User login
Early skin-to-skin contact promotes breastfeeding, benefits baby
ORLANDO – Early skin-to-skin contact between mothers and their newborns was associated with higher rates of exclusive breastfeeding in a retrospective study presented at the annual meeting of the American Academy of Pediatrics.
Of the 150 mothers included in the study, 72% intended to breastfeed exclusively, but only 28% did so. After adjustment for maternal age, mode of delivery, parity, and gestational age, the only factor significantly associated with exclusive breastfeeding other than intention to breastfeed exclusively was early skin-to-skin contact (odds ratio, 3.7), which occurred in 53% of cases, Dr. Darshna Bhatt of Cohen Children’s Medical Center of New York, New Hyde Park, reported.
For the study, Dr. Bhatt and her colleagues reviewed electronic medical records of consecutive admissions to the well baby nursery, including only singleton, late preterm, or term newborns whose records contained documentation regarding whether the newborn had early skin-to-skin contact with the mother. Early skin-to-skin contact is generally defined as mother-baby bare skin contact for a period of time right after delivery; exclusive breastfeeding was defined as receipt of no formula feedings during the hospital stay.
Early skin-to-skin contact between mother and infant in the delivery room has previously been shown to be associated with breastfeeding success, but not all newborns receive skin-to-skin contact in the critical postbirth period, Dr. Bhatt noted. The current findings suggest that promoting skin-to-skin contact in the delivery room may improve exclusive breastfeeding rates, she concluded.
Indeed, during a plenary session at the conference, Dr. Jae Kim, associate professor of pediatrics at the University of California, San Diego (UCSD), said that skin-to-skin contact promotes breastfeeding and provides a "rich experience in the first few minutes of life."
The benefits during this "early golden hour" are believed to be at least threefold, providing physical interaction that regulates the baby’s temperature and provides sensory stimuli; promoting an early breastfeeding response with access to colostrum, which improves both short- and long-term breastfeeding; and allowing for emotional bonding, which is difficult to measure but is "very, very critical to early infant development," he said.
Data suggest that this contact promotes body temperature regulation and physiological stability in the baby with respect to heart rate, breathing response, blood pressure, and blood sugar levels. It also is associated with less crying and a better breastfeeding response, Dr. Kim said, noting that a Cochrane review showed improved breastfeeding at 1 and 4 months, with trends toward longer duration of breastfeeding overall, in healthy term infants who experience early skin-to-skin contact. Improvement in terms of cardiorespiratory stability and blood glucose control also was seen in late pre-term infants.
Although better data – particularly on long-term effects – are needed, it is clear that skin-to-skin contact can "dramatically improve the breastfeeding success rate, halve the time to actually start breastfeeding, improve the satisfaction of both the mother and the family, and also [lead to] an increased amount of exclusive breastfeeding in those babies," he said.
Many hospitals, including his own institution, have moved toward a model that promotes early skin-to-skin contact, he said, adding that most babies at UCSD are coupled with their mother for early skin-to-skin contact.
The incidence of early skin-to-skin contact and establishment of breastfeeding at UCSD is very high for normal vaginal-birth babies and normal cesarean-section babies.
"We as pediatricians play an incredible role in really affecting this change. It’s not just the medical nurses that deliver this care, but it’s about the physicians sending a strong message about how important it is," he said, noting that the pediatricians at his hospital "make a very special point" to get babies back to their moms immediately after the physical examination and to emphasize the importance of skin-to-skin time.
Skin-to-skin contact can also be promoted in the neonatal intensive care unit (NICU), he said.
Data suggest that preterm and low-birth-weight infants do dramatically better with skin-to-skin contact, with improvements in mortality, sepsis, hypothermia, growth, mother-infant attachment, motor development, long-term cognitive development, stress and pain response, colic, sleep response, pain, breastfeeding, and length of stay.
This is an excellent model in limited-resource settings, and benefits have also been seen at UCSD.
"I think we can make a very strong case right now, especially in a family-centered model, the NICU, that we should be pushing for more and more skin-to-skin [contact time]," he said, noting that parents should be encouraged to request daily skin-to-skin therapy in the NICU.
A program at UCSD – the SPIN (Supporting Preterm Infant Nutrition) Program, which was designed to promote better preterm infant nutrition – has harnessed the benefits of early skin-to-skin contact and early human milk intake to move this approach from a regional program to a national platform, "where we can standardize how we deal with preterm infants and their nutrition," he said. Dialogue is encouraged to help improve standardization across the country, he said.
How can such a program be implemented?
It’s important to standardize the practice by gathering key stakeholders and empowering them to target certain objectives, take one step at a time, and develop a broad-based education program to teach everyone how to achieve the objectives. This is important for something like skin-to-skin contact, which involves the efforts of staff from many different areas (nurses from nursery, labor and delivery, NICU, etc.).
In addition, for quality improvement it is important to have some measure of the benchmarks you are targeting in order to measure success.
"A lot of the time, it’s just about getting everyone to the same table, having the same talk, and realizing the information is not that complicated, and that the practice is actually relatively easy to implement, even when it comes to very vulnerable babies in the NICU," he said.
Dr. Bhatt reported having no disclosures. Dr. Kim is on the speaker’s bureaus for Nestle Nutrition, Nutricia, Abbott Nutrition, and Medela, and has received honoraria or research grant support from Medela and GE Healthcare.
ORLANDO – Early skin-to-skin contact between mothers and their newborns was associated with higher rates of exclusive breastfeeding in a retrospective study presented at the annual meeting of the American Academy of Pediatrics.
Of the 150 mothers included in the study, 72% intended to breastfeed exclusively, but only 28% did so. After adjustment for maternal age, mode of delivery, parity, and gestational age, the only factor significantly associated with exclusive breastfeeding other than intention to breastfeed exclusively was early skin-to-skin contact (odds ratio, 3.7), which occurred in 53% of cases, Dr. Darshna Bhatt of Cohen Children’s Medical Center of New York, New Hyde Park, reported.
For the study, Dr. Bhatt and her colleagues reviewed electronic medical records of consecutive admissions to the well baby nursery, including only singleton, late preterm, or term newborns whose records contained documentation regarding whether the newborn had early skin-to-skin contact with the mother. Early skin-to-skin contact is generally defined as mother-baby bare skin contact for a period of time right after delivery; exclusive breastfeeding was defined as receipt of no formula feedings during the hospital stay.
Early skin-to-skin contact between mother and infant in the delivery room has previously been shown to be associated with breastfeeding success, but not all newborns receive skin-to-skin contact in the critical postbirth period, Dr. Bhatt noted. The current findings suggest that promoting skin-to-skin contact in the delivery room may improve exclusive breastfeeding rates, she concluded.
Indeed, during a plenary session at the conference, Dr. Jae Kim, associate professor of pediatrics at the University of California, San Diego (UCSD), said that skin-to-skin contact promotes breastfeeding and provides a "rich experience in the first few minutes of life."
The benefits during this "early golden hour" are believed to be at least threefold, providing physical interaction that regulates the baby’s temperature and provides sensory stimuli; promoting an early breastfeeding response with access to colostrum, which improves both short- and long-term breastfeeding; and allowing for emotional bonding, which is difficult to measure but is "very, very critical to early infant development," he said.
Data suggest that this contact promotes body temperature regulation and physiological stability in the baby with respect to heart rate, breathing response, blood pressure, and blood sugar levels. It also is associated with less crying and a better breastfeeding response, Dr. Kim said, noting that a Cochrane review showed improved breastfeeding at 1 and 4 months, with trends toward longer duration of breastfeeding overall, in healthy term infants who experience early skin-to-skin contact. Improvement in terms of cardiorespiratory stability and blood glucose control also was seen in late pre-term infants.
Although better data – particularly on long-term effects – are needed, it is clear that skin-to-skin contact can "dramatically improve the breastfeeding success rate, halve the time to actually start breastfeeding, improve the satisfaction of both the mother and the family, and also [lead to] an increased amount of exclusive breastfeeding in those babies," he said.
Many hospitals, including his own institution, have moved toward a model that promotes early skin-to-skin contact, he said, adding that most babies at UCSD are coupled with their mother for early skin-to-skin contact.
The incidence of early skin-to-skin contact and establishment of breastfeeding at UCSD is very high for normal vaginal-birth babies and normal cesarean-section babies.
"We as pediatricians play an incredible role in really affecting this change. It’s not just the medical nurses that deliver this care, but it’s about the physicians sending a strong message about how important it is," he said, noting that the pediatricians at his hospital "make a very special point" to get babies back to their moms immediately after the physical examination and to emphasize the importance of skin-to-skin time.
Skin-to-skin contact can also be promoted in the neonatal intensive care unit (NICU), he said.
Data suggest that preterm and low-birth-weight infants do dramatically better with skin-to-skin contact, with improvements in mortality, sepsis, hypothermia, growth, mother-infant attachment, motor development, long-term cognitive development, stress and pain response, colic, sleep response, pain, breastfeeding, and length of stay.
This is an excellent model in limited-resource settings, and benefits have also been seen at UCSD.
"I think we can make a very strong case right now, especially in a family-centered model, the NICU, that we should be pushing for more and more skin-to-skin [contact time]," he said, noting that parents should be encouraged to request daily skin-to-skin therapy in the NICU.
A program at UCSD – the SPIN (Supporting Preterm Infant Nutrition) Program, which was designed to promote better preterm infant nutrition – has harnessed the benefits of early skin-to-skin contact and early human milk intake to move this approach from a regional program to a national platform, "where we can standardize how we deal with preterm infants and their nutrition," he said. Dialogue is encouraged to help improve standardization across the country, he said.
How can such a program be implemented?
It’s important to standardize the practice by gathering key stakeholders and empowering them to target certain objectives, take one step at a time, and develop a broad-based education program to teach everyone how to achieve the objectives. This is important for something like skin-to-skin contact, which involves the efforts of staff from many different areas (nurses from nursery, labor and delivery, NICU, etc.).
In addition, for quality improvement it is important to have some measure of the benchmarks you are targeting in order to measure success.
"A lot of the time, it’s just about getting everyone to the same table, having the same talk, and realizing the information is not that complicated, and that the practice is actually relatively easy to implement, even when it comes to very vulnerable babies in the NICU," he said.
Dr. Bhatt reported having no disclosures. Dr. Kim is on the speaker’s bureaus for Nestle Nutrition, Nutricia, Abbott Nutrition, and Medela, and has received honoraria or research grant support from Medela and GE Healthcare.
ORLANDO – Early skin-to-skin contact between mothers and their newborns was associated with higher rates of exclusive breastfeeding in a retrospective study presented at the annual meeting of the American Academy of Pediatrics.
Of the 150 mothers included in the study, 72% intended to breastfeed exclusively, but only 28% did so. After adjustment for maternal age, mode of delivery, parity, and gestational age, the only factor significantly associated with exclusive breastfeeding other than intention to breastfeed exclusively was early skin-to-skin contact (odds ratio, 3.7), which occurred in 53% of cases, Dr. Darshna Bhatt of Cohen Children’s Medical Center of New York, New Hyde Park, reported.
For the study, Dr. Bhatt and her colleagues reviewed electronic medical records of consecutive admissions to the well baby nursery, including only singleton, late preterm, or term newborns whose records contained documentation regarding whether the newborn had early skin-to-skin contact with the mother. Early skin-to-skin contact is generally defined as mother-baby bare skin contact for a period of time right after delivery; exclusive breastfeeding was defined as receipt of no formula feedings during the hospital stay.
Early skin-to-skin contact between mother and infant in the delivery room has previously been shown to be associated with breastfeeding success, but not all newborns receive skin-to-skin contact in the critical postbirth period, Dr. Bhatt noted. The current findings suggest that promoting skin-to-skin contact in the delivery room may improve exclusive breastfeeding rates, she concluded.
Indeed, during a plenary session at the conference, Dr. Jae Kim, associate professor of pediatrics at the University of California, San Diego (UCSD), said that skin-to-skin contact promotes breastfeeding and provides a "rich experience in the first few minutes of life."
The benefits during this "early golden hour" are believed to be at least threefold, providing physical interaction that regulates the baby’s temperature and provides sensory stimuli; promoting an early breastfeeding response with access to colostrum, which improves both short- and long-term breastfeeding; and allowing for emotional bonding, which is difficult to measure but is "very, very critical to early infant development," he said.
Data suggest that this contact promotes body temperature regulation and physiological stability in the baby with respect to heart rate, breathing response, blood pressure, and blood sugar levels. It also is associated with less crying and a better breastfeeding response, Dr. Kim said, noting that a Cochrane review showed improved breastfeeding at 1 and 4 months, with trends toward longer duration of breastfeeding overall, in healthy term infants who experience early skin-to-skin contact. Improvement in terms of cardiorespiratory stability and blood glucose control also was seen in late pre-term infants.
Although better data – particularly on long-term effects – are needed, it is clear that skin-to-skin contact can "dramatically improve the breastfeeding success rate, halve the time to actually start breastfeeding, improve the satisfaction of both the mother and the family, and also [lead to] an increased amount of exclusive breastfeeding in those babies," he said.
Many hospitals, including his own institution, have moved toward a model that promotes early skin-to-skin contact, he said, adding that most babies at UCSD are coupled with their mother for early skin-to-skin contact.
The incidence of early skin-to-skin contact and establishment of breastfeeding at UCSD is very high for normal vaginal-birth babies and normal cesarean-section babies.
"We as pediatricians play an incredible role in really affecting this change. It’s not just the medical nurses that deliver this care, but it’s about the physicians sending a strong message about how important it is," he said, noting that the pediatricians at his hospital "make a very special point" to get babies back to their moms immediately after the physical examination and to emphasize the importance of skin-to-skin time.
Skin-to-skin contact can also be promoted in the neonatal intensive care unit (NICU), he said.
Data suggest that preterm and low-birth-weight infants do dramatically better with skin-to-skin contact, with improvements in mortality, sepsis, hypothermia, growth, mother-infant attachment, motor development, long-term cognitive development, stress and pain response, colic, sleep response, pain, breastfeeding, and length of stay.
This is an excellent model in limited-resource settings, and benefits have also been seen at UCSD.
"I think we can make a very strong case right now, especially in a family-centered model, the NICU, that we should be pushing for more and more skin-to-skin [contact time]," he said, noting that parents should be encouraged to request daily skin-to-skin therapy in the NICU.
A program at UCSD – the SPIN (Supporting Preterm Infant Nutrition) Program, which was designed to promote better preterm infant nutrition – has harnessed the benefits of early skin-to-skin contact and early human milk intake to move this approach from a regional program to a national platform, "where we can standardize how we deal with preterm infants and their nutrition," he said. Dialogue is encouraged to help improve standardization across the country, he said.
How can such a program be implemented?
It’s important to standardize the practice by gathering key stakeholders and empowering them to target certain objectives, take one step at a time, and develop a broad-based education program to teach everyone how to achieve the objectives. This is important for something like skin-to-skin contact, which involves the efforts of staff from many different areas (nurses from nursery, labor and delivery, NICU, etc.).
In addition, for quality improvement it is important to have some measure of the benchmarks you are targeting in order to measure success.
"A lot of the time, it’s just about getting everyone to the same table, having the same talk, and realizing the information is not that complicated, and that the practice is actually relatively easy to implement, even when it comes to very vulnerable babies in the NICU," he said.
Dr. Bhatt reported having no disclosures. Dr. Kim is on the speaker’s bureaus for Nestle Nutrition, Nutricia, Abbott Nutrition, and Medela, and has received honoraria or research grant support from Medela and GE Healthcare.
AT THE AAP NATIONAL CONFERENCE
Major finding: Early skin-to-skin contact was significantly associated with exclusive breastfeeding (odds ratio, 3.7).
Data source: A retrospective study of 150 mother-newborn pairs.
Disclosures: Dr. Bhatt reported having no disclosures. Dr. Kim is on the speaker’s bureaus for Nestle Nutrition, Nutricia, Abbott Nutrition, and Medela, and has received honoraria or research grant support from Medela and GE Healthcare.
New-onset hypertension in pregnancy boosts post-delivery risk
DALLAS – Previously normotensive women who develop a hypertensive disorder during pregnancy are at more than double the risk of being diagnosed with prehypertension or hypertension within the first year after delivery, according to a large California study.
"Early postpartum screening and improved follow-up of women with hypertensive disorders first identified during pregnancy may be necessary to identify those at risk for future hypertension or prehypertension," Mary Helen Black, Ph.D., concluded in presenting the results of her population-based study at the American Heart Association scientific sessions.
The study was a retrospective review of the comprehensive electronic health records of 5,960 women who received their prenatal care and subsequently delivered a live singleton neonate at 20 weeks’ gestation or more at a single Kaiser Permanente Southern California medical center during 2006-2010. All of these women were specifically identified as being normotensive prior to their pregnancy and 6% of them developed a hypertensive disorder in pregnancy; 215 of the 358 affected women had preeclampsia or eclampsia.

During the first year after delivery, 63 women, or 1.1% of the total study population, developed frank hypertension. Another 902, or 15%, developed prehypertension during that first year. Prehypertension was defined as a modestly elevated blood pressure of at least 120/80 mm Hg on two consecutive ambulatory visits.
After adjustment for potential confounders including age, race, parity, prepregnancy body mass index, and smoking status, previously normotensive women with hypertension in pregnancy had an adjusted 2.4-fold increased risk of developing hypertension or prehypertension in the year after delivery, compared with women without any hypertensive disorder in pregnancy. Women who developed preeclampsia or eclampsia had a 2.5-fold increased risk, according to Dr. Black, a research scientist at Kaiser Permanente Southern California in Pasadena.
Protocols exist for monitoring and treatment of pregnant women identified as having chronic hypertension prior to pregnancy. However, the new Kaiser study is one of the first to look at the downstream impact of hypertensive disorders in pregnancy arising among women with no preexisting indication of hypertension. The plan is to follow these women further to learn how their clinical outcomes progress. Long-term Scandinavian registry studies have linked hypertensive disorders in pregnancy to increased risk of eventual type 2 diabetes, hypertension, and cardiovascular disease.
Dr. Black and her coinvestigators are planning a postpartum intervention study aimed at preventing onset of type 2 diabetes and cardiovascular disease in previously normotensive women with hypertensive disorders in pregnancy. Serious consideration is being given to intervening with the DASH diet and other nonpharmacologic interventions, she said.
While women with chronic hypertension prior to pregnancy are known to be at increased risk for development of preeclampsia and other hypertensive disorders of pregnancy as well as for gestational diabetes mellitus, the situation regarding women with prepregnancy prehypertension has been less clear. Dr. Black and coworkers shed new light on this issue in a separate study presented at the AHA meeting. She reported that women with prepregnancy prehypertension are also at increased risk for these pregnancy complications.
This study involved 2,156 Kaiser Permanente patients with prepregnancy prehypertension and 5,646 who were normotensive. A total of 8.4% of the women developed a hypertensive disorder during pregnancy, including 373 with preeclampsia/eclampsia. In addition, 1,877 women developed gestational diabetes mellitus.
Women with prehypertension prior to pregnancy were an adjusted 2.7-fold more likely to develop a hypertensive disorder in pregnancy, 2.2-fold more likely to have preeclampsia/eclampsia, and 1.2-fold more likely to develop gestational diabetes than women who were normotensive before pregnancy.
The risk of preeclampsia/eclampsia among women with prepregnancy prehypertension was significantly greater if they were at least 30 years old than if they were younger.
Both studies were funded by Kaiser Permanente. Dr. Black is an employee of the company.
DALLAS – Previously normotensive women who develop a hypertensive disorder during pregnancy are at more than double the risk of being diagnosed with prehypertension or hypertension within the first year after delivery, according to a large California study.
"Early postpartum screening and improved follow-up of women with hypertensive disorders first identified during pregnancy may be necessary to identify those at risk for future hypertension or prehypertension," Mary Helen Black, Ph.D., concluded in presenting the results of her population-based study at the American Heart Association scientific sessions.
The study was a retrospective review of the comprehensive electronic health records of 5,960 women who received their prenatal care and subsequently delivered a live singleton neonate at 20 weeks’ gestation or more at a single Kaiser Permanente Southern California medical center during 2006-2010. All of these women were specifically identified as being normotensive prior to their pregnancy and 6% of them developed a hypertensive disorder in pregnancy; 215 of the 358 affected women had preeclampsia or eclampsia.
During the first year after delivery, 63 women, or 1.1% of the total study population, developed frank hypertension. Another 902, or 15%, developed prehypertension during that first year. Prehypertension was defined as a modestly elevated blood pressure of at least 120/80 mm Hg on two consecutive ambulatory visits.
After adjustment for potential confounders including age, race, parity, prepregnancy body mass index, and smoking status, previously normotensive women with hypertension in pregnancy had an adjusted 2.4-fold increased risk of developing hypertension or prehypertension in the year after delivery, compared with women without any hypertensive disorder in pregnancy. Women who developed preeclampsia or eclampsia had a 2.5-fold increased risk, according to Dr. Black, a research scientist at Kaiser Permanente Southern California in Pasadena.
Protocols exist for monitoring and treatment of pregnant women identified as having chronic hypertension prior to pregnancy. However, the new Kaiser study is one of the first to look at the downstream impact of hypertensive disorders in pregnancy arising among women with no preexisting indication of hypertension. The plan is to follow these women further to learn how their clinical outcomes progress. Long-term Scandinavian registry studies have linked hypertensive disorders in pregnancy to increased risk of eventual type 2 diabetes, hypertension, and cardiovascular disease.
Dr. Black and her coinvestigators are planning a postpartum intervention study aimed at preventing onset of type 2 diabetes and cardiovascular disease in previously normotensive women with hypertensive disorders in pregnancy. Serious consideration is being given to intervening with the DASH diet and other nonpharmacologic interventions, she said.
While women with chronic hypertension prior to pregnancy are known to be at increased risk for development of preeclampsia and other hypertensive disorders of pregnancy as well as for gestational diabetes mellitus, the situation regarding women with prepregnancy prehypertension has been less clear. Dr. Black and coworkers shed new light on this issue in a separate study presented at the AHA meeting. She reported that women with prepregnancy prehypertension are also at increased risk for these pregnancy complications.
This study involved 2,156 Kaiser Permanente patients with prepregnancy prehypertension and 5,646 who were normotensive. A total of 8.4% of the women developed a hypertensive disorder during pregnancy, including 373 with preeclampsia/eclampsia. In addition, 1,877 women developed gestational diabetes mellitus.
Women with prehypertension prior to pregnancy were an adjusted 2.7-fold more likely to develop a hypertensive disorder in pregnancy, 2.2-fold more likely to have preeclampsia/eclampsia, and 1.2-fold more likely to develop gestational diabetes than women who were normotensive before pregnancy.
The risk of preeclampsia/eclampsia among women with prepregnancy prehypertension was significantly greater if they were at least 30 years old than if they were younger.
Both studies were funded by Kaiser Permanente. Dr. Black is an employee of the company.
DALLAS – Previously normotensive women who develop a hypertensive disorder during pregnancy are at more than double the risk of being diagnosed with prehypertension or hypertension within the first year after delivery, according to a large California study.
"Early postpartum screening and improved follow-up of women with hypertensive disorders first identified during pregnancy may be necessary to identify those at risk for future hypertension or prehypertension," Mary Helen Black, Ph.D., concluded in presenting the results of her population-based study at the American Heart Association scientific sessions.
The study was a retrospective review of the comprehensive electronic health records of 5,960 women who received their prenatal care and subsequently delivered a live singleton neonate at 20 weeks’ gestation or more at a single Kaiser Permanente Southern California medical center during 2006-2010. All of these women were specifically identified as being normotensive prior to their pregnancy and 6% of them developed a hypertensive disorder in pregnancy; 215 of the 358 affected women had preeclampsia or eclampsia.
During the first year after delivery, 63 women, or 1.1% of the total study population, developed frank hypertension. Another 902, or 15%, developed prehypertension during that first year. Prehypertension was defined as a modestly elevated blood pressure of at least 120/80 mm Hg on two consecutive ambulatory visits.
After adjustment for potential confounders including age, race, parity, prepregnancy body mass index, and smoking status, previously normotensive women with hypertension in pregnancy had an adjusted 2.4-fold increased risk of developing hypertension or prehypertension in the year after delivery, compared with women without any hypertensive disorder in pregnancy. Women who developed preeclampsia or eclampsia had a 2.5-fold increased risk, according to Dr. Black, a research scientist at Kaiser Permanente Southern California in Pasadena.
Protocols exist for monitoring and treatment of pregnant women identified as having chronic hypertension prior to pregnancy. However, the new Kaiser study is one of the first to look at the downstream impact of hypertensive disorders in pregnancy arising among women with no preexisting indication of hypertension. The plan is to follow these women further to learn how their clinical outcomes progress. Long-term Scandinavian registry studies have linked hypertensive disorders in pregnancy to increased risk of eventual type 2 diabetes, hypertension, and cardiovascular disease.
Dr. Black and her coinvestigators are planning a postpartum intervention study aimed at preventing onset of type 2 diabetes and cardiovascular disease in previously normotensive women with hypertensive disorders in pregnancy. Serious consideration is being given to intervening with the DASH diet and other nonpharmacologic interventions, she said.
While women with chronic hypertension prior to pregnancy are known to be at increased risk for development of preeclampsia and other hypertensive disorders of pregnancy as well as for gestational diabetes mellitus, the situation regarding women with prepregnancy prehypertension has been less clear. Dr. Black and coworkers shed new light on this issue in a separate study presented at the AHA meeting. She reported that women with prepregnancy prehypertension are also at increased risk for these pregnancy complications.
This study involved 2,156 Kaiser Permanente patients with prepregnancy prehypertension and 5,646 who were normotensive. A total of 8.4% of the women developed a hypertensive disorder during pregnancy, including 373 with preeclampsia/eclampsia. In addition, 1,877 women developed gestational diabetes mellitus.
Women with prehypertension prior to pregnancy were an adjusted 2.7-fold more likely to develop a hypertensive disorder in pregnancy, 2.2-fold more likely to have preeclampsia/eclampsia, and 1.2-fold more likely to develop gestational diabetes than women who were normotensive before pregnancy.
The risk of preeclampsia/eclampsia among women with prepregnancy prehypertension was significantly greater if they were at least 30 years old than if they were younger.
Both studies were funded by Kaiser Permanente. Dr. Black is an employee of the company.
AT THE AHA SCIENTIFIC SESSIONS
Major finding: Women who were normotensive prepregnancy but developed a hypertensive disorder during pregnancy were at 2.4-fold increased risk of frank hypertension or prehypertension in their first year after delivery, compared with women who remained normotensive in pregnancy.
Data source: An observational study of 5,960 women who delivered a singleton neonate, 6% of whom developed a hypertensive disorder of pregnancy. All were known to be normotensive prior to pregnancy.
Disclosures: Dr. Black is an employee of Kaiser Permanente, which funded the study.

Multiple births declined in tandem with IVF reforms
The rate of triplet and higher-order births in the United States has declined since 1998, coincident with efforts to limit the number of embryos transferred during IVF procedures, according to a report published online Dec. 4 in the New England Journal of Medicine.
A similar effort to reduce multiple births resulting from non-IVF fertility treatments would decrease the rate even further, bringing it more into line with the "natural" rate of multiple births that occurred before fertility treatments became available in 1971, said Dr. Aniket D. Kulkarni of the women’s health and fertility branch at the Centers for Disease Control and Prevention, Atlanta, and her associates.

The investigators wanted to examine time trends in multiple births across the country, in particular the contribution that fertility treatments make to multiple births, but statistics regarding births that result from non-IVF fertility treatments are "not directly ascertainable" because there is no legal mandate to report those births, they noted. In contrast, multiple births resulting from IVF can be ascertained from a national registry of those births.
Dr. Kulkarni and her colleagues analyzed data on all live births that occurred from 1971 to 2011, then used statistical methods to estimate the proportion that occurred from natural conception, IVF, and non-IVF fertility treatments. They also used statistical methods to account for the effect of maternal age on multiple births.
The overall proportion of national births that were multiple births rose from 1.8% in 1971 to 3.5% in 2011.
This rate, however, did not show a continuous increase over the 4-decade study period, but rather showed a rise until approximately the last decade, followed by a steady decline.
By 2011, they estimated, 36% of twin births and 77% of triplet and higher-order births in the United States resulted from fertility treatments.
The rate of triplet and higher-order births increased from 1971 and reached its peak in 1998, the year that the Society for Assisted Reproductive Technology first issued practice guidelines designed to limit the number of embryos transferred during IVF cycles. The national rate of triplet and higher-order births then began to decline, going from 1.94 per 1,000 live births in 1998 to 1.37 per 1,000 in 2011.
This represents a 29% reduction, Dr. Kulkarni and her associates said (N. Engl. J. Med. 2013 [doi:10.1056/NEJMoa1301467]). The decline coincided with a 70% reduction in transfers of three or more embryos during IVF.
The trends for non-IVF fertility treatments were "less favorable," the researchers noted. In particular, ovulation induction and ovarian stimulation continue to contribute heavily to the national rate of triplet and higher-order multiple births.
Adherence to more prudent practice patterns, such as the use of low-dose gonadotropins, could reduce the rate of multiple births "while maintaining acceptable per-cycle pregnancy rates," they said, adding that mandating the public reporting of births resulting from non-IVF fertility treatments also would help by facilitating data analysis.
This study was supported by the U.S. Centers for Disease Control and Prevention. Dr. Kulkarni reported no financial conflicts of interest; an associate reported ties to Alere.
The rate of triplet and higher-order births in the United States has declined since 1998, coincident with efforts to limit the number of embryos transferred during IVF procedures, according to a report published online Dec. 4 in the New England Journal of Medicine.
A similar effort to reduce multiple births resulting from non-IVF fertility treatments would decrease the rate even further, bringing it more into line with the "natural" rate of multiple births that occurred before fertility treatments became available in 1971, said Dr. Aniket D. Kulkarni of the women’s health and fertility branch at the Centers for Disease Control and Prevention, Atlanta, and her associates.
The investigators wanted to examine time trends in multiple births across the country, in particular the contribution that fertility treatments make to multiple births, but statistics regarding births that result from non-IVF fertility treatments are "not directly ascertainable" because there is no legal mandate to report those births, they noted. In contrast, multiple births resulting from IVF can be ascertained from a national registry of those births.
Dr. Kulkarni and her colleagues analyzed data on all live births that occurred from 1971 to 2011, then used statistical methods to estimate the proportion that occurred from natural conception, IVF, and non-IVF fertility treatments. They also used statistical methods to account for the effect of maternal age on multiple births.
The overall proportion of national births that were multiple births rose from 1.8% in 1971 to 3.5% in 2011.
This rate, however, did not show a continuous increase over the 4-decade study period, but rather showed a rise until approximately the last decade, followed by a steady decline.
By 2011, they estimated, 36% of twin births and 77% of triplet and higher-order births in the United States resulted from fertility treatments.
The rate of triplet and higher-order births increased from 1971 and reached its peak in 1998, the year that the Society for Assisted Reproductive Technology first issued practice guidelines designed to limit the number of embryos transferred during IVF cycles. The national rate of triplet and higher-order births then began to decline, going from 1.94 per 1,000 live births in 1998 to 1.37 per 1,000 in 2011.
This represents a 29% reduction, Dr. Kulkarni and her associates said (N. Engl. J. Med. 2013 [doi:10.1056/NEJMoa1301467]). The decline coincided with a 70% reduction in transfers of three or more embryos during IVF.
The trends for non-IVF fertility treatments were "less favorable," the researchers noted. In particular, ovulation induction and ovarian stimulation continue to contribute heavily to the national rate of triplet and higher-order multiple births.
Adherence to more prudent practice patterns, such as the use of low-dose gonadotropins, could reduce the rate of multiple births "while maintaining acceptable per-cycle pregnancy rates," they said, adding that mandating the public reporting of births resulting from non-IVF fertility treatments also would help by facilitating data analysis.
This study was supported by the U.S. Centers for Disease Control and Prevention. Dr. Kulkarni reported no financial conflicts of interest; an associate reported ties to Alere.
The rate of triplet and higher-order births in the United States has declined since 1998, coincident with efforts to limit the number of embryos transferred during IVF procedures, according to a report published online Dec. 4 in the New England Journal of Medicine.
A similar effort to reduce multiple births resulting from non-IVF fertility treatments would decrease the rate even further, bringing it more into line with the "natural" rate of multiple births that occurred before fertility treatments became available in 1971, said Dr. Aniket D. Kulkarni of the women’s health and fertility branch at the Centers for Disease Control and Prevention, Atlanta, and her associates.
The investigators wanted to examine time trends in multiple births across the country, in particular the contribution that fertility treatments make to multiple births, but statistics regarding births that result from non-IVF fertility treatments are "not directly ascertainable" because there is no legal mandate to report those births, they noted. In contrast, multiple births resulting from IVF can be ascertained from a national registry of those births.
Dr. Kulkarni and her colleagues analyzed data on all live births that occurred from 1971 to 2011, then used statistical methods to estimate the proportion that occurred from natural conception, IVF, and non-IVF fertility treatments. They also used statistical methods to account for the effect of maternal age on multiple births.
The overall proportion of national births that were multiple births rose from 1.8% in 1971 to 3.5% in 2011.
This rate, however, did not show a continuous increase over the 4-decade study period, but rather showed a rise until approximately the last decade, followed by a steady decline.
By 2011, they estimated, 36% of twin births and 77% of triplet and higher-order births in the United States resulted from fertility treatments.
The rate of triplet and higher-order births increased from 1971 and reached its peak in 1998, the year that the Society for Assisted Reproductive Technology first issued practice guidelines designed to limit the number of embryos transferred during IVF cycles. The national rate of triplet and higher-order births then began to decline, going from 1.94 per 1,000 live births in 1998 to 1.37 per 1,000 in 2011.
This represents a 29% reduction, Dr. Kulkarni and her associates said (N. Engl. J. Med. 2013 [doi:10.1056/NEJMoa1301467]). The decline coincided with a 70% reduction in transfers of three or more embryos during IVF.
The trends for non-IVF fertility treatments were "less favorable," the researchers noted. In particular, ovulation induction and ovarian stimulation continue to contribute heavily to the national rate of triplet and higher-order multiple births.
Adherence to more prudent practice patterns, such as the use of low-dose gonadotropins, could reduce the rate of multiple births "while maintaining acceptable per-cycle pregnancy rates," they said, adding that mandating the public reporting of births resulting from non-IVF fertility treatments also would help by facilitating data analysis.
This study was supported by the U.S. Centers for Disease Control and Prevention. Dr. Kulkarni reported no financial conflicts of interest; an associate reported ties to Alere.
FROM THE NEW ENGLAND JOURNAL OF MEDICINE
Major Finding: The rate of triplet and higher-order births reached its peak in 1998 – the year that the Society for Assisted Reproductive Technology first issued practice guidelines designed to limit the number of embryos transferred during IVF cycles – and then began to decline, from 1.94 per 1,000 live births in 1998 to 1.37 per 1,000 in 2011.
Data Source: An analysis of national data on multiple births from 1971, when fertility treatments were first introduced, through 2011.
Disclosures: This study was supported by the U.S. Centers for Disease Control and Prevention. Ms. Kulkarni reported no financial conflicts of interest; an associate reported ties to Alere.

Point/Counterpoint – Should the IADPSG criteria for diagnosing gestational diabetes be adopted now worldwide?
POINT: Preventing adverse outcomes in newborns is imperative.
In March 2013, an independent panel at a National Institutes of Health consensus development conference recommended against adopting the one-step approach to diagnosis of gestational diabetes mellitus (GDM) that was recommended in 2008 by the International Association of Diabetes and Pregnancy Study Groups (IADPSG) and adopted by the American Diabetes Association, the World Health Organization, and organizations in other countries. The NIH panel voiced concerns about costs and interventions that would accompany an increased prevalence of GDM, as well as uncertainties about the benefits of identifying and treating so many additional new cases of GDM.
The panel’s recommendation is inconsistent with available data. There is more than sufficient evidence that the one-step approach should be used worldwide – without waiting for more research.

The study on which the IADPSG criteria were based – the Hyperglycemia and Adverse Pregnancy Outcomes (HAPO) Study (N. Engl. J. Med. 2008;358:1991-2002) – involved more than 23,000 pregnancies in nine different countries. All of the adverse pregnancy outcomes evaluated were related directly and significantly, and in a continuous fashion, to glucose concentrations at the fasting, 1-hour, and 2-hour points in a single 75-g, 2-hour oral glucose tolerance test (OGTT).
The IADPSG recommended that GDM be diagnosed when one or more of the plasma glucose values were met or exceeded: fasting, 92 mg/dL; 1-hour, 180 mg/dL; 2-hour, 153 mg/dL. According to the HAPO study data, patients with GDM have an approximate doubling of the likelihood of a birth weight above the 90th percentile compared to those without GDM, as well as a near-tripling of the likelihood of fetal hyperinsulinemia, twice the likelihood of preeclampsia, and a 50% increase in primary cesarean section, among other increased complication rates (Diabetes Care 2010;33:676-82).
The IADPSG diagnostic criteria are based on a predictive value of a 1.75 odds ratio above the mean for large for gestational age (LGA), neonatal body fat greater than 90th percentile, and cord blood hyperinsulinemia. This is equivalent to a doubling in the likelihood of these outcomes, because the 1.75 odds ratio is compared to the mean rather than to everyone without GDM.
HAPO was indeed an observational study, but we have solid data from other randomized trials demonstrating that intervention for mild GDM will prevent excess adverse outcomes.
In one of two recent randomized single-blinded trials on identifying and treating GDM, mild GDM was defined as a 2-hour, 75-g OGTT value between 140 and 198 mg/dL with a fasting plasma glucose value less than 140 mg/dL (mean, 86 mg/dL) – diagnostic criteria that, if anything, are lower than the IADPSG criteria. Patients randomized for intervention had a 66% reduction in "serious complications." Macrosomia was reduced by 50%, and preeclampsia by 30%. The cesarean rate was unchanged between the 1,000 women in the intervention and routine care groups (N. Engl. J. Med. 2005:352:2477-8).
In the second study of 958 women, identification and treatment lowered by half the rates of macrosomia, preeclampsia, and shoulder dystocia. There were other significant reductions in complications, and no difference in the rate of small-for-gestational-age infants (N. Engl. J. Med. 2009;361:1339-48). The criteria used to define mild GDM in this study meet the lower of two alternative sets of criteria recommended by the American College of Obstetricians and Gynecologists, but with a normal fasting plasma glucose concentration of 95 mg/dL or less.
Critics of the recommendations in the United States who say it is unreasonable and too expensive for such a large proportion of pregnant women to be identified as having a disease – 16%-18% in the HAPO population – need to look at the big picture.
Among women in the United States aged 18-44 years, 5% had diabetes and 26% had prediabetes from 2005 to 2008. Why, then, is 16%-18% called outrageously high, when the rate of prediabetes/diabetes outside of pregnancy is almost twice as high?
Undoubtedly, an increase in the number of mild GDM cases will increase costs – just as the broader epidemic of diabetes and prediabetes is increasing health care costs. Cost and resource issues are insufficient reasons, however, not to identify high-risk pregnancies in which adverse outcomes can be prevented with relatively simple interventions.
Indeed, we must develop more efficient ways to care for patients with GDM, but this is within our reach. We know from the trials of identifying and treating mild GDM that diet treatment is largely effective; only 8% and 20% women in these studies required insulin. This is reassuring. Group patient education may be helpful, and we have evidence that less frequent glucose monitoring – every second or third day, rather than daily – may be feasible.
We also must improve our level of postdelivery care; a cost-effectiveness analysis of the IADPSG criteria demonstrated that the new one-step approach will not be cost-effective without it. This is not surprising. Moreover, it’s a logical imperative: In addition to preventing adverse outcomes in newborns, an important benefit of diagnosing GDM is the opportunity to prevent diabetes in the future.
Dr. Coustan is professor of obstetrics and gynecology at the Warren Alpert Medical School of Brown University in Providence, R.I.
COUNTERPOINT: Not yet.
Diagnosing GDM with a single-step approach – rather than a two-step approach – is a positive change. The problem lies not with the one-step 75-g OGTT, but largely with the new diagnostic threshold values for GDM proposed by the IADPSG as part of this new one-step approach.

The HAPO study – the international observational study on which the IADPSG based its recommendations – was a beautiful study. It provided valuable data on the relationship between OGTT values and adverse perinatal outcomes. Unfortunately, but not surprisingly, there was a continuous linear relationship among fasting, 1-hour, and 2-hour glucose values and the frequency of adverse outcomes.
With this linear relationship and no clear-cut off values for normal and abnormal test results, the threshold values are by definition arbitrary. The IADPSG chose to base its diagnostic thresholds on a 1.75-fold increase in the incidence of fetal macrosomia. Using these criteria, approximately 18% of pregnant women worldwide, and 17%-25% of pregnant women in the United States, would be diagnosed as having GDM.
At the current time, there is insufficient evidence that the benefits of such an enormous increase in GDM patients would outweigh the disadvantages.
Two randomized studies have shown that treatment of GDM improves outcomes – lowering the incidence of fetal macrosomia, mortality, birth trauma, and in one study, cesarean delivery – but we do not have strong evidence yet that diagnosing and treating minor glucose abnormalities in all women will significantly improve outcomes.
There also is a real risk of "overmedicalization." A recent article that details driving factors – technological changes detecting even smaller abnormalities, for instance, and conflicted panels writing expanded disease definitions (BMJ 2012;344:e3502) – is acutely applicable to GDM. With lower thresholds, we run the risk of overdiagnosis, which could result in increases in labor inductions and in elective and secondary cesarean deliveries – without proven benefit.
This is starting to happen in Belgium: Data that are as yet unpublished in the medical literature show that the number of labor inductions in women with GDM – women whose diagnoses were made using lower thresholds than previously employed – has been rising. The interventions are driven by concern about presumed large babies, but thus far, signs are lacking of adverse effects in the babies.
With respect to prevention of childhood obesity, we need to consider the fact that while GDM is related to obesity in the offspring, this appears to be mainly in the case of coexisting maternal obesity.
A study from Finland showed that overweight and abdominal obesity in adolescents was associated with maternal obesity, and even more so with the combination of obesity and GDM, but not with GDM itself (Diabetes Care 2010:33;1115-21). Similar U.S. data on childhood metabolic syndrome have been published (Pediatrics 2005:115;e290-6), and a recent meta-analysis has shown that the relationship between diabetes in pregnancy and childhood obesity disappeared after adjustment for maternal BMI (Diabetologia 2011;54:1957-66).
We know from HAPO data too that GDM and obesity are independent risk factors with synergistic effects on short-term outcomes such as preeclampsia, primary cesarean deliveries, macrosomia, increased cord C-peptide levels, and newborn body fat.
As my colleague Dr. Harold W. de Valk and I point out in a recent article, it might be best to use stricter diagnostic thresholds for obese women rather than for all women, given what we know thus far about these synergistic effects and the possibility of a larger effect of obesity on long-term development of offspring (Am. J. Obstet. Gynecol. 2013:208;260-4).
This principle is part and parcel of the so-called Ryan recommendations, which may provide a more sensible alternative to the IADPSG approach. Dr. Ryan proposes that we use a threshold based on a twofold increase in large for gestational age (for an overall incidence of GDM around 10% instead of 18%), that we consider evidence insufficient for the treatment of very mild increases of glucose, except for increases in obese women, and that we continue to collect data and study outcomes (Diabetologia 2011;54:480-6).
A randomized controlled trial stratified for maternal BMI, in which half of the women with OGTT results in between the two proposed diagnostic threshold values are treated, is mandatory.
Dr. de Valk and I have reviewed the published arguments for and against changing the diagnostic criteria for GDM now, and we have other concerns, including the timing and poor reproducibility of the OGTT, the reliance on large for gestational age as an endpoint for setting diagnostic criteria, and the increase in use of oral antidiabetic drugs that could result from a vast increase in GDM.
Overall, we agree with the National Institutes of Health panel that real evidence for change is lacking, and that there is a lot to be done before we significantly expand GDM.
Dr. Visser is professor of obstetrics and gynecology at University Medical Center in Utrecht, the Netherlands.
Based on presentations made at the annual meeting of the Diabetes in Pregnancy Study Group of North America, Washington. Both Dr. Coustan and Dr. Visser reported that they had no conflicts of interest to disclose.
POINT: Preventing adverse outcomes in newborns is imperative.
In March 2013, an independent panel at a National Institutes of Health consensus development conference recommended against adopting the one-step approach to diagnosis of gestational diabetes mellitus (GDM) that was recommended in 2008 by the International Association of Diabetes and Pregnancy Study Groups (IADPSG) and adopted by the American Diabetes Association, the World Health Organization, and organizations in other countries. The NIH panel voiced concerns about costs and interventions that would accompany an increased prevalence of GDM, as well as uncertainties about the benefits of identifying and treating so many additional new cases of GDM.
The panel’s recommendation is inconsistent with available data. There is more than sufficient evidence that the one-step approach should be used worldwide – without waiting for more research.
The study on which the IADPSG criteria were based – the Hyperglycemia and Adverse Pregnancy Outcomes (HAPO) Study (N. Engl. J. Med. 2008;358:1991-2002) – involved more than 23,000 pregnancies in nine different countries. All of the adverse pregnancy outcomes evaluated were related directly and significantly, and in a continuous fashion, to glucose concentrations at the fasting, 1-hour, and 2-hour points in a single 75-g, 2-hour oral glucose tolerance test (OGTT).
The IADPSG recommended that GDM be diagnosed when one or more of the plasma glucose values were met or exceeded: fasting, 92 mg/dL; 1-hour, 180 mg/dL; 2-hour, 153 mg/dL. According to the HAPO study data, patients with GDM have an approximate doubling of the likelihood of a birth weight above the 90th percentile compared to those without GDM, as well as a near-tripling of the likelihood of fetal hyperinsulinemia, twice the likelihood of preeclampsia, and a 50% increase in primary cesarean section, among other increased complication rates (Diabetes Care 2010;33:676-82).
The IADPSG diagnostic criteria are based on a predictive value of a 1.75 odds ratio above the mean for large for gestational age (LGA), neonatal body fat greater than 90th percentile, and cord blood hyperinsulinemia. This is equivalent to a doubling in the likelihood of these outcomes, because the 1.75 odds ratio is compared to the mean rather than to everyone without GDM.
HAPO was indeed an observational study, but we have solid data from other randomized trials demonstrating that intervention for mild GDM will prevent excess adverse outcomes.
In one of two recent randomized single-blinded trials on identifying and treating GDM, mild GDM was defined as a 2-hour, 75-g OGTT value between 140 and 198 mg/dL with a fasting plasma glucose value less than 140 mg/dL (mean, 86 mg/dL) – diagnostic criteria that, if anything, are lower than the IADPSG criteria. Patients randomized for intervention had a 66% reduction in "serious complications." Macrosomia was reduced by 50%, and preeclampsia by 30%. The cesarean rate was unchanged between the 1,000 women in the intervention and routine care groups (N. Engl. J. Med. 2005:352:2477-8).
In the second study of 958 women, identification and treatment lowered by half the rates of macrosomia, preeclampsia, and shoulder dystocia. There were other significant reductions in complications, and no difference in the rate of small-for-gestational-age infants (N. Engl. J. Med. 2009;361:1339-48). The criteria used to define mild GDM in this study meet the lower of two alternative sets of criteria recommended by the American College of Obstetricians and Gynecologists, but with a normal fasting plasma glucose concentration of 95 mg/dL or less.
Critics of the recommendations in the United States who say it is unreasonable and too expensive for such a large proportion of pregnant women to be identified as having a disease – 16%-18% in the HAPO population – need to look at the big picture.
Among women in the United States aged 18-44 years, 5% had diabetes and 26% had prediabetes from 2005 to 2008. Why, then, is 16%-18% called outrageously high, when the rate of prediabetes/diabetes outside of pregnancy is almost twice as high?
Undoubtedly, an increase in the number of mild GDM cases will increase costs – just as the broader epidemic of diabetes and prediabetes is increasing health care costs. Cost and resource issues are insufficient reasons, however, not to identify high-risk pregnancies in which adverse outcomes can be prevented with relatively simple interventions.
Indeed, we must develop more efficient ways to care for patients with GDM, but this is within our reach. We know from the trials of identifying and treating mild GDM that diet treatment is largely effective; only 8% and 20% women in these studies required insulin. This is reassuring. Group patient education may be helpful, and we have evidence that less frequent glucose monitoring – every second or third day, rather than daily – may be feasible.
We also must improve our level of postdelivery care; a cost-effectiveness analysis of the IADPSG criteria demonstrated that the new one-step approach will not be cost-effective without it. This is not surprising. Moreover, it’s a logical imperative: In addition to preventing adverse outcomes in newborns, an important benefit of diagnosing GDM is the opportunity to prevent diabetes in the future.
Dr. Coustan is professor of obstetrics and gynecology at the Warren Alpert Medical School of Brown University in Providence, R.I.
COUNTERPOINT: Not yet.
Diagnosing GDM with a single-step approach – rather than a two-step approach – is a positive change. The problem lies not with the one-step 75-g OGTT, but largely with the new diagnostic threshold values for GDM proposed by the IADPSG as part of this new one-step approach.
The HAPO study – the international observational study on which the IADPSG based its recommendations – was a beautiful study. It provided valuable data on the relationship between OGTT values and adverse perinatal outcomes. Unfortunately, but not surprisingly, there was a continuous linear relationship among fasting, 1-hour, and 2-hour glucose values and the frequency of adverse outcomes.
With this linear relationship and no clear-cut off values for normal and abnormal test results, the threshold values are by definition arbitrary. The IADPSG chose to base its diagnostic thresholds on a 1.75-fold increase in the incidence of fetal macrosomia. Using these criteria, approximately 18% of pregnant women worldwide, and 17%-25% of pregnant women in the United States, would be diagnosed as having GDM.
At the current time, there is insufficient evidence that the benefits of such an enormous increase in GDM patients would outweigh the disadvantages.
Two randomized studies have shown that treatment of GDM improves outcomes – lowering the incidence of fetal macrosomia, mortality, birth trauma, and in one study, cesarean delivery – but we do not have strong evidence yet that diagnosing and treating minor glucose abnormalities in all women will significantly improve outcomes.
There also is a real risk of "overmedicalization." A recent article that details driving factors – technological changes detecting even smaller abnormalities, for instance, and conflicted panels writing expanded disease definitions (BMJ 2012;344:e3502) – is acutely applicable to GDM. With lower thresholds, we run the risk of overdiagnosis, which could result in increases in labor inductions and in elective and secondary cesarean deliveries – without proven benefit.
This is starting to happen in Belgium: Data that are as yet unpublished in the medical literature show that the number of labor inductions in women with GDM – women whose diagnoses were made using lower thresholds than previously employed – has been rising. The interventions are driven by concern about presumed large babies, but thus far, signs are lacking of adverse effects in the babies.
With respect to prevention of childhood obesity, we need to consider the fact that while GDM is related to obesity in the offspring, this appears to be mainly in the case of coexisting maternal obesity.
A study from Finland showed that overweight and abdominal obesity in adolescents was associated with maternal obesity, and even more so with the combination of obesity and GDM, but not with GDM itself (Diabetes Care 2010:33;1115-21). Similar U.S. data on childhood metabolic syndrome have been published (Pediatrics 2005:115;e290-6), and a recent meta-analysis has shown that the relationship between diabetes in pregnancy and childhood obesity disappeared after adjustment for maternal BMI (Diabetologia 2011;54:1957-66).
We know from HAPO data too that GDM and obesity are independent risk factors with synergistic effects on short-term outcomes such as preeclampsia, primary cesarean deliveries, macrosomia, increased cord C-peptide levels, and newborn body fat.
As my colleague Dr. Harold W. de Valk and I point out in a recent article, it might be best to use stricter diagnostic thresholds for obese women rather than for all women, given what we know thus far about these synergistic effects and the possibility of a larger effect of obesity on long-term development of offspring (Am. J. Obstet. Gynecol. 2013:208;260-4).
This principle is part and parcel of the so-called Ryan recommendations, which may provide a more sensible alternative to the IADPSG approach. Dr. Ryan proposes that we use a threshold based on a twofold increase in large for gestational age (for an overall incidence of GDM around 10% instead of 18%), that we consider evidence insufficient for the treatment of very mild increases of glucose, except for increases in obese women, and that we continue to collect data and study outcomes (Diabetologia 2011;54:480-6).
A randomized controlled trial stratified for maternal BMI, in which half of the women with OGTT results in between the two proposed diagnostic threshold values are treated, is mandatory.
Dr. de Valk and I have reviewed the published arguments for and against changing the diagnostic criteria for GDM now, and we have other concerns, including the timing and poor reproducibility of the OGTT, the reliance on large for gestational age as an endpoint for setting diagnostic criteria, and the increase in use of oral antidiabetic drugs that could result from a vast increase in GDM.
Overall, we agree with the National Institutes of Health panel that real evidence for change is lacking, and that there is a lot to be done before we significantly expand GDM.
Dr. Visser is professor of obstetrics and gynecology at University Medical Center in Utrecht, the Netherlands.
Based on presentations made at the annual meeting of the Diabetes in Pregnancy Study Group of North America, Washington. Both Dr. Coustan and Dr. Visser reported that they had no conflicts of interest to disclose.
POINT: Preventing adverse outcomes in newborns is imperative.
In March 2013, an independent panel at a National Institutes of Health consensus development conference recommended against adopting the one-step approach to diagnosis of gestational diabetes mellitus (GDM) that was recommended in 2008 by the International Association of Diabetes and Pregnancy Study Groups (IADPSG) and adopted by the American Diabetes Association, the World Health Organization, and organizations in other countries. The NIH panel voiced concerns about costs and interventions that would accompany an increased prevalence of GDM, as well as uncertainties about the benefits of identifying and treating so many additional new cases of GDM.
The panel’s recommendation is inconsistent with available data. There is more than sufficient evidence that the one-step approach should be used worldwide – without waiting for more research.
The study on which the IADPSG criteria were based – the Hyperglycemia and Adverse Pregnancy Outcomes (HAPO) Study (N. Engl. J. Med. 2008;358:1991-2002) – involved more than 23,000 pregnancies in nine different countries. All of the adverse pregnancy outcomes evaluated were related directly and significantly, and in a continuous fashion, to glucose concentrations at the fasting, 1-hour, and 2-hour points in a single 75-g, 2-hour oral glucose tolerance test (OGTT).
The IADPSG recommended that GDM be diagnosed when one or more of the plasma glucose values were met or exceeded: fasting, 92 mg/dL; 1-hour, 180 mg/dL; 2-hour, 153 mg/dL. According to the HAPO study data, patients with GDM have an approximate doubling of the likelihood of a birth weight above the 90th percentile compared to those without GDM, as well as a near-tripling of the likelihood of fetal hyperinsulinemia, twice the likelihood of preeclampsia, and a 50% increase in primary cesarean section, among other increased complication rates (Diabetes Care 2010;33:676-82).
The IADPSG diagnostic criteria are based on a predictive value of a 1.75 odds ratio above the mean for large for gestational age (LGA), neonatal body fat greater than 90th percentile, and cord blood hyperinsulinemia. This is equivalent to a doubling in the likelihood of these outcomes, because the 1.75 odds ratio is compared to the mean rather than to everyone without GDM.
HAPO was indeed an observational study, but we have solid data from other randomized trials demonstrating that intervention for mild GDM will prevent excess adverse outcomes.
In one of two recent randomized single-blinded trials on identifying and treating GDM, mild GDM was defined as a 2-hour, 75-g OGTT value between 140 and 198 mg/dL with a fasting plasma glucose value less than 140 mg/dL (mean, 86 mg/dL) – diagnostic criteria that, if anything, are lower than the IADPSG criteria. Patients randomized for intervention had a 66% reduction in "serious complications." Macrosomia was reduced by 50%, and preeclampsia by 30%. The cesarean rate was unchanged between the 1,000 women in the intervention and routine care groups (N. Engl. J. Med. 2005:352:2477-8).
In the second study of 958 women, identification and treatment lowered by half the rates of macrosomia, preeclampsia, and shoulder dystocia. There were other significant reductions in complications, and no difference in the rate of small-for-gestational-age infants (N. Engl. J. Med. 2009;361:1339-48). The criteria used to define mild GDM in this study meet the lower of two alternative sets of criteria recommended by the American College of Obstetricians and Gynecologists, but with a normal fasting plasma glucose concentration of 95 mg/dL or less.
Critics of the recommendations in the United States who say it is unreasonable and too expensive for such a large proportion of pregnant women to be identified as having a disease – 16%-18% in the HAPO population – need to look at the big picture.
Among women in the United States aged 18-44 years, 5% had diabetes and 26% had prediabetes from 2005 to 2008. Why, then, is 16%-18% called outrageously high, when the rate of prediabetes/diabetes outside of pregnancy is almost twice as high?
Undoubtedly, an increase in the number of mild GDM cases will increase costs – just as the broader epidemic of diabetes and prediabetes is increasing health care costs. Cost and resource issues are insufficient reasons, however, not to identify high-risk pregnancies in which adverse outcomes can be prevented with relatively simple interventions.
Indeed, we must develop more efficient ways to care for patients with GDM, but this is within our reach. We know from the trials of identifying and treating mild GDM that diet treatment is largely effective; only 8% and 20% women in these studies required insulin. This is reassuring. Group patient education may be helpful, and we have evidence that less frequent glucose monitoring – every second or third day, rather than daily – may be feasible.
We also must improve our level of postdelivery care; a cost-effectiveness analysis of the IADPSG criteria demonstrated that the new one-step approach will not be cost-effective without it. This is not surprising. Moreover, it’s a logical imperative: In addition to preventing adverse outcomes in newborns, an important benefit of diagnosing GDM is the opportunity to prevent diabetes in the future.
Dr. Coustan is professor of obstetrics and gynecology at the Warren Alpert Medical School of Brown University in Providence, R.I.
COUNTERPOINT: Not yet.
Diagnosing GDM with a single-step approach – rather than a two-step approach – is a positive change. The problem lies not with the one-step 75-g OGTT, but largely with the new diagnostic threshold values for GDM proposed by the IADPSG as part of this new one-step approach.
The HAPO study – the international observational study on which the IADPSG based its recommendations – was a beautiful study. It provided valuable data on the relationship between OGTT values and adverse perinatal outcomes. Unfortunately, but not surprisingly, there was a continuous linear relationship among fasting, 1-hour, and 2-hour glucose values and the frequency of adverse outcomes.
With this linear relationship and no clear-cut off values for normal and abnormal test results, the threshold values are by definition arbitrary. The IADPSG chose to base its diagnostic thresholds on a 1.75-fold increase in the incidence of fetal macrosomia. Using these criteria, approximately 18% of pregnant women worldwide, and 17%-25% of pregnant women in the United States, would be diagnosed as having GDM.
At the current time, there is insufficient evidence that the benefits of such an enormous increase in GDM patients would outweigh the disadvantages.
Two randomized studies have shown that treatment of GDM improves outcomes – lowering the incidence of fetal macrosomia, mortality, birth trauma, and in one study, cesarean delivery – but we do not have strong evidence yet that diagnosing and treating minor glucose abnormalities in all women will significantly improve outcomes.
There also is a real risk of "overmedicalization." A recent article that details driving factors – technological changes detecting even smaller abnormalities, for instance, and conflicted panels writing expanded disease definitions (BMJ 2012;344:e3502) – is acutely applicable to GDM. With lower thresholds, we run the risk of overdiagnosis, which could result in increases in labor inductions and in elective and secondary cesarean deliveries – without proven benefit.
This is starting to happen in Belgium: Data that are as yet unpublished in the medical literature show that the number of labor inductions in women with GDM – women whose diagnoses were made using lower thresholds than previously employed – has been rising. The interventions are driven by concern about presumed large babies, but thus far, signs are lacking of adverse effects in the babies.
With respect to prevention of childhood obesity, we need to consider the fact that while GDM is related to obesity in the offspring, this appears to be mainly in the case of coexisting maternal obesity.
A study from Finland showed that overweight and abdominal obesity in adolescents was associated with maternal obesity, and even more so with the combination of obesity and GDM, but not with GDM itself (Diabetes Care 2010:33;1115-21). Similar U.S. data on childhood metabolic syndrome have been published (Pediatrics 2005:115;e290-6), and a recent meta-analysis has shown that the relationship between diabetes in pregnancy and childhood obesity disappeared after adjustment for maternal BMI (Diabetologia 2011;54:1957-66).
We know from HAPO data too that GDM and obesity are independent risk factors with synergistic effects on short-term outcomes such as preeclampsia, primary cesarean deliveries, macrosomia, increased cord C-peptide levels, and newborn body fat.
As my colleague Dr. Harold W. de Valk and I point out in a recent article, it might be best to use stricter diagnostic thresholds for obese women rather than for all women, given what we know thus far about these synergistic effects and the possibility of a larger effect of obesity on long-term development of offspring (Am. J. Obstet. Gynecol. 2013:208;260-4).
This principle is part and parcel of the so-called Ryan recommendations, which may provide a more sensible alternative to the IADPSG approach. Dr. Ryan proposes that we use a threshold based on a twofold increase in large for gestational age (for an overall incidence of GDM around 10% instead of 18%), that we consider evidence insufficient for the treatment of very mild increases of glucose, except for increases in obese women, and that we continue to collect data and study outcomes (Diabetologia 2011;54:480-6).
A randomized controlled trial stratified for maternal BMI, in which half of the women with OGTT results in between the two proposed diagnostic threshold values are treated, is mandatory.
Dr. de Valk and I have reviewed the published arguments for and against changing the diagnostic criteria for GDM now, and we have other concerns, including the timing and poor reproducibility of the OGTT, the reliance on large for gestational age as an endpoint for setting diagnostic criteria, and the increase in use of oral antidiabetic drugs that could result from a vast increase in GDM.
Overall, we agree with the National Institutes of Health panel that real evidence for change is lacking, and that there is a lot to be done before we significantly expand GDM.
Dr. Visser is professor of obstetrics and gynecology at University Medical Center in Utrecht, the Netherlands.
Based on presentations made at the annual meeting of the Diabetes in Pregnancy Study Group of North America, Washington. Both Dr. Coustan and Dr. Visser reported that they had no conflicts of interest to disclose.

Is the risk of placenta accreta in a subsequent pregnancy higher after emergent primary cesarean or after elective primary cesarean?
Invasive disorders of the placenta (placenta accreta, increta, and percreta) are increasingly common. These conditions are associated with a high risk of massive obstetric hemorrhage, are the leading cause of peripartum hysterectomy, and are an important cause of pregnancy-related death in the United States and Western world.1 It is clear that strategies must be developed to reduce the incidence of these disorders, and that most of these strategies must focus on prevention.
Earlier studies have consistently found that cesarean delivery is the most important risk factor for placenta accreta in a subsequent pregnancy, with the risk rising with the number of prior cesarean deliveries.1 In recent years, the cesarean delivery rate has skyrocketed in most Western nations and is the major contributor to the increased incidence of placenta accreta.2 A major effort is in place to prevent the first cesarean delivery.2
In this study, Kamara and colleagues focused on the timing of cesarean delivery to determine the impact on the likelihood of placenta accreta in subsequent pregnancies.
Details of the study
Kamara and colleagues found that elective cesarean delivery carries a threefold increased risk of placenta accreta in a subsequent pregnancy, compared with cesarean delivery during labor. To my knowledge, until now, no one has attempted to determine whether the timing of cesarean delivery affects the risk of subsequent placenta accreta.
The investigators hypothesize that the increased risk arises when a thick, nonlaboring myometrium is incised, as opposed to the thinned-out myometrium that occurs in labor. This theory is in keeping with the theory that placenta accreta develops when a gestation implants into a cesarean scar.
Limitations of the study
The cases analyzed in this investigation came from a 15-year period, a time when practice patterns changed considerably.
The timing of cesareans performed during labor was not examined.
Primary cesarean was defined as the woman’s first cesarean delivery, regardless of whether she had vaginal deliveries before or after the cesarean.
Retrospective case-control study methodology cannot address causality and may not be ideally suited to provide definitive findings. However, the findings are novel and deserve further investigation.
Related Article: Evolving applications of first-trimester ultrasound Ilan E. Timor-Tritsch, MD, and Simi K. Gupta, MD (December 2012)
What this evidence means for practice
The rate of cesarean delivery continues to rise. It is increasingly performed on an elective basis for such reasons as maternal request, suspected macrosomia, and breech presentation (often without giving the patient the option of version). Although additional investigations are necessary to validate the findings of this study, patients should be counseled that elective primary cesarean is not without risk, and that placenta accreta in a subsequent pregnancy is a potential consequence.
This study provides one more reason to attempt to find methods to reduce the cesarean delivery rate, particularly the rate of elective cesarean.
--Yinka Oyelese, MD
- Oyelese Y, Smulian J. Placenta previa, placenta accreta, and vasa previa. Obstet Gynecol. 2006;107(4):927–941.
- Spong CY, Berghella V, Wenstrom KD, Mercer BM, Saade GR. Preventing the first cesarean delivery: Summary of a joint Eunice Kennedy Shriver National Institute of Child Health and Human Development, Society for Maternal-Fetal Medicine, and American College of Obstetricians and Gynecologists Workshop. Obstet Gynecol. 2012;120(5):1181–1193.
Invasive disorders of the placenta (placenta accreta, increta, and percreta) are increasingly common. These conditions are associated with a high risk of massive obstetric hemorrhage, are the leading cause of peripartum hysterectomy, and are an important cause of pregnancy-related death in the United States and Western world.1 It is clear that strategies must be developed to reduce the incidence of these disorders, and that most of these strategies must focus on prevention.
Earlier studies have consistently found that cesarean delivery is the most important risk factor for placenta accreta in a subsequent pregnancy, with the risk rising with the number of prior cesarean deliveries.1 In recent years, the cesarean delivery rate has skyrocketed in most Western nations and is the major contributor to the increased incidence of placenta accreta.2 A major effort is in place to prevent the first cesarean delivery.2
In this study, Kamara and colleagues focused on the timing of cesarean delivery to determine the impact on the likelihood of placenta accreta in subsequent pregnancies.
Details of the study
Kamara and colleagues found that elective cesarean delivery carries a threefold increased risk of placenta accreta in a subsequent pregnancy, compared with cesarean delivery during labor. To my knowledge, until now, no one has attempted to determine whether the timing of cesarean delivery affects the risk of subsequent placenta accreta.
The investigators hypothesize that the increased risk arises when a thick, nonlaboring myometrium is incised, as opposed to the thinned-out myometrium that occurs in labor. This theory is in keeping with the theory that placenta accreta develops when a gestation implants into a cesarean scar.
Limitations of the study
The cases analyzed in this investigation came from a 15-year period, a time when practice patterns changed considerably.
The timing of cesareans performed during labor was not examined.
Primary cesarean was defined as the woman’s first cesarean delivery, regardless of whether she had vaginal deliveries before or after the cesarean.
Retrospective case-control study methodology cannot address causality and may not be ideally suited to provide definitive findings. However, the findings are novel and deserve further investigation.
Related Article: Evolving applications of first-trimester ultrasound Ilan E. Timor-Tritsch, MD, and Simi K. Gupta, MD (December 2012)
What this evidence means for practice
The rate of cesarean delivery continues to rise. It is increasingly performed on an elective basis for such reasons as maternal request, suspected macrosomia, and breech presentation (often without giving the patient the option of version). Although additional investigations are necessary to validate the findings of this study, patients should be counseled that elective primary cesarean is not without risk, and that placenta accreta in a subsequent pregnancy is a potential consequence.
This study provides one more reason to attempt to find methods to reduce the cesarean delivery rate, particularly the rate of elective cesarean.
--Yinka Oyelese, MD
Invasive disorders of the placenta (placenta accreta, increta, and percreta) are increasingly common. These conditions are associated with a high risk of massive obstetric hemorrhage, are the leading cause of peripartum hysterectomy, and are an important cause of pregnancy-related death in the United States and Western world.1 It is clear that strategies must be developed to reduce the incidence of these disorders, and that most of these strategies must focus on prevention.
Earlier studies have consistently found that cesarean delivery is the most important risk factor for placenta accreta in a subsequent pregnancy, with the risk rising with the number of prior cesarean deliveries.1 In recent years, the cesarean delivery rate has skyrocketed in most Western nations and is the major contributor to the increased incidence of placenta accreta.2 A major effort is in place to prevent the first cesarean delivery.2
In this study, Kamara and colleagues focused on the timing of cesarean delivery to determine the impact on the likelihood of placenta accreta in subsequent pregnancies.
Details of the study
Kamara and colleagues found that elective cesarean delivery carries a threefold increased risk of placenta accreta in a subsequent pregnancy, compared with cesarean delivery during labor. To my knowledge, until now, no one has attempted to determine whether the timing of cesarean delivery affects the risk of subsequent placenta accreta.
The investigators hypothesize that the increased risk arises when a thick, nonlaboring myometrium is incised, as opposed to the thinned-out myometrium that occurs in labor. This theory is in keeping with the theory that placenta accreta develops when a gestation implants into a cesarean scar.
Limitations of the study
The cases analyzed in this investigation came from a 15-year period, a time when practice patterns changed considerably.
The timing of cesareans performed during labor was not examined.
Primary cesarean was defined as the woman’s first cesarean delivery, regardless of whether she had vaginal deliveries before or after the cesarean.
Retrospective case-control study methodology cannot address causality and may not be ideally suited to provide definitive findings. However, the findings are novel and deserve further investigation.
Related Article: Evolving applications of first-trimester ultrasound Ilan E. Timor-Tritsch, MD, and Simi K. Gupta, MD (December 2012)
What this evidence means for practice
The rate of cesarean delivery continues to rise. It is increasingly performed on an elective basis for such reasons as maternal request, suspected macrosomia, and breech presentation (often without giving the patient the option of version). Although additional investigations are necessary to validate the findings of this study, patients should be counseled that elective primary cesarean is not without risk, and that placenta accreta in a subsequent pregnancy is a potential consequence.
This study provides one more reason to attempt to find methods to reduce the cesarean delivery rate, particularly the rate of elective cesarean.
--Yinka Oyelese, MD
- Oyelese Y, Smulian J. Placenta previa, placenta accreta, and vasa previa. Obstet Gynecol. 2006;107(4):927–941.
- Spong CY, Berghella V, Wenstrom KD, Mercer BM, Saade GR. Preventing the first cesarean delivery: Summary of a joint Eunice Kennedy Shriver National Institute of Child Health and Human Development, Society for Maternal-Fetal Medicine, and American College of Obstetricians and Gynecologists Workshop. Obstet Gynecol. 2012;120(5):1181–1193.
- Oyelese Y, Smulian J. Placenta previa, placenta accreta, and vasa previa. Obstet Gynecol. 2006;107(4):927–941.
- Spong CY, Berghella V, Wenstrom KD, Mercer BM, Saade GR. Preventing the first cesarean delivery: Summary of a joint Eunice Kennedy Shriver National Institute of Child Health and Human Development, Society for Maternal-Fetal Medicine, and American College of Obstetricians and Gynecologists Workshop. Obstet Gynecol. 2012;120(5):1181–1193.
21st Century norms for assessing the progress of labor
For decades, clinicians used the normative findings reported by Friedman in 1954 to help manage labor.1 Recent observational research on labor progress, however, has identified a new set of norms for the 21st Century on assessing the progress of labor. These contemporary observations significantly influence how we manage labor. In this editorial, I outline the new standards, compared with the old, so you can effectively apply best obstetric practice.
PRACTICE CHANGER #1
Your patient may not be in the active phase of labor until she reaches a cervical dilation
of 6 cm
Friedman’s research identified two phases of the first stage of labor, the latent phase, where cervical dilation is slow, and the active phase, where cervical dilation is much faster. For clinicians managing labor, it is important to know the cervical dilation when most women are in the active phase of labor so that protraction and arrest disorders can be optimally diagnosed and treated.
Old norm: 4 cm; New norm: 6 cm
The standard Friedman partogram shows 4 cm as the cervical dilation where there is commonly a transition from the latent to the active phase. In a recent analysis of more than 62,000 labors, however, Zhang and colleagues reported the norms of 21st Century labor patterns.2 They found that most nulliparous women do not begin to dilate at a rate greater than 1 cm/hr (considered the active phase) until they reach a cervical dilation of 5 to 6 cm. The study data also show that there is no abrupt change in the rate of cervical dilation from the latent to the active phase. Rather, the increasing rate of cervical change is very gradual (FIGURE).
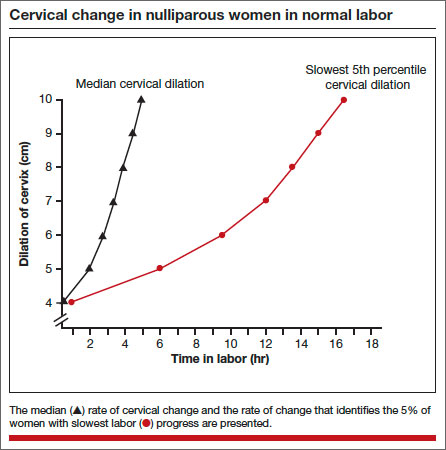
In 1998, Peisner and Rosen3 reported on the cervical dilation at which women entered the active phase, defined as a cervical change of more than 1.2 cm/hr in nulliparous women and more than 1.5 cm/hr in multiparous women. In this study, the percentages of women who entered the active phase at various degrees of cervical dilation were:
- ≤3 cm, 25%
- 4 cm, 25%
- 5 cm, 24%
- 6 cm, 15%
- ≥6 cm, 11%.
Based on these considerations, in contemporary practice it is best to use 6 cm of cervical dilation, not 4 cm, as the milestone in labor where a more rapid change in cervical dilation can be expected.
Related Article: Update on Obstetrics Jaimey M. Pauli, MD, and John T. Repke, MD (January 2013)
PRACTICE CHANGER #2
During the active phase of normal labor, the cervix may dilate as slowly as 0.5 cm/hr
It is important for obstetricians to know when labor is progressing too slowly, so that they can optimally manage protraction and arrest disorders of the first stage, thereby improving maternal and newborn outcomes. But, what is the slowest rate of cervical change we should expect in the active phase of the first stage of normal labor?
Old norm: as slow as 1.2 cm/hr; New norm: as slow as 0.5 cm/hr
Arbitrarily, an abnormally slow rate of cervical change during the active phase of labor can be defined as the rate of cervical change observed in the 5% of women with the slowest first stage of labor associated with a normal vaginal birth. Zhang and colleagues2 reported that the 5% of women with the slowest change during active labor had a rate of cervical dilation of:
- 0.45 to 0.70 cm/hr (nulliparous women) or
- 0.50 to 1.10 cm/hr (multiparous women).
Based on data from the mid-20th Century, Friedman reported that active labor was associated with a rate of cervical change of:
- >1.2 cm/hr in nulliparous and
- >1.5 cm/hr in multiparous women.
The data reported by Zhang and colleagues indicate that in the 21st Century, normal labor is associated with a much slower rate of cervical change, as slow as 0.5 cm/hr.
PRACTICE CHANGER #3
The normal second stage may last up to 3.6 hr in nulliparous women given an epidural anesthetic
Friedman1 reported that the second stage of normal labor was 3 hours or less in nulliparous women and 1 hour or less in multiparous women. Zhang and colleagues2 observed that in nulliparous women the second stage of normal labor was 3.6 hr or less with an epidural and 2.8 hr or less without an epidural anesthetic.
In multiparous women, the second stage of normal labor is less than 2.0 hr with an epidural and less than 1.3 hr without an epidural. These data suggest that we should reset our expectations of the length of a normal second stage in nulliparous women given an epidural from less than 3 hr to less than 3.6 hr.
Related Article: Develop and use a checklist for 3rd- and 4th-degree perineal lacerations
Robert L. Barbieri, MD (Editorial, August 2013)
ADJUST YOUR PRACTICE
Management of labor is a clinical art, requiring the integration of many diverse pieces of information, including the medical conditions affecting the parturient, the strength and frequency of uterine contractions, the physical characteristics of the birth canal, the size and position of the fetus, status of the membranes, and assessment of the fetal physiologic state. The bottom line of the Zhang report2 is that 21st Century labor has a pace that is slower than the pace reported by Friedman1 based on data from the mid-20th Century. Adjust your practice to integrate these new labor progress norms into your decision making.
INSTANT POLL
Do you favor the use of amniotomy and early oxytocin administration in the management of normal labor?
Tell us—at [email protected]
Please include your name and city and state.
- Friedman EA. The graphic analysis of labor. Am J Obstet Gynecol. 1954;68(6):1568–1575.
- Zhang J, Landy HJ, Branch DW, et al; Consortium on Safe Labor. Contemporary patterns of spontaneous labor with normal neonatal outcomes. Obstet Gynecol. 2010;116(6):1281–1287.
- Peisner DB, Rosen MG. Transition from latent to active labor. Obstet Gynecol. 1986;68(4):448–451.

Robert L. Barbieri, MD
Editor in Chief
Dr. Barbieri reports no financial relationships relevant to this article.
Robert L. Barbieri, MD
Editor in Chief
Dr. Barbieri reports no financial relationships relevant to this article.
Robert L. Barbieri, MD
Editor in Chief
Dr. Barbieri reports no financial relationships relevant to this article.
For decades, clinicians used the normative findings reported by Friedman in 1954 to help manage labor.1 Recent observational research on labor progress, however, has identified a new set of norms for the 21st Century on assessing the progress of labor. These contemporary observations significantly influence how we manage labor. In this editorial, I outline the new standards, compared with the old, so you can effectively apply best obstetric practice.
PRACTICE CHANGER #1
Your patient may not be in the active phase of labor until she reaches a cervical dilation
of 6 cm
Friedman’s research identified two phases of the first stage of labor, the latent phase, where cervical dilation is slow, and the active phase, where cervical dilation is much faster. For clinicians managing labor, it is important to know the cervical dilation when most women are in the active phase of labor so that protraction and arrest disorders can be optimally diagnosed and treated.
Old norm: 4 cm; New norm: 6 cm
The standard Friedman partogram shows 4 cm as the cervical dilation where there is commonly a transition from the latent to the active phase. In a recent analysis of more than 62,000 labors, however, Zhang and colleagues reported the norms of 21st Century labor patterns.2 They found that most nulliparous women do not begin to dilate at a rate greater than 1 cm/hr (considered the active phase) until they reach a cervical dilation of 5 to 6 cm. The study data also show that there is no abrupt change in the rate of cervical dilation from the latent to the active phase. Rather, the increasing rate of cervical change is very gradual (FIGURE).
In 1998, Peisner and Rosen3 reported on the cervical dilation at which women entered the active phase, defined as a cervical change of more than 1.2 cm/hr in nulliparous women and more than 1.5 cm/hr in multiparous women. In this study, the percentages of women who entered the active phase at various degrees of cervical dilation were:
- ≤3 cm, 25%
- 4 cm, 25%
- 5 cm, 24%
- 6 cm, 15%
- ≥6 cm, 11%.
Based on these considerations, in contemporary practice it is best to use 6 cm of cervical dilation, not 4 cm, as the milestone in labor where a more rapid change in cervical dilation can be expected.
Related Article: Update on Obstetrics Jaimey M. Pauli, MD, and John T. Repke, MD (January 2013)
PRACTICE CHANGER #2
During the active phase of normal labor, the cervix may dilate as slowly as 0.5 cm/hr
It is important for obstetricians to know when labor is progressing too slowly, so that they can optimally manage protraction and arrest disorders of the first stage, thereby improving maternal and newborn outcomes. But, what is the slowest rate of cervical change we should expect in the active phase of the first stage of normal labor?
Old norm: as slow as 1.2 cm/hr; New norm: as slow as 0.5 cm/hr
Arbitrarily, an abnormally slow rate of cervical change during the active phase of labor can be defined as the rate of cervical change observed in the 5% of women with the slowest first stage of labor associated with a normal vaginal birth. Zhang and colleagues2 reported that the 5% of women with the slowest change during active labor had a rate of cervical dilation of:
- 0.45 to 0.70 cm/hr (nulliparous women) or
- 0.50 to 1.10 cm/hr (multiparous women).
Based on data from the mid-20th Century, Friedman reported that active labor was associated with a rate of cervical change of:
- >1.2 cm/hr in nulliparous and
- >1.5 cm/hr in multiparous women.
The data reported by Zhang and colleagues indicate that in the 21st Century, normal labor is associated with a much slower rate of cervical change, as slow as 0.5 cm/hr.
PRACTICE CHANGER #3
The normal second stage may last up to 3.6 hr in nulliparous women given an epidural anesthetic
Friedman1 reported that the second stage of normal labor was 3 hours or less in nulliparous women and 1 hour or less in multiparous women. Zhang and colleagues2 observed that in nulliparous women the second stage of normal labor was 3.6 hr or less with an epidural and 2.8 hr or less without an epidural anesthetic.
In multiparous women, the second stage of normal labor is less than 2.0 hr with an epidural and less than 1.3 hr without an epidural. These data suggest that we should reset our expectations of the length of a normal second stage in nulliparous women given an epidural from less than 3 hr to less than 3.6 hr.
Related Article: Develop and use a checklist for 3rd- and 4th-degree perineal lacerations
Robert L. Barbieri, MD (Editorial, August 2013)
ADJUST YOUR PRACTICE
Management of labor is a clinical art, requiring the integration of many diverse pieces of information, including the medical conditions affecting the parturient, the strength and frequency of uterine contractions, the physical characteristics of the birth canal, the size and position of the fetus, status of the membranes, and assessment of the fetal physiologic state. The bottom line of the Zhang report2 is that 21st Century labor has a pace that is slower than the pace reported by Friedman1 based on data from the mid-20th Century. Adjust your practice to integrate these new labor progress norms into your decision making.
INSTANT POLL
Do you favor the use of amniotomy and early oxytocin administration in the management of normal labor?
Tell us—at [email protected]
Please include your name and city and state.
For decades, clinicians used the normative findings reported by Friedman in 1954 to help manage labor.1 Recent observational research on labor progress, however, has identified a new set of norms for the 21st Century on assessing the progress of labor. These contemporary observations significantly influence how we manage labor. In this editorial, I outline the new standards, compared with the old, so you can effectively apply best obstetric practice.
PRACTICE CHANGER #1
Your patient may not be in the active phase of labor until she reaches a cervical dilation
of 6 cm
Friedman’s research identified two phases of the first stage of labor, the latent phase, where cervical dilation is slow, and the active phase, where cervical dilation is much faster. For clinicians managing labor, it is important to know the cervical dilation when most women are in the active phase of labor so that protraction and arrest disorders can be optimally diagnosed and treated.
Old norm: 4 cm; New norm: 6 cm
The standard Friedman partogram shows 4 cm as the cervical dilation where there is commonly a transition from the latent to the active phase. In a recent analysis of more than 62,000 labors, however, Zhang and colleagues reported the norms of 21st Century labor patterns.2 They found that most nulliparous women do not begin to dilate at a rate greater than 1 cm/hr (considered the active phase) until they reach a cervical dilation of 5 to 6 cm. The study data also show that there is no abrupt change in the rate of cervical dilation from the latent to the active phase. Rather, the increasing rate of cervical change is very gradual (FIGURE).
In 1998, Peisner and Rosen3 reported on the cervical dilation at which women entered the active phase, defined as a cervical change of more than 1.2 cm/hr in nulliparous women and more than 1.5 cm/hr in multiparous women. In this study, the percentages of women who entered the active phase at various degrees of cervical dilation were:
- ≤3 cm, 25%
- 4 cm, 25%
- 5 cm, 24%
- 6 cm, 15%
- ≥6 cm, 11%.
Based on these considerations, in contemporary practice it is best to use 6 cm of cervical dilation, not 4 cm, as the milestone in labor where a more rapid change in cervical dilation can be expected.
Related Article: Update on Obstetrics Jaimey M. Pauli, MD, and John T. Repke, MD (January 2013)
PRACTICE CHANGER #2
During the active phase of normal labor, the cervix may dilate as slowly as 0.5 cm/hr
It is important for obstetricians to know when labor is progressing too slowly, so that they can optimally manage protraction and arrest disorders of the first stage, thereby improving maternal and newborn outcomes. But, what is the slowest rate of cervical change we should expect in the active phase of the first stage of normal labor?
Old norm: as slow as 1.2 cm/hr; New norm: as slow as 0.5 cm/hr
Arbitrarily, an abnormally slow rate of cervical change during the active phase of labor can be defined as the rate of cervical change observed in the 5% of women with the slowest first stage of labor associated with a normal vaginal birth. Zhang and colleagues2 reported that the 5% of women with the slowest change during active labor had a rate of cervical dilation of:
- 0.45 to 0.70 cm/hr (nulliparous women) or
- 0.50 to 1.10 cm/hr (multiparous women).
Based on data from the mid-20th Century, Friedman reported that active labor was associated with a rate of cervical change of:
- >1.2 cm/hr in nulliparous and
- >1.5 cm/hr in multiparous women.
The data reported by Zhang and colleagues indicate that in the 21st Century, normal labor is associated with a much slower rate of cervical change, as slow as 0.5 cm/hr.
PRACTICE CHANGER #3
The normal second stage may last up to 3.6 hr in nulliparous women given an epidural anesthetic
Friedman1 reported that the second stage of normal labor was 3 hours or less in nulliparous women and 1 hour or less in multiparous women. Zhang and colleagues2 observed that in nulliparous women the second stage of normal labor was 3.6 hr or less with an epidural and 2.8 hr or less without an epidural anesthetic.
In multiparous women, the second stage of normal labor is less than 2.0 hr with an epidural and less than 1.3 hr without an epidural. These data suggest that we should reset our expectations of the length of a normal second stage in nulliparous women given an epidural from less than 3 hr to less than 3.6 hr.
Related Article: Develop and use a checklist for 3rd- and 4th-degree perineal lacerations
Robert L. Barbieri, MD (Editorial, August 2013)
ADJUST YOUR PRACTICE
Management of labor is a clinical art, requiring the integration of many diverse pieces of information, including the medical conditions affecting the parturient, the strength and frequency of uterine contractions, the physical characteristics of the birth canal, the size and position of the fetus, status of the membranes, and assessment of the fetal physiologic state. The bottom line of the Zhang report2 is that 21st Century labor has a pace that is slower than the pace reported by Friedman1 based on data from the mid-20th Century. Adjust your practice to integrate these new labor progress norms into your decision making.
INSTANT POLL
Do you favor the use of amniotomy and early oxytocin administration in the management of normal labor?
Tell us—at [email protected]
Please include your name and city and state.
- Friedman EA. The graphic analysis of labor. Am J Obstet Gynecol. 1954;68(6):1568–1575.
- Zhang J, Landy HJ, Branch DW, et al; Consortium on Safe Labor. Contemporary patterns of spontaneous labor with normal neonatal outcomes. Obstet Gynecol. 2010;116(6):1281–1287.
- Peisner DB, Rosen MG. Transition from latent to active labor. Obstet Gynecol. 1986;68(4):448–451.
- Friedman EA. The graphic analysis of labor. Am J Obstet Gynecol. 1954;68(6):1568–1575.
- Zhang J, Landy HJ, Branch DW, et al; Consortium on Safe Labor. Contemporary patterns of spontaneous labor with normal neonatal outcomes. Obstet Gynecol. 2010;116(6):1281–1287.
- Peisner DB, Rosen MG. Transition from latent to active labor. Obstet Gynecol. 1986;68(4):448–451.
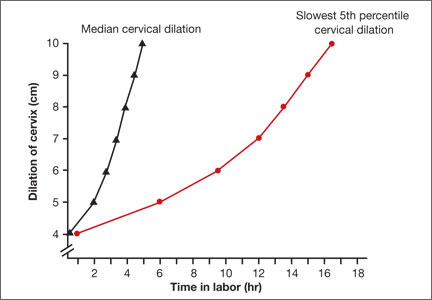
Don’t forget the chromosomes
The past year has seen tremendous media coverage surrounding genetic testing, sparking conversations regarding who should consider genetic testing – and with which genetic test – to determine if they have an increased risk for a particular condition such as cancer ("The Jolie effect on BRCA risks," Internal Medicine News, July 2013, p. 13).
Added to this is the recent Supreme Court ruling that overturned some of Myriad Genetics’ patents on BRCA1 and BRCA2 testing, arguably the best known hereditary cancer genes by patients and physicians ("Keep your patents off my genes!" Internal Medicine News, Oct. 1, 2013, p. 18). Many laboratories have jumped into the cancer testing arena, offering their version of genetic testing panels that examine a variety of genes based on cancer type. Some of these panels test for more than 50 genes related to hereditary cancers – and they go well beyond BRCA1 and BRCA2 testing, using next-generation sequencing (NGS) technology.
The emergence, promise, and application of NSG in cancer genetics have been discussed from numerous angles in this column, but it’s important not to forget chromosomal disorders.
Approximately 1 in 300 live births will carry chromosome abnormalities, and as medical care improves for these conditions, primary care physicians will see more children, such as those with Down syndrome, "graduate" from their pediatricians and require care from primary care physicians. New insight into adult-onset health issues (e.g., early-onset Alzheimer’s disease in Down syndrome) is emerging, but our understanding of the pathology and mechanism of disease remains a challenge. Although animal models exist, it has been a major challenge to recapitulate the effects of having an "extra copy" of an entire chromosome in order to study the biological effects, let alone develop a strategy to silence an entire extra chromosome in order to provide a potential therapy.
Exciting research by Jeanne Lawrence, Ph.D., and her colleagues was presented at the recent American Society of Human Genetics meeting in Boston regarding trisomy 21 (Down syndrome), and it caught my attention despite the onslaught of NSG data presented related to single-gene disorders. By using genome editing, they were able to silence the extra copy of chromosome 21 in Down syndrome pluripotent stem cells by taking advantage of the known genetic processes that silence X chromosomes.
In a normal female cell, there are two copies of the X chromosome; however, only one copy is active, because the other copy is "silenced" through a process called X-inactivation or Lyonization. This is driven by the X-inactivation gene (XIST), which produces a noncoding RNA that covers the entire X chromosome and essentially silences it – making it inactive and condensing it into what is termed a Barr body.
The investigators set out to determine if they could insert a copy of the XIST gene into the extra chromosome 21 – at a very specific location so as not to disrupt any known functional genes – and thereby silence the extra chromosome without affecting other chromosomes. After preliminary success in other cell lines, they attempted this in pluripotent stem cells from a Down syndrome patient, so that differentiation and different tissue subtypes could be studied.
Remarkably, Dr. Lawrence and her colleagues were able to accomplish this integration and overcome two major obstacles: the challenge of working with pluripotent stem cells, and inserting such a large amount of DNA (the XIST gene) via genomic editing. They demonstrated their successful silencing of the extra chromosome 21 through a variety of molecular, cellular, cytological, and genomic assays. Added to the elegance of their work, the strategy they used to insert the XIST gene created an inducible system – meaning they could turn on or off the chromosome 21 silencing based on whether the cells were exposed to doxycycline.
In essence, the investigators created a model to study human chromosome inactivation, which opens the doors to understanding the pathology and molecular pathways involved in chromosome abnormalities such as Down syndrome. This is the potential first step toward developing targeted "chromosomal therapies," something that was not thought to be feasible given the difficulty surrounding gene therapy for single-gene disorders.
While there have been many exciting advances in single-gene disorders and NGS technology, it is refreshing to see exciting research advance in other areas of genetics. I encourage readers to explore this groundbreaking research further.
Dr. Hulick is a medical geneticist at NorthShore University HealthSystem, Evanston, Ill., and a clinician educator at the University of Chicago. He reported having no conflicts of interest.
The past year has seen tremendous media coverage surrounding genetic testing, sparking conversations regarding who should consider genetic testing – and with which genetic test – to determine if they have an increased risk for a particular condition such as cancer ("The Jolie effect on BRCA risks," Internal Medicine News, July 2013, p. 13).
Added to this is the recent Supreme Court ruling that overturned some of Myriad Genetics’ patents on BRCA1 and BRCA2 testing, arguably the best known hereditary cancer genes by patients and physicians ("Keep your patents off my genes!" Internal Medicine News, Oct. 1, 2013, p. 18). Many laboratories have jumped into the cancer testing arena, offering their version of genetic testing panels that examine a variety of genes based on cancer type. Some of these panels test for more than 50 genes related to hereditary cancers – and they go well beyond BRCA1 and BRCA2 testing, using next-generation sequencing (NGS) technology.
The emergence, promise, and application of NSG in cancer genetics have been discussed from numerous angles in this column, but it’s important not to forget chromosomal disorders.
Approximately 1 in 300 live births will carry chromosome abnormalities, and as medical care improves for these conditions, primary care physicians will see more children, such as those with Down syndrome, "graduate" from their pediatricians and require care from primary care physicians. New insight into adult-onset health issues (e.g., early-onset Alzheimer’s disease in Down syndrome) is emerging, but our understanding of the pathology and mechanism of disease remains a challenge. Although animal models exist, it has been a major challenge to recapitulate the effects of having an "extra copy" of an entire chromosome in order to study the biological effects, let alone develop a strategy to silence an entire extra chromosome in order to provide a potential therapy.
Exciting research by Jeanne Lawrence, Ph.D., and her colleagues was presented at the recent American Society of Human Genetics meeting in Boston regarding trisomy 21 (Down syndrome), and it caught my attention despite the onslaught of NSG data presented related to single-gene disorders. By using genome editing, they were able to silence the extra copy of chromosome 21 in Down syndrome pluripotent stem cells by taking advantage of the known genetic processes that silence X chromosomes.
In a normal female cell, there are two copies of the X chromosome; however, only one copy is active, because the other copy is "silenced" through a process called X-inactivation or Lyonization. This is driven by the X-inactivation gene (XIST), which produces a noncoding RNA that covers the entire X chromosome and essentially silences it – making it inactive and condensing it into what is termed a Barr body.
The investigators set out to determine if they could insert a copy of the XIST gene into the extra chromosome 21 – at a very specific location so as not to disrupt any known functional genes – and thereby silence the extra chromosome without affecting other chromosomes. After preliminary success in other cell lines, they attempted this in pluripotent stem cells from a Down syndrome patient, so that differentiation and different tissue subtypes could be studied.
Remarkably, Dr. Lawrence and her colleagues were able to accomplish this integration and overcome two major obstacles: the challenge of working with pluripotent stem cells, and inserting such a large amount of DNA (the XIST gene) via genomic editing. They demonstrated their successful silencing of the extra chromosome 21 through a variety of molecular, cellular, cytological, and genomic assays. Added to the elegance of their work, the strategy they used to insert the XIST gene created an inducible system – meaning they could turn on or off the chromosome 21 silencing based on whether the cells were exposed to doxycycline.
In essence, the investigators created a model to study human chromosome inactivation, which opens the doors to understanding the pathology and molecular pathways involved in chromosome abnormalities such as Down syndrome. This is the potential first step toward developing targeted "chromosomal therapies," something that was not thought to be feasible given the difficulty surrounding gene therapy for single-gene disorders.
While there have been many exciting advances in single-gene disorders and NGS technology, it is refreshing to see exciting research advance in other areas of genetics. I encourage readers to explore this groundbreaking research further.
Dr. Hulick is a medical geneticist at NorthShore University HealthSystem, Evanston, Ill., and a clinician educator at the University of Chicago. He reported having no conflicts of interest.
The past year has seen tremendous media coverage surrounding genetic testing, sparking conversations regarding who should consider genetic testing – and with which genetic test – to determine if they have an increased risk for a particular condition such as cancer ("The Jolie effect on BRCA risks," Internal Medicine News, July 2013, p. 13).
Added to this is the recent Supreme Court ruling that overturned some of Myriad Genetics’ patents on BRCA1 and BRCA2 testing, arguably the best known hereditary cancer genes by patients and physicians ("Keep your patents off my genes!" Internal Medicine News, Oct. 1, 2013, p. 18). Many laboratories have jumped into the cancer testing arena, offering their version of genetic testing panels that examine a variety of genes based on cancer type. Some of these panels test for more than 50 genes related to hereditary cancers – and they go well beyond BRCA1 and BRCA2 testing, using next-generation sequencing (NGS) technology.
The emergence, promise, and application of NSG in cancer genetics have been discussed from numerous angles in this column, but it’s important not to forget chromosomal disorders.
Approximately 1 in 300 live births will carry chromosome abnormalities, and as medical care improves for these conditions, primary care physicians will see more children, such as those with Down syndrome, "graduate" from their pediatricians and require care from primary care physicians. New insight into adult-onset health issues (e.g., early-onset Alzheimer’s disease in Down syndrome) is emerging, but our understanding of the pathology and mechanism of disease remains a challenge. Although animal models exist, it has been a major challenge to recapitulate the effects of having an "extra copy" of an entire chromosome in order to study the biological effects, let alone develop a strategy to silence an entire extra chromosome in order to provide a potential therapy.
Exciting research by Jeanne Lawrence, Ph.D., and her colleagues was presented at the recent American Society of Human Genetics meeting in Boston regarding trisomy 21 (Down syndrome), and it caught my attention despite the onslaught of NSG data presented related to single-gene disorders. By using genome editing, they were able to silence the extra copy of chromosome 21 in Down syndrome pluripotent stem cells by taking advantage of the known genetic processes that silence X chromosomes.
In a normal female cell, there are two copies of the X chromosome; however, only one copy is active, because the other copy is "silenced" through a process called X-inactivation or Lyonization. This is driven by the X-inactivation gene (XIST), which produces a noncoding RNA that covers the entire X chromosome and essentially silences it – making it inactive and condensing it into what is termed a Barr body.
The investigators set out to determine if they could insert a copy of the XIST gene into the extra chromosome 21 – at a very specific location so as not to disrupt any known functional genes – and thereby silence the extra chromosome without affecting other chromosomes. After preliminary success in other cell lines, they attempted this in pluripotent stem cells from a Down syndrome patient, so that differentiation and different tissue subtypes could be studied.
Remarkably, Dr. Lawrence and her colleagues were able to accomplish this integration and overcome two major obstacles: the challenge of working with pluripotent stem cells, and inserting such a large amount of DNA (the XIST gene) via genomic editing. They demonstrated their successful silencing of the extra chromosome 21 through a variety of molecular, cellular, cytological, and genomic assays. Added to the elegance of their work, the strategy they used to insert the XIST gene created an inducible system – meaning they could turn on or off the chromosome 21 silencing based on whether the cells were exposed to doxycycline.
In essence, the investigators created a model to study human chromosome inactivation, which opens the doors to understanding the pathology and molecular pathways involved in chromosome abnormalities such as Down syndrome. This is the potential first step toward developing targeted "chromosomal therapies," something that was not thought to be feasible given the difficulty surrounding gene therapy for single-gene disorders.
While there have been many exciting advances in single-gene disorders and NGS technology, it is refreshing to see exciting research advance in other areas of genetics. I encourage readers to explore this groundbreaking research further.
Dr. Hulick is a medical geneticist at NorthShore University HealthSystem, Evanston, Ill., and a clinician educator at the University of Chicago. He reported having no conflicts of interest.

ACOG urges changes in diagnosis, management of preeclampsia
Proteinuria, or elevated protein in the urine, should no longer be considered the signature criterion besides new-onset hypertension in diagnosing preeclampsia, says the American College of Obstetricians and Gynecologists.
In exhaustive new clinical guidelines on hypertension in pregnancy, ACOG says that equal weight should be given to reduced platelet counts, renal insufficiency, severe headache, heart-lung compromise, and impaired liver function. Any one of these concurrent with new-onset hypertension at 20 weeks of pregnancy or beyond is enough to establish preeclampsia, even in the absence of proteinuria.
"Clinicians like hard numbers," said Dr. James N. Martin, chief of the division of maternal-fetal medicine at the University of Mississippi Medical Center in Jackson, a past ACOG president, and an author of the guidelines. "But sometimes we can be misled by them." Reviews of maternal mortality data have shown that waiting for proteinuria to present can result in delayed intervention or missed diagnosis, as not all women with preeclampsia will develop proteinuria.
The new guidelines replace recommendations from a 2002 ACOG Practice Bulletin (Obstet. Gynecol. 2002;99:159-67). In addition to the revised diagnostic recommendations and precisely defined measures to determine severity of disease, they address several important management challenges: preeclampsia on top of an existing hypertensive disorder; timing of induction for preeclampsia with and without severe symptoms; use of corticosteroids; and recognizing and managing preeclampsia in the postpartum period.
The guidelines do emphasize one hard number that should be useful to clinicians: Delivery at 37 weeks is advised for women with preeclampsia without severe features.
Dr. Martin said that the 37-week delivery recommendation was based largely on results from a 2009 trial in Holland in which 756 women were randomized to induction at the 36- to 37-week point or expectant monitoring to await labor; induction at 37 weeks was associated with poor outcomes in only 31% of subjects, compared with 44% of those receiving expectant monitoring.
The guidelines distinguish extensively between preeclampsia with and without severe features, but discourage the use of the phrase "mild preeclampsia," considering it misleading. "Preeclampsia in any form should never be minimized as ‘mild,’ " Dr. Martin said.
Proteinuria, in addition to being downgraded as the signature diagnostic finding in preeclampsia, should no longer be considered as useful in classifying preeclampsia as severe or in deciding whether to induce, the guidelines say, because the amount of protein in the urine has not been shown to predict either maternal or fetal outcomes.
Fetal growth restriction, once considered a major criterion to make the diagnosis of severe preeclampsia, is now to be used not for diagnosis of preeclampsia, but for indicated delivery in a patient with preeclampsia who also has an extremely small fetus (less than 5th centile) that is associated with abnormal blood flow findings in the umbilical cord connecting the fetus to the placenta.
The guidelines emphasize that preeclampsia can appear for the first time following delivery, or worsen rather than improve during in the postnatal period. It is advisable that all postpartum patients become educated about symptoms suggestive of new or worsening preeclampsia after leaving the hospital so that the patient’s doctors can be alerted and treatment begun in time to prevent problems.
On the prevention front, the guidelines have less to recommend. The use of vitamins C and E is not advised in preventing preeclampsia. Low-dose aspirin, however, is recommended starting late in the first trimester for patients who experience preterm severe preeclampsia.
"What we really need are biomarkers," Dr. Martin said, adding that despite encouraging science on placental growth factor and other potential early markers, none is yet ready for routine clinical use.
Some of the guidelines’ coauthors reported financial relationships or potential conflicts of interest. Dr. George Bakris disclosed associations with Takeda, CVRx, and other companies. Dr. John Barton disclosed relationships with Alere and Beckman Coulter. Dr. Ananth Karumanchi disclosed relationships with Beckman Coulter, Roche, and others. Dr. Baha Sibai disclosed a relationship with Alere. The remaining task force members said they had no relevant financial disclosures.
The report from the ACOG Task Force on Hypertension in Pregnancy marks an important departure from prior diagnostic and management criteria. Firstly, the diagnosis of preeclampsia no longer requires the presence of proteinuria, which can be relatively nonspecific and may also be associated with chronic hypertension. Rather, the task force includes evidence of maternal hepatic, renal, pulmonary, and cerebral end-organ disease in the diagnostic criteria – even in the absence of proteinuria. Once the diagnosis of preeclampsia has been established, the severity criteria no longer include fetal growth restriction, but rather focus on maternal symptoms. Thirdly, delivery is suggested for women with preeclampsia at 37 0/7 weeks’ gestation even in the absence of severe features, and special emphasis is placed on modifying analgesic therapy for women who fail to normalize their blood pressure after the first postpartum day.

|
|
These changes are based on evidence and partly choice. The choice to recognize nonproteinuric preeclampsia as a diagnostic entity follows in the footsteps of several international bodies. Now, women with new-onset hypertension and end-organ effects can be diagnosed with preeclampsia, and management can be based on severity criteria and gestational intervention thresholds without any potentially dangerous delay due to the absence of proteinuria. This important change has the potential to decrease maternal mortality that is attributable to delayed intervention.
The second important step is to remove fetal growth restriction as a severity criterion. This offers the advantage to manage maternal and fetal disease independently based on their individual severities. In the setting of disease-specific surveillance including umbilical artery Doppler ultrasound, this approach has the potential benefit of minimizing iatrogenic prematurity – an important contributor to adverse neonatal outcome.
One choice that the task force did not make is to emphasize the opportunity of first-trimester screening for preeclampsia. Standardized maternal blood pressure readings at this time both are an integral component of screening algorithms and provide additional diagnostic opportunity to document preexisting hypertension – critical for the later diagnosis of preeclampsia (Hypertension 2008;51:1027-33). In addition, the task force underemphasizes the importance of early initiation of low-dose aspirin, because the benefit is greatest for women initiating prophylaxis prior to 16 weeks, and risks for placental abruption increase with initiation in the second trimester (J. Obstet. Gynaecol. Can. 2009;31:818-26). This is important for those centers that choose to provide an early risk assessment, and based on that, initiate low-dose aspirin.
In summary, I think these changes offer a clear advantage by increasing the diagnostic specificity for preeclampsia and providing severity stratification that bears closer relevance to maternal and neonatal outcome. Accordingly, a simplified but clear management approach can be developed, tailored on the balance of disease severity and gestational age.
Dr. Ahmet A. Baschat is professor of obstetrics, gynecology, and reproductive sciences, and director of maternal fetal medicine and the section of fetal therapy at the University of Maryland in Baltimore. He was asked to comment on the task force report. Dr. Baschat said he had no financial disclosures relevant to the report.
The report from the ACOG Task Force on Hypertension in Pregnancy marks an important departure from prior diagnostic and management criteria. Firstly, the diagnosis of preeclampsia no longer requires the presence of proteinuria, which can be relatively nonspecific and may also be associated with chronic hypertension. Rather, the task force includes evidence of maternal hepatic, renal, pulmonary, and cerebral end-organ disease in the diagnostic criteria – even in the absence of proteinuria. Once the diagnosis of preeclampsia has been established, the severity criteria no longer include fetal growth restriction, but rather focus on maternal symptoms. Thirdly, delivery is suggested for women with preeclampsia at 37 0/7 weeks’ gestation even in the absence of severe features, and special emphasis is placed on modifying analgesic therapy for women who fail to normalize their blood pressure after the first postpartum day.
|
|
|
These changes are based on evidence and partly choice. The choice to recognize nonproteinuric preeclampsia as a diagnostic entity follows in the footsteps of several international bodies. Now, women with new-onset hypertension and end-organ effects can be diagnosed with preeclampsia, and management can be based on severity criteria and gestational intervention thresholds without any potentially dangerous delay due to the absence of proteinuria. This important change has the potential to decrease maternal mortality that is attributable to delayed intervention.
The second important step is to remove fetal growth restriction as a severity criterion. This offers the advantage to manage maternal and fetal disease independently based on their individual severities. In the setting of disease-specific surveillance including umbilical artery Doppler ultrasound, this approach has the potential benefit of minimizing iatrogenic prematurity – an important contributor to adverse neonatal outcome.
One choice that the task force did not make is to emphasize the opportunity of first-trimester screening for preeclampsia. Standardized maternal blood pressure readings at this time both are an integral component of screening algorithms and provide additional diagnostic opportunity to document preexisting hypertension – critical for the later diagnosis of preeclampsia (Hypertension 2008;51:1027-33). In addition, the task force underemphasizes the importance of early initiation of low-dose aspirin, because the benefit is greatest for women initiating prophylaxis prior to 16 weeks, and risks for placental abruption increase with initiation in the second trimester (J. Obstet. Gynaecol. Can. 2009;31:818-26). This is important for those centers that choose to provide an early risk assessment, and based on that, initiate low-dose aspirin.
In summary, I think these changes offer a clear advantage by increasing the diagnostic specificity for preeclampsia and providing severity stratification that bears closer relevance to maternal and neonatal outcome. Accordingly, a simplified but clear management approach can be developed, tailored on the balance of disease severity and gestational age.
Dr. Ahmet A. Baschat is professor of obstetrics, gynecology, and reproductive sciences, and director of maternal fetal medicine and the section of fetal therapy at the University of Maryland in Baltimore. He was asked to comment on the task force report. Dr. Baschat said he had no financial disclosures relevant to the report.
The report from the ACOG Task Force on Hypertension in Pregnancy marks an important departure from prior diagnostic and management criteria. Firstly, the diagnosis of preeclampsia no longer requires the presence of proteinuria, which can be relatively nonspecific and may also be associated with chronic hypertension. Rather, the task force includes evidence of maternal hepatic, renal, pulmonary, and cerebral end-organ disease in the diagnostic criteria – even in the absence of proteinuria. Once the diagnosis of preeclampsia has been established, the severity criteria no longer include fetal growth restriction, but rather focus on maternal symptoms. Thirdly, delivery is suggested for women with preeclampsia at 37 0/7 weeks’ gestation even in the absence of severe features, and special emphasis is placed on modifying analgesic therapy for women who fail to normalize their blood pressure after the first postpartum day.
|
|
|
These changes are based on evidence and partly choice. The choice to recognize nonproteinuric preeclampsia as a diagnostic entity follows in the footsteps of several international bodies. Now, women with new-onset hypertension and end-organ effects can be diagnosed with preeclampsia, and management can be based on severity criteria and gestational intervention thresholds without any potentially dangerous delay due to the absence of proteinuria. This important change has the potential to decrease maternal mortality that is attributable to delayed intervention.
The second important step is to remove fetal growth restriction as a severity criterion. This offers the advantage to manage maternal and fetal disease independently based on their individual severities. In the setting of disease-specific surveillance including umbilical artery Doppler ultrasound, this approach has the potential benefit of minimizing iatrogenic prematurity – an important contributor to adverse neonatal outcome.
One choice that the task force did not make is to emphasize the opportunity of first-trimester screening for preeclampsia. Standardized maternal blood pressure readings at this time both are an integral component of screening algorithms and provide additional diagnostic opportunity to document preexisting hypertension – critical for the later diagnosis of preeclampsia (Hypertension 2008;51:1027-33). In addition, the task force underemphasizes the importance of early initiation of low-dose aspirin, because the benefit is greatest for women initiating prophylaxis prior to 16 weeks, and risks for placental abruption increase with initiation in the second trimester (J. Obstet. Gynaecol. Can. 2009;31:818-26). This is important for those centers that choose to provide an early risk assessment, and based on that, initiate low-dose aspirin.
In summary, I think these changes offer a clear advantage by increasing the diagnostic specificity for preeclampsia and providing severity stratification that bears closer relevance to maternal and neonatal outcome. Accordingly, a simplified but clear management approach can be developed, tailored on the balance of disease severity and gestational age.
Dr. Ahmet A. Baschat is professor of obstetrics, gynecology, and reproductive sciences, and director of maternal fetal medicine and the section of fetal therapy at the University of Maryland in Baltimore. He was asked to comment on the task force report. Dr. Baschat said he had no financial disclosures relevant to the report.
Proteinuria, or elevated protein in the urine, should no longer be considered the signature criterion besides new-onset hypertension in diagnosing preeclampsia, says the American College of Obstetricians and Gynecologists.
In exhaustive new clinical guidelines on hypertension in pregnancy, ACOG says that equal weight should be given to reduced platelet counts, renal insufficiency, severe headache, heart-lung compromise, and impaired liver function. Any one of these concurrent with new-onset hypertension at 20 weeks of pregnancy or beyond is enough to establish preeclampsia, even in the absence of proteinuria.
"Clinicians like hard numbers," said Dr. James N. Martin, chief of the division of maternal-fetal medicine at the University of Mississippi Medical Center in Jackson, a past ACOG president, and an author of the guidelines. "But sometimes we can be misled by them." Reviews of maternal mortality data have shown that waiting for proteinuria to present can result in delayed intervention or missed diagnosis, as not all women with preeclampsia will develop proteinuria.
The new guidelines replace recommendations from a 2002 ACOG Practice Bulletin (Obstet. Gynecol. 2002;99:159-67). In addition to the revised diagnostic recommendations and precisely defined measures to determine severity of disease, they address several important management challenges: preeclampsia on top of an existing hypertensive disorder; timing of induction for preeclampsia with and without severe symptoms; use of corticosteroids; and recognizing and managing preeclampsia in the postpartum period.
The guidelines do emphasize one hard number that should be useful to clinicians: Delivery at 37 weeks is advised for women with preeclampsia without severe features.
Dr. Martin said that the 37-week delivery recommendation was based largely on results from a 2009 trial in Holland in which 756 women were randomized to induction at the 36- to 37-week point or expectant monitoring to await labor; induction at 37 weeks was associated with poor outcomes in only 31% of subjects, compared with 44% of those receiving expectant monitoring.
The guidelines distinguish extensively between preeclampsia with and without severe features, but discourage the use of the phrase "mild preeclampsia," considering it misleading. "Preeclampsia in any form should never be minimized as ‘mild,’ " Dr. Martin said.
Proteinuria, in addition to being downgraded as the signature diagnostic finding in preeclampsia, should no longer be considered as useful in classifying preeclampsia as severe or in deciding whether to induce, the guidelines say, because the amount of protein in the urine has not been shown to predict either maternal or fetal outcomes.
Fetal growth restriction, once considered a major criterion to make the diagnosis of severe preeclampsia, is now to be used not for diagnosis of preeclampsia, but for indicated delivery in a patient with preeclampsia who also has an extremely small fetus (less than 5th centile) that is associated with abnormal blood flow findings in the umbilical cord connecting the fetus to the placenta.
The guidelines emphasize that preeclampsia can appear for the first time following delivery, or worsen rather than improve during in the postnatal period. It is advisable that all postpartum patients become educated about symptoms suggestive of new or worsening preeclampsia after leaving the hospital so that the patient’s doctors can be alerted and treatment begun in time to prevent problems.
On the prevention front, the guidelines have less to recommend. The use of vitamins C and E is not advised in preventing preeclampsia. Low-dose aspirin, however, is recommended starting late in the first trimester for patients who experience preterm severe preeclampsia.
"What we really need are biomarkers," Dr. Martin said, adding that despite encouraging science on placental growth factor and other potential early markers, none is yet ready for routine clinical use.
Some of the guidelines’ coauthors reported financial relationships or potential conflicts of interest. Dr. George Bakris disclosed associations with Takeda, CVRx, and other companies. Dr. John Barton disclosed relationships with Alere and Beckman Coulter. Dr. Ananth Karumanchi disclosed relationships with Beckman Coulter, Roche, and others. Dr. Baha Sibai disclosed a relationship with Alere. The remaining task force members said they had no relevant financial disclosures.
Proteinuria, or elevated protein in the urine, should no longer be considered the signature criterion besides new-onset hypertension in diagnosing preeclampsia, says the American College of Obstetricians and Gynecologists.
In exhaustive new clinical guidelines on hypertension in pregnancy, ACOG says that equal weight should be given to reduced platelet counts, renal insufficiency, severe headache, heart-lung compromise, and impaired liver function. Any one of these concurrent with new-onset hypertension at 20 weeks of pregnancy or beyond is enough to establish preeclampsia, even in the absence of proteinuria.
"Clinicians like hard numbers," said Dr. James N. Martin, chief of the division of maternal-fetal medicine at the University of Mississippi Medical Center in Jackson, a past ACOG president, and an author of the guidelines. "But sometimes we can be misled by them." Reviews of maternal mortality data have shown that waiting for proteinuria to present can result in delayed intervention or missed diagnosis, as not all women with preeclampsia will develop proteinuria.
The new guidelines replace recommendations from a 2002 ACOG Practice Bulletin (Obstet. Gynecol. 2002;99:159-67). In addition to the revised diagnostic recommendations and precisely defined measures to determine severity of disease, they address several important management challenges: preeclampsia on top of an existing hypertensive disorder; timing of induction for preeclampsia with and without severe symptoms; use of corticosteroids; and recognizing and managing preeclampsia in the postpartum period.
The guidelines do emphasize one hard number that should be useful to clinicians: Delivery at 37 weeks is advised for women with preeclampsia without severe features.
Dr. Martin said that the 37-week delivery recommendation was based largely on results from a 2009 trial in Holland in which 756 women were randomized to induction at the 36- to 37-week point or expectant monitoring to await labor; induction at 37 weeks was associated with poor outcomes in only 31% of subjects, compared with 44% of those receiving expectant monitoring.
The guidelines distinguish extensively between preeclampsia with and without severe features, but discourage the use of the phrase "mild preeclampsia," considering it misleading. "Preeclampsia in any form should never be minimized as ‘mild,’ " Dr. Martin said.
Proteinuria, in addition to being downgraded as the signature diagnostic finding in preeclampsia, should no longer be considered as useful in classifying preeclampsia as severe or in deciding whether to induce, the guidelines say, because the amount of protein in the urine has not been shown to predict either maternal or fetal outcomes.
Fetal growth restriction, once considered a major criterion to make the diagnosis of severe preeclampsia, is now to be used not for diagnosis of preeclampsia, but for indicated delivery in a patient with preeclampsia who also has an extremely small fetus (less than 5th centile) that is associated with abnormal blood flow findings in the umbilical cord connecting the fetus to the placenta.
The guidelines emphasize that preeclampsia can appear for the first time following delivery, or worsen rather than improve during in the postnatal period. It is advisable that all postpartum patients become educated about symptoms suggestive of new or worsening preeclampsia after leaving the hospital so that the patient’s doctors can be alerted and treatment begun in time to prevent problems.
On the prevention front, the guidelines have less to recommend. The use of vitamins C and E is not advised in preventing preeclampsia. Low-dose aspirin, however, is recommended starting late in the first trimester for patients who experience preterm severe preeclampsia.
"What we really need are biomarkers," Dr. Martin said, adding that despite encouraging science on placental growth factor and other potential early markers, none is yet ready for routine clinical use.
Some of the guidelines’ coauthors reported financial relationships or potential conflicts of interest. Dr. George Bakris disclosed associations with Takeda, CVRx, and other companies. Dr. John Barton disclosed relationships with Alere and Beckman Coulter. Dr. Ananth Karumanchi disclosed relationships with Beckman Coulter, Roche, and others. Dr. Baha Sibai disclosed a relationship with Alere. The remaining task force members said they had no relevant financial disclosures.
FROM THE ACOG TASK FORCE REPORT ON HYPERTENSION IN PREGNANCY

Maternal lupus doubled autism risk
SAN DIEGO – The risk of autism spectrum disorders is more than doubled among children born to mothers with systemic lupus erythematosus, according to the first-ever controlled study to address the question.
That being said, women with SLE can be reassured that despite this elevated relative risk, the absolute risk that their child will be diagnosed with an autism spectrum disorder (ASD) is low – less than 1 in 50 – Dr. Evelyne Vinet said at the annual meeting of the American College of Rheumatology.
The increased risk of ASD in children born to women with SLE documented in this large study was not mediated by in utero exposure to medications for SLE, including antimalarials, immunosuppressive agents, corticosteroids, and antidepressants. Use of those drugs in pregnancy wasn’t associated with any increased risk. In light of this, further research is warranted into a highly promising alternative hypothesis: that in utero exposure to SLE-related autoantibodies, such as anti-DNA and antiphospholipid antibodies, may play a causative role, said Dr. Vinet, a rheumatologist at McGill University, Montreal.

Children born to mothers with SLE also had an increased likelihood of being diagnosed with attention-deficit/hyperactivity disorder in this study. However, in contrast to the situation with ASD, the increased risk of ADHD appeared to result from exposure to medications in utero – specifically, antidepressants and possibly immunosuppressives – rather than to maternal SLE per se, she added.
Dr. Vinet presented an analysis of the OSLER (Offspring of Systemic Lupus Erythematosus Mothers Registry) database, the world’s largest cohort of children born to mothers with SLE. OSLER includes all women with a diagnosis of SLE hospitalized for childbirth in the province of Quebec since 1989. This study included 509 women who had 719 children after they had been diagnosed with SLE, as well as 5,824 controls matched for age and year of delivery along with their 8,493 children. The mean maternal age was 30.3 years. The children were followed out to a mean age of 9.1 years.
ASD was diagnosed in 1.4% of children born to mothers with SLE, compared with 0.6% of control children. The mean age at diagnosis of ASD was noticeably lower in the offspring of mothers with SLE: 3.8 years, compared with 5.7 years in the control children.
Women with SLE had higher rates of hypertension, asthma, and diabetes than did controls at the time of delivery. They also had higher rates of obstetric complications, including preterm birth, small for gestational age, and gestational diabetes. In a multivariate analysis adjusted for these variables, maternal SLE remained independently associated with a 2.3-fold increased risk of diagnosis of an ASD in offspring.
Complete and reliable records of prescription drug use during pregnancy were available only for the roughly 20% of mothers belonging to the provincial medication public assistance program. Of the 18 cases of ASD diagnosed in the children of 1,925 mothers covered by the program, only one occurred among the 155 offspring of SLE mothers; that child had been exposed to corticosteroids in utero. Of the 17 cases of ASD diagnosed in the control group, 16 had no exposures to the medications under scrutiny, and one involved in utero exposure to an anticonvulsant.
The OSLER database doesn’t include information about maternal autoantibody levels, but Dr. Vinet and her coinvestigators have made the collection of such data a top priority in light of recent studies in animal models of SLE by other investigators. Those studies showed that SLE-related autoantibodies, including n-methyl-d-aspartate receptor antibodies and antiphospholipid antibodies, as well as interleukin-6 and other cytokines, alter fetal brain development and induce behavioral anomalies suggestive of autism, such as withdrawal, in the mouse offspring.
In addition, French investigators recently reported that 3 of 36 children born to mothers with antiphospholipid syndrome developed ASD, although Dr. Vinet noted that this small but intriguing study lacked a control group (Semin. Arthritis Rheum. 2013 Aug. 1 [doi: 10.1016/j.semarthrit.2013.07.001]).
ADHD was diagnosed in 9.9% of the children of mothers with SLE in the OSLER database, compared with 6.1% of controls. It was diagnosed when the children were older: at a mean age of 12.5 years, compared with 7.8 years in the controls. In a multivariate analysis adjusted for in utero drug exposures, the association between ADHD and maternal SLE was no longer significant. However, in utero exposure to antidepressant medication, regardless of whether or not a mother had SLE, was associated with a hefty 3.7-fold increase in ADHD in the offspring. Because of the relatively small number of mothers on antidepressant medication, Dr. Vinet is now collaborating with investigators in other Canadian provinces having more comprehensive maternal medication exposure data to take a closer look at this tentative link between in utero drug exposure and ADHD.
This study of the OSLER database was funded by the Canadian Institutes of Health Research. Dr. Vinet reported having no financial conflicts.
SAN DIEGO – The risk of autism spectrum disorders is more than doubled among children born to mothers with systemic lupus erythematosus, according to the first-ever controlled study to address the question.
That being said, women with SLE can be reassured that despite this elevated relative risk, the absolute risk that their child will be diagnosed with an autism spectrum disorder (ASD) is low – less than 1 in 50 – Dr. Evelyne Vinet said at the annual meeting of the American College of Rheumatology.
The increased risk of ASD in children born to women with SLE documented in this large study was not mediated by in utero exposure to medications for SLE, including antimalarials, immunosuppressive agents, corticosteroids, and antidepressants. Use of those drugs in pregnancy wasn’t associated with any increased risk. In light of this, further research is warranted into a highly promising alternative hypothesis: that in utero exposure to SLE-related autoantibodies, such as anti-DNA and antiphospholipid antibodies, may play a causative role, said Dr. Vinet, a rheumatologist at McGill University, Montreal.
Children born to mothers with SLE also had an increased likelihood of being diagnosed with attention-deficit/hyperactivity disorder in this study. However, in contrast to the situation with ASD, the increased risk of ADHD appeared to result from exposure to medications in utero – specifically, antidepressants and possibly immunosuppressives – rather than to maternal SLE per se, she added.
Dr. Vinet presented an analysis of the OSLER (Offspring of Systemic Lupus Erythematosus Mothers Registry) database, the world’s largest cohort of children born to mothers with SLE. OSLER includes all women with a diagnosis of SLE hospitalized for childbirth in the province of Quebec since 1989. This study included 509 women who had 719 children after they had been diagnosed with SLE, as well as 5,824 controls matched for age and year of delivery along with their 8,493 children. The mean maternal age was 30.3 years. The children were followed out to a mean age of 9.1 years.
ASD was diagnosed in 1.4% of children born to mothers with SLE, compared with 0.6% of control children. The mean age at diagnosis of ASD was noticeably lower in the offspring of mothers with SLE: 3.8 years, compared with 5.7 years in the control children.
Women with SLE had higher rates of hypertension, asthma, and diabetes than did controls at the time of delivery. They also had higher rates of obstetric complications, including preterm birth, small for gestational age, and gestational diabetes. In a multivariate analysis adjusted for these variables, maternal SLE remained independently associated with a 2.3-fold increased risk of diagnosis of an ASD in offspring.
Complete and reliable records of prescription drug use during pregnancy were available only for the roughly 20% of mothers belonging to the provincial medication public assistance program. Of the 18 cases of ASD diagnosed in the children of 1,925 mothers covered by the program, only one occurred among the 155 offspring of SLE mothers; that child had been exposed to corticosteroids in utero. Of the 17 cases of ASD diagnosed in the control group, 16 had no exposures to the medications under scrutiny, and one involved in utero exposure to an anticonvulsant.
The OSLER database doesn’t include information about maternal autoantibody levels, but Dr. Vinet and her coinvestigators have made the collection of such data a top priority in light of recent studies in animal models of SLE by other investigators. Those studies showed that SLE-related autoantibodies, including n-methyl-d-aspartate receptor antibodies and antiphospholipid antibodies, as well as interleukin-6 and other cytokines, alter fetal brain development and induce behavioral anomalies suggestive of autism, such as withdrawal, in the mouse offspring.
In addition, French investigators recently reported that 3 of 36 children born to mothers with antiphospholipid syndrome developed ASD, although Dr. Vinet noted that this small but intriguing study lacked a control group (Semin. Arthritis Rheum. 2013 Aug. 1 [doi: 10.1016/j.semarthrit.2013.07.001]).
ADHD was diagnosed in 9.9% of the children of mothers with SLE in the OSLER database, compared with 6.1% of controls. It was diagnosed when the children were older: at a mean age of 12.5 years, compared with 7.8 years in the controls. In a multivariate analysis adjusted for in utero drug exposures, the association between ADHD and maternal SLE was no longer significant. However, in utero exposure to antidepressant medication, regardless of whether or not a mother had SLE, was associated with a hefty 3.7-fold increase in ADHD in the offspring. Because of the relatively small number of mothers on antidepressant medication, Dr. Vinet is now collaborating with investigators in other Canadian provinces having more comprehensive maternal medication exposure data to take a closer look at this tentative link between in utero drug exposure and ADHD.
This study of the OSLER database was funded by the Canadian Institutes of Health Research. Dr. Vinet reported having no financial conflicts.
SAN DIEGO – The risk of autism spectrum disorders is more than doubled among children born to mothers with systemic lupus erythematosus, according to the first-ever controlled study to address the question.
That being said, women with SLE can be reassured that despite this elevated relative risk, the absolute risk that their child will be diagnosed with an autism spectrum disorder (ASD) is low – less than 1 in 50 – Dr. Evelyne Vinet said at the annual meeting of the American College of Rheumatology.
The increased risk of ASD in children born to women with SLE documented in this large study was not mediated by in utero exposure to medications for SLE, including antimalarials, immunosuppressive agents, corticosteroids, and antidepressants. Use of those drugs in pregnancy wasn’t associated with any increased risk. In light of this, further research is warranted into a highly promising alternative hypothesis: that in utero exposure to SLE-related autoantibodies, such as anti-DNA and antiphospholipid antibodies, may play a causative role, said Dr. Vinet, a rheumatologist at McGill University, Montreal.
Children born to mothers with SLE also had an increased likelihood of being diagnosed with attention-deficit/hyperactivity disorder in this study. However, in contrast to the situation with ASD, the increased risk of ADHD appeared to result from exposure to medications in utero – specifically, antidepressants and possibly immunosuppressives – rather than to maternal SLE per se, she added.
Dr. Vinet presented an analysis of the OSLER (Offspring of Systemic Lupus Erythematosus Mothers Registry) database, the world’s largest cohort of children born to mothers with SLE. OSLER includes all women with a diagnosis of SLE hospitalized for childbirth in the province of Quebec since 1989. This study included 509 women who had 719 children after they had been diagnosed with SLE, as well as 5,824 controls matched for age and year of delivery along with their 8,493 children. The mean maternal age was 30.3 years. The children were followed out to a mean age of 9.1 years.
ASD was diagnosed in 1.4% of children born to mothers with SLE, compared with 0.6% of control children. The mean age at diagnosis of ASD was noticeably lower in the offspring of mothers with SLE: 3.8 years, compared with 5.7 years in the control children.
Women with SLE had higher rates of hypertension, asthma, and diabetes than did controls at the time of delivery. They also had higher rates of obstetric complications, including preterm birth, small for gestational age, and gestational diabetes. In a multivariate analysis adjusted for these variables, maternal SLE remained independently associated with a 2.3-fold increased risk of diagnosis of an ASD in offspring.
Complete and reliable records of prescription drug use during pregnancy were available only for the roughly 20% of mothers belonging to the provincial medication public assistance program. Of the 18 cases of ASD diagnosed in the children of 1,925 mothers covered by the program, only one occurred among the 155 offspring of SLE mothers; that child had been exposed to corticosteroids in utero. Of the 17 cases of ASD diagnosed in the control group, 16 had no exposures to the medications under scrutiny, and one involved in utero exposure to an anticonvulsant.
The OSLER database doesn’t include information about maternal autoantibody levels, but Dr. Vinet and her coinvestigators have made the collection of such data a top priority in light of recent studies in animal models of SLE by other investigators. Those studies showed that SLE-related autoantibodies, including n-methyl-d-aspartate receptor antibodies and antiphospholipid antibodies, as well as interleukin-6 and other cytokines, alter fetal brain development and induce behavioral anomalies suggestive of autism, such as withdrawal, in the mouse offspring.
In addition, French investigators recently reported that 3 of 36 children born to mothers with antiphospholipid syndrome developed ASD, although Dr. Vinet noted that this small but intriguing study lacked a control group (Semin. Arthritis Rheum. 2013 Aug. 1 [doi: 10.1016/j.semarthrit.2013.07.001]).
ADHD was diagnosed in 9.9% of the children of mothers with SLE in the OSLER database, compared with 6.1% of controls. It was diagnosed when the children were older: at a mean age of 12.5 years, compared with 7.8 years in the controls. In a multivariate analysis adjusted for in utero drug exposures, the association between ADHD and maternal SLE was no longer significant. However, in utero exposure to antidepressant medication, regardless of whether or not a mother had SLE, was associated with a hefty 3.7-fold increase in ADHD in the offspring. Because of the relatively small number of mothers on antidepressant medication, Dr. Vinet is now collaborating with investigators in other Canadian provinces having more comprehensive maternal medication exposure data to take a closer look at this tentative link between in utero drug exposure and ADHD.
This study of the OSLER database was funded by the Canadian Institutes of Health Research. Dr. Vinet reported having no financial conflicts.
AT THE ACR ANNUAL MEETING
Major finding: Children born to mothers with systemic lupus erythematosus had an adjusted 2.3-fold increased risk of being diagnosed with an autism spectrum disorder, compared with controls.
Data source: This study from the world’s largest cohort of children born to mothers with SLE included 509 affected mothers and their 719 children, as well as 5,824 matched control mothers and their 8,493 children.
Disclosures: This study of the OSLER database was funded by the Canadian Institutes of Health Research. Dr. Vinet reported having no financial conflicts.

Why are well-educated women more likely to choose home birth?
In this audiocast, Dr. Norwitz discusses:
- His unique training and education, including his connection as an MD, PhD, to midwifery practice
- The increased number of women delivering at home in the United States
- Why older, well-educated, married, multiparous women are more likely to deliver at home
- What structure would support safe home care delivery
Dr. Norwitz is the author of What do the latest data reveal about the safety of home birth in the United States? (Examining the Evidence, November 2013).
Errol R. Norwitz, MD, PhD, is Louis E. Phaneuf Professor of Obstetrics and Gynecology, Tufts University School of Medicine, and Chairman of the Department of Obstetrics and Gynecology, Tufts Medical Center, Boston, Massachusetts. Dr. Norwitz serves on the OBG Management Board of Editors.
Errol R. Norwitz, MD, PhD, is Louis E. Phaneuf Professor of Obstetrics and Gynecology, Tufts University School of Medicine, and Chairman of the Department of Obstetrics and Gynecology, Tufts Medical Center, Boston, Massachusetts. Dr. Norwitz serves on the OBG Management Board of Editors.
Errol R. Norwitz, MD, PhD, is Louis E. Phaneuf Professor of Obstetrics and Gynecology, Tufts University School of Medicine, and Chairman of the Department of Obstetrics and Gynecology, Tufts Medical Center, Boston, Massachusetts. Dr. Norwitz serves on the OBG Management Board of Editors.
In this audiocast, Dr. Norwitz discusses:
- His unique training and education, including his connection as an MD, PhD, to midwifery practice
- The increased number of women delivering at home in the United States
- Why older, well-educated, married, multiparous women are more likely to deliver at home
- What structure would support safe home care delivery
Dr. Norwitz is the author of What do the latest data reveal about the safety of home birth in the United States? (Examining the Evidence, November 2013).
In this audiocast, Dr. Norwitz discusses:
- His unique training and education, including his connection as an MD, PhD, to midwifery practice
- The increased number of women delivering at home in the United States
- Why older, well-educated, married, multiparous women are more likely to deliver at home
- What structure would support safe home care delivery
Dr. Norwitz is the author of What do the latest data reveal about the safety of home birth in the United States? (Examining the Evidence, November 2013).