User login
Vibrating Belt Receives Approval to Help Women With Osteopenia Keep Bone Strength
The US Food and Drug Administration (FDA) has approved a wearable belt device for postmenopausal women with osteopenia, the precursor to osteoporosis, according to the company’s manufacturer, Bone Health Technologies.
According to the company, the device (Osteoboost) is the first nonpharmacologic device-based, prescription-only treatment for postmenopausal women with low bone density. It has not been tested for ability to reduce fracture risk.

The device is worn around the hips and delivers calibrated mild vibrations to the hips and lumbar spine to help preserve bone strength and density. A vibration pack is mounted to the back of the belt.
FDA approval, announced on January 18, was based on the findings of a National Institutes of Health–funded double-blinded, sham-controlled study of 126 women with low bone density conducted at the University of Nebraska Medical Center in Omaha. The data were shared at the 2023 Endocrine Society and American Society for Bone and Mineral Research annual meetings and published in the Journal of the Endocrine Society.
Lead investigator Laura D. Bilek, PT, PhD, associate dean for research and associate professor at the University of Nebraska, and colleagues wrote that the primary outcome measurement was the change in vertebral strength measured by CT scans for women who used the device a minimum of three times per week compared with a sham group who wore a belt that emitted sound but had no vibrations.
Compressive strength and volumetric density of the first lumbar vertebra were analyzed.
In the active-belt group, women lost, on average, 0.48% bone strength, while those in the sham group lost nearly 2.84% (P = .014), about five times as much. Results also showed that participants in the active treatment group who used the device three times per week lost 0.29% bone mineral density (BMD) compared with the 1.97% BMD lost in the control group. No adverse events were reported in the study.
Sonali Khandelwal, MD, a rheumatologist at Rush University in Chicago, told this news organization there’s considerable fear among some patients about long-term use of available medications for bone health, “so any modality that is nontherapeutic — not a pill — is always exciting.”
The endpoints of the study are one good measure, she said, but she emphasized that it will be important to show that the improved bone density from the belt that is described in this study “is a true marker of decreased fracture risk.”
Because there are no apparent side effects, she said it may be effective in combination with weight-bearing exercise, vitamin D and calcium, and/or medication, depending on severity of bone loss.
Current medications on the market for osteoporosis have been shown to improve bone strength and reduce fracture risk, she noted.
“It could help; I just don’t think we have enough evidence that it will completely treat the bone loss,” Dr. Khandelwal said.
She said she sees the potential population most interested in the belt as premenopausal women with a family history of bone loss who may not meet the level of bone loss for medical management but are interested in prevention.
“I also think of individuals who might already meet medication needs but are completely averse to being on medication,” she said. The bulk of her practice is treating bone loss, she said, estimating that 20% of her patients do not want to be on medication.
Bone Health Technologies CEO Laura Yecies, MBA, told this news organization the company has not yet set the price for the device and noted that because it will be available by prescription only, out-of-pocket costs and copays will differ. She said the company expects to begin shipping later this year. Requests for update notifications can be made at the company’s website.
Dr. Bilek told this news organization the device was tested for a year, so it’s unclear how long people with osteopenia would need to wear the belt for maximum benefit.
The theory behind the mechanism of action, she said, “is that the vibration actually inhibits the cells [osteoclasts] that take away bone mass.”
The researchers included only postmenopausal women with osteopenia in the study, but Dr. Bilek said she would like to test the device on other groups, such as men with prostate cancer getting testosterone-blocking therapy, which can result in loss of bone density. An estimated 34 million people in the United States have osteopenia.
Dr. Bilek said a next step for the study is to enroll a more diverse cohort at an additional center to test the device because most of the women in this one were White.
She noted that women’s bone mass peaks at age 30 and then starts to decline.
“When women hit menopause, there’s a really rapid decline [in bone strength] for the next 5-7 years and then the decline levels off. If we can slow that decline, hopefully that woman’s bone density is maintained at a higher level throughout their life,” Dr. Bilek said.
Dr. Bilek is a scientific adviser to Bone Health Technologies. She and many coauthors of the study received grants or fees from the company and own stock in or are employees of the company. Ms. Yecies is the founder and CEO of Bone Health Technologies. Dr. Khandelwal had no relevant financial relationships.
A version of this article first appeared on Medscape.com.
The US Food and Drug Administration (FDA) has approved a wearable belt device for postmenopausal women with osteopenia, the precursor to osteoporosis, according to the company’s manufacturer, Bone Health Technologies.
According to the company, the device (Osteoboost) is the first nonpharmacologic device-based, prescription-only treatment for postmenopausal women with low bone density. It has not been tested for ability to reduce fracture risk.
The device is worn around the hips and delivers calibrated mild vibrations to the hips and lumbar spine to help preserve bone strength and density. A vibration pack is mounted to the back of the belt.
FDA approval, announced on January 18, was based on the findings of a National Institutes of Health–funded double-blinded, sham-controlled study of 126 women with low bone density conducted at the University of Nebraska Medical Center in Omaha. The data were shared at the 2023 Endocrine Society and American Society for Bone and Mineral Research annual meetings and published in the Journal of the Endocrine Society.
Lead investigator Laura D. Bilek, PT, PhD, associate dean for research and associate professor at the University of Nebraska, and colleagues wrote that the primary outcome measurement was the change in vertebral strength measured by CT scans for women who used the device a minimum of three times per week compared with a sham group who wore a belt that emitted sound but had no vibrations.
Compressive strength and volumetric density of the first lumbar vertebra were analyzed.
In the active-belt group, women lost, on average, 0.48% bone strength, while those in the sham group lost nearly 2.84% (P = .014), about five times as much. Results also showed that participants in the active treatment group who used the device three times per week lost 0.29% bone mineral density (BMD) compared with the 1.97% BMD lost in the control group. No adverse events were reported in the study.
Sonali Khandelwal, MD, a rheumatologist at Rush University in Chicago, told this news organization there’s considerable fear among some patients about long-term use of available medications for bone health, “so any modality that is nontherapeutic — not a pill — is always exciting.”
The endpoints of the study are one good measure, she said, but she emphasized that it will be important to show that the improved bone density from the belt that is described in this study “is a true marker of decreased fracture risk.”
Because there are no apparent side effects, she said it may be effective in combination with weight-bearing exercise, vitamin D and calcium, and/or medication, depending on severity of bone loss.
Current medications on the market for osteoporosis have been shown to improve bone strength and reduce fracture risk, she noted.
“It could help; I just don’t think we have enough evidence that it will completely treat the bone loss,” Dr. Khandelwal said.
She said she sees the potential population most interested in the belt as premenopausal women with a family history of bone loss who may not meet the level of bone loss for medical management but are interested in prevention.
“I also think of individuals who might already meet medication needs but are completely averse to being on medication,” she said. The bulk of her practice is treating bone loss, she said, estimating that 20% of her patients do not want to be on medication.
Bone Health Technologies CEO Laura Yecies, MBA, told this news organization the company has not yet set the price for the device and noted that because it will be available by prescription only, out-of-pocket costs and copays will differ. She said the company expects to begin shipping later this year. Requests for update notifications can be made at the company’s website.
Dr. Bilek told this news organization the device was tested for a year, so it’s unclear how long people with osteopenia would need to wear the belt for maximum benefit.
The theory behind the mechanism of action, she said, “is that the vibration actually inhibits the cells [osteoclasts] that take away bone mass.”
The researchers included only postmenopausal women with osteopenia in the study, but Dr. Bilek said she would like to test the device on other groups, such as men with prostate cancer getting testosterone-blocking therapy, which can result in loss of bone density. An estimated 34 million people in the United States have osteopenia.
Dr. Bilek said a next step for the study is to enroll a more diverse cohort at an additional center to test the device because most of the women in this one were White.
She noted that women’s bone mass peaks at age 30 and then starts to decline.
“When women hit menopause, there’s a really rapid decline [in bone strength] for the next 5-7 years and then the decline levels off. If we can slow that decline, hopefully that woman’s bone density is maintained at a higher level throughout their life,” Dr. Bilek said.
Dr. Bilek is a scientific adviser to Bone Health Technologies. She and many coauthors of the study received grants or fees from the company and own stock in or are employees of the company. Ms. Yecies is the founder and CEO of Bone Health Technologies. Dr. Khandelwal had no relevant financial relationships.
A version of this article first appeared on Medscape.com.
The US Food and Drug Administration (FDA) has approved a wearable belt device for postmenopausal women with osteopenia, the precursor to osteoporosis, according to the company’s manufacturer, Bone Health Technologies.
According to the company, the device (Osteoboost) is the first nonpharmacologic device-based, prescription-only treatment for postmenopausal women with low bone density. It has not been tested for ability to reduce fracture risk.
The device is worn around the hips and delivers calibrated mild vibrations to the hips and lumbar spine to help preserve bone strength and density. A vibration pack is mounted to the back of the belt.
FDA approval, announced on January 18, was based on the findings of a National Institutes of Health–funded double-blinded, sham-controlled study of 126 women with low bone density conducted at the University of Nebraska Medical Center in Omaha. The data were shared at the 2023 Endocrine Society and American Society for Bone and Mineral Research annual meetings and published in the Journal of the Endocrine Society.
Lead investigator Laura D. Bilek, PT, PhD, associate dean for research and associate professor at the University of Nebraska, and colleagues wrote that the primary outcome measurement was the change in vertebral strength measured by CT scans for women who used the device a minimum of three times per week compared with a sham group who wore a belt that emitted sound but had no vibrations.
Compressive strength and volumetric density of the first lumbar vertebra were analyzed.
In the active-belt group, women lost, on average, 0.48% bone strength, while those in the sham group lost nearly 2.84% (P = .014), about five times as much. Results also showed that participants in the active treatment group who used the device three times per week lost 0.29% bone mineral density (BMD) compared with the 1.97% BMD lost in the control group. No adverse events were reported in the study.
Sonali Khandelwal, MD, a rheumatologist at Rush University in Chicago, told this news organization there’s considerable fear among some patients about long-term use of available medications for bone health, “so any modality that is nontherapeutic — not a pill — is always exciting.”
The endpoints of the study are one good measure, she said, but she emphasized that it will be important to show that the improved bone density from the belt that is described in this study “is a true marker of decreased fracture risk.”
Because there are no apparent side effects, she said it may be effective in combination with weight-bearing exercise, vitamin D and calcium, and/or medication, depending on severity of bone loss.
Current medications on the market for osteoporosis have been shown to improve bone strength and reduce fracture risk, she noted.
“It could help; I just don’t think we have enough evidence that it will completely treat the bone loss,” Dr. Khandelwal said.
She said she sees the potential population most interested in the belt as premenopausal women with a family history of bone loss who may not meet the level of bone loss for medical management but are interested in prevention.
“I also think of individuals who might already meet medication needs but are completely averse to being on medication,” she said. The bulk of her practice is treating bone loss, she said, estimating that 20% of her patients do not want to be on medication.
Bone Health Technologies CEO Laura Yecies, MBA, told this news organization the company has not yet set the price for the device and noted that because it will be available by prescription only, out-of-pocket costs and copays will differ. She said the company expects to begin shipping later this year. Requests for update notifications can be made at the company’s website.
Dr. Bilek told this news organization the device was tested for a year, so it’s unclear how long people with osteopenia would need to wear the belt for maximum benefit.
The theory behind the mechanism of action, she said, “is that the vibration actually inhibits the cells [osteoclasts] that take away bone mass.”
The researchers included only postmenopausal women with osteopenia in the study, but Dr. Bilek said she would like to test the device on other groups, such as men with prostate cancer getting testosterone-blocking therapy, which can result in loss of bone density. An estimated 34 million people in the United States have osteopenia.
Dr. Bilek said a next step for the study is to enroll a more diverse cohort at an additional center to test the device because most of the women in this one were White.
She noted that women’s bone mass peaks at age 30 and then starts to decline.
“When women hit menopause, there’s a really rapid decline [in bone strength] for the next 5-7 years and then the decline levels off. If we can slow that decline, hopefully that woman’s bone density is maintained at a higher level throughout their life,” Dr. Bilek said.
Dr. Bilek is a scientific adviser to Bone Health Technologies. She and many coauthors of the study received grants or fees from the company and own stock in or are employees of the company. Ms. Yecies is the founder and CEO of Bone Health Technologies. Dr. Khandelwal had no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Maternal Vegan Diet May Be Tied To Lower Birth Weight
Mothers on vegan diets during pregnancy may give birth to infants with lower mean birth weights than those of omnivorous mothers and may also have a greater risk of preeclampsia, a prospective study of Danish pregnant women suggests.
According to researchers led by Signe Hedegaard, MD, of the department of obstetrics and Gynecology at Rigshospitalet, Juliane Marie Center, University of Copenhagen, low protein intake may lie behind the observed association with birth weight. The report was published in Acta Obstetricia et Gynecologica Scandinavica.
While vegan-identifying mothers were very few in number, the authors conceded, their babies were more likely to weigh less on average than those of omnivorous mothers — 3441 g vs 3601 g — despite a mean gestation 5 days longer.
Prevalence rates of low birth weight (< 2500 g) in the two groups were 11.1% and 2.5%, respectively, and the prevalence of preeclampsia was 11.1% vs 2.6%. The mean birth weight of infants in the maternal vegan group was about 240 g lower than infants born to omnivorous mothers.
“The lower birth weight of around 240 g among vegans compared with omnivorous mothers in our study strengthens our observation that vegans may be at higher risk of giving birth to low-birth-weight infants. The observed effect size on birth weight is comparable to what is observed among daily smokers relative to nonsmokers in this cohort,“ Dr. Hedegaard and colleagues wrote. “Furthermore, the on-average 5-day longer gestation observed among vegans in our study would be indicative of reduced fetal growth rate rather than lower birth weight due to shorter gestation.”
These findings emerged from data on 66,738 pregnancies in the Danish National Birth Cohort, 1996-2002. A food frequency questionnaire characterized pregnant subjects as fish/poultry-vegetarians, lacto/ovo-vegetarians, vegans, or omnivores, based on their self-reporting in gestational week 30.
A total of 98.7% (n = 65,872) of participants were defined as omnivorous, while 1.0% (n = 666), 0.3% (n = 183), and 0.03% (n = 18) identified as fish/poultry vegetarians, lacto/ovo-vegetarians, or vegans, respectively.
Those following plant-based diets of all types were slightly older, more often parous, and less likely to smoke. This plant dietary group also had a somewhat lower prevalence of overweight and obesity (prepregnancy body mass index > 25 [kg/m2]) and a higher prevalence of underweight (prepregnancy BMI < 18.5).
Total energy intake was modestly lower from plant-based diets, for a mean difference of 0.3-0.7 MJ (72-167 kcal) per day.
As for total protein intake, this was substantially lower for lacto/ovo-vegetarians and vegans: 13.3% and 10.4% of energy, respectively, compared with 15.4% in omnivores.
Dietary intake of micronutrients was also considerably lower among vegans, but after factoring in intake from dietary supplements, no major differences emerged.
Mean birth weight, birth length, length of gestation, and rate of low birth weight (< 2500 g) were similar among omnivorous, fish/poultry-, and lacto/ovo-vegetarians. The prevalence of gestational diabetes, preeclampsia, and cesarean section was similar across groups, but the prevalence of anemia was higher among fish/poultry- and lacto/ovo-vegetarians than omnivorous participants.
As for preeclampsia, previous research in larger numbers of vegans found no indication of hypertensive disorders during pregnancy. Some studies, however, have suggested a link between preeclampsia and low intake of protein, calcium, or vitamin D, but the evidence is inconclusive, and the mechanism is unclear.
The observed associations, however, do not translate to causality, the authors cautioned. “Future studies should put more emphasis on characterizing the diet among those adhering to vegan diets and other forms of plant-based diets during pregnancy,” they wrote. “That would allow for stronger assumptions on possible causality between any association observed with birth or pregnancy outcomes in such studies and strengthen the basis for dietary recommendations.”
This study was funded by the Danish Council for Independent Research. The Danish National Birth Cohort Study is supported by the March of Dimes Birth Defects Foundation, the Danish Heart Association, Danish Medical Research Council, Sygekassernes Helsefond, the Innovation Fund Denmark, and the Danish National Research Foundation. The authors had no conflicts of interest to declare.
Mothers on vegan diets during pregnancy may give birth to infants with lower mean birth weights than those of omnivorous mothers and may also have a greater risk of preeclampsia, a prospective study of Danish pregnant women suggests.
According to researchers led by Signe Hedegaard, MD, of the department of obstetrics and Gynecology at Rigshospitalet, Juliane Marie Center, University of Copenhagen, low protein intake may lie behind the observed association with birth weight. The report was published in Acta Obstetricia et Gynecologica Scandinavica.
While vegan-identifying mothers were very few in number, the authors conceded, their babies were more likely to weigh less on average than those of omnivorous mothers — 3441 g vs 3601 g — despite a mean gestation 5 days longer.
Prevalence rates of low birth weight (< 2500 g) in the two groups were 11.1% and 2.5%, respectively, and the prevalence of preeclampsia was 11.1% vs 2.6%. The mean birth weight of infants in the maternal vegan group was about 240 g lower than infants born to omnivorous mothers.
“The lower birth weight of around 240 g among vegans compared with omnivorous mothers in our study strengthens our observation that vegans may be at higher risk of giving birth to low-birth-weight infants. The observed effect size on birth weight is comparable to what is observed among daily smokers relative to nonsmokers in this cohort,“ Dr. Hedegaard and colleagues wrote. “Furthermore, the on-average 5-day longer gestation observed among vegans in our study would be indicative of reduced fetal growth rate rather than lower birth weight due to shorter gestation.”
These findings emerged from data on 66,738 pregnancies in the Danish National Birth Cohort, 1996-2002. A food frequency questionnaire characterized pregnant subjects as fish/poultry-vegetarians, lacto/ovo-vegetarians, vegans, or omnivores, based on their self-reporting in gestational week 30.
A total of 98.7% (n = 65,872) of participants were defined as omnivorous, while 1.0% (n = 666), 0.3% (n = 183), and 0.03% (n = 18) identified as fish/poultry vegetarians, lacto/ovo-vegetarians, or vegans, respectively.
Those following plant-based diets of all types were slightly older, more often parous, and less likely to smoke. This plant dietary group also had a somewhat lower prevalence of overweight and obesity (prepregnancy body mass index > 25 [kg/m2]) and a higher prevalence of underweight (prepregnancy BMI < 18.5).
Total energy intake was modestly lower from plant-based diets, for a mean difference of 0.3-0.7 MJ (72-167 kcal) per day.
As for total protein intake, this was substantially lower for lacto/ovo-vegetarians and vegans: 13.3% and 10.4% of energy, respectively, compared with 15.4% in omnivores.
Dietary intake of micronutrients was also considerably lower among vegans, but after factoring in intake from dietary supplements, no major differences emerged.
Mean birth weight, birth length, length of gestation, and rate of low birth weight (< 2500 g) were similar among omnivorous, fish/poultry-, and lacto/ovo-vegetarians. The prevalence of gestational diabetes, preeclampsia, and cesarean section was similar across groups, but the prevalence of anemia was higher among fish/poultry- and lacto/ovo-vegetarians than omnivorous participants.
As for preeclampsia, previous research in larger numbers of vegans found no indication of hypertensive disorders during pregnancy. Some studies, however, have suggested a link between preeclampsia and low intake of protein, calcium, or vitamin D, but the evidence is inconclusive, and the mechanism is unclear.
The observed associations, however, do not translate to causality, the authors cautioned. “Future studies should put more emphasis on characterizing the diet among those adhering to vegan diets and other forms of plant-based diets during pregnancy,” they wrote. “That would allow for stronger assumptions on possible causality between any association observed with birth or pregnancy outcomes in such studies and strengthen the basis for dietary recommendations.”
This study was funded by the Danish Council for Independent Research. The Danish National Birth Cohort Study is supported by the March of Dimes Birth Defects Foundation, the Danish Heart Association, Danish Medical Research Council, Sygekassernes Helsefond, the Innovation Fund Denmark, and the Danish National Research Foundation. The authors had no conflicts of interest to declare.
Mothers on vegan diets during pregnancy may give birth to infants with lower mean birth weights than those of omnivorous mothers and may also have a greater risk of preeclampsia, a prospective study of Danish pregnant women suggests.
According to researchers led by Signe Hedegaard, MD, of the department of obstetrics and Gynecology at Rigshospitalet, Juliane Marie Center, University of Copenhagen, low protein intake may lie behind the observed association with birth weight. The report was published in Acta Obstetricia et Gynecologica Scandinavica.
While vegan-identifying mothers were very few in number, the authors conceded, their babies were more likely to weigh less on average than those of omnivorous mothers — 3441 g vs 3601 g — despite a mean gestation 5 days longer.
Prevalence rates of low birth weight (< 2500 g) in the two groups were 11.1% and 2.5%, respectively, and the prevalence of preeclampsia was 11.1% vs 2.6%. The mean birth weight of infants in the maternal vegan group was about 240 g lower than infants born to omnivorous mothers.
“The lower birth weight of around 240 g among vegans compared with omnivorous mothers in our study strengthens our observation that vegans may be at higher risk of giving birth to low-birth-weight infants. The observed effect size on birth weight is comparable to what is observed among daily smokers relative to nonsmokers in this cohort,“ Dr. Hedegaard and colleagues wrote. “Furthermore, the on-average 5-day longer gestation observed among vegans in our study would be indicative of reduced fetal growth rate rather than lower birth weight due to shorter gestation.”
These findings emerged from data on 66,738 pregnancies in the Danish National Birth Cohort, 1996-2002. A food frequency questionnaire characterized pregnant subjects as fish/poultry-vegetarians, lacto/ovo-vegetarians, vegans, or omnivores, based on their self-reporting in gestational week 30.
A total of 98.7% (n = 65,872) of participants were defined as omnivorous, while 1.0% (n = 666), 0.3% (n = 183), and 0.03% (n = 18) identified as fish/poultry vegetarians, lacto/ovo-vegetarians, or vegans, respectively.
Those following plant-based diets of all types were slightly older, more often parous, and less likely to smoke. This plant dietary group also had a somewhat lower prevalence of overweight and obesity (prepregnancy body mass index > 25 [kg/m2]) and a higher prevalence of underweight (prepregnancy BMI < 18.5).
Total energy intake was modestly lower from plant-based diets, for a mean difference of 0.3-0.7 MJ (72-167 kcal) per day.
As for total protein intake, this was substantially lower for lacto/ovo-vegetarians and vegans: 13.3% and 10.4% of energy, respectively, compared with 15.4% in omnivores.
Dietary intake of micronutrients was also considerably lower among vegans, but after factoring in intake from dietary supplements, no major differences emerged.
Mean birth weight, birth length, length of gestation, and rate of low birth weight (< 2500 g) were similar among omnivorous, fish/poultry-, and lacto/ovo-vegetarians. The prevalence of gestational diabetes, preeclampsia, and cesarean section was similar across groups, but the prevalence of anemia was higher among fish/poultry- and lacto/ovo-vegetarians than omnivorous participants.
As for preeclampsia, previous research in larger numbers of vegans found no indication of hypertensive disorders during pregnancy. Some studies, however, have suggested a link between preeclampsia and low intake of protein, calcium, or vitamin D, but the evidence is inconclusive, and the mechanism is unclear.
The observed associations, however, do not translate to causality, the authors cautioned. “Future studies should put more emphasis on characterizing the diet among those adhering to vegan diets and other forms of plant-based diets during pregnancy,” they wrote. “That would allow for stronger assumptions on possible causality between any association observed with birth or pregnancy outcomes in such studies and strengthen the basis for dietary recommendations.”
This study was funded by the Danish Council for Independent Research. The Danish National Birth Cohort Study is supported by the March of Dimes Birth Defects Foundation, the Danish Heart Association, Danish Medical Research Council, Sygekassernes Helsefond, the Innovation Fund Denmark, and the Danish National Research Foundation. The authors had no conflicts of interest to declare.
FROM ACTA OBSTETRICIA ET GYNECOLOGICA SCANDINAVICA
Buprenorphine Slightly Less Risky than Methadone for Fetal Malformation
Buprenorphine use, compared with methadone use, in pregnancy has been linked with a slightly lower risk of major congenital malformations in a new study of medications for opioid use disorder (OUD).
Elizabeth A. Suarez, PhD, MPH, with the Division of Pharmacoepidemiology and Pharmacoeconomics, Brigham and Women’s Hospital and Harvard Medical School in Boston, and colleagues published the findings in JAMA Internal Medicine.
The lower risk for buprenorphine was small (risk ratio, 0.82; 95% confidence interval [CI], 0.69-0.97), and methadone use should not be ruled out on that basis, the authors wrote. For some women, particularly those on stable treatment before pregnancy or women who do not respond well to buprenorphine, methadone may be the better choice, they explained.
Either Medication Better Than Not Treating
The authors noted that either medication “is strongly recommended over untreated OUD during pregnancy.”
JAMA Internal Medicine Deputy Editor Deborah Grady, MD, MPH, with the Department of Medicine, University of California, San Francisco, emphasized that recommendation in an editor’s note, highlighting that treatment for OUD is critical to prevent infections, overdose, and death in pregnant women as well as neonatal opioid withdrawal syndrome and fetal death.
She stressed that internists and other primary care physicians have a key role in ensuring pregnant women with OUD receive appropriate treatment.
Given the importance of the issue, she wrote, “we have taken the unusual step of publishing two accompanying invited commentaries.”
Two developments may help increase use of buprenorphine, the study authors wrote. One is a recent study showing lower risk of adverse neonatal outcomes when buprenorphine is used during pregnancy compared with methadone. Another is the removal last year of the prescribing waiver for buprenorphine.
Study Included Medicaid Data Over 18 Years
The population-based cohort study used data from publicly insured Medicaid beneficiaries from 2000 to 2018. Pregnancies with enrollment from 90 days before pregnancy through 1 month after delivery and first-trimester use of buprenorphine or methadone were included (n = 13,360). The data were linked with infants’ health data.
The study group included 9,514 pregnancies with first-trimester buprenorphine exposure and 3,846 with methadone exposure. The risk of malformations overall was 50.9 (95% CI, 46.5-55.3) per 1000 pregnancies for buprenorphine and 60.6 (95% CI, 53.0-68.1) per 1000 pregnancies for methadone.
Major malformations were any cardiac malformations, ventricular septal defect, secundum atrial septal defect/nonprematurity-related patent foramen ovale, neural tube defects, oral clefts, and clubfoot.
Two Invited Commentaries Urge Caution in Interpretation
The two invited commentaries Dr. Grady mentioned in her editor’s note point both to the importance of the team’s findings and the need for better understanding of factors that may affect the choice of which OUD medication to use.
A commentary by Max Jordan Nguemeni Tiako, MD, MS, with the Department of Medicine, Brigham and Women’s Hospital, and colleagues, said that while the Suarez et al. data are important to share with patients, “the ultimate treatment decision must be the result of shared decision-making between a knowledgeable clinician and the patient, rather than promoting one medication over another.”
They urge putting the findings in context given the study population, which comprises a relatively stable group of women with OUD, most of whom were taking OUD medications before they got pregnant. The study sample excludes a substantial number of women who are chronically underinsured or uninsured, Dr. Tiako’s team wrote, because those included were enrolled in Medicaid for 3 consecutive months before pregnancy.
“We urge caution when extrapolating these findings to newly pregnant individuals with untreated OUD,” they wrote.
Both Medications are Safe
Cara Poland, MD, MEd, with the Henry Ford Health + Michigan State University Health Sciences in Grand Rapids, and coauthors, added in another commentary that Suarez et al. didn’t include a comparison between the population-level congenital defect rate and the defect rate for people using medications for OUD in pregnancy.
That comparison, they wrote, would have better illustrated the safety of medications for OUD “instead of simply comparing two medications with long-standing safety data.”
When a clinician starts a woman on medication for OUD in pregnancy, it’s important to understand several factors, including individual access to and comfort with different treatment approaches, they noted. It’s also important to weigh whether changing medications is worth the potential drawbacks of disrupting their well-managed care.
They wrote that the paper by Suarez et al. does not make the case for switching medications based on their findings.
Internists, they added, are ideal experts to explain risk of fetal abnormalities in the wider context of supporting engagement with continuous medication for OUD.
“In the absence of other concerns, switching medications (methadone to buprenorphine) or — worse — discontinuing [medication for] OUD because of this study runs counter to the substantial evidence regarding the safety of these medications during pregnancy,” Dr. Poland’s team wrote. “No treatment is without risk in pregnancy.”
This study was supported by the National Institute on Drug Abuse. In the Suarez et al. study, coauthors Dr. Hernández-Díaz, Dr. Gray, Dr. Connery, Dr. Zhu, and Dr. Huybrechts reported grants, personal fees and consulting payments from several pharmaceutical companies. Dr. Grady reports no relevant financial relationships in her editor’s note. No relevant financial relationships were reported by authors of the Tiako et al. commentary.
Regarding the commentary by Poland et al., grants were reported from the Michigan Health Endowment Fund, the Michigan Department of Health and Human Services, the National Institute on Drug Abuse and Blue Cross Blue Shield of Michigan outside the submitted work. No other disclosures were reported.
Buprenorphine use, compared with methadone use, in pregnancy has been linked with a slightly lower risk of major congenital malformations in a new study of medications for opioid use disorder (OUD).
Elizabeth A. Suarez, PhD, MPH, with the Division of Pharmacoepidemiology and Pharmacoeconomics, Brigham and Women’s Hospital and Harvard Medical School in Boston, and colleagues published the findings in JAMA Internal Medicine.
The lower risk for buprenorphine was small (risk ratio, 0.82; 95% confidence interval [CI], 0.69-0.97), and methadone use should not be ruled out on that basis, the authors wrote. For some women, particularly those on stable treatment before pregnancy or women who do not respond well to buprenorphine, methadone may be the better choice, they explained.
Either Medication Better Than Not Treating
The authors noted that either medication “is strongly recommended over untreated OUD during pregnancy.”
JAMA Internal Medicine Deputy Editor Deborah Grady, MD, MPH, with the Department of Medicine, University of California, San Francisco, emphasized that recommendation in an editor’s note, highlighting that treatment for OUD is critical to prevent infections, overdose, and death in pregnant women as well as neonatal opioid withdrawal syndrome and fetal death.
She stressed that internists and other primary care physicians have a key role in ensuring pregnant women with OUD receive appropriate treatment.
Given the importance of the issue, she wrote, “we have taken the unusual step of publishing two accompanying invited commentaries.”
Two developments may help increase use of buprenorphine, the study authors wrote. One is a recent study showing lower risk of adverse neonatal outcomes when buprenorphine is used during pregnancy compared with methadone. Another is the removal last year of the prescribing waiver for buprenorphine.
Study Included Medicaid Data Over 18 Years
The population-based cohort study used data from publicly insured Medicaid beneficiaries from 2000 to 2018. Pregnancies with enrollment from 90 days before pregnancy through 1 month after delivery and first-trimester use of buprenorphine or methadone were included (n = 13,360). The data were linked with infants’ health data.
The study group included 9,514 pregnancies with first-trimester buprenorphine exposure and 3,846 with methadone exposure. The risk of malformations overall was 50.9 (95% CI, 46.5-55.3) per 1000 pregnancies for buprenorphine and 60.6 (95% CI, 53.0-68.1) per 1000 pregnancies for methadone.
Major malformations were any cardiac malformations, ventricular septal defect, secundum atrial septal defect/nonprematurity-related patent foramen ovale, neural tube defects, oral clefts, and clubfoot.
Two Invited Commentaries Urge Caution in Interpretation
The two invited commentaries Dr. Grady mentioned in her editor’s note point both to the importance of the team’s findings and the need for better understanding of factors that may affect the choice of which OUD medication to use.
A commentary by Max Jordan Nguemeni Tiako, MD, MS, with the Department of Medicine, Brigham and Women’s Hospital, and colleagues, said that while the Suarez et al. data are important to share with patients, “the ultimate treatment decision must be the result of shared decision-making between a knowledgeable clinician and the patient, rather than promoting one medication over another.”
They urge putting the findings in context given the study population, which comprises a relatively stable group of women with OUD, most of whom were taking OUD medications before they got pregnant. The study sample excludes a substantial number of women who are chronically underinsured or uninsured, Dr. Tiako’s team wrote, because those included were enrolled in Medicaid for 3 consecutive months before pregnancy.
“We urge caution when extrapolating these findings to newly pregnant individuals with untreated OUD,” they wrote.
Both Medications are Safe
Cara Poland, MD, MEd, with the Henry Ford Health + Michigan State University Health Sciences in Grand Rapids, and coauthors, added in another commentary that Suarez et al. didn’t include a comparison between the population-level congenital defect rate and the defect rate for people using medications for OUD in pregnancy.
That comparison, they wrote, would have better illustrated the safety of medications for OUD “instead of simply comparing two medications with long-standing safety data.”
When a clinician starts a woman on medication for OUD in pregnancy, it’s important to understand several factors, including individual access to and comfort with different treatment approaches, they noted. It’s also important to weigh whether changing medications is worth the potential drawbacks of disrupting their well-managed care.
They wrote that the paper by Suarez et al. does not make the case for switching medications based on their findings.
Internists, they added, are ideal experts to explain risk of fetal abnormalities in the wider context of supporting engagement with continuous medication for OUD.
“In the absence of other concerns, switching medications (methadone to buprenorphine) or — worse — discontinuing [medication for] OUD because of this study runs counter to the substantial evidence regarding the safety of these medications during pregnancy,” Dr. Poland’s team wrote. “No treatment is without risk in pregnancy.”
This study was supported by the National Institute on Drug Abuse. In the Suarez et al. study, coauthors Dr. Hernández-Díaz, Dr. Gray, Dr. Connery, Dr. Zhu, and Dr. Huybrechts reported grants, personal fees and consulting payments from several pharmaceutical companies. Dr. Grady reports no relevant financial relationships in her editor’s note. No relevant financial relationships were reported by authors of the Tiako et al. commentary.
Regarding the commentary by Poland et al., grants were reported from the Michigan Health Endowment Fund, the Michigan Department of Health and Human Services, the National Institute on Drug Abuse and Blue Cross Blue Shield of Michigan outside the submitted work. No other disclosures were reported.
Buprenorphine use, compared with methadone use, in pregnancy has been linked with a slightly lower risk of major congenital malformations in a new study of medications for opioid use disorder (OUD).
Elizabeth A. Suarez, PhD, MPH, with the Division of Pharmacoepidemiology and Pharmacoeconomics, Brigham and Women’s Hospital and Harvard Medical School in Boston, and colleagues published the findings in JAMA Internal Medicine.
The lower risk for buprenorphine was small (risk ratio, 0.82; 95% confidence interval [CI], 0.69-0.97), and methadone use should not be ruled out on that basis, the authors wrote. For some women, particularly those on stable treatment before pregnancy or women who do not respond well to buprenorphine, methadone may be the better choice, they explained.
Either Medication Better Than Not Treating
The authors noted that either medication “is strongly recommended over untreated OUD during pregnancy.”
JAMA Internal Medicine Deputy Editor Deborah Grady, MD, MPH, with the Department of Medicine, University of California, San Francisco, emphasized that recommendation in an editor’s note, highlighting that treatment for OUD is critical to prevent infections, overdose, and death in pregnant women as well as neonatal opioid withdrawal syndrome and fetal death.
She stressed that internists and other primary care physicians have a key role in ensuring pregnant women with OUD receive appropriate treatment.
Given the importance of the issue, she wrote, “we have taken the unusual step of publishing two accompanying invited commentaries.”
Two developments may help increase use of buprenorphine, the study authors wrote. One is a recent study showing lower risk of adverse neonatal outcomes when buprenorphine is used during pregnancy compared with methadone. Another is the removal last year of the prescribing waiver for buprenorphine.
Study Included Medicaid Data Over 18 Years
The population-based cohort study used data from publicly insured Medicaid beneficiaries from 2000 to 2018. Pregnancies with enrollment from 90 days before pregnancy through 1 month after delivery and first-trimester use of buprenorphine or methadone were included (n = 13,360). The data were linked with infants’ health data.
The study group included 9,514 pregnancies with first-trimester buprenorphine exposure and 3,846 with methadone exposure. The risk of malformations overall was 50.9 (95% CI, 46.5-55.3) per 1000 pregnancies for buprenorphine and 60.6 (95% CI, 53.0-68.1) per 1000 pregnancies for methadone.
Major malformations were any cardiac malformations, ventricular septal defect, secundum atrial septal defect/nonprematurity-related patent foramen ovale, neural tube defects, oral clefts, and clubfoot.
Two Invited Commentaries Urge Caution in Interpretation
The two invited commentaries Dr. Grady mentioned in her editor’s note point both to the importance of the team’s findings and the need for better understanding of factors that may affect the choice of which OUD medication to use.
A commentary by Max Jordan Nguemeni Tiako, MD, MS, with the Department of Medicine, Brigham and Women’s Hospital, and colleagues, said that while the Suarez et al. data are important to share with patients, “the ultimate treatment decision must be the result of shared decision-making between a knowledgeable clinician and the patient, rather than promoting one medication over another.”
They urge putting the findings in context given the study population, which comprises a relatively stable group of women with OUD, most of whom were taking OUD medications before they got pregnant. The study sample excludes a substantial number of women who are chronically underinsured or uninsured, Dr. Tiako’s team wrote, because those included were enrolled in Medicaid for 3 consecutive months before pregnancy.
“We urge caution when extrapolating these findings to newly pregnant individuals with untreated OUD,” they wrote.
Both Medications are Safe
Cara Poland, MD, MEd, with the Henry Ford Health + Michigan State University Health Sciences in Grand Rapids, and coauthors, added in another commentary that Suarez et al. didn’t include a comparison between the population-level congenital defect rate and the defect rate for people using medications for OUD in pregnancy.
That comparison, they wrote, would have better illustrated the safety of medications for OUD “instead of simply comparing two medications with long-standing safety data.”
When a clinician starts a woman on medication for OUD in pregnancy, it’s important to understand several factors, including individual access to and comfort with different treatment approaches, they noted. It’s also important to weigh whether changing medications is worth the potential drawbacks of disrupting their well-managed care.
They wrote that the paper by Suarez et al. does not make the case for switching medications based on their findings.
Internists, they added, are ideal experts to explain risk of fetal abnormalities in the wider context of supporting engagement with continuous medication for OUD.
“In the absence of other concerns, switching medications (methadone to buprenorphine) or — worse — discontinuing [medication for] OUD because of this study runs counter to the substantial evidence regarding the safety of these medications during pregnancy,” Dr. Poland’s team wrote. “No treatment is without risk in pregnancy.”
This study was supported by the National Institute on Drug Abuse. In the Suarez et al. study, coauthors Dr. Hernández-Díaz, Dr. Gray, Dr. Connery, Dr. Zhu, and Dr. Huybrechts reported grants, personal fees and consulting payments from several pharmaceutical companies. Dr. Grady reports no relevant financial relationships in her editor’s note. No relevant financial relationships were reported by authors of the Tiako et al. commentary.
Regarding the commentary by Poland et al., grants were reported from the Michigan Health Endowment Fund, the Michigan Department of Health and Human Services, the National Institute on Drug Abuse and Blue Cross Blue Shield of Michigan outside the submitted work. No other disclosures were reported.
FROM JAMA INTERNAL MEDICINE
Why Are Women More Likely to Get Long COVID?
Annette Gillaspie, a nurse in a small Oregon hospital, hoped she would be back working with patients by now. She contracted COVID-19 on the job early in the pandemic and ended up with long COVID.
After recovering a bit, her fatigue and dizziness returned, and today she is still working a desk job. She has also experienced more severe menstrual periods than before she had COVID.
“Being a female with long COVID definitely does add to the roller-coaster effect of symptoms,” Ms. Gillaspie said.
reported by the Centers for Disease Control and Prevention (CDC). Researchers are trying to determine why, what causes the gender disparity, and how best to treat it.
Scientists are also starting to look at the impact of long COVID on female reproductive health, including menstruation, pregnancy, and menopause.
Sex differences are common in infection-associated illnesses, said Beth Pollack, MS, a research scientist specializing in long COVID in the Massachusetts Institute of Technology’s Department of Biological Engineering, Cambridge, Massachusetts. “It informs research priorities and the lens with which we understand long COVID.”
For example, reproductive health issues for women, such as puberty, pregnancy, and menopause, can alter the course of illness in a subset of women in myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS) and postural orthostatic tachycardia syndrome (POTS), a condition that can cause dizziness and worse.
“This suggests that sex hormones may play key roles in immune responses to infections,” Ms. Pollack said.
ME/CFS and a Possible Link to Long COVID in Women
Some of the research into long COVID is being led by teams studying infection-associated chronic illnesses like ME/CFS.
The problem: Advocates say ME/CFS has been under-researched. Poorly understood for years, the condition is one of a handful of chronic illnesses linked to infections, including Lyme disease and now long COVID. Perhaps not coincidently, they are more likely to affect women.
Many of the research findings about long COVID mirror data that emerged in past ME/CFS research, said Jaime Seltzer, the scientific director at #MEAction, Santa Monica, California, an advocacy group. One point in particular: ME/CFS strikes women about twice as much as men, according to the CDC.
Ms. Seltzer said the response to long COVID could be much further ahead if the research community acknowledged the work done over the years on ME/CFS. Many of the potential biomarkers and risk factors emerging for long COVID were also suspected in ME/CFS, but not thoroughly studied, she said.
She also said not enough work has been done to unravel the links between gender and these chronic conditions.
“We’re stuck in this Groundhog Day situation,” she said. “There isn’t any research, so we can’t say anything definitively.”
Some New Research, Some New Clues
Scientists like Ms. Pollack are slowly making inroads. She was lead author on a 2023 review investigating the impact of long COVID on female reproductive health. The paper highlights long COVID links to ME/CFS, POTS, and Ehlers-Danlos syndrome (EDS), as well as a resulting laundry list of female reproductive health issues. The hope is physicians will examine how the menstrual cycle, pregnancy, and menopause affect symptoms and illness progression of long COVID.
The Tal Research group at MIT (where Ms. Pollack works) has also added long COVID to the list of infection-associated illnesses it studies. The lab is conducting a large study looking into both Lyme disease and long COVID. The goals are to identify biomarkers that can predict who will not recover and to advance available treatments.
Another MIT program, “SEXX + Immunity” holds seminars and networking sessions for scientists looking into the role of female and male biology in immune responses to infection.
Barriers to Progress Remain
On the clinical side, female patients with long COVID also have to deal with a historical bias that still lurks in medicine when it comes to women’s health, said Alba Azola, MD, an assistant professor of physical medicine at Johns Hopkins Medicine, Baltimore, Maryland.
Dr. Azola said she has discovered clinical descriptions of ME/CFE in the literature archives that describe it as “neurasthenia” and dismiss it as psychological.
Patients say that it is still happening, and while it may not be so blunt, “you can read between the lines,” Dr. Azola said.
Dr. Azola, who has worked with long COVID patients and is now seeing people with ME/CFS, said the symptoms of infection-associated chronic illness can mimic menopause, and many of her patients received that misdiagnosis. She recommends that doctors rule out long COVID for women with multiple symptoms before attributing symptoms to menopause.
Seeing that some long COVID patients were developing ME/CFS, staff at the Bateman Horne Center in Salt Lake City, Utah, set up a program for the condition in 2021. They were already treating patients with ME/CFS and what they call “multi-symptom chronic complex diseases.”
Jennifer Bell, a certified nurse practitioner at the center, said she has not seen any patients with ovarian failure but plenty with reproductive health issues.
“There definitely is a hormonal connection, but I don’t think there’s a good understanding about what is happening,” she said.
Most of her patients are female, and the more serious patients tend to go through a worsening of their symptoms in the week prior to getting a period, she said.
One thing Ms. Bell said she’s noticed in the past year is an increase in patients with EDS, which is also more common in women.
Like long COVID, many of the conditions traditionally treated at the center have no cure. But Ms. Bell said the center has developed an expertise in treating post-exertional malaise, a common symptom of long COVID, and keeps up with the literature for treatments to try, like the combination of guanfacine and the antioxidant N-acetyl cysteine to treat brain fog, an approach developed at Yale.
“It’s a very challenging illness to treat,” Ms. Bell said.
Since the emergence of long COVID, researchers have warned that symptoms vary so much from person to person that treatment will need to be targeted.
Ms. Pollack of MIT agrees and sees a big role for personalized medicine.
We need to “identify phenotypes within and across these overlapping and co-occurring illnesses so that we can identify the right therapeutics for each person,” she said.
As for Annette Gillaspie, she still hopes her long COVID will subside so she can get out from behind the desk and return to her normal nursing duties.
“I just got to a point where I realized I’m likely never going to be able to do my job,” she said. “It was incredibly heart breaking, but it’s the reality of long COVID, and I know I’m not the only one to have to step away from a job I loved.”
A version of this article appeared on Medscape.com.
Annette Gillaspie, a nurse in a small Oregon hospital, hoped she would be back working with patients by now. She contracted COVID-19 on the job early in the pandemic and ended up with long COVID.
After recovering a bit, her fatigue and dizziness returned, and today she is still working a desk job. She has also experienced more severe menstrual periods than before she had COVID.
“Being a female with long COVID definitely does add to the roller-coaster effect of symptoms,” Ms. Gillaspie said.
reported by the Centers for Disease Control and Prevention (CDC). Researchers are trying to determine why, what causes the gender disparity, and how best to treat it.
Scientists are also starting to look at the impact of long COVID on female reproductive health, including menstruation, pregnancy, and menopause.
Sex differences are common in infection-associated illnesses, said Beth Pollack, MS, a research scientist specializing in long COVID in the Massachusetts Institute of Technology’s Department of Biological Engineering, Cambridge, Massachusetts. “It informs research priorities and the lens with which we understand long COVID.”
For example, reproductive health issues for women, such as puberty, pregnancy, and menopause, can alter the course of illness in a subset of women in myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS) and postural orthostatic tachycardia syndrome (POTS), a condition that can cause dizziness and worse.
“This suggests that sex hormones may play key roles in immune responses to infections,” Ms. Pollack said.
ME/CFS and a Possible Link to Long COVID in Women
Some of the research into long COVID is being led by teams studying infection-associated chronic illnesses like ME/CFS.
The problem: Advocates say ME/CFS has been under-researched. Poorly understood for years, the condition is one of a handful of chronic illnesses linked to infections, including Lyme disease and now long COVID. Perhaps not coincidently, they are more likely to affect women.
Many of the research findings about long COVID mirror data that emerged in past ME/CFS research, said Jaime Seltzer, the scientific director at #MEAction, Santa Monica, California, an advocacy group. One point in particular: ME/CFS strikes women about twice as much as men, according to the CDC.
Ms. Seltzer said the response to long COVID could be much further ahead if the research community acknowledged the work done over the years on ME/CFS. Many of the potential biomarkers and risk factors emerging for long COVID were also suspected in ME/CFS, but not thoroughly studied, she said.
She also said not enough work has been done to unravel the links between gender and these chronic conditions.
“We’re stuck in this Groundhog Day situation,” she said. “There isn’t any research, so we can’t say anything definitively.”
Some New Research, Some New Clues
Scientists like Ms. Pollack are slowly making inroads. She was lead author on a 2023 review investigating the impact of long COVID on female reproductive health. The paper highlights long COVID links to ME/CFS, POTS, and Ehlers-Danlos syndrome (EDS), as well as a resulting laundry list of female reproductive health issues. The hope is physicians will examine how the menstrual cycle, pregnancy, and menopause affect symptoms and illness progression of long COVID.
The Tal Research group at MIT (where Ms. Pollack works) has also added long COVID to the list of infection-associated illnesses it studies. The lab is conducting a large study looking into both Lyme disease and long COVID. The goals are to identify biomarkers that can predict who will not recover and to advance available treatments.
Another MIT program, “SEXX + Immunity” holds seminars and networking sessions for scientists looking into the role of female and male biology in immune responses to infection.
Barriers to Progress Remain
On the clinical side, female patients with long COVID also have to deal with a historical bias that still lurks in medicine when it comes to women’s health, said Alba Azola, MD, an assistant professor of physical medicine at Johns Hopkins Medicine, Baltimore, Maryland.
Dr. Azola said she has discovered clinical descriptions of ME/CFE in the literature archives that describe it as “neurasthenia” and dismiss it as psychological.
Patients say that it is still happening, and while it may not be so blunt, “you can read between the lines,” Dr. Azola said.
Dr. Azola, who has worked with long COVID patients and is now seeing people with ME/CFS, said the symptoms of infection-associated chronic illness can mimic menopause, and many of her patients received that misdiagnosis. She recommends that doctors rule out long COVID for women with multiple symptoms before attributing symptoms to menopause.
Seeing that some long COVID patients were developing ME/CFS, staff at the Bateman Horne Center in Salt Lake City, Utah, set up a program for the condition in 2021. They were already treating patients with ME/CFS and what they call “multi-symptom chronic complex diseases.”
Jennifer Bell, a certified nurse practitioner at the center, said she has not seen any patients with ovarian failure but plenty with reproductive health issues.
“There definitely is a hormonal connection, but I don’t think there’s a good understanding about what is happening,” she said.
Most of her patients are female, and the more serious patients tend to go through a worsening of their symptoms in the week prior to getting a period, she said.
One thing Ms. Bell said she’s noticed in the past year is an increase in patients with EDS, which is also more common in women.
Like long COVID, many of the conditions traditionally treated at the center have no cure. But Ms. Bell said the center has developed an expertise in treating post-exertional malaise, a common symptom of long COVID, and keeps up with the literature for treatments to try, like the combination of guanfacine and the antioxidant N-acetyl cysteine to treat brain fog, an approach developed at Yale.
“It’s a very challenging illness to treat,” Ms. Bell said.
Since the emergence of long COVID, researchers have warned that symptoms vary so much from person to person that treatment will need to be targeted.
Ms. Pollack of MIT agrees and sees a big role for personalized medicine.
We need to “identify phenotypes within and across these overlapping and co-occurring illnesses so that we can identify the right therapeutics for each person,” she said.
As for Annette Gillaspie, she still hopes her long COVID will subside so she can get out from behind the desk and return to her normal nursing duties.
“I just got to a point where I realized I’m likely never going to be able to do my job,” she said. “It was incredibly heart breaking, but it’s the reality of long COVID, and I know I’m not the only one to have to step away from a job I loved.”
A version of this article appeared on Medscape.com.
Annette Gillaspie, a nurse in a small Oregon hospital, hoped she would be back working with patients by now. She contracted COVID-19 on the job early in the pandemic and ended up with long COVID.
After recovering a bit, her fatigue and dizziness returned, and today she is still working a desk job. She has also experienced more severe menstrual periods than before she had COVID.
“Being a female with long COVID definitely does add to the roller-coaster effect of symptoms,” Ms. Gillaspie said.
reported by the Centers for Disease Control and Prevention (CDC). Researchers are trying to determine why, what causes the gender disparity, and how best to treat it.
Scientists are also starting to look at the impact of long COVID on female reproductive health, including menstruation, pregnancy, and menopause.
Sex differences are common in infection-associated illnesses, said Beth Pollack, MS, a research scientist specializing in long COVID in the Massachusetts Institute of Technology’s Department of Biological Engineering, Cambridge, Massachusetts. “It informs research priorities and the lens with which we understand long COVID.”
For example, reproductive health issues for women, such as puberty, pregnancy, and menopause, can alter the course of illness in a subset of women in myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS) and postural orthostatic tachycardia syndrome (POTS), a condition that can cause dizziness and worse.
“This suggests that sex hormones may play key roles in immune responses to infections,” Ms. Pollack said.
ME/CFS and a Possible Link to Long COVID in Women
Some of the research into long COVID is being led by teams studying infection-associated chronic illnesses like ME/CFS.
The problem: Advocates say ME/CFS has been under-researched. Poorly understood for years, the condition is one of a handful of chronic illnesses linked to infections, including Lyme disease and now long COVID. Perhaps not coincidently, they are more likely to affect women.
Many of the research findings about long COVID mirror data that emerged in past ME/CFS research, said Jaime Seltzer, the scientific director at #MEAction, Santa Monica, California, an advocacy group. One point in particular: ME/CFS strikes women about twice as much as men, according to the CDC.
Ms. Seltzer said the response to long COVID could be much further ahead if the research community acknowledged the work done over the years on ME/CFS. Many of the potential biomarkers and risk factors emerging for long COVID were also suspected in ME/CFS, but not thoroughly studied, she said.
She also said not enough work has been done to unravel the links between gender and these chronic conditions.
“We’re stuck in this Groundhog Day situation,” she said. “There isn’t any research, so we can’t say anything definitively.”
Some New Research, Some New Clues
Scientists like Ms. Pollack are slowly making inroads. She was lead author on a 2023 review investigating the impact of long COVID on female reproductive health. The paper highlights long COVID links to ME/CFS, POTS, and Ehlers-Danlos syndrome (EDS), as well as a resulting laundry list of female reproductive health issues. The hope is physicians will examine how the menstrual cycle, pregnancy, and menopause affect symptoms and illness progression of long COVID.
The Tal Research group at MIT (where Ms. Pollack works) has also added long COVID to the list of infection-associated illnesses it studies. The lab is conducting a large study looking into both Lyme disease and long COVID. The goals are to identify biomarkers that can predict who will not recover and to advance available treatments.
Another MIT program, “SEXX + Immunity” holds seminars and networking sessions for scientists looking into the role of female and male biology in immune responses to infection.
Barriers to Progress Remain
On the clinical side, female patients with long COVID also have to deal with a historical bias that still lurks in medicine when it comes to women’s health, said Alba Azola, MD, an assistant professor of physical medicine at Johns Hopkins Medicine, Baltimore, Maryland.
Dr. Azola said she has discovered clinical descriptions of ME/CFE in the literature archives that describe it as “neurasthenia” and dismiss it as psychological.
Patients say that it is still happening, and while it may not be so blunt, “you can read between the lines,” Dr. Azola said.
Dr. Azola, who has worked with long COVID patients and is now seeing people with ME/CFS, said the symptoms of infection-associated chronic illness can mimic menopause, and many of her patients received that misdiagnosis. She recommends that doctors rule out long COVID for women with multiple symptoms before attributing symptoms to menopause.
Seeing that some long COVID patients were developing ME/CFS, staff at the Bateman Horne Center in Salt Lake City, Utah, set up a program for the condition in 2021. They were already treating patients with ME/CFS and what they call “multi-symptom chronic complex diseases.”
Jennifer Bell, a certified nurse practitioner at the center, said she has not seen any patients with ovarian failure but plenty with reproductive health issues.
“There definitely is a hormonal connection, but I don’t think there’s a good understanding about what is happening,” she said.
Most of her patients are female, and the more serious patients tend to go through a worsening of their symptoms in the week prior to getting a period, she said.
One thing Ms. Bell said she’s noticed in the past year is an increase in patients with EDS, which is also more common in women.
Like long COVID, many of the conditions traditionally treated at the center have no cure. But Ms. Bell said the center has developed an expertise in treating post-exertional malaise, a common symptom of long COVID, and keeps up with the literature for treatments to try, like the combination of guanfacine and the antioxidant N-acetyl cysteine to treat brain fog, an approach developed at Yale.
“It’s a very challenging illness to treat,” Ms. Bell said.
Since the emergence of long COVID, researchers have warned that symptoms vary so much from person to person that treatment will need to be targeted.
Ms. Pollack of MIT agrees and sees a big role for personalized medicine.
We need to “identify phenotypes within and across these overlapping and co-occurring illnesses so that we can identify the right therapeutics for each person,” she said.
As for Annette Gillaspie, she still hopes her long COVID will subside so she can get out from behind the desk and return to her normal nursing duties.
“I just got to a point where I realized I’m likely never going to be able to do my job,” she said. “It was incredibly heart breaking, but it’s the reality of long COVID, and I know I’m not the only one to have to step away from a job I loved.”
A version of this article appeared on Medscape.com.
Adequate Midlife Protein, Especially From Plants, Tied to Healthy Aging
Intake of protein, especially from plants, in middle age is associated with higher odds of healthy aging and positive mental and physical health status in older women, a recent analysis of the Nurses’ Health Study (NHS) data suggests.
The study is said to be the first to examine the long-term impact of midlife protein consumption on later health status.

Writing in the American Journal of Clinical Nutrition, a team led by Andres V. Ardisson Korat, DSc, a nutritional epidemiologist at the USDA Human Nutrition Research Center on Aging at Tufts University in Boston, Massachusetts, found the following midlife protein–related odds ratios (ORs) for later healthy aging measured at ages 70-93.
For each 3% energy increment from various protein sources:
- 1.05 (95% confidence interval, 1.01-1.10) for total protein
- 1.07 (1.02-1.11) for animal protein
- 1.14 (1.06-1.23) for dairy protein
- 1.38 (1.24-1.54) for plant protein
In substitution analyses, significant positive associations were observed for the isocaloric replacement of animal or dairy protein, carbohydrate, or fat with plant protein — with increased ORs for healthy aging of 1.22-1.58 for each 3% of energy replacement.
On the measure of physical function, for example, replacing calories from all macronutrient variables with equivalent calories from plant protein was associated with 20%-60% higher odds of having no physical function limitations. Plant protein was also associated with higher odds for good mental status.
“Other studies have looked at protein intake in older adults, but we felt midlife was a more relevant etiological window,” Dr. Ardisson Korat said in an interview. “Our findings generally align, however, with those of protein intake in older populations, which have shown that protein can reduce the risk of frailty.”
He added that the benefits of protein, especially from plant sources, would likely apply to men as well and increasing plant protein intake is not difficult. “If you want a snack during the day, eat a handful of nuts instead of potato chips,” he advised. And eating several meals a week featuring beans, peas, lentils, tofu, whole grains, or seeds is an easy way to boost dietary plant protein, which comes with health-promoting soluble and insoluble fiber as well as antioxidant and anti-inflammatory polyphenols and other phytochemicals.
Conversely, plant but not animal protein consumption in older adulthood was linked to a lower risk of frailty in a previous NHS trial.
Higher plant protein intake was associated with a better probability of achieving healthy aging defined by changes in functional impairments, self-reported health/vitality, mental health, and use of health services in the Spanish Seniors-Estudio Sobre Nutricion y Riesgo Cardiovascular.
In contrast, animal protein intake in middle adulthood has been linked to an increased risk of premature death from chronic diseases driven by cardiovascular disease mortality.
The present findings are consistent with those observed for protein intakes in older adulthood, Dr. Ardisson Korat said.
“This study underscores the health advantages for midlife adults consuming adequate dietary protein — particularly plant protein — as one component of pursuing a healthy lifestyle,” said Douglas R. Dirschl, MD, chair of orthopedic surgery at Baylor College of Medicine in Houston, Texas. Most Americans consume adequate amounts of protein, but according to Dr. Dirschl, who treats many older patients for osteoporotic fractures and other musculoskeletal conditions, many US diets are subpar in this nutrient.
While protein is essential for bone and muscle formation and maintenance, “a surprising number of Americans are protein deficient, even those who seem hale and are overweight,” he said.
Dietary Recommendations for Midlife Patients
Physicians should therefore advise midlife patients to meet or perhaps modestly exceed the recommended dietary allowance (RDA) for protein of 0.8 g/kg per day and to make plant protein a substantial component of daily dietary protein intake, Dr. Dirschl said.
Luke D. Kim, MD, MEd, a geriatrician at the Cleveland Clinic in Cleveland, Ohio, noted that patients with lower socioeconomic status or with difficulty in day-to-day functioning are likely to have suboptimal protein intake. Such patients may need encouragement to eat more protein. “But we should keep in mind that showing a higher associated odds ratio of better health with increased protein take does not mean causality,” he said.
According to Rachel L. Amdur, MD, an internist at Northwestern Medicine in Chicago, Illinois, the long-term follow-up data from the NHS are uniquely helpful. “Middle-aged persons may think they no longer need much dietary protein and need to be reminded. Sometimes eating carbohydrates is just easier,” she said in an interview. Physicians need to asses and counsel patients on nutrition at all stages of life. “As I tell my patients, it’s best to think of your future self now.”
In agreement is Louis J. Morledge, MD, an internist at Northwell Health in New York City. “I firmly counsel my patients about adequate and often increased protein intake in middle life. But this is always within a larger framework of overall nutritional health.” He added that middle-aged persons often find themselves “stuck in food ruts,” and one of his clinical focuses is to advise patients about the importance of healthier food choices so they can better adjust to mental, emotional, physical, and skeletal changes as they age.
Study Details
The NHS analysis drew on prospective data from 48,762 nurses under age 60 in 1984. Total protein, animal protein, dairy protein, and plant protein were derived from validated food-frequency questionnaires.
Adjusting for lifestyle, demographics, and health status, the investigators identified 3721 (7.6% of cohort) eligible participants. The mean age of participants at baseline was 48.6 years; 38.6% had body mass indexes (BMI; in kg/m2) greater than 25; 22.9% were current smokers; and 88.2% were married.
Healthy aging was defined as freedom from 11 major chronic diseases, good mental health, and no impairments in cognitive or physical function, as assessed in the 2014 or 2016 NHS participant questionnaires. Diseases/treatments included cancer, type 2 diabetes, myocardial infarction, coronary artery bypass graft or coronary angioplasty, congestive heart failure, stroke, kidney failure, chronic obstructive pulmonary disease, Parkinson disease, multiple sclerosis, and amyotrophic lateral sclerosis.
Mean total protein consumption as a percentage of energy was 18.3% (standard deviation 3%), slightly higher than the average 16% in the US diet. Of this, 13.3% derived from animals, 3.6% from dairy products, and 4.9% from plants.
Total protein intake was positively associated with higher education levels, being physically active, higher BMI, and a baseline history of hypertension and hypercholesterolemia. Conversely, total protein intake was inversely associated with intakes of total carbohydrates, nuts, alcohol, and sugar-sweetened beverages.
The associations between protein intake and healthy aging are complex and not fully understood, the authors stated.
Effects of Protein Intake
In studies of older adult populations lower protein intake has been associated with lean mass loss. Animal protein supplementation studies in older adults have shown lean mass gains potentially related to amino acid composition.
In terms of mechanisms, evidence suggests that protein-related activation of the rapamycin complex 1 pathway may play a role, the authors suggested. The activity of this signaling pathway decreases with age.
Rapamycin, a compound used to prevent organ transplant rejection, has been associated with delayed aging. In the body, dietary protein and exercise activate this pathway, thereby stimulating muscle protein synthesis and possibly improving physical function.
As for the differential associations of plant and animal protein on the chronic disease domain of the healthy aging phenotype, Dr. Ardisson Korat and coauthors said plant protein has been associated with favorable levels of important risk factors for cardiometabolic diseases, such as reduced LDL cholesterol, lower blood pressure, and insulin sensitivity, as well as decreased levels of proinflammatory markers.
Conversely, total and animal protein intakes have been positively associated with concentrations of insulin-like growth factor 1, which is implicated in the growth of malignant cells in breast and prostate tissue.
This study is the first step in evaluating the long-term health effect of protein intake in midlife, the relevant development window for most chronic conditions, the NHS study authors said. More research is needed, however, to corroborate the study findings in other populations and identify underlying mechanisms.
This study was supported by the USDA Agricultural Research Service and the National Institutes of Health. The authors reported no conflicts of interest. The commentators disclosed no relevant competing interests.
Intake of protein, especially from plants, in middle age is associated with higher odds of healthy aging and positive mental and physical health status in older women, a recent analysis of the Nurses’ Health Study (NHS) data suggests.
The study is said to be the first to examine the long-term impact of midlife protein consumption on later health status.
Writing in the American Journal of Clinical Nutrition, a team led by Andres V. Ardisson Korat, DSc, a nutritional epidemiologist at the USDA Human Nutrition Research Center on Aging at Tufts University in Boston, Massachusetts, found the following midlife protein–related odds ratios (ORs) for later healthy aging measured at ages 70-93.
For each 3% energy increment from various protein sources:
- 1.05 (95% confidence interval, 1.01-1.10) for total protein
- 1.07 (1.02-1.11) for animal protein
- 1.14 (1.06-1.23) for dairy protein
- 1.38 (1.24-1.54) for plant protein
In substitution analyses, significant positive associations were observed for the isocaloric replacement of animal or dairy protein, carbohydrate, or fat with plant protein — with increased ORs for healthy aging of 1.22-1.58 for each 3% of energy replacement.
On the measure of physical function, for example, replacing calories from all macronutrient variables with equivalent calories from plant protein was associated with 20%-60% higher odds of having no physical function limitations. Plant protein was also associated with higher odds for good mental status.
“Other studies have looked at protein intake in older adults, but we felt midlife was a more relevant etiological window,” Dr. Ardisson Korat said in an interview. “Our findings generally align, however, with those of protein intake in older populations, which have shown that protein can reduce the risk of frailty.”
He added that the benefits of protein, especially from plant sources, would likely apply to men as well and increasing plant protein intake is not difficult. “If you want a snack during the day, eat a handful of nuts instead of potato chips,” he advised. And eating several meals a week featuring beans, peas, lentils, tofu, whole grains, or seeds is an easy way to boost dietary plant protein, which comes with health-promoting soluble and insoluble fiber as well as antioxidant and anti-inflammatory polyphenols and other phytochemicals.
Conversely, plant but not animal protein consumption in older adulthood was linked to a lower risk of frailty in a previous NHS trial.
Higher plant protein intake was associated with a better probability of achieving healthy aging defined by changes in functional impairments, self-reported health/vitality, mental health, and use of health services in the Spanish Seniors-Estudio Sobre Nutricion y Riesgo Cardiovascular.
In contrast, animal protein intake in middle adulthood has been linked to an increased risk of premature death from chronic diseases driven by cardiovascular disease mortality.
The present findings are consistent with those observed for protein intakes in older adulthood, Dr. Ardisson Korat said.
“This study underscores the health advantages for midlife adults consuming adequate dietary protein — particularly plant protein — as one component of pursuing a healthy lifestyle,” said Douglas R. Dirschl, MD, chair of orthopedic surgery at Baylor College of Medicine in Houston, Texas. Most Americans consume adequate amounts of protein, but according to Dr. Dirschl, who treats many older patients for osteoporotic fractures and other musculoskeletal conditions, many US diets are subpar in this nutrient.
While protein is essential for bone and muscle formation and maintenance, “a surprising number of Americans are protein deficient, even those who seem hale and are overweight,” he said.
Dietary Recommendations for Midlife Patients
Physicians should therefore advise midlife patients to meet or perhaps modestly exceed the recommended dietary allowance (RDA) for protein of 0.8 g/kg per day and to make plant protein a substantial component of daily dietary protein intake, Dr. Dirschl said.
Luke D. Kim, MD, MEd, a geriatrician at the Cleveland Clinic in Cleveland, Ohio, noted that patients with lower socioeconomic status or with difficulty in day-to-day functioning are likely to have suboptimal protein intake. Such patients may need encouragement to eat more protein. “But we should keep in mind that showing a higher associated odds ratio of better health with increased protein take does not mean causality,” he said.
According to Rachel L. Amdur, MD, an internist at Northwestern Medicine in Chicago, Illinois, the long-term follow-up data from the NHS are uniquely helpful. “Middle-aged persons may think they no longer need much dietary protein and need to be reminded. Sometimes eating carbohydrates is just easier,” she said in an interview. Physicians need to asses and counsel patients on nutrition at all stages of life. “As I tell my patients, it’s best to think of your future self now.”
In agreement is Louis J. Morledge, MD, an internist at Northwell Health in New York City. “I firmly counsel my patients about adequate and often increased protein intake in middle life. But this is always within a larger framework of overall nutritional health.” He added that middle-aged persons often find themselves “stuck in food ruts,” and one of his clinical focuses is to advise patients about the importance of healthier food choices so they can better adjust to mental, emotional, physical, and skeletal changes as they age.
Study Details
The NHS analysis drew on prospective data from 48,762 nurses under age 60 in 1984. Total protein, animal protein, dairy protein, and plant protein were derived from validated food-frequency questionnaires.
Adjusting for lifestyle, demographics, and health status, the investigators identified 3721 (7.6% of cohort) eligible participants. The mean age of participants at baseline was 48.6 years; 38.6% had body mass indexes (BMI; in kg/m2) greater than 25; 22.9% were current smokers; and 88.2% were married.
Healthy aging was defined as freedom from 11 major chronic diseases, good mental health, and no impairments in cognitive or physical function, as assessed in the 2014 or 2016 NHS participant questionnaires. Diseases/treatments included cancer, type 2 diabetes, myocardial infarction, coronary artery bypass graft or coronary angioplasty, congestive heart failure, stroke, kidney failure, chronic obstructive pulmonary disease, Parkinson disease, multiple sclerosis, and amyotrophic lateral sclerosis.
Mean total protein consumption as a percentage of energy was 18.3% (standard deviation 3%), slightly higher than the average 16% in the US diet. Of this, 13.3% derived from animals, 3.6% from dairy products, and 4.9% from plants.
Total protein intake was positively associated with higher education levels, being physically active, higher BMI, and a baseline history of hypertension and hypercholesterolemia. Conversely, total protein intake was inversely associated with intakes of total carbohydrates, nuts, alcohol, and sugar-sweetened beverages.
The associations between protein intake and healthy aging are complex and not fully understood, the authors stated.
Effects of Protein Intake
In studies of older adult populations lower protein intake has been associated with lean mass loss. Animal protein supplementation studies in older adults have shown lean mass gains potentially related to amino acid composition.
In terms of mechanisms, evidence suggests that protein-related activation of the rapamycin complex 1 pathway may play a role, the authors suggested. The activity of this signaling pathway decreases with age.
Rapamycin, a compound used to prevent organ transplant rejection, has been associated with delayed aging. In the body, dietary protein and exercise activate this pathway, thereby stimulating muscle protein synthesis and possibly improving physical function.
As for the differential associations of plant and animal protein on the chronic disease domain of the healthy aging phenotype, Dr. Ardisson Korat and coauthors said plant protein has been associated with favorable levels of important risk factors for cardiometabolic diseases, such as reduced LDL cholesterol, lower blood pressure, and insulin sensitivity, as well as decreased levels of proinflammatory markers.
Conversely, total and animal protein intakes have been positively associated with concentrations of insulin-like growth factor 1, which is implicated in the growth of malignant cells in breast and prostate tissue.
This study is the first step in evaluating the long-term health effect of protein intake in midlife, the relevant development window for most chronic conditions, the NHS study authors said. More research is needed, however, to corroborate the study findings in other populations and identify underlying mechanisms.
This study was supported by the USDA Agricultural Research Service and the National Institutes of Health. The authors reported no conflicts of interest. The commentators disclosed no relevant competing interests.
Intake of protein, especially from plants, in middle age is associated with higher odds of healthy aging and positive mental and physical health status in older women, a recent analysis of the Nurses’ Health Study (NHS) data suggests.
The study is said to be the first to examine the long-term impact of midlife protein consumption on later health status.
Writing in the American Journal of Clinical Nutrition, a team led by Andres V. Ardisson Korat, DSc, a nutritional epidemiologist at the USDA Human Nutrition Research Center on Aging at Tufts University in Boston, Massachusetts, found the following midlife protein–related odds ratios (ORs) for later healthy aging measured at ages 70-93.
For each 3% energy increment from various protein sources:
- 1.05 (95% confidence interval, 1.01-1.10) for total protein
- 1.07 (1.02-1.11) for animal protein
- 1.14 (1.06-1.23) for dairy protein
- 1.38 (1.24-1.54) for plant protein
In substitution analyses, significant positive associations were observed for the isocaloric replacement of animal or dairy protein, carbohydrate, or fat with plant protein — with increased ORs for healthy aging of 1.22-1.58 for each 3% of energy replacement.
On the measure of physical function, for example, replacing calories from all macronutrient variables with equivalent calories from plant protein was associated with 20%-60% higher odds of having no physical function limitations. Plant protein was also associated with higher odds for good mental status.
“Other studies have looked at protein intake in older adults, but we felt midlife was a more relevant etiological window,” Dr. Ardisson Korat said in an interview. “Our findings generally align, however, with those of protein intake in older populations, which have shown that protein can reduce the risk of frailty.”
He added that the benefits of protein, especially from plant sources, would likely apply to men as well and increasing plant protein intake is not difficult. “If you want a snack during the day, eat a handful of nuts instead of potato chips,” he advised. And eating several meals a week featuring beans, peas, lentils, tofu, whole grains, or seeds is an easy way to boost dietary plant protein, which comes with health-promoting soluble and insoluble fiber as well as antioxidant and anti-inflammatory polyphenols and other phytochemicals.
Conversely, plant but not animal protein consumption in older adulthood was linked to a lower risk of frailty in a previous NHS trial.
Higher plant protein intake was associated with a better probability of achieving healthy aging defined by changes in functional impairments, self-reported health/vitality, mental health, and use of health services in the Spanish Seniors-Estudio Sobre Nutricion y Riesgo Cardiovascular.
In contrast, animal protein intake in middle adulthood has been linked to an increased risk of premature death from chronic diseases driven by cardiovascular disease mortality.
The present findings are consistent with those observed for protein intakes in older adulthood, Dr. Ardisson Korat said.
“This study underscores the health advantages for midlife adults consuming adequate dietary protein — particularly plant protein — as one component of pursuing a healthy lifestyle,” said Douglas R. Dirschl, MD, chair of orthopedic surgery at Baylor College of Medicine in Houston, Texas. Most Americans consume adequate amounts of protein, but according to Dr. Dirschl, who treats many older patients for osteoporotic fractures and other musculoskeletal conditions, many US diets are subpar in this nutrient.
While protein is essential for bone and muscle formation and maintenance, “a surprising number of Americans are protein deficient, even those who seem hale and are overweight,” he said.
Dietary Recommendations for Midlife Patients
Physicians should therefore advise midlife patients to meet or perhaps modestly exceed the recommended dietary allowance (RDA) for protein of 0.8 g/kg per day and to make plant protein a substantial component of daily dietary protein intake, Dr. Dirschl said.
Luke D. Kim, MD, MEd, a geriatrician at the Cleveland Clinic in Cleveland, Ohio, noted that patients with lower socioeconomic status or with difficulty in day-to-day functioning are likely to have suboptimal protein intake. Such patients may need encouragement to eat more protein. “But we should keep in mind that showing a higher associated odds ratio of better health with increased protein take does not mean causality,” he said.
According to Rachel L. Amdur, MD, an internist at Northwestern Medicine in Chicago, Illinois, the long-term follow-up data from the NHS are uniquely helpful. “Middle-aged persons may think they no longer need much dietary protein and need to be reminded. Sometimes eating carbohydrates is just easier,” she said in an interview. Physicians need to asses and counsel patients on nutrition at all stages of life. “As I tell my patients, it’s best to think of your future self now.”
In agreement is Louis J. Morledge, MD, an internist at Northwell Health in New York City. “I firmly counsel my patients about adequate and often increased protein intake in middle life. But this is always within a larger framework of overall nutritional health.” He added that middle-aged persons often find themselves “stuck in food ruts,” and one of his clinical focuses is to advise patients about the importance of healthier food choices so they can better adjust to mental, emotional, physical, and skeletal changes as they age.
Study Details
The NHS analysis drew on prospective data from 48,762 nurses under age 60 in 1984. Total protein, animal protein, dairy protein, and plant protein were derived from validated food-frequency questionnaires.
Adjusting for lifestyle, demographics, and health status, the investigators identified 3721 (7.6% of cohort) eligible participants. The mean age of participants at baseline was 48.6 years; 38.6% had body mass indexes (BMI; in kg/m2) greater than 25; 22.9% were current smokers; and 88.2% were married.
Healthy aging was defined as freedom from 11 major chronic diseases, good mental health, and no impairments in cognitive or physical function, as assessed in the 2014 or 2016 NHS participant questionnaires. Diseases/treatments included cancer, type 2 diabetes, myocardial infarction, coronary artery bypass graft or coronary angioplasty, congestive heart failure, stroke, kidney failure, chronic obstructive pulmonary disease, Parkinson disease, multiple sclerosis, and amyotrophic lateral sclerosis.
Mean total protein consumption as a percentage of energy was 18.3% (standard deviation 3%), slightly higher than the average 16% in the US diet. Of this, 13.3% derived from animals, 3.6% from dairy products, and 4.9% from plants.
Total protein intake was positively associated with higher education levels, being physically active, higher BMI, and a baseline history of hypertension and hypercholesterolemia. Conversely, total protein intake was inversely associated with intakes of total carbohydrates, nuts, alcohol, and sugar-sweetened beverages.
The associations between protein intake and healthy aging are complex and not fully understood, the authors stated.
Effects of Protein Intake
In studies of older adult populations lower protein intake has been associated with lean mass loss. Animal protein supplementation studies in older adults have shown lean mass gains potentially related to amino acid composition.
In terms of mechanisms, evidence suggests that protein-related activation of the rapamycin complex 1 pathway may play a role, the authors suggested. The activity of this signaling pathway decreases with age.
Rapamycin, a compound used to prevent organ transplant rejection, has been associated with delayed aging. In the body, dietary protein and exercise activate this pathway, thereby stimulating muscle protein synthesis and possibly improving physical function.
As for the differential associations of plant and animal protein on the chronic disease domain of the healthy aging phenotype, Dr. Ardisson Korat and coauthors said plant protein has been associated with favorable levels of important risk factors for cardiometabolic diseases, such as reduced LDL cholesterol, lower blood pressure, and insulin sensitivity, as well as decreased levels of proinflammatory markers.
Conversely, total and animal protein intakes have been positively associated with concentrations of insulin-like growth factor 1, which is implicated in the growth of malignant cells in breast and prostate tissue.
This study is the first step in evaluating the long-term health effect of protein intake in midlife, the relevant development window for most chronic conditions, the NHS study authors said. More research is needed, however, to corroborate the study findings in other populations and identify underlying mechanisms.
This study was supported by the USDA Agricultural Research Service and the National Institutes of Health. The authors reported no conflicts of interest. The commentators disclosed no relevant competing interests.

Magnesium Sulfate for Fetal Neuroprotection in Preterm Birth
Introduction: The Many Lanes of Research on Magnesium Sulfate
The research that improves human health in the most expedient and most impactful ways is multitiered, with basic or fundamental research, translational research, interventional studies, and retrospective research often occurring simultaneously. There should be no “single lane” of research and one type of research does not preclude the other.
Too often, we fall short in one of these lanes. While we have achieved many moonshots in obstetrics and maternal-fetal medicine, we have tended not to place a high priority on basic research, which can provide a strong understanding of the biology of major diseases and conditions affecting women and their offspring. When conducted with proper commitment and funding, such research can lead to biologically directed therapy.
Within our specialty, research on how we can effectively prevent preterm birth, prematurity, and preeclampsia has taken a long road, with various types of therapies being tried, but none being overwhelmingly effective — with an ongoing need for more basic or fundamental research. Nevertheless, we can benefit and gain great insights from retrospective and interventional studies associated with clinical therapies used to treat premature labor and preeclampsia when these therapies have an unanticipated and important secondary benefit.
This month our Master Class is focused on the neuroprotection of prematurity. Magnesium sulfate is a valuable tool for the treatment of both premature labor and preeclampsia, and more recently, also for neuroprotection of the fetus. Interestingly, this use stemmed from researchers looking retrospectively at outcomes in women who received the compound for other reasons. It took many years for researchers to prove its neuroprotective value through interventional trials, while researchers simultaneously strove to understand on a basic biologic level how magnesium sulfate works to prevent outcomes such as cerebral palsy.
Basic research underway today continues to improve our understanding of its precise mechanisms of action. Combined with other tiers of research — including more interventional studies and more translational research — we can improve its utility for the neuroprotection of prematurity. Alternatively, ongoing research may lead to different, even more effective treatments.
Our guest author is Irina Burd, MD, PhD, Sylvan Freiman, MD Endowed Professor and Chair of the department of obstetrics, gynecology, and reproductive sciences at the University of Maryland School of Medicine.* Dr. Burd is also a physician-scientist. She recounts the important story of magnesium sulfate and what is currently known about its biologic plausibility in neuroprotection — including through her own studies – as well as what may be coming in the future.

E. Albert Reece, MD, PhD, MBA, a maternal-fetal medicine specialist, is dean emeritus of the University of Maryland School of Medicine, former university executive vice president; currently the endowed professor and director of the Center for Advanced Research Training and Innovation (CARTI), and senior scientist in the Center for Birth Defects Research. Dr. Reece reported no relevant disclosures. He is the medical editor of this column. Contact him at [email protected].
Magnesium Sulfate for Fetal Neuroprotection in Preterm Birth
Without a doubt, magnesium sulfate (MgSO4) given before anticipated preterm birth reduces the risk of cerebral palsy. It is a valuable tool for fetal neuroprotection at a time when there are no proven alternatives. Yet without the persistent research that occurred over more than 20 years, it may not have won the endorsement of the American College of Obstetrics and Gynecologists in 2010 and worked its way into routine practice.
Its history is worthy of reflection. It took years of observational trials (not all of which showed neuroprotective effects), six randomized controlled trials (none of which met their primary endpoint), three meta-analyses, and a Cochrane Database Systematic Review to arrive at the conclusion that antenatal magnesium sulfate therapy given to women at risk of preterm birth has definitive neuroprotective benefit.

This history also holds lessons for our specialty given the dearth of drugs approved for use in pregnancy and the recent withdrawal from the market of Makena — one of only nine drugs to ever be approved by the Food and Drug Administration for use in pregnancy — after a second trial showed lack of benefit in preventing recurrent preterm birth. The story of MgSO4 tells us it’s acceptable to have major stumbling blocks: At one point, MgSO4 was considered to be not only not helpful, but harmful, causing neonatal death. Further research disproved this initial finding.
Moreover, the MgSO4 story is one that remains unfinished, as my laboratory and other researchers work to better understand its biologic plausibility and to discover additional neuroprotective agents for anticipated preterm birth that may further reduce the risk of cerebral palsy. This leading cause of chronic childhood disability is estimated by the United Cerebral Palsy Foundation to affect approximately 800,000 people in the United States.
Origins and Biologic Plausibility
The MgSO4 story is rooted in the late seventeenth century discovery by physician Nehemiah Grew that the compound was the key component of the then-famous medicinal spring waters in Epsom, England.1 MgSO4 was first used for eclampsia in 1906,2 and was first reported in the American literature for eclampsia in 1925.3 In 1959, its effect as a tocolytic agent was reported.4
More than 30 years later, in 1995, an observational study coauthored by Karin B. Nelson, MD, and Judith K. Grether, PhD of the National Institutes of Health, showed a reduced risk of cerebral palsy in very-low-birth-weight infants (VLBW).5 The report marked a turning point in research interest on neuroprotection for anticipated preterm birth.
The precise molecular mechanisms of action of MgSO4 for neuroprotection are still not well understood. However, research findings from the University of Maryland and other institutions have provided biologic plausibility for its use to prevent cerebral palsy. Our current thinking is that it involves the prevention of periventricular white matter injury and/or the prevention of oxidative stress and a neuronal injury mechanism called excitotoxicity.
Periventricular white matter injury involving injury to preoligodendrocytes before 32 weeks’ gestation is the most prevalent injury seen in cerebral palsy; preoligodendrocytes are precursors of myelinating oligodendrocytes, which constitute a major glial population in the white matter. Our research in a mouse model demonstrated that the intrauterine inflammation frequently associated with preterm birth can lead to neuronal injury as well as white matter damage, and that MgSO4 may ameliorate both.6,7
Excitotoxicity results from excessive stimulation of N-methyl-D-aspartate (NMDA) glutamatergic receptors on preoligodendrocytes and a rush of calcium through the voltage-gated channels. This calcium influx leads to the production of nitric oxide, oxidative stress, and subsequent mitochondrial damage and cell death. As a bivalent ion, MgSO4 sits in the voltage-gated channels of the NMDA receptors and reduces glutamatergic signaling, thus serving as a calcium antagonist and modulating calcium influx (See Figure).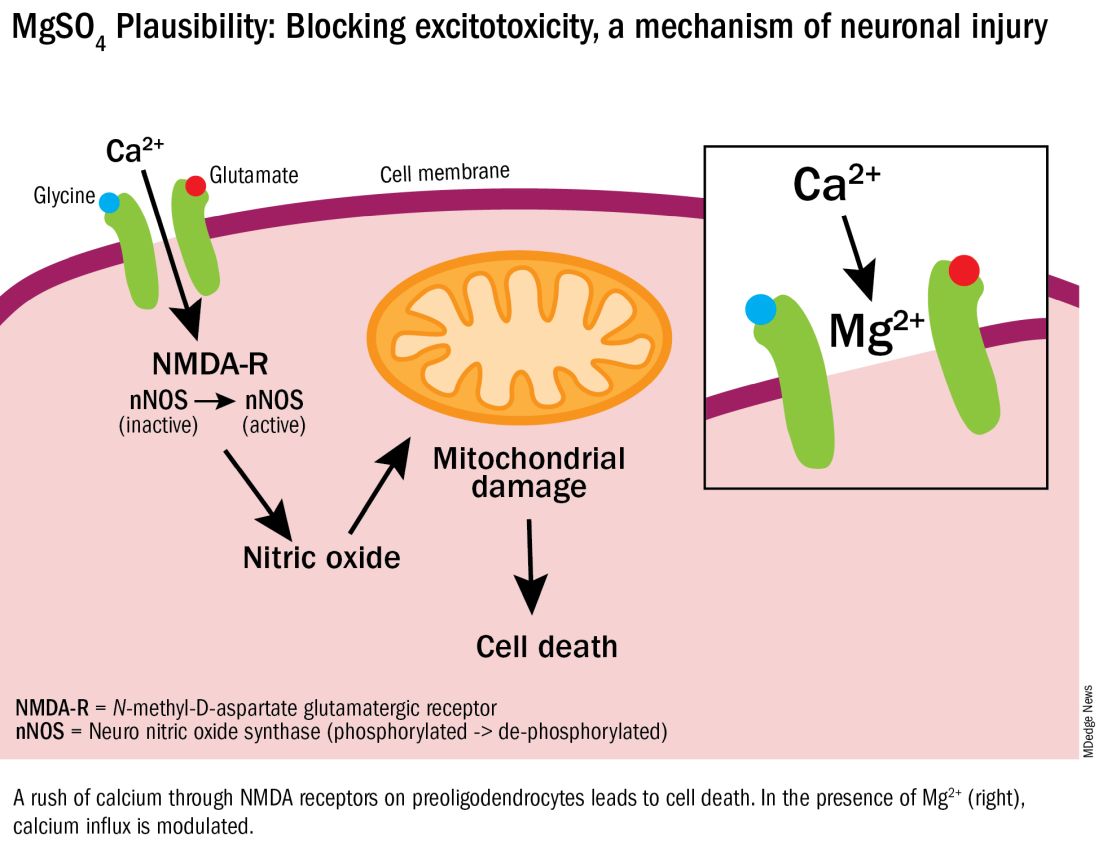
In vitro research in our laboratory has also shown that MgSO4 may dampen inflammatory reactions driven by intrauterine infections, which, like preterm birth, increase the risk of cerebral palsy and adverse neurodevelopmental outcomes.8 MgSO4 appears to do so by blocking the voltage-gated P2X7 receptor in umbilical vein endothelial cells, thus blocking endothelial secretion of the proinflammatory cytokine interleukin (IL)–1beta. Much more research is needed to determine whether MgSO4 could help prevent cerebral palsy through this mechanism.
The Long Route of Research
The 1995 Nelson-Grether study compared VLBW (< 1500 g) infants who survived and developed moderate/severe cerebral palsy within 3 years to randomly selected VLBW controls with respect to whether their mothers had received MgSO4 to prevent seizures in preeclampsia or as a tocolytic agent.5 In a population of more than 155,000 children born between 1983 and 1985, in utero exposure to MgSO4 was reported in 7.1% of 42 VLBW infants with cerebral palsy and 36% of 75 VLBW controls (odds ratio [OR], 0.14; 95% CI, 0.05-0.51). In women without preeclampsia the OR increased to 0.25.
This motivating study had been preceded by several observational studies showing that infants born to women with preeclampsia who received MgSO4 had significantly lower risks of developing intraventricular hemorrhage (IVH) and germinal matrix hemorrhage (GMH). In one of these studies, published in 1992, Karl C. Kuban, MD, and coauthors reported that “maternal receipt of magnesium sulfate was associated with diminished risk of GMH-IVH even in those babies born to mothers who apparently did not have preeclampsia.”9
In the several years following the 1995 Nelson-Grether study, several other case-control/observational studies were reported, with conflicting conclusions, and investigators around the world began designing and conducting needed randomized controlled trials.
The six published randomized controlled trials looking at MgSO4 and neuroprotection varied in their inclusion and exclusion criteria, their recruitment and enrollment style, the gestational ages for MgSO4 administration, loading and maintenance doses, how cerebral palsy or neuroprotection was assessed, and other factors (See Table for RCT characteristics and main outcomes).10-14 One of the trials aimed primarily at evaluating the efficacy of MgSO4 for preventing preeclampsia.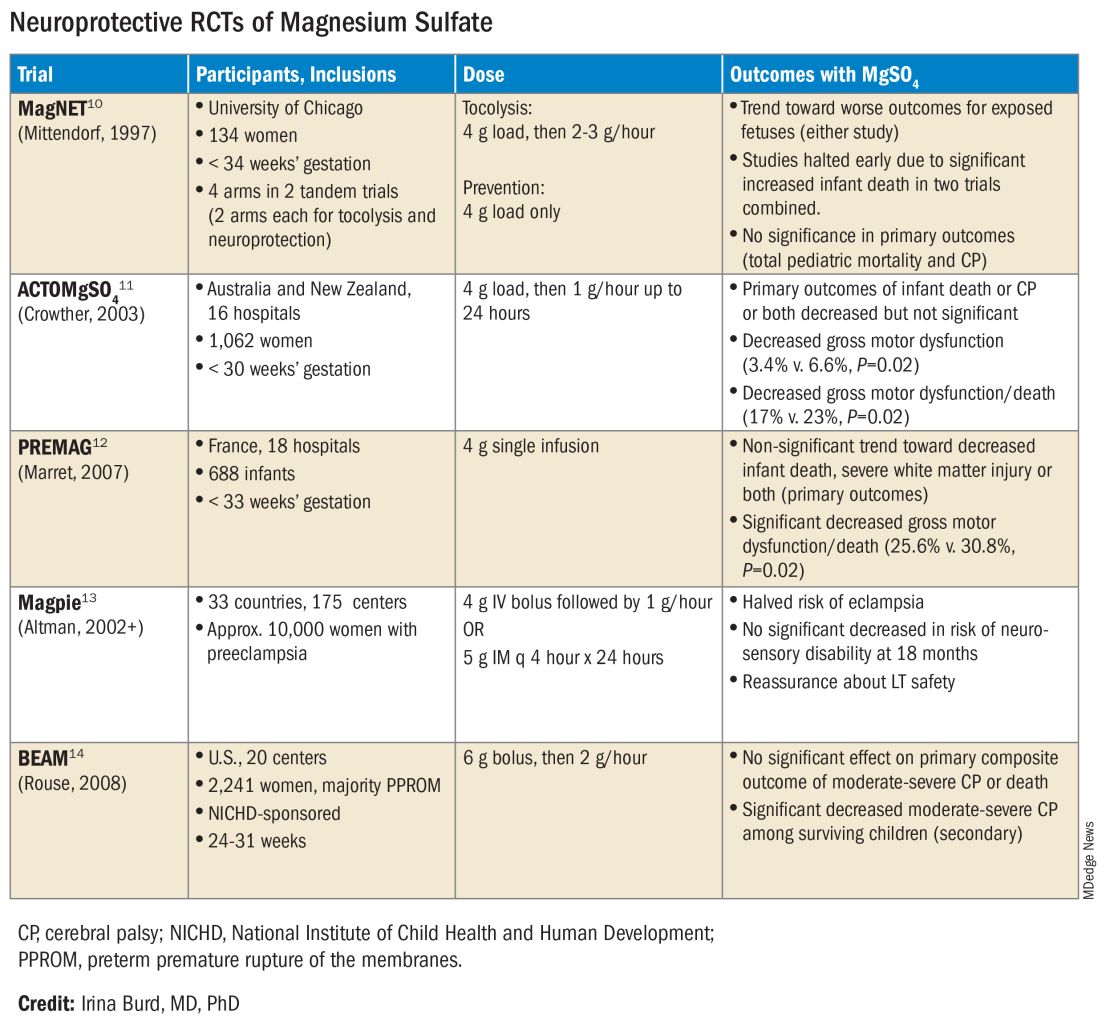
Again, none of the randomized controlled trials demonstrated statistical significance for their primary outcomes or concluded that there was a significant neuroprotective effect for cerebral palsy. Rather, most suggested benefit through secondary analyses. Moreover, as mentioned earlier, research that proceeded after the first published randomized controlled trial — the Magnesium and Neurologic Endpoints (MAGnet) trial — was suspended early when an interim analysis showed a significantly increased risk of mortality in MgSO4-exposed fetuses. All told, it wasn’t until researchers obtained unpublished data and conducted meta-analyses and systematic reviews that a significant effect of MgSO4 on cerebral palsy could be seen.
The three systematic reviews and the Cochrane review, each of which used slightly different methodologies, were published in rapid succession in 2009. One review calculated a relative risk of cerebral palsy of 0.71 (95% CI, 0.55-0.91) — and a relative risk for the combined outcome of death and cerebral palsy at 0.85 (95% CI, 0.74-0.98) — when women at risk of preterm birth were given MgSO4.15 The number needed to treat (NNT) to prevent one case of cerebral palsy was 63, investigators determined, and the NNT to prevent one case of cerebral palsy or infant death was 44.
Another review estimated the NNT for prevention of one case of cerebral palsy at 52 when MgSO4 is given at less than 34 weeks’ gestation, and similarly concluded that MgSO4 is associated with a significantly “reduced risk of moderate/severe CP and substantial gross motor dysfunction without any statistically significant effect on the risk of total pediatric mortality.”16
A third review, from the National Institute of Child Health and Human Development (NICHD) Maternal-Fetal Medicine Units Network (MFMU), estimated an NNT of 46 to prevent one case of cerebral palsy in infants exposed to MgSO4 before 30 weeks, and an NNT of 56 when exposure occurs before 32-34 weeks.17
The Cochrane Review, meanwhile, reported a relative reduction in the risk of cerebral palsy of 0.68 (95% CI, 0.54-0.87) when antenatal MgSO4 is given at less than 37 weeks’ gestation, as well as a significant reduction in the rate of substantial gross motor dysfunction (RR, 0.61; 95% CI, 0.44-0.85).18 The NNT to avoid one case of cerebral palsy, researchers reported, was 63.
Moving Forward
The NNTs calculated in these reviews — ranging from 44 to 63 — are convincing, and are comparable with evidence-based medicine data for prevention of other common diseases.19 For instance, the NNT for a life saved when aspirin is given immediately after a heart attack is 42. Statins given for 5 years in people with known heart disease have an NNT of 83 to save one life, an NNT of 39 to prevent one nonfatal heart attack, and an NNT of 125 to prevent one stroke. For oral anticoagulants used in nonvalvular atrial fibrillation for primary stroke prevention, the NNTs to prevent one stroke, and one death, are 22 and 42, respectively.19
In its 2010 Committee Opinion on Magnesium Sulfate Before Anticipated Preterm Birth for Neuroprotection (reaffirmed in 2020), the American College of Obstetricians and Gynecologists left it to institutions to develop their own guidelines “regarding inclusion criteria, treatment regimens, concurrent tocolysis, and monitoring in accordance with one of the larger trials.”20
Not surprisingly, most if not all hospitals have chosen a higher dose of MgSO4 administered up to 31 weeks’ gestation in keeping with the protocols employed in the NICHD-sponsored BEAM trial (See Table).
The hope moving forward is to expand treatment options for neuroprotection in cases of imminent preterm birth. Researchers have been assessing the ability of melatonin to provide neuroprotection in cases of growth restriction and neonatal asphyxia. Melatonin has anti-inflammatory and antioxidant properties and is known to mediate neuronal generation and synaptic plasticity.21
N-acetyl-L-cysteine is another potential neuroprotective agent. It acts as an antioxidant, a precursor to glutathione, and a modulator of the glutamate system and has been studied as a neuroprotective agent in cases of maternal chorioamnionitis.21 Both melatonin and N-acetyl-L-cysteine are regarded as safe in pregnancy, but much more clinical study is needed to prove their neuroprotective potential when given shortly before birth or earlier.
Dr. Burd is the Sylvan Freiman, MD Endowed Professor and Chair of the department of obstetrics, gynecology, and reproductive sciences at the University of Maryland School of Medicine, Baltimore. She has no conflicts of interest.
References
1. Clio Med. 1984;19(1-2):1-21.
2. Medicinsk Rev. (Bergen) 1906;32:264-272.
3. Am J Obstet Gynecol. 1996;174(4):1390-1391.
4. Am J Obstet Gynecol. 1959;78(1):27-32.
5. Pediatrics. 1995;95(2):263-269.
6. Am J Obstet Gynecol. 2009;201(3):279.e1-279.e8.
7. Am J Obstet Gynecol. 2010;202(3):292.e1-292.e9.
8. Pediatr Res. 2020;87(3):463-471.
9. J Child Neurol. 1992;7(1):70-76.
10. Lancet. 1997;350:1517-1518.
11. JAMA. 2003;290:2669-2676.
12. BJOG. 2007;114(3):310-318.
13. Lancet. 2002;359(9321):1877-1890.
14. N Engl J Med. 2008;359:895-905.
15. Obstet Gynecol. 2009;113(6):1327-1333.
16. Am J Obstet Gynecol. 2009;200(6):595-609.
17. Obstet Gynecol 2009;114:354-364.
18. Cochrane Database Syst Rev. 2009 Jan 21:(1):CD004661.
19. www.thennt.com.
20. Obstet Gynecol. 2010;115:669-671.
21. Front Synaptic Neurosci. 2012;13:680899.
*This story was corrected on June 10, 2024.
Introduction: The Many Lanes of Research on Magnesium Sulfate
The research that improves human health in the most expedient and most impactful ways is multitiered, with basic or fundamental research, translational research, interventional studies, and retrospective research often occurring simultaneously. There should be no “single lane” of research and one type of research does not preclude the other.
Too often, we fall short in one of these lanes. While we have achieved many moonshots in obstetrics and maternal-fetal medicine, we have tended not to place a high priority on basic research, which can provide a strong understanding of the biology of major diseases and conditions affecting women and their offspring. When conducted with proper commitment and funding, such research can lead to biologically directed therapy.
Within our specialty, research on how we can effectively prevent preterm birth, prematurity, and preeclampsia has taken a long road, with various types of therapies being tried, but none being overwhelmingly effective — with an ongoing need for more basic or fundamental research. Nevertheless, we can benefit and gain great insights from retrospective and interventional studies associated with clinical therapies used to treat premature labor and preeclampsia when these therapies have an unanticipated and important secondary benefit.
This month our Master Class is focused on the neuroprotection of prematurity. Magnesium sulfate is a valuable tool for the treatment of both premature labor and preeclampsia, and more recently, also for neuroprotection of the fetus. Interestingly, this use stemmed from researchers looking retrospectively at outcomes in women who received the compound for other reasons. It took many years for researchers to prove its neuroprotective value through interventional trials, while researchers simultaneously strove to understand on a basic biologic level how magnesium sulfate works to prevent outcomes such as cerebral palsy.
Basic research underway today continues to improve our understanding of its precise mechanisms of action. Combined with other tiers of research — including more interventional studies and more translational research — we can improve its utility for the neuroprotection of prematurity. Alternatively, ongoing research may lead to different, even more effective treatments.
Our guest author is Irina Burd, MD, PhD, Sylvan Freiman, MD Endowed Professor and Chair of the department of obstetrics, gynecology, and reproductive sciences at the University of Maryland School of Medicine.* Dr. Burd is also a physician-scientist. She recounts the important story of magnesium sulfate and what is currently known about its biologic plausibility in neuroprotection — including through her own studies – as well as what may be coming in the future.
E. Albert Reece, MD, PhD, MBA, a maternal-fetal medicine specialist, is dean emeritus of the University of Maryland School of Medicine, former university executive vice president; currently the endowed professor and director of the Center for Advanced Research Training and Innovation (CARTI), and senior scientist in the Center for Birth Defects Research. Dr. Reece reported no relevant disclosures. He is the medical editor of this column. Contact him at [email protected].
Magnesium Sulfate for Fetal Neuroprotection in Preterm Birth
Without a doubt, magnesium sulfate (MgSO4) given before anticipated preterm birth reduces the risk of cerebral palsy. It is a valuable tool for fetal neuroprotection at a time when there are no proven alternatives. Yet without the persistent research that occurred over more than 20 years, it may not have won the endorsement of the American College of Obstetrics and Gynecologists in 2010 and worked its way into routine practice.
Its history is worthy of reflection. It took years of observational trials (not all of which showed neuroprotective effects), six randomized controlled trials (none of which met their primary endpoint), three meta-analyses, and a Cochrane Database Systematic Review to arrive at the conclusion that antenatal magnesium sulfate therapy given to women at risk of preterm birth has definitive neuroprotective benefit.
This history also holds lessons for our specialty given the dearth of drugs approved for use in pregnancy and the recent withdrawal from the market of Makena — one of only nine drugs to ever be approved by the Food and Drug Administration for use in pregnancy — after a second trial showed lack of benefit in preventing recurrent preterm birth. The story of MgSO4 tells us it’s acceptable to have major stumbling blocks: At one point, MgSO4 was considered to be not only not helpful, but harmful, causing neonatal death. Further research disproved this initial finding.
Moreover, the MgSO4 story is one that remains unfinished, as my laboratory and other researchers work to better understand its biologic plausibility and to discover additional neuroprotective agents for anticipated preterm birth that may further reduce the risk of cerebral palsy. This leading cause of chronic childhood disability is estimated by the United Cerebral Palsy Foundation to affect approximately 800,000 people in the United States.
Origins and Biologic Plausibility
The MgSO4 story is rooted in the late seventeenth century discovery by physician Nehemiah Grew that the compound was the key component of the then-famous medicinal spring waters in Epsom, England.1 MgSO4 was first used for eclampsia in 1906,2 and was first reported in the American literature for eclampsia in 1925.3 In 1959, its effect as a tocolytic agent was reported.4
More than 30 years later, in 1995, an observational study coauthored by Karin B. Nelson, MD, and Judith K. Grether, PhD of the National Institutes of Health, showed a reduced risk of cerebral palsy in very-low-birth-weight infants (VLBW).5 The report marked a turning point in research interest on neuroprotection for anticipated preterm birth.
The precise molecular mechanisms of action of MgSO4 for neuroprotection are still not well understood. However, research findings from the University of Maryland and other institutions have provided biologic plausibility for its use to prevent cerebral palsy. Our current thinking is that it involves the prevention of periventricular white matter injury and/or the prevention of oxidative stress and a neuronal injury mechanism called excitotoxicity.
Periventricular white matter injury involving injury to preoligodendrocytes before 32 weeks’ gestation is the most prevalent injury seen in cerebral palsy; preoligodendrocytes are precursors of myelinating oligodendrocytes, which constitute a major glial population in the white matter. Our research in a mouse model demonstrated that the intrauterine inflammation frequently associated with preterm birth can lead to neuronal injury as well as white matter damage, and that MgSO4 may ameliorate both.6,7
Excitotoxicity results from excessive stimulation of N-methyl-D-aspartate (NMDA) glutamatergic receptors on preoligodendrocytes and a rush of calcium through the voltage-gated channels. This calcium influx leads to the production of nitric oxide, oxidative stress, and subsequent mitochondrial damage and cell death. As a bivalent ion, MgSO4 sits in the voltage-gated channels of the NMDA receptors and reduces glutamatergic signaling, thus serving as a calcium antagonist and modulating calcium influx (See Figure).
In vitro research in our laboratory has also shown that MgSO4 may dampen inflammatory reactions driven by intrauterine infections, which, like preterm birth, increase the risk of cerebral palsy and adverse neurodevelopmental outcomes.8 MgSO4 appears to do so by blocking the voltage-gated P2X7 receptor in umbilical vein endothelial cells, thus blocking endothelial secretion of the proinflammatory cytokine interleukin (IL)–1beta. Much more research is needed to determine whether MgSO4 could help prevent cerebral palsy through this mechanism.
The Long Route of Research
The 1995 Nelson-Grether study compared VLBW (< 1500 g) infants who survived and developed moderate/severe cerebral palsy within 3 years to randomly selected VLBW controls with respect to whether their mothers had received MgSO4 to prevent seizures in preeclampsia or as a tocolytic agent.5 In a population of more than 155,000 children born between 1983 and 1985, in utero exposure to MgSO4 was reported in 7.1% of 42 VLBW infants with cerebral palsy and 36% of 75 VLBW controls (odds ratio [OR], 0.14; 95% CI, 0.05-0.51). In women without preeclampsia the OR increased to 0.25.
This motivating study had been preceded by several observational studies showing that infants born to women with preeclampsia who received MgSO4 had significantly lower risks of developing intraventricular hemorrhage (IVH) and germinal matrix hemorrhage (GMH). In one of these studies, published in 1992, Karl C. Kuban, MD, and coauthors reported that “maternal receipt of magnesium sulfate was associated with diminished risk of GMH-IVH even in those babies born to mothers who apparently did not have preeclampsia.”9
In the several years following the 1995 Nelson-Grether study, several other case-control/observational studies were reported, with conflicting conclusions, and investigators around the world began designing and conducting needed randomized controlled trials.
The six published randomized controlled trials looking at MgSO4 and neuroprotection varied in their inclusion and exclusion criteria, their recruitment and enrollment style, the gestational ages for MgSO4 administration, loading and maintenance doses, how cerebral palsy or neuroprotection was assessed, and other factors (See Table for RCT characteristics and main outcomes).10-14 One of the trials aimed primarily at evaluating the efficacy of MgSO4 for preventing preeclampsia.
Again, none of the randomized controlled trials demonstrated statistical significance for their primary outcomes or concluded that there was a significant neuroprotective effect for cerebral palsy. Rather, most suggested benefit through secondary analyses. Moreover, as mentioned earlier, research that proceeded after the first published randomized controlled trial — the Magnesium and Neurologic Endpoints (MAGnet) trial — was suspended early when an interim analysis showed a significantly increased risk of mortality in MgSO4-exposed fetuses. All told, it wasn’t until researchers obtained unpublished data and conducted meta-analyses and systematic reviews that a significant effect of MgSO4 on cerebral palsy could be seen.
The three systematic reviews and the Cochrane review, each of which used slightly different methodologies, were published in rapid succession in 2009. One review calculated a relative risk of cerebral palsy of 0.71 (95% CI, 0.55-0.91) — and a relative risk for the combined outcome of death and cerebral palsy at 0.85 (95% CI, 0.74-0.98) — when women at risk of preterm birth were given MgSO4.15 The number needed to treat (NNT) to prevent one case of cerebral palsy was 63, investigators determined, and the NNT to prevent one case of cerebral palsy or infant death was 44.
Another review estimated the NNT for prevention of one case of cerebral palsy at 52 when MgSO4 is given at less than 34 weeks’ gestation, and similarly concluded that MgSO4 is associated with a significantly “reduced risk of moderate/severe CP and substantial gross motor dysfunction without any statistically significant effect on the risk of total pediatric mortality.”16
A third review, from the National Institute of Child Health and Human Development (NICHD) Maternal-Fetal Medicine Units Network (MFMU), estimated an NNT of 46 to prevent one case of cerebral palsy in infants exposed to MgSO4 before 30 weeks, and an NNT of 56 when exposure occurs before 32-34 weeks.17
The Cochrane Review, meanwhile, reported a relative reduction in the risk of cerebral palsy of 0.68 (95% CI, 0.54-0.87) when antenatal MgSO4 is given at less than 37 weeks’ gestation, as well as a significant reduction in the rate of substantial gross motor dysfunction (RR, 0.61; 95% CI, 0.44-0.85).18 The NNT to avoid one case of cerebral palsy, researchers reported, was 63.
Moving Forward
The NNTs calculated in these reviews — ranging from 44 to 63 — are convincing, and are comparable with evidence-based medicine data for prevention of other common diseases.19 For instance, the NNT for a life saved when aspirin is given immediately after a heart attack is 42. Statins given for 5 years in people with known heart disease have an NNT of 83 to save one life, an NNT of 39 to prevent one nonfatal heart attack, and an NNT of 125 to prevent one stroke. For oral anticoagulants used in nonvalvular atrial fibrillation for primary stroke prevention, the NNTs to prevent one stroke, and one death, are 22 and 42, respectively.19
In its 2010 Committee Opinion on Magnesium Sulfate Before Anticipated Preterm Birth for Neuroprotection (reaffirmed in 2020), the American College of Obstetricians and Gynecologists left it to institutions to develop their own guidelines “regarding inclusion criteria, treatment regimens, concurrent tocolysis, and monitoring in accordance with one of the larger trials.”20
Not surprisingly, most if not all hospitals have chosen a higher dose of MgSO4 administered up to 31 weeks’ gestation in keeping with the protocols employed in the NICHD-sponsored BEAM trial (See Table).
The hope moving forward is to expand treatment options for neuroprotection in cases of imminent preterm birth. Researchers have been assessing the ability of melatonin to provide neuroprotection in cases of growth restriction and neonatal asphyxia. Melatonin has anti-inflammatory and antioxidant properties and is known to mediate neuronal generation and synaptic plasticity.21
N-acetyl-L-cysteine is another potential neuroprotective agent. It acts as an antioxidant, a precursor to glutathione, and a modulator of the glutamate system and has been studied as a neuroprotective agent in cases of maternal chorioamnionitis.21 Both melatonin and N-acetyl-L-cysteine are regarded as safe in pregnancy, but much more clinical study is needed to prove their neuroprotective potential when given shortly before birth or earlier.
Dr. Burd is the Sylvan Freiman, MD Endowed Professor and Chair of the department of obstetrics, gynecology, and reproductive sciences at the University of Maryland School of Medicine, Baltimore. She has no conflicts of interest.
References
1. Clio Med. 1984;19(1-2):1-21.
2. Medicinsk Rev. (Bergen) 1906;32:264-272.
3. Am J Obstet Gynecol. 1996;174(4):1390-1391.
4. Am J Obstet Gynecol. 1959;78(1):27-32.
5. Pediatrics. 1995;95(2):263-269.
6. Am J Obstet Gynecol. 2009;201(3):279.e1-279.e8.
7. Am J Obstet Gynecol. 2010;202(3):292.e1-292.e9.
8. Pediatr Res. 2020;87(3):463-471.
9. J Child Neurol. 1992;7(1):70-76.
10. Lancet. 1997;350:1517-1518.
11. JAMA. 2003;290:2669-2676.
12. BJOG. 2007;114(3):310-318.
13. Lancet. 2002;359(9321):1877-1890.
14. N Engl J Med. 2008;359:895-905.
15. Obstet Gynecol. 2009;113(6):1327-1333.
16. Am J Obstet Gynecol. 2009;200(6):595-609.
17. Obstet Gynecol 2009;114:354-364.
18. Cochrane Database Syst Rev. 2009 Jan 21:(1):CD004661.
19. www.thennt.com.
20. Obstet Gynecol. 2010;115:669-671.
21. Front Synaptic Neurosci. 2012;13:680899.
*This story was corrected on June 10, 2024.
Introduction: The Many Lanes of Research on Magnesium Sulfate
The research that improves human health in the most expedient and most impactful ways is multitiered, with basic or fundamental research, translational research, interventional studies, and retrospective research often occurring simultaneously. There should be no “single lane” of research and one type of research does not preclude the other.
Too often, we fall short in one of these lanes. While we have achieved many moonshots in obstetrics and maternal-fetal medicine, we have tended not to place a high priority on basic research, which can provide a strong understanding of the biology of major diseases and conditions affecting women and their offspring. When conducted with proper commitment and funding, such research can lead to biologically directed therapy.
Within our specialty, research on how we can effectively prevent preterm birth, prematurity, and preeclampsia has taken a long road, with various types of therapies being tried, but none being overwhelmingly effective — with an ongoing need for more basic or fundamental research. Nevertheless, we can benefit and gain great insights from retrospective and interventional studies associated with clinical therapies used to treat premature labor and preeclampsia when these therapies have an unanticipated and important secondary benefit.
This month our Master Class is focused on the neuroprotection of prematurity. Magnesium sulfate is a valuable tool for the treatment of both premature labor and preeclampsia, and more recently, also for neuroprotection of the fetus. Interestingly, this use stemmed from researchers looking retrospectively at outcomes in women who received the compound for other reasons. It took many years for researchers to prove its neuroprotective value through interventional trials, while researchers simultaneously strove to understand on a basic biologic level how magnesium sulfate works to prevent outcomes such as cerebral palsy.
Basic research underway today continues to improve our understanding of its precise mechanisms of action. Combined with other tiers of research — including more interventional studies and more translational research — we can improve its utility for the neuroprotection of prematurity. Alternatively, ongoing research may lead to different, even more effective treatments.
Our guest author is Irina Burd, MD, PhD, Sylvan Freiman, MD Endowed Professor and Chair of the department of obstetrics, gynecology, and reproductive sciences at the University of Maryland School of Medicine.* Dr. Burd is also a physician-scientist. She recounts the important story of magnesium sulfate and what is currently known about its biologic plausibility in neuroprotection — including through her own studies – as well as what may be coming in the future.
E. Albert Reece, MD, PhD, MBA, a maternal-fetal medicine specialist, is dean emeritus of the University of Maryland School of Medicine, former university executive vice president; currently the endowed professor and director of the Center for Advanced Research Training and Innovation (CARTI), and senior scientist in the Center for Birth Defects Research. Dr. Reece reported no relevant disclosures. He is the medical editor of this column. Contact him at [email protected].
Magnesium Sulfate for Fetal Neuroprotection in Preterm Birth
Without a doubt, magnesium sulfate (MgSO4) given before anticipated preterm birth reduces the risk of cerebral palsy. It is a valuable tool for fetal neuroprotection at a time when there are no proven alternatives. Yet without the persistent research that occurred over more than 20 years, it may not have won the endorsement of the American College of Obstetrics and Gynecologists in 2010 and worked its way into routine practice.
Its history is worthy of reflection. It took years of observational trials (not all of which showed neuroprotective effects), six randomized controlled trials (none of which met their primary endpoint), three meta-analyses, and a Cochrane Database Systematic Review to arrive at the conclusion that antenatal magnesium sulfate therapy given to women at risk of preterm birth has definitive neuroprotective benefit.
This history also holds lessons for our specialty given the dearth of drugs approved for use in pregnancy and the recent withdrawal from the market of Makena — one of only nine drugs to ever be approved by the Food and Drug Administration for use in pregnancy — after a second trial showed lack of benefit in preventing recurrent preterm birth. The story of MgSO4 tells us it’s acceptable to have major stumbling blocks: At one point, MgSO4 was considered to be not only not helpful, but harmful, causing neonatal death. Further research disproved this initial finding.
Moreover, the MgSO4 story is one that remains unfinished, as my laboratory and other researchers work to better understand its biologic plausibility and to discover additional neuroprotective agents for anticipated preterm birth that may further reduce the risk of cerebral palsy. This leading cause of chronic childhood disability is estimated by the United Cerebral Palsy Foundation to affect approximately 800,000 people in the United States.
Origins and Biologic Plausibility
The MgSO4 story is rooted in the late seventeenth century discovery by physician Nehemiah Grew that the compound was the key component of the then-famous medicinal spring waters in Epsom, England.1 MgSO4 was first used for eclampsia in 1906,2 and was first reported in the American literature for eclampsia in 1925.3 In 1959, its effect as a tocolytic agent was reported.4
More than 30 years later, in 1995, an observational study coauthored by Karin B. Nelson, MD, and Judith K. Grether, PhD of the National Institutes of Health, showed a reduced risk of cerebral palsy in very-low-birth-weight infants (VLBW).5 The report marked a turning point in research interest on neuroprotection for anticipated preterm birth.
The precise molecular mechanisms of action of MgSO4 for neuroprotection are still not well understood. However, research findings from the University of Maryland and other institutions have provided biologic plausibility for its use to prevent cerebral palsy. Our current thinking is that it involves the prevention of periventricular white matter injury and/or the prevention of oxidative stress and a neuronal injury mechanism called excitotoxicity.
Periventricular white matter injury involving injury to preoligodendrocytes before 32 weeks’ gestation is the most prevalent injury seen in cerebral palsy; preoligodendrocytes are precursors of myelinating oligodendrocytes, which constitute a major glial population in the white matter. Our research in a mouse model demonstrated that the intrauterine inflammation frequently associated with preterm birth can lead to neuronal injury as well as white matter damage, and that MgSO4 may ameliorate both.6,7
Excitotoxicity results from excessive stimulation of N-methyl-D-aspartate (NMDA) glutamatergic receptors on preoligodendrocytes and a rush of calcium through the voltage-gated channels. This calcium influx leads to the production of nitric oxide, oxidative stress, and subsequent mitochondrial damage and cell death. As a bivalent ion, MgSO4 sits in the voltage-gated channels of the NMDA receptors and reduces glutamatergic signaling, thus serving as a calcium antagonist and modulating calcium influx (See Figure).
In vitro research in our laboratory has also shown that MgSO4 may dampen inflammatory reactions driven by intrauterine infections, which, like preterm birth, increase the risk of cerebral palsy and adverse neurodevelopmental outcomes.8 MgSO4 appears to do so by blocking the voltage-gated P2X7 receptor in umbilical vein endothelial cells, thus blocking endothelial secretion of the proinflammatory cytokine interleukin (IL)–1beta. Much more research is needed to determine whether MgSO4 could help prevent cerebral palsy through this mechanism.
The Long Route of Research
The 1995 Nelson-Grether study compared VLBW (< 1500 g) infants who survived and developed moderate/severe cerebral palsy within 3 years to randomly selected VLBW controls with respect to whether their mothers had received MgSO4 to prevent seizures in preeclampsia or as a tocolytic agent.5 In a population of more than 155,000 children born between 1983 and 1985, in utero exposure to MgSO4 was reported in 7.1% of 42 VLBW infants with cerebral palsy and 36% of 75 VLBW controls (odds ratio [OR], 0.14; 95% CI, 0.05-0.51). In women without preeclampsia the OR increased to 0.25.
This motivating study had been preceded by several observational studies showing that infants born to women with preeclampsia who received MgSO4 had significantly lower risks of developing intraventricular hemorrhage (IVH) and germinal matrix hemorrhage (GMH). In one of these studies, published in 1992, Karl C. Kuban, MD, and coauthors reported that “maternal receipt of magnesium sulfate was associated with diminished risk of GMH-IVH even in those babies born to mothers who apparently did not have preeclampsia.”9
In the several years following the 1995 Nelson-Grether study, several other case-control/observational studies were reported, with conflicting conclusions, and investigators around the world began designing and conducting needed randomized controlled trials.
The six published randomized controlled trials looking at MgSO4 and neuroprotection varied in their inclusion and exclusion criteria, their recruitment and enrollment style, the gestational ages for MgSO4 administration, loading and maintenance doses, how cerebral palsy or neuroprotection was assessed, and other factors (See Table for RCT characteristics and main outcomes).10-14 One of the trials aimed primarily at evaluating the efficacy of MgSO4 for preventing preeclampsia.
Again, none of the randomized controlled trials demonstrated statistical significance for their primary outcomes or concluded that there was a significant neuroprotective effect for cerebral palsy. Rather, most suggested benefit through secondary analyses. Moreover, as mentioned earlier, research that proceeded after the first published randomized controlled trial — the Magnesium and Neurologic Endpoints (MAGnet) trial — was suspended early when an interim analysis showed a significantly increased risk of mortality in MgSO4-exposed fetuses. All told, it wasn’t until researchers obtained unpublished data and conducted meta-analyses and systematic reviews that a significant effect of MgSO4 on cerebral palsy could be seen.
The three systematic reviews and the Cochrane review, each of which used slightly different methodologies, were published in rapid succession in 2009. One review calculated a relative risk of cerebral palsy of 0.71 (95% CI, 0.55-0.91) — and a relative risk for the combined outcome of death and cerebral palsy at 0.85 (95% CI, 0.74-0.98) — when women at risk of preterm birth were given MgSO4.15 The number needed to treat (NNT) to prevent one case of cerebral palsy was 63, investigators determined, and the NNT to prevent one case of cerebral palsy or infant death was 44.
Another review estimated the NNT for prevention of one case of cerebral palsy at 52 when MgSO4 is given at less than 34 weeks’ gestation, and similarly concluded that MgSO4 is associated with a significantly “reduced risk of moderate/severe CP and substantial gross motor dysfunction without any statistically significant effect on the risk of total pediatric mortality.”16
A third review, from the National Institute of Child Health and Human Development (NICHD) Maternal-Fetal Medicine Units Network (MFMU), estimated an NNT of 46 to prevent one case of cerebral palsy in infants exposed to MgSO4 before 30 weeks, and an NNT of 56 when exposure occurs before 32-34 weeks.17
The Cochrane Review, meanwhile, reported a relative reduction in the risk of cerebral palsy of 0.68 (95% CI, 0.54-0.87) when antenatal MgSO4 is given at less than 37 weeks’ gestation, as well as a significant reduction in the rate of substantial gross motor dysfunction (RR, 0.61; 95% CI, 0.44-0.85).18 The NNT to avoid one case of cerebral palsy, researchers reported, was 63.
Moving Forward
The NNTs calculated in these reviews — ranging from 44 to 63 — are convincing, and are comparable with evidence-based medicine data for prevention of other common diseases.19 For instance, the NNT for a life saved when aspirin is given immediately after a heart attack is 42. Statins given for 5 years in people with known heart disease have an NNT of 83 to save one life, an NNT of 39 to prevent one nonfatal heart attack, and an NNT of 125 to prevent one stroke. For oral anticoagulants used in nonvalvular atrial fibrillation for primary stroke prevention, the NNTs to prevent one stroke, and one death, are 22 and 42, respectively.19
In its 2010 Committee Opinion on Magnesium Sulfate Before Anticipated Preterm Birth for Neuroprotection (reaffirmed in 2020), the American College of Obstetricians and Gynecologists left it to institutions to develop their own guidelines “regarding inclusion criteria, treatment regimens, concurrent tocolysis, and monitoring in accordance with one of the larger trials.”20
Not surprisingly, most if not all hospitals have chosen a higher dose of MgSO4 administered up to 31 weeks’ gestation in keeping with the protocols employed in the NICHD-sponsored BEAM trial (See Table).
The hope moving forward is to expand treatment options for neuroprotection in cases of imminent preterm birth. Researchers have been assessing the ability of melatonin to provide neuroprotection in cases of growth restriction and neonatal asphyxia. Melatonin has anti-inflammatory and antioxidant properties and is known to mediate neuronal generation and synaptic plasticity.21
N-acetyl-L-cysteine is another potential neuroprotective agent. It acts as an antioxidant, a precursor to glutathione, and a modulator of the glutamate system and has been studied as a neuroprotective agent in cases of maternal chorioamnionitis.21 Both melatonin and N-acetyl-L-cysteine are regarded as safe in pregnancy, but much more clinical study is needed to prove their neuroprotective potential when given shortly before birth or earlier.
Dr. Burd is the Sylvan Freiman, MD Endowed Professor and Chair of the department of obstetrics, gynecology, and reproductive sciences at the University of Maryland School of Medicine, Baltimore. She has no conflicts of interest.
References
1. Clio Med. 1984;19(1-2):1-21.
2. Medicinsk Rev. (Bergen) 1906;32:264-272.
3. Am J Obstet Gynecol. 1996;174(4):1390-1391.
4. Am J Obstet Gynecol. 1959;78(1):27-32.
5. Pediatrics. 1995;95(2):263-269.
6. Am J Obstet Gynecol. 2009;201(3):279.e1-279.e8.
7. Am J Obstet Gynecol. 2010;202(3):292.e1-292.e9.
8. Pediatr Res. 2020;87(3):463-471.
9. J Child Neurol. 1992;7(1):70-76.
10. Lancet. 1997;350:1517-1518.
11. JAMA. 2003;290:2669-2676.
12. BJOG. 2007;114(3):310-318.
13. Lancet. 2002;359(9321):1877-1890.
14. N Engl J Med. 2008;359:895-905.
15. Obstet Gynecol. 2009;113(6):1327-1333.
16. Am J Obstet Gynecol. 2009;200(6):595-609.
17. Obstet Gynecol 2009;114:354-364.
18. Cochrane Database Syst Rev. 2009 Jan 21:(1):CD004661.
19. www.thennt.com.
20. Obstet Gynecol. 2010;115:669-671.
21. Front Synaptic Neurosci. 2012;13:680899.
*This story was corrected on June 10, 2024.
Gestational Diabetes May Double Chronic Kidney Disease Risk
TOPLINE:
Previous gestational diabetes mellitus (GDM) nearly doubles future chronic kidney disease (CKD) risk, irrespective of subsequent diabetes and hypertension, a study showed.
METHODOLOGY:
- A nationwide, cohort study was based on data from the Danish Medical Birth Register and included 697,622 women who gave birth between 1997 and 2018.
- Of all study participants, 3.4% reported GDM in at least one pregnancy, and 12.8% of women with GDM received insulin, a proxy for a more severe metabolic dysfunction.
- The women were followed up for a median of 11.9 years.
- Researchers studied CKD and acute kidney disease as the outcomes of interest, the mediating effects of subsequent diabetes and hypertension on future CKD, and how GDM severity affected later risk for kidney disease.
TAKEAWAY:
- Women with GDM showed significantly higher CKD risk than those without GDM (adjusted hazard ratio [aHR], 1.92; 95% CI, 1.67-2.21).
- Women who received insulin during pregnancy due to severe metabolic dysfunction but did not develop subsequent diabetes had a proportionally higher risk for CKD (aHR, 2.35; 95% CI, 1.39-3.97).
- Women with GDM who went on to develop diabetes or hypertension faced even higher risks for CKD, suggesting that preventing diabetes and hypertension after GDM may reduce the development of CKD.
- GDM did not affect the risk for acute kidney disease (aHR, 1.08; 95% CI, 0.90-1.29).
IN PRACTICE:
“Women with severe metabolic dysfunction during pregnancy constitute a high-risk group regarding future CKD,” the authors wrote. “The significantly elevated CKD risk was observed from 2 years after pregnancy and beyond.”
SOURCE:
The study, with first author Maria Hornstrup Christensen, of Odense University Hospital, Odense, Denmark, was published online on December 15 in Diabetes Care.
LIMITATIONS:
GDM may be underdiagnosed, and undiagnosed diabetes may be misclassified as GDM. The proxies of GDM and insulin treatment may not have captured the increasing severity of metabolic dysfunction. The prevalence of insulin treatment was lower than expected, perhaps due to the practice of providing a patient’s first insulin pen without a prescription and perhaps not recording it in a patient’s health record.
DISCLOSURES:
This work received financial support from the University of Southern Denmark, the Region of Southern Denmark, and the Danish Diabetes Academy, which is funded by the Novo Nordisk Foundation. The authors declared no conflicts of interest.
A version of this article appeared on Medscape.com.
TOPLINE:
Previous gestational diabetes mellitus (GDM) nearly doubles future chronic kidney disease (CKD) risk, irrespective of subsequent diabetes and hypertension, a study showed.
METHODOLOGY:
- A nationwide, cohort study was based on data from the Danish Medical Birth Register and included 697,622 women who gave birth between 1997 and 2018.
- Of all study participants, 3.4% reported GDM in at least one pregnancy, and 12.8% of women with GDM received insulin, a proxy for a more severe metabolic dysfunction.
- The women were followed up for a median of 11.9 years.
- Researchers studied CKD and acute kidney disease as the outcomes of interest, the mediating effects of subsequent diabetes and hypertension on future CKD, and how GDM severity affected later risk for kidney disease.
TAKEAWAY:
- Women with GDM showed significantly higher CKD risk than those without GDM (adjusted hazard ratio [aHR], 1.92; 95% CI, 1.67-2.21).
- Women who received insulin during pregnancy due to severe metabolic dysfunction but did not develop subsequent diabetes had a proportionally higher risk for CKD (aHR, 2.35; 95% CI, 1.39-3.97).
- Women with GDM who went on to develop diabetes or hypertension faced even higher risks for CKD, suggesting that preventing diabetes and hypertension after GDM may reduce the development of CKD.
- GDM did not affect the risk for acute kidney disease (aHR, 1.08; 95% CI, 0.90-1.29).
IN PRACTICE:
“Women with severe metabolic dysfunction during pregnancy constitute a high-risk group regarding future CKD,” the authors wrote. “The significantly elevated CKD risk was observed from 2 years after pregnancy and beyond.”
SOURCE:
The study, with first author Maria Hornstrup Christensen, of Odense University Hospital, Odense, Denmark, was published online on December 15 in Diabetes Care.
LIMITATIONS:
GDM may be underdiagnosed, and undiagnosed diabetes may be misclassified as GDM. The proxies of GDM and insulin treatment may not have captured the increasing severity of metabolic dysfunction. The prevalence of insulin treatment was lower than expected, perhaps due to the practice of providing a patient’s first insulin pen without a prescription and perhaps not recording it in a patient’s health record.
DISCLOSURES:
This work received financial support from the University of Southern Denmark, the Region of Southern Denmark, and the Danish Diabetes Academy, which is funded by the Novo Nordisk Foundation. The authors declared no conflicts of interest.
A version of this article appeared on Medscape.com.
TOPLINE:
Previous gestational diabetes mellitus (GDM) nearly doubles future chronic kidney disease (CKD) risk, irrespective of subsequent diabetes and hypertension, a study showed.
METHODOLOGY:
- A nationwide, cohort study was based on data from the Danish Medical Birth Register and included 697,622 women who gave birth between 1997 and 2018.
- Of all study participants, 3.4% reported GDM in at least one pregnancy, and 12.8% of women with GDM received insulin, a proxy for a more severe metabolic dysfunction.
- The women were followed up for a median of 11.9 years.
- Researchers studied CKD and acute kidney disease as the outcomes of interest, the mediating effects of subsequent diabetes and hypertension on future CKD, and how GDM severity affected later risk for kidney disease.
TAKEAWAY:
- Women with GDM showed significantly higher CKD risk than those without GDM (adjusted hazard ratio [aHR], 1.92; 95% CI, 1.67-2.21).
- Women who received insulin during pregnancy due to severe metabolic dysfunction but did not develop subsequent diabetes had a proportionally higher risk for CKD (aHR, 2.35; 95% CI, 1.39-3.97).
- Women with GDM who went on to develop diabetes or hypertension faced even higher risks for CKD, suggesting that preventing diabetes and hypertension after GDM may reduce the development of CKD.
- GDM did not affect the risk for acute kidney disease (aHR, 1.08; 95% CI, 0.90-1.29).
IN PRACTICE:
“Women with severe metabolic dysfunction during pregnancy constitute a high-risk group regarding future CKD,” the authors wrote. “The significantly elevated CKD risk was observed from 2 years after pregnancy and beyond.”
SOURCE:
The study, with first author Maria Hornstrup Christensen, of Odense University Hospital, Odense, Denmark, was published online on December 15 in Diabetes Care.
LIMITATIONS:
GDM may be underdiagnosed, and undiagnosed diabetes may be misclassified as GDM. The proxies of GDM and insulin treatment may not have captured the increasing severity of metabolic dysfunction. The prevalence of insulin treatment was lower than expected, perhaps due to the practice of providing a patient’s first insulin pen without a prescription and perhaps not recording it in a patient’s health record.
DISCLOSURES:
This work received financial support from the University of Southern Denmark, the Region of Southern Denmark, and the Danish Diabetes Academy, which is funded by the Novo Nordisk Foundation. The authors declared no conflicts of interest.
A version of this article appeared on Medscape.com.
Autoimmune Diseases and Perinatal Depression May Share Two-Way Link
Women with autoimmune disease are more likely to have perinatal depression (PND), according to findings from a new study that also suggested the reverse relationship is true: Women with a history of PND have a higher risk of developing autoimmune disease.
The research, published online on January 9, 2024, in Molecular Psychiatry, was led by Emma Bränn, PhD, Institute of Environmental Medicine, Karolinska Institute, Stockholm, Sweden.
The researchers used data from the Swedish Medical Birth Register and identified all women who had given birth in Sweden between 2001 and 2013. Out of the group of approximately 815,000 women and 1.3 million pregnancies, just more than 55,000 women had been diagnosed with depression during their pregnancy or within a year after delivery.
The researchers then compared the incidence of 41 autoimmune diseases in women who had and did not have PND. They controlled for factors including genetic makeup and childhood environment.
Results indicated that women with autoimmune disease were 30% more likely to have PND (odds ratio, 1.30; 95% CI, 1.25-1.35). Conversely, women with PND were 30% more likely than women with no PND to develop an autoimmune disease (hazard ratio, 1.30; 95% CI, 1.25-1.36).
A sibling comparison helped confirm the results by controlling for some shared genetic and early life environmental factors related to the household in which sisters grew up.
Potential Shared Biological Mechanisms
The association was independent of psychiatric comorbidities, suggesting there may be shared biological mechanisms.
Dr. Bränn told this news organization that the research team wanted to do the study because previous research has shown involvement of the immune system in depression, with similarities in both the symptoms of immune system–activated diseases and depression and the molecular pathways activated by the immune system.
“Adding on top of the tremendous changes in the immune system that we see in the body of the woman during the perinatal period, we hypothesized that autoimmune diseases could be associated to perinatal depression,” she said. “This had also been shown in some previous literature but not to the extent as what we have investigated in this paper.”
She said their results help make a case for counseling women at several points in healthcare interactions — before and after conception and childbirth — and in rheumatology visits to inform women with autoimmune diseases who are contemplating motherhood of the association with developing PND. The results may also demonstrate a need for monitoring women in these groups for depression or autoimmune disease.
Fred Miller, MD, PhD, retired Scientist Emeritus of the Environmental Autoimmunity Group at the National Institute of Environmental Health Sciences, who was not part of the study, said the results seem plausible as they build on early work that demonstrated selected associations between autoimmune conditions and mental illness.
“These associations may be the result of shared genetic and environmental risk factors, including stress, hormonal changes, medications, and the proinflammatory states that can lead to both,” he said.
The novelty, he said, is in the relatively strong associations of PND with autoimmune disease overall and with specific autoimmune diseases.
Strong Link Found With Multiple Sclerosis (MS)
According to the paper, a significant positive bidirectional link was found for autoimmune thyroid disease, psoriasis, MS, ulcerative colitis, and celiac disease.
Researchers found a particularly strong association — double the risk in both directions — between PND and MS.
Dr. Miller said though it is unclear from this study why the association of PND with MS was stronger than with other autoimmune diseases, people with MS are known to be at a high risk for depression in general. That may come from greater shared genetic and environmental risk factors, he added.
Additionally, MS is one of the more common autoimmune diseases, he noted, so the population is larger for study.
He said he was surprised the researchers didn’t investigate medication use because medications used in depression have immunologic effects and medications used in autoimmune diseases could have effects on mental conditions.
The study has implications for clinicians in a wide variety of specialties, Dr. Miller noted.
“It suggests that caregivers be more alert to the signs of developing autoimmune disease in women with perinatal depression and to the signs of developing perinatal depression in those with autoimmune disease,” Dr. Miller said, “so that appropriate screening, diagnostics, and interventions may be undertaken.”
The researchers say they will continue to examine the long-term effects of depression during pregnancy and in the year after childbirth.
“Depression during this sensitive period can have serious consequences for both the mother and the baby,” Dr. Bränn said. “We hope that our results will help decision-makers to steer funding toward maternal healthcare so that more women can get help and support in time.”
The study was financed by Karolinska Institute, Forte (the Swedish Research Council for Health, Working Life and Welfare), the Swedish Research Council, and the Icelandic Research Fund.
The researchers and Dr. Miller reported no relevant financial relationships.
A version of this article appeared on Medscape.com.
Women with autoimmune disease are more likely to have perinatal depression (PND), according to findings from a new study that also suggested the reverse relationship is true: Women with a history of PND have a higher risk of developing autoimmune disease.
The research, published online on January 9, 2024, in Molecular Psychiatry, was led by Emma Bränn, PhD, Institute of Environmental Medicine, Karolinska Institute, Stockholm, Sweden.
The researchers used data from the Swedish Medical Birth Register and identified all women who had given birth in Sweden between 2001 and 2013. Out of the group of approximately 815,000 women and 1.3 million pregnancies, just more than 55,000 women had been diagnosed with depression during their pregnancy or within a year after delivery.
The researchers then compared the incidence of 41 autoimmune diseases in women who had and did not have PND. They controlled for factors including genetic makeup and childhood environment.
Results indicated that women with autoimmune disease were 30% more likely to have PND (odds ratio, 1.30; 95% CI, 1.25-1.35). Conversely, women with PND were 30% more likely than women with no PND to develop an autoimmune disease (hazard ratio, 1.30; 95% CI, 1.25-1.36).
A sibling comparison helped confirm the results by controlling for some shared genetic and early life environmental factors related to the household in which sisters grew up.
Potential Shared Biological Mechanisms
The association was independent of psychiatric comorbidities, suggesting there may be shared biological mechanisms.
Dr. Bränn told this news organization that the research team wanted to do the study because previous research has shown involvement of the immune system in depression, with similarities in both the symptoms of immune system–activated diseases and depression and the molecular pathways activated by the immune system.
“Adding on top of the tremendous changes in the immune system that we see in the body of the woman during the perinatal period, we hypothesized that autoimmune diseases could be associated to perinatal depression,” she said. “This had also been shown in some previous literature but not to the extent as what we have investigated in this paper.”
She said their results help make a case for counseling women at several points in healthcare interactions — before and after conception and childbirth — and in rheumatology visits to inform women with autoimmune diseases who are contemplating motherhood of the association with developing PND. The results may also demonstrate a need for monitoring women in these groups for depression or autoimmune disease.
Fred Miller, MD, PhD, retired Scientist Emeritus of the Environmental Autoimmunity Group at the National Institute of Environmental Health Sciences, who was not part of the study, said the results seem plausible as they build on early work that demonstrated selected associations between autoimmune conditions and mental illness.
“These associations may be the result of shared genetic and environmental risk factors, including stress, hormonal changes, medications, and the proinflammatory states that can lead to both,” he said.
The novelty, he said, is in the relatively strong associations of PND with autoimmune disease overall and with specific autoimmune diseases.
Strong Link Found With Multiple Sclerosis (MS)
According to the paper, a significant positive bidirectional link was found for autoimmune thyroid disease, psoriasis, MS, ulcerative colitis, and celiac disease.
Researchers found a particularly strong association — double the risk in both directions — between PND and MS.
Dr. Miller said though it is unclear from this study why the association of PND with MS was stronger than with other autoimmune diseases, people with MS are known to be at a high risk for depression in general. That may come from greater shared genetic and environmental risk factors, he added.
Additionally, MS is one of the more common autoimmune diseases, he noted, so the population is larger for study.
He said he was surprised the researchers didn’t investigate medication use because medications used in depression have immunologic effects and medications used in autoimmune diseases could have effects on mental conditions.
The study has implications for clinicians in a wide variety of specialties, Dr. Miller noted.
“It suggests that caregivers be more alert to the signs of developing autoimmune disease in women with perinatal depression and to the signs of developing perinatal depression in those with autoimmune disease,” Dr. Miller said, “so that appropriate screening, diagnostics, and interventions may be undertaken.”
The researchers say they will continue to examine the long-term effects of depression during pregnancy and in the year after childbirth.
“Depression during this sensitive period can have serious consequences for both the mother and the baby,” Dr. Bränn said. “We hope that our results will help decision-makers to steer funding toward maternal healthcare so that more women can get help and support in time.”
The study was financed by Karolinska Institute, Forte (the Swedish Research Council for Health, Working Life and Welfare), the Swedish Research Council, and the Icelandic Research Fund.
The researchers and Dr. Miller reported no relevant financial relationships.
A version of this article appeared on Medscape.com.
Women with autoimmune disease are more likely to have perinatal depression (PND), according to findings from a new study that also suggested the reverse relationship is true: Women with a history of PND have a higher risk of developing autoimmune disease.
The research, published online on January 9, 2024, in Molecular Psychiatry, was led by Emma Bränn, PhD, Institute of Environmental Medicine, Karolinska Institute, Stockholm, Sweden.
The researchers used data from the Swedish Medical Birth Register and identified all women who had given birth in Sweden between 2001 and 2013. Out of the group of approximately 815,000 women and 1.3 million pregnancies, just more than 55,000 women had been diagnosed with depression during their pregnancy or within a year after delivery.
The researchers then compared the incidence of 41 autoimmune diseases in women who had and did not have PND. They controlled for factors including genetic makeup and childhood environment.
Results indicated that women with autoimmune disease were 30% more likely to have PND (odds ratio, 1.30; 95% CI, 1.25-1.35). Conversely, women with PND were 30% more likely than women with no PND to develop an autoimmune disease (hazard ratio, 1.30; 95% CI, 1.25-1.36).
A sibling comparison helped confirm the results by controlling for some shared genetic and early life environmental factors related to the household in which sisters grew up.
Potential Shared Biological Mechanisms
The association was independent of psychiatric comorbidities, suggesting there may be shared biological mechanisms.
Dr. Bränn told this news organization that the research team wanted to do the study because previous research has shown involvement of the immune system in depression, with similarities in both the symptoms of immune system–activated diseases and depression and the molecular pathways activated by the immune system.
“Adding on top of the tremendous changes in the immune system that we see in the body of the woman during the perinatal period, we hypothesized that autoimmune diseases could be associated to perinatal depression,” she said. “This had also been shown in some previous literature but not to the extent as what we have investigated in this paper.”
She said their results help make a case for counseling women at several points in healthcare interactions — before and after conception and childbirth — and in rheumatology visits to inform women with autoimmune diseases who are contemplating motherhood of the association with developing PND. The results may also demonstrate a need for monitoring women in these groups for depression or autoimmune disease.
Fred Miller, MD, PhD, retired Scientist Emeritus of the Environmental Autoimmunity Group at the National Institute of Environmental Health Sciences, who was not part of the study, said the results seem plausible as they build on early work that demonstrated selected associations between autoimmune conditions and mental illness.
“These associations may be the result of shared genetic and environmental risk factors, including stress, hormonal changes, medications, and the proinflammatory states that can lead to both,” he said.
The novelty, he said, is in the relatively strong associations of PND with autoimmune disease overall and with specific autoimmune diseases.
Strong Link Found With Multiple Sclerosis (MS)
According to the paper, a significant positive bidirectional link was found for autoimmune thyroid disease, psoriasis, MS, ulcerative colitis, and celiac disease.
Researchers found a particularly strong association — double the risk in both directions — between PND and MS.
Dr. Miller said though it is unclear from this study why the association of PND with MS was stronger than with other autoimmune diseases, people with MS are known to be at a high risk for depression in general. That may come from greater shared genetic and environmental risk factors, he added.
Additionally, MS is one of the more common autoimmune diseases, he noted, so the population is larger for study.
He said he was surprised the researchers didn’t investigate medication use because medications used in depression have immunologic effects and medications used in autoimmune diseases could have effects on mental conditions.
The study has implications for clinicians in a wide variety of specialties, Dr. Miller noted.
“It suggests that caregivers be more alert to the signs of developing autoimmune disease in women with perinatal depression and to the signs of developing perinatal depression in those with autoimmune disease,” Dr. Miller said, “so that appropriate screening, diagnostics, and interventions may be undertaken.”
The researchers say they will continue to examine the long-term effects of depression during pregnancy and in the year after childbirth.
“Depression during this sensitive period can have serious consequences for both the mother and the baby,” Dr. Bränn said. “We hope that our results will help decision-makers to steer funding toward maternal healthcare so that more women can get help and support in time.”
The study was financed by Karolinska Institute, Forte (the Swedish Research Council for Health, Working Life and Welfare), the Swedish Research Council, and the Icelandic Research Fund.
The researchers and Dr. Miller reported no relevant financial relationships.
A version of this article appeared on Medscape.com.
FROM MOLECULAR PSYCHIATRY
SUDs rates highest in head, neck, and gastric cancer survivors
.
The association between cancer and substance use is well known, but data on the prevalence of different substance use disorders (SUDs) in different types of cancer are limited, Katie F. Jones, PhD, of the VA Boston Healthcare System, and colleagues, wrote in their paper.
“Substance use and use disorders are on the rise in general and among older adults, who represent the majority of people diagnosed with cancer, and SUDs have significant potential to complicate cancer care and negatively impact cancer outcomes,” corresponding author Devon K. Check, PhD, of Duke University, Durham, N.C., said in an interview. “We thought it was important to understand whether SUDs are more common with certain types of cancer. We can use that information to guide resources toward populations where interventions to integrate SUD treatment and cancer treatment are most needed,” he said. “In addition, because different SUDs (opioid use disorder, alcohol use disorder) might complicate cancer treatment in different ways and necessitate different types of interventions, we thought it was important to understand the distribution of specific disorders,” he explained.
In the cross-sectional study published in JAMA Oncology, the researchers reviewed data from 6,101 adult cancer survivors who participated in the National Survey of Drug Use and Health (NSDUH) between 2015 and 2020.
The study population included survivors of solid tumor cancers. SUD was defined as meeting at least one of four criteria for substance abuse or at least 3 of 6 criteria for dependence based on the Diagnostic and Statistical Manual of Mental Disorders (Fourth Edition) criteria.
Overall, 3.83% of the participants met criteria for SUD. Survivors of head and neck cancers and survivors of gastric and esophageal cancers had the highest rates of SUDs (approximately 9%), followed by cervical cancer and melanoma survivors (approximately 6%).
Alcohol use disorder was the most common SUD both overall (2.8%) and among survivors of head and neck cancers, cervical cancers, and melanoma.
Cannabis use disorder was the most prevalent SUD among esophageal and gastric cancer survivors (approximately 9%).
The prevalence of SUDs overall and within the past year (active) was approximately 4%, but the prevalence of active SUDs was significantly higher for those with head and neck cancers and cervical cancer (18.73% and 15.70%, respectively). However, the distribution of specific SUDs was different in the newly diagnosed patients. Sedative use disorder took the top spot as the most common SUD for head and neck cancer survivors (9.81%), while alcohol use disorder was the most common SUD among cervical cancer survivors (10.49%).
Limitations and Implications
The findings were limited by several factors, including the nature of the study population and the data source, said Dr. Check.
“The average prevalence of SUD (or the prevalence across cancer types) was lower than we might have expected,” but the results make sense given the mainly older and female study population, he said. SUDs are less common among older adults compared with younger adults and among women compared with men, and the study’s data source (NSDUH) has been shown in other research to underestimate the prevalence of opioid use disorder, he added.
“Otherwise, the study findings were generally consistent with what we would expect,” Dr. Check said in an interview. “For example, alcohol use disorder is the most common SUD in the general U.S. population, and that was true for our study population of cancer survivors as well. In addition, SUD prevalence was higher in cancers such as cervical cancer and head and neck cancers that are causally linked to alcohol and/or tobacco use,” he said.
Integrated care is needed
“Among people diagnosed with certain types of cancers, including cervical and head and neck cancers, the estimated prevalence of SUD is similar to those [with] medical comorbidities such as diabetes and cardiopulmonary conditions,” said Dr. Check. “Within the field, there is an increasing emphasis on ensuring that people diagnosed with cancer have access to integrated care for their comorbid medical conditions. Similar efforts for people who concurrently manage cancer and SUD are largely absent but critically needed; these efforts should prioritize cancer populations where SUD prevalence is high,” he said.
Looking ahead, “We need to understand more about the specific challenges that arise at the intersection of cancer and SUD so we can design interventions and programs to better support both patients who concurrently manage cancer and SUD and the clinicians who care for them,” Dr. Check added.
Recognize risk factors
“It is very important to study overall substance use disorders in patients with cancer, because understanding the risks of developing these issues after treatment helps us develop approaches to best support these patients following their cancer therapies,” Henry S. Park, MD, a radiation oncologist at Yale University, New Haven, Connecticut, said in an interview.
The current study findings “are generally consistent with my experience and intuition, but it is still helpful to see the actual data,” said Dr. Park, who was not involved in the study. “This may be partially because of the baseline elevated risk of preexisting SUDs for certain patients from the higher-prevalence disease sites. However, it may also be related to the intense side effects that survivors of some types of cancers, such as head and neck cancer, gastroesophageal cancer, and cervical cancer, may experience soon after treatment, and even chronically long after treatment,” he said.
Individualize risk assessment
“Ultimately, clinicians should be aware that not all patients with cancer are the same, and that the majority do not necessarily develop SUDs,” Dr. Park said in an interview. “We should be careful to treat symptoms appropriately, and not withhold therapies purely because of an elevated risk of developing SUDs. However, there are some patients who are at higher risk of SUDs who will need extra support and care from physicians, advanced practice providers, nutritionists, social workers, psychologists, dietitians, and survivorship clinics, both in the short-term and long-term,” he emphasized.
As for additional research, “more work needs to be done on which particular patients within each disease subset are most likely to develop SUDs,” said Dr. Park. “Most importantly, once we identify our high-risk group as reliably as possible, we will have to study interventions that rely on supporting and partnering with patients to decrease the risk of developing SUDs as much as possible, while adequately treating residual symptoms and quality-of-life effects following cancer treatment,” he said.
The study received no outside funding. Dr. Check disclosed grants from Duke University during the study period and grants from the National Institutes of Health and AstraZeneca unrelated to the current study. Dr. Park had no financial conflicts to disclose.
.
The association between cancer and substance use is well known, but data on the prevalence of different substance use disorders (SUDs) in different types of cancer are limited, Katie F. Jones, PhD, of the VA Boston Healthcare System, and colleagues, wrote in their paper.
“Substance use and use disorders are on the rise in general and among older adults, who represent the majority of people diagnosed with cancer, and SUDs have significant potential to complicate cancer care and negatively impact cancer outcomes,” corresponding author Devon K. Check, PhD, of Duke University, Durham, N.C., said in an interview. “We thought it was important to understand whether SUDs are more common with certain types of cancer. We can use that information to guide resources toward populations where interventions to integrate SUD treatment and cancer treatment are most needed,” he said. “In addition, because different SUDs (opioid use disorder, alcohol use disorder) might complicate cancer treatment in different ways and necessitate different types of interventions, we thought it was important to understand the distribution of specific disorders,” he explained.
In the cross-sectional study published in JAMA Oncology, the researchers reviewed data from 6,101 adult cancer survivors who participated in the National Survey of Drug Use and Health (NSDUH) between 2015 and 2020.
The study population included survivors of solid tumor cancers. SUD was defined as meeting at least one of four criteria for substance abuse or at least 3 of 6 criteria for dependence based on the Diagnostic and Statistical Manual of Mental Disorders (Fourth Edition) criteria.
Overall, 3.83% of the participants met criteria for SUD. Survivors of head and neck cancers and survivors of gastric and esophageal cancers had the highest rates of SUDs (approximately 9%), followed by cervical cancer and melanoma survivors (approximately 6%).
Alcohol use disorder was the most common SUD both overall (2.8%) and among survivors of head and neck cancers, cervical cancers, and melanoma.
Cannabis use disorder was the most prevalent SUD among esophageal and gastric cancer survivors (approximately 9%).
The prevalence of SUDs overall and within the past year (active) was approximately 4%, but the prevalence of active SUDs was significantly higher for those with head and neck cancers and cervical cancer (18.73% and 15.70%, respectively). However, the distribution of specific SUDs was different in the newly diagnosed patients. Sedative use disorder took the top spot as the most common SUD for head and neck cancer survivors (9.81%), while alcohol use disorder was the most common SUD among cervical cancer survivors (10.49%).
Limitations and Implications
The findings were limited by several factors, including the nature of the study population and the data source, said Dr. Check.
“The average prevalence of SUD (or the prevalence across cancer types) was lower than we might have expected,” but the results make sense given the mainly older and female study population, he said. SUDs are less common among older adults compared with younger adults and among women compared with men, and the study’s data source (NSDUH) has been shown in other research to underestimate the prevalence of opioid use disorder, he added.
“Otherwise, the study findings were generally consistent with what we would expect,” Dr. Check said in an interview. “For example, alcohol use disorder is the most common SUD in the general U.S. population, and that was true for our study population of cancer survivors as well. In addition, SUD prevalence was higher in cancers such as cervical cancer and head and neck cancers that are causally linked to alcohol and/or tobacco use,” he said.
Integrated care is needed
“Among people diagnosed with certain types of cancers, including cervical and head and neck cancers, the estimated prevalence of SUD is similar to those [with] medical comorbidities such as diabetes and cardiopulmonary conditions,” said Dr. Check. “Within the field, there is an increasing emphasis on ensuring that people diagnosed with cancer have access to integrated care for their comorbid medical conditions. Similar efforts for people who concurrently manage cancer and SUD are largely absent but critically needed; these efforts should prioritize cancer populations where SUD prevalence is high,” he said.
Looking ahead, “We need to understand more about the specific challenges that arise at the intersection of cancer and SUD so we can design interventions and programs to better support both patients who concurrently manage cancer and SUD and the clinicians who care for them,” Dr. Check added.
Recognize risk factors
“It is very important to study overall substance use disorders in patients with cancer, because understanding the risks of developing these issues after treatment helps us develop approaches to best support these patients following their cancer therapies,” Henry S. Park, MD, a radiation oncologist at Yale University, New Haven, Connecticut, said in an interview.
The current study findings “are generally consistent with my experience and intuition, but it is still helpful to see the actual data,” said Dr. Park, who was not involved in the study. “This may be partially because of the baseline elevated risk of preexisting SUDs for certain patients from the higher-prevalence disease sites. However, it may also be related to the intense side effects that survivors of some types of cancers, such as head and neck cancer, gastroesophageal cancer, and cervical cancer, may experience soon after treatment, and even chronically long after treatment,” he said.
Individualize risk assessment
“Ultimately, clinicians should be aware that not all patients with cancer are the same, and that the majority do not necessarily develop SUDs,” Dr. Park said in an interview. “We should be careful to treat symptoms appropriately, and not withhold therapies purely because of an elevated risk of developing SUDs. However, there are some patients who are at higher risk of SUDs who will need extra support and care from physicians, advanced practice providers, nutritionists, social workers, psychologists, dietitians, and survivorship clinics, both in the short-term and long-term,” he emphasized.
As for additional research, “more work needs to be done on which particular patients within each disease subset are most likely to develop SUDs,” said Dr. Park. “Most importantly, once we identify our high-risk group as reliably as possible, we will have to study interventions that rely on supporting and partnering with patients to decrease the risk of developing SUDs as much as possible, while adequately treating residual symptoms and quality-of-life effects following cancer treatment,” he said.
The study received no outside funding. Dr. Check disclosed grants from Duke University during the study period and grants from the National Institutes of Health and AstraZeneca unrelated to the current study. Dr. Park had no financial conflicts to disclose.
.
The association between cancer and substance use is well known, but data on the prevalence of different substance use disorders (SUDs) in different types of cancer are limited, Katie F. Jones, PhD, of the VA Boston Healthcare System, and colleagues, wrote in their paper.
“Substance use and use disorders are on the rise in general and among older adults, who represent the majority of people diagnosed with cancer, and SUDs have significant potential to complicate cancer care and negatively impact cancer outcomes,” corresponding author Devon K. Check, PhD, of Duke University, Durham, N.C., said in an interview. “We thought it was important to understand whether SUDs are more common with certain types of cancer. We can use that information to guide resources toward populations where interventions to integrate SUD treatment and cancer treatment are most needed,” he said. “In addition, because different SUDs (opioid use disorder, alcohol use disorder) might complicate cancer treatment in different ways and necessitate different types of interventions, we thought it was important to understand the distribution of specific disorders,” he explained.
In the cross-sectional study published in JAMA Oncology, the researchers reviewed data from 6,101 adult cancer survivors who participated in the National Survey of Drug Use and Health (NSDUH) between 2015 and 2020.
The study population included survivors of solid tumor cancers. SUD was defined as meeting at least one of four criteria for substance abuse or at least 3 of 6 criteria for dependence based on the Diagnostic and Statistical Manual of Mental Disorders (Fourth Edition) criteria.
Overall, 3.83% of the participants met criteria for SUD. Survivors of head and neck cancers and survivors of gastric and esophageal cancers had the highest rates of SUDs (approximately 9%), followed by cervical cancer and melanoma survivors (approximately 6%).
Alcohol use disorder was the most common SUD both overall (2.8%) and among survivors of head and neck cancers, cervical cancers, and melanoma.
Cannabis use disorder was the most prevalent SUD among esophageal and gastric cancer survivors (approximately 9%).
The prevalence of SUDs overall and within the past year (active) was approximately 4%, but the prevalence of active SUDs was significantly higher for those with head and neck cancers and cervical cancer (18.73% and 15.70%, respectively). However, the distribution of specific SUDs was different in the newly diagnosed patients. Sedative use disorder took the top spot as the most common SUD for head and neck cancer survivors (9.81%), while alcohol use disorder was the most common SUD among cervical cancer survivors (10.49%).
Limitations and Implications
The findings were limited by several factors, including the nature of the study population and the data source, said Dr. Check.
“The average prevalence of SUD (or the prevalence across cancer types) was lower than we might have expected,” but the results make sense given the mainly older and female study population, he said. SUDs are less common among older adults compared with younger adults and among women compared with men, and the study’s data source (NSDUH) has been shown in other research to underestimate the prevalence of opioid use disorder, he added.
“Otherwise, the study findings were generally consistent with what we would expect,” Dr. Check said in an interview. “For example, alcohol use disorder is the most common SUD in the general U.S. population, and that was true for our study population of cancer survivors as well. In addition, SUD prevalence was higher in cancers such as cervical cancer and head and neck cancers that are causally linked to alcohol and/or tobacco use,” he said.
Integrated care is needed
“Among people diagnosed with certain types of cancers, including cervical and head and neck cancers, the estimated prevalence of SUD is similar to those [with] medical comorbidities such as diabetes and cardiopulmonary conditions,” said Dr. Check. “Within the field, there is an increasing emphasis on ensuring that people diagnosed with cancer have access to integrated care for their comorbid medical conditions. Similar efforts for people who concurrently manage cancer and SUD are largely absent but critically needed; these efforts should prioritize cancer populations where SUD prevalence is high,” he said.
Looking ahead, “We need to understand more about the specific challenges that arise at the intersection of cancer and SUD so we can design interventions and programs to better support both patients who concurrently manage cancer and SUD and the clinicians who care for them,” Dr. Check added.
Recognize risk factors
“It is very important to study overall substance use disorders in patients with cancer, because understanding the risks of developing these issues after treatment helps us develop approaches to best support these patients following their cancer therapies,” Henry S. Park, MD, a radiation oncologist at Yale University, New Haven, Connecticut, said in an interview.
The current study findings “are generally consistent with my experience and intuition, but it is still helpful to see the actual data,” said Dr. Park, who was not involved in the study. “This may be partially because of the baseline elevated risk of preexisting SUDs for certain patients from the higher-prevalence disease sites. However, it may also be related to the intense side effects that survivors of some types of cancers, such as head and neck cancer, gastroesophageal cancer, and cervical cancer, may experience soon after treatment, and even chronically long after treatment,” he said.
Individualize risk assessment
“Ultimately, clinicians should be aware that not all patients with cancer are the same, and that the majority do not necessarily develop SUDs,” Dr. Park said in an interview. “We should be careful to treat symptoms appropriately, and not withhold therapies purely because of an elevated risk of developing SUDs. However, there are some patients who are at higher risk of SUDs who will need extra support and care from physicians, advanced practice providers, nutritionists, social workers, psychologists, dietitians, and survivorship clinics, both in the short-term and long-term,” he emphasized.
As for additional research, “more work needs to be done on which particular patients within each disease subset are most likely to develop SUDs,” said Dr. Park. “Most importantly, once we identify our high-risk group as reliably as possible, we will have to study interventions that rely on supporting and partnering with patients to decrease the risk of developing SUDs as much as possible, while adequately treating residual symptoms and quality-of-life effects following cancer treatment,” he said.
The study received no outside funding. Dr. Check disclosed grants from Duke University during the study period and grants from the National Institutes of Health and AstraZeneca unrelated to the current study. Dr. Park had no financial conflicts to disclose.
FROM JAMA ONCOLOGY
A 27-year-old Haitian woman presented with a painful umbilical mass which had been growing in size for 5 months
Endometriosis is defined as the presence of endometrial tissue outside of the uterine cavity, commonly occurring in women of reproductive age. The condition usually affects the adnexa (ovaries, Fallopian tubes, and associated ligaments and connective tissue) but can also be seen in extrapelvic structures.
Cutaneous endometriosis is an uncommon subtype that accounts for 1% of endometriosis cases and occurs when endometrial tissue is found on the surface of the skin. It is divided into primary and secondary cutaneous endometriosis. The that may lead to seeding of endometrial tissue on the skin. In the case of our patient, it appears that her laparoscopic procedure 2 years ago was the cause of endometrial seeding in the umbilicus.
Clinically, the condition may present with a palpable mass, cyclic pain, and bloody discharge from the affected area. Due to the rarity of cutaneous endometriosis, it may be hard to distinguish from other diagnoses such as keloids, dermatofibromas, hernias, or cutaneous metastasis of cancers (Sister Mary Joseph nodules).

The definitive diagnosis can be made by biopsy and histopathological assessment showing a mixture of endometrial glands and stromal tissue. Imaging studies such as computed tomography (CT) scan and magnetic resonance imaging (MRI) are helpful in excluding more common diagnoses such as hernia or cutaneous metastasis. In this patient, the mass was surgically excised. Histopathological assessment established the diagnosis of cutaneous endometriosis.
Treatment options include surgical excision and medical therapy. Medical therapy entails the use of hormonal agents such as gonadotropin-releasing hormone agonists, danazol (a pituitary gonadotropin inhibitor), and oral contraceptives, which reduce the cyclical proliferation of endothelial tissue. These agents can be used preoperatively to reduce the size of the cutaneous mass before surgical excision, or as an alternative treatment for patients who wish to avoid surgery. The rate of recurrence is observed to be higher with medical therapy rather than surgical treatment.
The case and photo were submitted by Mina Ahmed, MBBS, Brooke Resh Sateesh MD, and Nathan Uebelhoer MD, of San Diego Family Dermatology, San Diego, California. The column was edited by Donna Bilu Martin, MD.
Dr. Bilu Martin is a board-certified dermatologist in private practice at Premier Dermatology, MD, in Aventura, Florida. More diagnostic cases are available at mdedge.com/dermatology. To submit a case for possible publication, send an email to [email protected].
References
1. Gonzalez RH et al. Am J Case Rep. 2021;22:e932493-1–e932493-4.
2. Raffi L et al. Int J Womens Dermatol. 2019 Dec;5(5):384-386.
3. Sharma A, Apostol R. Cutaneous endometriosis. Treasure Island, Fla: Statpearls Publishing, 2023.
Endometriosis is defined as the presence of endometrial tissue outside of the uterine cavity, commonly occurring in women of reproductive age. The condition usually affects the adnexa (ovaries, Fallopian tubes, and associated ligaments and connective tissue) but can also be seen in extrapelvic structures.
Cutaneous endometriosis is an uncommon subtype that accounts for 1% of endometriosis cases and occurs when endometrial tissue is found on the surface of the skin. It is divided into primary and secondary cutaneous endometriosis. The that may lead to seeding of endometrial tissue on the skin. In the case of our patient, it appears that her laparoscopic procedure 2 years ago was the cause of endometrial seeding in the umbilicus.
Clinically, the condition may present with a palpable mass, cyclic pain, and bloody discharge from the affected area. Due to the rarity of cutaneous endometriosis, it may be hard to distinguish from other diagnoses such as keloids, dermatofibromas, hernias, or cutaneous metastasis of cancers (Sister Mary Joseph nodules).
The definitive diagnosis can be made by biopsy and histopathological assessment showing a mixture of endometrial glands and stromal tissue. Imaging studies such as computed tomography (CT) scan and magnetic resonance imaging (MRI) are helpful in excluding more common diagnoses such as hernia or cutaneous metastasis. In this patient, the mass was surgically excised. Histopathological assessment established the diagnosis of cutaneous endometriosis.
Treatment options include surgical excision and medical therapy. Medical therapy entails the use of hormonal agents such as gonadotropin-releasing hormone agonists, danazol (a pituitary gonadotropin inhibitor), and oral contraceptives, which reduce the cyclical proliferation of endothelial tissue. These agents can be used preoperatively to reduce the size of the cutaneous mass before surgical excision, or as an alternative treatment for patients who wish to avoid surgery. The rate of recurrence is observed to be higher with medical therapy rather than surgical treatment.
The case and photo were submitted by Mina Ahmed, MBBS, Brooke Resh Sateesh MD, and Nathan Uebelhoer MD, of San Diego Family Dermatology, San Diego, California. The column was edited by Donna Bilu Martin, MD.
Dr. Bilu Martin is a board-certified dermatologist in private practice at Premier Dermatology, MD, in Aventura, Florida. More diagnostic cases are available at mdedge.com/dermatology. To submit a case for possible publication, send an email to [email protected].
References
1. Gonzalez RH et al. Am J Case Rep. 2021;22:e932493-1–e932493-4.
2. Raffi L et al. Int J Womens Dermatol. 2019 Dec;5(5):384-386.
3. Sharma A, Apostol R. Cutaneous endometriosis. Treasure Island, Fla: Statpearls Publishing, 2023.
Endometriosis is defined as the presence of endometrial tissue outside of the uterine cavity, commonly occurring in women of reproductive age. The condition usually affects the adnexa (ovaries, Fallopian tubes, and associated ligaments and connective tissue) but can also be seen in extrapelvic structures.
Cutaneous endometriosis is an uncommon subtype that accounts for 1% of endometriosis cases and occurs when endometrial tissue is found on the surface of the skin. It is divided into primary and secondary cutaneous endometriosis. The that may lead to seeding of endometrial tissue on the skin. In the case of our patient, it appears that her laparoscopic procedure 2 years ago was the cause of endometrial seeding in the umbilicus.
Clinically, the condition may present with a palpable mass, cyclic pain, and bloody discharge from the affected area. Due to the rarity of cutaneous endometriosis, it may be hard to distinguish from other diagnoses such as keloids, dermatofibromas, hernias, or cutaneous metastasis of cancers (Sister Mary Joseph nodules).
The definitive diagnosis can be made by biopsy and histopathological assessment showing a mixture of endometrial glands and stromal tissue. Imaging studies such as computed tomography (CT) scan and magnetic resonance imaging (MRI) are helpful in excluding more common diagnoses such as hernia or cutaneous metastasis. In this patient, the mass was surgically excised. Histopathological assessment established the diagnosis of cutaneous endometriosis.
Treatment options include surgical excision and medical therapy. Medical therapy entails the use of hormonal agents such as gonadotropin-releasing hormone agonists, danazol (a pituitary gonadotropin inhibitor), and oral contraceptives, which reduce the cyclical proliferation of endothelial tissue. These agents can be used preoperatively to reduce the size of the cutaneous mass before surgical excision, or as an alternative treatment for patients who wish to avoid surgery. The rate of recurrence is observed to be higher with medical therapy rather than surgical treatment.
The case and photo were submitted by Mina Ahmed, MBBS, Brooke Resh Sateesh MD, and Nathan Uebelhoer MD, of San Diego Family Dermatology, San Diego, California. The column was edited by Donna Bilu Martin, MD.
Dr. Bilu Martin is a board-certified dermatologist in private practice at Premier Dermatology, MD, in Aventura, Florida. More diagnostic cases are available at mdedge.com/dermatology. To submit a case for possible publication, send an email to [email protected].
References
1. Gonzalez RH et al. Am J Case Rep. 2021;22:e932493-1–e932493-4.
2. Raffi L et al. Int J Womens Dermatol. 2019 Dec;5(5):384-386.
3. Sharma A, Apostol R. Cutaneous endometriosis. Treasure Island, Fla: Statpearls Publishing, 2023.
