User login
Promising treatment option for incurable lung cancer described as ‘significant’
, according to researchers reporting earlier this month in Chicago at the annual meeting of the American Society of Clinical Oncology.
Advanced stage IIIA NSCLC is incurable in most patients with lung cancer, and with existing treatments only 30% of patients will live up to 5 years. In this study, neoadjuvant chemotherapy with nivolumab significantly increased the pathological complete response rate in 36.2% of patients, compared with 6.8% who received chemo alone, said study author Mariano Provencio-Pulla, MD, PhD, Instituto Investigacion Sanitaria Puerta de Hierro-Segovia de Arana, Spain. The major pathologic response (MPR) – which accounts for residual viable tumor of less than or equal to 10 – was better in the treatment group as compared with patients who received chemotherapy alone (52% vs 14%). The objective response rate (ORR) – or, the percentage of patients who had a partial or complete response to treatment – was 74% in the treatment group, compared with 48% among patients who received chemotherapy.
“In our opinion this should be the standard of care for patients,” Dr. Provencio-Pulla said during his presentation.
The ASCO treatment guidelines for stage III NSCLC, specify that some patients can receive immunotherapy for up to a year, but for resectable stage III disease, this therapy is still under investigation.
In this study, called NADIM II (NCT03838159), investigators enrolled 87 patients with resectable clinical stage IIIA disease between February 2019 and November 2021. NADIM II is an open-label, randomized, two-arm, phase 2, multicenter clinical trial. Patients had ECOG scores of 0-1 and no known EGFR/ALK alterations. Patients received either nivolumab 360 mg with paclitaxel 200 mg/m2 and carboplatin AUC5 for three cycles every 21 days as treatment before or after surgery. Patients who received a resection that left no microscopic tumor in the primary tumor bed, received adjuvant nivolumab between weeks 3 and 8 after surgery for 6 months.
At 91%, almost all patients who received the immunotherapy and chemotherapy treatment underwent surgery, compared with 69% of patients in the chemotherapy treatment group. In the treatment group, patients with pathological complete response (pCR) had higher PD-L1 tumor proportion score (TPS) scores (median 70%).
The primary endpoint was pathological complete response of 0% viable tumor cells in resected lung and lymph nodes. The major pathological response was no more than 10% viable tumor remaining. The secondary endpoints included overall response rate, toxicity profile, and potential predictive biomarkers.
The addition of neoadjuvant nivolumab to chemotherapy significantly improved pCR (odds ratio, 7.88). The safety profile was “tolerable” with a moderate increase in grade 3-4 toxicity; plus no surgery was delayed because of problems with the treatment, Dr. Provencio-Pulla said.
This study was funded by Fundación GECP. Dr. Provencio-Pulla has received funding from Bristol-Myers Squibb, the maker of Opdivo (nivolumab).
, according to researchers reporting earlier this month in Chicago at the annual meeting of the American Society of Clinical Oncology.
Advanced stage IIIA NSCLC is incurable in most patients with lung cancer, and with existing treatments only 30% of patients will live up to 5 years. In this study, neoadjuvant chemotherapy with nivolumab significantly increased the pathological complete response rate in 36.2% of patients, compared with 6.8% who received chemo alone, said study author Mariano Provencio-Pulla, MD, PhD, Instituto Investigacion Sanitaria Puerta de Hierro-Segovia de Arana, Spain. The major pathologic response (MPR) – which accounts for residual viable tumor of less than or equal to 10 – was better in the treatment group as compared with patients who received chemotherapy alone (52% vs 14%). The objective response rate (ORR) – or, the percentage of patients who had a partial or complete response to treatment – was 74% in the treatment group, compared with 48% among patients who received chemotherapy.
“In our opinion this should be the standard of care for patients,” Dr. Provencio-Pulla said during his presentation.
The ASCO treatment guidelines for stage III NSCLC, specify that some patients can receive immunotherapy for up to a year, but for resectable stage III disease, this therapy is still under investigation.
In this study, called NADIM II (NCT03838159), investigators enrolled 87 patients with resectable clinical stage IIIA disease between February 2019 and November 2021. NADIM II is an open-label, randomized, two-arm, phase 2, multicenter clinical trial. Patients had ECOG scores of 0-1 and no known EGFR/ALK alterations. Patients received either nivolumab 360 mg with paclitaxel 200 mg/m2 and carboplatin AUC5 for three cycles every 21 days as treatment before or after surgery. Patients who received a resection that left no microscopic tumor in the primary tumor bed, received adjuvant nivolumab between weeks 3 and 8 after surgery for 6 months.
At 91%, almost all patients who received the immunotherapy and chemotherapy treatment underwent surgery, compared with 69% of patients in the chemotherapy treatment group. In the treatment group, patients with pathological complete response (pCR) had higher PD-L1 tumor proportion score (TPS) scores (median 70%).
The primary endpoint was pathological complete response of 0% viable tumor cells in resected lung and lymph nodes. The major pathological response was no more than 10% viable tumor remaining. The secondary endpoints included overall response rate, toxicity profile, and potential predictive biomarkers.
The addition of neoadjuvant nivolumab to chemotherapy significantly improved pCR (odds ratio, 7.88). The safety profile was “tolerable” with a moderate increase in grade 3-4 toxicity; plus no surgery was delayed because of problems with the treatment, Dr. Provencio-Pulla said.
This study was funded by Fundación GECP. Dr. Provencio-Pulla has received funding from Bristol-Myers Squibb, the maker of Opdivo (nivolumab).
, according to researchers reporting earlier this month in Chicago at the annual meeting of the American Society of Clinical Oncology.
Advanced stage IIIA NSCLC is incurable in most patients with lung cancer, and with existing treatments only 30% of patients will live up to 5 years. In this study, neoadjuvant chemotherapy with nivolumab significantly increased the pathological complete response rate in 36.2% of patients, compared with 6.8% who received chemo alone, said study author Mariano Provencio-Pulla, MD, PhD, Instituto Investigacion Sanitaria Puerta de Hierro-Segovia de Arana, Spain. The major pathologic response (MPR) – which accounts for residual viable tumor of less than or equal to 10 – was better in the treatment group as compared with patients who received chemotherapy alone (52% vs 14%). The objective response rate (ORR) – or, the percentage of patients who had a partial or complete response to treatment – was 74% in the treatment group, compared with 48% among patients who received chemotherapy.
“In our opinion this should be the standard of care for patients,” Dr. Provencio-Pulla said during his presentation.
The ASCO treatment guidelines for stage III NSCLC, specify that some patients can receive immunotherapy for up to a year, but for resectable stage III disease, this therapy is still under investigation.
In this study, called NADIM II (NCT03838159), investigators enrolled 87 patients with resectable clinical stage IIIA disease between February 2019 and November 2021. NADIM II is an open-label, randomized, two-arm, phase 2, multicenter clinical trial. Patients had ECOG scores of 0-1 and no known EGFR/ALK alterations. Patients received either nivolumab 360 mg with paclitaxel 200 mg/m2 and carboplatin AUC5 for three cycles every 21 days as treatment before or after surgery. Patients who received a resection that left no microscopic tumor in the primary tumor bed, received adjuvant nivolumab between weeks 3 and 8 after surgery for 6 months.
At 91%, almost all patients who received the immunotherapy and chemotherapy treatment underwent surgery, compared with 69% of patients in the chemotherapy treatment group. In the treatment group, patients with pathological complete response (pCR) had higher PD-L1 tumor proportion score (TPS) scores (median 70%).
The primary endpoint was pathological complete response of 0% viable tumor cells in resected lung and lymph nodes. The major pathological response was no more than 10% viable tumor remaining. The secondary endpoints included overall response rate, toxicity profile, and potential predictive biomarkers.
The addition of neoadjuvant nivolumab to chemotherapy significantly improved pCR (odds ratio, 7.88). The safety profile was “tolerable” with a moderate increase in grade 3-4 toxicity; plus no surgery was delayed because of problems with the treatment, Dr. Provencio-Pulla said.
This study was funded by Fundación GECP. Dr. Provencio-Pulla has received funding from Bristol-Myers Squibb, the maker of Opdivo (nivolumab).
FROM ASCO 2022
Opioid use in the elderly a dementia risk factor?
in new findings that suggest exposure to these drugs may be another modifiable risk factor for dementia.
“Clinicians and others may want to consider that opioid exposure in those aged 75-80 increases dementia risk, and to balance the potential benefits of opioid use in old age with adverse side effects,” said Stephen Z. Levine, PhD, professor, department of community mental health, University of Haifa (Israel).
The study was published online in the American Journal of Geriatric Psychiatry.
Widespread use
Evidence points to a relatively high rate of opioid prescriptions among older adults. A Morbidity and Mortality Weekly Report noted 19.2% of the U.S. adult population filled an opioid prescription in 2018, with the rate in those over 65 double that of adults aged 20-24 years (25% vs. 11.2%).
Disorders and illnesses for which opioids might be prescribed, including cancer and some pain conditions, “are far more prevalent in old age than at a younger age,” said Dr. Levine.
This high rate of opioid use underscores the need to consider the risks of opioid use in old age, said Dr. Levine. “Unfortunately, studies of the association between opioid use and dementia risk in old age are few, and their results are inconsistent.”
The study included 91,307 Israeli citizens aged 60 and over without dementia who were enrolled in the Meuhedet Healthcare Services, a nonprofit health maintenance organization (HMO) serving 14% of the country’s population. Meuhedet has maintained an up-to-date dementia registry since 2002.
The average age of the study sample was 68.29 years at the start of the study (in 2012).
In Israel, opioids are prescribed for a 30-day period. In this study, opioid exposure was defined as opioid medication fills covering 60 days (or two prescriptions) within a 120-day interval.
The primary outcome was incident dementia during follow-up from Jan. 1, 2013 to Oct. 30, 2017. The analysis controlled for a number of factors, including age, sex, smoking status, health conditions such as arthritis, depression, diabetes, osteoporosis, cognitive decline, vitamin deficiencies, cancer, cardiovascular conditions, and hospitalizations for falls.
Researchers also accounted for the competing risk of mortality.
During the study, 3.1% of subjects were exposed to opioids at a mean age of 73.94 years, and 5.8% of subjects developed dementia at an average age of 78.07 years.
Increased dementia risk
The risk of incident dementia was significantly increased in those exposed to opioids versus unexposed individuals in the 75- to 80-year age group (adjusted hazard ratio, 1.39; 95% confidence interval, 1.01-1.92; z statistic = 2.02; P < .05).
The authors noted the effect size for opioid exposure in this elderly age group is like other potentially modifiable risk factors for dementia, including body mass index and smoking.
The current study could not determine the biological explanation for the increased dementia risk among older opioid users. “Causal notions are challenging in observational studies and should be viewed with caution,” Dr. Levine noted.
However, a plausible mechanism highlighted in the literature is that opioids promote apoptosis of microglia and neurons that contribute to neurodegenerative diseases, he said.
The study included 14 sensitivity analyses, including those that looked at females, subjects older than 70, smokers, and groups with and without comorbid health conditions. The only sensitivity analysis that didn’t have similar findings to the primary analysis looked at dementia risk restricted to subjects without a vitamin deficiency.
“It’s reassuring that 13 or 14 sensitivity analyses found a significant association between opioid exposure and dementia risk,” said Dr. Levine.
Some prior studies did not show an association between opioid exposure and dementia risk. One possible reason for the discrepancy with the current findings is that the previous research didn’t account for age-specific opioid use effects, or the competing risk of mortality, said Dr. Levine.
Clinicians have a number of potential alternatives to opioids to treat various conditions including acetaminophen, non-steroidal anti-inflammatory drugs, amine reuptake inhibitors (ARIs), membrane stabilizers, muscle relaxants, topical capsaicin, botulinum toxin, cannabinoids, and steroids.
A limitation of the study was that it didn’t adjust for all possible comorbid health conditions, including vascular conditions, or for use of benzodiazepines, and surgical procedures.
In addition, since up to 50% of dementia cases are undetected, it’s possible some in the unexposed opioid group may actually have undiagnosed dementia, thereby reducing the effect sizes in the results.
Reverse causality is also a possibility as the neuropathological process associated with dementia could have started prior to opioid exposure. In addition, the results are limited to prolonged opioid exposure.
Interpret with caution
Commenting on the study, David Knopman, MD, a neurologist at Mayo Clinic in Rochester, Minn., whose research involves late-life cognitive disorders, was skeptical.
“On the face of it, the fact that an association was seen only in one narrow age range – 75+ to 80 years – ought to raise serious suspicion about the reliability and validity of the claim that opioid use is a risk factor for dementia, he said.
Although the researchers performed several sensitivity analyses, including accounting for mortality, “pharmacoepidemiological studies are terribly sensitive to residual biases” related to physician and patient choices related to medication use, added Dr. Knopman.
The claim that opioids are a dementia risk “should be viewed with great caution” and should not influence use of opioids where they’re truly indicated, he said.
“It would be a great pity if patients with pain requiring opioids avoid them because of fears about dementia based on the dubious relationship between age and opioid use.”
Dr. Levine and Dr. Knopman report no relevant financial disclosures.
A version of this article first appeared on Medscape.com.
in new findings that suggest exposure to these drugs may be another modifiable risk factor for dementia.
“Clinicians and others may want to consider that opioid exposure in those aged 75-80 increases dementia risk, and to balance the potential benefits of opioid use in old age with adverse side effects,” said Stephen Z. Levine, PhD, professor, department of community mental health, University of Haifa (Israel).
The study was published online in the American Journal of Geriatric Psychiatry.
Widespread use
Evidence points to a relatively high rate of opioid prescriptions among older adults. A Morbidity and Mortality Weekly Report noted 19.2% of the U.S. adult population filled an opioid prescription in 2018, with the rate in those over 65 double that of adults aged 20-24 years (25% vs. 11.2%).
Disorders and illnesses for which opioids might be prescribed, including cancer and some pain conditions, “are far more prevalent in old age than at a younger age,” said Dr. Levine.
This high rate of opioid use underscores the need to consider the risks of opioid use in old age, said Dr. Levine. “Unfortunately, studies of the association between opioid use and dementia risk in old age are few, and their results are inconsistent.”
The study included 91,307 Israeli citizens aged 60 and over without dementia who were enrolled in the Meuhedet Healthcare Services, a nonprofit health maintenance organization (HMO) serving 14% of the country’s population. Meuhedet has maintained an up-to-date dementia registry since 2002.
The average age of the study sample was 68.29 years at the start of the study (in 2012).
In Israel, opioids are prescribed for a 30-day period. In this study, opioid exposure was defined as opioid medication fills covering 60 days (or two prescriptions) within a 120-day interval.
The primary outcome was incident dementia during follow-up from Jan. 1, 2013 to Oct. 30, 2017. The analysis controlled for a number of factors, including age, sex, smoking status, health conditions such as arthritis, depression, diabetes, osteoporosis, cognitive decline, vitamin deficiencies, cancer, cardiovascular conditions, and hospitalizations for falls.
Researchers also accounted for the competing risk of mortality.
During the study, 3.1% of subjects were exposed to opioids at a mean age of 73.94 years, and 5.8% of subjects developed dementia at an average age of 78.07 years.
Increased dementia risk
The risk of incident dementia was significantly increased in those exposed to opioids versus unexposed individuals in the 75- to 80-year age group (adjusted hazard ratio, 1.39; 95% confidence interval, 1.01-1.92; z statistic = 2.02; P < .05).
The authors noted the effect size for opioid exposure in this elderly age group is like other potentially modifiable risk factors for dementia, including body mass index and smoking.
The current study could not determine the biological explanation for the increased dementia risk among older opioid users. “Causal notions are challenging in observational studies and should be viewed with caution,” Dr. Levine noted.
However, a plausible mechanism highlighted in the literature is that opioids promote apoptosis of microglia and neurons that contribute to neurodegenerative diseases, he said.
The study included 14 sensitivity analyses, including those that looked at females, subjects older than 70, smokers, and groups with and without comorbid health conditions. The only sensitivity analysis that didn’t have similar findings to the primary analysis looked at dementia risk restricted to subjects without a vitamin deficiency.
“It’s reassuring that 13 or 14 sensitivity analyses found a significant association between opioid exposure and dementia risk,” said Dr. Levine.
Some prior studies did not show an association between opioid exposure and dementia risk. One possible reason for the discrepancy with the current findings is that the previous research didn’t account for age-specific opioid use effects, or the competing risk of mortality, said Dr. Levine.
Clinicians have a number of potential alternatives to opioids to treat various conditions including acetaminophen, non-steroidal anti-inflammatory drugs, amine reuptake inhibitors (ARIs), membrane stabilizers, muscle relaxants, topical capsaicin, botulinum toxin, cannabinoids, and steroids.
A limitation of the study was that it didn’t adjust for all possible comorbid health conditions, including vascular conditions, or for use of benzodiazepines, and surgical procedures.
In addition, since up to 50% of dementia cases are undetected, it’s possible some in the unexposed opioid group may actually have undiagnosed dementia, thereby reducing the effect sizes in the results.
Reverse causality is also a possibility as the neuropathological process associated with dementia could have started prior to opioid exposure. In addition, the results are limited to prolonged opioid exposure.
Interpret with caution
Commenting on the study, David Knopman, MD, a neurologist at Mayo Clinic in Rochester, Minn., whose research involves late-life cognitive disorders, was skeptical.
“On the face of it, the fact that an association was seen only in one narrow age range – 75+ to 80 years – ought to raise serious suspicion about the reliability and validity of the claim that opioid use is a risk factor for dementia, he said.
Although the researchers performed several sensitivity analyses, including accounting for mortality, “pharmacoepidemiological studies are terribly sensitive to residual biases” related to physician and patient choices related to medication use, added Dr. Knopman.
The claim that opioids are a dementia risk “should be viewed with great caution” and should not influence use of opioids where they’re truly indicated, he said.
“It would be a great pity if patients with pain requiring opioids avoid them because of fears about dementia based on the dubious relationship between age and opioid use.”
Dr. Levine and Dr. Knopman report no relevant financial disclosures.
A version of this article first appeared on Medscape.com.
in new findings that suggest exposure to these drugs may be another modifiable risk factor for dementia.
“Clinicians and others may want to consider that opioid exposure in those aged 75-80 increases dementia risk, and to balance the potential benefits of opioid use in old age with adverse side effects,” said Stephen Z. Levine, PhD, professor, department of community mental health, University of Haifa (Israel).
The study was published online in the American Journal of Geriatric Psychiatry.
Widespread use
Evidence points to a relatively high rate of opioid prescriptions among older adults. A Morbidity and Mortality Weekly Report noted 19.2% of the U.S. adult population filled an opioid prescription in 2018, with the rate in those over 65 double that of adults aged 20-24 years (25% vs. 11.2%).
Disorders and illnesses for which opioids might be prescribed, including cancer and some pain conditions, “are far more prevalent in old age than at a younger age,” said Dr. Levine.
This high rate of opioid use underscores the need to consider the risks of opioid use in old age, said Dr. Levine. “Unfortunately, studies of the association between opioid use and dementia risk in old age are few, and their results are inconsistent.”
The study included 91,307 Israeli citizens aged 60 and over without dementia who were enrolled in the Meuhedet Healthcare Services, a nonprofit health maintenance organization (HMO) serving 14% of the country’s population. Meuhedet has maintained an up-to-date dementia registry since 2002.
The average age of the study sample was 68.29 years at the start of the study (in 2012).
In Israel, opioids are prescribed for a 30-day period. In this study, opioid exposure was defined as opioid medication fills covering 60 days (or two prescriptions) within a 120-day interval.
The primary outcome was incident dementia during follow-up from Jan. 1, 2013 to Oct. 30, 2017. The analysis controlled for a number of factors, including age, sex, smoking status, health conditions such as arthritis, depression, diabetes, osteoporosis, cognitive decline, vitamin deficiencies, cancer, cardiovascular conditions, and hospitalizations for falls.
Researchers also accounted for the competing risk of mortality.
During the study, 3.1% of subjects were exposed to opioids at a mean age of 73.94 years, and 5.8% of subjects developed dementia at an average age of 78.07 years.
Increased dementia risk
The risk of incident dementia was significantly increased in those exposed to opioids versus unexposed individuals in the 75- to 80-year age group (adjusted hazard ratio, 1.39; 95% confidence interval, 1.01-1.92; z statistic = 2.02; P < .05).
The authors noted the effect size for opioid exposure in this elderly age group is like other potentially modifiable risk factors for dementia, including body mass index and smoking.
The current study could not determine the biological explanation for the increased dementia risk among older opioid users. “Causal notions are challenging in observational studies and should be viewed with caution,” Dr. Levine noted.
However, a plausible mechanism highlighted in the literature is that opioids promote apoptosis of microglia and neurons that contribute to neurodegenerative diseases, he said.
The study included 14 sensitivity analyses, including those that looked at females, subjects older than 70, smokers, and groups with and without comorbid health conditions. The only sensitivity analysis that didn’t have similar findings to the primary analysis looked at dementia risk restricted to subjects without a vitamin deficiency.
“It’s reassuring that 13 or 14 sensitivity analyses found a significant association between opioid exposure and dementia risk,” said Dr. Levine.
Some prior studies did not show an association between opioid exposure and dementia risk. One possible reason for the discrepancy with the current findings is that the previous research didn’t account for age-specific opioid use effects, or the competing risk of mortality, said Dr. Levine.
Clinicians have a number of potential alternatives to opioids to treat various conditions including acetaminophen, non-steroidal anti-inflammatory drugs, amine reuptake inhibitors (ARIs), membrane stabilizers, muscle relaxants, topical capsaicin, botulinum toxin, cannabinoids, and steroids.
A limitation of the study was that it didn’t adjust for all possible comorbid health conditions, including vascular conditions, or for use of benzodiazepines, and surgical procedures.
In addition, since up to 50% of dementia cases are undetected, it’s possible some in the unexposed opioid group may actually have undiagnosed dementia, thereby reducing the effect sizes in the results.
Reverse causality is also a possibility as the neuropathological process associated with dementia could have started prior to opioid exposure. In addition, the results are limited to prolonged opioid exposure.
Interpret with caution
Commenting on the study, David Knopman, MD, a neurologist at Mayo Clinic in Rochester, Minn., whose research involves late-life cognitive disorders, was skeptical.
“On the face of it, the fact that an association was seen only in one narrow age range – 75+ to 80 years – ought to raise serious suspicion about the reliability and validity of the claim that opioid use is a risk factor for dementia, he said.
Although the researchers performed several sensitivity analyses, including accounting for mortality, “pharmacoepidemiological studies are terribly sensitive to residual biases” related to physician and patient choices related to medication use, added Dr. Knopman.
The claim that opioids are a dementia risk “should be viewed with great caution” and should not influence use of opioids where they’re truly indicated, he said.
“It would be a great pity if patients with pain requiring opioids avoid them because of fears about dementia based on the dubious relationship between age and opioid use.”
Dr. Levine and Dr. Knopman report no relevant financial disclosures.
A version of this article first appeared on Medscape.com.
FROM AMERICAN JOURNAL OF GERIATRIC PSYCHIATRY
Genetic testing for best antidepressant accurate, cost effective
new research suggests.
CYP2D6 and CYP2C19, from the cytochrome P450 family, are involved in the metabolism and elimination of various molecules, including medications. Variants in the genes encoding these enzymes affect the speed at which drugs are metabolized, altering their pharmacokinetic profiles.
The researchers studied 125 patients with MDD and used CYP2D6 and CYP2C19 genotyping to determine the presence of actionable phenotypes in line with Food and Drug Administration labeling.
They found that, in many cases, pharmacogenetic testing could have predicted poor response to the initial treatment selection and could have helped guide subsequent choices to improve outcomes.
In addition, a pharmacoeconomic evaluation that combined direct and indirect costs resulting from MDD with the prevalence of CYP2D6 and CYP2C19 phenotypes showed that testing for functional variants in both genes would be cost effective at a national level.
Had psychiatrists who treated patients in the study known about their metabolizing profiles, it “might have contributed to switches in medication” and could have reduced “delays in response,” said lead researcher Alessio Squassina, PhD, associate professor of pharmacology at the University of Cagliari (Italy).
The findings were presented at the European Psychiatric Association 2022 Congress.
Highly variable response rates
Dr. Squassina noted that the response to antidepressants is a “highly variable trait,” and while it is known that genetics play a role, their contribution is “still not completely understood.”
He explained that the use of pharmacogenetics, which leverages genetic information to guide treatment decision-making, has increased significantly.
While regulatory bodies, including the FDA, have been “very active” in defining strict criteria for interpreting the information from pharmacogenetic tests, there remains some “discrepancy” in their clinical utility.
Dr. Squassina said the FDA provides guidance on use of genetic testing on the labels of 34 psychiatric medications. Of these, 79% relate to CYP2D6, 12% relate to CYP2C19, and 9% relate to other genes.
These labels provide guidance on when genetic testing is recommended or required, as well as potentially clinically actionable gene-drug associations in patients with certain functional alleles.
However, Dr. Squassina noted that the distribution of such alleles is not the same across Europe, so it’s possible that a psychiatrist in Italy may be less likely to treat a patient with a phenotype affecting response to treatment or risk of adverse events than one in Norway or Sweden.
For the study, the investigators examined the frequency of CYP2D6 and CYP2C19 phenotypes in psychiatric patients in Sardinia and their relationship with pharmacologic treatment and cost-effectiveness.
They set out to recruit 200 patients with MDD who had a documented 5-year medical and treatment history, including alterations in treatment, adverse events, hospitalizations, suicide, and symptom scores, as well as sociodemographic variables.
An interim analysis of the first 125 patients recruited to the study showed that the most common CYP2D6 phenotype was normal metabolizers (NM), at 60.5%, followed by intermediate metabolizers (IM), at 28.2%, ultrarapid metabolizers (UR), at 8.9%, and poor metabolizers (PM), at 2.4%.
For CYP2C19, the most common phenotype was NM (49%), followed by IM (29.0%), UR (25.0%), and PM (4.0%). While there were differences in the overall European averages, they were not significant.
To highlight the potential impact that pharmacogenetic testing could have had on patient care and outcome, Dr. Squassina highlighted two cases.
The first concerned a patient with a CYP2D6 IM and CYP2C19 UR phenotype, who did not respond to escitalopram. The FDA drug label indicates this phenotype is actionable and recommends an alternative drug.
The patient was subsequently switched to venlafaxine. The FDA drug label on venlafaxine notes that patients with this phenotype are likely to have a suboptimal response to this drug, and again, this patient did not respond to treatment.
Another patient with a CYP2D6 NM and CYP2C19 IM phenotype was also prescribed escitalopram. The FDA label on this drug notes that patients with this phenotype can try venlafaxine but may not respond. Indeed, this patient did not respond and was switched to venlafaxine and started responding.
“The psychiatrists [in these cases] may made have made different [drug] choices if they had known the genotypes in advance,” Dr. Squassina said.
Cost effective?
To determine the cost-effectiveness of screening for CYP2D6 and CYP2C19 phenotypes in patients with MDD, the researchers used real-world data to develop a Markov model with a hypothetical cohort of 2000 MDD patients, half of whom underwent pharmacogenetic testing, to determine the potential impact on outcomes over an 18-week period.
The model included the cost of medications and hospitalization, psychiatric counseling, loss of productivity, and the estimated probability of response and adverse events, adjusted for the patient’s likelihood of having a particular metabolizing phenotype.
Results showed that, for CYP2C19, compared to no testing, pharmacogenetic testing would be cost-effective at an incremental cost-effective ratio (ICER) of €60,000 ($64,000 USD) per quality-adjusted life-year (QALY).
This, Squassina said, is “below the willingness to pay threshold” for health authorities in developed countries.
For CYP2D6, pharmacogenetic testing would become cost-effective at an ICER of approximately €47,000 ($40,000 USD) per QALY.
The team plans to complete recruitment and perform a “detailed evaluation of all the variables, especially those relating to the medication history and changes in dosage, and adverse drug reactions.” The researchers would also like to study genetic phenotypes for other metabolizing enzymes and repeat the pharmacoeconomic analysis with the complete dataset.
A glimpse into the future
Approached for comment, Alessandro Serretti, MD, PhD, department of biomedical and neuromotor sciences, University of Bologna (Italy), who was not involved in the study, said the findings show there is a “small but evident benefit” from CYP profiling, “which makes sense.”
He added that in the Netherlands and other European countries, efforts are already underway to record the CYP status of patients at a national level. “Sooner or later, all Western countries will implement it as a routine,” he said in an interview.
He explained that, when such testing is widely available, electronic health record data will allow physicians to immediately select the optimal antidepressant for an individual patient. This will end the current trial-and-error process that leads to delayed treatment and will help avoid serious consequences, such as suicide.
While reducing a single patient’s treatment by a few weeks with the most appropriate antidepressant choice does not make a large difference in the cost per episode, at a population level, it has the potential to make a significant difference.
Dr. Serretti does not envisage genotyping all 333 million Europeans for the CYP phenotype at this point but imagines that in the future, individuals will undergo whole-genome sequencing to determine risks for cancer, dementia, and heart disease, at which point they will also undergo CYP functional allele profiling, and all these data will be recorded on individuals’ EHR.
“So, every doctor, a psychiatrist or cardiologist, can see everything, whenever they need it,” he said.
The study was funded by Fondazione di Sardegna and Regione Autonoma della Sardegna. The authors disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
new research suggests.
CYP2D6 and CYP2C19, from the cytochrome P450 family, are involved in the metabolism and elimination of various molecules, including medications. Variants in the genes encoding these enzymes affect the speed at which drugs are metabolized, altering their pharmacokinetic profiles.
The researchers studied 125 patients with MDD and used CYP2D6 and CYP2C19 genotyping to determine the presence of actionable phenotypes in line with Food and Drug Administration labeling.
They found that, in many cases, pharmacogenetic testing could have predicted poor response to the initial treatment selection and could have helped guide subsequent choices to improve outcomes.
In addition, a pharmacoeconomic evaluation that combined direct and indirect costs resulting from MDD with the prevalence of CYP2D6 and CYP2C19 phenotypes showed that testing for functional variants in both genes would be cost effective at a national level.
Had psychiatrists who treated patients in the study known about their metabolizing profiles, it “might have contributed to switches in medication” and could have reduced “delays in response,” said lead researcher Alessio Squassina, PhD, associate professor of pharmacology at the University of Cagliari (Italy).
The findings were presented at the European Psychiatric Association 2022 Congress.
Highly variable response rates
Dr. Squassina noted that the response to antidepressants is a “highly variable trait,” and while it is known that genetics play a role, their contribution is “still not completely understood.”
He explained that the use of pharmacogenetics, which leverages genetic information to guide treatment decision-making, has increased significantly.
While regulatory bodies, including the FDA, have been “very active” in defining strict criteria for interpreting the information from pharmacogenetic tests, there remains some “discrepancy” in their clinical utility.
Dr. Squassina said the FDA provides guidance on use of genetic testing on the labels of 34 psychiatric medications. Of these, 79% relate to CYP2D6, 12% relate to CYP2C19, and 9% relate to other genes.
These labels provide guidance on when genetic testing is recommended or required, as well as potentially clinically actionable gene-drug associations in patients with certain functional alleles.
However, Dr. Squassina noted that the distribution of such alleles is not the same across Europe, so it’s possible that a psychiatrist in Italy may be less likely to treat a patient with a phenotype affecting response to treatment or risk of adverse events than one in Norway or Sweden.
For the study, the investigators examined the frequency of CYP2D6 and CYP2C19 phenotypes in psychiatric patients in Sardinia and their relationship with pharmacologic treatment and cost-effectiveness.
They set out to recruit 200 patients with MDD who had a documented 5-year medical and treatment history, including alterations in treatment, adverse events, hospitalizations, suicide, and symptom scores, as well as sociodemographic variables.
An interim analysis of the first 125 patients recruited to the study showed that the most common CYP2D6 phenotype was normal metabolizers (NM), at 60.5%, followed by intermediate metabolizers (IM), at 28.2%, ultrarapid metabolizers (UR), at 8.9%, and poor metabolizers (PM), at 2.4%.
For CYP2C19, the most common phenotype was NM (49%), followed by IM (29.0%), UR (25.0%), and PM (4.0%). While there were differences in the overall European averages, they were not significant.
To highlight the potential impact that pharmacogenetic testing could have had on patient care and outcome, Dr. Squassina highlighted two cases.
The first concerned a patient with a CYP2D6 IM and CYP2C19 UR phenotype, who did not respond to escitalopram. The FDA drug label indicates this phenotype is actionable and recommends an alternative drug.
The patient was subsequently switched to venlafaxine. The FDA drug label on venlafaxine notes that patients with this phenotype are likely to have a suboptimal response to this drug, and again, this patient did not respond to treatment.
Another patient with a CYP2D6 NM and CYP2C19 IM phenotype was also prescribed escitalopram. The FDA label on this drug notes that patients with this phenotype can try venlafaxine but may not respond. Indeed, this patient did not respond and was switched to venlafaxine and started responding.
“The psychiatrists [in these cases] may made have made different [drug] choices if they had known the genotypes in advance,” Dr. Squassina said.
Cost effective?
To determine the cost-effectiveness of screening for CYP2D6 and CYP2C19 phenotypes in patients with MDD, the researchers used real-world data to develop a Markov model with a hypothetical cohort of 2000 MDD patients, half of whom underwent pharmacogenetic testing, to determine the potential impact on outcomes over an 18-week period.
The model included the cost of medications and hospitalization, psychiatric counseling, loss of productivity, and the estimated probability of response and adverse events, adjusted for the patient’s likelihood of having a particular metabolizing phenotype.
Results showed that, for CYP2C19, compared to no testing, pharmacogenetic testing would be cost-effective at an incremental cost-effective ratio (ICER) of €60,000 ($64,000 USD) per quality-adjusted life-year (QALY).
This, Squassina said, is “below the willingness to pay threshold” for health authorities in developed countries.
For CYP2D6, pharmacogenetic testing would become cost-effective at an ICER of approximately €47,000 ($40,000 USD) per QALY.
The team plans to complete recruitment and perform a “detailed evaluation of all the variables, especially those relating to the medication history and changes in dosage, and adverse drug reactions.” The researchers would also like to study genetic phenotypes for other metabolizing enzymes and repeat the pharmacoeconomic analysis with the complete dataset.
A glimpse into the future
Approached for comment, Alessandro Serretti, MD, PhD, department of biomedical and neuromotor sciences, University of Bologna (Italy), who was not involved in the study, said the findings show there is a “small but evident benefit” from CYP profiling, “which makes sense.”
He added that in the Netherlands and other European countries, efforts are already underway to record the CYP status of patients at a national level. “Sooner or later, all Western countries will implement it as a routine,” he said in an interview.
He explained that, when such testing is widely available, electronic health record data will allow physicians to immediately select the optimal antidepressant for an individual patient. This will end the current trial-and-error process that leads to delayed treatment and will help avoid serious consequences, such as suicide.
While reducing a single patient’s treatment by a few weeks with the most appropriate antidepressant choice does not make a large difference in the cost per episode, at a population level, it has the potential to make a significant difference.
Dr. Serretti does not envisage genotyping all 333 million Europeans for the CYP phenotype at this point but imagines that in the future, individuals will undergo whole-genome sequencing to determine risks for cancer, dementia, and heart disease, at which point they will also undergo CYP functional allele profiling, and all these data will be recorded on individuals’ EHR.
“So, every doctor, a psychiatrist or cardiologist, can see everything, whenever they need it,” he said.
The study was funded by Fondazione di Sardegna and Regione Autonoma della Sardegna. The authors disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
new research suggests.
CYP2D6 and CYP2C19, from the cytochrome P450 family, are involved in the metabolism and elimination of various molecules, including medications. Variants in the genes encoding these enzymes affect the speed at which drugs are metabolized, altering their pharmacokinetic profiles.
The researchers studied 125 patients with MDD and used CYP2D6 and CYP2C19 genotyping to determine the presence of actionable phenotypes in line with Food and Drug Administration labeling.
They found that, in many cases, pharmacogenetic testing could have predicted poor response to the initial treatment selection and could have helped guide subsequent choices to improve outcomes.
In addition, a pharmacoeconomic evaluation that combined direct and indirect costs resulting from MDD with the prevalence of CYP2D6 and CYP2C19 phenotypes showed that testing for functional variants in both genes would be cost effective at a national level.
Had psychiatrists who treated patients in the study known about their metabolizing profiles, it “might have contributed to switches in medication” and could have reduced “delays in response,” said lead researcher Alessio Squassina, PhD, associate professor of pharmacology at the University of Cagliari (Italy).
The findings were presented at the European Psychiatric Association 2022 Congress.
Highly variable response rates
Dr. Squassina noted that the response to antidepressants is a “highly variable trait,” and while it is known that genetics play a role, their contribution is “still not completely understood.”
He explained that the use of pharmacogenetics, which leverages genetic information to guide treatment decision-making, has increased significantly.
While regulatory bodies, including the FDA, have been “very active” in defining strict criteria for interpreting the information from pharmacogenetic tests, there remains some “discrepancy” in their clinical utility.
Dr. Squassina said the FDA provides guidance on use of genetic testing on the labels of 34 psychiatric medications. Of these, 79% relate to CYP2D6, 12% relate to CYP2C19, and 9% relate to other genes.
These labels provide guidance on when genetic testing is recommended or required, as well as potentially clinically actionable gene-drug associations in patients with certain functional alleles.
However, Dr. Squassina noted that the distribution of such alleles is not the same across Europe, so it’s possible that a psychiatrist in Italy may be less likely to treat a patient with a phenotype affecting response to treatment or risk of adverse events than one in Norway or Sweden.
For the study, the investigators examined the frequency of CYP2D6 and CYP2C19 phenotypes in psychiatric patients in Sardinia and their relationship with pharmacologic treatment and cost-effectiveness.
They set out to recruit 200 patients with MDD who had a documented 5-year medical and treatment history, including alterations in treatment, adverse events, hospitalizations, suicide, and symptom scores, as well as sociodemographic variables.
An interim analysis of the first 125 patients recruited to the study showed that the most common CYP2D6 phenotype was normal metabolizers (NM), at 60.5%, followed by intermediate metabolizers (IM), at 28.2%, ultrarapid metabolizers (UR), at 8.9%, and poor metabolizers (PM), at 2.4%.
For CYP2C19, the most common phenotype was NM (49%), followed by IM (29.0%), UR (25.0%), and PM (4.0%). While there were differences in the overall European averages, they were not significant.
To highlight the potential impact that pharmacogenetic testing could have had on patient care and outcome, Dr. Squassina highlighted two cases.
The first concerned a patient with a CYP2D6 IM and CYP2C19 UR phenotype, who did not respond to escitalopram. The FDA drug label indicates this phenotype is actionable and recommends an alternative drug.
The patient was subsequently switched to venlafaxine. The FDA drug label on venlafaxine notes that patients with this phenotype are likely to have a suboptimal response to this drug, and again, this patient did not respond to treatment.
Another patient with a CYP2D6 NM and CYP2C19 IM phenotype was also prescribed escitalopram. The FDA label on this drug notes that patients with this phenotype can try venlafaxine but may not respond. Indeed, this patient did not respond and was switched to venlafaxine and started responding.
“The psychiatrists [in these cases] may made have made different [drug] choices if they had known the genotypes in advance,” Dr. Squassina said.
Cost effective?
To determine the cost-effectiveness of screening for CYP2D6 and CYP2C19 phenotypes in patients with MDD, the researchers used real-world data to develop a Markov model with a hypothetical cohort of 2000 MDD patients, half of whom underwent pharmacogenetic testing, to determine the potential impact on outcomes over an 18-week period.
The model included the cost of medications and hospitalization, psychiatric counseling, loss of productivity, and the estimated probability of response and adverse events, adjusted for the patient’s likelihood of having a particular metabolizing phenotype.
Results showed that, for CYP2C19, compared to no testing, pharmacogenetic testing would be cost-effective at an incremental cost-effective ratio (ICER) of €60,000 ($64,000 USD) per quality-adjusted life-year (QALY).
This, Squassina said, is “below the willingness to pay threshold” for health authorities in developed countries.
For CYP2D6, pharmacogenetic testing would become cost-effective at an ICER of approximately €47,000 ($40,000 USD) per QALY.
The team plans to complete recruitment and perform a “detailed evaluation of all the variables, especially those relating to the medication history and changes in dosage, and adverse drug reactions.” The researchers would also like to study genetic phenotypes for other metabolizing enzymes and repeat the pharmacoeconomic analysis with the complete dataset.
A glimpse into the future
Approached for comment, Alessandro Serretti, MD, PhD, department of biomedical and neuromotor sciences, University of Bologna (Italy), who was not involved in the study, said the findings show there is a “small but evident benefit” from CYP profiling, “which makes sense.”
He added that in the Netherlands and other European countries, efforts are already underway to record the CYP status of patients at a national level. “Sooner or later, all Western countries will implement it as a routine,” he said in an interview.
He explained that, when such testing is widely available, electronic health record data will allow physicians to immediately select the optimal antidepressant for an individual patient. This will end the current trial-and-error process that leads to delayed treatment and will help avoid serious consequences, such as suicide.
While reducing a single patient’s treatment by a few weeks with the most appropriate antidepressant choice does not make a large difference in the cost per episode, at a population level, it has the potential to make a significant difference.
Dr. Serretti does not envisage genotyping all 333 million Europeans for the CYP phenotype at this point but imagines that in the future, individuals will undergo whole-genome sequencing to determine risks for cancer, dementia, and heart disease, at which point they will also undergo CYP functional allele profiling, and all these data will be recorded on individuals’ EHR.
“So, every doctor, a psychiatrist or cardiologist, can see everything, whenever they need it,” he said.
The study was funded by Fondazione di Sardegna and Regione Autonoma della Sardegna. The authors disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM EPA 2022
ADA updates on finerenone, SGLT2 inhibitors, and race-based eGFR
As it gears up for the first in-person scientific sessions for 3 years, the American Diabetes Association has issued an addendum to its most recent annual clinical practice recommendations published in December 2021, the 2022 Standards of Medical Care in Diabetes, based on recent trial evidence and consensus.
The update informs clinicians about:
- The effect of the nonsteroidal mineralocorticoid antagonist (Kerendia) on cardiovascular outcomes in patients with type 2 diabetes and chronic kidney disease.
- The effect of a sodium-glucose cotransporter 2 (SGLT2) inhibitor on heart failure and renal outcomes in patients with type 2 diabetes.
The National Kidney Foundation and the American Society of Nephrology Task Force recommendation to remove race in the formula for calculating estimated glomerular filtration rate (eGFR).

“This is the fifth year that we are able to update the Standards of Care after it has been published through our Living Standards of Care updates, making it possible to give diabetes care providers the most important information and the latest evidence relevant to their practice,” Robert A. Gabbay, MD, PhD, ADA chief scientific and medical officer, said in a press release from the organization.
The addendum, entitled, “Living Standards of Care,” updates Section 10, “Cardiovascular Disease and Risk Management,” and Section 11, “Chronic Kidney Disease and Risk Management” of the 2022 Standards of Medical Care in Diabetes.
The amendments were approved by the ADA Professional Practice Committee, which is responsible for developing the Standards of Care. The American College of Cardiology reviewed and endorsed the section on CVD and risk management.
The Living Standards Update was published online in Diabetes Care.
CVD and risk management
In the Addendum to Section 10, “Cardiovascular Disease and Risk Management,” the committee writes:
- “For patients with type 2 diabetes and chronic kidney disease treated with maximum tolerated doses of ACE inhibitors or angiotensin receptor blockers, addition of finerenone should be considered to improve cardiovascular outcomes and reduce the risk of chronic kidney disease progression. A”
- “Patients with type 2 diabetes and chronic kidney disease should be considered for treatment with finerenone to reduce cardiovascular outcomes and the risk of chronic kidney disease progression.”
- “In patients with type 2 diabetes and established heart failure with either preserved or reduced ejection fraction, an SGLT2 inhibitor [with proven benefit in this patient population] is recommended to reduce risk of worsening heart failure, hospitalizations for heart failure, and cardiovascular death. ”
In the section “Statin Treatment,” the addendum no longer states that “a prospective trial of a newer fibrate ... is ongoing,” because that trial investigating pemafibrate (Kowa), a novel selective peroxisome proliferator-activated receptor alpha modulator (or fibrate), has been discontinued.
Chronic kidney disease and risk management
In the Addendum to Section 11, “Chronic Kidney Disease and Risk Management,” the committee writes:
- “Traditionally, eGFR is calculated from serum creatinine using a validated formula. The Chronic Kidney Disease Epidemiology Collaboration (CKD-EPI) equation is preferred. ... Historically, a correction factor for muscle mass was included in a modified equation for African Americans; however, due to various issues with inequities, it was decided to the equation such that it applies to all. Hence, a committee was convened, resulting in the recommendation for immediate implementation of the CKD-EPI creatinine equation refit without the race variable in all laboratories in the U.S.” (This is based on an National Kidney Foundation and American Society of Nephrology Task Force recommendation.)
- “Additionally, increased use of cystatin C, especially to confirm estimated GFR in adults who are at risk for or have chronic kidney disease, because combining filtration markers (creatinine and cystatin C) is more accurate and would support better clinical decisions than either marker alone.”
Evidence from clinical trials
The update is based on findings from the following clinical trials:
- Efficacy and Safety of Finerenone in Subjects With Type 2 Diabetes Mellitus and Diabetic Kidney Disease (FIDELIO-DKD)
- Efficacy and Safety of Finerenone in Subjects With Type 2 Diabetes Mellitus and the Clinical Diagnosis of Diabetic Kidney Disease (FIGARO-DKD)
- FIDELITY, a prespecified pooled analysis of FIDELIO-DKD and FIGARO-DKD
- Empagliflozin Outcome Trial in Patients With Chronic Heart Failure With Preserved Ejection Fraction (EMPEROR-Preserved)
- Effects of Dapagliflozin on Biomarkers, Symptoms and Functional Status in Patients with PRESERVED Ejection Fraction Heart Failure (PRESERVED-HF)
- Pemafibrate to Reduce Cardiovascular Outcomes by Reducing Triglycerides in Patients with Diabetes (PROMINENT).
A version of this article first appeared on Medscape.com.
As it gears up for the first in-person scientific sessions for 3 years, the American Diabetes Association has issued an addendum to its most recent annual clinical practice recommendations published in December 2021, the 2022 Standards of Medical Care in Diabetes, based on recent trial evidence and consensus.
The update informs clinicians about:
- The effect of the nonsteroidal mineralocorticoid antagonist (Kerendia) on cardiovascular outcomes in patients with type 2 diabetes and chronic kidney disease.
- The effect of a sodium-glucose cotransporter 2 (SGLT2) inhibitor on heart failure and renal outcomes in patients with type 2 diabetes.
The National Kidney Foundation and the American Society of Nephrology Task Force recommendation to remove race in the formula for calculating estimated glomerular filtration rate (eGFR).
“This is the fifth year that we are able to update the Standards of Care after it has been published through our Living Standards of Care updates, making it possible to give diabetes care providers the most important information and the latest evidence relevant to their practice,” Robert A. Gabbay, MD, PhD, ADA chief scientific and medical officer, said in a press release from the organization.
The addendum, entitled, “Living Standards of Care,” updates Section 10, “Cardiovascular Disease and Risk Management,” and Section 11, “Chronic Kidney Disease and Risk Management” of the 2022 Standards of Medical Care in Diabetes.
The amendments were approved by the ADA Professional Practice Committee, which is responsible for developing the Standards of Care. The American College of Cardiology reviewed and endorsed the section on CVD and risk management.
The Living Standards Update was published online in Diabetes Care.
CVD and risk management
In the Addendum to Section 10, “Cardiovascular Disease and Risk Management,” the committee writes:
- “For patients with type 2 diabetes and chronic kidney disease treated with maximum tolerated doses of ACE inhibitors or angiotensin receptor blockers, addition of finerenone should be considered to improve cardiovascular outcomes and reduce the risk of chronic kidney disease progression. A”
- “Patients with type 2 diabetes and chronic kidney disease should be considered for treatment with finerenone to reduce cardiovascular outcomes and the risk of chronic kidney disease progression.”
- “In patients with type 2 diabetes and established heart failure with either preserved or reduced ejection fraction, an SGLT2 inhibitor [with proven benefit in this patient population] is recommended to reduce risk of worsening heart failure, hospitalizations for heart failure, and cardiovascular death. ”
In the section “Statin Treatment,” the addendum no longer states that “a prospective trial of a newer fibrate ... is ongoing,” because that trial investigating pemafibrate (Kowa), a novel selective peroxisome proliferator-activated receptor alpha modulator (or fibrate), has been discontinued.
Chronic kidney disease and risk management
In the Addendum to Section 11, “Chronic Kidney Disease and Risk Management,” the committee writes:
- “Traditionally, eGFR is calculated from serum creatinine using a validated formula. The Chronic Kidney Disease Epidemiology Collaboration (CKD-EPI) equation is preferred. ... Historically, a correction factor for muscle mass was included in a modified equation for African Americans; however, due to various issues with inequities, it was decided to the equation such that it applies to all. Hence, a committee was convened, resulting in the recommendation for immediate implementation of the CKD-EPI creatinine equation refit without the race variable in all laboratories in the U.S.” (This is based on an National Kidney Foundation and American Society of Nephrology Task Force recommendation.)
- “Additionally, increased use of cystatin C, especially to confirm estimated GFR in adults who are at risk for or have chronic kidney disease, because combining filtration markers (creatinine and cystatin C) is more accurate and would support better clinical decisions than either marker alone.”
Evidence from clinical trials
The update is based on findings from the following clinical trials:
- Efficacy and Safety of Finerenone in Subjects With Type 2 Diabetes Mellitus and Diabetic Kidney Disease (FIDELIO-DKD)
- Efficacy and Safety of Finerenone in Subjects With Type 2 Diabetes Mellitus and the Clinical Diagnosis of Diabetic Kidney Disease (FIGARO-DKD)
- FIDELITY, a prespecified pooled analysis of FIDELIO-DKD and FIGARO-DKD
- Empagliflozin Outcome Trial in Patients With Chronic Heart Failure With Preserved Ejection Fraction (EMPEROR-Preserved)
- Effects of Dapagliflozin on Biomarkers, Symptoms and Functional Status in Patients with PRESERVED Ejection Fraction Heart Failure (PRESERVED-HF)
- Pemafibrate to Reduce Cardiovascular Outcomes by Reducing Triglycerides in Patients with Diabetes (PROMINENT).
A version of this article first appeared on Medscape.com.
As it gears up for the first in-person scientific sessions for 3 years, the American Diabetes Association has issued an addendum to its most recent annual clinical practice recommendations published in December 2021, the 2022 Standards of Medical Care in Diabetes, based on recent trial evidence and consensus.
The update informs clinicians about:
- The effect of the nonsteroidal mineralocorticoid antagonist (Kerendia) on cardiovascular outcomes in patients with type 2 diabetes and chronic kidney disease.
- The effect of a sodium-glucose cotransporter 2 (SGLT2) inhibitor on heart failure and renal outcomes in patients with type 2 diabetes.
The National Kidney Foundation and the American Society of Nephrology Task Force recommendation to remove race in the formula for calculating estimated glomerular filtration rate (eGFR).
“This is the fifth year that we are able to update the Standards of Care after it has been published through our Living Standards of Care updates, making it possible to give diabetes care providers the most important information and the latest evidence relevant to their practice,” Robert A. Gabbay, MD, PhD, ADA chief scientific and medical officer, said in a press release from the organization.
The addendum, entitled, “Living Standards of Care,” updates Section 10, “Cardiovascular Disease and Risk Management,” and Section 11, “Chronic Kidney Disease and Risk Management” of the 2022 Standards of Medical Care in Diabetes.
The amendments were approved by the ADA Professional Practice Committee, which is responsible for developing the Standards of Care. The American College of Cardiology reviewed and endorsed the section on CVD and risk management.
The Living Standards Update was published online in Diabetes Care.
CVD and risk management
In the Addendum to Section 10, “Cardiovascular Disease and Risk Management,” the committee writes:
- “For patients with type 2 diabetes and chronic kidney disease treated with maximum tolerated doses of ACE inhibitors or angiotensin receptor blockers, addition of finerenone should be considered to improve cardiovascular outcomes and reduce the risk of chronic kidney disease progression. A”
- “Patients with type 2 diabetes and chronic kidney disease should be considered for treatment with finerenone to reduce cardiovascular outcomes and the risk of chronic kidney disease progression.”
- “In patients with type 2 diabetes and established heart failure with either preserved or reduced ejection fraction, an SGLT2 inhibitor [with proven benefit in this patient population] is recommended to reduce risk of worsening heart failure, hospitalizations for heart failure, and cardiovascular death. ”
In the section “Statin Treatment,” the addendum no longer states that “a prospective trial of a newer fibrate ... is ongoing,” because that trial investigating pemafibrate (Kowa), a novel selective peroxisome proliferator-activated receptor alpha modulator (or fibrate), has been discontinued.
Chronic kidney disease and risk management
In the Addendum to Section 11, “Chronic Kidney Disease and Risk Management,” the committee writes:
- “Traditionally, eGFR is calculated from serum creatinine using a validated formula. The Chronic Kidney Disease Epidemiology Collaboration (CKD-EPI) equation is preferred. ... Historically, a correction factor for muscle mass was included in a modified equation for African Americans; however, due to various issues with inequities, it was decided to the equation such that it applies to all. Hence, a committee was convened, resulting in the recommendation for immediate implementation of the CKD-EPI creatinine equation refit without the race variable in all laboratories in the U.S.” (This is based on an National Kidney Foundation and American Society of Nephrology Task Force recommendation.)
- “Additionally, increased use of cystatin C, especially to confirm estimated GFR in adults who are at risk for or have chronic kidney disease, because combining filtration markers (creatinine and cystatin C) is more accurate and would support better clinical decisions than either marker alone.”
Evidence from clinical trials
The update is based on findings from the following clinical trials:
- Efficacy and Safety of Finerenone in Subjects With Type 2 Diabetes Mellitus and Diabetic Kidney Disease (FIDELIO-DKD)
- Efficacy and Safety of Finerenone in Subjects With Type 2 Diabetes Mellitus and the Clinical Diagnosis of Diabetic Kidney Disease (FIGARO-DKD)
- FIDELITY, a prespecified pooled analysis of FIDELIO-DKD and FIGARO-DKD
- Empagliflozin Outcome Trial in Patients With Chronic Heart Failure With Preserved Ejection Fraction (EMPEROR-Preserved)
- Effects of Dapagliflozin on Biomarkers, Symptoms and Functional Status in Patients with PRESERVED Ejection Fraction Heart Failure (PRESERVED-HF)
- Pemafibrate to Reduce Cardiovascular Outcomes by Reducing Triglycerides in Patients with Diabetes (PROMINENT).
A version of this article first appeared on Medscape.com.
FROM DIABETES CARE
Schizophrenia patients in long-term facilities benefit from lower-dose antipsychotics
NEW ORLEANS –
“There is an argument by some experts in the field that state hospital populations represent a different set of patients who require higher antipsychotic dosages, with no alternative, but I don’t agree with that,” study lead author Mujeeb U. Shad, MD, GME-psychiatry program director and adjunct professor at the University of Nevada, Las Vegas, said in an interview.
In reducing doses, “patients appeared to blossom, becoming more active and less ‘zombie-like’; they started taking more interest in activities and their social [involvement] increased,” he said.

The study was among several presenting pros and cons of high antipsychotic doses at the 2022 annual meeting of the American Psychiatric Association.
Higher doses of antipsychotics are often relied upon when patients with acute psychosis fail to respond to standard treatment, however evidence supporting the approach is lacking.
And while some studies in fact show no benefit from the higher-dose maintenance therapy over conventional or even lower doses of antipsychotics, evidence regarding forensic patients hospitalized in long-term psychiatric facilities is also scant.
Meanwhile, the need to restore competency among those patients can be more pressing than normal.
“In a forensic population where executive cognitive function is one of the key elements to restore competency to stand trial, the continuation of high-dose therapy with excessive dopamine blockade may further compromise preexisting executive dysfunction to delay competency restoration,” Dr. Shad notes in the study.
The study describes a case series in which antipsychotic doses were lowered among 22 of Dr. Shad’s patients who had been determined to be incompetent to stand trial and referred to a state hospital to restore their competency.
With the objective of regaining the mental fitness to stand trial and being discharged from the facility, those on high doses of therapy, defined as a dose greater than 50% of the average package-insert dose, had their doses reduced to conventional dosages.
The approach led to as many as 68% of the patients being stabilized and discharged after having their competency restored, without symptom relapse, following an average antipsychotic dose reduction of 44%.
The average time to discharge following the dose reduction was just 2.3 months, after an average total hospitalization time of 11 months.
The shortest hospitalization durations (less than 7 months) were observed among those who did not receive changes in doses as they were already achieving efficacy with standard dosages.
Among two patients who were treated subtherapeutically, dose increases were required and they had the longest overall hospitalization (14.5 months)
Additional benefits of reduced dosages
Dr. Shad noted that, in addition to the earlier discharges, patients also had reductions in their polypharmacy, and in prolactin.
“We know that high prolactin level is such a huge problem, especially for female patients because it can cause osteoporosis, infertility, and abnormal menstruation, and the reductions in hyperprolactinemia can help reduce weight gain,” he said.
Dr. Shad added that he let some of those effects be his guide in making dose reductions.
“I was trying to gradually minimize the dose while monitoring the patients for relapse, and I used extrapyramidal symptoms and prolactin levels as my guide, looking for a sweet spot with the dosing,” he said.
“For example, if patients were taking an average of about 40-60 mg of a drug, I brought it down close to 20 mg, or close to the average package insert,” Dr. Shad said.
Key concerns among clinicians about reducing antipsychotic doses include the emergence of discontinuation or rebound symptoms, including psychosis, akathisia, or Parkinsonian symptoms, and studies, including a recent meta-analysis have supported those concerns, urging caution in reducing doses below standard levels.
However, Dr. Shad said his series suggests that reducing doses gradually while carefully monitoring extrapyramidal symptoms and prolactin levels may indeed pay off.
“They’re not the perfect guides, but they’re good guides, and with the right approach, [some] may be able to do this,” Dr. Shad said.
“However, the key to a successful dose reduction or discontinuation of an [antipsychotic medication] is to avoid abrupt discontinuation and follow a gradual dose reduction while monitoring symptoms and tolerability,” he said.

Commenting on the research, T. Scott Stroup, MD, a professor of psychiatry at Columbia University, New York, chimed in on the side of urging caution with higher doses and supporting possible benefits with the lower-dose approach.
“I agree that people who need antipsychotic medications should receive the lowest effective dose and that often this is identified by careful dose reduction,” he said in an interview.
Dr. Shad and Stroup had no disclosures to report.
NEW ORLEANS –
“There is an argument by some experts in the field that state hospital populations represent a different set of patients who require higher antipsychotic dosages, with no alternative, but I don’t agree with that,” study lead author Mujeeb U. Shad, MD, GME-psychiatry program director and adjunct professor at the University of Nevada, Las Vegas, said in an interview.
In reducing doses, “patients appeared to blossom, becoming more active and less ‘zombie-like’; they started taking more interest in activities and their social [involvement] increased,” he said.
The study was among several presenting pros and cons of high antipsychotic doses at the 2022 annual meeting of the American Psychiatric Association.
Higher doses of antipsychotics are often relied upon when patients with acute psychosis fail to respond to standard treatment, however evidence supporting the approach is lacking.
And while some studies in fact show no benefit from the higher-dose maintenance therapy over conventional or even lower doses of antipsychotics, evidence regarding forensic patients hospitalized in long-term psychiatric facilities is also scant.
Meanwhile, the need to restore competency among those patients can be more pressing than normal.
“In a forensic population where executive cognitive function is one of the key elements to restore competency to stand trial, the continuation of high-dose therapy with excessive dopamine blockade may further compromise preexisting executive dysfunction to delay competency restoration,” Dr. Shad notes in the study.
The study describes a case series in which antipsychotic doses were lowered among 22 of Dr. Shad’s patients who had been determined to be incompetent to stand trial and referred to a state hospital to restore their competency.
With the objective of regaining the mental fitness to stand trial and being discharged from the facility, those on high doses of therapy, defined as a dose greater than 50% of the average package-insert dose, had their doses reduced to conventional dosages.
The approach led to as many as 68% of the patients being stabilized and discharged after having their competency restored, without symptom relapse, following an average antipsychotic dose reduction of 44%.
The average time to discharge following the dose reduction was just 2.3 months, after an average total hospitalization time of 11 months.
The shortest hospitalization durations (less than 7 months) were observed among those who did not receive changes in doses as they were already achieving efficacy with standard dosages.
Among two patients who were treated subtherapeutically, dose increases were required and they had the longest overall hospitalization (14.5 months)
Additional benefits of reduced dosages
Dr. Shad noted that, in addition to the earlier discharges, patients also had reductions in their polypharmacy, and in prolactin.
“We know that high prolactin level is such a huge problem, especially for female patients because it can cause osteoporosis, infertility, and abnormal menstruation, and the reductions in hyperprolactinemia can help reduce weight gain,” he said.
Dr. Shad added that he let some of those effects be his guide in making dose reductions.
“I was trying to gradually minimize the dose while monitoring the patients for relapse, and I used extrapyramidal symptoms and prolactin levels as my guide, looking for a sweet spot with the dosing,” he said.
“For example, if patients were taking an average of about 40-60 mg of a drug, I brought it down close to 20 mg, or close to the average package insert,” Dr. Shad said.
Key concerns among clinicians about reducing antipsychotic doses include the emergence of discontinuation or rebound symptoms, including psychosis, akathisia, or Parkinsonian symptoms, and studies, including a recent meta-analysis have supported those concerns, urging caution in reducing doses below standard levels.
However, Dr. Shad said his series suggests that reducing doses gradually while carefully monitoring extrapyramidal symptoms and prolactin levels may indeed pay off.
“They’re not the perfect guides, but they’re good guides, and with the right approach, [some] may be able to do this,” Dr. Shad said.
“However, the key to a successful dose reduction or discontinuation of an [antipsychotic medication] is to avoid abrupt discontinuation and follow a gradual dose reduction while monitoring symptoms and tolerability,” he said.
Commenting on the research, T. Scott Stroup, MD, a professor of psychiatry at Columbia University, New York, chimed in on the side of urging caution with higher doses and supporting possible benefits with the lower-dose approach.
“I agree that people who need antipsychotic medications should receive the lowest effective dose and that often this is identified by careful dose reduction,” he said in an interview.
Dr. Shad and Stroup had no disclosures to report.
NEW ORLEANS –
“There is an argument by some experts in the field that state hospital populations represent a different set of patients who require higher antipsychotic dosages, with no alternative, but I don’t agree with that,” study lead author Mujeeb U. Shad, MD, GME-psychiatry program director and adjunct professor at the University of Nevada, Las Vegas, said in an interview.
In reducing doses, “patients appeared to blossom, becoming more active and less ‘zombie-like’; they started taking more interest in activities and their social [involvement] increased,” he said.
The study was among several presenting pros and cons of high antipsychotic doses at the 2022 annual meeting of the American Psychiatric Association.
Higher doses of antipsychotics are often relied upon when patients with acute psychosis fail to respond to standard treatment, however evidence supporting the approach is lacking.
And while some studies in fact show no benefit from the higher-dose maintenance therapy over conventional or even lower doses of antipsychotics, evidence regarding forensic patients hospitalized in long-term psychiatric facilities is also scant.
Meanwhile, the need to restore competency among those patients can be more pressing than normal.
“In a forensic population where executive cognitive function is one of the key elements to restore competency to stand trial, the continuation of high-dose therapy with excessive dopamine blockade may further compromise preexisting executive dysfunction to delay competency restoration,” Dr. Shad notes in the study.
The study describes a case series in which antipsychotic doses were lowered among 22 of Dr. Shad’s patients who had been determined to be incompetent to stand trial and referred to a state hospital to restore their competency.
With the objective of regaining the mental fitness to stand trial and being discharged from the facility, those on high doses of therapy, defined as a dose greater than 50% of the average package-insert dose, had their doses reduced to conventional dosages.
The approach led to as many as 68% of the patients being stabilized and discharged after having their competency restored, without symptom relapse, following an average antipsychotic dose reduction of 44%.
The average time to discharge following the dose reduction was just 2.3 months, after an average total hospitalization time of 11 months.
The shortest hospitalization durations (less than 7 months) were observed among those who did not receive changes in doses as they were already achieving efficacy with standard dosages.
Among two patients who were treated subtherapeutically, dose increases were required and they had the longest overall hospitalization (14.5 months)
Additional benefits of reduced dosages
Dr. Shad noted that, in addition to the earlier discharges, patients also had reductions in their polypharmacy, and in prolactin.
“We know that high prolactin level is such a huge problem, especially for female patients because it can cause osteoporosis, infertility, and abnormal menstruation, and the reductions in hyperprolactinemia can help reduce weight gain,” he said.
Dr. Shad added that he let some of those effects be his guide in making dose reductions.
“I was trying to gradually minimize the dose while monitoring the patients for relapse, and I used extrapyramidal symptoms and prolactin levels as my guide, looking for a sweet spot with the dosing,” he said.
“For example, if patients were taking an average of about 40-60 mg of a drug, I brought it down close to 20 mg, or close to the average package insert,” Dr. Shad said.
Key concerns among clinicians about reducing antipsychotic doses include the emergence of discontinuation or rebound symptoms, including psychosis, akathisia, or Parkinsonian symptoms, and studies, including a recent meta-analysis have supported those concerns, urging caution in reducing doses below standard levels.
However, Dr. Shad said his series suggests that reducing doses gradually while carefully monitoring extrapyramidal symptoms and prolactin levels may indeed pay off.
“They’re not the perfect guides, but they’re good guides, and with the right approach, [some] may be able to do this,” Dr. Shad said.
“However, the key to a successful dose reduction or discontinuation of an [antipsychotic medication] is to avoid abrupt discontinuation and follow a gradual dose reduction while monitoring symptoms and tolerability,” he said.
Commenting on the research, T. Scott Stroup, MD, a professor of psychiatry at Columbia University, New York, chimed in on the side of urging caution with higher doses and supporting possible benefits with the lower-dose approach.
“I agree that people who need antipsychotic medications should receive the lowest effective dose and that often this is identified by careful dose reduction,” he said in an interview.
Dr. Shad and Stroup had no disclosures to report.
FROM APA 2022
Novel drug ‘promising’ for concomitant depression, insomnia
In a randomized, placebo-controlled, adaptive dose–finding study conducted in more than 200 patients with MDD, those with more severe insomnia at baseline had a greater improvement in depressive symptoms versus those with less severe insomnia.
“As seltorexant is an orexin receptor antagonist, it is related to other medications that are marketed as sleeping pills, so it was important to show that its antidepressant efficacy was actually caused by improved sleep,” coinvestigator Michael E. Thase, MD, professor of psychiatry, Perelman School of Medicine, University of Pennsylvania, Philadelphia, told this news organization.

“This novel antidepressant may well turn out to be a treatment of choice for depressed patients with insomnia,” said Dr. Thase, who is also a member of the medical and research staff of the Corporal Michael J. Crescenz Department of Veterans Affairs Medical Center.
The findings were presented at the American Society of Clinical Psychopharmacology annual meeting.
Clinically meaningful?
In an earlier exploratory study, seltorexant showed antidepressant and sleep-promoting effects in patients with MDD. In a phase 2b study, a 20-mg dose of the drug showed clinically meaningful improvement in the Montgomery-Åsberg Depression Rating Scale (MADRS) total score after 6 weeks of treatment.
In the current analysis, the investigators evaluated the effect of seltorexant in improving depressive symptoms beyond sleep-related improvement in patients with MDD, using the MADRS-WOSI (MADRS without the sleep item).
They also used the six-item core MADRS subscale, which excludes sleep, anxiety, and appetite items.
The 283 participants were randomly assigned 3:3:1 to receive seltorexant 10 mg or 20 mg or placebo once daily. They were also stratified into two groups according to the severity of their insomnia: those with a baseline Insomnia Severity Index [ISI] score of 15 or higher (58%) and those with a baseline ISI score of less than 15 (42%).
Results showed that the group receiving the 20-mg/day dose of seltorexant (n = 61 patients) obtained a statistically and clinically meaningful response, compared with the placebo group (n = 137 patients) after removing the insomnia and other “not core items” of the MADRS. The effect was clearest among those with high insomnia ratings.
Improvement in the MADRS-WOSI score was also observed in the seltorexant 20-mg group at week 3 and week 6, compared with the placebo group.
The LSM average distance
The least squares mean (LSM) average difference between the treatment and placebo groups in the MADRS-WOSI score at week 3 was −3.8 (90% confidence interval, −5.98 to −1.57; P = .005).
At week 6, the LSM between the groups in the MADRS-WOSI score was −2.5 (90% CI, −5.24 to 0.15; P = .12).
The results were consistent with improvement in the MADRS total score. At week 3, the LSM in the MADRS total score was -4.5 (90% CI, -6.96 to -2.07; P = .003) and, at week 6, it was -3.1 (90% CI, -6.13 to -0.16; P = .083).
Seltorexant 20 mg was especially effective in patients who had more severe insomnia.
Commenting on the study, Nagy Youssef, MD, PhD, professor of psychiatry, The Ohio State University Wexner Medical Center, Columbus, said this was “a well-designed study examining a promising compound.”

“Especially if replicated, this study shows the promise of this molecule for this patient population,” said Dr. Youssef, who was not involved with the research.
The study was funded by Janssen Pharmaceutical of Johnson & Johnson. Dr. Thase reports financial relationships with numerous companies. Dr. Youssef reports no relevant financial relationships.
A version of this article first appeared on Medscape.com.
In a randomized, placebo-controlled, adaptive dose–finding study conducted in more than 200 patients with MDD, those with more severe insomnia at baseline had a greater improvement in depressive symptoms versus those with less severe insomnia.
“As seltorexant is an orexin receptor antagonist, it is related to other medications that are marketed as sleeping pills, so it was important to show that its antidepressant efficacy was actually caused by improved sleep,” coinvestigator Michael E. Thase, MD, professor of psychiatry, Perelman School of Medicine, University of Pennsylvania, Philadelphia, told this news organization.
“This novel antidepressant may well turn out to be a treatment of choice for depressed patients with insomnia,” said Dr. Thase, who is also a member of the medical and research staff of the Corporal Michael J. Crescenz Department of Veterans Affairs Medical Center.
The findings were presented at the American Society of Clinical Psychopharmacology annual meeting.
Clinically meaningful?
In an earlier exploratory study, seltorexant showed antidepressant and sleep-promoting effects in patients with MDD. In a phase 2b study, a 20-mg dose of the drug showed clinically meaningful improvement in the Montgomery-Åsberg Depression Rating Scale (MADRS) total score after 6 weeks of treatment.
In the current analysis, the investigators evaluated the effect of seltorexant in improving depressive symptoms beyond sleep-related improvement in patients with MDD, using the MADRS-WOSI (MADRS without the sleep item).
They also used the six-item core MADRS subscale, which excludes sleep, anxiety, and appetite items.
The 283 participants were randomly assigned 3:3:1 to receive seltorexant 10 mg or 20 mg or placebo once daily. They were also stratified into two groups according to the severity of their insomnia: those with a baseline Insomnia Severity Index [ISI] score of 15 or higher (58%) and those with a baseline ISI score of less than 15 (42%).
Results showed that the group receiving the 20-mg/day dose of seltorexant (n = 61 patients) obtained a statistically and clinically meaningful response, compared with the placebo group (n = 137 patients) after removing the insomnia and other “not core items” of the MADRS. The effect was clearest among those with high insomnia ratings.
Improvement in the MADRS-WOSI score was also observed in the seltorexant 20-mg group at week 3 and week 6, compared with the placebo group.
The LSM average distance
The least squares mean (LSM) average difference between the treatment and placebo groups in the MADRS-WOSI score at week 3 was −3.8 (90% confidence interval, −5.98 to −1.57; P = .005).
At week 6, the LSM between the groups in the MADRS-WOSI score was −2.5 (90% CI, −5.24 to 0.15; P = .12).
The results were consistent with improvement in the MADRS total score. At week 3, the LSM in the MADRS total score was -4.5 (90% CI, -6.96 to -2.07; P = .003) and, at week 6, it was -3.1 (90% CI, -6.13 to -0.16; P = .083).
Seltorexant 20 mg was especially effective in patients who had more severe insomnia.
Commenting on the study, Nagy Youssef, MD, PhD, professor of psychiatry, The Ohio State University Wexner Medical Center, Columbus, said this was “a well-designed study examining a promising compound.”
“Especially if replicated, this study shows the promise of this molecule for this patient population,” said Dr. Youssef, who was not involved with the research.
The study was funded by Janssen Pharmaceutical of Johnson & Johnson. Dr. Thase reports financial relationships with numerous companies. Dr. Youssef reports no relevant financial relationships.
A version of this article first appeared on Medscape.com.
In a randomized, placebo-controlled, adaptive dose–finding study conducted in more than 200 patients with MDD, those with more severe insomnia at baseline had a greater improvement in depressive symptoms versus those with less severe insomnia.
“As seltorexant is an orexin receptor antagonist, it is related to other medications that are marketed as sleeping pills, so it was important to show that its antidepressant efficacy was actually caused by improved sleep,” coinvestigator Michael E. Thase, MD, professor of psychiatry, Perelman School of Medicine, University of Pennsylvania, Philadelphia, told this news organization.
“This novel antidepressant may well turn out to be a treatment of choice for depressed patients with insomnia,” said Dr. Thase, who is also a member of the medical and research staff of the Corporal Michael J. Crescenz Department of Veterans Affairs Medical Center.
The findings were presented at the American Society of Clinical Psychopharmacology annual meeting.
Clinically meaningful?
In an earlier exploratory study, seltorexant showed antidepressant and sleep-promoting effects in patients with MDD. In a phase 2b study, a 20-mg dose of the drug showed clinically meaningful improvement in the Montgomery-Åsberg Depression Rating Scale (MADRS) total score after 6 weeks of treatment.
In the current analysis, the investigators evaluated the effect of seltorexant in improving depressive symptoms beyond sleep-related improvement in patients with MDD, using the MADRS-WOSI (MADRS without the sleep item).
They also used the six-item core MADRS subscale, which excludes sleep, anxiety, and appetite items.
The 283 participants were randomly assigned 3:3:1 to receive seltorexant 10 mg or 20 mg or placebo once daily. They were also stratified into two groups according to the severity of their insomnia: those with a baseline Insomnia Severity Index [ISI] score of 15 or higher (58%) and those with a baseline ISI score of less than 15 (42%).
Results showed that the group receiving the 20-mg/day dose of seltorexant (n = 61 patients) obtained a statistically and clinically meaningful response, compared with the placebo group (n = 137 patients) after removing the insomnia and other “not core items” of the MADRS. The effect was clearest among those with high insomnia ratings.
Improvement in the MADRS-WOSI score was also observed in the seltorexant 20-mg group at week 3 and week 6, compared with the placebo group.
The LSM average distance
The least squares mean (LSM) average difference between the treatment and placebo groups in the MADRS-WOSI score at week 3 was −3.8 (90% confidence interval, −5.98 to −1.57; P = .005).
At week 6, the LSM between the groups in the MADRS-WOSI score was −2.5 (90% CI, −5.24 to 0.15; P = .12).
The results were consistent with improvement in the MADRS total score. At week 3, the LSM in the MADRS total score was -4.5 (90% CI, -6.96 to -2.07; P = .003) and, at week 6, it was -3.1 (90% CI, -6.13 to -0.16; P = .083).
Seltorexant 20 mg was especially effective in patients who had more severe insomnia.
Commenting on the study, Nagy Youssef, MD, PhD, professor of psychiatry, The Ohio State University Wexner Medical Center, Columbus, said this was “a well-designed study examining a promising compound.”
“Especially if replicated, this study shows the promise of this molecule for this patient population,” said Dr. Youssef, who was not involved with the research.
The study was funded by Janssen Pharmaceutical of Johnson & Johnson. Dr. Thase reports financial relationships with numerous companies. Dr. Youssef reports no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM ASCP 2022
Acetaminophen linked to diminished response to immunotherapy in cancer
The team found a strong association between the use of acetaminophen and a decreased response to immune checkpoint inhibitors in a study of three clinical cohorts involving more than 600 patients with advanced cancer.
Patients who took acetaminophen at the start of immunotherapy – with acetaminophen exposure confirmed by plasma testing – were found to have worse overall survival and progression-free survival than patients who did not take the analgesic. Multivariate analysis confirmed the association independent of other prognostic factors. “It is unlikely that our data are the result of bias or unmeasured confounding,” the authors comment.
The findings “present a compelling case for caution” in using acetaminophen in patients with cancer who are receiving immune checkpoint blockers, senior investigator Antoine Italiano, MD, PhD, a medical oncologist at the University of Bordeaux (France), and colleagues concluded.
The study was presented at the annual meeting of the American Society of Clinical Oncology and published simultaneously in Annals of Oncology.
“Patients with advanced cancer taking [acetaminophen] during immunotherapy experience worse clinical outcomes, which suggests that [acetaminophen] decreases T cell–mediated antitumor immunity,” the authors comment.
They also report bench research and blood studies in four healthy volunteers, which showed an up-regulation of immunosuppressive regulatory T cells (Tregs) with acetaminophen, and other findings that together suggest that acetaminophen undermines the antitumor immune processes by which checkpoint inhibitors work.
Reconsider acetaminophen pretreatment
After hearing Dr. Italiano present the results at the meeting, a Polish oncologist in the audience said he was concerned that his clinic premedicates with acetaminophen before immune checkpoint blockade and wanted to know if they should stop doing it.
“I don’t think inducing Tregs ... in cancer patients is a good approach. I do a lot of clinical trials,” and “I do not understand why in several cases sponsors required mandatory premedication with acetaminophen. I think ... we should reconsider this approach,” Dr. Italiano said.
There’s precedence for the findings. Acetaminophen – also known as paracetamol – has been shown in some studies to limit immune cell proliferation, T-cell–dependent antibody response, and viral clearance, among other things. After a randomized trial showing blunted responses to vaccines in individuals who were taking acetaminophen, the World Health Organization recommended in 2015 against concurrent use of acetaminophen with vaccines.
Steroids, antibiotics, and proton pump inhibitors have also recently been shown to worsen outcomes with pembrolizumab, noted invited discussant, Margaret Gatti-Mays, MD, a medical oncologist at Ohio State University, Columbus.
“We are starting to understand that ... commonly used medications may have a larger impact on the efficacy and toxicity of immune checkpoint blockade than historically seen with chemotherapy,” she said.
However, she expressed some uncertainty over the French findings, as she was concerned that even the multivariate analysis didn’t completely rule out that acetaminophen users had worse disease to begin with and so would be expected to have worse outcomes.
She was also unsure of how much acetaminophen is too much.
Acetaminophen has a half-life of around 3 hours or less, where the immune checkpoint inhibitors have a half-life of around 20 days or more.
Given that, Dr. Gatti-Mays wondered whether “a single dose of acetaminophen [is] enough to derail the benefit of checkpoint inhibition? Does exposure need to be continuous?”
She allowed that acetaminophen use may turn out to be one more of the many patient-level factors emerging lately – such as chronic stress, diet, body flora, and physiological age, among others – that might help explain why checkpoint inhibition works in only about 20% of eligible patients with cancer.
Study details
Dr. Italiano and his team analyzed plasma samples from 297 participants in the CheckMate 025 trial of nivolumab for renal cancer; 34 participants in the BIP study into actionable molecular alterations in cancer; and 297 participants in the PREMIS immune-related adverse events study. The patients in these last two studies had a variety of cancers and were taking various agents.
All 628 patients were on checkpoint inhibitors. The investigators divided them according to who had acetaminophen or its metabolite acetaminophen glucuronide in their plasma when they started checkpoint inhibition and those who did not.
In CheckMate 025, overall survival was significantly worse among participants who had detectable acetaminophen or its metabolite in plasma (hazard ratio, 0.67; P = .004).
None of the acetaminophen-positive participants in the BIP study responded to checkpoint blockade, compared with almost 30% of those who were negative. Acetaminophen-positive participants also trended toward worse progression-free survival (median, 1.87 vs. 4.72 months) and overall survival (median, 7.87 vs. 16.56 months).
In PREMIS, progression-free survival was a median of 2.63 months in the acetaminophen group versus 5.03 months in negative participants (P = .009); median overall survival was 8.43 months versus 14.93 months, respectively (P < .0001).
A multivariate analysis was performed in PREMIS. Acetaminophen exposure was associated with both progression-free survival (hazard ratio, 1.43; P =.015) and overall survival (HR, 1.78; P =.006) independently of performance status, liver metastases, bone metastases, number of metastases sites, tumor type, number of previous lines of treatment, steroid/antibiotic use, lactate dehydrogenase levels, and other factors.
There was no funding for the work. Dr. Italiano is a consultant for AstraZeneca, Bayer, Chugai, Deciphera, Merck, Parthenon, Roche, and Springworks, He also has grants from AstraZeneca, Bayer, Bristol-Myers Squibb, Merck, MSD, Novartis, Pharmamar, and Roche. Two authors work for Explicyte and one works for Amgen. Dr. Gatti-Mays is a consultant for Seattle Genetics.
A version of this article first appeared on Medscape.com.
The team found a strong association between the use of acetaminophen and a decreased response to immune checkpoint inhibitors in a study of three clinical cohorts involving more than 600 patients with advanced cancer.
Patients who took acetaminophen at the start of immunotherapy – with acetaminophen exposure confirmed by plasma testing – were found to have worse overall survival and progression-free survival than patients who did not take the analgesic. Multivariate analysis confirmed the association independent of other prognostic factors. “It is unlikely that our data are the result of bias or unmeasured confounding,” the authors comment.
The findings “present a compelling case for caution” in using acetaminophen in patients with cancer who are receiving immune checkpoint blockers, senior investigator Antoine Italiano, MD, PhD, a medical oncologist at the University of Bordeaux (France), and colleagues concluded.
The study was presented at the annual meeting of the American Society of Clinical Oncology and published simultaneously in Annals of Oncology.
“Patients with advanced cancer taking [acetaminophen] during immunotherapy experience worse clinical outcomes, which suggests that [acetaminophen] decreases T cell–mediated antitumor immunity,” the authors comment.
They also report bench research and blood studies in four healthy volunteers, which showed an up-regulation of immunosuppressive regulatory T cells (Tregs) with acetaminophen, and other findings that together suggest that acetaminophen undermines the antitumor immune processes by which checkpoint inhibitors work.
Reconsider acetaminophen pretreatment
After hearing Dr. Italiano present the results at the meeting, a Polish oncologist in the audience said he was concerned that his clinic premedicates with acetaminophen before immune checkpoint blockade and wanted to know if they should stop doing it.
“I don’t think inducing Tregs ... in cancer patients is a good approach. I do a lot of clinical trials,” and “I do not understand why in several cases sponsors required mandatory premedication with acetaminophen. I think ... we should reconsider this approach,” Dr. Italiano said.
There’s precedence for the findings. Acetaminophen – also known as paracetamol – has been shown in some studies to limit immune cell proliferation, T-cell–dependent antibody response, and viral clearance, among other things. After a randomized trial showing blunted responses to vaccines in individuals who were taking acetaminophen, the World Health Organization recommended in 2015 against concurrent use of acetaminophen with vaccines.
Steroids, antibiotics, and proton pump inhibitors have also recently been shown to worsen outcomes with pembrolizumab, noted invited discussant, Margaret Gatti-Mays, MD, a medical oncologist at Ohio State University, Columbus.
“We are starting to understand that ... commonly used medications may have a larger impact on the efficacy and toxicity of immune checkpoint blockade than historically seen with chemotherapy,” she said.
However, she expressed some uncertainty over the French findings, as she was concerned that even the multivariate analysis didn’t completely rule out that acetaminophen users had worse disease to begin with and so would be expected to have worse outcomes.
She was also unsure of how much acetaminophen is too much.
Acetaminophen has a half-life of around 3 hours or less, where the immune checkpoint inhibitors have a half-life of around 20 days or more.
Given that, Dr. Gatti-Mays wondered whether “a single dose of acetaminophen [is] enough to derail the benefit of checkpoint inhibition? Does exposure need to be continuous?”
She allowed that acetaminophen use may turn out to be one more of the many patient-level factors emerging lately – such as chronic stress, diet, body flora, and physiological age, among others – that might help explain why checkpoint inhibition works in only about 20% of eligible patients with cancer.
Study details
Dr. Italiano and his team analyzed plasma samples from 297 participants in the CheckMate 025 trial of nivolumab for renal cancer; 34 participants in the BIP study into actionable molecular alterations in cancer; and 297 participants in the PREMIS immune-related adverse events study. The patients in these last two studies had a variety of cancers and were taking various agents.
All 628 patients were on checkpoint inhibitors. The investigators divided them according to who had acetaminophen or its metabolite acetaminophen glucuronide in their plasma when they started checkpoint inhibition and those who did not.
In CheckMate 025, overall survival was significantly worse among participants who had detectable acetaminophen or its metabolite in plasma (hazard ratio, 0.67; P = .004).
None of the acetaminophen-positive participants in the BIP study responded to checkpoint blockade, compared with almost 30% of those who were negative. Acetaminophen-positive participants also trended toward worse progression-free survival (median, 1.87 vs. 4.72 months) and overall survival (median, 7.87 vs. 16.56 months).
In PREMIS, progression-free survival was a median of 2.63 months in the acetaminophen group versus 5.03 months in negative participants (P = .009); median overall survival was 8.43 months versus 14.93 months, respectively (P < .0001).
A multivariate analysis was performed in PREMIS. Acetaminophen exposure was associated with both progression-free survival (hazard ratio, 1.43; P =.015) and overall survival (HR, 1.78; P =.006) independently of performance status, liver metastases, bone metastases, number of metastases sites, tumor type, number of previous lines of treatment, steroid/antibiotic use, lactate dehydrogenase levels, and other factors.
There was no funding for the work. Dr. Italiano is a consultant for AstraZeneca, Bayer, Chugai, Deciphera, Merck, Parthenon, Roche, and Springworks, He also has grants from AstraZeneca, Bayer, Bristol-Myers Squibb, Merck, MSD, Novartis, Pharmamar, and Roche. Two authors work for Explicyte and one works for Amgen. Dr. Gatti-Mays is a consultant for Seattle Genetics.
A version of this article first appeared on Medscape.com.
The team found a strong association between the use of acetaminophen and a decreased response to immune checkpoint inhibitors in a study of three clinical cohorts involving more than 600 patients with advanced cancer.
Patients who took acetaminophen at the start of immunotherapy – with acetaminophen exposure confirmed by plasma testing – were found to have worse overall survival and progression-free survival than patients who did not take the analgesic. Multivariate analysis confirmed the association independent of other prognostic factors. “It is unlikely that our data are the result of bias or unmeasured confounding,” the authors comment.
The findings “present a compelling case for caution” in using acetaminophen in patients with cancer who are receiving immune checkpoint blockers, senior investigator Antoine Italiano, MD, PhD, a medical oncologist at the University of Bordeaux (France), and colleagues concluded.
The study was presented at the annual meeting of the American Society of Clinical Oncology and published simultaneously in Annals of Oncology.
“Patients with advanced cancer taking [acetaminophen] during immunotherapy experience worse clinical outcomes, which suggests that [acetaminophen] decreases T cell–mediated antitumor immunity,” the authors comment.
They also report bench research and blood studies in four healthy volunteers, which showed an up-regulation of immunosuppressive regulatory T cells (Tregs) with acetaminophen, and other findings that together suggest that acetaminophen undermines the antitumor immune processes by which checkpoint inhibitors work.
Reconsider acetaminophen pretreatment
After hearing Dr. Italiano present the results at the meeting, a Polish oncologist in the audience said he was concerned that his clinic premedicates with acetaminophen before immune checkpoint blockade and wanted to know if they should stop doing it.
“I don’t think inducing Tregs ... in cancer patients is a good approach. I do a lot of clinical trials,” and “I do not understand why in several cases sponsors required mandatory premedication with acetaminophen. I think ... we should reconsider this approach,” Dr. Italiano said.
There’s precedence for the findings. Acetaminophen – also known as paracetamol – has been shown in some studies to limit immune cell proliferation, T-cell–dependent antibody response, and viral clearance, among other things. After a randomized trial showing blunted responses to vaccines in individuals who were taking acetaminophen, the World Health Organization recommended in 2015 against concurrent use of acetaminophen with vaccines.
Steroids, antibiotics, and proton pump inhibitors have also recently been shown to worsen outcomes with pembrolizumab, noted invited discussant, Margaret Gatti-Mays, MD, a medical oncologist at Ohio State University, Columbus.
“We are starting to understand that ... commonly used medications may have a larger impact on the efficacy and toxicity of immune checkpoint blockade than historically seen with chemotherapy,” she said.
However, she expressed some uncertainty over the French findings, as she was concerned that even the multivariate analysis didn’t completely rule out that acetaminophen users had worse disease to begin with and so would be expected to have worse outcomes.
She was also unsure of how much acetaminophen is too much.
Acetaminophen has a half-life of around 3 hours or less, where the immune checkpoint inhibitors have a half-life of around 20 days or more.
Given that, Dr. Gatti-Mays wondered whether “a single dose of acetaminophen [is] enough to derail the benefit of checkpoint inhibition? Does exposure need to be continuous?”
She allowed that acetaminophen use may turn out to be one more of the many patient-level factors emerging lately – such as chronic stress, diet, body flora, and physiological age, among others – that might help explain why checkpoint inhibition works in only about 20% of eligible patients with cancer.
Study details
Dr. Italiano and his team analyzed plasma samples from 297 participants in the CheckMate 025 trial of nivolumab for renal cancer; 34 participants in the BIP study into actionable molecular alterations in cancer; and 297 participants in the PREMIS immune-related adverse events study. The patients in these last two studies had a variety of cancers and were taking various agents.
All 628 patients were on checkpoint inhibitors. The investigators divided them according to who had acetaminophen or its metabolite acetaminophen glucuronide in their plasma when they started checkpoint inhibition and those who did not.
In CheckMate 025, overall survival was significantly worse among participants who had detectable acetaminophen or its metabolite in plasma (hazard ratio, 0.67; P = .004).
None of the acetaminophen-positive participants in the BIP study responded to checkpoint blockade, compared with almost 30% of those who were negative. Acetaminophen-positive participants also trended toward worse progression-free survival (median, 1.87 vs. 4.72 months) and overall survival (median, 7.87 vs. 16.56 months).
In PREMIS, progression-free survival was a median of 2.63 months in the acetaminophen group versus 5.03 months in negative participants (P = .009); median overall survival was 8.43 months versus 14.93 months, respectively (P < .0001).
A multivariate analysis was performed in PREMIS. Acetaminophen exposure was associated with both progression-free survival (hazard ratio, 1.43; P =.015) and overall survival (HR, 1.78; P =.006) independently of performance status, liver metastases, bone metastases, number of metastases sites, tumor type, number of previous lines of treatment, steroid/antibiotic use, lactate dehydrogenase levels, and other factors.
There was no funding for the work. Dr. Italiano is a consultant for AstraZeneca, Bayer, Chugai, Deciphera, Merck, Parthenon, Roche, and Springworks, He also has grants from AstraZeneca, Bayer, Bristol-Myers Squibb, Merck, MSD, Novartis, Pharmamar, and Roche. Two authors work for Explicyte and one works for Amgen. Dr. Gatti-Mays is a consultant for Seattle Genetics.
A version of this article first appeared on Medscape.com.
FROM ASCO 2022
Women are not being warned that anesthetic may reduce birth pill efficacy
The effectiveness of hormonal contraceptives, including the pill and mini-pill, may be compromised by sugammadex, a drug widely used in anesthesia for reversing neuromuscular blockade induced by rocuronium or vecuronium.
Yet women are not routinely informed that the drug may make their contraception less effective, delegates at Euroanaesthesia, the annual meeting of the European Society of Anaesthesiology and Intensive Care in Milan were told.
New research presented at the meeting supports the authors’ experience that “robust methods for identifying at-risk patients and informing them of the associated risk of contraceptive failures is not common practice across anesthetic departments within the United Kingdom, and likely further afield.”
This is according to a survey of almost 150 anesthetic professionals, including consultants, junior doctors, and physician assistants, working at University College London Hospitals NHS Foundation Trust.
Dr. Neha Passi, Dr. Matt Oliver, and colleagues at the trust’s department of anesthesiology sent out a seven-question survey to their 150 colleagues and received 82 responses, 94% of which claimed awareness of the risk of contraceptive failure with sugammadex. However, 70% of the respondents admitted that they do not routinely discuss this with patients who have received the drug.
Risk with all forms of hormonal contraceptive
Yet current guidance is to inform women of child-bearing age that they have received the drug and, because of increased risk of contraceptive failure, advise those taking oral hormonal contraceptives to follow the missed pill advice in the leaflet that comes with their contraceptives. It also counsels that clinicians should advise women using other types of hormonal contraceptive to use an additional nonhormonal means of contraception for 7 days.
The study authors also carried out a retrospective audit of sugammadex use in the trust and reported that during the 6 weeks covered by the audit, 234 patients were administered sugammadex of whom 65 (28%) were women of childbearing age. Of these, 17 had a medical history that meant they weren’t at risk of pregnancy, but the other 48 should have received advice on the risks of contraceptive failure – however there was no record in the medical notes of such advice having been given for any of the at-risk 48 women.
While sugammadex is the only anesthetic drug known to have this effect, it is recognized to interact with progesterone and so may reduce the effectiveness of hormonal contraceptives, including the progesterone-only pill, combined pill, vaginal rings, implants, and intrauterine devices.
Dr. Passi said: “It is concerning that we are so seldom informing patients of the risk of contraceptive failure following sugammadex use.
“Use of sugammadex is expected to rise as it becomes cheaper in the future, and ensuring that women receiving this medicine are aware it may increase their risk of unwanted pregnancy must be a priority.”
She added: “It is important to note, however, that most patients receiving an anesthetic do not need a muscle relaxant and that sugammadex is one of several drugs available to reverse muscle relaxation.”
Dr. Oliver said: “We only studied one hospital trust but we expect the results to be similar in elsewhere in the U.K.”
In response to their findings, the study’s authors have created patient information leaflets and letters and programmed the trust’s electronic patient record system to identify “at-risk” patients and deliver electronic prompts to the anesthetists caring for them in the perioperative period.
A version of this article first appeared on Medscape UK.
The effectiveness of hormonal contraceptives, including the pill and mini-pill, may be compromised by sugammadex, a drug widely used in anesthesia for reversing neuromuscular blockade induced by rocuronium or vecuronium.
Yet women are not routinely informed that the drug may make their contraception less effective, delegates at Euroanaesthesia, the annual meeting of the European Society of Anaesthesiology and Intensive Care in Milan were told.
New research presented at the meeting supports the authors’ experience that “robust methods for identifying at-risk patients and informing them of the associated risk of contraceptive failures is not common practice across anesthetic departments within the United Kingdom, and likely further afield.”
This is according to a survey of almost 150 anesthetic professionals, including consultants, junior doctors, and physician assistants, working at University College London Hospitals NHS Foundation Trust.
Dr. Neha Passi, Dr. Matt Oliver, and colleagues at the trust’s department of anesthesiology sent out a seven-question survey to their 150 colleagues and received 82 responses, 94% of which claimed awareness of the risk of contraceptive failure with sugammadex. However, 70% of the respondents admitted that they do not routinely discuss this with patients who have received the drug.
Risk with all forms of hormonal contraceptive
Yet current guidance is to inform women of child-bearing age that they have received the drug and, because of increased risk of contraceptive failure, advise those taking oral hormonal contraceptives to follow the missed pill advice in the leaflet that comes with their contraceptives. It also counsels that clinicians should advise women using other types of hormonal contraceptive to use an additional nonhormonal means of contraception for 7 days.
The study authors also carried out a retrospective audit of sugammadex use in the trust and reported that during the 6 weeks covered by the audit, 234 patients were administered sugammadex of whom 65 (28%) were women of childbearing age. Of these, 17 had a medical history that meant they weren’t at risk of pregnancy, but the other 48 should have received advice on the risks of contraceptive failure – however there was no record in the medical notes of such advice having been given for any of the at-risk 48 women.
While sugammadex is the only anesthetic drug known to have this effect, it is recognized to interact with progesterone and so may reduce the effectiveness of hormonal contraceptives, including the progesterone-only pill, combined pill, vaginal rings, implants, and intrauterine devices.
Dr. Passi said: “It is concerning that we are so seldom informing patients of the risk of contraceptive failure following sugammadex use.
“Use of sugammadex is expected to rise as it becomes cheaper in the future, and ensuring that women receiving this medicine are aware it may increase their risk of unwanted pregnancy must be a priority.”
She added: “It is important to note, however, that most patients receiving an anesthetic do not need a muscle relaxant and that sugammadex is one of several drugs available to reverse muscle relaxation.”
Dr. Oliver said: “We only studied one hospital trust but we expect the results to be similar in elsewhere in the U.K.”
In response to their findings, the study’s authors have created patient information leaflets and letters and programmed the trust’s electronic patient record system to identify “at-risk” patients and deliver electronic prompts to the anesthetists caring for them in the perioperative period.
A version of this article first appeared on Medscape UK.
The effectiveness of hormonal contraceptives, including the pill and mini-pill, may be compromised by sugammadex, a drug widely used in anesthesia for reversing neuromuscular blockade induced by rocuronium or vecuronium.
Yet women are not routinely informed that the drug may make their contraception less effective, delegates at Euroanaesthesia, the annual meeting of the European Society of Anaesthesiology and Intensive Care in Milan were told.
New research presented at the meeting supports the authors’ experience that “robust methods for identifying at-risk patients and informing them of the associated risk of contraceptive failures is not common practice across anesthetic departments within the United Kingdom, and likely further afield.”
This is according to a survey of almost 150 anesthetic professionals, including consultants, junior doctors, and physician assistants, working at University College London Hospitals NHS Foundation Trust.
Dr. Neha Passi, Dr. Matt Oliver, and colleagues at the trust’s department of anesthesiology sent out a seven-question survey to their 150 colleagues and received 82 responses, 94% of which claimed awareness of the risk of contraceptive failure with sugammadex. However, 70% of the respondents admitted that they do not routinely discuss this with patients who have received the drug.
Risk with all forms of hormonal contraceptive
Yet current guidance is to inform women of child-bearing age that they have received the drug and, because of increased risk of contraceptive failure, advise those taking oral hormonal contraceptives to follow the missed pill advice in the leaflet that comes with their contraceptives. It also counsels that clinicians should advise women using other types of hormonal contraceptive to use an additional nonhormonal means of contraception for 7 days.
The study authors also carried out a retrospective audit of sugammadex use in the trust and reported that during the 6 weeks covered by the audit, 234 patients were administered sugammadex of whom 65 (28%) were women of childbearing age. Of these, 17 had a medical history that meant they weren’t at risk of pregnancy, but the other 48 should have received advice on the risks of contraceptive failure – however there was no record in the medical notes of such advice having been given for any of the at-risk 48 women.
While sugammadex is the only anesthetic drug known to have this effect, it is recognized to interact with progesterone and so may reduce the effectiveness of hormonal contraceptives, including the progesterone-only pill, combined pill, vaginal rings, implants, and intrauterine devices.
Dr. Passi said: “It is concerning that we are so seldom informing patients of the risk of contraceptive failure following sugammadex use.
“Use of sugammadex is expected to rise as it becomes cheaper in the future, and ensuring that women receiving this medicine are aware it may increase their risk of unwanted pregnancy must be a priority.”
She added: “It is important to note, however, that most patients receiving an anesthetic do not need a muscle relaxant and that sugammadex is one of several drugs available to reverse muscle relaxation.”
Dr. Oliver said: “We only studied one hospital trust but we expect the results to be similar in elsewhere in the U.K.”
In response to their findings, the study’s authors have created patient information leaflets and letters and programmed the trust’s electronic patient record system to identify “at-risk” patients and deliver electronic prompts to the anesthetists caring for them in the perioperative period.
A version of this article first appeared on Medscape UK.
FROM EUROANAESTHESIA
Antipsychotic tied to dose-related weight gain, higher cholesterol
new research suggests.
Investigators analyzed 1-year data for more than 400 patients who were taking risperidone and/or its metabolite paliperidone (Invega). Results showed increments of 1 mg of risperidone-equivalent doses were associated with an increase of 0.25% of weight within a year of follow-up.
“Although our findings report a positive and statistically significant dose-dependence of weight gain and cholesterol, both total and LDL [cholesterol], the size of the predicted changes of metabolic effects is clinically nonrelevant,” lead author Marianna Piras, PharmD, Centre for Psychiatric Neuroscience, Lausanne (Switzerland) University Hospital, said in an interview.
“Therefore, dose lowering would not have a beneficial effect on attenuating weight gain or cholesterol increases and could lead to psychiatric decompensation,” said Ms. Piras, who is also a PhD candidate in the unit of pharmacogenetics and clinical psychopharmacology at the University of Lausanne.
However, she added that because dose increments could increase risk for significant weight gain in the first month of treatment – the dose can be increased typically in a range of 1-10 grams – and strong dose increments could contribute to metabolic worsening over time, “risperidone minimum effective doses should be preferred.”
The findings were published online in the Journal of Clinical Psychiatry.
‘Serious public health issue’
Compared with the general population, patients with mental illness present with a greater prevalence of metabolic disorders. In addition, several psychotropic medications, including antipsychotics, can induce metabolic alterations such as weight gain, the investigators noted.
Antipsychotic-induced metabolic adverse effects “constitute a serious public health issue” because they are risk factors for cardiovascular diseases such as obesity and/or dyslipidemia, “which have been associated with a 10-year reduced life expectancy in the psychiatric population,” Ms. Piras said.
“The dose-dependence of metabolic adverse effects is a debated subject that needs to be assessed for each psychotropic drug known to induce weight gain,” she added.
Several previous studies have examined whether there is a dose-related effect of antipsychotics on metabolic parameters, “with some results suggesting that [weight gain] seems to develop even when low off-label doses are prescribed,” Ms. Piras noted.
She and her colleagues had already studied dose-related metabolic effects of quetiapine (Seroquel) and olanzapine (Zyprexa).
Risperidone is an antipsychotic with a “medium to high metabolic risk profile,” the researchers note, and few studies have examined the impact of risperidone on metabolic parameters other than weight gain.
For the current analysis, they analyzed data from a longitudinal study that included 438 patients (mean age, 40.7 years; 50.7% men) who started treatment with risperidone and/or paliperidone between 2007 and 2018.
The participants had diagnoses of schizophrenia, schizoaffective disorder, bipolar disorder, depression, “other,” or “unknown.”
Clinical follow-up periods were up to a year, but were no shorter than 3 weeks. The investigators also assessed the data at different time intervals at 1, 3, 6, and 12 months “to appreciate the evolution of the metabolic parameters.”
In addition, they collected demographic and clinical information, such as comorbidities, and measured patients’ weight, height, waist circumference, blood pressure, plasma glucose, and lipids at baseline and at 1, 3, and 12 months and then annually. Weight, waist circumference, and BP were also assessed at 2 and 6 months.
Doses of paliperidone were converted into risperidone-equivalent doses.
Significant weight gain over time
The mean duration of follow-up for the participants, of whom 374 were being treated with risperidone and 64 with paliperidone, was 153 days. Close to half (48.2%) were taking other psychotropic medications known to be associated with some degree of metabolic risk.
Patients were divided into two cohorts based on their daily dose intake (DDI): less than 3 mg/day (n = 201) and at least 3 mg/day (n = 237).
In the overall cohort, a “significant effect of time on weight change was found for each time point,” the investigators reported.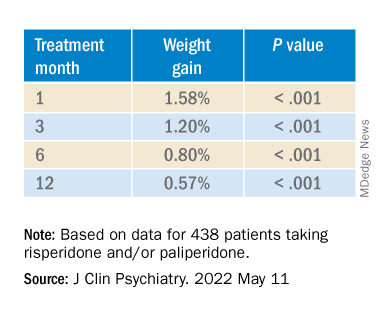
When the researchers looked at the changes according to DDI, they found that each 1-mg dose increase was associated with incremental weight gain at each time point.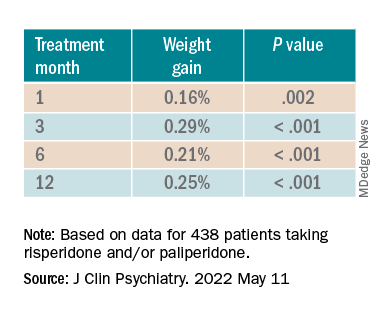
Patients who had 5% or greater weight gain in the first month continued to gain weight more than patients who did not reach that threshold, leading the researchers to call that early threshold a “strong predictor of important weight gain in the long term.” There was a weight gain of 6.68% at 3 months, of 7.36% at 6 months, and of 7.7% at 12 months.
After the patients were stratified by age, there were differences in the effect of DDI on various age groups at different time points.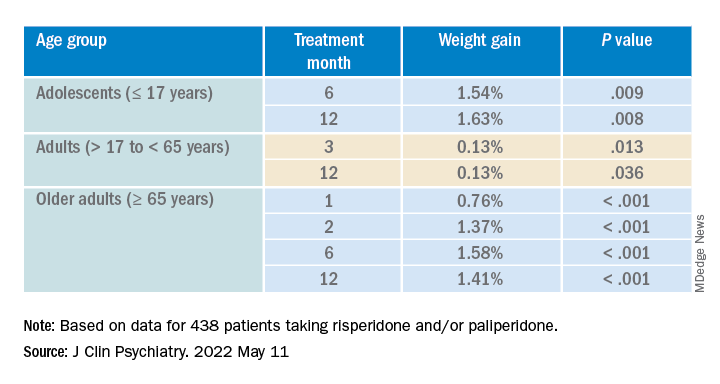
Dose was shown to have a significant effect on weight gain for women at all four time points (P ≥ .001), but for men only at 3 months (P = .003).
For each additional 1-mg dose, there was a 0.05 mmol/L (1.93 mg/dL) increase in total cholesterol (P = .018) after 1 year and a 0.04 mmol/L (1.54 mg/dL) increase in LDL cholesterol (P = .011).
There were no significant effects of time or DDI on triglycerides, HDL cholesterol, glucose levels, and systolic BP, and there was a negative effect of DDI on diastolic BP (P = .001).
The findings “provide evidence for a small dose effect of risperidone” on weight gain and total and LDL cholesterol levels, the investigators note.
Ms. Piras added that because each antipsychotic differs in its metabolic risk profile, “further analyses on other antipsychotics are ongoing in our laboratory, so far confirming our findings.”
Small increases, big changes
Commenting on the study, Erika Nurmi, MD, PhD, associate professor in the department of psychiatry and biobehavioral sciences at the Semel Institute for Neuroscience, University of California, Los Angeles, said the study is “unique in the field.”

It “leverages real-world data from a large patient registry to ask a long-unanswered question: Are weight and metabolic adverse effects proportional to dose? Big data approaches like these are very powerful, given the large number of participants that can be included,” said Dr. Nurmi, who was not involved with the research.
However, she cautioned, the “biggest drawback [is that] these data are by nature much more complex and prone to confounding effects.”
In this case, a “critical confounder” for the study was that the majority of individuals taking higher risperidone doses were also taking other drugs known to cause weight gain, whereas the majority of those on lower risperidone doses were not. “This difference may explain the dose relationship observed,” she said.
Because real-world, big data are “valuable but also messy, conclusions drawn from them must be interpreted with caution,” Dr. Nurmi said.
She added that it is generally wise to use the lowest effective dose possible.
“Clinicians should appreciate that even small doses of antipsychotics can cause big changes in weight. Risks and benefits of medications must be carefully considered in clinical practice,” Dr. Nurmi said.
The research was funded in part by the Swiss National Research Foundation. Piras reports no relevant financial relationships. The other investigators’ disclosures are listed in the original article. Dr. Nurmi reported no relevant financial relationships, but she is an unpaid member of the Tourette Association of America’s medical advisory board and of the Myriad Genetics scientific advisory board.
A version of this article first appeared on Medscape.com.
new research suggests.
Investigators analyzed 1-year data for more than 400 patients who were taking risperidone and/or its metabolite paliperidone (Invega). Results showed increments of 1 mg of risperidone-equivalent doses were associated with an increase of 0.25% of weight within a year of follow-up.
“Although our findings report a positive and statistically significant dose-dependence of weight gain and cholesterol, both total and LDL [cholesterol], the size of the predicted changes of metabolic effects is clinically nonrelevant,” lead author Marianna Piras, PharmD, Centre for Psychiatric Neuroscience, Lausanne (Switzerland) University Hospital, said in an interview.
“Therefore, dose lowering would not have a beneficial effect on attenuating weight gain or cholesterol increases and could lead to psychiatric decompensation,” said Ms. Piras, who is also a PhD candidate in the unit of pharmacogenetics and clinical psychopharmacology at the University of Lausanne.
However, she added that because dose increments could increase risk for significant weight gain in the first month of treatment – the dose can be increased typically in a range of 1-10 grams – and strong dose increments could contribute to metabolic worsening over time, “risperidone minimum effective doses should be preferred.”
The findings were published online in the Journal of Clinical Psychiatry.
‘Serious public health issue’
Compared with the general population, patients with mental illness present with a greater prevalence of metabolic disorders. In addition, several psychotropic medications, including antipsychotics, can induce metabolic alterations such as weight gain, the investigators noted.
Antipsychotic-induced metabolic adverse effects “constitute a serious public health issue” because they are risk factors for cardiovascular diseases such as obesity and/or dyslipidemia, “which have been associated with a 10-year reduced life expectancy in the psychiatric population,” Ms. Piras said.
“The dose-dependence of metabolic adverse effects is a debated subject that needs to be assessed for each psychotropic drug known to induce weight gain,” she added.
Several previous studies have examined whether there is a dose-related effect of antipsychotics on metabolic parameters, “with some results suggesting that [weight gain] seems to develop even when low off-label doses are prescribed,” Ms. Piras noted.
She and her colleagues had already studied dose-related metabolic effects of quetiapine (Seroquel) and olanzapine (Zyprexa).
Risperidone is an antipsychotic with a “medium to high metabolic risk profile,” the researchers note, and few studies have examined the impact of risperidone on metabolic parameters other than weight gain.
For the current analysis, they analyzed data from a longitudinal study that included 438 patients (mean age, 40.7 years; 50.7% men) who started treatment with risperidone and/or paliperidone between 2007 and 2018.
The participants had diagnoses of schizophrenia, schizoaffective disorder, bipolar disorder, depression, “other,” or “unknown.”
Clinical follow-up periods were up to a year, but were no shorter than 3 weeks. The investigators also assessed the data at different time intervals at 1, 3, 6, and 12 months “to appreciate the evolution of the metabolic parameters.”
In addition, they collected demographic and clinical information, such as comorbidities, and measured patients’ weight, height, waist circumference, blood pressure, plasma glucose, and lipids at baseline and at 1, 3, and 12 months and then annually. Weight, waist circumference, and BP were also assessed at 2 and 6 months.
Doses of paliperidone were converted into risperidone-equivalent doses.
Significant weight gain over time
The mean duration of follow-up for the participants, of whom 374 were being treated with risperidone and 64 with paliperidone, was 153 days. Close to half (48.2%) were taking other psychotropic medications known to be associated with some degree of metabolic risk.
Patients were divided into two cohorts based on their daily dose intake (DDI): less than 3 mg/day (n = 201) and at least 3 mg/day (n = 237).
In the overall cohort, a “significant effect of time on weight change was found for each time point,” the investigators reported.
When the researchers looked at the changes according to DDI, they found that each 1-mg dose increase was associated with incremental weight gain at each time point.
Patients who had 5% or greater weight gain in the first month continued to gain weight more than patients who did not reach that threshold, leading the researchers to call that early threshold a “strong predictor of important weight gain in the long term.” There was a weight gain of 6.68% at 3 months, of 7.36% at 6 months, and of 7.7% at 12 months.
After the patients were stratified by age, there were differences in the effect of DDI on various age groups at different time points.
Dose was shown to have a significant effect on weight gain for women at all four time points (P ≥ .001), but for men only at 3 months (P = .003).
For each additional 1-mg dose, there was a 0.05 mmol/L (1.93 mg/dL) increase in total cholesterol (P = .018) after 1 year and a 0.04 mmol/L (1.54 mg/dL) increase in LDL cholesterol (P = .011).
There were no significant effects of time or DDI on triglycerides, HDL cholesterol, glucose levels, and systolic BP, and there was a negative effect of DDI on diastolic BP (P = .001).
The findings “provide evidence for a small dose effect of risperidone” on weight gain and total and LDL cholesterol levels, the investigators note.
Ms. Piras added that because each antipsychotic differs in its metabolic risk profile, “further analyses on other antipsychotics are ongoing in our laboratory, so far confirming our findings.”
Small increases, big changes
Commenting on the study, Erika Nurmi, MD, PhD, associate professor in the department of psychiatry and biobehavioral sciences at the Semel Institute for Neuroscience, University of California, Los Angeles, said the study is “unique in the field.”
It “leverages real-world data from a large patient registry to ask a long-unanswered question: Are weight and metabolic adverse effects proportional to dose? Big data approaches like these are very powerful, given the large number of participants that can be included,” said Dr. Nurmi, who was not involved with the research.
However, she cautioned, the “biggest drawback [is that] these data are by nature much more complex and prone to confounding effects.”
In this case, a “critical confounder” for the study was that the majority of individuals taking higher risperidone doses were also taking other drugs known to cause weight gain, whereas the majority of those on lower risperidone doses were not. “This difference may explain the dose relationship observed,” she said.
Because real-world, big data are “valuable but also messy, conclusions drawn from them must be interpreted with caution,” Dr. Nurmi said.
She added that it is generally wise to use the lowest effective dose possible.
“Clinicians should appreciate that even small doses of antipsychotics can cause big changes in weight. Risks and benefits of medications must be carefully considered in clinical practice,” Dr. Nurmi said.
The research was funded in part by the Swiss National Research Foundation. Piras reports no relevant financial relationships. The other investigators’ disclosures are listed in the original article. Dr. Nurmi reported no relevant financial relationships, but she is an unpaid member of the Tourette Association of America’s medical advisory board and of the Myriad Genetics scientific advisory board.
A version of this article first appeared on Medscape.com.
new research suggests.
Investigators analyzed 1-year data for more than 400 patients who were taking risperidone and/or its metabolite paliperidone (Invega). Results showed increments of 1 mg of risperidone-equivalent doses were associated with an increase of 0.25% of weight within a year of follow-up.
“Although our findings report a positive and statistically significant dose-dependence of weight gain and cholesterol, both total and LDL [cholesterol], the size of the predicted changes of metabolic effects is clinically nonrelevant,” lead author Marianna Piras, PharmD, Centre for Psychiatric Neuroscience, Lausanne (Switzerland) University Hospital, said in an interview.
“Therefore, dose lowering would not have a beneficial effect on attenuating weight gain or cholesterol increases and could lead to psychiatric decompensation,” said Ms. Piras, who is also a PhD candidate in the unit of pharmacogenetics and clinical psychopharmacology at the University of Lausanne.
However, she added that because dose increments could increase risk for significant weight gain in the first month of treatment – the dose can be increased typically in a range of 1-10 grams – and strong dose increments could contribute to metabolic worsening over time, “risperidone minimum effective doses should be preferred.”
The findings were published online in the Journal of Clinical Psychiatry.
‘Serious public health issue’
Compared with the general population, patients with mental illness present with a greater prevalence of metabolic disorders. In addition, several psychotropic medications, including antipsychotics, can induce metabolic alterations such as weight gain, the investigators noted.
Antipsychotic-induced metabolic adverse effects “constitute a serious public health issue” because they are risk factors for cardiovascular diseases such as obesity and/or dyslipidemia, “which have been associated with a 10-year reduced life expectancy in the psychiatric population,” Ms. Piras said.
“The dose-dependence of metabolic adverse effects is a debated subject that needs to be assessed for each psychotropic drug known to induce weight gain,” she added.
Several previous studies have examined whether there is a dose-related effect of antipsychotics on metabolic parameters, “with some results suggesting that [weight gain] seems to develop even when low off-label doses are prescribed,” Ms. Piras noted.
She and her colleagues had already studied dose-related metabolic effects of quetiapine (Seroquel) and olanzapine (Zyprexa).
Risperidone is an antipsychotic with a “medium to high metabolic risk profile,” the researchers note, and few studies have examined the impact of risperidone on metabolic parameters other than weight gain.
For the current analysis, they analyzed data from a longitudinal study that included 438 patients (mean age, 40.7 years; 50.7% men) who started treatment with risperidone and/or paliperidone between 2007 and 2018.
The participants had diagnoses of schizophrenia, schizoaffective disorder, bipolar disorder, depression, “other,” or “unknown.”
Clinical follow-up periods were up to a year, but were no shorter than 3 weeks. The investigators also assessed the data at different time intervals at 1, 3, 6, and 12 months “to appreciate the evolution of the metabolic parameters.”
In addition, they collected demographic and clinical information, such as comorbidities, and measured patients’ weight, height, waist circumference, blood pressure, plasma glucose, and lipids at baseline and at 1, 3, and 12 months and then annually. Weight, waist circumference, and BP were also assessed at 2 and 6 months.
Doses of paliperidone were converted into risperidone-equivalent doses.
Significant weight gain over time
The mean duration of follow-up for the participants, of whom 374 were being treated with risperidone and 64 with paliperidone, was 153 days. Close to half (48.2%) were taking other psychotropic medications known to be associated with some degree of metabolic risk.
Patients were divided into two cohorts based on their daily dose intake (DDI): less than 3 mg/day (n = 201) and at least 3 mg/day (n = 237).
In the overall cohort, a “significant effect of time on weight change was found for each time point,” the investigators reported.
When the researchers looked at the changes according to DDI, they found that each 1-mg dose increase was associated with incremental weight gain at each time point.
Patients who had 5% or greater weight gain in the first month continued to gain weight more than patients who did not reach that threshold, leading the researchers to call that early threshold a “strong predictor of important weight gain in the long term.” There was a weight gain of 6.68% at 3 months, of 7.36% at 6 months, and of 7.7% at 12 months.
After the patients were stratified by age, there were differences in the effect of DDI on various age groups at different time points.
Dose was shown to have a significant effect on weight gain for women at all four time points (P ≥ .001), but for men only at 3 months (P = .003).
For each additional 1-mg dose, there was a 0.05 mmol/L (1.93 mg/dL) increase in total cholesterol (P = .018) after 1 year and a 0.04 mmol/L (1.54 mg/dL) increase in LDL cholesterol (P = .011).
There were no significant effects of time or DDI on triglycerides, HDL cholesterol, glucose levels, and systolic BP, and there was a negative effect of DDI on diastolic BP (P = .001).
The findings “provide evidence for a small dose effect of risperidone” on weight gain and total and LDL cholesterol levels, the investigators note.
Ms. Piras added that because each antipsychotic differs in its metabolic risk profile, “further analyses on other antipsychotics are ongoing in our laboratory, so far confirming our findings.”
Small increases, big changes
Commenting on the study, Erika Nurmi, MD, PhD, associate professor in the department of psychiatry and biobehavioral sciences at the Semel Institute for Neuroscience, University of California, Los Angeles, said the study is “unique in the field.”
It “leverages real-world data from a large patient registry to ask a long-unanswered question: Are weight and metabolic adverse effects proportional to dose? Big data approaches like these are very powerful, given the large number of participants that can be included,” said Dr. Nurmi, who was not involved with the research.
However, she cautioned, the “biggest drawback [is that] these data are by nature much more complex and prone to confounding effects.”
In this case, a “critical confounder” for the study was that the majority of individuals taking higher risperidone doses were also taking other drugs known to cause weight gain, whereas the majority of those on lower risperidone doses were not. “This difference may explain the dose relationship observed,” she said.
Because real-world, big data are “valuable but also messy, conclusions drawn from them must be interpreted with caution,” Dr. Nurmi said.
She added that it is generally wise to use the lowest effective dose possible.
“Clinicians should appreciate that even small doses of antipsychotics can cause big changes in weight. Risks and benefits of medications must be carefully considered in clinical practice,” Dr. Nurmi said.
The research was funded in part by the Swiss National Research Foundation. Piras reports no relevant financial relationships. The other investigators’ disclosures are listed in the original article. Dr. Nurmi reported no relevant financial relationships, but she is an unpaid member of the Tourette Association of America’s medical advisory board and of the Myriad Genetics scientific advisory board.
A version of this article first appeared on Medscape.com.
FROM THE JOURNAL OF CLINICAL PSYCHIATRY
‘Great optimism’ greets immunotherapy responses in dMMR rectal cancer
Thus far, the study has involved only 12 patients, but all of them have had a clinical complete response to treatment. They continue to show no signs of cancer (during follow-up ranging from 6 to 25 months) and have not undergone surgery or had radiation and chemotherapy, which are the standard treatment approaches.
The results were presented (Abstract 16) at the American Society of Clinical Oncology annual meeting and simultaneously published in the New England Journal of Medicine.
“In our study, the elimination of tumors after 6 months of therapy with PD-1 blockade enabled us to omit both chemoradiotherapy and surgery and to proceed with observation alone,” said the authors, led by Andrea Cercek, MD, Memorial Sloan Kettering Cancer Center, New York.
About 5%-10% of patients with rectal cancer have tumors with dMMR.
“The implications for quality of life are substantial, especially among patients in whom standard treatment would affect child-bearing potential [and] given that the incidence of rectal cancer is rising among young adults of childbearing age, the use of PD-1 blockade to eliminate the need for chemoradiotherapy and surgery may confer a particular benefit in that age group,” the authors wrote.
The results of the current study are cause for “great optimism, but such an approach cannot yet supplant our current curative treatment approach,” Dr. Hanna K. Sanoff, MD, University of North Carolina at Chapel Hill, wrote in an accompanying editorial.
Single-agent dostarlimab
For the study, all patients were treated with single-agent dostarlimab every 3 weeks for 6 months.
Dostarlimab is already approved by the Food and Drug Administration for use in the treatment of recurrent or advanced endometrial cancer with dMMR. Rectal cancer is an off-label use.
All patients had mismatch repair-deficient stage 2 or 3 rectal adenocarcinoma. The authors noted that these tumors respond poorly to standard chemotherapy regimens, including neoadjuvant chemotherapy. The median age of enrolled patients was 54 years and 62% were women.
For the study, investigators planned that patients who had a clinical complete response after completion of dostarlimab were to proceed to observation without undergoing either chemoradiotherapy or surgery, while those who did not have a complete response were to have received these standard treatments.
As it turned out, all 12 patients achieved a complete response and have been followed by observation alone. The median follow-up from time of enrollment to data cutoff for the 12 patients was 12 months.
“Therapeutic responses were rapid,” the authors noted, “with resolution of symptoms within 8 weeks after initiation of dostarlimab in 81% of the patients.”
To date, four patients have had 1 year of sustained clinical complete response after completion of the anti-PD-1 course.
In addition to the 12 patients documented in the study, another four patients have received at least one dose of dostarlimab and continue to receive treatment.
Adverse events occurred in most patients but none were grade 3 or higher. The most common grade 1 or 2 adverse events were rash or dermatitis, pruritus, fatigue, nausea and, in one patient, thyroid-function abnormalities.
The authors speculated that in addition to the extremely high tumor mutational burden associated with mismatch-repair deficiency, a tumor cell–extrinsic factor such as the gut microbiome may be driving the exceptionally good response to PD-1 blockade seen in this patient population.
Editorial commentary
In the editorial, Dr. Sanoff emphasized that the approach remains experimental and should not replace current curative treatment. She noted that cancer recurrences have been seen in other studies using both chemotherapy and immunotherapy.
For example, with chemotherapy and radiation, those patients who achieve a clinical complete response have a better prognosis compared with those who do not, but she cautioned that “cancer regrowth occurs in 20% to 30% of such patients when the cancer is managed nonoperatively.”
Dr. Sanoff noted that recurrences were seen when this approach of PD-1 inhibition has been used for metastatic colorectal cancer with dMMR. In the KEYNOTE-177 trial with pembrolizumab (Keytruda), only 55% of patients were reported to be alive without cancer progression at 12 months, and of the patients who initially had a strong response, only 70% had an ongoing response 3 years later.
“These recurrence dynamics may (or may not) differ between immunotherapy and chemoradiotherapy and between early and late-stage disease,” Dr. Sanoff said.
“In fact, very little is known about the duration of time needed to find out whether a clinical complete response to dostarlimab equates to cure,” she added.
In addition, Dr. Sanoff warned that the decision not to pursue further treatment and to follow patients with observation alone requires very close monitoring.
The current study was conducted at a top U.S. cancer center, Memorial Sloan Kettering Cancer Center. The authors noted that the complete responses (after a minimum of 6 months of follow-up) were measured by the combination of rectal MRI, visual endoscopic inspection, and digital rectal examination.
The completeness of these responses was further supported by the absence of residual tumor on serial endoscopic biopsies and the resolution of 18F-fluorodeoxyglucose uptake on PET scans, the authors added.
In the editorial, Dr. Sanoff said that “safe nonoperative management [also] involves access to specialty care for direct intraluminal visualization and expertise in interpretation of rectal magnetic resonance imaging ... Such expertise is not available in all communities and without it, patients could miss the opportunity for curative resection if tumor regrowth occurred.”
The study was sponsored by the Simon and Eve Colin Foundation, GlaxoSmithKline, and Stand Up to Cancer, among others.
A version of this article first appeared on Medscape.com.
Thus far, the study has involved only 12 patients, but all of them have had a clinical complete response to treatment. They continue to show no signs of cancer (during follow-up ranging from 6 to 25 months) and have not undergone surgery or had radiation and chemotherapy, which are the standard treatment approaches.
The results were presented (Abstract 16) at the American Society of Clinical Oncology annual meeting and simultaneously published in the New England Journal of Medicine.
“In our study, the elimination of tumors after 6 months of therapy with PD-1 blockade enabled us to omit both chemoradiotherapy and surgery and to proceed with observation alone,” said the authors, led by Andrea Cercek, MD, Memorial Sloan Kettering Cancer Center, New York.
About 5%-10% of patients with rectal cancer have tumors with dMMR.
“The implications for quality of life are substantial, especially among patients in whom standard treatment would affect child-bearing potential [and] given that the incidence of rectal cancer is rising among young adults of childbearing age, the use of PD-1 blockade to eliminate the need for chemoradiotherapy and surgery may confer a particular benefit in that age group,” the authors wrote.
The results of the current study are cause for “great optimism, but such an approach cannot yet supplant our current curative treatment approach,” Dr. Hanna K. Sanoff, MD, University of North Carolina at Chapel Hill, wrote in an accompanying editorial.
Single-agent dostarlimab
For the study, all patients were treated with single-agent dostarlimab every 3 weeks for 6 months.
Dostarlimab is already approved by the Food and Drug Administration for use in the treatment of recurrent or advanced endometrial cancer with dMMR. Rectal cancer is an off-label use.
All patients had mismatch repair-deficient stage 2 or 3 rectal adenocarcinoma. The authors noted that these tumors respond poorly to standard chemotherapy regimens, including neoadjuvant chemotherapy. The median age of enrolled patients was 54 years and 62% were women.
For the study, investigators planned that patients who had a clinical complete response after completion of dostarlimab were to proceed to observation without undergoing either chemoradiotherapy or surgery, while those who did not have a complete response were to have received these standard treatments.
As it turned out, all 12 patients achieved a complete response and have been followed by observation alone. The median follow-up from time of enrollment to data cutoff for the 12 patients was 12 months.
“Therapeutic responses were rapid,” the authors noted, “with resolution of symptoms within 8 weeks after initiation of dostarlimab in 81% of the patients.”
To date, four patients have had 1 year of sustained clinical complete response after completion of the anti-PD-1 course.
In addition to the 12 patients documented in the study, another four patients have received at least one dose of dostarlimab and continue to receive treatment.
Adverse events occurred in most patients but none were grade 3 or higher. The most common grade 1 or 2 adverse events were rash or dermatitis, pruritus, fatigue, nausea and, in one patient, thyroid-function abnormalities.
The authors speculated that in addition to the extremely high tumor mutational burden associated with mismatch-repair deficiency, a tumor cell–extrinsic factor such as the gut microbiome may be driving the exceptionally good response to PD-1 blockade seen in this patient population.
Editorial commentary
In the editorial, Dr. Sanoff emphasized that the approach remains experimental and should not replace current curative treatment. She noted that cancer recurrences have been seen in other studies using both chemotherapy and immunotherapy.
For example, with chemotherapy and radiation, those patients who achieve a clinical complete response have a better prognosis compared with those who do not, but she cautioned that “cancer regrowth occurs in 20% to 30% of such patients when the cancer is managed nonoperatively.”
Dr. Sanoff noted that recurrences were seen when this approach of PD-1 inhibition has been used for metastatic colorectal cancer with dMMR. In the KEYNOTE-177 trial with pembrolizumab (Keytruda), only 55% of patients were reported to be alive without cancer progression at 12 months, and of the patients who initially had a strong response, only 70% had an ongoing response 3 years later.
“These recurrence dynamics may (or may not) differ between immunotherapy and chemoradiotherapy and between early and late-stage disease,” Dr. Sanoff said.
“In fact, very little is known about the duration of time needed to find out whether a clinical complete response to dostarlimab equates to cure,” she added.
In addition, Dr. Sanoff warned that the decision not to pursue further treatment and to follow patients with observation alone requires very close monitoring.
The current study was conducted at a top U.S. cancer center, Memorial Sloan Kettering Cancer Center. The authors noted that the complete responses (after a minimum of 6 months of follow-up) were measured by the combination of rectal MRI, visual endoscopic inspection, and digital rectal examination.
The completeness of these responses was further supported by the absence of residual tumor on serial endoscopic biopsies and the resolution of 18F-fluorodeoxyglucose uptake on PET scans, the authors added.
In the editorial, Dr. Sanoff said that “safe nonoperative management [also] involves access to specialty care for direct intraluminal visualization and expertise in interpretation of rectal magnetic resonance imaging ... Such expertise is not available in all communities and without it, patients could miss the opportunity for curative resection if tumor regrowth occurred.”
The study was sponsored by the Simon and Eve Colin Foundation, GlaxoSmithKline, and Stand Up to Cancer, among others.
A version of this article first appeared on Medscape.com.
Thus far, the study has involved only 12 patients, but all of them have had a clinical complete response to treatment. They continue to show no signs of cancer (during follow-up ranging from 6 to 25 months) and have not undergone surgery or had radiation and chemotherapy, which are the standard treatment approaches.
The results were presented (Abstract 16) at the American Society of Clinical Oncology annual meeting and simultaneously published in the New England Journal of Medicine.
“In our study, the elimination of tumors after 6 months of therapy with PD-1 blockade enabled us to omit both chemoradiotherapy and surgery and to proceed with observation alone,” said the authors, led by Andrea Cercek, MD, Memorial Sloan Kettering Cancer Center, New York.
About 5%-10% of patients with rectal cancer have tumors with dMMR.
“The implications for quality of life are substantial, especially among patients in whom standard treatment would affect child-bearing potential [and] given that the incidence of rectal cancer is rising among young adults of childbearing age, the use of PD-1 blockade to eliminate the need for chemoradiotherapy and surgery may confer a particular benefit in that age group,” the authors wrote.
The results of the current study are cause for “great optimism, but such an approach cannot yet supplant our current curative treatment approach,” Dr. Hanna K. Sanoff, MD, University of North Carolina at Chapel Hill, wrote in an accompanying editorial.
Single-agent dostarlimab
For the study, all patients were treated with single-agent dostarlimab every 3 weeks for 6 months.
Dostarlimab is already approved by the Food and Drug Administration for use in the treatment of recurrent or advanced endometrial cancer with dMMR. Rectal cancer is an off-label use.
All patients had mismatch repair-deficient stage 2 or 3 rectal adenocarcinoma. The authors noted that these tumors respond poorly to standard chemotherapy regimens, including neoadjuvant chemotherapy. The median age of enrolled patients was 54 years and 62% were women.
For the study, investigators planned that patients who had a clinical complete response after completion of dostarlimab were to proceed to observation without undergoing either chemoradiotherapy or surgery, while those who did not have a complete response were to have received these standard treatments.
As it turned out, all 12 patients achieved a complete response and have been followed by observation alone. The median follow-up from time of enrollment to data cutoff for the 12 patients was 12 months.
“Therapeutic responses were rapid,” the authors noted, “with resolution of symptoms within 8 weeks after initiation of dostarlimab in 81% of the patients.”
To date, four patients have had 1 year of sustained clinical complete response after completion of the anti-PD-1 course.
In addition to the 12 patients documented in the study, another four patients have received at least one dose of dostarlimab and continue to receive treatment.
Adverse events occurred in most patients but none were grade 3 or higher. The most common grade 1 or 2 adverse events were rash or dermatitis, pruritus, fatigue, nausea and, in one patient, thyroid-function abnormalities.
The authors speculated that in addition to the extremely high tumor mutational burden associated with mismatch-repair deficiency, a tumor cell–extrinsic factor such as the gut microbiome may be driving the exceptionally good response to PD-1 blockade seen in this patient population.
Editorial commentary
In the editorial, Dr. Sanoff emphasized that the approach remains experimental and should not replace current curative treatment. She noted that cancer recurrences have been seen in other studies using both chemotherapy and immunotherapy.
For example, with chemotherapy and radiation, those patients who achieve a clinical complete response have a better prognosis compared with those who do not, but she cautioned that “cancer regrowth occurs in 20% to 30% of such patients when the cancer is managed nonoperatively.”
Dr. Sanoff noted that recurrences were seen when this approach of PD-1 inhibition has been used for metastatic colorectal cancer with dMMR. In the KEYNOTE-177 trial with pembrolizumab (Keytruda), only 55% of patients were reported to be alive without cancer progression at 12 months, and of the patients who initially had a strong response, only 70% had an ongoing response 3 years later.
“These recurrence dynamics may (or may not) differ between immunotherapy and chemoradiotherapy and between early and late-stage disease,” Dr. Sanoff said.
“In fact, very little is known about the duration of time needed to find out whether a clinical complete response to dostarlimab equates to cure,” she added.
In addition, Dr. Sanoff warned that the decision not to pursue further treatment and to follow patients with observation alone requires very close monitoring.
The current study was conducted at a top U.S. cancer center, Memorial Sloan Kettering Cancer Center. The authors noted that the complete responses (after a minimum of 6 months of follow-up) were measured by the combination of rectal MRI, visual endoscopic inspection, and digital rectal examination.
The completeness of these responses was further supported by the absence of residual tumor on serial endoscopic biopsies and the resolution of 18F-fluorodeoxyglucose uptake on PET scans, the authors added.
In the editorial, Dr. Sanoff said that “safe nonoperative management [also] involves access to specialty care for direct intraluminal visualization and expertise in interpretation of rectal magnetic resonance imaging ... Such expertise is not available in all communities and without it, patients could miss the opportunity for curative resection if tumor regrowth occurred.”
The study was sponsored by the Simon and Eve Colin Foundation, GlaxoSmithKline, and Stand Up to Cancer, among others.
A version of this article first appeared on Medscape.com.
FROM ASCO 2022