User login
Doug Brunk is a San Diego-based award-winning reporter who began covering health care in 1991. Before joining the company, he wrote for the health sciences division of Columbia University and was an associate editor at Contemporary Long Term Care magazine when it won a Jesse H. Neal Award. His work has been syndicated by the Los Angeles Times and he is the author of two books related to the University of Kentucky Wildcats men's basketball program. Doug has a master’s degree in magazine journalism from the S.I. Newhouse School of Public Communications at Syracuse University. Follow him on Twitter @dougbrunk.
Let Lip Defect Size Drive Treatment
SAN DIEGO – Principles for lip repair are based on size and location of the defect, etiology of the lesions, and patient age and gender, said Dr. Michael A. Keefe.
Surgical goals of lip reconstruction are to cover the skin and oral lining, leave a semblance of a vermilion and an adequate stomal diameter, make sure sensation is intact, and ensure that the patient has a competent oral sphincter. "The vermilion is the most visible component of the lips, and it’s also the sensory unit of the lip," Dr. Keefe said at a meeting on superficial anatomy and cutaneous surgery. The meeting was sponsored by the University of California, San Diego, School of Medicine and the Scripps Clinic.

"Scars are very well hidden at the vermilion-cutaneous border. If you have to cross the vermilion-cutaneous junction, cross at 90 degrees."
Lower Lip
The lower vermilion is the most affected target of solar radiation injury. In cases of premalignant lesions such as actinic cheilitis or leukoplakia, Dr. Keefe, a plastic surgeon with the division of head and neck surgery at Sharp Rees-Stealy Medical Group in San Diego, said he often performs a total vermilionectomy (lip shave). This involves resection from the white roll to the contact area with opposite lip. "Primary closure is possible," he said. "You can get tension and dehiscence and flattening of the lip, but generally it heals up pretty well. An option for vermilion reconstruction of larger defects is the buccal mucosal advancement flap, which involves elevating the mucosa deep to salivary glands and superficial to the orbicularis oris muscle."
An advantage of treating the lower lip is that there is increased soft tissue laxity and there is no Cupid’s bow, philtrum, or nose, "so it’s nice that there are no dominant central structures," he said. "The downside is that you have to be mindful of the effect of gravity on the repair, so there is a greater need for tone to prevent drooling and incompetence."

He recommends a staged approach based on the extent of the defect and the age of the patient. For small defects (those less than one-third of the lip size) he uses primary closure. Options for medium defects (those that involve one-third to two-thirds of the lip size) include the Estlander flap, the Abbe flap, Bernard Burow’s procedure, the Karapandzic flap, and the stairstep repair, while the options for large defects (those that involve more than two-thirds of the lip size) include Bernard Burow’s procedure, the Karapandzic flap, and the free flap. "You have a lot of tools, depending on what you feel comfortable with," Dr. Keefe said.
Upper Lip
Cancerous tumors of the upper lip are less common, "but there are some unique structures to pay attention to, including the nose, columella, Cupid’s bow, and the philtrum," he said. "In men there’s a hair-bearing skin issue, but scars can be disguised in a mustache."
The aesthetic subunits to keep in mind, he continued, are the medial subunit, which is one-half of the philtrum, and the lateral subunit, which consists of the philtral column, the nostril sill, the alar base, and the nasolabial crease. Primary closure is used for upper lip defects that involve less than one-third of the lip size. "You can make some perialar crescentic skin excisions, which can help advance things," Dr. Keefe said.
For centrally located medium-sized defects of the upper lip, he often uses primary closure with perialar crescentic skin excisions. "If it’s greater than one-half of the lip size, you can add an Abbe flap," he said. "That’s nice because that recreates the philtrum area."

For medially located medium-sized defects of the upper lip, "you can use the Abbe flap if the commissure is not involved and the Estlander flap if the commissure is involved."
Options for cases with large defects and adequate cheek tissue, he said, include the reverse Karapandzic flap, the reverse fan flap, inverted Bernard Burow’s procedure, superiorly based cheek flaps, and the bilateral levator anguli oris flap combined with the Abbe flap. Options for cases with inadequate cheek tissue include the distal pedicle flap and the free flap.
Repair Risks
A lot of these patients have medical problems," he said. "When you do your first injection to resect the tumor or put the lip back together, make sure you don’t cause a myocardial infarction. Generally you should be comfortable with patients who have an INR [International Normalized Ratio] of 2.5 and below."
For patients with large cancerous tumors of the lip, be mindful of lymphatic drainage, because larger tumors have an increased risk of metastases, said Dr. Keefe. For tumors larger than 2 cm in length or 6 mm in spread, or if there is perineural spread, the patient should be referred for radiation therapy.
Dr. Keefe said that he had no relevant financial conflicts to disclose.
SAN DIEGO – Principles for lip repair are based on size and location of the defect, etiology of the lesions, and patient age and gender, said Dr. Michael A. Keefe.
Surgical goals of lip reconstruction are to cover the skin and oral lining, leave a semblance of a vermilion and an adequate stomal diameter, make sure sensation is intact, and ensure that the patient has a competent oral sphincter. "The vermilion is the most visible component of the lips, and it’s also the sensory unit of the lip," Dr. Keefe said at a meeting on superficial anatomy and cutaneous surgery. The meeting was sponsored by the University of California, San Diego, School of Medicine and the Scripps Clinic.
"Scars are very well hidden at the vermilion-cutaneous border. If you have to cross the vermilion-cutaneous junction, cross at 90 degrees."
Lower Lip
The lower vermilion is the most affected target of solar radiation injury. In cases of premalignant lesions such as actinic cheilitis or leukoplakia, Dr. Keefe, a plastic surgeon with the division of head and neck surgery at Sharp Rees-Stealy Medical Group in San Diego, said he often performs a total vermilionectomy (lip shave). This involves resection from the white roll to the contact area with opposite lip. "Primary closure is possible," he said. "You can get tension and dehiscence and flattening of the lip, but generally it heals up pretty well. An option for vermilion reconstruction of larger defects is the buccal mucosal advancement flap, which involves elevating the mucosa deep to salivary glands and superficial to the orbicularis oris muscle."
An advantage of treating the lower lip is that there is increased soft tissue laxity and there is no Cupid’s bow, philtrum, or nose, "so it’s nice that there are no dominant central structures," he said. "The downside is that you have to be mindful of the effect of gravity on the repair, so there is a greater need for tone to prevent drooling and incompetence."
He recommends a staged approach based on the extent of the defect and the age of the patient. For small defects (those less than one-third of the lip size) he uses primary closure. Options for medium defects (those that involve one-third to two-thirds of the lip size) include the Estlander flap, the Abbe flap, Bernard Burow’s procedure, the Karapandzic flap, and the stairstep repair, while the options for large defects (those that involve more than two-thirds of the lip size) include Bernard Burow’s procedure, the Karapandzic flap, and the free flap. "You have a lot of tools, depending on what you feel comfortable with," Dr. Keefe said.
Upper Lip
Cancerous tumors of the upper lip are less common, "but there are some unique structures to pay attention to, including the nose, columella, Cupid’s bow, and the philtrum," he said. "In men there’s a hair-bearing skin issue, but scars can be disguised in a mustache."
The aesthetic subunits to keep in mind, he continued, are the medial subunit, which is one-half of the philtrum, and the lateral subunit, which consists of the philtral column, the nostril sill, the alar base, and the nasolabial crease. Primary closure is used for upper lip defects that involve less than one-third of the lip size. "You can make some perialar crescentic skin excisions, which can help advance things," Dr. Keefe said.
For centrally located medium-sized defects of the upper lip, he often uses primary closure with perialar crescentic skin excisions. "If it’s greater than one-half of the lip size, you can add an Abbe flap," he said. "That’s nice because that recreates the philtrum area."
For medially located medium-sized defects of the upper lip, "you can use the Abbe flap if the commissure is not involved and the Estlander flap if the commissure is involved."
Options for cases with large defects and adequate cheek tissue, he said, include the reverse Karapandzic flap, the reverse fan flap, inverted Bernard Burow’s procedure, superiorly based cheek flaps, and the bilateral levator anguli oris flap combined with the Abbe flap. Options for cases with inadequate cheek tissue include the distal pedicle flap and the free flap.
Repair Risks
A lot of these patients have medical problems," he said. "When you do your first injection to resect the tumor or put the lip back together, make sure you don’t cause a myocardial infarction. Generally you should be comfortable with patients who have an INR [International Normalized Ratio] of 2.5 and below."
For patients with large cancerous tumors of the lip, be mindful of lymphatic drainage, because larger tumors have an increased risk of metastases, said Dr. Keefe. For tumors larger than 2 cm in length or 6 mm in spread, or if there is perineural spread, the patient should be referred for radiation therapy.
Dr. Keefe said that he had no relevant financial conflicts to disclose.
SAN DIEGO – Principles for lip repair are based on size and location of the defect, etiology of the lesions, and patient age and gender, said Dr. Michael A. Keefe.
Surgical goals of lip reconstruction are to cover the skin and oral lining, leave a semblance of a vermilion and an adequate stomal diameter, make sure sensation is intact, and ensure that the patient has a competent oral sphincter. "The vermilion is the most visible component of the lips, and it’s also the sensory unit of the lip," Dr. Keefe said at a meeting on superficial anatomy and cutaneous surgery. The meeting was sponsored by the University of California, San Diego, School of Medicine and the Scripps Clinic.
"Scars are very well hidden at the vermilion-cutaneous border. If you have to cross the vermilion-cutaneous junction, cross at 90 degrees."
Lower Lip
The lower vermilion is the most affected target of solar radiation injury. In cases of premalignant lesions such as actinic cheilitis or leukoplakia, Dr. Keefe, a plastic surgeon with the division of head and neck surgery at Sharp Rees-Stealy Medical Group in San Diego, said he often performs a total vermilionectomy (lip shave). This involves resection from the white roll to the contact area with opposite lip. "Primary closure is possible," he said. "You can get tension and dehiscence and flattening of the lip, but generally it heals up pretty well. An option for vermilion reconstruction of larger defects is the buccal mucosal advancement flap, which involves elevating the mucosa deep to salivary glands and superficial to the orbicularis oris muscle."
An advantage of treating the lower lip is that there is increased soft tissue laxity and there is no Cupid’s bow, philtrum, or nose, "so it’s nice that there are no dominant central structures," he said. "The downside is that you have to be mindful of the effect of gravity on the repair, so there is a greater need for tone to prevent drooling and incompetence."
He recommends a staged approach based on the extent of the defect and the age of the patient. For small defects (those less than one-third of the lip size) he uses primary closure. Options for medium defects (those that involve one-third to two-thirds of the lip size) include the Estlander flap, the Abbe flap, Bernard Burow’s procedure, the Karapandzic flap, and the stairstep repair, while the options for large defects (those that involve more than two-thirds of the lip size) include Bernard Burow’s procedure, the Karapandzic flap, and the free flap. "You have a lot of tools, depending on what you feel comfortable with," Dr. Keefe said.
Upper Lip
Cancerous tumors of the upper lip are less common, "but there are some unique structures to pay attention to, including the nose, columella, Cupid’s bow, and the philtrum," he said. "In men there’s a hair-bearing skin issue, but scars can be disguised in a mustache."
The aesthetic subunits to keep in mind, he continued, are the medial subunit, which is one-half of the philtrum, and the lateral subunit, which consists of the philtral column, the nostril sill, the alar base, and the nasolabial crease. Primary closure is used for upper lip defects that involve less than one-third of the lip size. "You can make some perialar crescentic skin excisions, which can help advance things," Dr. Keefe said.
For centrally located medium-sized defects of the upper lip, he often uses primary closure with perialar crescentic skin excisions. "If it’s greater than one-half of the lip size, you can add an Abbe flap," he said. "That’s nice because that recreates the philtrum area."
For medially located medium-sized defects of the upper lip, "you can use the Abbe flap if the commissure is not involved and the Estlander flap if the commissure is involved."
Options for cases with large defects and adequate cheek tissue, he said, include the reverse Karapandzic flap, the reverse fan flap, inverted Bernard Burow’s procedure, superiorly based cheek flaps, and the bilateral levator anguli oris flap combined with the Abbe flap. Options for cases with inadequate cheek tissue include the distal pedicle flap and the free flap.
Repair Risks
A lot of these patients have medical problems," he said. "When you do your first injection to resect the tumor or put the lip back together, make sure you don’t cause a myocardial infarction. Generally you should be comfortable with patients who have an INR [International Normalized Ratio] of 2.5 and below."
For patients with large cancerous tumors of the lip, be mindful of lymphatic drainage, because larger tumors have an increased risk of metastases, said Dr. Keefe. For tumors larger than 2 cm in length or 6 mm in spread, or if there is perineural spread, the patient should be referred for radiation therapy.
Dr. Keefe said that he had no relevant financial conflicts to disclose.
AT A MEETING ON SUPERFICIAL ANATOMY AND CUTANEOUS SURGERY
Pretreatment ASPECTS Reading Affects Stroke Outcomes
SAN DIEGO – Interim results from an ongoing study demonstrated that that a higher pretreatment Alberta Stroke Program Early CT Score on computed tomography angiogram images is associated with better outcome following endovascular therapy.
"There is no standard imaging approach for endovascular therapy patient selection," Dr. Donald Frei said at the annual meeting of the Society of Neurointerventional Surgery. "We’re trying to improve time from door to CT imaging and time from imaging to groin puncture, but we also need to be a little bit more sophisticated about patient selection. That’s what we tried to do in this study."

For the analysis, Dr. Frei, director of neurointerventional surgery for Radiology Imaging Associates/Swedish Medical Center in Denver, and his associates at 15 centers evaluated the influence of pretreatment ASPECTS from CTA source image on outcomes following endovascular therapy in the START (Stroke Treatment and Revascularization Therapy) trial, a prospective, single-arm multicenter trial that set out to study the influence of pretreatment core infarct size in 147 patients undergoing endovascular stroke therapy with the Penumbra system.
Imaging methods were at the direction of each investigator and included noncontrast CT, CTA-SI (CTA source images), CT perfusion, or MRI diffuse imaging. The current analysis focused on the preliminary CTA-SI results. ASPECTS was graded in a blinded fashion and analyzed according to a prior classification (0-4, 5-7, or 8-10) and the entire scale. Clinical outcomes were dichotomized as 90-day modified Rankin Scale (mRS) scores of 0-2 (good) vs. 3-6.
Dr. Frei reported interim results from 77 patients who met study criteria. Their mean age was 66 years, 56% were women, and their mean National Institutes of Health Stroke Scale score was 19. The majority of target vessel occlusions were in the middle cerebral artery (75.3%), followed by internal carotid artery (22.1%), and other areas (2.6%). (Dr. Frei noted that results from all 147 patients are expected to be presented at the upcoming International Stroke Conference.)
The median pre-ASPECTS on CTA-SI was 6. Of the 77 patients, 20 (26%) had a score of 0-4, 43 (56%) had a score of 5-7, and 14 (18%) had a score of 8-10.
Dr. Frei, who is also a member of the SNIS Executive Committee, reported that the rate of TIMI (Thrombolysis in Myocardial Infarction) 2-3 revascularization was 85.3%, the median time from groin puncture to aspiration discontinuation was 71.5 minutes, and 48.1% of patients achieved a good 90-day clinical outcome.
The mortality rate was 28.6%, and 32.5% suffered from intracranial hemorrhage. Of these, 20.8% were asymptomatic.
In general, the higher the pretreatment ASPECTS on CTA-SI, the better the outcome. For example, the rate of good outcomes was 20% for those with a pretreatment ASPECTS of 0-4, 56% for 5-7, and 64% for 8-10 (P = .08 for all). After adjusting for age and stroke severity, the researchers determined that a pre-ASPECTS score of 5-10 was an independent predictor of good outcome (odds ratio, 6.8; P = .006).
Univariate analysis demonstrated the following significant predictors of good outcomes: pretreatment ASPECTS greater than 4 (P = .0043), younger age (P = .01), lower pretreatment NIHSS (P = .04), shorter time from groin puncture to discontinuation of aspiration (P = .0004), and revascularization time (P = .0001).
In a prepared statement, Dr. Frei noted that although thousands of men and women suffer a stroke every day, "only a small percentage of those affected are treated with endovascular therapy. This study strongly suggests that a simple ASPECTS reading from a fast, easy-to-obtain CTA source image can guide patient selection for endovascular therapy, particularly those most likely to benefit from the Penumbra System" beyond the 3- to 4.5-hour window.
The START trial was sponsored by Penumbra Inc.
Dr. Frei said that he had no relevant financial disclosures to make.
SAN DIEGO – Interim results from an ongoing study demonstrated that that a higher pretreatment Alberta Stroke Program Early CT Score on computed tomography angiogram images is associated with better outcome following endovascular therapy.
"There is no standard imaging approach for endovascular therapy patient selection," Dr. Donald Frei said at the annual meeting of the Society of Neurointerventional Surgery. "We’re trying to improve time from door to CT imaging and time from imaging to groin puncture, but we also need to be a little bit more sophisticated about patient selection. That’s what we tried to do in this study."
For the analysis, Dr. Frei, director of neurointerventional surgery for Radiology Imaging Associates/Swedish Medical Center in Denver, and his associates at 15 centers evaluated the influence of pretreatment ASPECTS from CTA source image on outcomes following endovascular therapy in the START (Stroke Treatment and Revascularization Therapy) trial, a prospective, single-arm multicenter trial that set out to study the influence of pretreatment core infarct size in 147 patients undergoing endovascular stroke therapy with the Penumbra system.
Imaging methods were at the direction of each investigator and included noncontrast CT, CTA-SI (CTA source images), CT perfusion, or MRI diffuse imaging. The current analysis focused on the preliminary CTA-SI results. ASPECTS was graded in a blinded fashion and analyzed according to a prior classification (0-4, 5-7, or 8-10) and the entire scale. Clinical outcomes were dichotomized as 90-day modified Rankin Scale (mRS) scores of 0-2 (good) vs. 3-6.
Dr. Frei reported interim results from 77 patients who met study criteria. Their mean age was 66 years, 56% were women, and their mean National Institutes of Health Stroke Scale score was 19. The majority of target vessel occlusions were in the middle cerebral artery (75.3%), followed by internal carotid artery (22.1%), and other areas (2.6%). (Dr. Frei noted that results from all 147 patients are expected to be presented at the upcoming International Stroke Conference.)
The median pre-ASPECTS on CTA-SI was 6. Of the 77 patients, 20 (26%) had a score of 0-4, 43 (56%) had a score of 5-7, and 14 (18%) had a score of 8-10.
Dr. Frei, who is also a member of the SNIS Executive Committee, reported that the rate of TIMI (Thrombolysis in Myocardial Infarction) 2-3 revascularization was 85.3%, the median time from groin puncture to aspiration discontinuation was 71.5 minutes, and 48.1% of patients achieved a good 90-day clinical outcome.
The mortality rate was 28.6%, and 32.5% suffered from intracranial hemorrhage. Of these, 20.8% were asymptomatic.
In general, the higher the pretreatment ASPECTS on CTA-SI, the better the outcome. For example, the rate of good outcomes was 20% for those with a pretreatment ASPECTS of 0-4, 56% for 5-7, and 64% for 8-10 (P = .08 for all). After adjusting for age and stroke severity, the researchers determined that a pre-ASPECTS score of 5-10 was an independent predictor of good outcome (odds ratio, 6.8; P = .006).
Univariate analysis demonstrated the following significant predictors of good outcomes: pretreatment ASPECTS greater than 4 (P = .0043), younger age (P = .01), lower pretreatment NIHSS (P = .04), shorter time from groin puncture to discontinuation of aspiration (P = .0004), and revascularization time (P = .0001).
In a prepared statement, Dr. Frei noted that although thousands of men and women suffer a stroke every day, "only a small percentage of those affected are treated with endovascular therapy. This study strongly suggests that a simple ASPECTS reading from a fast, easy-to-obtain CTA source image can guide patient selection for endovascular therapy, particularly those most likely to benefit from the Penumbra System" beyond the 3- to 4.5-hour window.
The START trial was sponsored by Penumbra Inc.
Dr. Frei said that he had no relevant financial disclosures to make.
SAN DIEGO – Interim results from an ongoing study demonstrated that that a higher pretreatment Alberta Stroke Program Early CT Score on computed tomography angiogram images is associated with better outcome following endovascular therapy.
"There is no standard imaging approach for endovascular therapy patient selection," Dr. Donald Frei said at the annual meeting of the Society of Neurointerventional Surgery. "We’re trying to improve time from door to CT imaging and time from imaging to groin puncture, but we also need to be a little bit more sophisticated about patient selection. That’s what we tried to do in this study."
For the analysis, Dr. Frei, director of neurointerventional surgery for Radiology Imaging Associates/Swedish Medical Center in Denver, and his associates at 15 centers evaluated the influence of pretreatment ASPECTS from CTA source image on outcomes following endovascular therapy in the START (Stroke Treatment and Revascularization Therapy) trial, a prospective, single-arm multicenter trial that set out to study the influence of pretreatment core infarct size in 147 patients undergoing endovascular stroke therapy with the Penumbra system.
Imaging methods were at the direction of each investigator and included noncontrast CT, CTA-SI (CTA source images), CT perfusion, or MRI diffuse imaging. The current analysis focused on the preliminary CTA-SI results. ASPECTS was graded in a blinded fashion and analyzed according to a prior classification (0-4, 5-7, or 8-10) and the entire scale. Clinical outcomes were dichotomized as 90-day modified Rankin Scale (mRS) scores of 0-2 (good) vs. 3-6.
Dr. Frei reported interim results from 77 patients who met study criteria. Their mean age was 66 years, 56% were women, and their mean National Institutes of Health Stroke Scale score was 19. The majority of target vessel occlusions were in the middle cerebral artery (75.3%), followed by internal carotid artery (22.1%), and other areas (2.6%). (Dr. Frei noted that results from all 147 patients are expected to be presented at the upcoming International Stroke Conference.)
The median pre-ASPECTS on CTA-SI was 6. Of the 77 patients, 20 (26%) had a score of 0-4, 43 (56%) had a score of 5-7, and 14 (18%) had a score of 8-10.
Dr. Frei, who is also a member of the SNIS Executive Committee, reported that the rate of TIMI (Thrombolysis in Myocardial Infarction) 2-3 revascularization was 85.3%, the median time from groin puncture to aspiration discontinuation was 71.5 minutes, and 48.1% of patients achieved a good 90-day clinical outcome.
The mortality rate was 28.6%, and 32.5% suffered from intracranial hemorrhage. Of these, 20.8% were asymptomatic.
In general, the higher the pretreatment ASPECTS on CTA-SI, the better the outcome. For example, the rate of good outcomes was 20% for those with a pretreatment ASPECTS of 0-4, 56% for 5-7, and 64% for 8-10 (P = .08 for all). After adjusting for age and stroke severity, the researchers determined that a pre-ASPECTS score of 5-10 was an independent predictor of good outcome (odds ratio, 6.8; P = .006).
Univariate analysis demonstrated the following significant predictors of good outcomes: pretreatment ASPECTS greater than 4 (P = .0043), younger age (P = .01), lower pretreatment NIHSS (P = .04), shorter time from groin puncture to discontinuation of aspiration (P = .0004), and revascularization time (P = .0001).
In a prepared statement, Dr. Frei noted that although thousands of men and women suffer a stroke every day, "only a small percentage of those affected are treated with endovascular therapy. This study strongly suggests that a simple ASPECTS reading from a fast, easy-to-obtain CTA source image can guide patient selection for endovascular therapy, particularly those most likely to benefit from the Penumbra System" beyond the 3- to 4.5-hour window.
The START trial was sponsored by Penumbra Inc.
Dr. Frei said that he had no relevant financial disclosures to make.
AT THE ANNUAL MEETING OF THE SOCIETY OF NEUROINTERVENTIONAL SURGERY
Major Finding: After adjustment for age and stroke severity, a pretreatment ASPECTS result of 5-10 was found to be an independent predictor of good stroke outcome after endovascular intervention (OR, 6.8; P = 0.006).
Data Source: This was based on interim results from a multicenter study of 77 patients that evaluated the influence of pretreatment ASPECTS from CTA-SI on outcomes following endovascular therapy in the START trial.
Disclosures: The START trial was sponsored by Penumbra Inc. Dr. Frei said that he had no relevant financial conflicts to disclose.

Understanding Elastic Recoil Key to Aging Skin
DANA POINT, CALIF. – Finding ways to restore elasticity of the skin is a better goal than is developing and refining ways to tighten the skin, according to Dr. R. Rox Anderson.
"The loss of natural skin tension with aging is due to a loss of its elasticity," Dr. Anderson said at the Summit in Aesthetic Medicine sponsored by Skin Disease Education Foundation (SDEF). "It’s the impressive loss of cutaneous elastic recoil with aging that accounts for the effectiveness of Botox, for example. A simple hypothesis is that restoring skin elasticity is a better goal than tightening the skin."

The "players" in cutaneous elastic recoil, he said, are numerous, but it remains unknown which are pivotal. Is it the extracellular matrix content and cross-linking, the fibril microstructure, or the active cytoskeleton?
"When you lose elastic recoil, we don’t know which ones of these are most important," said Dr. Anderson, professor of dermatology at Harvard Medical School, Boston. "If we knew that, we could design treatments that actually treat the cause as opposed to [treating] flabby skin."
He said that "powerful, verified" research tools are needed to improve understanding of cutaneous elastic recoil, including "composite, dynamic structural models" to expand understanding of the difference between microscopic and macroscopic skin. "Those exist; we don’t have to invent them," he said. "I’m an adjunct professor at Massachusetts Institute of Technology, [which has] an entire department that does nothing but material science and modeling. They’re really good at composite materials. That’s what we [humans] are: we are complex composite material."
Stress-strain component analysis is another key tool to improve understanding of elastic recoil. "Each of those components has its own structural and dynamic behavior," said Dr. Anderson, who also directs the Wellman Center for Photomedicine. "I think it’s important to recognize that the skin is a dynamic system that responds to stress. So Langer’s lines are due to particular strain receptors and fibroblasts. The genes that are strain inducible have been at least partially noted, but they have not been studied in the context of skin tightening and rejuvenation. I would love to see that: a dose response analysis for strain-mediated gene expression."
Studies involving in vivo microscopy will also be important. "Elastin, for example, is easy as pie to image in vivo in human skin," he said. "We should be able to map mechanical properties of skin."
Dr. Anderson said that he had no relevant financial conflicts to disclose.
DANA POINT, CALIF. – Finding ways to restore elasticity of the skin is a better goal than is developing and refining ways to tighten the skin, according to Dr. R. Rox Anderson.
"The loss of natural skin tension with aging is due to a loss of its elasticity," Dr. Anderson said at the Summit in Aesthetic Medicine sponsored by Skin Disease Education Foundation (SDEF). "It’s the impressive loss of cutaneous elastic recoil with aging that accounts for the effectiveness of Botox, for example. A simple hypothesis is that restoring skin elasticity is a better goal than tightening the skin."
The "players" in cutaneous elastic recoil, he said, are numerous, but it remains unknown which are pivotal. Is it the extracellular matrix content and cross-linking, the fibril microstructure, or the active cytoskeleton?
"When you lose elastic recoil, we don’t know which ones of these are most important," said Dr. Anderson, professor of dermatology at Harvard Medical School, Boston. "If we knew that, we could design treatments that actually treat the cause as opposed to [treating] flabby skin."
He said that "powerful, verified" research tools are needed to improve understanding of cutaneous elastic recoil, including "composite, dynamic structural models" to expand understanding of the difference between microscopic and macroscopic skin. "Those exist; we don’t have to invent them," he said. "I’m an adjunct professor at Massachusetts Institute of Technology, [which has] an entire department that does nothing but material science and modeling. They’re really good at composite materials. That’s what we [humans] are: we are complex composite material."
Stress-strain component analysis is another key tool to improve understanding of elastic recoil. "Each of those components has its own structural and dynamic behavior," said Dr. Anderson, who also directs the Wellman Center for Photomedicine. "I think it’s important to recognize that the skin is a dynamic system that responds to stress. So Langer’s lines are due to particular strain receptors and fibroblasts. The genes that are strain inducible have been at least partially noted, but they have not been studied in the context of skin tightening and rejuvenation. I would love to see that: a dose response analysis for strain-mediated gene expression."
Studies involving in vivo microscopy will also be important. "Elastin, for example, is easy as pie to image in vivo in human skin," he said. "We should be able to map mechanical properties of skin."
Dr. Anderson said that he had no relevant financial conflicts to disclose.
DANA POINT, CALIF. – Finding ways to restore elasticity of the skin is a better goal than is developing and refining ways to tighten the skin, according to Dr. R. Rox Anderson.
"The loss of natural skin tension with aging is due to a loss of its elasticity," Dr. Anderson said at the Summit in Aesthetic Medicine sponsored by Skin Disease Education Foundation (SDEF). "It’s the impressive loss of cutaneous elastic recoil with aging that accounts for the effectiveness of Botox, for example. A simple hypothesis is that restoring skin elasticity is a better goal than tightening the skin."
The "players" in cutaneous elastic recoil, he said, are numerous, but it remains unknown which are pivotal. Is it the extracellular matrix content and cross-linking, the fibril microstructure, or the active cytoskeleton?
"When you lose elastic recoil, we don’t know which ones of these are most important," said Dr. Anderson, professor of dermatology at Harvard Medical School, Boston. "If we knew that, we could design treatments that actually treat the cause as opposed to [treating] flabby skin."
He said that "powerful, verified" research tools are needed to improve understanding of cutaneous elastic recoil, including "composite, dynamic structural models" to expand understanding of the difference between microscopic and macroscopic skin. "Those exist; we don’t have to invent them," he said. "I’m an adjunct professor at Massachusetts Institute of Technology, [which has] an entire department that does nothing but material science and modeling. They’re really good at composite materials. That’s what we [humans] are: we are complex composite material."
Stress-strain component analysis is another key tool to improve understanding of elastic recoil. "Each of those components has its own structural and dynamic behavior," said Dr. Anderson, who also directs the Wellman Center for Photomedicine. "I think it’s important to recognize that the skin is a dynamic system that responds to stress. So Langer’s lines are due to particular strain receptors and fibroblasts. The genes that are strain inducible have been at least partially noted, but they have not been studied in the context of skin tightening and rejuvenation. I would love to see that: a dose response analysis for strain-mediated gene expression."
Studies involving in vivo microscopy will also be important. "Elastin, for example, is easy as pie to image in vivo in human skin," he said. "We should be able to map mechanical properties of skin."
Dr. Anderson said that he had no relevant financial conflicts to disclose.
EXPERT ANALYSIS AT THE SDEF SUMMIT IN AESTHETIC MEDICINE

Skin Flaps Remedy Defects of the Ear
SAN DIEGO – In the clinical experience of Dr. Michael A. Keefe, 70%-80% of ear defects from auricular cancer treatment can be easily remedied with skin flaps.
The most common locations of auricular cancer are the helix, the posterior auricle skin, and the antihelix, Dr. Keefe said at a meeting on superficial anatomy and cutaneous surgery.

"More than 70% of lesions are smaller than 3 cm in size, and auricular lesions make up an estimated 8% of all skin cancers," said Dr. Keefe, a plastic surgeon with the division of head and neck surgery at Sharp Rees-Stealy Medical Group in San Diego. "The defects are unique, and the underlying cartilage structure makes it all the more interesting."
And challenging – defects may be located on the skin of the ear only, on the lateral side, or on the posterior side, or they may involve a combination of skin and cartilage. Healing by secondary intention is effective for concave defects, but the size of the defect drives the reconstruction options. "If there is no perichondrium, punch holes through cartilage with a 2-3 mm punch to allow granulation tissue to grow through, and then use a skin graft or allow it to heal with secondary intention," he said. "Keep the area moist with antibiotic ointment."
Options for reconstruction of defects in the middle one-third of the ear include primary closure, full-thickness skin grafts (FTSGs), the helical advancement flap, and the retroauricular composite advancement flap, while options for defects in the lower one-third of the ear include primary closure and the preauricular tubed flap. Options for reconstruction of defects in the upper one-third of the ear include primary closure, FTSGs, the helical advancement flap, the retroauricular and preauricular tubed flaps, and constructing an autogenous cartilage framework with FTSGs.
Dr. Keefe said that most small helical rim defects limited to the skin can be closed primarily. "There might be slight rim asymmetry [after closure]," he said at the meeting, which was sponsored by the University of California, San Diego, School of Medicine and the Scripps Clinic. "Some patients might not care [about this], but you have to advise them of that," he added.
A bilobed advancement flap is another option for helical rim defects limited to the skin. This flap "works well for cutaneous defects 2 cm or smaller in the helical rim or the posterior auricle," he said. "The other thing you can do with these bilobed flaps is advance them over the edge to correct helical rim defects."
The banner flap is another effective flap for helical rim defects, especially those located on the superior helix. It does not replace cartilage, but it conceals the incision well. For small composite helix and anterior defects, Dr. Keefe favors the chondrocutaneous advancement flap.
He said that he favors using FTSGs on the anterior surface of the helix for skin defects whenever possible. "You can use a composite skin graft as well, especially to replace cartilage or skin defects that are smaller than 1 cm in size," he said. "A FTSG is easy to harvest and has minimal contraction. Common donor sites include the preauricular, postauricular, supraclavicular, and clavicular regions. Make sure you trim off the fat." For posterior surface defects, the bilobe or advancement flaps work well.
Grafts must be placed on tissue with an adequate blood supply. Effective grafts establish imbibition in the first 24 hours, inosculation within 48-72 hours, and restoration of circulation within 4-7 days.
Dr. Keefe said that he had no relevant financial conflicts to disclose.
SAN DIEGO – In the clinical experience of Dr. Michael A. Keefe, 70%-80% of ear defects from auricular cancer treatment can be easily remedied with skin flaps.
The most common locations of auricular cancer are the helix, the posterior auricle skin, and the antihelix, Dr. Keefe said at a meeting on superficial anatomy and cutaneous surgery.
"More than 70% of lesions are smaller than 3 cm in size, and auricular lesions make up an estimated 8% of all skin cancers," said Dr. Keefe, a plastic surgeon with the division of head and neck surgery at Sharp Rees-Stealy Medical Group in San Diego. "The defects are unique, and the underlying cartilage structure makes it all the more interesting."
And challenging – defects may be located on the skin of the ear only, on the lateral side, or on the posterior side, or they may involve a combination of skin and cartilage. Healing by secondary intention is effective for concave defects, but the size of the defect drives the reconstruction options. "If there is no perichondrium, punch holes through cartilage with a 2-3 mm punch to allow granulation tissue to grow through, and then use a skin graft or allow it to heal with secondary intention," he said. "Keep the area moist with antibiotic ointment."
Options for reconstruction of defects in the middle one-third of the ear include primary closure, full-thickness skin grafts (FTSGs), the helical advancement flap, and the retroauricular composite advancement flap, while options for defects in the lower one-third of the ear include primary closure and the preauricular tubed flap. Options for reconstruction of defects in the upper one-third of the ear include primary closure, FTSGs, the helical advancement flap, the retroauricular and preauricular tubed flaps, and constructing an autogenous cartilage framework with FTSGs.
Dr. Keefe said that most small helical rim defects limited to the skin can be closed primarily. "There might be slight rim asymmetry [after closure]," he said at the meeting, which was sponsored by the University of California, San Diego, School of Medicine and the Scripps Clinic. "Some patients might not care [about this], but you have to advise them of that," he added.
A bilobed advancement flap is another option for helical rim defects limited to the skin. This flap "works well for cutaneous defects 2 cm or smaller in the helical rim or the posterior auricle," he said. "The other thing you can do with these bilobed flaps is advance them over the edge to correct helical rim defects."
The banner flap is another effective flap for helical rim defects, especially those located on the superior helix. It does not replace cartilage, but it conceals the incision well. For small composite helix and anterior defects, Dr. Keefe favors the chondrocutaneous advancement flap.
He said that he favors using FTSGs on the anterior surface of the helix for skin defects whenever possible. "You can use a composite skin graft as well, especially to replace cartilage or skin defects that are smaller than 1 cm in size," he said. "A FTSG is easy to harvest and has minimal contraction. Common donor sites include the preauricular, postauricular, supraclavicular, and clavicular regions. Make sure you trim off the fat." For posterior surface defects, the bilobe or advancement flaps work well.
Grafts must be placed on tissue with an adequate blood supply. Effective grafts establish imbibition in the first 24 hours, inosculation within 48-72 hours, and restoration of circulation within 4-7 days.
Dr. Keefe said that he had no relevant financial conflicts to disclose.
SAN DIEGO – In the clinical experience of Dr. Michael A. Keefe, 70%-80% of ear defects from auricular cancer treatment can be easily remedied with skin flaps.
The most common locations of auricular cancer are the helix, the posterior auricle skin, and the antihelix, Dr. Keefe said at a meeting on superficial anatomy and cutaneous surgery.
"More than 70% of lesions are smaller than 3 cm in size, and auricular lesions make up an estimated 8% of all skin cancers," said Dr. Keefe, a plastic surgeon with the division of head and neck surgery at Sharp Rees-Stealy Medical Group in San Diego. "The defects are unique, and the underlying cartilage structure makes it all the more interesting."
And challenging – defects may be located on the skin of the ear only, on the lateral side, or on the posterior side, or they may involve a combination of skin and cartilage. Healing by secondary intention is effective for concave defects, but the size of the defect drives the reconstruction options. "If there is no perichondrium, punch holes through cartilage with a 2-3 mm punch to allow granulation tissue to grow through, and then use a skin graft or allow it to heal with secondary intention," he said. "Keep the area moist with antibiotic ointment."
Options for reconstruction of defects in the middle one-third of the ear include primary closure, full-thickness skin grafts (FTSGs), the helical advancement flap, and the retroauricular composite advancement flap, while options for defects in the lower one-third of the ear include primary closure and the preauricular tubed flap. Options for reconstruction of defects in the upper one-third of the ear include primary closure, FTSGs, the helical advancement flap, the retroauricular and preauricular tubed flaps, and constructing an autogenous cartilage framework with FTSGs.
Dr. Keefe said that most small helical rim defects limited to the skin can be closed primarily. "There might be slight rim asymmetry [after closure]," he said at the meeting, which was sponsored by the University of California, San Diego, School of Medicine and the Scripps Clinic. "Some patients might not care [about this], but you have to advise them of that," he added.
A bilobed advancement flap is another option for helical rim defects limited to the skin. This flap "works well for cutaneous defects 2 cm or smaller in the helical rim or the posterior auricle," he said. "The other thing you can do with these bilobed flaps is advance them over the edge to correct helical rim defects."
The banner flap is another effective flap for helical rim defects, especially those located on the superior helix. It does not replace cartilage, but it conceals the incision well. For small composite helix and anterior defects, Dr. Keefe favors the chondrocutaneous advancement flap.
He said that he favors using FTSGs on the anterior surface of the helix for skin defects whenever possible. "You can use a composite skin graft as well, especially to replace cartilage or skin defects that are smaller than 1 cm in size," he said. "A FTSG is easy to harvest and has minimal contraction. Common donor sites include the preauricular, postauricular, supraclavicular, and clavicular regions. Make sure you trim off the fat." For posterior surface defects, the bilobe or advancement flaps work well.
Grafts must be placed on tissue with an adequate blood supply. Effective grafts establish imbibition in the first 24 hours, inosculation within 48-72 hours, and restoration of circulation within 4-7 days.
Dr. Keefe said that he had no relevant financial conflicts to disclose.
EXPERT ANALYSIS FROM A MEETING ON SUPERFICIAL ANATOMY AND CUTANEOUS SURGERY

Early Scar Treatment Is 'Critical'
SAN DIEGO – The future of treating hypertrophic and keloidal scars will involve earlier intervention with new and existing technologies – even at the genesis of scar formation, said Dr. E. Victor Ross.
"I think you’re going to see a lot more in the future about scars, not just in the laser area, but also in the biologic arena, because we’re learning more about the way scars behave," Dr. Ross said at a meeting on superficial anatomy and cutaneous surgery. "Some physicians are treating scars as early as the time of Mohs surgery, for example, by applying the PDL [pulsed-dye laser] at the time of suture placement. That’s perhaps a bit extreme, but I think you are going to see newer technologies and drugs used synergistically to give us a better fighting chance to prevent and treat scars."

Dr. Ross of Scripps Clinic Laser and Cosmetic Dermatology Center in Carmel Valley, Calif., said that there is a lack of consensus regarding how the two main types of scars hypertrophic and keloidal – are defined. Historically, "we’ve said that hypertrophic scars don’t go beyond the boundary of where the scar tissue was, and keloidal scars go around the perimeter of where the scar boundaries were," he noted. "If the scar is red, even if it’s longstanding, I tend to call it a hypertrophic scar. If it tends to be more flesh colored, and aged like a fine wine, I tend to call it a keloidal scar. The critical thing with these scars is how long it takes the wound to heal. If an open wound takes more than 3-4 weeks to heal, often it will be hypertrophic."
Existing therapies that are commonly used to treat scars include intralesional steroids, intralesional 5-fluorouracil, oral antihistamines, cyclooxygenase-2 inhibitors, lasers, hydrogel sheeting, and compression. "The critical thing is to treat relatively early; you have to use all the weapons that are available to you," Dr. Ross said at the meeting, which was sponsored by the University of California San Diego School of Medicine and the Scripps Clinic.
He said that when treating scars, a modifiable approach should be taken. "You want to modify the scar. After it’s formed, you want to rehabilitate the scar and make it more like the skin around it."
When using intralesional steroids, Dr. Ross prefers to use very low volumes with a very high concentration of Kenalog, "typically 40 mg/mL in tiny amounts with a 3-gauge, half-inch needle," he said. "You want to keep the needle tip relatively superficial. If the steroid floats into the scar too easily you’re probably too deep or under the scar."
He favors using fractional lasers for scars whenever possible. These devices "create microscopic wounds in the skin," he said. "It turns out that if you fractionate a wound, the reservoirs of normal, undamaged skin act as ‘seeds’ to make the wounds heal quickly. I like to use purpuric settings with the pulsed-dye laser. They tend to give you better results than other settings."
For scars that form after thyroid surgery, Dr. Ross likes to use a PDL or IPL (intense pulsed light) to reduce the redness, followed by a nonablative fractional laser. With that tandem approach "you can almost make the scar go away, which is a complete rehabilitation of the scar," he said.
Innovative scar therapies include topical mitomycin C, which has worked well for postoperative keloids; oral and topical tamoxifen, which helps in the formation of fibroblasts; and oral methotrexate, which has demonstrated efficacy in the treatment and prevention of keloids. Imiquimod has also been used, "but I’m not a believer in it," Dr. Ross said. "We’ve tried it several times and we found that it irritated the skin most of the time. Retinoids are good and bad. They decrease fibroblast activity but also decrease collagenase."
Dr. Ross disclosed that he is a consultant for Cutera, Palomar Medical Technologies, and Lumenis. He has also received research support from Palomar, Sciton, and Syneron Medical.
SAN DIEGO – The future of treating hypertrophic and keloidal scars will involve earlier intervention with new and existing technologies – even at the genesis of scar formation, said Dr. E. Victor Ross.
"I think you’re going to see a lot more in the future about scars, not just in the laser area, but also in the biologic arena, because we’re learning more about the way scars behave," Dr. Ross said at a meeting on superficial anatomy and cutaneous surgery. "Some physicians are treating scars as early as the time of Mohs surgery, for example, by applying the PDL [pulsed-dye laser] at the time of suture placement. That’s perhaps a bit extreme, but I think you are going to see newer technologies and drugs used synergistically to give us a better fighting chance to prevent and treat scars."
Dr. Ross of Scripps Clinic Laser and Cosmetic Dermatology Center in Carmel Valley, Calif., said that there is a lack of consensus regarding how the two main types of scars hypertrophic and keloidal – are defined. Historically, "we’ve said that hypertrophic scars don’t go beyond the boundary of where the scar tissue was, and keloidal scars go around the perimeter of where the scar boundaries were," he noted. "If the scar is red, even if it’s longstanding, I tend to call it a hypertrophic scar. If it tends to be more flesh colored, and aged like a fine wine, I tend to call it a keloidal scar. The critical thing with these scars is how long it takes the wound to heal. If an open wound takes more than 3-4 weeks to heal, often it will be hypertrophic."
Existing therapies that are commonly used to treat scars include intralesional steroids, intralesional 5-fluorouracil, oral antihistamines, cyclooxygenase-2 inhibitors, lasers, hydrogel sheeting, and compression. "The critical thing is to treat relatively early; you have to use all the weapons that are available to you," Dr. Ross said at the meeting, which was sponsored by the University of California San Diego School of Medicine and the Scripps Clinic.
He said that when treating scars, a modifiable approach should be taken. "You want to modify the scar. After it’s formed, you want to rehabilitate the scar and make it more like the skin around it."
When using intralesional steroids, Dr. Ross prefers to use very low volumes with a very high concentration of Kenalog, "typically 40 mg/mL in tiny amounts with a 3-gauge, half-inch needle," he said. "You want to keep the needle tip relatively superficial. If the steroid floats into the scar too easily you’re probably too deep or under the scar."
He favors using fractional lasers for scars whenever possible. These devices "create microscopic wounds in the skin," he said. "It turns out that if you fractionate a wound, the reservoirs of normal, undamaged skin act as ‘seeds’ to make the wounds heal quickly. I like to use purpuric settings with the pulsed-dye laser. They tend to give you better results than other settings."
For scars that form after thyroid surgery, Dr. Ross likes to use a PDL or IPL (intense pulsed light) to reduce the redness, followed by a nonablative fractional laser. With that tandem approach "you can almost make the scar go away, which is a complete rehabilitation of the scar," he said.
Innovative scar therapies include topical mitomycin C, which has worked well for postoperative keloids; oral and topical tamoxifen, which helps in the formation of fibroblasts; and oral methotrexate, which has demonstrated efficacy in the treatment and prevention of keloids. Imiquimod has also been used, "but I’m not a believer in it," Dr. Ross said. "We’ve tried it several times and we found that it irritated the skin most of the time. Retinoids are good and bad. They decrease fibroblast activity but also decrease collagenase."
Dr. Ross disclosed that he is a consultant for Cutera, Palomar Medical Technologies, and Lumenis. He has also received research support from Palomar, Sciton, and Syneron Medical.
SAN DIEGO – The future of treating hypertrophic and keloidal scars will involve earlier intervention with new and existing technologies – even at the genesis of scar formation, said Dr. E. Victor Ross.
"I think you’re going to see a lot more in the future about scars, not just in the laser area, but also in the biologic arena, because we’re learning more about the way scars behave," Dr. Ross said at a meeting on superficial anatomy and cutaneous surgery. "Some physicians are treating scars as early as the time of Mohs surgery, for example, by applying the PDL [pulsed-dye laser] at the time of suture placement. That’s perhaps a bit extreme, but I think you are going to see newer technologies and drugs used synergistically to give us a better fighting chance to prevent and treat scars."
Dr. Ross of Scripps Clinic Laser and Cosmetic Dermatology Center in Carmel Valley, Calif., said that there is a lack of consensus regarding how the two main types of scars hypertrophic and keloidal – are defined. Historically, "we’ve said that hypertrophic scars don’t go beyond the boundary of where the scar tissue was, and keloidal scars go around the perimeter of where the scar boundaries were," he noted. "If the scar is red, even if it’s longstanding, I tend to call it a hypertrophic scar. If it tends to be more flesh colored, and aged like a fine wine, I tend to call it a keloidal scar. The critical thing with these scars is how long it takes the wound to heal. If an open wound takes more than 3-4 weeks to heal, often it will be hypertrophic."
Existing therapies that are commonly used to treat scars include intralesional steroids, intralesional 5-fluorouracil, oral antihistamines, cyclooxygenase-2 inhibitors, lasers, hydrogel sheeting, and compression. "The critical thing is to treat relatively early; you have to use all the weapons that are available to you," Dr. Ross said at the meeting, which was sponsored by the University of California San Diego School of Medicine and the Scripps Clinic.
He said that when treating scars, a modifiable approach should be taken. "You want to modify the scar. After it’s formed, you want to rehabilitate the scar and make it more like the skin around it."
When using intralesional steroids, Dr. Ross prefers to use very low volumes with a very high concentration of Kenalog, "typically 40 mg/mL in tiny amounts with a 3-gauge, half-inch needle," he said. "You want to keep the needle tip relatively superficial. If the steroid floats into the scar too easily you’re probably too deep or under the scar."
He favors using fractional lasers for scars whenever possible. These devices "create microscopic wounds in the skin," he said. "It turns out that if you fractionate a wound, the reservoirs of normal, undamaged skin act as ‘seeds’ to make the wounds heal quickly. I like to use purpuric settings with the pulsed-dye laser. They tend to give you better results than other settings."
For scars that form after thyroid surgery, Dr. Ross likes to use a PDL or IPL (intense pulsed light) to reduce the redness, followed by a nonablative fractional laser. With that tandem approach "you can almost make the scar go away, which is a complete rehabilitation of the scar," he said.
Innovative scar therapies include topical mitomycin C, which has worked well for postoperative keloids; oral and topical tamoxifen, which helps in the formation of fibroblasts; and oral methotrexate, which has demonstrated efficacy in the treatment and prevention of keloids. Imiquimod has also been used, "but I’m not a believer in it," Dr. Ross said. "We’ve tried it several times and we found that it irritated the skin most of the time. Retinoids are good and bad. They decrease fibroblast activity but also decrease collagenase."
Dr. Ross disclosed that he is a consultant for Cutera, Palomar Medical Technologies, and Lumenis. He has also received research support from Palomar, Sciton, and Syneron Medical.
EXPERT ANALYSIS FROM A MEETING ON SUPERFICIAL ANATOMY AND CUTANEOUS SURGERY

Gastric Bypass Tops Banding in Weight Loss
SAN DIEGO – Laparoscopic Roux-en-Y gastric bypass produced long-term weight loss results that were statistically superior to those of laparoscopic adjustable gastric banding, based on 10-years’ follow-up in a prospective randomized study.
Dr. Luigi Angrisani and his colleagues compared 10-year outcomes in 27 patients who underwent the Lap-Band via pars flaccida (group A) vs. those in 24 patients who underwent laparoscopic Roux-en-Y gastric bypass (group B) at San Giovanni Bosco Hospital, Naples, Italy, from January to November 2000.
Patients were included in the study if they had a body mass index (BMI) greater than 35 but less than 50 kg/m2, if they were older than age 19 years but younger than age 50, and if they lacked a hiatal hernia and had no previous abdominal surgery, Dr. Angrisani said at the annual meeting of the American Society for Metabolic and Bariatric Surgery.
At baseline, the mean age of patients was 34 years, their mean BMI was 44, their mean percentage of excess weight was 83%, and their mean weight was 118 kg.
Dr. Angrisani, who directs the general and laparoscopic surgery unit at San Giovanni Bosco Hospital, reported that the mean operative times were 60 minutes for group A and 220 minutes for group B (P greater than.001). There was no mortality, but five patients in group A and three in group B were lost to follow-up. The rate of reoperation was 41% in group A and 29% in group B.
After 10 years, the mean weight of patients in group A and B was 101 kg and 83 kg, respectively, their mean BMI was 37 vs. 30, and their mean loss of excess body weight was 46% vs. 69% (all P less than .05).
Reported compliance with the intake of multivitamins among patients in group B decreased over time. Compliance was 80% at 3 years, 66% at 5 years, 50% at 7 years, and just 33% at 10 years.
"Surgical complications in gastric bypass patients were life threatening, and long-term nutritional consequences remain to be defined, such as low compliance to vitamin supplementation," Dr. Angrisani said.
In his practice, potential candidates for gastric banding include "young and motivated" patients with a BMI of 40 or less; adolescents regardless of BMI; patients with BMI of 35 or less; high-risk patients, and those fearful of more-invasive procedures such as sleeve gastrectomy and Roux-en-Y gastric bypass.
Dr. Angrisani said that he had no relevant financial conflicts to disclose.
SAN DIEGO – Laparoscopic Roux-en-Y gastric bypass produced long-term weight loss results that were statistically superior to those of laparoscopic adjustable gastric banding, based on 10-years’ follow-up in a prospective randomized study.
Dr. Luigi Angrisani and his colleagues compared 10-year outcomes in 27 patients who underwent the Lap-Band via pars flaccida (group A) vs. those in 24 patients who underwent laparoscopic Roux-en-Y gastric bypass (group B) at San Giovanni Bosco Hospital, Naples, Italy, from January to November 2000.
Patients were included in the study if they had a body mass index (BMI) greater than 35 but less than 50 kg/m2, if they were older than age 19 years but younger than age 50, and if they lacked a hiatal hernia and had no previous abdominal surgery, Dr. Angrisani said at the annual meeting of the American Society for Metabolic and Bariatric Surgery.
At baseline, the mean age of patients was 34 years, their mean BMI was 44, their mean percentage of excess weight was 83%, and their mean weight was 118 kg.
Dr. Angrisani, who directs the general and laparoscopic surgery unit at San Giovanni Bosco Hospital, reported that the mean operative times were 60 minutes for group A and 220 minutes for group B (P greater than.001). There was no mortality, but five patients in group A and three in group B were lost to follow-up. The rate of reoperation was 41% in group A and 29% in group B.
After 10 years, the mean weight of patients in group A and B was 101 kg and 83 kg, respectively, their mean BMI was 37 vs. 30, and their mean loss of excess body weight was 46% vs. 69% (all P less than .05).
Reported compliance with the intake of multivitamins among patients in group B decreased over time. Compliance was 80% at 3 years, 66% at 5 years, 50% at 7 years, and just 33% at 10 years.
"Surgical complications in gastric bypass patients were life threatening, and long-term nutritional consequences remain to be defined, such as low compliance to vitamin supplementation," Dr. Angrisani said.
In his practice, potential candidates for gastric banding include "young and motivated" patients with a BMI of 40 or less; adolescents regardless of BMI; patients with BMI of 35 or less; high-risk patients, and those fearful of more-invasive procedures such as sleeve gastrectomy and Roux-en-Y gastric bypass.
Dr. Angrisani said that he had no relevant financial conflicts to disclose.
SAN DIEGO – Laparoscopic Roux-en-Y gastric bypass produced long-term weight loss results that were statistically superior to those of laparoscopic adjustable gastric banding, based on 10-years’ follow-up in a prospective randomized study.
Dr. Luigi Angrisani and his colleagues compared 10-year outcomes in 27 patients who underwent the Lap-Band via pars flaccida (group A) vs. those in 24 patients who underwent laparoscopic Roux-en-Y gastric bypass (group B) at San Giovanni Bosco Hospital, Naples, Italy, from January to November 2000.
Patients were included in the study if they had a body mass index (BMI) greater than 35 but less than 50 kg/m2, if they were older than age 19 years but younger than age 50, and if they lacked a hiatal hernia and had no previous abdominal surgery, Dr. Angrisani said at the annual meeting of the American Society for Metabolic and Bariatric Surgery.
At baseline, the mean age of patients was 34 years, their mean BMI was 44, their mean percentage of excess weight was 83%, and their mean weight was 118 kg.
Dr. Angrisani, who directs the general and laparoscopic surgery unit at San Giovanni Bosco Hospital, reported that the mean operative times were 60 minutes for group A and 220 minutes for group B (P greater than.001). There was no mortality, but five patients in group A and three in group B were lost to follow-up. The rate of reoperation was 41% in group A and 29% in group B.
After 10 years, the mean weight of patients in group A and B was 101 kg and 83 kg, respectively, their mean BMI was 37 vs. 30, and their mean loss of excess body weight was 46% vs. 69% (all P less than .05).
Reported compliance with the intake of multivitamins among patients in group B decreased over time. Compliance was 80% at 3 years, 66% at 5 years, 50% at 7 years, and just 33% at 10 years.
"Surgical complications in gastric bypass patients were life threatening, and long-term nutritional consequences remain to be defined, such as low compliance to vitamin supplementation," Dr. Angrisani said.
In his practice, potential candidates for gastric banding include "young and motivated" patients with a BMI of 40 or less; adolescents regardless of BMI; patients with BMI of 35 or less; high-risk patients, and those fearful of more-invasive procedures such as sleeve gastrectomy and Roux-en-Y gastric bypass.
Dr. Angrisani said that he had no relevant financial conflicts to disclose.
AT THE ANNUAL MEETING OF THE AMERICAN SOCIETY FOR METABOLIC AND BARIATRIC SURGERY
Major Finding: At 10 years of follow-up, the mean weight among patients who underwent gastric banding was 101 kg, compared with 83 kg among those who underwent laparoscopic Roux-en-Y gastric bypass. In addition, their mean BMI was 37 vs. 30, respectively, and their mean loss of excess body weight was 46% vs. 69% (all P less than .05).
Data Source: This was a randomized, single-center study of 51 patients who underwent either procedure from January to November 2000.
Disclosures: Dr. Angrisani said that he had no relevant financial conflicts to disclose.
Reversal of Lap-Band to Sleeve Gastrectomy Feasible
SAN DIEGO – Laparoscopic removal of the Lap-Band and reversal to sleeve gastrectomy is a safe and feasible operation, results from a two-center study showed.
"Since the Lap-Band was introduced in the United States in 2001, it has been a popular minimally invasive procedure for weight loss," Dr. Abdelkader A. Hawasli said at the annual meeting of the American Society for Metabolic and Bariatric Surgery. "However, recent reports have shown that there’s an increased rate of explantation (up to 49%)" because of complications or failure to lose weight. Options are removal, reversion, or reversal to a nonphysiological procedure, "such as Roux-en-Y gastric bypass or biliopancreatic diversion. However, recent reports have been showing that sleeve gastrectomy could be a possible physiologic alternative."
For the current study, Dr. Hawasli, a surgeon at St. John Hospital and Medical Center in Detroit and Beaumont Hospital in Grosse Pointe, Mich., and his associates set out to evaluate the safety of the laparoscopic reversal of the Lap-Band to sleeve gastrectomy, the feasibility of performing simultaneous laparoscopic removal of the Lap-Band and reversal to sleeve gastrectomy, and the results of the sleeve gastrectomy after reversal as the final bariatric procedure in continuing or maintaining weight loss.
Dr. Hawasli reported on 485 patients who had undergone Lap-Band placement at St. John Hospital and Medical Center and 4 who had undergone the procedure at another institution from January 2004 to October 2011.
Of the 489 patients, 34 (7%) had reversal of the Lap-Band to sleeve gastrectomy. Of these, 20 patients (group 1) underwent reversal because of slippage in 15 cases, erosion in 3 cases, and infection in 2 cases, whereas 14 patients (group 2) underwent reversal because they were dissatisfied with their weight loss. The mean time of the reversal to sleeve gastrectomy was more than 3 years from Lap-Band insertion among the slippage subset patients in group 1 and among all patients in group 2 (36.5 vs. 43.3 months, respectively).
The majority of patients (32) underwent simultaneous removal of the band with reversal to sleeve gastrectomy, whereas 2 underwent a staged sleeve gastrectomy.
Dr. Hawasli reported that there were just two complications in group 1: one leak, which occurred because of erosion, and one narrowing. Both cases were treated conservatively. There were no complications in group 2. There were no readmissions in group 1, whereas in group 2 one patient was readmitted for nausea and one for dehydration.
Patients in both groups lost weight after the reversal, but the loss was more pronounced in group 1, compared with group 2 (mean total body mass index loss, –15.8 kg/m2 vs. –10.8, respectively; mean percentage of excess BMI loss, –66.5% vs. –44.6%; all P less than .05).
To explain this difference in weight loss, Dr. Hawasli said that patients in group 1 lost most of their weight before the reversal (mean BMI loss, –11.7) and lost additional weight after the reversal (mean BMI loss, –3.8). However, group 2 patients struggled with weight loss before the reversal (mean BMI loss, –3.6) and they may have continued to struggle after the reversal, even though they lost more weight after the reversal than did group 1 patients (mean BMI loss, –7.2 vs. –3.8, respectively), which is expected.
"Another reason could be the short postreversal follow-up period (a mean of 9 months)," during which they did not get enough time to lose more weight, he explained.
In group 1, the mean operative time was 159 minutes for patients with Lap-Band slippage and 174 minutes for those with erosion or infection. The mean operative time in group 2 was 106 minutes.
Length of stay was about 2 days in both groups, but reached a mean of 3.6 days for the subset of group 1 patients who had reversal because of infection or erosion.
"The short-term results of weight loss after the reversal are better in patients who had the reversal secondary to complications," Dr. Hawasli concluded. "Concomitant removal of the band and reversal to sleeve gastrectomy did not increase the risk of complications except in patients with erosion. Thus, patients with erosion may benefit better from staged reversal."
Dr. Hawasli disclosed that he receives compensation from Covidien as a proctor.
SAN DIEGO – Laparoscopic removal of the Lap-Band and reversal to sleeve gastrectomy is a safe and feasible operation, results from a two-center study showed.
"Since the Lap-Band was introduced in the United States in 2001, it has been a popular minimally invasive procedure for weight loss," Dr. Abdelkader A. Hawasli said at the annual meeting of the American Society for Metabolic and Bariatric Surgery. "However, recent reports have shown that there’s an increased rate of explantation (up to 49%)" because of complications or failure to lose weight. Options are removal, reversion, or reversal to a nonphysiological procedure, "such as Roux-en-Y gastric bypass or biliopancreatic diversion. However, recent reports have been showing that sleeve gastrectomy could be a possible physiologic alternative."
For the current study, Dr. Hawasli, a surgeon at St. John Hospital and Medical Center in Detroit and Beaumont Hospital in Grosse Pointe, Mich., and his associates set out to evaluate the safety of the laparoscopic reversal of the Lap-Band to sleeve gastrectomy, the feasibility of performing simultaneous laparoscopic removal of the Lap-Band and reversal to sleeve gastrectomy, and the results of the sleeve gastrectomy after reversal as the final bariatric procedure in continuing or maintaining weight loss.
Dr. Hawasli reported on 485 patients who had undergone Lap-Band placement at St. John Hospital and Medical Center and 4 who had undergone the procedure at another institution from January 2004 to October 2011.
Of the 489 patients, 34 (7%) had reversal of the Lap-Band to sleeve gastrectomy. Of these, 20 patients (group 1) underwent reversal because of slippage in 15 cases, erosion in 3 cases, and infection in 2 cases, whereas 14 patients (group 2) underwent reversal because they were dissatisfied with their weight loss. The mean time of the reversal to sleeve gastrectomy was more than 3 years from Lap-Band insertion among the slippage subset patients in group 1 and among all patients in group 2 (36.5 vs. 43.3 months, respectively).
The majority of patients (32) underwent simultaneous removal of the band with reversal to sleeve gastrectomy, whereas 2 underwent a staged sleeve gastrectomy.
Dr. Hawasli reported that there were just two complications in group 1: one leak, which occurred because of erosion, and one narrowing. Both cases were treated conservatively. There were no complications in group 2. There were no readmissions in group 1, whereas in group 2 one patient was readmitted for nausea and one for dehydration.
Patients in both groups lost weight after the reversal, but the loss was more pronounced in group 1, compared with group 2 (mean total body mass index loss, –15.8 kg/m2 vs. –10.8, respectively; mean percentage of excess BMI loss, –66.5% vs. –44.6%; all P less than .05).
To explain this difference in weight loss, Dr. Hawasli said that patients in group 1 lost most of their weight before the reversal (mean BMI loss, –11.7) and lost additional weight after the reversal (mean BMI loss, –3.8). However, group 2 patients struggled with weight loss before the reversal (mean BMI loss, –3.6) and they may have continued to struggle after the reversal, even though they lost more weight after the reversal than did group 1 patients (mean BMI loss, –7.2 vs. –3.8, respectively), which is expected.
"Another reason could be the short postreversal follow-up period (a mean of 9 months)," during which they did not get enough time to lose more weight, he explained.
In group 1, the mean operative time was 159 minutes for patients with Lap-Band slippage and 174 minutes for those with erosion or infection. The mean operative time in group 2 was 106 minutes.
Length of stay was about 2 days in both groups, but reached a mean of 3.6 days for the subset of group 1 patients who had reversal because of infection or erosion.
"The short-term results of weight loss after the reversal are better in patients who had the reversal secondary to complications," Dr. Hawasli concluded. "Concomitant removal of the band and reversal to sleeve gastrectomy did not increase the risk of complications except in patients with erosion. Thus, patients with erosion may benefit better from staged reversal."
Dr. Hawasli disclosed that he receives compensation from Covidien as a proctor.
SAN DIEGO – Laparoscopic removal of the Lap-Band and reversal to sleeve gastrectomy is a safe and feasible operation, results from a two-center study showed.
"Since the Lap-Band was introduced in the United States in 2001, it has been a popular minimally invasive procedure for weight loss," Dr. Abdelkader A. Hawasli said at the annual meeting of the American Society for Metabolic and Bariatric Surgery. "However, recent reports have shown that there’s an increased rate of explantation (up to 49%)" because of complications or failure to lose weight. Options are removal, reversion, or reversal to a nonphysiological procedure, "such as Roux-en-Y gastric bypass or biliopancreatic diversion. However, recent reports have been showing that sleeve gastrectomy could be a possible physiologic alternative."
For the current study, Dr. Hawasli, a surgeon at St. John Hospital and Medical Center in Detroit and Beaumont Hospital in Grosse Pointe, Mich., and his associates set out to evaluate the safety of the laparoscopic reversal of the Lap-Band to sleeve gastrectomy, the feasibility of performing simultaneous laparoscopic removal of the Lap-Band and reversal to sleeve gastrectomy, and the results of the sleeve gastrectomy after reversal as the final bariatric procedure in continuing or maintaining weight loss.
Dr. Hawasli reported on 485 patients who had undergone Lap-Band placement at St. John Hospital and Medical Center and 4 who had undergone the procedure at another institution from January 2004 to October 2011.
Of the 489 patients, 34 (7%) had reversal of the Lap-Band to sleeve gastrectomy. Of these, 20 patients (group 1) underwent reversal because of slippage in 15 cases, erosion in 3 cases, and infection in 2 cases, whereas 14 patients (group 2) underwent reversal because they were dissatisfied with their weight loss. The mean time of the reversal to sleeve gastrectomy was more than 3 years from Lap-Band insertion among the slippage subset patients in group 1 and among all patients in group 2 (36.5 vs. 43.3 months, respectively).
The majority of patients (32) underwent simultaneous removal of the band with reversal to sleeve gastrectomy, whereas 2 underwent a staged sleeve gastrectomy.
Dr. Hawasli reported that there were just two complications in group 1: one leak, which occurred because of erosion, and one narrowing. Both cases were treated conservatively. There were no complications in group 2. There were no readmissions in group 1, whereas in group 2 one patient was readmitted for nausea and one for dehydration.
Patients in both groups lost weight after the reversal, but the loss was more pronounced in group 1, compared with group 2 (mean total body mass index loss, –15.8 kg/m2 vs. –10.8, respectively; mean percentage of excess BMI loss, –66.5% vs. –44.6%; all P less than .05).
To explain this difference in weight loss, Dr. Hawasli said that patients in group 1 lost most of their weight before the reversal (mean BMI loss, –11.7) and lost additional weight after the reversal (mean BMI loss, –3.8). However, group 2 patients struggled with weight loss before the reversal (mean BMI loss, –3.6) and they may have continued to struggle after the reversal, even though they lost more weight after the reversal than did group 1 patients (mean BMI loss, –7.2 vs. –3.8, respectively), which is expected.
"Another reason could be the short postreversal follow-up period (a mean of 9 months)," during which they did not get enough time to lose more weight, he explained.
In group 1, the mean operative time was 159 minutes for patients with Lap-Band slippage and 174 minutes for those with erosion or infection. The mean operative time in group 2 was 106 minutes.
Length of stay was about 2 days in both groups, but reached a mean of 3.6 days for the subset of group 1 patients who had reversal because of infection or erosion.
"The short-term results of weight loss after the reversal are better in patients who had the reversal secondary to complications," Dr. Hawasli concluded. "Concomitant removal of the band and reversal to sleeve gastrectomy did not increase the risk of complications except in patients with erosion. Thus, patients with erosion may benefit better from staged reversal."
Dr. Hawasli disclosed that he receives compensation from Covidien as a proctor.
AT THE ANNUAL MEETING OF THE AMERICAN SOCIETY FOR METABOLIC AND BARIATRIC SURGERY
Major Finding: Weight loss was more pronounced among patients who underwent reversal of Lap-Band to sleeve gastrectomy because of band slippage, erosion, or infection than because of dissatisfaction with weight loss (mean total BMI loss, –15.8 vs. –10.8, respectively; mean percentage of excess BMI loss, –66.5% vs. –44.6%; all P less than .05).
Data Source: The study consisted of 34 patients who underwent reversal of Lap-Band to sleeve gastrectomy at two centers from January 2004 to October 2011.
Disclosures: Dr. Hawasli disclosed that he receives compensation from Covidien as a proctor.
Bariatric Surgery Most Common Elective Surgical Procedure
SAN DIEGO – Within the setting of academic medical centers, bariatric surgery is the most common elective general surgical operation and it has the highest use of laparoscopy.
In addition, the in-hospital mortality rate of laparoscopic bariatric surgery is now comparable to those of laparoscopic appendectomy and antireflux surgery, and is currently lower than that of laparoscopic cholecystectomy.
Those are main findings from an analysis of data from the University HealthSystem Consortium database, which contains data from 114 academic centers and 250 major teaching affiliates in the United States.
"Laparoscopy has revolutionized the performance of most intra-abdominal operations [and] is now widely utilized in many different types of general surgical operations," Brian Nguyen, a research student at the University of California, Irvine, said at the annual meeting of the American Society for Metabolic and Bariatric Surgery.
He and his associates searched the University HealthSystem database to determine the rate of laparoscopy use in seven common elective general surgical operations performed between Oct. 1, 2008, and March 31, 2012: antireflux surgery for gastroesophageal reflux disease (GERD) or hiatal hernia, cholecystectomy for chronic cholecystitis, bariatric surgery for morbid obesity, ventral hernia repair for incisional hernia, appendectomy for acute appendicitis, rectal resection for rectal cancer, and colectomy for colon cancer or diverticulitis. Secondary objectives were to determine the rate of conversion to open surgery, length of stay, overall complications, and in-hospital mortality.
The most common elective surgical procedure performed during the study period was bariatric surgery (53,958 cases), followed by colectomy (29,934 cases), ventral hernia repair (17,749 cases), antireflux surgery (13,918 cases), appendectomy (8,654 cases), cholecystectomy (8,512 cases), and rectal resection (4,729). Bariatric surgery also led the way with the highest rate of laparoscopy use (94%), followed by antireflux surgery (83%), appendectomy (79%), cholecystectomy (77%), colectomy (52%), ventral hernia repair (28%), and rectal resection (18%).
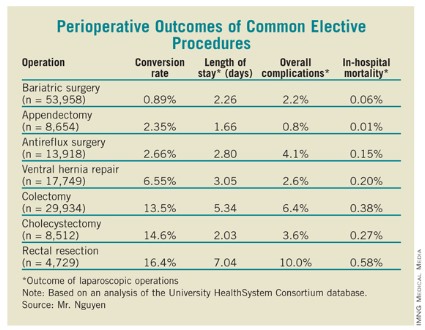
As for perioperative outcomes (see table), Mr. Nguyen reported that patients who underwent bariatric surgery had the lowest conversion rate to open procedures (0.89%). The overall complication rate of 2.2% and the in-hospital mortality rate of 0.06% associated with bariatric surgery were lower only in appendectomy, which had rates of 0.8% and 0.01%, respectively. The mean length of stay for bariatric surgery patients was 2.26 days, which was higher than that for appendectomy and cholecystectomy patients (a mean of 1.66 and 2.03 days, respectively), but lower than that for antireflux surgery (a mean of 2.80 days).
Mr. Nguyen acknowledged that the study was limited by the fact that it represented only inpatients at academic medical centers and affiliated hospitals.
He said that he had no relevant financial conflicts to disclose.
SAN DIEGO – Within the setting of academic medical centers, bariatric surgery is the most common elective general surgical operation and it has the highest use of laparoscopy.
In addition, the in-hospital mortality rate of laparoscopic bariatric surgery is now comparable to those of laparoscopic appendectomy and antireflux surgery, and is currently lower than that of laparoscopic cholecystectomy.
Those are main findings from an analysis of data from the University HealthSystem Consortium database, which contains data from 114 academic centers and 250 major teaching affiliates in the United States.
"Laparoscopy has revolutionized the performance of most intra-abdominal operations [and] is now widely utilized in many different types of general surgical operations," Brian Nguyen, a research student at the University of California, Irvine, said at the annual meeting of the American Society for Metabolic and Bariatric Surgery.
He and his associates searched the University HealthSystem database to determine the rate of laparoscopy use in seven common elective general surgical operations performed between Oct. 1, 2008, and March 31, 2012: antireflux surgery for gastroesophageal reflux disease (GERD) or hiatal hernia, cholecystectomy for chronic cholecystitis, bariatric surgery for morbid obesity, ventral hernia repair for incisional hernia, appendectomy for acute appendicitis, rectal resection for rectal cancer, and colectomy for colon cancer or diverticulitis. Secondary objectives were to determine the rate of conversion to open surgery, length of stay, overall complications, and in-hospital mortality.
The most common elective surgical procedure performed during the study period was bariatric surgery (53,958 cases), followed by colectomy (29,934 cases), ventral hernia repair (17,749 cases), antireflux surgery (13,918 cases), appendectomy (8,654 cases), cholecystectomy (8,512 cases), and rectal resection (4,729). Bariatric surgery also led the way with the highest rate of laparoscopy use (94%), followed by antireflux surgery (83%), appendectomy (79%), cholecystectomy (77%), colectomy (52%), ventral hernia repair (28%), and rectal resection (18%).
As for perioperative outcomes (see table), Mr. Nguyen reported that patients who underwent bariatric surgery had the lowest conversion rate to open procedures (0.89%). The overall complication rate of 2.2% and the in-hospital mortality rate of 0.06% associated with bariatric surgery were lower only in appendectomy, which had rates of 0.8% and 0.01%, respectively. The mean length of stay for bariatric surgery patients was 2.26 days, which was higher than that for appendectomy and cholecystectomy patients (a mean of 1.66 and 2.03 days, respectively), but lower than that for antireflux surgery (a mean of 2.80 days).
Mr. Nguyen acknowledged that the study was limited by the fact that it represented only inpatients at academic medical centers and affiliated hospitals.
He said that he had no relevant financial conflicts to disclose.
SAN DIEGO – Within the setting of academic medical centers, bariatric surgery is the most common elective general surgical operation and it has the highest use of laparoscopy.
In addition, the in-hospital mortality rate of laparoscopic bariatric surgery is now comparable to those of laparoscopic appendectomy and antireflux surgery, and is currently lower than that of laparoscopic cholecystectomy.
Those are main findings from an analysis of data from the University HealthSystem Consortium database, which contains data from 114 academic centers and 250 major teaching affiliates in the United States.
"Laparoscopy has revolutionized the performance of most intra-abdominal operations [and] is now widely utilized in many different types of general surgical operations," Brian Nguyen, a research student at the University of California, Irvine, said at the annual meeting of the American Society for Metabolic and Bariatric Surgery.
He and his associates searched the University HealthSystem database to determine the rate of laparoscopy use in seven common elective general surgical operations performed between Oct. 1, 2008, and March 31, 2012: antireflux surgery for gastroesophageal reflux disease (GERD) or hiatal hernia, cholecystectomy for chronic cholecystitis, bariatric surgery for morbid obesity, ventral hernia repair for incisional hernia, appendectomy for acute appendicitis, rectal resection for rectal cancer, and colectomy for colon cancer or diverticulitis. Secondary objectives were to determine the rate of conversion to open surgery, length of stay, overall complications, and in-hospital mortality.
The most common elective surgical procedure performed during the study period was bariatric surgery (53,958 cases), followed by colectomy (29,934 cases), ventral hernia repair (17,749 cases), antireflux surgery (13,918 cases), appendectomy (8,654 cases), cholecystectomy (8,512 cases), and rectal resection (4,729). Bariatric surgery also led the way with the highest rate of laparoscopy use (94%), followed by antireflux surgery (83%), appendectomy (79%), cholecystectomy (77%), colectomy (52%), ventral hernia repair (28%), and rectal resection (18%).
As for perioperative outcomes (see table), Mr. Nguyen reported that patients who underwent bariatric surgery had the lowest conversion rate to open procedures (0.89%). The overall complication rate of 2.2% and the in-hospital mortality rate of 0.06% associated with bariatric surgery were lower only in appendectomy, which had rates of 0.8% and 0.01%, respectively. The mean length of stay for bariatric surgery patients was 2.26 days, which was higher than that for appendectomy and cholecystectomy patients (a mean of 1.66 and 2.03 days, respectively), but lower than that for antireflux surgery (a mean of 2.80 days).
Mr. Nguyen acknowledged that the study was limited by the fact that it represented only inpatients at academic medical centers and affiliated hospitals.
He said that he had no relevant financial conflicts to disclose.
AT THE ANNUAL MEETING OF THE AMERICAN SOCIETY FOR METABOLIC AND BARIATRIC SURGERY
Major Finding: Between Oct. 1, 2008, and March 31, 2012, bariatric surgery ranked as the most common elective surgical procedure performed (53,958 cases), and led the way with use of laparoscopy (94% of cases).
Data Source: This study of seven common surgical elective procedures was based on a search of the University HealthSystem Consortium database, which is limited to 114 academic centers and 250 major teaching affiliates in the United States.
Disclosures: Mr. Nguyen said that he had no relevant financial conflicts to disclose.
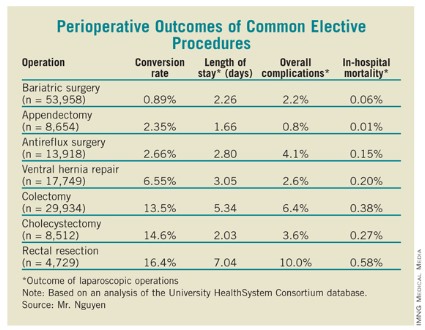
BMI Drives Body Contouring Results
DANA POINT, CALIF. – Three factors affect the results of body contouring outcomes after bariatric surgery: body mass index at presentation, fat deposition pattern, and quality of the skin-fat envelope, according to Dr. Al S. Aly.
"The fat deposition pattern is genetically controlled; we cannot alter that," Dr. Aly, professor and vice-chair of plastic surgery at the University of California, Irvine, said at the Summit in Aesthetic Medicine sponsored by Skin Disease Education Foundation (SDEF). "The quality of the skin-fat envelope is very important. If you have a very loose skin-fat envelope – meaning that they’ve had a tremendous drop in weight – you can do a lot more for them than with other patients."

The two main body contouring treatments for the lower trunk are abdominoplasty and circumferential belt lipectomy, said Dr. Aly. "Abdominoplasties are ideally suited for problems limited to the belly, or those located between the two anterior superior iliac spines. For larger patients you need to do something else."
The rehabilitation of larger patients involves a circumferential procedure commonly referred to as a body lift or belt lipectomy, which involves removing a circumferential wedge of tissue from around the trunk. "There are many reasons why we need circumferential excisions for these large patients, but the main one is that you need circumferential improvement above and below the area of resection as opposed to a regular tummy tuck," he explained.
Markings for the belt lipectomy "are the essence of the procedure," Dr. Aly said, who noted that about 10% of his patients are male. "The markings are adjustable guidelines, and they vary according to anatomy and desires. It’s a fairly complex set of issues but essentially you have to understand how tissues drape as the patient loses weight, and there are zones of adherence or areas of the body where the skin and the soft tissue envelope is stuck to the underlying musculoskeletal anatomy. It’s important to understand those before you can mark these patients. Surgical improvement is related to the amount of tension that you create above and below an area of excision."
Dr. Aly said that he routinely performs belt lipectomies with another surgeon and strives for surgical times under 6 hours. He uses a general anesthetic and an epidural for postoperative pain management. Moving patients into multiple positions during surgery is required, "otherwise you can’t accomplish the excisions," he said. "There is a variety of different approaches. Mine happens to be one of supine first then lateral/lateral."
Results of body contouring procedures generally correlate with the patient’s body mass index (BMI) at the time of surgery. "So people who present to us above a BMI of 35 kg/m2 ... their results are okay," he said. "Results are better for patients with a BMI of 30-35 kg/m2. If you’re lucky enough to get a patient at an ideal BMI – 26 kg/m2 and lower – then you can create almost normal anatomy."
He noted that, compared with abdominoplasties, results of belt lipectomies take longer than most procedures to mature. "However, their results are also far superior to those attainable with a tummy tuck," Dr. Aly said. Complications, including an increased risk for seroma and formation of hematoma, "correlate with BMI," he said. "If you’re not ready to deal with complications, massive weight loss patients are a tough group to deal with. It’s part of the nature of these patients."
Other areas that often need contouring include upper arm reductions, upper back roll reductions, reconstruction of the breasts (in women and men), and thigh reductions.
Dr. Aly said that he had no relevant conflicts to disclose. SDEF and this news organization are owned by Elsevier.
DANA POINT, CALIF. – Three factors affect the results of body contouring outcomes after bariatric surgery: body mass index at presentation, fat deposition pattern, and quality of the skin-fat envelope, according to Dr. Al S. Aly.
"The fat deposition pattern is genetically controlled; we cannot alter that," Dr. Aly, professor and vice-chair of plastic surgery at the University of California, Irvine, said at the Summit in Aesthetic Medicine sponsored by Skin Disease Education Foundation (SDEF). "The quality of the skin-fat envelope is very important. If you have a very loose skin-fat envelope – meaning that they’ve had a tremendous drop in weight – you can do a lot more for them than with other patients."
The two main body contouring treatments for the lower trunk are abdominoplasty and circumferential belt lipectomy, said Dr. Aly. "Abdominoplasties are ideally suited for problems limited to the belly, or those located between the two anterior superior iliac spines. For larger patients you need to do something else."
The rehabilitation of larger patients involves a circumferential procedure commonly referred to as a body lift or belt lipectomy, which involves removing a circumferential wedge of tissue from around the trunk. "There are many reasons why we need circumferential excisions for these large patients, but the main one is that you need circumferential improvement above and below the area of resection as opposed to a regular tummy tuck," he explained.
Markings for the belt lipectomy "are the essence of the procedure," Dr. Aly said, who noted that about 10% of his patients are male. "The markings are adjustable guidelines, and they vary according to anatomy and desires. It’s a fairly complex set of issues but essentially you have to understand how tissues drape as the patient loses weight, and there are zones of adherence or areas of the body where the skin and the soft tissue envelope is stuck to the underlying musculoskeletal anatomy. It’s important to understand those before you can mark these patients. Surgical improvement is related to the amount of tension that you create above and below an area of excision."
Dr. Aly said that he routinely performs belt lipectomies with another surgeon and strives for surgical times under 6 hours. He uses a general anesthetic and an epidural for postoperative pain management. Moving patients into multiple positions during surgery is required, "otherwise you can’t accomplish the excisions," he said. "There is a variety of different approaches. Mine happens to be one of supine first then lateral/lateral."
Results of body contouring procedures generally correlate with the patient’s body mass index (BMI) at the time of surgery. "So people who present to us above a BMI of 35 kg/m2 ... their results are okay," he said. "Results are better for patients with a BMI of 30-35 kg/m2. If you’re lucky enough to get a patient at an ideal BMI – 26 kg/m2 and lower – then you can create almost normal anatomy."
He noted that, compared with abdominoplasties, results of belt lipectomies take longer than most procedures to mature. "However, their results are also far superior to those attainable with a tummy tuck," Dr. Aly said. Complications, including an increased risk for seroma and formation of hematoma, "correlate with BMI," he said. "If you’re not ready to deal with complications, massive weight loss patients are a tough group to deal with. It’s part of the nature of these patients."
Other areas that often need contouring include upper arm reductions, upper back roll reductions, reconstruction of the breasts (in women and men), and thigh reductions.
Dr. Aly said that he had no relevant conflicts to disclose. SDEF and this news organization are owned by Elsevier.
DANA POINT, CALIF. – Three factors affect the results of body contouring outcomes after bariatric surgery: body mass index at presentation, fat deposition pattern, and quality of the skin-fat envelope, according to Dr. Al S. Aly.
"The fat deposition pattern is genetically controlled; we cannot alter that," Dr. Aly, professor and vice-chair of plastic surgery at the University of California, Irvine, said at the Summit in Aesthetic Medicine sponsored by Skin Disease Education Foundation (SDEF). "The quality of the skin-fat envelope is very important. If you have a very loose skin-fat envelope – meaning that they’ve had a tremendous drop in weight – you can do a lot more for them than with other patients."
The two main body contouring treatments for the lower trunk are abdominoplasty and circumferential belt lipectomy, said Dr. Aly. "Abdominoplasties are ideally suited for problems limited to the belly, or those located between the two anterior superior iliac spines. For larger patients you need to do something else."
The rehabilitation of larger patients involves a circumferential procedure commonly referred to as a body lift or belt lipectomy, which involves removing a circumferential wedge of tissue from around the trunk. "There are many reasons why we need circumferential excisions for these large patients, but the main one is that you need circumferential improvement above and below the area of resection as opposed to a regular tummy tuck," he explained.
Markings for the belt lipectomy "are the essence of the procedure," Dr. Aly said, who noted that about 10% of his patients are male. "The markings are adjustable guidelines, and they vary according to anatomy and desires. It’s a fairly complex set of issues but essentially you have to understand how tissues drape as the patient loses weight, and there are zones of adherence or areas of the body where the skin and the soft tissue envelope is stuck to the underlying musculoskeletal anatomy. It’s important to understand those before you can mark these patients. Surgical improvement is related to the amount of tension that you create above and below an area of excision."
Dr. Aly said that he routinely performs belt lipectomies with another surgeon and strives for surgical times under 6 hours. He uses a general anesthetic and an epidural for postoperative pain management. Moving patients into multiple positions during surgery is required, "otherwise you can’t accomplish the excisions," he said. "There is a variety of different approaches. Mine happens to be one of supine first then lateral/lateral."
Results of body contouring procedures generally correlate with the patient’s body mass index (BMI) at the time of surgery. "So people who present to us above a BMI of 35 kg/m2 ... their results are okay," he said. "Results are better for patients with a BMI of 30-35 kg/m2. If you’re lucky enough to get a patient at an ideal BMI – 26 kg/m2 and lower – then you can create almost normal anatomy."
He noted that, compared with abdominoplasties, results of belt lipectomies take longer than most procedures to mature. "However, their results are also far superior to those attainable with a tummy tuck," Dr. Aly said. Complications, including an increased risk for seroma and formation of hematoma, "correlate with BMI," he said. "If you’re not ready to deal with complications, massive weight loss patients are a tough group to deal with. It’s part of the nature of these patients."
Other areas that often need contouring include upper arm reductions, upper back roll reductions, reconstruction of the breasts (in women and men), and thigh reductions.
Dr. Aly said that he had no relevant conflicts to disclose. SDEF and this news organization are owned by Elsevier.
AT THE SDEF SUMMIT IN AESTHETIC MEDICINE
Sleeve Gastrectomy Feasible in Obese Transplant Candidates
SAN DIEGO – Laparoscopic sleeve gastrectomy is safe and effective in obese candidates for organ transplantation, results from a novel pilot study demonstrated.
Nationwide, 15%-20% of patients on the transplant waiting list are morbidly obese, with a body mass index of greater than 35 kg/m2, "but many cannot be transplanted unless they lose weight," said Dr. Matthew Y. Lin of the surgery department at the University of California, San Francisco (UCSF). "Morbid obesity can contribute to end-stage kidney or liver failure. For example, obesity-related nonalcoholic steatohepatitis is now the third most common indication for liver transplant in the United States and will likely become first in the future."

In what Dr. Lin said is the only reported case series of bariatric surgery in obese transplant candidates, he and his associates conducted a pilot study of 26 morbidly obese patients with liver or kidney failure who underwent laparoscopic sleeve gastrectomy at UCSF from 2006 to 2012. They chose sleeve gastrectomy over gastric banding "to avoid foreign body implantation, in anticipation of post-transplant immunosuppression," Dr. Lin explained at the annual meeting of the American Society for Metabolic and Bariatric Surgery.
"We chose sleeve gastrectomy over gastric bypass to maintain endoscopic access to the biliary system, to reduce surgical complexity, and to avoid unpredictable immunosuppression absorption," he said.
Morbid obesity is a relative contraindication for solid organ transplantation at most centers because of poor post-transplant outcomes, according to Dr. Lin. "At UCSF, the selection criteria are a BMI of less than 40 for liver transplant, less than 38 for kidney transplant, and less than 34 for kidney transplant in patients with diabetes." The researchers hypothesized that laparoscopic sleeve gastrectomy could be safely performed in high-risk patients with liver or kidney failure and achieve enough weight loss to allow for transplantation.
The 26 patients had a mean age of 57 years, 17 were women, 20 were white, and their average preoperative BMI was 48. Twenty patients had liver insufficiency with a mean Model for End-Stage Liver Disease (MELD) score of 11, and 6 had kidney insufficiency with a mean glomerular filtration rate of 10 mL/min. Five of these patients were on hemodialysis.
All 26 patients had laparoscopic sleeve gastrectomy performed by the same surgeon. The mean operative time was 151 minutes, and the mean length of stay was 4.2 days. Complications that occurred within 30 days were two cases of superficial wound infection and one case each of worsened hepatic encephalopathy, acute renal insufficiency, need for blood transfusion, and staple line leak. There was no mortality within 30 days, but after that period two patients died awaiting transplant and one patient died from complications of the staple line leak and progressive liver failure 4 years after surgery.
After 2 years, the average BMI of study participants dropped from a mean of 48 to a mean of 29. "Between the 6- and 12-month marks, most patients were able to achieve a BMI that would make them acceptable for transplant," Dr. Lin said.
At 1, 3, 12, and 24 months, the percent of excess body weight lost was 17%, 26%, 50%, and 66%, respectively. "The weight-loss profile is similar to [those of] the general bariatric sleeve gastrectomy population," he noted.
Of the 13 patients who had diabetes preoperatively, 7 had complete resolution after the procedure and 1 had partial resolution. Mean postoperative albumin levels for all 26 patients after sleeve gastrectomy were 3.1 g/dL at 6 months and 3.3 g/dL at 12 months.
Eight patients went on to receive their organ transplant, Dr. Lin said. Their mean age was 56 years, and six were women. They waited a mean of 17 months for their procedures, which included six liver transplants, one liver and kidney transplant, and one kidney transplant. Their mean BMI before sleeve gastrectomy was 46, and their mean BMI prior to transplantation was 31. Immediately before transplant, their mean albumin level was 3.2 g/dL, and the most current measurement remained the same. "No increased acute rejection or difficulty maintaining immunosuppression was observed," he said.
Dr. Lin acknowledged certain limitations of the study, including its single-center design, lack of a control population, and the fact that "there is very little statistical power to estimate the true complication rate in this high-risk surgical group. Furthermore, we only have short-term follow-up."
Dr. Lin said that he had no relevant financial conflicts to disclose.
SAN DIEGO – Laparoscopic sleeve gastrectomy is safe and effective in obese candidates for organ transplantation, results from a novel pilot study demonstrated.
Nationwide, 15%-20% of patients on the transplant waiting list are morbidly obese, with a body mass index of greater than 35 kg/m2, "but many cannot be transplanted unless they lose weight," said Dr. Matthew Y. Lin of the surgery department at the University of California, San Francisco (UCSF). "Morbid obesity can contribute to end-stage kidney or liver failure. For example, obesity-related nonalcoholic steatohepatitis is now the third most common indication for liver transplant in the United States and will likely become first in the future."
In what Dr. Lin said is the only reported case series of bariatric surgery in obese transplant candidates, he and his associates conducted a pilot study of 26 morbidly obese patients with liver or kidney failure who underwent laparoscopic sleeve gastrectomy at UCSF from 2006 to 2012. They chose sleeve gastrectomy over gastric banding "to avoid foreign body implantation, in anticipation of post-transplant immunosuppression," Dr. Lin explained at the annual meeting of the American Society for Metabolic and Bariatric Surgery.
"We chose sleeve gastrectomy over gastric bypass to maintain endoscopic access to the biliary system, to reduce surgical complexity, and to avoid unpredictable immunosuppression absorption," he said.
Morbid obesity is a relative contraindication for solid organ transplantation at most centers because of poor post-transplant outcomes, according to Dr. Lin. "At UCSF, the selection criteria are a BMI of less than 40 for liver transplant, less than 38 for kidney transplant, and less than 34 for kidney transplant in patients with diabetes." The researchers hypothesized that laparoscopic sleeve gastrectomy could be safely performed in high-risk patients with liver or kidney failure and achieve enough weight loss to allow for transplantation.
The 26 patients had a mean age of 57 years, 17 were women, 20 were white, and their average preoperative BMI was 48. Twenty patients had liver insufficiency with a mean Model for End-Stage Liver Disease (MELD) score of 11, and 6 had kidney insufficiency with a mean glomerular filtration rate of 10 mL/min. Five of these patients were on hemodialysis.
All 26 patients had laparoscopic sleeve gastrectomy performed by the same surgeon. The mean operative time was 151 minutes, and the mean length of stay was 4.2 days. Complications that occurred within 30 days were two cases of superficial wound infection and one case each of worsened hepatic encephalopathy, acute renal insufficiency, need for blood transfusion, and staple line leak. There was no mortality within 30 days, but after that period two patients died awaiting transplant and one patient died from complications of the staple line leak and progressive liver failure 4 years after surgery.
After 2 years, the average BMI of study participants dropped from a mean of 48 to a mean of 29. "Between the 6- and 12-month marks, most patients were able to achieve a BMI that would make them acceptable for transplant," Dr. Lin said.
At 1, 3, 12, and 24 months, the percent of excess body weight lost was 17%, 26%, 50%, and 66%, respectively. "The weight-loss profile is similar to [those of] the general bariatric sleeve gastrectomy population," he noted.
Of the 13 patients who had diabetes preoperatively, 7 had complete resolution after the procedure and 1 had partial resolution. Mean postoperative albumin levels for all 26 patients after sleeve gastrectomy were 3.1 g/dL at 6 months and 3.3 g/dL at 12 months.
Eight patients went on to receive their organ transplant, Dr. Lin said. Their mean age was 56 years, and six were women. They waited a mean of 17 months for their procedures, which included six liver transplants, one liver and kidney transplant, and one kidney transplant. Their mean BMI before sleeve gastrectomy was 46, and their mean BMI prior to transplantation was 31. Immediately before transplant, their mean albumin level was 3.2 g/dL, and the most current measurement remained the same. "No increased acute rejection or difficulty maintaining immunosuppression was observed," he said.
Dr. Lin acknowledged certain limitations of the study, including its single-center design, lack of a control population, and the fact that "there is very little statistical power to estimate the true complication rate in this high-risk surgical group. Furthermore, we only have short-term follow-up."
Dr. Lin said that he had no relevant financial conflicts to disclose.
SAN DIEGO – Laparoscopic sleeve gastrectomy is safe and effective in obese candidates for organ transplantation, results from a novel pilot study demonstrated.
Nationwide, 15%-20% of patients on the transplant waiting list are morbidly obese, with a body mass index of greater than 35 kg/m2, "but many cannot be transplanted unless they lose weight," said Dr. Matthew Y. Lin of the surgery department at the University of California, San Francisco (UCSF). "Morbid obesity can contribute to end-stage kidney or liver failure. For example, obesity-related nonalcoholic steatohepatitis is now the third most common indication for liver transplant in the United States and will likely become first in the future."
In what Dr. Lin said is the only reported case series of bariatric surgery in obese transplant candidates, he and his associates conducted a pilot study of 26 morbidly obese patients with liver or kidney failure who underwent laparoscopic sleeve gastrectomy at UCSF from 2006 to 2012. They chose sleeve gastrectomy over gastric banding "to avoid foreign body implantation, in anticipation of post-transplant immunosuppression," Dr. Lin explained at the annual meeting of the American Society for Metabolic and Bariatric Surgery.
"We chose sleeve gastrectomy over gastric bypass to maintain endoscopic access to the biliary system, to reduce surgical complexity, and to avoid unpredictable immunosuppression absorption," he said.
Morbid obesity is a relative contraindication for solid organ transplantation at most centers because of poor post-transplant outcomes, according to Dr. Lin. "At UCSF, the selection criteria are a BMI of less than 40 for liver transplant, less than 38 for kidney transplant, and less than 34 for kidney transplant in patients with diabetes." The researchers hypothesized that laparoscopic sleeve gastrectomy could be safely performed in high-risk patients with liver or kidney failure and achieve enough weight loss to allow for transplantation.
The 26 patients had a mean age of 57 years, 17 were women, 20 were white, and their average preoperative BMI was 48. Twenty patients had liver insufficiency with a mean Model for End-Stage Liver Disease (MELD) score of 11, and 6 had kidney insufficiency with a mean glomerular filtration rate of 10 mL/min. Five of these patients were on hemodialysis.
All 26 patients had laparoscopic sleeve gastrectomy performed by the same surgeon. The mean operative time was 151 minutes, and the mean length of stay was 4.2 days. Complications that occurred within 30 days were two cases of superficial wound infection and one case each of worsened hepatic encephalopathy, acute renal insufficiency, need for blood transfusion, and staple line leak. There was no mortality within 30 days, but after that period two patients died awaiting transplant and one patient died from complications of the staple line leak and progressive liver failure 4 years after surgery.
After 2 years, the average BMI of study participants dropped from a mean of 48 to a mean of 29. "Between the 6- and 12-month marks, most patients were able to achieve a BMI that would make them acceptable for transplant," Dr. Lin said.
At 1, 3, 12, and 24 months, the percent of excess body weight lost was 17%, 26%, 50%, and 66%, respectively. "The weight-loss profile is similar to [those of] the general bariatric sleeve gastrectomy population," he noted.
Of the 13 patients who had diabetes preoperatively, 7 had complete resolution after the procedure and 1 had partial resolution. Mean postoperative albumin levels for all 26 patients after sleeve gastrectomy were 3.1 g/dL at 6 months and 3.3 g/dL at 12 months.
Eight patients went on to receive their organ transplant, Dr. Lin said. Their mean age was 56 years, and six were women. They waited a mean of 17 months for their procedures, which included six liver transplants, one liver and kidney transplant, and one kidney transplant. Their mean BMI before sleeve gastrectomy was 46, and their mean BMI prior to transplantation was 31. Immediately before transplant, their mean albumin level was 3.2 g/dL, and the most current measurement remained the same. "No increased acute rejection or difficulty maintaining immunosuppression was observed," he said.
Dr. Lin acknowledged certain limitations of the study, including its single-center design, lack of a control population, and the fact that "there is very little statistical power to estimate the true complication rate in this high-risk surgical group. Furthermore, we only have short-term follow-up."
Dr. Lin said that he had no relevant financial conflicts to disclose.
AT THE ANNUAL MEETING OF THE AMERICAN SOCIETY FOR METABOLIC AND BARIATRIC SURGERY