User login
Survival varies widely for cardiac arrests in U.S. cath labs
The chance of surviving a cardiac arrest varies widely across hospitals in the United States, even when the arrest occurs in the highly controlled setting of a cardiac catheterization lab, a new study indicates.
Among 4,787 patients who arrested in the cath lab at 231 hospitals in the Get With The Guidelines (GWTG) Resuscitation registry, only about one-third survived to discharge. The median risk-adjusted survival rate (RASR) for all hospitals was 36%.
When stratified by RASR tertiles, however, median survival rates were 20%, 36%, and 52% for hospitals in the lowest, middle, and highest tertiles.
The odds of survival differed by 71% in similar patients presenting at two randomly selected hospitals (median odds ratio, 1.71; 95% confidence interval, 1.52-1.87).
“The good news is that cardiac arrests in the cath lab are relatively infrequent, but the bad news is that they still occur and the outcomes are, in general, pretty dismal,” senior author Deepak L. Bhatt, MD, MPH, said in an interview. “So anything that we can do as hospitals [and] health care systems to improve the care of these patients could go a long way.”

He noted that data are sparse on cardiac arrests in the cath lab but that recent studies examining in-hospital arrests in the same registry report lower hospital-wide survival rates, between 17% and 24%.
Nevertheless, the current study included only those hospitals motivated and with the resources to participate in the American Heart Association’s voluntary GWTG Resuscitation registry between January 2003 and December 2017.
“It probably does provide the best case scenario of what’s going on and, if we included every hospital in the United States or the world, probably the outcomes would be substantially worse,” said Dr. Bhatt, who was recently named director of Mount Sinai Heart and the first Dr. Valentin Fuster Professor of Cardiovascular Medicine, New York.
The results were published in JACC Cardiovascular Interventions.
Hospital and patient factors
Possible explanations for the wide disparity in survival are the small number of cardiac arrests in the cath lab, the increasing complexity of cases, and the fact that patients are often very sick and may experience a problem during a procedure, or both, Dr. Bhatt suggested. Cath labs also vary in how they handle resuscitative efforts and access to advanced mechanical support devices, such as extracorporeal membrane oxygenation (ECMO).
“It’s not available in every cath lab and, even in hospitals that have it, they may not have a given ECMO circuit available at the exact time the patient’s having a cardiac arrest,” he said. “That’s one example of something that can make, in my opinion, a big difference in whether a patient lives or dies if they’re having a cardiac arrest but may not always be easily deployed.”
When the investigators looked specifically at hospital-level factors, only yearly volume of cardiac arrests in the cath lab was significantly associated with risk-adjusted survival (P < .01), whereas hospital size, rural or urban setting, teaching status, and geographic location were not.
In multivariate adjusted analyses, factors associated with survival to discharge included age (OR, 0.78), Black race (OR, 0.68), respiratory insufficiency (OR, 0.75), and initial cardiac arrest rhythm (OR, 3.32).
The median hospital RASR was 27% higher for ventricular tachycardia or ventricular fibrillation arrests than for arrests with a nonshockable rhythm of asystole and pulseless electrical activity (55% vs. 28%).
Notably, hospitals in the lowest tertile of risk-adjusted survival rates had a higher prevalence of non-White patients, renal and respiratory comorbidity, and arrest with nonshockable rhythm.
“We want to make sure as we’re contemplating whether to resuscitate a patient or how aggressively to resuscitate, that we aren’t letting any of our own biases, whether they have to do with race or potentially sex and gender, interfere with more objective assessments of whether the patient can in fact be saved or not,” Dr. Bhatt said.
Reached for comment, Srihari S. Naidu, MD, who chaired the writing group for the Society for Cardiovascular Angiography and Interventions’ (SCAI) consensus statement on cardiogenic shock and co-authored its document on best practices in the cardiac cath lab, said the findings show that survival in the cath lab is higher than that seen in-hospital. “Still, there’s a lot of room for improvement,” he said.
He was particularly struck by the variability in survival. “Underprivileged individuals, so those who are non-White populations and have respiratory and renal problems, they seem to have a worse survival and that makes sense – patients with comorbidities – but it feeds into the issue of, ‘Are we treating our population similarly in terms of their baseline race and ethnicity as a gap in care?’ ”
Better survival at hospitals with high volumes likely reflects more experience in handling these events, a rapid response and personnel to help with resuscitation, and overall better critical care and cath lab environment, said Dr. Naidu, director of the cardiac cath lab at Westchester Medical Center and professor of medicine at New York Medical College, both in Valhalla, N.Y.
“So that leads into two things,” he said. “One is that probably we should be working on having all high-risk patients go to centers of excellence. So, for example, [for] patients in shock, patients with STEMI, regionalization of care to the high-volume cath labs that are experienced in cardiac arrest and critical care management may be a way to go.”
“Second, if experience counts, can that experience be simulated through drills and simulations in the cath lab?” Dr. Naidu said. “Should all cath labs have drills where we have a cardiac arrest patient, and how would we respond to that? Who’s going to do the compressions? Where’s the mechanical support device? What are the things we need to have a seamless cardiac arrest protocol for arrests during the cath lab?”
Dr. Bhatt and colleagues acknowledge that despite adjustment for many key variables, the study lacked procedural details that may affect survival and information related to resuscitation efforts.
“We really do need to focus more research efforts, potentially more in the way of quality-improvement efforts, to try and help patients get these sorts of patients who are in dire straits to the cath lab but hopefully also through the hospital discharge and back home,” Dr. Bhatt said.
In an editorial accompanying the study, Matthew L. Tomey, MD, Icahn School of Medicine at Mount Sinai, New York, writes that the “findings and limitations of this study together sound a call to action.”
He also signaled the need for more research and for registries and reporting instruments to capture variables particular to in-laboratory cardiac arrest and resuscitation in the cardiac cath lab. “A necessary first step is the development of consensus data elements for supplemental reporting in cases of ILCA,” such as indication for cath lab presentation, timing of arrest relative to procedure, and cause of arrest.
Dr. Bhatt reported numerous relationships with industry. Dr. Naidu and Dr. Tomey report having no relevant financial relationships.
A version of this article first appeared on Medscape.com.
The chance of surviving a cardiac arrest varies widely across hospitals in the United States, even when the arrest occurs in the highly controlled setting of a cardiac catheterization lab, a new study indicates.
Among 4,787 patients who arrested in the cath lab at 231 hospitals in the Get With The Guidelines (GWTG) Resuscitation registry, only about one-third survived to discharge. The median risk-adjusted survival rate (RASR) for all hospitals was 36%.
When stratified by RASR tertiles, however, median survival rates were 20%, 36%, and 52% for hospitals in the lowest, middle, and highest tertiles.
The odds of survival differed by 71% in similar patients presenting at two randomly selected hospitals (median odds ratio, 1.71; 95% confidence interval, 1.52-1.87).
“The good news is that cardiac arrests in the cath lab are relatively infrequent, but the bad news is that they still occur and the outcomes are, in general, pretty dismal,” senior author Deepak L. Bhatt, MD, MPH, said in an interview. “So anything that we can do as hospitals [and] health care systems to improve the care of these patients could go a long way.”
He noted that data are sparse on cardiac arrests in the cath lab but that recent studies examining in-hospital arrests in the same registry report lower hospital-wide survival rates, between 17% and 24%.
Nevertheless, the current study included only those hospitals motivated and with the resources to participate in the American Heart Association’s voluntary GWTG Resuscitation registry between January 2003 and December 2017.
“It probably does provide the best case scenario of what’s going on and, if we included every hospital in the United States or the world, probably the outcomes would be substantially worse,” said Dr. Bhatt, who was recently named director of Mount Sinai Heart and the first Dr. Valentin Fuster Professor of Cardiovascular Medicine, New York.
The results were published in JACC Cardiovascular Interventions.
Hospital and patient factors
Possible explanations for the wide disparity in survival are the small number of cardiac arrests in the cath lab, the increasing complexity of cases, and the fact that patients are often very sick and may experience a problem during a procedure, or both, Dr. Bhatt suggested. Cath labs also vary in how they handle resuscitative efforts and access to advanced mechanical support devices, such as extracorporeal membrane oxygenation (ECMO).
“It’s not available in every cath lab and, even in hospitals that have it, they may not have a given ECMO circuit available at the exact time the patient’s having a cardiac arrest,” he said. “That’s one example of something that can make, in my opinion, a big difference in whether a patient lives or dies if they’re having a cardiac arrest but may not always be easily deployed.”
When the investigators looked specifically at hospital-level factors, only yearly volume of cardiac arrests in the cath lab was significantly associated with risk-adjusted survival (P < .01), whereas hospital size, rural or urban setting, teaching status, and geographic location were not.
In multivariate adjusted analyses, factors associated with survival to discharge included age (OR, 0.78), Black race (OR, 0.68), respiratory insufficiency (OR, 0.75), and initial cardiac arrest rhythm (OR, 3.32).
The median hospital RASR was 27% higher for ventricular tachycardia or ventricular fibrillation arrests than for arrests with a nonshockable rhythm of asystole and pulseless electrical activity (55% vs. 28%).
Notably, hospitals in the lowest tertile of risk-adjusted survival rates had a higher prevalence of non-White patients, renal and respiratory comorbidity, and arrest with nonshockable rhythm.
“We want to make sure as we’re contemplating whether to resuscitate a patient or how aggressively to resuscitate, that we aren’t letting any of our own biases, whether they have to do with race or potentially sex and gender, interfere with more objective assessments of whether the patient can in fact be saved or not,” Dr. Bhatt said.
Reached for comment, Srihari S. Naidu, MD, who chaired the writing group for the Society for Cardiovascular Angiography and Interventions’ (SCAI) consensus statement on cardiogenic shock and co-authored its document on best practices in the cardiac cath lab, said the findings show that survival in the cath lab is higher than that seen in-hospital. “Still, there’s a lot of room for improvement,” he said.
He was particularly struck by the variability in survival. “Underprivileged individuals, so those who are non-White populations and have respiratory and renal problems, they seem to have a worse survival and that makes sense – patients with comorbidities – but it feeds into the issue of, ‘Are we treating our population similarly in terms of their baseline race and ethnicity as a gap in care?’ ”
Better survival at hospitals with high volumes likely reflects more experience in handling these events, a rapid response and personnel to help with resuscitation, and overall better critical care and cath lab environment, said Dr. Naidu, director of the cardiac cath lab at Westchester Medical Center and professor of medicine at New York Medical College, both in Valhalla, N.Y.
“So that leads into two things,” he said. “One is that probably we should be working on having all high-risk patients go to centers of excellence. So, for example, [for] patients in shock, patients with STEMI, regionalization of care to the high-volume cath labs that are experienced in cardiac arrest and critical care management may be a way to go.”
“Second, if experience counts, can that experience be simulated through drills and simulations in the cath lab?” Dr. Naidu said. “Should all cath labs have drills where we have a cardiac arrest patient, and how would we respond to that? Who’s going to do the compressions? Where’s the mechanical support device? What are the things we need to have a seamless cardiac arrest protocol for arrests during the cath lab?”
Dr. Bhatt and colleagues acknowledge that despite adjustment for many key variables, the study lacked procedural details that may affect survival and information related to resuscitation efforts.
“We really do need to focus more research efforts, potentially more in the way of quality-improvement efforts, to try and help patients get these sorts of patients who are in dire straits to the cath lab but hopefully also through the hospital discharge and back home,” Dr. Bhatt said.
In an editorial accompanying the study, Matthew L. Tomey, MD, Icahn School of Medicine at Mount Sinai, New York, writes that the “findings and limitations of this study together sound a call to action.”
He also signaled the need for more research and for registries and reporting instruments to capture variables particular to in-laboratory cardiac arrest and resuscitation in the cardiac cath lab. “A necessary first step is the development of consensus data elements for supplemental reporting in cases of ILCA,” such as indication for cath lab presentation, timing of arrest relative to procedure, and cause of arrest.
Dr. Bhatt reported numerous relationships with industry. Dr. Naidu and Dr. Tomey report having no relevant financial relationships.
A version of this article first appeared on Medscape.com.
The chance of surviving a cardiac arrest varies widely across hospitals in the United States, even when the arrest occurs in the highly controlled setting of a cardiac catheterization lab, a new study indicates.
Among 4,787 patients who arrested in the cath lab at 231 hospitals in the Get With The Guidelines (GWTG) Resuscitation registry, only about one-third survived to discharge. The median risk-adjusted survival rate (RASR) for all hospitals was 36%.
When stratified by RASR tertiles, however, median survival rates were 20%, 36%, and 52% for hospitals in the lowest, middle, and highest tertiles.
The odds of survival differed by 71% in similar patients presenting at two randomly selected hospitals (median odds ratio, 1.71; 95% confidence interval, 1.52-1.87).
“The good news is that cardiac arrests in the cath lab are relatively infrequent, but the bad news is that they still occur and the outcomes are, in general, pretty dismal,” senior author Deepak L. Bhatt, MD, MPH, said in an interview. “So anything that we can do as hospitals [and] health care systems to improve the care of these patients could go a long way.”
He noted that data are sparse on cardiac arrests in the cath lab but that recent studies examining in-hospital arrests in the same registry report lower hospital-wide survival rates, between 17% and 24%.
Nevertheless, the current study included only those hospitals motivated and with the resources to participate in the American Heart Association’s voluntary GWTG Resuscitation registry between January 2003 and December 2017.
“It probably does provide the best case scenario of what’s going on and, if we included every hospital in the United States or the world, probably the outcomes would be substantially worse,” said Dr. Bhatt, who was recently named director of Mount Sinai Heart and the first Dr. Valentin Fuster Professor of Cardiovascular Medicine, New York.
The results were published in JACC Cardiovascular Interventions.
Hospital and patient factors
Possible explanations for the wide disparity in survival are the small number of cardiac arrests in the cath lab, the increasing complexity of cases, and the fact that patients are often very sick and may experience a problem during a procedure, or both, Dr. Bhatt suggested. Cath labs also vary in how they handle resuscitative efforts and access to advanced mechanical support devices, such as extracorporeal membrane oxygenation (ECMO).
“It’s not available in every cath lab and, even in hospitals that have it, they may not have a given ECMO circuit available at the exact time the patient’s having a cardiac arrest,” he said. “That’s one example of something that can make, in my opinion, a big difference in whether a patient lives or dies if they’re having a cardiac arrest but may not always be easily deployed.”
When the investigators looked specifically at hospital-level factors, only yearly volume of cardiac arrests in the cath lab was significantly associated with risk-adjusted survival (P < .01), whereas hospital size, rural or urban setting, teaching status, and geographic location were not.
In multivariate adjusted analyses, factors associated with survival to discharge included age (OR, 0.78), Black race (OR, 0.68), respiratory insufficiency (OR, 0.75), and initial cardiac arrest rhythm (OR, 3.32).
The median hospital RASR was 27% higher for ventricular tachycardia or ventricular fibrillation arrests than for arrests with a nonshockable rhythm of asystole and pulseless electrical activity (55% vs. 28%).
Notably, hospitals in the lowest tertile of risk-adjusted survival rates had a higher prevalence of non-White patients, renal and respiratory comorbidity, and arrest with nonshockable rhythm.
“We want to make sure as we’re contemplating whether to resuscitate a patient or how aggressively to resuscitate, that we aren’t letting any of our own biases, whether they have to do with race or potentially sex and gender, interfere with more objective assessments of whether the patient can in fact be saved or not,” Dr. Bhatt said.
Reached for comment, Srihari S. Naidu, MD, who chaired the writing group for the Society for Cardiovascular Angiography and Interventions’ (SCAI) consensus statement on cardiogenic shock and co-authored its document on best practices in the cardiac cath lab, said the findings show that survival in the cath lab is higher than that seen in-hospital. “Still, there’s a lot of room for improvement,” he said.
He was particularly struck by the variability in survival. “Underprivileged individuals, so those who are non-White populations and have respiratory and renal problems, they seem to have a worse survival and that makes sense – patients with comorbidities – but it feeds into the issue of, ‘Are we treating our population similarly in terms of their baseline race and ethnicity as a gap in care?’ ”
Better survival at hospitals with high volumes likely reflects more experience in handling these events, a rapid response and personnel to help with resuscitation, and overall better critical care and cath lab environment, said Dr. Naidu, director of the cardiac cath lab at Westchester Medical Center and professor of medicine at New York Medical College, both in Valhalla, N.Y.
“So that leads into two things,” he said. “One is that probably we should be working on having all high-risk patients go to centers of excellence. So, for example, [for] patients in shock, patients with STEMI, regionalization of care to the high-volume cath labs that are experienced in cardiac arrest and critical care management may be a way to go.”
“Second, if experience counts, can that experience be simulated through drills and simulations in the cath lab?” Dr. Naidu said. “Should all cath labs have drills where we have a cardiac arrest patient, and how would we respond to that? Who’s going to do the compressions? Where’s the mechanical support device? What are the things we need to have a seamless cardiac arrest protocol for arrests during the cath lab?”
Dr. Bhatt and colleagues acknowledge that despite adjustment for many key variables, the study lacked procedural details that may affect survival and information related to resuscitation efforts.
“We really do need to focus more research efforts, potentially more in the way of quality-improvement efforts, to try and help patients get these sorts of patients who are in dire straits to the cath lab but hopefully also through the hospital discharge and back home,” Dr. Bhatt said.
In an editorial accompanying the study, Matthew L. Tomey, MD, Icahn School of Medicine at Mount Sinai, New York, writes that the “findings and limitations of this study together sound a call to action.”
He also signaled the need for more research and for registries and reporting instruments to capture variables particular to in-laboratory cardiac arrest and resuscitation in the cardiac cath lab. “A necessary first step is the development of consensus data elements for supplemental reporting in cases of ILCA,” such as indication for cath lab presentation, timing of arrest relative to procedure, and cause of arrest.
Dr. Bhatt reported numerous relationships with industry. Dr. Naidu and Dr. Tomey report having no relevant financial relationships.
A version of this article first appeared on Medscape.com.

Dispatching volunteer responders may not increase AED use in OHCA
Dispatching trained volunteer responders via smartphones to retrieve automated external defibrillators for patients in out-of-hospital cardiac arrest (OHCA) did not significantly increase bystander AED use in a randomized clinical trial in Sweden.
Most patients in OHCA can be saved if cardiopulmonary resuscitation and defibrillation are initiated within minutes, but despite the “substantial” public availability of AEDs and widespread CPR training among the Swedish public, use rates of both are low, Mattias Ringh, MD, PhD, of Karolinska Institutet in Stockholm, and colleagues wrote.
A previous study by the team showed that dispatching volunteer responders via a smartphone app significantly increased bystander CPR. The current study, called the Swedish AED and Mobile Bystander Activation (SAMBA) trial, aimed to see whether dispatching volunteer responders to collect a nearby AED would increase bystander AED use. A control group of volunteer responders was instructed to go straight to the scene and start CPR.
“The results showed that the volunteer responders were first to provide treatment with both CPR and AEDs in a large proportion of cases in both groups, thereby creating a ‘statistical’ dilutional effect,” Dr. Ringh said in an interview. In effect, the control arm also became an active arm.
“But if we agree that treatment with AEDs and CPR is saving lives, then dispatching volunteer responders is doing just that, although we could not fully measure the effect in our study,” he added.
The study was published online in JAMA Cardiology.
No significant differences
The SAMBA trial assessed outcomes of the smartphone dispatch system (Heartrunner), which is triggered at emergency dispatch centers in response to suspected OHCAs at the same time that an ambulance with advanced life support equipment is dispatched.
The volunteer responder system locates a maximum of 30 volunteer responders within a 1.3-km radius from the suspected out-of-hospital cardiac arrest, the researchers explained in their report. Volunteer responders are requested via their smartphone application to accept or decline the alert. If they accept an alert, the volunteer responders receive map-aided route directions to the location of the suspected arrest.
In patients allocated to intervention in this study, four of five of all volunteer responders who accepted the alert received instructions to collect the nearest available AED and then go directly to the patient with suspected out-of-hospital cardiac arrest, the authors noted. Route directions to the scene of the cardiac arrest and the AED were displayed on their smartphones. One of the 5 volunteer responders, closest to the arrest, was dispatched to go directly to initiate CPR.
In patients allocated to the control group, all volunteer responders who accepted the alert were instructed to go directly to the patient with suspected out-of-hospital cardiac arrest to perform CPR. No route directions to or locations of AEDs were displayed.
The study was conducted in Stockholm and in Västra Götaland from 2018 to 2020. At the start of the study, there were 3,123 AEDs and 24,493 volunteer responders in Stockholm and 3,195 AEDs and 19,117 volunteer responders in Västra Götaland.
Post-randomization exclusions included patients without OHCA, those with OHCAs not treated by emergency medical services, and those with OHCAs witnessed by EMS.
The primary outcome was overall bystander AED attachment before the arrival of EMS, including those attached by the volunteer responders but also by lay volunteers who did not use the smartphone app.
Volunteer responders were activated for 947 individuals with OHCA; 461 patients were randomized to the intervention group and 486 to the control group. In both groups, the patients’ median age was 73 and about 65% were men.
Attachment of the AED before the arrival of EMS or first responders occurred in 61 patients (13.2%) in the intervention group versus 46 (9.5%) in the control group (P = .08). However, the majority of all AEDs were attached by lay volunteers who were not volunteer responders using the smartphone app (37 in the intervention arm vs. 28 in the control arm), the researchers noted.
No significant differences were seen in secondary outcomes, which included bystander CPR (69% vs. 71.6%, respectively) and defibrillation before EMS arrival (3.7% vs. 3.9%) between groups.
Among the volunteer responders using the app, crossover was 11% and compliance to instructions was 31%. Overall, volunteer responders attached 38% of all bystander-attached AEDs and provided 45% of all bystander defibrillations and 43% of all bystander CPR.
Going forward, Dr. Ringh and colleagues will be further analyzing the results to understand how to better optimize the logistical challenges involved with smartphone dispatch to OHCA patients. “In the longer term, investigating the impact on survival is also warranted,” he concluded.
U.S. in worse shape
In a comment, Christopher Calandrella, DO, chair of emergency medicine at Long Island Jewish Forest Hills,, New York, part of Northwell Health, said: “Significant data are available to support the importance of prompt initiation of CPR and defibrillation for OHCA, and although this study did not demonstrate a meaningful increase in use of AEDs with the trial system, layperson CPR was initiated in approximately 70% of cases in the cohort as a whole. Because of this, I believe it is evident that patients still benefit from a system that encourages bystanders to provide aid prior to the arrival of EMS.”
Nevertheless, he noted, “despite the training of volunteers in applying an AED, overall, only a small percentage of patients in either group had placement and use of the device. While the reasons likely are multifactorial, it may be in part due to the significant stress and anxiety associated with OHCA.”
Additional research would be helpful, he said. “Future studies focusing on more rural areas with lower population density and limited availability of AEDs may be beneficial. Expanding the research outside of Europe to other countries would be useful. Next-phase trials looking at 30-day survival in these patients would also be important.”
Currently in the United States, research is underway to evaluate the use of smartphones to improve in-hospital cardiac arrests, he added, “but no nationwide programs are in place for OHCA.”
Similarly, Kevin G. Volpp, MD, PhD, and Benjamin S. Abella, MD, MPhil, both of the University of Pennsylvania, Philadelphia, wrote in a related editorial: “It is sobering to recognize that, in the U.S., it may be nearly impossible to even test an idea like this, given the lack of a supporting data infrastructure.”
Although there is an app in the United States to link OHCA events to bystander response, they noted, less than half of eligible 911 centers have linked to it.
“Furthermore, the bystander CPR rate in the U.S. is less than 35%, only about half of the Swedish rate, indicating far fewer people are trained in CPR and comfortable performing it in the U.S.,” they wrote. “A wealthy country like the U.S. should be able to develop a far more effective approach to preventing millions of ... families from having a loved one die of OHCA in the decade to come.”
The study was funded by unrestricted grant from the Swedish Heart-Lung Foundation and Stockholm County. The authors, editorialists, and Dr. Calandrella disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Dispatching trained volunteer responders via smartphones to retrieve automated external defibrillators for patients in out-of-hospital cardiac arrest (OHCA) did not significantly increase bystander AED use in a randomized clinical trial in Sweden.
Most patients in OHCA can be saved if cardiopulmonary resuscitation and defibrillation are initiated within minutes, but despite the “substantial” public availability of AEDs and widespread CPR training among the Swedish public, use rates of both are low, Mattias Ringh, MD, PhD, of Karolinska Institutet in Stockholm, and colleagues wrote.
A previous study by the team showed that dispatching volunteer responders via a smartphone app significantly increased bystander CPR. The current study, called the Swedish AED and Mobile Bystander Activation (SAMBA) trial, aimed to see whether dispatching volunteer responders to collect a nearby AED would increase bystander AED use. A control group of volunteer responders was instructed to go straight to the scene and start CPR.
“The results showed that the volunteer responders were first to provide treatment with both CPR and AEDs in a large proportion of cases in both groups, thereby creating a ‘statistical’ dilutional effect,” Dr. Ringh said in an interview. In effect, the control arm also became an active arm.
“But if we agree that treatment with AEDs and CPR is saving lives, then dispatching volunteer responders is doing just that, although we could not fully measure the effect in our study,” he added.
The study was published online in JAMA Cardiology.
No significant differences
The SAMBA trial assessed outcomes of the smartphone dispatch system (Heartrunner), which is triggered at emergency dispatch centers in response to suspected OHCAs at the same time that an ambulance with advanced life support equipment is dispatched.
The volunteer responder system locates a maximum of 30 volunteer responders within a 1.3-km radius from the suspected out-of-hospital cardiac arrest, the researchers explained in their report. Volunteer responders are requested via their smartphone application to accept or decline the alert. If they accept an alert, the volunteer responders receive map-aided route directions to the location of the suspected arrest.
In patients allocated to intervention in this study, four of five of all volunteer responders who accepted the alert received instructions to collect the nearest available AED and then go directly to the patient with suspected out-of-hospital cardiac arrest, the authors noted. Route directions to the scene of the cardiac arrest and the AED were displayed on their smartphones. One of the 5 volunteer responders, closest to the arrest, was dispatched to go directly to initiate CPR.
In patients allocated to the control group, all volunteer responders who accepted the alert were instructed to go directly to the patient with suspected out-of-hospital cardiac arrest to perform CPR. No route directions to or locations of AEDs were displayed.
The study was conducted in Stockholm and in Västra Götaland from 2018 to 2020. At the start of the study, there were 3,123 AEDs and 24,493 volunteer responders in Stockholm and 3,195 AEDs and 19,117 volunteer responders in Västra Götaland.
Post-randomization exclusions included patients without OHCA, those with OHCAs not treated by emergency medical services, and those with OHCAs witnessed by EMS.
The primary outcome was overall bystander AED attachment before the arrival of EMS, including those attached by the volunteer responders but also by lay volunteers who did not use the smartphone app.
Volunteer responders were activated for 947 individuals with OHCA; 461 patients were randomized to the intervention group and 486 to the control group. In both groups, the patients’ median age was 73 and about 65% were men.
Attachment of the AED before the arrival of EMS or first responders occurred in 61 patients (13.2%) in the intervention group versus 46 (9.5%) in the control group (P = .08). However, the majority of all AEDs were attached by lay volunteers who were not volunteer responders using the smartphone app (37 in the intervention arm vs. 28 in the control arm), the researchers noted.
No significant differences were seen in secondary outcomes, which included bystander CPR (69% vs. 71.6%, respectively) and defibrillation before EMS arrival (3.7% vs. 3.9%) between groups.
Among the volunteer responders using the app, crossover was 11% and compliance to instructions was 31%. Overall, volunteer responders attached 38% of all bystander-attached AEDs and provided 45% of all bystander defibrillations and 43% of all bystander CPR.
Going forward, Dr. Ringh and colleagues will be further analyzing the results to understand how to better optimize the logistical challenges involved with smartphone dispatch to OHCA patients. “In the longer term, investigating the impact on survival is also warranted,” he concluded.
U.S. in worse shape
In a comment, Christopher Calandrella, DO, chair of emergency medicine at Long Island Jewish Forest Hills,, New York, part of Northwell Health, said: “Significant data are available to support the importance of prompt initiation of CPR and defibrillation for OHCA, and although this study did not demonstrate a meaningful increase in use of AEDs with the trial system, layperson CPR was initiated in approximately 70% of cases in the cohort as a whole. Because of this, I believe it is evident that patients still benefit from a system that encourages bystanders to provide aid prior to the arrival of EMS.”
Nevertheless, he noted, “despite the training of volunteers in applying an AED, overall, only a small percentage of patients in either group had placement and use of the device. While the reasons likely are multifactorial, it may be in part due to the significant stress and anxiety associated with OHCA.”
Additional research would be helpful, he said. “Future studies focusing on more rural areas with lower population density and limited availability of AEDs may be beneficial. Expanding the research outside of Europe to other countries would be useful. Next-phase trials looking at 30-day survival in these patients would also be important.”
Currently in the United States, research is underway to evaluate the use of smartphones to improve in-hospital cardiac arrests, he added, “but no nationwide programs are in place for OHCA.”
Similarly, Kevin G. Volpp, MD, PhD, and Benjamin S. Abella, MD, MPhil, both of the University of Pennsylvania, Philadelphia, wrote in a related editorial: “It is sobering to recognize that, in the U.S., it may be nearly impossible to even test an idea like this, given the lack of a supporting data infrastructure.”
Although there is an app in the United States to link OHCA events to bystander response, they noted, less than half of eligible 911 centers have linked to it.
“Furthermore, the bystander CPR rate in the U.S. is less than 35%, only about half of the Swedish rate, indicating far fewer people are trained in CPR and comfortable performing it in the U.S.,” they wrote. “A wealthy country like the U.S. should be able to develop a far more effective approach to preventing millions of ... families from having a loved one die of OHCA in the decade to come.”
The study was funded by unrestricted grant from the Swedish Heart-Lung Foundation and Stockholm County. The authors, editorialists, and Dr. Calandrella disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Dispatching trained volunteer responders via smartphones to retrieve automated external defibrillators for patients in out-of-hospital cardiac arrest (OHCA) did not significantly increase bystander AED use in a randomized clinical trial in Sweden.
Most patients in OHCA can be saved if cardiopulmonary resuscitation and defibrillation are initiated within minutes, but despite the “substantial” public availability of AEDs and widespread CPR training among the Swedish public, use rates of both are low, Mattias Ringh, MD, PhD, of Karolinska Institutet in Stockholm, and colleagues wrote.
A previous study by the team showed that dispatching volunteer responders via a smartphone app significantly increased bystander CPR. The current study, called the Swedish AED and Mobile Bystander Activation (SAMBA) trial, aimed to see whether dispatching volunteer responders to collect a nearby AED would increase bystander AED use. A control group of volunteer responders was instructed to go straight to the scene and start CPR.
“The results showed that the volunteer responders were first to provide treatment with both CPR and AEDs in a large proportion of cases in both groups, thereby creating a ‘statistical’ dilutional effect,” Dr. Ringh said in an interview. In effect, the control arm also became an active arm.
“But if we agree that treatment with AEDs and CPR is saving lives, then dispatching volunteer responders is doing just that, although we could not fully measure the effect in our study,” he added.
The study was published online in JAMA Cardiology.
No significant differences
The SAMBA trial assessed outcomes of the smartphone dispatch system (Heartrunner), which is triggered at emergency dispatch centers in response to suspected OHCAs at the same time that an ambulance with advanced life support equipment is dispatched.
The volunteer responder system locates a maximum of 30 volunteer responders within a 1.3-km radius from the suspected out-of-hospital cardiac arrest, the researchers explained in their report. Volunteer responders are requested via their smartphone application to accept or decline the alert. If they accept an alert, the volunteer responders receive map-aided route directions to the location of the suspected arrest.
In patients allocated to intervention in this study, four of five of all volunteer responders who accepted the alert received instructions to collect the nearest available AED and then go directly to the patient with suspected out-of-hospital cardiac arrest, the authors noted. Route directions to the scene of the cardiac arrest and the AED were displayed on their smartphones. One of the 5 volunteer responders, closest to the arrest, was dispatched to go directly to initiate CPR.
In patients allocated to the control group, all volunteer responders who accepted the alert were instructed to go directly to the patient with suspected out-of-hospital cardiac arrest to perform CPR. No route directions to or locations of AEDs were displayed.
The study was conducted in Stockholm and in Västra Götaland from 2018 to 2020. At the start of the study, there were 3,123 AEDs and 24,493 volunteer responders in Stockholm and 3,195 AEDs and 19,117 volunteer responders in Västra Götaland.
Post-randomization exclusions included patients without OHCA, those with OHCAs not treated by emergency medical services, and those with OHCAs witnessed by EMS.
The primary outcome was overall bystander AED attachment before the arrival of EMS, including those attached by the volunteer responders but also by lay volunteers who did not use the smartphone app.
Volunteer responders were activated for 947 individuals with OHCA; 461 patients were randomized to the intervention group and 486 to the control group. In both groups, the patients’ median age was 73 and about 65% were men.
Attachment of the AED before the arrival of EMS or first responders occurred in 61 patients (13.2%) in the intervention group versus 46 (9.5%) in the control group (P = .08). However, the majority of all AEDs were attached by lay volunteers who were not volunteer responders using the smartphone app (37 in the intervention arm vs. 28 in the control arm), the researchers noted.
No significant differences were seen in secondary outcomes, which included bystander CPR (69% vs. 71.6%, respectively) and defibrillation before EMS arrival (3.7% vs. 3.9%) between groups.
Among the volunteer responders using the app, crossover was 11% and compliance to instructions was 31%. Overall, volunteer responders attached 38% of all bystander-attached AEDs and provided 45% of all bystander defibrillations and 43% of all bystander CPR.
Going forward, Dr. Ringh and colleagues will be further analyzing the results to understand how to better optimize the logistical challenges involved with smartphone dispatch to OHCA patients. “In the longer term, investigating the impact on survival is also warranted,” he concluded.
U.S. in worse shape
In a comment, Christopher Calandrella, DO, chair of emergency medicine at Long Island Jewish Forest Hills,, New York, part of Northwell Health, said: “Significant data are available to support the importance of prompt initiation of CPR and defibrillation for OHCA, and although this study did not demonstrate a meaningful increase in use of AEDs with the trial system, layperson CPR was initiated in approximately 70% of cases in the cohort as a whole. Because of this, I believe it is evident that patients still benefit from a system that encourages bystanders to provide aid prior to the arrival of EMS.”
Nevertheless, he noted, “despite the training of volunteers in applying an AED, overall, only a small percentage of patients in either group had placement and use of the device. While the reasons likely are multifactorial, it may be in part due to the significant stress and anxiety associated with OHCA.”
Additional research would be helpful, he said. “Future studies focusing on more rural areas with lower population density and limited availability of AEDs may be beneficial. Expanding the research outside of Europe to other countries would be useful. Next-phase trials looking at 30-day survival in these patients would also be important.”
Currently in the United States, research is underway to evaluate the use of smartphones to improve in-hospital cardiac arrests, he added, “but no nationwide programs are in place for OHCA.”
Similarly, Kevin G. Volpp, MD, PhD, and Benjamin S. Abella, MD, MPhil, both of the University of Pennsylvania, Philadelphia, wrote in a related editorial: “It is sobering to recognize that, in the U.S., it may be nearly impossible to even test an idea like this, given the lack of a supporting data infrastructure.”
Although there is an app in the United States to link OHCA events to bystander response, they noted, less than half of eligible 911 centers have linked to it.
“Furthermore, the bystander CPR rate in the U.S. is less than 35%, only about half of the Swedish rate, indicating far fewer people are trained in CPR and comfortable performing it in the U.S.,” they wrote. “A wealthy country like the U.S. should be able to develop a far more effective approach to preventing millions of ... families from having a loved one die of OHCA in the decade to come.”
The study was funded by unrestricted grant from the Swedish Heart-Lung Foundation and Stockholm County. The authors, editorialists, and Dr. Calandrella disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM JAMA CARDIOLOGY
‘Reassuring’ data on pregnancy with ischemic heart disease
Women with preexisting ischemic heart disease without another cardiac diagnosis have a higher risk of severe maternal morbidity and mortality than women with no cardiac disease, a new study suggests.
However, after adjustment for other comorbidities, the risk associated with isolated preexisting ischemic heart disease without additional evidence of cardiomyopathy was relatively similar to that of other low-risk cardiac diseases.
“These are reassuring findings,” lead author of the study, Anna E. Denoble, MD, Yale University, New Haven, Conn., told this news organization. “The risk is not zero. Women with preexisting ischemic heart disease are at a small increased risk compared to women without preexisting cardiac disease. But with good control of cardiovascular risk factors, these women have a good chance of a positive outcome.”
The study was published online in JACC: Advances.
“To our knowledge, this study provides the largest analysis to date examining the risk of severe morbidity and mortality among pregnant people with pre-existing ischemic heart disease,” the authors noted.
Dr. Denoble, a maternal and fetal medicine specialist, explained that in recent years, there has been an increase in the number of patients with preexisting ischemic heart disease who are considering pregnancy or who are pregnant when they present, but there is little information on outcomes for these patients.
The diagnosis of ischemic heart disease is not included in the main classification used for heart disease in pregnancy – the modified World Health Organization classification, Dr. Denoble noted. “This classification includes information on pregnancy outcomes in women with many cardiac conditions, including arrhythmias, congenital heart disease, heart failure, and aortic aneurysm, but ischemic heart disease is missing.”
She suggested this is probably because ischemic heart disease is regarded as a condition that occurs mainly in older people. “But we are seeing more and more women with ischemic heart disease who are pregnant or considering pregnancy. This could be because women are now often older when considering pregnancy, and also risk factors for ischemic heart disease, such as obesity and diabetes, are becoming more frequent in younger women.”
The researchers conducted the current study to investigate pregnancy outcomes for these women.
The retrospective cohort study analyzed data from the Nationwide Readmissions Database on women who had experienced a delivery hospitalization from Oct. 1, 2015, to Dec. 31, 2018. They compared outcomes for women with isolated preexisting ischemic heart disease with those of women who had no apparent cardiac condition and to those with mild or more severe cardiac conditions included in the mWHO classification after controlling for other comorbidities.
The primary outcome was severe maternal morbidity or death. Dr. Denoble explained that severe maternal morbidity includes mechanical ventilation, blood transfusion, and hysterectomy – the more severe maternal adverse outcomes of pregnancy.
Results showed that, of 11,556,136 delivery hospitalizations, 65,331 patients had another cardiac diagnosis, and 3,009 had ischemic heart disease alone. Patients with ischemic heart disease were older, and rates of diabetes and hypertension were higher.
In unadjusted analyses, adverse outcomes were more common among patients with ischemic heart disease alone than among patients with no cardiac disease and mild cardiac conditions (mWHO class I-II cardiac disease).
Of those with preexisting ischemic heart disease, 6.6% experienced severe maternal morbidity or death, compared with 1.5% of those without a cardiac disease (unadjusted relative risk vs. no cardiac disease, 4.3; 95% confidence interval, 3.5-5.2).
In comparison, 4.2% of women with mWHO I-II cardiac diseases and 23.1% of those with more severe mWHO II/III-IV cardiac diseases experienced severe maternal morbidity or death.
Similar differences were noted for nontransfusion severe maternal morbidity and mortality, as well as cardiac severe maternal morbidity and mortality.
After adjustment, ischemic heart disease alone was associated with a higher risk of severe maternal morbidity or death compared to no cardiac disease (adjusted RR, 1.51; 95% CI, 1.19-1.92).
In comparison, the aRR was 1.90 for WHO class I-II diseases and 5.87 (95% CI, 5.49-6.27) for more severe cardiac conditions defined as WHO II/III-IV diseases.
Risk for nontransfusion severe maternal morbidity or death (aRR, 1.60) and cardiac severe maternal morbidity or death (aRR, 2.98) were also higher for those with ischemic heart disease than for women without any cardiac disease.
There were no significant differences in preterm birth for those with preexisting ischemic heart disease compared to those with no cardiac disease after adjustment.
The risk of severe maternal morbidity and mortality, nontransfusion severe maternal morbidity and mortality, and cardiac severe maternal morbidity and mortality for ischemic heart disease alone most closely approximated that of mWHO class I or II cardiac diseases, the researchers said.
“We found that individuals with preexisting ischemic heart disease had a rate of severe maternal morbidity/mortality in the same range as those with other cardiac diagnoses in the mild cardiac disease classification (class I or II),” Dr. Denoble commented.
“This prognosis suggests it is very reasonable for these women to consider pregnancy. The risk of adverse outcomes is not so high that pregnancy is contraindicated,” she added.
Dr. Denoble said this information will be very helpful when counseling women with preexisting ischemic heart disease who are considering pregnancy. “These patients may need some extra monitoring, but in general, they have a high chance of a good outcome,” she noted.
“I would still advise these women to register with a high-risk obstetrics provider to have a baseline cardiovascular pregnancy evaluation. As long as that is reassuring, then further frequent intensive supervision may not be necessary,” she said.
However, the authors pointed out, “it is important to communicate to patients that while pregnancy may be considered low risk in the setting of pre-existing ischemic heart disease, 6.6% of patients with pre-existing ischemic heart disease alone did experience severe maternal morbidity or death during the delivery hospitalization.”
They added that other medical comorbidities should be factored into discussions regarding the risks of pregnancy.
The researchers also noted that the study was limited to evaluation of maternal outcomes occurring during the delivery hospitalization and that additional research that assesses rates of maternal adverse cardiac events and maternal morbidity occurring prior to or after the delivery hospitalization would be beneficial.
Future studies examining the potential gradation in risk associated with additional cardiac comorbidities in individuals with preexisting ischemic heart disease would also be worthwhile, they added.
The study was supported by funding from the National Institutes of Health and the Foundation for Women and Girls with Blood Disorders. The authors disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Women with preexisting ischemic heart disease without another cardiac diagnosis have a higher risk of severe maternal morbidity and mortality than women with no cardiac disease, a new study suggests.
However, after adjustment for other comorbidities, the risk associated with isolated preexisting ischemic heart disease without additional evidence of cardiomyopathy was relatively similar to that of other low-risk cardiac diseases.
“These are reassuring findings,” lead author of the study, Anna E. Denoble, MD, Yale University, New Haven, Conn., told this news organization. “The risk is not zero. Women with preexisting ischemic heart disease are at a small increased risk compared to women without preexisting cardiac disease. But with good control of cardiovascular risk factors, these women have a good chance of a positive outcome.”
The study was published online in JACC: Advances.
“To our knowledge, this study provides the largest analysis to date examining the risk of severe morbidity and mortality among pregnant people with pre-existing ischemic heart disease,” the authors noted.
Dr. Denoble, a maternal and fetal medicine specialist, explained that in recent years, there has been an increase in the number of patients with preexisting ischemic heart disease who are considering pregnancy or who are pregnant when they present, but there is little information on outcomes for these patients.
The diagnosis of ischemic heart disease is not included in the main classification used for heart disease in pregnancy – the modified World Health Organization classification, Dr. Denoble noted. “This classification includes information on pregnancy outcomes in women with many cardiac conditions, including arrhythmias, congenital heart disease, heart failure, and aortic aneurysm, but ischemic heart disease is missing.”
She suggested this is probably because ischemic heart disease is regarded as a condition that occurs mainly in older people. “But we are seeing more and more women with ischemic heart disease who are pregnant or considering pregnancy. This could be because women are now often older when considering pregnancy, and also risk factors for ischemic heart disease, such as obesity and diabetes, are becoming more frequent in younger women.”
The researchers conducted the current study to investigate pregnancy outcomes for these women.
The retrospective cohort study analyzed data from the Nationwide Readmissions Database on women who had experienced a delivery hospitalization from Oct. 1, 2015, to Dec. 31, 2018. They compared outcomes for women with isolated preexisting ischemic heart disease with those of women who had no apparent cardiac condition and to those with mild or more severe cardiac conditions included in the mWHO classification after controlling for other comorbidities.
The primary outcome was severe maternal morbidity or death. Dr. Denoble explained that severe maternal morbidity includes mechanical ventilation, blood transfusion, and hysterectomy – the more severe maternal adverse outcomes of pregnancy.
Results showed that, of 11,556,136 delivery hospitalizations, 65,331 patients had another cardiac diagnosis, and 3,009 had ischemic heart disease alone. Patients with ischemic heart disease were older, and rates of diabetes and hypertension were higher.
In unadjusted analyses, adverse outcomes were more common among patients with ischemic heart disease alone than among patients with no cardiac disease and mild cardiac conditions (mWHO class I-II cardiac disease).
Of those with preexisting ischemic heart disease, 6.6% experienced severe maternal morbidity or death, compared with 1.5% of those without a cardiac disease (unadjusted relative risk vs. no cardiac disease, 4.3; 95% confidence interval, 3.5-5.2).
In comparison, 4.2% of women with mWHO I-II cardiac diseases and 23.1% of those with more severe mWHO II/III-IV cardiac diseases experienced severe maternal morbidity or death.
Similar differences were noted for nontransfusion severe maternal morbidity and mortality, as well as cardiac severe maternal morbidity and mortality.
After adjustment, ischemic heart disease alone was associated with a higher risk of severe maternal morbidity or death compared to no cardiac disease (adjusted RR, 1.51; 95% CI, 1.19-1.92).
In comparison, the aRR was 1.90 for WHO class I-II diseases and 5.87 (95% CI, 5.49-6.27) for more severe cardiac conditions defined as WHO II/III-IV diseases.
Risk for nontransfusion severe maternal morbidity or death (aRR, 1.60) and cardiac severe maternal morbidity or death (aRR, 2.98) were also higher for those with ischemic heart disease than for women without any cardiac disease.
There were no significant differences in preterm birth for those with preexisting ischemic heart disease compared to those with no cardiac disease after adjustment.
The risk of severe maternal morbidity and mortality, nontransfusion severe maternal morbidity and mortality, and cardiac severe maternal morbidity and mortality for ischemic heart disease alone most closely approximated that of mWHO class I or II cardiac diseases, the researchers said.
“We found that individuals with preexisting ischemic heart disease had a rate of severe maternal morbidity/mortality in the same range as those with other cardiac diagnoses in the mild cardiac disease classification (class I or II),” Dr. Denoble commented.
“This prognosis suggests it is very reasonable for these women to consider pregnancy. The risk of adverse outcomes is not so high that pregnancy is contraindicated,” she added.
Dr. Denoble said this information will be very helpful when counseling women with preexisting ischemic heart disease who are considering pregnancy. “These patients may need some extra monitoring, but in general, they have a high chance of a good outcome,” she noted.
“I would still advise these women to register with a high-risk obstetrics provider to have a baseline cardiovascular pregnancy evaluation. As long as that is reassuring, then further frequent intensive supervision may not be necessary,” she said.
However, the authors pointed out, “it is important to communicate to patients that while pregnancy may be considered low risk in the setting of pre-existing ischemic heart disease, 6.6% of patients with pre-existing ischemic heart disease alone did experience severe maternal morbidity or death during the delivery hospitalization.”
They added that other medical comorbidities should be factored into discussions regarding the risks of pregnancy.
The researchers also noted that the study was limited to evaluation of maternal outcomes occurring during the delivery hospitalization and that additional research that assesses rates of maternal adverse cardiac events and maternal morbidity occurring prior to or after the delivery hospitalization would be beneficial.
Future studies examining the potential gradation in risk associated with additional cardiac comorbidities in individuals with preexisting ischemic heart disease would also be worthwhile, they added.
The study was supported by funding from the National Institutes of Health and the Foundation for Women and Girls with Blood Disorders. The authors disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Women with preexisting ischemic heart disease without another cardiac diagnosis have a higher risk of severe maternal morbidity and mortality than women with no cardiac disease, a new study suggests.
However, after adjustment for other comorbidities, the risk associated with isolated preexisting ischemic heart disease without additional evidence of cardiomyopathy was relatively similar to that of other low-risk cardiac diseases.
“These are reassuring findings,” lead author of the study, Anna E. Denoble, MD, Yale University, New Haven, Conn., told this news organization. “The risk is not zero. Women with preexisting ischemic heart disease are at a small increased risk compared to women without preexisting cardiac disease. But with good control of cardiovascular risk factors, these women have a good chance of a positive outcome.”
The study was published online in JACC: Advances.
“To our knowledge, this study provides the largest analysis to date examining the risk of severe morbidity and mortality among pregnant people with pre-existing ischemic heart disease,” the authors noted.
Dr. Denoble, a maternal and fetal medicine specialist, explained that in recent years, there has been an increase in the number of patients with preexisting ischemic heart disease who are considering pregnancy or who are pregnant when they present, but there is little information on outcomes for these patients.
The diagnosis of ischemic heart disease is not included in the main classification used for heart disease in pregnancy – the modified World Health Organization classification, Dr. Denoble noted. “This classification includes information on pregnancy outcomes in women with many cardiac conditions, including arrhythmias, congenital heart disease, heart failure, and aortic aneurysm, but ischemic heart disease is missing.”
She suggested this is probably because ischemic heart disease is regarded as a condition that occurs mainly in older people. “But we are seeing more and more women with ischemic heart disease who are pregnant or considering pregnancy. This could be because women are now often older when considering pregnancy, and also risk factors for ischemic heart disease, such as obesity and diabetes, are becoming more frequent in younger women.”
The researchers conducted the current study to investigate pregnancy outcomes for these women.
The retrospective cohort study analyzed data from the Nationwide Readmissions Database on women who had experienced a delivery hospitalization from Oct. 1, 2015, to Dec. 31, 2018. They compared outcomes for women with isolated preexisting ischemic heart disease with those of women who had no apparent cardiac condition and to those with mild or more severe cardiac conditions included in the mWHO classification after controlling for other comorbidities.
The primary outcome was severe maternal morbidity or death. Dr. Denoble explained that severe maternal morbidity includes mechanical ventilation, blood transfusion, and hysterectomy – the more severe maternal adverse outcomes of pregnancy.
Results showed that, of 11,556,136 delivery hospitalizations, 65,331 patients had another cardiac diagnosis, and 3,009 had ischemic heart disease alone. Patients with ischemic heart disease were older, and rates of diabetes and hypertension were higher.
In unadjusted analyses, adverse outcomes were more common among patients with ischemic heart disease alone than among patients with no cardiac disease and mild cardiac conditions (mWHO class I-II cardiac disease).
Of those with preexisting ischemic heart disease, 6.6% experienced severe maternal morbidity or death, compared with 1.5% of those without a cardiac disease (unadjusted relative risk vs. no cardiac disease, 4.3; 95% confidence interval, 3.5-5.2).
In comparison, 4.2% of women with mWHO I-II cardiac diseases and 23.1% of those with more severe mWHO II/III-IV cardiac diseases experienced severe maternal morbidity or death.
Similar differences were noted for nontransfusion severe maternal morbidity and mortality, as well as cardiac severe maternal morbidity and mortality.
After adjustment, ischemic heart disease alone was associated with a higher risk of severe maternal morbidity or death compared to no cardiac disease (adjusted RR, 1.51; 95% CI, 1.19-1.92).
In comparison, the aRR was 1.90 for WHO class I-II diseases and 5.87 (95% CI, 5.49-6.27) for more severe cardiac conditions defined as WHO II/III-IV diseases.
Risk for nontransfusion severe maternal morbidity or death (aRR, 1.60) and cardiac severe maternal morbidity or death (aRR, 2.98) were also higher for those with ischemic heart disease than for women without any cardiac disease.
There were no significant differences in preterm birth for those with preexisting ischemic heart disease compared to those with no cardiac disease after adjustment.
The risk of severe maternal morbidity and mortality, nontransfusion severe maternal morbidity and mortality, and cardiac severe maternal morbidity and mortality for ischemic heart disease alone most closely approximated that of mWHO class I or II cardiac diseases, the researchers said.
“We found that individuals with preexisting ischemic heart disease had a rate of severe maternal morbidity/mortality in the same range as those with other cardiac diagnoses in the mild cardiac disease classification (class I or II),” Dr. Denoble commented.
“This prognosis suggests it is very reasonable for these women to consider pregnancy. The risk of adverse outcomes is not so high that pregnancy is contraindicated,” she added.
Dr. Denoble said this information will be very helpful when counseling women with preexisting ischemic heart disease who are considering pregnancy. “These patients may need some extra monitoring, but in general, they have a high chance of a good outcome,” she noted.
“I would still advise these women to register with a high-risk obstetrics provider to have a baseline cardiovascular pregnancy evaluation. As long as that is reassuring, then further frequent intensive supervision may not be necessary,” she said.
However, the authors pointed out, “it is important to communicate to patients that while pregnancy may be considered low risk in the setting of pre-existing ischemic heart disease, 6.6% of patients with pre-existing ischemic heart disease alone did experience severe maternal morbidity or death during the delivery hospitalization.”
They added that other medical comorbidities should be factored into discussions regarding the risks of pregnancy.
The researchers also noted that the study was limited to evaluation of maternal outcomes occurring during the delivery hospitalization and that additional research that assesses rates of maternal adverse cardiac events and maternal morbidity occurring prior to or after the delivery hospitalization would be beneficial.
Future studies examining the potential gradation in risk associated with additional cardiac comorbidities in individuals with preexisting ischemic heart disease would also be worthwhile, they added.
The study was supported by funding from the National Institutes of Health and the Foundation for Women and Girls with Blood Disorders. The authors disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM JACC: ADVANCES
The 'Plaque Hypothesis': Focus on vulnerable lesions to cut events
A new strategy for the management of atherosclerotic plaque as a source of major adverse cardiac events is needed with the focus shifting from the flow-limiting coronary artery luminal lesions to the overall atherosclerotic burden, be it obstructive or nonobstructive, according to a review article.
The article, by Peter H. Stone, MD, and Peter Libby, MD, Brigham and Women’s Hospital, Boston, and William E. Boden, MD, Boston University School of Medicine, was published online in JAMA Cardiology.
The review explored new data from vascular biology, atherosclerosis imaging, natural history outcome studies, and large-scale clinical trials that support what the authors refer to as “The Plaque Hypothesis” – the idea that major adverse cardiac events such as myocardial infarction and cardiac death are triggered by destabilization of vulnerable plaque, which may be obstructive or nonobstructive.
“We need to consider embracing a new management strategy that directs our diagnostic and management focus to evaluate the entire length of the atheromatous coronary artery and broaden the target of our therapeutic intervention to include all regions of the plaque (both flow-limiting and non–flow-limiting), even those that are distant from the presumed ischemia-producing obstruction,” the authors concluded.
Dr. Stone explained to this news organization that, for several decades, the medical community has focused on plaques causing severe obstruction of coronary arteries as being responsible for major adverse cardiac events. This approach – known as the Ischemia Hypothesis – has been the accepted strategy for many years, with all guidelines advising the identification of the stenoses that cause the most obstruction for treatment with stenting.
However, the authors pointed out that a number of studies have now suggested that, while these severe obstructive stenoses cause angina, they do not seem to be responsible for the hard events of MI, acute coronary syndrome (ACS), and cardiac death.
Several studies including the COURAGE trial and BARI-2D, and the recent ISCHEMIA trial have all failed to show a reduction in these hard endpoints by intervening on these severe obstructive lesions, Dr. Stone noted.
“We present evidence for a new approach – that it is the composition and vascular biology of the atherosclerotic plaques that cause MI, ACS, and cardiac death, rather than simply how obstructive they are,” he said.
Dr. Stone pointed out that plaque seen on a coronary angiogram looks at only the lumen of the artery, but plaque is primarily based in the wall of the artery, and if that plaque is inflamed it can easily be the culprit responsible for adverse events even without encroaching into the lumen.
“Our paper describes many factors which can cause plaques to destabilize and cause an ACS. These include anatomical, biochemical, and biomechanical features that together cause plaque rupture or erosion and precipitate a clinical event. It is not sufficient to just look for obstructive plaques on a coronary angiogram,” he said. “We are barking up the wrong tree. We need to look for inflamed plaque in the whole wall of the coronary arteries.”
The authors described different factors that identify a plaque at high risk of destabilization. These include a large area of vulnerable plaque, a thin-cap atheroma, a severe inflamed core, macrocalcifications, a large plaque burden, and a physical profile that would encourage a thrombus to become trapped.
“Atherosclerotic plaques are very heterogeneous and complex structures and it is not just the mountain peaks but also the lower foothills that can precipitate a flow-limiting obstruction,” Dr. Stone noted.
“The slope of the mountain is probably very important in the ability for a thrombus to form. If the slope is gradual there isn’t a problem. But if the slope is jagged with sharp edges this can cause a thrombus to become trapped. We need to look at the entirety of plaque and all its risk features to identify the culprit areas that could cause MI or cardiac death. These are typically not the obstructive plaques we have all been fixated on for many years,” he added.
“We need to focus on plaque heterogeneity. Once plaque is old and just made up of scar tissue which is not inflamed it does not cause much [of] a problem – we can probably just leave it alone. Some of these obstructive plaques may cause some angina but many do not cause major cardiac events unless they have other high-risk features,” he said.
“Cardiac events are still caused by obstruction of blood flow but that can be an abrupt process where a thrombus attaches itself to an area of destabilized plaque. These areas of plaque were not necessarily obstructing to start with. We believe that this is the explanation behind the observation that 50% of all people who have an MI (half of which are fatal) do not have symptoms beforehand,” Dr. Stone commented.
Because these areas of destabilized plaque do not cause symptoms, he believes that vast populations of people with established cardiovascular risk factors should undergo screening. “At the moment we wait for people to experience chest pain or to have an MI – that is far too little too late.”
To identify these areas of high-risk plaques, imaging techniques looking inside the artery wall are needed such as intravascular ultrasound. However, this is an invasive procedure, and the noninvasive coronary CT angiography also gives a good picture, so it is probably the best way to begin as a wider screening modality, with more invasive screening methods then used in those found to be at risk, Dr. Stone suggested.
Plaques that are identified as likely to destabilize can be treated with percutaneous coronary intervention and stenting.
While systemic therapies are useful, those currently available are not sufficient, Dr. Stone noted. For example, there are still high levels of major cardiac events in patients treated with the PCSK9 inhibitors, which bring about very large reductions in LDL cholesterol. “These therapies are beneficial, but they are not enough on their own. So, these areas of unstable plaque would need to be treated with stenting or something similar. We believe that the intervention of stenting is good but at present it is targeted at the wrong areas,” he stated.
“Clearly what we’ve been doing – stenting only obstructive lesions – does not reduce hard clinical events. Imaging methods have improved so much in recent years that we can now identify high-risk areas of plaque. This whole field of studying the vulnerable plaque has been ongoing for many years, but it is only recently that imaging methods have become good enough to identify plaques at risk. This field is now coming of age,” he added.
The next steps are to start identifying these plaques in larger populations, more accurately characterizing those at the highest risk, and then performing randomized trials of preemptive intervention in those believed to be at highest risk, and follow up for clinical events, Dr. Stone explained.
Advances in detecting unstable plaque may also permit early evaluation of novel therapeutics and gauge the intensity of lifestyle and disease-modifying pharmacotherapy, the authors suggested.
This work was supported in part by the National Heart, Lung, and Blood Institute, the American Heart Association, the RRM Charitable Fund, the Simard Fund, and the Schaubert Family. Dr. Libby is an unpaid consultant to or involved in clinical trials with Amgen, AstraZeneca, Baim Institute, Beren Therapeutics, Esperion Therapeutics, Genentech, Kancera, Kowa Pharmaceuticals, MedImmune, Merck, Norvo Nordisk, Novartis, Pfizer, and Sanofi-Regeneron; and is a member of the scientific advisory board for Amgen, Caristo Diagnostics, Cartesian Therapeutics, CSL Behring, DalCor Pharmaceuticals, Dewpoint Therapeutics, Elucid Bioimaging, Kancera, Kowa Pharmaceuticals, Olatec Therapeutics, MedImmune, Moderna, Novartis, PlaqueTec, TenSixteen Bio, Soley Thereapeutics, and XBiotech.
A version of this article first appeared on Medscape.com.
A new strategy for the management of atherosclerotic plaque as a source of major adverse cardiac events is needed with the focus shifting from the flow-limiting coronary artery luminal lesions to the overall atherosclerotic burden, be it obstructive or nonobstructive, according to a review article.
The article, by Peter H. Stone, MD, and Peter Libby, MD, Brigham and Women’s Hospital, Boston, and William E. Boden, MD, Boston University School of Medicine, was published online in JAMA Cardiology.
The review explored new data from vascular biology, atherosclerosis imaging, natural history outcome studies, and large-scale clinical trials that support what the authors refer to as “The Plaque Hypothesis” – the idea that major adverse cardiac events such as myocardial infarction and cardiac death are triggered by destabilization of vulnerable plaque, which may be obstructive or nonobstructive.
“We need to consider embracing a new management strategy that directs our diagnostic and management focus to evaluate the entire length of the atheromatous coronary artery and broaden the target of our therapeutic intervention to include all regions of the plaque (both flow-limiting and non–flow-limiting), even those that are distant from the presumed ischemia-producing obstruction,” the authors concluded.
Dr. Stone explained to this news organization that, for several decades, the medical community has focused on plaques causing severe obstruction of coronary arteries as being responsible for major adverse cardiac events. This approach – known as the Ischemia Hypothesis – has been the accepted strategy for many years, with all guidelines advising the identification of the stenoses that cause the most obstruction for treatment with stenting.
However, the authors pointed out that a number of studies have now suggested that, while these severe obstructive stenoses cause angina, they do not seem to be responsible for the hard events of MI, acute coronary syndrome (ACS), and cardiac death.
Several studies including the COURAGE trial and BARI-2D, and the recent ISCHEMIA trial have all failed to show a reduction in these hard endpoints by intervening on these severe obstructive lesions, Dr. Stone noted.
“We present evidence for a new approach – that it is the composition and vascular biology of the atherosclerotic plaques that cause MI, ACS, and cardiac death, rather than simply how obstructive they are,” he said.
Dr. Stone pointed out that plaque seen on a coronary angiogram looks at only the lumen of the artery, but plaque is primarily based in the wall of the artery, and if that plaque is inflamed it can easily be the culprit responsible for adverse events even without encroaching into the lumen.
“Our paper describes many factors which can cause plaques to destabilize and cause an ACS. These include anatomical, biochemical, and biomechanical features that together cause plaque rupture or erosion and precipitate a clinical event. It is not sufficient to just look for obstructive plaques on a coronary angiogram,” he said. “We are barking up the wrong tree. We need to look for inflamed plaque in the whole wall of the coronary arteries.”
The authors described different factors that identify a plaque at high risk of destabilization. These include a large area of vulnerable plaque, a thin-cap atheroma, a severe inflamed core, macrocalcifications, a large plaque burden, and a physical profile that would encourage a thrombus to become trapped.
“Atherosclerotic plaques are very heterogeneous and complex structures and it is not just the mountain peaks but also the lower foothills that can precipitate a flow-limiting obstruction,” Dr. Stone noted.
“The slope of the mountain is probably very important in the ability for a thrombus to form. If the slope is gradual there isn’t a problem. But if the slope is jagged with sharp edges this can cause a thrombus to become trapped. We need to look at the entirety of plaque and all its risk features to identify the culprit areas that could cause MI or cardiac death. These are typically not the obstructive plaques we have all been fixated on for many years,” he added.
“We need to focus on plaque heterogeneity. Once plaque is old and just made up of scar tissue which is not inflamed it does not cause much [of] a problem – we can probably just leave it alone. Some of these obstructive plaques may cause some angina but many do not cause major cardiac events unless they have other high-risk features,” he said.
“Cardiac events are still caused by obstruction of blood flow but that can be an abrupt process where a thrombus attaches itself to an area of destabilized plaque. These areas of plaque were not necessarily obstructing to start with. We believe that this is the explanation behind the observation that 50% of all people who have an MI (half of which are fatal) do not have symptoms beforehand,” Dr. Stone commented.
Because these areas of destabilized plaque do not cause symptoms, he believes that vast populations of people with established cardiovascular risk factors should undergo screening. “At the moment we wait for people to experience chest pain or to have an MI – that is far too little too late.”
To identify these areas of high-risk plaques, imaging techniques looking inside the artery wall are needed such as intravascular ultrasound. However, this is an invasive procedure, and the noninvasive coronary CT angiography also gives a good picture, so it is probably the best way to begin as a wider screening modality, with more invasive screening methods then used in those found to be at risk, Dr. Stone suggested.
Plaques that are identified as likely to destabilize can be treated with percutaneous coronary intervention and stenting.
While systemic therapies are useful, those currently available are not sufficient, Dr. Stone noted. For example, there are still high levels of major cardiac events in patients treated with the PCSK9 inhibitors, which bring about very large reductions in LDL cholesterol. “These therapies are beneficial, but they are not enough on their own. So, these areas of unstable plaque would need to be treated with stenting or something similar. We believe that the intervention of stenting is good but at present it is targeted at the wrong areas,” he stated.
“Clearly what we’ve been doing – stenting only obstructive lesions – does not reduce hard clinical events. Imaging methods have improved so much in recent years that we can now identify high-risk areas of plaque. This whole field of studying the vulnerable plaque has been ongoing for many years, but it is only recently that imaging methods have become good enough to identify plaques at risk. This field is now coming of age,” he added.
The next steps are to start identifying these plaques in larger populations, more accurately characterizing those at the highest risk, and then performing randomized trials of preemptive intervention in those believed to be at highest risk, and follow up for clinical events, Dr. Stone explained.
Advances in detecting unstable plaque may also permit early evaluation of novel therapeutics and gauge the intensity of lifestyle and disease-modifying pharmacotherapy, the authors suggested.
This work was supported in part by the National Heart, Lung, and Blood Institute, the American Heart Association, the RRM Charitable Fund, the Simard Fund, and the Schaubert Family. Dr. Libby is an unpaid consultant to or involved in clinical trials with Amgen, AstraZeneca, Baim Institute, Beren Therapeutics, Esperion Therapeutics, Genentech, Kancera, Kowa Pharmaceuticals, MedImmune, Merck, Norvo Nordisk, Novartis, Pfizer, and Sanofi-Regeneron; and is a member of the scientific advisory board for Amgen, Caristo Diagnostics, Cartesian Therapeutics, CSL Behring, DalCor Pharmaceuticals, Dewpoint Therapeutics, Elucid Bioimaging, Kancera, Kowa Pharmaceuticals, Olatec Therapeutics, MedImmune, Moderna, Novartis, PlaqueTec, TenSixteen Bio, Soley Thereapeutics, and XBiotech.
A version of this article first appeared on Medscape.com.
A new strategy for the management of atherosclerotic plaque as a source of major adverse cardiac events is needed with the focus shifting from the flow-limiting coronary artery luminal lesions to the overall atherosclerotic burden, be it obstructive or nonobstructive, according to a review article.
The article, by Peter H. Stone, MD, and Peter Libby, MD, Brigham and Women’s Hospital, Boston, and William E. Boden, MD, Boston University School of Medicine, was published online in JAMA Cardiology.
The review explored new data from vascular biology, atherosclerosis imaging, natural history outcome studies, and large-scale clinical trials that support what the authors refer to as “The Plaque Hypothesis” – the idea that major adverse cardiac events such as myocardial infarction and cardiac death are triggered by destabilization of vulnerable plaque, which may be obstructive or nonobstructive.
“We need to consider embracing a new management strategy that directs our diagnostic and management focus to evaluate the entire length of the atheromatous coronary artery and broaden the target of our therapeutic intervention to include all regions of the plaque (both flow-limiting and non–flow-limiting), even those that are distant from the presumed ischemia-producing obstruction,” the authors concluded.
Dr. Stone explained to this news organization that, for several decades, the medical community has focused on plaques causing severe obstruction of coronary arteries as being responsible for major adverse cardiac events. This approach – known as the Ischemia Hypothesis – has been the accepted strategy for many years, with all guidelines advising the identification of the stenoses that cause the most obstruction for treatment with stenting.
However, the authors pointed out that a number of studies have now suggested that, while these severe obstructive stenoses cause angina, they do not seem to be responsible for the hard events of MI, acute coronary syndrome (ACS), and cardiac death.
Several studies including the COURAGE trial and BARI-2D, and the recent ISCHEMIA trial have all failed to show a reduction in these hard endpoints by intervening on these severe obstructive lesions, Dr. Stone noted.
“We present evidence for a new approach – that it is the composition and vascular biology of the atherosclerotic plaques that cause MI, ACS, and cardiac death, rather than simply how obstructive they are,” he said.
Dr. Stone pointed out that plaque seen on a coronary angiogram looks at only the lumen of the artery, but plaque is primarily based in the wall of the artery, and if that plaque is inflamed it can easily be the culprit responsible for adverse events even without encroaching into the lumen.
“Our paper describes many factors which can cause plaques to destabilize and cause an ACS. These include anatomical, biochemical, and biomechanical features that together cause plaque rupture or erosion and precipitate a clinical event. It is not sufficient to just look for obstructive plaques on a coronary angiogram,” he said. “We are barking up the wrong tree. We need to look for inflamed plaque in the whole wall of the coronary arteries.”
The authors described different factors that identify a plaque at high risk of destabilization. These include a large area of vulnerable plaque, a thin-cap atheroma, a severe inflamed core, macrocalcifications, a large plaque burden, and a physical profile that would encourage a thrombus to become trapped.
“Atherosclerotic plaques are very heterogeneous and complex structures and it is not just the mountain peaks but also the lower foothills that can precipitate a flow-limiting obstruction,” Dr. Stone noted.
“The slope of the mountain is probably very important in the ability for a thrombus to form. If the slope is gradual there isn’t a problem. But if the slope is jagged with sharp edges this can cause a thrombus to become trapped. We need to look at the entirety of plaque and all its risk features to identify the culprit areas that could cause MI or cardiac death. These are typically not the obstructive plaques we have all been fixated on for many years,” he added.
“We need to focus on plaque heterogeneity. Once plaque is old and just made up of scar tissue which is not inflamed it does not cause much [of] a problem – we can probably just leave it alone. Some of these obstructive plaques may cause some angina but many do not cause major cardiac events unless they have other high-risk features,” he said.
“Cardiac events are still caused by obstruction of blood flow but that can be an abrupt process where a thrombus attaches itself to an area of destabilized plaque. These areas of plaque were not necessarily obstructing to start with. We believe that this is the explanation behind the observation that 50% of all people who have an MI (half of which are fatal) do not have symptoms beforehand,” Dr. Stone commented.
Because these areas of destabilized plaque do not cause symptoms, he believes that vast populations of people with established cardiovascular risk factors should undergo screening. “At the moment we wait for people to experience chest pain or to have an MI – that is far too little too late.”
To identify these areas of high-risk plaques, imaging techniques looking inside the artery wall are needed such as intravascular ultrasound. However, this is an invasive procedure, and the noninvasive coronary CT angiography also gives a good picture, so it is probably the best way to begin as a wider screening modality, with more invasive screening methods then used in those found to be at risk, Dr. Stone suggested.
Plaques that are identified as likely to destabilize can be treated with percutaneous coronary intervention and stenting.
While systemic therapies are useful, those currently available are not sufficient, Dr. Stone noted. For example, there are still high levels of major cardiac events in patients treated with the PCSK9 inhibitors, which bring about very large reductions in LDL cholesterol. “These therapies are beneficial, but they are not enough on their own. So, these areas of unstable plaque would need to be treated with stenting or something similar. We believe that the intervention of stenting is good but at present it is targeted at the wrong areas,” he stated.
“Clearly what we’ve been doing – stenting only obstructive lesions – does not reduce hard clinical events. Imaging methods have improved so much in recent years that we can now identify high-risk areas of plaque. This whole field of studying the vulnerable plaque has been ongoing for many years, but it is only recently that imaging methods have become good enough to identify plaques at risk. This field is now coming of age,” he added.
The next steps are to start identifying these plaques in larger populations, more accurately characterizing those at the highest risk, and then performing randomized trials of preemptive intervention in those believed to be at highest risk, and follow up for clinical events, Dr. Stone explained.
Advances in detecting unstable plaque may also permit early evaluation of novel therapeutics and gauge the intensity of lifestyle and disease-modifying pharmacotherapy, the authors suggested.
This work was supported in part by the National Heart, Lung, and Blood Institute, the American Heart Association, the RRM Charitable Fund, the Simard Fund, and the Schaubert Family. Dr. Libby is an unpaid consultant to or involved in clinical trials with Amgen, AstraZeneca, Baim Institute, Beren Therapeutics, Esperion Therapeutics, Genentech, Kancera, Kowa Pharmaceuticals, MedImmune, Merck, Norvo Nordisk, Novartis, Pfizer, and Sanofi-Regeneron; and is a member of the scientific advisory board for Amgen, Caristo Diagnostics, Cartesian Therapeutics, CSL Behring, DalCor Pharmaceuticals, Dewpoint Therapeutics, Elucid Bioimaging, Kancera, Kowa Pharmaceuticals, Olatec Therapeutics, MedImmune, Moderna, Novartis, PlaqueTec, TenSixteen Bio, Soley Thereapeutics, and XBiotech.
A version of this article first appeared on Medscape.com.
New AHA statement on managing ACS in older adults
Age-related changes in general and cardiovascular health likely require modifications in how acute coronary syndrome (ACS) is diagnosed and managed in adults aged 75 and older, the American Heart Association says in a new scientific statement.
The statement outlines a framework to integrate geriatric risks into the management of ACS, including the diagnostic approach, pharmacotherapy, revascularization strategies, prevention of adverse events, and transition care planning.
The 31-page statement was published online in the AHA journal Circulation (2022 Dec 12. doi: 10.1161/CIR.0000000000001112). It updates a 2007 AHA statement on treatment of ACS in the elderly.
Complex patient group
Adults aged 75 and older make up roughly 30%-40% of all hospitalized patients with ACS and the majority of ACS-related deaths occur in this group, the writing group notes.

“Older patients have more pronounced anatomical changes and more severe functional impairment, and they are more likely to have additional health conditions,” writing group chair Abdulla A. Damluji, MD, PhD, director of the Inova Center of Outcomes Research in Fairfax, Va., notes in a news release.
“These include frailty, other chronic disorders (treated with multiple medications), physical dysfunction, cognitive decline and/or urinary incontinence – and these are not regularly studied in the context of ACS,” Dr. Damluji explained.
The writing group notes that the presence of one or more geriatric syndromes may substantially affect ACS clinical presentation, clinical course and prognosis, therapeutic decision-making, and response to treatment.
“It is therefore fundamental that clinicians caring for older patients with ACS be alert to the presence of geriatric syndromes and be able to integrate them into the care plan when appropriate,” they say.
They recommend a holistic, individualized, and patient-centered approach to ACS care in the elderly, taking into consideration coexisting and overlapping health issues.
Considerations for clinical care
The AHA statement offers several “considerations for clinical practice” with regard to ACS diagnosis and management in elderly adults. They include:
- ACS presentations without chest pain, such as shortness of breath, syncope, or sudden confusion, are more common in older adults.
- Many older adults have persistent elevations in cardiac troponin levels from myocardial fibrosis and kidney disease that diminish the positive predictive value of high-sensitivity cardiac troponin (hs-cTn) assays for identifying acute and chronic myocardial injury. For this reason, evaluating patterns of rise and fall is essential.
- Age-related changes in metabolism, weight, and muscle mass may require different choices in anticoagulant medications to lower bleeding risk.
- Clopidogrel (Plavix) is the preferred P2Y12 inhibitor because of a significantly lower bleeding profile than ticagrelor (Brilinta) or prasugrel (Effient). For patients with ST-segment myocardial infarction (STEMI) or complex anatomy, the use of ticagrelor is “reasonable.”
- Poor kidney function can increase the risk for contrast-induced acute kidney injury.
- Although the risks are greater, percutaneous coronary intervention or bypass surgery are beneficial in select older adults with ACS.
- Post-MI care should include cardiac rehabilitation tailored to address each patient’s circumstances and personal goals of care.
- For patients with cognitive difficulties and limited mobility, consider simplified medication plans with fewer doses per day and 90-day supplies to prevent the need for frequent refills.
- Patient care plans should be individualized, with input from a multidisciplinary team that may include cardiologists, surgeons, geriatricians, primary care clinicians, nutritionists, social workers, and family members.
- Determine a priori goals of care in older patients to help avoid an unwanted or futile intervention.
This scientific statement was prepared by the volunteer writing group on behalf of the AHA Cardiovascular Diseases in Older Populations Committee of the Council on Clinical Cardiology; the Council on Cardiovascular and Stroke Nursing; the Council on Cardiovascular Radiology and Intervention; and the Council on Lifestyle and Cardiometabolic Health.
A version of this article first appeared on Medscape.com.
Age-related changes in general and cardiovascular health likely require modifications in how acute coronary syndrome (ACS) is diagnosed and managed in adults aged 75 and older, the American Heart Association says in a new scientific statement.
The statement outlines a framework to integrate geriatric risks into the management of ACS, including the diagnostic approach, pharmacotherapy, revascularization strategies, prevention of adverse events, and transition care planning.
The 31-page statement was published online in the AHA journal Circulation (2022 Dec 12. doi: 10.1161/CIR.0000000000001112). It updates a 2007 AHA statement on treatment of ACS in the elderly.
Complex patient group
Adults aged 75 and older make up roughly 30%-40% of all hospitalized patients with ACS and the majority of ACS-related deaths occur in this group, the writing group notes.
“Older patients have more pronounced anatomical changes and more severe functional impairment, and they are more likely to have additional health conditions,” writing group chair Abdulla A. Damluji, MD, PhD, director of the Inova Center of Outcomes Research in Fairfax, Va., notes in a news release.
“These include frailty, other chronic disorders (treated with multiple medications), physical dysfunction, cognitive decline and/or urinary incontinence – and these are not regularly studied in the context of ACS,” Dr. Damluji explained.
The writing group notes that the presence of one or more geriatric syndromes may substantially affect ACS clinical presentation, clinical course and prognosis, therapeutic decision-making, and response to treatment.
“It is therefore fundamental that clinicians caring for older patients with ACS be alert to the presence of geriatric syndromes and be able to integrate them into the care plan when appropriate,” they say.
They recommend a holistic, individualized, and patient-centered approach to ACS care in the elderly, taking into consideration coexisting and overlapping health issues.
Considerations for clinical care
The AHA statement offers several “considerations for clinical practice” with regard to ACS diagnosis and management in elderly adults. They include:
- ACS presentations without chest pain, such as shortness of breath, syncope, or sudden confusion, are more common in older adults.
- Many older adults have persistent elevations in cardiac troponin levels from myocardial fibrosis and kidney disease that diminish the positive predictive value of high-sensitivity cardiac troponin (hs-cTn) assays for identifying acute and chronic myocardial injury. For this reason, evaluating patterns of rise and fall is essential.
- Age-related changes in metabolism, weight, and muscle mass may require different choices in anticoagulant medications to lower bleeding risk.
- Clopidogrel (Plavix) is the preferred P2Y12 inhibitor because of a significantly lower bleeding profile than ticagrelor (Brilinta) or prasugrel (Effient). For patients with ST-segment myocardial infarction (STEMI) or complex anatomy, the use of ticagrelor is “reasonable.”
- Poor kidney function can increase the risk for contrast-induced acute kidney injury.
- Although the risks are greater, percutaneous coronary intervention or bypass surgery are beneficial in select older adults with ACS.
- Post-MI care should include cardiac rehabilitation tailored to address each patient’s circumstances and personal goals of care.
- For patients with cognitive difficulties and limited mobility, consider simplified medication plans with fewer doses per day and 90-day supplies to prevent the need for frequent refills.
- Patient care plans should be individualized, with input from a multidisciplinary team that may include cardiologists, surgeons, geriatricians, primary care clinicians, nutritionists, social workers, and family members.
- Determine a priori goals of care in older patients to help avoid an unwanted or futile intervention.
This scientific statement was prepared by the volunteer writing group on behalf of the AHA Cardiovascular Diseases in Older Populations Committee of the Council on Clinical Cardiology; the Council on Cardiovascular and Stroke Nursing; the Council on Cardiovascular Radiology and Intervention; and the Council on Lifestyle and Cardiometabolic Health.
A version of this article first appeared on Medscape.com.
Age-related changes in general and cardiovascular health likely require modifications in how acute coronary syndrome (ACS) is diagnosed and managed in adults aged 75 and older, the American Heart Association says in a new scientific statement.
The statement outlines a framework to integrate geriatric risks into the management of ACS, including the diagnostic approach, pharmacotherapy, revascularization strategies, prevention of adverse events, and transition care planning.
The 31-page statement was published online in the AHA journal Circulation (2022 Dec 12. doi: 10.1161/CIR.0000000000001112). It updates a 2007 AHA statement on treatment of ACS in the elderly.
Complex patient group
Adults aged 75 and older make up roughly 30%-40% of all hospitalized patients with ACS and the majority of ACS-related deaths occur in this group, the writing group notes.
“Older patients have more pronounced anatomical changes and more severe functional impairment, and they are more likely to have additional health conditions,” writing group chair Abdulla A. Damluji, MD, PhD, director of the Inova Center of Outcomes Research in Fairfax, Va., notes in a news release.
“These include frailty, other chronic disorders (treated with multiple medications), physical dysfunction, cognitive decline and/or urinary incontinence – and these are not regularly studied in the context of ACS,” Dr. Damluji explained.
The writing group notes that the presence of one or more geriatric syndromes may substantially affect ACS clinical presentation, clinical course and prognosis, therapeutic decision-making, and response to treatment.
“It is therefore fundamental that clinicians caring for older patients with ACS be alert to the presence of geriatric syndromes and be able to integrate them into the care plan when appropriate,” they say.
They recommend a holistic, individualized, and patient-centered approach to ACS care in the elderly, taking into consideration coexisting and overlapping health issues.
Considerations for clinical care
The AHA statement offers several “considerations for clinical practice” with regard to ACS diagnosis and management in elderly adults. They include:
- ACS presentations without chest pain, such as shortness of breath, syncope, or sudden confusion, are more common in older adults.
- Many older adults have persistent elevations in cardiac troponin levels from myocardial fibrosis and kidney disease that diminish the positive predictive value of high-sensitivity cardiac troponin (hs-cTn) assays for identifying acute and chronic myocardial injury. For this reason, evaluating patterns of rise and fall is essential.
- Age-related changes in metabolism, weight, and muscle mass may require different choices in anticoagulant medications to lower bleeding risk.
- Clopidogrel (Plavix) is the preferred P2Y12 inhibitor because of a significantly lower bleeding profile than ticagrelor (Brilinta) or prasugrel (Effient). For patients with ST-segment myocardial infarction (STEMI) or complex anatomy, the use of ticagrelor is “reasonable.”
- Poor kidney function can increase the risk for contrast-induced acute kidney injury.
- Although the risks are greater, percutaneous coronary intervention or bypass surgery are beneficial in select older adults with ACS.
- Post-MI care should include cardiac rehabilitation tailored to address each patient’s circumstances and personal goals of care.
- For patients with cognitive difficulties and limited mobility, consider simplified medication plans with fewer doses per day and 90-day supplies to prevent the need for frequent refills.
- Patient care plans should be individualized, with input from a multidisciplinary team that may include cardiologists, surgeons, geriatricians, primary care clinicians, nutritionists, social workers, and family members.
- Determine a priori goals of care in older patients to help avoid an unwanted or futile intervention.
This scientific statement was prepared by the volunteer writing group on behalf of the AHA Cardiovascular Diseases in Older Populations Committee of the Council on Clinical Cardiology; the Council on Cardiovascular and Stroke Nursing; the Council on Cardiovascular Radiology and Intervention; and the Council on Lifestyle and Cardiometabolic Health.
A version of this article first appeared on Medscape.com.
Shorter fever prevention duration effective after cardiac arrest
a randomized trial shows.
“Since 2005, active fever prevention in comatose patients has been advocated by the guidelines for 72 hours after an out-of-hospital cardiac arrest,” Christian Hassager, MD, of the University of Copenhagen, told this news organization. “Our study is the first randomized trial ever on this subject – and it challenges the guidelines.”
At 90 days, a primary endpoint – a composite of death from any cause or hospital discharge with a high Cerebral Performance Category score – occurred in 32.4% of those in the 36-hour group and 33.6% of those in the 72-hour group; mortality was 29.5% versus 30.3%, respectively.
The study was published online in The New England Journal of Medicine. The results were also presented at the Resuscitation Science Symposium during the American Heart Association scientific sessions.
No significant differences
Assessment of the two device-based fever-prevention strategies for the duration was a predefined, additional randomly assigned open-label intervention in the Blood Pressure and Oxygenation Targets in Post Resuscitation Care (BOX) trial, which involved comatose adult patients who had been resuscitated after out-of-hospital cardiac arrest at two Danish cardiac arrest centers.
The main BOX analysis compared different primary strategies in these patients in a two-by-two factorial design: higher versus lower blood pressure targets and higher versus lower oxygenation targets. They found no difference between the various strategies in terms of death and discharge from hospital in a poor neurologic state. Those results were presented at the European Society of Cardiology Congress on Aug. 27, and simultaneously published in separate articles in The New England Journal of Medicine.
For this current analysis, a total of 789 comatose patients (mean age, 62; 80% men) received device-based temperature control targeting 36° C for 24 hours followed by 37° C for either 12 or 48 hours (total intervention times, 36 and 72 hours, respectively) or until the patient regained consciousness.
Patients were kept sedated and were receiving mechanical ventilation during the temperature control at 36° C, the authors note. Target core body temperature was controlled using commercially available surface cooling at one of the sites in 286 patients (Criticool and Allon, Belmont Medical Technologies) and using intravenous cooling in 503 patients at the other site (Thermogard XP, and Cool Line Catheter, Zoll).
Body temperature was maintained at 37° C with the same type of device that had been used for 36° C during the initial 24 hours. If the patient awakened, cooling was terminated.
Physicians in both groups were permitted to use non–device-based fever treatment (that is, for a body temperature > 37.5° C) with drugs such as paracetamol, by uncovering the patient’s body, or both, at the discretion of the treating physician. Ice packs or pads were not used.
The primary outcome was a composite of death from any cause or hospital discharge with a Cerebral Performance Category of 3 or 4 (range, 1 to 5, with higher scores indicating more severe disability) within 90 days after randomization.
Secondary outcomes at 90 days included death from any cause and the Montreal Cognitive Assessment score (range, 0 to 30, with higher scores indicating better cognitive ability).
A primary endpoint event occurred in 32.3% of patients in the 36-hour group and in 33.6% of those in the 72-hour group (hazard ratio, 0.99). Mortality was 29.5% in the 36-hour group and 30.3% in the 72-hour group.
The median Montreal Cognitive Assessment scores were 26 and 27, respectively. No significant between-group differences in the incidence of adverse events were observed.
The authors concluded that “active device-based fever prevention for 36 or 72 hours after cardiac arrest did not result in significantly different percentages of patients dying or having severe disability or coma.”
Dr. Hassager added, “We will continue with a new trial where we will randomize to treatment as usual or immediate wakeup call and no temperature intervention at all.”
Findings ‘very persuasive’
Intensivist Ken Parhar, MD, clinical associate professor, Critical Care Medicine at the University of Calgary (Alta.) and Alberta Health Services, Edmonton, and medical director, Cardiovascular Intensive Care Unit, commented on the study.
“The findings are very clear and very persuasive,” he said. “I think this should be incorporated into future guidelines, though it would be nice to see the trial repeated in another center.”
Dr. Parhar has kept comatose patients under temperature control for less than 72 hours, but mainly because those patients started to wake up. “This study provides clarity on the safety of that process – that we don’t have to unnecessarily keep somebody sedated just for an arbitrary timeline,” he said. “Beyond 36 hours, we need to continue to use our judgment.”
The study was supported by a grant from the Novo Nordisk Foundation, as was the work of one of the coauthors. Dr. Hassager’s work was funded by a grant from the Lundbeck Foundation; he also received an individual research grant from the Novo Nordisk Foundation, as well as honoraria from ABIOMED. No other disclosures were declared.
A version of this article first appeared on Medscape.com.
a randomized trial shows.
“Since 2005, active fever prevention in comatose patients has been advocated by the guidelines for 72 hours after an out-of-hospital cardiac arrest,” Christian Hassager, MD, of the University of Copenhagen, told this news organization. “Our study is the first randomized trial ever on this subject – and it challenges the guidelines.”
At 90 days, a primary endpoint – a composite of death from any cause or hospital discharge with a high Cerebral Performance Category score – occurred in 32.4% of those in the 36-hour group and 33.6% of those in the 72-hour group; mortality was 29.5% versus 30.3%, respectively.
The study was published online in The New England Journal of Medicine. The results were also presented at the Resuscitation Science Symposium during the American Heart Association scientific sessions.
No significant differences
Assessment of the two device-based fever-prevention strategies for the duration was a predefined, additional randomly assigned open-label intervention in the Blood Pressure and Oxygenation Targets in Post Resuscitation Care (BOX) trial, which involved comatose adult patients who had been resuscitated after out-of-hospital cardiac arrest at two Danish cardiac arrest centers.
The main BOX analysis compared different primary strategies in these patients in a two-by-two factorial design: higher versus lower blood pressure targets and higher versus lower oxygenation targets. They found no difference between the various strategies in terms of death and discharge from hospital in a poor neurologic state. Those results were presented at the European Society of Cardiology Congress on Aug. 27, and simultaneously published in separate articles in The New England Journal of Medicine.
For this current analysis, a total of 789 comatose patients (mean age, 62; 80% men) received device-based temperature control targeting 36° C for 24 hours followed by 37° C for either 12 or 48 hours (total intervention times, 36 and 72 hours, respectively) or until the patient regained consciousness.
Patients were kept sedated and were receiving mechanical ventilation during the temperature control at 36° C, the authors note. Target core body temperature was controlled using commercially available surface cooling at one of the sites in 286 patients (Criticool and Allon, Belmont Medical Technologies) and using intravenous cooling in 503 patients at the other site (Thermogard XP, and Cool Line Catheter, Zoll).
Body temperature was maintained at 37° C with the same type of device that had been used for 36° C during the initial 24 hours. If the patient awakened, cooling was terminated.
Physicians in both groups were permitted to use non–device-based fever treatment (that is, for a body temperature > 37.5° C) with drugs such as paracetamol, by uncovering the patient’s body, or both, at the discretion of the treating physician. Ice packs or pads were not used.
The primary outcome was a composite of death from any cause or hospital discharge with a Cerebral Performance Category of 3 or 4 (range, 1 to 5, with higher scores indicating more severe disability) within 90 days after randomization.
Secondary outcomes at 90 days included death from any cause and the Montreal Cognitive Assessment score (range, 0 to 30, with higher scores indicating better cognitive ability).
A primary endpoint event occurred in 32.3% of patients in the 36-hour group and in 33.6% of those in the 72-hour group (hazard ratio, 0.99). Mortality was 29.5% in the 36-hour group and 30.3% in the 72-hour group.
The median Montreal Cognitive Assessment scores were 26 and 27, respectively. No significant between-group differences in the incidence of adverse events were observed.
The authors concluded that “active device-based fever prevention for 36 or 72 hours after cardiac arrest did not result in significantly different percentages of patients dying or having severe disability or coma.”
Dr. Hassager added, “We will continue with a new trial where we will randomize to treatment as usual or immediate wakeup call and no temperature intervention at all.”
Findings ‘very persuasive’
Intensivist Ken Parhar, MD, clinical associate professor, Critical Care Medicine at the University of Calgary (Alta.) and Alberta Health Services, Edmonton, and medical director, Cardiovascular Intensive Care Unit, commented on the study.
“The findings are very clear and very persuasive,” he said. “I think this should be incorporated into future guidelines, though it would be nice to see the trial repeated in another center.”
Dr. Parhar has kept comatose patients under temperature control for less than 72 hours, but mainly because those patients started to wake up. “This study provides clarity on the safety of that process – that we don’t have to unnecessarily keep somebody sedated just for an arbitrary timeline,” he said. “Beyond 36 hours, we need to continue to use our judgment.”
The study was supported by a grant from the Novo Nordisk Foundation, as was the work of one of the coauthors. Dr. Hassager’s work was funded by a grant from the Lundbeck Foundation; he also received an individual research grant from the Novo Nordisk Foundation, as well as honoraria from ABIOMED. No other disclosures were declared.
A version of this article first appeared on Medscape.com.
a randomized trial shows.
“Since 2005, active fever prevention in comatose patients has been advocated by the guidelines for 72 hours after an out-of-hospital cardiac arrest,” Christian Hassager, MD, of the University of Copenhagen, told this news organization. “Our study is the first randomized trial ever on this subject – and it challenges the guidelines.”
At 90 days, a primary endpoint – a composite of death from any cause or hospital discharge with a high Cerebral Performance Category score – occurred in 32.4% of those in the 36-hour group and 33.6% of those in the 72-hour group; mortality was 29.5% versus 30.3%, respectively.
The study was published online in The New England Journal of Medicine. The results were also presented at the Resuscitation Science Symposium during the American Heart Association scientific sessions.
No significant differences
Assessment of the two device-based fever-prevention strategies for the duration was a predefined, additional randomly assigned open-label intervention in the Blood Pressure and Oxygenation Targets in Post Resuscitation Care (BOX) trial, which involved comatose adult patients who had been resuscitated after out-of-hospital cardiac arrest at two Danish cardiac arrest centers.
The main BOX analysis compared different primary strategies in these patients in a two-by-two factorial design: higher versus lower blood pressure targets and higher versus lower oxygenation targets. They found no difference between the various strategies in terms of death and discharge from hospital in a poor neurologic state. Those results were presented at the European Society of Cardiology Congress on Aug. 27, and simultaneously published in separate articles in The New England Journal of Medicine.
For this current analysis, a total of 789 comatose patients (mean age, 62; 80% men) received device-based temperature control targeting 36° C for 24 hours followed by 37° C for either 12 or 48 hours (total intervention times, 36 and 72 hours, respectively) or until the patient regained consciousness.
Patients were kept sedated and were receiving mechanical ventilation during the temperature control at 36° C, the authors note. Target core body temperature was controlled using commercially available surface cooling at one of the sites in 286 patients (Criticool and Allon, Belmont Medical Technologies) and using intravenous cooling in 503 patients at the other site (Thermogard XP, and Cool Line Catheter, Zoll).
Body temperature was maintained at 37° C with the same type of device that had been used for 36° C during the initial 24 hours. If the patient awakened, cooling was terminated.
Physicians in both groups were permitted to use non–device-based fever treatment (that is, for a body temperature > 37.5° C) with drugs such as paracetamol, by uncovering the patient’s body, or both, at the discretion of the treating physician. Ice packs or pads were not used.
The primary outcome was a composite of death from any cause or hospital discharge with a Cerebral Performance Category of 3 or 4 (range, 1 to 5, with higher scores indicating more severe disability) within 90 days after randomization.
Secondary outcomes at 90 days included death from any cause and the Montreal Cognitive Assessment score (range, 0 to 30, with higher scores indicating better cognitive ability).
A primary endpoint event occurred in 32.3% of patients in the 36-hour group and in 33.6% of those in the 72-hour group (hazard ratio, 0.99). Mortality was 29.5% in the 36-hour group and 30.3% in the 72-hour group.
The median Montreal Cognitive Assessment scores were 26 and 27, respectively. No significant between-group differences in the incidence of adverse events were observed.
The authors concluded that “active device-based fever prevention for 36 or 72 hours after cardiac arrest did not result in significantly different percentages of patients dying or having severe disability or coma.”
Dr. Hassager added, “We will continue with a new trial where we will randomize to treatment as usual or immediate wakeup call and no temperature intervention at all.”
Findings ‘very persuasive’
Intensivist Ken Parhar, MD, clinical associate professor, Critical Care Medicine at the University of Calgary (Alta.) and Alberta Health Services, Edmonton, and medical director, Cardiovascular Intensive Care Unit, commented on the study.
“The findings are very clear and very persuasive,” he said. “I think this should be incorporated into future guidelines, though it would be nice to see the trial repeated in another center.”
Dr. Parhar has kept comatose patients under temperature control for less than 72 hours, but mainly because those patients started to wake up. “This study provides clarity on the safety of that process – that we don’t have to unnecessarily keep somebody sedated just for an arbitrary timeline,” he said. “Beyond 36 hours, we need to continue to use our judgment.”
The study was supported by a grant from the Novo Nordisk Foundation, as was the work of one of the coauthors. Dr. Hassager’s work was funded by a grant from the Lundbeck Foundation; he also received an individual research grant from the Novo Nordisk Foundation, as well as honoraria from ABIOMED. No other disclosures were declared.
A version of this article first appeared on Medscape.com.
FROM NEJM
Single chest x-ray could predict 10-year CVD risk
who presented the results of their deep-learning model at the annual meeting of the Radiological Society of North America.
Current American College of Cardiologists and American Heart Association guidelines recommend estimating 10-year risk of major adverse cardiovascular events (MACE) to determine whether a patient should receive statins to help prevent atherosclerotic cardiovascular disease (ASCVD). Statins are recommended for patients with a 10-year risk of 7.5% or higher, the authors noted.
The current ASCVD risk score is determined with nine factors: age, sex, race, systolic blood pressure, hypertension treatment, smoking, type 2 diabetes, and a lipid panel.
Not all data points available in EHR
But not all of those data points may be available through the electronic health record, “which makes novel and easier approaches for population-wide screening desirable,” said lead researcher Jakob Weiss, MD, a radiologist affiliated with the Cardiovascular Imaging Research Center at Massachusetts General Hospital and the AI in medicine program at the Brigham and Women’s Hospital in Boston.
Chest x-ray images, on the other hand, are commonly available. The images carry rich information beyond diagnostic data but have not been used in this type of prediction model because AI models have been lacking, Dr. Weiss said.
The researchers trained a deep-learning model with single chest x-rays only.
They used 147,497 chest x-rays from 40,643 participants in the Prostate, Lung, Colorectal, and Ovarian Cancer (PLCO) Screening Trial, a multicenter, randomized controlled trial designed and sponsored by the National Cancer Institute.
Dr. Weiss acknowledged that the population used to train the model was heavily White and that should be a consideration in validating the model.
They compared their model’s ability to predict 10-year ASCVD risk with the standard ACC/AHA model.
“Based on a single chest radiograph image, deep learning can predict the risk of future cardiovascular events independent of cardiovascular risk factors and with similar performance to the established and guideline-recommended ASCVD risk score,” Dr. Weiss said.
Tested against independent group
They tested the model against an independent group of 11,430 outpatients (average age, 60 years; 42.9% male) who underwent a routine outpatient chest x-ray at Mass General Brigham and were potentially eligible to receive statins.
Of those 11,430 patients, 1,096 (9.6%) had a major adverse cardiac event over the median follow-up of 10.3 years.
There was a significant association of CXR-CVD risk and MACE among patients eligible to receive statins, the researchers found (hazard ratio, 2.03; 95% confidence interval, 1.81-2.30; P < .001), which remained significant after adjusting for cardiovascular risk factors (adjusted HR, 1.63; 95% CI, 1.43-1.86; P < .001).
Some of the variables were missing in the standard model, but in a subgroup of 2,401 patients, all the variables were available.
They calculated ASCVD risk in that subgroup using the standard model and the CXR model and found that the performance was similar (c-statistic, 0.64 vs. 0.65; P = .48) to the ASCVD risk score (aHR, 1.58; 95% CI, 1.20-2.09; P = .001).
Ritu R. Gill MD, MPH, associate professor of radiology at Harvard Medical School in Boston, who was not part of the study, said in an interview that “the predictive algorithm is promising and potentially translatable and could enhance the annual medical checkup in a select population.
“The algorithm was developed using the PLCO cohort with radiographs, which are likely subjects in the lung cancer screening arm,” she said. “This cohort would be at high risk of cardiovascular diseases, as smoking is a known risk factor for atherosclerotic disease, and therefore the results are expected.
“The algorithm needs to be validated in an independent database with inclusion of subjects with younger age groups and adjusted for gender and racial diversity,” Gill said.
David Cho, MD, a cardiologist at the University of California, Los Angeles, who also was not part of the study, said in an interview that “this work is a great example of AI being able to detect clinically relevant outcomes with a widely used and low-cost screening test.
“The volume of data needed to train these models is already out there,” Dr. Cho said. “It just needs to be mined.”
He noted that this tool, if validated in randomized trials, could help determine risk among patients living in places where access to specialized cardiac care is limited.
Dr. Weiss and Dr. Cho disclosed no relevant financial relationships. Dr. Gill has received research support from Cannon Inc and consultant fees from Imbio and WorldCare.
A version of this article first appeared on Medscape.com.
who presented the results of their deep-learning model at the annual meeting of the Radiological Society of North America.
Current American College of Cardiologists and American Heart Association guidelines recommend estimating 10-year risk of major adverse cardiovascular events (MACE) to determine whether a patient should receive statins to help prevent atherosclerotic cardiovascular disease (ASCVD). Statins are recommended for patients with a 10-year risk of 7.5% or higher, the authors noted.
The current ASCVD risk score is determined with nine factors: age, sex, race, systolic blood pressure, hypertension treatment, smoking, type 2 diabetes, and a lipid panel.
Not all data points available in EHR
But not all of those data points may be available through the electronic health record, “which makes novel and easier approaches for population-wide screening desirable,” said lead researcher Jakob Weiss, MD, a radiologist affiliated with the Cardiovascular Imaging Research Center at Massachusetts General Hospital and the AI in medicine program at the Brigham and Women’s Hospital in Boston.
Chest x-ray images, on the other hand, are commonly available. The images carry rich information beyond diagnostic data but have not been used in this type of prediction model because AI models have been lacking, Dr. Weiss said.
The researchers trained a deep-learning model with single chest x-rays only.
They used 147,497 chest x-rays from 40,643 participants in the Prostate, Lung, Colorectal, and Ovarian Cancer (PLCO) Screening Trial, a multicenter, randomized controlled trial designed and sponsored by the National Cancer Institute.
Dr. Weiss acknowledged that the population used to train the model was heavily White and that should be a consideration in validating the model.
They compared their model’s ability to predict 10-year ASCVD risk with the standard ACC/AHA model.
“Based on a single chest radiograph image, deep learning can predict the risk of future cardiovascular events independent of cardiovascular risk factors and with similar performance to the established and guideline-recommended ASCVD risk score,” Dr. Weiss said.
Tested against independent group
They tested the model against an independent group of 11,430 outpatients (average age, 60 years; 42.9% male) who underwent a routine outpatient chest x-ray at Mass General Brigham and were potentially eligible to receive statins.
Of those 11,430 patients, 1,096 (9.6%) had a major adverse cardiac event over the median follow-up of 10.3 years.
There was a significant association of CXR-CVD risk and MACE among patients eligible to receive statins, the researchers found (hazard ratio, 2.03; 95% confidence interval, 1.81-2.30; P < .001), which remained significant after adjusting for cardiovascular risk factors (adjusted HR, 1.63; 95% CI, 1.43-1.86; P < .001).
Some of the variables were missing in the standard model, but in a subgroup of 2,401 patients, all the variables were available.
They calculated ASCVD risk in that subgroup using the standard model and the CXR model and found that the performance was similar (c-statistic, 0.64 vs. 0.65; P = .48) to the ASCVD risk score (aHR, 1.58; 95% CI, 1.20-2.09; P = .001).
Ritu R. Gill MD, MPH, associate professor of radiology at Harvard Medical School in Boston, who was not part of the study, said in an interview that “the predictive algorithm is promising and potentially translatable and could enhance the annual medical checkup in a select population.
“The algorithm was developed using the PLCO cohort with radiographs, which are likely subjects in the lung cancer screening arm,” she said. “This cohort would be at high risk of cardiovascular diseases, as smoking is a known risk factor for atherosclerotic disease, and therefore the results are expected.
“The algorithm needs to be validated in an independent database with inclusion of subjects with younger age groups and adjusted for gender and racial diversity,” Gill said.
David Cho, MD, a cardiologist at the University of California, Los Angeles, who also was not part of the study, said in an interview that “this work is a great example of AI being able to detect clinically relevant outcomes with a widely used and low-cost screening test.
“The volume of data needed to train these models is already out there,” Dr. Cho said. “It just needs to be mined.”
He noted that this tool, if validated in randomized trials, could help determine risk among patients living in places where access to specialized cardiac care is limited.
Dr. Weiss and Dr. Cho disclosed no relevant financial relationships. Dr. Gill has received research support from Cannon Inc and consultant fees from Imbio and WorldCare.
A version of this article first appeared on Medscape.com.
who presented the results of their deep-learning model at the annual meeting of the Radiological Society of North America.
Current American College of Cardiologists and American Heart Association guidelines recommend estimating 10-year risk of major adverse cardiovascular events (MACE) to determine whether a patient should receive statins to help prevent atherosclerotic cardiovascular disease (ASCVD). Statins are recommended for patients with a 10-year risk of 7.5% or higher, the authors noted.
The current ASCVD risk score is determined with nine factors: age, sex, race, systolic blood pressure, hypertension treatment, smoking, type 2 diabetes, and a lipid panel.
Not all data points available in EHR
But not all of those data points may be available through the electronic health record, “which makes novel and easier approaches for population-wide screening desirable,” said lead researcher Jakob Weiss, MD, a radiologist affiliated with the Cardiovascular Imaging Research Center at Massachusetts General Hospital and the AI in medicine program at the Brigham and Women’s Hospital in Boston.
Chest x-ray images, on the other hand, are commonly available. The images carry rich information beyond diagnostic data but have not been used in this type of prediction model because AI models have been lacking, Dr. Weiss said.
The researchers trained a deep-learning model with single chest x-rays only.
They used 147,497 chest x-rays from 40,643 participants in the Prostate, Lung, Colorectal, and Ovarian Cancer (PLCO) Screening Trial, a multicenter, randomized controlled trial designed and sponsored by the National Cancer Institute.
Dr. Weiss acknowledged that the population used to train the model was heavily White and that should be a consideration in validating the model.
They compared their model’s ability to predict 10-year ASCVD risk with the standard ACC/AHA model.
“Based on a single chest radiograph image, deep learning can predict the risk of future cardiovascular events independent of cardiovascular risk factors and with similar performance to the established and guideline-recommended ASCVD risk score,” Dr. Weiss said.
Tested against independent group
They tested the model against an independent group of 11,430 outpatients (average age, 60 years; 42.9% male) who underwent a routine outpatient chest x-ray at Mass General Brigham and were potentially eligible to receive statins.
Of those 11,430 patients, 1,096 (9.6%) had a major adverse cardiac event over the median follow-up of 10.3 years.
There was a significant association of CXR-CVD risk and MACE among patients eligible to receive statins, the researchers found (hazard ratio, 2.03; 95% confidence interval, 1.81-2.30; P < .001), which remained significant after adjusting for cardiovascular risk factors (adjusted HR, 1.63; 95% CI, 1.43-1.86; P < .001).
Some of the variables were missing in the standard model, but in a subgroup of 2,401 patients, all the variables were available.
They calculated ASCVD risk in that subgroup using the standard model and the CXR model and found that the performance was similar (c-statistic, 0.64 vs. 0.65; P = .48) to the ASCVD risk score (aHR, 1.58; 95% CI, 1.20-2.09; P = .001).
Ritu R. Gill MD, MPH, associate professor of radiology at Harvard Medical School in Boston, who was not part of the study, said in an interview that “the predictive algorithm is promising and potentially translatable and could enhance the annual medical checkup in a select population.
“The algorithm was developed using the PLCO cohort with radiographs, which are likely subjects in the lung cancer screening arm,” she said. “This cohort would be at high risk of cardiovascular diseases, as smoking is a known risk factor for atherosclerotic disease, and therefore the results are expected.
“The algorithm needs to be validated in an independent database with inclusion of subjects with younger age groups and adjusted for gender and racial diversity,” Gill said.
David Cho, MD, a cardiologist at the University of California, Los Angeles, who also was not part of the study, said in an interview that “this work is a great example of AI being able to detect clinically relevant outcomes with a widely used and low-cost screening test.
“The volume of data needed to train these models is already out there,” Dr. Cho said. “It just needs to be mined.”
He noted that this tool, if validated in randomized trials, could help determine risk among patients living in places where access to specialized cardiac care is limited.
Dr. Weiss and Dr. Cho disclosed no relevant financial relationships. Dr. Gill has received research support from Cannon Inc and consultant fees from Imbio and WorldCare.
A version of this article first appeared on Medscape.com.
AT RSNA 2022
Lp(a) tied to more early CV events than familial hypercholesterolemia
Many more people are at risk for early cardiovascular events because of raised lipoprotein(a) levels than from having familial hypercholesterolemia (FH), a new study suggests.
The Danish study set out to try and establish a level of Lp(a) that would be associated with a cardiovascular risk similar to that seen with FH. As there are many different definitions of FH, results showed a large range of Lp(a) values that corresponded to risk levels of the different FH definitions.
However, if considering one of the broadest FH definitions (from MEDPED – Make Early Diagnoses, Prevent Early Deaths), which is the one most commonly used in the United States, results showed that the level of cardiovascular risk in patients with this definition of FH is similar to that associated with Lp(a) levels of around 70 mg/dL (0.7 g/L).
“While FH is fairly unusual, occurring in less than 1% of the population, levels of Lp(a) of 70 mg/dL or above are much more common, occurring in around 10% of the White population,” Børge Nordestgaard, MD, Copenhagen University Hospital, said in an interview. Around 20% of the Black population have such high levels, while levels in Hispanics are in between.
“Our results suggest that there will be many more individuals at risk of premature MI or cardiovascular death because of raised Lp(a) levels than because of FH,” added Dr. Nordestgaard, the senior author of the current study.
Dr. Nordestgaard explained that FH is well established to be a serious condition. “We consider FH to be the genetic disease that causes the most cases of early heart disease and early death worldwide.”
“But we know now that raised levels of Lp(a), which is also genetically determined, can also lead to an increased risk of cardiovascular events relatively early in life, and when you look into the numbers, it seems like high levels of Lp(a) could be more common than FH. We wanted to try and find the levels of Lp(a) that corresponded to similar cardiovascular risk as FH.”
The Danish study was published in the Journal of the American College of Cardiology.
The authors note that the 2019 joint European Society of Cardiology and European Atherosclerosis Society guidelines suggested that an Lp(a) level greater than 180 mg/dL (0.8 g/L) may confer a lifetime risk for heart disease equivalent to the risk associated with heterozygous FH, but they point out that this value was speculative and not based on a direct comparison of risk associated with the two conditions in the same population.
For their study, Dr. Nordestgaard and colleagues analyzed information from a large database of the Danish population, the Copenhagen General Population Study, including 69,644 individuals for whom data on FH and Lp(a) levels were available. As these conditions are genetically determined, and the study held records on individuals going back several decades, the researchers were able to analyze event rates over a median follow up time of 42 years. During this time, there were 4,166 cases of myocardial infarction and 11,464 cases of atherosclerotic cardiovascular disease (ASCVD).
Results showed that Lp(a) levels associated with MI risk equivalent to that of clinical FH ranged from 67 to 402 mg/dL depending on the definition used for FH. The Lp(a) level corresponding to the MI risk of genetically determined FH was 180 mg/dL.
In terms of risk of ASCVD events, the levels of Lp(a) corresponding to the risk associated with clinical FH ranged from 130 to 391 mg/dL, and the Lp(a) level corresponding to the ASCVD risk of genetically determined FH was 175 mg/dL.
“All these different definitions of FH may cause some confusion, but basically we are saying that if an individual is found to have an Lp(a) above 70 mg/dL, then they have a similar level of cardiovascular risk as that associated with the broadest definition of FH, and they should be taken as seriously as a patient diagnosed with FH,” Dr. Nordestgaard said.
He estimated that these individuals have approximately a doubling of cardiovascular risk, compared with the general population, and risk increases further with rising Lp(a) levels.
The researchers also found that if an individual has both FH and raised Lp(a) they are at very high risk, as these two conditions are independent of each other.
Although a specific treatment for lowering Lp(a) levels is not yet available, Dr. Nordestgaard stresses that it is still worth identifying individuals with raised Lp(a) as efforts can be made to address other cardiovascular risk factors.
“We know raised Lp(a) increases cardiovascular risk, but there are also many other factors that likewise increase this risk, and they are all additive. So, it is very important that individuals with raised Lp(a) levels address these other risk factors,” he said. “These include stopping smoking, being at healthy weight, exercising regularly, eating a heart-healthy diet, and aggressive treatment of raised LDL, hypertension, and diabetes. All these things will lower their overall risk of cardiovascular disease.”
And there is the promise of new drugs to lower Lp(a) on the horizon, with several such products now in clinical development.
Dr. Nordestgaard also points out that as Lp(a) is genetically determined, cascade screening of close relatives of the individual with raised Lp(a) should also take place to detect others who may be at risk.
Although a level of Lp(a) of around 70 mg/dL confers similar cardiovascular risk than some definitions of FH, Dr. Nordestgaard says lower levels than this should also be a signal for concern.
“We usually say Lp(a) levels of 50 mg/dL are when we need to start to take this seriously. And it’s estimated that about 20% of the White population will have levels of 50 mg/dL or over and even more in the Black population,” he added.
‘Screen for both conditions’
In an accompanying editorial, Pamela Morris, MD, Medical University of South Carolina, Charleston; Jagat Narula, MD, Icahn School of Medicine, New York; and Sotirios Tsimikas, MD, University of California, San Diego, say “the weight of evidence strongly supports that both genetic lipid disorders, elevated Lp(a) levels and FH, are causally associated with an increased risk of premature ASCVD and should be carefully considered in risk assessment and management for ASCVD risk reduction.”

Dr. Morris told this news organization that the current study found a very large range of Lp(a) levels that conferred a similar cardiovascular risk to FH, because of the many different definitions of FH in use.
“But this should not take away the importance of screening for raised Lp(a) levels,” she stressed.
“We know that increased Lp(a) levels signal a high risk of cardiovascular disease. A diagnosis of FH is also a high-risk condition,” she said. “Both are important, and we need to screen for both, but it is difficult to directly compare the two conditions because the different definitions of FH get in the way.”
Dr. Morris agrees with Dr. Nordestgaard that raised levels of Lp(a) may actually be more important for the population risk of cardiovascular disease than FH, as the prevalence of increased Lp(a) levels is higher.
“Because raised Lp(a) levels are more prevalent than confirmed FH, the risk to the population is greater,” she said.
Dr. Morris points out that cardiovascular risk starts to increase at Lp(a) levels of 30 mg/dL (75 nmol/L).
The editorialists recommend that “in addition to performing a lipid panel periodically according to evidence-based guidelines, measurement of Lp(a) levels should also be performed at least once in an individual’s lifetime for ASCVD risk assessment.”
They conclude that “it is vital to continue to raise awareness among clinicians and patients of these high-risk genetic lipid disorders. Our understanding of both disorders is rapidly expanding, and promising novel therapeutics may offer hope for prevention of cardiovascular disease in patients with elevated Lp(a) levels in the future.”
This work was supported by Copenhagen University Hospital – Herlev Gentofte, Denmark, and the Danish Beckett-Foundation. The Copenhagen General Population Study is supported by the Copenhagen County Foundation and Copenhagen University Hospital – Herlev Gentofte. Dr. Nordestgaard has been a consultant and a speaker for AstraZeneca, Sanofi, Regeneron, Akcea, Amgen, Kowa, Denka, Amarin, Novartis, Novo Nordisk, Silence Therapeutics, Abbott, and Esperion.
A version of this article first appeared on Medscape.com.
Many more people are at risk for early cardiovascular events because of raised lipoprotein(a) levels than from having familial hypercholesterolemia (FH), a new study suggests.
The Danish study set out to try and establish a level of Lp(a) that would be associated with a cardiovascular risk similar to that seen with FH. As there are many different definitions of FH, results showed a large range of Lp(a) values that corresponded to risk levels of the different FH definitions.
However, if considering one of the broadest FH definitions (from MEDPED – Make Early Diagnoses, Prevent Early Deaths), which is the one most commonly used in the United States, results showed that the level of cardiovascular risk in patients with this definition of FH is similar to that associated with Lp(a) levels of around 70 mg/dL (0.7 g/L).
“While FH is fairly unusual, occurring in less than 1% of the population, levels of Lp(a) of 70 mg/dL or above are much more common, occurring in around 10% of the White population,” Børge Nordestgaard, MD, Copenhagen University Hospital, said in an interview. Around 20% of the Black population have such high levels, while levels in Hispanics are in between.
“Our results suggest that there will be many more individuals at risk of premature MI or cardiovascular death because of raised Lp(a) levels than because of FH,” added Dr. Nordestgaard, the senior author of the current study.
Dr. Nordestgaard explained that FH is well established to be a serious condition. “We consider FH to be the genetic disease that causes the most cases of early heart disease and early death worldwide.”
“But we know now that raised levels of Lp(a), which is also genetically determined, can also lead to an increased risk of cardiovascular events relatively early in life, and when you look into the numbers, it seems like high levels of Lp(a) could be more common than FH. We wanted to try and find the levels of Lp(a) that corresponded to similar cardiovascular risk as FH.”
The Danish study was published in the Journal of the American College of Cardiology.
The authors note that the 2019 joint European Society of Cardiology and European Atherosclerosis Society guidelines suggested that an Lp(a) level greater than 180 mg/dL (0.8 g/L) may confer a lifetime risk for heart disease equivalent to the risk associated with heterozygous FH, but they point out that this value was speculative and not based on a direct comparison of risk associated with the two conditions in the same population.
For their study, Dr. Nordestgaard and colleagues analyzed information from a large database of the Danish population, the Copenhagen General Population Study, including 69,644 individuals for whom data on FH and Lp(a) levels were available. As these conditions are genetically determined, and the study held records on individuals going back several decades, the researchers were able to analyze event rates over a median follow up time of 42 years. During this time, there were 4,166 cases of myocardial infarction and 11,464 cases of atherosclerotic cardiovascular disease (ASCVD).
Results showed that Lp(a) levels associated with MI risk equivalent to that of clinical FH ranged from 67 to 402 mg/dL depending on the definition used for FH. The Lp(a) level corresponding to the MI risk of genetically determined FH was 180 mg/dL.
In terms of risk of ASCVD events, the levels of Lp(a) corresponding to the risk associated with clinical FH ranged from 130 to 391 mg/dL, and the Lp(a) level corresponding to the ASCVD risk of genetically determined FH was 175 mg/dL.
“All these different definitions of FH may cause some confusion, but basically we are saying that if an individual is found to have an Lp(a) above 70 mg/dL, then they have a similar level of cardiovascular risk as that associated with the broadest definition of FH, and they should be taken as seriously as a patient diagnosed with FH,” Dr. Nordestgaard said.
He estimated that these individuals have approximately a doubling of cardiovascular risk, compared with the general population, and risk increases further with rising Lp(a) levels.
The researchers also found that if an individual has both FH and raised Lp(a) they are at very high risk, as these two conditions are independent of each other.
Although a specific treatment for lowering Lp(a) levels is not yet available, Dr. Nordestgaard stresses that it is still worth identifying individuals with raised Lp(a) as efforts can be made to address other cardiovascular risk factors.
“We know raised Lp(a) increases cardiovascular risk, but there are also many other factors that likewise increase this risk, and they are all additive. So, it is very important that individuals with raised Lp(a) levels address these other risk factors,” he said. “These include stopping smoking, being at healthy weight, exercising regularly, eating a heart-healthy diet, and aggressive treatment of raised LDL, hypertension, and diabetes. All these things will lower their overall risk of cardiovascular disease.”
And there is the promise of new drugs to lower Lp(a) on the horizon, with several such products now in clinical development.
Dr. Nordestgaard also points out that as Lp(a) is genetically determined, cascade screening of close relatives of the individual with raised Lp(a) should also take place to detect others who may be at risk.
Although a level of Lp(a) of around 70 mg/dL confers similar cardiovascular risk than some definitions of FH, Dr. Nordestgaard says lower levels than this should also be a signal for concern.
“We usually say Lp(a) levels of 50 mg/dL are when we need to start to take this seriously. And it’s estimated that about 20% of the White population will have levels of 50 mg/dL or over and even more in the Black population,” he added.
‘Screen for both conditions’
In an accompanying editorial, Pamela Morris, MD, Medical University of South Carolina, Charleston; Jagat Narula, MD, Icahn School of Medicine, New York; and Sotirios Tsimikas, MD, University of California, San Diego, say “the weight of evidence strongly supports that both genetic lipid disorders, elevated Lp(a) levels and FH, are causally associated with an increased risk of premature ASCVD and should be carefully considered in risk assessment and management for ASCVD risk reduction.”
Dr. Morris told this news organization that the current study found a very large range of Lp(a) levels that conferred a similar cardiovascular risk to FH, because of the many different definitions of FH in use.
“But this should not take away the importance of screening for raised Lp(a) levels,” she stressed.
“We know that increased Lp(a) levels signal a high risk of cardiovascular disease. A diagnosis of FH is also a high-risk condition,” she said. “Both are important, and we need to screen for both, but it is difficult to directly compare the two conditions because the different definitions of FH get in the way.”
Dr. Morris agrees with Dr. Nordestgaard that raised levels of Lp(a) may actually be more important for the population risk of cardiovascular disease than FH, as the prevalence of increased Lp(a) levels is higher.
“Because raised Lp(a) levels are more prevalent than confirmed FH, the risk to the population is greater,” she said.
Dr. Morris points out that cardiovascular risk starts to increase at Lp(a) levels of 30 mg/dL (75 nmol/L).
The editorialists recommend that “in addition to performing a lipid panel periodically according to evidence-based guidelines, measurement of Lp(a) levels should also be performed at least once in an individual’s lifetime for ASCVD risk assessment.”
They conclude that “it is vital to continue to raise awareness among clinicians and patients of these high-risk genetic lipid disorders. Our understanding of both disorders is rapidly expanding, and promising novel therapeutics may offer hope for prevention of cardiovascular disease in patients with elevated Lp(a) levels in the future.”
This work was supported by Copenhagen University Hospital – Herlev Gentofte, Denmark, and the Danish Beckett-Foundation. The Copenhagen General Population Study is supported by the Copenhagen County Foundation and Copenhagen University Hospital – Herlev Gentofte. Dr. Nordestgaard has been a consultant and a speaker for AstraZeneca, Sanofi, Regeneron, Akcea, Amgen, Kowa, Denka, Amarin, Novartis, Novo Nordisk, Silence Therapeutics, Abbott, and Esperion.
A version of this article first appeared on Medscape.com.
Many more people are at risk for early cardiovascular events because of raised lipoprotein(a) levels than from having familial hypercholesterolemia (FH), a new study suggests.
The Danish study set out to try and establish a level of Lp(a) that would be associated with a cardiovascular risk similar to that seen with FH. As there are many different definitions of FH, results showed a large range of Lp(a) values that corresponded to risk levels of the different FH definitions.
However, if considering one of the broadest FH definitions (from MEDPED – Make Early Diagnoses, Prevent Early Deaths), which is the one most commonly used in the United States, results showed that the level of cardiovascular risk in patients with this definition of FH is similar to that associated with Lp(a) levels of around 70 mg/dL (0.7 g/L).
“While FH is fairly unusual, occurring in less than 1% of the population, levels of Lp(a) of 70 mg/dL or above are much more common, occurring in around 10% of the White population,” Børge Nordestgaard, MD, Copenhagen University Hospital, said in an interview. Around 20% of the Black population have such high levels, while levels in Hispanics are in between.
“Our results suggest that there will be many more individuals at risk of premature MI or cardiovascular death because of raised Lp(a) levels than because of FH,” added Dr. Nordestgaard, the senior author of the current study.
Dr. Nordestgaard explained that FH is well established to be a serious condition. “We consider FH to be the genetic disease that causes the most cases of early heart disease and early death worldwide.”
“But we know now that raised levels of Lp(a), which is also genetically determined, can also lead to an increased risk of cardiovascular events relatively early in life, and when you look into the numbers, it seems like high levels of Lp(a) could be more common than FH. We wanted to try and find the levels of Lp(a) that corresponded to similar cardiovascular risk as FH.”
The Danish study was published in the Journal of the American College of Cardiology.
The authors note that the 2019 joint European Society of Cardiology and European Atherosclerosis Society guidelines suggested that an Lp(a) level greater than 180 mg/dL (0.8 g/L) may confer a lifetime risk for heart disease equivalent to the risk associated with heterozygous FH, but they point out that this value was speculative and not based on a direct comparison of risk associated with the two conditions in the same population.
For their study, Dr. Nordestgaard and colleagues analyzed information from a large database of the Danish population, the Copenhagen General Population Study, including 69,644 individuals for whom data on FH and Lp(a) levels were available. As these conditions are genetically determined, and the study held records on individuals going back several decades, the researchers were able to analyze event rates over a median follow up time of 42 years. During this time, there were 4,166 cases of myocardial infarction and 11,464 cases of atherosclerotic cardiovascular disease (ASCVD).
Results showed that Lp(a) levels associated with MI risk equivalent to that of clinical FH ranged from 67 to 402 mg/dL depending on the definition used for FH. The Lp(a) level corresponding to the MI risk of genetically determined FH was 180 mg/dL.
In terms of risk of ASCVD events, the levels of Lp(a) corresponding to the risk associated with clinical FH ranged from 130 to 391 mg/dL, and the Lp(a) level corresponding to the ASCVD risk of genetically determined FH was 175 mg/dL.
“All these different definitions of FH may cause some confusion, but basically we are saying that if an individual is found to have an Lp(a) above 70 mg/dL, then they have a similar level of cardiovascular risk as that associated with the broadest definition of FH, and they should be taken as seriously as a patient diagnosed with FH,” Dr. Nordestgaard said.
He estimated that these individuals have approximately a doubling of cardiovascular risk, compared with the general population, and risk increases further with rising Lp(a) levels.
The researchers also found that if an individual has both FH and raised Lp(a) they are at very high risk, as these two conditions are independent of each other.
Although a specific treatment for lowering Lp(a) levels is not yet available, Dr. Nordestgaard stresses that it is still worth identifying individuals with raised Lp(a) as efforts can be made to address other cardiovascular risk factors.
“We know raised Lp(a) increases cardiovascular risk, but there are also many other factors that likewise increase this risk, and they are all additive. So, it is very important that individuals with raised Lp(a) levels address these other risk factors,” he said. “These include stopping smoking, being at healthy weight, exercising regularly, eating a heart-healthy diet, and aggressive treatment of raised LDL, hypertension, and diabetes. All these things will lower their overall risk of cardiovascular disease.”
And there is the promise of new drugs to lower Lp(a) on the horizon, with several such products now in clinical development.
Dr. Nordestgaard also points out that as Lp(a) is genetically determined, cascade screening of close relatives of the individual with raised Lp(a) should also take place to detect others who may be at risk.
Although a level of Lp(a) of around 70 mg/dL confers similar cardiovascular risk than some definitions of FH, Dr. Nordestgaard says lower levels than this should also be a signal for concern.
“We usually say Lp(a) levels of 50 mg/dL are when we need to start to take this seriously. And it’s estimated that about 20% of the White population will have levels of 50 mg/dL or over and even more in the Black population,” he added.
‘Screen for both conditions’
In an accompanying editorial, Pamela Morris, MD, Medical University of South Carolina, Charleston; Jagat Narula, MD, Icahn School of Medicine, New York; and Sotirios Tsimikas, MD, University of California, San Diego, say “the weight of evidence strongly supports that both genetic lipid disorders, elevated Lp(a) levels and FH, are causally associated with an increased risk of premature ASCVD and should be carefully considered in risk assessment and management for ASCVD risk reduction.”
Dr. Morris told this news organization that the current study found a very large range of Lp(a) levels that conferred a similar cardiovascular risk to FH, because of the many different definitions of FH in use.
“But this should not take away the importance of screening for raised Lp(a) levels,” she stressed.
“We know that increased Lp(a) levels signal a high risk of cardiovascular disease. A diagnosis of FH is also a high-risk condition,” she said. “Both are important, and we need to screen for both, but it is difficult to directly compare the two conditions because the different definitions of FH get in the way.”
Dr. Morris agrees with Dr. Nordestgaard that raised levels of Lp(a) may actually be more important for the population risk of cardiovascular disease than FH, as the prevalence of increased Lp(a) levels is higher.
“Because raised Lp(a) levels are more prevalent than confirmed FH, the risk to the population is greater,” she said.
Dr. Morris points out that cardiovascular risk starts to increase at Lp(a) levels of 30 mg/dL (75 nmol/L).
The editorialists recommend that “in addition to performing a lipid panel periodically according to evidence-based guidelines, measurement of Lp(a) levels should also be performed at least once in an individual’s lifetime for ASCVD risk assessment.”
They conclude that “it is vital to continue to raise awareness among clinicians and patients of these high-risk genetic lipid disorders. Our understanding of both disorders is rapidly expanding, and promising novel therapeutics may offer hope for prevention of cardiovascular disease in patients with elevated Lp(a) levels in the future.”
This work was supported by Copenhagen University Hospital – Herlev Gentofte, Denmark, and the Danish Beckett-Foundation. The Copenhagen General Population Study is supported by the Copenhagen County Foundation and Copenhagen University Hospital – Herlev Gentofte. Dr. Nordestgaard has been a consultant and a speaker for AstraZeneca, Sanofi, Regeneron, Akcea, Amgen, Kowa, Denka, Amarin, Novartis, Novo Nordisk, Silence Therapeutics, Abbott, and Esperion.
A version of this article first appeared on Medscape.com.
HDL cholesterol not linked to CHD risk in Blacks: REGARDS
High-density lipoprotein cholesterol may not be as effective a biomarker of cardiovascular disease risk as once thought, particularly in Black adults, according to results from a large biracial cohort study that also raised questions about the validity of high HDL cholesterol as a potentially protective factor in White and Black adults alike.
“I think this opens the door to suggest that every biomarker we use might have a race-specific association with disease outcome,” Nathalie Pamir, PhD, an associate professor at Oregon Health & Science University in Portland, said in an interview. “So, something as basic as HDL cholesterol – we’ve known about it since 1970 – has a race signature.”

Dr. Pamir and colleagues reported their findings from the REGARDS (Reasons for Geographic and Racial Differences in Stroke) cohort study that recruited 30,239 Black and White individuals aged 45 years and older from the contiguous United States from 2003 to 2007.
The study found that LDL cholesterol “modestly” predicted coronary heart disease (CHD) risk in Black and White adults. However, low HDL cholesterol, while associated with an increased risk in White patients (hazard ratio, 1.22; 95% confidence interval, 1.05-1.43), did not have a similar association in Blacks (HR, 0.94; 95% CI: 0.78-1.14). And high HDL cholesterol wasn’t found to be predictive in either group (HR, 0.96; 95% CI, 0.79-1.16 for White participants: HR, 0.91; 95% CI, 0.74-1.12 for Black participants).
Among 23,901 study participants who were CHD-risk free over a 10-year follow-up, 664 and 951 CHD events occurred in Black and White participants, respectively. The study cohort was 57.8% White and 58.4% women, with a mean age of 65 years.
The study noted that LDL cholesterol and triglycerides conferred similar risks for CHD in both White and Black participants.
Acknowledging that this study focused on Blacks, Dr. Pamir added that “we need to know about Asian Americans; we need to know about Hispanic Americans.”
Change of approach to lipid management called for
Dr. Pamir noted that the current understanding about HDL cholesterol and CHD risk comes from the Framingham heart study in the 1970s, whose population was 100% White.
Care algorithms derived from the Framingham study as well as the Multi-Ethnic Study of Atherosclerosis incorporate that association between HDL cholesterol and CHD risk, she noted, but these findings from REGARDS should change how cardiologists approach lipid management in Black and White patients.
“The conversation would go something like: High HDL cholesterol levels put you in a higher risk [bracket] but HDL cholesterol levels are not something we treat; we have no drugs for that,” Dr. Pamir said.
“The conversation would continue along the lines that: ‘You need to do more exercise, you need to change your diet, incorporate healthy fats, walnuts, and omega 3s.’
“But what might the conversation be for Black patients? ‘We don’t see the association that we see for White patients. Do adopt the good habits to exercise and dietary changes, but don’t get too worried about it.’ ”
The study report raises “caution” about using the Framingham, MESA, and other algorithms for evaluating CHD risk. Dr. Pamir explained what that means. “We might be underestimating risk, because what our study showed was that, when we looked at clinically high HDL cholesterol, about 60 mg/dL, it has no benefit for White and Black patients.”
She added, “So that pat on the back we get for patients that have high HDL-C levels? Maybe that pat on the back shouldn’t be there.”
In an invited commentary, Keith C. Ferdinand, MD, of Tulane University in New Orleans, wrote that using HDL cholesterol in risk calculations could inaccurately assess atherosclerotic cardiovascular risk in Black adults “and become a barrier to optimal care.”
In an interview, he said the REGARDS findings call for consideration of other biomarkers for evaluating CHD risk and point to the importance of socioeconomic factors in health outcomes.
“Physicians and other clinicians need to recognize the powerful impact of the social determinants of health and to also recognize the limits of HDL itself as either protective if it’s high or a definitive predictor of risk if it’s low, and focus on some more modern approaches, including coronary artery calcium scoring.”
He also said risk evaluation should include lipoprotein(a), which, he noted in the editorial, the European Atherosclerosis Society recommends measuring. “One of the reasons it’s underutilized is that we really don’t have a specific treatment for it,” he said of Lp(a) in the United States.
In his editorial comment, Dr. Ferdinand called for future research aimed at eliminating health disparities. “Regardless of the development of better tools for the assessment of risk, newer drugs to treat CVD, the use of coronary artery calcium, if we don’t apply evidence-based medicine equally across the population based on race, ethnicity, sex, gender, socioeconomic status, or geography, then the disparities are going to persist,” he said.
The National Institute of Neurological Disorders and Stroke and the National Institute on Aging provided funding for the study. Dr. Pamir has no relevant relationships to disclose. Dr. Ferdinand disclosed relationships with Boehringer Ingelheim, Novartis, Janssen, and Lilly.
High-density lipoprotein cholesterol may not be as effective a biomarker of cardiovascular disease risk as once thought, particularly in Black adults, according to results from a large biracial cohort study that also raised questions about the validity of high HDL cholesterol as a potentially protective factor in White and Black adults alike.
“I think this opens the door to suggest that every biomarker we use might have a race-specific association with disease outcome,” Nathalie Pamir, PhD, an associate professor at Oregon Health & Science University in Portland, said in an interview. “So, something as basic as HDL cholesterol – we’ve known about it since 1970 – has a race signature.”
Dr. Pamir and colleagues reported their findings from the REGARDS (Reasons for Geographic and Racial Differences in Stroke) cohort study that recruited 30,239 Black and White individuals aged 45 years and older from the contiguous United States from 2003 to 2007.
The study found that LDL cholesterol “modestly” predicted coronary heart disease (CHD) risk in Black and White adults. However, low HDL cholesterol, while associated with an increased risk in White patients (hazard ratio, 1.22; 95% confidence interval, 1.05-1.43), did not have a similar association in Blacks (HR, 0.94; 95% CI: 0.78-1.14). And high HDL cholesterol wasn’t found to be predictive in either group (HR, 0.96; 95% CI, 0.79-1.16 for White participants: HR, 0.91; 95% CI, 0.74-1.12 for Black participants).
Among 23,901 study participants who were CHD-risk free over a 10-year follow-up, 664 and 951 CHD events occurred in Black and White participants, respectively. The study cohort was 57.8% White and 58.4% women, with a mean age of 65 years.
The study noted that LDL cholesterol and triglycerides conferred similar risks for CHD in both White and Black participants.
Acknowledging that this study focused on Blacks, Dr. Pamir added that “we need to know about Asian Americans; we need to know about Hispanic Americans.”
Change of approach to lipid management called for
Dr. Pamir noted that the current understanding about HDL cholesterol and CHD risk comes from the Framingham heart study in the 1970s, whose population was 100% White.
Care algorithms derived from the Framingham study as well as the Multi-Ethnic Study of Atherosclerosis incorporate that association between HDL cholesterol and CHD risk, she noted, but these findings from REGARDS should change how cardiologists approach lipid management in Black and White patients.
“The conversation would go something like: High HDL cholesterol levels put you in a higher risk [bracket] but HDL cholesterol levels are not something we treat; we have no drugs for that,” Dr. Pamir said.
“The conversation would continue along the lines that: ‘You need to do more exercise, you need to change your diet, incorporate healthy fats, walnuts, and omega 3s.’
“But what might the conversation be for Black patients? ‘We don’t see the association that we see for White patients. Do adopt the good habits to exercise and dietary changes, but don’t get too worried about it.’ ”
The study report raises “caution” about using the Framingham, MESA, and other algorithms for evaluating CHD risk. Dr. Pamir explained what that means. “We might be underestimating risk, because what our study showed was that, when we looked at clinically high HDL cholesterol, about 60 mg/dL, it has no benefit for White and Black patients.”
She added, “So that pat on the back we get for patients that have high HDL-C levels? Maybe that pat on the back shouldn’t be there.”
In an invited commentary, Keith C. Ferdinand, MD, of Tulane University in New Orleans, wrote that using HDL cholesterol in risk calculations could inaccurately assess atherosclerotic cardiovascular risk in Black adults “and become a barrier to optimal care.”
In an interview, he said the REGARDS findings call for consideration of other biomarkers for evaluating CHD risk and point to the importance of socioeconomic factors in health outcomes.
“Physicians and other clinicians need to recognize the powerful impact of the social determinants of health and to also recognize the limits of HDL itself as either protective if it’s high or a definitive predictor of risk if it’s low, and focus on some more modern approaches, including coronary artery calcium scoring.”
He also said risk evaluation should include lipoprotein(a), which, he noted in the editorial, the European Atherosclerosis Society recommends measuring. “One of the reasons it’s underutilized is that we really don’t have a specific treatment for it,” he said of Lp(a) in the United States.
In his editorial comment, Dr. Ferdinand called for future research aimed at eliminating health disparities. “Regardless of the development of better tools for the assessment of risk, newer drugs to treat CVD, the use of coronary artery calcium, if we don’t apply evidence-based medicine equally across the population based on race, ethnicity, sex, gender, socioeconomic status, or geography, then the disparities are going to persist,” he said.
The National Institute of Neurological Disorders and Stroke and the National Institute on Aging provided funding for the study. Dr. Pamir has no relevant relationships to disclose. Dr. Ferdinand disclosed relationships with Boehringer Ingelheim, Novartis, Janssen, and Lilly.
High-density lipoprotein cholesterol may not be as effective a biomarker of cardiovascular disease risk as once thought, particularly in Black adults, according to results from a large biracial cohort study that also raised questions about the validity of high HDL cholesterol as a potentially protective factor in White and Black adults alike.
“I think this opens the door to suggest that every biomarker we use might have a race-specific association with disease outcome,” Nathalie Pamir, PhD, an associate professor at Oregon Health & Science University in Portland, said in an interview. “So, something as basic as HDL cholesterol – we’ve known about it since 1970 – has a race signature.”
Dr. Pamir and colleagues reported their findings from the REGARDS (Reasons for Geographic and Racial Differences in Stroke) cohort study that recruited 30,239 Black and White individuals aged 45 years and older from the contiguous United States from 2003 to 2007.
The study found that LDL cholesterol “modestly” predicted coronary heart disease (CHD) risk in Black and White adults. However, low HDL cholesterol, while associated with an increased risk in White patients (hazard ratio, 1.22; 95% confidence interval, 1.05-1.43), did not have a similar association in Blacks (HR, 0.94; 95% CI: 0.78-1.14). And high HDL cholesterol wasn’t found to be predictive in either group (HR, 0.96; 95% CI, 0.79-1.16 for White participants: HR, 0.91; 95% CI, 0.74-1.12 for Black participants).
Among 23,901 study participants who were CHD-risk free over a 10-year follow-up, 664 and 951 CHD events occurred in Black and White participants, respectively. The study cohort was 57.8% White and 58.4% women, with a mean age of 65 years.
The study noted that LDL cholesterol and triglycerides conferred similar risks for CHD in both White and Black participants.
Acknowledging that this study focused on Blacks, Dr. Pamir added that “we need to know about Asian Americans; we need to know about Hispanic Americans.”
Change of approach to lipid management called for
Dr. Pamir noted that the current understanding about HDL cholesterol and CHD risk comes from the Framingham heart study in the 1970s, whose population was 100% White.
Care algorithms derived from the Framingham study as well as the Multi-Ethnic Study of Atherosclerosis incorporate that association between HDL cholesterol and CHD risk, she noted, but these findings from REGARDS should change how cardiologists approach lipid management in Black and White patients.
“The conversation would go something like: High HDL cholesterol levels put you in a higher risk [bracket] but HDL cholesterol levels are not something we treat; we have no drugs for that,” Dr. Pamir said.
“The conversation would continue along the lines that: ‘You need to do more exercise, you need to change your diet, incorporate healthy fats, walnuts, and omega 3s.’
“But what might the conversation be for Black patients? ‘We don’t see the association that we see for White patients. Do adopt the good habits to exercise and dietary changes, but don’t get too worried about it.’ ”
The study report raises “caution” about using the Framingham, MESA, and other algorithms for evaluating CHD risk. Dr. Pamir explained what that means. “We might be underestimating risk, because what our study showed was that, when we looked at clinically high HDL cholesterol, about 60 mg/dL, it has no benefit for White and Black patients.”
She added, “So that pat on the back we get for patients that have high HDL-C levels? Maybe that pat on the back shouldn’t be there.”
In an invited commentary, Keith C. Ferdinand, MD, of Tulane University in New Orleans, wrote that using HDL cholesterol in risk calculations could inaccurately assess atherosclerotic cardiovascular risk in Black adults “and become a barrier to optimal care.”
In an interview, he said the REGARDS findings call for consideration of other biomarkers for evaluating CHD risk and point to the importance of socioeconomic factors in health outcomes.
“Physicians and other clinicians need to recognize the powerful impact of the social determinants of health and to also recognize the limits of HDL itself as either protective if it’s high or a definitive predictor of risk if it’s low, and focus on some more modern approaches, including coronary artery calcium scoring.”
He also said risk evaluation should include lipoprotein(a), which, he noted in the editorial, the European Atherosclerosis Society recommends measuring. “One of the reasons it’s underutilized is that we really don’t have a specific treatment for it,” he said of Lp(a) in the United States.
In his editorial comment, Dr. Ferdinand called for future research aimed at eliminating health disparities. “Regardless of the development of better tools for the assessment of risk, newer drugs to treat CVD, the use of coronary artery calcium, if we don’t apply evidence-based medicine equally across the population based on race, ethnicity, sex, gender, socioeconomic status, or geography, then the disparities are going to persist,” he said.
The National Institute of Neurological Disorders and Stroke and the National Institute on Aging provided funding for the study. Dr. Pamir has no relevant relationships to disclose. Dr. Ferdinand disclosed relationships with Boehringer Ingelheim, Novartis, Janssen, and Lilly.
FROM JOURNAL OF THE AMERICAN COLLEGE OF CARDIOLOGY
IRONMAN galvanizes case for IV iron repletion in heart failure
CHICAGO – Another major study appears to back the use of intravenous iron repletion in patients with heart failure (HF) and iron deficiency, strengthening largely consistent evidence, researchers say, that the treatment may improve symptoms and prevent some HF-related hospital admissions.
To be sure, the IRONMAN trial, which compared intravenous iron versus usual care in such patients – most with reduced ejection fraction and not hospitalized – failed to show a benefit for its primary endpoint. The 18% reduction in risk for HF hospitalization or cardiovascular (CV) death seen in the trial, however encouraging, can only be called a trend (P = .07).
But the intervention showed signs of benefit for some secondary endpoints, including quality of life scores, and hinted at such an effect on HF hospitalization. Risk for the latter endpoint dropped 20% (P = .085) over a median follow-up of 2.7 years.
The findings “build upon the other data we have that correcting iron deficiency can help improve well-being, and particularly reduce the risk of hospitalization, in a broad range of [HF] patients,” said Paul Kalra, MD, of the University of Glasgow and Portsmouth (England) Hospitals University NHS Trust.
The tested regimen “was well tolerated with no safety concerns” and offers “reassurance about the long-term safety” of the intravenous iron it used, ferric derisomaltose (MonoFerric), in patients with HF, Dr. Kalra said at a media briefing on the trial.
The remarks preceded his formal presentation of IRONMAN at the American Heart Association scientific sessions. Dr. Kalra is also lead author on the trial’s publication in The Lancet.
IRONMAN strengthens the base of evidence supporting intravenous iron in HF with iron deficiency, especially chronic HF in outpatients, Dr. Kalra and others said. It also supports efficacy for a form of intravenous iron not previously tested in a major HF trial.
Still, “the totality of data are now supporting intravenous iron per se,” regardless of the iron agent used, said Dr. Kalra. But ferric derisomaltose may have dosing advantages, he observed, “and we’ve now got these long-term safety data.”
The strongest prior support for intravenous iron in HF came from hospitalized patients who received it as ferric carboxymaltose (Ferinject) and were followed only 12 months. That was in the AFFIRM-AHF trial, published 2 years ago, which also missed its primary endpoint – the same one used in IRONMAN. Some outcomes in the two trials were similar.
The risk for HF hospitalization or CV death for intravenous iron therapy, compared with usual care, in AFFIRM-AHF fell 21% (P = .059), missing significance but apparently driven by a 26% drop in risk for HF readmissions (P = .013). But neither that trial nor IRONMAN suggested a benefit for CV mortality on its own.
The COVID effect
In IRONMAN, Dr. Kalra said, usual care could include oral iron supplementation, which 17% of patients in the control group received. That could potentially have kept the intravenous iron group from making a better showing for the primary endpoint, he proposed.
And some iron doses and other treatments were missed by a substantial number of patients in both groups who entered the trial after the United Kingdom’s national lockdown in response to the COVID-19 pandemic, he observed. “Patients were not able to come into hospitals for research visits, or in fact when they were able, may not have wanted to.”
So, the group conducted a “prespecified” sensitivity analysis that excluded the 9% of patients enrolled by the end of March 2020, about the time of the first lockdown, and followed the remainder for another 6 months.
In that analysis, risk for HF hospitalization or CV death declined 24% in the intravenous iron group, a marginal but significant result (P = .047) that was dominated by an improvement in HF hospitalizations.
Effects on guidelines
The intravenous iron recommendations in the European HF guidelines refer only to ferric carboxymaltose without mentioning other forms, such as ferric derisomaltose, “but this is now a class effect given the similarities between AFFIRM-AHF and IRONMAN,” said Gregory D. Lewis, MD, Mass General Brigham, Boston, invited discussant for Dr. Kalra’s presentation at the AHA session.
“In the United States, we relegate IV iron to improvement in functional capacity as a comorbidity of heart failure. Perhaps this role will expand,” added Dr. Lewis, who is medical director of his center’s heart transplant program.
He also wondered aloud whether the purported clinical benefits of intravenous iron in HF patients with iron deficiency, not as yet supported by a significant primary-endpoint showing in one of the major trials, currently justify expansion of its use in practice.
“With the benefits of IV iron on exercise capacity and quality of life, and the safety of administering high doses of IV iron,” potentially reducing HF polypharmacy, he noted, “should we be considering IV iron more commonly for utilization in our patients even if we find that heart failure hospitalizations and mortality are only modestly improved?”
IRONMAN “asked whether there’s benefit to IV iron in the longer term,” Kiran Musunuru, MD, PhD, MPH, University of Pennsylvania,Philadelphia, observed at the media briefing. As the trial was reported, “that does in fact, seem to be the case,” said Dr. Musunuru, who was not involved in IRONMAN.
Therefore, he said, “this study reinforces the message that we should be routinely monitoring our heart failure patients for iron deficiency and supplementing them as needed.”
A commentary linked to the IRONMAN publication agreed. The trial “increases the evidence base for the treatment of iron deficiency with intravenous iron supplementation,” wrote the editorialists, led by Theresa A. McDonagh, MD, King’s College Hospital and School of Cardiovascular Sciences, London.
Patients with acute or chronic HF, iron deficiency, and reduced or mildly reduced ejection fractions “should be offered treatment with intravenous iron to reduce their risk of hospital admission for heart failure,” they concluded.
Mostly reduced-EF outpatients
The open-label, blinded-endpoint IRONMAN trial, conducted at 70 centers in the United Kingdom, entered adults with HF, ejection fractions 45% or lower within the previous 2 years, and iron deficiency defined as transferrin saturation less than 20% or serum ferritin levels below 100 mcg/L, the report states. They were either hospitalized for HF, had such a hospitalization within the past 6 months, or were outpatients with elevated natriuretic peptide levels; the third category accounted for two thirds of the trial population.
Of the 1,137 randomized patients, 569 were assigned to receive intravenous ferric derisomaltose at weight- and hemoglobin-adjusted dosages; 568 went to the usual-care group.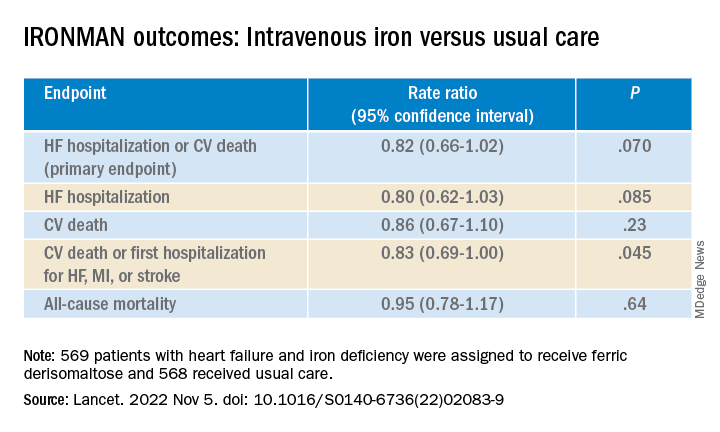
Those receiving intravenous iron visited the trial clinic 4 weeks later and then every 4 months. At those visits, they received a round of ferric derisomaltose if their ferritin levels were below 100 mcg/L, or 400 mcg/L or lower if transferrin saturation was below 25%, the published report states.
Mean scores on the Minnesota Living with Heart Failure Questionnaire improved by a marginally significant 3.33 points (P = .050) at 4 months in the intravenous iron group. The gain receded to a nonsignificant 2.57 points by 20 months (P = .23).
In COVID-related sensitivity analysis, the intravenous iron group showed a significant benefit for the primary endpoint and a trend for improved HF hospitalizations.
- HF hospitalization or CV death: RR, 0.76 (95% confidence interval, 0.58-1.00; P = .047)
- HF hospitalization: RR 0.76 (95% CI, 0.56-1.03; P = .077)
Fewer patients in the intravenous iron group experienced serious cardiac adverse events, 36% compared with 43% in for those on usual care, P = .016.
The recently updated European Society of Cardiology guidelines for HF made it a class 1 recommendation to assess iron status in every patient, Kalra observed. “It doesn›t specify how frequently, but I think we should be thinking about every 4-6 months.”
Dr. Kalra disclosed receiving research grants from Pharmacosmos; and consulting or lecturing for Amgen, AstraZeneca, Bayer, Boehringer Ingelheim, Novartis, Pfizer, Pharmacosmos, Servier, and Vifor Pharma. Dr. Musunuru disclosed significant ownership interest in Verve Therapeutics and Variant Bio. Dr. Lewis disclosed relationships with NXT, American Regent, and RIVUS; and receiving research grants from Cytokinetics and Amgen.
A version of this article first appeared on Medscape.com.
CHICAGO – Another major study appears to back the use of intravenous iron repletion in patients with heart failure (HF) and iron deficiency, strengthening largely consistent evidence, researchers say, that the treatment may improve symptoms and prevent some HF-related hospital admissions.
To be sure, the IRONMAN trial, which compared intravenous iron versus usual care in such patients – most with reduced ejection fraction and not hospitalized – failed to show a benefit for its primary endpoint. The 18% reduction in risk for HF hospitalization or cardiovascular (CV) death seen in the trial, however encouraging, can only be called a trend (P = .07).
But the intervention showed signs of benefit for some secondary endpoints, including quality of life scores, and hinted at such an effect on HF hospitalization. Risk for the latter endpoint dropped 20% (P = .085) over a median follow-up of 2.7 years.
The findings “build upon the other data we have that correcting iron deficiency can help improve well-being, and particularly reduce the risk of hospitalization, in a broad range of [HF] patients,” said Paul Kalra, MD, of the University of Glasgow and Portsmouth (England) Hospitals University NHS Trust.
The tested regimen “was well tolerated with no safety concerns” and offers “reassurance about the long-term safety” of the intravenous iron it used, ferric derisomaltose (MonoFerric), in patients with HF, Dr. Kalra said at a media briefing on the trial.
The remarks preceded his formal presentation of IRONMAN at the American Heart Association scientific sessions. Dr. Kalra is also lead author on the trial’s publication in The Lancet.
IRONMAN strengthens the base of evidence supporting intravenous iron in HF with iron deficiency, especially chronic HF in outpatients, Dr. Kalra and others said. It also supports efficacy for a form of intravenous iron not previously tested in a major HF trial.
Still, “the totality of data are now supporting intravenous iron per se,” regardless of the iron agent used, said Dr. Kalra. But ferric derisomaltose may have dosing advantages, he observed, “and we’ve now got these long-term safety data.”
The strongest prior support for intravenous iron in HF came from hospitalized patients who received it as ferric carboxymaltose (Ferinject) and were followed only 12 months. That was in the AFFIRM-AHF trial, published 2 years ago, which also missed its primary endpoint – the same one used in IRONMAN. Some outcomes in the two trials were similar.
The risk for HF hospitalization or CV death for intravenous iron therapy, compared with usual care, in AFFIRM-AHF fell 21% (P = .059), missing significance but apparently driven by a 26% drop in risk for HF readmissions (P = .013). But neither that trial nor IRONMAN suggested a benefit for CV mortality on its own.
The COVID effect
In IRONMAN, Dr. Kalra said, usual care could include oral iron supplementation, which 17% of patients in the control group received. That could potentially have kept the intravenous iron group from making a better showing for the primary endpoint, he proposed.
And some iron doses and other treatments were missed by a substantial number of patients in both groups who entered the trial after the United Kingdom’s national lockdown in response to the COVID-19 pandemic, he observed. “Patients were not able to come into hospitals for research visits, or in fact when they were able, may not have wanted to.”
So, the group conducted a “prespecified” sensitivity analysis that excluded the 9% of patients enrolled by the end of March 2020, about the time of the first lockdown, and followed the remainder for another 6 months.
In that analysis, risk for HF hospitalization or CV death declined 24% in the intravenous iron group, a marginal but significant result (P = .047) that was dominated by an improvement in HF hospitalizations.
Effects on guidelines
The intravenous iron recommendations in the European HF guidelines refer only to ferric carboxymaltose without mentioning other forms, such as ferric derisomaltose, “but this is now a class effect given the similarities between AFFIRM-AHF and IRONMAN,” said Gregory D. Lewis, MD, Mass General Brigham, Boston, invited discussant for Dr. Kalra’s presentation at the AHA session.
“In the United States, we relegate IV iron to improvement in functional capacity as a comorbidity of heart failure. Perhaps this role will expand,” added Dr. Lewis, who is medical director of his center’s heart transplant program.
He also wondered aloud whether the purported clinical benefits of intravenous iron in HF patients with iron deficiency, not as yet supported by a significant primary-endpoint showing in one of the major trials, currently justify expansion of its use in practice.
“With the benefits of IV iron on exercise capacity and quality of life, and the safety of administering high doses of IV iron,” potentially reducing HF polypharmacy, he noted, “should we be considering IV iron more commonly for utilization in our patients even if we find that heart failure hospitalizations and mortality are only modestly improved?”
IRONMAN “asked whether there’s benefit to IV iron in the longer term,” Kiran Musunuru, MD, PhD, MPH, University of Pennsylvania,Philadelphia, observed at the media briefing. As the trial was reported, “that does in fact, seem to be the case,” said Dr. Musunuru, who was not involved in IRONMAN.
Therefore, he said, “this study reinforces the message that we should be routinely monitoring our heart failure patients for iron deficiency and supplementing them as needed.”
A commentary linked to the IRONMAN publication agreed. The trial “increases the evidence base for the treatment of iron deficiency with intravenous iron supplementation,” wrote the editorialists, led by Theresa A. McDonagh, MD, King’s College Hospital and School of Cardiovascular Sciences, London.
Patients with acute or chronic HF, iron deficiency, and reduced or mildly reduced ejection fractions “should be offered treatment with intravenous iron to reduce their risk of hospital admission for heart failure,” they concluded.
Mostly reduced-EF outpatients
The open-label, blinded-endpoint IRONMAN trial, conducted at 70 centers in the United Kingdom, entered adults with HF, ejection fractions 45% or lower within the previous 2 years, and iron deficiency defined as transferrin saturation less than 20% or serum ferritin levels below 100 mcg/L, the report states. They were either hospitalized for HF, had such a hospitalization within the past 6 months, or were outpatients with elevated natriuretic peptide levels; the third category accounted for two thirds of the trial population.
Of the 1,137 randomized patients, 569 were assigned to receive intravenous ferric derisomaltose at weight- and hemoglobin-adjusted dosages; 568 went to the usual-care group.
Those receiving intravenous iron visited the trial clinic 4 weeks later and then every 4 months. At those visits, they received a round of ferric derisomaltose if their ferritin levels were below 100 mcg/L, or 400 mcg/L or lower if transferrin saturation was below 25%, the published report states.
Mean scores on the Minnesota Living with Heart Failure Questionnaire improved by a marginally significant 3.33 points (P = .050) at 4 months in the intravenous iron group. The gain receded to a nonsignificant 2.57 points by 20 months (P = .23).
In COVID-related sensitivity analysis, the intravenous iron group showed a significant benefit for the primary endpoint and a trend for improved HF hospitalizations.
- HF hospitalization or CV death: RR, 0.76 (95% confidence interval, 0.58-1.00; P = .047)
- HF hospitalization: RR 0.76 (95% CI, 0.56-1.03; P = .077)
Fewer patients in the intravenous iron group experienced serious cardiac adverse events, 36% compared with 43% in for those on usual care, P = .016.
The recently updated European Society of Cardiology guidelines for HF made it a class 1 recommendation to assess iron status in every patient, Kalra observed. “It doesn›t specify how frequently, but I think we should be thinking about every 4-6 months.”
Dr. Kalra disclosed receiving research grants from Pharmacosmos; and consulting or lecturing for Amgen, AstraZeneca, Bayer, Boehringer Ingelheim, Novartis, Pfizer, Pharmacosmos, Servier, and Vifor Pharma. Dr. Musunuru disclosed significant ownership interest in Verve Therapeutics and Variant Bio. Dr. Lewis disclosed relationships with NXT, American Regent, and RIVUS; and receiving research grants from Cytokinetics and Amgen.
A version of this article first appeared on Medscape.com.
CHICAGO – Another major study appears to back the use of intravenous iron repletion in patients with heart failure (HF) and iron deficiency, strengthening largely consistent evidence, researchers say, that the treatment may improve symptoms and prevent some HF-related hospital admissions.
To be sure, the IRONMAN trial, which compared intravenous iron versus usual care in such patients – most with reduced ejection fraction and not hospitalized – failed to show a benefit for its primary endpoint. The 18% reduction in risk for HF hospitalization or cardiovascular (CV) death seen in the trial, however encouraging, can only be called a trend (P = .07).
But the intervention showed signs of benefit for some secondary endpoints, including quality of life scores, and hinted at such an effect on HF hospitalization. Risk for the latter endpoint dropped 20% (P = .085) over a median follow-up of 2.7 years.
The findings “build upon the other data we have that correcting iron deficiency can help improve well-being, and particularly reduce the risk of hospitalization, in a broad range of [HF] patients,” said Paul Kalra, MD, of the University of Glasgow and Portsmouth (England) Hospitals University NHS Trust.
The tested regimen “was well tolerated with no safety concerns” and offers “reassurance about the long-term safety” of the intravenous iron it used, ferric derisomaltose (MonoFerric), in patients with HF, Dr. Kalra said at a media briefing on the trial.
The remarks preceded his formal presentation of IRONMAN at the American Heart Association scientific sessions. Dr. Kalra is also lead author on the trial’s publication in The Lancet.
IRONMAN strengthens the base of evidence supporting intravenous iron in HF with iron deficiency, especially chronic HF in outpatients, Dr. Kalra and others said. It also supports efficacy for a form of intravenous iron not previously tested in a major HF trial.
Still, “the totality of data are now supporting intravenous iron per se,” regardless of the iron agent used, said Dr. Kalra. But ferric derisomaltose may have dosing advantages, he observed, “and we’ve now got these long-term safety data.”
The strongest prior support for intravenous iron in HF came from hospitalized patients who received it as ferric carboxymaltose (Ferinject) and were followed only 12 months. That was in the AFFIRM-AHF trial, published 2 years ago, which also missed its primary endpoint – the same one used in IRONMAN. Some outcomes in the two trials were similar.
The risk for HF hospitalization or CV death for intravenous iron therapy, compared with usual care, in AFFIRM-AHF fell 21% (P = .059), missing significance but apparently driven by a 26% drop in risk for HF readmissions (P = .013). But neither that trial nor IRONMAN suggested a benefit for CV mortality on its own.
The COVID effect
In IRONMAN, Dr. Kalra said, usual care could include oral iron supplementation, which 17% of patients in the control group received. That could potentially have kept the intravenous iron group from making a better showing for the primary endpoint, he proposed.
And some iron doses and other treatments were missed by a substantial number of patients in both groups who entered the trial after the United Kingdom’s national lockdown in response to the COVID-19 pandemic, he observed. “Patients were not able to come into hospitals for research visits, or in fact when they were able, may not have wanted to.”
So, the group conducted a “prespecified” sensitivity analysis that excluded the 9% of patients enrolled by the end of March 2020, about the time of the first lockdown, and followed the remainder for another 6 months.
In that analysis, risk for HF hospitalization or CV death declined 24% in the intravenous iron group, a marginal but significant result (P = .047) that was dominated by an improvement in HF hospitalizations.
Effects on guidelines
The intravenous iron recommendations in the European HF guidelines refer only to ferric carboxymaltose without mentioning other forms, such as ferric derisomaltose, “but this is now a class effect given the similarities between AFFIRM-AHF and IRONMAN,” said Gregory D. Lewis, MD, Mass General Brigham, Boston, invited discussant for Dr. Kalra’s presentation at the AHA session.
“In the United States, we relegate IV iron to improvement in functional capacity as a comorbidity of heart failure. Perhaps this role will expand,” added Dr. Lewis, who is medical director of his center’s heart transplant program.
He also wondered aloud whether the purported clinical benefits of intravenous iron in HF patients with iron deficiency, not as yet supported by a significant primary-endpoint showing in one of the major trials, currently justify expansion of its use in practice.
“With the benefits of IV iron on exercise capacity and quality of life, and the safety of administering high doses of IV iron,” potentially reducing HF polypharmacy, he noted, “should we be considering IV iron more commonly for utilization in our patients even if we find that heart failure hospitalizations and mortality are only modestly improved?”
IRONMAN “asked whether there’s benefit to IV iron in the longer term,” Kiran Musunuru, MD, PhD, MPH, University of Pennsylvania,Philadelphia, observed at the media briefing. As the trial was reported, “that does in fact, seem to be the case,” said Dr. Musunuru, who was not involved in IRONMAN.
Therefore, he said, “this study reinforces the message that we should be routinely monitoring our heart failure patients for iron deficiency and supplementing them as needed.”
A commentary linked to the IRONMAN publication agreed. The trial “increases the evidence base for the treatment of iron deficiency with intravenous iron supplementation,” wrote the editorialists, led by Theresa A. McDonagh, MD, King’s College Hospital and School of Cardiovascular Sciences, London.
Patients with acute or chronic HF, iron deficiency, and reduced or mildly reduced ejection fractions “should be offered treatment with intravenous iron to reduce their risk of hospital admission for heart failure,” they concluded.
Mostly reduced-EF outpatients
The open-label, blinded-endpoint IRONMAN trial, conducted at 70 centers in the United Kingdom, entered adults with HF, ejection fractions 45% or lower within the previous 2 years, and iron deficiency defined as transferrin saturation less than 20% or serum ferritin levels below 100 mcg/L, the report states. They were either hospitalized for HF, had such a hospitalization within the past 6 months, or were outpatients with elevated natriuretic peptide levels; the third category accounted for two thirds of the trial population.
Of the 1,137 randomized patients, 569 were assigned to receive intravenous ferric derisomaltose at weight- and hemoglobin-adjusted dosages; 568 went to the usual-care group.
Those receiving intravenous iron visited the trial clinic 4 weeks later and then every 4 months. At those visits, they received a round of ferric derisomaltose if their ferritin levels were below 100 mcg/L, or 400 mcg/L or lower if transferrin saturation was below 25%, the published report states.
Mean scores on the Minnesota Living with Heart Failure Questionnaire improved by a marginally significant 3.33 points (P = .050) at 4 months in the intravenous iron group. The gain receded to a nonsignificant 2.57 points by 20 months (P = .23).
In COVID-related sensitivity analysis, the intravenous iron group showed a significant benefit for the primary endpoint and a trend for improved HF hospitalizations.
- HF hospitalization or CV death: RR, 0.76 (95% confidence interval, 0.58-1.00; P = .047)
- HF hospitalization: RR 0.76 (95% CI, 0.56-1.03; P = .077)
Fewer patients in the intravenous iron group experienced serious cardiac adverse events, 36% compared with 43% in for those on usual care, P = .016.
The recently updated European Society of Cardiology guidelines for HF made it a class 1 recommendation to assess iron status in every patient, Kalra observed. “It doesn›t specify how frequently, but I think we should be thinking about every 4-6 months.”
Dr. Kalra disclosed receiving research grants from Pharmacosmos; and consulting or lecturing for Amgen, AstraZeneca, Bayer, Boehringer Ingelheim, Novartis, Pfizer, Pharmacosmos, Servier, and Vifor Pharma. Dr. Musunuru disclosed significant ownership interest in Verve Therapeutics and Variant Bio. Dr. Lewis disclosed relationships with NXT, American Regent, and RIVUS; and receiving research grants from Cytokinetics and Amgen.
A version of this article first appeared on Medscape.com.
AT AHA 2022