User login
ASCO: String of Lackluster Results in ECOG Melanoma Trials
CHICAGO – A string of disappointing melanoma trials from the Eastern Cooperative Oncology Group left some seeing the proverbial glass as half empty, others as half full in an oral abstract session at the annual meeting of the American Society for Clinical Oncology.
No Benefit from GM-CSF
Updated data from the E4697 phase III cooperative trial in resected stage III and IV melanoma show only a hint of benefit for granulocyte-macrophage colony-stimulating factor (GM-CSF) in the adjuvant setting. The study was unblinded in April 2009, and an analysis reported later that year showed a significant improvement in disease-free survival for GM-CSF vs. placebo (P = .03), but no difference in overall survival.
In the updated analysis, with 86% of full data reported, the difference in disease-free survival at 9.2 months in 375 patients who were given placebo and 11.5 months in 368 patients who received GM-CSF was no longer significant (P = .14), Dr. David Lawson said. Again, there was no difference in overall survival.
GM-CSF also had no significant effect on either survival outcome in HLA A2–positive patients who also received peptide vaccination, said Dr. Lawson of Emory University in Atlanta.
A subset analysis that was stratified by disease stage, however, showed that GM-CSF did significantly improve disease-free survival in 258 patients with stage IV disease (hazard ratio 0.74, P = .04) but not overall survival (HR 0.72, P = .07).
Dr. Lawson said the data are worthy of further investigation and discussion. Invited discussant Dr. Michael S. Sabel of the University of Michigan in Ann Arbor said he is more skeptical, and would only go so far as to say that “you can’t take away the fact that there is some sort of immunologic effect potentially to these cytokines.”
Outcome Unchanged by Helper Peptides
Adding melanoma helper peptides to a multiepitope melanoma vaccination stimulated CD4+ and CD8+ T-cell responses, but did little to improve clinical outcome in the four-arm, phase II E1602 trial.
Patients with stage IV melanoma were vaccinated with 12 class I restricted melanoma peptides (arm A), plus either a tetanus peptide (arm B) or a mixture of six class II melanoma helper peptides (arm C), or with six class II melanoma helper peptides alone. Arm C was stopped early because of a lack of clinical response or disease stabilization.
The best overall response was partial response in 4% of 136 evaluable patients, said Dr. Craig L. Slingluff Jr., head of the surgical oncology division at the University of Virginia in Charlottesville. After a median follow-up of 21.4 months, median overall survival was 11.4 months, with no statistical differences between groups.
The trial can be viewed in two ways: as a success because it met the primary end point of stimulating T cells, but also as a requiem for peptide vaccines because “despite creating this army of antigen-specific T cells, the tumor continues to progress in the great majority of patients,” said invited discussant Dr. Antoni Ribas of the University of California, Los Angeles.
Adding Sorafenib Disappoints
There was little interpretation over the seventh and final analysis of the phase III E2603 trial of sorafenib (Nexavar) in combination with chemotherapy. Sorafenib does not improve overall survival, progression-free survival, or response rate when combined with carboplatin and paclitaxel in metastatic melanoma, reported Dr. Kevin Flaherty of Massachusetts General Hospital in Boston, who just 4 years ago set tongues wagging over sorafenib when he reported an 85% disease control rate in 105 melanoma patients.
Overall survival was 11.3 months, progression-free survival was 4.1 months, and the response rate was 16% with carboplatin/paclitaxel chemotherapy alone, compared with 11.1 months, 4.9 months, and 18%, respectively, for carboplatin/paclitaxel plus sorafenib. None of the differences was significantly different.
“There seem to be no additive effects, at least in melanoma,” said invited discussant Dr. Dirk Schadendorf, director of dermatology at University Hospital Essen (Germany). “What we have learned from the combination with chemotherapy, especially with carboplatin and paclitaxel, is that the progression-free survival time is around 4-5 months, which is interesting in patients who have rapid tumor progression and where you need a regimen to stop disease progression.”
Dr. Lawson reported a consultant/advisory role with Genzyme Corp. Dr. Slingluff reported a consultant/advisory role with and honoraria from Immatics Biotechnologies GmbH, research funding from Berlex Inc./Genzyme and GlaxoSmithKline, and other remuneration from the University of Virginia Patent Foundation. Dr. Ribas reported honoraria from Amgen Inc. and Roche. Dr. Flaherty disclosed no conflicts. Dr. Sabel reported a consultant/advisory role, honoraria, and research funding from Schering-Plough/Merck. Dr. Schadendorf disclosed consultant or advisory roles with AstraZeneca, Bristol-Myers Squibb Co., Plexxikon Inc., Roche, and Schering-Plough Corp., and research funding from Schering-Plough and Bayer-Schering.
CHICAGO – A string of disappointing melanoma trials from the Eastern Cooperative Oncology Group left some seeing the proverbial glass as half empty, others as half full in an oral abstract session at the annual meeting of the American Society for Clinical Oncology.
No Benefit from GM-CSF
Updated data from the E4697 phase III cooperative trial in resected stage III and IV melanoma show only a hint of benefit for granulocyte-macrophage colony-stimulating factor (GM-CSF) in the adjuvant setting. The study was unblinded in April 2009, and an analysis reported later that year showed a significant improvement in disease-free survival for GM-CSF vs. placebo (P = .03), but no difference in overall survival.
In the updated analysis, with 86% of full data reported, the difference in disease-free survival at 9.2 months in 375 patients who were given placebo and 11.5 months in 368 patients who received GM-CSF was no longer significant (P = .14), Dr. David Lawson said. Again, there was no difference in overall survival.
GM-CSF also had no significant effect on either survival outcome in HLA A2–positive patients who also received peptide vaccination, said Dr. Lawson of Emory University in Atlanta.
A subset analysis that was stratified by disease stage, however, showed that GM-CSF did significantly improve disease-free survival in 258 patients with stage IV disease (hazard ratio 0.74, P = .04) but not overall survival (HR 0.72, P = .07).
Dr. Lawson said the data are worthy of further investigation and discussion. Invited discussant Dr. Michael S. Sabel of the University of Michigan in Ann Arbor said he is more skeptical, and would only go so far as to say that “you can’t take away the fact that there is some sort of immunologic effect potentially to these cytokines.”
Outcome Unchanged by Helper Peptides
Adding melanoma helper peptides to a multiepitope melanoma vaccination stimulated CD4+ and CD8+ T-cell responses, but did little to improve clinical outcome in the four-arm, phase II E1602 trial.
Patients with stage IV melanoma were vaccinated with 12 class I restricted melanoma peptides (arm A), plus either a tetanus peptide (arm B) or a mixture of six class II melanoma helper peptides (arm C), or with six class II melanoma helper peptides alone. Arm C was stopped early because of a lack of clinical response or disease stabilization.
The best overall response was partial response in 4% of 136 evaluable patients, said Dr. Craig L. Slingluff Jr., head of the surgical oncology division at the University of Virginia in Charlottesville. After a median follow-up of 21.4 months, median overall survival was 11.4 months, with no statistical differences between groups.
The trial can be viewed in two ways: as a success because it met the primary end point of stimulating T cells, but also as a requiem for peptide vaccines because “despite creating this army of antigen-specific T cells, the tumor continues to progress in the great majority of patients,” said invited discussant Dr. Antoni Ribas of the University of California, Los Angeles.
Adding Sorafenib Disappoints
There was little interpretation over the seventh and final analysis of the phase III E2603 trial of sorafenib (Nexavar) in combination with chemotherapy. Sorafenib does not improve overall survival, progression-free survival, or response rate when combined with carboplatin and paclitaxel in metastatic melanoma, reported Dr. Kevin Flaherty of Massachusetts General Hospital in Boston, who just 4 years ago set tongues wagging over sorafenib when he reported an 85% disease control rate in 105 melanoma patients.
Overall survival was 11.3 months, progression-free survival was 4.1 months, and the response rate was 16% with carboplatin/paclitaxel chemotherapy alone, compared with 11.1 months, 4.9 months, and 18%, respectively, for carboplatin/paclitaxel plus sorafenib. None of the differences was significantly different.
“There seem to be no additive effects, at least in melanoma,” said invited discussant Dr. Dirk Schadendorf, director of dermatology at University Hospital Essen (Germany). “What we have learned from the combination with chemotherapy, especially with carboplatin and paclitaxel, is that the progression-free survival time is around 4-5 months, which is interesting in patients who have rapid tumor progression and where you need a regimen to stop disease progression.”
Dr. Lawson reported a consultant/advisory role with Genzyme Corp. Dr. Slingluff reported a consultant/advisory role with and honoraria from Immatics Biotechnologies GmbH, research funding from Berlex Inc./Genzyme and GlaxoSmithKline, and other remuneration from the University of Virginia Patent Foundation. Dr. Ribas reported honoraria from Amgen Inc. and Roche. Dr. Flaherty disclosed no conflicts. Dr. Sabel reported a consultant/advisory role, honoraria, and research funding from Schering-Plough/Merck. Dr. Schadendorf disclosed consultant or advisory roles with AstraZeneca, Bristol-Myers Squibb Co., Plexxikon Inc., Roche, and Schering-Plough Corp., and research funding from Schering-Plough and Bayer-Schering.
CHICAGO – A string of disappointing melanoma trials from the Eastern Cooperative Oncology Group left some seeing the proverbial glass as half empty, others as half full in an oral abstract session at the annual meeting of the American Society for Clinical Oncology.
No Benefit from GM-CSF
Updated data from the E4697 phase III cooperative trial in resected stage III and IV melanoma show only a hint of benefit for granulocyte-macrophage colony-stimulating factor (GM-CSF) in the adjuvant setting. The study was unblinded in April 2009, and an analysis reported later that year showed a significant improvement in disease-free survival for GM-CSF vs. placebo (P = .03), but no difference in overall survival.
In the updated analysis, with 86% of full data reported, the difference in disease-free survival at 9.2 months in 375 patients who were given placebo and 11.5 months in 368 patients who received GM-CSF was no longer significant (P = .14), Dr. David Lawson said. Again, there was no difference in overall survival.
GM-CSF also had no significant effect on either survival outcome in HLA A2–positive patients who also received peptide vaccination, said Dr. Lawson of Emory University in Atlanta.
A subset analysis that was stratified by disease stage, however, showed that GM-CSF did significantly improve disease-free survival in 258 patients with stage IV disease (hazard ratio 0.74, P = .04) but not overall survival (HR 0.72, P = .07).
Dr. Lawson said the data are worthy of further investigation and discussion. Invited discussant Dr. Michael S. Sabel of the University of Michigan in Ann Arbor said he is more skeptical, and would only go so far as to say that “you can’t take away the fact that there is some sort of immunologic effect potentially to these cytokines.”
Outcome Unchanged by Helper Peptides
Adding melanoma helper peptides to a multiepitope melanoma vaccination stimulated CD4+ and CD8+ T-cell responses, but did little to improve clinical outcome in the four-arm, phase II E1602 trial.
Patients with stage IV melanoma were vaccinated with 12 class I restricted melanoma peptides (arm A), plus either a tetanus peptide (arm B) or a mixture of six class II melanoma helper peptides (arm C), or with six class II melanoma helper peptides alone. Arm C was stopped early because of a lack of clinical response or disease stabilization.
The best overall response was partial response in 4% of 136 evaluable patients, said Dr. Craig L. Slingluff Jr., head of the surgical oncology division at the University of Virginia in Charlottesville. After a median follow-up of 21.4 months, median overall survival was 11.4 months, with no statistical differences between groups.
The trial can be viewed in two ways: as a success because it met the primary end point of stimulating T cells, but also as a requiem for peptide vaccines because “despite creating this army of antigen-specific T cells, the tumor continues to progress in the great majority of patients,” said invited discussant Dr. Antoni Ribas of the University of California, Los Angeles.
Adding Sorafenib Disappoints
There was little interpretation over the seventh and final analysis of the phase III E2603 trial of sorafenib (Nexavar) in combination with chemotherapy. Sorafenib does not improve overall survival, progression-free survival, or response rate when combined with carboplatin and paclitaxel in metastatic melanoma, reported Dr. Kevin Flaherty of Massachusetts General Hospital in Boston, who just 4 years ago set tongues wagging over sorafenib when he reported an 85% disease control rate in 105 melanoma patients.
Overall survival was 11.3 months, progression-free survival was 4.1 months, and the response rate was 16% with carboplatin/paclitaxel chemotherapy alone, compared with 11.1 months, 4.9 months, and 18%, respectively, for carboplatin/paclitaxel plus sorafenib. None of the differences was significantly different.
“There seem to be no additive effects, at least in melanoma,” said invited discussant Dr. Dirk Schadendorf, director of dermatology at University Hospital Essen (Germany). “What we have learned from the combination with chemotherapy, especially with carboplatin and paclitaxel, is that the progression-free survival time is around 4-5 months, which is interesting in patients who have rapid tumor progression and where you need a regimen to stop disease progression.”
Dr. Lawson reported a consultant/advisory role with Genzyme Corp. Dr. Slingluff reported a consultant/advisory role with and honoraria from Immatics Biotechnologies GmbH, research funding from Berlex Inc./Genzyme and GlaxoSmithKline, and other remuneration from the University of Virginia Patent Foundation. Dr. Ribas reported honoraria from Amgen Inc. and Roche. Dr. Flaherty disclosed no conflicts. Dr. Sabel reported a consultant/advisory role, honoraria, and research funding from Schering-Plough/Merck. Dr. Schadendorf disclosed consultant or advisory roles with AstraZeneca, Bristol-Myers Squibb Co., Plexxikon Inc., Roche, and Schering-Plough Corp., and research funding from Schering-Plough and Bayer-Schering.
Predicting Prognosis with Thin Melanoma

“Most patients do well at 5 years; 95% are doing fine,” Dr. Christopher J. Miller said at a summer symposium of the Alabama Dermatology Society.
This figure comes from a study (Arch. Dermatol. 2002:138:603-8) that found 95.3% of patients survive at least 5 years if they have thin (< 1 mm) melanoma, stage II/III disease, with no ulceration.
“About 10% are not doing as well,” Dr. Miller said, referring to a different group with thin melanoma (< 1 mm, stage IV/V with ulceration). In this group, study researchers found a 5-year survival rate of 90.9%.
So how do you estimate prognosis for your individual patient? Dr. Miller recommended www.melanomaprognosis.org, a fast and easy-to-use (I tried it!) instrument to estimate survival based on a few characteristics.
“This is a great tool … and a useful thing to have for your patients,” said Dr. Miller, director of dermatologic surgery at the University of Pennsylvania in Philadelphia. Using a number of factors to calculate survival is more accurate than relying on just one measure or using survival curves, he said.
I tried the site Dr. Miller recommended for a hypothetical patient with localized melanoma. I found that a 45-year-old with a 1-mm ulcerated lesion located on an axial site would have an estimate survival rate of:
98.8% at 1 year
96.8% at 2 years
86.5% at 5 years
73% at 10 years.
The online calculator was developed using the melanoma database of the American Joint Committee on Cancer.
–Damian McNamara @MedReporter on Twitter
“Most patients do well at 5 years; 95% are doing fine,” Dr. Christopher J. Miller said at a summer symposium of the Alabama Dermatology Society.
This figure comes from a study (Arch. Dermatol. 2002:138:603-8) that found 95.3% of patients survive at least 5 years if they have thin (< 1 mm) melanoma, stage II/III disease, with no ulceration.
“About 10% are not doing as well,” Dr. Miller said, referring to a different group with thin melanoma (< 1 mm, stage IV/V with ulceration). In this group, study researchers found a 5-year survival rate of 90.9%.
So how do you estimate prognosis for your individual patient? Dr. Miller recommended www.melanomaprognosis.org, a fast and easy-to-use (I tried it!) instrument to estimate survival based on a few characteristics.
“This is a great tool … and a useful thing to have for your patients,” said Dr. Miller, director of dermatologic surgery at the University of Pennsylvania in Philadelphia. Using a number of factors to calculate survival is more accurate than relying on just one measure or using survival curves, he said.
I tried the site Dr. Miller recommended for a hypothetical patient with localized melanoma. I found that a 45-year-old with a 1-mm ulcerated lesion located on an axial site would have an estimate survival rate of:
98.8% at 1 year
96.8% at 2 years
86.5% at 5 years
73% at 10 years.
The online calculator was developed using the melanoma database of the American Joint Committee on Cancer.
–Damian McNamara @MedReporter on Twitter
“Most patients do well at 5 years; 95% are doing fine,” Dr. Christopher J. Miller said at a summer symposium of the Alabama Dermatology Society.
This figure comes from a study (Arch. Dermatol. 2002:138:603-8) that found 95.3% of patients survive at least 5 years if they have thin (< 1 mm) melanoma, stage II/III disease, with no ulceration.
“About 10% are not doing as well,” Dr. Miller said, referring to a different group with thin melanoma (< 1 mm, stage IV/V with ulceration). In this group, study researchers found a 5-year survival rate of 90.9%.
So how do you estimate prognosis for your individual patient? Dr. Miller recommended www.melanomaprognosis.org, a fast and easy-to-use (I tried it!) instrument to estimate survival based on a few characteristics.
“This is a great tool … and a useful thing to have for your patients,” said Dr. Miller, director of dermatologic surgery at the University of Pennsylvania in Philadelphia. Using a number of factors to calculate survival is more accurate than relying on just one measure or using survival curves, he said.
I tried the site Dr. Miller recommended for a hypothetical patient with localized melanoma. I found that a 45-year-old with a 1-mm ulcerated lesion located on an axial site would have an estimate survival rate of:
98.8% at 1 year
96.8% at 2 years
86.5% at 5 years
73% at 10 years.
The online calculator was developed using the melanoma database of the American Joint Committee on Cancer.
–Damian McNamara @MedReporter on Twitter
ASCO: Percutaneous Hepatic Perfusion Offers Mixed Results in Metastatic Melanoma
CHICAGO — Percutaneous hepatic perfusion with melphalan improved local disease control, but not overall survival when compared with best available care in patients with ocular or cutaneous melanoma that had metastasized to the liver.
Chemoembolization is the standard of care in patients with hepatic metastases from ocular melanoma, a group that made up about 88% of the trial population. Systemic chemotherapy or immunotherapies do not appear to alter the natural history of the disease, which has a one-year survival of about 10%.
“Increased drug delivery achieved through novel regional therapeutic approaches may increase efficacy for a given agent (versus systemic administration) by overcoming a low therapeutic index,” said Dr. James Pingpank, Jr. who presented the late-breaking abstract at the annual meeting of the American Society of Clinical Oncology.
Forty-four patients were randomized to hepatic perfusion and 49 to best available care by the treating physician. More than half, 55%, of the control arm, crossed over to receive hepatic perfusion after hepatic progression.
High-dose melphalan at 3.0 mg/kg was infused into the hepatic artery via a percutaneously placed catheter with hepatic venous hemofiltration using a retrohepatic, double-balloon catheter and hemofiltration cartridges. Patients underwent 4 to 6 procedures at 28- to 35-day intervals.
The device and drug combination is under consideration by the Food and Drug Administration.
When compared with best available care, percutaneous hepatic perfusion increased median hepatic progression-free survival from 49 days to 245 days (hazard ratio 0.30, logrank P less than .0001), and overall progression-free survival from 46 days to 186 days (HR. 0.40, logrank P less than .0001).
No patients progressed while on hepatic perfusion with melphalan, and there were no differences in progression-free survival of ocular vs. cutaneous melanoma, said Dr. Pingpank of the University of Pittsburgh Hillman Cancer Center in Pittsburgh.
Median overall survival was similar at 301 days for best available care and 298 days for hepatic perfusion (HR 0.92, logrank P = .77). This was likely due to the high crossover rate, he said. When overall survival was examined in the control arm alone, it reached 398 days in patients who crossed over vs. 124 days for those who did not (logrank P = .0117).
Invited discussant Dr. Dirk Schadendorf, director of dermatology at University Hospital Essen in Essen, Germany, took issue with the high crossover rate and said a previous German trial (Br. J. Cancer 2002;87:840-5 also failed to show a significant survival advantage for intraarterial or IV fotemustine plus interferon-alpha and interleukin 2 in metastatic ocular melanoma.
“The clinical benefit besides local control is open and has not been answered by this trial,” he said. “The crossover in my view is a clear sign of bias and is not proving this treatment is of any benefit to the patient.”
Dr. Schadendorf said that additional relevant information is missing, such as the number of patients with liver-only metastases compared with other sites of metastasis, thus making it difficult to determine whether there is any potential patient imbalance between arms.
The most common therapy of the primary tumor was radiation in 52% of the experimental arm and 49% of the control arm, roughly 85% of patients had an ECOG performance status of 0, and their mean age was 55 years.
Expansion of the single-institution study to multiple centers proved safe and effective, Dr. Pingpank said. The most common grade 3/4 treatment-related toxicities in 40 evaluable patients receiving 116 perfusion treatments were thrombocytopenia (74%), neutropenia (61%), and anemia (47%). Three treatment-related deaths occurred, two due to neutropenic sepsis and one to hepatic failure.
Study sponsor Delcath Systems, Inc. provided melphalan and double-balloon catheters for the trial. The researchers disclosed serving on the scientific advisory board for and receiving research support from Delcath. Dr. Schadendorf disclosed honoraria or an advisory/consultancy role with AZD, Bristol-Myers Squibb, Plexxikon, Roche, Schering-Plough, and Bayer Schering Pharma.
CHICAGO — Percutaneous hepatic perfusion with melphalan improved local disease control, but not overall survival when compared with best available care in patients with ocular or cutaneous melanoma that had metastasized to the liver.
Chemoembolization is the standard of care in patients with hepatic metastases from ocular melanoma, a group that made up about 88% of the trial population. Systemic chemotherapy or immunotherapies do not appear to alter the natural history of the disease, which has a one-year survival of about 10%.
“Increased drug delivery achieved through novel regional therapeutic approaches may increase efficacy for a given agent (versus systemic administration) by overcoming a low therapeutic index,” said Dr. James Pingpank, Jr. who presented the late-breaking abstract at the annual meeting of the American Society of Clinical Oncology.
Forty-four patients were randomized to hepatic perfusion and 49 to best available care by the treating physician. More than half, 55%, of the control arm, crossed over to receive hepatic perfusion after hepatic progression.
High-dose melphalan at 3.0 mg/kg was infused into the hepatic artery via a percutaneously placed catheter with hepatic venous hemofiltration using a retrohepatic, double-balloon catheter and hemofiltration cartridges. Patients underwent 4 to 6 procedures at 28- to 35-day intervals.
The device and drug combination is under consideration by the Food and Drug Administration.
When compared with best available care, percutaneous hepatic perfusion increased median hepatic progression-free survival from 49 days to 245 days (hazard ratio 0.30, logrank P less than .0001), and overall progression-free survival from 46 days to 186 days (HR. 0.40, logrank P less than .0001).
No patients progressed while on hepatic perfusion with melphalan, and there were no differences in progression-free survival of ocular vs. cutaneous melanoma, said Dr. Pingpank of the University of Pittsburgh Hillman Cancer Center in Pittsburgh.
Median overall survival was similar at 301 days for best available care and 298 days for hepatic perfusion (HR 0.92, logrank P = .77). This was likely due to the high crossover rate, he said. When overall survival was examined in the control arm alone, it reached 398 days in patients who crossed over vs. 124 days for those who did not (logrank P = .0117).
Invited discussant Dr. Dirk Schadendorf, director of dermatology at University Hospital Essen in Essen, Germany, took issue with the high crossover rate and said a previous German trial (Br. J. Cancer 2002;87:840-5 also failed to show a significant survival advantage for intraarterial or IV fotemustine plus interferon-alpha and interleukin 2 in metastatic ocular melanoma.
“The clinical benefit besides local control is open and has not been answered by this trial,” he said. “The crossover in my view is a clear sign of bias and is not proving this treatment is of any benefit to the patient.”
Dr. Schadendorf said that additional relevant information is missing, such as the number of patients with liver-only metastases compared with other sites of metastasis, thus making it difficult to determine whether there is any potential patient imbalance between arms.
The most common therapy of the primary tumor was radiation in 52% of the experimental arm and 49% of the control arm, roughly 85% of patients had an ECOG performance status of 0, and their mean age was 55 years.
Expansion of the single-institution study to multiple centers proved safe and effective, Dr. Pingpank said. The most common grade 3/4 treatment-related toxicities in 40 evaluable patients receiving 116 perfusion treatments were thrombocytopenia (74%), neutropenia (61%), and anemia (47%). Three treatment-related deaths occurred, two due to neutropenic sepsis and one to hepatic failure.
Study sponsor Delcath Systems, Inc. provided melphalan and double-balloon catheters for the trial. The researchers disclosed serving on the scientific advisory board for and receiving research support from Delcath. Dr. Schadendorf disclosed honoraria or an advisory/consultancy role with AZD, Bristol-Myers Squibb, Plexxikon, Roche, Schering-Plough, and Bayer Schering Pharma.
CHICAGO — Percutaneous hepatic perfusion with melphalan improved local disease control, but not overall survival when compared with best available care in patients with ocular or cutaneous melanoma that had metastasized to the liver.
Chemoembolization is the standard of care in patients with hepatic metastases from ocular melanoma, a group that made up about 88% of the trial population. Systemic chemotherapy or immunotherapies do not appear to alter the natural history of the disease, which has a one-year survival of about 10%.
“Increased drug delivery achieved through novel regional therapeutic approaches may increase efficacy for a given agent (versus systemic administration) by overcoming a low therapeutic index,” said Dr. James Pingpank, Jr. who presented the late-breaking abstract at the annual meeting of the American Society of Clinical Oncology.
Forty-four patients were randomized to hepatic perfusion and 49 to best available care by the treating physician. More than half, 55%, of the control arm, crossed over to receive hepatic perfusion after hepatic progression.
High-dose melphalan at 3.0 mg/kg was infused into the hepatic artery via a percutaneously placed catheter with hepatic venous hemofiltration using a retrohepatic, double-balloon catheter and hemofiltration cartridges. Patients underwent 4 to 6 procedures at 28- to 35-day intervals.
The device and drug combination is under consideration by the Food and Drug Administration.
When compared with best available care, percutaneous hepatic perfusion increased median hepatic progression-free survival from 49 days to 245 days (hazard ratio 0.30, logrank P less than .0001), and overall progression-free survival from 46 days to 186 days (HR. 0.40, logrank P less than .0001).
No patients progressed while on hepatic perfusion with melphalan, and there were no differences in progression-free survival of ocular vs. cutaneous melanoma, said Dr. Pingpank of the University of Pittsburgh Hillman Cancer Center in Pittsburgh.
Median overall survival was similar at 301 days for best available care and 298 days for hepatic perfusion (HR 0.92, logrank P = .77). This was likely due to the high crossover rate, he said. When overall survival was examined in the control arm alone, it reached 398 days in patients who crossed over vs. 124 days for those who did not (logrank P = .0117).
Invited discussant Dr. Dirk Schadendorf, director of dermatology at University Hospital Essen in Essen, Germany, took issue with the high crossover rate and said a previous German trial (Br. J. Cancer 2002;87:840-5 also failed to show a significant survival advantage for intraarterial or IV fotemustine plus interferon-alpha and interleukin 2 in metastatic ocular melanoma.
“The clinical benefit besides local control is open and has not been answered by this trial,” he said. “The crossover in my view is a clear sign of bias and is not proving this treatment is of any benefit to the patient.”
Dr. Schadendorf said that additional relevant information is missing, such as the number of patients with liver-only metastases compared with other sites of metastasis, thus making it difficult to determine whether there is any potential patient imbalance between arms.
The most common therapy of the primary tumor was radiation in 52% of the experimental arm and 49% of the control arm, roughly 85% of patients had an ECOG performance status of 0, and their mean age was 55 years.
Expansion of the single-institution study to multiple centers proved safe and effective, Dr. Pingpank said. The most common grade 3/4 treatment-related toxicities in 40 evaluable patients receiving 116 perfusion treatments were thrombocytopenia (74%), neutropenia (61%), and anemia (47%). Three treatment-related deaths occurred, two due to neutropenic sepsis and one to hepatic failure.
Study sponsor Delcath Systems, Inc. provided melphalan and double-balloon catheters for the trial. The researchers disclosed serving on the scientific advisory board for and receiving research support from Delcath. Dr. Schadendorf disclosed honoraria or an advisory/consultancy role with AZD, Bristol-Myers Squibb, Plexxikon, Roche, Schering-Plough, and Bayer Schering Pharma.
Evidence Backs Imiquimod Tx for Melanoma in Situ
MIAMI — The topical immune response modulator imiquimod has a role in the treatment of melanoma in situ, particularly if patients refuse or fail surgery.
There are several concerns. The agent is only recommended for thinner lesions, and "failures do occur," said Dr. M. Shane Chapman of Darmouth-Hitchcock Medical Center in Lebanon, N.H. Also, "the 5-year follow-up data is not great—it's sparse. We are just not there yet."
Despite this, he said, imiquimod 5% cream (Aldara, Graceway) can have a role in the management of melanoma in situ, also known as lentigo maligna. Dr. Chapman acknowledged the controversial nature of his stance, and based his position on small case series, one "good prospective study" in the literature, and his own experience with more than 60 patients.
As an example, he discussed a 36-year-old man with metastatic melanoma. The patient had multiple surgeries and radiation therapy "and nothing seemed to work," he said. "I basically bathed him in imiquimod over several months." Six years later, the patient is doing well with no signs of nodal or metastatic disease. As with all melanoma patients, regardless of the therapy, they should be followed continuously for a lifetime, he said at the annual meeting of the American Academy of Dermatology.
In his regimen, imiquimod 5% cream is applied five times per week for 12 weeks, with a rest period on weekends. Inflammation can be intense with this aggressive protocol, so it is important to educate patients beforehand. Pretreatment with retinoids—such as tazarotene (Tazarac, Allergan) for 2 weeks—can increase the effectiveness of imiquimod in this setting, he added.
"The only good prospective study to date," Dr. Chapman said, is an open-label trial in which participants received daily treatment with topical 5% imiquimod for 3 months, followed by a biopsy 1 month post therapy (Br. J. Dermatol. 2003;149:66-70). The complete response rate was 93% in 28 patients with histologically confirmed lentigo maligna. Two patients were treatment failures.
Because of potential failures, "always go back and do a biopsy after clearance," he said.
For example, in a retrospective study of 40 patients pretreated with imiquimod (Dermatol. Surg. 2008;34:147-51), 30 appeared clinically clear after staged excision "but three of these had histologic evidence of disease—that is why I always do a follow-up biopsy."
One of his own patients failed after initial clearance of his lesion, Dr. Chapman said. The man had a large scalp lesion that cleared following use of topical imiquimod without retinoid treatment. "For 8 months, we thought he was cleared. He came back and had a node in middle of the lesion site—his third recurrence over 5 years." Dr. Chapman added, "He's doing well, but failures do occur."
It is important to realize that "we think we know when something is in situ, but we don't always know the entire lesion is in situ when we do this," Dr. Chapman said.
Even though surgical excision remains the first-line choice for most patients with melanoma in situ or thin melanoma lesions, surgery nonresponders or those who refuse resection can benefit from imiquimod. He cited three examples: a woman who did not want to have repeat surgery and whose lesion cleared with imiquimod; a man who did not want further surgery following two melanoma lesion excisions close together on his temple, who was treated well with imiquimod; and a patient with recurrent melanoma in situ at the forehead flap of the nose who is doing well 4 years out after imiquimod treatment.
In response to a question from the audience, Dr. Chapman said, "I don't think just any inflammatory response is going to make melanoma go away. Imiquimod is one of those serendipitous chemicals that is useful for a lot of skin tumors for some reason."
Dr. Chapman is a consultant for, and receives honoraria from, Graceway. He also receives honoraria from Abbott.
MIAMI — The topical immune response modulator imiquimod has a role in the treatment of melanoma in situ, particularly if patients refuse or fail surgery.
There are several concerns. The agent is only recommended for thinner lesions, and "failures do occur," said Dr. M. Shane Chapman of Darmouth-Hitchcock Medical Center in Lebanon, N.H. Also, "the 5-year follow-up data is not great—it's sparse. We are just not there yet."
Despite this, he said, imiquimod 5% cream (Aldara, Graceway) can have a role in the management of melanoma in situ, also known as lentigo maligna. Dr. Chapman acknowledged the controversial nature of his stance, and based his position on small case series, one "good prospective study" in the literature, and his own experience with more than 60 patients.
As an example, he discussed a 36-year-old man with metastatic melanoma. The patient had multiple surgeries and radiation therapy "and nothing seemed to work," he said. "I basically bathed him in imiquimod over several months." Six years later, the patient is doing well with no signs of nodal or metastatic disease. As with all melanoma patients, regardless of the therapy, they should be followed continuously for a lifetime, he said at the annual meeting of the American Academy of Dermatology.
In his regimen, imiquimod 5% cream is applied five times per week for 12 weeks, with a rest period on weekends. Inflammation can be intense with this aggressive protocol, so it is important to educate patients beforehand. Pretreatment with retinoids—such as tazarotene (Tazarac, Allergan) for 2 weeks—can increase the effectiveness of imiquimod in this setting, he added.
"The only good prospective study to date," Dr. Chapman said, is an open-label trial in which participants received daily treatment with topical 5% imiquimod for 3 months, followed by a biopsy 1 month post therapy (Br. J. Dermatol. 2003;149:66-70). The complete response rate was 93% in 28 patients with histologically confirmed lentigo maligna. Two patients were treatment failures.
Because of potential failures, "always go back and do a biopsy after clearance," he said.
For example, in a retrospective study of 40 patients pretreated with imiquimod (Dermatol. Surg. 2008;34:147-51), 30 appeared clinically clear after staged excision "but three of these had histologic evidence of disease—that is why I always do a follow-up biopsy."
One of his own patients failed after initial clearance of his lesion, Dr. Chapman said. The man had a large scalp lesion that cleared following use of topical imiquimod without retinoid treatment. "For 8 months, we thought he was cleared. He came back and had a node in middle of the lesion site—his third recurrence over 5 years." Dr. Chapman added, "He's doing well, but failures do occur."
It is important to realize that "we think we know when something is in situ, but we don't always know the entire lesion is in situ when we do this," Dr. Chapman said.
Even though surgical excision remains the first-line choice for most patients with melanoma in situ or thin melanoma lesions, surgery nonresponders or those who refuse resection can benefit from imiquimod. He cited three examples: a woman who did not want to have repeat surgery and whose lesion cleared with imiquimod; a man who did not want further surgery following two melanoma lesion excisions close together on his temple, who was treated well with imiquimod; and a patient with recurrent melanoma in situ at the forehead flap of the nose who is doing well 4 years out after imiquimod treatment.
In response to a question from the audience, Dr. Chapman said, "I don't think just any inflammatory response is going to make melanoma go away. Imiquimod is one of those serendipitous chemicals that is useful for a lot of skin tumors for some reason."
Dr. Chapman is a consultant for, and receives honoraria from, Graceway. He also receives honoraria from Abbott.
MIAMI — The topical immune response modulator imiquimod has a role in the treatment of melanoma in situ, particularly if patients refuse or fail surgery.
There are several concerns. The agent is only recommended for thinner lesions, and "failures do occur," said Dr. M. Shane Chapman of Darmouth-Hitchcock Medical Center in Lebanon, N.H. Also, "the 5-year follow-up data is not great—it's sparse. We are just not there yet."
Despite this, he said, imiquimod 5% cream (Aldara, Graceway) can have a role in the management of melanoma in situ, also known as lentigo maligna. Dr. Chapman acknowledged the controversial nature of his stance, and based his position on small case series, one "good prospective study" in the literature, and his own experience with more than 60 patients.
As an example, he discussed a 36-year-old man with metastatic melanoma. The patient had multiple surgeries and radiation therapy "and nothing seemed to work," he said. "I basically bathed him in imiquimod over several months." Six years later, the patient is doing well with no signs of nodal or metastatic disease. As with all melanoma patients, regardless of the therapy, they should be followed continuously for a lifetime, he said at the annual meeting of the American Academy of Dermatology.
In his regimen, imiquimod 5% cream is applied five times per week for 12 weeks, with a rest period on weekends. Inflammation can be intense with this aggressive protocol, so it is important to educate patients beforehand. Pretreatment with retinoids—such as tazarotene (Tazarac, Allergan) for 2 weeks—can increase the effectiveness of imiquimod in this setting, he added.
"The only good prospective study to date," Dr. Chapman said, is an open-label trial in which participants received daily treatment with topical 5% imiquimod for 3 months, followed by a biopsy 1 month post therapy (Br. J. Dermatol. 2003;149:66-70). The complete response rate was 93% in 28 patients with histologically confirmed lentigo maligna. Two patients were treatment failures.
Because of potential failures, "always go back and do a biopsy after clearance," he said.
For example, in a retrospective study of 40 patients pretreated with imiquimod (Dermatol. Surg. 2008;34:147-51), 30 appeared clinically clear after staged excision "but three of these had histologic evidence of disease—that is why I always do a follow-up biopsy."
One of his own patients failed after initial clearance of his lesion, Dr. Chapman said. The man had a large scalp lesion that cleared following use of topical imiquimod without retinoid treatment. "For 8 months, we thought he was cleared. He came back and had a node in middle of the lesion site—his third recurrence over 5 years." Dr. Chapman added, "He's doing well, but failures do occur."
It is important to realize that "we think we know when something is in situ, but we don't always know the entire lesion is in situ when we do this," Dr. Chapman said.
Even though surgical excision remains the first-line choice for most patients with melanoma in situ or thin melanoma lesions, surgery nonresponders or those who refuse resection can benefit from imiquimod. He cited three examples: a woman who did not want to have repeat surgery and whose lesion cleared with imiquimod; a man who did not want further surgery following two melanoma lesion excisions close together on his temple, who was treated well with imiquimod; and a patient with recurrent melanoma in situ at the forehead flap of the nose who is doing well 4 years out after imiquimod treatment.
In response to a question from the audience, Dr. Chapman said, "I don't think just any inflammatory response is going to make melanoma go away. Imiquimod is one of those serendipitous chemicals that is useful for a lot of skin tumors for some reason."
Dr. Chapman is a consultant for, and receives honoraria from, Graceway. He also receives honoraria from Abbott.
Sun Exposure May Offer Mortality Benefit in BCC Patients
MADRID - All-cause mortality is substantially lower in patients with basal cell carcinoma than in those with squamous cell carcinoma, according to a large Danish national registry study.
"In general, patients with basal cell carcinoma are in fact healthier than their counterparts with squamous cell carcinoma or age-matched controls," Dr. Gregor B. E. Jemec observed at the 13th World Congress on Cancers of the Skin, which was sponsored by the Skin Cancer Foundation.
He cited a study in which investigators at Aarhus (Denmark) University Hospital analyzed causes of death among patients with nonmelanoma skin cancer who were entered into the comprehensive Danish Cancer Registry in 1978-2001. The study population included all 82,837 Danes with basal cell carcinoma (BCC) and the 13,453 with squamous cell carcinoma (SCC) during the study years.
The all-cause mortality rate was 3% lower in the BCC cohort than the standardized rate in the general Danish population, whereas overall mortality in the SCC group was 30% greater than in the general population.
The increased all-cause mortality among patients with SCC was mainly due to excess deaths from chronic obstructive pulmonary disease, cardiovascular disease, cancer, and infectious diseases. In contrast, patients with BCC had below-average mortality from COPD, diabetes, and cardiovascular disease (Br. J. Dermatol. 2008;159:419-25).
The investigators speculated that the observed mortality benefit among patients with BCC might result in part from the salutary effects of increased serum vitamin D levels on a variety of chronic diseases.
BCC is a marker for increased sun exposure, which boosts serum vitamin D levels, which in turn has been linked in a growing number of epidemiologic studies to reduced risks of cardiovascular disease and other major causes of death.
However, the Danish registry didn't include data on vitamin D levels, so this is supposition.
Mortality from nonmelanoma skin cancer itself is quite limited. Investigators at the Danish Cancer Registry, using national data for 1984, estimated the lethality rates to be 4.3% for SCC and 0.12% for BCC (Br. J. Dermatol. 1991;125:580-2), noted Dr. Jemec, a dermatologist at the University of Copenhagen.
Nearly 74,000 deaths in the United States from 1969 to 2000 were attributed to nonmelanoma skin cancer, according to an analysis by investigators at Brown University in Providence, R.I. Almost 29,000 of these deaths were due to nonmelanoma skin cancers arising on genital skin, with a nearly 3:1 ratio of deaths attributed to vulvar and penile-scrotal cancers (J. Invest. Dermatol. 2007;127:2323-7).
Stressing avoidance of excessive sun exposure to prevent nonmelanoma skin cancer is important, but additional emphasis ought to be placed on reducing the mortality from genital nonmelanoma skin cancer, wrote Dr. Kevan G. Lewis and Dr. Martin A. Weinstock.
"The magnitude of the public health burden is great; nevertheless, efforts on the part of the dermatology community to prevent human papilloma virus infection in the United States have been slight compared to similar effort to reduce excess exposure to UV light," Dr. Lewis and Dr. Weinstock wrote.
"These data suggest that greater emphasis could be placed on the risk of mortality from genital skin cancer, both in efforts with patients and with physicians in related specialties such as family medicine and obstetrics-gynecology."
Dr. Jemec noted that the U.S. study showed sharply increasing nonmelanoma skin cancer mortality rates with each decade of age from middle age onward, and a general decline in nonmelanoma skin cancer-specific mortality during the study years.
Dr. Jemec reported having no conflicts of interest.
MADRID - All-cause mortality is substantially lower in patients with basal cell carcinoma than in those with squamous cell carcinoma, according to a large Danish national registry study.
"In general, patients with basal cell carcinoma are in fact healthier than their counterparts with squamous cell carcinoma or age-matched controls," Dr. Gregor B. E. Jemec observed at the 13th World Congress on Cancers of the Skin, which was sponsored by the Skin Cancer Foundation.
He cited a study in which investigators at Aarhus (Denmark) University Hospital analyzed causes of death among patients with nonmelanoma skin cancer who were entered into the comprehensive Danish Cancer Registry in 1978-2001. The study population included all 82,837 Danes with basal cell carcinoma (BCC) and the 13,453 with squamous cell carcinoma (SCC) during the study years.
The all-cause mortality rate was 3% lower in the BCC cohort than the standardized rate in the general Danish population, whereas overall mortality in the SCC group was 30% greater than in the general population.
The increased all-cause mortality among patients with SCC was mainly due to excess deaths from chronic obstructive pulmonary disease, cardiovascular disease, cancer, and infectious diseases. In contrast, patients with BCC had below-average mortality from COPD, diabetes, and cardiovascular disease (Br. J. Dermatol. 2008;159:419-25).
The investigators speculated that the observed mortality benefit among patients with BCC might result in part from the salutary effects of increased serum vitamin D levels on a variety of chronic diseases.
BCC is a marker for increased sun exposure, which boosts serum vitamin D levels, which in turn has been linked in a growing number of epidemiologic studies to reduced risks of cardiovascular disease and other major causes of death.
However, the Danish registry didn't include data on vitamin D levels, so this is supposition.
Mortality from nonmelanoma skin cancer itself is quite limited. Investigators at the Danish Cancer Registry, using national data for 1984, estimated the lethality rates to be 4.3% for SCC and 0.12% for BCC (Br. J. Dermatol. 1991;125:580-2), noted Dr. Jemec, a dermatologist at the University of Copenhagen.
Nearly 74,000 deaths in the United States from 1969 to 2000 were attributed to nonmelanoma skin cancer, according to an analysis by investigators at Brown University in Providence, R.I. Almost 29,000 of these deaths were due to nonmelanoma skin cancers arising on genital skin, with a nearly 3:1 ratio of deaths attributed to vulvar and penile-scrotal cancers (J. Invest. Dermatol. 2007;127:2323-7).
Stressing avoidance of excessive sun exposure to prevent nonmelanoma skin cancer is important, but additional emphasis ought to be placed on reducing the mortality from genital nonmelanoma skin cancer, wrote Dr. Kevan G. Lewis and Dr. Martin A. Weinstock.
"The magnitude of the public health burden is great; nevertheless, efforts on the part of the dermatology community to prevent human papilloma virus infection in the United States have been slight compared to similar effort to reduce excess exposure to UV light," Dr. Lewis and Dr. Weinstock wrote.
"These data suggest that greater emphasis could be placed on the risk of mortality from genital skin cancer, both in efforts with patients and with physicians in related specialties such as family medicine and obstetrics-gynecology."
Dr. Jemec noted that the U.S. study showed sharply increasing nonmelanoma skin cancer mortality rates with each decade of age from middle age onward, and a general decline in nonmelanoma skin cancer-specific mortality during the study years.
Dr. Jemec reported having no conflicts of interest.
MADRID - All-cause mortality is substantially lower in patients with basal cell carcinoma than in those with squamous cell carcinoma, according to a large Danish national registry study.
"In general, patients with basal cell carcinoma are in fact healthier than their counterparts with squamous cell carcinoma or age-matched controls," Dr. Gregor B. E. Jemec observed at the 13th World Congress on Cancers of the Skin, which was sponsored by the Skin Cancer Foundation.
He cited a study in which investigators at Aarhus (Denmark) University Hospital analyzed causes of death among patients with nonmelanoma skin cancer who were entered into the comprehensive Danish Cancer Registry in 1978-2001. The study population included all 82,837 Danes with basal cell carcinoma (BCC) and the 13,453 with squamous cell carcinoma (SCC) during the study years.
The all-cause mortality rate was 3% lower in the BCC cohort than the standardized rate in the general Danish population, whereas overall mortality in the SCC group was 30% greater than in the general population.
The increased all-cause mortality among patients with SCC was mainly due to excess deaths from chronic obstructive pulmonary disease, cardiovascular disease, cancer, and infectious diseases. In contrast, patients with BCC had below-average mortality from COPD, diabetes, and cardiovascular disease (Br. J. Dermatol. 2008;159:419-25).
The investigators speculated that the observed mortality benefit among patients with BCC might result in part from the salutary effects of increased serum vitamin D levels on a variety of chronic diseases.
BCC is a marker for increased sun exposure, which boosts serum vitamin D levels, which in turn has been linked in a growing number of epidemiologic studies to reduced risks of cardiovascular disease and other major causes of death.
However, the Danish registry didn't include data on vitamin D levels, so this is supposition.
Mortality from nonmelanoma skin cancer itself is quite limited. Investigators at the Danish Cancer Registry, using national data for 1984, estimated the lethality rates to be 4.3% for SCC and 0.12% for BCC (Br. J. Dermatol. 1991;125:580-2), noted Dr. Jemec, a dermatologist at the University of Copenhagen.
Nearly 74,000 deaths in the United States from 1969 to 2000 were attributed to nonmelanoma skin cancer, according to an analysis by investigators at Brown University in Providence, R.I. Almost 29,000 of these deaths were due to nonmelanoma skin cancers arising on genital skin, with a nearly 3:1 ratio of deaths attributed to vulvar and penile-scrotal cancers (J. Invest. Dermatol. 2007;127:2323-7).
Stressing avoidance of excessive sun exposure to prevent nonmelanoma skin cancer is important, but additional emphasis ought to be placed on reducing the mortality from genital nonmelanoma skin cancer, wrote Dr. Kevan G. Lewis and Dr. Martin A. Weinstock.
"The magnitude of the public health burden is great; nevertheless, efforts on the part of the dermatology community to prevent human papilloma virus infection in the United States have been slight compared to similar effort to reduce excess exposure to UV light," Dr. Lewis and Dr. Weinstock wrote.
"These data suggest that greater emphasis could be placed on the risk of mortality from genital skin cancer, both in efforts with patients and with physicians in related specialties such as family medicine and obstetrics-gynecology."
Dr. Jemec noted that the U.S. study showed sharply increasing nonmelanoma skin cancer mortality rates with each decade of age from middle age onward, and a general decline in nonmelanoma skin cancer-specific mortality during the study years.
Dr. Jemec reported having no conflicts of interest.
Sirolimus Cuts Skin Cancer After Renal Transplant
MADRID — Switching renal transplant recipients to sirolimus-based long-term immunosuppression markedly reduced their rate of nonmelanoma skin cancer in the first-ever randomized controlled trial of this cancer-prevention strategy.
This study is a landmark event because it shows that renal transplant teams are finally taking seriously the extraordinarily high risk of skin cancer in their patients, Dr. Julio Pascual observed at the 13th World Congress on Cancers of the Skin, which was sponsored by the Skin Cancer Foundation.
The blinded randomized trial, conducted at J.W. Goethe University in Frankfurt, Germany, follows a handful of prior uncontrolled studies by multiple transplant groups showing that converting renal transplant recipients from long-term immunosuppression with the calcineurin inhibitors cyclosporine and tacrolimus to the proliferation stimulation inhibitors sirolimus or everolimus often brings rapid improvement and prevents recurrence of multiple squamous cell carcinomas, basal cell carcinomas, melanoma, and Kaposi's sarcoma, said Dr. Pascual, a nephrologist and transplant physician at Hospital del Mar, Barcelona.
The Frankfurt study involved 44 renal transplant recipients with premalignant skin lesions who had been on calcineurin inhibitor-based immunosuppressive therapy for a mean of 3.8 years before they were randomized to a switch to sirolimus or continuation of their original immunosuppression.
Of 33 patients evaluable after 6 months of follow-up, only 1 of 16 on sirolimus developed nonmelanoma skin cancer, compared with 8 of 17 controls. Moreover, no one in the sirolimus group experienced worsening of preexisting premalignant lesions and five showed improvement. In contrast, five patients in the control group had progression of their preexisting premalignancies (Am. J. Transplant. 2010;10:1385-93).
Cancer accounts for 30% of all deaths in kidney transplant recipients, and squamous cell carcinoma is the cancer they develop most frequently. Indeed, registry studies show that the risk of nonmelanoma skin cancer is more than 20-fold greater in renal transplant recipients than the general population.
The duration, intensity, and type of immunosuppressive therapy play a crucial role in the development of these skin cancers. Use of azathioprine and the calcineurin inhibitors is a risk factor for skin cancer--they interfere with DNA repair and immunosurveillance. In addition, the calcineurin inhibitors are nephrotoxic. Sirolimus and everolimus are not only nonnephrotoxic, they inhibit angiogenesis and tumor growth, Dr. Pascual explained.
Nevertheless, he continued, most of his colleagues in renal transplant medicine have been slow to take their patients' elevated skin cancer risk as seriously as it deserves.
Dr. Pascual recalled last year's report on the 24-month results from the CONVERT trial, in which 830 renal transplant recipients were randomized 2:1 to convert from cyclosporine or tacrolimus to sirolimus or stay on their calcineurin inhibitor. This is a major study in the renal transplant field whose chief endpoints involved mortality, graft survival, urinary protein excretion, and glomerular filtration rate. Buried within the findings was the fact that the sirolimus group had a 3% incidence of neoplasia during follow-up, significantly less than the 9% rate in controls (Transplantation 2009;87:233-42).
"To me this is the most important finding in this trial, and it only gets about three lines in the results section," he said.
Dr. Pascual reported having no financial conflicts.
MADRID — Switching renal transplant recipients to sirolimus-based long-term immunosuppression markedly reduced their rate of nonmelanoma skin cancer in the first-ever randomized controlled trial of this cancer-prevention strategy.
This study is a landmark event because it shows that renal transplant teams are finally taking seriously the extraordinarily high risk of skin cancer in their patients, Dr. Julio Pascual observed at the 13th World Congress on Cancers of the Skin, which was sponsored by the Skin Cancer Foundation.
The blinded randomized trial, conducted at J.W. Goethe University in Frankfurt, Germany, follows a handful of prior uncontrolled studies by multiple transplant groups showing that converting renal transplant recipients from long-term immunosuppression with the calcineurin inhibitors cyclosporine and tacrolimus to the proliferation stimulation inhibitors sirolimus or everolimus often brings rapid improvement and prevents recurrence of multiple squamous cell carcinomas, basal cell carcinomas, melanoma, and Kaposi's sarcoma, said Dr. Pascual, a nephrologist and transplant physician at Hospital del Mar, Barcelona.
The Frankfurt study involved 44 renal transplant recipients with premalignant skin lesions who had been on calcineurin inhibitor-based immunosuppressive therapy for a mean of 3.8 years before they were randomized to a switch to sirolimus or continuation of their original immunosuppression.
Of 33 patients evaluable after 6 months of follow-up, only 1 of 16 on sirolimus developed nonmelanoma skin cancer, compared with 8 of 17 controls. Moreover, no one in the sirolimus group experienced worsening of preexisting premalignant lesions and five showed improvement. In contrast, five patients in the control group had progression of their preexisting premalignancies (Am. J. Transplant. 2010;10:1385-93).
Cancer accounts for 30% of all deaths in kidney transplant recipients, and squamous cell carcinoma is the cancer they develop most frequently. Indeed, registry studies show that the risk of nonmelanoma skin cancer is more than 20-fold greater in renal transplant recipients than the general population.
The duration, intensity, and type of immunosuppressive therapy play a crucial role in the development of these skin cancers. Use of azathioprine and the calcineurin inhibitors is a risk factor for skin cancer--they interfere with DNA repair and immunosurveillance. In addition, the calcineurin inhibitors are nephrotoxic. Sirolimus and everolimus are not only nonnephrotoxic, they inhibit angiogenesis and tumor growth, Dr. Pascual explained.
Nevertheless, he continued, most of his colleagues in renal transplant medicine have been slow to take their patients' elevated skin cancer risk as seriously as it deserves.
Dr. Pascual recalled last year's report on the 24-month results from the CONVERT trial, in which 830 renal transplant recipients were randomized 2:1 to convert from cyclosporine or tacrolimus to sirolimus or stay on their calcineurin inhibitor. This is a major study in the renal transplant field whose chief endpoints involved mortality, graft survival, urinary protein excretion, and glomerular filtration rate. Buried within the findings was the fact that the sirolimus group had a 3% incidence of neoplasia during follow-up, significantly less than the 9% rate in controls (Transplantation 2009;87:233-42).
"To me this is the most important finding in this trial, and it only gets about three lines in the results section," he said.
Dr. Pascual reported having no financial conflicts.
MADRID — Switching renal transplant recipients to sirolimus-based long-term immunosuppression markedly reduced their rate of nonmelanoma skin cancer in the first-ever randomized controlled trial of this cancer-prevention strategy.
This study is a landmark event because it shows that renal transplant teams are finally taking seriously the extraordinarily high risk of skin cancer in their patients, Dr. Julio Pascual observed at the 13th World Congress on Cancers of the Skin, which was sponsored by the Skin Cancer Foundation.
The blinded randomized trial, conducted at J.W. Goethe University in Frankfurt, Germany, follows a handful of prior uncontrolled studies by multiple transplant groups showing that converting renal transplant recipients from long-term immunosuppression with the calcineurin inhibitors cyclosporine and tacrolimus to the proliferation stimulation inhibitors sirolimus or everolimus often brings rapid improvement and prevents recurrence of multiple squamous cell carcinomas, basal cell carcinomas, melanoma, and Kaposi's sarcoma, said Dr. Pascual, a nephrologist and transplant physician at Hospital del Mar, Barcelona.
The Frankfurt study involved 44 renal transplant recipients with premalignant skin lesions who had been on calcineurin inhibitor-based immunosuppressive therapy for a mean of 3.8 years before they were randomized to a switch to sirolimus or continuation of their original immunosuppression.
Of 33 patients evaluable after 6 months of follow-up, only 1 of 16 on sirolimus developed nonmelanoma skin cancer, compared with 8 of 17 controls. Moreover, no one in the sirolimus group experienced worsening of preexisting premalignant lesions and five showed improvement. In contrast, five patients in the control group had progression of their preexisting premalignancies (Am. J. Transplant. 2010;10:1385-93).
Cancer accounts for 30% of all deaths in kidney transplant recipients, and squamous cell carcinoma is the cancer they develop most frequently. Indeed, registry studies show that the risk of nonmelanoma skin cancer is more than 20-fold greater in renal transplant recipients than the general population.
The duration, intensity, and type of immunosuppressive therapy play a crucial role in the development of these skin cancers. Use of azathioprine and the calcineurin inhibitors is a risk factor for skin cancer--they interfere with DNA repair and immunosurveillance. In addition, the calcineurin inhibitors are nephrotoxic. Sirolimus and everolimus are not only nonnephrotoxic, they inhibit angiogenesis and tumor growth, Dr. Pascual explained.
Nevertheless, he continued, most of his colleagues in renal transplant medicine have been slow to take their patients' elevated skin cancer risk as seriously as it deserves.
Dr. Pascual recalled last year's report on the 24-month results from the CONVERT trial, in which 830 renal transplant recipients were randomized 2:1 to convert from cyclosporine or tacrolimus to sirolimus or stay on their calcineurin inhibitor. This is a major study in the renal transplant field whose chief endpoints involved mortality, graft survival, urinary protein excretion, and glomerular filtration rate. Buried within the findings was the fact that the sirolimus group had a 3% incidence of neoplasia during follow-up, significantly less than the 9% rate in controls (Transplantation 2009;87:233-42).
"To me this is the most important finding in this trial, and it only gets about three lines in the results section," he said.
Dr. Pascual reported having no financial conflicts.
Deposits in Sentinel Nodes May Predict Prognosis
MADRID — The size and location of any microscopic metastatic deposits within the sentinel lymph node is an important predictor of prognosis in patients with cutaneous melanoma.
This conclusion is based upon detailed pathologic examination of 2,203 sentinel lymph nodes (SLNs) from 1,417 patients with cutaneous melanoma at MD Anderson Cancer Center in Houston. Sixteen percent of nodes were positive for metastases, Dr. Victor G. Prieto said at the 13th World Congress on Cancers of the Skin, which was sponsored by the Skin Cancer Foundation.

"The location of a metastatic deposit--subcapsular versus parenchymal--and the size of the largest focus should be reported in the pathology report, in my opinion, when examining sentinel lymph nodes from patients with cutaneous melanoma. We've been doing this for the last 8 years and we think it should be extended to other centers," declared Dr. Prieto, professor of dermatology and director of dermatopathology at M.D. Anderson.
In breast cancer, SLN tumor deposits less than 0.2 mm aren't considered significant by some pathologists. Melanoma is a different matter. There does not seem to be a definite cutoff below which tumor metastasis size doesn't matter. Dr. Prieto has seen cases in which a single melanoma cell detected in the SLN was followed by multiple distant metastases and death within 4 years of skin cancer diagnosis.
"I don't call histologic examination of the sentinel lymph nodes the standard of care in melanoma because that term has medicolegal ramifications. But even though it's not the standard of care, I think a sentinel lymph node examination is very important for our patients. It permits much more accurate staging," Dr. Prieto said.
Ongoing trials should eventually resolve the longstanding controversy as to whether there is any survival benefit to completion lymphadenectomy in patients with positive SLNs. Regardless of how that issue turns out, however, it's clear that staging SLNs provides very important prognostic information.
"We have to remember that a large number of these patients are … between 40 and 50 and they have children and may need to consider setting up college funds and providing for their families," the said.
It is his firm conviction that the entire SLN should be submitted for pathologic evaluation permanently embedded in paraffin rather than in frozen section.
"Even in the best laboratories, the quality of a frozen section is usually below that seen with permanent paraffin-embedded tissue. There's a loss of tissue when specimens are frozen. The subcapsular region, which is the most commonly affected by metastatic melanoma, may be lost," Dr. Prieto said.
Based upon the outcomes of patients with positive SLNs in the M.D. Anderson series, Dr. Prieto and coworkers stratify patients into three prognostic groups. The lowest-risk group is comprised of patients with involvement of one or two SLNs, a largest metastatic nest not more than 2 mm in size, and no ulceration of the primary lesion. Such patients constituted 39% of the SLN-positive population.
Ulceration was present in 43% of the primary melanomas with SLN involvement in this large series. SLN metastases were confined to the subcapsular region in 65% of affected patients.
The intermediate-risk group consisted of patients with ulceration in the primary tumor or any metastatic nest greater than 2 mm in size. The high-risk group, which included 28% of the total SLN-positive group, was made up of patients with involvement of three or more SLNs or ulceration in the primary lesion and any metastatic nest greater than 2 mm.
Ten-year survival was roughly 80% in the low-risk group, 60% in the intermediate-risk cohort, and 30% in the high-risk population.
It can be difficult to detect small numbers of melanoma cells in a SLN without the use of immunohistochemical stains.
At M.D. Anderson, the node is first "breadloafed," which allows evaluation of a relatively large surface area of the subcapsular region, and then the specimen is examined with routine hematoxylin and eosin staining.
If the results are negative, Dr. Prieto and colleagues utilize a cocktail of immunohistochemical stains comprised of HMB45, which is very specific but less than optimally sensitive, coupled with MART1, which is both very specific and more sensitive for melanoma than in HMB45. The flaw with MART1 is it can give false-positive results with macrophages.
If this cocktail proves negative, then and only then do the dermatopathologists resort to S100 protein staining, which is very sensitive but relatively nonspecific.
The Ki67 proliferation marker is employed to distinguish melanoma cells from benign capsular nevi, which should be Ki67-negative.
Dr. Prieto reported no financial conflicts.
MADRID — The size and location of any microscopic metastatic deposits within the sentinel lymph node is an important predictor of prognosis in patients with cutaneous melanoma.
This conclusion is based upon detailed pathologic examination of 2,203 sentinel lymph nodes (SLNs) from 1,417 patients with cutaneous melanoma at MD Anderson Cancer Center in Houston. Sixteen percent of nodes were positive for metastases, Dr. Victor G. Prieto said at the 13th World Congress on Cancers of the Skin, which was sponsored by the Skin Cancer Foundation.
"The location of a metastatic deposit--subcapsular versus parenchymal--and the size of the largest focus should be reported in the pathology report, in my opinion, when examining sentinel lymph nodes from patients with cutaneous melanoma. We've been doing this for the last 8 years and we think it should be extended to other centers," declared Dr. Prieto, professor of dermatology and director of dermatopathology at M.D. Anderson.
In breast cancer, SLN tumor deposits less than 0.2 mm aren't considered significant by some pathologists. Melanoma is a different matter. There does not seem to be a definite cutoff below which tumor metastasis size doesn't matter. Dr. Prieto has seen cases in which a single melanoma cell detected in the SLN was followed by multiple distant metastases and death within 4 years of skin cancer diagnosis.
"I don't call histologic examination of the sentinel lymph nodes the standard of care in melanoma because that term has medicolegal ramifications. But even though it's not the standard of care, I think a sentinel lymph node examination is very important for our patients. It permits much more accurate staging," Dr. Prieto said.
Ongoing trials should eventually resolve the longstanding controversy as to whether there is any survival benefit to completion lymphadenectomy in patients with positive SLNs. Regardless of how that issue turns out, however, it's clear that staging SLNs provides very important prognostic information.
"We have to remember that a large number of these patients are … between 40 and 50 and they have children and may need to consider setting up college funds and providing for their families," the said.
It is his firm conviction that the entire SLN should be submitted for pathologic evaluation permanently embedded in paraffin rather than in frozen section.
"Even in the best laboratories, the quality of a frozen section is usually below that seen with permanent paraffin-embedded tissue. There's a loss of tissue when specimens are frozen. The subcapsular region, which is the most commonly affected by metastatic melanoma, may be lost," Dr. Prieto said.
Based upon the outcomes of patients with positive SLNs in the M.D. Anderson series, Dr. Prieto and coworkers stratify patients into three prognostic groups. The lowest-risk group is comprised of patients with involvement of one or two SLNs, a largest metastatic nest not more than 2 mm in size, and no ulceration of the primary lesion. Such patients constituted 39% of the SLN-positive population.
Ulceration was present in 43% of the primary melanomas with SLN involvement in this large series. SLN metastases were confined to the subcapsular region in 65% of affected patients.
The intermediate-risk group consisted of patients with ulceration in the primary tumor or any metastatic nest greater than 2 mm in size. The high-risk group, which included 28% of the total SLN-positive group, was made up of patients with involvement of three or more SLNs or ulceration in the primary lesion and any metastatic nest greater than 2 mm.
Ten-year survival was roughly 80% in the low-risk group, 60% in the intermediate-risk cohort, and 30% in the high-risk population.
It can be difficult to detect small numbers of melanoma cells in a SLN without the use of immunohistochemical stains.
At M.D. Anderson, the node is first "breadloafed," which allows evaluation of a relatively large surface area of the subcapsular region, and then the specimen is examined with routine hematoxylin and eosin staining.
If the results are negative, Dr. Prieto and colleagues utilize a cocktail of immunohistochemical stains comprised of HMB45, which is very specific but less than optimally sensitive, coupled with MART1, which is both very specific and more sensitive for melanoma than in HMB45. The flaw with MART1 is it can give false-positive results with macrophages.
If this cocktail proves negative, then and only then do the dermatopathologists resort to S100 protein staining, which is very sensitive but relatively nonspecific.
The Ki67 proliferation marker is employed to distinguish melanoma cells from benign capsular nevi, which should be Ki67-negative.
Dr. Prieto reported no financial conflicts.
MADRID — The size and location of any microscopic metastatic deposits within the sentinel lymph node is an important predictor of prognosis in patients with cutaneous melanoma.
This conclusion is based upon detailed pathologic examination of 2,203 sentinel lymph nodes (SLNs) from 1,417 patients with cutaneous melanoma at MD Anderson Cancer Center in Houston. Sixteen percent of nodes were positive for metastases, Dr. Victor G. Prieto said at the 13th World Congress on Cancers of the Skin, which was sponsored by the Skin Cancer Foundation.
"The location of a metastatic deposit--subcapsular versus parenchymal--and the size of the largest focus should be reported in the pathology report, in my opinion, when examining sentinel lymph nodes from patients with cutaneous melanoma. We've been doing this for the last 8 years and we think it should be extended to other centers," declared Dr. Prieto, professor of dermatology and director of dermatopathology at M.D. Anderson.
In breast cancer, SLN tumor deposits less than 0.2 mm aren't considered significant by some pathologists. Melanoma is a different matter. There does not seem to be a definite cutoff below which tumor metastasis size doesn't matter. Dr. Prieto has seen cases in which a single melanoma cell detected in the SLN was followed by multiple distant metastases and death within 4 years of skin cancer diagnosis.
"I don't call histologic examination of the sentinel lymph nodes the standard of care in melanoma because that term has medicolegal ramifications. But even though it's not the standard of care, I think a sentinel lymph node examination is very important for our patients. It permits much more accurate staging," Dr. Prieto said.
Ongoing trials should eventually resolve the longstanding controversy as to whether there is any survival benefit to completion lymphadenectomy in patients with positive SLNs. Regardless of how that issue turns out, however, it's clear that staging SLNs provides very important prognostic information.
"We have to remember that a large number of these patients are … between 40 and 50 and they have children and may need to consider setting up college funds and providing for their families," the said.
It is his firm conviction that the entire SLN should be submitted for pathologic evaluation permanently embedded in paraffin rather than in frozen section.
"Even in the best laboratories, the quality of a frozen section is usually below that seen with permanent paraffin-embedded tissue. There's a loss of tissue when specimens are frozen. The subcapsular region, which is the most commonly affected by metastatic melanoma, may be lost," Dr. Prieto said.
Based upon the outcomes of patients with positive SLNs in the M.D. Anderson series, Dr. Prieto and coworkers stratify patients into three prognostic groups. The lowest-risk group is comprised of patients with involvement of one or two SLNs, a largest metastatic nest not more than 2 mm in size, and no ulceration of the primary lesion. Such patients constituted 39% of the SLN-positive population.
Ulceration was present in 43% of the primary melanomas with SLN involvement in this large series. SLN metastases were confined to the subcapsular region in 65% of affected patients.
The intermediate-risk group consisted of patients with ulceration in the primary tumor or any metastatic nest greater than 2 mm in size. The high-risk group, which included 28% of the total SLN-positive group, was made up of patients with involvement of three or more SLNs or ulceration in the primary lesion and any metastatic nest greater than 2 mm.
Ten-year survival was roughly 80% in the low-risk group, 60% in the intermediate-risk cohort, and 30% in the high-risk population.
It can be difficult to detect small numbers of melanoma cells in a SLN without the use of immunohistochemical stains.
At M.D. Anderson, the node is first "breadloafed," which allows evaluation of a relatively large surface area of the subcapsular region, and then the specimen is examined with routine hematoxylin and eosin staining.
If the results are negative, Dr. Prieto and colleagues utilize a cocktail of immunohistochemical stains comprised of HMB45, which is very specific but less than optimally sensitive, coupled with MART1, which is both very specific and more sensitive for melanoma than in HMB45. The flaw with MART1 is it can give false-positive results with macrophages.
If this cocktail proves negative, then and only then do the dermatopathologists resort to S100 protein staining, which is very sensitive but relatively nonspecific.
The Ki67 proliferation marker is employed to distinguish melanoma cells from benign capsular nevi, which should be Ki67-negative.
Dr. Prieto reported no financial conflicts.
Almost One-Third of Mohs Surgeons Employ PAs
NEW YORK — Roughly 30% of Moh's surgeons currently employ physician assistants in their practice for presurgical consults, postoperative assessments, intraoperative suturing, and more.
The data, from a small survey presented at the meeting, are among the first to assess the use of physician assistants (PAs) among Mohs surgeons.
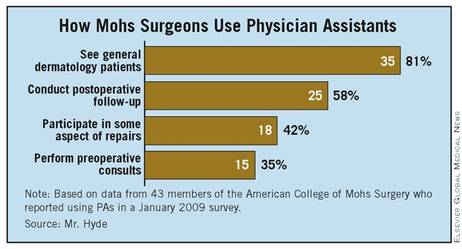
"The inherent tie between pathology and surgery in the Mohs specialty makes it very important that the PA act as an appendage of the Mohs surgeon," said Mr. Mark Hyde, a PA-C in the cutaneous oncology department at the Huntsman Cancer Institute at the University of Utah, Salt Lake City.
However, "with the employment of PAs in Mohs surgery, [physicians] can spend more face-to-face time with patients," he said at the annual meeting of the American College of Mohs Surgery.
Mr. Hyde mailed surveys to 576 members of the American College of Mohs Surgery in January 2009, asking whether the physician used a PA and if so, to do what. About a quarter of the physicians replied (143), and of those, 43 (30%) reported using a PA.
Mr. Hyde conceded that the response rate was low, but "because the data are not found anywhere else, we still felt this was important," he said.
Overall, 15 of 43 Moh's surgeons using PAs reported the PA at their practice performed preoperative consults. A total of 25 of the 43 surgeons, meanwhile, responded that their PA conducted postoperative follow-up.
Intraoperatively, 18 of 43 surgeons reported that PAs at their practice were participating in some aspect of repairs. These included primary repair design (8 of 43), dermal sutures on the primary tissue repair (12 of 43), epidermal sutures on the primary repair (18 of 43), dermal and epidermal sutures on the adjacent tissue transfer (8 and 14 of 43, respectively), and suturing of the skin graft (dermal, 10 of 43; epidermal, 16 of 43).
One surgeon reported that the PA at his facility excised Mohs sections, and another reported that their PA inked excised tissue.
No surgeons reported letting their PAs map Mohs sections, nor did any report letting PAs interpret pathology reports.
"There are some tasks that are rarely assigned to PAs in Mohs micrographic surgery--excision of the stages, mapping tissues, inking and grossing tissue, and interpreting pathology," said Mr. Hyde. However, "in our experience, PAs can ink and gross tissue, and increase efficiency by doing so."
He also pointed to an area in which PAs were especially useful to the physicians surveyed--seeing general dermatology patients. A total of 35 out of 43 surgeons, or more than 80%, reported using their PAs in this way.
In fact, he said, in the program at the University of Utah, PAs "act as a source of referrals for the Mohs surgeon."
Despite the use of the PAs in these practices, Mr. Hyde said there was no evidence to suggest that surgeons using PAs remove more tumors per week, or see more patients.
Nevertheless, as the use of PAs increases among Mohs surgeons, the need to identify which tasks PAs routinely perform is crucial to "allow PA programs and PA education providers to focus their training."
The survey was funded by the Society of Dermatology Physician Assistants with an unrestricted research grant. Mr. Hyde is on the board of the society.
NEW YORK — Roughly 30% of Moh's surgeons currently employ physician assistants in their practice for presurgical consults, postoperative assessments, intraoperative suturing, and more.
The data, from a small survey presented at the meeting, are among the first to assess the use of physician assistants (PAs) among Mohs surgeons.
"The inherent tie between pathology and surgery in the Mohs specialty makes it very important that the PA act as an appendage of the Mohs surgeon," said Mr. Mark Hyde, a PA-C in the cutaneous oncology department at the Huntsman Cancer Institute at the University of Utah, Salt Lake City.
However, "with the employment of PAs in Mohs surgery, [physicians] can spend more face-to-face time with patients," he said at the annual meeting of the American College of Mohs Surgery.
Mr. Hyde mailed surveys to 576 members of the American College of Mohs Surgery in January 2009, asking whether the physician used a PA and if so, to do what. About a quarter of the physicians replied (143), and of those, 43 (30%) reported using a PA.
Mr. Hyde conceded that the response rate was low, but "because the data are not found anywhere else, we still felt this was important," he said.
Overall, 15 of 43 Moh's surgeons using PAs reported the PA at their practice performed preoperative consults. A total of 25 of the 43 surgeons, meanwhile, responded that their PA conducted postoperative follow-up.
Intraoperatively, 18 of 43 surgeons reported that PAs at their practice were participating in some aspect of repairs. These included primary repair design (8 of 43), dermal sutures on the primary tissue repair (12 of 43), epidermal sutures on the primary repair (18 of 43), dermal and epidermal sutures on the adjacent tissue transfer (8 and 14 of 43, respectively), and suturing of the skin graft (dermal, 10 of 43; epidermal, 16 of 43).
One surgeon reported that the PA at his facility excised Mohs sections, and another reported that their PA inked excised tissue.
No surgeons reported letting their PAs map Mohs sections, nor did any report letting PAs interpret pathology reports.
"There are some tasks that are rarely assigned to PAs in Mohs micrographic surgery--excision of the stages, mapping tissues, inking and grossing tissue, and interpreting pathology," said Mr. Hyde. However, "in our experience, PAs can ink and gross tissue, and increase efficiency by doing so."
He also pointed to an area in which PAs were especially useful to the physicians surveyed--seeing general dermatology patients. A total of 35 out of 43 surgeons, or more than 80%, reported using their PAs in this way.
In fact, he said, in the program at the University of Utah, PAs "act as a source of referrals for the Mohs surgeon."
Despite the use of the PAs in these practices, Mr. Hyde said there was no evidence to suggest that surgeons using PAs remove more tumors per week, or see more patients.
Nevertheless, as the use of PAs increases among Mohs surgeons, the need to identify which tasks PAs routinely perform is crucial to "allow PA programs and PA education providers to focus their training."
The survey was funded by the Society of Dermatology Physician Assistants with an unrestricted research grant. Mr. Hyde is on the board of the society.
NEW YORK — Roughly 30% of Moh's surgeons currently employ physician assistants in their practice for presurgical consults, postoperative assessments, intraoperative suturing, and more.
The data, from a small survey presented at the meeting, are among the first to assess the use of physician assistants (PAs) among Mohs surgeons.
"The inherent tie between pathology and surgery in the Mohs specialty makes it very important that the PA act as an appendage of the Mohs surgeon," said Mr. Mark Hyde, a PA-C in the cutaneous oncology department at the Huntsman Cancer Institute at the University of Utah, Salt Lake City.
However, "with the employment of PAs in Mohs surgery, [physicians] can spend more face-to-face time with patients," he said at the annual meeting of the American College of Mohs Surgery.
Mr. Hyde mailed surveys to 576 members of the American College of Mohs Surgery in January 2009, asking whether the physician used a PA and if so, to do what. About a quarter of the physicians replied (143), and of those, 43 (30%) reported using a PA.
Mr. Hyde conceded that the response rate was low, but "because the data are not found anywhere else, we still felt this was important," he said.
Overall, 15 of 43 Moh's surgeons using PAs reported the PA at their practice performed preoperative consults. A total of 25 of the 43 surgeons, meanwhile, responded that their PA conducted postoperative follow-up.
Intraoperatively, 18 of 43 surgeons reported that PAs at their practice were participating in some aspect of repairs. These included primary repair design (8 of 43), dermal sutures on the primary tissue repair (12 of 43), epidermal sutures on the primary repair (18 of 43), dermal and epidermal sutures on the adjacent tissue transfer (8 and 14 of 43, respectively), and suturing of the skin graft (dermal, 10 of 43; epidermal, 16 of 43).
One surgeon reported that the PA at his facility excised Mohs sections, and another reported that their PA inked excised tissue.
No surgeons reported letting their PAs map Mohs sections, nor did any report letting PAs interpret pathology reports.
"There are some tasks that are rarely assigned to PAs in Mohs micrographic surgery--excision of the stages, mapping tissues, inking and grossing tissue, and interpreting pathology," said Mr. Hyde. However, "in our experience, PAs can ink and gross tissue, and increase efficiency by doing so."
He also pointed to an area in which PAs were especially useful to the physicians surveyed--seeing general dermatology patients. A total of 35 out of 43 surgeons, or more than 80%, reported using their PAs in this way.
In fact, he said, in the program at the University of Utah, PAs "act as a source of referrals for the Mohs surgeon."
Despite the use of the PAs in these practices, Mr. Hyde said there was no evidence to suggest that surgeons using PAs remove more tumors per week, or see more patients.
Nevertheless, as the use of PAs increases among Mohs surgeons, the need to identify which tasks PAs routinely perform is crucial to "allow PA programs and PA education providers to focus their training."
The survey was funded by the Society of Dermatology Physician Assistants with an unrestricted research grant. Mr. Hyde is on the board of the society.
After Mohs, Cancer Recurrence Less Than 2% in New Study
MADRID — Mohs surgery for lentigo maligna and lentigo maligna melanoma yields a substantially lower recurrence rate and smaller surgical deficit than does conventional surgery, according to Dr. Leonard H. Goldberg.
"It's especially useful on cosmetically sensitive areas of the body like the eyelids, where a 5-mm or 1-cm or 2-cm margin is virtually impossible because you'd destroy the patient's cosmetic appearance," Dr. Goldberg said at the 13th World Congress on Cancers of the Skin.
Of 708 cases of lentigo maligna and lentigo maligna melanoma that he treated using Mohs surgery from 1997 through 2007, the recurrence rate was 1.3%.
In contrast, conventional surgery is associated with recurrence rates of 8%-20%, he said. That's because the clinical margins of lentigo maligna are often indistinct, being masked by actinic keratoses or other sun-induced dysplastic changes.
The lentigines are "often much larger than what you'd expect," he said. "There's always the problem of where does the lentigo maligna end? Are those single cells in the periphery also lentigo maligna?"
Dr. Goldberg utilizes Dr. Helmut Breuninger's "Tübingen torte" technique of surgical specimen cutting using 90-degree sectioning, along with immunostaining. En-face (parallel) control of the entire surgical margin is considerably more reliable than bread-loafed cross-sectioning of the excised melanoma specimen.
"Bread-loafing doesn't always find the tumor. We don't bread-loaf tumors anymore," he said.
The change in practice came as a result of a study that Dr. Goldberg and his colleagues conducted in 36 patients with melanoma in situ treated with Mohs surgery with positive margins after initial excision with 5-mm margins (Dermatol. Surg. 2007;33:1434-9).
Because the average linear extent of melanoma at the surgical margin was 1.4 mm, they calculated that bread-loafing at 1-, 4-, and 10-mm intervals would have a 58%, 19%, and 7% chance, respectively, of detecting positive margins. To detect positive margins with 100% certainty, the bread-loafing would have to be done at 0.1-mm intervals, which is impractical, he said.
Dr. Goldberg noted that his personal 1.3% recurrence rate is in the same ballpark as outcomes reported by other Mohs surgeons. For example, researchers reported a 0.3% recurrence rate in 331 patients with melanoma in situ or lentigo maligna, compared with a 20% rate in 81 historical controls who underwent conventional surgery (J. Am. Acad. Dermatol. 2005;52:92-100).
In a separate review of four other published studies totaling 546 patients with lentigo maligna and lentigo maligna melanoma with margin control by various modifications of Mohs surgery, recurrence rates were 0.5%-2.8% (J. Am. Acad. Dermatol. 2007;57:659-64).
Dr. Goldberg reported no financial conflicts.
MADRID — Mohs surgery for lentigo maligna and lentigo maligna melanoma yields a substantially lower recurrence rate and smaller surgical deficit than does conventional surgery, according to Dr. Leonard H. Goldberg.
"It's especially useful on cosmetically sensitive areas of the body like the eyelids, where a 5-mm or 1-cm or 2-cm margin is virtually impossible because you'd destroy the patient's cosmetic appearance," Dr. Goldberg said at the 13th World Congress on Cancers of the Skin.
Of 708 cases of lentigo maligna and lentigo maligna melanoma that he treated using Mohs surgery from 1997 through 2007, the recurrence rate was 1.3%.
In contrast, conventional surgery is associated with recurrence rates of 8%-20%, he said. That's because the clinical margins of lentigo maligna are often indistinct, being masked by actinic keratoses or other sun-induced dysplastic changes.
The lentigines are "often much larger than what you'd expect," he said. "There's always the problem of where does the lentigo maligna end? Are those single cells in the periphery also lentigo maligna?"
Dr. Goldberg utilizes Dr. Helmut Breuninger's "Tübingen torte" technique of surgical specimen cutting using 90-degree sectioning, along with immunostaining. En-face (parallel) control of the entire surgical margin is considerably more reliable than bread-loafed cross-sectioning of the excised melanoma specimen.
"Bread-loafing doesn't always find the tumor. We don't bread-loaf tumors anymore," he said.
The change in practice came as a result of a study that Dr. Goldberg and his colleagues conducted in 36 patients with melanoma in situ treated with Mohs surgery with positive margins after initial excision with 5-mm margins (Dermatol. Surg. 2007;33:1434-9).
Because the average linear extent of melanoma at the surgical margin was 1.4 mm, they calculated that bread-loafing at 1-, 4-, and 10-mm intervals would have a 58%, 19%, and 7% chance, respectively, of detecting positive margins. To detect positive margins with 100% certainty, the bread-loafing would have to be done at 0.1-mm intervals, which is impractical, he said.
Dr. Goldberg noted that his personal 1.3% recurrence rate is in the same ballpark as outcomes reported by other Mohs surgeons. For example, researchers reported a 0.3% recurrence rate in 331 patients with melanoma in situ or lentigo maligna, compared with a 20% rate in 81 historical controls who underwent conventional surgery (J. Am. Acad. Dermatol. 2005;52:92-100).
In a separate review of four other published studies totaling 546 patients with lentigo maligna and lentigo maligna melanoma with margin control by various modifications of Mohs surgery, recurrence rates were 0.5%-2.8% (J. Am. Acad. Dermatol. 2007;57:659-64).
Dr. Goldberg reported no financial conflicts.
MADRID — Mohs surgery for lentigo maligna and lentigo maligna melanoma yields a substantially lower recurrence rate and smaller surgical deficit than does conventional surgery, according to Dr. Leonard H. Goldberg.
"It's especially useful on cosmetically sensitive areas of the body like the eyelids, where a 5-mm or 1-cm or 2-cm margin is virtually impossible because you'd destroy the patient's cosmetic appearance," Dr. Goldberg said at the 13th World Congress on Cancers of the Skin.
Of 708 cases of lentigo maligna and lentigo maligna melanoma that he treated using Mohs surgery from 1997 through 2007, the recurrence rate was 1.3%.
In contrast, conventional surgery is associated with recurrence rates of 8%-20%, he said. That's because the clinical margins of lentigo maligna are often indistinct, being masked by actinic keratoses or other sun-induced dysplastic changes.
The lentigines are "often much larger than what you'd expect," he said. "There's always the problem of where does the lentigo maligna end? Are those single cells in the periphery also lentigo maligna?"
Dr. Goldberg utilizes Dr. Helmut Breuninger's "Tübingen torte" technique of surgical specimen cutting using 90-degree sectioning, along with immunostaining. En-face (parallel) control of the entire surgical margin is considerably more reliable than bread-loafed cross-sectioning of the excised melanoma specimen.
"Bread-loafing doesn't always find the tumor. We don't bread-loaf tumors anymore," he said.
The change in practice came as a result of a study that Dr. Goldberg and his colleagues conducted in 36 patients with melanoma in situ treated with Mohs surgery with positive margins after initial excision with 5-mm margins (Dermatol. Surg. 2007;33:1434-9).
Because the average linear extent of melanoma at the surgical margin was 1.4 mm, they calculated that bread-loafing at 1-, 4-, and 10-mm intervals would have a 58%, 19%, and 7% chance, respectively, of detecting positive margins. To detect positive margins with 100% certainty, the bread-loafing would have to be done at 0.1-mm intervals, which is impractical, he said.
Dr. Goldberg noted that his personal 1.3% recurrence rate is in the same ballpark as outcomes reported by other Mohs surgeons. For example, researchers reported a 0.3% recurrence rate in 331 patients with melanoma in situ or lentigo maligna, compared with a 20% rate in 81 historical controls who underwent conventional surgery (J. Am. Acad. Dermatol. 2005;52:92-100).
In a separate review of four other published studies totaling 546 patients with lentigo maligna and lentigo maligna melanoma with margin control by various modifications of Mohs surgery, recurrence rates were 0.5%-2.8% (J. Am. Acad. Dermatol. 2007;57:659-64).
Dr. Goldberg reported no financial conflicts.
Could Aquaporins Be Next Skin Cancer Target?
MADRID — The Nobel Prize-winning discovery of aquaporins is having a trickle-down translational effect that could have a major impact upon the prevention and treatment of both melanoma and nonmelanoma skin cancers.
Aquaporins (AQPs) are also actively under study for potential utility in the treatment for a range of other diseases, including epilepsy, obesity, severe heart failure and various other edematous states, malaria, wound healing, glaucoma, Sjögren's syndrome, and for neuroprotection after brain or spinal cord injury, Dr. Julián S. Conejo-Mir said at the 13th World Congress on Cancers of the Skin, sponsored by the Skin Cancer Foundation.

There are also potential diagnostic applications, Dr. Conejo-Mir noted. The prototype is the discovery that AQP4 autoantibodies serve as a marker allowing for precise diagnosis of the neuromyelitis optica variant of multiple sclerosis.
However, while AQPs are now understood to have major influence in a wide range of diseases, no suitable AQP-modulator drugs have been identified.
Mercury and gold are pan-AQP inhibitors, but they are toxic and impractical in a therapeutic context, he noted. "It's early days," said Dr. Conejo-Mir, professor of dermatology at the University of Seville, Spain.
Aquaporins are a family of small cell membrane proteins that facilitate water transport in animals and plants. Thirteen mammalian AQPs have been identified. Dr. Peter C. Agre, the immediate past-president of the American Association for the Advancement of Science and a physician at Johns Hopkins University, Baltimore, who shared the 2003 Nobel Prize in Chemistry for his discovery of AQPs, called them "the plumbing system for cells."
AQP1 and AQP3 appear to be particularly relevant in skin cancer. They are involved in the key processes of cell migration, angiogenesis, cellular proliferation, and metastasis, said Dr. Conejo-Mir.
He presented a study in which he obtained 4-mm punch biopsies from 32 patients with various types of melanocytic skin lesions: 20 with malignant melanoma, 7 with common-acquired melanocytic nevi, and 5 with atypical or dysplastic nevi. The tissue specimens then underwent immunohistochemical staining for AQP1 and AQP3.
AQP1 was strongly expressed in the common melanocytic nevi but absent in the dysplastic nevi and all types of melanoma, which included six specimens of superficial spreading, four acral, five nodular, and five lentigo maligna melanomas.In contrast, AQP3 was upregulated in all of the melanocytic lesions, malignant or benign.
Dr. Conejo-Mir noted that his findings were consistent with prior studies by Dr. Alan S. Verkman and coworkers, who have done much of the early research on the role of AQPs in skin cancer.
AQP3 belongs to an AQP subgroup known as aquaglyceroporins, which transport glycerol as well as water. Dr. Verkman, who is professor of medicine and physiology at the University of California, San Francisco, and coworkers reported that AQP3 is normally expressed in plasma membranes of the basal epidermal cell layer of mammalian skin and is strongly overexpressed in human squamous cell carcinoma. They also demonstrated that AQP3-deficient mice have pathologically dry skin and slow recovery of the skin's barrier function after damage to the stratum corneum.
Dr. Verkman also found that AQP3-deficient mice are highly resistant to development of skin tumors when subjected to the standard multistage skin-tumor induction protocol widely utilized by bench scientists to study skin carcinogenesis.
"The remarkable resistance to skin tumorigenesis in AQP3 deficiency provides a rational basis for evaluation of AQP3 inhibitors for prevention and therapy of skin and other tumors associated with AQP3 overexpression," according to Dr. Verkman and Mariko Hara-Chikuma, Ph.D. (Mol. Cell. Biol. 2008;28:326-32).
The key roles AQPs play in glandular fluid secretion and urinary concentration were predictable based upon AQPs' function in transepithelial fluid transport. What was unanticipated, however, was aquaglyceroporins' involvement in fat metabolism, skin hydration, carcinogenesis, neural activity, and ocular function, which may mean translational possibilities for new treatments (J. Exp. Biol. June 2009; 212:1707-15).
Dr. Conejo-Mir had no conflicts of interest to disclose.
MADRID — The Nobel Prize-winning discovery of aquaporins is having a trickle-down translational effect that could have a major impact upon the prevention and treatment of both melanoma and nonmelanoma skin cancers.
Aquaporins (AQPs) are also actively under study for potential utility in the treatment for a range of other diseases, including epilepsy, obesity, severe heart failure and various other edematous states, malaria, wound healing, glaucoma, Sjögren's syndrome, and for neuroprotection after brain or spinal cord injury, Dr. Julián S. Conejo-Mir said at the 13th World Congress on Cancers of the Skin, sponsored by the Skin Cancer Foundation.
There are also potential diagnostic applications, Dr. Conejo-Mir noted. The prototype is the discovery that AQP4 autoantibodies serve as a marker allowing for precise diagnosis of the neuromyelitis optica variant of multiple sclerosis.
However, while AQPs are now understood to have major influence in a wide range of diseases, no suitable AQP-modulator drugs have been identified.
Mercury and gold are pan-AQP inhibitors, but they are toxic and impractical in a therapeutic context, he noted. "It's early days," said Dr. Conejo-Mir, professor of dermatology at the University of Seville, Spain.
Aquaporins are a family of small cell membrane proteins that facilitate water transport in animals and plants. Thirteen mammalian AQPs have been identified. Dr. Peter C. Agre, the immediate past-president of the American Association for the Advancement of Science and a physician at Johns Hopkins University, Baltimore, who shared the 2003 Nobel Prize in Chemistry for his discovery of AQPs, called them "the plumbing system for cells."
AQP1 and AQP3 appear to be particularly relevant in skin cancer. They are involved in the key processes of cell migration, angiogenesis, cellular proliferation, and metastasis, said Dr. Conejo-Mir.
He presented a study in which he obtained 4-mm punch biopsies from 32 patients with various types of melanocytic skin lesions: 20 with malignant melanoma, 7 with common-acquired melanocytic nevi, and 5 with atypical or dysplastic nevi. The tissue specimens then underwent immunohistochemical staining for AQP1 and AQP3.
AQP1 was strongly expressed in the common melanocytic nevi but absent in the dysplastic nevi and all types of melanoma, which included six specimens of superficial spreading, four acral, five nodular, and five lentigo maligna melanomas.In contrast, AQP3 was upregulated in all of the melanocytic lesions, malignant or benign.
Dr. Conejo-Mir noted that his findings were consistent with prior studies by Dr. Alan S. Verkman and coworkers, who have done much of the early research on the role of AQPs in skin cancer.
AQP3 belongs to an AQP subgroup known as aquaglyceroporins, which transport glycerol as well as water. Dr. Verkman, who is professor of medicine and physiology at the University of California, San Francisco, and coworkers reported that AQP3 is normally expressed in plasma membranes of the basal epidermal cell layer of mammalian skin and is strongly overexpressed in human squamous cell carcinoma. They also demonstrated that AQP3-deficient mice have pathologically dry skin and slow recovery of the skin's barrier function after damage to the stratum corneum.
Dr. Verkman also found that AQP3-deficient mice are highly resistant to development of skin tumors when subjected to the standard multistage skin-tumor induction protocol widely utilized by bench scientists to study skin carcinogenesis.
"The remarkable resistance to skin tumorigenesis in AQP3 deficiency provides a rational basis for evaluation of AQP3 inhibitors for prevention and therapy of skin and other tumors associated with AQP3 overexpression," according to Dr. Verkman and Mariko Hara-Chikuma, Ph.D. (Mol. Cell. Biol. 2008;28:326-32).
The key roles AQPs play in glandular fluid secretion and urinary concentration were predictable based upon AQPs' function in transepithelial fluid transport. What was unanticipated, however, was aquaglyceroporins' involvement in fat metabolism, skin hydration, carcinogenesis, neural activity, and ocular function, which may mean translational possibilities for new treatments (J. Exp. Biol. June 2009; 212:1707-15).
Dr. Conejo-Mir had no conflicts of interest to disclose.
MADRID — The Nobel Prize-winning discovery of aquaporins is having a trickle-down translational effect that could have a major impact upon the prevention and treatment of both melanoma and nonmelanoma skin cancers.
Aquaporins (AQPs) are also actively under study for potential utility in the treatment for a range of other diseases, including epilepsy, obesity, severe heart failure and various other edematous states, malaria, wound healing, glaucoma, Sjögren's syndrome, and for neuroprotection after brain or spinal cord injury, Dr. Julián S. Conejo-Mir said at the 13th World Congress on Cancers of the Skin, sponsored by the Skin Cancer Foundation.
There are also potential diagnostic applications, Dr. Conejo-Mir noted. The prototype is the discovery that AQP4 autoantibodies serve as a marker allowing for precise diagnosis of the neuromyelitis optica variant of multiple sclerosis.
However, while AQPs are now understood to have major influence in a wide range of diseases, no suitable AQP-modulator drugs have been identified.
Mercury and gold are pan-AQP inhibitors, but they are toxic and impractical in a therapeutic context, he noted. "It's early days," said Dr. Conejo-Mir, professor of dermatology at the University of Seville, Spain.
Aquaporins are a family of small cell membrane proteins that facilitate water transport in animals and plants. Thirteen mammalian AQPs have been identified. Dr. Peter C. Agre, the immediate past-president of the American Association for the Advancement of Science and a physician at Johns Hopkins University, Baltimore, who shared the 2003 Nobel Prize in Chemistry for his discovery of AQPs, called them "the plumbing system for cells."
AQP1 and AQP3 appear to be particularly relevant in skin cancer. They are involved in the key processes of cell migration, angiogenesis, cellular proliferation, and metastasis, said Dr. Conejo-Mir.
He presented a study in which he obtained 4-mm punch biopsies from 32 patients with various types of melanocytic skin lesions: 20 with malignant melanoma, 7 with common-acquired melanocytic nevi, and 5 with atypical or dysplastic nevi. The tissue specimens then underwent immunohistochemical staining for AQP1 and AQP3.
AQP1 was strongly expressed in the common melanocytic nevi but absent in the dysplastic nevi and all types of melanoma, which included six specimens of superficial spreading, four acral, five nodular, and five lentigo maligna melanomas.In contrast, AQP3 was upregulated in all of the melanocytic lesions, malignant or benign.
Dr. Conejo-Mir noted that his findings were consistent with prior studies by Dr. Alan S. Verkman and coworkers, who have done much of the early research on the role of AQPs in skin cancer.
AQP3 belongs to an AQP subgroup known as aquaglyceroporins, which transport glycerol as well as water. Dr. Verkman, who is professor of medicine and physiology at the University of California, San Francisco, and coworkers reported that AQP3 is normally expressed in plasma membranes of the basal epidermal cell layer of mammalian skin and is strongly overexpressed in human squamous cell carcinoma. They also demonstrated that AQP3-deficient mice have pathologically dry skin and slow recovery of the skin's barrier function after damage to the stratum corneum.
Dr. Verkman also found that AQP3-deficient mice are highly resistant to development of skin tumors when subjected to the standard multistage skin-tumor induction protocol widely utilized by bench scientists to study skin carcinogenesis.
"The remarkable resistance to skin tumorigenesis in AQP3 deficiency provides a rational basis for evaluation of AQP3 inhibitors for prevention and therapy of skin and other tumors associated with AQP3 overexpression," according to Dr. Verkman and Mariko Hara-Chikuma, Ph.D. (Mol. Cell. Biol. 2008;28:326-32).
The key roles AQPs play in glandular fluid secretion and urinary concentration were predictable based upon AQPs' function in transepithelial fluid transport. What was unanticipated, however, was aquaglyceroporins' involvement in fat metabolism, skin hydration, carcinogenesis, neural activity, and ocular function, which may mean translational possibilities for new treatments (J. Exp. Biol. June 2009; 212:1707-15).
Dr. Conejo-Mir had no conflicts of interest to disclose.