User login
New anticancer drugs linked to increased costs, life expectancy
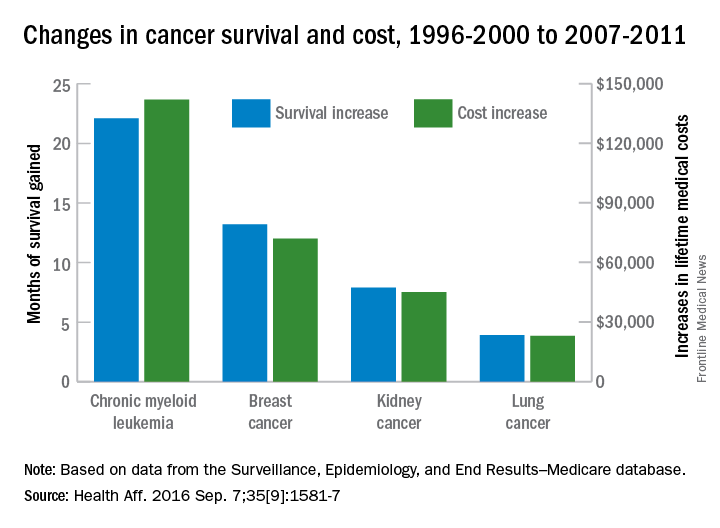
New anticancer drugs are often expensive and have been accompanied by large increases in the cost of medical treatment, but they also are associated with gains in life expectancy, according to an analysis of Medicare data published online.
Investigators looked at four different types of cancer – breast, kidney, lung, and chronic myeloid leukemia (CML) – over two time periods: 1996-2000 and 2007-2011. Patients treated for CML during 2007-2011 had the largest increases in both average lifetime medical cost ($142,000) and months of life gained (22.1) over those treated during 1996-2000, reported David H. Howard, PhD, of Emory University, Atlanta, and his associates.
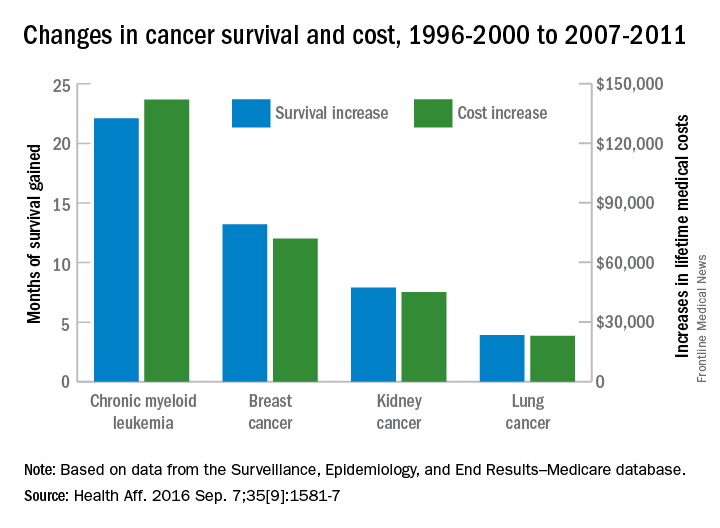
Breast cancer patients had the next-largest increases: 13.2 months of life expectancy and $72,000 in lifetime medical cost for those who received physician-administered intravenous drugs. For breast cancer patients who received only oral drugs, the increases were 2 months of life and $9,000 in lifetime cost, they noted.
Patients with kidney cancer had an average life-expectancy increase of 7.9 months and a cost increase of $45,000, but those estimates don’t fully reflect the effect of several oral drugs that were introduced after 2007 but did not come into widespread use during the entire study period, Dr. Howard and his associates noted (Health Aff. 2016 Sep 7;35[9]:1581-7).
Lung cancer patients experienced the smallest changes between the two time periods, with an increase in life expectancy of 3.9 months for those who received physician-administered anticancer drugs and a lifetime medical cost increase of $23,000. Patients with lung cancer who did not receive such drugs had increases of 0.7 months of life expectancy and $4,000 in lifetime medical costs.
The researchers used data from the Surveillance, Epidemiology, and End Results–Medicare database, and all costs are adjusted to 2012 dollars. Data collection was supported by the California Department of Health and funding for the study was provided by Pfizer. Three of Dr. Howard’s five coinvestigators are Pfizer employees.
New anticancer drugs are often expensive and have been accompanied by large increases in the cost of medical treatment, but they also are associated with gains in life expectancy, according to an analysis of Medicare data published online.
Investigators looked at four different types of cancer – breast, kidney, lung, and chronic myeloid leukemia (CML) – over two time periods: 1996-2000 and 2007-2011. Patients treated for CML during 2007-2011 had the largest increases in both average lifetime medical cost ($142,000) and months of life gained (22.1) over those treated during 1996-2000, reported David H. Howard, PhD, of Emory University, Atlanta, and his associates.
Breast cancer patients had the next-largest increases: 13.2 months of life expectancy and $72,000 in lifetime medical cost for those who received physician-administered intravenous drugs. For breast cancer patients who received only oral drugs, the increases were 2 months of life and $9,000 in lifetime cost, they noted.
Patients with kidney cancer had an average life-expectancy increase of 7.9 months and a cost increase of $45,000, but those estimates don’t fully reflect the effect of several oral drugs that were introduced after 2007 but did not come into widespread use during the entire study period, Dr. Howard and his associates noted (Health Aff. 2016 Sep 7;35[9]:1581-7).
Lung cancer patients experienced the smallest changes between the two time periods, with an increase in life expectancy of 3.9 months for those who received physician-administered anticancer drugs and a lifetime medical cost increase of $23,000. Patients with lung cancer who did not receive such drugs had increases of 0.7 months of life expectancy and $4,000 in lifetime medical costs.
The researchers used data from the Surveillance, Epidemiology, and End Results–Medicare database, and all costs are adjusted to 2012 dollars. Data collection was supported by the California Department of Health and funding for the study was provided by Pfizer. Three of Dr. Howard’s five coinvestigators are Pfizer employees.
New anticancer drugs are often expensive and have been accompanied by large increases in the cost of medical treatment, but they also are associated with gains in life expectancy, according to an analysis of Medicare data published online.
Investigators looked at four different types of cancer – breast, kidney, lung, and chronic myeloid leukemia (CML) – over two time periods: 1996-2000 and 2007-2011. Patients treated for CML during 2007-2011 had the largest increases in both average lifetime medical cost ($142,000) and months of life gained (22.1) over those treated during 1996-2000, reported David H. Howard, PhD, of Emory University, Atlanta, and his associates.
Breast cancer patients had the next-largest increases: 13.2 months of life expectancy and $72,000 in lifetime medical cost for those who received physician-administered intravenous drugs. For breast cancer patients who received only oral drugs, the increases were 2 months of life and $9,000 in lifetime cost, they noted.
Patients with kidney cancer had an average life-expectancy increase of 7.9 months and a cost increase of $45,000, but those estimates don’t fully reflect the effect of several oral drugs that were introduced after 2007 but did not come into widespread use during the entire study period, Dr. Howard and his associates noted (Health Aff. 2016 Sep 7;35[9]:1581-7).
Lung cancer patients experienced the smallest changes between the two time periods, with an increase in life expectancy of 3.9 months for those who received physician-administered anticancer drugs and a lifetime medical cost increase of $23,000. Patients with lung cancer who did not receive such drugs had increases of 0.7 months of life expectancy and $4,000 in lifetime medical costs.
The researchers used data from the Surveillance, Epidemiology, and End Results–Medicare database, and all costs are adjusted to 2012 dollars. Data collection was supported by the California Department of Health and funding for the study was provided by Pfizer. Three of Dr. Howard’s five coinvestigators are Pfizer employees.
FROM HEALTH AFFAIRS
Large retrospective study challenges updated ASCO-CAP HER2 categorizations
The most recent update of the American Society of Clinical Oncology and College of American Pathologists (ASCO-CAP) guidelines for interpreting HER2 diagnostic assays affected about 5% of breast cancer patients in three large clinical trials, researchers reported in the Journal of Clinical Oncology.
Although this is “a small minority of patients,” clinical correlates fail to support three of the five groups of patients that the updated guidelines designated based on HER2 FISH [fluorescent in situ hybridization] ratio and average number of HER2 gene copies per tumor cell, said Michael Press, MD, of the University of Southern California Norris Comprehensive Cancer Center, Los Angeles, and his associates.
“Our findings support the original categorizations of HER2 by FISH status in BCIRG [Breast Cancer International Research Group]/Translational Research in Oncology trials,” they said.
The most recent ASCO-CAP guidelines differ from Food and Drug Administration–approved package inserts for HER2 FISH companion diagnostic assays, which reflect the criteria used in clinical trials of the BCIRG/Translational Research in Oncology (TRIO) and previous (2007) ASCO-CAP guidelines, the researchers noted. In particular, the updated guidelines split patients into group 1 (in situ hybridization [ISH] positive, with a HER2-to-chromosome 17 centromere ratio of at least 2.0 and an average of at least four copies of the HER2 gene per tumor cell), group 2 (ISH positive, with a ratio of at least 2.0 and less than four HER2 gene copies), group 3 (ISH positive, with a ratio of less than 2.0 and at least six gene copies), group 4 (ISH equivocal, with a ratio of less than 2.0 and at least four but fewer than six gene copies), and group 5 (ISH negative, a ratio of less than 2.0 and fewer than four gene copies).
The researchers retrospectively analyzed detailed outcomes data from the BCIRG-005, BCIRG- 006, and BCIRG-007 clinical trials, which “now have long-term clinical follow-up data available that facilitate determination of whether the new HER2 guidelines for FISH are clinically useful and predictive of known outcomes,” they said.
The investigators counted cases in each of the five groups and looked to see if these groups correlated with the clinical implications of HER2 gene amplification, such as overexpression of HER2 protein and worse disease-free and overall survival without HER2 targeted therapy (J Clin Oncol. 2016 Aug 29. doi: 10.1200/JCO.2016.66.6693).
Among 10,468 patients in these trials, the vast majority fell into group 1 (41%) or 5 (54%), while 0.7% were in group 2, 0.5% were in group 3, and 4% were in group 4. HER2 amplification status did not change for most patients because the updated guidelines did not affect group 1 (amplified) or group 5 (not amplified). But groups 2 and 4, which the guidelines respectively designated as ISH positive and ISH equivocal, actually seemed to be HER2 not amplified, as neither group was associated with HER2 protein overexpression, group 2 showed a lack of response to trastuzumab therapy, and patients in group 4 who received only chemotherapy had a prognosis similar to that of group 5 in terms of disease-free and overall survival, the researchers reported.
“Overall, we observe approximately 99.3% agreement with initial FDA-approved guidelines and 94.7% agreement with current ASCO-CAP guidelines,” they wrote. “The 4.6% differential is related to only two groups, groups 3 and 4, introduced by ASCO-CAP that lead to different assessments of HER2 status, compared with FDA criteria. Finally, our observations indicate group 2, which represents 0.7% of breast cancers, is misclassified by both the FDA and ASCO-CAP guidelines as amplified and ISH positive.”
They also found that patients in group 3, which the guidelines designated as ISH positive, actually had both HER2 amplified and HER2 not-amplified breast cancers. “There are now nearly 3 decades of accumulated experience and published data studying this alteration in human breast cancers,” the investigators concluded. “Although guidelines are helpful, diagnostic judgment and long-term outcome data remain important in the evaluation of testing criteria.”
The most recent update of the American Society of Clinical Oncology and College of American Pathologists (ASCO-CAP) guidelines for interpreting HER2 diagnostic assays affected about 5% of breast cancer patients in three large clinical trials, researchers reported in the Journal of Clinical Oncology.
Although this is “a small minority of patients,” clinical correlates fail to support three of the five groups of patients that the updated guidelines designated based on HER2 FISH [fluorescent in situ hybridization] ratio and average number of HER2 gene copies per tumor cell, said Michael Press, MD, of the University of Southern California Norris Comprehensive Cancer Center, Los Angeles, and his associates.
“Our findings support the original categorizations of HER2 by FISH status in BCIRG [Breast Cancer International Research Group]/Translational Research in Oncology trials,” they said.
The most recent ASCO-CAP guidelines differ from Food and Drug Administration–approved package inserts for HER2 FISH companion diagnostic assays, which reflect the criteria used in clinical trials of the BCIRG/Translational Research in Oncology (TRIO) and previous (2007) ASCO-CAP guidelines, the researchers noted. In particular, the updated guidelines split patients into group 1 (in situ hybridization [ISH] positive, with a HER2-to-chromosome 17 centromere ratio of at least 2.0 and an average of at least four copies of the HER2 gene per tumor cell), group 2 (ISH positive, with a ratio of at least 2.0 and less than four HER2 gene copies), group 3 (ISH positive, with a ratio of less than 2.0 and at least six gene copies), group 4 (ISH equivocal, with a ratio of less than 2.0 and at least four but fewer than six gene copies), and group 5 (ISH negative, a ratio of less than 2.0 and fewer than four gene copies).
The researchers retrospectively analyzed detailed outcomes data from the BCIRG-005, BCIRG- 006, and BCIRG-007 clinical trials, which “now have long-term clinical follow-up data available that facilitate determination of whether the new HER2 guidelines for FISH are clinically useful and predictive of known outcomes,” they said.
The investigators counted cases in each of the five groups and looked to see if these groups correlated with the clinical implications of HER2 gene amplification, such as overexpression of HER2 protein and worse disease-free and overall survival without HER2 targeted therapy (J Clin Oncol. 2016 Aug 29. doi: 10.1200/JCO.2016.66.6693).
Among 10,468 patients in these trials, the vast majority fell into group 1 (41%) or 5 (54%), while 0.7% were in group 2, 0.5% were in group 3, and 4% were in group 4. HER2 amplification status did not change for most patients because the updated guidelines did not affect group 1 (amplified) or group 5 (not amplified). But groups 2 and 4, which the guidelines respectively designated as ISH positive and ISH equivocal, actually seemed to be HER2 not amplified, as neither group was associated with HER2 protein overexpression, group 2 showed a lack of response to trastuzumab therapy, and patients in group 4 who received only chemotherapy had a prognosis similar to that of group 5 in terms of disease-free and overall survival, the researchers reported.
“Overall, we observe approximately 99.3% agreement with initial FDA-approved guidelines and 94.7% agreement with current ASCO-CAP guidelines,” they wrote. “The 4.6% differential is related to only two groups, groups 3 and 4, introduced by ASCO-CAP that lead to different assessments of HER2 status, compared with FDA criteria. Finally, our observations indicate group 2, which represents 0.7% of breast cancers, is misclassified by both the FDA and ASCO-CAP guidelines as amplified and ISH positive.”
They also found that patients in group 3, which the guidelines designated as ISH positive, actually had both HER2 amplified and HER2 not-amplified breast cancers. “There are now nearly 3 decades of accumulated experience and published data studying this alteration in human breast cancers,” the investigators concluded. “Although guidelines are helpful, diagnostic judgment and long-term outcome data remain important in the evaluation of testing criteria.”
The most recent update of the American Society of Clinical Oncology and College of American Pathologists (ASCO-CAP) guidelines for interpreting HER2 diagnostic assays affected about 5% of breast cancer patients in three large clinical trials, researchers reported in the Journal of Clinical Oncology.
Although this is “a small minority of patients,” clinical correlates fail to support three of the five groups of patients that the updated guidelines designated based on HER2 FISH [fluorescent in situ hybridization] ratio and average number of HER2 gene copies per tumor cell, said Michael Press, MD, of the University of Southern California Norris Comprehensive Cancer Center, Los Angeles, and his associates.
“Our findings support the original categorizations of HER2 by FISH status in BCIRG [Breast Cancer International Research Group]/Translational Research in Oncology trials,” they said.
The most recent ASCO-CAP guidelines differ from Food and Drug Administration–approved package inserts for HER2 FISH companion diagnostic assays, which reflect the criteria used in clinical trials of the BCIRG/Translational Research in Oncology (TRIO) and previous (2007) ASCO-CAP guidelines, the researchers noted. In particular, the updated guidelines split patients into group 1 (in situ hybridization [ISH] positive, with a HER2-to-chromosome 17 centromere ratio of at least 2.0 and an average of at least four copies of the HER2 gene per tumor cell), group 2 (ISH positive, with a ratio of at least 2.0 and less than four HER2 gene copies), group 3 (ISH positive, with a ratio of less than 2.0 and at least six gene copies), group 4 (ISH equivocal, with a ratio of less than 2.0 and at least four but fewer than six gene copies), and group 5 (ISH negative, a ratio of less than 2.0 and fewer than four gene copies).
The researchers retrospectively analyzed detailed outcomes data from the BCIRG-005, BCIRG- 006, and BCIRG-007 clinical trials, which “now have long-term clinical follow-up data available that facilitate determination of whether the new HER2 guidelines for FISH are clinically useful and predictive of known outcomes,” they said.
The investigators counted cases in each of the five groups and looked to see if these groups correlated with the clinical implications of HER2 gene amplification, such as overexpression of HER2 protein and worse disease-free and overall survival without HER2 targeted therapy (J Clin Oncol. 2016 Aug 29. doi: 10.1200/JCO.2016.66.6693).
Among 10,468 patients in these trials, the vast majority fell into group 1 (41%) or 5 (54%), while 0.7% were in group 2, 0.5% were in group 3, and 4% were in group 4. HER2 amplification status did not change for most patients because the updated guidelines did not affect group 1 (amplified) or group 5 (not amplified). But groups 2 and 4, which the guidelines respectively designated as ISH positive and ISH equivocal, actually seemed to be HER2 not amplified, as neither group was associated with HER2 protein overexpression, group 2 showed a lack of response to trastuzumab therapy, and patients in group 4 who received only chemotherapy had a prognosis similar to that of group 5 in terms of disease-free and overall survival, the researchers reported.
“Overall, we observe approximately 99.3% agreement with initial FDA-approved guidelines and 94.7% agreement with current ASCO-CAP guidelines,” they wrote. “The 4.6% differential is related to only two groups, groups 3 and 4, introduced by ASCO-CAP that lead to different assessments of HER2 status, compared with FDA criteria. Finally, our observations indicate group 2, which represents 0.7% of breast cancers, is misclassified by both the FDA and ASCO-CAP guidelines as amplified and ISH positive.”
They also found that patients in group 3, which the guidelines designated as ISH positive, actually had both HER2 amplified and HER2 not-amplified breast cancers. “There are now nearly 3 decades of accumulated experience and published data studying this alteration in human breast cancers,” the investigators concluded. “Although guidelines are helpful, diagnostic judgment and long-term outcome data remain important in the evaluation of testing criteria.”
FROM THE JOURNAL OF CLINICAL ONCOLOGY
Key clinical point: Clinical trial data support the original ASCO-CAP categories for HER2 status, not the updated categories from the most recent guidelines.
Major finding: The guideline changes affect only about 5% of patients, but clinical correlates did not support three of five groups that the guidelines defined based on the HER2 FISH ratio and the average number of HER2 gene copies per tumor cell.
Data source: A retrospective analysis of data from 10,468 patients from three clinical trials of the Breast Cancer International Research Group.
Disclosures: The work was funded by the Breast Cancer Research Foundation; the California Breast Cancer Research Program; the Tower Cancer Research Foundation; Richard Blach, MD; the Entertainment Industry Foundation; the endowed Harold E. Lee Chair for Cancer Research; and the National Cancer Institute. Sanofi, Genentech, and F. Hoffman-La Roche supported the three clinical trials. Dr. Press disclosed ties to Biocartis, DAKO, Halozyme, Puma Biotechnology, Cepheid, and Ventana Medical Systems.
Breast density is key to appropriate screening intervals
Breast density is an important factor in determining the appropriate screening intervals for mammography after age 50 years, according to a report published online Aug. 22 in Annals of Internal Medicine.
Researchers from the Cancer Intervention and Surveillance Modeling Network, collaborating with the Breast Cancer Surveillance Consortium, assessed three separate, well-established microsimulation models that used different structures and underlying assumptions but the same data input to estimate the benefits and harms of various screening intervals. They applied the models to two hypothetical populations: Women aged 50 years and older who were initiating screening for the first time and women aged 65 years who had undergone biennial screening since age 50 years.

The models incorporated national data regarding breast cancer incidence, treatment efficacy, and survival. They assessed patient risk by including numerous factors, such as menopausal status, obesity status, age at menarche, nulliparity, and previous biopsy results, but didn’t include family history or genetic testing results. Screening strategies were compared among four possible breast-density levels, according to the American College of Radiology’s Breast Imaging Reporting and Data System (BI-RADS).
The principal finding was that two factors – breast density and risk for breast cancer – were key to determining the optimal screening interval. The optimal interval was the one that would yield the highest number of benefits (breast cancer deaths averted, life-years gained, and quality-adjusted life-years gained) while yielding the lowest number of harms (false-positive mammograms, benign biopsies, and overdiagnosis).
“For average-risk women in low-density subgroups, who comprise a large portion of the population, triennial screening provides a reasonable balance of benefits and harms and is cost effective. Annual screening has a favorable balance of benefits and harms and would be considered cost effective for subgroups of women ... with risk levels that are two to four times the average and with heterogeneously or extremely dense breasts,” the researchers wrote (Ann.Intern Med. 2016 Aug 22. doi: 10.7326/M16-0476).
After age 50 years, annual mammography was more beneficial than harmful only in two subgroups of women: those with greater breast density and those with higher risk for breast cancer. Such women are estimated to comprise less than 1% of the general population at both age 50 years and age 65 years. In contrast, biennial and even triennial mammography yielded fewer false-positives and fewer biopsies for average-risk women with low-density breasts without affecting the number of breast cancer deaths averted, the researchers noted.
The study was supported by grants from the National Institutes of Health and several state public health departments and cancer registries in the United States. The researchers reported receiving grants and other support from the NIH, the American Society of Breast Surgeons, Renaissance Rx, Ally Clinical Diagnostics, the Netherlands National Institute for Public Health and the Environment, SCOR Global Risk Center, and Genomic Health Canada.
The U.S. Preventive Services Task Force made a grade B recommendation for biennial mammography screening in average-risk women aged 50 to 74 years. This current work from the well-regarded Cancer Intervention and Surveillance Modeling Network and Breast Cancer Surveillance Consortium investigators helps women and clinicians to possibly individualize screening frequency based on risk and BI-RADS categories. It will be important to track outcomes in women who undergo alternative screening frequencies to validate this approach.
Christine D. Berg, MD, is in the department of radiation oncology at Johns Hopkins Hospital, Baltimore. She reported receiving personal fees from Medial Early Sign. These comments are excerpted from an editorial accompanying Dr. Trentham-Dietz’s report (Ann Intern Med. 2016 Aug 22. doi: 10.7326/M16-1791).
The U.S. Preventive Services Task Force made a grade B recommendation for biennial mammography screening in average-risk women aged 50 to 74 years. This current work from the well-regarded Cancer Intervention and Surveillance Modeling Network and Breast Cancer Surveillance Consortium investigators helps women and clinicians to possibly individualize screening frequency based on risk and BI-RADS categories. It will be important to track outcomes in women who undergo alternative screening frequencies to validate this approach.
Christine D. Berg, MD, is in the department of radiation oncology at Johns Hopkins Hospital, Baltimore. She reported receiving personal fees from Medial Early Sign. These comments are excerpted from an editorial accompanying Dr. Trentham-Dietz’s report (Ann Intern Med. 2016 Aug 22. doi: 10.7326/M16-1791).
The U.S. Preventive Services Task Force made a grade B recommendation for biennial mammography screening in average-risk women aged 50 to 74 years. This current work from the well-regarded Cancer Intervention and Surveillance Modeling Network and Breast Cancer Surveillance Consortium investigators helps women and clinicians to possibly individualize screening frequency based on risk and BI-RADS categories. It will be important to track outcomes in women who undergo alternative screening frequencies to validate this approach.
Christine D. Berg, MD, is in the department of radiation oncology at Johns Hopkins Hospital, Baltimore. She reported receiving personal fees from Medial Early Sign. These comments are excerpted from an editorial accompanying Dr. Trentham-Dietz’s report (Ann Intern Med. 2016 Aug 22. doi: 10.7326/M16-1791).
Breast density is an important factor in determining the appropriate screening intervals for mammography after age 50 years, according to a report published online Aug. 22 in Annals of Internal Medicine.
Researchers from the Cancer Intervention and Surveillance Modeling Network, collaborating with the Breast Cancer Surveillance Consortium, assessed three separate, well-established microsimulation models that used different structures and underlying assumptions but the same data input to estimate the benefits and harms of various screening intervals. They applied the models to two hypothetical populations: Women aged 50 years and older who were initiating screening for the first time and women aged 65 years who had undergone biennial screening since age 50 years.
The models incorporated national data regarding breast cancer incidence, treatment efficacy, and survival. They assessed patient risk by including numerous factors, such as menopausal status, obesity status, age at menarche, nulliparity, and previous biopsy results, but didn’t include family history or genetic testing results. Screening strategies were compared among four possible breast-density levels, according to the American College of Radiology’s Breast Imaging Reporting and Data System (BI-RADS).
The principal finding was that two factors – breast density and risk for breast cancer – were key to determining the optimal screening interval. The optimal interval was the one that would yield the highest number of benefits (breast cancer deaths averted, life-years gained, and quality-adjusted life-years gained) while yielding the lowest number of harms (false-positive mammograms, benign biopsies, and overdiagnosis).
“For average-risk women in low-density subgroups, who comprise a large portion of the population, triennial screening provides a reasonable balance of benefits and harms and is cost effective. Annual screening has a favorable balance of benefits and harms and would be considered cost effective for subgroups of women ... with risk levels that are two to four times the average and with heterogeneously or extremely dense breasts,” the researchers wrote (Ann.Intern Med. 2016 Aug 22. doi: 10.7326/M16-0476).
After age 50 years, annual mammography was more beneficial than harmful only in two subgroups of women: those with greater breast density and those with higher risk for breast cancer. Such women are estimated to comprise less than 1% of the general population at both age 50 years and age 65 years. In contrast, biennial and even triennial mammography yielded fewer false-positives and fewer biopsies for average-risk women with low-density breasts without affecting the number of breast cancer deaths averted, the researchers noted.
The study was supported by grants from the National Institutes of Health and several state public health departments and cancer registries in the United States. The researchers reported receiving grants and other support from the NIH, the American Society of Breast Surgeons, Renaissance Rx, Ally Clinical Diagnostics, the Netherlands National Institute for Public Health and the Environment, SCOR Global Risk Center, and Genomic Health Canada.
Breast density is an important factor in determining the appropriate screening intervals for mammography after age 50 years, according to a report published online Aug. 22 in Annals of Internal Medicine.
Researchers from the Cancer Intervention and Surveillance Modeling Network, collaborating with the Breast Cancer Surveillance Consortium, assessed three separate, well-established microsimulation models that used different structures and underlying assumptions but the same data input to estimate the benefits and harms of various screening intervals. They applied the models to two hypothetical populations: Women aged 50 years and older who were initiating screening for the first time and women aged 65 years who had undergone biennial screening since age 50 years.
The models incorporated national data regarding breast cancer incidence, treatment efficacy, and survival. They assessed patient risk by including numerous factors, such as menopausal status, obesity status, age at menarche, nulliparity, and previous biopsy results, but didn’t include family history or genetic testing results. Screening strategies were compared among four possible breast-density levels, according to the American College of Radiology’s Breast Imaging Reporting and Data System (BI-RADS).
The principal finding was that two factors – breast density and risk for breast cancer – were key to determining the optimal screening interval. The optimal interval was the one that would yield the highest number of benefits (breast cancer deaths averted, life-years gained, and quality-adjusted life-years gained) while yielding the lowest number of harms (false-positive mammograms, benign biopsies, and overdiagnosis).
“For average-risk women in low-density subgroups, who comprise a large portion of the population, triennial screening provides a reasonable balance of benefits and harms and is cost effective. Annual screening has a favorable balance of benefits and harms and would be considered cost effective for subgroups of women ... with risk levels that are two to four times the average and with heterogeneously or extremely dense breasts,” the researchers wrote (Ann.Intern Med. 2016 Aug 22. doi: 10.7326/M16-0476).
After age 50 years, annual mammography was more beneficial than harmful only in two subgroups of women: those with greater breast density and those with higher risk for breast cancer. Such women are estimated to comprise less than 1% of the general population at both age 50 years and age 65 years. In contrast, biennial and even triennial mammography yielded fewer false-positives and fewer biopsies for average-risk women with low-density breasts without affecting the number of breast cancer deaths averted, the researchers noted.
The study was supported by grants from the National Institutes of Health and several state public health departments and cancer registries in the United States. The researchers reported receiving grants and other support from the NIH, the American Society of Breast Surgeons, Renaissance Rx, Ally Clinical Diagnostics, the Netherlands National Institute for Public Health and the Environment, SCOR Global Risk Center, and Genomic Health Canada.
FROM ANNALS OF INTERNAL MEDICINE
Key clinical point: Breast density is a key factor in determining appropriate screening intervals for mammography after age 50.
Major finding: Annual mammography is beneficial only in women with greater breast density and higher risk for breast cancer, who comprise less than 1% of the general population.
Data source: A comparison of three separate microsimulation models for breast cancer screening after age 50 years.
Disclosures: The study was supported by grants from the National Institutes of Health and several state public health departments and cancer registries in the United States. The researchers reported receiving grants and other support from the NIH, the American Society of Breast Surgeons, Renaissance Rx, Ally Clinical Diagnostics, the Netherlands National Institute for Public Health and the Environment, SCOR Global Risk Center, and Genomic Health Canada.

Guideline recommends 2-mm negative margins for DCIS
Surgical excision with 2-mm clear margins combined with whole-breast irradiation may be the optimal standard to reduce recurrence in patients with ductal carcinoma in situ (DCIS), according to a multidisciplinary consensus panel.
Despite the widespread use of surgical excision in breast-conserving therapy among patients with DCIS, there is no consensus on the optimal negative margin to prevent recurrence and re-excision. Therefore, the Society of Surgical Oncology, the American Society for Radiation Oncology, and the American Society of Clinical Oncology convened a panel to answer the following question: What margin width minimizes the risk of ipsilateral breast tumor recurrence in patients with DCIS receiving breast-conserving surgery?

The guideline panel reviewed 20 studies including 7,883 DCIS patients. A median of 100% of patients received whole-breast radiation therapy and a median of 21% received endocrine therapy. Patients were followed for a median of 6.5 years and the median incidence of recurrence was 8.3%.
“There is no debate that a positive margin ... implies a potentially incomplete resection and is associated with a higher rate of [recurrence],” according to Monica Morrow, MD, of Memorial Sloan-Kettering Cancer Center, and her fellow panelists. Further, the addition of whole-breast irradiation did not negate this increased risk, the panelists noted (J Clin Oncol. 2016 Aug. doi: 10.1200/JCO.2016.68.3573).
According to the meta-analysis, patients with 2-mm negative margins plus whole-breast irradiation were significantly less likely to experience ipsilateral breast tumor recurrence compared with patients who had excisions with positive margins.
“Margins of at least 2 mm are associated with a reduced risk of [recurrence] relative to narrower negative margin widths in patients receiving [whole-breast radiotherapy]. The routine practice of obtaining negative margin widths wider than 2 mm is not supported by the evidence,” they wrote.
The panel also noted that treatment with excision alone is associated with higher rates of recurrence compared with treatment involving with both excision and whole-breast radiation therapy. However, if patients are treated with excision alone, the optimal margin, which is unknown for this subset of patients, should be at least 2 millimeters, according to the guideline.
Due to variability in specimen sampling and in margin evaluation and assessment, “clinical judgment must be used in determining whether patients with smaller negative margin widths (0 or 1 mm) require re-excision,” the panelists noted. “The findings should not be extrapolated to DCIS patients treated with [accelerated partial breast irradiation] or those with invasive carcinoma for whom a separate guideline has been developed,” Dr. Morrow and her associates wrote.
The guideline development process was funded by the Susan G. Komen Foundation. The authors had no relevant disclosures to report.
On Twitter @jessnicolecraig
Surgical excision with 2-mm clear margins combined with whole-breast irradiation may be the optimal standard to reduce recurrence in patients with ductal carcinoma in situ (DCIS), according to a multidisciplinary consensus panel.
Despite the widespread use of surgical excision in breast-conserving therapy among patients with DCIS, there is no consensus on the optimal negative margin to prevent recurrence and re-excision. Therefore, the Society of Surgical Oncology, the American Society for Radiation Oncology, and the American Society of Clinical Oncology convened a panel to answer the following question: What margin width minimizes the risk of ipsilateral breast tumor recurrence in patients with DCIS receiving breast-conserving surgery?
The guideline panel reviewed 20 studies including 7,883 DCIS patients. A median of 100% of patients received whole-breast radiation therapy and a median of 21% received endocrine therapy. Patients were followed for a median of 6.5 years and the median incidence of recurrence was 8.3%.
“There is no debate that a positive margin ... implies a potentially incomplete resection and is associated with a higher rate of [recurrence],” according to Monica Morrow, MD, of Memorial Sloan-Kettering Cancer Center, and her fellow panelists. Further, the addition of whole-breast irradiation did not negate this increased risk, the panelists noted (J Clin Oncol. 2016 Aug. doi: 10.1200/JCO.2016.68.3573).
According to the meta-analysis, patients with 2-mm negative margins plus whole-breast irradiation were significantly less likely to experience ipsilateral breast tumor recurrence compared with patients who had excisions with positive margins.
“Margins of at least 2 mm are associated with a reduced risk of [recurrence] relative to narrower negative margin widths in patients receiving [whole-breast radiotherapy]. The routine practice of obtaining negative margin widths wider than 2 mm is not supported by the evidence,” they wrote.
The panel also noted that treatment with excision alone is associated with higher rates of recurrence compared with treatment involving with both excision and whole-breast radiation therapy. However, if patients are treated with excision alone, the optimal margin, which is unknown for this subset of patients, should be at least 2 millimeters, according to the guideline.
Due to variability in specimen sampling and in margin evaluation and assessment, “clinical judgment must be used in determining whether patients with smaller negative margin widths (0 or 1 mm) require re-excision,” the panelists noted. “The findings should not be extrapolated to DCIS patients treated with [accelerated partial breast irradiation] or those with invasive carcinoma for whom a separate guideline has been developed,” Dr. Morrow and her associates wrote.
The guideline development process was funded by the Susan G. Komen Foundation. The authors had no relevant disclosures to report.
On Twitter @jessnicolecraig
Surgical excision with 2-mm clear margins combined with whole-breast irradiation may be the optimal standard to reduce recurrence in patients with ductal carcinoma in situ (DCIS), according to a multidisciplinary consensus panel.
Despite the widespread use of surgical excision in breast-conserving therapy among patients with DCIS, there is no consensus on the optimal negative margin to prevent recurrence and re-excision. Therefore, the Society of Surgical Oncology, the American Society for Radiation Oncology, and the American Society of Clinical Oncology convened a panel to answer the following question: What margin width minimizes the risk of ipsilateral breast tumor recurrence in patients with DCIS receiving breast-conserving surgery?
The guideline panel reviewed 20 studies including 7,883 DCIS patients. A median of 100% of patients received whole-breast radiation therapy and a median of 21% received endocrine therapy. Patients were followed for a median of 6.5 years and the median incidence of recurrence was 8.3%.
“There is no debate that a positive margin ... implies a potentially incomplete resection and is associated with a higher rate of [recurrence],” according to Monica Morrow, MD, of Memorial Sloan-Kettering Cancer Center, and her fellow panelists. Further, the addition of whole-breast irradiation did not negate this increased risk, the panelists noted (J Clin Oncol. 2016 Aug. doi: 10.1200/JCO.2016.68.3573).
According to the meta-analysis, patients with 2-mm negative margins plus whole-breast irradiation were significantly less likely to experience ipsilateral breast tumor recurrence compared with patients who had excisions with positive margins.
“Margins of at least 2 mm are associated with a reduced risk of [recurrence] relative to narrower negative margin widths in patients receiving [whole-breast radiotherapy]. The routine practice of obtaining negative margin widths wider than 2 mm is not supported by the evidence,” they wrote.
The panel also noted that treatment with excision alone is associated with higher rates of recurrence compared with treatment involving with both excision and whole-breast radiation therapy. However, if patients are treated with excision alone, the optimal margin, which is unknown for this subset of patients, should be at least 2 millimeters, according to the guideline.
Due to variability in specimen sampling and in margin evaluation and assessment, “clinical judgment must be used in determining whether patients with smaller negative margin widths (0 or 1 mm) require re-excision,” the panelists noted. “The findings should not be extrapolated to DCIS patients treated with [accelerated partial breast irradiation] or those with invasive carcinoma for whom a separate guideline has been developed,” Dr. Morrow and her associates wrote.
The guideline development process was funded by the Susan G. Komen Foundation. The authors had no relevant disclosures to report.
On Twitter @jessnicolecraig
FROM THE JOURNAL OF CLINICAL ONCOLOGY
Key clinical point: Surgical excision with 2-mm clear margins combined with whole-breast irradiation may be the optimal standard to reduce recurrence in patients with ductal carcinoma in situ.
Major finding: Patients with 2-mm clear margins were significantly less likely to experience ipsilateral breast tumor recurrence compared with patients who had excisions with positive margins.
Data source: Meta-analysis of 20 studies and other published literature.
Disclosures: The Susan G. Komen Foundation funded the guideline development process. The panel members had no relevant disclosures.

Unraveling the Causes of Breast Cancer Disparities
Why are black women more likely to develop certain aggressive subtypes of breast cancer than are white women? Also, why are black women more likely to die of breast cancer? The National Cancer Institute (NCI) has launched a collaborative research project to pinpoint genetic factors that underlie these and other disparities.
The Breast Cancer Genetic Study in African-Ancestry Populations is the largest study to date to investigate genetic and biological factors behind black women’s risk of breast cancer. It won’t enroll new patients but instead will bring together researchers and data from a variety of venues, including the African-American Breast Cancer Consortium, the African-American Breast Cancer Epidemiology and Risk Consortium, and the NCI Cohort Consortium. Minority scientists from various institutions are playing an important role in the study, NCI says.
The researchers will share biospecimens, data, and resources of the 20,000 black women involved in 18 previous studies. The genomes of those women will be compared with those of 20,000 black women who do not have breast cancer as well as with white women who have breast cancer. The project will investigate genetic variations associated with breast cancer risk in black women and gene expression in tumor samples to identify genetic pathways.
“This effort is about making sure that all Americans—no matter their background—reap the same benefits from the promising advances of precisions medicine,” said Douglas Lowy, MD, acting director of NCI. “I’m hopeful about where this new research can take us, not only in addressing the unique breast cancer profiles of African American women, but also in learning more about the origin of cancer disparities.”
Why are black women more likely to develop certain aggressive subtypes of breast cancer than are white women? Also, why are black women more likely to die of breast cancer? The National Cancer Institute (NCI) has launched a collaborative research project to pinpoint genetic factors that underlie these and other disparities.
The Breast Cancer Genetic Study in African-Ancestry Populations is the largest study to date to investigate genetic and biological factors behind black women’s risk of breast cancer. It won’t enroll new patients but instead will bring together researchers and data from a variety of venues, including the African-American Breast Cancer Consortium, the African-American Breast Cancer Epidemiology and Risk Consortium, and the NCI Cohort Consortium. Minority scientists from various institutions are playing an important role in the study, NCI says.
The researchers will share biospecimens, data, and resources of the 20,000 black women involved in 18 previous studies. The genomes of those women will be compared with those of 20,000 black women who do not have breast cancer as well as with white women who have breast cancer. The project will investigate genetic variations associated with breast cancer risk in black women and gene expression in tumor samples to identify genetic pathways.
“This effort is about making sure that all Americans—no matter their background—reap the same benefits from the promising advances of precisions medicine,” said Douglas Lowy, MD, acting director of NCI. “I’m hopeful about where this new research can take us, not only in addressing the unique breast cancer profiles of African American women, but also in learning more about the origin of cancer disparities.”
Why are black women more likely to develop certain aggressive subtypes of breast cancer than are white women? Also, why are black women more likely to die of breast cancer? The National Cancer Institute (NCI) has launched a collaborative research project to pinpoint genetic factors that underlie these and other disparities.
The Breast Cancer Genetic Study in African-Ancestry Populations is the largest study to date to investigate genetic and biological factors behind black women’s risk of breast cancer. It won’t enroll new patients but instead will bring together researchers and data from a variety of venues, including the African-American Breast Cancer Consortium, the African-American Breast Cancer Epidemiology and Risk Consortium, and the NCI Cohort Consortium. Minority scientists from various institutions are playing an important role in the study, NCI says.
The researchers will share biospecimens, data, and resources of the 20,000 black women involved in 18 previous studies. The genomes of those women will be compared with those of 20,000 black women who do not have breast cancer as well as with white women who have breast cancer. The project will investigate genetic variations associated with breast cancer risk in black women and gene expression in tumor samples to identify genetic pathways.
“This effort is about making sure that all Americans—no matter their background—reap the same benefits from the promising advances of precisions medicine,” said Douglas Lowy, MD, acting director of NCI. “I’m hopeful about where this new research can take us, not only in addressing the unique breast cancer profiles of African American women, but also in learning more about the origin of cancer disparities.”
Estrogen receptor mutations linked with worse outcomes in MBC
Estrogen receptor mutations in estrogen receptor–positive metastatic breast cancer are more prevalent than previous studies and methodologies suggest, investigators found during a secondary analysis of patients enrolled in the BOLERO-2 trial.
Furthermore, two specific estrogen receptor 1 (ESR1) mutations, D538G and Y537S, were associated with reduced overall survival.
Of the 724 patients enrolled in the BOLERO-2, a phase III trial of women with postmenopausal ER-positive, HER2-nonamplified advanced breast cancer refractory to nonsteroidal aromatase inhibitors, 541 had evaluable cell-free DNA from baseline plasma samples and consented to genomic testing. Cell-free DNA (cfDNA) was extracted from patient’s plasma samples and assayed (via BioRad’s QX200 Droplet Digital PCR [polymerase chain reaction] System) for two specific ESR1 mutations, D538G and Y537S.

ESR1 mutations were detected in 156 of the 541 patients (28.8%), with D538G mutations occurring in 114 patients (21.1%), Y537S mutations occurring in 72 patients (13.3%), and both mutations occurring in 30 patients (5.55%), according to Sarat Chandarlapaty, MD, PhD, of Memorial Sloan Kettering Cancer Center, New York, and his associates.
Frequency of ESR1 mutation did not differ by age, race, or site of metastatic disease. However, mutation prevalence was significantly associated with ECOG status (P = .04). Also, “there was a threefold increase in mutation prevalence in patients who had failed first-line therapy for metastatic disease (33% were mutant) compared with those who were initiating first-line treatment for MBC (11% were mutant), in whom exposure to AI therapy occurred only in the adjuvant setting,” the researchers wrote (JAMA Oncol. 2016 Aug 11. doi: 10.1001/jamaoncol.2016.1279).
Overall, patients with ESR1 mutations had shorter median overall survival times. Among patients with only D538G mutations, median overall survival was 25.99 months (95% CI, 19.19-32.36 months). Patients with only Y537S mutations had a median overall survival of 19.98 months (95% CI,13.01-29.31 months) whereas patients with neither mutation had an overall survival of 32.1 months (95% CI, 28.09-36.4 months). Patients carrying both mutations had an even further reduced median overall survival of 15.15 months (95% CI, 10.87-27.43).
Patients in BOLERO-2 had been randomized in a 2:1 ratio to receive either exemestane plus everolimus or exemestane plus placebo. For this secondary analysis, researchers found that patients who had received exemestane therapy and had the D538G mutation experienced a shorter median progression-free survival time (2.69 months; hazard ratio, 1.71; 95% CI, 1.09-2.68) compared with patients with no mutations who received exemestane therapy (3.94 months). Patients with no mutations who received everolimus had a median progression-free survival of 8.48 months, and patients with D538G mutations who received everolimus had a median progression-free survival of 5.78 months.
“One of the key findings of this work is the high prevalence of ER mutations in this patient population,” the investigators said.
The investigators also noted the ease, feasibility, and affordability with which cfDNA can be analyzed for these genetic mutations, and they believe the digital drop polymerase chain reaction assay used in this study could easily be implemented into regular clinical practice.
This study was funded by Novartis and supported by the Integrated Genomics Operation Core. Four of the investigators reported being employed by Novartis, and Dr. Chandarlapaty reported receiving financial compensation from AstraZeneca.
On Twitter @jessnicolecraig

|
Dr. Suzanne Fuqua |
The use of sensitive yet simple mutation monitoring of plasma as described in this study could provide indispensable predictive information for correcting the course of therapy in advanced or perhaps even early breast cancer. We eagerly await an illumination of what is not just evident on the surface, the “tip” of circulating cfDNA, but also what resistance networks lie beneath and drive the bulk of the metastatic ESR1 mutant-positive tumors in unique distant microenvironments.
Suzanne A.W. Fuqua, PhD, is a professor and researcher at the Lester and Sue Smith Breast Center at Baylor College of Medicine in Houston. Yassine Rechoum, PhD, is a postdoctoral fellow and Guowei Gu, PhD, is a postdoctoral associate at Baylor. These comments were excerpted from an invited commentary accompanying the study by Chandarlapaty et al. (JAMA Onc. 2016 Aug 11. doi:10.1001/jamaoncol.2016.1268).
|
|
Dr. Suzanne Fuqua |
The use of sensitive yet simple mutation monitoring of plasma as described in this study could provide indispensable predictive information for correcting the course of therapy in advanced or perhaps even early breast cancer. We eagerly await an illumination of what is not just evident on the surface, the “tip” of circulating cfDNA, but also what resistance networks lie beneath and drive the bulk of the metastatic ESR1 mutant-positive tumors in unique distant microenvironments.
Suzanne A.W. Fuqua, PhD, is a professor and researcher at the Lester and Sue Smith Breast Center at Baylor College of Medicine in Houston. Yassine Rechoum, PhD, is a postdoctoral fellow and Guowei Gu, PhD, is a postdoctoral associate at Baylor. These comments were excerpted from an invited commentary accompanying the study by Chandarlapaty et al. (JAMA Onc. 2016 Aug 11. doi:10.1001/jamaoncol.2016.1268).
|
|
Dr. Suzanne Fuqua |
The use of sensitive yet simple mutation monitoring of plasma as described in this study could provide indispensable predictive information for correcting the course of therapy in advanced or perhaps even early breast cancer. We eagerly await an illumination of what is not just evident on the surface, the “tip” of circulating cfDNA, but also what resistance networks lie beneath and drive the bulk of the metastatic ESR1 mutant-positive tumors in unique distant microenvironments.
Suzanne A.W. Fuqua, PhD, is a professor and researcher at the Lester and Sue Smith Breast Center at Baylor College of Medicine in Houston. Yassine Rechoum, PhD, is a postdoctoral fellow and Guowei Gu, PhD, is a postdoctoral associate at Baylor. These comments were excerpted from an invited commentary accompanying the study by Chandarlapaty et al. (JAMA Onc. 2016 Aug 11. doi:10.1001/jamaoncol.2016.1268).
Estrogen receptor mutations in estrogen receptor–positive metastatic breast cancer are more prevalent than previous studies and methodologies suggest, investigators found during a secondary analysis of patients enrolled in the BOLERO-2 trial.
Furthermore, two specific estrogen receptor 1 (ESR1) mutations, D538G and Y537S, were associated with reduced overall survival.
Of the 724 patients enrolled in the BOLERO-2, a phase III trial of women with postmenopausal ER-positive, HER2-nonamplified advanced breast cancer refractory to nonsteroidal aromatase inhibitors, 541 had evaluable cell-free DNA from baseline plasma samples and consented to genomic testing. Cell-free DNA (cfDNA) was extracted from patient’s plasma samples and assayed (via BioRad’s QX200 Droplet Digital PCR [polymerase chain reaction] System) for two specific ESR1 mutations, D538G and Y537S.
ESR1 mutations were detected in 156 of the 541 patients (28.8%), with D538G mutations occurring in 114 patients (21.1%), Y537S mutations occurring in 72 patients (13.3%), and both mutations occurring in 30 patients (5.55%), according to Sarat Chandarlapaty, MD, PhD, of Memorial Sloan Kettering Cancer Center, New York, and his associates.
Frequency of ESR1 mutation did not differ by age, race, or site of metastatic disease. However, mutation prevalence was significantly associated with ECOG status (P = .04). Also, “there was a threefold increase in mutation prevalence in patients who had failed first-line therapy for metastatic disease (33% were mutant) compared with those who were initiating first-line treatment for MBC (11% were mutant), in whom exposure to AI therapy occurred only in the adjuvant setting,” the researchers wrote (JAMA Oncol. 2016 Aug 11. doi: 10.1001/jamaoncol.2016.1279).
Overall, patients with ESR1 mutations had shorter median overall survival times. Among patients with only D538G mutations, median overall survival was 25.99 months (95% CI, 19.19-32.36 months). Patients with only Y537S mutations had a median overall survival of 19.98 months (95% CI,13.01-29.31 months) whereas patients with neither mutation had an overall survival of 32.1 months (95% CI, 28.09-36.4 months). Patients carrying both mutations had an even further reduced median overall survival of 15.15 months (95% CI, 10.87-27.43).
Patients in BOLERO-2 had been randomized in a 2:1 ratio to receive either exemestane plus everolimus or exemestane plus placebo. For this secondary analysis, researchers found that patients who had received exemestane therapy and had the D538G mutation experienced a shorter median progression-free survival time (2.69 months; hazard ratio, 1.71; 95% CI, 1.09-2.68) compared with patients with no mutations who received exemestane therapy (3.94 months). Patients with no mutations who received everolimus had a median progression-free survival of 8.48 months, and patients with D538G mutations who received everolimus had a median progression-free survival of 5.78 months.
“One of the key findings of this work is the high prevalence of ER mutations in this patient population,” the investigators said.
The investigators also noted the ease, feasibility, and affordability with which cfDNA can be analyzed for these genetic mutations, and they believe the digital drop polymerase chain reaction assay used in this study could easily be implemented into regular clinical practice.
This study was funded by Novartis and supported by the Integrated Genomics Operation Core. Four of the investigators reported being employed by Novartis, and Dr. Chandarlapaty reported receiving financial compensation from AstraZeneca.
On Twitter @jessnicolecraig
Estrogen receptor mutations in estrogen receptor–positive metastatic breast cancer are more prevalent than previous studies and methodologies suggest, investigators found during a secondary analysis of patients enrolled in the BOLERO-2 trial.
Furthermore, two specific estrogen receptor 1 (ESR1) mutations, D538G and Y537S, were associated with reduced overall survival.
Of the 724 patients enrolled in the BOLERO-2, a phase III trial of women with postmenopausal ER-positive, HER2-nonamplified advanced breast cancer refractory to nonsteroidal aromatase inhibitors, 541 had evaluable cell-free DNA from baseline plasma samples and consented to genomic testing. Cell-free DNA (cfDNA) was extracted from patient’s plasma samples and assayed (via BioRad’s QX200 Droplet Digital PCR [polymerase chain reaction] System) for two specific ESR1 mutations, D538G and Y537S.
ESR1 mutations were detected in 156 of the 541 patients (28.8%), with D538G mutations occurring in 114 patients (21.1%), Y537S mutations occurring in 72 patients (13.3%), and both mutations occurring in 30 patients (5.55%), according to Sarat Chandarlapaty, MD, PhD, of Memorial Sloan Kettering Cancer Center, New York, and his associates.
Frequency of ESR1 mutation did not differ by age, race, or site of metastatic disease. However, mutation prevalence was significantly associated with ECOG status (P = .04). Also, “there was a threefold increase in mutation prevalence in patients who had failed first-line therapy for metastatic disease (33% were mutant) compared with those who were initiating first-line treatment for MBC (11% were mutant), in whom exposure to AI therapy occurred only in the adjuvant setting,” the researchers wrote (JAMA Oncol. 2016 Aug 11. doi: 10.1001/jamaoncol.2016.1279).
Overall, patients with ESR1 mutations had shorter median overall survival times. Among patients with only D538G mutations, median overall survival was 25.99 months (95% CI, 19.19-32.36 months). Patients with only Y537S mutations had a median overall survival of 19.98 months (95% CI,13.01-29.31 months) whereas patients with neither mutation had an overall survival of 32.1 months (95% CI, 28.09-36.4 months). Patients carrying both mutations had an even further reduced median overall survival of 15.15 months (95% CI, 10.87-27.43).
Patients in BOLERO-2 had been randomized in a 2:1 ratio to receive either exemestane plus everolimus or exemestane plus placebo. For this secondary analysis, researchers found that patients who had received exemestane therapy and had the D538G mutation experienced a shorter median progression-free survival time (2.69 months; hazard ratio, 1.71; 95% CI, 1.09-2.68) compared with patients with no mutations who received exemestane therapy (3.94 months). Patients with no mutations who received everolimus had a median progression-free survival of 8.48 months, and patients with D538G mutations who received everolimus had a median progression-free survival of 5.78 months.
“One of the key findings of this work is the high prevalence of ER mutations in this patient population,” the investigators said.
The investigators also noted the ease, feasibility, and affordability with which cfDNA can be analyzed for these genetic mutations, and they believe the digital drop polymerase chain reaction assay used in this study could easily be implemented into regular clinical practice.
This study was funded by Novartis and supported by the Integrated Genomics Operation Core. Four of the investigators reported being employed by Novartis, and Dr. Chandarlapaty reported receiving financial compensation from AstraZeneca.
On Twitter @jessnicolecraig
FROM JAMA ONCOLOGY
Key clinical point: Estrogen receptor mutations in aromatase inhibitor–treated ER-positive metastatic breast cancer patients are common and are linked with worse outcomes.
Major finding: Estrogen receptor 1 mutations were detected in 156 patients (28.8% of 541 evaluable patients), with D538G mutations occurring in 114 patients (21.1%), Y537S mutations occurring in 72 patients (13.3%), and both mutations occurring in 30 patients (5.55%).
Data source: Plasma samples from 541 patients participating in BOLERO-2, a phase III trial of 724 women with postmenopausal ER-positive, HER2-nonamplified advanced breast cancer refractory to nonsteroidal aromatase inhibitors.
Disclosures: This study was funded by Novartis and supported by the Integrated Genomics Operation Core. Four of the investigators reported being employed by Novartis, and Dr. Chandarlapaty reported receiving financial compensation from AstraZeneca.

ESR1 mutations found prognostic but not predictive in metastatic breast cancer
CHICAGO – Mutation of the estrogen receptor 1 (ESR1) gene, one of the mechanisms whereby tumors become resistant to endocrine therapy, may be prognostic but not predictive in women with hormone receptor–positive advanced breast cancer that has progressed on this therapy, two studies showed.
In a cohort of women who had experienced progression on a first-line aromatase inhibitor, those with ESR1 mutations detected in circulating cell-free DNA at the time of progression had a 70% higher risk of progression-free survival events and a 90% higher risk of death thereafter. But the presence of this mutation did not predict benefit from subsequent therapy.
Similarly, in an analysis of women who had experienced progression on prior endocrine therapy and were treated on the randomized PALOMA-3 trial with fulvestrant plus either palbociclib (a cyclin-dependent kinase inhibitor) or placebo, adding the drug reduced the risk of progression-free survival events similarly, by about 50%, regardless of the presence of ESR1 mutations before starting therapy.
Findings in context

These new findings can help guide decisions about which patients should be tested for ESR1 mutations, according to invited discussant Sarat Chandarlapaty, MD, PhD, a medical oncologist at the Memorial Sloan Kettering Cancer Center in New York.
“Putting it all together … we see ESR1 mutations arise in the metastatic setting subclonally with prolonged exposure to low-estrogen environments,” he said. “If we are going to do testing, it makes sense to do it in the setting in which there is prior exposure to an aromatase inhibitor in metastatic ER-positive breast cancer.”
The studies’ results also help clarify what the finding of an ESR1 mutation means for patient prognosis and choice of next therapy, Dr. Chandarlapaty said at the annual meeting of the American Society of Clinical Oncology.
“It’s clear from two large studies that ESR1 mutation prognosticates poorer and shorter survival, so just the finding alone may aid as sort of a clinical risk assessment for physicians,” he said. “For the question of prediction, I would say the weight of evidence—even though the clinical studies are small—all the way from biology to clinic is that ESR1-mutant patients are unlikely to benefit from a second-line aromatase inhibitor.”
However, “the question of whether testing should be made available in practice on the basis of this particular clinical decision is more complicated,” Dr. Chandarlapaty said. “For one, is second-line aromatase inhibitor alone a widely used option? Secondly, does the adoption now of palbociclib in the first-line setting change the biology and the nature of resistance at this later line – in other words, are we going to see patients going on to a second-line aromatase inhibitor after they’ve had a prior aromatase inhibitor plus palbociclib?”
Mutations after progression on first-line aromatase inhibitors

In the first study, Florian Clatot, MD, PhD, a medical oncologist at the Centre Henri Becquerel, University of Normandy, Rouen, France, and colleagues retrospectively studied 144 women who had experienced progression on a first-line aromatase inhibitor.
The investigators used digital droplet polymerase chain reaction (PCR) testing to screen for four ESR-1 mutations in circulating cell-free DNA collected before, at the time of, and after the progression.
Overall, 30.6% of women were found to have at least one of these mutations at the time of progression, Dr. Clatot reported. The prevalence was higher the longer women had been on the aromatase inhibitor.
After progression, most women went on to receive chemotherapy or alternative endocrine therapy with either the selective estrogen receptor modulator tamoxifen or the estrogen receptor antagonist fulvestrant (Faslodex). With a median follow-up of 40 months, multivariate analyses showed that the group with ESR1 mutations at progression had higher risks of subsequent progression-free survival events (hazard ratio, 1.7; P = .008) and death (hazard ratio, 1.9; P = .002).
However, the mutations were not predictive: Women having one fared more poorly, whether given chemotherapy or given tamoxifen or fulvestrant.
Kinetic analyses showed that 75% of the ESR1 mutations seen at progression were already detectable in the 3 and even 6 months before that event. “Most of the mutations detected before progression increased while aromatase inhibitor therapy was ongoing,” Dr. Clatot commented. “These results suggest that the preclinical detection of ESR1 circulating mutation may [be of] clinical interest.”
Most women who had mutations at progression saw a decrease in the amount detectable over the subsequent 3 months with therapy, including to the point of not being detectable in about half of cases with a reduction. All of those having an increase in mutational burden had progression on their next therapy, compared with only about 40% of those having a decrease in burden.
“Taken together, these results suggest that the selection pressure provided by aromatase inhibitor exposure is one of the main mechanisms of ESR1 mutation increase,” concluded Dr. Clatot. “ESR1 mutations are a strong and independent marker of poor prognosis but do not have any predictive value with the treatments used in our cohort.”
Mutations after progression on prior endocrine therapy

In the second study, Nicholas C. Turner, MD, PhD, a medical oncologist at the Royal Marsden Hospital and Institute of Cancer Research, London, and colleagues analyzed data from a subset of 395 women from PALOMA-3.
The randomized phase III trial tested fulvestrant combined with palbociclib (Ibrance), an oral inhibitor of cyclin-dependent kinases 4 and 6, or placebo. All of the women enrolled had experienced progression on prior endocrine therapy in the adjuvant, advanced, or metastatic setting.
The investigators looked for 12 ESR1 mutations in circulating tumor DNA from baseline plasma samples using the BEAMing (beads, emulsion, amplification, magnetics) digital PCR technique and droplet digital PCR screening.
Overall, 27% of the women had ESR1 mutations before starting therapy on the trial, Dr. Turner reported. Mutations were seen in those who had received a prior aromatase inhibitor, but not in those who had received only prior tamoxifen. “So it’s quite clear these mutations are not a mechanism of resistance to tamoxifen, suggesting that tamoxifen must have at least some activity against these mutations,” he commented.
In addition, ESR1 mutations were more common in patients who had been sensitive versus not to prior endocrine therapy of any type (30.3% vs. 12.8%) and in patients who had been sensitive versus not specifically to prior aromatase inhibitor therapy (34.6% vs. 11.1%).
Stratified analyses showed that palbociclib was similarly superior to placebo in terms of progression-free survival whether patients were positive for an ESR1 mutation (9.4 vs. 4.1 months; hazard ratio, 0.52; P = .0052) or negative (9.5 vs. 3.8 months; hazard ratio, 0.44; P less than .0001).
“Detection of estrogen receptor mutations was strongly associated with acquired resistance to prior aromatase inhibitors,” Dr. Turner said.
“Palbociclib offered high efficacy regardless of the estrogen receptor mutation status,” he added. “And because in this patient population estrogen receptor mutations are detected frequently, the combination of palbociclib and fulvestrant presents an attractive treatment option for patients who have been previously treated with and progressed on aromatase inhibitors.”
CHICAGO – Mutation of the estrogen receptor 1 (ESR1) gene, one of the mechanisms whereby tumors become resistant to endocrine therapy, may be prognostic but not predictive in women with hormone receptor–positive advanced breast cancer that has progressed on this therapy, two studies showed.
In a cohort of women who had experienced progression on a first-line aromatase inhibitor, those with ESR1 mutations detected in circulating cell-free DNA at the time of progression had a 70% higher risk of progression-free survival events and a 90% higher risk of death thereafter. But the presence of this mutation did not predict benefit from subsequent therapy.
Similarly, in an analysis of women who had experienced progression on prior endocrine therapy and were treated on the randomized PALOMA-3 trial with fulvestrant plus either palbociclib (a cyclin-dependent kinase inhibitor) or placebo, adding the drug reduced the risk of progression-free survival events similarly, by about 50%, regardless of the presence of ESR1 mutations before starting therapy.
Findings in context
These new findings can help guide decisions about which patients should be tested for ESR1 mutations, according to invited discussant Sarat Chandarlapaty, MD, PhD, a medical oncologist at the Memorial Sloan Kettering Cancer Center in New York.
“Putting it all together … we see ESR1 mutations arise in the metastatic setting subclonally with prolonged exposure to low-estrogen environments,” he said. “If we are going to do testing, it makes sense to do it in the setting in which there is prior exposure to an aromatase inhibitor in metastatic ER-positive breast cancer.”
The studies’ results also help clarify what the finding of an ESR1 mutation means for patient prognosis and choice of next therapy, Dr. Chandarlapaty said at the annual meeting of the American Society of Clinical Oncology.
“It’s clear from two large studies that ESR1 mutation prognosticates poorer and shorter survival, so just the finding alone may aid as sort of a clinical risk assessment for physicians,” he said. “For the question of prediction, I would say the weight of evidence—even though the clinical studies are small—all the way from biology to clinic is that ESR1-mutant patients are unlikely to benefit from a second-line aromatase inhibitor.”
However, “the question of whether testing should be made available in practice on the basis of this particular clinical decision is more complicated,” Dr. Chandarlapaty said. “For one, is second-line aromatase inhibitor alone a widely used option? Secondly, does the adoption now of palbociclib in the first-line setting change the biology and the nature of resistance at this later line – in other words, are we going to see patients going on to a second-line aromatase inhibitor after they’ve had a prior aromatase inhibitor plus palbociclib?”
Mutations after progression on first-line aromatase inhibitors
In the first study, Florian Clatot, MD, PhD, a medical oncologist at the Centre Henri Becquerel, University of Normandy, Rouen, France, and colleagues retrospectively studied 144 women who had experienced progression on a first-line aromatase inhibitor.
The investigators used digital droplet polymerase chain reaction (PCR) testing to screen for four ESR-1 mutations in circulating cell-free DNA collected before, at the time of, and after the progression.
Overall, 30.6% of women were found to have at least one of these mutations at the time of progression, Dr. Clatot reported. The prevalence was higher the longer women had been on the aromatase inhibitor.
After progression, most women went on to receive chemotherapy or alternative endocrine therapy with either the selective estrogen receptor modulator tamoxifen or the estrogen receptor antagonist fulvestrant (Faslodex). With a median follow-up of 40 months, multivariate analyses showed that the group with ESR1 mutations at progression had higher risks of subsequent progression-free survival events (hazard ratio, 1.7; P = .008) and death (hazard ratio, 1.9; P = .002).
However, the mutations were not predictive: Women having one fared more poorly, whether given chemotherapy or given tamoxifen or fulvestrant.
Kinetic analyses showed that 75% of the ESR1 mutations seen at progression were already detectable in the 3 and even 6 months before that event. “Most of the mutations detected before progression increased while aromatase inhibitor therapy was ongoing,” Dr. Clatot commented. “These results suggest that the preclinical detection of ESR1 circulating mutation may [be of] clinical interest.”
Most women who had mutations at progression saw a decrease in the amount detectable over the subsequent 3 months with therapy, including to the point of not being detectable in about half of cases with a reduction. All of those having an increase in mutational burden had progression on their next therapy, compared with only about 40% of those having a decrease in burden.
“Taken together, these results suggest that the selection pressure provided by aromatase inhibitor exposure is one of the main mechanisms of ESR1 mutation increase,” concluded Dr. Clatot. “ESR1 mutations are a strong and independent marker of poor prognosis but do not have any predictive value with the treatments used in our cohort.”
Mutations after progression on prior endocrine therapy
In the second study, Nicholas C. Turner, MD, PhD, a medical oncologist at the Royal Marsden Hospital and Institute of Cancer Research, London, and colleagues analyzed data from a subset of 395 women from PALOMA-3.
The randomized phase III trial tested fulvestrant combined with palbociclib (Ibrance), an oral inhibitor of cyclin-dependent kinases 4 and 6, or placebo. All of the women enrolled had experienced progression on prior endocrine therapy in the adjuvant, advanced, or metastatic setting.
The investigators looked for 12 ESR1 mutations in circulating tumor DNA from baseline plasma samples using the BEAMing (beads, emulsion, amplification, magnetics) digital PCR technique and droplet digital PCR screening.
Overall, 27% of the women had ESR1 mutations before starting therapy on the trial, Dr. Turner reported. Mutations were seen in those who had received a prior aromatase inhibitor, but not in those who had received only prior tamoxifen. “So it’s quite clear these mutations are not a mechanism of resistance to tamoxifen, suggesting that tamoxifen must have at least some activity against these mutations,” he commented.
In addition, ESR1 mutations were more common in patients who had been sensitive versus not to prior endocrine therapy of any type (30.3% vs. 12.8%) and in patients who had been sensitive versus not specifically to prior aromatase inhibitor therapy (34.6% vs. 11.1%).
Stratified analyses showed that palbociclib was similarly superior to placebo in terms of progression-free survival whether patients were positive for an ESR1 mutation (9.4 vs. 4.1 months; hazard ratio, 0.52; P = .0052) or negative (9.5 vs. 3.8 months; hazard ratio, 0.44; P less than .0001).
“Detection of estrogen receptor mutations was strongly associated with acquired resistance to prior aromatase inhibitors,” Dr. Turner said.
“Palbociclib offered high efficacy regardless of the estrogen receptor mutation status,” he added. “And because in this patient population estrogen receptor mutations are detected frequently, the combination of palbociclib and fulvestrant presents an attractive treatment option for patients who have been previously treated with and progressed on aromatase inhibitors.”
CHICAGO – Mutation of the estrogen receptor 1 (ESR1) gene, one of the mechanisms whereby tumors become resistant to endocrine therapy, may be prognostic but not predictive in women with hormone receptor–positive advanced breast cancer that has progressed on this therapy, two studies showed.
In a cohort of women who had experienced progression on a first-line aromatase inhibitor, those with ESR1 mutations detected in circulating cell-free DNA at the time of progression had a 70% higher risk of progression-free survival events and a 90% higher risk of death thereafter. But the presence of this mutation did not predict benefit from subsequent therapy.
Similarly, in an analysis of women who had experienced progression on prior endocrine therapy and were treated on the randomized PALOMA-3 trial with fulvestrant plus either palbociclib (a cyclin-dependent kinase inhibitor) or placebo, adding the drug reduced the risk of progression-free survival events similarly, by about 50%, regardless of the presence of ESR1 mutations before starting therapy.
Findings in context
These new findings can help guide decisions about which patients should be tested for ESR1 mutations, according to invited discussant Sarat Chandarlapaty, MD, PhD, a medical oncologist at the Memorial Sloan Kettering Cancer Center in New York.
“Putting it all together … we see ESR1 mutations arise in the metastatic setting subclonally with prolonged exposure to low-estrogen environments,” he said. “If we are going to do testing, it makes sense to do it in the setting in which there is prior exposure to an aromatase inhibitor in metastatic ER-positive breast cancer.”
The studies’ results also help clarify what the finding of an ESR1 mutation means for patient prognosis and choice of next therapy, Dr. Chandarlapaty said at the annual meeting of the American Society of Clinical Oncology.
“It’s clear from two large studies that ESR1 mutation prognosticates poorer and shorter survival, so just the finding alone may aid as sort of a clinical risk assessment for physicians,” he said. “For the question of prediction, I would say the weight of evidence—even though the clinical studies are small—all the way from biology to clinic is that ESR1-mutant patients are unlikely to benefit from a second-line aromatase inhibitor.”
However, “the question of whether testing should be made available in practice on the basis of this particular clinical decision is more complicated,” Dr. Chandarlapaty said. “For one, is second-line aromatase inhibitor alone a widely used option? Secondly, does the adoption now of palbociclib in the first-line setting change the biology and the nature of resistance at this later line – in other words, are we going to see patients going on to a second-line aromatase inhibitor after they’ve had a prior aromatase inhibitor plus palbociclib?”
Mutations after progression on first-line aromatase inhibitors
In the first study, Florian Clatot, MD, PhD, a medical oncologist at the Centre Henri Becquerel, University of Normandy, Rouen, France, and colleagues retrospectively studied 144 women who had experienced progression on a first-line aromatase inhibitor.
The investigators used digital droplet polymerase chain reaction (PCR) testing to screen for four ESR-1 mutations in circulating cell-free DNA collected before, at the time of, and after the progression.
Overall, 30.6% of women were found to have at least one of these mutations at the time of progression, Dr. Clatot reported. The prevalence was higher the longer women had been on the aromatase inhibitor.
After progression, most women went on to receive chemotherapy or alternative endocrine therapy with either the selective estrogen receptor modulator tamoxifen or the estrogen receptor antagonist fulvestrant (Faslodex). With a median follow-up of 40 months, multivariate analyses showed that the group with ESR1 mutations at progression had higher risks of subsequent progression-free survival events (hazard ratio, 1.7; P = .008) and death (hazard ratio, 1.9; P = .002).
However, the mutations were not predictive: Women having one fared more poorly, whether given chemotherapy or given tamoxifen or fulvestrant.
Kinetic analyses showed that 75% of the ESR1 mutations seen at progression were already detectable in the 3 and even 6 months before that event. “Most of the mutations detected before progression increased while aromatase inhibitor therapy was ongoing,” Dr. Clatot commented. “These results suggest that the preclinical detection of ESR1 circulating mutation may [be of] clinical interest.”
Most women who had mutations at progression saw a decrease in the amount detectable over the subsequent 3 months with therapy, including to the point of not being detectable in about half of cases with a reduction. All of those having an increase in mutational burden had progression on their next therapy, compared with only about 40% of those having a decrease in burden.
“Taken together, these results suggest that the selection pressure provided by aromatase inhibitor exposure is one of the main mechanisms of ESR1 mutation increase,” concluded Dr. Clatot. “ESR1 mutations are a strong and independent marker of poor prognosis but do not have any predictive value with the treatments used in our cohort.”
Mutations after progression on prior endocrine therapy
In the second study, Nicholas C. Turner, MD, PhD, a medical oncologist at the Royal Marsden Hospital and Institute of Cancer Research, London, and colleagues analyzed data from a subset of 395 women from PALOMA-3.
The randomized phase III trial tested fulvestrant combined with palbociclib (Ibrance), an oral inhibitor of cyclin-dependent kinases 4 and 6, or placebo. All of the women enrolled had experienced progression on prior endocrine therapy in the adjuvant, advanced, or metastatic setting.
The investigators looked for 12 ESR1 mutations in circulating tumor DNA from baseline plasma samples using the BEAMing (beads, emulsion, amplification, magnetics) digital PCR technique and droplet digital PCR screening.
Overall, 27% of the women had ESR1 mutations before starting therapy on the trial, Dr. Turner reported. Mutations were seen in those who had received a prior aromatase inhibitor, but not in those who had received only prior tamoxifen. “So it’s quite clear these mutations are not a mechanism of resistance to tamoxifen, suggesting that tamoxifen must have at least some activity against these mutations,” he commented.
In addition, ESR1 mutations were more common in patients who had been sensitive versus not to prior endocrine therapy of any type (30.3% vs. 12.8%) and in patients who had been sensitive versus not specifically to prior aromatase inhibitor therapy (34.6% vs. 11.1%).
Stratified analyses showed that palbociclib was similarly superior to placebo in terms of progression-free survival whether patients were positive for an ESR1 mutation (9.4 vs. 4.1 months; hazard ratio, 0.52; P = .0052) or negative (9.5 vs. 3.8 months; hazard ratio, 0.44; P less than .0001).
“Detection of estrogen receptor mutations was strongly associated with acquired resistance to prior aromatase inhibitors,” Dr. Turner said.
“Palbociclib offered high efficacy regardless of the estrogen receptor mutation status,” he added. “And because in this patient population estrogen receptor mutations are detected frequently, the combination of palbociclib and fulvestrant presents an attractive treatment option for patients who have been previously treated with and progressed on aromatase inhibitors.”
AT THE 2016 ASCO ANNUAL MEETING
Key clinical point: An ESR1 mutation in circulating DNA after progression on endocrine therapy was a marker for poor prognosis but did not predict benefit from subsequent therapy.
Major finding: Women with ESR1 mutations had poorer progression-free and overall survival (hazard ratios, 1.7 and 1.9). Adding palbociclib to fulvestrant halved the risk of progression-free survival events, regardless of the presence of an ESR1 mutation.
Data source: A retrospective cohort study of 144 women with metastatic breast cancer who had experienced progression on a first-line aromatase inhibitor, and an analysis of 395 women with advanced breast cancer from a randomized trial testing addition of palbociclib to fulvestrant after progression on prior endocrine therapy (PALOMA-3 trial).
Disclosures: Dr. Clatot disclosed that he receives research funding from Novartis. Dr. Turner disclosed that he receives honoraria from and has a consulting or advisory role with AstraZeneca, Pfizer, and Roche Pharma; Pfizer sponsored PALOMA-3, and AstraZeneca provided the fulvestrant.

Does extending aromatase-inhibitor use from 5 to 10 years benefit menopausal women with hormone-positive breast cancer?
EXPERT COMMENTARY
Since the current treatment choice for hormone-receptor–positive early breast cancer in postmenopausal women is 5 years of aromatase inhibitor (AI) therapy, or AI therapy following initial tamoxifen treatment, could 10 years of an AI be beneficial to cancer recurrence? Goss and colleagues analyzed this question in the MA.17R trial, a North American Breast Cancer Group trial coordinated by the Canadian Cancer Trials Group. (Results of the prior MA.17 trial were published in 2003.1)
The randomized, double-blind, placebo-controlled trial evaluated the effect of 5 years of extended AI (letrozole 2.5 mg) treatment compared with placebo in menopausal women with hormone-receptor–positive breast cancer who had previously received 5 years of hormonal adjuvant therapy with tamoxifen alone or plus AIs. Of note, this study was funded in part by Novartis, the pharmaceutical manufacturer of letrozole, though the company had no role in either study design or writing of the manuscript. Seven of the 20 authors disclosed some sort of relationship with industry (some with the manufacturer of letrozole), including membership on advisory boards, board of directors, steering committees, or data and safety monitoring committees or receiving lecturer or consulting fees or grant support.
The trial’s primary end point was DFS. Secondary end points included overall survival, the incidence of contralateral breast cancer, quality of life (QOL), and long-term safety.
Details of the studyWomen were eligible to participate in the study if they were disease free after having completed 4.5 to 6 years of therapy with any AI and if their primary tumor was hormone-receptor positive. A total of 1,918 women were included in the trial and were randomly assigned to receive either letrozole treatment (n = 959) or placebo (n = 959).
Clinical evaluation was performed annually and included assessments of new bone fracture and new-onset osteoporosis, blood tests, mammography, and assessment of toxic effects. QOL measures were assessed with a validated health survey and a menopause-specific questionnaire. The Common Toxicity Criteria, version 2.0, was used to assess adverse events.
Impact on disease free, overall survivalThe rate of 5-year DFS was statistically improved in the letrozole group compared with the placebo group, 95% (95% confidence interval [CI], 93–96) versus 91% (95% CI, 89–93), respectively, a 4% improvement in DFS. However, there was no impact on disease-specific mortality and no benefit in overall survival (93% [95% CI, 92–95] with letrozole and 94% [95% CI, 92–95] with placebo), as competing causes of death become increasingly important in this older population. Among women who died during the study follow-up, more than half died of causes not related to breast cancer.
QOL measures. More than 85% of participants completed the QOL assessments at each time point. There was no difference in the various QOL measures between the letrozole and the placebo group.
Adverse effects. Expected adverse effects due to AIs were significantly higher in the letrozole group. For example, new-onset osteoporosis occurred in 109 (11%) of letrozole-treated women and in 54 (6%) of the placebo group (P<.001), and bone fracture occurred in 133 (14%) of the letrozole group and 88 (9%) of the placebo group (P = .001).
Of note, however, fewer toxicities/adverse effects were seen in the AI group in this study than in previously published reports. The authors suggested that these adverse effect data may be lower than expected because the majority of women eligible for this study likely had prior exposure to AIs, and those with significant adverse effects with aromatase inhibitor therapy may have self-selected out of this trial.
WHAT THIS EVIDENCE MEANS FOR PRACTICEWhile the study authors selected DFS as the primary outcome, the lack of overall survival, adverse effect profile, and the drug cost (average wholesale price, ~$33,050 for 5 years2) make the choice to routinely continue AIs in menopausal women with hormone-receptor–positive breast cancer less clear, and counseling on both the benefits and limitations of continuing hormonal adjuvant therapy will be important for these women.
Continued follow-up of the study participants over time would be useful to determine if, after 10 to 15 years, the benefit of extending AI therapy for an additional 5 years would provide an overall benefit in longevity, as competing causes of death (bone fracture, cardiovascular risk) actually may increase over time in the extended-treatment group compared with the placebo group.
— Mark D. Pearlman, MD
Share your thoughts! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.
- Goss PE, Ingle JN, Martino S, et al. A randomized trial of letrozole in postmenopausal women after five years of tamoxifen therapy for early-stage breast cancer. N Engl J Med. 2003;349(19):1793–1802.
- Average Wholesale Price (AWP) Policy. Truven Health Analytics. Red Book. http://sites.truvenhealth.com/redbook /awp/. Accessed July 18, 2016.
EXPERT COMMENTARY
Since the current treatment choice for hormone-receptor–positive early breast cancer in postmenopausal women is 5 years of aromatase inhibitor (AI) therapy, or AI therapy following initial tamoxifen treatment, could 10 years of an AI be beneficial to cancer recurrence? Goss and colleagues analyzed this question in the MA.17R trial, a North American Breast Cancer Group trial coordinated by the Canadian Cancer Trials Group. (Results of the prior MA.17 trial were published in 2003.1)
The randomized, double-blind, placebo-controlled trial evaluated the effect of 5 years of extended AI (letrozole 2.5 mg) treatment compared with placebo in menopausal women with hormone-receptor–positive breast cancer who had previously received 5 years of hormonal adjuvant therapy with tamoxifen alone or plus AIs. Of note, this study was funded in part by Novartis, the pharmaceutical manufacturer of letrozole, though the company had no role in either study design or writing of the manuscript. Seven of the 20 authors disclosed some sort of relationship with industry (some with the manufacturer of letrozole), including membership on advisory boards, board of directors, steering committees, or data and safety monitoring committees or receiving lecturer or consulting fees or grant support.
The trial’s primary end point was DFS. Secondary end points included overall survival, the incidence of contralateral breast cancer, quality of life (QOL), and long-term safety.
Details of the studyWomen were eligible to participate in the study if they were disease free after having completed 4.5 to 6 years of therapy with any AI and if their primary tumor was hormone-receptor positive. A total of 1,918 women were included in the trial and were randomly assigned to receive either letrozole treatment (n = 959) or placebo (n = 959).
Clinical evaluation was performed annually and included assessments of new bone fracture and new-onset osteoporosis, blood tests, mammography, and assessment of toxic effects. QOL measures were assessed with a validated health survey and a menopause-specific questionnaire. The Common Toxicity Criteria, version 2.0, was used to assess adverse events.
Impact on disease free, overall survivalThe rate of 5-year DFS was statistically improved in the letrozole group compared with the placebo group, 95% (95% confidence interval [CI], 93–96) versus 91% (95% CI, 89–93), respectively, a 4% improvement in DFS. However, there was no impact on disease-specific mortality and no benefit in overall survival (93% [95% CI, 92–95] with letrozole and 94% [95% CI, 92–95] with placebo), as competing causes of death become increasingly important in this older population. Among women who died during the study follow-up, more than half died of causes not related to breast cancer.
QOL measures. More than 85% of participants completed the QOL assessments at each time point. There was no difference in the various QOL measures between the letrozole and the placebo group.
Adverse effects. Expected adverse effects due to AIs were significantly higher in the letrozole group. For example, new-onset osteoporosis occurred in 109 (11%) of letrozole-treated women and in 54 (6%) of the placebo group (P<.001), and bone fracture occurred in 133 (14%) of the letrozole group and 88 (9%) of the placebo group (P = .001).
Of note, however, fewer toxicities/adverse effects were seen in the AI group in this study than in previously published reports. The authors suggested that these adverse effect data may be lower than expected because the majority of women eligible for this study likely had prior exposure to AIs, and those with significant adverse effects with aromatase inhibitor therapy may have self-selected out of this trial.
WHAT THIS EVIDENCE MEANS FOR PRACTICEWhile the study authors selected DFS as the primary outcome, the lack of overall survival, adverse effect profile, and the drug cost (average wholesale price, ~$33,050 for 5 years2) make the choice to routinely continue AIs in menopausal women with hormone-receptor–positive breast cancer less clear, and counseling on both the benefits and limitations of continuing hormonal adjuvant therapy will be important for these women.
Continued follow-up of the study participants over time would be useful to determine if, after 10 to 15 years, the benefit of extending AI therapy for an additional 5 years would provide an overall benefit in longevity, as competing causes of death (bone fracture, cardiovascular risk) actually may increase over time in the extended-treatment group compared with the placebo group.
— Mark D. Pearlman, MD
Share your thoughts! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.
EXPERT COMMENTARY
Since the current treatment choice for hormone-receptor–positive early breast cancer in postmenopausal women is 5 years of aromatase inhibitor (AI) therapy, or AI therapy following initial tamoxifen treatment, could 10 years of an AI be beneficial to cancer recurrence? Goss and colleagues analyzed this question in the MA.17R trial, a North American Breast Cancer Group trial coordinated by the Canadian Cancer Trials Group. (Results of the prior MA.17 trial were published in 2003.1)
The randomized, double-blind, placebo-controlled trial evaluated the effect of 5 years of extended AI (letrozole 2.5 mg) treatment compared with placebo in menopausal women with hormone-receptor–positive breast cancer who had previously received 5 years of hormonal adjuvant therapy with tamoxifen alone or plus AIs. Of note, this study was funded in part by Novartis, the pharmaceutical manufacturer of letrozole, though the company had no role in either study design or writing of the manuscript. Seven of the 20 authors disclosed some sort of relationship with industry (some with the manufacturer of letrozole), including membership on advisory boards, board of directors, steering committees, or data and safety monitoring committees or receiving lecturer or consulting fees or grant support.
The trial’s primary end point was DFS. Secondary end points included overall survival, the incidence of contralateral breast cancer, quality of life (QOL), and long-term safety.
Details of the studyWomen were eligible to participate in the study if they were disease free after having completed 4.5 to 6 years of therapy with any AI and if their primary tumor was hormone-receptor positive. A total of 1,918 women were included in the trial and were randomly assigned to receive either letrozole treatment (n = 959) or placebo (n = 959).
Clinical evaluation was performed annually and included assessments of new bone fracture and new-onset osteoporosis, blood tests, mammography, and assessment of toxic effects. QOL measures were assessed with a validated health survey and a menopause-specific questionnaire. The Common Toxicity Criteria, version 2.0, was used to assess adverse events.
Impact on disease free, overall survivalThe rate of 5-year DFS was statistically improved in the letrozole group compared with the placebo group, 95% (95% confidence interval [CI], 93–96) versus 91% (95% CI, 89–93), respectively, a 4% improvement in DFS. However, there was no impact on disease-specific mortality and no benefit in overall survival (93% [95% CI, 92–95] with letrozole and 94% [95% CI, 92–95] with placebo), as competing causes of death become increasingly important in this older population. Among women who died during the study follow-up, more than half died of causes not related to breast cancer.
QOL measures. More than 85% of participants completed the QOL assessments at each time point. There was no difference in the various QOL measures between the letrozole and the placebo group.
Adverse effects. Expected adverse effects due to AIs were significantly higher in the letrozole group. For example, new-onset osteoporosis occurred in 109 (11%) of letrozole-treated women and in 54 (6%) of the placebo group (P<.001), and bone fracture occurred in 133 (14%) of the letrozole group and 88 (9%) of the placebo group (P = .001).
Of note, however, fewer toxicities/adverse effects were seen in the AI group in this study than in previously published reports. The authors suggested that these adverse effect data may be lower than expected because the majority of women eligible for this study likely had prior exposure to AIs, and those with significant adverse effects with aromatase inhibitor therapy may have self-selected out of this trial.
WHAT THIS EVIDENCE MEANS FOR PRACTICEWhile the study authors selected DFS as the primary outcome, the lack of overall survival, adverse effect profile, and the drug cost (average wholesale price, ~$33,050 for 5 years2) make the choice to routinely continue AIs in menopausal women with hormone-receptor–positive breast cancer less clear, and counseling on both the benefits and limitations of continuing hormonal adjuvant therapy will be important for these women.
Continued follow-up of the study participants over time would be useful to determine if, after 10 to 15 years, the benefit of extending AI therapy for an additional 5 years would provide an overall benefit in longevity, as competing causes of death (bone fracture, cardiovascular risk) actually may increase over time in the extended-treatment group compared with the placebo group.
— Mark D. Pearlman, MD
Share your thoughts! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.
- Goss PE, Ingle JN, Martino S, et al. A randomized trial of letrozole in postmenopausal women after five years of tamoxifen therapy for early-stage breast cancer. N Engl J Med. 2003;349(19):1793–1802.
- Average Wholesale Price (AWP) Policy. Truven Health Analytics. Red Book. http://sites.truvenhealth.com/redbook /awp/. Accessed July 18, 2016.
- Goss PE, Ingle JN, Martino S, et al. A randomized trial of letrozole in postmenopausal women after five years of tamoxifen therapy for early-stage breast cancer. N Engl J Med. 2003;349(19):1793–1802.
- Average Wholesale Price (AWP) Policy. Truven Health Analytics. Red Book. http://sites.truvenhealth.com/redbook /awp/. Accessed July 18, 2016.

Young age, tumor subtype linked in breast cancer survival
Younger age at diagnosis of breast cancer predicts poor survival only with certain molecular subtypes of tumor, according to a report published online Aug. 1 in the Journal of Clinical Oncology.
An age of 40 years or younger “has long been considered a poor prognostic factor, because young women, on average, have an increased risk of disease recurrence and decreased survival. In recent years, however, with improved understanding of tumor biology, this assertion has been challenged with increased recognition of the prognostic and predictive role of tumor subtype and awareness that young women are more likely to develop more aggressive phenotypes,” said Ann H. Partridge, MD, of the Dana-Farber Cancer Institute, and Brigham and Women’s Hospital, both in Boston, and her associates.
To examine the relationships among patient age, tumor subtypes, and outcomes, they analyzed data for 17,575 women treated at eight U.S. cancer centers in 2000-2007 and enrolled in a National Comprehensive Cancer Network registry. The study participants (mean age, 35 years) all had newly diagnosed unilateral stage I, II, or III breast cancer and were followed for a median of 6.4 years. Their data were stratified by age at diagnosis: 40 years or younger, 41-50 years, 51-60 years, 61-70 years, or over 70 years.
In the initial analysis, younger women were 90% more likely to die of breast cancer than older women. This probability decreased to 50% when the data were adjusted to control for treatment, stage at diagnosis, and tumor grade, then decreased further to 30% when the data were further adjusted to control for tumor molecular subtype and method of detection, the investigators said (J Clin Oncol. 2016 Aug 1; doi:10.1200/JCO.2015.65.8013).
However, when the data were analyzed according to tumor subtype, women who had luminal A breast cancer (7,738 participants) were more than twice as likely to die of their disease if they were aged 40 or younger at diagnosis than if they were older (hazard ratio, 2.1). The age-related increase in risk was slightly lower for luminal B breast cancer (HR, 1.4), and appeared to be largely confined to those with HER2-negative luminal B tumors.
There also was a borderline increased risk of death in younger women who had triple-negative breast cancer (HR, 1.4), compared with older women who had that tumor subtype. In contrast, younger age did not correlate with increased breast cancer mortality among women with HER2-positive disease.
These findings “support the growing evidence that the relationship between age at diagnosis and breast-cancer-specific survival varies by tumor subtype, which has implications for both treatment decisions and future research directions. ....In women with luminal disease, younger age does have a substantial prognostic role, which may reflect inadequate therapy, including lower treatment efficacy and less therapeutic adherence and persistence, as well as residual differences in tumor biology,” Dr. Partridge and her associates said.
No specific source of funding was identified for this study. Dr. Partridge reported serving as a consultant for Pfizer; her associates reported ties to Pfizer, Tokai, Bristol-Myers Squibb, Carevive Systems, Oncothyreon, Amgen, and BeyondSpring Pharmaceuticals.
Younger age at diagnosis of breast cancer predicts poor survival only with certain molecular subtypes of tumor, according to a report published online Aug. 1 in the Journal of Clinical Oncology.
An age of 40 years or younger “has long been considered a poor prognostic factor, because young women, on average, have an increased risk of disease recurrence and decreased survival. In recent years, however, with improved understanding of tumor biology, this assertion has been challenged with increased recognition of the prognostic and predictive role of tumor subtype and awareness that young women are more likely to develop more aggressive phenotypes,” said Ann H. Partridge, MD, of the Dana-Farber Cancer Institute, and Brigham and Women’s Hospital, both in Boston, and her associates.
To examine the relationships among patient age, tumor subtypes, and outcomes, they analyzed data for 17,575 women treated at eight U.S. cancer centers in 2000-2007 and enrolled in a National Comprehensive Cancer Network registry. The study participants (mean age, 35 years) all had newly diagnosed unilateral stage I, II, or III breast cancer and were followed for a median of 6.4 years. Their data were stratified by age at diagnosis: 40 years or younger, 41-50 years, 51-60 years, 61-70 years, or over 70 years.
In the initial analysis, younger women were 90% more likely to die of breast cancer than older women. This probability decreased to 50% when the data were adjusted to control for treatment, stage at diagnosis, and tumor grade, then decreased further to 30% when the data were further adjusted to control for tumor molecular subtype and method of detection, the investigators said (J Clin Oncol. 2016 Aug 1; doi:10.1200/JCO.2015.65.8013).
However, when the data were analyzed according to tumor subtype, women who had luminal A breast cancer (7,738 participants) were more than twice as likely to die of their disease if they were aged 40 or younger at diagnosis than if they were older (hazard ratio, 2.1). The age-related increase in risk was slightly lower for luminal B breast cancer (HR, 1.4), and appeared to be largely confined to those with HER2-negative luminal B tumors.
There also was a borderline increased risk of death in younger women who had triple-negative breast cancer (HR, 1.4), compared with older women who had that tumor subtype. In contrast, younger age did not correlate with increased breast cancer mortality among women with HER2-positive disease.
These findings “support the growing evidence that the relationship between age at diagnosis and breast-cancer-specific survival varies by tumor subtype, which has implications for both treatment decisions and future research directions. ....In women with luminal disease, younger age does have a substantial prognostic role, which may reflect inadequate therapy, including lower treatment efficacy and less therapeutic adherence and persistence, as well as residual differences in tumor biology,” Dr. Partridge and her associates said.
No specific source of funding was identified for this study. Dr. Partridge reported serving as a consultant for Pfizer; her associates reported ties to Pfizer, Tokai, Bristol-Myers Squibb, Carevive Systems, Oncothyreon, Amgen, and BeyondSpring Pharmaceuticals.
Younger age at diagnosis of breast cancer predicts poor survival only with certain molecular subtypes of tumor, according to a report published online Aug. 1 in the Journal of Clinical Oncology.
An age of 40 years or younger “has long been considered a poor prognostic factor, because young women, on average, have an increased risk of disease recurrence and decreased survival. In recent years, however, with improved understanding of tumor biology, this assertion has been challenged with increased recognition of the prognostic and predictive role of tumor subtype and awareness that young women are more likely to develop more aggressive phenotypes,” said Ann H. Partridge, MD, of the Dana-Farber Cancer Institute, and Brigham and Women’s Hospital, both in Boston, and her associates.
To examine the relationships among patient age, tumor subtypes, and outcomes, they analyzed data for 17,575 women treated at eight U.S. cancer centers in 2000-2007 and enrolled in a National Comprehensive Cancer Network registry. The study participants (mean age, 35 years) all had newly diagnosed unilateral stage I, II, or III breast cancer and were followed for a median of 6.4 years. Their data were stratified by age at diagnosis: 40 years or younger, 41-50 years, 51-60 years, 61-70 years, or over 70 years.
In the initial analysis, younger women were 90% more likely to die of breast cancer than older women. This probability decreased to 50% when the data were adjusted to control for treatment, stage at diagnosis, and tumor grade, then decreased further to 30% when the data were further adjusted to control for tumor molecular subtype and method of detection, the investigators said (J Clin Oncol. 2016 Aug 1; doi:10.1200/JCO.2015.65.8013).
However, when the data were analyzed according to tumor subtype, women who had luminal A breast cancer (7,738 participants) were more than twice as likely to die of their disease if they were aged 40 or younger at diagnosis than if they were older (hazard ratio, 2.1). The age-related increase in risk was slightly lower for luminal B breast cancer (HR, 1.4), and appeared to be largely confined to those with HER2-negative luminal B tumors.
There also was a borderline increased risk of death in younger women who had triple-negative breast cancer (HR, 1.4), compared with older women who had that tumor subtype. In contrast, younger age did not correlate with increased breast cancer mortality among women with HER2-positive disease.
These findings “support the growing evidence that the relationship between age at diagnosis and breast-cancer-specific survival varies by tumor subtype, which has implications for both treatment decisions and future research directions. ....In women with luminal disease, younger age does have a substantial prognostic role, which may reflect inadequate therapy, including lower treatment efficacy and less therapeutic adherence and persistence, as well as residual differences in tumor biology,” Dr. Partridge and her associates said.
No specific source of funding was identified for this study. Dr. Partridge reported serving as a consultant for Pfizer; her associates reported ties to Pfizer, Tokai, Bristol-Myers Squibb, Carevive Systems, Oncothyreon, Amgen, and BeyondSpring Pharmaceuticals.
FROM THE JOURNAL OF CLINICAL ONCOLOGY
Key clinical point: Younger age at diagnosis of breast cancer predicts poor survival only with certain molecular subtypes of tumor.
Major finding: Women who had luminal A breast cancer (7,738 participants) were more than twice as likely to die of their disease if they were aged 40 or younger at diagnosis than if they were older (HR, 2.1).
Data source: A longitudinal cohort study assessing the role of age, tumor subtype, and survival among 17,575 breast cancer patients treated in 2000-2007 and followed for 6 years.
Disclosures: No specific source of funding was identified for this study. Dr. Partridge reported serving as a consultant for Pfizer; her associates reported ties to Pfizer, Tokai, Bristol-Myers Squibb, Carevive Systems, Oncothyreon, Amgen, and BeyondSpring Pharmaceuticals.
Clinical value of costly ER/PR testing of ductal carcinoma biopsies questioned
Limiting hormone receptor testing of diagnostic core biopisies containing ductal carcinoma in situ (DCIS) could save up to $35 million in associated health care costs every year in the United States.
The results of a cost analysis conducted by researchers at Johns Hopkins University were so striking that the hospital has now eliminated reflex testing of core needle biopsies for DCIS, Christopher J. VandenBussche, MD, and his colleagues wrote in the American Journal of Surgical Pathology (2016;40:1090-9).
“We suggest that reflex [hormone receptor] testing of core needle biopsy specimens harboring DCIS should not be performed, as the results do not guide the next step in therapy,” wrote Dr. VandenBussche of Johns Hopkins University, Baltimore. “On the basis of this study, we have convinced our clinicians and no longer reflexively perform estrogen- and progesterone-receptor [ER/PR] testing on core needle biopsy specimens with DCIS at Hopkins and encourage other institutions to follow suit.”
Conducting expensive hormone receptor testing of these biopsy samples before surgery doesn’t make clinical or financial sense, for several reasons, the team said:
• Hormone receptor status at biopsy has no effect on the next treatment step, as DCIS patients always progress first to surgical excision, not neoadjuvant hormone therapy.
• Surgery sometimes reveals extensive breast cancer in patents with pure DCIS, and these cancers will always need ER/PR testing, rendering irrelevant biopsy testing.
• Because ER and PR labeling are often heterogeneous in DCIS, negative results for ER/PR on small core needle biopsy specimens would have to be repeated anyway on surgical excision specimens with larger amounts of DCIS, to be sure that the result is truly negative.
• Hormone therapy for DCIS does decrease recurrence, but it doesn’t impact survival – and it does carry significant adverse effects. Therefore, many women refuse hormone therapy if they do have ER/PR-positive tumors.
• The independent role of PR status in DCIS is unproven, so testing for it is not supported by clinical evidence.
To examine the costs associated with reflexive ER/PR testing, the investigators reviewed 58 core needle biopsies of pure DCIS followed by surgical excision. None of the patients had neoadjuvant hormone therapy. Of the 58 tumors, 76% were pure DCIS, and 16% were DCIS with invasive breast cancer. Most of the DCIS (47) tumors were ER+/PR+; 6 were ER-/PR-; and 5 were ER+/PR-.
The team reviewed the records of 49 patients who underwent surgical excision and ended up with a diagnosis of pure DCIS. These included 46 ER-positive cases, and 3 that were ER-negative in both biopsy and excision.
The findings suggested that ER/PR results from either the biopsy and the surgical excision samples were relevant to therapy in only a portion of these patients.
“We found that the ER/PR results after surgical excision impacted therapy in at most only 16 of 49 cases (33%),” they said. These included the 3 ER-/PR-negative cases, which would, in any case, not have triggered hormone therapy; 10 patients who chose hormone therapy despite a Hopkins oncologist’s neutral recommendation; 1 of 2 who took hormone therapy on a Hopkins oncologist’s recommendation; and 2 of 3 who took it after seeing a non-Hopkins oncologist.
“In contrast,” the authors wrote, “in 33 of the cases (67%), the ER/PR result of the DCIS after surgical excision did not impact therapy.” All of these were ER-positive cases, including 4 patients who opted for bilateral mastectomies (no subsequent role for neoadjuvant therapy), 8 who declined to meet with an oncologist, 1 for whom hormone therapy was contraindicated, 8 (of 8) who declined hormone therapy when their Hopkins oncologist did not recommend it, 10 (of 20) who declined hormone therapy when their Hopkins oncologist was neutral about its risk/benefit ratio, 1 (of 2) who declined hormone therapy when the Hopkins oncologist recommended it, and the 1 patient (of 3) who declined hormone therapy after visiting a non-Hopkins oncologist.
After reviewing the costs associated with these cases, “we found that ER testing … costing $20,685.72 ($357 per patient) had been performed unnecessarily,” the investigators said. In addition, if the PR testing – which has never been proven clinically important in DCIS – had been eliminated, there would have been an additional $86.46 savings per patient, a total savings of $5,014.
“Extrapolating the increased cost of $583 per DCIS diagnosis on core needle biopsy to 60,000 new cases of DCIS in the United States each year, reflex core needle biopsy ER/PR testing unnecessarily increases costs by approximately $35 million,” the authors said. “We recommend that ER/PR not be reflexively ordered on core needle biopsy specimens or surgical excision specimens containing DCIS, but instead that ER alone be performed on surgical excision specimens only when hormone therapy is a serious consideration after medical oncology consultation.”
The group noted that this total reflects the total amount billed, not typical reimbursement. “Regardless,” they said, “the cost of this testing is staggering.”
The authors did not mention the study’s funding source. They had no relevant financial disclosures.
On Twitter @Alz_Gal
It is important to note that the authors are not recommending hormone receptor testing be completely abandoned for ductal carcinoma in situ. They are simply suggesting that the testing should be deferred to being performed on the surgical resection specimen rather than the diagnostic core needle biopsy tissue.
The sample size used (58 cases) is clearly extremely small and cannot be used as the basis for sweeping recommendations for the many thousands of DCIS cases that are diagnosed in the United States annually. This study is from a major academic program; other programs may run the risk of patients not having the ER testing done at all if it is no longer a routine component of pathology testing on DCIS tissue.
The case is probably stronger for abandoning PR testing in DCIS, since this value is very unlikely to influence management decisions on its own.

|
Dr. Lisa Newman |
Other institutions should be encouraged to perform their own analyses to monitor the cost-effectiveness of ER/PR testing on core needle biopsies revealing DCIS. A study of this type should also be considered for large, multisite data sets, such as the American College of Surgeons’ National Cancer Database.
Lisa Newman, MD, FACS, is director of the breast oncology program for the Henry Ford Health System, and medical director for the Henry Ford International Center for the Study of Breast Cancer Subtypes, both in Detroit. She also serves as adjunct professor of health management and policy at the University of Michigan School of Public Health, Detroit. She has no relevant financial disclosures.
It is important to note that the authors are not recommending hormone receptor testing be completely abandoned for ductal carcinoma in situ. They are simply suggesting that the testing should be deferred to being performed on the surgical resection specimen rather than the diagnostic core needle biopsy tissue.
The sample size used (58 cases) is clearly extremely small and cannot be used as the basis for sweeping recommendations for the many thousands of DCIS cases that are diagnosed in the United States annually. This study is from a major academic program; other programs may run the risk of patients not having the ER testing done at all if it is no longer a routine component of pathology testing on DCIS tissue.
The case is probably stronger for abandoning PR testing in DCIS, since this value is very unlikely to influence management decisions on its own.
|
|
Dr. Lisa Newman |
Other institutions should be encouraged to perform their own analyses to monitor the cost-effectiveness of ER/PR testing on core needle biopsies revealing DCIS. A study of this type should also be considered for large, multisite data sets, such as the American College of Surgeons’ National Cancer Database.
Lisa Newman, MD, FACS, is director of the breast oncology program for the Henry Ford Health System, and medical director for the Henry Ford International Center for the Study of Breast Cancer Subtypes, both in Detroit. She also serves as adjunct professor of health management and policy at the University of Michigan School of Public Health, Detroit. She has no relevant financial disclosures.
It is important to note that the authors are not recommending hormone receptor testing be completely abandoned for ductal carcinoma in situ. They are simply suggesting that the testing should be deferred to being performed on the surgical resection specimen rather than the diagnostic core needle biopsy tissue.
The sample size used (58 cases) is clearly extremely small and cannot be used as the basis for sweeping recommendations for the many thousands of DCIS cases that are diagnosed in the United States annually. This study is from a major academic program; other programs may run the risk of patients not having the ER testing done at all if it is no longer a routine component of pathology testing on DCIS tissue.
The case is probably stronger for abandoning PR testing in DCIS, since this value is very unlikely to influence management decisions on its own.
|
|
Dr. Lisa Newman |
Other institutions should be encouraged to perform their own analyses to monitor the cost-effectiveness of ER/PR testing on core needle biopsies revealing DCIS. A study of this type should also be considered for large, multisite data sets, such as the American College of Surgeons’ National Cancer Database.
Lisa Newman, MD, FACS, is director of the breast oncology program for the Henry Ford Health System, and medical director for the Henry Ford International Center for the Study of Breast Cancer Subtypes, both in Detroit. She also serves as adjunct professor of health management and policy at the University of Michigan School of Public Health, Detroit. She has no relevant financial disclosures.
Limiting hormone receptor testing of diagnostic core biopisies containing ductal carcinoma in situ (DCIS) could save up to $35 million in associated health care costs every year in the United States.
The results of a cost analysis conducted by researchers at Johns Hopkins University were so striking that the hospital has now eliminated reflex testing of core needle biopsies for DCIS, Christopher J. VandenBussche, MD, and his colleagues wrote in the American Journal of Surgical Pathology (2016;40:1090-9).
“We suggest that reflex [hormone receptor] testing of core needle biopsy specimens harboring DCIS should not be performed, as the results do not guide the next step in therapy,” wrote Dr. VandenBussche of Johns Hopkins University, Baltimore. “On the basis of this study, we have convinced our clinicians and no longer reflexively perform estrogen- and progesterone-receptor [ER/PR] testing on core needle biopsy specimens with DCIS at Hopkins and encourage other institutions to follow suit.”
Conducting expensive hormone receptor testing of these biopsy samples before surgery doesn’t make clinical or financial sense, for several reasons, the team said:
• Hormone receptor status at biopsy has no effect on the next treatment step, as DCIS patients always progress first to surgical excision, not neoadjuvant hormone therapy.
• Surgery sometimes reveals extensive breast cancer in patents with pure DCIS, and these cancers will always need ER/PR testing, rendering irrelevant biopsy testing.
• Because ER and PR labeling are often heterogeneous in DCIS, negative results for ER/PR on small core needle biopsy specimens would have to be repeated anyway on surgical excision specimens with larger amounts of DCIS, to be sure that the result is truly negative.
• Hormone therapy for DCIS does decrease recurrence, but it doesn’t impact survival – and it does carry significant adverse effects. Therefore, many women refuse hormone therapy if they do have ER/PR-positive tumors.
• The independent role of PR status in DCIS is unproven, so testing for it is not supported by clinical evidence.
To examine the costs associated with reflexive ER/PR testing, the investigators reviewed 58 core needle biopsies of pure DCIS followed by surgical excision. None of the patients had neoadjuvant hormone therapy. Of the 58 tumors, 76% were pure DCIS, and 16% were DCIS with invasive breast cancer. Most of the DCIS (47) tumors were ER+/PR+; 6 were ER-/PR-; and 5 were ER+/PR-.
The team reviewed the records of 49 patients who underwent surgical excision and ended up with a diagnosis of pure DCIS. These included 46 ER-positive cases, and 3 that were ER-negative in both biopsy and excision.
The findings suggested that ER/PR results from either the biopsy and the surgical excision samples were relevant to therapy in only a portion of these patients.
“We found that the ER/PR results after surgical excision impacted therapy in at most only 16 of 49 cases (33%),” they said. These included the 3 ER-/PR-negative cases, which would, in any case, not have triggered hormone therapy; 10 patients who chose hormone therapy despite a Hopkins oncologist’s neutral recommendation; 1 of 2 who took hormone therapy on a Hopkins oncologist’s recommendation; and 2 of 3 who took it after seeing a non-Hopkins oncologist.
“In contrast,” the authors wrote, “in 33 of the cases (67%), the ER/PR result of the DCIS after surgical excision did not impact therapy.” All of these were ER-positive cases, including 4 patients who opted for bilateral mastectomies (no subsequent role for neoadjuvant therapy), 8 who declined to meet with an oncologist, 1 for whom hormone therapy was contraindicated, 8 (of 8) who declined hormone therapy when their Hopkins oncologist did not recommend it, 10 (of 20) who declined hormone therapy when their Hopkins oncologist was neutral about its risk/benefit ratio, 1 (of 2) who declined hormone therapy when the Hopkins oncologist recommended it, and the 1 patient (of 3) who declined hormone therapy after visiting a non-Hopkins oncologist.
After reviewing the costs associated with these cases, “we found that ER testing … costing $20,685.72 ($357 per patient) had been performed unnecessarily,” the investigators said. In addition, if the PR testing – which has never been proven clinically important in DCIS – had been eliminated, there would have been an additional $86.46 savings per patient, a total savings of $5,014.
“Extrapolating the increased cost of $583 per DCIS diagnosis on core needle biopsy to 60,000 new cases of DCIS in the United States each year, reflex core needle biopsy ER/PR testing unnecessarily increases costs by approximately $35 million,” the authors said. “We recommend that ER/PR not be reflexively ordered on core needle biopsy specimens or surgical excision specimens containing DCIS, but instead that ER alone be performed on surgical excision specimens only when hormone therapy is a serious consideration after medical oncology consultation.”
The group noted that this total reflects the total amount billed, not typical reimbursement. “Regardless,” they said, “the cost of this testing is staggering.”
The authors did not mention the study’s funding source. They had no relevant financial disclosures.
On Twitter @Alz_Gal
Limiting hormone receptor testing of diagnostic core biopisies containing ductal carcinoma in situ (DCIS) could save up to $35 million in associated health care costs every year in the United States.
The results of a cost analysis conducted by researchers at Johns Hopkins University were so striking that the hospital has now eliminated reflex testing of core needle biopsies for DCIS, Christopher J. VandenBussche, MD, and his colleagues wrote in the American Journal of Surgical Pathology (2016;40:1090-9).
“We suggest that reflex [hormone receptor] testing of core needle biopsy specimens harboring DCIS should not be performed, as the results do not guide the next step in therapy,” wrote Dr. VandenBussche of Johns Hopkins University, Baltimore. “On the basis of this study, we have convinced our clinicians and no longer reflexively perform estrogen- and progesterone-receptor [ER/PR] testing on core needle biopsy specimens with DCIS at Hopkins and encourage other institutions to follow suit.”
Conducting expensive hormone receptor testing of these biopsy samples before surgery doesn’t make clinical or financial sense, for several reasons, the team said:
• Hormone receptor status at biopsy has no effect on the next treatment step, as DCIS patients always progress first to surgical excision, not neoadjuvant hormone therapy.
• Surgery sometimes reveals extensive breast cancer in patents with pure DCIS, and these cancers will always need ER/PR testing, rendering irrelevant biopsy testing.
• Because ER and PR labeling are often heterogeneous in DCIS, negative results for ER/PR on small core needle biopsy specimens would have to be repeated anyway on surgical excision specimens with larger amounts of DCIS, to be sure that the result is truly negative.
• Hormone therapy for DCIS does decrease recurrence, but it doesn’t impact survival – and it does carry significant adverse effects. Therefore, many women refuse hormone therapy if they do have ER/PR-positive tumors.
• The independent role of PR status in DCIS is unproven, so testing for it is not supported by clinical evidence.
To examine the costs associated with reflexive ER/PR testing, the investigators reviewed 58 core needle biopsies of pure DCIS followed by surgical excision. None of the patients had neoadjuvant hormone therapy. Of the 58 tumors, 76% were pure DCIS, and 16% were DCIS with invasive breast cancer. Most of the DCIS (47) tumors were ER+/PR+; 6 were ER-/PR-; and 5 were ER+/PR-.
The team reviewed the records of 49 patients who underwent surgical excision and ended up with a diagnosis of pure DCIS. These included 46 ER-positive cases, and 3 that were ER-negative in both biopsy and excision.
The findings suggested that ER/PR results from either the biopsy and the surgical excision samples were relevant to therapy in only a portion of these patients.
“We found that the ER/PR results after surgical excision impacted therapy in at most only 16 of 49 cases (33%),” they said. These included the 3 ER-/PR-negative cases, which would, in any case, not have triggered hormone therapy; 10 patients who chose hormone therapy despite a Hopkins oncologist’s neutral recommendation; 1 of 2 who took hormone therapy on a Hopkins oncologist’s recommendation; and 2 of 3 who took it after seeing a non-Hopkins oncologist.
“In contrast,” the authors wrote, “in 33 of the cases (67%), the ER/PR result of the DCIS after surgical excision did not impact therapy.” All of these were ER-positive cases, including 4 patients who opted for bilateral mastectomies (no subsequent role for neoadjuvant therapy), 8 who declined to meet with an oncologist, 1 for whom hormone therapy was contraindicated, 8 (of 8) who declined hormone therapy when their Hopkins oncologist did not recommend it, 10 (of 20) who declined hormone therapy when their Hopkins oncologist was neutral about its risk/benefit ratio, 1 (of 2) who declined hormone therapy when the Hopkins oncologist recommended it, and the 1 patient (of 3) who declined hormone therapy after visiting a non-Hopkins oncologist.
After reviewing the costs associated with these cases, “we found that ER testing … costing $20,685.72 ($357 per patient) had been performed unnecessarily,” the investigators said. In addition, if the PR testing – which has never been proven clinically important in DCIS – had been eliminated, there would have been an additional $86.46 savings per patient, a total savings of $5,014.
“Extrapolating the increased cost of $583 per DCIS diagnosis on core needle biopsy to 60,000 new cases of DCIS in the United States each year, reflex core needle biopsy ER/PR testing unnecessarily increases costs by approximately $35 million,” the authors said. “We recommend that ER/PR not be reflexively ordered on core needle biopsy specimens or surgical excision specimens containing DCIS, but instead that ER alone be performed on surgical excision specimens only when hormone therapy is a serious consideration after medical oncology consultation.”
The group noted that this total reflects the total amount billed, not typical reimbursement. “Regardless,” they said, “the cost of this testing is staggering.”
The authors did not mention the study’s funding source. They had no relevant financial disclosures.
On Twitter @Alz_Gal
FROM THE AMERICAN JOURNAL OF SURGICAL PATHOLOGY
Key clinical point: Hormone receptor testing of diagnostic core needle biopsies should not be automatic.
Major finding: Limiting testing to excised surgical section specimens could save up to $35 million a year in the United States.
Data source: The cost analysis examined testing and treatment of 58 patients with ductal carcinoma in situ.
Disclosures: The authors had no relevant financial disclosures.
