HT died, compared with 17.9% of former users. In contrast, 6.9% of women taking HT at the time of the baseline questionnaire died during follow-up.
Overall, current HT use was associated with a reduced risk of death from CHD (hazard ratio [HR], 0.84; 95% confidence interval, 0.74–0.95). This risk reduction was most notable (HR, 0.38) in the youngest HT users (36 to 59 years old). The risk of death from CHD gradually increased with the age of current HT users, reaching a hazard ratio of approximately 0.9 in current users who were 70 years and older. However, the CHD mortality hazard ratio did not reach or exceed the referent hazard ratio (1.0) assigned to never users of HT of any age.
The overall mortality rate was lowest for the youngest HT users (HR, 0.54) and approached 1.0 in the oldest current HT users.
The associations between overall and CHD mortality were similar among users of estrogen-only and estrogen-progestin HT.
As Allison and Manson point out in an editorial accompanying this study, the findings from the CTS are congruent with an extensive body of evidence from women and nonhuman primates. These data provide robust reassurance that HT does not increase the risk of death from CHD when it is used by recently menopausal women who have bothersome vasomotor symptoms.
Hormone therapy and dementia: Earlier use is better
Whitmer RA, Quesenberry CP, Zhou J, Yaffe K. Timing of hormone therapy and dementia: the critical window theory revisited. Ann Neurol. 2011;69(1):163–169.
Alzheimer’s disease is more common among women than men. In addition, caregivers to those who have dementia are more likely to be women. Therefore, it’s no surprise that women are especially concerned about their risk of dementia. Menopausal patients in my practice often ask whether use of HT might alter this risk.
Because vasomotor symptoms usually arise in late perimenopause or early menopause, women in observational studies (which reflect clinical practice) tend to begin HT when they are in their late 40s or early 50s. Overall, observational studies have suggested that HT is associated with a reduced risk of dementia. In contrast, the WHI clinical trial, in which the mean age of women who were randomized to HT or placebo was 63 years, found that the initiation of HT later in life increased the risk of dementia.
These observations led to the “critical window” theory regarding HT and dementia: Estrogen protects against dementia when it is taken by perimenopausal or early menopausal women, whereas it is not protective and may even accelerate cognitive decline when it is started many years after the onset of menopause.
In this recent study from the California Kaiser Permanente health maintenance organization, investigators assessed the long-term risk of dementia by timing of HT. From 1964 through 1973, menopausal “midlife” women who were 40 to 55 years old and free of dementia reported whether or not they used HT. Twenty-five to 30 years later, participants were reassessed for “late life” HT use.
Women who used HT in midlife only had the lowest prevalence of dementia, whereas those who used HT only in late life had the highest prevalence. Women who used HT at both time points had a prevalence of dementia similar to that of women who had never used HT.
Given these important findings, I believe it is now reasonable to counsel women in late perimenopause and early menopause that the use of HT may lower their risk of dementia. How long we should continue to prescribe HT depends on individual variables, including the presence of vasomotor symptoms, the risk of osteoporosis, and concerns about breast cancer.
I encourage women to taper their dosage of HT over time, aiming at complete discontinuation or a low maintenance dosage.
Are SRIs an effective alternative to HT for hot flushes?
Freeman EW, Guthrie K, Caan B, et al. Efficacy of escitalopram for hot flashes in healthy menopausal women: a randomized controlled trial. JAMA. 2011;305(3):267–274.
Interest in nonhormonal management of menopausal vasomotor symptoms continues to run high, although only hormonal therapy has FDA approval for this indication. Many trials of serotonin reuptake inhibitors (SRIs) for the treatment of vasomotor symptoms have focused on breast cancer survivors, many of whom use anti-estrogen agents that increase the prevalence of these symptoms. In contrast, this well-conducted multicenter trial, funded by the National Institutes of Health, enrolled healthy, symptomatic, menopausal women.
In the trial, 205 perimenopausal or postmenopausal women 40 to 62 years old who had at least 28 bothersome or severe episodes of hot flushes and night sweats a week were randomized to 10 mg daily of the SRI escitalopram (Lexapro) or placebo for 8 weeks. Women who did not report a reduction in hot flushes and night sweats of at least 50% at 4 weeks, or a decrease in the severity of these symptoms, were increased to a dosage of 20 mg daily of escitalopram or placebo. The mean baseline frequency of vasomotor symptoms was 9.79.
Within 1 week, women taking the SRI experienced significantly greater improvement than those taking placebo. By 8 weeks, the daily frequency of vasomotor symptoms had diminished by 4.6 hot flushes among women taking the SRI, compared with 3.20 among women taking placebo (P < .01).
Overall, adverse effects were reported by approximately 58% of participants. The pattern of these side effects was similar in the active and placebo treatment arms. No adverse events serious enough to require withdrawal from the study were reported in either arm.
Patient satisfaction with treatment was 70% in the SRI group, compared with 43% among women taking placebo (P < .001).
Although Freeman and colleagues convincingly demonstrate that escitalopram is more effective than placebo, the drug is less effective than HT. I agree with Nelson and coworkers, who, in a meta-analysis of nonhormonal treatments for vasomotor symptoms, concluded: “These therapies may be most useful for highly symptomatic women who cannot take estrogen but are not optimal choices for most women.”6
Unopposed estrogen appears to protect against breast cancer
LaCroix AZ, Chlebowski RT, Manson JE, et al; WHI Investigators. Health outcomes after stopping conjugated equine estrogens among postmenopausal women with prior hysterectomy. A randomized controlled trial. JAMA. 2011;305(13):1305–1314.
The WHI continues to surprise with its findings almost a decade after publication of initial data. In this brand new report from the estrogen-alone arm, postmenopausal, hysterectomized women who were followed for a mean of 10.7 years experienced a reduced risk of breast cancer after a mean of 5.9 years of use of conjugated equine estrogens (CEE).
They experienced no increased or diminished risk of coronary heart disease (CHD), deep venous thrombosis, stroke, hip fracture, colorectal cancer, or total mortality after post-intervention follow-up.
Keep in mind that the women in this arm were instructed to discontinue the study medication at the time the intervention phase was halted because of an increased risk of stroke among CEE users. The elevated risk of stroke attenuated with the longer follow-up.
All ages experienced a reduced risk of breast cancer
Some subgroup analyses from the WHI have found differential effects of HT by age of the user, with younger women experiencing fewer risks and more benefits than those who are more than 10 years past the menopausal transition. In this analysis, all three age groups (50–59 years, 60–69 years, and 70–79 years) of women who used CEE had a reduced risk of breast cancer, compared with placebo users.
Other risks did appear to differ by age. For example, the overall hazard ratio for CHD was 0.59 among CEE users 50 to 59 years old, but it approached unity among the older women.
As new and seemingly conflicting data are published, many clinicians and their menopausal patients may feel confused and frustrated. My perspective: It is becoming clear that age during HT use matters with respect to CHD and dementia, and that estrogen-only HT has a different impact on breast cancer risk than does combination estrogen-progestin HT. When this new information from the WHI is considered in aggregate with earlier WHI reports, as well as with data from the Nurses Health Study, the California Teachers Study, and Kaiser Permanente, we can, with growing confidence, advise our patients that menopausal HT does not increase the risk of fatal CHD and may reduce the risk of dementia when used by younger menopausal women with bothersome symptoms. I would define “younger” here as an age younger than 60 years or within 10 years of the onset of menopause.
In regard to breast cancer, it is now clear that, although estrogen-only HT lowers risk, use of combination estrogen-progestin therapy for more than approximately 5 years modestly elevates risk. Each menopausal woman may use this information to make an individual decision regarding use of HT.
In sum, current evidence allows me to feel comfortable counseling most young menopausal women who have bothersome symptoms that the initiation of HT for symptom relief is a safe and reasonable option.
We want to hear from you! Tell us what you think.
- Is hormone therapy still a valid option? 12 ObGyns address this question
Members of the OBG MANAGEMENT Virtual Board of Editors and Janelle Yates, Senior Editor (May 2011)
Dr. Kaunitz receives grant or research support from Bayer, Agile, Noven, Teva, and Medical Diagnostic Laboratories, is a consultant to Bayer, Merck, and Teva, and owns stock in Becton Dickinson.
Among the developments of the past year in the care of menopausal women are:
- updated guidelines from the Institute of Medicine regarding vitamin D requirements—suggesting that fewer women are deficient in this nutrient than experts had believed
- new data from Europe on hormone therapy (HT) that highlight the safety of transdermal estrogen in comparison with oral administration
- a recent analysis from the Women’s Health Initiative (WHI), confirming a small elevated risk of breast cancer mortality with use of combination estrogen-progestin HT
- confirmation that age at initiation of HT determines its effect on cardiovascular health
- clarification of the association between HT and dementia
- new data demonstrating modest improvement in hot flushes when the serotonin reuptake inhibitor (SRI) escitalopram is used
- a brand new report from the WHI estrogen-alone arm that shows a protective effect against breast cancer.
The new data on HT suggest that we still have much to learn about its benefits and risks. We also are reaching an understanding that, for many young, symptomatic, menopausal patients, HT can represent a safe choice, with much depending on the timing and duration of therapy.
For more on how your colleagues are managing menopausal patients with and without hormone therapy, see “Is hormone therapy still a valid option? 12 ObGyns address this question,” on the facing page.
Menopausal women need less vitamin D than we thought
Institute of Medicine. Dietary reference intakes for calcium and vitamin D. Washington, DC: IOM; December 2010. http://www.iom.edu/~/media/Files/Report%20Files/2010/Dietary-Reference-Intakes-for-Calcium-and-Vitamin-D/Vitamin%20D%20and%20Calcium%202010%20Report%20Brief.pdf. Accessed March 24, 2011.
In the 2010 Update on Menopause, I summarized recent findings on vitamin D requirements, including recommendations that menopausal women should take at least 800 IU of vitamin D daily. I also described the prevailing expert opinion that many North American women are deficient in this nutrient.
What a difference a year can make! In late November, the Institute of Medicine (IOM) released a comprehensive report on vitamin D. Here are some of its conclusions:
- Vitamin D plays an important role in skeletal health but its role in other areas, including cardiovascular disease and cancer, is uncertain
- An intake of 600 IU of vitamin D daily is appropriate for girls and for women as old as 70 years; an in-take of 800 IU daily is appropriate for women older than 70 years
- A serum level of 25-hydroxy vitamin D of 20 ng/mL is consistent with adequate vitamin D status; this is lower than the threshold many have recommended
- With few exceptions, all people who live in North America—including those who have minimal or no exposure to sunlight—are receiving adequate calcium and vitamin D
- Ingestion of more than 4,000 IU of vitamin D daily can cause renal damage and injure other tissues.
The IOM report will likely prompt multivitamin manufacturers to increase the amount of vitamin D contained in their supplements to 600 IU daily. In addition, the report will probably discourage the common practice of checking serum 25-hydroxy vitamin D levels and prescribing a high dosage of vitamin D supplementation when the level is below 30 ng/mL.
I continue to recommend multivitamin supplements that include calcium and vitamin D (but no iron) to my menopausal patients. However, I no longer routinely recommend that they take additional calcium and vitamin D or undergo assessment of serum vitamin D levels.
Is transdermal estrogen safer than oral administration?
Canonico M, Fournier A, Carcaillon L, et al. Postmenopausal hormone therapy and risk of idiopathic venous thromboembolism: results from the E3N cohort study. Arterioscler Thromb Vasc Biol. 2010;30(2):340–345.
Renoux C, Dell’aniello S, Garbe E, Suissa S. Transdermal and oral hormone replacement therapy and the risk of stroke: a nested case-control study. BMJ. 2010;340:c2519. doi: 10.1136/bmj.c2519.
In the WHI, the combination of oral conjugated equine estrogen and medroxyprogesterone acetate more than doubled the risk of deep venous thrombosis and pulmonary embolism and modestly increased the risk of stroke, compared with nonuse.1
A year after publication of the initial findings of the WHI estrogen-progestin arm, the Estrogen and THromboEmbolism Risk Study Group (ESTHER) case-control study from France provided evidence that transdermal estrogen does not increase the risk of venous thrombosis.2 In France, many menopausal women use HT, and the transdermal route of administration is common.
In 2010, the E3N cohort study from France also assessed the risk of thrombosis associated with oral and transdermal HT. Investigators followed more than 80,000 postmenopausal women and found that, unlike oral HT, the transdermal route did not increase the risk of venous thrombosis.
More recent evidence also suggests a safety advantage for transdermal HT. The newest data come from the United Kingdom General Practice Research Database, which includes information on more than 870,000 women who were 50 to 70 years old from 1987 to 2006. Investigators identified more than 15,000 women who were given a diagnosis of stroke during this period and compared the use of HT in these women with that of almost 60,000 women in a control group. The risk of stroke associated with current use of transdermal HT was similar to the risk associated with nonuse of HT. Women who used a patch containing 0.05 mg of estradiol or less had a risk of stroke 19% lower than women who did not use HT.
In contrast, the risk of stroke in users of patches that contained a higher dosage of estradiol was almost twice the risk in nonusers of HT. Current users of oral HT had a risk of stroke 28% higher than that of nonusers of HT.
The WHI assessed the risks and benefits of oral HT only. Although no randomized, clinical trial has compared cardiovascular risks among users of oral and transdermal HT, I believe that a preponderance of evidence points to a superior safety profile for the transdermal route, particularly at a dosage of 0.05 mg of estradiol or less.
I encourage my patients who are initiating HT to consider the transdermal route—particularly women who have an elevated risk of cardiovascular disease, including those who are overweight, smoke cigarettes, or who have hypertension or diabetes. I suggest the transdermal route despite its higher cost (oral micronized estradiol can be purchased for as little as $4 for a month’s supply at a chain pharmacy).
When a patient prefers to avoid a patch (because of local irritation), I offer her estradiol gel or spray or the vaginal ring. (Femring is systemic estradiol, whereas Estring is local.) These formulations should provide the same safety benefits as the patch.
Estrogen-progestin HT raises the risk of death from breast cancer
Chlebowski RT, Anderson GL, Gass M, et al. Estrogen plus progestin and breast cancer incidence and mortality in postmenopausal women. JAMA. 2010;304(15):1684–1692.
Toh S, Hernandez-Diaz S, Logan R, Rossouw JE, Hernan MA. Coronary heart disease in postmenopausal recipients of estrogen plus progestin: does the increased risk ever disappear? Ann Intern Med. 2010;152(4):211–217.
In the estrogen-progestin arm of the WHI, initially published in 2002, the risk of invasive breast cancer was modestly elevated (hazard ratio [HR], 1.26) among women who had used HT longer than 5 years.3
In 2010, investigators reported on breast cancer mortality in WHI participants at a mean follow-up of 11 years. They found that combination HT users had breast cancer histology similar to that of nonusers. However, the tumors were more likely to be node-positive in combination HT users (23.7% vs 16.2%). In addition, breast cancer mortality was slightly higher among users of HT (2.6 vs 1.3 deaths in every 10,000 woman-years) (HR, 1.96; 95% confidence interval, 1.00–4.04).
Earlier observational studies had suggested that the death rate from breast cancer is lower in users of combination HT than in nonusers. Consistent with the UK Million Women Study, however, a 2010 report from the WHI found a higher mortality rate among women who have used HT.4
These new WHI findings reinforce the importance of assessing whether micronized progesterone combined with estrogen might lower the risk of death from breast cancer—a possibility suggested by findings of the French E3N cohort study.5
In addition, given the possibility that HT may be cardioprotective when it is initiated within 10 years after the onset of menopause, a WHI report that addresses long-term all-cause mortality would allow us to better counsel our menopausal patients who are trying to decide whether to start or continue HT. See, for example, the data from the California Teachers Study (below) and the estrogen-alone arm of the WHI (page 46).
The findings of this important WHI publication have strengthened the resolve of some clinicians to stop prescribing HT for menopausal women. I continue to prescribe HT to patients who have bothersome vasomotor and related symptoms, however. I also counsel women about the other benefits of HT, which include alleviation of genital atrophy and prevention of osteoporotic fractures. For patients considering or using estrogen-progestin HT, I include discussion of the small increase in their risk of developing, and dying from, breast cancer.
Age at initiation of HT determines its effect on CHD
Stram DO, Liu Y, Henderson KD, et al. Age-specific effects of hormone therapy use on overall mortality and ischemic heart disease mortality among women in the California Teachers Study. Menopause 2011;18(3):253-261.
Allison MA, Manson JE. Age, hormone therapy use, coronary heart disease, and mortality [editorial]. Menopause. 2011;18(3):243-245.
The initial findings of the WHI estrogen-progestin arm suggested that menopausal HT increases the risk of CHD. Since then, however, further analyses from the WHI and other HT trials, as well as reports from the observational Nurses’ Health Study, have suggested that the timing of initiation of HT determines its effect on cardiovascular health.
In this study from the California Teachers Study (CTS), investigators explored the effect of age at initiation of HT on cardiovascular and overall mortality. The CTS is a prospective study of more than 133,000 current and retired female teachers and administrators who returned an initial questionnaire in 1995 and 1996. Participants were then followed until late 2004, or death, whichever came first. More than 71,000 participants were eligible for analysis.
Current HT users were leaner, less likely to smoke, and more likely to exercise and consume alcohol than nonusers were. The analysis was adjusted for a variety of potential cardiovascular and other confounders.
Youngest HT users had the lowest risk of death
During follow-up, 18.3% of never-users of HT died, compared with 17.9% of former users. In contrast, 6.9% of women taking HT at the time of the baseline questionnaire died during follow-up.
Overall, current HT use was associated with a reduced risk of death from CHD (hazard ratio [HR], 0.84; 95% confidence interval, 0.74–0.95). This risk reduction was most notable (HR, 0.38) in the youngest HT users (36 to 59 years old). The risk of death from CHD gradually increased with the age of current HT users, reaching a hazard ratio of approximately 0.9 in current users who were 70 years and older. However, the CHD mortality hazard ratio did not reach or exceed the referent hazard ratio (1.0) assigned to never users of HT of any age.
The overall mortality rate was lowest for the youngest HT users (HR, 0.54) and approached 1.0 in the oldest current HT users.
The associations between overall and CHD mortality were similar among users of estrogen-only and estrogen-progestin HT.
As Allison and Manson point out in an editorial accompanying this study, the findings from the CTS are congruent with an extensive body of evidence from women and nonhuman primates. These data provide robust reassurance that HT does not increase the risk of death from CHD when it is used by recently menopausal women who have bothersome vasomotor symptoms.
Hormone therapy and dementia: Earlier use is better
Whitmer RA, Quesenberry CP, Zhou J, Yaffe K. Timing of hormone therapy and dementia: the critical window theory revisited. Ann Neurol. 2011;69(1):163–169.
Alzheimer’s disease is more common among women than men. In addition, caregivers to those who have dementia are more likely to be women. Therefore, it’s no surprise that women are especially concerned about their risk of dementia. Menopausal patients in my practice often ask whether use of HT might alter this risk.
Because vasomotor symptoms usually arise in late perimenopause or early menopause, women in observational studies (which reflect clinical practice) tend to begin HT when they are in their late 40s or early 50s. Overall, observational studies have suggested that HT is associated with a reduced risk of dementia. In contrast, the WHI clinical trial, in which the mean age of women who were randomized to HT or placebo was 63 years, found that the initiation of HT later in life increased the risk of dementia.
These observations led to the “critical window” theory regarding HT and dementia: Estrogen protects against dementia when it is taken by perimenopausal or early menopausal women, whereas it is not protective and may even accelerate cognitive decline when it is started many years after the onset of menopause.
In this recent study from the California Kaiser Permanente health maintenance organization, investigators assessed the long-term risk of dementia by timing of HT. From 1964 through 1973, menopausal “midlife” women who were 40 to 55 years old and free of dementia reported whether or not they used HT. Twenty-five to 30 years later, participants were reassessed for “late life” HT use.
Women who used HT in midlife only had the lowest prevalence of dementia, whereas those who used HT only in late life had the highest prevalence. Women who used HT at both time points had a prevalence of dementia similar to that of women who had never used HT.
Given these important findings, I believe it is now reasonable to counsel women in late perimenopause and early menopause that the use of HT may lower their risk of dementia. How long we should continue to prescribe HT depends on individual variables, including the presence of vasomotor symptoms, the risk of osteoporosis, and concerns about breast cancer.
I encourage women to taper their dosage of HT over time, aiming at complete discontinuation or a low maintenance dosage.
Are SRIs an effective alternative to HT for hot flushes?
Freeman EW, Guthrie K, Caan B, et al. Efficacy of escitalopram for hot flashes in healthy menopausal women: a randomized controlled trial. JAMA. 2011;305(3):267–274.
Interest in nonhormonal management of menopausal vasomotor symptoms continues to run high, although only hormonal therapy has FDA approval for this indication. Many trials of serotonin reuptake inhibitors (SRIs) for the treatment of vasomotor symptoms have focused on breast cancer survivors, many of whom use anti-estrogen agents that increase the prevalence of these symptoms. In contrast, this well-conducted multicenter trial, funded by the National Institutes of Health, enrolled healthy, symptomatic, menopausal women.
In the trial, 205 perimenopausal or postmenopausal women 40 to 62 years old who had at least 28 bothersome or severe episodes of hot flushes and night sweats a week were randomized to 10 mg daily of the SRI escitalopram (Lexapro) or placebo for 8 weeks. Women who did not report a reduction in hot flushes and night sweats of at least 50% at 4 weeks, or a decrease in the severity of these symptoms, were increased to a dosage of 20 mg daily of escitalopram or placebo. The mean baseline frequency of vasomotor symptoms was 9.79.
Within 1 week, women taking the SRI experienced significantly greater improvement than those taking placebo. By 8 weeks, the daily frequency of vasomotor symptoms had diminished by 4.6 hot flushes among women taking the SRI, compared with 3.20 among women taking placebo (P < .01).
Overall, adverse effects were reported by approximately 58% of participants. The pattern of these side effects was similar in the active and placebo treatment arms. No adverse events serious enough to require withdrawal from the study were reported in either arm.
Patient satisfaction with treatment was 70% in the SRI group, compared with 43% among women taking placebo (P < .001).
Although Freeman and colleagues convincingly demonstrate that escitalopram is more effective than placebo, the drug is less effective than HT. I agree with Nelson and coworkers, who, in a meta-analysis of nonhormonal treatments for vasomotor symptoms, concluded: “These therapies may be most useful for highly symptomatic women who cannot take estrogen but are not optimal choices for most women.”6
Unopposed estrogen appears to protect against breast cancer
LaCroix AZ, Chlebowski RT, Manson JE, et al; WHI Investigators. Health outcomes after stopping conjugated equine estrogens among postmenopausal women with prior hysterectomy. A randomized controlled trial. JAMA. 2011;305(13):1305–1314.
The WHI continues to surprise with its findings almost a decade after publication of initial data. In this brand new report from the estrogen-alone arm, postmenopausal, hysterectomized women who were followed for a mean of 10.7 years experienced a reduced risk of breast cancer after a mean of 5.9 years of use of conjugated equine estrogens (CEE).
They experienced no increased or diminished risk of coronary heart disease (CHD), deep venous thrombosis, stroke, hip fracture, colorectal cancer, or total mortality after post-intervention follow-up.
Keep in mind that the women in this arm were instructed to discontinue the study medication at the time the intervention phase was halted because of an increased risk of stroke among CEE users. The elevated risk of stroke attenuated with the longer follow-up.
All ages experienced a reduced risk of breast cancer
Some subgroup analyses from the WHI have found differential effects of HT by age of the user, with younger women experiencing fewer risks and more benefits than those who are more than 10 years past the menopausal transition. In this analysis, all three age groups (50–59 years, 60–69 years, and 70–79 years) of women who used CEE had a reduced risk of breast cancer, compared with placebo users.
Other risks did appear to differ by age. For example, the overall hazard ratio for CHD was 0.59 among CEE users 50 to 59 years old, but it approached unity among the older women.
As new and seemingly conflicting data are published, many clinicians and their menopausal patients may feel confused and frustrated. My perspective: It is becoming clear that age during HT use matters with respect to CHD and dementia, and that estrogen-only HT has a different impact on breast cancer risk than does combination estrogen-progestin HT. When this new information from the WHI is considered in aggregate with earlier WHI reports, as well as with data from the Nurses Health Study, the California Teachers Study, and Kaiser Permanente, we can, with growing confidence, advise our patients that menopausal HT does not increase the risk of fatal CHD and may reduce the risk of dementia when used by younger menopausal women with bothersome symptoms. I would define “younger” here as an age younger than 60 years or within 10 years of the onset of menopause.
In regard to breast cancer, it is now clear that, although estrogen-only HT lowers risk, use of combination estrogen-progestin therapy for more than approximately 5 years modestly elevates risk. Each menopausal woman may use this information to make an individual decision regarding use of HT.
In sum, current evidence allows me to feel comfortable counseling most young menopausal women who have bothersome symptoms that the initiation of HT for symptom relief is a safe and reasonable option.
We want to hear from you! Tell us what you think.
1. Rossouw JE, Anderson GL, Prentice RL, et al. Writing Group for the Women’s Health Initiative Investigators. Risks and benefits of estrogen plus progestin in healthy postmenopausal women. Principal results from the Women’s Health Initiative Randomized Controlled Trial. JAMA. 2002;288(3):321-333.
2. Scarabin PY, Oger E, Plu-Bureau G. Estrogen and THromboembolism Risk (ESTHER) Study Group. Differential association of oral and transdermal oestrogen-replacement therapy with venous thromboembolism risk. Lancet. 2003;362(9382):428-432.
3. Anderson GL, Chlebowski RT, Rossouw JE, et al. Prior hormone therapy and breast cancer risk in the Women’s Health Initiative randomized trial of estrogen and progestin. Maturitas. 2006;55(2):103-115.
4. Million Women Study Collaborators. Breast cancer and hormone-replacement therapy in the Million Women Study. Lancet. 2003;362(9382):419-427.
5. Fournier A, Fabre A, Misrine S, et al. Use of different postmenopausal hormone therapies and risk of histology- and hormone receptor-defined invasive breast cancer. J Clin Oncol. 2008;26(8):1260-1268.
6. Nelson HD, Vesco KK, Haney E, et al. Nonhormonal therapies for menopausal hot flashes: systematic review and meta-analysis. JAMA. 2006;295(17):2057-2071.
1. Rossouw JE, Anderson GL, Prentice RL, et al. Writing Group for the Women’s Health Initiative Investigators. Risks and benefits of estrogen plus progestin in healthy postmenopausal women. Principal results from the Women’s Health Initiative Randomized Controlled Trial. JAMA. 2002;288(3):321-333.
2. Scarabin PY, Oger E, Plu-Bureau G. Estrogen and THromboembolism Risk (ESTHER) Study Group. Differential association of oral and transdermal oestrogen-replacement therapy with venous thromboembolism risk. Lancet. 2003;362(9382):428-432.
3. Anderson GL, Chlebowski RT, Rossouw JE, et al. Prior hormone therapy and breast cancer risk in the Women’s Health Initiative randomized trial of estrogen and progestin. Maturitas. 2006;55(2):103-115.
4. Million Women Study Collaborators. Breast cancer and hormone-replacement therapy in the Million Women Study. Lancet. 2003;362(9382):419-427.
5. Fournier A, Fabre A, Misrine S, et al. Use of different postmenopausal hormone therapies and risk of histology- and hormone receptor-defined invasive breast cancer. J Clin Oncol. 2008;26(8):1260-1268.
6. Nelson HD, Vesco KK, Haney E, et al. Nonhormonal therapies for menopausal hot flashes: systematic review and meta-analysis. JAMA. 2006;295(17):2057-2071.
A talk about, then a plan for, antidepressants in pregnancy
CAS: Depressive disorder, anticipating a pregnancy
Your patient Megan—well-educated, 29 years old, G0P0—has come to you to discuss her antidepressant (paroxetine [Paxil]) because she is planning her first pregnancy.
Megan has a history of recurrent major depressive disorder (MDD), which is in remission (see “What is MDD?”).
How will you begin the conversation with this patient about keeping MDD in remission during her pregnancy and ensuring the safety of her fetus?
- Major depressive disorder (MDD) is defined by criteria in the fourth edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-IV)
- The disorder varies in severity, 1) across an affected person’s lifetime and 2) within a depressive episode
- A current or prior episode of depression that includes 1) a significant impact on an individual’s functioning, 2) active suicidality, or 3) hospitalization signals severe MDD
- In women, average age at first episode of depression is 24 years
There is a 20% to 25% lifetime prevalence of depression in women; the disorder peaks during childbearing years, however.1 As of 2003, 13% of pregnant women had taken an antidepressant at some time during their pregnancy, a percentage that has doubled since it was assessed in 1999.2
You are faced with several quandaries in deciding whether to recommend that your patient continue, or discontinue, antidepressant therapy during pregnancy:
- As many as 68% of women who terminate antidepressant treatment before or during pregnancy relapse.
- Even 26% of women who continue antidepressant during pregnancy relapse—requiring a dosage adjustment or change in treatment.3
- Yet the possibly elevated cortisol levels of severe, untreated depression may harm the placenta and fetus.4,5
So, what do you need to know to assess the risks and benefits of “Megan” stopping, or continuing, paroxetine during her anticipated pregnancy? And what are the risks to Megan’s fetus of treating, or not treating, her depression with a serotonin reuptake inhibitor (SRI*)?
“Selective” has been dropped
from “SSRI” to yield simply “SRI.”
Gauging the risks of depression in pregnancy
In any given patient, her history and family history of depression are key to determining the likelihood that she will suffer ongoing or recurrent depression.
CASE continued Repeated treated episodes plus a family history
In obtaining Megan’s history, you learn that she has had three prior episodes of depression, all of which were successfully treated with paroxetine. Megan has been stable on paroxetine for 3 years.
Notably, the second episode of depression was initially treated with a 16-week trial of psychotherapy alone; when depressive symptoms did not remit, paroxetine was added. That episode was considered severe because it included pervasive thoughts of suicide.
You also learn that Megan’s mother suffered from postpartum depression and that her father and paternal grandmother were treated for depression.
Known risk factors for depression during pregnancy include: maternal anxiety; prior diagnosis of depression during pregnancy; history of postpartum anxiety or depression; prior diagnosis of either anxiety or depressive disorder; significant life stress (e.g., divorce, death of a loved one); degree of social support—particularly, intimate social support; “intendedness” of pregnancy; domestic violence; and insurance status.6
You review with Megan her risk factors for depression during pregnancy, namely: three prior episodes of MDD and a strong family history of mood disorder. Her MDD is considered “severe” because she has a history of suicidality. You tell Megan that, given these factors, she is at high risk of a recurrence of her depressive illness during pregnancy.
Megan asks: “Would getting depressed during pregnancy hurt the baby?”
Depression during pregnancy affects both infant and maternal well-being, although studies are in conflict about the extent of that morbidity. Multiple areas of potential risk to mother and infant have been studied, including the effect of depression on:
- maternal well-being
- growth of the infant
- spontaneous abortion
- preterm delivery
- neonatal physiologic and neurobehavioral measures
- long-term considerations for the developing infant and child.
Within these categories of risk, a diagnosis of depression during pregnancy has been associated (in some but not all studies) with a higher risk, or rate, of:
- postpartum depression
- preterm birth
- lower maternal weight gain
- maternal tobacco, alcohol, and other substance use
- lower infant gestational age at birth
- small-for-gestational age infant birth.7-10
In terms of long-term impact on offspring, studies differ in their estimation of risk; however, children exposed to untreated, maternal depression at 18 weeks’ and 32 weeks’ gestation did show a greater degree of developmental delay at 18 months than children who were born to a mother who was not depressed during pregnancy.11
You discuss these risks with Megan. She asks: “What treatment do you recommend for me?” You turn to the 2009 guidelines published jointly by the American Psychiatric Association (APA) and ACOG.
These guidelines recommend that you consider 1) the severity of her current depression, 2) her history of depression severity, and 3) her preference for treatment.12 For mild depression during pregnancy, when there is no history of severe depression, or for a history of depression that responded well to psychotherapy in the past, a trial of psychotherapy without medications is recommended.
But Megan’s history of depression falls into the “severe” category, and a prior episode of depression did not respond well to psychotherapy. Your recommendation to her, therefore, is that she should continue taking an antidepressant—unless she feels strongly that she should discontinue it.

Megan considers what you’ve discussed about her high risk of developing recurrent depression during pregnancy. She decides that she wants to continue taking her antidepressant during pregnancy, but she has concerns—based on what she has been reading on the Internet.
Megan hands you a detailed printout downloaded from a Web site unfamiliar to you and asks about risks to the baby of such medications as paroxetine.
What should you tell Megan about SRIs in pregnancy—paroxetine, specifically?
You preface your remarks to her by noting that the data physicians work with are imperfect—because randomized, controlled clinical trials pose an ethical dilemma as a method of study in pregnant women. You then discuss with her current scientific understanding of potential risks to her fetus.
The difference in the rates of structural malformation among SRI-exposed and SRI-unexposed groups has been studied; most studies have found no increased rate of major or specific cardiac malformations.12 However, first-trimester paroxetine appeared, in some studies, to be associated with an increased rate of cardiac malformations. That led to a category-“D” pregnancy classification in 2005 and an FDA “Public Health Advisory.”
Other large cohort studies have not uncovered such an association. It has been hypothesized that the methodology of data collection may have influenced this finding.13
Other malformations have been implicated in some studies but not others, and have included associations between specific SRIs and cardiac ventricular outflow defects, craniosynostosis, and omphalocele. The absolute risk of these defects remains extremely low, however, and close to the background rate seen in the general population.14
Megan asks: “With that risk-category ‘D’ for paroxetine, do you recommend I continue taking it or should I switch to another medication while I’m pregnant?”
You review again with Megan that, although some studies have linked first-trimester paroxetine to an increased risk of cardiac malformation, that finding has not been replicated in several large cohort studies. You explain that, if she had a history of recurrent depression that had failed to respond to many antidepressants and only paroxetine worked, an attempt at switching the SRI would not be recommended because of the potential for relapse.
Megan tells you that she would feel safer not taking a category-“D” drug. You agree and propose a judicious approach: Because she has come to see you before she became pregnant, with enough time to complete a slow crossover to an alternative SRI, and because she has not had any earlier trials of other SRIs, a slow taper of paroxetine, coupled with a crossover to an alternative SRI, is a reasonable option—with the caution that substitution always carries a risk of relapse.
Problems in newborns
Megan considers the risks you’ve discussed so far. She remembers a recent article in a magazine for pregnant women that described severe “respiratory” and “withdrawal” symptoms in infants who were born to mothers taking an SRI antidepressant. She wonders if she should consider discontinuing her SRI in the third trimester to try to mitigate those risks.
Megan is asking you about an SRI exposure risk that has been fairly consistent across studies, called neonatal abstinence syndrome (NAS) or poor neonatal adaptation.
NAS is a cluster of symptoms that occurs in 15% to 30% of newborns who have been exposed to an SRI during the third trimester of pregnancy.15 Signs include irritability, weak cry, tachypnea, temperature instability, and hypoglycemia—all of which are transient, peak during the first 48 hours after delivery, and resolve in less than 2 weeks.
Multiple hypotheses have been put forward to account for NAS, including the possibilities that it reflects a withdrawal syndrome, pharmacotoxicity, or an underlying gene–SRI interaction. The physiology behind NAS remains unknown, however.12
Megan next asks you about persistent pulmonary hypertension of the newborn (PPHN). You explain that PPHN is of recent concern in women who have been taking an SRI in the latter half of their pregnancy.
The rate of PPHN in the general population is 0.5 to 2 newborns for every 1,000. Associated mortality is approximately 10% to 20%.16-18 This rate is thought to rise to approximately 6 of every 1,000 newborns among those who have been exposed to an SRI in utero—with some evidence of increased risk conferred through SRI exposure during later pregnancy (studies define this as the second half of the pregnancy).15 Although the relative risk of PPHN is increased threefold to sixfold when an SRI is used in pregnancy, absolute risk remains extremely low.
Concerns have been raised over research methodology in the few studies that have looked into SRI exposure and PPHN. Not all such studies found a change in relative risk or absolute risk of PPHN in SRI- exposed infants, compared to what was found in non-SRI–exposed infants.15,19,20
Megan presses you, however, with the understandable question of whether she should taper her SRI during the last trimester (which the Web site she has found recommends). With the above information in mind, you explain that, given current understanding of the low absolute risk of PPHN, and given her illness history and severity of prior depression, you would not recommend that she taper the antidepressant in the third trimester.
Furthermore, the same counsel applies in regard to NAS: Given the risk of psychiatric morbidity caused by discontinuing an SRI during the third trimester, you do not recommend that she taper an SRI during that period to avoid NAS.
You explain that, instead, physicians now counsel women who take an SRI about the signs of NAS so that they can be prepared if they observe any of them in their infant.
Megan has one more question: “Will I be able to breastfeed while I’m taking an antidepressant?”
Given the inherent difficulties and risks of relapse associated with a crossover to an alternative antidepressant postpartum, it makes sense, when possible, for a woman to take an antidepressant during pregnancy that can safely be continued while she is breastfeeding.
You tell Megan that, even though the quality of the data in this area is also thin, SRIs that have a low maternal serum profile are considered safest in breastfeeding.
To date, two SRIs—sertraline and paroxetine—have not been detectable in the breast milk of women taking either of them.21
CASE Appointment concluded, overflowing with information,
advice, and optimism
Megan says that, taking into account all that you and she have talked about, and even though she wants to return with her husband, she would like to switch to sertraline before she becomes pregnant—while she gauges its effectiveness at keeping her disorder in remission.
A good outcome requires you to prevail over obstacles
Because a diagnosis of depression spans a continuum of severity and, often, is not perceived as an acutely life-threatening illness, evaluating the risks and benefits of treatment is a murky undertaking.
Our role as physicians is to, first, educate ourselves and our patients about these variables and, second, support our patients in the decisions that they make. Physicians who care for pregnant women must be aware of the benefits and limitations of treatments as reported in the most current literature if they are going to assist women with decisions about treatment in the best possible way.
Social stigma. There remains the impact of stigma. Depressive and anxiety disorders are often perceived to be either under the control of an affected person’s “free will” or not as serious as other forms of “medical” disease. Consequently, the role that cultural and social pressures play in the risk–benefit analysis conducted by pregnant women and their physicians can’t be discounted.
Customized decision-making. As more data emerge about the treatment of depression in pregnancy, it has become clear: Treatment algorithms meant to simplify our decisions must always be individualized and extended into the postpartum period.
Treatment selection. Management of mild depression during pregnancy does not always require medication. Multiple variables—the list is long, and includes a patient’s psychiatric history, family psychiatric history, response to prior treatment, severity of depression, severity of prior depression, degree of social support, and personal desires—must be considered in determining what treatment is appropriate before, during, and after a pregnancy.
For a woman who suffers mild or moderate depression, with few antenatal depression risk factors, a trial of psychotherapy is recommended as first-line treatment. For a woman suffering from severe depression, or one who has a history of severe depression that has not responded well to psychotherapy alone, continuation or initiation of an SRI antidepressant is the current recommendation.
We want to hear from you! Tell us what you think.
1. Kessler RC, Berglund P, Demler O, et al. National Comorbidity Survey Replication. The epidemiology of major depressive disorder: results from the National Comorbidity Survey Replication (NCS-R). JAMA. 2003;289(23):3095-3105.
2. Cooper W, Willy M, Pont S, Ray W. Increasing use of antidepressants in pregnancy. Am J Obstet Gynecol. 2007;196(6):544.e1-e5.
3. Cohen LS, Altshuler LL, Harlow BL, et al. Relapse of major depression during pregnancy in women who maintain or discontinue antidepressant treatment. JAMA. 2006;295(5):499-507.
4. Kramer MS, Lydon J, Séguin L, et al. Stress pathways to spontaneous preterm birth: the role of stressors, psychological distress, and stress hormones. Am J Epidemiol. 2009;169(11):1319-1326.
5. Ellman LM, Schetter CD, Hobel CJ, Chicz-Demet A, Glynn LM, Sandman CA. Timing of fetal exposure to stress hormones: effects on newborn physical and neuromuscular maturation. Dev Psychobiol. 2008;50(3):232-241.
6. Lancaster CA, Gold KJ, Flynn HA, Yoo H, Marcus SM, Davis MM. Risk factors for depressive symptoms during pregnancy: a systematic review. Am J Obstet Gynecol. 2010;202(1):5-14.
7. Suri R, Altshuler L, Hellemann G, Burt VK, Aquino A, Mintz J. Effects of antenatal depression and antidepressant treatment on gestational age at birth and risk of preterm birth. Am J Psychiatry. 2007;164(8):1206-1213.
8. Wisner KL, Sit DK, Hanusa BH, et al. Major depression and antidepressant treatment: impact no pregnancy and neonatal outcomes.” Am J Psychiatry. 2009;166(5):557-566.
9. Li D, Liu L, Odouli R. Presence of depressive symptoms during early pregnancy and the risk of preterm delivery: a prospective cohort study. Hum Reprod. 2009;24(1):146-153.
10. Zuckerman B, Amaro H, Bauchner H, Cabral H. Depressive symptoms during pregnancy: relationship to poor health behaviors. Am J Obstet Gynecol. 1989;150(5Pt 1):1107-1111.
11. Deave T, Heron J, Evans J, Emond A. The impact of maternal depression in pregnancy on early child development. BJOG. 2008;115(8):1043-1051.
12. Yonkers KA, Wisner KL, Stewart DE, et al. The management of depression during pregnancy: a report from the American Psychiatric Association and the American College of Obstetricians and Gynecologists. Obstet Gynecol. 2009;114(3):703-713.
13. Gentile S, Bellantuono C. Selective serotonin reuptake inhibitor exposure during early pregnancy and the risk of fetal major malformations: focus on paroxetine. J Clin Psychiatry. 2009;70(3):414-422.
14. Louik C, Lin AE, Werler MM, Hernandez-Diaz S, Mitchell AA. First-trimester use of selective serotonin-reuptake inhibitors and the risk of birth defects. New Engl J Med. 2007;356(26):2675-2683.
15. Chambers CD, Hernandez-Diaz S, Marter LJV, et al. Selective seroteonin-reuptake inhibitors and risk of persistent pulmonary hypertension of the newborn. New Engl J Med. 2006;354(6):579-587.
16. Chambers CD, Johnson KA, Dick LM, Felix RJ, Jones KL. Birth outcomes in pregnant women taking fluoxetine. New Engl J Med. 1996;335(14):1010-1015.
17. Hageman JR, Adams MA, Gardner TH. Persistent pulmonary hypertension of the newborn. Trends in incidence, diagnosis and management. Am J Dis Child. 1984;137(6):592-595.
18. Fricker J. Nitric oxide may reduce need for extracorporeal membrane oxygenation. Lancet. 1996;347(9012):1397.-
19. Kallen B, Olausson P. Maternal use of selective serotonin re-uptake inhibitors and persistent pulmonary hypertension of the newborn. Pharmacoepidemiol Drug Saf. 2008;17(8):801-806.
20. Andrade S, McPhillips H, Loren D, et al. Antidepressant medication use and risk of persistent pulmonary hypertension of the newborn. Pharmacoepidemiol Drug Saf. 2009;18(3):246-252.
21. Lanza di Scalea T, Wisner K. Antidepressant medication use during breastfeeding. Clin Obstet Gynecol. 2009;52(3):483-497.
CAS: Depressive disorder, anticipating a pregnancy
Your patient Megan—well-educated, 29 years old, G0P0—has come to you to discuss her antidepressant (paroxetine [Paxil]) because she is planning her first pregnancy.
Megan has a history of recurrent major depressive disorder (MDD), which is in remission (see “What is MDD?”).
How will you begin the conversation with this patient about keeping MDD in remission during her pregnancy and ensuring the safety of her fetus?
- Major depressive disorder (MDD) is defined by criteria in the fourth edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-IV)
- The disorder varies in severity, 1) across an affected person’s lifetime and 2) within a depressive episode
- A current or prior episode of depression that includes 1) a significant impact on an individual’s functioning, 2) active suicidality, or 3) hospitalization signals severe MDD
- In women, average age at first episode of depression is 24 years
There is a 20% to 25% lifetime prevalence of depression in women; the disorder peaks during childbearing years, however.1 As of 2003, 13% of pregnant women had taken an antidepressant at some time during their pregnancy, a percentage that has doubled since it was assessed in 1999.2
You are faced with several quandaries in deciding whether to recommend that your patient continue, or discontinue, antidepressant therapy during pregnancy:
- As many as 68% of women who terminate antidepressant treatment before or during pregnancy relapse.
- Even 26% of women who continue antidepressant during pregnancy relapse—requiring a dosage adjustment or change in treatment.3
- Yet the possibly elevated cortisol levels of severe, untreated depression may harm the placenta and fetus.4,5
So, what do you need to know to assess the risks and benefits of “Megan” stopping, or continuing, paroxetine during her anticipated pregnancy? And what are the risks to Megan’s fetus of treating, or not treating, her depression with a serotonin reuptake inhibitor (SRI*)?
“Selective” has been dropped
from “SSRI” to yield simply “SRI.”
Gauging the risks of depression in pregnancy
In any given patient, her history and family history of depression are key to determining the likelihood that she will suffer ongoing or recurrent depression.
CASE continued Repeated treated episodes plus a family history
In obtaining Megan’s history, you learn that she has had three prior episodes of depression, all of which were successfully treated with paroxetine. Megan has been stable on paroxetine for 3 years.
Notably, the second episode of depression was initially treated with a 16-week trial of psychotherapy alone; when depressive symptoms did not remit, paroxetine was added. That episode was considered severe because it included pervasive thoughts of suicide.
You also learn that Megan’s mother suffered from postpartum depression and that her father and paternal grandmother were treated for depression.
Known risk factors for depression during pregnancy include: maternal anxiety; prior diagnosis of depression during pregnancy; history of postpartum anxiety or depression; prior diagnosis of either anxiety or depressive disorder; significant life stress (e.g., divorce, death of a loved one); degree of social support—particularly, intimate social support; “intendedness” of pregnancy; domestic violence; and insurance status.6
You review with Megan her risk factors for depression during pregnancy, namely: three prior episodes of MDD and a strong family history of mood disorder. Her MDD is considered “severe” because she has a history of suicidality. You tell Megan that, given these factors, she is at high risk of a recurrence of her depressive illness during pregnancy.
Megan asks: “Would getting depressed during pregnancy hurt the baby?”
Depression during pregnancy affects both infant and maternal well-being, although studies are in conflict about the extent of that morbidity. Multiple areas of potential risk to mother and infant have been studied, including the effect of depression on:
- maternal well-being
- growth of the infant
- spontaneous abortion
- preterm delivery
- neonatal physiologic and neurobehavioral measures
- long-term considerations for the developing infant and child.
Within these categories of risk, a diagnosis of depression during pregnancy has been associated (in some but not all studies) with a higher risk, or rate, of:
- postpartum depression
- preterm birth
- lower maternal weight gain
- maternal tobacco, alcohol, and other substance use
- lower infant gestational age at birth
- small-for-gestational age infant birth.7-10
In terms of long-term impact on offspring, studies differ in their estimation of risk; however, children exposed to untreated, maternal depression at 18 weeks’ and 32 weeks’ gestation did show a greater degree of developmental delay at 18 months than children who were born to a mother who was not depressed during pregnancy.11
You discuss these risks with Megan. She asks: “What treatment do you recommend for me?” You turn to the 2009 guidelines published jointly by the American Psychiatric Association (APA) and ACOG.
These guidelines recommend that you consider 1) the severity of her current depression, 2) her history of depression severity, and 3) her preference for treatment.12 For mild depression during pregnancy, when there is no history of severe depression, or for a history of depression that responded well to psychotherapy in the past, a trial of psychotherapy without medications is recommended.
But Megan’s history of depression falls into the “severe” category, and a prior episode of depression did not respond well to psychotherapy. Your recommendation to her, therefore, is that she should continue taking an antidepressant—unless she feels strongly that she should discontinue it.
Megan considers what you’ve discussed about her high risk of developing recurrent depression during pregnancy. She decides that she wants to continue taking her antidepressant during pregnancy, but she has concerns—based on what she has been reading on the Internet.
Megan hands you a detailed printout downloaded from a Web site unfamiliar to you and asks about risks to the baby of such medications as paroxetine.
What should you tell Megan about SRIs in pregnancy—paroxetine, specifically?
You preface your remarks to her by noting that the data physicians work with are imperfect—because randomized, controlled clinical trials pose an ethical dilemma as a method of study in pregnant women. You then discuss with her current scientific understanding of potential risks to her fetus.
The difference in the rates of structural malformation among SRI-exposed and SRI-unexposed groups has been studied; most studies have found no increased rate of major or specific cardiac malformations.12 However, first-trimester paroxetine appeared, in some studies, to be associated with an increased rate of cardiac malformations. That led to a category-“D” pregnancy classification in 2005 and an FDA “Public Health Advisory.”
Other large cohort studies have not uncovered such an association. It has been hypothesized that the methodology of data collection may have influenced this finding.13
Other malformations have been implicated in some studies but not others, and have included associations between specific SRIs and cardiac ventricular outflow defects, craniosynostosis, and omphalocele. The absolute risk of these defects remains extremely low, however, and close to the background rate seen in the general population.14
Megan asks: “With that risk-category ‘D’ for paroxetine, do you recommend I continue taking it or should I switch to another medication while I’m pregnant?”
You review again with Megan that, although some studies have linked first-trimester paroxetine to an increased risk of cardiac malformation, that finding has not been replicated in several large cohort studies. You explain that, if she had a history of recurrent depression that had failed to respond to many antidepressants and only paroxetine worked, an attempt at switching the SRI would not be recommended because of the potential for relapse.
Megan tells you that she would feel safer not taking a category-“D” drug. You agree and propose a judicious approach: Because she has come to see you before she became pregnant, with enough time to complete a slow crossover to an alternative SRI, and because she has not had any earlier trials of other SRIs, a slow taper of paroxetine, coupled with a crossover to an alternative SRI, is a reasonable option—with the caution that substitution always carries a risk of relapse.
Problems in newborns
Megan considers the risks you’ve discussed so far. She remembers a recent article in a magazine for pregnant women that described severe “respiratory” and “withdrawal” symptoms in infants who were born to mothers taking an SRI antidepressant. She wonders if she should consider discontinuing her SRI in the third trimester to try to mitigate those risks.
Megan is asking you about an SRI exposure risk that has been fairly consistent across studies, called neonatal abstinence syndrome (NAS) or poor neonatal adaptation.
NAS is a cluster of symptoms that occurs in 15% to 30% of newborns who have been exposed to an SRI during the third trimester of pregnancy.15 Signs include irritability, weak cry, tachypnea, temperature instability, and hypoglycemia—all of which are transient, peak during the first 48 hours after delivery, and resolve in less than 2 weeks.
Multiple hypotheses have been put forward to account for NAS, including the possibilities that it reflects a withdrawal syndrome, pharmacotoxicity, or an underlying gene–SRI interaction. The physiology behind NAS remains unknown, however.12
Megan next asks you about persistent pulmonary hypertension of the newborn (PPHN). You explain that PPHN is of recent concern in women who have been taking an SRI in the latter half of their pregnancy.
The rate of PPHN in the general population is 0.5 to 2 newborns for every 1,000. Associated mortality is approximately 10% to 20%.16-18 This rate is thought to rise to approximately 6 of every 1,000 newborns among those who have been exposed to an SRI in utero—with some evidence of increased risk conferred through SRI exposure during later pregnancy (studies define this as the second half of the pregnancy).15 Although the relative risk of PPHN is increased threefold to sixfold when an SRI is used in pregnancy, absolute risk remains extremely low.
Concerns have been raised over research methodology in the few studies that have looked into SRI exposure and PPHN. Not all such studies found a change in relative risk or absolute risk of PPHN in SRI- exposed infants, compared to what was found in non-SRI–exposed infants.15,19,20
Megan presses you, however, with the understandable question of whether she should taper her SRI during the last trimester (which the Web site she has found recommends). With the above information in mind, you explain that, given current understanding of the low absolute risk of PPHN, and given her illness history and severity of prior depression, you would not recommend that she taper the antidepressant in the third trimester.
Furthermore, the same counsel applies in regard to NAS: Given the risk of psychiatric morbidity caused by discontinuing an SRI during the third trimester, you do not recommend that she taper an SRI during that period to avoid NAS.
You explain that, instead, physicians now counsel women who take an SRI about the signs of NAS so that they can be prepared if they observe any of them in their infant.
Megan has one more question: “Will I be able to breastfeed while I’m taking an antidepressant?”
Given the inherent difficulties and risks of relapse associated with a crossover to an alternative antidepressant postpartum, it makes sense, when possible, for a woman to take an antidepressant during pregnancy that can safely be continued while she is breastfeeding.
You tell Megan that, even though the quality of the data in this area is also thin, SRIs that have a low maternal serum profile are considered safest in breastfeeding.
To date, two SRIs—sertraline and paroxetine—have not been detectable in the breast milk of women taking either of them.21
CASE Appointment concluded, overflowing with information,
advice, and optimism
Megan says that, taking into account all that you and she have talked about, and even though she wants to return with her husband, she would like to switch to sertraline before she becomes pregnant—while she gauges its effectiveness at keeping her disorder in remission.
A good outcome requires you to prevail over obstacles
Because a diagnosis of depression spans a continuum of severity and, often, is not perceived as an acutely life-threatening illness, evaluating the risks and benefits of treatment is a murky undertaking.
Our role as physicians is to, first, educate ourselves and our patients about these variables and, second, support our patients in the decisions that they make. Physicians who care for pregnant women must be aware of the benefits and limitations of treatments as reported in the most current literature if they are going to assist women with decisions about treatment in the best possible way.
Social stigma. There remains the impact of stigma. Depressive and anxiety disorders are often perceived to be either under the control of an affected person’s “free will” or not as serious as other forms of “medical” disease. Consequently, the role that cultural and social pressures play in the risk–benefit analysis conducted by pregnant women and their physicians can’t be discounted.
Customized decision-making. As more data emerge about the treatment of depression in pregnancy, it has become clear: Treatment algorithms meant to simplify our decisions must always be individualized and extended into the postpartum period.
Treatment selection. Management of mild depression during pregnancy does not always require medication. Multiple variables—the list is long, and includes a patient’s psychiatric history, family psychiatric history, response to prior treatment, severity of depression, severity of prior depression, degree of social support, and personal desires—must be considered in determining what treatment is appropriate before, during, and after a pregnancy.
For a woman who suffers mild or moderate depression, with few antenatal depression risk factors, a trial of psychotherapy is recommended as first-line treatment. For a woman suffering from severe depression, or one who has a history of severe depression that has not responded well to psychotherapy alone, continuation or initiation of an SRI antidepressant is the current recommendation.
We want to hear from you! Tell us what you think.
CAS: Depressive disorder, anticipating a pregnancy
Your patient Megan—well-educated, 29 years old, G0P0—has come to you to discuss her antidepressant (paroxetine [Paxil]) because she is planning her first pregnancy.
Megan has a history of recurrent major depressive disorder (MDD), which is in remission (see “What is MDD?”).
How will you begin the conversation with this patient about keeping MDD in remission during her pregnancy and ensuring the safety of her fetus?
- Major depressive disorder (MDD) is defined by criteria in the fourth edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-IV)
- The disorder varies in severity, 1) across an affected person’s lifetime and 2) within a depressive episode
- A current or prior episode of depression that includes 1) a significant impact on an individual’s functioning, 2) active suicidality, or 3) hospitalization signals severe MDD
- In women, average age at first episode of depression is 24 years
There is a 20% to 25% lifetime prevalence of depression in women; the disorder peaks during childbearing years, however.1 As of 2003, 13% of pregnant women had taken an antidepressant at some time during their pregnancy, a percentage that has doubled since it was assessed in 1999.2
You are faced with several quandaries in deciding whether to recommend that your patient continue, or discontinue, antidepressant therapy during pregnancy:
- As many as 68% of women who terminate antidepressant treatment before or during pregnancy relapse.
- Even 26% of women who continue antidepressant during pregnancy relapse—requiring a dosage adjustment or change in treatment.3
- Yet the possibly elevated cortisol levels of severe, untreated depression may harm the placenta and fetus.4,5
So, what do you need to know to assess the risks and benefits of “Megan” stopping, or continuing, paroxetine during her anticipated pregnancy? And what are the risks to Megan’s fetus of treating, or not treating, her depression with a serotonin reuptake inhibitor (SRI*)?
“Selective” has been dropped
from “SSRI” to yield simply “SRI.”
Gauging the risks of depression in pregnancy
In any given patient, her history and family history of depression are key to determining the likelihood that she will suffer ongoing or recurrent depression.
CASE continued Repeated treated episodes plus a family history
In obtaining Megan’s history, you learn that she has had three prior episodes of depression, all of which were successfully treated with paroxetine. Megan has been stable on paroxetine for 3 years.
Notably, the second episode of depression was initially treated with a 16-week trial of psychotherapy alone; when depressive symptoms did not remit, paroxetine was added. That episode was considered severe because it included pervasive thoughts of suicide.
You also learn that Megan’s mother suffered from postpartum depression and that her father and paternal grandmother were treated for depression.
Known risk factors for depression during pregnancy include: maternal anxiety; prior diagnosis of depression during pregnancy; history of postpartum anxiety or depression; prior diagnosis of either anxiety or depressive disorder; significant life stress (e.g., divorce, death of a loved one); degree of social support—particularly, intimate social support; “intendedness” of pregnancy; domestic violence; and insurance status.6
You review with Megan her risk factors for depression during pregnancy, namely: three prior episodes of MDD and a strong family history of mood disorder. Her MDD is considered “severe” because she has a history of suicidality. You tell Megan that, given these factors, she is at high risk of a recurrence of her depressive illness during pregnancy.
Megan asks: “Would getting depressed during pregnancy hurt the baby?”
Depression during pregnancy affects both infant and maternal well-being, although studies are in conflict about the extent of that morbidity. Multiple areas of potential risk to mother and infant have been studied, including the effect of depression on:
- maternal well-being
- growth of the infant
- spontaneous abortion
- preterm delivery
- neonatal physiologic and neurobehavioral measures
- long-term considerations for the developing infant and child.
Within these categories of risk, a diagnosis of depression during pregnancy has been associated (in some but not all studies) with a higher risk, or rate, of:
- postpartum depression
- preterm birth
- lower maternal weight gain
- maternal tobacco, alcohol, and other substance use
- lower infant gestational age at birth
- small-for-gestational age infant birth.7-10
In terms of long-term impact on offspring, studies differ in their estimation of risk; however, children exposed to untreated, maternal depression at 18 weeks’ and 32 weeks’ gestation did show a greater degree of developmental delay at 18 months than children who were born to a mother who was not depressed during pregnancy.11
You discuss these risks with Megan. She asks: “What treatment do you recommend for me?” You turn to the 2009 guidelines published jointly by the American Psychiatric Association (APA) and ACOG.
These guidelines recommend that you consider 1) the severity of her current depression, 2) her history of depression severity, and 3) her preference for treatment.12 For mild depression during pregnancy, when there is no history of severe depression, or for a history of depression that responded well to psychotherapy in the past, a trial of psychotherapy without medications is recommended.
But Megan’s history of depression falls into the “severe” category, and a prior episode of depression did not respond well to psychotherapy. Your recommendation to her, therefore, is that she should continue taking an antidepressant—unless she feels strongly that she should discontinue it.
Megan considers what you’ve discussed about her high risk of developing recurrent depression during pregnancy. She decides that she wants to continue taking her antidepressant during pregnancy, but she has concerns—based on what she has been reading on the Internet.
Megan hands you a detailed printout downloaded from a Web site unfamiliar to you and asks about risks to the baby of such medications as paroxetine.
What should you tell Megan about SRIs in pregnancy—paroxetine, specifically?
You preface your remarks to her by noting that the data physicians work with are imperfect—because randomized, controlled clinical trials pose an ethical dilemma as a method of study in pregnant women. You then discuss with her current scientific understanding of potential risks to her fetus.
The difference in the rates of structural malformation among SRI-exposed and SRI-unexposed groups has been studied; most studies have found no increased rate of major or specific cardiac malformations.12 However, first-trimester paroxetine appeared, in some studies, to be associated with an increased rate of cardiac malformations. That led to a category-“D” pregnancy classification in 2005 and an FDA “Public Health Advisory.”
Other large cohort studies have not uncovered such an association. It has been hypothesized that the methodology of data collection may have influenced this finding.13
Other malformations have been implicated in some studies but not others, and have included associations between specific SRIs and cardiac ventricular outflow defects, craniosynostosis, and omphalocele. The absolute risk of these defects remains extremely low, however, and close to the background rate seen in the general population.14
Megan asks: “With that risk-category ‘D’ for paroxetine, do you recommend I continue taking it or should I switch to another medication while I’m pregnant?”
You review again with Megan that, although some studies have linked first-trimester paroxetine to an increased risk of cardiac malformation, that finding has not been replicated in several large cohort studies. You explain that, if she had a history of recurrent depression that had failed to respond to many antidepressants and only paroxetine worked, an attempt at switching the SRI would not be recommended because of the potential for relapse.
Megan tells you that she would feel safer not taking a category-“D” drug. You agree and propose a judicious approach: Because she has come to see you before she became pregnant, with enough time to complete a slow crossover to an alternative SRI, and because she has not had any earlier trials of other SRIs, a slow taper of paroxetine, coupled with a crossover to an alternative SRI, is a reasonable option—with the caution that substitution always carries a risk of relapse.
Problems in newborns
Megan considers the risks you’ve discussed so far. She remembers a recent article in a magazine for pregnant women that described severe “respiratory” and “withdrawal” symptoms in infants who were born to mothers taking an SRI antidepressant. She wonders if she should consider discontinuing her SRI in the third trimester to try to mitigate those risks.
Megan is asking you about an SRI exposure risk that has been fairly consistent across studies, called neonatal abstinence syndrome (NAS) or poor neonatal adaptation.
NAS is a cluster of symptoms that occurs in 15% to 30% of newborns who have been exposed to an SRI during the third trimester of pregnancy.15 Signs include irritability, weak cry, tachypnea, temperature instability, and hypoglycemia—all of which are transient, peak during the first 48 hours after delivery, and resolve in less than 2 weeks.
Multiple hypotheses have been put forward to account for NAS, including the possibilities that it reflects a withdrawal syndrome, pharmacotoxicity, or an underlying gene–SRI interaction. The physiology behind NAS remains unknown, however.12
Megan next asks you about persistent pulmonary hypertension of the newborn (PPHN). You explain that PPHN is of recent concern in women who have been taking an SRI in the latter half of their pregnancy.
The rate of PPHN in the general population is 0.5 to 2 newborns for every 1,000. Associated mortality is approximately 10% to 20%.16-18 This rate is thought to rise to approximately 6 of every 1,000 newborns among those who have been exposed to an SRI in utero—with some evidence of increased risk conferred through SRI exposure during later pregnancy (studies define this as the second half of the pregnancy).15 Although the relative risk of PPHN is increased threefold to sixfold when an SRI is used in pregnancy, absolute risk remains extremely low.
Concerns have been raised over research methodology in the few studies that have looked into SRI exposure and PPHN. Not all such studies found a change in relative risk or absolute risk of PPHN in SRI- exposed infants, compared to what was found in non-SRI–exposed infants.15,19,20
Megan presses you, however, with the understandable question of whether she should taper her SRI during the last trimester (which the Web site she has found recommends). With the above information in mind, you explain that, given current understanding of the low absolute risk of PPHN, and given her illness history and severity of prior depression, you would not recommend that she taper the antidepressant in the third trimester.
Furthermore, the same counsel applies in regard to NAS: Given the risk of psychiatric morbidity caused by discontinuing an SRI during the third trimester, you do not recommend that she taper an SRI during that period to avoid NAS.
You explain that, instead, physicians now counsel women who take an SRI about the signs of NAS so that they can be prepared if they observe any of them in their infant.
Megan has one more question: “Will I be able to breastfeed while I’m taking an antidepressant?”
Given the inherent difficulties and risks of relapse associated with a crossover to an alternative antidepressant postpartum, it makes sense, when possible, for a woman to take an antidepressant during pregnancy that can safely be continued while she is breastfeeding.
You tell Megan that, even though the quality of the data in this area is also thin, SRIs that have a low maternal serum profile are considered safest in breastfeeding.
To date, two SRIs—sertraline and paroxetine—have not been detectable in the breast milk of women taking either of them.21
CASE Appointment concluded, overflowing with information,
advice, and optimism
Megan says that, taking into account all that you and she have talked about, and even though she wants to return with her husband, she would like to switch to sertraline before she becomes pregnant—while she gauges its effectiveness at keeping her disorder in remission.
A good outcome requires you to prevail over obstacles
Because a diagnosis of depression spans a continuum of severity and, often, is not perceived as an acutely life-threatening illness, evaluating the risks and benefits of treatment is a murky undertaking.
Our role as physicians is to, first, educate ourselves and our patients about these variables and, second, support our patients in the decisions that they make. Physicians who care for pregnant women must be aware of the benefits and limitations of treatments as reported in the most current literature if they are going to assist women with decisions about treatment in the best possible way.
Social stigma. There remains the impact of stigma. Depressive and anxiety disorders are often perceived to be either under the control of an affected person’s “free will” or not as serious as other forms of “medical” disease. Consequently, the role that cultural and social pressures play in the risk–benefit analysis conducted by pregnant women and their physicians can’t be discounted.
Customized decision-making. As more data emerge about the treatment of depression in pregnancy, it has become clear: Treatment algorithms meant to simplify our decisions must always be individualized and extended into the postpartum period.
Treatment selection. Management of mild depression during pregnancy does not always require medication. Multiple variables—the list is long, and includes a patient’s psychiatric history, family psychiatric history, response to prior treatment, severity of depression, severity of prior depression, degree of social support, and personal desires—must be considered in determining what treatment is appropriate before, during, and after a pregnancy.
For a woman who suffers mild or moderate depression, with few antenatal depression risk factors, a trial of psychotherapy is recommended as first-line treatment. For a woman suffering from severe depression, or one who has a history of severe depression that has not responded well to psychotherapy alone, continuation or initiation of an SRI antidepressant is the current recommendation.
We want to hear from you! Tell us what you think.
1. Kessler RC, Berglund P, Demler O, et al. National Comorbidity Survey Replication. The epidemiology of major depressive disorder: results from the National Comorbidity Survey Replication (NCS-R). JAMA. 2003;289(23):3095-3105.
2. Cooper W, Willy M, Pont S, Ray W. Increasing use of antidepressants in pregnancy. Am J Obstet Gynecol. 2007;196(6):544.e1-e5.
3. Cohen LS, Altshuler LL, Harlow BL, et al. Relapse of major depression during pregnancy in women who maintain or discontinue antidepressant treatment. JAMA. 2006;295(5):499-507.
4. Kramer MS, Lydon J, Séguin L, et al. Stress pathways to spontaneous preterm birth: the role of stressors, psychological distress, and stress hormones. Am J Epidemiol. 2009;169(11):1319-1326.
5. Ellman LM, Schetter CD, Hobel CJ, Chicz-Demet A, Glynn LM, Sandman CA. Timing of fetal exposure to stress hormones: effects on newborn physical and neuromuscular maturation. Dev Psychobiol. 2008;50(3):232-241.
6. Lancaster CA, Gold KJ, Flynn HA, Yoo H, Marcus SM, Davis MM. Risk factors for depressive symptoms during pregnancy: a systematic review. Am J Obstet Gynecol. 2010;202(1):5-14.
7. Suri R, Altshuler L, Hellemann G, Burt VK, Aquino A, Mintz J. Effects of antenatal depression and antidepressant treatment on gestational age at birth and risk of preterm birth. Am J Psychiatry. 2007;164(8):1206-1213.
8. Wisner KL, Sit DK, Hanusa BH, et al. Major depression and antidepressant treatment: impact no pregnancy and neonatal outcomes.” Am J Psychiatry. 2009;166(5):557-566.
9. Li D, Liu L, Odouli R. Presence of depressive symptoms during early pregnancy and the risk of preterm delivery: a prospective cohort study. Hum Reprod. 2009;24(1):146-153.
10. Zuckerman B, Amaro H, Bauchner H, Cabral H. Depressive symptoms during pregnancy: relationship to poor health behaviors. Am J Obstet Gynecol. 1989;150(5Pt 1):1107-1111.
11. Deave T, Heron J, Evans J, Emond A. The impact of maternal depression in pregnancy on early child development. BJOG. 2008;115(8):1043-1051.
12. Yonkers KA, Wisner KL, Stewart DE, et al. The management of depression during pregnancy: a report from the American Psychiatric Association and the American College of Obstetricians and Gynecologists. Obstet Gynecol. 2009;114(3):703-713.
13. Gentile S, Bellantuono C. Selective serotonin reuptake inhibitor exposure during early pregnancy and the risk of fetal major malformations: focus on paroxetine. J Clin Psychiatry. 2009;70(3):414-422.
14. Louik C, Lin AE, Werler MM, Hernandez-Diaz S, Mitchell AA. First-trimester use of selective serotonin-reuptake inhibitors and the risk of birth defects. New Engl J Med. 2007;356(26):2675-2683.
15. Chambers CD, Hernandez-Diaz S, Marter LJV, et al. Selective seroteonin-reuptake inhibitors and risk of persistent pulmonary hypertension of the newborn. New Engl J Med. 2006;354(6):579-587.
16. Chambers CD, Johnson KA, Dick LM, Felix RJ, Jones KL. Birth outcomes in pregnant women taking fluoxetine. New Engl J Med. 1996;335(14):1010-1015.
17. Hageman JR, Adams MA, Gardner TH. Persistent pulmonary hypertension of the newborn. Trends in incidence, diagnosis and management. Am J Dis Child. 1984;137(6):592-595.
18. Fricker J. Nitric oxide may reduce need for extracorporeal membrane oxygenation. Lancet. 1996;347(9012):1397.-
19. Kallen B, Olausson P. Maternal use of selective serotonin re-uptake inhibitors and persistent pulmonary hypertension of the newborn. Pharmacoepidemiol Drug Saf. 2008;17(8):801-806.
20. Andrade S, McPhillips H, Loren D, et al. Antidepressant medication use and risk of persistent pulmonary hypertension of the newborn. Pharmacoepidemiol Drug Saf. 2009;18(3):246-252.
21. Lanza di Scalea T, Wisner K. Antidepressant medication use during breastfeeding. Clin Obstet Gynecol. 2009;52(3):483-497.
1. Kessler RC, Berglund P, Demler O, et al. National Comorbidity Survey Replication. The epidemiology of major depressive disorder: results from the National Comorbidity Survey Replication (NCS-R). JAMA. 2003;289(23):3095-3105.
2. Cooper W, Willy M, Pont S, Ray W. Increasing use of antidepressants in pregnancy. Am J Obstet Gynecol. 2007;196(6):544.e1-e5.
3. Cohen LS, Altshuler LL, Harlow BL, et al. Relapse of major depression during pregnancy in women who maintain or discontinue antidepressant treatment. JAMA. 2006;295(5):499-507.
4. Kramer MS, Lydon J, Séguin L, et al. Stress pathways to spontaneous preterm birth: the role of stressors, psychological distress, and stress hormones. Am J Epidemiol. 2009;169(11):1319-1326.
5. Ellman LM, Schetter CD, Hobel CJ, Chicz-Demet A, Glynn LM, Sandman CA. Timing of fetal exposure to stress hormones: effects on newborn physical and neuromuscular maturation. Dev Psychobiol. 2008;50(3):232-241.
6. Lancaster CA, Gold KJ, Flynn HA, Yoo H, Marcus SM, Davis MM. Risk factors for depressive symptoms during pregnancy: a systematic review. Am J Obstet Gynecol. 2010;202(1):5-14.
7. Suri R, Altshuler L, Hellemann G, Burt VK, Aquino A, Mintz J. Effects of antenatal depression and antidepressant treatment on gestational age at birth and risk of preterm birth. Am J Psychiatry. 2007;164(8):1206-1213.
8. Wisner KL, Sit DK, Hanusa BH, et al. Major depression and antidepressant treatment: impact no pregnancy and neonatal outcomes.” Am J Psychiatry. 2009;166(5):557-566.
9. Li D, Liu L, Odouli R. Presence of depressive symptoms during early pregnancy and the risk of preterm delivery: a prospective cohort study. Hum Reprod. 2009;24(1):146-153.
10. Zuckerman B, Amaro H, Bauchner H, Cabral H. Depressive symptoms during pregnancy: relationship to poor health behaviors. Am J Obstet Gynecol. 1989;150(5Pt 1):1107-1111.
11. Deave T, Heron J, Evans J, Emond A. The impact of maternal depression in pregnancy on early child development. BJOG. 2008;115(8):1043-1051.
12. Yonkers KA, Wisner KL, Stewart DE, et al. The management of depression during pregnancy: a report from the American Psychiatric Association and the American College of Obstetricians and Gynecologists. Obstet Gynecol. 2009;114(3):703-713.
13. Gentile S, Bellantuono C. Selective serotonin reuptake inhibitor exposure during early pregnancy and the risk of fetal major malformations: focus on paroxetine. J Clin Psychiatry. 2009;70(3):414-422.
14. Louik C, Lin AE, Werler MM, Hernandez-Diaz S, Mitchell AA. First-trimester use of selective serotonin-reuptake inhibitors and the risk of birth defects. New Engl J Med. 2007;356(26):2675-2683.
15. Chambers CD, Hernandez-Diaz S, Marter LJV, et al. Selective seroteonin-reuptake inhibitors and risk of persistent pulmonary hypertension of the newborn. New Engl J Med. 2006;354(6):579-587.
16. Chambers CD, Johnson KA, Dick LM, Felix RJ, Jones KL. Birth outcomes in pregnant women taking fluoxetine. New Engl J Med. 1996;335(14):1010-1015.
17. Hageman JR, Adams MA, Gardner TH. Persistent pulmonary hypertension of the newborn. Trends in incidence, diagnosis and management. Am J Dis Child. 1984;137(6):592-595.
18. Fricker J. Nitric oxide may reduce need for extracorporeal membrane oxygenation. Lancet. 1996;347(9012):1397.-
19. Kallen B, Olausson P. Maternal use of selective serotonin re-uptake inhibitors and persistent pulmonary hypertension of the newborn. Pharmacoepidemiol Drug Saf. 2008;17(8):801-806.
20. Andrade S, McPhillips H, Loren D, et al. Antidepressant medication use and risk of persistent pulmonary hypertension of the newborn. Pharmacoepidemiol Drug Saf. 2009;18(3):246-252.
21. Lanza di Scalea T, Wisner K. Antidepressant medication use during breastfeeding. Clin Obstet Gynecol. 2009;52(3):483-497.
Celiac Disease: A Storm of Gluten Intolerance
Celiac disease (CD), also known as gluten-sensitive enteropathy or celiac sprue, is an endocrine disorder whose effects are triggered by the ingestion of gluten—the principle storage protein in wheat, rye, and barley.1-3 CD inflicts damage to the mucosa of the small intestine and subsequently to systemic organ tissues. CD can affect any organ in the body.1 The responsible genetic factors are the human leukocyte antigens, HLA -DQ2 and -DQ8, which are present in 40% of the general population but are found in nearly 100% of patients with CD.1,3,4
Though previously considered uncommon, CD has been estimated to affect more than 1% of the general population worldwide.1,4,5 Currently, CD is most reliably identified by positive serum antibodies, specifically immunoglobulin A (IgA) anti-tissue transglutaminase (tTG) and IgA antiendomysial (EMA) antibodies,6 and by a finding of villous atrophy of the intestinal lining on biopsy. The spectrum of presentations of CD is broad, including the “typical” intestinal features of diarrhea, bloating, abdominal pain, and weight loss; or common “atypical” extraintestinal manifestations, such as anemia, osteoporosis, infertility, and neurologic disturbances (eg, peripheral neuropathy7).8 See Table 1.8,9
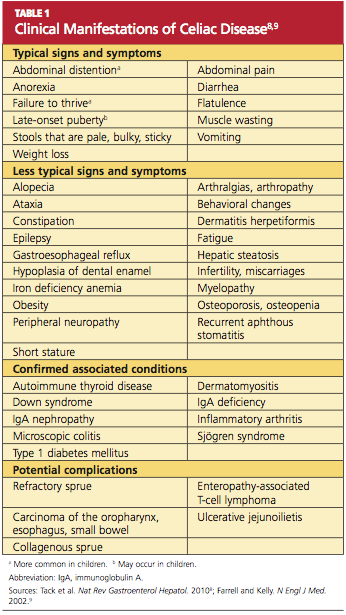
Prevalence of CD is greater among those with a family history of CD; with autoimmune diseases, especially type 1 diabetes mellitus (T1DM) and thyroiditis; and with certain genetic disorders (ie, Down, Turner, and Williams syndromes).8-15 Because atypical features dominate in older children and adults, many cases escape diagnosis, and patients may be exposed to serious long-term complications, such as infertility and cancer.1
CD is a lifelong condition, necessitating the complete exclusion of gluten-containing products from the diet. In the US food industry, gluten is used in numerous food applications, complicating the patient education and lifestyle changes needed to implement and maintain a gluten-free diet (GFD). However, if a GFD is not strictly followed, the patient’s quality of life can be seriously impaired.1,4,5
AWARENESS ESSENTIAL IN PRIMARY CARE
For the primary care provider (PCP), there is no shortage of patients with gastrointestinal (GI) disorders, thyroid disease, diabetes, anemia, fatigue, or dysmenorrhea; additionally, PCPs regularly treat patients for a number of associated disorders, including anxiety, irritability, and attention deficit. Yet how likely are PCPs to screen patients with these symptoms for CD? And how many patients with CD never receive a diagnosis of the disorder?
In fact, it has been estimated that more than 90% of persons affected by CD are currently undiagnosed.1,4 In one study involving mass screening of 1,000 children ages 2 to 18, it was determined that almost 90% of celiac-positive children had not previously been diagnosed.5 Similarly, in a cohort of 976 adults (median age, 54.3), the diagnostic rate for CD was initially low at 0.27 cases per thousand visits but increased to 11.6 cases per thousand visits after implementation of active screening.4 Based on these data, it has been estimated that more than 2.7 million Americans unknowingly carry this potentially life-threatening genetic disease.1,4,16
Given the potential patient population with undetected, untreated CD, some researchers consider the disorder one of the most common lifelong diseases in the US.1,8,16 CD is closely associated with T1DM and autoimmune thyroiditis, with cross- prevalence at 11% and 6.7%, respectively.8,12,17 The close association between T1DM and CD led the American Diabetes Association18 to amend guidelines in 2009, suggesting screening for CD in all patients newly diagnosed with T1DM.
PATIENT PRESENTATION: ADULTS VERSUS CHILDREN
Most infants and young children with CD present with the typical or “classic” triad of signs: short stature, failure to thrive, and diarrhea; in individual patients, however, the impact of genetics and exposure to gluten over time can cause considerable variation in patient presentation. As patients with undiagnosed CD age, they may present quite differently or even revert to a latent stage and become asymptomatic.19,20
In two separate reviews, it was noted that classic symptoms of CD are not evident in a majority of older children and adults; instead, anemia and fatigue were the predominating symptoms.12,20An important note: The patient with no symptoms or atypical signs of CD may still be experiencing significant damage, inflicted by gluten-induced antibodies, to the intestinal lining and/or mucosal linings in other organ systems—perhaps for years before the disease becomes evident.20
Clinical Findings Differ With Age, Gender
Historically, CD was considered a pediatric syndrome; however, a diagnosis of CD has become increasingly common among older children and adults, especially elderly patients, although symptoms in the latter group are subtle.21-23 Recent, active CD is being diagnosed among men older than 55 more commonly than in women of this age-group; women are generally younger at diagnosis but have experienced symptoms longer.22,23 This later onset in men suggests that antibody seropositivity and the associated active disease may be triggered later in life.8,22
A variety of findings have been reported in the history and physical exam of most patients who present with CD.The most prevalent signs and symptoms are abdominal pain, frequent loose stools, weight loss, joint pain, and weakness.8,11,16 Unlike the pediatric patient with the classic triad of symptoms, adults usually experience more generalized GI manifestations, such as irritable bowel syndrome (IBS), abdominal pain, or acid reflux.10
Many patients have no GI symptoms but may present solely with fatigue, arthralgias, or myalgia.20 In fact, more than 50% of adults with CD present with atypical or extraintestinal disorders, such as anemia, infertility, osteoporosis, neurologic problems, or other autoimmune disorders.8,16,23,24 It is important for clinicians to note that atypical is somewhat typical in the older patient who presents with CD.
Patients with asymptomatic or silent CD, (see “Classification and Pathology,” below) lack both classic and atypical symptoms but still have villous atrophy, usually discovered during endoscopy being conducted for other reasons.8 Because of its predominantly atypical presentations, CD is considered a multisystem endocrine condition rather than one that is mainly gastrointestinal.8,16,25,26
CLASSIFICATION AND PATHOLOGY
Though frequently a silent disorder, CD typically progresses through four stages: classical, atypical, latent, and silent. Clinicians should strive to become fully aware of each stage and its implications.8,26,27
The classical form is primarily diagnosed in children ages 6 to 18 months. It is characterized by villous atrophy and typical symptoms of intestinal malabsorption.8
The patient with atypical CD has minor intestinal symptoms, but architectural abnormalities can be found in the mucosa of the small intestine. This patient is likely to present with various extraintestinal disorders, including osteoporosis, anemia, infertility, and neuropathies.7,8
In the latent form of CD, the HLA-DQ2 and/or -DQ8 genetic markers are present. Serology for CD may be positive, but the intestinal mucosa may be normal. The patient may or may not be experiencing extraintestinal symptoms. In patients with latent CD, the gluten-associated changes appear later in life.8 The precise trigger for late activation of the disease, though apparently linked to genetics and gluten exposure, remains elusive.20,24
The silent form of CD is marked by mucosal abnormalities in the small intestine and usually by positive CD serology, but it is asymptomatic. The iceberg theory of celiac disease28 (see figure28) has been proposed to explain CD’s hidden manifestations over time.
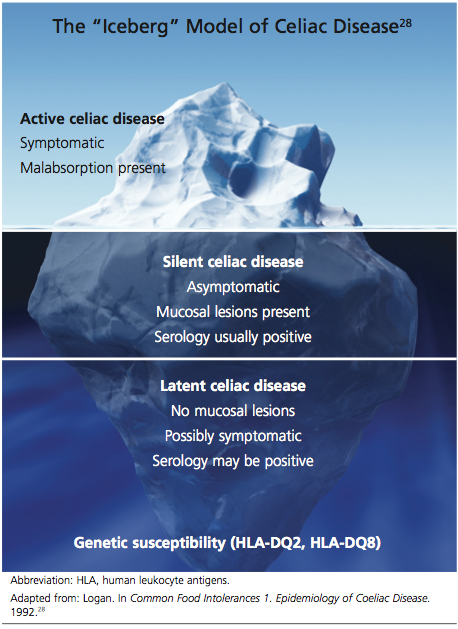
In patients with atypical, latent, or silent CD, the condition is sometimes detected incidentally during screening of at-risk groups or by endoscopy performed for other reasons.8 Most of these patients respond well to GFD therapy, noting both physical and psychological improvement—suggesting that these patients, even though asymptomatic and seemingly healthy, may have been experiencing minor manifestations of undiagnosed CD for many years: decreased appetite, fatigue, and even behavioral abnormalities.1,8
Histopathologic analysis of abnormalities found on biopsy of the small intestine relies on the four-stage Marsh classification29:
• Marsh 0: normal mucosa
• Marsh I: intraepithelial lymphocytosis
• Marsh II: intraepithelial lymphocytosis with crypt hyperplasia
• Marsh III: intraepithelial lymphocytosis with crypt hyperplasia and villous atrophy.8,29 Modifications to this classification have been made by Oberhuber30,31 to denote the degree of villous flattening32 (ie, IIIa, IIIb, IIIc).
Villous atrophy of the mucosa has long been considered the hallmark of CD, and its detection, according to the American Gastroenterological Association,2,26 remains the gold standard in confirming a diagnosis of CD.4,16,26 However, early screening (ie, serologic testing for tTG and EMA) is the necessary initial step in ensuring diagnostic accuracy, as other conditions can cause villous atrophy, and latent CD can coexist with normal intestinal mucosa.10
Avoiding Diagnostic Delays
Because of the broad spectrum of unrelated GI signs in all ages and the subtle presentation in adults, diagnosis of CD in this patient population is frequently delayed for estimated periods ranging from five to 11 years.4,11,23,33
Improving clinician awareness of the manifestations of CD is essential34; too frequently, the common symptoms of probable CD are treated as individual idiopathic disorders by both PCPs and secondary specialists, who prescribe proton pump inhibitors, antihistamines, cathartics, and/or antimotility drugs for years without ruling out a common, easily identified genetic disease. Even though the prevalence of CD has recently been shown to have increased more than fourfold since 1950,35 serologic testing for CD is not widely implemented by PCPs.4,11,20
Specialists, too, may be slow to recognize this treatable autoimmune disorder. In a recent nationwide study, it was found that gastroenterologists performed a small-bowel biopsy in less than 10% of their patients who underwent esophagogastroduodenoscopy (EGD) for likely symptoms of CD.36 Relying solely on clinical expertise and visual recognition of intestinal abnormalities can delay diagnosis for years.4,36 Many patients may never be given a correct diagnosis of CD.
The Role of Serologic Testing
Current data demonstrate that autoimmune diseases are on the rise,8,16,36 and CD can be the primary cause or a contributing factor in several other disorders (see Table 28,16,37,38). Gastroenterologists may be correct in stating that biopsy is the only way to make a diagnosis of CD or to stage CD-associated intestinal damage4,26; yet by implementing a protocol of serologic testing for tTG and EMA in at-risk patients, PCPs could prevent a missed diagnosis on EGD when biopsy has not been considered, as in the case of atypical CD; or when biopsy results are negative in a patient with latent CD.39,40
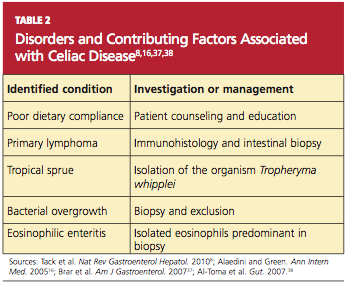
Because of its high negative predictive value, serologic testing should be conducted first to significantly reduce the probability of suspected CD. Such selective screening should be performed by the PCP before invasive testing by the gastroenterologist and before long-term empiric treatment for idiopathic GERD, IBS, or other unexplained disorders.32,40
Thus, it has been recommended that PCPs perform screening for CD in patients with unexplained chronic GI disturbances or a familial prevalence of CD, or in those who present with the atypical signs of CD or with associated disorders.1,10,16,20 Whether serologic screening results are positive or negative for CD, the patient with classic GI symptoms should undergo endoscopy with biopsy to confirm active disease and to evaluate the extent of intestinal damage—or to explore other causes.26,39 An algorithm2,4,8,11,16,26 illustrating suggested screening, treatment, and follow-up strategies for patients at high risk for CD is shown below.
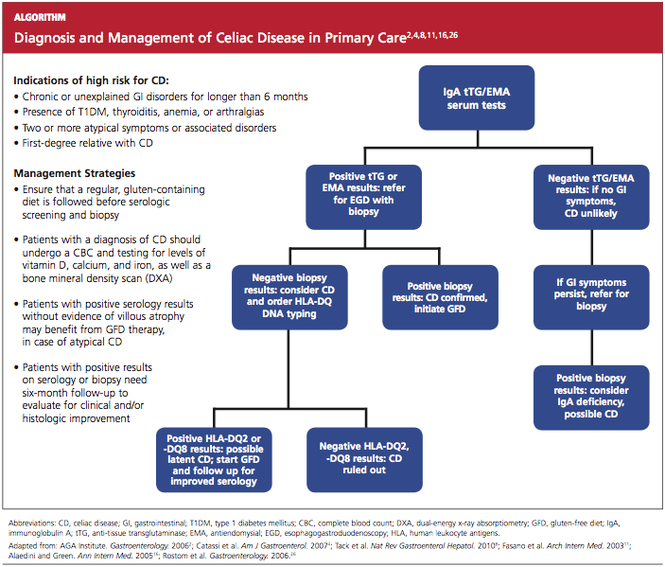
Catassi and Fasano34 recently proposed a “four out of five” rule, by which diagnosis of CD may be confirmed in patients with at least four of the following five criteria:
• Typical symptoms of CD
• Positive serology (ie, IgA tTG and IgA EMA antibodies)
• Genetic susceptibility (as confirmed by the presence of HLA-DQ2 and HLA-DQ8)
• Small intestine biopsy results indicating celiac enteropathy
• Improvement of CD signs and symptoms following implementation of the GFD.34
CURRENT TREATMENT AND ASSOCIATED CHALLENGES
Because gluten consumption is the principal trigger of CD pathology, a GFD is considered the safest, most effective therapy for the disorder.1,8,10,11,16,19 Implementing and maintaining the GFD involves a considerable learning curve for the patient, the patient’s family, and possibly the provider; to achieve complete recovery, all involved must become knowledgeable regarding gluten-free and gluten-containing products. The patient must be willing and able to avoid those that contain gluten and bear the potentially high costs8 of gluten-free foods.
Even for patients with CD who are determined to comply with the GFD, gluten monitoring can be difficult. There are ways to determine what is a safe level of gluten ingestion for each patient, but trace amounts of gluten are found in many products, including some that are marked “gluten-free.”1,41 The FDA has proposed that a product labeled gluten-free may contain no more than 20 parts per million (ppm, ie, 20 mg/kg) of gluten.42 In other countries, however, acceptable levels may be as high as 200 ppm (200 mg/kg)—which are considered well above the trigger amounts in the average patient with CD.1,41 The complex nature of each patient’s sensitivity to gluten and the ubiquitous presence of gluten as a food source in both industrialized and developing countries make adherence to the GFD challenging.10
It is critical for the PCP to help the patient review all of his or her prescription and OTC pharmaceuticals and nutritional supplements, as these may contain hidden gluten in the form of modified starches and other fillers.41 It may be also advisable to involve the patient’s pharmacist, requesting an assessment for agents that may be suspect.
A management team approach may ensure the most integrative care. In addition to the PCP and the pharmacist, such a team might include a gastroenterologist, an endocrinologist, a nutritionist, and a psychologist, who may be needed to help the patient confront the great life adjustment required, in addition to addressing other behavioral disorders that are common in patients with CD.10,26
See the box for resources that may be beneficial for both patients and their clinicians.
Alternative Medicine Options
Alternative medicine is gaining favor, especially when no drug therapy is currently available to alleviate gluten toxicity. Supplementation with the fat-soluble vitamins (A, D, E, and K), vitamin B12, folic acid, and the minerals calcium and iron, as indicated by serum deficiencies, is recommended.10,20 Supplementation with digestive enzymes, which are known to be deficient in patients with CD as a result of villous atrophy, may help break down undigested gluten proteins; research is under way to find a recombinant enzyme therapy.10 Researchers have recently shown that probiotics (specifically, Bifidobacterium lactis) significantly reduce the immune response when incidental exposure to gluten occurs.43
REFRACTORY CELIAC DISEASE
Patients with late-onset CD, especially those not diagnosed until after age 50, may have a diminished or absent response to dietary therapy. In some patients, histologic signs and clinical symptoms persist or relapse after a prior positive response to a strict GFD, despite continued adherence to the diet for longer than 12 months.44 Once other causes have been carefully excluded, these patients are considered to have refractory celiac disease (RCD). Exact prevalence of RCD is unknown, but Tack et al8 estimate it at 5% of all cases of CD. Relapsing CD resulting from poor adherence to the GFD is not considered true RCD.8,16,37,38
According to researchers for the European Celiac Disease working group,8,45 RCD can be divided into types I and II:
• RCD I, in which normal polyclonal T cells are present in the intestinal lumen
• RCD II, in which abnormal clonal T cells infiltrate the intestinal mucosa, representing premalignancy.45
The histologic picture of RCD mimics that of severe CD. Malabsorption complications, lesions in the intestinal mucosa, and inflammatory lymphocytosis are present.44 Some patients, like those with classical CD, have serology test results that are consistent with CD and an initial response to GFD therapy; after months or years, however, this response subsides. Other patients are immediately unresponsive to GFD and lack the serologic markers for CD.8
A differential diagnosis including other explanations for the manifestations of RCD must be carefully reviewed, with each excluded, through the strategies shown in Table 2. This review is essential, as patients with RCD II have a much worse prognosis than those with RCD I; the associated five-year survival rates are 44% to 58%, versus 85% or greater, respectively.36,46
Additionally, the continued autoimmune expansion of aberrant T cells in patients with RCD II causes early conversion to malignancy, usually within four to six years after diagnosis. Enteropathy-associated T-cell lymphoma is the most common malignancy, occurring in more than 50% of patients with RCD II, and a likely cause of death.3,8,46,47
Treatment for Refractory Celiac Disease
In addition to the GFD, patients with RCD I generally respond well to corticosteroids or other immunosuppressive treatment.8 Use of budesonide, a corticosteroid given in a once-daily, 9-mg dose, has led to almost complete recovery in most patients. Duration of therapy is response-dependent.37
Systemic corticosteroids or other immunosuppressant agents, such as azathioprine, should be reserved for patients with RCD I or RCD II who do not respond to budesonide, as lengthy treatment regimens are required, with considerable risk for adverse effects.35,48
Recently, promising results have been reported in a small, open-label cohort study involving patients with RCD II who underwent five days of treatment with IV cladribine (0.1 mg/kg/d).49
PREVENTION OF CD
A good nutritional start from birth could be the best means of preventing symptomatic CD. According to findings from a meta-analysis of data from four studies, children being breastfed at the time gluten was introduced had a 52% reduction in risk for CD, compared with their peers who were not being breastfed at that time.50
The protection breast milk appears to provide against CD is not clearly understood. One possible mechanism is that breast milk may protect an infant against CD by preventing gastrointestinal infections, as is the case with other infections. The presence of GI infections (eg, rotavirus) in early life could lead to increased permeability of the intestinal mucosa, allowing the passage of gluten into the lamina propria.3,8,50
Extended duration of breastfeeding is also associated with a reduced risk for CD.8,41,50 Long-term studies are needed, however, to determine whether breastfeeding delays CD onset or provides permanent protection against the disorder.
RECENT DEVELOPMENTS
A recently marketed OTC testing kit for CD is now available in Canada and other countries outside the US; this may be an indication of the growing awareness of the numbers of patients with undiagnosed CD. The test parallels the tTG serum test, which in the US is evaluated only in laboratories; it has comparable specificity and sensitivity, with results within 10 minutes. In the US, the FDA has not yet approved the kit, but domestic testing of the product may soon be under way.51
Alternative treatment modalities are currently focusing on the detoxification of wheat components, rapid enzymatic degradation to reduce exposure to gluten, inducing gluten tolerance, inhibiting permeability of the small intestine to gluten (which, it is thought, may prevent many of the systemic manifestations of CD), and finally, development of an immunomodulatory vaccine.8,33 None of these therapies is yet approved.
IMPLICATIONS OF DELAYED DIAGNOSIS
The unrecognized prevalence of CD is a growing issue, as many symptomatic but unscreened patients are frequently misdiagnosed with IBS, chronic fatigue, or other idiopathic disorders. The silent and latent forms of CD are of the greatest concern, as they show minimal signs and can lead to multiple organ system damage and are implicated in other autoimmune disorders. The longer diagnosis is delayed, the greater is patients’ resistance to dietary therapy, and the less likely that established intestinal and/or neurologic damage can be reversed.10,20,51
The large proportion of undiagnosed celiac patients may account for an accompanying underestimated cost to both the patient and the health care system because of repeated referrals to investigate unexplained disorders before an accurate diagnosis is made. In one recent analysis, mass screening for CD in a young adult population led to improved quality-of-life years by shortening the time to diagnosis and treatment; it was also found cost-effective.52 PCPs must be attentive to patients who may be at high risk for CD and implement combined serum tTG and EMA screening as the initial step in identification and treatment.4,10,11,20 Some form of standardized screening protocol may become inevitable.
CONCLUSION
The prevalence of CD has increased more than fourfold since 1950, and diagnosis is often significantly delayed. Increased awareness is needed among PCPs that CD in adults is likely to manifest with atypical (ie, nongastrointestinal) symptoms and signs. Judicious use of serologic screening for CD would lead to earlier diagnosis and more effective treatment, possibly preventing the potentially lethal refractory disease forms associated with chronic untreated CD.
REFERENCES
1. Ramos M, Orozovich P, Moser K, et al. Health 1. Catassi C, Fasano A. Celiac disease. Curr Opin Gastroenterol. 2008;24(6):687-691.
2. AGA Institute. AGA Institute medical position statement on the diagnosis and management of celiac disease. Gastroenterology. 2006;131(6):1977-1980.
3. Green PH, Jabri B. Coeliac disease. Lancet. 2003;362(9381):383-391.
4. Catassi C, Kryszak D, Louis-Jacques O, et al. Detection of celiac disease in primary care: a multicenter case-finding study in North America. Am J Gastroenterol. 2007;102(7);1454-1460.
5. Demirçeken FG, Kansu A, Kuloglu Z, et al. Human tissue transglutaminase antibody screening by immunochromatographic line immunoassay for early diagnosis of celiac disease in Turkish children. Turk J Gastroenterol. 2008;19(1):14-21.
6. van der Windt DA, Jellema P, Mulder CJ, et al. Diagnostic testing for celiac disease among patients with abdominal symptoms: a systematic review. JAMA. 2010;303(17):1738-1746.
7. Freeman HJ. Neurological disorders in adult celiac disease. Can J Gastroenterol. 2008; 22(11):909-911.
8. Tack GJ, Verbeek WHM, Schreurs MWJ, Mulder CJJ. The spectrum of celiac disease: epidemiology, clinical aspects and treatment. Nat Rev Gastroenterol Hepatol. 2010;7(4):204-213.
9. Farrell RJ, Kelly CP. Celiac sprue. N Engl J Med. 2002;346(3):180-188.
10. Green PHR, Cellier C. Celiac disease. N Engl J Med. 2007;357(17):1731-1743.
11. Fasano A, Berti I, Gerarduzzi T, et al. Prevalence of celiac disease in at-risk and not-at-risk groups in the United States: a large multicenter study. Arch Intern Med. 2003;163(3):286-292.
12. Sud S, Marcon M, Assor E, et al. Celiac disease and pediatric type 1 diabetes: diagnostic and treatment dilemmas. Int J Pediatr Endocrinol. 2010;2010:161285. Epub 2010 Jun 23.
13. Swigonski NL, Kuhlenschmidt HL, Bull MJ, et al. Screening for celiac disease in asymptomatic children with Down syndrome: cost-effectiveness of preventing lymphoma. Pediatrics. 2006;118(2):594-602.
14. Bonamico M, Pasquino AM, Mariani P, et al; Italian Society of Pediatric Gastroenterology Hepatology (SIGEP); Italian Study Group for Turner Syndrome (ISGTS). Prevalence and clinical picture of celiac disease in Turner syndrome. J Clin Endocrinol Metab. 2002;87(12): 5495-5498.
15. Giannotti A, Tiberio G, Castro M, et al. Coeliac disease in Williams syndrome. J Med Genet. 2001;38(11):767–768.
16. Alaedini A, Green P. Narrative review: celiac disease: understanding a complex autoimmune disorder. Ann Intern Med. 2005;142(4): 289-298.
17. Fröhlich-Reiterer EE, Hofer S, Kaspers S, et al. Screening frequency for celiac disease and autoimmune thyroiditis in children and adolescents with type 1 diabetes mellitus: data from a German/Austrian multicentre survey. Pediatr Diabetes. 2008;9(6):546-553.
18. American Diabetes Association. Standards of medical care in diabetes—2009. Diabetes Care. 2009;32(1):S13–S61.
19. Losowsky MS. A history of coeliac disease. Dig Dis. 2008;26(2):112-120.
20. Evans KE, Hadjivassilou M, Sanders DS. Understanding ‘silent’ coeliac disease: complications in diagnosis and treatment. Gastrointest Nurs. 2010;8(2):26-32.
21. Lurie Y, Landau DA, Pfeffer J, Oren R. Celiac disease diagnosed in the elderly. J Clin Gastroenterol. 2008;42(1):59-61.
22. Vilppula A, Kaukinen K, Luostarinen L, et al. Increasing prevalence and high incidence of celiac disease in elderly people: a population-based study. BMC Gastroenterol. 2009 Jun 29;9:49.
23. Lo W, Sano K, Lebwohl B, et al. Changing presentation of adult celiac disease. Dig Dis Sci. 2003;48(2):395-398.
24. Alaedini A, Okamoto H, Briani C, et al. Immune cross-reactivity in celiac disease: anti-gliadin antibodies bind to neuronal synapsin I. J Immunol. 2007;178(10):6590-6595.
25. Tursi A, Giorgetti G, Brandimarte G, et al. Prevalence and clinical presentation of subclinical/silent celiac disease in adults: an analysis on a 12-year observation. Hepatogastroenterology. 2001;48(38):462-464.
26. Rostom A, Murray JA, Kagnoff MF. American Gastroenterological Association (AGA) Institute technical review on the diagnosis and management of celiac disease. Gastroenterology. 2006;131(6):1981-2002.
27. Ferguson A, Arranz E, O’Mahony S. Clinical and pathological spectrum of coeliac disease—active, silent, latent, potential. Gut. 1993;34(2): 150-151.
28. Logan RFA. Problems and pitfalls in epidemiological studies of coeliac disease. In: Auricchio S, Visakorpi JK, eds. Common Food Intolerances 1. Epidemiology of Coeliac Disease (Dynamic Nutrition Research)(Pt 1). Basel, Switzerland: Karger; 1992:14-22.
29. Marsh MN. Gluten, major histocompatibility complex, and the small intestine: a molecular and immunobiologic approach to the spectrum of gluten sensitivity (‘celiac sprue’). Gastroenterology. 1992;102(1):330-354.
30. Oberhuber G, Granditsch G, Vogelsang H. The histopathology of coeliac disease: time for a standardized report scheme for pathologists. Eur J Gastroenterol Hepatol. 1999;11(10):1185-1194.
31. Corazza GR, Villanaci V. Coeliac disease.
J Clin Pathol. 2005;58(6):573-574.
32. Hadithi M, von Blomberg BM, Crusius JB, et al. Accuracy of serologic tests and HLA-DQ typing for diagnosing celiac disease. Ann Intern Med. 2007;147(5):294-302.
33. Lerner A. New therapeutic strategies for celiac disease. Autoimmun Rev. 2010;9(3):144-147.
34. Catassi C, Fasano A. Celiac disease diagnosis: simple rules are better than complicated algorithms. Am J Med. 2010;123(8):691-693.
35. Rubio-Tapia A, Kyle RA, Kaplan EL, et al. Increased prevalence and mortality in undiagnosed celiac disease. Gastroenterology. 2009; 137(1):88–93.
36. Harewood GC, Holub JL, Lieberman DA. Variation in small bowel biopsy performance among diverse endoscopy settings: results from a national endoscopic database. Am J Gastroenterol. 2004;99(9):1790-1794.
37. Brar P, Lee S, Lewis S, et al. Budesonide in the treatment of refractory celiac disease. Am J Gastroenterol. 2007;102(10):2265-2269.
38. Al-Toma A, Verbeek WHM, Hadithi M, et al. Survival in refractory coeliac disease and enteropathy-associated T-cell lymphoma: retrospective evaluation of single-centre experience. Gut. 2007;56(10):1373-1378.
39. Kaukinen K, Mäki M, Partanen J, et al. Celiac disease without villous atrophy: revision of criteria called for. Dig Dis Sci. 2001;46(4):879-887.
40. Mohamed BM, Feighery C, Coates C, et al. The absence of a mucosal lesion on standard histological examination does not exclude diagnosis of celiac disease. Dig Dis Sci. 2008; 53(1):52-61.
41. Fasano A, Catassi C. Current approaches to diagnosis and treatment of celiac disease: an evolving spectrum. Gastroenterology. 2001; 120(3):636-651.
42. US Food and Drug Administration. Topic-specific labeling information (2010). www.fda.gov/Food/LabelingNutrition/FoodLabeling GuidanceRegulatoryInformation/Topic-Specific LabelingInformation/default.htm. Accessed March 28, 2011.
43. Lindfors K, Blomqvist T, Juuti-Uusitalo K, et al. Live probiotic Bifidobacterium lactis bacteria inhibit the toxic effects induced by wheat gliadin in epithelial cell culture. Clin Exp Immunol. 2008;152(3):552-558.
44. Cellier C, Delabesse E, Helmer C, et al; French Coeliac Disease Study Group. Refractory sprue, coeliac disease, and enteropathy-associated T-cell lymphoma. Lancet. 2000;356(9225): 203-208.
45. United European Gastroenterology. When is a coeliac a coeliac? Report of a working group of the United European Gastroenterology Week in Amsterdam, 2001. Eur J Gastroenterol Hepatol. 2001;13(9):1123-1128.
46. Malamut G, Afchain P, Verkarre V, et al. Presentation and long-term follow-up of refractory celiac disease: comparison of type I with type II. Gastroenterology. 2009;136(1):81-90.
47. Al-Toma A, Goerres MS, Meijer JW, et al. Human leukocyte antigen-DQ2 homozygosity and the development of refractory celiac disease and enteropathy-associated T-cell lymphoma. Clin Gastroenterol Hepatol. 2006;4(3): 315-319.
48. Mauriño E, Niveloni S, Cherñavsky A, et al. Azathioprine in refractory sprue: results from a prospective, open-label study. Am J Gastroenterol. 2002;97(10):2595–2602.
49. Tack GJ, Verbeek WHM, Al-Toma A, et al. Evaluation of cladribine treatment in refractory celiac disease type II. World J Gastroenterol. 2011;17(4):506–513.
50. Akobeng AK, Ramanan AV, Buchan I, Heller RF. Effect of breast feeding on risk of coeliac disease: a systematic review and meta-analysis of observational studies. Arch Dis Child. 2006; 91(1):39-43.
51. Rashid M, Butzner JD, Warren R, et al. Home blood testing for celiac disease: recommendations for management. Can Fam Physician. 2009;55(2):151-153.
52. Hershcovici T, Leshno M, Goldin E, et al. Cost effectiveness of mass screening for coeliac disease is determined by time-delay to diagnosis and quality of life on a gluten-free diet. Aliment Pharmacol Ther. 2010;31(8):901-910.
Celiac disease (CD), also known as gluten-sensitive enteropathy or celiac sprue, is an endocrine disorder whose effects are triggered by the ingestion of gluten—the principle storage protein in wheat, rye, and barley.1-3 CD inflicts damage to the mucosa of the small intestine and subsequently to systemic organ tissues. CD can affect any organ in the body.1 The responsible genetic factors are the human leukocyte antigens, HLA -DQ2 and -DQ8, which are present in 40% of the general population but are found in nearly 100% of patients with CD.1,3,4
Though previously considered uncommon, CD has been estimated to affect more than 1% of the general population worldwide.1,4,5 Currently, CD is most reliably identified by positive serum antibodies, specifically immunoglobulin A (IgA) anti-tissue transglutaminase (tTG) and IgA antiendomysial (EMA) antibodies,6 and by a finding of villous atrophy of the intestinal lining on biopsy. The spectrum of presentations of CD is broad, including the “typical” intestinal features of diarrhea, bloating, abdominal pain, and weight loss; or common “atypical” extraintestinal manifestations, such as anemia, osteoporosis, infertility, and neurologic disturbances (eg, peripheral neuropathy7).8 See Table 1.8,9
Prevalence of CD is greater among those with a family history of CD; with autoimmune diseases, especially type 1 diabetes mellitus (T1DM) and thyroiditis; and with certain genetic disorders (ie, Down, Turner, and Williams syndromes).8-15 Because atypical features dominate in older children and adults, many cases escape diagnosis, and patients may be exposed to serious long-term complications, such as infertility and cancer.1
CD is a lifelong condition, necessitating the complete exclusion of gluten-containing products from the diet. In the US food industry, gluten is used in numerous food applications, complicating the patient education and lifestyle changes needed to implement and maintain a gluten-free diet (GFD). However, if a GFD is not strictly followed, the patient’s quality of life can be seriously impaired.1,4,5
AWARENESS ESSENTIAL IN PRIMARY CARE
For the primary care provider (PCP), there is no shortage of patients with gastrointestinal (GI) disorders, thyroid disease, diabetes, anemia, fatigue, or dysmenorrhea; additionally, PCPs regularly treat patients for a number of associated disorders, including anxiety, irritability, and attention deficit. Yet how likely are PCPs to screen patients with these symptoms for CD? And how many patients with CD never receive a diagnosis of the disorder?
In fact, it has been estimated that more than 90% of persons affected by CD are currently undiagnosed.1,4 In one study involving mass screening of 1,000 children ages 2 to 18, it was determined that almost 90% of celiac-positive children had not previously been diagnosed.5 Similarly, in a cohort of 976 adults (median age, 54.3), the diagnostic rate for CD was initially low at 0.27 cases per thousand visits but increased to 11.6 cases per thousand visits after implementation of active screening.4 Based on these data, it has been estimated that more than 2.7 million Americans unknowingly carry this potentially life-threatening genetic disease.1,4,16
Given the potential patient population with undetected, untreated CD, some researchers consider the disorder one of the most common lifelong diseases in the US.1,8,16 CD is closely associated with T1DM and autoimmune thyroiditis, with cross- prevalence at 11% and 6.7%, respectively.8,12,17 The close association between T1DM and CD led the American Diabetes Association18 to amend guidelines in 2009, suggesting screening for CD in all patients newly diagnosed with T1DM.
PATIENT PRESENTATION: ADULTS VERSUS CHILDREN
Most infants and young children with CD present with the typical or “classic” triad of signs: short stature, failure to thrive, and diarrhea; in individual patients, however, the impact of genetics and exposure to gluten over time can cause considerable variation in patient presentation. As patients with undiagnosed CD age, they may present quite differently or even revert to a latent stage and become asymptomatic.19,20
In two separate reviews, it was noted that classic symptoms of CD are not evident in a majority of older children and adults; instead, anemia and fatigue were the predominating symptoms.12,20An important note: The patient with no symptoms or atypical signs of CD may still be experiencing significant damage, inflicted by gluten-induced antibodies, to the intestinal lining and/or mucosal linings in other organ systems—perhaps for years before the disease becomes evident.20
Clinical Findings Differ With Age, Gender
Historically, CD was considered a pediatric syndrome; however, a diagnosis of CD has become increasingly common among older children and adults, especially elderly patients, although symptoms in the latter group are subtle.21-23 Recent, active CD is being diagnosed among men older than 55 more commonly than in women of this age-group; women are generally younger at diagnosis but have experienced symptoms longer.22,23 This later onset in men suggests that antibody seropositivity and the associated active disease may be triggered later in life.8,22
A variety of findings have been reported in the history and physical exam of most patients who present with CD.The most prevalent signs and symptoms are abdominal pain, frequent loose stools, weight loss, joint pain, and weakness.8,11,16 Unlike the pediatric patient with the classic triad of symptoms, adults usually experience more generalized GI manifestations, such as irritable bowel syndrome (IBS), abdominal pain, or acid reflux.10
Many patients have no GI symptoms but may present solely with fatigue, arthralgias, or myalgia.20 In fact, more than 50% of adults with CD present with atypical or extraintestinal disorders, such as anemia, infertility, osteoporosis, neurologic problems, or other autoimmune disorders.8,16,23,24 It is important for clinicians to note that atypical is somewhat typical in the older patient who presents with CD.
Patients with asymptomatic or silent CD, (see “Classification and Pathology,” below) lack both classic and atypical symptoms but still have villous atrophy, usually discovered during endoscopy being conducted for other reasons.8 Because of its predominantly atypical presentations, CD is considered a multisystem endocrine condition rather than one that is mainly gastrointestinal.8,16,25,26
CLASSIFICATION AND PATHOLOGY
Though frequently a silent disorder, CD typically progresses through four stages: classical, atypical, latent, and silent. Clinicians should strive to become fully aware of each stage and its implications.8,26,27
The classical form is primarily diagnosed in children ages 6 to 18 months. It is characterized by villous atrophy and typical symptoms of intestinal malabsorption.8
The patient with atypical CD has minor intestinal symptoms, but architectural abnormalities can be found in the mucosa of the small intestine. This patient is likely to present with various extraintestinal disorders, including osteoporosis, anemia, infertility, and neuropathies.7,8
In the latent form of CD, the HLA-DQ2 and/or -DQ8 genetic markers are present. Serology for CD may be positive, but the intestinal mucosa may be normal. The patient may or may not be experiencing extraintestinal symptoms. In patients with latent CD, the gluten-associated changes appear later in life.8 The precise trigger for late activation of the disease, though apparently linked to genetics and gluten exposure, remains elusive.20,24
The silent form of CD is marked by mucosal abnormalities in the small intestine and usually by positive CD serology, but it is asymptomatic. The iceberg theory of celiac disease28 (see figure28) has been proposed to explain CD’s hidden manifestations over time.
In patients with atypical, latent, or silent CD, the condition is sometimes detected incidentally during screening of at-risk groups or by endoscopy performed for other reasons.8 Most of these patients respond well to GFD therapy, noting both physical and psychological improvement—suggesting that these patients, even though asymptomatic and seemingly healthy, may have been experiencing minor manifestations of undiagnosed CD for many years: decreased appetite, fatigue, and even behavioral abnormalities.1,8
Histopathologic analysis of abnormalities found on biopsy of the small intestine relies on the four-stage Marsh classification29:
• Marsh 0: normal mucosa
• Marsh I: intraepithelial lymphocytosis
• Marsh II: intraepithelial lymphocytosis with crypt hyperplasia
• Marsh III: intraepithelial lymphocytosis with crypt hyperplasia and villous atrophy.8,29 Modifications to this classification have been made by Oberhuber30,31 to denote the degree of villous flattening32 (ie, IIIa, IIIb, IIIc).
Villous atrophy of the mucosa has long been considered the hallmark of CD, and its detection, according to the American Gastroenterological Association,2,26 remains the gold standard in confirming a diagnosis of CD.4,16,26 However, early screening (ie, serologic testing for tTG and EMA) is the necessary initial step in ensuring diagnostic accuracy, as other conditions can cause villous atrophy, and latent CD can coexist with normal intestinal mucosa.10
Avoiding Diagnostic Delays
Because of the broad spectrum of unrelated GI signs in all ages and the subtle presentation in adults, diagnosis of CD in this patient population is frequently delayed for estimated periods ranging from five to 11 years.4,11,23,33
Improving clinician awareness of the manifestations of CD is essential34; too frequently, the common symptoms of probable CD are treated as individual idiopathic disorders by both PCPs and secondary specialists, who prescribe proton pump inhibitors, antihistamines, cathartics, and/or antimotility drugs for years without ruling out a common, easily identified genetic disease. Even though the prevalence of CD has recently been shown to have increased more than fourfold since 1950,35 serologic testing for CD is not widely implemented by PCPs.4,11,20
Specialists, too, may be slow to recognize this treatable autoimmune disorder. In a recent nationwide study, it was found that gastroenterologists performed a small-bowel biopsy in less than 10% of their patients who underwent esophagogastroduodenoscopy (EGD) for likely symptoms of CD.36 Relying solely on clinical expertise and visual recognition of intestinal abnormalities can delay diagnosis for years.4,36 Many patients may never be given a correct diagnosis of CD.
The Role of Serologic Testing
Current data demonstrate that autoimmune diseases are on the rise,8,16,36 and CD can be the primary cause or a contributing factor in several other disorders (see Table 28,16,37,38). Gastroenterologists may be correct in stating that biopsy is the only way to make a diagnosis of CD or to stage CD-associated intestinal damage4,26; yet by implementing a protocol of serologic testing for tTG and EMA in at-risk patients, PCPs could prevent a missed diagnosis on EGD when biopsy has not been considered, as in the case of atypical CD; or when biopsy results are negative in a patient with latent CD.39,40
Because of its high negative predictive value, serologic testing should be conducted first to significantly reduce the probability of suspected CD. Such selective screening should be performed by the PCP before invasive testing by the gastroenterologist and before long-term empiric treatment for idiopathic GERD, IBS, or other unexplained disorders.32,40
Thus, it has been recommended that PCPs perform screening for CD in patients with unexplained chronic GI disturbances or a familial prevalence of CD, or in those who present with the atypical signs of CD or with associated disorders.1,10,16,20 Whether serologic screening results are positive or negative for CD, the patient with classic GI symptoms should undergo endoscopy with biopsy to confirm active disease and to evaluate the extent of intestinal damage—or to explore other causes.26,39 An algorithm2,4,8,11,16,26 illustrating suggested screening, treatment, and follow-up strategies for patients at high risk for CD is shown below.
Catassi and Fasano34 recently proposed a “four out of five” rule, by which diagnosis of CD may be confirmed in patients with at least four of the following five criteria:
• Typical symptoms of CD
• Positive serology (ie, IgA tTG and IgA EMA antibodies)
• Genetic susceptibility (as confirmed by the presence of HLA-DQ2 and HLA-DQ8)
• Small intestine biopsy results indicating celiac enteropathy
• Improvement of CD signs and symptoms following implementation of the GFD.34
CURRENT TREATMENT AND ASSOCIATED CHALLENGES
Because gluten consumption is the principal trigger of CD pathology, a GFD is considered the safest, most effective therapy for the disorder.1,8,10,11,16,19 Implementing and maintaining the GFD involves a considerable learning curve for the patient, the patient’s family, and possibly the provider; to achieve complete recovery, all involved must become knowledgeable regarding gluten-free and gluten-containing products. The patient must be willing and able to avoid those that contain gluten and bear the potentially high costs8 of gluten-free foods.
Even for patients with CD who are determined to comply with the GFD, gluten monitoring can be difficult. There are ways to determine what is a safe level of gluten ingestion for each patient, but trace amounts of gluten are found in many products, including some that are marked “gluten-free.”1,41 The FDA has proposed that a product labeled gluten-free may contain no more than 20 parts per million (ppm, ie, 20 mg/kg) of gluten.42 In other countries, however, acceptable levels may be as high as 200 ppm (200 mg/kg)—which are considered well above the trigger amounts in the average patient with CD.1,41 The complex nature of each patient’s sensitivity to gluten and the ubiquitous presence of gluten as a food source in both industrialized and developing countries make adherence to the GFD challenging.10
It is critical for the PCP to help the patient review all of his or her prescription and OTC pharmaceuticals and nutritional supplements, as these may contain hidden gluten in the form of modified starches and other fillers.41 It may be also advisable to involve the patient’s pharmacist, requesting an assessment for agents that may be suspect.
A management team approach may ensure the most integrative care. In addition to the PCP and the pharmacist, such a team might include a gastroenterologist, an endocrinologist, a nutritionist, and a psychologist, who may be needed to help the patient confront the great life adjustment required, in addition to addressing other behavioral disorders that are common in patients with CD.10,26
See the box for resources that may be beneficial for both patients and their clinicians.
Alternative Medicine Options
Alternative medicine is gaining favor, especially when no drug therapy is currently available to alleviate gluten toxicity. Supplementation with the fat-soluble vitamins (A, D, E, and K), vitamin B12, folic acid, and the minerals calcium and iron, as indicated by serum deficiencies, is recommended.10,20 Supplementation with digestive enzymes, which are known to be deficient in patients with CD as a result of villous atrophy, may help break down undigested gluten proteins; research is under way to find a recombinant enzyme therapy.10 Researchers have recently shown that probiotics (specifically, Bifidobacterium lactis) significantly reduce the immune response when incidental exposure to gluten occurs.43
REFRACTORY CELIAC DISEASE
Patients with late-onset CD, especially those not diagnosed until after age 50, may have a diminished or absent response to dietary therapy. In some patients, histologic signs and clinical symptoms persist or relapse after a prior positive response to a strict GFD, despite continued adherence to the diet for longer than 12 months.44 Once other causes have been carefully excluded, these patients are considered to have refractory celiac disease (RCD). Exact prevalence of RCD is unknown, but Tack et al8 estimate it at 5% of all cases of CD. Relapsing CD resulting from poor adherence to the GFD is not considered true RCD.8,16,37,38
According to researchers for the European Celiac Disease working group,8,45 RCD can be divided into types I and II:
• RCD I, in which normal polyclonal T cells are present in the intestinal lumen
• RCD II, in which abnormal clonal T cells infiltrate the intestinal mucosa, representing premalignancy.45
The histologic picture of RCD mimics that of severe CD. Malabsorption complications, lesions in the intestinal mucosa, and inflammatory lymphocytosis are present.44 Some patients, like those with classical CD, have serology test results that are consistent with CD and an initial response to GFD therapy; after months or years, however, this response subsides. Other patients are immediately unresponsive to GFD and lack the serologic markers for CD.8
A differential diagnosis including other explanations for the manifestations of RCD must be carefully reviewed, with each excluded, through the strategies shown in Table 2. This review is essential, as patients with RCD II have a much worse prognosis than those with RCD I; the associated five-year survival rates are 44% to 58%, versus 85% or greater, respectively.36,46
Additionally, the continued autoimmune expansion of aberrant T cells in patients with RCD II causes early conversion to malignancy, usually within four to six years after diagnosis. Enteropathy-associated T-cell lymphoma is the most common malignancy, occurring in more than 50% of patients with RCD II, and a likely cause of death.3,8,46,47
Treatment for Refractory Celiac Disease
In addition to the GFD, patients with RCD I generally respond well to corticosteroids or other immunosuppressive treatment.8 Use of budesonide, a corticosteroid given in a once-daily, 9-mg dose, has led to almost complete recovery in most patients. Duration of therapy is response-dependent.37
Systemic corticosteroids or other immunosuppressant agents, such as azathioprine, should be reserved for patients with RCD I or RCD II who do not respond to budesonide, as lengthy treatment regimens are required, with considerable risk for adverse effects.35,48
Recently, promising results have been reported in a small, open-label cohort study involving patients with RCD II who underwent five days of treatment with IV cladribine (0.1 mg/kg/d).49
PREVENTION OF CD
A good nutritional start from birth could be the best means of preventing symptomatic CD. According to findings from a meta-analysis of data from four studies, children being breastfed at the time gluten was introduced had a 52% reduction in risk for CD, compared with their peers who were not being breastfed at that time.50
The protection breast milk appears to provide against CD is not clearly understood. One possible mechanism is that breast milk may protect an infant against CD by preventing gastrointestinal infections, as is the case with other infections. The presence of GI infections (eg, rotavirus) in early life could lead to increased permeability of the intestinal mucosa, allowing the passage of gluten into the lamina propria.3,8,50
Extended duration of breastfeeding is also associated with a reduced risk for CD.8,41,50 Long-term studies are needed, however, to determine whether breastfeeding delays CD onset or provides permanent protection against the disorder.
RECENT DEVELOPMENTS
A recently marketed OTC testing kit for CD is now available in Canada and other countries outside the US; this may be an indication of the growing awareness of the numbers of patients with undiagnosed CD. The test parallels the tTG serum test, which in the US is evaluated only in laboratories; it has comparable specificity and sensitivity, with results within 10 minutes. In the US, the FDA has not yet approved the kit, but domestic testing of the product may soon be under way.51
Alternative treatment modalities are currently focusing on the detoxification of wheat components, rapid enzymatic degradation to reduce exposure to gluten, inducing gluten tolerance, inhibiting permeability of the small intestine to gluten (which, it is thought, may prevent many of the systemic manifestations of CD), and finally, development of an immunomodulatory vaccine.8,33 None of these therapies is yet approved.
IMPLICATIONS OF DELAYED DIAGNOSIS
The unrecognized prevalence of CD is a growing issue, as many symptomatic but unscreened patients are frequently misdiagnosed with IBS, chronic fatigue, or other idiopathic disorders. The silent and latent forms of CD are of the greatest concern, as they show minimal signs and can lead to multiple organ system damage and are implicated in other autoimmune disorders. The longer diagnosis is delayed, the greater is patients’ resistance to dietary therapy, and the less likely that established intestinal and/or neurologic damage can be reversed.10,20,51
The large proportion of undiagnosed celiac patients may account for an accompanying underestimated cost to both the patient and the health care system because of repeated referrals to investigate unexplained disorders before an accurate diagnosis is made. In one recent analysis, mass screening for CD in a young adult population led to improved quality-of-life years by shortening the time to diagnosis and treatment; it was also found cost-effective.52 PCPs must be attentive to patients who may be at high risk for CD and implement combined serum tTG and EMA screening as the initial step in identification and treatment.4,10,11,20 Some form of standardized screening protocol may become inevitable.
CONCLUSION
The prevalence of CD has increased more than fourfold since 1950, and diagnosis is often significantly delayed. Increased awareness is needed among PCPs that CD in adults is likely to manifest with atypical (ie, nongastrointestinal) symptoms and signs. Judicious use of serologic screening for CD would lead to earlier diagnosis and more effective treatment, possibly preventing the potentially lethal refractory disease forms associated with chronic untreated CD.
REFERENCES
1. Ramos M, Orozovich P, Moser K, et al. Health 1. Catassi C, Fasano A. Celiac disease. Curr Opin Gastroenterol. 2008;24(6):687-691.
2. AGA Institute. AGA Institute medical position statement on the diagnosis and management of celiac disease. Gastroenterology. 2006;131(6):1977-1980.
3. Green PH, Jabri B. Coeliac disease. Lancet. 2003;362(9381):383-391.
4. Catassi C, Kryszak D, Louis-Jacques O, et al. Detection of celiac disease in primary care: a multicenter case-finding study in North America. Am J Gastroenterol. 2007;102(7);1454-1460.
5. Demirçeken FG, Kansu A, Kuloglu Z, et al. Human tissue transglutaminase antibody screening by immunochromatographic line immunoassay for early diagnosis of celiac disease in Turkish children. Turk J Gastroenterol. 2008;19(1):14-21.
6. van der Windt DA, Jellema P, Mulder CJ, et al. Diagnostic testing for celiac disease among patients with abdominal symptoms: a systematic review. JAMA. 2010;303(17):1738-1746.
7. Freeman HJ. Neurological disorders in adult celiac disease. Can J Gastroenterol. 2008; 22(11):909-911.
8. Tack GJ, Verbeek WHM, Schreurs MWJ, Mulder CJJ. The spectrum of celiac disease: epidemiology, clinical aspects and treatment. Nat Rev Gastroenterol Hepatol. 2010;7(4):204-213.
9. Farrell RJ, Kelly CP. Celiac sprue. N Engl J Med. 2002;346(3):180-188.
10. Green PHR, Cellier C. Celiac disease. N Engl J Med. 2007;357(17):1731-1743.
11. Fasano A, Berti I, Gerarduzzi T, et al. Prevalence of celiac disease in at-risk and not-at-risk groups in the United States: a large multicenter study. Arch Intern Med. 2003;163(3):286-292.
12. Sud S, Marcon M, Assor E, et al. Celiac disease and pediatric type 1 diabetes: diagnostic and treatment dilemmas. Int J Pediatr Endocrinol. 2010;2010:161285. Epub 2010 Jun 23.
13. Swigonski NL, Kuhlenschmidt HL, Bull MJ, et al. Screening for celiac disease in asymptomatic children with Down syndrome: cost-effectiveness of preventing lymphoma. Pediatrics. 2006;118(2):594-602.
14. Bonamico M, Pasquino AM, Mariani P, et al; Italian Society of Pediatric Gastroenterology Hepatology (SIGEP); Italian Study Group for Turner Syndrome (ISGTS). Prevalence and clinical picture of celiac disease in Turner syndrome. J Clin Endocrinol Metab. 2002;87(12): 5495-5498.
15. Giannotti A, Tiberio G, Castro M, et al. Coeliac disease in Williams syndrome. J Med Genet. 2001;38(11):767–768.
16. Alaedini A, Green P. Narrative review: celiac disease: understanding a complex autoimmune disorder. Ann Intern Med. 2005;142(4): 289-298.
17. Fröhlich-Reiterer EE, Hofer S, Kaspers S, et al. Screening frequency for celiac disease and autoimmune thyroiditis in children and adolescents with type 1 diabetes mellitus: data from a German/Austrian multicentre survey. Pediatr Diabetes. 2008;9(6):546-553.
18. American Diabetes Association. Standards of medical care in diabetes—2009. Diabetes Care. 2009;32(1):S13–S61.
19. Losowsky MS. A history of coeliac disease. Dig Dis. 2008;26(2):112-120.
20. Evans KE, Hadjivassilou M, Sanders DS. Understanding ‘silent’ coeliac disease: complications in diagnosis and treatment. Gastrointest Nurs. 2010;8(2):26-32.
21. Lurie Y, Landau DA, Pfeffer J, Oren R. Celiac disease diagnosed in the elderly. J Clin Gastroenterol. 2008;42(1):59-61.
22. Vilppula A, Kaukinen K, Luostarinen L, et al. Increasing prevalence and high incidence of celiac disease in elderly people: a population-based study. BMC Gastroenterol. 2009 Jun 29;9:49.
23. Lo W, Sano K, Lebwohl B, et al. Changing presentation of adult celiac disease. Dig Dis Sci. 2003;48(2):395-398.
24. Alaedini A, Okamoto H, Briani C, et al. Immune cross-reactivity in celiac disease: anti-gliadin antibodies bind to neuronal synapsin I. J Immunol. 2007;178(10):6590-6595.
25. Tursi A, Giorgetti G, Brandimarte G, et al. Prevalence and clinical presentation of subclinical/silent celiac disease in adults: an analysis on a 12-year observation. Hepatogastroenterology. 2001;48(38):462-464.
26. Rostom A, Murray JA, Kagnoff MF. American Gastroenterological Association (AGA) Institute technical review on the diagnosis and management of celiac disease. Gastroenterology. 2006;131(6):1981-2002.
27. Ferguson A, Arranz E, O’Mahony S. Clinical and pathological spectrum of coeliac disease—active, silent, latent, potential. Gut. 1993;34(2): 150-151.
28. Logan RFA. Problems and pitfalls in epidemiological studies of coeliac disease. In: Auricchio S, Visakorpi JK, eds. Common Food Intolerances 1. Epidemiology of Coeliac Disease (Dynamic Nutrition Research)(Pt 1). Basel, Switzerland: Karger; 1992:14-22.
29. Marsh MN. Gluten, major histocompatibility complex, and the small intestine: a molecular and immunobiologic approach to the spectrum of gluten sensitivity (‘celiac sprue’). Gastroenterology. 1992;102(1):330-354.
30. Oberhuber G, Granditsch G, Vogelsang H. The histopathology of coeliac disease: time for a standardized report scheme for pathologists. Eur J Gastroenterol Hepatol. 1999;11(10):1185-1194.
31. Corazza GR, Villanaci V. Coeliac disease.
J Clin Pathol. 2005;58(6):573-574.
32. Hadithi M, von Blomberg BM, Crusius JB, et al. Accuracy of serologic tests and HLA-DQ typing for diagnosing celiac disease. Ann Intern Med. 2007;147(5):294-302.
33. Lerner A. New therapeutic strategies for celiac disease. Autoimmun Rev. 2010;9(3):144-147.
34. Catassi C, Fasano A. Celiac disease diagnosis: simple rules are better than complicated algorithms. Am J Med. 2010;123(8):691-693.
35. Rubio-Tapia A, Kyle RA, Kaplan EL, et al. Increased prevalence and mortality in undiagnosed celiac disease. Gastroenterology. 2009; 137(1):88–93.
36. Harewood GC, Holub JL, Lieberman DA. Variation in small bowel biopsy performance among diverse endoscopy settings: results from a national endoscopic database. Am J Gastroenterol. 2004;99(9):1790-1794.
37. Brar P, Lee S, Lewis S, et al. Budesonide in the treatment of refractory celiac disease. Am J Gastroenterol. 2007;102(10):2265-2269.
38. Al-Toma A, Verbeek WHM, Hadithi M, et al. Survival in refractory coeliac disease and enteropathy-associated T-cell lymphoma: retrospective evaluation of single-centre experience. Gut. 2007;56(10):1373-1378.
39. Kaukinen K, Mäki M, Partanen J, et al. Celiac disease without villous atrophy: revision of criteria called for. Dig Dis Sci. 2001;46(4):879-887.
40. Mohamed BM, Feighery C, Coates C, et al. The absence of a mucosal lesion on standard histological examination does not exclude diagnosis of celiac disease. Dig Dis Sci. 2008; 53(1):52-61.
41. Fasano A, Catassi C. Current approaches to diagnosis and treatment of celiac disease: an evolving spectrum. Gastroenterology. 2001; 120(3):636-651.
42. US Food and Drug Administration. Topic-specific labeling information (2010). www.fda.gov/Food/LabelingNutrition/FoodLabeling GuidanceRegulatoryInformation/Topic-Specific LabelingInformation/default.htm. Accessed March 28, 2011.
43. Lindfors K, Blomqvist T, Juuti-Uusitalo K, et al. Live probiotic Bifidobacterium lactis bacteria inhibit the toxic effects induced by wheat gliadin in epithelial cell culture. Clin Exp Immunol. 2008;152(3):552-558.
44. Cellier C, Delabesse E, Helmer C, et al; French Coeliac Disease Study Group. Refractory sprue, coeliac disease, and enteropathy-associated T-cell lymphoma. Lancet. 2000;356(9225): 203-208.
45. United European Gastroenterology. When is a coeliac a coeliac? Report of a working group of the United European Gastroenterology Week in Amsterdam, 2001. Eur J Gastroenterol Hepatol. 2001;13(9):1123-1128.
46. Malamut G, Afchain P, Verkarre V, et al. Presentation and long-term follow-up of refractory celiac disease: comparison of type I with type II. Gastroenterology. 2009;136(1):81-90.
47. Al-Toma A, Goerres MS, Meijer JW, et al. Human leukocyte antigen-DQ2 homozygosity and the development of refractory celiac disease and enteropathy-associated T-cell lymphoma. Clin Gastroenterol Hepatol. 2006;4(3): 315-319.
48. Mauriño E, Niveloni S, Cherñavsky A, et al. Azathioprine in refractory sprue: results from a prospective, open-label study. Am J Gastroenterol. 2002;97(10):2595–2602.
49. Tack GJ, Verbeek WHM, Al-Toma A, et al. Evaluation of cladribine treatment in refractory celiac disease type II. World J Gastroenterol. 2011;17(4):506–513.
50. Akobeng AK, Ramanan AV, Buchan I, Heller RF. Effect of breast feeding on risk of coeliac disease: a systematic review and meta-analysis of observational studies. Arch Dis Child. 2006; 91(1):39-43.
51. Rashid M, Butzner JD, Warren R, et al. Home blood testing for celiac disease: recommendations for management. Can Fam Physician. 2009;55(2):151-153.
52. Hershcovici T, Leshno M, Goldin E, et al. Cost effectiveness of mass screening for coeliac disease is determined by time-delay to diagnosis and quality of life on a gluten-free diet. Aliment Pharmacol Ther. 2010;31(8):901-910.
Celiac disease (CD), also known as gluten-sensitive enteropathy or celiac sprue, is an endocrine disorder whose effects are triggered by the ingestion of gluten—the principle storage protein in wheat, rye, and barley.1-3 CD inflicts damage to the mucosa of the small intestine and subsequently to systemic organ tissues. CD can affect any organ in the body.1 The responsible genetic factors are the human leukocyte antigens, HLA -DQ2 and -DQ8, which are present in 40% of the general population but are found in nearly 100% of patients with CD.1,3,4
Though previously considered uncommon, CD has been estimated to affect more than 1% of the general population worldwide.1,4,5 Currently, CD is most reliably identified by positive serum antibodies, specifically immunoglobulin A (IgA) anti-tissue transglutaminase (tTG) and IgA antiendomysial (EMA) antibodies,6 and by a finding of villous atrophy of the intestinal lining on biopsy. The spectrum of presentations of CD is broad, including the “typical” intestinal features of diarrhea, bloating, abdominal pain, and weight loss; or common “atypical” extraintestinal manifestations, such as anemia, osteoporosis, infertility, and neurologic disturbances (eg, peripheral neuropathy7).8 See Table 1.8,9
Prevalence of CD is greater among those with a family history of CD; with autoimmune diseases, especially type 1 diabetes mellitus (T1DM) and thyroiditis; and with certain genetic disorders (ie, Down, Turner, and Williams syndromes).8-15 Because atypical features dominate in older children and adults, many cases escape diagnosis, and patients may be exposed to serious long-term complications, such as infertility and cancer.1
CD is a lifelong condition, necessitating the complete exclusion of gluten-containing products from the diet. In the US food industry, gluten is used in numerous food applications, complicating the patient education and lifestyle changes needed to implement and maintain a gluten-free diet (GFD). However, if a GFD is not strictly followed, the patient’s quality of life can be seriously impaired.1,4,5
AWARENESS ESSENTIAL IN PRIMARY CARE
For the primary care provider (PCP), there is no shortage of patients with gastrointestinal (GI) disorders, thyroid disease, diabetes, anemia, fatigue, or dysmenorrhea; additionally, PCPs regularly treat patients for a number of associated disorders, including anxiety, irritability, and attention deficit. Yet how likely are PCPs to screen patients with these symptoms for CD? And how many patients with CD never receive a diagnosis of the disorder?
In fact, it has been estimated that more than 90% of persons affected by CD are currently undiagnosed.1,4 In one study involving mass screening of 1,000 children ages 2 to 18, it was determined that almost 90% of celiac-positive children had not previously been diagnosed.5 Similarly, in a cohort of 976 adults (median age, 54.3), the diagnostic rate for CD was initially low at 0.27 cases per thousand visits but increased to 11.6 cases per thousand visits after implementation of active screening.4 Based on these data, it has been estimated that more than 2.7 million Americans unknowingly carry this potentially life-threatening genetic disease.1,4,16
Given the potential patient population with undetected, untreated CD, some researchers consider the disorder one of the most common lifelong diseases in the US.1,8,16 CD is closely associated with T1DM and autoimmune thyroiditis, with cross- prevalence at 11% and 6.7%, respectively.8,12,17 The close association between T1DM and CD led the American Diabetes Association18 to amend guidelines in 2009, suggesting screening for CD in all patients newly diagnosed with T1DM.
PATIENT PRESENTATION: ADULTS VERSUS CHILDREN
Most infants and young children with CD present with the typical or “classic” triad of signs: short stature, failure to thrive, and diarrhea; in individual patients, however, the impact of genetics and exposure to gluten over time can cause considerable variation in patient presentation. As patients with undiagnosed CD age, they may present quite differently or even revert to a latent stage and become asymptomatic.19,20
In two separate reviews, it was noted that classic symptoms of CD are not evident in a majority of older children and adults; instead, anemia and fatigue were the predominating symptoms.12,20An important note: The patient with no symptoms or atypical signs of CD may still be experiencing significant damage, inflicted by gluten-induced antibodies, to the intestinal lining and/or mucosal linings in other organ systems—perhaps for years before the disease becomes evident.20
Clinical Findings Differ With Age, Gender
Historically, CD was considered a pediatric syndrome; however, a diagnosis of CD has become increasingly common among older children and adults, especially elderly patients, although symptoms in the latter group are subtle.21-23 Recent, active CD is being diagnosed among men older than 55 more commonly than in women of this age-group; women are generally younger at diagnosis but have experienced symptoms longer.22,23 This later onset in men suggests that antibody seropositivity and the associated active disease may be triggered later in life.8,22
A variety of findings have been reported in the history and physical exam of most patients who present with CD.The most prevalent signs and symptoms are abdominal pain, frequent loose stools, weight loss, joint pain, and weakness.8,11,16 Unlike the pediatric patient with the classic triad of symptoms, adults usually experience more generalized GI manifestations, such as irritable bowel syndrome (IBS), abdominal pain, or acid reflux.10
Many patients have no GI symptoms but may present solely with fatigue, arthralgias, or myalgia.20 In fact, more than 50% of adults with CD present with atypical or extraintestinal disorders, such as anemia, infertility, osteoporosis, neurologic problems, or other autoimmune disorders.8,16,23,24 It is important for clinicians to note that atypical is somewhat typical in the older patient who presents with CD.
Patients with asymptomatic or silent CD, (see “Classification and Pathology,” below) lack both classic and atypical symptoms but still have villous atrophy, usually discovered during endoscopy being conducted for other reasons.8 Because of its predominantly atypical presentations, CD is considered a multisystem endocrine condition rather than one that is mainly gastrointestinal.8,16,25,26
CLASSIFICATION AND PATHOLOGY
Though frequently a silent disorder, CD typically progresses through four stages: classical, atypical, latent, and silent. Clinicians should strive to become fully aware of each stage and its implications.8,26,27
The classical form is primarily diagnosed in children ages 6 to 18 months. It is characterized by villous atrophy and typical symptoms of intestinal malabsorption.8
The patient with atypical CD has minor intestinal symptoms, but architectural abnormalities can be found in the mucosa of the small intestine. This patient is likely to present with various extraintestinal disorders, including osteoporosis, anemia, infertility, and neuropathies.7,8
In the latent form of CD, the HLA-DQ2 and/or -DQ8 genetic markers are present. Serology for CD may be positive, but the intestinal mucosa may be normal. The patient may or may not be experiencing extraintestinal symptoms. In patients with latent CD, the gluten-associated changes appear later in life.8 The precise trigger for late activation of the disease, though apparently linked to genetics and gluten exposure, remains elusive.20,24
The silent form of CD is marked by mucosal abnormalities in the small intestine and usually by positive CD serology, but it is asymptomatic. The iceberg theory of celiac disease28 (see figure28) has been proposed to explain CD’s hidden manifestations over time.
In patients with atypical, latent, or silent CD, the condition is sometimes detected incidentally during screening of at-risk groups or by endoscopy performed for other reasons.8 Most of these patients respond well to GFD therapy, noting both physical and psychological improvement—suggesting that these patients, even though asymptomatic and seemingly healthy, may have been experiencing minor manifestations of undiagnosed CD for many years: decreased appetite, fatigue, and even behavioral abnormalities.1,8
Histopathologic analysis of abnormalities found on biopsy of the small intestine relies on the four-stage Marsh classification29:
• Marsh 0: normal mucosa
• Marsh I: intraepithelial lymphocytosis
• Marsh II: intraepithelial lymphocytosis with crypt hyperplasia
• Marsh III: intraepithelial lymphocytosis with crypt hyperplasia and villous atrophy.8,29 Modifications to this classification have been made by Oberhuber30,31 to denote the degree of villous flattening32 (ie, IIIa, IIIb, IIIc).
Villous atrophy of the mucosa has long been considered the hallmark of CD, and its detection, according to the American Gastroenterological Association,2,26 remains the gold standard in confirming a diagnosis of CD.4,16,26 However, early screening (ie, serologic testing for tTG and EMA) is the necessary initial step in ensuring diagnostic accuracy, as other conditions can cause villous atrophy, and latent CD can coexist with normal intestinal mucosa.10
Avoiding Diagnostic Delays
Because of the broad spectrum of unrelated GI signs in all ages and the subtle presentation in adults, diagnosis of CD in this patient population is frequently delayed for estimated periods ranging from five to 11 years.4,11,23,33
Improving clinician awareness of the manifestations of CD is essential34; too frequently, the common symptoms of probable CD are treated as individual idiopathic disorders by both PCPs and secondary specialists, who prescribe proton pump inhibitors, antihistamines, cathartics, and/or antimotility drugs for years without ruling out a common, easily identified genetic disease. Even though the prevalence of CD has recently been shown to have increased more than fourfold since 1950,35 serologic testing for CD is not widely implemented by PCPs.4,11,20
Specialists, too, may be slow to recognize this treatable autoimmune disorder. In a recent nationwide study, it was found that gastroenterologists performed a small-bowel biopsy in less than 10% of their patients who underwent esophagogastroduodenoscopy (EGD) for likely symptoms of CD.36 Relying solely on clinical expertise and visual recognition of intestinal abnormalities can delay diagnosis for years.4,36 Many patients may never be given a correct diagnosis of CD.
The Role of Serologic Testing
Current data demonstrate that autoimmune diseases are on the rise,8,16,36 and CD can be the primary cause or a contributing factor in several other disorders (see Table 28,16,37,38). Gastroenterologists may be correct in stating that biopsy is the only way to make a diagnosis of CD or to stage CD-associated intestinal damage4,26; yet by implementing a protocol of serologic testing for tTG and EMA in at-risk patients, PCPs could prevent a missed diagnosis on EGD when biopsy has not been considered, as in the case of atypical CD; or when biopsy results are negative in a patient with latent CD.39,40
Because of its high negative predictive value, serologic testing should be conducted first to significantly reduce the probability of suspected CD. Such selective screening should be performed by the PCP before invasive testing by the gastroenterologist and before long-term empiric treatment for idiopathic GERD, IBS, or other unexplained disorders.32,40
Thus, it has been recommended that PCPs perform screening for CD in patients with unexplained chronic GI disturbances or a familial prevalence of CD, or in those who present with the atypical signs of CD or with associated disorders.1,10,16,20 Whether serologic screening results are positive or negative for CD, the patient with classic GI symptoms should undergo endoscopy with biopsy to confirm active disease and to evaluate the extent of intestinal damage—or to explore other causes.26,39 An algorithm2,4,8,11,16,26 illustrating suggested screening, treatment, and follow-up strategies for patients at high risk for CD is shown below.
Catassi and Fasano34 recently proposed a “four out of five” rule, by which diagnosis of CD may be confirmed in patients with at least four of the following five criteria:
• Typical symptoms of CD
• Positive serology (ie, IgA tTG and IgA EMA antibodies)
• Genetic susceptibility (as confirmed by the presence of HLA-DQ2 and HLA-DQ8)
• Small intestine biopsy results indicating celiac enteropathy
• Improvement of CD signs and symptoms following implementation of the GFD.34
CURRENT TREATMENT AND ASSOCIATED CHALLENGES
Because gluten consumption is the principal trigger of CD pathology, a GFD is considered the safest, most effective therapy for the disorder.1,8,10,11,16,19 Implementing and maintaining the GFD involves a considerable learning curve for the patient, the patient’s family, and possibly the provider; to achieve complete recovery, all involved must become knowledgeable regarding gluten-free and gluten-containing products. The patient must be willing and able to avoid those that contain gluten and bear the potentially high costs8 of gluten-free foods.
Even for patients with CD who are determined to comply with the GFD, gluten monitoring can be difficult. There are ways to determine what is a safe level of gluten ingestion for each patient, but trace amounts of gluten are found in many products, including some that are marked “gluten-free.”1,41 The FDA has proposed that a product labeled gluten-free may contain no more than 20 parts per million (ppm, ie, 20 mg/kg) of gluten.42 In other countries, however, acceptable levels may be as high as 200 ppm (200 mg/kg)—which are considered well above the trigger amounts in the average patient with CD.1,41 The complex nature of each patient’s sensitivity to gluten and the ubiquitous presence of gluten as a food source in both industrialized and developing countries make adherence to the GFD challenging.10
It is critical for the PCP to help the patient review all of his or her prescription and OTC pharmaceuticals and nutritional supplements, as these may contain hidden gluten in the form of modified starches and other fillers.41 It may be also advisable to involve the patient’s pharmacist, requesting an assessment for agents that may be suspect.
A management team approach may ensure the most integrative care. In addition to the PCP and the pharmacist, such a team might include a gastroenterologist, an endocrinologist, a nutritionist, and a psychologist, who may be needed to help the patient confront the great life adjustment required, in addition to addressing other behavioral disorders that are common in patients with CD.10,26
See the box for resources that may be beneficial for both patients and their clinicians.
Alternative Medicine Options
Alternative medicine is gaining favor, especially when no drug therapy is currently available to alleviate gluten toxicity. Supplementation with the fat-soluble vitamins (A, D, E, and K), vitamin B12, folic acid, and the minerals calcium and iron, as indicated by serum deficiencies, is recommended.10,20 Supplementation with digestive enzymes, which are known to be deficient in patients with CD as a result of villous atrophy, may help break down undigested gluten proteins; research is under way to find a recombinant enzyme therapy.10 Researchers have recently shown that probiotics (specifically, Bifidobacterium lactis) significantly reduce the immune response when incidental exposure to gluten occurs.43
REFRACTORY CELIAC DISEASE
Patients with late-onset CD, especially those not diagnosed until after age 50, may have a diminished or absent response to dietary therapy. In some patients, histologic signs and clinical symptoms persist or relapse after a prior positive response to a strict GFD, despite continued adherence to the diet for longer than 12 months.44 Once other causes have been carefully excluded, these patients are considered to have refractory celiac disease (RCD). Exact prevalence of RCD is unknown, but Tack et al8 estimate it at 5% of all cases of CD. Relapsing CD resulting from poor adherence to the GFD is not considered true RCD.8,16,37,38
According to researchers for the European Celiac Disease working group,8,45 RCD can be divided into types I and II:
• RCD I, in which normal polyclonal T cells are present in the intestinal lumen
• RCD II, in which abnormal clonal T cells infiltrate the intestinal mucosa, representing premalignancy.45
The histologic picture of RCD mimics that of severe CD. Malabsorption complications, lesions in the intestinal mucosa, and inflammatory lymphocytosis are present.44 Some patients, like those with classical CD, have serology test results that are consistent with CD and an initial response to GFD therapy; after months or years, however, this response subsides. Other patients are immediately unresponsive to GFD and lack the serologic markers for CD.8
A differential diagnosis including other explanations for the manifestations of RCD must be carefully reviewed, with each excluded, through the strategies shown in Table 2. This review is essential, as patients with RCD II have a much worse prognosis than those with RCD I; the associated five-year survival rates are 44% to 58%, versus 85% or greater, respectively.36,46
Additionally, the continued autoimmune expansion of aberrant T cells in patients with RCD II causes early conversion to malignancy, usually within four to six years after diagnosis. Enteropathy-associated T-cell lymphoma is the most common malignancy, occurring in more than 50% of patients with RCD II, and a likely cause of death.3,8,46,47
Treatment for Refractory Celiac Disease
In addition to the GFD, patients with RCD I generally respond well to corticosteroids or other immunosuppressive treatment.8 Use of budesonide, a corticosteroid given in a once-daily, 9-mg dose, has led to almost complete recovery in most patients. Duration of therapy is response-dependent.37
Systemic corticosteroids or other immunosuppressant agents, such as azathioprine, should be reserved for patients with RCD I or RCD II who do not respond to budesonide, as lengthy treatment regimens are required, with considerable risk for adverse effects.35,48
Recently, promising results have been reported in a small, open-label cohort study involving patients with RCD II who underwent five days of treatment with IV cladribine (0.1 mg/kg/d).49
PREVENTION OF CD
A good nutritional start from birth could be the best means of preventing symptomatic CD. According to findings from a meta-analysis of data from four studies, children being breastfed at the time gluten was introduced had a 52% reduction in risk for CD, compared with their peers who were not being breastfed at that time.50
The protection breast milk appears to provide against CD is not clearly understood. One possible mechanism is that breast milk may protect an infant against CD by preventing gastrointestinal infections, as is the case with other infections. The presence of GI infections (eg, rotavirus) in early life could lead to increased permeability of the intestinal mucosa, allowing the passage of gluten into the lamina propria.3,8,50
Extended duration of breastfeeding is also associated with a reduced risk for CD.8,41,50 Long-term studies are needed, however, to determine whether breastfeeding delays CD onset or provides permanent protection against the disorder.
RECENT DEVELOPMENTS
A recently marketed OTC testing kit for CD is now available in Canada and other countries outside the US; this may be an indication of the growing awareness of the numbers of patients with undiagnosed CD. The test parallels the tTG serum test, which in the US is evaluated only in laboratories; it has comparable specificity and sensitivity, with results within 10 minutes. In the US, the FDA has not yet approved the kit, but domestic testing of the product may soon be under way.51
Alternative treatment modalities are currently focusing on the detoxification of wheat components, rapid enzymatic degradation to reduce exposure to gluten, inducing gluten tolerance, inhibiting permeability of the small intestine to gluten (which, it is thought, may prevent many of the systemic manifestations of CD), and finally, development of an immunomodulatory vaccine.8,33 None of these therapies is yet approved.
IMPLICATIONS OF DELAYED DIAGNOSIS
The unrecognized prevalence of CD is a growing issue, as many symptomatic but unscreened patients are frequently misdiagnosed with IBS, chronic fatigue, or other idiopathic disorders. The silent and latent forms of CD are of the greatest concern, as they show minimal signs and can lead to multiple organ system damage and are implicated in other autoimmune disorders. The longer diagnosis is delayed, the greater is patients’ resistance to dietary therapy, and the less likely that established intestinal and/or neurologic damage can be reversed.10,20,51
The large proportion of undiagnosed celiac patients may account for an accompanying underestimated cost to both the patient and the health care system because of repeated referrals to investigate unexplained disorders before an accurate diagnosis is made. In one recent analysis, mass screening for CD in a young adult population led to improved quality-of-life years by shortening the time to diagnosis and treatment; it was also found cost-effective.52 PCPs must be attentive to patients who may be at high risk for CD and implement combined serum tTG and EMA screening as the initial step in identification and treatment.4,10,11,20 Some form of standardized screening protocol may become inevitable.
CONCLUSION
The prevalence of CD has increased more than fourfold since 1950, and diagnosis is often significantly delayed. Increased awareness is needed among PCPs that CD in adults is likely to manifest with atypical (ie, nongastrointestinal) symptoms and signs. Judicious use of serologic screening for CD would lead to earlier diagnosis and more effective treatment, possibly preventing the potentially lethal refractory disease forms associated with chronic untreated CD.
REFERENCES
1. Ramos M, Orozovich P, Moser K, et al. Health 1. Catassi C, Fasano A. Celiac disease. Curr Opin Gastroenterol. 2008;24(6):687-691.
2. AGA Institute. AGA Institute medical position statement on the diagnosis and management of celiac disease. Gastroenterology. 2006;131(6):1977-1980.
3. Green PH, Jabri B. Coeliac disease. Lancet. 2003;362(9381):383-391.
4. Catassi C, Kryszak D, Louis-Jacques O, et al. Detection of celiac disease in primary care: a multicenter case-finding study in North America. Am J Gastroenterol. 2007;102(7);1454-1460.
5. Demirçeken FG, Kansu A, Kuloglu Z, et al. Human tissue transglutaminase antibody screening by immunochromatographic line immunoassay for early diagnosis of celiac disease in Turkish children. Turk J Gastroenterol. 2008;19(1):14-21.
6. van der Windt DA, Jellema P, Mulder CJ, et al. Diagnostic testing for celiac disease among patients with abdominal symptoms: a systematic review. JAMA. 2010;303(17):1738-1746.
7. Freeman HJ. Neurological disorders in adult celiac disease. Can J Gastroenterol. 2008; 22(11):909-911.
8. Tack GJ, Verbeek WHM, Schreurs MWJ, Mulder CJJ. The spectrum of celiac disease: epidemiology, clinical aspects and treatment. Nat Rev Gastroenterol Hepatol. 2010;7(4):204-213.
9. Farrell RJ, Kelly CP. Celiac sprue. N Engl J Med. 2002;346(3):180-188.
10. Green PHR, Cellier C. Celiac disease. N Engl J Med. 2007;357(17):1731-1743.
11. Fasano A, Berti I, Gerarduzzi T, et al. Prevalence of celiac disease in at-risk and not-at-risk groups in the United States: a large multicenter study. Arch Intern Med. 2003;163(3):286-292.
12. Sud S, Marcon M, Assor E, et al. Celiac disease and pediatric type 1 diabetes: diagnostic and treatment dilemmas. Int J Pediatr Endocrinol. 2010;2010:161285. Epub 2010 Jun 23.
13. Swigonski NL, Kuhlenschmidt HL, Bull MJ, et al. Screening for celiac disease in asymptomatic children with Down syndrome: cost-effectiveness of preventing lymphoma. Pediatrics. 2006;118(2):594-602.
14. Bonamico M, Pasquino AM, Mariani P, et al; Italian Society of Pediatric Gastroenterology Hepatology (SIGEP); Italian Study Group for Turner Syndrome (ISGTS). Prevalence and clinical picture of celiac disease in Turner syndrome. J Clin Endocrinol Metab. 2002;87(12): 5495-5498.
15. Giannotti A, Tiberio G, Castro M, et al. Coeliac disease in Williams syndrome. J Med Genet. 2001;38(11):767–768.
16. Alaedini A, Green P. Narrative review: celiac disease: understanding a complex autoimmune disorder. Ann Intern Med. 2005;142(4): 289-298.
17. Fröhlich-Reiterer EE, Hofer S, Kaspers S, et al. Screening frequency for celiac disease and autoimmune thyroiditis in children and adolescents with type 1 diabetes mellitus: data from a German/Austrian multicentre survey. Pediatr Diabetes. 2008;9(6):546-553.
18. American Diabetes Association. Standards of medical care in diabetes—2009. Diabetes Care. 2009;32(1):S13–S61.
19. Losowsky MS. A history of coeliac disease. Dig Dis. 2008;26(2):112-120.
20. Evans KE, Hadjivassilou M, Sanders DS. Understanding ‘silent’ coeliac disease: complications in diagnosis and treatment. Gastrointest Nurs. 2010;8(2):26-32.
21. Lurie Y, Landau DA, Pfeffer J, Oren R. Celiac disease diagnosed in the elderly. J Clin Gastroenterol. 2008;42(1):59-61.
22. Vilppula A, Kaukinen K, Luostarinen L, et al. Increasing prevalence and high incidence of celiac disease in elderly people: a population-based study. BMC Gastroenterol. 2009 Jun 29;9:49.
23. Lo W, Sano K, Lebwohl B, et al. Changing presentation of adult celiac disease. Dig Dis Sci. 2003;48(2):395-398.
24. Alaedini A, Okamoto H, Briani C, et al. Immune cross-reactivity in celiac disease: anti-gliadin antibodies bind to neuronal synapsin I. J Immunol. 2007;178(10):6590-6595.
25. Tursi A, Giorgetti G, Brandimarte G, et al. Prevalence and clinical presentation of subclinical/silent celiac disease in adults: an analysis on a 12-year observation. Hepatogastroenterology. 2001;48(38):462-464.
26. Rostom A, Murray JA, Kagnoff MF. American Gastroenterological Association (AGA) Institute technical review on the diagnosis and management of celiac disease. Gastroenterology. 2006;131(6):1981-2002.
27. Ferguson A, Arranz E, O’Mahony S. Clinical and pathological spectrum of coeliac disease—active, silent, latent, potential. Gut. 1993;34(2): 150-151.
28. Logan RFA. Problems and pitfalls in epidemiological studies of coeliac disease. In: Auricchio S, Visakorpi JK, eds. Common Food Intolerances 1. Epidemiology of Coeliac Disease (Dynamic Nutrition Research)(Pt 1). Basel, Switzerland: Karger; 1992:14-22.
29. Marsh MN. Gluten, major histocompatibility complex, and the small intestine: a molecular and immunobiologic approach to the spectrum of gluten sensitivity (‘celiac sprue’). Gastroenterology. 1992;102(1):330-354.
30. Oberhuber G, Granditsch G, Vogelsang H. The histopathology of coeliac disease: time for a standardized report scheme for pathologists. Eur J Gastroenterol Hepatol. 1999;11(10):1185-1194.
31. Corazza GR, Villanaci V. Coeliac disease.
J Clin Pathol. 2005;58(6):573-574.
32. Hadithi M, von Blomberg BM, Crusius JB, et al. Accuracy of serologic tests and HLA-DQ typing for diagnosing celiac disease. Ann Intern Med. 2007;147(5):294-302.
33. Lerner A. New therapeutic strategies for celiac disease. Autoimmun Rev. 2010;9(3):144-147.
34. Catassi C, Fasano A. Celiac disease diagnosis: simple rules are better than complicated algorithms. Am J Med. 2010;123(8):691-693.
35. Rubio-Tapia A, Kyle RA, Kaplan EL, et al. Increased prevalence and mortality in undiagnosed celiac disease. Gastroenterology. 2009; 137(1):88–93.
36. Harewood GC, Holub JL, Lieberman DA. Variation in small bowel biopsy performance among diverse endoscopy settings: results from a national endoscopic database. Am J Gastroenterol. 2004;99(9):1790-1794.
37. Brar P, Lee S, Lewis S, et al. Budesonide in the treatment of refractory celiac disease. Am J Gastroenterol. 2007;102(10):2265-2269.
38. Al-Toma A, Verbeek WHM, Hadithi M, et al. Survival in refractory coeliac disease and enteropathy-associated T-cell lymphoma: retrospective evaluation of single-centre experience. Gut. 2007;56(10):1373-1378.
39. Kaukinen K, Mäki M, Partanen J, et al. Celiac disease without villous atrophy: revision of criteria called for. Dig Dis Sci. 2001;46(4):879-887.
40. Mohamed BM, Feighery C, Coates C, et al. The absence of a mucosal lesion on standard histological examination does not exclude diagnosis of celiac disease. Dig Dis Sci. 2008; 53(1):52-61.
41. Fasano A, Catassi C. Current approaches to diagnosis and treatment of celiac disease: an evolving spectrum. Gastroenterology. 2001; 120(3):636-651.
42. US Food and Drug Administration. Topic-specific labeling information (2010). www.fda.gov/Food/LabelingNutrition/FoodLabeling GuidanceRegulatoryInformation/Topic-Specific LabelingInformation/default.htm. Accessed March 28, 2011.
43. Lindfors K, Blomqvist T, Juuti-Uusitalo K, et al. Live probiotic Bifidobacterium lactis bacteria inhibit the toxic effects induced by wheat gliadin in epithelial cell culture. Clin Exp Immunol. 2008;152(3):552-558.
44. Cellier C, Delabesse E, Helmer C, et al; French Coeliac Disease Study Group. Refractory sprue, coeliac disease, and enteropathy-associated T-cell lymphoma. Lancet. 2000;356(9225): 203-208.
45. United European Gastroenterology. When is a coeliac a coeliac? Report of a working group of the United European Gastroenterology Week in Amsterdam, 2001. Eur J Gastroenterol Hepatol. 2001;13(9):1123-1128.
46. Malamut G, Afchain P, Verkarre V, et al. Presentation and long-term follow-up of refractory celiac disease: comparison of type I with type II. Gastroenterology. 2009;136(1):81-90.
47. Al-Toma A, Goerres MS, Meijer JW, et al. Human leukocyte antigen-DQ2 homozygosity and the development of refractory celiac disease and enteropathy-associated T-cell lymphoma. Clin Gastroenterol Hepatol. 2006;4(3): 315-319.
48. Mauriño E, Niveloni S, Cherñavsky A, et al. Azathioprine in refractory sprue: results from a prospective, open-label study. Am J Gastroenterol. 2002;97(10):2595–2602.
49. Tack GJ, Verbeek WHM, Al-Toma A, et al. Evaluation of cladribine treatment in refractory celiac disease type II. World J Gastroenterol. 2011;17(4):506–513.
50. Akobeng AK, Ramanan AV, Buchan I, Heller RF. Effect of breast feeding on risk of coeliac disease: a systematic review and meta-analysis of observational studies. Arch Dis Child. 2006; 91(1):39-43.
51. Rashid M, Butzner JD, Warren R, et al. Home blood testing for celiac disease: recommendations for management. Can Fam Physician. 2009;55(2):151-153.
52. Hershcovici T, Leshno M, Goldin E, et al. Cost effectiveness of mass screening for coeliac disease is determined by time-delay to diagnosis and quality of life on a gluten-free diet. Aliment Pharmacol Ther. 2010;31(8):901-910.