User login
Perinatal depression rarely stands alone
Mental health conditions are the leading cause of pregnancy-related death in Illinois (40%) and across the United States (21%).1,2 Funding bodies, such as the Agency for Healthcare Research and Quality3 and the Health Resources and Service Administration,4 have spotlights on improving screening and access to care for depression and substance use disorders (SUDs). However, the needs of individuals with multiple mental health conditions still often go unrecognized and unaddressed in perinatal health settings.
The U.S. Preventive Services Task Force recommends that all adults be screened for depression, alcohol use, and drug use, and will be recommending screening for anxiety.5,6 The American College of Obstetrics and Gynecology recommends screening for perinatal mental health conditions including depression, anxiety, bipolar disorder, acute postpartum psychosis, and suicidality; however, despite these recommendations, screening and treatment for comorbid mental health disorders during pregnancy and the postpartum is not standard practice.7
Addressing perinatal mental health is critical because untreated mental health conditions during the perinatal period can cause long-term adverse psychiatric and medical outcomes for the birthing person, the baby, and the family.8 This commentary highlights the importance of recognizing and screening for perinatal mental health comorbidities, improving referral rates for mental health treatment, and raising awareness of the importance of addressing rural perinatal mental health.
Perinatal mental health comorbidities
Major depressive disorder is the most common mental health condition during the perinatal period9 and is often comorbid.10-12 In “Perinatal mental health in low-income urban and rural patients: The importance of screening for comorbidities,” Craemer et al.13 reported that nearly half of the perinatal patients who screened positive for MDD also screened positive for at least one other mental health condition, among them general anxiety disorder (GAD), SUD, posttraumatic stress disorder (PTSD), and suicidality.
Many (9%) of the perinatal patients with MDD had a severe comorbidity profile characterized by four diagnoses – MDD, GAD, SUD, and PTSD. In routine medical care these comorbidities often go undetected even though the risk to mothers and babies increases with more severe mental health symptoms.8
The high frequency of perinatal mental health comorbidities Craemer et al.13 found demonstrates a compelling need for comorbid mental health screening during the perinatal period, particularly for low-income Black, Hispanic, and rural birthing persons. Positive screens for perinatal mental health disorders may reflect the onset of these disorders in pregnancy or the postpartum, or preexisting disorders that have gone undetected or untreated before pregnancy.
For many patients, the perinatal period is the first time they are screened for any mental health disorder; typically, they are screened solely for depression. Screening alone can have a positive impact on perinatal mental health. In fact, the USPSTF found that programs to screen perinatal patients, with or without treatment-related support, resulted in a 2%-9% absolute reduction in depression prevalence.14 However, screening for MDD is too infrequent for many reasons, including the logistics of integrating screening into the clinic workflow and limited provider availability, time, and training in mental health.
We recommend screening perinatal patients for mental health comorbidities. This recommendation may seem impractical given the lack of screening tools for comorbid mental health conditions; however, the Computerized Adaptive Test for Mental Health (CAT-MH), the validated tool15-17 used in this study, is an ideal option. CAT-MH is uniquely capable of screening for MDD, GAD, PTSD, SUD, and suicidality in one platform and is routinely used in diverse settings including the Veterans Administration,18 foster care,19 and universities.20 The main limitation of this more comprehensive screening is that it takes about 10 minutes per patient. However, CAT-MH is self-administered and can be done in the waiting room or on a mobile device prior to a clinic visit.
CAT-MH can also be easily integrated into clinical workflow when added to the Electronic Medical Record21, and is a more comprehensive tool than existing perinatal depression tools such as the Perinatal Health Questionaire-9 (PHQ-9) and Edinburgh Perinatal Depression Scale (EPDS).22 Another limitation is cost – currently $5.00 per assessment – however, this is less than routine blood work.23 If CAT-MH is not an option, we recommend a stepped approach of screening for GAD when perinatal patients screen positive for MDD, as this is the most common comorbidity profile. The GAD-7 is a free and widely available tool.24
Barriers to care
In Craemer et al,13 nearly two-thirds (64.9%) of perinatal patients with a positive screen did not receive a referral to follow-up care or a medication prescription. These low referral rates may reflect a variety of widely recognized barriers to care, including lack of referral options, provider and/or patient reluctance to pursue referrals, barriers to insurance coverage, or inadequate behavioral health infrastructure to ensure referral and diagnostic follow-up.
Further, rural residing perinatal patients are an underserved population that need more resources and screening. Despite an on-site behavioral specialist at the rural clinic, Craemer et al13 found a stark disparity in referral rates: referrals to treatment for a positive diagnosis was over two times less at the rural clinic (23.9%), compared with the urban clinics (51.6%). The most common treatment offered at the rural clinic was a prescription for medication (17.4%), while referral to follow-up care was the most common at the urban clinics (35.5%). Rural areas not only have a shortage of health care providers, but community members seeking mental health care often encounter greater stigma, compared with urban residents.25,26
These data highlight an unmet need for referrals to treatment for patients in rural communities, particularly in Illinois where the pregnancy-related mortality ratio attributable to mental health conditions is three times greater in rural areas, compared with those residing in urban Cook County (Chicago).2 Increasing access and availability to mental health treatment and prevention resources in Illinois, especially in rural areas, is an opportunity to prevent pregnancy-related mortality attributable to mental health conditions.
Overall, there is a critical need for screening for perinatal mental health comorbidities, increased attention to low rates of referral to mental health treatment, and investing in rural perinatal mental health. Addressing perinatal mental health disorders is key to decreasing the burden of maternal mortality, particularly in Illinois.
Ms. Craemer and Ms. Sayah are senior research specialists at the Center for Research on Women & Gender, University of Illinois at Chicago. Dr. Duffecy is a professor of clinical psychiatry at the University of Illinois at Chicago. Dr. Geller is a professor of obstetrics & gynecology and director of the Center for Research on Women & Gender, University of Illinois at Chicago. Dr. Maki is a professor of psychiatry, psychology, and obstetrics & gynecology at the University of Illinois at Chicago.
References
1. Trost S et al. Pregnancy-related deaths: Data from maternal mortality review committees in 36 states, 2017-2019. Atlanta: Centers for Disease Control and Prevention, U.S. Department of Health & Human Services, 2022.
2. Illinois Department of Public Health. Illinois maternal morbidity and mortality report 2016-2017. 2021.
3. AHRQ. Funding opportunities to address opioid and other substance use disorders. Updated 2023.
4. HRSA. Screening and treatment for maternal mental health and substance use disorders.
5. U.S. Preventive Services Task Force. Recommendations for primary care practice. Accessed May 26, 2023.
6. U.S. Preventive Services Task Force. Draft recommendation statement: Anxiety in adults: Screening. 2022.
7. ACOG. Screening and diagnosis of mental health conditions during pregnancy and postpartum. Clinical Practice Guideline. Number 4. 2023 June.
8. Meltzer-Brody S and Stuebe A. The long-term psychiatric and medical prognosis of perinatal mental illness. Best Pract Res Clin Obstet Gynaecol. 2014 Jan. doi: 10.1016/j.bpobgyn.2013.08.009.
9. Van Niel MS and Payne JL. Perinatal depression: A review. Cleve Clin J Med. 2020 May. doi: 10.3949/ccjm.87a.19054.
10. Wisner KL et al. Onset timing, thoughts of self-harm, and diagnoses in postpartum women with screen-positive depression findings. 2013 May. doi: 10.1001/jamapsychiatry.2013.87.
11. Falah-Hassani K et al. The prevalence of antenatal and postnatal co-morbid anxiety and depression: A meta-analysis. Psychol Med. 2017 Sep. doi: 10.1017/S0033291717000617.
12. Pentecost R et al. Scoping review of the associations between perinatal substance use and perinatal depression and anxiety. J Obstet Gynecol Neonatal Nurs. 2021 Jul. doi: 10.1016/j.jogn.2021.02.008.
13. Craemer KA et al. Perinatal mental health in low-income urban and rural patients: The importance of screening for comorbidities. Gen Hosp Psychiatry. 2023 Jul-Aug. doi: 10.1016/j.genhosppsych.2023.05.007.
14. O’Connor E et al. Primary care screening for and treatment of depression in pregnant and postpartum women: Evidence report and systematic review for the U.S. Preventive Services Task Force. JAMA. 2016 Jan 26. doi: 10.1001/jama.2015.18948.
15. Kozhimannil KB et al. Racial and ethnic disparities in postpartum depression care among low-income women. Psychiatr Serv. 2011 Jun. doi: 10.1176/ps.62.6.pss6206_0619.
16. Wenzel ES et al. Depression and anxiety symptoms across pregnancy and the postpartum in low-income Black and Latina women. Arch Womens Ment Health. 2021 Dec. doi: 10.1007/s00737-021-01139-y.
17. Gibbons RD et al. Development of a computerized adaptive substance use disorder scale for screening and measurement: The CAT‐SUD. Addiction. 2020 Jul. doi: 10.1111/add.14938.
18. Brenner LA et al. Validation of a computerized adaptive test suicide scale (CAT-SS) among united states military veterans. PloS One. 2022 Jan 21. doi: 10.1371/journal.pone.0261920.
19. The Center for State Child Welfare Data. Using technology to diagnose and report on behavioral health challenges facing foster youth. 2018.
20. Kim JJ et al. The experience of depression, anxiety, and mania among perinatal women. Arch Womens Ment Health. 2016 Oct. doi: 10.1007/s00737-016-0632-6.
21. Tepper MC et al. Toward population health: Using a learning behavioral health system and measurement-based care to improve access, care, outcomes, and disparities. Community Ment Health J. 2022 Nov. doi: 10.1007/s10597-022-00957-3.
22. Wenzel E et al. Using computerised adaptive tests to screen for perinatal depression in underserved women of colour. Evid Based Ment Health. 2022 Feb. doi: 10.1136/ebmental-2021-300262.
23. Sanger-Katz M. They want it to be secret: How a common blood test can cost $11 or almost $1,000. New York Times. 2019 Apr 19.
24. Spitzer RL et al. A brief measure for assessing generalized anxiety disorder: The GAD-7. Arch Intern Med. 2006 May 22. doi: 10.1001/archinte.166.10.1092.
25. Mollard E et al. An integrative review of postpartum depression in rural US communities. Arch Psychiatr Nurs. 2016 Jun. doi: 10.1016/j.apnu.2015.12.003.
26. Anglim AJ and Radke SM. Rural maternal health care outcomes, drivers, and patient perspectives. Clin Obstet Gynecol. 2022 Dec 1. doi: 10.1097/GRF.0000000000000753.
Mental health conditions are the leading cause of pregnancy-related death in Illinois (40%) and across the United States (21%).1,2 Funding bodies, such as the Agency for Healthcare Research and Quality3 and the Health Resources and Service Administration,4 have spotlights on improving screening and access to care for depression and substance use disorders (SUDs). However, the needs of individuals with multiple mental health conditions still often go unrecognized and unaddressed in perinatal health settings.
The U.S. Preventive Services Task Force recommends that all adults be screened for depression, alcohol use, and drug use, and will be recommending screening for anxiety.5,6 The American College of Obstetrics and Gynecology recommends screening for perinatal mental health conditions including depression, anxiety, bipolar disorder, acute postpartum psychosis, and suicidality; however, despite these recommendations, screening and treatment for comorbid mental health disorders during pregnancy and the postpartum is not standard practice.7
Addressing perinatal mental health is critical because untreated mental health conditions during the perinatal period can cause long-term adverse psychiatric and medical outcomes for the birthing person, the baby, and the family.8 This commentary highlights the importance of recognizing and screening for perinatal mental health comorbidities, improving referral rates for mental health treatment, and raising awareness of the importance of addressing rural perinatal mental health.
Perinatal mental health comorbidities
Major depressive disorder is the most common mental health condition during the perinatal period9 and is often comorbid.10-12 In “Perinatal mental health in low-income urban and rural patients: The importance of screening for comorbidities,” Craemer et al.13 reported that nearly half of the perinatal patients who screened positive for MDD also screened positive for at least one other mental health condition, among them general anxiety disorder (GAD), SUD, posttraumatic stress disorder (PTSD), and suicidality.
Many (9%) of the perinatal patients with MDD had a severe comorbidity profile characterized by four diagnoses – MDD, GAD, SUD, and PTSD. In routine medical care these comorbidities often go undetected even though the risk to mothers and babies increases with more severe mental health symptoms.8
The high frequency of perinatal mental health comorbidities Craemer et al.13 found demonstrates a compelling need for comorbid mental health screening during the perinatal period, particularly for low-income Black, Hispanic, and rural birthing persons. Positive screens for perinatal mental health disorders may reflect the onset of these disorders in pregnancy or the postpartum, or preexisting disorders that have gone undetected or untreated before pregnancy.
For many patients, the perinatal period is the first time they are screened for any mental health disorder; typically, they are screened solely for depression. Screening alone can have a positive impact on perinatal mental health. In fact, the USPSTF found that programs to screen perinatal patients, with or without treatment-related support, resulted in a 2%-9% absolute reduction in depression prevalence.14 However, screening for MDD is too infrequent for many reasons, including the logistics of integrating screening into the clinic workflow and limited provider availability, time, and training in mental health.
We recommend screening perinatal patients for mental health comorbidities. This recommendation may seem impractical given the lack of screening tools for comorbid mental health conditions; however, the Computerized Adaptive Test for Mental Health (CAT-MH), the validated tool15-17 used in this study, is an ideal option. CAT-MH is uniquely capable of screening for MDD, GAD, PTSD, SUD, and suicidality in one platform and is routinely used in diverse settings including the Veterans Administration,18 foster care,19 and universities.20 The main limitation of this more comprehensive screening is that it takes about 10 minutes per patient. However, CAT-MH is self-administered and can be done in the waiting room or on a mobile device prior to a clinic visit.
CAT-MH can also be easily integrated into clinical workflow when added to the Electronic Medical Record21, and is a more comprehensive tool than existing perinatal depression tools such as the Perinatal Health Questionaire-9 (PHQ-9) and Edinburgh Perinatal Depression Scale (EPDS).22 Another limitation is cost – currently $5.00 per assessment – however, this is less than routine blood work.23 If CAT-MH is not an option, we recommend a stepped approach of screening for GAD when perinatal patients screen positive for MDD, as this is the most common comorbidity profile. The GAD-7 is a free and widely available tool.24
Barriers to care
In Craemer et al,13 nearly two-thirds (64.9%) of perinatal patients with a positive screen did not receive a referral to follow-up care or a medication prescription. These low referral rates may reflect a variety of widely recognized barriers to care, including lack of referral options, provider and/or patient reluctance to pursue referrals, barriers to insurance coverage, or inadequate behavioral health infrastructure to ensure referral and diagnostic follow-up.
Further, rural residing perinatal patients are an underserved population that need more resources and screening. Despite an on-site behavioral specialist at the rural clinic, Craemer et al13 found a stark disparity in referral rates: referrals to treatment for a positive diagnosis was over two times less at the rural clinic (23.9%), compared with the urban clinics (51.6%). The most common treatment offered at the rural clinic was a prescription for medication (17.4%), while referral to follow-up care was the most common at the urban clinics (35.5%). Rural areas not only have a shortage of health care providers, but community members seeking mental health care often encounter greater stigma, compared with urban residents.25,26
These data highlight an unmet need for referrals to treatment for patients in rural communities, particularly in Illinois where the pregnancy-related mortality ratio attributable to mental health conditions is three times greater in rural areas, compared with those residing in urban Cook County (Chicago).2 Increasing access and availability to mental health treatment and prevention resources in Illinois, especially in rural areas, is an opportunity to prevent pregnancy-related mortality attributable to mental health conditions.
Overall, there is a critical need for screening for perinatal mental health comorbidities, increased attention to low rates of referral to mental health treatment, and investing in rural perinatal mental health. Addressing perinatal mental health disorders is key to decreasing the burden of maternal mortality, particularly in Illinois.
Ms. Craemer and Ms. Sayah are senior research specialists at the Center for Research on Women & Gender, University of Illinois at Chicago. Dr. Duffecy is a professor of clinical psychiatry at the University of Illinois at Chicago. Dr. Geller is a professor of obstetrics & gynecology and director of the Center for Research on Women & Gender, University of Illinois at Chicago. Dr. Maki is a professor of psychiatry, psychology, and obstetrics & gynecology at the University of Illinois at Chicago.
References
1. Trost S et al. Pregnancy-related deaths: Data from maternal mortality review committees in 36 states, 2017-2019. Atlanta: Centers for Disease Control and Prevention, U.S. Department of Health & Human Services, 2022.
2. Illinois Department of Public Health. Illinois maternal morbidity and mortality report 2016-2017. 2021.
3. AHRQ. Funding opportunities to address opioid and other substance use disorders. Updated 2023.
4. HRSA. Screening and treatment for maternal mental health and substance use disorders.
5. U.S. Preventive Services Task Force. Recommendations for primary care practice. Accessed May 26, 2023.
6. U.S. Preventive Services Task Force. Draft recommendation statement: Anxiety in adults: Screening. 2022.
7. ACOG. Screening and diagnosis of mental health conditions during pregnancy and postpartum. Clinical Practice Guideline. Number 4. 2023 June.
8. Meltzer-Brody S and Stuebe A. The long-term psychiatric and medical prognosis of perinatal mental illness. Best Pract Res Clin Obstet Gynaecol. 2014 Jan. doi: 10.1016/j.bpobgyn.2013.08.009.
9. Van Niel MS and Payne JL. Perinatal depression: A review. Cleve Clin J Med. 2020 May. doi: 10.3949/ccjm.87a.19054.
10. Wisner KL et al. Onset timing, thoughts of self-harm, and diagnoses in postpartum women with screen-positive depression findings. 2013 May. doi: 10.1001/jamapsychiatry.2013.87.
11. Falah-Hassani K et al. The prevalence of antenatal and postnatal co-morbid anxiety and depression: A meta-analysis. Psychol Med. 2017 Sep. doi: 10.1017/S0033291717000617.
12. Pentecost R et al. Scoping review of the associations between perinatal substance use and perinatal depression and anxiety. J Obstet Gynecol Neonatal Nurs. 2021 Jul. doi: 10.1016/j.jogn.2021.02.008.
13. Craemer KA et al. Perinatal mental health in low-income urban and rural patients: The importance of screening for comorbidities. Gen Hosp Psychiatry. 2023 Jul-Aug. doi: 10.1016/j.genhosppsych.2023.05.007.
14. O’Connor E et al. Primary care screening for and treatment of depression in pregnant and postpartum women: Evidence report and systematic review for the U.S. Preventive Services Task Force. JAMA. 2016 Jan 26. doi: 10.1001/jama.2015.18948.
15. Kozhimannil KB et al. Racial and ethnic disparities in postpartum depression care among low-income women. Psychiatr Serv. 2011 Jun. doi: 10.1176/ps.62.6.pss6206_0619.
16. Wenzel ES et al. Depression and anxiety symptoms across pregnancy and the postpartum in low-income Black and Latina women. Arch Womens Ment Health. 2021 Dec. doi: 10.1007/s00737-021-01139-y.
17. Gibbons RD et al. Development of a computerized adaptive substance use disorder scale for screening and measurement: The CAT‐SUD. Addiction. 2020 Jul. doi: 10.1111/add.14938.
18. Brenner LA et al. Validation of a computerized adaptive test suicide scale (CAT-SS) among united states military veterans. PloS One. 2022 Jan 21. doi: 10.1371/journal.pone.0261920.
19. The Center for State Child Welfare Data. Using technology to diagnose and report on behavioral health challenges facing foster youth. 2018.
20. Kim JJ et al. The experience of depression, anxiety, and mania among perinatal women. Arch Womens Ment Health. 2016 Oct. doi: 10.1007/s00737-016-0632-6.
21. Tepper MC et al. Toward population health: Using a learning behavioral health system and measurement-based care to improve access, care, outcomes, and disparities. Community Ment Health J. 2022 Nov. doi: 10.1007/s10597-022-00957-3.
22. Wenzel E et al. Using computerised adaptive tests to screen for perinatal depression in underserved women of colour. Evid Based Ment Health. 2022 Feb. doi: 10.1136/ebmental-2021-300262.
23. Sanger-Katz M. They want it to be secret: How a common blood test can cost $11 or almost $1,000. New York Times. 2019 Apr 19.
24. Spitzer RL et al. A brief measure for assessing generalized anxiety disorder: The GAD-7. Arch Intern Med. 2006 May 22. doi: 10.1001/archinte.166.10.1092.
25. Mollard E et al. An integrative review of postpartum depression in rural US communities. Arch Psychiatr Nurs. 2016 Jun. doi: 10.1016/j.apnu.2015.12.003.
26. Anglim AJ and Radke SM. Rural maternal health care outcomes, drivers, and patient perspectives. Clin Obstet Gynecol. 2022 Dec 1. doi: 10.1097/GRF.0000000000000753.
Mental health conditions are the leading cause of pregnancy-related death in Illinois (40%) and across the United States (21%).1,2 Funding bodies, such as the Agency for Healthcare Research and Quality3 and the Health Resources and Service Administration,4 have spotlights on improving screening and access to care for depression and substance use disorders (SUDs). However, the needs of individuals with multiple mental health conditions still often go unrecognized and unaddressed in perinatal health settings.
The U.S. Preventive Services Task Force recommends that all adults be screened for depression, alcohol use, and drug use, and will be recommending screening for anxiety.5,6 The American College of Obstetrics and Gynecology recommends screening for perinatal mental health conditions including depression, anxiety, bipolar disorder, acute postpartum psychosis, and suicidality; however, despite these recommendations, screening and treatment for comorbid mental health disorders during pregnancy and the postpartum is not standard practice.7
Addressing perinatal mental health is critical because untreated mental health conditions during the perinatal period can cause long-term adverse psychiatric and medical outcomes for the birthing person, the baby, and the family.8 This commentary highlights the importance of recognizing and screening for perinatal mental health comorbidities, improving referral rates for mental health treatment, and raising awareness of the importance of addressing rural perinatal mental health.
Perinatal mental health comorbidities
Major depressive disorder is the most common mental health condition during the perinatal period9 and is often comorbid.10-12 In “Perinatal mental health in low-income urban and rural patients: The importance of screening for comorbidities,” Craemer et al.13 reported that nearly half of the perinatal patients who screened positive for MDD also screened positive for at least one other mental health condition, among them general anxiety disorder (GAD), SUD, posttraumatic stress disorder (PTSD), and suicidality.
Many (9%) of the perinatal patients with MDD had a severe comorbidity profile characterized by four diagnoses – MDD, GAD, SUD, and PTSD. In routine medical care these comorbidities often go undetected even though the risk to mothers and babies increases with more severe mental health symptoms.8
The high frequency of perinatal mental health comorbidities Craemer et al.13 found demonstrates a compelling need for comorbid mental health screening during the perinatal period, particularly for low-income Black, Hispanic, and rural birthing persons. Positive screens for perinatal mental health disorders may reflect the onset of these disorders in pregnancy or the postpartum, or preexisting disorders that have gone undetected or untreated before pregnancy.
For many patients, the perinatal period is the first time they are screened for any mental health disorder; typically, they are screened solely for depression. Screening alone can have a positive impact on perinatal mental health. In fact, the USPSTF found that programs to screen perinatal patients, with or without treatment-related support, resulted in a 2%-9% absolute reduction in depression prevalence.14 However, screening for MDD is too infrequent for many reasons, including the logistics of integrating screening into the clinic workflow and limited provider availability, time, and training in mental health.
We recommend screening perinatal patients for mental health comorbidities. This recommendation may seem impractical given the lack of screening tools for comorbid mental health conditions; however, the Computerized Adaptive Test for Mental Health (CAT-MH), the validated tool15-17 used in this study, is an ideal option. CAT-MH is uniquely capable of screening for MDD, GAD, PTSD, SUD, and suicidality in one platform and is routinely used in diverse settings including the Veterans Administration,18 foster care,19 and universities.20 The main limitation of this more comprehensive screening is that it takes about 10 minutes per patient. However, CAT-MH is self-administered and can be done in the waiting room or on a mobile device prior to a clinic visit.
CAT-MH can also be easily integrated into clinical workflow when added to the Electronic Medical Record21, and is a more comprehensive tool than existing perinatal depression tools such as the Perinatal Health Questionaire-9 (PHQ-9) and Edinburgh Perinatal Depression Scale (EPDS).22 Another limitation is cost – currently $5.00 per assessment – however, this is less than routine blood work.23 If CAT-MH is not an option, we recommend a stepped approach of screening for GAD when perinatal patients screen positive for MDD, as this is the most common comorbidity profile. The GAD-7 is a free and widely available tool.24
Barriers to care
In Craemer et al,13 nearly two-thirds (64.9%) of perinatal patients with a positive screen did not receive a referral to follow-up care or a medication prescription. These low referral rates may reflect a variety of widely recognized barriers to care, including lack of referral options, provider and/or patient reluctance to pursue referrals, barriers to insurance coverage, or inadequate behavioral health infrastructure to ensure referral and diagnostic follow-up.
Further, rural residing perinatal patients are an underserved population that need more resources and screening. Despite an on-site behavioral specialist at the rural clinic, Craemer et al13 found a stark disparity in referral rates: referrals to treatment for a positive diagnosis was over two times less at the rural clinic (23.9%), compared with the urban clinics (51.6%). The most common treatment offered at the rural clinic was a prescription for medication (17.4%), while referral to follow-up care was the most common at the urban clinics (35.5%). Rural areas not only have a shortage of health care providers, but community members seeking mental health care often encounter greater stigma, compared with urban residents.25,26
These data highlight an unmet need for referrals to treatment for patients in rural communities, particularly in Illinois where the pregnancy-related mortality ratio attributable to mental health conditions is three times greater in rural areas, compared with those residing in urban Cook County (Chicago).2 Increasing access and availability to mental health treatment and prevention resources in Illinois, especially in rural areas, is an opportunity to prevent pregnancy-related mortality attributable to mental health conditions.
Overall, there is a critical need for screening for perinatal mental health comorbidities, increased attention to low rates of referral to mental health treatment, and investing in rural perinatal mental health. Addressing perinatal mental health disorders is key to decreasing the burden of maternal mortality, particularly in Illinois.
Ms. Craemer and Ms. Sayah are senior research specialists at the Center for Research on Women & Gender, University of Illinois at Chicago. Dr. Duffecy is a professor of clinical psychiatry at the University of Illinois at Chicago. Dr. Geller is a professor of obstetrics & gynecology and director of the Center for Research on Women & Gender, University of Illinois at Chicago. Dr. Maki is a professor of psychiatry, psychology, and obstetrics & gynecology at the University of Illinois at Chicago.
References
1. Trost S et al. Pregnancy-related deaths: Data from maternal mortality review committees in 36 states, 2017-2019. Atlanta: Centers for Disease Control and Prevention, U.S. Department of Health & Human Services, 2022.
2. Illinois Department of Public Health. Illinois maternal morbidity and mortality report 2016-2017. 2021.
3. AHRQ. Funding opportunities to address opioid and other substance use disorders. Updated 2023.
4. HRSA. Screening and treatment for maternal mental health and substance use disorders.
5. U.S. Preventive Services Task Force. Recommendations for primary care practice. Accessed May 26, 2023.
6. U.S. Preventive Services Task Force. Draft recommendation statement: Anxiety in adults: Screening. 2022.
7. ACOG. Screening and diagnosis of mental health conditions during pregnancy and postpartum. Clinical Practice Guideline. Number 4. 2023 June.
8. Meltzer-Brody S and Stuebe A. The long-term psychiatric and medical prognosis of perinatal mental illness. Best Pract Res Clin Obstet Gynaecol. 2014 Jan. doi: 10.1016/j.bpobgyn.2013.08.009.
9. Van Niel MS and Payne JL. Perinatal depression: A review. Cleve Clin J Med. 2020 May. doi: 10.3949/ccjm.87a.19054.
10. Wisner KL et al. Onset timing, thoughts of self-harm, and diagnoses in postpartum women with screen-positive depression findings. 2013 May. doi: 10.1001/jamapsychiatry.2013.87.
11. Falah-Hassani K et al. The prevalence of antenatal and postnatal co-morbid anxiety and depression: A meta-analysis. Psychol Med. 2017 Sep. doi: 10.1017/S0033291717000617.
12. Pentecost R et al. Scoping review of the associations between perinatal substance use and perinatal depression and anxiety. J Obstet Gynecol Neonatal Nurs. 2021 Jul. doi: 10.1016/j.jogn.2021.02.008.
13. Craemer KA et al. Perinatal mental health in low-income urban and rural patients: The importance of screening for comorbidities. Gen Hosp Psychiatry. 2023 Jul-Aug. doi: 10.1016/j.genhosppsych.2023.05.007.
14. O’Connor E et al. Primary care screening for and treatment of depression in pregnant and postpartum women: Evidence report and systematic review for the U.S. Preventive Services Task Force. JAMA. 2016 Jan 26. doi: 10.1001/jama.2015.18948.
15. Kozhimannil KB et al. Racial and ethnic disparities in postpartum depression care among low-income women. Psychiatr Serv. 2011 Jun. doi: 10.1176/ps.62.6.pss6206_0619.
16. Wenzel ES et al. Depression and anxiety symptoms across pregnancy and the postpartum in low-income Black and Latina women. Arch Womens Ment Health. 2021 Dec. doi: 10.1007/s00737-021-01139-y.
17. Gibbons RD et al. Development of a computerized adaptive substance use disorder scale for screening and measurement: The CAT‐SUD. Addiction. 2020 Jul. doi: 10.1111/add.14938.
18. Brenner LA et al. Validation of a computerized adaptive test suicide scale (CAT-SS) among united states military veterans. PloS One. 2022 Jan 21. doi: 10.1371/journal.pone.0261920.
19. The Center for State Child Welfare Data. Using technology to diagnose and report on behavioral health challenges facing foster youth. 2018.
20. Kim JJ et al. The experience of depression, anxiety, and mania among perinatal women. Arch Womens Ment Health. 2016 Oct. doi: 10.1007/s00737-016-0632-6.
21. Tepper MC et al. Toward population health: Using a learning behavioral health system and measurement-based care to improve access, care, outcomes, and disparities. Community Ment Health J. 2022 Nov. doi: 10.1007/s10597-022-00957-3.
22. Wenzel E et al. Using computerised adaptive tests to screen for perinatal depression in underserved women of colour. Evid Based Ment Health. 2022 Feb. doi: 10.1136/ebmental-2021-300262.
23. Sanger-Katz M. They want it to be secret: How a common blood test can cost $11 or almost $1,000. New York Times. 2019 Apr 19.
24. Spitzer RL et al. A brief measure for assessing generalized anxiety disorder: The GAD-7. Arch Intern Med. 2006 May 22. doi: 10.1001/archinte.166.10.1092.
25. Mollard E et al. An integrative review of postpartum depression in rural US communities. Arch Psychiatr Nurs. 2016 Jun. doi: 10.1016/j.apnu.2015.12.003.
26. Anglim AJ and Radke SM. Rural maternal health care outcomes, drivers, and patient perspectives. Clin Obstet Gynecol. 2022 Dec 1. doi: 10.1097/GRF.0000000000000753.
Teens have easy online access to Delta-8 cannabinoid products
WASHINGTON – , researchers reported at the 2023 annual meeting of the American Academy of Pediatrics. Most of the products identified came in bright, colorful, kid-friendly packaging and cost less than $10, the researchers found, and only 2 out of 45 sites had a third-party age verification requirement for purchases.
Delta-8 THC, also called D8, is a synthetically produced cannabinoid whose chemical structure and effects are nearly identical to traditional THC, the authors explained, and past research has found that D8 products, such as e-cigarettes, can contain toxic byproducts and contaminants.
”Since D8 is not traditional THC, minors may underestimate its strength and potential danger,” wrote lead author Abhijeet Grewal, BS, a research assistant at Cohen Children’s Medical Center, New York, and senior author Ruth Milanaik, DO, director of the Neonatal Neurodevelopmental Program at Cohen Children’s and a developmental/behavioral pediatrician at Northwell Health, also in New York. “Although traditional THC is a federally banned substance, D8 is legal on a federal level and less restricted on a state by state basis, making it easier for individuals to acquire D8.”
Easily accessible
During the first seven moments of 2021, 77% of reports of accidental exposure occurred in people under age 18, including some children who required ICU admission. The U.S. Food and Drug Administration also received 104 reports of adverse events from products containing D8 between December 2020-February 2022, and more than half of those required medical intervention.
To better understand how easy it is to access D8, the authors collected data on 45 websites they identified that sold D8. The researchers looked for age verification questions for accessing the site, third-party age certification, what kinds of products (edibles, smoke products, or tinctures) were sold, the price and dosage of the cheapest product, and examples of packaging, flavors, marketing claims, and warning statements at each site.
More than a third of the sites (36%) did not ask for customers’ age and almost none of the sites asked for proof: 96% of the sites lacked formal third-party age verification procedures. All but one of the sites sold D8 edibles, and most (82%) sold D8 vaping or smoking products. Only 42% sold tinctures, a mix of concentrated D8 with oil that’s orally consumed.
The cheapest product was priced under $5 on one-third of the sites and under $10 on another third of the sites. The cheapest product was between $10-20 on 16% of the sites while the remaining nine sites’ cheapest product was more than $20. In assessing only the cheapest D8 products on each site, nearly half (47%) contained 51 mg or more of D8, and 20% of the products didn’t report the dosage. Another 22% contained 41-50 mg of D8, and the remaining five products contained 20-40 mg.
Kid-friendly D8
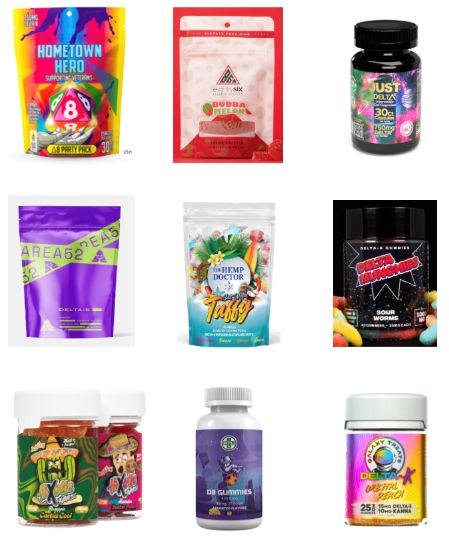
More than half of the D8 products were sold in kid-friendly packaging – packages with bright, colorful designs and fonts that resemble candy or snack food, sometimes cartoon characters or fun items like dice on the packaging. Further, 24% of the websites did not include any warnings or other health information about D8.
“The low prices, high dosages available, and eye-popping packaging make these products extremely attractive to teens who are looking for a high,” the researchers concluded. They advised clinicians to talk with teen patients about the dangers of D8 and advocated for policymakers to more strictly regulate online distributors of D8 products, particularly in requiring age verification procedures and prohibiting kid-friendly packaging.
Megan Moreno, MD, MSEd, MPH, an adolescent medicine physician and researcher at the University of Wisconsin, Madison, School of Medicine and Public Health and UWHealthKids, was particularly struck by how eye-catching the packaging was. “The bright colors and font choices are really designed to attract adolescents,” commented Dr. Moreno, who was not involved in the study. But she was not surprised overall by the findings.
“Other studies have found that the cannabis industry leverages online tools and social media, alongside youth-friendly packaging, to attract youth to their products,” she said. “What is disappointing is that these companies do not use industry standard approaches, such as the alcohol industry, to age-gate their websites.”
It’s important for providers who care for adolescents to ask about substance use but to especially include questions about substances that teens might not think of as “drugs,” such as Delta 8, Dr. Moreno said.
“Prior research on other types of substance such as these has found that teens can think these are less dangerous versions of cannabis, so providing accurate information and asking about these products can prevent harm to kids,” Dr. Moreno said. Although this study focused on websites that sell D8 products, she said that “another important area of influence to consider is social media messaging around these products, which may drive traffic to the purchasing site.” It’s clear this industry is not going to self-regulate without policy changes, Dr. Moreno added, so she noted the importance of advocating for policy that regulates these sites.
Mr. Grewal, Dr. Milanaik and Dr. Moreno had no disclosures. No external funding sources were noted.
WASHINGTON – , researchers reported at the 2023 annual meeting of the American Academy of Pediatrics. Most of the products identified came in bright, colorful, kid-friendly packaging and cost less than $10, the researchers found, and only 2 out of 45 sites had a third-party age verification requirement for purchases.
Delta-8 THC, also called D8, is a synthetically produced cannabinoid whose chemical structure and effects are nearly identical to traditional THC, the authors explained, and past research has found that D8 products, such as e-cigarettes, can contain toxic byproducts and contaminants.
”Since D8 is not traditional THC, minors may underestimate its strength and potential danger,” wrote lead author Abhijeet Grewal, BS, a research assistant at Cohen Children’s Medical Center, New York, and senior author Ruth Milanaik, DO, director of the Neonatal Neurodevelopmental Program at Cohen Children’s and a developmental/behavioral pediatrician at Northwell Health, also in New York. “Although traditional THC is a federally banned substance, D8 is legal on a federal level and less restricted on a state by state basis, making it easier for individuals to acquire D8.”
Easily accessible
During the first seven moments of 2021, 77% of reports of accidental exposure occurred in people under age 18, including some children who required ICU admission. The U.S. Food and Drug Administration also received 104 reports of adverse events from products containing D8 between December 2020-February 2022, and more than half of those required medical intervention.
To better understand how easy it is to access D8, the authors collected data on 45 websites they identified that sold D8. The researchers looked for age verification questions for accessing the site, third-party age certification, what kinds of products (edibles, smoke products, or tinctures) were sold, the price and dosage of the cheapest product, and examples of packaging, flavors, marketing claims, and warning statements at each site.
More than a third of the sites (36%) did not ask for customers’ age and almost none of the sites asked for proof: 96% of the sites lacked formal third-party age verification procedures. All but one of the sites sold D8 edibles, and most (82%) sold D8 vaping or smoking products. Only 42% sold tinctures, a mix of concentrated D8 with oil that’s orally consumed.
The cheapest product was priced under $5 on one-third of the sites and under $10 on another third of the sites. The cheapest product was between $10-20 on 16% of the sites while the remaining nine sites’ cheapest product was more than $20. In assessing only the cheapest D8 products on each site, nearly half (47%) contained 51 mg or more of D8, and 20% of the products didn’t report the dosage. Another 22% contained 41-50 mg of D8, and the remaining five products contained 20-40 mg.
Kid-friendly D8
More than half of the D8 products were sold in kid-friendly packaging – packages with bright, colorful designs and fonts that resemble candy or snack food, sometimes cartoon characters or fun items like dice on the packaging. Further, 24% of the websites did not include any warnings or other health information about D8.
“The low prices, high dosages available, and eye-popping packaging make these products extremely attractive to teens who are looking for a high,” the researchers concluded. They advised clinicians to talk with teen patients about the dangers of D8 and advocated for policymakers to more strictly regulate online distributors of D8 products, particularly in requiring age verification procedures and prohibiting kid-friendly packaging.
Megan Moreno, MD, MSEd, MPH, an adolescent medicine physician and researcher at the University of Wisconsin, Madison, School of Medicine and Public Health and UWHealthKids, was particularly struck by how eye-catching the packaging was. “The bright colors and font choices are really designed to attract adolescents,” commented Dr. Moreno, who was not involved in the study. But she was not surprised overall by the findings.
“Other studies have found that the cannabis industry leverages online tools and social media, alongside youth-friendly packaging, to attract youth to their products,” she said. “What is disappointing is that these companies do not use industry standard approaches, such as the alcohol industry, to age-gate their websites.”
It’s important for providers who care for adolescents to ask about substance use but to especially include questions about substances that teens might not think of as “drugs,” such as Delta 8, Dr. Moreno said.
“Prior research on other types of substance such as these has found that teens can think these are less dangerous versions of cannabis, so providing accurate information and asking about these products can prevent harm to kids,” Dr. Moreno said. Although this study focused on websites that sell D8 products, she said that “another important area of influence to consider is social media messaging around these products, which may drive traffic to the purchasing site.” It’s clear this industry is not going to self-regulate without policy changes, Dr. Moreno added, so she noted the importance of advocating for policy that regulates these sites.
Mr. Grewal, Dr. Milanaik and Dr. Moreno had no disclosures. No external funding sources were noted.
WASHINGTON – , researchers reported at the 2023 annual meeting of the American Academy of Pediatrics. Most of the products identified came in bright, colorful, kid-friendly packaging and cost less than $10, the researchers found, and only 2 out of 45 sites had a third-party age verification requirement for purchases.
Delta-8 THC, also called D8, is a synthetically produced cannabinoid whose chemical structure and effects are nearly identical to traditional THC, the authors explained, and past research has found that D8 products, such as e-cigarettes, can contain toxic byproducts and contaminants.
”Since D8 is not traditional THC, minors may underestimate its strength and potential danger,” wrote lead author Abhijeet Grewal, BS, a research assistant at Cohen Children’s Medical Center, New York, and senior author Ruth Milanaik, DO, director of the Neonatal Neurodevelopmental Program at Cohen Children’s and a developmental/behavioral pediatrician at Northwell Health, also in New York. “Although traditional THC is a federally banned substance, D8 is legal on a federal level and less restricted on a state by state basis, making it easier for individuals to acquire D8.”
Easily accessible
During the first seven moments of 2021, 77% of reports of accidental exposure occurred in people under age 18, including some children who required ICU admission. The U.S. Food and Drug Administration also received 104 reports of adverse events from products containing D8 between December 2020-February 2022, and more than half of those required medical intervention.
To better understand how easy it is to access D8, the authors collected data on 45 websites they identified that sold D8. The researchers looked for age verification questions for accessing the site, third-party age certification, what kinds of products (edibles, smoke products, or tinctures) were sold, the price and dosage of the cheapest product, and examples of packaging, flavors, marketing claims, and warning statements at each site.
More than a third of the sites (36%) did not ask for customers’ age and almost none of the sites asked for proof: 96% of the sites lacked formal third-party age verification procedures. All but one of the sites sold D8 edibles, and most (82%) sold D8 vaping or smoking products. Only 42% sold tinctures, a mix of concentrated D8 with oil that’s orally consumed.
The cheapest product was priced under $5 on one-third of the sites and under $10 on another third of the sites. The cheapest product was between $10-20 on 16% of the sites while the remaining nine sites’ cheapest product was more than $20. In assessing only the cheapest D8 products on each site, nearly half (47%) contained 51 mg or more of D8, and 20% of the products didn’t report the dosage. Another 22% contained 41-50 mg of D8, and the remaining five products contained 20-40 mg.
Kid-friendly D8
More than half of the D8 products were sold in kid-friendly packaging – packages with bright, colorful designs and fonts that resemble candy or snack food, sometimes cartoon characters or fun items like dice on the packaging. Further, 24% of the websites did not include any warnings or other health information about D8.
“The low prices, high dosages available, and eye-popping packaging make these products extremely attractive to teens who are looking for a high,” the researchers concluded. They advised clinicians to talk with teen patients about the dangers of D8 and advocated for policymakers to more strictly regulate online distributors of D8 products, particularly in requiring age verification procedures and prohibiting kid-friendly packaging.
Megan Moreno, MD, MSEd, MPH, an adolescent medicine physician and researcher at the University of Wisconsin, Madison, School of Medicine and Public Health and UWHealthKids, was particularly struck by how eye-catching the packaging was. “The bright colors and font choices are really designed to attract adolescents,” commented Dr. Moreno, who was not involved in the study. But she was not surprised overall by the findings.
“Other studies have found that the cannabis industry leverages online tools and social media, alongside youth-friendly packaging, to attract youth to their products,” she said. “What is disappointing is that these companies do not use industry standard approaches, such as the alcohol industry, to age-gate their websites.”
It’s important for providers who care for adolescents to ask about substance use but to especially include questions about substances that teens might not think of as “drugs,” such as Delta 8, Dr. Moreno said.
“Prior research on other types of substance such as these has found that teens can think these are less dangerous versions of cannabis, so providing accurate information and asking about these products can prevent harm to kids,” Dr. Moreno said. Although this study focused on websites that sell D8 products, she said that “another important area of influence to consider is social media messaging around these products, which may drive traffic to the purchasing site.” It’s clear this industry is not going to self-regulate without policy changes, Dr. Moreno added, so she noted the importance of advocating for policy that regulates these sites.
Mr. Grewal, Dr. Milanaik and Dr. Moreno had no disclosures. No external funding sources were noted.
At AAP 2023
Telehealth linked to better opioid treatment retention
TOPLINE:
METHODOLOGY:
- Researchers analyzed Medicaid claims data from November 2019 through the end of 2020 in Kentucky and Ohio to investigate the impact of a policy change implemented during the COVID-19 pandemic that allowed the use of telehealth to prescribe buprenorphine for OUD.
- The two main outcomes of interest were retention in treatment after initiation (telehealth vs. traditional) and opioid-related nonfatal overdose after initiation.
TAKEAWAY:
- For both states combined, nearly 92,000 adults had a buprenorphine prescription in at least one quarter in 2020, with nearly 43,000 of those individuals starting treatment in 2020.
- Sharp increases in telehealth delivery of buprenorphine were noted at the beginning of 2020 at the pandemic outset, and this was associated with greater retention in treatment (Kentucky adjusted odds ratio, 1.13; 95% confidence interval, 1.01-1.27 and Ohio aOR, 1.19; 95% CI, 1.06-1.32).
- Furthermore, 90-day retention rates were higher among those who started treatment via telehealth versus those who started treatment in nontelehealth settings in Kentucky (48% vs. 44%, respectively) and in Ohio (32% vs. 28%, respectively).
- There was no increased risk of nonfatal overdose with telehealth treatment, providing added evidence to suggest that patients were not harmed by having increased access to buprenorphine treatment via telehealth.
IN PRACTICE:
“These results offer important insights for states with a high burden of OUD looking to policies and methods to reduce barriers to treatment,” the authors write.
SOURCE:
The study, with first author Lindsey Hammerslag, PhD, with University of Kentucky College of Medicine, Lexington, was published online in JAMA Network Open, with an invited commentary by Lindsey Allen, PhD, Northwestern University, Chicago, on navigating the path to effective, equitable, and evidence-based telehealth for OUD treatment.
LIMITATIONS:
The analysis was limited to Medicaid patients in two states over 1 year and there may have been unmeasured confounders, such as perceived patient stability, that influenced the findings. Because Medicaid data were not linked to emergency services or death records, this study considered only medically treated overdose.
DISCLOSURES:
The study was supported by the National Institute on Drug Abuse and carried out in partnership with the Substance Abuse and Mental Health Services Administration. The authors report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
TOPLINE:
METHODOLOGY:
- Researchers analyzed Medicaid claims data from November 2019 through the end of 2020 in Kentucky and Ohio to investigate the impact of a policy change implemented during the COVID-19 pandemic that allowed the use of telehealth to prescribe buprenorphine for OUD.
- The two main outcomes of interest were retention in treatment after initiation (telehealth vs. traditional) and opioid-related nonfatal overdose after initiation.
TAKEAWAY:
- For both states combined, nearly 92,000 adults had a buprenorphine prescription in at least one quarter in 2020, with nearly 43,000 of those individuals starting treatment in 2020.
- Sharp increases in telehealth delivery of buprenorphine were noted at the beginning of 2020 at the pandemic outset, and this was associated with greater retention in treatment (Kentucky adjusted odds ratio, 1.13; 95% confidence interval, 1.01-1.27 and Ohio aOR, 1.19; 95% CI, 1.06-1.32).
- Furthermore, 90-day retention rates were higher among those who started treatment via telehealth versus those who started treatment in nontelehealth settings in Kentucky (48% vs. 44%, respectively) and in Ohio (32% vs. 28%, respectively).
- There was no increased risk of nonfatal overdose with telehealth treatment, providing added evidence to suggest that patients were not harmed by having increased access to buprenorphine treatment via telehealth.
IN PRACTICE:
“These results offer important insights for states with a high burden of OUD looking to policies and methods to reduce barriers to treatment,” the authors write.
SOURCE:
The study, with first author Lindsey Hammerslag, PhD, with University of Kentucky College of Medicine, Lexington, was published online in JAMA Network Open, with an invited commentary by Lindsey Allen, PhD, Northwestern University, Chicago, on navigating the path to effective, equitable, and evidence-based telehealth for OUD treatment.
LIMITATIONS:
The analysis was limited to Medicaid patients in two states over 1 year and there may have been unmeasured confounders, such as perceived patient stability, that influenced the findings. Because Medicaid data were not linked to emergency services or death records, this study considered only medically treated overdose.
DISCLOSURES:
The study was supported by the National Institute on Drug Abuse and carried out in partnership with the Substance Abuse and Mental Health Services Administration. The authors report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
TOPLINE:
METHODOLOGY:
- Researchers analyzed Medicaid claims data from November 2019 through the end of 2020 in Kentucky and Ohio to investigate the impact of a policy change implemented during the COVID-19 pandemic that allowed the use of telehealth to prescribe buprenorphine for OUD.
- The two main outcomes of interest were retention in treatment after initiation (telehealth vs. traditional) and opioid-related nonfatal overdose after initiation.
TAKEAWAY:
- For both states combined, nearly 92,000 adults had a buprenorphine prescription in at least one quarter in 2020, with nearly 43,000 of those individuals starting treatment in 2020.
- Sharp increases in telehealth delivery of buprenorphine were noted at the beginning of 2020 at the pandemic outset, and this was associated with greater retention in treatment (Kentucky adjusted odds ratio, 1.13; 95% confidence interval, 1.01-1.27 and Ohio aOR, 1.19; 95% CI, 1.06-1.32).
- Furthermore, 90-day retention rates were higher among those who started treatment via telehealth versus those who started treatment in nontelehealth settings in Kentucky (48% vs. 44%, respectively) and in Ohio (32% vs. 28%, respectively).
- There was no increased risk of nonfatal overdose with telehealth treatment, providing added evidence to suggest that patients were not harmed by having increased access to buprenorphine treatment via telehealth.
IN PRACTICE:
“These results offer important insights for states with a high burden of OUD looking to policies and methods to reduce barriers to treatment,” the authors write.
SOURCE:
The study, with first author Lindsey Hammerslag, PhD, with University of Kentucky College of Medicine, Lexington, was published online in JAMA Network Open, with an invited commentary by Lindsey Allen, PhD, Northwestern University, Chicago, on navigating the path to effective, equitable, and evidence-based telehealth for OUD treatment.
LIMITATIONS:
The analysis was limited to Medicaid patients in two states over 1 year and there may have been unmeasured confounders, such as perceived patient stability, that influenced the findings. Because Medicaid data were not linked to emergency services or death records, this study considered only medically treated overdose.
DISCLOSURES:
The study was supported by the National Institute on Drug Abuse and carried out in partnership with the Substance Abuse and Mental Health Services Administration. The authors report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM JAMA NETWORK OPEN
Predictors of prescription opioid overdose
A Canadian systematic review of 28 observational studies has identified 10 strong predictors of fatal and nonfatal prescription opioid overdose.
Published in CMAJ, the analysis found the risk of fatal and nonfatal opioid overdose was notably tied to such factors as high-dose and fentanyl prescriptions, multiple opioid prescribers or pharmacies, and several mental health issues. High-certainty evidence from 14 studies involving more than a million patients showed a linear dose-response relationship with opioid overdose.
“Our findings suggest that awareness of, and attention to, several patient and prescription characteristics may help reduce the risk of opioid overdose among people living with chronic pain,” wrote a research team led by Li Wang, PhD, a researcher at the Michael G. DeGroote Institute for Pain Research and Care and the department of anesthesia at McMaster University, Hamilton, Ont.
Predictors of fatal and nonfatal overdose
Reporting on studies of 103 possible predictors in a pooled cohort of almost 24 million patients, the review found moderate- to high-certainty evidence for large relative associations with the following 10 criteria:
- A history of overdose (odds ratio, 5.85; 95% confidence interval, 3.78-9.04).
- A higher opioid dosage (OR, 2.57; 95% CI, 2.08-3.18 per 90-mg increment).
- Three or more prescribers (OR, 4.68; 95% CI, 3.57-6.12).
- Four or more dispensing pharmacies (OR, 4.92; 95% CI, 4.35-5.57).
- Prescription for fentanyl (OR, 2.80; 95% CI, 2.30-3.41).
- Current substance use disorder (OR, 2.62; 95% CI, 2.09-3.27).
- Any mental health diagnosis (OR, 2.12; 95% CI, 1.73-2.61).
- Depression (OR, 2.22; 95% CI, 1.57-314).
- Bipolar disorder (OR, 2.07; 95% CI, 1.77-2.41).
- Pancreatitis (OR, 2.00; 95% CI,1.52-2.64).
Absolute risks in patients with the predictor ranged from 2 to 6 per 1,000 for fatal overdose and 4 to 12 per 1,000 for nonfatal overdose.
The authors noted that chronic pain affects 20% of the world’s population worldwide, and a 2021 meta-analysis of 60 observational studies revealed that opioids are prescribed for 27% of adults living with chronic pain, with a higher prevalence of prescribing in North America than in Europe.
International review
A total of 28 observational studies comprising 23,963,716 patients (52% female) with mean age of 52 years were enrolled. All used administrative databases. Twenty-four studies were conducted in the United States, three in Canada, and one in the United Kingdom. Twenty-one studies included only patients with noncancer chronic pain, while seven included patients with either cancer-related or noncancer chronic pain. Twenty-two studies accepted patients with previous or current substance use disorder and three excluded patients with comorbid substance use disorder. Twenty-three studies included patients with comorbid mental illness and five exclusively recruited veterans.
The median sample size was 43,885. As a limitation, 25 studies (89%) were at high risk of bias for at least one criterion, the authors acknowledged. Moderate-certainty evidence showed the pooled prevalence of fatal opioid overdose after prescription for chronic pain was 1.3 per 1,000 (95% CI, 0.6-2.3 per 1,000) for fatal overdose and 3.2 per 1,000 (95% CI, 2.0-4.7 per 1,000) for nonfatal overdose.
“Awareness of these predictors may facilitate shared decision-making regarding prescribing opioids for chronic pain and may inform harm-reduction strategies,” Dr. Wang and associates wrote.
This study was supported by a grant from Health Canada’s Substance Use and Addictions Program. Coauthor Dr. Corey Hayes was supported by Veterans Affairs Health Services Research and Development and the National Institute on Drug Abuse Clinical Trials Network. Dr. Jason Busse is supported by the Canadian Institutes of Health Research. Dr. David Juurlink has received travel support for presentations from the CIHR, Stanford University, and Texas Tech University Health Sciences Center.
A Canadian systematic review of 28 observational studies has identified 10 strong predictors of fatal and nonfatal prescription opioid overdose.
Published in CMAJ, the analysis found the risk of fatal and nonfatal opioid overdose was notably tied to such factors as high-dose and fentanyl prescriptions, multiple opioid prescribers or pharmacies, and several mental health issues. High-certainty evidence from 14 studies involving more than a million patients showed a linear dose-response relationship with opioid overdose.
“Our findings suggest that awareness of, and attention to, several patient and prescription characteristics may help reduce the risk of opioid overdose among people living with chronic pain,” wrote a research team led by Li Wang, PhD, a researcher at the Michael G. DeGroote Institute for Pain Research and Care and the department of anesthesia at McMaster University, Hamilton, Ont.
Predictors of fatal and nonfatal overdose
Reporting on studies of 103 possible predictors in a pooled cohort of almost 24 million patients, the review found moderate- to high-certainty evidence for large relative associations with the following 10 criteria:
- A history of overdose (odds ratio, 5.85; 95% confidence interval, 3.78-9.04).
- A higher opioid dosage (OR, 2.57; 95% CI, 2.08-3.18 per 90-mg increment).
- Three or more prescribers (OR, 4.68; 95% CI, 3.57-6.12).
- Four or more dispensing pharmacies (OR, 4.92; 95% CI, 4.35-5.57).
- Prescription for fentanyl (OR, 2.80; 95% CI, 2.30-3.41).
- Current substance use disorder (OR, 2.62; 95% CI, 2.09-3.27).
- Any mental health diagnosis (OR, 2.12; 95% CI, 1.73-2.61).
- Depression (OR, 2.22; 95% CI, 1.57-314).
- Bipolar disorder (OR, 2.07; 95% CI, 1.77-2.41).
- Pancreatitis (OR, 2.00; 95% CI,1.52-2.64).
Absolute risks in patients with the predictor ranged from 2 to 6 per 1,000 for fatal overdose and 4 to 12 per 1,000 for nonfatal overdose.
The authors noted that chronic pain affects 20% of the world’s population worldwide, and a 2021 meta-analysis of 60 observational studies revealed that opioids are prescribed for 27% of adults living with chronic pain, with a higher prevalence of prescribing in North America than in Europe.
International review
A total of 28 observational studies comprising 23,963,716 patients (52% female) with mean age of 52 years were enrolled. All used administrative databases. Twenty-four studies were conducted in the United States, three in Canada, and one in the United Kingdom. Twenty-one studies included only patients with noncancer chronic pain, while seven included patients with either cancer-related or noncancer chronic pain. Twenty-two studies accepted patients with previous or current substance use disorder and three excluded patients with comorbid substance use disorder. Twenty-three studies included patients with comorbid mental illness and five exclusively recruited veterans.
The median sample size was 43,885. As a limitation, 25 studies (89%) were at high risk of bias for at least one criterion, the authors acknowledged. Moderate-certainty evidence showed the pooled prevalence of fatal opioid overdose after prescription for chronic pain was 1.3 per 1,000 (95% CI, 0.6-2.3 per 1,000) for fatal overdose and 3.2 per 1,000 (95% CI, 2.0-4.7 per 1,000) for nonfatal overdose.
“Awareness of these predictors may facilitate shared decision-making regarding prescribing opioids for chronic pain and may inform harm-reduction strategies,” Dr. Wang and associates wrote.
This study was supported by a grant from Health Canada’s Substance Use and Addictions Program. Coauthor Dr. Corey Hayes was supported by Veterans Affairs Health Services Research and Development and the National Institute on Drug Abuse Clinical Trials Network. Dr. Jason Busse is supported by the Canadian Institutes of Health Research. Dr. David Juurlink has received travel support for presentations from the CIHR, Stanford University, and Texas Tech University Health Sciences Center.
A Canadian systematic review of 28 observational studies has identified 10 strong predictors of fatal and nonfatal prescription opioid overdose.
Published in CMAJ, the analysis found the risk of fatal and nonfatal opioid overdose was notably tied to such factors as high-dose and fentanyl prescriptions, multiple opioid prescribers or pharmacies, and several mental health issues. High-certainty evidence from 14 studies involving more than a million patients showed a linear dose-response relationship with opioid overdose.
“Our findings suggest that awareness of, and attention to, several patient and prescription characteristics may help reduce the risk of opioid overdose among people living with chronic pain,” wrote a research team led by Li Wang, PhD, a researcher at the Michael G. DeGroote Institute for Pain Research and Care and the department of anesthesia at McMaster University, Hamilton, Ont.
Predictors of fatal and nonfatal overdose
Reporting on studies of 103 possible predictors in a pooled cohort of almost 24 million patients, the review found moderate- to high-certainty evidence for large relative associations with the following 10 criteria:
- A history of overdose (odds ratio, 5.85; 95% confidence interval, 3.78-9.04).
- A higher opioid dosage (OR, 2.57; 95% CI, 2.08-3.18 per 90-mg increment).
- Three or more prescribers (OR, 4.68; 95% CI, 3.57-6.12).
- Four or more dispensing pharmacies (OR, 4.92; 95% CI, 4.35-5.57).
- Prescription for fentanyl (OR, 2.80; 95% CI, 2.30-3.41).
- Current substance use disorder (OR, 2.62; 95% CI, 2.09-3.27).
- Any mental health diagnosis (OR, 2.12; 95% CI, 1.73-2.61).
- Depression (OR, 2.22; 95% CI, 1.57-314).
- Bipolar disorder (OR, 2.07; 95% CI, 1.77-2.41).
- Pancreatitis (OR, 2.00; 95% CI,1.52-2.64).
Absolute risks in patients with the predictor ranged from 2 to 6 per 1,000 for fatal overdose and 4 to 12 per 1,000 for nonfatal overdose.
The authors noted that chronic pain affects 20% of the world’s population worldwide, and a 2021 meta-analysis of 60 observational studies revealed that opioids are prescribed for 27% of adults living with chronic pain, with a higher prevalence of prescribing in North America than in Europe.
International review
A total of 28 observational studies comprising 23,963,716 patients (52% female) with mean age of 52 years were enrolled. All used administrative databases. Twenty-four studies were conducted in the United States, three in Canada, and one in the United Kingdom. Twenty-one studies included only patients with noncancer chronic pain, while seven included patients with either cancer-related or noncancer chronic pain. Twenty-two studies accepted patients with previous or current substance use disorder and three excluded patients with comorbid substance use disorder. Twenty-three studies included patients with comorbid mental illness and five exclusively recruited veterans.
The median sample size was 43,885. As a limitation, 25 studies (89%) were at high risk of bias for at least one criterion, the authors acknowledged. Moderate-certainty evidence showed the pooled prevalence of fatal opioid overdose after prescription for chronic pain was 1.3 per 1,000 (95% CI, 0.6-2.3 per 1,000) for fatal overdose and 3.2 per 1,000 (95% CI, 2.0-4.7 per 1,000) for nonfatal overdose.
“Awareness of these predictors may facilitate shared decision-making regarding prescribing opioids for chronic pain and may inform harm-reduction strategies,” Dr. Wang and associates wrote.
This study was supported by a grant from Health Canada’s Substance Use and Addictions Program. Coauthor Dr. Corey Hayes was supported by Veterans Affairs Health Services Research and Development and the National Institute on Drug Abuse Clinical Trials Network. Dr. Jason Busse is supported by the Canadian Institutes of Health Research. Dr. David Juurlink has received travel support for presentations from the CIHR, Stanford University, and Texas Tech University Health Sciences Center.
FROM CMAJ
New Canadian guidelines for high-risk drinking, AUD
TOPLINE:
New Canadian guidelines for the management of high-risk drinking and alcohol use disorder (AUD) include 15 recommendations on screening, diagnosis, withdrawal management, and ongoing treatment including psychosocial interventions, drug therapies, and community-based programs.
METHODOLOGY:
- The Canadian Research Initiative in Substance Misuse convened a 36-member committee of clinicians, researchers, people with personal experience of alcohol use, and Indigenous or Métis individuals to develop the guidelines, using the Appraisal of Guidelines for Research and Evaluation Instrument.
- Risk assessment was based on Alcohol Use Disorders Identification Test-Consumption scores.
- The definition of AUD was based on patients experiencing “clinically significant impairment or distress” from their alcohol use, with severity being mild, moderate, or severe.
TAKEAWAY:
- All adult and youth patients at moderate or high risk for AUD should be screened annually for alcohol use, and those screening positive should receive a diagnostic interview for AUD and an individualized treatment plan.
- Assessment of severe alcohol withdrawal complications should include clinical parameters such as past seizures or delirium tremens and the Prediction of Alcohol Withdrawal Severity Scale, with treatment including nonbenzodiazepine medications for low-risk patients and a short-term benzodiazepine prescription for high-risk patients, ideally in an inpatient setting.
- All patients with AUD should be referred for psychosocial treatment, and those with moderate to severe AUD should be offered naltrexone, acamprosate, topiramate, or gabapentin, depending on contraindications and effectiveness.
- Antipsychotics or SSRI antidepressants have little benefit and may worsen outcomes and should not be prescribed for AUD.
IN PRACTICE:
The authors noted that more than half of people aged 15 years or older in Canada drink more than the recommended amount, and about 18% meet the definition for AUD. “The aim of this guideline is to support primary care providers and services to offer more effective treatments routinely to patients with AUD as the standard of practice, with resulting improvements in health as well as potential for considerable cost savings in health and social systems,” the investigators write. They also note that policy makers can substantially improve standards of care by promoting adoption of the guideline and its recommendations.
SOURCE:
The article was written by Evan Wood, MD, PhD, professor of medicine, University of British Columbia, Vancouver, and colleagues. It was published online in the Canadian Medical Association Journal.
LIMITATIONS:
The guideline was published more than 3 years after the initial literature search in September 2020 and did not include comprehensive guidance for AUD with co-occurring substance use disorders or with severe mental health conditions. Certain groups, including immigrant and refugee populations, were not represented.
DISCLOSURES:
Development of the guideline received support from Health Canada’s Substance Use and Addictions Program, Canadian Institutes of Health Research, and BC Centre on Substance Use. No committee members disclosed direct monetary or nonmonetary support from alcohol or pharmaceutical industry sources within the past 5 years, or that their clinical revenue would be influenced by the guideline recommendations.
A version of this article first appeared on Medscape.com.
TOPLINE:
New Canadian guidelines for the management of high-risk drinking and alcohol use disorder (AUD) include 15 recommendations on screening, diagnosis, withdrawal management, and ongoing treatment including psychosocial interventions, drug therapies, and community-based programs.
METHODOLOGY:
- The Canadian Research Initiative in Substance Misuse convened a 36-member committee of clinicians, researchers, people with personal experience of alcohol use, and Indigenous or Métis individuals to develop the guidelines, using the Appraisal of Guidelines for Research and Evaluation Instrument.
- Risk assessment was based on Alcohol Use Disorders Identification Test-Consumption scores.
- The definition of AUD was based on patients experiencing “clinically significant impairment or distress” from their alcohol use, with severity being mild, moderate, or severe.
TAKEAWAY:
- All adult and youth patients at moderate or high risk for AUD should be screened annually for alcohol use, and those screening positive should receive a diagnostic interview for AUD and an individualized treatment plan.
- Assessment of severe alcohol withdrawal complications should include clinical parameters such as past seizures or delirium tremens and the Prediction of Alcohol Withdrawal Severity Scale, with treatment including nonbenzodiazepine medications for low-risk patients and a short-term benzodiazepine prescription for high-risk patients, ideally in an inpatient setting.
- All patients with AUD should be referred for psychosocial treatment, and those with moderate to severe AUD should be offered naltrexone, acamprosate, topiramate, or gabapentin, depending on contraindications and effectiveness.
- Antipsychotics or SSRI antidepressants have little benefit and may worsen outcomes and should not be prescribed for AUD.
IN PRACTICE:
The authors noted that more than half of people aged 15 years or older in Canada drink more than the recommended amount, and about 18% meet the definition for AUD. “The aim of this guideline is to support primary care providers and services to offer more effective treatments routinely to patients with AUD as the standard of practice, with resulting improvements in health as well as potential for considerable cost savings in health and social systems,” the investigators write. They also note that policy makers can substantially improve standards of care by promoting adoption of the guideline and its recommendations.
SOURCE:
The article was written by Evan Wood, MD, PhD, professor of medicine, University of British Columbia, Vancouver, and colleagues. It was published online in the Canadian Medical Association Journal.
LIMITATIONS:
The guideline was published more than 3 years after the initial literature search in September 2020 and did not include comprehensive guidance for AUD with co-occurring substance use disorders or with severe mental health conditions. Certain groups, including immigrant and refugee populations, were not represented.
DISCLOSURES:
Development of the guideline received support from Health Canada’s Substance Use and Addictions Program, Canadian Institutes of Health Research, and BC Centre on Substance Use. No committee members disclosed direct monetary or nonmonetary support from alcohol or pharmaceutical industry sources within the past 5 years, or that their clinical revenue would be influenced by the guideline recommendations.
A version of this article first appeared on Medscape.com.
TOPLINE:
New Canadian guidelines for the management of high-risk drinking and alcohol use disorder (AUD) include 15 recommendations on screening, diagnosis, withdrawal management, and ongoing treatment including psychosocial interventions, drug therapies, and community-based programs.
METHODOLOGY:
- The Canadian Research Initiative in Substance Misuse convened a 36-member committee of clinicians, researchers, people with personal experience of alcohol use, and Indigenous or Métis individuals to develop the guidelines, using the Appraisal of Guidelines for Research and Evaluation Instrument.
- Risk assessment was based on Alcohol Use Disorders Identification Test-Consumption scores.
- The definition of AUD was based on patients experiencing “clinically significant impairment or distress” from their alcohol use, with severity being mild, moderate, or severe.
TAKEAWAY:
- All adult and youth patients at moderate or high risk for AUD should be screened annually for alcohol use, and those screening positive should receive a diagnostic interview for AUD and an individualized treatment plan.
- Assessment of severe alcohol withdrawal complications should include clinical parameters such as past seizures or delirium tremens and the Prediction of Alcohol Withdrawal Severity Scale, with treatment including nonbenzodiazepine medications for low-risk patients and a short-term benzodiazepine prescription for high-risk patients, ideally in an inpatient setting.
- All patients with AUD should be referred for psychosocial treatment, and those with moderate to severe AUD should be offered naltrexone, acamprosate, topiramate, or gabapentin, depending on contraindications and effectiveness.
- Antipsychotics or SSRI antidepressants have little benefit and may worsen outcomes and should not be prescribed for AUD.
IN PRACTICE:
The authors noted that more than half of people aged 15 years or older in Canada drink more than the recommended amount, and about 18% meet the definition for AUD. “The aim of this guideline is to support primary care providers and services to offer more effective treatments routinely to patients with AUD as the standard of practice, with resulting improvements in health as well as potential for considerable cost savings in health and social systems,” the investigators write. They also note that policy makers can substantially improve standards of care by promoting adoption of the guideline and its recommendations.
SOURCE:
The article was written by Evan Wood, MD, PhD, professor of medicine, University of British Columbia, Vancouver, and colleagues. It was published online in the Canadian Medical Association Journal.
LIMITATIONS:
The guideline was published more than 3 years after the initial literature search in September 2020 and did not include comprehensive guidance for AUD with co-occurring substance use disorders or with severe mental health conditions. Certain groups, including immigrant and refugee populations, were not represented.
DISCLOSURES:
Development of the guideline received support from Health Canada’s Substance Use and Addictions Program, Canadian Institutes of Health Research, and BC Centre on Substance Use. No committee members disclosed direct monetary or nonmonetary support from alcohol or pharmaceutical industry sources within the past 5 years, or that their clinical revenue would be influenced by the guideline recommendations.
A version of this article first appeared on Medscape.com.
Here’s how to help Black smokers quit
Black Americans attempt to quit smoking more often than their White counterparts but are less likely to succeed, and they pay the health consequences.
This knowledge has driven Kevin Choi, MD, acting scientific director of the National Institute on Minority Health and Health Disparities in Bethesda, Md., to dedicate his career to studying the patterns and disparities of smoking among these patients.
Dr. Choi wants primary care clinicians to know not just that they have the potential to educate patients on the harms of smoking – most patients already know smoking is unhealthy – but that aiding them will likely necessitate more assertive follow-up.
To do so, “we need to understand the bigger backdrop of racial and sociological stress experienced by the Black population, which stems from both interpersonal and structural racism,” Dr. Choi said.
Not only are Black smokers more likely to try to quit, but they also tend to smoke fewer cigarettes per day than other racial groups. Yet they experience higher rates of smoking-related mortality.
The reasons behind the attempts
Multiple factors play into Black smokers’ lower rates of successful quitting attempts than Asian, Hispanic, White, and Native American individuals.
One reason: An estimated 85% of Black smokers smoke highly addictive menthol cigarettes. According to Dr. Choi and other experts, the tobacco industry engages in targeted marketing of menthols by sponsoring community events in predominantly Black neighborhoods and colleges with historically Black populations and by using Black culture in advertising.
“The built environment really drives a change in behavior, and we have seen that chronically in the African American population being overly targeted and now being overly addicted to nicotine,” said Daniel Kortsch, MD, a family medicine physician and chair of the Tobacco Cessation Workgroup at Denver Health.
Menthol cigarettes are more addictive than traditional cigarettes, in part because they provide a less harsh feeling in the respiratory system, owing to anti-tussive, anti-irritant, and cooling properties that act as a cough suppressant and mask irritation and pain.
“You do not feel like you’re smoking that much or that it’s dangerous, and that’s exactly the reason why it’s harder to quit,” said Julia Adamian, MD, section chief of general internal medicine and clinical innovation at NYU Langone Tisch Hospital.
In addition, menthol cigarettes interact with the body in complex ways that make quitting harder, according to a study published in Nicotine & Tobacco Research. Menthol increases the amount of nicotine that the body absorbs and thus increases the risk of dependence on the drug.
According to Dr. Choi, rates of cigar and cigarillo use are higher among Black Americans, compared with other races, and these products are often left out of cessation programs. Smokers, regardless of race, may have a misguided belief that cigars and cigarillos are less harmful than cigarettes.
Research published in 2021 found that Black cigar smokers who were interested in cessation had not been asked by their health care provider if they smoked cigars, and those who were asked reported a lack of support for cessation.
Primary care providers should work to remove any misconceptions a patient has regarding the safety of cigarillos and cigars, Dr. Choi said.
These smokers are also at a disadvantage regarding cessation success because of the neighborhoods they may live in, according to Dr. Choi. Black Americans are more likely to earn less and to live in neighborhoods with lower housing values than other racial groups. Areas with more low-income households tend to have a higher density of tobacco outlets.
“If you’re trying to quit smoking, but you walk by three, four, or five gas stations, convenience stores, and other tobacco outlets with signs that advertise sales, it’s not going to make quitting easy,” Dr. Choi said.
Tailoring treatment to Black smokers
Considering the unique challenges Black patients may face in quitting, clinicians should provide more follow-up and consistent support, according to Dr. Adamian. The higher risk of tobacco-related death among Black smokers means clinicians need to be more aggressive in recommending every treatment possible if one treatment fails.
Pharmacotherapy, nicotine replacement therapy, and counseling are evidence-based options to help patients stop smoking.
Dr. Kortsch considers pharmacotherapy to be the most effective and evidence-based treatment for nicotine addiction. However, Black Americans are less likely than White smokers to try smoking cessation medications, and they express more suspicion about efficacy and potential addiction to the tools.
“African American populations simply do not use pharmacotherapy to the extent that other populations do to help them quit smoking; this is a problem,” Dr. Kortsch said.
Dr. Kortsch recommends the use of varenicline for all patients with nicotine addiction. He recommends varenicline in combination with tobacco replacement products such as lozenges, patches, gums, or inhalers if the patient is a heavy smoker as opposed to someone who has a few cigarettes on the weekends.
If a patient has anxiety or depression, Dr. Adamian advises initiating a pharmacologic treatment such as bupropion or varenicline more quickly, because mood disorders can hinder cessation.
Cessation counseling is another option, but clinicians may need to more thoroughly explain what it entails. According to Dr. Choi, Black patients may be more reluctant to try cessation counseling because of the negative stigma associated with the term “counseling.” But this treatment is not therapy – it involves identifying and coming up with strategies to manage smoking triggers and providing encouragement. Clinicians can eliminate any confusion patients may have between psychological therapy and cessation counseling.
“ ‘Counseling’ tends to have a somewhat negative connotation among racial minority populations, like you go to counseling because you’re crazy,” Dr. Choi said. “That needs to change.”
Clinicians also must clarify how each cessation tool works. For example, some patients may not realize that the nicotine patch isn’t an instant fix for a craving and that hours may pass before the user feels its effects, according to Dr. Choi.
Move past the ‘advise’ stage
While recommending to patients various forms of cessation, clinicians should be mindful of the U.S. Preventive Services Task Force’s guidelines for providers who treat patients who smoke. Those guidelines include a five-step process: Ask, Advise, Assess, Assist, and Arrange.
Dr. Choi said most providers stop at the “Advise” stage. In steps one and two, providers ask patients whether they smoke, then advise them to quit. Stage three involves asking whether or not a patient is ready to quit and where they are in their journey.
Clinicians shouldn’t give up when patients say they do not currently plan to quit. Instead, they can use the conversation to create an ongoing dialogue about the patient’s readiness to quit in future visits. Follow-up phone calls or text messages should be made 2-4 weeks after a patient makes an attempt to quit and at the same interval thereafter, Dr. Adamian advised.
“It takes a concerted effort on behalf of all people to be successful, and it is really uncommon for someone to be successful with only one attempt,” Dr. Kortsch said.
In a recent study published in the Journal of the American Medical Association, researchers identified three key factors that influence a Black smoker’s ability to stop smoking in early attempts. These factors have been shown to increase the chances of long-term cessation: fewer cigarettes per day, nonuse of other tobacco products, and lower levels of cotinine (a nicotine metabolite) at baseline.
“Using these predictors of early treatment response could allow providers to anticipate which smokers may benefit from a minimal, low-cost intervention and who may benefit from more intensive treatment,” said Eleanor Leavens, PhD, assistant professor in the department of population health at the University of Kansas School of Medicine, Kansas City, who led the study.
Dr. Leavens’ research also confirmed that early abstinence predicts long-term cessation success. Smokers who were able to forgo cigarettes within 2 weeks of their quit date were almost four times more likely to remain abstinent over the long term.
A quick phone call or message from the clinician or a staff member can help patients achieve early progress, enable changes in approach to quitting, and build a relationship with the patient, Dr. Adamian said.
“Have more empathy for what Black patients are going through,” Dr. Choi said. “Continue to cheer them on and to be a supporter of their smoking cessation journey.”
A version of this article first appeared on Medscape.com.
Black Americans attempt to quit smoking more often than their White counterparts but are less likely to succeed, and they pay the health consequences.
This knowledge has driven Kevin Choi, MD, acting scientific director of the National Institute on Minority Health and Health Disparities in Bethesda, Md., to dedicate his career to studying the patterns and disparities of smoking among these patients.
Dr. Choi wants primary care clinicians to know not just that they have the potential to educate patients on the harms of smoking – most patients already know smoking is unhealthy – but that aiding them will likely necessitate more assertive follow-up.
To do so, “we need to understand the bigger backdrop of racial and sociological stress experienced by the Black population, which stems from both interpersonal and structural racism,” Dr. Choi said.
Not only are Black smokers more likely to try to quit, but they also tend to smoke fewer cigarettes per day than other racial groups. Yet they experience higher rates of smoking-related mortality.
The reasons behind the attempts
Multiple factors play into Black smokers’ lower rates of successful quitting attempts than Asian, Hispanic, White, and Native American individuals.
One reason: An estimated 85% of Black smokers smoke highly addictive menthol cigarettes. According to Dr. Choi and other experts, the tobacco industry engages in targeted marketing of menthols by sponsoring community events in predominantly Black neighborhoods and colleges with historically Black populations and by using Black culture in advertising.
“The built environment really drives a change in behavior, and we have seen that chronically in the African American population being overly targeted and now being overly addicted to nicotine,” said Daniel Kortsch, MD, a family medicine physician and chair of the Tobacco Cessation Workgroup at Denver Health.
Menthol cigarettes are more addictive than traditional cigarettes, in part because they provide a less harsh feeling in the respiratory system, owing to anti-tussive, anti-irritant, and cooling properties that act as a cough suppressant and mask irritation and pain.
“You do not feel like you’re smoking that much or that it’s dangerous, and that’s exactly the reason why it’s harder to quit,” said Julia Adamian, MD, section chief of general internal medicine and clinical innovation at NYU Langone Tisch Hospital.
In addition, menthol cigarettes interact with the body in complex ways that make quitting harder, according to a study published in Nicotine & Tobacco Research. Menthol increases the amount of nicotine that the body absorbs and thus increases the risk of dependence on the drug.
According to Dr. Choi, rates of cigar and cigarillo use are higher among Black Americans, compared with other races, and these products are often left out of cessation programs. Smokers, regardless of race, may have a misguided belief that cigars and cigarillos are less harmful than cigarettes.
Research published in 2021 found that Black cigar smokers who were interested in cessation had not been asked by their health care provider if they smoked cigars, and those who were asked reported a lack of support for cessation.
Primary care providers should work to remove any misconceptions a patient has regarding the safety of cigarillos and cigars, Dr. Choi said.
These smokers are also at a disadvantage regarding cessation success because of the neighborhoods they may live in, according to Dr. Choi. Black Americans are more likely to earn less and to live in neighborhoods with lower housing values than other racial groups. Areas with more low-income households tend to have a higher density of tobacco outlets.
“If you’re trying to quit smoking, but you walk by three, four, or five gas stations, convenience stores, and other tobacco outlets with signs that advertise sales, it’s not going to make quitting easy,” Dr. Choi said.
Tailoring treatment to Black smokers
Considering the unique challenges Black patients may face in quitting, clinicians should provide more follow-up and consistent support, according to Dr. Adamian. The higher risk of tobacco-related death among Black smokers means clinicians need to be more aggressive in recommending every treatment possible if one treatment fails.
Pharmacotherapy, nicotine replacement therapy, and counseling are evidence-based options to help patients stop smoking.
Dr. Kortsch considers pharmacotherapy to be the most effective and evidence-based treatment for nicotine addiction. However, Black Americans are less likely than White smokers to try smoking cessation medications, and they express more suspicion about efficacy and potential addiction to the tools.
“African American populations simply do not use pharmacotherapy to the extent that other populations do to help them quit smoking; this is a problem,” Dr. Kortsch said.
Dr. Kortsch recommends the use of varenicline for all patients with nicotine addiction. He recommends varenicline in combination with tobacco replacement products such as lozenges, patches, gums, or inhalers if the patient is a heavy smoker as opposed to someone who has a few cigarettes on the weekends.
If a patient has anxiety or depression, Dr. Adamian advises initiating a pharmacologic treatment such as bupropion or varenicline more quickly, because mood disorders can hinder cessation.
Cessation counseling is another option, but clinicians may need to more thoroughly explain what it entails. According to Dr. Choi, Black patients may be more reluctant to try cessation counseling because of the negative stigma associated with the term “counseling.” But this treatment is not therapy – it involves identifying and coming up with strategies to manage smoking triggers and providing encouragement. Clinicians can eliminate any confusion patients may have between psychological therapy and cessation counseling.
“ ‘Counseling’ tends to have a somewhat negative connotation among racial minority populations, like you go to counseling because you’re crazy,” Dr. Choi said. “That needs to change.”
Clinicians also must clarify how each cessation tool works. For example, some patients may not realize that the nicotine patch isn’t an instant fix for a craving and that hours may pass before the user feels its effects, according to Dr. Choi.
Move past the ‘advise’ stage
While recommending to patients various forms of cessation, clinicians should be mindful of the U.S. Preventive Services Task Force’s guidelines for providers who treat patients who smoke. Those guidelines include a five-step process: Ask, Advise, Assess, Assist, and Arrange.
Dr. Choi said most providers stop at the “Advise” stage. In steps one and two, providers ask patients whether they smoke, then advise them to quit. Stage three involves asking whether or not a patient is ready to quit and where they are in their journey.
Clinicians shouldn’t give up when patients say they do not currently plan to quit. Instead, they can use the conversation to create an ongoing dialogue about the patient’s readiness to quit in future visits. Follow-up phone calls or text messages should be made 2-4 weeks after a patient makes an attempt to quit and at the same interval thereafter, Dr. Adamian advised.
“It takes a concerted effort on behalf of all people to be successful, and it is really uncommon for someone to be successful with only one attempt,” Dr. Kortsch said.
In a recent study published in the Journal of the American Medical Association, researchers identified three key factors that influence a Black smoker’s ability to stop smoking in early attempts. These factors have been shown to increase the chances of long-term cessation: fewer cigarettes per day, nonuse of other tobacco products, and lower levels of cotinine (a nicotine metabolite) at baseline.
“Using these predictors of early treatment response could allow providers to anticipate which smokers may benefit from a minimal, low-cost intervention and who may benefit from more intensive treatment,” said Eleanor Leavens, PhD, assistant professor in the department of population health at the University of Kansas School of Medicine, Kansas City, who led the study.
Dr. Leavens’ research also confirmed that early abstinence predicts long-term cessation success. Smokers who were able to forgo cigarettes within 2 weeks of their quit date were almost four times more likely to remain abstinent over the long term.
A quick phone call or message from the clinician or a staff member can help patients achieve early progress, enable changes in approach to quitting, and build a relationship with the patient, Dr. Adamian said.
“Have more empathy for what Black patients are going through,” Dr. Choi said. “Continue to cheer them on and to be a supporter of their smoking cessation journey.”
A version of this article first appeared on Medscape.com.
Black Americans attempt to quit smoking more often than their White counterparts but are less likely to succeed, and they pay the health consequences.
This knowledge has driven Kevin Choi, MD, acting scientific director of the National Institute on Minority Health and Health Disparities in Bethesda, Md., to dedicate his career to studying the patterns and disparities of smoking among these patients.
Dr. Choi wants primary care clinicians to know not just that they have the potential to educate patients on the harms of smoking – most patients already know smoking is unhealthy – but that aiding them will likely necessitate more assertive follow-up.
To do so, “we need to understand the bigger backdrop of racial and sociological stress experienced by the Black population, which stems from both interpersonal and structural racism,” Dr. Choi said.
Not only are Black smokers more likely to try to quit, but they also tend to smoke fewer cigarettes per day than other racial groups. Yet they experience higher rates of smoking-related mortality.
The reasons behind the attempts
Multiple factors play into Black smokers’ lower rates of successful quitting attempts than Asian, Hispanic, White, and Native American individuals.
One reason: An estimated 85% of Black smokers smoke highly addictive menthol cigarettes. According to Dr. Choi and other experts, the tobacco industry engages in targeted marketing of menthols by sponsoring community events in predominantly Black neighborhoods and colleges with historically Black populations and by using Black culture in advertising.
“The built environment really drives a change in behavior, and we have seen that chronically in the African American population being overly targeted and now being overly addicted to nicotine,” said Daniel Kortsch, MD, a family medicine physician and chair of the Tobacco Cessation Workgroup at Denver Health.
Menthol cigarettes are more addictive than traditional cigarettes, in part because they provide a less harsh feeling in the respiratory system, owing to anti-tussive, anti-irritant, and cooling properties that act as a cough suppressant and mask irritation and pain.
“You do not feel like you’re smoking that much or that it’s dangerous, and that’s exactly the reason why it’s harder to quit,” said Julia Adamian, MD, section chief of general internal medicine and clinical innovation at NYU Langone Tisch Hospital.
In addition, menthol cigarettes interact with the body in complex ways that make quitting harder, according to a study published in Nicotine & Tobacco Research. Menthol increases the amount of nicotine that the body absorbs and thus increases the risk of dependence on the drug.
According to Dr. Choi, rates of cigar and cigarillo use are higher among Black Americans, compared with other races, and these products are often left out of cessation programs. Smokers, regardless of race, may have a misguided belief that cigars and cigarillos are less harmful than cigarettes.
Research published in 2021 found that Black cigar smokers who were interested in cessation had not been asked by their health care provider if they smoked cigars, and those who were asked reported a lack of support for cessation.
Primary care providers should work to remove any misconceptions a patient has regarding the safety of cigarillos and cigars, Dr. Choi said.
These smokers are also at a disadvantage regarding cessation success because of the neighborhoods they may live in, according to Dr. Choi. Black Americans are more likely to earn less and to live in neighborhoods with lower housing values than other racial groups. Areas with more low-income households tend to have a higher density of tobacco outlets.
“If you’re trying to quit smoking, but you walk by three, four, or five gas stations, convenience stores, and other tobacco outlets with signs that advertise sales, it’s not going to make quitting easy,” Dr. Choi said.
Tailoring treatment to Black smokers
Considering the unique challenges Black patients may face in quitting, clinicians should provide more follow-up and consistent support, according to Dr. Adamian. The higher risk of tobacco-related death among Black smokers means clinicians need to be more aggressive in recommending every treatment possible if one treatment fails.
Pharmacotherapy, nicotine replacement therapy, and counseling are evidence-based options to help patients stop smoking.
Dr. Kortsch considers pharmacotherapy to be the most effective and evidence-based treatment for nicotine addiction. However, Black Americans are less likely than White smokers to try smoking cessation medications, and they express more suspicion about efficacy and potential addiction to the tools.
“African American populations simply do not use pharmacotherapy to the extent that other populations do to help them quit smoking; this is a problem,” Dr. Kortsch said.
Dr. Kortsch recommends the use of varenicline for all patients with nicotine addiction. He recommends varenicline in combination with tobacco replacement products such as lozenges, patches, gums, or inhalers if the patient is a heavy smoker as opposed to someone who has a few cigarettes on the weekends.
If a patient has anxiety or depression, Dr. Adamian advises initiating a pharmacologic treatment such as bupropion or varenicline more quickly, because mood disorders can hinder cessation.
Cessation counseling is another option, but clinicians may need to more thoroughly explain what it entails. According to Dr. Choi, Black patients may be more reluctant to try cessation counseling because of the negative stigma associated with the term “counseling.” But this treatment is not therapy – it involves identifying and coming up with strategies to manage smoking triggers and providing encouragement. Clinicians can eliminate any confusion patients may have between psychological therapy and cessation counseling.
“ ‘Counseling’ tends to have a somewhat negative connotation among racial minority populations, like you go to counseling because you’re crazy,” Dr. Choi said. “That needs to change.”
Clinicians also must clarify how each cessation tool works. For example, some patients may not realize that the nicotine patch isn’t an instant fix for a craving and that hours may pass before the user feels its effects, according to Dr. Choi.
Move past the ‘advise’ stage
While recommending to patients various forms of cessation, clinicians should be mindful of the U.S. Preventive Services Task Force’s guidelines for providers who treat patients who smoke. Those guidelines include a five-step process: Ask, Advise, Assess, Assist, and Arrange.
Dr. Choi said most providers stop at the “Advise” stage. In steps one and two, providers ask patients whether they smoke, then advise them to quit. Stage three involves asking whether or not a patient is ready to quit and where they are in their journey.
Clinicians shouldn’t give up when patients say they do not currently plan to quit. Instead, they can use the conversation to create an ongoing dialogue about the patient’s readiness to quit in future visits. Follow-up phone calls or text messages should be made 2-4 weeks after a patient makes an attempt to quit and at the same interval thereafter, Dr. Adamian advised.
“It takes a concerted effort on behalf of all people to be successful, and it is really uncommon for someone to be successful with only one attempt,” Dr. Kortsch said.
In a recent study published in the Journal of the American Medical Association, researchers identified three key factors that influence a Black smoker’s ability to stop smoking in early attempts. These factors have been shown to increase the chances of long-term cessation: fewer cigarettes per day, nonuse of other tobacco products, and lower levels of cotinine (a nicotine metabolite) at baseline.
“Using these predictors of early treatment response could allow providers to anticipate which smokers may benefit from a minimal, low-cost intervention and who may benefit from more intensive treatment,” said Eleanor Leavens, PhD, assistant professor in the department of population health at the University of Kansas School of Medicine, Kansas City, who led the study.
Dr. Leavens’ research also confirmed that early abstinence predicts long-term cessation success. Smokers who were able to forgo cigarettes within 2 weeks of their quit date were almost four times more likely to remain abstinent over the long term.
A quick phone call or message from the clinician or a staff member can help patients achieve early progress, enable changes in approach to quitting, and build a relationship with the patient, Dr. Adamian said.
“Have more empathy for what Black patients are going through,” Dr. Choi said. “Continue to cheer them on and to be a supporter of their smoking cessation journey.”
A version of this article first appeared on Medscape.com.
LSD use triples among young adults with depression
TOPLINE:
The increase was especially high among young adults and those earning less than $75,000 a year.
METHODOLOGY:
- Investigators analyzed responses of 478,500 adult respondents to the NSDUH, a cross-sectional, in-person survey administered by the Substance Abuse and Mental Health Services Administration between 2008 and 2019.
- Respondents were questioned about past-month and past-year LSD use and past-year depression.
- Investigators conducted statistical analysis between December 2022 and June 2023.
TAKEAWAY:
- Past-year use of LSD increased significantly more among adults with major depression, increasing from 0.5% in 2008 to 1.8% in 2019 (prevalence difference, 1.3% [95% confidence interval, 1.0%-1.6%]) compared with adults without major depression.
- This difference was particularly pronounced among young adults with depression age 34 years or younger (PD for age 18-25 years, 3.3% [95% CI, 2.5%-4.2%]; PD for age 26-34 years, 2.7% [95% CI, 1.6%-3.8%]).
- The increase was also higher among those earning less than $75,000 per year (PD for < $20,000, 1.9% [95% CI, 1.3%-2.6%]; PD for $20,000-$49,999, 1.5% [95% CI, 1.0%-2.1%]; PD for $50,000-$74,999, 1.3% [95% CI, 0.7%-2.0%]).
- Use of other hallucinogen classes either decreased or increased only among select age groups or time frames; the use of LSD consistently increased among every observed age group from 2002 to 2019.
IN PRACTICE:
“Future research should aim to understand the motivations for LSD use as well as the directionality between nonmedical LSD use and depression. As the evaluation of LSD as a potential psychiatric treatment continues, public health efforts to promote safe and evidence-based use of psychedelics are critical,” the investigators write.
SOURCE:

The study was led by Deborah S. Hasin, PhD, of Columbia University’s department of psychiatry, New York, and published online in JAMA Psychiatry.
LIMITATIONS:
Study limitations include the use of self-reporting measures in the NSDUH and the lack of information about motives for or doses of LSD use.
DISCLOSURES:
The authors have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
TOPLINE:
The increase was especially high among young adults and those earning less than $75,000 a year.
METHODOLOGY:
- Investigators analyzed responses of 478,500 adult respondents to the NSDUH, a cross-sectional, in-person survey administered by the Substance Abuse and Mental Health Services Administration between 2008 and 2019.
- Respondents were questioned about past-month and past-year LSD use and past-year depression.
- Investigators conducted statistical analysis between December 2022 and June 2023.
TAKEAWAY:
- Past-year use of LSD increased significantly more among adults with major depression, increasing from 0.5% in 2008 to 1.8% in 2019 (prevalence difference, 1.3% [95% confidence interval, 1.0%-1.6%]) compared with adults without major depression.
- This difference was particularly pronounced among young adults with depression age 34 years or younger (PD for age 18-25 years, 3.3% [95% CI, 2.5%-4.2%]; PD for age 26-34 years, 2.7% [95% CI, 1.6%-3.8%]).
- The increase was also higher among those earning less than $75,000 per year (PD for < $20,000, 1.9% [95% CI, 1.3%-2.6%]; PD for $20,000-$49,999, 1.5% [95% CI, 1.0%-2.1%]; PD for $50,000-$74,999, 1.3% [95% CI, 0.7%-2.0%]).
- Use of other hallucinogen classes either decreased or increased only among select age groups or time frames; the use of LSD consistently increased among every observed age group from 2002 to 2019.
IN PRACTICE:
“Future research should aim to understand the motivations for LSD use as well as the directionality between nonmedical LSD use and depression. As the evaluation of LSD as a potential psychiatric treatment continues, public health efforts to promote safe and evidence-based use of psychedelics are critical,” the investigators write.
SOURCE:
The study was led by Deborah S. Hasin, PhD, of Columbia University’s department of psychiatry, New York, and published online in JAMA Psychiatry.
LIMITATIONS:
Study limitations include the use of self-reporting measures in the NSDUH and the lack of information about motives for or doses of LSD use.
DISCLOSURES:
The authors have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
TOPLINE:
The increase was especially high among young adults and those earning less than $75,000 a year.
METHODOLOGY:
- Investigators analyzed responses of 478,500 adult respondents to the NSDUH, a cross-sectional, in-person survey administered by the Substance Abuse and Mental Health Services Administration between 2008 and 2019.
- Respondents were questioned about past-month and past-year LSD use and past-year depression.
- Investigators conducted statistical analysis between December 2022 and June 2023.
TAKEAWAY:
- Past-year use of LSD increased significantly more among adults with major depression, increasing from 0.5% in 2008 to 1.8% in 2019 (prevalence difference, 1.3% [95% confidence interval, 1.0%-1.6%]) compared with adults without major depression.
- This difference was particularly pronounced among young adults with depression age 34 years or younger (PD for age 18-25 years, 3.3% [95% CI, 2.5%-4.2%]; PD for age 26-34 years, 2.7% [95% CI, 1.6%-3.8%]).
- The increase was also higher among those earning less than $75,000 per year (PD for < $20,000, 1.9% [95% CI, 1.3%-2.6%]; PD for $20,000-$49,999, 1.5% [95% CI, 1.0%-2.1%]; PD for $50,000-$74,999, 1.3% [95% CI, 0.7%-2.0%]).
- Use of other hallucinogen classes either decreased or increased only among select age groups or time frames; the use of LSD consistently increased among every observed age group from 2002 to 2019.
IN PRACTICE:
“Future research should aim to understand the motivations for LSD use as well as the directionality between nonmedical LSD use and depression. As the evaluation of LSD as a potential psychiatric treatment continues, public health efforts to promote safe and evidence-based use of psychedelics are critical,” the investigators write.
SOURCE:
The study was led by Deborah S. Hasin, PhD, of Columbia University’s department of psychiatry, New York, and published online in JAMA Psychiatry.
LIMITATIONS:
Study limitations include the use of self-reporting measures in the NSDUH and the lack of information about motives for or doses of LSD use.
DISCLOSURES:
The authors have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM JAMA PSYCHIATRY
Why legal pot makes this physician sick
Last year, my husband and I took a 16-day road trip from Kentucky through Massachusetts to Maine. On our first morning in Boston, we exited the Park Street Station en route to Boston Common, but instead of being greeted by the aroma of molasses, we were hit full-on with a pungent, repulsive odor. “That’s skunk weed,” my husband chuckled as we stepped right into the middle of the Boston Freedom Rally, a celebration of all things cannabis.
As we boarded a hop-on-hop-off bus, we learned that this was the one week of the year that the city skips testing tour bus drivers for tetrahydrocannabinol (THC), “because we all test positive,” the driver quipped. As our open-air bus circled the Common, a crowd of pot enthusiasts displayed signs in support of relaxed regulation for public consumption.
The 34-year-old Boston Freedom Rally is a sign that U.S. culture has transformed forever. Mary Jane is no friend of emergency physicians nor of staff on hospital wards and offices.
Toking boomers and millennials
Researchers at the University of California, San Diego, looked at cannabis-related emergency department visits from all acute-care hospitals in the state from 2005 to 2019 and found an 1,808% increase in patients aged 65 or older (that is not a typo) who were there for complications from cannabis use.
The lead author said in an interview that, “older patients taking marijuana or related products may have dizziness and falls, heart palpitations, panic attacks, confusion, anxiety or worsening of underlying lung diseases, such as asthma or [chronic obstructive pulmonary disease].”
A recent study from Canada suggests that commercialization has been associated with an increase in related hospitalizations, including cannabis-induced psychosis.
According to a National Study of Drug Use and Health, marijuana use in young adults reached an all-time high (pun intended) in 2021. Nearly 10% of eighth graders and 20% of 10th graders reported using marijuana this past year.
The full downside of any drug, legal or illegal, is largely unknown until it infiltrates the mainstream market, but these are the typical cases we see:
Let’s start with the demotivated high school honors student who dropped out of college to work at the local cinema. He stumbled and broke his clavicle outside a bar at 2 AM, but he wasn’t sure if he passed out, so a cardiology consult was requested to “rule out” arrhythmia associated with syncope. He related that his plan to become a railway conductor had been upended because he knew he would be drug tested and just couldn’t give up pot. After a normal cardiac exam, ECG, labs, a Holter, and an echocardiogram were also requested and normal at a significant cost.
Cannabinoid hyperemesis syndrome
One of my Midwest colleagues related her encounter with two middle-aged pot users with ventricular tachycardia (VT). These episodes coincided with potassium levels less than 3.0 mEq/L in the setting of repetitive vomiting. The QTc interval didn’t normalize despite a corrected potassium level in one patient. They were both informed that they should never smoke pot because vomiting would predictably drop their K+ levels again and prolong their QTc intervals. Then began “the circular argument,” as my friend described it. The patient claims, “I smoke pot to relieve my nausea,” to which she explains that “in many folks, pot use induces nausea.” Of course, the classic reply is, “Not me.” Predictably one of these stoners soon returned with more VT, more puking, and more hypokalemia. “Consider yourself ‘allergic’ to pot smoke,” my friend advised, but “was met with no meaningful hint of understanding or hope for transformative change,” she told me.
I’ve seen cannabinoid hyperemesis syndrome several times in the past few years. It occurs in daily to weekly pot users. Very rarely, it can cause cerebral edema, but it is also associated with seizures and dehydration that can lead to hypovolemic shock and kidney failure.
Heart and brain harm
Then there are the young patients who for various reasons have developed heart failure. Unfortunately, some are repetitively tox screen positive with varying trifectas of methamphetamine (meth), cocaine, and THC; opiates, meth, and THC; alcohol, meth, and THC; or heroin, meth, and THC. THC, the ever present and essential third leg of the stool of stupor. These unfortunate patients often need heart failure medications that they can’t afford or won’t take because illicit drug use is expensive and dulls their ability to prioritize their health. Some desperately need a heart transplant, but the necessary negative drug screen is a pipe dream.
And it’s not just the heart that is affected. There are data linking cannabis use to a higher risk for both ischemic and hemorrhagic stroke. A retrospective study published in Stroke, of more than 1,000 people diagnosed with an aneurysmal subarachnoid hemorrhage, found that more than half of the 46 who tested positive for THC at admission developed delayed cerebral ischemia (DCI), which increases the risk for disability or early death. This was after adjusting for several patient characteristics as well as recent exposure to other illicit substances; cocaine, meth, and tobacco use were not associated with DCI.
Natural my ...
I’m certain my anti-cannabis stance will strike a nerve with those who love their recreational THC and push for its legal sale; after all, “It’s perfectly natural.” But I counter with the fact that tornadoes, earthquakes, cyanide, and appendicitis are all natural but certainly not optimal. And what we are seeing in the vascular specialties is completely unnatural. We are treating a different mix of complications than before pot was readily accessible across several states.
Our most effective action is to educate our patients. We should encourage those who don’t currently smoke cannabis to never start and those who do to quit. People who require marijuana for improved quality of life for terminal care or true (not supposed) disorders that mainstream medicine fails should be approached with empathy and caution.
A good rule of thumb is to never breathe anything you can see. Never put anything in your body that comes off the street: Drug dealers who sell cannabis cut with fentanyl will be ecstatic to take someone’s money then merely keep scrolling when their obituary comes up.
Let’s try to reverse the rise of vascular complications, orthopedic injuries, and vomiting across America. We can start by encouraging our patients to avoid “skunk weed” and get back to the sweet smells of nature in our cities and parks.
Some details have been changed to protect the patients’ identities, but the essence of their diagnoses has been preserved.
Dr. Walton-Shirley is a retired clinical cardiologist from Nashville, Tenn. She disclosed no relevant conflicts of interest.
A version of this article first appeared on Medscape.com.
Last year, my husband and I took a 16-day road trip from Kentucky through Massachusetts to Maine. On our first morning in Boston, we exited the Park Street Station en route to Boston Common, but instead of being greeted by the aroma of molasses, we were hit full-on with a pungent, repulsive odor. “That’s skunk weed,” my husband chuckled as we stepped right into the middle of the Boston Freedom Rally, a celebration of all things cannabis.
As we boarded a hop-on-hop-off bus, we learned that this was the one week of the year that the city skips testing tour bus drivers for tetrahydrocannabinol (THC), “because we all test positive,” the driver quipped. As our open-air bus circled the Common, a crowd of pot enthusiasts displayed signs in support of relaxed regulation for public consumption.
The 34-year-old Boston Freedom Rally is a sign that U.S. culture has transformed forever. Mary Jane is no friend of emergency physicians nor of staff on hospital wards and offices.
Toking boomers and millennials
Researchers at the University of California, San Diego, looked at cannabis-related emergency department visits from all acute-care hospitals in the state from 2005 to 2019 and found an 1,808% increase in patients aged 65 or older (that is not a typo) who were there for complications from cannabis use.
The lead author said in an interview that, “older patients taking marijuana or related products may have dizziness and falls, heart palpitations, panic attacks, confusion, anxiety or worsening of underlying lung diseases, such as asthma or [chronic obstructive pulmonary disease].”
A recent study from Canada suggests that commercialization has been associated with an increase in related hospitalizations, including cannabis-induced psychosis.
According to a National Study of Drug Use and Health, marijuana use in young adults reached an all-time high (pun intended) in 2021. Nearly 10% of eighth graders and 20% of 10th graders reported using marijuana this past year.
The full downside of any drug, legal or illegal, is largely unknown until it infiltrates the mainstream market, but these are the typical cases we see:
Let’s start with the demotivated high school honors student who dropped out of college to work at the local cinema. He stumbled and broke his clavicle outside a bar at 2 AM, but he wasn’t sure if he passed out, so a cardiology consult was requested to “rule out” arrhythmia associated with syncope. He related that his plan to become a railway conductor had been upended because he knew he would be drug tested and just couldn’t give up pot. After a normal cardiac exam, ECG, labs, a Holter, and an echocardiogram were also requested and normal at a significant cost.
Cannabinoid hyperemesis syndrome
One of my Midwest colleagues related her encounter with two middle-aged pot users with ventricular tachycardia (VT). These episodes coincided with potassium levels less than 3.0 mEq/L in the setting of repetitive vomiting. The QTc interval didn’t normalize despite a corrected potassium level in one patient. They were both informed that they should never smoke pot because vomiting would predictably drop their K+ levels again and prolong their QTc intervals. Then began “the circular argument,” as my friend described it. The patient claims, “I smoke pot to relieve my nausea,” to which she explains that “in many folks, pot use induces nausea.” Of course, the classic reply is, “Not me.” Predictably one of these stoners soon returned with more VT, more puking, and more hypokalemia. “Consider yourself ‘allergic’ to pot smoke,” my friend advised, but “was met with no meaningful hint of understanding or hope for transformative change,” she told me.
I’ve seen cannabinoid hyperemesis syndrome several times in the past few years. It occurs in daily to weekly pot users. Very rarely, it can cause cerebral edema, but it is also associated with seizures and dehydration that can lead to hypovolemic shock and kidney failure.
Heart and brain harm
Then there are the young patients who for various reasons have developed heart failure. Unfortunately, some are repetitively tox screen positive with varying trifectas of methamphetamine (meth), cocaine, and THC; opiates, meth, and THC; alcohol, meth, and THC; or heroin, meth, and THC. THC, the ever present and essential third leg of the stool of stupor. These unfortunate patients often need heart failure medications that they can’t afford or won’t take because illicit drug use is expensive and dulls their ability to prioritize their health. Some desperately need a heart transplant, but the necessary negative drug screen is a pipe dream.
And it’s not just the heart that is affected. There are data linking cannabis use to a higher risk for both ischemic and hemorrhagic stroke. A retrospective study published in Stroke, of more than 1,000 people diagnosed with an aneurysmal subarachnoid hemorrhage, found that more than half of the 46 who tested positive for THC at admission developed delayed cerebral ischemia (DCI), which increases the risk for disability or early death. This was after adjusting for several patient characteristics as well as recent exposure to other illicit substances; cocaine, meth, and tobacco use were not associated with DCI.
Natural my ...
I’m certain my anti-cannabis stance will strike a nerve with those who love their recreational THC and push for its legal sale; after all, “It’s perfectly natural.” But I counter with the fact that tornadoes, earthquakes, cyanide, and appendicitis are all natural but certainly not optimal. And what we are seeing in the vascular specialties is completely unnatural. We are treating a different mix of complications than before pot was readily accessible across several states.
Our most effective action is to educate our patients. We should encourage those who don’t currently smoke cannabis to never start and those who do to quit. People who require marijuana for improved quality of life for terminal care or true (not supposed) disorders that mainstream medicine fails should be approached with empathy and caution.
A good rule of thumb is to never breathe anything you can see. Never put anything in your body that comes off the street: Drug dealers who sell cannabis cut with fentanyl will be ecstatic to take someone’s money then merely keep scrolling when their obituary comes up.
Let’s try to reverse the rise of vascular complications, orthopedic injuries, and vomiting across America. We can start by encouraging our patients to avoid “skunk weed” and get back to the sweet smells of nature in our cities and parks.
Some details have been changed to protect the patients’ identities, but the essence of their diagnoses has been preserved.
Dr. Walton-Shirley is a retired clinical cardiologist from Nashville, Tenn. She disclosed no relevant conflicts of interest.
A version of this article first appeared on Medscape.com.
Last year, my husband and I took a 16-day road trip from Kentucky through Massachusetts to Maine. On our first morning in Boston, we exited the Park Street Station en route to Boston Common, but instead of being greeted by the aroma of molasses, we were hit full-on with a pungent, repulsive odor. “That’s skunk weed,” my husband chuckled as we stepped right into the middle of the Boston Freedom Rally, a celebration of all things cannabis.
As we boarded a hop-on-hop-off bus, we learned that this was the one week of the year that the city skips testing tour bus drivers for tetrahydrocannabinol (THC), “because we all test positive,” the driver quipped. As our open-air bus circled the Common, a crowd of pot enthusiasts displayed signs in support of relaxed regulation for public consumption.
The 34-year-old Boston Freedom Rally is a sign that U.S. culture has transformed forever. Mary Jane is no friend of emergency physicians nor of staff on hospital wards and offices.
Toking boomers and millennials
Researchers at the University of California, San Diego, looked at cannabis-related emergency department visits from all acute-care hospitals in the state from 2005 to 2019 and found an 1,808% increase in patients aged 65 or older (that is not a typo) who were there for complications from cannabis use.
The lead author said in an interview that, “older patients taking marijuana or related products may have dizziness and falls, heart palpitations, panic attacks, confusion, anxiety or worsening of underlying lung diseases, such as asthma or [chronic obstructive pulmonary disease].”
A recent study from Canada suggests that commercialization has been associated with an increase in related hospitalizations, including cannabis-induced psychosis.
According to a National Study of Drug Use and Health, marijuana use in young adults reached an all-time high (pun intended) in 2021. Nearly 10% of eighth graders and 20% of 10th graders reported using marijuana this past year.
The full downside of any drug, legal or illegal, is largely unknown until it infiltrates the mainstream market, but these are the typical cases we see:
Let’s start with the demotivated high school honors student who dropped out of college to work at the local cinema. He stumbled and broke his clavicle outside a bar at 2 AM, but he wasn’t sure if he passed out, so a cardiology consult was requested to “rule out” arrhythmia associated with syncope. He related that his plan to become a railway conductor had been upended because he knew he would be drug tested and just couldn’t give up pot. After a normal cardiac exam, ECG, labs, a Holter, and an echocardiogram were also requested and normal at a significant cost.
Cannabinoid hyperemesis syndrome
One of my Midwest colleagues related her encounter with two middle-aged pot users with ventricular tachycardia (VT). These episodes coincided with potassium levels less than 3.0 mEq/L in the setting of repetitive vomiting. The QTc interval didn’t normalize despite a corrected potassium level in one patient. They were both informed that they should never smoke pot because vomiting would predictably drop their K+ levels again and prolong their QTc intervals. Then began “the circular argument,” as my friend described it. The patient claims, “I smoke pot to relieve my nausea,” to which she explains that “in many folks, pot use induces nausea.” Of course, the classic reply is, “Not me.” Predictably one of these stoners soon returned with more VT, more puking, and more hypokalemia. “Consider yourself ‘allergic’ to pot smoke,” my friend advised, but “was met with no meaningful hint of understanding or hope for transformative change,” she told me.
I’ve seen cannabinoid hyperemesis syndrome several times in the past few years. It occurs in daily to weekly pot users. Very rarely, it can cause cerebral edema, but it is also associated with seizures and dehydration that can lead to hypovolemic shock and kidney failure.
Heart and brain harm
Then there are the young patients who for various reasons have developed heart failure. Unfortunately, some are repetitively tox screen positive with varying trifectas of methamphetamine (meth), cocaine, and THC; opiates, meth, and THC; alcohol, meth, and THC; or heroin, meth, and THC. THC, the ever present and essential third leg of the stool of stupor. These unfortunate patients often need heart failure medications that they can’t afford or won’t take because illicit drug use is expensive and dulls their ability to prioritize their health. Some desperately need a heart transplant, but the necessary negative drug screen is a pipe dream.
And it’s not just the heart that is affected. There are data linking cannabis use to a higher risk for both ischemic and hemorrhagic stroke. A retrospective study published in Stroke, of more than 1,000 people diagnosed with an aneurysmal subarachnoid hemorrhage, found that more than half of the 46 who tested positive for THC at admission developed delayed cerebral ischemia (DCI), which increases the risk for disability or early death. This was after adjusting for several patient characteristics as well as recent exposure to other illicit substances; cocaine, meth, and tobacco use were not associated with DCI.
Natural my ...
I’m certain my anti-cannabis stance will strike a nerve with those who love their recreational THC and push for its legal sale; after all, “It’s perfectly natural.” But I counter with the fact that tornadoes, earthquakes, cyanide, and appendicitis are all natural but certainly not optimal. And what we are seeing in the vascular specialties is completely unnatural. We are treating a different mix of complications than before pot was readily accessible across several states.
Our most effective action is to educate our patients. We should encourage those who don’t currently smoke cannabis to never start and those who do to quit. People who require marijuana for improved quality of life for terminal care or true (not supposed) disorders that mainstream medicine fails should be approached with empathy and caution.
A good rule of thumb is to never breathe anything you can see. Never put anything in your body that comes off the street: Drug dealers who sell cannabis cut with fentanyl will be ecstatic to take someone’s money then merely keep scrolling when their obituary comes up.
Let’s try to reverse the rise of vascular complications, orthopedic injuries, and vomiting across America. We can start by encouraging our patients to avoid “skunk weed” and get back to the sweet smells of nature in our cities and parks.
Some details have been changed to protect the patients’ identities, but the essence of their diagnoses has been preserved.
Dr. Walton-Shirley is a retired clinical cardiologist from Nashville, Tenn. She disclosed no relevant conflicts of interest.
A version of this article first appeared on Medscape.com.
Cannabis use growing among menopausal women
PHILADELPHIA – presented at the annual meeting of the Menopause Society (formerly The North American Menopause Society).
Though most women reported using cannabis for recreational reasons, 13% used it only for medical reasons, most often for chronic pain, anxiety, sleep, and stress.
“These findings highlight the importance of recognizing and discussing cannabis use in the health care setting, and the need for additional research to evaluate the potential harms and/or benefits of use in this vulnerable population,” Carolyn J. Gibson, PhD, MPH, a staff psychologist in women’s health at the San Francisco VA Health Care System and an assistant professor of psychiatry and behavioral sciences at the University of California, San Francisco, told attendees.
As cannabis has become more accessible, with its use legalized in 38 states and Washington, D.C., the proportion of U.S. adults using it has doubled over about a decade, from 6% in 2007 to 12% in 2019, Dr. Gibson said. Further, women aged 50 and older are among the fastest-growing groups of users of cannabis, and it’s being increasingly used – and marketed – for treating menopause-related and aging-related symptoms, including insomnia, anxiety, and chronic pain, she said.
“With these decisions to use cannabis, medically or for these other purposes, there’s this perception that it’s harmless,” Dr. Gibson said. Yet potential health risks associated with cannabis include the usual health effects associated with any kind of smoking as well as dependence in those who use it more frequently and/or develop a tolerance for it. She noted that average THC potency has increased over time, and acute risks for using cannabis with high levels of THC – at least 15% or at least 10 mg – can include anxiety/panic, confusion, disturbing/intrusive thoughts, psychosis, and effects on coordination and cognition. She also acknowledged, however, that most of the data available on risks come from studies of men and younger adults rather than older women.
Given the growing normalization of cannabis use, Dr. Gibson’s team sought to better understand prevalence of use as well as types of use and reasons for use in perimenopasual and postmenopausal women. They analyzed data from a cross-sectional survey of women and gender-diverse members, aged 45-64, of Ipsos KnowledgePanel, an online panel with more than 60,000 participating members in the United States.
All the respondents identified themselves as female at birth and had not used gender-affirming therapy or undergone gender-affirming surgery. The survey included questions on sociodemographics, menopause status, frequency of cannabis use, types of cannabis used, reasons for using cannabis, and use of cannabis in the previous 30 days. The 5,174 respondents were an average 55 years old and predominantly non-Hispanic white (63%), with 13% non-Hispanic Black and 16% Hispanic. Two-thirds of the women reported working full- or part-time (67%) and two-thirds were postmenopausal (68%), with 64% reporting experiencing menopause symptoms.
About two in five respondents (42%) had ever used cannabis in any form, most often smoking it (83%) or consuming edibles (51%). Among those who had ever used it, 30% reported having smoked it daily or nearly daily for at least a year at some point.
Ten percent of respondents had used cannabis in the past month, again primarily smoking (56%) or edibles (52%), though 39% said they used it in more than one form, including vaping, dabbing, or topical use. Nearly half (46%) of the respondents who smoked cannabis recently did not know the THC potency of what they consumed, and just over 20% of those consuming edibles didn’t know the THC potency of what they used. However, about a third of those taking edibles used cannabis with less than 10 mg of THC, and a little over a quarter used edibles with 10 mg of THC.
Within the 10% who had used cannabis in the past month, nearly a third (31%) of respondents – or around 3.1% of the total sample – reported smoking cannabis daily or almost daily, and 19% (or 1.9% of the overall sample) consumed cannabis edibles daily or almost daily.
Most of the respondents who used cannabis said it was for recreational use (62%), but a quarter (25%) reported using it for both recreational and medical reasons, and 13% used it only for medical reasons. The most common reason women used cannabis was to treat chronic pain (28%), followed by nearly as many women reporting cannabis use for anxiety (24%), sleep (22%), and stress (22%). Six percent of women used cannabis specifically for menopause-related sleep and mood problems.
Given the growing use of cannabis in this population and the dearth of data on its effects in older women, Dr. Gibson highlighted the need for research examining the potential benefits and harms of cannabis for menopausal women.
Not risk-free
Susan D. Reed, MD, MPH, MSCP, a professor emeritus of ob.gyn. at the University of Washington, Seattle, and president of the Menopause Society, found the study well-executed and was not surprised by how many respondents had ever used cannabis.

“What did surprise me was that nearly a third reported daily use for at least 1 year and that 38% were medical marijuana users, not just recreational,” Dr. Reed said in an interview. The proportions of women using cannabis for menopausal symptoms or using it daily are concerning, she added.
“These individuals are at risk for dependence and health risks related to marijuana use,” Dr. Reed said. “Providers should always ask patients about OTC products, herbals, supplements, cannabis use, and alternative management of menopausal symptoms to better understand patient preferences for menopausal symptom therapies, so that treatment plans can be discussed with individual patient preferences in mind. We need to start with where the patient is coming from.”
Data presented throughout the conference has shown how people are “disillusioned with the care they are receiving for menopause,” Dr. Reed added. “It is so difficult to distinguish truth from myths based on information gained through social media, family, and friends, and that often is where most people are getting their information.”
Physicians often have not received adequate training on how to provide people with accurate information about menopause and managing menopausal symptoms, so she advises patients and physicians to visit reliable sites such as the Menopause Society, the Swan Study, and My Menoplan.
The research was funded by the Tobacco-Related Disease Research Program and the Veterans Administration. Dr. Gibson has provided unpaid consultation to Astellas Pharmaceuticals. Dr. Reed has received research support from Bayer and receives royalties from UpToDate.
PHILADELPHIA – presented at the annual meeting of the Menopause Society (formerly The North American Menopause Society).
Though most women reported using cannabis for recreational reasons, 13% used it only for medical reasons, most often for chronic pain, anxiety, sleep, and stress.
“These findings highlight the importance of recognizing and discussing cannabis use in the health care setting, and the need for additional research to evaluate the potential harms and/or benefits of use in this vulnerable population,” Carolyn J. Gibson, PhD, MPH, a staff psychologist in women’s health at the San Francisco VA Health Care System and an assistant professor of psychiatry and behavioral sciences at the University of California, San Francisco, told attendees.
As cannabis has become more accessible, with its use legalized in 38 states and Washington, D.C., the proportion of U.S. adults using it has doubled over about a decade, from 6% in 2007 to 12% in 2019, Dr. Gibson said. Further, women aged 50 and older are among the fastest-growing groups of users of cannabis, and it’s being increasingly used – and marketed – for treating menopause-related and aging-related symptoms, including insomnia, anxiety, and chronic pain, she said.
“With these decisions to use cannabis, medically or for these other purposes, there’s this perception that it’s harmless,” Dr. Gibson said. Yet potential health risks associated with cannabis include the usual health effects associated with any kind of smoking as well as dependence in those who use it more frequently and/or develop a tolerance for it. She noted that average THC potency has increased over time, and acute risks for using cannabis with high levels of THC – at least 15% or at least 10 mg – can include anxiety/panic, confusion, disturbing/intrusive thoughts, psychosis, and effects on coordination and cognition. She also acknowledged, however, that most of the data available on risks come from studies of men and younger adults rather than older women.
Given the growing normalization of cannabis use, Dr. Gibson’s team sought to better understand prevalence of use as well as types of use and reasons for use in perimenopasual and postmenopausal women. They analyzed data from a cross-sectional survey of women and gender-diverse members, aged 45-64, of Ipsos KnowledgePanel, an online panel with more than 60,000 participating members in the United States.
All the respondents identified themselves as female at birth and had not used gender-affirming therapy or undergone gender-affirming surgery. The survey included questions on sociodemographics, menopause status, frequency of cannabis use, types of cannabis used, reasons for using cannabis, and use of cannabis in the previous 30 days. The 5,174 respondents were an average 55 years old and predominantly non-Hispanic white (63%), with 13% non-Hispanic Black and 16% Hispanic. Two-thirds of the women reported working full- or part-time (67%) and two-thirds were postmenopausal (68%), with 64% reporting experiencing menopause symptoms.
About two in five respondents (42%) had ever used cannabis in any form, most often smoking it (83%) or consuming edibles (51%). Among those who had ever used it, 30% reported having smoked it daily or nearly daily for at least a year at some point.
Ten percent of respondents had used cannabis in the past month, again primarily smoking (56%) or edibles (52%), though 39% said they used it in more than one form, including vaping, dabbing, or topical use. Nearly half (46%) of the respondents who smoked cannabis recently did not know the THC potency of what they consumed, and just over 20% of those consuming edibles didn’t know the THC potency of what they used. However, about a third of those taking edibles used cannabis with less than 10 mg of THC, and a little over a quarter used edibles with 10 mg of THC.
Within the 10% who had used cannabis in the past month, nearly a third (31%) of respondents – or around 3.1% of the total sample – reported smoking cannabis daily or almost daily, and 19% (or 1.9% of the overall sample) consumed cannabis edibles daily or almost daily.
Most of the respondents who used cannabis said it was for recreational use (62%), but a quarter (25%) reported using it for both recreational and medical reasons, and 13% used it only for medical reasons. The most common reason women used cannabis was to treat chronic pain (28%), followed by nearly as many women reporting cannabis use for anxiety (24%), sleep (22%), and stress (22%). Six percent of women used cannabis specifically for menopause-related sleep and mood problems.
Given the growing use of cannabis in this population and the dearth of data on its effects in older women, Dr. Gibson highlighted the need for research examining the potential benefits and harms of cannabis for menopausal women.
Not risk-free
Susan D. Reed, MD, MPH, MSCP, a professor emeritus of ob.gyn. at the University of Washington, Seattle, and president of the Menopause Society, found the study well-executed and was not surprised by how many respondents had ever used cannabis.
“What did surprise me was that nearly a third reported daily use for at least 1 year and that 38% were medical marijuana users, not just recreational,” Dr. Reed said in an interview. The proportions of women using cannabis for menopausal symptoms or using it daily are concerning, she added.
“These individuals are at risk for dependence and health risks related to marijuana use,” Dr. Reed said. “Providers should always ask patients about OTC products, herbals, supplements, cannabis use, and alternative management of menopausal symptoms to better understand patient preferences for menopausal symptom therapies, so that treatment plans can be discussed with individual patient preferences in mind. We need to start with where the patient is coming from.”
Data presented throughout the conference has shown how people are “disillusioned with the care they are receiving for menopause,” Dr. Reed added. “It is so difficult to distinguish truth from myths based on information gained through social media, family, and friends, and that often is where most people are getting their information.”
Physicians often have not received adequate training on how to provide people with accurate information about menopause and managing menopausal symptoms, so she advises patients and physicians to visit reliable sites such as the Menopause Society, the Swan Study, and My Menoplan.
The research was funded by the Tobacco-Related Disease Research Program and the Veterans Administration. Dr. Gibson has provided unpaid consultation to Astellas Pharmaceuticals. Dr. Reed has received research support from Bayer and receives royalties from UpToDate.
PHILADELPHIA – presented at the annual meeting of the Menopause Society (formerly The North American Menopause Society).
Though most women reported using cannabis for recreational reasons, 13% used it only for medical reasons, most often for chronic pain, anxiety, sleep, and stress.
“These findings highlight the importance of recognizing and discussing cannabis use in the health care setting, and the need for additional research to evaluate the potential harms and/or benefits of use in this vulnerable population,” Carolyn J. Gibson, PhD, MPH, a staff psychologist in women’s health at the San Francisco VA Health Care System and an assistant professor of psychiatry and behavioral sciences at the University of California, San Francisco, told attendees.
As cannabis has become more accessible, with its use legalized in 38 states and Washington, D.C., the proportion of U.S. adults using it has doubled over about a decade, from 6% in 2007 to 12% in 2019, Dr. Gibson said. Further, women aged 50 and older are among the fastest-growing groups of users of cannabis, and it’s being increasingly used – and marketed – for treating menopause-related and aging-related symptoms, including insomnia, anxiety, and chronic pain, she said.
“With these decisions to use cannabis, medically or for these other purposes, there’s this perception that it’s harmless,” Dr. Gibson said. Yet potential health risks associated with cannabis include the usual health effects associated with any kind of smoking as well as dependence in those who use it more frequently and/or develop a tolerance for it. She noted that average THC potency has increased over time, and acute risks for using cannabis with high levels of THC – at least 15% or at least 10 mg – can include anxiety/panic, confusion, disturbing/intrusive thoughts, psychosis, and effects on coordination and cognition. She also acknowledged, however, that most of the data available on risks come from studies of men and younger adults rather than older women.
Given the growing normalization of cannabis use, Dr. Gibson’s team sought to better understand prevalence of use as well as types of use and reasons for use in perimenopasual and postmenopausal women. They analyzed data from a cross-sectional survey of women and gender-diverse members, aged 45-64, of Ipsos KnowledgePanel, an online panel with more than 60,000 participating members in the United States.
All the respondents identified themselves as female at birth and had not used gender-affirming therapy or undergone gender-affirming surgery. The survey included questions on sociodemographics, menopause status, frequency of cannabis use, types of cannabis used, reasons for using cannabis, and use of cannabis in the previous 30 days. The 5,174 respondents were an average 55 years old and predominantly non-Hispanic white (63%), with 13% non-Hispanic Black and 16% Hispanic. Two-thirds of the women reported working full- or part-time (67%) and two-thirds were postmenopausal (68%), with 64% reporting experiencing menopause symptoms.
About two in five respondents (42%) had ever used cannabis in any form, most often smoking it (83%) or consuming edibles (51%). Among those who had ever used it, 30% reported having smoked it daily or nearly daily for at least a year at some point.
Ten percent of respondents had used cannabis in the past month, again primarily smoking (56%) or edibles (52%), though 39% said they used it in more than one form, including vaping, dabbing, or topical use. Nearly half (46%) of the respondents who smoked cannabis recently did not know the THC potency of what they consumed, and just over 20% of those consuming edibles didn’t know the THC potency of what they used. However, about a third of those taking edibles used cannabis with less than 10 mg of THC, and a little over a quarter used edibles with 10 mg of THC.
Within the 10% who had used cannabis in the past month, nearly a third (31%) of respondents – or around 3.1% of the total sample – reported smoking cannabis daily or almost daily, and 19% (or 1.9% of the overall sample) consumed cannabis edibles daily or almost daily.
Most of the respondents who used cannabis said it was for recreational use (62%), but a quarter (25%) reported using it for both recreational and medical reasons, and 13% used it only for medical reasons. The most common reason women used cannabis was to treat chronic pain (28%), followed by nearly as many women reporting cannabis use for anxiety (24%), sleep (22%), and stress (22%). Six percent of women used cannabis specifically for menopause-related sleep and mood problems.
Given the growing use of cannabis in this population and the dearth of data on its effects in older women, Dr. Gibson highlighted the need for research examining the potential benefits and harms of cannabis for menopausal women.
Not risk-free
Susan D. Reed, MD, MPH, MSCP, a professor emeritus of ob.gyn. at the University of Washington, Seattle, and president of the Menopause Society, found the study well-executed and was not surprised by how many respondents had ever used cannabis.
“What did surprise me was that nearly a third reported daily use for at least 1 year and that 38% were medical marijuana users, not just recreational,” Dr. Reed said in an interview. The proportions of women using cannabis for menopausal symptoms or using it daily are concerning, she added.
“These individuals are at risk for dependence and health risks related to marijuana use,” Dr. Reed said. “Providers should always ask patients about OTC products, herbals, supplements, cannabis use, and alternative management of menopausal symptoms to better understand patient preferences for menopausal symptom therapies, so that treatment plans can be discussed with individual patient preferences in mind. We need to start with where the patient is coming from.”
Data presented throughout the conference has shown how people are “disillusioned with the care they are receiving for menopause,” Dr. Reed added. “It is so difficult to distinguish truth from myths based on information gained through social media, family, and friends, and that often is where most people are getting their information.”
Physicians often have not received adequate training on how to provide people with accurate information about menopause and managing menopausal symptoms, so she advises patients and physicians to visit reliable sites such as the Menopause Society, the Swan Study, and My Menoplan.
The research was funded by the Tobacco-Related Disease Research Program and the Veterans Administration. Dr. Gibson has provided unpaid consultation to Astellas Pharmaceuticals. Dr. Reed has received research support from Bayer and receives royalties from UpToDate.
AT NAMS 2023
Growing ‘tranq’ threat poses challenges for PCPs
The widening threat of the animal tranquilizer xylazine, otherwise known as tranq, which has been found in illegally manufactured fentanyl, necessitates wider testing, a better understanding of its effects, and more research on treatment options, according to a narrative review published in the Annals of Internal Medicine.
“A lot of doctors and providers are asking about this drug,” said Joseph D’Orazio, MD, an addiction medicine specialist and medical toxicologist at Cooper University Healthcare, Camden, N.J., who led the review.
Xylazine is believed to prolong or intensify the effects of opioids, making it a popular additive to illegally produced opioids, particularly fentanyl, according to the Drug Enforcement Administration. Users end up in a zombie-like state with slowed breathing, and they sometimes develop skin ulcers. Because xylazine is not an opioid, common antidotes such as naloxone are ineffective. The White House has called the fentanyl-xylazine combo an “emerging threat.”
“Xylazine is making the deadliest drug threat our country has ever faced, fentanyl, even deadlier,” said DEA administrator Anne Milgram, in a statement on the agency’s website. “DEA has seized xylazine and fentanyl mixtures in 48 of 50 States. The DEA Laboratory System is reporting that in 2022 approximately 23% of fentanyl powder and 7% of fentanyl pills seized by the DEA contained xylazine.”
Dr. D’Orazio paired clinical experience with available research to provide guidance on the care of patients exposed to xylazine.
He and his team issued a call for more research on the drug’s effects, including more details on dependency and withdrawal.
Testing a patient who may have been exposed to xylazine requires forensic lab capabilities, which makes testing complicated and costly. The review found no evidence of the origin of the drug or why it causes open sores.
The review calls for more education of providers, including primary care physicians, on the treatment and care of patients who have used xylazine and fentanyl. The authors also call for expanding standard urine analysis to test for xylazine and for intensifying surveillance of the drug supply and distribution of xylazine test strips.
The authors of an editorial that accompanied the journal article urged the health care community to get ahead of xylazine before the crisis worsens.
“Not testing for xylazine in current unaffected areas and populations may lead to delays in responding if and when the drug becomes prevalent in the drug supply,” the authors wrote.
Xylazine was detected in 90% of street opioid samples tested in Philadelphia in 2021, and a toxic surveillance study of drug paraphernalia in Maryland found xylazine in 80% of samples tested between 2021 and 2022.
Dr. D’Orazio stressed that although Narcan is ineffective in treating xylazine, because the sedative is almost always mixed with fentanyl or another opiate, the opioid antagonist should still be used in emergencies.
Angelique Campen, MD, an emergency medicine physician at Providence St. Joseph Medical Center, Burbank, Calif., said she has seen an increase in patients entering the emergency department under the influence of what seems like fentanyl or heroin, but standard treatments such as Narcan have a limited effect. These patients remain in a prolonged period of sedation.
Recently, she admitted to her hospital’s intensive care unit a patient suspected of a xylazine overdose who was not responding to treatment.
Dr. Campen said that patients are screened for fentanyl, but because no test is available for xylazine, she presumed xylazine was causing the complication.
“It makes perfect medical sense to me that that’s what was going on,” Dr. Campen, who has worked at St. Joseph’s for 25 years, said. “I’m hoping with physicians being more aware of it that we can have that part of our regular urine drug screen.”
Dr. Campen also said she hopes an antidote is soon developed.
“If we can just keep delivering that message, hopefully, [to] more and more people, it will get through to them,” she said. “Every time you’re taking this, even though you may have taken it a week before and been fine, you never know: The next dose you take may be the lethal dose.”
A review author reports being awarded $1,000 to cover travel cost for Best Overall Abstract at the American Society of Addiction Medicine 2023 Annual Meeting. Another author reports receiving payments for training conducted as part of a NJDMAHS training grant to educate on substance use disorders. Dr. D’Orazio reports a $500 honorarium for a one-time lecture on xylazine at Yale; and a $500 honorarium for speaking one to three times per year on various topics regarding opioid use disorder at the Health Federation of Philadelphia. No other disclosures were reported.
A version of this article first appeared on Medscape.com.
The widening threat of the animal tranquilizer xylazine, otherwise known as tranq, which has been found in illegally manufactured fentanyl, necessitates wider testing, a better understanding of its effects, and more research on treatment options, according to a narrative review published in the Annals of Internal Medicine.
“A lot of doctors and providers are asking about this drug,” said Joseph D’Orazio, MD, an addiction medicine specialist and medical toxicologist at Cooper University Healthcare, Camden, N.J., who led the review.
Xylazine is believed to prolong or intensify the effects of opioids, making it a popular additive to illegally produced opioids, particularly fentanyl, according to the Drug Enforcement Administration. Users end up in a zombie-like state with slowed breathing, and they sometimes develop skin ulcers. Because xylazine is not an opioid, common antidotes such as naloxone are ineffective. The White House has called the fentanyl-xylazine combo an “emerging threat.”
“Xylazine is making the deadliest drug threat our country has ever faced, fentanyl, even deadlier,” said DEA administrator Anne Milgram, in a statement on the agency’s website. “DEA has seized xylazine and fentanyl mixtures in 48 of 50 States. The DEA Laboratory System is reporting that in 2022 approximately 23% of fentanyl powder and 7% of fentanyl pills seized by the DEA contained xylazine.”
Dr. D’Orazio paired clinical experience with available research to provide guidance on the care of patients exposed to xylazine.
He and his team issued a call for more research on the drug’s effects, including more details on dependency and withdrawal.
Testing a patient who may have been exposed to xylazine requires forensic lab capabilities, which makes testing complicated and costly. The review found no evidence of the origin of the drug or why it causes open sores.
The review calls for more education of providers, including primary care physicians, on the treatment and care of patients who have used xylazine and fentanyl. The authors also call for expanding standard urine analysis to test for xylazine and for intensifying surveillance of the drug supply and distribution of xylazine test strips.
The authors of an editorial that accompanied the journal article urged the health care community to get ahead of xylazine before the crisis worsens.
“Not testing for xylazine in current unaffected areas and populations may lead to delays in responding if and when the drug becomes prevalent in the drug supply,” the authors wrote.
Xylazine was detected in 90% of street opioid samples tested in Philadelphia in 2021, and a toxic surveillance study of drug paraphernalia in Maryland found xylazine in 80% of samples tested between 2021 and 2022.
Dr. D’Orazio stressed that although Narcan is ineffective in treating xylazine, because the sedative is almost always mixed with fentanyl or another opiate, the opioid antagonist should still be used in emergencies.
Angelique Campen, MD, an emergency medicine physician at Providence St. Joseph Medical Center, Burbank, Calif., said she has seen an increase in patients entering the emergency department under the influence of what seems like fentanyl or heroin, but standard treatments such as Narcan have a limited effect. These patients remain in a prolonged period of sedation.
Recently, she admitted to her hospital’s intensive care unit a patient suspected of a xylazine overdose who was not responding to treatment.
Dr. Campen said that patients are screened for fentanyl, but because no test is available for xylazine, she presumed xylazine was causing the complication.
“It makes perfect medical sense to me that that’s what was going on,” Dr. Campen, who has worked at St. Joseph’s for 25 years, said. “I’m hoping with physicians being more aware of it that we can have that part of our regular urine drug screen.”
Dr. Campen also said she hopes an antidote is soon developed.
“If we can just keep delivering that message, hopefully, [to] more and more people, it will get through to them,” she said. “Every time you’re taking this, even though you may have taken it a week before and been fine, you never know: The next dose you take may be the lethal dose.”
A review author reports being awarded $1,000 to cover travel cost for Best Overall Abstract at the American Society of Addiction Medicine 2023 Annual Meeting. Another author reports receiving payments for training conducted as part of a NJDMAHS training grant to educate on substance use disorders. Dr. D’Orazio reports a $500 honorarium for a one-time lecture on xylazine at Yale; and a $500 honorarium for speaking one to three times per year on various topics regarding opioid use disorder at the Health Federation of Philadelphia. No other disclosures were reported.
A version of this article first appeared on Medscape.com.
The widening threat of the animal tranquilizer xylazine, otherwise known as tranq, which has been found in illegally manufactured fentanyl, necessitates wider testing, a better understanding of its effects, and more research on treatment options, according to a narrative review published in the Annals of Internal Medicine.
“A lot of doctors and providers are asking about this drug,” said Joseph D’Orazio, MD, an addiction medicine specialist and medical toxicologist at Cooper University Healthcare, Camden, N.J., who led the review.
Xylazine is believed to prolong or intensify the effects of opioids, making it a popular additive to illegally produced opioids, particularly fentanyl, according to the Drug Enforcement Administration. Users end up in a zombie-like state with slowed breathing, and they sometimes develop skin ulcers. Because xylazine is not an opioid, common antidotes such as naloxone are ineffective. The White House has called the fentanyl-xylazine combo an “emerging threat.”
“Xylazine is making the deadliest drug threat our country has ever faced, fentanyl, even deadlier,” said DEA administrator Anne Milgram, in a statement on the agency’s website. “DEA has seized xylazine and fentanyl mixtures in 48 of 50 States. The DEA Laboratory System is reporting that in 2022 approximately 23% of fentanyl powder and 7% of fentanyl pills seized by the DEA contained xylazine.”
Dr. D’Orazio paired clinical experience with available research to provide guidance on the care of patients exposed to xylazine.
He and his team issued a call for more research on the drug’s effects, including more details on dependency and withdrawal.
Testing a patient who may have been exposed to xylazine requires forensic lab capabilities, which makes testing complicated and costly. The review found no evidence of the origin of the drug or why it causes open sores.
The review calls for more education of providers, including primary care physicians, on the treatment and care of patients who have used xylazine and fentanyl. The authors also call for expanding standard urine analysis to test for xylazine and for intensifying surveillance of the drug supply and distribution of xylazine test strips.
The authors of an editorial that accompanied the journal article urged the health care community to get ahead of xylazine before the crisis worsens.
“Not testing for xylazine in current unaffected areas and populations may lead to delays in responding if and when the drug becomes prevalent in the drug supply,” the authors wrote.
Xylazine was detected in 90% of street opioid samples tested in Philadelphia in 2021, and a toxic surveillance study of drug paraphernalia in Maryland found xylazine in 80% of samples tested between 2021 and 2022.
Dr. D’Orazio stressed that although Narcan is ineffective in treating xylazine, because the sedative is almost always mixed with fentanyl or another opiate, the opioid antagonist should still be used in emergencies.
Angelique Campen, MD, an emergency medicine physician at Providence St. Joseph Medical Center, Burbank, Calif., said she has seen an increase in patients entering the emergency department under the influence of what seems like fentanyl or heroin, but standard treatments such as Narcan have a limited effect. These patients remain in a prolonged period of sedation.
Recently, she admitted to her hospital’s intensive care unit a patient suspected of a xylazine overdose who was not responding to treatment.
Dr. Campen said that patients are screened for fentanyl, but because no test is available for xylazine, she presumed xylazine was causing the complication.
“It makes perfect medical sense to me that that’s what was going on,” Dr. Campen, who has worked at St. Joseph’s for 25 years, said. “I’m hoping with physicians being more aware of it that we can have that part of our regular urine drug screen.”
Dr. Campen also said she hopes an antidote is soon developed.
“If we can just keep delivering that message, hopefully, [to] more and more people, it will get through to them,” she said. “Every time you’re taking this, even though you may have taken it a week before and been fine, you never know: The next dose you take may be the lethal dose.”
A review author reports being awarded $1,000 to cover travel cost for Best Overall Abstract at the American Society of Addiction Medicine 2023 Annual Meeting. Another author reports receiving payments for training conducted as part of a NJDMAHS training grant to educate on substance use disorders. Dr. D’Orazio reports a $500 honorarium for a one-time lecture on xylazine at Yale; and a $500 honorarium for speaking one to three times per year on various topics regarding opioid use disorder at the Health Federation of Philadelphia. No other disclosures were reported.
A version of this article first appeared on Medscape.com.