User login
Chance to Diagnose Eosinophilic Esophagitis in the ED Commonly Missed
PHOENIX — The opportunity to diagnose eosinophilic esophagitis (EoE) when patients present to the emergency department (ED) with the classic symptom of esophageal food impaction (EFI) is commonly missed, with necessary biopsies provided at strikingly low rates, despite guideline recommendations, new research showed.
“This is the first study to assess the rate of biopsies at time of esophageal food impaction in a large, real-world dataset of community practices,” the authors explained in research presented at the American College of Gastroenterology (ACG) 2025 Annual Scientific Meeting.
The findings underscore that “.”
Research shows patients with EoE, a chronic and progressive type 2 inflammatory disease, have an average delay of 4 years before being diagnosed, with a delay of up to 10 years in about a third of cases. With those delays comes the likelihood of disease progression.
The latest guidelines from the ACG indicate that for diagnosis, “from a practical standpoint,” the preferred approach is to obtain at least two to four biopsies from at least two distinct esophageal areas, while targeting areas of visual inflammation.
However, prior evidence suggests that the biopsies are commonly not performed when patients present with the symptoms of EFI.
To further investigate the management of EFI during and after ED visits in a real-world setting, first author Walker D. Redd, MD, Center for Gastrointestinal Biology and Disease, UNC School of Medicine, Chapel Hill, North Carolina, and colleagues conducted a retrospective cohort study of 2566 patients in a multistate gastrointestinal practice group at 143 care centers in seven US states.

The patients were treated for esophageal food or foreign body removal between 2018 and 2024.
Among them, 1434 patients received evaluation with esophagogastroduodenoscopy (EGD), with 754 having no EGD and 378 receiving EGD for non-EFI.
The patients had a mean age of 63, with nearly 60% being older than 60 years, and 44.9% were women.
At the index EGD, only 19% had records of having esophageal biopsies. Among them, nearly half, 47%, were determined to have biopsy-confirmed EoE.
Of those who did not receive biopsies, only 7% had records of having received a follow-up EGD with an esophageal biopsy within 1 year, with 40% of those having EoE confirmed from a biopsy.
Among the remaining 93% of patients who had no record of such follow-up care within 1 year, 41% were lost to follow-up.
“We found that only about one fifth of patients had esophageal biopsies collected at the time of esophageal food impaction, which is similar to previous reports,” Redd said.
Overall, “esophageal biopsy rates at the time of esophageal food impaction remain low, and follow-up EGD with biopsy rates are also very low.”

Responding to a comment from the audience, Redd agreed that a limitation of the study was the scenario of patients from out of town being treated at an ED and then going back home, where their follow-up status may not be known.
Nevertheless, awareness of the low rates “represent an important opportunity to reduce the diagnostic delay and improve quality of care in EoE,” he said.
Commenting on the study, Danny Issa, MD, an interventional gastroenterologist at UCLA Health, agreed that the low rates of follow-up were troubling.
“Only 1 in 10 is a very low rate of follow-up endoscopy,” he told GI & Hepatology News.
“These results show we need to encourage quality improvement initiatives to make sure those patients are followed up,” he said.
Furthermore, “additional studies are needed to better understand the barriers behind the lack of follow-up, which were not addressed fully in the study.”
Co-moderator Sita S. Chokhavatia, MD, AGAF, a gastroenterologist at Valley Medical Group, in Paramus, New Jersey, added that “the point that needs to be made is that these patients need biopsies so you can diagnose and subsequently treat them.”
Redd reported having a consulting relationship with Sanofi. Issa reported having relationships with Boston Scientific and Eli Lilly. Chokhavatia had no disclosures to report.
A version of this article first appeared on Medscape.com.
PHOENIX — The opportunity to diagnose eosinophilic esophagitis (EoE) when patients present to the emergency department (ED) with the classic symptom of esophageal food impaction (EFI) is commonly missed, with necessary biopsies provided at strikingly low rates, despite guideline recommendations, new research showed.
“This is the first study to assess the rate of biopsies at time of esophageal food impaction in a large, real-world dataset of community practices,” the authors explained in research presented at the American College of Gastroenterology (ACG) 2025 Annual Scientific Meeting.
The findings underscore that “.”
Research shows patients with EoE, a chronic and progressive type 2 inflammatory disease, have an average delay of 4 years before being diagnosed, with a delay of up to 10 years in about a third of cases. With those delays comes the likelihood of disease progression.
The latest guidelines from the ACG indicate that for diagnosis, “from a practical standpoint,” the preferred approach is to obtain at least two to four biopsies from at least two distinct esophageal areas, while targeting areas of visual inflammation.
However, prior evidence suggests that the biopsies are commonly not performed when patients present with the symptoms of EFI.
To further investigate the management of EFI during and after ED visits in a real-world setting, first author Walker D. Redd, MD, Center for Gastrointestinal Biology and Disease, UNC School of Medicine, Chapel Hill, North Carolina, and colleagues conducted a retrospective cohort study of 2566 patients in a multistate gastrointestinal practice group at 143 care centers in seven US states.
The patients were treated for esophageal food or foreign body removal between 2018 and 2024.
Among them, 1434 patients received evaluation with esophagogastroduodenoscopy (EGD), with 754 having no EGD and 378 receiving EGD for non-EFI.
The patients had a mean age of 63, with nearly 60% being older than 60 years, and 44.9% were women.
At the index EGD, only 19% had records of having esophageal biopsies. Among them, nearly half, 47%, were determined to have biopsy-confirmed EoE.
Of those who did not receive biopsies, only 7% had records of having received a follow-up EGD with an esophageal biopsy within 1 year, with 40% of those having EoE confirmed from a biopsy.
Among the remaining 93% of patients who had no record of such follow-up care within 1 year, 41% were lost to follow-up.
“We found that only about one fifth of patients had esophageal biopsies collected at the time of esophageal food impaction, which is similar to previous reports,” Redd said.
Overall, “esophageal biopsy rates at the time of esophageal food impaction remain low, and follow-up EGD with biopsy rates are also very low.”
Responding to a comment from the audience, Redd agreed that a limitation of the study was the scenario of patients from out of town being treated at an ED and then going back home, where their follow-up status may not be known.
Nevertheless, awareness of the low rates “represent an important opportunity to reduce the diagnostic delay and improve quality of care in EoE,” he said.
Commenting on the study, Danny Issa, MD, an interventional gastroenterologist at UCLA Health, agreed that the low rates of follow-up were troubling.
“Only 1 in 10 is a very low rate of follow-up endoscopy,” he told GI & Hepatology News.
“These results show we need to encourage quality improvement initiatives to make sure those patients are followed up,” he said.
Furthermore, “additional studies are needed to better understand the barriers behind the lack of follow-up, which were not addressed fully in the study.”
Co-moderator Sita S. Chokhavatia, MD, AGAF, a gastroenterologist at Valley Medical Group, in Paramus, New Jersey, added that “the point that needs to be made is that these patients need biopsies so you can diagnose and subsequently treat them.”
Redd reported having a consulting relationship with Sanofi. Issa reported having relationships with Boston Scientific and Eli Lilly. Chokhavatia had no disclosures to report.
A version of this article first appeared on Medscape.com.
PHOENIX — The opportunity to diagnose eosinophilic esophagitis (EoE) when patients present to the emergency department (ED) with the classic symptom of esophageal food impaction (EFI) is commonly missed, with necessary biopsies provided at strikingly low rates, despite guideline recommendations, new research showed.
“This is the first study to assess the rate of biopsies at time of esophageal food impaction in a large, real-world dataset of community practices,” the authors explained in research presented at the American College of Gastroenterology (ACG) 2025 Annual Scientific Meeting.
The findings underscore that “.”
Research shows patients with EoE, a chronic and progressive type 2 inflammatory disease, have an average delay of 4 years before being diagnosed, with a delay of up to 10 years in about a third of cases. With those delays comes the likelihood of disease progression.
The latest guidelines from the ACG indicate that for diagnosis, “from a practical standpoint,” the preferred approach is to obtain at least two to four biopsies from at least two distinct esophageal areas, while targeting areas of visual inflammation.
However, prior evidence suggests that the biopsies are commonly not performed when patients present with the symptoms of EFI.
To further investigate the management of EFI during and after ED visits in a real-world setting, first author Walker D. Redd, MD, Center for Gastrointestinal Biology and Disease, UNC School of Medicine, Chapel Hill, North Carolina, and colleagues conducted a retrospective cohort study of 2566 patients in a multistate gastrointestinal practice group at 143 care centers in seven US states.
The patients were treated for esophageal food or foreign body removal between 2018 and 2024.
Among them, 1434 patients received evaluation with esophagogastroduodenoscopy (EGD), with 754 having no EGD and 378 receiving EGD for non-EFI.
The patients had a mean age of 63, with nearly 60% being older than 60 years, and 44.9% were women.
At the index EGD, only 19% had records of having esophageal biopsies. Among them, nearly half, 47%, were determined to have biopsy-confirmed EoE.
Of those who did not receive biopsies, only 7% had records of having received a follow-up EGD with an esophageal biopsy within 1 year, with 40% of those having EoE confirmed from a biopsy.
Among the remaining 93% of patients who had no record of such follow-up care within 1 year, 41% were lost to follow-up.
“We found that only about one fifth of patients had esophageal biopsies collected at the time of esophageal food impaction, which is similar to previous reports,” Redd said.
Overall, “esophageal biopsy rates at the time of esophageal food impaction remain low, and follow-up EGD with biopsy rates are also very low.”
Responding to a comment from the audience, Redd agreed that a limitation of the study was the scenario of patients from out of town being treated at an ED and then going back home, where their follow-up status may not be known.
Nevertheless, awareness of the low rates “represent an important opportunity to reduce the diagnostic delay and improve quality of care in EoE,” he said.
Commenting on the study, Danny Issa, MD, an interventional gastroenterologist at UCLA Health, agreed that the low rates of follow-up were troubling.
“Only 1 in 10 is a very low rate of follow-up endoscopy,” he told GI & Hepatology News.
“These results show we need to encourage quality improvement initiatives to make sure those patients are followed up,” he said.
Furthermore, “additional studies are needed to better understand the barriers behind the lack of follow-up, which were not addressed fully in the study.”
Co-moderator Sita S. Chokhavatia, MD, AGAF, a gastroenterologist at Valley Medical Group, in Paramus, New Jersey, added that “the point that needs to be made is that these patients need biopsies so you can diagnose and subsequently treat them.”
Redd reported having a consulting relationship with Sanofi. Issa reported having relationships with Boston Scientific and Eli Lilly. Chokhavatia had no disclosures to report.
A version of this article first appeared on Medscape.com.
FROM ACG 2025
Cholecystectomy Delay Linked to Substantially Increased Complication Risk
, regardless of the receipt of sphincterotomy or stenting, new research showed.
“These findings suggest an opportunity for systemic interventions, including prioritization algorithms and better perioperative coordination, to address preventable delays,” reported the authors in the study, presented at American College of Gastroenterology (ACG) 2025 Annual Scientific Meeting.
Choledocholithiasis can occur in up to 20% of symptomatic gallstone cases, and while guidelines recommend having a cholecystectomy concurrently with ERCP, data on the best timing is inconsistent and delays in gall bladder removal are consequently common.
One large study, for instance, the PONCHO trial conducted at 23 hospitals in Netherlands, showed complications to be significantly lower with same-admission vs interval cholecystectomy (4.7% vs 16.9%; P = .02).
Meanwhile, other research has suggested that delayed cholecystectomy is a preferred approach, allowing for removal when there is less inflammation.
Real world data meanwhile shows, despite the guidelines, the procedures are performed at the same time as ERCP only in about 41% of cases, first author Jessica El Halabi, MD, of the Johns Hopkins Hospital, Baltimore, said.
To further investigate outcomes associated with those delays, El Halabi and colleagues conducted a retrospective cohort study involving 507 patients admitted with choledocholithiasis at the hospital and community hospitals between 2005 and 2023 who had 12 months or more follow-up.
The patients had a mean age of 59 years and 59.4% were women.
Of the patients, 265 (52.3%) underwent early cholecystectomy, defined as surgery during the index admission, while 242 (47.7%) underwent delayed cholecystectomy, defined as postdischarge cholecystectomy or if cholecystectomy was not performed.
Overall, biliary complications occurred in as many as 23% of those who had delayed cholecystectomy compared with just 0.8% among those having the early cholecystectomy (P < .001).
Of patients who had delayed cholecystectomy and developed complications, 15.5% did so within 3 months, 6.5% by 6 months, and 1% by 12 months.
Among those who had ERCP with sphincterotomy, there were no significant differences in rates of biliary complications vs those who did not have sphincterotomy (26% vs 21%; P = .74), while stenting also did not reduce the risk (25% vs 27%; P = .81).
The leading reasons for delayed cholecystectomy included patients having a high surgical risk (27.3%), concurrent biliary pathology (19.2%), and physician preference (14%).
The findings underscore that “concurrent cholecystectomy is associated with the lowest risk of biliary complications,” El Halabi said.
“Delayed cholecystectomy is associated with an approximately 23% incidence of biliary complications with 1 year of initial admission, with the highest incidence occurring within 3 months,” she added. “Neither sphincterotomy nor stenting during ERCP mitigates this risk.”
“Early cholecystectomy during the index admission remains the most reliable strategy to reduce recurrent events.”
Findings Underscore Importance of Timing
Commenting on the study, Luis F. Lara, MD, division chief of digestive diseases at the University of Cincinnati, who co-moderated the session, agreed that evidence soundly supports early cholecystectomy.
“We also did a large study looking at this and there’s no doubt that doing it during the index admission has a tremendous effect on long-term outcomes,” Lara told GI & Hepatology News.
Lara noted that “part of it is people don’t show up again until they get sick again, so we don’t want to lose that opportunity the first time, during the index admission,” he said.
Lara’s previous studies have specifically documented how early cholecystectomy for acute biliary pancreatitis improves outcomes of hospitalization for cirrhosis and factors associated with early unplanned readmissions following same-admission cholecystectomy for acute biliary pancreatitis.
Akwi W. Asombang, MD, an interventional gastroenterologist at Massachusetts General Hospital and associate professor of medicine at Harvard Medical School, both in Boston, agreed that the findings are important.

“We know that if a cholecystectomy is not performed in the same admission as ERCP, the stones in the gallbladder remain and may migrate out into the bile duct, resulting in further complications as described in the study,” Asombang, also a session co-moderator, told GI & Hepatology News.
She noted that the practice can vary between institutions based on factors including the availability of physicians to perform the cholecystectomy.
Potential complications in delaying the procedure can range from inflammation and pancreatitis to obstruction of the bile duct, “which then can result in cholangitis and eventually sepsis or even death,” Asombang cautioned.
“So the timing of the procedure with ERCP is definitely significant,” she said.
El Halabi and Asombang had no disclosures to report. Lara reported a relationship with AbbVie.
A version of this article first appeared on Medscape.com.
, regardless of the receipt of sphincterotomy or stenting, new research showed.
“These findings suggest an opportunity for systemic interventions, including prioritization algorithms and better perioperative coordination, to address preventable delays,” reported the authors in the study, presented at American College of Gastroenterology (ACG) 2025 Annual Scientific Meeting.
Choledocholithiasis can occur in up to 20% of symptomatic gallstone cases, and while guidelines recommend having a cholecystectomy concurrently with ERCP, data on the best timing is inconsistent and delays in gall bladder removal are consequently common.
One large study, for instance, the PONCHO trial conducted at 23 hospitals in Netherlands, showed complications to be significantly lower with same-admission vs interval cholecystectomy (4.7% vs 16.9%; P = .02).
Meanwhile, other research has suggested that delayed cholecystectomy is a preferred approach, allowing for removal when there is less inflammation.
Real world data meanwhile shows, despite the guidelines, the procedures are performed at the same time as ERCP only in about 41% of cases, first author Jessica El Halabi, MD, of the Johns Hopkins Hospital, Baltimore, said.
To further investigate outcomes associated with those delays, El Halabi and colleagues conducted a retrospective cohort study involving 507 patients admitted with choledocholithiasis at the hospital and community hospitals between 2005 and 2023 who had 12 months or more follow-up.
The patients had a mean age of 59 years and 59.4% were women.
Of the patients, 265 (52.3%) underwent early cholecystectomy, defined as surgery during the index admission, while 242 (47.7%) underwent delayed cholecystectomy, defined as postdischarge cholecystectomy or if cholecystectomy was not performed.
Overall, biliary complications occurred in as many as 23% of those who had delayed cholecystectomy compared with just 0.8% among those having the early cholecystectomy (P < .001).
Of patients who had delayed cholecystectomy and developed complications, 15.5% did so within 3 months, 6.5% by 6 months, and 1% by 12 months.
Among those who had ERCP with sphincterotomy, there were no significant differences in rates of biliary complications vs those who did not have sphincterotomy (26% vs 21%; P = .74), while stenting also did not reduce the risk (25% vs 27%; P = .81).
The leading reasons for delayed cholecystectomy included patients having a high surgical risk (27.3%), concurrent biliary pathology (19.2%), and physician preference (14%).
The findings underscore that “concurrent cholecystectomy is associated with the lowest risk of biliary complications,” El Halabi said.
“Delayed cholecystectomy is associated with an approximately 23% incidence of biliary complications with 1 year of initial admission, with the highest incidence occurring within 3 months,” she added. “Neither sphincterotomy nor stenting during ERCP mitigates this risk.”
“Early cholecystectomy during the index admission remains the most reliable strategy to reduce recurrent events.”
Findings Underscore Importance of Timing
Commenting on the study, Luis F. Lara, MD, division chief of digestive diseases at the University of Cincinnati, who co-moderated the session, agreed that evidence soundly supports early cholecystectomy.
“We also did a large study looking at this and there’s no doubt that doing it during the index admission has a tremendous effect on long-term outcomes,” Lara told GI & Hepatology News.
Lara noted that “part of it is people don’t show up again until they get sick again, so we don’t want to lose that opportunity the first time, during the index admission,” he said.
Lara’s previous studies have specifically documented how early cholecystectomy for acute biliary pancreatitis improves outcomes of hospitalization for cirrhosis and factors associated with early unplanned readmissions following same-admission cholecystectomy for acute biliary pancreatitis.
Akwi W. Asombang, MD, an interventional gastroenterologist at Massachusetts General Hospital and associate professor of medicine at Harvard Medical School, both in Boston, agreed that the findings are important.
“We know that if a cholecystectomy is not performed in the same admission as ERCP, the stones in the gallbladder remain and may migrate out into the bile duct, resulting in further complications as described in the study,” Asombang, also a session co-moderator, told GI & Hepatology News.
She noted that the practice can vary between institutions based on factors including the availability of physicians to perform the cholecystectomy.
Potential complications in delaying the procedure can range from inflammation and pancreatitis to obstruction of the bile duct, “which then can result in cholangitis and eventually sepsis or even death,” Asombang cautioned.
“So the timing of the procedure with ERCP is definitely significant,” she said.
El Halabi and Asombang had no disclosures to report. Lara reported a relationship with AbbVie.
A version of this article first appeared on Medscape.com.
, regardless of the receipt of sphincterotomy or stenting, new research showed.
“These findings suggest an opportunity for systemic interventions, including prioritization algorithms and better perioperative coordination, to address preventable delays,” reported the authors in the study, presented at American College of Gastroenterology (ACG) 2025 Annual Scientific Meeting.
Choledocholithiasis can occur in up to 20% of symptomatic gallstone cases, and while guidelines recommend having a cholecystectomy concurrently with ERCP, data on the best timing is inconsistent and delays in gall bladder removal are consequently common.
One large study, for instance, the PONCHO trial conducted at 23 hospitals in Netherlands, showed complications to be significantly lower with same-admission vs interval cholecystectomy (4.7% vs 16.9%; P = .02).
Meanwhile, other research has suggested that delayed cholecystectomy is a preferred approach, allowing for removal when there is less inflammation.
Real world data meanwhile shows, despite the guidelines, the procedures are performed at the same time as ERCP only in about 41% of cases, first author Jessica El Halabi, MD, of the Johns Hopkins Hospital, Baltimore, said.
To further investigate outcomes associated with those delays, El Halabi and colleagues conducted a retrospective cohort study involving 507 patients admitted with choledocholithiasis at the hospital and community hospitals between 2005 and 2023 who had 12 months or more follow-up.
The patients had a mean age of 59 years and 59.4% were women.
Of the patients, 265 (52.3%) underwent early cholecystectomy, defined as surgery during the index admission, while 242 (47.7%) underwent delayed cholecystectomy, defined as postdischarge cholecystectomy or if cholecystectomy was not performed.
Overall, biliary complications occurred in as many as 23% of those who had delayed cholecystectomy compared with just 0.8% among those having the early cholecystectomy (P < .001).
Of patients who had delayed cholecystectomy and developed complications, 15.5% did so within 3 months, 6.5% by 6 months, and 1% by 12 months.
Among those who had ERCP with sphincterotomy, there were no significant differences in rates of biliary complications vs those who did not have sphincterotomy (26% vs 21%; P = .74), while stenting also did not reduce the risk (25% vs 27%; P = .81).
The leading reasons for delayed cholecystectomy included patients having a high surgical risk (27.3%), concurrent biliary pathology (19.2%), and physician preference (14%).
The findings underscore that “concurrent cholecystectomy is associated with the lowest risk of biliary complications,” El Halabi said.
“Delayed cholecystectomy is associated with an approximately 23% incidence of biliary complications with 1 year of initial admission, with the highest incidence occurring within 3 months,” she added. “Neither sphincterotomy nor stenting during ERCP mitigates this risk.”
“Early cholecystectomy during the index admission remains the most reliable strategy to reduce recurrent events.”
Findings Underscore Importance of Timing
Commenting on the study, Luis F. Lara, MD, division chief of digestive diseases at the University of Cincinnati, who co-moderated the session, agreed that evidence soundly supports early cholecystectomy.
“We also did a large study looking at this and there’s no doubt that doing it during the index admission has a tremendous effect on long-term outcomes,” Lara told GI & Hepatology News.
Lara noted that “part of it is people don’t show up again until they get sick again, so we don’t want to lose that opportunity the first time, during the index admission,” he said.
Lara’s previous studies have specifically documented how early cholecystectomy for acute biliary pancreatitis improves outcomes of hospitalization for cirrhosis and factors associated with early unplanned readmissions following same-admission cholecystectomy for acute biliary pancreatitis.
Akwi W. Asombang, MD, an interventional gastroenterologist at Massachusetts General Hospital and associate professor of medicine at Harvard Medical School, both in Boston, agreed that the findings are important.
“We know that if a cholecystectomy is not performed in the same admission as ERCP, the stones in the gallbladder remain and may migrate out into the bile duct, resulting in further complications as described in the study,” Asombang, also a session co-moderator, told GI & Hepatology News.
She noted that the practice can vary between institutions based on factors including the availability of physicians to perform the cholecystectomy.
Potential complications in delaying the procedure can range from inflammation and pancreatitis to obstruction of the bile duct, “which then can result in cholangitis and eventually sepsis or even death,” Asombang cautioned.
“So the timing of the procedure with ERCP is definitely significant,” she said.
El Halabi and Asombang had no disclosures to report. Lara reported a relationship with AbbVie.
A version of this article first appeared on Medscape.com.
FROM ACG 2025
Needle-Knife Fistulotomy is Safe During ERCP, Even for Trainees
, based on results of a randomized trial.
Across procedures conducted predominantly by trainees, safety outcomes were similar between NKF and standard cannulation, and all patients were successfully cannulated, suggesting this is a broadly accessible technique, reported lead author Aleksey Novikov, MD, of the University of Florida College of Medicine, Gainesville, and colleagues, reported.
Writing in Techniques and Innovations in Gastrointestinal Endoscopy, the investigators noted that standard cannulation fails in 5-20% of cases, which has led to development of various alternative techniques, including NKF. To perform the technique, the endoscopist makes a small incision in the intraduodenal biliary segment 3-6mm above the papillary orifice, with cephalad extension until bili-ary access is achieved.
To date, four prospective studies have evaluated NKF in the hands of expert advanced endoscopists.
“These studies showed that NKF is a safe and useful technique that significantly reduces the risk of PEP in the hands of expert advanced endoscopists,” the investigators wrote. ‘The suggestion that NKF should be restricted to expert advanced endoscopists likely limits widespread use.”
To determine whether NKF is a suitable technique for less experienced endoscopists, the investigators conducted the present single-center, prospective randomized controlled trial at Thomas Jefferson University Hospital in Philadelphia.
Adults undergoing ERCP for biliary indications were randomly assigned in a 1:1 ratio to undergo primary cannulation via NKF or standard cannulation. Patients with prior sphincterotomy, ampullectomy, or unfavorable anatomy were excluded.
A total of 186 patients were randomized, with 137 ultimately included in the per-protocol analysis after exclusions for anatomic factors. Most procedures (72.3%) were performed by advanced endoscopy trainees under direct supervision, 26 procedures (19.0%) were performed by attending endoscopists without substantive prior NKF experience, and 12 (8.8%) by an attending endoscopist with NKF expertise.
“It is important to note that the majority of procedures performed in the context of this study were performed by an advanced endoscopy trainee with no NKF experience or an attending advanced endoscopist with minimal NKF experience,” the investigators wrote.
All patients received prophylactic rectal indomethacin, and cannulation attempts were capped at 20 minutes before crossover to another technique was permitted.
The primary endpoint was incidence of post-ERCP pancreatitis. Secondary endpoints included successful biliary access, time to access, and rates of bleeding and perforation.
Post-ERCP pancreatitis occurred at similar rate across groups: 6 cases (8.2%) in the standard cannulation arm and 5 cases (7.8%) in the NKF arm (P = .93). Rates of bleeding and perforation were also similar for both techniques.
Within the initial 20-minute window, biliary access rates were comparable between groups, at 75.3% and 82.2% for standard cannulation and NKF, respectively (P = .89). Allowing additional attempts or crossover, overall success rose to 100% in both arms.
Mean time to access was longer with NKF, averaging 380 seconds compared with 268 seconds for standard cannulation (P less than .05).
“NKF was essentially equivalent to standard cannulation in many aspects,” the investigators wrote, calling the two techniques “complementary.”
They also suggested that the relative equivalence between techniques “carries more weight” after considering the low level of NKF experience among participating endoscopists.
“Overall, our data support teaching advanced endoscopy trainees NKF as a primary method of biliary access in patients with favorable anatomy,” the investigators concluded.
The investigators disclosed relationships with Medtronic, Boston Scientific, and Olympus.
, based on results of a randomized trial.
Across procedures conducted predominantly by trainees, safety outcomes were similar between NKF and standard cannulation, and all patients were successfully cannulated, suggesting this is a broadly accessible technique, reported lead author Aleksey Novikov, MD, of the University of Florida College of Medicine, Gainesville, and colleagues, reported.
Writing in Techniques and Innovations in Gastrointestinal Endoscopy, the investigators noted that standard cannulation fails in 5-20% of cases, which has led to development of various alternative techniques, including NKF. To perform the technique, the endoscopist makes a small incision in the intraduodenal biliary segment 3-6mm above the papillary orifice, with cephalad extension until bili-ary access is achieved.
To date, four prospective studies have evaluated NKF in the hands of expert advanced endoscopists.
“These studies showed that NKF is a safe and useful technique that significantly reduces the risk of PEP in the hands of expert advanced endoscopists,” the investigators wrote. ‘The suggestion that NKF should be restricted to expert advanced endoscopists likely limits widespread use.”
To determine whether NKF is a suitable technique for less experienced endoscopists, the investigators conducted the present single-center, prospective randomized controlled trial at Thomas Jefferson University Hospital in Philadelphia.
Adults undergoing ERCP for biliary indications were randomly assigned in a 1:1 ratio to undergo primary cannulation via NKF or standard cannulation. Patients with prior sphincterotomy, ampullectomy, or unfavorable anatomy were excluded.
A total of 186 patients were randomized, with 137 ultimately included in the per-protocol analysis after exclusions for anatomic factors. Most procedures (72.3%) were performed by advanced endoscopy trainees under direct supervision, 26 procedures (19.0%) were performed by attending endoscopists without substantive prior NKF experience, and 12 (8.8%) by an attending endoscopist with NKF expertise.
“It is important to note that the majority of procedures performed in the context of this study were performed by an advanced endoscopy trainee with no NKF experience or an attending advanced endoscopist with minimal NKF experience,” the investigators wrote.
All patients received prophylactic rectal indomethacin, and cannulation attempts were capped at 20 minutes before crossover to another technique was permitted.
The primary endpoint was incidence of post-ERCP pancreatitis. Secondary endpoints included successful biliary access, time to access, and rates of bleeding and perforation.
Post-ERCP pancreatitis occurred at similar rate across groups: 6 cases (8.2%) in the standard cannulation arm and 5 cases (7.8%) in the NKF arm (P = .93). Rates of bleeding and perforation were also similar for both techniques.
Within the initial 20-minute window, biliary access rates were comparable between groups, at 75.3% and 82.2% for standard cannulation and NKF, respectively (P = .89). Allowing additional attempts or crossover, overall success rose to 100% in both arms.
Mean time to access was longer with NKF, averaging 380 seconds compared with 268 seconds for standard cannulation (P less than .05).
“NKF was essentially equivalent to standard cannulation in many aspects,” the investigators wrote, calling the two techniques “complementary.”
They also suggested that the relative equivalence between techniques “carries more weight” after considering the low level of NKF experience among participating endoscopists.
“Overall, our data support teaching advanced endoscopy trainees NKF as a primary method of biliary access in patients with favorable anatomy,” the investigators concluded.
The investigators disclosed relationships with Medtronic, Boston Scientific, and Olympus.
, based on results of a randomized trial.
Across procedures conducted predominantly by trainees, safety outcomes were similar between NKF and standard cannulation, and all patients were successfully cannulated, suggesting this is a broadly accessible technique, reported lead author Aleksey Novikov, MD, of the University of Florida College of Medicine, Gainesville, and colleagues, reported.
Writing in Techniques and Innovations in Gastrointestinal Endoscopy, the investigators noted that standard cannulation fails in 5-20% of cases, which has led to development of various alternative techniques, including NKF. To perform the technique, the endoscopist makes a small incision in the intraduodenal biliary segment 3-6mm above the papillary orifice, with cephalad extension until bili-ary access is achieved.
To date, four prospective studies have evaluated NKF in the hands of expert advanced endoscopists.
“These studies showed that NKF is a safe and useful technique that significantly reduces the risk of PEP in the hands of expert advanced endoscopists,” the investigators wrote. ‘The suggestion that NKF should be restricted to expert advanced endoscopists likely limits widespread use.”
To determine whether NKF is a suitable technique for less experienced endoscopists, the investigators conducted the present single-center, prospective randomized controlled trial at Thomas Jefferson University Hospital in Philadelphia.
Adults undergoing ERCP for biliary indications were randomly assigned in a 1:1 ratio to undergo primary cannulation via NKF or standard cannulation. Patients with prior sphincterotomy, ampullectomy, or unfavorable anatomy were excluded.
A total of 186 patients were randomized, with 137 ultimately included in the per-protocol analysis after exclusions for anatomic factors. Most procedures (72.3%) were performed by advanced endoscopy trainees under direct supervision, 26 procedures (19.0%) were performed by attending endoscopists without substantive prior NKF experience, and 12 (8.8%) by an attending endoscopist with NKF expertise.
“It is important to note that the majority of procedures performed in the context of this study were performed by an advanced endoscopy trainee with no NKF experience or an attending advanced endoscopist with minimal NKF experience,” the investigators wrote.
All patients received prophylactic rectal indomethacin, and cannulation attempts were capped at 20 minutes before crossover to another technique was permitted.
The primary endpoint was incidence of post-ERCP pancreatitis. Secondary endpoints included successful biliary access, time to access, and rates of bleeding and perforation.
Post-ERCP pancreatitis occurred at similar rate across groups: 6 cases (8.2%) in the standard cannulation arm and 5 cases (7.8%) in the NKF arm (P = .93). Rates of bleeding and perforation were also similar for both techniques.
Within the initial 20-minute window, biliary access rates were comparable between groups, at 75.3% and 82.2% for standard cannulation and NKF, respectively (P = .89). Allowing additional attempts or crossover, overall success rose to 100% in both arms.
Mean time to access was longer with NKF, averaging 380 seconds compared with 268 seconds for standard cannulation (P less than .05).
“NKF was essentially equivalent to standard cannulation in many aspects,” the investigators wrote, calling the two techniques “complementary.”
They also suggested that the relative equivalence between techniques “carries more weight” after considering the low level of NKF experience among participating endoscopists.
“Overall, our data support teaching advanced endoscopy trainees NKF as a primary method of biliary access in patients with favorable anatomy,” the investigators concluded.
The investigators disclosed relationships with Medtronic, Boston Scientific, and Olympus.
FROM TECHNIQUES AND INNOVATIONS IN GASTROINTESTINAL ENDOSCOPY
Polypectomy Best Practices Not Routinely Followed in US
, an analysis of more than 1.8 million colonoscopies found.

“We expected to find some variations in polypectomy technique, but the results were surprising; overall, cold snare usage was much lower than expected, given that this is the recommended method for removing most small polyps,” Seth Crockett, MD, MPH, AGAF, professor of medicine, Division of Gastroenterology and Hepatology, Oregon Health & Science University, Portland, told GI & Hepatology News.
The study was published in the October issue of The American Journal of Gastroenterology.
Using Gastroenterology Quality Improvement Consortium Registry data, Crockett and colleagues analyzed more than 1.8 million colonoscopies performed by 4601 endoscopists between 2019 and 2022 across 702 sites. All colonoscopies involved removal of polyps < 1 cm; lesions of this size are commonly found in screening colonoscopies, and detection is crucial to early cancer prevention.
The researchers found striking variation in polypectomy technique. Guideline-based cold snare polypectomy (CSP) was used in only 58% of cases (and as a single device in only 51%), whereas cold forceps polypectomy (CFP) accounted for 35% and hot snare polypectomy (HSP) for 11%.
The fact that CSP was used in fewer than 60% of cases represents “an important quality gap,” the authors wrote, adding that the fact that more than 10% of colonoscopies used HSP suggests that “some patients harboring low-risk lesions may be exposed to excess risk related to these practice variations.”
And while recommendations around the use of CFP are more nuanced (based largely on forceps type and polyp size), the “high frequency of CFP also suggests nonadherence to best practices,” they noted.
Gastroenterologists More Apt to Follow Guidance
Polypectomy technique varied by polyp type. CFP was more common in cases where only hyperplastic polyps were removed compared with cases with tubular adenomas (45% vs 30%, respectively). CSP use was highest in cases where only sessile serrated lesions were removed (66%) compared with cases with only tubular adenomas (61%) or hyperplastic polyps (37%).
There was also considerable variation by provider specialty.
Gastroenterologists (compared with non-GI specialists) used HSP less (4% vs 8%) and CSP more (40% vs 34%). Colonoscopies performed with GI fellows were more likely to use CFP (31% vs 21%) and less likely to use HSP (1% vs 5%) compared with colonoscopies without fellows.
“It was somewhat reassuring that colonoscopies performed by gastroenterologists were more likely to adhere to guideline recommendations, which suggests that dedicated endoscopy training is likely an important factor driving high-quality colonoscopy,” Crockett told GI & Hepatology News.
“Unexpectedly,” polypectomy technique also differed dramatically by geographic region, he said. CFP was used more than twice as often in the Northeast (31%) as in the Midwest (14%), whereas CSP was used more frequently in the Midwest (52%) than in the Northeast (32%).
“We suspect that much of the variation is related to differences in training, preferences, habits, and evolution of colonoscopy practice over time,” Crockett said. “More research is needed on the underlying drivers of this variation, and how differences in polypectomy technique impact both the safety and efficacy of colonoscopy to prevent colorectal cancer,” he said.
“As a specialty, we need to continue to work on disseminating guideline recommendations regarding colonoscopy quality, monitoring adherence to evidence-based practices, and working to address gaps in quality where they exist,” he added.
‘Concerning, Surprising, and Disappointing’
David Johnson, MD, professor of medicine and chief of gastroenterology at Eastern Virginia Medical School and Old Dominion University in Norfolk, called the results “concerning, surprising, and disappointing” and not consistent with the most current quality recommendations that advocate cold snare for most polyps less than 1 cm in size.
“Cold snare polypectomy has been shown not only to be more effective but also takes less time to perform, relative to cold biopsy,” said Johnson, who wasn’t involved in the study.
Johnson told GI & Hepatology News, “Inadequate lesion resection and variation in resection quality are major issues for colonoscopy quality. Those who perform colonoscopies need to be up-to-date with evidence-based quality standards — as well as held accountable if [there is] discordant practice — if we are to optimize the cancer prevention benefits of quality colonoscopy.”
Limitations of the current analysis include lack of extensive patient information and inability to further stratify polyps < 1 cm by size.
The study had no commercial funding. Crockett had no disclosures. Johnson disclosed serving as a director, officer, partner, employee, advisor, consultant, or trustee for ISOThrive.
A version of this article appeared on Medscape.com.
, an analysis of more than 1.8 million colonoscopies found.
“We expected to find some variations in polypectomy technique, but the results were surprising; overall, cold snare usage was much lower than expected, given that this is the recommended method for removing most small polyps,” Seth Crockett, MD, MPH, AGAF, professor of medicine, Division of Gastroenterology and Hepatology, Oregon Health & Science University, Portland, told GI & Hepatology News.
The study was published in the October issue of The American Journal of Gastroenterology.
Using Gastroenterology Quality Improvement Consortium Registry data, Crockett and colleagues analyzed more than 1.8 million colonoscopies performed by 4601 endoscopists between 2019 and 2022 across 702 sites. All colonoscopies involved removal of polyps < 1 cm; lesions of this size are commonly found in screening colonoscopies, and detection is crucial to early cancer prevention.
The researchers found striking variation in polypectomy technique. Guideline-based cold snare polypectomy (CSP) was used in only 58% of cases (and as a single device in only 51%), whereas cold forceps polypectomy (CFP) accounted for 35% and hot snare polypectomy (HSP) for 11%.
The fact that CSP was used in fewer than 60% of cases represents “an important quality gap,” the authors wrote, adding that the fact that more than 10% of colonoscopies used HSP suggests that “some patients harboring low-risk lesions may be exposed to excess risk related to these practice variations.”
And while recommendations around the use of CFP are more nuanced (based largely on forceps type and polyp size), the “high frequency of CFP also suggests nonadherence to best practices,” they noted.
Gastroenterologists More Apt to Follow Guidance
Polypectomy technique varied by polyp type. CFP was more common in cases where only hyperplastic polyps were removed compared with cases with tubular adenomas (45% vs 30%, respectively). CSP use was highest in cases where only sessile serrated lesions were removed (66%) compared with cases with only tubular adenomas (61%) or hyperplastic polyps (37%).
There was also considerable variation by provider specialty.
Gastroenterologists (compared with non-GI specialists) used HSP less (4% vs 8%) and CSP more (40% vs 34%). Colonoscopies performed with GI fellows were more likely to use CFP (31% vs 21%) and less likely to use HSP (1% vs 5%) compared with colonoscopies without fellows.
“It was somewhat reassuring that colonoscopies performed by gastroenterologists were more likely to adhere to guideline recommendations, which suggests that dedicated endoscopy training is likely an important factor driving high-quality colonoscopy,” Crockett told GI & Hepatology News.
“Unexpectedly,” polypectomy technique also differed dramatically by geographic region, he said. CFP was used more than twice as often in the Northeast (31%) as in the Midwest (14%), whereas CSP was used more frequently in the Midwest (52%) than in the Northeast (32%).
“We suspect that much of the variation is related to differences in training, preferences, habits, and evolution of colonoscopy practice over time,” Crockett said. “More research is needed on the underlying drivers of this variation, and how differences in polypectomy technique impact both the safety and efficacy of colonoscopy to prevent colorectal cancer,” he said.
“As a specialty, we need to continue to work on disseminating guideline recommendations regarding colonoscopy quality, monitoring adherence to evidence-based practices, and working to address gaps in quality where they exist,” he added.
‘Concerning, Surprising, and Disappointing’
David Johnson, MD, professor of medicine and chief of gastroenterology at Eastern Virginia Medical School and Old Dominion University in Norfolk, called the results “concerning, surprising, and disappointing” and not consistent with the most current quality recommendations that advocate cold snare for most polyps less than 1 cm in size.
“Cold snare polypectomy has been shown not only to be more effective but also takes less time to perform, relative to cold biopsy,” said Johnson, who wasn’t involved in the study.
Johnson told GI & Hepatology News, “Inadequate lesion resection and variation in resection quality are major issues for colonoscopy quality. Those who perform colonoscopies need to be up-to-date with evidence-based quality standards — as well as held accountable if [there is] discordant practice — if we are to optimize the cancer prevention benefits of quality colonoscopy.”
Limitations of the current analysis include lack of extensive patient information and inability to further stratify polyps < 1 cm by size.
The study had no commercial funding. Crockett had no disclosures. Johnson disclosed serving as a director, officer, partner, employee, advisor, consultant, or trustee for ISOThrive.
A version of this article appeared on Medscape.com.
, an analysis of more than 1.8 million colonoscopies found.
“We expected to find some variations in polypectomy technique, but the results were surprising; overall, cold snare usage was much lower than expected, given that this is the recommended method for removing most small polyps,” Seth Crockett, MD, MPH, AGAF, professor of medicine, Division of Gastroenterology and Hepatology, Oregon Health & Science University, Portland, told GI & Hepatology News.
The study was published in the October issue of The American Journal of Gastroenterology.
Using Gastroenterology Quality Improvement Consortium Registry data, Crockett and colleagues analyzed more than 1.8 million colonoscopies performed by 4601 endoscopists between 2019 and 2022 across 702 sites. All colonoscopies involved removal of polyps < 1 cm; lesions of this size are commonly found in screening colonoscopies, and detection is crucial to early cancer prevention.
The researchers found striking variation in polypectomy technique. Guideline-based cold snare polypectomy (CSP) was used in only 58% of cases (and as a single device in only 51%), whereas cold forceps polypectomy (CFP) accounted for 35% and hot snare polypectomy (HSP) for 11%.
The fact that CSP was used in fewer than 60% of cases represents “an important quality gap,” the authors wrote, adding that the fact that more than 10% of colonoscopies used HSP suggests that “some patients harboring low-risk lesions may be exposed to excess risk related to these practice variations.”
And while recommendations around the use of CFP are more nuanced (based largely on forceps type and polyp size), the “high frequency of CFP also suggests nonadherence to best practices,” they noted.
Gastroenterologists More Apt to Follow Guidance
Polypectomy technique varied by polyp type. CFP was more common in cases where only hyperplastic polyps were removed compared with cases with tubular adenomas (45% vs 30%, respectively). CSP use was highest in cases where only sessile serrated lesions were removed (66%) compared with cases with only tubular adenomas (61%) or hyperplastic polyps (37%).
There was also considerable variation by provider specialty.
Gastroenterologists (compared with non-GI specialists) used HSP less (4% vs 8%) and CSP more (40% vs 34%). Colonoscopies performed with GI fellows were more likely to use CFP (31% vs 21%) and less likely to use HSP (1% vs 5%) compared with colonoscopies without fellows.
“It was somewhat reassuring that colonoscopies performed by gastroenterologists were more likely to adhere to guideline recommendations, which suggests that dedicated endoscopy training is likely an important factor driving high-quality colonoscopy,” Crockett told GI & Hepatology News.
“Unexpectedly,” polypectomy technique also differed dramatically by geographic region, he said. CFP was used more than twice as often in the Northeast (31%) as in the Midwest (14%), whereas CSP was used more frequently in the Midwest (52%) than in the Northeast (32%).
“We suspect that much of the variation is related to differences in training, preferences, habits, and evolution of colonoscopy practice over time,” Crockett said. “More research is needed on the underlying drivers of this variation, and how differences in polypectomy technique impact both the safety and efficacy of colonoscopy to prevent colorectal cancer,” he said.
“As a specialty, we need to continue to work on disseminating guideline recommendations regarding colonoscopy quality, monitoring adherence to evidence-based practices, and working to address gaps in quality where they exist,” he added.
‘Concerning, Surprising, and Disappointing’
David Johnson, MD, professor of medicine and chief of gastroenterology at Eastern Virginia Medical School and Old Dominion University in Norfolk, called the results “concerning, surprising, and disappointing” and not consistent with the most current quality recommendations that advocate cold snare for most polyps less than 1 cm in size.
“Cold snare polypectomy has been shown not only to be more effective but also takes less time to perform, relative to cold biopsy,” said Johnson, who wasn’t involved in the study.
Johnson told GI & Hepatology News, “Inadequate lesion resection and variation in resection quality are major issues for colonoscopy quality. Those who perform colonoscopies need to be up-to-date with evidence-based quality standards — as well as held accountable if [there is] discordant practice — if we are to optimize the cancer prevention benefits of quality colonoscopy.”
Limitations of the current analysis include lack of extensive patient information and inability to further stratify polyps < 1 cm by size.
The study had no commercial funding. Crockett had no disclosures. Johnson disclosed serving as a director, officer, partner, employee, advisor, consultant, or trustee for ISOThrive.
A version of this article appeared on Medscape.com.
AI in Gastroenterology and Endoscopy
Dear colleagues,
Since our last Perspectives feature on artificial intelligence (AI) in gastroenterology and hepatology, the field has experienced remarkable growth in both innovation and clinical adoption. AI tools that were once conceptual are now entering everyday practice, with many more on the horizon poised to transform how we diagnose, treat, and manage patients.
Dr. Yuvaraj Singh, Dr. Alessandro Colletta, and Dr. Neil Marya discuss how purpose-built AI models can reduce diagnostic uncertainty in advanced endoscopy. From cholangioscopy systems that outperform standard ERCP sampling in distinguishing malignant biliary strictures to EUS-based platforms that differentiate autoimmune pancreatitis from pancreatic cancer, they envision a near-term future in which machine intelligence enhances accuracy, accelerates decision-making, and refines interpretation—without replacing the clinician’s expertise.
Complementing this, Dr. Dennis Shung takes a broader view across the endoscopy unit and outpatient clinic. He highlights the promise of AI for polyp detection, digital biopsy, and automated reporting, while underscoring the importance of human oversight, workflow integration, and safeguards against misinformation. Dr. Shung also emphasizes the pivotal role professional societies can play in establishing clear standards, ethical boundaries, and trusted frameworks for AI deployment in GI practice.
We hope these perspectives spark practical conversations about when—and how—to integrate AI in your own practice. As always, we welcome your feedback and real-world experience. Join the conversation on X at @AGA_GIHN.

Gyanprakash A. Ketwaroo, MD, MSc, is associate professor of medicine, Yale University, New Haven, and chief of endoscopy at West Haven VA Medical Center, both in Connecticut. He is an associate editor for GI & Hepatology News.
AI Models in Advanced Endoscopy
BY YUVARAJ SINGH, MD; ALESSANDRO COLLETTA, MD; NEIL MARYA, MD
As the adage goes, “if tumor is the rumor, then tissue is the issue, because cancer may be the answer.”
Establishing an accurate diagnosis is the essential first step toward curing or palliating malignancy. From detecting an early neoplastic lesion, to distinguishing between malignant and benign pathology, or to determining when and where to obtain tissue, endoscopists are frequently faced with the challenge of transforming diagnostic suspicion into certainty.
Artificial intelligence (AI), designed to replicate human cognition such as pattern recognition and decision-making, has emerged as a technology to assist gastroenterologists in addressing a variety of different tasks during endoscopy. AI research in gastrointestinal endoscopy has initially focused on computer-aided detection (CADe) of colorectal polyps. More recently, however, there has been increased emphasis on developing AI to assist advanced endoscopists.
For instance, in biliary endoscopy, AI is being explored to improve the notoriously challenging diagnosis of cholangiocarcinoma, where conventional tissue sampling often falls short of providing a definitive diagnosis. Similarly, in the pancreas, AI models are showing potential to differentiate autoimmune pancreatitis (AIP) from pancreatic ductal adenocarcinoma (PDAC), a distinction with profound therapeutic implications. Even pancreatic cysts are beginning to benefit from AI models that refine risk stratification and guide management. Together, these advances underscore how AI is not merely an adjunct but a potentially massive catalyst for reimagining the diagnostic role of advanced endoscopists.
Classifying biliary strictures (MBS) accurately remains a challenge. Standard ERCP-based sampling techniques (forceps biopsy and brush cytology) are suboptimal diagnostic tools with false negative rates for detecting MBS of less than 50%. The diagnostic uncertainty related to biliary stricture classification carries significant consequences for patients. For example, patients with biliary cancer without positive cytology have treatments delayed until a malignant diagnosis is established.
Ancillary technologies to enhance ERCP-based tissue acquisition are still weighed down by low sensitivity and accuracy; even with ancillary use of fluorescent in situ hybridization (FISH), diagnostic yield remains limited. EUS-FNA can help with distal biliary strictures, but this technique risks needle-tract seeding in cases of perihilar disease. Cholangioscopy allows for direct visualization and targeted sampling; however, cholangioscopy-guided forceps biopsies are burdened by low sensitivities.1 Additionally, physician interpretation of visual findings during cholangioscopy often suffers from poor interobserver agreement and poor accuracy.2
To improve the classification of biliary strictures, several groups have studied the application of AI for cholangioscopy footage of biliary pathology. In our lab, we trained an AI incorporating over 2.3 million cholangioscopy still images and nearly 20,000 expert-annotated frames to enhance its development. The AI closely mirrored expert labeling of cholangioscopy images of malignant pathology and, when tested on full cholangioscopy videos of indeterminate biliary strictures, the AI achieved a diagnostic accuracy of 91%—outperforming both brush cytology (63%) and forceps biopsy (61%).3
The results from this initial study were later validated across multiple centers. AI-assisted cholangioscopy could thus offer a reproducible, real-world solution to one of the most persistent diagnostic dilemmas advanced endoscopists face—helping clinicians act earlier and with greater confidence when evaluating indeterminate strictures.
Moving from the biliary tree to the pancreas, autoimmune pancreatitis (AIP) is a benign fibro-inflammatory disease that often frustrates advanced endoscopists as it closely mimics the appearance of pancreatic ductal adenocarcinoma (PDAC). The stakes are high: despite modern diagnostic techniques, including advanced imaging, some patients with pancreatic resections for “suspected PDAC” are still found to have AIP on final pathology. Conventional tools to distinguish AIP from PDAC have gaps: serum IgG4 and EUS-guided biopsies are both specific but insensitive.
Using EUS videos and images of various pancreas pathologies at Mayo Clinic, we developed an AI to tackle this dilemma. After intensive training, the EUS AI achieved a greater accuracy for distinguishing AIP from PDAC than a group of expert Mayo clinic endosonographers.5 In practice, an EUS-AI can identify AIP patterns in real-time, guiding clinicians toward steroid trials or biopsies and reducing the need for unnecessary surgeries.
Looking ahead, there are multiple opportunities for integration of AI into advanced endoscopy practices. Ongoing research suggests that AI could soon assist with identification of pancreas cysts most at risk for malignant transformation, classification of high risk Barrett’s esophagus, and even help with rapid on-site assessment of cytologic specimens obtained during EUS. Beyond diagnosis, AI could likely play an important role in guiding therapeutic interventions. For example, an ERCP AI in the future may be able to provide cannulation assistance or an AI assistant could help endosonographers during deployments of lumen apposing metal stents.
By enhancing image interpretation and procedural consistency, AI has the potential to uphold the fundamental principle of primum non nocere, enabling us to intervene with precision while minimizing harm. AI can also bridge grey zones in clinical practice and narrow diagnostic uncertainty in real time. Importantly, these systems can help clinicians achieve expertise in a fraction of the time it traditionally takes to acquire comparable human proficiency, while offering wider availability across practice settings and reducing interobserver variability that has long challenged endoscopic interpretation.
Currently, adoption is limited by high bias risk, lack of external validation, and interpretability Still, the trajectory of AI suggests a future where these computer technologies will not only support but also elevate human expertise, reshaping the standards of care of diseases managed by advanced endoscopists.
Dr. Singh, Dr. Colletta, and Dr. Marya are based at the Division of Gastroenterology and Hepatology, UMass Chan Medical School, Worcester, Massachusetts. Dr. Marya is a consultant for Boston Scientific, and has no other disclosures. Dr. Singh and Dr. Colletta have no disclosures.
References
1. Navaneethan U, et al. Comparative effectiveness of biliary brush cytology and intraductal biopsy for detection of malignant biliary strictures: a systematic review and meta-analysis. Gastrointest Endosc. 2015 Jan. doi: 10.1016/j.gie.2014.09.017.
2. Stassen PMC, et al. Diagnostic accuracy and interobserver agreement of digital single-operator cholangioscopy for indeterminate biliary strictures. Gastrointest Endosc 2021 Dec. doi: 10.1016/j.gie.2021.06.027.
3. Marya NB, et al. Identification of patients with malignant biliary strictures using a cholangioscopy-based deep learning artificial intelligence (with video). Gastrointest Endosc. 2023 Feb. doi: 10.1016/j.gie.2022.08.021.
4. Marya NB, et al. Multicenter validation of a cholangioscopy artificial intelligence system for the evaluation of biliary tract disease. Endoscopy. 2025 Aug. doi: 10.1055/a-2650-0789.
5. Marya NB, et al. Utilisation of artificial intelligence for the development of an EUS-convolutional neural network model trained to enhance the diagnosis of autoimmune pancreatitis. Gut. 2021 Jul. doi: 10.1136/gutjnl-2020-322821.
AI in General GI and Endoscopy
BY DENNIS L. SHUNG, MD, MHS, PHD
The practice of gastroenterology is changing, but much of it will be rooted in the same – careful, focused attention on endoscopic procedures, and compassionate, attentive care in clinic. Artificial intelligence (AI), like the Industrial Revolution before, is going to transform our practice. This comes with upsides and downsides, and highlights the need for strong leadership from our societies to safeguard the technology for practitioners and patients.
What are the upsides?
AI has the potential to serve as a second set of eyes in detecting colon polyps, increasing the adenoma detection rate (ADR).1 AI can be applied to all areas of the gastrointestinal tract, providing digital biopsies, guiding resection, and ensuring quality, which are all now possible with powerful new endoscopy foundation models, such as GastroNet-5M.2
Additionally. the advent of automating the collection of data into reports may herald the end of our days as data entry clerks. Generative AI also has the potential to give us all the best information at our fingertips, suggesting guideline-based care, providing the most up to date evidence, and guiding the differential diagnosis. The potential for patient-facing AI systems could lead to better health literacy, more meaningful engagement, and improved patient satisfaction.3
What are the downsides?
For endoscopy, AI cannot make up for poor technique to ensure adequate mucosal exposure by the endoscopist, and an increase in AI-supported ADR does not yet convincingly translate into concrete gains in colorectal cancer-related mortality. For the foreseeable future, AI cannot make a connection with the patient in front of us, which is critical in diagnosing and treating patients.
Currently, AI appears to worsen loneliness4, and does not necessarily deepen the bonds or provide the positive touch that can heal, and which for many of us, was the reason we became physicians. Finally, as information proliferates, the information risk to patients and providers is growing – in the future, trusted sources to monitor, curate, and guide AI will be ever more important.
Black Swans
As AI begins to mature, there are risks that lurk beneath the surface. When regulatory bodies begin to look at AI-assisted diagnostics or therapeutics as the new standard of care, reimbursement models may adjust, and providers may be left behind. The rapid proliferation and haphazard adoption of AI could lead to overdependence and deskilling or result in weird and as yet unknown errors that are difficult to troubleshoot.
What is the role of the GI societies?
Specialty societies like AGA are taking leadership roles in determining the bounds of where AIs may tread, not just in providing information to their membership but also in digesting evidence and synthesizing recommendations. Societies must balance the real promise of AI in endoscopy with the practice realities for members, and provide living guidelines that reflect the consensus of members regarding scope of practice with the ability to update as new data become available.5
Societies also have a role as advocates for safety, taking ownership of high-quality content to prevent misinformation. AGA recently announced the development of a chat interface that will be focused on providing its members the highest quality information, and serve as a portal to identify and respond to its members’ information needs. By staying united rather than fragmenting, societies can maintain bounds to protect its members and their patients and advance areas where there is clinical need, together.
Dr. Shung is senior associate consultant, Division of Gastroenterology and Hepatology, and director of clinical generative artificial intelligence and informatics, Department of Medicine, at Mayo Clinic Rochester, Minnesota. He has no disclosures in regard to this article.
References
1. Soleymanjahi S, et al. Artificial Intelligence-Assisted Colonoscopy for Polyp Detection : A Systematic Review and Meta-analysis. Ann Intern Med. 2024 Dec. doi:10.7326/annals-24-00981.
2. Jong MR, et al. GastroNet-5M: A Multicenter Dataset for Developing Foundation Models in Gastrointestinal Endoscopy. Gastroenterology. 2025 Jul. doi: 10.1053/j.gastro.2025.07.030.
3. Soroush A, et al. Generative Artificial Intelligence in Clinical Medicine and Impact on Gastroenterology. Gastroenterology. 2025 Aug. doi: 10.1053/j.gastro.2025.03.038.
4. Mengying Fang C, et al. How AI and Human Behaviors Shape Psychosocial Effects of Extended Chatbot Use: A Longitudinal Randomized Controlled Study. arXiv e-prints. 2025 Mar. doi: 10.48550/arXiv.2503.17473.
5. Sultan S, et al. AGA Living Clinical Practice Guideline on Computer-Aided Detection-Assisted Colonoscopy. Gastroenterology. 2025 Apr. doi:10.1053/j.gastro.2025.01.002.
Dear colleagues,
Since our last Perspectives feature on artificial intelligence (AI) in gastroenterology and hepatology, the field has experienced remarkable growth in both innovation and clinical adoption. AI tools that were once conceptual are now entering everyday practice, with many more on the horizon poised to transform how we diagnose, treat, and manage patients.
Dr. Yuvaraj Singh, Dr. Alessandro Colletta, and Dr. Neil Marya discuss how purpose-built AI models can reduce diagnostic uncertainty in advanced endoscopy. From cholangioscopy systems that outperform standard ERCP sampling in distinguishing malignant biliary strictures to EUS-based platforms that differentiate autoimmune pancreatitis from pancreatic cancer, they envision a near-term future in which machine intelligence enhances accuracy, accelerates decision-making, and refines interpretation—without replacing the clinician’s expertise.
Complementing this, Dr. Dennis Shung takes a broader view across the endoscopy unit and outpatient clinic. He highlights the promise of AI for polyp detection, digital biopsy, and automated reporting, while underscoring the importance of human oversight, workflow integration, and safeguards against misinformation. Dr. Shung also emphasizes the pivotal role professional societies can play in establishing clear standards, ethical boundaries, and trusted frameworks for AI deployment in GI practice.
We hope these perspectives spark practical conversations about when—and how—to integrate AI in your own practice. As always, we welcome your feedback and real-world experience. Join the conversation on X at @AGA_GIHN.
Gyanprakash A. Ketwaroo, MD, MSc, is associate professor of medicine, Yale University, New Haven, and chief of endoscopy at West Haven VA Medical Center, both in Connecticut. He is an associate editor for GI & Hepatology News.
AI Models in Advanced Endoscopy
BY YUVARAJ SINGH, MD; ALESSANDRO COLLETTA, MD; NEIL MARYA, MD
As the adage goes, “if tumor is the rumor, then tissue is the issue, because cancer may be the answer.”
Establishing an accurate diagnosis is the essential first step toward curing or palliating malignancy. From detecting an early neoplastic lesion, to distinguishing between malignant and benign pathology, or to determining when and where to obtain tissue, endoscopists are frequently faced with the challenge of transforming diagnostic suspicion into certainty.
Artificial intelligence (AI), designed to replicate human cognition such as pattern recognition and decision-making, has emerged as a technology to assist gastroenterologists in addressing a variety of different tasks during endoscopy. AI research in gastrointestinal endoscopy has initially focused on computer-aided detection (CADe) of colorectal polyps. More recently, however, there has been increased emphasis on developing AI to assist advanced endoscopists.
For instance, in biliary endoscopy, AI is being explored to improve the notoriously challenging diagnosis of cholangiocarcinoma, where conventional tissue sampling often falls short of providing a definitive diagnosis. Similarly, in the pancreas, AI models are showing potential to differentiate autoimmune pancreatitis (AIP) from pancreatic ductal adenocarcinoma (PDAC), a distinction with profound therapeutic implications. Even pancreatic cysts are beginning to benefit from AI models that refine risk stratification and guide management. Together, these advances underscore how AI is not merely an adjunct but a potentially massive catalyst for reimagining the diagnostic role of advanced endoscopists.
Classifying biliary strictures (MBS) accurately remains a challenge. Standard ERCP-based sampling techniques (forceps biopsy and brush cytology) are suboptimal diagnostic tools with false negative rates for detecting MBS of less than 50%. The diagnostic uncertainty related to biliary stricture classification carries significant consequences for patients. For example, patients with biliary cancer without positive cytology have treatments delayed until a malignant diagnosis is established.
Ancillary technologies to enhance ERCP-based tissue acquisition are still weighed down by low sensitivity and accuracy; even with ancillary use of fluorescent in situ hybridization (FISH), diagnostic yield remains limited. EUS-FNA can help with distal biliary strictures, but this technique risks needle-tract seeding in cases of perihilar disease. Cholangioscopy allows for direct visualization and targeted sampling; however, cholangioscopy-guided forceps biopsies are burdened by low sensitivities.1 Additionally, physician interpretation of visual findings during cholangioscopy often suffers from poor interobserver agreement and poor accuracy.2
To improve the classification of biliary strictures, several groups have studied the application of AI for cholangioscopy footage of biliary pathology. In our lab, we trained an AI incorporating over 2.3 million cholangioscopy still images and nearly 20,000 expert-annotated frames to enhance its development. The AI closely mirrored expert labeling of cholangioscopy images of malignant pathology and, when tested on full cholangioscopy videos of indeterminate biliary strictures, the AI achieved a diagnostic accuracy of 91%—outperforming both brush cytology (63%) and forceps biopsy (61%).3
The results from this initial study were later validated across multiple centers. AI-assisted cholangioscopy could thus offer a reproducible, real-world solution to one of the most persistent diagnostic dilemmas advanced endoscopists face—helping clinicians act earlier and with greater confidence when evaluating indeterminate strictures.
Moving from the biliary tree to the pancreas, autoimmune pancreatitis (AIP) is a benign fibro-inflammatory disease that often frustrates advanced endoscopists as it closely mimics the appearance of pancreatic ductal adenocarcinoma (PDAC). The stakes are high: despite modern diagnostic techniques, including advanced imaging, some patients with pancreatic resections for “suspected PDAC” are still found to have AIP on final pathology. Conventional tools to distinguish AIP from PDAC have gaps: serum IgG4 and EUS-guided biopsies are both specific but insensitive.
Using EUS videos and images of various pancreas pathologies at Mayo Clinic, we developed an AI to tackle this dilemma. After intensive training, the EUS AI achieved a greater accuracy for distinguishing AIP from PDAC than a group of expert Mayo clinic endosonographers.5 In practice, an EUS-AI can identify AIP patterns in real-time, guiding clinicians toward steroid trials or biopsies and reducing the need for unnecessary surgeries.
Looking ahead, there are multiple opportunities for integration of AI into advanced endoscopy practices. Ongoing research suggests that AI could soon assist with identification of pancreas cysts most at risk for malignant transformation, classification of high risk Barrett’s esophagus, and even help with rapid on-site assessment of cytologic specimens obtained during EUS. Beyond diagnosis, AI could likely play an important role in guiding therapeutic interventions. For example, an ERCP AI in the future may be able to provide cannulation assistance or an AI assistant could help endosonographers during deployments of lumen apposing metal stents.
By enhancing image interpretation and procedural consistency, AI has the potential to uphold the fundamental principle of primum non nocere, enabling us to intervene with precision while minimizing harm. AI can also bridge grey zones in clinical practice and narrow diagnostic uncertainty in real time. Importantly, these systems can help clinicians achieve expertise in a fraction of the time it traditionally takes to acquire comparable human proficiency, while offering wider availability across practice settings and reducing interobserver variability that has long challenged endoscopic interpretation.
Currently, adoption is limited by high bias risk, lack of external validation, and interpretability Still, the trajectory of AI suggests a future where these computer technologies will not only support but also elevate human expertise, reshaping the standards of care of diseases managed by advanced endoscopists.
Dr. Singh, Dr. Colletta, and Dr. Marya are based at the Division of Gastroenterology and Hepatology, UMass Chan Medical School, Worcester, Massachusetts. Dr. Marya is a consultant for Boston Scientific, and has no other disclosures. Dr. Singh and Dr. Colletta have no disclosures.
References
1. Navaneethan U, et al. Comparative effectiveness of biliary brush cytology and intraductal biopsy for detection of malignant biliary strictures: a systematic review and meta-analysis. Gastrointest Endosc. 2015 Jan. doi: 10.1016/j.gie.2014.09.017.
2. Stassen PMC, et al. Diagnostic accuracy and interobserver agreement of digital single-operator cholangioscopy for indeterminate biliary strictures. Gastrointest Endosc 2021 Dec. doi: 10.1016/j.gie.2021.06.027.
3. Marya NB, et al. Identification of patients with malignant biliary strictures using a cholangioscopy-based deep learning artificial intelligence (with video). Gastrointest Endosc. 2023 Feb. doi: 10.1016/j.gie.2022.08.021.
4. Marya NB, et al. Multicenter validation of a cholangioscopy artificial intelligence system for the evaluation of biliary tract disease. Endoscopy. 2025 Aug. doi: 10.1055/a-2650-0789.
5. Marya NB, et al. Utilisation of artificial intelligence for the development of an EUS-convolutional neural network model trained to enhance the diagnosis of autoimmune pancreatitis. Gut. 2021 Jul. doi: 10.1136/gutjnl-2020-322821.
AI in General GI and Endoscopy
BY DENNIS L. SHUNG, MD, MHS, PHD
The practice of gastroenterology is changing, but much of it will be rooted in the same – careful, focused attention on endoscopic procedures, and compassionate, attentive care in clinic. Artificial intelligence (AI), like the Industrial Revolution before, is going to transform our practice. This comes with upsides and downsides, and highlights the need for strong leadership from our societies to safeguard the technology for practitioners and patients.
What are the upsides?
AI has the potential to serve as a second set of eyes in detecting colon polyps, increasing the adenoma detection rate (ADR).1 AI can be applied to all areas of the gastrointestinal tract, providing digital biopsies, guiding resection, and ensuring quality, which are all now possible with powerful new endoscopy foundation models, such as GastroNet-5M.2
Additionally. the advent of automating the collection of data into reports may herald the end of our days as data entry clerks. Generative AI also has the potential to give us all the best information at our fingertips, suggesting guideline-based care, providing the most up to date evidence, and guiding the differential diagnosis. The potential for patient-facing AI systems could lead to better health literacy, more meaningful engagement, and improved patient satisfaction.3
What are the downsides?
For endoscopy, AI cannot make up for poor technique to ensure adequate mucosal exposure by the endoscopist, and an increase in AI-supported ADR does not yet convincingly translate into concrete gains in colorectal cancer-related mortality. For the foreseeable future, AI cannot make a connection with the patient in front of us, which is critical in diagnosing and treating patients.
Currently, AI appears to worsen loneliness4, and does not necessarily deepen the bonds or provide the positive touch that can heal, and which for many of us, was the reason we became physicians. Finally, as information proliferates, the information risk to patients and providers is growing – in the future, trusted sources to monitor, curate, and guide AI will be ever more important.
Black Swans
As AI begins to mature, there are risks that lurk beneath the surface. When regulatory bodies begin to look at AI-assisted diagnostics or therapeutics as the new standard of care, reimbursement models may adjust, and providers may be left behind. The rapid proliferation and haphazard adoption of AI could lead to overdependence and deskilling or result in weird and as yet unknown errors that are difficult to troubleshoot.
What is the role of the GI societies?
Specialty societies like AGA are taking leadership roles in determining the bounds of where AIs may tread, not just in providing information to their membership but also in digesting evidence and synthesizing recommendations. Societies must balance the real promise of AI in endoscopy with the practice realities for members, and provide living guidelines that reflect the consensus of members regarding scope of practice with the ability to update as new data become available.5
Societies also have a role as advocates for safety, taking ownership of high-quality content to prevent misinformation. AGA recently announced the development of a chat interface that will be focused on providing its members the highest quality information, and serve as a portal to identify and respond to its members’ information needs. By staying united rather than fragmenting, societies can maintain bounds to protect its members and their patients and advance areas where there is clinical need, together.
Dr. Shung is senior associate consultant, Division of Gastroenterology and Hepatology, and director of clinical generative artificial intelligence and informatics, Department of Medicine, at Mayo Clinic Rochester, Minnesota. He has no disclosures in regard to this article.
References
1. Soleymanjahi S, et al. Artificial Intelligence-Assisted Colonoscopy for Polyp Detection : A Systematic Review and Meta-analysis. Ann Intern Med. 2024 Dec. doi:10.7326/annals-24-00981.
2. Jong MR, et al. GastroNet-5M: A Multicenter Dataset for Developing Foundation Models in Gastrointestinal Endoscopy. Gastroenterology. 2025 Jul. doi: 10.1053/j.gastro.2025.07.030.
3. Soroush A, et al. Generative Artificial Intelligence in Clinical Medicine and Impact on Gastroenterology. Gastroenterology. 2025 Aug. doi: 10.1053/j.gastro.2025.03.038.
4. Mengying Fang C, et al. How AI and Human Behaviors Shape Psychosocial Effects of Extended Chatbot Use: A Longitudinal Randomized Controlled Study. arXiv e-prints. 2025 Mar. doi: 10.48550/arXiv.2503.17473.
5. Sultan S, et al. AGA Living Clinical Practice Guideline on Computer-Aided Detection-Assisted Colonoscopy. Gastroenterology. 2025 Apr. doi:10.1053/j.gastro.2025.01.002.
Dear colleagues,
Since our last Perspectives feature on artificial intelligence (AI) in gastroenterology and hepatology, the field has experienced remarkable growth in both innovation and clinical adoption. AI tools that were once conceptual are now entering everyday practice, with many more on the horizon poised to transform how we diagnose, treat, and manage patients.
Dr. Yuvaraj Singh, Dr. Alessandro Colletta, and Dr. Neil Marya discuss how purpose-built AI models can reduce diagnostic uncertainty in advanced endoscopy. From cholangioscopy systems that outperform standard ERCP sampling in distinguishing malignant biliary strictures to EUS-based platforms that differentiate autoimmune pancreatitis from pancreatic cancer, they envision a near-term future in which machine intelligence enhances accuracy, accelerates decision-making, and refines interpretation—without replacing the clinician’s expertise.
Complementing this, Dr. Dennis Shung takes a broader view across the endoscopy unit and outpatient clinic. He highlights the promise of AI for polyp detection, digital biopsy, and automated reporting, while underscoring the importance of human oversight, workflow integration, and safeguards against misinformation. Dr. Shung also emphasizes the pivotal role professional societies can play in establishing clear standards, ethical boundaries, and trusted frameworks for AI deployment in GI practice.
We hope these perspectives spark practical conversations about when—and how—to integrate AI in your own practice. As always, we welcome your feedback and real-world experience. Join the conversation on X at @AGA_GIHN.
Gyanprakash A. Ketwaroo, MD, MSc, is associate professor of medicine, Yale University, New Haven, and chief of endoscopy at West Haven VA Medical Center, both in Connecticut. He is an associate editor for GI & Hepatology News.
AI Models in Advanced Endoscopy
BY YUVARAJ SINGH, MD; ALESSANDRO COLLETTA, MD; NEIL MARYA, MD
As the adage goes, “if tumor is the rumor, then tissue is the issue, because cancer may be the answer.”
Establishing an accurate diagnosis is the essential first step toward curing or palliating malignancy. From detecting an early neoplastic lesion, to distinguishing between malignant and benign pathology, or to determining when and where to obtain tissue, endoscopists are frequently faced with the challenge of transforming diagnostic suspicion into certainty.
Artificial intelligence (AI), designed to replicate human cognition such as pattern recognition and decision-making, has emerged as a technology to assist gastroenterologists in addressing a variety of different tasks during endoscopy. AI research in gastrointestinal endoscopy has initially focused on computer-aided detection (CADe) of colorectal polyps. More recently, however, there has been increased emphasis on developing AI to assist advanced endoscopists.
For instance, in biliary endoscopy, AI is being explored to improve the notoriously challenging diagnosis of cholangiocarcinoma, where conventional tissue sampling often falls short of providing a definitive diagnosis. Similarly, in the pancreas, AI models are showing potential to differentiate autoimmune pancreatitis (AIP) from pancreatic ductal adenocarcinoma (PDAC), a distinction with profound therapeutic implications. Even pancreatic cysts are beginning to benefit from AI models that refine risk stratification and guide management. Together, these advances underscore how AI is not merely an adjunct but a potentially massive catalyst for reimagining the diagnostic role of advanced endoscopists.
Classifying biliary strictures (MBS) accurately remains a challenge. Standard ERCP-based sampling techniques (forceps biopsy and brush cytology) are suboptimal diagnostic tools with false negative rates for detecting MBS of less than 50%. The diagnostic uncertainty related to biliary stricture classification carries significant consequences for patients. For example, patients with biliary cancer without positive cytology have treatments delayed until a malignant diagnosis is established.
Ancillary technologies to enhance ERCP-based tissue acquisition are still weighed down by low sensitivity and accuracy; even with ancillary use of fluorescent in situ hybridization (FISH), diagnostic yield remains limited. EUS-FNA can help with distal biliary strictures, but this technique risks needle-tract seeding in cases of perihilar disease. Cholangioscopy allows for direct visualization and targeted sampling; however, cholangioscopy-guided forceps biopsies are burdened by low sensitivities.1 Additionally, physician interpretation of visual findings during cholangioscopy often suffers from poor interobserver agreement and poor accuracy.2
To improve the classification of biliary strictures, several groups have studied the application of AI for cholangioscopy footage of biliary pathology. In our lab, we trained an AI incorporating over 2.3 million cholangioscopy still images and nearly 20,000 expert-annotated frames to enhance its development. The AI closely mirrored expert labeling of cholangioscopy images of malignant pathology and, when tested on full cholangioscopy videos of indeterminate biliary strictures, the AI achieved a diagnostic accuracy of 91%—outperforming both brush cytology (63%) and forceps biopsy (61%).3
The results from this initial study were later validated across multiple centers. AI-assisted cholangioscopy could thus offer a reproducible, real-world solution to one of the most persistent diagnostic dilemmas advanced endoscopists face—helping clinicians act earlier and with greater confidence when evaluating indeterminate strictures.
Moving from the biliary tree to the pancreas, autoimmune pancreatitis (AIP) is a benign fibro-inflammatory disease that often frustrates advanced endoscopists as it closely mimics the appearance of pancreatic ductal adenocarcinoma (PDAC). The stakes are high: despite modern diagnostic techniques, including advanced imaging, some patients with pancreatic resections for “suspected PDAC” are still found to have AIP on final pathology. Conventional tools to distinguish AIP from PDAC have gaps: serum IgG4 and EUS-guided biopsies are both specific but insensitive.
Using EUS videos and images of various pancreas pathologies at Mayo Clinic, we developed an AI to tackle this dilemma. After intensive training, the EUS AI achieved a greater accuracy for distinguishing AIP from PDAC than a group of expert Mayo clinic endosonographers.5 In practice, an EUS-AI can identify AIP patterns in real-time, guiding clinicians toward steroid trials or biopsies and reducing the need for unnecessary surgeries.
Looking ahead, there are multiple opportunities for integration of AI into advanced endoscopy practices. Ongoing research suggests that AI could soon assist with identification of pancreas cysts most at risk for malignant transformation, classification of high risk Barrett’s esophagus, and even help with rapid on-site assessment of cytologic specimens obtained during EUS. Beyond diagnosis, AI could likely play an important role in guiding therapeutic interventions. For example, an ERCP AI in the future may be able to provide cannulation assistance or an AI assistant could help endosonographers during deployments of lumen apposing metal stents.
By enhancing image interpretation and procedural consistency, AI has the potential to uphold the fundamental principle of primum non nocere, enabling us to intervene with precision while minimizing harm. AI can also bridge grey zones in clinical practice and narrow diagnostic uncertainty in real time. Importantly, these systems can help clinicians achieve expertise in a fraction of the time it traditionally takes to acquire comparable human proficiency, while offering wider availability across practice settings and reducing interobserver variability that has long challenged endoscopic interpretation.
Currently, adoption is limited by high bias risk, lack of external validation, and interpretability Still, the trajectory of AI suggests a future where these computer technologies will not only support but also elevate human expertise, reshaping the standards of care of diseases managed by advanced endoscopists.
Dr. Singh, Dr. Colletta, and Dr. Marya are based at the Division of Gastroenterology and Hepatology, UMass Chan Medical School, Worcester, Massachusetts. Dr. Marya is a consultant for Boston Scientific, and has no other disclosures. Dr. Singh and Dr. Colletta have no disclosures.
References
1. Navaneethan U, et al. Comparative effectiveness of biliary brush cytology and intraductal biopsy for detection of malignant biliary strictures: a systematic review and meta-analysis. Gastrointest Endosc. 2015 Jan. doi: 10.1016/j.gie.2014.09.017.
2. Stassen PMC, et al. Diagnostic accuracy and interobserver agreement of digital single-operator cholangioscopy for indeterminate biliary strictures. Gastrointest Endosc 2021 Dec. doi: 10.1016/j.gie.2021.06.027.
3. Marya NB, et al. Identification of patients with malignant biliary strictures using a cholangioscopy-based deep learning artificial intelligence (with video). Gastrointest Endosc. 2023 Feb. doi: 10.1016/j.gie.2022.08.021.
4. Marya NB, et al. Multicenter validation of a cholangioscopy artificial intelligence system for the evaluation of biliary tract disease. Endoscopy. 2025 Aug. doi: 10.1055/a-2650-0789.
5. Marya NB, et al. Utilisation of artificial intelligence for the development of an EUS-convolutional neural network model trained to enhance the diagnosis of autoimmune pancreatitis. Gut. 2021 Jul. doi: 10.1136/gutjnl-2020-322821.
AI in General GI and Endoscopy
BY DENNIS L. SHUNG, MD, MHS, PHD
The practice of gastroenterology is changing, but much of it will be rooted in the same – careful, focused attention on endoscopic procedures, and compassionate, attentive care in clinic. Artificial intelligence (AI), like the Industrial Revolution before, is going to transform our practice. This comes with upsides and downsides, and highlights the need for strong leadership from our societies to safeguard the technology for practitioners and patients.
What are the upsides?
AI has the potential to serve as a second set of eyes in detecting colon polyps, increasing the adenoma detection rate (ADR).1 AI can be applied to all areas of the gastrointestinal tract, providing digital biopsies, guiding resection, and ensuring quality, which are all now possible with powerful new endoscopy foundation models, such as GastroNet-5M.2
Additionally. the advent of automating the collection of data into reports may herald the end of our days as data entry clerks. Generative AI also has the potential to give us all the best information at our fingertips, suggesting guideline-based care, providing the most up to date evidence, and guiding the differential diagnosis. The potential for patient-facing AI systems could lead to better health literacy, more meaningful engagement, and improved patient satisfaction.3
What are the downsides?
For endoscopy, AI cannot make up for poor technique to ensure adequate mucosal exposure by the endoscopist, and an increase in AI-supported ADR does not yet convincingly translate into concrete gains in colorectal cancer-related mortality. For the foreseeable future, AI cannot make a connection with the patient in front of us, which is critical in diagnosing and treating patients.
Currently, AI appears to worsen loneliness4, and does not necessarily deepen the bonds or provide the positive touch that can heal, and which for many of us, was the reason we became physicians. Finally, as information proliferates, the information risk to patients and providers is growing – in the future, trusted sources to monitor, curate, and guide AI will be ever more important.
Black Swans
As AI begins to mature, there are risks that lurk beneath the surface. When regulatory bodies begin to look at AI-assisted diagnostics or therapeutics as the new standard of care, reimbursement models may adjust, and providers may be left behind. The rapid proliferation and haphazard adoption of AI could lead to overdependence and deskilling or result in weird and as yet unknown errors that are difficult to troubleshoot.
What is the role of the GI societies?
Specialty societies like AGA are taking leadership roles in determining the bounds of where AIs may tread, not just in providing information to their membership but also in digesting evidence and synthesizing recommendations. Societies must balance the real promise of AI in endoscopy with the practice realities for members, and provide living guidelines that reflect the consensus of members regarding scope of practice with the ability to update as new data become available.5
Societies also have a role as advocates for safety, taking ownership of high-quality content to prevent misinformation. AGA recently announced the development of a chat interface that will be focused on providing its members the highest quality information, and serve as a portal to identify and respond to its members’ information needs. By staying united rather than fragmenting, societies can maintain bounds to protect its members and their patients and advance areas where there is clinical need, together.
Dr. Shung is senior associate consultant, Division of Gastroenterology and Hepatology, and director of clinical generative artificial intelligence and informatics, Department of Medicine, at Mayo Clinic Rochester, Minnesota. He has no disclosures in regard to this article.
References
1. Soleymanjahi S, et al. Artificial Intelligence-Assisted Colonoscopy for Polyp Detection : A Systematic Review and Meta-analysis. Ann Intern Med. 2024 Dec. doi:10.7326/annals-24-00981.
2. Jong MR, et al. GastroNet-5M: A Multicenter Dataset for Developing Foundation Models in Gastrointestinal Endoscopy. Gastroenterology. 2025 Jul. doi: 10.1053/j.gastro.2025.07.030.
3. Soroush A, et al. Generative Artificial Intelligence in Clinical Medicine and Impact on Gastroenterology. Gastroenterology. 2025 Aug. doi: 10.1053/j.gastro.2025.03.038.
4. Mengying Fang C, et al. How AI and Human Behaviors Shape Psychosocial Effects of Extended Chatbot Use: A Longitudinal Randomized Controlled Study. arXiv e-prints. 2025 Mar. doi: 10.48550/arXiv.2503.17473.
5. Sultan S, et al. AGA Living Clinical Practice Guideline on Computer-Aided Detection-Assisted Colonoscopy. Gastroenterology. 2025 Apr. doi:10.1053/j.gastro.2025.01.002.
Impact of Retroactive Application of Updated Surveillance Guidelines on Endoscopy Center Capacity at a Large VA Health Care System
Impact of Retroactive Application of Updated Surveillance Guidelines on Endoscopy Center Capacity at a Large VA Health Care System
In 2020, the US Multi-Society Task Force (USMSTF) on Colorectal Cancer (CRC) increased the recommended colon polyp surveillance interval for 1 to 2 subcentimeter tubular adenomas from 5 to 10 years to 7 to 10 years.1 This change was prompted by emerging research indicating that rates of CRC and advanced neoplasia among patients with a history of only 1 to 2 subcentimeter tubular adenomas are lower than initially estimated.2,3 This extension provides an opportunity to increase endoscopy capacity and improve access to colonoscopies by retroactively applying the 2020 guidelines to surveillance interval recommendations made before their introduction. For example, based on the updated guidelines, patients previously recommended to undergo colon polyp surveillance colonoscopy 5 years after an index colonoscopy could extend their surveillance interval by 2 to 5 years. Increasing endoscopic capacity could address the growing demand for colonoscopies from new screening guidelines that reduced the age of initial CRC screening from 50 years to 45 years and the backlog of procedures due to COVID-19 restrictions.4
As part of a project to increase endoscopic capacity at the US Department of Veterans Affairs (VA) Pittsburgh Healthcare System (VAPHS), this study assessed the potential impact of retroactively applying the 2020 USMSTF polyp surveillance guidelines on endoscopic capacity. These results may be informative for other VA and private-sector health care systems seeking to identify strategies to improve endoscopy capacity.
Methods
VAPHS is an integrated health care system in the Veterans Health Administration (VHA) serving 85,000 patients across 8 health care institutions in Pennsylvania, Ohio, and West Virginia. VAPHS manages colorectal screening recommendations for patients receiving medical care in the health care system regardless of whether their prior colonoscopy was performed at VAPHS or external facilities. The VA maintains a national CRC screening and surveillance electronic medical record reminder that prompts health care practitioners to order colon polyp surveillance based on interval recommendations from the index colonoscopy. This study reviewed all patients from the VAPHS panel with a reminder to undergo colonoscopy for screening for CRC or surveillance of colon polyps within 12 months from September 1, 2022.
Among patients with a reminder, 3 investigators reviewed index colonoscopy and pathology reports to identify CRC risk category, colonoscopy indication, procedural quality, and recommended repeat colonoscopy interval. Per the USMSTF guidelines, patients with incomplete colonoscopy or pathology records, high-risk indications (ie, personal history of inflammatory bowel disease, personal history of CRC, or family history of CRC), or inadequate bowel preparation (Boston Bowel Preparation Score < 6) were excluded. Additionally, patients who had CRC screening or surveillance discontinued due to age or comorbidities, had completed a subsequent follow-up colonoscopy, or were deceased at the time of review were excluded.
Retroactive Interval Reclassification
Among eligible patients, this study compared the repeat colonoscopy interval recommended by the prior endoscopist with those from the 2020 USMSTF guidelines. In cases where the interval was documented as a range of years, the lower end was considered the recommendation. Similarly, the lower end of the range from the 2020 USMSTF guidelines was used for the reclassified surveillance interval. Years extended per patient were quantified relative to September 1, 2023 (ie, 1 year after the review date). For example, if the index colonoscopy was completed on September 1, 2016, the initial surveillance recommendation was 5 years, and the reclassified recommendation was 7 years, the interval extension beyond September 1, 2023, was 0 years.
Furthermore, because index surveillance recommendations are not always guideline concordant, the years extended per patient were calculated by harmonizing the index endoscopist’s recommendations with the guidelines at the time of the index colonoscopy.5 For example, if the index colonoscopy was completed on September 1, 2018, and the endoscopist recommended a 5-year follow-up for a patient with average risk for CRC, adequate bowel preparation, and no colorectal polyps, that patient is eligible to extend their colonoscopy to September 1, 2028, based on guideline recommendations at the time of index endoscopy recommending that the next colonoscopy occur in 10 years. In this analysis the 2012 USMSTF guidelines were applied to all index colonoscopies completed in 2021 or earlier to allow time for adoption of the 2020 guidelines.
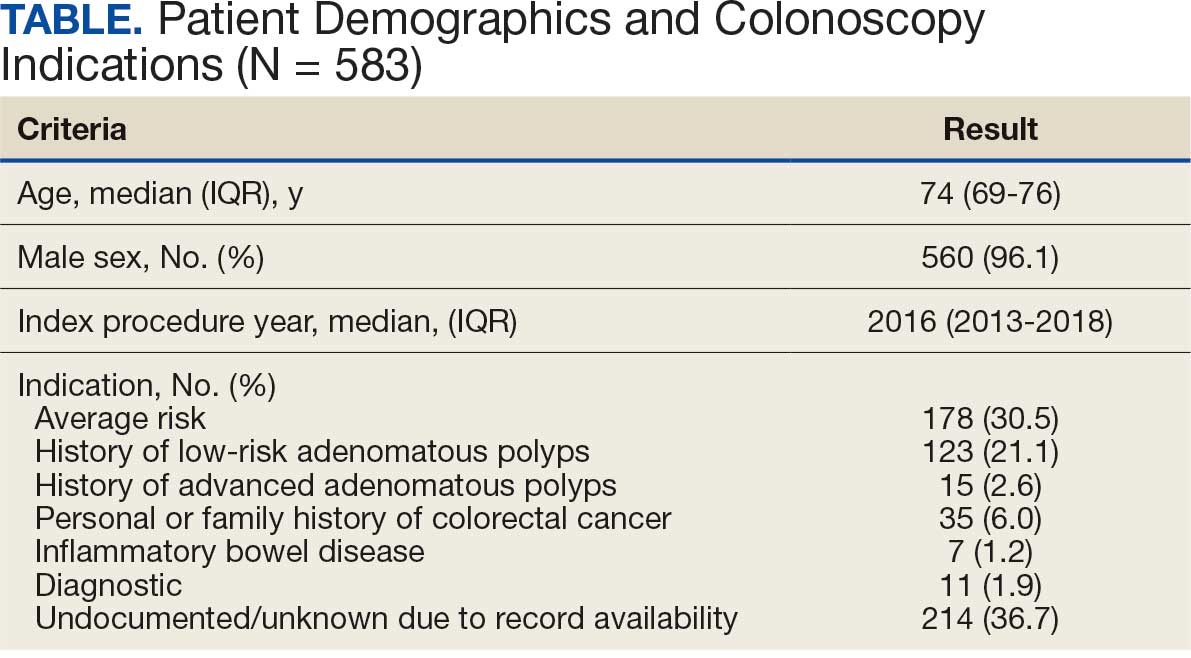
This project fulfilled a facility mandate to increase capacity to conduct endoscopic procedures. Institutional review board approval was not required by VAPHS policy relating to clinical operations projects. Approval for publication of clinical operations activity was obtained from the VAPHS facility director.
Results
Within 1 year of the September 1, 2022, review date, 637 patients receiving care at VAPHS had clinical reminders for an upcoming colonoscopy. Of these, 54 (8.4%) were already up to date or were deceased at the time of review. Of the 583 eligible patients, 96% were male, the median age was 74 years, the median index colonoscopy year was 2016, and 178 (30.5%) had an average-risk CRC screening indication at the index colonoscopy (Table).
Of the 583 patients due for colonoscopy, 331 (56.7%) had both colonoscopy and pathology reports available. The majority of those with incomplete records had the index colonoscopy completed outside VAPHS. Among these patients, 222 (67.0%) had adequate bowel preparation. Of those with adequate bowel preparation, 43 were not eligible for interval extension because of high-risk conditions and 13 were not eligible because there was no index surveillance interval recommendation from the index endoscopist. Of the patients due for colonoscopy, 166 (28.4%) were potentially eligible for surveillance interval extension (Figure).
Sixty-five (39.2%) of the 166 patients had 1 to 2 subcentimeter tubular adenomas on their index colonoscopy. Sixty-two patients were eligible for interval extension to 7 years, but this only resulted in ≥ 1 year of extension beyond the review date for 36 (6% of all 583 patients due for colonoscopy). The 36 patients were extended 63 years. By harmonizing the index endoscopists’ surveillance interval recommendation with the guideline at the time of the index colonoscopy, 29 additional patients could have their colonoscopy extended by ≥ 1 year. Harmonization extended colonoscopy intervals by 93 years. Retroactively applying the 2020 USMSTF polyp surveillance guidelines and harmonizing recommendations to guidelines extended the time of index colonoscopy by 153 years.
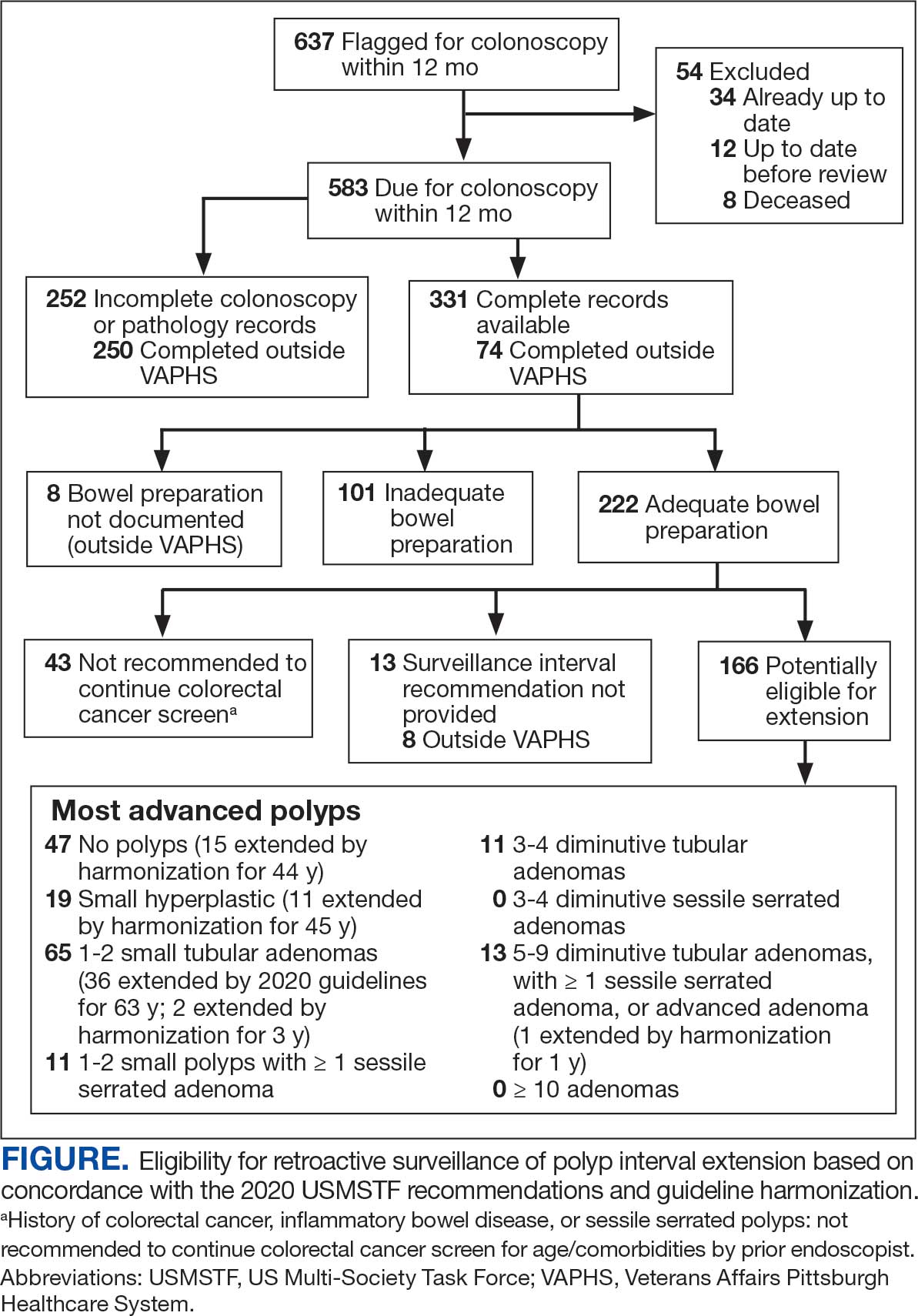
Discussion
With retroactive application of the 2020 USMSTF polyp surveillance guidelines, 6% of patients due for an upcoming colonoscopy could extend their follow-up by ≥ 1 year by extending the surveillance interval for 1 to 2 subcentimeter tubular adenomas to 7 years. An additional 5% of patients could extend their interval by harmonizing the index endoscopist’s interval recommendation with polyp surveillance guidelines at the time of the index colonoscopy. These findings are consistent with the results of 2 studies that demonstrated that about 14% of patients due for colonoscopy could have their interval extended.6,7 The current study enhances those insights by separating the contribution of 2020 USMSTF polyp surveillance guidelines from the contribution of harmonizing surveillance intervals with guidelines for other polyp histologies. This study found that there is an opportunity to improve endoscopic capacity by harmonizing recommendations with guidelines. This complements a 2023 study showing that even when knowledgeable about guidelines, clinicians do not necessarily follow recommendations.8 While this and previous research have identified that 11% to 14% of patients are eligible for extension, these individuals would also have to be willing to have their polyp surveillance intervals extended for there to be a real-world impact on endoscopic capacity. A 2024 study found that only 19% to 37% of patients with 1 to 2 small tubular adenomas were willing to have polyps surveillance interval extension.9 This suggests the actual effect on capacity may be even lower than reported.
Limitations
The overall impact of the 2020 USMSTF polyp surveillance guidelines on endoscopic capacity was blunted by the high prevalence of incomplete index colonoscopy records among the study population. Without data on bowel preparation quality or procedure indications, this study could not assess whether 43% of patients were eligible for surveillance interval extension. Most index colonoscopies with incomplete documentation were completed at community-care gastroenterology facilities. This high rate of incomplete documentation is likely generalizable to other VA health care systems—especially in the era of the Veterans Access, Choice, and Accountability Act of 2014, which increased veteran access to non-VA community care.10 Veterans due for colon polyp surveillance colonoscopies are more likely to have had their prior colonoscopy in community care compared with prior eras.11 Furthermore, because the VHA is among the most established integrated health care systems offering primary and subspecialty care in the US, private sector health care systems may have even greater rates of care fragmentation for longitudinal CRC screening and colon polyp surveillance, as these systems have only begun to regionally integrate recently.12,13
Another limitation is that nearly one-third of the individuals with documentation had inadequate bowel preparation for surveillance recommendations. This results in shorter surveillance follow-up colonoscopies and increases downstream demand for future colonoscopies. The low yield of extending colon polyp surveillance interval in this study emphasizes that improved efforts to obtain colonoscopy and pathology reports from community care, right-sizing the colon polyp surveillance intervals recommended by endoscopists, and improving quality of bowel preparation could have downstream health care system benefits in the future. These efforts could increase colonoscopy capacity at VA health care systems, thereby shortening colonoscopy wait times, decreasing fragmentation of care, and increasing the number of veterans who receive high-quality colonoscopies at VA health care systems.14
Conclusions
Eleven percent of patients in this study due for a colonoscopy could extend their follow-up by ≥ 1 year. About half of these extensions were directly due to the 2020 USMSTF polyp surveillance interval extension for 1 to 2 subcentimeter tubular adenomas. The rest resulted from harmonizing recommendations with guidelines at the time of the procedure. To determine whether retroactively applying polyp surveillance guidelines to follow-up interval recommendations will result in improved endoscopic capacity, health care system administrators should consider the degree of CRC screening care fragmentation in their patient population. Greater long-term gains in endoscopic capacity may be achieved by proactively supporting endoscopists in making guideline-concordant screening recommendations at the time of colonoscopy.
Gupta S, Lieberman D, Anderson JC, et al. Recommendations for follow-up after colonoscopy and polypectomy: a consensus update by the US Multi-Society Task Force on Colorectal Cancer. Gastrointest Endosc. 2020;91:463-485. doi:10.1016/j.gie.2020.01.014
Dubé C, Yakubu M, McCurdy BR, et al. Risk of advanced adenoma, colorectal cancer, and colorectal cancer mortality in people with low-risk adenomas at baseline colonoscopy: a systematic review and meta-analysis. Am J Gastroenterol. 2017;112:1790-1801. doi:10.1038/ajg.2017.360
Click B, Pinsky PF, Hickey T, Doroudi M, Shoen RE. Association of colonoscopy adenoma findings with long-term colorectal cancer incidence. JAMA. 2018;319:2021-2031. doi:10.1001/jama.2018.5809
US Preventive Services Task Force, Davidson KW, Barry MJ, et al. Screening for colorectal cancer: US Preventive Services Task Force recommendation statement. JAMA. 2021;325:1965-1977. doi:10.1001/jama.2021.6238
Djinbachian R, Dubé AJ, Durand M, et al. Adherence to post-polypectomy surveillance guidelines: a systematic review and meta-analysis. Endoscopy. 2019;51:673-683. doi:10.1055/a-0865-2082
Gawron AJ, Kaltenbach T, Dominitz JA. The impact of the coronavirus disease-19 pandemic on access to endoscopy procedures in the VA healthcare system. Gastroenterology. 2020;159:1216-1220.e1. doi:10.1053/j.gastro.2020.07.033
Xiao AH, Chang SY, Stevoff CG, Komanduri S, Pandolfino JE, Keswani RN. Adoption of multi-society guidelines facilitates value-based reduction in screening and surveillance colonoscopy volume during COVID-19 pandemic. Dig Dis Sci. 2021;66:2578-2584. doi:10.1007/s10620-020-06539-1
Dong J, Wang LF, Ardolino E, Feuerstein JD. Real-world compliance with the 2020 U.S. Multi-Society Task Force on Colorectal Cancer polypectomy surveillance guidelines: an observational study. Gastrointest Endosc. 2023;97:350-356.e3. doi:10.1016/j.gie.2022.08.020
Lee JK, Koripella PC, Jensen CD, et al. Randomized trial of patient outreach approaches to de-implement outdated colonoscopy surveillance intervals. Clin Gastroenterol Hepatol. 2024;22:1315-1322.e7. doi:10.1016/j.cgh.2023.12.027
Veterans Access, Choice, and Accountability Act of 2014, HR 3230, 113th Cong (2014). Accessed September 8, 2025. https://www.congress.gov/bill/113th-congress/house-bill/3230
Dueker JM, Khalid A. Performance of the Veterans Choice Program for improving access to colonoscopy at a tertiary VA facility. Fed Pract. 2020;37:224-228.
Oliver A. The Veterans Health Administration: an American success story? Milbank Q. 2007;85:5-35. doi:10.1111/j.1468-0009.2007.00475.x
Furukawa MF, Machta RM, Barrett KA, et al. Landscape of health systems in the United States. Med Care Res Rev. 2020;77:357-366. doi:10.1177/1077558718823130
Petros V, Tsambikos E, Madhoun M, Tierney WM. Impact of community referral on colonoscopy quality metrics in a Veterans Affairs Medical Center. Clin Transl Gastroenterol. 2022;13:e00460. doi:10.14309/ctg.0000000000000460
In 2020, the US Multi-Society Task Force (USMSTF) on Colorectal Cancer (CRC) increased the recommended colon polyp surveillance interval for 1 to 2 subcentimeter tubular adenomas from 5 to 10 years to 7 to 10 years.1 This change was prompted by emerging research indicating that rates of CRC and advanced neoplasia among patients with a history of only 1 to 2 subcentimeter tubular adenomas are lower than initially estimated.2,3 This extension provides an opportunity to increase endoscopy capacity and improve access to colonoscopies by retroactively applying the 2020 guidelines to surveillance interval recommendations made before their introduction. For example, based on the updated guidelines, patients previously recommended to undergo colon polyp surveillance colonoscopy 5 years after an index colonoscopy could extend their surveillance interval by 2 to 5 years. Increasing endoscopic capacity could address the growing demand for colonoscopies from new screening guidelines that reduced the age of initial CRC screening from 50 years to 45 years and the backlog of procedures due to COVID-19 restrictions.4
As part of a project to increase endoscopic capacity at the US Department of Veterans Affairs (VA) Pittsburgh Healthcare System (VAPHS), this study assessed the potential impact of retroactively applying the 2020 USMSTF polyp surveillance guidelines on endoscopic capacity. These results may be informative for other VA and private-sector health care systems seeking to identify strategies to improve endoscopy capacity.
Methods
VAPHS is an integrated health care system in the Veterans Health Administration (VHA) serving 85,000 patients across 8 health care institutions in Pennsylvania, Ohio, and West Virginia. VAPHS manages colorectal screening recommendations for patients receiving medical care in the health care system regardless of whether their prior colonoscopy was performed at VAPHS or external facilities. The VA maintains a national CRC screening and surveillance electronic medical record reminder that prompts health care practitioners to order colon polyp surveillance based on interval recommendations from the index colonoscopy. This study reviewed all patients from the VAPHS panel with a reminder to undergo colonoscopy for screening for CRC or surveillance of colon polyps within 12 months from September 1, 2022.
Among patients with a reminder, 3 investigators reviewed index colonoscopy and pathology reports to identify CRC risk category, colonoscopy indication, procedural quality, and recommended repeat colonoscopy interval. Per the USMSTF guidelines, patients with incomplete colonoscopy or pathology records, high-risk indications (ie, personal history of inflammatory bowel disease, personal history of CRC, or family history of CRC), or inadequate bowel preparation (Boston Bowel Preparation Score < 6) were excluded. Additionally, patients who had CRC screening or surveillance discontinued due to age or comorbidities, had completed a subsequent follow-up colonoscopy, or were deceased at the time of review were excluded.
Retroactive Interval Reclassification
Among eligible patients, this study compared the repeat colonoscopy interval recommended by the prior endoscopist with those from the 2020 USMSTF guidelines. In cases where the interval was documented as a range of years, the lower end was considered the recommendation. Similarly, the lower end of the range from the 2020 USMSTF guidelines was used for the reclassified surveillance interval. Years extended per patient were quantified relative to September 1, 2023 (ie, 1 year after the review date). For example, if the index colonoscopy was completed on September 1, 2016, the initial surveillance recommendation was 5 years, and the reclassified recommendation was 7 years, the interval extension beyond September 1, 2023, was 0 years.
Furthermore, because index surveillance recommendations are not always guideline concordant, the years extended per patient were calculated by harmonizing the index endoscopist’s recommendations with the guidelines at the time of the index colonoscopy.5 For example, if the index colonoscopy was completed on September 1, 2018, and the endoscopist recommended a 5-year follow-up for a patient with average risk for CRC, adequate bowel preparation, and no colorectal polyps, that patient is eligible to extend their colonoscopy to September 1, 2028, based on guideline recommendations at the time of index endoscopy recommending that the next colonoscopy occur in 10 years. In this analysis the 2012 USMSTF guidelines were applied to all index colonoscopies completed in 2021 or earlier to allow time for adoption of the 2020 guidelines.
This project fulfilled a facility mandate to increase capacity to conduct endoscopic procedures. Institutional review board approval was not required by VAPHS policy relating to clinical operations projects. Approval for publication of clinical operations activity was obtained from the VAPHS facility director.
Results
Within 1 year of the September 1, 2022, review date, 637 patients receiving care at VAPHS had clinical reminders for an upcoming colonoscopy. Of these, 54 (8.4%) were already up to date or were deceased at the time of review. Of the 583 eligible patients, 96% were male, the median age was 74 years, the median index colonoscopy year was 2016, and 178 (30.5%) had an average-risk CRC screening indication at the index colonoscopy (Table).
Of the 583 patients due for colonoscopy, 331 (56.7%) had both colonoscopy and pathology reports available. The majority of those with incomplete records had the index colonoscopy completed outside VAPHS. Among these patients, 222 (67.0%) had adequate bowel preparation. Of those with adequate bowel preparation, 43 were not eligible for interval extension because of high-risk conditions and 13 were not eligible because there was no index surveillance interval recommendation from the index endoscopist. Of the patients due for colonoscopy, 166 (28.4%) were potentially eligible for surveillance interval extension (Figure).
Sixty-five (39.2%) of the 166 patients had 1 to 2 subcentimeter tubular adenomas on their index colonoscopy. Sixty-two patients were eligible for interval extension to 7 years, but this only resulted in ≥ 1 year of extension beyond the review date for 36 (6% of all 583 patients due for colonoscopy). The 36 patients were extended 63 years. By harmonizing the index endoscopists’ surveillance interval recommendation with the guideline at the time of the index colonoscopy, 29 additional patients could have their colonoscopy extended by ≥ 1 year. Harmonization extended colonoscopy intervals by 93 years. Retroactively applying the 2020 USMSTF polyp surveillance guidelines and harmonizing recommendations to guidelines extended the time of index colonoscopy by 153 years.
Discussion
With retroactive application of the 2020 USMSTF polyp surveillance guidelines, 6% of patients due for an upcoming colonoscopy could extend their follow-up by ≥ 1 year by extending the surveillance interval for 1 to 2 subcentimeter tubular adenomas to 7 years. An additional 5% of patients could extend their interval by harmonizing the index endoscopist’s interval recommendation with polyp surveillance guidelines at the time of the index colonoscopy. These findings are consistent with the results of 2 studies that demonstrated that about 14% of patients due for colonoscopy could have their interval extended.6,7 The current study enhances those insights by separating the contribution of 2020 USMSTF polyp surveillance guidelines from the contribution of harmonizing surveillance intervals with guidelines for other polyp histologies. This study found that there is an opportunity to improve endoscopic capacity by harmonizing recommendations with guidelines. This complements a 2023 study showing that even when knowledgeable about guidelines, clinicians do not necessarily follow recommendations.8 While this and previous research have identified that 11% to 14% of patients are eligible for extension, these individuals would also have to be willing to have their polyp surveillance intervals extended for there to be a real-world impact on endoscopic capacity. A 2024 study found that only 19% to 37% of patients with 1 to 2 small tubular adenomas were willing to have polyps surveillance interval extension.9 This suggests the actual effect on capacity may be even lower than reported.
Limitations
The overall impact of the 2020 USMSTF polyp surveillance guidelines on endoscopic capacity was blunted by the high prevalence of incomplete index colonoscopy records among the study population. Without data on bowel preparation quality or procedure indications, this study could not assess whether 43% of patients were eligible for surveillance interval extension. Most index colonoscopies with incomplete documentation were completed at community-care gastroenterology facilities. This high rate of incomplete documentation is likely generalizable to other VA health care systems—especially in the era of the Veterans Access, Choice, and Accountability Act of 2014, which increased veteran access to non-VA community care.10 Veterans due for colon polyp surveillance colonoscopies are more likely to have had their prior colonoscopy in community care compared with prior eras.11 Furthermore, because the VHA is among the most established integrated health care systems offering primary and subspecialty care in the US, private sector health care systems may have even greater rates of care fragmentation for longitudinal CRC screening and colon polyp surveillance, as these systems have only begun to regionally integrate recently.12,13
Another limitation is that nearly one-third of the individuals with documentation had inadequate bowel preparation for surveillance recommendations. This results in shorter surveillance follow-up colonoscopies and increases downstream demand for future colonoscopies. The low yield of extending colon polyp surveillance interval in this study emphasizes that improved efforts to obtain colonoscopy and pathology reports from community care, right-sizing the colon polyp surveillance intervals recommended by endoscopists, and improving quality of bowel preparation could have downstream health care system benefits in the future. These efforts could increase colonoscopy capacity at VA health care systems, thereby shortening colonoscopy wait times, decreasing fragmentation of care, and increasing the number of veterans who receive high-quality colonoscopies at VA health care systems.14
Conclusions
Eleven percent of patients in this study due for a colonoscopy could extend their follow-up by ≥ 1 year. About half of these extensions were directly due to the 2020 USMSTF polyp surveillance interval extension for 1 to 2 subcentimeter tubular adenomas. The rest resulted from harmonizing recommendations with guidelines at the time of the procedure. To determine whether retroactively applying polyp surveillance guidelines to follow-up interval recommendations will result in improved endoscopic capacity, health care system administrators should consider the degree of CRC screening care fragmentation in their patient population. Greater long-term gains in endoscopic capacity may be achieved by proactively supporting endoscopists in making guideline-concordant screening recommendations at the time of colonoscopy.
In 2020, the US Multi-Society Task Force (USMSTF) on Colorectal Cancer (CRC) increased the recommended colon polyp surveillance interval for 1 to 2 subcentimeter tubular adenomas from 5 to 10 years to 7 to 10 years.1 This change was prompted by emerging research indicating that rates of CRC and advanced neoplasia among patients with a history of only 1 to 2 subcentimeter tubular adenomas are lower than initially estimated.2,3 This extension provides an opportunity to increase endoscopy capacity and improve access to colonoscopies by retroactively applying the 2020 guidelines to surveillance interval recommendations made before their introduction. For example, based on the updated guidelines, patients previously recommended to undergo colon polyp surveillance colonoscopy 5 years after an index colonoscopy could extend their surveillance interval by 2 to 5 years. Increasing endoscopic capacity could address the growing demand for colonoscopies from new screening guidelines that reduced the age of initial CRC screening from 50 years to 45 years and the backlog of procedures due to COVID-19 restrictions.4
As part of a project to increase endoscopic capacity at the US Department of Veterans Affairs (VA) Pittsburgh Healthcare System (VAPHS), this study assessed the potential impact of retroactively applying the 2020 USMSTF polyp surveillance guidelines on endoscopic capacity. These results may be informative for other VA and private-sector health care systems seeking to identify strategies to improve endoscopy capacity.
Methods
VAPHS is an integrated health care system in the Veterans Health Administration (VHA) serving 85,000 patients across 8 health care institutions in Pennsylvania, Ohio, and West Virginia. VAPHS manages colorectal screening recommendations for patients receiving medical care in the health care system regardless of whether their prior colonoscopy was performed at VAPHS or external facilities. The VA maintains a national CRC screening and surveillance electronic medical record reminder that prompts health care practitioners to order colon polyp surveillance based on interval recommendations from the index colonoscopy. This study reviewed all patients from the VAPHS panel with a reminder to undergo colonoscopy for screening for CRC or surveillance of colon polyps within 12 months from September 1, 2022.
Among patients with a reminder, 3 investigators reviewed index colonoscopy and pathology reports to identify CRC risk category, colonoscopy indication, procedural quality, and recommended repeat colonoscopy interval. Per the USMSTF guidelines, patients with incomplete colonoscopy or pathology records, high-risk indications (ie, personal history of inflammatory bowel disease, personal history of CRC, or family history of CRC), or inadequate bowel preparation (Boston Bowel Preparation Score < 6) were excluded. Additionally, patients who had CRC screening or surveillance discontinued due to age or comorbidities, had completed a subsequent follow-up colonoscopy, or were deceased at the time of review were excluded.
Retroactive Interval Reclassification
Among eligible patients, this study compared the repeat colonoscopy interval recommended by the prior endoscopist with those from the 2020 USMSTF guidelines. In cases where the interval was documented as a range of years, the lower end was considered the recommendation. Similarly, the lower end of the range from the 2020 USMSTF guidelines was used for the reclassified surveillance interval. Years extended per patient were quantified relative to September 1, 2023 (ie, 1 year after the review date). For example, if the index colonoscopy was completed on September 1, 2016, the initial surveillance recommendation was 5 years, and the reclassified recommendation was 7 years, the interval extension beyond September 1, 2023, was 0 years.
Furthermore, because index surveillance recommendations are not always guideline concordant, the years extended per patient were calculated by harmonizing the index endoscopist’s recommendations with the guidelines at the time of the index colonoscopy.5 For example, if the index colonoscopy was completed on September 1, 2018, and the endoscopist recommended a 5-year follow-up for a patient with average risk for CRC, adequate bowel preparation, and no colorectal polyps, that patient is eligible to extend their colonoscopy to September 1, 2028, based on guideline recommendations at the time of index endoscopy recommending that the next colonoscopy occur in 10 years. In this analysis the 2012 USMSTF guidelines were applied to all index colonoscopies completed in 2021 or earlier to allow time for adoption of the 2020 guidelines.
This project fulfilled a facility mandate to increase capacity to conduct endoscopic procedures. Institutional review board approval was not required by VAPHS policy relating to clinical operations projects. Approval for publication of clinical operations activity was obtained from the VAPHS facility director.
Results
Within 1 year of the September 1, 2022, review date, 637 patients receiving care at VAPHS had clinical reminders for an upcoming colonoscopy. Of these, 54 (8.4%) were already up to date or were deceased at the time of review. Of the 583 eligible patients, 96% were male, the median age was 74 years, the median index colonoscopy year was 2016, and 178 (30.5%) had an average-risk CRC screening indication at the index colonoscopy (Table).
Of the 583 patients due for colonoscopy, 331 (56.7%) had both colonoscopy and pathology reports available. The majority of those with incomplete records had the index colonoscopy completed outside VAPHS. Among these patients, 222 (67.0%) had adequate bowel preparation. Of those with adequate bowel preparation, 43 were not eligible for interval extension because of high-risk conditions and 13 were not eligible because there was no index surveillance interval recommendation from the index endoscopist. Of the patients due for colonoscopy, 166 (28.4%) were potentially eligible for surveillance interval extension (Figure).
Sixty-five (39.2%) of the 166 patients had 1 to 2 subcentimeter tubular adenomas on their index colonoscopy. Sixty-two patients were eligible for interval extension to 7 years, but this only resulted in ≥ 1 year of extension beyond the review date for 36 (6% of all 583 patients due for colonoscopy). The 36 patients were extended 63 years. By harmonizing the index endoscopists’ surveillance interval recommendation with the guideline at the time of the index colonoscopy, 29 additional patients could have their colonoscopy extended by ≥ 1 year. Harmonization extended colonoscopy intervals by 93 years. Retroactively applying the 2020 USMSTF polyp surveillance guidelines and harmonizing recommendations to guidelines extended the time of index colonoscopy by 153 years.
Discussion
With retroactive application of the 2020 USMSTF polyp surveillance guidelines, 6% of patients due for an upcoming colonoscopy could extend their follow-up by ≥ 1 year by extending the surveillance interval for 1 to 2 subcentimeter tubular adenomas to 7 years. An additional 5% of patients could extend their interval by harmonizing the index endoscopist’s interval recommendation with polyp surveillance guidelines at the time of the index colonoscopy. These findings are consistent with the results of 2 studies that demonstrated that about 14% of patients due for colonoscopy could have their interval extended.6,7 The current study enhances those insights by separating the contribution of 2020 USMSTF polyp surveillance guidelines from the contribution of harmonizing surveillance intervals with guidelines for other polyp histologies. This study found that there is an opportunity to improve endoscopic capacity by harmonizing recommendations with guidelines. This complements a 2023 study showing that even when knowledgeable about guidelines, clinicians do not necessarily follow recommendations.8 While this and previous research have identified that 11% to 14% of patients are eligible for extension, these individuals would also have to be willing to have their polyp surveillance intervals extended for there to be a real-world impact on endoscopic capacity. A 2024 study found that only 19% to 37% of patients with 1 to 2 small tubular adenomas were willing to have polyps surveillance interval extension.9 This suggests the actual effect on capacity may be even lower than reported.
Limitations
The overall impact of the 2020 USMSTF polyp surveillance guidelines on endoscopic capacity was blunted by the high prevalence of incomplete index colonoscopy records among the study population. Without data on bowel preparation quality or procedure indications, this study could not assess whether 43% of patients were eligible for surveillance interval extension. Most index colonoscopies with incomplete documentation were completed at community-care gastroenterology facilities. This high rate of incomplete documentation is likely generalizable to other VA health care systems—especially in the era of the Veterans Access, Choice, and Accountability Act of 2014, which increased veteran access to non-VA community care.10 Veterans due for colon polyp surveillance colonoscopies are more likely to have had their prior colonoscopy in community care compared with prior eras.11 Furthermore, because the VHA is among the most established integrated health care systems offering primary and subspecialty care in the US, private sector health care systems may have even greater rates of care fragmentation for longitudinal CRC screening and colon polyp surveillance, as these systems have only begun to regionally integrate recently.12,13
Another limitation is that nearly one-third of the individuals with documentation had inadequate bowel preparation for surveillance recommendations. This results in shorter surveillance follow-up colonoscopies and increases downstream demand for future colonoscopies. The low yield of extending colon polyp surveillance interval in this study emphasizes that improved efforts to obtain colonoscopy and pathology reports from community care, right-sizing the colon polyp surveillance intervals recommended by endoscopists, and improving quality of bowel preparation could have downstream health care system benefits in the future. These efforts could increase colonoscopy capacity at VA health care systems, thereby shortening colonoscopy wait times, decreasing fragmentation of care, and increasing the number of veterans who receive high-quality colonoscopies at VA health care systems.14
Conclusions
Eleven percent of patients in this study due for a colonoscopy could extend their follow-up by ≥ 1 year. About half of these extensions were directly due to the 2020 USMSTF polyp surveillance interval extension for 1 to 2 subcentimeter tubular adenomas. The rest resulted from harmonizing recommendations with guidelines at the time of the procedure. To determine whether retroactively applying polyp surveillance guidelines to follow-up interval recommendations will result in improved endoscopic capacity, health care system administrators should consider the degree of CRC screening care fragmentation in their patient population. Greater long-term gains in endoscopic capacity may be achieved by proactively supporting endoscopists in making guideline-concordant screening recommendations at the time of colonoscopy.
Gupta S, Lieberman D, Anderson JC, et al. Recommendations for follow-up after colonoscopy and polypectomy: a consensus update by the US Multi-Society Task Force on Colorectal Cancer. Gastrointest Endosc. 2020;91:463-485. doi:10.1016/j.gie.2020.01.014
Dubé C, Yakubu M, McCurdy BR, et al. Risk of advanced adenoma, colorectal cancer, and colorectal cancer mortality in people with low-risk adenomas at baseline colonoscopy: a systematic review and meta-analysis. Am J Gastroenterol. 2017;112:1790-1801. doi:10.1038/ajg.2017.360
Click B, Pinsky PF, Hickey T, Doroudi M, Shoen RE. Association of colonoscopy adenoma findings with long-term colorectal cancer incidence. JAMA. 2018;319:2021-2031. doi:10.1001/jama.2018.5809
US Preventive Services Task Force, Davidson KW, Barry MJ, et al. Screening for colorectal cancer: US Preventive Services Task Force recommendation statement. JAMA. 2021;325:1965-1977. doi:10.1001/jama.2021.6238
Djinbachian R, Dubé AJ, Durand M, et al. Adherence to post-polypectomy surveillance guidelines: a systematic review and meta-analysis. Endoscopy. 2019;51:673-683. doi:10.1055/a-0865-2082
Gawron AJ, Kaltenbach T, Dominitz JA. The impact of the coronavirus disease-19 pandemic on access to endoscopy procedures in the VA healthcare system. Gastroenterology. 2020;159:1216-1220.e1. doi:10.1053/j.gastro.2020.07.033
Xiao AH, Chang SY, Stevoff CG, Komanduri S, Pandolfino JE, Keswani RN. Adoption of multi-society guidelines facilitates value-based reduction in screening and surveillance colonoscopy volume during COVID-19 pandemic. Dig Dis Sci. 2021;66:2578-2584. doi:10.1007/s10620-020-06539-1
Dong J, Wang LF, Ardolino E, Feuerstein JD. Real-world compliance with the 2020 U.S. Multi-Society Task Force on Colorectal Cancer polypectomy surveillance guidelines: an observational study. Gastrointest Endosc. 2023;97:350-356.e3. doi:10.1016/j.gie.2022.08.020
Lee JK, Koripella PC, Jensen CD, et al. Randomized trial of patient outreach approaches to de-implement outdated colonoscopy surveillance intervals. Clin Gastroenterol Hepatol. 2024;22:1315-1322.e7. doi:10.1016/j.cgh.2023.12.027
Veterans Access, Choice, and Accountability Act of 2014, HR 3230, 113th Cong (2014). Accessed September 8, 2025. https://www.congress.gov/bill/113th-congress/house-bill/3230
Dueker JM, Khalid A. Performance of the Veterans Choice Program for improving access to colonoscopy at a tertiary VA facility. Fed Pract. 2020;37:224-228.
Oliver A. The Veterans Health Administration: an American success story? Milbank Q. 2007;85:5-35. doi:10.1111/j.1468-0009.2007.00475.x
Furukawa MF, Machta RM, Barrett KA, et al. Landscape of health systems in the United States. Med Care Res Rev. 2020;77:357-366. doi:10.1177/1077558718823130
Petros V, Tsambikos E, Madhoun M, Tierney WM. Impact of community referral on colonoscopy quality metrics in a Veterans Affairs Medical Center. Clin Transl Gastroenterol. 2022;13:e00460. doi:10.14309/ctg.0000000000000460
Gupta S, Lieberman D, Anderson JC, et al. Recommendations for follow-up after colonoscopy and polypectomy: a consensus update by the US Multi-Society Task Force on Colorectal Cancer. Gastrointest Endosc. 2020;91:463-485. doi:10.1016/j.gie.2020.01.014
Dubé C, Yakubu M, McCurdy BR, et al. Risk of advanced adenoma, colorectal cancer, and colorectal cancer mortality in people with low-risk adenomas at baseline colonoscopy: a systematic review and meta-analysis. Am J Gastroenterol. 2017;112:1790-1801. doi:10.1038/ajg.2017.360
Click B, Pinsky PF, Hickey T, Doroudi M, Shoen RE. Association of colonoscopy adenoma findings with long-term colorectal cancer incidence. JAMA. 2018;319:2021-2031. doi:10.1001/jama.2018.5809
US Preventive Services Task Force, Davidson KW, Barry MJ, et al. Screening for colorectal cancer: US Preventive Services Task Force recommendation statement. JAMA. 2021;325:1965-1977. doi:10.1001/jama.2021.6238
Djinbachian R, Dubé AJ, Durand M, et al. Adherence to post-polypectomy surveillance guidelines: a systematic review and meta-analysis. Endoscopy. 2019;51:673-683. doi:10.1055/a-0865-2082
Gawron AJ, Kaltenbach T, Dominitz JA. The impact of the coronavirus disease-19 pandemic on access to endoscopy procedures in the VA healthcare system. Gastroenterology. 2020;159:1216-1220.e1. doi:10.1053/j.gastro.2020.07.033
Xiao AH, Chang SY, Stevoff CG, Komanduri S, Pandolfino JE, Keswani RN. Adoption of multi-society guidelines facilitates value-based reduction in screening and surveillance colonoscopy volume during COVID-19 pandemic. Dig Dis Sci. 2021;66:2578-2584. doi:10.1007/s10620-020-06539-1
Dong J, Wang LF, Ardolino E, Feuerstein JD. Real-world compliance with the 2020 U.S. Multi-Society Task Force on Colorectal Cancer polypectomy surveillance guidelines: an observational study. Gastrointest Endosc. 2023;97:350-356.e3. doi:10.1016/j.gie.2022.08.020
Lee JK, Koripella PC, Jensen CD, et al. Randomized trial of patient outreach approaches to de-implement outdated colonoscopy surveillance intervals. Clin Gastroenterol Hepatol. 2024;22:1315-1322.e7. doi:10.1016/j.cgh.2023.12.027
Veterans Access, Choice, and Accountability Act of 2014, HR 3230, 113th Cong (2014). Accessed September 8, 2025. https://www.congress.gov/bill/113th-congress/house-bill/3230
Dueker JM, Khalid A. Performance of the Veterans Choice Program for improving access to colonoscopy at a tertiary VA facility. Fed Pract. 2020;37:224-228.
Oliver A. The Veterans Health Administration: an American success story? Milbank Q. 2007;85:5-35. doi:10.1111/j.1468-0009.2007.00475.x
Furukawa MF, Machta RM, Barrett KA, et al. Landscape of health systems in the United States. Med Care Res Rev. 2020;77:357-366. doi:10.1177/1077558718823130
Petros V, Tsambikos E, Madhoun M, Tierney WM. Impact of community referral on colonoscopy quality metrics in a Veterans Affairs Medical Center. Clin Transl Gastroenterol. 2022;13:e00460. doi:10.14309/ctg.0000000000000460
Impact of Retroactive Application of Updated Surveillance Guidelines on Endoscopy Center Capacity at a Large VA Health Care System
Impact of Retroactive Application of Updated Surveillance Guidelines on Endoscopy Center Capacity at a Large VA Health Care System

A Case Report of Unanticipated Difficult Intubation Due to Posterior Tracheal Angulation
A Case Report of Unanticipated Difficult Intubation Due to Posterior Tracheal Angulation
Tracheal deviation mostly occurs from mechanical compression of the trachea, and can be caused by a variety of clinical conditions, including trauma,¹ pharyngeal abscess,² neck hematoma,³ thyroid enlargement,4 and kyphoscoliosis.5 These conditions often result in lateral tracheal deviation, which can be associated with tracheal compression and reduction in tracheal caliber.
Anterior-posterior (A-P) tracheal deviation has rarely been reported. Kyphoscoliosis, scarring after a tracheostomy, or innominate vein compression are probable causes of A-P tracheal deviation and can be associated with tracheal narrowing and vascular fistula formation. This report describes a case of difficult endotracheal tube (ETT) advancement secondary to unexpected acute posterior tracheal deviation encountered during cardiopulmonary resuscitation (CPR). A waiver of patient consent was obtained from the Human Research Protection Program at the US Department of Veterans Affairs (VA) Puget Sound Health Care System.
Case Presentation
A 50-year-old male with a history of chronic cerebral venous sinus thrombosis and taking enoxaparin, presented to the emergency department for recurrent headaches. He experienced sudden cardiac arrest, and CPR in the form of chest compression and bag mask ventilation was immediately initiated. With the patient's head in an extended position and using a video laryngoscope, a Cormack–Lehane grade 1 view of the glottic opening was obtained and the trachea was intubated with an 8 mm (internal diameter) polyvinyl chloride ETT. Tracheal intubation was confirmed by utilizing continuous EtCO2 monitoring. The ETT was secured at 22 cm measured at the teeth.
After about 40 minutes of CPR, spontaneous circulation restarted and a portable A-P chest X-ray with the head in a neutral position indicated the ETT tip was at the level of the first rib (Figure 1). This finding, along with a persistent air leak, prompted blind advancement of the ETT to 26 cm at the teeth, but resistance to advancement was noted. A subsequent chest computed tomography (CT) with the head in a neutral position revealed the ETT remained inappropriately positioned with the tip measured 8.2 cm above the carina (Figure 2A). Concurrently, a sagittal CT view demonstrated significant posterior deviation of the mid and lower trachea. This deviation was determined to be the most likely cause of the difficulty encountered in advancing the ETT. No masses or lesions contributing to the acute tracheal angulation could be identified. Comparing CT imaging from 2 months prior, the trachea was of normal caliber and ordinarily aligned with the vertebral column (Figure 2B).
With the patient in Fowler position with the head midline, a flexible fiber-optic bronchoscopy was performed. Acute, almost 90-degree tracheal angulation was encountered and navigated by retroflexion of the flexible bronchoscope. Once the posterior tracheal wall was encountered, retroflexion was relaxed and the carina was visualized. The bronchoscope tip was placed near the carina, and the ETT was advanced over the fiber-optic bronchoscope to terminate 3 cm above the carina. A subsequent chest X-ray confirmed appropriate ETT position (Figure 3).
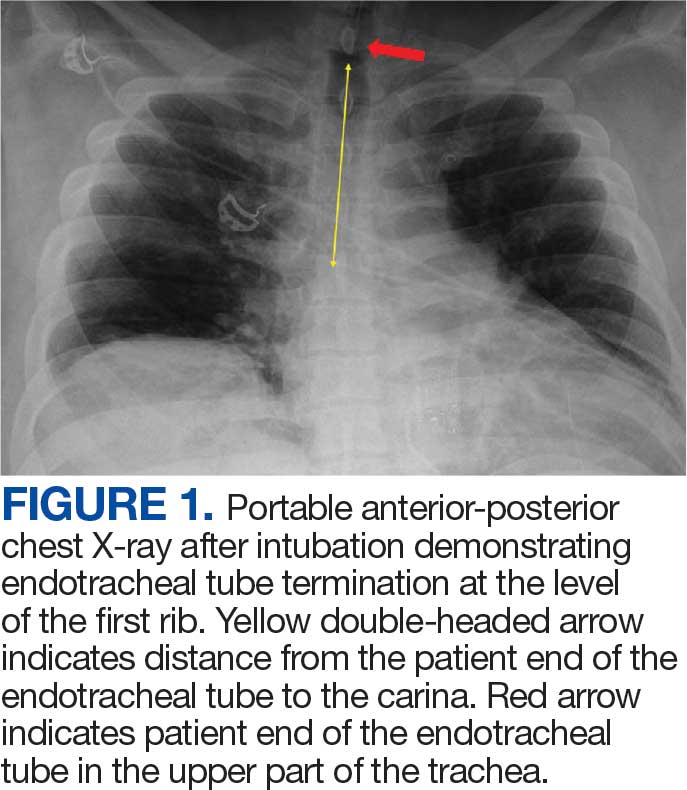
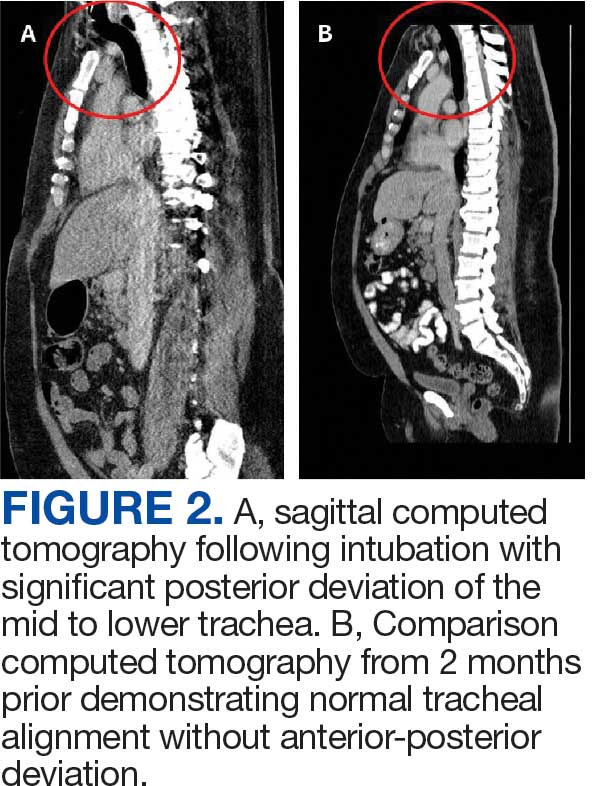
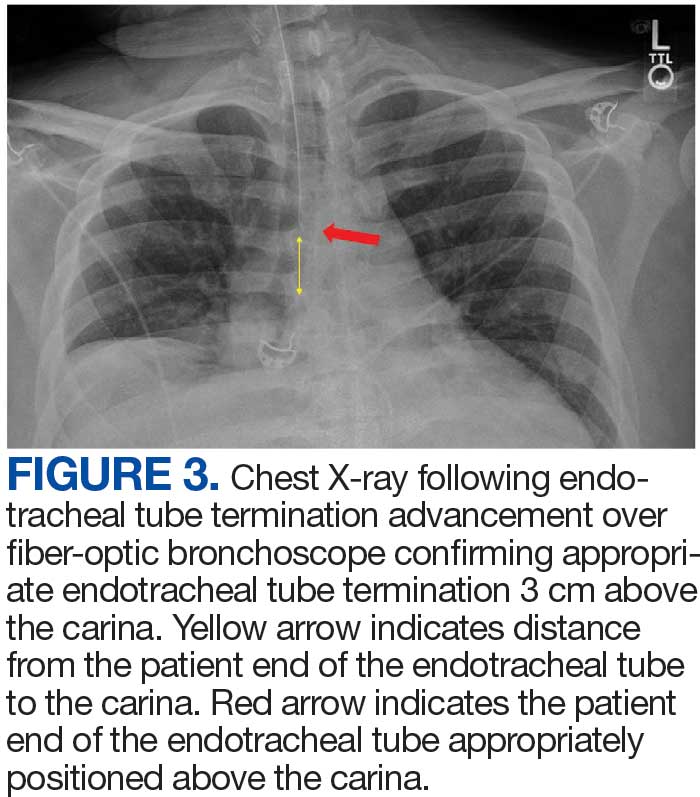
Discussion
Tracheal deviation in the A-P dimension resulting in difficult tracheal intubation has rarely been reported. Previous reports have described anatomical lesions contributing to similar tracheal deviation, such as retro-tracheal thyroid tissue, pronounced cervical lordosis, and severe kyphoscoliosis with destructive cervical fusion.5-8 In a study of the anatomical correlation of double lumen tube placement while using positron emission tomography CT, Cameron et al evaluated the size and angulation of the glottis and proximal trachea using calibrated CT measurements and an online digital protractor and note nearly perfect alignment of the pharynx and glottis.9 However, the trachea turned posteriorly relative to the glottis, resulting in an overall posterior angle of the proximal trachea compared to the glottis of 30.4 to 50.1 degrees, with no sex differences. The need to maneuver similar proximal tracheal angulation during endotracheal intubation has been reported as a cause of difficult intubation.10
In this case, the posterior angulation was not encountered in the proximal trachea but rather in the more distal trachea. The extreme A-P tracheal deviation was not associated with any identifiable masses or lesions. A CT performed 2 months prior demonstrated normal tracheal anatomy, and there was no interval history of neck trauma or tracheal obstruction suggestive of a likely cause for this deviation. This change in the patient’s tracheal anatomy was only discovered after CPR had been performed and as part of the workup for cardiac arrest. Iatrogenic injuries are known to occur during CPR. Common CPR-related airway injuries include tracheal mucosal injury from traumatic intubation and bony injuries to the chest wall from compressions.11 Laryngeal cartilage damage from intubation may also occur, but tracheal displacement following CPR has not been previously reported.11
This case of tracheal deviation is unlikely to be related to patient positioning, as the A-P deviation persisted in 3 separate head and neck alignments. First, during indirect laryngoscopy, performed in a standard sniffing position. Second, during the CT, performed in the supine position, with no head support. The acute A-P deviation seen in Figure 2 was clearly noted in this position. Lastly, flexible fiber-optic bronchoscopy was performed in a semiupright position with the head supported on a pillow. A-P deviation was encountered and navigated in this position during flexible fiber-optic guided ETT repositioning.
Using magnetic resonance imaging, alterations in the alignment of pharyngeal and tracheal axes have been described with changes in neck positioning; however, tracheal deviation has not been described with changes in head and neck alignment.12 Although the clinical presentation in this case was consistent with prior reports, we were unable to identify any previously reported anatomic cause for the tracheal deviation.5,6,8 Initial glottic visualization with a video laryngoscope was unremarkable, but resistance to sufficient ETT advancement past the vocal cords and a persistent air leak due to cuff herniation through the glottic opening was noticeable. The ETT was maneuvered to an appropriate position in the trachea using a flexible fiber-optic bronchoscope. The acute angulation of the trachea that was appreciated on bronchoscopy did not result in kinking of the ETT both initially and after in-situ thermosoftening of the polyvinyl chloride tube.13 Previously reported instances of A-P tracheal deviation have outlined the necessity of using alternative techniques to establish a patent airway, including the use of a laryngeal mask airway and a cuffless ETT with saline-soaked gauze packing.5,8 In 1 reported case, awake fiber-optic intubation was performed when difficult tracheal intubation was anticipated due to known A-P tracheal deviation.6
Failure of ETT advancement can be due to obstruction from the arytenoids and at the level of the vocal cords.14 When the ETT has been visualized to have traversed the vocal cords, tracheal A-P deviation should be considered as a cause of difficult ETT advancement. If an adequate endotracheal airway cannot be established, prompt consideration should be given to placement of a supraglottic airway. Early fiber-optic bronchoscopy should be used to establish the diagnosis and assist with proper ETT positioning.
Conclusions
This case illustrates the rare occurrence of A-P tracheal deviation leading to difficult intubation during CPR. The findings underscore the importance of considering A-P deviation as a potential cause of airway complications in emergency settings, especially in patients with previously normal tracheal anatomy. The successful use of flexible fiber-optic bronchoscopy in this case provides a valuable technique for addressing acute tracheal angulation. This report contributes to the limited literature on A-P tracheal deviation and serves as a reminder for clinicians to maintain a high index of suspicion for unusual airway challenges during critical interventions.
Creasy JD, Chiles C, Routh WD, et al. Overview of traumatic injury of the thoracic aorta. Radiogr Rev Publ Radiol Soc N Am Inc. 1997;17:27-45. doi:10.1148/radiographics.17.1.9017797
Yee AM, Christensen DN, Waterbrook AL, et al. Parapharyngeal abscess with tracheal deviation. Intern Emerg Med. 2017;12:1077-1078.doi:10.1007/s11739-017-1634-8
Querney J, Singh SI, Sebbag I. Tracheal deviation with phrenic nerve palsy after brachial plexus block. Anaesth Rep. 2021;9:41-43. doi:10.1002/anr3.12100
Geissler B, Wagner T, Dorn R, et al. Extensive sterile abscess in an invasive fibrous thyroiditis (Riedel’s thyroiditis) caused by an occlusive vasculitis. J Endocrinol Invest. 2001;24:111-115. doi:10.1007/BF03343824
Kim HJ, Choi YS, Park SH, et al. Difficult endotracheal intubation secondary to tracheal deviation and stenosis in a patient with severe kyphoscoliosis: a case report. Korean J Anesthesiol. 2016;69:386-389. doi:10.4097/kjae.2016.69.4.386
Crabb IJ. Anterior deviation of the trachea. Anaesthesia. 2001;56:284-286.doi:10.1046/j.1365-2044.2001.01918-17.x
De Cassai A, Boscolo A, Rose K, et al. Predictive parameters of difficult intubation in thyroid surgery: a meta-analysis. Minerva Anestesiol. 2020;86:317-326. doi:10.23736/S0375-9393.19.14127-2
Davies R. Difficult tracheal intubation secondary to a tracheal diverticulum and a 90 degree deviation in the trachea. Anaesthesia. 2000;55:923-925. doi:10.1046/j.1365-2044.2000.01664-18.x
Cameron RB, Peacock WJ, Chang XG, et al. Double lumen endobronchial tube intubation: lessons learned from anatomy. BMC Anesthesiol. 2024;24:150. doi:10.1186/s12871-024-02517-6
Walls RM, Samuels-Kalow M, Perkins A. A new maneuver for endotracheal tube insertion during difficult GlideScope intubation. J Emerg Med. 2010;39:86-88. doi:10.1016/j.jemermed.2009.11.005
Buschmann CT, Tsokos M. Frequent and rare complications of resuscitation attempts. Intensive Care Med. 2009;35:397-404. doi:10.1007/s00134-008-1255-9
Greenland KB, Edwards MJ, Hutton NJ, et al. Changes in airway configuration with different head and neck positions using magnetic resonance imaging of normal airways: a new concept with possible clinical applications. Br J Anaesth. 2010;105:683-690. doi:10.1093/bja/aeq239
Takasugi Y, Futagawa K, Umeda T, et al. Thermophysical Properties of Thermosoftening Nasotracheal Tubes. Anesth Prog. 2018;65:100-105. doi:10.2344/anpr-65-02-06
Phelan MP. Use of the endotracheal bougie introducer for difficult intubations. Am J Emerg Med. 2004;22:479-482. doi:10.1016/j.ajem.2004.07.017
Tracheal deviation mostly occurs from mechanical compression of the trachea, and can be caused by a variety of clinical conditions, including trauma,¹ pharyngeal abscess,² neck hematoma,³ thyroid enlargement,4 and kyphoscoliosis.5 These conditions often result in lateral tracheal deviation, which can be associated with tracheal compression and reduction in tracheal caliber.
Anterior-posterior (A-P) tracheal deviation has rarely been reported. Kyphoscoliosis, scarring after a tracheostomy, or innominate vein compression are probable causes of A-P tracheal deviation and can be associated with tracheal narrowing and vascular fistula formation. This report describes a case of difficult endotracheal tube (ETT) advancement secondary to unexpected acute posterior tracheal deviation encountered during cardiopulmonary resuscitation (CPR). A waiver of patient consent was obtained from the Human Research Protection Program at the US Department of Veterans Affairs (VA) Puget Sound Health Care System.
Case Presentation
A 50-year-old male with a history of chronic cerebral venous sinus thrombosis and taking enoxaparin, presented to the emergency department for recurrent headaches. He experienced sudden cardiac arrest, and CPR in the form of chest compression and bag mask ventilation was immediately initiated. With the patient's head in an extended position and using a video laryngoscope, a Cormack–Lehane grade 1 view of the glottic opening was obtained and the trachea was intubated with an 8 mm (internal diameter) polyvinyl chloride ETT. Tracheal intubation was confirmed by utilizing continuous EtCO2 monitoring. The ETT was secured at 22 cm measured at the teeth.
After about 40 minutes of CPR, spontaneous circulation restarted and a portable A-P chest X-ray with the head in a neutral position indicated the ETT tip was at the level of the first rib (Figure 1). This finding, along with a persistent air leak, prompted blind advancement of the ETT to 26 cm at the teeth, but resistance to advancement was noted. A subsequent chest computed tomography (CT) with the head in a neutral position revealed the ETT remained inappropriately positioned with the tip measured 8.2 cm above the carina (Figure 2A). Concurrently, a sagittal CT view demonstrated significant posterior deviation of the mid and lower trachea. This deviation was determined to be the most likely cause of the difficulty encountered in advancing the ETT. No masses or lesions contributing to the acute tracheal angulation could be identified. Comparing CT imaging from 2 months prior, the trachea was of normal caliber and ordinarily aligned with the vertebral column (Figure 2B).
With the patient in Fowler position with the head midline, a flexible fiber-optic bronchoscopy was performed. Acute, almost 90-degree tracheal angulation was encountered and navigated by retroflexion of the flexible bronchoscope. Once the posterior tracheal wall was encountered, retroflexion was relaxed and the carina was visualized. The bronchoscope tip was placed near the carina, and the ETT was advanced over the fiber-optic bronchoscope to terminate 3 cm above the carina. A subsequent chest X-ray confirmed appropriate ETT position (Figure 3).
Discussion
Tracheal deviation in the A-P dimension resulting in difficult tracheal intubation has rarely been reported. Previous reports have described anatomical lesions contributing to similar tracheal deviation, such as retro-tracheal thyroid tissue, pronounced cervical lordosis, and severe kyphoscoliosis with destructive cervical fusion.5-8 In a study of the anatomical correlation of double lumen tube placement while using positron emission tomography CT, Cameron et al evaluated the size and angulation of the glottis and proximal trachea using calibrated CT measurements and an online digital protractor and note nearly perfect alignment of the pharynx and glottis.9 However, the trachea turned posteriorly relative to the glottis, resulting in an overall posterior angle of the proximal trachea compared to the glottis of 30.4 to 50.1 degrees, with no sex differences. The need to maneuver similar proximal tracheal angulation during endotracheal intubation has been reported as a cause of difficult intubation.10
In this case, the posterior angulation was not encountered in the proximal trachea but rather in the more distal trachea. The extreme A-P tracheal deviation was not associated with any identifiable masses or lesions. A CT performed 2 months prior demonstrated normal tracheal anatomy, and there was no interval history of neck trauma or tracheal obstruction suggestive of a likely cause for this deviation. This change in the patient’s tracheal anatomy was only discovered after CPR had been performed and as part of the workup for cardiac arrest. Iatrogenic injuries are known to occur during CPR. Common CPR-related airway injuries include tracheal mucosal injury from traumatic intubation and bony injuries to the chest wall from compressions.11 Laryngeal cartilage damage from intubation may also occur, but tracheal displacement following CPR has not been previously reported.11
This case of tracheal deviation is unlikely to be related to patient positioning, as the A-P deviation persisted in 3 separate head and neck alignments. First, during indirect laryngoscopy, performed in a standard sniffing position. Second, during the CT, performed in the supine position, with no head support. The acute A-P deviation seen in Figure 2 was clearly noted in this position. Lastly, flexible fiber-optic bronchoscopy was performed in a semiupright position with the head supported on a pillow. A-P deviation was encountered and navigated in this position during flexible fiber-optic guided ETT repositioning.
Using magnetic resonance imaging, alterations in the alignment of pharyngeal and tracheal axes have been described with changes in neck positioning; however, tracheal deviation has not been described with changes in head and neck alignment.12 Although the clinical presentation in this case was consistent with prior reports, we were unable to identify any previously reported anatomic cause for the tracheal deviation.5,6,8 Initial glottic visualization with a video laryngoscope was unremarkable, but resistance to sufficient ETT advancement past the vocal cords and a persistent air leak due to cuff herniation through the glottic opening was noticeable. The ETT was maneuvered to an appropriate position in the trachea using a flexible fiber-optic bronchoscope. The acute angulation of the trachea that was appreciated on bronchoscopy did not result in kinking of the ETT both initially and after in-situ thermosoftening of the polyvinyl chloride tube.13 Previously reported instances of A-P tracheal deviation have outlined the necessity of using alternative techniques to establish a patent airway, including the use of a laryngeal mask airway and a cuffless ETT with saline-soaked gauze packing.5,8 In 1 reported case, awake fiber-optic intubation was performed when difficult tracheal intubation was anticipated due to known A-P tracheal deviation.6
Failure of ETT advancement can be due to obstruction from the arytenoids and at the level of the vocal cords.14 When the ETT has been visualized to have traversed the vocal cords, tracheal A-P deviation should be considered as a cause of difficult ETT advancement. If an adequate endotracheal airway cannot be established, prompt consideration should be given to placement of a supraglottic airway. Early fiber-optic bronchoscopy should be used to establish the diagnosis and assist with proper ETT positioning.
Conclusions
This case illustrates the rare occurrence of A-P tracheal deviation leading to difficult intubation during CPR. The findings underscore the importance of considering A-P deviation as a potential cause of airway complications in emergency settings, especially in patients with previously normal tracheal anatomy. The successful use of flexible fiber-optic bronchoscopy in this case provides a valuable technique for addressing acute tracheal angulation. This report contributes to the limited literature on A-P tracheal deviation and serves as a reminder for clinicians to maintain a high index of suspicion for unusual airway challenges during critical interventions.
Tracheal deviation mostly occurs from mechanical compression of the trachea, and can be caused by a variety of clinical conditions, including trauma,¹ pharyngeal abscess,² neck hematoma,³ thyroid enlargement,4 and kyphoscoliosis.5 These conditions often result in lateral tracheal deviation, which can be associated with tracheal compression and reduction in tracheal caliber.
Anterior-posterior (A-P) tracheal deviation has rarely been reported. Kyphoscoliosis, scarring after a tracheostomy, or innominate vein compression are probable causes of A-P tracheal deviation and can be associated with tracheal narrowing and vascular fistula formation. This report describes a case of difficult endotracheal tube (ETT) advancement secondary to unexpected acute posterior tracheal deviation encountered during cardiopulmonary resuscitation (CPR). A waiver of patient consent was obtained from the Human Research Protection Program at the US Department of Veterans Affairs (VA) Puget Sound Health Care System.
Case Presentation
A 50-year-old male with a history of chronic cerebral venous sinus thrombosis and taking enoxaparin, presented to the emergency department for recurrent headaches. He experienced sudden cardiac arrest, and CPR in the form of chest compression and bag mask ventilation was immediately initiated. With the patient's head in an extended position and using a video laryngoscope, a Cormack–Lehane grade 1 view of the glottic opening was obtained and the trachea was intubated with an 8 mm (internal diameter) polyvinyl chloride ETT. Tracheal intubation was confirmed by utilizing continuous EtCO2 monitoring. The ETT was secured at 22 cm measured at the teeth.
After about 40 minutes of CPR, spontaneous circulation restarted and a portable A-P chest X-ray with the head in a neutral position indicated the ETT tip was at the level of the first rib (Figure 1). This finding, along with a persistent air leak, prompted blind advancement of the ETT to 26 cm at the teeth, but resistance to advancement was noted. A subsequent chest computed tomography (CT) with the head in a neutral position revealed the ETT remained inappropriately positioned with the tip measured 8.2 cm above the carina (Figure 2A). Concurrently, a sagittal CT view demonstrated significant posterior deviation of the mid and lower trachea. This deviation was determined to be the most likely cause of the difficulty encountered in advancing the ETT. No masses or lesions contributing to the acute tracheal angulation could be identified. Comparing CT imaging from 2 months prior, the trachea was of normal caliber and ordinarily aligned with the vertebral column (Figure 2B).
With the patient in Fowler position with the head midline, a flexible fiber-optic bronchoscopy was performed. Acute, almost 90-degree tracheal angulation was encountered and navigated by retroflexion of the flexible bronchoscope. Once the posterior tracheal wall was encountered, retroflexion was relaxed and the carina was visualized. The bronchoscope tip was placed near the carina, and the ETT was advanced over the fiber-optic bronchoscope to terminate 3 cm above the carina. A subsequent chest X-ray confirmed appropriate ETT position (Figure 3).
Discussion
Tracheal deviation in the A-P dimension resulting in difficult tracheal intubation has rarely been reported. Previous reports have described anatomical lesions contributing to similar tracheal deviation, such as retro-tracheal thyroid tissue, pronounced cervical lordosis, and severe kyphoscoliosis with destructive cervical fusion.5-8 In a study of the anatomical correlation of double lumen tube placement while using positron emission tomography CT, Cameron et al evaluated the size and angulation of the glottis and proximal trachea using calibrated CT measurements and an online digital protractor and note nearly perfect alignment of the pharynx and glottis.9 However, the trachea turned posteriorly relative to the glottis, resulting in an overall posterior angle of the proximal trachea compared to the glottis of 30.4 to 50.1 degrees, with no sex differences. The need to maneuver similar proximal tracheal angulation during endotracheal intubation has been reported as a cause of difficult intubation.10
In this case, the posterior angulation was not encountered in the proximal trachea but rather in the more distal trachea. The extreme A-P tracheal deviation was not associated with any identifiable masses or lesions. A CT performed 2 months prior demonstrated normal tracheal anatomy, and there was no interval history of neck trauma or tracheal obstruction suggestive of a likely cause for this deviation. This change in the patient’s tracheal anatomy was only discovered after CPR had been performed and as part of the workup for cardiac arrest. Iatrogenic injuries are known to occur during CPR. Common CPR-related airway injuries include tracheal mucosal injury from traumatic intubation and bony injuries to the chest wall from compressions.11 Laryngeal cartilage damage from intubation may also occur, but tracheal displacement following CPR has not been previously reported.11
This case of tracheal deviation is unlikely to be related to patient positioning, as the A-P deviation persisted in 3 separate head and neck alignments. First, during indirect laryngoscopy, performed in a standard sniffing position. Second, during the CT, performed in the supine position, with no head support. The acute A-P deviation seen in Figure 2 was clearly noted in this position. Lastly, flexible fiber-optic bronchoscopy was performed in a semiupright position with the head supported on a pillow. A-P deviation was encountered and navigated in this position during flexible fiber-optic guided ETT repositioning.
Using magnetic resonance imaging, alterations in the alignment of pharyngeal and tracheal axes have been described with changes in neck positioning; however, tracheal deviation has not been described with changes in head and neck alignment.12 Although the clinical presentation in this case was consistent with prior reports, we were unable to identify any previously reported anatomic cause for the tracheal deviation.5,6,8 Initial glottic visualization with a video laryngoscope was unremarkable, but resistance to sufficient ETT advancement past the vocal cords and a persistent air leak due to cuff herniation through the glottic opening was noticeable. The ETT was maneuvered to an appropriate position in the trachea using a flexible fiber-optic bronchoscope. The acute angulation of the trachea that was appreciated on bronchoscopy did not result in kinking of the ETT both initially and after in-situ thermosoftening of the polyvinyl chloride tube.13 Previously reported instances of A-P tracheal deviation have outlined the necessity of using alternative techniques to establish a patent airway, including the use of a laryngeal mask airway and a cuffless ETT with saline-soaked gauze packing.5,8 In 1 reported case, awake fiber-optic intubation was performed when difficult tracheal intubation was anticipated due to known A-P tracheal deviation.6
Failure of ETT advancement can be due to obstruction from the arytenoids and at the level of the vocal cords.14 When the ETT has been visualized to have traversed the vocal cords, tracheal A-P deviation should be considered as a cause of difficult ETT advancement. If an adequate endotracheal airway cannot be established, prompt consideration should be given to placement of a supraglottic airway. Early fiber-optic bronchoscopy should be used to establish the diagnosis and assist with proper ETT positioning.
Conclusions
This case illustrates the rare occurrence of A-P tracheal deviation leading to difficult intubation during CPR. The findings underscore the importance of considering A-P deviation as a potential cause of airway complications in emergency settings, especially in patients with previously normal tracheal anatomy. The successful use of flexible fiber-optic bronchoscopy in this case provides a valuable technique for addressing acute tracheal angulation. This report contributes to the limited literature on A-P tracheal deviation and serves as a reminder for clinicians to maintain a high index of suspicion for unusual airway challenges during critical interventions.
Creasy JD, Chiles C, Routh WD, et al. Overview of traumatic injury of the thoracic aorta. Radiogr Rev Publ Radiol Soc N Am Inc. 1997;17:27-45. doi:10.1148/radiographics.17.1.9017797
Yee AM, Christensen DN, Waterbrook AL, et al. Parapharyngeal abscess with tracheal deviation. Intern Emerg Med. 2017;12:1077-1078.doi:10.1007/s11739-017-1634-8
Querney J, Singh SI, Sebbag I. Tracheal deviation with phrenic nerve palsy after brachial plexus block. Anaesth Rep. 2021;9:41-43. doi:10.1002/anr3.12100
Geissler B, Wagner T, Dorn R, et al. Extensive sterile abscess in an invasive fibrous thyroiditis (Riedel’s thyroiditis) caused by an occlusive vasculitis. J Endocrinol Invest. 2001;24:111-115. doi:10.1007/BF03343824
Kim HJ, Choi YS, Park SH, et al. Difficult endotracheal intubation secondary to tracheal deviation and stenosis in a patient with severe kyphoscoliosis: a case report. Korean J Anesthesiol. 2016;69:386-389. doi:10.4097/kjae.2016.69.4.386
Crabb IJ. Anterior deviation of the trachea. Anaesthesia. 2001;56:284-286.doi:10.1046/j.1365-2044.2001.01918-17.x
De Cassai A, Boscolo A, Rose K, et al. Predictive parameters of difficult intubation in thyroid surgery: a meta-analysis. Minerva Anestesiol. 2020;86:317-326. doi:10.23736/S0375-9393.19.14127-2
Davies R. Difficult tracheal intubation secondary to a tracheal diverticulum and a 90 degree deviation in the trachea. Anaesthesia. 2000;55:923-925. doi:10.1046/j.1365-2044.2000.01664-18.x
Cameron RB, Peacock WJ, Chang XG, et al. Double lumen endobronchial tube intubation: lessons learned from anatomy. BMC Anesthesiol. 2024;24:150. doi:10.1186/s12871-024-02517-6
Walls RM, Samuels-Kalow M, Perkins A. A new maneuver for endotracheal tube insertion during difficult GlideScope intubation. J Emerg Med. 2010;39:86-88. doi:10.1016/j.jemermed.2009.11.005
Buschmann CT, Tsokos M. Frequent and rare complications of resuscitation attempts. Intensive Care Med. 2009;35:397-404. doi:10.1007/s00134-008-1255-9
Greenland KB, Edwards MJ, Hutton NJ, et al. Changes in airway configuration with different head and neck positions using magnetic resonance imaging of normal airways: a new concept with possible clinical applications. Br J Anaesth. 2010;105:683-690. doi:10.1093/bja/aeq239
Takasugi Y, Futagawa K, Umeda T, et al. Thermophysical Properties of Thermosoftening Nasotracheal Tubes. Anesth Prog. 2018;65:100-105. doi:10.2344/anpr-65-02-06
Phelan MP. Use of the endotracheal bougie introducer for difficult intubations. Am J Emerg Med. 2004;22:479-482. doi:10.1016/j.ajem.2004.07.017
Creasy JD, Chiles C, Routh WD, et al. Overview of traumatic injury of the thoracic aorta. Radiogr Rev Publ Radiol Soc N Am Inc. 1997;17:27-45. doi:10.1148/radiographics.17.1.9017797
Yee AM, Christensen DN, Waterbrook AL, et al. Parapharyngeal abscess with tracheal deviation. Intern Emerg Med. 2017;12:1077-1078.doi:10.1007/s11739-017-1634-8
Querney J, Singh SI, Sebbag I. Tracheal deviation with phrenic nerve palsy after brachial plexus block. Anaesth Rep. 2021;9:41-43. doi:10.1002/anr3.12100
Geissler B, Wagner T, Dorn R, et al. Extensive sterile abscess in an invasive fibrous thyroiditis (Riedel’s thyroiditis) caused by an occlusive vasculitis. J Endocrinol Invest. 2001;24:111-115. doi:10.1007/BF03343824
Kim HJ, Choi YS, Park SH, et al. Difficult endotracheal intubation secondary to tracheal deviation and stenosis in a patient with severe kyphoscoliosis: a case report. Korean J Anesthesiol. 2016;69:386-389. doi:10.4097/kjae.2016.69.4.386
Crabb IJ. Anterior deviation of the trachea. Anaesthesia. 2001;56:284-286.doi:10.1046/j.1365-2044.2001.01918-17.x
De Cassai A, Boscolo A, Rose K, et al. Predictive parameters of difficult intubation in thyroid surgery: a meta-analysis. Minerva Anestesiol. 2020;86:317-326. doi:10.23736/S0375-9393.19.14127-2
Davies R. Difficult tracheal intubation secondary to a tracheal diverticulum and a 90 degree deviation in the trachea. Anaesthesia. 2000;55:923-925. doi:10.1046/j.1365-2044.2000.01664-18.x
Cameron RB, Peacock WJ, Chang XG, et al. Double lumen endobronchial tube intubation: lessons learned from anatomy. BMC Anesthesiol. 2024;24:150. doi:10.1186/s12871-024-02517-6
Walls RM, Samuels-Kalow M, Perkins A. A new maneuver for endotracheal tube insertion during difficult GlideScope intubation. J Emerg Med. 2010;39:86-88. doi:10.1016/j.jemermed.2009.11.005
Buschmann CT, Tsokos M. Frequent and rare complications of resuscitation attempts. Intensive Care Med. 2009;35:397-404. doi:10.1007/s00134-008-1255-9
Greenland KB, Edwards MJ, Hutton NJ, et al. Changes in airway configuration with different head and neck positions using magnetic resonance imaging of normal airways: a new concept with possible clinical applications. Br J Anaesth. 2010;105:683-690. doi:10.1093/bja/aeq239
Takasugi Y, Futagawa K, Umeda T, et al. Thermophysical Properties of Thermosoftening Nasotracheal Tubes. Anesth Prog. 2018;65:100-105. doi:10.2344/anpr-65-02-06
Phelan MP. Use of the endotracheal bougie introducer for difficult intubations. Am J Emerg Med. 2004;22:479-482. doi:10.1016/j.ajem.2004.07.017
A Case Report of Unanticipated Difficult Intubation Due to Posterior Tracheal Angulation
A Case Report of Unanticipated Difficult Intubation Due to Posterior Tracheal Angulation

Combining Upper-Lower GI Screening Feasible, Effective
BERLIN — , including malignancies and lesions requiring ongoing surveillance, according to an interim analysis from the TOGAS study.
“There was an abundance of benign but clinically relevant findings,” said lead investigator Jan Bornschein, MD, gastroenterologist at Oxford University Hospitals NHS Foundation Trust, Oxford, England, who presented the interim resuts of the study at United European Gastroenterology (UEG) Week 2025.
While the study found upper GI neoplasia in only 1.4% of participants, 17.8% of individuals were marked for upper GI endoscopic surveillance.
The results may inform how Europe develops gastric cancer prevention programs alongside those for colorectal cancer, said Bornschein. “If we can combine the upper GI endoscopy with other modalities [colonoscopy], the more likelihood there is that you can have a one-stop test package,” he said. “A combination, particularly for bowel and stomach, is more feasible and also more cost-effective. So far, the findings show that it’s definitely a strategy that, in my opinion, is worth implementing.”
Bornschein and the TOGAS study group hope that the combined approach will prove workable across diverse European settings and will help identify a spectrum of upper GI pathology, from cancers and dysplasia to atrophy and intestinal metaplasia, that can meaningfully affect follow-up surveillance.
Mixed Rates of GI Cancers Across Europe and the US
These findings come amid data showing rising rates of early-onset (younger than 50 years) GI cancers in the US, including colorectal, gastric, pancreatic, and esophageal tumors. These trends, previously reported by this news organization, point to environmental and lifestyle drivers, strengthening the case for earlier detection and risk-tailored strategies for upper GI neoplasia and preneoplastic conditions detected during existing colorectal cancer screening pathways.
However, Bornschein noted that prevalence varies considerably across Europe. “There are areas, particularly in the Eastern regions, and in some parts of the West, for example, Portugal, that have a very high incidence of GI cancers. In the UK or in Germany, we have noticed a decline over the years, so the numbers are actually much better than they used to be.”
The study is the second in a series of three TOGAS pilot studies and was conducted across eight centers (France, Germany, Ireland, Latvia, Lithuania, the Netherlands, Portugal, and Spain) in adults aged 50-74 years attending screening or polyp-surveillance colonoscopy.
A European Society of Gastrointestinal Endoscopy-aligned protocol defining image documentation, biopsy sampling, and quality parameters was followed to ensure a standardized approach. “Marked preneoplastic change” was defined as gastric glandular atrophy or intestinal metaplasia at the Operative Link on Gastritis Assessment/Operative Link on Gastric Intestinal Metaplasia Assessment stage III-IV and/or Endoscopic Grading of Gastric Intestinal Metaplasia > 5, triggering a need for endoscopic surveillance.
Data were gathered on colonoscopy findings (including polyp surveillance and family history), EGD findings plus biopsies, serum pepsinogen, and Helicobacter pylori serology. Outcome measures included the prevalence of gastric cancer and preneoplastic conditions, the diagnostic accuracy of pepsinogen testing, comparisons between national settings, the relevance of upper endoscopy in fecal immunochemical test-positive cases, and overall H pylori prevalence.
Neoplasia and Preneoplasia Found
A total of 846 participants were analyzed. At baseline, the mean age was 62 years, 52.2% were men, and 84.2% were White, despite efforts to recruit a more diverse population. Around 390 participants drank alcohol, and 190 smoked tobacco.
A total of 37.8% of participants had undergone prior EGD, of which 94.7% were performed more than 3 years before the study start. The history of GI surgery was 13.7%, and the history of cancer was 14.5%. Around 11% took aspirin, and 14% took proton pump inhibitors (PPIs). “We were surprised at the low prevalence of PPI use,” remarked Bornschein. “It was also good news that around half were never smokers.”
Key results for upper GI neoplasia included six patients (0.7%) with gastric cancers, three (0.4%) with esophageal cancers, and five (0.6%) with duodenal tumors. H pylori positivity was found in 303 patients (35.8%), with an additional 81 (9.6%) reporting a history of eradication.
Colorectal findings included 15 patients (1.8%) with cancers and colon polyps in 503 (59.5%) participants.
Regarding preneoplastic conditions, endoscopy identified intestinal metaplasia in 174 patients (20.6%), of which 65 (7.7%) were multifocal. Atrophy was observed in 220 patients (26.0%), with 59 (7.0%) showing multifocal atrophic changes. Both intestinal metaplasia and atrophy were found together in 105 (12.4%) patients. Barrett’s esophagus was detected in 31 (3.7%) patients.
“I’d really like to highlight these further benign gastric findings,” said Bornschein. These included gastric ulcers in 28 (3.3%) patients, erosive gastritis in 245 (29.0%) patients, esophageal ulcers in three (0.4%) patients, Los Angeles Community College District classification esophagitis in 13 (1.5%) patients, and duodenal ulcers in 10 (1.2%) patients. “These were asymptomatic, but we were able to identify them,” he noted.
“We’ve had a very low rate of complications (0.01%),” he added.” I don’t want to jinx that now. These were basically related to sedation.”
PROSPERO: Early Detection of Upper GI Conditions in a UK Population
Massimiliano di Pietro, MD, consultant gastroenterologist at Addenbrooke’s Hospital, Cambridge, England, and the principal investigator of the PROSPERO study, which aimed to determine the prevalence of premalignant upper GI conditions in routine endoscopy in the UK, commented on the findings. The TOGAS study focuses on asymptomatic individuals referred for colonoscopy and examines the value of performing an upper GI endoscopy at the same time, he explained. “This approach might identify upper GI conditions that require monitoring, in particular early cancer.”
“On the other hand, the PROSPERO study focuses on patients referred for upper GI symptoms and diagnosis,” he said. Preliminary data from that study, presented during the same session as the TOGAS trial, showed a 13.6% prevalence of premalignant upper GI conditions in a symptomatic UK patient population referred for endoscopy.
“In some respects, the findings were similar, particularly the rate of upper GI cancer at 1.4%, although there were differences in the prevalence of premalignant conditions,” he noted. “This may be explained by the fact that TOGAS is a European study, while PROSPERO is UK-based, where the distribution of upper GI cancers differs, with more esophageal adenocarcinoma vs gastric adenocarcinoma.”
Reflecting on both of the studies, Di Pietro said they are “really important in fulfilling an unmet need in the quality of upper GI endoscopy. Currently, there are no diagnostic quality indicators in upper GI endoscopy, so it’s difficult to rate the performance of endoscopists in the same way as we can in lower GI. It’s really important to understand the population prevalence, both in symptomatic and asymptomatic individuals, of premalignant and malignant upper GI conditions.”
TOGAS 2 is recruiting until February 2026, with 1200 of a potential 1600 participants recruited to date. The data will be used for implementation modeling and to inform quality indicators for future screening programs. Final results and plans for a follow-up study are expected in 2026.
Bornschein declared receiving advisory and speaker fees from Flynn Pharma and Juvisé Pharmaceuticals. Di Pietro reported having no disclosures relevant to the studies discussed.
A version of this article first appeared on Medscape.com.
BERLIN — , including malignancies and lesions requiring ongoing surveillance, according to an interim analysis from the TOGAS study.
“There was an abundance of benign but clinically relevant findings,” said lead investigator Jan Bornschein, MD, gastroenterologist at Oxford University Hospitals NHS Foundation Trust, Oxford, England, who presented the interim resuts of the study at United European Gastroenterology (UEG) Week 2025.
While the study found upper GI neoplasia in only 1.4% of participants, 17.8% of individuals were marked for upper GI endoscopic surveillance.
The results may inform how Europe develops gastric cancer prevention programs alongside those for colorectal cancer, said Bornschein. “If we can combine the upper GI endoscopy with other modalities [colonoscopy], the more likelihood there is that you can have a one-stop test package,” he said. “A combination, particularly for bowel and stomach, is more feasible and also more cost-effective. So far, the findings show that it’s definitely a strategy that, in my opinion, is worth implementing.”
Bornschein and the TOGAS study group hope that the combined approach will prove workable across diverse European settings and will help identify a spectrum of upper GI pathology, from cancers and dysplasia to atrophy and intestinal metaplasia, that can meaningfully affect follow-up surveillance.
Mixed Rates of GI Cancers Across Europe and the US
These findings come amid data showing rising rates of early-onset (younger than 50 years) GI cancers in the US, including colorectal, gastric, pancreatic, and esophageal tumors. These trends, previously reported by this news organization, point to environmental and lifestyle drivers, strengthening the case for earlier detection and risk-tailored strategies for upper GI neoplasia and preneoplastic conditions detected during existing colorectal cancer screening pathways.
However, Bornschein noted that prevalence varies considerably across Europe. “There are areas, particularly in the Eastern regions, and in some parts of the West, for example, Portugal, that have a very high incidence of GI cancers. In the UK or in Germany, we have noticed a decline over the years, so the numbers are actually much better than they used to be.”
The study is the second in a series of three TOGAS pilot studies and was conducted across eight centers (France, Germany, Ireland, Latvia, Lithuania, the Netherlands, Portugal, and Spain) in adults aged 50-74 years attending screening or polyp-surveillance colonoscopy.
A European Society of Gastrointestinal Endoscopy-aligned protocol defining image documentation, biopsy sampling, and quality parameters was followed to ensure a standardized approach. “Marked preneoplastic change” was defined as gastric glandular atrophy or intestinal metaplasia at the Operative Link on Gastritis Assessment/Operative Link on Gastric Intestinal Metaplasia Assessment stage III-IV and/or Endoscopic Grading of Gastric Intestinal Metaplasia > 5, triggering a need for endoscopic surveillance.
Data were gathered on colonoscopy findings (including polyp surveillance and family history), EGD findings plus biopsies, serum pepsinogen, and Helicobacter pylori serology. Outcome measures included the prevalence of gastric cancer and preneoplastic conditions, the diagnostic accuracy of pepsinogen testing, comparisons between national settings, the relevance of upper endoscopy in fecal immunochemical test-positive cases, and overall H pylori prevalence.
Neoplasia and Preneoplasia Found
A total of 846 participants were analyzed. At baseline, the mean age was 62 years, 52.2% were men, and 84.2% were White, despite efforts to recruit a more diverse population. Around 390 participants drank alcohol, and 190 smoked tobacco.
A total of 37.8% of participants had undergone prior EGD, of which 94.7% were performed more than 3 years before the study start. The history of GI surgery was 13.7%, and the history of cancer was 14.5%. Around 11% took aspirin, and 14% took proton pump inhibitors (PPIs). “We were surprised at the low prevalence of PPI use,” remarked Bornschein. “It was also good news that around half were never smokers.”
Key results for upper GI neoplasia included six patients (0.7%) with gastric cancers, three (0.4%) with esophageal cancers, and five (0.6%) with duodenal tumors. H pylori positivity was found in 303 patients (35.8%), with an additional 81 (9.6%) reporting a history of eradication.
Colorectal findings included 15 patients (1.8%) with cancers and colon polyps in 503 (59.5%) participants.
Regarding preneoplastic conditions, endoscopy identified intestinal metaplasia in 174 patients (20.6%), of which 65 (7.7%) were multifocal. Atrophy was observed in 220 patients (26.0%), with 59 (7.0%) showing multifocal atrophic changes. Both intestinal metaplasia and atrophy were found together in 105 (12.4%) patients. Barrett’s esophagus was detected in 31 (3.7%) patients.
“I’d really like to highlight these further benign gastric findings,” said Bornschein. These included gastric ulcers in 28 (3.3%) patients, erosive gastritis in 245 (29.0%) patients, esophageal ulcers in three (0.4%) patients, Los Angeles Community College District classification esophagitis in 13 (1.5%) patients, and duodenal ulcers in 10 (1.2%) patients. “These were asymptomatic, but we were able to identify them,” he noted.
“We’ve had a very low rate of complications (0.01%),” he added.” I don’t want to jinx that now. These were basically related to sedation.”
PROSPERO: Early Detection of Upper GI Conditions in a UK Population
Massimiliano di Pietro, MD, consultant gastroenterologist at Addenbrooke’s Hospital, Cambridge, England, and the principal investigator of the PROSPERO study, which aimed to determine the prevalence of premalignant upper GI conditions in routine endoscopy in the UK, commented on the findings. The TOGAS study focuses on asymptomatic individuals referred for colonoscopy and examines the value of performing an upper GI endoscopy at the same time, he explained. “This approach might identify upper GI conditions that require monitoring, in particular early cancer.”
“On the other hand, the PROSPERO study focuses on patients referred for upper GI symptoms and diagnosis,” he said. Preliminary data from that study, presented during the same session as the TOGAS trial, showed a 13.6% prevalence of premalignant upper GI conditions in a symptomatic UK patient population referred for endoscopy.
“In some respects, the findings were similar, particularly the rate of upper GI cancer at 1.4%, although there were differences in the prevalence of premalignant conditions,” he noted. “This may be explained by the fact that TOGAS is a European study, while PROSPERO is UK-based, where the distribution of upper GI cancers differs, with more esophageal adenocarcinoma vs gastric adenocarcinoma.”
Reflecting on both of the studies, Di Pietro said they are “really important in fulfilling an unmet need in the quality of upper GI endoscopy. Currently, there are no diagnostic quality indicators in upper GI endoscopy, so it’s difficult to rate the performance of endoscopists in the same way as we can in lower GI. It’s really important to understand the population prevalence, both in symptomatic and asymptomatic individuals, of premalignant and malignant upper GI conditions.”
TOGAS 2 is recruiting until February 2026, with 1200 of a potential 1600 participants recruited to date. The data will be used for implementation modeling and to inform quality indicators for future screening programs. Final results and plans for a follow-up study are expected in 2026.
Bornschein declared receiving advisory and speaker fees from Flynn Pharma and Juvisé Pharmaceuticals. Di Pietro reported having no disclosures relevant to the studies discussed.
A version of this article first appeared on Medscape.com.
BERLIN — , including malignancies and lesions requiring ongoing surveillance, according to an interim analysis from the TOGAS study.
“There was an abundance of benign but clinically relevant findings,” said lead investigator Jan Bornschein, MD, gastroenterologist at Oxford University Hospitals NHS Foundation Trust, Oxford, England, who presented the interim resuts of the study at United European Gastroenterology (UEG) Week 2025.
While the study found upper GI neoplasia in only 1.4% of participants, 17.8% of individuals were marked for upper GI endoscopic surveillance.
The results may inform how Europe develops gastric cancer prevention programs alongside those for colorectal cancer, said Bornschein. “If we can combine the upper GI endoscopy with other modalities [colonoscopy], the more likelihood there is that you can have a one-stop test package,” he said. “A combination, particularly for bowel and stomach, is more feasible and also more cost-effective. So far, the findings show that it’s definitely a strategy that, in my opinion, is worth implementing.”
Bornschein and the TOGAS study group hope that the combined approach will prove workable across diverse European settings and will help identify a spectrum of upper GI pathology, from cancers and dysplasia to atrophy and intestinal metaplasia, that can meaningfully affect follow-up surveillance.
Mixed Rates of GI Cancers Across Europe and the US
These findings come amid data showing rising rates of early-onset (younger than 50 years) GI cancers in the US, including colorectal, gastric, pancreatic, and esophageal tumors. These trends, previously reported by this news organization, point to environmental and lifestyle drivers, strengthening the case for earlier detection and risk-tailored strategies for upper GI neoplasia and preneoplastic conditions detected during existing colorectal cancer screening pathways.
However, Bornschein noted that prevalence varies considerably across Europe. “There are areas, particularly in the Eastern regions, and in some parts of the West, for example, Portugal, that have a very high incidence of GI cancers. In the UK or in Germany, we have noticed a decline over the years, so the numbers are actually much better than they used to be.”
The study is the second in a series of three TOGAS pilot studies and was conducted across eight centers (France, Germany, Ireland, Latvia, Lithuania, the Netherlands, Portugal, and Spain) in adults aged 50-74 years attending screening or polyp-surveillance colonoscopy.
A European Society of Gastrointestinal Endoscopy-aligned protocol defining image documentation, biopsy sampling, and quality parameters was followed to ensure a standardized approach. “Marked preneoplastic change” was defined as gastric glandular atrophy or intestinal metaplasia at the Operative Link on Gastritis Assessment/Operative Link on Gastric Intestinal Metaplasia Assessment stage III-IV and/or Endoscopic Grading of Gastric Intestinal Metaplasia > 5, triggering a need for endoscopic surveillance.
Data were gathered on colonoscopy findings (including polyp surveillance and family history), EGD findings plus biopsies, serum pepsinogen, and Helicobacter pylori serology. Outcome measures included the prevalence of gastric cancer and preneoplastic conditions, the diagnostic accuracy of pepsinogen testing, comparisons between national settings, the relevance of upper endoscopy in fecal immunochemical test-positive cases, and overall H pylori prevalence.
Neoplasia and Preneoplasia Found
A total of 846 participants were analyzed. At baseline, the mean age was 62 years, 52.2% were men, and 84.2% were White, despite efforts to recruit a more diverse population. Around 390 participants drank alcohol, and 190 smoked tobacco.
A total of 37.8% of participants had undergone prior EGD, of which 94.7% were performed more than 3 years before the study start. The history of GI surgery was 13.7%, and the history of cancer was 14.5%. Around 11% took aspirin, and 14% took proton pump inhibitors (PPIs). “We were surprised at the low prevalence of PPI use,” remarked Bornschein. “It was also good news that around half were never smokers.”
Key results for upper GI neoplasia included six patients (0.7%) with gastric cancers, three (0.4%) with esophageal cancers, and five (0.6%) with duodenal tumors. H pylori positivity was found in 303 patients (35.8%), with an additional 81 (9.6%) reporting a history of eradication.
Colorectal findings included 15 patients (1.8%) with cancers and colon polyps in 503 (59.5%) participants.
Regarding preneoplastic conditions, endoscopy identified intestinal metaplasia in 174 patients (20.6%), of which 65 (7.7%) were multifocal. Atrophy was observed in 220 patients (26.0%), with 59 (7.0%) showing multifocal atrophic changes. Both intestinal metaplasia and atrophy were found together in 105 (12.4%) patients. Barrett’s esophagus was detected in 31 (3.7%) patients.
“I’d really like to highlight these further benign gastric findings,” said Bornschein. These included gastric ulcers in 28 (3.3%) patients, erosive gastritis in 245 (29.0%) patients, esophageal ulcers in three (0.4%) patients, Los Angeles Community College District classification esophagitis in 13 (1.5%) patients, and duodenal ulcers in 10 (1.2%) patients. “These were asymptomatic, but we were able to identify them,” he noted.
“We’ve had a very low rate of complications (0.01%),” he added.” I don’t want to jinx that now. These were basically related to sedation.”
PROSPERO: Early Detection of Upper GI Conditions in a UK Population
Massimiliano di Pietro, MD, consultant gastroenterologist at Addenbrooke’s Hospital, Cambridge, England, and the principal investigator of the PROSPERO study, which aimed to determine the prevalence of premalignant upper GI conditions in routine endoscopy in the UK, commented on the findings. The TOGAS study focuses on asymptomatic individuals referred for colonoscopy and examines the value of performing an upper GI endoscopy at the same time, he explained. “This approach might identify upper GI conditions that require monitoring, in particular early cancer.”
“On the other hand, the PROSPERO study focuses on patients referred for upper GI symptoms and diagnosis,” he said. Preliminary data from that study, presented during the same session as the TOGAS trial, showed a 13.6% prevalence of premalignant upper GI conditions in a symptomatic UK patient population referred for endoscopy.
“In some respects, the findings were similar, particularly the rate of upper GI cancer at 1.4%, although there were differences in the prevalence of premalignant conditions,” he noted. “This may be explained by the fact that TOGAS is a European study, while PROSPERO is UK-based, where the distribution of upper GI cancers differs, with more esophageal adenocarcinoma vs gastric adenocarcinoma.”
Reflecting on both of the studies, Di Pietro said they are “really important in fulfilling an unmet need in the quality of upper GI endoscopy. Currently, there are no diagnostic quality indicators in upper GI endoscopy, so it’s difficult to rate the performance of endoscopists in the same way as we can in lower GI. It’s really important to understand the population prevalence, both in symptomatic and asymptomatic individuals, of premalignant and malignant upper GI conditions.”
TOGAS 2 is recruiting until February 2026, with 1200 of a potential 1600 participants recruited to date. The data will be used for implementation modeling and to inform quality indicators for future screening programs. Final results and plans for a follow-up study are expected in 2026.
Bornschein declared receiving advisory and speaker fees from Flynn Pharma and Juvisé Pharmaceuticals. Di Pietro reported having no disclosures relevant to the studies discussed.
A version of this article first appeared on Medscape.com.
Is AI Use Causing Endoscopists to Lose Their Skills?
, a large observational study suggested.
“The extent and consistency of the adenoma detection rate (ADR) drop after long-term AI use were not expected,” study authors Krzysztof Budzyń, MD, and Marcin Romańczyk, MD, of the Academy of Silesia, Katowice, Poland, told GI & Hepatology News. “We thought there might be a small effect, but the 6% absolute decrease — observed in several centers and among most endoscopists — points to a genuine change in behavior. This was especially notable because all participants were very experienced, with more than 2000 colonoscopies each.”
Another unexpected result, they said, “was that the decrease was stronger in centers with higher starting ADRs and in certain patient groups, such as women under 60. We had assumed experienced clinicians would be less affected, but our results show that even highly skilled practitioners can be influenced.”
The study was published online in The Lancet Gastroenterology & Hepatology.
ADR Reduced After AI Use
To assess how endoscopists who used AI regularly performed colonoscopy when AI was not in use, researchers conducted a retrospective, observational study at four endoscopy centers in Poland taking part in the ACCEPT trial.
These centers introduced AI tools for polyp detection at the end of 2021, after which colonoscopies were randomly assigned to be done with or without AI assistance.
The researchers assessed colonoscopy quality by comparing two different phases: 3 months before and 3 months after AI implementation. All diagnostic colonoscopies were included, except for those involving intensive anticoagulant use, pregnancy, or a history of colorectal resection or inflammatory bowel disease.
The primary outcome was the change in the ADR of standard, non-AI-assisted colonoscopy before and after AI exposure.
Between September 2021 and March 2022, a total of 2177 colonoscopies were conducted, including 1443 without AI use and 734 with AI. The current analysis focused on the 795 patients who underwent non-AI-assisted colonoscopy before the introduction of AI and the 648 who underwent non-AI-assisted colonoscopy after.
Participants’ median age was 61 years, and 59% were women. The colonoscopies were performed by 19 experienced endoscopists who had conducted over 2000 colonoscopies each.
The ADR of standard colonoscopy decreased significantly from 28.4% (226 of 795) before the introduction of AI to 22.4% (145 of 648) after, corresponding to a 20% relative and 6% absolute reduction in the ADR.
The ADR for AI-assisted colonoscopies was 25.3% (186 of 734).
The number of adenomas per colonoscopy (APC) in patients with at least one adenoma detected did not change significantly between the groups before and after AI exposure, with a mean of 1.91 before vs 1.92 after. Similarly, the number of mean advanced APC was comparable between the two periods (0.062 vs 0.063).
The mean advanced APC detection on standard colonoscopy in patients with at least one adenoma detected was 0.22 before AI exposure and 0.28 after AI exposure.
Colorectal cancers were detected in 6 (0.8%) of 795 colonoscopies before AI exposure and in 8 (1.2%) of 648 after AI exposure.
In multivariable logistic regression analysis, exposure to AI (odds ratio [OR], 0.69), patient’s male sex (OR, 1.78), and patient age at least 60 years (OR, 3.60) were independent factors significantly associated with ADR.
In all centers, the ADR for standard, non-AI-assisted colonoscopy was reduced after AI exposure, although the magnitude of ADR reduction varied greatly between centers, according to the authors.
“Clinicians should be aware that while AI can boost detection rates, prolonged reliance may subtly affect their performance when the technology is not available,” Budzyń and Romańczyk said. “This does not mean AI should be avoided — rather, it highlights the need for conscious engagement with the task, even when AI is assisting. Monitoring one’s own detection rates in both AI-assisted and non-AI-assisted procedures can help identify changes early.”
“Endoscopists should view AI as a collaborative partner, not a replacement for their vigilance and judgment,” they concluded. “Integrating AI effectively means using it to complement, not substitute, core observational and diagnostic skills. In short, enjoy the benefits of AI, but keep your skills sharp — your patients depend on both.”
Omer Ahmed, MD, of University College London, London, England, gives a similar message in a related editorial. The study “compels us to carefully consider the effect of AI integration into routine endoscopic practice,” he wrote. “Although AI continues to offer great promise to enhance clinical outcomes, we must also safeguard against the quiet erosion of fundamental skills required for high-quality endoscopy.”
‘Certainly a Signal’
Commenting on the study for GI & Hepatology News, Rajiv Bhuta, MD, assistant professor of clinical gastroenterology and hepatology at Temple University and a gastroenterologist at Temple University Hospital, both in Philadelphia, said, “On the face of it, these findings would seem to correlate with all our lived experiences as humans. Any skill or task that we give to a machine will inherently ‘de-skill’ or weaken our ability to perform it.”

“The only way to miss a polyp is either due to lack of attention/recognition of a polyp in the field of view or a lack of fold exposure and cleansing,” said Bhuta, who was not involved in the study. “For AI to specifically de-skill polyp detection, it would mean the AI is conditioning physicians to pay less active attention during the procedure, similar to the way a driver may pay less attention in a car that has self-driving capabilities.”
That said, he noted that this is a small retrospective observational study with a short timeframe and an average of fewer than 100 colonoscopies per physician.
“My own ADR may vary by 8% or more by random chance in such a small dataset,” he said. “It’s hard to draw any real conclusions, but it is certainly a signal.”
The issue of de-skilling goes beyond gastroenterology and medicine, Bhuta noted. “We have invented millions of machines that have ‘de-skilled’ us in thousands of small ways, and mostly, we have benefited as a society. However, we’ve never had a machine that can de-skill our attention, our creativity, and our reason.”
“The question is not whether AI will de-skill us but when, where, and how do we set the boundaries of what we want a machine to do for us,” he said. “What is lost and what is gained by AI taking over these roles, and is that an acceptable trade-off?”
The study was funded by the European Commission and the Japan Society for the Promotion of Science. Budzyń, Romańczyk, and Bhuta declared having no competing interests. Ahmed declared receiving medical consultancy fees from Olympus, Odin Vision, Medtronic, and Norgine.
A version of this article appeared on Medscape.com.
, a large observational study suggested.
“The extent and consistency of the adenoma detection rate (ADR) drop after long-term AI use were not expected,” study authors Krzysztof Budzyń, MD, and Marcin Romańczyk, MD, of the Academy of Silesia, Katowice, Poland, told GI & Hepatology News. “We thought there might be a small effect, but the 6% absolute decrease — observed in several centers and among most endoscopists — points to a genuine change in behavior. This was especially notable because all participants were very experienced, with more than 2000 colonoscopies each.”
Another unexpected result, they said, “was that the decrease was stronger in centers with higher starting ADRs and in certain patient groups, such as women under 60. We had assumed experienced clinicians would be less affected, but our results show that even highly skilled practitioners can be influenced.”
The study was published online in The Lancet Gastroenterology & Hepatology.
ADR Reduced After AI Use
To assess how endoscopists who used AI regularly performed colonoscopy when AI was not in use, researchers conducted a retrospective, observational study at four endoscopy centers in Poland taking part in the ACCEPT trial.
These centers introduced AI tools for polyp detection at the end of 2021, after which colonoscopies were randomly assigned to be done with or without AI assistance.
The researchers assessed colonoscopy quality by comparing two different phases: 3 months before and 3 months after AI implementation. All diagnostic colonoscopies were included, except for those involving intensive anticoagulant use, pregnancy, or a history of colorectal resection or inflammatory bowel disease.
The primary outcome was the change in the ADR of standard, non-AI-assisted colonoscopy before and after AI exposure.
Between September 2021 and March 2022, a total of 2177 colonoscopies were conducted, including 1443 without AI use and 734 with AI. The current analysis focused on the 795 patients who underwent non-AI-assisted colonoscopy before the introduction of AI and the 648 who underwent non-AI-assisted colonoscopy after.
Participants’ median age was 61 years, and 59% were women. The colonoscopies were performed by 19 experienced endoscopists who had conducted over 2000 colonoscopies each.
The ADR of standard colonoscopy decreased significantly from 28.4% (226 of 795) before the introduction of AI to 22.4% (145 of 648) after, corresponding to a 20% relative and 6% absolute reduction in the ADR.
The ADR for AI-assisted colonoscopies was 25.3% (186 of 734).
The number of adenomas per colonoscopy (APC) in patients with at least one adenoma detected did not change significantly between the groups before and after AI exposure, with a mean of 1.91 before vs 1.92 after. Similarly, the number of mean advanced APC was comparable between the two periods (0.062 vs 0.063).
The mean advanced APC detection on standard colonoscopy in patients with at least one adenoma detected was 0.22 before AI exposure and 0.28 after AI exposure.
Colorectal cancers were detected in 6 (0.8%) of 795 colonoscopies before AI exposure and in 8 (1.2%) of 648 after AI exposure.
In multivariable logistic regression analysis, exposure to AI (odds ratio [OR], 0.69), patient’s male sex (OR, 1.78), and patient age at least 60 years (OR, 3.60) were independent factors significantly associated with ADR.
In all centers, the ADR for standard, non-AI-assisted colonoscopy was reduced after AI exposure, although the magnitude of ADR reduction varied greatly between centers, according to the authors.
“Clinicians should be aware that while AI can boost detection rates, prolonged reliance may subtly affect their performance when the technology is not available,” Budzyń and Romańczyk said. “This does not mean AI should be avoided — rather, it highlights the need for conscious engagement with the task, even when AI is assisting. Monitoring one’s own detection rates in both AI-assisted and non-AI-assisted procedures can help identify changes early.”
“Endoscopists should view AI as a collaborative partner, not a replacement for their vigilance and judgment,” they concluded. “Integrating AI effectively means using it to complement, not substitute, core observational and diagnostic skills. In short, enjoy the benefits of AI, but keep your skills sharp — your patients depend on both.”
Omer Ahmed, MD, of University College London, London, England, gives a similar message in a related editorial. The study “compels us to carefully consider the effect of AI integration into routine endoscopic practice,” he wrote. “Although AI continues to offer great promise to enhance clinical outcomes, we must also safeguard against the quiet erosion of fundamental skills required for high-quality endoscopy.”
‘Certainly a Signal’
Commenting on the study for GI & Hepatology News, Rajiv Bhuta, MD, assistant professor of clinical gastroenterology and hepatology at Temple University and a gastroenterologist at Temple University Hospital, both in Philadelphia, said, “On the face of it, these findings would seem to correlate with all our lived experiences as humans. Any skill or task that we give to a machine will inherently ‘de-skill’ or weaken our ability to perform it.”
“The only way to miss a polyp is either due to lack of attention/recognition of a polyp in the field of view or a lack of fold exposure and cleansing,” said Bhuta, who was not involved in the study. “For AI to specifically de-skill polyp detection, it would mean the AI is conditioning physicians to pay less active attention during the procedure, similar to the way a driver may pay less attention in a car that has self-driving capabilities.”
That said, he noted that this is a small retrospective observational study with a short timeframe and an average of fewer than 100 colonoscopies per physician.
“My own ADR may vary by 8% or more by random chance in such a small dataset,” he said. “It’s hard to draw any real conclusions, but it is certainly a signal.”
The issue of de-skilling goes beyond gastroenterology and medicine, Bhuta noted. “We have invented millions of machines that have ‘de-skilled’ us in thousands of small ways, and mostly, we have benefited as a society. However, we’ve never had a machine that can de-skill our attention, our creativity, and our reason.”
“The question is not whether AI will de-skill us but when, where, and how do we set the boundaries of what we want a machine to do for us,” he said. “What is lost and what is gained by AI taking over these roles, and is that an acceptable trade-off?”
The study was funded by the European Commission and the Japan Society for the Promotion of Science. Budzyń, Romańczyk, and Bhuta declared having no competing interests. Ahmed declared receiving medical consultancy fees from Olympus, Odin Vision, Medtronic, and Norgine.
A version of this article appeared on Medscape.com.
, a large observational study suggested.
“The extent and consistency of the adenoma detection rate (ADR) drop after long-term AI use were not expected,” study authors Krzysztof Budzyń, MD, and Marcin Romańczyk, MD, of the Academy of Silesia, Katowice, Poland, told GI & Hepatology News. “We thought there might be a small effect, but the 6% absolute decrease — observed in several centers and among most endoscopists — points to a genuine change in behavior. This was especially notable because all participants were very experienced, with more than 2000 colonoscopies each.”
Another unexpected result, they said, “was that the decrease was stronger in centers with higher starting ADRs and in certain patient groups, such as women under 60. We had assumed experienced clinicians would be less affected, but our results show that even highly skilled practitioners can be influenced.”
The study was published online in The Lancet Gastroenterology & Hepatology.
ADR Reduced After AI Use
To assess how endoscopists who used AI regularly performed colonoscopy when AI was not in use, researchers conducted a retrospective, observational study at four endoscopy centers in Poland taking part in the ACCEPT trial.
These centers introduced AI tools for polyp detection at the end of 2021, after which colonoscopies were randomly assigned to be done with or without AI assistance.
The researchers assessed colonoscopy quality by comparing two different phases: 3 months before and 3 months after AI implementation. All diagnostic colonoscopies were included, except for those involving intensive anticoagulant use, pregnancy, or a history of colorectal resection or inflammatory bowel disease.
The primary outcome was the change in the ADR of standard, non-AI-assisted colonoscopy before and after AI exposure.
Between September 2021 and March 2022, a total of 2177 colonoscopies were conducted, including 1443 without AI use and 734 with AI. The current analysis focused on the 795 patients who underwent non-AI-assisted colonoscopy before the introduction of AI and the 648 who underwent non-AI-assisted colonoscopy after.
Participants’ median age was 61 years, and 59% were women. The colonoscopies were performed by 19 experienced endoscopists who had conducted over 2000 colonoscopies each.
The ADR of standard colonoscopy decreased significantly from 28.4% (226 of 795) before the introduction of AI to 22.4% (145 of 648) after, corresponding to a 20% relative and 6% absolute reduction in the ADR.
The ADR for AI-assisted colonoscopies was 25.3% (186 of 734).
The number of adenomas per colonoscopy (APC) in patients with at least one adenoma detected did not change significantly between the groups before and after AI exposure, with a mean of 1.91 before vs 1.92 after. Similarly, the number of mean advanced APC was comparable between the two periods (0.062 vs 0.063).
The mean advanced APC detection on standard colonoscopy in patients with at least one adenoma detected was 0.22 before AI exposure and 0.28 after AI exposure.
Colorectal cancers were detected in 6 (0.8%) of 795 colonoscopies before AI exposure and in 8 (1.2%) of 648 after AI exposure.
In multivariable logistic regression analysis, exposure to AI (odds ratio [OR], 0.69), patient’s male sex (OR, 1.78), and patient age at least 60 years (OR, 3.60) were independent factors significantly associated with ADR.
In all centers, the ADR for standard, non-AI-assisted colonoscopy was reduced after AI exposure, although the magnitude of ADR reduction varied greatly between centers, according to the authors.
“Clinicians should be aware that while AI can boost detection rates, prolonged reliance may subtly affect their performance when the technology is not available,” Budzyń and Romańczyk said. “This does not mean AI should be avoided — rather, it highlights the need for conscious engagement with the task, even when AI is assisting. Monitoring one’s own detection rates in both AI-assisted and non-AI-assisted procedures can help identify changes early.”
“Endoscopists should view AI as a collaborative partner, not a replacement for their vigilance and judgment,” they concluded. “Integrating AI effectively means using it to complement, not substitute, core observational and diagnostic skills. In short, enjoy the benefits of AI, but keep your skills sharp — your patients depend on both.”
Omer Ahmed, MD, of University College London, London, England, gives a similar message in a related editorial. The study “compels us to carefully consider the effect of AI integration into routine endoscopic practice,” he wrote. “Although AI continues to offer great promise to enhance clinical outcomes, we must also safeguard against the quiet erosion of fundamental skills required for high-quality endoscopy.”
‘Certainly a Signal’
Commenting on the study for GI & Hepatology News, Rajiv Bhuta, MD, assistant professor of clinical gastroenterology and hepatology at Temple University and a gastroenterologist at Temple University Hospital, both in Philadelphia, said, “On the face of it, these findings would seem to correlate with all our lived experiences as humans. Any skill or task that we give to a machine will inherently ‘de-skill’ or weaken our ability to perform it.”
“The only way to miss a polyp is either due to lack of attention/recognition of a polyp in the field of view or a lack of fold exposure and cleansing,” said Bhuta, who was not involved in the study. “For AI to specifically de-skill polyp detection, it would mean the AI is conditioning physicians to pay less active attention during the procedure, similar to the way a driver may pay less attention in a car that has self-driving capabilities.”
That said, he noted that this is a small retrospective observational study with a short timeframe and an average of fewer than 100 colonoscopies per physician.
“My own ADR may vary by 8% or more by random chance in such a small dataset,” he said. “It’s hard to draw any real conclusions, but it is certainly a signal.”
The issue of de-skilling goes beyond gastroenterology and medicine, Bhuta noted. “We have invented millions of machines that have ‘de-skilled’ us in thousands of small ways, and mostly, we have benefited as a society. However, we’ve never had a machine that can de-skill our attention, our creativity, and our reason.”
“The question is not whether AI will de-skill us but when, where, and how do we set the boundaries of what we want a machine to do for us,” he said. “What is lost and what is gained by AI taking over these roles, and is that an acceptable trade-off?”
The study was funded by the European Commission and the Japan Society for the Promotion of Science. Budzyń, Romańczyk, and Bhuta declared having no competing interests. Ahmed declared receiving medical consultancy fees from Olympus, Odin Vision, Medtronic, and Norgine.
A version of this article appeared on Medscape.com.
Repeat Intubation of the Sigmoid Colon Improves Adenoma Detection
, new research showed.
“After eliminating the impact of time, the adenoma-detection rate [with a second intubation vs standard withdrawal] was still significantly increased, indicating that the second intubation technique could enhance the visualization of the sigmoid colon mucosa and reduce the rate of missed lesions,” reported the authors of the study, published in The American Journal of Gastroenterology.
When precancerous polyps are removed during standard colonoscopies, as many as 70%-90% of colorectal cancers can be prevented; however, rates of missed polyps during colonoscopy are notoriously high.
Recent studies have shown improved adenoma-detection rates with the use of Endocuff, water-assisted colonoscopy, full-spectrum endoscopy, and repeat withdrawal examinations, which include retroflexion and forward-viewing methods.
The repeat colonoscopy examinations may represent “the easiest and most practical option for endoscopists as they do not require additional tools, staff, or funding,” the authors explained.
However, most studies on the issue have focused mainly on the right colon and forward-viewing examinations, whereas the sigmoid colon, which has the most turns and is the most easily compressed, can be easily missed during withdrawal observation.
To investigate if use of a second colon intubation of the sigmoid colon could improve detection rates, senior author Jianning Yao, MD, of the Department of Gastroenterology, The First Affiliated Hospital of Zhengzhou University, Zhengzhou, China, conducted a randomized trial, enrolling 650 patients between December 2023 and April 2024 who were aged 45 or older and had overweight or obesity (BMI ≥ 24).
At the time of the first withdrawal during the colonoscopy, the patients were randomized 1:1 to groups of 325 each to either receive standard withdrawal, with withdrawal to the anus, or to receive a second intubation, with reinsertion into the sigmoid colon.
In the second intubation, the colonoscope was pushed forward without straightening, “allowing for slight looping that could be used to flatten the colonic folds as the tip of the instrument was advanced,” they explained.
The patients had a mean age of 55; about 25% had a smoking habit, and the mean BMI was about 28. There were no significant differences in other baseline characteristics.
The results showed that patients in the second-intubation group vs standard-withdrawal group had a substantially higher adenoma-detection rate (24.3% vs 14.5%) and polyp-detection rate (29.2% vs 17.8%, P = .001 for both) in the sigmoid colon.
In the second-intubation group, 85% of the adenomas discovered throughout the second inspection in the sigmoid colon were 5 mm or smaller in size. In addition, 90% of the 40 adenomas were somewhat raised or pedunculated, and all were tubular adenomas.
No high-grade dysplasia adenomas were discovered.
Of note, the colonoscopy in the second-intubation group’s colonoscopic examinations took just 1.47 minute longer overall than the standard-withdrawal group’s examinations.
Factors that were determined in a multivariate analysis to be independent predictors of higher adenoma detection in the second-intubation group included older age, smoking habit, longer duration of the second inspection, and the identification of lesions during the initial withdrawal from the sigmoid colon.
Patients’ vital signs were monitored at intervals of 3 minutes throughout the colonoscopy procedure, and patients were followed up to monitor for any adverse events occurring within 2 weeks after the examination, with no notable disparities observed between the two groups.
Alternative to AKS Approach in Second Intubation
The authors explained that, in their approach in the second intubation, the common axis-keeping shortening (AKS) was not utilized, and instead they pushed the colonoscope forward without straightening it, which offers important advantages.
“In this way, slight looping of the colonoscope can be used to flatten the colonic folds as the tip of the instrument is advanced, thereby achieving an observation effect that cannot be reached by any number of withdrawal examinations.”
In general, the stimulation of peristalsis during a second examination allows for the observation of the colonic mucosa from different angles, thereby reducing the rate of missed lesions, the authors added.
“Although the detection of these lesions may not significantly affect clinical outcomes, it serves as a reminder for patients regarding regular follow-ups and lifestyle adjustments,” they explained. “Additionally, it may reduce the likelihood of missing some smaller lesions that progress rapidly, such as de novo cancer.”
Based on the results, the authors concluded that older patients, patients who smoke, or those with lesions found on the first sigmoid inspection have a higher chance of having missed adenomas discovered in the sigmoid colon during the second intubation examination.
“If one of these risk factors is present, a second examination of the sigmoid colon may be considered to detect missed lesions,” they said.
The added time commitment of just 1.47 minutes can be a worthwhile tradeoff, they added.
“Considering the improvements in the adenoma-detection rate provided by the second intubation, this modest time increase may be acceptable.”
The authors had no disclosures to report.
A version of this article appeared on Medscape.com.
, new research showed.
“After eliminating the impact of time, the adenoma-detection rate [with a second intubation vs standard withdrawal] was still significantly increased, indicating that the second intubation technique could enhance the visualization of the sigmoid colon mucosa and reduce the rate of missed lesions,” reported the authors of the study, published in The American Journal of Gastroenterology.
When precancerous polyps are removed during standard colonoscopies, as many as 70%-90% of colorectal cancers can be prevented; however, rates of missed polyps during colonoscopy are notoriously high.
Recent studies have shown improved adenoma-detection rates with the use of Endocuff, water-assisted colonoscopy, full-spectrum endoscopy, and repeat withdrawal examinations, which include retroflexion and forward-viewing methods.
The repeat colonoscopy examinations may represent “the easiest and most practical option for endoscopists as they do not require additional tools, staff, or funding,” the authors explained.
However, most studies on the issue have focused mainly on the right colon and forward-viewing examinations, whereas the sigmoid colon, which has the most turns and is the most easily compressed, can be easily missed during withdrawal observation.
To investigate if use of a second colon intubation of the sigmoid colon could improve detection rates, senior author Jianning Yao, MD, of the Department of Gastroenterology, The First Affiliated Hospital of Zhengzhou University, Zhengzhou, China, conducted a randomized trial, enrolling 650 patients between December 2023 and April 2024 who were aged 45 or older and had overweight or obesity (BMI ≥ 24).
At the time of the first withdrawal during the colonoscopy, the patients were randomized 1:1 to groups of 325 each to either receive standard withdrawal, with withdrawal to the anus, or to receive a second intubation, with reinsertion into the sigmoid colon.
In the second intubation, the colonoscope was pushed forward without straightening, “allowing for slight looping that could be used to flatten the colonic folds as the tip of the instrument was advanced,” they explained.
The patients had a mean age of 55; about 25% had a smoking habit, and the mean BMI was about 28. There were no significant differences in other baseline characteristics.
The results showed that patients in the second-intubation group vs standard-withdrawal group had a substantially higher adenoma-detection rate (24.3% vs 14.5%) and polyp-detection rate (29.2% vs 17.8%, P = .001 for both) in the sigmoid colon.
In the second-intubation group, 85% of the adenomas discovered throughout the second inspection in the sigmoid colon were 5 mm or smaller in size. In addition, 90% of the 40 adenomas were somewhat raised or pedunculated, and all were tubular adenomas.
No high-grade dysplasia adenomas were discovered.
Of note, the colonoscopy in the second-intubation group’s colonoscopic examinations took just 1.47 minute longer overall than the standard-withdrawal group’s examinations.
Factors that were determined in a multivariate analysis to be independent predictors of higher adenoma detection in the second-intubation group included older age, smoking habit, longer duration of the second inspection, and the identification of lesions during the initial withdrawal from the sigmoid colon.
Patients’ vital signs were monitored at intervals of 3 minutes throughout the colonoscopy procedure, and patients were followed up to monitor for any adverse events occurring within 2 weeks after the examination, with no notable disparities observed between the two groups.
Alternative to AKS Approach in Second Intubation
The authors explained that, in their approach in the second intubation, the common axis-keeping shortening (AKS) was not utilized, and instead they pushed the colonoscope forward without straightening it, which offers important advantages.
“In this way, slight looping of the colonoscope can be used to flatten the colonic folds as the tip of the instrument is advanced, thereby achieving an observation effect that cannot be reached by any number of withdrawal examinations.”
In general, the stimulation of peristalsis during a second examination allows for the observation of the colonic mucosa from different angles, thereby reducing the rate of missed lesions, the authors added.
“Although the detection of these lesions may not significantly affect clinical outcomes, it serves as a reminder for patients regarding regular follow-ups and lifestyle adjustments,” they explained. “Additionally, it may reduce the likelihood of missing some smaller lesions that progress rapidly, such as de novo cancer.”
Based on the results, the authors concluded that older patients, patients who smoke, or those with lesions found on the first sigmoid inspection have a higher chance of having missed adenomas discovered in the sigmoid colon during the second intubation examination.
“If one of these risk factors is present, a second examination of the sigmoid colon may be considered to detect missed lesions,” they said.
The added time commitment of just 1.47 minutes can be a worthwhile tradeoff, they added.
“Considering the improvements in the adenoma-detection rate provided by the second intubation, this modest time increase may be acceptable.”
The authors had no disclosures to report.
A version of this article appeared on Medscape.com.
, new research showed.
“After eliminating the impact of time, the adenoma-detection rate [with a second intubation vs standard withdrawal] was still significantly increased, indicating that the second intubation technique could enhance the visualization of the sigmoid colon mucosa and reduce the rate of missed lesions,” reported the authors of the study, published in The American Journal of Gastroenterology.
When precancerous polyps are removed during standard colonoscopies, as many as 70%-90% of colorectal cancers can be prevented; however, rates of missed polyps during colonoscopy are notoriously high.
Recent studies have shown improved adenoma-detection rates with the use of Endocuff, water-assisted colonoscopy, full-spectrum endoscopy, and repeat withdrawal examinations, which include retroflexion and forward-viewing methods.
The repeat colonoscopy examinations may represent “the easiest and most practical option for endoscopists as they do not require additional tools, staff, or funding,” the authors explained.
However, most studies on the issue have focused mainly on the right colon and forward-viewing examinations, whereas the sigmoid colon, which has the most turns and is the most easily compressed, can be easily missed during withdrawal observation.
To investigate if use of a second colon intubation of the sigmoid colon could improve detection rates, senior author Jianning Yao, MD, of the Department of Gastroenterology, The First Affiliated Hospital of Zhengzhou University, Zhengzhou, China, conducted a randomized trial, enrolling 650 patients between December 2023 and April 2024 who were aged 45 or older and had overweight or obesity (BMI ≥ 24).
At the time of the first withdrawal during the colonoscopy, the patients were randomized 1:1 to groups of 325 each to either receive standard withdrawal, with withdrawal to the anus, or to receive a second intubation, with reinsertion into the sigmoid colon.
In the second intubation, the colonoscope was pushed forward without straightening, “allowing for slight looping that could be used to flatten the colonic folds as the tip of the instrument was advanced,” they explained.
The patients had a mean age of 55; about 25% had a smoking habit, and the mean BMI was about 28. There were no significant differences in other baseline characteristics.
The results showed that patients in the second-intubation group vs standard-withdrawal group had a substantially higher adenoma-detection rate (24.3% vs 14.5%) and polyp-detection rate (29.2% vs 17.8%, P = .001 for both) in the sigmoid colon.
In the second-intubation group, 85% of the adenomas discovered throughout the second inspection in the sigmoid colon were 5 mm or smaller in size. In addition, 90% of the 40 adenomas were somewhat raised or pedunculated, and all were tubular adenomas.
No high-grade dysplasia adenomas were discovered.
Of note, the colonoscopy in the second-intubation group’s colonoscopic examinations took just 1.47 minute longer overall than the standard-withdrawal group’s examinations.
Factors that were determined in a multivariate analysis to be independent predictors of higher adenoma detection in the second-intubation group included older age, smoking habit, longer duration of the second inspection, and the identification of lesions during the initial withdrawal from the sigmoid colon.
Patients’ vital signs were monitored at intervals of 3 minutes throughout the colonoscopy procedure, and patients were followed up to monitor for any adverse events occurring within 2 weeks after the examination, with no notable disparities observed between the two groups.
Alternative to AKS Approach in Second Intubation
The authors explained that, in their approach in the second intubation, the common axis-keeping shortening (AKS) was not utilized, and instead they pushed the colonoscope forward without straightening it, which offers important advantages.
“In this way, slight looping of the colonoscope can be used to flatten the colonic folds as the tip of the instrument is advanced, thereby achieving an observation effect that cannot be reached by any number of withdrawal examinations.”
In general, the stimulation of peristalsis during a second examination allows for the observation of the colonic mucosa from different angles, thereby reducing the rate of missed lesions, the authors added.
“Although the detection of these lesions may not significantly affect clinical outcomes, it serves as a reminder for patients regarding regular follow-ups and lifestyle adjustments,” they explained. “Additionally, it may reduce the likelihood of missing some smaller lesions that progress rapidly, such as de novo cancer.”
Based on the results, the authors concluded that older patients, patients who smoke, or those with lesions found on the first sigmoid inspection have a higher chance of having missed adenomas discovered in the sigmoid colon during the second intubation examination.
“If one of these risk factors is present, a second examination of the sigmoid colon may be considered to detect missed lesions,” they said.
The added time commitment of just 1.47 minutes can be a worthwhile tradeoff, they added.
“Considering the improvements in the adenoma-detection rate provided by the second intubation, this modest time increase may be acceptable.”
The authors had no disclosures to report.
A version of this article appeared on Medscape.com.