User login
Nothing Is Sacred: The Need for Unceasing Questioning in Scientific Research
As we look at the trauma articles lined up in this issue of The American Journal of Orthopedics, we are reminded of one of the principle missions of our academic journals, the evaluation and dissemination of new knowledge. All 4 trauma articles offer an improvement in treatment or new perspective in the evaluation of musculoskeletal injury. As an Associate Editor of the journal, I often hear comments from reviewers like “nothing new here,” “retrospective study,” or “has been done before.” But I’m continually reminded that we can never get enough quality information in our quest to provide truth and knowledge to our readership.
Things are not always as they seem. Nothing reminds us of this as much as the revelations seen in the recent work showcased on the front page of The New York Times on August 27, 2015.1 A research group at the Center for Open Science in Charlottesville, Virginia, attempted to reproduce 100 studies published in leading psychology journals and discovered that only 35% could be verified.1 No fraud was inferred, just the “conclusion” that the results were not as definitive as originally felt to be. Interesting, shocking, or stimulating? I would contend it’s the latter. Though many things written in major and respected journals are held as sacred tenets of our craft, all should be challenged. Clinical science particularly needs to be continually refined, as one study is rarely powerful enough to be definitive.
There is nothing so true that it should not be retested. For centuries great academicians accepted and repeatedly published on the “fact” that the earth was the center of our universe. Phlebotomy was an accepted and practiced treatment for febrile illness for centuries. It is alleged to have played a significant role in the death of our country’s first president, George Washington, who succumbed to suppurative pharyngitis.2 Needless to say, we no longer hold these truths to be valid.
Even in our own recent literature, clinical solutions held to be advances, such as metal-on-metal arthroplasty, bone morphogenetic proteins (BMPs), and the aggressive arthroscopic treatment of superior labrum, anterior to posterior (SLAP) lesions, have been properly and helpfully challenged, clarifying their role in our armamentarium. Consider this issue of the journal to be a salute to the investigators and authors who honestly report their findings to us in hopes of better understanding.
But we should never be dissuaded from taking a second look, or even a third, at a clinical principle or basic science belief. In his comments to The New York Times, Brian Nosek, psychology professor at the University of Virginia and director of the Center for Open Science stated, “We see this is a call to action…to the research community to do more replication.”1 I could not agree more. Continued curiosity and constructive criticism should be encouraged. We should never be cowed into complacency because something “has already been done.” We encourage investigators to unceasingly question and work to test their hypotheses. They help us add to our fund of knowledge. Without their continued diligence we will have nothing to fill these pages. We thank them.
1. Carey B. Many psychology findings not as strong as claimed, study says. New York Times. August 27, 2015:A1. http://www.nytimes.com/2015/08/28/science/many-social-science-findings-not-as-strong-as-claimed-study-says.html?_r=0. Accessed September 11, 2015.
2. Wallenborn WM. George Washington’s terminal illness: a modern medical analysis of the last illness and death of George Washington. Papers of George Washington website. http://gwpapers.virginia.edu/history/articles/illness. Published November 5, 1997. Accessed September 11, 2015.
As we look at the trauma articles lined up in this issue of The American Journal of Orthopedics, we are reminded of one of the principle missions of our academic journals, the evaluation and dissemination of new knowledge. All 4 trauma articles offer an improvement in treatment or new perspective in the evaluation of musculoskeletal injury. As an Associate Editor of the journal, I often hear comments from reviewers like “nothing new here,” “retrospective study,” or “has been done before.” But I’m continually reminded that we can never get enough quality information in our quest to provide truth and knowledge to our readership.
Things are not always as they seem. Nothing reminds us of this as much as the revelations seen in the recent work showcased on the front page of The New York Times on August 27, 2015.1 A research group at the Center for Open Science in Charlottesville, Virginia, attempted to reproduce 100 studies published in leading psychology journals and discovered that only 35% could be verified.1 No fraud was inferred, just the “conclusion” that the results were not as definitive as originally felt to be. Interesting, shocking, or stimulating? I would contend it’s the latter. Though many things written in major and respected journals are held as sacred tenets of our craft, all should be challenged. Clinical science particularly needs to be continually refined, as one study is rarely powerful enough to be definitive.
There is nothing so true that it should not be retested. For centuries great academicians accepted and repeatedly published on the “fact” that the earth was the center of our universe. Phlebotomy was an accepted and practiced treatment for febrile illness for centuries. It is alleged to have played a significant role in the death of our country’s first president, George Washington, who succumbed to suppurative pharyngitis.2 Needless to say, we no longer hold these truths to be valid.
Even in our own recent literature, clinical solutions held to be advances, such as metal-on-metal arthroplasty, bone morphogenetic proteins (BMPs), and the aggressive arthroscopic treatment of superior labrum, anterior to posterior (SLAP) lesions, have been properly and helpfully challenged, clarifying their role in our armamentarium. Consider this issue of the journal to be a salute to the investigators and authors who honestly report their findings to us in hopes of better understanding.
But we should never be dissuaded from taking a second look, or even a third, at a clinical principle or basic science belief. In his comments to The New York Times, Brian Nosek, psychology professor at the University of Virginia and director of the Center for Open Science stated, “We see this is a call to action…to the research community to do more replication.”1 I could not agree more. Continued curiosity and constructive criticism should be encouraged. We should never be cowed into complacency because something “has already been done.” We encourage investigators to unceasingly question and work to test their hypotheses. They help us add to our fund of knowledge. Without their continued diligence we will have nothing to fill these pages. We thank them.
As we look at the trauma articles lined up in this issue of The American Journal of Orthopedics, we are reminded of one of the principle missions of our academic journals, the evaluation and dissemination of new knowledge. All 4 trauma articles offer an improvement in treatment or new perspective in the evaluation of musculoskeletal injury. As an Associate Editor of the journal, I often hear comments from reviewers like “nothing new here,” “retrospective study,” or “has been done before.” But I’m continually reminded that we can never get enough quality information in our quest to provide truth and knowledge to our readership.
Things are not always as they seem. Nothing reminds us of this as much as the revelations seen in the recent work showcased on the front page of The New York Times on August 27, 2015.1 A research group at the Center for Open Science in Charlottesville, Virginia, attempted to reproduce 100 studies published in leading psychology journals and discovered that only 35% could be verified.1 No fraud was inferred, just the “conclusion” that the results were not as definitive as originally felt to be. Interesting, shocking, or stimulating? I would contend it’s the latter. Though many things written in major and respected journals are held as sacred tenets of our craft, all should be challenged. Clinical science particularly needs to be continually refined, as one study is rarely powerful enough to be definitive.
There is nothing so true that it should not be retested. For centuries great academicians accepted and repeatedly published on the “fact” that the earth was the center of our universe. Phlebotomy was an accepted and practiced treatment for febrile illness for centuries. It is alleged to have played a significant role in the death of our country’s first president, George Washington, who succumbed to suppurative pharyngitis.2 Needless to say, we no longer hold these truths to be valid.
Even in our own recent literature, clinical solutions held to be advances, such as metal-on-metal arthroplasty, bone morphogenetic proteins (BMPs), and the aggressive arthroscopic treatment of superior labrum, anterior to posterior (SLAP) lesions, have been properly and helpfully challenged, clarifying their role in our armamentarium. Consider this issue of the journal to be a salute to the investigators and authors who honestly report their findings to us in hopes of better understanding.
But we should never be dissuaded from taking a second look, or even a third, at a clinical principle or basic science belief. In his comments to The New York Times, Brian Nosek, psychology professor at the University of Virginia and director of the Center for Open Science stated, “We see this is a call to action…to the research community to do more replication.”1 I could not agree more. Continued curiosity and constructive criticism should be encouraged. We should never be cowed into complacency because something “has already been done.” We encourage investigators to unceasingly question and work to test their hypotheses. They help us add to our fund of knowledge. Without their continued diligence we will have nothing to fill these pages. We thank them.
1. Carey B. Many psychology findings not as strong as claimed, study says. New York Times. August 27, 2015:A1. http://www.nytimes.com/2015/08/28/science/many-social-science-findings-not-as-strong-as-claimed-study-says.html?_r=0. Accessed September 11, 2015.
2. Wallenborn WM. George Washington’s terminal illness: a modern medical analysis of the last illness and death of George Washington. Papers of George Washington website. http://gwpapers.virginia.edu/history/articles/illness. Published November 5, 1997. Accessed September 11, 2015.
1. Carey B. Many psychology findings not as strong as claimed, study says. New York Times. August 27, 2015:A1. http://www.nytimes.com/2015/08/28/science/many-social-science-findings-not-as-strong-as-claimed-study-says.html?_r=0. Accessed September 11, 2015.
2. Wallenborn WM. George Washington’s terminal illness: a modern medical analysis of the last illness and death of George Washington. Papers of George Washington website. http://gwpapers.virginia.edu/history/articles/illness. Published November 5, 1997. Accessed September 11, 2015.

PsA, PsC do not affect total hip replacement outcomes
Neither psoriatic arthritis (PsA) nor cutaneous psoriasis (PsC) is an independent predictor of poor postoperative pain or function following a total hip arthroplasty, according to the results of a case-control study by Dr. Lisa A. Mandl and her colleagues.
The study’s participants underwent surgery between May 1, 2007, and Dec. 31, 2010, in a center that performs more than 4,300 THAs annually. All subjects lived for at least 2 years after their operations. The researchers compared pre- and postoperative data from patients in the following three categories: those with PsA, those with PsC without evidence of inflammatory arthritis, and those with osteoarthritis (OA). Patients with OA comprised the control group, which excluded any patient who self-reported a history of PsA, rheumatoid arthritis, lupus erythematosus, or any other systematic rheumatic disease, or who had documentation of skin psoriasis. The researchers acquired postoperative self-report data from 47 PsA patients, 106 PsC patients, and 864 OA patients. Seventeen percent of patients submitted information on their status at 1 year, 69% at 2 years, and 14% at 3-5 years.

The primary outcomes of interest were postoperative pain and function, which were assessed via the Hip Osteoarthritis Outcome Score (HOOS), from which the Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) was derived.
There were no statistically significant differences in postoperative WOMAC pain or function scores between the three groups of patients (P = .78 and .96, respectively). The mean pain scores were 14.9, 6.1, and 15.8 for patients with PsA, PsC, and OA, respectively. These patients’ mean function scores were 16.3, 19.6, and 18.8 for the PsA, PsC and OA groups, respectively.
Overall levels of satisfaction with the surgery were similar among the three groups (P = .54). Ninety-three percent of the PsA patients, 79% of the PsC patients, and 84% of the OA patients were “very satisfied” with their total hip arthroplasty. Between 1% and 3% of each group reported being “very dissatisfied” with their surgery. The researchers found that extent of skin disease was not associated with worse postoperative pain or function.
“Further work needs to be done to better understand the interplay of disease activity and quality of life on the outcomes of [total hip arthroplasty] in PsA and PsC,” they wrote.
Read the report in Arthritis & Rheumatology (doi: 10.1002/art.39431).
Neither psoriatic arthritis (PsA) nor cutaneous psoriasis (PsC) is an independent predictor of poor postoperative pain or function following a total hip arthroplasty, according to the results of a case-control study by Dr. Lisa A. Mandl and her colleagues.
The study’s participants underwent surgery between May 1, 2007, and Dec. 31, 2010, in a center that performs more than 4,300 THAs annually. All subjects lived for at least 2 years after their operations. The researchers compared pre- and postoperative data from patients in the following three categories: those with PsA, those with PsC without evidence of inflammatory arthritis, and those with osteoarthritis (OA). Patients with OA comprised the control group, which excluded any patient who self-reported a history of PsA, rheumatoid arthritis, lupus erythematosus, or any other systematic rheumatic disease, or who had documentation of skin psoriasis. The researchers acquired postoperative self-report data from 47 PsA patients, 106 PsC patients, and 864 OA patients. Seventeen percent of patients submitted information on their status at 1 year, 69% at 2 years, and 14% at 3-5 years.
The primary outcomes of interest were postoperative pain and function, which were assessed via the Hip Osteoarthritis Outcome Score (HOOS), from which the Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) was derived.
There were no statistically significant differences in postoperative WOMAC pain or function scores between the three groups of patients (P = .78 and .96, respectively). The mean pain scores were 14.9, 6.1, and 15.8 for patients with PsA, PsC, and OA, respectively. These patients’ mean function scores were 16.3, 19.6, and 18.8 for the PsA, PsC and OA groups, respectively.
Overall levels of satisfaction with the surgery were similar among the three groups (P = .54). Ninety-three percent of the PsA patients, 79% of the PsC patients, and 84% of the OA patients were “very satisfied” with their total hip arthroplasty. Between 1% and 3% of each group reported being “very dissatisfied” with their surgery. The researchers found that extent of skin disease was not associated with worse postoperative pain or function.
“Further work needs to be done to better understand the interplay of disease activity and quality of life on the outcomes of [total hip arthroplasty] in PsA and PsC,” they wrote.
Read the report in Arthritis & Rheumatology (doi: 10.1002/art.39431).
Neither psoriatic arthritis (PsA) nor cutaneous psoriasis (PsC) is an independent predictor of poor postoperative pain or function following a total hip arthroplasty, according to the results of a case-control study by Dr. Lisa A. Mandl and her colleagues.
The study’s participants underwent surgery between May 1, 2007, and Dec. 31, 2010, in a center that performs more than 4,300 THAs annually. All subjects lived for at least 2 years after their operations. The researchers compared pre- and postoperative data from patients in the following three categories: those with PsA, those with PsC without evidence of inflammatory arthritis, and those with osteoarthritis (OA). Patients with OA comprised the control group, which excluded any patient who self-reported a history of PsA, rheumatoid arthritis, lupus erythematosus, or any other systematic rheumatic disease, or who had documentation of skin psoriasis. The researchers acquired postoperative self-report data from 47 PsA patients, 106 PsC patients, and 864 OA patients. Seventeen percent of patients submitted information on their status at 1 year, 69% at 2 years, and 14% at 3-5 years.
The primary outcomes of interest were postoperative pain and function, which were assessed via the Hip Osteoarthritis Outcome Score (HOOS), from which the Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) was derived.
There were no statistically significant differences in postoperative WOMAC pain or function scores between the three groups of patients (P = .78 and .96, respectively). The mean pain scores were 14.9, 6.1, and 15.8 for patients with PsA, PsC, and OA, respectively. These patients’ mean function scores were 16.3, 19.6, and 18.8 for the PsA, PsC and OA groups, respectively.
Overall levels of satisfaction with the surgery were similar among the three groups (P = .54). Ninety-three percent of the PsA patients, 79% of the PsC patients, and 84% of the OA patients were “very satisfied” with their total hip arthroplasty. Between 1% and 3% of each group reported being “very dissatisfied” with their surgery. The researchers found that extent of skin disease was not associated with worse postoperative pain or function.
“Further work needs to be done to better understand the interplay of disease activity and quality of life on the outcomes of [total hip arthroplasty] in PsA and PsC,” they wrote.
Read the report in Arthritis & Rheumatology (doi: 10.1002/art.39431).
FROM ARTHRITIS & RHEUMATOLOGY

Smoother orthopedic implants may minimize bacterial adherence
SAN DIEGO – Rough materials used for orthopedic implants, such as cobalt chromium and titanium, increased bacterial adherence, while smoother materials such as stainless steel did not, results from an image analysis demonstrated.
“In light of these results, it is important to question why we utilize the types of materials we use for various orthopedic procedures,” Dioscaris R. Garcia, Ph.D., said in an interview in advance of the annual Interscience Conference on Antimicrobial Agents and Chemotherapy. “There was no one-size-fits-all material to minimize adherence per the findings of this study, but the findings may suggest that having a smoother surface may minimize the ability of bacterial pathogens to adhere to the surface.”

He characterized the topic of bacterial adherence to orthopedic implants as “an issue of great interest due to how little is known about the biological implications of the materials utilized. The most researched of these materials is titanium, which is touted for its biocompatibility. This study aims to provide a base and a glimpse into how the most commonly utilized orthopedic-relevant materials interact with some of the most commonly encountered pathogens.”
For the study, Dr. Garcia, a molecular pharmacologist at Rhode Island Hospital in Providence, Dr. Alan H. Daniels, an orthopedic surgeon at the hospital, and their associates used scanning electron microscopy and confocal laser scanning microscopy to evaluate the adherence pattern, density, and propagation of six commonly encountered bacterial pathogens (methicillin-sensitive Staphylococcus aureus, methicillin-resistant S. aureus, coagulase-negative Staphylococcus epidermidis, multidrug-resistant Acinetobacter baumannii, Propionibacterium acnes, and vancomycin-resistant Enterococcus faecalis) on five commonly used spinal implant materials (titanium, titanium alloy, stainless steel, cobalt chromium, and polyetherether ketone). The samples were fixed and dehydrated via ethanol dehydration gradient and critical point drying.
The researchers found that some pathogens, such as vancomycin-resistant E. faecalis and multidrug-resistant A. baumannii, were more likely to adhere to more textured materials such as cobalt chromium and titanium, compared with smoother materials such as stainless steel. “Additionally, the findings suggest that the microtopography of these materials may be the driving force behind the adherence of pathogens on the materials themselves,” Dr. Garcia said. Compared with smoother, polished materials, he explained, the rougher materials were more likely to harbor dense proliferation of bacterial pathogens, which could be characterized as biofilms.
“This study has been successful in providing a platform for future studies to build upon and expand to study additional parameters and statistical tools to give further insight into additional driving forces behind adherence and means for improvement of material design,” Dr. Garcia concluded.
Dr. Christopher T. Born, head of the Diane N. Weiss Center for Orthopedic Trauma Research at Rhode Island Hospital, was the study’s principal investigator. The study was supported by Stryker Corp.*
*Correction, 9/19/2015: Dr. Born is a consultant for Stryker. He also has stock ownership in Biointraface, does consulting for the company, and is a member of its board.
SAN DIEGO – Rough materials used for orthopedic implants, such as cobalt chromium and titanium, increased bacterial adherence, while smoother materials such as stainless steel did not, results from an image analysis demonstrated.
“In light of these results, it is important to question why we utilize the types of materials we use for various orthopedic procedures,” Dioscaris R. Garcia, Ph.D., said in an interview in advance of the annual Interscience Conference on Antimicrobial Agents and Chemotherapy. “There was no one-size-fits-all material to minimize adherence per the findings of this study, but the findings may suggest that having a smoother surface may minimize the ability of bacterial pathogens to adhere to the surface.”
He characterized the topic of bacterial adherence to orthopedic implants as “an issue of great interest due to how little is known about the biological implications of the materials utilized. The most researched of these materials is titanium, which is touted for its biocompatibility. This study aims to provide a base and a glimpse into how the most commonly utilized orthopedic-relevant materials interact with some of the most commonly encountered pathogens.”
For the study, Dr. Garcia, a molecular pharmacologist at Rhode Island Hospital in Providence, Dr. Alan H. Daniels, an orthopedic surgeon at the hospital, and their associates used scanning electron microscopy and confocal laser scanning microscopy to evaluate the adherence pattern, density, and propagation of six commonly encountered bacterial pathogens (methicillin-sensitive Staphylococcus aureus, methicillin-resistant S. aureus, coagulase-negative Staphylococcus epidermidis, multidrug-resistant Acinetobacter baumannii, Propionibacterium acnes, and vancomycin-resistant Enterococcus faecalis) on five commonly used spinal implant materials (titanium, titanium alloy, stainless steel, cobalt chromium, and polyetherether ketone). The samples were fixed and dehydrated via ethanol dehydration gradient and critical point drying.
The researchers found that some pathogens, such as vancomycin-resistant E. faecalis and multidrug-resistant A. baumannii, were more likely to adhere to more textured materials such as cobalt chromium and titanium, compared with smoother materials such as stainless steel. “Additionally, the findings suggest that the microtopography of these materials may be the driving force behind the adherence of pathogens on the materials themselves,” Dr. Garcia said. Compared with smoother, polished materials, he explained, the rougher materials were more likely to harbor dense proliferation of bacterial pathogens, which could be characterized as biofilms.
“This study has been successful in providing a platform for future studies to build upon and expand to study additional parameters and statistical tools to give further insight into additional driving forces behind adherence and means for improvement of material design,” Dr. Garcia concluded.
Dr. Christopher T. Born, head of the Diane N. Weiss Center for Orthopedic Trauma Research at Rhode Island Hospital, was the study’s principal investigator. The study was supported by Stryker Corp.*
*Correction, 9/19/2015: Dr. Born is a consultant for Stryker. He also has stock ownership in Biointraface, does consulting for the company, and is a member of its board.
SAN DIEGO – Rough materials used for orthopedic implants, such as cobalt chromium and titanium, increased bacterial adherence, while smoother materials such as stainless steel did not, results from an image analysis demonstrated.
“In light of these results, it is important to question why we utilize the types of materials we use for various orthopedic procedures,” Dioscaris R. Garcia, Ph.D., said in an interview in advance of the annual Interscience Conference on Antimicrobial Agents and Chemotherapy. “There was no one-size-fits-all material to minimize adherence per the findings of this study, but the findings may suggest that having a smoother surface may minimize the ability of bacterial pathogens to adhere to the surface.”
He characterized the topic of bacterial adherence to orthopedic implants as “an issue of great interest due to how little is known about the biological implications of the materials utilized. The most researched of these materials is titanium, which is touted for its biocompatibility. This study aims to provide a base and a glimpse into how the most commonly utilized orthopedic-relevant materials interact with some of the most commonly encountered pathogens.”
For the study, Dr. Garcia, a molecular pharmacologist at Rhode Island Hospital in Providence, Dr. Alan H. Daniels, an orthopedic surgeon at the hospital, and their associates used scanning electron microscopy and confocal laser scanning microscopy to evaluate the adherence pattern, density, and propagation of six commonly encountered bacterial pathogens (methicillin-sensitive Staphylococcus aureus, methicillin-resistant S. aureus, coagulase-negative Staphylococcus epidermidis, multidrug-resistant Acinetobacter baumannii, Propionibacterium acnes, and vancomycin-resistant Enterococcus faecalis) on five commonly used spinal implant materials (titanium, titanium alloy, stainless steel, cobalt chromium, and polyetherether ketone). The samples were fixed and dehydrated via ethanol dehydration gradient and critical point drying.
The researchers found that some pathogens, such as vancomycin-resistant E. faecalis and multidrug-resistant A. baumannii, were more likely to adhere to more textured materials such as cobalt chromium and titanium, compared with smoother materials such as stainless steel. “Additionally, the findings suggest that the microtopography of these materials may be the driving force behind the adherence of pathogens on the materials themselves,” Dr. Garcia said. Compared with smoother, polished materials, he explained, the rougher materials were more likely to harbor dense proliferation of bacterial pathogens, which could be characterized as biofilms.
“This study has been successful in providing a platform for future studies to build upon and expand to study additional parameters and statistical tools to give further insight into additional driving forces behind adherence and means for improvement of material design,” Dr. Garcia concluded.
Dr. Christopher T. Born, head of the Diane N. Weiss Center for Orthopedic Trauma Research at Rhode Island Hospital, was the study’s principal investigator. The study was supported by Stryker Corp.*
*Correction, 9/19/2015: Dr. Born is a consultant for Stryker. He also has stock ownership in Biointraface, does consulting for the company, and is a member of its board.
AT ICAAC 2015
Key clinical point: Orthopedic implants made from smoother material may minimize bacterial adherence.
Major finding: Some pathogens, such as vancomycin-resistant Enterococcus faecalis and multidrug-resistant Acinetobacter baumannii, were more likely to adhere to more textured materials like cobalt chromium and titanium, compared with smoother materials such as stainless steel.
Data source: A study that used scanning electron microscopy and confocal laser scanning microscopy to evaluate the adherence pattern, density, and propagation of six commonly encountered bacterial pathogens on five commonly used spinal implant materials.
Disclosures: The study was supported by Stryker Corp. Dr. Born is a consultant for Stryker. He also has stock ownership in Biointraface, does consulting for the company, and is a member of its board.*

Complementary and Alternative Medicine for Chronic Musculoskeletal Pain
Musculoskeletal pain affects one-quarter of the adult population and is the most common reason for self-medication and for seeking health care.1-3 It is also cited as the most common reason for the use of complementary and alternative medicine (CAM), and the lower back, head, neck, and knee are the most commonly reported areas of pain.4-8 In 2007, the estimated annual cost of managing chronic pain, adjusted for inflation, ranged from $560 to $635 billion; whereas the direct out-of-pocket cost for patients with back pain was $34 billion.9 Chronic pain persists beyond the usual course of disease or healing; generally about 3 months or longer.10-12 The most common forms of pain include those associated with musculoskeletal disorders, such as degenerative arthritis, rheumatoid arthritis, osteoarthritis, myofascial pain, chronic headache, low back pain, and bone pain.11,13-15
A large number of returning Operation Iraqi Freedom (OIF) and Operation Enduring Freedom (OEF) veterans have reported chronic pain symptoms, with back and head being the most common pain locations.7 They experienced pain related to wearing heavy gear every day, being transported in armored vehicles over crater-ridden roads, and enduring less than optimal sleeping conditions.16 Studies have found a significant number of subjects in this population who reported using CAM therapy. The OIF/OEF veterans were likely to have outpatient visits for musculoskeletal system disorders and to use CAM as an additional tool in pain management—not as a reaction to perceived inadequacies of conventional care.17,18
Complementary and alternative medicine is often used to describe various substances, procedures, and approaches outside of mainstream, Western, or conventional medicine for health promotion, treating injuries, symptoms, and illnesses.18,19 Although complementary and alternative are often used interchangeably, the 2 terms refer to different concepts. Complementary refers to the use of a nonmainstream approach with conventional medicine, whereas alternative refers to the use of a nonmainstream approach instead of conventional medicine.19 About 40% of Americans use CAM for various reasons.19
The services and self-care forms of CAM account for a large portion of out-of-pocket costs; patients are willing to pay for it themselves. In 2007, the U.S. spent $33.9 billion on out-of-pocket expenses for CAM classes, products, materials, and visits to CAM providers.20 The costs are comparable with those of conventional health care services and prescription drug use.20 One national study concluded that many patients use CAM in accordance with their beliefs, values, and philosophy concerning health and life.21 Other studies found that many patients use CAM not only because of functional status, pain severity, or self-efficacy, but also because they perceive significant benefits in pain relief.6,17,22-25 Some authors reported that CAM is used to augment and not replace conventional medicine and that it has now become part of the accepted armamentarium for managing chronic musculoskeletal pain.6,17,25
The National Center for Complementary and Alternative Medicine at the National Institutes of Health (NIH) classifies CAM in 2 ways: (1) Mind and body practices, such as acupuncture, massage therapy, meditation, movement therapies, relaxation techniques, spinal manipulation, tai chi and qi gong, yoga, healing touch, and hypnotherapy; and (2) natural products, including probiotics, herbs, and vitamins and minerals usually sold as dietary supplements.19 These products are regulated by the FDA but not as drugs. They have a different set of regulations under the Dietary Supplement Health and Education Act of 1994.26
Mind and body practices or provider-based CAM therapies such as chiropractic care, acupuncture, and massage increased significantly between 2002 and 2007, and many more patients may be willing to try these therapies for chronic low back pain if they do not have to pay out of pocket.27,28 Multiple studies have also found that these treatments in addition to herbal medicine are the most commonly reported CAM treatments used for pain relief in adults.3,17,22,23
Other commonly reported CAM therapies are garlic preparations, exercise, and yoga and meditation.22,23 A large number of veterans have reported previous use or willingness to try chiropractic care, massage therapy, herbal medicines, and acupuncture for chronic noncancer pain.17 In addition to acute care with conventional treatment, the VHA has now expanded services to allow for CAM as available treatment options for chronic musculoskeletal pain.29 The majority of VHA facilities also provide and refer patients to CAM service providers.30
This review article explores the evidence supporting the use of the most commonly reported CAM therapies; specifically acupuncture, massage therapy, and spinal manipulation for musculoskeletal pain relief. Because of the plethora of herbs and dietary supplements in the literature, these were not included in this review, although they are also reported among the most commonly used CAM therapies.1,23,31 The investigators sought to examine the effectiveness of acupuncture, spinal manipulation, or massage compared with no treatment, sham therapy, or current noninvasive first-line treatment for chronic musculoskeletal pain.
Study Selection
To find research addressing this question, the authors searched the PubMed, MEDLINE, and Cumulative Index to Nursing and Allied Health Literature (CINAHL) databases and the Cochrane Library for all relevant studies published between October 31, 2003, and October 31, 2013. The combined search from all sources for randomized controlled trials (RCTs) resulted in 1,157 studies with acupuncture and chronic pain, 343 studies with spinal manipulation and chronic pain, and 416 studies with massage and chronic pain. Acupuncture and chronic musculoskeletal pain yielded 94 studies, spinal manipulation and chronic musculoskeletal pain yielded 29 studies, and massage and chronic musculoskeletal pain yielded 55 RCTs.
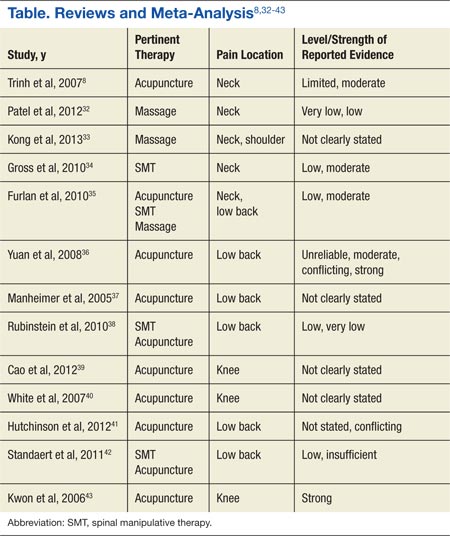
Targeted searches were then conducted within the results for systematic reviews and meta-analysis of relevant studies of RCTs, focus on adults with any type of musculoskeletal pain, written in English, and had pain level or level of pain-related improvement as its primary outcome. The results were assessed for relevance to the review based on the information provided in the title, abstract, and the National Library of Medicine Medical Subject Headings. References of the search results were also searched manually for additional studies relevant to the review. Duplicated studies and those that looked at only acute or cancer pain were excluded. Thirteen systematic reviews and meta-analyses met the inclusion criteria (Table). The investigators reviewed the full reports and agreed to use the data that were abstracted from the studies.
Study Parameters
Four different categories of outcome measuring points for posttreatment follow-up are reported in the CAM studies: immediate, short-term, intermediate, and long-term. There are inconsistencies across studies for the timing of these 4 categories. Immediate posttreatment is defined as up to 1 day.8,32-34 The duration for the short-term follow-up period is defined as between 1 day and 3 months8,32,33; ≤ 3 months35,36; closest to 3 weeks37; closest to 4 weeks34; 1 month38; closest to 8 weeks, but < 3 months after randomization39; or up to 25 weeks, but nearest to 12 weeks.40Intermediate follow-up is between 3 months and 1 year8,33,35; between 3 and 6 months38; ≥ 3 months, but < 1 year36; or closest to 6 months.34Long term is defined as >12 months8,35; closest to 6 months37; 12 months38; 1 year or more36; closest to 6 months, but >3 months after randomization34,39; or between 26 weeks and 56 weeks.40
Pain intensity and pain relief was the treatment efficacy outcome for all the studies. A variety of measuring tools were reported across studies. Eight of the 13 studies reported measurement of pain intensity using the visual analog scale (VAS).8,33,35-37,41-43 In addition to the VAS, 2 studies also used the numerical rating scale (NRS).8,36 One study used the NRS alone.38 Other studies used the McGill Pain Questionnaire35; the SF-36 bodily pain dimension, Von Korff chronic pain grading scale, or low back pain rating scale36; or the Western Ontario and McMaster Universities Osteoarthritis Index subscale for pain.39,40,43
Authors from 8 of the systematic reviews and meta-analysis reported levels of evidence, or GRADE (Grades of Recommendation, Assessment, Development, and Evaluation), used to evaluate the overall quality of the evidence and the strength of the recommendations.8,32,34-36,38,42,43 Levels of evidence were based on RCTs. The various levels were (1) “strong evidence,” consistent findings in multiple high-quality RCTs; (2) “moderate evidence,” consistent findings among multiple high-quality RTCs and/or 1 high-quality RCT; (3) “limited evidence,” low-quality RCT; (4) “conflicting evidence,” inconsistent findings among multiple RCTs; and (5) “no evidence,” no RCTs or no studies.8,36
Most studies expressed the overall strength of the body of literature in 6 different categories: (1) “high quality,” confidence that the evidence reflected the true effect and that further research is very unlikely to change confidence in the effect of size; (2) “moderate quality,” further research is likely to have an impact on confidence in the estimate of effect and may change the estimate; (3) “low quality,” further research is very likely to have an important impact on confidence in the estimate of effect and is likely to change it; (4) “very low quality,” great uncertainty about the estimate; (5) “insufficient evidence,” either the evidence is unavailable or does not allow for a conclusion; and (6)“no evidence,” no evidence from RTCs.32,34,35,38,42,43 Kwon and colleagues reported using a modified jaded score where a total of 5 points was awarded if a study was described as randomized, used an appropriate method, if subjects were blinded to the intervention, if the evaluator was blinded to the intervention, and if there was a description of withdrawals and dropouts.43
Acupuncture
About 3 million American adults receive acupuncture each year.44 The most commonly reported reason for its use is chronic pain.44,45 Trials that examined the characteristics of those seeking and using acupuncture as adjunct to conventional treatment have found that patients who experienced positive outcomes, such as improvement in pain subscale, included females, previous failure of other therapies, and prior positive acupuncture encounters.46
Six of the studies in this review examined the evidence of acupuncture for chronic low back pain.35-38,41,42 Two of those studies found moderate evidence that acupuncture was more effective than no treatment for short-term pain relief.35,36 Manheimer and colleagues found it to be significantly more effective than no additional treatment or sham treatment for short-term pain relief.37 They however, reported a lack of evidence to suggest that it was more effective than were other active therapies.37 Hutchinson and colleagues did not differentiate among data points for intermediate, short-term, or long-term follow-up in their study.41 However, they concluded that there was some evidence to support acupuncture as more effective than no treatment and conflicting evidence of its effectiveness over other treatment modalities. Different levels of evidence were reported for intermediate pain relief with 2 of the other studies. One study found that the evidence was limited.35 The other study reported conflicting evidence that it was more effective than no treatment for immediate pain relief for those with chronic low back pain.36
Rubinstein and colleagues reported low- to very-low-quality evidence that acupuncture provided a short-term clinically relevant effect compared with waiting list control or when it was added to another intervention for chronic low back pain.38 Standaert and colleagues concluded that there was insufficient evidence to determine the relative effectiveness of acupuncture compared with either exercise or spinal manipulative therapy (SMT) in relieving chronic low back pain.42 Yuan and colleagues reported strong evidence that acupuncture combined with conventional therapy was more effective than conventional therapy alone.36
Furlan and colleagues found moderate evidence for significant improvement in pain intensity compared with subjects in physical therapy or usual care groups at short-term or immediate follow-up for chronic back pain.35 Studies that evaluated the efficacy of acupuncture for knee osteoarthritis compared acupuncture with sham acupuncture controls or no additional treatment and found that acupuncture was significantly better at relieving knee pain.39,40,43 Cao and colleagues found it to be effective both in the short term and long term.39 White and colleagues and Kwon and colleagues were unable to draw a conclusion concerning long-term effects due to the data point included in the study or the heterogeneity in the results.40,43
Trinh and colleagues reported moderate evidence that acupuncture is more effective for relief of chronic neck pain compared with inactive, sham treatments at immediate posttreatment.8 They also found moderate evidence that acupuncture was more effective than some other types of sham controls immediately posttreatment and limited evidence that it was more effective than massage at short-term follow-up.8 Furlan and colleagues found trials that applied sham acupuncture tended to produce nonstatistically significant results.35 Their meta-analysis of 2 studies indicated no significant difference between acupuncture and sham acupuncture for immediate posttreatment pain intensity. They also reported inconsistent results for the effects of acupuncture compared with medication or with spinal manipulation for chronic neck pain.35
Massage
Massage promotes health and well-being through the use of mechanical manipulation of body tissues with rhythmic pressure and stroking.47 Treatment techniques include Hoffa massage, friction massage, connective tissue massage, transverse friction massage, and trigger point massage.48 Massage is one of the most popular CAM therapies for neck and back pain.49 In their survey, White and colleagues reported that active-duty military personnel listed massage as the most frequently used CAM therapy in the previous 12 months.18
Patel and colleagues reported that the overall methodology of the trials assessed in their study was either low- or very-low-GRADE level.32 They found very-low to low-quality evidence that there is no difference in effectiveness of 3 approaches of massage therapies (ischemic compression to upper fibre of trapezius trigger point, transverse friction massage to upper fibre of trapezius, and ischemic compression to upper fibre of trapezius) for neck muscle pain. They also reported no difference between conventional Western massage and acupuncture for generalized neck muscle pain at short-term follow-up, and no difference in pain intensity compared with other therapies such as acupuncture, manual therapy, exercise, education, and multimodal interventions. The investigators concluded that the effectiveness of massage therapy for improving neck pain remains unclear, as results could not be combined due to the wide range of techniques and comparative treatments. They were unable to make any firm statement to guide clinical practice.32
Two other studies compared massage to no treatment and found it significantly improved chronic neck pain immediately after the end of treatment.33,35 Kong and colleagues also found similar effects for shoulder pain at immediate and short-term
follow-up but not for neck or shoulder pain when massage was compared with active therapies.33 Furlan and colleagues’ meta-analysis found that massage compared with relaxation or physical therapy was significantly better at reducing chronic nonspecific low back pain immediately after treatment.35
Spinal Manipultaion
Spinal manipulation is high-velocity and low-amplitude localized force directed at specific spinal segments.34 It is performed by using the hands or a device to apply a controlled force to a joint of the spine and is practiced by osteopathic physicians, naturopathic physicians, chiropractors, physical therapists, and some medical doctors.19
In a study to assess its effectiveness, Rubinstein and colleagues found low-quality evidence to very-low-quality evidence to suggest that SMT does not provide a more clinically beneficial effect compared with sham, passive modalities, or other interventions for the relief of chronic low back pain.38 Comparative interventions included usual medical care, physical therapy, exercise, physiotherapy, and multimodal treatments. Standaert and colleagues also found no difference between motor control exercise and SMT in pain relief.42 They concluded that although the evidence is low, there is an indication that structured exercise and SMT seem to offer equivalent benefits in terms of pain for those with chronic lower back pain with clinical benefits evident within 8 weeks of care.42
Gross and colleagues found that when cervical manipulation was compared with control for chronic mechanical neck pain, there was moderate-quality evidence for similar effects at short-term and intermediate follow-up.34 They also reported low-quality evidence in support of thoracic manipulation alone or in combination with electrothermal or individualized physiotherapy and suggested cervical manipulation may provide short-term but not long-term pain relief.34 Furlan and colleagues reported moderate-quality evidence that spinal manipulation provided significantly better posttreatment neck pain relief compared with placebo.35 They also found low evidence that it was significantly better than placebo, acupuncture, and pain medication at immediate follow-up.35
Conclusion
Considerable effort was made to retrieve all studies; however, the authors cannot be certain that the review was exhaustive. They also relied on other analyses of primary studies for the conclusion.
The 3 types of musculoskeletal pain in the review were low back, neck, and knee pain related to osteoarthritis. The authors found that the most common CAM modality studied for chronic musculoskeletal pain was acupuncture. Studies on massage therapy and SMT that were relevant to the review were limited.
Two studies reported strong level of evidence for acupuncture.36,40 One study reported that acupuncture was superior to no treatment or to sham acupuncture for relief of chronic knee pain.40 The other study reported that acupuncture was more effective than conventional therapy alone when it was combined with conventional therapy for chronic low back pain, but there was no difference when compared with sham acupuncture for short-term pain relief.36 The strength of the evidence for acupuncture combined with conventional treatment for low back pain was conflicting. One other review found low evidence for its benefit. Similar to Hopton and MacPherson, this review found that acupuncture treatment seemed to provide effective short-term relief of chronic low back pain.14 Evidence would also seem to support acupuncture for the short-term relief of chronic neck pain and knee pain associated with osteoarthritis.
This review also found immediate and short-term benefits, although mostly with weak evidence, for the use of SMT in the treatment of chronic neck and low back pain. There was conflicting evidence for the support of massage therapy. Furlan and colleagues, however, found that acupuncture, SMT, and massage treatments were significantly more efficacious than no treatment, placebo, physical therapy, or usual care in reducing pain immediately or at short-term after treatment.35 Inconsistencies may be related to the methodologic and clinical diversity of RCTs, which limit the extent of quantitative synthesis and complicates result interpretation.35 Also, better conclusions could be drawn if future studies use head-to-head comparisons of CAM treatments and trials comparing CAM to widely used active treatments that report on all clinically relevant outcomes.35
Although the relationship between conventional treatment and the world of CAM remains equivocal, review of the evidence suggests acupuncture and SMT may be effective treatment for various chronic painful musculoskeletal conditions.35,44,50,51 These CAM modalities are reasonable referral options to supplement conventional therapy for the treatment of chronic musculoskeletal pain when conventional therapy has not yielded satisfactory results.
Author disclosures
The authors report no actual or potential conflicts of interest with regard to this article.
Disclaimer
The opinions expressed herein are those of the authors and do not necessarily reflect those of Federal Practitioner, Frontline Medical Communications Inc., the U.S. Government, or any of its agencies. This article may discuss unlabeled or investigational use of certain drugs. Please review the complete prescribing information for specific drugs or drug combinations—including indications, contraindications, warnings, and adverse effects—before administering pharmacologic therapy to patients.
1. Callahan LF, Wiley-Exley EK, Mielenz TJ, et al. Use of complementary and alternative medicine among patients with arthritis. Prev Chronic Dis. 2009;6(2):A44.
2. Walsh NE, Brooks P, Hazes JM, et al; Bone and Joint Decade Task Force for Standards of Care for Acute and Chronic Musculoskeletal Pain. Standards of care for acute and chronic musculoskeletal pain: the Bone and Joint Decade (2000-2010). Arch Phys Med Rehabil. 2008;89(9):1830-1845.
3. Williamson AT, Fletcher PC, Dawson KA. Complementary and alternative medicine. Use in an older population. J Gerontol Nurs. 2003;29(5):20-28.
4. Artus M, Croft P, Lewis M. The use of CAM and conventional treatments among primary care consulters with chronic musculoskeletal pain. BMC Fam Pract. 2007;8:26.
5. Cherkin DC, Sherman KJ, Kahn J, et al. A comparison of the effects of 2 types of massage and usual care on chronic low back pain: a randomized controlled trial. Ann Intern Med. 2011;155(1):1-9.
6. Fleming S, Rabago DP, Mundt MP, Fleming MF. CAM therapies among primary care patients using opioid therapy for chronic pain. BMC Complement Altern Med. 2007;7:15.
7. Lew HL, Otis JD, Tun C, Kerns RD, Clark ME, Cifu DX. Prevalence of chronic pain, posttraumatic stress disorder, and persistent post concussive symptoms in OIF/OEF veterans: polytrauma clinical triad. J Rehabil Res Dev. 2009;46(6):697-702.
8. Trinh K, Graham N, Gross A, et al. Acupuncture for neck disorders. Spine (Phila PA 1976). 2007;32(2):236-243.
9. Gaskin DJ, Richard P. Appendix C: The economic costs of pain in the United States. In: Institute of Medicine (US) Committee on Advancing Pain Research, Care, and Education. Relieving Pain in America: A Blueprint for Transforming Prevention, Care, Education, and Research. Washington, DC: National Academies Press; 2011. National Center for Biotechnology Information Website. http://www. ncbi.nlm.nih.gov/books/NBK92521. Accessed July 31, 2015.
10. American Academy of Pain Medicine. AAPM facts and figures on pain. American Academy of Pain Medicine Website. http://www.painmed.org/files/facts-and-figures-on-pain.pdf. Accessed July 31, 2015.
11. Rosenquist RW, Vrooman MD. Chronic pain management. In: Butterworth JF, Mackey DC, Wasnick JD, eds. Morgan & Mikhail’s Clinical Anesthesiology. 5th ed. New York, NY: McGraw-Hill; 2013:chap 47.
12. Rasu RS, Sohraby R, Cunningham L, Knell ME. Assessing chronic pain treatment practices and evaluating adherence to chronic pain clinical guidelines in outpatient practices in the United States. J Pain. 2013;14(6):568-578.
13. Gureje O, Von Korff M, Simon, GE, Grater R. Persistent pain and well-being: a World Health Organization study in primary care. JAMA. 1998;280(2):147-151.
14. Hopton A, MacPherson H. Acupuncture for chronic pain: is acupuncture more than an effective placebo? A systematic review of pooled data from meta-analyses. Pain Pract. 2010;10(2):94-102.
15. Kumar N. WHO Normative guidelines on pain management. World Health Organization Website. http://www.who.int/medicines/areas/quality_safety/delphi_study_pain_guidelines.pdf. Published June 2007. Accessed August 3, 2015.
16. Koffman RL. Downrange acupuncture. Med Acupunct. 2011;23(4):215-218.
17. Denneson LM, Corson K, Dobscha SK. Complementary and alternative medicine use among veterans with chronic noncancer pain. J Rehabil Res Dev. 2011;(48)9:1119-1128.
18. White MR, Jacobson IG, Smith B, et al; Millennium Cohort Study Team. Health care utilization among complementary and alternative medicine users in a large military cohort. BMC Complement Alternat Med. 2011;11:27.
19. U.S. Department of Health and Human Services, National Institutes of Health, National Center for Complementary and Alternative Medicine. Complementary, alternative, or integrative health: What’s in a name? National Center for Complementary and Alternative Medicine Website. http://nccam.nih.gov/health/whatiscam. Updated March 2015. Modified July 8, 2015. Accessed August 4, 2015.
20. Nahin RL, Barnes PM, Stussman BJ, Bloom B. Costs of complementary and alternative medicine (CAM) and frequency of visits to CAM practitioners: United States, 2007. Natl Health Stat Report. 2009;30(18):1-14.
21. Astin JA. Why patients use alternative medicine: results of a national study. JAMA. 1998;279(19):1548-1553.
22. Rosenberg EI, Genao I, Chen I, et al. Complementary and alternative medicine use in primary care patients with chronic pain. Pain Med. 2008;9(8):1065-1072.
23. Alaaeddine N, Okais J, Ballane L, Baddoura RM. Use of complementary and alternative therapy among patients with rheumatoid arthritis and osteoarthritis. J Clin Nurs. 2012;21(21-22):3198-3204.
24. Tan MG, Win MT, Khan SA. The use of complementary and alternative medicine in chronic pain patients in Singapore: a single-centre study. Ann Acad Med Singapore. 2013;42(3):133-137.
25. White P. A background to acupuncture and its use in chronic painful musculoskeletal conditions. J R Soc Promot Health. 2006;126(5):219-227.
26. U.S. Department of Health and Human Services, National Institutes of Health, Office of Dietary Supplements. Dietary Supplement Health and Education Act of 1994. National Institutes of Health Website. http://ods.od.nih.gov/About/DSHEA_Wording.aspx. Published October 25, 1994. Accessed August 4, 2015.
27. Su D, Li L. Trends in the use of complementary and alternative medicine in the United States: 2002-2007. J Health Care Poor Underserved. 2011;22(1):296-310.
28. Sherman KJ, Cherkin DC, Connelly MT, et al. Complementary and alternative medical therapies for chronic low back pain: what treatments are patients willing to try? BMC Complement Alternat Med. 2004;4:9.
29. Smeeding SJ, Bradshaw DH, Kumpfer KL, Trevithick S, Stoddard GJ. Outcome evaluation of the Veterans Affairs Salt Lake City Integrative Health Clinic for Chronic Nonmalignant Pain. Clin J Pain. 2011;27(2):146-155.
30. U.S. Department of Veterans Affairs, Veterans Health Administration, Office of the Assistant Deputy Under Secretary for Health for Policy and Planning. 2011 complementary and alternative medicine. U.S. Department of Veterans Affairs Office of Research and Development Website. http://www.research.va.gov/research_topics/2011cam_finalreport.pdf. Published September 2011. Accessed August 4, 2015.
31. Unsal A, Gözüm S. Use of complementary and alternative medicine by patients with arthritis. J Clin Nurs. 2010;19(7-8):1129-1138.
32. Patel KC, Gross A, Graham N, et al. Massage for mechanical neck disorder. Cochrane Database Syst Rev. 2012;9:CD004871.
33. Kong LJ, Zhan HS, Cheng YW, Yuan WA, Chen B, Fang M. Massage therapy for neck and shoulder pain: a systematic review and meta-analysis. Evid Based Complement Alternat Med. 2013;2013:613279.
34. Gross A, Miller J, D’Sylva J, et al; COG. Manipulation or mobilisation for neck pain: a Cochrane review. Man Ther. 2010;15(4):315-333.
35. Furlan A, Yazdi F, Tsertsvadze A, et al. Complementary and alternative therapies for back Pain II. Evidence report/technology assessment No. 194. (Prepared by the University of Ottawa Evidence-based Practice Center under Contract No. 290-2007-10059-I (EPCIII). AHRQ Publication No. 10(11)E007. Rockville, MD: Agency for Healthcare Research and Quality; 2010.
36. Yuan J, Purepong N, Kerr DP, Park J, Bradbury I, McDonough S. Effectiveness of acupuncture for low back pain. Spine (Phila PA 1976). 2008;33(23):E887-E900.
37. Manheimer E, White A, Berman B, Forys K, Ernst E. Meta-analysis: acupuncture for low back pain. Ann Intern Med. 2005;142(8):651-663.
38. Rubinstein SM, van Middelkoop M, Kuijpers T, et al. A systematic review on the effectiveness of complementary and alternative medicine for chronic non-specific low-back pain. Eur Spine J. 2010;19(8):1213-1228.
39. Cao L, Zhang XL, Gao YS, Jiang Y. Needle acupuncture for osteoarthritis of the knee. A systematic review and updated meta-analysis. Saudi Med J. 2012;33(5):526-532.
40. White A, Foster NE, Cummings M, Barlas P. Acupuncture treatment for chronic knee pain: a systematic review. Rheumatology (Oxford). 2007;46(3):384-390.
41. Hutchinson AJ, Ball S, Andrews JC, Jones GG. The effectiveness of acupuncture in treating chronic non-specific low back pain: a systematic review of the literature. J Orthop Surg Res. 2012;7:36.
42. Standaert, CJ, Friedly J, Erwin MW, et al. Comparative effectiveness of exercise, acupuncture, and spinal manipulation for low back pain. Spine (Phila PA 1976). 2011;36(21 suppl):S120-S130.
43. Kwon YD, Pittler MH, Ernst E. Acupuncture for peripheral joint osteoarthritis: a systematic review and meta-analysis. Rheumatology (Oxford). 2006;45(11):1331-1337.
44. Vickers AJ, Cronin AM, Maschino AC, et al; Acupuncture Trialists’ Collaboration. Individual patient data meta-analysis of acupuncture for chronic pain: protocol of the Acupuncture Trialists’ Collaboration. Trials. 2010;11:90.
45. Kelly RB. Acupuncture for pain. Am Fam Physician. 2009;80(5):481-484.
46. Witt CM, Schützler L, Lüdtke R, Wegscheider K, Willich SN. Patient characteristics and variation in treatment outcomes: which patients benefit most from acupuncture for chronic pain? Clin J Pain. 2011;27(6):550-555.
47. Cafarelli E, Flint F. The role of massage in preparation for and recovery from exercise: an overview. Sports Med. 1992;14(1):1-9.
48. Prentice WE. Therapeutic massage. In: Prentice WE. Therapeutic Modalities in Rehabilitation. 4th ed. New York, NY: McGraw-Hill; 2011:chap 16.
49. Wolsko PM, Eisenberg DM, Davis RB, Kessler R, Phillips RS. Patterns and perceptions of care for treatment of back and neck pain: results of a national survey. Spine (Phila PA 1976). 2003;28(3):292-297.
50. Perlman AI, Sabina A, Williams AL, Njike VY, Katz DL. Massage therapy for osteoarthritis of the knee: a randomized controlled trial. Arch Intern Med. 2006;166(22):2533-2538.
51. Tsao JCI. Effectiveness of massage therapy for chronic, non-malignant pain: a review. Evid Based Complement Alternat Med. 2007;4(2):165-179.
Musculoskeletal pain affects one-quarter of the adult population and is the most common reason for self-medication and for seeking health care.1-3 It is also cited as the most common reason for the use of complementary and alternative medicine (CAM), and the lower back, head, neck, and knee are the most commonly reported areas of pain.4-8 In 2007, the estimated annual cost of managing chronic pain, adjusted for inflation, ranged from $560 to $635 billion; whereas the direct out-of-pocket cost for patients with back pain was $34 billion.9 Chronic pain persists beyond the usual course of disease or healing; generally about 3 months or longer.10-12 The most common forms of pain include those associated with musculoskeletal disorders, such as degenerative arthritis, rheumatoid arthritis, osteoarthritis, myofascial pain, chronic headache, low back pain, and bone pain.11,13-15
A large number of returning Operation Iraqi Freedom (OIF) and Operation Enduring Freedom (OEF) veterans have reported chronic pain symptoms, with back and head being the most common pain locations.7 They experienced pain related to wearing heavy gear every day, being transported in armored vehicles over crater-ridden roads, and enduring less than optimal sleeping conditions.16 Studies have found a significant number of subjects in this population who reported using CAM therapy. The OIF/OEF veterans were likely to have outpatient visits for musculoskeletal system disorders and to use CAM as an additional tool in pain management—not as a reaction to perceived inadequacies of conventional care.17,18
Complementary and alternative medicine is often used to describe various substances, procedures, and approaches outside of mainstream, Western, or conventional medicine for health promotion, treating injuries, symptoms, and illnesses.18,19 Although complementary and alternative are often used interchangeably, the 2 terms refer to different concepts. Complementary refers to the use of a nonmainstream approach with conventional medicine, whereas alternative refers to the use of a nonmainstream approach instead of conventional medicine.19 About 40% of Americans use CAM for various reasons.19
The services and self-care forms of CAM account for a large portion of out-of-pocket costs; patients are willing to pay for it themselves. In 2007, the U.S. spent $33.9 billion on out-of-pocket expenses for CAM classes, products, materials, and visits to CAM providers.20 The costs are comparable with those of conventional health care services and prescription drug use.20 One national study concluded that many patients use CAM in accordance with their beliefs, values, and philosophy concerning health and life.21 Other studies found that many patients use CAM not only because of functional status, pain severity, or self-efficacy, but also because they perceive significant benefits in pain relief.6,17,22-25 Some authors reported that CAM is used to augment and not replace conventional medicine and that it has now become part of the accepted armamentarium for managing chronic musculoskeletal pain.6,17,25
The National Center for Complementary and Alternative Medicine at the National Institutes of Health (NIH) classifies CAM in 2 ways: (1) Mind and body practices, such as acupuncture, massage therapy, meditation, movement therapies, relaxation techniques, spinal manipulation, tai chi and qi gong, yoga, healing touch, and hypnotherapy; and (2) natural products, including probiotics, herbs, and vitamins and minerals usually sold as dietary supplements.19 These products are regulated by the FDA but not as drugs. They have a different set of regulations under the Dietary Supplement Health and Education Act of 1994.26
Mind and body practices or provider-based CAM therapies such as chiropractic care, acupuncture, and massage increased significantly between 2002 and 2007, and many more patients may be willing to try these therapies for chronic low back pain if they do not have to pay out of pocket.27,28 Multiple studies have also found that these treatments in addition to herbal medicine are the most commonly reported CAM treatments used for pain relief in adults.3,17,22,23
Other commonly reported CAM therapies are garlic preparations, exercise, and yoga and meditation.22,23 A large number of veterans have reported previous use or willingness to try chiropractic care, massage therapy, herbal medicines, and acupuncture for chronic noncancer pain.17 In addition to acute care with conventional treatment, the VHA has now expanded services to allow for CAM as available treatment options for chronic musculoskeletal pain.29 The majority of VHA facilities also provide and refer patients to CAM service providers.30
This review article explores the evidence supporting the use of the most commonly reported CAM therapies; specifically acupuncture, massage therapy, and spinal manipulation for musculoskeletal pain relief. Because of the plethora of herbs and dietary supplements in the literature, these were not included in this review, although they are also reported among the most commonly used CAM therapies.1,23,31 The investigators sought to examine the effectiveness of acupuncture, spinal manipulation, or massage compared with no treatment, sham therapy, or current noninvasive first-line treatment for chronic musculoskeletal pain.
Study Selection
To find research addressing this question, the authors searched the PubMed, MEDLINE, and Cumulative Index to Nursing and Allied Health Literature (CINAHL) databases and the Cochrane Library for all relevant studies published between October 31, 2003, and October 31, 2013. The combined search from all sources for randomized controlled trials (RCTs) resulted in 1,157 studies with acupuncture and chronic pain, 343 studies with spinal manipulation and chronic pain, and 416 studies with massage and chronic pain. Acupuncture and chronic musculoskeletal pain yielded 94 studies, spinal manipulation and chronic musculoskeletal pain yielded 29 studies, and massage and chronic musculoskeletal pain yielded 55 RCTs.
Targeted searches were then conducted within the results for systematic reviews and meta-analysis of relevant studies of RCTs, focus on adults with any type of musculoskeletal pain, written in English, and had pain level or level of pain-related improvement as its primary outcome. The results were assessed for relevance to the review based on the information provided in the title, abstract, and the National Library of Medicine Medical Subject Headings. References of the search results were also searched manually for additional studies relevant to the review. Duplicated studies and those that looked at only acute or cancer pain were excluded. Thirteen systematic reviews and meta-analyses met the inclusion criteria (Table). The investigators reviewed the full reports and agreed to use the data that were abstracted from the studies.
Study Parameters
Four different categories of outcome measuring points for posttreatment follow-up are reported in the CAM studies: immediate, short-term, intermediate, and long-term. There are inconsistencies across studies for the timing of these 4 categories. Immediate posttreatment is defined as up to 1 day.8,32-34 The duration for the short-term follow-up period is defined as between 1 day and 3 months8,32,33; ≤ 3 months35,36; closest to 3 weeks37; closest to 4 weeks34; 1 month38; closest to 8 weeks, but < 3 months after randomization39; or up to 25 weeks, but nearest to 12 weeks.40Intermediate follow-up is between 3 months and 1 year8,33,35; between 3 and 6 months38; ≥ 3 months, but < 1 year36; or closest to 6 months.34Long term is defined as >12 months8,35; closest to 6 months37; 12 months38; 1 year or more36; closest to 6 months, but >3 months after randomization34,39; or between 26 weeks and 56 weeks.40
Pain intensity and pain relief was the treatment efficacy outcome for all the studies. A variety of measuring tools were reported across studies. Eight of the 13 studies reported measurement of pain intensity using the visual analog scale (VAS).8,33,35-37,41-43 In addition to the VAS, 2 studies also used the numerical rating scale (NRS).8,36 One study used the NRS alone.38 Other studies used the McGill Pain Questionnaire35; the SF-36 bodily pain dimension, Von Korff chronic pain grading scale, or low back pain rating scale36; or the Western Ontario and McMaster Universities Osteoarthritis Index subscale for pain.39,40,43
Authors from 8 of the systematic reviews and meta-analysis reported levels of evidence, or GRADE (Grades of Recommendation, Assessment, Development, and Evaluation), used to evaluate the overall quality of the evidence and the strength of the recommendations.8,32,34-36,38,42,43 Levels of evidence were based on RCTs. The various levels were (1) “strong evidence,” consistent findings in multiple high-quality RCTs; (2) “moderate evidence,” consistent findings among multiple high-quality RTCs and/or 1 high-quality RCT; (3) “limited evidence,” low-quality RCT; (4) “conflicting evidence,” inconsistent findings among multiple RCTs; and (5) “no evidence,” no RCTs or no studies.8,36
Most studies expressed the overall strength of the body of literature in 6 different categories: (1) “high quality,” confidence that the evidence reflected the true effect and that further research is very unlikely to change confidence in the effect of size; (2) “moderate quality,” further research is likely to have an impact on confidence in the estimate of effect and may change the estimate; (3) “low quality,” further research is very likely to have an important impact on confidence in the estimate of effect and is likely to change it; (4) “very low quality,” great uncertainty about the estimate; (5) “insufficient evidence,” either the evidence is unavailable or does not allow for a conclusion; and (6)“no evidence,” no evidence from RTCs.32,34,35,38,42,43 Kwon and colleagues reported using a modified jaded score where a total of 5 points was awarded if a study was described as randomized, used an appropriate method, if subjects were blinded to the intervention, if the evaluator was blinded to the intervention, and if there was a description of withdrawals and dropouts.43
Acupuncture
About 3 million American adults receive acupuncture each year.44 The most commonly reported reason for its use is chronic pain.44,45 Trials that examined the characteristics of those seeking and using acupuncture as adjunct to conventional treatment have found that patients who experienced positive outcomes, such as improvement in pain subscale, included females, previous failure of other therapies, and prior positive acupuncture encounters.46
Six of the studies in this review examined the evidence of acupuncture for chronic low back pain.35-38,41,42 Two of those studies found moderate evidence that acupuncture was more effective than no treatment for short-term pain relief.35,36 Manheimer and colleagues found it to be significantly more effective than no additional treatment or sham treatment for short-term pain relief.37 They however, reported a lack of evidence to suggest that it was more effective than were other active therapies.37 Hutchinson and colleagues did not differentiate among data points for intermediate, short-term, or long-term follow-up in their study.41 However, they concluded that there was some evidence to support acupuncture as more effective than no treatment and conflicting evidence of its effectiveness over other treatment modalities. Different levels of evidence were reported for intermediate pain relief with 2 of the other studies. One study found that the evidence was limited.35 The other study reported conflicting evidence that it was more effective than no treatment for immediate pain relief for those with chronic low back pain.36
Rubinstein and colleagues reported low- to very-low-quality evidence that acupuncture provided a short-term clinically relevant effect compared with waiting list control or when it was added to another intervention for chronic low back pain.38 Standaert and colleagues concluded that there was insufficient evidence to determine the relative effectiveness of acupuncture compared with either exercise or spinal manipulative therapy (SMT) in relieving chronic low back pain.42 Yuan and colleagues reported strong evidence that acupuncture combined with conventional therapy was more effective than conventional therapy alone.36
Furlan and colleagues found moderate evidence for significant improvement in pain intensity compared with subjects in physical therapy or usual care groups at short-term or immediate follow-up for chronic back pain.35 Studies that evaluated the efficacy of acupuncture for knee osteoarthritis compared acupuncture with sham acupuncture controls or no additional treatment and found that acupuncture was significantly better at relieving knee pain.39,40,43 Cao and colleagues found it to be effective both in the short term and long term.39 White and colleagues and Kwon and colleagues were unable to draw a conclusion concerning long-term effects due to the data point included in the study or the heterogeneity in the results.40,43
Trinh and colleagues reported moderate evidence that acupuncture is more effective for relief of chronic neck pain compared with inactive, sham treatments at immediate posttreatment.8 They also found moderate evidence that acupuncture was more effective than some other types of sham controls immediately posttreatment and limited evidence that it was more effective than massage at short-term follow-up.8 Furlan and colleagues found trials that applied sham acupuncture tended to produce nonstatistically significant results.35 Their meta-analysis of 2 studies indicated no significant difference between acupuncture and sham acupuncture for immediate posttreatment pain intensity. They also reported inconsistent results for the effects of acupuncture compared with medication or with spinal manipulation for chronic neck pain.35
Massage
Massage promotes health and well-being through the use of mechanical manipulation of body tissues with rhythmic pressure and stroking.47 Treatment techniques include Hoffa massage, friction massage, connective tissue massage, transverse friction massage, and trigger point massage.48 Massage is one of the most popular CAM therapies for neck and back pain.49 In their survey, White and colleagues reported that active-duty military personnel listed massage as the most frequently used CAM therapy in the previous 12 months.18
Patel and colleagues reported that the overall methodology of the trials assessed in their study was either low- or very-low-GRADE level.32 They found very-low to low-quality evidence that there is no difference in effectiveness of 3 approaches of massage therapies (ischemic compression to upper fibre of trapezius trigger point, transverse friction massage to upper fibre of trapezius, and ischemic compression to upper fibre of trapezius) for neck muscle pain. They also reported no difference between conventional Western massage and acupuncture for generalized neck muscle pain at short-term follow-up, and no difference in pain intensity compared with other therapies such as acupuncture, manual therapy, exercise, education, and multimodal interventions. The investigators concluded that the effectiveness of massage therapy for improving neck pain remains unclear, as results could not be combined due to the wide range of techniques and comparative treatments. They were unable to make any firm statement to guide clinical practice.32
Two other studies compared massage to no treatment and found it significantly improved chronic neck pain immediately after the end of treatment.33,35 Kong and colleagues also found similar effects for shoulder pain at immediate and short-term
follow-up but not for neck or shoulder pain when massage was compared with active therapies.33 Furlan and colleagues’ meta-analysis found that massage compared with relaxation or physical therapy was significantly better at reducing chronic nonspecific low back pain immediately after treatment.35
Spinal Manipultaion
Spinal manipulation is high-velocity and low-amplitude localized force directed at specific spinal segments.34 It is performed by using the hands or a device to apply a controlled force to a joint of the spine and is practiced by osteopathic physicians, naturopathic physicians, chiropractors, physical therapists, and some medical doctors.19
In a study to assess its effectiveness, Rubinstein and colleagues found low-quality evidence to very-low-quality evidence to suggest that SMT does not provide a more clinically beneficial effect compared with sham, passive modalities, or other interventions for the relief of chronic low back pain.38 Comparative interventions included usual medical care, physical therapy, exercise, physiotherapy, and multimodal treatments. Standaert and colleagues also found no difference between motor control exercise and SMT in pain relief.42 They concluded that although the evidence is low, there is an indication that structured exercise and SMT seem to offer equivalent benefits in terms of pain for those with chronic lower back pain with clinical benefits evident within 8 weeks of care.42
Gross and colleagues found that when cervical manipulation was compared with control for chronic mechanical neck pain, there was moderate-quality evidence for similar effects at short-term and intermediate follow-up.34 They also reported low-quality evidence in support of thoracic manipulation alone or in combination with electrothermal or individualized physiotherapy and suggested cervical manipulation may provide short-term but not long-term pain relief.34 Furlan and colleagues reported moderate-quality evidence that spinal manipulation provided significantly better posttreatment neck pain relief compared with placebo.35 They also found low evidence that it was significantly better than placebo, acupuncture, and pain medication at immediate follow-up.35
Conclusion
Considerable effort was made to retrieve all studies; however, the authors cannot be certain that the review was exhaustive. They also relied on other analyses of primary studies for the conclusion.
The 3 types of musculoskeletal pain in the review were low back, neck, and knee pain related to osteoarthritis. The authors found that the most common CAM modality studied for chronic musculoskeletal pain was acupuncture. Studies on massage therapy and SMT that were relevant to the review were limited.
Two studies reported strong level of evidence for acupuncture.36,40 One study reported that acupuncture was superior to no treatment or to sham acupuncture for relief of chronic knee pain.40 The other study reported that acupuncture was more effective than conventional therapy alone when it was combined with conventional therapy for chronic low back pain, but there was no difference when compared with sham acupuncture for short-term pain relief.36 The strength of the evidence for acupuncture combined with conventional treatment for low back pain was conflicting. One other review found low evidence for its benefit. Similar to Hopton and MacPherson, this review found that acupuncture treatment seemed to provide effective short-term relief of chronic low back pain.14 Evidence would also seem to support acupuncture for the short-term relief of chronic neck pain and knee pain associated with osteoarthritis.
This review also found immediate and short-term benefits, although mostly with weak evidence, for the use of SMT in the treatment of chronic neck and low back pain. There was conflicting evidence for the support of massage therapy. Furlan and colleagues, however, found that acupuncture, SMT, and massage treatments were significantly more efficacious than no treatment, placebo, physical therapy, or usual care in reducing pain immediately or at short-term after treatment.35 Inconsistencies may be related to the methodologic and clinical diversity of RCTs, which limit the extent of quantitative synthesis and complicates result interpretation.35 Also, better conclusions could be drawn if future studies use head-to-head comparisons of CAM treatments and trials comparing CAM to widely used active treatments that report on all clinically relevant outcomes.35
Although the relationship between conventional treatment and the world of CAM remains equivocal, review of the evidence suggests acupuncture and SMT may be effective treatment for various chronic painful musculoskeletal conditions.35,44,50,51 These CAM modalities are reasonable referral options to supplement conventional therapy for the treatment of chronic musculoskeletal pain when conventional therapy has not yielded satisfactory results.
Author disclosures
The authors report no actual or potential conflicts of interest with regard to this article.
Disclaimer
The opinions expressed herein are those of the authors and do not necessarily reflect those of Federal Practitioner, Frontline Medical Communications Inc., the U.S. Government, or any of its agencies. This article may discuss unlabeled or investigational use of certain drugs. Please review the complete prescribing information for specific drugs or drug combinations—including indications, contraindications, warnings, and adverse effects—before administering pharmacologic therapy to patients.
Musculoskeletal pain affects one-quarter of the adult population and is the most common reason for self-medication and for seeking health care.1-3 It is also cited as the most common reason for the use of complementary and alternative medicine (CAM), and the lower back, head, neck, and knee are the most commonly reported areas of pain.4-8 In 2007, the estimated annual cost of managing chronic pain, adjusted for inflation, ranged from $560 to $635 billion; whereas the direct out-of-pocket cost for patients with back pain was $34 billion.9 Chronic pain persists beyond the usual course of disease or healing; generally about 3 months or longer.10-12 The most common forms of pain include those associated with musculoskeletal disorders, such as degenerative arthritis, rheumatoid arthritis, osteoarthritis, myofascial pain, chronic headache, low back pain, and bone pain.11,13-15
A large number of returning Operation Iraqi Freedom (OIF) and Operation Enduring Freedom (OEF) veterans have reported chronic pain symptoms, with back and head being the most common pain locations.7 They experienced pain related to wearing heavy gear every day, being transported in armored vehicles over crater-ridden roads, and enduring less than optimal sleeping conditions.16 Studies have found a significant number of subjects in this population who reported using CAM therapy. The OIF/OEF veterans were likely to have outpatient visits for musculoskeletal system disorders and to use CAM as an additional tool in pain management—not as a reaction to perceived inadequacies of conventional care.17,18
Complementary and alternative medicine is often used to describe various substances, procedures, and approaches outside of mainstream, Western, or conventional medicine for health promotion, treating injuries, symptoms, and illnesses.18,19 Although complementary and alternative are often used interchangeably, the 2 terms refer to different concepts. Complementary refers to the use of a nonmainstream approach with conventional medicine, whereas alternative refers to the use of a nonmainstream approach instead of conventional medicine.19 About 40% of Americans use CAM for various reasons.19
The services and self-care forms of CAM account for a large portion of out-of-pocket costs; patients are willing to pay for it themselves. In 2007, the U.S. spent $33.9 billion on out-of-pocket expenses for CAM classes, products, materials, and visits to CAM providers.20 The costs are comparable with those of conventional health care services and prescription drug use.20 One national study concluded that many patients use CAM in accordance with their beliefs, values, and philosophy concerning health and life.21 Other studies found that many patients use CAM not only because of functional status, pain severity, or self-efficacy, but also because they perceive significant benefits in pain relief.6,17,22-25 Some authors reported that CAM is used to augment and not replace conventional medicine and that it has now become part of the accepted armamentarium for managing chronic musculoskeletal pain.6,17,25
The National Center for Complementary and Alternative Medicine at the National Institutes of Health (NIH) classifies CAM in 2 ways: (1) Mind and body practices, such as acupuncture, massage therapy, meditation, movement therapies, relaxation techniques, spinal manipulation, tai chi and qi gong, yoga, healing touch, and hypnotherapy; and (2) natural products, including probiotics, herbs, and vitamins and minerals usually sold as dietary supplements.19 These products are regulated by the FDA but not as drugs. They have a different set of regulations under the Dietary Supplement Health and Education Act of 1994.26
Mind and body practices or provider-based CAM therapies such as chiropractic care, acupuncture, and massage increased significantly between 2002 and 2007, and many more patients may be willing to try these therapies for chronic low back pain if they do not have to pay out of pocket.27,28 Multiple studies have also found that these treatments in addition to herbal medicine are the most commonly reported CAM treatments used for pain relief in adults.3,17,22,23
Other commonly reported CAM therapies are garlic preparations, exercise, and yoga and meditation.22,23 A large number of veterans have reported previous use or willingness to try chiropractic care, massage therapy, herbal medicines, and acupuncture for chronic noncancer pain.17 In addition to acute care with conventional treatment, the VHA has now expanded services to allow for CAM as available treatment options for chronic musculoskeletal pain.29 The majority of VHA facilities also provide and refer patients to CAM service providers.30
This review article explores the evidence supporting the use of the most commonly reported CAM therapies; specifically acupuncture, massage therapy, and spinal manipulation for musculoskeletal pain relief. Because of the plethora of herbs and dietary supplements in the literature, these were not included in this review, although they are also reported among the most commonly used CAM therapies.1,23,31 The investigators sought to examine the effectiveness of acupuncture, spinal manipulation, or massage compared with no treatment, sham therapy, or current noninvasive first-line treatment for chronic musculoskeletal pain.
Study Selection
To find research addressing this question, the authors searched the PubMed, MEDLINE, and Cumulative Index to Nursing and Allied Health Literature (CINAHL) databases and the Cochrane Library for all relevant studies published between October 31, 2003, and October 31, 2013. The combined search from all sources for randomized controlled trials (RCTs) resulted in 1,157 studies with acupuncture and chronic pain, 343 studies with spinal manipulation and chronic pain, and 416 studies with massage and chronic pain. Acupuncture and chronic musculoskeletal pain yielded 94 studies, spinal manipulation and chronic musculoskeletal pain yielded 29 studies, and massage and chronic musculoskeletal pain yielded 55 RCTs.
Targeted searches were then conducted within the results for systematic reviews and meta-analysis of relevant studies of RCTs, focus on adults with any type of musculoskeletal pain, written in English, and had pain level or level of pain-related improvement as its primary outcome. The results were assessed for relevance to the review based on the information provided in the title, abstract, and the National Library of Medicine Medical Subject Headings. References of the search results were also searched manually for additional studies relevant to the review. Duplicated studies and those that looked at only acute or cancer pain were excluded. Thirteen systematic reviews and meta-analyses met the inclusion criteria (Table). The investigators reviewed the full reports and agreed to use the data that were abstracted from the studies.
Study Parameters
Four different categories of outcome measuring points for posttreatment follow-up are reported in the CAM studies: immediate, short-term, intermediate, and long-term. There are inconsistencies across studies for the timing of these 4 categories. Immediate posttreatment is defined as up to 1 day.8,32-34 The duration for the short-term follow-up period is defined as between 1 day and 3 months8,32,33; ≤ 3 months35,36; closest to 3 weeks37; closest to 4 weeks34; 1 month38; closest to 8 weeks, but < 3 months after randomization39; or up to 25 weeks, but nearest to 12 weeks.40Intermediate follow-up is between 3 months and 1 year8,33,35; between 3 and 6 months38; ≥ 3 months, but < 1 year36; or closest to 6 months.34Long term is defined as >12 months8,35; closest to 6 months37; 12 months38; 1 year or more36; closest to 6 months, but >3 months after randomization34,39; or between 26 weeks and 56 weeks.40
Pain intensity and pain relief was the treatment efficacy outcome for all the studies. A variety of measuring tools were reported across studies. Eight of the 13 studies reported measurement of pain intensity using the visual analog scale (VAS).8,33,35-37,41-43 In addition to the VAS, 2 studies also used the numerical rating scale (NRS).8,36 One study used the NRS alone.38 Other studies used the McGill Pain Questionnaire35; the SF-36 bodily pain dimension, Von Korff chronic pain grading scale, or low back pain rating scale36; or the Western Ontario and McMaster Universities Osteoarthritis Index subscale for pain.39,40,43
Authors from 8 of the systematic reviews and meta-analysis reported levels of evidence, or GRADE (Grades of Recommendation, Assessment, Development, and Evaluation), used to evaluate the overall quality of the evidence and the strength of the recommendations.8,32,34-36,38,42,43 Levels of evidence were based on RCTs. The various levels were (1) “strong evidence,” consistent findings in multiple high-quality RCTs; (2) “moderate evidence,” consistent findings among multiple high-quality RTCs and/or 1 high-quality RCT; (3) “limited evidence,” low-quality RCT; (4) “conflicting evidence,” inconsistent findings among multiple RCTs; and (5) “no evidence,” no RCTs or no studies.8,36
Most studies expressed the overall strength of the body of literature in 6 different categories: (1) “high quality,” confidence that the evidence reflected the true effect and that further research is very unlikely to change confidence in the effect of size; (2) “moderate quality,” further research is likely to have an impact on confidence in the estimate of effect and may change the estimate; (3) “low quality,” further research is very likely to have an important impact on confidence in the estimate of effect and is likely to change it; (4) “very low quality,” great uncertainty about the estimate; (5) “insufficient evidence,” either the evidence is unavailable or does not allow for a conclusion; and (6)“no evidence,” no evidence from RTCs.32,34,35,38,42,43 Kwon and colleagues reported using a modified jaded score where a total of 5 points was awarded if a study was described as randomized, used an appropriate method, if subjects were blinded to the intervention, if the evaluator was blinded to the intervention, and if there was a description of withdrawals and dropouts.43
Acupuncture
About 3 million American adults receive acupuncture each year.44 The most commonly reported reason for its use is chronic pain.44,45 Trials that examined the characteristics of those seeking and using acupuncture as adjunct to conventional treatment have found that patients who experienced positive outcomes, such as improvement in pain subscale, included females, previous failure of other therapies, and prior positive acupuncture encounters.46
Six of the studies in this review examined the evidence of acupuncture for chronic low back pain.35-38,41,42 Two of those studies found moderate evidence that acupuncture was more effective than no treatment for short-term pain relief.35,36 Manheimer and colleagues found it to be significantly more effective than no additional treatment or sham treatment for short-term pain relief.37 They however, reported a lack of evidence to suggest that it was more effective than were other active therapies.37 Hutchinson and colleagues did not differentiate among data points for intermediate, short-term, or long-term follow-up in their study.41 However, they concluded that there was some evidence to support acupuncture as more effective than no treatment and conflicting evidence of its effectiveness over other treatment modalities. Different levels of evidence were reported for intermediate pain relief with 2 of the other studies. One study found that the evidence was limited.35 The other study reported conflicting evidence that it was more effective than no treatment for immediate pain relief for those with chronic low back pain.36
Rubinstein and colleagues reported low- to very-low-quality evidence that acupuncture provided a short-term clinically relevant effect compared with waiting list control or when it was added to another intervention for chronic low back pain.38 Standaert and colleagues concluded that there was insufficient evidence to determine the relative effectiveness of acupuncture compared with either exercise or spinal manipulative therapy (SMT) in relieving chronic low back pain.42 Yuan and colleagues reported strong evidence that acupuncture combined with conventional therapy was more effective than conventional therapy alone.36
Furlan and colleagues found moderate evidence for significant improvement in pain intensity compared with subjects in physical therapy or usual care groups at short-term or immediate follow-up for chronic back pain.35 Studies that evaluated the efficacy of acupuncture for knee osteoarthritis compared acupuncture with sham acupuncture controls or no additional treatment and found that acupuncture was significantly better at relieving knee pain.39,40,43 Cao and colleagues found it to be effective both in the short term and long term.39 White and colleagues and Kwon and colleagues were unable to draw a conclusion concerning long-term effects due to the data point included in the study or the heterogeneity in the results.40,43
Trinh and colleagues reported moderate evidence that acupuncture is more effective for relief of chronic neck pain compared with inactive, sham treatments at immediate posttreatment.8 They also found moderate evidence that acupuncture was more effective than some other types of sham controls immediately posttreatment and limited evidence that it was more effective than massage at short-term follow-up.8 Furlan and colleagues found trials that applied sham acupuncture tended to produce nonstatistically significant results.35 Their meta-analysis of 2 studies indicated no significant difference between acupuncture and sham acupuncture for immediate posttreatment pain intensity. They also reported inconsistent results for the effects of acupuncture compared with medication or with spinal manipulation for chronic neck pain.35
Massage
Massage promotes health and well-being through the use of mechanical manipulation of body tissues with rhythmic pressure and stroking.47 Treatment techniques include Hoffa massage, friction massage, connective tissue massage, transverse friction massage, and trigger point massage.48 Massage is one of the most popular CAM therapies for neck and back pain.49 In their survey, White and colleagues reported that active-duty military personnel listed massage as the most frequently used CAM therapy in the previous 12 months.18
Patel and colleagues reported that the overall methodology of the trials assessed in their study was either low- or very-low-GRADE level.32 They found very-low to low-quality evidence that there is no difference in effectiveness of 3 approaches of massage therapies (ischemic compression to upper fibre of trapezius trigger point, transverse friction massage to upper fibre of trapezius, and ischemic compression to upper fibre of trapezius) for neck muscle pain. They also reported no difference between conventional Western massage and acupuncture for generalized neck muscle pain at short-term follow-up, and no difference in pain intensity compared with other therapies such as acupuncture, manual therapy, exercise, education, and multimodal interventions. The investigators concluded that the effectiveness of massage therapy for improving neck pain remains unclear, as results could not be combined due to the wide range of techniques and comparative treatments. They were unable to make any firm statement to guide clinical practice.32
Two other studies compared massage to no treatment and found it significantly improved chronic neck pain immediately after the end of treatment.33,35 Kong and colleagues also found similar effects for shoulder pain at immediate and short-term
follow-up but not for neck or shoulder pain when massage was compared with active therapies.33 Furlan and colleagues’ meta-analysis found that massage compared with relaxation or physical therapy was significantly better at reducing chronic nonspecific low back pain immediately after treatment.35
Spinal Manipultaion
Spinal manipulation is high-velocity and low-amplitude localized force directed at specific spinal segments.34 It is performed by using the hands or a device to apply a controlled force to a joint of the spine and is practiced by osteopathic physicians, naturopathic physicians, chiropractors, physical therapists, and some medical doctors.19
In a study to assess its effectiveness, Rubinstein and colleagues found low-quality evidence to very-low-quality evidence to suggest that SMT does not provide a more clinically beneficial effect compared with sham, passive modalities, or other interventions for the relief of chronic low back pain.38 Comparative interventions included usual medical care, physical therapy, exercise, physiotherapy, and multimodal treatments. Standaert and colleagues also found no difference between motor control exercise and SMT in pain relief.42 They concluded that although the evidence is low, there is an indication that structured exercise and SMT seem to offer equivalent benefits in terms of pain for those with chronic lower back pain with clinical benefits evident within 8 weeks of care.42
Gross and colleagues found that when cervical manipulation was compared with control for chronic mechanical neck pain, there was moderate-quality evidence for similar effects at short-term and intermediate follow-up.34 They also reported low-quality evidence in support of thoracic manipulation alone or in combination with electrothermal or individualized physiotherapy and suggested cervical manipulation may provide short-term but not long-term pain relief.34 Furlan and colleagues reported moderate-quality evidence that spinal manipulation provided significantly better posttreatment neck pain relief compared with placebo.35 They also found low evidence that it was significantly better than placebo, acupuncture, and pain medication at immediate follow-up.35
Conclusion
Considerable effort was made to retrieve all studies; however, the authors cannot be certain that the review was exhaustive. They also relied on other analyses of primary studies for the conclusion.
The 3 types of musculoskeletal pain in the review were low back, neck, and knee pain related to osteoarthritis. The authors found that the most common CAM modality studied for chronic musculoskeletal pain was acupuncture. Studies on massage therapy and SMT that were relevant to the review were limited.
Two studies reported strong level of evidence for acupuncture.36,40 One study reported that acupuncture was superior to no treatment or to sham acupuncture for relief of chronic knee pain.40 The other study reported that acupuncture was more effective than conventional therapy alone when it was combined with conventional therapy for chronic low back pain, but there was no difference when compared with sham acupuncture for short-term pain relief.36 The strength of the evidence for acupuncture combined with conventional treatment for low back pain was conflicting. One other review found low evidence for its benefit. Similar to Hopton and MacPherson, this review found that acupuncture treatment seemed to provide effective short-term relief of chronic low back pain.14 Evidence would also seem to support acupuncture for the short-term relief of chronic neck pain and knee pain associated with osteoarthritis.
This review also found immediate and short-term benefits, although mostly with weak evidence, for the use of SMT in the treatment of chronic neck and low back pain. There was conflicting evidence for the support of massage therapy. Furlan and colleagues, however, found that acupuncture, SMT, and massage treatments were significantly more efficacious than no treatment, placebo, physical therapy, or usual care in reducing pain immediately or at short-term after treatment.35 Inconsistencies may be related to the methodologic and clinical diversity of RCTs, which limit the extent of quantitative synthesis and complicates result interpretation.35 Also, better conclusions could be drawn if future studies use head-to-head comparisons of CAM treatments and trials comparing CAM to widely used active treatments that report on all clinically relevant outcomes.35
Although the relationship between conventional treatment and the world of CAM remains equivocal, review of the evidence suggests acupuncture and SMT may be effective treatment for various chronic painful musculoskeletal conditions.35,44,50,51 These CAM modalities are reasonable referral options to supplement conventional therapy for the treatment of chronic musculoskeletal pain when conventional therapy has not yielded satisfactory results.
Author disclosures
The authors report no actual or potential conflicts of interest with regard to this article.
Disclaimer
The opinions expressed herein are those of the authors and do not necessarily reflect those of Federal Practitioner, Frontline Medical Communications Inc., the U.S. Government, or any of its agencies. This article may discuss unlabeled or investigational use of certain drugs. Please review the complete prescribing information for specific drugs or drug combinations—including indications, contraindications, warnings, and adverse effects—before administering pharmacologic therapy to patients.
1. Callahan LF, Wiley-Exley EK, Mielenz TJ, et al. Use of complementary and alternative medicine among patients with arthritis. Prev Chronic Dis. 2009;6(2):A44.
2. Walsh NE, Brooks P, Hazes JM, et al; Bone and Joint Decade Task Force for Standards of Care for Acute and Chronic Musculoskeletal Pain. Standards of care for acute and chronic musculoskeletal pain: the Bone and Joint Decade (2000-2010). Arch Phys Med Rehabil. 2008;89(9):1830-1845.
3. Williamson AT, Fletcher PC, Dawson KA. Complementary and alternative medicine. Use in an older population. J Gerontol Nurs. 2003;29(5):20-28.
4. Artus M, Croft P, Lewis M. The use of CAM and conventional treatments among primary care consulters with chronic musculoskeletal pain. BMC Fam Pract. 2007;8:26.
5. Cherkin DC, Sherman KJ, Kahn J, et al. A comparison of the effects of 2 types of massage and usual care on chronic low back pain: a randomized controlled trial. Ann Intern Med. 2011;155(1):1-9.
6. Fleming S, Rabago DP, Mundt MP, Fleming MF. CAM therapies among primary care patients using opioid therapy for chronic pain. BMC Complement Altern Med. 2007;7:15.
7. Lew HL, Otis JD, Tun C, Kerns RD, Clark ME, Cifu DX. Prevalence of chronic pain, posttraumatic stress disorder, and persistent post concussive symptoms in OIF/OEF veterans: polytrauma clinical triad. J Rehabil Res Dev. 2009;46(6):697-702.
8. Trinh K, Graham N, Gross A, et al. Acupuncture for neck disorders. Spine (Phila PA 1976). 2007;32(2):236-243.
9. Gaskin DJ, Richard P. Appendix C: The economic costs of pain in the United States. In: Institute of Medicine (US) Committee on Advancing Pain Research, Care, and Education. Relieving Pain in America: A Blueprint for Transforming Prevention, Care, Education, and Research. Washington, DC: National Academies Press; 2011. National Center for Biotechnology Information Website. http://www. ncbi.nlm.nih.gov/books/NBK92521. Accessed July 31, 2015.
10. American Academy of Pain Medicine. AAPM facts and figures on pain. American Academy of Pain Medicine Website. http://www.painmed.org/files/facts-and-figures-on-pain.pdf. Accessed July 31, 2015.
11. Rosenquist RW, Vrooman MD. Chronic pain management. In: Butterworth JF, Mackey DC, Wasnick JD, eds. Morgan & Mikhail’s Clinical Anesthesiology. 5th ed. New York, NY: McGraw-Hill; 2013:chap 47.
12. Rasu RS, Sohraby R, Cunningham L, Knell ME. Assessing chronic pain treatment practices and evaluating adherence to chronic pain clinical guidelines in outpatient practices in the United States. J Pain. 2013;14(6):568-578.
13. Gureje O, Von Korff M, Simon, GE, Grater R. Persistent pain and well-being: a World Health Organization study in primary care. JAMA. 1998;280(2):147-151.
14. Hopton A, MacPherson H. Acupuncture for chronic pain: is acupuncture more than an effective placebo? A systematic review of pooled data from meta-analyses. Pain Pract. 2010;10(2):94-102.
15. Kumar N. WHO Normative guidelines on pain management. World Health Organization Website. http://www.who.int/medicines/areas/quality_safety/delphi_study_pain_guidelines.pdf. Published June 2007. Accessed August 3, 2015.
16. Koffman RL. Downrange acupuncture. Med Acupunct. 2011;23(4):215-218.
17. Denneson LM, Corson K, Dobscha SK. Complementary and alternative medicine use among veterans with chronic noncancer pain. J Rehabil Res Dev. 2011;(48)9:1119-1128.
18. White MR, Jacobson IG, Smith B, et al; Millennium Cohort Study Team. Health care utilization among complementary and alternative medicine users in a large military cohort. BMC Complement Alternat Med. 2011;11:27.
19. U.S. Department of Health and Human Services, National Institutes of Health, National Center for Complementary and Alternative Medicine. Complementary, alternative, or integrative health: What’s in a name? National Center for Complementary and Alternative Medicine Website. http://nccam.nih.gov/health/whatiscam. Updated March 2015. Modified July 8, 2015. Accessed August 4, 2015.
20. Nahin RL, Barnes PM, Stussman BJ, Bloom B. Costs of complementary and alternative medicine (CAM) and frequency of visits to CAM practitioners: United States, 2007. Natl Health Stat Report. 2009;30(18):1-14.
21. Astin JA. Why patients use alternative medicine: results of a national study. JAMA. 1998;279(19):1548-1553.
22. Rosenberg EI, Genao I, Chen I, et al. Complementary and alternative medicine use in primary care patients with chronic pain. Pain Med. 2008;9(8):1065-1072.
23. Alaaeddine N, Okais J, Ballane L, Baddoura RM. Use of complementary and alternative therapy among patients with rheumatoid arthritis and osteoarthritis. J Clin Nurs. 2012;21(21-22):3198-3204.
24. Tan MG, Win MT, Khan SA. The use of complementary and alternative medicine in chronic pain patients in Singapore: a single-centre study. Ann Acad Med Singapore. 2013;42(3):133-137.
25. White P. A background to acupuncture and its use in chronic painful musculoskeletal conditions. J R Soc Promot Health. 2006;126(5):219-227.
26. U.S. Department of Health and Human Services, National Institutes of Health, Office of Dietary Supplements. Dietary Supplement Health and Education Act of 1994. National Institutes of Health Website. http://ods.od.nih.gov/About/DSHEA_Wording.aspx. Published October 25, 1994. Accessed August 4, 2015.
27. Su D, Li L. Trends in the use of complementary and alternative medicine in the United States: 2002-2007. J Health Care Poor Underserved. 2011;22(1):296-310.
28. Sherman KJ, Cherkin DC, Connelly MT, et al. Complementary and alternative medical therapies for chronic low back pain: what treatments are patients willing to try? BMC Complement Alternat Med. 2004;4:9.
29. Smeeding SJ, Bradshaw DH, Kumpfer KL, Trevithick S, Stoddard GJ. Outcome evaluation of the Veterans Affairs Salt Lake City Integrative Health Clinic for Chronic Nonmalignant Pain. Clin J Pain. 2011;27(2):146-155.
30. U.S. Department of Veterans Affairs, Veterans Health Administration, Office of the Assistant Deputy Under Secretary for Health for Policy and Planning. 2011 complementary and alternative medicine. U.S. Department of Veterans Affairs Office of Research and Development Website. http://www.research.va.gov/research_topics/2011cam_finalreport.pdf. Published September 2011. Accessed August 4, 2015.
31. Unsal A, Gözüm S. Use of complementary and alternative medicine by patients with arthritis. J Clin Nurs. 2010;19(7-8):1129-1138.
32. Patel KC, Gross A, Graham N, et al. Massage for mechanical neck disorder. Cochrane Database Syst Rev. 2012;9:CD004871.
33. Kong LJ, Zhan HS, Cheng YW, Yuan WA, Chen B, Fang M. Massage therapy for neck and shoulder pain: a systematic review and meta-analysis. Evid Based Complement Alternat Med. 2013;2013:613279.
34. Gross A, Miller J, D’Sylva J, et al; COG. Manipulation or mobilisation for neck pain: a Cochrane review. Man Ther. 2010;15(4):315-333.
35. Furlan A, Yazdi F, Tsertsvadze A, et al. Complementary and alternative therapies for back Pain II. Evidence report/technology assessment No. 194. (Prepared by the University of Ottawa Evidence-based Practice Center under Contract No. 290-2007-10059-I (EPCIII). AHRQ Publication No. 10(11)E007. Rockville, MD: Agency for Healthcare Research and Quality; 2010.
36. Yuan J, Purepong N, Kerr DP, Park J, Bradbury I, McDonough S. Effectiveness of acupuncture for low back pain. Spine (Phila PA 1976). 2008;33(23):E887-E900.
37. Manheimer E, White A, Berman B, Forys K, Ernst E. Meta-analysis: acupuncture for low back pain. Ann Intern Med. 2005;142(8):651-663.
38. Rubinstein SM, van Middelkoop M, Kuijpers T, et al. A systematic review on the effectiveness of complementary and alternative medicine for chronic non-specific low-back pain. Eur Spine J. 2010;19(8):1213-1228.
39. Cao L, Zhang XL, Gao YS, Jiang Y. Needle acupuncture for osteoarthritis of the knee. A systematic review and updated meta-analysis. Saudi Med J. 2012;33(5):526-532.
40. White A, Foster NE, Cummings M, Barlas P. Acupuncture treatment for chronic knee pain: a systematic review. Rheumatology (Oxford). 2007;46(3):384-390.
41. Hutchinson AJ, Ball S, Andrews JC, Jones GG. The effectiveness of acupuncture in treating chronic non-specific low back pain: a systematic review of the literature. J Orthop Surg Res. 2012;7:36.
42. Standaert, CJ, Friedly J, Erwin MW, et al. Comparative effectiveness of exercise, acupuncture, and spinal manipulation for low back pain. Spine (Phila PA 1976). 2011;36(21 suppl):S120-S130.
43. Kwon YD, Pittler MH, Ernst E. Acupuncture for peripheral joint osteoarthritis: a systematic review and meta-analysis. Rheumatology (Oxford). 2006;45(11):1331-1337.
44. Vickers AJ, Cronin AM, Maschino AC, et al; Acupuncture Trialists’ Collaboration. Individual patient data meta-analysis of acupuncture for chronic pain: protocol of the Acupuncture Trialists’ Collaboration. Trials. 2010;11:90.
45. Kelly RB. Acupuncture for pain. Am Fam Physician. 2009;80(5):481-484.
46. Witt CM, Schützler L, Lüdtke R, Wegscheider K, Willich SN. Patient characteristics and variation in treatment outcomes: which patients benefit most from acupuncture for chronic pain? Clin J Pain. 2011;27(6):550-555.
47. Cafarelli E, Flint F. The role of massage in preparation for and recovery from exercise: an overview. Sports Med. 1992;14(1):1-9.
48. Prentice WE. Therapeutic massage. In: Prentice WE. Therapeutic Modalities in Rehabilitation. 4th ed. New York, NY: McGraw-Hill; 2011:chap 16.
49. Wolsko PM, Eisenberg DM, Davis RB, Kessler R, Phillips RS. Patterns and perceptions of care for treatment of back and neck pain: results of a national survey. Spine (Phila PA 1976). 2003;28(3):292-297.
50. Perlman AI, Sabina A, Williams AL, Njike VY, Katz DL. Massage therapy for osteoarthritis of the knee: a randomized controlled trial. Arch Intern Med. 2006;166(22):2533-2538.
51. Tsao JCI. Effectiveness of massage therapy for chronic, non-malignant pain: a review. Evid Based Complement Alternat Med. 2007;4(2):165-179.
1. Callahan LF, Wiley-Exley EK, Mielenz TJ, et al. Use of complementary and alternative medicine among patients with arthritis. Prev Chronic Dis. 2009;6(2):A44.
2. Walsh NE, Brooks P, Hazes JM, et al; Bone and Joint Decade Task Force for Standards of Care for Acute and Chronic Musculoskeletal Pain. Standards of care for acute and chronic musculoskeletal pain: the Bone and Joint Decade (2000-2010). Arch Phys Med Rehabil. 2008;89(9):1830-1845.
3. Williamson AT, Fletcher PC, Dawson KA. Complementary and alternative medicine. Use in an older population. J Gerontol Nurs. 2003;29(5):20-28.
4. Artus M, Croft P, Lewis M. The use of CAM and conventional treatments among primary care consulters with chronic musculoskeletal pain. BMC Fam Pract. 2007;8:26.
5. Cherkin DC, Sherman KJ, Kahn J, et al. A comparison of the effects of 2 types of massage and usual care on chronic low back pain: a randomized controlled trial. Ann Intern Med. 2011;155(1):1-9.
6. Fleming S, Rabago DP, Mundt MP, Fleming MF. CAM therapies among primary care patients using opioid therapy for chronic pain. BMC Complement Altern Med. 2007;7:15.
7. Lew HL, Otis JD, Tun C, Kerns RD, Clark ME, Cifu DX. Prevalence of chronic pain, posttraumatic stress disorder, and persistent post concussive symptoms in OIF/OEF veterans: polytrauma clinical triad. J Rehabil Res Dev. 2009;46(6):697-702.
8. Trinh K, Graham N, Gross A, et al. Acupuncture for neck disorders. Spine (Phila PA 1976). 2007;32(2):236-243.
9. Gaskin DJ, Richard P. Appendix C: The economic costs of pain in the United States. In: Institute of Medicine (US) Committee on Advancing Pain Research, Care, and Education. Relieving Pain in America: A Blueprint for Transforming Prevention, Care, Education, and Research. Washington, DC: National Academies Press; 2011. National Center for Biotechnology Information Website. http://www. ncbi.nlm.nih.gov/books/NBK92521. Accessed July 31, 2015.
10. American Academy of Pain Medicine. AAPM facts and figures on pain. American Academy of Pain Medicine Website. http://www.painmed.org/files/facts-and-figures-on-pain.pdf. Accessed July 31, 2015.
11. Rosenquist RW, Vrooman MD. Chronic pain management. In: Butterworth JF, Mackey DC, Wasnick JD, eds. Morgan & Mikhail’s Clinical Anesthesiology. 5th ed. New York, NY: McGraw-Hill; 2013:chap 47.
12. Rasu RS, Sohraby R, Cunningham L, Knell ME. Assessing chronic pain treatment practices and evaluating adherence to chronic pain clinical guidelines in outpatient practices in the United States. J Pain. 2013;14(6):568-578.
13. Gureje O, Von Korff M, Simon, GE, Grater R. Persistent pain and well-being: a World Health Organization study in primary care. JAMA. 1998;280(2):147-151.
14. Hopton A, MacPherson H. Acupuncture for chronic pain: is acupuncture more than an effective placebo? A systematic review of pooled data from meta-analyses. Pain Pract. 2010;10(2):94-102.
15. Kumar N. WHO Normative guidelines on pain management. World Health Organization Website. http://www.who.int/medicines/areas/quality_safety/delphi_study_pain_guidelines.pdf. Published June 2007. Accessed August 3, 2015.
16. Koffman RL. Downrange acupuncture. Med Acupunct. 2011;23(4):215-218.
17. Denneson LM, Corson K, Dobscha SK. Complementary and alternative medicine use among veterans with chronic noncancer pain. J Rehabil Res Dev. 2011;(48)9:1119-1128.
18. White MR, Jacobson IG, Smith B, et al; Millennium Cohort Study Team. Health care utilization among complementary and alternative medicine users in a large military cohort. BMC Complement Alternat Med. 2011;11:27.
19. U.S. Department of Health and Human Services, National Institutes of Health, National Center for Complementary and Alternative Medicine. Complementary, alternative, or integrative health: What’s in a name? National Center for Complementary and Alternative Medicine Website. http://nccam.nih.gov/health/whatiscam. Updated March 2015. Modified July 8, 2015. Accessed August 4, 2015.
20. Nahin RL, Barnes PM, Stussman BJ, Bloom B. Costs of complementary and alternative medicine (CAM) and frequency of visits to CAM practitioners: United States, 2007. Natl Health Stat Report. 2009;30(18):1-14.
21. Astin JA. Why patients use alternative medicine: results of a national study. JAMA. 1998;279(19):1548-1553.
22. Rosenberg EI, Genao I, Chen I, et al. Complementary and alternative medicine use in primary care patients with chronic pain. Pain Med. 2008;9(8):1065-1072.
23. Alaaeddine N, Okais J, Ballane L, Baddoura RM. Use of complementary and alternative therapy among patients with rheumatoid arthritis and osteoarthritis. J Clin Nurs. 2012;21(21-22):3198-3204.
24. Tan MG, Win MT, Khan SA. The use of complementary and alternative medicine in chronic pain patients in Singapore: a single-centre study. Ann Acad Med Singapore. 2013;42(3):133-137.
25. White P. A background to acupuncture and its use in chronic painful musculoskeletal conditions. J R Soc Promot Health. 2006;126(5):219-227.
26. U.S. Department of Health and Human Services, National Institutes of Health, Office of Dietary Supplements. Dietary Supplement Health and Education Act of 1994. National Institutes of Health Website. http://ods.od.nih.gov/About/DSHEA_Wording.aspx. Published October 25, 1994. Accessed August 4, 2015.
27. Su D, Li L. Trends in the use of complementary and alternative medicine in the United States: 2002-2007. J Health Care Poor Underserved. 2011;22(1):296-310.
28. Sherman KJ, Cherkin DC, Connelly MT, et al. Complementary and alternative medical therapies for chronic low back pain: what treatments are patients willing to try? BMC Complement Alternat Med. 2004;4:9.
29. Smeeding SJ, Bradshaw DH, Kumpfer KL, Trevithick S, Stoddard GJ. Outcome evaluation of the Veterans Affairs Salt Lake City Integrative Health Clinic for Chronic Nonmalignant Pain. Clin J Pain. 2011;27(2):146-155.
30. U.S. Department of Veterans Affairs, Veterans Health Administration, Office of the Assistant Deputy Under Secretary for Health for Policy and Planning. 2011 complementary and alternative medicine. U.S. Department of Veterans Affairs Office of Research and Development Website. http://www.research.va.gov/research_topics/2011cam_finalreport.pdf. Published September 2011. Accessed August 4, 2015.
31. Unsal A, Gözüm S. Use of complementary and alternative medicine by patients with arthritis. J Clin Nurs. 2010;19(7-8):1129-1138.
32. Patel KC, Gross A, Graham N, et al. Massage for mechanical neck disorder. Cochrane Database Syst Rev. 2012;9:CD004871.
33. Kong LJ, Zhan HS, Cheng YW, Yuan WA, Chen B, Fang M. Massage therapy for neck and shoulder pain: a systematic review and meta-analysis. Evid Based Complement Alternat Med. 2013;2013:613279.
34. Gross A, Miller J, D’Sylva J, et al; COG. Manipulation or mobilisation for neck pain: a Cochrane review. Man Ther. 2010;15(4):315-333.
35. Furlan A, Yazdi F, Tsertsvadze A, et al. Complementary and alternative therapies for back Pain II. Evidence report/technology assessment No. 194. (Prepared by the University of Ottawa Evidence-based Practice Center under Contract No. 290-2007-10059-I (EPCIII). AHRQ Publication No. 10(11)E007. Rockville, MD: Agency for Healthcare Research and Quality; 2010.
36. Yuan J, Purepong N, Kerr DP, Park J, Bradbury I, McDonough S. Effectiveness of acupuncture for low back pain. Spine (Phila PA 1976). 2008;33(23):E887-E900.
37. Manheimer E, White A, Berman B, Forys K, Ernst E. Meta-analysis: acupuncture for low back pain. Ann Intern Med. 2005;142(8):651-663.
38. Rubinstein SM, van Middelkoop M, Kuijpers T, et al. A systematic review on the effectiveness of complementary and alternative medicine for chronic non-specific low-back pain. Eur Spine J. 2010;19(8):1213-1228.
39. Cao L, Zhang XL, Gao YS, Jiang Y. Needle acupuncture for osteoarthritis of the knee. A systematic review and updated meta-analysis. Saudi Med J. 2012;33(5):526-532.
40. White A, Foster NE, Cummings M, Barlas P. Acupuncture treatment for chronic knee pain: a systematic review. Rheumatology (Oxford). 2007;46(3):384-390.
41. Hutchinson AJ, Ball S, Andrews JC, Jones GG. The effectiveness of acupuncture in treating chronic non-specific low back pain: a systematic review of the literature. J Orthop Surg Res. 2012;7:36.
42. Standaert, CJ, Friedly J, Erwin MW, et al. Comparative effectiveness of exercise, acupuncture, and spinal manipulation for low back pain. Spine (Phila PA 1976). 2011;36(21 suppl):S120-S130.
43. Kwon YD, Pittler MH, Ernst E. Acupuncture for peripheral joint osteoarthritis: a systematic review and meta-analysis. Rheumatology (Oxford). 2006;45(11):1331-1337.
44. Vickers AJ, Cronin AM, Maschino AC, et al; Acupuncture Trialists’ Collaboration. Individual patient data meta-analysis of acupuncture for chronic pain: protocol of the Acupuncture Trialists’ Collaboration. Trials. 2010;11:90.
45. Kelly RB. Acupuncture for pain. Am Fam Physician. 2009;80(5):481-484.
46. Witt CM, Schützler L, Lüdtke R, Wegscheider K, Willich SN. Patient characteristics and variation in treatment outcomes: which patients benefit most from acupuncture for chronic pain? Clin J Pain. 2011;27(6):550-555.
47. Cafarelli E, Flint F. The role of massage in preparation for and recovery from exercise: an overview. Sports Med. 1992;14(1):1-9.
48. Prentice WE. Therapeutic massage. In: Prentice WE. Therapeutic Modalities in Rehabilitation. 4th ed. New York, NY: McGraw-Hill; 2011:chap 16.
49. Wolsko PM, Eisenberg DM, Davis RB, Kessler R, Phillips RS. Patterns and perceptions of care for treatment of back and neck pain: results of a national survey. Spine (Phila PA 1976). 2003;28(3):292-297.
50. Perlman AI, Sabina A, Williams AL, Njike VY, Katz DL. Massage therapy for osteoarthritis of the knee: a randomized controlled trial. Arch Intern Med. 2006;166(22):2533-2538.
51. Tsao JCI. Effectiveness of massage therapy for chronic, non-malignant pain: a review. Evid Based Complement Alternat Med. 2007;4(2):165-179.
Commentary to "CDC Will Soon Issue Guidelines for the Prevention of Surgical Site Infection"
Analyzing the Guidelines: It Can't All Be Level I
The demand for total joint arthroplasty continues to rise, resulting in a steady increase in the number of primary total hip and knee replacements every year. Unfortunately, as these numbers rise, so will the number of periprosthetic joint infections (PJIs). The economic burden and patient morbidity associated with PJI has resulted in the creation of multiple orthopedic societies and committees focused on formulating “best practice” guidelines in order to reduce the rates of PJI as much as possible.
The new guidelines for surgical site infection (SSI) prevention by the Centers for Disease Control and Prevention (CDC) recently forced the orthopedic community to critically analyze the current literature. Dr. Javad Parvizi’s editorial elegantly notes that many areas of infection prevention and treatment are not well evaluated, and many of our day-to-day practices are based on low levels of evidence. Level I studies continue to be a costly and time-consuming challenge due to the already very low SSI rate, and, in order to show an improvement in this rate, thousands of patients are required for study. This makes a multicenter approach necessary to ensure adequate power, and a multicenter study often requires significant resources and funding outlets. These requirements have resulted in many of our practice recommendations being based on retrospective reviews, which have inherent methodological limitations. The retrospective nature of these studies lacks the experimental design necessary to confidently make treatment recommendations; however, they do allow us to look at what strategies have been tried, and in essence, how well they worked. Although level III and IV studies do not allow us to compare treatments head to head, they do give us some insights into viable treatment strategies and should not be completely disregarded. The results of retrospective studies allow us to design prospective experiments based on what we have observed as successful treatment modalities in particular patient cohorts.
An alternative approach for evaluating new and existing treatment strategies is through basic science translational research. Future advancements in PJI diagnosis and treatment will likely be founded upon translational research efforts from clinician scientists testing treatment protocols both on the benchtop and in animal models. The most glaring knowledge gaps in PJI should be identified through the combined efforts of the CDC, the Musculoskeletal Infection Society, the American Academy of Orthopaedic Surgeons, and the Orthopaedic Research Society. Coordinated efforts should be made and strategies executed to systematically fund translational projects that answer these questions. Translational studies will be able to safely and methodically evaluate new and even established treatment protocols for PJI in a cost-effective manner.
We have made great strides in the prevention and treatment of PJI over the past 2 decades. When working together as a cohesive profession, we will undoubtedly continue to advance our knowledge base and improve treatment recommendations for our patients.
Analyzing the Guidelines: It Can't All Be Level I
The demand for total joint arthroplasty continues to rise, resulting in a steady increase in the number of primary total hip and knee replacements every year. Unfortunately, as these numbers rise, so will the number of periprosthetic joint infections (PJIs). The economic burden and patient morbidity associated with PJI has resulted in the creation of multiple orthopedic societies and committees focused on formulating “best practice” guidelines in order to reduce the rates of PJI as much as possible.
The new guidelines for surgical site infection (SSI) prevention by the Centers for Disease Control and Prevention (CDC) recently forced the orthopedic community to critically analyze the current literature. Dr. Javad Parvizi’s editorial elegantly notes that many areas of infection prevention and treatment are not well evaluated, and many of our day-to-day practices are based on low levels of evidence. Level I studies continue to be a costly and time-consuming challenge due to the already very low SSI rate, and, in order to show an improvement in this rate, thousands of patients are required for study. This makes a multicenter approach necessary to ensure adequate power, and a multicenter study often requires significant resources and funding outlets. These requirements have resulted in many of our practice recommendations being based on retrospective reviews, which have inherent methodological limitations. The retrospective nature of these studies lacks the experimental design necessary to confidently make treatment recommendations; however, they do allow us to look at what strategies have been tried, and in essence, how well they worked. Although level III and IV studies do not allow us to compare treatments head to head, they do give us some insights into viable treatment strategies and should not be completely disregarded. The results of retrospective studies allow us to design prospective experiments based on what we have observed as successful treatment modalities in particular patient cohorts.
An alternative approach for evaluating new and existing treatment strategies is through basic science translational research. Future advancements in PJI diagnosis and treatment will likely be founded upon translational research efforts from clinician scientists testing treatment protocols both on the benchtop and in animal models. The most glaring knowledge gaps in PJI should be identified through the combined efforts of the CDC, the Musculoskeletal Infection Society, the American Academy of Orthopaedic Surgeons, and the Orthopaedic Research Society. Coordinated efforts should be made and strategies executed to systematically fund translational projects that answer these questions. Translational studies will be able to safely and methodically evaluate new and even established treatment protocols for PJI in a cost-effective manner.
We have made great strides in the prevention and treatment of PJI over the past 2 decades. When working together as a cohesive profession, we will undoubtedly continue to advance our knowledge base and improve treatment recommendations for our patients.
Analyzing the Guidelines: It Can't All Be Level I
The demand for total joint arthroplasty continues to rise, resulting in a steady increase in the number of primary total hip and knee replacements every year. Unfortunately, as these numbers rise, so will the number of periprosthetic joint infections (PJIs). The economic burden and patient morbidity associated with PJI has resulted in the creation of multiple orthopedic societies and committees focused on formulating “best practice” guidelines in order to reduce the rates of PJI as much as possible.
The new guidelines for surgical site infection (SSI) prevention by the Centers for Disease Control and Prevention (CDC) recently forced the orthopedic community to critically analyze the current literature. Dr. Javad Parvizi’s editorial elegantly notes that many areas of infection prevention and treatment are not well evaluated, and many of our day-to-day practices are based on low levels of evidence. Level I studies continue to be a costly and time-consuming challenge due to the already very low SSI rate, and, in order to show an improvement in this rate, thousands of patients are required for study. This makes a multicenter approach necessary to ensure adequate power, and a multicenter study often requires significant resources and funding outlets. These requirements have resulted in many of our practice recommendations being based on retrospective reviews, which have inherent methodological limitations. The retrospective nature of these studies lacks the experimental design necessary to confidently make treatment recommendations; however, they do allow us to look at what strategies have been tried, and in essence, how well they worked. Although level III and IV studies do not allow us to compare treatments head to head, they do give us some insights into viable treatment strategies and should not be completely disregarded. The results of retrospective studies allow us to design prospective experiments based on what we have observed as successful treatment modalities in particular patient cohorts.
An alternative approach for evaluating new and existing treatment strategies is through basic science translational research. Future advancements in PJI diagnosis and treatment will likely be founded upon translational research efforts from clinician scientists testing treatment protocols both on the benchtop and in animal models. The most glaring knowledge gaps in PJI should be identified through the combined efforts of the CDC, the Musculoskeletal Infection Society, the American Academy of Orthopaedic Surgeons, and the Orthopaedic Research Society. Coordinated efforts should be made and strategies executed to systematically fund translational projects that answer these questions. Translational studies will be able to safely and methodically evaluate new and even established treatment protocols for PJI in a cost-effective manner.
We have made great strides in the prevention and treatment of PJI over the past 2 decades. When working together as a cohesive profession, we will undoubtedly continue to advance our knowledge base and improve treatment recommendations for our patients.

Total Knee Replacement Is Effective in Patients With Rheumatoid Arthritis
According to a new study, total knee arthroplasty is highly effective in reducing clinically relevant knee pain to a greater extent than other subjective health-related quality-of-life indicies in patients with rheumatoid arthritis, although this improvement is less marked as compared to outcomes in patients with osteoarthritis. These study findings were published online ahead of print July 20 in Arthritis & Rheumatology.
The study included patients with rheumatologist-diagnosed arthritis undergoing primary total knee arthroplasty during 1999 to 2012. Indices of pain knee, and health-related quality of life were obtained in 3 consecutive 6-month intervals: preoperative, perioperative, and postoperative. Descriptive statistics and 1-way analysis of variance were used to compare total knee arthroplasty outcomes by diagnosis. Effect sizes and standardized response means were calculated between baseline and recovery.

Of the participating 18,897 patients, 834 people with rheumatoid arthritis, and 315 people with osteoarthritis had undergone index total knee arthroplasty at mean ages 65 and 68. Post total knee arthroplasty, significant improvements were observed for most domains of pain, function, and health-related quality of life within both disease groups, with greater impact in osteoarthritis. Based on the standardized response means, the maximum improvement was shown in index knee pain.
The Health Assessment Questionnaire II and the Short Form 36 physical component summary were the most responsive health-related quality of life indices in detecting post-total knee arthroplasty improvement in rheumatoid arthritis. A diagnosis of rheumatoid arthritis, lower income, and preoperative anxiety were independently associated with a lower degree of improvement in index knee pain following total knee arthroplasty.
Senior author Kaleb D. Michaud, PhD, Associate Professor in the Division of Rheumatology and Immunology at the University of Nebraska Medical Center in Omaha, and colleagues said that total knee replacement can serve as a “time machine” by which patients can return to a less disabled lifestyle, before the arthritic process catches up.
“A new knee can give osteoarthritis patients 10 to 20 years of painless use, whereas rheumatoid arthritis continues to affect the joint soon afterward,” the researchers said. “It’s an important and effective treatment, but patients with rheumatoid arthritis shouldn’t expect the same, often dramatic results experienced by their osteoarthritis counterparts,” Dr. Michaud said.
Suggested Reading
Dusad A, Pedro S, Mikuls TR, et al. Impact of total knee arthroplasty as assessed using patient-reported pain and health-related quality of life indices: rheumatoid arthritis versus osteoarthritis. Arthritis Rheumatol. 2015 July 20 [Epub ahead of print].
According to a new study, total knee arthroplasty is highly effective in reducing clinically relevant knee pain to a greater extent than other subjective health-related quality-of-life indicies in patients with rheumatoid arthritis, although this improvement is less marked as compared to outcomes in patients with osteoarthritis. These study findings were published online ahead of print July 20 in Arthritis & Rheumatology.
The study included patients with rheumatologist-diagnosed arthritis undergoing primary total knee arthroplasty during 1999 to 2012. Indices of pain knee, and health-related quality of life were obtained in 3 consecutive 6-month intervals: preoperative, perioperative, and postoperative. Descriptive statistics and 1-way analysis of variance were used to compare total knee arthroplasty outcomes by diagnosis. Effect sizes and standardized response means were calculated between baseline and recovery.
Of the participating 18,897 patients, 834 people with rheumatoid arthritis, and 315 people with osteoarthritis had undergone index total knee arthroplasty at mean ages 65 and 68. Post total knee arthroplasty, significant improvements were observed for most domains of pain, function, and health-related quality of life within both disease groups, with greater impact in osteoarthritis. Based on the standardized response means, the maximum improvement was shown in index knee pain.
The Health Assessment Questionnaire II and the Short Form 36 physical component summary were the most responsive health-related quality of life indices in detecting post-total knee arthroplasty improvement in rheumatoid arthritis. A diagnosis of rheumatoid arthritis, lower income, and preoperative anxiety were independently associated with a lower degree of improvement in index knee pain following total knee arthroplasty.
Senior author Kaleb D. Michaud, PhD, Associate Professor in the Division of Rheumatology and Immunology at the University of Nebraska Medical Center in Omaha, and colleagues said that total knee replacement can serve as a “time machine” by which patients can return to a less disabled lifestyle, before the arthritic process catches up.
“A new knee can give osteoarthritis patients 10 to 20 years of painless use, whereas rheumatoid arthritis continues to affect the joint soon afterward,” the researchers said. “It’s an important and effective treatment, but patients with rheumatoid arthritis shouldn’t expect the same, often dramatic results experienced by their osteoarthritis counterparts,” Dr. Michaud said.
According to a new study, total knee arthroplasty is highly effective in reducing clinically relevant knee pain to a greater extent than other subjective health-related quality-of-life indicies in patients with rheumatoid arthritis, although this improvement is less marked as compared to outcomes in patients with osteoarthritis. These study findings were published online ahead of print July 20 in Arthritis & Rheumatology.
The study included patients with rheumatologist-diagnosed arthritis undergoing primary total knee arthroplasty during 1999 to 2012. Indices of pain knee, and health-related quality of life were obtained in 3 consecutive 6-month intervals: preoperative, perioperative, and postoperative. Descriptive statistics and 1-way analysis of variance were used to compare total knee arthroplasty outcomes by diagnosis. Effect sizes and standardized response means were calculated between baseline and recovery.
Of the participating 18,897 patients, 834 people with rheumatoid arthritis, and 315 people with osteoarthritis had undergone index total knee arthroplasty at mean ages 65 and 68. Post total knee arthroplasty, significant improvements were observed for most domains of pain, function, and health-related quality of life within both disease groups, with greater impact in osteoarthritis. Based on the standardized response means, the maximum improvement was shown in index knee pain.
The Health Assessment Questionnaire II and the Short Form 36 physical component summary were the most responsive health-related quality of life indices in detecting post-total knee arthroplasty improvement in rheumatoid arthritis. A diagnosis of rheumatoid arthritis, lower income, and preoperative anxiety were independently associated with a lower degree of improvement in index knee pain following total knee arthroplasty.
Senior author Kaleb D. Michaud, PhD, Associate Professor in the Division of Rheumatology and Immunology at the University of Nebraska Medical Center in Omaha, and colleagues said that total knee replacement can serve as a “time machine” by which patients can return to a less disabled lifestyle, before the arthritic process catches up.
“A new knee can give osteoarthritis patients 10 to 20 years of painless use, whereas rheumatoid arthritis continues to affect the joint soon afterward,” the researchers said. “It’s an important and effective treatment, but patients with rheumatoid arthritis shouldn’t expect the same, often dramatic results experienced by their osteoarthritis counterparts,” Dr. Michaud said.
Suggested Reading
Dusad A, Pedro S, Mikuls TR, et al. Impact of total knee arthroplasty as assessed using patient-reported pain and health-related quality of life indices: rheumatoid arthritis versus osteoarthritis. Arthritis Rheumatol. 2015 July 20 [Epub ahead of print].
Suggested Reading
Dusad A, Pedro S, Mikuls TR, et al. Impact of total knee arthroplasty as assessed using patient-reported pain and health-related quality of life indices: rheumatoid arthritis versus osteoarthritis. Arthritis Rheumatol. 2015 July 20 [Epub ahead of print].

Kidney and Bladder Stones Do Not Increase Postmenopausal Women’s Risk of Osteoporosis
Postmenopausal women with kidney or bladder stones are not at increased risk for osteoporosis, but they do have about a 15% increased risk of another painful stone, according to a study published online ahead of print May 19 in the Journal of Bone and Mineral Research.
Researchers examined data on approximately 150,000 postmenopausal women and found, despite the 2 conditions being clearly associated in men, the same did not hold true for women. “We know in men that if you have a kidney stone, you are more likely to have osteoporosis,” said Laura D. Carbone, MD, MS, Division Chief Chief of Rheumatology in the Department of Medicine at the Medical College of Georgia at Georgia Regents University in Augusta. What Dr. Carbone and colleagues found was that “unlike what has been reported in men, a woman having a kidney stone is not a risk factor for osteoporosis. However, having one urinary tract stone does put women at increased risk for a second stone.”

Data came from participants in the National Institutes of Health Women’s Health Initiative. Out of more than 150,000 women followed in the Women’s Health Initiative, 9,856 women reported urinary tract stones at the start of or over the course of the study. The women were followed for about 8 years, on average.
Dr. Carbone and colleagues looked at the data several different ways, adjusting for factors that could also influence outcome, such as physical inactivity. Investigators only looked at whether urinary tract stones increased the risk of osteoporosis, not the reverse. In unadjusted models there was a significant association of urinary tract stones with incident total fractures (hazard ratio, 1.10) However, in covariate adjusted analyses, urinary tract stones were not significantly related to changes in bone mineral density at any skeletal site or to incident fractures.
The Osteoporotic Fractures in Men study, which looked at nearly 6,000 men with a mean age of 73.7 to determine risk factors for osteoporosis, identified urinary tract stones are a risk factor.
One link between the seemingly disparate conditions of stones and weak bones is an excess of calcium in the urine, which tends to be more common in men, Dr. Carbone said. Sodium and calcium share a common transport mechanism in the kidney, the researchers pointed out, and sodium affects reabsorption of calcium by that organ. When sodium levels are high, more calcium in eliminated in the urine. “Overactivity of the parathyroid glands, which regulate levels of calcium in the blood, is associated with both urinary tract stones and fractures of the vertebra in the spine,” the researchers said.
Some treatments for osteoporosis, including calcium supplementation, can increase the risk of stones. Conversely, individuals who’ve already experienced a urinary tract stone might avoid calcium to help avoid another a subsequent stone and inadvertently increase their osteoporosis risk, the researchers wrote.
“Women with a stone likely should work with their physician to reduce their increased risk of a subsequent stone,” the physicians said, noting that low water and fluid intake, and a high-salt, high-calorie diet are common stone risks.
Suggested Reading
Carbone LD, Hovey KM, Andrews CA, et al. Urinary tract stones and osteoporosis: findings from the women’s health initiative. J Bone Miner Res. 2015 May 19 [Epub ahead of print].
Postmenopausal women with kidney or bladder stones are not at increased risk for osteoporosis, but they do have about a 15% increased risk of another painful stone, according to a study published online ahead of print May 19 in the Journal of Bone and Mineral Research.
Researchers examined data on approximately 150,000 postmenopausal women and found, despite the 2 conditions being clearly associated in men, the same did not hold true for women. “We know in men that if you have a kidney stone, you are more likely to have osteoporosis,” said Laura D. Carbone, MD, MS, Division Chief Chief of Rheumatology in the Department of Medicine at the Medical College of Georgia at Georgia Regents University in Augusta. What Dr. Carbone and colleagues found was that “unlike what has been reported in men, a woman having a kidney stone is not a risk factor for osteoporosis. However, having one urinary tract stone does put women at increased risk for a second stone.”
Data came from participants in the National Institutes of Health Women’s Health Initiative. Out of more than 150,000 women followed in the Women’s Health Initiative, 9,856 women reported urinary tract stones at the start of or over the course of the study. The women were followed for about 8 years, on average.
Dr. Carbone and colleagues looked at the data several different ways, adjusting for factors that could also influence outcome, such as physical inactivity. Investigators only looked at whether urinary tract stones increased the risk of osteoporosis, not the reverse. In unadjusted models there was a significant association of urinary tract stones with incident total fractures (hazard ratio, 1.10) However, in covariate adjusted analyses, urinary tract stones were not significantly related to changes in bone mineral density at any skeletal site or to incident fractures.
The Osteoporotic Fractures in Men study, which looked at nearly 6,000 men with a mean age of 73.7 to determine risk factors for osteoporosis, identified urinary tract stones are a risk factor.
One link between the seemingly disparate conditions of stones and weak bones is an excess of calcium in the urine, which tends to be more common in men, Dr. Carbone said. Sodium and calcium share a common transport mechanism in the kidney, the researchers pointed out, and sodium affects reabsorption of calcium by that organ. When sodium levels are high, more calcium in eliminated in the urine. “Overactivity of the parathyroid glands, which regulate levels of calcium in the blood, is associated with both urinary tract stones and fractures of the vertebra in the spine,” the researchers said.
Some treatments for osteoporosis, including calcium supplementation, can increase the risk of stones. Conversely, individuals who’ve already experienced a urinary tract stone might avoid calcium to help avoid another a subsequent stone and inadvertently increase their osteoporosis risk, the researchers wrote.
“Women with a stone likely should work with their physician to reduce their increased risk of a subsequent stone,” the physicians said, noting that low water and fluid intake, and a high-salt, high-calorie diet are common stone risks.
Postmenopausal women with kidney or bladder stones are not at increased risk for osteoporosis, but they do have about a 15% increased risk of another painful stone, according to a study published online ahead of print May 19 in the Journal of Bone and Mineral Research.
Researchers examined data on approximately 150,000 postmenopausal women and found, despite the 2 conditions being clearly associated in men, the same did not hold true for women. “We know in men that if you have a kidney stone, you are more likely to have osteoporosis,” said Laura D. Carbone, MD, MS, Division Chief Chief of Rheumatology in the Department of Medicine at the Medical College of Georgia at Georgia Regents University in Augusta. What Dr. Carbone and colleagues found was that “unlike what has been reported in men, a woman having a kidney stone is not a risk factor for osteoporosis. However, having one urinary tract stone does put women at increased risk for a second stone.”
Data came from participants in the National Institutes of Health Women’s Health Initiative. Out of more than 150,000 women followed in the Women’s Health Initiative, 9,856 women reported urinary tract stones at the start of or over the course of the study. The women were followed for about 8 years, on average.
Dr. Carbone and colleagues looked at the data several different ways, adjusting for factors that could also influence outcome, such as physical inactivity. Investigators only looked at whether urinary tract stones increased the risk of osteoporosis, not the reverse. In unadjusted models there was a significant association of urinary tract stones with incident total fractures (hazard ratio, 1.10) However, in covariate adjusted analyses, urinary tract stones were not significantly related to changes in bone mineral density at any skeletal site or to incident fractures.
The Osteoporotic Fractures in Men study, which looked at nearly 6,000 men with a mean age of 73.7 to determine risk factors for osteoporosis, identified urinary tract stones are a risk factor.
One link between the seemingly disparate conditions of stones and weak bones is an excess of calcium in the urine, which tends to be more common in men, Dr. Carbone said. Sodium and calcium share a common transport mechanism in the kidney, the researchers pointed out, and sodium affects reabsorption of calcium by that organ. When sodium levels are high, more calcium in eliminated in the urine. “Overactivity of the parathyroid glands, which regulate levels of calcium in the blood, is associated with both urinary tract stones and fractures of the vertebra in the spine,” the researchers said.
Some treatments for osteoporosis, including calcium supplementation, can increase the risk of stones. Conversely, individuals who’ve already experienced a urinary tract stone might avoid calcium to help avoid another a subsequent stone and inadvertently increase their osteoporosis risk, the researchers wrote.
“Women with a stone likely should work with their physician to reduce their increased risk of a subsequent stone,” the physicians said, noting that low water and fluid intake, and a high-salt, high-calorie diet are common stone risks.
Suggested Reading
Carbone LD, Hovey KM, Andrews CA, et al. Urinary tract stones and osteoporosis: findings from the women’s health initiative. J Bone Miner Res. 2015 May 19 [Epub ahead of print].
Suggested Reading
Carbone LD, Hovey KM, Andrews CA, et al. Urinary tract stones and osteoporosis: findings from the women’s health initiative. J Bone Miner Res. 2015 May 19 [Epub ahead of print].

Calisthenics May Reverse Age-Related Bone Loss in Middle-Aged Men
Certain types of weight-lifting and jumping exercises, when completed for at least 6 months, improve bone density in active, healthy, middle-aged men with low bone mass, according to a study published online ahead of print June 16 in Bone.
“Weight-lifting programs exist to increase muscular strength, but less research has examined what happens to bones during these types of exercises,” said Pam Hinton, PhD, Associate Professor and Director of Nutritional Sciences Graduate Studies in the University of Missouri Department of Nutrition and Exercise Physiology in Columbia, Missouri. “Our study is the first to show that exercise-based interventions work to increase bone density in middle-aged men with low bone mass who are otherwise healthy. These exercises could be prescribed to reverse bone loss associated with aging.”

Dr. Hinton and colleagues studied 38 physically active, middle-aged men with osteopenia of the hip or spine who completed either a weight-lifting program or a jumping program for 1 year. Both programs required participants to complete 60 to 120 minutes of targeted exercise each week. The participants took calcium (1200 mg/day) and vitamin D (10 mcg/day) supplements throughout their training programs. The researchers measured the men’s bone mass at the beginning of the study and again at 6 and 12 months using DXA scans of the whole body, total hip, and lumbar spine.
The investigators found the bone mass of the whole body and lumbar spine significantly increased after 6 months of completing the weight-lifting or jumping programs, and this increase was maintained at 12 months. Hip-bone density only increased among those who completed the weight-lifting program.
Dr. Hinton said the study results do not indicate that all kinds of weight-lifting will help improve bone mass; rather, targeted exercises made the training programs effective.
“Only the bone experiencing the mechanical load is going to get stronger, so we specifically chose exercises that would load the hip and the spine, which is why we had participants do squats, deadlifts, lunges, and the overhead press,” Dr. Hinton said. “Also, the intensity of the loading needs to increase over time to build strength. Both of the training programs gradually increased in intensity, and our participants also had rest weeks. Bones need to rest to continue to maximize the response.”
Throughout their training programs, participants rated pain and fatigue after completing their exercises. The participants reported minimal pain and fatigue, and these ratings decreased over the year. Dr. Hinton said individuals who want to use similar training programs to improve bone density should consider their current activity levels and exercise preferences as well as time and equipment constraints.
“The interventions we studied are effective, safe, and take 60 to 120 minutes per week to complete, which is feasible for most people,” Dr. Hinton said. “Also, the exercises can be done at home and require minimal exercise equipment, which adds to the ease of implementing and continuing these interventions.”
Suggested Reading
Hinton PS, Nigh P, Thyfault J. Effectiveness of resistance training or jumping-exercise to increase bone mineral density in men with low bone mass: a 12-month randomized, clinical trial. Bone. 2015 June 16 [Epub ahead of print].
Certain types of weight-lifting and jumping exercises, when completed for at least 6 months, improve bone density in active, healthy, middle-aged men with low bone mass, according to a study published online ahead of print June 16 in Bone.
“Weight-lifting programs exist to increase muscular strength, but less research has examined what happens to bones during these types of exercises,” said Pam Hinton, PhD, Associate Professor and Director of Nutritional Sciences Graduate Studies in the University of Missouri Department of Nutrition and Exercise Physiology in Columbia, Missouri. “Our study is the first to show that exercise-based interventions work to increase bone density in middle-aged men with low bone mass who are otherwise healthy. These exercises could be prescribed to reverse bone loss associated with aging.”
Dr. Hinton and colleagues studied 38 physically active, middle-aged men with osteopenia of the hip or spine who completed either a weight-lifting program or a jumping program for 1 year. Both programs required participants to complete 60 to 120 minutes of targeted exercise each week. The participants took calcium (1200 mg/day) and vitamin D (10 mcg/day) supplements throughout their training programs. The researchers measured the men’s bone mass at the beginning of the study and again at 6 and 12 months using DXA scans of the whole body, total hip, and lumbar spine.
The investigators found the bone mass of the whole body and lumbar spine significantly increased after 6 months of completing the weight-lifting or jumping programs, and this increase was maintained at 12 months. Hip-bone density only increased among those who completed the weight-lifting program.
Dr. Hinton said the study results do not indicate that all kinds of weight-lifting will help improve bone mass; rather, targeted exercises made the training programs effective.
“Only the bone experiencing the mechanical load is going to get stronger, so we specifically chose exercises that would load the hip and the spine, which is why we had participants do squats, deadlifts, lunges, and the overhead press,” Dr. Hinton said. “Also, the intensity of the loading needs to increase over time to build strength. Both of the training programs gradually increased in intensity, and our participants also had rest weeks. Bones need to rest to continue to maximize the response.”
Throughout their training programs, participants rated pain and fatigue after completing their exercises. The participants reported minimal pain and fatigue, and these ratings decreased over the year. Dr. Hinton said individuals who want to use similar training programs to improve bone density should consider their current activity levels and exercise preferences as well as time and equipment constraints.
“The interventions we studied are effective, safe, and take 60 to 120 minutes per week to complete, which is feasible for most people,” Dr. Hinton said. “Also, the exercises can be done at home and require minimal exercise equipment, which adds to the ease of implementing and continuing these interventions.”
Certain types of weight-lifting and jumping exercises, when completed for at least 6 months, improve bone density in active, healthy, middle-aged men with low bone mass, according to a study published online ahead of print June 16 in Bone.
“Weight-lifting programs exist to increase muscular strength, but less research has examined what happens to bones during these types of exercises,” said Pam Hinton, PhD, Associate Professor and Director of Nutritional Sciences Graduate Studies in the University of Missouri Department of Nutrition and Exercise Physiology in Columbia, Missouri. “Our study is the first to show that exercise-based interventions work to increase bone density in middle-aged men with low bone mass who are otherwise healthy. These exercises could be prescribed to reverse bone loss associated with aging.”
Dr. Hinton and colleagues studied 38 physically active, middle-aged men with osteopenia of the hip or spine who completed either a weight-lifting program or a jumping program for 1 year. Both programs required participants to complete 60 to 120 minutes of targeted exercise each week. The participants took calcium (1200 mg/day) and vitamin D (10 mcg/day) supplements throughout their training programs. The researchers measured the men’s bone mass at the beginning of the study and again at 6 and 12 months using DXA scans of the whole body, total hip, and lumbar spine.
The investigators found the bone mass of the whole body and lumbar spine significantly increased after 6 months of completing the weight-lifting or jumping programs, and this increase was maintained at 12 months. Hip-bone density only increased among those who completed the weight-lifting program.
Dr. Hinton said the study results do not indicate that all kinds of weight-lifting will help improve bone mass; rather, targeted exercises made the training programs effective.
“Only the bone experiencing the mechanical load is going to get stronger, so we specifically chose exercises that would load the hip and the spine, which is why we had participants do squats, deadlifts, lunges, and the overhead press,” Dr. Hinton said. “Also, the intensity of the loading needs to increase over time to build strength. Both of the training programs gradually increased in intensity, and our participants also had rest weeks. Bones need to rest to continue to maximize the response.”
Throughout their training programs, participants rated pain and fatigue after completing their exercises. The participants reported minimal pain and fatigue, and these ratings decreased over the year. Dr. Hinton said individuals who want to use similar training programs to improve bone density should consider their current activity levels and exercise preferences as well as time and equipment constraints.
“The interventions we studied are effective, safe, and take 60 to 120 minutes per week to complete, which is feasible for most people,” Dr. Hinton said. “Also, the exercises can be done at home and require minimal exercise equipment, which adds to the ease of implementing and continuing these interventions.”
Suggested Reading
Hinton PS, Nigh P, Thyfault J. Effectiveness of resistance training or jumping-exercise to increase bone mineral density in men with low bone mass: a 12-month randomized, clinical trial. Bone. 2015 June 16 [Epub ahead of print].
Suggested Reading
Hinton PS, Nigh P, Thyfault J. Effectiveness of resistance training or jumping-exercise to increase bone mineral density in men with low bone mass: a 12-month randomized, clinical trial. Bone. 2015 June 16 [Epub ahead of print].

Knee Replacement Proves Effective for Degeneration Caused by Blount Disease
Total knee replacements can effectively treat degeneration caused by Blount disease, according to a study published online ahead of print July 11 in the Journal of Arthroplasty.
Middle-aged patients with Blount disease who underwent joint replacements on 1 or both knees were found to have stable knees, excellent range of motion, and no need for pain medications, according to the study conducted at Loyola University Medical Center in Illinois.
“With proper attention paid to technical details, patients with Blount or Blount-like deformity can undergo successful total knee arthroplasty,” said Harold Rees, MD, Assistant Professor of Reconstructive Surgery and Joint Replacement at Loyola University Chicago Stritch School of Medicine in Maywood, Illinois, and colleagues.

For the study, Dr. Rees and colleagues reviewed the records of 5 patients with Blount disease. Three patients had replacements on both knees and 2 patients had replacements on 1 knee. Four patients were African American and 4 were male. All were obese. The average age at the time of the knee replacements was 49.9. Patients were followed-up an average of 75.2 months after their knee replacements.
Mean proximal tibial metaphyseal-diaphyseal angle was 20.75 degrees. Each patient had substantial posteromedial tibial bony defects and 6 knees required extensive medial releases. Two knees required increased constraint at index procedure. One patient underwent bilateral revision surgery with rotating hinge prostheses.
The researchers used a scoring system, devised by the Knee Society, that combines clinical, functional, and satisfaction scores. The mean Knee Society score was 212.5, out of a maximum possible score of 255. Patients also were rated on the Western Ontario and McMaster Universities Osteoarthritis Index.
“The main purpose was to highlight surgical considerations in performing total knee arthroplasty in patients with Blount disease or Blount-like deformity. Despite a challenging patient population in which to perform total knee arthroplasty, we show that it can be done with a low risk of complication and reasonable medium-term results,” said the study authors. “Surgeons should be prepared to address posteromedial tibial bony defects and consider constrained arthroplasty at the index procedure,” they said.
Suggested Reading
Natoli RM, Nypaver CM, Schiff AP, et al. Total knee arthroplasty in patients with blount disease or blount-like deformity. J Arthroplasty. 2015 Jul 11 [Epub ahead of print].
Total knee replacements can effectively treat degeneration caused by Blount disease, according to a study published online ahead of print July 11 in the Journal of Arthroplasty.
Middle-aged patients with Blount disease who underwent joint replacements on 1 or both knees were found to have stable knees, excellent range of motion, and no need for pain medications, according to the study conducted at Loyola University Medical Center in Illinois.
“With proper attention paid to technical details, patients with Blount or Blount-like deformity can undergo successful total knee arthroplasty,” said Harold Rees, MD, Assistant Professor of Reconstructive Surgery and Joint Replacement at Loyola University Chicago Stritch School of Medicine in Maywood, Illinois, and colleagues.
For the study, Dr. Rees and colleagues reviewed the records of 5 patients with Blount disease. Three patients had replacements on both knees and 2 patients had replacements on 1 knee. Four patients were African American and 4 were male. All were obese. The average age at the time of the knee replacements was 49.9. Patients were followed-up an average of 75.2 months after their knee replacements.
Mean proximal tibial metaphyseal-diaphyseal angle was 20.75 degrees. Each patient had substantial posteromedial tibial bony defects and 6 knees required extensive medial releases. Two knees required increased constraint at index procedure. One patient underwent bilateral revision surgery with rotating hinge prostheses.
The researchers used a scoring system, devised by the Knee Society, that combines clinical, functional, and satisfaction scores. The mean Knee Society score was 212.5, out of a maximum possible score of 255. Patients also were rated on the Western Ontario and McMaster Universities Osteoarthritis Index.
“The main purpose was to highlight surgical considerations in performing total knee arthroplasty in patients with Blount disease or Blount-like deformity. Despite a challenging patient population in which to perform total knee arthroplasty, we show that it can be done with a low risk of complication and reasonable medium-term results,” said the study authors. “Surgeons should be prepared to address posteromedial tibial bony defects and consider constrained arthroplasty at the index procedure,” they said.
Total knee replacements can effectively treat degeneration caused by Blount disease, according to a study published online ahead of print July 11 in the Journal of Arthroplasty.
Middle-aged patients with Blount disease who underwent joint replacements on 1 or both knees were found to have stable knees, excellent range of motion, and no need for pain medications, according to the study conducted at Loyola University Medical Center in Illinois.
“With proper attention paid to technical details, patients with Blount or Blount-like deformity can undergo successful total knee arthroplasty,” said Harold Rees, MD, Assistant Professor of Reconstructive Surgery and Joint Replacement at Loyola University Chicago Stritch School of Medicine in Maywood, Illinois, and colleagues.
For the study, Dr. Rees and colleagues reviewed the records of 5 patients with Blount disease. Three patients had replacements on both knees and 2 patients had replacements on 1 knee. Four patients were African American and 4 were male. All were obese. The average age at the time of the knee replacements was 49.9. Patients were followed-up an average of 75.2 months after their knee replacements.
Mean proximal tibial metaphyseal-diaphyseal angle was 20.75 degrees. Each patient had substantial posteromedial tibial bony defects and 6 knees required extensive medial releases. Two knees required increased constraint at index procedure. One patient underwent bilateral revision surgery with rotating hinge prostheses.
The researchers used a scoring system, devised by the Knee Society, that combines clinical, functional, and satisfaction scores. The mean Knee Society score was 212.5, out of a maximum possible score of 255. Patients also were rated on the Western Ontario and McMaster Universities Osteoarthritis Index.
“The main purpose was to highlight surgical considerations in performing total knee arthroplasty in patients with Blount disease or Blount-like deformity. Despite a challenging patient population in which to perform total knee arthroplasty, we show that it can be done with a low risk of complication and reasonable medium-term results,” said the study authors. “Surgeons should be prepared to address posteromedial tibial bony defects and consider constrained arthroplasty at the index procedure,” they said.
Suggested Reading
Natoli RM, Nypaver CM, Schiff AP, et al. Total knee arthroplasty in patients with blount disease or blount-like deformity. J Arthroplasty. 2015 Jul 11 [Epub ahead of print].
Suggested Reading
Natoli RM, Nypaver CM, Schiff AP, et al. Total knee arthroplasty in patients with blount disease or blount-like deformity. J Arthroplasty. 2015 Jul 11 [Epub ahead of print].

A Picture Is Worth a Thousand Words: Unconscious Bias in the Residency Application Process?
Applying for a residency program can be a stressful process for medical students. It is a combination of applying for a job in the “real world” and applying to a college or medical school. In certain fields of medicine or surgery, there may be over 600 residency applications for 40 to 80 interviewee slots. Different specialties, as well as programs within a given specialty, take a different number of residents per year. This can vary from 1 to over 20 available spots, depending on the field of medicine or surgery as well as the specific program. Orthopedic surgery residencies, for example, can match between 2 and 12 residents each year. During the 2013–2014 academic year at our institution, there were over 600 applications received for approximately 50 interview slots for a class of 5 orthopedic surgery residents. Nationally, according to publicly available 2013 National Resident Matching Program (NRMP) data, a total of 1038 applicants (833 US medical school seniors) applied for 693 spots in orthopedic surgery, of which 692 were filled, indicating that orthopedic surgery remains one of the most desired fields among medical school seniors.1 Looking at the statistics provided by the NRMP data, orthopedic applicants remain some of the most competitive, with proportionally higher board scores, publication numbers, and grades, among other factors.1
Each individual program has its own method for sifting through the applications. At some institutions, the individual “in charge” of the selection committee may look through all applications initially, narrow them down, and then distribute them to the other members of the selection committee to determine the final interviewee list. At other institutions, the initial group of applications may be divided and distributed to the committee members so that each member reviews the applications and ultimately decides upon the interview candidates.
The Electronic Residency Application Service (ERAS) application includes the applicant’s name, birth city, current place of residence, education history, standardized test scores, grades achieved during medical school, letters of recommendation, personal statement, extracurricular activities, volunteer activities, research experience, and languages spoken, along with several other pieces of data, all intended to be able to give the committee a better understanding of the applicant. Interestingly, however, the application also includes a photograph of the applicant.
Countless authors have demonstrated that we make assumptions and reach conclusions without even being aware that this is occurring. This is the theory of “unconscious bias.”2-5 Unconscious bias applies to how we perceive other people, and occurs when subconscious beliefs or unrecognized stereotypes about specific characteristics, including gender, ethnicity, religion, socioeconomic status, age, and sexual orientation, result in an automatic and unconscious reaction and/or behavior.6 Unconscious bias has the ability to affect everything from how health care is delivered to how employees are hired.7-12 We are all biased, and becoming aware of our biases will help us mitigate them in the workplace.
Title VII of the Civil Rights Act of 1964 requires that employers rely solely on job-related qualifications, and not physical characteristics, in their interviewing and hiring process. The US Equal Employment Opportunity Commission (EEOC), the federal agency that enforces Title VII, includes asking for photographs during the application stage on its list of prohibited practices for employers.13 It is our belief that including a photograph in the ERAS application, prior to the selection of interview candidates, may produce unconscious bias in the decision for granting (or not granting) an interview, and this component of the application should be eliminated.
Using a wide spectrum of cultural backgrounds in employers, Dion and colleagues14 demonstrated that the “what is beautiful is good” bias is present in all cultures when prospective employees are closely matched in qualification. Attractive individuals are thought to have better professional lives and stable marital relationships and personalities, according to previous studies.14 There has been much research aimed at determining if physical attractiveness is a factor in hiring, and the evidence suggests that the more attractive the applicant is, the greater the chances of being hired.15 Specifically, Watkins and Johnston15 have found that attractive people are thought to have better personalities than less attractive people, and that a photograph can influence the hiring decision process.
Bradley Ruffle at Ben-Gurion University and Ze’ev Shtudiner at Ariel University looked at what happens when job hunters include photographs with their curricula vitae (CV), as is the norm in much of Europe and Asia.16 For over 2500 job postings, they sent 2 identical résumés: one with a photograph and one without a photograph. An equal number of male and female applicants were sent to each posting, as were an equal number of attractive and plain-looking photographs; applications without photographs were also sent as a control group. For men, the results were as expected: CVs of “attractive” men were more likely to elicit a response from the employer (19.7%) compared with those of no-picture men (13.7%) and plain-looking men (9.2%). Interestingly, men who were viewed as “plain-looking” were better off not including a photograph. For the female applicants, however, the results were unexpected: CVs of women without a picture elicited the highest response rate (16.6%), while CVs of “plain-looking” women (13.6%) and of “attractive” women (12.8%) were less likely to receive a response.16
It is an unfortunate reality that personal preference, bias, and, in some cases, discriminatory hiring practices all factor into the selection process.17 This is why, as described above, the EEOC includes asking for photographs during the application stage on its list of prohibited practices for employers.13 The EEOC website also states: “If needed for identification purposes, a photograph may be obtained after an offer of employment is made and accepted.”13 In the residency application scenario, once an applicant has been granted an interview, a photograph can be taken on the day of the interview. With so many interviewees, this may help the interviewers to remember the interviewee. At this point in the process, the applicant has already been granted the interview. The bias associated with merely looking at a photograph is thus eliminated. This is in accordance with Title VII and is clearly different than including a photograph in the initial application, which directly violates Title VII.
Reviewers of applicants may have an unconscious bias due to the applicant’s attractiveness, race, sex, ethnicity, etc. Other, subtler forms of bias may also be present. Without realizing it, people may judge the quality of the photograph, or even what the applicant was wearing in the photograph. In orthopedic surgery, for example, there may be bias in the “size” of the applicant regardless of sex. Reviewers may unconsciously think how is he/she going to hold the leg, cut a rod, reduce a hip, etc. Without even realizing it, this may sway the person reviewing the application to choose one applicant over another. This may occur regardless of the applicant’s actual qualifications as based on the previously described factors, including test scores, grades during medical school, letters of recommendation, personal statement, extracurricular activities, volunteer activities, and research experience.
Unconscious bias is present in everyone. In an ideal world, one would be able to eliminate all sources of unconscious bias in the application process. Bias due to attending an Ivy League school versus a state school, bias due to where the applicant is from, bias due to who wrote the letter of recommendation, along with various other sources of unconscious bias, would be able to be eliminated. Unfortunately, this is not possible. What is possible, however, is to remove the photograph from the application process and to comply with Title VII of the Civil Rights Act of 1964.
1. National Resident Matching Program, Data Release and Research Committee. Results of the 2013 NRMP Applicant Survey by Preferred Specialty and Applicant Type. Washington, DC: National Resident Matching Program; 2013. www.nrmp.org/wp-content/uploads/2013/08/applicantresultsbyspecialty2013.pdf. Accessed July 20, 2015.
2. Santry HP, Wren SM. The role of unconscious bias in surgical safety and outcomes. Surg Clin North Am. 2012;92(1):137–151.
3. Greenwald AG, McGhee DE, Schwartz JL. Measuring individual differences in implicit cognition: the implicit association test. J Pers Soc Psychol. 1998;74(6):1464–1480.
4. Greenwald AG, Poehlman TA, Uhlmann EL, Banaji MR. Understanding and using the Implicit Association Test: III. Meta-analysis of predictive validity. J Pers Soc Psychol. 2009;97(1):17–41.
5. Plessner H, Banse R. Attitude measurement using the Implicit Association Test (IAT). Z Exp Psychol. 2001;48(2):82–84.
6. Chapman EN, Kaatz A, Carnes M. Physicians and implicit bias: how doctors may unwittingly perpetuate health care disparities. J Gen Intern Med. 2013;28(11):1504–1510.
7. What you don’t know: the science of unconscious bias and what to do about it in the search and recruitment process [e-learning seminar]. Association of American Medical Colleges website. https://www.aamc.org/members/leadership/catalog/178420/unconscious_bias.html. Accessed July 14, 2015.
8. Haider AH, Schneider EB, Sriram N, et al. Unconscious race and class bias: its association with decision making by trauma and acute care surgeons. J Trauma Acute Care Surg. 2014;77(3):409–416.
9. Blair IV, Steiner JF, Hanratty R, et al. An investigation of associations between clinicians’ ethnic or racial bias and hypertension treatment, medication adherence and blood pressure control. J Gen Intern Med. 2014;29(7):987–995.
10. Ravenell J, Ogedegbe G. Unconscious bias and real-world hypertension outcomes: advancing disparities research. J Gen Intern Med. 2014;29(7):973–975.
11. van Ryn M, Saha S. Exploring unconscious bias in disparities research and medical education. JAMA. 2011;306(9):995–996.
12. Puhl RM, Moss-Racusin CA, Schwartz MB, Brownell KD. Weight stigmatization and bias reduction: perspectives of overweight and obese adults. Health Educ Res. 2008;23(2):347–358.
13. Prohibited employment policies/practices. US Equal Employment Opportunity Commission website. http://www.eeoc.gov/laws/practices/. Accessed July 14, 2015.
14. Dion K, Berscheid E, Walster E. What is beautiful is good. J Pers Soc Psychol. 1972;24(3):285–290.
15. Watkins LM, Johnston L. Screening job applicants: the impact of physical attractiveness and application quality. Int J Selection Assess. 2000;8(2):76–84.
16. Ruffle BJ, Shtudiner Z. Are good-looking people more employable? Manage Sci. http://dx.doi.org/10.1287/mnsc.2014.1927. Published May 29, 2014. Accessed July 14, 2015.
17. Lemay EP Jr, Clark MS, Greenberg A. What is beautiful is good because what is beautiful is desired: physical attractiveness stereotyping as projection of interpersonal goals. Pers Soc Psychol Bull. 2010;36(3):339–353.
Applying for a residency program can be a stressful process for medical students. It is a combination of applying for a job in the “real world” and applying to a college or medical school. In certain fields of medicine or surgery, there may be over 600 residency applications for 40 to 80 interviewee slots. Different specialties, as well as programs within a given specialty, take a different number of residents per year. This can vary from 1 to over 20 available spots, depending on the field of medicine or surgery as well as the specific program. Orthopedic surgery residencies, for example, can match between 2 and 12 residents each year. During the 2013–2014 academic year at our institution, there were over 600 applications received for approximately 50 interview slots for a class of 5 orthopedic surgery residents. Nationally, according to publicly available 2013 National Resident Matching Program (NRMP) data, a total of 1038 applicants (833 US medical school seniors) applied for 693 spots in orthopedic surgery, of which 692 were filled, indicating that orthopedic surgery remains one of the most desired fields among medical school seniors.1 Looking at the statistics provided by the NRMP data, orthopedic applicants remain some of the most competitive, with proportionally higher board scores, publication numbers, and grades, among other factors.1
Each individual program has its own method for sifting through the applications. At some institutions, the individual “in charge” of the selection committee may look through all applications initially, narrow them down, and then distribute them to the other members of the selection committee to determine the final interviewee list. At other institutions, the initial group of applications may be divided and distributed to the committee members so that each member reviews the applications and ultimately decides upon the interview candidates.
The Electronic Residency Application Service (ERAS) application includes the applicant’s name, birth city, current place of residence, education history, standardized test scores, grades achieved during medical school, letters of recommendation, personal statement, extracurricular activities, volunteer activities, research experience, and languages spoken, along with several other pieces of data, all intended to be able to give the committee a better understanding of the applicant. Interestingly, however, the application also includes a photograph of the applicant.
Countless authors have demonstrated that we make assumptions and reach conclusions without even being aware that this is occurring. This is the theory of “unconscious bias.”2-5 Unconscious bias applies to how we perceive other people, and occurs when subconscious beliefs or unrecognized stereotypes about specific characteristics, including gender, ethnicity, religion, socioeconomic status, age, and sexual orientation, result in an automatic and unconscious reaction and/or behavior.6 Unconscious bias has the ability to affect everything from how health care is delivered to how employees are hired.7-12 We are all biased, and becoming aware of our biases will help us mitigate them in the workplace.
Title VII of the Civil Rights Act of 1964 requires that employers rely solely on job-related qualifications, and not physical characteristics, in their interviewing and hiring process. The US Equal Employment Opportunity Commission (EEOC), the federal agency that enforces Title VII, includes asking for photographs during the application stage on its list of prohibited practices for employers.13 It is our belief that including a photograph in the ERAS application, prior to the selection of interview candidates, may produce unconscious bias in the decision for granting (or not granting) an interview, and this component of the application should be eliminated.
Using a wide spectrum of cultural backgrounds in employers, Dion and colleagues14 demonstrated that the “what is beautiful is good” bias is present in all cultures when prospective employees are closely matched in qualification. Attractive individuals are thought to have better professional lives and stable marital relationships and personalities, according to previous studies.14 There has been much research aimed at determining if physical attractiveness is a factor in hiring, and the evidence suggests that the more attractive the applicant is, the greater the chances of being hired.15 Specifically, Watkins and Johnston15 have found that attractive people are thought to have better personalities than less attractive people, and that a photograph can influence the hiring decision process.
Bradley Ruffle at Ben-Gurion University and Ze’ev Shtudiner at Ariel University looked at what happens when job hunters include photographs with their curricula vitae (CV), as is the norm in much of Europe and Asia.16 For over 2500 job postings, they sent 2 identical résumés: one with a photograph and one without a photograph. An equal number of male and female applicants were sent to each posting, as were an equal number of attractive and plain-looking photographs; applications without photographs were also sent as a control group. For men, the results were as expected: CVs of “attractive” men were more likely to elicit a response from the employer (19.7%) compared with those of no-picture men (13.7%) and plain-looking men (9.2%). Interestingly, men who were viewed as “plain-looking” were better off not including a photograph. For the female applicants, however, the results were unexpected: CVs of women without a picture elicited the highest response rate (16.6%), while CVs of “plain-looking” women (13.6%) and of “attractive” women (12.8%) were less likely to receive a response.16
It is an unfortunate reality that personal preference, bias, and, in some cases, discriminatory hiring practices all factor into the selection process.17 This is why, as described above, the EEOC includes asking for photographs during the application stage on its list of prohibited practices for employers.13 The EEOC website also states: “If needed for identification purposes, a photograph may be obtained after an offer of employment is made and accepted.”13 In the residency application scenario, once an applicant has been granted an interview, a photograph can be taken on the day of the interview. With so many interviewees, this may help the interviewers to remember the interviewee. At this point in the process, the applicant has already been granted the interview. The bias associated with merely looking at a photograph is thus eliminated. This is in accordance with Title VII and is clearly different than including a photograph in the initial application, which directly violates Title VII.
Reviewers of applicants may have an unconscious bias due to the applicant’s attractiveness, race, sex, ethnicity, etc. Other, subtler forms of bias may also be present. Without realizing it, people may judge the quality of the photograph, or even what the applicant was wearing in the photograph. In orthopedic surgery, for example, there may be bias in the “size” of the applicant regardless of sex. Reviewers may unconsciously think how is he/she going to hold the leg, cut a rod, reduce a hip, etc. Without even realizing it, this may sway the person reviewing the application to choose one applicant over another. This may occur regardless of the applicant’s actual qualifications as based on the previously described factors, including test scores, grades during medical school, letters of recommendation, personal statement, extracurricular activities, volunteer activities, and research experience.
Unconscious bias is present in everyone. In an ideal world, one would be able to eliminate all sources of unconscious bias in the application process. Bias due to attending an Ivy League school versus a state school, bias due to where the applicant is from, bias due to who wrote the letter of recommendation, along with various other sources of unconscious bias, would be able to be eliminated. Unfortunately, this is not possible. What is possible, however, is to remove the photograph from the application process and to comply with Title VII of the Civil Rights Act of 1964.
Applying for a residency program can be a stressful process for medical students. It is a combination of applying for a job in the “real world” and applying to a college or medical school. In certain fields of medicine or surgery, there may be over 600 residency applications for 40 to 80 interviewee slots. Different specialties, as well as programs within a given specialty, take a different number of residents per year. This can vary from 1 to over 20 available spots, depending on the field of medicine or surgery as well as the specific program. Orthopedic surgery residencies, for example, can match between 2 and 12 residents each year. During the 2013–2014 academic year at our institution, there were over 600 applications received for approximately 50 interview slots for a class of 5 orthopedic surgery residents. Nationally, according to publicly available 2013 National Resident Matching Program (NRMP) data, a total of 1038 applicants (833 US medical school seniors) applied for 693 spots in orthopedic surgery, of which 692 were filled, indicating that orthopedic surgery remains one of the most desired fields among medical school seniors.1 Looking at the statistics provided by the NRMP data, orthopedic applicants remain some of the most competitive, with proportionally higher board scores, publication numbers, and grades, among other factors.1
Each individual program has its own method for sifting through the applications. At some institutions, the individual “in charge” of the selection committee may look through all applications initially, narrow them down, and then distribute them to the other members of the selection committee to determine the final interviewee list. At other institutions, the initial group of applications may be divided and distributed to the committee members so that each member reviews the applications and ultimately decides upon the interview candidates.
The Electronic Residency Application Service (ERAS) application includes the applicant’s name, birth city, current place of residence, education history, standardized test scores, grades achieved during medical school, letters of recommendation, personal statement, extracurricular activities, volunteer activities, research experience, and languages spoken, along with several other pieces of data, all intended to be able to give the committee a better understanding of the applicant. Interestingly, however, the application also includes a photograph of the applicant.
Countless authors have demonstrated that we make assumptions and reach conclusions without even being aware that this is occurring. This is the theory of “unconscious bias.”2-5 Unconscious bias applies to how we perceive other people, and occurs when subconscious beliefs or unrecognized stereotypes about specific characteristics, including gender, ethnicity, religion, socioeconomic status, age, and sexual orientation, result in an automatic and unconscious reaction and/or behavior.6 Unconscious bias has the ability to affect everything from how health care is delivered to how employees are hired.7-12 We are all biased, and becoming aware of our biases will help us mitigate them in the workplace.
Title VII of the Civil Rights Act of 1964 requires that employers rely solely on job-related qualifications, and not physical characteristics, in their interviewing and hiring process. The US Equal Employment Opportunity Commission (EEOC), the federal agency that enforces Title VII, includes asking for photographs during the application stage on its list of prohibited practices for employers.13 It is our belief that including a photograph in the ERAS application, prior to the selection of interview candidates, may produce unconscious bias in the decision for granting (or not granting) an interview, and this component of the application should be eliminated.
Using a wide spectrum of cultural backgrounds in employers, Dion and colleagues14 demonstrated that the “what is beautiful is good” bias is present in all cultures when prospective employees are closely matched in qualification. Attractive individuals are thought to have better professional lives and stable marital relationships and personalities, according to previous studies.14 There has been much research aimed at determining if physical attractiveness is a factor in hiring, and the evidence suggests that the more attractive the applicant is, the greater the chances of being hired.15 Specifically, Watkins and Johnston15 have found that attractive people are thought to have better personalities than less attractive people, and that a photograph can influence the hiring decision process.
Bradley Ruffle at Ben-Gurion University and Ze’ev Shtudiner at Ariel University looked at what happens when job hunters include photographs with their curricula vitae (CV), as is the norm in much of Europe and Asia.16 For over 2500 job postings, they sent 2 identical résumés: one with a photograph and one without a photograph. An equal number of male and female applicants were sent to each posting, as were an equal number of attractive and plain-looking photographs; applications without photographs were also sent as a control group. For men, the results were as expected: CVs of “attractive” men were more likely to elicit a response from the employer (19.7%) compared with those of no-picture men (13.7%) and plain-looking men (9.2%). Interestingly, men who were viewed as “plain-looking” were better off not including a photograph. For the female applicants, however, the results were unexpected: CVs of women without a picture elicited the highest response rate (16.6%), while CVs of “plain-looking” women (13.6%) and of “attractive” women (12.8%) were less likely to receive a response.16
It is an unfortunate reality that personal preference, bias, and, in some cases, discriminatory hiring practices all factor into the selection process.17 This is why, as described above, the EEOC includes asking for photographs during the application stage on its list of prohibited practices for employers.13 The EEOC website also states: “If needed for identification purposes, a photograph may be obtained after an offer of employment is made and accepted.”13 In the residency application scenario, once an applicant has been granted an interview, a photograph can be taken on the day of the interview. With so many interviewees, this may help the interviewers to remember the interviewee. At this point in the process, the applicant has already been granted the interview. The bias associated with merely looking at a photograph is thus eliminated. This is in accordance with Title VII and is clearly different than including a photograph in the initial application, which directly violates Title VII.
Reviewers of applicants may have an unconscious bias due to the applicant’s attractiveness, race, sex, ethnicity, etc. Other, subtler forms of bias may also be present. Without realizing it, people may judge the quality of the photograph, or even what the applicant was wearing in the photograph. In orthopedic surgery, for example, there may be bias in the “size” of the applicant regardless of sex. Reviewers may unconsciously think how is he/she going to hold the leg, cut a rod, reduce a hip, etc. Without even realizing it, this may sway the person reviewing the application to choose one applicant over another. This may occur regardless of the applicant’s actual qualifications as based on the previously described factors, including test scores, grades during medical school, letters of recommendation, personal statement, extracurricular activities, volunteer activities, and research experience.
Unconscious bias is present in everyone. In an ideal world, one would be able to eliminate all sources of unconscious bias in the application process. Bias due to attending an Ivy League school versus a state school, bias due to where the applicant is from, bias due to who wrote the letter of recommendation, along with various other sources of unconscious bias, would be able to be eliminated. Unfortunately, this is not possible. What is possible, however, is to remove the photograph from the application process and to comply with Title VII of the Civil Rights Act of 1964.
1. National Resident Matching Program, Data Release and Research Committee. Results of the 2013 NRMP Applicant Survey by Preferred Specialty and Applicant Type. Washington, DC: National Resident Matching Program; 2013. www.nrmp.org/wp-content/uploads/2013/08/applicantresultsbyspecialty2013.pdf. Accessed July 20, 2015.
2. Santry HP, Wren SM. The role of unconscious bias in surgical safety and outcomes. Surg Clin North Am. 2012;92(1):137–151.
3. Greenwald AG, McGhee DE, Schwartz JL. Measuring individual differences in implicit cognition: the implicit association test. J Pers Soc Psychol. 1998;74(6):1464–1480.
4. Greenwald AG, Poehlman TA, Uhlmann EL, Banaji MR. Understanding and using the Implicit Association Test: III. Meta-analysis of predictive validity. J Pers Soc Psychol. 2009;97(1):17–41.
5. Plessner H, Banse R. Attitude measurement using the Implicit Association Test (IAT). Z Exp Psychol. 2001;48(2):82–84.
6. Chapman EN, Kaatz A, Carnes M. Physicians and implicit bias: how doctors may unwittingly perpetuate health care disparities. J Gen Intern Med. 2013;28(11):1504–1510.
7. What you don’t know: the science of unconscious bias and what to do about it in the search and recruitment process [e-learning seminar]. Association of American Medical Colleges website. https://www.aamc.org/members/leadership/catalog/178420/unconscious_bias.html. Accessed July 14, 2015.
8. Haider AH, Schneider EB, Sriram N, et al. Unconscious race and class bias: its association with decision making by trauma and acute care surgeons. J Trauma Acute Care Surg. 2014;77(3):409–416.
9. Blair IV, Steiner JF, Hanratty R, et al. An investigation of associations between clinicians’ ethnic or racial bias and hypertension treatment, medication adherence and blood pressure control. J Gen Intern Med. 2014;29(7):987–995.
10. Ravenell J, Ogedegbe G. Unconscious bias and real-world hypertension outcomes: advancing disparities research. J Gen Intern Med. 2014;29(7):973–975.
11. van Ryn M, Saha S. Exploring unconscious bias in disparities research and medical education. JAMA. 2011;306(9):995–996.
12. Puhl RM, Moss-Racusin CA, Schwartz MB, Brownell KD. Weight stigmatization and bias reduction: perspectives of overweight and obese adults. Health Educ Res. 2008;23(2):347–358.
13. Prohibited employment policies/practices. US Equal Employment Opportunity Commission website. http://www.eeoc.gov/laws/practices/. Accessed July 14, 2015.
14. Dion K, Berscheid E, Walster E. What is beautiful is good. J Pers Soc Psychol. 1972;24(3):285–290.
15. Watkins LM, Johnston L. Screening job applicants: the impact of physical attractiveness and application quality. Int J Selection Assess. 2000;8(2):76–84.
16. Ruffle BJ, Shtudiner Z. Are good-looking people more employable? Manage Sci. http://dx.doi.org/10.1287/mnsc.2014.1927. Published May 29, 2014. Accessed July 14, 2015.
17. Lemay EP Jr, Clark MS, Greenberg A. What is beautiful is good because what is beautiful is desired: physical attractiveness stereotyping as projection of interpersonal goals. Pers Soc Psychol Bull. 2010;36(3):339–353.
1. National Resident Matching Program, Data Release and Research Committee. Results of the 2013 NRMP Applicant Survey by Preferred Specialty and Applicant Type. Washington, DC: National Resident Matching Program; 2013. www.nrmp.org/wp-content/uploads/2013/08/applicantresultsbyspecialty2013.pdf. Accessed July 20, 2015.
2. Santry HP, Wren SM. The role of unconscious bias in surgical safety and outcomes. Surg Clin North Am. 2012;92(1):137–151.
3. Greenwald AG, McGhee DE, Schwartz JL. Measuring individual differences in implicit cognition: the implicit association test. J Pers Soc Psychol. 1998;74(6):1464–1480.
4. Greenwald AG, Poehlman TA, Uhlmann EL, Banaji MR. Understanding and using the Implicit Association Test: III. Meta-analysis of predictive validity. J Pers Soc Psychol. 2009;97(1):17–41.
5. Plessner H, Banse R. Attitude measurement using the Implicit Association Test (IAT). Z Exp Psychol. 2001;48(2):82–84.
6. Chapman EN, Kaatz A, Carnes M. Physicians and implicit bias: how doctors may unwittingly perpetuate health care disparities. J Gen Intern Med. 2013;28(11):1504–1510.
7. What you don’t know: the science of unconscious bias and what to do about it in the search and recruitment process [e-learning seminar]. Association of American Medical Colleges website. https://www.aamc.org/members/leadership/catalog/178420/unconscious_bias.html. Accessed July 14, 2015.
8. Haider AH, Schneider EB, Sriram N, et al. Unconscious race and class bias: its association with decision making by trauma and acute care surgeons. J Trauma Acute Care Surg. 2014;77(3):409–416.
9. Blair IV, Steiner JF, Hanratty R, et al. An investigation of associations between clinicians’ ethnic or racial bias and hypertension treatment, medication adherence and blood pressure control. J Gen Intern Med. 2014;29(7):987–995.
10. Ravenell J, Ogedegbe G. Unconscious bias and real-world hypertension outcomes: advancing disparities research. J Gen Intern Med. 2014;29(7):973–975.
11. van Ryn M, Saha S. Exploring unconscious bias in disparities research and medical education. JAMA. 2011;306(9):995–996.
12. Puhl RM, Moss-Racusin CA, Schwartz MB, Brownell KD. Weight stigmatization and bias reduction: perspectives of overweight and obese adults. Health Educ Res. 2008;23(2):347–358.
13. Prohibited employment policies/practices. US Equal Employment Opportunity Commission website. http://www.eeoc.gov/laws/practices/. Accessed July 14, 2015.
14. Dion K, Berscheid E, Walster E. What is beautiful is good. J Pers Soc Psychol. 1972;24(3):285–290.
15. Watkins LM, Johnston L. Screening job applicants: the impact of physical attractiveness and application quality. Int J Selection Assess. 2000;8(2):76–84.
16. Ruffle BJ, Shtudiner Z. Are good-looking people more employable? Manage Sci. http://dx.doi.org/10.1287/mnsc.2014.1927. Published May 29, 2014. Accessed July 14, 2015.
17. Lemay EP Jr, Clark MS, Greenberg A. What is beautiful is good because what is beautiful is desired: physical attractiveness stereotyping as projection of interpersonal goals. Pers Soc Psychol Bull. 2010;36(3):339–353.
