User login
Tigger and end-of-life talk
My wife texted, "Tigger is having problems. Call me."
Tigger is our beloved (and bouncy) 9½-year-old boxer. My wife had just finished putting our 16-month-old son down for his nap when she heard a commotion in the foyer. She looked downstairs and saw Tigger struggling to get up. She ran down the steps and sat down beside him. It was clear that his hind legs were not working. Wide-eyed, he looked terrified to her. As she stroked his back, he eventually settled down and rested for several minutes. After about 10 minutes, he was able to get up and slowly walk around the house.
I came home from work, followed shortly thereafter by one of our friends and two of his young boys. While my wife and I had drinks and pizza with our friend, and the boys and our daughter played in the yard. Tigger, normally in the center of the action, lay off to the side of the patio. When I brought out a bowl of food for him, he did not budge. This was a first – he has never passed up a meal. Instead, he usually looks to supplement his food with anything he can steal from unsuspecting members of our family.
That evening, my wife and I had a long conversation about Tigger. We were going to take him to the vet and have him evaluated, but we were very realistic about what we might find. On average, boxers live just shy of 10 years. We’ve noticed that he had been slowing down, and the events of that evening – keeping to himself and passing up dinner – made us concerned that the end was close. We agreed that our primary goal is to keep him comfortable. He is a valued member of our family, and we do not want him to suffer.
Thankfully, Tigger rebounded from that initial episode, although he had a similar episode in the weeks that followed. We know the end is coming for him and we are working to maximize our time with him. We are retelling stories from his younger days and enjoying some of his behavioral quirks (read: stealing food) more than we had in the past. Again, our focus remains on his comfort. When he appears to be struggling too much – when his pain and discomfort exceeds – we will make that difficult decision that most every pet owner has to eventually make.
These discussions made me think of the patients I have cared for over the years who were never encouraged to think in such terms about their own lives. Many were being treated for underlying malignancies, yet had no conversations with their physicians about goals of care or end-of-life decisions.
I have written in the past about the need for these discussions and how we, as physicians, often die differently from our patients. Allow this to be a reminder to everyone to discuss goals of care with your patients. The conversations are an important investment in your relationship with that patient and are vital to providing the best possible care for them.
Dr. Pistoria is chief of hospital medicine at Coordinated Health in Bethlehem, Pa., and an adviser to Hospitalist News. He believes that the best care is always personal.
My wife texted, "Tigger is having problems. Call me."
Tigger is our beloved (and bouncy) 9½-year-old boxer. My wife had just finished putting our 16-month-old son down for his nap when she heard a commotion in the foyer. She looked downstairs and saw Tigger struggling to get up. She ran down the steps and sat down beside him. It was clear that his hind legs were not working. Wide-eyed, he looked terrified to her. As she stroked his back, he eventually settled down and rested for several minutes. After about 10 minutes, he was able to get up and slowly walk around the house.
I came home from work, followed shortly thereafter by one of our friends and two of his young boys. While my wife and I had drinks and pizza with our friend, and the boys and our daughter played in the yard. Tigger, normally in the center of the action, lay off to the side of the patio. When I brought out a bowl of food for him, he did not budge. This was a first – he has never passed up a meal. Instead, he usually looks to supplement his food with anything he can steal from unsuspecting members of our family.
That evening, my wife and I had a long conversation about Tigger. We were going to take him to the vet and have him evaluated, but we were very realistic about what we might find. On average, boxers live just shy of 10 years. We’ve noticed that he had been slowing down, and the events of that evening – keeping to himself and passing up dinner – made us concerned that the end was close. We agreed that our primary goal is to keep him comfortable. He is a valued member of our family, and we do not want him to suffer.
Thankfully, Tigger rebounded from that initial episode, although he had a similar episode in the weeks that followed. We know the end is coming for him and we are working to maximize our time with him. We are retelling stories from his younger days and enjoying some of his behavioral quirks (read: stealing food) more than we had in the past. Again, our focus remains on his comfort. When he appears to be struggling too much – when his pain and discomfort exceeds – we will make that difficult decision that most every pet owner has to eventually make.
These discussions made me think of the patients I have cared for over the years who were never encouraged to think in such terms about their own lives. Many were being treated for underlying malignancies, yet had no conversations with their physicians about goals of care or end-of-life decisions.
I have written in the past about the need for these discussions and how we, as physicians, often die differently from our patients. Allow this to be a reminder to everyone to discuss goals of care with your patients. The conversations are an important investment in your relationship with that patient and are vital to providing the best possible care for them.
Dr. Pistoria is chief of hospital medicine at Coordinated Health in Bethlehem, Pa., and an adviser to Hospitalist News. He believes that the best care is always personal.
My wife texted, "Tigger is having problems. Call me."
Tigger is our beloved (and bouncy) 9½-year-old boxer. My wife had just finished putting our 16-month-old son down for his nap when she heard a commotion in the foyer. She looked downstairs and saw Tigger struggling to get up. She ran down the steps and sat down beside him. It was clear that his hind legs were not working. Wide-eyed, he looked terrified to her. As she stroked his back, he eventually settled down and rested for several minutes. After about 10 minutes, he was able to get up and slowly walk around the house.
I came home from work, followed shortly thereafter by one of our friends and two of his young boys. While my wife and I had drinks and pizza with our friend, and the boys and our daughter played in the yard. Tigger, normally in the center of the action, lay off to the side of the patio. When I brought out a bowl of food for him, he did not budge. This was a first – he has never passed up a meal. Instead, he usually looks to supplement his food with anything he can steal from unsuspecting members of our family.
That evening, my wife and I had a long conversation about Tigger. We were going to take him to the vet and have him evaluated, but we were very realistic about what we might find. On average, boxers live just shy of 10 years. We’ve noticed that he had been slowing down, and the events of that evening – keeping to himself and passing up dinner – made us concerned that the end was close. We agreed that our primary goal is to keep him comfortable. He is a valued member of our family, and we do not want him to suffer.
Thankfully, Tigger rebounded from that initial episode, although he had a similar episode in the weeks that followed. We know the end is coming for him and we are working to maximize our time with him. We are retelling stories from his younger days and enjoying some of his behavioral quirks (read: stealing food) more than we had in the past. Again, our focus remains on his comfort. When he appears to be struggling too much – when his pain and discomfort exceeds – we will make that difficult decision that most every pet owner has to eventually make.
These discussions made me think of the patients I have cared for over the years who were never encouraged to think in such terms about their own lives. Many were being treated for underlying malignancies, yet had no conversations with their physicians about goals of care or end-of-life decisions.
I have written in the past about the need for these discussions and how we, as physicians, often die differently from our patients. Allow this to be a reminder to everyone to discuss goals of care with your patients. The conversations are an important investment in your relationship with that patient and are vital to providing the best possible care for them.
Dr. Pistoria is chief of hospital medicine at Coordinated Health in Bethlehem, Pa., and an adviser to Hospitalist News. He believes that the best care is always personal.

More hospitals providing palliative care
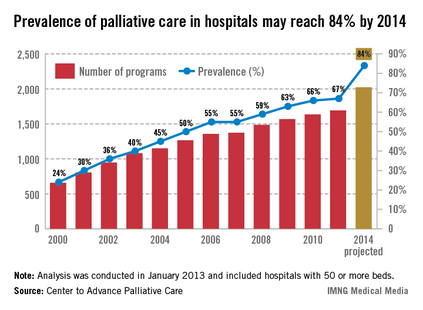
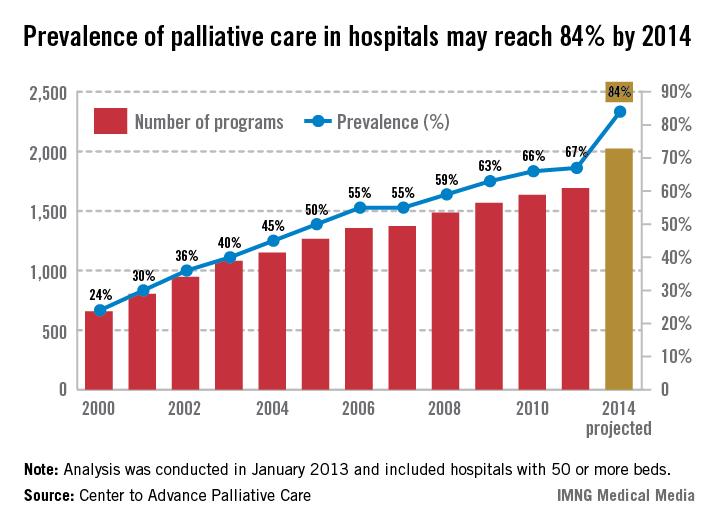
The prevalence of palliative care programs in U.S. hospitals is expected to reach 84% by 2014, according to an analysis from the Center to Advance Palliative Care.
From 2000 to 2011, the number of hospitals with 50 or more beds that had a palliative care program went from 658 to 1,692, an increase of 157%. If that trend continues, there should be 2,023 hospitals – approximately 84% – providing palliative care in the United States by 2014, the CAPC reported.
The CAPC analysis, conducted in January 2013, involved data from the American Hospital Association and the center’s own National Palliative Care Registry.
The prevalence of palliative care programs in U.S. hospitals is expected to reach 84% by 2014, according to an analysis from the Center to Advance Palliative Care.
From 2000 to 2011, the number of hospitals with 50 or more beds that had a palliative care program went from 658 to 1,692, an increase of 157%. If that trend continues, there should be 2,023 hospitals – approximately 84% – providing palliative care in the United States by 2014, the CAPC reported.
The CAPC analysis, conducted in January 2013, involved data from the American Hospital Association and the center’s own National Palliative Care Registry.
The prevalence of palliative care programs in U.S. hospitals is expected to reach 84% by 2014, according to an analysis from the Center to Advance Palliative Care.
From 2000 to 2011, the number of hospitals with 50 or more beds that had a palliative care program went from 658 to 1,692, an increase of 157%. If that trend continues, there should be 2,023 hospitals – approximately 84% – providing palliative care in the United States by 2014, the CAPC reported.
The CAPC analysis, conducted in January 2013, involved data from the American Hospital Association and the center’s own National Palliative Care Registry.
Palliative care training and associations with burnout in oncology fellows
ABSTRACT
Background Burnout among physicians can lead to decreased career satisfaction, physical and emotional exhaustion, and increased medical errors. In oncologists, high exposure to fatal illness is associated with burnout.
Methods The Maslach Burnout Inventory, measuring Emotional Exhaustion (EE), Depersonalization (DP), and Personal Accomplishment (PA), was administered to second-year US oncology fellows. Bivariate and multivariate analyses explored associations between burnout and fellow demographics, attitudes, and educational experiences.
Results A total of 254 fellows out of 402 eligible US fellows responded (63.2%) and 24.2% reported high EE, 30.0% reported high DP, and 26.8% reported low PA. Over half of the fellows reported burnout in at least one domain. Lower EE scores were associated with the fellows’ perceptions of having received better teaching, explicit teaching about certain end-of-life topics, and receipt of direct observation of goals-of-care discussions. Fellows who reported better overall teaching quality and more frequent observation of their skills had less depersonalization. Fellows who felt a responsibility to help patients at the end of life to prepare for death had higher PA.
Limitations This survey relies on the fellows’ self-reported perceptions without an objective measure for validation. Factors associated with burnout may not be causal. The number of analyses performed raises the concern for Type I errors; therefore, a stringent P value (.01) was used.
Conclusions Burnout is prevalent during oncology training. Higher-quality teaching is associated with less burnout among fellows. Fellowship programs should recognize the prevalence of burnout among oncology fellows as well as components of training that may protect against burnout.
*For a PDF of the full article, click on the link to the left of this introduction.
Life, Communication
ABSTRACT
Background Burnout among physicians can lead to decreased career satisfaction, physical and emotional exhaustion, and increased medical errors. In oncologists, high exposure to fatal illness is associated with burnout.
Methods The Maslach Burnout Inventory, measuring Emotional Exhaustion (EE), Depersonalization (DP), and Personal Accomplishment (PA), was administered to second-year US oncology fellows. Bivariate and multivariate analyses explored associations between burnout and fellow demographics, attitudes, and educational experiences.
Results A total of 254 fellows out of 402 eligible US fellows responded (63.2%) and 24.2% reported high EE, 30.0% reported high DP, and 26.8% reported low PA. Over half of the fellows reported burnout in at least one domain. Lower EE scores were associated with the fellows’ perceptions of having received better teaching, explicit teaching about certain end-of-life topics, and receipt of direct observation of goals-of-care discussions. Fellows who reported better overall teaching quality and more frequent observation of their skills had less depersonalization. Fellows who felt a responsibility to help patients at the end of life to prepare for death had higher PA.
Limitations This survey relies on the fellows’ self-reported perceptions without an objective measure for validation. Factors associated with burnout may not be causal. The number of analyses performed raises the concern for Type I errors; therefore, a stringent P value (.01) was used.
Conclusions Burnout is prevalent during oncology training. Higher-quality teaching is associated with less burnout among fellows. Fellowship programs should recognize the prevalence of burnout among oncology fellows as well as components of training that may protect against burnout.
*For a PDF of the full article, click on the link to the left of this introduction.
ABSTRACT
Background Burnout among physicians can lead to decreased career satisfaction, physical and emotional exhaustion, and increased medical errors. In oncologists, high exposure to fatal illness is associated with burnout.
Methods The Maslach Burnout Inventory, measuring Emotional Exhaustion (EE), Depersonalization (DP), and Personal Accomplishment (PA), was administered to second-year US oncology fellows. Bivariate and multivariate analyses explored associations between burnout and fellow demographics, attitudes, and educational experiences.
Results A total of 254 fellows out of 402 eligible US fellows responded (63.2%) and 24.2% reported high EE, 30.0% reported high DP, and 26.8% reported low PA. Over half of the fellows reported burnout in at least one domain. Lower EE scores were associated with the fellows’ perceptions of having received better teaching, explicit teaching about certain end-of-life topics, and receipt of direct observation of goals-of-care discussions. Fellows who reported better overall teaching quality and more frequent observation of their skills had less depersonalization. Fellows who felt a responsibility to help patients at the end of life to prepare for death had higher PA.
Limitations This survey relies on the fellows’ self-reported perceptions without an objective measure for validation. Factors associated with burnout may not be causal. The number of analyses performed raises the concern for Type I errors; therefore, a stringent P value (.01) was used.
Conclusions Burnout is prevalent during oncology training. Higher-quality teaching is associated with less burnout among fellows. Fellowship programs should recognize the prevalence of burnout among oncology fellows as well as components of training that may protect against burnout.
*For a PDF of the full article, click on the link to the left of this introduction.
Life, Communication
Life, Communication
Checking up on advance care planning - and charting, too
Earlier today our team was consulted to see an 85-year-old gentleman. A request was made that we conduct a family meeting to elicit the goals of care.
The patient had several underlying illnesses including diastolic heart failure, chronic renal insufficiency, and COPD. He was admitted after experiencing a complication from an outpatient procedure aimed at alleviating his chronic low back pain. After paging through his chart, it was clear that he suffered multiple setbacks throughout his admission, and that over the last 12 hours he was rapidly decompensating from hospital-acquired pneumonia and subsequent sepsis.
Though I was quite certain that his family had been approached about treatment goals, there was no documentation of this in the chart or reflection of these goals in the care plan. This was hospital day No. 32.
Two decades are behind us after being confronted with the impressive discord between what patients with advanced illnesses desire for themselves, what we think they want, and the actual care we deliver to them(JAMA 1995;274(20):1591-98). Where are we today when it comes to having dialogue with patients and families about advance care planning (ACP) or code status and our documentation of these critical decisions?
Recently, a study from 12 hospitals spanning Canada set out to see how often seriously ill elderly patients in the hospital were engaged in ACP (JAMA Intern. Med. 2013 April 1 [doi: 10.1001/jamainternmed.2013.203]). The mean age of the patients was 80 years, and they all had advanced illnesses that were not expected to be curable. Over 75% of the almost 300 patients enrolled reflected on end-of-life preferences prior to hospitalization, and only 12% were interested in life-prolonging care versus care that focused on quality of life. While in the prehospital period patients are completing advance directives (AD) and identifying a surrogate (48% and 73% respectively), the disconnect comes when looking at whether the documentation in the medical record is in agreement with patient preferences. It is not. The medical record accurately reflects the patient choice only 30% of the time. This led the invited commentary to declare that this disregard be classified as a medical error(JAMA Intern. Med. 2013 April 1 [doi: 10.1001/jamainternmed.2013.203]).
Are we the barriers to seeing ACP take place and properly chart the results?
Clearly that is part of the problem (the patient side of this equation will be explored in a future piece). In 2010, a group of hospitalists were audio-recorded during their initial encounter with a newly admitted patient (J. Gen. Intern. Med. 2011 26(4):359-66). During a total of 80 encounters, ACP was brought up less than 20% of the time. When it was addressed, the median length of a code status discussion was 1 minute. Prognosis was mentioned in only one encounter. No physician made a quantitative estimate of prognosis, nor did anyone make recommendations on whether or not CPR was medically appropriate.
Here is a sample from the recording with a hospitalist discussing code status with a patient diagnosed with cholangiocarcinoma:
Physician: "... If for some reason you got so sick that your heart stopped beating or your lungs got so sick that they couldn’t breathe on their own, would you want us to attempt to bring you back to life with electricity shocks and other things?"
Patient: "Yes."
Physician: "Yes. Okay. Okay. I think that’s all my questions."
How does the lack of ACP and documentation impact the hospitalist in 2013? Two big-ticket items come to mind: HCAHPS (Hospital Consumer Assessment of Healthcare Providers and Systems) and 30-day readmissions. Both of these will be explored in the next column, along with what we can do to make both immediate and long-term positive impacts on ACP.
Dr. Bekanich and Dr. Fredholm are codirectors of Seton Health Palliative Care, part of the University of Texas Southwestern Residency Programs in Austin.
Earlier today our team was consulted to see an 85-year-old gentleman. A request was made that we conduct a family meeting to elicit the goals of care.
The patient had several underlying illnesses including diastolic heart failure, chronic renal insufficiency, and COPD. He was admitted after experiencing a complication from an outpatient procedure aimed at alleviating his chronic low back pain. After paging through his chart, it was clear that he suffered multiple setbacks throughout his admission, and that over the last 12 hours he was rapidly decompensating from hospital-acquired pneumonia and subsequent sepsis.
Though I was quite certain that his family had been approached about treatment goals, there was no documentation of this in the chart or reflection of these goals in the care plan. This was hospital day No. 32.
Two decades are behind us after being confronted with the impressive discord between what patients with advanced illnesses desire for themselves, what we think they want, and the actual care we deliver to them(JAMA 1995;274(20):1591-98). Where are we today when it comes to having dialogue with patients and families about advance care planning (ACP) or code status and our documentation of these critical decisions?
Recently, a study from 12 hospitals spanning Canada set out to see how often seriously ill elderly patients in the hospital were engaged in ACP (JAMA Intern. Med. 2013 April 1 [doi: 10.1001/jamainternmed.2013.203]). The mean age of the patients was 80 years, and they all had advanced illnesses that were not expected to be curable. Over 75% of the almost 300 patients enrolled reflected on end-of-life preferences prior to hospitalization, and only 12% were interested in life-prolonging care versus care that focused on quality of life. While in the prehospital period patients are completing advance directives (AD) and identifying a surrogate (48% and 73% respectively), the disconnect comes when looking at whether the documentation in the medical record is in agreement with patient preferences. It is not. The medical record accurately reflects the patient choice only 30% of the time. This led the invited commentary to declare that this disregard be classified as a medical error(JAMA Intern. Med. 2013 April 1 [doi: 10.1001/jamainternmed.2013.203]).
Are we the barriers to seeing ACP take place and properly chart the results?
Clearly that is part of the problem (the patient side of this equation will be explored in a future piece). In 2010, a group of hospitalists were audio-recorded during their initial encounter with a newly admitted patient (J. Gen. Intern. Med. 2011 26(4):359-66). During a total of 80 encounters, ACP was brought up less than 20% of the time. When it was addressed, the median length of a code status discussion was 1 minute. Prognosis was mentioned in only one encounter. No physician made a quantitative estimate of prognosis, nor did anyone make recommendations on whether or not CPR was medically appropriate.
Here is a sample from the recording with a hospitalist discussing code status with a patient diagnosed with cholangiocarcinoma:
Physician: "... If for some reason you got so sick that your heart stopped beating or your lungs got so sick that they couldn’t breathe on their own, would you want us to attempt to bring you back to life with electricity shocks and other things?"
Patient: "Yes."
Physician: "Yes. Okay. Okay. I think that’s all my questions."
How does the lack of ACP and documentation impact the hospitalist in 2013? Two big-ticket items come to mind: HCAHPS (Hospital Consumer Assessment of Healthcare Providers and Systems) and 30-day readmissions. Both of these will be explored in the next column, along with what we can do to make both immediate and long-term positive impacts on ACP.
Dr. Bekanich and Dr. Fredholm are codirectors of Seton Health Palliative Care, part of the University of Texas Southwestern Residency Programs in Austin.
Earlier today our team was consulted to see an 85-year-old gentleman. A request was made that we conduct a family meeting to elicit the goals of care.
The patient had several underlying illnesses including diastolic heart failure, chronic renal insufficiency, and COPD. He was admitted after experiencing a complication from an outpatient procedure aimed at alleviating his chronic low back pain. After paging through his chart, it was clear that he suffered multiple setbacks throughout his admission, and that over the last 12 hours he was rapidly decompensating from hospital-acquired pneumonia and subsequent sepsis.
Though I was quite certain that his family had been approached about treatment goals, there was no documentation of this in the chart or reflection of these goals in the care plan. This was hospital day No. 32.
Two decades are behind us after being confronted with the impressive discord between what patients with advanced illnesses desire for themselves, what we think they want, and the actual care we deliver to them(JAMA 1995;274(20):1591-98). Where are we today when it comes to having dialogue with patients and families about advance care planning (ACP) or code status and our documentation of these critical decisions?
Recently, a study from 12 hospitals spanning Canada set out to see how often seriously ill elderly patients in the hospital were engaged in ACP (JAMA Intern. Med. 2013 April 1 [doi: 10.1001/jamainternmed.2013.203]). The mean age of the patients was 80 years, and they all had advanced illnesses that were not expected to be curable. Over 75% of the almost 300 patients enrolled reflected on end-of-life preferences prior to hospitalization, and only 12% were interested in life-prolonging care versus care that focused on quality of life. While in the prehospital period patients are completing advance directives (AD) and identifying a surrogate (48% and 73% respectively), the disconnect comes when looking at whether the documentation in the medical record is in agreement with patient preferences. It is not. The medical record accurately reflects the patient choice only 30% of the time. This led the invited commentary to declare that this disregard be classified as a medical error(JAMA Intern. Med. 2013 April 1 [doi: 10.1001/jamainternmed.2013.203]).
Are we the barriers to seeing ACP take place and properly chart the results?
Clearly that is part of the problem (the patient side of this equation will be explored in a future piece). In 2010, a group of hospitalists were audio-recorded during their initial encounter with a newly admitted patient (J. Gen. Intern. Med. 2011 26(4):359-66). During a total of 80 encounters, ACP was brought up less than 20% of the time. When it was addressed, the median length of a code status discussion was 1 minute. Prognosis was mentioned in only one encounter. No physician made a quantitative estimate of prognosis, nor did anyone make recommendations on whether or not CPR was medically appropriate.
Here is a sample from the recording with a hospitalist discussing code status with a patient diagnosed with cholangiocarcinoma:
Physician: "... If for some reason you got so sick that your heart stopped beating or your lungs got so sick that they couldn’t breathe on their own, would you want us to attempt to bring you back to life with electricity shocks and other things?"
Patient: "Yes."
Physician: "Yes. Okay. Okay. I think that’s all my questions."
How does the lack of ACP and documentation impact the hospitalist in 2013? Two big-ticket items come to mind: HCAHPS (Hospital Consumer Assessment of Healthcare Providers and Systems) and 30-day readmissions. Both of these will be explored in the next column, along with what we can do to make both immediate and long-term positive impacts on ACP.
Dr. Bekanich and Dr. Fredholm are codirectors of Seton Health Palliative Care, part of the University of Texas Southwestern Residency Programs in Austin.

Timely palliative consult affects end-of-life care in gynecologic cancer patients
LOS ANGELES – A palliative care consultation within the last month of life improves a variety of end-of-life outcomes in patients dying from gynecologic cancers, based on a retrospective analysis.
Among the 100 patients studied, about one-fourth had a timely palliative care consultation, defined in one study as 14 days before death and in another study as 30 days before death, lead investigator Dr. Nicole S. Nevadunsky of Montefiore Medical Center, New York, reported at the annual meeting of the Society of Gynecologic Oncology.

Compared with their counterparts who had late or no consultations, patients who had timely consultations had lower scores for aggressive end-of-life events such as emergency department visits, chemotherapy, and death in an acute care setting.
In addition, in their last 14 days of life, this group had median direct inpatient hospital costs that were $5,106 less, and they were half as likely to be admitted.
"Our data suggest that early palliative medicine consultation results in decreased aggressive measures at the end of life [and] was associated with decreased direct inpatient costs for women who died from gynecologic malignancies," Dr. Nevadunsky noted. "Further research is needed to evaluate the quality of life in relation to [the aggressiveness of care] for patients and their families."
While it is unclear how many gynecologic oncologists are also board certified in palliative care, "I think more clinicians actually do palliative medicine as part of their everyday practice," Dr. Nevadunsky said. Also, palliative care is truly a multidisciplinary undertaking involving, for example, nurses, pastoral care personnel, social workers, and others.
"As far as the best metric for palliative medicine, I think it is quality of life. But how to define that is extremely complicated and still evolving," she added.
"I think it’s an experience where the patient is getting what they want most out of things, and sometimes that’s saying to the patient, ‘If we can’t cure you, what is the most important thing to you?’ " she replied. "Each patient is different, and that’s what makes (defining quality of life) so complicated."
The American Society of Clinical Oncology recommends consideration of palliative care early in the course of metastatic or symptomatic disease.
"This is a very vague recommendation: who, what, when, where, how? How will patients respond to this? Who’s going to pay for this? What’s the patient going to get out of this?" Dr. Nevadunsky commented.
She and her colleagues studied 100 consecutive patients who died from gynecologic cancer between 2006 and 2009 and received care at Montefiore in the year before death.
In the first study, they defined a timely palliative care consultation as one occurring more than 30 days before death.
"The ideal timing for palliative medicine consultation is unknown; however, 30 days was chosen as the minimal exposure time because the standard metrics utilized to compare aggressive measures at the end of life included a minimum of 30 days," Dr. Nevadunsky explained.
"Overall, I was surprised to find that 49 of the 100 women actually had a palliative medicine consultation at some time or another during their care," she said.
However, the median number of days between consultation and death was 16, and only 18% of patients had a timely consultation.
Late diagnosis did not explain this finding, as less than 10% of patients received their diagnosis in the month before they died.
"The scope of this study was not inclusive to determine why this [late palliative care consultation] was happening," Dr. Nevadunsky said. Data showed that although the two groups were demographically similar, the patients who received a timely consultation were more likely to be married.
The group with timely consultations were less likely to receive aggressive end-of-life care, based on measures of eight indicators of aggressive care (0 vs. 2, P = .025).
The difference between those patients who had timely consultation and those with untimely or no consultation was greatest for the indicators of a hospital stay lasting more than 14 days in the last month of life (22% vs. 40%) and death in the acute care setting (28% vs. 45%).
In the second study, the investigators found that 29% of patients had a timely palliative care consultation, defined in this case as one occurring 14 days or more before death.
Patients with a timely consultation had lower median direct hospital inpatient costs per day in the last 30 days of life ($613 vs. $702, P = .02). They also had lower median direct hospital inpatient costs in the last 14 days overall ($0 vs. $5,106, P = .007) and on a per-day basis ($0 vs. $676, P = .007).
"The patients who had the timely consultations actually weren’t admitted to the hospital as often," Dr. Nevadunsky noted. In fact, they were half as likely to be admitted in the last 14 days (35% vs. 71%, P = .001).
"Shortcomings [of the study] include small numbers and the retrospective collection of data. Also, our study did not account for outpatient costs, including those assumed by families, or for those costs incurred by loss of time out of work by families to care for the patient," acknowledged Dr. Nevadunsky, who disclosed no relevant conflicts of interest.
LOS ANGELES – A palliative care consultation within the last month of life improves a variety of end-of-life outcomes in patients dying from gynecologic cancers, based on a retrospective analysis.
Among the 100 patients studied, about one-fourth had a timely palliative care consultation, defined in one study as 14 days before death and in another study as 30 days before death, lead investigator Dr. Nicole S. Nevadunsky of Montefiore Medical Center, New York, reported at the annual meeting of the Society of Gynecologic Oncology.
Compared with their counterparts who had late or no consultations, patients who had timely consultations had lower scores for aggressive end-of-life events such as emergency department visits, chemotherapy, and death in an acute care setting.
In addition, in their last 14 days of life, this group had median direct inpatient hospital costs that were $5,106 less, and they were half as likely to be admitted.
"Our data suggest that early palliative medicine consultation results in decreased aggressive measures at the end of life [and] was associated with decreased direct inpatient costs for women who died from gynecologic malignancies," Dr. Nevadunsky noted. "Further research is needed to evaluate the quality of life in relation to [the aggressiveness of care] for patients and their families."
While it is unclear how many gynecologic oncologists are also board certified in palliative care, "I think more clinicians actually do palliative medicine as part of their everyday practice," Dr. Nevadunsky said. Also, palliative care is truly a multidisciplinary undertaking involving, for example, nurses, pastoral care personnel, social workers, and others.
"As far as the best metric for palliative medicine, I think it is quality of life. But how to define that is extremely complicated and still evolving," she added.
"I think it’s an experience where the patient is getting what they want most out of things, and sometimes that’s saying to the patient, ‘If we can’t cure you, what is the most important thing to you?’ " she replied. "Each patient is different, and that’s what makes (defining quality of life) so complicated."
The American Society of Clinical Oncology recommends consideration of palliative care early in the course of metastatic or symptomatic disease.
"This is a very vague recommendation: who, what, when, where, how? How will patients respond to this? Who’s going to pay for this? What’s the patient going to get out of this?" Dr. Nevadunsky commented.
She and her colleagues studied 100 consecutive patients who died from gynecologic cancer between 2006 and 2009 and received care at Montefiore in the year before death.
In the first study, they defined a timely palliative care consultation as one occurring more than 30 days before death.
"The ideal timing for palliative medicine consultation is unknown; however, 30 days was chosen as the minimal exposure time because the standard metrics utilized to compare aggressive measures at the end of life included a minimum of 30 days," Dr. Nevadunsky explained.
"Overall, I was surprised to find that 49 of the 100 women actually had a palliative medicine consultation at some time or another during their care," she said.
However, the median number of days between consultation and death was 16, and only 18% of patients had a timely consultation.
Late diagnosis did not explain this finding, as less than 10% of patients received their diagnosis in the month before they died.
"The scope of this study was not inclusive to determine why this [late palliative care consultation] was happening," Dr. Nevadunsky said. Data showed that although the two groups were demographically similar, the patients who received a timely consultation were more likely to be married.
The group with timely consultations were less likely to receive aggressive end-of-life care, based on measures of eight indicators of aggressive care (0 vs. 2, P = .025).
The difference between those patients who had timely consultation and those with untimely or no consultation was greatest for the indicators of a hospital stay lasting more than 14 days in the last month of life (22% vs. 40%) and death in the acute care setting (28% vs. 45%).
In the second study, the investigators found that 29% of patients had a timely palliative care consultation, defined in this case as one occurring 14 days or more before death.
Patients with a timely consultation had lower median direct hospital inpatient costs per day in the last 30 days of life ($613 vs. $702, P = .02). They also had lower median direct hospital inpatient costs in the last 14 days overall ($0 vs. $5,106, P = .007) and on a per-day basis ($0 vs. $676, P = .007).
"The patients who had the timely consultations actually weren’t admitted to the hospital as often," Dr. Nevadunsky noted. In fact, they were half as likely to be admitted in the last 14 days (35% vs. 71%, P = .001).
"Shortcomings [of the study] include small numbers and the retrospective collection of data. Also, our study did not account for outpatient costs, including those assumed by families, or for those costs incurred by loss of time out of work by families to care for the patient," acknowledged Dr. Nevadunsky, who disclosed no relevant conflicts of interest.
LOS ANGELES – A palliative care consultation within the last month of life improves a variety of end-of-life outcomes in patients dying from gynecologic cancers, based on a retrospective analysis.
Among the 100 patients studied, about one-fourth had a timely palliative care consultation, defined in one study as 14 days before death and in another study as 30 days before death, lead investigator Dr. Nicole S. Nevadunsky of Montefiore Medical Center, New York, reported at the annual meeting of the Society of Gynecologic Oncology.
Compared with their counterparts who had late or no consultations, patients who had timely consultations had lower scores for aggressive end-of-life events such as emergency department visits, chemotherapy, and death in an acute care setting.
In addition, in their last 14 days of life, this group had median direct inpatient hospital costs that were $5,106 less, and they were half as likely to be admitted.
"Our data suggest that early palliative medicine consultation results in decreased aggressive measures at the end of life [and] was associated with decreased direct inpatient costs for women who died from gynecologic malignancies," Dr. Nevadunsky noted. "Further research is needed to evaluate the quality of life in relation to [the aggressiveness of care] for patients and their families."
While it is unclear how many gynecologic oncologists are also board certified in palliative care, "I think more clinicians actually do palliative medicine as part of their everyday practice," Dr. Nevadunsky said. Also, palliative care is truly a multidisciplinary undertaking involving, for example, nurses, pastoral care personnel, social workers, and others.
"As far as the best metric for palliative medicine, I think it is quality of life. But how to define that is extremely complicated and still evolving," she added.
"I think it’s an experience where the patient is getting what they want most out of things, and sometimes that’s saying to the patient, ‘If we can’t cure you, what is the most important thing to you?’ " she replied. "Each patient is different, and that’s what makes (defining quality of life) so complicated."
The American Society of Clinical Oncology recommends consideration of palliative care early in the course of metastatic or symptomatic disease.
"This is a very vague recommendation: who, what, when, where, how? How will patients respond to this? Who’s going to pay for this? What’s the patient going to get out of this?" Dr. Nevadunsky commented.
She and her colleagues studied 100 consecutive patients who died from gynecologic cancer between 2006 and 2009 and received care at Montefiore in the year before death.
In the first study, they defined a timely palliative care consultation as one occurring more than 30 days before death.
"The ideal timing for palliative medicine consultation is unknown; however, 30 days was chosen as the minimal exposure time because the standard metrics utilized to compare aggressive measures at the end of life included a minimum of 30 days," Dr. Nevadunsky explained.
"Overall, I was surprised to find that 49 of the 100 women actually had a palliative medicine consultation at some time or another during their care," she said.
However, the median number of days between consultation and death was 16, and only 18% of patients had a timely consultation.
Late diagnosis did not explain this finding, as less than 10% of patients received their diagnosis in the month before they died.
"The scope of this study was not inclusive to determine why this [late palliative care consultation] was happening," Dr. Nevadunsky said. Data showed that although the two groups were demographically similar, the patients who received a timely consultation were more likely to be married.
The group with timely consultations were less likely to receive aggressive end-of-life care, based on measures of eight indicators of aggressive care (0 vs. 2, P = .025).
The difference between those patients who had timely consultation and those with untimely or no consultation was greatest for the indicators of a hospital stay lasting more than 14 days in the last month of life (22% vs. 40%) and death in the acute care setting (28% vs. 45%).
In the second study, the investigators found that 29% of patients had a timely palliative care consultation, defined in this case as one occurring 14 days or more before death.
Patients with a timely consultation had lower median direct hospital inpatient costs per day in the last 30 days of life ($613 vs. $702, P = .02). They also had lower median direct hospital inpatient costs in the last 14 days overall ($0 vs. $5,106, P = .007) and on a per-day basis ($0 vs. $676, P = .007).
"The patients who had the timely consultations actually weren’t admitted to the hospital as often," Dr. Nevadunsky noted. In fact, they were half as likely to be admitted in the last 14 days (35% vs. 71%, P = .001).
"Shortcomings [of the study] include small numbers and the retrospective collection of data. Also, our study did not account for outpatient costs, including those assumed by families, or for those costs incurred by loss of time out of work by families to care for the patient," acknowledged Dr. Nevadunsky, who disclosed no relevant conflicts of interest.
AT THE ANNUAL MEETING ON WOMEN'S CANCER
Major finding: Patients receiving timely palliative care had lower scores for aggressive care at the end of life (0 vs. 2) and, in their last 14 days, had lower median direct inpatient hospital costs ($0 vs. $5,106) and were half as likely to be admitted (35% vs. 71%).
Data source: A pair of retrospective cohort studies among 100 patients who died from gynecologic cancers.
Disclosures: Dr. Nevadunsky disclosed no relevant conflicts of interest.

Lower costs documented in hospitals with palliative care programs
NEW ORLEANS – Hospitals with palliative care programs had lower treatment intensity on average at the end of life than did those without palliative care, in a national sample of 3,593 hospitals.
ICU length of stay in the last 6 months of life was 0.4 days shorter (P less than .001) and hospice length of stay 1.6 days longer (P = .013) at hospitals with palliative care versus those without.
The study strengthens claims that palliative care cuts costs, and is the first to examine the impact of palliative care in such a large national sample of hospitals, Jay R. Horton said at the annual meeting of the American Academy of Hospice and Palliative Medicine.
Prior studies focused on the effects of palliative care. Mr. Horton’s study considers outcomes for the entire older adult population in the hospital.

The researchers considered data from 3,593 hospitals with a palliative care status noted on the 2008 American Hospital Association survey. In all, 1,657 hospitals had palliative care programs and 1,936 hospitals did not. The researchers then linked the hospital data with the data from the Dartmouth Atlas on 896,097 fee-for-service Medicare patients, aged 67-99 years, with one or more chronic illnesses, who died in 2007. Patients were assigned to a hospital where they received the majority of their care in the last 2 years of life.
Covariates predictive of outcomes such as age, sex, race and comorbidities were already corrected for in the Dartmouth Atlas. Propensity scoring was used for variables predictive of outcomes or the presence of palliative care in the AHA survey such as Joint Commission Accreditation and total bed count. Finally, propensity scores were used to reweight the sample to reduce selection bias.
The effect of palliative care would very likely be stronger if the data had identified those patients who actually received palliative care, said Mr. Horton , director of the palliative care consult service at The Lilian and Benjamin Hertzberg Palliative Care Institute, Icahn School of Medicine at Mount Sinai Hospital, New York. Ongoing research uses data from the National Palliative Care Registry to better identify palliative care programs and socioeconomic factors to further reduce potential selection bias.
Treatment intensity for patients with serious illness varies widely across the country. One study showed that more than 40% of the variation is due to the supply of specialists and hospital capacity (BMJ 2002;325:961-4). Put another way, the greater the supply of physicians, the greater the utilization, even after adjustment for factors that should drive utilization, such as patient preference and disease severity.
"This supply-sensitive care, as it is sometimes called, is at the discretion of clinicians and to a certain extent at the discretion of patients, but more troubling is that much of this care may be unnecessary," said Mr. Horton.
Mr. Horton reported having no financial disclosures.
NEW ORLEANS – Hospitals with palliative care programs had lower treatment intensity on average at the end of life than did those without palliative care, in a national sample of 3,593 hospitals.
ICU length of stay in the last 6 months of life was 0.4 days shorter (P less than .001) and hospice length of stay 1.6 days longer (P = .013) at hospitals with palliative care versus those without.
The study strengthens claims that palliative care cuts costs, and is the first to examine the impact of palliative care in such a large national sample of hospitals, Jay R. Horton said at the annual meeting of the American Academy of Hospice and Palliative Medicine.
Prior studies focused on the effects of palliative care. Mr. Horton’s study considers outcomes for the entire older adult population in the hospital.
The researchers considered data from 3,593 hospitals with a palliative care status noted on the 2008 American Hospital Association survey. In all, 1,657 hospitals had palliative care programs and 1,936 hospitals did not. The researchers then linked the hospital data with the data from the Dartmouth Atlas on 896,097 fee-for-service Medicare patients, aged 67-99 years, with one or more chronic illnesses, who died in 2007. Patients were assigned to a hospital where they received the majority of their care in the last 2 years of life.
Covariates predictive of outcomes such as age, sex, race and comorbidities were already corrected for in the Dartmouth Atlas. Propensity scoring was used for variables predictive of outcomes or the presence of palliative care in the AHA survey such as Joint Commission Accreditation and total bed count. Finally, propensity scores were used to reweight the sample to reduce selection bias.
The effect of palliative care would very likely be stronger if the data had identified those patients who actually received palliative care, said Mr. Horton , director of the palliative care consult service at The Lilian and Benjamin Hertzberg Palliative Care Institute, Icahn School of Medicine at Mount Sinai Hospital, New York. Ongoing research uses data from the National Palliative Care Registry to better identify palliative care programs and socioeconomic factors to further reduce potential selection bias.
Treatment intensity for patients with serious illness varies widely across the country. One study showed that more than 40% of the variation is due to the supply of specialists and hospital capacity (BMJ 2002;325:961-4). Put another way, the greater the supply of physicians, the greater the utilization, even after adjustment for factors that should drive utilization, such as patient preference and disease severity.
"This supply-sensitive care, as it is sometimes called, is at the discretion of clinicians and to a certain extent at the discretion of patients, but more troubling is that much of this care may be unnecessary," said Mr. Horton.
Mr. Horton reported having no financial disclosures.
NEW ORLEANS – Hospitals with palliative care programs had lower treatment intensity on average at the end of life than did those without palliative care, in a national sample of 3,593 hospitals.
ICU length of stay in the last 6 months of life was 0.4 days shorter (P less than .001) and hospice length of stay 1.6 days longer (P = .013) at hospitals with palliative care versus those without.
The study strengthens claims that palliative care cuts costs, and is the first to examine the impact of palliative care in such a large national sample of hospitals, Jay R. Horton said at the annual meeting of the American Academy of Hospice and Palliative Medicine.
Prior studies focused on the effects of palliative care. Mr. Horton’s study considers outcomes for the entire older adult population in the hospital.
The researchers considered data from 3,593 hospitals with a palliative care status noted on the 2008 American Hospital Association survey. In all, 1,657 hospitals had palliative care programs and 1,936 hospitals did not. The researchers then linked the hospital data with the data from the Dartmouth Atlas on 896,097 fee-for-service Medicare patients, aged 67-99 years, with one or more chronic illnesses, who died in 2007. Patients were assigned to a hospital where they received the majority of their care in the last 2 years of life.
Covariates predictive of outcomes such as age, sex, race and comorbidities were already corrected for in the Dartmouth Atlas. Propensity scoring was used for variables predictive of outcomes or the presence of palliative care in the AHA survey such as Joint Commission Accreditation and total bed count. Finally, propensity scores were used to reweight the sample to reduce selection bias.
The effect of palliative care would very likely be stronger if the data had identified those patients who actually received palliative care, said Mr. Horton , director of the palliative care consult service at The Lilian and Benjamin Hertzberg Palliative Care Institute, Icahn School of Medicine at Mount Sinai Hospital, New York. Ongoing research uses data from the National Palliative Care Registry to better identify palliative care programs and socioeconomic factors to further reduce potential selection bias.
Treatment intensity for patients with serious illness varies widely across the country. One study showed that more than 40% of the variation is due to the supply of specialists and hospital capacity (BMJ 2002;325:961-4). Put another way, the greater the supply of physicians, the greater the utilization, even after adjustment for factors that should drive utilization, such as patient preference and disease severity.
"This supply-sensitive care, as it is sometimes called, is at the discretion of clinicians and to a certain extent at the discretion of patients, but more troubling is that much of this care may be unnecessary," said Mr. Horton.
Mr. Horton reported having no financial disclosures.
AT THE AAHPM ANNUAL ASSEMBLY
Major finding: ICU length of stay in the last 6 months of life was 0.4 days shorter and hospice length of stay was 1.6 days longer at hospitals with palliative care (P less than .001, P = .013).
Data source: A retrospective analysis of 3,593 hospitals with palliative care data.
Disclosures: Mr. Horton reported having no financial disclosures.

SPIKES protocol offers guidance for 'active listening' when talking to cancer patients
Mr. William Goeren provides personal insight and practical tips for communicating with cancer patients using the SPIKES method. Mr. Goeren is a recent cancer survivor and director of clinical services at CancerCare, a national nonprofit organization that provides counseling, educational programs, and practical and financial assistance to people affected by cancer.
The Oncology Practice Summit was the 8th annual meeting of Community Oncology, the journal of clinical issues in community practice. The conference was hosted this year by Community Oncology as well as The Journal of Supportive Oncology and The Oncology Report.
Mr. William Goeren provides personal insight and practical tips for communicating with cancer patients using the SPIKES method. Mr. Goeren is a recent cancer survivor and director of clinical services at CancerCare, a national nonprofit organization that provides counseling, educational programs, and practical and financial assistance to people affected by cancer.
The Oncology Practice Summit was the 8th annual meeting of Community Oncology, the journal of clinical issues in community practice. The conference was hosted this year by Community Oncology as well as The Journal of Supportive Oncology and The Oncology Report.
Mr. William Goeren provides personal insight and practical tips for communicating with cancer patients using the SPIKES method. Mr. Goeren is a recent cancer survivor and director of clinical services at CancerCare, a national nonprofit organization that provides counseling, educational programs, and practical and financial assistance to people affected by cancer.
The Oncology Practice Summit was the 8th annual meeting of Community Oncology, the journal of clinical issues in community practice. The conference was hosted this year by Community Oncology as well as The Journal of Supportive Oncology and The Oncology Report.
Need is dire for palliative care in disaster planning
NEW ORLEANS – In a room filled with roughly 2,000 health care providers, just a dozen or so hands went up when the audience was asked whether their hospital or state had a "crisis standards of care" protocol.
"That’s actually very common, because the problem with some of these protocols is that very few people know that they exist, which makes it hard to implement them in a time of crisis," Dr. Sheri Fink said during a disaster preparedness plenary session at the annual meeting of the American Academy of Hospice and Palliative Medicine.

Dr. Fink and other experts made the case for a wider discussion of the often agonizing decisions health care providers face when natural disasters disrupt delivery of care. For example: After "superstorm" Hurricane Sandy last fall, providers at one hospital were warned of the possibility they might be faced with having just six functioning power outlets for 56 ICU patients. No one should have to make that kind of call alone, the experts contend.
The Institute of Medicine (IOM) issued a 2009 report in the wake of Hurricane Katrina defining crisis standards of care (CSC), and followed it up last year with a series of templates to guide those responsible for CSC planning and implementation.
Many CSC protocols call for withdrawing patients from scarce resources, and offer guidance on how to score patients for resource allocation and evacuation. Very little research is available, however, to support these triage protocols, and most fail to discuss the practical removal of care, according to Dr. Fink, a senior fellow at the Harvard Humanitarian Initiative who earned a 2010 Pulitzer prize for investigative reporting on the deadly choices made after Katrina at Memorial Medical Center in New Orleans.
"All of you here who have engaged in end-of-life discussions, who’ve dealt with withdrawing patients from ventilators where the care is futile, know just how hard it is to help the family wrap their mind around that," she said. "Just imagine being in a disaster when you have to do that, and there’s a reasonable chance that the patient could survive."
In New Orleans, the sickest of the sick with a DNR (do not resuscitate) order were taken out last from Memorial Hospital – but no one asked them or their families, thus violating patient autonomy. Some families who found out about the decision begged to have the DNR rescinded and their loved ones moved. After Sandy, some hospitals planned to evacuate the sickest; but after triaging patients and explaining the scope of the disaster to families, they found that many families let other patients go first, Dr. Fink said.
"DNR orders aren’t necessarily a great triage," she said. "They tell you about the patient’s foresight about dying, not about their ability to survive."
Hospitals understand the need to have redundant communication systems and off-site drug supplies, but they may not think about such practical issues as the weight of their patients, said Marianne Matzo, Ph.D., chair of palliative care nursing at the University of Oklahoma Health Sciences Center College of Nursing in Oklahoma City, and a member of the IOM committee that crafted the CSC templates.
During Katrina, emergency cots broke under the weight of obese patients, while helicopter pilots told hospital staff they could evacuate two obese patients or four normal-weight patients. After Sandy, two obese patients had to be sheltered in place at Bellevue Hospital in New York because they were too heavy to be transported out once the electricity went out.
In the face of America’s obesity epidemic, a first step in triage may be to move heavier patients to lower floors, before the elevators stop working, she said.
The IOM has convened a new committee to look at what triggers the activation of CSC protocols. During Sandy, the trigger was the same, but the responses varied. The Veterans Health Administration evacuated its patients before the storm, Bellevue evacuated patients after the storm and, unfortunately, New York University evacuated patients during the storm, Dr. Matzo said.

Both women pointed to the need for greater discourse and education among physicians and the public about disaster planning, response, and recovery.
Vital education for all first responders and providers should include how to access medication stockpiles, how to titrate opiates for patients in pain and near death, how to use medications to manage symptoms so an individual experiences a comfortable death, and basics in psychosocial counseling and support for peer-to-peer and provider/patient services under mass casualty event scenarios, Dr. Matzo said.
When disaster planners make decisions about which patients will and will not get access to lifesaving resources without the help of palliative care experts, Dr. Fink said, "it’s just sort of assumed that the default is that everyone else will get palliated."
However, the lesson learned from New Orleans and other recent U.S. disasters is that few actually do.
Dr. Fink and Dr. Matzo reported no relevant disclosures.
It seems that there are two broad categories of disasters: mass-casualty events (in which our existing health care infrastructure is not compromised) and natural disasters (in which the infrastructure as well as safety of patients, health care providers and their families may be at risk).
In both cases, we are learning from each successive event (as demonstrated by the Dr. Fink reporting and by efforts to standardize the approach to ethical dilemmas, triage, etc). Having been at war for the last 10 or so years has improved coordination of response at the community and health care system level.
During a disaster, we can really only follow our training and care for the patients in our institutions. Going forward, it is imperative that hospitalists be involved in disaster-planning efforts in their respective institutions.
Hospitalists may be asked to help determine when and if to deploy scarce resources, and as such should advocate for institutional or perhaps statewide standards. This keeps the onus for making these decisions off individual physicians. The Institute of Medicine's initial efforts at producing such standards can be found at tinyurl.com/IOMCrisis.
Leigh Fredholm, M.D., is a codirector of Seton Health Palliative Care, part of the University of Texas Southwestern Residency Programs in Austin. She is coauthor of the Palliatively Speaking blog for Hospitalist News.
It seems that there are two broad categories of disasters: mass-casualty events (in which our existing health care infrastructure is not compromised) and natural disasters (in which the infrastructure as well as safety of patients, health care providers and their families may be at risk).
In both cases, we are learning from each successive event (as demonstrated by the Dr. Fink reporting and by efforts to standardize the approach to ethical dilemmas, triage, etc). Having been at war for the last 10 or so years has improved coordination of response at the community and health care system level.
During a disaster, we can really only follow our training and care for the patients in our institutions. Going forward, it is imperative that hospitalists be involved in disaster-planning efforts in their respective institutions.
Hospitalists may be asked to help determine when and if to deploy scarce resources, and as such should advocate for institutional or perhaps statewide standards. This keeps the onus for making these decisions off individual physicians. The Institute of Medicine's initial efforts at producing such standards can be found at tinyurl.com/IOMCrisis.
Leigh Fredholm, M.D., is a codirector of Seton Health Palliative Care, part of the University of Texas Southwestern Residency Programs in Austin. She is coauthor of the Palliatively Speaking blog for Hospitalist News.
It seems that there are two broad categories of disasters: mass-casualty events (in which our existing health care infrastructure is not compromised) and natural disasters (in which the infrastructure as well as safety of patients, health care providers and their families may be at risk).
In both cases, we are learning from each successive event (as demonstrated by the Dr. Fink reporting and by efforts to standardize the approach to ethical dilemmas, triage, etc). Having been at war for the last 10 or so years has improved coordination of response at the community and health care system level.
During a disaster, we can really only follow our training and care for the patients in our institutions. Going forward, it is imperative that hospitalists be involved in disaster-planning efforts in their respective institutions.
Hospitalists may be asked to help determine when and if to deploy scarce resources, and as such should advocate for institutional or perhaps statewide standards. This keeps the onus for making these decisions off individual physicians. The Institute of Medicine's initial efforts at producing such standards can be found at tinyurl.com/IOMCrisis.
Leigh Fredholm, M.D., is a codirector of Seton Health Palliative Care, part of the University of Texas Southwestern Residency Programs in Austin. She is coauthor of the Palliatively Speaking blog for Hospitalist News.
NEW ORLEANS – In a room filled with roughly 2,000 health care providers, just a dozen or so hands went up when the audience was asked whether their hospital or state had a "crisis standards of care" protocol.
"That’s actually very common, because the problem with some of these protocols is that very few people know that they exist, which makes it hard to implement them in a time of crisis," Dr. Sheri Fink said during a disaster preparedness plenary session at the annual meeting of the American Academy of Hospice and Palliative Medicine.
Dr. Fink and other experts made the case for a wider discussion of the often agonizing decisions health care providers face when natural disasters disrupt delivery of care. For example: After "superstorm" Hurricane Sandy last fall, providers at one hospital were warned of the possibility they might be faced with having just six functioning power outlets for 56 ICU patients. No one should have to make that kind of call alone, the experts contend.
The Institute of Medicine (IOM) issued a 2009 report in the wake of Hurricane Katrina defining crisis standards of care (CSC), and followed it up last year with a series of templates to guide those responsible for CSC planning and implementation.
Many CSC protocols call for withdrawing patients from scarce resources, and offer guidance on how to score patients for resource allocation and evacuation. Very little research is available, however, to support these triage protocols, and most fail to discuss the practical removal of care, according to Dr. Fink, a senior fellow at the Harvard Humanitarian Initiative who earned a 2010 Pulitzer prize for investigative reporting on the deadly choices made after Katrina at Memorial Medical Center in New Orleans.
"All of you here who have engaged in end-of-life discussions, who’ve dealt with withdrawing patients from ventilators where the care is futile, know just how hard it is to help the family wrap their mind around that," she said. "Just imagine being in a disaster when you have to do that, and there’s a reasonable chance that the patient could survive."
In New Orleans, the sickest of the sick with a DNR (do not resuscitate) order were taken out last from Memorial Hospital – but no one asked them or their families, thus violating patient autonomy. Some families who found out about the decision begged to have the DNR rescinded and their loved ones moved. After Sandy, some hospitals planned to evacuate the sickest; but after triaging patients and explaining the scope of the disaster to families, they found that many families let other patients go first, Dr. Fink said.
"DNR orders aren’t necessarily a great triage," she said. "They tell you about the patient’s foresight about dying, not about their ability to survive."
Hospitals understand the need to have redundant communication systems and off-site drug supplies, but they may not think about such practical issues as the weight of their patients, said Marianne Matzo, Ph.D., chair of palliative care nursing at the University of Oklahoma Health Sciences Center College of Nursing in Oklahoma City, and a member of the IOM committee that crafted the CSC templates.
During Katrina, emergency cots broke under the weight of obese patients, while helicopter pilots told hospital staff they could evacuate two obese patients or four normal-weight patients. After Sandy, two obese patients had to be sheltered in place at Bellevue Hospital in New York because they were too heavy to be transported out once the electricity went out.
In the face of America’s obesity epidemic, a first step in triage may be to move heavier patients to lower floors, before the elevators stop working, she said.
The IOM has convened a new committee to look at what triggers the activation of CSC protocols. During Sandy, the trigger was the same, but the responses varied. The Veterans Health Administration evacuated its patients before the storm, Bellevue evacuated patients after the storm and, unfortunately, New York University evacuated patients during the storm, Dr. Matzo said.
Both women pointed to the need for greater discourse and education among physicians and the public about disaster planning, response, and recovery.
Vital education for all first responders and providers should include how to access medication stockpiles, how to titrate opiates for patients in pain and near death, how to use medications to manage symptoms so an individual experiences a comfortable death, and basics in psychosocial counseling and support for peer-to-peer and provider/patient services under mass casualty event scenarios, Dr. Matzo said.
When disaster planners make decisions about which patients will and will not get access to lifesaving resources without the help of palliative care experts, Dr. Fink said, "it’s just sort of assumed that the default is that everyone else will get palliated."
However, the lesson learned from New Orleans and other recent U.S. disasters is that few actually do.
Dr. Fink and Dr. Matzo reported no relevant disclosures.
NEW ORLEANS – In a room filled with roughly 2,000 health care providers, just a dozen or so hands went up when the audience was asked whether their hospital or state had a "crisis standards of care" protocol.
"That’s actually very common, because the problem with some of these protocols is that very few people know that they exist, which makes it hard to implement them in a time of crisis," Dr. Sheri Fink said during a disaster preparedness plenary session at the annual meeting of the American Academy of Hospice and Palliative Medicine.
Dr. Fink and other experts made the case for a wider discussion of the often agonizing decisions health care providers face when natural disasters disrupt delivery of care. For example: After "superstorm" Hurricane Sandy last fall, providers at one hospital were warned of the possibility they might be faced with having just six functioning power outlets for 56 ICU patients. No one should have to make that kind of call alone, the experts contend.
The Institute of Medicine (IOM) issued a 2009 report in the wake of Hurricane Katrina defining crisis standards of care (CSC), and followed it up last year with a series of templates to guide those responsible for CSC planning and implementation.
Many CSC protocols call for withdrawing patients from scarce resources, and offer guidance on how to score patients for resource allocation and evacuation. Very little research is available, however, to support these triage protocols, and most fail to discuss the practical removal of care, according to Dr. Fink, a senior fellow at the Harvard Humanitarian Initiative who earned a 2010 Pulitzer prize for investigative reporting on the deadly choices made after Katrina at Memorial Medical Center in New Orleans.
"All of you here who have engaged in end-of-life discussions, who’ve dealt with withdrawing patients from ventilators where the care is futile, know just how hard it is to help the family wrap their mind around that," she said. "Just imagine being in a disaster when you have to do that, and there’s a reasonable chance that the patient could survive."
In New Orleans, the sickest of the sick with a DNR (do not resuscitate) order were taken out last from Memorial Hospital – but no one asked them or their families, thus violating patient autonomy. Some families who found out about the decision begged to have the DNR rescinded and their loved ones moved. After Sandy, some hospitals planned to evacuate the sickest; but after triaging patients and explaining the scope of the disaster to families, they found that many families let other patients go first, Dr. Fink said.
"DNR orders aren’t necessarily a great triage," she said. "They tell you about the patient’s foresight about dying, not about their ability to survive."
Hospitals understand the need to have redundant communication systems and off-site drug supplies, but they may not think about such practical issues as the weight of their patients, said Marianne Matzo, Ph.D., chair of palliative care nursing at the University of Oklahoma Health Sciences Center College of Nursing in Oklahoma City, and a member of the IOM committee that crafted the CSC templates.
During Katrina, emergency cots broke under the weight of obese patients, while helicopter pilots told hospital staff they could evacuate two obese patients or four normal-weight patients. After Sandy, two obese patients had to be sheltered in place at Bellevue Hospital in New York because they were too heavy to be transported out once the electricity went out.
In the face of America’s obesity epidemic, a first step in triage may be to move heavier patients to lower floors, before the elevators stop working, she said.
The IOM has convened a new committee to look at what triggers the activation of CSC protocols. During Sandy, the trigger was the same, but the responses varied. The Veterans Health Administration evacuated its patients before the storm, Bellevue evacuated patients after the storm and, unfortunately, New York University evacuated patients during the storm, Dr. Matzo said.
Both women pointed to the need for greater discourse and education among physicians and the public about disaster planning, response, and recovery.
Vital education for all first responders and providers should include how to access medication stockpiles, how to titrate opiates for patients in pain and near death, how to use medications to manage symptoms so an individual experiences a comfortable death, and basics in psychosocial counseling and support for peer-to-peer and provider/patient services under mass casualty event scenarios, Dr. Matzo said.
When disaster planners make decisions about which patients will and will not get access to lifesaving resources without the help of palliative care experts, Dr. Fink said, "it’s just sort of assumed that the default is that everyone else will get palliated."
However, the lesson learned from New Orleans and other recent U.S. disasters is that few actually do.
Dr. Fink and Dr. Matzo reported no relevant disclosures.
AT THE AAHPM ANNUAL ASSEMBLY

Dexamethasone eases end-of-life cancer-related fatigue
NEW ORLEANS – Dexamethasone was more effective than was placebo in relieving cancer-related fatigue in a double-blind randomized trial of patients with advanced cancer.
After 14 days of treatment, scores on the Functional Assessment of Chronic Illness Therapy (FACIT) fatigue subscale improved by nearly 6 points in the dexamethasone group (9.0 vs. 3.1; P = .008).

"[Treatment] duration is very important in our patient population because when they are referred to us, it’s very late. They typically have a survival of just 28 to 7 days," Dr. Sriram Yennu said at the annual meeting of the American Academy of Hospice and Palliative Medicine.
Although 20%-50% of palliative care patients receive some form of corticosteroid, no steroid study to date has used cancer-related fatigue (CRF) as a primary outcome or assessed CRF with a validated outcome measure, he said. Fatigue is ubiquitous, however, contributing up to one-third of symptom distress in patients with advanced cancer.
The study enrolled 132 outpatients with a life expectancy of at least 4 weeks with three or more cancer-related symptoms (fatigue, pain, nausea, loss of appetite, depression, anxiety, or sleep disturbance), and randomly assigned them to oral dexamethasone 4 mg twice daily or placebo for 14 days.
The most common diagnosis was head and neck/lung cancer in 45 patients, followed by gastrointestinal cancer in 39, breast cancer in 13, and genitourinary in 10. Median patient age was 60; 81 patients were white, and the average FACIT fatigue score was 19.6, where 52 denotes no fatigue and 0 is severe fatigue.
Among 84 evaluable patients, total scores on FACIT favored the dexamethasone group (18.16 vs. 7.87; P = .03), as did scores on its physical subscale (5.25 vs. 1.32; P = .002), said Dr. Yennu of the department of palliative care and rehabilitation medicine, University of Texas MD Anderson Cancer Center, Houston.
Scores on the physical domain of the Edmonton Symptom Assessment Scale (ESAS) were better in the dexamethasone group than in the placebo group (–10.15 vs. –5.39; P = .04), according to the study, which earned Dr. Yennu a young investigator award.
Notably, scores were similar between the dexamethasone and placebo groups on the emotional subscale of FACIT (1.85 vs. 1.18; P = .49) and the ESAS psychological subscale (–1.48 vs. –2.08; P = .76). The emotional domain of the FACIT-F is measured by six items using a 0-4 scale where 0 is "not at all" and 4 includes statements like "I am losing hope in the fight against my illness." The finding suggests that the improvement in fatigue was likely not just a euphoric effect, as observed before in other steroid trials, Dr. Yennu said.
He expressed concern that corticosteroid use would increase toxicity, particularly insomnia, but no significant differences were observed between the dexamethasone and placebo groups regarding insomnia (3 vs. 4), overall adverse events (41 vs. 44) or serious adverse events (17 vs. 11).
Larger, long-term safety and efficacy studies are needed to address steroid dose and duration, and whether dexamethasone should be coupled with interventions targeting the psychological domain, he said. A 3-point difference in the FACIT is considered clinically important, but research in press in the Journal of Clinical Oncology, by Dr. Yennu and his colleagues, suggests a 10-point difference is more meaningful.
The American Cancer Society supported the study. Dr. Yennu reported having no financial disclosures.
NEW ORLEANS – Dexamethasone was more effective than was placebo in relieving cancer-related fatigue in a double-blind randomized trial of patients with advanced cancer.
After 14 days of treatment, scores on the Functional Assessment of Chronic Illness Therapy (FACIT) fatigue subscale improved by nearly 6 points in the dexamethasone group (9.0 vs. 3.1; P = .008).
"[Treatment] duration is very important in our patient population because when they are referred to us, it’s very late. They typically have a survival of just 28 to 7 days," Dr. Sriram Yennu said at the annual meeting of the American Academy of Hospice and Palliative Medicine.
Although 20%-50% of palliative care patients receive some form of corticosteroid, no steroid study to date has used cancer-related fatigue (CRF) as a primary outcome or assessed CRF with a validated outcome measure, he said. Fatigue is ubiquitous, however, contributing up to one-third of symptom distress in patients with advanced cancer.
The study enrolled 132 outpatients with a life expectancy of at least 4 weeks with three or more cancer-related symptoms (fatigue, pain, nausea, loss of appetite, depression, anxiety, or sleep disturbance), and randomly assigned them to oral dexamethasone 4 mg twice daily or placebo for 14 days.
The most common diagnosis was head and neck/lung cancer in 45 patients, followed by gastrointestinal cancer in 39, breast cancer in 13, and genitourinary in 10. Median patient age was 60; 81 patients were white, and the average FACIT fatigue score was 19.6, where 52 denotes no fatigue and 0 is severe fatigue.
Among 84 evaluable patients, total scores on FACIT favored the dexamethasone group (18.16 vs. 7.87; P = .03), as did scores on its physical subscale (5.25 vs. 1.32; P = .002), said Dr. Yennu of the department of palliative care and rehabilitation medicine, University of Texas MD Anderson Cancer Center, Houston.
Scores on the physical domain of the Edmonton Symptom Assessment Scale (ESAS) were better in the dexamethasone group than in the placebo group (–10.15 vs. –5.39; P = .04), according to the study, which earned Dr. Yennu a young investigator award.
Notably, scores were similar between the dexamethasone and placebo groups on the emotional subscale of FACIT (1.85 vs. 1.18; P = .49) and the ESAS psychological subscale (–1.48 vs. –2.08; P = .76). The emotional domain of the FACIT-F is measured by six items using a 0-4 scale where 0 is "not at all" and 4 includes statements like "I am losing hope in the fight against my illness." The finding suggests that the improvement in fatigue was likely not just a euphoric effect, as observed before in other steroid trials, Dr. Yennu said.
He expressed concern that corticosteroid use would increase toxicity, particularly insomnia, but no significant differences were observed between the dexamethasone and placebo groups regarding insomnia (3 vs. 4), overall adverse events (41 vs. 44) or serious adverse events (17 vs. 11).
Larger, long-term safety and efficacy studies are needed to address steroid dose and duration, and whether dexamethasone should be coupled with interventions targeting the psychological domain, he said. A 3-point difference in the FACIT is considered clinically important, but research in press in the Journal of Clinical Oncology, by Dr. Yennu and his colleagues, suggests a 10-point difference is more meaningful.
The American Cancer Society supported the study. Dr. Yennu reported having no financial disclosures.
NEW ORLEANS – Dexamethasone was more effective than was placebo in relieving cancer-related fatigue in a double-blind randomized trial of patients with advanced cancer.
After 14 days of treatment, scores on the Functional Assessment of Chronic Illness Therapy (FACIT) fatigue subscale improved by nearly 6 points in the dexamethasone group (9.0 vs. 3.1; P = .008).
"[Treatment] duration is very important in our patient population because when they are referred to us, it’s very late. They typically have a survival of just 28 to 7 days," Dr. Sriram Yennu said at the annual meeting of the American Academy of Hospice and Palliative Medicine.
Although 20%-50% of palliative care patients receive some form of corticosteroid, no steroid study to date has used cancer-related fatigue (CRF) as a primary outcome or assessed CRF with a validated outcome measure, he said. Fatigue is ubiquitous, however, contributing up to one-third of symptom distress in patients with advanced cancer.
The study enrolled 132 outpatients with a life expectancy of at least 4 weeks with three or more cancer-related symptoms (fatigue, pain, nausea, loss of appetite, depression, anxiety, or sleep disturbance), and randomly assigned them to oral dexamethasone 4 mg twice daily or placebo for 14 days.
The most common diagnosis was head and neck/lung cancer in 45 patients, followed by gastrointestinal cancer in 39, breast cancer in 13, and genitourinary in 10. Median patient age was 60; 81 patients were white, and the average FACIT fatigue score was 19.6, where 52 denotes no fatigue and 0 is severe fatigue.
Among 84 evaluable patients, total scores on FACIT favored the dexamethasone group (18.16 vs. 7.87; P = .03), as did scores on its physical subscale (5.25 vs. 1.32; P = .002), said Dr. Yennu of the department of palliative care and rehabilitation medicine, University of Texas MD Anderson Cancer Center, Houston.
Scores on the physical domain of the Edmonton Symptom Assessment Scale (ESAS) were better in the dexamethasone group than in the placebo group (–10.15 vs. –5.39; P = .04), according to the study, which earned Dr. Yennu a young investigator award.
Notably, scores were similar between the dexamethasone and placebo groups on the emotional subscale of FACIT (1.85 vs. 1.18; P = .49) and the ESAS psychological subscale (–1.48 vs. –2.08; P = .76). The emotional domain of the FACIT-F is measured by six items using a 0-4 scale where 0 is "not at all" and 4 includes statements like "I am losing hope in the fight against my illness." The finding suggests that the improvement in fatigue was likely not just a euphoric effect, as observed before in other steroid trials, Dr. Yennu said.
He expressed concern that corticosteroid use would increase toxicity, particularly insomnia, but no significant differences were observed between the dexamethasone and placebo groups regarding insomnia (3 vs. 4), overall adverse events (41 vs. 44) or serious adverse events (17 vs. 11).
Larger, long-term safety and efficacy studies are needed to address steroid dose and duration, and whether dexamethasone should be coupled with interventions targeting the psychological domain, he said. A 3-point difference in the FACIT is considered clinically important, but research in press in the Journal of Clinical Oncology, by Dr. Yennu and his colleagues, suggests a 10-point difference is more meaningful.
The American Cancer Society supported the study. Dr. Yennu reported having no financial disclosures.
AT THE AAHPM ANNUAL ASSEMBLY
Major finding: Scores on the FACIT fatigue subscale improved by an average of 6 points in patients treated with dexamethasone, compared with 3 points in patients treated with placebo.
Data source: Double-blind, randomized trial of 132 patients with advanced cancer.
Disclosures: The American Cancer Society supported the study. Dr. Yennu reported having no financial disclosures.

Cancer patients embrace pioneer assisted-suicide program
The Death with Dignity program, a pioneering program that includes medically assisted suicide for competent, terminally ill adults treated at a comprehensive cancer center in Seattle, has been well accepted by patients, families, and clinicians, according to a report published online April 11 in the New England Journal of Medicine.
The report details the experience in 2009-2011 with the Death with Dignity program at the Seattle Cancer Care Alliance, which serves all of the Pacific Northwest. The program, "designed to adhere to legal regulations, maintain safety, and ensure the quality of patient care," allows patients with a life expectancy of 6 months or less because of a diagnosed medical condition (usually cancer) to request and self-administer lethal medication prescribed by a physician.
This experience may help to inform efforts to introduce similar programs in other states. At present, Hawaii, Pennsylvania, and Vermont are all considering pertinent legislation, said Dr. Elizabeth Trice Loggers of the Fred Hutchinson Cancer Research Center, Seattle, and her associates.
The program’s policy – written by the Seattle Cancer Care Alliance’s medical director and approved by a majority of the medical executive committee members, as with any clinical policy – requires that patients request information about medically assisted suicide from their physicians, or that these clinicians raise the topic, to be considered for referral. Participation is entirely voluntary for medical staff and faculty members.
Every patient who is a potential participant is first assigned an advocate, a licensed social worker employed by the Alliance, who assists patients, family members, pharmacists, and physicians throughout a multistep process of participating. This advocate also tracks compliance with required documentation for the state Department of Health.
The advocate, as well as the attending physician, ensures that all potential participants are aware of alternatives to medically assisted suicide, such as palliative care and hospice care. The patient’s terminal status is verified, and if the attending physician doesn’t wish to participate, a prescribing physician and a consulting physician are chosen from a group of willing providers.
Psychosocial and psychological assessments are required to ensure the patient’s competence to make the choice of assisted suicide and to identify any depression, which would make the patient ineligible to participate. The patient’s preferences for interventions and health-care directives are documented. Grief support, legacy support, and bereavement support are offered through periodic calls and visits.
The patient and his or her family meet with the prescribing clinician and the consulting clinician to review the diagnosis, prognosis, treatment alternatives, and end-of-life issues. After a mandatory waiting period of 15 days, a written prescription is then sent to the pharmacy, and the pharmacist schedules another appointment with the patient and family to discuss preparation of the drug(s), potential side effects, and the concomitant use of prescription antiemetics.
Patients are then free to fill the prescription or not and to take the drug(s) or not, as they wish.
To date, 114 patients have inquired about the Death with Dignity program, and 44 (38%) either did not pursue the matter further or were deemed ineligible to participate.
Thirty patients (26%) have made a first oral request to initiate the process but either decided not to participate or died before completing the process. Forty patients (35% of those who made an initial inquiry) received prescriptions for lethal medication, and all 40 have died. Twenty-four chose to die by ingesting the medication (secobarbital).
Thus, only 21% of the participants actually used assisted suicide. Death with Dignity participants accounted for 2.4% of all annual deaths among patients at the Seattle Cancer Center Alliance.*
The reasons patients gave most often for participating in the assisted-suicide program were loss of autonomy (97%), inability to engage in enjoyable activities (89%), and loss of dignity (75%).
"We have not received any complaints from family members or caregivers regarding our process or the manner of death. Anecdotally, families describe the death as peaceful (even when death has taken longer than the average of approximately 35 minutes)," Dr. Loggers and her associates wrote physician (N. Engl. J. Med. 2013 April 11;368:1417-24 [doi:10.1056/NEJMsa1213398]).
"Both patients and families frequently express gratitude after the patient received the prescription, regardless of whether it is ever filled or ingested, typically referencing an important sense of control in an uncertain situation," they noted.
Opponents of medically assisted suicide have argued that legislation would disproportionately affect vulnerable populations, such as racial or ethnic minorities, low-income groups, or cognitively impaired patients. The Death with Dignity experience refutes this argument, as most participants were white, male, and well educated, the investigators said.
There have been no unexpected complications among patients who chose assisted suicide, but one patient remained alive for a day after taking the medication. This protracted dying process caused distress to both the family members and the clinicians involved. Similar cases have been reported previously, they added.
*Correction, 4/12/13: An earlier version of this story described findings from a study (citation) in the New England Journal of Medicine. That study misstated the percentage of Death with Dignity patients among all annual patient deaths reported at the Seattle Cancer Center Alliance.
The Death with Dignity program, a pioneering program that includes medically assisted suicide for competent, terminally ill adults treated at a comprehensive cancer center in Seattle, has been well accepted by patients, families, and clinicians, according to a report published online April 11 in the New England Journal of Medicine.
The report details the experience in 2009-2011 with the Death with Dignity program at the Seattle Cancer Care Alliance, which serves all of the Pacific Northwest. The program, "designed to adhere to legal regulations, maintain safety, and ensure the quality of patient care," allows patients with a life expectancy of 6 months or less because of a diagnosed medical condition (usually cancer) to request and self-administer lethal medication prescribed by a physician.
This experience may help to inform efforts to introduce similar programs in other states. At present, Hawaii, Pennsylvania, and Vermont are all considering pertinent legislation, said Dr. Elizabeth Trice Loggers of the Fred Hutchinson Cancer Research Center, Seattle, and her associates.
The program’s policy – written by the Seattle Cancer Care Alliance’s medical director and approved by a majority of the medical executive committee members, as with any clinical policy – requires that patients request information about medically assisted suicide from their physicians, or that these clinicians raise the topic, to be considered for referral. Participation is entirely voluntary for medical staff and faculty members.
Every patient who is a potential participant is first assigned an advocate, a licensed social worker employed by the Alliance, who assists patients, family members, pharmacists, and physicians throughout a multistep process of participating. This advocate also tracks compliance with required documentation for the state Department of Health.
The advocate, as well as the attending physician, ensures that all potential participants are aware of alternatives to medically assisted suicide, such as palliative care and hospice care. The patient’s terminal status is verified, and if the attending physician doesn’t wish to participate, a prescribing physician and a consulting physician are chosen from a group of willing providers.
Psychosocial and psychological assessments are required to ensure the patient’s competence to make the choice of assisted suicide and to identify any depression, which would make the patient ineligible to participate. The patient’s preferences for interventions and health-care directives are documented. Grief support, legacy support, and bereavement support are offered through periodic calls and visits.
The patient and his or her family meet with the prescribing clinician and the consulting clinician to review the diagnosis, prognosis, treatment alternatives, and end-of-life issues. After a mandatory waiting period of 15 days, a written prescription is then sent to the pharmacy, and the pharmacist schedules another appointment with the patient and family to discuss preparation of the drug(s), potential side effects, and the concomitant use of prescription antiemetics.
Patients are then free to fill the prescription or not and to take the drug(s) or not, as they wish.
To date, 114 patients have inquired about the Death with Dignity program, and 44 (38%) either did not pursue the matter further or were deemed ineligible to participate.
Thirty patients (26%) have made a first oral request to initiate the process but either decided not to participate or died before completing the process. Forty patients (35% of those who made an initial inquiry) received prescriptions for lethal medication, and all 40 have died. Twenty-four chose to die by ingesting the medication (secobarbital).
Thus, only 21% of the participants actually used assisted suicide. Death with Dignity participants accounted for 2.4% of all annual deaths among patients at the Seattle Cancer Center Alliance.*
The reasons patients gave most often for participating in the assisted-suicide program were loss of autonomy (97%), inability to engage in enjoyable activities (89%), and loss of dignity (75%).
"We have not received any complaints from family members or caregivers regarding our process or the manner of death. Anecdotally, families describe the death as peaceful (even when death has taken longer than the average of approximately 35 minutes)," Dr. Loggers and her associates wrote physician (N. Engl. J. Med. 2013 April 11;368:1417-24 [doi:10.1056/NEJMsa1213398]).
"Both patients and families frequently express gratitude after the patient received the prescription, regardless of whether it is ever filled or ingested, typically referencing an important sense of control in an uncertain situation," they noted.
Opponents of medically assisted suicide have argued that legislation would disproportionately affect vulnerable populations, such as racial or ethnic minorities, low-income groups, or cognitively impaired patients. The Death with Dignity experience refutes this argument, as most participants were white, male, and well educated, the investigators said.
There have been no unexpected complications among patients who chose assisted suicide, but one patient remained alive for a day after taking the medication. This protracted dying process caused distress to both the family members and the clinicians involved. Similar cases have been reported previously, they added.
*Correction, 4/12/13: An earlier version of this story described findings from a study (citation) in the New England Journal of Medicine. That study misstated the percentage of Death with Dignity patients among all annual patient deaths reported at the Seattle Cancer Center Alliance.
The Death with Dignity program, a pioneering program that includes medically assisted suicide for competent, terminally ill adults treated at a comprehensive cancer center in Seattle, has been well accepted by patients, families, and clinicians, according to a report published online April 11 in the New England Journal of Medicine.
The report details the experience in 2009-2011 with the Death with Dignity program at the Seattle Cancer Care Alliance, which serves all of the Pacific Northwest. The program, "designed to adhere to legal regulations, maintain safety, and ensure the quality of patient care," allows patients with a life expectancy of 6 months or less because of a diagnosed medical condition (usually cancer) to request and self-administer lethal medication prescribed by a physician.
This experience may help to inform efforts to introduce similar programs in other states. At present, Hawaii, Pennsylvania, and Vermont are all considering pertinent legislation, said Dr. Elizabeth Trice Loggers of the Fred Hutchinson Cancer Research Center, Seattle, and her associates.
The program’s policy – written by the Seattle Cancer Care Alliance’s medical director and approved by a majority of the medical executive committee members, as with any clinical policy – requires that patients request information about medically assisted suicide from their physicians, or that these clinicians raise the topic, to be considered for referral. Participation is entirely voluntary for medical staff and faculty members.
Every patient who is a potential participant is first assigned an advocate, a licensed social worker employed by the Alliance, who assists patients, family members, pharmacists, and physicians throughout a multistep process of participating. This advocate also tracks compliance with required documentation for the state Department of Health.
The advocate, as well as the attending physician, ensures that all potential participants are aware of alternatives to medically assisted suicide, such as palliative care and hospice care. The patient’s terminal status is verified, and if the attending physician doesn’t wish to participate, a prescribing physician and a consulting physician are chosen from a group of willing providers.
Psychosocial and psychological assessments are required to ensure the patient’s competence to make the choice of assisted suicide and to identify any depression, which would make the patient ineligible to participate. The patient’s preferences for interventions and health-care directives are documented. Grief support, legacy support, and bereavement support are offered through periodic calls and visits.
The patient and his or her family meet with the prescribing clinician and the consulting clinician to review the diagnosis, prognosis, treatment alternatives, and end-of-life issues. After a mandatory waiting period of 15 days, a written prescription is then sent to the pharmacy, and the pharmacist schedules another appointment with the patient and family to discuss preparation of the drug(s), potential side effects, and the concomitant use of prescription antiemetics.
Patients are then free to fill the prescription or not and to take the drug(s) or not, as they wish.
To date, 114 patients have inquired about the Death with Dignity program, and 44 (38%) either did not pursue the matter further or were deemed ineligible to participate.
Thirty patients (26%) have made a first oral request to initiate the process but either decided not to participate or died before completing the process. Forty patients (35% of those who made an initial inquiry) received prescriptions for lethal medication, and all 40 have died. Twenty-four chose to die by ingesting the medication (secobarbital).
Thus, only 21% of the participants actually used assisted suicide. Death with Dignity participants accounted for 2.4% of all annual deaths among patients at the Seattle Cancer Center Alliance.*
The reasons patients gave most often for participating in the assisted-suicide program were loss of autonomy (97%), inability to engage in enjoyable activities (89%), and loss of dignity (75%).
"We have not received any complaints from family members or caregivers regarding our process or the manner of death. Anecdotally, families describe the death as peaceful (even when death has taken longer than the average of approximately 35 minutes)," Dr. Loggers and her associates wrote physician (N. Engl. J. Med. 2013 April 11;368:1417-24 [doi:10.1056/NEJMsa1213398]).
"Both patients and families frequently express gratitude after the patient received the prescription, regardless of whether it is ever filled or ingested, typically referencing an important sense of control in an uncertain situation," they noted.
Opponents of medically assisted suicide have argued that legislation would disproportionately affect vulnerable populations, such as racial or ethnic minorities, low-income groups, or cognitively impaired patients. The Death with Dignity experience refutes this argument, as most participants were white, male, and well educated, the investigators said.
There have been no unexpected complications among patients who chose assisted suicide, but one patient remained alive for a day after taking the medication. This protracted dying process caused distress to both the family members and the clinicians involved. Similar cases have been reported previously, they added.
*Correction, 4/12/13: An earlier version of this story described findings from a study (citation) in the New England Journal of Medicine. That study misstated the percentage of Death with Dignity patients among all annual patient deaths reported at the Seattle Cancer Center Alliance.
FROM THE NEW ENGLAND JOURNAL OF MEDICINE
Major finding: None of the 114 patients who participated in the Death with Dignity (assisted-suicide) program during a 2-year period, nor their family members and caregivers, have complained about the process or manner of death.
Data source: A descriptive study of the experience to date concerning the Death with Dignity program serving patients throughout the Pacific Northwest at a comprehensive cancer center.
Disclosures: No financial conflicts of interest were reported.