User login
Teens' Experience With Acne Varies by Ethnicity, Race
Acne severity, frequency, and beliefs about the effect of external factors, such as cleansing habits, all play a part in how likely adolescents are to seek help for their acne.
The findings come from a survey of more than 1,000 middle and high school–aged teens in New Jersey. The study was published online in the journal Pediatric Dermatology (2010 Aug. 26 [doi:10.1111/j.1525-1470.2010.01286.x]).

"Our study demonstrated that grade of acne, knowledge, and beliefs play a role in help-seeking behaviors, which vary to a significant extent by race and ethnicity," wrote Carol E. Cheng and her coinvestigators. Ms. Cheng is a medical student at Boston University. "Better education about how to manage their acne effectively, and guiding appropriate patients to health care providers, may be important ways to decrease the risk of racial disparities in acne morbidity."
Students at five middle schools and three high schools in New Jersey were asked to complete an anonymous survey, in which they were asked questions about their acne severity, frequency, treatment, beliefs about external factors affecting acne, and perception of the psychosocial impact of acne. Students self-reported demographic information on age, gender, grade, ethnicity (Hispanic, not Hispanic, don't know), and race (American Indian, Native Hawaiian, white, black/African American, more than one race, or unknown).
A total of 1,214 students in grades 6-12 completed the survey; their ages ranged from 10 to 18 years. Roughly half (52%) were male. Almost a quarter of the students (24%) were Hispanic, 40% were white, 14% were Asian, and 10% were black.
Students were asked to rate their acne frequency as never, rarely, sometimes, often, or always. Roughly three-quarters (76%) reported that they had acne of some frequency. They were also asked to rate the severity of their acne as none, mild, moderate, or severe. In all, 65% reported that they had acne of some severity.
"The largest differences appeared in the frequency and severity of black respondents, compared with other races, which suggest that this population may be less affected or may perceive themselves to be less affected," the investigators wrote. Black students were 14% less likely than nonblack students to report acne of any frequency. Similarly, black students were 18% less likely than white students to report acne of any severity.
Participants were also asked to report whether they visited a pediatrician, dermatologist, or another type of health professional, or had never seen a health professional for their acne. Most (83%) reported they had not seen a health professional for their acne. This value was similar across ethnicities and races.
Self-reported acne had an impact on the likelihood of respondents having seen a physician and also on the type of physician seen. Students who reported having acne of some severity were more likely to have seen a physician, compared with those who reported not having acne (21% vs. 8%, respectively). Increased acne severity corresponded with increased likelihood of seeing a dermatologist.
Black students with mild or moderate acne were more likely to have seen a health care professional for their acne, compared with white students (relative risk 3.63 and 3.06, respectively). In contrast, Hispanic students with mild or moderate acne were less likely to see a health professional for their acne, compared with non-Hispanic students (RR 0.56 and 0.47, respectively).
Students were also asked if they treated their own acne, followed a health professional's advice, did both, or did something else. There were no significant differences by race or ethnicity with regard to treatment advice.
The researchers asked the students to rate how much they believed that certain factors affected their acne. These included poor cleansing habits, poor dietary habits, decreased sleep, increased stress, increased exercise, increased drinking of water, increased face touching, increased face washing, increased tanning, and pimple popping.
A majority of students believed that the following factors worsened acne: poor cleansing habits (77%), poor dietary habits (56%), stress (60%), increased face touching (70%), and pimple popping (70%).
"Notably, black respondents in 6/10 cases were least likely to believe that a given factor worsened acne relative to other groups, whereas Asian respondents in 7/10 cases were more likely to believe that a given factor worsened acne relative to other groups," the researchers noted.
White students were more likely to have seen a health care professional and follow a treatment suggestion from a physician if they believed external factors affected acne. Black students who believed external factors affected acne were also more likely to follow a treatment suggestion from a physician. "Notably, Asian respondents did not attribute their help-seeking behavior or treatment decisions to any external factors," the investigators reported.
Disclosures: The investigators did not report whether they had any relevant financial relationships.
Acne severity, frequency, and beliefs about the effect of external factors, such as cleansing habits, all play a part in how likely adolescents are to seek help for their acne.
The findings come from a survey of more than 1,000 middle and high school–aged teens in New Jersey. The study was published online in the journal Pediatric Dermatology (2010 Aug. 26 [doi:10.1111/j.1525-1470.2010.01286.x]).
"Our study demonstrated that grade of acne, knowledge, and beliefs play a role in help-seeking behaviors, which vary to a significant extent by race and ethnicity," wrote Carol E. Cheng and her coinvestigators. Ms. Cheng is a medical student at Boston University. "Better education about how to manage their acne effectively, and guiding appropriate patients to health care providers, may be important ways to decrease the risk of racial disparities in acne morbidity."
Students at five middle schools and three high schools in New Jersey were asked to complete an anonymous survey, in which they were asked questions about their acne severity, frequency, treatment, beliefs about external factors affecting acne, and perception of the psychosocial impact of acne. Students self-reported demographic information on age, gender, grade, ethnicity (Hispanic, not Hispanic, don't know), and race (American Indian, Native Hawaiian, white, black/African American, more than one race, or unknown).
A total of 1,214 students in grades 6-12 completed the survey; their ages ranged from 10 to 18 years. Roughly half (52%) were male. Almost a quarter of the students (24%) were Hispanic, 40% were white, 14% were Asian, and 10% were black.
Students were asked to rate their acne frequency as never, rarely, sometimes, often, or always. Roughly three-quarters (76%) reported that they had acne of some frequency. They were also asked to rate the severity of their acne as none, mild, moderate, or severe. In all, 65% reported that they had acne of some severity.
"The largest differences appeared in the frequency and severity of black respondents, compared with other races, which suggest that this population may be less affected or may perceive themselves to be less affected," the investigators wrote. Black students were 14% less likely than nonblack students to report acne of any frequency. Similarly, black students were 18% less likely than white students to report acne of any severity.
Participants were also asked to report whether they visited a pediatrician, dermatologist, or another type of health professional, or had never seen a health professional for their acne. Most (83%) reported they had not seen a health professional for their acne. This value was similar across ethnicities and races.
Self-reported acne had an impact on the likelihood of respondents having seen a physician and also on the type of physician seen. Students who reported having acne of some severity were more likely to have seen a physician, compared with those who reported not having acne (21% vs. 8%, respectively). Increased acne severity corresponded with increased likelihood of seeing a dermatologist.
Black students with mild or moderate acne were more likely to have seen a health care professional for their acne, compared with white students (relative risk 3.63 and 3.06, respectively). In contrast, Hispanic students with mild or moderate acne were less likely to see a health professional for their acne, compared with non-Hispanic students (RR 0.56 and 0.47, respectively).
Students were also asked if they treated their own acne, followed a health professional's advice, did both, or did something else. There were no significant differences by race or ethnicity with regard to treatment advice.
The researchers asked the students to rate how much they believed that certain factors affected their acne. These included poor cleansing habits, poor dietary habits, decreased sleep, increased stress, increased exercise, increased drinking of water, increased face touching, increased face washing, increased tanning, and pimple popping.
A majority of students believed that the following factors worsened acne: poor cleansing habits (77%), poor dietary habits (56%), stress (60%), increased face touching (70%), and pimple popping (70%).
"Notably, black respondents in 6/10 cases were least likely to believe that a given factor worsened acne relative to other groups, whereas Asian respondents in 7/10 cases were more likely to believe that a given factor worsened acne relative to other groups," the researchers noted.
White students were more likely to have seen a health care professional and follow a treatment suggestion from a physician if they believed external factors affected acne. Black students who believed external factors affected acne were also more likely to follow a treatment suggestion from a physician. "Notably, Asian respondents did not attribute their help-seeking behavior or treatment decisions to any external factors," the investigators reported.
Disclosures: The investigators did not report whether they had any relevant financial relationships.
Acne severity, frequency, and beliefs about the effect of external factors, such as cleansing habits, all play a part in how likely adolescents are to seek help for their acne.
The findings come from a survey of more than 1,000 middle and high school–aged teens in New Jersey. The study was published online in the journal Pediatric Dermatology (2010 Aug. 26 [doi:10.1111/j.1525-1470.2010.01286.x]).
"Our study demonstrated that grade of acne, knowledge, and beliefs play a role in help-seeking behaviors, which vary to a significant extent by race and ethnicity," wrote Carol E. Cheng and her coinvestigators. Ms. Cheng is a medical student at Boston University. "Better education about how to manage their acne effectively, and guiding appropriate patients to health care providers, may be important ways to decrease the risk of racial disparities in acne morbidity."
Students at five middle schools and three high schools in New Jersey were asked to complete an anonymous survey, in which they were asked questions about their acne severity, frequency, treatment, beliefs about external factors affecting acne, and perception of the psychosocial impact of acne. Students self-reported demographic information on age, gender, grade, ethnicity (Hispanic, not Hispanic, don't know), and race (American Indian, Native Hawaiian, white, black/African American, more than one race, or unknown).
A total of 1,214 students in grades 6-12 completed the survey; their ages ranged from 10 to 18 years. Roughly half (52%) were male. Almost a quarter of the students (24%) were Hispanic, 40% were white, 14% were Asian, and 10% were black.
Students were asked to rate their acne frequency as never, rarely, sometimes, often, or always. Roughly three-quarters (76%) reported that they had acne of some frequency. They were also asked to rate the severity of their acne as none, mild, moderate, or severe. In all, 65% reported that they had acne of some severity.
"The largest differences appeared in the frequency and severity of black respondents, compared with other races, which suggest that this population may be less affected or may perceive themselves to be less affected," the investigators wrote. Black students were 14% less likely than nonblack students to report acne of any frequency. Similarly, black students were 18% less likely than white students to report acne of any severity.
Participants were also asked to report whether they visited a pediatrician, dermatologist, or another type of health professional, or had never seen a health professional for their acne. Most (83%) reported they had not seen a health professional for their acne. This value was similar across ethnicities and races.
Self-reported acne had an impact on the likelihood of respondents having seen a physician and also on the type of physician seen. Students who reported having acne of some severity were more likely to have seen a physician, compared with those who reported not having acne (21% vs. 8%, respectively). Increased acne severity corresponded with increased likelihood of seeing a dermatologist.
Black students with mild or moderate acne were more likely to have seen a health care professional for their acne, compared with white students (relative risk 3.63 and 3.06, respectively). In contrast, Hispanic students with mild or moderate acne were less likely to see a health professional for their acne, compared with non-Hispanic students (RR 0.56 and 0.47, respectively).
Students were also asked if they treated their own acne, followed a health professional's advice, did both, or did something else. There were no significant differences by race or ethnicity with regard to treatment advice.
The researchers asked the students to rate how much they believed that certain factors affected their acne. These included poor cleansing habits, poor dietary habits, decreased sleep, increased stress, increased exercise, increased drinking of water, increased face touching, increased face washing, increased tanning, and pimple popping.
A majority of students believed that the following factors worsened acne: poor cleansing habits (77%), poor dietary habits (56%), stress (60%), increased face touching (70%), and pimple popping (70%).
"Notably, black respondents in 6/10 cases were least likely to believe that a given factor worsened acne relative to other groups, whereas Asian respondents in 7/10 cases were more likely to believe that a given factor worsened acne relative to other groups," the researchers noted.
White students were more likely to have seen a health care professional and follow a treatment suggestion from a physician if they believed external factors affected acne. Black students who believed external factors affected acne were also more likely to follow a treatment suggestion from a physician. "Notably, Asian respondents did not attribute their help-seeking behavior or treatment decisions to any external factors," the investigators reported.
Disclosures: The investigators did not report whether they had any relevant financial relationships.
Combination Oral Contraceptives Tackle Tough Acne in Some Women
CHICAGO – Patients with severe acne are missing out on the skin-clearing benefits of oral contraceptives and need to know that OCs can be prescribed for acne without a pelvic examination by a gynecologist, according to Dr. Bethanee Schlosser.
"When talking to teens and their parents, it's important to explain that a pelvic exam is not necessary before giving these medications to young women," she said.

It appears that patients aren't privy to this information, and are reluctant to ask for oral contraceptives as acne medication.
"That may be the biggest hurdle keeping these patients from getting adequate treatment for their acne," she said.
In 2004, the World Health Organization released guidelines stating that pelvic exams and Pap smears are no longer required before administering combination oral contraceptives.
Dr. Schlosser noted, however, that she does ask all of her female patients when they had their last full gynecologic exam, Pap smear included, and encourages them to stay current.
Oral Contraceptives
Three combination oral contraceptives are approved for the treatment of acne in women in the United States: ethinyl estradiol and norgestimate, ethinyl estradiol and norethindrone, and ethinyl estradiol and drospirenone.
Drospironone, an analogue of spironolactone, reduces sebum production and increases sex hormone–binding globulin, thus reducing circulating androgens, Dr. Schlosser said. "Some women will come to me, though, and say that their ob.gyn. has told them they can’t take any pill containing drospirenone or spironolactone," because of its possible effect on potassium levels, especially in combination with other drugs that increase serum potassium (ACE inhibitors, angiotensin receptor blockers, potassium-sparing diuretics, heparin, aldosterone antagonists, and nonsteroidal anti-inflammatories).
Dr. Schlosser pointed to a 2009 study of 27 women with either severe papular or nodulocystic acne who were treated with a combined oral contraceptive containing 30 mg ethinyl estradiol, 3 mg drospirenone, and 100 mg spironolactone. None of the patients had a significant elevation in serum potassium level; there were no reports of adverse events serious enough to require discontinuation of treatment. At follow up, 85% of subjects were entirely clear of acne lesions or had excellent improvement, 7% were mildly improved, and 7% were not improved (J. Am. Acad. Derm. 2880;58:60-2).
A 2008 study looked only at the risk of hyperkalemia among 22,429 women who used the drospirenone-containing contraceptive compared with 44,858 who used other oral contraceptives (Contraception 2008;78:377-83). There was no significant between-group difference in the incidence of hyperkalemia.
This type of treatment is not an overnight acne cure, Dr. Schlosser stressed. “I tell women you have to allow at least three cycles of use before you start to judge efficacy. Patients can continue to get more benefit from 3-6 months of use, too.”
A 2007 Cochrane review of the three U.S. Food and Drug Administration–approved acne-fighting oral contraceptives found no significant differences in effectiveness, she said.
The Role of Androgen Testing
Elevated androgens are a large contributor to acne in women, and both the estradiol and progestins in combination oral contraceptives work to decrease them, said Dr. Schlosser, director of the women’s skin health program at Northwestern University, Chicago. Androgen testing may be appropriate for some women.
"If a woman complains of sudden onset of acne, or acne that is severe or recalcitrant to traditional therapy, I would say testing is a good idea. You might also consider it for women with androgenic features – hirsutism, deep voice, muscular habitus, or androgenic alopecia," she said.
Because these features can also be symptoms of polycystic ovary syndrome, Dr. Schlosser also suggested checking for acanthosis nigricans, central obesity, irregular menses, and infertility.
Androgen testing is most informative when performed at the onset of menses. "This is because androgen secretion follows the same pattern as estradiol, which peaks in midcycle and falls to a nadir at the beginning of menstruation," Dr. Schlosser said. "I print out a lab request, and tell the patient to have her blood drawn on the first day of her period." Morning testing is better, if possible, because of the hormone’s diurnal secretion.
Total testosterone is the most sensitive test for androgen levels in women with acne. However, "it’s important to note that the levels associated with acne can be elevated compared to controls, but still within the normal reference ranges," she said. Total testosterone level can also be falsely elevated in obese women, "because insulin reduces the liver’s secretion of sex hormone–binding globulin," she said.
Treatment Risks
There are some contraindications to the use of oral contraceptives for the treatment of acne, Dr. Schlosser noted. Hypercoagulability, a history of venous thromboembolism (VTE), stroke or coronary artery disease, any gynecologic cancer, uncontrolled hypertension, abnormal liver function tests, pregnancy, or abnormal vaginal bleeding should be considered before prescribing.
Oral contraceptives do increase the risk of venous thromboembolism, although that risk is highly dependent on other factors as well, including advancing age and tobacco use. Dr. Schlosser said a concrete, direct link between oral contraceptives and VTE risk has yet to be found, but he hopes an ongoing case-control study of more than 50,000 oral contraceptive users (including up to 5 years of follow-up data) will provide answers.
Finally, Dr. Schlosser added, the single greatest risk of VTE among women is pregnancy and the postpartum period. "So I would say if you’re treating acne in a woman of childbearing age with an oral contraceptive, you are also protecting her from the biggest risk factor she has for thromboembolic events."
Disclosures: Dr. Schlosser said she had no relevant financial disclosures.
CHICAGO – Patients with severe acne are missing out on the skin-clearing benefits of oral contraceptives and need to know that OCs can be prescribed for acne without a pelvic examination by a gynecologist, according to Dr. Bethanee Schlosser.
"When talking to teens and their parents, it's important to explain that a pelvic exam is not necessary before giving these medications to young women," she said.
It appears that patients aren't privy to this information, and are reluctant to ask for oral contraceptives as acne medication.
"That may be the biggest hurdle keeping these patients from getting adequate treatment for their acne," she said.
In 2004, the World Health Organization released guidelines stating that pelvic exams and Pap smears are no longer required before administering combination oral contraceptives.
Dr. Schlosser noted, however, that she does ask all of her female patients when they had their last full gynecologic exam, Pap smear included, and encourages them to stay current.
Oral Contraceptives
Three combination oral contraceptives are approved for the treatment of acne in women in the United States: ethinyl estradiol and norgestimate, ethinyl estradiol and norethindrone, and ethinyl estradiol and drospirenone.
Drospironone, an analogue of spironolactone, reduces sebum production and increases sex hormone–binding globulin, thus reducing circulating androgens, Dr. Schlosser said. "Some women will come to me, though, and say that their ob.gyn. has told them they can’t take any pill containing drospirenone or spironolactone," because of its possible effect on potassium levels, especially in combination with other drugs that increase serum potassium (ACE inhibitors, angiotensin receptor blockers, potassium-sparing diuretics, heparin, aldosterone antagonists, and nonsteroidal anti-inflammatories).
Dr. Schlosser pointed to a 2009 study of 27 women with either severe papular or nodulocystic acne who were treated with a combined oral contraceptive containing 30 mg ethinyl estradiol, 3 mg drospirenone, and 100 mg spironolactone. None of the patients had a significant elevation in serum potassium level; there were no reports of adverse events serious enough to require discontinuation of treatment. At follow up, 85% of subjects were entirely clear of acne lesions or had excellent improvement, 7% were mildly improved, and 7% were not improved (J. Am. Acad. Derm. 2880;58:60-2).
A 2008 study looked only at the risk of hyperkalemia among 22,429 women who used the drospirenone-containing contraceptive compared with 44,858 who used other oral contraceptives (Contraception 2008;78:377-83). There was no significant between-group difference in the incidence of hyperkalemia.
This type of treatment is not an overnight acne cure, Dr. Schlosser stressed. “I tell women you have to allow at least three cycles of use before you start to judge efficacy. Patients can continue to get more benefit from 3-6 months of use, too.”
A 2007 Cochrane review of the three U.S. Food and Drug Administration–approved acne-fighting oral contraceptives found no significant differences in effectiveness, she said.
The Role of Androgen Testing
Elevated androgens are a large contributor to acne in women, and both the estradiol and progestins in combination oral contraceptives work to decrease them, said Dr. Schlosser, director of the women’s skin health program at Northwestern University, Chicago. Androgen testing may be appropriate for some women.
"If a woman complains of sudden onset of acne, or acne that is severe or recalcitrant to traditional therapy, I would say testing is a good idea. You might also consider it for women with androgenic features – hirsutism, deep voice, muscular habitus, or androgenic alopecia," she said.
Because these features can also be symptoms of polycystic ovary syndrome, Dr. Schlosser also suggested checking for acanthosis nigricans, central obesity, irregular menses, and infertility.
Androgen testing is most informative when performed at the onset of menses. "This is because androgen secretion follows the same pattern as estradiol, which peaks in midcycle and falls to a nadir at the beginning of menstruation," Dr. Schlosser said. "I print out a lab request, and tell the patient to have her blood drawn on the first day of her period." Morning testing is better, if possible, because of the hormone’s diurnal secretion.
Total testosterone is the most sensitive test for androgen levels in women with acne. However, "it’s important to note that the levels associated with acne can be elevated compared to controls, but still within the normal reference ranges," she said. Total testosterone level can also be falsely elevated in obese women, "because insulin reduces the liver’s secretion of sex hormone–binding globulin," she said.
Treatment Risks
There are some contraindications to the use of oral contraceptives for the treatment of acne, Dr. Schlosser noted. Hypercoagulability, a history of venous thromboembolism (VTE), stroke or coronary artery disease, any gynecologic cancer, uncontrolled hypertension, abnormal liver function tests, pregnancy, or abnormal vaginal bleeding should be considered before prescribing.
Oral contraceptives do increase the risk of venous thromboembolism, although that risk is highly dependent on other factors as well, including advancing age and tobacco use. Dr. Schlosser said a concrete, direct link between oral contraceptives and VTE risk has yet to be found, but he hopes an ongoing case-control study of more than 50,000 oral contraceptive users (including up to 5 years of follow-up data) will provide answers.
Finally, Dr. Schlosser added, the single greatest risk of VTE among women is pregnancy and the postpartum period. "So I would say if you’re treating acne in a woman of childbearing age with an oral contraceptive, you are also protecting her from the biggest risk factor she has for thromboembolic events."
Disclosures: Dr. Schlosser said she had no relevant financial disclosures.
CHICAGO – Patients with severe acne are missing out on the skin-clearing benefits of oral contraceptives and need to know that OCs can be prescribed for acne without a pelvic examination by a gynecologist, according to Dr. Bethanee Schlosser.
"When talking to teens and their parents, it's important to explain that a pelvic exam is not necessary before giving these medications to young women," she said.
It appears that patients aren't privy to this information, and are reluctant to ask for oral contraceptives as acne medication.
"That may be the biggest hurdle keeping these patients from getting adequate treatment for their acne," she said.
In 2004, the World Health Organization released guidelines stating that pelvic exams and Pap smears are no longer required before administering combination oral contraceptives.
Dr. Schlosser noted, however, that she does ask all of her female patients when they had their last full gynecologic exam, Pap smear included, and encourages them to stay current.
Oral Contraceptives
Three combination oral contraceptives are approved for the treatment of acne in women in the United States: ethinyl estradiol and norgestimate, ethinyl estradiol and norethindrone, and ethinyl estradiol and drospirenone.
Drospironone, an analogue of spironolactone, reduces sebum production and increases sex hormone–binding globulin, thus reducing circulating androgens, Dr. Schlosser said. "Some women will come to me, though, and say that their ob.gyn. has told them they can’t take any pill containing drospirenone or spironolactone," because of its possible effect on potassium levels, especially in combination with other drugs that increase serum potassium (ACE inhibitors, angiotensin receptor blockers, potassium-sparing diuretics, heparin, aldosterone antagonists, and nonsteroidal anti-inflammatories).
Dr. Schlosser pointed to a 2009 study of 27 women with either severe papular or nodulocystic acne who were treated with a combined oral contraceptive containing 30 mg ethinyl estradiol, 3 mg drospirenone, and 100 mg spironolactone. None of the patients had a significant elevation in serum potassium level; there were no reports of adverse events serious enough to require discontinuation of treatment. At follow up, 85% of subjects were entirely clear of acne lesions or had excellent improvement, 7% were mildly improved, and 7% were not improved (J. Am. Acad. Derm. 2880;58:60-2).
A 2008 study looked only at the risk of hyperkalemia among 22,429 women who used the drospirenone-containing contraceptive compared with 44,858 who used other oral contraceptives (Contraception 2008;78:377-83). There was no significant between-group difference in the incidence of hyperkalemia.
This type of treatment is not an overnight acne cure, Dr. Schlosser stressed. “I tell women you have to allow at least three cycles of use before you start to judge efficacy. Patients can continue to get more benefit from 3-6 months of use, too.”
A 2007 Cochrane review of the three U.S. Food and Drug Administration–approved acne-fighting oral contraceptives found no significant differences in effectiveness, she said.
The Role of Androgen Testing
Elevated androgens are a large contributor to acne in women, and both the estradiol and progestins in combination oral contraceptives work to decrease them, said Dr. Schlosser, director of the women’s skin health program at Northwestern University, Chicago. Androgen testing may be appropriate for some women.
"If a woman complains of sudden onset of acne, or acne that is severe or recalcitrant to traditional therapy, I would say testing is a good idea. You might also consider it for women with androgenic features – hirsutism, deep voice, muscular habitus, or androgenic alopecia," she said.
Because these features can also be symptoms of polycystic ovary syndrome, Dr. Schlosser also suggested checking for acanthosis nigricans, central obesity, irregular menses, and infertility.
Androgen testing is most informative when performed at the onset of menses. "This is because androgen secretion follows the same pattern as estradiol, which peaks in midcycle and falls to a nadir at the beginning of menstruation," Dr. Schlosser said. "I print out a lab request, and tell the patient to have her blood drawn on the first day of her period." Morning testing is better, if possible, because of the hormone’s diurnal secretion.
Total testosterone is the most sensitive test for androgen levels in women with acne. However, "it’s important to note that the levels associated with acne can be elevated compared to controls, but still within the normal reference ranges," she said. Total testosterone level can also be falsely elevated in obese women, "because insulin reduces the liver’s secretion of sex hormone–binding globulin," she said.
Treatment Risks
There are some contraindications to the use of oral contraceptives for the treatment of acne, Dr. Schlosser noted. Hypercoagulability, a history of venous thromboembolism (VTE), stroke or coronary artery disease, any gynecologic cancer, uncontrolled hypertension, abnormal liver function tests, pregnancy, or abnormal vaginal bleeding should be considered before prescribing.
Oral contraceptives do increase the risk of venous thromboembolism, although that risk is highly dependent on other factors as well, including advancing age and tobacco use. Dr. Schlosser said a concrete, direct link between oral contraceptives and VTE risk has yet to be found, but he hopes an ongoing case-control study of more than 50,000 oral contraceptive users (including up to 5 years of follow-up data) will provide answers.
Finally, Dr. Schlosser added, the single greatest risk of VTE among women is pregnancy and the postpartum period. "So I would say if you’re treating acne in a woman of childbearing age with an oral contraceptive, you are also protecting her from the biggest risk factor she has for thromboembolic events."
Disclosures: Dr. Schlosser said she had no relevant financial disclosures.
Acne Scar Patients Give Thumbs Up to CO2 Laser Treatment
Single treatment with a carbon dioxide fractional laser was as effective for acne scars as a nonablative fractional system, according to results of a randomized split-face study.
Fractional lasers are well tolerated and widely used to treat scarring, but patients often need multiple sessions to achieve clinical improvement, reported Dr. S.B. Cho of Yonsei University College of Medicine in Seoul, Korea, and colleagues.
However, previous studies have shown that carbon dioxide fractional laser systems can improve scars in as few as three treatments.
In this study, the researchers directly compared improvements in acne scarring after half of a patient’s face underwent a single treatment with a nonablative 1550-nm erbium-doped fractional photothermolysis system (FPS) and the other half underwent a single treatment with an ablative 10,600-nm carbon dioxide fractional laser system (CO2 FS).
The eight patients in the study were Asian males (Fitzpatrick skin type IV) aged 20 to 23 years with mild to severe atrophic acne scars.
At follow-up 3 months after FPS treatment, six of the eight patients showed clinical improvements of 26%-50% from baseline, one patient showed a clinical improvement of 51%-75%, and one showed no clinical improvement (J. Eur. Acad. Dermatol. Venereol. 2010;24:921-5). As for CO2 FS results at 3 months, five of the eight patients had a 26%-50% clinical improvement from baseline, two patients had a 51%-75% improvement, and one had an improvement of over 76%.
The level of clinical improvement was not affected by the type of acne scar (boxcar, icepick, or rolling).
The average VAS pain score on a scale of 0, no pain, to 10, severe pain, was significantly higher after the CO2 FS treatment, compared with the FPS treatment (7.0 vs. 3.9, respectively). However, patient-reported satisfaction was higher after the CO2 FS treatment. Two patients (25%) were “very satisfied,” four (50%) were “satisfied,” one (12.5%) was “slightly satisfied,” and one (12.5%) was “unsatisfied.” After the FPS treatment, none of the patients were very satisfied, two (25%) were satisfied, five (62.5%) were slightly satisfied, and one (12.5%) was unsatisfied.
Common side effects associated with both treatments included crusting, scaling, and erythema. The average duration of crusting or scaling was significantly longer in the CO2 FS group, compared with the FPS group (7.4 days vs. 2.3 days, respectively). However, the difference in post-therapy erythema was not significantly different between the two groups (11.5 days vs. 7.5 days, respectively).
“We could not completely eliminate the possibility of subject bias as the participants experienced different posttreatment responses with FPS and CO2 FS,” the researchers wrote. But the results suggest that a single treatment with CO2 FS might be more effective than a single treatment with FPS.
Although the findings are not conclusive, given the study’s small size, they could serve as a reference for clinicians choosing among laser options for acne scar treatment, the researchers added.
Dr. Cho and colleagues had no financial conflicts to disclose.
Single treatment with a carbon dioxide fractional laser was as effective for acne scars as a nonablative fractional system, according to results of a randomized split-face study.
Fractional lasers are well tolerated and widely used to treat scarring, but patients often need multiple sessions to achieve clinical improvement, reported Dr. S.B. Cho of Yonsei University College of Medicine in Seoul, Korea, and colleagues.
However, previous studies have shown that carbon dioxide fractional laser systems can improve scars in as few as three treatments.
In this study, the researchers directly compared improvements in acne scarring after half of a patient’s face underwent a single treatment with a nonablative 1550-nm erbium-doped fractional photothermolysis system (FPS) and the other half underwent a single treatment with an ablative 10,600-nm carbon dioxide fractional laser system (CO2 FS).
The eight patients in the study were Asian males (Fitzpatrick skin type IV) aged 20 to 23 years with mild to severe atrophic acne scars.
At follow-up 3 months after FPS treatment, six of the eight patients showed clinical improvements of 26%-50% from baseline, one patient showed a clinical improvement of 51%-75%, and one showed no clinical improvement (J. Eur. Acad. Dermatol. Venereol. 2010;24:921-5). As for CO2 FS results at 3 months, five of the eight patients had a 26%-50% clinical improvement from baseline, two patients had a 51%-75% improvement, and one had an improvement of over 76%.
The level of clinical improvement was not affected by the type of acne scar (boxcar, icepick, or rolling).
The average VAS pain score on a scale of 0, no pain, to 10, severe pain, was significantly higher after the CO2 FS treatment, compared with the FPS treatment (7.0 vs. 3.9, respectively). However, patient-reported satisfaction was higher after the CO2 FS treatment. Two patients (25%) were “very satisfied,” four (50%) were “satisfied,” one (12.5%) was “slightly satisfied,” and one (12.5%) was “unsatisfied.” After the FPS treatment, none of the patients were very satisfied, two (25%) were satisfied, five (62.5%) were slightly satisfied, and one (12.5%) was unsatisfied.
Common side effects associated with both treatments included crusting, scaling, and erythema. The average duration of crusting or scaling was significantly longer in the CO2 FS group, compared with the FPS group (7.4 days vs. 2.3 days, respectively). However, the difference in post-therapy erythema was not significantly different between the two groups (11.5 days vs. 7.5 days, respectively).
“We could not completely eliminate the possibility of subject bias as the participants experienced different posttreatment responses with FPS and CO2 FS,” the researchers wrote. But the results suggest that a single treatment with CO2 FS might be more effective than a single treatment with FPS.
Although the findings are not conclusive, given the study’s small size, they could serve as a reference for clinicians choosing among laser options for acne scar treatment, the researchers added.
Dr. Cho and colleagues had no financial conflicts to disclose.
Single treatment with a carbon dioxide fractional laser was as effective for acne scars as a nonablative fractional system, according to results of a randomized split-face study.
Fractional lasers are well tolerated and widely used to treat scarring, but patients often need multiple sessions to achieve clinical improvement, reported Dr. S.B. Cho of Yonsei University College of Medicine in Seoul, Korea, and colleagues.
However, previous studies have shown that carbon dioxide fractional laser systems can improve scars in as few as three treatments.
In this study, the researchers directly compared improvements in acne scarring after half of a patient’s face underwent a single treatment with a nonablative 1550-nm erbium-doped fractional photothermolysis system (FPS) and the other half underwent a single treatment with an ablative 10,600-nm carbon dioxide fractional laser system (CO2 FS).
The eight patients in the study were Asian males (Fitzpatrick skin type IV) aged 20 to 23 years with mild to severe atrophic acne scars.
At follow-up 3 months after FPS treatment, six of the eight patients showed clinical improvements of 26%-50% from baseline, one patient showed a clinical improvement of 51%-75%, and one showed no clinical improvement (J. Eur. Acad. Dermatol. Venereol. 2010;24:921-5). As for CO2 FS results at 3 months, five of the eight patients had a 26%-50% clinical improvement from baseline, two patients had a 51%-75% improvement, and one had an improvement of over 76%.
The level of clinical improvement was not affected by the type of acne scar (boxcar, icepick, or rolling).
The average VAS pain score on a scale of 0, no pain, to 10, severe pain, was significantly higher after the CO2 FS treatment, compared with the FPS treatment (7.0 vs. 3.9, respectively). However, patient-reported satisfaction was higher after the CO2 FS treatment. Two patients (25%) were “very satisfied,” four (50%) were “satisfied,” one (12.5%) was “slightly satisfied,” and one (12.5%) was “unsatisfied.” After the FPS treatment, none of the patients were very satisfied, two (25%) were satisfied, five (62.5%) were slightly satisfied, and one (12.5%) was unsatisfied.
Common side effects associated with both treatments included crusting, scaling, and erythema. The average duration of crusting or scaling was significantly longer in the CO2 FS group, compared with the FPS group (7.4 days vs. 2.3 days, respectively). However, the difference in post-therapy erythema was not significantly different between the two groups (11.5 days vs. 7.5 days, respectively).
“We could not completely eliminate the possibility of subject bias as the participants experienced different posttreatment responses with FPS and CO2 FS,” the researchers wrote. But the results suggest that a single treatment with CO2 FS might be more effective than a single treatment with FPS.
Although the findings are not conclusive, given the study’s small size, they could serve as a reference for clinicians choosing among laser options for acne scar treatment, the researchers added.
Dr. Cho and colleagues had no financial conflicts to disclose.
Ablative Fractional Resurfacing Appears Effective for Acne Scars in Asians
Ablative fractional resurfacing appears to be safe and effective in Asians with mild to moderate atrophic acne scarring, according to a study of 13 patients.
While 12 of the 13 patients experienced some postinflammatory hyperpigmentation, this resolved in all patients in an average of 5 weeks.
The Asian patients underwent three sessions of ablative fractional resurfacing (AFR) with the Ellipse Juvia 15-W CO2 laser, wrote Dr. Woraphong Manuskiatti and colleagues of Mahidol University, Bangkok. All patients had skin phototype IV. Intervals between treatments averaged 7 weeks. All patients were followed for 6 months after the third treatment.
Independent physicians blinded to the order in which clinical photos had been taken judged the improvement in scarring to be excellent in 8% of the patients, good in 38.5% of them, fair in 38.5%, and slight in 15%. None of the patients worsened (J. Am. Acad. Dermatol. 2010;63:274-83).
By the patients’ own evaluations, 46% judged their overall improvement to be fair, 23% judged it to be good, and 31% judged it to be excellent. In both physician and patient evaluations, “slight” was defined as less than 25% improvement, “fair” as 25%-50% improvement, good as 51%-75% improvement, and excellent as 76%-100% improvement.
Postinflammatory hyperpigmentation (PIH) was the most common side effect, seen in 12 of the 13 (92%) patients and after 20 of the 39 (51%) treatment sessions. All cases of PIH were graded as mild except for one that was graded as moderate. After treatment with 4% hydroquinone cream once daily, PIH resolved in all patients within 2-16 weeks (average 5 weeks).
Other adverse events were acneiform eruptions in four patients, allergic contact dermatitis in two patients, and herpes simplex infection in one patient.
Each treatment consisted of a full-face single-pass treatment with a 5-7 ms pulse width. Investigators adjusted the laser to deliver 49 microthermal zones (MTZs) per square centimeter, with each individual MTZ 500 mcm in diameter. The average percent coverage was 9.6%, and the investigators set the laser to deliver energies between 75-105 mJ/MTZ depending on the severity of scarring.
Although physicians prepared the patients for 1 hour before each treatment with a topical anesthetic applied to the full face with occlusion, on average patients rated their pain as 8.1 on a scale of 1-10. Pain scores tended to decrease for the second and third treatments.
The investigators described AFR as offering a treatment alternative midway between nonablative fractional resurfacing (NAFR) and fractional photothermolysis (FP). “Although NAFR has a patient-friendly advantage,” the investigators wrote, “the outcomes of most NAFR lasers still leave much to be desired in the treatment of photodamaged skin, rhytides, and atrophic scars. ... By depositing a pixelated pattern of microscopic ablative wounds surrounded by healthy tissue in a manner similar to that of [the] NAFR method, AFR combines the increased efficacy of ablative techniques with the safety and reduced downtime associated with FP.”
The investigators declared that they had no conflicts of interest. The study was supported by a research grant from Ellipse A/S, which manufactures the laser used in the study.
Ablative fractional resurfacing appears to be safe and effective in Asians with mild to moderate atrophic acne scarring, according to a study of 13 patients.
While 12 of the 13 patients experienced some postinflammatory hyperpigmentation, this resolved in all patients in an average of 5 weeks.
The Asian patients underwent three sessions of ablative fractional resurfacing (AFR) with the Ellipse Juvia 15-W CO2 laser, wrote Dr. Woraphong Manuskiatti and colleagues of Mahidol University, Bangkok. All patients had skin phototype IV. Intervals between treatments averaged 7 weeks. All patients were followed for 6 months after the third treatment.
Independent physicians blinded to the order in which clinical photos had been taken judged the improvement in scarring to be excellent in 8% of the patients, good in 38.5% of them, fair in 38.5%, and slight in 15%. None of the patients worsened (J. Am. Acad. Dermatol. 2010;63:274-83).
By the patients’ own evaluations, 46% judged their overall improvement to be fair, 23% judged it to be good, and 31% judged it to be excellent. In both physician and patient evaluations, “slight” was defined as less than 25% improvement, “fair” as 25%-50% improvement, good as 51%-75% improvement, and excellent as 76%-100% improvement.
Postinflammatory hyperpigmentation (PIH) was the most common side effect, seen in 12 of the 13 (92%) patients and after 20 of the 39 (51%) treatment sessions. All cases of PIH were graded as mild except for one that was graded as moderate. After treatment with 4% hydroquinone cream once daily, PIH resolved in all patients within 2-16 weeks (average 5 weeks).
Other adverse events were acneiform eruptions in four patients, allergic contact dermatitis in two patients, and herpes simplex infection in one patient.
Each treatment consisted of a full-face single-pass treatment with a 5-7 ms pulse width. Investigators adjusted the laser to deliver 49 microthermal zones (MTZs) per square centimeter, with each individual MTZ 500 mcm in diameter. The average percent coverage was 9.6%, and the investigators set the laser to deliver energies between 75-105 mJ/MTZ depending on the severity of scarring.
Although physicians prepared the patients for 1 hour before each treatment with a topical anesthetic applied to the full face with occlusion, on average patients rated their pain as 8.1 on a scale of 1-10. Pain scores tended to decrease for the second and third treatments.
The investigators described AFR as offering a treatment alternative midway between nonablative fractional resurfacing (NAFR) and fractional photothermolysis (FP). “Although NAFR has a patient-friendly advantage,” the investigators wrote, “the outcomes of most NAFR lasers still leave much to be desired in the treatment of photodamaged skin, rhytides, and atrophic scars. ... By depositing a pixelated pattern of microscopic ablative wounds surrounded by healthy tissue in a manner similar to that of [the] NAFR method, AFR combines the increased efficacy of ablative techniques with the safety and reduced downtime associated with FP.”
The investigators declared that they had no conflicts of interest. The study was supported by a research grant from Ellipse A/S, which manufactures the laser used in the study.
Ablative fractional resurfacing appears to be safe and effective in Asians with mild to moderate atrophic acne scarring, according to a study of 13 patients.
While 12 of the 13 patients experienced some postinflammatory hyperpigmentation, this resolved in all patients in an average of 5 weeks.
The Asian patients underwent three sessions of ablative fractional resurfacing (AFR) with the Ellipse Juvia 15-W CO2 laser, wrote Dr. Woraphong Manuskiatti and colleagues of Mahidol University, Bangkok. All patients had skin phototype IV. Intervals between treatments averaged 7 weeks. All patients were followed for 6 months after the third treatment.
Independent physicians blinded to the order in which clinical photos had been taken judged the improvement in scarring to be excellent in 8% of the patients, good in 38.5% of them, fair in 38.5%, and slight in 15%. None of the patients worsened (J. Am. Acad. Dermatol. 2010;63:274-83).
By the patients’ own evaluations, 46% judged their overall improvement to be fair, 23% judged it to be good, and 31% judged it to be excellent. In both physician and patient evaluations, “slight” was defined as less than 25% improvement, “fair” as 25%-50% improvement, good as 51%-75% improvement, and excellent as 76%-100% improvement.
Postinflammatory hyperpigmentation (PIH) was the most common side effect, seen in 12 of the 13 (92%) patients and after 20 of the 39 (51%) treatment sessions. All cases of PIH were graded as mild except for one that was graded as moderate. After treatment with 4% hydroquinone cream once daily, PIH resolved in all patients within 2-16 weeks (average 5 weeks).
Other adverse events were acneiform eruptions in four patients, allergic contact dermatitis in two patients, and herpes simplex infection in one patient.
Each treatment consisted of a full-face single-pass treatment with a 5-7 ms pulse width. Investigators adjusted the laser to deliver 49 microthermal zones (MTZs) per square centimeter, with each individual MTZ 500 mcm in diameter. The average percent coverage was 9.6%, and the investigators set the laser to deliver energies between 75-105 mJ/MTZ depending on the severity of scarring.
Although physicians prepared the patients for 1 hour before each treatment with a topical anesthetic applied to the full face with occlusion, on average patients rated their pain as 8.1 on a scale of 1-10. Pain scores tended to decrease for the second and third treatments.
The investigators described AFR as offering a treatment alternative midway between nonablative fractional resurfacing (NAFR) and fractional photothermolysis (FP). “Although NAFR has a patient-friendly advantage,” the investigators wrote, “the outcomes of most NAFR lasers still leave much to be desired in the treatment of photodamaged skin, rhytides, and atrophic scars. ... By depositing a pixelated pattern of microscopic ablative wounds surrounded by healthy tissue in a manner similar to that of [the] NAFR method, AFR combines the increased efficacy of ablative techniques with the safety and reduced downtime associated with FP.”
The investigators declared that they had no conflicts of interest. The study was supported by a research grant from Ellipse A/S, which manufactures the laser used in the study.
FDA: Veltin Gel Approved for Acne
The Food and Drug Administration has approved Veltin, a gel containing clindamycin phosphate and tretinoin, for the topical treatment of acne vulgaris in patients aged 12 years and older.
The treatment brings together a topical retinoid and an antibiotic - which are often recommended for the treatment of acne vulgaris - in a water-based gel.
Veltin (1.2% clindamycin phosphate and 0.025% tretinoin) should not be used by patients who have Crohn’s disease or ulcerative colitis or have developed colitis with past antibiotic use. Patients using the treatment should avoid exposure to sunlight and sun lamps and should wear sunscreen daily.
Stiefel Laboratories Inc., a GlaxoSmithKline company, expects the gel to be available by prescription later this year.
For more information, including complete prescribing information, contact Stiefel by calling 919-483-2839.
The Food and Drug Administration has approved Veltin, a gel containing clindamycin phosphate and tretinoin, for the topical treatment of acne vulgaris in patients aged 12 years and older.
The treatment brings together a topical retinoid and an antibiotic - which are often recommended for the treatment of acne vulgaris - in a water-based gel.
Veltin (1.2% clindamycin phosphate and 0.025% tretinoin) should not be used by patients who have Crohn’s disease or ulcerative colitis or have developed colitis with past antibiotic use. Patients using the treatment should avoid exposure to sunlight and sun lamps and should wear sunscreen daily.
Stiefel Laboratories Inc., a GlaxoSmithKline company, expects the gel to be available by prescription later this year.
For more information, including complete prescribing information, contact Stiefel by calling 919-483-2839.
The Food and Drug Administration has approved Veltin, a gel containing clindamycin phosphate and tretinoin, for the topical treatment of acne vulgaris in patients aged 12 years and older.
The treatment brings together a topical retinoid and an antibiotic - which are often recommended for the treatment of acne vulgaris - in a water-based gel.
Veltin (1.2% clindamycin phosphate and 0.025% tretinoin) should not be used by patients who have Crohn’s disease or ulcerative colitis or have developed colitis with past antibiotic use. Patients using the treatment should avoid exposure to sunlight and sun lamps and should wear sunscreen daily.
Stiefel Laboratories Inc., a GlaxoSmithKline company, expects the gel to be available by prescription later this year.
For more information, including complete prescribing information, contact Stiefel by calling 919-483-2839.
Rosacea in Patients With Skin of Color: Uncommon But Not Rare [editorial]
Tips for Treating Acne Scarring in Darker Skinned Patients
PHOENIX — Educate darker skinned patients who seek treatment for acne scars that there is no remedy to make the scars completely disappear.
"Depending on the patient's skin type, the sensitivity of their skin, and how aggressively you treat them, the risk of hyperpigmentation can be relatively modest, or well over 50%. The expected degree of improvement, on the other hand, even with multiple modalities and multiple treatments, is 40%-50%. I think it's very important to explain that," said Dr. Murad Alam at the annual meeting of the American Society for Laser Medicine and Surgery.

Dr. Alam, chief of cutaneous and aesthetic surgery at Northwestern University, Chicago, said that clinicians face certain challenges in treating acne scars in patients of color, including the risk of exacerbation of active acne, risk of focal or diffuse hyperpigmentation or hypopigmentation, risk of nodularity or surface texture change, and risk of minimal effect.
To mitigate risks, Dr. Alam considers oral antibiotics in patients who have any degree of active acne, "even if they get one or two acne pimples once in a blue moon," he said. "If the acne is more than very mild, you may wish to target that as the primary goal and defer treatment of the acne scarring until the acne is under good control."
If the acne is mild, "you can start oral antibiotics at least 1 month before the acne scarring intervention, so they do have something on board to reduce the risk of an acne flare," he said. "You may also consider pretreatment with bleaching agents. I'm personally not that convinced that pre-treatment is that helpful, but post-treatment with bleaching agents is of definite efficacy in mitigating postinflammatory hyperpigmentation."
As for treatment, nonablative resurfacing with mid-infrared lasers, including 1320-nm, 1450-nm, and 1540-nm devices, has been shown to be effective in patients with lighter skin. "This heating process causes collagen remodeling, and can have a modest effect on so-called rolling scars, which can be quite disfiguring," he said.
Another option is ablative resurfacing with non-CO2 fractional lasers such as the 1550-nm laser. "This is one of the most gentle devices in this category, but even so you have risks of postinflammatory hyperpigmentation," Dr. Alam said. "I like to err on the side of being very modest with regard to fluences. It's much better to do more treatments than to push each individual treatment at the risk of having pigmentary abnormalities."
A more aggressive approach is ablative resurfacing with CO2 fractional lasers, which "should be restricted to patients who are of lighter skin type. If they do choose this [modality], they need to understand the significant risk of postinflammatory hyperpigmentation. I would say that virtually every patient of skin of color who undergoes this treatment will have some degree of postinflammatory hyperpigmentation. In some cases they might consider that worth it if it makes their scarring better and if it can be managed after treatment so it eventually goes away."
Perhaps the most beneficial treatment for acne scars in patients of color, Dr. Alam said, is subdermal manipulation.
In one procedure, known as subcision, clinicians insert a needle with a sphere-like tip, often an 18-guage Nokor needle, underneath the skin. "By debriding the underside of the skin, you can cause some of the acne scars to float upward," he explained. "You want to ensure very good hemostasis before doing this—lidocaine with epinephrine—because you want to avoid bruising during the procedure. If done properly, this can result in modest improvement of rolling scars, and it can be done repeatedly."
Dermal fillers can be used as an adjunct. About a month after subcision procedures Dr. Alam considers collagen for fine defects, hyaluronic acid for medium defects, and calcium hydroxylapatite for deeper defects.
The best way to develop a treatment plan for acne scarring, he said, is to assess the patient's commitment to improvement and their tolerance for adverse events.
"How much annoyance and disfigurement are they willing to tolerate?" Dr. Alam asked. "If both of these are low, you might wish to restrict yourself to subcision with or without fillers, because if done properly, that almost eliminates the risk of adverse events like hyperpigmentation, and it does provide some modest improvement with relatively little cost."
If the patient is highly committed to achieving improvement but is wary of adverse events, "then you might consider subcision and fillers, followed by nonablative laser or repeated low energy non-CO2 fractional laser treatments."
In those rare patients with a high tolerance for adverse events, he said, consider CO2 fractional laser treatments "at very modest settings."
Dr. Alam said that he had no relevant financial conflicts.
PHOENIX — Educate darker skinned patients who seek treatment for acne scars that there is no remedy to make the scars completely disappear.
"Depending on the patient's skin type, the sensitivity of their skin, and how aggressively you treat them, the risk of hyperpigmentation can be relatively modest, or well over 50%. The expected degree of improvement, on the other hand, even with multiple modalities and multiple treatments, is 40%-50%. I think it's very important to explain that," said Dr. Murad Alam at the annual meeting of the American Society for Laser Medicine and Surgery.
Dr. Alam, chief of cutaneous and aesthetic surgery at Northwestern University, Chicago, said that clinicians face certain challenges in treating acne scars in patients of color, including the risk of exacerbation of active acne, risk of focal or diffuse hyperpigmentation or hypopigmentation, risk of nodularity or surface texture change, and risk of minimal effect.
To mitigate risks, Dr. Alam considers oral antibiotics in patients who have any degree of active acne, "even if they get one or two acne pimples once in a blue moon," he said. "If the acne is more than very mild, you may wish to target that as the primary goal and defer treatment of the acne scarring until the acne is under good control."
If the acne is mild, "you can start oral antibiotics at least 1 month before the acne scarring intervention, so they do have something on board to reduce the risk of an acne flare," he said. "You may also consider pretreatment with bleaching agents. I'm personally not that convinced that pre-treatment is that helpful, but post-treatment with bleaching agents is of definite efficacy in mitigating postinflammatory hyperpigmentation."
As for treatment, nonablative resurfacing with mid-infrared lasers, including 1320-nm, 1450-nm, and 1540-nm devices, has been shown to be effective in patients with lighter skin. "This heating process causes collagen remodeling, and can have a modest effect on so-called rolling scars, which can be quite disfiguring," he said.
Another option is ablative resurfacing with non-CO2 fractional lasers such as the 1550-nm laser. "This is one of the most gentle devices in this category, but even so you have risks of postinflammatory hyperpigmentation," Dr. Alam said. "I like to err on the side of being very modest with regard to fluences. It's much better to do more treatments than to push each individual treatment at the risk of having pigmentary abnormalities."
A more aggressive approach is ablative resurfacing with CO2 fractional lasers, which "should be restricted to patients who are of lighter skin type. If they do choose this [modality], they need to understand the significant risk of postinflammatory hyperpigmentation. I would say that virtually every patient of skin of color who undergoes this treatment will have some degree of postinflammatory hyperpigmentation. In some cases they might consider that worth it if it makes their scarring better and if it can be managed after treatment so it eventually goes away."
Perhaps the most beneficial treatment for acne scars in patients of color, Dr. Alam said, is subdermal manipulation.
In one procedure, known as subcision, clinicians insert a needle with a sphere-like tip, often an 18-guage Nokor needle, underneath the skin. "By debriding the underside of the skin, you can cause some of the acne scars to float upward," he explained. "You want to ensure very good hemostasis before doing this—lidocaine with epinephrine—because you want to avoid bruising during the procedure. If done properly, this can result in modest improvement of rolling scars, and it can be done repeatedly."
Dermal fillers can be used as an adjunct. About a month after subcision procedures Dr. Alam considers collagen for fine defects, hyaluronic acid for medium defects, and calcium hydroxylapatite for deeper defects.
The best way to develop a treatment plan for acne scarring, he said, is to assess the patient's commitment to improvement and their tolerance for adverse events.
"How much annoyance and disfigurement are they willing to tolerate?" Dr. Alam asked. "If both of these are low, you might wish to restrict yourself to subcision with or without fillers, because if done properly, that almost eliminates the risk of adverse events like hyperpigmentation, and it does provide some modest improvement with relatively little cost."
If the patient is highly committed to achieving improvement but is wary of adverse events, "then you might consider subcision and fillers, followed by nonablative laser or repeated low energy non-CO2 fractional laser treatments."
In those rare patients with a high tolerance for adverse events, he said, consider CO2 fractional laser treatments "at very modest settings."
Dr. Alam said that he had no relevant financial conflicts.
PHOENIX — Educate darker skinned patients who seek treatment for acne scars that there is no remedy to make the scars completely disappear.
"Depending on the patient's skin type, the sensitivity of their skin, and how aggressively you treat them, the risk of hyperpigmentation can be relatively modest, or well over 50%. The expected degree of improvement, on the other hand, even with multiple modalities and multiple treatments, is 40%-50%. I think it's very important to explain that," said Dr. Murad Alam at the annual meeting of the American Society for Laser Medicine and Surgery.
Dr. Alam, chief of cutaneous and aesthetic surgery at Northwestern University, Chicago, said that clinicians face certain challenges in treating acne scars in patients of color, including the risk of exacerbation of active acne, risk of focal or diffuse hyperpigmentation or hypopigmentation, risk of nodularity or surface texture change, and risk of minimal effect.
To mitigate risks, Dr. Alam considers oral antibiotics in patients who have any degree of active acne, "even if they get one or two acne pimples once in a blue moon," he said. "If the acne is more than very mild, you may wish to target that as the primary goal and defer treatment of the acne scarring until the acne is under good control."
If the acne is mild, "you can start oral antibiotics at least 1 month before the acne scarring intervention, so they do have something on board to reduce the risk of an acne flare," he said. "You may also consider pretreatment with bleaching agents. I'm personally not that convinced that pre-treatment is that helpful, but post-treatment with bleaching agents is of definite efficacy in mitigating postinflammatory hyperpigmentation."
As for treatment, nonablative resurfacing with mid-infrared lasers, including 1320-nm, 1450-nm, and 1540-nm devices, has been shown to be effective in patients with lighter skin. "This heating process causes collagen remodeling, and can have a modest effect on so-called rolling scars, which can be quite disfiguring," he said.
Another option is ablative resurfacing with non-CO2 fractional lasers such as the 1550-nm laser. "This is one of the most gentle devices in this category, but even so you have risks of postinflammatory hyperpigmentation," Dr. Alam said. "I like to err on the side of being very modest with regard to fluences. It's much better to do more treatments than to push each individual treatment at the risk of having pigmentary abnormalities."
A more aggressive approach is ablative resurfacing with CO2 fractional lasers, which "should be restricted to patients who are of lighter skin type. If they do choose this [modality], they need to understand the significant risk of postinflammatory hyperpigmentation. I would say that virtually every patient of skin of color who undergoes this treatment will have some degree of postinflammatory hyperpigmentation. In some cases they might consider that worth it if it makes their scarring better and if it can be managed after treatment so it eventually goes away."
Perhaps the most beneficial treatment for acne scars in patients of color, Dr. Alam said, is subdermal manipulation.
In one procedure, known as subcision, clinicians insert a needle with a sphere-like tip, often an 18-guage Nokor needle, underneath the skin. "By debriding the underside of the skin, you can cause some of the acne scars to float upward," he explained. "You want to ensure very good hemostasis before doing this—lidocaine with epinephrine—because you want to avoid bruising during the procedure. If done properly, this can result in modest improvement of rolling scars, and it can be done repeatedly."
Dermal fillers can be used as an adjunct. About a month after subcision procedures Dr. Alam considers collagen for fine defects, hyaluronic acid for medium defects, and calcium hydroxylapatite for deeper defects.
The best way to develop a treatment plan for acne scarring, he said, is to assess the patient's commitment to improvement and their tolerance for adverse events.
"How much annoyance and disfigurement are they willing to tolerate?" Dr. Alam asked. "If both of these are low, you might wish to restrict yourself to subcision with or without fillers, because if done properly, that almost eliminates the risk of adverse events like hyperpigmentation, and it does provide some modest improvement with relatively little cost."
If the patient is highly committed to achieving improvement but is wary of adverse events, "then you might consider subcision and fillers, followed by nonablative laser or repeated low energy non-CO2 fractional laser treatments."
In those rare patients with a high tolerance for adverse events, he said, consider CO2 fractional laser treatments "at very modest settings."
Dr. Alam said that he had no relevant financial conflicts.
Novel Device Uses Ultrasound to Treat Acne
PHOENIX – An investigational intense-therapy ultrasound device safely and effectively treated mild to moderate acne in a preliminary study.
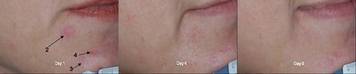
The device, manufactured by Xthetix Inc., was used to treat 5-15 active acne lesions on one side of the face for 5 consecutive days in 18 women and 7 men with a mean age of 26 years. Of the patients, about 84% showed significant improvement after five treatment sessions.
According to a poster presented during the annual meeting of the American Society for Laser Medicine and Surgery, energy generated by the device is delivered to the level of the sebaceous gland, "raising the temperature 5-15 degrees Celsius above ambient skin temperature. It is designed not to cause thermal coagulation, but to increase the tissue temperature for a period of time sufficient to produce a therapeutic effect."
In an interview, lead investigator Dr. Bill Halmi said that although there are a few devices currently on the market that use heat to reduce the duration of an inflammatory acne papule, the machine uses ultrasound to heat the targeted area.
"Putting the energy intradermally into the pilosebaceous unit is the unique aspect of the device," he said. "It changes the inner workings of the gland, kills bacteria, [and] peaks the inflammatory process, among other things."
Each treatment session lasted about 15 minutes. The contralateral side of the face did not receive any ultrasound treatment and served as the control.
The researchers took photographs on all visit days and a masked reviewer conducted posttreatment and facial acne assessments at every visit. Each patient completed daily pain and acne assessments.
Dr. Halmi, who practices dermatology in Phoenix, reported that the greatest percentage of lesion clearance (30%) occurred on day 4 of treatment. "This differs from 'blue light' devices that expect to see improvements after at least 1 week of treatment," he said. "Going into the study we really weren't certain that we would see an immediate effect from the device. We were certainly pleased to discover that this ultrasound device measurably reduced the duration of an acne lesion."
A majority of patients (84%) reported moderate to significant improvement of their treated sides during the course of treatment, while 40% experienced mild transient erythema that lasted less than 30 minutes. The average pain score was 3 on a scale of 1-10, with 10 being the most severe.
The findings suggest that "there is a role for heat in reducing the duration of an acne lesion," Dr. Halmi said. "The advantage ultrasound has is that it can target that heat to the depth desired."
He cautioned that the study is preliminary and that, while encouraging, "repeated studies using more patients will help confirm our findings. Additionally, the role of ultrasound in the prophylactic treatment of acne remains to be revealed."
Dr. Halmi disclosed that he is a paid consultant for Xthetix.
PHOENIX – An investigational intense-therapy ultrasound device safely and effectively treated mild to moderate acne in a preliminary study.
The device, manufactured by Xthetix Inc., was used to treat 5-15 active acne lesions on one side of the face for 5 consecutive days in 18 women and 7 men with a mean age of 26 years. Of the patients, about 84% showed significant improvement after five treatment sessions.
According to a poster presented during the annual meeting of the American Society for Laser Medicine and Surgery, energy generated by the device is delivered to the level of the sebaceous gland, "raising the temperature 5-15 degrees Celsius above ambient skin temperature. It is designed not to cause thermal coagulation, but to increase the tissue temperature for a period of time sufficient to produce a therapeutic effect."
In an interview, lead investigator Dr. Bill Halmi said that although there are a few devices currently on the market that use heat to reduce the duration of an inflammatory acne papule, the machine uses ultrasound to heat the targeted area.
"Putting the energy intradermally into the pilosebaceous unit is the unique aspect of the device," he said. "It changes the inner workings of the gland, kills bacteria, [and] peaks the inflammatory process, among other things."
Each treatment session lasted about 15 minutes. The contralateral side of the face did not receive any ultrasound treatment and served as the control.
The researchers took photographs on all visit days and a masked reviewer conducted posttreatment and facial acne assessments at every visit. Each patient completed daily pain and acne assessments.
Dr. Halmi, who practices dermatology in Phoenix, reported that the greatest percentage of lesion clearance (30%) occurred on day 4 of treatment. "This differs from 'blue light' devices that expect to see improvements after at least 1 week of treatment," he said. "Going into the study we really weren't certain that we would see an immediate effect from the device. We were certainly pleased to discover that this ultrasound device measurably reduced the duration of an acne lesion."
A majority of patients (84%) reported moderate to significant improvement of their treated sides during the course of treatment, while 40% experienced mild transient erythema that lasted less than 30 minutes. The average pain score was 3 on a scale of 1-10, with 10 being the most severe.
The findings suggest that "there is a role for heat in reducing the duration of an acne lesion," Dr. Halmi said. "The advantage ultrasound has is that it can target that heat to the depth desired."
He cautioned that the study is preliminary and that, while encouraging, "repeated studies using more patients will help confirm our findings. Additionally, the role of ultrasound in the prophylactic treatment of acne remains to be revealed."
Dr. Halmi disclosed that he is a paid consultant for Xthetix.
PHOENIX – An investigational intense-therapy ultrasound device safely and effectively treated mild to moderate acne in a preliminary study.
The device, manufactured by Xthetix Inc., was used to treat 5-15 active acne lesions on one side of the face for 5 consecutive days in 18 women and 7 men with a mean age of 26 years. Of the patients, about 84% showed significant improvement after five treatment sessions.
According to a poster presented during the annual meeting of the American Society for Laser Medicine and Surgery, energy generated by the device is delivered to the level of the sebaceous gland, "raising the temperature 5-15 degrees Celsius above ambient skin temperature. It is designed not to cause thermal coagulation, but to increase the tissue temperature for a period of time sufficient to produce a therapeutic effect."
In an interview, lead investigator Dr. Bill Halmi said that although there are a few devices currently on the market that use heat to reduce the duration of an inflammatory acne papule, the machine uses ultrasound to heat the targeted area.
"Putting the energy intradermally into the pilosebaceous unit is the unique aspect of the device," he said. "It changes the inner workings of the gland, kills bacteria, [and] peaks the inflammatory process, among other things."
Each treatment session lasted about 15 minutes. The contralateral side of the face did not receive any ultrasound treatment and served as the control.
The researchers took photographs on all visit days and a masked reviewer conducted posttreatment and facial acne assessments at every visit. Each patient completed daily pain and acne assessments.
Dr. Halmi, who practices dermatology in Phoenix, reported that the greatest percentage of lesion clearance (30%) occurred on day 4 of treatment. "This differs from 'blue light' devices that expect to see improvements after at least 1 week of treatment," he said. "Going into the study we really weren't certain that we would see an immediate effect from the device. We were certainly pleased to discover that this ultrasound device measurably reduced the duration of an acne lesion."
A majority of patients (84%) reported moderate to significant improvement of their treated sides during the course of treatment, while 40% experienced mild transient erythema that lasted less than 30 minutes. The average pain score was 3 on a scale of 1-10, with 10 being the most severe.
The findings suggest that "there is a role for heat in reducing the duration of an acne lesion," Dr. Halmi said. "The advantage ultrasound has is that it can target that heat to the depth desired."
He cautioned that the study is preliminary and that, while encouraging, "repeated studies using more patients will help confirm our findings. Additionally, the role of ultrasound in the prophylactic treatment of acne remains to be revealed."
Dr. Halmi disclosed that he is a paid consultant for Xthetix.