User login
Mnemonics in a mnutshell: 32 aids to psychiatric diagnosis
From SIG: E CAPS to CAGE and WWHHHHIMPS, mnemonics help practitioners and trainees recall important lists (such as criteria for depression, screening questions for alcoholism, or life-threatening causes of delirium, respectively). Mnemonics’ efficacy rests on the principle that grouped information is easier to remember than individual points of data.
Not everyone loves mnemonics, but recollecting diagnostic criteria is useful in clinical practice and research, on board examinations, and for insurance reimbursement. Thus, tools that assist in recalling diagnostic criteria have a role in psychiatric practice and teaching.
In this article, we present 32 mnemonics to help clinicians diagnose:
- affective disorders (Box 1)1,2
- anxiety disorders (Box 2)3-6
- medication adverse effects (Box 3)7,8
- personality disorders (Box 4)9-11
- addiction disorders (Box 5)12,13
- causes of delirium (Box 6).14
We also discuss how mnemonics improve one’s memory, based on the principles of learning theory.
How mnemonics work
A mnemonic—from the Greek word “mnemonikos” (“of memory”)—links new data with previously learned information. Mnemonics assist in learning by reducing the amount of information (“cognitive load”) that needs to be stored for long-term processing and retrieval.15
Memory, defined as the “persistence of learning in a state that can be revealed at a later time,”16 can be divided into 2 types:
- declarative (a conscious recollection of facts, such as remembering a relative’s birthday)
- procedural (skills-based learning, such as riding a bicycle).
Declarative memory has a conscious component and may be mediated by the medial temporal lobe and cortical association structures. Procedural memory has less of a conscious component; it may involve the basal ganglia, cerebellum, and a variety of cortical sensory-perceptive regions.17
| Depression SIG: E CAPS* Suicidal thoughts Interests decreased Guilt Energy decreased Concentration decreased Appetite disturbance (increased or decreased) Psychomotor changes (agitation or retardation) Sleep disturbance (increased or decreased) * Created by Carey Gross, MD | Dysthymia HE’S 2 SAD2 Hopelessness Energy loss or fatigue Self-esteem is low 2 years minimum of depressed mood most of the day, for more days than not Sleep is increased or decreased Appetite is increased or decreased Decision-making or concentration is impaired | Mania DIG FAST Distractibility Indiscretion Grandiosity Flight of ideas Activity increase Sleep deficit Talkativeness |
| Depression C GASP DIE1 Concentration decreased Guilt Appetite Sleep disturbance Psychomotor agitation or retardation Death or suicide (thoughts or acts of) Interests decreased Energy decreased | Hypomania TAD HIGH Talkative Attention deficit Decreased need for sleep High self-esteem/grandiosity Ideas that race Goal-directed activity increased High-risk activity | Mania DeTeR the HIGH* Distractibility Talkativeness Reckless behavior Hyposomnia Ideas that race Grandiosity Hypersexuality * Created by Carey Gross, MD |
Declarative memory can be subdivided into working memory and long-term memory.
With working memory, new items of information are held briefly so that encoding and eventual storage can take place.
Working memory guides decision-making and future planning and is intricately related to attention.18-21 Functional MRI and positron emission tomography as well as neurocognitive testing have shown that working memory tasks activate the prefrontal cortex and brain regions specific to language and visuospatial memory.
The hippocampus is thought to rapidly absorb new information, and this data is consolidated and permanently stored via the prefrontal cortex.22-26 Given the hippocampus’ limited storage capacity, new information (such as what you ate for breakfast 3 weeks ago) will disappear if it is not repeated regularly.17
Long-term memory, on the other hand, is encoded knowledge that is linked to facts learned in the past; it is consolidated in the brain and can be readily retrieved. Neuroimaging studies have demonstrated opposing patterns of activation in the hippocampus and prefrontal cortex, depending on whether the memory being recalled is:
- new (high hippocampal activity, low prefrontal cortex activity)
- old (low hippocampal activity, high prefrontal cortex activity).27
Mnemonics are thought to affect working memory by reducing the introduced cognitive load and increasing the efficiency of memory acquisition and encoding. They reduce cognitive load by grouping objects into a single verbal or visual cue that can be introduced into working memory. Learning is optimized when the load on working memory is minimized, enabling long-term memory to be facilitated.28
| Generalized anxiety disorder Worry WARTS3 Wound up Worn-out Absentminded Restless Touchy Sleepless | Posttraumatic stress disorder TRAUMA5 Traumatic event Re-experience Avoidance Unable to function Month or more of symptoms Arousal increased | Anxiety disorder due to a general medical condition Physical Diseases That Have Commonly Appeared Anxious: Pheochromocytoma Diabetes mellitus Temporal lobe epilepsy Hyperthyroidism Carcinoid Alcohol withdrawal Arrhythmias |
| Generalized anxiety disorder WATCHERS4 Worry Anxiety Tension in muscles Concentration difficulty Hyperarousal (or irritability) Energy loss Restlessness Sleep disturbance | Posttraumatic stress disorder DREAMS6 Disinterest in usual activities Re-experience Event preceding symptoms Avoidance Month or more of symptoms Sympathetic arousal |
| Antidepressant discontinuation syndrome FINISH7 Flu-like symptoms Insomnia Nausea Imbalance Sensory disturbances Hyperarousal (anxiety/agitation) | Neuroleptic malignant syndrome FEVER8 Fever Encephalopathy Vital sign instability Elevated WBC/CPK Rigidity WBC: white blood cell count CPK: creatine phosphokinase | Serotonin syndrome HARMED Hyperthermia Autonomic instability Rigidity Myoclonus Encephalopathy Diaphoresis |
Mnemonics may use rhyme, music, or visual cues to enhance memory. Most mnemonics used in medical practice and education are word-based, including:
- Acronyms—words, each letter of which stands for a particular piece of information to be recalled (such as RICE for treatment of a sprained joint: rest, ice, compression, elevation).
- Acrostics—sentences with the first letter of each word prompting the desired recollection (such as “To Zanzibar by motor car” for the branches of the facial nerve: temporal, zygomatic, buccal, mandibular, cervical).
- Alphabetical sequences (such as ABCDE of trauma assessment: airway, breathing, circulation, disability, exposure).29
An appropriate teaching tool?
Dozens of mnemonics addressing psychiatric diagnosis and treatment have been published, but relatively few are widely used. Psychiatric educators may resist teaching with mnemonics, believing they might erode a humanistic approach to patients by reducing psychopathology to “a laundry list” of symptoms and the art of psychiatric diagnosis to a “check-box” endeavor. Mnemonics that use humor may be rejected as irreverent or unprofessional.30 Publishing a novel mnemonic may be viewed with disdain by some as an “easy” way of padding a curriculum vitae.
| Paranoid personality disorder SUSPECT9 Spousal infidelity suspected Unforgiving (bears grudges) Suspicious Perceives attacks (and reacts quickly) Enemy or friend? (suspects associates and friends) Confiding in others is feared Threats perceived in benign events | Schizotypal personality disorder ME PECULIAR9 Magical thinking Experiences unusual perceptions Paranoid ideation Eccentric behavior or appearance Constricted or inappropriate affect Unusual thinking or speech Lacks close friends Ideas of reference Anxiety in social situations Rule out psychotic or pervasive developmental disorders | Borderline personality disorder IMPULSIVE10 Impulsive Moodiness Paranoia or dissociation under stress Unstable self-image Labile intense relationships Suicidal gestures Inappropriate anger Vulnerability to abandonment Emptiness (feelings of) | Histrionic personality disorder PRAISE ME9 Provocative or seductive behavior Relationships considered more intimate than they are Attention (need to be the center of) Influenced easily Style of speech (impressionistic, lacking detail) Emotions (rapidly shifting, shallow) Make up (physical appearance used to draw attention to self) Emotions exaggerated | Narcissistic personality disorder GRANDIOSE11 Grandiose Requires attention Arrogant Need to be special Dreams of success and power Interpersonally exploitative Others (unable to recognize feelings/needs of) Sense of entitlement Envious | Dependent personality disorder RELIANCE9 Reassurance required Expressing disagreement difficult Life responsibilities assumed by others Initiating projects difficult Alone (feels helpless and uncomfortable when alone) Nurturance (goes to excessive lengths to obtain) Companionship sought urgently when a relationship ends Exaggerated fears of being left to care for self |
| Schizoid personality disorder DISTANT9 Detached or flattened affect Indifferent to criticism or praise Sexual experiences of little interest Tasks done solitarily Absence of close friends Neither desires nor enjoys close relationships Takes pleasure in few activities | Antisocial personality disorder CORRUPT9 Cannot conform to law Obligations ignored Reckless disregard for safety Remorseless Underhanded (deceitful) Planning insufficient (impulsive) Temper (irritable and aggressive) | Borderline personality disorder DESPAIRER* Disturbance of identity Emotionally labile Suicidal behavior Paranoia or dissociation Abandonment (fear of) Impulsive Relationships unstable Emptiness (feelings of) Rage (inappropriate) * Created by Jason P. Caplan, MD | Histrionic personality disorder ACTRESSS* Appearance focused Center of attention Theatrical Relationships (believed to be more intimate than they are) Easily influenced Seductive behavior Shallow emotions Speech (impressionistic and vague) * Created by Jason P. Caplan, MD | Avoidant personality disorder CRINGES9 Criticism or rejection preoccupies thoughts in social situations Restraint in relationships due to fear of shame Inhibited in new relationships Needs to be sure of being liked before engaging socially Gets around occupational activities with need for interpersonal contact Embarrassment prevents new activity or taking risks Self viewed as unappealing or inferior | Obsessive-compulsive personality disorder SCRIMPER* Stubborn Cannot discard worthless objects Rule obsessed Inflexible Miserly Perfectionistic Excludes leisure due to devotion to work Reluctant to delegate to others * Created by Jason P. Caplan, MD |
Entire Web sites exist to share mnemonics for medical education (see Related Resources). Thus it is likely that trainees are using them with or without their teachers’ supervision. Psychiatric educators need to be aware of the mnemonics their trainees are using and to:
- screen these tools for factual errors (such as incomplete diagnostic criteria)
- remind trainees that although mnemonics are useful, psychiatrists should approach patients as individuals without the prejudice of a potentially pejorative label.
Our methodology
In preparing this article, we gathered numerous mnemonics (some published and some novel) designed to capture the learner’s attention and impart information pertinent to psychiatric diagnosis and treatment. Whenever possible, we credited each mnemonic to its creator, but—given the difficulty in confirming authorship of (what in many cases has become) oral history—we’ve listed some mnemonics without citation.
Our list is far from complete because we likely are unaware of many mnemonics, and we have excluded some that seemed obscure, unwieldy, or redundant. We have not excluded mnemonics that some may view as pejorative but merely report their existence. Including them does not mean that we endorse them.
This article lists 32 mnemonics related to psychiatric diagnosis. Thus, it seems odd that an informal survey of >60 residents at the Massachusetts General Hospital (MGH)/McLean Residency Training Program in Psychiatry revealed that most were aware of only 2 or 3 psychiatric mnemonics, typically:
- SIG: E CAPS (a tool to recall the criteria for depression)
- DIG FAST (a list of criteria for diagnosing mania)
- WWHHHHIMPS (a tool for recalling life-threatening causes of delirium).
Although this unscientific survey may be biased because faculty or trainees at MGH created the above 3 mnemonics, it nonetheless begs the question of what qualities make a mnemonic memorable.
Learning theory provides several clues. George Miller’s classic 1956 paper, “The magical number seven, plus or minus two: some limits on our capacity for processing information,” discussed the finding that 7 seems to be the upper limit of individual pieces of data that can be easily remembered.31 Research also has shown that recruiting the limbic system (potentially through the use of humor) aids in the recall of otherwise dry, cortical information.32,33
Intuitively, it would seem that nonrepeating letters would facilitate the recall of the linked data, allowing each letter to provide a distinct cue, without any clouding by redundancy. Of the 3 most popular psychiatric mnemonics, however, only DIG FAST fits the learning theory. It contains 7 letters, repeats no letters, and has the limbic cue of allowing the learner to imagine a person with mania digging furiously.
| Substance dependence ADDICTeD12 Activities are given up or reduced Dependence, physical: tolerance Dependence, physical: withdrawal Intrapersonal (Internal) consequences, physical or psychological Can’t cut down or control use Time-consuming Duration or amount of use is greater than intended | Substance abuse WILD12 Work, school, or home role obligation failures Interpersonal or social consequences Legal problems Dangerous use | Alcohol abuse CAGE13 Have you ever felt you should CUT DOWN your drinking? Have people ANNOYED you by criticizing your drinking? Have you ever felt bad or GUILTY about your drinking? Have you ever had a drink first thing in the morning to steady your nerves or get rid of a hangover (EYE-OPENER)? |
SIG: E CAPS falls within the range of 7 plus or minus 2, includes a limbic cue (although often forgotten, it refers to the prescription of energy capsules for depression), but repeats the letter S.
WWHHHHIMPS, with 10 letters, exceeds the recommended range, repeats the W (appearing twice) and the H (appearing 4 times), and provides no clear limbic cue.
| Causes I WATCH DEATH Infection Withdrawal Acute metabolic Trauma CNS pathology Hypoxia Deficiencies Endocrinopathies Acute vascular Toxins or drugs Heavy metals | Life-threatening causes WWHHHHIMPS* Wernicke’s encephalopathy Withdrawal Hypertensive crisis Hypoperfusion/hypoxia of the brain Hypoglycemia Hyper/hypothermia Intracranial process/infection Metabolic/meningitis Poisons Status epilepticus * Created by Gary W. Small, MD | Deliriogenic medications ACUTE CHANGE IN MS14 Antibiotics Cardiac drugs Urinary incontinence drugs Theophylline Ethanol Corticosteroids H2 blockers Antiparkinsonian drugs Narcotics Geriatric psychiatric drugs ENT drugs Insomnia drugs NSAIDs Muscle relaxants Seizure medicines |
It may be that recruiting the limbic system provides the greatest likelihood of recall. Recruiting this system may add increased valence to a particular mnemonic for a specific individual, but this same limbic valence may limit its usefulness in a professional context.
- Free searchable database of medical mnemonics. www.medicalmnemonics.com.
- Robinson DJ. Mnemonics and more for psychiatry. Port Huron, MI: Rapid Psychler Press, 2001.
1. Abraham PF, Shirley ER. New mnemonic for depressive symptoms. Am J Psychiatry 2006;163(2):329-30.
2. Christman DS. “HE’S 2 SAD” detects dysthymic disorder. Current Psychiatry 2008;7(3):120.-
3. Coupland NJ. Worry WARTS have generalized anxiety disorder. Can J Psychiatry 2002;47(2):197.-
4. Berber MJ. WATCHERS: recognizing generalized anxiety disorder. J Clin Psychiatry 2000;61(6):447.-
5. Khouzam HR. A simple mnemonic for the diagnostic criteria for post-traumatic stress disorder. West J Med 2001;174(6):424.-
6. Short DD, Workman EA, Morse JH, Turner RL. Mnemonics for eight DSM-III-R disorders. Hosp Community Psychiatry 1992;43(6):642-4.
7. Berber MJ. FINISH: remembering the discontinuation syndrome. Flu-like symptoms, Insomnia, Nausea, Imbalance, Sensory disturbances, and Hyperarousal (anxiety/agitation). J Clin Psychiatry 1998;59(5):255.-
8. Christensen RC. Identify neuroleptic malignant syndrome with FEVER. Current Psychiatry 2005;4(7):102.-
9. Pinkofsky HB. Mnemonics for DSM-IV personality disorders. Psychiatr Serv 1997;48(9):1197-8.
10. Senger HL. Borderline mnemonic. Am J Psychiatry 1997;154(9):1321.-
11. Kim SI, Swanson TA, Caplan JP, eds. Underground clinical vignettes step 2: psychiatry. 4th ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2007:130.
12. Bogenschutz MP, Quinn DK. Acronyms for substance use disorders. J Clin Psychiatry 2001;62(6):474-5.
13. Ewing JA. Detecting alcoholism. The CAGE questionnaire. JAMA 1984;252(14):1905-7.
14. Flaherty JH. Psychotherapeutic agents in older adults. Commonly prescribed and over-the-counter remedies: causes of confusion. Clin Geriatr Med 1998;14:101-27.
15. Sweller J. Cognitive load theory, learning difficulty, and instructional design. Learn Instr 1994;4:295-312.
16. Squire LR. Memory and brain. New York, NY: Oxford University Press; 1987.
17. DeLuca J, Lengenfelder J, Eslinger P. Memory and learning. In: Rizzo M, Eslinger P, eds. Principles and practice of behavioral neurology and neuropsychology. Philadelphia, PA: Saunders; 2004:251.
18. Dash PK, Moore AN, Kobori N, et al. Molecular activity underlying working memory. Learn Mem 2007;14:554-63.
19. Awh E, Vogel EK, Oh SH. Interactions between attention and working memory. Neuroscience 2006;139:201-8.
20. Knudson EI. Fundamental components of attention. Ann Rev Neurosci 2007;30:57-78.
21. Postle BR. Working memory as an emergent property of the mind and brain. Neuroscience 2006;139:23-36.
22. Fletcher PC, Henson RN. Frontal lobes and human memory: Insights from functional neuroimaging. Brain 2001;124:849-81.
23. Miller EK, Cohen JD. An integrative theory of prefrontal cortex function. Ann Rev Neurosci 2001;24:167-202.
24. Schumacher EH, Lauber E, Awh E, et al. PET evidence for a modal verbal working memory system. Neuroimage 1996;3:79-88.
25. Smith EE, Jonides J, Koeppe RA. Dissociating verbal and spatial working memory using PET. Cereb Cortex 1996;6:11-20.
26. Wager TD, Smith EE. Neuroimaging studies of working memory: a meta-analysis. Cogn Affect Behav Neurosci 2003;3(4):255-74.
27. Frankland PW, Bontempi B. The organization of recent and remote memories. Nat Rev Neurosci 2005;6:119-30.
28. Sweller J. Cognitive load during problem solving: effects on learning. Cogn Sci 1988;12(1):257-85.
29. Beitz JM. Unleashing the power of memory: the mighty mnemonic. Nurse Educ 1997;22(2):25-9.
30. Larson EW. Criticism of mnemonic device. Am J Psychiatry 1990;147(7):963-4.
31. Miller GA. The magical number seven, plus or minus two: some limits on our capacity for processing information. Psychol Rev 1956;63:81-97.
32. Schmidt SR. Effects of humor on sentence memory. J Exp Psychol Learn Mem Cogn 1994;20(4):953-67.
33. Lippman LG, Dunn ML. Contextual connections within puns: effects on perceived humor and memory. J Gen Psychol 2000;127(2):185-97.
From SIG: E CAPS to CAGE and WWHHHHIMPS, mnemonics help practitioners and trainees recall important lists (such as criteria for depression, screening questions for alcoholism, or life-threatening causes of delirium, respectively). Mnemonics’ efficacy rests on the principle that grouped information is easier to remember than individual points of data.
Not everyone loves mnemonics, but recollecting diagnostic criteria is useful in clinical practice and research, on board examinations, and for insurance reimbursement. Thus, tools that assist in recalling diagnostic criteria have a role in psychiatric practice and teaching.
In this article, we present 32 mnemonics to help clinicians diagnose:
- affective disorders (Box 1)1,2
- anxiety disorders (Box 2)3-6
- medication adverse effects (Box 3)7,8
- personality disorders (Box 4)9-11
- addiction disorders (Box 5)12,13
- causes of delirium (Box 6).14
We also discuss how mnemonics improve one’s memory, based on the principles of learning theory.
How mnemonics work
A mnemonic—from the Greek word “mnemonikos” (“of memory”)—links new data with previously learned information. Mnemonics assist in learning by reducing the amount of information (“cognitive load”) that needs to be stored for long-term processing and retrieval.15
Memory, defined as the “persistence of learning in a state that can be revealed at a later time,”16 can be divided into 2 types:
- declarative (a conscious recollection of facts, such as remembering a relative’s birthday)
- procedural (skills-based learning, such as riding a bicycle).
Declarative memory has a conscious component and may be mediated by the medial temporal lobe and cortical association structures. Procedural memory has less of a conscious component; it may involve the basal ganglia, cerebellum, and a variety of cortical sensory-perceptive regions.17
| Depression SIG: E CAPS* Suicidal thoughts Interests decreased Guilt Energy decreased Concentration decreased Appetite disturbance (increased or decreased) Psychomotor changes (agitation or retardation) Sleep disturbance (increased or decreased) * Created by Carey Gross, MD | Dysthymia HE’S 2 SAD2 Hopelessness Energy loss or fatigue Self-esteem is low 2 years minimum of depressed mood most of the day, for more days than not Sleep is increased or decreased Appetite is increased or decreased Decision-making or concentration is impaired | Mania DIG FAST Distractibility Indiscretion Grandiosity Flight of ideas Activity increase Sleep deficit Talkativeness |
| Depression C GASP DIE1 Concentration decreased Guilt Appetite Sleep disturbance Psychomotor agitation or retardation Death or suicide (thoughts or acts of) Interests decreased Energy decreased | Hypomania TAD HIGH Talkative Attention deficit Decreased need for sleep High self-esteem/grandiosity Ideas that race Goal-directed activity increased High-risk activity | Mania DeTeR the HIGH* Distractibility Talkativeness Reckless behavior Hyposomnia Ideas that race Grandiosity Hypersexuality * Created by Carey Gross, MD |
Declarative memory can be subdivided into working memory and long-term memory.
With working memory, new items of information are held briefly so that encoding and eventual storage can take place.
Working memory guides decision-making and future planning and is intricately related to attention.18-21 Functional MRI and positron emission tomography as well as neurocognitive testing have shown that working memory tasks activate the prefrontal cortex and brain regions specific to language and visuospatial memory.
The hippocampus is thought to rapidly absorb new information, and this data is consolidated and permanently stored via the prefrontal cortex.22-26 Given the hippocampus’ limited storage capacity, new information (such as what you ate for breakfast 3 weeks ago) will disappear if it is not repeated regularly.17
Long-term memory, on the other hand, is encoded knowledge that is linked to facts learned in the past; it is consolidated in the brain and can be readily retrieved. Neuroimaging studies have demonstrated opposing patterns of activation in the hippocampus and prefrontal cortex, depending on whether the memory being recalled is:
- new (high hippocampal activity, low prefrontal cortex activity)
- old (low hippocampal activity, high prefrontal cortex activity).27
Mnemonics are thought to affect working memory by reducing the introduced cognitive load and increasing the efficiency of memory acquisition and encoding. They reduce cognitive load by grouping objects into a single verbal or visual cue that can be introduced into working memory. Learning is optimized when the load on working memory is minimized, enabling long-term memory to be facilitated.28
| Generalized anxiety disorder Worry WARTS3 Wound up Worn-out Absentminded Restless Touchy Sleepless | Posttraumatic stress disorder TRAUMA5 Traumatic event Re-experience Avoidance Unable to function Month or more of symptoms Arousal increased | Anxiety disorder due to a general medical condition Physical Diseases That Have Commonly Appeared Anxious: Pheochromocytoma Diabetes mellitus Temporal lobe epilepsy Hyperthyroidism Carcinoid Alcohol withdrawal Arrhythmias |
| Generalized anxiety disorder WATCHERS4 Worry Anxiety Tension in muscles Concentration difficulty Hyperarousal (or irritability) Energy loss Restlessness Sleep disturbance | Posttraumatic stress disorder DREAMS6 Disinterest in usual activities Re-experience Event preceding symptoms Avoidance Month or more of symptoms Sympathetic arousal |
| Antidepressant discontinuation syndrome FINISH7 Flu-like symptoms Insomnia Nausea Imbalance Sensory disturbances Hyperarousal (anxiety/agitation) | Neuroleptic malignant syndrome FEVER8 Fever Encephalopathy Vital sign instability Elevated WBC/CPK Rigidity WBC: white blood cell count CPK: creatine phosphokinase | Serotonin syndrome HARMED Hyperthermia Autonomic instability Rigidity Myoclonus Encephalopathy Diaphoresis |
Mnemonics may use rhyme, music, or visual cues to enhance memory. Most mnemonics used in medical practice and education are word-based, including:
- Acronyms—words, each letter of which stands for a particular piece of information to be recalled (such as RICE for treatment of a sprained joint: rest, ice, compression, elevation).
- Acrostics—sentences with the first letter of each word prompting the desired recollection (such as “To Zanzibar by motor car” for the branches of the facial nerve: temporal, zygomatic, buccal, mandibular, cervical).
- Alphabetical sequences (such as ABCDE of trauma assessment: airway, breathing, circulation, disability, exposure).29
An appropriate teaching tool?
Dozens of mnemonics addressing psychiatric diagnosis and treatment have been published, but relatively few are widely used. Psychiatric educators may resist teaching with mnemonics, believing they might erode a humanistic approach to patients by reducing psychopathology to “a laundry list” of symptoms and the art of psychiatric diagnosis to a “check-box” endeavor. Mnemonics that use humor may be rejected as irreverent or unprofessional.30 Publishing a novel mnemonic may be viewed with disdain by some as an “easy” way of padding a curriculum vitae.
| Paranoid personality disorder SUSPECT9 Spousal infidelity suspected Unforgiving (bears grudges) Suspicious Perceives attacks (and reacts quickly) Enemy or friend? (suspects associates and friends) Confiding in others is feared Threats perceived in benign events | Schizotypal personality disorder ME PECULIAR9 Magical thinking Experiences unusual perceptions Paranoid ideation Eccentric behavior or appearance Constricted or inappropriate affect Unusual thinking or speech Lacks close friends Ideas of reference Anxiety in social situations Rule out psychotic or pervasive developmental disorders | Borderline personality disorder IMPULSIVE10 Impulsive Moodiness Paranoia or dissociation under stress Unstable self-image Labile intense relationships Suicidal gestures Inappropriate anger Vulnerability to abandonment Emptiness (feelings of) | Histrionic personality disorder PRAISE ME9 Provocative or seductive behavior Relationships considered more intimate than they are Attention (need to be the center of) Influenced easily Style of speech (impressionistic, lacking detail) Emotions (rapidly shifting, shallow) Make up (physical appearance used to draw attention to self) Emotions exaggerated | Narcissistic personality disorder GRANDIOSE11 Grandiose Requires attention Arrogant Need to be special Dreams of success and power Interpersonally exploitative Others (unable to recognize feelings/needs of) Sense of entitlement Envious | Dependent personality disorder RELIANCE9 Reassurance required Expressing disagreement difficult Life responsibilities assumed by others Initiating projects difficult Alone (feels helpless and uncomfortable when alone) Nurturance (goes to excessive lengths to obtain) Companionship sought urgently when a relationship ends Exaggerated fears of being left to care for self |
| Schizoid personality disorder DISTANT9 Detached or flattened affect Indifferent to criticism or praise Sexual experiences of little interest Tasks done solitarily Absence of close friends Neither desires nor enjoys close relationships Takes pleasure in few activities | Antisocial personality disorder CORRUPT9 Cannot conform to law Obligations ignored Reckless disregard for safety Remorseless Underhanded (deceitful) Planning insufficient (impulsive) Temper (irritable and aggressive) | Borderline personality disorder DESPAIRER* Disturbance of identity Emotionally labile Suicidal behavior Paranoia or dissociation Abandonment (fear of) Impulsive Relationships unstable Emptiness (feelings of) Rage (inappropriate) * Created by Jason P. Caplan, MD | Histrionic personality disorder ACTRESSS* Appearance focused Center of attention Theatrical Relationships (believed to be more intimate than they are) Easily influenced Seductive behavior Shallow emotions Speech (impressionistic and vague) * Created by Jason P. Caplan, MD | Avoidant personality disorder CRINGES9 Criticism or rejection preoccupies thoughts in social situations Restraint in relationships due to fear of shame Inhibited in new relationships Needs to be sure of being liked before engaging socially Gets around occupational activities with need for interpersonal contact Embarrassment prevents new activity or taking risks Self viewed as unappealing or inferior | Obsessive-compulsive personality disorder SCRIMPER* Stubborn Cannot discard worthless objects Rule obsessed Inflexible Miserly Perfectionistic Excludes leisure due to devotion to work Reluctant to delegate to others * Created by Jason P. Caplan, MD |
Entire Web sites exist to share mnemonics for medical education (see Related Resources). Thus it is likely that trainees are using them with or without their teachers’ supervision. Psychiatric educators need to be aware of the mnemonics their trainees are using and to:
- screen these tools for factual errors (such as incomplete diagnostic criteria)
- remind trainees that although mnemonics are useful, psychiatrists should approach patients as individuals without the prejudice of a potentially pejorative label.
Our methodology
In preparing this article, we gathered numerous mnemonics (some published and some novel) designed to capture the learner’s attention and impart information pertinent to psychiatric diagnosis and treatment. Whenever possible, we credited each mnemonic to its creator, but—given the difficulty in confirming authorship of (what in many cases has become) oral history—we’ve listed some mnemonics without citation.
Our list is far from complete because we likely are unaware of many mnemonics, and we have excluded some that seemed obscure, unwieldy, or redundant. We have not excluded mnemonics that some may view as pejorative but merely report their existence. Including them does not mean that we endorse them.
This article lists 32 mnemonics related to psychiatric diagnosis. Thus, it seems odd that an informal survey of >60 residents at the Massachusetts General Hospital (MGH)/McLean Residency Training Program in Psychiatry revealed that most were aware of only 2 or 3 psychiatric mnemonics, typically:
- SIG: E CAPS (a tool to recall the criteria for depression)
- DIG FAST (a list of criteria for diagnosing mania)
- WWHHHHIMPS (a tool for recalling life-threatening causes of delirium).
Although this unscientific survey may be biased because faculty or trainees at MGH created the above 3 mnemonics, it nonetheless begs the question of what qualities make a mnemonic memorable.
Learning theory provides several clues. George Miller’s classic 1956 paper, “The magical number seven, plus or minus two: some limits on our capacity for processing information,” discussed the finding that 7 seems to be the upper limit of individual pieces of data that can be easily remembered.31 Research also has shown that recruiting the limbic system (potentially through the use of humor) aids in the recall of otherwise dry, cortical information.32,33
Intuitively, it would seem that nonrepeating letters would facilitate the recall of the linked data, allowing each letter to provide a distinct cue, without any clouding by redundancy. Of the 3 most popular psychiatric mnemonics, however, only DIG FAST fits the learning theory. It contains 7 letters, repeats no letters, and has the limbic cue of allowing the learner to imagine a person with mania digging furiously.
| Substance dependence ADDICTeD12 Activities are given up or reduced Dependence, physical: tolerance Dependence, physical: withdrawal Intrapersonal (Internal) consequences, physical or psychological Can’t cut down or control use Time-consuming Duration or amount of use is greater than intended | Substance abuse WILD12 Work, school, or home role obligation failures Interpersonal or social consequences Legal problems Dangerous use | Alcohol abuse CAGE13 Have you ever felt you should CUT DOWN your drinking? Have people ANNOYED you by criticizing your drinking? Have you ever felt bad or GUILTY about your drinking? Have you ever had a drink first thing in the morning to steady your nerves or get rid of a hangover (EYE-OPENER)? |
SIG: E CAPS falls within the range of 7 plus or minus 2, includes a limbic cue (although often forgotten, it refers to the prescription of energy capsules for depression), but repeats the letter S.
WWHHHHIMPS, with 10 letters, exceeds the recommended range, repeats the W (appearing twice) and the H (appearing 4 times), and provides no clear limbic cue.
| Causes I WATCH DEATH Infection Withdrawal Acute metabolic Trauma CNS pathology Hypoxia Deficiencies Endocrinopathies Acute vascular Toxins or drugs Heavy metals | Life-threatening causes WWHHHHIMPS* Wernicke’s encephalopathy Withdrawal Hypertensive crisis Hypoperfusion/hypoxia of the brain Hypoglycemia Hyper/hypothermia Intracranial process/infection Metabolic/meningitis Poisons Status epilepticus * Created by Gary W. Small, MD | Deliriogenic medications ACUTE CHANGE IN MS14 Antibiotics Cardiac drugs Urinary incontinence drugs Theophylline Ethanol Corticosteroids H2 blockers Antiparkinsonian drugs Narcotics Geriatric psychiatric drugs ENT drugs Insomnia drugs NSAIDs Muscle relaxants Seizure medicines |
It may be that recruiting the limbic system provides the greatest likelihood of recall. Recruiting this system may add increased valence to a particular mnemonic for a specific individual, but this same limbic valence may limit its usefulness in a professional context.
- Free searchable database of medical mnemonics. www.medicalmnemonics.com.
- Robinson DJ. Mnemonics and more for psychiatry. Port Huron, MI: Rapid Psychler Press, 2001.
From SIG: E CAPS to CAGE and WWHHHHIMPS, mnemonics help practitioners and trainees recall important lists (such as criteria for depression, screening questions for alcoholism, or life-threatening causes of delirium, respectively). Mnemonics’ efficacy rests on the principle that grouped information is easier to remember than individual points of data.
Not everyone loves mnemonics, but recollecting diagnostic criteria is useful in clinical practice and research, on board examinations, and for insurance reimbursement. Thus, tools that assist in recalling diagnostic criteria have a role in psychiatric practice and teaching.
In this article, we present 32 mnemonics to help clinicians diagnose:
- affective disorders (Box 1)1,2
- anxiety disorders (Box 2)3-6
- medication adverse effects (Box 3)7,8
- personality disorders (Box 4)9-11
- addiction disorders (Box 5)12,13
- causes of delirium (Box 6).14
We also discuss how mnemonics improve one’s memory, based on the principles of learning theory.
How mnemonics work
A mnemonic—from the Greek word “mnemonikos” (“of memory”)—links new data with previously learned information. Mnemonics assist in learning by reducing the amount of information (“cognitive load”) that needs to be stored for long-term processing and retrieval.15
Memory, defined as the “persistence of learning in a state that can be revealed at a later time,”16 can be divided into 2 types:
- declarative (a conscious recollection of facts, such as remembering a relative’s birthday)
- procedural (skills-based learning, such as riding a bicycle).
Declarative memory has a conscious component and may be mediated by the medial temporal lobe and cortical association structures. Procedural memory has less of a conscious component; it may involve the basal ganglia, cerebellum, and a variety of cortical sensory-perceptive regions.17
| Depression SIG: E CAPS* Suicidal thoughts Interests decreased Guilt Energy decreased Concentration decreased Appetite disturbance (increased or decreased) Psychomotor changes (agitation or retardation) Sleep disturbance (increased or decreased) * Created by Carey Gross, MD | Dysthymia HE’S 2 SAD2 Hopelessness Energy loss or fatigue Self-esteem is low 2 years minimum of depressed mood most of the day, for more days than not Sleep is increased or decreased Appetite is increased or decreased Decision-making or concentration is impaired | Mania DIG FAST Distractibility Indiscretion Grandiosity Flight of ideas Activity increase Sleep deficit Talkativeness |
| Depression C GASP DIE1 Concentration decreased Guilt Appetite Sleep disturbance Psychomotor agitation or retardation Death or suicide (thoughts or acts of) Interests decreased Energy decreased | Hypomania TAD HIGH Talkative Attention deficit Decreased need for sleep High self-esteem/grandiosity Ideas that race Goal-directed activity increased High-risk activity | Mania DeTeR the HIGH* Distractibility Talkativeness Reckless behavior Hyposomnia Ideas that race Grandiosity Hypersexuality * Created by Carey Gross, MD |
Declarative memory can be subdivided into working memory and long-term memory.
With working memory, new items of information are held briefly so that encoding and eventual storage can take place.
Working memory guides decision-making and future planning and is intricately related to attention.18-21 Functional MRI and positron emission tomography as well as neurocognitive testing have shown that working memory tasks activate the prefrontal cortex and brain regions specific to language and visuospatial memory.
The hippocampus is thought to rapidly absorb new information, and this data is consolidated and permanently stored via the prefrontal cortex.22-26 Given the hippocampus’ limited storage capacity, new information (such as what you ate for breakfast 3 weeks ago) will disappear if it is not repeated regularly.17
Long-term memory, on the other hand, is encoded knowledge that is linked to facts learned in the past; it is consolidated in the brain and can be readily retrieved. Neuroimaging studies have demonstrated opposing patterns of activation in the hippocampus and prefrontal cortex, depending on whether the memory being recalled is:
- new (high hippocampal activity, low prefrontal cortex activity)
- old (low hippocampal activity, high prefrontal cortex activity).27
Mnemonics are thought to affect working memory by reducing the introduced cognitive load and increasing the efficiency of memory acquisition and encoding. They reduce cognitive load by grouping objects into a single verbal or visual cue that can be introduced into working memory. Learning is optimized when the load on working memory is minimized, enabling long-term memory to be facilitated.28
| Generalized anxiety disorder Worry WARTS3 Wound up Worn-out Absentminded Restless Touchy Sleepless | Posttraumatic stress disorder TRAUMA5 Traumatic event Re-experience Avoidance Unable to function Month or more of symptoms Arousal increased | Anxiety disorder due to a general medical condition Physical Diseases That Have Commonly Appeared Anxious: Pheochromocytoma Diabetes mellitus Temporal lobe epilepsy Hyperthyroidism Carcinoid Alcohol withdrawal Arrhythmias |
| Generalized anxiety disorder WATCHERS4 Worry Anxiety Tension in muscles Concentration difficulty Hyperarousal (or irritability) Energy loss Restlessness Sleep disturbance | Posttraumatic stress disorder DREAMS6 Disinterest in usual activities Re-experience Event preceding symptoms Avoidance Month or more of symptoms Sympathetic arousal |
| Antidepressant discontinuation syndrome FINISH7 Flu-like symptoms Insomnia Nausea Imbalance Sensory disturbances Hyperarousal (anxiety/agitation) | Neuroleptic malignant syndrome FEVER8 Fever Encephalopathy Vital sign instability Elevated WBC/CPK Rigidity WBC: white blood cell count CPK: creatine phosphokinase | Serotonin syndrome HARMED Hyperthermia Autonomic instability Rigidity Myoclonus Encephalopathy Diaphoresis |
Mnemonics may use rhyme, music, or visual cues to enhance memory. Most mnemonics used in medical practice and education are word-based, including:
- Acronyms—words, each letter of which stands for a particular piece of information to be recalled (such as RICE for treatment of a sprained joint: rest, ice, compression, elevation).
- Acrostics—sentences with the first letter of each word prompting the desired recollection (such as “To Zanzibar by motor car” for the branches of the facial nerve: temporal, zygomatic, buccal, mandibular, cervical).
- Alphabetical sequences (such as ABCDE of trauma assessment: airway, breathing, circulation, disability, exposure).29
An appropriate teaching tool?
Dozens of mnemonics addressing psychiatric diagnosis and treatment have been published, but relatively few are widely used. Psychiatric educators may resist teaching with mnemonics, believing they might erode a humanistic approach to patients by reducing psychopathology to “a laundry list” of symptoms and the art of psychiatric diagnosis to a “check-box” endeavor. Mnemonics that use humor may be rejected as irreverent or unprofessional.30 Publishing a novel mnemonic may be viewed with disdain by some as an “easy” way of padding a curriculum vitae.
| Paranoid personality disorder SUSPECT9 Spousal infidelity suspected Unforgiving (bears grudges) Suspicious Perceives attacks (and reacts quickly) Enemy or friend? (suspects associates and friends) Confiding in others is feared Threats perceived in benign events | Schizotypal personality disorder ME PECULIAR9 Magical thinking Experiences unusual perceptions Paranoid ideation Eccentric behavior or appearance Constricted or inappropriate affect Unusual thinking or speech Lacks close friends Ideas of reference Anxiety in social situations Rule out psychotic or pervasive developmental disorders | Borderline personality disorder IMPULSIVE10 Impulsive Moodiness Paranoia or dissociation under stress Unstable self-image Labile intense relationships Suicidal gestures Inappropriate anger Vulnerability to abandonment Emptiness (feelings of) | Histrionic personality disorder PRAISE ME9 Provocative or seductive behavior Relationships considered more intimate than they are Attention (need to be the center of) Influenced easily Style of speech (impressionistic, lacking detail) Emotions (rapidly shifting, shallow) Make up (physical appearance used to draw attention to self) Emotions exaggerated | Narcissistic personality disorder GRANDIOSE11 Grandiose Requires attention Arrogant Need to be special Dreams of success and power Interpersonally exploitative Others (unable to recognize feelings/needs of) Sense of entitlement Envious | Dependent personality disorder RELIANCE9 Reassurance required Expressing disagreement difficult Life responsibilities assumed by others Initiating projects difficult Alone (feels helpless and uncomfortable when alone) Nurturance (goes to excessive lengths to obtain) Companionship sought urgently when a relationship ends Exaggerated fears of being left to care for self |
| Schizoid personality disorder DISTANT9 Detached or flattened affect Indifferent to criticism or praise Sexual experiences of little interest Tasks done solitarily Absence of close friends Neither desires nor enjoys close relationships Takes pleasure in few activities | Antisocial personality disorder CORRUPT9 Cannot conform to law Obligations ignored Reckless disregard for safety Remorseless Underhanded (deceitful) Planning insufficient (impulsive) Temper (irritable and aggressive) | Borderline personality disorder DESPAIRER* Disturbance of identity Emotionally labile Suicidal behavior Paranoia or dissociation Abandonment (fear of) Impulsive Relationships unstable Emptiness (feelings of) Rage (inappropriate) * Created by Jason P. Caplan, MD | Histrionic personality disorder ACTRESSS* Appearance focused Center of attention Theatrical Relationships (believed to be more intimate than they are) Easily influenced Seductive behavior Shallow emotions Speech (impressionistic and vague) * Created by Jason P. Caplan, MD | Avoidant personality disorder CRINGES9 Criticism or rejection preoccupies thoughts in social situations Restraint in relationships due to fear of shame Inhibited in new relationships Needs to be sure of being liked before engaging socially Gets around occupational activities with need for interpersonal contact Embarrassment prevents new activity or taking risks Self viewed as unappealing or inferior | Obsessive-compulsive personality disorder SCRIMPER* Stubborn Cannot discard worthless objects Rule obsessed Inflexible Miserly Perfectionistic Excludes leisure due to devotion to work Reluctant to delegate to others * Created by Jason P. Caplan, MD |
Entire Web sites exist to share mnemonics for medical education (see Related Resources). Thus it is likely that trainees are using them with or without their teachers’ supervision. Psychiatric educators need to be aware of the mnemonics their trainees are using and to:
- screen these tools for factual errors (such as incomplete diagnostic criteria)
- remind trainees that although mnemonics are useful, psychiatrists should approach patients as individuals without the prejudice of a potentially pejorative label.
Our methodology
In preparing this article, we gathered numerous mnemonics (some published and some novel) designed to capture the learner’s attention and impart information pertinent to psychiatric diagnosis and treatment. Whenever possible, we credited each mnemonic to its creator, but—given the difficulty in confirming authorship of (what in many cases has become) oral history—we’ve listed some mnemonics without citation.
Our list is far from complete because we likely are unaware of many mnemonics, and we have excluded some that seemed obscure, unwieldy, or redundant. We have not excluded mnemonics that some may view as pejorative but merely report their existence. Including them does not mean that we endorse them.
This article lists 32 mnemonics related to psychiatric diagnosis. Thus, it seems odd that an informal survey of >60 residents at the Massachusetts General Hospital (MGH)/McLean Residency Training Program in Psychiatry revealed that most were aware of only 2 or 3 psychiatric mnemonics, typically:
- SIG: E CAPS (a tool to recall the criteria for depression)
- DIG FAST (a list of criteria for diagnosing mania)
- WWHHHHIMPS (a tool for recalling life-threatening causes of delirium).
Although this unscientific survey may be biased because faculty or trainees at MGH created the above 3 mnemonics, it nonetheless begs the question of what qualities make a mnemonic memorable.
Learning theory provides several clues. George Miller’s classic 1956 paper, “The magical number seven, plus or minus two: some limits on our capacity for processing information,” discussed the finding that 7 seems to be the upper limit of individual pieces of data that can be easily remembered.31 Research also has shown that recruiting the limbic system (potentially through the use of humor) aids in the recall of otherwise dry, cortical information.32,33
Intuitively, it would seem that nonrepeating letters would facilitate the recall of the linked data, allowing each letter to provide a distinct cue, without any clouding by redundancy. Of the 3 most popular psychiatric mnemonics, however, only DIG FAST fits the learning theory. It contains 7 letters, repeats no letters, and has the limbic cue of allowing the learner to imagine a person with mania digging furiously.
| Substance dependence ADDICTeD12 Activities are given up or reduced Dependence, physical: tolerance Dependence, physical: withdrawal Intrapersonal (Internal) consequences, physical or psychological Can’t cut down or control use Time-consuming Duration or amount of use is greater than intended | Substance abuse WILD12 Work, school, or home role obligation failures Interpersonal or social consequences Legal problems Dangerous use | Alcohol abuse CAGE13 Have you ever felt you should CUT DOWN your drinking? Have people ANNOYED you by criticizing your drinking? Have you ever felt bad or GUILTY about your drinking? Have you ever had a drink first thing in the morning to steady your nerves or get rid of a hangover (EYE-OPENER)? |
SIG: E CAPS falls within the range of 7 plus or minus 2, includes a limbic cue (although often forgotten, it refers to the prescription of energy capsules for depression), but repeats the letter S.
WWHHHHIMPS, with 10 letters, exceeds the recommended range, repeats the W (appearing twice) and the H (appearing 4 times), and provides no clear limbic cue.
| Causes I WATCH DEATH Infection Withdrawal Acute metabolic Trauma CNS pathology Hypoxia Deficiencies Endocrinopathies Acute vascular Toxins or drugs Heavy metals | Life-threatening causes WWHHHHIMPS* Wernicke’s encephalopathy Withdrawal Hypertensive crisis Hypoperfusion/hypoxia of the brain Hypoglycemia Hyper/hypothermia Intracranial process/infection Metabolic/meningitis Poisons Status epilepticus * Created by Gary W. Small, MD | Deliriogenic medications ACUTE CHANGE IN MS14 Antibiotics Cardiac drugs Urinary incontinence drugs Theophylline Ethanol Corticosteroids H2 blockers Antiparkinsonian drugs Narcotics Geriatric psychiatric drugs ENT drugs Insomnia drugs NSAIDs Muscle relaxants Seizure medicines |
It may be that recruiting the limbic system provides the greatest likelihood of recall. Recruiting this system may add increased valence to a particular mnemonic for a specific individual, but this same limbic valence may limit its usefulness in a professional context.
- Free searchable database of medical mnemonics. www.medicalmnemonics.com.
- Robinson DJ. Mnemonics and more for psychiatry. Port Huron, MI: Rapid Psychler Press, 2001.
1. Abraham PF, Shirley ER. New mnemonic for depressive symptoms. Am J Psychiatry 2006;163(2):329-30.
2. Christman DS. “HE’S 2 SAD” detects dysthymic disorder. Current Psychiatry 2008;7(3):120.-
3. Coupland NJ. Worry WARTS have generalized anxiety disorder. Can J Psychiatry 2002;47(2):197.-
4. Berber MJ. WATCHERS: recognizing generalized anxiety disorder. J Clin Psychiatry 2000;61(6):447.-
5. Khouzam HR. A simple mnemonic for the diagnostic criteria for post-traumatic stress disorder. West J Med 2001;174(6):424.-
6. Short DD, Workman EA, Morse JH, Turner RL. Mnemonics for eight DSM-III-R disorders. Hosp Community Psychiatry 1992;43(6):642-4.
7. Berber MJ. FINISH: remembering the discontinuation syndrome. Flu-like symptoms, Insomnia, Nausea, Imbalance, Sensory disturbances, and Hyperarousal (anxiety/agitation). J Clin Psychiatry 1998;59(5):255.-
8. Christensen RC. Identify neuroleptic malignant syndrome with FEVER. Current Psychiatry 2005;4(7):102.-
9. Pinkofsky HB. Mnemonics for DSM-IV personality disorders. Psychiatr Serv 1997;48(9):1197-8.
10. Senger HL. Borderline mnemonic. Am J Psychiatry 1997;154(9):1321.-
11. Kim SI, Swanson TA, Caplan JP, eds. Underground clinical vignettes step 2: psychiatry. 4th ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2007:130.
12. Bogenschutz MP, Quinn DK. Acronyms for substance use disorders. J Clin Psychiatry 2001;62(6):474-5.
13. Ewing JA. Detecting alcoholism. The CAGE questionnaire. JAMA 1984;252(14):1905-7.
14. Flaherty JH. Psychotherapeutic agents in older adults. Commonly prescribed and over-the-counter remedies: causes of confusion. Clin Geriatr Med 1998;14:101-27.
15. Sweller J. Cognitive load theory, learning difficulty, and instructional design. Learn Instr 1994;4:295-312.
16. Squire LR. Memory and brain. New York, NY: Oxford University Press; 1987.
17. DeLuca J, Lengenfelder J, Eslinger P. Memory and learning. In: Rizzo M, Eslinger P, eds. Principles and practice of behavioral neurology and neuropsychology. Philadelphia, PA: Saunders; 2004:251.
18. Dash PK, Moore AN, Kobori N, et al. Molecular activity underlying working memory. Learn Mem 2007;14:554-63.
19. Awh E, Vogel EK, Oh SH. Interactions between attention and working memory. Neuroscience 2006;139:201-8.
20. Knudson EI. Fundamental components of attention. Ann Rev Neurosci 2007;30:57-78.
21. Postle BR. Working memory as an emergent property of the mind and brain. Neuroscience 2006;139:23-36.
22. Fletcher PC, Henson RN. Frontal lobes and human memory: Insights from functional neuroimaging. Brain 2001;124:849-81.
23. Miller EK, Cohen JD. An integrative theory of prefrontal cortex function. Ann Rev Neurosci 2001;24:167-202.
24. Schumacher EH, Lauber E, Awh E, et al. PET evidence for a modal verbal working memory system. Neuroimage 1996;3:79-88.
25. Smith EE, Jonides J, Koeppe RA. Dissociating verbal and spatial working memory using PET. Cereb Cortex 1996;6:11-20.
26. Wager TD, Smith EE. Neuroimaging studies of working memory: a meta-analysis. Cogn Affect Behav Neurosci 2003;3(4):255-74.
27. Frankland PW, Bontempi B. The organization of recent and remote memories. Nat Rev Neurosci 2005;6:119-30.
28. Sweller J. Cognitive load during problem solving: effects on learning. Cogn Sci 1988;12(1):257-85.
29. Beitz JM. Unleashing the power of memory: the mighty mnemonic. Nurse Educ 1997;22(2):25-9.
30. Larson EW. Criticism of mnemonic device. Am J Psychiatry 1990;147(7):963-4.
31. Miller GA. The magical number seven, plus or minus two: some limits on our capacity for processing information. Psychol Rev 1956;63:81-97.
32. Schmidt SR. Effects of humor on sentence memory. J Exp Psychol Learn Mem Cogn 1994;20(4):953-67.
33. Lippman LG, Dunn ML. Contextual connections within puns: effects on perceived humor and memory. J Gen Psychol 2000;127(2):185-97.
1. Abraham PF, Shirley ER. New mnemonic for depressive symptoms. Am J Psychiatry 2006;163(2):329-30.
2. Christman DS. “HE’S 2 SAD” detects dysthymic disorder. Current Psychiatry 2008;7(3):120.-
3. Coupland NJ. Worry WARTS have generalized anxiety disorder. Can J Psychiatry 2002;47(2):197.-
4. Berber MJ. WATCHERS: recognizing generalized anxiety disorder. J Clin Psychiatry 2000;61(6):447.-
5. Khouzam HR. A simple mnemonic for the diagnostic criteria for post-traumatic stress disorder. West J Med 2001;174(6):424.-
6. Short DD, Workman EA, Morse JH, Turner RL. Mnemonics for eight DSM-III-R disorders. Hosp Community Psychiatry 1992;43(6):642-4.
7. Berber MJ. FINISH: remembering the discontinuation syndrome. Flu-like symptoms, Insomnia, Nausea, Imbalance, Sensory disturbances, and Hyperarousal (anxiety/agitation). J Clin Psychiatry 1998;59(5):255.-
8. Christensen RC. Identify neuroleptic malignant syndrome with FEVER. Current Psychiatry 2005;4(7):102.-
9. Pinkofsky HB. Mnemonics for DSM-IV personality disorders. Psychiatr Serv 1997;48(9):1197-8.
10. Senger HL. Borderline mnemonic. Am J Psychiatry 1997;154(9):1321.-
11. Kim SI, Swanson TA, Caplan JP, eds. Underground clinical vignettes step 2: psychiatry. 4th ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2007:130.
12. Bogenschutz MP, Quinn DK. Acronyms for substance use disorders. J Clin Psychiatry 2001;62(6):474-5.
13. Ewing JA. Detecting alcoholism. The CAGE questionnaire. JAMA 1984;252(14):1905-7.
14. Flaherty JH. Psychotherapeutic agents in older adults. Commonly prescribed and over-the-counter remedies: causes of confusion. Clin Geriatr Med 1998;14:101-27.
15. Sweller J. Cognitive load theory, learning difficulty, and instructional design. Learn Instr 1994;4:295-312.
16. Squire LR. Memory and brain. New York, NY: Oxford University Press; 1987.
17. DeLuca J, Lengenfelder J, Eslinger P. Memory and learning. In: Rizzo M, Eslinger P, eds. Principles and practice of behavioral neurology and neuropsychology. Philadelphia, PA: Saunders; 2004:251.
18. Dash PK, Moore AN, Kobori N, et al. Molecular activity underlying working memory. Learn Mem 2007;14:554-63.
19. Awh E, Vogel EK, Oh SH. Interactions between attention and working memory. Neuroscience 2006;139:201-8.
20. Knudson EI. Fundamental components of attention. Ann Rev Neurosci 2007;30:57-78.
21. Postle BR. Working memory as an emergent property of the mind and brain. Neuroscience 2006;139:23-36.
22. Fletcher PC, Henson RN. Frontal lobes and human memory: Insights from functional neuroimaging. Brain 2001;124:849-81.
23. Miller EK, Cohen JD. An integrative theory of prefrontal cortex function. Ann Rev Neurosci 2001;24:167-202.
24. Schumacher EH, Lauber E, Awh E, et al. PET evidence for a modal verbal working memory system. Neuroimage 1996;3:79-88.
25. Smith EE, Jonides J, Koeppe RA. Dissociating verbal and spatial working memory using PET. Cereb Cortex 1996;6:11-20.
26. Wager TD, Smith EE. Neuroimaging studies of working memory: a meta-analysis. Cogn Affect Behav Neurosci 2003;3(4):255-74.
27. Frankland PW, Bontempi B. The organization of recent and remote memories. Nat Rev Neurosci 2005;6:119-30.
28. Sweller J. Cognitive load during problem solving: effects on learning. Cogn Sci 1988;12(1):257-85.
29. Beitz JM. Unleashing the power of memory: the mighty mnemonic. Nurse Educ 1997;22(2):25-9.
30. Larson EW. Criticism of mnemonic device. Am J Psychiatry 1990;147(7):963-4.
31. Miller GA. The magical number seven, plus or minus two: some limits on our capacity for processing information. Psychol Rev 1956;63:81-97.
32. Schmidt SR. Effects of humor on sentence memory. J Exp Psychol Learn Mem Cogn 1994;20(4):953-67.
33. Lippman LG, Dunn ML. Contextual connections within puns: effects on perceived humor and memory. J Gen Psychol 2000;127(2):185-97.
Put your patients to sleep: Useful nondrug strategies for chronic insomnia
Ms. H, age 53, has a 20-year history of recurrent major depressive disorder. She seeks treatment for insomnia; her primary complaint is that “no medicine has really ever helped me to sleep for very long.” She reports that every night she experiences a 2-hour sleep onset delay and an average of 5 awakenings that last 10 to 60 minutes each. Her mood is stable.
After failed trials of zolpidem, mirtazapine, amitriptyline, and sertraline plus trazodone, she improves with quetiapine, 50 mg at bedtime, plus sertraline, 150 mg at bedtime. Unfortunately, over the next 6 months Ms. H gains 20 pounds and her physician becomes concerned about her fasting serum glucose levels, which suggest borderline diabetes.
After Ms. H discontinues quetiapine, onset and maintenance insomnia remain clinically significant. Polysomnography reveals moderately loud snoring, a normal respiratory disturbance index of 4.5 per hour, no periodic leg movements of sleep, 32-minute sleep onset, total sleep time of 389 minutes (6.5 hours), and a sleep efficiency of 72%. Ms. H estimates that it took her 120 minutes to fall asleep and that she slept only 270 minutes (4.5 hours) of the 540 minutes (9 hours) in bed. The sleep specialist recommends cognitive-behavioral therapy for insomnia.
For some chronic insomnia patients—such as Ms. H—pharmacotherapy is ineffective or causes intolerable side effects. In any year, >50% of adults in the general population report experiencing difficulty falling asleep, staying asleep, early awakening, or poorly restorative sleep, but these symptoms are usually time-limited and have only a small impact on daytime alertness and function. Chronic insomnia, on the other hand, lasts ≥1 month and has substantial impact on daytime alertness and attention, cognitive function, depressed and anxious mood, and focused performance (Box).1
Medications used to treat insomnia include FDA-approved drugs such as eszopiclone and zolpidem and off-label agents such as mirtazapine and trazodone. The cognitive, behavioral, and other nonpharmacologic therapies described below can be effective options, either alone or in combination with medication.
One in 10 adults in industrialized nations experiences chronic insomnia. Women are affected twice as often as men, with higher rates also reported in older patients and those in lower socioeconomic groups.
Among adults with chronic insomnia, 35% to 45% have psychiatric comorbidities, such as anxiety or mood disorders, and 15% have primary insomnia—sleep disturbance with no identifiable cause, which traditional medical literature described as conditioned or psychophysiologic insomnia.
In the remaining cases, chronic insomnia is associated with:
- medical and sleep disorders (restless legs syndrome, periodic leg movements of sleep, and sleep apnea)
- general medical disorders, particularly those that cause pain
- use of medications that disrupt normal CNS sleep mechanisms.
Source: Reference 1
Assessing insomnia
Start by performing a thorough assessment and history. I have described this process in previous reviews,1,2 as has Neubauer in Current Psychiatry.3
Before initiating therapy for insomnia, assess and address the following:
- significant ongoing depression, mania, hypomania, generalized anxiety, panic, or obsessive-compulsive symptoms that impact sleep
- primary medical disorders of sleep, including restless legs syndrome, increased motor activity during sleep such as periodic leg movements of sleep, and the snoring/snorting of sleep apnea
- prescribed or self-administered medications or substances that can disrupt sleep, such as alcohol, caffeine, stimulants, corticosteroids, or beta blockers.
Recommended nondrug therapies
In 2006, the Standards of Practice Committee of the American Academy of Sleep Medicine (AASM) updated a comprehensive literature review of psychological and behavioral treatments of primary and secondary insomnia. On the basis of this peer-reviewed, graded evidence, the AASM recommended:
- stimulus control therapy
- relaxation training
- cognitive-behavioral therapy for insomnia (CBTi).4
The AASM also offered guidelines for sleep restriction therapy, multi-component therapy without cognitive therapy, paradoxical intention, and biofeedback. Evidence for sleep hygiene, imaging training, or cognitive therapy alone was insufficient, and the AASM neither recommended nor excluded these methods. Psychological and behavioral interventions were considered effective for treating insomnia in older adults and patients withdrawing from hypnotics.
Stimulus control therapy. Bootzin et al5 first evaluated stimulus control therapy for conditioned insomnia (subsequently identified as primary insomnia). This therapy’s goal is to interrupt the conditioned activation that occurs at bedtime. Patients are instructed to:
- go to bed when sleepy
- remain in bed for no more than 10 minutes (20 minutes if elderly) without sleeping
- if unable to sleep, get up, do something boring, and return to bed only when sleepy
- repeat getting up and returning as frequently as necessary until sleep onset.
For the first 2 weeks of stimulus control therapy, patients are required to self-monitor their sleep behaviors using a sleep diary. Stimulus control therapy is beneficial for primary insomnia and insomnia related to anxious preoccupation. About 70% of patients with conditioned insomnia will improve using stimulus control therapy,4 but it is not clear whether the primary effective intervention is:
- patients dissociating conditioned responses at bedtime, or
- the inevitable sleep restriction caused by getting out of bed.
Relaxation training. Progressive muscle relaxation is a common behavioral treatment of insomnia. Patients learn to tense and then relax individual muscles, beginning at the feet or head and working their way up or down the body. Patients are taught the difference between tension and relaxation to facilitate a relaxation response at bedtime. Another method is the body scanning technique, in which the patient “talks” to each body part, telling it to “relax… relax… relax.”
Relaxation training is predicated on the belief that insomnia is caused by somatized tension and psychophysiologic arousal. The greatest challenge to effective relaxation training is that patients need extensive daytime practice before they can bring the method to the bedroom.
Remind patients that “practice makes perfect.” Therapists often instruct patients to start practicing their relaxation method during the day while self-monitoring by sleep diary and restricting time in bed at night.2
CBTi is the most extensively investigated nonpharmacologic therapy for insomnia.6 It has been used to effectively manage comorbid insomnia in patients with psychiatric disorders,7,8 such as depression,9 generalized anxiety,10 and alcohol dependence,11 as well as those with breast cancer,12 traumatic brain injury,13 and fibromyalgia.14 Age does not appear to be a limitation; research trials show the technique is effective in elderly patients.15
CBTi incorporates cognitive strategies and behavioral interventions to improve sleep quality. Patient self-monitoring with sleep diaries and worksheets is essential.
CBTi commonly is provided in 5 to 8 sessions over 8 to 12 weeks, although studies have described abbreviated practices that used 2 sessions16 and CBTi delivered over the Internet.17 Highly trained clinical psychologists are at the forefront of therapy, but counselors and nurses in primary care settings have administered CBTi.18 For primary insomnia, CBTi is superior in efficacy to pharmacotherapy:
- as initial treatment19
- for long-term management4
- in assisting discontinuation of hypnotic medication.20
CASE CONTINUED: An effective approach
You refer Ms. H to a clinical psychologist who specializes in CBTi. Ms. H begins self-monitoring with a sleep diary and has 5 CBTi sessions over 8 weeks. Initial interventions reduce time in bed from 9 hours to 7 hours per night. Ms. H learns simple relaxation methods that she practices for 2 weeks before attempting to use them to sleep. The psychologist addresses her dysfunctional beliefs about sleep.
During the last 2 weeks of therapy, Ms. H’s sleep diary reveals a sleep efficiency of 92% and improvements in well being, energy, and perceived work efficiency. At a 3-month booster visit, Ms. H has sustained these gains in sleep and daytime function.
Implementing nondrug therapy
I recommend the following steps when offering psychological and behavioral treatment of chronic insomnia, such as CBTi.
Initial visit. Determine whether your patient needs treatment for depressive or anxiety symptoms. Assess the need for polysomnography. Does the patient have a history of an urge to move the legs (restless legs syndrome), increased kicking behavior at night (periodic leg movements of sleep), or loud, disruptive snoring (obstructive sleep apnea)? It is often helpful to have patients think back to when they were consistently sleeping well to identify factors that might be exacerbating poor sleep.
Session 1 (Week 0). Teach patients about normal sleep, how it changes over the life cycle, and common dysfunctional beliefs and behaviors that worsen sleep. Tell patients that every morning when they wake up they should complete a sleep diary (Table 1); you can download a sample sleep diary by visiting this article on CurrentPsychiatry.com.
Table 1
Insomnia: What to document on a sleep diary
| Daytime fatigue |
| Minutes spent napping |
| Medication use |
| Time the patient first tried to fall asleep |
| How long it took to fall asleep |
| How many times the patient woke up |
| Final waking time |
| Hours slept |
| Sleep quality rating |
| How refreshed the patient feels on awakening |
Session 2 (Week 1). Review the sleep diary. Address infractions of sleep hygiene, such as working until bedtime, using caffeine or alcohol in the evening, excessive smoking, or eating in bed. Discuss and specify mutual therapeutic goals for:
- minutes to sleep onset
- minutes of nighttime wakefulness
- number of awakenings
- improvements in sleep efficiency, morning refreshment/alertness, and daytime functioning.
Therapeutic intervention: Instruct patients to reduce their total time in bed (TIB) to their estimated total sleep time, unless they report <6 hours. Insomnia patients commonly overestimate their amount of wakefulness. Because research indicates daytime performance is adversely affected when sleep falls below 6 hours per night,21 I initially limit TIB to 6 hours and further restrict TIB in future sessions as needed to improve sleep efficiency.
Session 3 (Week 2). Review the sleep diary, and calculate the average time to sleep onset and sleep efficiency (divide total minutes of reported sleep by the total minutes spent in bed). Typical goals include an average onset of 10 to 20 minutes and an average efficiency of >90%.
Therapeutic intervention: If sleep efficiency falls below 80%, further restrict TIB by 15 minutes; if sleep efficiency is >90%, increase TIB by 15 minutes (no TIB change is needed with efficiencies between 80% and 90%). Identify dysfunctional beliefs about sleep, and provide strategies to interrupt cognitive overactivation—the pressured “talking to oneself” in hopes of falling asleep.
Session 4 (Week 3). Review the sleep diary, and calculate the average time to sleep onset and sleep efficiency. Increase or decrease TIB based on sleep efficiency as described above. Determine if the patient has dysfunctional beliefs regarding sleep.
Therapeutic intervention: Reframe the patient’s dysfunctional beliefs/concepts by comparing sleep diary entries with dysfunctional beliefs (Table 2). Remind patients about strategies to address cognitive overactivation, and have them practice daily to apply the appropriate reframe response from Table 2 that improves sleep. Review progressive muscular relaxation to address somatized tension and arousal, but instruct patients to practice relaxation only during the day at this point.
Table 2
Correcting patients’ dysfunctional sleep beliefs/concepts
| Belief/concept | Reframe responses |
|---|---|
| ‘I need 8 hours sleep per night’ | 1. Nightly sleep need varies among individuals from 5 to 9 hours, particularly with aging 2. Employed adults sleep 6.5 to 7 hours per workweek night 3. For the ‘average’ person, it takes <6 hours of sleep to reduce performance |
| ‘If I don’t sleep, I can’t _____ (work, socialize, take care of the kids, etc.) or ‘If I don’t sleep tonight, I won’t be able to ____’ | 1. Every day one-third of Americans sleep <6.5 hours and yet work, socialize, and live their lives 2. ‘You told me that on ____ you had a terrible night, yet you did ____ (that presentation, meeting, activity with family, etc.)’ |
| ‘If I don’t sleep, I feel _____’ | Explore situations where the person has felt tired, irritable, angry, anxious, etc. independent from lack of sleep |
| ‘If X happens, I won’t sleep’ | Explore situations where X or something like it happened, yet sleep occurred |
| ‘I don’t sleep at all’ | 1. Explore whether a bed partner reports the patient was sleeping or snoring when the person was convinced he or she was awake 2. Tell patients that if they remain in bed for >30 minutes, it is likely they slept, particularly if anxious or frustrated (older depressed patients may be an exception) 3. Teach patients that ‘don’t at all’ statements often represent an excessive focus on wakefulness, and that self-monitoring by sleep diary is helpful |
Session 5 (Week 4). Review the sleep diary. Adjust TIB as necessary. Emphasize the patient’s mastery of dysfunctional beliefs, and highlight progress on the sleep diary. Spend much of this session helping patients improve their relaxation practice and preparing them to bring it to bedtime.
Therapeutic intervention: Tell the patient to apply the relaxation training to bedtime and nocturnal awakenings.
Session 6 (Week 6). Review the sleep diary. Emphasize progress. Address any problem areas regarding dysfunctional beliefs, maladaptive behaviors, or relaxation methods.
Therapeutic intervention: Prepare patients to maintain sleep gains on their own.
Session 7 (Week 8). Review the sleep diary. Have patients identify areas of mastery. Discuss scenarios that might be expected to result in a temporary return of insomnia—such as difficulties with work or home life, stress of job change, or medical illness—and strategies they could apply to improve sleep. Such strategies might include a “safety net” of a sedative/hypnotic agent to use after ≥2 nights of poor sleep.
‘Booster’ session. Three months later, schedule a booster session to determine whether the patient has maintained mastery of improved sleep. Patients who are doing well often cancel this session because they are satisfied with their progress.
Related resource
- American Academy of Sleep Medicine. www.aasmnet.org.
Drug brand names
- Amitriptyline • Elavil, Endep
- Eszopiclone • Lunesta
- Mirtazapine • Remeron
- Quetiapine • Seroquel
- Sertraline • Zoloft
- Trazodone • Desyrel
- Zolpidem • Ambien
Disclosure
Dr. Becker receives research/grant support from sanofi-aventis and is a speaker for Sepracor Inc. and Takeda Pharmaceutical.
1. Becker PM. Insomnia: prevalence, impact, pathogenesis, differential diagnosis, and evaluation. Psychiatr Clin North Am 2006;29(4):855-70.
2. Becker PM. Pharmacologic and nonpharmacologic treatments of insomnia. Neurol Clin 2005;23(4):1149-63.
3. Neubauer DN. Treatment resistant-insomnia: ask yourself 8 questions. Current Psychiatry 2007;6(12):46-54.
4. Morgenthaler T, Kramer M, Alessi C, et al. American Academy of Sleep Medicine. Practice parameters for the psychological and behavioral treatment of insomnia: an update. An American Academy of Sleep Medicine report. Sleep 2006;29(11):1415-9.
5. Bootzin RR, Perlis ML. Nonpharmacologic treatments of insomnia. J Clin Psychiatry 1992;53(suppl):37-41.
6. Morin CM, Bootzin RR, Buysse DJ, et al. Psychological and behavioral treatment of insomnia: update of the recent evidence (1998-2004). Sleep 2006;29(11):1398-414.
7. Smith MT, Huang MI, Manber R. Cognitive behavior therapy for chronic insomnia occurring within the context of medical and psychiatric disorders. Clin Psychol Rev 2005;25(5):559-92.
8. Dopke CA, Lehner RK, Wells AM. Cognitive-behavioral group therapy for insomnia in individuals with serious mental illnesses: a preliminary evaluation. Psychiatr Rehabil J 2004;27(3):235-42.
9. Carney CE, Segal ZV, Edinger JD, Krystal AD. A comparison of rates of residual insomnia symptoms following pharmacotherapy or cognitive-behavioral therapy for major depressive disorder. J Clin Psychiatry 2007;68(2):254-60.
10. Bélanger L, Morin CM, Langlois F, Ladouceur R. Insomnia and generalized anxiety disorder: effects of cognitive behavior therapy for GAD on insomnia symptoms. J Anxiety Disord 2004;18(4):561-71.
11. Currie SR, Clark S, Hodgins DC, El-Guebaly N. Randomized controlled trial of brief cognitive-behavioural interventions for insomnia in recovering alcoholics. Addiction 2004;99(9):1121-32.
12. Epstein DR, Dirksen SR. Randomized trial of a cognitive-behavioral intervention for insomnia in breast cancer survivors. Oncol Nurs Forum 2007;34(5):E51-9.
13. Ouellet MC, Morin CM. Efficacy of cognitive-behavioral therapy for insomnia associated with traumatic brain injury: a single-case experimental design. Arch Phys Med Rehabil 2007;88(12):1581-92.
14. Edinger JD, Wohlgemuth WK, Krystal AD, Rice JR. Behavioral insomnia therapy for fibromyalgia patients: a randomized clinical trial. Arch Intern Med 2005;165(21):2527-35.
15. Irwin MR, Cole JC, Nicassio PM. Comparative meta-analysis of behavioral interventions for insomnia and their efficacy in middle-aged adults and in older adults 55+ years of age. Health Psychol 2006;25(1):3-14.
16. Edinger JD, Wohlgemuth WK, Radtke RA, et al. Dose-response effects of cognitive-behavioral insomnia therapy: a randomized clinical trial. Sleep 2007;30(2):203-12.
17. Ström L, Pettersson R, Andersson G. Internet-based treatment for insomnia: a controlled evaluation. J Consult Clin Psychol 2004;72(1):113-20.
18. Espie CA, MacMahon KM, Kelly HL, et al. Randomized clinical effectiveness trial of nurse-administered small-group cognitive behavior therapy for persistent insomnia in general practice. Sleep 2007;30(5):574-84.
19. Jacobs GD, Pace-Schott EF, Stickgold R, Otto MW. Cognitive behavior therapy and pharmacotherapy for insomnia: a randomized controlled trial and direct comparison. Arch Intern Med 2004;164(17):1888-96.
20. Morin CM, Bélanger L, Bastien C, Vallières A. Long-term outcome after discontinuation of benzodiazepines for insomnia: a survival analysis of relapse. Behav Res Ther 2005;43(1):1-14.
21. Lim J, Dinges DF. Sleep deprivation and vigilant attention. Ann N Y Acad Sci 2008;1129:305-22.
Ms. H, age 53, has a 20-year history of recurrent major depressive disorder. She seeks treatment for insomnia; her primary complaint is that “no medicine has really ever helped me to sleep for very long.” She reports that every night she experiences a 2-hour sleep onset delay and an average of 5 awakenings that last 10 to 60 minutes each. Her mood is stable.
After failed trials of zolpidem, mirtazapine, amitriptyline, and sertraline plus trazodone, she improves with quetiapine, 50 mg at bedtime, plus sertraline, 150 mg at bedtime. Unfortunately, over the next 6 months Ms. H gains 20 pounds and her physician becomes concerned about her fasting serum glucose levels, which suggest borderline diabetes.
After Ms. H discontinues quetiapine, onset and maintenance insomnia remain clinically significant. Polysomnography reveals moderately loud snoring, a normal respiratory disturbance index of 4.5 per hour, no periodic leg movements of sleep, 32-minute sleep onset, total sleep time of 389 minutes (6.5 hours), and a sleep efficiency of 72%. Ms. H estimates that it took her 120 minutes to fall asleep and that she slept only 270 minutes (4.5 hours) of the 540 minutes (9 hours) in bed. The sleep specialist recommends cognitive-behavioral therapy for insomnia.
For some chronic insomnia patients—such as Ms. H—pharmacotherapy is ineffective or causes intolerable side effects. In any year, >50% of adults in the general population report experiencing difficulty falling asleep, staying asleep, early awakening, or poorly restorative sleep, but these symptoms are usually time-limited and have only a small impact on daytime alertness and function. Chronic insomnia, on the other hand, lasts ≥1 month and has substantial impact on daytime alertness and attention, cognitive function, depressed and anxious mood, and focused performance (Box).1
Medications used to treat insomnia include FDA-approved drugs such as eszopiclone and zolpidem and off-label agents such as mirtazapine and trazodone. The cognitive, behavioral, and other nonpharmacologic therapies described below can be effective options, either alone or in combination with medication.
One in 10 adults in industrialized nations experiences chronic insomnia. Women are affected twice as often as men, with higher rates also reported in older patients and those in lower socioeconomic groups.
Among adults with chronic insomnia, 35% to 45% have psychiatric comorbidities, such as anxiety or mood disorders, and 15% have primary insomnia—sleep disturbance with no identifiable cause, which traditional medical literature described as conditioned or psychophysiologic insomnia.
In the remaining cases, chronic insomnia is associated with:
- medical and sleep disorders (restless legs syndrome, periodic leg movements of sleep, and sleep apnea)
- general medical disorders, particularly those that cause pain
- use of medications that disrupt normal CNS sleep mechanisms.
Source: Reference 1
Assessing insomnia
Start by performing a thorough assessment and history. I have described this process in previous reviews,1,2 as has Neubauer in Current Psychiatry.3
Before initiating therapy for insomnia, assess and address the following:
- significant ongoing depression, mania, hypomania, generalized anxiety, panic, or obsessive-compulsive symptoms that impact sleep
- primary medical disorders of sleep, including restless legs syndrome, increased motor activity during sleep such as periodic leg movements of sleep, and the snoring/snorting of sleep apnea
- prescribed or self-administered medications or substances that can disrupt sleep, such as alcohol, caffeine, stimulants, corticosteroids, or beta blockers.
Recommended nondrug therapies
In 2006, the Standards of Practice Committee of the American Academy of Sleep Medicine (AASM) updated a comprehensive literature review of psychological and behavioral treatments of primary and secondary insomnia. On the basis of this peer-reviewed, graded evidence, the AASM recommended:
- stimulus control therapy
- relaxation training
- cognitive-behavioral therapy for insomnia (CBTi).4
The AASM also offered guidelines for sleep restriction therapy, multi-component therapy without cognitive therapy, paradoxical intention, and biofeedback. Evidence for sleep hygiene, imaging training, or cognitive therapy alone was insufficient, and the AASM neither recommended nor excluded these methods. Psychological and behavioral interventions were considered effective for treating insomnia in older adults and patients withdrawing from hypnotics.
Stimulus control therapy. Bootzin et al5 first evaluated stimulus control therapy for conditioned insomnia (subsequently identified as primary insomnia). This therapy’s goal is to interrupt the conditioned activation that occurs at bedtime. Patients are instructed to:
- go to bed when sleepy
- remain in bed for no more than 10 minutes (20 minutes if elderly) without sleeping
- if unable to sleep, get up, do something boring, and return to bed only when sleepy
- repeat getting up and returning as frequently as necessary until sleep onset.
For the first 2 weeks of stimulus control therapy, patients are required to self-monitor their sleep behaviors using a sleep diary. Stimulus control therapy is beneficial for primary insomnia and insomnia related to anxious preoccupation. About 70% of patients with conditioned insomnia will improve using stimulus control therapy,4 but it is not clear whether the primary effective intervention is:
- patients dissociating conditioned responses at bedtime, or
- the inevitable sleep restriction caused by getting out of bed.
Relaxation training. Progressive muscle relaxation is a common behavioral treatment of insomnia. Patients learn to tense and then relax individual muscles, beginning at the feet or head and working their way up or down the body. Patients are taught the difference between tension and relaxation to facilitate a relaxation response at bedtime. Another method is the body scanning technique, in which the patient “talks” to each body part, telling it to “relax… relax… relax.”
Relaxation training is predicated on the belief that insomnia is caused by somatized tension and psychophysiologic arousal. The greatest challenge to effective relaxation training is that patients need extensive daytime practice before they can bring the method to the bedroom.
Remind patients that “practice makes perfect.” Therapists often instruct patients to start practicing their relaxation method during the day while self-monitoring by sleep diary and restricting time in bed at night.2
CBTi is the most extensively investigated nonpharmacologic therapy for insomnia.6 It has been used to effectively manage comorbid insomnia in patients with psychiatric disorders,7,8 such as depression,9 generalized anxiety,10 and alcohol dependence,11 as well as those with breast cancer,12 traumatic brain injury,13 and fibromyalgia.14 Age does not appear to be a limitation; research trials show the technique is effective in elderly patients.15
CBTi incorporates cognitive strategies and behavioral interventions to improve sleep quality. Patient self-monitoring with sleep diaries and worksheets is essential.
CBTi commonly is provided in 5 to 8 sessions over 8 to 12 weeks, although studies have described abbreviated practices that used 2 sessions16 and CBTi delivered over the Internet.17 Highly trained clinical psychologists are at the forefront of therapy, but counselors and nurses in primary care settings have administered CBTi.18 For primary insomnia, CBTi is superior in efficacy to pharmacotherapy:
- as initial treatment19
- for long-term management4
- in assisting discontinuation of hypnotic medication.20
CASE CONTINUED: An effective approach
You refer Ms. H to a clinical psychologist who specializes in CBTi. Ms. H begins self-monitoring with a sleep diary and has 5 CBTi sessions over 8 weeks. Initial interventions reduce time in bed from 9 hours to 7 hours per night. Ms. H learns simple relaxation methods that she practices for 2 weeks before attempting to use them to sleep. The psychologist addresses her dysfunctional beliefs about sleep.
During the last 2 weeks of therapy, Ms. H’s sleep diary reveals a sleep efficiency of 92% and improvements in well being, energy, and perceived work efficiency. At a 3-month booster visit, Ms. H has sustained these gains in sleep and daytime function.
Implementing nondrug therapy
I recommend the following steps when offering psychological and behavioral treatment of chronic insomnia, such as CBTi.
Initial visit. Determine whether your patient needs treatment for depressive or anxiety symptoms. Assess the need for polysomnography. Does the patient have a history of an urge to move the legs (restless legs syndrome), increased kicking behavior at night (periodic leg movements of sleep), or loud, disruptive snoring (obstructive sleep apnea)? It is often helpful to have patients think back to when they were consistently sleeping well to identify factors that might be exacerbating poor sleep.
Session 1 (Week 0). Teach patients about normal sleep, how it changes over the life cycle, and common dysfunctional beliefs and behaviors that worsen sleep. Tell patients that every morning when they wake up they should complete a sleep diary (Table 1); you can download a sample sleep diary by visiting this article on CurrentPsychiatry.com.
Table 1
Insomnia: What to document on a sleep diary
| Daytime fatigue |
| Minutes spent napping |
| Medication use |
| Time the patient first tried to fall asleep |
| How long it took to fall asleep |
| How many times the patient woke up |
| Final waking time |
| Hours slept |
| Sleep quality rating |
| How refreshed the patient feels on awakening |
Session 2 (Week 1). Review the sleep diary. Address infractions of sleep hygiene, such as working until bedtime, using caffeine or alcohol in the evening, excessive smoking, or eating in bed. Discuss and specify mutual therapeutic goals for:
- minutes to sleep onset
- minutes of nighttime wakefulness
- number of awakenings
- improvements in sleep efficiency, morning refreshment/alertness, and daytime functioning.
Therapeutic intervention: Instruct patients to reduce their total time in bed (TIB) to their estimated total sleep time, unless they report <6 hours. Insomnia patients commonly overestimate their amount of wakefulness. Because research indicates daytime performance is adversely affected when sleep falls below 6 hours per night,21 I initially limit TIB to 6 hours and further restrict TIB in future sessions as needed to improve sleep efficiency.
Session 3 (Week 2). Review the sleep diary, and calculate the average time to sleep onset and sleep efficiency (divide total minutes of reported sleep by the total minutes spent in bed). Typical goals include an average onset of 10 to 20 minutes and an average efficiency of >90%.
Therapeutic intervention: If sleep efficiency falls below 80%, further restrict TIB by 15 minutes; if sleep efficiency is >90%, increase TIB by 15 minutes (no TIB change is needed with efficiencies between 80% and 90%). Identify dysfunctional beliefs about sleep, and provide strategies to interrupt cognitive overactivation—the pressured “talking to oneself” in hopes of falling asleep.
Session 4 (Week 3). Review the sleep diary, and calculate the average time to sleep onset and sleep efficiency. Increase or decrease TIB based on sleep efficiency as described above. Determine if the patient has dysfunctional beliefs regarding sleep.
Therapeutic intervention: Reframe the patient’s dysfunctional beliefs/concepts by comparing sleep diary entries with dysfunctional beliefs (Table 2). Remind patients about strategies to address cognitive overactivation, and have them practice daily to apply the appropriate reframe response from Table 2 that improves sleep. Review progressive muscular relaxation to address somatized tension and arousal, but instruct patients to practice relaxation only during the day at this point.
Table 2
Correcting patients’ dysfunctional sleep beliefs/concepts
| Belief/concept | Reframe responses |
|---|---|
| ‘I need 8 hours sleep per night’ | 1. Nightly sleep need varies among individuals from 5 to 9 hours, particularly with aging 2. Employed adults sleep 6.5 to 7 hours per workweek night 3. For the ‘average’ person, it takes <6 hours of sleep to reduce performance |
| ‘If I don’t sleep, I can’t _____ (work, socialize, take care of the kids, etc.) or ‘If I don’t sleep tonight, I won’t be able to ____’ | 1. Every day one-third of Americans sleep <6.5 hours and yet work, socialize, and live their lives 2. ‘You told me that on ____ you had a terrible night, yet you did ____ (that presentation, meeting, activity with family, etc.)’ |
| ‘If I don’t sleep, I feel _____’ | Explore situations where the person has felt tired, irritable, angry, anxious, etc. independent from lack of sleep |
| ‘If X happens, I won’t sleep’ | Explore situations where X or something like it happened, yet sleep occurred |
| ‘I don’t sleep at all’ | 1. Explore whether a bed partner reports the patient was sleeping or snoring when the person was convinced he or she was awake 2. Tell patients that if they remain in bed for >30 minutes, it is likely they slept, particularly if anxious or frustrated (older depressed patients may be an exception) 3. Teach patients that ‘don’t at all’ statements often represent an excessive focus on wakefulness, and that self-monitoring by sleep diary is helpful |
Session 5 (Week 4). Review the sleep diary. Adjust TIB as necessary. Emphasize the patient’s mastery of dysfunctional beliefs, and highlight progress on the sleep diary. Spend much of this session helping patients improve their relaxation practice and preparing them to bring it to bedtime.
Therapeutic intervention: Tell the patient to apply the relaxation training to bedtime and nocturnal awakenings.
Session 6 (Week 6). Review the sleep diary. Emphasize progress. Address any problem areas regarding dysfunctional beliefs, maladaptive behaviors, or relaxation methods.
Therapeutic intervention: Prepare patients to maintain sleep gains on their own.
Session 7 (Week 8). Review the sleep diary. Have patients identify areas of mastery. Discuss scenarios that might be expected to result in a temporary return of insomnia—such as difficulties with work or home life, stress of job change, or medical illness—and strategies they could apply to improve sleep. Such strategies might include a “safety net” of a sedative/hypnotic agent to use after ≥2 nights of poor sleep.
‘Booster’ session. Three months later, schedule a booster session to determine whether the patient has maintained mastery of improved sleep. Patients who are doing well often cancel this session because they are satisfied with their progress.
Related resource
- American Academy of Sleep Medicine. www.aasmnet.org.
Drug brand names
- Amitriptyline • Elavil, Endep
- Eszopiclone • Lunesta
- Mirtazapine • Remeron
- Quetiapine • Seroquel
- Sertraline • Zoloft
- Trazodone • Desyrel
- Zolpidem • Ambien
Disclosure
Dr. Becker receives research/grant support from sanofi-aventis and is a speaker for Sepracor Inc. and Takeda Pharmaceutical.
Ms. H, age 53, has a 20-year history of recurrent major depressive disorder. She seeks treatment for insomnia; her primary complaint is that “no medicine has really ever helped me to sleep for very long.” She reports that every night she experiences a 2-hour sleep onset delay and an average of 5 awakenings that last 10 to 60 minutes each. Her mood is stable.
After failed trials of zolpidem, mirtazapine, amitriptyline, and sertraline plus trazodone, she improves with quetiapine, 50 mg at bedtime, plus sertraline, 150 mg at bedtime. Unfortunately, over the next 6 months Ms. H gains 20 pounds and her physician becomes concerned about her fasting serum glucose levels, which suggest borderline diabetes.
After Ms. H discontinues quetiapine, onset and maintenance insomnia remain clinically significant. Polysomnography reveals moderately loud snoring, a normal respiratory disturbance index of 4.5 per hour, no periodic leg movements of sleep, 32-minute sleep onset, total sleep time of 389 minutes (6.5 hours), and a sleep efficiency of 72%. Ms. H estimates that it took her 120 minutes to fall asleep and that she slept only 270 minutes (4.5 hours) of the 540 minutes (9 hours) in bed. The sleep specialist recommends cognitive-behavioral therapy for insomnia.
For some chronic insomnia patients—such as Ms. H—pharmacotherapy is ineffective or causes intolerable side effects. In any year, >50% of adults in the general population report experiencing difficulty falling asleep, staying asleep, early awakening, or poorly restorative sleep, but these symptoms are usually time-limited and have only a small impact on daytime alertness and function. Chronic insomnia, on the other hand, lasts ≥1 month and has substantial impact on daytime alertness and attention, cognitive function, depressed and anxious mood, and focused performance (Box).1
Medications used to treat insomnia include FDA-approved drugs such as eszopiclone and zolpidem and off-label agents such as mirtazapine and trazodone. The cognitive, behavioral, and other nonpharmacologic therapies described below can be effective options, either alone or in combination with medication.
One in 10 adults in industrialized nations experiences chronic insomnia. Women are affected twice as often as men, with higher rates also reported in older patients and those in lower socioeconomic groups.
Among adults with chronic insomnia, 35% to 45% have psychiatric comorbidities, such as anxiety or mood disorders, and 15% have primary insomnia—sleep disturbance with no identifiable cause, which traditional medical literature described as conditioned or psychophysiologic insomnia.
In the remaining cases, chronic insomnia is associated with:
- medical and sleep disorders (restless legs syndrome, periodic leg movements of sleep, and sleep apnea)
- general medical disorders, particularly those that cause pain
- use of medications that disrupt normal CNS sleep mechanisms.
Source: Reference 1
Assessing insomnia
Start by performing a thorough assessment and history. I have described this process in previous reviews,1,2 as has Neubauer in Current Psychiatry.3
Before initiating therapy for insomnia, assess and address the following:
- significant ongoing depression, mania, hypomania, generalized anxiety, panic, or obsessive-compulsive symptoms that impact sleep
- primary medical disorders of sleep, including restless legs syndrome, increased motor activity during sleep such as periodic leg movements of sleep, and the snoring/snorting of sleep apnea
- prescribed or self-administered medications or substances that can disrupt sleep, such as alcohol, caffeine, stimulants, corticosteroids, or beta blockers.
Recommended nondrug therapies
In 2006, the Standards of Practice Committee of the American Academy of Sleep Medicine (AASM) updated a comprehensive literature review of psychological and behavioral treatments of primary and secondary insomnia. On the basis of this peer-reviewed, graded evidence, the AASM recommended:
- stimulus control therapy
- relaxation training
- cognitive-behavioral therapy for insomnia (CBTi).4
The AASM also offered guidelines for sleep restriction therapy, multi-component therapy without cognitive therapy, paradoxical intention, and biofeedback. Evidence for sleep hygiene, imaging training, or cognitive therapy alone was insufficient, and the AASM neither recommended nor excluded these methods. Psychological and behavioral interventions were considered effective for treating insomnia in older adults and patients withdrawing from hypnotics.
Stimulus control therapy. Bootzin et al5 first evaluated stimulus control therapy for conditioned insomnia (subsequently identified as primary insomnia). This therapy’s goal is to interrupt the conditioned activation that occurs at bedtime. Patients are instructed to:
- go to bed when sleepy
- remain in bed for no more than 10 minutes (20 minutes if elderly) without sleeping
- if unable to sleep, get up, do something boring, and return to bed only when sleepy
- repeat getting up and returning as frequently as necessary until sleep onset.
For the first 2 weeks of stimulus control therapy, patients are required to self-monitor their sleep behaviors using a sleep diary. Stimulus control therapy is beneficial for primary insomnia and insomnia related to anxious preoccupation. About 70% of patients with conditioned insomnia will improve using stimulus control therapy,4 but it is not clear whether the primary effective intervention is:
- patients dissociating conditioned responses at bedtime, or
- the inevitable sleep restriction caused by getting out of bed.
Relaxation training. Progressive muscle relaxation is a common behavioral treatment of insomnia. Patients learn to tense and then relax individual muscles, beginning at the feet or head and working their way up or down the body. Patients are taught the difference between tension and relaxation to facilitate a relaxation response at bedtime. Another method is the body scanning technique, in which the patient “talks” to each body part, telling it to “relax… relax… relax.”
Relaxation training is predicated on the belief that insomnia is caused by somatized tension and psychophysiologic arousal. The greatest challenge to effective relaxation training is that patients need extensive daytime practice before they can bring the method to the bedroom.
Remind patients that “practice makes perfect.” Therapists often instruct patients to start practicing their relaxation method during the day while self-monitoring by sleep diary and restricting time in bed at night.2
CBTi is the most extensively investigated nonpharmacologic therapy for insomnia.6 It has been used to effectively manage comorbid insomnia in patients with psychiatric disorders,7,8 such as depression,9 generalized anxiety,10 and alcohol dependence,11 as well as those with breast cancer,12 traumatic brain injury,13 and fibromyalgia.14 Age does not appear to be a limitation; research trials show the technique is effective in elderly patients.15
CBTi incorporates cognitive strategies and behavioral interventions to improve sleep quality. Patient self-monitoring with sleep diaries and worksheets is essential.
CBTi commonly is provided in 5 to 8 sessions over 8 to 12 weeks, although studies have described abbreviated practices that used 2 sessions16 and CBTi delivered over the Internet.17 Highly trained clinical psychologists are at the forefront of therapy, but counselors and nurses in primary care settings have administered CBTi.18 For primary insomnia, CBTi is superior in efficacy to pharmacotherapy:
- as initial treatment19
- for long-term management4
- in assisting discontinuation of hypnotic medication.20
CASE CONTINUED: An effective approach
You refer Ms. H to a clinical psychologist who specializes in CBTi. Ms. H begins self-monitoring with a sleep diary and has 5 CBTi sessions over 8 weeks. Initial interventions reduce time in bed from 9 hours to 7 hours per night. Ms. H learns simple relaxation methods that she practices for 2 weeks before attempting to use them to sleep. The psychologist addresses her dysfunctional beliefs about sleep.
During the last 2 weeks of therapy, Ms. H’s sleep diary reveals a sleep efficiency of 92% and improvements in well being, energy, and perceived work efficiency. At a 3-month booster visit, Ms. H has sustained these gains in sleep and daytime function.
Implementing nondrug therapy
I recommend the following steps when offering psychological and behavioral treatment of chronic insomnia, such as CBTi.
Initial visit. Determine whether your patient needs treatment for depressive or anxiety symptoms. Assess the need for polysomnography. Does the patient have a history of an urge to move the legs (restless legs syndrome), increased kicking behavior at night (periodic leg movements of sleep), or loud, disruptive snoring (obstructive sleep apnea)? It is often helpful to have patients think back to when they were consistently sleeping well to identify factors that might be exacerbating poor sleep.
Session 1 (Week 0). Teach patients about normal sleep, how it changes over the life cycle, and common dysfunctional beliefs and behaviors that worsen sleep. Tell patients that every morning when they wake up they should complete a sleep diary (Table 1); you can download a sample sleep diary by visiting this article on CurrentPsychiatry.com.
Table 1
Insomnia: What to document on a sleep diary
| Daytime fatigue |
| Minutes spent napping |
| Medication use |
| Time the patient first tried to fall asleep |
| How long it took to fall asleep |
| How many times the patient woke up |
| Final waking time |
| Hours slept |
| Sleep quality rating |
| How refreshed the patient feels on awakening |
Session 2 (Week 1). Review the sleep diary. Address infractions of sleep hygiene, such as working until bedtime, using caffeine or alcohol in the evening, excessive smoking, or eating in bed. Discuss and specify mutual therapeutic goals for:
- minutes to sleep onset
- minutes of nighttime wakefulness
- number of awakenings
- improvements in sleep efficiency, morning refreshment/alertness, and daytime functioning.
Therapeutic intervention: Instruct patients to reduce their total time in bed (TIB) to their estimated total sleep time, unless they report <6 hours. Insomnia patients commonly overestimate their amount of wakefulness. Because research indicates daytime performance is adversely affected when sleep falls below 6 hours per night,21 I initially limit TIB to 6 hours and further restrict TIB in future sessions as needed to improve sleep efficiency.
Session 3 (Week 2). Review the sleep diary, and calculate the average time to sleep onset and sleep efficiency (divide total minutes of reported sleep by the total minutes spent in bed). Typical goals include an average onset of 10 to 20 minutes and an average efficiency of >90%.
Therapeutic intervention: If sleep efficiency falls below 80%, further restrict TIB by 15 minutes; if sleep efficiency is >90%, increase TIB by 15 minutes (no TIB change is needed with efficiencies between 80% and 90%). Identify dysfunctional beliefs about sleep, and provide strategies to interrupt cognitive overactivation—the pressured “talking to oneself” in hopes of falling asleep.
Session 4 (Week 3). Review the sleep diary, and calculate the average time to sleep onset and sleep efficiency. Increase or decrease TIB based on sleep efficiency as described above. Determine if the patient has dysfunctional beliefs regarding sleep.
Therapeutic intervention: Reframe the patient’s dysfunctional beliefs/concepts by comparing sleep diary entries with dysfunctional beliefs (Table 2). Remind patients about strategies to address cognitive overactivation, and have them practice daily to apply the appropriate reframe response from Table 2 that improves sleep. Review progressive muscular relaxation to address somatized tension and arousal, but instruct patients to practice relaxation only during the day at this point.
Table 2
Correcting patients’ dysfunctional sleep beliefs/concepts
| Belief/concept | Reframe responses |
|---|---|
| ‘I need 8 hours sleep per night’ | 1. Nightly sleep need varies among individuals from 5 to 9 hours, particularly with aging 2. Employed adults sleep 6.5 to 7 hours per workweek night 3. For the ‘average’ person, it takes <6 hours of sleep to reduce performance |
| ‘If I don’t sleep, I can’t _____ (work, socialize, take care of the kids, etc.) or ‘If I don’t sleep tonight, I won’t be able to ____’ | 1. Every day one-third of Americans sleep <6.5 hours and yet work, socialize, and live their lives 2. ‘You told me that on ____ you had a terrible night, yet you did ____ (that presentation, meeting, activity with family, etc.)’ |
| ‘If I don’t sleep, I feel _____’ | Explore situations where the person has felt tired, irritable, angry, anxious, etc. independent from lack of sleep |
| ‘If X happens, I won’t sleep’ | Explore situations where X or something like it happened, yet sleep occurred |
| ‘I don’t sleep at all’ | 1. Explore whether a bed partner reports the patient was sleeping or snoring when the person was convinced he or she was awake 2. Tell patients that if they remain in bed for >30 minutes, it is likely they slept, particularly if anxious or frustrated (older depressed patients may be an exception) 3. Teach patients that ‘don’t at all’ statements often represent an excessive focus on wakefulness, and that self-monitoring by sleep diary is helpful |
Session 5 (Week 4). Review the sleep diary. Adjust TIB as necessary. Emphasize the patient’s mastery of dysfunctional beliefs, and highlight progress on the sleep diary. Spend much of this session helping patients improve their relaxation practice and preparing them to bring it to bedtime.
Therapeutic intervention: Tell the patient to apply the relaxation training to bedtime and nocturnal awakenings.
Session 6 (Week 6). Review the sleep diary. Emphasize progress. Address any problem areas regarding dysfunctional beliefs, maladaptive behaviors, or relaxation methods.
Therapeutic intervention: Prepare patients to maintain sleep gains on their own.
Session 7 (Week 8). Review the sleep diary. Have patients identify areas of mastery. Discuss scenarios that might be expected to result in a temporary return of insomnia—such as difficulties with work or home life, stress of job change, or medical illness—and strategies they could apply to improve sleep. Such strategies might include a “safety net” of a sedative/hypnotic agent to use after ≥2 nights of poor sleep.
‘Booster’ session. Three months later, schedule a booster session to determine whether the patient has maintained mastery of improved sleep. Patients who are doing well often cancel this session because they are satisfied with their progress.
Related resource
- American Academy of Sleep Medicine. www.aasmnet.org.
Drug brand names
- Amitriptyline • Elavil, Endep
- Eszopiclone • Lunesta
- Mirtazapine • Remeron
- Quetiapine • Seroquel
- Sertraline • Zoloft
- Trazodone • Desyrel
- Zolpidem • Ambien
Disclosure
Dr. Becker receives research/grant support from sanofi-aventis and is a speaker for Sepracor Inc. and Takeda Pharmaceutical.
1. Becker PM. Insomnia: prevalence, impact, pathogenesis, differential diagnosis, and evaluation. Psychiatr Clin North Am 2006;29(4):855-70.
2. Becker PM. Pharmacologic and nonpharmacologic treatments of insomnia. Neurol Clin 2005;23(4):1149-63.
3. Neubauer DN. Treatment resistant-insomnia: ask yourself 8 questions. Current Psychiatry 2007;6(12):46-54.
4. Morgenthaler T, Kramer M, Alessi C, et al. American Academy of Sleep Medicine. Practice parameters for the psychological and behavioral treatment of insomnia: an update. An American Academy of Sleep Medicine report. Sleep 2006;29(11):1415-9.
5. Bootzin RR, Perlis ML. Nonpharmacologic treatments of insomnia. J Clin Psychiatry 1992;53(suppl):37-41.
6. Morin CM, Bootzin RR, Buysse DJ, et al. Psychological and behavioral treatment of insomnia: update of the recent evidence (1998-2004). Sleep 2006;29(11):1398-414.
7. Smith MT, Huang MI, Manber R. Cognitive behavior therapy for chronic insomnia occurring within the context of medical and psychiatric disorders. Clin Psychol Rev 2005;25(5):559-92.
8. Dopke CA, Lehner RK, Wells AM. Cognitive-behavioral group therapy for insomnia in individuals with serious mental illnesses: a preliminary evaluation. Psychiatr Rehabil J 2004;27(3):235-42.
9. Carney CE, Segal ZV, Edinger JD, Krystal AD. A comparison of rates of residual insomnia symptoms following pharmacotherapy or cognitive-behavioral therapy for major depressive disorder. J Clin Psychiatry 2007;68(2):254-60.
10. Bélanger L, Morin CM, Langlois F, Ladouceur R. Insomnia and generalized anxiety disorder: effects of cognitive behavior therapy for GAD on insomnia symptoms. J Anxiety Disord 2004;18(4):561-71.
11. Currie SR, Clark S, Hodgins DC, El-Guebaly N. Randomized controlled trial of brief cognitive-behavioural interventions for insomnia in recovering alcoholics. Addiction 2004;99(9):1121-32.
12. Epstein DR, Dirksen SR. Randomized trial of a cognitive-behavioral intervention for insomnia in breast cancer survivors. Oncol Nurs Forum 2007;34(5):E51-9.
13. Ouellet MC, Morin CM. Efficacy of cognitive-behavioral therapy for insomnia associated with traumatic brain injury: a single-case experimental design. Arch Phys Med Rehabil 2007;88(12):1581-92.
14. Edinger JD, Wohlgemuth WK, Krystal AD, Rice JR. Behavioral insomnia therapy for fibromyalgia patients: a randomized clinical trial. Arch Intern Med 2005;165(21):2527-35.
15. Irwin MR, Cole JC, Nicassio PM. Comparative meta-analysis of behavioral interventions for insomnia and their efficacy in middle-aged adults and in older adults 55+ years of age. Health Psychol 2006;25(1):3-14.
16. Edinger JD, Wohlgemuth WK, Radtke RA, et al. Dose-response effects of cognitive-behavioral insomnia therapy: a randomized clinical trial. Sleep 2007;30(2):203-12.
17. Ström L, Pettersson R, Andersson G. Internet-based treatment for insomnia: a controlled evaluation. J Consult Clin Psychol 2004;72(1):113-20.
18. Espie CA, MacMahon KM, Kelly HL, et al. Randomized clinical effectiveness trial of nurse-administered small-group cognitive behavior therapy for persistent insomnia in general practice. Sleep 2007;30(5):574-84.
19. Jacobs GD, Pace-Schott EF, Stickgold R, Otto MW. Cognitive behavior therapy and pharmacotherapy for insomnia: a randomized controlled trial and direct comparison. Arch Intern Med 2004;164(17):1888-96.
20. Morin CM, Bélanger L, Bastien C, Vallières A. Long-term outcome after discontinuation of benzodiazepines for insomnia: a survival analysis of relapse. Behav Res Ther 2005;43(1):1-14.
21. Lim J, Dinges DF. Sleep deprivation and vigilant attention. Ann N Y Acad Sci 2008;1129:305-22.
1. Becker PM. Insomnia: prevalence, impact, pathogenesis, differential diagnosis, and evaluation. Psychiatr Clin North Am 2006;29(4):855-70.
2. Becker PM. Pharmacologic and nonpharmacologic treatments of insomnia. Neurol Clin 2005;23(4):1149-63.
3. Neubauer DN. Treatment resistant-insomnia: ask yourself 8 questions. Current Psychiatry 2007;6(12):46-54.
4. Morgenthaler T, Kramer M, Alessi C, et al. American Academy of Sleep Medicine. Practice parameters for the psychological and behavioral treatment of insomnia: an update. An American Academy of Sleep Medicine report. Sleep 2006;29(11):1415-9.
5. Bootzin RR, Perlis ML. Nonpharmacologic treatments of insomnia. J Clin Psychiatry 1992;53(suppl):37-41.
6. Morin CM, Bootzin RR, Buysse DJ, et al. Psychological and behavioral treatment of insomnia: update of the recent evidence (1998-2004). Sleep 2006;29(11):1398-414.
7. Smith MT, Huang MI, Manber R. Cognitive behavior therapy for chronic insomnia occurring within the context of medical and psychiatric disorders. Clin Psychol Rev 2005;25(5):559-92.
8. Dopke CA, Lehner RK, Wells AM. Cognitive-behavioral group therapy for insomnia in individuals with serious mental illnesses: a preliminary evaluation. Psychiatr Rehabil J 2004;27(3):235-42.
9. Carney CE, Segal ZV, Edinger JD, Krystal AD. A comparison of rates of residual insomnia symptoms following pharmacotherapy or cognitive-behavioral therapy for major depressive disorder. J Clin Psychiatry 2007;68(2):254-60.
10. Bélanger L, Morin CM, Langlois F, Ladouceur R. Insomnia and generalized anxiety disorder: effects of cognitive behavior therapy for GAD on insomnia symptoms. J Anxiety Disord 2004;18(4):561-71.
11. Currie SR, Clark S, Hodgins DC, El-Guebaly N. Randomized controlled trial of brief cognitive-behavioural interventions for insomnia in recovering alcoholics. Addiction 2004;99(9):1121-32.
12. Epstein DR, Dirksen SR. Randomized trial of a cognitive-behavioral intervention for insomnia in breast cancer survivors. Oncol Nurs Forum 2007;34(5):E51-9.
13. Ouellet MC, Morin CM. Efficacy of cognitive-behavioral therapy for insomnia associated with traumatic brain injury: a single-case experimental design. Arch Phys Med Rehabil 2007;88(12):1581-92.
14. Edinger JD, Wohlgemuth WK, Krystal AD, Rice JR. Behavioral insomnia therapy for fibromyalgia patients: a randomized clinical trial. Arch Intern Med 2005;165(21):2527-35.
15. Irwin MR, Cole JC, Nicassio PM. Comparative meta-analysis of behavioral interventions for insomnia and their efficacy in middle-aged adults and in older adults 55+ years of age. Health Psychol 2006;25(1):3-14.
16. Edinger JD, Wohlgemuth WK, Radtke RA, et al. Dose-response effects of cognitive-behavioral insomnia therapy: a randomized clinical trial. Sleep 2007;30(2):203-12.
17. Ström L, Pettersson R, Andersson G. Internet-based treatment for insomnia: a controlled evaluation. J Consult Clin Psychol 2004;72(1):113-20.
18. Espie CA, MacMahon KM, Kelly HL, et al. Randomized clinical effectiveness trial of nurse-administered small-group cognitive behavior therapy for persistent insomnia in general practice. Sleep 2007;30(5):574-84.
19. Jacobs GD, Pace-Schott EF, Stickgold R, Otto MW. Cognitive behavior therapy and pharmacotherapy for insomnia: a randomized controlled trial and direct comparison. Arch Intern Med 2004;164(17):1888-96.
20. Morin CM, Bélanger L, Bastien C, Vallières A. Long-term outcome after discontinuation of benzodiazepines for insomnia: a survival analysis of relapse. Behav Res Ther 2005;43(1):1-14.
21. Lim J, Dinges DF. Sleep deprivation and vigilant attention. Ann N Y Acad Sci 2008;1129:305-22.
How seizure disorders change depression treatment
Ms. A, age 29, has had depression for 6 years and has taken antidepressants with inconsistent response. For 3 weeks, while not taking any antidepressant, she reports loss of energy; feeling sad, subdued, and tearful; poor concentration; and reduced interest in enjoyable activities including sex, the same symptoms she ?rst reported 6 years ago. She has no appetite but has not lost weight.
Several times a month Ms. A “loses” short periods of time. For example she says sometimes she cannot remember what happens between parking her car and sitting at her desk at work. After these episodes, which began 9 years ago, her speech is slightly slurred, and coworkers tease her about being “hungover.” She feels fuzzy-headed, but her speech and thinking clear after a few hours. At other times she smells burning rubber and feels that everything she does repeats what she has done before. Sometimes she feels “out of body” and can watch herself from the ceiling.
Ms. A’s symptoms suggest a seizure disorder. Her depressive features appeared after these ictal episodes began 9 years ago.
Recognizing mood disorders in patients with epilepsy is important because these disorders can be successfully treated within the context of the medical condition.
Many cases of comorbid depression in epilepsy are undiagnosed. A study of 100 patients with refractory epilepsy and depression severe enough for pharmacotherapy found that referral for psychiatric treatment was delayed >1 year in 75% of patients with spontaneous mood disorders and 89% of patients with depression secondary to antiepileptic drugs (AEDs).1
Psychiatrists often are called on to evaluate and treat depression in epilepsy patients or to assess for nonadherence to AEDs. Successfully treating these patients requires understanding:
- the relationship between epilepsy and depression
- the etiology of depression in patients with seizure disorder
- how to treat depression in this population.
High comorbidity
Depression rates are higher in epilepsy patients than in the general population (1% to 3% of men, 2% to 9% of women).2 Depression can be diagnosed in:
- 20% to 30% of patients with recurrent seizures
- 6% to 9% of patients in remission
- 50% to 55% of patients attending hospital epilepsy clinics and video telemetry units.3
Temporal relationship. Depression can be preictal, ictal, postictal, or interictal.4 One-third of patients with partial seizures report premonitory symptoms, usually before secondary generalized tonic clonic seizures.5
- Preictal depression occurs hours to days before a seizure and often is relieved by the convulsion.
- Ictal depression—more common in TLE—occurs as an aura in approximately 1% of patients. Onset is sudden and ranges from mild sadness to profound helplessness and despair. Treating the seizures also treats the depression.
- Postictal depression in TLE patients lasts hours to days after a seizure.
- Interictal depression affects up to two-thirds of epilepsy patients, especially those with severe or frequent seizures. Treat interictal depression separately from the Seizures.
Differential diagnosis
Search for seizure cause. Although 70% of epilepsies are idiopathic, search for the cause of a patient’s seizures. Neuroimaging can rule out a stroke, cerebral tumor, or traumatic brain injury as the cause of both depression and epilepsy.4 Even after exhaustive study, 10% to 20% of epilepsy cases cannot be identified by electroencephalography (EEG).
Seizure type and location, severity, laterality of seizure focus, and frequency are important variables in the etiology of depression in patients with epilepsy.6 Similar changes in neurotransmitters—serotonin, noradrenaline, dopamine, and gamma-aminobutyric acid—are observed in both depression and epilepsy.5
Characterize depressive symptoms. Consider involving the patient’s spouse or partner in the discussion to validate and augment the patient’s report. Often patients describe depressive symptoms— such as sleep problems, changes in appetite, loss of libido, and impaired cognition—that could be side effects of AEDs or symptoms of epilepsy.
Depression associated with epilepsy has distinct features. Blumer7 coined the term interictal dysphoric disorder (IDD), characterized by these types of symptoms:
- somatoform (anergia, pain, and insomnia)
- affective (irritability, euphoric moods, fear, and anxiety).
Is it bipolar depression? Determine if your patient’s depression might be part of a bipolar disorder. This diagnosis may modify your treatment plan because antidepressants could trigger a manic or hypomanic episode. Also look for untreated psychotic features, which are associated with a suicide completion rate of 19% in bipolar epilepsy patients.6
Screen for suicidal behavior. Ask about suicidal ideation, plans, and attempts within the past month and in the patient’s lifetime.4 Compared with the general population, the risk of suicide is 4 to 5 times higher in depressed persons with epilepsy8 and 25 times higher in those with TLE (Table 1).9 Overdoses are used in 80% to 90% of suicide attempts among patients with epilepsy, perhaps because of the availability of AEDs.3
Perceived social stigma, inability to drive, AEDs’ effects on cognition, and interpersonal and psychosocial issues may contribute to the patient’s depression. Ask about social support, recent stressful events, and financial and vocational impact of the seizure disorder.6
Table 1
Risk factors for suicide among epilepsy patients
| Age 25 to 49 years |
| Male gender |
| Coexisting psychopathology, including personality disorders |
| Temporal lobe epilepsy |
| Personal difficulties such as social or workrelated problems |
| Prolonged duration of epilepsy |
| Poor seizure control |
| Source: Reference 3 |
CASE CONTINUED: Searching for a cause
Previously Ms. A worked steadily and led an active life. She does not have a history of mania or hypomania. She is alert, neat, and cooperative. She sits calmly, gestures appropriately when speaking, and has no abnormal movements. She is subdued but says she is a bit anxious.
Her workup includes routine hematologic and biochemical parameters, EEG, and brain MRI. All are negative.
Her episodes are sudden, brief, and involve altered awareness followed by amnesia. She describes déjà vu, perceptual changes, and motor speech problems.
Ms. A’s behavioral syndrome is consistent with complex partial seizure with frontal and temporal foci. Her dominant brain hemisphere likely is involved because speech is affected. We classify her depression as postictal because of the temporal relationship with the seizures. Thus, controlling the seizures should prevent the depression.
Depression as a side effect
Depression in epilepsy is multifactorial, and pharmacotherapy is one of many biologic and psychosocial risk factors.
AED’s negative effects such as depression and cognitive changes may be caused by polypharmacy, drug- induced folate deficiency, drug titration and dosage, or withdrawal.6 Patients receiving combination therapies are more likely to be depressed.4 AED polypharmacy might be a marker for refractory epilepsy, and thus depression can be caused by both the neurologic illness and its treatment. Shorvon et al10 reported improved alertness, concentration, drive, mood, and sociability after patients’ polytherapy was reduced to monotherapy, especially carbamazepine monotherapy.
Onset or worsening of depression could coincide with starting a new AED.6 Phenobarbital and topiramate are most closely associated with acute depression during initial treatment.3 One study noted that depressed patients taking barbiturates as part of polytherapy were significantly more depressed than those taking carbamazepine.8 Phenobarbital can produce depression, suicidal ideation, and suicidal and parasuicidal behavior.
Patients starting tiagabine might develop agitation, withdrawal, and mood disturbance that could suggest depression.3 With topiramate the rate of affective symptoms is dose-dependent, with an incidence of 9% with 200 mg/d and 19% with 1,000 mg/d.11
Some patients (11% to 15%) receiving polytherapy that includes liver enzyme -inducing AEDs (carbamazepine, oxcarbazepine, phenobarbital, phenytoin, primidone, and topiramate) present with decreased serum, erythrocyte, and cerebrospinal fluid folate levels, which is associated with depression.4
Bipolar depression. AEDs such as carbamazepine, valproic acid, and lamotrigine are used for bipolar maintenance therapy in patients without a seizure disorder. Lamotrigine is used to treat bipolar depression in non-epilepsy patients. Therefore, these AEDs are first-line treatment for comorbid epilepsy and bipolar depression.12
Using antidepressants
Effectively treating depression in epilepsy patients (Algorithm) encompasses assessment of prescribed AEDs and the use of antidepressants, electroconvulsive therapy (ECT), and psychotherapy. No evidence indicates that any 1 antidepressant is more effective than others for treating depression in patients with epilepsy. When starting an antidepressant, consider the drug’s effect on seizure threshold, its efficacy, and drug-drug interactions.
Seizure risk. Seizures are a rare but serious adverse effect of most antidepressants (Table 2).13 Compared with the incidence of first seizures in the general population (4 Generalized tonic-clonic seizures are associated with increased mortality in tricyclic antidepressant (TCA) overdose, especially with amitriptyline, maprotiline, and clomipramine.
Desipramine, monoamine oxidase inhibitors (MAOIs), selective serotonin reuptake inhibitors (SSRIs), and trazodone are preferred options for depressed epilepsy patients because these drugs lower the seizure threshold less than other antidepressants, with a 1% to 1.5% incidence of seizures during the first 2 years of treatment.14 Because most seizures reported with these medications are dose-related, blood level monitoring is helpful. Avoid bupropion, which has a seizure rate double that of other antidepressants.6
Clinical trial experience and EEG studies suggest that the SSRIs are less epileptogenic than TCAs. MAOIs also are less likely than TCAs to cause seizures but can cause excessive sedation when coadministered with barbiturates. The only double-blind trial of antidepressants (amitriptyline, nomifensine, and placebo) to treat comorbid depression and epilepsy found no significant differences among drugs or placebo.8
Drug-drug interactions. Consider the cytochrome P450 enzyme system when choosing an antidepressant for an epilepsy patient.6 Antidepressants can alter serum levels of phenobarbital and carbamazepine, and AEDs usually reduce antidepressant levels.8 For example, carbamazepine could lower TCA levels, valproic acid might elevate TCA levels,15 and imipramine and nortriptyline might increase phenytoin levels. Similarly, monitor TCA levels during AED withdrawal, as increased TCA concentrations can result in toxicity and concomitant behavioral effects.13
Start antidepressants at doses lower than used in patients without epilepsy, and gradually increase until depression remits. Periodically check AED levels during antidepressant treatment, and adjust dosages to maintain a therapeutic level.
Algorithm
Stepwise approach to treating
comorbid psychiatric disorders and epilepsy
| Step 1 |
| Determine the etiology of depression |
| ↓ |
| Step 2 |
| Assess AED regimen Avoid polytherapy Consider the adverse psychotropic effects with phenobarbital and primidone Consider changing to carbamazepine or valproic acid, if clinically appropriate; modified release preparations usually are better tolerated Monitor total plasma levels of AEDs Screen erythrocyte folate levels |
| ↓ |
| Step 3 |
| Start the antidepressant at a low dose and then increase slowly Start with drugs of choice such as selective serotonin reuptake inhibitors Bupropion, maprotiline, and clomipramine are contraindicated in patients with a history of seizures, brain injury, or EEG abnormality Assess for antidepressant-AED interactions Continue to monitor plasma levels of AEDs Remember that all antidepressants can lower the seizure threshold |
| ↓ |
| Step 4 |
| Consider ECT for refractory or severe depression |
| ↓ |
| Step 5 |
| Recommend support groups and cognitivebehavioral therapy Communicate regularly with patient’s neurologist, primary care physician, and other specialists involved in his or her care |
| AEDs: antiepileptic drugs; ECT: electroconvulsive therapy; |
| EEG: electroencephalography |
Antidepressants’ seizure potential in any patient
| Antidepressant | Risk of seizures (%) |
|---|---|
| High risk (not indicated for epilepsy patients) | |
| Bupropion 450 to 650 mg | 0.4 0.6 to2.19 |
| Clomipramine | 0.5 to 1.66 |
| Maprotiline | 0.4 to 15.6 |
| Intermediate risk | |
| Tricyclics | 0.1 to 15.6 |
| Amitriptyline | 0.4 to 0.5 |
| Imipramine | 0.6 to 0.9 |
| Low risk | |
| Citalopram | |
| Fluoxetine | |
| Fluvoxamine | 0.2 |
| Paroxetine | 0.1 |
| Sertraline | |
| Trazodone | |
| Venlafaxine | 0.1 to 0.2 |
| Mirtazapine | |
| Duloxetine | 0.2 |
| Source: References 6,3 | |
Nondrug therapies
ECT. Consider ECT for patients with refractory or severe depression. ECT can be lifesaving—especially in patients with psychotic depression—and is a viable and safe alternative to antidepressants for patients with epilepsy.3
ECT can raise a patient’s seizure threshold.13 Unilateral nondominant electrode placement is recommended to minimize the combined cognitive side effects of AEDs and ECT. Except for those at high risk of status epilepticus, advise patients not to take their AEDs the morning of ECT treatments.
Support groups. Epilepsy can affect many aspects of a patient’s life, including education, employment, family life, and selfesteem.13 Epilepsy support groups can provide emotional support by introducing patients to others with a seizure disorder. Patients often experience a sense of relief when they discover that they are not alone and other group members share similar dilemmas. Becu et al16 reported that self-help group intervention characterized by education, support, and socialization significantly reduced depression scores in epilepsy patients. These groups often offer education about the nature of the patient’s illness.
Psychotherapy. Because psychosocial factors can play a role in the expression of depression in patients with epilepsy, cognitive, behavioral, and interpersonal therapy may be useful.6 These treatment modalities provide an opportunity to educate patients and families about epilepsy, explore emotional reactions to the condition, and correct false beliefs about the illness. Goldstein17 showed that after 12 sessions of cognitive-behavioral therapy, 6 patients with chronic, poorly controlled epilepsy reported reduced depression scores. Their initial epilepsy-related problem had less impact on their daily lives and self-rated work and social adjustment improved significantly.
CASE CONTINUED: Seeing results
We treat Ms. A’s mood episodes with carbamazepine, titrated up to 400 mg bid. Her seizures decrease in frequency, and after 1 month her depressive symptoms subside. Her coworkers describe Ms. A as more outgoing and full of energy.
We refer Ms. A to an epilepsy support group that meets twice a month, and she is relieved to know other patients experience similar symptoms. She continues individual psychotherapy, which helps her adjust to epilepsy’s chronic nature and complications.
- Epilepsy Foundation. Epilepsy and mood disorders. www.epilepsyfoundation.org/programs/mood.
- Epilepsy Foundation. Neurological Disorders Depression Inventory for Epilepsy Screening Tool. www.epilepsyfoundation.org/about/related/mood/nddietool.cfm.
- Amitriptyline • Elavil
- Amoxapine • Asendin
- Bupropion • Wellbutrin
- Carbamazepine • Tegretol
- Citalopram • Celexa
- Clomipramine • Anafranil
- Desipramine • Norpramin
- Doxepin • Sinequan
- Duloxetine • Cymbalta
- Fluoxetine • Prozac
- Fluvoxamine • Luvox
- Imipramine • Tofranill
- Lamotrigine • Lamictal
- Lithium • Eskalith, Lithobid
- Nomifensine • Merital
- Maprotiline • Ludiomil
- Mirtazapine • Remeron
- Nefazodone • Serzone
- Nortriptyline • Aventyl, Pamelor
- Oxcarbazepine • Trileptal
- Paroxetine • Paxil
- Phenytoin • Dilantin
- Primidone • Mysoline
- Sertraline • Zoloft
- Tiagabine • Gabitril
- Topiramate • Topamax
- Trazodone • Desyrel
- Valproic acid • Depakote
- Venlafaxine • Effexor
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Kanner AM. Should neurologists be trained to recognize and treat comorbid depression of neurologic disorders? Yes. Epilepsy Behav 2005;6(3):303-11.
2. Gilliam FG. Diagnosis and treatment of mood disorders in persons with epilepsy. Curr Opin Neurol 2005;18(2):129-33.
3. Jackson MJ, Turkington D. Depression and anxiety in epilepsy. J Neurol Neurosurg Psychiatry 2005;76(suppl 1):45-7.
4. Lambert MV, Robertson MM. Depression in epilepsy: etiology, phenomenology, and treatment. Epilepsia 1999;40(suppl 10):S21-S47.
5. Gaitatzis A, Trimble MR, Sander JW. The psychiatric comorbidity of epilepsy. Acta Neurol Scand 2004;110(4):207-20.
6. Barry JJ. The recognition and management of mood disorders as a comorbidity of epilepsy. Epilepsia 2003;44(suppl 4):30-40.
7. Blumer D, Montouris G, Davies K. The interictal dysphoric disorder: recognition, pathogenesis, and treatment of the major psychiatric disorder of epilepsy. Epilepsy Behav 2004;5(6):826-40.
8. Robertson M. Mood disorders associated with epilepsy. In: McConnell HW, Snyder PJ, eds. Psychiatric comorbidity in epilepsy: basic mechanisms, diagnosis, and treatment. Washington DC: American Psychiatric Publishing; 1998:133-67.
9. Harris EC, Barraclough B. Suicide as an outcome for mental disorders. A meta-analysis. Br J Psychiatry 1997;170:205-28.
10. Shorvon SD, Reynolds EH. Reduction in polypharmacy for epilepsy. Br Med J 1979;2(6197):1023-5.
11. Mula M, Trimle MR, Lhatoo SD, Sander JW. Topiramate and psychiatric adverse events in patients with epilepsy. Epilepsia 2003;44(5):659-63.
12. Selai C, Bannister D, Trimble M. Antiepileptic drugs and the regulation of mood and quality (QOL): the evidence from epilepsy. Epilepsia 2005;46(suppl 4):50-7.
13. McConnell H, Duncan D. Treatment of psychiatric comorbidity in epilepsy. In: McConnell HW, Snyder PJ, eds. Psychiatric comorbidity in epilepsy: basic mechanisms, diagnosis, and treatment. Washington DC: American Psychiatric Publishing; 1998:245-361.
14. Charney DS, Berman RM, Miller HL. Treatment of depression. In: Schatzberg AF, Nemeroff CB, eds. Essentials of clinical psychopharmacology. Washington DC: American Psychiatric Publishing; 2001:359.
15. Tucker GJ. Neuropsychiatric aspects of seizure disorders. In: Yudofsky SC, Hales RE, eds. Essentials of neuropsychiatry and clinical neurosciences. Washington DC: American Psychiatric Publishing; 2004:293-313.
16. Becu M, Becu N, Manzur G, Kochen S. Self-help epilepsy groups: an evaluation of effect on depression and schizophrenia. Epilepsia 1993;34(5):841-5.
17. Goldstein LH, McAlpine M, Deale A, et al. Cognitive behaviour therapy with adults with intractable epilepsy and psychiatric co-morbidity: preliminary observations on changes in psychological state and seizure frequency. Behav Res Ther 2003;41(4):447-6.
Ms. A, age 29, has had depression for 6 years and has taken antidepressants with inconsistent response. For 3 weeks, while not taking any antidepressant, she reports loss of energy; feeling sad, subdued, and tearful; poor concentration; and reduced interest in enjoyable activities including sex, the same symptoms she ?rst reported 6 years ago. She has no appetite but has not lost weight.
Several times a month Ms. A “loses” short periods of time. For example she says sometimes she cannot remember what happens between parking her car and sitting at her desk at work. After these episodes, which began 9 years ago, her speech is slightly slurred, and coworkers tease her about being “hungover.” She feels fuzzy-headed, but her speech and thinking clear after a few hours. At other times she smells burning rubber and feels that everything she does repeats what she has done before. Sometimes she feels “out of body” and can watch herself from the ceiling.
Ms. A’s symptoms suggest a seizure disorder. Her depressive features appeared after these ictal episodes began 9 years ago.
Recognizing mood disorders in patients with epilepsy is important because these disorders can be successfully treated within the context of the medical condition.
Many cases of comorbid depression in epilepsy are undiagnosed. A study of 100 patients with refractory epilepsy and depression severe enough for pharmacotherapy found that referral for psychiatric treatment was delayed >1 year in 75% of patients with spontaneous mood disorders and 89% of patients with depression secondary to antiepileptic drugs (AEDs).1
Psychiatrists often are called on to evaluate and treat depression in epilepsy patients or to assess for nonadherence to AEDs. Successfully treating these patients requires understanding:
- the relationship between epilepsy and depression
- the etiology of depression in patients with seizure disorder
- how to treat depression in this population.
High comorbidity
Depression rates are higher in epilepsy patients than in the general population (1% to 3% of men, 2% to 9% of women).2 Depression can be diagnosed in:
- 20% to 30% of patients with recurrent seizures
- 6% to 9% of patients in remission
- 50% to 55% of patients attending hospital epilepsy clinics and video telemetry units.3
Temporal relationship. Depression can be preictal, ictal, postictal, or interictal.4 One-third of patients with partial seizures report premonitory symptoms, usually before secondary generalized tonic clonic seizures.5
- Preictal depression occurs hours to days before a seizure and often is relieved by the convulsion.
- Ictal depression—more common in TLE—occurs as an aura in approximately 1% of patients. Onset is sudden and ranges from mild sadness to profound helplessness and despair. Treating the seizures also treats the depression.
- Postictal depression in TLE patients lasts hours to days after a seizure.
- Interictal depression affects up to two-thirds of epilepsy patients, especially those with severe or frequent seizures. Treat interictal depression separately from the Seizures.
Differential diagnosis
Search for seizure cause. Although 70% of epilepsies are idiopathic, search for the cause of a patient’s seizures. Neuroimaging can rule out a stroke, cerebral tumor, or traumatic brain injury as the cause of both depression and epilepsy.4 Even after exhaustive study, 10% to 20% of epilepsy cases cannot be identified by electroencephalography (EEG).
Seizure type and location, severity, laterality of seizure focus, and frequency are important variables in the etiology of depression in patients with epilepsy.6 Similar changes in neurotransmitters—serotonin, noradrenaline, dopamine, and gamma-aminobutyric acid—are observed in both depression and epilepsy.5
Characterize depressive symptoms. Consider involving the patient’s spouse or partner in the discussion to validate and augment the patient’s report. Often patients describe depressive symptoms— such as sleep problems, changes in appetite, loss of libido, and impaired cognition—that could be side effects of AEDs or symptoms of epilepsy.
Depression associated with epilepsy has distinct features. Blumer7 coined the term interictal dysphoric disorder (IDD), characterized by these types of symptoms:
- somatoform (anergia, pain, and insomnia)
- affective (irritability, euphoric moods, fear, and anxiety).
Is it bipolar depression? Determine if your patient’s depression might be part of a bipolar disorder. This diagnosis may modify your treatment plan because antidepressants could trigger a manic or hypomanic episode. Also look for untreated psychotic features, which are associated with a suicide completion rate of 19% in bipolar epilepsy patients.6
Screen for suicidal behavior. Ask about suicidal ideation, plans, and attempts within the past month and in the patient’s lifetime.4 Compared with the general population, the risk of suicide is 4 to 5 times higher in depressed persons with epilepsy8 and 25 times higher in those with TLE (Table 1).9 Overdoses are used in 80% to 90% of suicide attempts among patients with epilepsy, perhaps because of the availability of AEDs.3
Perceived social stigma, inability to drive, AEDs’ effects on cognition, and interpersonal and psychosocial issues may contribute to the patient’s depression. Ask about social support, recent stressful events, and financial and vocational impact of the seizure disorder.6
Table 1
Risk factors for suicide among epilepsy patients
| Age 25 to 49 years |
| Male gender |
| Coexisting psychopathology, including personality disorders |
| Temporal lobe epilepsy |
| Personal difficulties such as social or workrelated problems |
| Prolonged duration of epilepsy |
| Poor seizure control |
| Source: Reference 3 |
CASE CONTINUED: Searching for a cause
Previously Ms. A worked steadily and led an active life. She does not have a history of mania or hypomania. She is alert, neat, and cooperative. She sits calmly, gestures appropriately when speaking, and has no abnormal movements. She is subdued but says she is a bit anxious.
Her workup includes routine hematologic and biochemical parameters, EEG, and brain MRI. All are negative.
Her episodes are sudden, brief, and involve altered awareness followed by amnesia. She describes déjà vu, perceptual changes, and motor speech problems.
Ms. A’s behavioral syndrome is consistent with complex partial seizure with frontal and temporal foci. Her dominant brain hemisphere likely is involved because speech is affected. We classify her depression as postictal because of the temporal relationship with the seizures. Thus, controlling the seizures should prevent the depression.
Depression as a side effect
Depression in epilepsy is multifactorial, and pharmacotherapy is one of many biologic and psychosocial risk factors.
AED’s negative effects such as depression and cognitive changes may be caused by polypharmacy, drug- induced folate deficiency, drug titration and dosage, or withdrawal.6 Patients receiving combination therapies are more likely to be depressed.4 AED polypharmacy might be a marker for refractory epilepsy, and thus depression can be caused by both the neurologic illness and its treatment. Shorvon et al10 reported improved alertness, concentration, drive, mood, and sociability after patients’ polytherapy was reduced to monotherapy, especially carbamazepine monotherapy.
Onset or worsening of depression could coincide with starting a new AED.6 Phenobarbital and topiramate are most closely associated with acute depression during initial treatment.3 One study noted that depressed patients taking barbiturates as part of polytherapy were significantly more depressed than those taking carbamazepine.8 Phenobarbital can produce depression, suicidal ideation, and suicidal and parasuicidal behavior.
Patients starting tiagabine might develop agitation, withdrawal, and mood disturbance that could suggest depression.3 With topiramate the rate of affective symptoms is dose-dependent, with an incidence of 9% with 200 mg/d and 19% with 1,000 mg/d.11
Some patients (11% to 15%) receiving polytherapy that includes liver enzyme -inducing AEDs (carbamazepine, oxcarbazepine, phenobarbital, phenytoin, primidone, and topiramate) present with decreased serum, erythrocyte, and cerebrospinal fluid folate levels, which is associated with depression.4
Bipolar depression. AEDs such as carbamazepine, valproic acid, and lamotrigine are used for bipolar maintenance therapy in patients without a seizure disorder. Lamotrigine is used to treat bipolar depression in non-epilepsy patients. Therefore, these AEDs are first-line treatment for comorbid epilepsy and bipolar depression.12
Using antidepressants
Effectively treating depression in epilepsy patients (Algorithm) encompasses assessment of prescribed AEDs and the use of antidepressants, electroconvulsive therapy (ECT), and psychotherapy. No evidence indicates that any 1 antidepressant is more effective than others for treating depression in patients with epilepsy. When starting an antidepressant, consider the drug’s effect on seizure threshold, its efficacy, and drug-drug interactions.
Seizure risk. Seizures are a rare but serious adverse effect of most antidepressants (Table 2).13 Compared with the incidence of first seizures in the general population (4 Generalized tonic-clonic seizures are associated with increased mortality in tricyclic antidepressant (TCA) overdose, especially with amitriptyline, maprotiline, and clomipramine.
Desipramine, monoamine oxidase inhibitors (MAOIs), selective serotonin reuptake inhibitors (SSRIs), and trazodone are preferred options for depressed epilepsy patients because these drugs lower the seizure threshold less than other antidepressants, with a 1% to 1.5% incidence of seizures during the first 2 years of treatment.14 Because most seizures reported with these medications are dose-related, blood level monitoring is helpful. Avoid bupropion, which has a seizure rate double that of other antidepressants.6
Clinical trial experience and EEG studies suggest that the SSRIs are less epileptogenic than TCAs. MAOIs also are less likely than TCAs to cause seizures but can cause excessive sedation when coadministered with barbiturates. The only double-blind trial of antidepressants (amitriptyline, nomifensine, and placebo) to treat comorbid depression and epilepsy found no significant differences among drugs or placebo.8
Drug-drug interactions. Consider the cytochrome P450 enzyme system when choosing an antidepressant for an epilepsy patient.6 Antidepressants can alter serum levels of phenobarbital and carbamazepine, and AEDs usually reduce antidepressant levels.8 For example, carbamazepine could lower TCA levels, valproic acid might elevate TCA levels,15 and imipramine and nortriptyline might increase phenytoin levels. Similarly, monitor TCA levels during AED withdrawal, as increased TCA concentrations can result in toxicity and concomitant behavioral effects.13
Start antidepressants at doses lower than used in patients without epilepsy, and gradually increase until depression remits. Periodically check AED levels during antidepressant treatment, and adjust dosages to maintain a therapeutic level.
Algorithm
Stepwise approach to treating
comorbid psychiatric disorders and epilepsy
| Step 1 |
| Determine the etiology of depression |
| ↓ |
| Step 2 |
| Assess AED regimen Avoid polytherapy Consider the adverse psychotropic effects with phenobarbital and primidone Consider changing to carbamazepine or valproic acid, if clinically appropriate; modified release preparations usually are better tolerated Monitor total plasma levels of AEDs Screen erythrocyte folate levels |
| ↓ |
| Step 3 |
| Start the antidepressant at a low dose and then increase slowly Start with drugs of choice such as selective serotonin reuptake inhibitors Bupropion, maprotiline, and clomipramine are contraindicated in patients with a history of seizures, brain injury, or EEG abnormality Assess for antidepressant-AED interactions Continue to monitor plasma levels of AEDs Remember that all antidepressants can lower the seizure threshold |
| ↓ |
| Step 4 |
| Consider ECT for refractory or severe depression |
| ↓ |
| Step 5 |
| Recommend support groups and cognitivebehavioral therapy Communicate regularly with patient’s neurologist, primary care physician, and other specialists involved in his or her care |
| AEDs: antiepileptic drugs; ECT: electroconvulsive therapy; |
| EEG: electroencephalography |
Antidepressants’ seizure potential in any patient
| Antidepressant | Risk of seizures (%) |
|---|---|
| High risk (not indicated for epilepsy patients) | |
| Bupropion 450 to 650 mg | 0.4 0.6 to2.19 |
| Clomipramine | 0.5 to 1.66 |
| Maprotiline | 0.4 to 15.6 |
| Intermediate risk | |
| Tricyclics | 0.1 to 15.6 |
| Amitriptyline | 0.4 to 0.5 |
| Imipramine | 0.6 to 0.9 |
| Low risk | |
| Citalopram | |
| Fluoxetine | |
| Fluvoxamine | 0.2 |
| Paroxetine | 0.1 |
| Sertraline | |
| Trazodone | |
| Venlafaxine | 0.1 to 0.2 |
| Mirtazapine | |
| Duloxetine | 0.2 |
| Source: References 6,3 | |
Nondrug therapies
ECT. Consider ECT for patients with refractory or severe depression. ECT can be lifesaving—especially in patients with psychotic depression—and is a viable and safe alternative to antidepressants for patients with epilepsy.3
ECT can raise a patient’s seizure threshold.13 Unilateral nondominant electrode placement is recommended to minimize the combined cognitive side effects of AEDs and ECT. Except for those at high risk of status epilepticus, advise patients not to take their AEDs the morning of ECT treatments.
Support groups. Epilepsy can affect many aspects of a patient’s life, including education, employment, family life, and selfesteem.13 Epilepsy support groups can provide emotional support by introducing patients to others with a seizure disorder. Patients often experience a sense of relief when they discover that they are not alone and other group members share similar dilemmas. Becu et al16 reported that self-help group intervention characterized by education, support, and socialization significantly reduced depression scores in epilepsy patients. These groups often offer education about the nature of the patient’s illness.
Psychotherapy. Because psychosocial factors can play a role in the expression of depression in patients with epilepsy, cognitive, behavioral, and interpersonal therapy may be useful.6 These treatment modalities provide an opportunity to educate patients and families about epilepsy, explore emotional reactions to the condition, and correct false beliefs about the illness. Goldstein17 showed that after 12 sessions of cognitive-behavioral therapy, 6 patients with chronic, poorly controlled epilepsy reported reduced depression scores. Their initial epilepsy-related problem had less impact on their daily lives and self-rated work and social adjustment improved significantly.
CASE CONTINUED: Seeing results
We treat Ms. A’s mood episodes with carbamazepine, titrated up to 400 mg bid. Her seizures decrease in frequency, and after 1 month her depressive symptoms subside. Her coworkers describe Ms. A as more outgoing and full of energy.
We refer Ms. A to an epilepsy support group that meets twice a month, and she is relieved to know other patients experience similar symptoms. She continues individual psychotherapy, which helps her adjust to epilepsy’s chronic nature and complications.
- Epilepsy Foundation. Epilepsy and mood disorders. www.epilepsyfoundation.org/programs/mood.
- Epilepsy Foundation. Neurological Disorders Depression Inventory for Epilepsy Screening Tool. www.epilepsyfoundation.org/about/related/mood/nddietool.cfm.
- Amitriptyline • Elavil
- Amoxapine • Asendin
- Bupropion • Wellbutrin
- Carbamazepine • Tegretol
- Citalopram • Celexa
- Clomipramine • Anafranil
- Desipramine • Norpramin
- Doxepin • Sinequan
- Duloxetine • Cymbalta
- Fluoxetine • Prozac
- Fluvoxamine • Luvox
- Imipramine • Tofranill
- Lamotrigine • Lamictal
- Lithium • Eskalith, Lithobid
- Nomifensine • Merital
- Maprotiline • Ludiomil
- Mirtazapine • Remeron
- Nefazodone • Serzone
- Nortriptyline • Aventyl, Pamelor
- Oxcarbazepine • Trileptal
- Paroxetine • Paxil
- Phenytoin • Dilantin
- Primidone • Mysoline
- Sertraline • Zoloft
- Tiagabine • Gabitril
- Topiramate • Topamax
- Trazodone • Desyrel
- Valproic acid • Depakote
- Venlafaxine • Effexor
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Ms. A, age 29, has had depression for 6 years and has taken antidepressants with inconsistent response. For 3 weeks, while not taking any antidepressant, she reports loss of energy; feeling sad, subdued, and tearful; poor concentration; and reduced interest in enjoyable activities including sex, the same symptoms she ?rst reported 6 years ago. She has no appetite but has not lost weight.
Several times a month Ms. A “loses” short periods of time. For example she says sometimes she cannot remember what happens between parking her car and sitting at her desk at work. After these episodes, which began 9 years ago, her speech is slightly slurred, and coworkers tease her about being “hungover.” She feels fuzzy-headed, but her speech and thinking clear after a few hours. At other times she smells burning rubber and feels that everything she does repeats what she has done before. Sometimes she feels “out of body” and can watch herself from the ceiling.
Ms. A’s symptoms suggest a seizure disorder. Her depressive features appeared after these ictal episodes began 9 years ago.
Recognizing mood disorders in patients with epilepsy is important because these disorders can be successfully treated within the context of the medical condition.
Many cases of comorbid depression in epilepsy are undiagnosed. A study of 100 patients with refractory epilepsy and depression severe enough for pharmacotherapy found that referral for psychiatric treatment was delayed >1 year in 75% of patients with spontaneous mood disorders and 89% of patients with depression secondary to antiepileptic drugs (AEDs).1
Psychiatrists often are called on to evaluate and treat depression in epilepsy patients or to assess for nonadherence to AEDs. Successfully treating these patients requires understanding:
- the relationship between epilepsy and depression
- the etiology of depression in patients with seizure disorder
- how to treat depression in this population.
High comorbidity
Depression rates are higher in epilepsy patients than in the general population (1% to 3% of men, 2% to 9% of women).2 Depression can be diagnosed in:
- 20% to 30% of patients with recurrent seizures
- 6% to 9% of patients in remission
- 50% to 55% of patients attending hospital epilepsy clinics and video telemetry units.3
Temporal relationship. Depression can be preictal, ictal, postictal, or interictal.4 One-third of patients with partial seizures report premonitory symptoms, usually before secondary generalized tonic clonic seizures.5
- Preictal depression occurs hours to days before a seizure and often is relieved by the convulsion.
- Ictal depression—more common in TLE—occurs as an aura in approximately 1% of patients. Onset is sudden and ranges from mild sadness to profound helplessness and despair. Treating the seizures also treats the depression.
- Postictal depression in TLE patients lasts hours to days after a seizure.
- Interictal depression affects up to two-thirds of epilepsy patients, especially those with severe or frequent seizures. Treat interictal depression separately from the Seizures.
Differential diagnosis
Search for seizure cause. Although 70% of epilepsies are idiopathic, search for the cause of a patient’s seizures. Neuroimaging can rule out a stroke, cerebral tumor, or traumatic brain injury as the cause of both depression and epilepsy.4 Even after exhaustive study, 10% to 20% of epilepsy cases cannot be identified by electroencephalography (EEG).
Seizure type and location, severity, laterality of seizure focus, and frequency are important variables in the etiology of depression in patients with epilepsy.6 Similar changes in neurotransmitters—serotonin, noradrenaline, dopamine, and gamma-aminobutyric acid—are observed in both depression and epilepsy.5
Characterize depressive symptoms. Consider involving the patient’s spouse or partner in the discussion to validate and augment the patient’s report. Often patients describe depressive symptoms— such as sleep problems, changes in appetite, loss of libido, and impaired cognition—that could be side effects of AEDs or symptoms of epilepsy.
Depression associated with epilepsy has distinct features. Blumer7 coined the term interictal dysphoric disorder (IDD), characterized by these types of symptoms:
- somatoform (anergia, pain, and insomnia)
- affective (irritability, euphoric moods, fear, and anxiety).
Is it bipolar depression? Determine if your patient’s depression might be part of a bipolar disorder. This diagnosis may modify your treatment plan because antidepressants could trigger a manic or hypomanic episode. Also look for untreated psychotic features, which are associated with a suicide completion rate of 19% in bipolar epilepsy patients.6
Screen for suicidal behavior. Ask about suicidal ideation, plans, and attempts within the past month and in the patient’s lifetime.4 Compared with the general population, the risk of suicide is 4 to 5 times higher in depressed persons with epilepsy8 and 25 times higher in those with TLE (Table 1).9 Overdoses are used in 80% to 90% of suicide attempts among patients with epilepsy, perhaps because of the availability of AEDs.3
Perceived social stigma, inability to drive, AEDs’ effects on cognition, and interpersonal and psychosocial issues may contribute to the patient’s depression. Ask about social support, recent stressful events, and financial and vocational impact of the seizure disorder.6
Table 1
Risk factors for suicide among epilepsy patients
| Age 25 to 49 years |
| Male gender |
| Coexisting psychopathology, including personality disorders |
| Temporal lobe epilepsy |
| Personal difficulties such as social or workrelated problems |
| Prolonged duration of epilepsy |
| Poor seizure control |
| Source: Reference 3 |
CASE CONTINUED: Searching for a cause
Previously Ms. A worked steadily and led an active life. She does not have a history of mania or hypomania. She is alert, neat, and cooperative. She sits calmly, gestures appropriately when speaking, and has no abnormal movements. She is subdued but says she is a bit anxious.
Her workup includes routine hematologic and biochemical parameters, EEG, and brain MRI. All are negative.
Her episodes are sudden, brief, and involve altered awareness followed by amnesia. She describes déjà vu, perceptual changes, and motor speech problems.
Ms. A’s behavioral syndrome is consistent with complex partial seizure with frontal and temporal foci. Her dominant brain hemisphere likely is involved because speech is affected. We classify her depression as postictal because of the temporal relationship with the seizures. Thus, controlling the seizures should prevent the depression.
Depression as a side effect
Depression in epilepsy is multifactorial, and pharmacotherapy is one of many biologic and psychosocial risk factors.
AED’s negative effects such as depression and cognitive changes may be caused by polypharmacy, drug- induced folate deficiency, drug titration and dosage, or withdrawal.6 Patients receiving combination therapies are more likely to be depressed.4 AED polypharmacy might be a marker for refractory epilepsy, and thus depression can be caused by both the neurologic illness and its treatment. Shorvon et al10 reported improved alertness, concentration, drive, mood, and sociability after patients’ polytherapy was reduced to monotherapy, especially carbamazepine monotherapy.
Onset or worsening of depression could coincide with starting a new AED.6 Phenobarbital and topiramate are most closely associated with acute depression during initial treatment.3 One study noted that depressed patients taking barbiturates as part of polytherapy were significantly more depressed than those taking carbamazepine.8 Phenobarbital can produce depression, suicidal ideation, and suicidal and parasuicidal behavior.
Patients starting tiagabine might develop agitation, withdrawal, and mood disturbance that could suggest depression.3 With topiramate the rate of affective symptoms is dose-dependent, with an incidence of 9% with 200 mg/d and 19% with 1,000 mg/d.11
Some patients (11% to 15%) receiving polytherapy that includes liver enzyme -inducing AEDs (carbamazepine, oxcarbazepine, phenobarbital, phenytoin, primidone, and topiramate) present with decreased serum, erythrocyte, and cerebrospinal fluid folate levels, which is associated with depression.4
Bipolar depression. AEDs such as carbamazepine, valproic acid, and lamotrigine are used for bipolar maintenance therapy in patients without a seizure disorder. Lamotrigine is used to treat bipolar depression in non-epilepsy patients. Therefore, these AEDs are first-line treatment for comorbid epilepsy and bipolar depression.12
Using antidepressants
Effectively treating depression in epilepsy patients (Algorithm) encompasses assessment of prescribed AEDs and the use of antidepressants, electroconvulsive therapy (ECT), and psychotherapy. No evidence indicates that any 1 antidepressant is more effective than others for treating depression in patients with epilepsy. When starting an antidepressant, consider the drug’s effect on seizure threshold, its efficacy, and drug-drug interactions.
Seizure risk. Seizures are a rare but serious adverse effect of most antidepressants (Table 2).13 Compared with the incidence of first seizures in the general population (4 Generalized tonic-clonic seizures are associated with increased mortality in tricyclic antidepressant (TCA) overdose, especially with amitriptyline, maprotiline, and clomipramine.
Desipramine, monoamine oxidase inhibitors (MAOIs), selective serotonin reuptake inhibitors (SSRIs), and trazodone are preferred options for depressed epilepsy patients because these drugs lower the seizure threshold less than other antidepressants, with a 1% to 1.5% incidence of seizures during the first 2 years of treatment.14 Because most seizures reported with these medications are dose-related, blood level monitoring is helpful. Avoid bupropion, which has a seizure rate double that of other antidepressants.6
Clinical trial experience and EEG studies suggest that the SSRIs are less epileptogenic than TCAs. MAOIs also are less likely than TCAs to cause seizures but can cause excessive sedation when coadministered with barbiturates. The only double-blind trial of antidepressants (amitriptyline, nomifensine, and placebo) to treat comorbid depression and epilepsy found no significant differences among drugs or placebo.8
Drug-drug interactions. Consider the cytochrome P450 enzyme system when choosing an antidepressant for an epilepsy patient.6 Antidepressants can alter serum levels of phenobarbital and carbamazepine, and AEDs usually reduce antidepressant levels.8 For example, carbamazepine could lower TCA levels, valproic acid might elevate TCA levels,15 and imipramine and nortriptyline might increase phenytoin levels. Similarly, monitor TCA levels during AED withdrawal, as increased TCA concentrations can result in toxicity and concomitant behavioral effects.13
Start antidepressants at doses lower than used in patients without epilepsy, and gradually increase until depression remits. Periodically check AED levels during antidepressant treatment, and adjust dosages to maintain a therapeutic level.
Algorithm
Stepwise approach to treating
comorbid psychiatric disorders and epilepsy
| Step 1 |
| Determine the etiology of depression |
| ↓ |
| Step 2 |
| Assess AED regimen Avoid polytherapy Consider the adverse psychotropic effects with phenobarbital and primidone Consider changing to carbamazepine or valproic acid, if clinically appropriate; modified release preparations usually are better tolerated Monitor total plasma levels of AEDs Screen erythrocyte folate levels |
| ↓ |
| Step 3 |
| Start the antidepressant at a low dose and then increase slowly Start with drugs of choice such as selective serotonin reuptake inhibitors Bupropion, maprotiline, and clomipramine are contraindicated in patients with a history of seizures, brain injury, or EEG abnormality Assess for antidepressant-AED interactions Continue to monitor plasma levels of AEDs Remember that all antidepressants can lower the seizure threshold |
| ↓ |
| Step 4 |
| Consider ECT for refractory or severe depression |
| ↓ |
| Step 5 |
| Recommend support groups and cognitivebehavioral therapy Communicate regularly with patient’s neurologist, primary care physician, and other specialists involved in his or her care |
| AEDs: antiepileptic drugs; ECT: electroconvulsive therapy; |
| EEG: electroencephalography |
Antidepressants’ seizure potential in any patient
| Antidepressant | Risk of seizures (%) |
|---|---|
| High risk (not indicated for epilepsy patients) | |
| Bupropion 450 to 650 mg | 0.4 0.6 to2.19 |
| Clomipramine | 0.5 to 1.66 |
| Maprotiline | 0.4 to 15.6 |
| Intermediate risk | |
| Tricyclics | 0.1 to 15.6 |
| Amitriptyline | 0.4 to 0.5 |
| Imipramine | 0.6 to 0.9 |
| Low risk | |
| Citalopram | |
| Fluoxetine | |
| Fluvoxamine | 0.2 |
| Paroxetine | 0.1 |
| Sertraline | |
| Trazodone | |
| Venlafaxine | 0.1 to 0.2 |
| Mirtazapine | |
| Duloxetine | 0.2 |
| Source: References 6,3 | |
Nondrug therapies
ECT. Consider ECT for patients with refractory or severe depression. ECT can be lifesaving—especially in patients with psychotic depression—and is a viable and safe alternative to antidepressants for patients with epilepsy.3
ECT can raise a patient’s seizure threshold.13 Unilateral nondominant electrode placement is recommended to minimize the combined cognitive side effects of AEDs and ECT. Except for those at high risk of status epilepticus, advise patients not to take their AEDs the morning of ECT treatments.
Support groups. Epilepsy can affect many aspects of a patient’s life, including education, employment, family life, and selfesteem.13 Epilepsy support groups can provide emotional support by introducing patients to others with a seizure disorder. Patients often experience a sense of relief when they discover that they are not alone and other group members share similar dilemmas. Becu et al16 reported that self-help group intervention characterized by education, support, and socialization significantly reduced depression scores in epilepsy patients. These groups often offer education about the nature of the patient’s illness.
Psychotherapy. Because psychosocial factors can play a role in the expression of depression in patients with epilepsy, cognitive, behavioral, and interpersonal therapy may be useful.6 These treatment modalities provide an opportunity to educate patients and families about epilepsy, explore emotional reactions to the condition, and correct false beliefs about the illness. Goldstein17 showed that after 12 sessions of cognitive-behavioral therapy, 6 patients with chronic, poorly controlled epilepsy reported reduced depression scores. Their initial epilepsy-related problem had less impact on their daily lives and self-rated work and social adjustment improved significantly.
CASE CONTINUED: Seeing results
We treat Ms. A’s mood episodes with carbamazepine, titrated up to 400 mg bid. Her seizures decrease in frequency, and after 1 month her depressive symptoms subside. Her coworkers describe Ms. A as more outgoing and full of energy.
We refer Ms. A to an epilepsy support group that meets twice a month, and she is relieved to know other patients experience similar symptoms. She continues individual psychotherapy, which helps her adjust to epilepsy’s chronic nature and complications.
- Epilepsy Foundation. Epilepsy and mood disorders. www.epilepsyfoundation.org/programs/mood.
- Epilepsy Foundation. Neurological Disorders Depression Inventory for Epilepsy Screening Tool. www.epilepsyfoundation.org/about/related/mood/nddietool.cfm.
- Amitriptyline • Elavil
- Amoxapine • Asendin
- Bupropion • Wellbutrin
- Carbamazepine • Tegretol
- Citalopram • Celexa
- Clomipramine • Anafranil
- Desipramine • Norpramin
- Doxepin • Sinequan
- Duloxetine • Cymbalta
- Fluoxetine • Prozac
- Fluvoxamine • Luvox
- Imipramine • Tofranill
- Lamotrigine • Lamictal
- Lithium • Eskalith, Lithobid
- Nomifensine • Merital
- Maprotiline • Ludiomil
- Mirtazapine • Remeron
- Nefazodone • Serzone
- Nortriptyline • Aventyl, Pamelor
- Oxcarbazepine • Trileptal
- Paroxetine • Paxil
- Phenytoin • Dilantin
- Primidone • Mysoline
- Sertraline • Zoloft
- Tiagabine • Gabitril
- Topiramate • Topamax
- Trazodone • Desyrel
- Valproic acid • Depakote
- Venlafaxine • Effexor
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Kanner AM. Should neurologists be trained to recognize and treat comorbid depression of neurologic disorders? Yes. Epilepsy Behav 2005;6(3):303-11.
2. Gilliam FG. Diagnosis and treatment of mood disorders in persons with epilepsy. Curr Opin Neurol 2005;18(2):129-33.
3. Jackson MJ, Turkington D. Depression and anxiety in epilepsy. J Neurol Neurosurg Psychiatry 2005;76(suppl 1):45-7.
4. Lambert MV, Robertson MM. Depression in epilepsy: etiology, phenomenology, and treatment. Epilepsia 1999;40(suppl 10):S21-S47.
5. Gaitatzis A, Trimble MR, Sander JW. The psychiatric comorbidity of epilepsy. Acta Neurol Scand 2004;110(4):207-20.
6. Barry JJ. The recognition and management of mood disorders as a comorbidity of epilepsy. Epilepsia 2003;44(suppl 4):30-40.
7. Blumer D, Montouris G, Davies K. The interictal dysphoric disorder: recognition, pathogenesis, and treatment of the major psychiatric disorder of epilepsy. Epilepsy Behav 2004;5(6):826-40.
8. Robertson M. Mood disorders associated with epilepsy. In: McConnell HW, Snyder PJ, eds. Psychiatric comorbidity in epilepsy: basic mechanisms, diagnosis, and treatment. Washington DC: American Psychiatric Publishing; 1998:133-67.
9. Harris EC, Barraclough B. Suicide as an outcome for mental disorders. A meta-analysis. Br J Psychiatry 1997;170:205-28.
10. Shorvon SD, Reynolds EH. Reduction in polypharmacy for epilepsy. Br Med J 1979;2(6197):1023-5.
11. Mula M, Trimle MR, Lhatoo SD, Sander JW. Topiramate and psychiatric adverse events in patients with epilepsy. Epilepsia 2003;44(5):659-63.
12. Selai C, Bannister D, Trimble M. Antiepileptic drugs and the regulation of mood and quality (QOL): the evidence from epilepsy. Epilepsia 2005;46(suppl 4):50-7.
13. McConnell H, Duncan D. Treatment of psychiatric comorbidity in epilepsy. In: McConnell HW, Snyder PJ, eds. Psychiatric comorbidity in epilepsy: basic mechanisms, diagnosis, and treatment. Washington DC: American Psychiatric Publishing; 1998:245-361.
14. Charney DS, Berman RM, Miller HL. Treatment of depression. In: Schatzberg AF, Nemeroff CB, eds. Essentials of clinical psychopharmacology. Washington DC: American Psychiatric Publishing; 2001:359.
15. Tucker GJ. Neuropsychiatric aspects of seizure disorders. In: Yudofsky SC, Hales RE, eds. Essentials of neuropsychiatry and clinical neurosciences. Washington DC: American Psychiatric Publishing; 2004:293-313.
16. Becu M, Becu N, Manzur G, Kochen S. Self-help epilepsy groups: an evaluation of effect on depression and schizophrenia. Epilepsia 1993;34(5):841-5.
17. Goldstein LH, McAlpine M, Deale A, et al. Cognitive behaviour therapy with adults with intractable epilepsy and psychiatric co-morbidity: preliminary observations on changes in psychological state and seizure frequency. Behav Res Ther 2003;41(4):447-6.
1. Kanner AM. Should neurologists be trained to recognize and treat comorbid depression of neurologic disorders? Yes. Epilepsy Behav 2005;6(3):303-11.
2. Gilliam FG. Diagnosis and treatment of mood disorders in persons with epilepsy. Curr Opin Neurol 2005;18(2):129-33.
3. Jackson MJ, Turkington D. Depression and anxiety in epilepsy. J Neurol Neurosurg Psychiatry 2005;76(suppl 1):45-7.
4. Lambert MV, Robertson MM. Depression in epilepsy: etiology, phenomenology, and treatment. Epilepsia 1999;40(suppl 10):S21-S47.
5. Gaitatzis A, Trimble MR, Sander JW. The psychiatric comorbidity of epilepsy. Acta Neurol Scand 2004;110(4):207-20.
6. Barry JJ. The recognition and management of mood disorders as a comorbidity of epilepsy. Epilepsia 2003;44(suppl 4):30-40.
7. Blumer D, Montouris G, Davies K. The interictal dysphoric disorder: recognition, pathogenesis, and treatment of the major psychiatric disorder of epilepsy. Epilepsy Behav 2004;5(6):826-40.
8. Robertson M. Mood disorders associated with epilepsy. In: McConnell HW, Snyder PJ, eds. Psychiatric comorbidity in epilepsy: basic mechanisms, diagnosis, and treatment. Washington DC: American Psychiatric Publishing; 1998:133-67.
9. Harris EC, Barraclough B. Suicide as an outcome for mental disorders. A meta-analysis. Br J Psychiatry 1997;170:205-28.
10. Shorvon SD, Reynolds EH. Reduction in polypharmacy for epilepsy. Br Med J 1979;2(6197):1023-5.
11. Mula M, Trimle MR, Lhatoo SD, Sander JW. Topiramate and psychiatric adverse events in patients with epilepsy. Epilepsia 2003;44(5):659-63.
12. Selai C, Bannister D, Trimble M. Antiepileptic drugs and the regulation of mood and quality (QOL): the evidence from epilepsy. Epilepsia 2005;46(suppl 4):50-7.
13. McConnell H, Duncan D. Treatment of psychiatric comorbidity in epilepsy. In: McConnell HW, Snyder PJ, eds. Psychiatric comorbidity in epilepsy: basic mechanisms, diagnosis, and treatment. Washington DC: American Psychiatric Publishing; 1998:245-361.
14. Charney DS, Berman RM, Miller HL. Treatment of depression. In: Schatzberg AF, Nemeroff CB, eds. Essentials of clinical psychopharmacology. Washington DC: American Psychiatric Publishing; 2001:359.
15. Tucker GJ. Neuropsychiatric aspects of seizure disorders. In: Yudofsky SC, Hales RE, eds. Essentials of neuropsychiatry and clinical neurosciences. Washington DC: American Psychiatric Publishing; 2004:293-313.
16. Becu M, Becu N, Manzur G, Kochen S. Self-help epilepsy groups: an evaluation of effect on depression and schizophrenia. Epilepsia 1993;34(5):841-5.
17. Goldstein LH, McAlpine M, Deale A, et al. Cognitive behaviour therapy with adults with intractable epilepsy and psychiatric co-morbidity: preliminary observations on changes in psychological state and seizure frequency. Behav Res Ther 2003;41(4):447-6.
ADHD in adults: Matching therapies with patients’ needs
Mr. Z, age 42, is referred by his primary care physician with symptoms suggesting attention-deficit/hyperactivity disorder (ADHD). Mr. Z has seen his physician sporadically for 10 years and acknowledges not following dietary and exercise advice. He has had intermittent “minor” depression, is overweight, and is a smoker with a family history of cardiovascular disease and diabetes.
A salesman, Mr. Z recently was promoted to an administrative position that substantially increased his paperwork. He is having difficulty performing his job because of longstanding forgetfulness and disorganization. He says he feels “like I’m in grade school again, lost in paperwork.” He also describes a recent educational assessment for his son, age 7, who may have ADHD. Similarities between Mr. Z’s and his son’s early childhood academic struggles are striking.
Like Mr. Z, adults with ADHD commonly seek treatment when increasing stressors and demands overwhelm their cognitive-attentional abilities. Some may be “healthy” men and women without psychiatric histories, whose disorganization, forgetfulness, or impulsivity contributes to functional impairment, including nonadherence with medical advice. For others, such as those with known psychiatric disorders, ADHD may be a hidden comorbidity contributing to seemingly refractory depression or anxiety disorder.
Despite growing evidence related to adult ADHD, individualizing and maintaining treatment over time can be challenging for clinicians and patients. Fortunately, new tools and multiple stimulant and nonstimulant medications can help you screen for, assess, and treat adult ADHD.
ADHD diagnosis
To diagnose ADHD in an adult patient, first establish that symptoms have existed from childhood to adulthood. One approach is to review DSM-IV-TR criteria for ADHD with your patient and ask him or her to reflect on childhood symptoms and dysfunction. Begin with orienting questions, such as “Do you remember your first grade teacher, your school, where you lived?” ADHD symptoms might have been present even if the patient maintained acceptable grades, particularly in elementary school, as dedicated parents or teachers might have contributed to early academic success.
Next, turn to diagnostic language that captures ADHD symptoms in adults. For example, the 18-item World Health Organization Adult ADHD Self-Report Scale (ASRS-v1.1) prompts individuals to self-report DSM-IV ADHD symptoms, and a 6-item subset (Table 1) is a highly specific screener (see Related Resources). The ASRS is most reliable in adults with limited psychiatric comorbidity.1
Adults often describe fluctuations in symptom severity over time. Symptoms may have less impact with more physically demanding work—such as sales—and greater impact with organizationally demanding work—such as administration.
Base your summary ADHD diagnosis on DSM-IV-TR criteria, including:
- lifetime persistence of symptoms, beginning before age 7
- functional impairment in ≥2 life settings, such as work, school, or home
- lack of another medical or psychiatric condition sufficient to explain the symptoms.
Table 1
Adult Self-Report Scale-v1.1 WHO 6-question screening tool for ADHD*
| Check the box that best describes how you have felt and conducted yourself over the past 6 months. Please give the completed questionnaire to your healthcare professional during your next appointment to discuss the results | Never | Rarely | Sometimes | Often | Very often |
|---|---|---|---|---|---|
| 1. How often do you have trouble wrapping up the final details of a project, once the challenging parts have been done? | |||||
| 2. How often do you have difficulty getting things in order when you have to do a task that requires organization? | |||||
| 3. How often do you have problems remembering appointments or obligations? | |||||
| 4. When you have a task that requires a lot of thought, how often do you avoid or delay getting started? | |||||
| 5. How often do you fidget or squirm with your hands or feet when you have to sit down for a long time? | |||||
| 6. How often do you feel overly active and compelled to do things, like you were driven by a motor? | |||||
| Add the number of checkmarks that appear in the darkly shaded area. Four (4) or more checkmarks indicate that your symptoms may be consistent with adult ADHD. It may be beneficial for you to talk with your healthcare provider about an evaluation. | |||||
| * Intended for use by persons age 18 and older ADHD: attention-deficit/hyperactivity disorder; WHO: World Health Organization | |||||
| Source: Reprinted with permission. World Health Organization Copyright 2003. All rights reserved | |||||
CASE CONTINUED: ‘All the time, every day’
Mr. Z completes the ASRS self-report symptom checklist and brings his wife to the next appointment. He rated all 6 screening symptoms and most others as occurring “often” or “very often.” He describes functional impairments “essentially all the time, basically every day” at work, home, and socially. His wife confirms these symptoms and the frustrations and conflicts they have caused.
Mr. Z describes ADHD symptoms from early elementary school to college. He was held back in kindergarten for being “immature,” his academic performance was inconsistent, and he “just got by…by cramming” in high school and college. His school performance pattern does not suggest a learning disability; he did not need special help in 1 subject more than others, and under pressure he could achieve average grades.
Medical review excludes explanations other than ADHD for his inattention, restlessness, and impulsivity. You conclude that Mr. Z meets criteria for ADHD, combined subtype, and discuss medication treatment.
FDA-approved medications
Medication for ADHD is appropriate only if symptoms are impairing. Five effective and generally well-tolerated medications are FDA-approved for adults with ADHD (Table 2):
- extended-release mixed amphetamine (Adderall XR)
- extended-release OROS methylphenidate (Concerta)
- extended-release dexmethylphenidate (Focalin XR)
- atomoxetine (Strattera)
- lisdexamfetamine (Vyvanse).
Efficacy. A meta-analysis of 29 pediatric ADHD trials across 30 years demonstrated greater effect size for stimulant class medications (immediate- and long-acting), compared with nonstimulant medications (including bupropion, atomoxetine, and modafinil).2 This finding is consistent with the American Academy of Child and Adolescent Psychiatry’s recommendation of stimulant medications as first-line agents for pediatric ADHD.3 A similar meta-analysis of 6 controlled studies of methylphenidate-class medications in adults found a large mean effect size (0.9), with greater effects associated with higher doses.4
Atomoxetine, a norepinephrine reuptake inhibitor, is the only nonstimulant medication FDA-approved for ADHD in adults. More than 6,000 children, adolescents, and adults have taken atomoxetine in clinical trials for ADHD (Lilly, prescribing information), with 4 years of open treatment data showing benefit being maintained over time.5
Tolerability. Although ADHD medications are generally well-tolerated by healthy adults, assess for a history of potential contraindications:
- unstable medical condition, hyperthyroidism, glaucoma
- treatment with a monoamine oxidase inhibitor or other pressor agents because of possible effects on blood pressure and heart rate
- use of cytochrome P450 2D6 inhibitors, which may increase atomoxetine steady-state plasma concentrations
- cardiovascular disease or family history of early cardiac disease (Box 1)6,7
- history of or active substance use disorder, such as alcohol dependence, cocaine or heroin abuse
- history of psychosis, bipolar disorder, or an active clinically significant psychiatric comorbidity (major depression, agitated state, suicidality).
Clinically, some patients appear to tolerate 1 class of stimulant (such as methylphenidate or amphetamine) over another. Consider switching to an alternate stimulant if your patient has bothersome side effects—mild low appetite, insomnia, tension, or jitteriness—or has received limited or partial benefit during an initial stimulant trial.
Serious cardiovascular events and sudden death have occurred in adults and children treated with stimulants.6 Agents used for attention-deficit/hyperactivity disorder (ADHD) have not been shown to cause sudden cardiac death, but the FDA requires stimulants’ labeling to warn about this risk in patients with structural cardiac abnormalities. The warning advises against using stimulants in adults with cardiomyopathy, serious heart rhythm abnormalities, or coronary artery disease.
When treating adults with ADHD, look to advisories about cardiovascular monitoring in children with ADHD. Before initiating medications, do a physical exam focused on cardiovascular disease risk factors and obtain a patient and family health history of:
- fainting or dizziness
- sudden or unexplained death in someone young
- sudden cardiac death or “heart attack” in family members age <35 years.
The American Academy of Pediatrics, American Academy of Child and Adolescent Psychiatry, and American Heart Association concur that electrocardiography (ECG) is not mandatory in cardiovascular assessment and monitoring during ADHD pharmacotherapy.7 This author (PH) refers cardiovascular questions to a primary care physician or cardiologist.
During ADHD treatment, monitor vital signs and refer patients with emergent cardiac symptoms or concerns to a cardiologist. Expect increases in blood pressure (1 to 4 mm Hg) and heart rate (2 to 6 bpm) during treatment with methylphenidate and amphetamine-class stimulants as well as with atomoxetine. Do not expect significant changes in ECG parameters (PR, QRS, and QTC intervals).
Extended-release formulations. Early adult studies demonstrated the efficacy of immediate-release stimulants, but adults with ADHD’s inherent deficits in organization and memory may have higher adherence rates and greater success with once-daily, extended-release formulations.8-11 Unless your patient wants to begin with small, short-acting dosages (5 to 10 mg) or desires to target treatment to specific times of day (such as in the morning for administrative work only), many appreciate once-daily formulations. Extended-release formulations also may be the simplest stimulants with which to begin ADHD treatment.
Over time, patients may benefit from an immediate-release form:
- added for certain times of day—such as in late afternoon, when the morning extended-release dose has worn off (Box 2)12,13
- to use as an alternative to extended-release formulations when more or less flexibly is desired, such as on weekends.
Table 2
Administering medications approved for adult ADHD
| Drug | Recommended dosage* | Comments |
|---|---|---|
| Stimulants | ||
| Extended-release mixed amphetamine (Adderall XR) | 20 mg | Initial prescription of 10-mg XR capsules allows gradual titration |
| Extended-release OROS methylphenidate (Concerta) | 18 to 72 mg/d | Initial prescription of 18-mg OROS MPH capsules allows gradual titration |
| Extended-release dexmethylphenidate (Focalin XR) | 10 mg/d; maximum 20 mg/d | Dosing is one-half the typical dosing of racemic MPH |
| Lisdexamfetamine (Vyvanse) | 30 mg/d; maximum 70 mg/d | May be adjusted weekly in 10-mg or 20-mg increments |
| Nonstimulant | ||
| Atomoxetine (Strattera) | 80 mg/d; maximum 100 mg/d | Initial dosage of 40 mg/d can be increased to target dosage after a minimum of 3 days; can be given as a morning dose or divided evenly between morning and evening doses |
| * FDA-approved dosages as listed in the package inserts of these medications ADHD: attention-deficit/hyperactivity disorder; MPH: methylphenidate; OROS: osmotic release oral system; XR: extended-release formulation | ||
CASE CONTINUED: Feeling ‘calm, less frenetic’
During the next 6 months, you start Mr. Z on stimulant treatment at robust dosing consistent with his weight (90 kg). He complains that extended-duration methylphenidate (MPH)—titrated to 90 mg/d—doesn’t last into the late afternoon, and he feels mildly tense with a low appetite. Because of an apparent partial response and relatively mild adverse effects, you discontinue MPH and try an extended-duration amphetamine, titrated to 60 mg.
Mr. Z’s blood pressure and heart rate remain stable. He begins to exercise regularly and reduce his use of tobacco and caffeine drinks, as you recommend. He says he feels “calm, less frenetic.” He reports no tension on this medication and only mild reduced appetite. With a plan to continue taking the stimulant medication with regular monitoring, he then disappears from treatment.
Promoting adherence
Treatment nonadherence is an issue throughout medicine, and individuals with disorganization, forgetfulness, and impulsivity may be at higher-than-usual risk of not following through on medication regimens.
Combining short- and long-acting stimulants may cover hours when attention-deficit/hyperactivity (ADHD) symptoms emerge despite therapy with a long-acting agent.12,13 Ask patients who report lack of full-day coverage if the once-daily, extended-duration formulation they are taking works well until a certain time of day. Then consider adding a similar-class immediate-release stimulant at this time to cover the later hours.
If a patient reports partial response throughout the day—such as early in treatment—begin by optimizing the long-acting agent’s dosage. Keep a target daily dose in mind, based on FDA recommendations and clinical trial data. For example, an adult weighing 80 kg may respond optimally to a combination of 60 mg of a long-acting methylphenidate (MPH) in the morning, followed by 10 to 20 mg of an immediate-release MPH in mid-afternoon.
The later stimulants are taken in the day, the more likely insomnia may emerge as an adverse effect. Some patients adjust to this problem within the first weeks of treatment. If insomnia remains impairing, reduce the stimulant dose or consider switching to a shorter duration medication or to the nonstimulant atomoxetine.
In addition, restrictions on stimulant-class medications do not permit multiple-month prescribing (refills), as is allowed with non-scheduled medications such as atomoxetine. Discuss with patients how they will obtain stimulant medications on a regular, monthly or bimonthly basis. In our experience, the practical challenges of remaining in treatment at times may limit patients’ adherence to ADHD medications more than a lack of response or tolerability concerns.
Explain to patients early in treatment that they might need to try several different medications before settling on 1 that is optimally tolerated and efficacious. Because stimulants are generally quite effective for ADHD symptoms, set your goal to identify adverse effects and aim for a patient response of “this works well, and I don’t feel any different on it.”
CASE CONTINUED: Ready to try again
Three years later, Mr. Z returns and reports gradually discontinuing the stimulant because he “wanted to go it on my own.” He functioned relatively well at first, but errors and conflicts at his job led to his dismissal.
Since then, he has been unemployed. He is increasingly depressed and reports drinking and smoking “more heavily than in college.” He asks about resuming ADHD treatment.
Mr. Z does not meet DSM-IV-TR criteria for major depressive disorder or alcohol abuse/dependence. His depressed mood appears to be linked to his marked ADHD symptoms. Mr. Z agrees to a new treatment plan that includes starting atomoxetine at 25 mg to allow for flexible titration and psychotherapy to monitor his mood and achieve sobriety.
ADHD and substance abuse
Clinical judgment determines whether an adult with ADHD and a history of substance use disorders may safely benefit from treatment with a stimulant. The relationship between ADHD and substance use disorders is of clinical concern, but ADHD medications have not been shown to increase risk for later substance use disorders in children.14 Conversely, effective ADHD treatment appears to reduce later cigarette and substance use.15
Consider using a nonstimulant-class medication in adults with ADHD and active substance use disorders. In a 12-week, double-blind, controlled trial, atomoxetine improved ADHD symptoms significantly more than placebo in adults meeting DS-MIV-TR criteria for comorbid alcohol use disorders. After 4 to 30 days of alcohol abstinence, 72 patients were randomly assigned to atomoxetine, 25 to 100 mg/d (mean final dose 90 mg/d), and 75 patients to placebo. Although estimated times to initial relapse to heavy drinking did not differ:
- atomoxetine-treated subjects had 26% fewer cumulative heavy drinking days than placebo-treated subjects (P=0.023)
- the difference in cumulative heavy drinking days between the atomoxetine and placebo groups became statistically significant after 55 days of treatment.16
- World Health Organization Adult Self-Report Scale (ASRS) 18-item instrument and 6-item screener. www.med.nyu.edu/psych/psychiatrist/adhd.html.
- Volkow ND, Swanson JM. Does childhood treatment of ADHD with stimulant medication affect substance abuse in adulthood? Am J Psychiatry 2008;165:553-5.
- Adler LA, Spencer TJ, Levine LR, et al. Functional outcomes in the treatment of adults with ADHD. J Atten Disord 2008; 11:720-7.
Drug brand names
- Atomoxetine • Strattera
- Bupropion • Wellbutrin
- Extended-release mixed amphetamine • Adderall XR
- Extended duration OROS methylphenidate • Concerta
- Extended-release dexmethylphenidate • Focalin XR
- Lisdexamfetamine • Vyvanse
- Modafinil • Provigil
Disclosure
Dr. Hammerness has received research support from and is on the speakers bureau for Shire Pharmaceuticals. He has received support for CME activities and talks from Shire Pharmaceuticals, Ortho-McNeil, and Abbott Laboratories.
Dr. Surman receives research support and/or is a speaker for Abbott Laboratories, Cephalon, Eli Lilly and Company, Janssen, Ortho-McNeil, Merck, New River Pharmaceuticals, Novartis, Pfizer Inc., Shire Pharmaceuticals, and Takeda Pharmaceutical Company.
Dr. Sassi reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Acknowledgement
Clinical research assistant Katherine Miller, BA, contributed to the literature review for this article and assisted in preparing the manuscript.
1. Kessler RC, Adler L, Ames M, et al. The World Health Organization Adult ADHD Self-Report Scale (ASRS): a short screening scale for use in the general population. Psychol Med 2005;35:245-56.
2. Faraone SV, Biederman J, Spencer TJ, Aleardi M. Comparing the efficacy of medications for ADHD using meta-analysis. MedGenMed 2006;8(4):4.-
3. Greenhill L, Pliszka S, Dulcan M, et al. Summary of the practice parameter for the use of stimulant medications in the treatment of children, adolescents, and adults. J Am Acad Child Adolesc Psychiatry 2001;40(11):1352-5.
4. Faraone SV, Spencer T, Aleardi M, et al. Meta-analysis of the efficacy of methylphenidate for treating adult attention-deficit/hyperactivity disorder. J Clin Psychopharmacol 2004;24:24-9.
5. Adler LA, Spencer TJ, Williams DW, et al. Long-term, open-label safety and efficacy of atomoxetine in adults with ADHD: final report of a 4-year study. J Atten Disord Epub 2008 April 30.
6. Nissen SE. ADHD drugs and cardiovascular risk. N Engl J Med 2006;354:1445-8.
7. American Academy of Pediatrics/American Heart Association clarification of statement on cardiovascular evaluation and monitoring of children and adolescents with heart disease receiving medications for ADHD May 16, 2008. Available at: http://www.aap.org/pressroom/aap-ahastatement.htm. Accessed August 14, 2008.
8. Biederman J, Mick E, Surman C, et al. A randomized, placebo-controlled trial of OROS methylphenidate in adults with attention-deficit/hyperactivity disorder. Biol Psychiatry 2006;59(9):829-35.
9. Biederman J, Mick E, Surman C, et al. Comparative acute efficacy and tolerability of OROS and immediate release formulations of methylphenidate in the treatment of adults with attention-deficit/hyperactivity disorder. BMC Psychiatry 2007;7:49.-
10. Mick E, Spencer TJ, Surman C, et al. Randomized single-blind substitution study of methylphenidate in ADHD adults receiving immediate-release methylphenidate. NR357. Poster presented at: Annual Meeting of the American Psychiatric Association; May 19-24, 2007; San Diego, CA.
11. Capone N, McDonnel T. Medication persistence among agents used to treat attention-deficit/hyperactivity disorder, diabetes, and elevated serum cholesterol. NR 639. Poster presented at: Annual Meeting of the American Psychiatric Association; May 20-25, 2006; Toronto, Ontario, Canada.
12. Adler L, Morrill M, Reingold B. d-methylphenidate augmentation of extended-release stimulant therapy in ADHD. NR 619. Poster presented at: Annual Meeting of the American Psychiatric Association; May 20-25, 2006; Toronto, Ontario, Canada.
13. Adler L, Reingold LS, Morrill MS, Wilens TE. Combination pharmacotherapy for adult ADHD. Curr Psychiatry Rep 2006;8:409-15.
14. Biederman J, Monuteaux MC, Spencer T, et al. Stimulant therapy and risk for subsequent substance use disorders in male adults with ADHD: a naturalistic controlled 10-year follow-up study. Am J Psychiatry 2008;165:597-603.
15. Faraone SV, Wilens TE. Effect of stimulant medications for attention-deficit/hyperactivity disorder on later substance use and the potential for stimulant misuse, abuse, and diversion. J Clin Psychiatry 2007;68(suppl 11):15-22.
16. Wilens TE, Adler LA, Weiss MD, et al. Atomoxetine treatment of adults with ADHD and comorbid alcohol use disorders. Drug Alcohol Depend 2008;96:145-54.
Mr. Z, age 42, is referred by his primary care physician with symptoms suggesting attention-deficit/hyperactivity disorder (ADHD). Mr. Z has seen his physician sporadically for 10 years and acknowledges not following dietary and exercise advice. He has had intermittent “minor” depression, is overweight, and is a smoker with a family history of cardiovascular disease and diabetes.
A salesman, Mr. Z recently was promoted to an administrative position that substantially increased his paperwork. He is having difficulty performing his job because of longstanding forgetfulness and disorganization. He says he feels “like I’m in grade school again, lost in paperwork.” He also describes a recent educational assessment for his son, age 7, who may have ADHD. Similarities between Mr. Z’s and his son’s early childhood academic struggles are striking.
Like Mr. Z, adults with ADHD commonly seek treatment when increasing stressors and demands overwhelm their cognitive-attentional abilities. Some may be “healthy” men and women without psychiatric histories, whose disorganization, forgetfulness, or impulsivity contributes to functional impairment, including nonadherence with medical advice. For others, such as those with known psychiatric disorders, ADHD may be a hidden comorbidity contributing to seemingly refractory depression or anxiety disorder.
Despite growing evidence related to adult ADHD, individualizing and maintaining treatment over time can be challenging for clinicians and patients. Fortunately, new tools and multiple stimulant and nonstimulant medications can help you screen for, assess, and treat adult ADHD.
ADHD diagnosis
To diagnose ADHD in an adult patient, first establish that symptoms have existed from childhood to adulthood. One approach is to review DSM-IV-TR criteria for ADHD with your patient and ask him or her to reflect on childhood symptoms and dysfunction. Begin with orienting questions, such as “Do you remember your first grade teacher, your school, where you lived?” ADHD symptoms might have been present even if the patient maintained acceptable grades, particularly in elementary school, as dedicated parents or teachers might have contributed to early academic success.
Next, turn to diagnostic language that captures ADHD symptoms in adults. For example, the 18-item World Health Organization Adult ADHD Self-Report Scale (ASRS-v1.1) prompts individuals to self-report DSM-IV ADHD symptoms, and a 6-item subset (Table 1) is a highly specific screener (see Related Resources). The ASRS is most reliable in adults with limited psychiatric comorbidity.1
Adults often describe fluctuations in symptom severity over time. Symptoms may have less impact with more physically demanding work—such as sales—and greater impact with organizationally demanding work—such as administration.
Base your summary ADHD diagnosis on DSM-IV-TR criteria, including:
- lifetime persistence of symptoms, beginning before age 7
- functional impairment in ≥2 life settings, such as work, school, or home
- lack of another medical or psychiatric condition sufficient to explain the symptoms.
Table 1
Adult Self-Report Scale-v1.1 WHO 6-question screening tool for ADHD*
| Check the box that best describes how you have felt and conducted yourself over the past 6 months. Please give the completed questionnaire to your healthcare professional during your next appointment to discuss the results | Never | Rarely | Sometimes | Often | Very often |
|---|---|---|---|---|---|
| 1. How often do you have trouble wrapping up the final details of a project, once the challenging parts have been done? | |||||
| 2. How often do you have difficulty getting things in order when you have to do a task that requires organization? | |||||
| 3. How often do you have problems remembering appointments or obligations? | |||||
| 4. When you have a task that requires a lot of thought, how often do you avoid or delay getting started? | |||||
| 5. How often do you fidget or squirm with your hands or feet when you have to sit down for a long time? | |||||
| 6. How often do you feel overly active and compelled to do things, like you were driven by a motor? | |||||
| Add the number of checkmarks that appear in the darkly shaded area. Four (4) or more checkmarks indicate that your symptoms may be consistent with adult ADHD. It may be beneficial for you to talk with your healthcare provider about an evaluation. | |||||
| * Intended for use by persons age 18 and older ADHD: attention-deficit/hyperactivity disorder; WHO: World Health Organization | |||||
| Source: Reprinted with permission. World Health Organization Copyright 2003. All rights reserved | |||||
CASE CONTINUED: ‘All the time, every day’
Mr. Z completes the ASRS self-report symptom checklist and brings his wife to the next appointment. He rated all 6 screening symptoms and most others as occurring “often” or “very often.” He describes functional impairments “essentially all the time, basically every day” at work, home, and socially. His wife confirms these symptoms and the frustrations and conflicts they have caused.
Mr. Z describes ADHD symptoms from early elementary school to college. He was held back in kindergarten for being “immature,” his academic performance was inconsistent, and he “just got by…by cramming” in high school and college. His school performance pattern does not suggest a learning disability; he did not need special help in 1 subject more than others, and under pressure he could achieve average grades.
Medical review excludes explanations other than ADHD for his inattention, restlessness, and impulsivity. You conclude that Mr. Z meets criteria for ADHD, combined subtype, and discuss medication treatment.
FDA-approved medications
Medication for ADHD is appropriate only if symptoms are impairing. Five effective and generally well-tolerated medications are FDA-approved for adults with ADHD (Table 2):
- extended-release mixed amphetamine (Adderall XR)
- extended-release OROS methylphenidate (Concerta)
- extended-release dexmethylphenidate (Focalin XR)
- atomoxetine (Strattera)
- lisdexamfetamine (Vyvanse).
Efficacy. A meta-analysis of 29 pediatric ADHD trials across 30 years demonstrated greater effect size for stimulant class medications (immediate- and long-acting), compared with nonstimulant medications (including bupropion, atomoxetine, and modafinil).2 This finding is consistent with the American Academy of Child and Adolescent Psychiatry’s recommendation of stimulant medications as first-line agents for pediatric ADHD.3 A similar meta-analysis of 6 controlled studies of methylphenidate-class medications in adults found a large mean effect size (0.9), with greater effects associated with higher doses.4
Atomoxetine, a norepinephrine reuptake inhibitor, is the only nonstimulant medication FDA-approved for ADHD in adults. More than 6,000 children, adolescents, and adults have taken atomoxetine in clinical trials for ADHD (Lilly, prescribing information), with 4 years of open treatment data showing benefit being maintained over time.5
Tolerability. Although ADHD medications are generally well-tolerated by healthy adults, assess for a history of potential contraindications:
- unstable medical condition, hyperthyroidism, glaucoma
- treatment with a monoamine oxidase inhibitor or other pressor agents because of possible effects on blood pressure and heart rate
- use of cytochrome P450 2D6 inhibitors, which may increase atomoxetine steady-state plasma concentrations
- cardiovascular disease or family history of early cardiac disease (Box 1)6,7
- history of or active substance use disorder, such as alcohol dependence, cocaine or heroin abuse
- history of psychosis, bipolar disorder, or an active clinically significant psychiatric comorbidity (major depression, agitated state, suicidality).
Clinically, some patients appear to tolerate 1 class of stimulant (such as methylphenidate or amphetamine) over another. Consider switching to an alternate stimulant if your patient has bothersome side effects—mild low appetite, insomnia, tension, or jitteriness—or has received limited or partial benefit during an initial stimulant trial.
Serious cardiovascular events and sudden death have occurred in adults and children treated with stimulants.6 Agents used for attention-deficit/hyperactivity disorder (ADHD) have not been shown to cause sudden cardiac death, but the FDA requires stimulants’ labeling to warn about this risk in patients with structural cardiac abnormalities. The warning advises against using stimulants in adults with cardiomyopathy, serious heart rhythm abnormalities, or coronary artery disease.
When treating adults with ADHD, look to advisories about cardiovascular monitoring in children with ADHD. Before initiating medications, do a physical exam focused on cardiovascular disease risk factors and obtain a patient and family health history of:
- fainting or dizziness
- sudden or unexplained death in someone young
- sudden cardiac death or “heart attack” in family members age <35 years.
The American Academy of Pediatrics, American Academy of Child and Adolescent Psychiatry, and American Heart Association concur that electrocardiography (ECG) is not mandatory in cardiovascular assessment and monitoring during ADHD pharmacotherapy.7 This author (PH) refers cardiovascular questions to a primary care physician or cardiologist.
During ADHD treatment, monitor vital signs and refer patients with emergent cardiac symptoms or concerns to a cardiologist. Expect increases in blood pressure (1 to 4 mm Hg) and heart rate (2 to 6 bpm) during treatment with methylphenidate and amphetamine-class stimulants as well as with atomoxetine. Do not expect significant changes in ECG parameters (PR, QRS, and QTC intervals).
Extended-release formulations. Early adult studies demonstrated the efficacy of immediate-release stimulants, but adults with ADHD’s inherent deficits in organization and memory may have higher adherence rates and greater success with once-daily, extended-release formulations.8-11 Unless your patient wants to begin with small, short-acting dosages (5 to 10 mg) or desires to target treatment to specific times of day (such as in the morning for administrative work only), many appreciate once-daily formulations. Extended-release formulations also may be the simplest stimulants with which to begin ADHD treatment.
Over time, patients may benefit from an immediate-release form:
- added for certain times of day—such as in late afternoon, when the morning extended-release dose has worn off (Box 2)12,13
- to use as an alternative to extended-release formulations when more or less flexibly is desired, such as on weekends.
Table 2
Administering medications approved for adult ADHD
| Drug | Recommended dosage* | Comments |
|---|---|---|
| Stimulants | ||
| Extended-release mixed amphetamine (Adderall XR) | 20 mg | Initial prescription of 10-mg XR capsules allows gradual titration |
| Extended-release OROS methylphenidate (Concerta) | 18 to 72 mg/d | Initial prescription of 18-mg OROS MPH capsules allows gradual titration |
| Extended-release dexmethylphenidate (Focalin XR) | 10 mg/d; maximum 20 mg/d | Dosing is one-half the typical dosing of racemic MPH |
| Lisdexamfetamine (Vyvanse) | 30 mg/d; maximum 70 mg/d | May be adjusted weekly in 10-mg or 20-mg increments |
| Nonstimulant | ||
| Atomoxetine (Strattera) | 80 mg/d; maximum 100 mg/d | Initial dosage of 40 mg/d can be increased to target dosage after a minimum of 3 days; can be given as a morning dose or divided evenly between morning and evening doses |
| * FDA-approved dosages as listed in the package inserts of these medications ADHD: attention-deficit/hyperactivity disorder; MPH: methylphenidate; OROS: osmotic release oral system; XR: extended-release formulation | ||
CASE CONTINUED: Feeling ‘calm, less frenetic’
During the next 6 months, you start Mr. Z on stimulant treatment at robust dosing consistent with his weight (90 kg). He complains that extended-duration methylphenidate (MPH)—titrated to 90 mg/d—doesn’t last into the late afternoon, and he feels mildly tense with a low appetite. Because of an apparent partial response and relatively mild adverse effects, you discontinue MPH and try an extended-duration amphetamine, titrated to 60 mg.
Mr. Z’s blood pressure and heart rate remain stable. He begins to exercise regularly and reduce his use of tobacco and caffeine drinks, as you recommend. He says he feels “calm, less frenetic.” He reports no tension on this medication and only mild reduced appetite. With a plan to continue taking the stimulant medication with regular monitoring, he then disappears from treatment.
Promoting adherence
Treatment nonadherence is an issue throughout medicine, and individuals with disorganization, forgetfulness, and impulsivity may be at higher-than-usual risk of not following through on medication regimens.
Combining short- and long-acting stimulants may cover hours when attention-deficit/hyperactivity (ADHD) symptoms emerge despite therapy with a long-acting agent.12,13 Ask patients who report lack of full-day coverage if the once-daily, extended-duration formulation they are taking works well until a certain time of day. Then consider adding a similar-class immediate-release stimulant at this time to cover the later hours.
If a patient reports partial response throughout the day—such as early in treatment—begin by optimizing the long-acting agent’s dosage. Keep a target daily dose in mind, based on FDA recommendations and clinical trial data. For example, an adult weighing 80 kg may respond optimally to a combination of 60 mg of a long-acting methylphenidate (MPH) in the morning, followed by 10 to 20 mg of an immediate-release MPH in mid-afternoon.
The later stimulants are taken in the day, the more likely insomnia may emerge as an adverse effect. Some patients adjust to this problem within the first weeks of treatment. If insomnia remains impairing, reduce the stimulant dose or consider switching to a shorter duration medication or to the nonstimulant atomoxetine.
In addition, restrictions on stimulant-class medications do not permit multiple-month prescribing (refills), as is allowed with non-scheduled medications such as atomoxetine. Discuss with patients how they will obtain stimulant medications on a regular, monthly or bimonthly basis. In our experience, the practical challenges of remaining in treatment at times may limit patients’ adherence to ADHD medications more than a lack of response or tolerability concerns.
Explain to patients early in treatment that they might need to try several different medications before settling on 1 that is optimally tolerated and efficacious. Because stimulants are generally quite effective for ADHD symptoms, set your goal to identify adverse effects and aim for a patient response of “this works well, and I don’t feel any different on it.”
CASE CONTINUED: Ready to try again
Three years later, Mr. Z returns and reports gradually discontinuing the stimulant because he “wanted to go it on my own.” He functioned relatively well at first, but errors and conflicts at his job led to his dismissal.
Since then, he has been unemployed. He is increasingly depressed and reports drinking and smoking “more heavily than in college.” He asks about resuming ADHD treatment.
Mr. Z does not meet DSM-IV-TR criteria for major depressive disorder or alcohol abuse/dependence. His depressed mood appears to be linked to his marked ADHD symptoms. Mr. Z agrees to a new treatment plan that includes starting atomoxetine at 25 mg to allow for flexible titration and psychotherapy to monitor his mood and achieve sobriety.
ADHD and substance abuse
Clinical judgment determines whether an adult with ADHD and a history of substance use disorders may safely benefit from treatment with a stimulant. The relationship between ADHD and substance use disorders is of clinical concern, but ADHD medications have not been shown to increase risk for later substance use disorders in children.14 Conversely, effective ADHD treatment appears to reduce later cigarette and substance use.15
Consider using a nonstimulant-class medication in adults with ADHD and active substance use disorders. In a 12-week, double-blind, controlled trial, atomoxetine improved ADHD symptoms significantly more than placebo in adults meeting DS-MIV-TR criteria for comorbid alcohol use disorders. After 4 to 30 days of alcohol abstinence, 72 patients were randomly assigned to atomoxetine, 25 to 100 mg/d (mean final dose 90 mg/d), and 75 patients to placebo. Although estimated times to initial relapse to heavy drinking did not differ:
- atomoxetine-treated subjects had 26% fewer cumulative heavy drinking days than placebo-treated subjects (P=0.023)
- the difference in cumulative heavy drinking days between the atomoxetine and placebo groups became statistically significant after 55 days of treatment.16
- World Health Organization Adult Self-Report Scale (ASRS) 18-item instrument and 6-item screener. www.med.nyu.edu/psych/psychiatrist/adhd.html.
- Volkow ND, Swanson JM. Does childhood treatment of ADHD with stimulant medication affect substance abuse in adulthood? Am J Psychiatry 2008;165:553-5.
- Adler LA, Spencer TJ, Levine LR, et al. Functional outcomes in the treatment of adults with ADHD. J Atten Disord 2008; 11:720-7.
Drug brand names
- Atomoxetine • Strattera
- Bupropion • Wellbutrin
- Extended-release mixed amphetamine • Adderall XR
- Extended duration OROS methylphenidate • Concerta
- Extended-release dexmethylphenidate • Focalin XR
- Lisdexamfetamine • Vyvanse
- Modafinil • Provigil
Disclosure
Dr. Hammerness has received research support from and is on the speakers bureau for Shire Pharmaceuticals. He has received support for CME activities and talks from Shire Pharmaceuticals, Ortho-McNeil, and Abbott Laboratories.
Dr. Surman receives research support and/or is a speaker for Abbott Laboratories, Cephalon, Eli Lilly and Company, Janssen, Ortho-McNeil, Merck, New River Pharmaceuticals, Novartis, Pfizer Inc., Shire Pharmaceuticals, and Takeda Pharmaceutical Company.
Dr. Sassi reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Acknowledgement
Clinical research assistant Katherine Miller, BA, contributed to the literature review for this article and assisted in preparing the manuscript.
Mr. Z, age 42, is referred by his primary care physician with symptoms suggesting attention-deficit/hyperactivity disorder (ADHD). Mr. Z has seen his physician sporadically for 10 years and acknowledges not following dietary and exercise advice. He has had intermittent “minor” depression, is overweight, and is a smoker with a family history of cardiovascular disease and diabetes.
A salesman, Mr. Z recently was promoted to an administrative position that substantially increased his paperwork. He is having difficulty performing his job because of longstanding forgetfulness and disorganization. He says he feels “like I’m in grade school again, lost in paperwork.” He also describes a recent educational assessment for his son, age 7, who may have ADHD. Similarities between Mr. Z’s and his son’s early childhood academic struggles are striking.
Like Mr. Z, adults with ADHD commonly seek treatment when increasing stressors and demands overwhelm their cognitive-attentional abilities. Some may be “healthy” men and women without psychiatric histories, whose disorganization, forgetfulness, or impulsivity contributes to functional impairment, including nonadherence with medical advice. For others, such as those with known psychiatric disorders, ADHD may be a hidden comorbidity contributing to seemingly refractory depression or anxiety disorder.
Despite growing evidence related to adult ADHD, individualizing and maintaining treatment over time can be challenging for clinicians and patients. Fortunately, new tools and multiple stimulant and nonstimulant medications can help you screen for, assess, and treat adult ADHD.
ADHD diagnosis
To diagnose ADHD in an adult patient, first establish that symptoms have existed from childhood to adulthood. One approach is to review DSM-IV-TR criteria for ADHD with your patient and ask him or her to reflect on childhood symptoms and dysfunction. Begin with orienting questions, such as “Do you remember your first grade teacher, your school, where you lived?” ADHD symptoms might have been present even if the patient maintained acceptable grades, particularly in elementary school, as dedicated parents or teachers might have contributed to early academic success.
Next, turn to diagnostic language that captures ADHD symptoms in adults. For example, the 18-item World Health Organization Adult ADHD Self-Report Scale (ASRS-v1.1) prompts individuals to self-report DSM-IV ADHD symptoms, and a 6-item subset (Table 1) is a highly specific screener (see Related Resources). The ASRS is most reliable in adults with limited psychiatric comorbidity.1
Adults often describe fluctuations in symptom severity over time. Symptoms may have less impact with more physically demanding work—such as sales—and greater impact with organizationally demanding work—such as administration.
Base your summary ADHD diagnosis on DSM-IV-TR criteria, including:
- lifetime persistence of symptoms, beginning before age 7
- functional impairment in ≥2 life settings, such as work, school, or home
- lack of another medical or psychiatric condition sufficient to explain the symptoms.
Table 1
Adult Self-Report Scale-v1.1 WHO 6-question screening tool for ADHD*
| Check the box that best describes how you have felt and conducted yourself over the past 6 months. Please give the completed questionnaire to your healthcare professional during your next appointment to discuss the results | Never | Rarely | Sometimes | Often | Very often |
|---|---|---|---|---|---|
| 1. How often do you have trouble wrapping up the final details of a project, once the challenging parts have been done? | |||||
| 2. How often do you have difficulty getting things in order when you have to do a task that requires organization? | |||||
| 3. How often do you have problems remembering appointments or obligations? | |||||
| 4. When you have a task that requires a lot of thought, how often do you avoid or delay getting started? | |||||
| 5. How often do you fidget or squirm with your hands or feet when you have to sit down for a long time? | |||||
| 6. How often do you feel overly active and compelled to do things, like you were driven by a motor? | |||||
| Add the number of checkmarks that appear in the darkly shaded area. Four (4) or more checkmarks indicate that your symptoms may be consistent with adult ADHD. It may be beneficial for you to talk with your healthcare provider about an evaluation. | |||||
| * Intended for use by persons age 18 and older ADHD: attention-deficit/hyperactivity disorder; WHO: World Health Organization | |||||
| Source: Reprinted with permission. World Health Organization Copyright 2003. All rights reserved | |||||
CASE CONTINUED: ‘All the time, every day’
Mr. Z completes the ASRS self-report symptom checklist and brings his wife to the next appointment. He rated all 6 screening symptoms and most others as occurring “often” or “very often.” He describes functional impairments “essentially all the time, basically every day” at work, home, and socially. His wife confirms these symptoms and the frustrations and conflicts they have caused.
Mr. Z describes ADHD symptoms from early elementary school to college. He was held back in kindergarten for being “immature,” his academic performance was inconsistent, and he “just got by…by cramming” in high school and college. His school performance pattern does not suggest a learning disability; he did not need special help in 1 subject more than others, and under pressure he could achieve average grades.
Medical review excludes explanations other than ADHD for his inattention, restlessness, and impulsivity. You conclude that Mr. Z meets criteria for ADHD, combined subtype, and discuss medication treatment.
FDA-approved medications
Medication for ADHD is appropriate only if symptoms are impairing. Five effective and generally well-tolerated medications are FDA-approved for adults with ADHD (Table 2):
- extended-release mixed amphetamine (Adderall XR)
- extended-release OROS methylphenidate (Concerta)
- extended-release dexmethylphenidate (Focalin XR)
- atomoxetine (Strattera)
- lisdexamfetamine (Vyvanse).
Efficacy. A meta-analysis of 29 pediatric ADHD trials across 30 years demonstrated greater effect size for stimulant class medications (immediate- and long-acting), compared with nonstimulant medications (including bupropion, atomoxetine, and modafinil).2 This finding is consistent with the American Academy of Child and Adolescent Psychiatry’s recommendation of stimulant medications as first-line agents for pediatric ADHD.3 A similar meta-analysis of 6 controlled studies of methylphenidate-class medications in adults found a large mean effect size (0.9), with greater effects associated with higher doses.4
Atomoxetine, a norepinephrine reuptake inhibitor, is the only nonstimulant medication FDA-approved for ADHD in adults. More than 6,000 children, adolescents, and adults have taken atomoxetine in clinical trials for ADHD (Lilly, prescribing information), with 4 years of open treatment data showing benefit being maintained over time.5
Tolerability. Although ADHD medications are generally well-tolerated by healthy adults, assess for a history of potential contraindications:
- unstable medical condition, hyperthyroidism, glaucoma
- treatment with a monoamine oxidase inhibitor or other pressor agents because of possible effects on blood pressure and heart rate
- use of cytochrome P450 2D6 inhibitors, which may increase atomoxetine steady-state plasma concentrations
- cardiovascular disease or family history of early cardiac disease (Box 1)6,7
- history of or active substance use disorder, such as alcohol dependence, cocaine or heroin abuse
- history of psychosis, bipolar disorder, or an active clinically significant psychiatric comorbidity (major depression, agitated state, suicidality).
Clinically, some patients appear to tolerate 1 class of stimulant (such as methylphenidate or amphetamine) over another. Consider switching to an alternate stimulant if your patient has bothersome side effects—mild low appetite, insomnia, tension, or jitteriness—or has received limited or partial benefit during an initial stimulant trial.
Serious cardiovascular events and sudden death have occurred in adults and children treated with stimulants.6 Agents used for attention-deficit/hyperactivity disorder (ADHD) have not been shown to cause sudden cardiac death, but the FDA requires stimulants’ labeling to warn about this risk in patients with structural cardiac abnormalities. The warning advises against using stimulants in adults with cardiomyopathy, serious heart rhythm abnormalities, or coronary artery disease.
When treating adults with ADHD, look to advisories about cardiovascular monitoring in children with ADHD. Before initiating medications, do a physical exam focused on cardiovascular disease risk factors and obtain a patient and family health history of:
- fainting or dizziness
- sudden or unexplained death in someone young
- sudden cardiac death or “heart attack” in family members age <35 years.
The American Academy of Pediatrics, American Academy of Child and Adolescent Psychiatry, and American Heart Association concur that electrocardiography (ECG) is not mandatory in cardiovascular assessment and monitoring during ADHD pharmacotherapy.7 This author (PH) refers cardiovascular questions to a primary care physician or cardiologist.
During ADHD treatment, monitor vital signs and refer patients with emergent cardiac symptoms or concerns to a cardiologist. Expect increases in blood pressure (1 to 4 mm Hg) and heart rate (2 to 6 bpm) during treatment with methylphenidate and amphetamine-class stimulants as well as with atomoxetine. Do not expect significant changes in ECG parameters (PR, QRS, and QTC intervals).
Extended-release formulations. Early adult studies demonstrated the efficacy of immediate-release stimulants, but adults with ADHD’s inherent deficits in organization and memory may have higher adherence rates and greater success with once-daily, extended-release formulations.8-11 Unless your patient wants to begin with small, short-acting dosages (5 to 10 mg) or desires to target treatment to specific times of day (such as in the morning for administrative work only), many appreciate once-daily formulations. Extended-release formulations also may be the simplest stimulants with which to begin ADHD treatment.
Over time, patients may benefit from an immediate-release form:
- added for certain times of day—such as in late afternoon, when the morning extended-release dose has worn off (Box 2)12,13
- to use as an alternative to extended-release formulations when more or less flexibly is desired, such as on weekends.
Table 2
Administering medications approved for adult ADHD
| Drug | Recommended dosage* | Comments |
|---|---|---|
| Stimulants | ||
| Extended-release mixed amphetamine (Adderall XR) | 20 mg | Initial prescription of 10-mg XR capsules allows gradual titration |
| Extended-release OROS methylphenidate (Concerta) | 18 to 72 mg/d | Initial prescription of 18-mg OROS MPH capsules allows gradual titration |
| Extended-release dexmethylphenidate (Focalin XR) | 10 mg/d; maximum 20 mg/d | Dosing is one-half the typical dosing of racemic MPH |
| Lisdexamfetamine (Vyvanse) | 30 mg/d; maximum 70 mg/d | May be adjusted weekly in 10-mg or 20-mg increments |
| Nonstimulant | ||
| Atomoxetine (Strattera) | 80 mg/d; maximum 100 mg/d | Initial dosage of 40 mg/d can be increased to target dosage after a minimum of 3 days; can be given as a morning dose or divided evenly between morning and evening doses |
| * FDA-approved dosages as listed in the package inserts of these medications ADHD: attention-deficit/hyperactivity disorder; MPH: methylphenidate; OROS: osmotic release oral system; XR: extended-release formulation | ||
CASE CONTINUED: Feeling ‘calm, less frenetic’
During the next 6 months, you start Mr. Z on stimulant treatment at robust dosing consistent with his weight (90 kg). He complains that extended-duration methylphenidate (MPH)—titrated to 90 mg/d—doesn’t last into the late afternoon, and he feels mildly tense with a low appetite. Because of an apparent partial response and relatively mild adverse effects, you discontinue MPH and try an extended-duration amphetamine, titrated to 60 mg.
Mr. Z’s blood pressure and heart rate remain stable. He begins to exercise regularly and reduce his use of tobacco and caffeine drinks, as you recommend. He says he feels “calm, less frenetic.” He reports no tension on this medication and only mild reduced appetite. With a plan to continue taking the stimulant medication with regular monitoring, he then disappears from treatment.
Promoting adherence
Treatment nonadherence is an issue throughout medicine, and individuals with disorganization, forgetfulness, and impulsivity may be at higher-than-usual risk of not following through on medication regimens.
Combining short- and long-acting stimulants may cover hours when attention-deficit/hyperactivity (ADHD) symptoms emerge despite therapy with a long-acting agent.12,13 Ask patients who report lack of full-day coverage if the once-daily, extended-duration formulation they are taking works well until a certain time of day. Then consider adding a similar-class immediate-release stimulant at this time to cover the later hours.
If a patient reports partial response throughout the day—such as early in treatment—begin by optimizing the long-acting agent’s dosage. Keep a target daily dose in mind, based on FDA recommendations and clinical trial data. For example, an adult weighing 80 kg may respond optimally to a combination of 60 mg of a long-acting methylphenidate (MPH) in the morning, followed by 10 to 20 mg of an immediate-release MPH in mid-afternoon.
The later stimulants are taken in the day, the more likely insomnia may emerge as an adverse effect. Some patients adjust to this problem within the first weeks of treatment. If insomnia remains impairing, reduce the stimulant dose or consider switching to a shorter duration medication or to the nonstimulant atomoxetine.
In addition, restrictions on stimulant-class medications do not permit multiple-month prescribing (refills), as is allowed with non-scheduled medications such as atomoxetine. Discuss with patients how they will obtain stimulant medications on a regular, monthly or bimonthly basis. In our experience, the practical challenges of remaining in treatment at times may limit patients’ adherence to ADHD medications more than a lack of response or tolerability concerns.
Explain to patients early in treatment that they might need to try several different medications before settling on 1 that is optimally tolerated and efficacious. Because stimulants are generally quite effective for ADHD symptoms, set your goal to identify adverse effects and aim for a patient response of “this works well, and I don’t feel any different on it.”
CASE CONTINUED: Ready to try again
Three years later, Mr. Z returns and reports gradually discontinuing the stimulant because he “wanted to go it on my own.” He functioned relatively well at first, but errors and conflicts at his job led to his dismissal.
Since then, he has been unemployed. He is increasingly depressed and reports drinking and smoking “more heavily than in college.” He asks about resuming ADHD treatment.
Mr. Z does not meet DSM-IV-TR criteria for major depressive disorder or alcohol abuse/dependence. His depressed mood appears to be linked to his marked ADHD symptoms. Mr. Z agrees to a new treatment plan that includes starting atomoxetine at 25 mg to allow for flexible titration and psychotherapy to monitor his mood and achieve sobriety.
ADHD and substance abuse
Clinical judgment determines whether an adult with ADHD and a history of substance use disorders may safely benefit from treatment with a stimulant. The relationship between ADHD and substance use disorders is of clinical concern, but ADHD medications have not been shown to increase risk for later substance use disorders in children.14 Conversely, effective ADHD treatment appears to reduce later cigarette and substance use.15
Consider using a nonstimulant-class medication in adults with ADHD and active substance use disorders. In a 12-week, double-blind, controlled trial, atomoxetine improved ADHD symptoms significantly more than placebo in adults meeting DS-MIV-TR criteria for comorbid alcohol use disorders. After 4 to 30 days of alcohol abstinence, 72 patients were randomly assigned to atomoxetine, 25 to 100 mg/d (mean final dose 90 mg/d), and 75 patients to placebo. Although estimated times to initial relapse to heavy drinking did not differ:
- atomoxetine-treated subjects had 26% fewer cumulative heavy drinking days than placebo-treated subjects (P=0.023)
- the difference in cumulative heavy drinking days between the atomoxetine and placebo groups became statistically significant after 55 days of treatment.16
- World Health Organization Adult Self-Report Scale (ASRS) 18-item instrument and 6-item screener. www.med.nyu.edu/psych/psychiatrist/adhd.html.
- Volkow ND, Swanson JM. Does childhood treatment of ADHD with stimulant medication affect substance abuse in adulthood? Am J Psychiatry 2008;165:553-5.
- Adler LA, Spencer TJ, Levine LR, et al. Functional outcomes in the treatment of adults with ADHD. J Atten Disord 2008; 11:720-7.
Drug brand names
- Atomoxetine • Strattera
- Bupropion • Wellbutrin
- Extended-release mixed amphetamine • Adderall XR
- Extended duration OROS methylphenidate • Concerta
- Extended-release dexmethylphenidate • Focalin XR
- Lisdexamfetamine • Vyvanse
- Modafinil • Provigil
Disclosure
Dr. Hammerness has received research support from and is on the speakers bureau for Shire Pharmaceuticals. He has received support for CME activities and talks from Shire Pharmaceuticals, Ortho-McNeil, and Abbott Laboratories.
Dr. Surman receives research support and/or is a speaker for Abbott Laboratories, Cephalon, Eli Lilly and Company, Janssen, Ortho-McNeil, Merck, New River Pharmaceuticals, Novartis, Pfizer Inc., Shire Pharmaceuticals, and Takeda Pharmaceutical Company.
Dr. Sassi reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Acknowledgement
Clinical research assistant Katherine Miller, BA, contributed to the literature review for this article and assisted in preparing the manuscript.
1. Kessler RC, Adler L, Ames M, et al. The World Health Organization Adult ADHD Self-Report Scale (ASRS): a short screening scale for use in the general population. Psychol Med 2005;35:245-56.
2. Faraone SV, Biederman J, Spencer TJ, Aleardi M. Comparing the efficacy of medications for ADHD using meta-analysis. MedGenMed 2006;8(4):4.-
3. Greenhill L, Pliszka S, Dulcan M, et al. Summary of the practice parameter for the use of stimulant medications in the treatment of children, adolescents, and adults. J Am Acad Child Adolesc Psychiatry 2001;40(11):1352-5.
4. Faraone SV, Spencer T, Aleardi M, et al. Meta-analysis of the efficacy of methylphenidate for treating adult attention-deficit/hyperactivity disorder. J Clin Psychopharmacol 2004;24:24-9.
5. Adler LA, Spencer TJ, Williams DW, et al. Long-term, open-label safety and efficacy of atomoxetine in adults with ADHD: final report of a 4-year study. J Atten Disord Epub 2008 April 30.
6. Nissen SE. ADHD drugs and cardiovascular risk. N Engl J Med 2006;354:1445-8.
7. American Academy of Pediatrics/American Heart Association clarification of statement on cardiovascular evaluation and monitoring of children and adolescents with heart disease receiving medications for ADHD May 16, 2008. Available at: http://www.aap.org/pressroom/aap-ahastatement.htm. Accessed August 14, 2008.
8. Biederman J, Mick E, Surman C, et al. A randomized, placebo-controlled trial of OROS methylphenidate in adults with attention-deficit/hyperactivity disorder. Biol Psychiatry 2006;59(9):829-35.
9. Biederman J, Mick E, Surman C, et al. Comparative acute efficacy and tolerability of OROS and immediate release formulations of methylphenidate in the treatment of adults with attention-deficit/hyperactivity disorder. BMC Psychiatry 2007;7:49.-
10. Mick E, Spencer TJ, Surman C, et al. Randomized single-blind substitution study of methylphenidate in ADHD adults receiving immediate-release methylphenidate. NR357. Poster presented at: Annual Meeting of the American Psychiatric Association; May 19-24, 2007; San Diego, CA.
11. Capone N, McDonnel T. Medication persistence among agents used to treat attention-deficit/hyperactivity disorder, diabetes, and elevated serum cholesterol. NR 639. Poster presented at: Annual Meeting of the American Psychiatric Association; May 20-25, 2006; Toronto, Ontario, Canada.
12. Adler L, Morrill M, Reingold B. d-methylphenidate augmentation of extended-release stimulant therapy in ADHD. NR 619. Poster presented at: Annual Meeting of the American Psychiatric Association; May 20-25, 2006; Toronto, Ontario, Canada.
13. Adler L, Reingold LS, Morrill MS, Wilens TE. Combination pharmacotherapy for adult ADHD. Curr Psychiatry Rep 2006;8:409-15.
14. Biederman J, Monuteaux MC, Spencer T, et al. Stimulant therapy and risk for subsequent substance use disorders in male adults with ADHD: a naturalistic controlled 10-year follow-up study. Am J Psychiatry 2008;165:597-603.
15. Faraone SV, Wilens TE. Effect of stimulant medications for attention-deficit/hyperactivity disorder on later substance use and the potential for stimulant misuse, abuse, and diversion. J Clin Psychiatry 2007;68(suppl 11):15-22.
16. Wilens TE, Adler LA, Weiss MD, et al. Atomoxetine treatment of adults with ADHD and comorbid alcohol use disorders. Drug Alcohol Depend 2008;96:145-54.
1. Kessler RC, Adler L, Ames M, et al. The World Health Organization Adult ADHD Self-Report Scale (ASRS): a short screening scale for use in the general population. Psychol Med 2005;35:245-56.
2. Faraone SV, Biederman J, Spencer TJ, Aleardi M. Comparing the efficacy of medications for ADHD using meta-analysis. MedGenMed 2006;8(4):4.-
3. Greenhill L, Pliszka S, Dulcan M, et al. Summary of the practice parameter for the use of stimulant medications in the treatment of children, adolescents, and adults. J Am Acad Child Adolesc Psychiatry 2001;40(11):1352-5.
4. Faraone SV, Spencer T, Aleardi M, et al. Meta-analysis of the efficacy of methylphenidate for treating adult attention-deficit/hyperactivity disorder. J Clin Psychopharmacol 2004;24:24-9.
5. Adler LA, Spencer TJ, Williams DW, et al. Long-term, open-label safety and efficacy of atomoxetine in adults with ADHD: final report of a 4-year study. J Atten Disord Epub 2008 April 30.
6. Nissen SE. ADHD drugs and cardiovascular risk. N Engl J Med 2006;354:1445-8.
7. American Academy of Pediatrics/American Heart Association clarification of statement on cardiovascular evaluation and monitoring of children and adolescents with heart disease receiving medications for ADHD May 16, 2008. Available at: http://www.aap.org/pressroom/aap-ahastatement.htm. Accessed August 14, 2008.
8. Biederman J, Mick E, Surman C, et al. A randomized, placebo-controlled trial of OROS methylphenidate in adults with attention-deficit/hyperactivity disorder. Biol Psychiatry 2006;59(9):829-35.
9. Biederman J, Mick E, Surman C, et al. Comparative acute efficacy and tolerability of OROS and immediate release formulations of methylphenidate in the treatment of adults with attention-deficit/hyperactivity disorder. BMC Psychiatry 2007;7:49.-
10. Mick E, Spencer TJ, Surman C, et al. Randomized single-blind substitution study of methylphenidate in ADHD adults receiving immediate-release methylphenidate. NR357. Poster presented at: Annual Meeting of the American Psychiatric Association; May 19-24, 2007; San Diego, CA.
11. Capone N, McDonnel T. Medication persistence among agents used to treat attention-deficit/hyperactivity disorder, diabetes, and elevated serum cholesterol. NR 639. Poster presented at: Annual Meeting of the American Psychiatric Association; May 20-25, 2006; Toronto, Ontario, Canada.
12. Adler L, Morrill M, Reingold B. d-methylphenidate augmentation of extended-release stimulant therapy in ADHD. NR 619. Poster presented at: Annual Meeting of the American Psychiatric Association; May 20-25, 2006; Toronto, Ontario, Canada.
13. Adler L, Reingold LS, Morrill MS, Wilens TE. Combination pharmacotherapy for adult ADHD. Curr Psychiatry Rep 2006;8:409-15.
14. Biederman J, Monuteaux MC, Spencer T, et al. Stimulant therapy and risk for subsequent substance use disorders in male adults with ADHD: a naturalistic controlled 10-year follow-up study. Am J Psychiatry 2008;165:597-603.
15. Faraone SV, Wilens TE. Effect of stimulant medications for attention-deficit/hyperactivity disorder on later substance use and the potential for stimulant misuse, abuse, and diversion. J Clin Psychiatry 2007;68(suppl 11):15-22.
16. Wilens TE, Adler LA, Weiss MD, et al. Atomoxetine treatment of adults with ADHD and comorbid alcohol use disorders. Drug Alcohol Depend 2008;96:145-54.
‘I’m sober, Doctor, really’: Best biomarkers for underreported alcohol use
Hospitalized patients who are not truthful about their alcohol consumption may be at risk for an unplanned withdrawal. Self-reports of alcohol use—such as CAGE and the Alcohol Use Disorders Identification Test (AUDIT)—are valid, inexpensive, and noninvasive, but patients easily can feign results.1 Biochemical measures are more objective, and combinations of markers are an effective tool to detect recent heavy drinking in the 10% to 25% of patients who underreport alcohol use.2
Biochemical measures can detect acute alcohol intoxication and recent prolonged drinking. Because marker levels return to normal after long-term abstinence, ongoing monitoring can help detect a relapse before a patient admits to it.3
This article presents 3 cases in which biochemical markers helped prevent alcohol withdrawal in patients who denied alcohol abuse. We discuss why we ordered biochemical tests and which combinations provided highly sensitive results.
CASE 1: Depression and substance abuse
Ms. C, age 39, presents with bleeding gums due to excessive warfarin, which she takes prophylactically for a history of deep vein thrombosis. She is seen by the psychiatric consultation service for depression—which she says she has experienced since “the day I was born”—and substance abuse that includes a history binge drinking. Ms. C says she has stopped drinking and remained abstinent for the past year because she is fearful of further damaging her kidneys. She also denies psychosis. She does not have a history or symptoms of hepatobiliary or hematologic disease.
Challenge. Despite Ms. C’s self-reported 1 year of sobriety, her history of binge drinking and depression calls for evaluating her alcohol withdrawal risk. Laboratory markers of alcohol abuse are the only means to assess her recent drinking behavior.
Discussion. Lab results include serum albumin of 3.4 g/dL, total bilirubin of 0.3 mg/dL, total protein of 6.3 g/dL, aspartate aminotransferase (AST) of 13 U/L, alanine aminotransferase (ALT) of 19 U/L, alkaline phosphatase of 136 U/L, and blood ammonia level of 37 μg/dL. Gamma-glutamyl transferase (GGT) is elevated at 104 U/L (normal range for women: 0 to 45 U/L). Mean corpuscular volume (MCV) is elevated at 101 fL (normal range 80 to 100 fL).
The combination of elevated MCV and GGT has a 95% sensitivity for alcohol abuse.4 GGT levels become elevated after 24 hours to 2 weeks of heavy alcohol consumption and return to normal within 2 to 6 weeks of abstinence, which allows them to detect binge drinking. MCV takes 6 to 8 weeks of heavy drinking—we which we define as consuming ≥40 grams of alcohol/day5—to become elevated and returns to normal within 3 months of abstinence.
These data provide evidence that Ms. C recently consumed substantial amounts of alcohol. As a result, we start her on alcohol withdrawal precautions (AWP).
Markers of alcohol abuse
Biochemical markers commonly used to detect alcohol abuse (Table 1) include:
- blood alcohol level (BAL)
- MCV
- liver function tests (LFTs) such as ALT, AST, and GGT
- carbohydrate deficient transferrin (CDT).
Table 1
By the numbers: Biomarkers of excessive alcohol consumption
| Biomarker | |||||
|---|---|---|---|---|---|
| CDT | GGT | AST | ALT | MCV | |
| Blood test normal range | Women: 0 to 45 U/L Men: 0 to 53 U/L | 10 to 34 U/L | 8 to 37 U/L | 80 to 100 fL | |
| Blood test abnormal range | >1.3% of total transferrin concentration | Women: >45 U/L Men: >53 U/L | Levels rarely exceed 500 U/L | Levels rarely exceed 300 U/L | >100 fL |
| Time to elevation | 2 to 3 weeks | 24 hours to 2 weeks | 3 to 7 days | 3 to 7 days | After 6 weeks |
| Time to descent to normal levels | 2 to 4 weeks of abstinence | 2 to 6 weeks of abstinence | Half-life 12 to 24 hours | Half-life 37 to 57 hours | 3 months |
| Dose-response of alcohol | 60 g/d | 80 to 200 g/d | ≥40 g/d | ≥40 g/d | ≥40 g/d |
| Sensitivity | 55% to 90%a-e | 37% to 85%b, f, g | AST:ALT ratio >2:1 has a 70% sensitivity and 92% to 100% specificity for alcoholic-induced liver diseaseh-j | 20% to 70%b,k | |
| Relapse sensitivity | 55% to 76%a,l,m | 50%a,e | 20%a,n | ||
| Specificity | 92% to 97%a,b | 18% to 93%a,b,e | 64% to 66%b,k,n | ||
| Positive predictive value | 46% to 75%c,g | 41%g | 36%g | ||
| Negative predictive value | 72% to 98%a,c,g | 69% to 92%a,e,g | 67%g | ||
| AST: aspartate aminotransferase; ALT: alanine aminotransferase; CDT: carbohydrate deficient transferrin; GGT: gamma-glutamyl transferase; MCV: mean corpuscular volume | |||||
| Source: Reference Citations: click here | |||||
BAL can document acute alcohol intoxication, but its use is limited because alcohol has a 4-hour half-life and an elimination rate of 7 grams/hour—equivalent to 1 drink/hour.6 (A “drink” typically is defined as a 12-ounce bottle of beer or wine cooler, a 5-ounce glass of wine, or 1.5 ounces of 80-proof distilled spirits.) Therefore, BAL will identify as false negatives alcohol-dependent patients who abstain from alcohol within 24 hours of testing.
MCV is an index of the average volume of erythrocytes. Macrocytosis occurs when the volume exceeds 100 fL. Elevated MCV is the most typical morphologic abnormality associated with excessive alcohol consumption7,8 and macrocytosis—sometimes without associated anemia—is often evident in persons with alcoholism. MCV elevates after 6 weeks of alcohol misuse and may remain elevated for up to 3 months after a person has stopped drinking.9
Because patients with disorders unrelated to alcohol use can have elevated MCV, alone it is not a useful screening marker for alcohol abuse.10 Additionally, because macrocytosis can persist under strictly controlled alcohol abstinence, MCV is not a reliable clinical indicator of relapse.11
LFTs measure enzymes and proteins. ALT, AST, and GGT are the most relevant for detecting heavy drinking. An AST:ALT ratio >2:1 supports a suspicion of alcohol abuse.12 More than 90% of patients with an AST:ALT ratio of 2:1 have alcoholic liver disease. This increases to more than 96% if the ratio is 3:1.13
GGT is an enzyme concentrated in the liver, bile ducts, and kidneys; normal range is 0 to 45 U/L (for females) or 53 U/L (for males).14 GGT levels >30 U/L correlate with alcohol consumption of >4 drinks per day.15 GGT has a half-life of 14 to 26 days and remains elevated for 4 to 6 weeks after drinking cessation, which make it useful for monitoring abstinence in treatment programs.16 Sensitivity ranges from 37% to 85% and specificity is as high as 93% in nonmedical populations.17 Although nonalcoholic liver disease can elevate GGT in persons who do not abuse alcohol, 50% to 72% of GGT elevations can be explained by excessive alcohol consumption.18
CDT is a newer biomarker used to monitor alcohol consumption. The most accurate way to express CDT level is as a percentage of total transferrin concentration. This method accounts for individual variations in transferrin levels, thus minimizing false positives.18 In persons who consume >4 or 5 drinks per day for 2 weeks or more, CDT is >1.3% of total transferrin.19 Unfortunately, because it is expensive and requires sophisticated test methodology, CDT testing is not available at most hospitals.20
Combinations improve detection
Each biochemical measure has strengths and weaknesses as a marker for determining patients’ alcohol consumption (Table 2). CDT and GGT show the highest sensitivity for heavy drinking, and CDT has a higher specificity than GGT (Table 3).21,22 Relapse to alcohol use after abstinence may be best identified by a simultaneous 30% increase in CDT and GGT.5
Because GGT has a longer half-life than CDT, its diagnostic efficiency in detecting alcohol relapse may not develop until 4 weeks after alcohol detoxification, whereas CDT may become clinically useful for detecting relapse as early as 1 week after detoxification.23
Table 2
Biomarkers of alcohol use: Strengths and weaknesses
| Biomarker | Strengths | Weaknesses |
|---|---|---|
| CDT | High specificity for alcohol use; few factors cause false positives High sensitivity in distinguishing alcoholics from social drinkers Marker of relapse and abstinence from drinking Confirmatory test for patients suspected of alcohol abuse | Low sensitivity; more valuable to confirm than exclude heavy drinking Cost (average $30/assay) and low availability of testing Likely less sensitive for women and younger patients compared with men Poor screening tool for alcohol use in general population |
| GGT | Elevations precede alcohol-induced liver damage High specificity in patients with suspected alcohol abuse Effective marker for patients suspected of binge drinking Inexpensive ( | Can be falsely elevated by liver and biliary disease, smoking, obesity, and medications that induce microsomal enzymes Low sensitivity makes it a poor screening tool in general population Poor marker of relapse |
| AST:ALT >2:1 | Highly sensitive and specific for alcohol-induced liver damage | Enzyme elevations can be detected only after periods of heavy drinking Elevations secondary to liver damage at the hepatocellular level (after fatty changes) |
| MCV | Accuracy similar in male and female patients Elevations in suspected cases of alcohol use indicate chronicity of drinking Routine laboratory test | Poor biomarker for relapse False positives caused by liver disease, hemolysis, bleeding disorders, anemia, folate deficiency, and medications that reduce folate Low sensitivity and specificity for alcohol use make it a poor screening tool for alcohol abuse |
| AST: aspartate aminotransferase; ALT: alanine aminotransferase; CDT: carbohydrate deficient transferrin; GGT: gamma-glutamyl transferase; MCV: mean corpuscular volume | ||
Table 3
Interpreting diagnostic test performance
| Term | Definition | Applicability |
|---|---|---|
| Sensitivity | Percent of persons with disease who test positive | High value is desirable for ruling out disease (low false-negative rate) |
| Specificity | Percent of persons without disease who test negative | High value is desirable for ruling in disease (low false-positive rate) |
| Positive predictive value | Percent of positive test results that are true positives | Probability that a person with a positive test result has the disease |
| Negative predictive value | Percent of negative test results that are true negatives | Probability that a person with a negative test result is disease-free |
| Source: References 21,22 | ||
There is evidence that combining tests can improve alcohol use detection.24 For example, Dolman et al25 found that the ability of the AUDIT questionnaire to correctly predict which patients would experience alcohol withdrawal increases when it is used in combination with biochemical markers. Specifically, the positive predictive value of an AUDIT score ≥8 increased from 17% to 47% when found in combination with ≥2 abnormal biochemical marker levels; the study looked at GGT, ALT, AST, and MCV. Sensitivity was 94% and specificity was 98%.
Similarly, combinations of biochemical markers—especially CDT and GGT—have improved detection of alcohol use and subsequent risk of withdrawal.26Table 4 provides a summary of studies that evaluated using combinations of biochemical markers.4,5,27-31
Table 4
Combining biomarker tests: An effective approach
| Combination | Study | Sensitivity* |
|---|---|---|
| GGT + MCV | Morgan et al4 | 95% |
| GGT + CDT | Hietala et al5 | 90% |
| Mundle et al29 | 90% | |
| Bell et al30 | 90% | |
| Sillanaukee et al31 | 95% | |
| GGT + AST:ALT >2:1 | Gluud et al27 | 92% |
| Morgan et al4 | 100% | |
| MCV + AST:ALT >2:1 | Kawachi et al28 | 97% |
| Morgan et al4 | 95% | |
| GGT + MCV + AST:ALT >2:1 | Morgan et al4 | 100% |
| GGT + MCV + CDT | Sillanaukee et al31 | 70% |
| * Sensitivity for detecting excessive alcohol consumption | ||
| AST: aspartate aminotransferase; ALT: alanine aminotransferase; CDT: carbohydrate deficient transferrin; GGT: gamma-glutamyl transferase; MCV: mean corpuscular volume | ||
Consider patients’ comorbidities
Patients at risk for underreporting alcohol use include those with unemployment histories, previous alcohol treatment, and higher scores on the Alcohol Dependence Scale (18.5, SD=8.1).2 Interpret biochemical testing results in the context of a patient’s overall clinical picture.
The following 2 case patients denied or underreported recent alcohol use but we determined they were at high risk for an alcohol disorder because of their medical and/or psychiatric histories. Analysis of biochemical markers helped assess the risk of alcohol withdrawal.
CASE 2: Altered mental status
Family members bring Mr. N, age 44, to the hospital because of his odd behavior. He presents with paranoid delusions and an inappropriate elated mood. His medical history includes acquired immune deficiency syndrome (AIDS). After cerebrospinal fluid analysis, computed tomography of the head, electroencephalogram, and metabolic workup are within normal limits, the patient is diagnosed with human immunodeficiency virus (HIV) mania and is admitted.
On admission, Mr. N denies alcohol use. A blood alcohol/urine toxicity screen is negative. One day after admission, Mr. M develops elevated blood pressure and tachycardia and reports headache and nausea.
Challenge. Gathering a valid history of Mr. N’s alcohol use is difficult because of his acutely altered mental status and manic-like state. We use laboratory data to assess his risk of alcohol withdrawal. His liver function tests include an AST of 33 U/L, ALT of 30 U/L, and an alkaline phosphatase of 94 U/L. MCV is normal at 90 fL. Interestingly, the GGT level is elevated almost 4 times normal at 164 U/L.
Discussion. Although Mr. N denied alcohol use and presented with a negative BAL, laboratory data support alcohol dependence. His GGT was elevated well beyond normal limits, without evidence of hepatobiliary disease. GGT has a sensitivity as high as 85%32 and limited specificity for alcohol abuse. Because of his high probability of recent alcohol consumption, we place Mr. N on AWP.
We postulate that our patient’s autonomic instability, headache, and nausea are related to alcohol withdrawal. We are aware that delirium occurs frequently in patients with HIV infection, and although Mr. N’s medical workup is negative, HIV infection can produce an acute encephalopathy that could resemble our patient’s clinical picture.33
Mr. N’s autonomic instability, headache, and nausea abated after treatment for alcohol withdrawal.
CASE 3: Suicide attempt?
Mr. S, age 28, presents to the trauma service with a self-inflicted gunshot wound to the face. He reports feeling depressed for the last year but denies a history of psychotic symptoms or heroin withdrawal symptoms. He also denies recent or past alcohol abuse and does not have a history of biliary tract disease or megaloblastic anemia. His mother tells us Mr. S has had a history of depression since childhood.
Challenge. Based on Mr. S’ apparent suicide attempt and history, we feel he is at high risk for alcohol abuse. We use laboratory markers to assess the likelihood of alcohol consumption and possibly decrease his risk of alcohol withdrawal.
Discussion. Mr. S’ lab data show an MCV of 91 fL, AST of 95 U/L, alanine ALT of 156 U/L, and alkaline phosphatase of 160 U/L. GGT was elevated at 122 U/L.
Although Mr. S’ MCV is within the normal range, his GGT is elevated, and the combination of an elevated GGT and MCV has a 95% sensitivity for the diagnosis of alcohol abuse. We place Mr. S on alcohol withdrawal precautions and discuss with him the potential life-threatening complications of alcohol withdrawal. Confronted with this information and the possible implication of his elevated LFTs, the patient admits his alcohol history—which consists of drinking 12 beers/day for at least the past 2 years. He admits this despite exhibiting no signs or symptoms of alcohol withdrawal.
Related Resources
- National Institute on Alcohol Abuse and Alcoholism Data/Statistical Tables. www.niaaa.nih.gov/Resources/DatabaseResources/QuickFacts.
- Maisto SA, Connors GJ, Allen JP. Contrasting self-report screens for alcohol problems: a review. Alcohol Clin Exp Res 1995;19(6):1510-6.
- Coulton S, Drummond C, James D, et al. Opportunistic screening for alcohol use disorders in primary care: comparative study. BMJ 2006;332:511-7.
Bottom line
Because CDT—the most accurate biomarker—is not available at most hospitals, we recommend using combinations of other measures to detect unreported recent alcohol consumption. If GGT and MCV are elevated, GGT is elevated and AST:ALT is >2:1, or MCV is elevated and AST:ALT is >2:1, consider initiating alcohol withdrawal precautions.
Acknowledgement
The authors acknowledge Daiana Radac, BA, a third-year medical student at Eastern Virginia Medical School, for her contributions to this article.
1. Allen JP, Anthenelli RM. Getting to the bottom of problem drinking: the case for routine screening. Current Psychiatry 2003;2(6):26-44.
2. Killeen TK, Brady KT, Gold PB, et al. Comparison of self-report versus agency records of service utilization in a community sample of individuals with alcohol use disorders. Drug Alcohol Depend 2004;73(2):141-7.
3. Alcohol withdrawal syndrome: how to predict, prevent, diagnose and treat it. Prescrire Int 2007;16(87):24-31.
4. Morgan MY, Colman JC, Sherlock S. The use of a combination of peripheral markers for diagnosing alcoholism and monitoring for continued abuse. Alcohol Alcohol 1981;16:167-77.
5. Hietala J, Koivisto H, Anttila P, et al. Comparison of the combined marker GGT-CDT and the conventional laboratory markers of alcohol abuse in heavy drinkers, moderate drinkers and abstainers. Alcohol Alcohol 2006;41(5):528-33.
6. Swift R. Direct measurement of alcohol and its metabolites. Addiction 2003;98:73-80.
7. Koivisto H, Hietala J, Anttila P, et al. Long-term ethanol consumption and macrocytosis: diagnostic and pathogenic implications. J Lab Clin Med 2005;147(4):191-6.
8. Savage DG, Ogundipe A, Allen RH, et al. Etiology and diagnostic evaluation of macrocytosis. Am J Med Sci 2000;319(6):343-52.
9. Gordon H. Detection of alcoholic liver disease. World J Gastroenterol 2001;7(3):297-302.
10. Bernadt M, Mumford J, Taylor C, et al. Comparison of questionnaire and laboratory tests in the detection of excessive drinking and alcoholism. Lancet 1982;1:325-8.
11. Hasselblatt M, Martin F, Maul O, et al. Persistent macrocytosis following abstinence from chronic alcohol use. JAMA 2001;286:2946.-
12. Prati D, Taioli E, Zanella A, et al. Updated definitions of healthy ranges for serum alanine aminotransferase levels. Ann Intern Med 2002;137:1-9.
13. Fancher T, Kamboj A, Onate J. Interpreting liver function tests. Current Psychiatry 2007;6(5):61-8.
14. Puukka K, Hietala J, Koivisto H, et al. Obesity and the clinical use of serum GGT activity as a marker of heavy drinking. Scand J Clin Lab Invest 2007;67(5):480-8.
15. Litten RZ, Allen JP, Fertig JB. y-glutamyl transpeptidase and carbohydrate deficient transferrin: alternative measures of excessive alcohol consumption. Alcohol Clin Exp Res 1995;19(6):1541-6.
16. National Institute on Alcohol Abuse and Alcoholism. Screening for alcohol problems—an update. Alcohol Alert No 56 Available at: http://pubs.niaaa.nih.gov/publications/aa56.htm. Accessed May 5, 2007.
17. DiMartini A. A clinical guide to assessing alcohol use and problems. Available at: http://www.alcoholmedicalscholars.org/clin-asmt.ppt. Accessed June 30, 2008.
18. Wolff K, Marshall E. Biological markers of alcohol use. Psychiatry 2006;5(12):437-8.
19. ARUP Laboratories. Carbohydrate-deficient transferrin (CDT) for alcohol use. 2006. Available at: http://www.aruplab.com/TestDirectory/resources/TechnicalBulletins/Carbohydrate-Deficient%20Transferrin%20(CDT)%20Mar%202006.pdf. Accessed July 30, 2008.
20. Allen JP, Litten RZ. The role of laboratory testing in alcoholism treatment. J Subst Abuse Treat 2001;20:81-5.
21. Bhushan V, Le T, Ozturk A, et al. Behavioral Science. In: Le T, Bhushan V, Rao DA, eds. First aid for the USMLE step 1: a student to student guide. New York, NY: McGraw Hill Medical Publishing Division; 2007.
22. Miller PM, Anton RF. Biochemical alcohol screening in primary care. Addict Behav 2004;29(7):1427-37.
23. Schmidt LG, Schmidt K, Dufeu P, et al. Superiority of carbohydrate-deficient transferrin to gamma-glutamyltransferase in detecting relapse in alcoholism. Am J Psychiatry 1997;154(1):75-80.
24. Salaspuro M. Carbohydrate-deficient transferrin as compared to other markers of alcoholism: a systematic review. Alcohol 1999;19(3):261-71.
25. Dolman JM, Hawkes ND. Combining the AUDIT questionnaire and biochemical markers to assess alcohol use and risk of alcohol withdrawal in medical patients. Alcohol Alcohol 2005;40(6):515-9.
26. Helander A, Carlsson AV, Borg S. Longitudinal comparison of carbohydrate-deficient transferrin and gamma-glutamyl transferase: complementary markers of excessive alcohol consumption. Alcohol Alcohol 1996;31(1):101-7.
27. Gluud C, Andersen I, Dietrichson O, et al. Gamma-glutamyltransferase, aspartate aminotransferase and alkaline phosphatase as markers of alcohol consumption in out-patient alcoholics. Eur J Clin Invest 1981;11(3):171-6.
28. Kawachi I, Robinson GM, Stace NH. A combination of raised serum AST: ALT ratio and erythrocyte mean cell volume level detects excessive alcohol consumption. N Z Med J 1990;103(887):145-8.
29. Mundle G, Ackerman K, Mann K. Biological markers as indicators for relapse in alcohol-dependent patients. Addict Biol 1999;4(2):209-14.
30. Bell H, Tallaksen C, Sjåheim T, et al. Serum carbohydrate-deficient transferrin as a marker of alcohol consumption in patients with chronic liver diseases. Alcohol Clin Exp Res 1993;17(2):246-52.
31. Sillanaukee P, Aalto M, Seppa K. Carbohydrate-deficient transferrin and conventional alcohol markers as indicators for brief intervention among heavy drinkers in primary health care. Alcohol Clin Exp Res 1998;22(4):892-6.
32. Salaspuro S. Conventional and coming laboratory markers of alcoholism and heavy drinking. Alcohol Clin Exp Res 1986;10(6 suppl):5-12.
33. Della Penna ND, Treisman GJ. HIV/AIDS. In: Levenson J, ed. Essentials of psychosomatic medicine. Washington, DC: American Psychiatric Publishing, Inc; 2007.
Hospitalized patients who are not truthful about their alcohol consumption may be at risk for an unplanned withdrawal. Self-reports of alcohol use—such as CAGE and the Alcohol Use Disorders Identification Test (AUDIT)—are valid, inexpensive, and noninvasive, but patients easily can feign results.1 Biochemical measures are more objective, and combinations of markers are an effective tool to detect recent heavy drinking in the 10% to 25% of patients who underreport alcohol use.2
Biochemical measures can detect acute alcohol intoxication and recent prolonged drinking. Because marker levels return to normal after long-term abstinence, ongoing monitoring can help detect a relapse before a patient admits to it.3
This article presents 3 cases in which biochemical markers helped prevent alcohol withdrawal in patients who denied alcohol abuse. We discuss why we ordered biochemical tests and which combinations provided highly sensitive results.
CASE 1: Depression and substance abuse
Ms. C, age 39, presents with bleeding gums due to excessive warfarin, which she takes prophylactically for a history of deep vein thrombosis. She is seen by the psychiatric consultation service for depression—which she says she has experienced since “the day I was born”—and substance abuse that includes a history binge drinking. Ms. C says she has stopped drinking and remained abstinent for the past year because she is fearful of further damaging her kidneys. She also denies psychosis. She does not have a history or symptoms of hepatobiliary or hematologic disease.
Challenge. Despite Ms. C’s self-reported 1 year of sobriety, her history of binge drinking and depression calls for evaluating her alcohol withdrawal risk. Laboratory markers of alcohol abuse are the only means to assess her recent drinking behavior.
Discussion. Lab results include serum albumin of 3.4 g/dL, total bilirubin of 0.3 mg/dL, total protein of 6.3 g/dL, aspartate aminotransferase (AST) of 13 U/L, alanine aminotransferase (ALT) of 19 U/L, alkaline phosphatase of 136 U/L, and blood ammonia level of 37 μg/dL. Gamma-glutamyl transferase (GGT) is elevated at 104 U/L (normal range for women: 0 to 45 U/L). Mean corpuscular volume (MCV) is elevated at 101 fL (normal range 80 to 100 fL).
The combination of elevated MCV and GGT has a 95% sensitivity for alcohol abuse.4 GGT levels become elevated after 24 hours to 2 weeks of heavy alcohol consumption and return to normal within 2 to 6 weeks of abstinence, which allows them to detect binge drinking. MCV takes 6 to 8 weeks of heavy drinking—we which we define as consuming ≥40 grams of alcohol/day5—to become elevated and returns to normal within 3 months of abstinence.
These data provide evidence that Ms. C recently consumed substantial amounts of alcohol. As a result, we start her on alcohol withdrawal precautions (AWP).
Markers of alcohol abuse
Biochemical markers commonly used to detect alcohol abuse (Table 1) include:
- blood alcohol level (BAL)
- MCV
- liver function tests (LFTs) such as ALT, AST, and GGT
- carbohydrate deficient transferrin (CDT).
Table 1
By the numbers: Biomarkers of excessive alcohol consumption
| Biomarker | |||||
|---|---|---|---|---|---|
| CDT | GGT | AST | ALT | MCV | |
| Blood test normal range | Women: 0 to 45 U/L Men: 0 to 53 U/L | 10 to 34 U/L | 8 to 37 U/L | 80 to 100 fL | |
| Blood test abnormal range | >1.3% of total transferrin concentration | Women: >45 U/L Men: >53 U/L | Levels rarely exceed 500 U/L | Levels rarely exceed 300 U/L | >100 fL |
| Time to elevation | 2 to 3 weeks | 24 hours to 2 weeks | 3 to 7 days | 3 to 7 days | After 6 weeks |
| Time to descent to normal levels | 2 to 4 weeks of abstinence | 2 to 6 weeks of abstinence | Half-life 12 to 24 hours | Half-life 37 to 57 hours | 3 months |
| Dose-response of alcohol | 60 g/d | 80 to 200 g/d | ≥40 g/d | ≥40 g/d | ≥40 g/d |
| Sensitivity | 55% to 90%a-e | 37% to 85%b, f, g | AST:ALT ratio >2:1 has a 70% sensitivity and 92% to 100% specificity for alcoholic-induced liver diseaseh-j | 20% to 70%b,k | |
| Relapse sensitivity | 55% to 76%a,l,m | 50%a,e | 20%a,n | ||
| Specificity | 92% to 97%a,b | 18% to 93%a,b,e | 64% to 66%b,k,n | ||
| Positive predictive value | 46% to 75%c,g | 41%g | 36%g | ||
| Negative predictive value | 72% to 98%a,c,g | 69% to 92%a,e,g | 67%g | ||
| AST: aspartate aminotransferase; ALT: alanine aminotransferase; CDT: carbohydrate deficient transferrin; GGT: gamma-glutamyl transferase; MCV: mean corpuscular volume | |||||
| Source: Reference Citations: click here | |||||
BAL can document acute alcohol intoxication, but its use is limited because alcohol has a 4-hour half-life and an elimination rate of 7 grams/hour—equivalent to 1 drink/hour.6 (A “drink” typically is defined as a 12-ounce bottle of beer or wine cooler, a 5-ounce glass of wine, or 1.5 ounces of 80-proof distilled spirits.) Therefore, BAL will identify as false negatives alcohol-dependent patients who abstain from alcohol within 24 hours of testing.
MCV is an index of the average volume of erythrocytes. Macrocytosis occurs when the volume exceeds 100 fL. Elevated MCV is the most typical morphologic abnormality associated with excessive alcohol consumption7,8 and macrocytosis—sometimes without associated anemia—is often evident in persons with alcoholism. MCV elevates after 6 weeks of alcohol misuse and may remain elevated for up to 3 months after a person has stopped drinking.9
Because patients with disorders unrelated to alcohol use can have elevated MCV, alone it is not a useful screening marker for alcohol abuse.10 Additionally, because macrocytosis can persist under strictly controlled alcohol abstinence, MCV is not a reliable clinical indicator of relapse.11
LFTs measure enzymes and proteins. ALT, AST, and GGT are the most relevant for detecting heavy drinking. An AST:ALT ratio >2:1 supports a suspicion of alcohol abuse.12 More than 90% of patients with an AST:ALT ratio of 2:1 have alcoholic liver disease. This increases to more than 96% if the ratio is 3:1.13
GGT is an enzyme concentrated in the liver, bile ducts, and kidneys; normal range is 0 to 45 U/L (for females) or 53 U/L (for males).14 GGT levels >30 U/L correlate with alcohol consumption of >4 drinks per day.15 GGT has a half-life of 14 to 26 days and remains elevated for 4 to 6 weeks after drinking cessation, which make it useful for monitoring abstinence in treatment programs.16 Sensitivity ranges from 37% to 85% and specificity is as high as 93% in nonmedical populations.17 Although nonalcoholic liver disease can elevate GGT in persons who do not abuse alcohol, 50% to 72% of GGT elevations can be explained by excessive alcohol consumption.18
CDT is a newer biomarker used to monitor alcohol consumption. The most accurate way to express CDT level is as a percentage of total transferrin concentration. This method accounts for individual variations in transferrin levels, thus minimizing false positives.18 In persons who consume >4 or 5 drinks per day for 2 weeks or more, CDT is >1.3% of total transferrin.19 Unfortunately, because it is expensive and requires sophisticated test methodology, CDT testing is not available at most hospitals.20
Combinations improve detection
Each biochemical measure has strengths and weaknesses as a marker for determining patients’ alcohol consumption (Table 2). CDT and GGT show the highest sensitivity for heavy drinking, and CDT has a higher specificity than GGT (Table 3).21,22 Relapse to alcohol use after abstinence may be best identified by a simultaneous 30% increase in CDT and GGT.5
Because GGT has a longer half-life than CDT, its diagnostic efficiency in detecting alcohol relapse may not develop until 4 weeks after alcohol detoxification, whereas CDT may become clinically useful for detecting relapse as early as 1 week after detoxification.23
Table 2
Biomarkers of alcohol use: Strengths and weaknesses
| Biomarker | Strengths | Weaknesses |
|---|---|---|
| CDT | High specificity for alcohol use; few factors cause false positives High sensitivity in distinguishing alcoholics from social drinkers Marker of relapse and abstinence from drinking Confirmatory test for patients suspected of alcohol abuse | Low sensitivity; more valuable to confirm than exclude heavy drinking Cost (average $30/assay) and low availability of testing Likely less sensitive for women and younger patients compared with men Poor screening tool for alcohol use in general population |
| GGT | Elevations precede alcohol-induced liver damage High specificity in patients with suspected alcohol abuse Effective marker for patients suspected of binge drinking Inexpensive ( | Can be falsely elevated by liver and biliary disease, smoking, obesity, and medications that induce microsomal enzymes Low sensitivity makes it a poor screening tool in general population Poor marker of relapse |
| AST:ALT >2:1 | Highly sensitive and specific for alcohol-induced liver damage | Enzyme elevations can be detected only after periods of heavy drinking Elevations secondary to liver damage at the hepatocellular level (after fatty changes) |
| MCV | Accuracy similar in male and female patients Elevations in suspected cases of alcohol use indicate chronicity of drinking Routine laboratory test | Poor biomarker for relapse False positives caused by liver disease, hemolysis, bleeding disorders, anemia, folate deficiency, and medications that reduce folate Low sensitivity and specificity for alcohol use make it a poor screening tool for alcohol abuse |
| AST: aspartate aminotransferase; ALT: alanine aminotransferase; CDT: carbohydrate deficient transferrin; GGT: gamma-glutamyl transferase; MCV: mean corpuscular volume | ||
Table 3
Interpreting diagnostic test performance
| Term | Definition | Applicability |
|---|---|---|
| Sensitivity | Percent of persons with disease who test positive | High value is desirable for ruling out disease (low false-negative rate) |
| Specificity | Percent of persons without disease who test negative | High value is desirable for ruling in disease (low false-positive rate) |
| Positive predictive value | Percent of positive test results that are true positives | Probability that a person with a positive test result has the disease |
| Negative predictive value | Percent of negative test results that are true negatives | Probability that a person with a negative test result is disease-free |
| Source: References 21,22 | ||
There is evidence that combining tests can improve alcohol use detection.24 For example, Dolman et al25 found that the ability of the AUDIT questionnaire to correctly predict which patients would experience alcohol withdrawal increases when it is used in combination with biochemical markers. Specifically, the positive predictive value of an AUDIT score ≥8 increased from 17% to 47% when found in combination with ≥2 abnormal biochemical marker levels; the study looked at GGT, ALT, AST, and MCV. Sensitivity was 94% and specificity was 98%.
Similarly, combinations of biochemical markers—especially CDT and GGT—have improved detection of alcohol use and subsequent risk of withdrawal.26Table 4 provides a summary of studies that evaluated using combinations of biochemical markers.4,5,27-31
Table 4
Combining biomarker tests: An effective approach
| Combination | Study | Sensitivity* |
|---|---|---|
| GGT + MCV | Morgan et al4 | 95% |
| GGT + CDT | Hietala et al5 | 90% |
| Mundle et al29 | 90% | |
| Bell et al30 | 90% | |
| Sillanaukee et al31 | 95% | |
| GGT + AST:ALT >2:1 | Gluud et al27 | 92% |
| Morgan et al4 | 100% | |
| MCV + AST:ALT >2:1 | Kawachi et al28 | 97% |
| Morgan et al4 | 95% | |
| GGT + MCV + AST:ALT >2:1 | Morgan et al4 | 100% |
| GGT + MCV + CDT | Sillanaukee et al31 | 70% |
| * Sensitivity for detecting excessive alcohol consumption | ||
| AST: aspartate aminotransferase; ALT: alanine aminotransferase; CDT: carbohydrate deficient transferrin; GGT: gamma-glutamyl transferase; MCV: mean corpuscular volume | ||
Consider patients’ comorbidities
Patients at risk for underreporting alcohol use include those with unemployment histories, previous alcohol treatment, and higher scores on the Alcohol Dependence Scale (18.5, SD=8.1).2 Interpret biochemical testing results in the context of a patient’s overall clinical picture.
The following 2 case patients denied or underreported recent alcohol use but we determined they were at high risk for an alcohol disorder because of their medical and/or psychiatric histories. Analysis of biochemical markers helped assess the risk of alcohol withdrawal.
CASE 2: Altered mental status
Family members bring Mr. N, age 44, to the hospital because of his odd behavior. He presents with paranoid delusions and an inappropriate elated mood. His medical history includes acquired immune deficiency syndrome (AIDS). After cerebrospinal fluid analysis, computed tomography of the head, electroencephalogram, and metabolic workup are within normal limits, the patient is diagnosed with human immunodeficiency virus (HIV) mania and is admitted.
On admission, Mr. N denies alcohol use. A blood alcohol/urine toxicity screen is negative. One day after admission, Mr. M develops elevated blood pressure and tachycardia and reports headache and nausea.
Challenge. Gathering a valid history of Mr. N’s alcohol use is difficult because of his acutely altered mental status and manic-like state. We use laboratory data to assess his risk of alcohol withdrawal. His liver function tests include an AST of 33 U/L, ALT of 30 U/L, and an alkaline phosphatase of 94 U/L. MCV is normal at 90 fL. Interestingly, the GGT level is elevated almost 4 times normal at 164 U/L.
Discussion. Although Mr. N denied alcohol use and presented with a negative BAL, laboratory data support alcohol dependence. His GGT was elevated well beyond normal limits, without evidence of hepatobiliary disease. GGT has a sensitivity as high as 85%32 and limited specificity for alcohol abuse. Because of his high probability of recent alcohol consumption, we place Mr. N on AWP.
We postulate that our patient’s autonomic instability, headache, and nausea are related to alcohol withdrawal. We are aware that delirium occurs frequently in patients with HIV infection, and although Mr. N’s medical workup is negative, HIV infection can produce an acute encephalopathy that could resemble our patient’s clinical picture.33
Mr. N’s autonomic instability, headache, and nausea abated after treatment for alcohol withdrawal.
CASE 3: Suicide attempt?
Mr. S, age 28, presents to the trauma service with a self-inflicted gunshot wound to the face. He reports feeling depressed for the last year but denies a history of psychotic symptoms or heroin withdrawal symptoms. He also denies recent or past alcohol abuse and does not have a history of biliary tract disease or megaloblastic anemia. His mother tells us Mr. S has had a history of depression since childhood.
Challenge. Based on Mr. S’ apparent suicide attempt and history, we feel he is at high risk for alcohol abuse. We use laboratory markers to assess the likelihood of alcohol consumption and possibly decrease his risk of alcohol withdrawal.
Discussion. Mr. S’ lab data show an MCV of 91 fL, AST of 95 U/L, alanine ALT of 156 U/L, and alkaline phosphatase of 160 U/L. GGT was elevated at 122 U/L.
Although Mr. S’ MCV is within the normal range, his GGT is elevated, and the combination of an elevated GGT and MCV has a 95% sensitivity for the diagnosis of alcohol abuse. We place Mr. S on alcohol withdrawal precautions and discuss with him the potential life-threatening complications of alcohol withdrawal. Confronted with this information and the possible implication of his elevated LFTs, the patient admits his alcohol history—which consists of drinking 12 beers/day for at least the past 2 years. He admits this despite exhibiting no signs or symptoms of alcohol withdrawal.
Related Resources
- National Institute on Alcohol Abuse and Alcoholism Data/Statistical Tables. www.niaaa.nih.gov/Resources/DatabaseResources/QuickFacts.
- Maisto SA, Connors GJ, Allen JP. Contrasting self-report screens for alcohol problems: a review. Alcohol Clin Exp Res 1995;19(6):1510-6.
- Coulton S, Drummond C, James D, et al. Opportunistic screening for alcohol use disorders in primary care: comparative study. BMJ 2006;332:511-7.
Bottom line
Because CDT—the most accurate biomarker—is not available at most hospitals, we recommend using combinations of other measures to detect unreported recent alcohol consumption. If GGT and MCV are elevated, GGT is elevated and AST:ALT is >2:1, or MCV is elevated and AST:ALT is >2:1, consider initiating alcohol withdrawal precautions.
Acknowledgement
The authors acknowledge Daiana Radac, BA, a third-year medical student at Eastern Virginia Medical School, for her contributions to this article.
Hospitalized patients who are not truthful about their alcohol consumption may be at risk for an unplanned withdrawal. Self-reports of alcohol use—such as CAGE and the Alcohol Use Disorders Identification Test (AUDIT)—are valid, inexpensive, and noninvasive, but patients easily can feign results.1 Biochemical measures are more objective, and combinations of markers are an effective tool to detect recent heavy drinking in the 10% to 25% of patients who underreport alcohol use.2
Biochemical measures can detect acute alcohol intoxication and recent prolonged drinking. Because marker levels return to normal after long-term abstinence, ongoing monitoring can help detect a relapse before a patient admits to it.3
This article presents 3 cases in which biochemical markers helped prevent alcohol withdrawal in patients who denied alcohol abuse. We discuss why we ordered biochemical tests and which combinations provided highly sensitive results.
CASE 1: Depression and substance abuse
Ms. C, age 39, presents with bleeding gums due to excessive warfarin, which she takes prophylactically for a history of deep vein thrombosis. She is seen by the psychiatric consultation service for depression—which she says she has experienced since “the day I was born”—and substance abuse that includes a history binge drinking. Ms. C says she has stopped drinking and remained abstinent for the past year because she is fearful of further damaging her kidneys. She also denies psychosis. She does not have a history or symptoms of hepatobiliary or hematologic disease.
Challenge. Despite Ms. C’s self-reported 1 year of sobriety, her history of binge drinking and depression calls for evaluating her alcohol withdrawal risk. Laboratory markers of alcohol abuse are the only means to assess her recent drinking behavior.
Discussion. Lab results include serum albumin of 3.4 g/dL, total bilirubin of 0.3 mg/dL, total protein of 6.3 g/dL, aspartate aminotransferase (AST) of 13 U/L, alanine aminotransferase (ALT) of 19 U/L, alkaline phosphatase of 136 U/L, and blood ammonia level of 37 μg/dL. Gamma-glutamyl transferase (GGT) is elevated at 104 U/L (normal range for women: 0 to 45 U/L). Mean corpuscular volume (MCV) is elevated at 101 fL (normal range 80 to 100 fL).
The combination of elevated MCV and GGT has a 95% sensitivity for alcohol abuse.4 GGT levels become elevated after 24 hours to 2 weeks of heavy alcohol consumption and return to normal within 2 to 6 weeks of abstinence, which allows them to detect binge drinking. MCV takes 6 to 8 weeks of heavy drinking—we which we define as consuming ≥40 grams of alcohol/day5—to become elevated and returns to normal within 3 months of abstinence.
These data provide evidence that Ms. C recently consumed substantial amounts of alcohol. As a result, we start her on alcohol withdrawal precautions (AWP).
Markers of alcohol abuse
Biochemical markers commonly used to detect alcohol abuse (Table 1) include:
- blood alcohol level (BAL)
- MCV
- liver function tests (LFTs) such as ALT, AST, and GGT
- carbohydrate deficient transferrin (CDT).
Table 1
By the numbers: Biomarkers of excessive alcohol consumption
| Biomarker | |||||
|---|---|---|---|---|---|
| CDT | GGT | AST | ALT | MCV | |
| Blood test normal range | Women: 0 to 45 U/L Men: 0 to 53 U/L | 10 to 34 U/L | 8 to 37 U/L | 80 to 100 fL | |
| Blood test abnormal range | >1.3% of total transferrin concentration | Women: >45 U/L Men: >53 U/L | Levels rarely exceed 500 U/L | Levels rarely exceed 300 U/L | >100 fL |
| Time to elevation | 2 to 3 weeks | 24 hours to 2 weeks | 3 to 7 days | 3 to 7 days | After 6 weeks |
| Time to descent to normal levels | 2 to 4 weeks of abstinence | 2 to 6 weeks of abstinence | Half-life 12 to 24 hours | Half-life 37 to 57 hours | 3 months |
| Dose-response of alcohol | 60 g/d | 80 to 200 g/d | ≥40 g/d | ≥40 g/d | ≥40 g/d |
| Sensitivity | 55% to 90%a-e | 37% to 85%b, f, g | AST:ALT ratio >2:1 has a 70% sensitivity and 92% to 100% specificity for alcoholic-induced liver diseaseh-j | 20% to 70%b,k | |
| Relapse sensitivity | 55% to 76%a,l,m | 50%a,e | 20%a,n | ||
| Specificity | 92% to 97%a,b | 18% to 93%a,b,e | 64% to 66%b,k,n | ||
| Positive predictive value | 46% to 75%c,g | 41%g | 36%g | ||
| Negative predictive value | 72% to 98%a,c,g | 69% to 92%a,e,g | 67%g | ||
| AST: aspartate aminotransferase; ALT: alanine aminotransferase; CDT: carbohydrate deficient transferrin; GGT: gamma-glutamyl transferase; MCV: mean corpuscular volume | |||||
| Source: Reference Citations: click here | |||||
BAL can document acute alcohol intoxication, but its use is limited because alcohol has a 4-hour half-life and an elimination rate of 7 grams/hour—equivalent to 1 drink/hour.6 (A “drink” typically is defined as a 12-ounce bottle of beer or wine cooler, a 5-ounce glass of wine, or 1.5 ounces of 80-proof distilled spirits.) Therefore, BAL will identify as false negatives alcohol-dependent patients who abstain from alcohol within 24 hours of testing.
MCV is an index of the average volume of erythrocytes. Macrocytosis occurs when the volume exceeds 100 fL. Elevated MCV is the most typical morphologic abnormality associated with excessive alcohol consumption7,8 and macrocytosis—sometimes without associated anemia—is often evident in persons with alcoholism. MCV elevates after 6 weeks of alcohol misuse and may remain elevated for up to 3 months after a person has stopped drinking.9
Because patients with disorders unrelated to alcohol use can have elevated MCV, alone it is not a useful screening marker for alcohol abuse.10 Additionally, because macrocytosis can persist under strictly controlled alcohol abstinence, MCV is not a reliable clinical indicator of relapse.11
LFTs measure enzymes and proteins. ALT, AST, and GGT are the most relevant for detecting heavy drinking. An AST:ALT ratio >2:1 supports a suspicion of alcohol abuse.12 More than 90% of patients with an AST:ALT ratio of 2:1 have alcoholic liver disease. This increases to more than 96% if the ratio is 3:1.13
GGT is an enzyme concentrated in the liver, bile ducts, and kidneys; normal range is 0 to 45 U/L (for females) or 53 U/L (for males).14 GGT levels >30 U/L correlate with alcohol consumption of >4 drinks per day.15 GGT has a half-life of 14 to 26 days and remains elevated for 4 to 6 weeks after drinking cessation, which make it useful for monitoring abstinence in treatment programs.16 Sensitivity ranges from 37% to 85% and specificity is as high as 93% in nonmedical populations.17 Although nonalcoholic liver disease can elevate GGT in persons who do not abuse alcohol, 50% to 72% of GGT elevations can be explained by excessive alcohol consumption.18
CDT is a newer biomarker used to monitor alcohol consumption. The most accurate way to express CDT level is as a percentage of total transferrin concentration. This method accounts for individual variations in transferrin levels, thus minimizing false positives.18 In persons who consume >4 or 5 drinks per day for 2 weeks or more, CDT is >1.3% of total transferrin.19 Unfortunately, because it is expensive and requires sophisticated test methodology, CDT testing is not available at most hospitals.20
Combinations improve detection
Each biochemical measure has strengths and weaknesses as a marker for determining patients’ alcohol consumption (Table 2). CDT and GGT show the highest sensitivity for heavy drinking, and CDT has a higher specificity than GGT (Table 3).21,22 Relapse to alcohol use after abstinence may be best identified by a simultaneous 30% increase in CDT and GGT.5
Because GGT has a longer half-life than CDT, its diagnostic efficiency in detecting alcohol relapse may not develop until 4 weeks after alcohol detoxification, whereas CDT may become clinically useful for detecting relapse as early as 1 week after detoxification.23
Table 2
Biomarkers of alcohol use: Strengths and weaknesses
| Biomarker | Strengths | Weaknesses |
|---|---|---|
| CDT | High specificity for alcohol use; few factors cause false positives High sensitivity in distinguishing alcoholics from social drinkers Marker of relapse and abstinence from drinking Confirmatory test for patients suspected of alcohol abuse | Low sensitivity; more valuable to confirm than exclude heavy drinking Cost (average $30/assay) and low availability of testing Likely less sensitive for women and younger patients compared with men Poor screening tool for alcohol use in general population |
| GGT | Elevations precede alcohol-induced liver damage High specificity in patients with suspected alcohol abuse Effective marker for patients suspected of binge drinking Inexpensive ( | Can be falsely elevated by liver and biliary disease, smoking, obesity, and medications that induce microsomal enzymes Low sensitivity makes it a poor screening tool in general population Poor marker of relapse |
| AST:ALT >2:1 | Highly sensitive and specific for alcohol-induced liver damage | Enzyme elevations can be detected only after periods of heavy drinking Elevations secondary to liver damage at the hepatocellular level (after fatty changes) |
| MCV | Accuracy similar in male and female patients Elevations in suspected cases of alcohol use indicate chronicity of drinking Routine laboratory test | Poor biomarker for relapse False positives caused by liver disease, hemolysis, bleeding disorders, anemia, folate deficiency, and medications that reduce folate Low sensitivity and specificity for alcohol use make it a poor screening tool for alcohol abuse |
| AST: aspartate aminotransferase; ALT: alanine aminotransferase; CDT: carbohydrate deficient transferrin; GGT: gamma-glutamyl transferase; MCV: mean corpuscular volume | ||
Table 3
Interpreting diagnostic test performance
| Term | Definition | Applicability |
|---|---|---|
| Sensitivity | Percent of persons with disease who test positive | High value is desirable for ruling out disease (low false-negative rate) |
| Specificity | Percent of persons without disease who test negative | High value is desirable for ruling in disease (low false-positive rate) |
| Positive predictive value | Percent of positive test results that are true positives | Probability that a person with a positive test result has the disease |
| Negative predictive value | Percent of negative test results that are true negatives | Probability that a person with a negative test result is disease-free |
| Source: References 21,22 | ||
There is evidence that combining tests can improve alcohol use detection.24 For example, Dolman et al25 found that the ability of the AUDIT questionnaire to correctly predict which patients would experience alcohol withdrawal increases when it is used in combination with biochemical markers. Specifically, the positive predictive value of an AUDIT score ≥8 increased from 17% to 47% when found in combination with ≥2 abnormal biochemical marker levels; the study looked at GGT, ALT, AST, and MCV. Sensitivity was 94% and specificity was 98%.
Similarly, combinations of biochemical markers—especially CDT and GGT—have improved detection of alcohol use and subsequent risk of withdrawal.26Table 4 provides a summary of studies that evaluated using combinations of biochemical markers.4,5,27-31
Table 4
Combining biomarker tests: An effective approach
| Combination | Study | Sensitivity* |
|---|---|---|
| GGT + MCV | Morgan et al4 | 95% |
| GGT + CDT | Hietala et al5 | 90% |
| Mundle et al29 | 90% | |
| Bell et al30 | 90% | |
| Sillanaukee et al31 | 95% | |
| GGT + AST:ALT >2:1 | Gluud et al27 | 92% |
| Morgan et al4 | 100% | |
| MCV + AST:ALT >2:1 | Kawachi et al28 | 97% |
| Morgan et al4 | 95% | |
| GGT + MCV + AST:ALT >2:1 | Morgan et al4 | 100% |
| GGT + MCV + CDT | Sillanaukee et al31 | 70% |
| * Sensitivity for detecting excessive alcohol consumption | ||
| AST: aspartate aminotransferase; ALT: alanine aminotransferase; CDT: carbohydrate deficient transferrin; GGT: gamma-glutamyl transferase; MCV: mean corpuscular volume | ||
Consider patients’ comorbidities
Patients at risk for underreporting alcohol use include those with unemployment histories, previous alcohol treatment, and higher scores on the Alcohol Dependence Scale (18.5, SD=8.1).2 Interpret biochemical testing results in the context of a patient’s overall clinical picture.
The following 2 case patients denied or underreported recent alcohol use but we determined they were at high risk for an alcohol disorder because of their medical and/or psychiatric histories. Analysis of biochemical markers helped assess the risk of alcohol withdrawal.
CASE 2: Altered mental status
Family members bring Mr. N, age 44, to the hospital because of his odd behavior. He presents with paranoid delusions and an inappropriate elated mood. His medical history includes acquired immune deficiency syndrome (AIDS). After cerebrospinal fluid analysis, computed tomography of the head, electroencephalogram, and metabolic workup are within normal limits, the patient is diagnosed with human immunodeficiency virus (HIV) mania and is admitted.
On admission, Mr. N denies alcohol use. A blood alcohol/urine toxicity screen is negative. One day after admission, Mr. M develops elevated blood pressure and tachycardia and reports headache and nausea.
Challenge. Gathering a valid history of Mr. N’s alcohol use is difficult because of his acutely altered mental status and manic-like state. We use laboratory data to assess his risk of alcohol withdrawal. His liver function tests include an AST of 33 U/L, ALT of 30 U/L, and an alkaline phosphatase of 94 U/L. MCV is normal at 90 fL. Interestingly, the GGT level is elevated almost 4 times normal at 164 U/L.
Discussion. Although Mr. N denied alcohol use and presented with a negative BAL, laboratory data support alcohol dependence. His GGT was elevated well beyond normal limits, without evidence of hepatobiliary disease. GGT has a sensitivity as high as 85%32 and limited specificity for alcohol abuse. Because of his high probability of recent alcohol consumption, we place Mr. N on AWP.
We postulate that our patient’s autonomic instability, headache, and nausea are related to alcohol withdrawal. We are aware that delirium occurs frequently in patients with HIV infection, and although Mr. N’s medical workup is negative, HIV infection can produce an acute encephalopathy that could resemble our patient’s clinical picture.33
Mr. N’s autonomic instability, headache, and nausea abated after treatment for alcohol withdrawal.
CASE 3: Suicide attempt?
Mr. S, age 28, presents to the trauma service with a self-inflicted gunshot wound to the face. He reports feeling depressed for the last year but denies a history of psychotic symptoms or heroin withdrawal symptoms. He also denies recent or past alcohol abuse and does not have a history of biliary tract disease or megaloblastic anemia. His mother tells us Mr. S has had a history of depression since childhood.
Challenge. Based on Mr. S’ apparent suicide attempt and history, we feel he is at high risk for alcohol abuse. We use laboratory markers to assess the likelihood of alcohol consumption and possibly decrease his risk of alcohol withdrawal.
Discussion. Mr. S’ lab data show an MCV of 91 fL, AST of 95 U/L, alanine ALT of 156 U/L, and alkaline phosphatase of 160 U/L. GGT was elevated at 122 U/L.
Although Mr. S’ MCV is within the normal range, his GGT is elevated, and the combination of an elevated GGT and MCV has a 95% sensitivity for the diagnosis of alcohol abuse. We place Mr. S on alcohol withdrawal precautions and discuss with him the potential life-threatening complications of alcohol withdrawal. Confronted with this information and the possible implication of his elevated LFTs, the patient admits his alcohol history—which consists of drinking 12 beers/day for at least the past 2 years. He admits this despite exhibiting no signs or symptoms of alcohol withdrawal.
Related Resources
- National Institute on Alcohol Abuse and Alcoholism Data/Statistical Tables. www.niaaa.nih.gov/Resources/DatabaseResources/QuickFacts.
- Maisto SA, Connors GJ, Allen JP. Contrasting self-report screens for alcohol problems: a review. Alcohol Clin Exp Res 1995;19(6):1510-6.
- Coulton S, Drummond C, James D, et al. Opportunistic screening for alcohol use disorders in primary care: comparative study. BMJ 2006;332:511-7.
Bottom line
Because CDT—the most accurate biomarker—is not available at most hospitals, we recommend using combinations of other measures to detect unreported recent alcohol consumption. If GGT and MCV are elevated, GGT is elevated and AST:ALT is >2:1, or MCV is elevated and AST:ALT is >2:1, consider initiating alcohol withdrawal precautions.
Acknowledgement
The authors acknowledge Daiana Radac, BA, a third-year medical student at Eastern Virginia Medical School, for her contributions to this article.
1. Allen JP, Anthenelli RM. Getting to the bottom of problem drinking: the case for routine screening. Current Psychiatry 2003;2(6):26-44.
2. Killeen TK, Brady KT, Gold PB, et al. Comparison of self-report versus agency records of service utilization in a community sample of individuals with alcohol use disorders. Drug Alcohol Depend 2004;73(2):141-7.
3. Alcohol withdrawal syndrome: how to predict, prevent, diagnose and treat it. Prescrire Int 2007;16(87):24-31.
4. Morgan MY, Colman JC, Sherlock S. The use of a combination of peripheral markers for diagnosing alcoholism and monitoring for continued abuse. Alcohol Alcohol 1981;16:167-77.
5. Hietala J, Koivisto H, Anttila P, et al. Comparison of the combined marker GGT-CDT and the conventional laboratory markers of alcohol abuse in heavy drinkers, moderate drinkers and abstainers. Alcohol Alcohol 2006;41(5):528-33.
6. Swift R. Direct measurement of alcohol and its metabolites. Addiction 2003;98:73-80.
7. Koivisto H, Hietala J, Anttila P, et al. Long-term ethanol consumption and macrocytosis: diagnostic and pathogenic implications. J Lab Clin Med 2005;147(4):191-6.
8. Savage DG, Ogundipe A, Allen RH, et al. Etiology and diagnostic evaluation of macrocytosis. Am J Med Sci 2000;319(6):343-52.
9. Gordon H. Detection of alcoholic liver disease. World J Gastroenterol 2001;7(3):297-302.
10. Bernadt M, Mumford J, Taylor C, et al. Comparison of questionnaire and laboratory tests in the detection of excessive drinking and alcoholism. Lancet 1982;1:325-8.
11. Hasselblatt M, Martin F, Maul O, et al. Persistent macrocytosis following abstinence from chronic alcohol use. JAMA 2001;286:2946.-
12. Prati D, Taioli E, Zanella A, et al. Updated definitions of healthy ranges for serum alanine aminotransferase levels. Ann Intern Med 2002;137:1-9.
13. Fancher T, Kamboj A, Onate J. Interpreting liver function tests. Current Psychiatry 2007;6(5):61-8.
14. Puukka K, Hietala J, Koivisto H, et al. Obesity and the clinical use of serum GGT activity as a marker of heavy drinking. Scand J Clin Lab Invest 2007;67(5):480-8.
15. Litten RZ, Allen JP, Fertig JB. y-glutamyl transpeptidase and carbohydrate deficient transferrin: alternative measures of excessive alcohol consumption. Alcohol Clin Exp Res 1995;19(6):1541-6.
16. National Institute on Alcohol Abuse and Alcoholism. Screening for alcohol problems—an update. Alcohol Alert No 56 Available at: http://pubs.niaaa.nih.gov/publications/aa56.htm. Accessed May 5, 2007.
17. DiMartini A. A clinical guide to assessing alcohol use and problems. Available at: http://www.alcoholmedicalscholars.org/clin-asmt.ppt. Accessed June 30, 2008.
18. Wolff K, Marshall E. Biological markers of alcohol use. Psychiatry 2006;5(12):437-8.
19. ARUP Laboratories. Carbohydrate-deficient transferrin (CDT) for alcohol use. 2006. Available at: http://www.aruplab.com/TestDirectory/resources/TechnicalBulletins/Carbohydrate-Deficient%20Transferrin%20(CDT)%20Mar%202006.pdf. Accessed July 30, 2008.
20. Allen JP, Litten RZ. The role of laboratory testing in alcoholism treatment. J Subst Abuse Treat 2001;20:81-5.
21. Bhushan V, Le T, Ozturk A, et al. Behavioral Science. In: Le T, Bhushan V, Rao DA, eds. First aid for the USMLE step 1: a student to student guide. New York, NY: McGraw Hill Medical Publishing Division; 2007.
22. Miller PM, Anton RF. Biochemical alcohol screening in primary care. Addict Behav 2004;29(7):1427-37.
23. Schmidt LG, Schmidt K, Dufeu P, et al. Superiority of carbohydrate-deficient transferrin to gamma-glutamyltransferase in detecting relapse in alcoholism. Am J Psychiatry 1997;154(1):75-80.
24. Salaspuro M. Carbohydrate-deficient transferrin as compared to other markers of alcoholism: a systematic review. Alcohol 1999;19(3):261-71.
25. Dolman JM, Hawkes ND. Combining the AUDIT questionnaire and biochemical markers to assess alcohol use and risk of alcohol withdrawal in medical patients. Alcohol Alcohol 2005;40(6):515-9.
26. Helander A, Carlsson AV, Borg S. Longitudinal comparison of carbohydrate-deficient transferrin and gamma-glutamyl transferase: complementary markers of excessive alcohol consumption. Alcohol Alcohol 1996;31(1):101-7.
27. Gluud C, Andersen I, Dietrichson O, et al. Gamma-glutamyltransferase, aspartate aminotransferase and alkaline phosphatase as markers of alcohol consumption in out-patient alcoholics. Eur J Clin Invest 1981;11(3):171-6.
28. Kawachi I, Robinson GM, Stace NH. A combination of raised serum AST: ALT ratio and erythrocyte mean cell volume level detects excessive alcohol consumption. N Z Med J 1990;103(887):145-8.
29. Mundle G, Ackerman K, Mann K. Biological markers as indicators for relapse in alcohol-dependent patients. Addict Biol 1999;4(2):209-14.
30. Bell H, Tallaksen C, Sjåheim T, et al. Serum carbohydrate-deficient transferrin as a marker of alcohol consumption in patients with chronic liver diseases. Alcohol Clin Exp Res 1993;17(2):246-52.
31. Sillanaukee P, Aalto M, Seppa K. Carbohydrate-deficient transferrin and conventional alcohol markers as indicators for brief intervention among heavy drinkers in primary health care. Alcohol Clin Exp Res 1998;22(4):892-6.
32. Salaspuro S. Conventional and coming laboratory markers of alcoholism and heavy drinking. Alcohol Clin Exp Res 1986;10(6 suppl):5-12.
33. Della Penna ND, Treisman GJ. HIV/AIDS. In: Levenson J, ed. Essentials of psychosomatic medicine. Washington, DC: American Psychiatric Publishing, Inc; 2007.
1. Allen JP, Anthenelli RM. Getting to the bottom of problem drinking: the case for routine screening. Current Psychiatry 2003;2(6):26-44.
2. Killeen TK, Brady KT, Gold PB, et al. Comparison of self-report versus agency records of service utilization in a community sample of individuals with alcohol use disorders. Drug Alcohol Depend 2004;73(2):141-7.
3. Alcohol withdrawal syndrome: how to predict, prevent, diagnose and treat it. Prescrire Int 2007;16(87):24-31.
4. Morgan MY, Colman JC, Sherlock S. The use of a combination of peripheral markers for diagnosing alcoholism and monitoring for continued abuse. Alcohol Alcohol 1981;16:167-77.
5. Hietala J, Koivisto H, Anttila P, et al. Comparison of the combined marker GGT-CDT and the conventional laboratory markers of alcohol abuse in heavy drinkers, moderate drinkers and abstainers. Alcohol Alcohol 2006;41(5):528-33.
6. Swift R. Direct measurement of alcohol and its metabolites. Addiction 2003;98:73-80.
7. Koivisto H, Hietala J, Anttila P, et al. Long-term ethanol consumption and macrocytosis: diagnostic and pathogenic implications. J Lab Clin Med 2005;147(4):191-6.
8. Savage DG, Ogundipe A, Allen RH, et al. Etiology and diagnostic evaluation of macrocytosis. Am J Med Sci 2000;319(6):343-52.
9. Gordon H. Detection of alcoholic liver disease. World J Gastroenterol 2001;7(3):297-302.
10. Bernadt M, Mumford J, Taylor C, et al. Comparison of questionnaire and laboratory tests in the detection of excessive drinking and alcoholism. Lancet 1982;1:325-8.
11. Hasselblatt M, Martin F, Maul O, et al. Persistent macrocytosis following abstinence from chronic alcohol use. JAMA 2001;286:2946.-
12. Prati D, Taioli E, Zanella A, et al. Updated definitions of healthy ranges for serum alanine aminotransferase levels. Ann Intern Med 2002;137:1-9.
13. Fancher T, Kamboj A, Onate J. Interpreting liver function tests. Current Psychiatry 2007;6(5):61-8.
14. Puukka K, Hietala J, Koivisto H, et al. Obesity and the clinical use of serum GGT activity as a marker of heavy drinking. Scand J Clin Lab Invest 2007;67(5):480-8.
15. Litten RZ, Allen JP, Fertig JB. y-glutamyl transpeptidase and carbohydrate deficient transferrin: alternative measures of excessive alcohol consumption. Alcohol Clin Exp Res 1995;19(6):1541-6.
16. National Institute on Alcohol Abuse and Alcoholism. Screening for alcohol problems—an update. Alcohol Alert No 56 Available at: http://pubs.niaaa.nih.gov/publications/aa56.htm. Accessed May 5, 2007.
17. DiMartini A. A clinical guide to assessing alcohol use and problems. Available at: http://www.alcoholmedicalscholars.org/clin-asmt.ppt. Accessed June 30, 2008.
18. Wolff K, Marshall E. Biological markers of alcohol use. Psychiatry 2006;5(12):437-8.
19. ARUP Laboratories. Carbohydrate-deficient transferrin (CDT) for alcohol use. 2006. Available at: http://www.aruplab.com/TestDirectory/resources/TechnicalBulletins/Carbohydrate-Deficient%20Transferrin%20(CDT)%20Mar%202006.pdf. Accessed July 30, 2008.
20. Allen JP, Litten RZ. The role of laboratory testing in alcoholism treatment. J Subst Abuse Treat 2001;20:81-5.
21. Bhushan V, Le T, Ozturk A, et al. Behavioral Science. In: Le T, Bhushan V, Rao DA, eds. First aid for the USMLE step 1: a student to student guide. New York, NY: McGraw Hill Medical Publishing Division; 2007.
22. Miller PM, Anton RF. Biochemical alcohol screening in primary care. Addict Behav 2004;29(7):1427-37.
23. Schmidt LG, Schmidt K, Dufeu P, et al. Superiority of carbohydrate-deficient transferrin to gamma-glutamyltransferase in detecting relapse in alcoholism. Am J Psychiatry 1997;154(1):75-80.
24. Salaspuro M. Carbohydrate-deficient transferrin as compared to other markers of alcoholism: a systematic review. Alcohol 1999;19(3):261-71.
25. Dolman JM, Hawkes ND. Combining the AUDIT questionnaire and biochemical markers to assess alcohol use and risk of alcohol withdrawal in medical patients. Alcohol Alcohol 2005;40(6):515-9.
26. Helander A, Carlsson AV, Borg S. Longitudinal comparison of carbohydrate-deficient transferrin and gamma-glutamyl transferase: complementary markers of excessive alcohol consumption. Alcohol Alcohol 1996;31(1):101-7.
27. Gluud C, Andersen I, Dietrichson O, et al. Gamma-glutamyltransferase, aspartate aminotransferase and alkaline phosphatase as markers of alcohol consumption in out-patient alcoholics. Eur J Clin Invest 1981;11(3):171-6.
28. Kawachi I, Robinson GM, Stace NH. A combination of raised serum AST: ALT ratio and erythrocyte mean cell volume level detects excessive alcohol consumption. N Z Med J 1990;103(887):145-8.
29. Mundle G, Ackerman K, Mann K. Biological markers as indicators for relapse in alcohol-dependent patients. Addict Biol 1999;4(2):209-14.
30. Bell H, Tallaksen C, Sjåheim T, et al. Serum carbohydrate-deficient transferrin as a marker of alcohol consumption in patients with chronic liver diseases. Alcohol Clin Exp Res 1993;17(2):246-52.
31. Sillanaukee P, Aalto M, Seppa K. Carbohydrate-deficient transferrin and conventional alcohol markers as indicators for brief intervention among heavy drinkers in primary health care. Alcohol Clin Exp Res 1998;22(4):892-6.
32. Salaspuro S. Conventional and coming laboratory markers of alcoholism and heavy drinking. Alcohol Clin Exp Res 1986;10(6 suppl):5-12.
33. Della Penna ND, Treisman GJ. HIV/AIDS. In: Levenson J, ed. Essentials of psychosomatic medicine. Washington, DC: American Psychiatric Publishing, Inc; 2007.
Psychiatrist/patient boundaries: When it’s OK to stretch the line
Dr. M is facing financial challenges with his fledgling private practice and begins consulting at a weight loss clinic to supplement his income. He finds him-self attracted to Ms. Y, a weight-loss patient he is treating. They seem to click interpersonally, and he extends his office visits with her. Ms. Y clearly enjoys this extra attention, and Dr. M begins including personal disclosures in his conversations with her.
In his residency training, Dr. M was taught never to date a current or former patient, but he views this situation as different. Ms. Y is seeing him only for weight loss, and he rationalizes that he is providing her with medical care, not “psychiatric” care. On 2 occasions he gives her a limited quantity of benzodiazepines for mild anxiety, which he considers a transitory stress-related condition and not an “official” DSM-IV-TR disorder.
Eventually, Dr. M asks Ms. Y to dinner and she accepts. After they begin dating, he decides to transfer her to another clinic physician “just to be safe.”
Although many psychiatrists assume that psychiatrist/patient boundaries are well defined by ethical and legal standards, boundary issues are a complex and controversial aspect of clinical practice. Psychoanalysts initially defined psychiatrist/patient boundaries as a way of structuring the unique and intimate relationship that evolves during analysis.1,2 The introduction of other therapeutic techniques and changes in health care funding have combined to make psychiatrist/patient boundaries far more complex.
Boundary violations are about exploitation. Both the American Medical Association (AMA) and the Canadian Medical Association warn members to “scrupulously avoid using the physician/patient relationship to gratify their own emotional, financial, and sexual needs.”3
Boundaries represent the edge of appropriate behavior and serve 2 important purposes:
- They separate the therapeutic relationship from social, sexual, romantic, and business relationships and from relationships that transform into caretaking of the psychiatrist by the patient.
- They structure the professional relationship in ways that maintain the identity and roles of the patient and the professional.4
Psychiatry’s unique dilemmas
As are all physicians, psychiatrists are governed by the 9 biomedical ethics set forth in the AMA’s Principles of Medical Ethics. The American Psychiatric Association (APA), however, acknowledges that psychiatry has a “broader set of moral and ethical problems and dilemmas” that are unique to and magnified by the mental health setting.5 The APA has adopted 39 standards in addition to those set forth by the AMA. The first standard captures the unique responsibilities inherent in the psychiatrist/ patient relationship: A psychiatrist shall not gratify his or her own needs by exploiting the patient (Box).6
Sexual contact with patients is inherently harmful to patients, always unethical, and usually illegal.7 The rate of sexual misconduct among psychiatrists is unknown. National Practitioner Data Bank information is not available to the general public.8 Based on literature reviews and data from individual states9,10 and government agencies,11 an estimated 6% to10% of psychiatrists have had inappropriate sexual relations with patients.12 Estimates of sexual misconduct by psychiatrists:
All physicians are required to practice in accordance with the American Medical Association’s Principles of Medical Ethics. Because these guidelines can be difficult to interpret for psychiatry, the American Psychiatric Association provides further guidance with The Principles of Medical Ethics with Annotations Especially Applicable to Psychiatry. The following excerpts from annotations to the first 2 principles spell out the basic concepts underlying appropriate psychiatrist/patient boundaries:
‘A psychiatrist shall not gratify his or her own needs by exploiting the patient. The psychiatrist shall be ever vigilant about the impact that his or her conduct has upon the boundaries of the doctor/patient relationship, and thus upon the well-being of the patient. These requirements become particularly important because of the essentially private, highly personal, and sometimes intensely emotional nature of the relationship established with the psychiatrist.
‘The requirement that the physician conduct himself/herself with propriety in his or her profession and in all the actions of his or her life is especially important in the case of the psychiatrist because the patient tends to model his or her behavior after that of his or her psychiatrist by identification. Further, the necessary intensity of the treatment relationship may tend to activate sexual and other needs and fantasies on the part of both patient and psychiatrist, while weakening the objectivity necessary for control. Additionally, the inherent inequality in the doctor-patient relationship may lead to exploitation of the patient. Sexual activity with a current or former patient is unethical.’
Source: Reference 6
- increase if misconduct is based on patient complaints
- decrease if self-reports are used
- decrease even further if based on official investigations.4
American psychoanalyst Frieda Fromm-Reichman reportedly offered her colleagues a not-so-humorous admonition: “Don’t have sex with your patients; you will only disappoint them.”4
Nonsexual boundary violations—such as accepting gifts, entering into business arrangements, or trying to influence a patient’s political or religious beliefs or sexual orientation—occur more frequently than sexual misconduct.12 Although the impact of nonsexual violations generally is less serious, any relationship that coexists with the therapeutic relationship has the potential to impair your judgment and contaminate your ability to focus exclusively on your patient’s well-being.13 Be cautious about any decision that could affect the treatment relationship.14
Triangle relationships.Originally, this term referred to the patient/therapist/psychiatrist triad. The term now has a broader meaning that includes:
- encroachments into care by managed care companies and government regulatory agencies
- interactions with the patient’s family members
- providing psychiatric care in non-traditional settings such as schools or prisons
- serving as an expert witness.15
The framework of trust once considered a core feature of the psychiatrist/patient relationship is being undermined by a funding system that demands efficiency and economy.16 Recognizing that some settings sacrifice patients’ clinical needs to the interests of the organization, the APA’s Guidelines for Ethical Practice in Organized Settings stipulate that the psychiatrist must “strive to resolve these conflicts in a manner that is likely to be of greatest benefit to the patient” by (for example):
- informing a patient of financial incentives or penalties that limit your ability to provide appropriate treatment
- not with holding information the patient could use to make informed treatment decisions, including treatment options not provided by you.6
Psychiatrists who doubt that the system—such as a mental health clinic, hospital, or managed care contract provider or reviewer—upholds the standard of acceptable care have the “ethical responsibility” to improve the system.6
Another change in mental health care attempts to limit psychiatrists to “medication management” so that less expensive professionals can provide adjunctive therapies. The treating psychiatrist bears some responsibility, however, for the appropriateness of the patient’s therapeutic options.6 According to Reid,17 psychiatrists are responsible for knowing something about the care, treatment style, credentials, and even ethics of those with whom they share treatment or to whom they refer patients.
The American Academy of Child and Adolescent Psychiatry (AACAP) Code of Ethics addresses the unique challenges encountered when a patient’s opinions differ from those of parents and other authority figures, such as school staff. The AACAP standards consistently direct the psychiatrist to keep the child’s interest primary, explaining that “the child and adolescent psychiatrist may be called upon to participate in attempts to control or change the behavior of children or adolescents…[but] the child and adolescent psychiatrist will avoid acting solely as an agent of the parents, guardians, or agencies.”18
Another triangle can occur when a treating psychiatrist serves as an expert witness or other evaluator for forensic or disability purposes. The American Academy of Psychiatry and the Law (AAPL) recommends that psychiatrists avoid acting as expert witnesses for their patients or performing patient evaluations for legal purposes.19 While recognizing that certain situations may require a psychiatrist to serve a dual role, the AAPL stresses that sensitivity to differences between clinical and legal obligations remains important.
Avoid serving as an expert witness for your patient. The intrusion of another role into the doctor/patient relationship can alter the treatment process and permanently color future inter actions. Likewise, treating an individual whom you previously evaluated for forensic purposes raises similar concerns, including the possibility of a mercenary motivation. Even when no such motivation exists, these situations can create the appearance that you have conscripted a vulnerable individual into your practice.
Emerging trends
Crossings vs violations. Efforts to distinguish when an action is unethical or illegal have led some to differentiate boundary crossings from boundary violations. Unfortunately, the 2 terms continue to be used synonymously, which confuses rather than clarifies the issue:
- Boundary crossings are aimed at enhancing the therapist’s treatment efforts—such as a hug instead of a hand shake at the end of a particularly difficult treatment session.
- Boundary violations are invariably harmful and unethical because they serve the therapist’s needs rather than the patient’s needs or the therapeutic process.20
Rather than trying to differentiate between crossings and violations or to determine under what circumstances changing boundaries is acceptable, Sheets21 conceptualizes a boundary not as a line to cross, but as a continuum of behavior. Under-involvement is at one end, over-involvement at the other, and a “zone of helpfulness” is in the middle.
Glass uses a Venn diagram to illustrate that although most boundary crossings probably fall within the realm of ethical practice, gray areas alert therapists that they are approaching a violation (Figure).20 Five factors have been found to increase psychiatrists’ vulnerability to boundary violations (Table 1).22
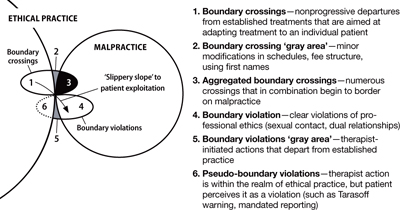
Figure Beware the ‘gray areas’ between boundary crossings, violations
Source: Glass L. The gray areas of boundary crossings and violations. Am J Psychother 2003;57(4):429-44. Republished with permission of the Association for the Advancement of PsychotherapyTable 1
Boundary violations: Factors that increase your vulnerability
| Life crises—effects of aging, career disappointments, unfulfilled hopes, or marital conflicts |
| Transitions—job changes or job loss |
| Medical illness |
| Arrogance—the belief that a boundary violation couldn’t happen to you and not recognizing the need for consultation |
| Stress points shared by the patient |
| Source: Reference 22 |
CASE CONTINUED: Board investigation
Dr. M’s relationship with Ms. Y grows intense, and he becomes increasingly concerned about her “clinginess.” After several months, Dr. M feels emotionally suffocated and ends the relationship. Despondent and suicidal, she seeks treatment in the local emergency room. Ms. Y tells the ER psychiatrist about her relationship with Dr. M and that she cannot go on without him in her life. The ER psychiatrist refers her to another psychiatrist for outpatient care, and, with Ms. Y’s permission, files a complaint about Dr. M with the state medical board and the district branch ethics committee.
The state medical board investigates Dr. M. He is contrite about his actions and their effect on Ms. Y. The state board refers Dr. M to an impaired physician’s program. He is required to attend a boundary violations course and undergo 1 year of practice supervision by a local psychiatrist. Several years later, Dr. M is doing well in his practice and has had no further complaints lodged against him.
Boundaries vs relationships. Using boundaries as a metaphor for maintaining the separation of therapist and patient was intended to serve the analytic process and to protect the patient’s welfare.2 Clearly, certain boundaries—such as sexual contact between psychiatrist and patient—must remain sacrosanct. Yet certain practices avoided in analysis may be appropriate for other therapeutic interventions. For example, whereas psychoanalysis has strict prohibitions against seeing patients anywhere except in the office, cognitive-behavioral therapists may find it useful to conduct sessions in public, or—under carefully arranged circumstances—even in a patient’s home. Other examples include accompanying a patient with agoraphobia to a public gathering or dining with a patient with anorexia.
Exercise caution when you decide to alter traditional boundaries. Even minor crossings that are not likely to progress to violations have the potential to contaminate the therapeutic relationship and place the psychiatrist on a “slippery slope” to patient exploitation.22,23 Some boundary issues are ambiguous, and extenuating circumstances can create a context that temporarily stretches a boundary beyond its normal limits,24 especially in small communities and rural settings where patients and treating psychiatrists are likely to know and encounter each other in social settings.25 Our recommendations for avoiding boundary violations appear in Table 2.
Except in clear cases of malfeasance, determining whether or not you have crossed a boundary is not a straightforward decision based on a single theoretical perspective or absolute standard.26 Regardless of whether a given boundary’s edge is well defined, 2 things are clear:
- unlike patients, psychiatrists have a professional code to honor27
- harm is determined by the meaning of the behavior to the patient and not the psychiatrist’s intentions.4
Table 2
Simple steps help avoid boundary violations
| Dos |
| Know your state’s statutes regarding medical ethics |
| Stay abreast of the American Psychiatric Association’s Principles of Medical Ethics |
| Consult with colleagues |
| Be aware of your weaknesses |
| Avoid ‘slippery slopes’ |
| Use objective documentation |
| Build a satisfying personal life |
| Don’ts |
| Don’t foster dependency |
| Don’t use patients for your own gratification |
| Don’t engage in extra-therapeutic contacts |
| Avoid physical contact |
| Don’t accept gifts or services |
Related Resources
- American Medical Association. Principles of medical ethics. www.ama-assn.org/ama/pub/category/2512.html.
- American Psychiatric Association. The principles of medical ethics with annotations especially applicable to psychiatry. Washington, DC: American Psychiatric Association; 2008.
Disclosures
Drs. Marshall and Myers report no financial relationship with any company whose products are mentioned in this article, or with manufacturers of competing products.
Dr. Teston is a speaker for Shire US, Inc.
1. Margison F. Boundary violations and psychotherapy. Curr Opin Psychiatry 1996;9(3):204-8.
2. Smith D, Fitzpatrick M. Patient-therapist boundary issues: an integrative review of theory and research. Prof Psychol Res Pr 1995;26(5):499-506.
3. Canadian Medical Association. Canadian Medical Association code of ethics. Ottawa, ON: Canadian Medical Association; 1996.
4. Sarkar S. Boundary violation and sexual exploitation in psychiatry and psychotherapy: a review. Advances in Psychiatric Treatment 2004;10:312-20.
5. Radeen J. The debate continues: unique ethics for psychiatry. Aust N Z J Psychiatry 2003;38:115-8.
6. American Psychiatric Association The principles of medical ethics with annotations especially applicable to psychiatry. Washington, DC: American Psychiatric Association; 2008.
7. Zur O. To cross or not to cross: do boundaries in therapy protect or harm? The Psychotherapy Bulletin 2004;39(3):27-32.
8. Spickard W, Swiggart W, Manley G, et al. A continuing medical education approach to improve sexual boundaries of physicians. Bull Menninger Clin 2008;72(1):38-53.
9. Morrison J, Morrison T. Psychiatrists disciplined by a state medical board. Am J Psychiatry 2001;158:474-8.
10. Beecher L, Altchuler S. Sexual boundary violations. Minn Med 2005;88:42-4.
11. Dehlendorf C. Physicians disciplined for sex-related offenses. JAMA 1998;279(23):1883-8.
12. Garfinkel P, Dorian B, Sadavoy J, Bagby R. Boundary violations and departments of psychiatry. Can J Psychiatry 1997;42:764-70.
13. Gabbard G, Nadelson C. Professional boundaries in the physician-patient relationship. JAMA 1995;273(18):1445-9.
14. Nadelson C, Notman M. Boundaries in the doctor-patient relationship. Theor Med 2002;23:191-201.
15. Sarkar S, Adshead G. Ethics in forensic psychiatry. Curr Opin Psychiatry 2002;15:527-31.
16. Green S, Bloch S. Working in a flawed mental health care system: an ethical challenge. Am J Psychiatry 2001;158(9):1378-83.
17. Reid W. Treating clinicians and expert testimony. Journal of Practical Psychiatry and Behavioral Health 1998;4(2):121-4.
18. American Academy of Child and Adolescent Psychiatry. American Academy of Child and Adolescent Psychiatry code of ethics. Annotations to AACAP ethical code with special reference to evolving health care delivery and reimbursement systems. Washington, DC: American Academy of Child and Adolescent Psychiatry; 1995.
19. American Academy of Psychiatry and the Law. Ethics guidelines for the practice of forensic psychiatry. 2005. Available at: http://www.aapl.org/pdf/ETHICSGDLNS. pdf. Accessed June 3, 2008.
20. Glass L. The gray areas of boundary crossings and violations. Am J Psychother 2003;57(4):429-44.
21. Sheets V. Teach nurses how to maintain professional boundaries, recognize potential problems, and make better patient care decisions. Nurs Manage 2000;31(8):28-34.
22. Norris D, Gutheil T, Strasburger L. This couldn’t happen to me: boundary problems and sexual misconduct in the psychotherapy relationship. Psychiatr Serv 2003;54:517-22.
23. Galletly C. Crossing professional boundaries in medicine: the slippery slope to patient sexual exploitation. Med J Aust 2004;181(7):380-3.
24. Gutheil T, Gabbard G. Misuses and misunderstandings of boundary theory in clinical and regulatory settings. Am J Psychiatry 1998;155(3):409-14.
25. Simon R, Williams I. Maintaining treatment boundaries in small communities and rural areas. Psychiatr Serv 1999;50:1440-6.
26. Dvoskin J. Commentary: two sides to every story—the need for objectivity and evidence. J Am Acad Psychiatry Law 2005;33(4):482-3.
27. Gutheil T. Boundary issues and personality disorders. J Psychiatr Pract 2005;11(2):88-96.
Dr. M is facing financial challenges with his fledgling private practice and begins consulting at a weight loss clinic to supplement his income. He finds him-self attracted to Ms. Y, a weight-loss patient he is treating. They seem to click interpersonally, and he extends his office visits with her. Ms. Y clearly enjoys this extra attention, and Dr. M begins including personal disclosures in his conversations with her.
In his residency training, Dr. M was taught never to date a current or former patient, but he views this situation as different. Ms. Y is seeing him only for weight loss, and he rationalizes that he is providing her with medical care, not “psychiatric” care. On 2 occasions he gives her a limited quantity of benzodiazepines for mild anxiety, which he considers a transitory stress-related condition and not an “official” DSM-IV-TR disorder.
Eventually, Dr. M asks Ms. Y to dinner and she accepts. After they begin dating, he decides to transfer her to another clinic physician “just to be safe.”
Although many psychiatrists assume that psychiatrist/patient boundaries are well defined by ethical and legal standards, boundary issues are a complex and controversial aspect of clinical practice. Psychoanalysts initially defined psychiatrist/patient boundaries as a way of structuring the unique and intimate relationship that evolves during analysis.1,2 The introduction of other therapeutic techniques and changes in health care funding have combined to make psychiatrist/patient boundaries far more complex.
Boundary violations are about exploitation. Both the American Medical Association (AMA) and the Canadian Medical Association warn members to “scrupulously avoid using the physician/patient relationship to gratify their own emotional, financial, and sexual needs.”3
Boundaries represent the edge of appropriate behavior and serve 2 important purposes:
- They separate the therapeutic relationship from social, sexual, romantic, and business relationships and from relationships that transform into caretaking of the psychiatrist by the patient.
- They structure the professional relationship in ways that maintain the identity and roles of the patient and the professional.4
Psychiatry’s unique dilemmas
As are all physicians, psychiatrists are governed by the 9 biomedical ethics set forth in the AMA’s Principles of Medical Ethics. The American Psychiatric Association (APA), however, acknowledges that psychiatry has a “broader set of moral and ethical problems and dilemmas” that are unique to and magnified by the mental health setting.5 The APA has adopted 39 standards in addition to those set forth by the AMA. The first standard captures the unique responsibilities inherent in the psychiatrist/ patient relationship: A psychiatrist shall not gratify his or her own needs by exploiting the patient (Box).6
Sexual contact with patients is inherently harmful to patients, always unethical, and usually illegal.7 The rate of sexual misconduct among psychiatrists is unknown. National Practitioner Data Bank information is not available to the general public.8 Based on literature reviews and data from individual states9,10 and government agencies,11 an estimated 6% to10% of psychiatrists have had inappropriate sexual relations with patients.12 Estimates of sexual misconduct by psychiatrists:
All physicians are required to practice in accordance with the American Medical Association’s Principles of Medical Ethics. Because these guidelines can be difficult to interpret for psychiatry, the American Psychiatric Association provides further guidance with The Principles of Medical Ethics with Annotations Especially Applicable to Psychiatry. The following excerpts from annotations to the first 2 principles spell out the basic concepts underlying appropriate psychiatrist/patient boundaries:
‘A psychiatrist shall not gratify his or her own needs by exploiting the patient. The psychiatrist shall be ever vigilant about the impact that his or her conduct has upon the boundaries of the doctor/patient relationship, and thus upon the well-being of the patient. These requirements become particularly important because of the essentially private, highly personal, and sometimes intensely emotional nature of the relationship established with the psychiatrist.
‘The requirement that the physician conduct himself/herself with propriety in his or her profession and in all the actions of his or her life is especially important in the case of the psychiatrist because the patient tends to model his or her behavior after that of his or her psychiatrist by identification. Further, the necessary intensity of the treatment relationship may tend to activate sexual and other needs and fantasies on the part of both patient and psychiatrist, while weakening the objectivity necessary for control. Additionally, the inherent inequality in the doctor-patient relationship may lead to exploitation of the patient. Sexual activity with a current or former patient is unethical.’
Source: Reference 6
- increase if misconduct is based on patient complaints
- decrease if self-reports are used
- decrease even further if based on official investigations.4
American psychoanalyst Frieda Fromm-Reichman reportedly offered her colleagues a not-so-humorous admonition: “Don’t have sex with your patients; you will only disappoint them.”4
Nonsexual boundary violations—such as accepting gifts, entering into business arrangements, or trying to influence a patient’s political or religious beliefs or sexual orientation—occur more frequently than sexual misconduct.12 Although the impact of nonsexual violations generally is less serious, any relationship that coexists with the therapeutic relationship has the potential to impair your judgment and contaminate your ability to focus exclusively on your patient’s well-being.13 Be cautious about any decision that could affect the treatment relationship.14
Triangle relationships.Originally, this term referred to the patient/therapist/psychiatrist triad. The term now has a broader meaning that includes:
- encroachments into care by managed care companies and government regulatory agencies
- interactions with the patient’s family members
- providing psychiatric care in non-traditional settings such as schools or prisons
- serving as an expert witness.15
The framework of trust once considered a core feature of the psychiatrist/patient relationship is being undermined by a funding system that demands efficiency and economy.16 Recognizing that some settings sacrifice patients’ clinical needs to the interests of the organization, the APA’s Guidelines for Ethical Practice in Organized Settings stipulate that the psychiatrist must “strive to resolve these conflicts in a manner that is likely to be of greatest benefit to the patient” by (for example):
- informing a patient of financial incentives or penalties that limit your ability to provide appropriate treatment
- not with holding information the patient could use to make informed treatment decisions, including treatment options not provided by you.6
Psychiatrists who doubt that the system—such as a mental health clinic, hospital, or managed care contract provider or reviewer—upholds the standard of acceptable care have the “ethical responsibility” to improve the system.6
Another change in mental health care attempts to limit psychiatrists to “medication management” so that less expensive professionals can provide adjunctive therapies. The treating psychiatrist bears some responsibility, however, for the appropriateness of the patient’s therapeutic options.6 According to Reid,17 psychiatrists are responsible for knowing something about the care, treatment style, credentials, and even ethics of those with whom they share treatment or to whom they refer patients.
The American Academy of Child and Adolescent Psychiatry (AACAP) Code of Ethics addresses the unique challenges encountered when a patient’s opinions differ from those of parents and other authority figures, such as school staff. The AACAP standards consistently direct the psychiatrist to keep the child’s interest primary, explaining that “the child and adolescent psychiatrist may be called upon to participate in attempts to control or change the behavior of children or adolescents…[but] the child and adolescent psychiatrist will avoid acting solely as an agent of the parents, guardians, or agencies.”18
Another triangle can occur when a treating psychiatrist serves as an expert witness or other evaluator for forensic or disability purposes. The American Academy of Psychiatry and the Law (AAPL) recommends that psychiatrists avoid acting as expert witnesses for their patients or performing patient evaluations for legal purposes.19 While recognizing that certain situations may require a psychiatrist to serve a dual role, the AAPL stresses that sensitivity to differences between clinical and legal obligations remains important.
Avoid serving as an expert witness for your patient. The intrusion of another role into the doctor/patient relationship can alter the treatment process and permanently color future inter actions. Likewise, treating an individual whom you previously evaluated for forensic purposes raises similar concerns, including the possibility of a mercenary motivation. Even when no such motivation exists, these situations can create the appearance that you have conscripted a vulnerable individual into your practice.
Emerging trends
Crossings vs violations. Efforts to distinguish when an action is unethical or illegal have led some to differentiate boundary crossings from boundary violations. Unfortunately, the 2 terms continue to be used synonymously, which confuses rather than clarifies the issue:
- Boundary crossings are aimed at enhancing the therapist’s treatment efforts—such as a hug instead of a hand shake at the end of a particularly difficult treatment session.
- Boundary violations are invariably harmful and unethical because they serve the therapist’s needs rather than the patient’s needs or the therapeutic process.20
Rather than trying to differentiate between crossings and violations or to determine under what circumstances changing boundaries is acceptable, Sheets21 conceptualizes a boundary not as a line to cross, but as a continuum of behavior. Under-involvement is at one end, over-involvement at the other, and a “zone of helpfulness” is in the middle.
Glass uses a Venn diagram to illustrate that although most boundary crossings probably fall within the realm of ethical practice, gray areas alert therapists that they are approaching a violation (Figure).20 Five factors have been found to increase psychiatrists’ vulnerability to boundary violations (Table 1).22
Figure Beware the ‘gray areas’ between boundary crossings, violations
Source: Glass L. The gray areas of boundary crossings and violations. Am J Psychother 2003;57(4):429-44. Republished with permission of the Association for the Advancement of PsychotherapyTable 1
Boundary violations: Factors that increase your vulnerability
| Life crises—effects of aging, career disappointments, unfulfilled hopes, or marital conflicts |
| Transitions—job changes or job loss |
| Medical illness |
| Arrogance—the belief that a boundary violation couldn’t happen to you and not recognizing the need for consultation |
| Stress points shared by the patient |
| Source: Reference 22 |
CASE CONTINUED: Board investigation
Dr. M’s relationship with Ms. Y grows intense, and he becomes increasingly concerned about her “clinginess.” After several months, Dr. M feels emotionally suffocated and ends the relationship. Despondent and suicidal, she seeks treatment in the local emergency room. Ms. Y tells the ER psychiatrist about her relationship with Dr. M and that she cannot go on without him in her life. The ER psychiatrist refers her to another psychiatrist for outpatient care, and, with Ms. Y’s permission, files a complaint about Dr. M with the state medical board and the district branch ethics committee.
The state medical board investigates Dr. M. He is contrite about his actions and their effect on Ms. Y. The state board refers Dr. M to an impaired physician’s program. He is required to attend a boundary violations course and undergo 1 year of practice supervision by a local psychiatrist. Several years later, Dr. M is doing well in his practice and has had no further complaints lodged against him.
Boundaries vs relationships. Using boundaries as a metaphor for maintaining the separation of therapist and patient was intended to serve the analytic process and to protect the patient’s welfare.2 Clearly, certain boundaries—such as sexual contact between psychiatrist and patient—must remain sacrosanct. Yet certain practices avoided in analysis may be appropriate for other therapeutic interventions. For example, whereas psychoanalysis has strict prohibitions against seeing patients anywhere except in the office, cognitive-behavioral therapists may find it useful to conduct sessions in public, or—under carefully arranged circumstances—even in a patient’s home. Other examples include accompanying a patient with agoraphobia to a public gathering or dining with a patient with anorexia.
Exercise caution when you decide to alter traditional boundaries. Even minor crossings that are not likely to progress to violations have the potential to contaminate the therapeutic relationship and place the psychiatrist on a “slippery slope” to patient exploitation.22,23 Some boundary issues are ambiguous, and extenuating circumstances can create a context that temporarily stretches a boundary beyond its normal limits,24 especially in small communities and rural settings where patients and treating psychiatrists are likely to know and encounter each other in social settings.25 Our recommendations for avoiding boundary violations appear in Table 2.
Except in clear cases of malfeasance, determining whether or not you have crossed a boundary is not a straightforward decision based on a single theoretical perspective or absolute standard.26 Regardless of whether a given boundary’s edge is well defined, 2 things are clear:
- unlike patients, psychiatrists have a professional code to honor27
- harm is determined by the meaning of the behavior to the patient and not the psychiatrist’s intentions.4
Table 2
Simple steps help avoid boundary violations
| Dos |
| Know your state’s statutes regarding medical ethics |
| Stay abreast of the American Psychiatric Association’s Principles of Medical Ethics |
| Consult with colleagues |
| Be aware of your weaknesses |
| Avoid ‘slippery slopes’ |
| Use objective documentation |
| Build a satisfying personal life |
| Don’ts |
| Don’t foster dependency |
| Don’t use patients for your own gratification |
| Don’t engage in extra-therapeutic contacts |
| Avoid physical contact |
| Don’t accept gifts or services |
Related Resources
- American Medical Association. Principles of medical ethics. www.ama-assn.org/ama/pub/category/2512.html.
- American Psychiatric Association. The principles of medical ethics with annotations especially applicable to psychiatry. Washington, DC: American Psychiatric Association; 2008.
Disclosures
Drs. Marshall and Myers report no financial relationship with any company whose products are mentioned in this article, or with manufacturers of competing products.
Dr. Teston is a speaker for Shire US, Inc.
Dr. M is facing financial challenges with his fledgling private practice and begins consulting at a weight loss clinic to supplement his income. He finds him-self attracted to Ms. Y, a weight-loss patient he is treating. They seem to click interpersonally, and he extends his office visits with her. Ms. Y clearly enjoys this extra attention, and Dr. M begins including personal disclosures in his conversations with her.
In his residency training, Dr. M was taught never to date a current or former patient, but he views this situation as different. Ms. Y is seeing him only for weight loss, and he rationalizes that he is providing her with medical care, not “psychiatric” care. On 2 occasions he gives her a limited quantity of benzodiazepines for mild anxiety, which he considers a transitory stress-related condition and not an “official” DSM-IV-TR disorder.
Eventually, Dr. M asks Ms. Y to dinner and she accepts. After they begin dating, he decides to transfer her to another clinic physician “just to be safe.”
Although many psychiatrists assume that psychiatrist/patient boundaries are well defined by ethical and legal standards, boundary issues are a complex and controversial aspect of clinical practice. Psychoanalysts initially defined psychiatrist/patient boundaries as a way of structuring the unique and intimate relationship that evolves during analysis.1,2 The introduction of other therapeutic techniques and changes in health care funding have combined to make psychiatrist/patient boundaries far more complex.
Boundary violations are about exploitation. Both the American Medical Association (AMA) and the Canadian Medical Association warn members to “scrupulously avoid using the physician/patient relationship to gratify their own emotional, financial, and sexual needs.”3
Boundaries represent the edge of appropriate behavior and serve 2 important purposes:
- They separate the therapeutic relationship from social, sexual, romantic, and business relationships and from relationships that transform into caretaking of the psychiatrist by the patient.
- They structure the professional relationship in ways that maintain the identity and roles of the patient and the professional.4
Psychiatry’s unique dilemmas
As are all physicians, psychiatrists are governed by the 9 biomedical ethics set forth in the AMA’s Principles of Medical Ethics. The American Psychiatric Association (APA), however, acknowledges that psychiatry has a “broader set of moral and ethical problems and dilemmas” that are unique to and magnified by the mental health setting.5 The APA has adopted 39 standards in addition to those set forth by the AMA. The first standard captures the unique responsibilities inherent in the psychiatrist/ patient relationship: A psychiatrist shall not gratify his or her own needs by exploiting the patient (Box).6
Sexual contact with patients is inherently harmful to patients, always unethical, and usually illegal.7 The rate of sexual misconduct among psychiatrists is unknown. National Practitioner Data Bank information is not available to the general public.8 Based on literature reviews and data from individual states9,10 and government agencies,11 an estimated 6% to10% of psychiatrists have had inappropriate sexual relations with patients.12 Estimates of sexual misconduct by psychiatrists:
All physicians are required to practice in accordance with the American Medical Association’s Principles of Medical Ethics. Because these guidelines can be difficult to interpret for psychiatry, the American Psychiatric Association provides further guidance with The Principles of Medical Ethics with Annotations Especially Applicable to Psychiatry. The following excerpts from annotations to the first 2 principles spell out the basic concepts underlying appropriate psychiatrist/patient boundaries:
‘A psychiatrist shall not gratify his or her own needs by exploiting the patient. The psychiatrist shall be ever vigilant about the impact that his or her conduct has upon the boundaries of the doctor/patient relationship, and thus upon the well-being of the patient. These requirements become particularly important because of the essentially private, highly personal, and sometimes intensely emotional nature of the relationship established with the psychiatrist.
‘The requirement that the physician conduct himself/herself with propriety in his or her profession and in all the actions of his or her life is especially important in the case of the psychiatrist because the patient tends to model his or her behavior after that of his or her psychiatrist by identification. Further, the necessary intensity of the treatment relationship may tend to activate sexual and other needs and fantasies on the part of both patient and psychiatrist, while weakening the objectivity necessary for control. Additionally, the inherent inequality in the doctor-patient relationship may lead to exploitation of the patient. Sexual activity with a current or former patient is unethical.’
Source: Reference 6
- increase if misconduct is based on patient complaints
- decrease if self-reports are used
- decrease even further if based on official investigations.4
American psychoanalyst Frieda Fromm-Reichman reportedly offered her colleagues a not-so-humorous admonition: “Don’t have sex with your patients; you will only disappoint them.”4
Nonsexual boundary violations—such as accepting gifts, entering into business arrangements, or trying to influence a patient’s political or religious beliefs or sexual orientation—occur more frequently than sexual misconduct.12 Although the impact of nonsexual violations generally is less serious, any relationship that coexists with the therapeutic relationship has the potential to impair your judgment and contaminate your ability to focus exclusively on your patient’s well-being.13 Be cautious about any decision that could affect the treatment relationship.14
Triangle relationships.Originally, this term referred to the patient/therapist/psychiatrist triad. The term now has a broader meaning that includes:
- encroachments into care by managed care companies and government regulatory agencies
- interactions with the patient’s family members
- providing psychiatric care in non-traditional settings such as schools or prisons
- serving as an expert witness.15
The framework of trust once considered a core feature of the psychiatrist/patient relationship is being undermined by a funding system that demands efficiency and economy.16 Recognizing that some settings sacrifice patients’ clinical needs to the interests of the organization, the APA’s Guidelines for Ethical Practice in Organized Settings stipulate that the psychiatrist must “strive to resolve these conflicts in a manner that is likely to be of greatest benefit to the patient” by (for example):
- informing a patient of financial incentives or penalties that limit your ability to provide appropriate treatment
- not with holding information the patient could use to make informed treatment decisions, including treatment options not provided by you.6
Psychiatrists who doubt that the system—such as a mental health clinic, hospital, or managed care contract provider or reviewer—upholds the standard of acceptable care have the “ethical responsibility” to improve the system.6
Another change in mental health care attempts to limit psychiatrists to “medication management” so that less expensive professionals can provide adjunctive therapies. The treating psychiatrist bears some responsibility, however, for the appropriateness of the patient’s therapeutic options.6 According to Reid,17 psychiatrists are responsible for knowing something about the care, treatment style, credentials, and even ethics of those with whom they share treatment or to whom they refer patients.
The American Academy of Child and Adolescent Psychiatry (AACAP) Code of Ethics addresses the unique challenges encountered when a patient’s opinions differ from those of parents and other authority figures, such as school staff. The AACAP standards consistently direct the psychiatrist to keep the child’s interest primary, explaining that “the child and adolescent psychiatrist may be called upon to participate in attempts to control or change the behavior of children or adolescents…[but] the child and adolescent psychiatrist will avoid acting solely as an agent of the parents, guardians, or agencies.”18
Another triangle can occur when a treating psychiatrist serves as an expert witness or other evaluator for forensic or disability purposes. The American Academy of Psychiatry and the Law (AAPL) recommends that psychiatrists avoid acting as expert witnesses for their patients or performing patient evaluations for legal purposes.19 While recognizing that certain situations may require a psychiatrist to serve a dual role, the AAPL stresses that sensitivity to differences between clinical and legal obligations remains important.
Avoid serving as an expert witness for your patient. The intrusion of another role into the doctor/patient relationship can alter the treatment process and permanently color future inter actions. Likewise, treating an individual whom you previously evaluated for forensic purposes raises similar concerns, including the possibility of a mercenary motivation. Even when no such motivation exists, these situations can create the appearance that you have conscripted a vulnerable individual into your practice.
Emerging trends
Crossings vs violations. Efforts to distinguish when an action is unethical or illegal have led some to differentiate boundary crossings from boundary violations. Unfortunately, the 2 terms continue to be used synonymously, which confuses rather than clarifies the issue:
- Boundary crossings are aimed at enhancing the therapist’s treatment efforts—such as a hug instead of a hand shake at the end of a particularly difficult treatment session.
- Boundary violations are invariably harmful and unethical because they serve the therapist’s needs rather than the patient’s needs or the therapeutic process.20
Rather than trying to differentiate between crossings and violations or to determine under what circumstances changing boundaries is acceptable, Sheets21 conceptualizes a boundary not as a line to cross, but as a continuum of behavior. Under-involvement is at one end, over-involvement at the other, and a “zone of helpfulness” is in the middle.
Glass uses a Venn diagram to illustrate that although most boundary crossings probably fall within the realm of ethical practice, gray areas alert therapists that they are approaching a violation (Figure).20 Five factors have been found to increase psychiatrists’ vulnerability to boundary violations (Table 1).22
Figure Beware the ‘gray areas’ between boundary crossings, violations
Source: Glass L. The gray areas of boundary crossings and violations. Am J Psychother 2003;57(4):429-44. Republished with permission of the Association for the Advancement of PsychotherapyTable 1
Boundary violations: Factors that increase your vulnerability
| Life crises—effects of aging, career disappointments, unfulfilled hopes, or marital conflicts |
| Transitions—job changes or job loss |
| Medical illness |
| Arrogance—the belief that a boundary violation couldn’t happen to you and not recognizing the need for consultation |
| Stress points shared by the patient |
| Source: Reference 22 |
CASE CONTINUED: Board investigation
Dr. M’s relationship with Ms. Y grows intense, and he becomes increasingly concerned about her “clinginess.” After several months, Dr. M feels emotionally suffocated and ends the relationship. Despondent and suicidal, she seeks treatment in the local emergency room. Ms. Y tells the ER psychiatrist about her relationship with Dr. M and that she cannot go on without him in her life. The ER psychiatrist refers her to another psychiatrist for outpatient care, and, with Ms. Y’s permission, files a complaint about Dr. M with the state medical board and the district branch ethics committee.
The state medical board investigates Dr. M. He is contrite about his actions and their effect on Ms. Y. The state board refers Dr. M to an impaired physician’s program. He is required to attend a boundary violations course and undergo 1 year of practice supervision by a local psychiatrist. Several years later, Dr. M is doing well in his practice and has had no further complaints lodged against him.
Boundaries vs relationships. Using boundaries as a metaphor for maintaining the separation of therapist and patient was intended to serve the analytic process and to protect the patient’s welfare.2 Clearly, certain boundaries—such as sexual contact between psychiatrist and patient—must remain sacrosanct. Yet certain practices avoided in analysis may be appropriate for other therapeutic interventions. For example, whereas psychoanalysis has strict prohibitions against seeing patients anywhere except in the office, cognitive-behavioral therapists may find it useful to conduct sessions in public, or—under carefully arranged circumstances—even in a patient’s home. Other examples include accompanying a patient with agoraphobia to a public gathering or dining with a patient with anorexia.
Exercise caution when you decide to alter traditional boundaries. Even minor crossings that are not likely to progress to violations have the potential to contaminate the therapeutic relationship and place the psychiatrist on a “slippery slope” to patient exploitation.22,23 Some boundary issues are ambiguous, and extenuating circumstances can create a context that temporarily stretches a boundary beyond its normal limits,24 especially in small communities and rural settings where patients and treating psychiatrists are likely to know and encounter each other in social settings.25 Our recommendations for avoiding boundary violations appear in Table 2.
Except in clear cases of malfeasance, determining whether or not you have crossed a boundary is not a straightforward decision based on a single theoretical perspective or absolute standard.26 Regardless of whether a given boundary’s edge is well defined, 2 things are clear:
- unlike patients, psychiatrists have a professional code to honor27
- harm is determined by the meaning of the behavior to the patient and not the psychiatrist’s intentions.4
Table 2
Simple steps help avoid boundary violations
| Dos |
| Know your state’s statutes regarding medical ethics |
| Stay abreast of the American Psychiatric Association’s Principles of Medical Ethics |
| Consult with colleagues |
| Be aware of your weaknesses |
| Avoid ‘slippery slopes’ |
| Use objective documentation |
| Build a satisfying personal life |
| Don’ts |
| Don’t foster dependency |
| Don’t use patients for your own gratification |
| Don’t engage in extra-therapeutic contacts |
| Avoid physical contact |
| Don’t accept gifts or services |
Related Resources
- American Medical Association. Principles of medical ethics. www.ama-assn.org/ama/pub/category/2512.html.
- American Psychiatric Association. The principles of medical ethics with annotations especially applicable to psychiatry. Washington, DC: American Psychiatric Association; 2008.
Disclosures
Drs. Marshall and Myers report no financial relationship with any company whose products are mentioned in this article, or with manufacturers of competing products.
Dr. Teston is a speaker for Shire US, Inc.
1. Margison F. Boundary violations and psychotherapy. Curr Opin Psychiatry 1996;9(3):204-8.
2. Smith D, Fitzpatrick M. Patient-therapist boundary issues: an integrative review of theory and research. Prof Psychol Res Pr 1995;26(5):499-506.
3. Canadian Medical Association. Canadian Medical Association code of ethics. Ottawa, ON: Canadian Medical Association; 1996.
4. Sarkar S. Boundary violation and sexual exploitation in psychiatry and psychotherapy: a review. Advances in Psychiatric Treatment 2004;10:312-20.
5. Radeen J. The debate continues: unique ethics for psychiatry. Aust N Z J Psychiatry 2003;38:115-8.
6. American Psychiatric Association The principles of medical ethics with annotations especially applicable to psychiatry. Washington, DC: American Psychiatric Association; 2008.
7. Zur O. To cross or not to cross: do boundaries in therapy protect or harm? The Psychotherapy Bulletin 2004;39(3):27-32.
8. Spickard W, Swiggart W, Manley G, et al. A continuing medical education approach to improve sexual boundaries of physicians. Bull Menninger Clin 2008;72(1):38-53.
9. Morrison J, Morrison T. Psychiatrists disciplined by a state medical board. Am J Psychiatry 2001;158:474-8.
10. Beecher L, Altchuler S. Sexual boundary violations. Minn Med 2005;88:42-4.
11. Dehlendorf C. Physicians disciplined for sex-related offenses. JAMA 1998;279(23):1883-8.
12. Garfinkel P, Dorian B, Sadavoy J, Bagby R. Boundary violations and departments of psychiatry. Can J Psychiatry 1997;42:764-70.
13. Gabbard G, Nadelson C. Professional boundaries in the physician-patient relationship. JAMA 1995;273(18):1445-9.
14. Nadelson C, Notman M. Boundaries in the doctor-patient relationship. Theor Med 2002;23:191-201.
15. Sarkar S, Adshead G. Ethics in forensic psychiatry. Curr Opin Psychiatry 2002;15:527-31.
16. Green S, Bloch S. Working in a flawed mental health care system: an ethical challenge. Am J Psychiatry 2001;158(9):1378-83.
17. Reid W. Treating clinicians and expert testimony. Journal of Practical Psychiatry and Behavioral Health 1998;4(2):121-4.
18. American Academy of Child and Adolescent Psychiatry. American Academy of Child and Adolescent Psychiatry code of ethics. Annotations to AACAP ethical code with special reference to evolving health care delivery and reimbursement systems. Washington, DC: American Academy of Child and Adolescent Psychiatry; 1995.
19. American Academy of Psychiatry and the Law. Ethics guidelines for the practice of forensic psychiatry. 2005. Available at: http://www.aapl.org/pdf/ETHICSGDLNS. pdf. Accessed June 3, 2008.
20. Glass L. The gray areas of boundary crossings and violations. Am J Psychother 2003;57(4):429-44.
21. Sheets V. Teach nurses how to maintain professional boundaries, recognize potential problems, and make better patient care decisions. Nurs Manage 2000;31(8):28-34.
22. Norris D, Gutheil T, Strasburger L. This couldn’t happen to me: boundary problems and sexual misconduct in the psychotherapy relationship. Psychiatr Serv 2003;54:517-22.
23. Galletly C. Crossing professional boundaries in medicine: the slippery slope to patient sexual exploitation. Med J Aust 2004;181(7):380-3.
24. Gutheil T, Gabbard G. Misuses and misunderstandings of boundary theory in clinical and regulatory settings. Am J Psychiatry 1998;155(3):409-14.
25. Simon R, Williams I. Maintaining treatment boundaries in small communities and rural areas. Psychiatr Serv 1999;50:1440-6.
26. Dvoskin J. Commentary: two sides to every story—the need for objectivity and evidence. J Am Acad Psychiatry Law 2005;33(4):482-3.
27. Gutheil T. Boundary issues and personality disorders. J Psychiatr Pract 2005;11(2):88-96.
1. Margison F. Boundary violations and psychotherapy. Curr Opin Psychiatry 1996;9(3):204-8.
2. Smith D, Fitzpatrick M. Patient-therapist boundary issues: an integrative review of theory and research. Prof Psychol Res Pr 1995;26(5):499-506.
3. Canadian Medical Association. Canadian Medical Association code of ethics. Ottawa, ON: Canadian Medical Association; 1996.
4. Sarkar S. Boundary violation and sexual exploitation in psychiatry and psychotherapy: a review. Advances in Psychiatric Treatment 2004;10:312-20.
5. Radeen J. The debate continues: unique ethics for psychiatry. Aust N Z J Psychiatry 2003;38:115-8.
6. American Psychiatric Association The principles of medical ethics with annotations especially applicable to psychiatry. Washington, DC: American Psychiatric Association; 2008.
7. Zur O. To cross or not to cross: do boundaries in therapy protect or harm? The Psychotherapy Bulletin 2004;39(3):27-32.
8. Spickard W, Swiggart W, Manley G, et al. A continuing medical education approach to improve sexual boundaries of physicians. Bull Menninger Clin 2008;72(1):38-53.
9. Morrison J, Morrison T. Psychiatrists disciplined by a state medical board. Am J Psychiatry 2001;158:474-8.
10. Beecher L, Altchuler S. Sexual boundary violations. Minn Med 2005;88:42-4.
11. Dehlendorf C. Physicians disciplined for sex-related offenses. JAMA 1998;279(23):1883-8.
12. Garfinkel P, Dorian B, Sadavoy J, Bagby R. Boundary violations and departments of psychiatry. Can J Psychiatry 1997;42:764-70.
13. Gabbard G, Nadelson C. Professional boundaries in the physician-patient relationship. JAMA 1995;273(18):1445-9.
14. Nadelson C, Notman M. Boundaries in the doctor-patient relationship. Theor Med 2002;23:191-201.
15. Sarkar S, Adshead G. Ethics in forensic psychiatry. Curr Opin Psychiatry 2002;15:527-31.
16. Green S, Bloch S. Working in a flawed mental health care system: an ethical challenge. Am J Psychiatry 2001;158(9):1378-83.
17. Reid W. Treating clinicians and expert testimony. Journal of Practical Psychiatry and Behavioral Health 1998;4(2):121-4.
18. American Academy of Child and Adolescent Psychiatry. American Academy of Child and Adolescent Psychiatry code of ethics. Annotations to AACAP ethical code with special reference to evolving health care delivery and reimbursement systems. Washington, DC: American Academy of Child and Adolescent Psychiatry; 1995.
19. American Academy of Psychiatry and the Law. Ethics guidelines for the practice of forensic psychiatry. 2005. Available at: http://www.aapl.org/pdf/ETHICSGDLNS. pdf. Accessed June 3, 2008.
20. Glass L. The gray areas of boundary crossings and violations. Am J Psychother 2003;57(4):429-44.
21. Sheets V. Teach nurses how to maintain professional boundaries, recognize potential problems, and make better patient care decisions. Nurs Manage 2000;31(8):28-34.
22. Norris D, Gutheil T, Strasburger L. This couldn’t happen to me: boundary problems and sexual misconduct in the psychotherapy relationship. Psychiatr Serv 2003;54:517-22.
23. Galletly C. Crossing professional boundaries in medicine: the slippery slope to patient sexual exploitation. Med J Aust 2004;181(7):380-3.
24. Gutheil T, Gabbard G. Misuses and misunderstandings of boundary theory in clinical and regulatory settings. Am J Psychiatry 1998;155(3):409-14.
25. Simon R, Williams I. Maintaining treatment boundaries in small communities and rural areas. Psychiatr Serv 1999;50:1440-6.
26. Dvoskin J. Commentary: two sides to every story—the need for objectivity and evidence. J Am Acad Psychiatry Law 2005;33(4):482-3.
27. Gutheil T. Boundary issues and personality disorders. J Psychiatr Pract 2005;11(2):88-96.
Subsyndromal depression
Mr. W, a 53-year-old divorced entrepreneur, presents to you for evaluation of poor concentration, decreased self-esteem, and difficulty making decisions that are interfering with his work. A longtime patient of another psychiatrist, Mr. W has a 26-year history of bipolar I disorder. He has not had a manic episode for 5 years but has had several depressive episodes.
During his last manic episode, Mr. W was hospitalized with expansive and irritable mood, racing thoughts, impulsive sexual behavior, psychomotor agitation, elevated self-esteem, marked distractibility, and paranoid ideas about his business partners. His discharge regimen included lithium titrated to 0.9 mEq/L and divalproex sodium, 1,500 mg/d, with lamotrigine, 200 mg/d, added to reduce depressive relapse risk. After several years of stable treatment, Mr. W complained of cognitive impairment. His psychiatrist discontinued lithium and added a low-dose stimulant—methylphenidate, 20 mg bid—to address Mr. W’s complaints of poor concentration.
Mr. W also is taking zolpidem, 10 mg as needed for onset insomnia, and receives weekly psychodynamic psychotherapy. His work performance problems persist despite these treatments, and his company is failing.
A poor course in bipolar disorder—as in Mr. W’s case—is frequently characterized by persistent or relapsing depression. Bipolar disorder is diagnosed by a manic, mixed, or hypomanic episode, but depression and depressive symptoms are most prominent in clinical practice. Likewise, major observational studies blame depression for most of the time spent ill in bipolar types I and II.1-8
A good deal of bipolar symptom burden is associated with subsyndromal depression—defined as having >2 but 5 and depressive symptoms are disproportionately responsible—compared with manic symptoms—for the impact of bipolar illness on patients and their families.9
This article offers clinically useful strategies to minimize subsyndromal depression in patients with bipolar disorder (Table 1). These strategies include an evidence-based approach to medication, the use of validated psychotherapies, regular sleep and socialization schedules, and careful monitoring of mood symptoms.
Table 1
How to minimize bipolar subsyndromal depression
| Monitor symptoms using validated clinician- and patient-rated tools at all visits |
| Use evidence-based treatments first |
| Eliminate ineffective medications |
| Use adequate doses of medications for different mood states |
| Monitor and treat adverse effects of successful treatments |
| Monitor and minimize medications that can worsen symptoms |
| Watch for the impact of medical conditions on mood |
| Be attentive to alcohol and substance use (including caffeine, nicotine, and energy drinks) |
| Monitor psychotherapies for symptom worsening |
| Address comorbid psychiatric conditions |
| Regularize social rhythms |
| Initiate validated psychosocial treatments |
| Engage the patient as a active participant in treatment |
Persistent depression
Randomized, controlled trials designed to obtain FDA approval of bipolar medications inadequately reflect the disabling, confounding nature of bipolar illness. Nearly all of these large studies of acute treatments for mood episodes are placebo-controlled trials with narrow inclusion and broad exclusion criteria. Eliminating subsyndromal symptoms is not their goal, and they are of little help in understanding how to manage residual symptoms.
A more realistic view of bipolar disorder comes from large observational studies that have examined its longitudinal course in outpatients under more or less ideal treatment conditions.10 These studies show that bipolar disorder is almost always recurrent and relapsing, but full recovery and functioning between episodes is not the norm. Most patients never achieve prolonged recovery, complete symptom relief, or return to full functioning.5,8,11
STEP-BD. Most patients in the Systematic Treatment Enhancement Program for Bipolar Disorder (STEP-BD) never recovered from a depressed episode during 2 years of prospective follow-up under optimal care. Only 58% of patients who entered the study during an episode of illness achieved 8 consecutive weeks of euthymia.5
Collaborative Depression study. Longitudinal data from the National Institute of Mental Health’s Collaborative Depression Study6,7 showed:
- patients with bipolar I disorder had depressive symptoms in approximately three-quarters of the weeks in which they reported significant symptoms
- patients with bipolar II disorder were depressed in nearly all sick weeks.
The Stanley Foundation Bipolar Network had similar findings, with bipolar disorder patients reporting 3 times as much time spent with depressed mood as with elevated mood.8 Poor social and occupational functioning predicted poor outcomes, suggesting an interplay between subsyndromal depression, poor functioning, and relapse.
Risk factors
Rapid cycling may be a marker for persistent, subsyndromal symptoms. Rapid cycling is defined clinically as 4 distinct mood episodes—switching to the opposite pole or 2 episodes of the same pole separated by ≥8 weeks of partial or full recovery—in the previous 12 months. Rapid cycling usually is diagnosed retrospectively—introducing patients’ recall bias—but may be more of a marker for symptom persistence than for defined episodes.
In STEP-BD, 32% of study entrants reported ≥4 mood episodes in the previous year, yet only 6% of that subgroup had ≥4 episodes after 1 year of prospective follow-up.12 This suggests:
- patients who retrospectively report rapid cycling may be chronically and persistently ill, rather than experiencing multiple discrete episodes
- rapid cycling is a marker for symptom persistence, subsyndromal depression, and lack of sustained remission.
- comorbid anxiety disorders (present in ≤50% of patients with bipolar I and II disorder)
- active and past substance use disorders (including nicotine dependence)
- early age of onset of the mood disorder.13-16
CASE CONTINUED: Restoring the cornerstone
You review Mr. W’s records. Recent lab values were essentially normal, with thyroid stimulating hormone 2.3 mIU/mL and stable renal function. He scores 11 on the Quick Inventory of Depressive Symptoms–self-rated version (QIDS-SR), indicating mild to moderate depressive symptom burden.
His mood chart and interview reveal that he has been depressed and anhedonic most of the day for 4 of the last 10 days. By systematically asking the depression questions in the DSM-IV-TR, you find that he does not meet criteria for depressed mood or anhedonia but has difficulty concentrating most of the day, persistent low self-esteem, and feeling “slowed.”
After you discuss lithium’s pros and cons with Mr. W, he agrees to try this mood stabilizer again. You explain the importance of preventing relapse to mania and of monitoring his cognitive performance at work.
Over time, you titrate lithium to a moderate serum level (0.5 to 0.7 mEq/L) and treat a resulting mild tremor with propranolol, 20 to 40 mg/d. Mr. W is tolerating lamotrigine well, so you continue this medication because of its potential to decrease the probability of relapse to depression. You also continue zolpidem, as needed, but discontinue methylphenidate because you think it may be contributing to sleep difficulties.
Managing medication
Nine drugs are FDA-approved for acute bipolar mania, but treatments for bipolar depression, maintenance treatment, and relapse prevention are far fewer, often partially effective, or effective for a limited number of patients. When depressive symptoms fail to resolve, a reasonable approach is to review patients’ medications and suggest alternatives with proven efficacy for bipolar disorder (Table 2). Patients can then accept or reject various options based on personal preference.
Combination strategies. Antimanic treatment is the cornerstone of treating bipolar I disorder, and preventing manic episodes should be a primary treatment goal. Thus, consider continuing treatments that have prevented mania for your patient—as lithium did in Mr. W’s case—while adding treatments aimed at depression. For example, adding lamotrigine to any antimanic agent is reasonable, especially if doing so does not add substantially to your patient’s side-effect burden.
Minimize antidepressants. Given the predominance and persistence of depressive symptoms in bipolar disorder, one can understand why clinicians and patients might try standard antidepressants without clear evidence supporting this practice. Antidepressants—especially venlafaxine and tricyclic antidepressants—are the most common and likely suspects when patients experience switching to mania, rapid cycling, and symptom persistence.17 Antidepressants’ negative effect has not been clearly defined, however, and may be patient-specific (related to patient factors rather than intrinsic to the compound).
In my clinical experience, minimizing antidepressant use in bipolar depression hastens rather than delays patients’ recovery. A prudent approach would be to use the minimum dose necessary and discontinue the antidepressant if possible. Also minimize medical pharmacotherapies—including corticosteroids and oral contraceptives—that may worsen mood symptoms, especially in patients with this history.
Avoid under-dosing. Inadequate dosing and duration often are overlooked as causes of treatment resistance in bipolar disorder and other illnesses.18 Bipolar disorder medications are hardly benign; every drug approved for any phase of bipolar disorder has a black-box warning. Understandably, clinicians and patients try to choose medications and dosages perceived to be most tolerable. Full-dose treatment trials may be warranted, however, given the high probability of incomplete recovery, impaired functioning, and risk of relapse with ineffective dosing.
Address iatrogenic causes. In addition, identify and eliminate medications and treatments that may be perpetuating patients’ bipolar symptoms. Stimulants such as methylphenidate and amphetamines may contribute to sleep disturbance and manic relapse and might be minimized or eliminated in a patient with continued symptoms and sleep disturbance.19
- Two trials of aripiprazole for bipolar depression failed to show benefit.20
- A trial that compared risperidone with lamotrigine and inositol for treatment-resistant bipolar depression suggested that risperidone may have hindered recovery.21
Table 2
Subsyndromal bipolar depression: Recommended medications*
| Medication | Initial and maximum dosages | Clinically important side effects |
|---|---|---|
| Quetiapine | Start at 50 mg and titrate to 300 mg within 4 to 7 days; maximum 600 mg | Sedation, somnolence, weight gain, gastrointestinal side effects, lipid abnormalities, increased fasting glucose, increased risk of diabetes |
| Olanzapine/fluoxetine | Start at 6 mg/25 mg; maximum 12 mg/50 mg | Weight gain, sedation, gastrointestinal side effects, lipid abnormalities, increased fasting glucose, increased risk of diabetes |
| Lamotrigine | Must be titrated per package labeling; start at 25 mg and titrate to 200 mg (12.5 mg titrated to 100 mg if patient is on valproate, 50 mg titrated to 400 mg if on carbamazepine or other enzyme inducer); maximum (per label) 500 mg | Rash, headache, balance difficulties, clumsiness; Stevens-Johnson syndrome or toxic epidermal necrolysis are rare but potentially fatal |
| Lithium | Start at 300 to 600 mg and use moderate blood levels (0.4 to 0.7 mEq/L); if no improvement in 4 to 8 weeks, titrate to 0.8 to 1.1 mEq/L | Tremor, nausea, diarrhea, increased thirst, increased urination, hair loss, thyroid abnormalities, weight gain, acne, worsening of psoriasis, diabetes insipidus, renal insufficiency |
| Divalproex | Start at 500 to 750 mg and increase to 15 to 20 mg/kg; usual target blood levels are >50 mg/dL | Nausea, abnormal liver function tests, weight gain, hair loss |
| Olanzapine | Start at 5 mg; maximum 30 mg | Weight gain, sedation, somnolence, lipid abnormalities, increased fasting glucose, increased risk of diabetes |
| Modafinil | Start at 50 to 100 mg and increase to 200 mg; higher dosages have not been systematically studied in bipolar disorder | Nervousness, insomnia |
| EPS: extrapyramidal symptoms | ||
| * Medications are listed in from most to least evidence supporting their use in treating bipolar depression | ||
CASE CONTINUED: Distressed by psychotherapy
You ask Mr. W about his psychodynamic psychotherapy, and he says that exploring his early life experiences and his work difficulty is increasing his anxiety. You recommend switching to cognitive-behavioral therapy (CBT) to work on delegating tasks that are not his strong areas and focusing on his marketing talents. You also encourage him to maintain regular sleep-wake cycles.
Some psychodynamic psychotherapies are thought to increase anxiety and mood instability in bipolar disorder patients. Examine the form and content of psychosocial approaches for their role in worsening your patients’ symptoms. As with medications, validated psychotherapeutic interventions—such as CBT for bipolar disorder, family-focused treatment, interpersonal social rhythm therapy, and long-term group psychotherapy23,24—are preferred over those not specifically studied in bipolar disorder.
- Establish a social rhythm that includes a regularized sleep-wake cycle and predictable daily schedules, with planned contact with people and organized activities.
- Decrease behaviors associated with mood fluctuation, such as substance use, irregular hours of sleep, conflicts in relationships and work, poor adherence to medications, and lack of regard for physical health.
CASE CONTINUED: Changes for the better
After several months of CBT and medication changes, Mr. W is continuing to work and shows some symptom improvement. His QIDS-SR scores have decreased to 6, indicating minimal to mild depressive symptom burden. He reports that most weeks he has no depressive symptoms, but he remains unable to focus on specific tasks for long periods. He continues to have difficulties when his work requires detailed, intensive activities.
Mr. W has developed a new relationship but gives high priority to keeping a regular schedule. Before going to sleep most nights, he records his mood in a diary to monitor his progress.
Mr. W may show additional improvement in work performance with continued daily mood monitoring and a regularized routine. The care of most patients with bipolar disorder must be systematically optimized over years, not weeks or months.26 Because medication adherence during well periods is essential, discuss and address adverse effects such as weight gain or urinary symptoms.
- minimize or eliminate ineffective and harmful treatments
- continue effective treatments, whether psychopharmacologic or psychosocial.
Tools for monitoring subsyndromal symptoms
| Encourage patient to keep a daily mood chart, including sleep-wake times |
Use standardized depression rating scales to monitor symptom changes:
|
| Use the Structured Clinical Interview for DSM-IV, Mood Module to verify whether or not the patient is in a mood episode |
| Use the Clinical Global Impression Severity Scale (BP version) as a measure of illness severity |
| Monitor use of caffeine, nicotine, alcohol, and other drugs of abuse by asking about the frequency and amounts used |
| Calculate body mass index at each visit to monitor for weight gain |
- Otto M, Reilly-Harrington N, Kogan JN, Henin A. Managing bipolar disorder: a cognitive behavior treatment program therapist guide (treatments that work). Oxford, UK: Oxford University Press; 2008.
- Inventory of Depressive Symptomatology (IDS) and Quick Inventory of Depressive Symptomatology (QIDS). Validity, reliability, administration, and scoring. www.ids-qids.org.
- Bipolar Clinic and Research Program, Massachusetts General Hospital. Resources for clinicians and patients, plus links to information on bipolar disorder. www.manicdepressive.org.
- Aripiprazole • Abilify
- Carbamazepine • Tegretol
- Divalproex • Depakote
- Lamotrigine • Lamictal
- Lithium • various
- Methylphenidate • various
- Modafinil • Provigil
- Olanzapine • Zyprexa
- Olanzapine/fluoxetine • Symbyax
- Propranolol • Inderal
- Quetiapine • Seroquel
- Valproate • Depacon
- Venlafaxine • Effexor
- Zolpidem • Ambien
Dr. Ostacher is a speaker for AstraZeneca, Bristol-Myers Squibb, Eli Lilly and Company, GlaxoSmithKline, and Pfizer Inc.
1. Royal Australian and New Zealand College of Psychiatrists Clinical Practice Guidelines Team for Bipolar Disorder. Australian and New Zealand clinical practice guidelines for the treatment of bipolar disorder. Aust N Z J Psychiatry 2004;38:280-305.
2. Yatham LN, Kennedy SH, O’Donovan C, et al. Canadian Network for Mood and Anxiety Treatments (CANMAT) guidelines for the management of patients with bipolar disorder: consensus and controversies. Bipolar Disord 2005;7(suppl 3):5-69.
3. American Psychiatric Association. Practice guidelines for the treatment of patients with bipolar disorder. 2nd ed. Washington, DC: American Psychiatric Publishing, Inc; 2002.
4. Goodwin GM. And the Consensus Group of the British Association for Psychopharmacology. Evidence-based guidelines for treating bipolar disorder: recommendations from the British Association for Psychopharmacology. J Psychopharmacol 2003;17:149-73.
5. Perlis RH, Ostacher MJ, Patel J, et al. Predictors of recurrence in bipolar disorder: primary outcomes from the Systematic Treatment Enhancement Program for Bipolar Disorder (STEP-BD). Am J Psychiatry 2006;163:217-24.
6. Judd LL, Akiskal HS, Schettler PJ, et al. The long-term natural history of the weekly symptomatic status of bipolar I disorder. Arch Gen Psychiatry 2002;59:530-7.
7. Judd LL, Akiskal HS, Schettler PJ, et al. A prospective investigation of the natural history of the long-term weekly symptomatic status of bipolar II disorder. Arch Gen Psychiatry 2003;60:261-9.
8. Post RM, Denicoff KD, Leverich GS, et al. Morbidity in 258 bipolar outpatients followed for 1 year with daily prospective ratings on the NIMH life chart method. J Clin Psychiatry 2003;64:680-90.
9. Ostacher MJ, Nierenberg AA, Iosifescu D, et al. And the STEP-BD Family Experience Collaborative Study Group. Correlates of subjective and objective burden among caregivers of patients with bipolar disorder. Acta Psychiatr Scand 2008;118:49-56.
10. Sachs GS, Thase ME, Otto MW, et al. Rationale, design, and methods of the Systematic Treatment Enhancement Program for Bipolar Disorder (STEP-BD). Biol Psychiatry 2003;53:1028-42.
11. Tohen M, Zarate CA, Jr, Hennen J, et al. The McLean-Harvard First-Episode Mania Study: prediction of recovery and first recurrence. Am J Psychiatry 2003;160:2099-107.
12. Schneck C. What is the best treatment for rapid cycling? Presented at: Annual Meeting of the American Psychiatric Association; May 21-26, 2005; Atlanta, GA.
13. Perlis RH, Miyahara S, Marangell LB, et al. For the STEP-BD Investigators. Long-term implications of early onset in bipolar disorder: data from the first 1000 participants in the Systematic Treatment Enhancement Program for Bipolar Disorder (STEP-BD). Biol Psychiatry 2004;55:875-81.
14. Weiss RD, Ostacher MJ, Otto MW, et al. For the STEP-BD Investigators. Does recovery from substance use disorder matter in patients with bipolar disorder? J Clin Psychiatry 2005;66:730-5.
15. Simon NM, Otto MW, Wisniewski SR, et al. Anxiety disorder comorbidity in bipolar disorder patients: data from the first 500 participants in the Systematic Treatment Enhancement Program for Bipolar Disorder (STEP-BD). Am J Psychiatry 2004;161:2222-9.
16. Waxmonsky JA, Thomas MR, Miklowitz DJ, et al. Prevalence and correlates of tobacco use in bipolar disorder: data from the first 2000 participants in the Systematic Treatment Enhancement Program. Gen Hosp Psychiatry 2005;27:321-8.
17. Leverich GS, Altshuler LL, Frye MA, et al. Risk of switch in mood polarity to hypomania or mania in patients with bipolar depression during acute and continuation trials of venlafaxine, sertraline, and bupropion as adjuncts to mood stabilizers. Am J Psychiatry 2006;163:232-9.
18. Simon NM, Otto MW, Weiss RD, et al. Pharmacotherapy for bipolar disorder and comorbid conditions: baseline data from STEP-BD. J Clin Psychopharmacol 2004;24:512-20.
19. Ghaemi SN, Hsu DJ, Soldani F, Goodwin FK. Antidepressants in bipolar disorder: the case for caution. Bipolar Disord 2003;5:421-33.
20. Thase ME, Jonas A, Khan A, et al. Aripiprazole monotherapy in nonpsychotic bipolar I depression: results of 2 randomized, placebo-controlled studies. J Clin Psychopharmacol 2008;28:13-20.
21. Nierenberg AA, Ostacher MJ, Calabrese JR, et al. Treatment-resistant bipolar depression: a STEP-BD equipoise randomized effectiveness trial of antidepressant augmentation with lamotrigine, inositol, or risperidone. Am J Psychiatry 2006;163:210-6.
22. Frye MA, Grunze H, Suppes T, et al. A placebo-controlled evaluation of adjunctive modafinil in the treatment of bipolar depression. Am J Psychiatry 2007;164:1242-9.
23. Colom F, Vieta E, Martinez-Aran A, et al. A randomized trial on the efficacy of group psychoeducation in the prophylaxis of recurrences in bipolar patients whose disease is in remission. Arch Gen Psychiatry 2003;60:402-7.
24. Sachs GS, Nierenberg AA, Calabrese JR, et al. Effectiveness of adjunctive antidepressant treatment for bipolar depression. N Engl J Med 2007;356:1711-22.
25. Frank E, Gonzalez JM, Fagiolini A. The importance of routine for preventing recurrence in bipolar disorder. Am J Psychiatry 2006;163:981-5.
26. Nierenberg AA, Ostacher MJ, Borrelli DJ, et al. The integration of measurement and management for the treatment of bipolar disorder: a STEP-BD model of collaborative care in psychiatry. J Clin Psychiatry 2006;67(suppl 11):3-7.
Mr. W, a 53-year-old divorced entrepreneur, presents to you for evaluation of poor concentration, decreased self-esteem, and difficulty making decisions that are interfering with his work. A longtime patient of another psychiatrist, Mr. W has a 26-year history of bipolar I disorder. He has not had a manic episode for 5 years but has had several depressive episodes.
During his last manic episode, Mr. W was hospitalized with expansive and irritable mood, racing thoughts, impulsive sexual behavior, psychomotor agitation, elevated self-esteem, marked distractibility, and paranoid ideas about his business partners. His discharge regimen included lithium titrated to 0.9 mEq/L and divalproex sodium, 1,500 mg/d, with lamotrigine, 200 mg/d, added to reduce depressive relapse risk. After several years of stable treatment, Mr. W complained of cognitive impairment. His psychiatrist discontinued lithium and added a low-dose stimulant—methylphenidate, 20 mg bid—to address Mr. W’s complaints of poor concentration.
Mr. W also is taking zolpidem, 10 mg as needed for onset insomnia, and receives weekly psychodynamic psychotherapy. His work performance problems persist despite these treatments, and his company is failing.
A poor course in bipolar disorder—as in Mr. W’s case—is frequently characterized by persistent or relapsing depression. Bipolar disorder is diagnosed by a manic, mixed, or hypomanic episode, but depression and depressive symptoms are most prominent in clinical practice. Likewise, major observational studies blame depression for most of the time spent ill in bipolar types I and II.1-8
A good deal of bipolar symptom burden is associated with subsyndromal depression—defined as having >2 but 5 and depressive symptoms are disproportionately responsible—compared with manic symptoms—for the impact of bipolar illness on patients and their families.9
This article offers clinically useful strategies to minimize subsyndromal depression in patients with bipolar disorder (Table 1). These strategies include an evidence-based approach to medication, the use of validated psychotherapies, regular sleep and socialization schedules, and careful monitoring of mood symptoms.
Table 1
How to minimize bipolar subsyndromal depression
| Monitor symptoms using validated clinician- and patient-rated tools at all visits |
| Use evidence-based treatments first |
| Eliminate ineffective medications |
| Use adequate doses of medications for different mood states |
| Monitor and treat adverse effects of successful treatments |
| Monitor and minimize medications that can worsen symptoms |
| Watch for the impact of medical conditions on mood |
| Be attentive to alcohol and substance use (including caffeine, nicotine, and energy drinks) |
| Monitor psychotherapies for symptom worsening |
| Address comorbid psychiatric conditions |
| Regularize social rhythms |
| Initiate validated psychosocial treatments |
| Engage the patient as a active participant in treatment |
Persistent depression
Randomized, controlled trials designed to obtain FDA approval of bipolar medications inadequately reflect the disabling, confounding nature of bipolar illness. Nearly all of these large studies of acute treatments for mood episodes are placebo-controlled trials with narrow inclusion and broad exclusion criteria. Eliminating subsyndromal symptoms is not their goal, and they are of little help in understanding how to manage residual symptoms.
A more realistic view of bipolar disorder comes from large observational studies that have examined its longitudinal course in outpatients under more or less ideal treatment conditions.10 These studies show that bipolar disorder is almost always recurrent and relapsing, but full recovery and functioning between episodes is not the norm. Most patients never achieve prolonged recovery, complete symptom relief, or return to full functioning.5,8,11
STEP-BD. Most patients in the Systematic Treatment Enhancement Program for Bipolar Disorder (STEP-BD) never recovered from a depressed episode during 2 years of prospective follow-up under optimal care. Only 58% of patients who entered the study during an episode of illness achieved 8 consecutive weeks of euthymia.5
Collaborative Depression study. Longitudinal data from the National Institute of Mental Health’s Collaborative Depression Study6,7 showed:
- patients with bipolar I disorder had depressive symptoms in approximately three-quarters of the weeks in which they reported significant symptoms
- patients with bipolar II disorder were depressed in nearly all sick weeks.
The Stanley Foundation Bipolar Network had similar findings, with bipolar disorder patients reporting 3 times as much time spent with depressed mood as with elevated mood.8 Poor social and occupational functioning predicted poor outcomes, suggesting an interplay between subsyndromal depression, poor functioning, and relapse.
Risk factors
Rapid cycling may be a marker for persistent, subsyndromal symptoms. Rapid cycling is defined clinically as 4 distinct mood episodes—switching to the opposite pole or 2 episodes of the same pole separated by ≥8 weeks of partial or full recovery—in the previous 12 months. Rapid cycling usually is diagnosed retrospectively—introducing patients’ recall bias—but may be more of a marker for symptom persistence than for defined episodes.
In STEP-BD, 32% of study entrants reported ≥4 mood episodes in the previous year, yet only 6% of that subgroup had ≥4 episodes after 1 year of prospective follow-up.12 This suggests:
- patients who retrospectively report rapid cycling may be chronically and persistently ill, rather than experiencing multiple discrete episodes
- rapid cycling is a marker for symptom persistence, subsyndromal depression, and lack of sustained remission.
- comorbid anxiety disorders (present in ≤50% of patients with bipolar I and II disorder)
- active and past substance use disorders (including nicotine dependence)
- early age of onset of the mood disorder.13-16
CASE CONTINUED: Restoring the cornerstone
You review Mr. W’s records. Recent lab values were essentially normal, with thyroid stimulating hormone 2.3 mIU/mL and stable renal function. He scores 11 on the Quick Inventory of Depressive Symptoms–self-rated version (QIDS-SR), indicating mild to moderate depressive symptom burden.
His mood chart and interview reveal that he has been depressed and anhedonic most of the day for 4 of the last 10 days. By systematically asking the depression questions in the DSM-IV-TR, you find that he does not meet criteria for depressed mood or anhedonia but has difficulty concentrating most of the day, persistent low self-esteem, and feeling “slowed.”
After you discuss lithium’s pros and cons with Mr. W, he agrees to try this mood stabilizer again. You explain the importance of preventing relapse to mania and of monitoring his cognitive performance at work.
Over time, you titrate lithium to a moderate serum level (0.5 to 0.7 mEq/L) and treat a resulting mild tremor with propranolol, 20 to 40 mg/d. Mr. W is tolerating lamotrigine well, so you continue this medication because of its potential to decrease the probability of relapse to depression. You also continue zolpidem, as needed, but discontinue methylphenidate because you think it may be contributing to sleep difficulties.
Managing medication
Nine drugs are FDA-approved for acute bipolar mania, but treatments for bipolar depression, maintenance treatment, and relapse prevention are far fewer, often partially effective, or effective for a limited number of patients. When depressive symptoms fail to resolve, a reasonable approach is to review patients’ medications and suggest alternatives with proven efficacy for bipolar disorder (Table 2). Patients can then accept or reject various options based on personal preference.
Combination strategies. Antimanic treatment is the cornerstone of treating bipolar I disorder, and preventing manic episodes should be a primary treatment goal. Thus, consider continuing treatments that have prevented mania for your patient—as lithium did in Mr. W’s case—while adding treatments aimed at depression. For example, adding lamotrigine to any antimanic agent is reasonable, especially if doing so does not add substantially to your patient’s side-effect burden.
Minimize antidepressants. Given the predominance and persistence of depressive symptoms in bipolar disorder, one can understand why clinicians and patients might try standard antidepressants without clear evidence supporting this practice. Antidepressants—especially venlafaxine and tricyclic antidepressants—are the most common and likely suspects when patients experience switching to mania, rapid cycling, and symptom persistence.17 Antidepressants’ negative effect has not been clearly defined, however, and may be patient-specific (related to patient factors rather than intrinsic to the compound).
In my clinical experience, minimizing antidepressant use in bipolar depression hastens rather than delays patients’ recovery. A prudent approach would be to use the minimum dose necessary and discontinue the antidepressant if possible. Also minimize medical pharmacotherapies—including corticosteroids and oral contraceptives—that may worsen mood symptoms, especially in patients with this history.
Avoid under-dosing. Inadequate dosing and duration often are overlooked as causes of treatment resistance in bipolar disorder and other illnesses.18 Bipolar disorder medications are hardly benign; every drug approved for any phase of bipolar disorder has a black-box warning. Understandably, clinicians and patients try to choose medications and dosages perceived to be most tolerable. Full-dose treatment trials may be warranted, however, given the high probability of incomplete recovery, impaired functioning, and risk of relapse with ineffective dosing.
Address iatrogenic causes. In addition, identify and eliminate medications and treatments that may be perpetuating patients’ bipolar symptoms. Stimulants such as methylphenidate and amphetamines may contribute to sleep disturbance and manic relapse and might be minimized or eliminated in a patient with continued symptoms and sleep disturbance.19
- Two trials of aripiprazole for bipolar depression failed to show benefit.20
- A trial that compared risperidone with lamotrigine and inositol for treatment-resistant bipolar depression suggested that risperidone may have hindered recovery.21
Table 2
Subsyndromal bipolar depression: Recommended medications*
| Medication | Initial and maximum dosages | Clinically important side effects |
|---|---|---|
| Quetiapine | Start at 50 mg and titrate to 300 mg within 4 to 7 days; maximum 600 mg | Sedation, somnolence, weight gain, gastrointestinal side effects, lipid abnormalities, increased fasting glucose, increased risk of diabetes |
| Olanzapine/fluoxetine | Start at 6 mg/25 mg; maximum 12 mg/50 mg | Weight gain, sedation, gastrointestinal side effects, lipid abnormalities, increased fasting glucose, increased risk of diabetes |
| Lamotrigine | Must be titrated per package labeling; start at 25 mg and titrate to 200 mg (12.5 mg titrated to 100 mg if patient is on valproate, 50 mg titrated to 400 mg if on carbamazepine or other enzyme inducer); maximum (per label) 500 mg | Rash, headache, balance difficulties, clumsiness; Stevens-Johnson syndrome or toxic epidermal necrolysis are rare but potentially fatal |
| Lithium | Start at 300 to 600 mg and use moderate blood levels (0.4 to 0.7 mEq/L); if no improvement in 4 to 8 weeks, titrate to 0.8 to 1.1 mEq/L | Tremor, nausea, diarrhea, increased thirst, increased urination, hair loss, thyroid abnormalities, weight gain, acne, worsening of psoriasis, diabetes insipidus, renal insufficiency |
| Divalproex | Start at 500 to 750 mg and increase to 15 to 20 mg/kg; usual target blood levels are >50 mg/dL | Nausea, abnormal liver function tests, weight gain, hair loss |
| Olanzapine | Start at 5 mg; maximum 30 mg | Weight gain, sedation, somnolence, lipid abnormalities, increased fasting glucose, increased risk of diabetes |
| Modafinil | Start at 50 to 100 mg and increase to 200 mg; higher dosages have not been systematically studied in bipolar disorder | Nervousness, insomnia |
| EPS: extrapyramidal symptoms | ||
| * Medications are listed in from most to least evidence supporting their use in treating bipolar depression | ||
CASE CONTINUED: Distressed by psychotherapy
You ask Mr. W about his psychodynamic psychotherapy, and he says that exploring his early life experiences and his work difficulty is increasing his anxiety. You recommend switching to cognitive-behavioral therapy (CBT) to work on delegating tasks that are not his strong areas and focusing on his marketing talents. You also encourage him to maintain regular sleep-wake cycles.
Some psychodynamic psychotherapies are thought to increase anxiety and mood instability in bipolar disorder patients. Examine the form and content of psychosocial approaches for their role in worsening your patients’ symptoms. As with medications, validated psychotherapeutic interventions—such as CBT for bipolar disorder, family-focused treatment, interpersonal social rhythm therapy, and long-term group psychotherapy23,24—are preferred over those not specifically studied in bipolar disorder.
- Establish a social rhythm that includes a regularized sleep-wake cycle and predictable daily schedules, with planned contact with people and organized activities.
- Decrease behaviors associated with mood fluctuation, such as substance use, irregular hours of sleep, conflicts in relationships and work, poor adherence to medications, and lack of regard for physical health.
CASE CONTINUED: Changes for the better
After several months of CBT and medication changes, Mr. W is continuing to work and shows some symptom improvement. His QIDS-SR scores have decreased to 6, indicating minimal to mild depressive symptom burden. He reports that most weeks he has no depressive symptoms, but he remains unable to focus on specific tasks for long periods. He continues to have difficulties when his work requires detailed, intensive activities.
Mr. W has developed a new relationship but gives high priority to keeping a regular schedule. Before going to sleep most nights, he records his mood in a diary to monitor his progress.
Mr. W may show additional improvement in work performance with continued daily mood monitoring and a regularized routine. The care of most patients with bipolar disorder must be systematically optimized over years, not weeks or months.26 Because medication adherence during well periods is essential, discuss and address adverse effects such as weight gain or urinary symptoms.
- minimize or eliminate ineffective and harmful treatments
- continue effective treatments, whether psychopharmacologic or psychosocial.
Tools for monitoring subsyndromal symptoms
| Encourage patient to keep a daily mood chart, including sleep-wake times |
Use standardized depression rating scales to monitor symptom changes:
|
| Use the Structured Clinical Interview for DSM-IV, Mood Module to verify whether or not the patient is in a mood episode |
| Use the Clinical Global Impression Severity Scale (BP version) as a measure of illness severity |
| Monitor use of caffeine, nicotine, alcohol, and other drugs of abuse by asking about the frequency and amounts used |
| Calculate body mass index at each visit to monitor for weight gain |
- Otto M, Reilly-Harrington N, Kogan JN, Henin A. Managing bipolar disorder: a cognitive behavior treatment program therapist guide (treatments that work). Oxford, UK: Oxford University Press; 2008.
- Inventory of Depressive Symptomatology (IDS) and Quick Inventory of Depressive Symptomatology (QIDS). Validity, reliability, administration, and scoring. www.ids-qids.org.
- Bipolar Clinic and Research Program, Massachusetts General Hospital. Resources for clinicians and patients, plus links to information on bipolar disorder. www.manicdepressive.org.
- Aripiprazole • Abilify
- Carbamazepine • Tegretol
- Divalproex • Depakote
- Lamotrigine • Lamictal
- Lithium • various
- Methylphenidate • various
- Modafinil • Provigil
- Olanzapine • Zyprexa
- Olanzapine/fluoxetine • Symbyax
- Propranolol • Inderal
- Quetiapine • Seroquel
- Valproate • Depacon
- Venlafaxine • Effexor
- Zolpidem • Ambien
Dr. Ostacher is a speaker for AstraZeneca, Bristol-Myers Squibb, Eli Lilly and Company, GlaxoSmithKline, and Pfizer Inc.
Mr. W, a 53-year-old divorced entrepreneur, presents to you for evaluation of poor concentration, decreased self-esteem, and difficulty making decisions that are interfering with his work. A longtime patient of another psychiatrist, Mr. W has a 26-year history of bipolar I disorder. He has not had a manic episode for 5 years but has had several depressive episodes.
During his last manic episode, Mr. W was hospitalized with expansive and irritable mood, racing thoughts, impulsive sexual behavior, psychomotor agitation, elevated self-esteem, marked distractibility, and paranoid ideas about his business partners. His discharge regimen included lithium titrated to 0.9 mEq/L and divalproex sodium, 1,500 mg/d, with lamotrigine, 200 mg/d, added to reduce depressive relapse risk. After several years of stable treatment, Mr. W complained of cognitive impairment. His psychiatrist discontinued lithium and added a low-dose stimulant—methylphenidate, 20 mg bid—to address Mr. W’s complaints of poor concentration.
Mr. W also is taking zolpidem, 10 mg as needed for onset insomnia, and receives weekly psychodynamic psychotherapy. His work performance problems persist despite these treatments, and his company is failing.
A poor course in bipolar disorder—as in Mr. W’s case—is frequently characterized by persistent or relapsing depression. Bipolar disorder is diagnosed by a manic, mixed, or hypomanic episode, but depression and depressive symptoms are most prominent in clinical practice. Likewise, major observational studies blame depression for most of the time spent ill in bipolar types I and II.1-8
A good deal of bipolar symptom burden is associated with subsyndromal depression—defined as having >2 but 5 and depressive symptoms are disproportionately responsible—compared with manic symptoms—for the impact of bipolar illness on patients and their families.9
This article offers clinically useful strategies to minimize subsyndromal depression in patients with bipolar disorder (Table 1). These strategies include an evidence-based approach to medication, the use of validated psychotherapies, regular sleep and socialization schedules, and careful monitoring of mood symptoms.
Table 1
How to minimize bipolar subsyndromal depression
| Monitor symptoms using validated clinician- and patient-rated tools at all visits |
| Use evidence-based treatments first |
| Eliminate ineffective medications |
| Use adequate doses of medications for different mood states |
| Monitor and treat adverse effects of successful treatments |
| Monitor and minimize medications that can worsen symptoms |
| Watch for the impact of medical conditions on mood |
| Be attentive to alcohol and substance use (including caffeine, nicotine, and energy drinks) |
| Monitor psychotherapies for symptom worsening |
| Address comorbid psychiatric conditions |
| Regularize social rhythms |
| Initiate validated psychosocial treatments |
| Engage the patient as a active participant in treatment |
Persistent depression
Randomized, controlled trials designed to obtain FDA approval of bipolar medications inadequately reflect the disabling, confounding nature of bipolar illness. Nearly all of these large studies of acute treatments for mood episodes are placebo-controlled trials with narrow inclusion and broad exclusion criteria. Eliminating subsyndromal symptoms is not their goal, and they are of little help in understanding how to manage residual symptoms.
A more realistic view of bipolar disorder comes from large observational studies that have examined its longitudinal course in outpatients under more or less ideal treatment conditions.10 These studies show that bipolar disorder is almost always recurrent and relapsing, but full recovery and functioning between episodes is not the norm. Most patients never achieve prolonged recovery, complete symptom relief, or return to full functioning.5,8,11
STEP-BD. Most patients in the Systematic Treatment Enhancement Program for Bipolar Disorder (STEP-BD) never recovered from a depressed episode during 2 years of prospective follow-up under optimal care. Only 58% of patients who entered the study during an episode of illness achieved 8 consecutive weeks of euthymia.5
Collaborative Depression study. Longitudinal data from the National Institute of Mental Health’s Collaborative Depression Study6,7 showed:
- patients with bipolar I disorder had depressive symptoms in approximately three-quarters of the weeks in which they reported significant symptoms
- patients with bipolar II disorder were depressed in nearly all sick weeks.
The Stanley Foundation Bipolar Network had similar findings, with bipolar disorder patients reporting 3 times as much time spent with depressed mood as with elevated mood.8 Poor social and occupational functioning predicted poor outcomes, suggesting an interplay between subsyndromal depression, poor functioning, and relapse.
Risk factors
Rapid cycling may be a marker for persistent, subsyndromal symptoms. Rapid cycling is defined clinically as 4 distinct mood episodes—switching to the opposite pole or 2 episodes of the same pole separated by ≥8 weeks of partial or full recovery—in the previous 12 months. Rapid cycling usually is diagnosed retrospectively—introducing patients’ recall bias—but may be more of a marker for symptom persistence than for defined episodes.
In STEP-BD, 32% of study entrants reported ≥4 mood episodes in the previous year, yet only 6% of that subgroup had ≥4 episodes after 1 year of prospective follow-up.12 This suggests:
- patients who retrospectively report rapid cycling may be chronically and persistently ill, rather than experiencing multiple discrete episodes
- rapid cycling is a marker for symptom persistence, subsyndromal depression, and lack of sustained remission.
- comorbid anxiety disorders (present in ≤50% of patients with bipolar I and II disorder)
- active and past substance use disorders (including nicotine dependence)
- early age of onset of the mood disorder.13-16
CASE CONTINUED: Restoring the cornerstone
You review Mr. W’s records. Recent lab values were essentially normal, with thyroid stimulating hormone 2.3 mIU/mL and stable renal function. He scores 11 on the Quick Inventory of Depressive Symptoms–self-rated version (QIDS-SR), indicating mild to moderate depressive symptom burden.
His mood chart and interview reveal that he has been depressed and anhedonic most of the day for 4 of the last 10 days. By systematically asking the depression questions in the DSM-IV-TR, you find that he does not meet criteria for depressed mood or anhedonia but has difficulty concentrating most of the day, persistent low self-esteem, and feeling “slowed.”
After you discuss lithium’s pros and cons with Mr. W, he agrees to try this mood stabilizer again. You explain the importance of preventing relapse to mania and of monitoring his cognitive performance at work.
Over time, you titrate lithium to a moderate serum level (0.5 to 0.7 mEq/L) and treat a resulting mild tremor with propranolol, 20 to 40 mg/d. Mr. W is tolerating lamotrigine well, so you continue this medication because of its potential to decrease the probability of relapse to depression. You also continue zolpidem, as needed, but discontinue methylphenidate because you think it may be contributing to sleep difficulties.
Managing medication
Nine drugs are FDA-approved for acute bipolar mania, but treatments for bipolar depression, maintenance treatment, and relapse prevention are far fewer, often partially effective, or effective for a limited number of patients. When depressive symptoms fail to resolve, a reasonable approach is to review patients’ medications and suggest alternatives with proven efficacy for bipolar disorder (Table 2). Patients can then accept or reject various options based on personal preference.
Combination strategies. Antimanic treatment is the cornerstone of treating bipolar I disorder, and preventing manic episodes should be a primary treatment goal. Thus, consider continuing treatments that have prevented mania for your patient—as lithium did in Mr. W’s case—while adding treatments aimed at depression. For example, adding lamotrigine to any antimanic agent is reasonable, especially if doing so does not add substantially to your patient’s side-effect burden.
Minimize antidepressants. Given the predominance and persistence of depressive symptoms in bipolar disorder, one can understand why clinicians and patients might try standard antidepressants without clear evidence supporting this practice. Antidepressants—especially venlafaxine and tricyclic antidepressants—are the most common and likely suspects when patients experience switching to mania, rapid cycling, and symptom persistence.17 Antidepressants’ negative effect has not been clearly defined, however, and may be patient-specific (related to patient factors rather than intrinsic to the compound).
In my clinical experience, minimizing antidepressant use in bipolar depression hastens rather than delays patients’ recovery. A prudent approach would be to use the minimum dose necessary and discontinue the antidepressant if possible. Also minimize medical pharmacotherapies—including corticosteroids and oral contraceptives—that may worsen mood symptoms, especially in patients with this history.
Avoid under-dosing. Inadequate dosing and duration often are overlooked as causes of treatment resistance in bipolar disorder and other illnesses.18 Bipolar disorder medications are hardly benign; every drug approved for any phase of bipolar disorder has a black-box warning. Understandably, clinicians and patients try to choose medications and dosages perceived to be most tolerable. Full-dose treatment trials may be warranted, however, given the high probability of incomplete recovery, impaired functioning, and risk of relapse with ineffective dosing.
Address iatrogenic causes. In addition, identify and eliminate medications and treatments that may be perpetuating patients’ bipolar symptoms. Stimulants such as methylphenidate and amphetamines may contribute to sleep disturbance and manic relapse and might be minimized or eliminated in a patient with continued symptoms and sleep disturbance.19
- Two trials of aripiprazole for bipolar depression failed to show benefit.20
- A trial that compared risperidone with lamotrigine and inositol for treatment-resistant bipolar depression suggested that risperidone may have hindered recovery.21
Table 2
Subsyndromal bipolar depression: Recommended medications*
| Medication | Initial and maximum dosages | Clinically important side effects |
|---|---|---|
| Quetiapine | Start at 50 mg and titrate to 300 mg within 4 to 7 days; maximum 600 mg | Sedation, somnolence, weight gain, gastrointestinal side effects, lipid abnormalities, increased fasting glucose, increased risk of diabetes |
| Olanzapine/fluoxetine | Start at 6 mg/25 mg; maximum 12 mg/50 mg | Weight gain, sedation, gastrointestinal side effects, lipid abnormalities, increased fasting glucose, increased risk of diabetes |
| Lamotrigine | Must be titrated per package labeling; start at 25 mg and titrate to 200 mg (12.5 mg titrated to 100 mg if patient is on valproate, 50 mg titrated to 400 mg if on carbamazepine or other enzyme inducer); maximum (per label) 500 mg | Rash, headache, balance difficulties, clumsiness; Stevens-Johnson syndrome or toxic epidermal necrolysis are rare but potentially fatal |
| Lithium | Start at 300 to 600 mg and use moderate blood levels (0.4 to 0.7 mEq/L); if no improvement in 4 to 8 weeks, titrate to 0.8 to 1.1 mEq/L | Tremor, nausea, diarrhea, increased thirst, increased urination, hair loss, thyroid abnormalities, weight gain, acne, worsening of psoriasis, diabetes insipidus, renal insufficiency |
| Divalproex | Start at 500 to 750 mg and increase to 15 to 20 mg/kg; usual target blood levels are >50 mg/dL | Nausea, abnormal liver function tests, weight gain, hair loss |
| Olanzapine | Start at 5 mg; maximum 30 mg | Weight gain, sedation, somnolence, lipid abnormalities, increased fasting glucose, increased risk of diabetes |
| Modafinil | Start at 50 to 100 mg and increase to 200 mg; higher dosages have not been systematically studied in bipolar disorder | Nervousness, insomnia |
| EPS: extrapyramidal symptoms | ||
| * Medications are listed in from most to least evidence supporting their use in treating bipolar depression | ||
CASE CONTINUED: Distressed by psychotherapy
You ask Mr. W about his psychodynamic psychotherapy, and he says that exploring his early life experiences and his work difficulty is increasing his anxiety. You recommend switching to cognitive-behavioral therapy (CBT) to work on delegating tasks that are not his strong areas and focusing on his marketing talents. You also encourage him to maintain regular sleep-wake cycles.
Some psychodynamic psychotherapies are thought to increase anxiety and mood instability in bipolar disorder patients. Examine the form and content of psychosocial approaches for their role in worsening your patients’ symptoms. As with medications, validated psychotherapeutic interventions—such as CBT for bipolar disorder, family-focused treatment, interpersonal social rhythm therapy, and long-term group psychotherapy23,24—are preferred over those not specifically studied in bipolar disorder.
- Establish a social rhythm that includes a regularized sleep-wake cycle and predictable daily schedules, with planned contact with people and organized activities.
- Decrease behaviors associated with mood fluctuation, such as substance use, irregular hours of sleep, conflicts in relationships and work, poor adherence to medications, and lack of regard for physical health.
CASE CONTINUED: Changes for the better
After several months of CBT and medication changes, Mr. W is continuing to work and shows some symptom improvement. His QIDS-SR scores have decreased to 6, indicating minimal to mild depressive symptom burden. He reports that most weeks he has no depressive symptoms, but he remains unable to focus on specific tasks for long periods. He continues to have difficulties when his work requires detailed, intensive activities.
Mr. W has developed a new relationship but gives high priority to keeping a regular schedule. Before going to sleep most nights, he records his mood in a diary to monitor his progress.
Mr. W may show additional improvement in work performance with continued daily mood monitoring and a regularized routine. The care of most patients with bipolar disorder must be systematically optimized over years, not weeks or months.26 Because medication adherence during well periods is essential, discuss and address adverse effects such as weight gain or urinary symptoms.
- minimize or eliminate ineffective and harmful treatments
- continue effective treatments, whether psychopharmacologic or psychosocial.
Tools for monitoring subsyndromal symptoms
| Encourage patient to keep a daily mood chart, including sleep-wake times |
Use standardized depression rating scales to monitor symptom changes:
|
| Use the Structured Clinical Interview for DSM-IV, Mood Module to verify whether or not the patient is in a mood episode |
| Use the Clinical Global Impression Severity Scale (BP version) as a measure of illness severity |
| Monitor use of caffeine, nicotine, alcohol, and other drugs of abuse by asking about the frequency and amounts used |
| Calculate body mass index at each visit to monitor for weight gain |
- Otto M, Reilly-Harrington N, Kogan JN, Henin A. Managing bipolar disorder: a cognitive behavior treatment program therapist guide (treatments that work). Oxford, UK: Oxford University Press; 2008.
- Inventory of Depressive Symptomatology (IDS) and Quick Inventory of Depressive Symptomatology (QIDS). Validity, reliability, administration, and scoring. www.ids-qids.org.
- Bipolar Clinic and Research Program, Massachusetts General Hospital. Resources for clinicians and patients, plus links to information on bipolar disorder. www.manicdepressive.org.
- Aripiprazole • Abilify
- Carbamazepine • Tegretol
- Divalproex • Depakote
- Lamotrigine • Lamictal
- Lithium • various
- Methylphenidate • various
- Modafinil • Provigil
- Olanzapine • Zyprexa
- Olanzapine/fluoxetine • Symbyax
- Propranolol • Inderal
- Quetiapine • Seroquel
- Valproate • Depacon
- Venlafaxine • Effexor
- Zolpidem • Ambien
Dr. Ostacher is a speaker for AstraZeneca, Bristol-Myers Squibb, Eli Lilly and Company, GlaxoSmithKline, and Pfizer Inc.
1. Royal Australian and New Zealand College of Psychiatrists Clinical Practice Guidelines Team for Bipolar Disorder. Australian and New Zealand clinical practice guidelines for the treatment of bipolar disorder. Aust N Z J Psychiatry 2004;38:280-305.
2. Yatham LN, Kennedy SH, O’Donovan C, et al. Canadian Network for Mood and Anxiety Treatments (CANMAT) guidelines for the management of patients with bipolar disorder: consensus and controversies. Bipolar Disord 2005;7(suppl 3):5-69.
3. American Psychiatric Association. Practice guidelines for the treatment of patients with bipolar disorder. 2nd ed. Washington, DC: American Psychiatric Publishing, Inc; 2002.
4. Goodwin GM. And the Consensus Group of the British Association for Psychopharmacology. Evidence-based guidelines for treating bipolar disorder: recommendations from the British Association for Psychopharmacology. J Psychopharmacol 2003;17:149-73.
5. Perlis RH, Ostacher MJ, Patel J, et al. Predictors of recurrence in bipolar disorder: primary outcomes from the Systematic Treatment Enhancement Program for Bipolar Disorder (STEP-BD). Am J Psychiatry 2006;163:217-24.
6. Judd LL, Akiskal HS, Schettler PJ, et al. The long-term natural history of the weekly symptomatic status of bipolar I disorder. Arch Gen Psychiatry 2002;59:530-7.
7. Judd LL, Akiskal HS, Schettler PJ, et al. A prospective investigation of the natural history of the long-term weekly symptomatic status of bipolar II disorder. Arch Gen Psychiatry 2003;60:261-9.
8. Post RM, Denicoff KD, Leverich GS, et al. Morbidity in 258 bipolar outpatients followed for 1 year with daily prospective ratings on the NIMH life chart method. J Clin Psychiatry 2003;64:680-90.
9. Ostacher MJ, Nierenberg AA, Iosifescu D, et al. And the STEP-BD Family Experience Collaborative Study Group. Correlates of subjective and objective burden among caregivers of patients with bipolar disorder. Acta Psychiatr Scand 2008;118:49-56.
10. Sachs GS, Thase ME, Otto MW, et al. Rationale, design, and methods of the Systematic Treatment Enhancement Program for Bipolar Disorder (STEP-BD). Biol Psychiatry 2003;53:1028-42.
11. Tohen M, Zarate CA, Jr, Hennen J, et al. The McLean-Harvard First-Episode Mania Study: prediction of recovery and first recurrence. Am J Psychiatry 2003;160:2099-107.
12. Schneck C. What is the best treatment for rapid cycling? Presented at: Annual Meeting of the American Psychiatric Association; May 21-26, 2005; Atlanta, GA.
13. Perlis RH, Miyahara S, Marangell LB, et al. For the STEP-BD Investigators. Long-term implications of early onset in bipolar disorder: data from the first 1000 participants in the Systematic Treatment Enhancement Program for Bipolar Disorder (STEP-BD). Biol Psychiatry 2004;55:875-81.
14. Weiss RD, Ostacher MJ, Otto MW, et al. For the STEP-BD Investigators. Does recovery from substance use disorder matter in patients with bipolar disorder? J Clin Psychiatry 2005;66:730-5.
15. Simon NM, Otto MW, Wisniewski SR, et al. Anxiety disorder comorbidity in bipolar disorder patients: data from the first 500 participants in the Systematic Treatment Enhancement Program for Bipolar Disorder (STEP-BD). Am J Psychiatry 2004;161:2222-9.
16. Waxmonsky JA, Thomas MR, Miklowitz DJ, et al. Prevalence and correlates of tobacco use in bipolar disorder: data from the first 2000 participants in the Systematic Treatment Enhancement Program. Gen Hosp Psychiatry 2005;27:321-8.
17. Leverich GS, Altshuler LL, Frye MA, et al. Risk of switch in mood polarity to hypomania or mania in patients with bipolar depression during acute and continuation trials of venlafaxine, sertraline, and bupropion as adjuncts to mood stabilizers. Am J Psychiatry 2006;163:232-9.
18. Simon NM, Otto MW, Weiss RD, et al. Pharmacotherapy for bipolar disorder and comorbid conditions: baseline data from STEP-BD. J Clin Psychopharmacol 2004;24:512-20.
19. Ghaemi SN, Hsu DJ, Soldani F, Goodwin FK. Antidepressants in bipolar disorder: the case for caution. Bipolar Disord 2003;5:421-33.
20. Thase ME, Jonas A, Khan A, et al. Aripiprazole monotherapy in nonpsychotic bipolar I depression: results of 2 randomized, placebo-controlled studies. J Clin Psychopharmacol 2008;28:13-20.
21. Nierenberg AA, Ostacher MJ, Calabrese JR, et al. Treatment-resistant bipolar depression: a STEP-BD equipoise randomized effectiveness trial of antidepressant augmentation with lamotrigine, inositol, or risperidone. Am J Psychiatry 2006;163:210-6.
22. Frye MA, Grunze H, Suppes T, et al. A placebo-controlled evaluation of adjunctive modafinil in the treatment of bipolar depression. Am J Psychiatry 2007;164:1242-9.
23. Colom F, Vieta E, Martinez-Aran A, et al. A randomized trial on the efficacy of group psychoeducation in the prophylaxis of recurrences in bipolar patients whose disease is in remission. Arch Gen Psychiatry 2003;60:402-7.
24. Sachs GS, Nierenberg AA, Calabrese JR, et al. Effectiveness of adjunctive antidepressant treatment for bipolar depression. N Engl J Med 2007;356:1711-22.
25. Frank E, Gonzalez JM, Fagiolini A. The importance of routine for preventing recurrence in bipolar disorder. Am J Psychiatry 2006;163:981-5.
26. Nierenberg AA, Ostacher MJ, Borrelli DJ, et al. The integration of measurement and management for the treatment of bipolar disorder: a STEP-BD model of collaborative care in psychiatry. J Clin Psychiatry 2006;67(suppl 11):3-7.
1. Royal Australian and New Zealand College of Psychiatrists Clinical Practice Guidelines Team for Bipolar Disorder. Australian and New Zealand clinical practice guidelines for the treatment of bipolar disorder. Aust N Z J Psychiatry 2004;38:280-305.
2. Yatham LN, Kennedy SH, O’Donovan C, et al. Canadian Network for Mood and Anxiety Treatments (CANMAT) guidelines for the management of patients with bipolar disorder: consensus and controversies. Bipolar Disord 2005;7(suppl 3):5-69.
3. American Psychiatric Association. Practice guidelines for the treatment of patients with bipolar disorder. 2nd ed. Washington, DC: American Psychiatric Publishing, Inc; 2002.
4. Goodwin GM. And the Consensus Group of the British Association for Psychopharmacology. Evidence-based guidelines for treating bipolar disorder: recommendations from the British Association for Psychopharmacology. J Psychopharmacol 2003;17:149-73.
5. Perlis RH, Ostacher MJ, Patel J, et al. Predictors of recurrence in bipolar disorder: primary outcomes from the Systematic Treatment Enhancement Program for Bipolar Disorder (STEP-BD). Am J Psychiatry 2006;163:217-24.
6. Judd LL, Akiskal HS, Schettler PJ, et al. The long-term natural history of the weekly symptomatic status of bipolar I disorder. Arch Gen Psychiatry 2002;59:530-7.
7. Judd LL, Akiskal HS, Schettler PJ, et al. A prospective investigation of the natural history of the long-term weekly symptomatic status of bipolar II disorder. Arch Gen Psychiatry 2003;60:261-9.
8. Post RM, Denicoff KD, Leverich GS, et al. Morbidity in 258 bipolar outpatients followed for 1 year with daily prospective ratings on the NIMH life chart method. J Clin Psychiatry 2003;64:680-90.
9. Ostacher MJ, Nierenberg AA, Iosifescu D, et al. And the STEP-BD Family Experience Collaborative Study Group. Correlates of subjective and objective burden among caregivers of patients with bipolar disorder. Acta Psychiatr Scand 2008;118:49-56.
10. Sachs GS, Thase ME, Otto MW, et al. Rationale, design, and methods of the Systematic Treatment Enhancement Program for Bipolar Disorder (STEP-BD). Biol Psychiatry 2003;53:1028-42.
11. Tohen M, Zarate CA, Jr, Hennen J, et al. The McLean-Harvard First-Episode Mania Study: prediction of recovery and first recurrence. Am J Psychiatry 2003;160:2099-107.
12. Schneck C. What is the best treatment for rapid cycling? Presented at: Annual Meeting of the American Psychiatric Association; May 21-26, 2005; Atlanta, GA.
13. Perlis RH, Miyahara S, Marangell LB, et al. For the STEP-BD Investigators. Long-term implications of early onset in bipolar disorder: data from the first 1000 participants in the Systematic Treatment Enhancement Program for Bipolar Disorder (STEP-BD). Biol Psychiatry 2004;55:875-81.
14. Weiss RD, Ostacher MJ, Otto MW, et al. For the STEP-BD Investigators. Does recovery from substance use disorder matter in patients with bipolar disorder? J Clin Psychiatry 2005;66:730-5.
15. Simon NM, Otto MW, Wisniewski SR, et al. Anxiety disorder comorbidity in bipolar disorder patients: data from the first 500 participants in the Systematic Treatment Enhancement Program for Bipolar Disorder (STEP-BD). Am J Psychiatry 2004;161:2222-9.
16. Waxmonsky JA, Thomas MR, Miklowitz DJ, et al. Prevalence and correlates of tobacco use in bipolar disorder: data from the first 2000 participants in the Systematic Treatment Enhancement Program. Gen Hosp Psychiatry 2005;27:321-8.
17. Leverich GS, Altshuler LL, Frye MA, et al. Risk of switch in mood polarity to hypomania or mania in patients with bipolar depression during acute and continuation trials of venlafaxine, sertraline, and bupropion as adjuncts to mood stabilizers. Am J Psychiatry 2006;163:232-9.
18. Simon NM, Otto MW, Weiss RD, et al. Pharmacotherapy for bipolar disorder and comorbid conditions: baseline data from STEP-BD. J Clin Psychopharmacol 2004;24:512-20.
19. Ghaemi SN, Hsu DJ, Soldani F, Goodwin FK. Antidepressants in bipolar disorder: the case for caution. Bipolar Disord 2003;5:421-33.
20. Thase ME, Jonas A, Khan A, et al. Aripiprazole monotherapy in nonpsychotic bipolar I depression: results of 2 randomized, placebo-controlled studies. J Clin Psychopharmacol 2008;28:13-20.
21. Nierenberg AA, Ostacher MJ, Calabrese JR, et al. Treatment-resistant bipolar depression: a STEP-BD equipoise randomized effectiveness trial of antidepressant augmentation with lamotrigine, inositol, or risperidone. Am J Psychiatry 2006;163:210-6.
22. Frye MA, Grunze H, Suppes T, et al. A placebo-controlled evaluation of adjunctive modafinil in the treatment of bipolar depression. Am J Psychiatry 2007;164:1242-9.
23. Colom F, Vieta E, Martinez-Aran A, et al. A randomized trial on the efficacy of group psychoeducation in the prophylaxis of recurrences in bipolar patients whose disease is in remission. Arch Gen Psychiatry 2003;60:402-7.
24. Sachs GS, Nierenberg AA, Calabrese JR, et al. Effectiveness of adjunctive antidepressant treatment for bipolar depression. N Engl J Med 2007;356:1711-22.
25. Frank E, Gonzalez JM, Fagiolini A. The importance of routine for preventing recurrence in bipolar disorder. Am J Psychiatry 2006;163:981-5.
26. Nierenberg AA, Ostacher MJ, Borrelli DJ, et al. The integration of measurement and management for the treatment of bipolar disorder: a STEP-BD model of collaborative care in psychiatry. J Clin Psychiatry 2006;67(suppl 11):3-7.
Chronic nonmalignant pain: How to ‘turn down’ its physiologic triggers
Mrs. A, age 50, reports recurrent headaches and neck pain from a motor vehicle accident in 1999. At the time, MRI revealed degenerative changes at the C5-C6 vertebrae without bony stenosis or spinal injury. Treatment consisted of conservative measures and physical therapy; she was not a candidate for surgical intervention.
Although Mrs. A can manage activities of daily living, pain prevents her from pastimes she previously enjoyed, including painting and pottery, and is causing problems in her marriage.
Mrs. A’s pain became much worse approximately 1 year ago. In the past year, its severity has lead to multiple clinical presentations and consultations. She uses transdermal fentanyl, 75 mcg/hr every 72 hours, and acetaminophen/ hydrocodone, 5 mg/500 mg every 4 hours up to 6 times a day for breakthrough pain. Even so, she still rates her pain as 7 on a 10-point scale.
Pain is a complex perception with psychological and sensory components. It is the most common reason patients seek treatment at ambulatory medical settings.1 Most pain remits spontaneously or responds to simple treatment, but up to 25% of symptoms remain chronic.1
Chronic pain—defined as pain at ≥1 anatomic sites for ≥6 months—can substantially impair adaptation and vocational and interpersonal functioning. Treatments that focus solely on analgesics are shortsighted and often of limited benefit. Patients with chronic pain need a rehabilitative approach that incorporates psychiatric and psychological intervention.
Complex chronic pain
Most individuals with chronic pain can maintain basic functioning, work, relationships, and interests. They work with healthcare providers and obtain relief from medications or other interventions.
Some, however, are preoccupied with—and entirely debilitated by—their pain. For them, life revolves around the pain and perceived disability. Many if not all aspects of this patient’s life are contingent on pain and fears it might worsen.2 Preoccupation with pain can profoundly affect social activities and prevent employment. The patient may become dependent on others, and being a patient can become a primary psychosocial state. A chronic pain patient also may become increasingly preoccupied with medication use and possibly abuse.
- a general medical condition
- psychological factors
- both.
Pain disorder criteria often are perceived as insufficiently operationalized—there is no checklist of symptoms that collectively define the syndrome.5,6 The clinician must infer whether—and to what extent—psychological factors are involved in the pain.5 There are no guidelines to help psychiatrists ascertain whether psychological factors “have an important role” in pain (criteria C) or if pain is “not better accounted for” by a mood disorder (criteria E).6 This distinction can be indecipherable because of frequent comorbidity of mood disturbances with pain.7,8 Some clinicians have suggested that pain disorder be removed from the somato-form disorder classification and instead confined to Axis III.9
Table 1
DSM-IV-TR diagnostic criteria for pain disorder
| A. Pain in ≥1 anatomical sites |
| B. Produces distress or impairs social, occupational, or other functioning |
| C. Psychological factors have an important role in pain onset, severity, exacerbation, or maintenance |
| D. Not intentionally produced or feigned (as in factitious disorder or malingering) |
| E. Not better accounted for by a mood, anxiety, or psychotic disorder and does not meet criteria for dyspareunia |
| Subtypes |
| Pain disorder associated with psychological factors, which are judged to have the major role in pain onset, severity, exacerbation, or maintenance |
| Pain disorder associated with both psychological factors and a general medical condition, which are judged to have important roles in pain onset, severity, exacerbation, or maintenance |
| Pain disorder associated with a general medical condition.* If psychological factors are present, they do not have a major role in pain onset, severity, exacerbation, or maintenance |
| * Not considered a mental disorder (encoded on Axis III) Source: Adapted from Diagnostic and statistical manual of mental disorders. 4th ed, text rev. Washington, DC: American Psychiatric Association; 2000 |
What are the risk factors?
Psychological and social covariates play a substantial role in the chronic pain experience (Table 2). How patients experience chronic pain also is influenced by personality and premorbid, semi-dormant characteristics that become activated by the stress of unremitting pain.7
- mood
- thought patterns
- perceptions
- coping abilities
- personality.
Table 2
Patient factors that contribute to or perpetuate chronic pain
| Poor modulation of emotions (anger, depression, anxiety) |
| Somatization (using pain to avoid confl icts, express anger, or punish others) |
| Problematic cognitive styles (catastrophizing, perceived loss of control) |
| Poor coping skills |
| Psychiatric comorbidities |
Social/interpersonal variables:
|
Reinforcement for remaining sick and/or disabled:
|
| Source: Adapted from reference 3 |
CASE CONTINUED: Underlying causes
Psychological and psychosocial factors appear to play an important role in Mrs. A’s pain. After her husband’s job was restructured, the couple moved away from Mrs. A’s mother, which she found distressing. Additionally, Mrs. A reports that her son has incurred substantial gambling debt.
Mrs. A admits she has “a hard time” accepting these events, but she cannot acknowledge anger or frustration. She avoids questions about such feelings and focuses on her pain. She reports, “The pain is always there and ruins my entire life. Absolutely nothing gives me relief.”
She does not endorse depressive or psychotic symptoms. She sometimes has passive thoughts of death when she feels hopeless about her persistent pain, but she vehemently denies suicidal ideas, intent, or plans. She has smoked 1 pack of cigarettes per day for 12 years but denies alcohol abuse or use of illicit substances.
Biopsychosocial assessment
Assessing a chronic pain patient includes evaluating somatic, psychological, and social factors (Table 3).3 A biopsychosocial approach recognizes that the patient’s experience of pain, presentation, and response to treatment are determined by the interaction of:
- biological factors
- the patient’s psychological makeup
- psychological comorbidities
- the extent of social support
- extenuating environmental circumstances.3,10
A thorough psychiatric assessment may reveal psychiatric comorbidity and psychological conditions that mediate pain.8 Recognizing and treating coexisting psychiatric disorders often will enhance effective pain management.
Subsyndromal psychological factors—such as troubling affective states, problematic cognitive styles,14 and ineffective coping strategies and interpersonal skills—can accompany pain. If unattended, such factors can heighten the patient’s pain awareness and compromise rehabilitation.
For example, patients such as Mrs. A can aggravate pain by catastrophizing.15 Having a tendency to exaggerate pain and the significance of related life events interferes with their ability to attend to matters within their control and pursue productive activities.16 Catastrophizing is associated with increased pain and perceived disability, poor adjustment to pain, and marked emotional distress.17,18
How pain shapes beliefs. Pain can shape the manner with which patients make sense of events in their lives by altering the way they perceive themselves and the world. Problematic beliefs of the self (inadequacy and helplessness), of the world (dangerousness), and of the future (hopelessness) can produce significant distress. A patient with such beliefs may experience a loss of self-esteem, self-efficacy, and connections with others and may experience marked disappointment and disillusionment.
- substance abuse
- nonadherence with treatment
- withdrawal from support systems
- incapacitating emotional states, such as marked dysphoria, anger, or anxiety.
Table 3
Biopsychosocial assessment of chronic pain patients: 3 components
| Somatic factors |
| Determine pain onset/duration, location, quality, intensity, associated features, aggravating and alleviating factors |
| Single-dimension pain rating scales, such as Numeric Rating Scale or Visual Analog Scale |
| Review prescribed and over-the-counter analgesic use (adherence, excess use, impact on functional adaptation) |
| Psychological factors |
| Mood and affect, cognitive content and processes, coping skills |
| Psychiatric comorbidities (substance abuse/dependence; anxiety, sleep, and somatoform disorders; delirium; depression; sexual dysfunction) |
| Suicide risk assessment |
| Multidimensional pain rating scales, such as Coping Strategies Questionnaire or Multidimensional Pain Inventory |
| Social factors |
| Impact on relationships, including capacity for intimacy, mutuality, and sexuality |
| Impact on activities of daily living, vocational and recreational functioning |
| Determine functions patient can perform despite pain |
| Source: Adapted from reference 3 |
CASE CONTINUED: Multifaceted treatment
You prescribe amitriptyline, 20 mg at bed-time, for pain and refer Mrs. A for cognitive-behavioral therapy (CBT). The emphasis of therapy is to identify affective states and cognitive distortions that are temporally related to pain exacerbations, to develop coping skills to deal with stressors, and to effectively express her anger. Mrs. A learns relaxation techniques and self-hypnosis to reduce distress. These measures help reduce her pain severity ratings to 3 on a 10-point scale. She also participates in physical therapy and yoga classes, which increase her endurance.
Psychiatrists’ role in treatment
Many chronic nonmalignant pain syndromes—including arthritic conditions, back pain, and fibromyalgia—are tenacious and not easily cured. Treatment goals are to relieve pain and maximize the patient’s functioning and quality of life while minimizing risks of iatrogenic harm. As part of a biopsychosocial approach to care:
- diagnose and treat psychiatric comorbidities
- assess responses to treatment interventions
- refine treatment measures when patients do not achieve functional and adaptational goals
- initiate pharmacologic interventions for pain
- address subsyndromal emotional and cognitive impediments to functional restoration.
In initial CBT sessions, the goal is to elicit the patient’s:
- perception of pain
- life situations
- beliefs about his or her life, relationships, and the future
- coping measures.
Self-regulatory techniques—including relaxation training, biofeedback, and hypnosis—can facilitate relaxation and “turn down” the physiologic triggers that cause and perpetuate pain.25,26 Hypnosis can lead to dissociative states that modify how a patient experiences pain. There is modest evidence that self-regulatory techniques are effective for treating pain.27,28
Pharmacotherapy. Multiple pathophysiologic mechanisms—including ion channel up-regulation, spinal hyperexcitability, and descending neurotransmitter pathway impairment—play a role in chronic pain states. Several classes of psychoactive agents can mitigate pain (Table 4), and some psychotropics are FDA-approved for specific pain conditions (Table 5).
Individualize medication selection, considering:
- cost
- ease of use
- tolerability
- interactions with coadministered medications
- clinical comorbidities.
- opioid therapy fails
- patients become dependent on escalating doses of opioids.
Antidepressants influence pain by blocking monoamine reuptake. Those that influence noradrenergic and serotonergic transmission may have greater analgesic effects than those that affect serotonin or norepinephrine reuptake alone.31-33
Anticonvulsants mitigate pain by influencing sodium or calcium channel regulation, GABA activity, or combinations of the 3.
In randomized controlled trials that included patients with diabetic and postherpetic neuropathies:
- one-third of patients achieved ≥50% pain relief with tricyclic antidepressants (TCAs) or anticonvulsants
- adverse effects were slightly more common with TCAs.34,35
Because antidepressants and anticonvulsants have different presumed mechanisms of action for pain relief, anticonvulsants might be useful for patients whose pain persists despite optimal antidepressant dosing or for whom antidepressants are in-tolerable. Alternately, coadministering antidepressants and anticonvulsants might capitalize on complimentary mechanisms of action. With coadministration, lower doses may be sufficiently analgesic and avoid adverse effects.
Benzodiazepines have been used short-term to mitigate muscle spasm pain as in fibromyalgia, phantom limb pain, and restless legs syndrome.36,37 Long-term benzodiazepine use can lead to low activity levels, high use of ambulatory medical services, and high disability levels, however.38 if required for muscle spasm or restless legs syndrome, benzodiazepines may best be confined to short-term use.
Antipsychotics. Limited studies have evaluated antipsychotics’ efficacy for chronic pain.39,40 Some have been found to be useful in neuropathic pain.40 Antipsychotics are seldom used to treat pain because of limited efficacy data, potential side effects, and an abundance of alternate agents. Because risks—most notably extrapyramidal side effects and tardive dyskinesia—appear to outweigh analgesic efficacy, I would confine antipsychotics to pain patients with delirium or psychosis. Antipsychotics’ potential role in treating refractory pain might warrant further investigation.40
Stimulants may reduce sedation, dysphoria, and cognitive inefficiency that can accompany opioid use.
Table 4
Uses of psychotropics in patients with chronic pain
| Class/drug | Uses | Limitations |
|---|---|---|
| Antidepressants | Neuropathic pain, tension and migraine headache, FM, functional GI disorders, pain comorbid with depression/anxiety | NE/5-HT reuptake inhibitors are most effective for analgesia; side effects (TCAs may be least tolerable); drug interactions |
| Anticonvulsants | Neuropathic pain, migraine headache, central pain, phantom limb pain | Side effects (sedation, motor and GI effects, rash); drug interactions |
| Benzodiazepines | Muscle relaxation, restless legs syndrome, anxiety, insomnia | Abuse/dependence potential; sedation |
| Lithium | Cluster headache prophylaxis | Not effective for episodic cluster headache; risk of toxicity if dehydration occurs or with certain drug combinations |
| Stimulants | Opioid analgesia augmentation, opioid-induced fatigue and sedation | Abuse/dependence potential; overstimulation, anorexia, insomnia |
| Stimulants | Opioid analgesia augmentation, opioid-induced fatigue and sedation | Abuse/dependence potential; overstimulation, anorexia, insomnia |
| Antipsychotics | Neuropathic pain, migraine, cancer pain, delirium | Limited data; risks such as EPS and TD may outweigh benefi ts |
| EPS: extrapyramidal symptoms; FM: fibromyalgia; GI: gastrointestinal; NE: norepinephrine; 5-HT: serotonin; TCAs: tricyclic antidepressants; TD: tardive dyskinesia | ||
| Source: Adapted from reference 3 | ||
Table 5
Psychotropics approved for managing pain
| Drug | Indication |
|---|---|
| Carbamazepine | Trigeminal neuralgia |
| Divalproex | Migraine prophylaxis |
| Duloxetine | Diabetic neuropathy |
| Gabapentin | Postherpetic neuralgia |
| Pregabalin | Postherpetic neuralgia, diabetic neuropathy, fibromyalgia |
| Source: Adapted from reference 3 | |
- International Association for the Study of Pain. www.iasp-pain.org.
- Leo RJ. Clinical manual of pain management in psychiatry. Washington, DC: American Psychiatric Publishing; 2007.
- Loeser JD, Butler SH, Chapman CR, Turk DC. Bonica’s management of pain. 3rd ed. Philadelphia, PA: Lippincott, Williams & Wilkins; 2001.
- Acetaminophen/hydrocodone • Lortab, others
- Amitriptyline • Elavil, Endep
- Carbamazepine • Tegretol
- Divalproex • Depakote
- Duloxetine • Cymbalta
- Fentanyl transdermal • Duragesic
- Gabapentin • Neurontin
- Lithium • Eskalith, Lithobid
- Pregabalin • Lyrica
Dr. Leo reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Schappert SM. National Ambulatory Medical Care Survey: 1989 summary. Vital Health Stat 13 1992;(110):1-80.
2. Sternbach RA. Pain patients: traits and treatment. New York, NY: Academic Press; 1974.
3. Leo RJ. Clinical manual of pain management in psychiatry. Washington, DC: American Psychiatric Publishing; 2007.
4. Aigner M, Bach M. Clinical utility of DSM-IV pain disorder. Compr Psychiatry 1999;40(5):353-7.
5. Boland RJ. How could the validity of the DSM-IV pain disorder be improved in reference to the concept that it is supposed to identify? Curr Pain Headache Rep 2002;6(1):23-9.
6. Sullivan MD. DSM-IV pain disorder: a case against the diagnosis. Int Rev Psychiatry 2000;12:91-8.
7. Dersh J, Polatin PB, Gatchel RJ. Chronic pain and psychopathology: research findings and theoretical considerations. Psychosom Med 2002;64:773-86.
8. Fishbain DA. Approaches to treatment decisions for psychiatric comorbidity in the management of the chronic pain patient. Med Clin North Am 1999;83:737-60.
9. Mayou R, Kirmayer LJ, Simon G, et al. Somatoform disorders: time for a new approach in DSM-V. Am J Psychiatry 2005;162(5):847-55.
10. Gallagher RM. Treatment planning in pain medicine—integrating medical, physical, and behavioral therapies. Med Clin North Am 1999;83(3):823-49.
11. Jensen MP, Karoly P, Braver S. The measurement of clinical pain intensity: a comparison of six methods. Pain 1986;27:117-26.
12. Rosenstiel AK, Keefe FJ. The use of coping strategies in chronic low back pain patients: relationship to patient characteristics and current adjustment. Pain 1983;17:33-44.
13. Kerns RD, Turk DC, Rudy TE. The West Haven-Yale multidimensional pain inventory (WHYMPI). Pain 1985;23:345-56.
14. Jensen MP, Turner JA, Romano JM, et al. Coping with chronic pain: a critical review. Pain 1991;47:249-83.
15. Sullivan MJL, Stanish W, Waite H, et al. Catastrophizing, pain, and disability in patients with soft-tissue injuries. Pain 1998;77:253-60.
16. Crombez G, Eccleston C, Baeyens F, et al. When somatic information threatens, catastrophic thinking enhances attentional interference. Pain 1998;75:187-98.
17. Hasenbring M, Hallner D, Klasen B. Psychological mechanisms in the transition from acute to chronic pain: over-or underrated? Schmerz. 2001;15:442-7.
18. Sullivan MJ, Thorn B, Haythornthwaite JA, et al. Theoretical perspectives on the relation between catastrophizing and pain. Clin J Pain 2001;17:52-64.
19. Arnstein P. The mediation of disability by self efficacy in different samples of chronic pain patients. Disabil Rehabil 2000;22(17):794-801.
20. Fishbain DA. The association of chronic pain and suicide. Semin Clin Neuropsychiatry 1999;4(3):221-7.
21. Astin JA, Beckner W, Soeken K, et al. Psychological interventions for rheumatoid arthritis: a meta-analysis of randomized controlled trials. Arthritis Rheum 2002;47:291-302.
22. Goldenberg DL, Burckhardt C, Crofford L. Management of fibromyalgia syndrome. JAMA 2004;292(19):2388-95.
23. Morley S, Eccleston C, Williams A. Systematic review and meta-analysis of randomized controlled trials of cognitive behaviour therapy and behaviour therapy for chronic pain in adults, excluding headache. Pain 1999;80:1-13.
24. Hoffman BM, Papas RK, Chatkoff DK, Kerns RD. Meta-analysis of psychological interventions for chronic low back pain. Health Psychol 2007;26(1):1-9.
25. Turner JA, Chapman CR. Psychological interventions for chronic pain: a critical review, II: operant conditioning, hypnosis, and cognitive-behavioral therapy. Pain 1982;12:23-46.
26. Turner JA, Chapman CR. Psychological interventions for chronic pain: a critical review, I: relaxation training and biofeedback. Pain 1982;12:1-21.
27. Carroll D, Seers K. Relaxation for the relief of chronic pain: a systematic review. J Adv Nurs 1998;27:476-87.
28. Keel PJ, Bodoky C, Gerhard U, et al. Comparison of integrated group therapy and group relaxation training for fibromyalgia. Clin J Pain 1998;14:232-8.
29. Eriksen J, Sjogren P, Bruera E, et al. Critical issues on opioids in chronic non-cancer pain: an epidemiological study. Pain 2006;125:172-9.
30. Ballantyne JC, Mao J. Opioid therapy for chronic pain. N Engl J Med 2003;349:1943-53.
31. Lynch ME. Antidepressants as analgesics: a review of randomized controlled trials. J Psychiatry Neurosci 2001;26(1):30-6.
32. McQuay HJ, Tramer M, Nye BA, et al. A systematic review of antidepressants in neuropathic pain. Pain 1996;68:217-27.
33. Sussman N. SNRI’s versus SSRI’s: mechanisms of action in treating depression and painful physical symptoms. Prim Care Companion J Clin Psychiatry 2003;5(suppl 7):19-26.
34. Collins SL, Moore RA, McQuay HJ, et al. Antidepressants and anticonvulsants for diabetic neuropathy and postherpetic neuralgia: a quantitative systematic review. J Pain Symptom Manage 2000;20:449-58.
35. McQuay HJ. Neuropathic pain: evidence matters. Eur J Pain 2002;6(suppl A):11-8.
36. Bartusch SL, Sanders BJ, D’Alessio JG, et al. Clonazepam for the treatment of lancinating phantom limb pain. Clin J Pain 1996;12:59-62.
37. Dellemijn PL, Fields HL. Do benzodiazepines have a role in chronic pain management? Pain 1994;57:137-52.
38. Ciccone DS, Just N, Bandilla EB, et al. Psychological correlates of opioid use in patients with chronic nonmalignant pain: a preliminary test of the downhill spiral hypothesis. J Pain Symptom Manage 2000;20:180-92.
39. Gomez-Perez FJ, Rull JA, Dies H, et al. Nortriptyline and fluphenazine in the symptomatic treatment of diabetic neuropathy: a double-blind cross-over study. Pain 1985;23:395-400.
40. Fishbain DA, Cutler RB, Lewis J, et al. Do the second-generation “atypical neuroleptics” have analgesic properties? A structured evidence-based review. Pain Med 2004;5:359-65.
Mrs. A, age 50, reports recurrent headaches and neck pain from a motor vehicle accident in 1999. At the time, MRI revealed degenerative changes at the C5-C6 vertebrae without bony stenosis or spinal injury. Treatment consisted of conservative measures and physical therapy; she was not a candidate for surgical intervention.
Although Mrs. A can manage activities of daily living, pain prevents her from pastimes she previously enjoyed, including painting and pottery, and is causing problems in her marriage.
Mrs. A’s pain became much worse approximately 1 year ago. In the past year, its severity has lead to multiple clinical presentations and consultations. She uses transdermal fentanyl, 75 mcg/hr every 72 hours, and acetaminophen/ hydrocodone, 5 mg/500 mg every 4 hours up to 6 times a day for breakthrough pain. Even so, she still rates her pain as 7 on a 10-point scale.
Pain is a complex perception with psychological and sensory components. It is the most common reason patients seek treatment at ambulatory medical settings.1 Most pain remits spontaneously or responds to simple treatment, but up to 25% of symptoms remain chronic.1
Chronic pain—defined as pain at ≥1 anatomic sites for ≥6 months—can substantially impair adaptation and vocational and interpersonal functioning. Treatments that focus solely on analgesics are shortsighted and often of limited benefit. Patients with chronic pain need a rehabilitative approach that incorporates psychiatric and psychological intervention.
Complex chronic pain
Most individuals with chronic pain can maintain basic functioning, work, relationships, and interests. They work with healthcare providers and obtain relief from medications or other interventions.
Some, however, are preoccupied with—and entirely debilitated by—their pain. For them, life revolves around the pain and perceived disability. Many if not all aspects of this patient’s life are contingent on pain and fears it might worsen.2 Preoccupation with pain can profoundly affect social activities and prevent employment. The patient may become dependent on others, and being a patient can become a primary psychosocial state. A chronic pain patient also may become increasingly preoccupied with medication use and possibly abuse.
- a general medical condition
- psychological factors
- both.
Pain disorder criteria often are perceived as insufficiently operationalized—there is no checklist of symptoms that collectively define the syndrome.5,6 The clinician must infer whether—and to what extent—psychological factors are involved in the pain.5 There are no guidelines to help psychiatrists ascertain whether psychological factors “have an important role” in pain (criteria C) or if pain is “not better accounted for” by a mood disorder (criteria E).6 This distinction can be indecipherable because of frequent comorbidity of mood disturbances with pain.7,8 Some clinicians have suggested that pain disorder be removed from the somato-form disorder classification and instead confined to Axis III.9
Table 1
DSM-IV-TR diagnostic criteria for pain disorder
| A. Pain in ≥1 anatomical sites |
| B. Produces distress or impairs social, occupational, or other functioning |
| C. Psychological factors have an important role in pain onset, severity, exacerbation, or maintenance |
| D. Not intentionally produced or feigned (as in factitious disorder or malingering) |
| E. Not better accounted for by a mood, anxiety, or psychotic disorder and does not meet criteria for dyspareunia |
| Subtypes |
| Pain disorder associated with psychological factors, which are judged to have the major role in pain onset, severity, exacerbation, or maintenance |
| Pain disorder associated with both psychological factors and a general medical condition, which are judged to have important roles in pain onset, severity, exacerbation, or maintenance |
| Pain disorder associated with a general medical condition.* If psychological factors are present, they do not have a major role in pain onset, severity, exacerbation, or maintenance |
| * Not considered a mental disorder (encoded on Axis III) Source: Adapted from Diagnostic and statistical manual of mental disorders. 4th ed, text rev. Washington, DC: American Psychiatric Association; 2000 |
What are the risk factors?
Psychological and social covariates play a substantial role in the chronic pain experience (Table 2). How patients experience chronic pain also is influenced by personality and premorbid, semi-dormant characteristics that become activated by the stress of unremitting pain.7
- mood
- thought patterns
- perceptions
- coping abilities
- personality.
Table 2
Patient factors that contribute to or perpetuate chronic pain
| Poor modulation of emotions (anger, depression, anxiety) |
| Somatization (using pain to avoid confl icts, express anger, or punish others) |
| Problematic cognitive styles (catastrophizing, perceived loss of control) |
| Poor coping skills |
| Psychiatric comorbidities |
Social/interpersonal variables:
|
Reinforcement for remaining sick and/or disabled:
|
| Source: Adapted from reference 3 |
CASE CONTINUED: Underlying causes
Psychological and psychosocial factors appear to play an important role in Mrs. A’s pain. After her husband’s job was restructured, the couple moved away from Mrs. A’s mother, which she found distressing. Additionally, Mrs. A reports that her son has incurred substantial gambling debt.
Mrs. A admits she has “a hard time” accepting these events, but she cannot acknowledge anger or frustration. She avoids questions about such feelings and focuses on her pain. She reports, “The pain is always there and ruins my entire life. Absolutely nothing gives me relief.”
She does not endorse depressive or psychotic symptoms. She sometimes has passive thoughts of death when she feels hopeless about her persistent pain, but she vehemently denies suicidal ideas, intent, or plans. She has smoked 1 pack of cigarettes per day for 12 years but denies alcohol abuse or use of illicit substances.
Biopsychosocial assessment
Assessing a chronic pain patient includes evaluating somatic, psychological, and social factors (Table 3).3 A biopsychosocial approach recognizes that the patient’s experience of pain, presentation, and response to treatment are determined by the interaction of:
- biological factors
- the patient’s psychological makeup
- psychological comorbidities
- the extent of social support
- extenuating environmental circumstances.3,10
A thorough psychiatric assessment may reveal psychiatric comorbidity and psychological conditions that mediate pain.8 Recognizing and treating coexisting psychiatric disorders often will enhance effective pain management.
Subsyndromal psychological factors—such as troubling affective states, problematic cognitive styles,14 and ineffective coping strategies and interpersonal skills—can accompany pain. If unattended, such factors can heighten the patient’s pain awareness and compromise rehabilitation.
For example, patients such as Mrs. A can aggravate pain by catastrophizing.15 Having a tendency to exaggerate pain and the significance of related life events interferes with their ability to attend to matters within their control and pursue productive activities.16 Catastrophizing is associated with increased pain and perceived disability, poor adjustment to pain, and marked emotional distress.17,18
How pain shapes beliefs. Pain can shape the manner with which patients make sense of events in their lives by altering the way they perceive themselves and the world. Problematic beliefs of the self (inadequacy and helplessness), of the world (dangerousness), and of the future (hopelessness) can produce significant distress. A patient with such beliefs may experience a loss of self-esteem, self-efficacy, and connections with others and may experience marked disappointment and disillusionment.
- substance abuse
- nonadherence with treatment
- withdrawal from support systems
- incapacitating emotional states, such as marked dysphoria, anger, or anxiety.
Table 3
Biopsychosocial assessment of chronic pain patients: 3 components
| Somatic factors |
| Determine pain onset/duration, location, quality, intensity, associated features, aggravating and alleviating factors |
| Single-dimension pain rating scales, such as Numeric Rating Scale or Visual Analog Scale |
| Review prescribed and over-the-counter analgesic use (adherence, excess use, impact on functional adaptation) |
| Psychological factors |
| Mood and affect, cognitive content and processes, coping skills |
| Psychiatric comorbidities (substance abuse/dependence; anxiety, sleep, and somatoform disorders; delirium; depression; sexual dysfunction) |
| Suicide risk assessment |
| Multidimensional pain rating scales, such as Coping Strategies Questionnaire or Multidimensional Pain Inventory |
| Social factors |
| Impact on relationships, including capacity for intimacy, mutuality, and sexuality |
| Impact on activities of daily living, vocational and recreational functioning |
| Determine functions patient can perform despite pain |
| Source: Adapted from reference 3 |
CASE CONTINUED: Multifaceted treatment
You prescribe amitriptyline, 20 mg at bed-time, for pain and refer Mrs. A for cognitive-behavioral therapy (CBT). The emphasis of therapy is to identify affective states and cognitive distortions that are temporally related to pain exacerbations, to develop coping skills to deal with stressors, and to effectively express her anger. Mrs. A learns relaxation techniques and self-hypnosis to reduce distress. These measures help reduce her pain severity ratings to 3 on a 10-point scale. She also participates in physical therapy and yoga classes, which increase her endurance.
Psychiatrists’ role in treatment
Many chronic nonmalignant pain syndromes—including arthritic conditions, back pain, and fibromyalgia—are tenacious and not easily cured. Treatment goals are to relieve pain and maximize the patient’s functioning and quality of life while minimizing risks of iatrogenic harm. As part of a biopsychosocial approach to care:
- diagnose and treat psychiatric comorbidities
- assess responses to treatment interventions
- refine treatment measures when patients do not achieve functional and adaptational goals
- initiate pharmacologic interventions for pain
- address subsyndromal emotional and cognitive impediments to functional restoration.
In initial CBT sessions, the goal is to elicit the patient’s:
- perception of pain
- life situations
- beliefs about his or her life, relationships, and the future
- coping measures.
Self-regulatory techniques—including relaxation training, biofeedback, and hypnosis—can facilitate relaxation and “turn down” the physiologic triggers that cause and perpetuate pain.25,26 Hypnosis can lead to dissociative states that modify how a patient experiences pain. There is modest evidence that self-regulatory techniques are effective for treating pain.27,28
Pharmacotherapy. Multiple pathophysiologic mechanisms—including ion channel up-regulation, spinal hyperexcitability, and descending neurotransmitter pathway impairment—play a role in chronic pain states. Several classes of psychoactive agents can mitigate pain (Table 4), and some psychotropics are FDA-approved for specific pain conditions (Table 5).
Individualize medication selection, considering:
- cost
- ease of use
- tolerability
- interactions with coadministered medications
- clinical comorbidities.
- opioid therapy fails
- patients become dependent on escalating doses of opioids.
Antidepressants influence pain by blocking monoamine reuptake. Those that influence noradrenergic and serotonergic transmission may have greater analgesic effects than those that affect serotonin or norepinephrine reuptake alone.31-33
Anticonvulsants mitigate pain by influencing sodium or calcium channel regulation, GABA activity, or combinations of the 3.
In randomized controlled trials that included patients with diabetic and postherpetic neuropathies:
- one-third of patients achieved ≥50% pain relief with tricyclic antidepressants (TCAs) or anticonvulsants
- adverse effects were slightly more common with TCAs.34,35
Because antidepressants and anticonvulsants have different presumed mechanisms of action for pain relief, anticonvulsants might be useful for patients whose pain persists despite optimal antidepressant dosing or for whom antidepressants are in-tolerable. Alternately, coadministering antidepressants and anticonvulsants might capitalize on complimentary mechanisms of action. With coadministration, lower doses may be sufficiently analgesic and avoid adverse effects.
Benzodiazepines have been used short-term to mitigate muscle spasm pain as in fibromyalgia, phantom limb pain, and restless legs syndrome.36,37 Long-term benzodiazepine use can lead to low activity levels, high use of ambulatory medical services, and high disability levels, however.38 if required for muscle spasm or restless legs syndrome, benzodiazepines may best be confined to short-term use.
Antipsychotics. Limited studies have evaluated antipsychotics’ efficacy for chronic pain.39,40 Some have been found to be useful in neuropathic pain.40 Antipsychotics are seldom used to treat pain because of limited efficacy data, potential side effects, and an abundance of alternate agents. Because risks—most notably extrapyramidal side effects and tardive dyskinesia—appear to outweigh analgesic efficacy, I would confine antipsychotics to pain patients with delirium or psychosis. Antipsychotics’ potential role in treating refractory pain might warrant further investigation.40
Stimulants may reduce sedation, dysphoria, and cognitive inefficiency that can accompany opioid use.
Table 4
Uses of psychotropics in patients with chronic pain
| Class/drug | Uses | Limitations |
|---|---|---|
| Antidepressants | Neuropathic pain, tension and migraine headache, FM, functional GI disorders, pain comorbid with depression/anxiety | NE/5-HT reuptake inhibitors are most effective for analgesia; side effects (TCAs may be least tolerable); drug interactions |
| Anticonvulsants | Neuropathic pain, migraine headache, central pain, phantom limb pain | Side effects (sedation, motor and GI effects, rash); drug interactions |
| Benzodiazepines | Muscle relaxation, restless legs syndrome, anxiety, insomnia | Abuse/dependence potential; sedation |
| Lithium | Cluster headache prophylaxis | Not effective for episodic cluster headache; risk of toxicity if dehydration occurs or with certain drug combinations |
| Stimulants | Opioid analgesia augmentation, opioid-induced fatigue and sedation | Abuse/dependence potential; overstimulation, anorexia, insomnia |
| Stimulants | Opioid analgesia augmentation, opioid-induced fatigue and sedation | Abuse/dependence potential; overstimulation, anorexia, insomnia |
| Antipsychotics | Neuropathic pain, migraine, cancer pain, delirium | Limited data; risks such as EPS and TD may outweigh benefi ts |
| EPS: extrapyramidal symptoms; FM: fibromyalgia; GI: gastrointestinal; NE: norepinephrine; 5-HT: serotonin; TCAs: tricyclic antidepressants; TD: tardive dyskinesia | ||
| Source: Adapted from reference 3 | ||
Table 5
Psychotropics approved for managing pain
| Drug | Indication |
|---|---|
| Carbamazepine | Trigeminal neuralgia |
| Divalproex | Migraine prophylaxis |
| Duloxetine | Diabetic neuropathy |
| Gabapentin | Postherpetic neuralgia |
| Pregabalin | Postherpetic neuralgia, diabetic neuropathy, fibromyalgia |
| Source: Adapted from reference 3 | |
- International Association for the Study of Pain. www.iasp-pain.org.
- Leo RJ. Clinical manual of pain management in psychiatry. Washington, DC: American Psychiatric Publishing; 2007.
- Loeser JD, Butler SH, Chapman CR, Turk DC. Bonica’s management of pain. 3rd ed. Philadelphia, PA: Lippincott, Williams & Wilkins; 2001.
- Acetaminophen/hydrocodone • Lortab, others
- Amitriptyline • Elavil, Endep
- Carbamazepine • Tegretol
- Divalproex • Depakote
- Duloxetine • Cymbalta
- Fentanyl transdermal • Duragesic
- Gabapentin • Neurontin
- Lithium • Eskalith, Lithobid
- Pregabalin • Lyrica
Dr. Leo reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Mrs. A, age 50, reports recurrent headaches and neck pain from a motor vehicle accident in 1999. At the time, MRI revealed degenerative changes at the C5-C6 vertebrae without bony stenosis or spinal injury. Treatment consisted of conservative measures and physical therapy; she was not a candidate for surgical intervention.
Although Mrs. A can manage activities of daily living, pain prevents her from pastimes she previously enjoyed, including painting and pottery, and is causing problems in her marriage.
Mrs. A’s pain became much worse approximately 1 year ago. In the past year, its severity has lead to multiple clinical presentations and consultations. She uses transdermal fentanyl, 75 mcg/hr every 72 hours, and acetaminophen/ hydrocodone, 5 mg/500 mg every 4 hours up to 6 times a day for breakthrough pain. Even so, she still rates her pain as 7 on a 10-point scale.
Pain is a complex perception with psychological and sensory components. It is the most common reason patients seek treatment at ambulatory medical settings.1 Most pain remits spontaneously or responds to simple treatment, but up to 25% of symptoms remain chronic.1
Chronic pain—defined as pain at ≥1 anatomic sites for ≥6 months—can substantially impair adaptation and vocational and interpersonal functioning. Treatments that focus solely on analgesics are shortsighted and often of limited benefit. Patients with chronic pain need a rehabilitative approach that incorporates psychiatric and psychological intervention.
Complex chronic pain
Most individuals with chronic pain can maintain basic functioning, work, relationships, and interests. They work with healthcare providers and obtain relief from medications or other interventions.
Some, however, are preoccupied with—and entirely debilitated by—their pain. For them, life revolves around the pain and perceived disability. Many if not all aspects of this patient’s life are contingent on pain and fears it might worsen.2 Preoccupation with pain can profoundly affect social activities and prevent employment. The patient may become dependent on others, and being a patient can become a primary psychosocial state. A chronic pain patient also may become increasingly preoccupied with medication use and possibly abuse.
- a general medical condition
- psychological factors
- both.
Pain disorder criteria often are perceived as insufficiently operationalized—there is no checklist of symptoms that collectively define the syndrome.5,6 The clinician must infer whether—and to what extent—psychological factors are involved in the pain.5 There are no guidelines to help psychiatrists ascertain whether psychological factors “have an important role” in pain (criteria C) or if pain is “not better accounted for” by a mood disorder (criteria E).6 This distinction can be indecipherable because of frequent comorbidity of mood disturbances with pain.7,8 Some clinicians have suggested that pain disorder be removed from the somato-form disorder classification and instead confined to Axis III.9
Table 1
DSM-IV-TR diagnostic criteria for pain disorder
| A. Pain in ≥1 anatomical sites |
| B. Produces distress or impairs social, occupational, or other functioning |
| C. Psychological factors have an important role in pain onset, severity, exacerbation, or maintenance |
| D. Not intentionally produced or feigned (as in factitious disorder or malingering) |
| E. Not better accounted for by a mood, anxiety, or psychotic disorder and does not meet criteria for dyspareunia |
| Subtypes |
| Pain disorder associated with psychological factors, which are judged to have the major role in pain onset, severity, exacerbation, or maintenance |
| Pain disorder associated with both psychological factors and a general medical condition, which are judged to have important roles in pain onset, severity, exacerbation, or maintenance |
| Pain disorder associated with a general medical condition.* If psychological factors are present, they do not have a major role in pain onset, severity, exacerbation, or maintenance |
| * Not considered a mental disorder (encoded on Axis III) Source: Adapted from Diagnostic and statistical manual of mental disorders. 4th ed, text rev. Washington, DC: American Psychiatric Association; 2000 |
What are the risk factors?
Psychological and social covariates play a substantial role in the chronic pain experience (Table 2). How patients experience chronic pain also is influenced by personality and premorbid, semi-dormant characteristics that become activated by the stress of unremitting pain.7
- mood
- thought patterns
- perceptions
- coping abilities
- personality.
Table 2
Patient factors that contribute to or perpetuate chronic pain
| Poor modulation of emotions (anger, depression, anxiety) |
| Somatization (using pain to avoid confl icts, express anger, or punish others) |
| Problematic cognitive styles (catastrophizing, perceived loss of control) |
| Poor coping skills |
| Psychiatric comorbidities |
Social/interpersonal variables:
|
Reinforcement for remaining sick and/or disabled:
|
| Source: Adapted from reference 3 |
CASE CONTINUED: Underlying causes
Psychological and psychosocial factors appear to play an important role in Mrs. A’s pain. After her husband’s job was restructured, the couple moved away from Mrs. A’s mother, which she found distressing. Additionally, Mrs. A reports that her son has incurred substantial gambling debt.
Mrs. A admits she has “a hard time” accepting these events, but she cannot acknowledge anger or frustration. She avoids questions about such feelings and focuses on her pain. She reports, “The pain is always there and ruins my entire life. Absolutely nothing gives me relief.”
She does not endorse depressive or psychotic symptoms. She sometimes has passive thoughts of death when she feels hopeless about her persistent pain, but she vehemently denies suicidal ideas, intent, or plans. She has smoked 1 pack of cigarettes per day for 12 years but denies alcohol abuse or use of illicit substances.
Biopsychosocial assessment
Assessing a chronic pain patient includes evaluating somatic, psychological, and social factors (Table 3).3 A biopsychosocial approach recognizes that the patient’s experience of pain, presentation, and response to treatment are determined by the interaction of:
- biological factors
- the patient’s psychological makeup
- psychological comorbidities
- the extent of social support
- extenuating environmental circumstances.3,10
A thorough psychiatric assessment may reveal psychiatric comorbidity and psychological conditions that mediate pain.8 Recognizing and treating coexisting psychiatric disorders often will enhance effective pain management.
Subsyndromal psychological factors—such as troubling affective states, problematic cognitive styles,14 and ineffective coping strategies and interpersonal skills—can accompany pain. If unattended, such factors can heighten the patient’s pain awareness and compromise rehabilitation.
For example, patients such as Mrs. A can aggravate pain by catastrophizing.15 Having a tendency to exaggerate pain and the significance of related life events interferes with their ability to attend to matters within their control and pursue productive activities.16 Catastrophizing is associated with increased pain and perceived disability, poor adjustment to pain, and marked emotional distress.17,18
How pain shapes beliefs. Pain can shape the manner with which patients make sense of events in their lives by altering the way they perceive themselves and the world. Problematic beliefs of the self (inadequacy and helplessness), of the world (dangerousness), and of the future (hopelessness) can produce significant distress. A patient with such beliefs may experience a loss of self-esteem, self-efficacy, and connections with others and may experience marked disappointment and disillusionment.
- substance abuse
- nonadherence with treatment
- withdrawal from support systems
- incapacitating emotional states, such as marked dysphoria, anger, or anxiety.
Table 3
Biopsychosocial assessment of chronic pain patients: 3 components
| Somatic factors |
| Determine pain onset/duration, location, quality, intensity, associated features, aggravating and alleviating factors |
| Single-dimension pain rating scales, such as Numeric Rating Scale or Visual Analog Scale |
| Review prescribed and over-the-counter analgesic use (adherence, excess use, impact on functional adaptation) |
| Psychological factors |
| Mood and affect, cognitive content and processes, coping skills |
| Psychiatric comorbidities (substance abuse/dependence; anxiety, sleep, and somatoform disorders; delirium; depression; sexual dysfunction) |
| Suicide risk assessment |
| Multidimensional pain rating scales, such as Coping Strategies Questionnaire or Multidimensional Pain Inventory |
| Social factors |
| Impact on relationships, including capacity for intimacy, mutuality, and sexuality |
| Impact on activities of daily living, vocational and recreational functioning |
| Determine functions patient can perform despite pain |
| Source: Adapted from reference 3 |
CASE CONTINUED: Multifaceted treatment
You prescribe amitriptyline, 20 mg at bed-time, for pain and refer Mrs. A for cognitive-behavioral therapy (CBT). The emphasis of therapy is to identify affective states and cognitive distortions that are temporally related to pain exacerbations, to develop coping skills to deal with stressors, and to effectively express her anger. Mrs. A learns relaxation techniques and self-hypnosis to reduce distress. These measures help reduce her pain severity ratings to 3 on a 10-point scale. She also participates in physical therapy and yoga classes, which increase her endurance.
Psychiatrists’ role in treatment
Many chronic nonmalignant pain syndromes—including arthritic conditions, back pain, and fibromyalgia—are tenacious and not easily cured. Treatment goals are to relieve pain and maximize the patient’s functioning and quality of life while minimizing risks of iatrogenic harm. As part of a biopsychosocial approach to care:
- diagnose and treat psychiatric comorbidities
- assess responses to treatment interventions
- refine treatment measures when patients do not achieve functional and adaptational goals
- initiate pharmacologic interventions for pain
- address subsyndromal emotional and cognitive impediments to functional restoration.
In initial CBT sessions, the goal is to elicit the patient’s:
- perception of pain
- life situations
- beliefs about his or her life, relationships, and the future
- coping measures.
Self-regulatory techniques—including relaxation training, biofeedback, and hypnosis—can facilitate relaxation and “turn down” the physiologic triggers that cause and perpetuate pain.25,26 Hypnosis can lead to dissociative states that modify how a patient experiences pain. There is modest evidence that self-regulatory techniques are effective for treating pain.27,28
Pharmacotherapy. Multiple pathophysiologic mechanisms—including ion channel up-regulation, spinal hyperexcitability, and descending neurotransmitter pathway impairment—play a role in chronic pain states. Several classes of psychoactive agents can mitigate pain (Table 4), and some psychotropics are FDA-approved for specific pain conditions (Table 5).
Individualize medication selection, considering:
- cost
- ease of use
- tolerability
- interactions with coadministered medications
- clinical comorbidities.
- opioid therapy fails
- patients become dependent on escalating doses of opioids.
Antidepressants influence pain by blocking monoamine reuptake. Those that influence noradrenergic and serotonergic transmission may have greater analgesic effects than those that affect serotonin or norepinephrine reuptake alone.31-33
Anticonvulsants mitigate pain by influencing sodium or calcium channel regulation, GABA activity, or combinations of the 3.
In randomized controlled trials that included patients with diabetic and postherpetic neuropathies:
- one-third of patients achieved ≥50% pain relief with tricyclic antidepressants (TCAs) or anticonvulsants
- adverse effects were slightly more common with TCAs.34,35
Because antidepressants and anticonvulsants have different presumed mechanisms of action for pain relief, anticonvulsants might be useful for patients whose pain persists despite optimal antidepressant dosing or for whom antidepressants are in-tolerable. Alternately, coadministering antidepressants and anticonvulsants might capitalize on complimentary mechanisms of action. With coadministration, lower doses may be sufficiently analgesic and avoid adverse effects.
Benzodiazepines have been used short-term to mitigate muscle spasm pain as in fibromyalgia, phantom limb pain, and restless legs syndrome.36,37 Long-term benzodiazepine use can lead to low activity levels, high use of ambulatory medical services, and high disability levels, however.38 if required for muscle spasm or restless legs syndrome, benzodiazepines may best be confined to short-term use.
Antipsychotics. Limited studies have evaluated antipsychotics’ efficacy for chronic pain.39,40 Some have been found to be useful in neuropathic pain.40 Antipsychotics are seldom used to treat pain because of limited efficacy data, potential side effects, and an abundance of alternate agents. Because risks—most notably extrapyramidal side effects and tardive dyskinesia—appear to outweigh analgesic efficacy, I would confine antipsychotics to pain patients with delirium or psychosis. Antipsychotics’ potential role in treating refractory pain might warrant further investigation.40
Stimulants may reduce sedation, dysphoria, and cognitive inefficiency that can accompany opioid use.
Table 4
Uses of psychotropics in patients with chronic pain
| Class/drug | Uses | Limitations |
|---|---|---|
| Antidepressants | Neuropathic pain, tension and migraine headache, FM, functional GI disorders, pain comorbid with depression/anxiety | NE/5-HT reuptake inhibitors are most effective for analgesia; side effects (TCAs may be least tolerable); drug interactions |
| Anticonvulsants | Neuropathic pain, migraine headache, central pain, phantom limb pain | Side effects (sedation, motor and GI effects, rash); drug interactions |
| Benzodiazepines | Muscle relaxation, restless legs syndrome, anxiety, insomnia | Abuse/dependence potential; sedation |
| Lithium | Cluster headache prophylaxis | Not effective for episodic cluster headache; risk of toxicity if dehydration occurs or with certain drug combinations |
| Stimulants | Opioid analgesia augmentation, opioid-induced fatigue and sedation | Abuse/dependence potential; overstimulation, anorexia, insomnia |
| Stimulants | Opioid analgesia augmentation, opioid-induced fatigue and sedation | Abuse/dependence potential; overstimulation, anorexia, insomnia |
| Antipsychotics | Neuropathic pain, migraine, cancer pain, delirium | Limited data; risks such as EPS and TD may outweigh benefi ts |
| EPS: extrapyramidal symptoms; FM: fibromyalgia; GI: gastrointestinal; NE: norepinephrine; 5-HT: serotonin; TCAs: tricyclic antidepressants; TD: tardive dyskinesia | ||
| Source: Adapted from reference 3 | ||
Table 5
Psychotropics approved for managing pain
| Drug | Indication |
|---|---|
| Carbamazepine | Trigeminal neuralgia |
| Divalproex | Migraine prophylaxis |
| Duloxetine | Diabetic neuropathy |
| Gabapentin | Postherpetic neuralgia |
| Pregabalin | Postherpetic neuralgia, diabetic neuropathy, fibromyalgia |
| Source: Adapted from reference 3 | |
- International Association for the Study of Pain. www.iasp-pain.org.
- Leo RJ. Clinical manual of pain management in psychiatry. Washington, DC: American Psychiatric Publishing; 2007.
- Loeser JD, Butler SH, Chapman CR, Turk DC. Bonica’s management of pain. 3rd ed. Philadelphia, PA: Lippincott, Williams & Wilkins; 2001.
- Acetaminophen/hydrocodone • Lortab, others
- Amitriptyline • Elavil, Endep
- Carbamazepine • Tegretol
- Divalproex • Depakote
- Duloxetine • Cymbalta
- Fentanyl transdermal • Duragesic
- Gabapentin • Neurontin
- Lithium • Eskalith, Lithobid
- Pregabalin • Lyrica
Dr. Leo reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Schappert SM. National Ambulatory Medical Care Survey: 1989 summary. Vital Health Stat 13 1992;(110):1-80.
2. Sternbach RA. Pain patients: traits and treatment. New York, NY: Academic Press; 1974.
3. Leo RJ. Clinical manual of pain management in psychiatry. Washington, DC: American Psychiatric Publishing; 2007.
4. Aigner M, Bach M. Clinical utility of DSM-IV pain disorder. Compr Psychiatry 1999;40(5):353-7.
5. Boland RJ. How could the validity of the DSM-IV pain disorder be improved in reference to the concept that it is supposed to identify? Curr Pain Headache Rep 2002;6(1):23-9.
6. Sullivan MD. DSM-IV pain disorder: a case against the diagnosis. Int Rev Psychiatry 2000;12:91-8.
7. Dersh J, Polatin PB, Gatchel RJ. Chronic pain and psychopathology: research findings and theoretical considerations. Psychosom Med 2002;64:773-86.
8. Fishbain DA. Approaches to treatment decisions for psychiatric comorbidity in the management of the chronic pain patient. Med Clin North Am 1999;83:737-60.
9. Mayou R, Kirmayer LJ, Simon G, et al. Somatoform disorders: time for a new approach in DSM-V. Am J Psychiatry 2005;162(5):847-55.
10. Gallagher RM. Treatment planning in pain medicine—integrating medical, physical, and behavioral therapies. Med Clin North Am 1999;83(3):823-49.
11. Jensen MP, Karoly P, Braver S. The measurement of clinical pain intensity: a comparison of six methods. Pain 1986;27:117-26.
12. Rosenstiel AK, Keefe FJ. The use of coping strategies in chronic low back pain patients: relationship to patient characteristics and current adjustment. Pain 1983;17:33-44.
13. Kerns RD, Turk DC, Rudy TE. The West Haven-Yale multidimensional pain inventory (WHYMPI). Pain 1985;23:345-56.
14. Jensen MP, Turner JA, Romano JM, et al. Coping with chronic pain: a critical review. Pain 1991;47:249-83.
15. Sullivan MJL, Stanish W, Waite H, et al. Catastrophizing, pain, and disability in patients with soft-tissue injuries. Pain 1998;77:253-60.
16. Crombez G, Eccleston C, Baeyens F, et al. When somatic information threatens, catastrophic thinking enhances attentional interference. Pain 1998;75:187-98.
17. Hasenbring M, Hallner D, Klasen B. Psychological mechanisms in the transition from acute to chronic pain: over-or underrated? Schmerz. 2001;15:442-7.
18. Sullivan MJ, Thorn B, Haythornthwaite JA, et al. Theoretical perspectives on the relation between catastrophizing and pain. Clin J Pain 2001;17:52-64.
19. Arnstein P. The mediation of disability by self efficacy in different samples of chronic pain patients. Disabil Rehabil 2000;22(17):794-801.
20. Fishbain DA. The association of chronic pain and suicide. Semin Clin Neuropsychiatry 1999;4(3):221-7.
21. Astin JA, Beckner W, Soeken K, et al. Psychological interventions for rheumatoid arthritis: a meta-analysis of randomized controlled trials. Arthritis Rheum 2002;47:291-302.
22. Goldenberg DL, Burckhardt C, Crofford L. Management of fibromyalgia syndrome. JAMA 2004;292(19):2388-95.
23. Morley S, Eccleston C, Williams A. Systematic review and meta-analysis of randomized controlled trials of cognitive behaviour therapy and behaviour therapy for chronic pain in adults, excluding headache. Pain 1999;80:1-13.
24. Hoffman BM, Papas RK, Chatkoff DK, Kerns RD. Meta-analysis of psychological interventions for chronic low back pain. Health Psychol 2007;26(1):1-9.
25. Turner JA, Chapman CR. Psychological interventions for chronic pain: a critical review, II: operant conditioning, hypnosis, and cognitive-behavioral therapy. Pain 1982;12:23-46.
26. Turner JA, Chapman CR. Psychological interventions for chronic pain: a critical review, I: relaxation training and biofeedback. Pain 1982;12:1-21.
27. Carroll D, Seers K. Relaxation for the relief of chronic pain: a systematic review. J Adv Nurs 1998;27:476-87.
28. Keel PJ, Bodoky C, Gerhard U, et al. Comparison of integrated group therapy and group relaxation training for fibromyalgia. Clin J Pain 1998;14:232-8.
29. Eriksen J, Sjogren P, Bruera E, et al. Critical issues on opioids in chronic non-cancer pain: an epidemiological study. Pain 2006;125:172-9.
30. Ballantyne JC, Mao J. Opioid therapy for chronic pain. N Engl J Med 2003;349:1943-53.
31. Lynch ME. Antidepressants as analgesics: a review of randomized controlled trials. J Psychiatry Neurosci 2001;26(1):30-6.
32. McQuay HJ, Tramer M, Nye BA, et al. A systematic review of antidepressants in neuropathic pain. Pain 1996;68:217-27.
33. Sussman N. SNRI’s versus SSRI’s: mechanisms of action in treating depression and painful physical symptoms. Prim Care Companion J Clin Psychiatry 2003;5(suppl 7):19-26.
34. Collins SL, Moore RA, McQuay HJ, et al. Antidepressants and anticonvulsants for diabetic neuropathy and postherpetic neuralgia: a quantitative systematic review. J Pain Symptom Manage 2000;20:449-58.
35. McQuay HJ. Neuropathic pain: evidence matters. Eur J Pain 2002;6(suppl A):11-8.
36. Bartusch SL, Sanders BJ, D’Alessio JG, et al. Clonazepam for the treatment of lancinating phantom limb pain. Clin J Pain 1996;12:59-62.
37. Dellemijn PL, Fields HL. Do benzodiazepines have a role in chronic pain management? Pain 1994;57:137-52.
38. Ciccone DS, Just N, Bandilla EB, et al. Psychological correlates of opioid use in patients with chronic nonmalignant pain: a preliminary test of the downhill spiral hypothesis. J Pain Symptom Manage 2000;20:180-92.
39. Gomez-Perez FJ, Rull JA, Dies H, et al. Nortriptyline and fluphenazine in the symptomatic treatment of diabetic neuropathy: a double-blind cross-over study. Pain 1985;23:395-400.
40. Fishbain DA, Cutler RB, Lewis J, et al. Do the second-generation “atypical neuroleptics” have analgesic properties? A structured evidence-based review. Pain Med 2004;5:359-65.
1. Schappert SM. National Ambulatory Medical Care Survey: 1989 summary. Vital Health Stat 13 1992;(110):1-80.
2. Sternbach RA. Pain patients: traits and treatment. New York, NY: Academic Press; 1974.
3. Leo RJ. Clinical manual of pain management in psychiatry. Washington, DC: American Psychiatric Publishing; 2007.
4. Aigner M, Bach M. Clinical utility of DSM-IV pain disorder. Compr Psychiatry 1999;40(5):353-7.
5. Boland RJ. How could the validity of the DSM-IV pain disorder be improved in reference to the concept that it is supposed to identify? Curr Pain Headache Rep 2002;6(1):23-9.
6. Sullivan MD. DSM-IV pain disorder: a case against the diagnosis. Int Rev Psychiatry 2000;12:91-8.
7. Dersh J, Polatin PB, Gatchel RJ. Chronic pain and psychopathology: research findings and theoretical considerations. Psychosom Med 2002;64:773-86.
8. Fishbain DA. Approaches to treatment decisions for psychiatric comorbidity in the management of the chronic pain patient. Med Clin North Am 1999;83:737-60.
9. Mayou R, Kirmayer LJ, Simon G, et al. Somatoform disorders: time for a new approach in DSM-V. Am J Psychiatry 2005;162(5):847-55.
10. Gallagher RM. Treatment planning in pain medicine—integrating medical, physical, and behavioral therapies. Med Clin North Am 1999;83(3):823-49.
11. Jensen MP, Karoly P, Braver S. The measurement of clinical pain intensity: a comparison of six methods. Pain 1986;27:117-26.
12. Rosenstiel AK, Keefe FJ. The use of coping strategies in chronic low back pain patients: relationship to patient characteristics and current adjustment. Pain 1983;17:33-44.
13. Kerns RD, Turk DC, Rudy TE. The West Haven-Yale multidimensional pain inventory (WHYMPI). Pain 1985;23:345-56.
14. Jensen MP, Turner JA, Romano JM, et al. Coping with chronic pain: a critical review. Pain 1991;47:249-83.
15. Sullivan MJL, Stanish W, Waite H, et al. Catastrophizing, pain, and disability in patients with soft-tissue injuries. Pain 1998;77:253-60.
16. Crombez G, Eccleston C, Baeyens F, et al. When somatic information threatens, catastrophic thinking enhances attentional interference. Pain 1998;75:187-98.
17. Hasenbring M, Hallner D, Klasen B. Psychological mechanisms in the transition from acute to chronic pain: over-or underrated? Schmerz. 2001;15:442-7.
18. Sullivan MJ, Thorn B, Haythornthwaite JA, et al. Theoretical perspectives on the relation between catastrophizing and pain. Clin J Pain 2001;17:52-64.
19. Arnstein P. The mediation of disability by self efficacy in different samples of chronic pain patients. Disabil Rehabil 2000;22(17):794-801.
20. Fishbain DA. The association of chronic pain and suicide. Semin Clin Neuropsychiatry 1999;4(3):221-7.
21. Astin JA, Beckner W, Soeken K, et al. Psychological interventions for rheumatoid arthritis: a meta-analysis of randomized controlled trials. Arthritis Rheum 2002;47:291-302.
22. Goldenberg DL, Burckhardt C, Crofford L. Management of fibromyalgia syndrome. JAMA 2004;292(19):2388-95.
23. Morley S, Eccleston C, Williams A. Systematic review and meta-analysis of randomized controlled trials of cognitive behaviour therapy and behaviour therapy for chronic pain in adults, excluding headache. Pain 1999;80:1-13.
24. Hoffman BM, Papas RK, Chatkoff DK, Kerns RD. Meta-analysis of psychological interventions for chronic low back pain. Health Psychol 2007;26(1):1-9.
25. Turner JA, Chapman CR. Psychological interventions for chronic pain: a critical review, II: operant conditioning, hypnosis, and cognitive-behavioral therapy. Pain 1982;12:23-46.
26. Turner JA, Chapman CR. Psychological interventions for chronic pain: a critical review, I: relaxation training and biofeedback. Pain 1982;12:1-21.
27. Carroll D, Seers K. Relaxation for the relief of chronic pain: a systematic review. J Adv Nurs 1998;27:476-87.
28. Keel PJ, Bodoky C, Gerhard U, et al. Comparison of integrated group therapy and group relaxation training for fibromyalgia. Clin J Pain 1998;14:232-8.
29. Eriksen J, Sjogren P, Bruera E, et al. Critical issues on opioids in chronic non-cancer pain: an epidemiological study. Pain 2006;125:172-9.
30. Ballantyne JC, Mao J. Opioid therapy for chronic pain. N Engl J Med 2003;349:1943-53.
31. Lynch ME. Antidepressants as analgesics: a review of randomized controlled trials. J Psychiatry Neurosci 2001;26(1):30-6.
32. McQuay HJ, Tramer M, Nye BA, et al. A systematic review of antidepressants in neuropathic pain. Pain 1996;68:217-27.
33. Sussman N. SNRI’s versus SSRI’s: mechanisms of action in treating depression and painful physical symptoms. Prim Care Companion J Clin Psychiatry 2003;5(suppl 7):19-26.
34. Collins SL, Moore RA, McQuay HJ, et al. Antidepressants and anticonvulsants for diabetic neuropathy and postherpetic neuralgia: a quantitative systematic review. J Pain Symptom Manage 2000;20:449-58.
35. McQuay HJ. Neuropathic pain: evidence matters. Eur J Pain 2002;6(suppl A):11-8.
36. Bartusch SL, Sanders BJ, D’Alessio JG, et al. Clonazepam for the treatment of lancinating phantom limb pain. Clin J Pain 1996;12:59-62.
37. Dellemijn PL, Fields HL. Do benzodiazepines have a role in chronic pain management? Pain 1994;57:137-52.
38. Ciccone DS, Just N, Bandilla EB, et al. Psychological correlates of opioid use in patients with chronic nonmalignant pain: a preliminary test of the downhill spiral hypothesis. J Pain Symptom Manage 2000;20:180-92.
39. Gomez-Perez FJ, Rull JA, Dies H, et al. Nortriptyline and fluphenazine in the symptomatic treatment of diabetic neuropathy: a double-blind cross-over study. Pain 1985;23:395-400.
40. Fishbain DA, Cutler RB, Lewis J, et al. Do the second-generation “atypical neuroleptics” have analgesic properties? A structured evidence-based review. Pain Med 2004;5:359-65.
Did Internet-purchased diet pills cause serotonin syndrome?
Ms. G, age 28, presents to a tertiary care hospital with altered mental status. Six weeks ago she started taking phentermine, 37.5 mg/d, to lose weight. Her body mass index is 24 kg/m2 (normal range), and she obtained the stimulant agent via the Internet. Her family reports Ms. G was very busy in the past week, staying up until 2 AM cleaning. They say she also was irritable with her 5-year-old son.
Two days ago, Ms. G complained of fatigue and nausea without emesis. She went to bed early and did not awaken the next morning. Her sister found her in bed, minimally responsive to verbal stimuli, and brought her to the hospital.
Patients have used phentermine as a weight-reducing agent since the FDA approved this amphetamine-like compound in 1960.1 Phentermine’s mechanism of action is thought to involve dopaminergic, noradrenergic, and serotonergic effects.2 Stimulation of norepinephrine (NE) release is its most potent effect, followed by NE reuptake inhibition, stimulation of dopamine (DA) release, DA reuptake inhibition, stimulation of serotonin (5-HT) release, and 5-HT reuptake inhibition (weak).3
Because phentermine could in theory cause serotonin syndrome,4 its use is contraindicated with monoamine oxidase inhibitors (MAOIs) and not recommended with selective serotonin reuptake inhibitors (SSRIs).5 One case report describes an interaction between fluoxetine and phentermine that appears consistent with serotonin syndrome.6 We are aware of no case reports of serotonin syndrome caused by phentermine alone.
This article reports the case of Ms. G, who presented with probable serotonin syndrome associated with phentermine use and subsequently developed a rapid-onset, superimposed neuroleptic malignant syndrome (NMS). We hypothesize that phentermine use may increase NMS risk through adverse drug events and discuss potential pathophysiologic mechanisms and treatment implications.
Serotonin syndrome vs NMS
Serotonin syndrome is an infrequent and potentially life-threatening adverse drug reaction that presumably results from excess serotonin activity (Box 1).7-10 NMS also is an infrequent and potentially life-threatening neurologic emergency (Box 2).11-18 Similarities between disorders of increased serotonergic activity and disorders of low dopaminergic activity (Table 1) suggest both may result from an imbalance between the serotonergic and dopaminergic systems, which have reciprocal relationships in the CNS.19
Differentiating between serotonin syndrome and NMS is further complicated when both antipsychotics and serotonergic agents may be implicated.20 Clinical trials are not feasible because NMS and serotonin syndrome rarely occur.
Sternbach7 first summarized serotonin syndrome’s clinical presentation in a review of 38 cases. The most frequent clinical features include changes in mental status, restlessness, myoclonus, hyperreflexia, diaphoresis, shivering, and tremor (Table 1).
The clinical syndrome varies in scope and intensity. Animal models suggest the pathophysiologic mechanism involves brainstem and spinal cord inundation with serotonin, acting on 5-HT1A and 5-HT2A receptors. Recent evidence supports a greater role for 5-HT2A receptors.8
Primary treatment calls for discontinuing the suspected serotonergic agent and instituting supportive measures. Case reports also suggest using serotonin receptor antagonists—such as cyproheptadine, methysergide, chlorpromazine, or propranolol—to clinically manage serotonin syndrome, although empiric support is limited.9
The syndrome often improves within 24 hours of primary treatment, although confusion sometimes last for days and death has been reported.10
NMS—characterized by fever, extrapyramidal rigidity, and disturbances of autonomic function and consciousness—was first described with the use of haloperidol.11 Risk factors include catatonia, disorganized presentation, and dehydration.12 NMS is thought to result from deficient compensatory mechanisms following blockade of dopaminergic regulation of muscle tone and autonomic function.13
Although possibly idiosyncratic, the reaction has been associated with:
- intramuscular, higher total dose, or abruptly increasing doses of antipsychotics14
- withdrawal of dopaminergic agents, such as those used to treat Parkinson’s disease.15
Akin to serotonin syndrome, managing NMS focuses on removing the offending agent(s) and providing supportive care. Severe cases require intensive monitoring, aggressive IV hydration, and respiratory support. Dopaminergics such as bromocriptine16 and skeletal muscle relaxants such as dantrolene17 also have been used to manage NMS.
Unlike serotonin syndrome, NMS often resolves slowly (typically >1 week). NMS’ mortality rate of 11% to 38% appears to be declining in recent years, perhaps because it is being recognized more rapidly.18
Signs and symptoms of NMS vs serotonin syndrome
| NMS | Serotonin syndrome | |
|---|---|---|
| Onset | Insidious, days to weeks | Acute (minutes to hours) |
| Resolution | Slow, often >1 week | Improvement or resolution often within 24 hours |
| Autonomic | Fever, tachycardia, diaphoresis, elevated or labile blood pressure, sialorrhea, tachypnea, incontinence | Diaphoresis, shivering, fever, tachycardia, hypertension, mydriasis |
| Gastrointestinal | Dysphagia, elevated transaminases | Diarrhea, nausea, vomiting, elevated ammonia and transaminases |
| Neuromuscular | Rigidity, bradykinesia, dysarthria, dyskinesias, coarse tremor, ataxia, opisthotonos, oculogyric crisis, rhabdomyolysis | Clonus, myoclonus, hyperreflexia, ataxia, incoordination, rigidity, tremor |
| Psychiatric | Altered mental status, stupor, somnolence, mutism | Altered mental status, agitation, hypomania, hyperactivity, restlessness, somnolence (less common) |
| Other | Leukocytosis, elevated creatine kinase (significant), elevated serum creatinine, proteinuria, renal failure, disseminated intravascular coagulation | Leukocytosis (rarely >20K cells/mm3), elevated creatine kinase (less common), disseminated intravascular coagulation, metabolic acidosis |
| NMS: neuroleptic malignant syndrome | ||
| Note: Classically reported symptoms are italicized | ||
CASE CONTINUED: Fever follows haloperidol
Initial workup. Ms. G has no significant medical or psychiatric history. She has no history of seizures, head trauma, changes in mental status, recent travel, tick bites, or mosquito bites. Family history is relevant only for a maternal aunt with a history of 1 seizure. Ms. G is employed and lives with her husband and son. She is not taking other medications, herbal supplements, or vitamins and does not use tobacco, alcohol, caffeine, or illicit drugs.
On admission, she is somnolent and arousable only to painful stimuli. Temperature is 36.7°C, blood pressure 89/58 mm Hg, heart rate 73 bpm, and respirations 21/minute. She does not talk but is cooperative to physical examination, which is otherwise unremarkable.
Neurologic exam also is unremarkable, with no evidence of meningeal irritation, abnormal reflexes, or muscle tone. Serum ammonia (51 µmol/L; normal range 7 to 42 µmol/L) is slightly elevated. Liver function tests, electrolytes, blood urea nitrogen, creatinine, complete blood counts, urinalysis, urine culture, and blood cultures are unremarkable. Ethanol, salicylate, and acetaminophen levels are negative. Evaluation reveals a positive urine drug screen only for amphetamines, attributed to use of phentermine. Chest radiography and head CT are unremarkable.
Electroencephalography (EEG) 17 hours after admission reveals left anterior temporal spikes suggestive of seizure activity lasting 50 seconds. The patient is described as stuporous but arousable during EEG, and diffuse delta slow waves are superimposed on an alpha rhythm with intermittent diffuse delta bursts. Brain MRI is unremarkable.
Despite no clinical evidence of seizure, Ms. G is transferred to the cardiac telemetry ward to monitor for potential side effects from IV phenytoin loading, at which time (24 hours after admission) she is found to have intermittent sinus tachycardia ≤140 bpm.
Antipsychotic therapy. Thirty hours after admission—after phenytoin loading and normalized EEG—Ms. G shows periodic episodes of sudden startling, with repetitive leg shaking. Continuous ankle clonus is present bilaterally. She complains of severe paresthesias in her legs and is unable to urinate on her own.
NMS signs emerge. Forty-eight hours after admission, Ms. G becomes febrile (38.3°C) and shows tachycardia, with heart rate consistently >130 bpm. Her vital signs did not normalize before the fever developed. She remains somnolent and continues to have spastic lower leg and ankle clonus. She shows no seizure activity on video EEG monitoring during later episodes of repetitive leg shaking, approximately 60 hours after admission.
Ms. G receives empiric vancomycin, ceftriaxone, ampicillin, and acyclovir for possible infectious encephalitis, and lumbar puncture is done emergently. Further laboratory tests reveal creatine kinase (CK) elevation (17,282 U/L, from 270 on admission), leukocytosis (white blood cell count 16.1K/mm3, from 7.2K on admission), and elevated transaminases (AST 199 U/L, up from 21 on admission; ALT 84 U/L, up from 19 on admission).
She is transferred to the ICU with a preliminary diagnosis of NMS. Again, continuous EEG monitoring does not show seizure activity. CSF specimen is negative for infection (negative cultures, negative herpes simplex virus PCR, protein 31 mg/dl, glucose 75 mg/dl). She is started on dantrolene, bromocriptine, and levodopa but shows no initial improvement.
Intubation. On hospital day 8, the patient is intubated to protect her airway and placed in a pentobarbital coma for 2 days, with no improvement. On hospital day 9, cyproheptadine, 24 mg/d, is added for possible serotonin syndrome, and continued for 9 days.
On day 11, the addition of IV diazepam, 10 mg per hour, is followed by gradual improvement in rigidity. Ms. G remains on continuous EEG, with no evidence of seizure activity before diazepam was added or after it is tapered off by day 23.
Discharge. Ms. G is extubated on hospital day 18. On day 23 she can follow commands but is not fully oriented, and levodopa, phenytoin, bromocriptine, and dantrolene are tapered off. She is discharged to a rehabilitation facility, where she again requires phenytoin for a witnessed seizure, attributed to anticonvulsant withdrawal.
On follow-up phone interviews 4 and 18 months after hospitalization, Ms. G says she remains seizure-free without taking anticonvulsants. She reports a subjective, interval improvement in cognitive function, which has since returned to baseline.
Evidence for serotonin syndrome
This case involves a young woman with a several-week history of phentermine use for weight reduction who presented with confusion, sedation, mutism, and nausea. She was initially found to have an abnormal EEG, for which she was loaded with the anticonvulsant phenytoin. However, she continued to exhibit altered mental status, myoclonus, and hyperreflexia along with autonomic dysregulation—such as urinary retention and tachycardia—despite a negative EEG on continuous monitoring.
On retrospective review, we believe she likely was experiencing serotonin toxicity from phentermine. She later developed NMS within several hours of receiving the antipsychotic haloperidol.
Even though phentermine is thought to have a relatively weak serotonergic effect,3 it has been shown to markedly increase serotonin efflux in the rat hypothalamus (to a greater degree than the SSRI fluoxetine).23 Although Ms. G did not report having consumed foods or supplements that could have interfered with phentermine’s metabolism, such use could have contributed to or prolonged a serotonin syndrome.20 Phentermine misuse also cannot be ruled out.
Excess phentermine or concomitant use of other serotonergic agents may have precipitated serotonin syndrome. Ms. G’s hyperactivity a few days before she complained of fatigue and somnolence may represent:
- a sign of phentermine intoxication or overuse
- a harbinger of serotonin syndrome, because these symptoms were followed by overt serotonin syndrome signs such as confusion, disorientation, myoclonus, and autonomic dysfunction.
Evidence for NMS
Ms. G received haloperidol because her agitation obstructed urgent evaluation. After several doses, she rapidly developed signs and symptoms highly consistent with NMS. Onset was rapid compared with the typically described, more insidious NMS evolution of 24 to 72 hours, however.25 Rapid NMS onset may have been precipitated in 2 ways:
- dopaminergic (phentermine) withdrawal combined with dopamine antagonist challenge (haloperidol)25,26
- background serotonin syndrome caused by amphetamine (phentermine) predisposing the patient to develop NMS.27
Although phentermine-induced sympathetic hyperactivity also could have predisposed Ms. G to NMS,31 we think this is unlikely because phentermine was discontinued 3 to 4 days before she developed NMS. Nonetheless, sympathetic hyperactivity secondary to phentermine or serotonin syndrome may increase the risk of developing NMS.
Treatment strategy
Because serotonin syndrome and NMS share many clinical findings, differentiating between the 2 syndromes may be difficult, especially when the patient’s medication history does not implicate a specific agent. A detailed history and physical may help distinguish the syndromes. Clonus may be particularly specific and is important in the diagnosis of serotonin syndrome.32 If you are unable to differentiate between serotonin syndrome and NMS in a patient with this acute neurotoxic abnormal behavior syndrome,33 consider a common treatment strategy (Table 2).19,25
In Ms. G’s case, she probably should not have received bromocriptine for NMS,20 given the potential role of serotonin syndrome in precipitating her symptoms.
Case reports support our hypotheses of an increased predilection for NMS with dopaminergic withdrawal or serotonin syndrome. Growing evidence supports the use of chlorpromazine for serotonin syndrome,34 but consider its use contraindicated in patients with NMS.
Table 2
Serotonin syndrome or NMS?
When in doubt, follow 4 management principles
| Avoid serotonin agonists and dopamine antagonists when a patient presents with features of serotonin syndrome or neuroleptic malignant syndrome (NMS) and the diagnosis is unclear20 |
| Provide supportive care with monitoring, cooling blankets as needed, and hydration |
| Avoid using antipsychotics for agitation, when possible; benzodiazepines may be preferable, although their use in NMS is controversial25 |
| Avoid using bromocriptine, given its contraindication in serotonin syndrome, but consider cyproheptadine for the serotonin syndrome component and dantrolene for skeletal muscle rigidity20 |
Related resources
- Carbone JR. The neuroleptic malignant and serotonin syndromes. Emerg Med Clin North Am 2000;18:317-25.
- Gillman PK. The serotonin syndrome and its treatment. J Psychopharmacol 1999;13:100-9.
- Neuroleptic Malignant Syndrome Information Service (NMSIS). www.nmsis.org. NMS hotline for medical professionals (toll-free 888-667-8367) handles calls on NMS, serotonin syndrome, heat stroke, malignant catatonia, and other drug-induced heat-related disorders.
This paper was among those entered in the 2007 Promising New Investigators competition sponsored by the Neuroleptic Malignant Syndrome Information Service (NMSIS). The theme of this year’s competition was “New insights on psychotropic drug safety and side effects.”
Current Psychiatry is honored to publish this peer-reviewed, evidence-based article on a clinically important topic for practicing psychiatrists.
- Acyclovir • Zovirax
- Ampicillin • various
- Bromocriptine • Parlodel
- Ceftriaxone • Rocephin
- Chlorpromazine • Thorazine
- Cyproheptadine • Periactin
- Dantrolene • Dantrium
- Diazepam • Valium
- Dextroamphetamine • Dexedrine
- Fluoxetine • Prozac
- Haloperidol • Haldol
- Levodopa • various
- Methysergide • Sansert
- Pentobarbital • Nembutal
- Phentermine • various
- Phenytoin • Dilantin
- Propranolol • Inderal
- Vancomycin • various
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Mosby’s Drug Consult, 16th ed. St. Louis, MO: Mosby; 2006.
2. McEvoy G. AHFS drug information. Bethesda, MD: American Society of Health-System Pharmacists; 2006.
3. Rothman RB, Baumann MH, Dersch CM, et al. Amphetamine-type central nervous system stimulants release norepinephrine more potently than they release dopamine and serotonin. Synapse 2001;39:32-41.
4. Ener RA, Meglathery SB, Van Decker WA, Gallagher RM. Serotonin syndrome and other serotonergic disorders. Pain Med 2003;4:63-74.
5. Phentermine hydrochloride. Physicians’ Desk Reference, 53rd ed. Montvale, NJ: Medical Economics; 1999:3055-6.
6. Bostwick JM, Brown TM. A toxic reaction from combining fluoxetine and phentermine. J Clin Psychopharmacol 1996;16:189-90.
7. Sternbach H. The serotonin syndrome. Am J Psychiatry 1991;148(6):705-13.
8. Nisijima K, Yoshino T, Yui K, Katoh S. Potent serotonin (5-HT)(2A) receptor antagonists completely prevent the development of hyperthermia in an animal model of the 5-HT syndrome. Brain Res 2001;890:23-31.
9. Mason PJ, Morris VA, Balcezak TJ. Serotonin syndrome. Presentation of 2 cases and review of the literature. Medicine (Baltimore) 2000;79:201-9.
10. Boyer EW, Shannon M. The serotonin syndrome. N Engl J Med 2005;352:1112-20.
11. Delay J, Pichot P, Lemperiere T, et al. [A non-phenothiazine and non-reserpine major neuroleptic, haloperidol, in the treatment of psychoses.] Ann Med Psychol (Paris). 1960;118:145-52.
12. Berardi D, Dell’Atti M, Amore M, et al. Clinical risk factors for neuroleptic malignant syndrome. Hum Psychopharmacol 2002;17:99-102.
13. Pearlman CA. Neuroleptic malignant syndrome: a review of the literature. J Clin Psychopharmacol 1986;6:257-73.
14. Viejo LF, Morales V, Punal P, et al. Risk factors in neuroleptic malignant syndrome. A case-control study. Acta Psychiatr Scand 2003;107:45-9.
15. Ikebe S, Harada T, Hashimoto T, et al. Prevention and treatment of malignant syndrome in Parkinson’s disease: a consensus statement of the Malignant Syndrome Research Group. Parkinsonism Relat Disord 2003;9(suppl 1):S47-9.
16. Mueller PS, Vester JW, Fermaglich J. Neuroleptic malignant syndrome. Successful treatment with bromocriptine. JAMA 1983;249:386-8.
17. Coons DJ, Hillman FJ, Marshall RW. Treatment of neuroleptic malignant syndrome with dantrolene sodium: a case report. Am J Psychiatry 1982;139:944-5.
18. Spivak B, Maline DI, Kozyrev VN, et al. Frequency of neuroleptic malignant syndrome in a large psychiatric hospital in Moscow. Eur Psychiatry 2000;15:330-3.
19. Gerber PE, Lynd LD. Selective serotonin-reuptake inhibitor-induced movement disorders. Ann Pharmacother 1998;32:692-8.
20. Kaufman KR, Levitt MJ, Schiltz JF, Sunderram J. Neuroleptic malignant syndrome and serotonin syndrome in the critical care setting: case analysis. Ann Clin Psychiatry 2006;18:201-4.
21. Spencer DC, Hwang J, Morrell MJ. Fenfluramine-phentermine (Fen-Phen) and seizures: evidence for an association. Epilepsy Behav 2000;1(6):448-52.
22. Mills KC. Serotonin syndrome. A clinical update. Crit Care Clin 1997;13(4):763-83.
23. Tao R, Fray A, Aspley S, et al. Effects on serotonin in rat hypothalamus of D-fenfluramine, aminorex, phentermine and fluoxetine. Eur J Pharmacol 2002;445(1-2):69-81.
24. Gillman PK. Serotonin syndrome: history and risk. Fundam Clin Pharmacol 1998;12:482-91.
25. Bhanushali MJ, Tuite PJ. The evaluation and management of patients with neuroleptic malignant syndrome. Neurol Clin 2004;22:389-411.
26. Ebadi M, Pfeiffer RF, Murrin LC. Pathogenesis and treatment of neuroleptic malignant syndrome. Gen Pharmacol 1990;21:367-86.
27. Green AR, Cross AJ, Goodwin GM. Review of the pharmacology and clinical pharmacology of 3,4-methylenedioxymethamphetamine (MDMA or “Ecstasy”). Psychopharmacology (Berl) 1995;119:247-60.
28. Chayasirisobhon S, Cullis P, Veeramasuneni RR. Occurrence of neuroleptic malignant syndrome in a narcoleptic patient. Hosp Community Psychiatry 1983;34:548-50.
29. Serrano-Dueñas M. Neuroleptic malignant syndrome-like, or—dopaminergic malignant syndrome—due to levodopa therapy withdrawal. Clinical features in 11 patients. Parkinsonism Relat Disord 2003;9:175-8.
30. Kline SS, Mauro LS, Scala-Barnett DM, Zick D. Serotonin syndrome versus neuroleptic malignant syndrome as a cause of death. Clin Pharm 1989;8(7):510-14.
31. Gurrera RJ. Sympathoadrenal hyperactivity and the etiology of neuroleptic malignant syndrome. Am J Psychiatry 1999;156:169-80.
32. Dunkley EJ, Isbister GK, Sibbritt D, et al. The Hunter Serotonin Toxicity Criteria: simple and accurate diagnostic decision rules for serotonin toxicity. QJM 2003;96:635-42.
33. Fink M. Toxic serotonin syndrome or neuroleptic malignant syndrome? Pharmacopsychiatry 1996;29:159-61.
34. Gillman PK. Serotonin syndrome treated with chlorpromazine. J Clin Psychopharmacol 1997;17:128-9.
Ms. G, age 28, presents to a tertiary care hospital with altered mental status. Six weeks ago she started taking phentermine, 37.5 mg/d, to lose weight. Her body mass index is 24 kg/m2 (normal range), and she obtained the stimulant agent via the Internet. Her family reports Ms. G was very busy in the past week, staying up until 2 AM cleaning. They say she also was irritable with her 5-year-old son.
Two days ago, Ms. G complained of fatigue and nausea without emesis. She went to bed early and did not awaken the next morning. Her sister found her in bed, minimally responsive to verbal stimuli, and brought her to the hospital.
Patients have used phentermine as a weight-reducing agent since the FDA approved this amphetamine-like compound in 1960.1 Phentermine’s mechanism of action is thought to involve dopaminergic, noradrenergic, and serotonergic effects.2 Stimulation of norepinephrine (NE) release is its most potent effect, followed by NE reuptake inhibition, stimulation of dopamine (DA) release, DA reuptake inhibition, stimulation of serotonin (5-HT) release, and 5-HT reuptake inhibition (weak).3
Because phentermine could in theory cause serotonin syndrome,4 its use is contraindicated with monoamine oxidase inhibitors (MAOIs) and not recommended with selective serotonin reuptake inhibitors (SSRIs).5 One case report describes an interaction between fluoxetine and phentermine that appears consistent with serotonin syndrome.6 We are aware of no case reports of serotonin syndrome caused by phentermine alone.
This article reports the case of Ms. G, who presented with probable serotonin syndrome associated with phentermine use and subsequently developed a rapid-onset, superimposed neuroleptic malignant syndrome (NMS). We hypothesize that phentermine use may increase NMS risk through adverse drug events and discuss potential pathophysiologic mechanisms and treatment implications.
Serotonin syndrome vs NMS
Serotonin syndrome is an infrequent and potentially life-threatening adverse drug reaction that presumably results from excess serotonin activity (Box 1).7-10 NMS also is an infrequent and potentially life-threatening neurologic emergency (Box 2).11-18 Similarities between disorders of increased serotonergic activity and disorders of low dopaminergic activity (Table 1) suggest both may result from an imbalance between the serotonergic and dopaminergic systems, which have reciprocal relationships in the CNS.19
Differentiating between serotonin syndrome and NMS is further complicated when both antipsychotics and serotonergic agents may be implicated.20 Clinical trials are not feasible because NMS and serotonin syndrome rarely occur.
Sternbach7 first summarized serotonin syndrome’s clinical presentation in a review of 38 cases. The most frequent clinical features include changes in mental status, restlessness, myoclonus, hyperreflexia, diaphoresis, shivering, and tremor (Table 1).
The clinical syndrome varies in scope and intensity. Animal models suggest the pathophysiologic mechanism involves brainstem and spinal cord inundation with serotonin, acting on 5-HT1A and 5-HT2A receptors. Recent evidence supports a greater role for 5-HT2A receptors.8
Primary treatment calls for discontinuing the suspected serotonergic agent and instituting supportive measures. Case reports also suggest using serotonin receptor antagonists—such as cyproheptadine, methysergide, chlorpromazine, or propranolol—to clinically manage serotonin syndrome, although empiric support is limited.9
The syndrome often improves within 24 hours of primary treatment, although confusion sometimes last for days and death has been reported.10
NMS—characterized by fever, extrapyramidal rigidity, and disturbances of autonomic function and consciousness—was first described with the use of haloperidol.11 Risk factors include catatonia, disorganized presentation, and dehydration.12 NMS is thought to result from deficient compensatory mechanisms following blockade of dopaminergic regulation of muscle tone and autonomic function.13
Although possibly idiosyncratic, the reaction has been associated with:
- intramuscular, higher total dose, or abruptly increasing doses of antipsychotics14
- withdrawal of dopaminergic agents, such as those used to treat Parkinson’s disease.15
Akin to serotonin syndrome, managing NMS focuses on removing the offending agent(s) and providing supportive care. Severe cases require intensive monitoring, aggressive IV hydration, and respiratory support. Dopaminergics such as bromocriptine16 and skeletal muscle relaxants such as dantrolene17 also have been used to manage NMS.
Unlike serotonin syndrome, NMS often resolves slowly (typically >1 week). NMS’ mortality rate of 11% to 38% appears to be declining in recent years, perhaps because it is being recognized more rapidly.18
Signs and symptoms of NMS vs serotonin syndrome
| NMS | Serotonin syndrome | |
|---|---|---|
| Onset | Insidious, days to weeks | Acute (minutes to hours) |
| Resolution | Slow, often >1 week | Improvement or resolution often within 24 hours |
| Autonomic | Fever, tachycardia, diaphoresis, elevated or labile blood pressure, sialorrhea, tachypnea, incontinence | Diaphoresis, shivering, fever, tachycardia, hypertension, mydriasis |
| Gastrointestinal | Dysphagia, elevated transaminases | Diarrhea, nausea, vomiting, elevated ammonia and transaminases |
| Neuromuscular | Rigidity, bradykinesia, dysarthria, dyskinesias, coarse tremor, ataxia, opisthotonos, oculogyric crisis, rhabdomyolysis | Clonus, myoclonus, hyperreflexia, ataxia, incoordination, rigidity, tremor |
| Psychiatric | Altered mental status, stupor, somnolence, mutism | Altered mental status, agitation, hypomania, hyperactivity, restlessness, somnolence (less common) |
| Other | Leukocytosis, elevated creatine kinase (significant), elevated serum creatinine, proteinuria, renal failure, disseminated intravascular coagulation | Leukocytosis (rarely >20K cells/mm3), elevated creatine kinase (less common), disseminated intravascular coagulation, metabolic acidosis |
| NMS: neuroleptic malignant syndrome | ||
| Note: Classically reported symptoms are italicized | ||
CASE CONTINUED: Fever follows haloperidol
Initial workup. Ms. G has no significant medical or psychiatric history. She has no history of seizures, head trauma, changes in mental status, recent travel, tick bites, or mosquito bites. Family history is relevant only for a maternal aunt with a history of 1 seizure. Ms. G is employed and lives with her husband and son. She is not taking other medications, herbal supplements, or vitamins and does not use tobacco, alcohol, caffeine, or illicit drugs.
On admission, she is somnolent and arousable only to painful stimuli. Temperature is 36.7°C, blood pressure 89/58 mm Hg, heart rate 73 bpm, and respirations 21/minute. She does not talk but is cooperative to physical examination, which is otherwise unremarkable.
Neurologic exam also is unremarkable, with no evidence of meningeal irritation, abnormal reflexes, or muscle tone. Serum ammonia (51 µmol/L; normal range 7 to 42 µmol/L) is slightly elevated. Liver function tests, electrolytes, blood urea nitrogen, creatinine, complete blood counts, urinalysis, urine culture, and blood cultures are unremarkable. Ethanol, salicylate, and acetaminophen levels are negative. Evaluation reveals a positive urine drug screen only for amphetamines, attributed to use of phentermine. Chest radiography and head CT are unremarkable.
Electroencephalography (EEG) 17 hours after admission reveals left anterior temporal spikes suggestive of seizure activity lasting 50 seconds. The patient is described as stuporous but arousable during EEG, and diffuse delta slow waves are superimposed on an alpha rhythm with intermittent diffuse delta bursts. Brain MRI is unremarkable.
Despite no clinical evidence of seizure, Ms. G is transferred to the cardiac telemetry ward to monitor for potential side effects from IV phenytoin loading, at which time (24 hours after admission) she is found to have intermittent sinus tachycardia ≤140 bpm.
Antipsychotic therapy. Thirty hours after admission—after phenytoin loading and normalized EEG—Ms. G shows periodic episodes of sudden startling, with repetitive leg shaking. Continuous ankle clonus is present bilaterally. She complains of severe paresthesias in her legs and is unable to urinate on her own.
NMS signs emerge. Forty-eight hours after admission, Ms. G becomes febrile (38.3°C) and shows tachycardia, with heart rate consistently >130 bpm. Her vital signs did not normalize before the fever developed. She remains somnolent and continues to have spastic lower leg and ankle clonus. She shows no seizure activity on video EEG monitoring during later episodes of repetitive leg shaking, approximately 60 hours after admission.
Ms. G receives empiric vancomycin, ceftriaxone, ampicillin, and acyclovir for possible infectious encephalitis, and lumbar puncture is done emergently. Further laboratory tests reveal creatine kinase (CK) elevation (17,282 U/L, from 270 on admission), leukocytosis (white blood cell count 16.1K/mm3, from 7.2K on admission), and elevated transaminases (AST 199 U/L, up from 21 on admission; ALT 84 U/L, up from 19 on admission).
She is transferred to the ICU with a preliminary diagnosis of NMS. Again, continuous EEG monitoring does not show seizure activity. CSF specimen is negative for infection (negative cultures, negative herpes simplex virus PCR, protein 31 mg/dl, glucose 75 mg/dl). She is started on dantrolene, bromocriptine, and levodopa but shows no initial improvement.
Intubation. On hospital day 8, the patient is intubated to protect her airway and placed in a pentobarbital coma for 2 days, with no improvement. On hospital day 9, cyproheptadine, 24 mg/d, is added for possible serotonin syndrome, and continued for 9 days.
On day 11, the addition of IV diazepam, 10 mg per hour, is followed by gradual improvement in rigidity. Ms. G remains on continuous EEG, with no evidence of seizure activity before diazepam was added or after it is tapered off by day 23.
Discharge. Ms. G is extubated on hospital day 18. On day 23 she can follow commands but is not fully oriented, and levodopa, phenytoin, bromocriptine, and dantrolene are tapered off. She is discharged to a rehabilitation facility, where she again requires phenytoin for a witnessed seizure, attributed to anticonvulsant withdrawal.
On follow-up phone interviews 4 and 18 months after hospitalization, Ms. G says she remains seizure-free without taking anticonvulsants. She reports a subjective, interval improvement in cognitive function, which has since returned to baseline.
Evidence for serotonin syndrome
This case involves a young woman with a several-week history of phentermine use for weight reduction who presented with confusion, sedation, mutism, and nausea. She was initially found to have an abnormal EEG, for which she was loaded with the anticonvulsant phenytoin. However, she continued to exhibit altered mental status, myoclonus, and hyperreflexia along with autonomic dysregulation—such as urinary retention and tachycardia—despite a negative EEG on continuous monitoring.
On retrospective review, we believe she likely was experiencing serotonin toxicity from phentermine. She later developed NMS within several hours of receiving the antipsychotic haloperidol.
Even though phentermine is thought to have a relatively weak serotonergic effect,3 it has been shown to markedly increase serotonin efflux in the rat hypothalamus (to a greater degree than the SSRI fluoxetine).23 Although Ms. G did not report having consumed foods or supplements that could have interfered with phentermine’s metabolism, such use could have contributed to or prolonged a serotonin syndrome.20 Phentermine misuse also cannot be ruled out.
Excess phentermine or concomitant use of other serotonergic agents may have precipitated serotonin syndrome. Ms. G’s hyperactivity a few days before she complained of fatigue and somnolence may represent:
- a sign of phentermine intoxication or overuse
- a harbinger of serotonin syndrome, because these symptoms were followed by overt serotonin syndrome signs such as confusion, disorientation, myoclonus, and autonomic dysfunction.
Evidence for NMS
Ms. G received haloperidol because her agitation obstructed urgent evaluation. After several doses, she rapidly developed signs and symptoms highly consistent with NMS. Onset was rapid compared with the typically described, more insidious NMS evolution of 24 to 72 hours, however.25 Rapid NMS onset may have been precipitated in 2 ways:
- dopaminergic (phentermine) withdrawal combined with dopamine antagonist challenge (haloperidol)25,26
- background serotonin syndrome caused by amphetamine (phentermine) predisposing the patient to develop NMS.27
Although phentermine-induced sympathetic hyperactivity also could have predisposed Ms. G to NMS,31 we think this is unlikely because phentermine was discontinued 3 to 4 days before she developed NMS. Nonetheless, sympathetic hyperactivity secondary to phentermine or serotonin syndrome may increase the risk of developing NMS.
Treatment strategy
Because serotonin syndrome and NMS share many clinical findings, differentiating between the 2 syndromes may be difficult, especially when the patient’s medication history does not implicate a specific agent. A detailed history and physical may help distinguish the syndromes. Clonus may be particularly specific and is important in the diagnosis of serotonin syndrome.32 If you are unable to differentiate between serotonin syndrome and NMS in a patient with this acute neurotoxic abnormal behavior syndrome,33 consider a common treatment strategy (Table 2).19,25
In Ms. G’s case, she probably should not have received bromocriptine for NMS,20 given the potential role of serotonin syndrome in precipitating her symptoms.
Case reports support our hypotheses of an increased predilection for NMS with dopaminergic withdrawal or serotonin syndrome. Growing evidence supports the use of chlorpromazine for serotonin syndrome,34 but consider its use contraindicated in patients with NMS.
Table 2
Serotonin syndrome or NMS?
When in doubt, follow 4 management principles
| Avoid serotonin agonists and dopamine antagonists when a patient presents with features of serotonin syndrome or neuroleptic malignant syndrome (NMS) and the diagnosis is unclear20 |
| Provide supportive care with monitoring, cooling blankets as needed, and hydration |
| Avoid using antipsychotics for agitation, when possible; benzodiazepines may be preferable, although their use in NMS is controversial25 |
| Avoid using bromocriptine, given its contraindication in serotonin syndrome, but consider cyproheptadine for the serotonin syndrome component and dantrolene for skeletal muscle rigidity20 |
Related resources
- Carbone JR. The neuroleptic malignant and serotonin syndromes. Emerg Med Clin North Am 2000;18:317-25.
- Gillman PK. The serotonin syndrome and its treatment. J Psychopharmacol 1999;13:100-9.
- Neuroleptic Malignant Syndrome Information Service (NMSIS). www.nmsis.org. NMS hotline for medical professionals (toll-free 888-667-8367) handles calls on NMS, serotonin syndrome, heat stroke, malignant catatonia, and other drug-induced heat-related disorders.
This paper was among those entered in the 2007 Promising New Investigators competition sponsored by the Neuroleptic Malignant Syndrome Information Service (NMSIS). The theme of this year’s competition was “New insights on psychotropic drug safety and side effects.”
Current Psychiatry is honored to publish this peer-reviewed, evidence-based article on a clinically important topic for practicing psychiatrists.
- Acyclovir • Zovirax
- Ampicillin • various
- Bromocriptine • Parlodel
- Ceftriaxone • Rocephin
- Chlorpromazine • Thorazine
- Cyproheptadine • Periactin
- Dantrolene • Dantrium
- Diazepam • Valium
- Dextroamphetamine • Dexedrine
- Fluoxetine • Prozac
- Haloperidol • Haldol
- Levodopa • various
- Methysergide • Sansert
- Pentobarbital • Nembutal
- Phentermine • various
- Phenytoin • Dilantin
- Propranolol • Inderal
- Vancomycin • various
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Ms. G, age 28, presents to a tertiary care hospital with altered mental status. Six weeks ago she started taking phentermine, 37.5 mg/d, to lose weight. Her body mass index is 24 kg/m2 (normal range), and she obtained the stimulant agent via the Internet. Her family reports Ms. G was very busy in the past week, staying up until 2 AM cleaning. They say she also was irritable with her 5-year-old son.
Two days ago, Ms. G complained of fatigue and nausea without emesis. She went to bed early and did not awaken the next morning. Her sister found her in bed, minimally responsive to verbal stimuli, and brought her to the hospital.
Patients have used phentermine as a weight-reducing agent since the FDA approved this amphetamine-like compound in 1960.1 Phentermine’s mechanism of action is thought to involve dopaminergic, noradrenergic, and serotonergic effects.2 Stimulation of norepinephrine (NE) release is its most potent effect, followed by NE reuptake inhibition, stimulation of dopamine (DA) release, DA reuptake inhibition, stimulation of serotonin (5-HT) release, and 5-HT reuptake inhibition (weak).3
Because phentermine could in theory cause serotonin syndrome,4 its use is contraindicated with monoamine oxidase inhibitors (MAOIs) and not recommended with selective serotonin reuptake inhibitors (SSRIs).5 One case report describes an interaction between fluoxetine and phentermine that appears consistent with serotonin syndrome.6 We are aware of no case reports of serotonin syndrome caused by phentermine alone.
This article reports the case of Ms. G, who presented with probable serotonin syndrome associated with phentermine use and subsequently developed a rapid-onset, superimposed neuroleptic malignant syndrome (NMS). We hypothesize that phentermine use may increase NMS risk through adverse drug events and discuss potential pathophysiologic mechanisms and treatment implications.
Serotonin syndrome vs NMS
Serotonin syndrome is an infrequent and potentially life-threatening adverse drug reaction that presumably results from excess serotonin activity (Box 1).7-10 NMS also is an infrequent and potentially life-threatening neurologic emergency (Box 2).11-18 Similarities between disorders of increased serotonergic activity and disorders of low dopaminergic activity (Table 1) suggest both may result from an imbalance between the serotonergic and dopaminergic systems, which have reciprocal relationships in the CNS.19
Differentiating between serotonin syndrome and NMS is further complicated when both antipsychotics and serotonergic agents may be implicated.20 Clinical trials are not feasible because NMS and serotonin syndrome rarely occur.
Sternbach7 first summarized serotonin syndrome’s clinical presentation in a review of 38 cases. The most frequent clinical features include changes in mental status, restlessness, myoclonus, hyperreflexia, diaphoresis, shivering, and tremor (Table 1).
The clinical syndrome varies in scope and intensity. Animal models suggest the pathophysiologic mechanism involves brainstem and spinal cord inundation with serotonin, acting on 5-HT1A and 5-HT2A receptors. Recent evidence supports a greater role for 5-HT2A receptors.8
Primary treatment calls for discontinuing the suspected serotonergic agent and instituting supportive measures. Case reports also suggest using serotonin receptor antagonists—such as cyproheptadine, methysergide, chlorpromazine, or propranolol—to clinically manage serotonin syndrome, although empiric support is limited.9
The syndrome often improves within 24 hours of primary treatment, although confusion sometimes last for days and death has been reported.10
NMS—characterized by fever, extrapyramidal rigidity, and disturbances of autonomic function and consciousness—was first described with the use of haloperidol.11 Risk factors include catatonia, disorganized presentation, and dehydration.12 NMS is thought to result from deficient compensatory mechanisms following blockade of dopaminergic regulation of muscle tone and autonomic function.13
Although possibly idiosyncratic, the reaction has been associated with:
- intramuscular, higher total dose, or abruptly increasing doses of antipsychotics14
- withdrawal of dopaminergic agents, such as those used to treat Parkinson’s disease.15
Akin to serotonin syndrome, managing NMS focuses on removing the offending agent(s) and providing supportive care. Severe cases require intensive monitoring, aggressive IV hydration, and respiratory support. Dopaminergics such as bromocriptine16 and skeletal muscle relaxants such as dantrolene17 also have been used to manage NMS.
Unlike serotonin syndrome, NMS often resolves slowly (typically >1 week). NMS’ mortality rate of 11% to 38% appears to be declining in recent years, perhaps because it is being recognized more rapidly.18
Signs and symptoms of NMS vs serotonin syndrome
| NMS | Serotonin syndrome | |
|---|---|---|
| Onset | Insidious, days to weeks | Acute (minutes to hours) |
| Resolution | Slow, often >1 week | Improvement or resolution often within 24 hours |
| Autonomic | Fever, tachycardia, diaphoresis, elevated or labile blood pressure, sialorrhea, tachypnea, incontinence | Diaphoresis, shivering, fever, tachycardia, hypertension, mydriasis |
| Gastrointestinal | Dysphagia, elevated transaminases | Diarrhea, nausea, vomiting, elevated ammonia and transaminases |
| Neuromuscular | Rigidity, bradykinesia, dysarthria, dyskinesias, coarse tremor, ataxia, opisthotonos, oculogyric crisis, rhabdomyolysis | Clonus, myoclonus, hyperreflexia, ataxia, incoordination, rigidity, tremor |
| Psychiatric | Altered mental status, stupor, somnolence, mutism | Altered mental status, agitation, hypomania, hyperactivity, restlessness, somnolence (less common) |
| Other | Leukocytosis, elevated creatine kinase (significant), elevated serum creatinine, proteinuria, renal failure, disseminated intravascular coagulation | Leukocytosis (rarely >20K cells/mm3), elevated creatine kinase (less common), disseminated intravascular coagulation, metabolic acidosis |
| NMS: neuroleptic malignant syndrome | ||
| Note: Classically reported symptoms are italicized | ||
CASE CONTINUED: Fever follows haloperidol
Initial workup. Ms. G has no significant medical or psychiatric history. She has no history of seizures, head trauma, changes in mental status, recent travel, tick bites, or mosquito bites. Family history is relevant only for a maternal aunt with a history of 1 seizure. Ms. G is employed and lives with her husband and son. She is not taking other medications, herbal supplements, or vitamins and does not use tobacco, alcohol, caffeine, or illicit drugs.
On admission, she is somnolent and arousable only to painful stimuli. Temperature is 36.7°C, blood pressure 89/58 mm Hg, heart rate 73 bpm, and respirations 21/minute. She does not talk but is cooperative to physical examination, which is otherwise unremarkable.
Neurologic exam also is unremarkable, with no evidence of meningeal irritation, abnormal reflexes, or muscle tone. Serum ammonia (51 µmol/L; normal range 7 to 42 µmol/L) is slightly elevated. Liver function tests, electrolytes, blood urea nitrogen, creatinine, complete blood counts, urinalysis, urine culture, and blood cultures are unremarkable. Ethanol, salicylate, and acetaminophen levels are negative. Evaluation reveals a positive urine drug screen only for amphetamines, attributed to use of phentermine. Chest radiography and head CT are unremarkable.
Electroencephalography (EEG) 17 hours after admission reveals left anterior temporal spikes suggestive of seizure activity lasting 50 seconds. The patient is described as stuporous but arousable during EEG, and diffuse delta slow waves are superimposed on an alpha rhythm with intermittent diffuse delta bursts. Brain MRI is unremarkable.
Despite no clinical evidence of seizure, Ms. G is transferred to the cardiac telemetry ward to monitor for potential side effects from IV phenytoin loading, at which time (24 hours after admission) she is found to have intermittent sinus tachycardia ≤140 bpm.
Antipsychotic therapy. Thirty hours after admission—after phenytoin loading and normalized EEG—Ms. G shows periodic episodes of sudden startling, with repetitive leg shaking. Continuous ankle clonus is present bilaterally. She complains of severe paresthesias in her legs and is unable to urinate on her own.
NMS signs emerge. Forty-eight hours after admission, Ms. G becomes febrile (38.3°C) and shows tachycardia, with heart rate consistently >130 bpm. Her vital signs did not normalize before the fever developed. She remains somnolent and continues to have spastic lower leg and ankle clonus. She shows no seizure activity on video EEG monitoring during later episodes of repetitive leg shaking, approximately 60 hours after admission.
Ms. G receives empiric vancomycin, ceftriaxone, ampicillin, and acyclovir for possible infectious encephalitis, and lumbar puncture is done emergently. Further laboratory tests reveal creatine kinase (CK) elevation (17,282 U/L, from 270 on admission), leukocytosis (white blood cell count 16.1K/mm3, from 7.2K on admission), and elevated transaminases (AST 199 U/L, up from 21 on admission; ALT 84 U/L, up from 19 on admission).
She is transferred to the ICU with a preliminary diagnosis of NMS. Again, continuous EEG monitoring does not show seizure activity. CSF specimen is negative for infection (negative cultures, negative herpes simplex virus PCR, protein 31 mg/dl, glucose 75 mg/dl). She is started on dantrolene, bromocriptine, and levodopa but shows no initial improvement.
Intubation. On hospital day 8, the patient is intubated to protect her airway and placed in a pentobarbital coma for 2 days, with no improvement. On hospital day 9, cyproheptadine, 24 mg/d, is added for possible serotonin syndrome, and continued for 9 days.
On day 11, the addition of IV diazepam, 10 mg per hour, is followed by gradual improvement in rigidity. Ms. G remains on continuous EEG, with no evidence of seizure activity before diazepam was added or after it is tapered off by day 23.
Discharge. Ms. G is extubated on hospital day 18. On day 23 she can follow commands but is not fully oriented, and levodopa, phenytoin, bromocriptine, and dantrolene are tapered off. She is discharged to a rehabilitation facility, where she again requires phenytoin for a witnessed seizure, attributed to anticonvulsant withdrawal.
On follow-up phone interviews 4 and 18 months after hospitalization, Ms. G says she remains seizure-free without taking anticonvulsants. She reports a subjective, interval improvement in cognitive function, which has since returned to baseline.
Evidence for serotonin syndrome
This case involves a young woman with a several-week history of phentermine use for weight reduction who presented with confusion, sedation, mutism, and nausea. She was initially found to have an abnormal EEG, for which she was loaded with the anticonvulsant phenytoin. However, she continued to exhibit altered mental status, myoclonus, and hyperreflexia along with autonomic dysregulation—such as urinary retention and tachycardia—despite a negative EEG on continuous monitoring.
On retrospective review, we believe she likely was experiencing serotonin toxicity from phentermine. She later developed NMS within several hours of receiving the antipsychotic haloperidol.
Even though phentermine is thought to have a relatively weak serotonergic effect,3 it has been shown to markedly increase serotonin efflux in the rat hypothalamus (to a greater degree than the SSRI fluoxetine).23 Although Ms. G did not report having consumed foods or supplements that could have interfered with phentermine’s metabolism, such use could have contributed to or prolonged a serotonin syndrome.20 Phentermine misuse also cannot be ruled out.
Excess phentermine or concomitant use of other serotonergic agents may have precipitated serotonin syndrome. Ms. G’s hyperactivity a few days before she complained of fatigue and somnolence may represent:
- a sign of phentermine intoxication or overuse
- a harbinger of serotonin syndrome, because these symptoms were followed by overt serotonin syndrome signs such as confusion, disorientation, myoclonus, and autonomic dysfunction.
Evidence for NMS
Ms. G received haloperidol because her agitation obstructed urgent evaluation. After several doses, she rapidly developed signs and symptoms highly consistent with NMS. Onset was rapid compared with the typically described, more insidious NMS evolution of 24 to 72 hours, however.25 Rapid NMS onset may have been precipitated in 2 ways:
- dopaminergic (phentermine) withdrawal combined with dopamine antagonist challenge (haloperidol)25,26
- background serotonin syndrome caused by amphetamine (phentermine) predisposing the patient to develop NMS.27
Although phentermine-induced sympathetic hyperactivity also could have predisposed Ms. G to NMS,31 we think this is unlikely because phentermine was discontinued 3 to 4 days before she developed NMS. Nonetheless, sympathetic hyperactivity secondary to phentermine or serotonin syndrome may increase the risk of developing NMS.
Treatment strategy
Because serotonin syndrome and NMS share many clinical findings, differentiating between the 2 syndromes may be difficult, especially when the patient’s medication history does not implicate a specific agent. A detailed history and physical may help distinguish the syndromes. Clonus may be particularly specific and is important in the diagnosis of serotonin syndrome.32 If you are unable to differentiate between serotonin syndrome and NMS in a patient with this acute neurotoxic abnormal behavior syndrome,33 consider a common treatment strategy (Table 2).19,25
In Ms. G’s case, she probably should not have received bromocriptine for NMS,20 given the potential role of serotonin syndrome in precipitating her symptoms.
Case reports support our hypotheses of an increased predilection for NMS with dopaminergic withdrawal or serotonin syndrome. Growing evidence supports the use of chlorpromazine for serotonin syndrome,34 but consider its use contraindicated in patients with NMS.
Table 2
Serotonin syndrome or NMS?
When in doubt, follow 4 management principles
| Avoid serotonin agonists and dopamine antagonists when a patient presents with features of serotonin syndrome or neuroleptic malignant syndrome (NMS) and the diagnosis is unclear20 |
| Provide supportive care with monitoring, cooling blankets as needed, and hydration |
| Avoid using antipsychotics for agitation, when possible; benzodiazepines may be preferable, although their use in NMS is controversial25 |
| Avoid using bromocriptine, given its contraindication in serotonin syndrome, but consider cyproheptadine for the serotonin syndrome component and dantrolene for skeletal muscle rigidity20 |
Related resources
- Carbone JR. The neuroleptic malignant and serotonin syndromes. Emerg Med Clin North Am 2000;18:317-25.
- Gillman PK. The serotonin syndrome and its treatment. J Psychopharmacol 1999;13:100-9.
- Neuroleptic Malignant Syndrome Information Service (NMSIS). www.nmsis.org. NMS hotline for medical professionals (toll-free 888-667-8367) handles calls on NMS, serotonin syndrome, heat stroke, malignant catatonia, and other drug-induced heat-related disorders.
This paper was among those entered in the 2007 Promising New Investigators competition sponsored by the Neuroleptic Malignant Syndrome Information Service (NMSIS). The theme of this year’s competition was “New insights on psychotropic drug safety and side effects.”
Current Psychiatry is honored to publish this peer-reviewed, evidence-based article on a clinically important topic for practicing psychiatrists.
- Acyclovir • Zovirax
- Ampicillin • various
- Bromocriptine • Parlodel
- Ceftriaxone • Rocephin
- Chlorpromazine • Thorazine
- Cyproheptadine • Periactin
- Dantrolene • Dantrium
- Diazepam • Valium
- Dextroamphetamine • Dexedrine
- Fluoxetine • Prozac
- Haloperidol • Haldol
- Levodopa • various
- Methysergide • Sansert
- Pentobarbital • Nembutal
- Phentermine • various
- Phenytoin • Dilantin
- Propranolol • Inderal
- Vancomycin • various
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Mosby’s Drug Consult, 16th ed. St. Louis, MO: Mosby; 2006.
2. McEvoy G. AHFS drug information. Bethesda, MD: American Society of Health-System Pharmacists; 2006.
3. Rothman RB, Baumann MH, Dersch CM, et al. Amphetamine-type central nervous system stimulants release norepinephrine more potently than they release dopamine and serotonin. Synapse 2001;39:32-41.
4. Ener RA, Meglathery SB, Van Decker WA, Gallagher RM. Serotonin syndrome and other serotonergic disorders. Pain Med 2003;4:63-74.
5. Phentermine hydrochloride. Physicians’ Desk Reference, 53rd ed. Montvale, NJ: Medical Economics; 1999:3055-6.
6. Bostwick JM, Brown TM. A toxic reaction from combining fluoxetine and phentermine. J Clin Psychopharmacol 1996;16:189-90.
7. Sternbach H. The serotonin syndrome. Am J Psychiatry 1991;148(6):705-13.
8. Nisijima K, Yoshino T, Yui K, Katoh S. Potent serotonin (5-HT)(2A) receptor antagonists completely prevent the development of hyperthermia in an animal model of the 5-HT syndrome. Brain Res 2001;890:23-31.
9. Mason PJ, Morris VA, Balcezak TJ. Serotonin syndrome. Presentation of 2 cases and review of the literature. Medicine (Baltimore) 2000;79:201-9.
10. Boyer EW, Shannon M. The serotonin syndrome. N Engl J Med 2005;352:1112-20.
11. Delay J, Pichot P, Lemperiere T, et al. [A non-phenothiazine and non-reserpine major neuroleptic, haloperidol, in the treatment of psychoses.] Ann Med Psychol (Paris). 1960;118:145-52.
12. Berardi D, Dell’Atti M, Amore M, et al. Clinical risk factors for neuroleptic malignant syndrome. Hum Psychopharmacol 2002;17:99-102.
13. Pearlman CA. Neuroleptic malignant syndrome: a review of the literature. J Clin Psychopharmacol 1986;6:257-73.
14. Viejo LF, Morales V, Punal P, et al. Risk factors in neuroleptic malignant syndrome. A case-control study. Acta Psychiatr Scand 2003;107:45-9.
15. Ikebe S, Harada T, Hashimoto T, et al. Prevention and treatment of malignant syndrome in Parkinson’s disease: a consensus statement of the Malignant Syndrome Research Group. Parkinsonism Relat Disord 2003;9(suppl 1):S47-9.
16. Mueller PS, Vester JW, Fermaglich J. Neuroleptic malignant syndrome. Successful treatment with bromocriptine. JAMA 1983;249:386-8.
17. Coons DJ, Hillman FJ, Marshall RW. Treatment of neuroleptic malignant syndrome with dantrolene sodium: a case report. Am J Psychiatry 1982;139:944-5.
18. Spivak B, Maline DI, Kozyrev VN, et al. Frequency of neuroleptic malignant syndrome in a large psychiatric hospital in Moscow. Eur Psychiatry 2000;15:330-3.
19. Gerber PE, Lynd LD. Selective serotonin-reuptake inhibitor-induced movement disorders. Ann Pharmacother 1998;32:692-8.
20. Kaufman KR, Levitt MJ, Schiltz JF, Sunderram J. Neuroleptic malignant syndrome and serotonin syndrome in the critical care setting: case analysis. Ann Clin Psychiatry 2006;18:201-4.
21. Spencer DC, Hwang J, Morrell MJ. Fenfluramine-phentermine (Fen-Phen) and seizures: evidence for an association. Epilepsy Behav 2000;1(6):448-52.
22. Mills KC. Serotonin syndrome. A clinical update. Crit Care Clin 1997;13(4):763-83.
23. Tao R, Fray A, Aspley S, et al. Effects on serotonin in rat hypothalamus of D-fenfluramine, aminorex, phentermine and fluoxetine. Eur J Pharmacol 2002;445(1-2):69-81.
24. Gillman PK. Serotonin syndrome: history and risk. Fundam Clin Pharmacol 1998;12:482-91.
25. Bhanushali MJ, Tuite PJ. The evaluation and management of patients with neuroleptic malignant syndrome. Neurol Clin 2004;22:389-411.
26. Ebadi M, Pfeiffer RF, Murrin LC. Pathogenesis and treatment of neuroleptic malignant syndrome. Gen Pharmacol 1990;21:367-86.
27. Green AR, Cross AJ, Goodwin GM. Review of the pharmacology and clinical pharmacology of 3,4-methylenedioxymethamphetamine (MDMA or “Ecstasy”). Psychopharmacology (Berl) 1995;119:247-60.
28. Chayasirisobhon S, Cullis P, Veeramasuneni RR. Occurrence of neuroleptic malignant syndrome in a narcoleptic patient. Hosp Community Psychiatry 1983;34:548-50.
29. Serrano-Dueñas M. Neuroleptic malignant syndrome-like, or—dopaminergic malignant syndrome—due to levodopa therapy withdrawal. Clinical features in 11 patients. Parkinsonism Relat Disord 2003;9:175-8.
30. Kline SS, Mauro LS, Scala-Barnett DM, Zick D. Serotonin syndrome versus neuroleptic malignant syndrome as a cause of death. Clin Pharm 1989;8(7):510-14.
31. Gurrera RJ. Sympathoadrenal hyperactivity and the etiology of neuroleptic malignant syndrome. Am J Psychiatry 1999;156:169-80.
32. Dunkley EJ, Isbister GK, Sibbritt D, et al. The Hunter Serotonin Toxicity Criteria: simple and accurate diagnostic decision rules for serotonin toxicity. QJM 2003;96:635-42.
33. Fink M. Toxic serotonin syndrome or neuroleptic malignant syndrome? Pharmacopsychiatry 1996;29:159-61.
34. Gillman PK. Serotonin syndrome treated with chlorpromazine. J Clin Psychopharmacol 1997;17:128-9.
1. Mosby’s Drug Consult, 16th ed. St. Louis, MO: Mosby; 2006.
2. McEvoy G. AHFS drug information. Bethesda, MD: American Society of Health-System Pharmacists; 2006.
3. Rothman RB, Baumann MH, Dersch CM, et al. Amphetamine-type central nervous system stimulants release norepinephrine more potently than they release dopamine and serotonin. Synapse 2001;39:32-41.
4. Ener RA, Meglathery SB, Van Decker WA, Gallagher RM. Serotonin syndrome and other serotonergic disorders. Pain Med 2003;4:63-74.
5. Phentermine hydrochloride. Physicians’ Desk Reference, 53rd ed. Montvale, NJ: Medical Economics; 1999:3055-6.
6. Bostwick JM, Brown TM. A toxic reaction from combining fluoxetine and phentermine. J Clin Psychopharmacol 1996;16:189-90.
7. Sternbach H. The serotonin syndrome. Am J Psychiatry 1991;148(6):705-13.
8. Nisijima K, Yoshino T, Yui K, Katoh S. Potent serotonin (5-HT)(2A) receptor antagonists completely prevent the development of hyperthermia in an animal model of the 5-HT syndrome. Brain Res 2001;890:23-31.
9. Mason PJ, Morris VA, Balcezak TJ. Serotonin syndrome. Presentation of 2 cases and review of the literature. Medicine (Baltimore) 2000;79:201-9.
10. Boyer EW, Shannon M. The serotonin syndrome. N Engl J Med 2005;352:1112-20.
11. Delay J, Pichot P, Lemperiere T, et al. [A non-phenothiazine and non-reserpine major neuroleptic, haloperidol, in the treatment of psychoses.] Ann Med Psychol (Paris). 1960;118:145-52.
12. Berardi D, Dell’Atti M, Amore M, et al. Clinical risk factors for neuroleptic malignant syndrome. Hum Psychopharmacol 2002;17:99-102.
13. Pearlman CA. Neuroleptic malignant syndrome: a review of the literature. J Clin Psychopharmacol 1986;6:257-73.
14. Viejo LF, Morales V, Punal P, et al. Risk factors in neuroleptic malignant syndrome. A case-control study. Acta Psychiatr Scand 2003;107:45-9.
15. Ikebe S, Harada T, Hashimoto T, et al. Prevention and treatment of malignant syndrome in Parkinson’s disease: a consensus statement of the Malignant Syndrome Research Group. Parkinsonism Relat Disord 2003;9(suppl 1):S47-9.
16. Mueller PS, Vester JW, Fermaglich J. Neuroleptic malignant syndrome. Successful treatment with bromocriptine. JAMA 1983;249:386-8.
17. Coons DJ, Hillman FJ, Marshall RW. Treatment of neuroleptic malignant syndrome with dantrolene sodium: a case report. Am J Psychiatry 1982;139:944-5.
18. Spivak B, Maline DI, Kozyrev VN, et al. Frequency of neuroleptic malignant syndrome in a large psychiatric hospital in Moscow. Eur Psychiatry 2000;15:330-3.
19. Gerber PE, Lynd LD. Selective serotonin-reuptake inhibitor-induced movement disorders. Ann Pharmacother 1998;32:692-8.
20. Kaufman KR, Levitt MJ, Schiltz JF, Sunderram J. Neuroleptic malignant syndrome and serotonin syndrome in the critical care setting: case analysis. Ann Clin Psychiatry 2006;18:201-4.
21. Spencer DC, Hwang J, Morrell MJ. Fenfluramine-phentermine (Fen-Phen) and seizures: evidence for an association. Epilepsy Behav 2000;1(6):448-52.
22. Mills KC. Serotonin syndrome. A clinical update. Crit Care Clin 1997;13(4):763-83.
23. Tao R, Fray A, Aspley S, et al. Effects on serotonin in rat hypothalamus of D-fenfluramine, aminorex, phentermine and fluoxetine. Eur J Pharmacol 2002;445(1-2):69-81.
24. Gillman PK. Serotonin syndrome: history and risk. Fundam Clin Pharmacol 1998;12:482-91.
25. Bhanushali MJ, Tuite PJ. The evaluation and management of patients with neuroleptic malignant syndrome. Neurol Clin 2004;22:389-411.
26. Ebadi M, Pfeiffer RF, Murrin LC. Pathogenesis and treatment of neuroleptic malignant syndrome. Gen Pharmacol 1990;21:367-86.
27. Green AR, Cross AJ, Goodwin GM. Review of the pharmacology and clinical pharmacology of 3,4-methylenedioxymethamphetamine (MDMA or “Ecstasy”). Psychopharmacology (Berl) 1995;119:247-60.
28. Chayasirisobhon S, Cullis P, Veeramasuneni RR. Occurrence of neuroleptic malignant syndrome in a narcoleptic patient. Hosp Community Psychiatry 1983;34:548-50.
29. Serrano-Dueñas M. Neuroleptic malignant syndrome-like, or—dopaminergic malignant syndrome—due to levodopa therapy withdrawal. Clinical features in 11 patients. Parkinsonism Relat Disord 2003;9:175-8.
30. Kline SS, Mauro LS, Scala-Barnett DM, Zick D. Serotonin syndrome versus neuroleptic malignant syndrome as a cause of death. Clin Pharm 1989;8(7):510-14.
31. Gurrera RJ. Sympathoadrenal hyperactivity and the etiology of neuroleptic malignant syndrome. Am J Psychiatry 1999;156:169-80.
32. Dunkley EJ, Isbister GK, Sibbritt D, et al. The Hunter Serotonin Toxicity Criteria: simple and accurate diagnostic decision rules for serotonin toxicity. QJM 2003;96:635-42.
33. Fink M. Toxic serotonin syndrome or neuroleptic malignant syndrome? Pharmacopsychiatry 1996;29:159-61.
34. Gillman PK. Serotonin syndrome treated with chlorpromazine. J Clin Psychopharmacol 1997;17:128-9.
Antipsychotic combinations: Blind step or logical?
In a perfect world, every treatment decision would fall under the protective umbrella of evidence-based medicine. The reality is that up to 30% of schizophrenia patients respond poorly to antipsychotic monotherapy,1 and addressing their chronic debilitating illness requires clinicians to step outside the realm of evidence.
This does not have to be a blind step, however. Guided by logic, you can apply knowledge of receptor binding profiles, adverse effects, and kinetic considerations when choosing antipsychotic polypharmacy. This article offers evidence to answer 2 questions:
- What clinical evidence and/or pharmacologic rationale support using >1 antipsychotic?
- When might it be appropriate to use 2 antipsychotics in patients with treatment-resistant psychosis?
Antipsychotic polypharmacy defined
“Polypharmacy” can carry a negative connotation, but not all forms are bad. In some circumstances, antipsychotic polypharmacy may be necessary to provide optimum benefit and prevent harm to the patient and/or staff.
Short-term polypharmacy often occurs when switching patients from 1 antipsychotic to another. This “crossover phase” is justified to provide a smooth transition between the 2 agents, as abrupt antipsychotic discontinuation may cause a rebound worsening of psychosis. Other short-term antipsychotic polypharmacy strategies may be necessary in inpatient settings, particularly for a patient who is acutely psychotic or aggressive.
The use of a first-generation antipsychotic (FGA) to lead in a second-generation antipsychotic (SGA) is a justifiable treatment strategy. In addition, sedative antipsychotics such as quetiapine often are used during initial treatment of acutely ill patients and subsequently withdrawn.
As our understanding of psychosis’ pathophysiology of improves, more options will come for treatment-resistant cases. Changes in the glutamatergic system, for example, have been implicated in schizophrenia’s pathophysiology.15
Lamotrigine—a second-generation anticonvulsant with antiglutamatergic activity—has been studied as augmentation to antipsychotics in patients with schizophrenia. Several randomized, controlled trials suggested clinical benefit from adjunctive lamotrigine,16-18 but 2 recent multicenter, randomized, double-blind trials failed to support that finding.19
Although not adequately studied, other possible augmentation options may include GABA agonists, COX-2 inhibitors, and selective serotonin reuptake inhibitors.20
Experience-based treatment?
Antipsychotic polypharmacy is prevalent (reported in up to 25% of outpatients and 50% of inpatients with schizophrenia),2-7 costly for patients and insurers,8 and likely to be associated with increased risk of adverse effects and drug-drug interactions. Despite what is known, a wide gap exists between the science and clinical practice of combination antipsychotic therapy in schizophrenia (Table 1).
Clinical trials. The efficacy and safety of antipsychotic combinations in schizophrenia (with options including FGA + FGA, FGA + SGA, and SGA + SGA) has not been studied adequately in well-controlled, systematic trials. Four short-term—6 to 26 weeks—randomized, double-blind, controlled studies9-12 have examined antipsychotic polypharmacy (clozapine + risperidone) in patients with schizophrenia:
- In 3 studies,9,11,12 adding risperidone to clozapine did not significantly improve positive or negative symptoms.
- In all 4 studies, clozapine + risperidone was associated with increased sedation, akathisia, hyperprolactinemia, and elevated fasting blood glucose.
Not all combinations make pharmacologic sense, however, such as adding haloperidol to aripiprazole. Haloperidol’s pharmacologic binding profile (potent D2 blockade) may cancel out any benefits with regard to extrapyramidal symptoms and hyperprolactinemia from aripiprazole’s receptor binding profile (D2 agonist/antagonist). In theory, any displacement of antipsychotic medication from D2 receptors because of competing inhibition may increase risk of symptom exacerbation.
Mortality risk? Two independent, longitudinal cohort studies have found antipsychotic polypharmacy to be a statistically significant predictor of reduced survival.21,22 Although these studies have identified a possible association, additional research is required to determine whether increased mortality in schizophrenia is attributable to the disorder, comorbid medical conditions, antipsychotic medications, or a complex interaction of factors.
Treatment guidelines—such as the Texas Medication Algorithm Project’s updated treatment algorithm for schizophrenia23—reflect the paucity of controlled studies of antipsychotic combinations. The expert consensus panel that developed the TMAP algorithm recommends clozapine augmentation with an FGA or SGA, or electroconvulsive therapy after adequate trials of antipsychotic monotherapy, including clozapine. The panel recommends reserving other antipsychotic combinations as a last-line strategy (see Related Resources).
Table 1
Take-home points about antipsychotic polypharmacy
| Long-term antipsychotic polypharmacy is common, even in schizophrenia patients without treatment-refractory psychosis |
| Controlled clinical trials do not support antipsychotic polypharmacy; many clinicians use this strategy, however, so it may have perceived value |
| Which antipsychotic combinations are best—in terms of efficacy and safety—is unclear |
| Controlled trials of combination antipsychotic therapy are difficult to conduct, which limits the availability of evidence to inform clinical practice |
| Whenever you initiate antipsychotic polypharmacy, document your rationale and the alternatives you considered |
‘Sensible’ pharmacology
Despite the lack of supporting evidence, many clinicians apparently are using antipsychotic polypharmacy for schizophrenia patients with treatment-resistant psychosis. Moreover, reports that up to one-fourth of outpatients and one-half of inpatients may receive antipsychotic polypharmacy2-7 suggest that this approach is not being reserved for treatment-resistant psychosis. Rather, it is being used in non-treatment-refractory schizophrenia patients as well—a practice Stahl labeled a “dirty little secret.”24
Before you consider using antipsychotic polypharmacy for a schizophrenia patient, we suggest that you answer a series of questions to rationalize your decision (Table 2). These questions seem intuitive, but they represent appropriate clinical practice and may support the use of multiple antipsychotics in selected patients.
Which combination? If you determine that a patient is an appropriate candidate for antipsychotic polypharmacy, think about the pharmacologic profiles of available agents. Administering 2 antipsychotics may augment pharmacologic activity, provide an additive effect, or worsen your patient’s symptoms.
Although data from well-controlled studies of clozapine + risperidone do not support its efficacy,9-12 this combination is rational from a pharmacologic perspective. Clozapine shows a lower D2 receptor occupancy (16% to 68%) than that of risperidone (63% to 89%),25 so risperidone’s additional D2 receptor occupancy may enhance a patient’s response to clozapine. Table 3 lists other potentially “sensible” antipsychoticantipsychotic combinations.
Table 2
Questions to consider before initiating antipsychotic polypharmacy
| Ask yourself, ‘Have I… |
|---|
| Determined if my patient is taking the prescribed medication correctly or even at all? |
| Allowed for an adequate trial—dosage and duration—of antipsychotic monotherapy? |
| Maximized the dosage of the current antipsychotic? |
| Tried at least 2 to 3 trials of a first-generation and/or second-generation antipsychotic? |
| Tried an adequate trial of clozapine? |
| Re-evaluated my patient’s diagnosis? |
| Considered tolerability and safety issues associated with adding another antipsychotic? |
| Considered drug-drug interactions that may occur as a result of adding another antipsychotic? |
| Considered nonpharmacologic alternatives, including psychosocial interventions? |
| Augmented with a nonantipsychotic medication, such as valproic acid? |
| Considered my patient’s ability to pay for an additional antipsychotic? |
| Considered whether I can monitor my patient more closely while he/she is on multiple antipsychotics? |
Theoretically beneficial antipsychotic combinations
| Antipsychotic #1 | Antipsychotic #2 | Theoretical pharmacologic benefit | Theoretical safety/tolerability concerns |
|---|---|---|---|
| Clozapine | Olanzapine | Additional D2 receptor occupancy | Anticholinergic effects, metabolic adverse events, orthostasis, sedation |
| Aripiprazole | Quetiapine | D2 agonist/antagonist in addition to ‘fast on/fast off’ D2 blockade; unique 5HT activity | Sedation |
| Quetiapine | Olanzapine | Differing D2 blockade properties with minimal increase in EPS risk; 2 agents with structural similarity to clozapine | Anticholinergic effects, metabolic adverse events, orthostasis, sedation |
| Aripiprazole | Loxapine | D2 agonist/antagonist plus a typical antipsychotic that has atypical properties at low doses; 2 agents thought to not potentiate weight gain | Orthostasis, sedation |
| D2: dopamine; 5HT: serotonergic; EPS: extrapyramidal symptoms | |||
Safety/tolerability
Reduced dosages. Combining antipsychotics may allow you to increase treatment efficacy and improve patient tolerability. Lower dosages of 2 antipsychotics may cause fewer side effects than a high dosage of 1 antipsychotic.
For example, case reports and retrospective studies26,27 suggest that adding aripiprazole to clozapine may improve antipsychotic efficacy and reduce metabolic adverse events in treatment-resistant patients. In these cases, clozapine dosages were lower than those usually used in patients with schizophrenia.
Metabolic effects. Carefully weigh the propensity of some antipsychotics to induce weight gain, hyperlipidemia, or glucose dysregulation if you plan to use these agents as part of a polypharmacy regimen. Among SGAs, clozapine and olanzapine are associated with the highest risks of metabolic adverse effects, followed by quetiapine and risperidone. Aripiprazole and ziprasidone are less likely than other SGAs to cause these effects.28
A recent study found a higher incidence of metabolic syndrome in patients receiving antipsychotic polypharmacy. The increased incidence was linked to demographics and clinical risk factors, however, and was not independently associated with the use of multiple antipsychotics.29
Because evidence is scarce and inconclusive, the risk of metabolic adverse events is unknown when antipsychotics are combined. Exercise caution when combining antipsychotics—particularly those known to cause adverse metabolic effects—in case the risk is additive.
Tardive dyskinesia (TD). SGAs are associated with a lower incidence of TD compared with FGAs, but adding an FGA to an SGA may increase the patient’s TD risk.30 Also assess patients regularly (as often as weekly during acute treatment and every 6 to 12 months during maintenance treatment)31 for extrapyramidal symptoms, including akathisia. Administer appropriate rating scales (such as the Abnormal Involuntary Movements Scale [AIMS], Barnes Akathisia Rating Scale [BARS], or Simpson-Angus Rating Scale [SARS]), and treat these adverse events as clinically indicated.
Other adverse effects. The concurrent use of 2 antipsychotics may amplify side effects that are generally considered mild, such as sedation. For example, risperidone and ziprasidone are considered to cause low to moderate sedation. This combination may result in an additive sedative effect that could negatively impact the patient’s psychosocial functioning.
Anticholinergic effects may also be potentiated, especially if a particular combination of antipsychotics warrants anticholinergic medication use for extrapyramidal symptoms.
- Texas Medication Algorithm Project (TMAP). Schizophrenia antipsychotic treatment algorithm. www.dshs.state.tx.us/mhprograms/TIMA.shtm.
- Lehman AF, Lieberman JA, Dixon LB, et al. Practice guideline for the treatment of patients with schizophrenia, 2nd ed. Am J Psychiatry 2004;161(suppl):1-56.
- Aripiprazole • Abilify
- Clozapine • Clozaril
- Haloperidol • Haldol
- Lamotrigine • Lamictal
- Loxapine • Loxitane
- Olanzapine • Zyprexa
- Quetiapine • Seroquel
- Risperidone • Risperdal
- Valproic acid • Depakene
- Ziprasidone • Geodon
Dr. Gibson reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products. He receives research support from the PhRMA Foundation.
Dr. Patel receives grant support from Takeda Pharmaceuticals and is a consultant for Eli Lilly and Company and Shire Pharmaceuticals.
Dr. Lauriello receives grant support from Eli Lilly and Company and serves as a consultant to Eli Lilly and Company and Vanda Pharmaceuticals.
Dr. Buckley receives grant support from AstraZeneca, National Institute of Mental Health, Pfizer Inc., Solvay, and Wyeth and is a consultant for AstraZeneca, Bristol-Myers Squibb, Eli Lilly and Company, Janssen Pharmaceutica, Lundbeck, Pfizer Inc., Solvay, and Wyeth. He receives honoraria from Bristol Myers-Squibb, Janssen Pharmaceutica, Lundbeck, and Pfizer Inc.
1. Lieberman JA, Stroup TS, McEvoy JP, et al. Effectiveness of antipsychotic drugs in patients with chronic schizophrenia. N Engl J Med 2005;353(12):1209-23.
2. Chakos MH, Glick ID, Miller AL, et al. Baseline use of concomitant psychotropic medications to treat schizophrenia in the CATIE trial. Psychiatr Serv 2006;57(8):1094-101.
3. Botts S, Hines H, Littrell R. Antipsychotic polypharmacy in the ambulatory care setting, 1993-2000. Psychiatr Serv 2003;54(8):1086.-
4. Tapp A, Wood AE, Secrest L, et al. Combination antipsychotic therapy in clinical practice. Psychiatr Serv 2003;54(1):55-9.
5. Paton C, Lelliott P, Harrington M, et al. Patterns of antipsychotic and anticholinergic prescribing for hospital inpatients. J Psychopharmacol 2003;17(2):223-9.
6. Tempier RP, Pawliuk NH. Conventional, atypical, and combination antipsychotic prescriptions: a 2-year comparison. J Clin Psychiatry 2003;64(6):673-9.
7. Jaffe AB, Levine J. Antipsychotic medication coprescribing in a large state hospital system. Pharmacoepidemiol Drug Saf 2003;12(1):41-8.
8. Valuck RJ, Morrato EH, Dodd S, et al. How expensive is antipsychotic polypharmacy? Experience from five US state Medicaid programs. Curr Med Res Opin 2007;23(10):2567-76.
9. Freudenreich O, Henderson DC, Walsh JP, et al. Risperidone augmentation for schizophrenia partially responsive to clozapine: a double-blind, placebo-controlled trial. Schizophr Res 2007;92(1-3):90-4.
10. Josiassen RC, Joseph A, Kohegyi E, et al. Clozapine augmented with risperidone in the treatment of schizophrenia: a randomized, double-blind, placebo-controlled trial. Am J Psychiatry 2005;162(1):130-6.
11. Honer WG, Thornton AE, Chen EY, et al. Clozapine alone versus clozapine and risperidone with refractory schizophrenia. N Engl J Med 2006;354(5):472-82.
12. Anil Yağcioğlu AE, Kivircik Akdede BB, Turgut TI, et al. A double-blind controlled study of adjunctive treatment with risperidone in schizophrenic patients partially responsive to clozapine: efficacy and safety. J Clin Psychiatry 2005;66(1):63-72.
13. Chan J, Sweeting M. Combination therapy with nonclozapine atypical antipsychotic medication: a review of current evidence. J Psychopharmacol 2007;21(6):657-64.
14. Lerner V, Libov I, Kotler M, Strous RD. Combination of “atypical” antipsychotic medication in the management of treatment-resistant schizophrenia and schizoaffective disorder. Prog Neuropsychopharmacol Biol Psychiatry 2004;28(1):89-98.
15. Goff DC, Coyle JT. The emerging role of glutamate in the pathophysiology and treatment of schizophrenia. Am J Psychiatry 2001;158(9):1367-77.
16. Kremer I, Vass A, Gorelik I, et al. Placebo-controlled trial of lamotrigine added to conventional and atypical antipsychotics in schizophrenia. Biol Psychiatry 2004;56(6):441-6.
17. Tiihonen J, Hallikainen T, Ryynänen OP, et al. Lamotrigine in treatment-resistant schizophrenia: a randomized placebo-controlled crossover trial. Biol Psychiatry 2003;54(11):1241-8.
18. Zoccali R, Muscatello MR, Bruno A, et al. The effect of lamotrigine augmentation of clozapine in a sample of treatment-resistant schizophrenic patients: a double-blind, placebo-controlled study. Schizophr Res 2007;93(1-3):109-16.
19. Goff DC, Keefe R, Citrome L, et al. Lamotrigine as add-on therapy in schizophrenia: results of 2 placebo-controlled trials. J Clin Psychopharmacol 2007;27(6):582-9.
20. Nasrallah HA. Innovative polypharmacy: when dopamine blockade is not enough [editorial]. Current Psychiatry 2007;6(11):17-18.
21. Waddington JL, Youssef HA, Kinsella A. Mortality in schizophrenia. Antipsychotic polypharmacy and absence of adjunctive anticholinergics over the course of a 10-year prospective study. Br J Psychiatry 1998;173:325-9.
22. Joukamaa M, Heliovaara M, Knekt P, et al. Schizophrenia, neuroleptic medication and mortality. Br J Psychiatry 2006;188:122-7.
23. Moore TA, Buchanan RW, Buckley PF, et al. The Texas Medication Algorithm Project antipsychotic algorithm for schizophrenia: 2006 update. J Clin Psychiatry 2007;68(11):1751-62.
24. Stahl SM. Antipsychotic polypharmacy, part 1: therapeutic option or dirty little secret? J Clin Psychiatry 1999;60(7):425-6.
25. Kapur S, Zipursky RB, Remington G. Clinical and theoretical implications of 5-HT2 and D2 receptor occupancy of clozapine, risperidone, and olanzapine in schizophrenia. Am J Psychiatry 1999;156(2):286-93.
26. Lim S, Pralea C, Schnitt J, et al. Possible increased efficacy of low-dosed clozapine when combined with aripiprazole. J Clin Psychiatry 2004;65(9):1284-5.
27. Karunakaran K, Tungaraza TE, Harborne GC. Is clozapine-aripiprazole combination a useful regimen in the management of treatment-resistant schizophrenia? J Psychopharmacol 2007;21(4):453-6.
28. Haddad PM, Sharma SG. Adverse effects of atypical antipsychotics: differential risk and clinical implications. CNS Drugs 2007;21(11):911-36.
29. Correll CU, Frederickson AM, Kane JM, et al. Does antipsychotic polypharmacy increase the risk of metabolic syndrome? Schizophr Res 2007;89(1-3):91-100.
30. Haddad PM, Dursun SM. Neurologic complications of psychiatric drugs: clinical features and management. Hum Psychopharmacol 2008;23(suppl 1):15-26.
31. Marder SR, Essock S, Miller AL, et al. Physical health monitoring of patients with schizophrenia. Am J Psychiatry 2004;161(8):1334-49.
In a perfect world, every treatment decision would fall under the protective umbrella of evidence-based medicine. The reality is that up to 30% of schizophrenia patients respond poorly to antipsychotic monotherapy,1 and addressing their chronic debilitating illness requires clinicians to step outside the realm of evidence.
This does not have to be a blind step, however. Guided by logic, you can apply knowledge of receptor binding profiles, adverse effects, and kinetic considerations when choosing antipsychotic polypharmacy. This article offers evidence to answer 2 questions:
- What clinical evidence and/or pharmacologic rationale support using >1 antipsychotic?
- When might it be appropriate to use 2 antipsychotics in patients with treatment-resistant psychosis?
Antipsychotic polypharmacy defined
“Polypharmacy” can carry a negative connotation, but not all forms are bad. In some circumstances, antipsychotic polypharmacy may be necessary to provide optimum benefit and prevent harm to the patient and/or staff.
Short-term polypharmacy often occurs when switching patients from 1 antipsychotic to another. This “crossover phase” is justified to provide a smooth transition between the 2 agents, as abrupt antipsychotic discontinuation may cause a rebound worsening of psychosis. Other short-term antipsychotic polypharmacy strategies may be necessary in inpatient settings, particularly for a patient who is acutely psychotic or aggressive.
The use of a first-generation antipsychotic (FGA) to lead in a second-generation antipsychotic (SGA) is a justifiable treatment strategy. In addition, sedative antipsychotics such as quetiapine often are used during initial treatment of acutely ill patients and subsequently withdrawn.
As our understanding of psychosis’ pathophysiology of improves, more options will come for treatment-resistant cases. Changes in the glutamatergic system, for example, have been implicated in schizophrenia’s pathophysiology.15
Lamotrigine—a second-generation anticonvulsant with antiglutamatergic activity—has been studied as augmentation to antipsychotics in patients with schizophrenia. Several randomized, controlled trials suggested clinical benefit from adjunctive lamotrigine,16-18 but 2 recent multicenter, randomized, double-blind trials failed to support that finding.19
Although not adequately studied, other possible augmentation options may include GABA agonists, COX-2 inhibitors, and selective serotonin reuptake inhibitors.20
Experience-based treatment?
Antipsychotic polypharmacy is prevalent (reported in up to 25% of outpatients and 50% of inpatients with schizophrenia),2-7 costly for patients and insurers,8 and likely to be associated with increased risk of adverse effects and drug-drug interactions. Despite what is known, a wide gap exists between the science and clinical practice of combination antipsychotic therapy in schizophrenia (Table 1).
Clinical trials. The efficacy and safety of antipsychotic combinations in schizophrenia (with options including FGA + FGA, FGA + SGA, and SGA + SGA) has not been studied adequately in well-controlled, systematic trials. Four short-term—6 to 26 weeks—randomized, double-blind, controlled studies9-12 have examined antipsychotic polypharmacy (clozapine + risperidone) in patients with schizophrenia:
- In 3 studies,9,11,12 adding risperidone to clozapine did not significantly improve positive or negative symptoms.
- In all 4 studies, clozapine + risperidone was associated with increased sedation, akathisia, hyperprolactinemia, and elevated fasting blood glucose.
Not all combinations make pharmacologic sense, however, such as adding haloperidol to aripiprazole. Haloperidol’s pharmacologic binding profile (potent D2 blockade) may cancel out any benefits with regard to extrapyramidal symptoms and hyperprolactinemia from aripiprazole’s receptor binding profile (D2 agonist/antagonist). In theory, any displacement of antipsychotic medication from D2 receptors because of competing inhibition may increase risk of symptom exacerbation.
Mortality risk? Two independent, longitudinal cohort studies have found antipsychotic polypharmacy to be a statistically significant predictor of reduced survival.21,22 Although these studies have identified a possible association, additional research is required to determine whether increased mortality in schizophrenia is attributable to the disorder, comorbid medical conditions, antipsychotic medications, or a complex interaction of factors.
Treatment guidelines—such as the Texas Medication Algorithm Project’s updated treatment algorithm for schizophrenia23—reflect the paucity of controlled studies of antipsychotic combinations. The expert consensus panel that developed the TMAP algorithm recommends clozapine augmentation with an FGA or SGA, or electroconvulsive therapy after adequate trials of antipsychotic monotherapy, including clozapine. The panel recommends reserving other antipsychotic combinations as a last-line strategy (see Related Resources).
Table 1
Take-home points about antipsychotic polypharmacy
| Long-term antipsychotic polypharmacy is common, even in schizophrenia patients without treatment-refractory psychosis |
| Controlled clinical trials do not support antipsychotic polypharmacy; many clinicians use this strategy, however, so it may have perceived value |
| Which antipsychotic combinations are best—in terms of efficacy and safety—is unclear |
| Controlled trials of combination antipsychotic therapy are difficult to conduct, which limits the availability of evidence to inform clinical practice |
| Whenever you initiate antipsychotic polypharmacy, document your rationale and the alternatives you considered |
‘Sensible’ pharmacology
Despite the lack of supporting evidence, many clinicians apparently are using antipsychotic polypharmacy for schizophrenia patients with treatment-resistant psychosis. Moreover, reports that up to one-fourth of outpatients and one-half of inpatients may receive antipsychotic polypharmacy2-7 suggest that this approach is not being reserved for treatment-resistant psychosis. Rather, it is being used in non-treatment-refractory schizophrenia patients as well—a practice Stahl labeled a “dirty little secret.”24
Before you consider using antipsychotic polypharmacy for a schizophrenia patient, we suggest that you answer a series of questions to rationalize your decision (Table 2). These questions seem intuitive, but they represent appropriate clinical practice and may support the use of multiple antipsychotics in selected patients.
Which combination? If you determine that a patient is an appropriate candidate for antipsychotic polypharmacy, think about the pharmacologic profiles of available agents. Administering 2 antipsychotics may augment pharmacologic activity, provide an additive effect, or worsen your patient’s symptoms.
Although data from well-controlled studies of clozapine + risperidone do not support its efficacy,9-12 this combination is rational from a pharmacologic perspective. Clozapine shows a lower D2 receptor occupancy (16% to 68%) than that of risperidone (63% to 89%),25 so risperidone’s additional D2 receptor occupancy may enhance a patient’s response to clozapine. Table 3 lists other potentially “sensible” antipsychoticantipsychotic combinations.
Table 2
Questions to consider before initiating antipsychotic polypharmacy
| Ask yourself, ‘Have I… |
|---|
| Determined if my patient is taking the prescribed medication correctly or even at all? |
| Allowed for an adequate trial—dosage and duration—of antipsychotic monotherapy? |
| Maximized the dosage of the current antipsychotic? |
| Tried at least 2 to 3 trials of a first-generation and/or second-generation antipsychotic? |
| Tried an adequate trial of clozapine? |
| Re-evaluated my patient’s diagnosis? |
| Considered tolerability and safety issues associated with adding another antipsychotic? |
| Considered drug-drug interactions that may occur as a result of adding another antipsychotic? |
| Considered nonpharmacologic alternatives, including psychosocial interventions? |
| Augmented with a nonantipsychotic medication, such as valproic acid? |
| Considered my patient’s ability to pay for an additional antipsychotic? |
| Considered whether I can monitor my patient more closely while he/she is on multiple antipsychotics? |
Theoretically beneficial antipsychotic combinations
| Antipsychotic #1 | Antipsychotic #2 | Theoretical pharmacologic benefit | Theoretical safety/tolerability concerns |
|---|---|---|---|
| Clozapine | Olanzapine | Additional D2 receptor occupancy | Anticholinergic effects, metabolic adverse events, orthostasis, sedation |
| Aripiprazole | Quetiapine | D2 agonist/antagonist in addition to ‘fast on/fast off’ D2 blockade; unique 5HT activity | Sedation |
| Quetiapine | Olanzapine | Differing D2 blockade properties with minimal increase in EPS risk; 2 agents with structural similarity to clozapine | Anticholinergic effects, metabolic adverse events, orthostasis, sedation |
| Aripiprazole | Loxapine | D2 agonist/antagonist plus a typical antipsychotic that has atypical properties at low doses; 2 agents thought to not potentiate weight gain | Orthostasis, sedation |
| D2: dopamine; 5HT: serotonergic; EPS: extrapyramidal symptoms | |||
Safety/tolerability
Reduced dosages. Combining antipsychotics may allow you to increase treatment efficacy and improve patient tolerability. Lower dosages of 2 antipsychotics may cause fewer side effects than a high dosage of 1 antipsychotic.
For example, case reports and retrospective studies26,27 suggest that adding aripiprazole to clozapine may improve antipsychotic efficacy and reduce metabolic adverse events in treatment-resistant patients. In these cases, clozapine dosages were lower than those usually used in patients with schizophrenia.
Metabolic effects. Carefully weigh the propensity of some antipsychotics to induce weight gain, hyperlipidemia, or glucose dysregulation if you plan to use these agents as part of a polypharmacy regimen. Among SGAs, clozapine and olanzapine are associated with the highest risks of metabolic adverse effects, followed by quetiapine and risperidone. Aripiprazole and ziprasidone are less likely than other SGAs to cause these effects.28
A recent study found a higher incidence of metabolic syndrome in patients receiving antipsychotic polypharmacy. The increased incidence was linked to demographics and clinical risk factors, however, and was not independently associated with the use of multiple antipsychotics.29
Because evidence is scarce and inconclusive, the risk of metabolic adverse events is unknown when antipsychotics are combined. Exercise caution when combining antipsychotics—particularly those known to cause adverse metabolic effects—in case the risk is additive.
Tardive dyskinesia (TD). SGAs are associated with a lower incidence of TD compared with FGAs, but adding an FGA to an SGA may increase the patient’s TD risk.30 Also assess patients regularly (as often as weekly during acute treatment and every 6 to 12 months during maintenance treatment)31 for extrapyramidal symptoms, including akathisia. Administer appropriate rating scales (such as the Abnormal Involuntary Movements Scale [AIMS], Barnes Akathisia Rating Scale [BARS], or Simpson-Angus Rating Scale [SARS]), and treat these adverse events as clinically indicated.
Other adverse effects. The concurrent use of 2 antipsychotics may amplify side effects that are generally considered mild, such as sedation. For example, risperidone and ziprasidone are considered to cause low to moderate sedation. This combination may result in an additive sedative effect that could negatively impact the patient’s psychosocial functioning.
Anticholinergic effects may also be potentiated, especially if a particular combination of antipsychotics warrants anticholinergic medication use for extrapyramidal symptoms.
- Texas Medication Algorithm Project (TMAP). Schizophrenia antipsychotic treatment algorithm. www.dshs.state.tx.us/mhprograms/TIMA.shtm.
- Lehman AF, Lieberman JA, Dixon LB, et al. Practice guideline for the treatment of patients with schizophrenia, 2nd ed. Am J Psychiatry 2004;161(suppl):1-56.
- Aripiprazole • Abilify
- Clozapine • Clozaril
- Haloperidol • Haldol
- Lamotrigine • Lamictal
- Loxapine • Loxitane
- Olanzapine • Zyprexa
- Quetiapine • Seroquel
- Risperidone • Risperdal
- Valproic acid • Depakene
- Ziprasidone • Geodon
Dr. Gibson reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products. He receives research support from the PhRMA Foundation.
Dr. Patel receives grant support from Takeda Pharmaceuticals and is a consultant for Eli Lilly and Company and Shire Pharmaceuticals.
Dr. Lauriello receives grant support from Eli Lilly and Company and serves as a consultant to Eli Lilly and Company and Vanda Pharmaceuticals.
Dr. Buckley receives grant support from AstraZeneca, National Institute of Mental Health, Pfizer Inc., Solvay, and Wyeth and is a consultant for AstraZeneca, Bristol-Myers Squibb, Eli Lilly and Company, Janssen Pharmaceutica, Lundbeck, Pfizer Inc., Solvay, and Wyeth. He receives honoraria from Bristol Myers-Squibb, Janssen Pharmaceutica, Lundbeck, and Pfizer Inc.
In a perfect world, every treatment decision would fall under the protective umbrella of evidence-based medicine. The reality is that up to 30% of schizophrenia patients respond poorly to antipsychotic monotherapy,1 and addressing their chronic debilitating illness requires clinicians to step outside the realm of evidence.
This does not have to be a blind step, however. Guided by logic, you can apply knowledge of receptor binding profiles, adverse effects, and kinetic considerations when choosing antipsychotic polypharmacy. This article offers evidence to answer 2 questions:
- What clinical evidence and/or pharmacologic rationale support using >1 antipsychotic?
- When might it be appropriate to use 2 antipsychotics in patients with treatment-resistant psychosis?
Antipsychotic polypharmacy defined
“Polypharmacy” can carry a negative connotation, but not all forms are bad. In some circumstances, antipsychotic polypharmacy may be necessary to provide optimum benefit and prevent harm to the patient and/or staff.
Short-term polypharmacy often occurs when switching patients from 1 antipsychotic to another. This “crossover phase” is justified to provide a smooth transition between the 2 agents, as abrupt antipsychotic discontinuation may cause a rebound worsening of psychosis. Other short-term antipsychotic polypharmacy strategies may be necessary in inpatient settings, particularly for a patient who is acutely psychotic or aggressive.
The use of a first-generation antipsychotic (FGA) to lead in a second-generation antipsychotic (SGA) is a justifiable treatment strategy. In addition, sedative antipsychotics such as quetiapine often are used during initial treatment of acutely ill patients and subsequently withdrawn.
As our understanding of psychosis’ pathophysiology of improves, more options will come for treatment-resistant cases. Changes in the glutamatergic system, for example, have been implicated in schizophrenia’s pathophysiology.15
Lamotrigine—a second-generation anticonvulsant with antiglutamatergic activity—has been studied as augmentation to antipsychotics in patients with schizophrenia. Several randomized, controlled trials suggested clinical benefit from adjunctive lamotrigine,16-18 but 2 recent multicenter, randomized, double-blind trials failed to support that finding.19
Although not adequately studied, other possible augmentation options may include GABA agonists, COX-2 inhibitors, and selective serotonin reuptake inhibitors.20
Experience-based treatment?
Antipsychotic polypharmacy is prevalent (reported in up to 25% of outpatients and 50% of inpatients with schizophrenia),2-7 costly for patients and insurers,8 and likely to be associated with increased risk of adverse effects and drug-drug interactions. Despite what is known, a wide gap exists between the science and clinical practice of combination antipsychotic therapy in schizophrenia (Table 1).
Clinical trials. The efficacy and safety of antipsychotic combinations in schizophrenia (with options including FGA + FGA, FGA + SGA, and SGA + SGA) has not been studied adequately in well-controlled, systematic trials. Four short-term—6 to 26 weeks—randomized, double-blind, controlled studies9-12 have examined antipsychotic polypharmacy (clozapine + risperidone) in patients with schizophrenia:
- In 3 studies,9,11,12 adding risperidone to clozapine did not significantly improve positive or negative symptoms.
- In all 4 studies, clozapine + risperidone was associated with increased sedation, akathisia, hyperprolactinemia, and elevated fasting blood glucose.
Not all combinations make pharmacologic sense, however, such as adding haloperidol to aripiprazole. Haloperidol’s pharmacologic binding profile (potent D2 blockade) may cancel out any benefits with regard to extrapyramidal symptoms and hyperprolactinemia from aripiprazole’s receptor binding profile (D2 agonist/antagonist). In theory, any displacement of antipsychotic medication from D2 receptors because of competing inhibition may increase risk of symptom exacerbation.
Mortality risk? Two independent, longitudinal cohort studies have found antipsychotic polypharmacy to be a statistically significant predictor of reduced survival.21,22 Although these studies have identified a possible association, additional research is required to determine whether increased mortality in schizophrenia is attributable to the disorder, comorbid medical conditions, antipsychotic medications, or a complex interaction of factors.
Treatment guidelines—such as the Texas Medication Algorithm Project’s updated treatment algorithm for schizophrenia23—reflect the paucity of controlled studies of antipsychotic combinations. The expert consensus panel that developed the TMAP algorithm recommends clozapine augmentation with an FGA or SGA, or electroconvulsive therapy after adequate trials of antipsychotic monotherapy, including clozapine. The panel recommends reserving other antipsychotic combinations as a last-line strategy (see Related Resources).
Table 1
Take-home points about antipsychotic polypharmacy
| Long-term antipsychotic polypharmacy is common, even in schizophrenia patients without treatment-refractory psychosis |
| Controlled clinical trials do not support antipsychotic polypharmacy; many clinicians use this strategy, however, so it may have perceived value |
| Which antipsychotic combinations are best—in terms of efficacy and safety—is unclear |
| Controlled trials of combination antipsychotic therapy are difficult to conduct, which limits the availability of evidence to inform clinical practice |
| Whenever you initiate antipsychotic polypharmacy, document your rationale and the alternatives you considered |
‘Sensible’ pharmacology
Despite the lack of supporting evidence, many clinicians apparently are using antipsychotic polypharmacy for schizophrenia patients with treatment-resistant psychosis. Moreover, reports that up to one-fourth of outpatients and one-half of inpatients may receive antipsychotic polypharmacy2-7 suggest that this approach is not being reserved for treatment-resistant psychosis. Rather, it is being used in non-treatment-refractory schizophrenia patients as well—a practice Stahl labeled a “dirty little secret.”24
Before you consider using antipsychotic polypharmacy for a schizophrenia patient, we suggest that you answer a series of questions to rationalize your decision (Table 2). These questions seem intuitive, but they represent appropriate clinical practice and may support the use of multiple antipsychotics in selected patients.
Which combination? If you determine that a patient is an appropriate candidate for antipsychotic polypharmacy, think about the pharmacologic profiles of available agents. Administering 2 antipsychotics may augment pharmacologic activity, provide an additive effect, or worsen your patient’s symptoms.
Although data from well-controlled studies of clozapine + risperidone do not support its efficacy,9-12 this combination is rational from a pharmacologic perspective. Clozapine shows a lower D2 receptor occupancy (16% to 68%) than that of risperidone (63% to 89%),25 so risperidone’s additional D2 receptor occupancy may enhance a patient’s response to clozapine. Table 3 lists other potentially “sensible” antipsychoticantipsychotic combinations.
Table 2
Questions to consider before initiating antipsychotic polypharmacy
| Ask yourself, ‘Have I… |
|---|
| Determined if my patient is taking the prescribed medication correctly or even at all? |
| Allowed for an adequate trial—dosage and duration—of antipsychotic monotherapy? |
| Maximized the dosage of the current antipsychotic? |
| Tried at least 2 to 3 trials of a first-generation and/or second-generation antipsychotic? |
| Tried an adequate trial of clozapine? |
| Re-evaluated my patient’s diagnosis? |
| Considered tolerability and safety issues associated with adding another antipsychotic? |
| Considered drug-drug interactions that may occur as a result of adding another antipsychotic? |
| Considered nonpharmacologic alternatives, including psychosocial interventions? |
| Augmented with a nonantipsychotic medication, such as valproic acid? |
| Considered my patient’s ability to pay for an additional antipsychotic? |
| Considered whether I can monitor my patient more closely while he/she is on multiple antipsychotics? |
Theoretically beneficial antipsychotic combinations
| Antipsychotic #1 | Antipsychotic #2 | Theoretical pharmacologic benefit | Theoretical safety/tolerability concerns |
|---|---|---|---|
| Clozapine | Olanzapine | Additional D2 receptor occupancy | Anticholinergic effects, metabolic adverse events, orthostasis, sedation |
| Aripiprazole | Quetiapine | D2 agonist/antagonist in addition to ‘fast on/fast off’ D2 blockade; unique 5HT activity | Sedation |
| Quetiapine | Olanzapine | Differing D2 blockade properties with minimal increase in EPS risk; 2 agents with structural similarity to clozapine | Anticholinergic effects, metabolic adverse events, orthostasis, sedation |
| Aripiprazole | Loxapine | D2 agonist/antagonist plus a typical antipsychotic that has atypical properties at low doses; 2 agents thought to not potentiate weight gain | Orthostasis, sedation |
| D2: dopamine; 5HT: serotonergic; EPS: extrapyramidal symptoms | |||
Safety/tolerability
Reduced dosages. Combining antipsychotics may allow you to increase treatment efficacy and improve patient tolerability. Lower dosages of 2 antipsychotics may cause fewer side effects than a high dosage of 1 antipsychotic.
For example, case reports and retrospective studies26,27 suggest that adding aripiprazole to clozapine may improve antipsychotic efficacy and reduce metabolic adverse events in treatment-resistant patients. In these cases, clozapine dosages were lower than those usually used in patients with schizophrenia.
Metabolic effects. Carefully weigh the propensity of some antipsychotics to induce weight gain, hyperlipidemia, or glucose dysregulation if you plan to use these agents as part of a polypharmacy regimen. Among SGAs, clozapine and olanzapine are associated with the highest risks of metabolic adverse effects, followed by quetiapine and risperidone. Aripiprazole and ziprasidone are less likely than other SGAs to cause these effects.28
A recent study found a higher incidence of metabolic syndrome in patients receiving antipsychotic polypharmacy. The increased incidence was linked to demographics and clinical risk factors, however, and was not independently associated with the use of multiple antipsychotics.29
Because evidence is scarce and inconclusive, the risk of metabolic adverse events is unknown when antipsychotics are combined. Exercise caution when combining antipsychotics—particularly those known to cause adverse metabolic effects—in case the risk is additive.
Tardive dyskinesia (TD). SGAs are associated with a lower incidence of TD compared with FGAs, but adding an FGA to an SGA may increase the patient’s TD risk.30 Also assess patients regularly (as often as weekly during acute treatment and every 6 to 12 months during maintenance treatment)31 for extrapyramidal symptoms, including akathisia. Administer appropriate rating scales (such as the Abnormal Involuntary Movements Scale [AIMS], Barnes Akathisia Rating Scale [BARS], or Simpson-Angus Rating Scale [SARS]), and treat these adverse events as clinically indicated.
Other adverse effects. The concurrent use of 2 antipsychotics may amplify side effects that are generally considered mild, such as sedation. For example, risperidone and ziprasidone are considered to cause low to moderate sedation. This combination may result in an additive sedative effect that could negatively impact the patient’s psychosocial functioning.
Anticholinergic effects may also be potentiated, especially if a particular combination of antipsychotics warrants anticholinergic medication use for extrapyramidal symptoms.
- Texas Medication Algorithm Project (TMAP). Schizophrenia antipsychotic treatment algorithm. www.dshs.state.tx.us/mhprograms/TIMA.shtm.
- Lehman AF, Lieberman JA, Dixon LB, et al. Practice guideline for the treatment of patients with schizophrenia, 2nd ed. Am J Psychiatry 2004;161(suppl):1-56.
- Aripiprazole • Abilify
- Clozapine • Clozaril
- Haloperidol • Haldol
- Lamotrigine • Lamictal
- Loxapine • Loxitane
- Olanzapine • Zyprexa
- Quetiapine • Seroquel
- Risperidone • Risperdal
- Valproic acid • Depakene
- Ziprasidone • Geodon
Dr. Gibson reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products. He receives research support from the PhRMA Foundation.
Dr. Patel receives grant support from Takeda Pharmaceuticals and is a consultant for Eli Lilly and Company and Shire Pharmaceuticals.
Dr. Lauriello receives grant support from Eli Lilly and Company and serves as a consultant to Eli Lilly and Company and Vanda Pharmaceuticals.
Dr. Buckley receives grant support from AstraZeneca, National Institute of Mental Health, Pfizer Inc., Solvay, and Wyeth and is a consultant for AstraZeneca, Bristol-Myers Squibb, Eli Lilly and Company, Janssen Pharmaceutica, Lundbeck, Pfizer Inc., Solvay, and Wyeth. He receives honoraria from Bristol Myers-Squibb, Janssen Pharmaceutica, Lundbeck, and Pfizer Inc.
1. Lieberman JA, Stroup TS, McEvoy JP, et al. Effectiveness of antipsychotic drugs in patients with chronic schizophrenia. N Engl J Med 2005;353(12):1209-23.
2. Chakos MH, Glick ID, Miller AL, et al. Baseline use of concomitant psychotropic medications to treat schizophrenia in the CATIE trial. Psychiatr Serv 2006;57(8):1094-101.
3. Botts S, Hines H, Littrell R. Antipsychotic polypharmacy in the ambulatory care setting, 1993-2000. Psychiatr Serv 2003;54(8):1086.-
4. Tapp A, Wood AE, Secrest L, et al. Combination antipsychotic therapy in clinical practice. Psychiatr Serv 2003;54(1):55-9.
5. Paton C, Lelliott P, Harrington M, et al. Patterns of antipsychotic and anticholinergic prescribing for hospital inpatients. J Psychopharmacol 2003;17(2):223-9.
6. Tempier RP, Pawliuk NH. Conventional, atypical, and combination antipsychotic prescriptions: a 2-year comparison. J Clin Psychiatry 2003;64(6):673-9.
7. Jaffe AB, Levine J. Antipsychotic medication coprescribing in a large state hospital system. Pharmacoepidemiol Drug Saf 2003;12(1):41-8.
8. Valuck RJ, Morrato EH, Dodd S, et al. How expensive is antipsychotic polypharmacy? Experience from five US state Medicaid programs. Curr Med Res Opin 2007;23(10):2567-76.
9. Freudenreich O, Henderson DC, Walsh JP, et al. Risperidone augmentation for schizophrenia partially responsive to clozapine: a double-blind, placebo-controlled trial. Schizophr Res 2007;92(1-3):90-4.
10. Josiassen RC, Joseph A, Kohegyi E, et al. Clozapine augmented with risperidone in the treatment of schizophrenia: a randomized, double-blind, placebo-controlled trial. Am J Psychiatry 2005;162(1):130-6.
11. Honer WG, Thornton AE, Chen EY, et al. Clozapine alone versus clozapine and risperidone with refractory schizophrenia. N Engl J Med 2006;354(5):472-82.
12. Anil Yağcioğlu AE, Kivircik Akdede BB, Turgut TI, et al. A double-blind controlled study of adjunctive treatment with risperidone in schizophrenic patients partially responsive to clozapine: efficacy and safety. J Clin Psychiatry 2005;66(1):63-72.
13. Chan J, Sweeting M. Combination therapy with nonclozapine atypical antipsychotic medication: a review of current evidence. J Psychopharmacol 2007;21(6):657-64.
14. Lerner V, Libov I, Kotler M, Strous RD. Combination of “atypical” antipsychotic medication in the management of treatment-resistant schizophrenia and schizoaffective disorder. Prog Neuropsychopharmacol Biol Psychiatry 2004;28(1):89-98.
15. Goff DC, Coyle JT. The emerging role of glutamate in the pathophysiology and treatment of schizophrenia. Am J Psychiatry 2001;158(9):1367-77.
16. Kremer I, Vass A, Gorelik I, et al. Placebo-controlled trial of lamotrigine added to conventional and atypical antipsychotics in schizophrenia. Biol Psychiatry 2004;56(6):441-6.
17. Tiihonen J, Hallikainen T, Ryynänen OP, et al. Lamotrigine in treatment-resistant schizophrenia: a randomized placebo-controlled crossover trial. Biol Psychiatry 2003;54(11):1241-8.
18. Zoccali R, Muscatello MR, Bruno A, et al. The effect of lamotrigine augmentation of clozapine in a sample of treatment-resistant schizophrenic patients: a double-blind, placebo-controlled study. Schizophr Res 2007;93(1-3):109-16.
19. Goff DC, Keefe R, Citrome L, et al. Lamotrigine as add-on therapy in schizophrenia: results of 2 placebo-controlled trials. J Clin Psychopharmacol 2007;27(6):582-9.
20. Nasrallah HA. Innovative polypharmacy: when dopamine blockade is not enough [editorial]. Current Psychiatry 2007;6(11):17-18.
21. Waddington JL, Youssef HA, Kinsella A. Mortality in schizophrenia. Antipsychotic polypharmacy and absence of adjunctive anticholinergics over the course of a 10-year prospective study. Br J Psychiatry 1998;173:325-9.
22. Joukamaa M, Heliovaara M, Knekt P, et al. Schizophrenia, neuroleptic medication and mortality. Br J Psychiatry 2006;188:122-7.
23. Moore TA, Buchanan RW, Buckley PF, et al. The Texas Medication Algorithm Project antipsychotic algorithm for schizophrenia: 2006 update. J Clin Psychiatry 2007;68(11):1751-62.
24. Stahl SM. Antipsychotic polypharmacy, part 1: therapeutic option or dirty little secret? J Clin Psychiatry 1999;60(7):425-6.
25. Kapur S, Zipursky RB, Remington G. Clinical and theoretical implications of 5-HT2 and D2 receptor occupancy of clozapine, risperidone, and olanzapine in schizophrenia. Am J Psychiatry 1999;156(2):286-93.
26. Lim S, Pralea C, Schnitt J, et al. Possible increased efficacy of low-dosed clozapine when combined with aripiprazole. J Clin Psychiatry 2004;65(9):1284-5.
27. Karunakaran K, Tungaraza TE, Harborne GC. Is clozapine-aripiprazole combination a useful regimen in the management of treatment-resistant schizophrenia? J Psychopharmacol 2007;21(4):453-6.
28. Haddad PM, Sharma SG. Adverse effects of atypical antipsychotics: differential risk and clinical implications. CNS Drugs 2007;21(11):911-36.
29. Correll CU, Frederickson AM, Kane JM, et al. Does antipsychotic polypharmacy increase the risk of metabolic syndrome? Schizophr Res 2007;89(1-3):91-100.
30. Haddad PM, Dursun SM. Neurologic complications of psychiatric drugs: clinical features and management. Hum Psychopharmacol 2008;23(suppl 1):15-26.
31. Marder SR, Essock S, Miller AL, et al. Physical health monitoring of patients with schizophrenia. Am J Psychiatry 2004;161(8):1334-49.
1. Lieberman JA, Stroup TS, McEvoy JP, et al. Effectiveness of antipsychotic drugs in patients with chronic schizophrenia. N Engl J Med 2005;353(12):1209-23.
2. Chakos MH, Glick ID, Miller AL, et al. Baseline use of concomitant psychotropic medications to treat schizophrenia in the CATIE trial. Psychiatr Serv 2006;57(8):1094-101.
3. Botts S, Hines H, Littrell R. Antipsychotic polypharmacy in the ambulatory care setting, 1993-2000. Psychiatr Serv 2003;54(8):1086.-
4. Tapp A, Wood AE, Secrest L, et al. Combination antipsychotic therapy in clinical practice. Psychiatr Serv 2003;54(1):55-9.
5. Paton C, Lelliott P, Harrington M, et al. Patterns of antipsychotic and anticholinergic prescribing for hospital inpatients. J Psychopharmacol 2003;17(2):223-9.
6. Tempier RP, Pawliuk NH. Conventional, atypical, and combination antipsychotic prescriptions: a 2-year comparison. J Clin Psychiatry 2003;64(6):673-9.
7. Jaffe AB, Levine J. Antipsychotic medication coprescribing in a large state hospital system. Pharmacoepidemiol Drug Saf 2003;12(1):41-8.
8. Valuck RJ, Morrato EH, Dodd S, et al. How expensive is antipsychotic polypharmacy? Experience from five US state Medicaid programs. Curr Med Res Opin 2007;23(10):2567-76.
9. Freudenreich O, Henderson DC, Walsh JP, et al. Risperidone augmentation for schizophrenia partially responsive to clozapine: a double-blind, placebo-controlled trial. Schizophr Res 2007;92(1-3):90-4.
10. Josiassen RC, Joseph A, Kohegyi E, et al. Clozapine augmented with risperidone in the treatment of schizophrenia: a randomized, double-blind, placebo-controlled trial. Am J Psychiatry 2005;162(1):130-6.
11. Honer WG, Thornton AE, Chen EY, et al. Clozapine alone versus clozapine and risperidone with refractory schizophrenia. N Engl J Med 2006;354(5):472-82.
12. Anil Yağcioğlu AE, Kivircik Akdede BB, Turgut TI, et al. A double-blind controlled study of adjunctive treatment with risperidone in schizophrenic patients partially responsive to clozapine: efficacy and safety. J Clin Psychiatry 2005;66(1):63-72.
13. Chan J, Sweeting M. Combination therapy with nonclozapine atypical antipsychotic medication: a review of current evidence. J Psychopharmacol 2007;21(6):657-64.
14. Lerner V, Libov I, Kotler M, Strous RD. Combination of “atypical” antipsychotic medication in the management of treatment-resistant schizophrenia and schizoaffective disorder. Prog Neuropsychopharmacol Biol Psychiatry 2004;28(1):89-98.
15. Goff DC, Coyle JT. The emerging role of glutamate in the pathophysiology and treatment of schizophrenia. Am J Psychiatry 2001;158(9):1367-77.
16. Kremer I, Vass A, Gorelik I, et al. Placebo-controlled trial of lamotrigine added to conventional and atypical antipsychotics in schizophrenia. Biol Psychiatry 2004;56(6):441-6.
17. Tiihonen J, Hallikainen T, Ryynänen OP, et al. Lamotrigine in treatment-resistant schizophrenia: a randomized placebo-controlled crossover trial. Biol Psychiatry 2003;54(11):1241-8.
18. Zoccali R, Muscatello MR, Bruno A, et al. The effect of lamotrigine augmentation of clozapine in a sample of treatment-resistant schizophrenic patients: a double-blind, placebo-controlled study. Schizophr Res 2007;93(1-3):109-16.
19. Goff DC, Keefe R, Citrome L, et al. Lamotrigine as add-on therapy in schizophrenia: results of 2 placebo-controlled trials. J Clin Psychopharmacol 2007;27(6):582-9.
20. Nasrallah HA. Innovative polypharmacy: when dopamine blockade is not enough [editorial]. Current Psychiatry 2007;6(11):17-18.
21. Waddington JL, Youssef HA, Kinsella A. Mortality in schizophrenia. Antipsychotic polypharmacy and absence of adjunctive anticholinergics over the course of a 10-year prospective study. Br J Psychiatry 1998;173:325-9.
22. Joukamaa M, Heliovaara M, Knekt P, et al. Schizophrenia, neuroleptic medication and mortality. Br J Psychiatry 2006;188:122-7.
23. Moore TA, Buchanan RW, Buckley PF, et al. The Texas Medication Algorithm Project antipsychotic algorithm for schizophrenia: 2006 update. J Clin Psychiatry 2007;68(11):1751-62.
24. Stahl SM. Antipsychotic polypharmacy, part 1: therapeutic option or dirty little secret? J Clin Psychiatry 1999;60(7):425-6.
25. Kapur S, Zipursky RB, Remington G. Clinical and theoretical implications of 5-HT2 and D2 receptor occupancy of clozapine, risperidone, and olanzapine in schizophrenia. Am J Psychiatry 1999;156(2):286-93.
26. Lim S, Pralea C, Schnitt J, et al. Possible increased efficacy of low-dosed clozapine when combined with aripiprazole. J Clin Psychiatry 2004;65(9):1284-5.
27. Karunakaran K, Tungaraza TE, Harborne GC. Is clozapine-aripiprazole combination a useful regimen in the management of treatment-resistant schizophrenia? J Psychopharmacol 2007;21(4):453-6.
28. Haddad PM, Sharma SG. Adverse effects of atypical antipsychotics: differential risk and clinical implications. CNS Drugs 2007;21(11):911-36.
29. Correll CU, Frederickson AM, Kane JM, et al. Does antipsychotic polypharmacy increase the risk of metabolic syndrome? Schizophr Res 2007;89(1-3):91-100.
30. Haddad PM, Dursun SM. Neurologic complications of psychiatric drugs: clinical features and management. Hum Psychopharmacol 2008;23(suppl 1):15-26.
31. Marder SR, Essock S, Miller AL, et al. Physical health monitoring of patients with schizophrenia. Am J Psychiatry 2004;161(8):1334-49.