User login
Pembrolizumab shows activity against advanced TNBC
Early data from a phase Ib trial suggest that the immune checkpoint inhibitor pembrolizumab has modest activity against heavily pretreated metastatic triple-negative breast cancer (mTNBC).
Among 27 women with advanced triple-negative breast cancer (tumors lacking HER2, estrogen, and progesterone receptors) enrolled in a basket trial for cancers expressing the programmed death-1 ligand (PD-L1), the overall response rate to biweekly pembrolizumab (Keytruda) was 18.5%, reported Dr. Rita Nanda of the University of Chicago and colleagues (J Clin Oncol. 2016 May 2. doi: 10.1200/JCO.2015.64.8931).

“Overall, these results support further development of pembrolizumab for the treatment of mTNBC,” they said.
The TNBC study was included in the open-label, multicohort Keynote 012 study looking at the use of pembrolizumab in patients with advanced solid tumors expressing PD-L1.
The investigators evaluated PD-L1 status in 111 women with mTNBC, and identified 65 with tumors expressing the target, 32 of whom were enrolled in the trial.
The patients were treated with pembrolizumab 10 mg/kg intravenously every 2 weeks until unacceptable toxicity or disease progression, or at the discretion of the investigator. Clinically stable patients with first radiologic evidence of disease progression according to Response Evaluation Criteria for Solid Tumors (RECIST) could be continued on the checkpoint inhibitor until evidence of progression could be shown on a second scan 4 or more weeks later.
The patients received a median of five doses (range, 1-36). After a median follow-up of 10 months, the overall response rate among 27 patients evaluable for response was 18.5%, consisting of one complete response, four partial responses, and seven cases of stable disease. Thirteen patients had disease progression on pembrolizumab, and two patients discontinued therapy before the first scan.
The median time to response was 17.9 weeks; the median duration of response had not been reached by the time of data cut-off on March 25, 2015.
The adverse event profile was similar to that seen with pembrolizumab in the other study cohorts (gastric, urothelial, and head and neck cancers), with generally mild arthralgia, fatigue, myalgia, and nausea. However, there were five grade 3 or greater toxicities, including anemia, aseptic meningitis, lymphopenia, headache, and pyrexia, and one patient died from treatment-related disseminated intravascular coagulation accompanied by a grade 4 decrease in blood fibrinogen.
The investigators noted that the overall response rate seen in the TNBC cohort “makes it the first published report showing clinical activity for an immune checkpoint inhibitor in a heavily pretreated mTNBC population.”
Overall response rates for the other cohorts in the study were 21.4% for patients with head and neck cancers, 22.2% for those with gastric cancers, and 27.6% for those with urothelial cancers.
The study was sponsored by Merck & Co. Dr. Nanda and several coauthors disclosed consulting, research funding, and/or honoraria from the company, and four of the 12 coauthors are employees.
Early data from a phase Ib trial suggest that the immune checkpoint inhibitor pembrolizumab has modest activity against heavily pretreated metastatic triple-negative breast cancer (mTNBC).
Among 27 women with advanced triple-negative breast cancer (tumors lacking HER2, estrogen, and progesterone receptors) enrolled in a basket trial for cancers expressing the programmed death-1 ligand (PD-L1), the overall response rate to biweekly pembrolizumab (Keytruda) was 18.5%, reported Dr. Rita Nanda of the University of Chicago and colleagues (J Clin Oncol. 2016 May 2. doi: 10.1200/JCO.2015.64.8931).
“Overall, these results support further development of pembrolizumab for the treatment of mTNBC,” they said.
The TNBC study was included in the open-label, multicohort Keynote 012 study looking at the use of pembrolizumab in patients with advanced solid tumors expressing PD-L1.
The investigators evaluated PD-L1 status in 111 women with mTNBC, and identified 65 with tumors expressing the target, 32 of whom were enrolled in the trial.
The patients were treated with pembrolizumab 10 mg/kg intravenously every 2 weeks until unacceptable toxicity or disease progression, or at the discretion of the investigator. Clinically stable patients with first radiologic evidence of disease progression according to Response Evaluation Criteria for Solid Tumors (RECIST) could be continued on the checkpoint inhibitor until evidence of progression could be shown on a second scan 4 or more weeks later.
The patients received a median of five doses (range, 1-36). After a median follow-up of 10 months, the overall response rate among 27 patients evaluable for response was 18.5%, consisting of one complete response, four partial responses, and seven cases of stable disease. Thirteen patients had disease progression on pembrolizumab, and two patients discontinued therapy before the first scan.
The median time to response was 17.9 weeks; the median duration of response had not been reached by the time of data cut-off on March 25, 2015.
The adverse event profile was similar to that seen with pembrolizumab in the other study cohorts (gastric, urothelial, and head and neck cancers), with generally mild arthralgia, fatigue, myalgia, and nausea. However, there were five grade 3 or greater toxicities, including anemia, aseptic meningitis, lymphopenia, headache, and pyrexia, and one patient died from treatment-related disseminated intravascular coagulation accompanied by a grade 4 decrease in blood fibrinogen.
The investigators noted that the overall response rate seen in the TNBC cohort “makes it the first published report showing clinical activity for an immune checkpoint inhibitor in a heavily pretreated mTNBC population.”
Overall response rates for the other cohorts in the study were 21.4% for patients with head and neck cancers, 22.2% for those with gastric cancers, and 27.6% for those with urothelial cancers.
The study was sponsored by Merck & Co. Dr. Nanda and several coauthors disclosed consulting, research funding, and/or honoraria from the company, and four of the 12 coauthors are employees.
Early data from a phase Ib trial suggest that the immune checkpoint inhibitor pembrolizumab has modest activity against heavily pretreated metastatic triple-negative breast cancer (mTNBC).
Among 27 women with advanced triple-negative breast cancer (tumors lacking HER2, estrogen, and progesterone receptors) enrolled in a basket trial for cancers expressing the programmed death-1 ligand (PD-L1), the overall response rate to biweekly pembrolizumab (Keytruda) was 18.5%, reported Dr. Rita Nanda of the University of Chicago and colleagues (J Clin Oncol. 2016 May 2. doi: 10.1200/JCO.2015.64.8931).
“Overall, these results support further development of pembrolizumab for the treatment of mTNBC,” they said.
The TNBC study was included in the open-label, multicohort Keynote 012 study looking at the use of pembrolizumab in patients with advanced solid tumors expressing PD-L1.
The investigators evaluated PD-L1 status in 111 women with mTNBC, and identified 65 with tumors expressing the target, 32 of whom were enrolled in the trial.
The patients were treated with pembrolizumab 10 mg/kg intravenously every 2 weeks until unacceptable toxicity or disease progression, or at the discretion of the investigator. Clinically stable patients with first radiologic evidence of disease progression according to Response Evaluation Criteria for Solid Tumors (RECIST) could be continued on the checkpoint inhibitor until evidence of progression could be shown on a second scan 4 or more weeks later.
The patients received a median of five doses (range, 1-36). After a median follow-up of 10 months, the overall response rate among 27 patients evaluable for response was 18.5%, consisting of one complete response, four partial responses, and seven cases of stable disease. Thirteen patients had disease progression on pembrolizumab, and two patients discontinued therapy before the first scan.
The median time to response was 17.9 weeks; the median duration of response had not been reached by the time of data cut-off on March 25, 2015.
The adverse event profile was similar to that seen with pembrolizumab in the other study cohorts (gastric, urothelial, and head and neck cancers), with generally mild arthralgia, fatigue, myalgia, and nausea. However, there were five grade 3 or greater toxicities, including anemia, aseptic meningitis, lymphopenia, headache, and pyrexia, and one patient died from treatment-related disseminated intravascular coagulation accompanied by a grade 4 decrease in blood fibrinogen.
The investigators noted that the overall response rate seen in the TNBC cohort “makes it the first published report showing clinical activity for an immune checkpoint inhibitor in a heavily pretreated mTNBC population.”
Overall response rates for the other cohorts in the study were 21.4% for patients with head and neck cancers, 22.2% for those with gastric cancers, and 27.6% for those with urothelial cancers.
The study was sponsored by Merck & Co. Dr. Nanda and several coauthors disclosed consulting, research funding, and/or honoraria from the company, and four of the 12 coauthors are employees.
FROM JOURNAL OF CLINICAL ONCOLOGY
Key clinical point: The immune checkpoint inhibitor pembrolizumab may be effective against metastatic triple-negative breast cancer.
Major finding: The overall response rate to pembrolizumab therapy among 27 women with metastatic TNBC evaluable for response was 18.5%.
Data source: Open-label, multicohort, phase Ib study in patients with solid tumors expressing PD-L1.
Disclosures: The study was sponsored by Merck & Co. Dr. Nanda and several coauthors disclosed consulting, research funding, and/or honoraria from the company, and four of the 12 coauthors are employees.

ACOSOG Z0011: Good long-term results with SLND without ALND
CHICAGO – Sentinel lymph node dissection without axillary lymph node dissection offers excellent regional control in select patients with early metastatic breast cancer who are treated using breast-conserving therapy and adjuvant systemic therapy, according to 10-year results from the American College of Surgeons Oncology Group (ACOSOG) Z0011 Randomized Trial. ACOSOG is now part of Alliance for Clinical Trials in Oncology.
The findings confirm the previously reported 5-year outcomes, which demonstrated no significant difference in locoregional recurrence for patients with positive sentinel nodes who were randomized to undergo axillary lymph node dissection (ALND) or no further axillary treatment, Dr. Armando E. Giuliano of Cedars-Sinai Medical Center, Los Angeles, reported at the annual meeting of the American Surgical Association.

“In fact, the [5-year] results were highly significant showing noninferiority of sentinel lymph node dissection,” he said.
At a median follow-up of 9.25 years, there still was no statistically significant difference between 446 sentinel lymph node dissection (SLND)–only patients and 445 completion ALND patients with respect to the rate of locoregional recurrence, Dr. Giuliano said.
“The 10-year locoregional recurrence incidence after axillary lymph node dissection is 6.2%, compared to 5.3% after sentinel lymph node dissection alone,” he said, noting that most recurrences were seen in the first 5 years.
Of the ALND patients, 27% had additional positive nodes removed beyond the sentinel nodes.
“Therefore, about 27% of patients who underwent sentinel node dissection alone had residual disease remaining in the axilla undissected. Despite this high possibility of residual disease, very few regional recurrences were seen in either arm,” he noted.
Local recurrences occurred in 19 (5.6%) of patients in the ALND group and 12 (3.8%) in the SLND group, and regional recurrence was seen in 2 (0.5%) patients in the ALND group and 5 (1.5%) in the SLND group. The differences were not statistically significant.
Only hormone receptor status, Bloom-Richardson score, and tumor size were associated with locoregional recurrence. Omission of radiation increased local but not regional recurrence, but numbers were too few to draw further conclusions, he said.
“We can conclude, however, that sentinel lymph node dissection provides excellent locoregional control comparable to completion axillary lymph node dissection in these selected patients,” he said.
ACOSOG Z0011 subjects were patients with hematoxylin-eosin (H&E)–detected sentinel lymph node metastases undergoing breast-conserving therapy. The groups randomized to undergo ALND or to receive no further axillary treatment were similar with respect to age, Bloom-Richardson score, estrogen-receptor status, adjuvant systemic therapy, histology, and tumor size.
Nearly all patients had adjuvant systemic therapy (96% and 97% in the ALND and SLND groups, respectively), and about 60% in each group received chemotherapy.
Dr. Giuliano concluded that, despite the potential for residual axillary disease after SLND, SLND without ALND offers excellent regional control for selected patients with early metastatic breast cancer treated with breast-conserving therapy and adjuvant systemic therapy.
“Axillary lymph node dissection is not necessary for patients with early metastatic breast cancer and should be abandoned,” he said.
Dr. Giuliano had no disclosures.
The complete manuscript of this presentation is anticipated to be published in the Annals of Surgery pending editorial review
CHICAGO – Sentinel lymph node dissection without axillary lymph node dissection offers excellent regional control in select patients with early metastatic breast cancer who are treated using breast-conserving therapy and adjuvant systemic therapy, according to 10-year results from the American College of Surgeons Oncology Group (ACOSOG) Z0011 Randomized Trial. ACOSOG is now part of Alliance for Clinical Trials in Oncology.
The findings confirm the previously reported 5-year outcomes, which demonstrated no significant difference in locoregional recurrence for patients with positive sentinel nodes who were randomized to undergo axillary lymph node dissection (ALND) or no further axillary treatment, Dr. Armando E. Giuliano of Cedars-Sinai Medical Center, Los Angeles, reported at the annual meeting of the American Surgical Association.
“In fact, the [5-year] results were highly significant showing noninferiority of sentinel lymph node dissection,” he said.
At a median follow-up of 9.25 years, there still was no statistically significant difference between 446 sentinel lymph node dissection (SLND)–only patients and 445 completion ALND patients with respect to the rate of locoregional recurrence, Dr. Giuliano said.
“The 10-year locoregional recurrence incidence after axillary lymph node dissection is 6.2%, compared to 5.3% after sentinel lymph node dissection alone,” he said, noting that most recurrences were seen in the first 5 years.
Of the ALND patients, 27% had additional positive nodes removed beyond the sentinel nodes.
“Therefore, about 27% of patients who underwent sentinel node dissection alone had residual disease remaining in the axilla undissected. Despite this high possibility of residual disease, very few regional recurrences were seen in either arm,” he noted.
Local recurrences occurred in 19 (5.6%) of patients in the ALND group and 12 (3.8%) in the SLND group, and regional recurrence was seen in 2 (0.5%) patients in the ALND group and 5 (1.5%) in the SLND group. The differences were not statistically significant.
Only hormone receptor status, Bloom-Richardson score, and tumor size were associated with locoregional recurrence. Omission of radiation increased local but not regional recurrence, but numbers were too few to draw further conclusions, he said.
“We can conclude, however, that sentinel lymph node dissection provides excellent locoregional control comparable to completion axillary lymph node dissection in these selected patients,” he said.
ACOSOG Z0011 subjects were patients with hematoxylin-eosin (H&E)–detected sentinel lymph node metastases undergoing breast-conserving therapy. The groups randomized to undergo ALND or to receive no further axillary treatment were similar with respect to age, Bloom-Richardson score, estrogen-receptor status, adjuvant systemic therapy, histology, and tumor size.
Nearly all patients had adjuvant systemic therapy (96% and 97% in the ALND and SLND groups, respectively), and about 60% in each group received chemotherapy.
Dr. Giuliano concluded that, despite the potential for residual axillary disease after SLND, SLND without ALND offers excellent regional control for selected patients with early metastatic breast cancer treated with breast-conserving therapy and adjuvant systemic therapy.
“Axillary lymph node dissection is not necessary for patients with early metastatic breast cancer and should be abandoned,” he said.
Dr. Giuliano had no disclosures.
The complete manuscript of this presentation is anticipated to be published in the Annals of Surgery pending editorial review
CHICAGO – Sentinel lymph node dissection without axillary lymph node dissection offers excellent regional control in select patients with early metastatic breast cancer who are treated using breast-conserving therapy and adjuvant systemic therapy, according to 10-year results from the American College of Surgeons Oncology Group (ACOSOG) Z0011 Randomized Trial. ACOSOG is now part of Alliance for Clinical Trials in Oncology.
The findings confirm the previously reported 5-year outcomes, which demonstrated no significant difference in locoregional recurrence for patients with positive sentinel nodes who were randomized to undergo axillary lymph node dissection (ALND) or no further axillary treatment, Dr. Armando E. Giuliano of Cedars-Sinai Medical Center, Los Angeles, reported at the annual meeting of the American Surgical Association.
“In fact, the [5-year] results were highly significant showing noninferiority of sentinel lymph node dissection,” he said.
At a median follow-up of 9.25 years, there still was no statistically significant difference between 446 sentinel lymph node dissection (SLND)–only patients and 445 completion ALND patients with respect to the rate of locoregional recurrence, Dr. Giuliano said.
“The 10-year locoregional recurrence incidence after axillary lymph node dissection is 6.2%, compared to 5.3% after sentinel lymph node dissection alone,” he said, noting that most recurrences were seen in the first 5 years.
Of the ALND patients, 27% had additional positive nodes removed beyond the sentinel nodes.
“Therefore, about 27% of patients who underwent sentinel node dissection alone had residual disease remaining in the axilla undissected. Despite this high possibility of residual disease, very few regional recurrences were seen in either arm,” he noted.
Local recurrences occurred in 19 (5.6%) of patients in the ALND group and 12 (3.8%) in the SLND group, and regional recurrence was seen in 2 (0.5%) patients in the ALND group and 5 (1.5%) in the SLND group. The differences were not statistically significant.
Only hormone receptor status, Bloom-Richardson score, and tumor size were associated with locoregional recurrence. Omission of radiation increased local but not regional recurrence, but numbers were too few to draw further conclusions, he said.
“We can conclude, however, that sentinel lymph node dissection provides excellent locoregional control comparable to completion axillary lymph node dissection in these selected patients,” he said.
ACOSOG Z0011 subjects were patients with hematoxylin-eosin (H&E)–detected sentinel lymph node metastases undergoing breast-conserving therapy. The groups randomized to undergo ALND or to receive no further axillary treatment were similar with respect to age, Bloom-Richardson score, estrogen-receptor status, adjuvant systemic therapy, histology, and tumor size.
Nearly all patients had adjuvant systemic therapy (96% and 97% in the ALND and SLND groups, respectively), and about 60% in each group received chemotherapy.
Dr. Giuliano concluded that, despite the potential for residual axillary disease after SLND, SLND without ALND offers excellent regional control for selected patients with early metastatic breast cancer treated with breast-conserving therapy and adjuvant systemic therapy.
“Axillary lymph node dissection is not necessary for patients with early metastatic breast cancer and should be abandoned,” he said.
Dr. Giuliano had no disclosures.
The complete manuscript of this presentation is anticipated to be published in the Annals of Surgery pending editorial review
AT THE ASA ANNUAL MEETING
Key clinical point: Sentinel lymph node dissection without axillary lymph node dissection offers excellent long-term regional control in select patients with early metastatic breast cancer who are treated using breast-conserving therapy and adjuvant systemic therapy.
Major finding: The 10-year locoregional recurrence after axillary lymph node dissection was 6.2%, compared with 5.3% after SLND alone.
Data source: The American College of Surgeons Oncology Group (ACOSOG) Z0011 Randomized Trial involving 891 patients.
Disclosures: Dr. Giuliano had no disclosures.

Reaching high-risk underserved individuals for cancer genetic counseling by video-teleconferencing
Background Breast and colorectal cancers are common cancers for which genetic risk assessment and counseling are available. However, these services are often limited to metropolitan areas and are not readily accessible to underserved populations. Moreover, ethnic and racial disparities present additional obstacles to identifying and screening high-risk individuals and have a bearing on treatment outcomes.
Objective To provide cancer genetic risk assessment and counseling through telemedicine to the remote, underserved primarily Hispanic population of the Texas-Mexico border region.
Methods Program participants were mailed a questionnaire to assess their satisfaction with the program so that we could determine the acceptability of video-teleconferencing for cancer risk assessment.
Results The overall level of satisfaction with the program was very high, demonstrating the acceptability of a cancer genetic risk assessment program that relied on telemedicine to reach and underserved minority community.
Limitations Delivery model requires the availability of and access to communication technologies; trained staff are needed at remote sites for sample collection and patient handling.
Conclusion Video-teleconferencing is an acceptable method of providing cancer risk assessment in a remote, underserved population.
Funding Supported primarily by a grant from the Cancer Prevention and Research Institute of Texas (PP120089 [GT]), NIH-NCI P30 CA54174 (CTRC at UTHSCSA); and a grant from the Valley Baptist Legacy Foundation.
Click on the PDF icon at the top of this introduction to read the full article.
Background Breast and colorectal cancers are common cancers for which genetic risk assessment and counseling are available. However, these services are often limited to metropolitan areas and are not readily accessible to underserved populations. Moreover, ethnic and racial disparities present additional obstacles to identifying and screening high-risk individuals and have a bearing on treatment outcomes.
Objective To provide cancer genetic risk assessment and counseling through telemedicine to the remote, underserved primarily Hispanic population of the Texas-Mexico border region.
Methods Program participants were mailed a questionnaire to assess their satisfaction with the program so that we could determine the acceptability of video-teleconferencing for cancer risk assessment.
Results The overall level of satisfaction with the program was very high, demonstrating the acceptability of a cancer genetic risk assessment program that relied on telemedicine to reach and underserved minority community.
Limitations Delivery model requires the availability of and access to communication technologies; trained staff are needed at remote sites for sample collection and patient handling.
Conclusion Video-teleconferencing is an acceptable method of providing cancer risk assessment in a remote, underserved population.
Funding Supported primarily by a grant from the Cancer Prevention and Research Institute of Texas (PP120089 [GT]), NIH-NCI P30 CA54174 (CTRC at UTHSCSA); and a grant from the Valley Baptist Legacy Foundation.
Click on the PDF icon at the top of this introduction to read the full article.
Background Breast and colorectal cancers are common cancers for which genetic risk assessment and counseling are available. However, these services are often limited to metropolitan areas and are not readily accessible to underserved populations. Moreover, ethnic and racial disparities present additional obstacles to identifying and screening high-risk individuals and have a bearing on treatment outcomes.
Objective To provide cancer genetic risk assessment and counseling through telemedicine to the remote, underserved primarily Hispanic population of the Texas-Mexico border region.
Methods Program participants were mailed a questionnaire to assess their satisfaction with the program so that we could determine the acceptability of video-teleconferencing for cancer risk assessment.
Results The overall level of satisfaction with the program was very high, demonstrating the acceptability of a cancer genetic risk assessment program that relied on telemedicine to reach and underserved minority community.
Limitations Delivery model requires the availability of and access to communication technologies; trained staff are needed at remote sites for sample collection and patient handling.
Conclusion Video-teleconferencing is an acceptable method of providing cancer risk assessment in a remote, underserved population.
Funding Supported primarily by a grant from the Cancer Prevention and Research Institute of Texas (PP120089 [GT]), NIH-NCI P30 CA54174 (CTRC at UTHSCSA); and a grant from the Valley Baptist Legacy Foundation.
Click on the PDF icon at the top of this introduction to read the full article.
Adding tomosynthesis may benefit women with dense breasts
Women with dense breasts may benefit from additional screening at the time of digital mammography, but the messages notifying these women of potential risks and benefits of more screening are often poorly written and understood, according to a pair of studies published online in JAMA on April 26.
Adding tomosynthesis to screening digital mammography significantly increased cancer detection rates in women with dense and nondense breasts, based on data from a retrospective study of 452,320 examinations.

Dense breast tissue may be an independent risk factor for breast cancer, but the impact of additional treatment modalities on women with dense breasts has not been well studied, wrote Dr. Elizabeth A. Rafferty of L&M Radiology in West Acton, Mass., and associates. Dr. Rafferty conducted the study with colleagues while affiliated with Massachusetts General Hospital in Boston (JAMA 2016 Apr 26. doi: 10.1001/jama.2016.1708).
The researchers reviewed data from an earlier multicenter study involving 13 U.S. institutions, with data reported for 12 months that included 278,906 digital mammographies and 173,414 digital mammographies plus tomosynthesis. A total of 2,157 cancers were diagnosed. Cancer detection rates increased in both groups with the addition of tomosynthesis: Invasive cancer detection increased from 3.0 to 4.0 per 1,000 screens in nondense breasts and from 2.9 to 4.2 per 1,000 screens in dense breasts.
In addition, recall rates decreased from 90 to 79 per 1,000 screens in nondense breasts and from 127 to 109 per 1,000 screens in dense breasts.
Although the study was limited by its retrospective design, the results suggest that the “combined gains were largest for women with heterogeneously dense breasts, potentially addressing limitations in cancer detection seen with digital mammography alone in this group, but were not significant in women with extremely dense breasts,” the researchers noted.
The researchers had no financial conflicts to disclose, and the study was supported by a research grant from Hologic.
Meanwhile, a separate study published in JAMA found that most messages sent to notify women of breast density are poorly understood.
Nancy R. Kressin, Ph.D., of Veterans Affairs Boston Healthcare System and Boston University and colleagues examined the dense breast notifications sent to women following screening mammography in 23 of the 24 states that required such notifications as of January 2016. They assessed the messages for content, readability, and understandability (JAMA 2016 Apr 26. doi: 10.1001/jama.2016.1712).
Although all the notifications reviewed mentioned masking bias (how dense breasts can mask cancer on mammography), the researchers found considerable variation in other content: 74% of notifications mentioned increased cancer risk and 65% mentioned the option of additional screening. Of the 15 states that require supplemental screening to be mentioned, six state notifications explained that the women might benefit from such screening and four state notifications mentioned specific screening modalities.
Only three states’ notifications were written at grade 8 reading level or below, although approximately 20% of the U.S. population reads at grade 5 level or below, the researchers noted. All states’ notifications scored between 11% and 33% on a measure of readability.
“Many [dense breast notifications] appropriately encourage discussions and shared decision making between patients and physicians,” the researchers noted. However, “efforts should focus on enhancing the understandability of [dense breast notifications] so that all women are clearly and accurately informed about their density status, its effect on their breast cancer risk, and the harms and benefits of supplemental screening,” they wrote.
Dr. Kressin reported receiving a Research Career Scientist award from the Department of Veterans Affairs, and coauthor Dr. Tracy Battaglia is the chair elect of the American Cancer Society of New England.
Women with dense breasts may benefit from additional screening at the time of digital mammography, but the messages notifying these women of potential risks and benefits of more screening are often poorly written and understood, according to a pair of studies published online in JAMA on April 26.
Adding tomosynthesis to screening digital mammography significantly increased cancer detection rates in women with dense and nondense breasts, based on data from a retrospective study of 452,320 examinations.
Dense breast tissue may be an independent risk factor for breast cancer, but the impact of additional treatment modalities on women with dense breasts has not been well studied, wrote Dr. Elizabeth A. Rafferty of L&M Radiology in West Acton, Mass., and associates. Dr. Rafferty conducted the study with colleagues while affiliated with Massachusetts General Hospital in Boston (JAMA 2016 Apr 26. doi: 10.1001/jama.2016.1708).
The researchers reviewed data from an earlier multicenter study involving 13 U.S. institutions, with data reported for 12 months that included 278,906 digital mammographies and 173,414 digital mammographies plus tomosynthesis. A total of 2,157 cancers were diagnosed. Cancer detection rates increased in both groups with the addition of tomosynthesis: Invasive cancer detection increased from 3.0 to 4.0 per 1,000 screens in nondense breasts and from 2.9 to 4.2 per 1,000 screens in dense breasts.
In addition, recall rates decreased from 90 to 79 per 1,000 screens in nondense breasts and from 127 to 109 per 1,000 screens in dense breasts.
Although the study was limited by its retrospective design, the results suggest that the “combined gains were largest for women with heterogeneously dense breasts, potentially addressing limitations in cancer detection seen with digital mammography alone in this group, but were not significant in women with extremely dense breasts,” the researchers noted.
The researchers had no financial conflicts to disclose, and the study was supported by a research grant from Hologic.
Meanwhile, a separate study published in JAMA found that most messages sent to notify women of breast density are poorly understood.
Nancy R. Kressin, Ph.D., of Veterans Affairs Boston Healthcare System and Boston University and colleagues examined the dense breast notifications sent to women following screening mammography in 23 of the 24 states that required such notifications as of January 2016. They assessed the messages for content, readability, and understandability (JAMA 2016 Apr 26. doi: 10.1001/jama.2016.1712).
Although all the notifications reviewed mentioned masking bias (how dense breasts can mask cancer on mammography), the researchers found considerable variation in other content: 74% of notifications mentioned increased cancer risk and 65% mentioned the option of additional screening. Of the 15 states that require supplemental screening to be mentioned, six state notifications explained that the women might benefit from such screening and four state notifications mentioned specific screening modalities.
Only three states’ notifications were written at grade 8 reading level or below, although approximately 20% of the U.S. population reads at grade 5 level or below, the researchers noted. All states’ notifications scored between 11% and 33% on a measure of readability.
“Many [dense breast notifications] appropriately encourage discussions and shared decision making between patients and physicians,” the researchers noted. However, “efforts should focus on enhancing the understandability of [dense breast notifications] so that all women are clearly and accurately informed about their density status, its effect on their breast cancer risk, and the harms and benefits of supplemental screening,” they wrote.
Dr. Kressin reported receiving a Research Career Scientist award from the Department of Veterans Affairs, and coauthor Dr. Tracy Battaglia is the chair elect of the American Cancer Society of New England.
Women with dense breasts may benefit from additional screening at the time of digital mammography, but the messages notifying these women of potential risks and benefits of more screening are often poorly written and understood, according to a pair of studies published online in JAMA on April 26.
Adding tomosynthesis to screening digital mammography significantly increased cancer detection rates in women with dense and nondense breasts, based on data from a retrospective study of 452,320 examinations.
Dense breast tissue may be an independent risk factor for breast cancer, but the impact of additional treatment modalities on women with dense breasts has not been well studied, wrote Dr. Elizabeth A. Rafferty of L&M Radiology in West Acton, Mass., and associates. Dr. Rafferty conducted the study with colleagues while affiliated with Massachusetts General Hospital in Boston (JAMA 2016 Apr 26. doi: 10.1001/jama.2016.1708).
The researchers reviewed data from an earlier multicenter study involving 13 U.S. institutions, with data reported for 12 months that included 278,906 digital mammographies and 173,414 digital mammographies plus tomosynthesis. A total of 2,157 cancers were diagnosed. Cancer detection rates increased in both groups with the addition of tomosynthesis: Invasive cancer detection increased from 3.0 to 4.0 per 1,000 screens in nondense breasts and from 2.9 to 4.2 per 1,000 screens in dense breasts.
In addition, recall rates decreased from 90 to 79 per 1,000 screens in nondense breasts and from 127 to 109 per 1,000 screens in dense breasts.
Although the study was limited by its retrospective design, the results suggest that the “combined gains were largest for women with heterogeneously dense breasts, potentially addressing limitations in cancer detection seen with digital mammography alone in this group, but were not significant in women with extremely dense breasts,” the researchers noted.
The researchers had no financial conflicts to disclose, and the study was supported by a research grant from Hologic.
Meanwhile, a separate study published in JAMA found that most messages sent to notify women of breast density are poorly understood.
Nancy R. Kressin, Ph.D., of Veterans Affairs Boston Healthcare System and Boston University and colleagues examined the dense breast notifications sent to women following screening mammography in 23 of the 24 states that required such notifications as of January 2016. They assessed the messages for content, readability, and understandability (JAMA 2016 Apr 26. doi: 10.1001/jama.2016.1712).
Although all the notifications reviewed mentioned masking bias (how dense breasts can mask cancer on mammography), the researchers found considerable variation in other content: 74% of notifications mentioned increased cancer risk and 65% mentioned the option of additional screening. Of the 15 states that require supplemental screening to be mentioned, six state notifications explained that the women might benefit from such screening and four state notifications mentioned specific screening modalities.
Only three states’ notifications were written at grade 8 reading level or below, although approximately 20% of the U.S. population reads at grade 5 level or below, the researchers noted. All states’ notifications scored between 11% and 33% on a measure of readability.
“Many [dense breast notifications] appropriately encourage discussions and shared decision making between patients and physicians,” the researchers noted. However, “efforts should focus on enhancing the understandability of [dense breast notifications] so that all women are clearly and accurately informed about their density status, its effect on their breast cancer risk, and the harms and benefits of supplemental screening,” they wrote.
Dr. Kressin reported receiving a Research Career Scientist award from the Department of Veterans Affairs, and coauthor Dr. Tracy Battaglia is the chair elect of the American Cancer Society of New England.
FROM JAMA
Key clinical point: Women with dense breasts may benefit from additional screening, but state-mandated density notification messages are often hard for them to understand.
Major finding: Invasive cancer detection increased from 3.0 to 4.0 per 1,000 screens in nondense breasts, and from 2.9 to 4.2 per 1,000 screens in dense breasts, with the addition of tomosynthesis to digital screening mammography. In another study, 65% of dense breast notifications mentioned the option of additional screening.
Data source: A retrospective study of 452,320 breast cancer screening examinations, and a review of dense breast notifications sent to women in 23 states as of January 2016.
Disclosures: Dr. Rafferty had no financial conflicts to disclose, and the study was supported by a research grant from Hologic. Dr. Kressin disclosed support from a Research Career Scientist award from the Department of Veterans Affairs, and coauthor Dr. Tracy Battaglia is the chair elect of the American Cancer Society of New England.

MammaPrint bests clinical factors in sparing patients from chemotherapy
A large multinational European trial shows that genetic analysis of breast tumors can spare women unnecessary adjuvant chemotherapy, even when clinical factors indicate a high risk of recurrence.
Using MammaPrint, a 70-gene signature test, led to a 14% absolute reduction in the use of chemotherapy, compared with a clinical strategy, according to the highly anticipated results of the Phase III Microarray in Node-negative and 1 to 3 positive lymph node Disease may Avoid Chemo Therapy (MINDACT) trial, presented at the annual meeting of the American Association for Cancer Research.

While three decades of clinical trials have shown survival benefits of adjuvant chemotherapy, it carries later risks. “And it will happen when the survival gain associated with adjuvant chemotherapy is small, in the range of 2%-3% – it happens in good prognosis patients – and is counterbalanced by the long-term severe risks of adjuvant chemotherapy,” said Dr. Martine Piccart, director of medicine at the Jules Bordet Institute in Brussels, and principal investigator for the trial.
Risks include secondary cancers, cardiotoxicity, early menopause, and a decline in cognitive function, as well as negative socioeconomic effects. So avoiding chemotherapy when outcomes would be nearly the same without it is a reasonable goal.
To investigate the best method to determine which breast cancer patients could do just as well without adjuvant chemotherapy, European investigators at 111 centers in 9 countries screened 11,288 patients with early-stage disease and enrolled 6,693 in the MINDACT trial. Speaking at a news conference during the annual meeting, Dr. Piccart said MINDACT compared tumor genetic testing with clinical and pathology parameters to gauge the risk of disease recurrence and is the only trial to date to compare the utility of the two strategies.
MammaPrint is a genetic test (G) of early stage breast cancer tumors that produces a 70-gene signature indicating a high or low 10-year risk of metastatic recurrence. The Adjuvant! Online tool takes into account clinical factors and pathology markers, including a patient’s age and comorbidities and a tumor’s estrogen receptor status, grade, size, and the number of positive lymph nodes, to calculate a ten-year “clinical risk” (C) of negative outcomes with or without adjuvant chemotherapy or hormonal therapy.
After surgery, tissue samples underwent local pathology examination to determine tumor stage and nodal, hormone receptor, and HER2 status. Samples were also sent to a central facility for MammaPrint testing. For women with low-risk tumors by both tests, no chemotherapy was indicated. For high-risk tumors by both tests, chemotherapy was prescribed. But those with discordant results were randomized equally to receive chemotherapy or not.
MammaPrint better predictor than clinical factors
The median age of patients at enrollment was 55 years, 80% of tumors were node-negative, 58% were T1, 88% hormone receptor–positive, and 10% HER2-positive. At a median follow-up of 5 years, 362 (5.4%) women had distant metastases or had died.
Among 3,356 patients classified as high risk based on the Adjuvant! Online test, there were 1,550 classified by genetic criteria as low risk (C-High/G-Low), including 48% with positive nodes. For this C-High/G-Low group, the 5-year distant metastasis-free survival was greater than 94% regardless of adjuvant chemotherapy and was not statistically different for the two groups. These are patients who would normally be prescribed adjuvant chemotherapy if based solely on the C criteria.
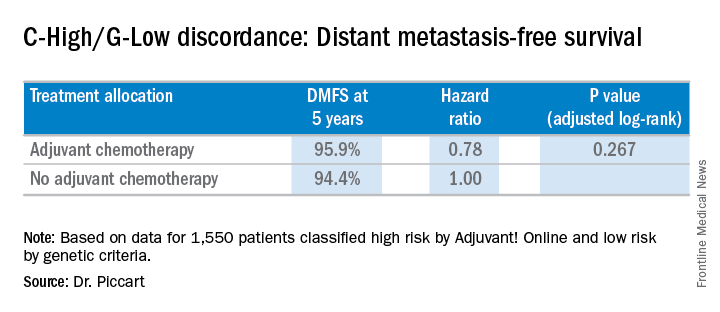
Going by MammaPrint test results would thereby reduce chemotherapy prescriptions by 46% (1,550/3,356) for the study cohort. Considering the entire initial 11,288 patients screened, the genomic strategy would lead to a 14% absolute reduction in chemotherapy, compared with the clinical strategy, according to Dr. Piccart. “MINDACT results provide level 1A evidence of the clinical utility of MammaPrint for assessing the lack of a clinically relevant chemotherapy benefit in the clinically high-risk population,” she said.
When asked about the use of MammaPrint in the United States, she said it is more common in Europe and other places in the world, whereas the use of Oncotype DX genetic testing seems to be more prevalent in the U.S.
News conference moderator Dr. Nancy Davidson, director of the University of Pittsburgh Cancer Institute, said that both tests are used at her institution. “I would say Oncotype is probably the dominant test that’s ordered,” she said. “But there are folks who are big fans of MammaPrint, and they’re going to be very excited to see these major results come out from this trial to help us to discuss this further and to think about how to guide our thinking and our patients.”
Entities and funding sources involved in the study included Adjuvant! Online, Agendia, Novartis, Roche, Sanofi-Aventis, Veridex, and Eli Lilly. Dr. Piccart disclosed that she is a board member of Radius, and a consultant for AstraZeneca, Eli Lilly, Invivus, Merck Sharp & Dohme, Novartis, Pfizer, Roche-Genentech, Synthon, Debiopharm, and PharmaMar. The Jules Bordet Institute receives grant/research funds from most companies in the field.
A large multinational European trial shows that genetic analysis of breast tumors can spare women unnecessary adjuvant chemotherapy, even when clinical factors indicate a high risk of recurrence.
Using MammaPrint, a 70-gene signature test, led to a 14% absolute reduction in the use of chemotherapy, compared with a clinical strategy, according to the highly anticipated results of the Phase III Microarray in Node-negative and 1 to 3 positive lymph node Disease may Avoid Chemo Therapy (MINDACT) trial, presented at the annual meeting of the American Association for Cancer Research.
While three decades of clinical trials have shown survival benefits of adjuvant chemotherapy, it carries later risks. “And it will happen when the survival gain associated with adjuvant chemotherapy is small, in the range of 2%-3% – it happens in good prognosis patients – and is counterbalanced by the long-term severe risks of adjuvant chemotherapy,” said Dr. Martine Piccart, director of medicine at the Jules Bordet Institute in Brussels, and principal investigator for the trial.
Risks include secondary cancers, cardiotoxicity, early menopause, and a decline in cognitive function, as well as negative socioeconomic effects. So avoiding chemotherapy when outcomes would be nearly the same without it is a reasonable goal.
To investigate the best method to determine which breast cancer patients could do just as well without adjuvant chemotherapy, European investigators at 111 centers in 9 countries screened 11,288 patients with early-stage disease and enrolled 6,693 in the MINDACT trial. Speaking at a news conference during the annual meeting, Dr. Piccart said MINDACT compared tumor genetic testing with clinical and pathology parameters to gauge the risk of disease recurrence and is the only trial to date to compare the utility of the two strategies.
MammaPrint is a genetic test (G) of early stage breast cancer tumors that produces a 70-gene signature indicating a high or low 10-year risk of metastatic recurrence. The Adjuvant! Online tool takes into account clinical factors and pathology markers, including a patient’s age and comorbidities and a tumor’s estrogen receptor status, grade, size, and the number of positive lymph nodes, to calculate a ten-year “clinical risk” (C) of negative outcomes with or without adjuvant chemotherapy or hormonal therapy.
After surgery, tissue samples underwent local pathology examination to determine tumor stage and nodal, hormone receptor, and HER2 status. Samples were also sent to a central facility for MammaPrint testing. For women with low-risk tumors by both tests, no chemotherapy was indicated. For high-risk tumors by both tests, chemotherapy was prescribed. But those with discordant results were randomized equally to receive chemotherapy or not.
MammaPrint better predictor than clinical factors
The median age of patients at enrollment was 55 years, 80% of tumors were node-negative, 58% were T1, 88% hormone receptor–positive, and 10% HER2-positive. At a median follow-up of 5 years, 362 (5.4%) women had distant metastases or had died.
Among 3,356 patients classified as high risk based on the Adjuvant! Online test, there were 1,550 classified by genetic criteria as low risk (C-High/G-Low), including 48% with positive nodes. For this C-High/G-Low group, the 5-year distant metastasis-free survival was greater than 94% regardless of adjuvant chemotherapy and was not statistically different for the two groups. These are patients who would normally be prescribed adjuvant chemotherapy if based solely on the C criteria.
Going by MammaPrint test results would thereby reduce chemotherapy prescriptions by 46% (1,550/3,356) for the study cohort. Considering the entire initial 11,288 patients screened, the genomic strategy would lead to a 14% absolute reduction in chemotherapy, compared with the clinical strategy, according to Dr. Piccart. “MINDACT results provide level 1A evidence of the clinical utility of MammaPrint for assessing the lack of a clinically relevant chemotherapy benefit in the clinically high-risk population,” she said.
When asked about the use of MammaPrint in the United States, she said it is more common in Europe and other places in the world, whereas the use of Oncotype DX genetic testing seems to be more prevalent in the U.S.
News conference moderator Dr. Nancy Davidson, director of the University of Pittsburgh Cancer Institute, said that both tests are used at her institution. “I would say Oncotype is probably the dominant test that’s ordered,” she said. “But there are folks who are big fans of MammaPrint, and they’re going to be very excited to see these major results come out from this trial to help us to discuss this further and to think about how to guide our thinking and our patients.”
Entities and funding sources involved in the study included Adjuvant! Online, Agendia, Novartis, Roche, Sanofi-Aventis, Veridex, and Eli Lilly. Dr. Piccart disclosed that she is a board member of Radius, and a consultant for AstraZeneca, Eli Lilly, Invivus, Merck Sharp & Dohme, Novartis, Pfizer, Roche-Genentech, Synthon, Debiopharm, and PharmaMar. The Jules Bordet Institute receives grant/research funds from most companies in the field.
A large multinational European trial shows that genetic analysis of breast tumors can spare women unnecessary adjuvant chemotherapy, even when clinical factors indicate a high risk of recurrence.
Using MammaPrint, a 70-gene signature test, led to a 14% absolute reduction in the use of chemotherapy, compared with a clinical strategy, according to the highly anticipated results of the Phase III Microarray in Node-negative and 1 to 3 positive lymph node Disease may Avoid Chemo Therapy (MINDACT) trial, presented at the annual meeting of the American Association for Cancer Research.
While three decades of clinical trials have shown survival benefits of adjuvant chemotherapy, it carries later risks. “And it will happen when the survival gain associated with adjuvant chemotherapy is small, in the range of 2%-3% – it happens in good prognosis patients – and is counterbalanced by the long-term severe risks of adjuvant chemotherapy,” said Dr. Martine Piccart, director of medicine at the Jules Bordet Institute in Brussels, and principal investigator for the trial.
Risks include secondary cancers, cardiotoxicity, early menopause, and a decline in cognitive function, as well as negative socioeconomic effects. So avoiding chemotherapy when outcomes would be nearly the same without it is a reasonable goal.
To investigate the best method to determine which breast cancer patients could do just as well without adjuvant chemotherapy, European investigators at 111 centers in 9 countries screened 11,288 patients with early-stage disease and enrolled 6,693 in the MINDACT trial. Speaking at a news conference during the annual meeting, Dr. Piccart said MINDACT compared tumor genetic testing with clinical and pathology parameters to gauge the risk of disease recurrence and is the only trial to date to compare the utility of the two strategies.
MammaPrint is a genetic test (G) of early stage breast cancer tumors that produces a 70-gene signature indicating a high or low 10-year risk of metastatic recurrence. The Adjuvant! Online tool takes into account clinical factors and pathology markers, including a patient’s age and comorbidities and a tumor’s estrogen receptor status, grade, size, and the number of positive lymph nodes, to calculate a ten-year “clinical risk” (C) of negative outcomes with or without adjuvant chemotherapy or hormonal therapy.
After surgery, tissue samples underwent local pathology examination to determine tumor stage and nodal, hormone receptor, and HER2 status. Samples were also sent to a central facility for MammaPrint testing. For women with low-risk tumors by both tests, no chemotherapy was indicated. For high-risk tumors by both tests, chemotherapy was prescribed. But those with discordant results were randomized equally to receive chemotherapy or not.
MammaPrint better predictor than clinical factors
The median age of patients at enrollment was 55 years, 80% of tumors were node-negative, 58% were T1, 88% hormone receptor–positive, and 10% HER2-positive. At a median follow-up of 5 years, 362 (5.4%) women had distant metastases or had died.
Among 3,356 patients classified as high risk based on the Adjuvant! Online test, there were 1,550 classified by genetic criteria as low risk (C-High/G-Low), including 48% with positive nodes. For this C-High/G-Low group, the 5-year distant metastasis-free survival was greater than 94% regardless of adjuvant chemotherapy and was not statistically different for the two groups. These are patients who would normally be prescribed adjuvant chemotherapy if based solely on the C criteria.
Going by MammaPrint test results would thereby reduce chemotherapy prescriptions by 46% (1,550/3,356) for the study cohort. Considering the entire initial 11,288 patients screened, the genomic strategy would lead to a 14% absolute reduction in chemotherapy, compared with the clinical strategy, according to Dr. Piccart. “MINDACT results provide level 1A evidence of the clinical utility of MammaPrint for assessing the lack of a clinically relevant chemotherapy benefit in the clinically high-risk population,” she said.
When asked about the use of MammaPrint in the United States, she said it is more common in Europe and other places in the world, whereas the use of Oncotype DX genetic testing seems to be more prevalent in the U.S.
News conference moderator Dr. Nancy Davidson, director of the University of Pittsburgh Cancer Institute, said that both tests are used at her institution. “I would say Oncotype is probably the dominant test that’s ordered,” she said. “But there are folks who are big fans of MammaPrint, and they’re going to be very excited to see these major results come out from this trial to help us to discuss this further and to think about how to guide our thinking and our patients.”
Entities and funding sources involved in the study included Adjuvant! Online, Agendia, Novartis, Roche, Sanofi-Aventis, Veridex, and Eli Lilly. Dr. Piccart disclosed that she is a board member of Radius, and a consultant for AstraZeneca, Eli Lilly, Invivus, Merck Sharp & Dohme, Novartis, Pfizer, Roche-Genentech, Synthon, Debiopharm, and PharmaMar. The Jules Bordet Institute receives grant/research funds from most companies in the field.
FROM THE AACR ANNUAL MEETING
Key clinical point: MammaPrint bests Adjuvant! Online for sparing low-risk patients from chemotherapy.
Major finding: Genotyping results in a 14% reduction in the use of chemotherapy, compared with a clinical strategy.
Data source: Phase III randomized controlled study of 6,693 women with early stage breast cancer.
Disclosures: Entities and funding sources involved in the study include Adjuvant! Online, Agendia, Novartis, Roche, Sanofi-Aventis, Veridex, and Eli Lilly. Dr. Piccart disclosed that she is a board member of Radius, and a consultant for AstraZeneca, Eli Lilly, Invivus, Merck Sharp & Dohme, Novartis, Pfizer, Roche-Genentech, Synthon, Debiopharm, and PharmaMar. The Jules Bordet Institute receives grant/research funds from most companies in the field.

Neratinib not superior to trastuzumab
Neratinib plus paclitaxel was found not superior to trastuzumab plus paclitaxel as first-line therapy for ERBB2-positive metastatic breast cancer in an international phase II trial, according to investigators.
Recent research had suggested that small-molecule ERBB2 kinase inhibitors might be particularly effective against CNS metastases in such cases, so investigators performed the open-label randomized clinical trial in 479 women at 188 medical centers. After a median follow-up of 23 months, the primary endpoint – median progression-free survival – was 12.9 months for both neratinib-paclitaxel and trastuzumab-paclitaxel, said Dr. Ahmad Awada of the Medical Oncology Clinic, Jules Bordet Institute, Brussels, and his associates.
This outcome was consistent across all subgroups of patients, regardless of age, race, area of residence, hormone receptor status, or prior exposure to trastuzumab. Neratinib also was not superior to trastuzumab in any of the secondary study endpoints, including objective response rate, duration of response, and clinical benefit rate. These findings suggest that the two agents have similar efficacy in this patient population, the investigators said (JAMA Oncol. 2016 April 14. [doi: 10.1001/jamaoncol.2016.0237).
However, neratinib was associated with a reduced frequency of symptomatic or progressive CNS recurrences (RR, 0.48), as well as a delayed onset of such recurrences (HR, 0.45), compared with trastuzumab. This finding warrants further investigation in a larger trial with predefined CNS end points, they noted.
Neratinib was associated with more frequent adverse effects than trastuzumab, chiefly diarrhea (92.5% vs 33.3%) and nausea (44.2% vs 30.3%). Grade 3 diarrhea developed in 30.4% of patients receiving neratinib, compared with 3.8% of those receiving trastuzumab, and diarrhea accounted for discontinuation of study treatment in 3.8% of patients receiving neratinib, compared with 0.4% of those receiving trastuzumab. Aggressive primary prophylaxis of diarrhea should now be required for the first cycle of neratinib therapy, Dr. Awada and his associates added.
Neratinib’s benefits regarding CNS progression could prove to be an important therapeutic advance, given the debilitating sequelae of brain metastases and the especially poor prognosis associated with CNS progression.
However, the agent’s toxic effects are considerable. Grade 2-3 diarrhea, which developed in 65.4% of the neratinib arm of this study and 11.1% of the trastuzumab arm, should be considered clinically unacceptable.
Dr. Mark D. Pegram is at Stanford (Calif.) University’s Women’s Cancer Center. He reported serving as a consultant to Pfizer and Genentech/Roche, on the data and safety monitoring committee for a trial of neratinib monotherapy, and on the steering committee for a trial sponsored by Oncothyreon. Dr. Pegram made these remarks in an editorial accompanying Dr. Awada’s report (JAMA Oncol. 2016 April 14. doi: 10.1001/jamaoncol.2016.0238).
Neratinib’s benefits regarding CNS progression could prove to be an important therapeutic advance, given the debilitating sequelae of brain metastases and the especially poor prognosis associated with CNS progression.
However, the agent’s toxic effects are considerable. Grade 2-3 diarrhea, which developed in 65.4% of the neratinib arm of this study and 11.1% of the trastuzumab arm, should be considered clinically unacceptable.
Dr. Mark D. Pegram is at Stanford (Calif.) University’s Women’s Cancer Center. He reported serving as a consultant to Pfizer and Genentech/Roche, on the data and safety monitoring committee for a trial of neratinib monotherapy, and on the steering committee for a trial sponsored by Oncothyreon. Dr. Pegram made these remarks in an editorial accompanying Dr. Awada’s report (JAMA Oncol. 2016 April 14. doi: 10.1001/jamaoncol.2016.0238).
Neratinib’s benefits regarding CNS progression could prove to be an important therapeutic advance, given the debilitating sequelae of brain metastases and the especially poor prognosis associated with CNS progression.
However, the agent’s toxic effects are considerable. Grade 2-3 diarrhea, which developed in 65.4% of the neratinib arm of this study and 11.1% of the trastuzumab arm, should be considered clinically unacceptable.
Dr. Mark D. Pegram is at Stanford (Calif.) University’s Women’s Cancer Center. He reported serving as a consultant to Pfizer and Genentech/Roche, on the data and safety monitoring committee for a trial of neratinib monotherapy, and on the steering committee for a trial sponsored by Oncothyreon. Dr. Pegram made these remarks in an editorial accompanying Dr. Awada’s report (JAMA Oncol. 2016 April 14. doi: 10.1001/jamaoncol.2016.0238).
Neratinib plus paclitaxel was found not superior to trastuzumab plus paclitaxel as first-line therapy for ERBB2-positive metastatic breast cancer in an international phase II trial, according to investigators.
Recent research had suggested that small-molecule ERBB2 kinase inhibitors might be particularly effective against CNS metastases in such cases, so investigators performed the open-label randomized clinical trial in 479 women at 188 medical centers. After a median follow-up of 23 months, the primary endpoint – median progression-free survival – was 12.9 months for both neratinib-paclitaxel and trastuzumab-paclitaxel, said Dr. Ahmad Awada of the Medical Oncology Clinic, Jules Bordet Institute, Brussels, and his associates.
This outcome was consistent across all subgroups of patients, regardless of age, race, area of residence, hormone receptor status, or prior exposure to trastuzumab. Neratinib also was not superior to trastuzumab in any of the secondary study endpoints, including objective response rate, duration of response, and clinical benefit rate. These findings suggest that the two agents have similar efficacy in this patient population, the investigators said (JAMA Oncol. 2016 April 14. [doi: 10.1001/jamaoncol.2016.0237).
However, neratinib was associated with a reduced frequency of symptomatic or progressive CNS recurrences (RR, 0.48), as well as a delayed onset of such recurrences (HR, 0.45), compared with trastuzumab. This finding warrants further investigation in a larger trial with predefined CNS end points, they noted.
Neratinib was associated with more frequent adverse effects than trastuzumab, chiefly diarrhea (92.5% vs 33.3%) and nausea (44.2% vs 30.3%). Grade 3 diarrhea developed in 30.4% of patients receiving neratinib, compared with 3.8% of those receiving trastuzumab, and diarrhea accounted for discontinuation of study treatment in 3.8% of patients receiving neratinib, compared with 0.4% of those receiving trastuzumab. Aggressive primary prophylaxis of diarrhea should now be required for the first cycle of neratinib therapy, Dr. Awada and his associates added.
Neratinib plus paclitaxel was found not superior to trastuzumab plus paclitaxel as first-line therapy for ERBB2-positive metastatic breast cancer in an international phase II trial, according to investigators.
Recent research had suggested that small-molecule ERBB2 kinase inhibitors might be particularly effective against CNS metastases in such cases, so investigators performed the open-label randomized clinical trial in 479 women at 188 medical centers. After a median follow-up of 23 months, the primary endpoint – median progression-free survival – was 12.9 months for both neratinib-paclitaxel and trastuzumab-paclitaxel, said Dr. Ahmad Awada of the Medical Oncology Clinic, Jules Bordet Institute, Brussels, and his associates.
This outcome was consistent across all subgroups of patients, regardless of age, race, area of residence, hormone receptor status, or prior exposure to trastuzumab. Neratinib also was not superior to trastuzumab in any of the secondary study endpoints, including objective response rate, duration of response, and clinical benefit rate. These findings suggest that the two agents have similar efficacy in this patient population, the investigators said (JAMA Oncol. 2016 April 14. [doi: 10.1001/jamaoncol.2016.0237).
However, neratinib was associated with a reduced frequency of symptomatic or progressive CNS recurrences (RR, 0.48), as well as a delayed onset of such recurrences (HR, 0.45), compared with trastuzumab. This finding warrants further investigation in a larger trial with predefined CNS end points, they noted.
Neratinib was associated with more frequent adverse effects than trastuzumab, chiefly diarrhea (92.5% vs 33.3%) and nausea (44.2% vs 30.3%). Grade 3 diarrhea developed in 30.4% of patients receiving neratinib, compared with 3.8% of those receiving trastuzumab, and diarrhea accounted for discontinuation of study treatment in 3.8% of patients receiving neratinib, compared with 0.4% of those receiving trastuzumab. Aggressive primary prophylaxis of diarrhea should now be required for the first cycle of neratinib therapy, Dr. Awada and his associates added.
FROM JAMA ONCOLOGY
Key clinical point: Neratinib plus paclitaxel was found not superior to trastuzumab plus paclitaxel for ERBB2-positive metastatic breast cancer.
Major finding: Median progression-free survival was 12.9 months for both neratinib-paclitaxel and trastuzumab-paclitaxel.
Data source: An international randomized controlled open-label phase II trial involving 479 patients followed for 2 years.
Disclosures: This trial was sponsored by Wyeth, Pfizer, and Puma Biotechnology, which were involved in the design and conduct of the study; the collection, analysis, and interpretation of the data; and the preparation of the report. Dr. Awada reported receiving an honorarium from Wyeth; his associates reported ties to numerous industry sources.
Racial disparities found in HER2-positive breast cancer care
There are significant racial disparities in the delivery of HER2-targeted therapy for breast cancer, investigators have found.
A review of Medicare beneficiaries with incident stage I-III HER2-positive breast cancer showed that black women were 25% less likely than white women to receive adjuvant trastuzumab (Herceptin) within a year of diagnosis, reported Dr. Katherine Reeder-Hayes and her colleagues at the University of North Carolina at Chapel Hill.
In addition, the investigators found that about one-half of Medicare-insured patients with HER2-positive tumors did not receive HER2-targeted therapy, despite the well-known clinical benefits in this population.
“These findings have several troubling implications. First, although this study did not examine survival outcomes, the low overall rates of use among patients with stage II and III disease raise concerns for widespread underuse of trastuzumab in this age group. Second, the racial findings suggest that the presence of a clear biologic predictor of treatment benefit, in this case the HER2 marker, does not mitigate the overall pattern of treatment disparity observed among black women with breast cancer,” they wrote (J Clin Oncol. 2016 April 11. doi: 10.1200/JCO.2015.65.8716).
The authors reviewed Surveillance, Epidemiology and End Results (SEER) Medicare data on 1,362 women with incidence stages I-III HER2-positive breast cancers in 2010 and 2011, and used insurance claims data to identify the use of adjuvant trastuzumab and chemotherapy agents within 12 months of diagnosis. The sample included 1,162 white women, 104 black women, and 96 women described as “other.”
The investigators found that just half of all white women (50%) and 40% of black women received at least some trastuzumab therapy.
In logistic regression analysis controlling for tumor characteristics, socioeconomic factors, and comorbidities, they found that compared with white women, black women had a risk ratio for receiving trastuzumab of 0.745 (P = .0097).
The investigators noted that in addition to the racial disparities, older women and those with more comorbidities were also less likely to get trastuzumab.
“However, given the sizeable benefit of trastuzumab, the overall aggressive biology of this subtype, and extensive literature documenting undertreatment of even healthy older patients, the hypothesis that age is used inappropriately to withhold trastuzumab-based therapy deserves further exploration,” they wrote.
The investigators called for the development of system-level interventions that can objectively identify patients eligible for HER2-targeted therapy, and for ongoing efforts to eradicate racial disparities in care.
The study was supported by grants from the National Institutes of Health and the University (NC) Cancer Research Fund.
There are significant racial disparities in the delivery of HER2-targeted therapy for breast cancer, investigators have found.
A review of Medicare beneficiaries with incident stage I-III HER2-positive breast cancer showed that black women were 25% less likely than white women to receive adjuvant trastuzumab (Herceptin) within a year of diagnosis, reported Dr. Katherine Reeder-Hayes and her colleagues at the University of North Carolina at Chapel Hill.
In addition, the investigators found that about one-half of Medicare-insured patients with HER2-positive tumors did not receive HER2-targeted therapy, despite the well-known clinical benefits in this population.
“These findings have several troubling implications. First, although this study did not examine survival outcomes, the low overall rates of use among patients with stage II and III disease raise concerns for widespread underuse of trastuzumab in this age group. Second, the racial findings suggest that the presence of a clear biologic predictor of treatment benefit, in this case the HER2 marker, does not mitigate the overall pattern of treatment disparity observed among black women with breast cancer,” they wrote (J Clin Oncol. 2016 April 11. doi: 10.1200/JCO.2015.65.8716).
The authors reviewed Surveillance, Epidemiology and End Results (SEER) Medicare data on 1,362 women with incidence stages I-III HER2-positive breast cancers in 2010 and 2011, and used insurance claims data to identify the use of adjuvant trastuzumab and chemotherapy agents within 12 months of diagnosis. The sample included 1,162 white women, 104 black women, and 96 women described as “other.”
The investigators found that just half of all white women (50%) and 40% of black women received at least some trastuzumab therapy.
In logistic regression analysis controlling for tumor characteristics, socioeconomic factors, and comorbidities, they found that compared with white women, black women had a risk ratio for receiving trastuzumab of 0.745 (P = .0097).
The investigators noted that in addition to the racial disparities, older women and those with more comorbidities were also less likely to get trastuzumab.
“However, given the sizeable benefit of trastuzumab, the overall aggressive biology of this subtype, and extensive literature documenting undertreatment of even healthy older patients, the hypothesis that age is used inappropriately to withhold trastuzumab-based therapy deserves further exploration,” they wrote.
The investigators called for the development of system-level interventions that can objectively identify patients eligible for HER2-targeted therapy, and for ongoing efforts to eradicate racial disparities in care.
The study was supported by grants from the National Institutes of Health and the University (NC) Cancer Research Fund.
There are significant racial disparities in the delivery of HER2-targeted therapy for breast cancer, investigators have found.
A review of Medicare beneficiaries with incident stage I-III HER2-positive breast cancer showed that black women were 25% less likely than white women to receive adjuvant trastuzumab (Herceptin) within a year of diagnosis, reported Dr. Katherine Reeder-Hayes and her colleagues at the University of North Carolina at Chapel Hill.
In addition, the investigators found that about one-half of Medicare-insured patients with HER2-positive tumors did not receive HER2-targeted therapy, despite the well-known clinical benefits in this population.
“These findings have several troubling implications. First, although this study did not examine survival outcomes, the low overall rates of use among patients with stage II and III disease raise concerns for widespread underuse of trastuzumab in this age group. Second, the racial findings suggest that the presence of a clear biologic predictor of treatment benefit, in this case the HER2 marker, does not mitigate the overall pattern of treatment disparity observed among black women with breast cancer,” they wrote (J Clin Oncol. 2016 April 11. doi: 10.1200/JCO.2015.65.8716).
The authors reviewed Surveillance, Epidemiology and End Results (SEER) Medicare data on 1,362 women with incidence stages I-III HER2-positive breast cancers in 2010 and 2011, and used insurance claims data to identify the use of adjuvant trastuzumab and chemotherapy agents within 12 months of diagnosis. The sample included 1,162 white women, 104 black women, and 96 women described as “other.”
The investigators found that just half of all white women (50%) and 40% of black women received at least some trastuzumab therapy.
In logistic regression analysis controlling for tumor characteristics, socioeconomic factors, and comorbidities, they found that compared with white women, black women had a risk ratio for receiving trastuzumab of 0.745 (P = .0097).
The investigators noted that in addition to the racial disparities, older women and those with more comorbidities were also less likely to get trastuzumab.
“However, given the sizeable benefit of trastuzumab, the overall aggressive biology of this subtype, and extensive literature documenting undertreatment of even healthy older patients, the hypothesis that age is used inappropriately to withhold trastuzumab-based therapy deserves further exploration,” they wrote.
The investigators called for the development of system-level interventions that can objectively identify patients eligible for HER2-targeted therapy, and for ongoing efforts to eradicate racial disparities in care.
The study was supported by grants from the National Institutes of Health and the University (NC) Cancer Research Fund.
FROM THE JOURNAL OF CLINICAL ONCOLOGY
Key clinical point: Trastuzumab is known to be beneficial in women with HER2-positive breast cancer, but black women were less likely to receive it than white women.
Major finding: Only 50% of white women and 40% of black women with HER2-positive cancers received trastuzumab.
Data source: A retrospective study of SEER Medicare data on 1,362 women with stage I-III HER2-positive breast cancer.
Disclosures: The study was supported by grants from the National Institutes of Health and the University (NC) Cancer Research Fund.
NCCN breast cancer RT guidelines: hypofractionation preferred
HOLLYWOOD, FLA. – No huge surprises here, but newly revised National Comprehensive Cancer Network guidelines for locoregional therapy of breast cancer help clarify the optimal use of adjuvant radiation.
For example, updates to the pages on principles of radiation therapy in invasive breast cancer contain new information on optimal dosing, fractionation, treatment planning, and techniques for minimizing radiation of surrounding normal tissues, noted Dr. Kilian E. Salerno, director of breast radiation and soft tissue/melanoma radiation at the Roswell Park Cancer Institute in Buffalo, New York.

“There are a number of treatment options, many more now than ever before,” she said at the annual conference of the National Comprehensive Cancer Network.
The guidelines emphasize the importance of individualized radiation therapy planning and delivery. A CT-based treatment plan can help clinicians choose target volumes and identify adjacent organs and tissues that may be at risk for radiation spill.
Recommended options for reducing radiation doses to adjacent tissues include deep breath holds and prone positioning so that the treated breast hangs down, helping to isolate it from the heart and lungs.
Whole breast irradiation
Whole breast irradiation is the standard for radiation therapy of early breast cancer following breast-conserving surgery, although partial breast irradiation, typically of lumpectomy cavities, is also commonly performed, Dr. Salerno said.
Boost radiation in conjunction with breast conserving therapy can be delivered via en face electron fields, photons, or brachytherapy; boost dosing to chest wall scar is usually treated with photons or electrons, the guidelines note.
The guidelines recommend weekly imaging to ensure that daily treatment setup is consistent, but caution against routine use of daily imaging.
For whole breast irradiation, the guidelines recommend either doses of 46-50 Gy divided into 23-25 fractions (conventional fractionation), or, preferably, hypofractionated radiation delivered in doses of 40-42.5 Gy over 15-16 fractions, with all doses given 5 days per week. Patients at higher risk for recurrence should receive boost doses to the tumor bed, typically at doses of 10-16 Gy delivered in 4-8 fractions.
The guidelines now favor hypofractionation based on long-term results from clinical trials conducted in Ontario, Canada, and in London.
In the Canadian trial (N Engl J Med. 2010;362:513-20), patients were treated with whole-breast irradiation at doses of 42.5 Gy in 16 fractions, with no boost dose.
In the Standardisation of Breast Radiotherapy B (START B) trial (Lancet Oncol. 14;11:1086-94), in London, patients received 40 Gy in 15 fractions without a boost dose.
Both trials showed that hypofractionation was associated with disease outcomes that were equivalent or better to those seen with conventional fractionation schedules, as well as equivalent or better cosmesis and adverse event profiles, Dr. Salerno said.
“This is for whole breast radiation; it is not to be routinely used in the post-mastectomy setting or when you’re treating regional nodes,” she said.
Accelerated partial breast irradiation
For accelerated partial breast irradiation (APBI), the guidelines recommend a hypofractionated schedule of 34 Gy divided into 10 fractions delivered twice daily for 5 days for brachytherapy, or 38.5 Gy in 10 twice daily fractions with external beam therapy to the tumor bed.
The NCCN guidelines for APBI are based on the American Society of Radiation Oncology (ASTRO) consensus statement for APBI. An updated statement is planned for 2017.
Omit radiation?
Results from the CALGB 9343 trial and other studies suggest that in selected women with lower risk for recurrence, radiation can be omitted without compromising survival. These include women aged 70 or older with small primary breast cancers, negative nodes, negative surgical margins, and hormone-receptor-positive disease who are treated with breast conserving surgery and go on to tamoxifen maintenance.
Post-mastectomy radiation
Following total mastectomy with surgical axillary staging, with our without reconstruction, the guidelines recommend specific steps based on the number of nodes involved and the tumor size and/or margin status.
Thus, women with four or more positive axillary nodes should receive radiation to the chest wall and infraclavicular region, supraclavicular area, internal mammary nodes, and any at-risk part of the axillary bed. If adjuvant chemotherapy is prescribed, radiation usually is given following chemotherapy completion.
For women with one to three positive axillary nodes, the guidelines urge clinicians to “strongly consider” treating them as they would women with four or more positive nodes. The same advice applies to women with negative nodes but tumors larger than 5 cm or positive surgical margins as defined by ink on tumor.
For patients with negative nodes, tumors 5 cm or smaller and negative but narrow margins (less than 1 mm), the guidelines recommend consideration of radiation to the chest wall. Patients with small tumors, no nodal involvement, and margins 1 mm or greater can be spared radiation therapy.
Recurrence
For women with local-only recurrence, the guidelines recommend mastectomy with axillary lymph node staging for those with recurrences after initial lumpectomy and radiation, or if the initial treatment was mastectomy with no radiation, surgical resection with radiation, or surgical resection alone for those women previously treated with mastectomy and radiation.
For regional or locoregional recurrences, the guidelines recommend that axillary recurrences be treated with surgery and radiation if possible, and that supraclavicular or internal mammary node recurrences be treated with radiation therapy, if possible.
HOLLYWOOD, FLA. – No huge surprises here, but newly revised National Comprehensive Cancer Network guidelines for locoregional therapy of breast cancer help clarify the optimal use of adjuvant radiation.
For example, updates to the pages on principles of radiation therapy in invasive breast cancer contain new information on optimal dosing, fractionation, treatment planning, and techniques for minimizing radiation of surrounding normal tissues, noted Dr. Kilian E. Salerno, director of breast radiation and soft tissue/melanoma radiation at the Roswell Park Cancer Institute in Buffalo, New York.
“There are a number of treatment options, many more now than ever before,” she said at the annual conference of the National Comprehensive Cancer Network.
The guidelines emphasize the importance of individualized radiation therapy planning and delivery. A CT-based treatment plan can help clinicians choose target volumes and identify adjacent organs and tissues that may be at risk for radiation spill.
Recommended options for reducing radiation doses to adjacent tissues include deep breath holds and prone positioning so that the treated breast hangs down, helping to isolate it from the heart and lungs.
Whole breast irradiation
Whole breast irradiation is the standard for radiation therapy of early breast cancer following breast-conserving surgery, although partial breast irradiation, typically of lumpectomy cavities, is also commonly performed, Dr. Salerno said.
Boost radiation in conjunction with breast conserving therapy can be delivered via en face electron fields, photons, or brachytherapy; boost dosing to chest wall scar is usually treated with photons or electrons, the guidelines note.
The guidelines recommend weekly imaging to ensure that daily treatment setup is consistent, but caution against routine use of daily imaging.
For whole breast irradiation, the guidelines recommend either doses of 46-50 Gy divided into 23-25 fractions (conventional fractionation), or, preferably, hypofractionated radiation delivered in doses of 40-42.5 Gy over 15-16 fractions, with all doses given 5 days per week. Patients at higher risk for recurrence should receive boost doses to the tumor bed, typically at doses of 10-16 Gy delivered in 4-8 fractions.
The guidelines now favor hypofractionation based on long-term results from clinical trials conducted in Ontario, Canada, and in London.
In the Canadian trial (N Engl J Med. 2010;362:513-20), patients were treated with whole-breast irradiation at doses of 42.5 Gy in 16 fractions, with no boost dose.
In the Standardisation of Breast Radiotherapy B (START B) trial (Lancet Oncol. 14;11:1086-94), in London, patients received 40 Gy in 15 fractions without a boost dose.
Both trials showed that hypofractionation was associated with disease outcomes that were equivalent or better to those seen with conventional fractionation schedules, as well as equivalent or better cosmesis and adverse event profiles, Dr. Salerno said.
“This is for whole breast radiation; it is not to be routinely used in the post-mastectomy setting or when you’re treating regional nodes,” she said.
Accelerated partial breast irradiation
For accelerated partial breast irradiation (APBI), the guidelines recommend a hypofractionated schedule of 34 Gy divided into 10 fractions delivered twice daily for 5 days for brachytherapy, or 38.5 Gy in 10 twice daily fractions with external beam therapy to the tumor bed.
The NCCN guidelines for APBI are based on the American Society of Radiation Oncology (ASTRO) consensus statement for APBI. An updated statement is planned for 2017.
Omit radiation?
Results from the CALGB 9343 trial and other studies suggest that in selected women with lower risk for recurrence, radiation can be omitted without compromising survival. These include women aged 70 or older with small primary breast cancers, negative nodes, negative surgical margins, and hormone-receptor-positive disease who are treated with breast conserving surgery and go on to tamoxifen maintenance.
Post-mastectomy radiation
Following total mastectomy with surgical axillary staging, with our without reconstruction, the guidelines recommend specific steps based on the number of nodes involved and the tumor size and/or margin status.
Thus, women with four or more positive axillary nodes should receive radiation to the chest wall and infraclavicular region, supraclavicular area, internal mammary nodes, and any at-risk part of the axillary bed. If adjuvant chemotherapy is prescribed, radiation usually is given following chemotherapy completion.
For women with one to three positive axillary nodes, the guidelines urge clinicians to “strongly consider” treating them as they would women with four or more positive nodes. The same advice applies to women with negative nodes but tumors larger than 5 cm or positive surgical margins as defined by ink on tumor.
For patients with negative nodes, tumors 5 cm or smaller and negative but narrow margins (less than 1 mm), the guidelines recommend consideration of radiation to the chest wall. Patients with small tumors, no nodal involvement, and margins 1 mm or greater can be spared radiation therapy.
Recurrence
For women with local-only recurrence, the guidelines recommend mastectomy with axillary lymph node staging for those with recurrences after initial lumpectomy and radiation, or if the initial treatment was mastectomy with no radiation, surgical resection with radiation, or surgical resection alone for those women previously treated with mastectomy and radiation.
For regional or locoregional recurrences, the guidelines recommend that axillary recurrences be treated with surgery and radiation if possible, and that supraclavicular or internal mammary node recurrences be treated with radiation therapy, if possible.
HOLLYWOOD, FLA. – No huge surprises here, but newly revised National Comprehensive Cancer Network guidelines for locoregional therapy of breast cancer help clarify the optimal use of adjuvant radiation.
For example, updates to the pages on principles of radiation therapy in invasive breast cancer contain new information on optimal dosing, fractionation, treatment planning, and techniques for minimizing radiation of surrounding normal tissues, noted Dr. Kilian E. Salerno, director of breast radiation and soft tissue/melanoma radiation at the Roswell Park Cancer Institute in Buffalo, New York.
“There are a number of treatment options, many more now than ever before,” she said at the annual conference of the National Comprehensive Cancer Network.
The guidelines emphasize the importance of individualized radiation therapy planning and delivery. A CT-based treatment plan can help clinicians choose target volumes and identify adjacent organs and tissues that may be at risk for radiation spill.
Recommended options for reducing radiation doses to adjacent tissues include deep breath holds and prone positioning so that the treated breast hangs down, helping to isolate it from the heart and lungs.
Whole breast irradiation
Whole breast irradiation is the standard for radiation therapy of early breast cancer following breast-conserving surgery, although partial breast irradiation, typically of lumpectomy cavities, is also commonly performed, Dr. Salerno said.
Boost radiation in conjunction with breast conserving therapy can be delivered via en face electron fields, photons, or brachytherapy; boost dosing to chest wall scar is usually treated with photons or electrons, the guidelines note.
The guidelines recommend weekly imaging to ensure that daily treatment setup is consistent, but caution against routine use of daily imaging.
For whole breast irradiation, the guidelines recommend either doses of 46-50 Gy divided into 23-25 fractions (conventional fractionation), or, preferably, hypofractionated radiation delivered in doses of 40-42.5 Gy over 15-16 fractions, with all doses given 5 days per week. Patients at higher risk for recurrence should receive boost doses to the tumor bed, typically at doses of 10-16 Gy delivered in 4-8 fractions.
The guidelines now favor hypofractionation based on long-term results from clinical trials conducted in Ontario, Canada, and in London.
In the Canadian trial (N Engl J Med. 2010;362:513-20), patients were treated with whole-breast irradiation at doses of 42.5 Gy in 16 fractions, with no boost dose.
In the Standardisation of Breast Radiotherapy B (START B) trial (Lancet Oncol. 14;11:1086-94), in London, patients received 40 Gy in 15 fractions without a boost dose.
Both trials showed that hypofractionation was associated with disease outcomes that were equivalent or better to those seen with conventional fractionation schedules, as well as equivalent or better cosmesis and adverse event profiles, Dr. Salerno said.
“This is for whole breast radiation; it is not to be routinely used in the post-mastectomy setting or when you’re treating regional nodes,” she said.
Accelerated partial breast irradiation
For accelerated partial breast irradiation (APBI), the guidelines recommend a hypofractionated schedule of 34 Gy divided into 10 fractions delivered twice daily for 5 days for brachytherapy, or 38.5 Gy in 10 twice daily fractions with external beam therapy to the tumor bed.
The NCCN guidelines for APBI are based on the American Society of Radiation Oncology (ASTRO) consensus statement for APBI. An updated statement is planned for 2017.
Omit radiation?
Results from the CALGB 9343 trial and other studies suggest that in selected women with lower risk for recurrence, radiation can be omitted without compromising survival. These include women aged 70 or older with small primary breast cancers, negative nodes, negative surgical margins, and hormone-receptor-positive disease who are treated with breast conserving surgery and go on to tamoxifen maintenance.
Post-mastectomy radiation
Following total mastectomy with surgical axillary staging, with our without reconstruction, the guidelines recommend specific steps based on the number of nodes involved and the tumor size and/or margin status.
Thus, women with four or more positive axillary nodes should receive radiation to the chest wall and infraclavicular region, supraclavicular area, internal mammary nodes, and any at-risk part of the axillary bed. If adjuvant chemotherapy is prescribed, radiation usually is given following chemotherapy completion.
For women with one to three positive axillary nodes, the guidelines urge clinicians to “strongly consider” treating them as they would women with four or more positive nodes. The same advice applies to women with negative nodes but tumors larger than 5 cm or positive surgical margins as defined by ink on tumor.
For patients with negative nodes, tumors 5 cm or smaller and negative but narrow margins (less than 1 mm), the guidelines recommend consideration of radiation to the chest wall. Patients with small tumors, no nodal involvement, and margins 1 mm or greater can be spared radiation therapy.
Recurrence
For women with local-only recurrence, the guidelines recommend mastectomy with axillary lymph node staging for those with recurrences after initial lumpectomy and radiation, or if the initial treatment was mastectomy with no radiation, surgical resection with radiation, or surgical resection alone for those women previously treated with mastectomy and radiation.
For regional or locoregional recurrences, the guidelines recommend that axillary recurrences be treated with surgery and radiation if possible, and that supraclavicular or internal mammary node recurrences be treated with radiation therapy, if possible.
AT THE NCCN ANNUAL CONFERENCE
Key clinical point: NCCN guidelines on radiation therapy for locoregional treatment of breast cancer emphasize hypofractionated whole-breast irradiation for treatment of early disease.
Major finding: In clinical trials, hypofractionated whole-breast irradiation was equivalent to or better than conventional fractionation for disease control, cosmesis, and adverse events.
Data source: Review of updated NCCN guidelines and supporting evidence.
Disclosures: Dr. Salerno reported having no relevant disclosures.

NCCN fine-tunes breast cancer guidelines
HOLLYWOOD, FLA. – The latest updates to the National Comprehensive Cancer Network guidelines on breast cancer reflect a more nuanced approach to the use of systemic therapy in both the pre- and postoperative settings, with increasing emphasis on tailoring therapies to the unique clinical profiles of individual patients, according to Dr. William Gradishar.
The revised guidelines include new recommendations about preoperative endocrine and HER2-directed therapies, optimizing adjuvant endocrine therapy in both pre- and postmenopausal women, targeted agents as partner drugs for endocrine therapy in women with metastatic breast cancer, and recommendations about preservation of fertility in younger patients, said Dr. Gradishar, chair of the Robert H. Lurie Comprehensive Cancer Center at Northwestern University in Chicago.

“There have been some tweaks but I wouldn’t say major, major changes within the guidelines,” he said at the annual conference of the National Comprehensive Cancer Network.
Neoadjuvant therapy
One of the larger changes to this year’s guidelines is the addition of a page devoted to the principles of preoperative systemic therapy. The guidelines note that randomized clinical trials have shown similar long-term outcomes when patients receive the same treatment in either the pre- or post-op setting.
They add, however, that neoadjuvant systemic therapy “can render surgically inoperable tumors operable and offers potential benefits for patients with operable breast cancer. Importantly, preoperative systemic therapy can improve rates of breast conservation therapy eligibility and provides an opportunity to observe clinical and pathologic response to systemic therapy in an individual patient.”
The guidelines also note that a pathologic complete response to preoperative systemic therapy is predictive of “extremely favorable” disease-free and overall survival.
Patients who may be good candidates for neoadjuvant endocrine therapy include those with estrogen receptor–rich tumors (Allred score, 7 or 8), older postmenopausal women, and younger, premenopausal women with significant comorbidities that may make them poor candidates for chemotherapy, Dr. Gradishar said.
Adjuvant therapy
Regarding adjuvant therapy, the guidelines reflect data from recent clinical trials showing the benefits of both extended tamoxifen therapy, and for women who are premenopausal at diagnosis and are at high risk of recurrence, an aromatase inhibitor (AI) or steroidal aromatase inactivator plus ovarian suppression or ablation.
The recommendation to consider an AI and ovarian suppression in this population is based on data from the SOFT and TEXT trials (N Engl J Med. 2014; 371:107-18), which showed a significant reduction in the recurrence of hormone receptor–positive early breast cancer in premenopausal women treated with exemestane (Aromasin) and ovarian suppression, compared with tamoxifen and ovarian suppression.
Although data supporting the use of endocrine therapy and ovarian suppression are compelling, “we have to individualize our choice of which patient is appropriate for this, because there is a price to pay in terms of side effects, and we have to figure out if that balance is right for an individual patient,” Dr. Gradishar commented.
Anti-HER2 therapy
The guidelines state that patients with HER2-positive tumors should receive neoadjuvant systemic therapy with trastuzumab (Herceptin) for at least 9 weeks prior to surgery. For patients with stage T2 or greater or nodal status N1 or greater HER2-positive disease, a pertuzumab (Perjeta)-containing regimen may be considered.
Recurrent/Stage IV disease
Premenopausal women with recurrent or stage IV hormone receptor–positive disease should have ovarian ablation or suppression, and then be treated with a regimen for postmenopausal women, the guidelines say. Agents used in therapy for advanced disease have included a nonsteroidal or steroidal AI, a combination of exmestane and everolimus, palbociclib (Ibrance) plus letrozole (Femara), palbociclib plus fulvestrant, tamoxifen, or toremafine, megesterol acetate fluoxymesterone, or ethinyl estradiol.
The updated guidelines note that “a single study (S0226) in women with hormone receptor–positive breast cancer and no prior chemotherapy, biological therapy, or endocrine therapy for metastatic disease demonstrated that the addition of fulvestrant to anastrozole resulted in prolongation of time to progression. Subset analysis suggested that patients without prior adjuvant tamoxifen and more than 10 years since diagnosis experienced the greatest benefit. Two studies with similar design (FACT and SOFEA) demonstrated no advantage in time to progression with the addition of fulvestrant to anastrozole.”
Chemotherapy regimens for recurrent/metastatic breast cancer include various combination regimens, as well as single-agent therapy with anthracyclines, taxanes, antimetabolites, or microtubule inhibitors (all of the above preferred single agents), or with cyclophosphamide, carboplatin, docetaxel, albumin-bound paclitaxel, cisplatin, epirubicin, or ixabepilone.
For HER2-positive disease, preferred agents include pertuzumab and trastuzumab with either docetaxel (category 1 recommendation) or paclitaxel. Trastuzumab can also be combined with other agents such as paclitaxel with or without cisplatin, docetaxel, vinorelbine, or capecitabine.
For patients with recurrent HER2-positve disease with prior trastuzumab exposure, combinations may include lapatinin with capecitabine, or trastuzumab with capecitabine, lapatinib (without cytoxic therapy), or other agents.
Fertility preservation
Lastly, the revised guidelines note that all premenopausal patients should be informed about the potential effects of chemotherapy on fertility, with women who express the wish to have future pregnancies referred to fertility specialists. The options presented should be “based on patient specifics, disease stage, and biology (which determine the urgency and type and sequence of treatment). Timing and duration allowed for fertility preservation, options inclusive of oocyte and embryo cryopreservation as well as evolving technologies, and the probability of successful pregnancies subsequent to completion of breast cancer therapy are also to be discussed,” the guidelines say.
HOLLYWOOD, FLA. – The latest updates to the National Comprehensive Cancer Network guidelines on breast cancer reflect a more nuanced approach to the use of systemic therapy in both the pre- and postoperative settings, with increasing emphasis on tailoring therapies to the unique clinical profiles of individual patients, according to Dr. William Gradishar.
The revised guidelines include new recommendations about preoperative endocrine and HER2-directed therapies, optimizing adjuvant endocrine therapy in both pre- and postmenopausal women, targeted agents as partner drugs for endocrine therapy in women with metastatic breast cancer, and recommendations about preservation of fertility in younger patients, said Dr. Gradishar, chair of the Robert H. Lurie Comprehensive Cancer Center at Northwestern University in Chicago.
“There have been some tweaks but I wouldn’t say major, major changes within the guidelines,” he said at the annual conference of the National Comprehensive Cancer Network.
Neoadjuvant therapy
One of the larger changes to this year’s guidelines is the addition of a page devoted to the principles of preoperative systemic therapy. The guidelines note that randomized clinical trials have shown similar long-term outcomes when patients receive the same treatment in either the pre- or post-op setting.
They add, however, that neoadjuvant systemic therapy “can render surgically inoperable tumors operable and offers potential benefits for patients with operable breast cancer. Importantly, preoperative systemic therapy can improve rates of breast conservation therapy eligibility and provides an opportunity to observe clinical and pathologic response to systemic therapy in an individual patient.”
The guidelines also note that a pathologic complete response to preoperative systemic therapy is predictive of “extremely favorable” disease-free and overall survival.
Patients who may be good candidates for neoadjuvant endocrine therapy include those with estrogen receptor–rich tumors (Allred score, 7 or 8), older postmenopausal women, and younger, premenopausal women with significant comorbidities that may make them poor candidates for chemotherapy, Dr. Gradishar said.
Adjuvant therapy
Regarding adjuvant therapy, the guidelines reflect data from recent clinical trials showing the benefits of both extended tamoxifen therapy, and for women who are premenopausal at diagnosis and are at high risk of recurrence, an aromatase inhibitor (AI) or steroidal aromatase inactivator plus ovarian suppression or ablation.
The recommendation to consider an AI and ovarian suppression in this population is based on data from the SOFT and TEXT trials (N Engl J Med. 2014; 371:107-18), which showed a significant reduction in the recurrence of hormone receptor–positive early breast cancer in premenopausal women treated with exemestane (Aromasin) and ovarian suppression, compared with tamoxifen and ovarian suppression.
Although data supporting the use of endocrine therapy and ovarian suppression are compelling, “we have to individualize our choice of which patient is appropriate for this, because there is a price to pay in terms of side effects, and we have to figure out if that balance is right for an individual patient,” Dr. Gradishar commented.
Anti-HER2 therapy
The guidelines state that patients with HER2-positive tumors should receive neoadjuvant systemic therapy with trastuzumab (Herceptin) for at least 9 weeks prior to surgery. For patients with stage T2 or greater or nodal status N1 or greater HER2-positive disease, a pertuzumab (Perjeta)-containing regimen may be considered.
Recurrent/Stage IV disease
Premenopausal women with recurrent or stage IV hormone receptor–positive disease should have ovarian ablation or suppression, and then be treated with a regimen for postmenopausal women, the guidelines say. Agents used in therapy for advanced disease have included a nonsteroidal or steroidal AI, a combination of exmestane and everolimus, palbociclib (Ibrance) plus letrozole (Femara), palbociclib plus fulvestrant, tamoxifen, or toremafine, megesterol acetate fluoxymesterone, or ethinyl estradiol.
The updated guidelines note that “a single study (S0226) in women with hormone receptor–positive breast cancer and no prior chemotherapy, biological therapy, or endocrine therapy for metastatic disease demonstrated that the addition of fulvestrant to anastrozole resulted in prolongation of time to progression. Subset analysis suggested that patients without prior adjuvant tamoxifen and more than 10 years since diagnosis experienced the greatest benefit. Two studies with similar design (FACT and SOFEA) demonstrated no advantage in time to progression with the addition of fulvestrant to anastrozole.”
Chemotherapy regimens for recurrent/metastatic breast cancer include various combination regimens, as well as single-agent therapy with anthracyclines, taxanes, antimetabolites, or microtubule inhibitors (all of the above preferred single agents), or with cyclophosphamide, carboplatin, docetaxel, albumin-bound paclitaxel, cisplatin, epirubicin, or ixabepilone.
For HER2-positive disease, preferred agents include pertuzumab and trastuzumab with either docetaxel (category 1 recommendation) or paclitaxel. Trastuzumab can also be combined with other agents such as paclitaxel with or without cisplatin, docetaxel, vinorelbine, or capecitabine.
For patients with recurrent HER2-positve disease with prior trastuzumab exposure, combinations may include lapatinin with capecitabine, or trastuzumab with capecitabine, lapatinib (without cytoxic therapy), or other agents.
Fertility preservation
Lastly, the revised guidelines note that all premenopausal patients should be informed about the potential effects of chemotherapy on fertility, with women who express the wish to have future pregnancies referred to fertility specialists. The options presented should be “based on patient specifics, disease stage, and biology (which determine the urgency and type and sequence of treatment). Timing and duration allowed for fertility preservation, options inclusive of oocyte and embryo cryopreservation as well as evolving technologies, and the probability of successful pregnancies subsequent to completion of breast cancer therapy are also to be discussed,” the guidelines say.
HOLLYWOOD, FLA. – The latest updates to the National Comprehensive Cancer Network guidelines on breast cancer reflect a more nuanced approach to the use of systemic therapy in both the pre- and postoperative settings, with increasing emphasis on tailoring therapies to the unique clinical profiles of individual patients, according to Dr. William Gradishar.
The revised guidelines include new recommendations about preoperative endocrine and HER2-directed therapies, optimizing adjuvant endocrine therapy in both pre- and postmenopausal women, targeted agents as partner drugs for endocrine therapy in women with metastatic breast cancer, and recommendations about preservation of fertility in younger patients, said Dr. Gradishar, chair of the Robert H. Lurie Comprehensive Cancer Center at Northwestern University in Chicago.
“There have been some tweaks but I wouldn’t say major, major changes within the guidelines,” he said at the annual conference of the National Comprehensive Cancer Network.
Neoadjuvant therapy
One of the larger changes to this year’s guidelines is the addition of a page devoted to the principles of preoperative systemic therapy. The guidelines note that randomized clinical trials have shown similar long-term outcomes when patients receive the same treatment in either the pre- or post-op setting.
They add, however, that neoadjuvant systemic therapy “can render surgically inoperable tumors operable and offers potential benefits for patients with operable breast cancer. Importantly, preoperative systemic therapy can improve rates of breast conservation therapy eligibility and provides an opportunity to observe clinical and pathologic response to systemic therapy in an individual patient.”
The guidelines also note that a pathologic complete response to preoperative systemic therapy is predictive of “extremely favorable” disease-free and overall survival.
Patients who may be good candidates for neoadjuvant endocrine therapy include those with estrogen receptor–rich tumors (Allred score, 7 or 8), older postmenopausal women, and younger, premenopausal women with significant comorbidities that may make them poor candidates for chemotherapy, Dr. Gradishar said.
Adjuvant therapy
Regarding adjuvant therapy, the guidelines reflect data from recent clinical trials showing the benefits of both extended tamoxifen therapy, and for women who are premenopausal at diagnosis and are at high risk of recurrence, an aromatase inhibitor (AI) or steroidal aromatase inactivator plus ovarian suppression or ablation.
The recommendation to consider an AI and ovarian suppression in this population is based on data from the SOFT and TEXT trials (N Engl J Med. 2014; 371:107-18), which showed a significant reduction in the recurrence of hormone receptor–positive early breast cancer in premenopausal women treated with exemestane (Aromasin) and ovarian suppression, compared with tamoxifen and ovarian suppression.
Although data supporting the use of endocrine therapy and ovarian suppression are compelling, “we have to individualize our choice of which patient is appropriate for this, because there is a price to pay in terms of side effects, and we have to figure out if that balance is right for an individual patient,” Dr. Gradishar commented.
Anti-HER2 therapy
The guidelines state that patients with HER2-positive tumors should receive neoadjuvant systemic therapy with trastuzumab (Herceptin) for at least 9 weeks prior to surgery. For patients with stage T2 or greater or nodal status N1 or greater HER2-positive disease, a pertuzumab (Perjeta)-containing regimen may be considered.
Recurrent/Stage IV disease
Premenopausal women with recurrent or stage IV hormone receptor–positive disease should have ovarian ablation or suppression, and then be treated with a regimen for postmenopausal women, the guidelines say. Agents used in therapy for advanced disease have included a nonsteroidal or steroidal AI, a combination of exmestane and everolimus, palbociclib (Ibrance) plus letrozole (Femara), palbociclib plus fulvestrant, tamoxifen, or toremafine, megesterol acetate fluoxymesterone, or ethinyl estradiol.
The updated guidelines note that “a single study (S0226) in women with hormone receptor–positive breast cancer and no prior chemotherapy, biological therapy, or endocrine therapy for metastatic disease demonstrated that the addition of fulvestrant to anastrozole resulted in prolongation of time to progression. Subset analysis suggested that patients without prior adjuvant tamoxifen and more than 10 years since diagnosis experienced the greatest benefit. Two studies with similar design (FACT and SOFEA) demonstrated no advantage in time to progression with the addition of fulvestrant to anastrozole.”
Chemotherapy regimens for recurrent/metastatic breast cancer include various combination regimens, as well as single-agent therapy with anthracyclines, taxanes, antimetabolites, or microtubule inhibitors (all of the above preferred single agents), or with cyclophosphamide, carboplatin, docetaxel, albumin-bound paclitaxel, cisplatin, epirubicin, or ixabepilone.
For HER2-positive disease, preferred agents include pertuzumab and trastuzumab with either docetaxel (category 1 recommendation) or paclitaxel. Trastuzumab can also be combined with other agents such as paclitaxel with or without cisplatin, docetaxel, vinorelbine, or capecitabine.
For patients with recurrent HER2-positve disease with prior trastuzumab exposure, combinations may include lapatinin with capecitabine, or trastuzumab with capecitabine, lapatinib (without cytoxic therapy), or other agents.
Fertility preservation
Lastly, the revised guidelines note that all premenopausal patients should be informed about the potential effects of chemotherapy on fertility, with women who express the wish to have future pregnancies referred to fertility specialists. The options presented should be “based on patient specifics, disease stage, and biology (which determine the urgency and type and sequence of treatment). Timing and duration allowed for fertility preservation, options inclusive of oocyte and embryo cryopreservation as well as evolving technologies, and the probability of successful pregnancies subsequent to completion of breast cancer therapy are also to be discussed,” the guidelines say.
AT THE NCCN ANNUAL CONFERENCE

Feds advance cancer moonshot with expert panel, outline of goals
Federal officials took the next step in their moonshot to end cancer by announcing on April 4 a blue ribbon panel to guide the effort.
A total of 28 leading researchers, clinicians, and patient advocates have been named to the panel charged with informing the scientific direction and goals of the National Cancer Moonshot Initiative, led by Vice President Joe Biden.
“This Blue Ribbon Panel will ensure that, as [the National Institutes of Health] allocates new resources through the Moonshot, decisions will be grounded in the best science,” Vice President Biden said in a statement. “I look forward to working with this panel and many others involved with the Moonshot to make unprecedented improvements in prevention, diagnosis, and treatment of cancer.”
The key goals of the initiative were set out simultaneously in a perspective from Dr. Francis S. Collins, NIH director, and Dr. Douglas R. Lowy, director of the National Cancer Institute. The editorial was published in the New England Journal of Medicine.
“Fueled by an additional $680 million in the proposed fiscal year 2017 budget for the NIH, plus additional resources for the Food and Drug Administration, the initiative will aim to accelerate progress toward the next generation of interventions that we hope will substantially reduce cancer incidence and dramatically improve patient outcomes,” Dr. Collins and Dr. Lowy wrote. “The NIH’s most compelling opportunities for progress will be set forth by late summer 2016 in a research plan informed by the deliberations of a blue-ribbon panel of experts, which will provide scientific input to the National Cancer Advisory Board. Some possible opportunities include vaccine development, early-detection technology, single-cell genomic analysis, immunotherapy, a focus on pediatric cancer, and enhanced data sharing.”
To read the full editorial, click here.
On Twitter @denisefulton
Federal officials took the next step in their moonshot to end cancer by announcing on April 4 a blue ribbon panel to guide the effort.
A total of 28 leading researchers, clinicians, and patient advocates have been named to the panel charged with informing the scientific direction and goals of the National Cancer Moonshot Initiative, led by Vice President Joe Biden.
“This Blue Ribbon Panel will ensure that, as [the National Institutes of Health] allocates new resources through the Moonshot, decisions will be grounded in the best science,” Vice President Biden said in a statement. “I look forward to working with this panel and many others involved with the Moonshot to make unprecedented improvements in prevention, diagnosis, and treatment of cancer.”
The key goals of the initiative were set out simultaneously in a perspective from Dr. Francis S. Collins, NIH director, and Dr. Douglas R. Lowy, director of the National Cancer Institute. The editorial was published in the New England Journal of Medicine.
“Fueled by an additional $680 million in the proposed fiscal year 2017 budget for the NIH, plus additional resources for the Food and Drug Administration, the initiative will aim to accelerate progress toward the next generation of interventions that we hope will substantially reduce cancer incidence and dramatically improve patient outcomes,” Dr. Collins and Dr. Lowy wrote. “The NIH’s most compelling opportunities for progress will be set forth by late summer 2016 in a research plan informed by the deliberations of a blue-ribbon panel of experts, which will provide scientific input to the National Cancer Advisory Board. Some possible opportunities include vaccine development, early-detection technology, single-cell genomic analysis, immunotherapy, a focus on pediatric cancer, and enhanced data sharing.”
To read the full editorial, click here.
On Twitter @denisefulton
Federal officials took the next step in their moonshot to end cancer by announcing on April 4 a blue ribbon panel to guide the effort.
A total of 28 leading researchers, clinicians, and patient advocates have been named to the panel charged with informing the scientific direction and goals of the National Cancer Moonshot Initiative, led by Vice President Joe Biden.
“This Blue Ribbon Panel will ensure that, as [the National Institutes of Health] allocates new resources through the Moonshot, decisions will be grounded in the best science,” Vice President Biden said in a statement. “I look forward to working with this panel and many others involved with the Moonshot to make unprecedented improvements in prevention, diagnosis, and treatment of cancer.”
The key goals of the initiative were set out simultaneously in a perspective from Dr. Francis S. Collins, NIH director, and Dr. Douglas R. Lowy, director of the National Cancer Institute. The editorial was published in the New England Journal of Medicine.
“Fueled by an additional $680 million in the proposed fiscal year 2017 budget for the NIH, plus additional resources for the Food and Drug Administration, the initiative will aim to accelerate progress toward the next generation of interventions that we hope will substantially reduce cancer incidence and dramatically improve patient outcomes,” Dr. Collins and Dr. Lowy wrote. “The NIH’s most compelling opportunities for progress will be set forth by late summer 2016 in a research plan informed by the deliberations of a blue-ribbon panel of experts, which will provide scientific input to the National Cancer Advisory Board. Some possible opportunities include vaccine development, early-detection technology, single-cell genomic analysis, immunotherapy, a focus on pediatric cancer, and enhanced data sharing.”
To read the full editorial, click here.
On Twitter @denisefulton
FROM NEJM