User login
MDedge conference coverage features onsite reporting of the latest study results and expert perspectives from leading researchers.
Circulating tumor DNA may predict poor prognosis in breast cancer
a new meta-analysis and systematic review found.
“Circulating tumor DNA (ctDNA) has been extensively studied as a prognostic biomarker in early breast cancer. However, there is a significant heterogeneity in the study results, which is probably related to the fact that each individual study included different patient populations, collected blood at different time points, and used different methods (assays) for ctDNA analysis,” said Guilherme Nader Marta, MD, of the Institut Jules Bordet, Anderlecht, Belgium, in an interview.
“The aim of our study was to summarize the available evidence that has been presented so far on this topic by performing a systematic review and meta-analysis including studies that reported the association between ctDNA detection and long-term outcomes,” said Dr. Nader Marta, who coauthored the new research, which was presented as a poster (Poster 26P) at the European Society for Medical Oncology (ESMO) Breast Cancer annual congress.
Methods and results
The authors identified 57 studies including data from 5,729 individuals with early breast cancer. The 44.5% for whom stages were reported consisted of 18.3% with stage I disease, 60.0% with stage II, and 21.5% with stage III. Patients’ ctDNA collection was divided into three groups: baseline, after neoadjuvant therapy (End-of-NAT), and during follow-up care; ctDNA assays were classified as tumor-informed or non–tumor-informed.
The detection of ctDNA at any time point during diagnosis and treatment was associated with worse disease-free survival (DFS) and overall survival (OS), compared with no ctDNA. The association was stronger in tumor-informed assays, the researchers said.
For disease-free survival, the overall multivariate hazard ratios were 2.5, 5.5, and 7.2 for ctDNA detection at baseline, End-of-NAT, and follow-up, respectively.
For overall survival, the overall multivariate hazard ratios were 3.0, 12.9, and 5.6, for ctDNA detection at baseline, End-of-NAT, and follow-up, respectively.
The pooled hazard ratios were numerically higher for both DFS and OS when ctDNA was detected at either End-of-NAT or follow-up.
In addition, detection of ctDNA was associated with a high degree of specificity (from 0.7 to 1.0) for breast cancer relapse; sensitivity ranged from 0.31 to 1.0, the researchers noted. The mean lead time from ctDNA detection to breast cancer recurrence in these cases was approximately 10 months.
Results show ctDNA detection is associated with worse survival
“Our study results demonstrate that ctDNA detection is associated with worse disease-free survival and overall survival in patients with early breast cancer, particularly when measured after treatment with tumor-informed assays,” Dr. Nader Marta said in an interview.
“As next steps, we need to build on this evidence to bring the potential benefits of this powerful prognostic tool to our patients,” said Dr. Nader Marta. “Ongoing studies exploring different management strategies based on serial ctDNA assessments will help us understand the exact role of this technology in our clinical practice.”
The study received no outside funding. Dr. Nader Marta disclosed relationships with companies including Roche and Bayer.
a new meta-analysis and systematic review found.
“Circulating tumor DNA (ctDNA) has been extensively studied as a prognostic biomarker in early breast cancer. However, there is a significant heterogeneity in the study results, which is probably related to the fact that each individual study included different patient populations, collected blood at different time points, and used different methods (assays) for ctDNA analysis,” said Guilherme Nader Marta, MD, of the Institut Jules Bordet, Anderlecht, Belgium, in an interview.
“The aim of our study was to summarize the available evidence that has been presented so far on this topic by performing a systematic review and meta-analysis including studies that reported the association between ctDNA detection and long-term outcomes,” said Dr. Nader Marta, who coauthored the new research, which was presented as a poster (Poster 26P) at the European Society for Medical Oncology (ESMO) Breast Cancer annual congress.
Methods and results
The authors identified 57 studies including data from 5,729 individuals with early breast cancer. The 44.5% for whom stages were reported consisted of 18.3% with stage I disease, 60.0% with stage II, and 21.5% with stage III. Patients’ ctDNA collection was divided into three groups: baseline, after neoadjuvant therapy (End-of-NAT), and during follow-up care; ctDNA assays were classified as tumor-informed or non–tumor-informed.
The detection of ctDNA at any time point during diagnosis and treatment was associated with worse disease-free survival (DFS) and overall survival (OS), compared with no ctDNA. The association was stronger in tumor-informed assays, the researchers said.
For disease-free survival, the overall multivariate hazard ratios were 2.5, 5.5, and 7.2 for ctDNA detection at baseline, End-of-NAT, and follow-up, respectively.
For overall survival, the overall multivariate hazard ratios were 3.0, 12.9, and 5.6, for ctDNA detection at baseline, End-of-NAT, and follow-up, respectively.
The pooled hazard ratios were numerically higher for both DFS and OS when ctDNA was detected at either End-of-NAT or follow-up.
In addition, detection of ctDNA was associated with a high degree of specificity (from 0.7 to 1.0) for breast cancer relapse; sensitivity ranged from 0.31 to 1.0, the researchers noted. The mean lead time from ctDNA detection to breast cancer recurrence in these cases was approximately 10 months.
Results show ctDNA detection is associated with worse survival
“Our study results demonstrate that ctDNA detection is associated with worse disease-free survival and overall survival in patients with early breast cancer, particularly when measured after treatment with tumor-informed assays,” Dr. Nader Marta said in an interview.
“As next steps, we need to build on this evidence to bring the potential benefits of this powerful prognostic tool to our patients,” said Dr. Nader Marta. “Ongoing studies exploring different management strategies based on serial ctDNA assessments will help us understand the exact role of this technology in our clinical practice.”
The study received no outside funding. Dr. Nader Marta disclosed relationships with companies including Roche and Bayer.
a new meta-analysis and systematic review found.
“Circulating tumor DNA (ctDNA) has been extensively studied as a prognostic biomarker in early breast cancer. However, there is a significant heterogeneity in the study results, which is probably related to the fact that each individual study included different patient populations, collected blood at different time points, and used different methods (assays) for ctDNA analysis,” said Guilherme Nader Marta, MD, of the Institut Jules Bordet, Anderlecht, Belgium, in an interview.
“The aim of our study was to summarize the available evidence that has been presented so far on this topic by performing a systematic review and meta-analysis including studies that reported the association between ctDNA detection and long-term outcomes,” said Dr. Nader Marta, who coauthored the new research, which was presented as a poster (Poster 26P) at the European Society for Medical Oncology (ESMO) Breast Cancer annual congress.
Methods and results
The authors identified 57 studies including data from 5,729 individuals with early breast cancer. The 44.5% for whom stages were reported consisted of 18.3% with stage I disease, 60.0% with stage II, and 21.5% with stage III. Patients’ ctDNA collection was divided into three groups: baseline, after neoadjuvant therapy (End-of-NAT), and during follow-up care; ctDNA assays were classified as tumor-informed or non–tumor-informed.
The detection of ctDNA at any time point during diagnosis and treatment was associated with worse disease-free survival (DFS) and overall survival (OS), compared with no ctDNA. The association was stronger in tumor-informed assays, the researchers said.
For disease-free survival, the overall multivariate hazard ratios were 2.5, 5.5, and 7.2 for ctDNA detection at baseline, End-of-NAT, and follow-up, respectively.
For overall survival, the overall multivariate hazard ratios were 3.0, 12.9, and 5.6, for ctDNA detection at baseline, End-of-NAT, and follow-up, respectively.
The pooled hazard ratios were numerically higher for both DFS and OS when ctDNA was detected at either End-of-NAT or follow-up.
In addition, detection of ctDNA was associated with a high degree of specificity (from 0.7 to 1.0) for breast cancer relapse; sensitivity ranged from 0.31 to 1.0, the researchers noted. The mean lead time from ctDNA detection to breast cancer recurrence in these cases was approximately 10 months.
Results show ctDNA detection is associated with worse survival
“Our study results demonstrate that ctDNA detection is associated with worse disease-free survival and overall survival in patients with early breast cancer, particularly when measured after treatment with tumor-informed assays,” Dr. Nader Marta said in an interview.
“As next steps, we need to build on this evidence to bring the potential benefits of this powerful prognostic tool to our patients,” said Dr. Nader Marta. “Ongoing studies exploring different management strategies based on serial ctDNA assessments will help us understand the exact role of this technology in our clinical practice.”
The study received no outside funding. Dr. Nader Marta disclosed relationships with companies including Roche and Bayer.
ESMO BREAST CANCER 2023
Breast cancer outcomes are worse for Black men
A new study finds that racial disparities in male breast cancer are persisting in the United States.
From 2000 to 2019, Black men were diagnosed at later ages than White males (median ages, 69 and 63 years, respectively) and were more likely to die from the disease (22.4% vs. 16.8%, respectively). Male breast cancer (MBC) was more likely to kill Black men in rural vs. urban areas (hazard ratio = 1.4; 95% confidence interval, 1.0-2.1; P less than .05). Among White males, in contrast, there was no difference on that front, according to the research, which was presented in a poster (Abstract No. 87P) at the European Society for Medical Oncology (ESMO) Breast Cancer annual congress.
It’s not clear why the disparities exist, said lead author Lekha Yadukumar, MBBS, an internal medicine resident at the Wright Center for Graduate Medical Education in Scranton, Penn., in an interview.
“Several potential factors may contribute to the higher rate of breast cancer diagnosis in older [Black] men, including the pathology of the disease, limited awareness about breast cancer, and potential barriers to accessibility,” she said. “The increased mortality among [Black men] may be linked to variations in tumor pathology and molecular biology. Social factors may also potentially impact survival rates, including [having] limited access to health care in rural areas and inadequate social support.”
Male breast cancer is rare, accounting for less than 1% of all breast cancer cases in the United States, according to the Breast Cancer Research Foundation. An estimated 2,700 men are diagnosed each year, and about 530 will die. Previous research has suggested Black men have worse outcomes than White men, but the data covered earlier years than the new study.
Methods and results
Dr. Yadukumar and colleagues retrospectively analyzed statistics from the Surveillance, Epidemiology, and End Results database for patients diagnosed with primary male breast cancer from 2000 to 2019 (n = 8,373; Black men, 1,111 [13.26%]; White men, 6,817 [81.41%]).
Median income didn’t affect mortality, whereas men in both racial groups were less likely to die if they were married vs. single/divorced (hazard ratio = 0.6; P less than .05).
Other studies have shown that “[Black American] men diagnosed with breast cancer experience longer time intervals before receiving treatment, encounter more severe disease manifestations, and exhibit lower rates of survivorship,” Dr. Yadukumar said. “Despite these findings, there remains a scarcity of genetic studies aimed at comprehending the underlying causes of these disparities. Moreover, there is a dearth of research investigating other factors that may influence survival outcomes among men with breast cancer.”
Findings reflect the disparities in female breast cancer
In an interview, Duke University, Durham, N.C., oncologist Arif Kamal, MD, MBA, MHS, the chief patient officer at the American Cancer Society, said the study is impressive since the number of patients is large for a rare cancer and the population is diverse. Plus, the findings reflect the disparities in female breast cancer, he noted.
“We know that Black women’s mortality is worse vs. White women in breast cancer, and we believe that most of that has nothing to do with cancer screening,” said Dr. Kamal, who was not involved in the new study. “When the clock starts from diagnosis onwards, you start to see less introduction to clinical trials and standard care medications and more time to treatment, surgery, and radiation,” he said.
“You see similar disparities as related to mortality in Black vs. White men,” he noted.
The new findings about higher death rates for Black men, especially in rural areas, suggest that “distance matters, and race matters,” he said. In rural areas, it can be hard to access pathologists, radiologists, and surgeons with more experience with breast cancer, he said.
But, he noted, the study finds that income doesn’t appear to be a factor.
In the big picture, he said, the results suggest that when it comes to barriers to better outcomes, “things that are systemic don’t make exceptions because you are a man vs. a woman.”
No study funding was reported. The study authors and Dr. Kamal have no relevant financial disclosures.
A new study finds that racial disparities in male breast cancer are persisting in the United States.
From 2000 to 2019, Black men were diagnosed at later ages than White males (median ages, 69 and 63 years, respectively) and were more likely to die from the disease (22.4% vs. 16.8%, respectively). Male breast cancer (MBC) was more likely to kill Black men in rural vs. urban areas (hazard ratio = 1.4; 95% confidence interval, 1.0-2.1; P less than .05). Among White males, in contrast, there was no difference on that front, according to the research, which was presented in a poster (Abstract No. 87P) at the European Society for Medical Oncology (ESMO) Breast Cancer annual congress.
It’s not clear why the disparities exist, said lead author Lekha Yadukumar, MBBS, an internal medicine resident at the Wright Center for Graduate Medical Education in Scranton, Penn., in an interview.
“Several potential factors may contribute to the higher rate of breast cancer diagnosis in older [Black] men, including the pathology of the disease, limited awareness about breast cancer, and potential barriers to accessibility,” she said. “The increased mortality among [Black men] may be linked to variations in tumor pathology and molecular biology. Social factors may also potentially impact survival rates, including [having] limited access to health care in rural areas and inadequate social support.”
Male breast cancer is rare, accounting for less than 1% of all breast cancer cases in the United States, according to the Breast Cancer Research Foundation. An estimated 2,700 men are diagnosed each year, and about 530 will die. Previous research has suggested Black men have worse outcomes than White men, but the data covered earlier years than the new study.
Methods and results
Dr. Yadukumar and colleagues retrospectively analyzed statistics from the Surveillance, Epidemiology, and End Results database for patients diagnosed with primary male breast cancer from 2000 to 2019 (n = 8,373; Black men, 1,111 [13.26%]; White men, 6,817 [81.41%]).
Median income didn’t affect mortality, whereas men in both racial groups were less likely to die if they were married vs. single/divorced (hazard ratio = 0.6; P less than .05).
Other studies have shown that “[Black American] men diagnosed with breast cancer experience longer time intervals before receiving treatment, encounter more severe disease manifestations, and exhibit lower rates of survivorship,” Dr. Yadukumar said. “Despite these findings, there remains a scarcity of genetic studies aimed at comprehending the underlying causes of these disparities. Moreover, there is a dearth of research investigating other factors that may influence survival outcomes among men with breast cancer.”
Findings reflect the disparities in female breast cancer
In an interview, Duke University, Durham, N.C., oncologist Arif Kamal, MD, MBA, MHS, the chief patient officer at the American Cancer Society, said the study is impressive since the number of patients is large for a rare cancer and the population is diverse. Plus, the findings reflect the disparities in female breast cancer, he noted.
“We know that Black women’s mortality is worse vs. White women in breast cancer, and we believe that most of that has nothing to do with cancer screening,” said Dr. Kamal, who was not involved in the new study. “When the clock starts from diagnosis onwards, you start to see less introduction to clinical trials and standard care medications and more time to treatment, surgery, and radiation,” he said.
“You see similar disparities as related to mortality in Black vs. White men,” he noted.
The new findings about higher death rates for Black men, especially in rural areas, suggest that “distance matters, and race matters,” he said. In rural areas, it can be hard to access pathologists, radiologists, and surgeons with more experience with breast cancer, he said.
But, he noted, the study finds that income doesn’t appear to be a factor.
In the big picture, he said, the results suggest that when it comes to barriers to better outcomes, “things that are systemic don’t make exceptions because you are a man vs. a woman.”
No study funding was reported. The study authors and Dr. Kamal have no relevant financial disclosures.
A new study finds that racial disparities in male breast cancer are persisting in the United States.
From 2000 to 2019, Black men were diagnosed at later ages than White males (median ages, 69 and 63 years, respectively) and were more likely to die from the disease (22.4% vs. 16.8%, respectively). Male breast cancer (MBC) was more likely to kill Black men in rural vs. urban areas (hazard ratio = 1.4; 95% confidence interval, 1.0-2.1; P less than .05). Among White males, in contrast, there was no difference on that front, according to the research, which was presented in a poster (Abstract No. 87P) at the European Society for Medical Oncology (ESMO) Breast Cancer annual congress.
It’s not clear why the disparities exist, said lead author Lekha Yadukumar, MBBS, an internal medicine resident at the Wright Center for Graduate Medical Education in Scranton, Penn., in an interview.
“Several potential factors may contribute to the higher rate of breast cancer diagnosis in older [Black] men, including the pathology of the disease, limited awareness about breast cancer, and potential barriers to accessibility,” she said. “The increased mortality among [Black men] may be linked to variations in tumor pathology and molecular biology. Social factors may also potentially impact survival rates, including [having] limited access to health care in rural areas and inadequate social support.”
Male breast cancer is rare, accounting for less than 1% of all breast cancer cases in the United States, according to the Breast Cancer Research Foundation. An estimated 2,700 men are diagnosed each year, and about 530 will die. Previous research has suggested Black men have worse outcomes than White men, but the data covered earlier years than the new study.
Methods and results
Dr. Yadukumar and colleagues retrospectively analyzed statistics from the Surveillance, Epidemiology, and End Results database for patients diagnosed with primary male breast cancer from 2000 to 2019 (n = 8,373; Black men, 1,111 [13.26%]; White men, 6,817 [81.41%]).
Median income didn’t affect mortality, whereas men in both racial groups were less likely to die if they were married vs. single/divorced (hazard ratio = 0.6; P less than .05).
Other studies have shown that “[Black American] men diagnosed with breast cancer experience longer time intervals before receiving treatment, encounter more severe disease manifestations, and exhibit lower rates of survivorship,” Dr. Yadukumar said. “Despite these findings, there remains a scarcity of genetic studies aimed at comprehending the underlying causes of these disparities. Moreover, there is a dearth of research investigating other factors that may influence survival outcomes among men with breast cancer.”
Findings reflect the disparities in female breast cancer
In an interview, Duke University, Durham, N.C., oncologist Arif Kamal, MD, MBA, MHS, the chief patient officer at the American Cancer Society, said the study is impressive since the number of patients is large for a rare cancer and the population is diverse. Plus, the findings reflect the disparities in female breast cancer, he noted.
“We know that Black women’s mortality is worse vs. White women in breast cancer, and we believe that most of that has nothing to do with cancer screening,” said Dr. Kamal, who was not involved in the new study. “When the clock starts from diagnosis onwards, you start to see less introduction to clinical trials and standard care medications and more time to treatment, surgery, and radiation,” he said.
“You see similar disparities as related to mortality in Black vs. White men,” he noted.
The new findings about higher death rates for Black men, especially in rural areas, suggest that “distance matters, and race matters,” he said. In rural areas, it can be hard to access pathologists, radiologists, and surgeons with more experience with breast cancer, he said.
But, he noted, the study finds that income doesn’t appear to be a factor.
In the big picture, he said, the results suggest that when it comes to barriers to better outcomes, “things that are systemic don’t make exceptions because you are a man vs. a woman.”
No study funding was reported. The study authors and Dr. Kamal have no relevant financial disclosures.
FROM ESMO BREAST CANCER 2023
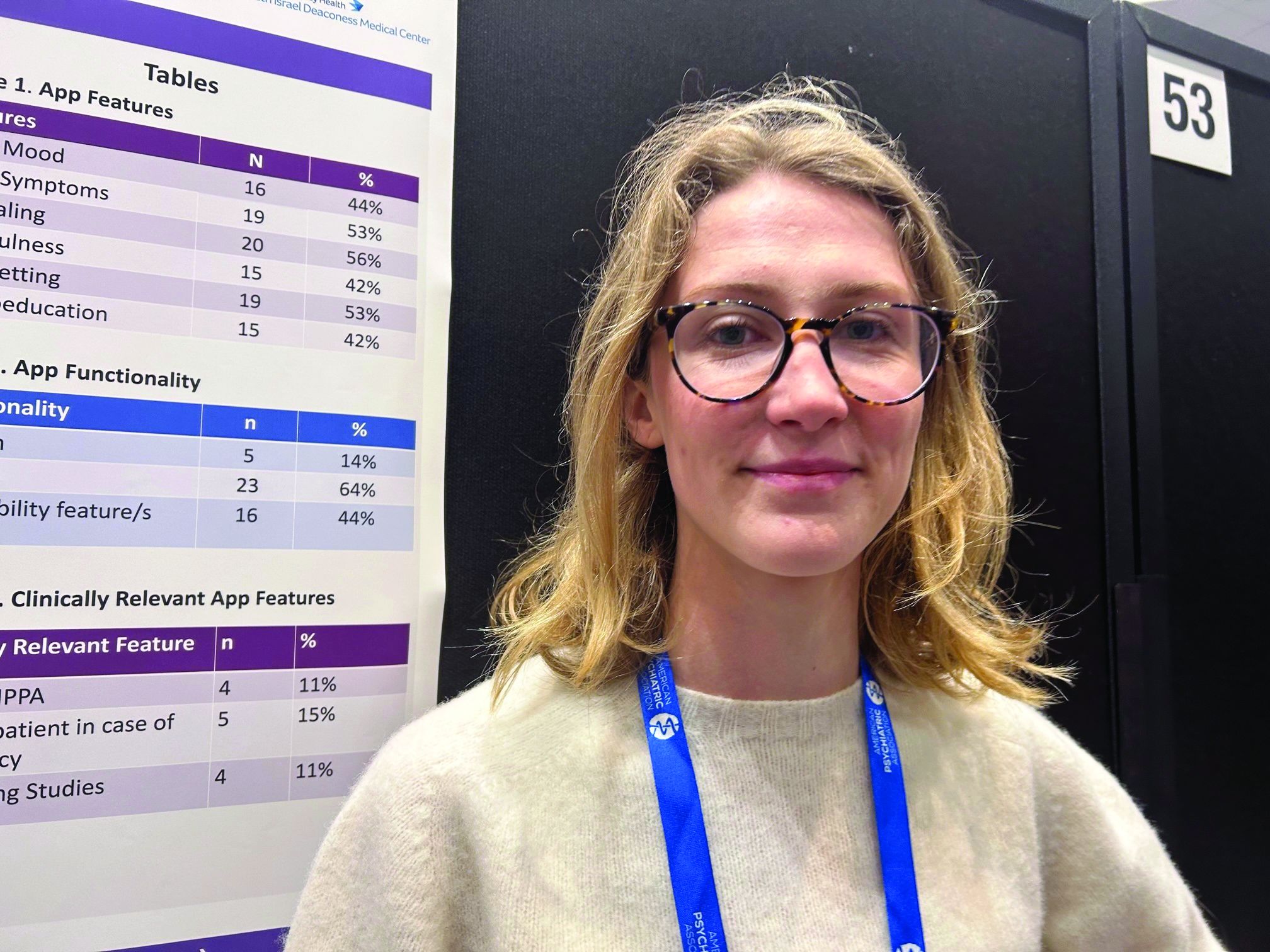
Eating disorder apps fall short when it comes to privacy
SAN FRANCISCO –
Federal laws require those handling sensitive health information to have policies and security safeguards in place to protect such information, whether it’s stored on paper or electronically.
“As it stands right now, there’s not enough evidence to support using these apps as an adjunct to clinical care,” study author Theodora O’Leary, a 4th-year medical student at Tufts University, Boston, said in an interview. “We need more research on the efficacy of these apps because right now not enough of them meet HIPAA [standards] and don’t have privacy and security measures.”
The findings were presented at the annual meeting of the American Psychiatric Association.
Eating disorders (EDs) are a common mental health condition affecting almost 1 in 10 Americans over their lifetime. Yet only about a third of patients with an eating disorder receive adequate treatment.
The pandemic saw a rise in eating disorders and in the use of mental health apps “to kind of fill the gap because people couldn’t be seen in person,” said Ms. O’Leary.
Inexpensive and accessible
Smartphone apps have a lot of advantages for patients with an ED. For one thing, they’re relatively inexpensive and accessible; most Americans already own one or more devices on which these apps can be used.
They’re also a feasible means of delivering psychological interventions, which are often recommended for EDs. Among these interventions, cognitive-behavioral therapy (CBT) has the largest evidence base for this condition.
Also, as many individuals with an ED may be reluctant to seek treatment because of stigma and shame, the anonymity afforded by an app could increase access to the help they seek.
But Ms. O’Leary warned the Food and Drug Administration does not regulate these apps, and people are sharing their personal health information on them.
The researchers conducted a review of commercially available eating disorder apps by searching the Apple and Google play stores using key phrases such as “eating disorder,” “anorexia,” and “binge eating disorder.”
They found 16 relevant apps that they added to the publicly available apps already in a database at Tufts, for a total of about 36 that were evaluated in the study (the number fluctuates as apps are deleted.)
They then reviewed the apps using the 105 questions based on the APA’s app evaluation model, which covers categories such as efficacy, privacy, accessibility, and clinical applicability. And they used filters to group apps by characteristics such as function, cost, and features.
The vast majority were self-help apps, which include things like journaling, meditation, and information on CBT. Others were reference apps that provide related definitions and sometimes include surveys to determine, for example, if the user has an eating disorder.
About 44% of the apps track mood, and 53% track symptoms. Some 56% include journaling, 42% mindfulness, 53% goal setting, and 42% psychoeducation.
Hybrid care
Only 5% of apps allow for “hybrid” care. This, explained Ms. O’Leary, is when clinicians use their own app to access patients’ apps, allowing them to track food restrictions and therapies, and make comments.
“The hybrid is viewed as the best form of app”, she said. “It’s almost like an adjunct to clinical care.”
Hybrid apps also tend to have patient safety features, she added. And these apps meet HIPAA standards, which only 11% of the apps in the study did.
Only 15% of apps advised patients to take steps in case of an emergency, and 11% had supporting studies. And where there was supporting research, much of it was funded by the app creators, said Ms. O’Leary.
For example, an app provided by Noom (the weight loss program that promises to help change habits and mindsets around food) “has a bunch of feasibility studies but they’re all funded by Noom”, which can introduce bias, she explained.
None of the apps were created by an accredited health care institution, she noted. “And I think only one app out of all the eating disorder apps we looked at was from a nonprofit.”
About 17% of the apps offer help with a “coach” or “expert”. However, these apps often fail to disclose the definition of a coach or state they’re not a replacement for medical care.
Coaching apps more expensive
Additionally, these coaching apps are often some of the most expensive, said Ms. O’Leary.
Daniel E. Gih, MD, associate professor at the University of Nebraska Medical Center, Omaha, helped start an eating disorders program at the University of Michigan and continues to treat patients with eating disorders. He said the increase in the use of eating disorder apps isn’t surprising as the incidence of these disorders increased in the wake of pandemic restrictions, especially among young people.
“Patients are likely doing more research on their medical conditions and trying to crowdsource information or self-treat,” Dr. Gih said.
It’s unclear whether “shame or just the general lack of specialized eating disorder professionals,” including physicians, is driving some of the interest in these apps, he added.
Dr. Gih stressed eating disorder apps should not only include screening for suicidality, but also explicitly tell patients to seek immediate attention if they show certain signs – for example, fainting, chest pain, or blood in emesis.
“The apps may be giving patients false hope or delaying medical care,” he said. “Apps are likely not sufficient enough to replace a multidisciplinary team with experience and expertise in eating disorders.”
Ms. O’Leary and Dr. Gih report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
SAN FRANCISCO –
Federal laws require those handling sensitive health information to have policies and security safeguards in place to protect such information, whether it’s stored on paper or electronically.
“As it stands right now, there’s not enough evidence to support using these apps as an adjunct to clinical care,” study author Theodora O’Leary, a 4th-year medical student at Tufts University, Boston, said in an interview. “We need more research on the efficacy of these apps because right now not enough of them meet HIPAA [standards] and don’t have privacy and security measures.”
The findings were presented at the annual meeting of the American Psychiatric Association.
Eating disorders (EDs) are a common mental health condition affecting almost 1 in 10 Americans over their lifetime. Yet only about a third of patients with an eating disorder receive adequate treatment.
The pandemic saw a rise in eating disorders and in the use of mental health apps “to kind of fill the gap because people couldn’t be seen in person,” said Ms. O’Leary.
Inexpensive and accessible
Smartphone apps have a lot of advantages for patients with an ED. For one thing, they’re relatively inexpensive and accessible; most Americans already own one or more devices on which these apps can be used.
They’re also a feasible means of delivering psychological interventions, which are often recommended for EDs. Among these interventions, cognitive-behavioral therapy (CBT) has the largest evidence base for this condition.
Also, as many individuals with an ED may be reluctant to seek treatment because of stigma and shame, the anonymity afforded by an app could increase access to the help they seek.
But Ms. O’Leary warned the Food and Drug Administration does not regulate these apps, and people are sharing their personal health information on them.
The researchers conducted a review of commercially available eating disorder apps by searching the Apple and Google play stores using key phrases such as “eating disorder,” “anorexia,” and “binge eating disorder.”
They found 16 relevant apps that they added to the publicly available apps already in a database at Tufts, for a total of about 36 that were evaluated in the study (the number fluctuates as apps are deleted.)
They then reviewed the apps using the 105 questions based on the APA’s app evaluation model, which covers categories such as efficacy, privacy, accessibility, and clinical applicability. And they used filters to group apps by characteristics such as function, cost, and features.
The vast majority were self-help apps, which include things like journaling, meditation, and information on CBT. Others were reference apps that provide related definitions and sometimes include surveys to determine, for example, if the user has an eating disorder.
About 44% of the apps track mood, and 53% track symptoms. Some 56% include journaling, 42% mindfulness, 53% goal setting, and 42% psychoeducation.
Hybrid care
Only 5% of apps allow for “hybrid” care. This, explained Ms. O’Leary, is when clinicians use their own app to access patients’ apps, allowing them to track food restrictions and therapies, and make comments.
“The hybrid is viewed as the best form of app”, she said. “It’s almost like an adjunct to clinical care.”
Hybrid apps also tend to have patient safety features, she added. And these apps meet HIPAA standards, which only 11% of the apps in the study did.
Only 15% of apps advised patients to take steps in case of an emergency, and 11% had supporting studies. And where there was supporting research, much of it was funded by the app creators, said Ms. O’Leary.
For example, an app provided by Noom (the weight loss program that promises to help change habits and mindsets around food) “has a bunch of feasibility studies but they’re all funded by Noom”, which can introduce bias, she explained.
None of the apps were created by an accredited health care institution, she noted. “And I think only one app out of all the eating disorder apps we looked at was from a nonprofit.”
About 17% of the apps offer help with a “coach” or “expert”. However, these apps often fail to disclose the definition of a coach or state they’re not a replacement for medical care.
Coaching apps more expensive
Additionally, these coaching apps are often some of the most expensive, said Ms. O’Leary.
Daniel E. Gih, MD, associate professor at the University of Nebraska Medical Center, Omaha, helped start an eating disorders program at the University of Michigan and continues to treat patients with eating disorders. He said the increase in the use of eating disorder apps isn’t surprising as the incidence of these disorders increased in the wake of pandemic restrictions, especially among young people.
“Patients are likely doing more research on their medical conditions and trying to crowdsource information or self-treat,” Dr. Gih said.
It’s unclear whether “shame or just the general lack of specialized eating disorder professionals,” including physicians, is driving some of the interest in these apps, he added.
Dr. Gih stressed eating disorder apps should not only include screening for suicidality, but also explicitly tell patients to seek immediate attention if they show certain signs – for example, fainting, chest pain, or blood in emesis.
“The apps may be giving patients false hope or delaying medical care,” he said. “Apps are likely not sufficient enough to replace a multidisciplinary team with experience and expertise in eating disorders.”
Ms. O’Leary and Dr. Gih report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
SAN FRANCISCO –
Federal laws require those handling sensitive health information to have policies and security safeguards in place to protect such information, whether it’s stored on paper or electronically.
“As it stands right now, there’s not enough evidence to support using these apps as an adjunct to clinical care,” study author Theodora O’Leary, a 4th-year medical student at Tufts University, Boston, said in an interview. “We need more research on the efficacy of these apps because right now not enough of them meet HIPAA [standards] and don’t have privacy and security measures.”
The findings were presented at the annual meeting of the American Psychiatric Association.
Eating disorders (EDs) are a common mental health condition affecting almost 1 in 10 Americans over their lifetime. Yet only about a third of patients with an eating disorder receive adequate treatment.
The pandemic saw a rise in eating disorders and in the use of mental health apps “to kind of fill the gap because people couldn’t be seen in person,” said Ms. O’Leary.
Inexpensive and accessible
Smartphone apps have a lot of advantages for patients with an ED. For one thing, they’re relatively inexpensive and accessible; most Americans already own one or more devices on which these apps can be used.
They’re also a feasible means of delivering psychological interventions, which are often recommended for EDs. Among these interventions, cognitive-behavioral therapy (CBT) has the largest evidence base for this condition.
Also, as many individuals with an ED may be reluctant to seek treatment because of stigma and shame, the anonymity afforded by an app could increase access to the help they seek.
But Ms. O’Leary warned the Food and Drug Administration does not regulate these apps, and people are sharing their personal health information on them.
The researchers conducted a review of commercially available eating disorder apps by searching the Apple and Google play stores using key phrases such as “eating disorder,” “anorexia,” and “binge eating disorder.”
They found 16 relevant apps that they added to the publicly available apps already in a database at Tufts, for a total of about 36 that were evaluated in the study (the number fluctuates as apps are deleted.)
They then reviewed the apps using the 105 questions based on the APA’s app evaluation model, which covers categories such as efficacy, privacy, accessibility, and clinical applicability. And they used filters to group apps by characteristics such as function, cost, and features.
The vast majority were self-help apps, which include things like journaling, meditation, and information on CBT. Others were reference apps that provide related definitions and sometimes include surveys to determine, for example, if the user has an eating disorder.
About 44% of the apps track mood, and 53% track symptoms. Some 56% include journaling, 42% mindfulness, 53% goal setting, and 42% psychoeducation.
Hybrid care
Only 5% of apps allow for “hybrid” care. This, explained Ms. O’Leary, is when clinicians use their own app to access patients’ apps, allowing them to track food restrictions and therapies, and make comments.
“The hybrid is viewed as the best form of app”, she said. “It’s almost like an adjunct to clinical care.”
Hybrid apps also tend to have patient safety features, she added. And these apps meet HIPAA standards, which only 11% of the apps in the study did.
Only 15% of apps advised patients to take steps in case of an emergency, and 11% had supporting studies. And where there was supporting research, much of it was funded by the app creators, said Ms. O’Leary.
For example, an app provided by Noom (the weight loss program that promises to help change habits and mindsets around food) “has a bunch of feasibility studies but they’re all funded by Noom”, which can introduce bias, she explained.
None of the apps were created by an accredited health care institution, she noted. “And I think only one app out of all the eating disorder apps we looked at was from a nonprofit.”
About 17% of the apps offer help with a “coach” or “expert”. However, these apps often fail to disclose the definition of a coach or state they’re not a replacement for medical care.
Coaching apps more expensive
Additionally, these coaching apps are often some of the most expensive, said Ms. O’Leary.
Daniel E. Gih, MD, associate professor at the University of Nebraska Medical Center, Omaha, helped start an eating disorders program at the University of Michigan and continues to treat patients with eating disorders. He said the increase in the use of eating disorder apps isn’t surprising as the incidence of these disorders increased in the wake of pandemic restrictions, especially among young people.
“Patients are likely doing more research on their medical conditions and trying to crowdsource information or self-treat,” Dr. Gih said.
It’s unclear whether “shame or just the general lack of specialized eating disorder professionals,” including physicians, is driving some of the interest in these apps, he added.
Dr. Gih stressed eating disorder apps should not only include screening for suicidality, but also explicitly tell patients to seek immediate attention if they show certain signs – for example, fainting, chest pain, or blood in emesis.
“The apps may be giving patients false hope or delaying medical care,” he said. “Apps are likely not sufficient enough to replace a multidisciplinary team with experience and expertise in eating disorders.”
Ms. O’Leary and Dr. Gih report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
AT APA 2023
Tweaking food delivery apps can lower calories purchased
DUBLIN – , show three new randomized trials from the United Kingdom.
The prominent positioning of low-calorie menu items, and restaurants with low-calorie main meals, on a food app emerged as the most promising approach to promote healthier eating, followed by preselecting smaller portions by default, and finally calorie labels, Anna Keleher, MPA, a behavioral scientist at Nesta, London, reported at the European Congress on Obesity (ECO) meeting.
“Many out-of-home meals have more calories than meals cooked in-home and using delivery apps is linked with a higher risk of becoming overweight or obese,” she remarked. “We’re interested in understanding more about delivery apps because they can be modified at scale easily and can reach millions of people with interventions to promote healthier and more nutritious options in these settings.”
Food delivery apps have surged in use in the United Kingdom with a 55% increase since 2015; examples include Uber Eats, Just Eat, and Deliveroo. “This trend is similar in the United States, with more and more consumers using delivery apps to buy food,” said Ms. Keleher, a senior adviser at the Behavioral Insights Team, New York.
Emma Boyland, PhD, an obesity psychologist from Liverpool (England) University, said: “Apps are an increasingly popular way for people to buy food and the virtual food environment is becoming as prominent as the physical food environment in how we go about obtaining meals.”
She highlighted the need to understand more about how food apps change the way we purchase and eat, but noted that “the work presented today” showed that “moving the position of food choices and information, as well as the brand name and imagery, influences what people end up buying and consuming.
“I think there’s a place for interventions that challenge these things and improve dietary health,” said Dr. Boyland, who chaired the session during which Ms. Keleher presented her results. “However, as we’ve seen with calorie labeling, they don’t always have the biggest effect on their own, so as is often the case, we need to take multiple actions, incorporating all the elements of the environment to make a meaningful difference.”
Three trials changing displays on simulated food delivery apps
“Delivery apps could reach millions of people and help us select healthier food options, and yet there is very little research looking at what works to promote healthier and more nutritious options in these settings,” Filippo Bianchi, MD, a colleague working with Ms. Keleher, said in a press release issued by ECO.
So the research team carried out a proof-of-concept testing of health-promoting interventions by developing a simulated food delivery app and asking 23,783 adults who typically use such services to choose a meal for themselves as if it were a real-life food delivery order.
“As a first step, we developed a simulated online food delivery platform to generate evidence on the effectiveness of our interventions,” Ms. Keleher explained, noting that the simulated platform included 21 restaurants and almost 600 food and drink items to choose from.
The research evaluated 14 interventions across three randomized controlled trials, displaying various food-ordering options that promoted lower-calorie options against a control. The trials investigated default choices (promoting the selection of small portion sizes through defaults, n = 6,000); positioning (promoting the selection of less calorie-dense options through positioning, n = 9,003); and labeling (promoting the selection of less calorific options through calorie labels, n = 8,780).
The primary outcome was the total number of calories in the basket at checkout. The results were adjusted for potentially confounding factors, such as body mass index, age, gender, and income.
For the trial that promoted smaller portions by default, “all of our interventions significantly reduced calorie purchases, with each additional intervention element increasing the effect sizes, which ranged from a 6% to 13% reduction in calories [–5.5% to –12.5% kcal/order; P < .05],” reported Ms. Keleher.
The second trial varied the position of both items on the menu and the order of restaurants – effectively, lower-calorie menu options were more prominent, and restaurant options with lower-calorie main meals were placed at the top of the restaurant selection page.
Ms. Keleher noted that there have been some concerns about whether this strategy would negatively affect restaurant business, so the research team counteracted this by also incorporating an option where low-calorie but high-price options were placed near the top of the display to promote healthier options but without loss of income for participating restaurants. This last intervention with low-calorie/high-price options placed near the top also led to reduced calorie intake.
“This showed that promoting low-calorie options does not necessarily mean damaging business revenue,” she said. “We hope that the industry can evolve to meet the widely recognized needs of society and consumers.”
Repositioning restaurants emerged as more effective than repositioning foods on the menu, while all interventions significantly reduced calorie purchases. “Effect sizes ranged from 6% to 15% reductions in calories purchased per order [P < .05],” reported Ms. Keleher.
The last trial tested seven calorie labels: four that changed the font size and location of the label, two that added a switch on/off filter for calorie label display, and one that was a calorie summary at checkout.
“All these standard calorie labels directionally reduced the number of excess calories with two [options] reaching statistical significance. Five out of seven labels significantly reduced calorie purchases with effect sizes ranging from 4.3% to –7.8% kcal/order (P < .05),” reported Ms. Keleher.
“This research is important for policymakers so they can understand the best way for companies to display calorie labels and what to include in regulations and guidelines,” she summarized.
Qualitative think-aloud study explored views around food delivery apps
Another piece of research, the think-aloud study, by the same authors, was presented at ECO, and explored how best to enhance the effectiveness and acceptability of calorie labels in food delivery apps in consultation with 20 adult delivery app users in the United Kingdom.
Researchers tried to document the range of views people have about calorie labels, including variation both between people and within an individual.
“For example, on a weekend, people might not want to engage with calories at all because they are more concerned to treat themselves, whereas at a mid-week lunch that same person might really want the ability to check the calorie content of their food,” Ms. Keleher reported.
She said that considerations varied significantly between people such that they described different ways in which calorie labeling impacted their food-ordering experience.
“Some people felt labels supported their existing intentions, whereas others felt labels built their knowledge. Still others felt calorie labels were insufficient to support their health and wanted more information, such as on macronutrients,” said Ms. Keleher, quoting one participant: “There’s no situation in which I would look at [calories]. I look at nutrients. I prefer the traffic light system [color-coding salt, fat, and sugar content],” she relayed.
The key recommendations based on the think-aloud study included providing a filter that allows users to switch calorie labels on and off; communicating recommended energy intake per meal (that is, 600 kcal) and not just per day (that is, 2,000 kcal); and avoiding framing calorie label messaging or formatting as judgmental (for example, red fonts).
“These studies provide encouraging proof-of-concept evidence that small tweaks in delivery apps could help many people to identify and select healthier foods. Testing similar initiatives with real restaurants and delivery apps will be important to assess the long-term impact of these interventions in the real world. Further research should also explore the best way to balance desired health impacts while minimizing effects on businesses and on cost-of-living concerns for consumers,” concluded Dr. Bianchi.
A version of this article first appeared on Medscape.com.
DUBLIN – , show three new randomized trials from the United Kingdom.
The prominent positioning of low-calorie menu items, and restaurants with low-calorie main meals, on a food app emerged as the most promising approach to promote healthier eating, followed by preselecting smaller portions by default, and finally calorie labels, Anna Keleher, MPA, a behavioral scientist at Nesta, London, reported at the European Congress on Obesity (ECO) meeting.
“Many out-of-home meals have more calories than meals cooked in-home and using delivery apps is linked with a higher risk of becoming overweight or obese,” she remarked. “We’re interested in understanding more about delivery apps because they can be modified at scale easily and can reach millions of people with interventions to promote healthier and more nutritious options in these settings.”
Food delivery apps have surged in use in the United Kingdom with a 55% increase since 2015; examples include Uber Eats, Just Eat, and Deliveroo. “This trend is similar in the United States, with more and more consumers using delivery apps to buy food,” said Ms. Keleher, a senior adviser at the Behavioral Insights Team, New York.
Emma Boyland, PhD, an obesity psychologist from Liverpool (England) University, said: “Apps are an increasingly popular way for people to buy food and the virtual food environment is becoming as prominent as the physical food environment in how we go about obtaining meals.”
She highlighted the need to understand more about how food apps change the way we purchase and eat, but noted that “the work presented today” showed that “moving the position of food choices and information, as well as the brand name and imagery, influences what people end up buying and consuming.
“I think there’s a place for interventions that challenge these things and improve dietary health,” said Dr. Boyland, who chaired the session during which Ms. Keleher presented her results. “However, as we’ve seen with calorie labeling, they don’t always have the biggest effect on their own, so as is often the case, we need to take multiple actions, incorporating all the elements of the environment to make a meaningful difference.”
Three trials changing displays on simulated food delivery apps
“Delivery apps could reach millions of people and help us select healthier food options, and yet there is very little research looking at what works to promote healthier and more nutritious options in these settings,” Filippo Bianchi, MD, a colleague working with Ms. Keleher, said in a press release issued by ECO.
So the research team carried out a proof-of-concept testing of health-promoting interventions by developing a simulated food delivery app and asking 23,783 adults who typically use such services to choose a meal for themselves as if it were a real-life food delivery order.
“As a first step, we developed a simulated online food delivery platform to generate evidence on the effectiveness of our interventions,” Ms. Keleher explained, noting that the simulated platform included 21 restaurants and almost 600 food and drink items to choose from.
The research evaluated 14 interventions across three randomized controlled trials, displaying various food-ordering options that promoted lower-calorie options against a control. The trials investigated default choices (promoting the selection of small portion sizes through defaults, n = 6,000); positioning (promoting the selection of less calorie-dense options through positioning, n = 9,003); and labeling (promoting the selection of less calorific options through calorie labels, n = 8,780).
The primary outcome was the total number of calories in the basket at checkout. The results were adjusted for potentially confounding factors, such as body mass index, age, gender, and income.
For the trial that promoted smaller portions by default, “all of our interventions significantly reduced calorie purchases, with each additional intervention element increasing the effect sizes, which ranged from a 6% to 13% reduction in calories [–5.5% to –12.5% kcal/order; P < .05],” reported Ms. Keleher.
The second trial varied the position of both items on the menu and the order of restaurants – effectively, lower-calorie menu options were more prominent, and restaurant options with lower-calorie main meals were placed at the top of the restaurant selection page.
Ms. Keleher noted that there have been some concerns about whether this strategy would negatively affect restaurant business, so the research team counteracted this by also incorporating an option where low-calorie but high-price options were placed near the top of the display to promote healthier options but without loss of income for participating restaurants. This last intervention with low-calorie/high-price options placed near the top also led to reduced calorie intake.
“This showed that promoting low-calorie options does not necessarily mean damaging business revenue,” she said. “We hope that the industry can evolve to meet the widely recognized needs of society and consumers.”
Repositioning restaurants emerged as more effective than repositioning foods on the menu, while all interventions significantly reduced calorie purchases. “Effect sizes ranged from 6% to 15% reductions in calories purchased per order [P < .05],” reported Ms. Keleher.
The last trial tested seven calorie labels: four that changed the font size and location of the label, two that added a switch on/off filter for calorie label display, and one that was a calorie summary at checkout.
“All these standard calorie labels directionally reduced the number of excess calories with two [options] reaching statistical significance. Five out of seven labels significantly reduced calorie purchases with effect sizes ranging from 4.3% to –7.8% kcal/order (P < .05),” reported Ms. Keleher.
“This research is important for policymakers so they can understand the best way for companies to display calorie labels and what to include in regulations and guidelines,” she summarized.
Qualitative think-aloud study explored views around food delivery apps
Another piece of research, the think-aloud study, by the same authors, was presented at ECO, and explored how best to enhance the effectiveness and acceptability of calorie labels in food delivery apps in consultation with 20 adult delivery app users in the United Kingdom.
Researchers tried to document the range of views people have about calorie labels, including variation both between people and within an individual.
“For example, on a weekend, people might not want to engage with calories at all because they are more concerned to treat themselves, whereas at a mid-week lunch that same person might really want the ability to check the calorie content of their food,” Ms. Keleher reported.
She said that considerations varied significantly between people such that they described different ways in which calorie labeling impacted their food-ordering experience.
“Some people felt labels supported their existing intentions, whereas others felt labels built their knowledge. Still others felt calorie labels were insufficient to support their health and wanted more information, such as on macronutrients,” said Ms. Keleher, quoting one participant: “There’s no situation in which I would look at [calories]. I look at nutrients. I prefer the traffic light system [color-coding salt, fat, and sugar content],” she relayed.
The key recommendations based on the think-aloud study included providing a filter that allows users to switch calorie labels on and off; communicating recommended energy intake per meal (that is, 600 kcal) and not just per day (that is, 2,000 kcal); and avoiding framing calorie label messaging or formatting as judgmental (for example, red fonts).
“These studies provide encouraging proof-of-concept evidence that small tweaks in delivery apps could help many people to identify and select healthier foods. Testing similar initiatives with real restaurants and delivery apps will be important to assess the long-term impact of these interventions in the real world. Further research should also explore the best way to balance desired health impacts while minimizing effects on businesses and on cost-of-living concerns for consumers,” concluded Dr. Bianchi.
A version of this article first appeared on Medscape.com.
DUBLIN – , show three new randomized trials from the United Kingdom.
The prominent positioning of low-calorie menu items, and restaurants with low-calorie main meals, on a food app emerged as the most promising approach to promote healthier eating, followed by preselecting smaller portions by default, and finally calorie labels, Anna Keleher, MPA, a behavioral scientist at Nesta, London, reported at the European Congress on Obesity (ECO) meeting.
“Many out-of-home meals have more calories than meals cooked in-home and using delivery apps is linked with a higher risk of becoming overweight or obese,” she remarked. “We’re interested in understanding more about delivery apps because they can be modified at scale easily and can reach millions of people with interventions to promote healthier and more nutritious options in these settings.”
Food delivery apps have surged in use in the United Kingdom with a 55% increase since 2015; examples include Uber Eats, Just Eat, and Deliveroo. “This trend is similar in the United States, with more and more consumers using delivery apps to buy food,” said Ms. Keleher, a senior adviser at the Behavioral Insights Team, New York.
Emma Boyland, PhD, an obesity psychologist from Liverpool (England) University, said: “Apps are an increasingly popular way for people to buy food and the virtual food environment is becoming as prominent as the physical food environment in how we go about obtaining meals.”
She highlighted the need to understand more about how food apps change the way we purchase and eat, but noted that “the work presented today” showed that “moving the position of food choices and information, as well as the brand name and imagery, influences what people end up buying and consuming.
“I think there’s a place for interventions that challenge these things and improve dietary health,” said Dr. Boyland, who chaired the session during which Ms. Keleher presented her results. “However, as we’ve seen with calorie labeling, they don’t always have the biggest effect on their own, so as is often the case, we need to take multiple actions, incorporating all the elements of the environment to make a meaningful difference.”
Three trials changing displays on simulated food delivery apps
“Delivery apps could reach millions of people and help us select healthier food options, and yet there is very little research looking at what works to promote healthier and more nutritious options in these settings,” Filippo Bianchi, MD, a colleague working with Ms. Keleher, said in a press release issued by ECO.
So the research team carried out a proof-of-concept testing of health-promoting interventions by developing a simulated food delivery app and asking 23,783 adults who typically use such services to choose a meal for themselves as if it were a real-life food delivery order.
“As a first step, we developed a simulated online food delivery platform to generate evidence on the effectiveness of our interventions,” Ms. Keleher explained, noting that the simulated platform included 21 restaurants and almost 600 food and drink items to choose from.
The research evaluated 14 interventions across three randomized controlled trials, displaying various food-ordering options that promoted lower-calorie options against a control. The trials investigated default choices (promoting the selection of small portion sizes through defaults, n = 6,000); positioning (promoting the selection of less calorie-dense options through positioning, n = 9,003); and labeling (promoting the selection of less calorific options through calorie labels, n = 8,780).
The primary outcome was the total number of calories in the basket at checkout. The results were adjusted for potentially confounding factors, such as body mass index, age, gender, and income.
For the trial that promoted smaller portions by default, “all of our interventions significantly reduced calorie purchases, with each additional intervention element increasing the effect sizes, which ranged from a 6% to 13% reduction in calories [–5.5% to –12.5% kcal/order; P < .05],” reported Ms. Keleher.
The second trial varied the position of both items on the menu and the order of restaurants – effectively, lower-calorie menu options were more prominent, and restaurant options with lower-calorie main meals were placed at the top of the restaurant selection page.
Ms. Keleher noted that there have been some concerns about whether this strategy would negatively affect restaurant business, so the research team counteracted this by also incorporating an option where low-calorie but high-price options were placed near the top of the display to promote healthier options but without loss of income for participating restaurants. This last intervention with low-calorie/high-price options placed near the top also led to reduced calorie intake.
“This showed that promoting low-calorie options does not necessarily mean damaging business revenue,” she said. “We hope that the industry can evolve to meet the widely recognized needs of society and consumers.”
Repositioning restaurants emerged as more effective than repositioning foods on the menu, while all interventions significantly reduced calorie purchases. “Effect sizes ranged from 6% to 15% reductions in calories purchased per order [P < .05],” reported Ms. Keleher.
The last trial tested seven calorie labels: four that changed the font size and location of the label, two that added a switch on/off filter for calorie label display, and one that was a calorie summary at checkout.
“All these standard calorie labels directionally reduced the number of excess calories with two [options] reaching statistical significance. Five out of seven labels significantly reduced calorie purchases with effect sizes ranging from 4.3% to –7.8% kcal/order (P < .05),” reported Ms. Keleher.
“This research is important for policymakers so they can understand the best way for companies to display calorie labels and what to include in regulations and guidelines,” she summarized.
Qualitative think-aloud study explored views around food delivery apps
Another piece of research, the think-aloud study, by the same authors, was presented at ECO, and explored how best to enhance the effectiveness and acceptability of calorie labels in food delivery apps in consultation with 20 adult delivery app users in the United Kingdom.
Researchers tried to document the range of views people have about calorie labels, including variation both between people and within an individual.
“For example, on a weekend, people might not want to engage with calories at all because they are more concerned to treat themselves, whereas at a mid-week lunch that same person might really want the ability to check the calorie content of their food,” Ms. Keleher reported.
She said that considerations varied significantly between people such that they described different ways in which calorie labeling impacted their food-ordering experience.
“Some people felt labels supported their existing intentions, whereas others felt labels built their knowledge. Still others felt calorie labels were insufficient to support their health and wanted more information, such as on macronutrients,” said Ms. Keleher, quoting one participant: “There’s no situation in which I would look at [calories]. I look at nutrients. I prefer the traffic light system [color-coding salt, fat, and sugar content],” she relayed.
The key recommendations based on the think-aloud study included providing a filter that allows users to switch calorie labels on and off; communicating recommended energy intake per meal (that is, 600 kcal) and not just per day (that is, 2,000 kcal); and avoiding framing calorie label messaging or formatting as judgmental (for example, red fonts).
“These studies provide encouraging proof-of-concept evidence that small tweaks in delivery apps could help many people to identify and select healthier foods. Testing similar initiatives with real restaurants and delivery apps will be important to assess the long-term impact of these interventions in the real world. Further research should also explore the best way to balance desired health impacts while minimizing effects on businesses and on cost-of-living concerns for consumers,” concluded Dr. Bianchi.
A version of this article first appeared on Medscape.com.
AT ECO 2023
Urology groups endorse two prostate biopsy approaches
CHICAGO - , endorsing both transperineal and transrectal biopsy instead of choosing one over the other.
The new guidelines, issued at the annual meeting of the American Urological Association, contrast with 2021 recommendations from the European Association of Urologists (EAU), which regard the transperineal approach as superior to and safer than the transrectal approach.
The new guidelines state: “Clinicians may use either a transrectal or transperineal biopsy route when performing a biopsy. (Conditional Recommendation; Evidence Level: Grade C).” Grade C is the lowest grade of acceptance the guideline committee could issue, according to Daniel Lin, MD, vice-chair of the AUA guideline panel.
“The AUA looked at all the higher-level data comparing the two procedures. There was a lack of that data,” Dr. Lin, chief of urologic oncology at the University of Washington, Seattle, said in an interview. He said the literature consists mainly of systematic single-center reviews, rather than multicenter randomized trials.
But Hendrik Van Poppel, MD, policy chief for the EAU, said that in Europe, transrectal biopsies are now considered “medical malpractice.”
Philip Cornford, MD, associate professor of urology at the University of Liverpool, England, and chair of the prostate biopsy guidelines panel for the EAU, said the society in 2021 concluded that the transperineal approach is the preferred one.
The EAU stated that transperineal prostate biopsies should be performed “due to the lower risk of infectious complications.” The EAU described the evidence as strong: A meta-analysis of seven studies that included 1,330 patients showed that for patients undergoing transperineal biopsy, infectious complications were significantly reduced.
Dr. Cornford said in essence, the EAU made its decision out of concern about infections, whereas the AUA and SUO based their decision on the ability of the methods to detect cancer.
Advocates for transperineal procedures cite several studies that show that the rate of infection, including sepsis, with such biopsies is virtually zero.
However, Dr. Lin noted that the committee said existing data on infection did not support this position. He also cited a “a fairly compelling” single-center randomized study with 750 patients that showed no difference in infection rates. The study was presented at the AUA meeting.
Agents of death and destruction?
Badar Mian, MD, professor of surgery at Albany (N.Y.) Medical College, who led the study, told an AUA session that urology has been trapped in an “echo chamber” regarding the relative safety of biopsies.
Clinicians hear “loud proclamations, which get repeated and magnified, that there is a real zero risk of complications after transperineal biopsies as compared to the horrendous 5% to 10% or higher rate of transrectal biopsy complications and that you, with your transrectal biopsies, are the cause of death and destruction all around,” Dr. Mian said. “Well, if you step out of the echo chamber, what you’ll find is that the accurate complications amongst the two procedures are not that dramatically different, much less dramatic than what you’ve been told to believe.”
The campaign to end transrectal biopsies in Europe started in 2018 with the death of a Norwegian man who experienced an infection after the procedure. Truls Bjerklund Johansen, MD, who’d performed the biopsy on the patient and who worked with the man’s daughter to change national practice, persuaded the EAU to look at the issue.
Advocates also say transperineal biopsies are better at detecting anterior and apical cancers.
“I would agree the data on cancer detection is less convincing, but that is not the basis of the EAU recommendation,” Dr. Cornford said.
Arvin George, MD, leads the transperineal biopsy program at the University of Michigan, Ann Arbor, and directs the transperineal training program at the AUA’s annual meeting. He said his course was sold out early and included about 60 trainees.
Dr. George said the new guideline statement “is not an unequivocal endorsement for transperineal biopsy as the preferred approach for diagnostic sampling but rather an acknowledgment of this approach as an alternative option.”
He said that although the new position statement should increase awareness of the transperineal approach in the United States, “without a strong recommendation, the guideline statement is unlikely to spark a large switch to the transperineal biopsy but rather supports the continued slow and steady adoption.”
Matthew Allaway, DO, founder of Perineologic, developer of the PrecisionPoint Transperineal Access System, said industry figures show that about 10% of the 1.5 million prostate biopsies performed in the United States annually are performed transperineally, a doubling in 2 years.
Jeremy Grummet, MD, clinical professor of urology at Monash University, Melbourne, and leader of the TREXIT (Transperineal Exit) movement to abandon transrectal procedures, said the AUA guidelines are biased toward “physician convenience.”
Lack of training
The AUA said another reason it did not endorse the transperineal approach was that currently, American urologists lack training and experience with transperineal procedures.
Dr. Grummet blamed major medical centers for any gap in the familiarity of clinicians with transperineal biopsies, which have been available for more than a decade.
“It is incumbent on the leaders of urology departments globally to ensure that their colleagues are trained in transperineal biopsy and have access to the appropriate equipment,” he said in an interview. “Lack of training didn’t seem to prevent the rapid uptake of robotic prostatectomy – a far more complex procedure.”
The authors have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
CHICAGO - , endorsing both transperineal and transrectal biopsy instead of choosing one over the other.
The new guidelines, issued at the annual meeting of the American Urological Association, contrast with 2021 recommendations from the European Association of Urologists (EAU), which regard the transperineal approach as superior to and safer than the transrectal approach.
The new guidelines state: “Clinicians may use either a transrectal or transperineal biopsy route when performing a biopsy. (Conditional Recommendation; Evidence Level: Grade C).” Grade C is the lowest grade of acceptance the guideline committee could issue, according to Daniel Lin, MD, vice-chair of the AUA guideline panel.
“The AUA looked at all the higher-level data comparing the two procedures. There was a lack of that data,” Dr. Lin, chief of urologic oncology at the University of Washington, Seattle, said in an interview. He said the literature consists mainly of systematic single-center reviews, rather than multicenter randomized trials.
But Hendrik Van Poppel, MD, policy chief for the EAU, said that in Europe, transrectal biopsies are now considered “medical malpractice.”
Philip Cornford, MD, associate professor of urology at the University of Liverpool, England, and chair of the prostate biopsy guidelines panel for the EAU, said the society in 2021 concluded that the transperineal approach is the preferred one.
The EAU stated that transperineal prostate biopsies should be performed “due to the lower risk of infectious complications.” The EAU described the evidence as strong: A meta-analysis of seven studies that included 1,330 patients showed that for patients undergoing transperineal biopsy, infectious complications were significantly reduced.
Dr. Cornford said in essence, the EAU made its decision out of concern about infections, whereas the AUA and SUO based their decision on the ability of the methods to detect cancer.
Advocates for transperineal procedures cite several studies that show that the rate of infection, including sepsis, with such biopsies is virtually zero.
However, Dr. Lin noted that the committee said existing data on infection did not support this position. He also cited a “a fairly compelling” single-center randomized study with 750 patients that showed no difference in infection rates. The study was presented at the AUA meeting.
Agents of death and destruction?
Badar Mian, MD, professor of surgery at Albany (N.Y.) Medical College, who led the study, told an AUA session that urology has been trapped in an “echo chamber” regarding the relative safety of biopsies.
Clinicians hear “loud proclamations, which get repeated and magnified, that there is a real zero risk of complications after transperineal biopsies as compared to the horrendous 5% to 10% or higher rate of transrectal biopsy complications and that you, with your transrectal biopsies, are the cause of death and destruction all around,” Dr. Mian said. “Well, if you step out of the echo chamber, what you’ll find is that the accurate complications amongst the two procedures are not that dramatically different, much less dramatic than what you’ve been told to believe.”
The campaign to end transrectal biopsies in Europe started in 2018 with the death of a Norwegian man who experienced an infection after the procedure. Truls Bjerklund Johansen, MD, who’d performed the biopsy on the patient and who worked with the man’s daughter to change national practice, persuaded the EAU to look at the issue.
Advocates also say transperineal biopsies are better at detecting anterior and apical cancers.
“I would agree the data on cancer detection is less convincing, but that is not the basis of the EAU recommendation,” Dr. Cornford said.
Arvin George, MD, leads the transperineal biopsy program at the University of Michigan, Ann Arbor, and directs the transperineal training program at the AUA’s annual meeting. He said his course was sold out early and included about 60 trainees.
Dr. George said the new guideline statement “is not an unequivocal endorsement for transperineal biopsy as the preferred approach for diagnostic sampling but rather an acknowledgment of this approach as an alternative option.”
He said that although the new position statement should increase awareness of the transperineal approach in the United States, “without a strong recommendation, the guideline statement is unlikely to spark a large switch to the transperineal biopsy but rather supports the continued slow and steady adoption.”
Matthew Allaway, DO, founder of Perineologic, developer of the PrecisionPoint Transperineal Access System, said industry figures show that about 10% of the 1.5 million prostate biopsies performed in the United States annually are performed transperineally, a doubling in 2 years.
Jeremy Grummet, MD, clinical professor of urology at Monash University, Melbourne, and leader of the TREXIT (Transperineal Exit) movement to abandon transrectal procedures, said the AUA guidelines are biased toward “physician convenience.”
Lack of training
The AUA said another reason it did not endorse the transperineal approach was that currently, American urologists lack training and experience with transperineal procedures.
Dr. Grummet blamed major medical centers for any gap in the familiarity of clinicians with transperineal biopsies, which have been available for more than a decade.
“It is incumbent on the leaders of urology departments globally to ensure that their colleagues are trained in transperineal biopsy and have access to the appropriate equipment,” he said in an interview. “Lack of training didn’t seem to prevent the rapid uptake of robotic prostatectomy – a far more complex procedure.”
The authors have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
CHICAGO - , endorsing both transperineal and transrectal biopsy instead of choosing one over the other.
The new guidelines, issued at the annual meeting of the American Urological Association, contrast with 2021 recommendations from the European Association of Urologists (EAU), which regard the transperineal approach as superior to and safer than the transrectal approach.
The new guidelines state: “Clinicians may use either a transrectal or transperineal biopsy route when performing a biopsy. (Conditional Recommendation; Evidence Level: Grade C).” Grade C is the lowest grade of acceptance the guideline committee could issue, according to Daniel Lin, MD, vice-chair of the AUA guideline panel.
“The AUA looked at all the higher-level data comparing the two procedures. There was a lack of that data,” Dr. Lin, chief of urologic oncology at the University of Washington, Seattle, said in an interview. He said the literature consists mainly of systematic single-center reviews, rather than multicenter randomized trials.
But Hendrik Van Poppel, MD, policy chief for the EAU, said that in Europe, transrectal biopsies are now considered “medical malpractice.”
Philip Cornford, MD, associate professor of urology at the University of Liverpool, England, and chair of the prostate biopsy guidelines panel for the EAU, said the society in 2021 concluded that the transperineal approach is the preferred one.
The EAU stated that transperineal prostate biopsies should be performed “due to the lower risk of infectious complications.” The EAU described the evidence as strong: A meta-analysis of seven studies that included 1,330 patients showed that for patients undergoing transperineal biopsy, infectious complications were significantly reduced.
Dr. Cornford said in essence, the EAU made its decision out of concern about infections, whereas the AUA and SUO based their decision on the ability of the methods to detect cancer.
Advocates for transperineal procedures cite several studies that show that the rate of infection, including sepsis, with such biopsies is virtually zero.
However, Dr. Lin noted that the committee said existing data on infection did not support this position. He also cited a “a fairly compelling” single-center randomized study with 750 patients that showed no difference in infection rates. The study was presented at the AUA meeting.
Agents of death and destruction?
Badar Mian, MD, professor of surgery at Albany (N.Y.) Medical College, who led the study, told an AUA session that urology has been trapped in an “echo chamber” regarding the relative safety of biopsies.
Clinicians hear “loud proclamations, which get repeated and magnified, that there is a real zero risk of complications after transperineal biopsies as compared to the horrendous 5% to 10% or higher rate of transrectal biopsy complications and that you, with your transrectal biopsies, are the cause of death and destruction all around,” Dr. Mian said. “Well, if you step out of the echo chamber, what you’ll find is that the accurate complications amongst the two procedures are not that dramatically different, much less dramatic than what you’ve been told to believe.”
The campaign to end transrectal biopsies in Europe started in 2018 with the death of a Norwegian man who experienced an infection after the procedure. Truls Bjerklund Johansen, MD, who’d performed the biopsy on the patient and who worked with the man’s daughter to change national practice, persuaded the EAU to look at the issue.
Advocates also say transperineal biopsies are better at detecting anterior and apical cancers.
“I would agree the data on cancer detection is less convincing, but that is not the basis of the EAU recommendation,” Dr. Cornford said.
Arvin George, MD, leads the transperineal biopsy program at the University of Michigan, Ann Arbor, and directs the transperineal training program at the AUA’s annual meeting. He said his course was sold out early and included about 60 trainees.
Dr. George said the new guideline statement “is not an unequivocal endorsement for transperineal biopsy as the preferred approach for diagnostic sampling but rather an acknowledgment of this approach as an alternative option.”
He said that although the new position statement should increase awareness of the transperineal approach in the United States, “without a strong recommendation, the guideline statement is unlikely to spark a large switch to the transperineal biopsy but rather supports the continued slow and steady adoption.”
Matthew Allaway, DO, founder of Perineologic, developer of the PrecisionPoint Transperineal Access System, said industry figures show that about 10% of the 1.5 million prostate biopsies performed in the United States annually are performed transperineally, a doubling in 2 years.
Jeremy Grummet, MD, clinical professor of urology at Monash University, Melbourne, and leader of the TREXIT (Transperineal Exit) movement to abandon transrectal procedures, said the AUA guidelines are biased toward “physician convenience.”
Lack of training
The AUA said another reason it did not endorse the transperineal approach was that currently, American urologists lack training and experience with transperineal procedures.
Dr. Grummet blamed major medical centers for any gap in the familiarity of clinicians with transperineal biopsies, which have been available for more than a decade.
“It is incumbent on the leaders of urology departments globally to ensure that their colleagues are trained in transperineal biopsy and have access to the appropriate equipment,” he said in an interview. “Lack of training didn’t seem to prevent the rapid uptake of robotic prostatectomy – a far more complex procedure.”
The authors have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
AT AUA 2023
CardioMEMS boosts QoL, curbs HF hospitalizations: MONITOR-HF
In the first randomized clinical trial of remote pulmonary artery pressure–guided monitoring and management of chronic heart failure (HF) in Europe, the intervention “substantially” improved quality of life (QoL) and reduced HF hospitalizations, new data show.
The CardioMEMS-HF system (Abbot Laboratories) used in the trial, called MONITOR-HF, remotely monitors changes in pulmonary artery pressure and provides an early warning of worsening HF.
Jasper Brugts, MD, PhD, of Erasmus MC University Medical Centre, Rotterdam, the Netherlands, said in an interview, “The concordance on outcomes of the three CardioMEMS trials across different eras, evolving GDMT [guideline-directed medical therapy], different conditions (pandemic), and different health care systems is reassuring and supportive of technologies such as CardioMEMS to improve patient monitoring to prevent HF hospitalizations and improve QoL.”
Dr. Brugts presented the study at the Heart Failure Association of the European Society of Cardiology (HFA-ESC) 2023 sessions.
(11 vs. 17), in comparison with standard of care, Dr. Brugts told meeting attendees.
Furthermore, CardioMEMS monitors hypervolemia as well as hypovolemia, enabling “fine-tuning of diuretics.”
The presentation drew such applause that one chairperson described it as “close to a standing ovation.” The study was published simultaneously in The Lancet.
Aggregate evidence
Early clinical evidence of the benefits of remote monitoring with the CardioMEMS-HF system was provided by the CHAMPION trial, which included patients with New York Heart Association (NYHA) class III heart failure.
Results of the subsequent GUIDE-HF trial, which aimed to test a broader population of patients with NYHA class II–IV heart failure and either increased N-terminal-pro-B-type natriuretic peptide (NT-proBNP) concentrations or hospitalization, were inconclusive.
However, a pre–COVID-19 impact analysis of GUIDE-HF indicated a possible benefit, which was primarily driven by a lower HF hospitalization rate, compared with the control group. That finding was the basis for an expanded indication for the system from the U.S. Food and Drug Administration.
The 2022 FDA indication permits the use of CardioMEMS for patients with NYHA class II HF and for those with worsening HF, as assessed by elevated natriuretic peptide levels.
From United States to Europe
Aware that most CardioMEMS data came from U.S. trials, the investigators embarked on the current trial, MONITOR-HF, an open-label, randomized trial in 25 centers in the Netherlands. Eligible patients had chronic NYHA class III HF, irrespective of ejection fraction, and had previously undergone hospitalization for HF.
A total of 348 patients were randomly assigned to either CardioMEMS-HF or standard of care (SoC) between 2019 and 2022.The median age of the patients was 69 years, and the median ejection fraction was 30%.
All patients were scheduled to be seen by their clinician at 3 months, 6 months, and every 6 months thereafter for up to 48 months.
The primary endpoint was the mean difference in the Kansas City Cardiomyopathy Questionnaire (KCCQ) summary score at 12 months
That difference between groups was 7.13 (+7.05 in the CardioMEMS group and –0.08 in the SoC group).
In the responder analysis, the odds ratio of an improvement of at least 5 points in the KCCQ overall summary score was 1.69 in the CardioMEMS group vs. the SoC group; the OR of a deterioration of at least 5 points was 0.45.
Subgroup analyses showed no relevant heterogeneity in the treatment effect on total HF hospitalizations and, notably, no significant interaction in patients with an EF below 40% and an EF above 40%.
There was a significant reduction in the median NT-proBNP change from baseline only in the remote monitoring group (800 pg/mL) and a smaller, nonsignificant difference with SoC.
Both groups received highly appropriate background guideline–directed medical therapy throughout the study. There were no significant between-group differences at 12 months.
Freedom from device-related or system-related complications and sensor failure were 97.7% and 98.8%, respectively.
Two sensor failures occurred during a mean follow-up 1.8 years. The percentage of failures was comparable to CHAMPION and GUIDE-HF trials.
The trial was not powered to assess a mortality benefit.
Pick the right patients
“As in the U.S. trials, there will be side effects, so select the right patients, because [remote monitoring] is not without risk,” Dr. Brugts told meeting attendees.
That point also was made by Christiane E. Angermann of University and University Hospital Würzburg, Germany, in a related editorial in The Lancet.
“To reproduce these results on a large scale in real-life health care, diligent patient selection should identify those at high risk of heart failure–related hospitalization who agree with the concept of daily data collection and are able and motivated to comply with treatment recommendations even if asymptomatic,” Dr. Angermann writes.
“Without direct interaction between health care providers and patients, and timely treatment modification triggered by abnormal monitoring results, the care cycle might break and the potential benefits from early detection of decompensation would be lost.”
Val Rakita, MD, assistant professor of medicine at Temple University, Philadelphia, a specialist in advanced heart failure and main implanter of the CardioMEMS device at Temple University Hospital, commented on the study for this article.
“This study confirms the previous data that the device is very safe and effective in preventing HF hospitalizations and improving patients’ quality of life, even in a different population with more modern background guideline-directed medical therapy.”
Nevertheless, he noted, “Studies have yet to confirm a mortality benefit, despite logic telling us that preventing heart failure hospitalizations should also improve patient survival. More studies are needed to see if a survival benefit can be proven over a longer follow-up period.”
Overall, he said, “Remote monitoring allows more precise management of medications, prevention of hospitalizations, and improvement in quality of life, and I am an advocate for it in my practice.”
Not everyone is an advocate, however. In a commentary published last year, John M. Mandrola, MD, a cardiac electrophysiologist at Baptist Medical Associates in Louisville, Ky., said the expanded FDA indication for the device is the result of “dubious trial analysis, spin, lax regulation, and the growth of low-value care.”
Others also have questioned the device’s value in the clinic.
But at least for now, as Dr. Angermann writes, “Scientific evidence supports the use of the CardioMEMS-HF system to enhance remote patient management in heart failure care. For more widespread application, technological advancements are desirable to provide more comfort for patients and reusable external device components, thereby improving care experience and saving resources.”
The MONITOR-HF trial is funded by the Dutch Ministry of Health and Health Care institute. Dr. Brugts has an independent research grant from Abbott (investigator-sponsored study) and has had speaker engagements or has participated in advisory boards for Abbott and other pharmaceutical companies. Dr. Angermann has received personal fees from Abbott for serving as chair of the steering committee for the CardioMEMS European Monitoring Study for Heart Failure (MEMS-HF) and consulting fees, honoraria, and travel costs from Abbott. Dr. Rakita has disclosed no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
In the first randomized clinical trial of remote pulmonary artery pressure–guided monitoring and management of chronic heart failure (HF) in Europe, the intervention “substantially” improved quality of life (QoL) and reduced HF hospitalizations, new data show.
The CardioMEMS-HF system (Abbot Laboratories) used in the trial, called MONITOR-HF, remotely monitors changes in pulmonary artery pressure and provides an early warning of worsening HF.
Jasper Brugts, MD, PhD, of Erasmus MC University Medical Centre, Rotterdam, the Netherlands, said in an interview, “The concordance on outcomes of the three CardioMEMS trials across different eras, evolving GDMT [guideline-directed medical therapy], different conditions (pandemic), and different health care systems is reassuring and supportive of technologies such as CardioMEMS to improve patient monitoring to prevent HF hospitalizations and improve QoL.”
Dr. Brugts presented the study at the Heart Failure Association of the European Society of Cardiology (HFA-ESC) 2023 sessions.
(11 vs. 17), in comparison with standard of care, Dr. Brugts told meeting attendees.
Furthermore, CardioMEMS monitors hypervolemia as well as hypovolemia, enabling “fine-tuning of diuretics.”
The presentation drew such applause that one chairperson described it as “close to a standing ovation.” The study was published simultaneously in The Lancet.
Aggregate evidence
Early clinical evidence of the benefits of remote monitoring with the CardioMEMS-HF system was provided by the CHAMPION trial, which included patients with New York Heart Association (NYHA) class III heart failure.
Results of the subsequent GUIDE-HF trial, which aimed to test a broader population of patients with NYHA class II–IV heart failure and either increased N-terminal-pro-B-type natriuretic peptide (NT-proBNP) concentrations or hospitalization, were inconclusive.
However, a pre–COVID-19 impact analysis of GUIDE-HF indicated a possible benefit, which was primarily driven by a lower HF hospitalization rate, compared with the control group. That finding was the basis for an expanded indication for the system from the U.S. Food and Drug Administration.
The 2022 FDA indication permits the use of CardioMEMS for patients with NYHA class II HF and for those with worsening HF, as assessed by elevated natriuretic peptide levels.
From United States to Europe
Aware that most CardioMEMS data came from U.S. trials, the investigators embarked on the current trial, MONITOR-HF, an open-label, randomized trial in 25 centers in the Netherlands. Eligible patients had chronic NYHA class III HF, irrespective of ejection fraction, and had previously undergone hospitalization for HF.
A total of 348 patients were randomly assigned to either CardioMEMS-HF or standard of care (SoC) between 2019 and 2022.The median age of the patients was 69 years, and the median ejection fraction was 30%.
All patients were scheduled to be seen by their clinician at 3 months, 6 months, and every 6 months thereafter for up to 48 months.
The primary endpoint was the mean difference in the Kansas City Cardiomyopathy Questionnaire (KCCQ) summary score at 12 months
That difference between groups was 7.13 (+7.05 in the CardioMEMS group and –0.08 in the SoC group).
In the responder analysis, the odds ratio of an improvement of at least 5 points in the KCCQ overall summary score was 1.69 in the CardioMEMS group vs. the SoC group; the OR of a deterioration of at least 5 points was 0.45.
Subgroup analyses showed no relevant heterogeneity in the treatment effect on total HF hospitalizations and, notably, no significant interaction in patients with an EF below 40% and an EF above 40%.
There was a significant reduction in the median NT-proBNP change from baseline only in the remote monitoring group (800 pg/mL) and a smaller, nonsignificant difference with SoC.
Both groups received highly appropriate background guideline–directed medical therapy throughout the study. There were no significant between-group differences at 12 months.
Freedom from device-related or system-related complications and sensor failure were 97.7% and 98.8%, respectively.
Two sensor failures occurred during a mean follow-up 1.8 years. The percentage of failures was comparable to CHAMPION and GUIDE-HF trials.
The trial was not powered to assess a mortality benefit.
Pick the right patients
“As in the U.S. trials, there will be side effects, so select the right patients, because [remote monitoring] is not without risk,” Dr. Brugts told meeting attendees.
That point also was made by Christiane E. Angermann of University and University Hospital Würzburg, Germany, in a related editorial in The Lancet.
“To reproduce these results on a large scale in real-life health care, diligent patient selection should identify those at high risk of heart failure–related hospitalization who agree with the concept of daily data collection and are able and motivated to comply with treatment recommendations even if asymptomatic,” Dr. Angermann writes.
“Without direct interaction between health care providers and patients, and timely treatment modification triggered by abnormal monitoring results, the care cycle might break and the potential benefits from early detection of decompensation would be lost.”
Val Rakita, MD, assistant professor of medicine at Temple University, Philadelphia, a specialist in advanced heart failure and main implanter of the CardioMEMS device at Temple University Hospital, commented on the study for this article.
“This study confirms the previous data that the device is very safe and effective in preventing HF hospitalizations and improving patients’ quality of life, even in a different population with more modern background guideline-directed medical therapy.”
Nevertheless, he noted, “Studies have yet to confirm a mortality benefit, despite logic telling us that preventing heart failure hospitalizations should also improve patient survival. More studies are needed to see if a survival benefit can be proven over a longer follow-up period.”
Overall, he said, “Remote monitoring allows more precise management of medications, prevention of hospitalizations, and improvement in quality of life, and I am an advocate for it in my practice.”
Not everyone is an advocate, however. In a commentary published last year, John M. Mandrola, MD, a cardiac electrophysiologist at Baptist Medical Associates in Louisville, Ky., said the expanded FDA indication for the device is the result of “dubious trial analysis, spin, lax regulation, and the growth of low-value care.”
Others also have questioned the device’s value in the clinic.
But at least for now, as Dr. Angermann writes, “Scientific evidence supports the use of the CardioMEMS-HF system to enhance remote patient management in heart failure care. For more widespread application, technological advancements are desirable to provide more comfort for patients and reusable external device components, thereby improving care experience and saving resources.”
The MONITOR-HF trial is funded by the Dutch Ministry of Health and Health Care institute. Dr. Brugts has an independent research grant from Abbott (investigator-sponsored study) and has had speaker engagements or has participated in advisory boards for Abbott and other pharmaceutical companies. Dr. Angermann has received personal fees from Abbott for serving as chair of the steering committee for the CardioMEMS European Monitoring Study for Heart Failure (MEMS-HF) and consulting fees, honoraria, and travel costs from Abbott. Dr. Rakita has disclosed no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
In the first randomized clinical trial of remote pulmonary artery pressure–guided monitoring and management of chronic heart failure (HF) in Europe, the intervention “substantially” improved quality of life (QoL) and reduced HF hospitalizations, new data show.
The CardioMEMS-HF system (Abbot Laboratories) used in the trial, called MONITOR-HF, remotely monitors changes in pulmonary artery pressure and provides an early warning of worsening HF.
Jasper Brugts, MD, PhD, of Erasmus MC University Medical Centre, Rotterdam, the Netherlands, said in an interview, “The concordance on outcomes of the three CardioMEMS trials across different eras, evolving GDMT [guideline-directed medical therapy], different conditions (pandemic), and different health care systems is reassuring and supportive of technologies such as CardioMEMS to improve patient monitoring to prevent HF hospitalizations and improve QoL.”
Dr. Brugts presented the study at the Heart Failure Association of the European Society of Cardiology (HFA-ESC) 2023 sessions.
(11 vs. 17), in comparison with standard of care, Dr. Brugts told meeting attendees.
Furthermore, CardioMEMS monitors hypervolemia as well as hypovolemia, enabling “fine-tuning of diuretics.”
The presentation drew such applause that one chairperson described it as “close to a standing ovation.” The study was published simultaneously in The Lancet.
Aggregate evidence
Early clinical evidence of the benefits of remote monitoring with the CardioMEMS-HF system was provided by the CHAMPION trial, which included patients with New York Heart Association (NYHA) class III heart failure.
Results of the subsequent GUIDE-HF trial, which aimed to test a broader population of patients with NYHA class II–IV heart failure and either increased N-terminal-pro-B-type natriuretic peptide (NT-proBNP) concentrations or hospitalization, were inconclusive.
However, a pre–COVID-19 impact analysis of GUIDE-HF indicated a possible benefit, which was primarily driven by a lower HF hospitalization rate, compared with the control group. That finding was the basis for an expanded indication for the system from the U.S. Food and Drug Administration.
The 2022 FDA indication permits the use of CardioMEMS for patients with NYHA class II HF and for those with worsening HF, as assessed by elevated natriuretic peptide levels.
From United States to Europe
Aware that most CardioMEMS data came from U.S. trials, the investigators embarked on the current trial, MONITOR-HF, an open-label, randomized trial in 25 centers in the Netherlands. Eligible patients had chronic NYHA class III HF, irrespective of ejection fraction, and had previously undergone hospitalization for HF.
A total of 348 patients were randomly assigned to either CardioMEMS-HF or standard of care (SoC) between 2019 and 2022.The median age of the patients was 69 years, and the median ejection fraction was 30%.
All patients were scheduled to be seen by their clinician at 3 months, 6 months, and every 6 months thereafter for up to 48 months.
The primary endpoint was the mean difference in the Kansas City Cardiomyopathy Questionnaire (KCCQ) summary score at 12 months
That difference between groups was 7.13 (+7.05 in the CardioMEMS group and –0.08 in the SoC group).
In the responder analysis, the odds ratio of an improvement of at least 5 points in the KCCQ overall summary score was 1.69 in the CardioMEMS group vs. the SoC group; the OR of a deterioration of at least 5 points was 0.45.
Subgroup analyses showed no relevant heterogeneity in the treatment effect on total HF hospitalizations and, notably, no significant interaction in patients with an EF below 40% and an EF above 40%.
There was a significant reduction in the median NT-proBNP change from baseline only in the remote monitoring group (800 pg/mL) and a smaller, nonsignificant difference with SoC.
Both groups received highly appropriate background guideline–directed medical therapy throughout the study. There were no significant between-group differences at 12 months.
Freedom from device-related or system-related complications and sensor failure were 97.7% and 98.8%, respectively.
Two sensor failures occurred during a mean follow-up 1.8 years. The percentage of failures was comparable to CHAMPION and GUIDE-HF trials.
The trial was not powered to assess a mortality benefit.
Pick the right patients
“As in the U.S. trials, there will be side effects, so select the right patients, because [remote monitoring] is not without risk,” Dr. Brugts told meeting attendees.
That point also was made by Christiane E. Angermann of University and University Hospital Würzburg, Germany, in a related editorial in The Lancet.
“To reproduce these results on a large scale in real-life health care, diligent patient selection should identify those at high risk of heart failure–related hospitalization who agree with the concept of daily data collection and are able and motivated to comply with treatment recommendations even if asymptomatic,” Dr. Angermann writes.
“Without direct interaction between health care providers and patients, and timely treatment modification triggered by abnormal monitoring results, the care cycle might break and the potential benefits from early detection of decompensation would be lost.”
Val Rakita, MD, assistant professor of medicine at Temple University, Philadelphia, a specialist in advanced heart failure and main implanter of the CardioMEMS device at Temple University Hospital, commented on the study for this article.
“This study confirms the previous data that the device is very safe and effective in preventing HF hospitalizations and improving patients’ quality of life, even in a different population with more modern background guideline-directed medical therapy.”
Nevertheless, he noted, “Studies have yet to confirm a mortality benefit, despite logic telling us that preventing heart failure hospitalizations should also improve patient survival. More studies are needed to see if a survival benefit can be proven over a longer follow-up period.”
Overall, he said, “Remote monitoring allows more precise management of medications, prevention of hospitalizations, and improvement in quality of life, and I am an advocate for it in my practice.”
Not everyone is an advocate, however. In a commentary published last year, John M. Mandrola, MD, a cardiac electrophysiologist at Baptist Medical Associates in Louisville, Ky., said the expanded FDA indication for the device is the result of “dubious trial analysis, spin, lax regulation, and the growth of low-value care.”
Others also have questioned the device’s value in the clinic.
But at least for now, as Dr. Angermann writes, “Scientific evidence supports the use of the CardioMEMS-HF system to enhance remote patient management in heart failure care. For more widespread application, technological advancements are desirable to provide more comfort for patients and reusable external device components, thereby improving care experience and saving resources.”
The MONITOR-HF trial is funded by the Dutch Ministry of Health and Health Care institute. Dr. Brugts has an independent research grant from Abbott (investigator-sponsored study) and has had speaker engagements or has participated in advisory boards for Abbott and other pharmaceutical companies. Dr. Angermann has received personal fees from Abbott for serving as chair of the steering committee for the CardioMEMS European Monitoring Study for Heart Failure (MEMS-HF) and consulting fees, honoraria, and travel costs from Abbott. Dr. Rakita has disclosed no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
FROM ESC HEART FAILURE 2023
Losing weight may bolster AFib ablation’s chances for success: LEAF interim results
, a new analysis suggests.
The finding comes from a small study that entered such patients with paroxysmal and especially persistent AFib who were candidates for ablation. Those shedding at least 3% of body weight in the months before the procedure while engaged in a structured risk-factor modification (RFM) program were “dramatically” more likely to be AFib-free 6 months later.
The improved ablation efficacy, compared with results in similar patients who didn’t lose as much weight, was most pronounced among those whose AFib had been the persistent form, reported investigators at the annual scientific sessions of the Heart Rhythm Society, held in New Orleans.
Of note, ablations in the study were consistently limited, as much as possible, to standard pulmonary-vein isolation (PVI).
Associations between AFib and obesity and other behavioral and lifestyle-related risk factors are well recognized, but the limited studies of their effect on AFib ablation success have been inconsistent. The current analysis, the group says, points specifically to preablation weight loss as means to improving AFib-ablation outcomes.
“Adjunctive therapy focused on weight loss should be incorporated in the treatment plan for obese patients undergoing ablation for atrial fibrillation,” Jeffrey J. Goldberger, MD, MBA, of the University of Miami, said when presenting the new results at the HRS sessions.
Such a plan is entirely consistent with recent guidelines and especially a 2020 American Heart Association (AHA) consensus statement, but is inconsistently and perhaps even seldom realized in clinical practice.
Dramatic increase in success
Even modest weight loss before ablation may help, proposed Dr. Goldberger, who directs his institution’s Center for Atrial Fibrillation. Decreases for the greater-weight-loss group actually averaged less than 6% of baseline body weight.
Yet it was apparently enough to improve ablation outcomes significantly: Eighty-eight percent were free of AFib 6 months after the procedure, compared with 61% for patients who lost less than 3% of their preablation weight.
For improving ablation success, he said, “We’re talking about a moderate amount of weight loss. These patients are not going from being obese to being thin. They’re still quite overweight.”
In an analysis limited to the four-fifths of patients with persistent AFib, “we saw the same pattern,” Dr. Goldberger said at a media presentation prior to his formal report at the HRS sessions.
Moreover, that subgroup’s benefit persisted out to 12 months, at which time 42% and 81% of patients with less and greater weight loss, respectively, were free of AFib. That represents, he said, “a really tremendous – dramatic, actually – increase in success of pulmonary vein isolation in those who lost weight.”
“We’ve known for a long time that weight loss is important for preventing atrial fibrillation or increasing the success rates of the different treatments we use,” Cynthia M. Tracy, MD, said in an interview. “Probably in some studies, weight loss has been as effective as antiarrhythmics.”
A loss of 3% body weight “is not a lot,” she said. In the current analysis, “It’s notable that it made that much difference with even a fairly modest amount of weight loss.”
Now when asked, “ ‘How much do I have to lose before you’ll consider doing my ablation?’ we have a bit more concrete data to give patients and doctors as to what amount might be beneficial,” said Dr. Tracy of George Washington University Hospital, Washington, who is not associated with the study.
Evolving view of AFib
The findings are emblematic of the profession’s evolving view of AFib and its management, Dr. Goldberger observed at the press conference. Should clinicians think of AFib as similar to “a disease like Wolff-Parkinson-White syndrome,” in which the patient usually has a successful ablation, and then “we expect that to last in perpetuity with no further interventions?”
Or, he said, “is atrial fibrillation more a disease like coronary artery disease, where even if they have an intervention, the disease process is still ongoing and requires long-term disease management? I think it’s pretty clear that we’re dealing with the latter case.”
Dr. Goldberger’s report was an interim analysis of an ongoing randomized trial called LEAF (Liraglutide Effect on Atrial Fibrillation), which is comparing patients with AFib assigned to “take” vs. “not take” the GLP-1 receptor agonist liraglutide, an antidiabetic (Victoza) and weight-loss (Saxenda) drug. The trial aims to assess the drug’s apparent ability to shrink atrial epicardial adipose tissue which, Dr. Goldberger said, is thought to contribute to AFib development and influence AFib-ablation outcomes.
It’s unknown and a limitation of the current analysis, he said, whether the observed link between improved preablation–weight ablation success “is specifically related to weight loss, liraglutide treatment, or both.”
As the invited discussant for Dr. Goldberger’s presentation, David Frankel, MD, observed that studies have been inconsistent on whether substantial weight loss may improve the results of AFib rhythm-control therapy.
Those finding such an association, including LEAF and the influential LEGACY study, differed from others showing a null effect by including “a comprehensive risk factor management” program, observed Dr. Frankel, of the Hospital of the University of Pennsylvania and Penn Heart and Vascular Center, Philadelphia.
Rather than focusing solely on weight loss or sleep apnea as AFib risk factors, he said, the studies linking weight loss to AFib rhythm control also included “hypertension, diabetes, hyperlipidemia, smoking cessation, and alcohol reduction,” Dr. Frankel said. “So it seems clear that to significantly impact AF recurrence, we need to focus on all these contributors to metabolic syndrome.”
Comprehensive risk-factor management
LEAF entered patients with AFib, 79% of whom had persistent AF and the rest paroxysmal AF, who followed the RFM program and were randomly assigned also to take liraglutide or placebo. The “nurse-practitioner-led” RFM program, conducted both in-clinic and online, featured “established goals for each patient” using AHA diet and lifestyle recommendations, an exercise prescription, dietary counseling, evaluation and treatment of sleep apnea, and measures to control any diabetes, hyperlipidemia, or hypertension, Dr. Goldberger said. And patients “were counseled on alcohol reduction and smoking cessation as necessary.”
After 3 months, 29 and 30 patients – regardless of randomization assignment – had lost < 3% and at least 3% of baseline body weight, respectively.
Catheter ablation achieved PVI in all patients. A 3-month blanking period followed, after which they went off antiarrhythmic meds.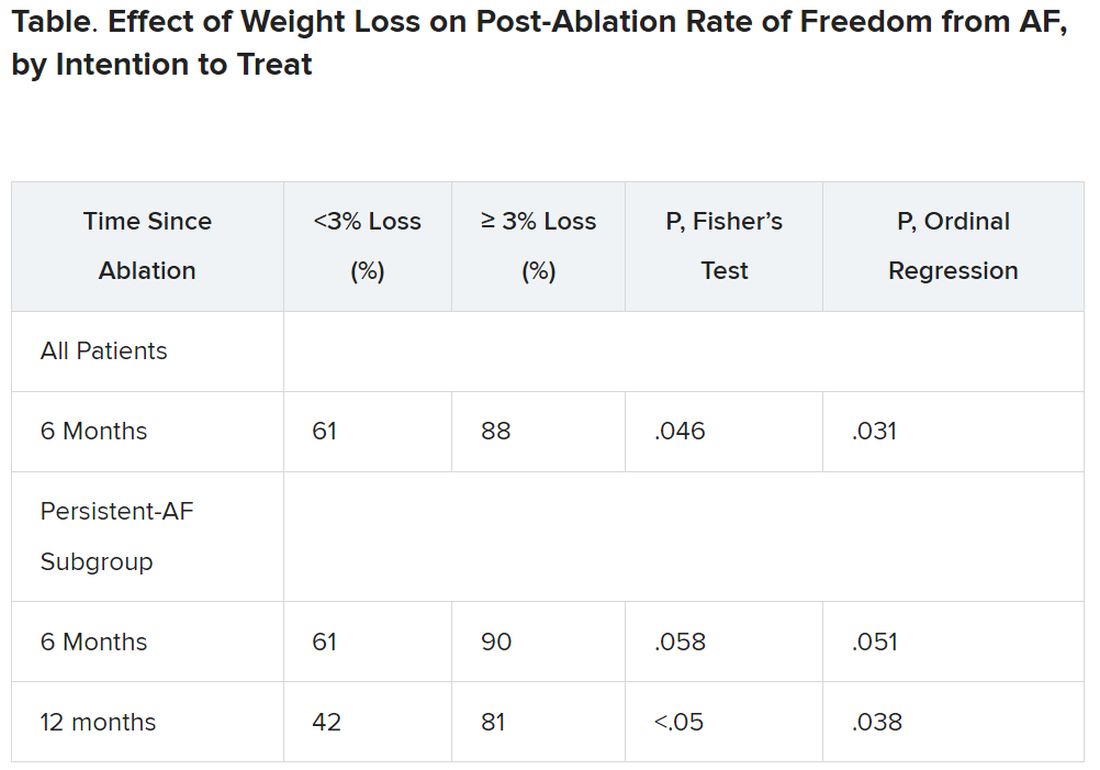
It’s very difficult for patients to lose 10% or more of body weight, “and it would not happen overnight,” Dr. Tracy observed. “These are symptomatic patients, for the most part, if they get referred to an electrophysiologist. So you don’t want to defer them indefinitely.”
The current findings, she said, point to “a more realistic target,” suggesting that weight loss of at least 3% should improve AFib ablation’s chances for success.
Dr. Goldberger disclosed ties to Medtronic. Dr. Frankel disclosed ties to Medtronic, Stryker, Biosense Webster, and Boston Scientific. Dr. Tracy reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
, a new analysis suggests.
The finding comes from a small study that entered such patients with paroxysmal and especially persistent AFib who were candidates for ablation. Those shedding at least 3% of body weight in the months before the procedure while engaged in a structured risk-factor modification (RFM) program were “dramatically” more likely to be AFib-free 6 months later.
The improved ablation efficacy, compared with results in similar patients who didn’t lose as much weight, was most pronounced among those whose AFib had been the persistent form, reported investigators at the annual scientific sessions of the Heart Rhythm Society, held in New Orleans.
Of note, ablations in the study were consistently limited, as much as possible, to standard pulmonary-vein isolation (PVI).
Associations between AFib and obesity and other behavioral and lifestyle-related risk factors are well recognized, but the limited studies of their effect on AFib ablation success have been inconsistent. The current analysis, the group says, points specifically to preablation weight loss as means to improving AFib-ablation outcomes.
“Adjunctive therapy focused on weight loss should be incorporated in the treatment plan for obese patients undergoing ablation for atrial fibrillation,” Jeffrey J. Goldberger, MD, MBA, of the University of Miami, said when presenting the new results at the HRS sessions.
Such a plan is entirely consistent with recent guidelines and especially a 2020 American Heart Association (AHA) consensus statement, but is inconsistently and perhaps even seldom realized in clinical practice.
Dramatic increase in success
Even modest weight loss before ablation may help, proposed Dr. Goldberger, who directs his institution’s Center for Atrial Fibrillation. Decreases for the greater-weight-loss group actually averaged less than 6% of baseline body weight.
Yet it was apparently enough to improve ablation outcomes significantly: Eighty-eight percent were free of AFib 6 months after the procedure, compared with 61% for patients who lost less than 3% of their preablation weight.
For improving ablation success, he said, “We’re talking about a moderate amount of weight loss. These patients are not going from being obese to being thin. They’re still quite overweight.”
In an analysis limited to the four-fifths of patients with persistent AFib, “we saw the same pattern,” Dr. Goldberger said at a media presentation prior to his formal report at the HRS sessions.
Moreover, that subgroup’s benefit persisted out to 12 months, at which time 42% and 81% of patients with less and greater weight loss, respectively, were free of AFib. That represents, he said, “a really tremendous – dramatic, actually – increase in success of pulmonary vein isolation in those who lost weight.”
“We’ve known for a long time that weight loss is important for preventing atrial fibrillation or increasing the success rates of the different treatments we use,” Cynthia M. Tracy, MD, said in an interview. “Probably in some studies, weight loss has been as effective as antiarrhythmics.”
A loss of 3% body weight “is not a lot,” she said. In the current analysis, “It’s notable that it made that much difference with even a fairly modest amount of weight loss.”
Now when asked, “ ‘How much do I have to lose before you’ll consider doing my ablation?’ we have a bit more concrete data to give patients and doctors as to what amount might be beneficial,” said Dr. Tracy of George Washington University Hospital, Washington, who is not associated with the study.
Evolving view of AFib
The findings are emblematic of the profession’s evolving view of AFib and its management, Dr. Goldberger observed at the press conference. Should clinicians think of AFib as similar to “a disease like Wolff-Parkinson-White syndrome,” in which the patient usually has a successful ablation, and then “we expect that to last in perpetuity with no further interventions?”
Or, he said, “is atrial fibrillation more a disease like coronary artery disease, where even if they have an intervention, the disease process is still ongoing and requires long-term disease management? I think it’s pretty clear that we’re dealing with the latter case.”
Dr. Goldberger’s report was an interim analysis of an ongoing randomized trial called LEAF (Liraglutide Effect on Atrial Fibrillation), which is comparing patients with AFib assigned to “take” vs. “not take” the GLP-1 receptor agonist liraglutide, an antidiabetic (Victoza) and weight-loss (Saxenda) drug. The trial aims to assess the drug’s apparent ability to shrink atrial epicardial adipose tissue which, Dr. Goldberger said, is thought to contribute to AFib development and influence AFib-ablation outcomes.
It’s unknown and a limitation of the current analysis, he said, whether the observed link between improved preablation–weight ablation success “is specifically related to weight loss, liraglutide treatment, or both.”
As the invited discussant for Dr. Goldberger’s presentation, David Frankel, MD, observed that studies have been inconsistent on whether substantial weight loss may improve the results of AFib rhythm-control therapy.
Those finding such an association, including LEAF and the influential LEGACY study, differed from others showing a null effect by including “a comprehensive risk factor management” program, observed Dr. Frankel, of the Hospital of the University of Pennsylvania and Penn Heart and Vascular Center, Philadelphia.
Rather than focusing solely on weight loss or sleep apnea as AFib risk factors, he said, the studies linking weight loss to AFib rhythm control also included “hypertension, diabetes, hyperlipidemia, smoking cessation, and alcohol reduction,” Dr. Frankel said. “So it seems clear that to significantly impact AF recurrence, we need to focus on all these contributors to metabolic syndrome.”
Comprehensive risk-factor management
LEAF entered patients with AFib, 79% of whom had persistent AF and the rest paroxysmal AF, who followed the RFM program and were randomly assigned also to take liraglutide or placebo. The “nurse-practitioner-led” RFM program, conducted both in-clinic and online, featured “established goals for each patient” using AHA diet and lifestyle recommendations, an exercise prescription, dietary counseling, evaluation and treatment of sleep apnea, and measures to control any diabetes, hyperlipidemia, or hypertension, Dr. Goldberger said. And patients “were counseled on alcohol reduction and smoking cessation as necessary.”
After 3 months, 29 and 30 patients – regardless of randomization assignment – had lost < 3% and at least 3% of baseline body weight, respectively.
Catheter ablation achieved PVI in all patients. A 3-month blanking period followed, after which they went off antiarrhythmic meds.
It’s very difficult for patients to lose 10% or more of body weight, “and it would not happen overnight,” Dr. Tracy observed. “These are symptomatic patients, for the most part, if they get referred to an electrophysiologist. So you don’t want to defer them indefinitely.”
The current findings, she said, point to “a more realistic target,” suggesting that weight loss of at least 3% should improve AFib ablation’s chances for success.
Dr. Goldberger disclosed ties to Medtronic. Dr. Frankel disclosed ties to Medtronic, Stryker, Biosense Webster, and Boston Scientific. Dr. Tracy reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
, a new analysis suggests.
The finding comes from a small study that entered such patients with paroxysmal and especially persistent AFib who were candidates for ablation. Those shedding at least 3% of body weight in the months before the procedure while engaged in a structured risk-factor modification (RFM) program were “dramatically” more likely to be AFib-free 6 months later.
The improved ablation efficacy, compared with results in similar patients who didn’t lose as much weight, was most pronounced among those whose AFib had been the persistent form, reported investigators at the annual scientific sessions of the Heart Rhythm Society, held in New Orleans.
Of note, ablations in the study were consistently limited, as much as possible, to standard pulmonary-vein isolation (PVI).
Associations between AFib and obesity and other behavioral and lifestyle-related risk factors are well recognized, but the limited studies of their effect on AFib ablation success have been inconsistent. The current analysis, the group says, points specifically to preablation weight loss as means to improving AFib-ablation outcomes.
“Adjunctive therapy focused on weight loss should be incorporated in the treatment plan for obese patients undergoing ablation for atrial fibrillation,” Jeffrey J. Goldberger, MD, MBA, of the University of Miami, said when presenting the new results at the HRS sessions.
Such a plan is entirely consistent with recent guidelines and especially a 2020 American Heart Association (AHA) consensus statement, but is inconsistently and perhaps even seldom realized in clinical practice.
Dramatic increase in success
Even modest weight loss before ablation may help, proposed Dr. Goldberger, who directs his institution’s Center for Atrial Fibrillation. Decreases for the greater-weight-loss group actually averaged less than 6% of baseline body weight.
Yet it was apparently enough to improve ablation outcomes significantly: Eighty-eight percent were free of AFib 6 months after the procedure, compared with 61% for patients who lost less than 3% of their preablation weight.
For improving ablation success, he said, “We’re talking about a moderate amount of weight loss. These patients are not going from being obese to being thin. They’re still quite overweight.”
In an analysis limited to the four-fifths of patients with persistent AFib, “we saw the same pattern,” Dr. Goldberger said at a media presentation prior to his formal report at the HRS sessions.
Moreover, that subgroup’s benefit persisted out to 12 months, at which time 42% and 81% of patients with less and greater weight loss, respectively, were free of AFib. That represents, he said, “a really tremendous – dramatic, actually – increase in success of pulmonary vein isolation in those who lost weight.”
“We’ve known for a long time that weight loss is important for preventing atrial fibrillation or increasing the success rates of the different treatments we use,” Cynthia M. Tracy, MD, said in an interview. “Probably in some studies, weight loss has been as effective as antiarrhythmics.”
A loss of 3% body weight “is not a lot,” she said. In the current analysis, “It’s notable that it made that much difference with even a fairly modest amount of weight loss.”
Now when asked, “ ‘How much do I have to lose before you’ll consider doing my ablation?’ we have a bit more concrete data to give patients and doctors as to what amount might be beneficial,” said Dr. Tracy of George Washington University Hospital, Washington, who is not associated with the study.
Evolving view of AFib
The findings are emblematic of the profession’s evolving view of AFib and its management, Dr. Goldberger observed at the press conference. Should clinicians think of AFib as similar to “a disease like Wolff-Parkinson-White syndrome,” in which the patient usually has a successful ablation, and then “we expect that to last in perpetuity with no further interventions?”
Or, he said, “is atrial fibrillation more a disease like coronary artery disease, where even if they have an intervention, the disease process is still ongoing and requires long-term disease management? I think it’s pretty clear that we’re dealing with the latter case.”
Dr. Goldberger’s report was an interim analysis of an ongoing randomized trial called LEAF (Liraglutide Effect on Atrial Fibrillation), which is comparing patients with AFib assigned to “take” vs. “not take” the GLP-1 receptor agonist liraglutide, an antidiabetic (Victoza) and weight-loss (Saxenda) drug. The trial aims to assess the drug’s apparent ability to shrink atrial epicardial adipose tissue which, Dr. Goldberger said, is thought to contribute to AFib development and influence AFib-ablation outcomes.
It’s unknown and a limitation of the current analysis, he said, whether the observed link between improved preablation–weight ablation success “is specifically related to weight loss, liraglutide treatment, or both.”
As the invited discussant for Dr. Goldberger’s presentation, David Frankel, MD, observed that studies have been inconsistent on whether substantial weight loss may improve the results of AFib rhythm-control therapy.
Those finding such an association, including LEAF and the influential LEGACY study, differed from others showing a null effect by including “a comprehensive risk factor management” program, observed Dr. Frankel, of the Hospital of the University of Pennsylvania and Penn Heart and Vascular Center, Philadelphia.
Rather than focusing solely on weight loss or sleep apnea as AFib risk factors, he said, the studies linking weight loss to AFib rhythm control also included “hypertension, diabetes, hyperlipidemia, smoking cessation, and alcohol reduction,” Dr. Frankel said. “So it seems clear that to significantly impact AF recurrence, we need to focus on all these contributors to metabolic syndrome.”
Comprehensive risk-factor management
LEAF entered patients with AFib, 79% of whom had persistent AF and the rest paroxysmal AF, who followed the RFM program and were randomly assigned also to take liraglutide or placebo. The “nurse-practitioner-led” RFM program, conducted both in-clinic and online, featured “established goals for each patient” using AHA diet and lifestyle recommendations, an exercise prescription, dietary counseling, evaluation and treatment of sleep apnea, and measures to control any diabetes, hyperlipidemia, or hypertension, Dr. Goldberger said. And patients “were counseled on alcohol reduction and smoking cessation as necessary.”
After 3 months, 29 and 30 patients – regardless of randomization assignment – had lost < 3% and at least 3% of baseline body weight, respectively.
Catheter ablation achieved PVI in all patients. A 3-month blanking period followed, after which they went off antiarrhythmic meds.
It’s very difficult for patients to lose 10% or more of body weight, “and it would not happen overnight,” Dr. Tracy observed. “These are symptomatic patients, for the most part, if they get referred to an electrophysiologist. So you don’t want to defer them indefinitely.”
The current findings, she said, point to “a more realistic target,” suggesting that weight loss of at least 3% should improve AFib ablation’s chances for success.
Dr. Goldberger disclosed ties to Medtronic. Dr. Frankel disclosed ties to Medtronic, Stryker, Biosense Webster, and Boston Scientific. Dr. Tracy reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM HEART RHYTHM 2023
AxSpA effects may be more severe for Black patients
CLEVELAND – Documenting the prevalence of axial spondyloarthritis (axSpA) among Black Americans has been difficult because of little published data, but new research suggests that when Black Americans do have the disease, it seems to be more severe.
Iman Abutineh, MD, of the University of Tennessee, Memphis, discussed her team’s work at the annual meeting of the Spondyloarthritis Research and Treatment Network (SPARTAN).
A total of 244 patients with axSpA were identified, including 168 (69%) males, 78 (32%) Black patients, and 143 (59%) White patients.
Average age of onset for patients overall was 27.7 years, and age at diagnosis was 36.1 years with a 7-year delay in diagnosis. Sixty-six (27%) patients had nonradiographic axSpA, 83% were on tumor necrosis factor inhibitors, and 38% were prescribed glucocorticoids.
The researchers found several differences by race.
White patients were more likely to be HLA-B27 positive (77% vs. 59%; P = .010). White patients also had higher prevalence of psoriasis, coronary artery disease, and family history of SpA. White females had a higher prevalence of inflammatory bowel disease, fibromyalgia, depression, and lower grades of sacroiliitis.
Black patients had more hip involvement
A higher percentage of Black patients had elevated erythrocyte sedimentation rate (ESR), C-reactive protein (CRP), and hip involvement. In comparing hip involvement, the researchers found that 39 (39%) White males had hip involvement as did 9 (21%) White females. In comparison, 22 (45%) Black men in the study and 14 (54%) Black women showed hip involvement (P = .035).
After adjustment for age, sex, HLA-B27, and insurance status, Black patients had higher grades of sacroiliitis with an odds ratio of 2.32 (95% confidence interval, 1.23-4.44). Black patients had a numerically longer delay in diagnosis, compared with Whites (7.93 vs. 6.64 years), but this did not achieve statistical significance (P = .454), the researchers wrote.
Study addresses racial disparities
“Traditionally we think of axial spondyloarthritis largely in Caucasian males who are HLA-B27 positive,” Dr. Abutineh said, “and we found that there is still a significant portion of patients who don’t meet the criteria that do have disease that is very significant.”
Although actual prevalence was not clear from this study, Dr. Abutineh said their data suggest a 3-to-1 ratio of White-to-Black patients with spondyloarthritis, “but of the Black patients who are diagnosed, their disease is almost always more severe. That points to why it’s important to have a high index of suspicion for this disease in that patient population because if you miss it, it could be detrimental to the patients.”
Swetha Alexander, MD, a rheumatology fellow at the University of Utah, Salt Lake City, who was not part of the study, said in an interview, “It is an excellent and timely study addressing the racial disparities and inequities surrounding axSpA diagnosis. It highlights the delay in diagnosis and increased burden of disease among Black Americans.”
She said the study may prompt a further look into barriers to care for Black Americans and their beliefs regarding seeking health care for their pain.
Higher rates of nonradiographic axSpA among Black patients
The rate of nonradiographic axSpA among Black Americans was more than twice that of their White counterparts, which, Dr. Alexander noted, could make it more difficult to diagnose axSpA in that population.
The odds ratio for Black patients having nonradiographic axSpA, compared with Whites, was 2.265 (95% CI, 1.082-4.999; P = .035), after adjustment for age, sex, and HLA-B27 status.
Adult patients with axSpA were identified from rheumatology clinics at four major hospital systems and one private clinic in Shelby County, Tenn., between 2011 and 2021. Patients met modified New York (mNY) or Assessment of Spondyloarthritis International Society (ASAS) criteria as assessed by reviewers.
The authors and Dr. Alexander reported no relevant financial relationships.
CLEVELAND – Documenting the prevalence of axial spondyloarthritis (axSpA) among Black Americans has been difficult because of little published data, but new research suggests that when Black Americans do have the disease, it seems to be more severe.
Iman Abutineh, MD, of the University of Tennessee, Memphis, discussed her team’s work at the annual meeting of the Spondyloarthritis Research and Treatment Network (SPARTAN).
A total of 244 patients with axSpA were identified, including 168 (69%) males, 78 (32%) Black patients, and 143 (59%) White patients.
Average age of onset for patients overall was 27.7 years, and age at diagnosis was 36.1 years with a 7-year delay in diagnosis. Sixty-six (27%) patients had nonradiographic axSpA, 83% were on tumor necrosis factor inhibitors, and 38% were prescribed glucocorticoids.
The researchers found several differences by race.
White patients were more likely to be HLA-B27 positive (77% vs. 59%; P = .010). White patients also had higher prevalence of psoriasis, coronary artery disease, and family history of SpA. White females had a higher prevalence of inflammatory bowel disease, fibromyalgia, depression, and lower grades of sacroiliitis.
Black patients had more hip involvement
A higher percentage of Black patients had elevated erythrocyte sedimentation rate (ESR), C-reactive protein (CRP), and hip involvement. In comparing hip involvement, the researchers found that 39 (39%) White males had hip involvement as did 9 (21%) White females. In comparison, 22 (45%) Black men in the study and 14 (54%) Black women showed hip involvement (P = .035).
After adjustment for age, sex, HLA-B27, and insurance status, Black patients had higher grades of sacroiliitis with an odds ratio of 2.32 (95% confidence interval, 1.23-4.44). Black patients had a numerically longer delay in diagnosis, compared with Whites (7.93 vs. 6.64 years), but this did not achieve statistical significance (P = .454), the researchers wrote.
Study addresses racial disparities
“Traditionally we think of axial spondyloarthritis largely in Caucasian males who are HLA-B27 positive,” Dr. Abutineh said, “and we found that there is still a significant portion of patients who don’t meet the criteria that do have disease that is very significant.”
Although actual prevalence was not clear from this study, Dr. Abutineh said their data suggest a 3-to-1 ratio of White-to-Black patients with spondyloarthritis, “but of the Black patients who are diagnosed, their disease is almost always more severe. That points to why it’s important to have a high index of suspicion for this disease in that patient population because if you miss it, it could be detrimental to the patients.”
Swetha Alexander, MD, a rheumatology fellow at the University of Utah, Salt Lake City, who was not part of the study, said in an interview, “It is an excellent and timely study addressing the racial disparities and inequities surrounding axSpA diagnosis. It highlights the delay in diagnosis and increased burden of disease among Black Americans.”
She said the study may prompt a further look into barriers to care for Black Americans and their beliefs regarding seeking health care for their pain.
Higher rates of nonradiographic axSpA among Black patients
The rate of nonradiographic axSpA among Black Americans was more than twice that of their White counterparts, which, Dr. Alexander noted, could make it more difficult to diagnose axSpA in that population.
The odds ratio for Black patients having nonradiographic axSpA, compared with Whites, was 2.265 (95% CI, 1.082-4.999; P = .035), after adjustment for age, sex, and HLA-B27 status.
Adult patients with axSpA were identified from rheumatology clinics at four major hospital systems and one private clinic in Shelby County, Tenn., between 2011 and 2021. Patients met modified New York (mNY) or Assessment of Spondyloarthritis International Society (ASAS) criteria as assessed by reviewers.
The authors and Dr. Alexander reported no relevant financial relationships.
CLEVELAND – Documenting the prevalence of axial spondyloarthritis (axSpA) among Black Americans has been difficult because of little published data, but new research suggests that when Black Americans do have the disease, it seems to be more severe.
Iman Abutineh, MD, of the University of Tennessee, Memphis, discussed her team’s work at the annual meeting of the Spondyloarthritis Research and Treatment Network (SPARTAN).
A total of 244 patients with axSpA were identified, including 168 (69%) males, 78 (32%) Black patients, and 143 (59%) White patients.
Average age of onset for patients overall was 27.7 years, and age at diagnosis was 36.1 years with a 7-year delay in diagnosis. Sixty-six (27%) patients had nonradiographic axSpA, 83% were on tumor necrosis factor inhibitors, and 38% were prescribed glucocorticoids.
The researchers found several differences by race.
White patients were more likely to be HLA-B27 positive (77% vs. 59%; P = .010). White patients also had higher prevalence of psoriasis, coronary artery disease, and family history of SpA. White females had a higher prevalence of inflammatory bowel disease, fibromyalgia, depression, and lower grades of sacroiliitis.
Black patients had more hip involvement
A higher percentage of Black patients had elevated erythrocyte sedimentation rate (ESR), C-reactive protein (CRP), and hip involvement. In comparing hip involvement, the researchers found that 39 (39%) White males had hip involvement as did 9 (21%) White females. In comparison, 22 (45%) Black men in the study and 14 (54%) Black women showed hip involvement (P = .035).
After adjustment for age, sex, HLA-B27, and insurance status, Black patients had higher grades of sacroiliitis with an odds ratio of 2.32 (95% confidence interval, 1.23-4.44). Black patients had a numerically longer delay in diagnosis, compared with Whites (7.93 vs. 6.64 years), but this did not achieve statistical significance (P = .454), the researchers wrote.
Study addresses racial disparities
“Traditionally we think of axial spondyloarthritis largely in Caucasian males who are HLA-B27 positive,” Dr. Abutineh said, “and we found that there is still a significant portion of patients who don’t meet the criteria that do have disease that is very significant.”
Although actual prevalence was not clear from this study, Dr. Abutineh said their data suggest a 3-to-1 ratio of White-to-Black patients with spondyloarthritis, “but of the Black patients who are diagnosed, their disease is almost always more severe. That points to why it’s important to have a high index of suspicion for this disease in that patient population because if you miss it, it could be detrimental to the patients.”
Swetha Alexander, MD, a rheumatology fellow at the University of Utah, Salt Lake City, who was not part of the study, said in an interview, “It is an excellent and timely study addressing the racial disparities and inequities surrounding axSpA diagnosis. It highlights the delay in diagnosis and increased burden of disease among Black Americans.”
She said the study may prompt a further look into barriers to care for Black Americans and their beliefs regarding seeking health care for their pain.
Higher rates of nonradiographic axSpA among Black patients
The rate of nonradiographic axSpA among Black Americans was more than twice that of their White counterparts, which, Dr. Alexander noted, could make it more difficult to diagnose axSpA in that population.
The odds ratio for Black patients having nonradiographic axSpA, compared with Whites, was 2.265 (95% CI, 1.082-4.999; P = .035), after adjustment for age, sex, and HLA-B27 status.
Adult patients with axSpA were identified from rheumatology clinics at four major hospital systems and one private clinic in Shelby County, Tenn., between 2011 and 2021. Patients met modified New York (mNY) or Assessment of Spondyloarthritis International Society (ASAS) criteria as assessed by reviewers.
The authors and Dr. Alexander reported no relevant financial relationships.
AT SPARTAN 2023
Novel antibody safe, promising for ATTR in phase 1 trial
, a new study suggests.
Currently, the only drug approved to treat ATTR is tafamidis, which improves survival and reduces hospitalizations, but does not reverse disease symptoms, the authors noted.
NI006 is a recombinant human anti-ATTR antibody given by infusion that was developed to trigger removal of ATTR by the body’s phagocytic immune cells.
Use of the drug was not associated with serious drug-related adverse events, though mild and moderate adverse events did occur.
Median N-terminal pro–B-type natriuretic peptide (NT-proBNP) and troponin T levels also seemed to be reduced over the study period.
Given the success of the antibody in this initial 40-patient trial, a larger phase-3 placebo-controlled trial is planned and expected to launch in the second half of 2023, said lead author Pablo Garcia-Pavia, MD, of Hospital Universitario Puerta de Hierro and the Spanish National Cardiovascular Research Institute, Madrid.
However, “The design of appropriate phase-3 trials to demonstrate efficacy of drugs for ATTR-CM is becoming more complicated and challenging,” he said.
“Increased awareness of the disease and advances in cardiac imaging techniques have led to recognition of a larger number of patients with ATTR-CM who have a different clinical profile and a different prognosis than the patients who were diagnosed in previous years and were enrolled in the initial trials of stabilizers,” Dr. Garcia-Pavia added.
“Moreover, the availability of tafamidis, and hopefully soon other medications to treat ATTR-CM has complicated the design of new clinical trials because of the heterogenicity of treatments that patients might receive,” he said. “Therefore, it is critical to plan the design very well.”
Dr. Garcia-Pavia presented the findings on NI006 at the Heart Failure Association of the European Society of Cardiology (HFA-ESC) 2023 sessions. The study was published simultaneously in the New England Journal of Medicine.
No serious adverse events
For the phase-1, double-blind, multicenter study, the investigators randomly assigned (2:1 ratio) 40 patients (median age, 72 years; 98% men) with wild-type or variant ATTR cardiomyopathy and chronic heart failure to receive IV infusions of either NI006, at one of six doses ranging from 0.3 mg/kg to 60 mg/kg of body weight, or placebo every 4 weeks for 4 months.
After the four infusions, participants were enrolled in an open-label extension phase in which they received eight NI006 infusions with stepwise increases in the dose.
Participants had a confirmed diagnosis of ATTR-CM; left ventricular wall thickness of at least 14 mm; left ventricular ejection fraction of at least 40%; New York Heart Association class I, II, or III; estimated glomerular filtration rate of more than 30 mL/min per 1.73 m2; and an NT-proBNP level of 600 to 6,000 pg/mL.
Most (36) were receiving tafamidis, with a median treatment duration of 7 months; other ATTR-specific drugs were not permitted. Patients randomly assigned to receive NI006 seemed to have more advanced disease compared with those assigned to placebo.
Adherence to the trial protocol was high: Thirty-four patients received the four scheduled infusions during the ascending-dose phase, and 34 of 35 patients who completed this phase subsequently enrolled in the open-label extension.
No apparent drug-related serious adverse events were reported. However, during the ascending-dose phase, 38 patients had at least one adverse event, most of which were mild or moderate; of the 191 total events, 124 were grade 1 and 60 were grade 2 (most commonly heart failure and arrhythmias). Three patients had cytokine release syndrome; all three completed treatment through the extension phase.
Musculoskeletal events increased with ascending doses of NI006, which led two patients to withdraw from the trial.
At doses of at least 10 mg/kg, cardiac tracer uptake on scintigraphy and extracellular volume on cardiac MRI, both of which are imaging-based surrogate markers of cardiac amyloid load, appeared to be reduced over 12 months.
Because NI006 stimulates the patient’s own immune system to eliminate cardiac amyloid fibrils, one session chair at the meeting wondered whether NI006 represented the “rise of immunology in cardiology,” and whether biologics might follow.
Another questioned how removing amyloid might affect cardiac function. The echocardiographic findings gathered so far don’t indicate dysfunction, “but this is a small trial, and we need more data,” Dr. Garcia-Pavia said.
Tempered excitement
In a comment, Ronald Witteles, MD, professor of cardiovascular medicine, Stanford (Calif.) University, and founder/codirector of the Stanford Amyloid Center, said that “antibody-based amyloid removal strategies are not currently clinically available and represent a fundamentally different mechanism to treat the disease from what we currently have.
“While the data are encouraging and will generate excitement for later-phase studies, we’re talking about small numbers of patients and nothing definitive should be drawn from this data,” said Dr. Witteles, deputy editor of JACC: CardioOncology.
“The biggest caveat is that similar approaches of antibody removal of amyloid deposits for other forms of amyloidosis — most notably AL amyloidosis (amyloid light chain or primary amyloidosis) – have failed in late-phase trials. Although there is reason to believe that ATTR amyloidosis may be more amenable to improvements with amyloid fibril removal than AL amyloidosis, the unimpressive results in other forms of amyloidosis still do temper the excitement to a degree.”
Like Dr. Garcia-Pavia, Dr. Witteles said, “Ultimately, we are going to need to see a phase 3 clinical trial which shows that NI006 – on top of standard-of-care treatment – improves hard outcomes in the disease. As treatment options likely expand in the coming years, that is likely to be a harder and harder bar to reach.”
Furthermore, although the safety profile was favorable overall, it “wasn’t entirely clean,” given cytokine release syndrome in three patients, a lowering of platelet counts in a couple of patients, and musculoskeletal side effects that triggered two to withdraw from the study. “Unless that changes,” he said, “that will be a barrier for some patients.”
Overall, he noted, “With the vast majority of patients being able to be diagnosed noninvasively, and with treatment options now available, we have seen a true explosion in the number of patients being diagnosed.
“But we also know that the large majority ... are still not getting diagnosed or are having huge delays in diagnosis. As such, the biggest thing we can do for patients with the disease is to continue to educate people about it,” Dr. Witteles concluded.
The study was funded by Neurimmune. Dr. Garcia-Pavia disclosed ties to Alexion, Alnylam Pharmaceuticals, AstraZeneca, Attralus, BridgeBio, General Electric, Intellia, Ionis Pharmaceuticals, Neurimmune, Novo Nordisk, and Pfizer. Dr. Witteles reported ties to Alexion, Alnylam, AstraZeneca, BridgeBio, Intellia, Ionis, Janssen, Novo Nordisk, and Pfizer.
A version of this article first appeared on Medscape.com.
, a new study suggests.
Currently, the only drug approved to treat ATTR is tafamidis, which improves survival and reduces hospitalizations, but does not reverse disease symptoms, the authors noted.
NI006 is a recombinant human anti-ATTR antibody given by infusion that was developed to trigger removal of ATTR by the body’s phagocytic immune cells.
Use of the drug was not associated with serious drug-related adverse events, though mild and moderate adverse events did occur.
Median N-terminal pro–B-type natriuretic peptide (NT-proBNP) and troponin T levels also seemed to be reduced over the study period.
Given the success of the antibody in this initial 40-patient trial, a larger phase-3 placebo-controlled trial is planned and expected to launch in the second half of 2023, said lead author Pablo Garcia-Pavia, MD, of Hospital Universitario Puerta de Hierro and the Spanish National Cardiovascular Research Institute, Madrid.
However, “The design of appropriate phase-3 trials to demonstrate efficacy of drugs for ATTR-CM is becoming more complicated and challenging,” he said.
“Increased awareness of the disease and advances in cardiac imaging techniques have led to recognition of a larger number of patients with ATTR-CM who have a different clinical profile and a different prognosis than the patients who were diagnosed in previous years and were enrolled in the initial trials of stabilizers,” Dr. Garcia-Pavia added.
“Moreover, the availability of tafamidis, and hopefully soon other medications to treat ATTR-CM has complicated the design of new clinical trials because of the heterogenicity of treatments that patients might receive,” he said. “Therefore, it is critical to plan the design very well.”
Dr. Garcia-Pavia presented the findings on NI006 at the Heart Failure Association of the European Society of Cardiology (HFA-ESC) 2023 sessions. The study was published simultaneously in the New England Journal of Medicine.
No serious adverse events
For the phase-1, double-blind, multicenter study, the investigators randomly assigned (2:1 ratio) 40 patients (median age, 72 years; 98% men) with wild-type or variant ATTR cardiomyopathy and chronic heart failure to receive IV infusions of either NI006, at one of six doses ranging from 0.3 mg/kg to 60 mg/kg of body weight, or placebo every 4 weeks for 4 months.
After the four infusions, participants were enrolled in an open-label extension phase in which they received eight NI006 infusions with stepwise increases in the dose.
Participants had a confirmed diagnosis of ATTR-CM; left ventricular wall thickness of at least 14 mm; left ventricular ejection fraction of at least 40%; New York Heart Association class I, II, or III; estimated glomerular filtration rate of more than 30 mL/min per 1.73 m2; and an NT-proBNP level of 600 to 6,000 pg/mL.
Most (36) were receiving tafamidis, with a median treatment duration of 7 months; other ATTR-specific drugs were not permitted. Patients randomly assigned to receive NI006 seemed to have more advanced disease compared with those assigned to placebo.
Adherence to the trial protocol was high: Thirty-four patients received the four scheduled infusions during the ascending-dose phase, and 34 of 35 patients who completed this phase subsequently enrolled in the open-label extension.
No apparent drug-related serious adverse events were reported. However, during the ascending-dose phase, 38 patients had at least one adverse event, most of which were mild or moderate; of the 191 total events, 124 were grade 1 and 60 were grade 2 (most commonly heart failure and arrhythmias). Three patients had cytokine release syndrome; all three completed treatment through the extension phase.
Musculoskeletal events increased with ascending doses of NI006, which led two patients to withdraw from the trial.
At doses of at least 10 mg/kg, cardiac tracer uptake on scintigraphy and extracellular volume on cardiac MRI, both of which are imaging-based surrogate markers of cardiac amyloid load, appeared to be reduced over 12 months.
Because NI006 stimulates the patient’s own immune system to eliminate cardiac amyloid fibrils, one session chair at the meeting wondered whether NI006 represented the “rise of immunology in cardiology,” and whether biologics might follow.
Another questioned how removing amyloid might affect cardiac function. The echocardiographic findings gathered so far don’t indicate dysfunction, “but this is a small trial, and we need more data,” Dr. Garcia-Pavia said.
Tempered excitement
In a comment, Ronald Witteles, MD, professor of cardiovascular medicine, Stanford (Calif.) University, and founder/codirector of the Stanford Amyloid Center, said that “antibody-based amyloid removal strategies are not currently clinically available and represent a fundamentally different mechanism to treat the disease from what we currently have.
“While the data are encouraging and will generate excitement for later-phase studies, we’re talking about small numbers of patients and nothing definitive should be drawn from this data,” said Dr. Witteles, deputy editor of JACC: CardioOncology.
“The biggest caveat is that similar approaches of antibody removal of amyloid deposits for other forms of amyloidosis — most notably AL amyloidosis (amyloid light chain or primary amyloidosis) – have failed in late-phase trials. Although there is reason to believe that ATTR amyloidosis may be more amenable to improvements with amyloid fibril removal than AL amyloidosis, the unimpressive results in other forms of amyloidosis still do temper the excitement to a degree.”
Like Dr. Garcia-Pavia, Dr. Witteles said, “Ultimately, we are going to need to see a phase 3 clinical trial which shows that NI006 – on top of standard-of-care treatment – improves hard outcomes in the disease. As treatment options likely expand in the coming years, that is likely to be a harder and harder bar to reach.”
Furthermore, although the safety profile was favorable overall, it “wasn’t entirely clean,” given cytokine release syndrome in three patients, a lowering of platelet counts in a couple of patients, and musculoskeletal side effects that triggered two to withdraw from the study. “Unless that changes,” he said, “that will be a barrier for some patients.”
Overall, he noted, “With the vast majority of patients being able to be diagnosed noninvasively, and with treatment options now available, we have seen a true explosion in the number of patients being diagnosed.
“But we also know that the large majority ... are still not getting diagnosed or are having huge delays in diagnosis. As such, the biggest thing we can do for patients with the disease is to continue to educate people about it,” Dr. Witteles concluded.
The study was funded by Neurimmune. Dr. Garcia-Pavia disclosed ties to Alexion, Alnylam Pharmaceuticals, AstraZeneca, Attralus, BridgeBio, General Electric, Intellia, Ionis Pharmaceuticals, Neurimmune, Novo Nordisk, and Pfizer. Dr. Witteles reported ties to Alexion, Alnylam, AstraZeneca, BridgeBio, Intellia, Ionis, Janssen, Novo Nordisk, and Pfizer.
A version of this article first appeared on Medscape.com.
, a new study suggests.
Currently, the only drug approved to treat ATTR is tafamidis, which improves survival and reduces hospitalizations, but does not reverse disease symptoms, the authors noted.
NI006 is a recombinant human anti-ATTR antibody given by infusion that was developed to trigger removal of ATTR by the body’s phagocytic immune cells.
Use of the drug was not associated with serious drug-related adverse events, though mild and moderate adverse events did occur.
Median N-terminal pro–B-type natriuretic peptide (NT-proBNP) and troponin T levels also seemed to be reduced over the study period.
Given the success of the antibody in this initial 40-patient trial, a larger phase-3 placebo-controlled trial is planned and expected to launch in the second half of 2023, said lead author Pablo Garcia-Pavia, MD, of Hospital Universitario Puerta de Hierro and the Spanish National Cardiovascular Research Institute, Madrid.
However, “The design of appropriate phase-3 trials to demonstrate efficacy of drugs for ATTR-CM is becoming more complicated and challenging,” he said.
“Increased awareness of the disease and advances in cardiac imaging techniques have led to recognition of a larger number of patients with ATTR-CM who have a different clinical profile and a different prognosis than the patients who were diagnosed in previous years and were enrolled in the initial trials of stabilizers,” Dr. Garcia-Pavia added.
“Moreover, the availability of tafamidis, and hopefully soon other medications to treat ATTR-CM has complicated the design of new clinical trials because of the heterogenicity of treatments that patients might receive,” he said. “Therefore, it is critical to plan the design very well.”
Dr. Garcia-Pavia presented the findings on NI006 at the Heart Failure Association of the European Society of Cardiology (HFA-ESC) 2023 sessions. The study was published simultaneously in the New England Journal of Medicine.
No serious adverse events
For the phase-1, double-blind, multicenter study, the investigators randomly assigned (2:1 ratio) 40 patients (median age, 72 years; 98% men) with wild-type or variant ATTR cardiomyopathy and chronic heart failure to receive IV infusions of either NI006, at one of six doses ranging from 0.3 mg/kg to 60 mg/kg of body weight, or placebo every 4 weeks for 4 months.
After the four infusions, participants were enrolled in an open-label extension phase in which they received eight NI006 infusions with stepwise increases in the dose.
Participants had a confirmed diagnosis of ATTR-CM; left ventricular wall thickness of at least 14 mm; left ventricular ejection fraction of at least 40%; New York Heart Association class I, II, or III; estimated glomerular filtration rate of more than 30 mL/min per 1.73 m2; and an NT-proBNP level of 600 to 6,000 pg/mL.
Most (36) were receiving tafamidis, with a median treatment duration of 7 months; other ATTR-specific drugs were not permitted. Patients randomly assigned to receive NI006 seemed to have more advanced disease compared with those assigned to placebo.
Adherence to the trial protocol was high: Thirty-four patients received the four scheduled infusions during the ascending-dose phase, and 34 of 35 patients who completed this phase subsequently enrolled in the open-label extension.
No apparent drug-related serious adverse events were reported. However, during the ascending-dose phase, 38 patients had at least one adverse event, most of which were mild or moderate; of the 191 total events, 124 were grade 1 and 60 were grade 2 (most commonly heart failure and arrhythmias). Three patients had cytokine release syndrome; all three completed treatment through the extension phase.
Musculoskeletal events increased with ascending doses of NI006, which led two patients to withdraw from the trial.
At doses of at least 10 mg/kg, cardiac tracer uptake on scintigraphy and extracellular volume on cardiac MRI, both of which are imaging-based surrogate markers of cardiac amyloid load, appeared to be reduced over 12 months.
Because NI006 stimulates the patient’s own immune system to eliminate cardiac amyloid fibrils, one session chair at the meeting wondered whether NI006 represented the “rise of immunology in cardiology,” and whether biologics might follow.
Another questioned how removing amyloid might affect cardiac function. The echocardiographic findings gathered so far don’t indicate dysfunction, “but this is a small trial, and we need more data,” Dr. Garcia-Pavia said.
Tempered excitement
In a comment, Ronald Witteles, MD, professor of cardiovascular medicine, Stanford (Calif.) University, and founder/codirector of the Stanford Amyloid Center, said that “antibody-based amyloid removal strategies are not currently clinically available and represent a fundamentally different mechanism to treat the disease from what we currently have.
“While the data are encouraging and will generate excitement for later-phase studies, we’re talking about small numbers of patients and nothing definitive should be drawn from this data,” said Dr. Witteles, deputy editor of JACC: CardioOncology.
“The biggest caveat is that similar approaches of antibody removal of amyloid deposits for other forms of amyloidosis — most notably AL amyloidosis (amyloid light chain or primary amyloidosis) – have failed in late-phase trials. Although there is reason to believe that ATTR amyloidosis may be more amenable to improvements with amyloid fibril removal than AL amyloidosis, the unimpressive results in other forms of amyloidosis still do temper the excitement to a degree.”
Like Dr. Garcia-Pavia, Dr. Witteles said, “Ultimately, we are going to need to see a phase 3 clinical trial which shows that NI006 – on top of standard-of-care treatment – improves hard outcomes in the disease. As treatment options likely expand in the coming years, that is likely to be a harder and harder bar to reach.”
Furthermore, although the safety profile was favorable overall, it “wasn’t entirely clean,” given cytokine release syndrome in three patients, a lowering of platelet counts in a couple of patients, and musculoskeletal side effects that triggered two to withdraw from the study. “Unless that changes,” he said, “that will be a barrier for some patients.”
Overall, he noted, “With the vast majority of patients being able to be diagnosed noninvasively, and with treatment options now available, we have seen a true explosion in the number of patients being diagnosed.
“But we also know that the large majority ... are still not getting diagnosed or are having huge delays in diagnosis. As such, the biggest thing we can do for patients with the disease is to continue to educate people about it,” Dr. Witteles concluded.
The study was funded by Neurimmune. Dr. Garcia-Pavia disclosed ties to Alexion, Alnylam Pharmaceuticals, AstraZeneca, Attralus, BridgeBio, General Electric, Intellia, Ionis Pharmaceuticals, Neurimmune, Novo Nordisk, and Pfizer. Dr. Witteles reported ties to Alexion, Alnylam, AstraZeneca, BridgeBio, Intellia, Ionis, Janssen, Novo Nordisk, and Pfizer.
A version of this article first appeared on Medscape.com.
FROM ESC HEART FAILURE 2023
Docs can help combat TikTok misinformation on rare psychiatric disorder
SAN FRANCISCO – , new research shows.
These findings, say investigators, underscore the need for mental health professionals to help counter the spread of false information by creating accurate content and posting it on the popular social media platform.

“Health care professionals need to make engaging content to post on social media platforms like YouTube and especially TikTok, to reach wider audiences and combat misinformation about DID,” study investigator Isreal Bladimir Munoz, a fourth-year medical student at University of Texas, Galveston, said in an interview.
The findings were presented at the annual meeting of the American Psychiatric Association.
Popularized by the media
A rare condition affecting less than 1% of the general population, DID involves two or more distinct personality states, along with changes in behavior and memory gaps.
The condition has been popularized in books and the media. Movies such as “Split,” “Psycho,” and “Fight Club” all feature characters with DID.
“These bring awareness about the condition, but also often sensationalize or stigmatize it and reinforce stereotypes,” said Mr. Munoz.
In recent years, social media has become an integral part of everyday life. An estimated 4.2 billion people actively frequent sites such as YouTube, TikTok, Twitter, and Meta.
Although social media allows for instant communication and the opportunity for self-expression, there are mounting concerns about the spread of misinformation and its potential impact on mental health and privacy, said Mr. Munoz.
To evaluate the quality and accuracy of information about DID on social media, investigators analyzed 60 YouTube and 97 TikTok videos on the condition.
To evaluate the reliability and the intent and reliability of videos, researchers used the modified DISCERN instrument and the Global Quality Scale, a five-point rating system.
Using these tools, the researchers determined whether the selected videos were useful, misleading, or neither. Mr. Munoz said videos were classified as useful if they contained accurate information about the condition and its pathogenesis, treatment, and management.
Researchers determined that for YouTube videos, 51.7% were useful, 6.6% were misleading, and 34.7% were neither. About 43.3% of these videos involved interviews, 21.7% were educational, 15% involved personal stories, 8.3% were films/TV programs, 5% were comedy skits, and 3.3% were another content type.
The highest quality YouTube videos were from educational organizations and health care professionals. The least accurate videos came from independent users and film/TV sources.
As for TikTok videos on DID, only 5.2% were useful, 10.3% were misleading, and 41.7% were neither.
The main sources for TikTok videos were independent organizations, whereas podcasts and film/TV were the least common sources.
The findings, said Mr. Munoz, underscore the need for medical professionals to develop high-quality content about DID and post it on TikTok to counter misinformation on social media.
Call to action
In a comment, Howard Y. Liu, MD, a child and adolescent psychiatrist and chair of the department of psychiatry, University of Nebraska, Omaha, described the study as “compelling.”

When it comes to public health messages, it’s important to know what social media people are using. Today’s parents are on Twitter and Facebook, whereas their children are more likely to be checking out YouTube and TikTok, said Dr. Liu, chair of the APA’s Council on Communications.
“TikTok is critical because that’s where all the youth eyeballs are,” he said.
The medical profession needs to engage with the platform to reach this next-generation audience and help stop the spread of misinformation about DID, said Dr. Liu. He noted that the APA is looking into undertaking such an initiative.
The study investigators report no relevant disclosures. Dr. Liu reports no relevant disclosures.
A version of this article first appeared on Medscape.com.
SAN FRANCISCO – , new research shows.
These findings, say investigators, underscore the need for mental health professionals to help counter the spread of false information by creating accurate content and posting it on the popular social media platform.
“Health care professionals need to make engaging content to post on social media platforms like YouTube and especially TikTok, to reach wider audiences and combat misinformation about DID,” study investigator Isreal Bladimir Munoz, a fourth-year medical student at University of Texas, Galveston, said in an interview.
The findings were presented at the annual meeting of the American Psychiatric Association.
Popularized by the media
A rare condition affecting less than 1% of the general population, DID involves two or more distinct personality states, along with changes in behavior and memory gaps.
The condition has been popularized in books and the media. Movies such as “Split,” “Psycho,” and “Fight Club” all feature characters with DID.
“These bring awareness about the condition, but also often sensationalize or stigmatize it and reinforce stereotypes,” said Mr. Munoz.
In recent years, social media has become an integral part of everyday life. An estimated 4.2 billion people actively frequent sites such as YouTube, TikTok, Twitter, and Meta.
Although social media allows for instant communication and the opportunity for self-expression, there are mounting concerns about the spread of misinformation and its potential impact on mental health and privacy, said Mr. Munoz.
To evaluate the quality and accuracy of information about DID on social media, investigators analyzed 60 YouTube and 97 TikTok videos on the condition.
To evaluate the reliability and the intent and reliability of videos, researchers used the modified DISCERN instrument and the Global Quality Scale, a five-point rating system.
Using these tools, the researchers determined whether the selected videos were useful, misleading, or neither. Mr. Munoz said videos were classified as useful if they contained accurate information about the condition and its pathogenesis, treatment, and management.
Researchers determined that for YouTube videos, 51.7% were useful, 6.6% were misleading, and 34.7% were neither. About 43.3% of these videos involved interviews, 21.7% were educational, 15% involved personal stories, 8.3% were films/TV programs, 5% were comedy skits, and 3.3% were another content type.
The highest quality YouTube videos were from educational organizations and health care professionals. The least accurate videos came from independent users and film/TV sources.
As for TikTok videos on DID, only 5.2% were useful, 10.3% were misleading, and 41.7% were neither.
The main sources for TikTok videos were independent organizations, whereas podcasts and film/TV were the least common sources.
The findings, said Mr. Munoz, underscore the need for medical professionals to develop high-quality content about DID and post it on TikTok to counter misinformation on social media.
Call to action
In a comment, Howard Y. Liu, MD, a child and adolescent psychiatrist and chair of the department of psychiatry, University of Nebraska, Omaha, described the study as “compelling.”
When it comes to public health messages, it’s important to know what social media people are using. Today’s parents are on Twitter and Facebook, whereas their children are more likely to be checking out YouTube and TikTok, said Dr. Liu, chair of the APA’s Council on Communications.
“TikTok is critical because that’s where all the youth eyeballs are,” he said.
The medical profession needs to engage with the platform to reach this next-generation audience and help stop the spread of misinformation about DID, said Dr. Liu. He noted that the APA is looking into undertaking such an initiative.
The study investigators report no relevant disclosures. Dr. Liu reports no relevant disclosures.
A version of this article first appeared on Medscape.com.
SAN FRANCISCO – , new research shows.
These findings, say investigators, underscore the need for mental health professionals to help counter the spread of false information by creating accurate content and posting it on the popular social media platform.
“Health care professionals need to make engaging content to post on social media platforms like YouTube and especially TikTok, to reach wider audiences and combat misinformation about DID,” study investigator Isreal Bladimir Munoz, a fourth-year medical student at University of Texas, Galveston, said in an interview.
The findings were presented at the annual meeting of the American Psychiatric Association.
Popularized by the media
A rare condition affecting less than 1% of the general population, DID involves two or more distinct personality states, along with changes in behavior and memory gaps.
The condition has been popularized in books and the media. Movies such as “Split,” “Psycho,” and “Fight Club” all feature characters with DID.
“These bring awareness about the condition, but also often sensationalize or stigmatize it and reinforce stereotypes,” said Mr. Munoz.
In recent years, social media has become an integral part of everyday life. An estimated 4.2 billion people actively frequent sites such as YouTube, TikTok, Twitter, and Meta.
Although social media allows for instant communication and the opportunity for self-expression, there are mounting concerns about the spread of misinformation and its potential impact on mental health and privacy, said Mr. Munoz.
To evaluate the quality and accuracy of information about DID on social media, investigators analyzed 60 YouTube and 97 TikTok videos on the condition.
To evaluate the reliability and the intent and reliability of videos, researchers used the modified DISCERN instrument and the Global Quality Scale, a five-point rating system.
Using these tools, the researchers determined whether the selected videos were useful, misleading, or neither. Mr. Munoz said videos were classified as useful if they contained accurate information about the condition and its pathogenesis, treatment, and management.
Researchers determined that for YouTube videos, 51.7% were useful, 6.6% were misleading, and 34.7% were neither. About 43.3% of these videos involved interviews, 21.7% were educational, 15% involved personal stories, 8.3% were films/TV programs, 5% were comedy skits, and 3.3% were another content type.
The highest quality YouTube videos were from educational organizations and health care professionals. The least accurate videos came from independent users and film/TV sources.
As for TikTok videos on DID, only 5.2% were useful, 10.3% were misleading, and 41.7% were neither.
The main sources for TikTok videos were independent organizations, whereas podcasts and film/TV were the least common sources.
The findings, said Mr. Munoz, underscore the need for medical professionals to develop high-quality content about DID and post it on TikTok to counter misinformation on social media.
Call to action
In a comment, Howard Y. Liu, MD, a child and adolescent psychiatrist and chair of the department of psychiatry, University of Nebraska, Omaha, described the study as “compelling.”
When it comes to public health messages, it’s important to know what social media people are using. Today’s parents are on Twitter and Facebook, whereas their children are more likely to be checking out YouTube and TikTok, said Dr. Liu, chair of the APA’s Council on Communications.
“TikTok is critical because that’s where all the youth eyeballs are,” he said.
The medical profession needs to engage with the platform to reach this next-generation audience and help stop the spread of misinformation about DID, said Dr. Liu. He noted that the APA is looking into undertaking such an initiative.
The study investigators report no relevant disclosures. Dr. Liu reports no relevant disclosures.
A version of this article first appeared on Medscape.com.
AT APA 2023