User login
Downturn in reoperation after breast conservation surgery
Rates of reoperation after breast conservation surgery have declined significantly since 2003, but nearly 25% of women are still undergoing repeat operations, new data suggest.
Researchers analyzed data from a population-based sample of 89,448 women undergoing primary breast conservation surgery for breast cancer in New York State from 2003 to 2013.
According to a study published online Feb.17 in JAMA Surgery, the mean 90-day reoperation rate declined from 39.5% in 2003-2004 to 23.1% in 2011-2013 (P less than .001), with an overall rate of 30.9% for the entire study period.
“We believe that the findings of reduced occurrence of reoperations are encouraging and imply improvements in training and patient selection for BCS,” wrote Abby J. Isaacs of Cornell University, New York, and her coauthors.
Reoperation rates were highest in younger women (37.7%), compared with women aged over 65 years (26.3%).
However, the study also showed that women aged 50-64 years were less likely than were older or younger women to undergo breast conservation surgery, compared with mastectomy as a repeat procedure (JAMA Surg 2016 Feb 17. doi:10.1001/jamasurg.2015.5535).
Breast conservation surgery was more common than was mastectomy as a repeat procedure in women who were white, had commercial insurance, had low comorbidity scores, or had in situ disease.
Researchers observed significant surgeon-level variation in rates of reoperation after breast conservation surgery, which they described as “novel and unprecedented.” The rates of reoperation among surgeons ranged from 0% to nearly 100%.
Overall, the mean rate of reoperation for surgeons was 30.8%, but nearly 20% of surgeons had reoperation rates above 50% and 6.1% had reoperation rates above the 99.8% limits.
Similarly, 6% of surgeons had reoperation rates below the 95% confidence limits and 2.9% were below the 99.8% limits.
Reoperation rates were independently associated with surgical volume; surgeons performing fewer than 14 breast conservation surgery procedures had a mean reoperation rate of 35.2% while those who performed 34 or more procedures had a reoperation rate of 27.5%.
Over the entire study period, the overall rate of breast conservation surgery peaked in 2004 with more than 8,500 cases, then decreased to a mean number of 8,078 for 2011-2013.
The decrease in primary breast conservation surgery was significantly greater in women aged 20-49 years (P less than .001) with 1,416 women in this age group undergoing breast conservation surgery in 2013, compared with 3,644 women aged 65 years or older.
“The reduction in the use of BCS in women younger than 50 years and a corresponding reduction in overall reoperation rates over time implies that surgeons may be selecting more appropriate patients for the procedures,” the authors wrote.
They acknowledged that they did not have access to information on tumor size, grade, and staging, which are variables known to have an important influence on margin rates and reoperation rates. “We believe, however, in the context of physician-level outcomes, that these factors will not bias the results; the recommendation for BCS will be made by surgeons based on their knowledge of the patients’ disease, and we have no reason to believe that unknowable patient characteristics will be unbalanced between surgeons.”
Two authors reported involvement with the Food and Drug Administration–funded MDEpiNet Science and Infrastructure Center; no other conflicts of interest were declared.
The recent Society for Surgical Oncology–American Society for Radiation Oncology (SSO-ASTRO) consensus guidelines encourage the use of “no ink on tumor” as the current standard in an era of multimodal treatment and evolving understanding of tumor biology along with tumor burden.
|
Dr. E. Shelley Hwang |
Establishing a rational, evidence-based approach to reexcision as originally proposed by Fisher et al. and supported by the new SSO-ASTRO guidelines can provide substantial national cost savings by eliminating reexcisions for close but negative margins.
Dr. Uttara Nag and Dr. E. Shelley Hwang are with the department of health policy and management in the department of surgery, Duke University, Durham, N.C. These comments are taken from an editorial (JAMA Surg. 2016 Feb 17. doi:10.1001/jamasurg.2015.5555). No conflicts of interest were declared.
The recent Society for Surgical Oncology–American Society for Radiation Oncology (SSO-ASTRO) consensus guidelines encourage the use of “no ink on tumor” as the current standard in an era of multimodal treatment and evolving understanding of tumor biology along with tumor burden.
|
|
Dr. E. Shelley Hwang |
Establishing a rational, evidence-based approach to reexcision as originally proposed by Fisher et al. and supported by the new SSO-ASTRO guidelines can provide substantial national cost savings by eliminating reexcisions for close but negative margins.
Dr. Uttara Nag and Dr. E. Shelley Hwang are with the department of health policy and management in the department of surgery, Duke University, Durham, N.C. These comments are taken from an editorial (JAMA Surg. 2016 Feb 17. doi:10.1001/jamasurg.2015.5555). No conflicts of interest were declared.
The recent Society for Surgical Oncology–American Society for Radiation Oncology (SSO-ASTRO) consensus guidelines encourage the use of “no ink on tumor” as the current standard in an era of multimodal treatment and evolving understanding of tumor biology along with tumor burden.
|
|
Dr. E. Shelley Hwang |
Establishing a rational, evidence-based approach to reexcision as originally proposed by Fisher et al. and supported by the new SSO-ASTRO guidelines can provide substantial national cost savings by eliminating reexcisions for close but negative margins.
Dr. Uttara Nag and Dr. E. Shelley Hwang are with the department of health policy and management in the department of surgery, Duke University, Durham, N.C. These comments are taken from an editorial (JAMA Surg. 2016 Feb 17. doi:10.1001/jamasurg.2015.5555). No conflicts of interest were declared.
Rates of reoperation after breast conservation surgery have declined significantly since 2003, but nearly 25% of women are still undergoing repeat operations, new data suggest.
Researchers analyzed data from a population-based sample of 89,448 women undergoing primary breast conservation surgery for breast cancer in New York State from 2003 to 2013.
According to a study published online Feb.17 in JAMA Surgery, the mean 90-day reoperation rate declined from 39.5% in 2003-2004 to 23.1% in 2011-2013 (P less than .001), with an overall rate of 30.9% for the entire study period.
“We believe that the findings of reduced occurrence of reoperations are encouraging and imply improvements in training and patient selection for BCS,” wrote Abby J. Isaacs of Cornell University, New York, and her coauthors.
Reoperation rates were highest in younger women (37.7%), compared with women aged over 65 years (26.3%).
However, the study also showed that women aged 50-64 years were less likely than were older or younger women to undergo breast conservation surgery, compared with mastectomy as a repeat procedure (JAMA Surg 2016 Feb 17. doi:10.1001/jamasurg.2015.5535).
Breast conservation surgery was more common than was mastectomy as a repeat procedure in women who were white, had commercial insurance, had low comorbidity scores, or had in situ disease.
Researchers observed significant surgeon-level variation in rates of reoperation after breast conservation surgery, which they described as “novel and unprecedented.” The rates of reoperation among surgeons ranged from 0% to nearly 100%.
Overall, the mean rate of reoperation for surgeons was 30.8%, but nearly 20% of surgeons had reoperation rates above 50% and 6.1% had reoperation rates above the 99.8% limits.
Similarly, 6% of surgeons had reoperation rates below the 95% confidence limits and 2.9% were below the 99.8% limits.
Reoperation rates were independently associated with surgical volume; surgeons performing fewer than 14 breast conservation surgery procedures had a mean reoperation rate of 35.2% while those who performed 34 or more procedures had a reoperation rate of 27.5%.
Over the entire study period, the overall rate of breast conservation surgery peaked in 2004 with more than 8,500 cases, then decreased to a mean number of 8,078 for 2011-2013.
The decrease in primary breast conservation surgery was significantly greater in women aged 20-49 years (P less than .001) with 1,416 women in this age group undergoing breast conservation surgery in 2013, compared with 3,644 women aged 65 years or older.
“The reduction in the use of BCS in women younger than 50 years and a corresponding reduction in overall reoperation rates over time implies that surgeons may be selecting more appropriate patients for the procedures,” the authors wrote.
They acknowledged that they did not have access to information on tumor size, grade, and staging, which are variables known to have an important influence on margin rates and reoperation rates. “We believe, however, in the context of physician-level outcomes, that these factors will not bias the results; the recommendation for BCS will be made by surgeons based on their knowledge of the patients’ disease, and we have no reason to believe that unknowable patient characteristics will be unbalanced between surgeons.”
Two authors reported involvement with the Food and Drug Administration–funded MDEpiNet Science and Infrastructure Center; no other conflicts of interest were declared.
Rates of reoperation after breast conservation surgery have declined significantly since 2003, but nearly 25% of women are still undergoing repeat operations, new data suggest.
Researchers analyzed data from a population-based sample of 89,448 women undergoing primary breast conservation surgery for breast cancer in New York State from 2003 to 2013.
According to a study published online Feb.17 in JAMA Surgery, the mean 90-day reoperation rate declined from 39.5% in 2003-2004 to 23.1% in 2011-2013 (P less than .001), with an overall rate of 30.9% for the entire study period.
“We believe that the findings of reduced occurrence of reoperations are encouraging and imply improvements in training and patient selection for BCS,” wrote Abby J. Isaacs of Cornell University, New York, and her coauthors.
Reoperation rates were highest in younger women (37.7%), compared with women aged over 65 years (26.3%).
However, the study also showed that women aged 50-64 years were less likely than were older or younger women to undergo breast conservation surgery, compared with mastectomy as a repeat procedure (JAMA Surg 2016 Feb 17. doi:10.1001/jamasurg.2015.5535).
Breast conservation surgery was more common than was mastectomy as a repeat procedure in women who were white, had commercial insurance, had low comorbidity scores, or had in situ disease.
Researchers observed significant surgeon-level variation in rates of reoperation after breast conservation surgery, which they described as “novel and unprecedented.” The rates of reoperation among surgeons ranged from 0% to nearly 100%.
Overall, the mean rate of reoperation for surgeons was 30.8%, but nearly 20% of surgeons had reoperation rates above 50% and 6.1% had reoperation rates above the 99.8% limits.
Similarly, 6% of surgeons had reoperation rates below the 95% confidence limits and 2.9% were below the 99.8% limits.
Reoperation rates were independently associated with surgical volume; surgeons performing fewer than 14 breast conservation surgery procedures had a mean reoperation rate of 35.2% while those who performed 34 or more procedures had a reoperation rate of 27.5%.
Over the entire study period, the overall rate of breast conservation surgery peaked in 2004 with more than 8,500 cases, then decreased to a mean number of 8,078 for 2011-2013.
The decrease in primary breast conservation surgery was significantly greater in women aged 20-49 years (P less than .001) with 1,416 women in this age group undergoing breast conservation surgery in 2013, compared with 3,644 women aged 65 years or older.
“The reduction in the use of BCS in women younger than 50 years and a corresponding reduction in overall reoperation rates over time implies that surgeons may be selecting more appropriate patients for the procedures,” the authors wrote.
They acknowledged that they did not have access to information on tumor size, grade, and staging, which are variables known to have an important influence on margin rates and reoperation rates. “We believe, however, in the context of physician-level outcomes, that these factors will not bias the results; the recommendation for BCS will be made by surgeons based on their knowledge of the patients’ disease, and we have no reason to believe that unknowable patient characteristics will be unbalanced between surgeons.”
Two authors reported involvement with the Food and Drug Administration–funded MDEpiNet Science and Infrastructure Center; no other conflicts of interest were declared.
FROM JAMA SURGERY
Key clinical point: Rates of reoperation after breast conservation surgery are declining but vary significantly between surgeons.
Major finding: The mean 90-day reoperation rate after breast conservation surgery declined from 39.5% in 2003-2004 to 23.1% in 2011-2013.
Data source: Population-based sample of 89,448 women undergoing primary breast conservation surgery for breast cancer.
Disclosures: Two authors reported involvement with the Food and Drug Administration–funded MDEpiNet Science and Infrastructure Center; no other conflicts of interest were declared.
Encouraging data on immunotherapy, cardiotoxicity, and DFS
Click on the PDF icon at the top of this introduction to read the full article.
Click on the PDF icon at the top of this introduction to read the full article.
Click on the PDF icon at the top of this introduction to read the full article.
Making immunotherapy part of routine breast cancer treatment
Cancer treatment is evolving rapidly, and 2015 was no exception. It was the year of immunotherapy. Following the approval by the US Food and Drug Administration in 2014 of pembrolizumab for melanoma, 2015 saw approvals of nivolumab for melanoma, lung cancer, and kidney cancer; pembrolizumab for lung cancer; and the combination of ipilimumab and nivolimab for melanoma. That’s an impressive list of immunotherapy approvals for a single year.
Click on the PDF icon at the top of this introduction to read the full article.
Cancer treatment is evolving rapidly, and 2015 was no exception. It was the year of immunotherapy. Following the approval by the US Food and Drug Administration in 2014 of pembrolizumab for melanoma, 2015 saw approvals of nivolumab for melanoma, lung cancer, and kidney cancer; pembrolizumab for lung cancer; and the combination of ipilimumab and nivolimab for melanoma. That’s an impressive list of immunotherapy approvals for a single year.
Click on the PDF icon at the top of this introduction to read the full article.
Cancer treatment is evolving rapidly, and 2015 was no exception. It was the year of immunotherapy. Following the approval by the US Food and Drug Administration in 2014 of pembrolizumab for melanoma, 2015 saw approvals of nivolumab for melanoma, lung cancer, and kidney cancer; pembrolizumab for lung cancer; and the combination of ipilimumab and nivolimab for melanoma. That’s an impressive list of immunotherapy approvals for a single year.
Click on the PDF icon at the top of this introduction to read the full article.
Breast cancer patients at increased risk of colorectal cancer
Women previously diagnosed with breast cancer had a 60% increased risk of colorectal cancer, according to analysis of Swedish cancer registries, and breast cancer therapy had no effect on risk.
Women previously diagnosed with breast cancer had a higher risk of colorectal adenocarcinoma, compared with the general population (standardized incidence ratio, 1.59; 95% confidence interval, 1.53-1.65). Higher risk was observed for adenocarcinoma of the proximal colon, compared with the distal colon (SIR, 1.72; 95% CI, 1.61-1.82 vs. SIR, 1.46; 95% CI, 1.34-1.58).
Risk for adenocarcinoma of the proximal colon, the predominant subtype in women, increased with age at breast cancer diagnosis, from an SIR of 1.60 for women diagnosed between the ages of 15 and 49 years, to an SIR of 1.51 for 50-59 years, to an SIR of 1.82 for age 60 years or greater. By contrast, the SIR for general colorectal adenocarcinoma dipped in the 50-59 age group, a finding that may point to the role of estrogen in colorectal carcinoma (Cancer Epidemiol. 2016 Feb 15. doi: 10.1016/j.canep.2016.01.006).
“It is well known that estrogen levels are elevated in breast cancer patients, which may contribute to the increased risk of colorectal cancer in this population. Interestingly, our results showed that the SIRs of colorectal adenocarcinoma changed in different age groups, compared with the general population. Specifically, the SIRs showed a drop in the 50-59 age group but increased again after the age of 60,” wrote Dr. Yunxia Lu, associate professor in the department of molecular medicine and surgery, Karolinska Institute, Stockholm, and colleagues. The researchers noted previous reports of endogenous estrogen levels decreasing after menopause for a short period, while exogenous hormones may take effect some time after menopause.
The study found no association between different types of breast cancer treatment, including antihormonal therapy, and the risk of colorectal cancer.
The retrospective analysis used data from the Swedish Cancer Register, including 179,733 patients diagnosed with breast cancer from 1961 to 2010, and 2,571 colorectal cancers identified. Analysis of treatment effects on colorectal cancer risk used data from the Stockholm-Gotland Breast Cancer Register of 20,171 patients with breast cancer and relevant treatment information.
Dr. Lu and coauthors reported having no disclosures.
Women previously diagnosed with breast cancer had a 60% increased risk of colorectal cancer, according to analysis of Swedish cancer registries, and breast cancer therapy had no effect on risk.
Women previously diagnosed with breast cancer had a higher risk of colorectal adenocarcinoma, compared with the general population (standardized incidence ratio, 1.59; 95% confidence interval, 1.53-1.65). Higher risk was observed for adenocarcinoma of the proximal colon, compared with the distal colon (SIR, 1.72; 95% CI, 1.61-1.82 vs. SIR, 1.46; 95% CI, 1.34-1.58).
Risk for adenocarcinoma of the proximal colon, the predominant subtype in women, increased with age at breast cancer diagnosis, from an SIR of 1.60 for women diagnosed between the ages of 15 and 49 years, to an SIR of 1.51 for 50-59 years, to an SIR of 1.82 for age 60 years or greater. By contrast, the SIR for general colorectal adenocarcinoma dipped in the 50-59 age group, a finding that may point to the role of estrogen in colorectal carcinoma (Cancer Epidemiol. 2016 Feb 15. doi: 10.1016/j.canep.2016.01.006).
“It is well known that estrogen levels are elevated in breast cancer patients, which may contribute to the increased risk of colorectal cancer in this population. Interestingly, our results showed that the SIRs of colorectal adenocarcinoma changed in different age groups, compared with the general population. Specifically, the SIRs showed a drop in the 50-59 age group but increased again after the age of 60,” wrote Dr. Yunxia Lu, associate professor in the department of molecular medicine and surgery, Karolinska Institute, Stockholm, and colleagues. The researchers noted previous reports of endogenous estrogen levels decreasing after menopause for a short period, while exogenous hormones may take effect some time after menopause.
The study found no association between different types of breast cancer treatment, including antihormonal therapy, and the risk of colorectal cancer.
The retrospective analysis used data from the Swedish Cancer Register, including 179,733 patients diagnosed with breast cancer from 1961 to 2010, and 2,571 colorectal cancers identified. Analysis of treatment effects on colorectal cancer risk used data from the Stockholm-Gotland Breast Cancer Register of 20,171 patients with breast cancer and relevant treatment information.
Dr. Lu and coauthors reported having no disclosures.
Women previously diagnosed with breast cancer had a 60% increased risk of colorectal cancer, according to analysis of Swedish cancer registries, and breast cancer therapy had no effect on risk.
Women previously diagnosed with breast cancer had a higher risk of colorectal adenocarcinoma, compared with the general population (standardized incidence ratio, 1.59; 95% confidence interval, 1.53-1.65). Higher risk was observed for adenocarcinoma of the proximal colon, compared with the distal colon (SIR, 1.72; 95% CI, 1.61-1.82 vs. SIR, 1.46; 95% CI, 1.34-1.58).
Risk for adenocarcinoma of the proximal colon, the predominant subtype in women, increased with age at breast cancer diagnosis, from an SIR of 1.60 for women diagnosed between the ages of 15 and 49 years, to an SIR of 1.51 for 50-59 years, to an SIR of 1.82 for age 60 years or greater. By contrast, the SIR for general colorectal adenocarcinoma dipped in the 50-59 age group, a finding that may point to the role of estrogen in colorectal carcinoma (Cancer Epidemiol. 2016 Feb 15. doi: 10.1016/j.canep.2016.01.006).
“It is well known that estrogen levels are elevated in breast cancer patients, which may contribute to the increased risk of colorectal cancer in this population. Interestingly, our results showed that the SIRs of colorectal adenocarcinoma changed in different age groups, compared with the general population. Specifically, the SIRs showed a drop in the 50-59 age group but increased again after the age of 60,” wrote Dr. Yunxia Lu, associate professor in the department of molecular medicine and surgery, Karolinska Institute, Stockholm, and colleagues. The researchers noted previous reports of endogenous estrogen levels decreasing after menopause for a short period, while exogenous hormones may take effect some time after menopause.
The study found no association between different types of breast cancer treatment, including antihormonal therapy, and the risk of colorectal cancer.
The retrospective analysis used data from the Swedish Cancer Register, including 179,733 patients diagnosed with breast cancer from 1961 to 2010, and 2,571 colorectal cancers identified. Analysis of treatment effects on colorectal cancer risk used data from the Stockholm-Gotland Breast Cancer Register of 20,171 patients with breast cancer and relevant treatment information.
Dr. Lu and coauthors reported having no disclosures.
FROM CANCER EPIDEMIOLOGY
Key clinical point: Colorectal cancer risk was significantly increased in patients previously diagnosed with breast cancer.
Major finding: Standardized incidence ratio for the breast cancer cohort compared with the general population was 1.59 (95% CI, 1.53-1.65).
Data source: The Swedish Cancer Register included 179,733 patients with breast cancer; the Stockholm-Gotland Breast Cancer Register included 20,171 patients with breast cancer and relevant treatment information.
Disclosures: Dr. Lu and coauthors reported having no disclosures.
Cancer death rates show wide geographic variation
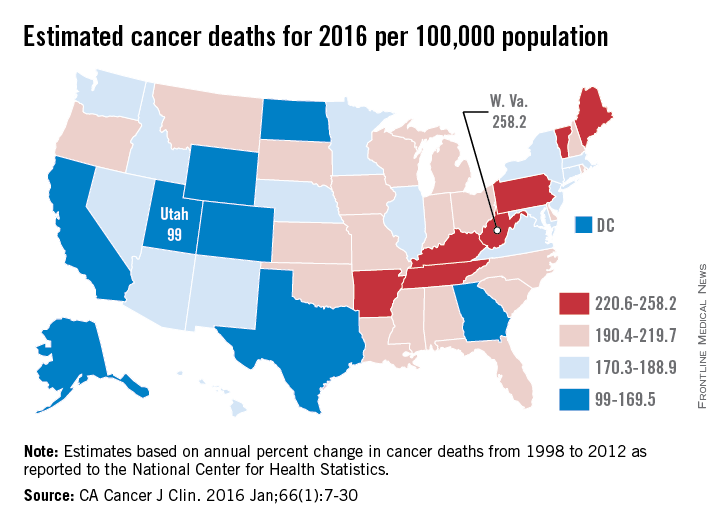
Over 595,000 cancer deaths – an average of about 1,600 each day – are expected in the United States in 2016, but those deaths are not evenly distributed among the states, according to investigators from the American Cancer Society.
Estimates from the ACS show that, in 2016, Utah will have a cancer death rate of 99 per 100,000 population, the lowest in the country. Those same estimates predict that West Virginia will have a highest-in-the-country death rate of 258.2 per 100,000 – 2.6 times higher than Utah’s. Other states with high estimated death rates include Maine, Kentucky, Arkansas, and Pennsylvania, noted Rebecca L. Siegel and her associates at the ACS (CA Cancer J Clin. 2016 Jan;66[1]:7-30).
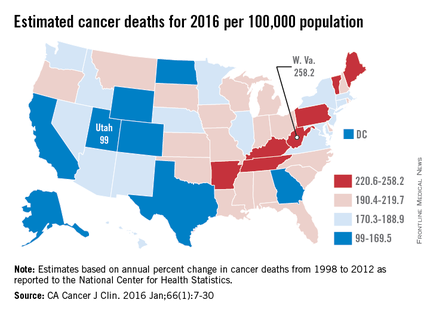
Besides Utah, the states with the lowest estimated cancer death rates in 2016 are Colorado, Texas, and Alaska, along with the District of Columbia. The national death rate for cancer has dropped 23% since 1991, the investigators said, but cancer is now the leading cause of death in 21 states. This good news/bad news situation comes about mainly as a result of “exceptionally large reductions in death from heart disease,” they added.
Ms. Siegel and her associates calculated the expected number of cancer deaths “based on the annual percent change in reported numbers of cancer deaths from 1998 through 2012 at the state and national levels as reported to the [National Center for Health Statistics].” Death rates were calculated here using estimated populations for 2015 from the U.S. Census Bureau.
Over 595,000 cancer deaths – an average of about 1,600 each day – are expected in the United States in 2016, but those deaths are not evenly distributed among the states, according to investigators from the American Cancer Society.
Estimates from the ACS show that, in 2016, Utah will have a cancer death rate of 99 per 100,000 population, the lowest in the country. Those same estimates predict that West Virginia will have a highest-in-the-country death rate of 258.2 per 100,000 – 2.6 times higher than Utah’s. Other states with high estimated death rates include Maine, Kentucky, Arkansas, and Pennsylvania, noted Rebecca L. Siegel and her associates at the ACS (CA Cancer J Clin. 2016 Jan;66[1]:7-30).
Besides Utah, the states with the lowest estimated cancer death rates in 2016 are Colorado, Texas, and Alaska, along with the District of Columbia. The national death rate for cancer has dropped 23% since 1991, the investigators said, but cancer is now the leading cause of death in 21 states. This good news/bad news situation comes about mainly as a result of “exceptionally large reductions in death from heart disease,” they added.
Ms. Siegel and her associates calculated the expected number of cancer deaths “based on the annual percent change in reported numbers of cancer deaths from 1998 through 2012 at the state and national levels as reported to the [National Center for Health Statistics].” Death rates were calculated here using estimated populations for 2015 from the U.S. Census Bureau.
Over 595,000 cancer deaths – an average of about 1,600 each day – are expected in the United States in 2016, but those deaths are not evenly distributed among the states, according to investigators from the American Cancer Society.
Estimates from the ACS show that, in 2016, Utah will have a cancer death rate of 99 per 100,000 population, the lowest in the country. Those same estimates predict that West Virginia will have a highest-in-the-country death rate of 258.2 per 100,000 – 2.6 times higher than Utah’s. Other states with high estimated death rates include Maine, Kentucky, Arkansas, and Pennsylvania, noted Rebecca L. Siegel and her associates at the ACS (CA Cancer J Clin. 2016 Jan;66[1]:7-30).
Besides Utah, the states with the lowest estimated cancer death rates in 2016 are Colorado, Texas, and Alaska, along with the District of Columbia. The national death rate for cancer has dropped 23% since 1991, the investigators said, but cancer is now the leading cause of death in 21 states. This good news/bad news situation comes about mainly as a result of “exceptionally large reductions in death from heart disease,” they added.
Ms. Siegel and her associates calculated the expected number of cancer deaths “based on the annual percent change in reported numbers of cancer deaths from 1998 through 2012 at the state and national levels as reported to the [National Center for Health Statistics].” Death rates were calculated here using estimated populations for 2015 from the U.S. Census Bureau.
Rate of BRCA testing up among young women with breast cancer
The rate at which young women diagnosed with breast cancer are undergoing genetic testing for BRCA1 and BRCA2 mutations has increased, investigators report online in JAMA Oncology.
In a study of 897 women aged 40 years and younger diagnosed with breast cancer at any one of 11 academic or community medical centers, 780 (87%) reported undergoing BRCA testing within the first year after diagnosis, reported Dr. Ann H. Partridge of the Dana-Farber Cancer Institute, Boston, and her associates (JAMA Onc. 2016 Feb 11. doi: 10.1001/jamaoncol.2015.5941).

Among the 780 women who had BRCA testing, 59 (7.6%) reported a BRCA1 mutation, 35 (4.5%) reported a BRCA2 mutation, and 35 (4.6%) reported an indeterminate result or variant of unknown clinical significance, the investigators said.
The frequency of testing increased over time. Of 39 women diagnosed with breast cancer in 2006, 30 (76.9%) elected to have testing, but by 2013, 123 (95.3%) of 129 women diagnosed with breast cancer reported BRCA testing.
The investigators attribute the increasing frequency of BRCA testing to the fact that most women in the group were insured, educated, and treated at cancer centers where comprehensive genetic counseling and testing services were widely available, but they also acknowledged the possibility that media attention to genetic breast cancer (in other words, the Angelina Jolie effect) may have motivated more women to bring up the issue of genetic risk with their physician or genetic counselor.
The study can be found online here.
On Twitter @NikolaidesLaura
The rate at which young women diagnosed with breast cancer are undergoing genetic testing for BRCA1 and BRCA2 mutations has increased, investigators report online in JAMA Oncology.
In a study of 897 women aged 40 years and younger diagnosed with breast cancer at any one of 11 academic or community medical centers, 780 (87%) reported undergoing BRCA testing within the first year after diagnosis, reported Dr. Ann H. Partridge of the Dana-Farber Cancer Institute, Boston, and her associates (JAMA Onc. 2016 Feb 11. doi: 10.1001/jamaoncol.2015.5941).
Among the 780 women who had BRCA testing, 59 (7.6%) reported a BRCA1 mutation, 35 (4.5%) reported a BRCA2 mutation, and 35 (4.6%) reported an indeterminate result or variant of unknown clinical significance, the investigators said.
The frequency of testing increased over time. Of 39 women diagnosed with breast cancer in 2006, 30 (76.9%) elected to have testing, but by 2013, 123 (95.3%) of 129 women diagnosed with breast cancer reported BRCA testing.
The investigators attribute the increasing frequency of BRCA testing to the fact that most women in the group were insured, educated, and treated at cancer centers where comprehensive genetic counseling and testing services were widely available, but they also acknowledged the possibility that media attention to genetic breast cancer (in other words, the Angelina Jolie effect) may have motivated more women to bring up the issue of genetic risk with their physician or genetic counselor.
The study can be found online here.
On Twitter @NikolaidesLaura
The rate at which young women diagnosed with breast cancer are undergoing genetic testing for BRCA1 and BRCA2 mutations has increased, investigators report online in JAMA Oncology.
In a study of 897 women aged 40 years and younger diagnosed with breast cancer at any one of 11 academic or community medical centers, 780 (87%) reported undergoing BRCA testing within the first year after diagnosis, reported Dr. Ann H. Partridge of the Dana-Farber Cancer Institute, Boston, and her associates (JAMA Onc. 2016 Feb 11. doi: 10.1001/jamaoncol.2015.5941).
Among the 780 women who had BRCA testing, 59 (7.6%) reported a BRCA1 mutation, 35 (4.5%) reported a BRCA2 mutation, and 35 (4.6%) reported an indeterminate result or variant of unknown clinical significance, the investigators said.
The frequency of testing increased over time. Of 39 women diagnosed with breast cancer in 2006, 30 (76.9%) elected to have testing, but by 2013, 123 (95.3%) of 129 women diagnosed with breast cancer reported BRCA testing.
The investigators attribute the increasing frequency of BRCA testing to the fact that most women in the group were insured, educated, and treated at cancer centers where comprehensive genetic counseling and testing services were widely available, but they also acknowledged the possibility that media attention to genetic breast cancer (in other words, the Angelina Jolie effect) may have motivated more women to bring up the issue of genetic risk with their physician or genetic counselor.
The study can be found online here.
On Twitter @NikolaidesLaura
FROM JAMA ONCOLOGY

Epoetin alfa missed its safety endpoint in metastatic breast cancer
A randomized phase III trial failed to allay safety concerns about the use of erythropoietin-stimulating agents in cancer patients, researchers reported online Feb. 8 in the Journal of Clinical Oncology.
The analysis could not rule out a 15% increase in the risk of progressive disease or death when women with metastatic breast cancer received epoetin alfa (EPO) instead of best standard of care for anemia, said Dr. Brian Leyland-Jones of Avera Cancer Institute in Sioux Falls, S.D., and his associates. Red blood cell transfusions should remain the preferred treatment for anemia in these patients, and any use of epoetin alfa for advanced cases “should be done with caution and based on careful risk-benefit assessment,” the researchers said.
Erythropoietin-stimulating agents can effectively treat cancer-associated anemia but have been linked to worse survival and locoregional control. However, the agents were used off label in several of these trials, the researchers noted. Therefore, they studied 2,098 women undergoing first- or second-line chemotherapy for metastatic breast cancer who had less than 11 mg/dL hemoglobin, an ECOG performance status of 0 or 1, and a life expectancy of at least 6 months. They randomly assigned patients to receive either standard treatment or 40,000 IU EPO once weekly until disease progression or the end of chemotherapy (J Clin Onc. 2016 Feb 8. doi: 10.1200/JCO.2015.63.5649). Median progression-free survival (PFS) was 7.4 months in both groups, but the EPO group was 9% more likely to die or develop progressive disease during the study, and the upper bound of the hazard ratio exceeded the prespecified noninferiority margin of 1.15 (hazard ratio, 1.089; 95% confidence interval, 0.988-1.200). An independent review committee calculated a median PFS of 7.6 months for both groups, and a hazard ratio whose upper bound fell just within the prespecified noninferiority margin (1.146). The EPO group needed about half as many red blood cell transfusions as did the control group (P less than .001), but experienced twice as many thrombotic vascular events (2.8% vs. 1.4%; P = .04).
“The results of this study do not suggest any new safety signal associated with EPO treatment and are consistent with the known safety risk to patients,” the researchers concluded. An ongoing randomized phase III study comparing darbepoetin with best standard of care for anemia in patients undergoing platinum-based treatment of stage IV non–small cell lung cancer “will further inform the benefit-risk profile of erythropoietin-stimulating agents in the oncology setting,” they said.
A randomized phase III trial failed to allay safety concerns about the use of erythropoietin-stimulating agents in cancer patients, researchers reported online Feb. 8 in the Journal of Clinical Oncology.
The analysis could not rule out a 15% increase in the risk of progressive disease or death when women with metastatic breast cancer received epoetin alfa (EPO) instead of best standard of care for anemia, said Dr. Brian Leyland-Jones of Avera Cancer Institute in Sioux Falls, S.D., and his associates. Red blood cell transfusions should remain the preferred treatment for anemia in these patients, and any use of epoetin alfa for advanced cases “should be done with caution and based on careful risk-benefit assessment,” the researchers said.
Erythropoietin-stimulating agents can effectively treat cancer-associated anemia but have been linked to worse survival and locoregional control. However, the agents were used off label in several of these trials, the researchers noted. Therefore, they studied 2,098 women undergoing first- or second-line chemotherapy for metastatic breast cancer who had less than 11 mg/dL hemoglobin, an ECOG performance status of 0 or 1, and a life expectancy of at least 6 months. They randomly assigned patients to receive either standard treatment or 40,000 IU EPO once weekly until disease progression or the end of chemotherapy (J Clin Onc. 2016 Feb 8. doi: 10.1200/JCO.2015.63.5649). Median progression-free survival (PFS) was 7.4 months in both groups, but the EPO group was 9% more likely to die or develop progressive disease during the study, and the upper bound of the hazard ratio exceeded the prespecified noninferiority margin of 1.15 (hazard ratio, 1.089; 95% confidence interval, 0.988-1.200). An independent review committee calculated a median PFS of 7.6 months for both groups, and a hazard ratio whose upper bound fell just within the prespecified noninferiority margin (1.146). The EPO group needed about half as many red blood cell transfusions as did the control group (P less than .001), but experienced twice as many thrombotic vascular events (2.8% vs. 1.4%; P = .04).
“The results of this study do not suggest any new safety signal associated with EPO treatment and are consistent with the known safety risk to patients,” the researchers concluded. An ongoing randomized phase III study comparing darbepoetin with best standard of care for anemia in patients undergoing platinum-based treatment of stage IV non–small cell lung cancer “will further inform the benefit-risk profile of erythropoietin-stimulating agents in the oncology setting,” they said.
A randomized phase III trial failed to allay safety concerns about the use of erythropoietin-stimulating agents in cancer patients, researchers reported online Feb. 8 in the Journal of Clinical Oncology.
The analysis could not rule out a 15% increase in the risk of progressive disease or death when women with metastatic breast cancer received epoetin alfa (EPO) instead of best standard of care for anemia, said Dr. Brian Leyland-Jones of Avera Cancer Institute in Sioux Falls, S.D., and his associates. Red blood cell transfusions should remain the preferred treatment for anemia in these patients, and any use of epoetin alfa for advanced cases “should be done with caution and based on careful risk-benefit assessment,” the researchers said.
Erythropoietin-stimulating agents can effectively treat cancer-associated anemia but have been linked to worse survival and locoregional control. However, the agents were used off label in several of these trials, the researchers noted. Therefore, they studied 2,098 women undergoing first- or second-line chemotherapy for metastatic breast cancer who had less than 11 mg/dL hemoglobin, an ECOG performance status of 0 or 1, and a life expectancy of at least 6 months. They randomly assigned patients to receive either standard treatment or 40,000 IU EPO once weekly until disease progression or the end of chemotherapy (J Clin Onc. 2016 Feb 8. doi: 10.1200/JCO.2015.63.5649). Median progression-free survival (PFS) was 7.4 months in both groups, but the EPO group was 9% more likely to die or develop progressive disease during the study, and the upper bound of the hazard ratio exceeded the prespecified noninferiority margin of 1.15 (hazard ratio, 1.089; 95% confidence interval, 0.988-1.200). An independent review committee calculated a median PFS of 7.6 months for both groups, and a hazard ratio whose upper bound fell just within the prespecified noninferiority margin (1.146). The EPO group needed about half as many red blood cell transfusions as did the control group (P less than .001), but experienced twice as many thrombotic vascular events (2.8% vs. 1.4%; P = .04).
“The results of this study do not suggest any new safety signal associated with EPO treatment and are consistent with the known safety risk to patients,” the researchers concluded. An ongoing randomized phase III study comparing darbepoetin with best standard of care for anemia in patients undergoing platinum-based treatment of stage IV non–small cell lung cancer “will further inform the benefit-risk profile of erythropoietin-stimulating agents in the oncology setting,” they said.
FROM THE JOURNAL OF CLINICAL ONCOLOGY
Key clinical point: The erythropoietin-stimulating agent epoetin alfa was associated with lower rates of progression-free survival, compared with best standard of care for anemia in women with metastatic breast cancer.
Major finding: The 95% confidence interval for the hazard ratio had an upper limit of 1.20, exceeding the prespecified noninferiority margin of 1.15.
Data source: An open-label, randomized, controlled, noninferiority trial of 2,098 patients.
Disclosures: Janssen Research and Development makes epoetin alfa and supported the study. Dr. Leyland-Jones reported receiving honoraria from Janssen Research and Development, and other funding from Genentech, GlaxoSmithKline, Amgen, and Johnson & Johnson. Seven coinvestigators reported employment with Janssen Research and Development. The other 15 coinvestigators had no disclosures.
A Perfect Storm: Tumor biology and genomics
This is the second installment of a five-part monthly series that will discuss the pathologic, genomic, and clinical factors that contribute to the racial survival disparity in breast cancer. The series, which is adapted from an article that originally appeared in CA: A Cancer Journal for Clinicians1, a journal of the American Cancer Society, will also review exciting and innovative interventions to close this survival gap. This month’s column reviews tumor biology and genomics—the first element in the perfect storm.
Hormone receptor status and human epidermal growth factor receptor 2 (HER2)/neu
Breast cancer is not a single disease, and breast cancer subtype classifications are used in the clinical setting to determine prognosis and guide management. These different molecular subtypes are based on tumor markers, which include the presence or absence of three proteins: estrogen receptor (ER), progesterone receptor (PR), and HER2/neu. Hormone receptor status is a main factor in planning breast cancer treatment. Hormone receptor–positive breast tumors benefit from hormone therapies, such as selective ER modulators (for example, tamoxifen) and aromatase inhibitors (for example, anastrozole). Thus, these tumors have a more favorable disease-specific survival than do hormone receptor–negative tumors.2
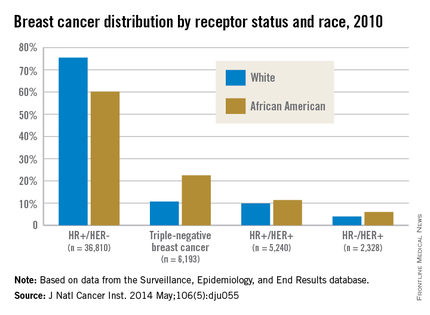
African American women are more likely to present with hormone receptor-negative tumors. In an analysis of the California Cancer Registry, which has collected patient ER and PR status since 1990, whites had a higher proportion of tumors that were ER positive or PR positive (or both) and HER2 negative (72% vs. 53%).3 DeSantis et al.4 reported similar results for this tumor type, with 76% of non-Hispanic whites having hormone receptor–positive, HER2-negative tumors vs. 62% of non-Hispanic blacks. Even with stratification by tumor stage, African Americans continue to have a significantly higher proportion of hormone receptor–negative tumors than do whites for localized and advanced disease.5
Although hormone receptor status varies significantly by race, HER2 status does not show the same divergence. HER2 overexpression is present in approximately 20% of invasive breast cancers. HER2-positive, hormone receptor–negative tumors demonstrate more-aggressive features and worse breast cancer–specific survival than do hormone receptor–positive and HER2-negative tumors,2 although survival has vastly improved with new HER2-targeted therapies such as trastuzumab and pertuzumab. Unlike hormone receptor status, there was no association between race and HER2-positive/ER-negative tumors in the Carolina Breast Cancer Study.2
Triple-negative breast cancer (TNBC)
TNBC is the subtype of breast cancer with the worst prognosis. TNBC gets its name because its tumor cells lack the markers for ER, PR, and HER2 overexpression. Thus, TNBC tumors are estrogen receptor negative (ER), progesterone receptor negative (PR), and HER2/neu negative (HER2). While other subtypes of breast cancer have benefited from drug development regarding hormonal therapies and HER2-targeted treatments, TNBC has not experienced the same pharmacologic breakthroughs.
As such, even after analyses control for the stage at diagnosis, women with this subtype have poorer survival than those with other breast cancers.6 African American women have a higher incidence of TNBC than white women.7 DeSantis et al.4 reported that 22% of breast cancers were triple negative in non-Hispanic black patients vs. only 11% in non-Hispanic white patients. The Carolina Breast Cancer Study found that 26% of African American women had TNBC, whereas 16% of non-African American women did.2 This subtype was most common among younger, premenopausal African American women (39% of diagnosed cancer subtypes). When TNBC patients were excluded from analysis in the Carolina Breast Cancer Study, breast cancer–specific survival remained significantly worse among premenopausal African American women, suggesting that although tumor biology in part explains the poor outcomes, the survival disparity story is more complex.
Germline mutations: BRCA1 and BRCA2 Mutations
In addition to tumor biology, cancer genomics has become increasingly important in determining cancer prognosis and guiding treatment. Approximately 5%-10% of breast cancer cases present in individuals with inherited mutations in autosomal dominant, highly penetrant breast cancer susceptibility genes.8 Accounting for 80%-90% of families containing multiple cases of breast and ovarian cancer, BRCA1 and BRCA2 germline mutations are the most common of the breast cancer susceptibility genes.9 These patients often are younger and have a higher-grade tumor that is hormone receptor negative, which also often matches the profile of the African American breast cancer patient.10
Despite similarities between BRCA1-associated breast cancers and breast cancer in African Americans, genetic abnormalities in African American breast cancer patients remain underresearched. Nanda et al.11 found that BRCA1 and BRCA2 mutations occur with appreciable frequency in high-risk families of African ancestry, with 28% testing positive for a deleterious mutation in one of these genes. This frequency was at a lower rate than that found in non-Hispanic, non-Jewish whites, who had a rate of 46%, because African Americans had a higher rate of polymorphisms or variants of unknown significance (44% vs. 12%). This large percentage of variants of unknown significance indicates that more analysis is needed to understand the clinical implications of these genetic variations. In another study from the Northern California site of the Breast Cancer Family Registry, the BRCA1 mutation prevalence was 16.7% in African American cases diagnosed under the age of 35 years vs. 7.2% in non-Hispanic, non-Ashkenazi Jewish whites in the same age category.12 High frequencies of mutations in BRCA1 and BRCA2 have also been reported in breast cancer patients of African ancestry from Nigeria and the Bahamas.13, 14
These results in African American patients highlight the need for further study of breast cancer genomics in minority populations. However, Armstrong et al.15 illuminated the existence of racial/ethnic disparities in patterns of referral to cancer risk clinics. In their study, African American women with a family history of breast or ovarian cancer were significantly less likely to undergo genetic counseling for BRCA1/2 testing than were white women with this family history. The results of this study were noteworthy for the magnitude of the disparity, with white women having almost five times greater odds of undergoing this clinically important evaluation. More than two decades after BRCA1 and BRCA2 genes were identified, larger studies are still needed in diverse populations to derive true estimates of the burden of mutations in both genes in underserved and understudied populations.
Although these differences in tumor biology and genomics tell part of the mortality disparity story, there is more to be told. In a study of African American and white patients in South Carolina, Adams et al.16 determined survival rates by ethnicity that were adjusted for disease stage and other prognostic characteristics. After they controlled for age, stage, ER, and HER2 expression as well as insurance status, African American women still had a twofold excess risk of death from breast cancer. Thus, in addition to differences in the innate characteristics of the breast tumors, racial differences in patterns of care for women with breast cancer must be considered in unraveling the observed disparity in mortality. The third installment of this series will discuss the second element of the perfect storm – patterns of care.
Other installments of this column can be found in the Related Content box.
1. Daly B, Olopade OI. A perfect storm: How tumor biology, genomics, and health care delivery patterns collide to create a racial survival disparity in breast cancer and proposed interventions for change. CA Cancer J Clin. 2015;65(3):221-238.
2. Carey LA, Perou CM, Livasy CA, et al. Race, breast cancer subtypes, and survival in the Carolina Breast Cancer Study. JAMA. 2006;295(21):2492-502.
3. Kurian AW, Fish K, Shema SJ, Clarke CA. Lifetime risks of specific breast cancer subtypes among women in four racial/ethnic groups. Breast Cancer Res. 2010;12(6):R99.
4. DeSantis CE, Fedewa SA, Goding Sauer A, Kramer JL, Smith RA, Jemal A. Breast cancer statistics, 2015: Convergence of incidence rates between black and white women. CA Cancer J Clin. 2015 Oct 29. doi: 10.3322/caac.21320. [Epub ahead of print]
5. Setiawan VW, Monroe KR, Wilkens LR, Kolonel LN, Pike MC, Henderson BE. Breast cancer risk factors defined by estrogen and progesterone receptor status: the multiethnic cohort study. Am J Epidemiol. 2009;169(10):1251-9.
6. Bauer KR, Brown M, Cress RD, Parise CA, Caggiano V. Descriptive analysis of estrogen receptor (ER)-negative, progesterone receptor (PR)-negative, and HER2-negative invasive breast cancer, the so-called triple-negative phenotype: a population-based study from the California cancer Registry. Cancer. 2007;109(9):1721-8.
7. Ray M, Polite BN. Triple-negative breast cancers: a view from 10,000 feet. Cancer J. 2010;16(1):17-22.
8. Claus EB, Schildkraut JM, Thompson WD, Risch NJ. The genetic attributable risk of breast and ovarian cancer. Cancer. 1996;77(11):2318-24.
9. Easton DF, Bishop DT, Ford D, Crockford GP. Genetic linkage analysis in familial breast and ovarian cancer: results from 214 families. The Breast Cancer Linkage Consortium. Am J Hum Genet. 1993;52(4):678-701.
10. Polite BN, Olopade OI. Breast cancer and race: a rising tide does not lift all boats equally. Perspect Biol Med. 2005;48(1 Suppl):S166-75.
11. Nanda R, Schumm LP, Cummings S, et al. Genetic testing in an ethnically diverse cohort of high-risk women: a comparative analysis of BRCA1 and BRCA2 mutations in American families of European and African ancestry. JAMA. 2005;294(15):1925-33.
12. John EM, Miron A, Gong G, et al. Prevalence of pathogenic BRCA1 mutation carriers in 5 US racial/ethnic groups. JAMA. 2007;298(24):2869-76.
13. Fackenthal JD, Zhang J, Zhang B, et al. High prevalence of BRCA1 and BRCA2 mutations in unselected Nigerian breast cancer patients. Int J Cancer. 2012;131(5):1114-23.
14. Donenberg T, Lunn J, Curling D, et al. A high prevalence of BRCA1 mutations among breast cancer patients from the Bahamas. Breast Cancer Res Treat. 2011;125(2):591-6.
15. Armstrong K, Micco E, Carney A, Stopfer J, Putt M. Racial differences in the use of BRCA1/2 testing among women with a family history of breast or ovarian cancer. JAMA. 2005;293(14):1729-36.
16. Adams SA, Butler WM, Fulton J, et al. Racial disparities in breast cancer mortality in a multi-ethnic cohort in the Southeast. Cancer. 2012;118(10):2693-9.

Bobby Daly, MD, MBA, is the chief fellow in the section of hematology/oncology at the University of Chicago Medicine. His clinical focus is breast and thoracic oncology, and his research focus is health services. Specifically, Dr. Daly researches disparities in oncology care delivery, oncology health care utilization, aggressive end-of-life oncology care, and oncology payment models. He received his MD and MBA from Harvard Medical School and Harvard Business School, both in Boston, and a BA in Economics and History from Stanford (Calif.) University. He was the recipient of the Dean’s Award at Harvard Medical and Business Schools.

Olufunmilayo Olopade, MD, FACP, OON, is the Walter L. Palmer Distinguished Service Professor of Medicine and Human Genetics, and director, Center for Global Health at the University of Chicago. She is adopting emerging high throughput genomic and informatics strategies to identify genetic and nongenetic risk factors for breast cancer in order to implement precision health care in diverse populations. This innovative approach has the potential to improve the quality of care and reduce costs while saving more lives.
Disclosures: Dr. Olopade serves on the Medical Advisory Board for CancerIQ. Dr. Daly serves as a director of Quadrant Holdings Corporation and receives compensation from this entity. Frontline Medical Communications is a subsidiary of Quadrant Holdings Corporation.
Published in conjunction with Susan G. Komen®.
This is the second installment of a five-part monthly series that will discuss the pathologic, genomic, and clinical factors that contribute to the racial survival disparity in breast cancer. The series, which is adapted from an article that originally appeared in CA: A Cancer Journal for Clinicians1, a journal of the American Cancer Society, will also review exciting and innovative interventions to close this survival gap. This month’s column reviews tumor biology and genomics—the first element in the perfect storm.
Hormone receptor status and human epidermal growth factor receptor 2 (HER2)/neu
Breast cancer is not a single disease, and breast cancer subtype classifications are used in the clinical setting to determine prognosis and guide management. These different molecular subtypes are based on tumor markers, which include the presence or absence of three proteins: estrogen receptor (ER), progesterone receptor (PR), and HER2/neu. Hormone receptor status is a main factor in planning breast cancer treatment. Hormone receptor–positive breast tumors benefit from hormone therapies, such as selective ER modulators (for example, tamoxifen) and aromatase inhibitors (for example, anastrozole). Thus, these tumors have a more favorable disease-specific survival than do hormone receptor–negative tumors.2
African American women are more likely to present with hormone receptor-negative tumors. In an analysis of the California Cancer Registry, which has collected patient ER and PR status since 1990, whites had a higher proportion of tumors that were ER positive or PR positive (or both) and HER2 negative (72% vs. 53%).3 DeSantis et al.4 reported similar results for this tumor type, with 76% of non-Hispanic whites having hormone receptor–positive, HER2-negative tumors vs. 62% of non-Hispanic blacks. Even with stratification by tumor stage, African Americans continue to have a significantly higher proportion of hormone receptor–negative tumors than do whites for localized and advanced disease.5
Although hormone receptor status varies significantly by race, HER2 status does not show the same divergence. HER2 overexpression is present in approximately 20% of invasive breast cancers. HER2-positive, hormone receptor–negative tumors demonstrate more-aggressive features and worse breast cancer–specific survival than do hormone receptor–positive and HER2-negative tumors,2 although survival has vastly improved with new HER2-targeted therapies such as trastuzumab and pertuzumab. Unlike hormone receptor status, there was no association between race and HER2-positive/ER-negative tumors in the Carolina Breast Cancer Study.2
Triple-negative breast cancer (TNBC)
TNBC is the subtype of breast cancer with the worst prognosis. TNBC gets its name because its tumor cells lack the markers for ER, PR, and HER2 overexpression. Thus, TNBC tumors are estrogen receptor negative (ER), progesterone receptor negative (PR), and HER2/neu negative (HER2). While other subtypes of breast cancer have benefited from drug development regarding hormonal therapies and HER2-targeted treatments, TNBC has not experienced the same pharmacologic breakthroughs.
As such, even after analyses control for the stage at diagnosis, women with this subtype have poorer survival than those with other breast cancers.6 African American women have a higher incidence of TNBC than white women.7 DeSantis et al.4 reported that 22% of breast cancers were triple negative in non-Hispanic black patients vs. only 11% in non-Hispanic white patients. The Carolina Breast Cancer Study found that 26% of African American women had TNBC, whereas 16% of non-African American women did.2 This subtype was most common among younger, premenopausal African American women (39% of diagnosed cancer subtypes). When TNBC patients were excluded from analysis in the Carolina Breast Cancer Study, breast cancer–specific survival remained significantly worse among premenopausal African American women, suggesting that although tumor biology in part explains the poor outcomes, the survival disparity story is more complex.
Germline mutations: BRCA1 and BRCA2 Mutations
In addition to tumor biology, cancer genomics has become increasingly important in determining cancer prognosis and guiding treatment. Approximately 5%-10% of breast cancer cases present in individuals with inherited mutations in autosomal dominant, highly penetrant breast cancer susceptibility genes.8 Accounting for 80%-90% of families containing multiple cases of breast and ovarian cancer, BRCA1 and BRCA2 germline mutations are the most common of the breast cancer susceptibility genes.9 These patients often are younger and have a higher-grade tumor that is hormone receptor negative, which also often matches the profile of the African American breast cancer patient.10
Despite similarities between BRCA1-associated breast cancers and breast cancer in African Americans, genetic abnormalities in African American breast cancer patients remain underresearched. Nanda et al.11 found that BRCA1 and BRCA2 mutations occur with appreciable frequency in high-risk families of African ancestry, with 28% testing positive for a deleterious mutation in one of these genes. This frequency was at a lower rate than that found in non-Hispanic, non-Jewish whites, who had a rate of 46%, because African Americans had a higher rate of polymorphisms or variants of unknown significance (44% vs. 12%). This large percentage of variants of unknown significance indicates that more analysis is needed to understand the clinical implications of these genetic variations. In another study from the Northern California site of the Breast Cancer Family Registry, the BRCA1 mutation prevalence was 16.7% in African American cases diagnosed under the age of 35 years vs. 7.2% in non-Hispanic, non-Ashkenazi Jewish whites in the same age category.12 High frequencies of mutations in BRCA1 and BRCA2 have also been reported in breast cancer patients of African ancestry from Nigeria and the Bahamas.13, 14
These results in African American patients highlight the need for further study of breast cancer genomics in minority populations. However, Armstrong et al.15 illuminated the existence of racial/ethnic disparities in patterns of referral to cancer risk clinics. In their study, African American women with a family history of breast or ovarian cancer were significantly less likely to undergo genetic counseling for BRCA1/2 testing than were white women with this family history. The results of this study were noteworthy for the magnitude of the disparity, with white women having almost five times greater odds of undergoing this clinically important evaluation. More than two decades after BRCA1 and BRCA2 genes were identified, larger studies are still needed in diverse populations to derive true estimates of the burden of mutations in both genes in underserved and understudied populations.
Although these differences in tumor biology and genomics tell part of the mortality disparity story, there is more to be told. In a study of African American and white patients in South Carolina, Adams et al.16 determined survival rates by ethnicity that were adjusted for disease stage and other prognostic characteristics. After they controlled for age, stage, ER, and HER2 expression as well as insurance status, African American women still had a twofold excess risk of death from breast cancer. Thus, in addition to differences in the innate characteristics of the breast tumors, racial differences in patterns of care for women with breast cancer must be considered in unraveling the observed disparity in mortality. The third installment of this series will discuss the second element of the perfect storm – patterns of care.
Other installments of this column can be found in the Related Content box.
1. Daly B, Olopade OI. A perfect storm: How tumor biology, genomics, and health care delivery patterns collide to create a racial survival disparity in breast cancer and proposed interventions for change. CA Cancer J Clin. 2015;65(3):221-238.
2. Carey LA, Perou CM, Livasy CA, et al. Race, breast cancer subtypes, and survival in the Carolina Breast Cancer Study. JAMA. 2006;295(21):2492-502.
3. Kurian AW, Fish K, Shema SJ, Clarke CA. Lifetime risks of specific breast cancer subtypes among women in four racial/ethnic groups. Breast Cancer Res. 2010;12(6):R99.
4. DeSantis CE, Fedewa SA, Goding Sauer A, Kramer JL, Smith RA, Jemal A. Breast cancer statistics, 2015: Convergence of incidence rates between black and white women. CA Cancer J Clin. 2015 Oct 29. doi: 10.3322/caac.21320. [Epub ahead of print]
5. Setiawan VW, Monroe KR, Wilkens LR, Kolonel LN, Pike MC, Henderson BE. Breast cancer risk factors defined by estrogen and progesterone receptor status: the multiethnic cohort study. Am J Epidemiol. 2009;169(10):1251-9.
6. Bauer KR, Brown M, Cress RD, Parise CA, Caggiano V. Descriptive analysis of estrogen receptor (ER)-negative, progesterone receptor (PR)-negative, and HER2-negative invasive breast cancer, the so-called triple-negative phenotype: a population-based study from the California cancer Registry. Cancer. 2007;109(9):1721-8.
7. Ray M, Polite BN. Triple-negative breast cancers: a view from 10,000 feet. Cancer J. 2010;16(1):17-22.
8. Claus EB, Schildkraut JM, Thompson WD, Risch NJ. The genetic attributable risk of breast and ovarian cancer. Cancer. 1996;77(11):2318-24.
9. Easton DF, Bishop DT, Ford D, Crockford GP. Genetic linkage analysis in familial breast and ovarian cancer: results from 214 families. The Breast Cancer Linkage Consortium. Am J Hum Genet. 1993;52(4):678-701.
10. Polite BN, Olopade OI. Breast cancer and race: a rising tide does not lift all boats equally. Perspect Biol Med. 2005;48(1 Suppl):S166-75.
11. Nanda R, Schumm LP, Cummings S, et al. Genetic testing in an ethnically diverse cohort of high-risk women: a comparative analysis of BRCA1 and BRCA2 mutations in American families of European and African ancestry. JAMA. 2005;294(15):1925-33.
12. John EM, Miron A, Gong G, et al. Prevalence of pathogenic BRCA1 mutation carriers in 5 US racial/ethnic groups. JAMA. 2007;298(24):2869-76.
13. Fackenthal JD, Zhang J, Zhang B, et al. High prevalence of BRCA1 and BRCA2 mutations in unselected Nigerian breast cancer patients. Int J Cancer. 2012;131(5):1114-23.
14. Donenberg T, Lunn J, Curling D, et al. A high prevalence of BRCA1 mutations among breast cancer patients from the Bahamas. Breast Cancer Res Treat. 2011;125(2):591-6.
15. Armstrong K, Micco E, Carney A, Stopfer J, Putt M. Racial differences in the use of BRCA1/2 testing among women with a family history of breast or ovarian cancer. JAMA. 2005;293(14):1729-36.
16. Adams SA, Butler WM, Fulton J, et al. Racial disparities in breast cancer mortality in a multi-ethnic cohort in the Southeast. Cancer. 2012;118(10):2693-9.
Bobby Daly, MD, MBA, is the chief fellow in the section of hematology/oncology at the University of Chicago Medicine. His clinical focus is breast and thoracic oncology, and his research focus is health services. Specifically, Dr. Daly researches disparities in oncology care delivery, oncology health care utilization, aggressive end-of-life oncology care, and oncology payment models. He received his MD and MBA from Harvard Medical School and Harvard Business School, both in Boston, and a BA in Economics and History from Stanford (Calif.) University. He was the recipient of the Dean’s Award at Harvard Medical and Business Schools.
Olufunmilayo Olopade, MD, FACP, OON, is the Walter L. Palmer Distinguished Service Professor of Medicine and Human Genetics, and director, Center for Global Health at the University of Chicago. She is adopting emerging high throughput genomic and informatics strategies to identify genetic and nongenetic risk factors for breast cancer in order to implement precision health care in diverse populations. This innovative approach has the potential to improve the quality of care and reduce costs while saving more lives.
Disclosures: Dr. Olopade serves on the Medical Advisory Board for CancerIQ. Dr. Daly serves as a director of Quadrant Holdings Corporation and receives compensation from this entity. Frontline Medical Communications is a subsidiary of Quadrant Holdings Corporation.
Published in conjunction with Susan G. Komen®.
This is the second installment of a five-part monthly series that will discuss the pathologic, genomic, and clinical factors that contribute to the racial survival disparity in breast cancer. The series, which is adapted from an article that originally appeared in CA: A Cancer Journal for Clinicians1, a journal of the American Cancer Society, will also review exciting and innovative interventions to close this survival gap. This month’s column reviews tumor biology and genomics—the first element in the perfect storm.
Hormone receptor status and human epidermal growth factor receptor 2 (HER2)/neu
Breast cancer is not a single disease, and breast cancer subtype classifications are used in the clinical setting to determine prognosis and guide management. These different molecular subtypes are based on tumor markers, which include the presence or absence of three proteins: estrogen receptor (ER), progesterone receptor (PR), and HER2/neu. Hormone receptor status is a main factor in planning breast cancer treatment. Hormone receptor–positive breast tumors benefit from hormone therapies, such as selective ER modulators (for example, tamoxifen) and aromatase inhibitors (for example, anastrozole). Thus, these tumors have a more favorable disease-specific survival than do hormone receptor–negative tumors.2
African American women are more likely to present with hormone receptor-negative tumors. In an analysis of the California Cancer Registry, which has collected patient ER and PR status since 1990, whites had a higher proportion of tumors that were ER positive or PR positive (or both) and HER2 negative (72% vs. 53%).3 DeSantis et al.4 reported similar results for this tumor type, with 76% of non-Hispanic whites having hormone receptor–positive, HER2-negative tumors vs. 62% of non-Hispanic blacks. Even with stratification by tumor stage, African Americans continue to have a significantly higher proportion of hormone receptor–negative tumors than do whites for localized and advanced disease.5
Although hormone receptor status varies significantly by race, HER2 status does not show the same divergence. HER2 overexpression is present in approximately 20% of invasive breast cancers. HER2-positive, hormone receptor–negative tumors demonstrate more-aggressive features and worse breast cancer–specific survival than do hormone receptor–positive and HER2-negative tumors,2 although survival has vastly improved with new HER2-targeted therapies such as trastuzumab and pertuzumab. Unlike hormone receptor status, there was no association between race and HER2-positive/ER-negative tumors in the Carolina Breast Cancer Study.2
Triple-negative breast cancer (TNBC)
TNBC is the subtype of breast cancer with the worst prognosis. TNBC gets its name because its tumor cells lack the markers for ER, PR, and HER2 overexpression. Thus, TNBC tumors are estrogen receptor negative (ER), progesterone receptor negative (PR), and HER2/neu negative (HER2). While other subtypes of breast cancer have benefited from drug development regarding hormonal therapies and HER2-targeted treatments, TNBC has not experienced the same pharmacologic breakthroughs.
As such, even after analyses control for the stage at diagnosis, women with this subtype have poorer survival than those with other breast cancers.6 African American women have a higher incidence of TNBC than white women.7 DeSantis et al.4 reported that 22% of breast cancers were triple negative in non-Hispanic black patients vs. only 11% in non-Hispanic white patients. The Carolina Breast Cancer Study found that 26% of African American women had TNBC, whereas 16% of non-African American women did.2 This subtype was most common among younger, premenopausal African American women (39% of diagnosed cancer subtypes). When TNBC patients were excluded from analysis in the Carolina Breast Cancer Study, breast cancer–specific survival remained significantly worse among premenopausal African American women, suggesting that although tumor biology in part explains the poor outcomes, the survival disparity story is more complex.
Germline mutations: BRCA1 and BRCA2 Mutations
In addition to tumor biology, cancer genomics has become increasingly important in determining cancer prognosis and guiding treatment. Approximately 5%-10% of breast cancer cases present in individuals with inherited mutations in autosomal dominant, highly penetrant breast cancer susceptibility genes.8 Accounting for 80%-90% of families containing multiple cases of breast and ovarian cancer, BRCA1 and BRCA2 germline mutations are the most common of the breast cancer susceptibility genes.9 These patients often are younger and have a higher-grade tumor that is hormone receptor negative, which also often matches the profile of the African American breast cancer patient.10
Despite similarities between BRCA1-associated breast cancers and breast cancer in African Americans, genetic abnormalities in African American breast cancer patients remain underresearched. Nanda et al.11 found that BRCA1 and BRCA2 mutations occur with appreciable frequency in high-risk families of African ancestry, with 28% testing positive for a deleterious mutation in one of these genes. This frequency was at a lower rate than that found in non-Hispanic, non-Jewish whites, who had a rate of 46%, because African Americans had a higher rate of polymorphisms or variants of unknown significance (44% vs. 12%). This large percentage of variants of unknown significance indicates that more analysis is needed to understand the clinical implications of these genetic variations. In another study from the Northern California site of the Breast Cancer Family Registry, the BRCA1 mutation prevalence was 16.7% in African American cases diagnosed under the age of 35 years vs. 7.2% in non-Hispanic, non-Ashkenazi Jewish whites in the same age category.12 High frequencies of mutations in BRCA1 and BRCA2 have also been reported in breast cancer patients of African ancestry from Nigeria and the Bahamas.13, 14
These results in African American patients highlight the need for further study of breast cancer genomics in minority populations. However, Armstrong et al.15 illuminated the existence of racial/ethnic disparities in patterns of referral to cancer risk clinics. In their study, African American women with a family history of breast or ovarian cancer were significantly less likely to undergo genetic counseling for BRCA1/2 testing than were white women with this family history. The results of this study were noteworthy for the magnitude of the disparity, with white women having almost five times greater odds of undergoing this clinically important evaluation. More than two decades after BRCA1 and BRCA2 genes were identified, larger studies are still needed in diverse populations to derive true estimates of the burden of mutations in both genes in underserved and understudied populations.
Although these differences in tumor biology and genomics tell part of the mortality disparity story, there is more to be told. In a study of African American and white patients in South Carolina, Adams et al.16 determined survival rates by ethnicity that were adjusted for disease stage and other prognostic characteristics. After they controlled for age, stage, ER, and HER2 expression as well as insurance status, African American women still had a twofold excess risk of death from breast cancer. Thus, in addition to differences in the innate characteristics of the breast tumors, racial differences in patterns of care for women with breast cancer must be considered in unraveling the observed disparity in mortality. The third installment of this series will discuss the second element of the perfect storm – patterns of care.
Other installments of this column can be found in the Related Content box.
1. Daly B, Olopade OI. A perfect storm: How tumor biology, genomics, and health care delivery patterns collide to create a racial survival disparity in breast cancer and proposed interventions for change. CA Cancer J Clin. 2015;65(3):221-238.
2. Carey LA, Perou CM, Livasy CA, et al. Race, breast cancer subtypes, and survival in the Carolina Breast Cancer Study. JAMA. 2006;295(21):2492-502.
3. Kurian AW, Fish K, Shema SJ, Clarke CA. Lifetime risks of specific breast cancer subtypes among women in four racial/ethnic groups. Breast Cancer Res. 2010;12(6):R99.
4. DeSantis CE, Fedewa SA, Goding Sauer A, Kramer JL, Smith RA, Jemal A. Breast cancer statistics, 2015: Convergence of incidence rates between black and white women. CA Cancer J Clin. 2015 Oct 29. doi: 10.3322/caac.21320. [Epub ahead of print]
5. Setiawan VW, Monroe KR, Wilkens LR, Kolonel LN, Pike MC, Henderson BE. Breast cancer risk factors defined by estrogen and progesterone receptor status: the multiethnic cohort study. Am J Epidemiol. 2009;169(10):1251-9.
6. Bauer KR, Brown M, Cress RD, Parise CA, Caggiano V. Descriptive analysis of estrogen receptor (ER)-negative, progesterone receptor (PR)-negative, and HER2-negative invasive breast cancer, the so-called triple-negative phenotype: a population-based study from the California cancer Registry. Cancer. 2007;109(9):1721-8.
7. Ray M, Polite BN. Triple-negative breast cancers: a view from 10,000 feet. Cancer J. 2010;16(1):17-22.
8. Claus EB, Schildkraut JM, Thompson WD, Risch NJ. The genetic attributable risk of breast and ovarian cancer. Cancer. 1996;77(11):2318-24.
9. Easton DF, Bishop DT, Ford D, Crockford GP. Genetic linkage analysis in familial breast and ovarian cancer: results from 214 families. The Breast Cancer Linkage Consortium. Am J Hum Genet. 1993;52(4):678-701.
10. Polite BN, Olopade OI. Breast cancer and race: a rising tide does not lift all boats equally. Perspect Biol Med. 2005;48(1 Suppl):S166-75.
11. Nanda R, Schumm LP, Cummings S, et al. Genetic testing in an ethnically diverse cohort of high-risk women: a comparative analysis of BRCA1 and BRCA2 mutations in American families of European and African ancestry. JAMA. 2005;294(15):1925-33.
12. John EM, Miron A, Gong G, et al. Prevalence of pathogenic BRCA1 mutation carriers in 5 US racial/ethnic groups. JAMA. 2007;298(24):2869-76.
13. Fackenthal JD, Zhang J, Zhang B, et al. High prevalence of BRCA1 and BRCA2 mutations in unselected Nigerian breast cancer patients. Int J Cancer. 2012;131(5):1114-23.
14. Donenberg T, Lunn J, Curling D, et al. A high prevalence of BRCA1 mutations among breast cancer patients from the Bahamas. Breast Cancer Res Treat. 2011;125(2):591-6.
15. Armstrong K, Micco E, Carney A, Stopfer J, Putt M. Racial differences in the use of BRCA1/2 testing among women with a family history of breast or ovarian cancer. JAMA. 2005;293(14):1729-36.
16. Adams SA, Butler WM, Fulton J, et al. Racial disparities in breast cancer mortality in a multi-ethnic cohort in the Southeast. Cancer. 2012;118(10):2693-9.
Bobby Daly, MD, MBA, is the chief fellow in the section of hematology/oncology at the University of Chicago Medicine. His clinical focus is breast and thoracic oncology, and his research focus is health services. Specifically, Dr. Daly researches disparities in oncology care delivery, oncology health care utilization, aggressive end-of-life oncology care, and oncology payment models. He received his MD and MBA from Harvard Medical School and Harvard Business School, both in Boston, and a BA in Economics and History from Stanford (Calif.) University. He was the recipient of the Dean’s Award at Harvard Medical and Business Schools.
Olufunmilayo Olopade, MD, FACP, OON, is the Walter L. Palmer Distinguished Service Professor of Medicine and Human Genetics, and director, Center for Global Health at the University of Chicago. She is adopting emerging high throughput genomic and informatics strategies to identify genetic and nongenetic risk factors for breast cancer in order to implement precision health care in diverse populations. This innovative approach has the potential to improve the quality of care and reduce costs while saving more lives.
Disclosures: Dr. Olopade serves on the Medical Advisory Board for CancerIQ. Dr. Daly serves as a director of Quadrant Holdings Corporation and receives compensation from this entity. Frontline Medical Communications is a subsidiary of Quadrant Holdings Corporation.
Published in conjunction with Susan G. Komen®.
Reader reactions to modified American Cancer Society mammography guidelines

Why is ACOG so late?I am quite dismayed that the American College of Obstetricians and Gynecologists (ACOG), again, is the last kid on the block to accept data on a major recommendation like mammography. (ACOG was late to respond to cervical cancer screening changes.) There are growing data supporting the concept that we have over-done mammography and ignored the warnings that mammograms do not meet usual criteria for a good screening test, especially for those aged younger than 50 years. In the 70s and 80s, Dr. John Bailar of the National Cancer Institute warned of the dangers of radiation in “breast x-rays”.1,2 We must move forward and develop a more unified approach for this deadly disease.
James Kolter, MD
Paoli, Pennsylvania
References
- Bailar JC 3rd. Mammography: a time for caution. JAMA. 1977;237(10):997–998.
- Bailar JC 3rd. Mammography before age 50 years? JAMA. 1988;259(10):1548–1549.
Help me accept that we must let these women dieI have been a frontline gynecologist for about 40 years. When I was trained, the goal was to screen everyone. We sought to find diseases early enough to successfully treat and cure before they were too far advanced. In my years thus far I have seen it work: early breast cancers have been found on mammography and during clinical breast examinations. Many lives saved.
I have known most of my patients for 25 to 35 years. I am embarrassed to send an academic journal these experiential and anecdotal stories without numbers and percentages, but I treat individual people and not populations. I cannot get it into my brain that it is not worth saving these women.
Janet, a 37-year-old woman, had just lost her husband to a sudden heart attack, leaving her with 5- and 7-year-old daughters. At that time, baseline mammograms were ordered between ages 35 and 40 years. We were shocked when her mammography revealed breast cancer; she had no family history of breast cancer. Five years later it recurred, and 5 years after that, she was found to have something no one had known about earlier: the BRCA gene mutation. She has since had bilateral mastectomies and bilateral oophorectomies. Last week, at her annual check-up at age 62, she showed me pictures of her grandchildren.
I cannot help but feel that Janet would not be here today if we had not done that screening mammography years ago. But now I am asked to let someone like her go, so that the system does not have to pay for all the “normals.” There are many stories of lumps found during routine examination, of an aggressive cancer found on mammogram 1 year (not 2) after a perfectly normal mammogram.
Help me accept that we must let these people die, or identify their disease at a much more advanced state given these new guidelines. I cannot be the only bread-and-butter gynecologist who is having trouble agreeing with this new approach.
Are there not other ways to cut medical costs? Can we eliminate the “middlemen” in the system? Is there any way other than not screening to save women’s lives?
If a patient gets breast cancer before age 45 or within the 2-year interval between mammograms, would she sue their doctor for not recommending annual screening? We all know cases of women who have died of cervical cancer after having normal Papanicolaou (Pap) test results 2 years before. (Their survivors sued, and won). But if they had had a Pap after only 1 year, would their disease have been discovered and successfully treated?
Perhaps I reveal myself as politically incorrect or not “cost-effective” in this letter. But rest assured, many of my colleagues are retiring (as will I in time), so those trained in my era will disappear. The younger crop is thoroughly trained in this new way. I wonder what the pendulum will do, if after these guidelines sink in, advanced cancers that cannot be treated successfully reveal themselves.
Lois S. Goodman, MD
Weston, Massachusetts
Prevent rather than detectEarly detection is not prevention. Until medicine actually wants to work on prevention, the American Cancer Society guidelines are just more of the same old story, focusing on the symptoms rather than on the root causes. Using genomics and personalized, functional medicine in combination with breast thermography, many more breast cancers can potentially be prevented in the first place, with mammography (and ultrasonography) used as a diagnostic tool. This would be much more powerful than focusing only on early detection. ObGyns need to learn how to apply these new skills and help women get much more value from their preventive care. Until physicians reclaim their ability to think and evaluate critically with open, curious minds, they will continue to fail the very people they aim to serve—their patients.
Roberta Kline, MD
Santa Fe, New Mexico
Guidelines written by statisticians, not ObGynsI was happy to see Dr. Kopan’s article, as well as others about the new American Cancer Society (ACS) screening mammography guidelines. Initially, I was infuriated when I read the guidelines. Looking at the composition of the ACS committee, I can understand some of the conclusions: I believe there were 4 statisticians among the members.
Statisticians look at mammography statistics as numbers and significant figures. They do not consider that these numbers represent lives. In the guidelines it was stated that earlier and more frequent screening, as well as discontinuing screening after the age of 74, only saved the lives of 10 women out of 100,000. That would certainly be significant for the 10 women who are saved. What if one of them was a relative of one of the committee members?
Another silly recommendation was that women no longer have clinical breast examinations. The committee obviously does not realize how frequently cancers are found by clinical exam.
Norman D. Lindley, MD
Alamogordo, New Mexico
“MANUAL VACUUM ASPIRATION: A SAFE AND EFFECTIVE TREATMENT FOR EARLY MISCARRIAGE”PIYAPA PRADITPAN, MD, MPH, AND ANNE R. DAVIS, MD, MPH (NOVEMBER 2015)
Which antibiotic for prophylaxis at vacuum aspiration for miscarriage?Thank you to Drs. Praditpan and Davis for a great article. I think, however, there is more evidence for azithromycin 1 g PO (than doxycycline as the authors recommend) as prophylaxis for surgical abortion and no antibiotic prophylaxis for medi‑ cal abortion.
Tirun (Ty) Gopal, MD
San Francisco, California
Drs. Praditpan and Davis respond Thank you for your comment and for allowing us to provide clarification on the topic of antibiotic prophylaxis at the time of vacuum aspiration for miscarriage management. Few studies address the question of antibiotic prophylaxis at the time of surgical management of miscarriage, and a meta-analysis found insufficient data to yield a conclusion.1 Recommendations for infection prophylaxis in miscarriage management have been extrapolated from the abundance of data for induced abortion, since the surgical procedure is the same for both.
The 2011 Society of Family Planning (SFP) clinical guidelines on prevention of infection after induced abortion identified 14 randomized trials that examined the efficacy of antibiotic regimens administered preoperatively to prevent upper genital tract infection after first trimester surgical procedures.2 Five studies (involving a total of 5,380 patients) examined tetracyclines, while only 1 study (N = 378) examined macrolides. The trials comparing tetracycline prophylaxis with placebo showed significant risk reduction in upper genital tract infection in tetracycline users (up to 88%), with an overall postinfection rate similar to that reported in the United States (<1%). Regardless of antibiotic choice or duration, the risk of infection was lower in women who received any prophylactic antibiotics compared with women who received placebo.
Based on these data and doxycycline’s cost effectiveness and its minimal adverse effects, the SFP recommends doxycycline as the antibiotic of choice for prevention of infection after induced abortion. Antibiotics should be administered on the day of the procedure and, if clinicians prefer, for no more than 3 days afterwards. Azithromycin is a macrolide that can be used for presumptive treatment of chlamydia at the time of surgical abortion.3 No trials compare azithromycin to doxycycline for prevention of infection after vacuum aspiration.
References
- May W, Gulmezoglu AM, Ba-Thike K. Antibiotics for incomplete abortion. Cochrane Database Syst Rev. 2007;(4):CD001779.
- Achilles SL, Reeve MF; Society of Family Planning. Prevention of infection after induced abortion: release date October 2010: SFP Guideline 2010. Contraception. 2011;83(4):295–309.
- Royal College of Obstetricians and Gynaecologists. The care of women requesting induced abortion: Evidence-based clinical guideline number 7. https://www.rcog.org.uk/globalassets/documents/guidelines/abortion-guideline_web_1.pdf. Published November 2011. Accessed December 18, 2015.
Why is ACOG so late?I am quite dismayed that the American College of Obstetricians and Gynecologists (ACOG), again, is the last kid on the block to accept data on a major recommendation like mammography. (ACOG was late to respond to cervical cancer screening changes.) There are growing data supporting the concept that we have over-done mammography and ignored the warnings that mammograms do not meet usual criteria for a good screening test, especially for those aged younger than 50 years. In the 70s and 80s, Dr. John Bailar of the National Cancer Institute warned of the dangers of radiation in “breast x-rays”.1,2 We must move forward and develop a more unified approach for this deadly disease.
James Kolter, MD
Paoli, Pennsylvania
References
- Bailar JC 3rd. Mammography: a time for caution. JAMA. 1977;237(10):997–998.
- Bailar JC 3rd. Mammography before age 50 years? JAMA. 1988;259(10):1548–1549.
Help me accept that we must let these women dieI have been a frontline gynecologist for about 40 years. When I was trained, the goal was to screen everyone. We sought to find diseases early enough to successfully treat and cure before they were too far advanced. In my years thus far I have seen it work: early breast cancers have been found on mammography and during clinical breast examinations. Many lives saved.
I have known most of my patients for 25 to 35 years. I am embarrassed to send an academic journal these experiential and anecdotal stories without numbers and percentages, but I treat individual people and not populations. I cannot get it into my brain that it is not worth saving these women.
Janet, a 37-year-old woman, had just lost her husband to a sudden heart attack, leaving her with 5- and 7-year-old daughters. At that time, baseline mammograms were ordered between ages 35 and 40 years. We were shocked when her mammography revealed breast cancer; she had no family history of breast cancer. Five years later it recurred, and 5 years after that, she was found to have something no one had known about earlier: the BRCA gene mutation. She has since had bilateral mastectomies and bilateral oophorectomies. Last week, at her annual check-up at age 62, she showed me pictures of her grandchildren.
I cannot help but feel that Janet would not be here today if we had not done that screening mammography years ago. But now I am asked to let someone like her go, so that the system does not have to pay for all the “normals.” There are many stories of lumps found during routine examination, of an aggressive cancer found on mammogram 1 year (not 2) after a perfectly normal mammogram.
Help me accept that we must let these people die, or identify their disease at a much more advanced state given these new guidelines. I cannot be the only bread-and-butter gynecologist who is having trouble agreeing with this new approach.
Are there not other ways to cut medical costs? Can we eliminate the “middlemen” in the system? Is there any way other than not screening to save women’s lives?
If a patient gets breast cancer before age 45 or within the 2-year interval between mammograms, would she sue their doctor for not recommending annual screening? We all know cases of women who have died of cervical cancer after having normal Papanicolaou (Pap) test results 2 years before. (Their survivors sued, and won). But if they had had a Pap after only 1 year, would their disease have been discovered and successfully treated?
Perhaps I reveal myself as politically incorrect or not “cost-effective” in this letter. But rest assured, many of my colleagues are retiring (as will I in time), so those trained in my era will disappear. The younger crop is thoroughly trained in this new way. I wonder what the pendulum will do, if after these guidelines sink in, advanced cancers that cannot be treated successfully reveal themselves.
Lois S. Goodman, MD
Weston, Massachusetts
Prevent rather than detectEarly detection is not prevention. Until medicine actually wants to work on prevention, the American Cancer Society guidelines are just more of the same old story, focusing on the symptoms rather than on the root causes. Using genomics and personalized, functional medicine in combination with breast thermography, many more breast cancers can potentially be prevented in the first place, with mammography (and ultrasonography) used as a diagnostic tool. This would be much more powerful than focusing only on early detection. ObGyns need to learn how to apply these new skills and help women get much more value from their preventive care. Until physicians reclaim their ability to think and evaluate critically with open, curious minds, they will continue to fail the very people they aim to serve—their patients.
Roberta Kline, MD
Santa Fe, New Mexico
Guidelines written by statisticians, not ObGynsI was happy to see Dr. Kopan’s article, as well as others about the new American Cancer Society (ACS) screening mammography guidelines. Initially, I was infuriated when I read the guidelines. Looking at the composition of the ACS committee, I can understand some of the conclusions: I believe there were 4 statisticians among the members.
Statisticians look at mammography statistics as numbers and significant figures. They do not consider that these numbers represent lives. In the guidelines it was stated that earlier and more frequent screening, as well as discontinuing screening after the age of 74, only saved the lives of 10 women out of 100,000. That would certainly be significant for the 10 women who are saved. What if one of them was a relative of one of the committee members?
Another silly recommendation was that women no longer have clinical breast examinations. The committee obviously does not realize how frequently cancers are found by clinical exam.
Norman D. Lindley, MD
Alamogordo, New Mexico
“MANUAL VACUUM ASPIRATION: A SAFE AND EFFECTIVE TREATMENT FOR EARLY MISCARRIAGE”PIYAPA PRADITPAN, MD, MPH, AND ANNE R. DAVIS, MD, MPH (NOVEMBER 2015)
Which antibiotic for prophylaxis at vacuum aspiration for miscarriage?Thank you to Drs. Praditpan and Davis for a great article. I think, however, there is more evidence for azithromycin 1 g PO (than doxycycline as the authors recommend) as prophylaxis for surgical abortion and no antibiotic prophylaxis for medi‑ cal abortion.
Tirun (Ty) Gopal, MD
San Francisco, California
Drs. Praditpan and Davis respond Thank you for your comment and for allowing us to provide clarification on the topic of antibiotic prophylaxis at the time of vacuum aspiration for miscarriage management. Few studies address the question of antibiotic prophylaxis at the time of surgical management of miscarriage, and a meta-analysis found insufficient data to yield a conclusion.1 Recommendations for infection prophylaxis in miscarriage management have been extrapolated from the abundance of data for induced abortion, since the surgical procedure is the same for both.
The 2011 Society of Family Planning (SFP) clinical guidelines on prevention of infection after induced abortion identified 14 randomized trials that examined the efficacy of antibiotic regimens administered preoperatively to prevent upper genital tract infection after first trimester surgical procedures.2 Five studies (involving a total of 5,380 patients) examined tetracyclines, while only 1 study (N = 378) examined macrolides. The trials comparing tetracycline prophylaxis with placebo showed significant risk reduction in upper genital tract infection in tetracycline users (up to 88%), with an overall postinfection rate similar to that reported in the United States (<1%). Regardless of antibiotic choice or duration, the risk of infection was lower in women who received any prophylactic antibiotics compared with women who received placebo.
Based on these data and doxycycline’s cost effectiveness and its minimal adverse effects, the SFP recommends doxycycline as the antibiotic of choice for prevention of infection after induced abortion. Antibiotics should be administered on the day of the procedure and, if clinicians prefer, for no more than 3 days afterwards. Azithromycin is a macrolide that can be used for presumptive treatment of chlamydia at the time of surgical abortion.3 No trials compare azithromycin to doxycycline for prevention of infection after vacuum aspiration.
References
- May W, Gulmezoglu AM, Ba-Thike K. Antibiotics for incomplete abortion. Cochrane Database Syst Rev. 2007;(4):CD001779.
- Achilles SL, Reeve MF; Society of Family Planning. Prevention of infection after induced abortion: release date October 2010: SFP Guideline 2010. Contraception. 2011;83(4):295–309.
- Royal College of Obstetricians and Gynaecologists. The care of women requesting induced abortion: Evidence-based clinical guideline number 7. https://www.rcog.org.uk/globalassets/documents/guidelines/abortion-guideline_web_1.pdf. Published November 2011. Accessed December 18, 2015.
Why is ACOG so late?I am quite dismayed that the American College of Obstetricians and Gynecologists (ACOG), again, is the last kid on the block to accept data on a major recommendation like mammography. (ACOG was late to respond to cervical cancer screening changes.) There are growing data supporting the concept that we have over-done mammography and ignored the warnings that mammograms do not meet usual criteria for a good screening test, especially for those aged younger than 50 years. In the 70s and 80s, Dr. John Bailar of the National Cancer Institute warned of the dangers of radiation in “breast x-rays”.1,2 We must move forward and develop a more unified approach for this deadly disease.
James Kolter, MD
Paoli, Pennsylvania
References
- Bailar JC 3rd. Mammography: a time for caution. JAMA. 1977;237(10):997–998.
- Bailar JC 3rd. Mammography before age 50 years? JAMA. 1988;259(10):1548–1549.
Help me accept that we must let these women dieI have been a frontline gynecologist for about 40 years. When I was trained, the goal was to screen everyone. We sought to find diseases early enough to successfully treat and cure before they were too far advanced. In my years thus far I have seen it work: early breast cancers have been found on mammography and during clinical breast examinations. Many lives saved.
I have known most of my patients for 25 to 35 years. I am embarrassed to send an academic journal these experiential and anecdotal stories without numbers and percentages, but I treat individual people and not populations. I cannot get it into my brain that it is not worth saving these women.
Janet, a 37-year-old woman, had just lost her husband to a sudden heart attack, leaving her with 5- and 7-year-old daughters. At that time, baseline mammograms were ordered between ages 35 and 40 years. We were shocked when her mammography revealed breast cancer; she had no family history of breast cancer. Five years later it recurred, and 5 years after that, she was found to have something no one had known about earlier: the BRCA gene mutation. She has since had bilateral mastectomies and bilateral oophorectomies. Last week, at her annual check-up at age 62, she showed me pictures of her grandchildren.
I cannot help but feel that Janet would not be here today if we had not done that screening mammography years ago. But now I am asked to let someone like her go, so that the system does not have to pay for all the “normals.” There are many stories of lumps found during routine examination, of an aggressive cancer found on mammogram 1 year (not 2) after a perfectly normal mammogram.
Help me accept that we must let these people die, or identify their disease at a much more advanced state given these new guidelines. I cannot be the only bread-and-butter gynecologist who is having trouble agreeing with this new approach.
Are there not other ways to cut medical costs? Can we eliminate the “middlemen” in the system? Is there any way other than not screening to save women’s lives?
If a patient gets breast cancer before age 45 or within the 2-year interval between mammograms, would she sue their doctor for not recommending annual screening? We all know cases of women who have died of cervical cancer after having normal Papanicolaou (Pap) test results 2 years before. (Their survivors sued, and won). But if they had had a Pap after only 1 year, would their disease have been discovered and successfully treated?
Perhaps I reveal myself as politically incorrect or not “cost-effective” in this letter. But rest assured, many of my colleagues are retiring (as will I in time), so those trained in my era will disappear. The younger crop is thoroughly trained in this new way. I wonder what the pendulum will do, if after these guidelines sink in, advanced cancers that cannot be treated successfully reveal themselves.
Lois S. Goodman, MD
Weston, Massachusetts
Prevent rather than detectEarly detection is not prevention. Until medicine actually wants to work on prevention, the American Cancer Society guidelines are just more of the same old story, focusing on the symptoms rather than on the root causes. Using genomics and personalized, functional medicine in combination with breast thermography, many more breast cancers can potentially be prevented in the first place, with mammography (and ultrasonography) used as a diagnostic tool. This would be much more powerful than focusing only on early detection. ObGyns need to learn how to apply these new skills and help women get much more value from their preventive care. Until physicians reclaim their ability to think and evaluate critically with open, curious minds, they will continue to fail the very people they aim to serve—their patients.
Roberta Kline, MD
Santa Fe, New Mexico
Guidelines written by statisticians, not ObGynsI was happy to see Dr. Kopan’s article, as well as others about the new American Cancer Society (ACS) screening mammography guidelines. Initially, I was infuriated when I read the guidelines. Looking at the composition of the ACS committee, I can understand some of the conclusions: I believe there were 4 statisticians among the members.
Statisticians look at mammography statistics as numbers and significant figures. They do not consider that these numbers represent lives. In the guidelines it was stated that earlier and more frequent screening, as well as discontinuing screening after the age of 74, only saved the lives of 10 women out of 100,000. That would certainly be significant for the 10 women who are saved. What if one of them was a relative of one of the committee members?
Another silly recommendation was that women no longer have clinical breast examinations. The committee obviously does not realize how frequently cancers are found by clinical exam.
Norman D. Lindley, MD
Alamogordo, New Mexico
“MANUAL VACUUM ASPIRATION: A SAFE AND EFFECTIVE TREATMENT FOR EARLY MISCARRIAGE”PIYAPA PRADITPAN, MD, MPH, AND ANNE R. DAVIS, MD, MPH (NOVEMBER 2015)
Which antibiotic for prophylaxis at vacuum aspiration for miscarriage?Thank you to Drs. Praditpan and Davis for a great article. I think, however, there is more evidence for azithromycin 1 g PO (than doxycycline as the authors recommend) as prophylaxis for surgical abortion and no antibiotic prophylaxis for medi‑ cal abortion.
Tirun (Ty) Gopal, MD
San Francisco, California
Drs. Praditpan and Davis respond Thank you for your comment and for allowing us to provide clarification on the topic of antibiotic prophylaxis at the time of vacuum aspiration for miscarriage management. Few studies address the question of antibiotic prophylaxis at the time of surgical management of miscarriage, and a meta-analysis found insufficient data to yield a conclusion.1 Recommendations for infection prophylaxis in miscarriage management have been extrapolated from the abundance of data for induced abortion, since the surgical procedure is the same for both.
The 2011 Society of Family Planning (SFP) clinical guidelines on prevention of infection after induced abortion identified 14 randomized trials that examined the efficacy of antibiotic regimens administered preoperatively to prevent upper genital tract infection after first trimester surgical procedures.2 Five studies (involving a total of 5,380 patients) examined tetracyclines, while only 1 study (N = 378) examined macrolides. The trials comparing tetracycline prophylaxis with placebo showed significant risk reduction in upper genital tract infection in tetracycline users (up to 88%), with an overall postinfection rate similar to that reported in the United States (<1%). Regardless of antibiotic choice or duration, the risk of infection was lower in women who received any prophylactic antibiotics compared with women who received placebo.
Based on these data and doxycycline’s cost effectiveness and its minimal adverse effects, the SFP recommends doxycycline as the antibiotic of choice for prevention of infection after induced abortion. Antibiotics should be administered on the day of the procedure and, if clinicians prefer, for no more than 3 days afterwards. Azithromycin is a macrolide that can be used for presumptive treatment of chlamydia at the time of surgical abortion.3 No trials compare azithromycin to doxycycline for prevention of infection after vacuum aspiration.
References
- May W, Gulmezoglu AM, Ba-Thike K. Antibiotics for incomplete abortion. Cochrane Database Syst Rev. 2007;(4):CD001779.
- Achilles SL, Reeve MF; Society of Family Planning. Prevention of infection after induced abortion: release date October 2010: SFP Guideline 2010. Contraception. 2011;83(4):295–309.
- Royal College of Obstetricians and Gynaecologists. The care of women requesting induced abortion: Evidence-based clinical guideline number 7. https://www.rcog.org.uk/globalassets/documents/guidelines/abortion-guideline_web_1.pdf. Published November 2011. Accessed December 18, 2015.

Patient prognostic score may lessen DCIS overtreatment
A prognostic score based on tumor size, age, and nuclear grade indicated the magnitude of survival benefit from radiation therapy (RT) after breast-conserving surgery for ductal carcinoma in situ (DCIS).
For patients of younger age with larger tumors and higher nuclear grade, survival among those who received radiation therapy was significantly better than among those who did not. In the absence of these risk factors, survival was similar for the RT and non-RT groups. The magnitude of the survival improvement with RT was significantly correlated with the patient prognostic score: for score 0, hazard ratio (HR) was 1.2 (95% CI, 0.67 to 2.06); for score 5, HR was 0.29 (95% CI, 0.09 to 0.91).
“Overall [breast cancer mortality] was only approximately 1%, whereas mortality from other causes was approximately 10% in our study. These results, when taken together with our earlier findings on DCIS, suggest that further research investigating the overdiagnosis and overtreatment of breast cancer is warranted and that a less invasive and more individualized local treatment strategy on the basis of one’s probability of local recurrence should be considered,” wrote Dr. Yasuaki Sagara of Brigham and Women’s Hospital and Dana-Farber/Brigham and Women’s Cancer Center, Boston, and colleagues (J Clin Oncol. 2016 Feb 1. doi: 10.1200/JCO.2015.65.1869).
The retrospective longitudinal cohort study used SEER data of 32,144 patients with DCIS: 20,329 (63.2%) received radiation therapy and 11,815 (36.8%) did not. At a median 8-year follow up, there were 304 breast-cancer specific deaths (0.9%).
The patient prognostic score is based on three factors: age, tumor size, and histology, with a cumulative score ranging from 0 (lowest risk) to 6 (highest risk). Patient age categories are 61 years or greater (0 points), 40-60 years (1 point), and 40 years or less (2 points); size categories are less than 16 mm (0), 16 mm to 40 mm (1), and 41 mm or greater (2); histology categories are low grade (0), intermediate grade (1), and high grade (2).
Investigators cautioned that this retrospective study was unable to measure potential confounders, such as surgical margin status, endocrine therapy, patient comorbidities, and reasons for treatment selection, which are factors that can significantly impact overall survival outcome measures.
The researchers highlighted the utility of the prognostic score in predicting survival benefit of RT, which can guide individual treatment decisions.
“As an oncology community, we must be cognizant of overtreatment for this disease process that has low [breast cancer mortality],” they wrote.
A prognostic score based on tumor size, age, and nuclear grade indicated the magnitude of survival benefit from radiation therapy (RT) after breast-conserving surgery for ductal carcinoma in situ (DCIS).
For patients of younger age with larger tumors and higher nuclear grade, survival among those who received radiation therapy was significantly better than among those who did not. In the absence of these risk factors, survival was similar for the RT and non-RT groups. The magnitude of the survival improvement with RT was significantly correlated with the patient prognostic score: for score 0, hazard ratio (HR) was 1.2 (95% CI, 0.67 to 2.06); for score 5, HR was 0.29 (95% CI, 0.09 to 0.91).
“Overall [breast cancer mortality] was only approximately 1%, whereas mortality from other causes was approximately 10% in our study. These results, when taken together with our earlier findings on DCIS, suggest that further research investigating the overdiagnosis and overtreatment of breast cancer is warranted and that a less invasive and more individualized local treatment strategy on the basis of one’s probability of local recurrence should be considered,” wrote Dr. Yasuaki Sagara of Brigham and Women’s Hospital and Dana-Farber/Brigham and Women’s Cancer Center, Boston, and colleagues (J Clin Oncol. 2016 Feb 1. doi: 10.1200/JCO.2015.65.1869).
The retrospective longitudinal cohort study used SEER data of 32,144 patients with DCIS: 20,329 (63.2%) received radiation therapy and 11,815 (36.8%) did not. At a median 8-year follow up, there were 304 breast-cancer specific deaths (0.9%).
The patient prognostic score is based on three factors: age, tumor size, and histology, with a cumulative score ranging from 0 (lowest risk) to 6 (highest risk). Patient age categories are 61 years or greater (0 points), 40-60 years (1 point), and 40 years or less (2 points); size categories are less than 16 mm (0), 16 mm to 40 mm (1), and 41 mm or greater (2); histology categories are low grade (0), intermediate grade (1), and high grade (2).
Investigators cautioned that this retrospective study was unable to measure potential confounders, such as surgical margin status, endocrine therapy, patient comorbidities, and reasons for treatment selection, which are factors that can significantly impact overall survival outcome measures.
The researchers highlighted the utility of the prognostic score in predicting survival benefit of RT, which can guide individual treatment decisions.
“As an oncology community, we must be cognizant of overtreatment for this disease process that has low [breast cancer mortality],” they wrote.
A prognostic score based on tumor size, age, and nuclear grade indicated the magnitude of survival benefit from radiation therapy (RT) after breast-conserving surgery for ductal carcinoma in situ (DCIS).
For patients of younger age with larger tumors and higher nuclear grade, survival among those who received radiation therapy was significantly better than among those who did not. In the absence of these risk factors, survival was similar for the RT and non-RT groups. The magnitude of the survival improvement with RT was significantly correlated with the patient prognostic score: for score 0, hazard ratio (HR) was 1.2 (95% CI, 0.67 to 2.06); for score 5, HR was 0.29 (95% CI, 0.09 to 0.91).
“Overall [breast cancer mortality] was only approximately 1%, whereas mortality from other causes was approximately 10% in our study. These results, when taken together with our earlier findings on DCIS, suggest that further research investigating the overdiagnosis and overtreatment of breast cancer is warranted and that a less invasive and more individualized local treatment strategy on the basis of one’s probability of local recurrence should be considered,” wrote Dr. Yasuaki Sagara of Brigham and Women’s Hospital and Dana-Farber/Brigham and Women’s Cancer Center, Boston, and colleagues (J Clin Oncol. 2016 Feb 1. doi: 10.1200/JCO.2015.65.1869).
The retrospective longitudinal cohort study used SEER data of 32,144 patients with DCIS: 20,329 (63.2%) received radiation therapy and 11,815 (36.8%) did not. At a median 8-year follow up, there were 304 breast-cancer specific deaths (0.9%).
The patient prognostic score is based on three factors: age, tumor size, and histology, with a cumulative score ranging from 0 (lowest risk) to 6 (highest risk). Patient age categories are 61 years or greater (0 points), 40-60 years (1 point), and 40 years or less (2 points); size categories are less than 16 mm (0), 16 mm to 40 mm (1), and 41 mm or greater (2); histology categories are low grade (0), intermediate grade (1), and high grade (2).
Investigators cautioned that this retrospective study was unable to measure potential confounders, such as surgical margin status, endocrine therapy, patient comorbidities, and reasons for treatment selection, which are factors that can significantly impact overall survival outcome measures.
The researchers highlighted the utility of the prognostic score in predicting survival benefit of RT, which can guide individual treatment decisions.
“As an oncology community, we must be cognizant of overtreatment for this disease process that has low [breast cancer mortality],” they wrote.
FROM JOURNAL OF CLINICAL ONCOLOGY
Key clinical point: A recurrence risk score based on clinicopathologic features of ductal carcinoma in situ (DCIS) was associated with survival benefit of radiation therapy after breast-conserving surgery.
Major finding: For patients of younger age with larger tumors and higher nuclear grade, survival among those who received radiation therapy was significantly better than among those who did not; in the absence of the risk factors, survival was similar for the two groups.
Data source: Retrospective longitudinal cohort study using SEER data of 32,144 patients with DCIS: 20,329 received radiation therapy and 11,815 did not.
Disclosures: Dr. Sagara reported having no disclosures. Two of his coauthors reported ties to industry.