User login
In U.S., lockdowns added 2 pounds per month
Americans gained nearly 2 pounds per month under COVID-19 shelter-in-place orders in 2020, according to a new study published March 22, 2021, in JAMA Network Open.
Those who kept the same lockdown habits could have gained 20 pounds during the past year, the study authors said.
“We know that weight gain is a public health problem in the U.S. already, so anything making it worse is definitely concerning, and shelter-in-place orders are so ubiquitous that the sheer number of people affected by this makes it extremely relevant,” Gregory Marcus, MD, the senior author and a cardiologist at the University of California, San Francisco, told the New York Times.
Dr. Marcus and colleagues analyzed more than 7,000 weight measurements from 269 people in 37 states who used Bluetooth-connected scales from Feb. 1 to June 1, 2020. Among the participants, about 52% were women, 77% were White, and they had an average age of 52 years.
The research team found that participants had a steady weight gain of more than half a pound every 10 days. That equals about 1.5-2 pounds per month.
Many of the participants were losing weight before the shelter-in-place orders went into effect, Dr. Marcus said. The lockdown effects could be even greater for those who weren’t losing weight before.
“It’s reasonable to assume these individuals are more engaged with their health in general, and more disciplined and on top of things,” he said. “That suggests we could be underestimating – that this is the tip of the iceberg.”
The small study doesn’t represent all of the nation and can’t be generalized to the U.S. population, the study authors noted, but it’s an indicator of what happened during the pandemic. The participants’ weight increased regardless of their location and chronic medical conditions.
Overall, people don’t move around as much during lockdowns, the UCSF researchers reported in another study published in Annals of Internal Medicine in November 2020. According to smartphone data, daily step counts decreased by 27% in March 2020. The step counts increased again throughout the summer but still remained lower than before the COVID-19 pandemic.
“The detrimental health outcomes suggested by these data demonstrate a need to identify concurrent strategies to mitigate weight gain,” the authors wrote in the JAMA Network Open study, “such as encouraging healthy diets and exploring ways to enhance physical activity, as local governments consider new constraints in response to SARS-CoV-2 and potential future pandemics.”
A version of this article first appeared on WebMD.com.
Americans gained nearly 2 pounds per month under COVID-19 shelter-in-place orders in 2020, according to a new study published March 22, 2021, in JAMA Network Open.
Those who kept the same lockdown habits could have gained 20 pounds during the past year, the study authors said.
“We know that weight gain is a public health problem in the U.S. already, so anything making it worse is definitely concerning, and shelter-in-place orders are so ubiquitous that the sheer number of people affected by this makes it extremely relevant,” Gregory Marcus, MD, the senior author and a cardiologist at the University of California, San Francisco, told the New York Times.
Dr. Marcus and colleagues analyzed more than 7,000 weight measurements from 269 people in 37 states who used Bluetooth-connected scales from Feb. 1 to June 1, 2020. Among the participants, about 52% were women, 77% were White, and they had an average age of 52 years.
The research team found that participants had a steady weight gain of more than half a pound every 10 days. That equals about 1.5-2 pounds per month.
Many of the participants were losing weight before the shelter-in-place orders went into effect, Dr. Marcus said. The lockdown effects could be even greater for those who weren’t losing weight before.
“It’s reasonable to assume these individuals are more engaged with their health in general, and more disciplined and on top of things,” he said. “That suggests we could be underestimating – that this is the tip of the iceberg.”
The small study doesn’t represent all of the nation and can’t be generalized to the U.S. population, the study authors noted, but it’s an indicator of what happened during the pandemic. The participants’ weight increased regardless of their location and chronic medical conditions.
Overall, people don’t move around as much during lockdowns, the UCSF researchers reported in another study published in Annals of Internal Medicine in November 2020. According to smartphone data, daily step counts decreased by 27% in March 2020. The step counts increased again throughout the summer but still remained lower than before the COVID-19 pandemic.
“The detrimental health outcomes suggested by these data demonstrate a need to identify concurrent strategies to mitigate weight gain,” the authors wrote in the JAMA Network Open study, “such as encouraging healthy diets and exploring ways to enhance physical activity, as local governments consider new constraints in response to SARS-CoV-2 and potential future pandemics.”
A version of this article first appeared on WebMD.com.
Americans gained nearly 2 pounds per month under COVID-19 shelter-in-place orders in 2020, according to a new study published March 22, 2021, in JAMA Network Open.
Those who kept the same lockdown habits could have gained 20 pounds during the past year, the study authors said.
“We know that weight gain is a public health problem in the U.S. already, so anything making it worse is definitely concerning, and shelter-in-place orders are so ubiquitous that the sheer number of people affected by this makes it extremely relevant,” Gregory Marcus, MD, the senior author and a cardiologist at the University of California, San Francisco, told the New York Times.
Dr. Marcus and colleagues analyzed more than 7,000 weight measurements from 269 people in 37 states who used Bluetooth-connected scales from Feb. 1 to June 1, 2020. Among the participants, about 52% were women, 77% were White, and they had an average age of 52 years.
The research team found that participants had a steady weight gain of more than half a pound every 10 days. That equals about 1.5-2 pounds per month.
Many of the participants were losing weight before the shelter-in-place orders went into effect, Dr. Marcus said. The lockdown effects could be even greater for those who weren’t losing weight before.
“It’s reasonable to assume these individuals are more engaged with their health in general, and more disciplined and on top of things,” he said. “That suggests we could be underestimating – that this is the tip of the iceberg.”
The small study doesn’t represent all of the nation and can’t be generalized to the U.S. population, the study authors noted, but it’s an indicator of what happened during the pandemic. The participants’ weight increased regardless of their location and chronic medical conditions.
Overall, people don’t move around as much during lockdowns, the UCSF researchers reported in another study published in Annals of Internal Medicine in November 2020. According to smartphone data, daily step counts decreased by 27% in March 2020. The step counts increased again throughout the summer but still remained lower than before the COVID-19 pandemic.
“The detrimental health outcomes suggested by these data demonstrate a need to identify concurrent strategies to mitigate weight gain,” the authors wrote in the JAMA Network Open study, “such as encouraging healthy diets and exploring ways to enhance physical activity, as local governments consider new constraints in response to SARS-CoV-2 and potential future pandemics.”
A version of this article first appeared on WebMD.com.
Obesity pegged as source of marked increased risk of diabetes in PCOS
The increased risk of type 2 diabetes in women with polycystic ovary syndrome is well established, but a new analysis has shown that obesity is the major mediator and a target for preventing or reversing this comorbidity.
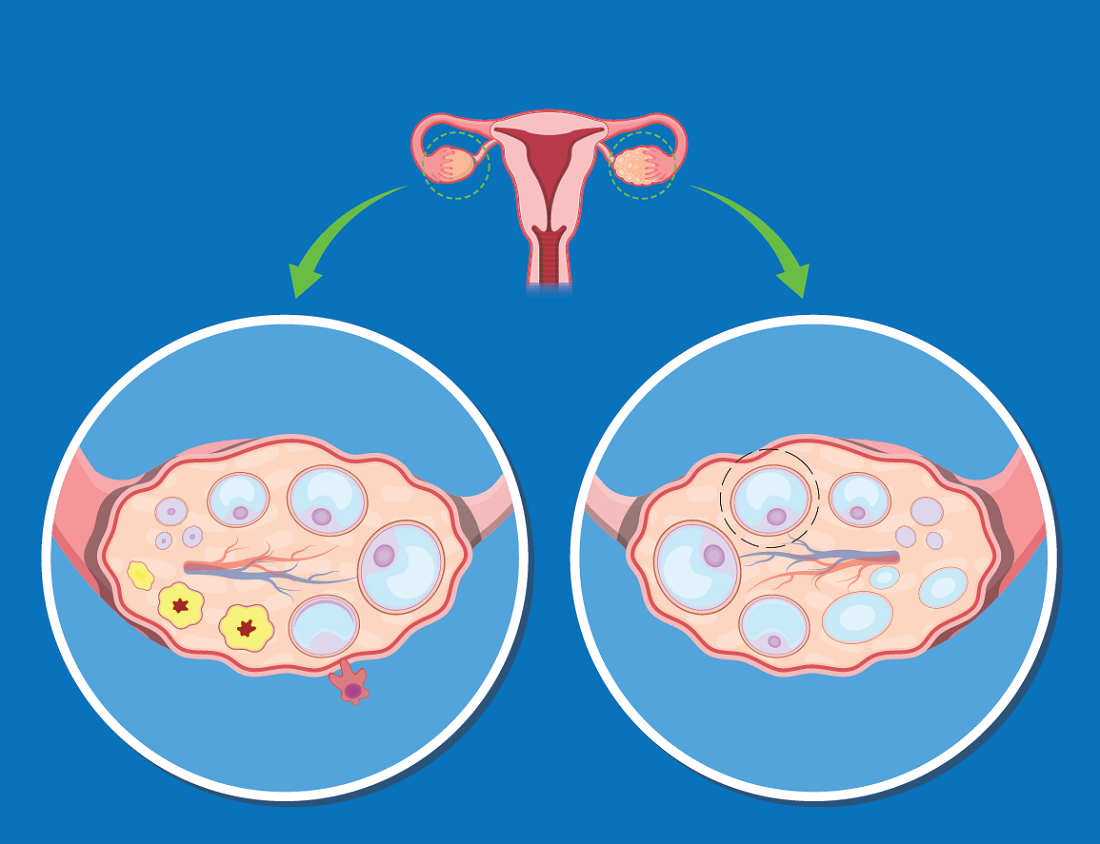
“Most women with PCOS are obese, complicating the effort to understand whether high rates of diabetes in this population are due to PCOS or excess weight, but our study now suggest that obesity isa targetable risk factor,” reported Panagiotis Anagnostis, MD, PhD, a reproductive endocrinologist at the Medical School of Aristotle University, Thessaloniki, Greece.
Obesity is also a known risk factor for type 2 diabetes (T2D), but there is reason to suspect that PCOS, which is associated with abnormal carbohydrate metabolism, has a direct impact on the risk of developing T2D, according to Dr. Anagnostis. It is also reasonable to expect “a synergistic deleterious effect” from PCOS and obesity on adverse changes in glucose metabolism that lead to T2D.
Even though rates of obesity among women with PCOS reach 80% in some studies, Dr. Anagnostis attempted to disentangle the relationship between obesity, PCOS, and risk of T2D using a large set of data drawn from a comprehensive search of published studies.
After screening with predefined criteria, 12 studies provided data on 224,284 women, of whom 45,361 had PCOS and 5,717 had T2D. Not least of the criteria for inclusion in this analysis, all studies stratified women as obese, defined as a body mass index (BMI) greater than 30 kg/m2, or nonobese, he reported at the annual meeting of the Endocrine Society.
Diabetes risk tripled in PCOS
When compared without regard to BMI, the relative risk of having T2D among those with PCOS relative to those without this condition was more than three times greater (RR 3.13; P < .001). When women with PCOS were stratified for BMI, obesity was associated with a more than fourfold increased risk relative to controls without PCOS (RR, 4.06; P < .001).
In women who were nonobese, the risk of T2D was numerically higher for those with PCOS than those without (RR, 2.68), but it was only a trend with a large confidence interval (95% confidence interval, 0.97-7.49).
Among women with PCOS, those who were obese also had a more than fourfold and highly significant increased risk of T2D relative to those who were not obese (RR, 4.20; P < .001).
The message from these data is that obesity is a major and potentially modifiable risk factor for diabetes in women with PCOS, according to Dr. Anagnostis.
He said these data provide the basis for recommending weight loss specifically for managing this common PCOS comorbidity.
Almost the same relative risk of diabetes was derived from an analysis of a women’s health database published 2 years ago in Diabetes Care. In that study with 1,916 person-years of follow-up, the hazard ratio for T2D was also more than three times greater (HR, 3.23; P < .001) for those with PCOS relative to those without the syndrome.
However, normal BMI did not eliminate risk of developing diabetes in this study. Rather, the relative risk of T2D in women with PCOS was higher in those of normal weight, compared with those who were obese (HR, 4.68 vs. 2.36; P < .005). The investigators recommend screening all women with PCOS at least every 3 years with more frequent screening in those with risk factors.
PCOS complexity challenges simple conclusions
The complexity of disturbed metabolic pathways in patients with PCOS and obesity might explain some of the difficulty in unraveling the relationship between these two disease states and diabetes risk. In one recent review, it was suggested that obesity and PCOS share interrelated adverse effects on glucose metabolism. As a result, these associations are “more complex than a simple cause-and-effect process.” the authors of that article concluded.
Furthermore, in their examination of metabolic pathways, genetic susceptibility, and behavioral factors that might link PCOS, weight gain, and T2D, the authors did not ignore the psychological impact of PCOS in causing obesity and, as a byproduct, diabetes. These psychological factors might be relevant to treatment.
For example, depression and stress “might hamper ongoing attempts at lifestyle change and therefore effective weight loss” in at least some women, they cautioned.
However, in encouraging weight loss in overweight women with PCOS, the debate about cause of T2D might be moot in practical terms, according to Michael Dansinger, MD, founding director of the diabetes reversal program at Tufts Medical Center, Boston.
“Reducing excess body fat reduces the risk of type 2 diabetes,” Dr. Dansinger said in an interview. “Since women with obesity and PCOS are clearly at risk for future type 2 diabetes, that’s another reason to lose excess body fat through healthy eating and exercise.”
Dr. Anagnostis and Dr. Dansinger reported no relevant conflicts of interest.
The increased risk of type 2 diabetes in women with polycystic ovary syndrome is well established, but a new analysis has shown that obesity is the major mediator and a target for preventing or reversing this comorbidity.
“Most women with PCOS are obese, complicating the effort to understand whether high rates of diabetes in this population are due to PCOS or excess weight, but our study now suggest that obesity isa targetable risk factor,” reported Panagiotis Anagnostis, MD, PhD, a reproductive endocrinologist at the Medical School of Aristotle University, Thessaloniki, Greece.
Obesity is also a known risk factor for type 2 diabetes (T2D), but there is reason to suspect that PCOS, which is associated with abnormal carbohydrate metabolism, has a direct impact on the risk of developing T2D, according to Dr. Anagnostis. It is also reasonable to expect “a synergistic deleterious effect” from PCOS and obesity on adverse changes in glucose metabolism that lead to T2D.
Even though rates of obesity among women with PCOS reach 80% in some studies, Dr. Anagnostis attempted to disentangle the relationship between obesity, PCOS, and risk of T2D using a large set of data drawn from a comprehensive search of published studies.
After screening with predefined criteria, 12 studies provided data on 224,284 women, of whom 45,361 had PCOS and 5,717 had T2D. Not least of the criteria for inclusion in this analysis, all studies stratified women as obese, defined as a body mass index (BMI) greater than 30 kg/m2, or nonobese, he reported at the annual meeting of the Endocrine Society.
Diabetes risk tripled in PCOS
When compared without regard to BMI, the relative risk of having T2D among those with PCOS relative to those without this condition was more than three times greater (RR 3.13; P < .001). When women with PCOS were stratified for BMI, obesity was associated with a more than fourfold increased risk relative to controls without PCOS (RR, 4.06; P < .001).
In women who were nonobese, the risk of T2D was numerically higher for those with PCOS than those without (RR, 2.68), but it was only a trend with a large confidence interval (95% confidence interval, 0.97-7.49).
Among women with PCOS, those who were obese also had a more than fourfold and highly significant increased risk of T2D relative to those who were not obese (RR, 4.20; P < .001).
The message from these data is that obesity is a major and potentially modifiable risk factor for diabetes in women with PCOS, according to Dr. Anagnostis.
He said these data provide the basis for recommending weight loss specifically for managing this common PCOS comorbidity.
Almost the same relative risk of diabetes was derived from an analysis of a women’s health database published 2 years ago in Diabetes Care. In that study with 1,916 person-years of follow-up, the hazard ratio for T2D was also more than three times greater (HR, 3.23; P < .001) for those with PCOS relative to those without the syndrome.
However, normal BMI did not eliminate risk of developing diabetes in this study. Rather, the relative risk of T2D in women with PCOS was higher in those of normal weight, compared with those who were obese (HR, 4.68 vs. 2.36; P < .005). The investigators recommend screening all women with PCOS at least every 3 years with more frequent screening in those with risk factors.
PCOS complexity challenges simple conclusions
The complexity of disturbed metabolic pathways in patients with PCOS and obesity might explain some of the difficulty in unraveling the relationship between these two disease states and diabetes risk. In one recent review, it was suggested that obesity and PCOS share interrelated adverse effects on glucose metabolism. As a result, these associations are “more complex than a simple cause-and-effect process.” the authors of that article concluded.
Furthermore, in their examination of metabolic pathways, genetic susceptibility, and behavioral factors that might link PCOS, weight gain, and T2D, the authors did not ignore the psychological impact of PCOS in causing obesity and, as a byproduct, diabetes. These psychological factors might be relevant to treatment.
For example, depression and stress “might hamper ongoing attempts at lifestyle change and therefore effective weight loss” in at least some women, they cautioned.
However, in encouraging weight loss in overweight women with PCOS, the debate about cause of T2D might be moot in practical terms, according to Michael Dansinger, MD, founding director of the diabetes reversal program at Tufts Medical Center, Boston.
“Reducing excess body fat reduces the risk of type 2 diabetes,” Dr. Dansinger said in an interview. “Since women with obesity and PCOS are clearly at risk for future type 2 diabetes, that’s another reason to lose excess body fat through healthy eating and exercise.”
Dr. Anagnostis and Dr. Dansinger reported no relevant conflicts of interest.
The increased risk of type 2 diabetes in women with polycystic ovary syndrome is well established, but a new analysis has shown that obesity is the major mediator and a target for preventing or reversing this comorbidity.
“Most women with PCOS are obese, complicating the effort to understand whether high rates of diabetes in this population are due to PCOS or excess weight, but our study now suggest that obesity isa targetable risk factor,” reported Panagiotis Anagnostis, MD, PhD, a reproductive endocrinologist at the Medical School of Aristotle University, Thessaloniki, Greece.
Obesity is also a known risk factor for type 2 diabetes (T2D), but there is reason to suspect that PCOS, which is associated with abnormal carbohydrate metabolism, has a direct impact on the risk of developing T2D, according to Dr. Anagnostis. It is also reasonable to expect “a synergistic deleterious effect” from PCOS and obesity on adverse changes in glucose metabolism that lead to T2D.
Even though rates of obesity among women with PCOS reach 80% in some studies, Dr. Anagnostis attempted to disentangle the relationship between obesity, PCOS, and risk of T2D using a large set of data drawn from a comprehensive search of published studies.
After screening with predefined criteria, 12 studies provided data on 224,284 women, of whom 45,361 had PCOS and 5,717 had T2D. Not least of the criteria for inclusion in this analysis, all studies stratified women as obese, defined as a body mass index (BMI) greater than 30 kg/m2, or nonobese, he reported at the annual meeting of the Endocrine Society.
Diabetes risk tripled in PCOS
When compared without regard to BMI, the relative risk of having T2D among those with PCOS relative to those without this condition was more than three times greater (RR 3.13; P < .001). When women with PCOS were stratified for BMI, obesity was associated with a more than fourfold increased risk relative to controls without PCOS (RR, 4.06; P < .001).
In women who were nonobese, the risk of T2D was numerically higher for those with PCOS than those without (RR, 2.68), but it was only a trend with a large confidence interval (95% confidence interval, 0.97-7.49).
Among women with PCOS, those who were obese also had a more than fourfold and highly significant increased risk of T2D relative to those who were not obese (RR, 4.20; P < .001).
The message from these data is that obesity is a major and potentially modifiable risk factor for diabetes in women with PCOS, according to Dr. Anagnostis.
He said these data provide the basis for recommending weight loss specifically for managing this common PCOS comorbidity.
Almost the same relative risk of diabetes was derived from an analysis of a women’s health database published 2 years ago in Diabetes Care. In that study with 1,916 person-years of follow-up, the hazard ratio for T2D was also more than three times greater (HR, 3.23; P < .001) for those with PCOS relative to those without the syndrome.
However, normal BMI did not eliminate risk of developing diabetes in this study. Rather, the relative risk of T2D in women with PCOS was higher in those of normal weight, compared with those who were obese (HR, 4.68 vs. 2.36; P < .005). The investigators recommend screening all women with PCOS at least every 3 years with more frequent screening in those with risk factors.
PCOS complexity challenges simple conclusions
The complexity of disturbed metabolic pathways in patients with PCOS and obesity might explain some of the difficulty in unraveling the relationship between these two disease states and diabetes risk. In one recent review, it was suggested that obesity and PCOS share interrelated adverse effects on glucose metabolism. As a result, these associations are “more complex than a simple cause-and-effect process.” the authors of that article concluded.
Furthermore, in their examination of metabolic pathways, genetic susceptibility, and behavioral factors that might link PCOS, weight gain, and T2D, the authors did not ignore the psychological impact of PCOS in causing obesity and, as a byproduct, diabetes. These psychological factors might be relevant to treatment.
For example, depression and stress “might hamper ongoing attempts at lifestyle change and therefore effective weight loss” in at least some women, they cautioned.
However, in encouraging weight loss in overweight women with PCOS, the debate about cause of T2D might be moot in practical terms, according to Michael Dansinger, MD, founding director of the diabetes reversal program at Tufts Medical Center, Boston.
“Reducing excess body fat reduces the risk of type 2 diabetes,” Dr. Dansinger said in an interview. “Since women with obesity and PCOS are clearly at risk for future type 2 diabetes, that’s another reason to lose excess body fat through healthy eating and exercise.”
Dr. Anagnostis and Dr. Dansinger reported no relevant conflicts of interest.
FROM ENDO 2021
ApoB may better predict mortality risk in statin-treated patients
A new study shows apolipoprotein B (apoB) and non-HDL cholesterol – but not LDL cholesterol – are associated with increased risk for all-cause mortality and myocardial infarction in patients taking statins.

Moreover, apoB was a more accurate marker of all-cause mortality risk than non-HDL or LDL cholesterol and was more accurate at identifying MI risk than LDL cholesterol.
“Any patient that comes to a doctor for evaluation, if statin treatment is sufficient, the doctor should look not only at LDL cholesterol but HDL cholesterol and apoB, if its available – that is the take-home message,” senior author Børge Grønne Nordestgaard, MD, DMSC, University of Copenhagen, said in an interview.
The findings are very relevant to clinical practice because international guidelines focus on LDL cholesterol and “many doctors are brainwashed that that is the only thing they should look at, just to keep LDL cholesterol down,” he said. “I’ve worked for years with triglyceride lipoproteins, what I call remnant cholesterol, and I think that the risk is very high also when you have high remnant cholesterol.”
Previous work has shown that apoB and non-HDL cholesterol better reflect atherosclerotic cardiovascular disease risk than LDL cholesterol. This is the first study, however, to show that elevated apoB and non-HDL cholesterol are associated with a higher risk for all-cause death in statin-treated patients with low LDL cholesterol, Dr. Nordestgaard noted.
The investigators compared outcomes among 13,015 statin-treated participants in the Copenhagen General Population Study using median baseline values of 92 mg/dL for apoB, 3.1 mmol/L (120 mg/dL) for non-HDL cholesterol, and 2.3 mmol/L (89 mg/dL) for LDL cholesterol. Over a median follow-up of 8 years, there were 2,499 deaths and 537 MIs.
As reported in the Journal of the American College of Cardiology, discordant apoB above the median with LDL cholesterol below was associated with a 21% increased risk for all-cause mortality (hazard ratio, 1.21; 95% confidence interval, 1.07-1.36) and 49% increased risk for MI (HR, 1.49; 95% CI, 1.15-1.92), compared with concordant apoB and LDL cholesterol below the medians.
Similar results were found for discordant non-HDL cholesterol above the median with low LDL cholesterol for all-cause mortality (HR, 1.18; 95% CI, 1.02-1.36) and MI (1.78; 95% CI, 1.35-2.34).
No such associations with mortality or MI were observed when LDL cholesterol was above the median and apoB or non-HDL below.
Additional analyses showed that high apoB with low non-HDL cholesterol was associated with a higher risk for all-cause mortality (HR, 1.21; 95% CI, 1.03-1.41), whereas high non-HDL cholesterol with low apoB was associated with a lower risk (HR, 0.75; 95% CI, 0.62-0.92).
Current guidelines define apoB greater than 130 mg/dL as a risk modifier in patients not using statins but, the authors wrote, “based on our results, the threshold for apoB as a risk modifier in statin-treated patients should be closer to 92 mg/dL than to 130 mg/dL.”
In an accompanying editorial, Neil J. Stone, MD, and Donald Lloyd-Jones, MD, both from Northwestern University, Chicago, said that American and European guidelines acknowledge the usefulness of apoB and non-HDL cholesterol in their risk algorithms and as possible targets to indicate efficacy, but don’t give a strong recommendation for apoB to assess residual risk.

“This paper suggests that, in the next iteration, we’ve got to give a stronger thought to measuring apoB for residual risk in those with secondary prevention,” Dr. Stone, vice chair of the 2018 American Heart Association/ACC cholesterol guidelines, said in an interview.
“The whole part of the guidelines was not to focus on any one number but to focus on the clinical risk as a whole,” he said. “You can enlarge your understanding of the patient by looking at their non-HDL, which you have anyway, and in certain circumstances, for example, people with metabolic syndrome, diabetes, obesity, or high triglycerides, those people might very well benefit from an apoB to further understand their risk. This paper simply highlights that and, therefore, was very valuable.”
Dr. Stone and Dr. Lloyd-Jones, however, pointed out that statin use was self-reported and information was lacking on adherence, dose intensity, and the amount of LDL cholesterol lowering from baseline. LDL cholesterol levels were also above current recommendations for optimizing risk reduction. “If statin dosing and LDL [cholesterol] were not optimized already, then there may have been ‘room’ for non-HDL [cholesterol] and apoB to add value in understanding residual risk,” they wrote.
The editorialists suggested that sequential use, rather than regular use, of apoB and non-HDL cholesterol may be best and that incorporating this information may be particularly beneficial for patients with metabolic disorders and elevated triglycerides after statin therapy.
“Maybe this paper is a wake-up call that there are other markers out there that can tell you that you still have higher risk and need to tighten up lifestyle and maybe be more adherent,” Dr. Stone said. “I think this is a wonderful chance to say that preventive cardiology isn’t just ‘set it and forget it’.”
C. Noel Bairey Merz, MD, who coauthored the 2018 cholesterol guidelines, agreed there’s “an overexuberant focus on LDL [cholesterol] for residual risk” and highlighted a recent systematic review of statins, ezetimibe, and PCSK9 cardiovascular outcomes trials that showed very little gain from aggressively driving down LDL below 100 mg/dL, unless the patient is at extremely high risk.
“If I, as a treating cardiologist who spends a lot of time on lipids, had a patient on a high-intensity statin and they didn’t drop [their LDL cholesterol] 50% and I already had them going to cardiac rehab and they were already losing weight, would I measure apoB? Yeah, I might, to motivate them to do more or to take Vascepa,” she said.
“This study is a useful addition to a relatively important problem, which is residual risk, and really supports personalized or precision medicine,” added Bairey Merz, MD, Cedars-Sinai Medical Center, Los Angeles. “But now we have to do the work and do an intervention trial in these people and see whether these markers make a difference.”
The study was supported by Herlev and Gentofte Hospital’s Research Fund and the department of clinical biochemistry, Herlev and Gentofte Hospital, Copenhagen University Hospital. Dr. Nordestgaard has had consultancies or talks sponsored by AstraZeneca, Sanofi, Regeneron, Akcea, Amarin, Amgen, Esperion, Kowa, Novartis, Novo Nordisk, and Silence Therapeutics. All other authors, Dr. Stone, and Dr. Lloyd-Jones reported no conflicts. Dr. Merz reported no relevant disclosures.
A version of this article first appeared on Medscape.com.
A new study shows apolipoprotein B (apoB) and non-HDL cholesterol – but not LDL cholesterol – are associated with increased risk for all-cause mortality and myocardial infarction in patients taking statins.
Moreover, apoB was a more accurate marker of all-cause mortality risk than non-HDL or LDL cholesterol and was more accurate at identifying MI risk than LDL cholesterol.
“Any patient that comes to a doctor for evaluation, if statin treatment is sufficient, the doctor should look not only at LDL cholesterol but HDL cholesterol and apoB, if its available – that is the take-home message,” senior author Børge Grønne Nordestgaard, MD, DMSC, University of Copenhagen, said in an interview.
The findings are very relevant to clinical practice because international guidelines focus on LDL cholesterol and “many doctors are brainwashed that that is the only thing they should look at, just to keep LDL cholesterol down,” he said. “I’ve worked for years with triglyceride lipoproteins, what I call remnant cholesterol, and I think that the risk is very high also when you have high remnant cholesterol.”
Previous work has shown that apoB and non-HDL cholesterol better reflect atherosclerotic cardiovascular disease risk than LDL cholesterol. This is the first study, however, to show that elevated apoB and non-HDL cholesterol are associated with a higher risk for all-cause death in statin-treated patients with low LDL cholesterol, Dr. Nordestgaard noted.
The investigators compared outcomes among 13,015 statin-treated participants in the Copenhagen General Population Study using median baseline values of 92 mg/dL for apoB, 3.1 mmol/L (120 mg/dL) for non-HDL cholesterol, and 2.3 mmol/L (89 mg/dL) for LDL cholesterol. Over a median follow-up of 8 years, there were 2,499 deaths and 537 MIs.
As reported in the Journal of the American College of Cardiology, discordant apoB above the median with LDL cholesterol below was associated with a 21% increased risk for all-cause mortality (hazard ratio, 1.21; 95% confidence interval, 1.07-1.36) and 49% increased risk for MI (HR, 1.49; 95% CI, 1.15-1.92), compared with concordant apoB and LDL cholesterol below the medians.
Similar results were found for discordant non-HDL cholesterol above the median with low LDL cholesterol for all-cause mortality (HR, 1.18; 95% CI, 1.02-1.36) and MI (1.78; 95% CI, 1.35-2.34).
No such associations with mortality or MI were observed when LDL cholesterol was above the median and apoB or non-HDL below.
Additional analyses showed that high apoB with low non-HDL cholesterol was associated with a higher risk for all-cause mortality (HR, 1.21; 95% CI, 1.03-1.41), whereas high non-HDL cholesterol with low apoB was associated with a lower risk (HR, 0.75; 95% CI, 0.62-0.92).
Current guidelines define apoB greater than 130 mg/dL as a risk modifier in patients not using statins but, the authors wrote, “based on our results, the threshold for apoB as a risk modifier in statin-treated patients should be closer to 92 mg/dL than to 130 mg/dL.”
In an accompanying editorial, Neil J. Stone, MD, and Donald Lloyd-Jones, MD, both from Northwestern University, Chicago, said that American and European guidelines acknowledge the usefulness of apoB and non-HDL cholesterol in their risk algorithms and as possible targets to indicate efficacy, but don’t give a strong recommendation for apoB to assess residual risk.
“This paper suggests that, in the next iteration, we’ve got to give a stronger thought to measuring apoB for residual risk in those with secondary prevention,” Dr. Stone, vice chair of the 2018 American Heart Association/ACC cholesterol guidelines, said in an interview.
“The whole part of the guidelines was not to focus on any one number but to focus on the clinical risk as a whole,” he said. “You can enlarge your understanding of the patient by looking at their non-HDL, which you have anyway, and in certain circumstances, for example, people with metabolic syndrome, diabetes, obesity, or high triglycerides, those people might very well benefit from an apoB to further understand their risk. This paper simply highlights that and, therefore, was very valuable.”
Dr. Stone and Dr. Lloyd-Jones, however, pointed out that statin use was self-reported and information was lacking on adherence, dose intensity, and the amount of LDL cholesterol lowering from baseline. LDL cholesterol levels were also above current recommendations for optimizing risk reduction. “If statin dosing and LDL [cholesterol] were not optimized already, then there may have been ‘room’ for non-HDL [cholesterol] and apoB to add value in understanding residual risk,” they wrote.
The editorialists suggested that sequential use, rather than regular use, of apoB and non-HDL cholesterol may be best and that incorporating this information may be particularly beneficial for patients with metabolic disorders and elevated triglycerides after statin therapy.
“Maybe this paper is a wake-up call that there are other markers out there that can tell you that you still have higher risk and need to tighten up lifestyle and maybe be more adherent,” Dr. Stone said. “I think this is a wonderful chance to say that preventive cardiology isn’t just ‘set it and forget it’.”
C. Noel Bairey Merz, MD, who coauthored the 2018 cholesterol guidelines, agreed there’s “an overexuberant focus on LDL [cholesterol] for residual risk” and highlighted a recent systematic review of statins, ezetimibe, and PCSK9 cardiovascular outcomes trials that showed very little gain from aggressively driving down LDL below 100 mg/dL, unless the patient is at extremely high risk.
“If I, as a treating cardiologist who spends a lot of time on lipids, had a patient on a high-intensity statin and they didn’t drop [their LDL cholesterol] 50% and I already had them going to cardiac rehab and they were already losing weight, would I measure apoB? Yeah, I might, to motivate them to do more or to take Vascepa,” she said.
“This study is a useful addition to a relatively important problem, which is residual risk, and really supports personalized or precision medicine,” added Bairey Merz, MD, Cedars-Sinai Medical Center, Los Angeles. “But now we have to do the work and do an intervention trial in these people and see whether these markers make a difference.”
The study was supported by Herlev and Gentofte Hospital’s Research Fund and the department of clinical biochemistry, Herlev and Gentofte Hospital, Copenhagen University Hospital. Dr. Nordestgaard has had consultancies or talks sponsored by AstraZeneca, Sanofi, Regeneron, Akcea, Amarin, Amgen, Esperion, Kowa, Novartis, Novo Nordisk, and Silence Therapeutics. All other authors, Dr. Stone, and Dr. Lloyd-Jones reported no conflicts. Dr. Merz reported no relevant disclosures.
A version of this article first appeared on Medscape.com.
A new study shows apolipoprotein B (apoB) and non-HDL cholesterol – but not LDL cholesterol – are associated with increased risk for all-cause mortality and myocardial infarction in patients taking statins.
Moreover, apoB was a more accurate marker of all-cause mortality risk than non-HDL or LDL cholesterol and was more accurate at identifying MI risk than LDL cholesterol.
“Any patient that comes to a doctor for evaluation, if statin treatment is sufficient, the doctor should look not only at LDL cholesterol but HDL cholesterol and apoB, if its available – that is the take-home message,” senior author Børge Grønne Nordestgaard, MD, DMSC, University of Copenhagen, said in an interview.
The findings are very relevant to clinical practice because international guidelines focus on LDL cholesterol and “many doctors are brainwashed that that is the only thing they should look at, just to keep LDL cholesterol down,” he said. “I’ve worked for years with triglyceride lipoproteins, what I call remnant cholesterol, and I think that the risk is very high also when you have high remnant cholesterol.”
Previous work has shown that apoB and non-HDL cholesterol better reflect atherosclerotic cardiovascular disease risk than LDL cholesterol. This is the first study, however, to show that elevated apoB and non-HDL cholesterol are associated with a higher risk for all-cause death in statin-treated patients with low LDL cholesterol, Dr. Nordestgaard noted.
The investigators compared outcomes among 13,015 statin-treated participants in the Copenhagen General Population Study using median baseline values of 92 mg/dL for apoB, 3.1 mmol/L (120 mg/dL) for non-HDL cholesterol, and 2.3 mmol/L (89 mg/dL) for LDL cholesterol. Over a median follow-up of 8 years, there were 2,499 deaths and 537 MIs.
As reported in the Journal of the American College of Cardiology, discordant apoB above the median with LDL cholesterol below was associated with a 21% increased risk for all-cause mortality (hazard ratio, 1.21; 95% confidence interval, 1.07-1.36) and 49% increased risk for MI (HR, 1.49; 95% CI, 1.15-1.92), compared with concordant apoB and LDL cholesterol below the medians.
Similar results were found for discordant non-HDL cholesterol above the median with low LDL cholesterol for all-cause mortality (HR, 1.18; 95% CI, 1.02-1.36) and MI (1.78; 95% CI, 1.35-2.34).
No such associations with mortality or MI were observed when LDL cholesterol was above the median and apoB or non-HDL below.
Additional analyses showed that high apoB with low non-HDL cholesterol was associated with a higher risk for all-cause mortality (HR, 1.21; 95% CI, 1.03-1.41), whereas high non-HDL cholesterol with low apoB was associated with a lower risk (HR, 0.75; 95% CI, 0.62-0.92).
Current guidelines define apoB greater than 130 mg/dL as a risk modifier in patients not using statins but, the authors wrote, “based on our results, the threshold for apoB as a risk modifier in statin-treated patients should be closer to 92 mg/dL than to 130 mg/dL.”
In an accompanying editorial, Neil J. Stone, MD, and Donald Lloyd-Jones, MD, both from Northwestern University, Chicago, said that American and European guidelines acknowledge the usefulness of apoB and non-HDL cholesterol in their risk algorithms and as possible targets to indicate efficacy, but don’t give a strong recommendation for apoB to assess residual risk.
“This paper suggests that, in the next iteration, we’ve got to give a stronger thought to measuring apoB for residual risk in those with secondary prevention,” Dr. Stone, vice chair of the 2018 American Heart Association/ACC cholesterol guidelines, said in an interview.
“The whole part of the guidelines was not to focus on any one number but to focus on the clinical risk as a whole,” he said. “You can enlarge your understanding of the patient by looking at their non-HDL, which you have anyway, and in certain circumstances, for example, people with metabolic syndrome, diabetes, obesity, or high triglycerides, those people might very well benefit from an apoB to further understand their risk. This paper simply highlights that and, therefore, was very valuable.”
Dr. Stone and Dr. Lloyd-Jones, however, pointed out that statin use was self-reported and information was lacking on adherence, dose intensity, and the amount of LDL cholesterol lowering from baseline. LDL cholesterol levels were also above current recommendations for optimizing risk reduction. “If statin dosing and LDL [cholesterol] were not optimized already, then there may have been ‘room’ for non-HDL [cholesterol] and apoB to add value in understanding residual risk,” they wrote.
The editorialists suggested that sequential use, rather than regular use, of apoB and non-HDL cholesterol may be best and that incorporating this information may be particularly beneficial for patients with metabolic disorders and elevated triglycerides after statin therapy.
“Maybe this paper is a wake-up call that there are other markers out there that can tell you that you still have higher risk and need to tighten up lifestyle and maybe be more adherent,” Dr. Stone said. “I think this is a wonderful chance to say that preventive cardiology isn’t just ‘set it and forget it’.”
C. Noel Bairey Merz, MD, who coauthored the 2018 cholesterol guidelines, agreed there’s “an overexuberant focus on LDL [cholesterol] for residual risk” and highlighted a recent systematic review of statins, ezetimibe, and PCSK9 cardiovascular outcomes trials that showed very little gain from aggressively driving down LDL below 100 mg/dL, unless the patient is at extremely high risk.
“If I, as a treating cardiologist who spends a lot of time on lipids, had a patient on a high-intensity statin and they didn’t drop [their LDL cholesterol] 50% and I already had them going to cardiac rehab and they were already losing weight, would I measure apoB? Yeah, I might, to motivate them to do more or to take Vascepa,” she said.
“This study is a useful addition to a relatively important problem, which is residual risk, and really supports personalized or precision medicine,” added Bairey Merz, MD, Cedars-Sinai Medical Center, Los Angeles. “But now we have to do the work and do an intervention trial in these people and see whether these markers make a difference.”
The study was supported by Herlev and Gentofte Hospital’s Research Fund and the department of clinical biochemistry, Herlev and Gentofte Hospital, Copenhagen University Hospital. Dr. Nordestgaard has had consultancies or talks sponsored by AstraZeneca, Sanofi, Regeneron, Akcea, Amarin, Amgen, Esperion, Kowa, Novartis, Novo Nordisk, and Silence Therapeutics. All other authors, Dr. Stone, and Dr. Lloyd-Jones reported no conflicts. Dr. Merz reported no relevant disclosures.
A version of this article first appeared on Medscape.com.
PCOS equivalent in men: No ovaries required
The concept that there is a male equivalent of polycystic ovary syndrome (PCOS) was first described more than 15 years ago; a new study has further validated the principle using a polygenic risk score.
By demonstrating a high rates of cardiometabolic dysfunction and androgenic conditions in men with a high PCOS risk score, “we have shown that these genetic risk factors can act independently of ovarian function,” reported Jia Zhu, MD, a clinical endocrinology fellow at Boston Children’s Hospital.
The characterization of a male equivalent of PCOS has implications for both men and women, according to Dr. Zhu. For men, better definition of a phenotype has potential to accelerate the recognition and treatment of an inherited metabolic disorder. For women, this direction of study might help to unravel the relationship between the metabolic pathology and symptoms involving the reproductive system.
Affecting up to 10% of women, PCOS is characterized by ovulatory dysfunction and hyperandrogenism commonly associated with insulin resistance, obesity, and elevation in cardiovascular risk factors. Familial clustering implies an important genetic component, but the relationship between metabolic and ovulatory dysfunction remains incompletely understood.
“Both ovarian-related and ovarian-independent factors have been implicated in the pathogenesis of PCOS, but it remains to be determined which are the inciting events and which are the secondary consequences,” Dr. Zhu explained during his presentation of the study at the annual meeting of the Endocrine Society.
Polygenic risk score applied to men
In this study, a polygenic risk score algorithm developed to predict PCOS in women was applied to men. The risk score was developed through genetic testing in 206,851 unrelated women in the UK Biobank. This algorithm was then applied to stratify risk in 176,360 men from the same biobank. For males, several adjustments were made, including those for age and genetic components relevant to ancestry.
When stratified into quintiles, those at highest risk, relative to those at lower risk, had numerically modest but highly significant increased odds ratio for obesity defined by a body mass index (BMI) of at least 30 kg/m2 (OR, 1.17; P < .13 x 10–29) and type 2 diabetes (OR, 1.15; P = .53 x 10–7). Those in the highest risk group were also more likely to have coronary artery disease (HR, 1.05; P = .01) as well as androgenic alopecia (OR, 1.05; P = .03).
When stratified into deciles of risk, a stepwise increase was observed for the prevalence of several cardiovascular risk factors. These included hemoglobin A1c, triglycerides, BMI, and free androgen, reported Dr. Zhu.
The relationship between the risk score and both coronary artery disease and several dyslipidemias appeared to be mediated by BMI, but the relationship between the PCOS polygenic risk score and type 2 diabetes persisted after adjusting for BMI.
For women, the implication of this analysis is that the reproductive dysfunction associated with PCOS might arise in at least some cases “secondarily from the genetically determined disruption of biological pathways common to both men and women,” Dr. Zhu said. She suggested that efforts to dissect these biological pathways might provide a path to under-standing the underlying mechanism of the ovarian complications, such as irregular menstrual periods, infertility, and ovarian cysts.
Family history of PCOS central to male risk
For men, a family history of PCOS might be relevant to predicting increased risk of type 2 diabetes, obesity and cardiovascular disease, Dr. Zhu indicated. In addition, this syndrome is also likely relevant to such signs of hyperandrogenism as hair loss and low testosterone levels in males with the PCOS-equivalent syndrome.
Other investigators have also suggested that male-equivalent PCOS exists and might be clinically relevant. According to Frederica Di Guardio, MD, a gynecologist in the department of medical surgical specialties, University of Catania (Italy), there is enough evidence for a PCOS-equivalent syndrome in men to consider asking males with obesity or other evidence of the metabolic abnormalities about a family history of PCOS.
“These patients have a high risk of developing cardiovascular disease, metabolic syndrome, and carotid atherosclerotic plaques,” she advised on the basis of her own and previous studies. By asking about a family history of PCOS in males, it can raise clinical suspicion and permit early intervention.
Not least important, identifying males at risk can allow them “to adopt a healthy lifestyle, preventing the risk of metabolic and cardiovascular events,” Dr. Di Guardio said.
In a recent review article on the male PCOS syndrome, Dr. Di Guardio traced the male PCOS-equivalent syndrome to a 2004 article. She reported that more than 30 articles have been published subsequently.
There is no formal clinical definition of male equivalent PCOS. According to her review of published studies, Dr. Di Guardio acknowledged that there has been considerable heterogeneity in the prevalence of the associated features, but the unifying factor is the presence of a set of genes associated with PCOS. In men, as well as in women, these appear to drive an increased risk of metabolic abnormalities and cardiovascular disease.
Dr. Zhu and Dr. Di Guardio reported no relevant conflicts of interest.
The concept that there is a male equivalent of polycystic ovary syndrome (PCOS) was first described more than 15 years ago; a new study has further validated the principle using a polygenic risk score.
By demonstrating a high rates of cardiometabolic dysfunction and androgenic conditions in men with a high PCOS risk score, “we have shown that these genetic risk factors can act independently of ovarian function,” reported Jia Zhu, MD, a clinical endocrinology fellow at Boston Children’s Hospital.
The characterization of a male equivalent of PCOS has implications for both men and women, according to Dr. Zhu. For men, better definition of a phenotype has potential to accelerate the recognition and treatment of an inherited metabolic disorder. For women, this direction of study might help to unravel the relationship between the metabolic pathology and symptoms involving the reproductive system.
Affecting up to 10% of women, PCOS is characterized by ovulatory dysfunction and hyperandrogenism commonly associated with insulin resistance, obesity, and elevation in cardiovascular risk factors. Familial clustering implies an important genetic component, but the relationship between metabolic and ovulatory dysfunction remains incompletely understood.
“Both ovarian-related and ovarian-independent factors have been implicated in the pathogenesis of PCOS, but it remains to be determined which are the inciting events and which are the secondary consequences,” Dr. Zhu explained during his presentation of the study at the annual meeting of the Endocrine Society.
Polygenic risk score applied to men
In this study, a polygenic risk score algorithm developed to predict PCOS in women was applied to men. The risk score was developed through genetic testing in 206,851 unrelated women in the UK Biobank. This algorithm was then applied to stratify risk in 176,360 men from the same biobank. For males, several adjustments were made, including those for age and genetic components relevant to ancestry.
When stratified into quintiles, those at highest risk, relative to those at lower risk, had numerically modest but highly significant increased odds ratio for obesity defined by a body mass index (BMI) of at least 30 kg/m2 (OR, 1.17; P < .13 x 10–29) and type 2 diabetes (OR, 1.15; P = .53 x 10–7). Those in the highest risk group were also more likely to have coronary artery disease (HR, 1.05; P = .01) as well as androgenic alopecia (OR, 1.05; P = .03).
When stratified into deciles of risk, a stepwise increase was observed for the prevalence of several cardiovascular risk factors. These included hemoglobin A1c, triglycerides, BMI, and free androgen, reported Dr. Zhu.
The relationship between the risk score and both coronary artery disease and several dyslipidemias appeared to be mediated by BMI, but the relationship between the PCOS polygenic risk score and type 2 diabetes persisted after adjusting for BMI.
For women, the implication of this analysis is that the reproductive dysfunction associated with PCOS might arise in at least some cases “secondarily from the genetically determined disruption of biological pathways common to both men and women,” Dr. Zhu said. She suggested that efforts to dissect these biological pathways might provide a path to under-standing the underlying mechanism of the ovarian complications, such as irregular menstrual periods, infertility, and ovarian cysts.
Family history of PCOS central to male risk
For men, a family history of PCOS might be relevant to predicting increased risk of type 2 diabetes, obesity and cardiovascular disease, Dr. Zhu indicated. In addition, this syndrome is also likely relevant to such signs of hyperandrogenism as hair loss and low testosterone levels in males with the PCOS-equivalent syndrome.
Other investigators have also suggested that male-equivalent PCOS exists and might be clinically relevant. According to Frederica Di Guardio, MD, a gynecologist in the department of medical surgical specialties, University of Catania (Italy), there is enough evidence for a PCOS-equivalent syndrome in men to consider asking males with obesity or other evidence of the metabolic abnormalities about a family history of PCOS.
“These patients have a high risk of developing cardiovascular disease, metabolic syndrome, and carotid atherosclerotic plaques,” she advised on the basis of her own and previous studies. By asking about a family history of PCOS in males, it can raise clinical suspicion and permit early intervention.
Not least important, identifying males at risk can allow them “to adopt a healthy lifestyle, preventing the risk of metabolic and cardiovascular events,” Dr. Di Guardio said.
In a recent review article on the male PCOS syndrome, Dr. Di Guardio traced the male PCOS-equivalent syndrome to a 2004 article. She reported that more than 30 articles have been published subsequently.
There is no formal clinical definition of male equivalent PCOS. According to her review of published studies, Dr. Di Guardio acknowledged that there has been considerable heterogeneity in the prevalence of the associated features, but the unifying factor is the presence of a set of genes associated with PCOS. In men, as well as in women, these appear to drive an increased risk of metabolic abnormalities and cardiovascular disease.
Dr. Zhu and Dr. Di Guardio reported no relevant conflicts of interest.
The concept that there is a male equivalent of polycystic ovary syndrome (PCOS) was first described more than 15 years ago; a new study has further validated the principle using a polygenic risk score.
By demonstrating a high rates of cardiometabolic dysfunction and androgenic conditions in men with a high PCOS risk score, “we have shown that these genetic risk factors can act independently of ovarian function,” reported Jia Zhu, MD, a clinical endocrinology fellow at Boston Children’s Hospital.
The characterization of a male equivalent of PCOS has implications for both men and women, according to Dr. Zhu. For men, better definition of a phenotype has potential to accelerate the recognition and treatment of an inherited metabolic disorder. For women, this direction of study might help to unravel the relationship between the metabolic pathology and symptoms involving the reproductive system.
Affecting up to 10% of women, PCOS is characterized by ovulatory dysfunction and hyperandrogenism commonly associated with insulin resistance, obesity, and elevation in cardiovascular risk factors. Familial clustering implies an important genetic component, but the relationship between metabolic and ovulatory dysfunction remains incompletely understood.
“Both ovarian-related and ovarian-independent factors have been implicated in the pathogenesis of PCOS, but it remains to be determined which are the inciting events and which are the secondary consequences,” Dr. Zhu explained during his presentation of the study at the annual meeting of the Endocrine Society.
Polygenic risk score applied to men
In this study, a polygenic risk score algorithm developed to predict PCOS in women was applied to men. The risk score was developed through genetic testing in 206,851 unrelated women in the UK Biobank. This algorithm was then applied to stratify risk in 176,360 men from the same biobank. For males, several adjustments were made, including those for age and genetic components relevant to ancestry.
When stratified into quintiles, those at highest risk, relative to those at lower risk, had numerically modest but highly significant increased odds ratio for obesity defined by a body mass index (BMI) of at least 30 kg/m2 (OR, 1.17; P < .13 x 10–29) and type 2 diabetes (OR, 1.15; P = .53 x 10–7). Those in the highest risk group were also more likely to have coronary artery disease (HR, 1.05; P = .01) as well as androgenic alopecia (OR, 1.05; P = .03).
When stratified into deciles of risk, a stepwise increase was observed for the prevalence of several cardiovascular risk factors. These included hemoglobin A1c, triglycerides, BMI, and free androgen, reported Dr. Zhu.
The relationship between the risk score and both coronary artery disease and several dyslipidemias appeared to be mediated by BMI, but the relationship between the PCOS polygenic risk score and type 2 diabetes persisted after adjusting for BMI.
For women, the implication of this analysis is that the reproductive dysfunction associated with PCOS might arise in at least some cases “secondarily from the genetically determined disruption of biological pathways common to both men and women,” Dr. Zhu said. She suggested that efforts to dissect these biological pathways might provide a path to under-standing the underlying mechanism of the ovarian complications, such as irregular menstrual periods, infertility, and ovarian cysts.
Family history of PCOS central to male risk
For men, a family history of PCOS might be relevant to predicting increased risk of type 2 diabetes, obesity and cardiovascular disease, Dr. Zhu indicated. In addition, this syndrome is also likely relevant to such signs of hyperandrogenism as hair loss and low testosterone levels in males with the PCOS-equivalent syndrome.
Other investigators have also suggested that male-equivalent PCOS exists and might be clinically relevant. According to Frederica Di Guardio, MD, a gynecologist in the department of medical surgical specialties, University of Catania (Italy), there is enough evidence for a PCOS-equivalent syndrome in men to consider asking males with obesity or other evidence of the metabolic abnormalities about a family history of PCOS.
“These patients have a high risk of developing cardiovascular disease, metabolic syndrome, and carotid atherosclerotic plaques,” she advised on the basis of her own and previous studies. By asking about a family history of PCOS in males, it can raise clinical suspicion and permit early intervention.
Not least important, identifying males at risk can allow them “to adopt a healthy lifestyle, preventing the risk of metabolic and cardiovascular events,” Dr. Di Guardio said.
In a recent review article on the male PCOS syndrome, Dr. Di Guardio traced the male PCOS-equivalent syndrome to a 2004 article. She reported that more than 30 articles have been published subsequently.
There is no formal clinical definition of male equivalent PCOS. According to her review of published studies, Dr. Di Guardio acknowledged that there has been considerable heterogeneity in the prevalence of the associated features, but the unifying factor is the presence of a set of genes associated with PCOS. In men, as well as in women, these appear to drive an increased risk of metabolic abnormalities and cardiovascular disease.
Dr. Zhu and Dr. Di Guardio reported no relevant conflicts of interest.
FROM ENDO 2021
High-intensity interval training cuts cardiometabolic risks in women with PCOS
High-intensity interval training (HIIT) was better than moderate-intensity continuous training (MICT) for improving several measures of cardiometabolic health in women with polycystic ovary syndrome (PCOS) in a prospective, randomized, single-center study with 27 women.

After 12 weeks on a supervised exercise regimen, the women with PCOS who followed the HIIT program had significantly better improvements in aerobic capacity, insulin sensitivity, and level of sex hormone–binding globulin, Rhiannon K. Patten, MSc, said at the annual meeting of the Endocrine Society.
“HIIT can offer superior improvements in health outcomes, and should be considered as an effective tool to reduce cardiometabolic risk in women with PCOS,” concluded Ms. Patten, a researcher in the Institute for Health and Sport at Victoria University in Melbourne in her presentation (Abstract OR10-1).
“The changes we see [after 12 weeks on the HIIT regimen] seem to occur despite no change in body mass index, so rather than focus on weight loss we encourage participants to focus on the health improvements that seem to be greater with HIIT. We actively encourage the HIIT protocol right now,” she said.
Both regimens use a stationary cycle ergometer. In the HIIT protocol patients twice weekly pedal through 12 1-minute intervals at a heart rate of 90%-100% maximum, interspersed with 1 minute rest intervals. On a third day per week, patients pedal to a heart rate of 90%-95% maximum for 6-8 intervals maintained for 2 minutes and interspersed with rest intervals of 2 minutes. The MICT regimen used as a comparator has participants pedal to 60%-70% of their maximum heart rate continuously for 50 minutes 3 days weekly.
HIIT saves time
“These findings are relevant to clinical practice, because they demonstrate that HIIT is effective in women with PCOS. Reducing the time devoted to exercise to achieve fitness goals is attractive to patients. The reduced time to achieve training benefits with HIIT should improve patient compliance,” commented Andrea Dunaif, MD, professor and chief of the division of endocrinology, diabetes, and bone disease of the Mount Sinai Health System in New York, who was not involved with the study.
The overall weekly exercise time on the MICT regimen, 150 minutes, halves down to 75 minutes a week in the HIIT program. Guideline recommendations released in 2018 by the International PCOS Network recommended these as acceptable alternative exercise strategies. Ms. Patten and her associates sought to determine whether one strategy surpassed the other, the first time this has been examined in women with PCOS, she said.
They randomized 27 sedentary women 18-45 years old with a body mass index (BMI) above 25 kg/m2 and diagnosed with PCOS by the Rotterdam criteria to a 12-week supervised exercise program on either the HIIT or MICT protocol. Their average BMI at entry was 36-37 kg/m2. The study excluded women who smoked, were pregnant, had an illness or injury that would prevent exercise, or were on an oral contraceptive or insulin-sensitizing medication.
At the end of 12 weeks, neither group had a significant change in average weight or BMI, and waist circumference dropped by an average of just over 2 cm in both treatment groups. Lean mass increased by a mean 1 kg in the HIIT group, a significant change, compared with a nonsignificant 0.3 kg average increase in the MICT group.
Increased aerobic capacity ‘partially explains’ improved insulin sensitivity
Aerobic capacity, measured as peak oxygen consumption (VO2peak), increased by an average 5.7 mL/kg per min among the HIIT patients, significantly more than the mean 3.2 mL/kg per min increase among those in the MICT program.
The insulin sensitivity index rose by a significant, relative 35% among the HIIT patients, but barely budged in the MICT group. Fasting glucose fell significantly and the glucose infusion rate increased significantly among the women who performed HIIT, but again showed little change among those doing MICT.
Analysis showed a significant link between the increase in VO2peak and the increase in insulin sensitivity among the women engaged in HIIT, Ms. Patten reported. The improvement in the insulin sensitivity index was “partially explained” by the increase in VO2peak, she said.
Assessment of hormone levels showed a significant increase in sex hormone–binding globulin in the HIIT patients while those in the MICT group showed a small decline in this level. The free androgen index fell by a relative 39% on average in the HIIT group, a significant drop, but decreased by a much smaller and not significant amount among the women who did MICT. The women who performed HIIT also showed a significant drop in their free testosterone level, a change not seen with MICT.
Women who performed the HIIT protocol also had a significant improvement in their menstrual cyclicity, and significant improvements in depression, stress, and anxiety, Ms Patten reported. She next plans to do longer follow-up on study participants, out to 6 and 12 months after the end of the exercise protocol.
“Overall, the findings suggest that HIIT is superior to MICT for improving fitness and insulin sensitivity in the short term. Results from a number of studies in individuals without PCOS suggest that HIIT is superior to MICT for improving fitness short term,” commented Dr. Dunaif. “This study makes an important contribution by directly investigating the impact of training intensity in women with PCOS. Larger studies will be needed before the superiority of HIIT is established for women with PCOS, and study durations of at least several months will be needed to assess the impact on reproductive outcomes such as ovulation,” she said in an interview. She also called for assessing the effects of HIIT in more diverse populations of women with PCOS.
Ms. Patten had no disclosures. Dr. Dunaif has been a consultant to Equator Therapeutics, Fractyl Laboratories, and Globe Life Sciences.
High-intensity interval training (HIIT) was better than moderate-intensity continuous training (MICT) for improving several measures of cardiometabolic health in women with polycystic ovary syndrome (PCOS) in a prospective, randomized, single-center study with 27 women.
After 12 weeks on a supervised exercise regimen, the women with PCOS who followed the HIIT program had significantly better improvements in aerobic capacity, insulin sensitivity, and level of sex hormone–binding globulin, Rhiannon K. Patten, MSc, said at the annual meeting of the Endocrine Society.
“HIIT can offer superior improvements in health outcomes, and should be considered as an effective tool to reduce cardiometabolic risk in women with PCOS,” concluded Ms. Patten, a researcher in the Institute for Health and Sport at Victoria University in Melbourne in her presentation (Abstract OR10-1).
“The changes we see [after 12 weeks on the HIIT regimen] seem to occur despite no change in body mass index, so rather than focus on weight loss we encourage participants to focus on the health improvements that seem to be greater with HIIT. We actively encourage the HIIT protocol right now,” she said.
Both regimens use a stationary cycle ergometer. In the HIIT protocol patients twice weekly pedal through 12 1-minute intervals at a heart rate of 90%-100% maximum, interspersed with 1 minute rest intervals. On a third day per week, patients pedal to a heart rate of 90%-95% maximum for 6-8 intervals maintained for 2 minutes and interspersed with rest intervals of 2 minutes. The MICT regimen used as a comparator has participants pedal to 60%-70% of their maximum heart rate continuously for 50 minutes 3 days weekly.
HIIT saves time
“These findings are relevant to clinical practice, because they demonstrate that HIIT is effective in women with PCOS. Reducing the time devoted to exercise to achieve fitness goals is attractive to patients. The reduced time to achieve training benefits with HIIT should improve patient compliance,” commented Andrea Dunaif, MD, professor and chief of the division of endocrinology, diabetes, and bone disease of the Mount Sinai Health System in New York, who was not involved with the study.
The overall weekly exercise time on the MICT regimen, 150 minutes, halves down to 75 minutes a week in the HIIT program. Guideline recommendations released in 2018 by the International PCOS Network recommended these as acceptable alternative exercise strategies. Ms. Patten and her associates sought to determine whether one strategy surpassed the other, the first time this has been examined in women with PCOS, she said.
They randomized 27 sedentary women 18-45 years old with a body mass index (BMI) above 25 kg/m2 and diagnosed with PCOS by the Rotterdam criteria to a 12-week supervised exercise program on either the HIIT or MICT protocol. Their average BMI at entry was 36-37 kg/m2. The study excluded women who smoked, were pregnant, had an illness or injury that would prevent exercise, or were on an oral contraceptive or insulin-sensitizing medication.
At the end of 12 weeks, neither group had a significant change in average weight or BMI, and waist circumference dropped by an average of just over 2 cm in both treatment groups. Lean mass increased by a mean 1 kg in the HIIT group, a significant change, compared with a nonsignificant 0.3 kg average increase in the MICT group.
Increased aerobic capacity ‘partially explains’ improved insulin sensitivity
Aerobic capacity, measured as peak oxygen consumption (VO2peak), increased by an average 5.7 mL/kg per min among the HIIT patients, significantly more than the mean 3.2 mL/kg per min increase among those in the MICT program.
The insulin sensitivity index rose by a significant, relative 35% among the HIIT patients, but barely budged in the MICT group. Fasting glucose fell significantly and the glucose infusion rate increased significantly among the women who performed HIIT, but again showed little change among those doing MICT.
Analysis showed a significant link between the increase in VO2peak and the increase in insulin sensitivity among the women engaged in HIIT, Ms. Patten reported. The improvement in the insulin sensitivity index was “partially explained” by the increase in VO2peak, she said.
Assessment of hormone levels showed a significant increase in sex hormone–binding globulin in the HIIT patients while those in the MICT group showed a small decline in this level. The free androgen index fell by a relative 39% on average in the HIIT group, a significant drop, but decreased by a much smaller and not significant amount among the women who did MICT. The women who performed HIIT also showed a significant drop in their free testosterone level, a change not seen with MICT.
Women who performed the HIIT protocol also had a significant improvement in their menstrual cyclicity, and significant improvements in depression, stress, and anxiety, Ms Patten reported. She next plans to do longer follow-up on study participants, out to 6 and 12 months after the end of the exercise protocol.
“Overall, the findings suggest that HIIT is superior to MICT for improving fitness and insulin sensitivity in the short term. Results from a number of studies in individuals without PCOS suggest that HIIT is superior to MICT for improving fitness short term,” commented Dr. Dunaif. “This study makes an important contribution by directly investigating the impact of training intensity in women with PCOS. Larger studies will be needed before the superiority of HIIT is established for women with PCOS, and study durations of at least several months will be needed to assess the impact on reproductive outcomes such as ovulation,” she said in an interview. She also called for assessing the effects of HIIT in more diverse populations of women with PCOS.
Ms. Patten had no disclosures. Dr. Dunaif has been a consultant to Equator Therapeutics, Fractyl Laboratories, and Globe Life Sciences.
High-intensity interval training (HIIT) was better than moderate-intensity continuous training (MICT) for improving several measures of cardiometabolic health in women with polycystic ovary syndrome (PCOS) in a prospective, randomized, single-center study with 27 women.
After 12 weeks on a supervised exercise regimen, the women with PCOS who followed the HIIT program had significantly better improvements in aerobic capacity, insulin sensitivity, and level of sex hormone–binding globulin, Rhiannon K. Patten, MSc, said at the annual meeting of the Endocrine Society.
“HIIT can offer superior improvements in health outcomes, and should be considered as an effective tool to reduce cardiometabolic risk in women with PCOS,” concluded Ms. Patten, a researcher in the Institute for Health and Sport at Victoria University in Melbourne in her presentation (Abstract OR10-1).
“The changes we see [after 12 weeks on the HIIT regimen] seem to occur despite no change in body mass index, so rather than focus on weight loss we encourage participants to focus on the health improvements that seem to be greater with HIIT. We actively encourage the HIIT protocol right now,” she said.
Both regimens use a stationary cycle ergometer. In the HIIT protocol patients twice weekly pedal through 12 1-minute intervals at a heart rate of 90%-100% maximum, interspersed with 1 minute rest intervals. On a third day per week, patients pedal to a heart rate of 90%-95% maximum for 6-8 intervals maintained for 2 minutes and interspersed with rest intervals of 2 minutes. The MICT regimen used as a comparator has participants pedal to 60%-70% of their maximum heart rate continuously for 50 minutes 3 days weekly.
HIIT saves time
“These findings are relevant to clinical practice, because they demonstrate that HIIT is effective in women with PCOS. Reducing the time devoted to exercise to achieve fitness goals is attractive to patients. The reduced time to achieve training benefits with HIIT should improve patient compliance,” commented Andrea Dunaif, MD, professor and chief of the division of endocrinology, diabetes, and bone disease of the Mount Sinai Health System in New York, who was not involved with the study.
The overall weekly exercise time on the MICT regimen, 150 minutes, halves down to 75 minutes a week in the HIIT program. Guideline recommendations released in 2018 by the International PCOS Network recommended these as acceptable alternative exercise strategies. Ms. Patten and her associates sought to determine whether one strategy surpassed the other, the first time this has been examined in women with PCOS, she said.
They randomized 27 sedentary women 18-45 years old with a body mass index (BMI) above 25 kg/m2 and diagnosed with PCOS by the Rotterdam criteria to a 12-week supervised exercise program on either the HIIT or MICT protocol. Their average BMI at entry was 36-37 kg/m2. The study excluded women who smoked, were pregnant, had an illness or injury that would prevent exercise, or were on an oral contraceptive or insulin-sensitizing medication.
At the end of 12 weeks, neither group had a significant change in average weight or BMI, and waist circumference dropped by an average of just over 2 cm in both treatment groups. Lean mass increased by a mean 1 kg in the HIIT group, a significant change, compared with a nonsignificant 0.3 kg average increase in the MICT group.
Increased aerobic capacity ‘partially explains’ improved insulin sensitivity
Aerobic capacity, measured as peak oxygen consumption (VO2peak), increased by an average 5.7 mL/kg per min among the HIIT patients, significantly more than the mean 3.2 mL/kg per min increase among those in the MICT program.
The insulin sensitivity index rose by a significant, relative 35% among the HIIT patients, but barely budged in the MICT group. Fasting glucose fell significantly and the glucose infusion rate increased significantly among the women who performed HIIT, but again showed little change among those doing MICT.
Analysis showed a significant link between the increase in VO2peak and the increase in insulin sensitivity among the women engaged in HIIT, Ms. Patten reported. The improvement in the insulin sensitivity index was “partially explained” by the increase in VO2peak, she said.
Assessment of hormone levels showed a significant increase in sex hormone–binding globulin in the HIIT patients while those in the MICT group showed a small decline in this level. The free androgen index fell by a relative 39% on average in the HIIT group, a significant drop, but decreased by a much smaller and not significant amount among the women who did MICT. The women who performed HIIT also showed a significant drop in their free testosterone level, a change not seen with MICT.
Women who performed the HIIT protocol also had a significant improvement in their menstrual cyclicity, and significant improvements in depression, stress, and anxiety, Ms Patten reported. She next plans to do longer follow-up on study participants, out to 6 and 12 months after the end of the exercise protocol.
“Overall, the findings suggest that HIIT is superior to MICT for improving fitness and insulin sensitivity in the short term. Results from a number of studies in individuals without PCOS suggest that HIIT is superior to MICT for improving fitness short term,” commented Dr. Dunaif. “This study makes an important contribution by directly investigating the impact of training intensity in women with PCOS. Larger studies will be needed before the superiority of HIIT is established for women with PCOS, and study durations of at least several months will be needed to assess the impact on reproductive outcomes such as ovulation,” she said in an interview. She also called for assessing the effects of HIIT in more diverse populations of women with PCOS.
Ms. Patten had no disclosures. Dr. Dunaif has been a consultant to Equator Therapeutics, Fractyl Laboratories, and Globe Life Sciences.
FROM ENDO 2021
Ultraprocessed foods, many marketed as healthy, raise CVD risk
Eating ultraprocessed foods poses a significant risk to cardiovascular and coronary heart health, according to prospective data from about 3,000 people in the Framingham Offspring Cohort, the second generation of participants in the Framingham Heart Study.

Each regular, daily serving of ultraprocessed food was linked with significant elevations of 5%-9% in the relative rates of “hard” cardiovascular disease (CVD) events, hard coronary heart disease (CHD) events, overall CVD events, and CVD death, after adjustments for numerous potential confounders including energy intake, body mass index, waist circumference, and blood pressure, Filippa Juul, PhD, and associates wrote in a report published in the Journal of the American College of Cardiology.
“Consumption of ultraprocessed foods makes up over half of the daily calories in the average American diet and are increasingly consumed worldwide. As poor diet is a major modifiable risk factor for heart disease, it represents a critical target in prevention efforts,” said Dr. Juul, a nutritional epidemiologist at New York University, in a statement released by the American College of Cardiology.
“Our findings add to a growing body of evidence suggesting cardiovascular benefits of limiting ultraprocessed foods. Ultraprocessed foods are ubiquitous and include many foods that are marketed as healthy, such as protein bars, breakfast cereals, and most industrially produced breads,” she added. Other commonplace members of the ultraprocessed food group include carbonated soft drinks, packaged snacks, candies, sausages, margarines, and energy drinks. The concept of ultraprocessed foods as a distinct, wide-ranging, and dangerous food category first appeared in 2010, and then received an update from a United Nations panel in 2019 as what’s now called the NOVA classification system.
Ultraprocessed foods fly under the radar
“Although cardiovascular guidelines emphasize consuming minimally processed foods, such as fruits, vegetables, whole grains, and nuts, they give less attention to the importance of minimizing ultraprocessed food,” wrote Robert J. Ostfeld, MD, and Kathleen E. Allen, MS, in an editorial that accompanied the new report. This reduced attention may be because of a “paucity of studies examining the association cardiovascular outcomes and ultraprocessed foods.”
The new evidence demands new policies, educational efforts, and labeling changes, suggested Dr. Ostfeld, director of preventive cardiology at Montefiore Health System in New York, and Ms. Allen, a dietitian at the Geisel School of Medicine at Dartmouth, Hanover, N.H. “The goal should be to make the unhealthy choice the hard choice and the healthy choice the easy choice.”
The new analysis used data collected from people enrolled the Framingham Offspring Cohort, with their clinical metrics and diet information collected during 1991-1995 serving as their baseline. After excluding participants with prevalent CVD at baseline and those with incomplete follow-up of CVD events, the researchers had a cohort of 3,003 adults with an average follow-up of 18 years. At baseline, the cohort averaged 54 years of age; 55% were women, their average body mass index was 27.3 kg/m2, and about 6% had diabetes. They reported eating, on average, 7.5 servings of ultraprocessed food daily.
During follow-up, the cohort tallied 648 incident CVD events, including 251 hard CVD events (coronary death, MI, or stroke) and 163 hard CHD events (coronary death or MI), and 713 total deaths including 108 CVD deaths. Other CVD events recorded but not considered hard included heart failure, intermittent claudication, and transient ischemic attack.
In a multivariate-adjusted analysis, each average daily portion of ultraprocessed food was linked with an significant 7% relative increase in the incidence of a hard CVD event, compared with participants who ate fewer ultraprocessed food portions, and a 9% relative increase in the rate of hard CHD events, the study’s two prespecified primary outcomes. The researchers also found that each ultraprocessed serving significantly was associated with a 5% relative increased rate of total CVD events, and a 9% relative rise in CVD deaths. The analysis showed no significant association between total mortality and ultraprocessed food intake. (Average follow-up for the mortality analyses was 20 years.)
The authors also reported endpoint associations with intake of specific types of ultraprocessed foods, and found significantly increased associations specifically for portions of bread, ultraprocessed meat, salty snacks, and low-calorie soft drinks.
Convenient, omnipresent, and affordable
The authors acknowledged that the associations they found need examination in ethnically diverse populations, but nonetheless the findings “suggest the need for increased efforts to implement population-wide strategies” to lower consumption of ultraprocessed foods. “Given the convenience, omnipresence, and affordability of ultraprocessed foods, careful nutrition counseling is needed to design individualized, patient-centered, heart-healthy diets,” they concluded.
“Population-wide strategies such as taxation on sugar-sweetened beverages and other ultraprocessed foods and recommendations regarding processing levels in national dietary guidelines are needed to reduce the intake of ultraprocessed foods,” added Dr. Juul in her statement. “Of course, we must also implement policies that increase the availability, accessibility, and affordability of nutritious, minimally processed foods, especially in disadvantaged populations. At the clinical level, there is a need for increased commitment to individualized nutrition counseling for adopting sustainable heart-healthy diets.”
The study had no commercial funding. Dr. Juul and coauthors, Dr. Ostfeld, and Ms. Allen had no disclosures.
Eating ultraprocessed foods poses a significant risk to cardiovascular and coronary heart health, according to prospective data from about 3,000 people in the Framingham Offspring Cohort, the second generation of participants in the Framingham Heart Study.
Each regular, daily serving of ultraprocessed food was linked with significant elevations of 5%-9% in the relative rates of “hard” cardiovascular disease (CVD) events, hard coronary heart disease (CHD) events, overall CVD events, and CVD death, after adjustments for numerous potential confounders including energy intake, body mass index, waist circumference, and blood pressure, Filippa Juul, PhD, and associates wrote in a report published in the Journal of the American College of Cardiology.
“Consumption of ultraprocessed foods makes up over half of the daily calories in the average American diet and are increasingly consumed worldwide. As poor diet is a major modifiable risk factor for heart disease, it represents a critical target in prevention efforts,” said Dr. Juul, a nutritional epidemiologist at New York University, in a statement released by the American College of Cardiology.
“Our findings add to a growing body of evidence suggesting cardiovascular benefits of limiting ultraprocessed foods. Ultraprocessed foods are ubiquitous and include many foods that are marketed as healthy, such as protein bars, breakfast cereals, and most industrially produced breads,” she added. Other commonplace members of the ultraprocessed food group include carbonated soft drinks, packaged snacks, candies, sausages, margarines, and energy drinks. The concept of ultraprocessed foods as a distinct, wide-ranging, and dangerous food category first appeared in 2010, and then received an update from a United Nations panel in 2019 as what’s now called the NOVA classification system.
Ultraprocessed foods fly under the radar
“Although cardiovascular guidelines emphasize consuming minimally processed foods, such as fruits, vegetables, whole grains, and nuts, they give less attention to the importance of minimizing ultraprocessed food,” wrote Robert J. Ostfeld, MD, and Kathleen E. Allen, MS, in an editorial that accompanied the new report. This reduced attention may be because of a “paucity of studies examining the association cardiovascular outcomes and ultraprocessed foods.”
The new evidence demands new policies, educational efforts, and labeling changes, suggested Dr. Ostfeld, director of preventive cardiology at Montefiore Health System in New York, and Ms. Allen, a dietitian at the Geisel School of Medicine at Dartmouth, Hanover, N.H. “The goal should be to make the unhealthy choice the hard choice and the healthy choice the easy choice.”
The new analysis used data collected from people enrolled the Framingham Offspring Cohort, with their clinical metrics and diet information collected during 1991-1995 serving as their baseline. After excluding participants with prevalent CVD at baseline and those with incomplete follow-up of CVD events, the researchers had a cohort of 3,003 adults with an average follow-up of 18 years. At baseline, the cohort averaged 54 years of age; 55% were women, their average body mass index was 27.3 kg/m2, and about 6% had diabetes. They reported eating, on average, 7.5 servings of ultraprocessed food daily.
During follow-up, the cohort tallied 648 incident CVD events, including 251 hard CVD events (coronary death, MI, or stroke) and 163 hard CHD events (coronary death or MI), and 713 total deaths including 108 CVD deaths. Other CVD events recorded but not considered hard included heart failure, intermittent claudication, and transient ischemic attack.
In a multivariate-adjusted analysis, each average daily portion of ultraprocessed food was linked with an significant 7% relative increase in the incidence of a hard CVD event, compared with participants who ate fewer ultraprocessed food portions, and a 9% relative increase in the rate of hard CHD events, the study’s two prespecified primary outcomes. The researchers also found that each ultraprocessed serving significantly was associated with a 5% relative increased rate of total CVD events, and a 9% relative rise in CVD deaths. The analysis showed no significant association between total mortality and ultraprocessed food intake. (Average follow-up for the mortality analyses was 20 years.)
The authors also reported endpoint associations with intake of specific types of ultraprocessed foods, and found significantly increased associations specifically for portions of bread, ultraprocessed meat, salty snacks, and low-calorie soft drinks.
Convenient, omnipresent, and affordable
The authors acknowledged that the associations they found need examination in ethnically diverse populations, but nonetheless the findings “suggest the need for increased efforts to implement population-wide strategies” to lower consumption of ultraprocessed foods. “Given the convenience, omnipresence, and affordability of ultraprocessed foods, careful nutrition counseling is needed to design individualized, patient-centered, heart-healthy diets,” they concluded.
“Population-wide strategies such as taxation on sugar-sweetened beverages and other ultraprocessed foods and recommendations regarding processing levels in national dietary guidelines are needed to reduce the intake of ultraprocessed foods,” added Dr. Juul in her statement. “Of course, we must also implement policies that increase the availability, accessibility, and affordability of nutritious, minimally processed foods, especially in disadvantaged populations. At the clinical level, there is a need for increased commitment to individualized nutrition counseling for adopting sustainable heart-healthy diets.”
The study had no commercial funding. Dr. Juul and coauthors, Dr. Ostfeld, and Ms. Allen had no disclosures.
Eating ultraprocessed foods poses a significant risk to cardiovascular and coronary heart health, according to prospective data from about 3,000 people in the Framingham Offspring Cohort, the second generation of participants in the Framingham Heart Study.
Each regular, daily serving of ultraprocessed food was linked with significant elevations of 5%-9% in the relative rates of “hard” cardiovascular disease (CVD) events, hard coronary heart disease (CHD) events, overall CVD events, and CVD death, after adjustments for numerous potential confounders including energy intake, body mass index, waist circumference, and blood pressure, Filippa Juul, PhD, and associates wrote in a report published in the Journal of the American College of Cardiology.
“Consumption of ultraprocessed foods makes up over half of the daily calories in the average American diet and are increasingly consumed worldwide. As poor diet is a major modifiable risk factor for heart disease, it represents a critical target in prevention efforts,” said Dr. Juul, a nutritional epidemiologist at New York University, in a statement released by the American College of Cardiology.
“Our findings add to a growing body of evidence suggesting cardiovascular benefits of limiting ultraprocessed foods. Ultraprocessed foods are ubiquitous and include many foods that are marketed as healthy, such as protein bars, breakfast cereals, and most industrially produced breads,” she added. Other commonplace members of the ultraprocessed food group include carbonated soft drinks, packaged snacks, candies, sausages, margarines, and energy drinks. The concept of ultraprocessed foods as a distinct, wide-ranging, and dangerous food category first appeared in 2010, and then received an update from a United Nations panel in 2019 as what’s now called the NOVA classification system.
Ultraprocessed foods fly under the radar
“Although cardiovascular guidelines emphasize consuming minimally processed foods, such as fruits, vegetables, whole grains, and nuts, they give less attention to the importance of minimizing ultraprocessed food,” wrote Robert J. Ostfeld, MD, and Kathleen E. Allen, MS, in an editorial that accompanied the new report. This reduced attention may be because of a “paucity of studies examining the association cardiovascular outcomes and ultraprocessed foods.”
The new evidence demands new policies, educational efforts, and labeling changes, suggested Dr. Ostfeld, director of preventive cardiology at Montefiore Health System in New York, and Ms. Allen, a dietitian at the Geisel School of Medicine at Dartmouth, Hanover, N.H. “The goal should be to make the unhealthy choice the hard choice and the healthy choice the easy choice.”
The new analysis used data collected from people enrolled the Framingham Offspring Cohort, with their clinical metrics and diet information collected during 1991-1995 serving as their baseline. After excluding participants with prevalent CVD at baseline and those with incomplete follow-up of CVD events, the researchers had a cohort of 3,003 adults with an average follow-up of 18 years. At baseline, the cohort averaged 54 years of age; 55% were women, their average body mass index was 27.3 kg/m2, and about 6% had diabetes. They reported eating, on average, 7.5 servings of ultraprocessed food daily.
During follow-up, the cohort tallied 648 incident CVD events, including 251 hard CVD events (coronary death, MI, or stroke) and 163 hard CHD events (coronary death or MI), and 713 total deaths including 108 CVD deaths. Other CVD events recorded but not considered hard included heart failure, intermittent claudication, and transient ischemic attack.
In a multivariate-adjusted analysis, each average daily portion of ultraprocessed food was linked with an significant 7% relative increase in the incidence of a hard CVD event, compared with participants who ate fewer ultraprocessed food portions, and a 9% relative increase in the rate of hard CHD events, the study’s two prespecified primary outcomes. The researchers also found that each ultraprocessed serving significantly was associated with a 5% relative increased rate of total CVD events, and a 9% relative rise in CVD deaths. The analysis showed no significant association between total mortality and ultraprocessed food intake. (Average follow-up for the mortality analyses was 20 years.)
The authors also reported endpoint associations with intake of specific types of ultraprocessed foods, and found significantly increased associations specifically for portions of bread, ultraprocessed meat, salty snacks, and low-calorie soft drinks.
Convenient, omnipresent, and affordable
The authors acknowledged that the associations they found need examination in ethnically diverse populations, but nonetheless the findings “suggest the need for increased efforts to implement population-wide strategies” to lower consumption of ultraprocessed foods. “Given the convenience, omnipresence, and affordability of ultraprocessed foods, careful nutrition counseling is needed to design individualized, patient-centered, heart-healthy diets,” they concluded.
“Population-wide strategies such as taxation on sugar-sweetened beverages and other ultraprocessed foods and recommendations regarding processing levels in national dietary guidelines are needed to reduce the intake of ultraprocessed foods,” added Dr. Juul in her statement. “Of course, we must also implement policies that increase the availability, accessibility, and affordability of nutritious, minimally processed foods, especially in disadvantaged populations. At the clinical level, there is a need for increased commitment to individualized nutrition counseling for adopting sustainable heart-healthy diets.”
The study had no commercial funding. Dr. Juul and coauthors, Dr. Ostfeld, and Ms. Allen had no disclosures.
FROM THE JOURNAL OF THE AMERICAN COLLEGE OF CARDIOLOGY
Dose-related AFib risk with omega-3 fatty acids?
There may be a dose-related risk for atrial fibrillation (AFib) with omega-3 fatty acid intake, data from four randomized clinical trials suggest.

The latest trial to evaluate the association, the VITAL-RHYTHM study, showed that using a low dose of omega-3 fatty acids or a vitamin D supplement had no significant effect on the risks of developing incident AFib.
The trial, first reported at last year’s American Heart Association meeting, was published online March 16 in the Journal of the American Medical Association.
Together with three other randomized clinical trials, however, these results suggest a possible dose-related effect of omega-3 fatty acids on the risk for AFib, an accompanying “Editor’s Note” suggests.
The note, by JAMA deputy editor Gregory Curfman, MD, points out that in the past 2 years, four randomized clinical trials have provided data on the risk of AFib with omega-3 fatty acid intake.
In the STRENGTH and REDUCE-IT trials, both of which evaluated high doses (4 g/day) of omega-3 fatty acids in patients with heart disease (or at high risk for it), there was a highly statistically significant increase in risk for AFib in the omega-3 groups vs. controls in both trials.
In the OMEMI trial in elderly patients with a recent myocardial infarction, an intermediate dose (1.8 g/day) of omega-3 fatty acids also showed an increase in AFib risk (hazard ratio, 1.84) but this was not significant. And now, the VITAL-RHYTHM trial shows no significant effect of a low dose (840 mg/day) of omega-3 fatty acids on the risk of developing AFib in a primary prevention population.
“Patients who choose to take omega-3 fatty acids, especially in high doses, should be informed of the risk of AF [AFib] and followed up for the possible development of this common and potentially hazardous arrhythmia,” Dr. Curfman concludes.
The authors of the VITAL-RHYTHM trial, led by Christine M. Albert, MD, MPH, Cedars-Sinai Medical Center, Los Angeles, Calif., explain that the trial was conducted after observational studies had shown that individuals with low blood levels of omega-3 fatty acids, eicosapentaenoic acid (EPA) and docosahexaenoic acid (DHA), and vitamin D3 have higher risks of incident AFib, but data on dietary or supplemental intake of these nutrients on AFib risk were mixed.
“To our knowledge, this study is the first randomized, placebo-controlled trial to prospectively test the effect of any intervention on incident AF and is the only trial to test alternative upstream preventive agents for AF in a large enough population over a long enough time period to provide an assessment of the plausible benefits and risks,” they write.
The VITAL-RHYTHM study was an ancillary trial embedded within the Vitamin D and Omega-3 (VITAL) trial, which used a 2 x 2 factorial design to evaluate daily supplementation with 2,000 IU of vitamin D3 and/or 840 mg of marine omega-3 fatty acids (460 mg EPA and 380 mg DHA), in the primary prevention of cardiovascular disease and cancer in 25,871 men and women age 50 and older in the United States.
Results showed that over a median 5.3 years of treatment and follow-up, the primary endpoint of incident AFib occurred in 3.6% of the study population. For the omega-3 part of the trial, incident AFib events occurred in 3.7% of patients taking EPA/DHA vs. 3.4% of the placebo group, giving a hazard ratio of 1.09, which was not significant (P = .19).
For the vitamin D3 vs. placebo comparison, results were very similar, with incident AFib events occurring in 3.7% vs. 3.4% of participants, respectively, giving a hazard ratio of 1.09, which was again not significant (P = .19). There was no evidence for interaction between the two study agents.
“Overall, these findings do not support the use of supplemental EPA-DHA or vitamin D3 for the primary prevention of AFib and provide reassurance regarding lack of a major risk of AFib incidence associated with these commonly used supplements at these doses,” the authors conclude.
Noting that significant increases in AFib have been seen with much higher doses of omega-3 fatty acids in the REDUCE-IT and STRENGTH trials, they add: “Potentially, the adverse effect on AF risk may be dose related, and the higher dosages of EPA used in these other studies might account for the significant adverse effect on AF.”
The researchers say that, to their knowledge, this is the only randomized trial to assess the effect of vitamin D3 supplementation on AFib risk and results suggest a null effect. They add that subgroup analyses in patients with vitamin D levels considered deficient (<20 ng/mL) did not suggest a benefit; however, the power to detect a benefit in this much smaller subset of the population was limited.
They point out that, while there were no significant differences in incident AFib for either omega-3 fatty acid or vitamin D in the overall study population, an increased risk for incident AFib associated with randomized treatment was observed in selected subgroups.
For omega-3 fatty acids, AFib risk was modestly increased in taller individuals, and for vitamin D3, elevations in AFib risk were observed in younger individuals and participants who drank less alcohol.
“Although the hazard ratios and tests for interaction were significant, the P values associated with these subgroup analyses have not been adjusted for multiple comparisons. Thus, these findings should be interpreted with caution and considered hypothesis generating,” they warn.
The VITAL Rhythm Study was supported by a grant from the National Heart, Lung, and Blood Institute. Dr. Albert reported receipt of grants from St Jude Medical, Abbott, and Roche Diagnostics. Dr. Curfman reports no relevant disclosures.
A version of this article first appeared on Medscape.com.
There may be a dose-related risk for atrial fibrillation (AFib) with omega-3 fatty acid intake, data from four randomized clinical trials suggest.
The latest trial to evaluate the association, the VITAL-RHYTHM study, showed that using a low dose of omega-3 fatty acids or a vitamin D supplement had no significant effect on the risks of developing incident AFib.
The trial, first reported at last year’s American Heart Association meeting, was published online March 16 in the Journal of the American Medical Association.
Together with three other randomized clinical trials, however, these results suggest a possible dose-related effect of omega-3 fatty acids on the risk for AFib, an accompanying “Editor’s Note” suggests.
The note, by JAMA deputy editor Gregory Curfman, MD, points out that in the past 2 years, four randomized clinical trials have provided data on the risk of AFib with omega-3 fatty acid intake.
In the STRENGTH and REDUCE-IT trials, both of which evaluated high doses (4 g/day) of omega-3 fatty acids in patients with heart disease (or at high risk for it), there was a highly statistically significant increase in risk for AFib in the omega-3 groups vs. controls in both trials.
In the OMEMI trial in elderly patients with a recent myocardial infarction, an intermediate dose (1.8 g/day) of omega-3 fatty acids also showed an increase in AFib risk (hazard ratio, 1.84) but this was not significant. And now, the VITAL-RHYTHM trial shows no significant effect of a low dose (840 mg/day) of omega-3 fatty acids on the risk of developing AFib in a primary prevention population.
“Patients who choose to take omega-3 fatty acids, especially in high doses, should be informed of the risk of AF [AFib] and followed up for the possible development of this common and potentially hazardous arrhythmia,” Dr. Curfman concludes.
The authors of the VITAL-RHYTHM trial, led by Christine M. Albert, MD, MPH, Cedars-Sinai Medical Center, Los Angeles, Calif., explain that the trial was conducted after observational studies had shown that individuals with low blood levels of omega-3 fatty acids, eicosapentaenoic acid (EPA) and docosahexaenoic acid (DHA), and vitamin D3 have higher risks of incident AFib, but data on dietary or supplemental intake of these nutrients on AFib risk were mixed.
“To our knowledge, this study is the first randomized, placebo-controlled trial to prospectively test the effect of any intervention on incident AF and is the only trial to test alternative upstream preventive agents for AF in a large enough population over a long enough time period to provide an assessment of the plausible benefits and risks,” they write.
The VITAL-RHYTHM study was an ancillary trial embedded within the Vitamin D and Omega-3 (VITAL) trial, which used a 2 x 2 factorial design to evaluate daily supplementation with 2,000 IU of vitamin D3 and/or 840 mg of marine omega-3 fatty acids (460 mg EPA and 380 mg DHA), in the primary prevention of cardiovascular disease and cancer in 25,871 men and women age 50 and older in the United States.
Results showed that over a median 5.3 years of treatment and follow-up, the primary endpoint of incident AFib occurred in 3.6% of the study population. For the omega-3 part of the trial, incident AFib events occurred in 3.7% of patients taking EPA/DHA vs. 3.4% of the placebo group, giving a hazard ratio of 1.09, which was not significant (P = .19).
For the vitamin D3 vs. placebo comparison, results were very similar, with incident AFib events occurring in 3.7% vs. 3.4% of participants, respectively, giving a hazard ratio of 1.09, which was again not significant (P = .19). There was no evidence for interaction between the two study agents.
“Overall, these findings do not support the use of supplemental EPA-DHA or vitamin D3 for the primary prevention of AFib and provide reassurance regarding lack of a major risk of AFib incidence associated with these commonly used supplements at these doses,” the authors conclude.
Noting that significant increases in AFib have been seen with much higher doses of omega-3 fatty acids in the REDUCE-IT and STRENGTH trials, they add: “Potentially, the adverse effect on AF risk may be dose related, and the higher dosages of EPA used in these other studies might account for the significant adverse effect on AF.”
The researchers say that, to their knowledge, this is the only randomized trial to assess the effect of vitamin D3 supplementation on AFib risk and results suggest a null effect. They add that subgroup analyses in patients with vitamin D levels considered deficient (<20 ng/mL) did not suggest a benefit; however, the power to detect a benefit in this much smaller subset of the population was limited.
They point out that, while there were no significant differences in incident AFib for either omega-3 fatty acid or vitamin D in the overall study population, an increased risk for incident AFib associated with randomized treatment was observed in selected subgroups.
For omega-3 fatty acids, AFib risk was modestly increased in taller individuals, and for vitamin D3, elevations in AFib risk were observed in younger individuals and participants who drank less alcohol.
“Although the hazard ratios and tests for interaction were significant, the P values associated with these subgroup analyses have not been adjusted for multiple comparisons. Thus, these findings should be interpreted with caution and considered hypothesis generating,” they warn.
The VITAL Rhythm Study was supported by a grant from the National Heart, Lung, and Blood Institute. Dr. Albert reported receipt of grants from St Jude Medical, Abbott, and Roche Diagnostics. Dr. Curfman reports no relevant disclosures.
A version of this article first appeared on Medscape.com.
There may be a dose-related risk for atrial fibrillation (AFib) with omega-3 fatty acid intake, data from four randomized clinical trials suggest.
The latest trial to evaluate the association, the VITAL-RHYTHM study, showed that using a low dose of omega-3 fatty acids or a vitamin D supplement had no significant effect on the risks of developing incident AFib.
The trial, first reported at last year’s American Heart Association meeting, was published online March 16 in the Journal of the American Medical Association.
Together with three other randomized clinical trials, however, these results suggest a possible dose-related effect of omega-3 fatty acids on the risk for AFib, an accompanying “Editor’s Note” suggests.
The note, by JAMA deputy editor Gregory Curfman, MD, points out that in the past 2 years, four randomized clinical trials have provided data on the risk of AFib with omega-3 fatty acid intake.
In the STRENGTH and REDUCE-IT trials, both of which evaluated high doses (4 g/day) of omega-3 fatty acids in patients with heart disease (or at high risk for it), there was a highly statistically significant increase in risk for AFib in the omega-3 groups vs. controls in both trials.
In the OMEMI trial in elderly patients with a recent myocardial infarction, an intermediate dose (1.8 g/day) of omega-3 fatty acids also showed an increase in AFib risk (hazard ratio, 1.84) but this was not significant. And now, the VITAL-RHYTHM trial shows no significant effect of a low dose (840 mg/day) of omega-3 fatty acids on the risk of developing AFib in a primary prevention population.
“Patients who choose to take omega-3 fatty acids, especially in high doses, should be informed of the risk of AF [AFib] and followed up for the possible development of this common and potentially hazardous arrhythmia,” Dr. Curfman concludes.
The authors of the VITAL-RHYTHM trial, led by Christine M. Albert, MD, MPH, Cedars-Sinai Medical Center, Los Angeles, Calif., explain that the trial was conducted after observational studies had shown that individuals with low blood levels of omega-3 fatty acids, eicosapentaenoic acid (EPA) and docosahexaenoic acid (DHA), and vitamin D3 have higher risks of incident AFib, but data on dietary or supplemental intake of these nutrients on AFib risk were mixed.
“To our knowledge, this study is the first randomized, placebo-controlled trial to prospectively test the effect of any intervention on incident AF and is the only trial to test alternative upstream preventive agents for AF in a large enough population over a long enough time period to provide an assessment of the plausible benefits and risks,” they write.
The VITAL-RHYTHM study was an ancillary trial embedded within the Vitamin D and Omega-3 (VITAL) trial, which used a 2 x 2 factorial design to evaluate daily supplementation with 2,000 IU of vitamin D3 and/or 840 mg of marine omega-3 fatty acids (460 mg EPA and 380 mg DHA), in the primary prevention of cardiovascular disease and cancer in 25,871 men and women age 50 and older in the United States.
Results showed that over a median 5.3 years of treatment and follow-up, the primary endpoint of incident AFib occurred in 3.6% of the study population. For the omega-3 part of the trial, incident AFib events occurred in 3.7% of patients taking EPA/DHA vs. 3.4% of the placebo group, giving a hazard ratio of 1.09, which was not significant (P = .19).
For the vitamin D3 vs. placebo comparison, results were very similar, with incident AFib events occurring in 3.7% vs. 3.4% of participants, respectively, giving a hazard ratio of 1.09, which was again not significant (P = .19). There was no evidence for interaction between the two study agents.
“Overall, these findings do not support the use of supplemental EPA-DHA or vitamin D3 for the primary prevention of AFib and provide reassurance regarding lack of a major risk of AFib incidence associated with these commonly used supplements at these doses,” the authors conclude.
Noting that significant increases in AFib have been seen with much higher doses of omega-3 fatty acids in the REDUCE-IT and STRENGTH trials, they add: “Potentially, the adverse effect on AF risk may be dose related, and the higher dosages of EPA used in these other studies might account for the significant adverse effect on AF.”
The researchers say that, to their knowledge, this is the only randomized trial to assess the effect of vitamin D3 supplementation on AFib risk and results suggest a null effect. They add that subgroup analyses in patients with vitamin D levels considered deficient (<20 ng/mL) did not suggest a benefit; however, the power to detect a benefit in this much smaller subset of the population was limited.
They point out that, while there were no significant differences in incident AFib for either omega-3 fatty acid or vitamin D in the overall study population, an increased risk for incident AFib associated with randomized treatment was observed in selected subgroups.
For omega-3 fatty acids, AFib risk was modestly increased in taller individuals, and for vitamin D3, elevations in AFib risk were observed in younger individuals and participants who drank less alcohol.
“Although the hazard ratios and tests for interaction were significant, the P values associated with these subgroup analyses have not been adjusted for multiple comparisons. Thus, these findings should be interpreted with caution and considered hypothesis generating,” they warn.
The VITAL Rhythm Study was supported by a grant from the National Heart, Lung, and Blood Institute. Dr. Albert reported receipt of grants from St Jude Medical, Abbott, and Roche Diagnostics. Dr. Curfman reports no relevant disclosures.
A version of this article first appeared on Medscape.com.
High obesity rates in Southern states magnify COVID threats
In January, as Mississippi health officials planned for their incoming shipments of COVID-19 vaccine, they assessed the state’s most vulnerable: health care workers, of course, and elderly people in nursing homes. But among those who needed urgent protection from the virus ripping across the Magnolia State were 1 million Mississippians with obesity.
Obesity and weight-related illnesses have been deadly liabilities in the COVID era. A report released this month by the World Obesity Federation found that increased body weight is the second-greatest predictor of COVID-related hospitalization and death across the globe, trailing only old age as a risk factor.
As a fixture of life in the American South – home to 9 of the nation’s 12 heaviest states – obesity is playing a role not only in COVID outcomes, but in the calculus of the vaccination rollout. Mississippi was one of the first states to add a body mass index of 30 or more (a rough gauge of obesity tied to height and weight) to the list of qualifying medical conditions for a shot. About 40% of the state’s adults meet that definition, according to federal health survey data, and combined with the risk group already eligible for vaccination – residents 65 and older – that means fully half of Mississippi’s adults are entitled to vie for a restricted allotment of shots.
At least 29 states have green-lighted obesity for inclusion in the first phases of the vaccine rollout, according to KFF – a vast widening of eligibility that has the potential to overwhelm government efforts and heighten competition for scarce doses.
“We have a lifesaving intervention, and we don’t have enough of it,” said Jen Kates, PhD, director of global health and HIV policy for Kaiser Family Foundation. “Hard choices are being made about who should go first, and there is no right answer.”
The sheer prevalence of obesity in the nation – two in three Americans exceed what is considered a healthy weight – was a public health concern well before the pandemic. But COVID-19 dramatically fast-tracked the discussion from warnings about the long-term damage excess fat tissue can pose to heart, lung and metabolic functions to far more immediate threats.
In the United Kingdom, for example, overweight COVID patients were 67% more likely to require intensive care, and obese patients three times likelier, according to the World Obesity Federation report. A Centers for Disease Control and Prevention study released Monday found a similar trend among U.S. patients and noted that the risk of COVID-related hospitalization, ventilation and death increased with patients’ obesity level.
The counties that hug the southern Mississippi River are home to some of the most concentrated pockets of extreme obesity in the United States. Coronavirus infections began surging in Southern states early last summer, and hospitalizations rose in step.
Deaths in rural stretches of Arkansas, Louisiana, Mississippi, and Tennessee have been overshadowed by the sheer number of deaths in metropolitan areas like New York, Los Angeles, and Essex County, N.J. But as a share of the population, the coronavirus has been similarly unsparing in many Southern communities. In sparsely populated Claiborne County, Miss., on the floodplains of the Mississippi River, 30 residents – about 1 in 300 – had died as of early March. In East Feliciana Parish, La., north of Baton Rouge, with 106 deaths, about 1 in 180 had died by then.
“It’s just math. If the population is more obese and obesity clearly contributes to worse outcomes, then neighborhoods, cities, states and countries that are more obese will have a greater toll from COVID,” said Dr. James de Lemos, MD, a professor of internal medicine at UT Southwestern Medical Center in Dallas who led a study of hospitalized COVID patients published in the medical journal Circulation.
And, because in the U.S. obesity rates tend to be relatively high among African Americans and Latinos who are poor, with diminished access to health care, “it’s a triple whammy,” Dr. de Lemos said. “All these things intersect.”
Poverty and limited access to medical care are common features in the South, where residents like Michelle Antonyshyn, a former registered nurse and mother of seven in Salem, Ark., say they are afraid of the virus. Ms. Antonyshyn, 49, has obesity and debilitating pain in her knees and back, though she does not have high blood pressure or diabetes, two underlying conditions that federal health officials have determined are added risk factors for severe cases of COVID-19.
Still, she said, she “was very concerned just knowing that being obese puts you more at risk for bad outcomes such as being on a ventilator and death.” As a precaution, Ms. Antonyshyn said, she and her large brood locked down early and stopped attending church services in person, watching online instead.
“It’s not the same as having fellowship, but the risk for me was enough,” said Ms. Antonyshyn.
Governors throughout the South seem to recognize that weight can contribute to COVID-19 complications and have pushed for vaccine eligibility rules that prioritize obesity. But on the ground, local health officials are girding for having to tell newly eligible people who qualify as obese that there aren’t enough shots to go around.
In Port Gibson, Miss., Mheja Williams, MD, medical director of the Claiborne County Family Health Center, has been receiving barely enough doses to inoculate the health workers and oldest seniors in her county of 9,600. One week in early February, she received 100 doses.
Obesity and extreme obesity are endemic in Claiborne County, and health officials say the “normalization” of obesity means people often don’t register their weight as a risk factor, whether for COVID or other health issues. The risks are exacerbated by a general flouting of pandemic etiquette: Dr. Williams said that middle-aged and younger residents are not especially vigilant about physical distancing and that mask use is rare.
The rise of obesity in the United States is well documented over the past half-century, as the nation turned from a diet of fruits, vegetables and limited meats to one laden with ultra-processed foods and rich with salt, fat, sugar, and flavorings, along with copious amounts of meat, fast food, and soda. The U.S. has generally led the global obesity race, setting records as even toddlers and young children grew implausibly, dangerously overweight.
Well before COVID, obesity was a leading cause of preventable death in the United States. The National Institutes of Health declared it a disease in 1998, one that fosters heart disease, stroke, type 2 diabetes, and breast, colon, and other cancers.
Researchers say it is no coincidence that nations like the United States, the United Kingdom, and Italy, with relatively high obesity rates, have proved particularly vulnerable to the novel coronavirus.
They believe the virus may exploit underlying metabolic and physiological impairments that often exist in concert with obesity. Extra fat can lead to a cascade of metabolic disruptions, chronic systemic inflammation, and hormonal dysregulation that may thwart the body’s response to infection.
Other respiratory viruses, like influenza and SARS, which appeared in China in 2002, rely on cholesterol to spread enveloped RNA virus to neighboring cells, and researchers have proposed that a similar mechanism may play a role in the spread of the novel coronavirus.
There are also practical problems for coronavirus patients with obesity admitted to the hospital. They can be more difficult to intubate because of excess central weight pressing down on the diaphragm, making breathing with infected lungs even more difficult.
Physicians who specialize in treating patients with obesity say public health officials need to be more forthright and urgent in their messaging, telegraphing the risks of this COVID era.
“It should be explicit and direct,” said Fatima Stanford, MD, an obesity medicine specialist at Massachusetts General Hospital, Boston, and a Harvard Medical School instructor.
Dr. Stanford denounces the fat-shaming and bullying that people with obesity often experience. But telling patients – and the public – that obesity increases the risk of hospitalization and death is crucial, she said.
“I don’t think it’s stigmatizing,” she said. “If you tell them in that way, it’s not to scare you, it’s just giving information. Sometimes people are just unaware.”
KHN (Kaiser Health News) is a national newsroom that produces in-depth journalism about health issues. Together with Policy Analysis and Polling, KHN is one of the three major operating programs at KFF (Kaiser Family Foundation). KFF is an endowed nonprofit organization providing information on health issues to the nation.
In January, as Mississippi health officials planned for their incoming shipments of COVID-19 vaccine, they assessed the state’s most vulnerable: health care workers, of course, and elderly people in nursing homes. But among those who needed urgent protection from the virus ripping across the Magnolia State were 1 million Mississippians with obesity.
Obesity and weight-related illnesses have been deadly liabilities in the COVID era. A report released this month by the World Obesity Federation found that increased body weight is the second-greatest predictor of COVID-related hospitalization and death across the globe, trailing only old age as a risk factor.
As a fixture of life in the American South – home to 9 of the nation’s 12 heaviest states – obesity is playing a role not only in COVID outcomes, but in the calculus of the vaccination rollout. Mississippi was one of the first states to add a body mass index of 30 or more (a rough gauge of obesity tied to height and weight) to the list of qualifying medical conditions for a shot. About 40% of the state’s adults meet that definition, according to federal health survey data, and combined with the risk group already eligible for vaccination – residents 65 and older – that means fully half of Mississippi’s adults are entitled to vie for a restricted allotment of shots.
At least 29 states have green-lighted obesity for inclusion in the first phases of the vaccine rollout, according to KFF – a vast widening of eligibility that has the potential to overwhelm government efforts and heighten competition for scarce doses.
“We have a lifesaving intervention, and we don’t have enough of it,” said Jen Kates, PhD, director of global health and HIV policy for Kaiser Family Foundation. “Hard choices are being made about who should go first, and there is no right answer.”
The sheer prevalence of obesity in the nation – two in three Americans exceed what is considered a healthy weight – was a public health concern well before the pandemic. But COVID-19 dramatically fast-tracked the discussion from warnings about the long-term damage excess fat tissue can pose to heart, lung and metabolic functions to far more immediate threats.
In the United Kingdom, for example, overweight COVID patients were 67% more likely to require intensive care, and obese patients three times likelier, according to the World Obesity Federation report. A Centers for Disease Control and Prevention study released Monday found a similar trend among U.S. patients and noted that the risk of COVID-related hospitalization, ventilation and death increased with patients’ obesity level.
The counties that hug the southern Mississippi River are home to some of the most concentrated pockets of extreme obesity in the United States. Coronavirus infections began surging in Southern states early last summer, and hospitalizations rose in step.
Deaths in rural stretches of Arkansas, Louisiana, Mississippi, and Tennessee have been overshadowed by the sheer number of deaths in metropolitan areas like New York, Los Angeles, and Essex County, N.J. But as a share of the population, the coronavirus has been similarly unsparing in many Southern communities. In sparsely populated Claiborne County, Miss., on the floodplains of the Mississippi River, 30 residents – about 1 in 300 – had died as of early March. In East Feliciana Parish, La., north of Baton Rouge, with 106 deaths, about 1 in 180 had died by then.
“It’s just math. If the population is more obese and obesity clearly contributes to worse outcomes, then neighborhoods, cities, states and countries that are more obese will have a greater toll from COVID,” said Dr. James de Lemos, MD, a professor of internal medicine at UT Southwestern Medical Center in Dallas who led a study of hospitalized COVID patients published in the medical journal Circulation.
And, because in the U.S. obesity rates tend to be relatively high among African Americans and Latinos who are poor, with diminished access to health care, “it’s a triple whammy,” Dr. de Lemos said. “All these things intersect.”
Poverty and limited access to medical care are common features in the South, where residents like Michelle Antonyshyn, a former registered nurse and mother of seven in Salem, Ark., say they are afraid of the virus. Ms. Antonyshyn, 49, has obesity and debilitating pain in her knees and back, though she does not have high blood pressure or diabetes, two underlying conditions that federal health officials have determined are added risk factors for severe cases of COVID-19.
Still, she said, she “was very concerned just knowing that being obese puts you more at risk for bad outcomes such as being on a ventilator and death.” As a precaution, Ms. Antonyshyn said, she and her large brood locked down early and stopped attending church services in person, watching online instead.
“It’s not the same as having fellowship, but the risk for me was enough,” said Ms. Antonyshyn.
Governors throughout the South seem to recognize that weight can contribute to COVID-19 complications and have pushed for vaccine eligibility rules that prioritize obesity. But on the ground, local health officials are girding for having to tell newly eligible people who qualify as obese that there aren’t enough shots to go around.
In Port Gibson, Miss., Mheja Williams, MD, medical director of the Claiborne County Family Health Center, has been receiving barely enough doses to inoculate the health workers and oldest seniors in her county of 9,600. One week in early February, she received 100 doses.
Obesity and extreme obesity are endemic in Claiborne County, and health officials say the “normalization” of obesity means people often don’t register their weight as a risk factor, whether for COVID or other health issues. The risks are exacerbated by a general flouting of pandemic etiquette: Dr. Williams said that middle-aged and younger residents are not especially vigilant about physical distancing and that mask use is rare.
The rise of obesity in the United States is well documented over the past half-century, as the nation turned from a diet of fruits, vegetables and limited meats to one laden with ultra-processed foods and rich with salt, fat, sugar, and flavorings, along with copious amounts of meat, fast food, and soda. The U.S. has generally led the global obesity race, setting records as even toddlers and young children grew implausibly, dangerously overweight.
Well before COVID, obesity was a leading cause of preventable death in the United States. The National Institutes of Health declared it a disease in 1998, one that fosters heart disease, stroke, type 2 diabetes, and breast, colon, and other cancers.
Researchers say it is no coincidence that nations like the United States, the United Kingdom, and Italy, with relatively high obesity rates, have proved particularly vulnerable to the novel coronavirus.
They believe the virus may exploit underlying metabolic and physiological impairments that often exist in concert with obesity. Extra fat can lead to a cascade of metabolic disruptions, chronic systemic inflammation, and hormonal dysregulation that may thwart the body’s response to infection.
Other respiratory viruses, like influenza and SARS, which appeared in China in 2002, rely on cholesterol to spread enveloped RNA virus to neighboring cells, and researchers have proposed that a similar mechanism may play a role in the spread of the novel coronavirus.
There are also practical problems for coronavirus patients with obesity admitted to the hospital. They can be more difficult to intubate because of excess central weight pressing down on the diaphragm, making breathing with infected lungs even more difficult.
Physicians who specialize in treating patients with obesity say public health officials need to be more forthright and urgent in their messaging, telegraphing the risks of this COVID era.
“It should be explicit and direct,” said Fatima Stanford, MD, an obesity medicine specialist at Massachusetts General Hospital, Boston, and a Harvard Medical School instructor.
Dr. Stanford denounces the fat-shaming and bullying that people with obesity often experience. But telling patients – and the public – that obesity increases the risk of hospitalization and death is crucial, she said.
“I don’t think it’s stigmatizing,” she said. “If you tell them in that way, it’s not to scare you, it’s just giving information. Sometimes people are just unaware.”
KHN (Kaiser Health News) is a national newsroom that produces in-depth journalism about health issues. Together with Policy Analysis and Polling, KHN is one of the three major operating programs at KFF (Kaiser Family Foundation). KFF is an endowed nonprofit organization providing information on health issues to the nation.
In January, as Mississippi health officials planned for their incoming shipments of COVID-19 vaccine, they assessed the state’s most vulnerable: health care workers, of course, and elderly people in nursing homes. But among those who needed urgent protection from the virus ripping across the Magnolia State were 1 million Mississippians with obesity.
Obesity and weight-related illnesses have been deadly liabilities in the COVID era. A report released this month by the World Obesity Federation found that increased body weight is the second-greatest predictor of COVID-related hospitalization and death across the globe, trailing only old age as a risk factor.
As a fixture of life in the American South – home to 9 of the nation’s 12 heaviest states – obesity is playing a role not only in COVID outcomes, but in the calculus of the vaccination rollout. Mississippi was one of the first states to add a body mass index of 30 or more (a rough gauge of obesity tied to height and weight) to the list of qualifying medical conditions for a shot. About 40% of the state’s adults meet that definition, according to federal health survey data, and combined with the risk group already eligible for vaccination – residents 65 and older – that means fully half of Mississippi’s adults are entitled to vie for a restricted allotment of shots.
At least 29 states have green-lighted obesity for inclusion in the first phases of the vaccine rollout, according to KFF – a vast widening of eligibility that has the potential to overwhelm government efforts and heighten competition for scarce doses.
“We have a lifesaving intervention, and we don’t have enough of it,” said Jen Kates, PhD, director of global health and HIV policy for Kaiser Family Foundation. “Hard choices are being made about who should go first, and there is no right answer.”
The sheer prevalence of obesity in the nation – two in three Americans exceed what is considered a healthy weight – was a public health concern well before the pandemic. But COVID-19 dramatically fast-tracked the discussion from warnings about the long-term damage excess fat tissue can pose to heart, lung and metabolic functions to far more immediate threats.
In the United Kingdom, for example, overweight COVID patients were 67% more likely to require intensive care, and obese patients three times likelier, according to the World Obesity Federation report. A Centers for Disease Control and Prevention study released Monday found a similar trend among U.S. patients and noted that the risk of COVID-related hospitalization, ventilation and death increased with patients’ obesity level.
The counties that hug the southern Mississippi River are home to some of the most concentrated pockets of extreme obesity in the United States. Coronavirus infections began surging in Southern states early last summer, and hospitalizations rose in step.
Deaths in rural stretches of Arkansas, Louisiana, Mississippi, and Tennessee have been overshadowed by the sheer number of deaths in metropolitan areas like New York, Los Angeles, and Essex County, N.J. But as a share of the population, the coronavirus has been similarly unsparing in many Southern communities. In sparsely populated Claiborne County, Miss., on the floodplains of the Mississippi River, 30 residents – about 1 in 300 – had died as of early March. In East Feliciana Parish, La., north of Baton Rouge, with 106 deaths, about 1 in 180 had died by then.
“It’s just math. If the population is more obese and obesity clearly contributes to worse outcomes, then neighborhoods, cities, states and countries that are more obese will have a greater toll from COVID,” said Dr. James de Lemos, MD, a professor of internal medicine at UT Southwestern Medical Center in Dallas who led a study of hospitalized COVID patients published in the medical journal Circulation.
And, because in the U.S. obesity rates tend to be relatively high among African Americans and Latinos who are poor, with diminished access to health care, “it’s a triple whammy,” Dr. de Lemos said. “All these things intersect.”
Poverty and limited access to medical care are common features in the South, where residents like Michelle Antonyshyn, a former registered nurse and mother of seven in Salem, Ark., say they are afraid of the virus. Ms. Antonyshyn, 49, has obesity and debilitating pain in her knees and back, though she does not have high blood pressure or diabetes, two underlying conditions that federal health officials have determined are added risk factors for severe cases of COVID-19.
Still, she said, she “was very concerned just knowing that being obese puts you more at risk for bad outcomes such as being on a ventilator and death.” As a precaution, Ms. Antonyshyn said, she and her large brood locked down early and stopped attending church services in person, watching online instead.
“It’s not the same as having fellowship, but the risk for me was enough,” said Ms. Antonyshyn.
Governors throughout the South seem to recognize that weight can contribute to COVID-19 complications and have pushed for vaccine eligibility rules that prioritize obesity. But on the ground, local health officials are girding for having to tell newly eligible people who qualify as obese that there aren’t enough shots to go around.
In Port Gibson, Miss., Mheja Williams, MD, medical director of the Claiborne County Family Health Center, has been receiving barely enough doses to inoculate the health workers and oldest seniors in her county of 9,600. One week in early February, she received 100 doses.
Obesity and extreme obesity are endemic in Claiborne County, and health officials say the “normalization” of obesity means people often don’t register their weight as a risk factor, whether for COVID or other health issues. The risks are exacerbated by a general flouting of pandemic etiquette: Dr. Williams said that middle-aged and younger residents are not especially vigilant about physical distancing and that mask use is rare.
The rise of obesity in the United States is well documented over the past half-century, as the nation turned from a diet of fruits, vegetables and limited meats to one laden with ultra-processed foods and rich with salt, fat, sugar, and flavorings, along with copious amounts of meat, fast food, and soda. The U.S. has generally led the global obesity race, setting records as even toddlers and young children grew implausibly, dangerously overweight.
Well before COVID, obesity was a leading cause of preventable death in the United States. The National Institutes of Health declared it a disease in 1998, one that fosters heart disease, stroke, type 2 diabetes, and breast, colon, and other cancers.
Researchers say it is no coincidence that nations like the United States, the United Kingdom, and Italy, with relatively high obesity rates, have proved particularly vulnerable to the novel coronavirus.
They believe the virus may exploit underlying metabolic and physiological impairments that often exist in concert with obesity. Extra fat can lead to a cascade of metabolic disruptions, chronic systemic inflammation, and hormonal dysregulation that may thwart the body’s response to infection.
Other respiratory viruses, like influenza and SARS, which appeared in China in 2002, rely on cholesterol to spread enveloped RNA virus to neighboring cells, and researchers have proposed that a similar mechanism may play a role in the spread of the novel coronavirus.
There are also practical problems for coronavirus patients with obesity admitted to the hospital. They can be more difficult to intubate because of excess central weight pressing down on the diaphragm, making breathing with infected lungs even more difficult.
Physicians who specialize in treating patients with obesity say public health officials need to be more forthright and urgent in their messaging, telegraphing the risks of this COVID era.
“It should be explicit and direct,” said Fatima Stanford, MD, an obesity medicine specialist at Massachusetts General Hospital, Boston, and a Harvard Medical School instructor.
Dr. Stanford denounces the fat-shaming and bullying that people with obesity often experience. But telling patients – and the public – that obesity increases the risk of hospitalization and death is crucial, she said.
“I don’t think it’s stigmatizing,” she said. “If you tell them in that way, it’s not to scare you, it’s just giving information. Sometimes people are just unaware.”
KHN (Kaiser Health News) is a national newsroom that produces in-depth journalism about health issues. Together with Policy Analysis and Polling, KHN is one of the three major operating programs at KFF (Kaiser Family Foundation). KFF is an endowed nonprofit organization providing information on health issues to the nation.
Type 2 diabetes linked to increased risk for Parkinson’s
New analyses of both observational and genetic data have provided “convincing evidence” that type 2 diabetes is associated with an increased risk for Parkinson’s disease.

“The fact that we see the same effects in both types of analysis separately makes it more likely that these results are real – that type 2 diabetes really is a driver of Parkinson’s disease risk,” Alastair Noyce, PhD, senior author of the new studies, said in an interview.
The two analyses are reported in one paper published online March 8 in the journal Movement Disorders.
Dr. Noyce, clinical senior lecturer in the preventive neurology unit at the Wolfson Institute of Preventive Medicine, Queen Mary University of London, explained that his group is interested in risk factors for Parkinson’s disease, particularly those relevant at the population level and which might be modifiable.
“Several studies have looked at diabetes as a risk factor for Parkinson’s but very few have focused on type 2 diabetes, and, as this is such a growing health issue, we wanted to look at that in more detail,” he said.
The researchers performed two different analyses: a meta-analysis of observational studies investigating an association between type 2 diabetes and Parkinson’s; and a separate Mendelian randomization analysis of genetic data on the two conditions.
They found similar results in both studies, with the observational data suggesting type 2 diabetes was associated with a 21% increased risk for Parkinson’s disease and the genetic data suggesting an 8% increased risk. There were also hints that type 2 diabetes might also be associated with faster progression of Parkinson’s symptoms.
“I don’t think type 2 diabetes is a major cause of Parkinson’s, but it probably makes some contribution and may increase the risk of a more aggressive form of the condition,” Dr. Noyce said.
“I would say the increased risk of Parkinson’s disease attributable to type 2 diabetes may be similar to that of head injury or pesticide exposure, but it is important, as type 2 diabetes is very prevalent and is increasing,” he added. “As we see the growth in type 2 diabetes, this could lead to a later increase in Parkinson’s, which is already one of the fastest-growing diseases worldwide.”
For the meta-analysis of observational data, the researchers included nine studies that investigated preceding type 2 diabetes specifically and its effect on the risk for Parkinson’s disease and progression.
The pooled effect estimates showed that type 2 diabetes was associated with an increased risk for Parkinson’s disease (odds ratio, 1.21; 95% confidence interval, 1.07-1.36), and there was some evidence that type 2 diabetes was associated with faster progression of motor symptoms (standardized mean difference [SMD], 0.55) and cognitive decline (SMD, −0.92).
The observational meta-analysis included seven cohort studies and two case-control studies, and these different types of studies showed different results in regard to the association between diabetes and Parkinson’s. While the cohort studies showed a detrimental effect of diabetes on Parkinson’s risk (OR, 1.29), the case-control studies suggested protective effect (OR, 0.51).
Addressing this, Dr. Noyce noted that the case-control studies may be less reliable as they suffered more from survivor bias. “Diabetes may cause deaths in mid-life before people go on to develop Parkinson’s, and this would cause a protective effect to be seen, but we believe this to be a spurious result. Cohort studies are generally more reliable and are less susceptible to survivor bias,” he said.
For the genetic analysis, the researchers combined results from two large publicly available genome-wide association studies – one for type 2 diabetes and one for Parkinson’s disease to assess whether individuals with a genetic tendency to type 2 diabetes had a higher risk of developing Parkinson’s.
Results showed an increased risk for Parkinson’s in those individuals with genetic variants associated with type 2 diabetes, with an odds ratio of 1.08 (P = .010). There was also some evidence of an effect on motor progression (OR, 1.10; P = .032) but not on cognitive progression.
On the possible mechanism behind this observation, Dr. Noyce noted type 2 diabetes and Parkinson’s have some similarities in biology, including abnormal protein aggregation.
In the study, the authors also suggest that circulating insulin may have a neuroprotective role, whereas systemic and local insulin resistance can influence pathways known to be important in Parkinson’s pathogenesis, including those that relate to mitochondrial dysfunction, neuroinflammation, synaptic plasticity, and mitochondrial dysfunction.
Dr. Noyce further pointed out that several drugs used for the treatment of type 2 diabetes have been repurposed as possible treatments for Parkinson’s disease and are now being tested for this new indication. “Our results support that approach and raise the idea that some of these drugs may even prevent Parkinson’s in people at risk,” he said.
Most people who have type 2 diabetes won’t get Parkinson’s disease, he added. Other outcomes such as heart disease, kidney disease, and microvascular complications are far more likely, and the main aim of preventing and treating type 2 diabetes is to prevent these far more common outcomes. “But our data suggests that this could also have a possible benefit in reducing future Parkinson’s risk,” he said.
Not on the horizon at present is the possibility of screening patients with type 2 diabetes for signs of early Parkinson’s, Dr. Noyce said.
“There isn’t a test for identifying presymptomatic neurodegenerative diseases such as Parkinson’s yet, but perhaps in the future there will be, and type 2 diabetes may be one risk factor to take into account when considering such screening,” he added.
This work was financially supported by grants from The Michael J. Fox Foundation; the Canadian Consortium on Neurodegeneration in Aging (CCNA); the Canada First Research Excellence Fund (CFREF), awarded to McGill University for the Healthy Brains for Healthy Lives (HBHL) initiative; and Parkinson Canada, and the Intramural Research Program of the NIH, National Institute on Aging.
Dr. Noyce reports grants from the Barts Charity, Parkinson’s UK, Aligning Science Across Parkinson’s and Michael J. Fox Foundation, and the Virginia Keiley Benefaction; and personal fees/honoraria from Britannia, BIAL, AbbVie, Global Kinetics Corporation, Profile, Biogen, Roche, and UCB outside of the submitted work.
A version of this article first appeared on Medscape.com.
New analyses of both observational and genetic data have provided “convincing evidence” that type 2 diabetes is associated with an increased risk for Parkinson’s disease.
“The fact that we see the same effects in both types of analysis separately makes it more likely that these results are real – that type 2 diabetes really is a driver of Parkinson’s disease risk,” Alastair Noyce, PhD, senior author of the new studies, said in an interview.
The two analyses are reported in one paper published online March 8 in the journal Movement Disorders.
Dr. Noyce, clinical senior lecturer in the preventive neurology unit at the Wolfson Institute of Preventive Medicine, Queen Mary University of London, explained that his group is interested in risk factors for Parkinson’s disease, particularly those relevant at the population level and which might be modifiable.
“Several studies have looked at diabetes as a risk factor for Parkinson’s but very few have focused on type 2 diabetes, and, as this is such a growing health issue, we wanted to look at that in more detail,” he said.
The researchers performed two different analyses: a meta-analysis of observational studies investigating an association between type 2 diabetes and Parkinson’s; and a separate Mendelian randomization analysis of genetic data on the two conditions.
They found similar results in both studies, with the observational data suggesting type 2 diabetes was associated with a 21% increased risk for Parkinson’s disease and the genetic data suggesting an 8% increased risk. There were also hints that type 2 diabetes might also be associated with faster progression of Parkinson’s symptoms.
“I don’t think type 2 diabetes is a major cause of Parkinson’s, but it probably makes some contribution and may increase the risk of a more aggressive form of the condition,” Dr. Noyce said.
“I would say the increased risk of Parkinson’s disease attributable to type 2 diabetes may be similar to that of head injury or pesticide exposure, but it is important, as type 2 diabetes is very prevalent and is increasing,” he added. “As we see the growth in type 2 diabetes, this could lead to a later increase in Parkinson’s, which is already one of the fastest-growing diseases worldwide.”
For the meta-analysis of observational data, the researchers included nine studies that investigated preceding type 2 diabetes specifically and its effect on the risk for Parkinson’s disease and progression.
The pooled effect estimates showed that type 2 diabetes was associated with an increased risk for Parkinson’s disease (odds ratio, 1.21; 95% confidence interval, 1.07-1.36), and there was some evidence that type 2 diabetes was associated with faster progression of motor symptoms (standardized mean difference [SMD], 0.55) and cognitive decline (SMD, −0.92).
The observational meta-analysis included seven cohort studies and two case-control studies, and these different types of studies showed different results in regard to the association between diabetes and Parkinson’s. While the cohort studies showed a detrimental effect of diabetes on Parkinson’s risk (OR, 1.29), the case-control studies suggested protective effect (OR, 0.51).
Addressing this, Dr. Noyce noted that the case-control studies may be less reliable as they suffered more from survivor bias. “Diabetes may cause deaths in mid-life before people go on to develop Parkinson’s, and this would cause a protective effect to be seen, but we believe this to be a spurious result. Cohort studies are generally more reliable and are less susceptible to survivor bias,” he said.
For the genetic analysis, the researchers combined results from two large publicly available genome-wide association studies – one for type 2 diabetes and one for Parkinson’s disease to assess whether individuals with a genetic tendency to type 2 diabetes had a higher risk of developing Parkinson’s.
Results showed an increased risk for Parkinson’s in those individuals with genetic variants associated with type 2 diabetes, with an odds ratio of 1.08 (P = .010). There was also some evidence of an effect on motor progression (OR, 1.10; P = .032) but not on cognitive progression.
On the possible mechanism behind this observation, Dr. Noyce noted type 2 diabetes and Parkinson’s have some similarities in biology, including abnormal protein aggregation.
In the study, the authors also suggest that circulating insulin may have a neuroprotective role, whereas systemic and local insulin resistance can influence pathways known to be important in Parkinson’s pathogenesis, including those that relate to mitochondrial dysfunction, neuroinflammation, synaptic plasticity, and mitochondrial dysfunction.
Dr. Noyce further pointed out that several drugs used for the treatment of type 2 diabetes have been repurposed as possible treatments for Parkinson’s disease and are now being tested for this new indication. “Our results support that approach and raise the idea that some of these drugs may even prevent Parkinson’s in people at risk,” he said.
Most people who have type 2 diabetes won’t get Parkinson’s disease, he added. Other outcomes such as heart disease, kidney disease, and microvascular complications are far more likely, and the main aim of preventing and treating type 2 diabetes is to prevent these far more common outcomes. “But our data suggests that this could also have a possible benefit in reducing future Parkinson’s risk,” he said.
Not on the horizon at present is the possibility of screening patients with type 2 diabetes for signs of early Parkinson’s, Dr. Noyce said.
“There isn’t a test for identifying presymptomatic neurodegenerative diseases such as Parkinson’s yet, but perhaps in the future there will be, and type 2 diabetes may be one risk factor to take into account when considering such screening,” he added.
This work was financially supported by grants from The Michael J. Fox Foundation; the Canadian Consortium on Neurodegeneration in Aging (CCNA); the Canada First Research Excellence Fund (CFREF), awarded to McGill University for the Healthy Brains for Healthy Lives (HBHL) initiative; and Parkinson Canada, and the Intramural Research Program of the NIH, National Institute on Aging.
Dr. Noyce reports grants from the Barts Charity, Parkinson’s UK, Aligning Science Across Parkinson’s and Michael J. Fox Foundation, and the Virginia Keiley Benefaction; and personal fees/honoraria from Britannia, BIAL, AbbVie, Global Kinetics Corporation, Profile, Biogen, Roche, and UCB outside of the submitted work.
A version of this article first appeared on Medscape.com.
New analyses of both observational and genetic data have provided “convincing evidence” that type 2 diabetes is associated with an increased risk for Parkinson’s disease.
“The fact that we see the same effects in both types of analysis separately makes it more likely that these results are real – that type 2 diabetes really is a driver of Parkinson’s disease risk,” Alastair Noyce, PhD, senior author of the new studies, said in an interview.
The two analyses are reported in one paper published online March 8 in the journal Movement Disorders.
Dr. Noyce, clinical senior lecturer in the preventive neurology unit at the Wolfson Institute of Preventive Medicine, Queen Mary University of London, explained that his group is interested in risk factors for Parkinson’s disease, particularly those relevant at the population level and which might be modifiable.
“Several studies have looked at diabetes as a risk factor for Parkinson’s but very few have focused on type 2 diabetes, and, as this is such a growing health issue, we wanted to look at that in more detail,” he said.
The researchers performed two different analyses: a meta-analysis of observational studies investigating an association between type 2 diabetes and Parkinson’s; and a separate Mendelian randomization analysis of genetic data on the two conditions.
They found similar results in both studies, with the observational data suggesting type 2 diabetes was associated with a 21% increased risk for Parkinson’s disease and the genetic data suggesting an 8% increased risk. There were also hints that type 2 diabetes might also be associated with faster progression of Parkinson’s symptoms.
“I don’t think type 2 diabetes is a major cause of Parkinson’s, but it probably makes some contribution and may increase the risk of a more aggressive form of the condition,” Dr. Noyce said.
“I would say the increased risk of Parkinson’s disease attributable to type 2 diabetes may be similar to that of head injury or pesticide exposure, but it is important, as type 2 diabetes is very prevalent and is increasing,” he added. “As we see the growth in type 2 diabetes, this could lead to a later increase in Parkinson’s, which is already one of the fastest-growing diseases worldwide.”
For the meta-analysis of observational data, the researchers included nine studies that investigated preceding type 2 diabetes specifically and its effect on the risk for Parkinson’s disease and progression.
The pooled effect estimates showed that type 2 diabetes was associated with an increased risk for Parkinson’s disease (odds ratio, 1.21; 95% confidence interval, 1.07-1.36), and there was some evidence that type 2 diabetes was associated with faster progression of motor symptoms (standardized mean difference [SMD], 0.55) and cognitive decline (SMD, −0.92).
The observational meta-analysis included seven cohort studies and two case-control studies, and these different types of studies showed different results in regard to the association between diabetes and Parkinson’s. While the cohort studies showed a detrimental effect of diabetes on Parkinson’s risk (OR, 1.29), the case-control studies suggested protective effect (OR, 0.51).
Addressing this, Dr. Noyce noted that the case-control studies may be less reliable as they suffered more from survivor bias. “Diabetes may cause deaths in mid-life before people go on to develop Parkinson’s, and this would cause a protective effect to be seen, but we believe this to be a spurious result. Cohort studies are generally more reliable and are less susceptible to survivor bias,” he said.
For the genetic analysis, the researchers combined results from two large publicly available genome-wide association studies – one for type 2 diabetes and one for Parkinson’s disease to assess whether individuals with a genetic tendency to type 2 diabetes had a higher risk of developing Parkinson’s.
Results showed an increased risk for Parkinson’s in those individuals with genetic variants associated with type 2 diabetes, with an odds ratio of 1.08 (P = .010). There was also some evidence of an effect on motor progression (OR, 1.10; P = .032) but not on cognitive progression.
On the possible mechanism behind this observation, Dr. Noyce noted type 2 diabetes and Parkinson’s have some similarities in biology, including abnormal protein aggregation.
In the study, the authors also suggest that circulating insulin may have a neuroprotective role, whereas systemic and local insulin resistance can influence pathways known to be important in Parkinson’s pathogenesis, including those that relate to mitochondrial dysfunction, neuroinflammation, synaptic plasticity, and mitochondrial dysfunction.
Dr. Noyce further pointed out that several drugs used for the treatment of type 2 diabetes have been repurposed as possible treatments for Parkinson’s disease and are now being tested for this new indication. “Our results support that approach and raise the idea that some of these drugs may even prevent Parkinson’s in people at risk,” he said.
Most people who have type 2 diabetes won’t get Parkinson’s disease, he added. Other outcomes such as heart disease, kidney disease, and microvascular complications are far more likely, and the main aim of preventing and treating type 2 diabetes is to prevent these far more common outcomes. “But our data suggests that this could also have a possible benefit in reducing future Parkinson’s risk,” he said.
Not on the horizon at present is the possibility of screening patients with type 2 diabetes for signs of early Parkinson’s, Dr. Noyce said.
“There isn’t a test for identifying presymptomatic neurodegenerative diseases such as Parkinson’s yet, but perhaps in the future there will be, and type 2 diabetes may be one risk factor to take into account when considering such screening,” he added.
This work was financially supported by grants from The Michael J. Fox Foundation; the Canadian Consortium on Neurodegeneration in Aging (CCNA); the Canada First Research Excellence Fund (CFREF), awarded to McGill University for the Healthy Brains for Healthy Lives (HBHL) initiative; and Parkinson Canada, and the Intramural Research Program of the NIH, National Institute on Aging.
Dr. Noyce reports grants from the Barts Charity, Parkinson’s UK, Aligning Science Across Parkinson’s and Michael J. Fox Foundation, and the Virginia Keiley Benefaction; and personal fees/honoraria from Britannia, BIAL, AbbVie, Global Kinetics Corporation, Profile, Biogen, Roche, and UCB outside of the submitted work.
A version of this article first appeared on Medscape.com.
Evidence grows for food as RA treatment
Patients with rheumatoid arthritis are often eager to try dietary interventions in an effort to improve their symptoms. For guidance, they turn to their rheumatologists, who typically can offer little in terms of concrete evidence-based recommendations. That’s because their training didn’t emphasize the role of nutrients in rheumatic diseases, the scientific evidence has historically been sketchy, and the topic of diet and disease is rife with fad diets, inflated Internet claims, and hucksterism.
But that’s changing. Indeed, recent annual meetings of the American College of Rheumatology have featured randomized, controlled trials that bring welcome rigor to the field and provide findings of practical interest to clinicians and their patients, Orrin M. Troum, MD, said at the 2021 Rheumatology Winter Clinical Symposium.
He highlighted some of this work, including positive randomized trials of the dietary supplements Biqi – a traditional Chinese herbal medicine – as well as turmeric, along with reported progress in efforts to design a palatable anti-inflammatory diet that favorably alters the gut microbiome and systemic metabolome while improving clinical outcomes in patients with RA.
Dr. Troum, a rheumatologist at the University of Southern California, Los Angeles, and in private practice in Santa Monica, described a typical patient encounter in his clinic that appeared to resonate with his audience from throughout the country: “You can tell people to take another medicine and they’ll start shaking their head no before you’re finished. But when you say there are natural supplements that can help you, they’re saying ‘Yes!’ ”
RA improvement on an ITIS diet
Many physicians recommend a Mediterranean-style diet, first popularized in the landmark Seven Countries Study launched by the late Dr. Ancel Keys. This familiar plant-based regimen emphasizes liberal consumption of extra-virgin olive oil, legumes, fruits and vegetables, whole grains, fish, nuts, and moderate alcohol intake, with very limited intake of red and processed meats, refined grains, and sugar. There is strong evidence that the Mediterranean diet is cardioprotective, which is relevant to patients with RA since they are known to be at elevated cardiovascular risk.
However, investigators at the University of California, San Diego, became convinced that the Mediterranean diet is lacking in key anti-inflammatory ingredients from other parts of the world. These include ginger, green tea, black pepper, turmeric, miso, flax seeds, and tahini, all of which are backed by evidence – from animal models and/or interventional diet studies in patients – that suggests beneficial effects in pain and joint swelling in RA. The researchers also suspected that certain vegetables embraced in the Mediterranean diet – notably eggplant, tomatoes, and potatoes – might be problematic for RA patients because they contain solanine, thought to increase intestinal permeability, which might have arthritogenic effects on the gut microbiome.
The investigators set out to develop an anti-inflammatory diet they call the ITIS diet, essentially tweaking the Mediterranean-style diet by incorporating these additions and subtractions. Importantly, they designed the ITIS diet in conjunction with a multiracial local group of RA patients strongly enthusiastic about the potential for dietary interventions aimed at improving their symptoms. The patients provided feedback that enabled the investigators to fine-tune the anti-inflammatory diet so as to boost palatability and acceptance.
As an illustrative example of the ITIS diet, a typical day might start off with a homemade smoothie of parsley, pineapple, strawberries, and water, followed by a breakfast consisting of one or two corn tortillas spread with avocado, linseed oil, and sesame seeds, accompanied by green tea. Following a mid-morning snack of plain Greek-style yogurt, lunch might be a choice of a large salad, legumes with vegetables, or whole grains with vegetables. For the afternoon snack: four walnuts plus mango, banana, pear, papaya, apple, or pineapple. And for dinner, the options are vegetable soup and a protein; salad plus a protein; or miso soup, cooked vegetables, and a protein.
At the 2020 ACR annual meeting, Roxana Coras, MD, presented the positive findings of an open-label, pilot study of the ITIS diet in which 17 patients with active RA involving at least three tender and three swollen joints adopted the diet for 2 weeks . The ITIS diet turned out to be not too much of a stretch for Southern California RA patients interested in dietary complementary and alternative medicine. Many had already adopted some elements of the anti-inflammatory diet. Dietary adherence in the study was good, as monitored in food logs and by mass spectrometry metabolic profiling of fecal and plasma samples.
Eleven patients were categorized as responders to the anti-inflammatory diet as defined by at least a 50% improvement in pain scores from baseline to 2 weeks; six patients were nonresponders. In the overall study population, mean pain scores on a 0-10 visual analog scale improved from 3.9 to 2.45. Scores on the Clinical Disease Activity Index (CDAI) also improved significantly on the ITIS diet, from 29 to 12.7, reported Dr. Coras, a rheumatologist at the University of California, San Diego.
The mechanisms for the clinical improvement on the diet are under study. Significant differences in the gut microbiome and metabolome were seen between the responders and nonresponders. For example, Mollicutes were increased and Coriobacteriales decreased in clinical responders versus nonresponders. A significant increase in circulating levels of anti-inflammatory oxylipins was also seen in responders. Longer-term controlled studies of the ITIS diet are planned.
Biqi is big in China, gaining ground in the U.S.
Ayurvedic medicine in India and Chinese traditional herbal medicine have richly documented 4,500-year histories.
“It’s so common in my neck of the woods, where there are large Asian communities, for Chinese or Korean or Japanese or Indian medicines to be combined with our medicines. And if you don’t ask about them, you’re never going to find out what these patients are taking,” Dr. Troum said.
If they’re taking Biqi capsules, readily available on the Internet, be advised that there is randomized trial evidence to show that they’re using an efficacious and safe herbal medicine for RA. In China, the combination of Biqi capsules and a conventional disease-modifying antirheumatic drug such as methotrexate is now widely used for treatment of RA. And at the 2019 ACR annual meeting, Runyue Huang, MD, of Guangzhou University of Chinese Medicine, presented the results of a 24-week, randomized, multicenter, open-label clinical trial in which 70 RA patients were assigned to methotrexate plus a 1.2-g Biqi capsule twice daily or to methotrexate plus leflunomide (Arava) at 20 mg/day. The primary outcome – achievement of a 20% improvement in the ACR criteria, or ACR20 response, at week 24 – was achieved in 77% of the Biqi group, not significantly different from the 83% rate in the comparator group. However, the Biqi plus methotrexate group had significantly fewer adverse events and the combination was better tolerated than was leflunomide plus methotrexate.
In addition, a systematic review of earlier clinical trials concluded that Biqi in combination with methotrexate was more effective and had fewer adverse events than methotrexate alone.
“Biqi capsule with methotrexate appears to be a promising combination for RA if you can rest assured that what’s found in the Biqi capsule is exactly what they say. And that’s the main issue: You don’t really know what you’re getting unless it’s in a trial,” Dr. Troum said.
American RA patients embrace turmeric
Turmeric has played a prominent role in Ayurvedic medicine for millenia. The most medicinally important component of turmeric root is curcumin, which has potent anti-inflammatory and antioxidant properties. Americans with RA have gotten on the bandwagon, as demonstrated in a survey of 291 patients with RA or psoriatic arthritis presented at ACR 2020 by investigators from the University of Central Florida, Orlando. Among the respondents, 37% reported having taken curcumin, with no predilection based upon age, gender, or diagnosis. Fifty-nine percent took their curcumin in the form of capsules, with the rest took it as an oil or powder. Fifty-four percent got their curcumin at a local store.
Thirty-six percent of curcumin users reported improvement in pain after going on the herbal supplement. Twenty-five percent reported reduced swelling, 23% had less stiffness, and 16% reported improvement in fatigue. Patients taking 200-1,000 mg/day reported significantly greater improvement in symptoms than that of those taking less than 200 mg/day. Onset of benefits was slow: Patients on curcumin for a year or longer reported greater symptomatic improvement than did those on the supplement for less time.
Asked what he recommends to his RA patients who express interest in supplements aimed at achieving symptomatic improvement, Dr. Troum replied that he’s comfortable suggesting curcumin capsules at 500 mg twice daily, which should be labeled as containing black pepper extract to aid in absorption. He also recommends fish oil both for its cardioprotective benefits and because of randomized trial evidence that it enhances the chances of achieving ACR remission in patients on conventional disease-modifying antirheumatic drugs.
What about osteoarthritis?
Investigators with the National Institutes of Health–sponsored Osteoarthritis Initiative found in an analysis of the dietary patterns of 2,757 patients with mild to moderate knee OA who were followed annually for 6 years that participants could be grouped into two broad categories: Those who consumed what was termed the prudent diet, with high intake of fruits and vegetables, legumes, fish, and whole grains; and fans of the Western diet, characterized by lots of red meat, refined grains, and liberal consumption of French fries. Knee symptoms increased over time in dose-response fashion with greater adherence to the Western diet and decreased with higher prudent diet scores.
Also at ACR 2019, Australian investigators presented the results of the double-blind CurKOA trial, in which 70 participants with knee OA and moderate baseline effusion/synovitis by ultrasound were randomized to take a capsule containing 500 mg of turmeric root extract or identical placebo twice daily for 12 weeks. The group on turmeric plant extract experienced 9.11-mm greater reduction in knee pain on a 0- to 100-mm visual analog scale than did controls, which translates to a moderate standard effect size deemed by investigators to be “greater than other conventional pharmacologic therapies.” Overall, 63% of the turmeric group achieved a treatment response by OARSI-OMERACT criteria, a significantly better outcome than the 38% rate in controls. However, there was no significant between-group difference in knee structural measures as assessed by MRI in this relatively brief trial.
Anne M. Stevens, MD, PhD, senior director of immunology translational medicine at Janssen Pharmaceuticals and a pediatric rheumatologist at Seattle Children’s Hospital, rose from the audience to share that she recommends that her patients on high-dose curcumin not take NSAIDs because the two share a similar mechanism of action involving COX-2 inhibition, and the combination might therefore increase bleeding risk. But Dr. Troum said he hasn’t seen any increase in bleeding in his patients on both agents.
Dr. Troum has financial relationships with numerous pharmaceutical companies, but reported having no financial conflicts of interest regarding his presentation.
Patients with rheumatoid arthritis are often eager to try dietary interventions in an effort to improve their symptoms. For guidance, they turn to their rheumatologists, who typically can offer little in terms of concrete evidence-based recommendations. That’s because their training didn’t emphasize the role of nutrients in rheumatic diseases, the scientific evidence has historically been sketchy, and the topic of diet and disease is rife with fad diets, inflated Internet claims, and hucksterism.
But that’s changing. Indeed, recent annual meetings of the American College of Rheumatology have featured randomized, controlled trials that bring welcome rigor to the field and provide findings of practical interest to clinicians and their patients, Orrin M. Troum, MD, said at the 2021 Rheumatology Winter Clinical Symposium.
He highlighted some of this work, including positive randomized trials of the dietary supplements Biqi – a traditional Chinese herbal medicine – as well as turmeric, along with reported progress in efforts to design a palatable anti-inflammatory diet that favorably alters the gut microbiome and systemic metabolome while improving clinical outcomes in patients with RA.
Dr. Troum, a rheumatologist at the University of Southern California, Los Angeles, and in private practice in Santa Monica, described a typical patient encounter in his clinic that appeared to resonate with his audience from throughout the country: “You can tell people to take another medicine and they’ll start shaking their head no before you’re finished. But when you say there are natural supplements that can help you, they’re saying ‘Yes!’ ”
RA improvement on an ITIS diet
Many physicians recommend a Mediterranean-style diet, first popularized in the landmark Seven Countries Study launched by the late Dr. Ancel Keys. This familiar plant-based regimen emphasizes liberal consumption of extra-virgin olive oil, legumes, fruits and vegetables, whole grains, fish, nuts, and moderate alcohol intake, with very limited intake of red and processed meats, refined grains, and sugar. There is strong evidence that the Mediterranean diet is cardioprotective, which is relevant to patients with RA since they are known to be at elevated cardiovascular risk.
However, investigators at the University of California, San Diego, became convinced that the Mediterranean diet is lacking in key anti-inflammatory ingredients from other parts of the world. These include ginger, green tea, black pepper, turmeric, miso, flax seeds, and tahini, all of which are backed by evidence – from animal models and/or interventional diet studies in patients – that suggests beneficial effects in pain and joint swelling in RA. The researchers also suspected that certain vegetables embraced in the Mediterranean diet – notably eggplant, tomatoes, and potatoes – might be problematic for RA patients because they contain solanine, thought to increase intestinal permeability, which might have arthritogenic effects on the gut microbiome.
The investigators set out to develop an anti-inflammatory diet they call the ITIS diet, essentially tweaking the Mediterranean-style diet by incorporating these additions and subtractions. Importantly, they designed the ITIS diet in conjunction with a multiracial local group of RA patients strongly enthusiastic about the potential for dietary interventions aimed at improving their symptoms. The patients provided feedback that enabled the investigators to fine-tune the anti-inflammatory diet so as to boost palatability and acceptance.
As an illustrative example of the ITIS diet, a typical day might start off with a homemade smoothie of parsley, pineapple, strawberries, and water, followed by a breakfast consisting of one or two corn tortillas spread with avocado, linseed oil, and sesame seeds, accompanied by green tea. Following a mid-morning snack of plain Greek-style yogurt, lunch might be a choice of a large salad, legumes with vegetables, or whole grains with vegetables. For the afternoon snack: four walnuts plus mango, banana, pear, papaya, apple, or pineapple. And for dinner, the options are vegetable soup and a protein; salad plus a protein; or miso soup, cooked vegetables, and a protein.
At the 2020 ACR annual meeting, Roxana Coras, MD, presented the positive findings of an open-label, pilot study of the ITIS diet in which 17 patients with active RA involving at least three tender and three swollen joints adopted the diet for 2 weeks . The ITIS diet turned out to be not too much of a stretch for Southern California RA patients interested in dietary complementary and alternative medicine. Many had already adopted some elements of the anti-inflammatory diet. Dietary adherence in the study was good, as monitored in food logs and by mass spectrometry metabolic profiling of fecal and plasma samples.
Eleven patients were categorized as responders to the anti-inflammatory diet as defined by at least a 50% improvement in pain scores from baseline to 2 weeks; six patients were nonresponders. In the overall study population, mean pain scores on a 0-10 visual analog scale improved from 3.9 to 2.45. Scores on the Clinical Disease Activity Index (CDAI) also improved significantly on the ITIS diet, from 29 to 12.7, reported Dr. Coras, a rheumatologist at the University of California, San Diego.
The mechanisms for the clinical improvement on the diet are under study. Significant differences in the gut microbiome and metabolome were seen between the responders and nonresponders. For example, Mollicutes were increased and Coriobacteriales decreased in clinical responders versus nonresponders. A significant increase in circulating levels of anti-inflammatory oxylipins was also seen in responders. Longer-term controlled studies of the ITIS diet are planned.
Biqi is big in China, gaining ground in the U.S.
Ayurvedic medicine in India and Chinese traditional herbal medicine have richly documented 4,500-year histories.
“It’s so common in my neck of the woods, where there are large Asian communities, for Chinese or Korean or Japanese or Indian medicines to be combined with our medicines. And if you don’t ask about them, you’re never going to find out what these patients are taking,” Dr. Troum said.
If they’re taking Biqi capsules, readily available on the Internet, be advised that there is randomized trial evidence to show that they’re using an efficacious and safe herbal medicine for RA. In China, the combination of Biqi capsules and a conventional disease-modifying antirheumatic drug such as methotrexate is now widely used for treatment of RA. And at the 2019 ACR annual meeting, Runyue Huang, MD, of Guangzhou University of Chinese Medicine, presented the results of a 24-week, randomized, multicenter, open-label clinical trial in which 70 RA patients were assigned to methotrexate plus a 1.2-g Biqi capsule twice daily or to methotrexate plus leflunomide (Arava) at 20 mg/day. The primary outcome – achievement of a 20% improvement in the ACR criteria, or ACR20 response, at week 24 – was achieved in 77% of the Biqi group, not significantly different from the 83% rate in the comparator group. However, the Biqi plus methotrexate group had significantly fewer adverse events and the combination was better tolerated than was leflunomide plus methotrexate.
In addition, a systematic review of earlier clinical trials concluded that Biqi in combination with methotrexate was more effective and had fewer adverse events than methotrexate alone.
“Biqi capsule with methotrexate appears to be a promising combination for RA if you can rest assured that what’s found in the Biqi capsule is exactly what they say. And that’s the main issue: You don’t really know what you’re getting unless it’s in a trial,” Dr. Troum said.
American RA patients embrace turmeric
Turmeric has played a prominent role in Ayurvedic medicine for millenia. The most medicinally important component of turmeric root is curcumin, which has potent anti-inflammatory and antioxidant properties. Americans with RA have gotten on the bandwagon, as demonstrated in a survey of 291 patients with RA or psoriatic arthritis presented at ACR 2020 by investigators from the University of Central Florida, Orlando. Among the respondents, 37% reported having taken curcumin, with no predilection based upon age, gender, or diagnosis. Fifty-nine percent took their curcumin in the form of capsules, with the rest took it as an oil or powder. Fifty-four percent got their curcumin at a local store.
Thirty-six percent of curcumin users reported improvement in pain after going on the herbal supplement. Twenty-five percent reported reduced swelling, 23% had less stiffness, and 16% reported improvement in fatigue. Patients taking 200-1,000 mg/day reported significantly greater improvement in symptoms than that of those taking less than 200 mg/day. Onset of benefits was slow: Patients on curcumin for a year or longer reported greater symptomatic improvement than did those on the supplement for less time.
Asked what he recommends to his RA patients who express interest in supplements aimed at achieving symptomatic improvement, Dr. Troum replied that he’s comfortable suggesting curcumin capsules at 500 mg twice daily, which should be labeled as containing black pepper extract to aid in absorption. He also recommends fish oil both for its cardioprotective benefits and because of randomized trial evidence that it enhances the chances of achieving ACR remission in patients on conventional disease-modifying antirheumatic drugs.
What about osteoarthritis?
Investigators with the National Institutes of Health–sponsored Osteoarthritis Initiative found in an analysis of the dietary patterns of 2,757 patients with mild to moderate knee OA who were followed annually for 6 years that participants could be grouped into two broad categories: Those who consumed what was termed the prudent diet, with high intake of fruits and vegetables, legumes, fish, and whole grains; and fans of the Western diet, characterized by lots of red meat, refined grains, and liberal consumption of French fries. Knee symptoms increased over time in dose-response fashion with greater adherence to the Western diet and decreased with higher prudent diet scores.
Also at ACR 2019, Australian investigators presented the results of the double-blind CurKOA trial, in which 70 participants with knee OA and moderate baseline effusion/synovitis by ultrasound were randomized to take a capsule containing 500 mg of turmeric root extract or identical placebo twice daily for 12 weeks. The group on turmeric plant extract experienced 9.11-mm greater reduction in knee pain on a 0- to 100-mm visual analog scale than did controls, which translates to a moderate standard effect size deemed by investigators to be “greater than other conventional pharmacologic therapies.” Overall, 63% of the turmeric group achieved a treatment response by OARSI-OMERACT criteria, a significantly better outcome than the 38% rate in controls. However, there was no significant between-group difference in knee structural measures as assessed by MRI in this relatively brief trial.
Anne M. Stevens, MD, PhD, senior director of immunology translational medicine at Janssen Pharmaceuticals and a pediatric rheumatologist at Seattle Children’s Hospital, rose from the audience to share that she recommends that her patients on high-dose curcumin not take NSAIDs because the two share a similar mechanism of action involving COX-2 inhibition, and the combination might therefore increase bleeding risk. But Dr. Troum said he hasn’t seen any increase in bleeding in his patients on both agents.
Dr. Troum has financial relationships with numerous pharmaceutical companies, but reported having no financial conflicts of interest regarding his presentation.
Patients with rheumatoid arthritis are often eager to try dietary interventions in an effort to improve their symptoms. For guidance, they turn to their rheumatologists, who typically can offer little in terms of concrete evidence-based recommendations. That’s because their training didn’t emphasize the role of nutrients in rheumatic diseases, the scientific evidence has historically been sketchy, and the topic of diet and disease is rife with fad diets, inflated Internet claims, and hucksterism.
But that’s changing. Indeed, recent annual meetings of the American College of Rheumatology have featured randomized, controlled trials that bring welcome rigor to the field and provide findings of practical interest to clinicians and their patients, Orrin M. Troum, MD, said at the 2021 Rheumatology Winter Clinical Symposium.
He highlighted some of this work, including positive randomized trials of the dietary supplements Biqi – a traditional Chinese herbal medicine – as well as turmeric, along with reported progress in efforts to design a palatable anti-inflammatory diet that favorably alters the gut microbiome and systemic metabolome while improving clinical outcomes in patients with RA.
Dr. Troum, a rheumatologist at the University of Southern California, Los Angeles, and in private practice in Santa Monica, described a typical patient encounter in his clinic that appeared to resonate with his audience from throughout the country: “You can tell people to take another medicine and they’ll start shaking their head no before you’re finished. But when you say there are natural supplements that can help you, they’re saying ‘Yes!’ ”
RA improvement on an ITIS diet
Many physicians recommend a Mediterranean-style diet, first popularized in the landmark Seven Countries Study launched by the late Dr. Ancel Keys. This familiar plant-based regimen emphasizes liberal consumption of extra-virgin olive oil, legumes, fruits and vegetables, whole grains, fish, nuts, and moderate alcohol intake, with very limited intake of red and processed meats, refined grains, and sugar. There is strong evidence that the Mediterranean diet is cardioprotective, which is relevant to patients with RA since they are known to be at elevated cardiovascular risk.
However, investigators at the University of California, San Diego, became convinced that the Mediterranean diet is lacking in key anti-inflammatory ingredients from other parts of the world. These include ginger, green tea, black pepper, turmeric, miso, flax seeds, and tahini, all of which are backed by evidence – from animal models and/or interventional diet studies in patients – that suggests beneficial effects in pain and joint swelling in RA. The researchers also suspected that certain vegetables embraced in the Mediterranean diet – notably eggplant, tomatoes, and potatoes – might be problematic for RA patients because they contain solanine, thought to increase intestinal permeability, which might have arthritogenic effects on the gut microbiome.
The investigators set out to develop an anti-inflammatory diet they call the ITIS diet, essentially tweaking the Mediterranean-style diet by incorporating these additions and subtractions. Importantly, they designed the ITIS diet in conjunction with a multiracial local group of RA patients strongly enthusiastic about the potential for dietary interventions aimed at improving their symptoms. The patients provided feedback that enabled the investigators to fine-tune the anti-inflammatory diet so as to boost palatability and acceptance.
As an illustrative example of the ITIS diet, a typical day might start off with a homemade smoothie of parsley, pineapple, strawberries, and water, followed by a breakfast consisting of one or two corn tortillas spread with avocado, linseed oil, and sesame seeds, accompanied by green tea. Following a mid-morning snack of plain Greek-style yogurt, lunch might be a choice of a large salad, legumes with vegetables, or whole grains with vegetables. For the afternoon snack: four walnuts plus mango, banana, pear, papaya, apple, or pineapple. And for dinner, the options are vegetable soup and a protein; salad plus a protein; or miso soup, cooked vegetables, and a protein.
At the 2020 ACR annual meeting, Roxana Coras, MD, presented the positive findings of an open-label, pilot study of the ITIS diet in which 17 patients with active RA involving at least three tender and three swollen joints adopted the diet for 2 weeks . The ITIS diet turned out to be not too much of a stretch for Southern California RA patients interested in dietary complementary and alternative medicine. Many had already adopted some elements of the anti-inflammatory diet. Dietary adherence in the study was good, as monitored in food logs and by mass spectrometry metabolic profiling of fecal and plasma samples.
Eleven patients were categorized as responders to the anti-inflammatory diet as defined by at least a 50% improvement in pain scores from baseline to 2 weeks; six patients were nonresponders. In the overall study population, mean pain scores on a 0-10 visual analog scale improved from 3.9 to 2.45. Scores on the Clinical Disease Activity Index (CDAI) also improved significantly on the ITIS diet, from 29 to 12.7, reported Dr. Coras, a rheumatologist at the University of California, San Diego.
The mechanisms for the clinical improvement on the diet are under study. Significant differences in the gut microbiome and metabolome were seen between the responders and nonresponders. For example, Mollicutes were increased and Coriobacteriales decreased in clinical responders versus nonresponders. A significant increase in circulating levels of anti-inflammatory oxylipins was also seen in responders. Longer-term controlled studies of the ITIS diet are planned.
Biqi is big in China, gaining ground in the U.S.
Ayurvedic medicine in India and Chinese traditional herbal medicine have richly documented 4,500-year histories.
“It’s so common in my neck of the woods, where there are large Asian communities, for Chinese or Korean or Japanese or Indian medicines to be combined with our medicines. And if you don’t ask about them, you’re never going to find out what these patients are taking,” Dr. Troum said.
If they’re taking Biqi capsules, readily available on the Internet, be advised that there is randomized trial evidence to show that they’re using an efficacious and safe herbal medicine for RA. In China, the combination of Biqi capsules and a conventional disease-modifying antirheumatic drug such as methotrexate is now widely used for treatment of RA. And at the 2019 ACR annual meeting, Runyue Huang, MD, of Guangzhou University of Chinese Medicine, presented the results of a 24-week, randomized, multicenter, open-label clinical trial in which 70 RA patients were assigned to methotrexate plus a 1.2-g Biqi capsule twice daily or to methotrexate plus leflunomide (Arava) at 20 mg/day. The primary outcome – achievement of a 20% improvement in the ACR criteria, or ACR20 response, at week 24 – was achieved in 77% of the Biqi group, not significantly different from the 83% rate in the comparator group. However, the Biqi plus methotrexate group had significantly fewer adverse events and the combination was better tolerated than was leflunomide plus methotrexate.
In addition, a systematic review of earlier clinical trials concluded that Biqi in combination with methotrexate was more effective and had fewer adverse events than methotrexate alone.
“Biqi capsule with methotrexate appears to be a promising combination for RA if you can rest assured that what’s found in the Biqi capsule is exactly what they say. And that’s the main issue: You don’t really know what you’re getting unless it’s in a trial,” Dr. Troum said.
American RA patients embrace turmeric
Turmeric has played a prominent role in Ayurvedic medicine for millenia. The most medicinally important component of turmeric root is curcumin, which has potent anti-inflammatory and antioxidant properties. Americans with RA have gotten on the bandwagon, as demonstrated in a survey of 291 patients with RA or psoriatic arthritis presented at ACR 2020 by investigators from the University of Central Florida, Orlando. Among the respondents, 37% reported having taken curcumin, with no predilection based upon age, gender, or diagnosis. Fifty-nine percent took their curcumin in the form of capsules, with the rest took it as an oil or powder. Fifty-four percent got their curcumin at a local store.
Thirty-six percent of curcumin users reported improvement in pain after going on the herbal supplement. Twenty-five percent reported reduced swelling, 23% had less stiffness, and 16% reported improvement in fatigue. Patients taking 200-1,000 mg/day reported significantly greater improvement in symptoms than that of those taking less than 200 mg/day. Onset of benefits was slow: Patients on curcumin for a year or longer reported greater symptomatic improvement than did those on the supplement for less time.
Asked what he recommends to his RA patients who express interest in supplements aimed at achieving symptomatic improvement, Dr. Troum replied that he’s comfortable suggesting curcumin capsules at 500 mg twice daily, which should be labeled as containing black pepper extract to aid in absorption. He also recommends fish oil both for its cardioprotective benefits and because of randomized trial evidence that it enhances the chances of achieving ACR remission in patients on conventional disease-modifying antirheumatic drugs.
What about osteoarthritis?
Investigators with the National Institutes of Health–sponsored Osteoarthritis Initiative found in an analysis of the dietary patterns of 2,757 patients with mild to moderate knee OA who were followed annually for 6 years that participants could be grouped into two broad categories: Those who consumed what was termed the prudent diet, with high intake of fruits and vegetables, legumes, fish, and whole grains; and fans of the Western diet, characterized by lots of red meat, refined grains, and liberal consumption of French fries. Knee symptoms increased over time in dose-response fashion with greater adherence to the Western diet and decreased with higher prudent diet scores.
Also at ACR 2019, Australian investigators presented the results of the double-blind CurKOA trial, in which 70 participants with knee OA and moderate baseline effusion/synovitis by ultrasound were randomized to take a capsule containing 500 mg of turmeric root extract or identical placebo twice daily for 12 weeks. The group on turmeric plant extract experienced 9.11-mm greater reduction in knee pain on a 0- to 100-mm visual analog scale than did controls, which translates to a moderate standard effect size deemed by investigators to be “greater than other conventional pharmacologic therapies.” Overall, 63% of the turmeric group achieved a treatment response by OARSI-OMERACT criteria, a significantly better outcome than the 38% rate in controls. However, there was no significant between-group difference in knee structural measures as assessed by MRI in this relatively brief trial.
Anne M. Stevens, MD, PhD, senior director of immunology translational medicine at Janssen Pharmaceuticals and a pediatric rheumatologist at Seattle Children’s Hospital, rose from the audience to share that she recommends that her patients on high-dose curcumin not take NSAIDs because the two share a similar mechanism of action involving COX-2 inhibition, and the combination might therefore increase bleeding risk. But Dr. Troum said he hasn’t seen any increase in bleeding in his patients on both agents.
Dr. Troum has financial relationships with numerous pharmaceutical companies, but reported having no financial conflicts of interest regarding his presentation.
FROM RWCS 2021