User login
A disease that strikes close to home

Besides caring for these patients, many of us also have a parent, spouse, or a close relative with dementia. My 90-year-old mother has multi-infarct dementia from her diabetes and vascular disease, but is still able to live in an apartment with my 91-year-old father, with assistance from wonderful home aides. Despite her profound dementia, she can still play the piano and read music.
Menchola and Weiss are to be congratulated for their excellent, evidence-based review of the diagnosis, treatment, and prevention of Alzheimer’s disease (AD). (See "Addressing Alzheimer’s: A pragmatic approach.") They do not get caught up in unjustified enthusiasm for screening and drug treatment. Some of their important recommendations bear repeating here:
Do not routinely screen for AD. This may seem like heresy in these days of early detection and prevention. But for screening to be useful, there must be effective early interventions, and so far, early treatments for AD have been disappointing. Cholinesterase inhibitors and N-methyl-D-aspartate glutamate receptor blockers provide very small improvements in cognitive function and have significant adverse effects. Some behavioral interventions to delay onset of cognitive decline show promise—but are unproven.
Although routine screening is not recommended, “case finding” remains important. We need to be alert to signs and symptoms that suggest early dementia in our patients, and we need to evaluate these patients carefully or refer them for neurologic testing if the diagnosis is in doubt.
Use drugs sparingly, especially when treating behavioral problems. They have serious adverse effects, and behavioral interventions should always be used first. Encourage caregivers to seek out social support. My father attends an Alzheimer’s support group each month, and this has lifted some of the burden.
Address prognosis and end-of-life care, and avoid unnecessary and aggressive treatments that are likely to cause more harm than benefit. Hospice care is suitable and beneficial for those with late-stage Alzheimer’s, but feeding tubes are not.
With many new advances in research techniques, it is likely that investigators will develop better methods of diagnosis and treatment of AD. In the meantime, there is already much we can do to alleviate the suffering of these patients and support their caregivers. This knowledge will likely serve us at home, as well.
Besides caring for these patients, many of us also have a parent, spouse, or a close relative with dementia. My 90-year-old mother has multi-infarct dementia from her diabetes and vascular disease, but is still able to live in an apartment with my 91-year-old father, with assistance from wonderful home aides. Despite her profound dementia, she can still play the piano and read music.
Menchola and Weiss are to be congratulated for their excellent, evidence-based review of the diagnosis, treatment, and prevention of Alzheimer’s disease (AD). (See "Addressing Alzheimer’s: A pragmatic approach.") They do not get caught up in unjustified enthusiasm for screening and drug treatment. Some of their important recommendations bear repeating here:
Do not routinely screen for AD. This may seem like heresy in these days of early detection and prevention. But for screening to be useful, there must be effective early interventions, and so far, early treatments for AD have been disappointing. Cholinesterase inhibitors and N-methyl-D-aspartate glutamate receptor blockers provide very small improvements in cognitive function and have significant adverse effects. Some behavioral interventions to delay onset of cognitive decline show promise—but are unproven.
Although routine screening is not recommended, “case finding” remains important. We need to be alert to signs and symptoms that suggest early dementia in our patients, and we need to evaluate these patients carefully or refer them for neurologic testing if the diagnosis is in doubt.
Use drugs sparingly, especially when treating behavioral problems. They have serious adverse effects, and behavioral interventions should always be used first. Encourage caregivers to seek out social support. My father attends an Alzheimer’s support group each month, and this has lifted some of the burden.
Address prognosis and end-of-life care, and avoid unnecessary and aggressive treatments that are likely to cause more harm than benefit. Hospice care is suitable and beneficial for those with late-stage Alzheimer’s, but feeding tubes are not.
With many new advances in research techniques, it is likely that investigators will develop better methods of diagnosis and treatment of AD. In the meantime, there is already much we can do to alleviate the suffering of these patients and support their caregivers. This knowledge will likely serve us at home, as well.
Besides caring for these patients, many of us also have a parent, spouse, or a close relative with dementia. My 90-year-old mother has multi-infarct dementia from her diabetes and vascular disease, but is still able to live in an apartment with my 91-year-old father, with assistance from wonderful home aides. Despite her profound dementia, she can still play the piano and read music.
Menchola and Weiss are to be congratulated for their excellent, evidence-based review of the diagnosis, treatment, and prevention of Alzheimer’s disease (AD). (See "Addressing Alzheimer’s: A pragmatic approach.") They do not get caught up in unjustified enthusiasm for screening and drug treatment. Some of their important recommendations bear repeating here:
Do not routinely screen for AD. This may seem like heresy in these days of early detection and prevention. But for screening to be useful, there must be effective early interventions, and so far, early treatments for AD have been disappointing. Cholinesterase inhibitors and N-methyl-D-aspartate glutamate receptor blockers provide very small improvements in cognitive function and have significant adverse effects. Some behavioral interventions to delay onset of cognitive decline show promise—but are unproven.
Although routine screening is not recommended, “case finding” remains important. We need to be alert to signs and symptoms that suggest early dementia in our patients, and we need to evaluate these patients carefully or refer them for neurologic testing if the diagnosis is in doubt.
Use drugs sparingly, especially when treating behavioral problems. They have serious adverse effects, and behavioral interventions should always be used first. Encourage caregivers to seek out social support. My father attends an Alzheimer’s support group each month, and this has lifted some of the burden.
Address prognosis and end-of-life care, and avoid unnecessary and aggressive treatments that are likely to cause more harm than benefit. Hospice care is suitable and beneficial for those with late-stage Alzheimer’s, but feeding tubes are not.
With many new advances in research techniques, it is likely that investigators will develop better methods of diagnosis and treatment of AD. In the meantime, there is already much we can do to alleviate the suffering of these patients and support their caregivers. This knowledge will likely serve us at home, as well.
Use baby formula to check for bladder integrity

“FAREWELL TO INDIGO CARMINE”
ROBERT L. BARBIERI, MD (EDITORIAL; SEPTEMBER 2014)
Use baby formula to check for bladder integrity
There is an additional method that can be used to check for bladder injury that some of us “older” gynecologists have employed. Baby formula is packaged in sterile bottles. I have had the rare occasion to need to check for bladder integrity and have had the circulating nurse inject diluted formula through the indwelling urinary catheter. I have yet to encounter (or read about) an allergic response from this technique.
Martin E. Kanoff, DO
Sewell, New Jersey
I found Dr. Barbieri’s editorial on the indigo carmine shortage very appropriate and timely.
When intraoperatively testing a bladder repair or looking for a possible bladder injury, administration of phenazopyridine or instillation of dilute methylene blue as noted are reasonable approaches. Due to tissue staining, which can make repeat bladder assessment more difficult, I have found that instilling sterile formula, usually easily available on the obstetric unit, will allow detection of “leaks” and easily can be rinsed out of the pelvis with saline, allowing repeat instillation if necessary.
Also, if the bladder is distended with fluid when looking for defects, it pays to wait a few minutes before decompressing, as small leaks may gradually deflate the bladder and alert the surgeon to the need for further investigation.
William J. Mann, Jr, MD
Executive Medical Director
Olde Towne Medical and Dental Center
Clinical Professor, ObGyn
Virginia Commonwealth School of Medicine
Richmond, Virginia
What about using sterile milk?
Dr. Barbieri, what is your opinion and do you have any ideas on sourcing sterile milk for use in diagnostic cystoscopy and tubal patency in gynecology?
Donna G. Ivery, MD
Titusville, Florida
Is there a methylene blue shortage too?
I commonly perform chromotubation for my infertility patients and for tubal reversals. I have been substituting methylene blue for indigo carmine. Recently, I was told by my surgical center that methylene blue is on back order. Have you noticed the methylene blue shortage? Do you have suggestions for a replacement for my indications of chromotubation and tubal reversal surgeries?
Online I have seen mention of isosulfan blue being injected into lymphatic tissue to identify sentinel nodes—although it is more expensive. I will be searching now for a supplier of isosulfan blue. Sterile milk has been used to identify bladder fistulas. Can it be used for chromotubation?
Peter G. Van Deerlin, MD
South Jersey Fertility Center
Marlton, New Jersey
Can we brainstorm a solution to the shortage?
Dr. Barbieri, once again you have demonstrated your clear thinking and reasoned approach to what is a clinical problem.
I would add the following thought: Perhaps a group of physicians from major specialty/subspecialty organizations could meet with the present manufacturers and brainstorm for a solution. Self-interest is clearly the practical path and patient safety/customer satisfaction can come into play also.
Stephen S. Schuster, MD
Queens, New York
Another way to diagnose PROM
I read with interest the editorial covering the shortage of indigo carmine. In the section “Options to diagnose PROM … ”, you stated NONE as the option for diagnosing premature rupture of membranes (PROM) when standard clinical testing is equivocal.
A recent article in Journal of Perinatal Medicine suggests that placental alpha microglobulin-1 (PAMG-1) testing is as reliable as dye studies.1 This was a 140-patient prospective study and is certainly encouraging.
I don’t use PAMG-1 as a first-line agent for diagnosing rupture of membranes (ROM). Speculum examination with pooling of amniotic fluid, nitrozine testing, and microscopic examination for ferning confirm or rule out ROM in most cases. This article points toward avoiding the more invasive dye study. The data are timely in light of the indigo carmine shortage.
John R. Hannig, MD
Salem, Oregon
Reference
- Sosa CG, Herrera E, Restrepo JC, Strauss A, Alonso J. Comparison of placental alpha macroglobulin-1 in vaginal fluid with intra-amniotic injection of indigo carmine for the diagnosis of rupture of membranes. J Perinat Med. 2014;42(5):611–616.
Dr. Barbieri responds
I appreciate the great suggestion by Drs. Kanoff, Mann, and Ivery to use sterile baby formula to test bladder integrity. Sterile baby formula is usually available on an obstetric unit, and less available in a main operating room environment. One small caveat about the use of the word “sterile.” Baby formula is “sterile” using criteria for a commercial food product. Injectable agents typically need to be both sterile, using criteria for a pharmaceutical agent, and pyrogen free. These criteria are more stringent than for a food product. Some surgical nursing and pharmacy administrators may focus on this technical difference and resist the use of sterile baby formula to test bladder integrity.
First it was indigo carmine, now methylene blue is on back order. As Dr. Van Deerlin suspects, isosulfan blue is expensive. A 5-mL vial of isosulfan blue has a list price of $714. If no dye were available to test tubal patency, I would consider using saline or lactated Ringer’s solution. I would hesitate to use sterile baby formula because I would be concerned about peritoneal and tubal epithelial inflammation.
Dr. Schuster has a great suggestion to better coordinate the capabilities of manufacturers with the needs of clinicians and patients. We will forward your suggestion to the ACOG leadership.
I agree with Dr. Hannig’s suggestion that measurement of placental alpha macroglobulin-1 in vaginal fluid is an excellent option for replacing intra-amniotic injection of indigo carmine. Some obstetric units have not yet deployed this test because, in many centers, only a few cases per year needed this test. With the loss of access to indigo carmine, it is a good option to consider measurement of placental alpha macroglobulin-1 in vaginal fluid in cases where it is unclear if the membranes have ruptured.
“PREVENTING POSTOPERATIVE NEUROPATHIES: PATIENT POSITIONING FOR MINIMALLY INVASIVE PROCEDURES”
TIFFANY JACKSON, MD; BICH-VAN TRAN, MD; ARNOLD ADVINCULA, MD; KAREN WIERCINSKI, RN, BSN; JULIO LOPEZ (VIDEO; SEPTEMBER 2014)
May I share the video?
The video on patient positioning to prevent postoperative neuropathies is a great resource for physicians and nurses! May I share this video with our gynecologic operative room staff as a teaching tool?
Christinne D. Canela, MD
Roanoke, Virginia
The Editors respond
This, and all of the videos at obgmanagement.com are meant to be shared with your colleagues.

“TISSUE EXTRACTION DURING MINIMALLY INVASIVE GYN SURGERY. SECOND OF 2 PARTS: COUNSELING THE PATIENT”
(ROUNDTABLE; OCTOBER 2014)
May I morcellate your uterus please?
The laparoscopic approach to the fibroid uterus is currently a puzzle. After the FDA released a statement in April postulating that the use of power morcellation to remove uterine fibroids should be “discouraged,” a great controversy developed in the minimally invasive surgical community.
Subsequently in July, the Obstetrics and Gynecology Devices Advisory Panel of the FDA held a 2-day meeting to analyze risks, benefits, and the overall clinical role of laparoscopic power morcellation in gynecology. One recommendation was to include in the informed consent a disclosure of the risks of disseminating an occult uterine malignancy. I salute the efforts of the panel and agree on the necessity for a comprehensive consent process that discloses risks that could worsen the patient’s prognosis.
Soon after that FDA panel met in July, Ethicon, a division of Johnson and Johnson, made a business decision to initiate a worldwide withdrawal of the company’s morcellation devices.
Now, on November 24, the FDA issued an updated Safety Communication recommending that the use of power morcellators is contraindicated for removal of uterine tissue containing suspected fibroids in patients who are peri- or post-menopausal, or are candidates for en bloc tissue removal. They also said that laparoscopic power morcellators are contraindicated in gynecologic surgery in which the tissue to be morcellated is known or suspected to contain malignancy. The FDA is issuing a boxed warning, and recommends that surgeons thoroughly discuss the benefits and risks of all treatment to patients, including younger women who want to maintain their fertility or women not yet perimenopausal who wish to keep their uterus.
How will having a patient sign a consent form change the risk of unfortunate dispersion? How will it protect the surgeon from the subsequent liability? Who will be responsible for worsening the patient’s survival?
Month after month in the Medical Verdicts column, we see cases of unfortunate patients who suffer well-known surgical complications that are litigated, with different outcomes and compensations. I am certain that in most of these cases, the patients had signed at least a standard consent form that lists the most commonly known complications. Having a patient sign a consent form does not reduce the incidence of complications nor protect the physician from liability.
In my opinion, effort should be concentrated on finding a way to better preoperatively identify the patient at risk of occult uterine malignancy so that the surgical approach can be modified accordingly.
The controversy regarding morcellation is far from over. Perhaps the last tissue extractor remaining in the market should be used to morcellate the tort system and finally build a system that will protect patients and physicians.
Jose Carugno, MD
Miami, Florida
Dr. Iglesia responds
Dr. Carugno is correct. A “consent form” does not protect the surgeon from potential liability nor the patient from potential harm. Informed decision-making is a process wherein providers and patients discuss the diagnoses and conditions; the treatment options and alternatives ranging from expectant management, medical management or surgical intervention; and the potential risks and benefits of each of those options. Physicians should perform an adequate preoperative evaluation, and patients should be given the opportunity to ask questions with the understanding that no treatment is without risks (including the option for watchful waiting). Physicians should describe the steps that will be taken during the preoperative, intraoperative, and postoperative periods to mitigate those risks.
“TOTAL ABDOMINAL HYSTERECTOMY THE MAYO CLINIC WAY” JOHN B. GEBHART, MD, MS (SURGICAL TECHNIQUE; OCTOBER 2014)
We need to focus on improving vaginal hysterectomy
I found Dr. Gebhart’s article on abdominal hysterectomy technically very accurate and well written. It is with the greatest respect that I write to express my concern with the author’s response that because of the restriction of power morcellation devices, the rate of abdominal hysterectomy will increase.
Rather than focus on the improvement of the most common gynecologic surgical procedure, we should be focusing on improving techniques of vaginal hysterectomy, a route that unfortunately is under-taught in the United States.
I have been a practicing ObGyn for more than 20 years, and exclusively as a gynecologist for the last 4 years. I perform vaginal hysterectomies more than 90% of the time. My total abdominal hysterectomy and laparoscopic-assisted vaginal hysterectomy rates remain less than 5%; laparoscopic supracervical hysterectomy and total laparoscopic hysterectomy rates: 0%; and power morcellation rate: 0%.
In conclusion, why abdominal hysterectomy?
Robert C. Raymond, MD, MBA
Fort Payne, Alabama
Dr. Gebhart responds
Dr. Raymond, I thank you for your comments and question. I applaud your surgical skill set and approach to hysterectomy. My preferred route of hysterectomy for benign disease is the vaginal route. A few years ago we published an article in OBG Management on keys to success in vaginal hysterectomy.1 Indeed, the vaginal approach remains the least expensive and least morbid approach to hysterectomy, yet the least common. I continue to publish and lecture on the benefits of a vaginal approach and societies, such as the Society of Gynecologic Surgeons (SGS), remain committed to teaching and advocating this well-established, evidence-based yet underutilized approach.
Given the interest and controversy in the use of power morcellation after the FDA’s Safety Communication last April,2 it was felt that a good technical review of abdominal hysterectomy was cogent. If surgeons have a concern about using power morcellation or their institution has banned use of a power morcellator, then the abdominal route is the most likely alternative for removing the enlarged uterus intact. As you state, the abdominal approach remains the most common route of hysterectomy. My sense is that most providers faced with an enlarged uterus that cannot be removed via laparoscopic morcellation (for reasons stated previously) are likely to turn to abdominal hysterectomy. Hopefully, the article gives readers a chance to assess and develop their technical approach to abdominal hysterectomy.
References
- Occhino JA, Gebhart JB. The difficult vaginal hysterectomy: 5 keys to success. OBG Manag. 2010;22(11):32–47.
- US Food and Drug Administration. Laparoscopic uterine power morcellation in hysterectomy and myomectomy: FDA Safety Communication. http://www.fda.gov/MedicalDevices/Safety/AlertsandNotices/ucm393576.htm. Published April 17, 2014. Accessed December 8, 2014.
Share your thoughts on these letters or on another article! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.
“FAREWELL TO INDIGO CARMINE”
ROBERT L. BARBIERI, MD (EDITORIAL; SEPTEMBER 2014)
Use baby formula to check for bladder integrity
There is an additional method that can be used to check for bladder injury that some of us “older” gynecologists have employed. Baby formula is packaged in sterile bottles. I have had the rare occasion to need to check for bladder integrity and have had the circulating nurse inject diluted formula through the indwelling urinary catheter. I have yet to encounter (or read about) an allergic response from this technique.
Martin E. Kanoff, DO
Sewell, New Jersey
I found Dr. Barbieri’s editorial on the indigo carmine shortage very appropriate and timely.
When intraoperatively testing a bladder repair or looking for a possible bladder injury, administration of phenazopyridine or instillation of dilute methylene blue as noted are reasonable approaches. Due to tissue staining, which can make repeat bladder assessment more difficult, I have found that instilling sterile formula, usually easily available on the obstetric unit, will allow detection of “leaks” and easily can be rinsed out of the pelvis with saline, allowing repeat instillation if necessary.
Also, if the bladder is distended with fluid when looking for defects, it pays to wait a few minutes before decompressing, as small leaks may gradually deflate the bladder and alert the surgeon to the need for further investigation.
William J. Mann, Jr, MD
Executive Medical Director
Olde Towne Medical and Dental Center
Clinical Professor, ObGyn
Virginia Commonwealth School of Medicine
Richmond, Virginia
What about using sterile milk?
Dr. Barbieri, what is your opinion and do you have any ideas on sourcing sterile milk for use in diagnostic cystoscopy and tubal patency in gynecology?
Donna G. Ivery, MD
Titusville, Florida
Is there a methylene blue shortage too?
I commonly perform chromotubation for my infertility patients and for tubal reversals. I have been substituting methylene blue for indigo carmine. Recently, I was told by my surgical center that methylene blue is on back order. Have you noticed the methylene blue shortage? Do you have suggestions for a replacement for my indications of chromotubation and tubal reversal surgeries?
Online I have seen mention of isosulfan blue being injected into lymphatic tissue to identify sentinel nodes—although it is more expensive. I will be searching now for a supplier of isosulfan blue. Sterile milk has been used to identify bladder fistulas. Can it be used for chromotubation?
Peter G. Van Deerlin, MD
South Jersey Fertility Center
Marlton, New Jersey
Can we brainstorm a solution to the shortage?
Dr. Barbieri, once again you have demonstrated your clear thinking and reasoned approach to what is a clinical problem.
I would add the following thought: Perhaps a group of physicians from major specialty/subspecialty organizations could meet with the present manufacturers and brainstorm for a solution. Self-interest is clearly the practical path and patient safety/customer satisfaction can come into play also.
Stephen S. Schuster, MD
Queens, New York
Another way to diagnose PROM
I read with interest the editorial covering the shortage of indigo carmine. In the section “Options to diagnose PROM … ”, you stated NONE as the option for diagnosing premature rupture of membranes (PROM) when standard clinical testing is equivocal.
A recent article in Journal of Perinatal Medicine suggests that placental alpha microglobulin-1 (PAMG-1) testing is as reliable as dye studies.1 This was a 140-patient prospective study and is certainly encouraging.
I don’t use PAMG-1 as a first-line agent for diagnosing rupture of membranes (ROM). Speculum examination with pooling of amniotic fluid, nitrozine testing, and microscopic examination for ferning confirm or rule out ROM in most cases. This article points toward avoiding the more invasive dye study. The data are timely in light of the indigo carmine shortage.
John R. Hannig, MD
Salem, Oregon
Reference
- Sosa CG, Herrera E, Restrepo JC, Strauss A, Alonso J. Comparison of placental alpha macroglobulin-1 in vaginal fluid with intra-amniotic injection of indigo carmine for the diagnosis of rupture of membranes. J Perinat Med. 2014;42(5):611–616.
Dr. Barbieri responds
I appreciate the great suggestion by Drs. Kanoff, Mann, and Ivery to use sterile baby formula to test bladder integrity. Sterile baby formula is usually available on an obstetric unit, and less available in a main operating room environment. One small caveat about the use of the word “sterile.” Baby formula is “sterile” using criteria for a commercial food product. Injectable agents typically need to be both sterile, using criteria for a pharmaceutical agent, and pyrogen free. These criteria are more stringent than for a food product. Some surgical nursing and pharmacy administrators may focus on this technical difference and resist the use of sterile baby formula to test bladder integrity.
First it was indigo carmine, now methylene blue is on back order. As Dr. Van Deerlin suspects, isosulfan blue is expensive. A 5-mL vial of isosulfan blue has a list price of $714. If no dye were available to test tubal patency, I would consider using saline or lactated Ringer’s solution. I would hesitate to use sterile baby formula because I would be concerned about peritoneal and tubal epithelial inflammation.
Dr. Schuster has a great suggestion to better coordinate the capabilities of manufacturers with the needs of clinicians and patients. We will forward your suggestion to the ACOG leadership.
I agree with Dr. Hannig’s suggestion that measurement of placental alpha macroglobulin-1 in vaginal fluid is an excellent option for replacing intra-amniotic injection of indigo carmine. Some obstetric units have not yet deployed this test because, in many centers, only a few cases per year needed this test. With the loss of access to indigo carmine, it is a good option to consider measurement of placental alpha macroglobulin-1 in vaginal fluid in cases where it is unclear if the membranes have ruptured.
“PREVENTING POSTOPERATIVE NEUROPATHIES: PATIENT POSITIONING FOR MINIMALLY INVASIVE PROCEDURES”
TIFFANY JACKSON, MD; BICH-VAN TRAN, MD; ARNOLD ADVINCULA, MD; KAREN WIERCINSKI, RN, BSN; JULIO LOPEZ (VIDEO; SEPTEMBER 2014)
May I share the video?
The video on patient positioning to prevent postoperative neuropathies is a great resource for physicians and nurses! May I share this video with our gynecologic operative room staff as a teaching tool?
Christinne D. Canela, MD
Roanoke, Virginia
The Editors respond
This, and all of the videos at obgmanagement.com are meant to be shared with your colleagues.
“TISSUE EXTRACTION DURING MINIMALLY INVASIVE GYN SURGERY. SECOND OF 2 PARTS: COUNSELING THE PATIENT”
(ROUNDTABLE; OCTOBER 2014)
May I morcellate your uterus please?
The laparoscopic approach to the fibroid uterus is currently a puzzle. After the FDA released a statement in April postulating that the use of power morcellation to remove uterine fibroids should be “discouraged,” a great controversy developed in the minimally invasive surgical community.
Subsequently in July, the Obstetrics and Gynecology Devices Advisory Panel of the FDA held a 2-day meeting to analyze risks, benefits, and the overall clinical role of laparoscopic power morcellation in gynecology. One recommendation was to include in the informed consent a disclosure of the risks of disseminating an occult uterine malignancy. I salute the efforts of the panel and agree on the necessity for a comprehensive consent process that discloses risks that could worsen the patient’s prognosis.
Soon after that FDA panel met in July, Ethicon, a division of Johnson and Johnson, made a business decision to initiate a worldwide withdrawal of the company’s morcellation devices.
Now, on November 24, the FDA issued an updated Safety Communication recommending that the use of power morcellators is contraindicated for removal of uterine tissue containing suspected fibroids in patients who are peri- or post-menopausal, or are candidates for en bloc tissue removal. They also said that laparoscopic power morcellators are contraindicated in gynecologic surgery in which the tissue to be morcellated is known or suspected to contain malignancy. The FDA is issuing a boxed warning, and recommends that surgeons thoroughly discuss the benefits and risks of all treatment to patients, including younger women who want to maintain their fertility or women not yet perimenopausal who wish to keep their uterus.
How will having a patient sign a consent form change the risk of unfortunate dispersion? How will it protect the surgeon from the subsequent liability? Who will be responsible for worsening the patient’s survival?
Month after month in the Medical Verdicts column, we see cases of unfortunate patients who suffer well-known surgical complications that are litigated, with different outcomes and compensations. I am certain that in most of these cases, the patients had signed at least a standard consent form that lists the most commonly known complications. Having a patient sign a consent form does not reduce the incidence of complications nor protect the physician from liability.
In my opinion, effort should be concentrated on finding a way to better preoperatively identify the patient at risk of occult uterine malignancy so that the surgical approach can be modified accordingly.
The controversy regarding morcellation is far from over. Perhaps the last tissue extractor remaining in the market should be used to morcellate the tort system and finally build a system that will protect patients and physicians.
Jose Carugno, MD
Miami, Florida
Dr. Iglesia responds
Dr. Carugno is correct. A “consent form” does not protect the surgeon from potential liability nor the patient from potential harm. Informed decision-making is a process wherein providers and patients discuss the diagnoses and conditions; the treatment options and alternatives ranging from expectant management, medical management or surgical intervention; and the potential risks and benefits of each of those options. Physicians should perform an adequate preoperative evaluation, and patients should be given the opportunity to ask questions with the understanding that no treatment is without risks (including the option for watchful waiting). Physicians should describe the steps that will be taken during the preoperative, intraoperative, and postoperative periods to mitigate those risks.
“TOTAL ABDOMINAL HYSTERECTOMY THE MAYO CLINIC WAY” JOHN B. GEBHART, MD, MS (SURGICAL TECHNIQUE; OCTOBER 2014)
We need to focus on improving vaginal hysterectomy
I found Dr. Gebhart’s article on abdominal hysterectomy technically very accurate and well written. It is with the greatest respect that I write to express my concern with the author’s response that because of the restriction of power morcellation devices, the rate of abdominal hysterectomy will increase.
Rather than focus on the improvement of the most common gynecologic surgical procedure, we should be focusing on improving techniques of vaginal hysterectomy, a route that unfortunately is under-taught in the United States.
I have been a practicing ObGyn for more than 20 years, and exclusively as a gynecologist for the last 4 years. I perform vaginal hysterectomies more than 90% of the time. My total abdominal hysterectomy and laparoscopic-assisted vaginal hysterectomy rates remain less than 5%; laparoscopic supracervical hysterectomy and total laparoscopic hysterectomy rates: 0%; and power morcellation rate: 0%.
In conclusion, why abdominal hysterectomy?
Robert C. Raymond, MD, MBA
Fort Payne, Alabama
Dr. Gebhart responds
Dr. Raymond, I thank you for your comments and question. I applaud your surgical skill set and approach to hysterectomy. My preferred route of hysterectomy for benign disease is the vaginal route. A few years ago we published an article in OBG Management on keys to success in vaginal hysterectomy.1 Indeed, the vaginal approach remains the least expensive and least morbid approach to hysterectomy, yet the least common. I continue to publish and lecture on the benefits of a vaginal approach and societies, such as the Society of Gynecologic Surgeons (SGS), remain committed to teaching and advocating this well-established, evidence-based yet underutilized approach.
Given the interest and controversy in the use of power morcellation after the FDA’s Safety Communication last April,2 it was felt that a good technical review of abdominal hysterectomy was cogent. If surgeons have a concern about using power morcellation or their institution has banned use of a power morcellator, then the abdominal route is the most likely alternative for removing the enlarged uterus intact. As you state, the abdominal approach remains the most common route of hysterectomy. My sense is that most providers faced with an enlarged uterus that cannot be removed via laparoscopic morcellation (for reasons stated previously) are likely to turn to abdominal hysterectomy. Hopefully, the article gives readers a chance to assess and develop their technical approach to abdominal hysterectomy.
References
- Occhino JA, Gebhart JB. The difficult vaginal hysterectomy: 5 keys to success. OBG Manag. 2010;22(11):32–47.
- US Food and Drug Administration. Laparoscopic uterine power morcellation in hysterectomy and myomectomy: FDA Safety Communication. http://www.fda.gov/MedicalDevices/Safety/AlertsandNotices/ucm393576.htm. Published April 17, 2014. Accessed December 8, 2014.
Share your thoughts on these letters or on another article! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.
“FAREWELL TO INDIGO CARMINE”
ROBERT L. BARBIERI, MD (EDITORIAL; SEPTEMBER 2014)
Use baby formula to check for bladder integrity
There is an additional method that can be used to check for bladder injury that some of us “older” gynecologists have employed. Baby formula is packaged in sterile bottles. I have had the rare occasion to need to check for bladder integrity and have had the circulating nurse inject diluted formula through the indwelling urinary catheter. I have yet to encounter (or read about) an allergic response from this technique.
Martin E. Kanoff, DO
Sewell, New Jersey
I found Dr. Barbieri’s editorial on the indigo carmine shortage very appropriate and timely.
When intraoperatively testing a bladder repair or looking for a possible bladder injury, administration of phenazopyridine or instillation of dilute methylene blue as noted are reasonable approaches. Due to tissue staining, which can make repeat bladder assessment more difficult, I have found that instilling sterile formula, usually easily available on the obstetric unit, will allow detection of “leaks” and easily can be rinsed out of the pelvis with saline, allowing repeat instillation if necessary.
Also, if the bladder is distended with fluid when looking for defects, it pays to wait a few minutes before decompressing, as small leaks may gradually deflate the bladder and alert the surgeon to the need for further investigation.
William J. Mann, Jr, MD
Executive Medical Director
Olde Towne Medical and Dental Center
Clinical Professor, ObGyn
Virginia Commonwealth School of Medicine
Richmond, Virginia
What about using sterile milk?
Dr. Barbieri, what is your opinion and do you have any ideas on sourcing sterile milk for use in diagnostic cystoscopy and tubal patency in gynecology?
Donna G. Ivery, MD
Titusville, Florida
Is there a methylene blue shortage too?
I commonly perform chromotubation for my infertility patients and for tubal reversals. I have been substituting methylene blue for indigo carmine. Recently, I was told by my surgical center that methylene blue is on back order. Have you noticed the methylene blue shortage? Do you have suggestions for a replacement for my indications of chromotubation and tubal reversal surgeries?
Online I have seen mention of isosulfan blue being injected into lymphatic tissue to identify sentinel nodes—although it is more expensive. I will be searching now for a supplier of isosulfan blue. Sterile milk has been used to identify bladder fistulas. Can it be used for chromotubation?
Peter G. Van Deerlin, MD
South Jersey Fertility Center
Marlton, New Jersey
Can we brainstorm a solution to the shortage?
Dr. Barbieri, once again you have demonstrated your clear thinking and reasoned approach to what is a clinical problem.
I would add the following thought: Perhaps a group of physicians from major specialty/subspecialty organizations could meet with the present manufacturers and brainstorm for a solution. Self-interest is clearly the practical path and patient safety/customer satisfaction can come into play also.
Stephen S. Schuster, MD
Queens, New York
Another way to diagnose PROM
I read with interest the editorial covering the shortage of indigo carmine. In the section “Options to diagnose PROM … ”, you stated NONE as the option for diagnosing premature rupture of membranes (PROM) when standard clinical testing is equivocal.
A recent article in Journal of Perinatal Medicine suggests that placental alpha microglobulin-1 (PAMG-1) testing is as reliable as dye studies.1 This was a 140-patient prospective study and is certainly encouraging.
I don’t use PAMG-1 as a first-line agent for diagnosing rupture of membranes (ROM). Speculum examination with pooling of amniotic fluid, nitrozine testing, and microscopic examination for ferning confirm or rule out ROM in most cases. This article points toward avoiding the more invasive dye study. The data are timely in light of the indigo carmine shortage.
John R. Hannig, MD
Salem, Oregon
Reference
- Sosa CG, Herrera E, Restrepo JC, Strauss A, Alonso J. Comparison of placental alpha macroglobulin-1 in vaginal fluid with intra-amniotic injection of indigo carmine for the diagnosis of rupture of membranes. J Perinat Med. 2014;42(5):611–616.
Dr. Barbieri responds
I appreciate the great suggestion by Drs. Kanoff, Mann, and Ivery to use sterile baby formula to test bladder integrity. Sterile baby formula is usually available on an obstetric unit, and less available in a main operating room environment. One small caveat about the use of the word “sterile.” Baby formula is “sterile” using criteria for a commercial food product. Injectable agents typically need to be both sterile, using criteria for a pharmaceutical agent, and pyrogen free. These criteria are more stringent than for a food product. Some surgical nursing and pharmacy administrators may focus on this technical difference and resist the use of sterile baby formula to test bladder integrity.
First it was indigo carmine, now methylene blue is on back order. As Dr. Van Deerlin suspects, isosulfan blue is expensive. A 5-mL vial of isosulfan blue has a list price of $714. If no dye were available to test tubal patency, I would consider using saline or lactated Ringer’s solution. I would hesitate to use sterile baby formula because I would be concerned about peritoneal and tubal epithelial inflammation.
Dr. Schuster has a great suggestion to better coordinate the capabilities of manufacturers with the needs of clinicians and patients. We will forward your suggestion to the ACOG leadership.
I agree with Dr. Hannig’s suggestion that measurement of placental alpha macroglobulin-1 in vaginal fluid is an excellent option for replacing intra-amniotic injection of indigo carmine. Some obstetric units have not yet deployed this test because, in many centers, only a few cases per year needed this test. With the loss of access to indigo carmine, it is a good option to consider measurement of placental alpha macroglobulin-1 in vaginal fluid in cases where it is unclear if the membranes have ruptured.
“PREVENTING POSTOPERATIVE NEUROPATHIES: PATIENT POSITIONING FOR MINIMALLY INVASIVE PROCEDURES”
TIFFANY JACKSON, MD; BICH-VAN TRAN, MD; ARNOLD ADVINCULA, MD; KAREN WIERCINSKI, RN, BSN; JULIO LOPEZ (VIDEO; SEPTEMBER 2014)
May I share the video?
The video on patient positioning to prevent postoperative neuropathies is a great resource for physicians and nurses! May I share this video with our gynecologic operative room staff as a teaching tool?
Christinne D. Canela, MD
Roanoke, Virginia
The Editors respond
This, and all of the videos at obgmanagement.com are meant to be shared with your colleagues.
“TISSUE EXTRACTION DURING MINIMALLY INVASIVE GYN SURGERY. SECOND OF 2 PARTS: COUNSELING THE PATIENT”
(ROUNDTABLE; OCTOBER 2014)
May I morcellate your uterus please?
The laparoscopic approach to the fibroid uterus is currently a puzzle. After the FDA released a statement in April postulating that the use of power morcellation to remove uterine fibroids should be “discouraged,” a great controversy developed in the minimally invasive surgical community.
Subsequently in July, the Obstetrics and Gynecology Devices Advisory Panel of the FDA held a 2-day meeting to analyze risks, benefits, and the overall clinical role of laparoscopic power morcellation in gynecology. One recommendation was to include in the informed consent a disclosure of the risks of disseminating an occult uterine malignancy. I salute the efforts of the panel and agree on the necessity for a comprehensive consent process that discloses risks that could worsen the patient’s prognosis.
Soon after that FDA panel met in July, Ethicon, a division of Johnson and Johnson, made a business decision to initiate a worldwide withdrawal of the company’s morcellation devices.
Now, on November 24, the FDA issued an updated Safety Communication recommending that the use of power morcellators is contraindicated for removal of uterine tissue containing suspected fibroids in patients who are peri- or post-menopausal, or are candidates for en bloc tissue removal. They also said that laparoscopic power morcellators are contraindicated in gynecologic surgery in which the tissue to be morcellated is known or suspected to contain malignancy. The FDA is issuing a boxed warning, and recommends that surgeons thoroughly discuss the benefits and risks of all treatment to patients, including younger women who want to maintain their fertility or women not yet perimenopausal who wish to keep their uterus.
How will having a patient sign a consent form change the risk of unfortunate dispersion? How will it protect the surgeon from the subsequent liability? Who will be responsible for worsening the patient’s survival?
Month after month in the Medical Verdicts column, we see cases of unfortunate patients who suffer well-known surgical complications that are litigated, with different outcomes and compensations. I am certain that in most of these cases, the patients had signed at least a standard consent form that lists the most commonly known complications. Having a patient sign a consent form does not reduce the incidence of complications nor protect the physician from liability.
In my opinion, effort should be concentrated on finding a way to better preoperatively identify the patient at risk of occult uterine malignancy so that the surgical approach can be modified accordingly.
The controversy regarding morcellation is far from over. Perhaps the last tissue extractor remaining in the market should be used to morcellate the tort system and finally build a system that will protect patients and physicians.
Jose Carugno, MD
Miami, Florida
Dr. Iglesia responds
Dr. Carugno is correct. A “consent form” does not protect the surgeon from potential liability nor the patient from potential harm. Informed decision-making is a process wherein providers and patients discuss the diagnoses and conditions; the treatment options and alternatives ranging from expectant management, medical management or surgical intervention; and the potential risks and benefits of each of those options. Physicians should perform an adequate preoperative evaluation, and patients should be given the opportunity to ask questions with the understanding that no treatment is without risks (including the option for watchful waiting). Physicians should describe the steps that will be taken during the preoperative, intraoperative, and postoperative periods to mitigate those risks.
“TOTAL ABDOMINAL HYSTERECTOMY THE MAYO CLINIC WAY” JOHN B. GEBHART, MD, MS (SURGICAL TECHNIQUE; OCTOBER 2014)
We need to focus on improving vaginal hysterectomy
I found Dr. Gebhart’s article on abdominal hysterectomy technically very accurate and well written. It is with the greatest respect that I write to express my concern with the author’s response that because of the restriction of power morcellation devices, the rate of abdominal hysterectomy will increase.
Rather than focus on the improvement of the most common gynecologic surgical procedure, we should be focusing on improving techniques of vaginal hysterectomy, a route that unfortunately is under-taught in the United States.
I have been a practicing ObGyn for more than 20 years, and exclusively as a gynecologist for the last 4 years. I perform vaginal hysterectomies more than 90% of the time. My total abdominal hysterectomy and laparoscopic-assisted vaginal hysterectomy rates remain less than 5%; laparoscopic supracervical hysterectomy and total laparoscopic hysterectomy rates: 0%; and power morcellation rate: 0%.
In conclusion, why abdominal hysterectomy?
Robert C. Raymond, MD, MBA
Fort Payne, Alabama
Dr. Gebhart responds
Dr. Raymond, I thank you for your comments and question. I applaud your surgical skill set and approach to hysterectomy. My preferred route of hysterectomy for benign disease is the vaginal route. A few years ago we published an article in OBG Management on keys to success in vaginal hysterectomy.1 Indeed, the vaginal approach remains the least expensive and least morbid approach to hysterectomy, yet the least common. I continue to publish and lecture on the benefits of a vaginal approach and societies, such as the Society of Gynecologic Surgeons (SGS), remain committed to teaching and advocating this well-established, evidence-based yet underutilized approach.
Given the interest and controversy in the use of power morcellation after the FDA’s Safety Communication last April,2 it was felt that a good technical review of abdominal hysterectomy was cogent. If surgeons have a concern about using power morcellation or their institution has banned use of a power morcellator, then the abdominal route is the most likely alternative for removing the enlarged uterus intact. As you state, the abdominal approach remains the most common route of hysterectomy. My sense is that most providers faced with an enlarged uterus that cannot be removed via laparoscopic morcellation (for reasons stated previously) are likely to turn to abdominal hysterectomy. Hopefully, the article gives readers a chance to assess and develop their technical approach to abdominal hysterectomy.
References
- Occhino JA, Gebhart JB. The difficult vaginal hysterectomy: 5 keys to success. OBG Manag. 2010;22(11):32–47.
- US Food and Drug Administration. Laparoscopic uterine power morcellation in hysterectomy and myomectomy: FDA Safety Communication. http://www.fda.gov/MedicalDevices/Safety/AlertsandNotices/ucm393576.htm. Published April 17, 2014. Accessed December 8, 2014.
Share your thoughts on these letters or on another article! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.
Featured letters:
– Use baby formula to check for bladder integrity
– What about using sterile milk?
– Is there a methylene blue shortage too?
– Can we brainstorm a solution to the shortage?
– Another way to diagnose PROM
– May I share the video?
– May I morcellate your uterus please?
– We need to focus on improving vaginal hysterectomy
Protecting adolescents from radicalization, recruitment
Why do young people go to war zones – especially if their parents brought them to the United States for a new start? To stop adolescents from being lured to places such as Syria, Iraq, or Somalia, we need answers to that question.
One answer we hear from Somali Americans is, “We are the generation that was supposed to fix Somalia.” They were not presented with good options for doing so in a peaceful way, however, and this has made it relatively easy for terrorist organizations to exploit their passion. In 2007 and 2008, at least 17 Somali American adolescent boys and young men living in Minneapolis–St. Paul secretly left their homes and flew to Somalia to join militant extremist training camps run by Al Shabaab (Dynamics of Asymmetric Conflict 2009;2:181-200).

To better understand why this happened and how it can be prevented, we conducted a research study of Somali Americans funded by the U.S. Department of Homeland Security. We interviewed 57 people in Minneapolis–St. Paul who were either Somali American males aged 16-30 years, Somali American parents or adult family members, or service providers who worked within that community.
Multiple risks found
What we found is that no single risk factor explains violent radicalization. Instead, a combination of multiple risks at the individual, family, community, and societal levels are implicated.
To explain how to address these risks, we built a model called Diminishing Opportunities for Violent Extremism, or DOVE. This model shows that building community resilience to violent extremism depends on sustaining and strengthening (or in some cases initiating) protective resources through collaborations between family and youth, community, and government.
According to the DOVE model, these protective resources should focus on three risk levels:
• Diminishing youth’s unaccountable times and unobserved spaces (the times when adolescents and young adults are not answerable to parents or other adults and are in spaces where they are out of the sight of adults).
• Diminishing the perceived social legitimacy of violent extremism (perceptions of the appropriateness and necessity of violent extremist ideology and actions).
• Diminishing contact with recruiters or associates (adolescents and young adults interacting directly with either recruiters or companions who facilitate their increased involvement in violent extremism).
The U.S. government, state and local law enforcement, and local communities have been trying to organize prevention activities to address these and other risks. In Pres. Barack Obama’s Sept. 24, 2014, address to the United Nations, he stated: “There is no military solution to the problem of misguided individuals seeking to join terrorist organizations.” He supported a strategy called countering violent extremism, or CVE. This strategy is concerned with preventing violent ideologies from taking hold of people in the first place, and intervening and dissuading people from crossing the line toward actual violence.
The DOVE model supports the basic claim of CVE that government can’t do it alone, and it is going to require changes in communities. Meaningful preventive responses to radicalization must originate from within communities. One promising example is the Safe Spaces Initiative, a community-led preventive intervention developed by the Muslim Public Affairs Council. Safe Spaces leaves it up to communities to intervene with young people who might be getting involved with radicalization but have not yet entered into criminal space. It calls for communities to form Critical Inquiry Teams that include the participation of mental health professionals.
Role of mental health professionals
Incorporating mental health into CVE holds significant potential for enhancing both intervention and prevention capabilities with adolescents and young adults. In the United Kingdom, a national strategy called Prevent includes Channel, a multiagency program aimed at providing support to people at risk of being drawn into radicalization. One key component of Channel is for mental health professionals to be involved in assessment and support, but in order for mental health, law enforcement, and communities to be able to work together on radicalization and recruitment in the United States, we are going to have to invest in developing, implementing, and evaluating new collaborative models.
The threat of recruitment and radicalization has heightened significantly with the rise of ISIS (Islamic State of Iraq and Syria). ISIS uses propaganda videos and social media messages to appeal to a range of audiences, including would-be violent avengers, humanitarians, immigrants and refugees, and converts – males and females. Hundreds of U.S. foreign fighters reportedly have gone to ISIS. U.S. law enforcement agencies are concerned that more Americans will join ISIS, and that those foreign fighters who have joined and traveled abroad might pose security threats here at home.
To compete with ISIS to prevent more young people from going to Syria and Iraq, implementing CVE programs and policies is a national priority. This could be an opportunity for psychiatry and other mental health professionals to contribute to national and local response strategies.
One new initiative is a project recently begun by our team that is funded by the Science and Technology Directorate of the Homeland Security Dept. as part of a broader research portfolio on CVE conducted by the START Consortium, which aims to better understand how to integrate mental health professionals into countering violent extremism. This project presents an opportunity for psychiatrists and other mental health professionals to contribute to national and local response strategies to radicalization and recruitment.
Dr. Weine is professor of psychiatry at the University of Illinois at Chicago. He will address the issue of radicalization and recruitment to violence among Muslim-American teens at the upcoming joint meeting between the American Society for Adolescent Psychiatry (ASAP) and the Internal Society for Adolescent Psychiatry March 26-29 in New York. The meeting, which is themed “The Art and Science of Adolescent Psychiatry and Psychotherapy,” also will include resumption of ASAP’s Certification Examination in Adolescent Psychiatry.
Why do young people go to war zones – especially if their parents brought them to the United States for a new start? To stop adolescents from being lured to places such as Syria, Iraq, or Somalia, we need answers to that question.
One answer we hear from Somali Americans is, “We are the generation that was supposed to fix Somalia.” They were not presented with good options for doing so in a peaceful way, however, and this has made it relatively easy for terrorist organizations to exploit their passion. In 2007 and 2008, at least 17 Somali American adolescent boys and young men living in Minneapolis–St. Paul secretly left their homes and flew to Somalia to join militant extremist training camps run by Al Shabaab (Dynamics of Asymmetric Conflict 2009;2:181-200).
To better understand why this happened and how it can be prevented, we conducted a research study of Somali Americans funded by the U.S. Department of Homeland Security. We interviewed 57 people in Minneapolis–St. Paul who were either Somali American males aged 16-30 years, Somali American parents or adult family members, or service providers who worked within that community.
Multiple risks found
What we found is that no single risk factor explains violent radicalization. Instead, a combination of multiple risks at the individual, family, community, and societal levels are implicated.
To explain how to address these risks, we built a model called Diminishing Opportunities for Violent Extremism, or DOVE. This model shows that building community resilience to violent extremism depends on sustaining and strengthening (or in some cases initiating) protective resources through collaborations between family and youth, community, and government.
According to the DOVE model, these protective resources should focus on three risk levels:
• Diminishing youth’s unaccountable times and unobserved spaces (the times when adolescents and young adults are not answerable to parents or other adults and are in spaces where they are out of the sight of adults).
• Diminishing the perceived social legitimacy of violent extremism (perceptions of the appropriateness and necessity of violent extremist ideology and actions).
• Diminishing contact with recruiters or associates (adolescents and young adults interacting directly with either recruiters or companions who facilitate their increased involvement in violent extremism).
The U.S. government, state and local law enforcement, and local communities have been trying to organize prevention activities to address these and other risks. In Pres. Barack Obama’s Sept. 24, 2014, address to the United Nations, he stated: “There is no military solution to the problem of misguided individuals seeking to join terrorist organizations.” He supported a strategy called countering violent extremism, or CVE. This strategy is concerned with preventing violent ideologies from taking hold of people in the first place, and intervening and dissuading people from crossing the line toward actual violence.
The DOVE model supports the basic claim of CVE that government can’t do it alone, and it is going to require changes in communities. Meaningful preventive responses to radicalization must originate from within communities. One promising example is the Safe Spaces Initiative, a community-led preventive intervention developed by the Muslim Public Affairs Council. Safe Spaces leaves it up to communities to intervene with young people who might be getting involved with radicalization but have not yet entered into criminal space. It calls for communities to form Critical Inquiry Teams that include the participation of mental health professionals.
Role of mental health professionals
Incorporating mental health into CVE holds significant potential for enhancing both intervention and prevention capabilities with adolescents and young adults. In the United Kingdom, a national strategy called Prevent includes Channel, a multiagency program aimed at providing support to people at risk of being drawn into radicalization. One key component of Channel is for mental health professionals to be involved in assessment and support, but in order for mental health, law enforcement, and communities to be able to work together on radicalization and recruitment in the United States, we are going to have to invest in developing, implementing, and evaluating new collaborative models.
The threat of recruitment and radicalization has heightened significantly with the rise of ISIS (Islamic State of Iraq and Syria). ISIS uses propaganda videos and social media messages to appeal to a range of audiences, including would-be violent avengers, humanitarians, immigrants and refugees, and converts – males and females. Hundreds of U.S. foreign fighters reportedly have gone to ISIS. U.S. law enforcement agencies are concerned that more Americans will join ISIS, and that those foreign fighters who have joined and traveled abroad might pose security threats here at home.
To compete with ISIS to prevent more young people from going to Syria and Iraq, implementing CVE programs and policies is a national priority. This could be an opportunity for psychiatry and other mental health professionals to contribute to national and local response strategies.
One new initiative is a project recently begun by our team that is funded by the Science and Technology Directorate of the Homeland Security Dept. as part of a broader research portfolio on CVE conducted by the START Consortium, which aims to better understand how to integrate mental health professionals into countering violent extremism. This project presents an opportunity for psychiatrists and other mental health professionals to contribute to national and local response strategies to radicalization and recruitment.
Dr. Weine is professor of psychiatry at the University of Illinois at Chicago. He will address the issue of radicalization and recruitment to violence among Muslim-American teens at the upcoming joint meeting between the American Society for Adolescent Psychiatry (ASAP) and the Internal Society for Adolescent Psychiatry March 26-29 in New York. The meeting, which is themed “The Art and Science of Adolescent Psychiatry and Psychotherapy,” also will include resumption of ASAP’s Certification Examination in Adolescent Psychiatry.
Why do young people go to war zones – especially if their parents brought them to the United States for a new start? To stop adolescents from being lured to places such as Syria, Iraq, or Somalia, we need answers to that question.
One answer we hear from Somali Americans is, “We are the generation that was supposed to fix Somalia.” They were not presented with good options for doing so in a peaceful way, however, and this has made it relatively easy for terrorist organizations to exploit their passion. In 2007 and 2008, at least 17 Somali American adolescent boys and young men living in Minneapolis–St. Paul secretly left their homes and flew to Somalia to join militant extremist training camps run by Al Shabaab (Dynamics of Asymmetric Conflict 2009;2:181-200).
To better understand why this happened and how it can be prevented, we conducted a research study of Somali Americans funded by the U.S. Department of Homeland Security. We interviewed 57 people in Minneapolis–St. Paul who were either Somali American males aged 16-30 years, Somali American parents or adult family members, or service providers who worked within that community.
Multiple risks found
What we found is that no single risk factor explains violent radicalization. Instead, a combination of multiple risks at the individual, family, community, and societal levels are implicated.
To explain how to address these risks, we built a model called Diminishing Opportunities for Violent Extremism, or DOVE. This model shows that building community resilience to violent extremism depends on sustaining and strengthening (or in some cases initiating) protective resources through collaborations between family and youth, community, and government.
According to the DOVE model, these protective resources should focus on three risk levels:
• Diminishing youth’s unaccountable times and unobserved spaces (the times when adolescents and young adults are not answerable to parents or other adults and are in spaces where they are out of the sight of adults).
• Diminishing the perceived social legitimacy of violent extremism (perceptions of the appropriateness and necessity of violent extremist ideology and actions).
• Diminishing contact with recruiters or associates (adolescents and young adults interacting directly with either recruiters or companions who facilitate their increased involvement in violent extremism).
The U.S. government, state and local law enforcement, and local communities have been trying to organize prevention activities to address these and other risks. In Pres. Barack Obama’s Sept. 24, 2014, address to the United Nations, he stated: “There is no military solution to the problem of misguided individuals seeking to join terrorist organizations.” He supported a strategy called countering violent extremism, or CVE. This strategy is concerned with preventing violent ideologies from taking hold of people in the first place, and intervening and dissuading people from crossing the line toward actual violence.
The DOVE model supports the basic claim of CVE that government can’t do it alone, and it is going to require changes in communities. Meaningful preventive responses to radicalization must originate from within communities. One promising example is the Safe Spaces Initiative, a community-led preventive intervention developed by the Muslim Public Affairs Council. Safe Spaces leaves it up to communities to intervene with young people who might be getting involved with radicalization but have not yet entered into criminal space. It calls for communities to form Critical Inquiry Teams that include the participation of mental health professionals.
Role of mental health professionals
Incorporating mental health into CVE holds significant potential for enhancing both intervention and prevention capabilities with adolescents and young adults. In the United Kingdom, a national strategy called Prevent includes Channel, a multiagency program aimed at providing support to people at risk of being drawn into radicalization. One key component of Channel is for mental health professionals to be involved in assessment and support, but in order for mental health, law enforcement, and communities to be able to work together on radicalization and recruitment in the United States, we are going to have to invest in developing, implementing, and evaluating new collaborative models.
The threat of recruitment and radicalization has heightened significantly with the rise of ISIS (Islamic State of Iraq and Syria). ISIS uses propaganda videos and social media messages to appeal to a range of audiences, including would-be violent avengers, humanitarians, immigrants and refugees, and converts – males and females. Hundreds of U.S. foreign fighters reportedly have gone to ISIS. U.S. law enforcement agencies are concerned that more Americans will join ISIS, and that those foreign fighters who have joined and traveled abroad might pose security threats here at home.
To compete with ISIS to prevent more young people from going to Syria and Iraq, implementing CVE programs and policies is a national priority. This could be an opportunity for psychiatry and other mental health professionals to contribute to national and local response strategies.
One new initiative is a project recently begun by our team that is funded by the Science and Technology Directorate of the Homeland Security Dept. as part of a broader research portfolio on CVE conducted by the START Consortium, which aims to better understand how to integrate mental health professionals into countering violent extremism. This project presents an opportunity for psychiatrists and other mental health professionals to contribute to national and local response strategies to radicalization and recruitment.
Dr. Weine is professor of psychiatry at the University of Illinois at Chicago. He will address the issue of radicalization and recruitment to violence among Muslim-American teens at the upcoming joint meeting between the American Society for Adolescent Psychiatry (ASAP) and the Internal Society for Adolescent Psychiatry March 26-29 in New York. The meeting, which is themed “The Art and Science of Adolescent Psychiatry and Psychotherapy,” also will include resumption of ASAP’s Certification Examination in Adolescent Psychiatry.

When cardiologists attend meetings, do patients benefit?
Can the high-intensity care given acutely ill, high-risk U.S. patients with cardiac disease actually harm them?
Results from an unusual analysis of cardiology-meeting times seem to suggest that sobering possibility. Patient outcomes improved when thousands of high-level, American cardiologists left their practices for a few days each year to attend either of the two major U.S. heart disease meetings.
Researchers led by Dr. Anupam B. Jena of Harvard University, Boston, used Medicare data to examine mortality rates among patients hospitalized for cardiac arrest, heart failure, or acute myocardial infarction during 2002-2011. They focused on patients admitted during the annual meetings of the American College of Cardiology (usually in March) or the American Heart Association (during November).

As controls in their case-control analyses, they used data from patients admitted on similar days of the week during the 3 weeks immediately before or after these two meetings. This gave them roughly 11,000 total patients with cardiac arrest, nearly 134,000 with heart failure, and about 60,000 with acute MI – about 14% of patients in each disease category admitted during a meeting and the other 86% (controls) admitted when there was no meeting.
The results showed some statistically significant differences indicating that patients did better during the meetings, presumably when many cardiologists were away from their hospitals. These associations only occurred at teaching hospitals and among patients at high risk for inpatient mortality. The investigators saw no statistically significant differences, after adjustment, in mortality during meetings among patients treated at nonteaching hospitals or among patients with a low risk for inpatient mortality.
In analyses that adjusted for baseline differences in risk factors, the 30-day mortality rate for patients admitted to teaching hospitals with cardiac arrest was 69% during control dates and 59% during the meetings. Thirty-day mortality for patients admitted with heart failure was 25% during control dates and 18% during the meetings, researchers reported in an article published online on Dec. 22 (JAMA Intern. Med. 2014 [doi:10.1001/jamainternmed.2014.6781]).
Although 30-day mortality among patients admitted with an acute MI did not differ significantly at teaching hospitals between patients who presented during a major meeting and those who did not, the results showed that these similar mortality rates were achieved despite a statistically significant difference in the rate of percutaneous coronary interventions (PCI) that patients received: During the major meetings, 21% of the acute MI patients underwent PCI, but when a meeting was not in progress, the PCI rate jumped to 28% of all acute MI patients.
“One explanation for these findings is that the intensity of care provided during meeting dates is lower, and that for high-risk patients with cardiovascular disease, the harms of this care may unexpectedly outweigh the benefits,” Dr. Jena concluded.
It’s a remarkable and surprising finding, but can it be taken seriously? At least one expert said yes, at least seriously enough to warrant further study and consideration.
An editor’s note published with the new report suggested a plausible explanation for the findings is that “more interventions in high-risk patients with heart failure and cardiac arrest leads to higher mortality.” In her note, Dr. Rita F. Redberg, a cardiologist at the University of California, San Francisco, and editor of JAMA Internal Medicine, concluded, “It is reassuring that patient outcomes do not suffer while many cardiologists are away. More important, this analysis may help us to understand how we could lower mortality throughout the year.”
It will be interesting to see if anyone takes up the challenge to further explore this relationship and tries to find ways to apply throughout the year the protective effect of having fewer teaching-hospital cardiologists around. If a drug had this beneficial effect on mortality, the pharmaceutical industry would be all over it.
On Twitter @mitchelzoler
Can the high-intensity care given acutely ill, high-risk U.S. patients with cardiac disease actually harm them?
Results from an unusual analysis of cardiology-meeting times seem to suggest that sobering possibility. Patient outcomes improved when thousands of high-level, American cardiologists left their practices for a few days each year to attend either of the two major U.S. heart disease meetings.
Researchers led by Dr. Anupam B. Jena of Harvard University, Boston, used Medicare data to examine mortality rates among patients hospitalized for cardiac arrest, heart failure, or acute myocardial infarction during 2002-2011. They focused on patients admitted during the annual meetings of the American College of Cardiology (usually in March) or the American Heart Association (during November).
As controls in their case-control analyses, they used data from patients admitted on similar days of the week during the 3 weeks immediately before or after these two meetings. This gave them roughly 11,000 total patients with cardiac arrest, nearly 134,000 with heart failure, and about 60,000 with acute MI – about 14% of patients in each disease category admitted during a meeting and the other 86% (controls) admitted when there was no meeting.
The results showed some statistically significant differences indicating that patients did better during the meetings, presumably when many cardiologists were away from their hospitals. These associations only occurred at teaching hospitals and among patients at high risk for inpatient mortality. The investigators saw no statistically significant differences, after adjustment, in mortality during meetings among patients treated at nonteaching hospitals or among patients with a low risk for inpatient mortality.
In analyses that adjusted for baseline differences in risk factors, the 30-day mortality rate for patients admitted to teaching hospitals with cardiac arrest was 69% during control dates and 59% during the meetings. Thirty-day mortality for patients admitted with heart failure was 25% during control dates and 18% during the meetings, researchers reported in an article published online on Dec. 22 (JAMA Intern. Med. 2014 [doi:10.1001/jamainternmed.2014.6781]).
Although 30-day mortality among patients admitted with an acute MI did not differ significantly at teaching hospitals between patients who presented during a major meeting and those who did not, the results showed that these similar mortality rates were achieved despite a statistically significant difference in the rate of percutaneous coronary interventions (PCI) that patients received: During the major meetings, 21% of the acute MI patients underwent PCI, but when a meeting was not in progress, the PCI rate jumped to 28% of all acute MI patients.
“One explanation for these findings is that the intensity of care provided during meeting dates is lower, and that for high-risk patients with cardiovascular disease, the harms of this care may unexpectedly outweigh the benefits,” Dr. Jena concluded.
It’s a remarkable and surprising finding, but can it be taken seriously? At least one expert said yes, at least seriously enough to warrant further study and consideration.
An editor’s note published with the new report suggested a plausible explanation for the findings is that “more interventions in high-risk patients with heart failure and cardiac arrest leads to higher mortality.” In her note, Dr. Rita F. Redberg, a cardiologist at the University of California, San Francisco, and editor of JAMA Internal Medicine, concluded, “It is reassuring that patient outcomes do not suffer while many cardiologists are away. More important, this analysis may help us to understand how we could lower mortality throughout the year.”
It will be interesting to see if anyone takes up the challenge to further explore this relationship and tries to find ways to apply throughout the year the protective effect of having fewer teaching-hospital cardiologists around. If a drug had this beneficial effect on mortality, the pharmaceutical industry would be all over it.
On Twitter @mitchelzoler
Can the high-intensity care given acutely ill, high-risk U.S. patients with cardiac disease actually harm them?
Results from an unusual analysis of cardiology-meeting times seem to suggest that sobering possibility. Patient outcomes improved when thousands of high-level, American cardiologists left their practices for a few days each year to attend either of the two major U.S. heart disease meetings.
Researchers led by Dr. Anupam B. Jena of Harvard University, Boston, used Medicare data to examine mortality rates among patients hospitalized for cardiac arrest, heart failure, or acute myocardial infarction during 2002-2011. They focused on patients admitted during the annual meetings of the American College of Cardiology (usually in March) or the American Heart Association (during November).
As controls in their case-control analyses, they used data from patients admitted on similar days of the week during the 3 weeks immediately before or after these two meetings. This gave them roughly 11,000 total patients with cardiac arrest, nearly 134,000 with heart failure, and about 60,000 with acute MI – about 14% of patients in each disease category admitted during a meeting and the other 86% (controls) admitted when there was no meeting.
The results showed some statistically significant differences indicating that patients did better during the meetings, presumably when many cardiologists were away from their hospitals. These associations only occurred at teaching hospitals and among patients at high risk for inpatient mortality. The investigators saw no statistically significant differences, after adjustment, in mortality during meetings among patients treated at nonteaching hospitals or among patients with a low risk for inpatient mortality.
In analyses that adjusted for baseline differences in risk factors, the 30-day mortality rate for patients admitted to teaching hospitals with cardiac arrest was 69% during control dates and 59% during the meetings. Thirty-day mortality for patients admitted with heart failure was 25% during control dates and 18% during the meetings, researchers reported in an article published online on Dec. 22 (JAMA Intern. Med. 2014 [doi:10.1001/jamainternmed.2014.6781]).
Although 30-day mortality among patients admitted with an acute MI did not differ significantly at teaching hospitals between patients who presented during a major meeting and those who did not, the results showed that these similar mortality rates were achieved despite a statistically significant difference in the rate of percutaneous coronary interventions (PCI) that patients received: During the major meetings, 21% of the acute MI patients underwent PCI, but when a meeting was not in progress, the PCI rate jumped to 28% of all acute MI patients.
“One explanation for these findings is that the intensity of care provided during meeting dates is lower, and that for high-risk patients with cardiovascular disease, the harms of this care may unexpectedly outweigh the benefits,” Dr. Jena concluded.
It’s a remarkable and surprising finding, but can it be taken seriously? At least one expert said yes, at least seriously enough to warrant further study and consideration.
An editor’s note published with the new report suggested a plausible explanation for the findings is that “more interventions in high-risk patients with heart failure and cardiac arrest leads to higher mortality.” In her note, Dr. Rita F. Redberg, a cardiologist at the University of California, San Francisco, and editor of JAMA Internal Medicine, concluded, “It is reassuring that patient outcomes do not suffer while many cardiologists are away. More important, this analysis may help us to understand how we could lower mortality throughout the year.”
It will be interesting to see if anyone takes up the challenge to further explore this relationship and tries to find ways to apply throughout the year the protective effect of having fewer teaching-hospital cardiologists around. If a drug had this beneficial effect on mortality, the pharmaceutical industry would be all over it.
On Twitter @mitchelzoler

Why Travel Health Belongs in Primary Care
Chelsea had been stationed with the Peace Corps in Ghana and decided to take her 7-year-old daughter, Amber, with her on a return trip to visit friends she had made there. They planned to spend three weeks in the African nation.
Since Amber was home-schooled, Chelsea had not felt it necessary to follow the CDC guidelines for routine childhood immunizations. Once they planned to travel abroad, however, she made appointments with their primary care provider (PCP) to update Amber’s immunizations and with the travel clinic—where I practice—for yellow fever vaccines (required for entry to Ghana) for both of them.
Chelsea explained their travel plans to the PCP, adding that she intended to get the yellow fever vaccine at another clinic. The PCP administered Amber’s varicella and MMR vaccines.
Aware that it takes 10 days for yellow fever vaccine to be effective, Chelsea scheduled their appointments with me at the travel clinic for two weeks prior to their departure—which was also one week after their visit to the PCP. Did I mention they had nonrefundable tickets?
Chelsea became very upset when I told her I could not give Amber her yellow fever vaccine. I explained the live virus vaccine rule, which states that live virus vaccines must be given either on the same day or 28 days apart.1 If they are not given 28 days apart, the second vaccine—in this case, Amber’s yellow fever immunization—is not considered effective.
Chelsea and Amber were not able to travel to Ghana as planned, because her PCP did not know enough about the administration of yellow fever vaccine. As a result, Chelsea lost $5,000 in airline tickets and cancellation fees. She insisted that her PCP pay her expenses, and her PCP did. But how easily could this have happened in your practice?
Continue for pretravel immunizations >>
It’s been only 100 years since the first commercial airline service began. Today, the travel industry is the largest service industry in the world; 1 billion people traveled internationally in 2013.2 We travel for pleasure, business, education, adventure, adoption, and humanitarian reasons (not to mention visiting friends and family). It is now possible to travel around the world in less than 36 hours.2
Study results vary, but many report that 50% or more of all international travelers will become sick or injured because of their travel.3 Travel health now plays a larger role in public health as travelers bring home more than just souvenirs. Measles outbreaks are at a 30-year high, with many cases attributed to importation by international travelers.4 Many microbes—including SARS, novel influenza strains, and Ebola—are able to spread more easily because of advances in international travel.
The field of travel health grew from the recognition that many of the conditions being treated in infectious disease clinics could have been prevented by pretravel interventions. To address these issues, travel health—a new multidisciplinary specialty—was created, and in 1985 the International Society for Travel Medicine was formed. As a result, the practice of travel health has been concentrated in specialist-led clinics, often in the infectious disease departments of hospitals.
Research indicates that most international travelers do not seek any pretravel health advice.5 When they do, they consult their PCP more often than a travel clinic. Yet most PCPs are woefully undereducated in travel health. Patients such as Chelsea think it is less expensive to consult a PCP first to catch up on routine immunizations before going to a travel clinic for required vaccines. But it makes more sense to consult a travel clinic expert first.
The travel health specialist, who could be an NP, PA, registered pharmacist, RN, or MD, can devise a travel immunization plan that can be coordinated with a PCP to save costs. Many travel clinics don’t accept insurance because most payers do not cover travel health services or immunizations. This includes most private third-party insurers, Medicaid, and Medicare.
But what if Chelsea’s PCP could have provided her travel health needs? It is possible for PCPs to gain knowledge and expertise about travel health, even if they don’t choose to provide every travel immunization.
For example, yellow fever vaccine can only be provided at a certified yellow fever center. Certification requirements are determined at the state level and therefore vary by state. It is possible for PCPs to become certified to administer yellow fever vaccine, if they so choose.
But since not all international travelers require yellow fever vaccine, a PCP could still meet the needs of the majority of patients traveling internationally without taking that step. PCPs can provide vaccination against hepatitis A, typhoid, adult polio, meningococcal disease, Japanese encephalitis, and rabies (preexposure)—not to mention what I consider the most important travel vaccine, influenza. PCPs can counsel patients about food and water safety and insect precautions and provide strategies for self-treatment of traveler’s diarrhea and malaria chemoprophylaxis.
Patients go to a travel clinic because they recognize that they are exposing themselves to risk and want to mitigate that risk. In a primary care office, the PCP has an opportunity to identify patients who don’t know they are at risk and intervene.
Since I also work in a primary care setting, I look for opportunities to identify patients who may be traveling and evaluate their immunization status in that broader context. When I see patients who were born in other countries, I ask if they plan to travel back home. When patients ask for extra prescription refills because they are traveling, I ask where they are going. As part of wellness visits, I ask if my patient has any plans to travel outside the United States in the next year as I assess their vaccine needs. None of these interventions takes much time.
The foundations of travel health include immunization, patient education on food- and waterborne diseases, insect-borne diseases, and safety. PCPs are experts at patient education, risk identification and management, and immunizations.
So ask your patients if they are planning to travel. Make sure everyone’s routine immunizations are current at every visit. Provide every patient with a personal immunization record to take with them when they visit any other provider and when they travel.
More information on travel health is available from the CDC (www.cdc.gov/travel), the International Society of Travel Medicine (www.istm.org), and the American Travel Health Nurses Association (www.athna.org). By availing yourself of these resources, you will protect the health of your community and keep your traveling patients well, wherever they go.
REFERENCES
1. CDC. General recommendations on immunization. www.cdc.gov/vaccines/pubs/pink book/downloads/genrec.pdf. Accessed December 15, 2014.
2. World Tourism Organization. UNWTO Tourism Highlights: 2014 Edition. http://dtxtq4w60xqpw.cloudfront.net/sites/all/file/pdf/unwto_highlights14_en.pdf. Accessed December 15, 2014.
3. Freedman DO. Travel epidemiology. In: Brunette GW, ed. CDC Health Information for International Travel. Atlanta, GA: CDC; 2014:8-11. wwwnc.cdc.gov/travel/yellowbook/2014/chapter-1-introduction/travel-epidemiology. Accessed December 15, 2014.
4. Measles—United States, January 1–August 24, 2013. MMWR Morbid Mortal Wkly Rep. 2013;62(36):741-743.
5. LaRoque RC, Rao SR, Tribris A, et al. Pre-travel health advice-seeking behavior among US international travelers departing from Boston Logan International Airport. J Travel Med. 2010;17(6):387-391.
Chelsea had been stationed with the Peace Corps in Ghana and decided to take her 7-year-old daughter, Amber, with her on a return trip to visit friends she had made there. They planned to spend three weeks in the African nation.
Since Amber was home-schooled, Chelsea had not felt it necessary to follow the CDC guidelines for routine childhood immunizations. Once they planned to travel abroad, however, she made appointments with their primary care provider (PCP) to update Amber’s immunizations and with the travel clinic—where I practice—for yellow fever vaccines (required for entry to Ghana) for both of them.
Chelsea explained their travel plans to the PCP, adding that she intended to get the yellow fever vaccine at another clinic. The PCP administered Amber’s varicella and MMR vaccines.
Aware that it takes 10 days for yellow fever vaccine to be effective, Chelsea scheduled their appointments with me at the travel clinic for two weeks prior to their departure—which was also one week after their visit to the PCP. Did I mention they had nonrefundable tickets?
Chelsea became very upset when I told her I could not give Amber her yellow fever vaccine. I explained the live virus vaccine rule, which states that live virus vaccines must be given either on the same day or 28 days apart.1 If they are not given 28 days apart, the second vaccine—in this case, Amber’s yellow fever immunization—is not considered effective.
Chelsea and Amber were not able to travel to Ghana as planned, because her PCP did not know enough about the administration of yellow fever vaccine. As a result, Chelsea lost $5,000 in airline tickets and cancellation fees. She insisted that her PCP pay her expenses, and her PCP did. But how easily could this have happened in your practice?
Continue for pretravel immunizations >>
It’s been only 100 years since the first commercial airline service began. Today, the travel industry is the largest service industry in the world; 1 billion people traveled internationally in 2013.2 We travel for pleasure, business, education, adventure, adoption, and humanitarian reasons (not to mention visiting friends and family). It is now possible to travel around the world in less than 36 hours.2
Study results vary, but many report that 50% or more of all international travelers will become sick or injured because of their travel.3 Travel health now plays a larger role in public health as travelers bring home more than just souvenirs. Measles outbreaks are at a 30-year high, with many cases attributed to importation by international travelers.4 Many microbes—including SARS, novel influenza strains, and Ebola—are able to spread more easily because of advances in international travel.
The field of travel health grew from the recognition that many of the conditions being treated in infectious disease clinics could have been prevented by pretravel interventions. To address these issues, travel health—a new multidisciplinary specialty—was created, and in 1985 the International Society for Travel Medicine was formed. As a result, the practice of travel health has been concentrated in specialist-led clinics, often in the infectious disease departments of hospitals.
Research indicates that most international travelers do not seek any pretravel health advice.5 When they do, they consult their PCP more often than a travel clinic. Yet most PCPs are woefully undereducated in travel health. Patients such as Chelsea think it is less expensive to consult a PCP first to catch up on routine immunizations before going to a travel clinic for required vaccines. But it makes more sense to consult a travel clinic expert first.
The travel health specialist, who could be an NP, PA, registered pharmacist, RN, or MD, can devise a travel immunization plan that can be coordinated with a PCP to save costs. Many travel clinics don’t accept insurance because most payers do not cover travel health services or immunizations. This includes most private third-party insurers, Medicaid, and Medicare.
But what if Chelsea’s PCP could have provided her travel health needs? It is possible for PCPs to gain knowledge and expertise about travel health, even if they don’t choose to provide every travel immunization.
For example, yellow fever vaccine can only be provided at a certified yellow fever center. Certification requirements are determined at the state level and therefore vary by state. It is possible for PCPs to become certified to administer yellow fever vaccine, if they so choose.
But since not all international travelers require yellow fever vaccine, a PCP could still meet the needs of the majority of patients traveling internationally without taking that step. PCPs can provide vaccination against hepatitis A, typhoid, adult polio, meningococcal disease, Japanese encephalitis, and rabies (preexposure)—not to mention what I consider the most important travel vaccine, influenza. PCPs can counsel patients about food and water safety and insect precautions and provide strategies for self-treatment of traveler’s diarrhea and malaria chemoprophylaxis.
Patients go to a travel clinic because they recognize that they are exposing themselves to risk and want to mitigate that risk. In a primary care office, the PCP has an opportunity to identify patients who don’t know they are at risk and intervene.
Since I also work in a primary care setting, I look for opportunities to identify patients who may be traveling and evaluate their immunization status in that broader context. When I see patients who were born in other countries, I ask if they plan to travel back home. When patients ask for extra prescription refills because they are traveling, I ask where they are going. As part of wellness visits, I ask if my patient has any plans to travel outside the United States in the next year as I assess their vaccine needs. None of these interventions takes much time.
The foundations of travel health include immunization, patient education on food- and waterborne diseases, insect-borne diseases, and safety. PCPs are experts at patient education, risk identification and management, and immunizations.
So ask your patients if they are planning to travel. Make sure everyone’s routine immunizations are current at every visit. Provide every patient with a personal immunization record to take with them when they visit any other provider and when they travel.
More information on travel health is available from the CDC (www.cdc.gov/travel), the International Society of Travel Medicine (www.istm.org), and the American Travel Health Nurses Association (www.athna.org). By availing yourself of these resources, you will protect the health of your community and keep your traveling patients well, wherever they go.
REFERENCES
1. CDC. General recommendations on immunization. www.cdc.gov/vaccines/pubs/pink book/downloads/genrec.pdf. Accessed December 15, 2014.
2. World Tourism Organization. UNWTO Tourism Highlights: 2014 Edition. http://dtxtq4w60xqpw.cloudfront.net/sites/all/file/pdf/unwto_highlights14_en.pdf. Accessed December 15, 2014.
3. Freedman DO. Travel epidemiology. In: Brunette GW, ed. CDC Health Information for International Travel. Atlanta, GA: CDC; 2014:8-11. wwwnc.cdc.gov/travel/yellowbook/2014/chapter-1-introduction/travel-epidemiology. Accessed December 15, 2014.
4. Measles—United States, January 1–August 24, 2013. MMWR Morbid Mortal Wkly Rep. 2013;62(36):741-743.
5. LaRoque RC, Rao SR, Tribris A, et al. Pre-travel health advice-seeking behavior among US international travelers departing from Boston Logan International Airport. J Travel Med. 2010;17(6):387-391.
Chelsea had been stationed with the Peace Corps in Ghana and decided to take her 7-year-old daughter, Amber, with her on a return trip to visit friends she had made there. They planned to spend three weeks in the African nation.
Since Amber was home-schooled, Chelsea had not felt it necessary to follow the CDC guidelines for routine childhood immunizations. Once they planned to travel abroad, however, she made appointments with their primary care provider (PCP) to update Amber’s immunizations and with the travel clinic—where I practice—for yellow fever vaccines (required for entry to Ghana) for both of them.
Chelsea explained their travel plans to the PCP, adding that she intended to get the yellow fever vaccine at another clinic. The PCP administered Amber’s varicella and MMR vaccines.
Aware that it takes 10 days for yellow fever vaccine to be effective, Chelsea scheduled their appointments with me at the travel clinic for two weeks prior to their departure—which was also one week after their visit to the PCP. Did I mention they had nonrefundable tickets?
Chelsea became very upset when I told her I could not give Amber her yellow fever vaccine. I explained the live virus vaccine rule, which states that live virus vaccines must be given either on the same day or 28 days apart.1 If they are not given 28 days apart, the second vaccine—in this case, Amber’s yellow fever immunization—is not considered effective.
Chelsea and Amber were not able to travel to Ghana as planned, because her PCP did not know enough about the administration of yellow fever vaccine. As a result, Chelsea lost $5,000 in airline tickets and cancellation fees. She insisted that her PCP pay her expenses, and her PCP did. But how easily could this have happened in your practice?
Continue for pretravel immunizations >>
It’s been only 100 years since the first commercial airline service began. Today, the travel industry is the largest service industry in the world; 1 billion people traveled internationally in 2013.2 We travel for pleasure, business, education, adventure, adoption, and humanitarian reasons (not to mention visiting friends and family). It is now possible to travel around the world in less than 36 hours.2
Study results vary, but many report that 50% or more of all international travelers will become sick or injured because of their travel.3 Travel health now plays a larger role in public health as travelers bring home more than just souvenirs. Measles outbreaks are at a 30-year high, with many cases attributed to importation by international travelers.4 Many microbes—including SARS, novel influenza strains, and Ebola—are able to spread more easily because of advances in international travel.
The field of travel health grew from the recognition that many of the conditions being treated in infectious disease clinics could have been prevented by pretravel interventions. To address these issues, travel health—a new multidisciplinary specialty—was created, and in 1985 the International Society for Travel Medicine was formed. As a result, the practice of travel health has been concentrated in specialist-led clinics, often in the infectious disease departments of hospitals.
Research indicates that most international travelers do not seek any pretravel health advice.5 When they do, they consult their PCP more often than a travel clinic. Yet most PCPs are woefully undereducated in travel health. Patients such as Chelsea think it is less expensive to consult a PCP first to catch up on routine immunizations before going to a travel clinic for required vaccines. But it makes more sense to consult a travel clinic expert first.
The travel health specialist, who could be an NP, PA, registered pharmacist, RN, or MD, can devise a travel immunization plan that can be coordinated with a PCP to save costs. Many travel clinics don’t accept insurance because most payers do not cover travel health services or immunizations. This includes most private third-party insurers, Medicaid, and Medicare.
But what if Chelsea’s PCP could have provided her travel health needs? It is possible for PCPs to gain knowledge and expertise about travel health, even if they don’t choose to provide every travel immunization.
For example, yellow fever vaccine can only be provided at a certified yellow fever center. Certification requirements are determined at the state level and therefore vary by state. It is possible for PCPs to become certified to administer yellow fever vaccine, if they so choose.
But since not all international travelers require yellow fever vaccine, a PCP could still meet the needs of the majority of patients traveling internationally without taking that step. PCPs can provide vaccination against hepatitis A, typhoid, adult polio, meningococcal disease, Japanese encephalitis, and rabies (preexposure)—not to mention what I consider the most important travel vaccine, influenza. PCPs can counsel patients about food and water safety and insect precautions and provide strategies for self-treatment of traveler’s diarrhea and malaria chemoprophylaxis.
Patients go to a travel clinic because they recognize that they are exposing themselves to risk and want to mitigate that risk. In a primary care office, the PCP has an opportunity to identify patients who don’t know they are at risk and intervene.
Since I also work in a primary care setting, I look for opportunities to identify patients who may be traveling and evaluate their immunization status in that broader context. When I see patients who were born in other countries, I ask if they plan to travel back home. When patients ask for extra prescription refills because they are traveling, I ask where they are going. As part of wellness visits, I ask if my patient has any plans to travel outside the United States in the next year as I assess their vaccine needs. None of these interventions takes much time.
The foundations of travel health include immunization, patient education on food- and waterborne diseases, insect-borne diseases, and safety. PCPs are experts at patient education, risk identification and management, and immunizations.
So ask your patients if they are planning to travel. Make sure everyone’s routine immunizations are current at every visit. Provide every patient with a personal immunization record to take with them when they visit any other provider and when they travel.
More information on travel health is available from the CDC (www.cdc.gov/travel), the International Society of Travel Medicine (www.istm.org), and the American Travel Health Nurses Association (www.athna.org). By availing yourself of these resources, you will protect the health of your community and keep your traveling patients well, wherever they go.
REFERENCES
1. CDC. General recommendations on immunization. www.cdc.gov/vaccines/pubs/pink book/downloads/genrec.pdf. Accessed December 15, 2014.
2. World Tourism Organization. UNWTO Tourism Highlights: 2014 Edition. http://dtxtq4w60xqpw.cloudfront.net/sites/all/file/pdf/unwto_highlights14_en.pdf. Accessed December 15, 2014.
3. Freedman DO. Travel epidemiology. In: Brunette GW, ed. CDC Health Information for International Travel. Atlanta, GA: CDC; 2014:8-11. wwwnc.cdc.gov/travel/yellowbook/2014/chapter-1-introduction/travel-epidemiology. Accessed December 15, 2014.
4. Measles—United States, January 1–August 24, 2013. MMWR Morbid Mortal Wkly Rep. 2013;62(36):741-743.
5. LaRoque RC, Rao SR, Tribris A, et al. Pre-travel health advice-seeking behavior among US international travelers departing from Boston Logan International Airport. J Travel Med. 2010;17(6):387-391.
A step away from immediate umbilical cord clamping
The common practice of immediate cord clamping, which generally means clamping within 15-20 seconds after birth, was fueled by efforts to reduce the risk of postpartum hemorrhage, a leading cause of maternal death worldwide. Immediate clamping was part of a full active management intervention recommended in 2007 by the World Health Organization, along with the use of uterotonics (generally oxytocin) immediately after birth and controlled cord traction to quickly deliver the placenta.
Adoption of the WHO-recommended “active management during the third stage of labor” (AMTSL) worked, leading to a 70% reduction in postpartum hemorrhage and a 60% reduction in blood transfusion over passive management. However, it appears that immediate cord clamping has not played an important role in these reductions. Several randomized controlled trials have shown that early clamping does not impact the risk of postpartum hemorrhage (> 1000 cc or > 500 cc), nor does it impact the need for manual removal of the placenta or the need for blood transfusion.
Instead, the critical component of the AMTSL package appears to be administration of a uterotonic, as reported in a large WHO-directed multicenter clinical trial published in 2012. The study also found that women who received controlled cord traction bled an average of 11 cc less – an insignificant difference – than did women who delivered their placentas by their own effort. Moreover, they had a third stage of labor that was an average of 6 minutes shorter (Lancet 2012;379:1721-7).

With assurance that the timing of umbilical cord clamping does not impact maternal outcomes, investigators have begun to look more at the impact of immediate versus delayed cord clamping on the health of the baby.
Thus far, the issues in this arena are a bit more complicated than on the maternal side. There are indications, however, that slight delays in umbilical cord clamping may be beneficial for the newborn – particularly for preterm infants, who appear in systemic reviews to have a nearly 50% reduction in intraventricular hemorrhage when clamping is delayed.
Timing in term infants
The theoretical benefits of delayed cord clamping include increased neonatal blood volume (improved perfusion and decreased organ injury), more time for spontaneous breathing (reduced risks of resuscitation and a smoother transition of cardiopulmonary and cerebral circulation), and increased stem cells for the infant (anti-inflammatory, neurotropic, and neuroprotective effects).

Theoretically, delayed clamping will increase the infant’s iron stores and lower the incidence of iron deficiency anemia during infancy. This is particularly relevant in developing countries, where up to 50% of infants have anemia by 1 year of age. Anemia is consistently associated with abnormal neurodevelopment, and treatment may not always reverse developmental issues.
On the negative side, delayed clamping is associated with theoretical concerns about hyperbilirubinemia and jaundice, hypothermia, polycythemia, and delays in the bonding of infants and mothers.
For term infants, our best reading on the benefits and risks of delayed umbilical cord clamping comes from a 2013 Cochrane systematic review that assessed results from 15 randomized controlled trials involving 3,911 women and infant pairs. Early cord clamping was generally carried out within 60 seconds of birth, whereas delayed cord clamping involved clamping the umbilical cord more than 1 minute after birth or when cord pulsation has ceased.
The review found that delayed clamping was associated with a significantly higher neonatal hemoglobin concentration at 24-48 hours postpartum (a weighted mean difference of 2 g/dL) and increased iron reserves up to 6 months after birth. Infants in the early clamping group were more than twice as likely to be iron deficient at 3-6 months compared with infants whose cord clamping was delayed (Cochrane Database Syst. Rev. 2013;7:CD004074)
There were no significant differences between early and late clamping in neonatal mortality or for most other neonatal morbidity outcomes. Delayed clamping also did not increase the risk of severe postpartum hemorrhage, blood loss, or reduced hemoglobin levels in mothers.
The downside to delayed cord clamping was an increased risk of jaundice requiring phototherapy. Infants in the later cord clamping group were 40% more likely to need phototherapy – a difference that equates to 3% of infants in the early clamping group and 5% of infants in the late clamping group.
Data were insufficient in the Cochrane review to draw reliable conclusions about the comparative effects on other short-term outcomes such as symptomatic polycythemia, respiratory problems, hypothermia, and infection, as data were limited on long-term outcomes.
In practice, this means that the risk of jaundice must be weighed against the risk of iron deficiency. In developed countries we have the resources both to increase iron stores of infants and to provide phototherapy. While the WHO recommends umbilical cord clamping after 1-3 minutes to improve an infant’s iron status, I do not believe the evidence is strong enough to universally adopt such delayed cord clamping in the United States.
Considering the risks of jaundice and the relative infrequency of iron deficiency in the United States, we should not routinely delay clamping for term infants at this point.
A recent committee opinion developed by the American College of Obstetricians and Gynecologists and endorsed by the American Academy of Pediatrics (No. 543, December 2012) captures this view by concluding that “insufficient evidence exists to support or to refute the benefits from delayed umbilical cord clamping for term infants that are born in settings with rich resources.” Although the ACOG opinion preceded the Cochrane review, the committee, of which I was a member, reviewed much of the same literature.
Timing in preterm infants
Preterm neonates are at increased risk of temperature dysregulation, hypotension, and the need for rapid initial pediatric care and blood transfusion. The increased risk of intraventricular hemorrhage and necrotizing enterocolitis in preterm infants is possibly related to the increased risk of hypotension.
As with term infants, a 2012 Cochrane systematic review offers good insight on our current knowledge. This review of umbilical cord clamping at preterm birth covers 15 studies that included 738 infants delivered between 24 and 36 weeks of gestation. The timing of umbilical cord clamping ranged from 25 seconds to a maximum of 180 seconds (Cochrane Database Syst. Rev. 2012;8:CD003248).
Delayed cord clamping was associated with fewer transfusions for anemia or low blood pressure, less intraventricular hemorrhage of all grades (relative risk 0.59), and a lower risk for necrotizing enterocolitis (relative risk 0.62), compared with immediate clamping.
While there were no clear differences with respect to severe intraventricular hemorrhage (grades 3-4), the nearly 50% reduction in intraventricular hemorrhage overall among deliveries with delayed clamping was significant enough to prompt ACOG to conclude that delayed cord clamping should be considered for preterm infants. This reduction in intraventricular hemorrhage appears to be the single most important benefit, based on current findings.
The data on cord clamping in preterm infants are suggestive of benefit, but are not robust. The studies published thus far have been small, and many of them, as the 2012 Cochrane review points out, involved incomplete reporting and wide confidence intervals. Moreover, just as with the studies on term infants, there has been a lack of long-term follow-up in most of the published trials.
When considering delayed cord clamping in preterm infants, as the ACOG Committee Opinion recommends, I urge focusing on earlier gestational ages. Allowing more placental transfusion at births that occur at or after 36 weeks of gestation may not make much sense because by that point the risk of intraventricular hemorrhage is almost nonexistent.
Our practice and the future
At our institution, births that occur at less than 32 weeks of gestation are eligible for delayed umbilical cord clamping, usually at 30-45 seconds after birth. The main contraindications are placental abruption and multiples.
We do not perform any milking or stripping of the umbilical cord, as the risks are unknown and it is not yet clear whether such practices are equivalent to delayed cord clamping. Compared with delayed cord clamping, which is a natural passive transfusion of placental blood to the infant, milking and stripping are not physiologic.
Additional data from an ongoing large international multicenter study, the Australian Placental Transfusion Study, may resolve some of the current controversy. This study is evaluating the cord clamping in neonates < 30 weeks’ gestation. Another study ongoing in Europe should also provide more information.
These studies – and other trials that are larger and longer than the trials published thus far – are necessary to evaluate long-term outcomes and to establish the ideal timing for umbilical cord clamping. Research is also needed to evaluate the management of the third stage of labor relative to umbilical cord clamping as well as the timing in relation to the initiation of voluntary or assisted ventilation.
Dr. Macones said he had no relevant financial disclosures.
Dr. Macones is the Mitchell and Elaine Yanow Professor and Chair, and director of the division of maternal-fetal medicine and ultrasound in the department of obstetrics and gynecology at Washington University, St. Louis.
The common practice of immediate cord clamping, which generally means clamping within 15-20 seconds after birth, was fueled by efforts to reduce the risk of postpartum hemorrhage, a leading cause of maternal death worldwide. Immediate clamping was part of a full active management intervention recommended in 2007 by the World Health Organization, along with the use of uterotonics (generally oxytocin) immediately after birth and controlled cord traction to quickly deliver the placenta.
Adoption of the WHO-recommended “active management during the third stage of labor” (AMTSL) worked, leading to a 70% reduction in postpartum hemorrhage and a 60% reduction in blood transfusion over passive management. However, it appears that immediate cord clamping has not played an important role in these reductions. Several randomized controlled trials have shown that early clamping does not impact the risk of postpartum hemorrhage (> 1000 cc or > 500 cc), nor does it impact the need for manual removal of the placenta or the need for blood transfusion.
Instead, the critical component of the AMTSL package appears to be administration of a uterotonic, as reported in a large WHO-directed multicenter clinical trial published in 2012. The study also found that women who received controlled cord traction bled an average of 11 cc less – an insignificant difference – than did women who delivered their placentas by their own effort. Moreover, they had a third stage of labor that was an average of 6 minutes shorter (Lancet 2012;379:1721-7).
With assurance that the timing of umbilical cord clamping does not impact maternal outcomes, investigators have begun to look more at the impact of immediate versus delayed cord clamping on the health of the baby.
Thus far, the issues in this arena are a bit more complicated than on the maternal side. There are indications, however, that slight delays in umbilical cord clamping may be beneficial for the newborn – particularly for preterm infants, who appear in systemic reviews to have a nearly 50% reduction in intraventricular hemorrhage when clamping is delayed.
Timing in term infants
The theoretical benefits of delayed cord clamping include increased neonatal blood volume (improved perfusion and decreased organ injury), more time for spontaneous breathing (reduced risks of resuscitation and a smoother transition of cardiopulmonary and cerebral circulation), and increased stem cells for the infant (anti-inflammatory, neurotropic, and neuroprotective effects).
Theoretically, delayed clamping will increase the infant’s iron stores and lower the incidence of iron deficiency anemia during infancy. This is particularly relevant in developing countries, where up to 50% of infants have anemia by 1 year of age. Anemia is consistently associated with abnormal neurodevelopment, and treatment may not always reverse developmental issues.
On the negative side, delayed clamping is associated with theoretical concerns about hyperbilirubinemia and jaundice, hypothermia, polycythemia, and delays in the bonding of infants and mothers.
For term infants, our best reading on the benefits and risks of delayed umbilical cord clamping comes from a 2013 Cochrane systematic review that assessed results from 15 randomized controlled trials involving 3,911 women and infant pairs. Early cord clamping was generally carried out within 60 seconds of birth, whereas delayed cord clamping involved clamping the umbilical cord more than 1 minute after birth or when cord pulsation has ceased.
The review found that delayed clamping was associated with a significantly higher neonatal hemoglobin concentration at 24-48 hours postpartum (a weighted mean difference of 2 g/dL) and increased iron reserves up to 6 months after birth. Infants in the early clamping group were more than twice as likely to be iron deficient at 3-6 months compared with infants whose cord clamping was delayed (Cochrane Database Syst. Rev. 2013;7:CD004074)
There were no significant differences between early and late clamping in neonatal mortality or for most other neonatal morbidity outcomes. Delayed clamping also did not increase the risk of severe postpartum hemorrhage, blood loss, or reduced hemoglobin levels in mothers.
The downside to delayed cord clamping was an increased risk of jaundice requiring phototherapy. Infants in the later cord clamping group were 40% more likely to need phototherapy – a difference that equates to 3% of infants in the early clamping group and 5% of infants in the late clamping group.
Data were insufficient in the Cochrane review to draw reliable conclusions about the comparative effects on other short-term outcomes such as symptomatic polycythemia, respiratory problems, hypothermia, and infection, as data were limited on long-term outcomes.
In practice, this means that the risk of jaundice must be weighed against the risk of iron deficiency. In developed countries we have the resources both to increase iron stores of infants and to provide phototherapy. While the WHO recommends umbilical cord clamping after 1-3 minutes to improve an infant’s iron status, I do not believe the evidence is strong enough to universally adopt such delayed cord clamping in the United States.
Considering the risks of jaundice and the relative infrequency of iron deficiency in the United States, we should not routinely delay clamping for term infants at this point.
A recent committee opinion developed by the American College of Obstetricians and Gynecologists and endorsed by the American Academy of Pediatrics (No. 543, December 2012) captures this view by concluding that “insufficient evidence exists to support or to refute the benefits from delayed umbilical cord clamping for term infants that are born in settings with rich resources.” Although the ACOG opinion preceded the Cochrane review, the committee, of which I was a member, reviewed much of the same literature.
Timing in preterm infants
Preterm neonates are at increased risk of temperature dysregulation, hypotension, and the need for rapid initial pediatric care and blood transfusion. The increased risk of intraventricular hemorrhage and necrotizing enterocolitis in preterm infants is possibly related to the increased risk of hypotension.
As with term infants, a 2012 Cochrane systematic review offers good insight on our current knowledge. This review of umbilical cord clamping at preterm birth covers 15 studies that included 738 infants delivered between 24 and 36 weeks of gestation. The timing of umbilical cord clamping ranged from 25 seconds to a maximum of 180 seconds (Cochrane Database Syst. Rev. 2012;8:CD003248).
Delayed cord clamping was associated with fewer transfusions for anemia or low blood pressure, less intraventricular hemorrhage of all grades (relative risk 0.59), and a lower risk for necrotizing enterocolitis (relative risk 0.62), compared with immediate clamping.
While there were no clear differences with respect to severe intraventricular hemorrhage (grades 3-4), the nearly 50% reduction in intraventricular hemorrhage overall among deliveries with delayed clamping was significant enough to prompt ACOG to conclude that delayed cord clamping should be considered for preterm infants. This reduction in intraventricular hemorrhage appears to be the single most important benefit, based on current findings.
The data on cord clamping in preterm infants are suggestive of benefit, but are not robust. The studies published thus far have been small, and many of them, as the 2012 Cochrane review points out, involved incomplete reporting and wide confidence intervals. Moreover, just as with the studies on term infants, there has been a lack of long-term follow-up in most of the published trials.
When considering delayed cord clamping in preterm infants, as the ACOG Committee Opinion recommends, I urge focusing on earlier gestational ages. Allowing more placental transfusion at births that occur at or after 36 weeks of gestation may not make much sense because by that point the risk of intraventricular hemorrhage is almost nonexistent.
Our practice and the future
At our institution, births that occur at less than 32 weeks of gestation are eligible for delayed umbilical cord clamping, usually at 30-45 seconds after birth. The main contraindications are placental abruption and multiples.
We do not perform any milking or stripping of the umbilical cord, as the risks are unknown and it is not yet clear whether such practices are equivalent to delayed cord clamping. Compared with delayed cord clamping, which is a natural passive transfusion of placental blood to the infant, milking and stripping are not physiologic.
Additional data from an ongoing large international multicenter study, the Australian Placental Transfusion Study, may resolve some of the current controversy. This study is evaluating the cord clamping in neonates < 30 weeks’ gestation. Another study ongoing in Europe should also provide more information.
These studies – and other trials that are larger and longer than the trials published thus far – are necessary to evaluate long-term outcomes and to establish the ideal timing for umbilical cord clamping. Research is also needed to evaluate the management of the third stage of labor relative to umbilical cord clamping as well as the timing in relation to the initiation of voluntary or assisted ventilation.
Dr. Macones said he had no relevant financial disclosures.
Dr. Macones is the Mitchell and Elaine Yanow Professor and Chair, and director of the division of maternal-fetal medicine and ultrasound in the department of obstetrics and gynecology at Washington University, St. Louis.
The common practice of immediate cord clamping, which generally means clamping within 15-20 seconds after birth, was fueled by efforts to reduce the risk of postpartum hemorrhage, a leading cause of maternal death worldwide. Immediate clamping was part of a full active management intervention recommended in 2007 by the World Health Organization, along with the use of uterotonics (generally oxytocin) immediately after birth and controlled cord traction to quickly deliver the placenta.
Adoption of the WHO-recommended “active management during the third stage of labor” (AMTSL) worked, leading to a 70% reduction in postpartum hemorrhage and a 60% reduction in blood transfusion over passive management. However, it appears that immediate cord clamping has not played an important role in these reductions. Several randomized controlled trials have shown that early clamping does not impact the risk of postpartum hemorrhage (> 1000 cc or > 500 cc), nor does it impact the need for manual removal of the placenta or the need for blood transfusion.
Instead, the critical component of the AMTSL package appears to be administration of a uterotonic, as reported in a large WHO-directed multicenter clinical trial published in 2012. The study also found that women who received controlled cord traction bled an average of 11 cc less – an insignificant difference – than did women who delivered their placentas by their own effort. Moreover, they had a third stage of labor that was an average of 6 minutes shorter (Lancet 2012;379:1721-7).
With assurance that the timing of umbilical cord clamping does not impact maternal outcomes, investigators have begun to look more at the impact of immediate versus delayed cord clamping on the health of the baby.
Thus far, the issues in this arena are a bit more complicated than on the maternal side. There are indications, however, that slight delays in umbilical cord clamping may be beneficial for the newborn – particularly for preterm infants, who appear in systemic reviews to have a nearly 50% reduction in intraventricular hemorrhage when clamping is delayed.
Timing in term infants
The theoretical benefits of delayed cord clamping include increased neonatal blood volume (improved perfusion and decreased organ injury), more time for spontaneous breathing (reduced risks of resuscitation and a smoother transition of cardiopulmonary and cerebral circulation), and increased stem cells for the infant (anti-inflammatory, neurotropic, and neuroprotective effects).
Theoretically, delayed clamping will increase the infant’s iron stores and lower the incidence of iron deficiency anemia during infancy. This is particularly relevant in developing countries, where up to 50% of infants have anemia by 1 year of age. Anemia is consistently associated with abnormal neurodevelopment, and treatment may not always reverse developmental issues.
On the negative side, delayed clamping is associated with theoretical concerns about hyperbilirubinemia and jaundice, hypothermia, polycythemia, and delays in the bonding of infants and mothers.
For term infants, our best reading on the benefits and risks of delayed umbilical cord clamping comes from a 2013 Cochrane systematic review that assessed results from 15 randomized controlled trials involving 3,911 women and infant pairs. Early cord clamping was generally carried out within 60 seconds of birth, whereas delayed cord clamping involved clamping the umbilical cord more than 1 minute after birth or when cord pulsation has ceased.
The review found that delayed clamping was associated with a significantly higher neonatal hemoglobin concentration at 24-48 hours postpartum (a weighted mean difference of 2 g/dL) and increased iron reserves up to 6 months after birth. Infants in the early clamping group were more than twice as likely to be iron deficient at 3-6 months compared with infants whose cord clamping was delayed (Cochrane Database Syst. Rev. 2013;7:CD004074)
There were no significant differences between early and late clamping in neonatal mortality or for most other neonatal morbidity outcomes. Delayed clamping also did not increase the risk of severe postpartum hemorrhage, blood loss, or reduced hemoglobin levels in mothers.
The downside to delayed cord clamping was an increased risk of jaundice requiring phototherapy. Infants in the later cord clamping group were 40% more likely to need phototherapy – a difference that equates to 3% of infants in the early clamping group and 5% of infants in the late clamping group.
Data were insufficient in the Cochrane review to draw reliable conclusions about the comparative effects on other short-term outcomes such as symptomatic polycythemia, respiratory problems, hypothermia, and infection, as data were limited on long-term outcomes.
In practice, this means that the risk of jaundice must be weighed against the risk of iron deficiency. In developed countries we have the resources both to increase iron stores of infants and to provide phototherapy. While the WHO recommends umbilical cord clamping after 1-3 minutes to improve an infant’s iron status, I do not believe the evidence is strong enough to universally adopt such delayed cord clamping in the United States.
Considering the risks of jaundice and the relative infrequency of iron deficiency in the United States, we should not routinely delay clamping for term infants at this point.
A recent committee opinion developed by the American College of Obstetricians and Gynecologists and endorsed by the American Academy of Pediatrics (No. 543, December 2012) captures this view by concluding that “insufficient evidence exists to support or to refute the benefits from delayed umbilical cord clamping for term infants that are born in settings with rich resources.” Although the ACOG opinion preceded the Cochrane review, the committee, of which I was a member, reviewed much of the same literature.
Timing in preterm infants
Preterm neonates are at increased risk of temperature dysregulation, hypotension, and the need for rapid initial pediatric care and blood transfusion. The increased risk of intraventricular hemorrhage and necrotizing enterocolitis in preterm infants is possibly related to the increased risk of hypotension.
As with term infants, a 2012 Cochrane systematic review offers good insight on our current knowledge. This review of umbilical cord clamping at preterm birth covers 15 studies that included 738 infants delivered between 24 and 36 weeks of gestation. The timing of umbilical cord clamping ranged from 25 seconds to a maximum of 180 seconds (Cochrane Database Syst. Rev. 2012;8:CD003248).
Delayed cord clamping was associated with fewer transfusions for anemia or low blood pressure, less intraventricular hemorrhage of all grades (relative risk 0.59), and a lower risk for necrotizing enterocolitis (relative risk 0.62), compared with immediate clamping.
While there were no clear differences with respect to severe intraventricular hemorrhage (grades 3-4), the nearly 50% reduction in intraventricular hemorrhage overall among deliveries with delayed clamping was significant enough to prompt ACOG to conclude that delayed cord clamping should be considered for preterm infants. This reduction in intraventricular hemorrhage appears to be the single most important benefit, based on current findings.
The data on cord clamping in preterm infants are suggestive of benefit, but are not robust. The studies published thus far have been small, and many of them, as the 2012 Cochrane review points out, involved incomplete reporting and wide confidence intervals. Moreover, just as with the studies on term infants, there has been a lack of long-term follow-up in most of the published trials.
When considering delayed cord clamping in preterm infants, as the ACOG Committee Opinion recommends, I urge focusing on earlier gestational ages. Allowing more placental transfusion at births that occur at or after 36 weeks of gestation may not make much sense because by that point the risk of intraventricular hemorrhage is almost nonexistent.
Our practice and the future
At our institution, births that occur at less than 32 weeks of gestation are eligible for delayed umbilical cord clamping, usually at 30-45 seconds after birth. The main contraindications are placental abruption and multiples.
We do not perform any milking or stripping of the umbilical cord, as the risks are unknown and it is not yet clear whether such practices are equivalent to delayed cord clamping. Compared with delayed cord clamping, which is a natural passive transfusion of placental blood to the infant, milking and stripping are not physiologic.
Additional data from an ongoing large international multicenter study, the Australian Placental Transfusion Study, may resolve some of the current controversy. This study is evaluating the cord clamping in neonates < 30 weeks’ gestation. Another study ongoing in Europe should also provide more information.
These studies – and other trials that are larger and longer than the trials published thus far – are necessary to evaluate long-term outcomes and to establish the ideal timing for umbilical cord clamping. Research is also needed to evaluate the management of the third stage of labor relative to umbilical cord clamping as well as the timing in relation to the initiation of voluntary or assisted ventilation.
Dr. Macones said he had no relevant financial disclosures.
Dr. Macones is the Mitchell and Elaine Yanow Professor and Chair, and director of the division of maternal-fetal medicine and ultrasound in the department of obstetrics and gynecology at Washington University, St. Louis.
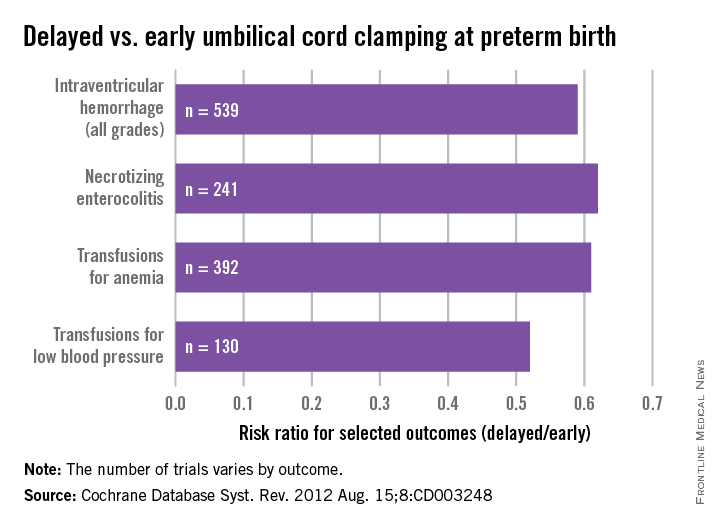
College transition
Perhaps the greatest transition in an adolescent’s life is the transition to college. The process of preparation, investigation, application, interviewing, waiting, choosing, and preparing to leave for college is one of the most exciting, exhausting, and challenging experiences in the life of an adolescent and his or her family. The final selection of a school can mark a shorthand summary of accomplishment and builds a major piece of a young adult’s identity.
Although there are certainly many steps to autonomy through childhood – walking, starting school, being home alone, driving a car – none compares to leaving the warmth and structure of home for the college experience. Once in the dorm, teens are probably more alone and independent than they have ever been before, likely without any long-standing friends, in an unfamiliar setting, and facing high expectations. College offers structure and support to help with this transition, and most adolescents are ready and even eager to start to manage their own lives pragmatically, academically, and socially. But there will be setbacks and failures, big and small, as they navigate new territory with virtually full independence. This transition would be a challenge to a mature adult and is daunting to someone who is doing this for the first time and with an identity that is still forming.
We know that most teenagers make this transition successfully. However, we also know that this new level of independence and responsibility and the loss of supervision and structure can place adolescents at risk for several problems. Some adolescents make poor or risky choices with serious consequences. Depression affects about 20% of all freshmen, with consequences that range from mild to severe, sometimes requiring a leave of absence. Many students who have managed mild problems with anxiety or body image may find that with more stress and less support, these problems grow into eating disorders and substance abuse disorders. It now appears that sexual assaults on campuses, often during “frat” parties and in the setting of substance use, are far more prevalent than previously acknowledged. Recently in the news was the tragic accident of a young woman under the influence of substances who was seriously injured when she fell out of a window. Finally, we know the most prevalent morbidity and mortality are from car accidents, many of which are related to risk taking and substance use.
Clearly there are critical developmental gains toward healthy adulthood when this transition goes well, and quite substantial risks when it does not. Pediatricians quite commonly follow their patients well into the college years, and at least treat patients during the time in which they are preparing to leave for college. Therefore the transition from high school to college can be considered a part of pediatric primary care. How can a pediatrician contribute to the adolescent’s preparations for this transition to essentially full, day-to-day autonomy? The pediatrician is in a position to offer meaningful guidance to these adolescent patients, and in some cases to their parents as well, particularly on the subjects of substance use, mental health, and sexuality. This process starts in early high school, with progressively more detailed and frank discussions into and through college.
Substance use
For purposes of this discussion, let’s focus on alcohol use. Talking about the risks of alcohol probably should start in late junior high and upon entry to high school. But if you have not yet had a discussion with your adolescent patient about drugs and alcohol, it is not too late to have one during the time before they start college. It would be helpful to learn about their personal and family history of alcohol and drug use. How has alcohol been discussed, and more importantly, used in the home by parents? What are your patients’ attitudes to drinking and related social pressure? Have they needed to be “rescued,” or have they needed to rescue friends? Have they been the designated driver? Have they passed out or seen someone pass out at a party? In these situations, how have they coped? What decisions have they made? Is there a pattern of self-monitoring or largely one of risk taking? What do they imagine college will be like with regard to drinking?
For your patients who have been decidedly sober through high school, it will be important to find out if they are curious about trying alcohol once they are on campus. Even if they voice shocked refusal, you might speak generally with them about the easy availability of alcohol at many parties on campus, particularly if they join a fraternity or sorority or even plan to be on a varsity sports team. Superior athletes are often surrounded by older students and often gain access to parties as freshmen or sophomores surrounded by far more experienced seniors. Speaking generally about how common it is to try alcohol in college, while offering details on how easy it can be for first-time drinkers to become drunk, can be very valuable. You might even offer them data and strategies on how to pace themselves: one drink per hour, no hard alcohol or “mysterious punch,” or two glasses of water for every beer are a few such strategies. You might note how quickly alcohol is absorbed and the risks of rapid ingestion of larger quantities. You should be clear that you are not endorsing underage drinking. Your goal is to ensure that they are equipped with knowledge about smart self-care, especially as intoxication can put them at risk for being victimized or exploited sexually, for serious accidents, for administrative problems, and even for medical consequences.
For your patients who have been risk takers, especially if they have had trouble with drugs or alcohol in high school, it will be important to speak with them about the likelihood that a risky pattern of substance use in high school will grow into a more serious problem in the less-supervised college setting. While this may sound to them like the exciting chance to have easier access and fewer restrictions or punishments, you have the opportunity to complicate their thinking about what this will actually mean. In all likelihood, their use will grow into a problem of abuse or dependence and could easily threaten their ability to succeed at college, landing them back in a far more restrictive setting. It may be valuable to talk with your patients about how they would know if their drug or alcohol use was becoming a problem. When would they say they have reached a limit they are concerned about? Would they be willing to see a therapist or psychiatrist about their substance use before leaving for college to make thoughtful plans for how to manage it? If they are willing, it may be protective to invite their parents into this conversation so that there is a better chance that they may discuss this with their parents outside of your office and once they are on campus.
Mental health
The prevalence of depressive and anxiety symptoms in the college years is very high, likely because of a combination of external stressors, loss of external supports, and continued rapid physical and neurologic development. For adolescents who have not experienced any mental health problems, it can be protective to have a conversation with them about the real risks of developing a mental health problem while they are at school and the value and efficacy of early treatment. You might tell them that while some anxiety and sadness are to be expected during a challenging transition, experiencing intense anxiety or sadness that is sustained (2 weeks or more) and that interferes with their functioning should prompt them to seek help from the student health services. They should be on the lookout for sustained disruptions in their sleep and loss of appetite and energy (the classic neurovegetative symptoms), and of course, any emerging hopelessness or suicidal preoccupation also should prompt them to turn to student health services for evaluation and support.
For your patients who have a history of psychiatric problems and treatment, it is critical – even if they are in remission – that you review with them when they should turn to the campus student health services for evaluation. What symptoms have indicated a worsening problem or relapse for them in the past? What might be the earliest signs of deterioration? If they are in active treatment, you should ensure that the treatment provider has built a transition plan for their treatment to continue on campus. Helping these patients to be smart about their self-care, just as you would if they were responsible for continuing treatment of their diabetes away from the supports of home, can be a powerful preventative intervention.
Sexuality
In all likelihood, you have already had a conversation about sex, even a brief one, with your adolescent patients by the time they are packing for college. But this is a key time to revisit the subject with them. You can begin an open-ended discussion about the fact that the years in college are commonly a time when adolescents start having sex (if they have not already done so). As such, it is important for them to learn about birth control and protection against sexually transmitted infections. This is normally a developmental stage in which sex becomes a more fully integrated part of their emerging identity and their healthy adult life. They may find that they develop a fuller awareness of whom they are attracted to and what they enjoy, and it is commonly a time of some experimentation or exploration. It is very meaningful for your young patients to hear about this nonjudgmentally from their pediatrician. This discussion should include some prevention, in the form of talk about the risks of sexual assault on campus. Help your patients, both male and female, to consider how new independence and access to alcohol can be a dangerous mix with the intense social scene on college campuses. Many situations in which they will be socializing with strangers will involve alcohol, even drugs. Would they have sex with someone if they or their partner were intoxicated? How would they know if the person they were connecting with was actually very intoxicated? How might they think about protecting a friend who seemed to be very intoxicated and at risk for sexual exploitation or assault? If they think they are witnessing a sexual assault or a risky situation, what could they do? If they are considering sex with someone, is it because they are attracted to and interested in that person, or are they feeling pressured, anxious, or bullied? Remind them that while exploration is healthy and should be fun, it also is wise to go slowly when something is new, and to be especially cautious when substance use is involved. They can protect themselves and their friends from the trauma of assault or of being accused of assaulting someone who could not meaningfully consent to sex with some thoughtful anticipation and planning. They took great care to arrange to get into college, and they can take equally great care with their own health and well-being.
Progressively relevant and honest discussions between a pediatrician and teenage patient can have a meaningful impact. Consider how teens could have access to you during their freshman year. Should they have your pager or your cell phone number if they feel they need your help? Should you schedule a psychosocial follow-up visit during a holiday break first semester and again as indicated? Doing what you can to anticipate and prevent harm during the transition to college is highly relevant to many if not all of your patients.
Dr. Swick is an attending psychiatrist in the division of child psychiatry at Massachusetts General Hospital, Boston, and director of the Parenting at a Challenging Time (PACT) Program at the Vernon Cancer Center at Newton Wellesley Hospital, also in Boston. Dr. Jellinek is professor of psychiatry and of pediatrics at Harvard Medical School, Boston. E-mail them at [email protected].
Perhaps the greatest transition in an adolescent’s life is the transition to college. The process of preparation, investigation, application, interviewing, waiting, choosing, and preparing to leave for college is one of the most exciting, exhausting, and challenging experiences in the life of an adolescent and his or her family. The final selection of a school can mark a shorthand summary of accomplishment and builds a major piece of a young adult’s identity.
Although there are certainly many steps to autonomy through childhood – walking, starting school, being home alone, driving a car – none compares to leaving the warmth and structure of home for the college experience. Once in the dorm, teens are probably more alone and independent than they have ever been before, likely without any long-standing friends, in an unfamiliar setting, and facing high expectations. College offers structure and support to help with this transition, and most adolescents are ready and even eager to start to manage their own lives pragmatically, academically, and socially. But there will be setbacks and failures, big and small, as they navigate new territory with virtually full independence. This transition would be a challenge to a mature adult and is daunting to someone who is doing this for the first time and with an identity that is still forming.
We know that most teenagers make this transition successfully. However, we also know that this new level of independence and responsibility and the loss of supervision and structure can place adolescents at risk for several problems. Some adolescents make poor or risky choices with serious consequences. Depression affects about 20% of all freshmen, with consequences that range from mild to severe, sometimes requiring a leave of absence. Many students who have managed mild problems with anxiety or body image may find that with more stress and less support, these problems grow into eating disorders and substance abuse disorders. It now appears that sexual assaults on campuses, often during “frat” parties and in the setting of substance use, are far more prevalent than previously acknowledged. Recently in the news was the tragic accident of a young woman under the influence of substances who was seriously injured when she fell out of a window. Finally, we know the most prevalent morbidity and mortality are from car accidents, many of which are related to risk taking and substance use.
Clearly there are critical developmental gains toward healthy adulthood when this transition goes well, and quite substantial risks when it does not. Pediatricians quite commonly follow their patients well into the college years, and at least treat patients during the time in which they are preparing to leave for college. Therefore the transition from high school to college can be considered a part of pediatric primary care. How can a pediatrician contribute to the adolescent’s preparations for this transition to essentially full, day-to-day autonomy? The pediatrician is in a position to offer meaningful guidance to these adolescent patients, and in some cases to their parents as well, particularly on the subjects of substance use, mental health, and sexuality. This process starts in early high school, with progressively more detailed and frank discussions into and through college.
Substance use
For purposes of this discussion, let’s focus on alcohol use. Talking about the risks of alcohol probably should start in late junior high and upon entry to high school. But if you have not yet had a discussion with your adolescent patient about drugs and alcohol, it is not too late to have one during the time before they start college. It would be helpful to learn about their personal and family history of alcohol and drug use. How has alcohol been discussed, and more importantly, used in the home by parents? What are your patients’ attitudes to drinking and related social pressure? Have they needed to be “rescued,” or have they needed to rescue friends? Have they been the designated driver? Have they passed out or seen someone pass out at a party? In these situations, how have they coped? What decisions have they made? Is there a pattern of self-monitoring or largely one of risk taking? What do they imagine college will be like with regard to drinking?
For your patients who have been decidedly sober through high school, it will be important to find out if they are curious about trying alcohol once they are on campus. Even if they voice shocked refusal, you might speak generally with them about the easy availability of alcohol at many parties on campus, particularly if they join a fraternity or sorority or even plan to be on a varsity sports team. Superior athletes are often surrounded by older students and often gain access to parties as freshmen or sophomores surrounded by far more experienced seniors. Speaking generally about how common it is to try alcohol in college, while offering details on how easy it can be for first-time drinkers to become drunk, can be very valuable. You might even offer them data and strategies on how to pace themselves: one drink per hour, no hard alcohol or “mysterious punch,” or two glasses of water for every beer are a few such strategies. You might note how quickly alcohol is absorbed and the risks of rapid ingestion of larger quantities. You should be clear that you are not endorsing underage drinking. Your goal is to ensure that they are equipped with knowledge about smart self-care, especially as intoxication can put them at risk for being victimized or exploited sexually, for serious accidents, for administrative problems, and even for medical consequences.
For your patients who have been risk takers, especially if they have had trouble with drugs or alcohol in high school, it will be important to speak with them about the likelihood that a risky pattern of substance use in high school will grow into a more serious problem in the less-supervised college setting. While this may sound to them like the exciting chance to have easier access and fewer restrictions or punishments, you have the opportunity to complicate their thinking about what this will actually mean. In all likelihood, their use will grow into a problem of abuse or dependence and could easily threaten their ability to succeed at college, landing them back in a far more restrictive setting. It may be valuable to talk with your patients about how they would know if their drug or alcohol use was becoming a problem. When would they say they have reached a limit they are concerned about? Would they be willing to see a therapist or psychiatrist about their substance use before leaving for college to make thoughtful plans for how to manage it? If they are willing, it may be protective to invite their parents into this conversation so that there is a better chance that they may discuss this with their parents outside of your office and once they are on campus.
Mental health
The prevalence of depressive and anxiety symptoms in the college years is very high, likely because of a combination of external stressors, loss of external supports, and continued rapid physical and neurologic development. For adolescents who have not experienced any mental health problems, it can be protective to have a conversation with them about the real risks of developing a mental health problem while they are at school and the value and efficacy of early treatment. You might tell them that while some anxiety and sadness are to be expected during a challenging transition, experiencing intense anxiety or sadness that is sustained (2 weeks or more) and that interferes with their functioning should prompt them to seek help from the student health services. They should be on the lookout for sustained disruptions in their sleep and loss of appetite and energy (the classic neurovegetative symptoms), and of course, any emerging hopelessness or suicidal preoccupation also should prompt them to turn to student health services for evaluation and support.
For your patients who have a history of psychiatric problems and treatment, it is critical – even if they are in remission – that you review with them when they should turn to the campus student health services for evaluation. What symptoms have indicated a worsening problem or relapse for them in the past? What might be the earliest signs of deterioration? If they are in active treatment, you should ensure that the treatment provider has built a transition plan for their treatment to continue on campus. Helping these patients to be smart about their self-care, just as you would if they were responsible for continuing treatment of their diabetes away from the supports of home, can be a powerful preventative intervention.
Sexuality
In all likelihood, you have already had a conversation about sex, even a brief one, with your adolescent patients by the time they are packing for college. But this is a key time to revisit the subject with them. You can begin an open-ended discussion about the fact that the years in college are commonly a time when adolescents start having sex (if they have not already done so). As such, it is important for them to learn about birth control and protection against sexually transmitted infections. This is normally a developmental stage in which sex becomes a more fully integrated part of their emerging identity and their healthy adult life. They may find that they develop a fuller awareness of whom they are attracted to and what they enjoy, and it is commonly a time of some experimentation or exploration. It is very meaningful for your young patients to hear about this nonjudgmentally from their pediatrician. This discussion should include some prevention, in the form of talk about the risks of sexual assault on campus. Help your patients, both male and female, to consider how new independence and access to alcohol can be a dangerous mix with the intense social scene on college campuses. Many situations in which they will be socializing with strangers will involve alcohol, even drugs. Would they have sex with someone if they or their partner were intoxicated? How would they know if the person they were connecting with was actually very intoxicated? How might they think about protecting a friend who seemed to be very intoxicated and at risk for sexual exploitation or assault? If they think they are witnessing a sexual assault or a risky situation, what could they do? If they are considering sex with someone, is it because they are attracted to and interested in that person, or are they feeling pressured, anxious, or bullied? Remind them that while exploration is healthy and should be fun, it also is wise to go slowly when something is new, and to be especially cautious when substance use is involved. They can protect themselves and their friends from the trauma of assault or of being accused of assaulting someone who could not meaningfully consent to sex with some thoughtful anticipation and planning. They took great care to arrange to get into college, and they can take equally great care with their own health and well-being.
Progressively relevant and honest discussions between a pediatrician and teenage patient can have a meaningful impact. Consider how teens could have access to you during their freshman year. Should they have your pager or your cell phone number if they feel they need your help? Should you schedule a psychosocial follow-up visit during a holiday break first semester and again as indicated? Doing what you can to anticipate and prevent harm during the transition to college is highly relevant to many if not all of your patients.
Dr. Swick is an attending psychiatrist in the division of child psychiatry at Massachusetts General Hospital, Boston, and director of the Parenting at a Challenging Time (PACT) Program at the Vernon Cancer Center at Newton Wellesley Hospital, also in Boston. Dr. Jellinek is professor of psychiatry and of pediatrics at Harvard Medical School, Boston. E-mail them at [email protected].
Perhaps the greatest transition in an adolescent’s life is the transition to college. The process of preparation, investigation, application, interviewing, waiting, choosing, and preparing to leave for college is one of the most exciting, exhausting, and challenging experiences in the life of an adolescent and his or her family. The final selection of a school can mark a shorthand summary of accomplishment and builds a major piece of a young adult’s identity.
Although there are certainly many steps to autonomy through childhood – walking, starting school, being home alone, driving a car – none compares to leaving the warmth and structure of home for the college experience. Once in the dorm, teens are probably more alone and independent than they have ever been before, likely without any long-standing friends, in an unfamiliar setting, and facing high expectations. College offers structure and support to help with this transition, and most adolescents are ready and even eager to start to manage their own lives pragmatically, academically, and socially. But there will be setbacks and failures, big and small, as they navigate new territory with virtually full independence. This transition would be a challenge to a mature adult and is daunting to someone who is doing this for the first time and with an identity that is still forming.
We know that most teenagers make this transition successfully. However, we also know that this new level of independence and responsibility and the loss of supervision and structure can place adolescents at risk for several problems. Some adolescents make poor or risky choices with serious consequences. Depression affects about 20% of all freshmen, with consequences that range from mild to severe, sometimes requiring a leave of absence. Many students who have managed mild problems with anxiety or body image may find that with more stress and less support, these problems grow into eating disorders and substance abuse disorders. It now appears that sexual assaults on campuses, often during “frat” parties and in the setting of substance use, are far more prevalent than previously acknowledged. Recently in the news was the tragic accident of a young woman under the influence of substances who was seriously injured when she fell out of a window. Finally, we know the most prevalent morbidity and mortality are from car accidents, many of which are related to risk taking and substance use.
Clearly there are critical developmental gains toward healthy adulthood when this transition goes well, and quite substantial risks when it does not. Pediatricians quite commonly follow their patients well into the college years, and at least treat patients during the time in which they are preparing to leave for college. Therefore the transition from high school to college can be considered a part of pediatric primary care. How can a pediatrician contribute to the adolescent’s preparations for this transition to essentially full, day-to-day autonomy? The pediatrician is in a position to offer meaningful guidance to these adolescent patients, and in some cases to their parents as well, particularly on the subjects of substance use, mental health, and sexuality. This process starts in early high school, with progressively more detailed and frank discussions into and through college.
Substance use
For purposes of this discussion, let’s focus on alcohol use. Talking about the risks of alcohol probably should start in late junior high and upon entry to high school. But if you have not yet had a discussion with your adolescent patient about drugs and alcohol, it is not too late to have one during the time before they start college. It would be helpful to learn about their personal and family history of alcohol and drug use. How has alcohol been discussed, and more importantly, used in the home by parents? What are your patients’ attitudes to drinking and related social pressure? Have they needed to be “rescued,” or have they needed to rescue friends? Have they been the designated driver? Have they passed out or seen someone pass out at a party? In these situations, how have they coped? What decisions have they made? Is there a pattern of self-monitoring or largely one of risk taking? What do they imagine college will be like with regard to drinking?
For your patients who have been decidedly sober through high school, it will be important to find out if they are curious about trying alcohol once they are on campus. Even if they voice shocked refusal, you might speak generally with them about the easy availability of alcohol at many parties on campus, particularly if they join a fraternity or sorority or even plan to be on a varsity sports team. Superior athletes are often surrounded by older students and often gain access to parties as freshmen or sophomores surrounded by far more experienced seniors. Speaking generally about how common it is to try alcohol in college, while offering details on how easy it can be for first-time drinkers to become drunk, can be very valuable. You might even offer them data and strategies on how to pace themselves: one drink per hour, no hard alcohol or “mysterious punch,” or two glasses of water for every beer are a few such strategies. You might note how quickly alcohol is absorbed and the risks of rapid ingestion of larger quantities. You should be clear that you are not endorsing underage drinking. Your goal is to ensure that they are equipped with knowledge about smart self-care, especially as intoxication can put them at risk for being victimized or exploited sexually, for serious accidents, for administrative problems, and even for medical consequences.
For your patients who have been risk takers, especially if they have had trouble with drugs or alcohol in high school, it will be important to speak with them about the likelihood that a risky pattern of substance use in high school will grow into a more serious problem in the less-supervised college setting. While this may sound to them like the exciting chance to have easier access and fewer restrictions or punishments, you have the opportunity to complicate their thinking about what this will actually mean. In all likelihood, their use will grow into a problem of abuse or dependence and could easily threaten their ability to succeed at college, landing them back in a far more restrictive setting. It may be valuable to talk with your patients about how they would know if their drug or alcohol use was becoming a problem. When would they say they have reached a limit they are concerned about? Would they be willing to see a therapist or psychiatrist about their substance use before leaving for college to make thoughtful plans for how to manage it? If they are willing, it may be protective to invite their parents into this conversation so that there is a better chance that they may discuss this with their parents outside of your office and once they are on campus.
Mental health
The prevalence of depressive and anxiety symptoms in the college years is very high, likely because of a combination of external stressors, loss of external supports, and continued rapid physical and neurologic development. For adolescents who have not experienced any mental health problems, it can be protective to have a conversation with them about the real risks of developing a mental health problem while they are at school and the value and efficacy of early treatment. You might tell them that while some anxiety and sadness are to be expected during a challenging transition, experiencing intense anxiety or sadness that is sustained (2 weeks or more) and that interferes with their functioning should prompt them to seek help from the student health services. They should be on the lookout for sustained disruptions in their sleep and loss of appetite and energy (the classic neurovegetative symptoms), and of course, any emerging hopelessness or suicidal preoccupation also should prompt them to turn to student health services for evaluation and support.
For your patients who have a history of psychiatric problems and treatment, it is critical – even if they are in remission – that you review with them when they should turn to the campus student health services for evaluation. What symptoms have indicated a worsening problem or relapse for them in the past? What might be the earliest signs of deterioration? If they are in active treatment, you should ensure that the treatment provider has built a transition plan for their treatment to continue on campus. Helping these patients to be smart about their self-care, just as you would if they were responsible for continuing treatment of their diabetes away from the supports of home, can be a powerful preventative intervention.
Sexuality
In all likelihood, you have already had a conversation about sex, even a brief one, with your adolescent patients by the time they are packing for college. But this is a key time to revisit the subject with them. You can begin an open-ended discussion about the fact that the years in college are commonly a time when adolescents start having sex (if they have not already done so). As such, it is important for them to learn about birth control and protection against sexually transmitted infections. This is normally a developmental stage in which sex becomes a more fully integrated part of their emerging identity and their healthy adult life. They may find that they develop a fuller awareness of whom they are attracted to and what they enjoy, and it is commonly a time of some experimentation or exploration. It is very meaningful for your young patients to hear about this nonjudgmentally from their pediatrician. This discussion should include some prevention, in the form of talk about the risks of sexual assault on campus. Help your patients, both male and female, to consider how new independence and access to alcohol can be a dangerous mix with the intense social scene on college campuses. Many situations in which they will be socializing with strangers will involve alcohol, even drugs. Would they have sex with someone if they or their partner were intoxicated? How would they know if the person they were connecting with was actually very intoxicated? How might they think about protecting a friend who seemed to be very intoxicated and at risk for sexual exploitation or assault? If they think they are witnessing a sexual assault or a risky situation, what could they do? If they are considering sex with someone, is it because they are attracted to and interested in that person, or are they feeling pressured, anxious, or bullied? Remind them that while exploration is healthy and should be fun, it also is wise to go slowly when something is new, and to be especially cautious when substance use is involved. They can protect themselves and their friends from the trauma of assault or of being accused of assaulting someone who could not meaningfully consent to sex with some thoughtful anticipation and planning. They took great care to arrange to get into college, and they can take equally great care with their own health and well-being.
Progressively relevant and honest discussions between a pediatrician and teenage patient can have a meaningful impact. Consider how teens could have access to you during their freshman year. Should they have your pager or your cell phone number if they feel they need your help? Should you schedule a psychosocial follow-up visit during a holiday break first semester and again as indicated? Doing what you can to anticipate and prevent harm during the transition to college is highly relevant to many if not all of your patients.
Dr. Swick is an attending psychiatrist in the division of child psychiatry at Massachusetts General Hospital, Boston, and director of the Parenting at a Challenging Time (PACT) Program at the Vernon Cancer Center at Newton Wellesley Hospital, also in Boston. Dr. Jellinek is professor of psychiatry and of pediatrics at Harvard Medical School, Boston. E-mail them at [email protected].

Join Us in Celebrating
Clinician Reviews is celebrating its 25th year of publication in 2015. As the journal’s PA and NP Editors-in-Chief, we would like to be among the first to congratulate the publication on this milestone anniversary.
Paging through the inaugural issue (February 1991) today is an indication of how much has changed in 25 years (and, at the same time, how much hasn’t). In that issue, the editors acknowledged the service of military PAs and NPs who were deployed during Operation Desert Storm (at the time, a current conflict) and introduced an AIDS Update department because “the spread of human immunodeficiency virus (HIV) shows little sign of abating.”
Despite the passage of time, CR remains faithful to the editorial purpose established more than two decades ago. It was “designed to provide you with the information you need to keep abreast of the changes in medicine that occur on a daily basis.” And to the present day, the editorial staff and the editorial board have maintained their commitment to providing peer-reviewed, clinician-authored content that helps NPs and PAs provide the best possible patient care in an increasingly challenging environment. The journal has never lost its focus on primary care—the heart of health care in the United States—while acknowledging that primary care clinicians manage a wide variety of disease states and conditions.
The true strength of the journal has always been, and continues to be, the people affiliated with it. Special thanks to the dedicated editorial staff: Karen J. Clemments (Editor), Ann M. Hoppel (Managing Editor), Fran Hopkins (Senior Editor), and Kristen Garafano (Web Editor). This noteworthy anniversary would not be complete without extending special thanks to past Editors Robert E. De Donato, Jean Paternoster, and Maura Griffin, and longtime Senior Editor Christine Mooney Lukesh, who retired last year.
In addition, we acknowledge that no journal can be successful without the support and guidance of its editorial board. We have been especially blessed with colleagues from both the PA and NP professions—many of whom have been on the board for a decade or longer. Their names are listed here.
We, as Editors-in-Chief, would particularly like to thank you—our readers and colleagues—for your thoughtful feedback on our monthly editorials. It is rewarding to think that we have fostered discussion and fruitful debate on issues relevant to our professions—and we gain just as much perspective as we hope to impart. To those of you who have contributed manuscripts over the years, know that we are grateful for your professionalism, generosity with your time and expertise, and commitment to enhancing the knowledge of your fellow practitioners.
So, as CR marks its 25th anniversary, we invite our authors, peer reviewers, and readers to join us in celebrating. Thank you for your support for the past 25 years. Here’s to many more.
Clinician Reviews is celebrating its 25th year of publication in 2015. As the journal’s PA and NP Editors-in-Chief, we would like to be among the first to congratulate the publication on this milestone anniversary.
Paging through the inaugural issue (February 1991) today is an indication of how much has changed in 25 years (and, at the same time, how much hasn’t). In that issue, the editors acknowledged the service of military PAs and NPs who were deployed during Operation Desert Storm (at the time, a current conflict) and introduced an AIDS Update department because “the spread of human immunodeficiency virus (HIV) shows little sign of abating.”
Despite the passage of time, CR remains faithful to the editorial purpose established more than two decades ago. It was “designed to provide you with the information you need to keep abreast of the changes in medicine that occur on a daily basis.” And to the present day, the editorial staff and the editorial board have maintained their commitment to providing peer-reviewed, clinician-authored content that helps NPs and PAs provide the best possible patient care in an increasingly challenging environment. The journal has never lost its focus on primary care—the heart of health care in the United States—while acknowledging that primary care clinicians manage a wide variety of disease states and conditions.
The true strength of the journal has always been, and continues to be, the people affiliated with it. Special thanks to the dedicated editorial staff: Karen J. Clemments (Editor), Ann M. Hoppel (Managing Editor), Fran Hopkins (Senior Editor), and Kristen Garafano (Web Editor). This noteworthy anniversary would not be complete without extending special thanks to past Editors Robert E. De Donato, Jean Paternoster, and Maura Griffin, and longtime Senior Editor Christine Mooney Lukesh, who retired last year.
In addition, we acknowledge that no journal can be successful without the support and guidance of its editorial board. We have been especially blessed with colleagues from both the PA and NP professions—many of whom have been on the board for a decade or longer. Their names are listed here.
We, as Editors-in-Chief, would particularly like to thank you—our readers and colleagues—for your thoughtful feedback on our monthly editorials. It is rewarding to think that we have fostered discussion and fruitful debate on issues relevant to our professions—and we gain just as much perspective as we hope to impart. To those of you who have contributed manuscripts over the years, know that we are grateful for your professionalism, generosity with your time and expertise, and commitment to enhancing the knowledge of your fellow practitioners.
So, as CR marks its 25th anniversary, we invite our authors, peer reviewers, and readers to join us in celebrating. Thank you for your support for the past 25 years. Here’s to many more.
Clinician Reviews is celebrating its 25th year of publication in 2015. As the journal’s PA and NP Editors-in-Chief, we would like to be among the first to congratulate the publication on this milestone anniversary.
Paging through the inaugural issue (February 1991) today is an indication of how much has changed in 25 years (and, at the same time, how much hasn’t). In that issue, the editors acknowledged the service of military PAs and NPs who were deployed during Operation Desert Storm (at the time, a current conflict) and introduced an AIDS Update department because “the spread of human immunodeficiency virus (HIV) shows little sign of abating.”
Despite the passage of time, CR remains faithful to the editorial purpose established more than two decades ago. It was “designed to provide you with the information you need to keep abreast of the changes in medicine that occur on a daily basis.” And to the present day, the editorial staff and the editorial board have maintained their commitment to providing peer-reviewed, clinician-authored content that helps NPs and PAs provide the best possible patient care in an increasingly challenging environment. The journal has never lost its focus on primary care—the heart of health care in the United States—while acknowledging that primary care clinicians manage a wide variety of disease states and conditions.
The true strength of the journal has always been, and continues to be, the people affiliated with it. Special thanks to the dedicated editorial staff: Karen J. Clemments (Editor), Ann M. Hoppel (Managing Editor), Fran Hopkins (Senior Editor), and Kristen Garafano (Web Editor). This noteworthy anniversary would not be complete without extending special thanks to past Editors Robert E. De Donato, Jean Paternoster, and Maura Griffin, and longtime Senior Editor Christine Mooney Lukesh, who retired last year.
In addition, we acknowledge that no journal can be successful without the support and guidance of its editorial board. We have been especially blessed with colleagues from both the PA and NP professions—many of whom have been on the board for a decade or longer. Their names are listed here.
We, as Editors-in-Chief, would particularly like to thank you—our readers and colleagues—for your thoughtful feedback on our monthly editorials. It is rewarding to think that we have fostered discussion and fruitful debate on issues relevant to our professions—and we gain just as much perspective as we hope to impart. To those of you who have contributed manuscripts over the years, know that we are grateful for your professionalism, generosity with your time and expertise, and commitment to enhancing the knowledge of your fellow practitioners.
So, as CR marks its 25th anniversary, we invite our authors, peer reviewers, and readers to join us in celebrating. Thank you for your support for the past 25 years. Here’s to many more.
Raising the Bar for Online Physician Review Sites
There are more than 60 websites that review physicians online, with the number growing each year. A staggering number of physician searches—in excess of 3 million—are done each day in the United States. They have increased 68% from 2013 to 2014.1 All online physician review sites provide some type of structured doctor experience rating score, and many allow comments from patients. Some sites also provide information about physician education, board certification, and hospital affiliation. The quality of physician review sites varies, just like the quality of those reviewed.
Physician review sites have not been embraced by the medical community and are often regarded by physicians with apathy, if not antipathy. There are many reasons for this reaction. The information on the sites—often gathered from flawed public and payer databases—can be very inaccurate; the number of patient reviews for each physician—orthopedic surgeons have an average of 12—is too limited to accurately represent a practice; and a single scathing review—frequently anonymous—can damage a physician’s reputation. First Amendment free speech laws allow patients to place their reviews anonymously, and the Health Insurance Portability and Accountability Act (HIPAA) prevents a physician from answering a negative review in anything but general terms. Under the federal Communications Decency Act, website providers aren’t liable for the postings of those who comment. Legitimate rave reviews may be deemed fake by certain websites and removed, and customer service is often a charade, with no one to speak to but a website computer. Most importantly, the review sites rarely represent the full breadth of a physician’s practice and reduce the physician to a simple star or numerical rating.
Like it or not, physician review sites are here to stay. In part as a result of the insurance changes created by the Affordable Care Act, patients are searching for new doctors online in unprecedented numbers. According to the Pew Research Internet Project, 72% of Internet users say they go online for health information.2 A 2014 study in the Journal of the American Medical Association reported that 59% of respondents indicated that physician rating sites were “somewhat or very important” when choosing a physician; 35% reported selection of a physician based on good ratings; and 37% reported avoidance of a physician based on bad ones.3 This is important information for an orthopedic surgeon to consider. Orthopedic surgery is the most frequently searched physician specialty on the Internet, and it is not uncommon for a busy orthopedist to have more than 1000 searches per year on just 1 review site. Consumer research data indicates that as many as 50% of patients who visit a review site call that physician for an appointment within 1 week.4 When a physician’s name is entered into a search engine such as Google, physician review sites are often listed above the physician’s own website.
Last year the California Orthopaedic Association (COA), responding to its members’ concerns, reviewed online physician review sites. As part of this initiative, the COA approached Healthgrades, a leader in online medical reporting of physicians, hospitals, and other health care providers. The goal was to understand Healthgrades’ perspective and to see if they were open to orthopedic input. The COA was concerned that review sites often had incomplete and inaccurate information about physicians’ practices, lacked orthopedic subspecialty designation, and precluded physicians from posting comprehensive information about their practices in their own words. Personalized practice information provided by the physician, the COA reasoned, especially if displayed prominently, would complement the patients’ 1- to 5-star physician rating. Both prospective patients and physicians would benefit.
Three months ago, as a direct result of these collaborative efforts, Healthgrades made major changes to its review site. They increased the number of searchable orthopedic subspecialties, so that a patient with a specific problem is more likely to find an orthopedic surgeon with the right expertise. Physicians or their practice managers can now more easily update information about their practice, either online or by phone. Most importantly, Healthgrades added a featured section—“Your Voice”—prominently positioned next to their star rating, where a physician can describe who he/she is and what he/she does. This addition is not to be underestimated. No other major review site provides this opportunity to the physician.
Healthgrades should be applauded for their collaboration with the COA and the highly successful improvement of their physician review site. They have raised the bar and set an example that other review sites will hopefully follow.
References
1. Leslie J. Patient use of online reviews: IndustryView 2014. Software Advice. http://www.softwareadvice.com/medical/industryview/online-reviews-report-2014. Published November 19, 2014. Accessed December 8, 2014.
2. Fox S, Duggan M. Health online 2013. Pew Research Center’s Internet & American Life Project. http://www.pewinternet.org/2013/01/15/health-online-2013. Published January 15, 2013. Accessed December 8, 2014.
3. Hanauer DA, Zheng K, Singer DC, Gebremariam A, Davis MM. Public awareness, perception, and use of online physician rating sites. JAMA. 2014;311(7):734-735.
4. Stax, Inc. Assessing Objectives & Actions Taken Among Users of Healthgrades. Unpublished data, April 2012.
There are more than 60 websites that review physicians online, with the number growing each year. A staggering number of physician searches—in excess of 3 million—are done each day in the United States. They have increased 68% from 2013 to 2014.1 All online physician review sites provide some type of structured doctor experience rating score, and many allow comments from patients. Some sites also provide information about physician education, board certification, and hospital affiliation. The quality of physician review sites varies, just like the quality of those reviewed.
Physician review sites have not been embraced by the medical community and are often regarded by physicians with apathy, if not antipathy. There are many reasons for this reaction. The information on the sites—often gathered from flawed public and payer databases—can be very inaccurate; the number of patient reviews for each physician—orthopedic surgeons have an average of 12—is too limited to accurately represent a practice; and a single scathing review—frequently anonymous—can damage a physician’s reputation. First Amendment free speech laws allow patients to place their reviews anonymously, and the Health Insurance Portability and Accountability Act (HIPAA) prevents a physician from answering a negative review in anything but general terms. Under the federal Communications Decency Act, website providers aren’t liable for the postings of those who comment. Legitimate rave reviews may be deemed fake by certain websites and removed, and customer service is often a charade, with no one to speak to but a website computer. Most importantly, the review sites rarely represent the full breadth of a physician’s practice and reduce the physician to a simple star or numerical rating.
Like it or not, physician review sites are here to stay. In part as a result of the insurance changes created by the Affordable Care Act, patients are searching for new doctors online in unprecedented numbers. According to the Pew Research Internet Project, 72% of Internet users say they go online for health information.2 A 2014 study in the Journal of the American Medical Association reported that 59% of respondents indicated that physician rating sites were “somewhat or very important” when choosing a physician; 35% reported selection of a physician based on good ratings; and 37% reported avoidance of a physician based on bad ones.3 This is important information for an orthopedic surgeon to consider. Orthopedic surgery is the most frequently searched physician specialty on the Internet, and it is not uncommon for a busy orthopedist to have more than 1000 searches per year on just 1 review site. Consumer research data indicates that as many as 50% of patients who visit a review site call that physician for an appointment within 1 week.4 When a physician’s name is entered into a search engine such as Google, physician review sites are often listed above the physician’s own website.
Last year the California Orthopaedic Association (COA), responding to its members’ concerns, reviewed online physician review sites. As part of this initiative, the COA approached Healthgrades, a leader in online medical reporting of physicians, hospitals, and other health care providers. The goal was to understand Healthgrades’ perspective and to see if they were open to orthopedic input. The COA was concerned that review sites often had incomplete and inaccurate information about physicians’ practices, lacked orthopedic subspecialty designation, and precluded physicians from posting comprehensive information about their practices in their own words. Personalized practice information provided by the physician, the COA reasoned, especially if displayed prominently, would complement the patients’ 1- to 5-star physician rating. Both prospective patients and physicians would benefit.
Three months ago, as a direct result of these collaborative efforts, Healthgrades made major changes to its review site. They increased the number of searchable orthopedic subspecialties, so that a patient with a specific problem is more likely to find an orthopedic surgeon with the right expertise. Physicians or their practice managers can now more easily update information about their practice, either online or by phone. Most importantly, Healthgrades added a featured section—“Your Voice”—prominently positioned next to their star rating, where a physician can describe who he/she is and what he/she does. This addition is not to be underestimated. No other major review site provides this opportunity to the physician.
Healthgrades should be applauded for their collaboration with the COA and the highly successful improvement of their physician review site. They have raised the bar and set an example that other review sites will hopefully follow.
References
1. Leslie J. Patient use of online reviews: IndustryView 2014. Software Advice. http://www.softwareadvice.com/medical/industryview/online-reviews-report-2014. Published November 19, 2014. Accessed December 8, 2014.
2. Fox S, Duggan M. Health online 2013. Pew Research Center’s Internet & American Life Project. http://www.pewinternet.org/2013/01/15/health-online-2013. Published January 15, 2013. Accessed December 8, 2014.
3. Hanauer DA, Zheng K, Singer DC, Gebremariam A, Davis MM. Public awareness, perception, and use of online physician rating sites. JAMA. 2014;311(7):734-735.
4. Stax, Inc. Assessing Objectives & Actions Taken Among Users of Healthgrades. Unpublished data, April 2012.
There are more than 60 websites that review physicians online, with the number growing each year. A staggering number of physician searches—in excess of 3 million—are done each day in the United States. They have increased 68% from 2013 to 2014.1 All online physician review sites provide some type of structured doctor experience rating score, and many allow comments from patients. Some sites also provide information about physician education, board certification, and hospital affiliation. The quality of physician review sites varies, just like the quality of those reviewed.
Physician review sites have not been embraced by the medical community and are often regarded by physicians with apathy, if not antipathy. There are many reasons for this reaction. The information on the sites—often gathered from flawed public and payer databases—can be very inaccurate; the number of patient reviews for each physician—orthopedic surgeons have an average of 12—is too limited to accurately represent a practice; and a single scathing review—frequently anonymous—can damage a physician’s reputation. First Amendment free speech laws allow patients to place their reviews anonymously, and the Health Insurance Portability and Accountability Act (HIPAA) prevents a physician from answering a negative review in anything but general terms. Under the federal Communications Decency Act, website providers aren’t liable for the postings of those who comment. Legitimate rave reviews may be deemed fake by certain websites and removed, and customer service is often a charade, with no one to speak to but a website computer. Most importantly, the review sites rarely represent the full breadth of a physician’s practice and reduce the physician to a simple star or numerical rating.
Like it or not, physician review sites are here to stay. In part as a result of the insurance changes created by the Affordable Care Act, patients are searching for new doctors online in unprecedented numbers. According to the Pew Research Internet Project, 72% of Internet users say they go online for health information.2 A 2014 study in the Journal of the American Medical Association reported that 59% of respondents indicated that physician rating sites were “somewhat or very important” when choosing a physician; 35% reported selection of a physician based on good ratings; and 37% reported avoidance of a physician based on bad ones.3 This is important information for an orthopedic surgeon to consider. Orthopedic surgery is the most frequently searched physician specialty on the Internet, and it is not uncommon for a busy orthopedist to have more than 1000 searches per year on just 1 review site. Consumer research data indicates that as many as 50% of patients who visit a review site call that physician for an appointment within 1 week.4 When a physician’s name is entered into a search engine such as Google, physician review sites are often listed above the physician’s own website.
Last year the California Orthopaedic Association (COA), responding to its members’ concerns, reviewed online physician review sites. As part of this initiative, the COA approached Healthgrades, a leader in online medical reporting of physicians, hospitals, and other health care providers. The goal was to understand Healthgrades’ perspective and to see if they were open to orthopedic input. The COA was concerned that review sites often had incomplete and inaccurate information about physicians’ practices, lacked orthopedic subspecialty designation, and precluded physicians from posting comprehensive information about their practices in their own words. Personalized practice information provided by the physician, the COA reasoned, especially if displayed prominently, would complement the patients’ 1- to 5-star physician rating. Both prospective patients and physicians would benefit.
Three months ago, as a direct result of these collaborative efforts, Healthgrades made major changes to its review site. They increased the number of searchable orthopedic subspecialties, so that a patient with a specific problem is more likely to find an orthopedic surgeon with the right expertise. Physicians or their practice managers can now more easily update information about their practice, either online or by phone. Most importantly, Healthgrades added a featured section—“Your Voice”—prominently positioned next to their star rating, where a physician can describe who he/she is and what he/she does. This addition is not to be underestimated. No other major review site provides this opportunity to the physician.
Healthgrades should be applauded for their collaboration with the COA and the highly successful improvement of their physician review site. They have raised the bar and set an example that other review sites will hopefully follow.
References
1. Leslie J. Patient use of online reviews: IndustryView 2014. Software Advice. http://www.softwareadvice.com/medical/industryview/online-reviews-report-2014. Published November 19, 2014. Accessed December 8, 2014.
2. Fox S, Duggan M. Health online 2013. Pew Research Center’s Internet & American Life Project. http://www.pewinternet.org/2013/01/15/health-online-2013. Published January 15, 2013. Accessed December 8, 2014.
3. Hanauer DA, Zheng K, Singer DC, Gebremariam A, Davis MM. Public awareness, perception, and use of online physician rating sites. JAMA. 2014;311(7):734-735.
4. Stax, Inc. Assessing Objectives & Actions Taken Among Users of Healthgrades. Unpublished data, April 2012.

Where’s the line on refusing to treat smokers?
We all dismiss patients who are noncompliant with treatment. The threshold varies between us, but all of us have fired (for example) an epilepsy patient who won’t take the meds and is in and out of the emergency department.
What about smokers? Do they count?
A recent article in Anesthesiology News (2014 September) featured a surgical group that won’t do elective hernia repairs on patients who don’t quit smoking. I can see their point. Smoking increases the risk of complications, which hurt the patient. So, having a good patient outcome depends on their condition, too. And, honestly, I don’t blame the surgeons for refusing to do nonurgent cases under these circumstances.
What about neurologists, though?
Smoking is a big one. The literature has no shortage of data on it worsening migraines and multiple sclerosis, increasing the risk of stroke and peripheral vascular disease, contributing to vascular dementia ... and many other things.
I always tell smokers that they should quit, but should I be going beyond that? Refuse to treat migraines until someone quits smoking? The other conditions I mentioned have enough serious health risks that I don’t think it’s ethical to withhold care over smoking.
At my first job, I had a partner who took this approach. She routinely told migraineurs who smoked that they couldn’t return to her until they’d quit. Her view was that then she could treat them to her best ability without tobacco as a confounding factor, or they’d simply not come back.
I can understand this approach, and, in a perfect world, would do it myself. I certainly don’t support tobacco use and wish I had a magic bullet to help them quit. But I don’t. I can preach it, explain why they should quit, review the risks, send them to their internist for cessation ... but I’m still not sure I’d flat out turn them away.
I’m trying to help them. Refusing to provide care, even in the name of quitting smoking, is only going to alienate them. They may get turned off to seeing doctors altogether and consequently develop other issues. I don’t want them to smoke, but none of us is without our vices, either.
I’m also not them, and don’t know what’s going on in their lives. Maybe they are taking care of a parent with a terminal condition, going through a divorce, have a terrible job, or a million other stressors and just don’t have the will right now to quit tobacco.
Migraines, in the grand scheme of medicine, are certainly a lower-risk issue than surgical complications. So, while I disapprove of tobacco and encourage smokers to stop, my door remains open to them. Part of caring for my patients is accepting them as they are and trying to work with them inside that framework.
Dr. Block has a solo neurology practice in Scottsdale, Ariz.
We all dismiss patients who are noncompliant with treatment. The threshold varies between us, but all of us have fired (for example) an epilepsy patient who won’t take the meds and is in and out of the emergency department.
What about smokers? Do they count?
A recent article in Anesthesiology News (2014 September) featured a surgical group that won’t do elective hernia repairs on patients who don’t quit smoking. I can see their point. Smoking increases the risk of complications, which hurt the patient. So, having a good patient outcome depends on their condition, too. And, honestly, I don’t blame the surgeons for refusing to do nonurgent cases under these circumstances.
What about neurologists, though?
Smoking is a big one. The literature has no shortage of data on it worsening migraines and multiple sclerosis, increasing the risk of stroke and peripheral vascular disease, contributing to vascular dementia ... and many other things.
I always tell smokers that they should quit, but should I be going beyond that? Refuse to treat migraines until someone quits smoking? The other conditions I mentioned have enough serious health risks that I don’t think it’s ethical to withhold care over smoking.
At my first job, I had a partner who took this approach. She routinely told migraineurs who smoked that they couldn’t return to her until they’d quit. Her view was that then she could treat them to her best ability without tobacco as a confounding factor, or they’d simply not come back.
I can understand this approach, and, in a perfect world, would do it myself. I certainly don’t support tobacco use and wish I had a magic bullet to help them quit. But I don’t. I can preach it, explain why they should quit, review the risks, send them to their internist for cessation ... but I’m still not sure I’d flat out turn them away.
I’m trying to help them. Refusing to provide care, even in the name of quitting smoking, is only going to alienate them. They may get turned off to seeing doctors altogether and consequently develop other issues. I don’t want them to smoke, but none of us is without our vices, either.
I’m also not them, and don’t know what’s going on in their lives. Maybe they are taking care of a parent with a terminal condition, going through a divorce, have a terrible job, or a million other stressors and just don’t have the will right now to quit tobacco.
Migraines, in the grand scheme of medicine, are certainly a lower-risk issue than surgical complications. So, while I disapprove of tobacco and encourage smokers to stop, my door remains open to them. Part of caring for my patients is accepting them as they are and trying to work with them inside that framework.
Dr. Block has a solo neurology practice in Scottsdale, Ariz.
We all dismiss patients who are noncompliant with treatment. The threshold varies between us, but all of us have fired (for example) an epilepsy patient who won’t take the meds and is in and out of the emergency department.
What about smokers? Do they count?
A recent article in Anesthesiology News (2014 September) featured a surgical group that won’t do elective hernia repairs on patients who don’t quit smoking. I can see their point. Smoking increases the risk of complications, which hurt the patient. So, having a good patient outcome depends on their condition, too. And, honestly, I don’t blame the surgeons for refusing to do nonurgent cases under these circumstances.
What about neurologists, though?
Smoking is a big one. The literature has no shortage of data on it worsening migraines and multiple sclerosis, increasing the risk of stroke and peripheral vascular disease, contributing to vascular dementia ... and many other things.
I always tell smokers that they should quit, but should I be going beyond that? Refuse to treat migraines until someone quits smoking? The other conditions I mentioned have enough serious health risks that I don’t think it’s ethical to withhold care over smoking.
At my first job, I had a partner who took this approach. She routinely told migraineurs who smoked that they couldn’t return to her until they’d quit. Her view was that then she could treat them to her best ability without tobacco as a confounding factor, or they’d simply not come back.
I can understand this approach, and, in a perfect world, would do it myself. I certainly don’t support tobacco use and wish I had a magic bullet to help them quit. But I don’t. I can preach it, explain why they should quit, review the risks, send them to their internist for cessation ... but I’m still not sure I’d flat out turn them away.
I’m trying to help them. Refusing to provide care, even in the name of quitting smoking, is only going to alienate them. They may get turned off to seeing doctors altogether and consequently develop other issues. I don’t want them to smoke, but none of us is without our vices, either.
I’m also not them, and don’t know what’s going on in their lives. Maybe they are taking care of a parent with a terminal condition, going through a divorce, have a terrible job, or a million other stressors and just don’t have the will right now to quit tobacco.
Migraines, in the grand scheme of medicine, are certainly a lower-risk issue than surgical complications. So, while I disapprove of tobacco and encourage smokers to stop, my door remains open to them. Part of caring for my patients is accepting them as they are and trying to work with them inside that framework.
Dr. Block has a solo neurology practice in Scottsdale, Ariz.
