User login
Medicare subsidies eliminate disparities in adherence to hormonal
The low-income subsidy in Medicare Part D is helping to eliminate racial disparities in adherence to hormonal therapy among breast cancer patients.
Investigators identified a nationwide cohort of 25,111 Medicare D enrollees with a breast cancer operation between 2006 and 2007 and at least one prescription filled for oral breast cancer hormonal therapy. Women not receiving the low-income subsidy “were 60%-200% more likely to discontinue hormonal therapy in the first 35 months, compared with low-income subsidy recipients of the same race or ethnicity,” reported Alana Biggers, MD, of University of Illinois at Chicago, and her colleagues, in the Journal of Clinical Oncology.
The study found that overall, it took 14 months for 25% of the cohort to discontinue medication (unadjusted). When the researchers broke it down by race/ethnicity, they found that it took 12 months for 25% of unsubsidized whites to discontinue medication, compared with 24 months for subsidized whites. For unsubsidized blacks, it was 9 months, compared with 24 months for subsidized blacks. For unsubsidized Hispanics, it was 10 months vs. 29 months for subsidized Hispanics.
“Our findings regarding the relatively large difference in persistence in adherence between subsidized and unsubsidized women are consistent with large reductions in out-of-pocket costs for aromatase inhibitors with the subsidy,” the authors state.
More effort should be placed on ensuring that women eligible for the low-income subsidy are enrolled, and legislative and advocacy efforts for those outside of Medicare “should focus on lowering out-of-pocket costs for younger women. Given the high costs of oral oncologic and supportive medications, the impact on disparities of other initiatives to reduce out-of-pocket costs deserves urgent study,” they said.
The authors reported no relevant conflicts of interest related to this study, which was supported by grants from the National Institutes of Health and the American Cancer Society.
The low-income subsidy in Medicare Part D is helping to eliminate racial disparities in adherence to hormonal therapy among breast cancer patients.
Investigators identified a nationwide cohort of 25,111 Medicare D enrollees with a breast cancer operation between 2006 and 2007 and at least one prescription filled for oral breast cancer hormonal therapy. Women not receiving the low-income subsidy “were 60%-200% more likely to discontinue hormonal therapy in the first 35 months, compared with low-income subsidy recipients of the same race or ethnicity,” reported Alana Biggers, MD, of University of Illinois at Chicago, and her colleagues, in the Journal of Clinical Oncology.
The study found that overall, it took 14 months for 25% of the cohort to discontinue medication (unadjusted). When the researchers broke it down by race/ethnicity, they found that it took 12 months for 25% of unsubsidized whites to discontinue medication, compared with 24 months for subsidized whites. For unsubsidized blacks, it was 9 months, compared with 24 months for subsidized blacks. For unsubsidized Hispanics, it was 10 months vs. 29 months for subsidized Hispanics.
“Our findings regarding the relatively large difference in persistence in adherence between subsidized and unsubsidized women are consistent with large reductions in out-of-pocket costs for aromatase inhibitors with the subsidy,” the authors state.
More effort should be placed on ensuring that women eligible for the low-income subsidy are enrolled, and legislative and advocacy efforts for those outside of Medicare “should focus on lowering out-of-pocket costs for younger women. Given the high costs of oral oncologic and supportive medications, the impact on disparities of other initiatives to reduce out-of-pocket costs deserves urgent study,” they said.
The authors reported no relevant conflicts of interest related to this study, which was supported by grants from the National Institutes of Health and the American Cancer Society.
The low-income subsidy in Medicare Part D is helping to eliminate racial disparities in adherence to hormonal therapy among breast cancer patients.
Investigators identified a nationwide cohort of 25,111 Medicare D enrollees with a breast cancer operation between 2006 and 2007 and at least one prescription filled for oral breast cancer hormonal therapy. Women not receiving the low-income subsidy “were 60%-200% more likely to discontinue hormonal therapy in the first 35 months, compared with low-income subsidy recipients of the same race or ethnicity,” reported Alana Biggers, MD, of University of Illinois at Chicago, and her colleagues, in the Journal of Clinical Oncology.
The study found that overall, it took 14 months for 25% of the cohort to discontinue medication (unadjusted). When the researchers broke it down by race/ethnicity, they found that it took 12 months for 25% of unsubsidized whites to discontinue medication, compared with 24 months for subsidized whites. For unsubsidized blacks, it was 9 months, compared with 24 months for subsidized blacks. For unsubsidized Hispanics, it was 10 months vs. 29 months for subsidized Hispanics.
“Our findings regarding the relatively large difference in persistence in adherence between subsidized and unsubsidized women are consistent with large reductions in out-of-pocket costs for aromatase inhibitors with the subsidy,” the authors state.
More effort should be placed on ensuring that women eligible for the low-income subsidy are enrolled, and legislative and advocacy efforts for those outside of Medicare “should focus on lowering out-of-pocket costs for younger women. Given the high costs of oral oncologic and supportive medications, the impact on disparities of other initiatives to reduce out-of-pocket costs deserves urgent study,” they said.
The authors reported no relevant conflicts of interest related to this study, which was supported by grants from the National Institutes of Health and the American Cancer Society.
FALCON airs PFS edge for fulvestrant in ER+ breast cancer
COPENHAGEN – Fulvestrant continues to show superiority over anastrozole in treatment of hormone receptor-positive breast cancer, particularly in women with lower-volume disease, reported investigators in the phase III FALCON trial.
At a median follow-up of 25 months, median progression-free survival (PFS) for women assigned to receive the selective estrogen-receptor degrader fulvestrant (Faslodex) was 16.6 months, compared with 13.8 months for women assigned to receive the aromatase inhibitor anastrozole (Arimidex), reported Matthew J. Ellis, PhD, of the Lester and Sue Smith Breast Center at Baylor College of Medicine in Houston.
“These results are consistent with data from the FIRST study and confirm that fulvestrant is more efficacious than anastrozole in postmenopausal women with hormone receptor–positive locally advanced or metastatic breast cancer who have not received prior endocrine therapy,” he said at the European Society for Medical Oncology Congress.
The benefit of fulvestrant appeared to be only among patients who did not have visceral metastases, however.
In the FIRST study, results of which were reported at the San Antonio Breast Cancer Symposium in 2014, median overall survival at a median follow-up of 48.8 months was 54.1 months in patients on fulvestrant, vs. 48.4 months with anastrozole (hazard ratio [HR] 0.70, P = .04). The median PFS durations were 23.4 months vs. 13.1 months, respectively (HR 0.66, P = .01).
The FALCON (Fulvestrant and Anastrozole Compared in Hormonal Therapy-Naive Advanced Breast Cancer) trial was a phase III study designed to confirm the PFS benefit seen with fulvestrant in the earlier trial.
Postmenopausal women with locally advanced or metastatic breast cancer positive for the estrogen and/or progesterone receptor and negative for HER2 who had not previously received endocrine therapy were enrolled. They were randomly assigned to receive fulvestrant 500 mg intramuscularly on days 0, 14, and 28 then every 28 days plus an anastrozole placebo (232 patients), or oral anastrozole 1 mg daily plus fulvestrant placebo (230 patients).
Women with life-threatening visceral metastases, systemic estrogen-containing hormone replacement therapy within 6 months of randomization, or prior systemic treatment for breast cancer other than one line of chemotherapy or radiotherapy within 28 days of randomization (except radiation for control of bone pain) were excluded.
As noted, the primary endpoint of PFS was 16.6 months in the fulvestrant arm vs. 13.8 months in the anastrozole arm, translating into an HR for progression on fulvestrant of 0.797 (P = .0486).
Among the 208 patients with no visceral disease, median PFS with fulvestrant was 22.3 months, vs. 13.8 months (HR 0.59, P less than .01). In contrast, among the 254 patients with visceral disease, the respective median PFS durations were 13.8 and 15.9 months (nonsignificant).
For the secondary endpoint of overall survival, at 31% maturity (longest follow-up out to 39 months), there was no significant difference between the study arms.
There were also no significant differences in the secondary endpoints of overall response rate (among patients with measurable disease at baseline), clinical benefit rate, median duration of response, median duration of clinical benefit, or median time to deterioration of total score on the Functional Assessment of Cancer Therapy–Breast (FACT-B) patient-reported outcomes instrument.
Only estimated duration of response (11.4 vs. 7.5 months) and estimated duration of clinical benefit (21.9 vs. 17.5 months) were significantly better with fulvestrant (P less than .001 for each).

Grade 3 or greater adverse events occurred in 22.4% vs. 17.7%. Deaths from adverse events occurred in six patients on fulvestrant vs. seven on anastrozole. None of these deaths were considered to be related.
The FALCON results, which showed a benefit for fulvestrant only for those patients without visceral disease, point to a need for investigating whether patients with visceral metastases should receive other therapies, but this observation is hypothesis-generating only, said invited discussant Peter Schmid, MD, PhD, of Barts Cancer Institute at St. Bartholomew’s Hospital at Queen Mary University of London.
COPENHAGEN – Fulvestrant continues to show superiority over anastrozole in treatment of hormone receptor-positive breast cancer, particularly in women with lower-volume disease, reported investigators in the phase III FALCON trial.
At a median follow-up of 25 months, median progression-free survival (PFS) for women assigned to receive the selective estrogen-receptor degrader fulvestrant (Faslodex) was 16.6 months, compared with 13.8 months for women assigned to receive the aromatase inhibitor anastrozole (Arimidex), reported Matthew J. Ellis, PhD, of the Lester and Sue Smith Breast Center at Baylor College of Medicine in Houston.
“These results are consistent with data from the FIRST study and confirm that fulvestrant is more efficacious than anastrozole in postmenopausal women with hormone receptor–positive locally advanced or metastatic breast cancer who have not received prior endocrine therapy,” he said at the European Society for Medical Oncology Congress.
The benefit of fulvestrant appeared to be only among patients who did not have visceral metastases, however.
In the FIRST study, results of which were reported at the San Antonio Breast Cancer Symposium in 2014, median overall survival at a median follow-up of 48.8 months was 54.1 months in patients on fulvestrant, vs. 48.4 months with anastrozole (hazard ratio [HR] 0.70, P = .04). The median PFS durations were 23.4 months vs. 13.1 months, respectively (HR 0.66, P = .01).
The FALCON (Fulvestrant and Anastrozole Compared in Hormonal Therapy-Naive Advanced Breast Cancer) trial was a phase III study designed to confirm the PFS benefit seen with fulvestrant in the earlier trial.
Postmenopausal women with locally advanced or metastatic breast cancer positive for the estrogen and/or progesterone receptor and negative for HER2 who had not previously received endocrine therapy were enrolled. They were randomly assigned to receive fulvestrant 500 mg intramuscularly on days 0, 14, and 28 then every 28 days plus an anastrozole placebo (232 patients), or oral anastrozole 1 mg daily plus fulvestrant placebo (230 patients).
Women with life-threatening visceral metastases, systemic estrogen-containing hormone replacement therapy within 6 months of randomization, or prior systemic treatment for breast cancer other than one line of chemotherapy or radiotherapy within 28 days of randomization (except radiation for control of bone pain) were excluded.
As noted, the primary endpoint of PFS was 16.6 months in the fulvestrant arm vs. 13.8 months in the anastrozole arm, translating into an HR for progression on fulvestrant of 0.797 (P = .0486).
Among the 208 patients with no visceral disease, median PFS with fulvestrant was 22.3 months, vs. 13.8 months (HR 0.59, P less than .01). In contrast, among the 254 patients with visceral disease, the respective median PFS durations were 13.8 and 15.9 months (nonsignificant).
For the secondary endpoint of overall survival, at 31% maturity (longest follow-up out to 39 months), there was no significant difference between the study arms.
There were also no significant differences in the secondary endpoints of overall response rate (among patients with measurable disease at baseline), clinical benefit rate, median duration of response, median duration of clinical benefit, or median time to deterioration of total score on the Functional Assessment of Cancer Therapy–Breast (FACT-B) patient-reported outcomes instrument.
Only estimated duration of response (11.4 vs. 7.5 months) and estimated duration of clinical benefit (21.9 vs. 17.5 months) were significantly better with fulvestrant (P less than .001 for each).
Grade 3 or greater adverse events occurred in 22.4% vs. 17.7%. Deaths from adverse events occurred in six patients on fulvestrant vs. seven on anastrozole. None of these deaths were considered to be related.
The FALCON results, which showed a benefit for fulvestrant only for those patients without visceral disease, point to a need for investigating whether patients with visceral metastases should receive other therapies, but this observation is hypothesis-generating only, said invited discussant Peter Schmid, MD, PhD, of Barts Cancer Institute at St. Bartholomew’s Hospital at Queen Mary University of London.
COPENHAGEN – Fulvestrant continues to show superiority over anastrozole in treatment of hormone receptor-positive breast cancer, particularly in women with lower-volume disease, reported investigators in the phase III FALCON trial.
At a median follow-up of 25 months, median progression-free survival (PFS) for women assigned to receive the selective estrogen-receptor degrader fulvestrant (Faslodex) was 16.6 months, compared with 13.8 months for women assigned to receive the aromatase inhibitor anastrozole (Arimidex), reported Matthew J. Ellis, PhD, of the Lester and Sue Smith Breast Center at Baylor College of Medicine in Houston.
“These results are consistent with data from the FIRST study and confirm that fulvestrant is more efficacious than anastrozole in postmenopausal women with hormone receptor–positive locally advanced or metastatic breast cancer who have not received prior endocrine therapy,” he said at the European Society for Medical Oncology Congress.
The benefit of fulvestrant appeared to be only among patients who did not have visceral metastases, however.
In the FIRST study, results of which were reported at the San Antonio Breast Cancer Symposium in 2014, median overall survival at a median follow-up of 48.8 months was 54.1 months in patients on fulvestrant, vs. 48.4 months with anastrozole (hazard ratio [HR] 0.70, P = .04). The median PFS durations were 23.4 months vs. 13.1 months, respectively (HR 0.66, P = .01).
The FALCON (Fulvestrant and Anastrozole Compared in Hormonal Therapy-Naive Advanced Breast Cancer) trial was a phase III study designed to confirm the PFS benefit seen with fulvestrant in the earlier trial.
Postmenopausal women with locally advanced or metastatic breast cancer positive for the estrogen and/or progesterone receptor and negative for HER2 who had not previously received endocrine therapy were enrolled. They were randomly assigned to receive fulvestrant 500 mg intramuscularly on days 0, 14, and 28 then every 28 days plus an anastrozole placebo (232 patients), or oral anastrozole 1 mg daily plus fulvestrant placebo (230 patients).
Women with life-threatening visceral metastases, systemic estrogen-containing hormone replacement therapy within 6 months of randomization, or prior systemic treatment for breast cancer other than one line of chemotherapy or radiotherapy within 28 days of randomization (except radiation for control of bone pain) were excluded.
As noted, the primary endpoint of PFS was 16.6 months in the fulvestrant arm vs. 13.8 months in the anastrozole arm, translating into an HR for progression on fulvestrant of 0.797 (P = .0486).
Among the 208 patients with no visceral disease, median PFS with fulvestrant was 22.3 months, vs. 13.8 months (HR 0.59, P less than .01). In contrast, among the 254 patients with visceral disease, the respective median PFS durations were 13.8 and 15.9 months (nonsignificant).
For the secondary endpoint of overall survival, at 31% maturity (longest follow-up out to 39 months), there was no significant difference between the study arms.
There were also no significant differences in the secondary endpoints of overall response rate (among patients with measurable disease at baseline), clinical benefit rate, median duration of response, median duration of clinical benefit, or median time to deterioration of total score on the Functional Assessment of Cancer Therapy–Breast (FACT-B) patient-reported outcomes instrument.
Only estimated duration of response (11.4 vs. 7.5 months) and estimated duration of clinical benefit (21.9 vs. 17.5 months) were significantly better with fulvestrant (P less than .001 for each).
Grade 3 or greater adverse events occurred in 22.4% vs. 17.7%. Deaths from adverse events occurred in six patients on fulvestrant vs. seven on anastrozole. None of these deaths were considered to be related.
The FALCON results, which showed a benefit for fulvestrant only for those patients without visceral disease, point to a need for investigating whether patients with visceral metastases should receive other therapies, but this observation is hypothesis-generating only, said invited discussant Peter Schmid, MD, PhD, of Barts Cancer Institute at St. Bartholomew’s Hospital at Queen Mary University of London.
AT ESMO 2016
Key clinical point: The selective estrogen receptor degrader fulvestrant continues to offer improved progression-free survival (PFS) compared with the aromatase inhibitor anastrozole.
Major finding: At a median 25 months’ follow-up, median PFS was 16.6 months for fulvestrant vs. 13.8 months for anastrozole.
Data source: Randomized phase III trial of 462 women with endocrine therapy–naive locally advanced metastatic hormone receptor–positive breast cancer.
Disclosures: FALCON was sponsored by AstraZeneca. Dr. Ellis reported consulting for AstraZeneca, and Dr. Schmid reported honoraria or consultation fees from the company.
Overdiagnosis more likely than early detection of threatening cancer with mammography screening
Following the introduction of mammography, women were considerably more likely to have tumors that were overdiagnosed than to have earlier detection of a tumor that was destined to become large, according to an analysis of trends from the Surveillance, Epidemiology, and End Results (SEER) database.
To assess the effectiveness of screening mammography in the real-world clinical and community setting, H. Gilbert Welch, MD, of the Dartmouth Institute for Health Policy and Clinical Practice and his associates examined trends in breast tumor size between the years of 1975 and 2012, a span of time that can be broken down into two distinct periods: a baseline period that predated the widespread use of screening mammography (1975-1979) and a period encompassing the most recent years for which 10 years of follow-up data were available (2000 through 2002).

Retrospective analysis of the SEER database revealed a shift in the size distribution of breast tumors: Large tumors, defined as invasive tumors measuring two centimeters or more, predominated in the period before widespread screening mammography, and small tumors, defined as in situ carcinomas or invasive tumors measuring less than two centimeters, predominated after.
This shift, the researchers noted, can, in part, be attributed to the use of screening mammography.
Overall, from 1975 to 2012, the proportion of breast tumors that were small increased from 36% to 68%. In that same time period, the proportion of large tumors decreased from 64% to 32%.
“This shift in size distribution was less the result of a substantial decrease in the incidence of large tumors and more the result of substantial increases in the detection of small tumors,” Dr. Welch and his associates wrote.
Put another way, the incidence of small tumors increased by 162 cases of cancer per 100,000 women, from 82 to 244 cases, while the incidence of large tumors decreased by 30 cases of cancer per 100,000 women, from 145 to 115 cases. “Assuming that the underlying burden of clinically meaningful breast cancer was unchanged, these data suggest that 30 cases of cancer per 100,000 women were destined to become large but were detected earlier, and the remaining 132 cases of cancer per 100,000 women were overdiagnosed,” the researchers wrote.
“The magnitude of the imbalance indicates that women were considerably more likely to have tumors that were overdiagnosed than to have earlier detection of a tumor that was destined to become large,” the researchers continued. “Our analysis of size-specific incidence highlights the fact that the introduction of screening mammography has produced a mixture of effects,” Dr. Welch and his associates added.
The Dartmouth Institute for Health Policy and Clinical Practice, Dartmouth’s Geisel School of Medicine, and the National Cancer Institute supported this study. The investigators had no relevant disclosures.
Overdiagnosis of breast cancer has been suggested on the basis of multiple studies that used different designs and approaches and is acknowledged by national organizations such as the American Cancer Society and the U.S. Preventive Services Task Force. Although Dr. Welch and his associates present powerful data on a large number of women in a very clear fashion, they also rely on data with extensive missing values, make assumptions about underlying disease burden that cannot be verified, and acknowledge that their estimates are imprecise.
Rather than focusing on statistical issues and study design, we should move forward by agreeing that overdiagnosis does occur, even though the exact percentage of overdiagnosed cases remains unknown. Some consider overdiagnosis to be an intractable problem. No single approach will adequately address the issue. Instead, a multilevel approach ranging from research and education at the population level to intensified focus at the patient level is needed. One way to reduce overdiagnosis is targeted, precision screening of persons who have a higher risk of breast cancer rather than screening large populations in which the majority of persons are at a lower risk for harmful disease.
At the provider level, we need better tools to evaluate medical data and classify findings on the basis of clinical judgment. Previous research has documented extensive diagnostic variability among radiologists in their interpretation of mammograms and among pathologists in their interpretation of breast biopsy specimens. We are using archaic disease-classification systems with inadequate vetting and defective nosologic boundaries. Diagnostic thresholds for “abnormality” need to be revised because the middle and lower boundaries of these classification systems have expanded without a clear benefit to patients.
Rigorous analytic methods are required for the development of disease nosologies, and physicians need more sophisticated tools to improve diagnostic precision and accuracy. At the patient level, we need better methods of distinguishing biologically self-limited tumors from harmful tumors that progress. We must also improve communication regarding overdiagnosis at all levels, from dissemination of scientific findings at a population level to education of patients before they undergo screening.
Clinicians face time constraints and lack experience in communicating screening nuances. Better training may help. Building trust in science and medicine starts by taking ownership of all aspects of the screening cascade, including the collateral damage of our well-intentioned efforts.
Dr. Elmore is a professor of medicine and adjunct professor of epidemiology at the University of Washington. Dr. Elmore reported having no relevant disclosures related to this commentary but did report receiving financial compensation from UpToDate and Healthwise/Informed Medical Decisions Foundation. These comments are excerpted from an accompanying editorial (N Engl J Med. 2016 Oct 12;375[15]:1483-6).
Overdiagnosis of breast cancer has been suggested on the basis of multiple studies that used different designs and approaches and is acknowledged by national organizations such as the American Cancer Society and the U.S. Preventive Services Task Force. Although Dr. Welch and his associates present powerful data on a large number of women in a very clear fashion, they also rely on data with extensive missing values, make assumptions about underlying disease burden that cannot be verified, and acknowledge that their estimates are imprecise.
Rather than focusing on statistical issues and study design, we should move forward by agreeing that overdiagnosis does occur, even though the exact percentage of overdiagnosed cases remains unknown. Some consider overdiagnosis to be an intractable problem. No single approach will adequately address the issue. Instead, a multilevel approach ranging from research and education at the population level to intensified focus at the patient level is needed. One way to reduce overdiagnosis is targeted, precision screening of persons who have a higher risk of breast cancer rather than screening large populations in which the majority of persons are at a lower risk for harmful disease.
At the provider level, we need better tools to evaluate medical data and classify findings on the basis of clinical judgment. Previous research has documented extensive diagnostic variability among radiologists in their interpretation of mammograms and among pathologists in their interpretation of breast biopsy specimens. We are using archaic disease-classification systems with inadequate vetting and defective nosologic boundaries. Diagnostic thresholds for “abnormality” need to be revised because the middle and lower boundaries of these classification systems have expanded without a clear benefit to patients.
Rigorous analytic methods are required for the development of disease nosologies, and physicians need more sophisticated tools to improve diagnostic precision and accuracy. At the patient level, we need better methods of distinguishing biologically self-limited tumors from harmful tumors that progress. We must also improve communication regarding overdiagnosis at all levels, from dissemination of scientific findings at a population level to education of patients before they undergo screening.
Clinicians face time constraints and lack experience in communicating screening nuances. Better training may help. Building trust in science and medicine starts by taking ownership of all aspects of the screening cascade, including the collateral damage of our well-intentioned efforts.
Dr. Elmore is a professor of medicine and adjunct professor of epidemiology at the University of Washington. Dr. Elmore reported having no relevant disclosures related to this commentary but did report receiving financial compensation from UpToDate and Healthwise/Informed Medical Decisions Foundation. These comments are excerpted from an accompanying editorial (N Engl J Med. 2016 Oct 12;375[15]:1483-6).
Overdiagnosis of breast cancer has been suggested on the basis of multiple studies that used different designs and approaches and is acknowledged by national organizations such as the American Cancer Society and the U.S. Preventive Services Task Force. Although Dr. Welch and his associates present powerful data on a large number of women in a very clear fashion, they also rely on data with extensive missing values, make assumptions about underlying disease burden that cannot be verified, and acknowledge that their estimates are imprecise.
Rather than focusing on statistical issues and study design, we should move forward by agreeing that overdiagnosis does occur, even though the exact percentage of overdiagnosed cases remains unknown. Some consider overdiagnosis to be an intractable problem. No single approach will adequately address the issue. Instead, a multilevel approach ranging from research and education at the population level to intensified focus at the patient level is needed. One way to reduce overdiagnosis is targeted, precision screening of persons who have a higher risk of breast cancer rather than screening large populations in which the majority of persons are at a lower risk for harmful disease.
At the provider level, we need better tools to evaluate medical data and classify findings on the basis of clinical judgment. Previous research has documented extensive diagnostic variability among radiologists in their interpretation of mammograms and among pathologists in their interpretation of breast biopsy specimens. We are using archaic disease-classification systems with inadequate vetting and defective nosologic boundaries. Diagnostic thresholds for “abnormality” need to be revised because the middle and lower boundaries of these classification systems have expanded without a clear benefit to patients.
Rigorous analytic methods are required for the development of disease nosologies, and physicians need more sophisticated tools to improve diagnostic precision and accuracy. At the patient level, we need better methods of distinguishing biologically self-limited tumors from harmful tumors that progress. We must also improve communication regarding overdiagnosis at all levels, from dissemination of scientific findings at a population level to education of patients before they undergo screening.
Clinicians face time constraints and lack experience in communicating screening nuances. Better training may help. Building trust in science and medicine starts by taking ownership of all aspects of the screening cascade, including the collateral damage of our well-intentioned efforts.
Dr. Elmore is a professor of medicine and adjunct professor of epidemiology at the University of Washington. Dr. Elmore reported having no relevant disclosures related to this commentary but did report receiving financial compensation from UpToDate and Healthwise/Informed Medical Decisions Foundation. These comments are excerpted from an accompanying editorial (N Engl J Med. 2016 Oct 12;375[15]:1483-6).
Following the introduction of mammography, women were considerably more likely to have tumors that were overdiagnosed than to have earlier detection of a tumor that was destined to become large, according to an analysis of trends from the Surveillance, Epidemiology, and End Results (SEER) database.
To assess the effectiveness of screening mammography in the real-world clinical and community setting, H. Gilbert Welch, MD, of the Dartmouth Institute for Health Policy and Clinical Practice and his associates examined trends in breast tumor size between the years of 1975 and 2012, a span of time that can be broken down into two distinct periods: a baseline period that predated the widespread use of screening mammography (1975-1979) and a period encompassing the most recent years for which 10 years of follow-up data were available (2000 through 2002).
Retrospective analysis of the SEER database revealed a shift in the size distribution of breast tumors: Large tumors, defined as invasive tumors measuring two centimeters or more, predominated in the period before widespread screening mammography, and small tumors, defined as in situ carcinomas or invasive tumors measuring less than two centimeters, predominated after.
This shift, the researchers noted, can, in part, be attributed to the use of screening mammography.
Overall, from 1975 to 2012, the proportion of breast tumors that were small increased from 36% to 68%. In that same time period, the proportion of large tumors decreased from 64% to 32%.
“This shift in size distribution was less the result of a substantial decrease in the incidence of large tumors and more the result of substantial increases in the detection of small tumors,” Dr. Welch and his associates wrote.
Put another way, the incidence of small tumors increased by 162 cases of cancer per 100,000 women, from 82 to 244 cases, while the incidence of large tumors decreased by 30 cases of cancer per 100,000 women, from 145 to 115 cases. “Assuming that the underlying burden of clinically meaningful breast cancer was unchanged, these data suggest that 30 cases of cancer per 100,000 women were destined to become large but were detected earlier, and the remaining 132 cases of cancer per 100,000 women were overdiagnosed,” the researchers wrote.
“The magnitude of the imbalance indicates that women were considerably more likely to have tumors that were overdiagnosed than to have earlier detection of a tumor that was destined to become large,” the researchers continued. “Our analysis of size-specific incidence highlights the fact that the introduction of screening mammography has produced a mixture of effects,” Dr. Welch and his associates added.
The Dartmouth Institute for Health Policy and Clinical Practice, Dartmouth’s Geisel School of Medicine, and the National Cancer Institute supported this study. The investigators had no relevant disclosures.
Following the introduction of mammography, women were considerably more likely to have tumors that were overdiagnosed than to have earlier detection of a tumor that was destined to become large, according to an analysis of trends from the Surveillance, Epidemiology, and End Results (SEER) database.
To assess the effectiveness of screening mammography in the real-world clinical and community setting, H. Gilbert Welch, MD, of the Dartmouth Institute for Health Policy and Clinical Practice and his associates examined trends in breast tumor size between the years of 1975 and 2012, a span of time that can be broken down into two distinct periods: a baseline period that predated the widespread use of screening mammography (1975-1979) and a period encompassing the most recent years for which 10 years of follow-up data were available (2000 through 2002).
Retrospective analysis of the SEER database revealed a shift in the size distribution of breast tumors: Large tumors, defined as invasive tumors measuring two centimeters or more, predominated in the period before widespread screening mammography, and small tumors, defined as in situ carcinomas or invasive tumors measuring less than two centimeters, predominated after.
This shift, the researchers noted, can, in part, be attributed to the use of screening mammography.
Overall, from 1975 to 2012, the proportion of breast tumors that were small increased from 36% to 68%. In that same time period, the proportion of large tumors decreased from 64% to 32%.
“This shift in size distribution was less the result of a substantial decrease in the incidence of large tumors and more the result of substantial increases in the detection of small tumors,” Dr. Welch and his associates wrote.
Put another way, the incidence of small tumors increased by 162 cases of cancer per 100,000 women, from 82 to 244 cases, while the incidence of large tumors decreased by 30 cases of cancer per 100,000 women, from 145 to 115 cases. “Assuming that the underlying burden of clinically meaningful breast cancer was unchanged, these data suggest that 30 cases of cancer per 100,000 women were destined to become large but were detected earlier, and the remaining 132 cases of cancer per 100,000 women were overdiagnosed,” the researchers wrote.
“The magnitude of the imbalance indicates that women were considerably more likely to have tumors that were overdiagnosed than to have earlier detection of a tumor that was destined to become large,” the researchers continued. “Our analysis of size-specific incidence highlights the fact that the introduction of screening mammography has produced a mixture of effects,” Dr. Welch and his associates added.
The Dartmouth Institute for Health Policy and Clinical Practice, Dartmouth’s Geisel School of Medicine, and the National Cancer Institute supported this study. The investigators had no relevant disclosures.
Key clinical point:
Major finding: Of a population of 100,000 women, mammography detected 30 small tumors that were destined to become large but were detected earlier, while 132 cases of cancer were overdiagnosed.
Data source: Retrospective analysis of SEER data from 1975 to 2012.
Disclosures: The Dartmouth Institute for Health Policy and Clinical Practice, Dartmouth’s Geisel School of Medicine, and the National Cancer Institute supported this study. The investigators had no relevant disclosures.
CDC: Improvement in breast cancer mortality slower among black women
Breast cancer mortality rates decreased for both white and black women from 2000 to 2014, but the decrease was slower for black women, according to a report by investigators with the Centers for Disease Control and Prevention.
The mortality rate decreased an average of 1.9% per year for white women, compared with an average decrease of 1.5% per year for black women, in an analysis of data from United States Cancer Statistics (USCS). Between 2010 and 2014, breast cancer mortality was 41% higher among black women (29.2 deaths per 100,000 people) than among white women (20.6 deaths per 100,000 population), reported Lisa C. Richardson, MD, and her associates at the CDC’s National Center for Chronic Disease Prevention and Health Promotion (MMWR. 2016 Oct 14;65[40]:1093-8).![]()
Between 1999 and 2004, mortality rates decreased only for white woman older than 50 years.
USCS includes incidence data from the CDC’s National Program of Cancer Registries and the National Cancer Institute’s Surveillance, Epidemiology, and End Results Program, and mortality data from the National Vital Statistics System.
“When combined with population-based approaches to increase knowledge of family history of cancer, increase physical activity, promote a healthy diet to maintain a healthy bodyweight, and increase screening for breast cancer, targeted treatment interventions could reduce racial disparities in breast cancer,” the investigators said. “A fuller understanding of [breast cancer’s] exact mechanisms might lead to more tailored interventions that could decrease mortality disparities.”
[email protected]
On Twitter @jessnicolecraig
Breast cancer mortality rates decreased for both white and black women from 2000 to 2014, but the decrease was slower for black women, according to a report by investigators with the Centers for Disease Control and Prevention.
The mortality rate decreased an average of 1.9% per year for white women, compared with an average decrease of 1.5% per year for black women, in an analysis of data from United States Cancer Statistics (USCS). Between 2010 and 2014, breast cancer mortality was 41% higher among black women (29.2 deaths per 100,000 people) than among white women (20.6 deaths per 100,000 population), reported Lisa C. Richardson, MD, and her associates at the CDC’s National Center for Chronic Disease Prevention and Health Promotion (MMWR. 2016 Oct 14;65[40]:1093-8).![]()
Between 1999 and 2004, mortality rates decreased only for white woman older than 50 years.
USCS includes incidence data from the CDC’s National Program of Cancer Registries and the National Cancer Institute’s Surveillance, Epidemiology, and End Results Program, and mortality data from the National Vital Statistics System.
“When combined with population-based approaches to increase knowledge of family history of cancer, increase physical activity, promote a healthy diet to maintain a healthy bodyweight, and increase screening for breast cancer, targeted treatment interventions could reduce racial disparities in breast cancer,” the investigators said. “A fuller understanding of [breast cancer’s] exact mechanisms might lead to more tailored interventions that could decrease mortality disparities.”
[email protected]
On Twitter @jessnicolecraig
Breast cancer mortality rates decreased for both white and black women from 2000 to 2014, but the decrease was slower for black women, according to a report by investigators with the Centers for Disease Control and Prevention.
The mortality rate decreased an average of 1.9% per year for white women, compared with an average decrease of 1.5% per year for black women, in an analysis of data from United States Cancer Statistics (USCS). Between 2010 and 2014, breast cancer mortality was 41% higher among black women (29.2 deaths per 100,000 people) than among white women (20.6 deaths per 100,000 population), reported Lisa C. Richardson, MD, and her associates at the CDC’s National Center for Chronic Disease Prevention and Health Promotion (MMWR. 2016 Oct 14;65[40]:1093-8).![]()
Between 1999 and 2004, mortality rates decreased only for white woman older than 50 years.
USCS includes incidence data from the CDC’s National Program of Cancer Registries and the National Cancer Institute’s Surveillance, Epidemiology, and End Results Program, and mortality data from the National Vital Statistics System.
“When combined with population-based approaches to increase knowledge of family history of cancer, increase physical activity, promote a healthy diet to maintain a healthy bodyweight, and increase screening for breast cancer, targeted treatment interventions could reduce racial disparities in breast cancer,” the investigators said. “A fuller understanding of [breast cancer’s] exact mechanisms might lead to more tailored interventions that could decrease mortality disparities.”
[email protected]
On Twitter @jessnicolecraig
Key clinical point:
Major finding: The mortality rate decreased an average of 1.9% per year for white women, compared with an average decrease of 1.5% per year for black women.
Data source: United States Cancer Statistics (USCS).
Disclosures: The CDC supported this study.
Ribociclib/letrozole combo a ‘game changer’ in advanced breast cancer
COPENHAGEN – Progression-free survival for postmenopausal women with hormone receptor–positive advanced breast cancer was significantly improved when the cyclin-dependent kinase inhibitor ribociclib was added to standard therapy with the aromatase inhibitor letrozole, interim analysis from a phase III randomized trial shows.
After 18 months of follow-up, the risk of progression-free survival (PFS) among patients assigned to receive letrozole (Femara) and ribociclib was 44% lower than for patients assigned to receive letrozole and placebo, reported Gabriel N. Hortobagyi, MD, of the University of Texas MD Anderson Cancer Center, Houston, on behalf of coinvestigators in the MONALEESA-2 trial.

“We concluded that patients who received ribociclib with letrozole had a statistically significant and a clinically meaningful increase in progress-free survival compared to letrozole plus placebo, or letrozole alone,” he said at the European Society for Medical Oncology Congress.
“Is this a game changer? I think it probably is,” said invited discussant Stephen R.D. Johnston, MD, PhD, professor of breast cancer medicine and consultant oncologist at Royal Marsden Hospital in London.

Results of the first interim analysis of MONALEESA-2 (Mammary Oncology Assessment of LEE011’s Efficacy and Safety) were published simultaneously in the New England Journal of Medicine.
CDK 4 and 6 are frequently overexpressed in hormone receptor–positive breast cancer, and are key mediators of endocrine resistance, Dr. Hortobagyi explained.
Ribociclib is an oral small-molecule inhibitor of the pathway that includes CDK4/6 and the retinoblastoma protein, and has been shown to have efficacy in previously untreated HR-positive advanced breast cancer, and in patients with progressive disease on other therapies.
The MONALEESA-2 study is a phase III, double-blind, placebo-controlled trial of 668 postmenopausal women with HR-positive, HER2-negative advanced breast cancer who had not received prior therapy for advanced disease. Patients were stratified by the presence or absence of liver and/or lung metastases, and then assigned to receive letrozole 2.5 mg/day plus either ribociclib 600 mg/day for 3 weeks followed by 1 week off, or placebo on the same schedule.
At a preplanned interim analysis, after 243 events (disease progression or death) had occurred, the investigators found that the trial met its primary endpoint of locally assessed PFS, with a hazard ratio for ribociclib of 0.556 (P = .0000329 for superiority).
At the time of the analysis, median PFS had not been reached in the combination arm, compared with 14.7 months for the letrozole/placebo arm.
At 18 months’ follow-up (median 15.3 months), the PFS rate for ribociclib and letrozole was 63%, compared with 42.2% in the placebo group.
Respective response rates for patients with measurable disease at baseline were 52.7% vs. 37.1% (P less than .001).
Grade 3 or 4 adverse events occurring in more than 10% of patients included neutropenia in nearly two-thirds (59.3%) of the women who received ribociclib vs. 0.9% of those who received placebo, and leukopenia in 21% vs. 0.6%, respectively. In all, 7.5% of patients in the ribociclib group discontinued therapy because of adverse events, compared with 2.1% in the placebo group.
The challenge, Dr. Johnston said, will be to figure out how to integrate the findings from this trial and similar results with the CDK4/6 inhibitor palbociclib and letrozole seen in the PALOMA-2 trial into clinical practice.
Clinicians will be faced with deciding how to select various patient groups – endocrine sensitive, endocrine resistant, and treatment-naive – for targeted combinations or perhaps, for some patients, an aromatase inhibitor alone.
It also remains to be seen whether the CDK4/6 inhibitor/AI combination will be cost effective or affordable in many countries, and the pattern of resistance to CDK 4/6 inhibition is sill unknown, Dr. Johnston said.
The study was funded by Novartis. Dr. Hortobagyi disclosed grants and personal fees from the company during the conduct of the study, and personal fees from Eli Lilly and Pfizer outside the submitted work. Dr. Johnston disclosed consulting and/or research funding with AstraZeneca, GlaxoSmithKline, Novartis, Pfizer, Eli Lilly, Roche/Genentech and Puma
COPENHAGEN – Progression-free survival for postmenopausal women with hormone receptor–positive advanced breast cancer was significantly improved when the cyclin-dependent kinase inhibitor ribociclib was added to standard therapy with the aromatase inhibitor letrozole, interim analysis from a phase III randomized trial shows.
After 18 months of follow-up, the risk of progression-free survival (PFS) among patients assigned to receive letrozole (Femara) and ribociclib was 44% lower than for patients assigned to receive letrozole and placebo, reported Gabriel N. Hortobagyi, MD, of the University of Texas MD Anderson Cancer Center, Houston, on behalf of coinvestigators in the MONALEESA-2 trial.
“We concluded that patients who received ribociclib with letrozole had a statistically significant and a clinically meaningful increase in progress-free survival compared to letrozole plus placebo, or letrozole alone,” he said at the European Society for Medical Oncology Congress.
“Is this a game changer? I think it probably is,” said invited discussant Stephen R.D. Johnston, MD, PhD, professor of breast cancer medicine and consultant oncologist at Royal Marsden Hospital in London.
Results of the first interim analysis of MONALEESA-2 (Mammary Oncology Assessment of LEE011’s Efficacy and Safety) were published simultaneously in the New England Journal of Medicine.
CDK 4 and 6 are frequently overexpressed in hormone receptor–positive breast cancer, and are key mediators of endocrine resistance, Dr. Hortobagyi explained.
Ribociclib is an oral small-molecule inhibitor of the pathway that includes CDK4/6 and the retinoblastoma protein, and has been shown to have efficacy in previously untreated HR-positive advanced breast cancer, and in patients with progressive disease on other therapies.
The MONALEESA-2 study is a phase III, double-blind, placebo-controlled trial of 668 postmenopausal women with HR-positive, HER2-negative advanced breast cancer who had not received prior therapy for advanced disease. Patients were stratified by the presence or absence of liver and/or lung metastases, and then assigned to receive letrozole 2.5 mg/day plus either ribociclib 600 mg/day for 3 weeks followed by 1 week off, or placebo on the same schedule.
At a preplanned interim analysis, after 243 events (disease progression or death) had occurred, the investigators found that the trial met its primary endpoint of locally assessed PFS, with a hazard ratio for ribociclib of 0.556 (P = .0000329 for superiority).
At the time of the analysis, median PFS had not been reached in the combination arm, compared with 14.7 months for the letrozole/placebo arm.
At 18 months’ follow-up (median 15.3 months), the PFS rate for ribociclib and letrozole was 63%, compared with 42.2% in the placebo group.
Respective response rates for patients with measurable disease at baseline were 52.7% vs. 37.1% (P less than .001).
Grade 3 or 4 adverse events occurring in more than 10% of patients included neutropenia in nearly two-thirds (59.3%) of the women who received ribociclib vs. 0.9% of those who received placebo, and leukopenia in 21% vs. 0.6%, respectively. In all, 7.5% of patients in the ribociclib group discontinued therapy because of adverse events, compared with 2.1% in the placebo group.
The challenge, Dr. Johnston said, will be to figure out how to integrate the findings from this trial and similar results with the CDK4/6 inhibitor palbociclib and letrozole seen in the PALOMA-2 trial into clinical practice.
Clinicians will be faced with deciding how to select various patient groups – endocrine sensitive, endocrine resistant, and treatment-naive – for targeted combinations or perhaps, for some patients, an aromatase inhibitor alone.
It also remains to be seen whether the CDK4/6 inhibitor/AI combination will be cost effective or affordable in many countries, and the pattern of resistance to CDK 4/6 inhibition is sill unknown, Dr. Johnston said.
The study was funded by Novartis. Dr. Hortobagyi disclosed grants and personal fees from the company during the conduct of the study, and personal fees from Eli Lilly and Pfizer outside the submitted work. Dr. Johnston disclosed consulting and/or research funding with AstraZeneca, GlaxoSmithKline, Novartis, Pfizer, Eli Lilly, Roche/Genentech and Puma
COPENHAGEN – Progression-free survival for postmenopausal women with hormone receptor–positive advanced breast cancer was significantly improved when the cyclin-dependent kinase inhibitor ribociclib was added to standard therapy with the aromatase inhibitor letrozole, interim analysis from a phase III randomized trial shows.
After 18 months of follow-up, the risk of progression-free survival (PFS) among patients assigned to receive letrozole (Femara) and ribociclib was 44% lower than for patients assigned to receive letrozole and placebo, reported Gabriel N. Hortobagyi, MD, of the University of Texas MD Anderson Cancer Center, Houston, on behalf of coinvestigators in the MONALEESA-2 trial.
“We concluded that patients who received ribociclib with letrozole had a statistically significant and a clinically meaningful increase in progress-free survival compared to letrozole plus placebo, or letrozole alone,” he said at the European Society for Medical Oncology Congress.
“Is this a game changer? I think it probably is,” said invited discussant Stephen R.D. Johnston, MD, PhD, professor of breast cancer medicine and consultant oncologist at Royal Marsden Hospital in London.
Results of the first interim analysis of MONALEESA-2 (Mammary Oncology Assessment of LEE011’s Efficacy and Safety) were published simultaneously in the New England Journal of Medicine.
CDK 4 and 6 are frequently overexpressed in hormone receptor–positive breast cancer, and are key mediators of endocrine resistance, Dr. Hortobagyi explained.
Ribociclib is an oral small-molecule inhibitor of the pathway that includes CDK4/6 and the retinoblastoma protein, and has been shown to have efficacy in previously untreated HR-positive advanced breast cancer, and in patients with progressive disease on other therapies.
The MONALEESA-2 study is a phase III, double-blind, placebo-controlled trial of 668 postmenopausal women with HR-positive, HER2-negative advanced breast cancer who had not received prior therapy for advanced disease. Patients were stratified by the presence or absence of liver and/or lung metastases, and then assigned to receive letrozole 2.5 mg/day plus either ribociclib 600 mg/day for 3 weeks followed by 1 week off, or placebo on the same schedule.
At a preplanned interim analysis, after 243 events (disease progression or death) had occurred, the investigators found that the trial met its primary endpoint of locally assessed PFS, with a hazard ratio for ribociclib of 0.556 (P = .0000329 for superiority).
At the time of the analysis, median PFS had not been reached in the combination arm, compared with 14.7 months for the letrozole/placebo arm.
At 18 months’ follow-up (median 15.3 months), the PFS rate for ribociclib and letrozole was 63%, compared with 42.2% in the placebo group.
Respective response rates for patients with measurable disease at baseline were 52.7% vs. 37.1% (P less than .001).
Grade 3 or 4 adverse events occurring in more than 10% of patients included neutropenia in nearly two-thirds (59.3%) of the women who received ribociclib vs. 0.9% of those who received placebo, and leukopenia in 21% vs. 0.6%, respectively. In all, 7.5% of patients in the ribociclib group discontinued therapy because of adverse events, compared with 2.1% in the placebo group.
The challenge, Dr. Johnston said, will be to figure out how to integrate the findings from this trial and similar results with the CDK4/6 inhibitor palbociclib and letrozole seen in the PALOMA-2 trial into clinical practice.
Clinicians will be faced with deciding how to select various patient groups – endocrine sensitive, endocrine resistant, and treatment-naive – for targeted combinations or perhaps, for some patients, an aromatase inhibitor alone.
It also remains to be seen whether the CDK4/6 inhibitor/AI combination will be cost effective or affordable in many countries, and the pattern of resistance to CDK 4/6 inhibition is sill unknown, Dr. Johnston said.
The study was funded by Novartis. Dr. Hortobagyi disclosed grants and personal fees from the company during the conduct of the study, and personal fees from Eli Lilly and Pfizer outside the submitted work. Dr. Johnston disclosed consulting and/or research funding with AstraZeneca, GlaxoSmithKline, Novartis, Pfizer, Eli Lilly, Roche/Genentech and Puma
Key clinical point: Adding the CDK 4/6 inhibitor ribociclib to an aromatase inhibitor significantly improved PFS in postmenopausal women with HR+/HER2- advanced breast cancer.
Major finding: The hazard ratio for progression with the combination of ribociclib and letrozole was 0.556 compared with letrozole/placebo.
Data source: Randomized phase III, placebo controlled trial in 668 postmenopausal women with untreated HR-positive/HER2- advanced breast cancer.
Disclosures: The study was funded by Novartis. Dr. Hortobagyi disclosed grants and personal fees from the company during the conduct of the study, and personal fees from Eli Lilly and Pfizer outside the submitted work. Dr. Johnston disclosed consulting and/or research funding with AstraZeneca, GlaxoSmithKline, Novartis, Pfizer, Eli Lilly, Roche/Genentech and Puma.
Partial-breast irradiation alternative to mastectomy following recurrence
BOSTON – In women with in-breast failures following breast-conserving surgery and whole-breast irradiation, partial-breast irradiation with 3D conformal radiation appears to be an effective and safe alternative to mastectomy, results of a phase II trial indicate.
At a median follow-up of 3.6 years, there were only two ipsilateral breast recurrences, and four mastectomies required among 58 women treated with partial-breast irradiation after a second lumpectomy, reported Douglas W. Arthur, MD, chair of radiation oncology at Virginia Commonwealth University in Richmond.

“I think this information adds to the growing data supporting this treatment approach as an alternative to mastectomy for those who continue to want to preserve the breast,” he said at a late-breaking abstracts session at the annual meeting of the American Society of Radiation Oncology.
The NRG/RTOG 1014 study is a prospective phase II trial designed to evaluate skin, breast, and chest wall events occurring within 1 year of re-irradiation. One-year toxicity results from the trial were reported at the 2015 ASTRO annual meeting.
Dr. Arthur presented 3-year efficacy results from the trial. The investigators enrolled women with in-breast recurrences more than 1 year after whole-breast irradiation (WBI), with tumors that were smaller than 3 cm, unifocal, and resected with negative margins. Axillary involvement was limited to pathologic NO or N1 without extracapsular extension.
Partial-breast irradiation was targeted to the surgical cavity with a safety margin of plus 1.5 cm for the clinical target volume, and an additional 1-cm expansion. The prescribed dose was 45 Gy in 1.5-Gy fractions delivered via 3D conformal radiotherapy in 30 treatments.
Of 65 patients accrued, 58 completed treatment and were evaluable for efficacy. The median age was 67.5 years. In all, 23 patients had ductal carcinoma in situ, and 35 had invasive cancers. All patients were node negative.
A total of four patients (6.9%) reported late grade 3 toxicities, which included breast infection, fibrous deep connective tissue, skin induration, and breast atrophy, pain, and volume loss. There were no grade 4 toxicities, and no treatment-related deaths.
Two patients had in-breast recurrences, which translated into a year estimate of 3.7%. Four patients underwent mastectomies, for a 3-year estimated mastectomy failure rate of 5.2%. Two of the mastectomies were for the in-breast recurrences, one for a nonhealing wound, and one occurred in a patient who developed cancer in the contralateral breast and opted for a bilateral mastectomy.
BOSTON – In women with in-breast failures following breast-conserving surgery and whole-breast irradiation, partial-breast irradiation with 3D conformal radiation appears to be an effective and safe alternative to mastectomy, results of a phase II trial indicate.
At a median follow-up of 3.6 years, there were only two ipsilateral breast recurrences, and four mastectomies required among 58 women treated with partial-breast irradiation after a second lumpectomy, reported Douglas W. Arthur, MD, chair of radiation oncology at Virginia Commonwealth University in Richmond.
“I think this information adds to the growing data supporting this treatment approach as an alternative to mastectomy for those who continue to want to preserve the breast,” he said at a late-breaking abstracts session at the annual meeting of the American Society of Radiation Oncology.
The NRG/RTOG 1014 study is a prospective phase II trial designed to evaluate skin, breast, and chest wall events occurring within 1 year of re-irradiation. One-year toxicity results from the trial were reported at the 2015 ASTRO annual meeting.
Dr. Arthur presented 3-year efficacy results from the trial. The investigators enrolled women with in-breast recurrences more than 1 year after whole-breast irradiation (WBI), with tumors that were smaller than 3 cm, unifocal, and resected with negative margins. Axillary involvement was limited to pathologic NO or N1 without extracapsular extension.
Partial-breast irradiation was targeted to the surgical cavity with a safety margin of plus 1.5 cm for the clinical target volume, and an additional 1-cm expansion. The prescribed dose was 45 Gy in 1.5-Gy fractions delivered via 3D conformal radiotherapy in 30 treatments.
Of 65 patients accrued, 58 completed treatment and were evaluable for efficacy. The median age was 67.5 years. In all, 23 patients had ductal carcinoma in situ, and 35 had invasive cancers. All patients were node negative.
A total of four patients (6.9%) reported late grade 3 toxicities, which included breast infection, fibrous deep connective tissue, skin induration, and breast atrophy, pain, and volume loss. There were no grade 4 toxicities, and no treatment-related deaths.
Two patients had in-breast recurrences, which translated into a year estimate of 3.7%. Four patients underwent mastectomies, for a 3-year estimated mastectomy failure rate of 5.2%. Two of the mastectomies were for the in-breast recurrences, one for a nonhealing wound, and one occurred in a patient who developed cancer in the contralateral breast and opted for a bilateral mastectomy.
BOSTON – In women with in-breast failures following breast-conserving surgery and whole-breast irradiation, partial-breast irradiation with 3D conformal radiation appears to be an effective and safe alternative to mastectomy, results of a phase II trial indicate.
At a median follow-up of 3.6 years, there were only two ipsilateral breast recurrences, and four mastectomies required among 58 women treated with partial-breast irradiation after a second lumpectomy, reported Douglas W. Arthur, MD, chair of radiation oncology at Virginia Commonwealth University in Richmond.
“I think this information adds to the growing data supporting this treatment approach as an alternative to mastectomy for those who continue to want to preserve the breast,” he said at a late-breaking abstracts session at the annual meeting of the American Society of Radiation Oncology.
The NRG/RTOG 1014 study is a prospective phase II trial designed to evaluate skin, breast, and chest wall events occurring within 1 year of re-irradiation. One-year toxicity results from the trial were reported at the 2015 ASTRO annual meeting.
Dr. Arthur presented 3-year efficacy results from the trial. The investigators enrolled women with in-breast recurrences more than 1 year after whole-breast irradiation (WBI), with tumors that were smaller than 3 cm, unifocal, and resected with negative margins. Axillary involvement was limited to pathologic NO or N1 without extracapsular extension.
Partial-breast irradiation was targeted to the surgical cavity with a safety margin of plus 1.5 cm for the clinical target volume, and an additional 1-cm expansion. The prescribed dose was 45 Gy in 1.5-Gy fractions delivered via 3D conformal radiotherapy in 30 treatments.
Of 65 patients accrued, 58 completed treatment and were evaluable for efficacy. The median age was 67.5 years. In all, 23 patients had ductal carcinoma in situ, and 35 had invasive cancers. All patients were node negative.
A total of four patients (6.9%) reported late grade 3 toxicities, which included breast infection, fibrous deep connective tissue, skin induration, and breast atrophy, pain, and volume loss. There were no grade 4 toxicities, and no treatment-related deaths.
Two patients had in-breast recurrences, which translated into a year estimate of 3.7%. Four patients underwent mastectomies, for a 3-year estimated mastectomy failure rate of 5.2%. Two of the mastectomies were for the in-breast recurrences, one for a nonhealing wound, and one occurred in a patient who developed cancer in the contralateral breast and opted for a bilateral mastectomy.
AT ASTRO 2016
Key clinical point: Re-irradiation following second lumpectomy after in-breast cancer recurrences appears to be a safe and effective alternative to mastectomy.
Major finding: The 3-year estimated in-breast recurrence rate was 3.7%.
Data source: Phase II nonrandomized study in 58 women with in-breast failures following breast-conserving surgery and whole-breast irradiation.
Disclosures: The study was supported by the National Cancer Institute. Dr. Arthur reported formerly serving on the medical advisory board of Impedimed,
Boost dose pays off long term after surgery, WBRT for DCIS
BOSTON – Adding a boost dose after surgery and whole-breast radiation therapy (WBRT) for ductal carcinoma in situ offers a small but significant reduction in long-term risk of same-breast recurrence, according to results of a multicenter study.
An analysis of pooled data from 10 institutions showed that after 15 years of follow-up, 91.6% of women who had been treated with breast-conserving surgery, WBRT, and a boost dose remained free of ipsilateral breast tumor recurrence (IBTR), compared with 88% of women who received WBRT alone, reported Meena Savur Moran, MD, director of the breast cancer radiotherapy program at Smilow Cancer Hospital, Yale New Haven, Connecticut.

The absolute differences between the groups – 3% at 10 years, and 4% at 15 years – “don’t seem like a lot, but it is clinically important for patients, because what we’ve learned from the invasive cancer data is that this small, incremental decrease results in about a 40% less mastectomy rate for salvage mastectomies for recurrences,” she said.
It is common practice in many centers to give a radiation boost to the tumor bed of 8-16 Gy in 4-8 additional fractions following breast-conserving surgery and WBRT. This has been shown in invasive cancers to be associated with a statistically significant decrease in risk for IBTR in all age groups of about 4% at 20 years.
Yet because DCIS generally has an excellent prognosis with very few recurrences after whole-breast irradiation, it has been harder to determine whether radiation boosting would offer similar benefit to that seen in invasive cancers,
In an attempt to answer this question, investigators from 10 centers collaborated to create a DCIS database of patients treated with WBRT either with or without boost, and then analyzed the results.
The final cohort included 4,131 patients, far exceeding the minimum sample size the statisticians calculated would be needed to detect a benefit.
The median age of patients at the time of therapy was 56.1 years, median follow-up was 9 years, and the median boost dose was 14 Gy. In all, 4% of patients had positive tumor margins after surgery.
Rates of IBTR-free survival with boost vs. no boost were 97.1% vs. 96.3% at 5 years, 94.1% vs. 92.5% at 10 years, and, as noted before, 91.6% vs. 88% at 15 years (P = .0389).
In both univariate and in multivariate analysis controlling for tumor grade, comedo carcinoma, tamoxifen use, margin status, and age, IBTR was significantly associated with lower risk for recurrence.
The investigators also conducted a boost/no boost analysis stratified by margin status using both the National Surgical Adjuvant Breast and Bowel Project (NSABP) definition of negative margins as no ink on tumor, and the joint Society of Surgical Oncology, ASTRO, and American Society of Clinical Oncology guideline definition as less than 2 mm, and in each case found that among patients with negative margins, boosting offered a significant recurrence-free advantage.
Finally, they found that boosting offered a significant advantage both for patients 50 and older (P = .0073) and those 49 and younger (P = .0166).
“For DCIS, most of who treat breast cancer have used a boost, but we really extrapolated from the treatment from invasive breast cancer. Evidence for this practice until now in specific for DCIS has been lacking,” said Geraldine Jacobson, MD, MPH, professor and chair of radiation oncology at West Virginia University, Morgantown. Dr. Jacobson moderated the briefing.
She noted that the large sample size and long follow-up of the study was necessary for the treatment benefit to emerge.
BOSTON – Adding a boost dose after surgery and whole-breast radiation therapy (WBRT) for ductal carcinoma in situ offers a small but significant reduction in long-term risk of same-breast recurrence, according to results of a multicenter study.
An analysis of pooled data from 10 institutions showed that after 15 years of follow-up, 91.6% of women who had been treated with breast-conserving surgery, WBRT, and a boost dose remained free of ipsilateral breast tumor recurrence (IBTR), compared with 88% of women who received WBRT alone, reported Meena Savur Moran, MD, director of the breast cancer radiotherapy program at Smilow Cancer Hospital, Yale New Haven, Connecticut.
The absolute differences between the groups – 3% at 10 years, and 4% at 15 years – “don’t seem like a lot, but it is clinically important for patients, because what we’ve learned from the invasive cancer data is that this small, incremental decrease results in about a 40% less mastectomy rate for salvage mastectomies for recurrences,” she said.
It is common practice in many centers to give a radiation boost to the tumor bed of 8-16 Gy in 4-8 additional fractions following breast-conserving surgery and WBRT. This has been shown in invasive cancers to be associated with a statistically significant decrease in risk for IBTR in all age groups of about 4% at 20 years.
Yet because DCIS generally has an excellent prognosis with very few recurrences after whole-breast irradiation, it has been harder to determine whether radiation boosting would offer similar benefit to that seen in invasive cancers,
In an attempt to answer this question, investigators from 10 centers collaborated to create a DCIS database of patients treated with WBRT either with or without boost, and then analyzed the results.
The final cohort included 4,131 patients, far exceeding the minimum sample size the statisticians calculated would be needed to detect a benefit.
The median age of patients at the time of therapy was 56.1 years, median follow-up was 9 years, and the median boost dose was 14 Gy. In all, 4% of patients had positive tumor margins after surgery.
Rates of IBTR-free survival with boost vs. no boost were 97.1% vs. 96.3% at 5 years, 94.1% vs. 92.5% at 10 years, and, as noted before, 91.6% vs. 88% at 15 years (P = .0389).
In both univariate and in multivariate analysis controlling for tumor grade, comedo carcinoma, tamoxifen use, margin status, and age, IBTR was significantly associated with lower risk for recurrence.
The investigators also conducted a boost/no boost analysis stratified by margin status using both the National Surgical Adjuvant Breast and Bowel Project (NSABP) definition of negative margins as no ink on tumor, and the joint Society of Surgical Oncology, ASTRO, and American Society of Clinical Oncology guideline definition as less than 2 mm, and in each case found that among patients with negative margins, boosting offered a significant recurrence-free advantage.
Finally, they found that boosting offered a significant advantage both for patients 50 and older (P = .0073) and those 49 and younger (P = .0166).
“For DCIS, most of who treat breast cancer have used a boost, but we really extrapolated from the treatment from invasive breast cancer. Evidence for this practice until now in specific for DCIS has been lacking,” said Geraldine Jacobson, MD, MPH, professor and chair of radiation oncology at West Virginia University, Morgantown. Dr. Jacobson moderated the briefing.
She noted that the large sample size and long follow-up of the study was necessary for the treatment benefit to emerge.
BOSTON – Adding a boost dose after surgery and whole-breast radiation therapy (WBRT) for ductal carcinoma in situ offers a small but significant reduction in long-term risk of same-breast recurrence, according to results of a multicenter study.
An analysis of pooled data from 10 institutions showed that after 15 years of follow-up, 91.6% of women who had been treated with breast-conserving surgery, WBRT, and a boost dose remained free of ipsilateral breast tumor recurrence (IBTR), compared with 88% of women who received WBRT alone, reported Meena Savur Moran, MD, director of the breast cancer radiotherapy program at Smilow Cancer Hospital, Yale New Haven, Connecticut.
The absolute differences between the groups – 3% at 10 years, and 4% at 15 years – “don’t seem like a lot, but it is clinically important for patients, because what we’ve learned from the invasive cancer data is that this small, incremental decrease results in about a 40% less mastectomy rate for salvage mastectomies for recurrences,” she said.
It is common practice in many centers to give a radiation boost to the tumor bed of 8-16 Gy in 4-8 additional fractions following breast-conserving surgery and WBRT. This has been shown in invasive cancers to be associated with a statistically significant decrease in risk for IBTR in all age groups of about 4% at 20 years.
Yet because DCIS generally has an excellent prognosis with very few recurrences after whole-breast irradiation, it has been harder to determine whether radiation boosting would offer similar benefit to that seen in invasive cancers,
In an attempt to answer this question, investigators from 10 centers collaborated to create a DCIS database of patients treated with WBRT either with or without boost, and then analyzed the results.
The final cohort included 4,131 patients, far exceeding the minimum sample size the statisticians calculated would be needed to detect a benefit.
The median age of patients at the time of therapy was 56.1 years, median follow-up was 9 years, and the median boost dose was 14 Gy. In all, 4% of patients had positive tumor margins after surgery.
Rates of IBTR-free survival with boost vs. no boost were 97.1% vs. 96.3% at 5 years, 94.1% vs. 92.5% at 10 years, and, as noted before, 91.6% vs. 88% at 15 years (P = .0389).
In both univariate and in multivariate analysis controlling for tumor grade, comedo carcinoma, tamoxifen use, margin status, and age, IBTR was significantly associated with lower risk for recurrence.
The investigators also conducted a boost/no boost analysis stratified by margin status using both the National Surgical Adjuvant Breast and Bowel Project (NSABP) definition of negative margins as no ink on tumor, and the joint Society of Surgical Oncology, ASTRO, and American Society of Clinical Oncology guideline definition as less than 2 mm, and in each case found that among patients with negative margins, boosting offered a significant recurrence-free advantage.
Finally, they found that boosting offered a significant advantage both for patients 50 and older (P = .0073) and those 49 and younger (P = .0166).
“For DCIS, most of who treat breast cancer have used a boost, but we really extrapolated from the treatment from invasive breast cancer. Evidence for this practice until now in specific for DCIS has been lacking,” said Geraldine Jacobson, MD, MPH, professor and chair of radiation oncology at West Virginia University, Morgantown. Dr. Jacobson moderated the briefing.
She noted that the large sample size and long follow-up of the study was necessary for the treatment benefit to emerge.
AT THE ASTRO ANNUAL MEETING 2016
Key clinical point: This study shows a significant benefit for adding a boost radiation dose following breast-conserving surgery and whole-breast radiation for ductal carcinoma in situ (DCIS).
Major finding: After 15 years of follow-up, 91.6% of women who had received a boost dose were free of ipsilateral breast recurrence, compared with 88% of women who did not have a boost.
Data source: Analysis of pooled data on 4,131 patients with DCIS treated at 10 academic medical centers.
Disclosures: The study was supported by participating institutions. Dr. Moran and Dr. Jacobson reported no conflicts of interest.
Modern breast surgery: What you should know
In a striking trend, the rate of contralateral prophylactic mastectomy (CPM) has risen by 30% over the last 10 years in the United States.1 Many women undergo CPM because of the fear and anxiety of cancer recurrence and their perceived risk of contralateral breast cancer; however, few women have a medical condition that necessitates removal of the contralateral breast. The medical indications for CPM include having a pathogenic genetic mutation (eg, BRCA1 and BRCA2), a strong family history of breast cancer, or prior mediastina chest radiation.
The actual risk of contralateral breast cancer is much lower than perceived. In women without a genetic mutation, the 10-year risk of contralateral breast cancer is only 3% to 5%.1 Also, CPM does not prevent the development of metastatic disease and offers no survival benefit over breast conservation or unilateral mastectomy.2 Furthermore, compared with unilateral therapeutic mastectomy, the “upgrade” to a CPM carries a 2.7-fold risk of a major surgical complication.3 It is therefore important that patients receive appropriate counseling regarding CPM, and that this counseling include cancer stage at diagnosis, family history and genetic risk, and cancer versus surgical risk (see “Counseling patients on contralateral prophylactic mastectomy” for key points to cover in patient discussions).
Counseling patients on contralateral prophylactic mastectomy
Commonly, patients diagnosed with breast cancer consider having their contralateral healthy breast removed as part of a bilateral mastectomy. They often experience severe anxiety about the cancer coming back and believe that removing both breasts will enable them to live longer. Keep the following key facts in mind when discussing treatment options with breast cancer patients.
Cancer stage at diagnosis. How long a patient lives from the time of her breast cancer diagnosis depends on the stage of the cancer at diagnosis, not the type of surgery performed. A woman with early stage I or stage II breast cancer has an 80% to 90% chance of being cancer free in 5 years.1 The chance of cancer recurring in the bones, liver, or lungs (metastatic breast cancer) will not be changed by removing the healthy breast. The risk of metastatic recurrence can be reduced, however, with chemotherapy and/or with hormone-blocker therapy.
Family history and genetic risk. Few women have a strong family history of breast and/or ovarian and other cancers, and this issue should be addressed with genetic counseling and testing prior to surgery. Those who carry a cancer-causing gene, such as BRCA1 or BRCA2, are at increased risk (40% to 60%) for a second or third breast cancer, especially if they are diagnosed at a young age (<50 years).2,3 In women who have a genetic mutation, removing both breasts and sometimes the ovaries can prevent development of another breast cancer. But this will not prevent spread of the cancer that is already present. Only chemotherapy and hormone blockers can prevent the spread of cancer.
Cancer risk versus surgical risk. For women with no family history of breast cancer, no genetic mutation, and no prior chest wall radiation, the risk of developing a new breast cancer in their other breast is only 3% to 5% every 10 years.3,4 This means that they have a 95% chance of not developing a new breast cancer in their healthy breast. Notably, removing the healthy breast can double the risk of postsurgical complications, including bleeding, infection, and loss of tissue and implant. The mastectomy site will be numb and the skin and nipple areola will not have any function other than cosmetic. Finally, wound complications from surgery could delay the start of important cancer treatment, such as chemotherapy or radiation.
The bottom line. Unless a woman has a strong family history of breast cancer, is diagnosed at a very young age, or has a genetic cancer-causing mutation, removing the contralateral healthy breast is not medically necessary and is not routinely recommended.
References
- Hennigs A, Riedel F, Gondos A, et al. Prognosis of breast cancer molecular subtypes in routine clinical care: a large prospective cohort study. BMC Cancer. 2016;16(1):734.
- Graeser MK, Engel C, Rhiem K, et al. Contralateral breast cancer risk in BRCA1 and BRCA2 mutation carriers. J Clin Oncol. 2009;27(35):5887–5992.
- Curtis RE, Ron E, Hankey BF, Hoover RN. New malignancies following breast cancer. In: Curtis RE, Freedman DM, Ron E, et al, eds. New Malignancies Among Cancer Survivors: SEER Cancer Registries, 1973-2000. Bethesda, MD: National Cancer Institute. NIH Publ. No. 05-5302. 2006:181–205. http://seer.cancer.gov/archive/publications/mpmono. Accessed September 18, 2016.
- Nichols HB, Berrington de Gonzalez A, Lacey JV Jr, Rosenberg PS, Anderson WF. Declining incidence of contralateral breast cancer in the United States from 1975 to 2006. J Clin Oncol. 2011;29(12):1564–1569.
Women should be made aware that there are alternatives to mastectomy that have similar, or even better, outcomes with improved quality of life. Furthermore, a multi‑disciplinary, team-oriented approach with emphasis on minimally invasive biopsy and better cosmetic outcomes has enhanced quality of care. Knowledge of this team approach and of modern breast cancer treatments is essential for general ObGyns as this understanding improves the overall care and guidance—specifically regarding referral to expert, high-volume breast surgeons—provided to those women most in need.
Expanded treatment options for breast cancer
Advancements in breast surgery, better imaging, and targeted therapies are changing the paradigm of breast cancer treatment.
Image-guided biopsy is key in decision making
When an abnormality is found in the breast, surgical excision of an undiagnosed breast lesion is no longer considered an appropriate first step. Use of image-guided biopsy or minimally invasive core needle biopsy allows for accurate diagnosis of a breast lesion while avoiding a potentially breast deforming and expensive surgical operation. It is always better to go into the operating room (OR) with a diagnosis and do the right operation the first time.
A core needle biopsy, results of which demonstrate a benign lesion, helps avoid breast surgery in women who do not need it. If cancer is diagnosed on biopsy, the extent of disease can be better evaluated and decision making can be more informed, with a multidisciplinary approach used to consider the various options, including genetic counseling, plastic surgery consultation, or neoadjuvant therapy. Some lesions, such as those too close to the skin, chest wall, or an implant, may not be amenable to core needle biopsy and therefore require surgical excision for diagnosis.
Benefits of a multidisciplinary tumor conference
It is important for a multidisciplinary group of cancer specialists to review a patient’s case and discuss the ideal treatment plan prior to surgery. Some breast cancer subtypes (such as human epidermal growth factor receptor 2 [HER2]–overamplified breast cancer and many triple-negative breast cancers) are very sensitive to chemotherapy, and patients with these tumor types may benefit from receiving neoadjuvant chemotherapy prior to surgery. New types of chemotherapy may allow up to 60% of some breast cancers to diminish almost completely, with subsequent improved cosmetic results of breast surgery.4 It may also allow time for genetic counseling and testing prior to surgery. (See “How to code for a multidisciplinary tumor conference” for appropriate coding procedure.)
How to code for a multidisciplinary tumor conference
Melanie Witt, RN, MA
There are two coding choices for team conferences involving physician participation. If the patient and/or family is present, the CPT instruction is to bill a problem E/M service code (99201-99215) based on the time spent during this coordination of care/counseling. Documentation would include details about the conference decisions and implications for care, rather than history or examination.
If the patient is not present, report 99367 (Medical team conference with interdisciplinary team of health care professionals, patient and/or family not present, 30 minutes or more; participation by physician), but note that this code was developed under the assumption that the conference would be performed in a facility setting. Diagnostic coding would be breast cancer.
Ms. Witt is an independent coding and documentation consultant and former program manager, department of coding and nomenclature, American Congress of Obstetricians and Gynecologists.
The author reports no financial relationships relevant to this article.
This is an excerpt from a companion coding resource for breast cancer–related procedures by Ms. Witt. To read the companion article, “Coding for breast cancer–related procedures: A how-to guide,” in its entirety, click here.
Image-guided lumpectomy
Advances in breast imaging have led to increased identification of nonpalpable breast cancers. Surgical excision of nonpalpable breast lesions requires image guidance, which can be done using a variety of techniques.
Wire-guided localization (WGL) has been used in practice for the past 40 years. The procedure involves placement of a hooked wire under local anesthesia using either mammographic or ultrasound guidance. This procedure is mostly done in the radiology department on the same day as the surgery and requires that the radiologist coordinate with the OR schedule. Besides scheduling conflicts and delays in surgery, this procedure can be complicated by wires becoming dislodged, transected, or migrated, and limits the surgeon’s ability to cosmetically hide the scar in relation to position of the wire. It is uncomfortable for the patient, who must be transported from the radiology department to the OR with a wire extruding from her breast.
An alternative localization technique is placement of a radioactive source within the tumor, which can then be identified in the OR with a gamma probe.
Iodine I 125 Radioactive seed localization (RSL) involves placing a 4-mm titanium radiolabeled seed into the breast lesion under mammographic or ultrasound guidance (FIGURES 1 and 2). The procedure can be performed a few days before surgery in the radiology department, and there is less chance for the seed to become displaced or dislodged. This technique provides scheduling flexibility for the radiologist and reduces OR delays. The surgeon uses the same gamma probe for sentinel node biopsy to find the lesion in the breast, using the setting specific for iodine I 125. Incisions can be tailored anywhere in the breast, and the seed is detected by a focal gamma signal. Once the lumpectomy is performed, the specimen is probed and radiographed to confirm removal of the seed and adequate margins.
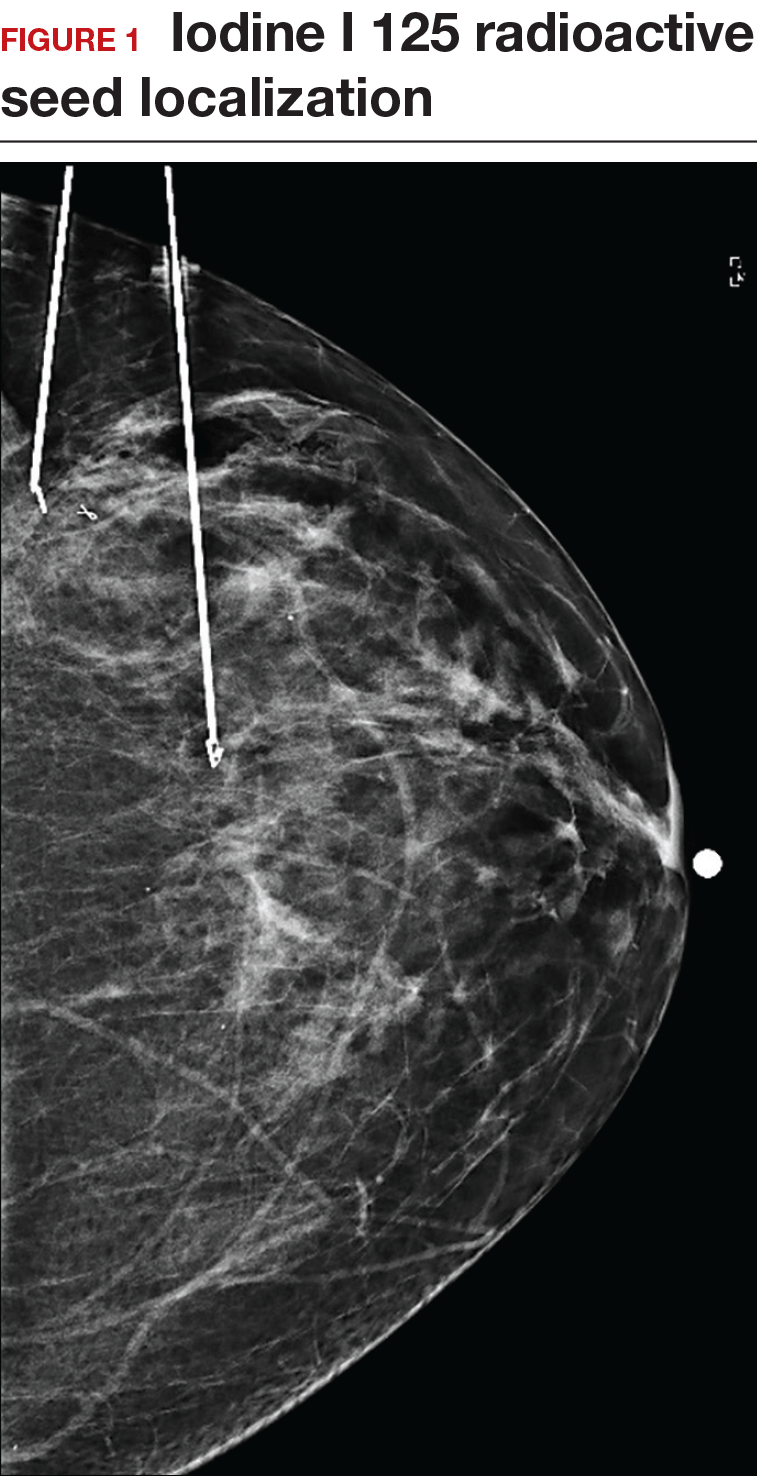
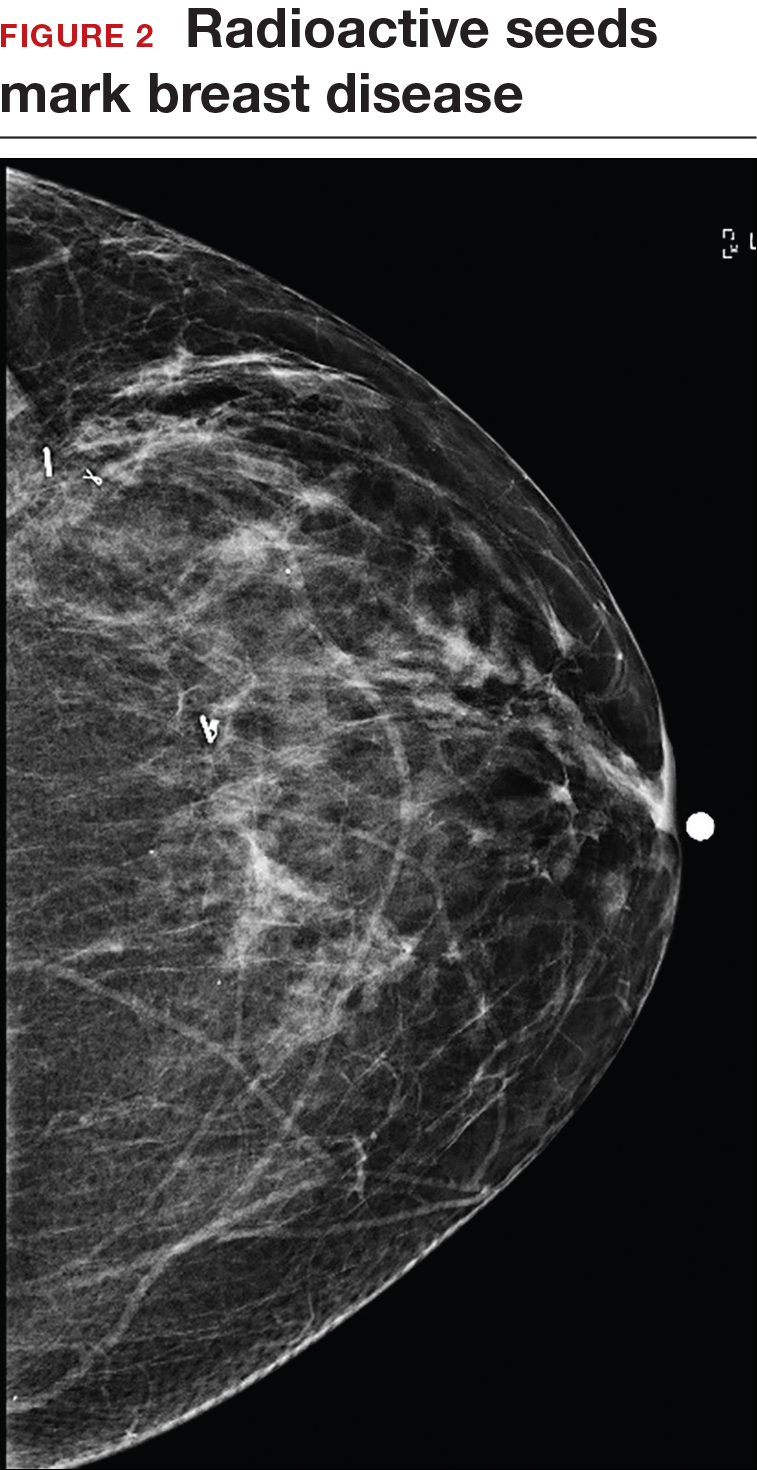
Limitations of this procedure include potential loss of the seed during the operation and radiation safety issues regarding handling and disposal of the radioactive isotope. Once the seed has been placed in the patient’s body, it must be removed surgically, as the half-life of iodine I 125 is long (60 days).5 Care must therefore be taken to optimize medical clearance prior to seed placement and to avoid surgery cancellations.
Intraoperative ultrasound (IOUS) allows the surgeon to identify the lesion under general anesthesia in the OR, which is more comfortable for the patient. The surgical incision can be tailored cosmetically and the lumpectomy can be performed with real-time ultrasound visualization of the tumor during dissection. This technique eliminates the need for a separate preoperative seed or wire localization in radiology. However, it can be used only for lesions or clips that are visible by ultrasound. The excised specimen can be evaluated for confirmation of tumor removal and adequate margins via ultrasound and re-excision of close margins can be accomplished immediately if needed.
Results of a meta-analysis of WGL versus IOUS demonstrated a significant reduction of positive margins with the use of IOUS.6 Results of the COBALT trial, in which patients were assigned randomly to excision of palpable breast cancers with either IOUS or palpation, demonstrated a 14% reduction in positive margins in favor of IOUS.7 Surgeon-performed breast ultrasound requires advanced training and accreditation in breast ultrasound through a rigorous certification process offered by the American Society of Breast Surgeons (www.breastsurgeons.org).
Oncoplastic lumpectomy
This approach to lumpectomy combines adequate oncologist resection of the breast tumor with plastic surgery techniques to achieve superior cosmesis. This approach allows complete removal of the tumor with negative margins, yet maintains the normal shape and contour of the breast. Two techniques have been described: volume displacement and volume replacement.
With the volume displacement technique, the surgeon uses adjacent tissue advancement to fill the lumpectomy cavity with the patient’s own surrounding breast tissue (FIGURE 3). The volume replacement technique requires the transposition of autologous tissue from elsewhere in the body.

Oncoplastic lumpectomy allows more women with larger tumors to undergo breast conservation with better cosmetic results. It reduces the number of mastectomies performed without compromising local control and avoids the need for extensive plastic surgery reconstruction and implants. Special effort and attention must be paid to ensure adequate margins utilizing intraoperative specimen radiograph and pathology evaluation.
This procedure requires that the surgeon acquire specialized skills and knowledge of oncologic and plastic surgery techniques, and it is best performed with the collaboration of a multidisciplinary team. Compared with conventional lumpectomy or mastectomy, oncoplastic breast conservation has been shown to reduce re-excision rates, and it has similar rates of local and distant recurrence and similar disease-free survival and overall survival.8,9
Total skin- and nipple-sparing mastectomy
Some patients do not have the option of breast conservation. Women with multicentric breast cancer (more than 1 tumor in different quadrants of the breast) are better served with mastectomy. Surgical techniques for mastectomy have improved and provide women with various options. One option is skin- and nipple-sparing mastectomy, which preserves the skin envelope overlying the breast (including the skin of the nipple and areola) while removing the glandular elements of the breast and the majority of ductal tissue beneath the nipple-areola complex (FIGURE 4). This surgery can be performed via hidden scars at the inframammary crease or periareolar and is combined with immediate reconstruction, which provides an excellent cosmetic result.
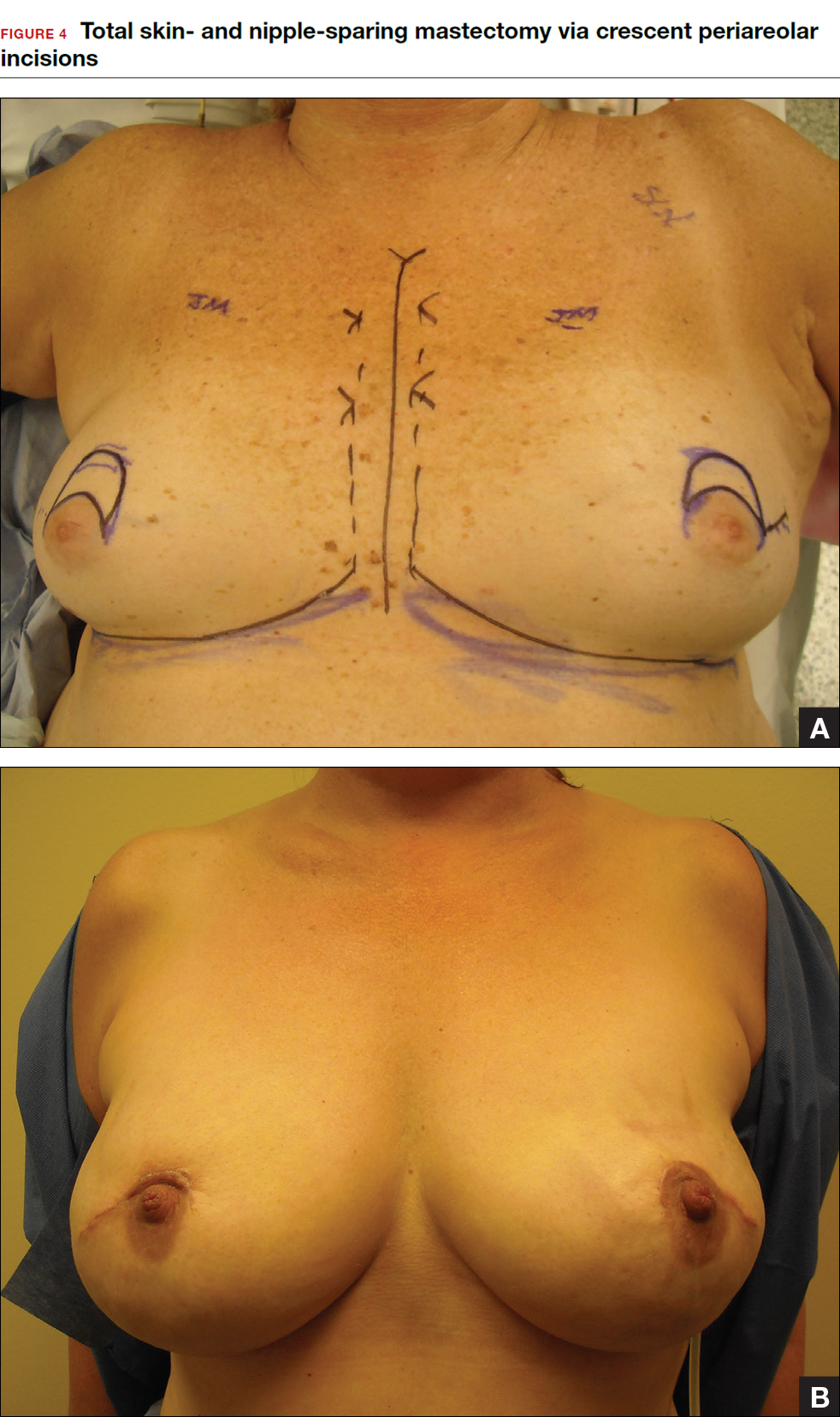
Surgical considerations include removing glandular breast tissue within its anatomic boundaries while maintaining the blood supply to the skin and nipple-areola complex. Furthermore, there must be close dissection of ductal tissue beneath the nipple-areola complex and intraoperative frozen section of the nipple margin in cancer cases. Nipple-sparing mastectomy is oncologically safe in carefully selected patients who do not have cancer near or within the skin or nipple (eg, Paget disease).10 It is also safe as a prophylactic procedure for patients with genetic mutations, such as BRCA1 and BRCA2.11 The procedure is not ideal for smokers or patients with large, pendulous breasts. There is a 3% risk of breast cancer recurrence at the nipple or in the skin or muscle.10 Surgical complications include a 10% to 20% risk of skin or nipple necrosis.12
How do we manage the lymph nodes: Axillary dissection vs sentinel node biopsy?
Evaluation of the axillary nodes is currently part of breast cancer staging and can help the clinician determine the need for adjuvant chemotherapy. It also may assist in assessing the need for extending the radiation field beyond the breast to include the regional lymph nodes. Patients with early stage (stage I and II) breast cancer who do not have abnormal palpable lymph nodes or biopsy-proven metastasis to axillary nodes qualify for sentinel lymph node (SLN) biopsy.
Sentinel node biopsy = less morbidity with no loss of accuracy. Compared with axillary lymph node dissection (ALND; removing all the level I and II nodes in the axilla), SLN biopsy has a 98% accuracy and is associated with less morbidity from lymphedema. The procedure involves injecting the breast with 2 tracers: a radioactive isotope, injected into the breast within 24 hours of the operation, and isosulfan blue dye, injected into the breast in the OR at the time of surgery (see illustration). Both tracers travel through the breast lymphatics and concentrate in the first few lymph nodes that drain the breast. The surgery is performed through a separate axillary incision, and the blue and radioactive lymph nodes are individually dissected and removed for pathologic evaluation. On average, 2 to 4 sentinel nodes are removed, including any suspicious palpable nodes. In experienced hands, this procedure has a false-negative rate of less than 5% to 10%.13
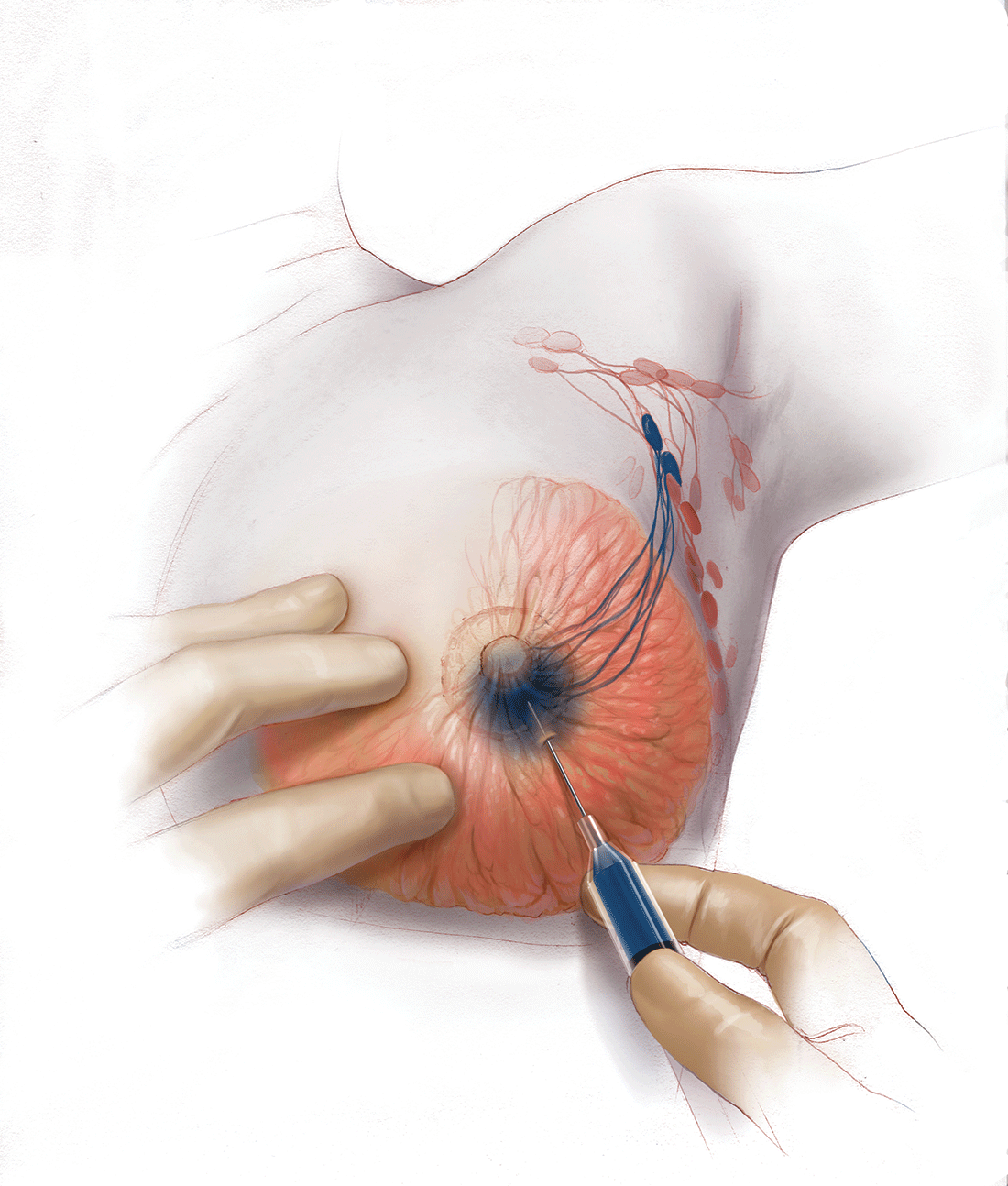
Axillary node dissection no longer standard of care. The indication for a completion ALND has changed based on the results of the randomized trial, ACOSOG Z0011.14 In this trial, patients with early stage breast cancer and 1 to 2 positive SLNs who were undergoing breast conservation therapy with radiation and adjuvant systemic therapy were randomly assigned to ALND or no ALND. (The trial did not include patients who were undergoing mastectomy, neoadjuvant chemotherapy, or who had more than 2 metastatic lymph nodes.) The investigators found no difference in overall or disease-free survival or local-regional recurrence between the 2 treatment groups over 9.2 years of follow up.14
Based on this practice-changing trial result, guidelines of the National Comprehensive Cancer Network no longer recommend completion ALND for patients who meet the ACOSOG Z0011 criteria. For patients who do not meet ACOSOG Z0011 criteria, we do intraoperative pathologic lymph node assessment with either frozen section or imprint cytology, and we perform immediate ALND when results are positive.
Indications for SLN biopsy include:
- invasive breast cancer with clinically negative axillary nodes
- ductal carcinoma in situ (DCIS) with microinvasion or extensive enough to require mastectomy
- clinically negative axillary nodes after neoadjuvant chemotherapy.
Contraindications for SLN biopsy include:
- bulky palpable lymphadenopathy
- pregnancy, as the safety of radioactive isotope and blue dye is not well studied; in isotope mapping the radiation dose is small and within safety limits for pregnant patients
- inflammatory breast cancer.
Complications of any axillary surgery may include risk of lymphedema (5% with SLN biopsy and 30% to 40% with ALND).15 Other complications include neuropathy of the affected arm with chronic pain and numbness of the skin.
Positive trends: Improved patient outcomes, specialized clinician training
Management of breast cancer has changed dramatically over the past several decades. More women are surviving breast cancer thanks to improvements in early detection, an individualized treatment approach with less aggressive surgery, and more effective targeted systemic therapies. A multidisciplinary, team-oriented approach with emphasis on minimally invasive biopsy and better cosmetic outcomes has enhanced quality of care.
Complexity in breast disease management has led to the development of formal fellowship training in breast surgical oncology. Studies have demonstrated that patients treated by high-volume breast surgeons are more satisfied with their care and have improved cancer outcomes.16,17 Women should be aware that they have different options for their breast cancer care, and surgeons with advanced specialization in this field may provide optimal results and better quality of care.
Share your thoughts! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.
- Nichols HB, Berrington de Gonzalez A, Lacey JV Jr, Rosenberg PS, Anderson WF. Declining incidence of contralateral breast cancer in the United States from 1975 to 2006. J Clin Oncol. 2011;29(12):1564–1569.
- Wong SM, Freedman RA, Sagara Y, Aydogan F, Barry WT, Golshan M. Growing use of contralateral prophylactic mastectomy despite no improvement in long-term survival for invasive breast cancer [published online ahead of print March 8, 2016]. Ann Surg. doi:10.1097/SLA.0000000000001698.
- Miller ME, Czechura T, Martz B, et al. Operative risks associated with contralateral prophylactic mastectomy: a single institution experience. Ann Surg Oncol. 2013;20(13):4113–4120.
- Zhang X, Zhang XJ, Zhang TY, et al. Effect and safety of dual anti-human epidermal growth factor receptor 2 therapy compared to monotherapy in patients with human epidermal growth factor receptor 2-positive breast cancer: a systematic review. BMC Cancer. 2014;14:625.
- Ahmed M, Rubio IT, Klaase JM, Douek M. Surgical treatment of nonpalpable primary invasive and in situ breast cancer. Nat Rev Clin Oncol. 2015;12(11):645–663.
- Ahmed M, Douek M. Intra-operative ultrasound versus wire-guided localization in the surgical management of non-palpable breast cancers: systemic review and meta-analysis. Breast Cancer Res Treat. 2013;140(3):435–446.
- Krekel NM, Haloua MH, Lopes Cardozo AM, et al. Intraoperative ultrasound guidance for palpable breast cancer excision (COBALT trial): a multicentre, randomised controlled trial. Lancet Oncol. 2013;14(1):48–54.
- Chakravorty A, Shrestha AK, Sanmugalingam N, et al. How safe is oncoplastic breast conservation? Comparative analysis with standard breast conserving surgery. Eur J Surg Oncol. 2012;38(5):395–398.
- De Lorenzi F, Hubner G, Rotmensz N, et al. Oncological results of oncoplastic breast-conserving surgery: long term follow-up of a large series at a single institution: a matched-cohort analysis. Eur J Surg Oncol. 2016;42(1):71–77.
- De La Cruz L, Moody AM, Tappy EE, Blankenship AA, Hecht EM. Overall survival, disease-free survival, local recurrence, and nipple-areolar recurrence in the setting of nipple-sparing mastectomy: a meta-analysis and systematic review. Ann Surg Oncol. 2015;22(10):3241–3249.
- Yao K, Liederbach E, Tang R, et al. Nipple-sparing mastectomy in BRCA1/2 mutation carriers: an interim analysis and review of the literature. Ann Surg Oncol. 2015;22(2):370–376.
- Fortunato L, Loreti A, Andrich R, et al. When mastectomy is needed: is the nipple-sparing procedure a new standard with very few contraindications? J Surg Oncol. 2013;108(4):207–212.
- Veronesi U, Viale G, Paganelli G, et al. Sentinel lymph node biopsy in breast cancer: ten-year results of a randomized controlled study. Ann Surg. 2010;251(4):595–600.
- Giuliano AE, Hunt K, Ballman KV, et al. Ten-year survival results of ACOSOG Z0011: a randomized trial of axillary node dissection in women with clinical T1-2 N0 M0 breast cancer who have a positive sentinel node (Alliance). In: 2016 ASCO Annual Meeting; June 3-7, 2016. J Clin Oncol. 2016;34(15; May 20 suppl): Abstract 1007.
- DiSipio T, Rye S, Newman B, Hayes S. Incidence of unilateral arm lymphedema after breast cancer: a systematic review and meta-analysis. Lancet Oncol. 2013;14(6):500–515.
- Skinner KA, Helsper JT, Deapen D, Ye W, Sposto R. Breast cancer: do specialists make a difference? Ann Surg Oncol. 2003;10(6):606–615.
- Waljee JF, Hawley S, Alderman AK, Morrow M, Katz SJ. Patient satisfaction with treatment of breast cancer: does surgeon specialization matter? J Clin Oncol. 2007;25(24):3694–3698.

The author reports no financial relationships relevant to this article.
The author reports no financial relationships relevant to this article.
The author reports no financial relationships relevant to this article.
In a striking trend, the rate of contralateral prophylactic mastectomy (CPM) has risen by 30% over the last 10 years in the United States.1 Many women undergo CPM because of the fear and anxiety of cancer recurrence and their perceived risk of contralateral breast cancer; however, few women have a medical condition that necessitates removal of the contralateral breast. The medical indications for CPM include having a pathogenic genetic mutation (eg, BRCA1 and BRCA2), a strong family history of breast cancer, or prior mediastina chest radiation.
The actual risk of contralateral breast cancer is much lower than perceived. In women without a genetic mutation, the 10-year risk of contralateral breast cancer is only 3% to 5%.1 Also, CPM does not prevent the development of metastatic disease and offers no survival benefit over breast conservation or unilateral mastectomy.2 Furthermore, compared with unilateral therapeutic mastectomy, the “upgrade” to a CPM carries a 2.7-fold risk of a major surgical complication.3 It is therefore important that patients receive appropriate counseling regarding CPM, and that this counseling include cancer stage at diagnosis, family history and genetic risk, and cancer versus surgical risk (see “Counseling patients on contralateral prophylactic mastectomy” for key points to cover in patient discussions).
Counseling patients on contralateral prophylactic mastectomy
Commonly, patients diagnosed with breast cancer consider having their contralateral healthy breast removed as part of a bilateral mastectomy. They often experience severe anxiety about the cancer coming back and believe that removing both breasts will enable them to live longer. Keep the following key facts in mind when discussing treatment options with breast cancer patients.
Cancer stage at diagnosis. How long a patient lives from the time of her breast cancer diagnosis depends on the stage of the cancer at diagnosis, not the type of surgery performed. A woman with early stage I or stage II breast cancer has an 80% to 90% chance of being cancer free in 5 years.1 The chance of cancer recurring in the bones, liver, or lungs (metastatic breast cancer) will not be changed by removing the healthy breast. The risk of metastatic recurrence can be reduced, however, with chemotherapy and/or with hormone-blocker therapy.
Family history and genetic risk. Few women have a strong family history of breast and/or ovarian and other cancers, and this issue should be addressed with genetic counseling and testing prior to surgery. Those who carry a cancer-causing gene, such as BRCA1 or BRCA2, are at increased risk (40% to 60%) for a second or third breast cancer, especially if they are diagnosed at a young age (<50 years).2,3 In women who have a genetic mutation, removing both breasts and sometimes the ovaries can prevent development of another breast cancer. But this will not prevent spread of the cancer that is already present. Only chemotherapy and hormone blockers can prevent the spread of cancer.
Cancer risk versus surgical risk. For women with no family history of breast cancer, no genetic mutation, and no prior chest wall radiation, the risk of developing a new breast cancer in their other breast is only 3% to 5% every 10 years.3,4 This means that they have a 95% chance of not developing a new breast cancer in their healthy breast. Notably, removing the healthy breast can double the risk of postsurgical complications, including bleeding, infection, and loss of tissue and implant. The mastectomy site will be numb and the skin and nipple areola will not have any function other than cosmetic. Finally, wound complications from surgery could delay the start of important cancer treatment, such as chemotherapy or radiation.
The bottom line. Unless a woman has a strong family history of breast cancer, is diagnosed at a very young age, or has a genetic cancer-causing mutation, removing the contralateral healthy breast is not medically necessary and is not routinely recommended.
References
- Hennigs A, Riedel F, Gondos A, et al. Prognosis of breast cancer molecular subtypes in routine clinical care: a large prospective cohort study. BMC Cancer. 2016;16(1):734.
- Graeser MK, Engel C, Rhiem K, et al. Contralateral breast cancer risk in BRCA1 and BRCA2 mutation carriers. J Clin Oncol. 2009;27(35):5887–5992.
- Curtis RE, Ron E, Hankey BF, Hoover RN. New malignancies following breast cancer. In: Curtis RE, Freedman DM, Ron E, et al, eds. New Malignancies Among Cancer Survivors: SEER Cancer Registries, 1973-2000. Bethesda, MD: National Cancer Institute. NIH Publ. No. 05-5302. 2006:181–205. http://seer.cancer.gov/archive/publications/mpmono. Accessed September 18, 2016.
- Nichols HB, Berrington de Gonzalez A, Lacey JV Jr, Rosenberg PS, Anderson WF. Declining incidence of contralateral breast cancer in the United States from 1975 to 2006. J Clin Oncol. 2011;29(12):1564–1569.
Women should be made aware that there are alternatives to mastectomy that have similar, or even better, outcomes with improved quality of life. Furthermore, a multi‑disciplinary, team-oriented approach with emphasis on minimally invasive biopsy and better cosmetic outcomes has enhanced quality of care. Knowledge of this team approach and of modern breast cancer treatments is essential for general ObGyns as this understanding improves the overall care and guidance—specifically regarding referral to expert, high-volume breast surgeons—provided to those women most in need.
Expanded treatment options for breast cancer
Advancements in breast surgery, better imaging, and targeted therapies are changing the paradigm of breast cancer treatment.
Image-guided biopsy is key in decision making
When an abnormality is found in the breast, surgical excision of an undiagnosed breast lesion is no longer considered an appropriate first step. Use of image-guided biopsy or minimally invasive core needle biopsy allows for accurate diagnosis of a breast lesion while avoiding a potentially breast deforming and expensive surgical operation. It is always better to go into the operating room (OR) with a diagnosis and do the right operation the first time.
A core needle biopsy, results of which demonstrate a benign lesion, helps avoid breast surgery in women who do not need it. If cancer is diagnosed on biopsy, the extent of disease can be better evaluated and decision making can be more informed, with a multidisciplinary approach used to consider the various options, including genetic counseling, plastic surgery consultation, or neoadjuvant therapy. Some lesions, such as those too close to the skin, chest wall, or an implant, may not be amenable to core needle biopsy and therefore require surgical excision for diagnosis.
Benefits of a multidisciplinary tumor conference
It is important for a multidisciplinary group of cancer specialists to review a patient’s case and discuss the ideal treatment plan prior to surgery. Some breast cancer subtypes (such as human epidermal growth factor receptor 2 [HER2]–overamplified breast cancer and many triple-negative breast cancers) are very sensitive to chemotherapy, and patients with these tumor types may benefit from receiving neoadjuvant chemotherapy prior to surgery. New types of chemotherapy may allow up to 60% of some breast cancers to diminish almost completely, with subsequent improved cosmetic results of breast surgery.4 It may also allow time for genetic counseling and testing prior to surgery. (See “How to code for a multidisciplinary tumor conference” for appropriate coding procedure.)
How to code for a multidisciplinary tumor conference
Melanie Witt, RN, MA
There are two coding choices for team conferences involving physician participation. If the patient and/or family is present, the CPT instruction is to bill a problem E/M service code (99201-99215) based on the time spent during this coordination of care/counseling. Documentation would include details about the conference decisions and implications for care, rather than history or examination.
If the patient is not present, report 99367 (Medical team conference with interdisciplinary team of health care professionals, patient and/or family not present, 30 minutes or more; participation by physician), but note that this code was developed under the assumption that the conference would be performed in a facility setting. Diagnostic coding would be breast cancer.
Ms. Witt is an independent coding and documentation consultant and former program manager, department of coding and nomenclature, American Congress of Obstetricians and Gynecologists.
The author reports no financial relationships relevant to this article.
This is an excerpt from a companion coding resource for breast cancer–related procedures by Ms. Witt. To read the companion article, “Coding for breast cancer–related procedures: A how-to guide,” in its entirety, click here.
Image-guided lumpectomy
Advances in breast imaging have led to increased identification of nonpalpable breast cancers. Surgical excision of nonpalpable breast lesions requires image guidance, which can be done using a variety of techniques.
Wire-guided localization (WGL) has been used in practice for the past 40 years. The procedure involves placement of a hooked wire under local anesthesia using either mammographic or ultrasound guidance. This procedure is mostly done in the radiology department on the same day as the surgery and requires that the radiologist coordinate with the OR schedule. Besides scheduling conflicts and delays in surgery, this procedure can be complicated by wires becoming dislodged, transected, or migrated, and limits the surgeon’s ability to cosmetically hide the scar in relation to position of the wire. It is uncomfortable for the patient, who must be transported from the radiology department to the OR with a wire extruding from her breast.
An alternative localization technique is placement of a radioactive source within the tumor, which can then be identified in the OR with a gamma probe.
Iodine I 125 Radioactive seed localization (RSL) involves placing a 4-mm titanium radiolabeled seed into the breast lesion under mammographic or ultrasound guidance (FIGURES 1 and 2). The procedure can be performed a few days before surgery in the radiology department, and there is less chance for the seed to become displaced or dislodged. This technique provides scheduling flexibility for the radiologist and reduces OR delays. The surgeon uses the same gamma probe for sentinel node biopsy to find the lesion in the breast, using the setting specific for iodine I 125. Incisions can be tailored anywhere in the breast, and the seed is detected by a focal gamma signal. Once the lumpectomy is performed, the specimen is probed and radiographed to confirm removal of the seed and adequate margins.
Limitations of this procedure include potential loss of the seed during the operation and radiation safety issues regarding handling and disposal of the radioactive isotope. Once the seed has been placed in the patient’s body, it must be removed surgically, as the half-life of iodine I 125 is long (60 days).5 Care must therefore be taken to optimize medical clearance prior to seed placement and to avoid surgery cancellations.
Intraoperative ultrasound (IOUS) allows the surgeon to identify the lesion under general anesthesia in the OR, which is more comfortable for the patient. The surgical incision can be tailored cosmetically and the lumpectomy can be performed with real-time ultrasound visualization of the tumor during dissection. This technique eliminates the need for a separate preoperative seed or wire localization in radiology. However, it can be used only for lesions or clips that are visible by ultrasound. The excised specimen can be evaluated for confirmation of tumor removal and adequate margins via ultrasound and re-excision of close margins can be accomplished immediately if needed.
Results of a meta-analysis of WGL versus IOUS demonstrated a significant reduction of positive margins with the use of IOUS.6 Results of the COBALT trial, in which patients were assigned randomly to excision of palpable breast cancers with either IOUS or palpation, demonstrated a 14% reduction in positive margins in favor of IOUS.7 Surgeon-performed breast ultrasound requires advanced training and accreditation in breast ultrasound through a rigorous certification process offered by the American Society of Breast Surgeons (www.breastsurgeons.org).
Oncoplastic lumpectomy
This approach to lumpectomy combines adequate oncologist resection of the breast tumor with plastic surgery techniques to achieve superior cosmesis. This approach allows complete removal of the tumor with negative margins, yet maintains the normal shape and contour of the breast. Two techniques have been described: volume displacement and volume replacement.
With the volume displacement technique, the surgeon uses adjacent tissue advancement to fill the lumpectomy cavity with the patient’s own surrounding breast tissue (FIGURE 3). The volume replacement technique requires the transposition of autologous tissue from elsewhere in the body.
Oncoplastic lumpectomy allows more women with larger tumors to undergo breast conservation with better cosmetic results. It reduces the number of mastectomies performed without compromising local control and avoids the need for extensive plastic surgery reconstruction and implants. Special effort and attention must be paid to ensure adequate margins utilizing intraoperative specimen radiograph and pathology evaluation.
This procedure requires that the surgeon acquire specialized skills and knowledge of oncologic and plastic surgery techniques, and it is best performed with the collaboration of a multidisciplinary team. Compared with conventional lumpectomy or mastectomy, oncoplastic breast conservation has been shown to reduce re-excision rates, and it has similar rates of local and distant recurrence and similar disease-free survival and overall survival.8,9
Total skin- and nipple-sparing mastectomy
Some patients do not have the option of breast conservation. Women with multicentric breast cancer (more than 1 tumor in different quadrants of the breast) are better served with mastectomy. Surgical techniques for mastectomy have improved and provide women with various options. One option is skin- and nipple-sparing mastectomy, which preserves the skin envelope overlying the breast (including the skin of the nipple and areola) while removing the glandular elements of the breast and the majority of ductal tissue beneath the nipple-areola complex (FIGURE 4). This surgery can be performed via hidden scars at the inframammary crease or periareolar and is combined with immediate reconstruction, which provides an excellent cosmetic result.
Surgical considerations include removing glandular breast tissue within its anatomic boundaries while maintaining the blood supply to the skin and nipple-areola complex. Furthermore, there must be close dissection of ductal tissue beneath the nipple-areola complex and intraoperative frozen section of the nipple margin in cancer cases. Nipple-sparing mastectomy is oncologically safe in carefully selected patients who do not have cancer near or within the skin or nipple (eg, Paget disease).10 It is also safe as a prophylactic procedure for patients with genetic mutations, such as BRCA1 and BRCA2.11 The procedure is not ideal for smokers or patients with large, pendulous breasts. There is a 3% risk of breast cancer recurrence at the nipple or in the skin or muscle.10 Surgical complications include a 10% to 20% risk of skin or nipple necrosis.12
How do we manage the lymph nodes: Axillary dissection vs sentinel node biopsy?
Evaluation of the axillary nodes is currently part of breast cancer staging and can help the clinician determine the need for adjuvant chemotherapy. It also may assist in assessing the need for extending the radiation field beyond the breast to include the regional lymph nodes. Patients with early stage (stage I and II) breast cancer who do not have abnormal palpable lymph nodes or biopsy-proven metastasis to axillary nodes qualify for sentinel lymph node (SLN) biopsy.
Sentinel node biopsy = less morbidity with no loss of accuracy. Compared with axillary lymph node dissection (ALND; removing all the level I and II nodes in the axilla), SLN biopsy has a 98% accuracy and is associated with less morbidity from lymphedema. The procedure involves injecting the breast with 2 tracers: a radioactive isotope, injected into the breast within 24 hours of the operation, and isosulfan blue dye, injected into the breast in the OR at the time of surgery (see illustration). Both tracers travel through the breast lymphatics and concentrate in the first few lymph nodes that drain the breast. The surgery is performed through a separate axillary incision, and the blue and radioactive lymph nodes are individually dissected and removed for pathologic evaluation. On average, 2 to 4 sentinel nodes are removed, including any suspicious palpable nodes. In experienced hands, this procedure has a false-negative rate of less than 5% to 10%.13
Axillary node dissection no longer standard of care. The indication for a completion ALND has changed based on the results of the randomized trial, ACOSOG Z0011.14 In this trial, patients with early stage breast cancer and 1 to 2 positive SLNs who were undergoing breast conservation therapy with radiation and adjuvant systemic therapy were randomly assigned to ALND or no ALND. (The trial did not include patients who were undergoing mastectomy, neoadjuvant chemotherapy, or who had more than 2 metastatic lymph nodes.) The investigators found no difference in overall or disease-free survival or local-regional recurrence between the 2 treatment groups over 9.2 years of follow up.14
Based on this practice-changing trial result, guidelines of the National Comprehensive Cancer Network no longer recommend completion ALND for patients who meet the ACOSOG Z0011 criteria. For patients who do not meet ACOSOG Z0011 criteria, we do intraoperative pathologic lymph node assessment with either frozen section or imprint cytology, and we perform immediate ALND when results are positive.
Indications for SLN biopsy include:
- invasive breast cancer with clinically negative axillary nodes
- ductal carcinoma in situ (DCIS) with microinvasion or extensive enough to require mastectomy
- clinically negative axillary nodes after neoadjuvant chemotherapy.
Contraindications for SLN biopsy include:
- bulky palpable lymphadenopathy
- pregnancy, as the safety of radioactive isotope and blue dye is not well studied; in isotope mapping the radiation dose is small and within safety limits for pregnant patients
- inflammatory breast cancer.
Complications of any axillary surgery may include risk of lymphedema (5% with SLN biopsy and 30% to 40% with ALND).15 Other complications include neuropathy of the affected arm with chronic pain and numbness of the skin.
Positive trends: Improved patient outcomes, specialized clinician training
Management of breast cancer has changed dramatically over the past several decades. More women are surviving breast cancer thanks to improvements in early detection, an individualized treatment approach with less aggressive surgery, and more effective targeted systemic therapies. A multidisciplinary, team-oriented approach with emphasis on minimally invasive biopsy and better cosmetic outcomes has enhanced quality of care.
Complexity in breast disease management has led to the development of formal fellowship training in breast surgical oncology. Studies have demonstrated that patients treated by high-volume breast surgeons are more satisfied with their care and have improved cancer outcomes.16,17 Women should be aware that they have different options for their breast cancer care, and surgeons with advanced specialization in this field may provide optimal results and better quality of care.
Share your thoughts! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.
In a striking trend, the rate of contralateral prophylactic mastectomy (CPM) has risen by 30% over the last 10 years in the United States.1 Many women undergo CPM because of the fear and anxiety of cancer recurrence and their perceived risk of contralateral breast cancer; however, few women have a medical condition that necessitates removal of the contralateral breast. The medical indications for CPM include having a pathogenic genetic mutation (eg, BRCA1 and BRCA2), a strong family history of breast cancer, or prior mediastina chest radiation.
The actual risk of contralateral breast cancer is much lower than perceived. In women without a genetic mutation, the 10-year risk of contralateral breast cancer is only 3% to 5%.1 Also, CPM does not prevent the development of metastatic disease and offers no survival benefit over breast conservation or unilateral mastectomy.2 Furthermore, compared with unilateral therapeutic mastectomy, the “upgrade” to a CPM carries a 2.7-fold risk of a major surgical complication.3 It is therefore important that patients receive appropriate counseling regarding CPM, and that this counseling include cancer stage at diagnosis, family history and genetic risk, and cancer versus surgical risk (see “Counseling patients on contralateral prophylactic mastectomy” for key points to cover in patient discussions).
Counseling patients on contralateral prophylactic mastectomy
Commonly, patients diagnosed with breast cancer consider having their contralateral healthy breast removed as part of a bilateral mastectomy. They often experience severe anxiety about the cancer coming back and believe that removing both breasts will enable them to live longer. Keep the following key facts in mind when discussing treatment options with breast cancer patients.
Cancer stage at diagnosis. How long a patient lives from the time of her breast cancer diagnosis depends on the stage of the cancer at diagnosis, not the type of surgery performed. A woman with early stage I or stage II breast cancer has an 80% to 90% chance of being cancer free in 5 years.1 The chance of cancer recurring in the bones, liver, or lungs (metastatic breast cancer) will not be changed by removing the healthy breast. The risk of metastatic recurrence can be reduced, however, with chemotherapy and/or with hormone-blocker therapy.
Family history and genetic risk. Few women have a strong family history of breast and/or ovarian and other cancers, and this issue should be addressed with genetic counseling and testing prior to surgery. Those who carry a cancer-causing gene, such as BRCA1 or BRCA2, are at increased risk (40% to 60%) for a second or third breast cancer, especially if they are diagnosed at a young age (<50 years).2,3 In women who have a genetic mutation, removing both breasts and sometimes the ovaries can prevent development of another breast cancer. But this will not prevent spread of the cancer that is already present. Only chemotherapy and hormone blockers can prevent the spread of cancer.
Cancer risk versus surgical risk. For women with no family history of breast cancer, no genetic mutation, and no prior chest wall radiation, the risk of developing a new breast cancer in their other breast is only 3% to 5% every 10 years.3,4 This means that they have a 95% chance of not developing a new breast cancer in their healthy breast. Notably, removing the healthy breast can double the risk of postsurgical complications, including bleeding, infection, and loss of tissue and implant. The mastectomy site will be numb and the skin and nipple areola will not have any function other than cosmetic. Finally, wound complications from surgery could delay the start of important cancer treatment, such as chemotherapy or radiation.
The bottom line. Unless a woman has a strong family history of breast cancer, is diagnosed at a very young age, or has a genetic cancer-causing mutation, removing the contralateral healthy breast is not medically necessary and is not routinely recommended.
References
- Hennigs A, Riedel F, Gondos A, et al. Prognosis of breast cancer molecular subtypes in routine clinical care: a large prospective cohort study. BMC Cancer. 2016;16(1):734.
- Graeser MK, Engel C, Rhiem K, et al. Contralateral breast cancer risk in BRCA1 and BRCA2 mutation carriers. J Clin Oncol. 2009;27(35):5887–5992.
- Curtis RE, Ron E, Hankey BF, Hoover RN. New malignancies following breast cancer. In: Curtis RE, Freedman DM, Ron E, et al, eds. New Malignancies Among Cancer Survivors: SEER Cancer Registries, 1973-2000. Bethesda, MD: National Cancer Institute. NIH Publ. No. 05-5302. 2006:181–205. http://seer.cancer.gov/archive/publications/mpmono. Accessed September 18, 2016.
- Nichols HB, Berrington de Gonzalez A, Lacey JV Jr, Rosenberg PS, Anderson WF. Declining incidence of contralateral breast cancer in the United States from 1975 to 2006. J Clin Oncol. 2011;29(12):1564–1569.
Women should be made aware that there are alternatives to mastectomy that have similar, or even better, outcomes with improved quality of life. Furthermore, a multi‑disciplinary, team-oriented approach with emphasis on minimally invasive biopsy and better cosmetic outcomes has enhanced quality of care. Knowledge of this team approach and of modern breast cancer treatments is essential for general ObGyns as this understanding improves the overall care and guidance—specifically regarding referral to expert, high-volume breast surgeons—provided to those women most in need.
Expanded treatment options for breast cancer
Advancements in breast surgery, better imaging, and targeted therapies are changing the paradigm of breast cancer treatment.
Image-guided biopsy is key in decision making
When an abnormality is found in the breast, surgical excision of an undiagnosed breast lesion is no longer considered an appropriate first step. Use of image-guided biopsy or minimally invasive core needle biopsy allows for accurate diagnosis of a breast lesion while avoiding a potentially breast deforming and expensive surgical operation. It is always better to go into the operating room (OR) with a diagnosis and do the right operation the first time.
A core needle biopsy, results of which demonstrate a benign lesion, helps avoid breast surgery in women who do not need it. If cancer is diagnosed on biopsy, the extent of disease can be better evaluated and decision making can be more informed, with a multidisciplinary approach used to consider the various options, including genetic counseling, plastic surgery consultation, or neoadjuvant therapy. Some lesions, such as those too close to the skin, chest wall, or an implant, may not be amenable to core needle biopsy and therefore require surgical excision for diagnosis.
Benefits of a multidisciplinary tumor conference
It is important for a multidisciplinary group of cancer specialists to review a patient’s case and discuss the ideal treatment plan prior to surgery. Some breast cancer subtypes (such as human epidermal growth factor receptor 2 [HER2]–overamplified breast cancer and many triple-negative breast cancers) are very sensitive to chemotherapy, and patients with these tumor types may benefit from receiving neoadjuvant chemotherapy prior to surgery. New types of chemotherapy may allow up to 60% of some breast cancers to diminish almost completely, with subsequent improved cosmetic results of breast surgery.4 It may also allow time for genetic counseling and testing prior to surgery. (See “How to code for a multidisciplinary tumor conference” for appropriate coding procedure.)
How to code for a multidisciplinary tumor conference
Melanie Witt, RN, MA
There are two coding choices for team conferences involving physician participation. If the patient and/or family is present, the CPT instruction is to bill a problem E/M service code (99201-99215) based on the time spent during this coordination of care/counseling. Documentation would include details about the conference decisions and implications for care, rather than history or examination.
If the patient is not present, report 99367 (Medical team conference with interdisciplinary team of health care professionals, patient and/or family not present, 30 minutes or more; participation by physician), but note that this code was developed under the assumption that the conference would be performed in a facility setting. Diagnostic coding would be breast cancer.
Ms. Witt is an independent coding and documentation consultant and former program manager, department of coding and nomenclature, American Congress of Obstetricians and Gynecologists.
The author reports no financial relationships relevant to this article.
This is an excerpt from a companion coding resource for breast cancer–related procedures by Ms. Witt. To read the companion article, “Coding for breast cancer–related procedures: A how-to guide,” in its entirety, click here.
Image-guided lumpectomy
Advances in breast imaging have led to increased identification of nonpalpable breast cancers. Surgical excision of nonpalpable breast lesions requires image guidance, which can be done using a variety of techniques.
Wire-guided localization (WGL) has been used in practice for the past 40 years. The procedure involves placement of a hooked wire under local anesthesia using either mammographic or ultrasound guidance. This procedure is mostly done in the radiology department on the same day as the surgery and requires that the radiologist coordinate with the OR schedule. Besides scheduling conflicts and delays in surgery, this procedure can be complicated by wires becoming dislodged, transected, or migrated, and limits the surgeon’s ability to cosmetically hide the scar in relation to position of the wire. It is uncomfortable for the patient, who must be transported from the radiology department to the OR with a wire extruding from her breast.
An alternative localization technique is placement of a radioactive source within the tumor, which can then be identified in the OR with a gamma probe.
Iodine I 125 Radioactive seed localization (RSL) involves placing a 4-mm titanium radiolabeled seed into the breast lesion under mammographic or ultrasound guidance (FIGURES 1 and 2). The procedure can be performed a few days before surgery in the radiology department, and there is less chance for the seed to become displaced or dislodged. This technique provides scheduling flexibility for the radiologist and reduces OR delays. The surgeon uses the same gamma probe for sentinel node biopsy to find the lesion in the breast, using the setting specific for iodine I 125. Incisions can be tailored anywhere in the breast, and the seed is detected by a focal gamma signal. Once the lumpectomy is performed, the specimen is probed and radiographed to confirm removal of the seed and adequate margins.
Limitations of this procedure include potential loss of the seed during the operation and radiation safety issues regarding handling and disposal of the radioactive isotope. Once the seed has been placed in the patient’s body, it must be removed surgically, as the half-life of iodine I 125 is long (60 days).5 Care must therefore be taken to optimize medical clearance prior to seed placement and to avoid surgery cancellations.
Intraoperative ultrasound (IOUS) allows the surgeon to identify the lesion under general anesthesia in the OR, which is more comfortable for the patient. The surgical incision can be tailored cosmetically and the lumpectomy can be performed with real-time ultrasound visualization of the tumor during dissection. This technique eliminates the need for a separate preoperative seed or wire localization in radiology. However, it can be used only for lesions or clips that are visible by ultrasound. The excised specimen can be evaluated for confirmation of tumor removal and adequate margins via ultrasound and re-excision of close margins can be accomplished immediately if needed.
Results of a meta-analysis of WGL versus IOUS demonstrated a significant reduction of positive margins with the use of IOUS.6 Results of the COBALT trial, in which patients were assigned randomly to excision of palpable breast cancers with either IOUS or palpation, demonstrated a 14% reduction in positive margins in favor of IOUS.7 Surgeon-performed breast ultrasound requires advanced training and accreditation in breast ultrasound through a rigorous certification process offered by the American Society of Breast Surgeons (www.breastsurgeons.org).
Oncoplastic lumpectomy
This approach to lumpectomy combines adequate oncologist resection of the breast tumor with plastic surgery techniques to achieve superior cosmesis. This approach allows complete removal of the tumor with negative margins, yet maintains the normal shape and contour of the breast. Two techniques have been described: volume displacement and volume replacement.
With the volume displacement technique, the surgeon uses adjacent tissue advancement to fill the lumpectomy cavity with the patient’s own surrounding breast tissue (FIGURE 3). The volume replacement technique requires the transposition of autologous tissue from elsewhere in the body.
Oncoplastic lumpectomy allows more women with larger tumors to undergo breast conservation with better cosmetic results. It reduces the number of mastectomies performed without compromising local control and avoids the need for extensive plastic surgery reconstruction and implants. Special effort and attention must be paid to ensure adequate margins utilizing intraoperative specimen radiograph and pathology evaluation.
This procedure requires that the surgeon acquire specialized skills and knowledge of oncologic and plastic surgery techniques, and it is best performed with the collaboration of a multidisciplinary team. Compared with conventional lumpectomy or mastectomy, oncoplastic breast conservation has been shown to reduce re-excision rates, and it has similar rates of local and distant recurrence and similar disease-free survival and overall survival.8,9
Total skin- and nipple-sparing mastectomy
Some patients do not have the option of breast conservation. Women with multicentric breast cancer (more than 1 tumor in different quadrants of the breast) are better served with mastectomy. Surgical techniques for mastectomy have improved and provide women with various options. One option is skin- and nipple-sparing mastectomy, which preserves the skin envelope overlying the breast (including the skin of the nipple and areola) while removing the glandular elements of the breast and the majority of ductal tissue beneath the nipple-areola complex (FIGURE 4). This surgery can be performed via hidden scars at the inframammary crease or periareolar and is combined with immediate reconstruction, which provides an excellent cosmetic result.
Surgical considerations include removing glandular breast tissue within its anatomic boundaries while maintaining the blood supply to the skin and nipple-areola complex. Furthermore, there must be close dissection of ductal tissue beneath the nipple-areola complex and intraoperative frozen section of the nipple margin in cancer cases. Nipple-sparing mastectomy is oncologically safe in carefully selected patients who do not have cancer near or within the skin or nipple (eg, Paget disease).10 It is also safe as a prophylactic procedure for patients with genetic mutations, such as BRCA1 and BRCA2.11 The procedure is not ideal for smokers or patients with large, pendulous breasts. There is a 3% risk of breast cancer recurrence at the nipple or in the skin or muscle.10 Surgical complications include a 10% to 20% risk of skin or nipple necrosis.12
How do we manage the lymph nodes: Axillary dissection vs sentinel node biopsy?
Evaluation of the axillary nodes is currently part of breast cancer staging and can help the clinician determine the need for adjuvant chemotherapy. It also may assist in assessing the need for extending the radiation field beyond the breast to include the regional lymph nodes. Patients with early stage (stage I and II) breast cancer who do not have abnormal palpable lymph nodes or biopsy-proven metastasis to axillary nodes qualify for sentinel lymph node (SLN) biopsy.
Sentinel node biopsy = less morbidity with no loss of accuracy. Compared with axillary lymph node dissection (ALND; removing all the level I and II nodes in the axilla), SLN biopsy has a 98% accuracy and is associated with less morbidity from lymphedema. The procedure involves injecting the breast with 2 tracers: a radioactive isotope, injected into the breast within 24 hours of the operation, and isosulfan blue dye, injected into the breast in the OR at the time of surgery (see illustration). Both tracers travel through the breast lymphatics and concentrate in the first few lymph nodes that drain the breast. The surgery is performed through a separate axillary incision, and the blue and radioactive lymph nodes are individually dissected and removed for pathologic evaluation. On average, 2 to 4 sentinel nodes are removed, including any suspicious palpable nodes. In experienced hands, this procedure has a false-negative rate of less than 5% to 10%.13
Axillary node dissection no longer standard of care. The indication for a completion ALND has changed based on the results of the randomized trial, ACOSOG Z0011.14 In this trial, patients with early stage breast cancer and 1 to 2 positive SLNs who were undergoing breast conservation therapy with radiation and adjuvant systemic therapy were randomly assigned to ALND or no ALND. (The trial did not include patients who were undergoing mastectomy, neoadjuvant chemotherapy, or who had more than 2 metastatic lymph nodes.) The investigators found no difference in overall or disease-free survival or local-regional recurrence between the 2 treatment groups over 9.2 years of follow up.14
Based on this practice-changing trial result, guidelines of the National Comprehensive Cancer Network no longer recommend completion ALND for patients who meet the ACOSOG Z0011 criteria. For patients who do not meet ACOSOG Z0011 criteria, we do intraoperative pathologic lymph node assessment with either frozen section or imprint cytology, and we perform immediate ALND when results are positive.
Indications for SLN biopsy include:
- invasive breast cancer with clinically negative axillary nodes
- ductal carcinoma in situ (DCIS) with microinvasion or extensive enough to require mastectomy
- clinically negative axillary nodes after neoadjuvant chemotherapy.
Contraindications for SLN biopsy include:
- bulky palpable lymphadenopathy
- pregnancy, as the safety of radioactive isotope and blue dye is not well studied; in isotope mapping the radiation dose is small and within safety limits for pregnant patients
- inflammatory breast cancer.
Complications of any axillary surgery may include risk of lymphedema (5% with SLN biopsy and 30% to 40% with ALND).15 Other complications include neuropathy of the affected arm with chronic pain and numbness of the skin.
Positive trends: Improved patient outcomes, specialized clinician training
Management of breast cancer has changed dramatically over the past several decades. More women are surviving breast cancer thanks to improvements in early detection, an individualized treatment approach with less aggressive surgery, and more effective targeted systemic therapies. A multidisciplinary, team-oriented approach with emphasis on minimally invasive biopsy and better cosmetic outcomes has enhanced quality of care.
Complexity in breast disease management has led to the development of formal fellowship training in breast surgical oncology. Studies have demonstrated that patients treated by high-volume breast surgeons are more satisfied with their care and have improved cancer outcomes.16,17 Women should be aware that they have different options for their breast cancer care, and surgeons with advanced specialization in this field may provide optimal results and better quality of care.
Share your thoughts! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.
- Nichols HB, Berrington de Gonzalez A, Lacey JV Jr, Rosenberg PS, Anderson WF. Declining incidence of contralateral breast cancer in the United States from 1975 to 2006. J Clin Oncol. 2011;29(12):1564–1569.
- Wong SM, Freedman RA, Sagara Y, Aydogan F, Barry WT, Golshan M. Growing use of contralateral prophylactic mastectomy despite no improvement in long-term survival for invasive breast cancer [published online ahead of print March 8, 2016]. Ann Surg. doi:10.1097/SLA.0000000000001698.
- Miller ME, Czechura T, Martz B, et al. Operative risks associated with contralateral prophylactic mastectomy: a single institution experience. Ann Surg Oncol. 2013;20(13):4113–4120.
- Zhang X, Zhang XJ, Zhang TY, et al. Effect and safety of dual anti-human epidermal growth factor receptor 2 therapy compared to monotherapy in patients with human epidermal growth factor receptor 2-positive breast cancer: a systematic review. BMC Cancer. 2014;14:625.
- Ahmed M, Rubio IT, Klaase JM, Douek M. Surgical treatment of nonpalpable primary invasive and in situ breast cancer. Nat Rev Clin Oncol. 2015;12(11):645–663.
- Ahmed M, Douek M. Intra-operative ultrasound versus wire-guided localization in the surgical management of non-palpable breast cancers: systemic review and meta-analysis. Breast Cancer Res Treat. 2013;140(3):435–446.
- Krekel NM, Haloua MH, Lopes Cardozo AM, et al. Intraoperative ultrasound guidance for palpable breast cancer excision (COBALT trial): a multicentre, randomised controlled trial. Lancet Oncol. 2013;14(1):48–54.
- Chakravorty A, Shrestha AK, Sanmugalingam N, et al. How safe is oncoplastic breast conservation? Comparative analysis with standard breast conserving surgery. Eur J Surg Oncol. 2012;38(5):395–398.
- De Lorenzi F, Hubner G, Rotmensz N, et al. Oncological results of oncoplastic breast-conserving surgery: long term follow-up of a large series at a single institution: a matched-cohort analysis. Eur J Surg Oncol. 2016;42(1):71–77.
- De La Cruz L, Moody AM, Tappy EE, Blankenship AA, Hecht EM. Overall survival, disease-free survival, local recurrence, and nipple-areolar recurrence in the setting of nipple-sparing mastectomy: a meta-analysis and systematic review. Ann Surg Oncol. 2015;22(10):3241–3249.
- Yao K, Liederbach E, Tang R, et al. Nipple-sparing mastectomy in BRCA1/2 mutation carriers: an interim analysis and review of the literature. Ann Surg Oncol. 2015;22(2):370–376.
- Fortunato L, Loreti A, Andrich R, et al. When mastectomy is needed: is the nipple-sparing procedure a new standard with very few contraindications? J Surg Oncol. 2013;108(4):207–212.
- Veronesi U, Viale G, Paganelli G, et al. Sentinel lymph node biopsy in breast cancer: ten-year results of a randomized controlled study. Ann Surg. 2010;251(4):595–600.
- Giuliano AE, Hunt K, Ballman KV, et al. Ten-year survival results of ACOSOG Z0011: a randomized trial of axillary node dissection in women with clinical T1-2 N0 M0 breast cancer who have a positive sentinel node (Alliance). In: 2016 ASCO Annual Meeting; June 3-7, 2016. J Clin Oncol. 2016;34(15; May 20 suppl): Abstract 1007.
- DiSipio T, Rye S, Newman B, Hayes S. Incidence of unilateral arm lymphedema after breast cancer: a systematic review and meta-analysis. Lancet Oncol. 2013;14(6):500–515.
- Skinner KA, Helsper JT, Deapen D, Ye W, Sposto R. Breast cancer: do specialists make a difference? Ann Surg Oncol. 2003;10(6):606–615.
- Waljee JF, Hawley S, Alderman AK, Morrow M, Katz SJ. Patient satisfaction with treatment of breast cancer: does surgeon specialization matter? J Clin Oncol. 2007;25(24):3694–3698.
- Nichols HB, Berrington de Gonzalez A, Lacey JV Jr, Rosenberg PS, Anderson WF. Declining incidence of contralateral breast cancer in the United States from 1975 to 2006. J Clin Oncol. 2011;29(12):1564–1569.
- Wong SM, Freedman RA, Sagara Y, Aydogan F, Barry WT, Golshan M. Growing use of contralateral prophylactic mastectomy despite no improvement in long-term survival for invasive breast cancer [published online ahead of print March 8, 2016]. Ann Surg. doi:10.1097/SLA.0000000000001698.
- Miller ME, Czechura T, Martz B, et al. Operative risks associated with contralateral prophylactic mastectomy: a single institution experience. Ann Surg Oncol. 2013;20(13):4113–4120.
- Zhang X, Zhang XJ, Zhang TY, et al. Effect and safety of dual anti-human epidermal growth factor receptor 2 therapy compared to monotherapy in patients with human epidermal growth factor receptor 2-positive breast cancer: a systematic review. BMC Cancer. 2014;14:625.
- Ahmed M, Rubio IT, Klaase JM, Douek M. Surgical treatment of nonpalpable primary invasive and in situ breast cancer. Nat Rev Clin Oncol. 2015;12(11):645–663.
- Ahmed M, Douek M. Intra-operative ultrasound versus wire-guided localization in the surgical management of non-palpable breast cancers: systemic review and meta-analysis. Breast Cancer Res Treat. 2013;140(3):435–446.
- Krekel NM, Haloua MH, Lopes Cardozo AM, et al. Intraoperative ultrasound guidance for palpable breast cancer excision (COBALT trial): a multicentre, randomised controlled trial. Lancet Oncol. 2013;14(1):48–54.
- Chakravorty A, Shrestha AK, Sanmugalingam N, et al. How safe is oncoplastic breast conservation? Comparative analysis with standard breast conserving surgery. Eur J Surg Oncol. 2012;38(5):395–398.
- De Lorenzi F, Hubner G, Rotmensz N, et al. Oncological results of oncoplastic breast-conserving surgery: long term follow-up of a large series at a single institution: a matched-cohort analysis. Eur J Surg Oncol. 2016;42(1):71–77.
- De La Cruz L, Moody AM, Tappy EE, Blankenship AA, Hecht EM. Overall survival, disease-free survival, local recurrence, and nipple-areolar recurrence in the setting of nipple-sparing mastectomy: a meta-analysis and systematic review. Ann Surg Oncol. 2015;22(10):3241–3249.
- Yao K, Liederbach E, Tang R, et al. Nipple-sparing mastectomy in BRCA1/2 mutation carriers: an interim analysis and review of the literature. Ann Surg Oncol. 2015;22(2):370–376.
- Fortunato L, Loreti A, Andrich R, et al. When mastectomy is needed: is the nipple-sparing procedure a new standard with very few contraindications? J Surg Oncol. 2013;108(4):207–212.
- Veronesi U, Viale G, Paganelli G, et al. Sentinel lymph node biopsy in breast cancer: ten-year results of a randomized controlled study. Ann Surg. 2010;251(4):595–600.
- Giuliano AE, Hunt K, Ballman KV, et al. Ten-year survival results of ACOSOG Z0011: a randomized trial of axillary node dissection in women with clinical T1-2 N0 M0 breast cancer who have a positive sentinel node (Alliance). In: 2016 ASCO Annual Meeting; June 3-7, 2016. J Clin Oncol. 2016;34(15; May 20 suppl): Abstract 1007.
- DiSipio T, Rye S, Newman B, Hayes S. Incidence of unilateral arm lymphedema after breast cancer: a systematic review and meta-analysis. Lancet Oncol. 2013;14(6):500–515.
- Skinner KA, Helsper JT, Deapen D, Ye W, Sposto R. Breast cancer: do specialists make a difference? Ann Surg Oncol. 2003;10(6):606–615.
- Waljee JF, Hawley S, Alderman AK, Morrow M, Katz SJ. Patient satisfaction with treatment of breast cancer: does surgeon specialization matter? J Clin Oncol. 2007;25(24):3694–3698.
In this Article
- Counseling patients on CPM
- Oncoplastic lumpectomy approach
- How to manage the lymph nodes
Long-term breast cancer studies yield encouraging data for recurrence, survival
Four pivotal breast cancer trials were presented at the 2016 annual meeting of the American Society of Clinical Oncology in Chicago. The MA.17R trial, which was the plenary talk by Dr Paul Goss, looked at extending adjuvant aromatase inhibitors to 10 years or beyond in postmenopausal women; two presentations reported on mutations after progression in metastatic breast cancer, one on first-line AIs and the other on prior endocrine therapy (PALOMA-3); and results from the Z0011 trial showed that sentinel lymph node dissection without axillary lymph node dissection might show promising 10-year loco-regional control and survival outcomes.
Click on the PDF icon at the top of this introduction to read the full article.
Four pivotal breast cancer trials were presented at the 2016 annual meeting of the American Society of Clinical Oncology in Chicago. The MA.17R trial, which was the plenary talk by Dr Paul Goss, looked at extending adjuvant aromatase inhibitors to 10 years or beyond in postmenopausal women; two presentations reported on mutations after progression in metastatic breast cancer, one on first-line AIs and the other on prior endocrine therapy (PALOMA-3); and results from the Z0011 trial showed that sentinel lymph node dissection without axillary lymph node dissection might show promising 10-year loco-regional control and survival outcomes.
Click on the PDF icon at the top of this introduction to read the full article.
Four pivotal breast cancer trials were presented at the 2016 annual meeting of the American Society of Clinical Oncology in Chicago. The MA.17R trial, which was the plenary talk by Dr Paul Goss, looked at extending adjuvant aromatase inhibitors to 10 years or beyond in postmenopausal women; two presentations reported on mutations after progression in metastatic breast cancer, one on first-line AIs and the other on prior endocrine therapy (PALOMA-3); and results from the Z0011 trial showed that sentinel lymph node dissection without axillary lymph node dissection might show promising 10-year loco-regional control and survival outcomes.
Click on the PDF icon at the top of this introduction to read the full article.
ASCO updates postmastectomy radiotherapy guideline
The 2001 American Society of Clinical Oncology clinical practice guideline on postmastectomy radiotherapy has been updated to help clinicians and patients decide which cases of T1-T2 breast cancer with one-three positive axillary lymph nodes will not benefit from the treatment. Recent evidence suggests that some subsets of this patient group are likely to have such a low risk of locoregional recurrence that the potential adverse effects of radiotherapy would outweigh its benefit.
“We still don’t have a single, validated formula that can determine who needs postmastectomy radiotherapy, but we hope that the research evidence summarized in this guideline update will help doctors and patients make more informed decisions,” Abram Recht, MD, cochair of the expert panel that developed the update, said in a press statement.
“Thanks to advances in systemic therapy, fewer women need radiation therapy after a mastectomy. This means we can be more selective when recommending this treatment to our patients,” said Dr. Recht of Beth Israel Deaconess Medical Center, Boston.
ASCO, in collaboration with the American Society for Radiation Oncology and the Society of Surgical Oncology, reviewed the literature since 2001, including a meta-analysis of 22 clinical trials involving 8,135 patients who were randomly assigned to receive or not receive postmastectomy radiotherapy. “Our panel focused on the results for the 3,786 women who underwent axillary dissection.” The 10-year rate of locoregional treatment failure was only 4.3% with irradiation, compared with 21.0% without irradiation. The 10-year rate of local or distant treatment failure was 33.8% with irradiation and 45.5% without it, and the 20-year rates of breast cancer mortality were 41.5% and 49.4%, respectively.
“The panel unanimously agreed that the available evidence shows that postmastectomy radiotherapy reduces the risks of locoregional failure, any recurrence, and breast cancer mortality for patients with T1-T2 breast cancer and one-three positive lymph nodes,” according to the guideline.
However, clinicians and patients “should consider factors that may decrease the risk of locoregional failure, attenuate the benefit of reduced breast cancer–specific mortality, and/or increase the risk of complications.” These include older patient age, limited life expectancy, coexisting conditions that affect the risk of complications, small tumor size, absence of lymphovascular invasion, small nodal metastases, substantial response to neoadjuvant systemic therapy, low tumor grade, or strong tumor sensitivity to hormonal therapy, Dr. Recht and his associates said (J Clin Oncol. 2016 Sep 19. doi: 10.1200/JCO.2016.69.1188).
The guideline also addressed other areas of controversy.
Some clinicians now omit performing axillary lymph node dissection if one-two sentinel nodes are positive, “primarily based on extrapolation of data from randomized trials of patients treated exclusively or predominantly with breast-conserving surgery.” In such cases, the updated guideline “recommends that these patients receive postmastectomy radiotherapy only if there is already sufficient information to justify its use without needing to know that additional axillary nodes are involved.”
Many clinicians are uncertain whether to pursue postmastectomy radiotherapy in patients who have received neoadjuvant systemic therapy, because observational studies suggest the risk of locoregional recurrence is low for those who either have clinically negative nodes before undergoing the treatment or have a complete pathologic response to it in the lymph nodes. The panel decided that current evidence is insufficient to recommend whether radiotherapy should be administered or can be omitted in these groups.
The guideline also recommends that regional nodal irradiation generally should target both the internal mammary and the supraclavicular-axillary apical nodes, in addition to the chest wall or reconstructed breast. “There may be subgroups that will experience limited, if any, benefits from treating both these nodal areas, compared with treating only one or perhaps treating only the chest wall or reconstructed breast. [However,] there is insufficient evidence at this time to define such subgroups in detail.”
Copies of the updated guideline, as well as additional information such as details regarding the panel’s methodology, evidence tables, and clinical tools, are avail at www.asco.org/pmrt-guideline and www.asco.org/guidelineswiki.
This work was supported by the American Society of Clinical Oncology, the American Society for Radiation Oncology, and the Society of Surgical Oncology. Dr. Recht reported serving as a consultant or advisor to CareCore and U.S. Oncology and receiving research funding from Genomic Health; his associates reported ties to numerous industry sources.
The 2001 American Society of Clinical Oncology clinical practice guideline on postmastectomy radiotherapy has been updated to help clinicians and patients decide which cases of T1-T2 breast cancer with one-three positive axillary lymph nodes will not benefit from the treatment. Recent evidence suggests that some subsets of this patient group are likely to have such a low risk of locoregional recurrence that the potential adverse effects of radiotherapy would outweigh its benefit.
“We still don’t have a single, validated formula that can determine who needs postmastectomy radiotherapy, but we hope that the research evidence summarized in this guideline update will help doctors and patients make more informed decisions,” Abram Recht, MD, cochair of the expert panel that developed the update, said in a press statement.
“Thanks to advances in systemic therapy, fewer women need radiation therapy after a mastectomy. This means we can be more selective when recommending this treatment to our patients,” said Dr. Recht of Beth Israel Deaconess Medical Center, Boston.
ASCO, in collaboration with the American Society for Radiation Oncology and the Society of Surgical Oncology, reviewed the literature since 2001, including a meta-analysis of 22 clinical trials involving 8,135 patients who were randomly assigned to receive or not receive postmastectomy radiotherapy. “Our panel focused on the results for the 3,786 women who underwent axillary dissection.” The 10-year rate of locoregional treatment failure was only 4.3% with irradiation, compared with 21.0% without irradiation. The 10-year rate of local or distant treatment failure was 33.8% with irradiation and 45.5% without it, and the 20-year rates of breast cancer mortality were 41.5% and 49.4%, respectively.
“The panel unanimously agreed that the available evidence shows that postmastectomy radiotherapy reduces the risks of locoregional failure, any recurrence, and breast cancer mortality for patients with T1-T2 breast cancer and one-three positive lymph nodes,” according to the guideline.
However, clinicians and patients “should consider factors that may decrease the risk of locoregional failure, attenuate the benefit of reduced breast cancer–specific mortality, and/or increase the risk of complications.” These include older patient age, limited life expectancy, coexisting conditions that affect the risk of complications, small tumor size, absence of lymphovascular invasion, small nodal metastases, substantial response to neoadjuvant systemic therapy, low tumor grade, or strong tumor sensitivity to hormonal therapy, Dr. Recht and his associates said (J Clin Oncol. 2016 Sep 19. doi: 10.1200/JCO.2016.69.1188).
The guideline also addressed other areas of controversy.
Some clinicians now omit performing axillary lymph node dissection if one-two sentinel nodes are positive, “primarily based on extrapolation of data from randomized trials of patients treated exclusively or predominantly with breast-conserving surgery.” In such cases, the updated guideline “recommends that these patients receive postmastectomy radiotherapy only if there is already sufficient information to justify its use without needing to know that additional axillary nodes are involved.”
Many clinicians are uncertain whether to pursue postmastectomy radiotherapy in patients who have received neoadjuvant systemic therapy, because observational studies suggest the risk of locoregional recurrence is low for those who either have clinically negative nodes before undergoing the treatment or have a complete pathologic response to it in the lymph nodes. The panel decided that current evidence is insufficient to recommend whether radiotherapy should be administered or can be omitted in these groups.
The guideline also recommends that regional nodal irradiation generally should target both the internal mammary and the supraclavicular-axillary apical nodes, in addition to the chest wall or reconstructed breast. “There may be subgroups that will experience limited, if any, benefits from treating both these nodal areas, compared with treating only one or perhaps treating only the chest wall or reconstructed breast. [However,] there is insufficient evidence at this time to define such subgroups in detail.”
Copies of the updated guideline, as well as additional information such as details regarding the panel’s methodology, evidence tables, and clinical tools, are avail at www.asco.org/pmrt-guideline and www.asco.org/guidelineswiki.
This work was supported by the American Society of Clinical Oncology, the American Society for Radiation Oncology, and the Society of Surgical Oncology. Dr. Recht reported serving as a consultant or advisor to CareCore and U.S. Oncology and receiving research funding from Genomic Health; his associates reported ties to numerous industry sources.
The 2001 American Society of Clinical Oncology clinical practice guideline on postmastectomy radiotherapy has been updated to help clinicians and patients decide which cases of T1-T2 breast cancer with one-three positive axillary lymph nodes will not benefit from the treatment. Recent evidence suggests that some subsets of this patient group are likely to have such a low risk of locoregional recurrence that the potential adverse effects of radiotherapy would outweigh its benefit.
“We still don’t have a single, validated formula that can determine who needs postmastectomy radiotherapy, but we hope that the research evidence summarized in this guideline update will help doctors and patients make more informed decisions,” Abram Recht, MD, cochair of the expert panel that developed the update, said in a press statement.
“Thanks to advances in systemic therapy, fewer women need radiation therapy after a mastectomy. This means we can be more selective when recommending this treatment to our patients,” said Dr. Recht of Beth Israel Deaconess Medical Center, Boston.
ASCO, in collaboration with the American Society for Radiation Oncology and the Society of Surgical Oncology, reviewed the literature since 2001, including a meta-analysis of 22 clinical trials involving 8,135 patients who were randomly assigned to receive or not receive postmastectomy radiotherapy. “Our panel focused on the results for the 3,786 women who underwent axillary dissection.” The 10-year rate of locoregional treatment failure was only 4.3% with irradiation, compared with 21.0% without irradiation. The 10-year rate of local or distant treatment failure was 33.8% with irradiation and 45.5% without it, and the 20-year rates of breast cancer mortality were 41.5% and 49.4%, respectively.
“The panel unanimously agreed that the available evidence shows that postmastectomy radiotherapy reduces the risks of locoregional failure, any recurrence, and breast cancer mortality for patients with T1-T2 breast cancer and one-three positive lymph nodes,” according to the guideline.
However, clinicians and patients “should consider factors that may decrease the risk of locoregional failure, attenuate the benefit of reduced breast cancer–specific mortality, and/or increase the risk of complications.” These include older patient age, limited life expectancy, coexisting conditions that affect the risk of complications, small tumor size, absence of lymphovascular invasion, small nodal metastases, substantial response to neoadjuvant systemic therapy, low tumor grade, or strong tumor sensitivity to hormonal therapy, Dr. Recht and his associates said (J Clin Oncol. 2016 Sep 19. doi: 10.1200/JCO.2016.69.1188).
The guideline also addressed other areas of controversy.
Some clinicians now omit performing axillary lymph node dissection if one-two sentinel nodes are positive, “primarily based on extrapolation of data from randomized trials of patients treated exclusively or predominantly with breast-conserving surgery.” In such cases, the updated guideline “recommends that these patients receive postmastectomy radiotherapy only if there is already sufficient information to justify its use without needing to know that additional axillary nodes are involved.”
Many clinicians are uncertain whether to pursue postmastectomy radiotherapy in patients who have received neoadjuvant systemic therapy, because observational studies suggest the risk of locoregional recurrence is low for those who either have clinically negative nodes before undergoing the treatment or have a complete pathologic response to it in the lymph nodes. The panel decided that current evidence is insufficient to recommend whether radiotherapy should be administered or can be omitted in these groups.
The guideline also recommends that regional nodal irradiation generally should target both the internal mammary and the supraclavicular-axillary apical nodes, in addition to the chest wall or reconstructed breast. “There may be subgroups that will experience limited, if any, benefits from treating both these nodal areas, compared with treating only one or perhaps treating only the chest wall or reconstructed breast. [However,] there is insufficient evidence at this time to define such subgroups in detail.”
Copies of the updated guideline, as well as additional information such as details regarding the panel’s methodology, evidence tables, and clinical tools, are avail at www.asco.org/pmrt-guideline and www.asco.org/guidelineswiki.
This work was supported by the American Society of Clinical Oncology, the American Society for Radiation Oncology, and the Society of Surgical Oncology. Dr. Recht reported serving as a consultant or advisor to CareCore and U.S. Oncology and receiving research funding from Genomic Health; his associates reported ties to numerous industry sources.
FROM THE JOURNAL OF CLINICAL ONCOLOGY
Key clinical point: The ASCO clinical practice guideline on postmastectomy radiotherapy has been updated to help clinicians decide which patients who have T1-T2 breast cancer with one-three positive axillary lymph nodes will not benefit from the treatment.
Major finding: The 10-year rate of locoregional treatment failure was only 4.3% with irradiation, compared with 21.0% without irradiation, and the 10-year rate of local or distant treatment failure was 33.8% with irradiation and 45.5% without it.
Data source: A review of the literature and compilation of several treatment recommendations.
Disclosures: This work was supported by the American Society of Clinical Oncology, the American Society for Radiation Oncology, and the Society of Surgical Oncology. Dr. Recht reported serving as a consultant or advisor to CareCore and U.S. Oncology and receiving research funding from Genomic Health; his associates reported ties to numerous industry sources.