User login
Bringing you the latest news, research and reviews, exclusive interviews, podcasts, quizzes, and more.
div[contains(@class, 'read-next-article')]
div[contains(@class, 'nav-primary')]
nav[contains(@class, 'nav-primary')]
section[contains(@class, 'footer-nav-section-wrapper')]
nav[contains(@class, 'nav-ce-stack nav-ce-stack__large-screen')]
header[@id='header']
div[contains(@class, 'header__large-screen')]
div[contains(@class, 'read-next-article')]
div[contains(@class, 'main-prefix')]
div[contains(@class, 'nav-primary')]
nav[contains(@class, 'nav-primary')]
section[contains(@class, 'footer-nav-section-wrapper')]
footer[@id='footer']
section[contains(@class, 'nav-hidden')]
div[contains(@class, 'ce-card-content')]
nav[contains(@class, 'nav-ce-stack')]
div[contains(@class, 'view-medstat-quiz-listing-panes')]
div[contains(@class, 'pane-article-sidebar-latest-news')]
Student loan forgiveness plans exclude physicians
In the run up to the midterm elections in November, President Biden has warmed to student loan forgiveness. However, before even being proposed,
What was the plan?
During the 2020 election, student loan forgiveness was a hot topic as the COVID epidemic raged. The CARES Act has placed all federal student loans in forbearance, with no payments made and the interest rate set to 0% to prevent further accrual. While this was tremendously useful to 45 million borrowers around the country (including the author), nothing material was done to deal with the loans.
The Biden Administration’s approach at that time was multi-tiered and chaotic. Plans were put forward that either expanded Public Service Loan Forgiveness (PSLF) or capped it. Plans were put forward that either extended free undergraduate or severely limited it through Pell Grants. Unfortunately, that duality continues today, with current plans not having a clear goal or a target group of beneficiaries.
Necessary CARES Act extensions
The Biden Administration has attempted repeatedly to turn the student loan apparatus back on, restarting payments en masse. However, each time, they are beset by challenges, ranging from repeat COVID spikes to servicer withdrawals or macroeconomic indicators of a recession.
At each step, the administration has had little choice but to extend the CARES Act forbearance, lest they suffer retribution for hastily resuming payments for 45 million borrowers without the apparatus to do so. Two years ago, the major federal servicers laid off hundreds, if not thousands, of staffers responsible for payment processing, accounting, customer care, and taxation. Hiring, training, and staffing these positions is nontrivial.
The administration has been out of step with servicers such that three of the largest have chosen not to renew their contracts: Navient, MyFedLoan, and Granite State Management and Resources. This has left 15 million borrowers in the lurch, not knowing who their servicer is – and, even worse, losing track of qualifying payments toward programs like PSLF.
Avenues of forgiveness
There are two major pathways to forgiveness. It is widely believed that the executive branch has the authority to broadly forgive student loans under executive order and managed through the U.S. Department of Education.
The alternative is through congressional action, voting on forgiveness as an economic stimulus plan. There is little appetite in Congress for forgiveness, and prominent congresspeople like Senator Warren and Senator Schumer have both pushed the executive branch for forgiveness in recognition of this.
What has been proposed?
First, it’s important to state that as headline-grabbing as it is to see that $50,000 of forgiveness has been proposed, the reality is that President Biden has repeatedly stated that he will not be in favor of that level of forgiveness. Instead, the number most commonly being discussed is $10,000. This would represent an unprecedented amount of support, alleviating 35% of borrowers of all student debt.
The impact of proposed forgiveness plans for physicians
For the medical community, sadly, this doesn’t represent a significant amount of forgiveness. At graduation, the average MD has $203,000 in debt, and the average DO has $258,000 in debt. These numbers grow during residency for years before any meaningful payments are made.
Further weakening forgiveness plans for physicians has been two caps proposed by the administration in recent days. The first is an income cap of $125,000. While this would maintain forgiveness for nearly all residents and fellows, this would exclude nearly every practicing physician. The alternative to an income cap is specific exclusion of certain careers seen to be high-earning: doctors and lawyers.
The bottom line
Physicians are unlikely to be included in any forgiveness plans being proposed recently by the Biden Administration. If they are considered, it will be for exclusion from any forgiveness offered.
For physicians no longer eligible for PSLF, this exclusion needs to be considered in managing the student loan debt associated with becoming a doctor.
Dr. Palmer is a part-time instructor, department of pediatrics, Harvard Medical School, Boston, and staff physician, department of medical critical care, Boston Children’s Hospital. He disclosed that he serves as director for Panacea Financial.
A version of this article first appeared on Medscape.com.
In the run up to the midterm elections in November, President Biden has warmed to student loan forgiveness. However, before even being proposed,
What was the plan?
During the 2020 election, student loan forgiveness was a hot topic as the COVID epidemic raged. The CARES Act has placed all federal student loans in forbearance, with no payments made and the interest rate set to 0% to prevent further accrual. While this was tremendously useful to 45 million borrowers around the country (including the author), nothing material was done to deal with the loans.
The Biden Administration’s approach at that time was multi-tiered and chaotic. Plans were put forward that either expanded Public Service Loan Forgiveness (PSLF) or capped it. Plans were put forward that either extended free undergraduate or severely limited it through Pell Grants. Unfortunately, that duality continues today, with current plans not having a clear goal or a target group of beneficiaries.
Necessary CARES Act extensions
The Biden Administration has attempted repeatedly to turn the student loan apparatus back on, restarting payments en masse. However, each time, they are beset by challenges, ranging from repeat COVID spikes to servicer withdrawals or macroeconomic indicators of a recession.
At each step, the administration has had little choice but to extend the CARES Act forbearance, lest they suffer retribution for hastily resuming payments for 45 million borrowers without the apparatus to do so. Two years ago, the major federal servicers laid off hundreds, if not thousands, of staffers responsible for payment processing, accounting, customer care, and taxation. Hiring, training, and staffing these positions is nontrivial.
The administration has been out of step with servicers such that three of the largest have chosen not to renew their contracts: Navient, MyFedLoan, and Granite State Management and Resources. This has left 15 million borrowers in the lurch, not knowing who their servicer is – and, even worse, losing track of qualifying payments toward programs like PSLF.
Avenues of forgiveness
There are two major pathways to forgiveness. It is widely believed that the executive branch has the authority to broadly forgive student loans under executive order and managed through the U.S. Department of Education.
The alternative is through congressional action, voting on forgiveness as an economic stimulus plan. There is little appetite in Congress for forgiveness, and prominent congresspeople like Senator Warren and Senator Schumer have both pushed the executive branch for forgiveness in recognition of this.
What has been proposed?
First, it’s important to state that as headline-grabbing as it is to see that $50,000 of forgiveness has been proposed, the reality is that President Biden has repeatedly stated that he will not be in favor of that level of forgiveness. Instead, the number most commonly being discussed is $10,000. This would represent an unprecedented amount of support, alleviating 35% of borrowers of all student debt.
The impact of proposed forgiveness plans for physicians
For the medical community, sadly, this doesn’t represent a significant amount of forgiveness. At graduation, the average MD has $203,000 in debt, and the average DO has $258,000 in debt. These numbers grow during residency for years before any meaningful payments are made.
Further weakening forgiveness plans for physicians has been two caps proposed by the administration in recent days. The first is an income cap of $125,000. While this would maintain forgiveness for nearly all residents and fellows, this would exclude nearly every practicing physician. The alternative to an income cap is specific exclusion of certain careers seen to be high-earning: doctors and lawyers.
The bottom line
Physicians are unlikely to be included in any forgiveness plans being proposed recently by the Biden Administration. If they are considered, it will be for exclusion from any forgiveness offered.
For physicians no longer eligible for PSLF, this exclusion needs to be considered in managing the student loan debt associated with becoming a doctor.
Dr. Palmer is a part-time instructor, department of pediatrics, Harvard Medical School, Boston, and staff physician, department of medical critical care, Boston Children’s Hospital. He disclosed that he serves as director for Panacea Financial.
A version of this article first appeared on Medscape.com.
In the run up to the midterm elections in November, President Biden has warmed to student loan forgiveness. However, before even being proposed,
What was the plan?
During the 2020 election, student loan forgiveness was a hot topic as the COVID epidemic raged. The CARES Act has placed all federal student loans in forbearance, with no payments made and the interest rate set to 0% to prevent further accrual. While this was tremendously useful to 45 million borrowers around the country (including the author), nothing material was done to deal with the loans.
The Biden Administration’s approach at that time was multi-tiered and chaotic. Plans were put forward that either expanded Public Service Loan Forgiveness (PSLF) or capped it. Plans were put forward that either extended free undergraduate or severely limited it through Pell Grants. Unfortunately, that duality continues today, with current plans not having a clear goal or a target group of beneficiaries.
Necessary CARES Act extensions
The Biden Administration has attempted repeatedly to turn the student loan apparatus back on, restarting payments en masse. However, each time, they are beset by challenges, ranging from repeat COVID spikes to servicer withdrawals or macroeconomic indicators of a recession.
At each step, the administration has had little choice but to extend the CARES Act forbearance, lest they suffer retribution for hastily resuming payments for 45 million borrowers without the apparatus to do so. Two years ago, the major federal servicers laid off hundreds, if not thousands, of staffers responsible for payment processing, accounting, customer care, and taxation. Hiring, training, and staffing these positions is nontrivial.
The administration has been out of step with servicers such that three of the largest have chosen not to renew their contracts: Navient, MyFedLoan, and Granite State Management and Resources. This has left 15 million borrowers in the lurch, not knowing who their servicer is – and, even worse, losing track of qualifying payments toward programs like PSLF.
Avenues of forgiveness
There are two major pathways to forgiveness. It is widely believed that the executive branch has the authority to broadly forgive student loans under executive order and managed through the U.S. Department of Education.
The alternative is through congressional action, voting on forgiveness as an economic stimulus plan. There is little appetite in Congress for forgiveness, and prominent congresspeople like Senator Warren and Senator Schumer have both pushed the executive branch for forgiveness in recognition of this.
What has been proposed?
First, it’s important to state that as headline-grabbing as it is to see that $50,000 of forgiveness has been proposed, the reality is that President Biden has repeatedly stated that he will not be in favor of that level of forgiveness. Instead, the number most commonly being discussed is $10,000. This would represent an unprecedented amount of support, alleviating 35% of borrowers of all student debt.
The impact of proposed forgiveness plans for physicians
For the medical community, sadly, this doesn’t represent a significant amount of forgiveness. At graduation, the average MD has $203,000 in debt, and the average DO has $258,000 in debt. These numbers grow during residency for years before any meaningful payments are made.
Further weakening forgiveness plans for physicians has been two caps proposed by the administration in recent days. The first is an income cap of $125,000. While this would maintain forgiveness for nearly all residents and fellows, this would exclude nearly every practicing physician. The alternative to an income cap is specific exclusion of certain careers seen to be high-earning: doctors and lawyers.
The bottom line
Physicians are unlikely to be included in any forgiveness plans being proposed recently by the Biden Administration. If they are considered, it will be for exclusion from any forgiveness offered.
For physicians no longer eligible for PSLF, this exclusion needs to be considered in managing the student loan debt associated with becoming a doctor.
Dr. Palmer is a part-time instructor, department of pediatrics, Harvard Medical School, Boston, and staff physician, department of medical critical care, Boston Children’s Hospital. He disclosed that he serves as director for Panacea Financial.
A version of this article first appeared on Medscape.com.
FDA authorizes Pfizer’s COVID booster for kids ages 5 to 11
emergency use authorization (EUA), allowing the Pfizer-BioNTech COVID-19 booster shot for children ages 5 to 11 who are at least 5 months out from their first vaccine series.

According to the most recent data from the Centers for Disease Control and Prevention, 28.6% of children in this age group have received both initial doses of Pfizer’s COVID-19 vaccine, and 35.3% have received their first dose.
Pfizer’s vaccine trial involving 4,500 children showed few side effects among children younger than 12 who received a booster, or third dose, according to a company statement.
Pfizer asked the FDA for an amended authorization in April, after submitting data showing that a third dose in children between 5 and 11 raised antibodies targeting the Omicron variant by 36 times.
“While it has largely been the case that COVID-19 tends to be less severe in children than adults, the omicron wave has seen more kids getting sick with the disease and being hospitalized, and children may also experience longer-term effects, even following initially mild disease,” FDA Commissioner Robert M. Califf, MD, said in a news release.
A study done by the New York State Department of Health showed the effectiveness of Pfizer’s two-dose vaccine series fell from 68% to 12% 4-5 months after the second dose was given to children 5 to 11 during the Omicron surge. A CDC study published in March also showed that the Pfizer shot reduced the risk of Omicron by 31% in children 5 to 11, a significantly lower rate than for kids 12 to 15, who had a 59% risk reduction after receiving two doses.
To some experts, this data suggest an even greater need for children under 12 to be eligible for a third dose.
“Since authorizing the vaccine for children down to 5 years of age in October 2021, emerging data suggest that vaccine effectiveness against COVID-19 wanes after the second dose of the vaccine in all authorized populations,” says Peter Marks, MD, PhD, the director of the FDA’s Center for Biologics Evaluation and Research.
The CDC still needs to sign off on the shots before they can be allowed. The agency’s Advisory Committee on Immunization Practices is set to meet on May 19 to discuss boosters in this age group.
FDA advisory panels plan to meet next month to discuss allowing Pfizer’s and Moderna’s COVID-19 vaccines for children under 6 years old.
A version of this article first appeared on WebMD.com.
emergency use authorization (EUA), allowing the Pfizer-BioNTech COVID-19 booster shot for children ages 5 to 11 who are at least 5 months out from their first vaccine series.
According to the most recent data from the Centers for Disease Control and Prevention, 28.6% of children in this age group have received both initial doses of Pfizer’s COVID-19 vaccine, and 35.3% have received their first dose.
Pfizer’s vaccine trial involving 4,500 children showed few side effects among children younger than 12 who received a booster, or third dose, according to a company statement.
Pfizer asked the FDA for an amended authorization in April, after submitting data showing that a third dose in children between 5 and 11 raised antibodies targeting the Omicron variant by 36 times.
“While it has largely been the case that COVID-19 tends to be less severe in children than adults, the omicron wave has seen more kids getting sick with the disease and being hospitalized, and children may also experience longer-term effects, even following initially mild disease,” FDA Commissioner Robert M. Califf, MD, said in a news release.
A study done by the New York State Department of Health showed the effectiveness of Pfizer’s two-dose vaccine series fell from 68% to 12% 4-5 months after the second dose was given to children 5 to 11 during the Omicron surge. A CDC study published in March also showed that the Pfizer shot reduced the risk of Omicron by 31% in children 5 to 11, a significantly lower rate than for kids 12 to 15, who had a 59% risk reduction after receiving two doses.
To some experts, this data suggest an even greater need for children under 12 to be eligible for a third dose.
“Since authorizing the vaccine for children down to 5 years of age in October 2021, emerging data suggest that vaccine effectiveness against COVID-19 wanes after the second dose of the vaccine in all authorized populations,” says Peter Marks, MD, PhD, the director of the FDA’s Center for Biologics Evaluation and Research.
The CDC still needs to sign off on the shots before they can be allowed. The agency’s Advisory Committee on Immunization Practices is set to meet on May 19 to discuss boosters in this age group.
FDA advisory panels plan to meet next month to discuss allowing Pfizer’s and Moderna’s COVID-19 vaccines for children under 6 years old.
A version of this article first appeared on WebMD.com.
emergency use authorization (EUA), allowing the Pfizer-BioNTech COVID-19 booster shot for children ages 5 to 11 who are at least 5 months out from their first vaccine series.
According to the most recent data from the Centers for Disease Control and Prevention, 28.6% of children in this age group have received both initial doses of Pfizer’s COVID-19 vaccine, and 35.3% have received their first dose.
Pfizer’s vaccine trial involving 4,500 children showed few side effects among children younger than 12 who received a booster, or third dose, according to a company statement.
Pfizer asked the FDA for an amended authorization in April, after submitting data showing that a third dose in children between 5 and 11 raised antibodies targeting the Omicron variant by 36 times.
“While it has largely been the case that COVID-19 tends to be less severe in children than adults, the omicron wave has seen more kids getting sick with the disease and being hospitalized, and children may also experience longer-term effects, even following initially mild disease,” FDA Commissioner Robert M. Califf, MD, said in a news release.
A study done by the New York State Department of Health showed the effectiveness of Pfizer’s two-dose vaccine series fell from 68% to 12% 4-5 months after the second dose was given to children 5 to 11 during the Omicron surge. A CDC study published in March also showed that the Pfizer shot reduced the risk of Omicron by 31% in children 5 to 11, a significantly lower rate than for kids 12 to 15, who had a 59% risk reduction after receiving two doses.
To some experts, this data suggest an even greater need for children under 12 to be eligible for a third dose.
“Since authorizing the vaccine for children down to 5 years of age in October 2021, emerging data suggest that vaccine effectiveness against COVID-19 wanes after the second dose of the vaccine in all authorized populations,” says Peter Marks, MD, PhD, the director of the FDA’s Center for Biologics Evaluation and Research.
The CDC still needs to sign off on the shots before they can be allowed. The agency’s Advisory Committee on Immunization Practices is set to meet on May 19 to discuss boosters in this age group.
FDA advisory panels plan to meet next month to discuss allowing Pfizer’s and Moderna’s COVID-19 vaccines for children under 6 years old.
A version of this article first appeared on WebMD.com.
Why do clinical trials still underrepresent minority groups?
It’s no secret that, for decades, the participants in clinical trials for new drugs and medical devices haven’t accurately represented the diverse groups of patients the drugs and devices were designed for.
In a recently published draft guidance, the Food and Drug Administration recommended that companies in charge of running these trials should submit a proposal to the agency that would address how they plan to enroll more “clinically relevant populations” and historically underrepresented racial and ethnic groups.
It’s an issue that the U.S. has been trying to fix for years. In 1993, the NIH Revitalization Act was passed into law. It mandated the appropriate inclusion of women and racial minorities in all National Institutes of Health–funded research.
Since then, the FDA has put out plans that encourage trial sponsors to recruit more diverse enrollees, offering strategies and best practices rather than establishing requirements or quotas that companies would be forced to meet. Despite its efforts to encourage inclusion, people of color continue to be largely underrepresented in clinical trials.
Experts aren’t just calling for trial cohorts to reflect U.S. census data. Rather, the demographics of participants should match those of the diagnosis being studied. An analysis of 24 clinical trials of cardiovascular drugs, for example, found that Black Americans made up 2.9% of trial participants, compared with 83.1% for White people. Given that cardiovascular diseases affect Black Americans at almost the same rate as Whites (23.5% and 23.7%, respectively) – and keeping in mind that Black Americans make up 13.4% of the population and White people represent 76.3% – the degree of underrepresentation is glaring.
One commonly cited reason for this lack of representation is that people of color, especially Black Americans, have lingering feelings of mistrust toward the medical field. The U.S.-run Tuskegee study – during which researchers documented the natural progression of syphilis in hundreds of Black men who were kept from life-saving treatment – is, justifiably, often named as a notable source of that suspicion.
But blaming the disproportionately low numbers of Black participants in clinical trials on medical mistrust is an easy answer to a much more complicated issue, said cardiologist Clyde Yancy, MD, who also serves as the vice dean for diversity and inclusion at Northwestern University’s Feinberg School of Medicine, Chicago.
“We need to not put the onus on the back of the patient cohort, and say they are the problem,” Dr. Yancy said, adding that many trials add financial barriers and don’t provide proper transportation for participants who may live farther away.
The diversity of the study team itself – the institutions, researchers, and recruiters – also contributes to a lack of diversity in the participant pool. When considering all of these factors, “you begin to understand the complexity and the multidimensionality of why we have underrepresentation,” said Dr. Yancy. “So I would not promulgate the notion that this is simply because patients don’t trust the system.”
Soumya Niranjan, PhD, worked as a study coordinator at the Tulane Cancer Center in New Orleans, La., where she recruited patients for a prostate cancer study. After researching the impact of clinicians’ biases on the recruitment of racial and ethnic minorities in oncology trials, she found that some recruiters view patients of color as less promising participants.
“Who ends up being approached for a clinical trial is based on a preset rubric that one has in mind about a patient who may be eligible for a cancer study,” said Dr. Niranjan. “There is a characterization of, ‘we want to make sure this patient is compliant, that they will be a good historian and seem responsible.’ ... Our study showed that it kind of fell along racial lines.”
In her study, published in the journal Cancer in 2020, Dr. Niranjan wrote that researchers sometimes “perceived racial minority groups to have low knowledge of cancer clinical trials. This was considered to be a hindrance while explaining cancer clinical trials in the face of limited provider time during a clinical encounter.”
Some researchers believed minority participants, especially Black women, would be less likely to file study protocols. Others said people of color are more likely to be selfish.
She quoted one research investigator as saying Black people are less knowledgeable.
“African Americans I think have less knowledge,” the unnamed researcher said. “We take a little bit more time to explain to African American [sic]. I think ... they have more questions because we know they are not more knowledgeable so I think it takes time. They have a lot of questions.”
Progress over the years
The FDA’s recent draft builds upon a guidance from 2016, which already recommended that trial teams submit an inclusion plan to the agency at the earliest phase of development. While the recent announcement is another step in the right direction, it may not be substantial enough.
“There’s always an enrollment plan,” Dr. Niranjan said. “But those enrollment plans are not enforced. So if it’s not enforced, what does that look like?”
In an emailed statement to this news organization, Lola Fashoyin-Aje, MD, the deputy director of the FDA Oncology Center of Excellence’s division to expand diversity, emphasized that the draft guidance does not require anything, but that the agency “expect[s] sponsors will follow FDA’s recommendations as described in the draft guidance.”
Without requirements, it’s up to the sponsor to make the effort to enroll people with varied racial and ethnic backgrounds. During the development of the COVID-19 vaccine, Moderna announced that the company would slow the trial’s enrollment to ensure minority groups were properly represented.
Not every sponsor is as motivated to make this a concerted effort, and some simply don’t have the funds to allocate to strengthening the enrollment process.
“There’s so much red tape and paperwork to get the funding for a clinical trial,” said Julie Silver, MD, professor of physical medicine and rehabilitation at Harvard Medical School, Boston, who studies workforce diversity and inclusion. “Even when people are equitably included, the amount of funding they have to do the trial might not be enough to do an analysis that shows potential differences.”
Whether the FDA will enforce enrollment plans in the future remains an open question; however, Dr. Yancy said the most effective way to do this would be through incentives, rather than penalties.
According to Dr. Fashoyin-Aje, the FDA and sponsors “will learn from these submissions and over time, whether and how these diversity plans lead to meaningful changes in clinical trial representation will need to be assessed, including whether additional steps need to be taken.”
A version of this article first appeared on Medscape.com.
It’s no secret that, for decades, the participants in clinical trials for new drugs and medical devices haven’t accurately represented the diverse groups of patients the drugs and devices were designed for.
In a recently published draft guidance, the Food and Drug Administration recommended that companies in charge of running these trials should submit a proposal to the agency that would address how they plan to enroll more “clinically relevant populations” and historically underrepresented racial and ethnic groups.
It’s an issue that the U.S. has been trying to fix for years. In 1993, the NIH Revitalization Act was passed into law. It mandated the appropriate inclusion of women and racial minorities in all National Institutes of Health–funded research.
Since then, the FDA has put out plans that encourage trial sponsors to recruit more diverse enrollees, offering strategies and best practices rather than establishing requirements or quotas that companies would be forced to meet. Despite its efforts to encourage inclusion, people of color continue to be largely underrepresented in clinical trials.
Experts aren’t just calling for trial cohorts to reflect U.S. census data. Rather, the demographics of participants should match those of the diagnosis being studied. An analysis of 24 clinical trials of cardiovascular drugs, for example, found that Black Americans made up 2.9% of trial participants, compared with 83.1% for White people. Given that cardiovascular diseases affect Black Americans at almost the same rate as Whites (23.5% and 23.7%, respectively) – and keeping in mind that Black Americans make up 13.4% of the population and White people represent 76.3% – the degree of underrepresentation is glaring.
One commonly cited reason for this lack of representation is that people of color, especially Black Americans, have lingering feelings of mistrust toward the medical field. The U.S.-run Tuskegee study – during which researchers documented the natural progression of syphilis in hundreds of Black men who were kept from life-saving treatment – is, justifiably, often named as a notable source of that suspicion.
But blaming the disproportionately low numbers of Black participants in clinical trials on medical mistrust is an easy answer to a much more complicated issue, said cardiologist Clyde Yancy, MD, who also serves as the vice dean for diversity and inclusion at Northwestern University’s Feinberg School of Medicine, Chicago.
“We need to not put the onus on the back of the patient cohort, and say they are the problem,” Dr. Yancy said, adding that many trials add financial barriers and don’t provide proper transportation for participants who may live farther away.
The diversity of the study team itself – the institutions, researchers, and recruiters – also contributes to a lack of diversity in the participant pool. When considering all of these factors, “you begin to understand the complexity and the multidimensionality of why we have underrepresentation,” said Dr. Yancy. “So I would not promulgate the notion that this is simply because patients don’t trust the system.”
Soumya Niranjan, PhD, worked as a study coordinator at the Tulane Cancer Center in New Orleans, La., where she recruited patients for a prostate cancer study. After researching the impact of clinicians’ biases on the recruitment of racial and ethnic minorities in oncology trials, she found that some recruiters view patients of color as less promising participants.
“Who ends up being approached for a clinical trial is based on a preset rubric that one has in mind about a patient who may be eligible for a cancer study,” said Dr. Niranjan. “There is a characterization of, ‘we want to make sure this patient is compliant, that they will be a good historian and seem responsible.’ ... Our study showed that it kind of fell along racial lines.”
In her study, published in the journal Cancer in 2020, Dr. Niranjan wrote that researchers sometimes “perceived racial minority groups to have low knowledge of cancer clinical trials. This was considered to be a hindrance while explaining cancer clinical trials in the face of limited provider time during a clinical encounter.”
Some researchers believed minority participants, especially Black women, would be less likely to file study protocols. Others said people of color are more likely to be selfish.
She quoted one research investigator as saying Black people are less knowledgeable.
“African Americans I think have less knowledge,” the unnamed researcher said. “We take a little bit more time to explain to African American [sic]. I think ... they have more questions because we know they are not more knowledgeable so I think it takes time. They have a lot of questions.”
Progress over the years
The FDA’s recent draft builds upon a guidance from 2016, which already recommended that trial teams submit an inclusion plan to the agency at the earliest phase of development. While the recent announcement is another step in the right direction, it may not be substantial enough.
“There’s always an enrollment plan,” Dr. Niranjan said. “But those enrollment plans are not enforced. So if it’s not enforced, what does that look like?”
In an emailed statement to this news organization, Lola Fashoyin-Aje, MD, the deputy director of the FDA Oncology Center of Excellence’s division to expand diversity, emphasized that the draft guidance does not require anything, but that the agency “expect[s] sponsors will follow FDA’s recommendations as described in the draft guidance.”
Without requirements, it’s up to the sponsor to make the effort to enroll people with varied racial and ethnic backgrounds. During the development of the COVID-19 vaccine, Moderna announced that the company would slow the trial’s enrollment to ensure minority groups were properly represented.
Not every sponsor is as motivated to make this a concerted effort, and some simply don’t have the funds to allocate to strengthening the enrollment process.
“There’s so much red tape and paperwork to get the funding for a clinical trial,” said Julie Silver, MD, professor of physical medicine and rehabilitation at Harvard Medical School, Boston, who studies workforce diversity and inclusion. “Even when people are equitably included, the amount of funding they have to do the trial might not be enough to do an analysis that shows potential differences.”
Whether the FDA will enforce enrollment plans in the future remains an open question; however, Dr. Yancy said the most effective way to do this would be through incentives, rather than penalties.
According to Dr. Fashoyin-Aje, the FDA and sponsors “will learn from these submissions and over time, whether and how these diversity plans lead to meaningful changes in clinical trial representation will need to be assessed, including whether additional steps need to be taken.”
A version of this article first appeared on Medscape.com.
It’s no secret that, for decades, the participants in clinical trials for new drugs and medical devices haven’t accurately represented the diverse groups of patients the drugs and devices were designed for.
In a recently published draft guidance, the Food and Drug Administration recommended that companies in charge of running these trials should submit a proposal to the agency that would address how they plan to enroll more “clinically relevant populations” and historically underrepresented racial and ethnic groups.
It’s an issue that the U.S. has been trying to fix for years. In 1993, the NIH Revitalization Act was passed into law. It mandated the appropriate inclusion of women and racial minorities in all National Institutes of Health–funded research.
Since then, the FDA has put out plans that encourage trial sponsors to recruit more diverse enrollees, offering strategies and best practices rather than establishing requirements or quotas that companies would be forced to meet. Despite its efforts to encourage inclusion, people of color continue to be largely underrepresented in clinical trials.
Experts aren’t just calling for trial cohorts to reflect U.S. census data. Rather, the demographics of participants should match those of the diagnosis being studied. An analysis of 24 clinical trials of cardiovascular drugs, for example, found that Black Americans made up 2.9% of trial participants, compared with 83.1% for White people. Given that cardiovascular diseases affect Black Americans at almost the same rate as Whites (23.5% and 23.7%, respectively) – and keeping in mind that Black Americans make up 13.4% of the population and White people represent 76.3% – the degree of underrepresentation is glaring.
One commonly cited reason for this lack of representation is that people of color, especially Black Americans, have lingering feelings of mistrust toward the medical field. The U.S.-run Tuskegee study – during which researchers documented the natural progression of syphilis in hundreds of Black men who were kept from life-saving treatment – is, justifiably, often named as a notable source of that suspicion.
But blaming the disproportionately low numbers of Black participants in clinical trials on medical mistrust is an easy answer to a much more complicated issue, said cardiologist Clyde Yancy, MD, who also serves as the vice dean for diversity and inclusion at Northwestern University’s Feinberg School of Medicine, Chicago.
“We need to not put the onus on the back of the patient cohort, and say they are the problem,” Dr. Yancy said, adding that many trials add financial barriers and don’t provide proper transportation for participants who may live farther away.
The diversity of the study team itself – the institutions, researchers, and recruiters – also contributes to a lack of diversity in the participant pool. When considering all of these factors, “you begin to understand the complexity and the multidimensionality of why we have underrepresentation,” said Dr. Yancy. “So I would not promulgate the notion that this is simply because patients don’t trust the system.”
Soumya Niranjan, PhD, worked as a study coordinator at the Tulane Cancer Center in New Orleans, La., where she recruited patients for a prostate cancer study. After researching the impact of clinicians’ biases on the recruitment of racial and ethnic minorities in oncology trials, she found that some recruiters view patients of color as less promising participants.
“Who ends up being approached for a clinical trial is based on a preset rubric that one has in mind about a patient who may be eligible for a cancer study,” said Dr. Niranjan. “There is a characterization of, ‘we want to make sure this patient is compliant, that they will be a good historian and seem responsible.’ ... Our study showed that it kind of fell along racial lines.”
In her study, published in the journal Cancer in 2020, Dr. Niranjan wrote that researchers sometimes “perceived racial minority groups to have low knowledge of cancer clinical trials. This was considered to be a hindrance while explaining cancer clinical trials in the face of limited provider time during a clinical encounter.”
Some researchers believed minority participants, especially Black women, would be less likely to file study protocols. Others said people of color are more likely to be selfish.
She quoted one research investigator as saying Black people are less knowledgeable.
“African Americans I think have less knowledge,” the unnamed researcher said. “We take a little bit more time to explain to African American [sic]. I think ... they have more questions because we know they are not more knowledgeable so I think it takes time. They have a lot of questions.”
Progress over the years
The FDA’s recent draft builds upon a guidance from 2016, which already recommended that trial teams submit an inclusion plan to the agency at the earliest phase of development. While the recent announcement is another step in the right direction, it may not be substantial enough.
“There’s always an enrollment plan,” Dr. Niranjan said. “But those enrollment plans are not enforced. So if it’s not enforced, what does that look like?”
In an emailed statement to this news organization, Lola Fashoyin-Aje, MD, the deputy director of the FDA Oncology Center of Excellence’s division to expand diversity, emphasized that the draft guidance does not require anything, but that the agency “expect[s] sponsors will follow FDA’s recommendations as described in the draft guidance.”
Without requirements, it’s up to the sponsor to make the effort to enroll people with varied racial and ethnic backgrounds. During the development of the COVID-19 vaccine, Moderna announced that the company would slow the trial’s enrollment to ensure minority groups were properly represented.
Not every sponsor is as motivated to make this a concerted effort, and some simply don’t have the funds to allocate to strengthening the enrollment process.
“There’s so much red tape and paperwork to get the funding for a clinical trial,” said Julie Silver, MD, professor of physical medicine and rehabilitation at Harvard Medical School, Boston, who studies workforce diversity and inclusion. “Even when people are equitably included, the amount of funding they have to do the trial might not be enough to do an analysis that shows potential differences.”
Whether the FDA will enforce enrollment plans in the future remains an open question; however, Dr. Yancy said the most effective way to do this would be through incentives, rather than penalties.
According to Dr. Fashoyin-Aje, the FDA and sponsors “will learn from these submissions and over time, whether and how these diversity plans lead to meaningful changes in clinical trial representation will need to be assessed, including whether additional steps need to be taken.”
A version of this article first appeared on Medscape.com.
Advancing digital health care past pandemic-driven telemedicine
COVID-19 forced consumers to adopt digital and virtual platforms to receive medical care, and more than 2 years after the start of the pandemic, it doesn’t appear that that will change.
“During the pandemic we witnessed a very steep rise in the utilization of digital health care transactions. And as we have now witnessed a plateau, we see that digital health care transactions have not fallen back to the way things were prepandemic,” said Bart M. Demaerschalk, MD, professor and chair of cerebrovascular diseases for digital health research at the Mayo Clinic in Phoenix, Ariz. “At Mayo Clinic and other health care organizations, approximately 20% ... of the composite care is occurring by digital means.”
Dr. Demaerschalk was among a panel representing retail and traditional health care organizations at the American Telemedicine Association conference in Boston.
The pandemic created this new reality, and health care leaders are now trying to make the most of all digital tools. Marcus Osborne, former senior vice president at Walmart Health, said that to progress, the health care industry needs to move beyond the conception of a world in which consumers interact with care providers via one-off in-person or digital experiences.

“What we’re actually seeing in other sectors and in life in general is that the world is not multichannel. The world is omnichannel,” Mr. Osborne said. Under an omnichannel paradigm, provider organizations integrate multiple digital and in-person health delivery methods, making it possible to “create whole new experiences for consumers that no one channel could deliver,” he added.
Creagh Milford, DO, vice president and head of enterprise virtual care at CVS Health, agreed and added that “the retail footprint will evolve” from offering separate physical and virtual care experiences to a “blended” experience.

To move in this direction, health care leaders need to “stop talking about the site of care so much,” said Christopher McCann, MBChB, CEO and cofounder of the health IT firm Current Health. Instead of “fixating” on either brick-and-mortar or digital experiences, leaders should meet “the consumer where they are and deliver what is the most appropriate care to that consumer in the most appropriate setting,” Dr. McCann said.
Three key digital technology strategies
In addition to supporting an omnichannel experience, the panelists pointed out that traditional and retail health care providers can make the most of digital technologies in a few different ways.
One is by helping consumers manage innovation. With venture capital investments in digital technologies at an all-time high, the health care industry is drowning in innovation, <r/ Osborne pointed out.
“So on one hand, we have been blessed with this eruption of innovation. On the other hand – and I’m saying this as a consumer – it [doesn’t] really matter. I’m overwhelmed, and I think the market is overwhelmed,” Mr. Osborne said. “So if we’re overwhelmed, it means we’re not going to leverage that innovation as effectively as we should.” The challenge, then, is to find a way to “not get overwhelmed by the sheer force of innovations occurring” and to instead leverage these new technologies to drive real transformation in our health care system.
To meet this challenge, health care organizations will have to provide consumers with “some guidance as to how to tailor that journey,” Dr. Demaerschalk said. “It’s the responsibility of all of us to be creating that tailored and individual guidance for our patients.” By doing so, health care organizations ultimately can help consumers feel less overwhelmed.
Another strategy is to ensure that the use of technology promotes health equity. Mr. Osborne pointed out that events such as the pandemic and George Floyd’s murder have resulted in a “much more robust conversation around the need to address health inequities in America. I’ve also heard a lot of people say they believe that digital health solutions are the answer.”
As such, health care organizations need to ensure that digital innovations are leveraged to “fundamentally address the inequities that we’re facing today and support the care of all Americans,” Mr. Osborne noted.
To move in this direction, leaders need to address one glaring gap: “We talk all the time about fancy technology, like artificial intelligence. Most of my clients, they’re just trying to get basic Internet access at home,” Dr. McCann said. “So, there’s a technology challenge we first have to solve.”
Once this hurdle is overcome, however, digital technologies could pay off in spades, especially for consumers who struggle to access in-person services because they live 2 or 3 hours away from the hospital, are working two jobs, and have child care responsibilities, Dr. McCann noted.
Health care must also address staffing issues, said the panelists. Leaders need to create new career paths for clinicians as digital care delivery becomes more prominent.
Some health care organizations have already discovered that using digital technologies to support hospital-at-home programs can also enhance the work lives of clinicians.
When working in hospital-at-home programs, clinicians can “deliver care in the way that they have always wanted to but have never been able to within an acute inpatient facility. They’re able to go into patients’ homes and spend an hour with them, actually develop a proper relationship and look at social determinants of health and medications and do things in a way they’ve never been able to do before. And that has dramatically reduced rates of burnout,” Dr. McCann said.
While these strategies will help organizations support “this exciting digital ecosystem,” health care technology innovators need to “really study the costs and the health outcomes related to these digital health transactions in order to move the entire field and the science forward,” Dr. Demaerschalk concluded.
A version of this article first appeared on Medscape.com.
COVID-19 forced consumers to adopt digital and virtual platforms to receive medical care, and more than 2 years after the start of the pandemic, it doesn’t appear that that will change.
“During the pandemic we witnessed a very steep rise in the utilization of digital health care transactions. And as we have now witnessed a plateau, we see that digital health care transactions have not fallen back to the way things were prepandemic,” said Bart M. Demaerschalk, MD, professor and chair of cerebrovascular diseases for digital health research at the Mayo Clinic in Phoenix, Ariz. “At Mayo Clinic and other health care organizations, approximately 20% ... of the composite care is occurring by digital means.”
Dr. Demaerschalk was among a panel representing retail and traditional health care organizations at the American Telemedicine Association conference in Boston.
The pandemic created this new reality, and health care leaders are now trying to make the most of all digital tools. Marcus Osborne, former senior vice president at Walmart Health, said that to progress, the health care industry needs to move beyond the conception of a world in which consumers interact with care providers via one-off in-person or digital experiences.
“What we’re actually seeing in other sectors and in life in general is that the world is not multichannel. The world is omnichannel,” Mr. Osborne said. Under an omnichannel paradigm, provider organizations integrate multiple digital and in-person health delivery methods, making it possible to “create whole new experiences for consumers that no one channel could deliver,” he added.
Creagh Milford, DO, vice president and head of enterprise virtual care at CVS Health, agreed and added that “the retail footprint will evolve” from offering separate physical and virtual care experiences to a “blended” experience.
To move in this direction, health care leaders need to “stop talking about the site of care so much,” said Christopher McCann, MBChB, CEO and cofounder of the health IT firm Current Health. Instead of “fixating” on either brick-and-mortar or digital experiences, leaders should meet “the consumer where they are and deliver what is the most appropriate care to that consumer in the most appropriate setting,” Dr. McCann said.
Three key digital technology strategies
In addition to supporting an omnichannel experience, the panelists pointed out that traditional and retail health care providers can make the most of digital technologies in a few different ways.
One is by helping consumers manage innovation. With venture capital investments in digital technologies at an all-time high, the health care industry is drowning in innovation, <r/ Osborne pointed out.
“So on one hand, we have been blessed with this eruption of innovation. On the other hand – and I’m saying this as a consumer – it [doesn’t] really matter. I’m overwhelmed, and I think the market is overwhelmed,” Mr. Osborne said. “So if we’re overwhelmed, it means we’re not going to leverage that innovation as effectively as we should.” The challenge, then, is to find a way to “not get overwhelmed by the sheer force of innovations occurring” and to instead leverage these new technologies to drive real transformation in our health care system.
To meet this challenge, health care organizations will have to provide consumers with “some guidance as to how to tailor that journey,” Dr. Demaerschalk said. “It’s the responsibility of all of us to be creating that tailored and individual guidance for our patients.” By doing so, health care organizations ultimately can help consumers feel less overwhelmed.
Another strategy is to ensure that the use of technology promotes health equity. Mr. Osborne pointed out that events such as the pandemic and George Floyd’s murder have resulted in a “much more robust conversation around the need to address health inequities in America. I’ve also heard a lot of people say they believe that digital health solutions are the answer.”
As such, health care organizations need to ensure that digital innovations are leveraged to “fundamentally address the inequities that we’re facing today and support the care of all Americans,” Mr. Osborne noted.
To move in this direction, leaders need to address one glaring gap: “We talk all the time about fancy technology, like artificial intelligence. Most of my clients, they’re just trying to get basic Internet access at home,” Dr. McCann said. “So, there’s a technology challenge we first have to solve.”
Once this hurdle is overcome, however, digital technologies could pay off in spades, especially for consumers who struggle to access in-person services because they live 2 or 3 hours away from the hospital, are working two jobs, and have child care responsibilities, Dr. McCann noted.
Health care must also address staffing issues, said the panelists. Leaders need to create new career paths for clinicians as digital care delivery becomes more prominent.
Some health care organizations have already discovered that using digital technologies to support hospital-at-home programs can also enhance the work lives of clinicians.
When working in hospital-at-home programs, clinicians can “deliver care in the way that they have always wanted to but have never been able to within an acute inpatient facility. They’re able to go into patients’ homes and spend an hour with them, actually develop a proper relationship and look at social determinants of health and medications and do things in a way they’ve never been able to do before. And that has dramatically reduced rates of burnout,” Dr. McCann said.
While these strategies will help organizations support “this exciting digital ecosystem,” health care technology innovators need to “really study the costs and the health outcomes related to these digital health transactions in order to move the entire field and the science forward,” Dr. Demaerschalk concluded.
A version of this article first appeared on Medscape.com.
COVID-19 forced consumers to adopt digital and virtual platforms to receive medical care, and more than 2 years after the start of the pandemic, it doesn’t appear that that will change.
“During the pandemic we witnessed a very steep rise in the utilization of digital health care transactions. And as we have now witnessed a plateau, we see that digital health care transactions have not fallen back to the way things were prepandemic,” said Bart M. Demaerschalk, MD, professor and chair of cerebrovascular diseases for digital health research at the Mayo Clinic in Phoenix, Ariz. “At Mayo Clinic and other health care organizations, approximately 20% ... of the composite care is occurring by digital means.”
Dr. Demaerschalk was among a panel representing retail and traditional health care organizations at the American Telemedicine Association conference in Boston.
The pandemic created this new reality, and health care leaders are now trying to make the most of all digital tools. Marcus Osborne, former senior vice president at Walmart Health, said that to progress, the health care industry needs to move beyond the conception of a world in which consumers interact with care providers via one-off in-person or digital experiences.
“What we’re actually seeing in other sectors and in life in general is that the world is not multichannel. The world is omnichannel,” Mr. Osborne said. Under an omnichannel paradigm, provider organizations integrate multiple digital and in-person health delivery methods, making it possible to “create whole new experiences for consumers that no one channel could deliver,” he added.
Creagh Milford, DO, vice president and head of enterprise virtual care at CVS Health, agreed and added that “the retail footprint will evolve” from offering separate physical and virtual care experiences to a “blended” experience.
To move in this direction, health care leaders need to “stop talking about the site of care so much,” said Christopher McCann, MBChB, CEO and cofounder of the health IT firm Current Health. Instead of “fixating” on either brick-and-mortar or digital experiences, leaders should meet “the consumer where they are and deliver what is the most appropriate care to that consumer in the most appropriate setting,” Dr. McCann said.
Three key digital technology strategies
In addition to supporting an omnichannel experience, the panelists pointed out that traditional and retail health care providers can make the most of digital technologies in a few different ways.
One is by helping consumers manage innovation. With venture capital investments in digital technologies at an all-time high, the health care industry is drowning in innovation, <r/ Osborne pointed out.
“So on one hand, we have been blessed with this eruption of innovation. On the other hand – and I’m saying this as a consumer – it [doesn’t] really matter. I’m overwhelmed, and I think the market is overwhelmed,” Mr. Osborne said. “So if we’re overwhelmed, it means we’re not going to leverage that innovation as effectively as we should.” The challenge, then, is to find a way to “not get overwhelmed by the sheer force of innovations occurring” and to instead leverage these new technologies to drive real transformation in our health care system.
To meet this challenge, health care organizations will have to provide consumers with “some guidance as to how to tailor that journey,” Dr. Demaerschalk said. “It’s the responsibility of all of us to be creating that tailored and individual guidance for our patients.” By doing so, health care organizations ultimately can help consumers feel less overwhelmed.
Another strategy is to ensure that the use of technology promotes health equity. Mr. Osborne pointed out that events such as the pandemic and George Floyd’s murder have resulted in a “much more robust conversation around the need to address health inequities in America. I’ve also heard a lot of people say they believe that digital health solutions are the answer.”
As such, health care organizations need to ensure that digital innovations are leveraged to “fundamentally address the inequities that we’re facing today and support the care of all Americans,” Mr. Osborne noted.
To move in this direction, leaders need to address one glaring gap: “We talk all the time about fancy technology, like artificial intelligence. Most of my clients, they’re just trying to get basic Internet access at home,” Dr. McCann said. “So, there’s a technology challenge we first have to solve.”
Once this hurdle is overcome, however, digital technologies could pay off in spades, especially for consumers who struggle to access in-person services because they live 2 or 3 hours away from the hospital, are working two jobs, and have child care responsibilities, Dr. McCann noted.
Health care must also address staffing issues, said the panelists. Leaders need to create new career paths for clinicians as digital care delivery becomes more prominent.
Some health care organizations have already discovered that using digital technologies to support hospital-at-home programs can also enhance the work lives of clinicians.
When working in hospital-at-home programs, clinicians can “deliver care in the way that they have always wanted to but have never been able to within an acute inpatient facility. They’re able to go into patients’ homes and spend an hour with them, actually develop a proper relationship and look at social determinants of health and medications and do things in a way they’ve never been able to do before. And that has dramatically reduced rates of burnout,” Dr. McCann said.
While these strategies will help organizations support “this exciting digital ecosystem,” health care technology innovators need to “really study the costs and the health outcomes related to these digital health transactions in order to move the entire field and the science forward,” Dr. Demaerschalk concluded.
A version of this article first appeared on Medscape.com.
FROM ATA 2022
Administrative hassle hacks: Strategies to curb physician stress
The American Medical Association estimates that physician burnout costs the country $4.6 billion annually, and that doesn’t include the cost for nurses and other clinicians. In addition, physicians note too many bureaucratic tasks as a main contributor to their daily stress.
Such revelations have prompted many in the health care industry to focus on clinician burnout, including a panel at the recent American Telemedicine Association annual conference in Boston.

Not surprisingly, the discussion quickly turned to the COVID-19 pandemic, commonly cited as an event that has exacerbated existing clinician burnout and caused what has become known as the “great resignation.”
Peter Yellowlees, MBBS, MD, professor of psychiatry and chief wellness officer at the University of California, Davis, said his health system has experienced a lot of its nursing staff resigning or moving to other employment, particularly from intensive care units and the emergency department.
“We actually haven’t had too many physicians go, but I have a funny feeling we’re going to see that over the next year or so because I think a lot of people have just put their head down during the pandemic and they’ve worked themselves hard,” he said. “They’re now sort of putting their heads up above the wall,” and could realize that they want a change.
In his role as the wellness officer at the academic medical center, Dr. Yellowlees is proactively addressing burnout among the organization’s 14,000 employees. For example, during the pandemic, he developed a peer responder program. Under this initiative, 600 staff members received training in “psychological first aid,” essentially utilizing staff to become therapists for peers.
For example, if a clinician is struggling emotionally while dealing with a patient who has had significant trauma, a peer responder could talk with the clinician, helping him or her to better deal with the situation.
Marlene McDermott, senior director of therapy services at Array Behavioral Care, a national telepsychiatry provider with offices in New Jersey and Illinois, noted that her organization also addresses burnout by creating opportunities for peer-to-peer support.
“We’ve got hundreds of clinicians and we’ll take 10 to 15 of them, put them in small treatment teams and they have a live chat, a one-off virtual meeting with each other to vent and to ask clinical questions. It’s all clinicians, there’s no administrative staff in there,” Ms. McDermott said. The clinicians have found value in these meetings, as they can share their concerns as well as “silly images or quotes, just to keep things light at times. That’s made a big difference.”
Retraining, technology can help curb administrative burdens
In addition to providing peer support, both Dr. Yellowlees and Ms. McDermott are addressing the significant administrative burden that plagues physicians.
This burden is especially onerous for physicians in the United States, according to a study that compared the number of keystrokes required to produce clinical notes among physicians in several countries.
“What [the study] discovered was that the American notes were three to five times longer than the notes of the Australian or U.K. physicians. I’ve worked in all three countries and I can promise you there’s no difference in the quality of the doctors across those places,” Dr. Yellowlees said.
To address this issue, Dr. Yellowlees is training physicians to reduce the length of their clinical documentation.
“I am trying to retrain physicians who for many years have been trained to be defensive in their documentation – to write absurd amounts just to justify billing,” Dr. Yellowlees said. “We are trying to go back in some respects to the way that we used to write notes 20 years ago ... so much shorter. This is a huge retraining exercise but it’s an exercise that is essential.”
Ms. McDermott also is tackling the administrative burden at her organization.
“We are trying to make the workflow as efficient as possible, doing some asynchronous work where consumers are completing information before a session ... so clinicians are essentially reconciling information instead of gathering all nonpertinent information. They can just work at the top of the license and not be burdened by some of the questions that don’t directly affect treatment,” Ms. McDermott noted.
Encouraging and training physicians in concurrent documentation also can help reduce administrative burden.
“Being proficient at remaining in session and documenting as much as you can during a session can help. So that at the end, you’re pressing the button, closing the encounter and you’ve finished documenting,” Ms. McDermott said. “It’s definitely possible to do that without losing the connection with the patient.”
To accomplish this, physicians need to leverage touch-typing – the practice of typing without looking at the keyboard. Fortunately, telehealth makes this mode of documentation easily achievable. Consider the following: During an online session, clinicians can place the patient’s picture “right underneath the camera and make it small. And then you type with the note floating behind it. So you’re actually staring at the note and the person all at the same time,” Ms. McDermott said.
The continued uptake of telehealth in general could also reduce stress for physicians, added Dr. Yellowlees.
“One of the interesting things about that is just how much time we save the physicians because it actually takes quite a lot of time to room patients,” Dr. Yellowlees concluded. “We are now doing about 20% of all our outpatient visits in all disciplines by video. We were higher than that midway through COVID. I’m hoping we’ll go back to being higher than that.”
A version of this article first appeared on Medscape.com.
The American Medical Association estimates that physician burnout costs the country $4.6 billion annually, and that doesn’t include the cost for nurses and other clinicians. In addition, physicians note too many bureaucratic tasks as a main contributor to their daily stress.
Such revelations have prompted many in the health care industry to focus on clinician burnout, including a panel at the recent American Telemedicine Association annual conference in Boston.
Not surprisingly, the discussion quickly turned to the COVID-19 pandemic, commonly cited as an event that has exacerbated existing clinician burnout and caused what has become known as the “great resignation.”
Peter Yellowlees, MBBS, MD, professor of psychiatry and chief wellness officer at the University of California, Davis, said his health system has experienced a lot of its nursing staff resigning or moving to other employment, particularly from intensive care units and the emergency department.
“We actually haven’t had too many physicians go, but I have a funny feeling we’re going to see that over the next year or so because I think a lot of people have just put their head down during the pandemic and they’ve worked themselves hard,” he said. “They’re now sort of putting their heads up above the wall,” and could realize that they want a change.
In his role as the wellness officer at the academic medical center, Dr. Yellowlees is proactively addressing burnout among the organization’s 14,000 employees. For example, during the pandemic, he developed a peer responder program. Under this initiative, 600 staff members received training in “psychological first aid,” essentially utilizing staff to become therapists for peers.
For example, if a clinician is struggling emotionally while dealing with a patient who has had significant trauma, a peer responder could talk with the clinician, helping him or her to better deal with the situation.
Marlene McDermott, senior director of therapy services at Array Behavioral Care, a national telepsychiatry provider with offices in New Jersey and Illinois, noted that her organization also addresses burnout by creating opportunities for peer-to-peer support.
“We’ve got hundreds of clinicians and we’ll take 10 to 15 of them, put them in small treatment teams and they have a live chat, a one-off virtual meeting with each other to vent and to ask clinical questions. It’s all clinicians, there’s no administrative staff in there,” Ms. McDermott said. The clinicians have found value in these meetings, as they can share their concerns as well as “silly images or quotes, just to keep things light at times. That’s made a big difference.”
Retraining, technology can help curb administrative burdens
In addition to providing peer support, both Dr. Yellowlees and Ms. McDermott are addressing the significant administrative burden that plagues physicians.
This burden is especially onerous for physicians in the United States, according to a study that compared the number of keystrokes required to produce clinical notes among physicians in several countries.
“What [the study] discovered was that the American notes were three to five times longer than the notes of the Australian or U.K. physicians. I’ve worked in all three countries and I can promise you there’s no difference in the quality of the doctors across those places,” Dr. Yellowlees said.
To address this issue, Dr. Yellowlees is training physicians to reduce the length of their clinical documentation.
“I am trying to retrain physicians who for many years have been trained to be defensive in their documentation – to write absurd amounts just to justify billing,” Dr. Yellowlees said. “We are trying to go back in some respects to the way that we used to write notes 20 years ago ... so much shorter. This is a huge retraining exercise but it’s an exercise that is essential.”
Ms. McDermott also is tackling the administrative burden at her organization.
“We are trying to make the workflow as efficient as possible, doing some asynchronous work where consumers are completing information before a session ... so clinicians are essentially reconciling information instead of gathering all nonpertinent information. They can just work at the top of the license and not be burdened by some of the questions that don’t directly affect treatment,” Ms. McDermott noted.
Encouraging and training physicians in concurrent documentation also can help reduce administrative burden.
“Being proficient at remaining in session and documenting as much as you can during a session can help. So that at the end, you’re pressing the button, closing the encounter and you’ve finished documenting,” Ms. McDermott said. “It’s definitely possible to do that without losing the connection with the patient.”
To accomplish this, physicians need to leverage touch-typing – the practice of typing without looking at the keyboard. Fortunately, telehealth makes this mode of documentation easily achievable. Consider the following: During an online session, clinicians can place the patient’s picture “right underneath the camera and make it small. And then you type with the note floating behind it. So you’re actually staring at the note and the person all at the same time,” Ms. McDermott said.
The continued uptake of telehealth in general could also reduce stress for physicians, added Dr. Yellowlees.
“One of the interesting things about that is just how much time we save the physicians because it actually takes quite a lot of time to room patients,” Dr. Yellowlees concluded. “We are now doing about 20% of all our outpatient visits in all disciplines by video. We were higher than that midway through COVID. I’m hoping we’ll go back to being higher than that.”
A version of this article first appeared on Medscape.com.
The American Medical Association estimates that physician burnout costs the country $4.6 billion annually, and that doesn’t include the cost for nurses and other clinicians. In addition, physicians note too many bureaucratic tasks as a main contributor to their daily stress.
Such revelations have prompted many in the health care industry to focus on clinician burnout, including a panel at the recent American Telemedicine Association annual conference in Boston.
Not surprisingly, the discussion quickly turned to the COVID-19 pandemic, commonly cited as an event that has exacerbated existing clinician burnout and caused what has become known as the “great resignation.”
Peter Yellowlees, MBBS, MD, professor of psychiatry and chief wellness officer at the University of California, Davis, said his health system has experienced a lot of its nursing staff resigning or moving to other employment, particularly from intensive care units and the emergency department.
“We actually haven’t had too many physicians go, but I have a funny feeling we’re going to see that over the next year or so because I think a lot of people have just put their head down during the pandemic and they’ve worked themselves hard,” he said. “They’re now sort of putting their heads up above the wall,” and could realize that they want a change.
In his role as the wellness officer at the academic medical center, Dr. Yellowlees is proactively addressing burnout among the organization’s 14,000 employees. For example, during the pandemic, he developed a peer responder program. Under this initiative, 600 staff members received training in “psychological first aid,” essentially utilizing staff to become therapists for peers.
For example, if a clinician is struggling emotionally while dealing with a patient who has had significant trauma, a peer responder could talk with the clinician, helping him or her to better deal with the situation.
Marlene McDermott, senior director of therapy services at Array Behavioral Care, a national telepsychiatry provider with offices in New Jersey and Illinois, noted that her organization also addresses burnout by creating opportunities for peer-to-peer support.
“We’ve got hundreds of clinicians and we’ll take 10 to 15 of them, put them in small treatment teams and they have a live chat, a one-off virtual meeting with each other to vent and to ask clinical questions. It’s all clinicians, there’s no administrative staff in there,” Ms. McDermott said. The clinicians have found value in these meetings, as they can share their concerns as well as “silly images or quotes, just to keep things light at times. That’s made a big difference.”
Retraining, technology can help curb administrative burdens
In addition to providing peer support, both Dr. Yellowlees and Ms. McDermott are addressing the significant administrative burden that plagues physicians.
This burden is especially onerous for physicians in the United States, according to a study that compared the number of keystrokes required to produce clinical notes among physicians in several countries.
“What [the study] discovered was that the American notes were three to five times longer than the notes of the Australian or U.K. physicians. I’ve worked in all three countries and I can promise you there’s no difference in the quality of the doctors across those places,” Dr. Yellowlees said.
To address this issue, Dr. Yellowlees is training physicians to reduce the length of their clinical documentation.
“I am trying to retrain physicians who for many years have been trained to be defensive in their documentation – to write absurd amounts just to justify billing,” Dr. Yellowlees said. “We are trying to go back in some respects to the way that we used to write notes 20 years ago ... so much shorter. This is a huge retraining exercise but it’s an exercise that is essential.”
Ms. McDermott also is tackling the administrative burden at her organization.
“We are trying to make the workflow as efficient as possible, doing some asynchronous work where consumers are completing information before a session ... so clinicians are essentially reconciling information instead of gathering all nonpertinent information. They can just work at the top of the license and not be burdened by some of the questions that don’t directly affect treatment,” Ms. McDermott noted.
Encouraging and training physicians in concurrent documentation also can help reduce administrative burden.
“Being proficient at remaining in session and documenting as much as you can during a session can help. So that at the end, you’re pressing the button, closing the encounter and you’ve finished documenting,” Ms. McDermott said. “It’s definitely possible to do that without losing the connection with the patient.”
To accomplish this, physicians need to leverage touch-typing – the practice of typing without looking at the keyboard. Fortunately, telehealth makes this mode of documentation easily achievable. Consider the following: During an online session, clinicians can place the patient’s picture “right underneath the camera and make it small. And then you type with the note floating behind it. So you’re actually staring at the note and the person all at the same time,” Ms. McDermott said.
The continued uptake of telehealth in general could also reduce stress for physicians, added Dr. Yellowlees.
“One of the interesting things about that is just how much time we save the physicians because it actually takes quite a lot of time to room patients,” Dr. Yellowlees concluded. “We are now doing about 20% of all our outpatient visits in all disciplines by video. We were higher than that midway through COVID. I’m hoping we’ll go back to being higher than that.”
A version of this article first appeared on Medscape.com.
Spell it out: Writing out common medical terms boosts patient understanding, says study
MI. HTN. hx. Although these abbreviations might make it easier for physicians and other health care professionals to create and consume clinical documentation, the shorthand confuses patients, according to a study published in JAMA Network Open.
Researchers, who conducted clinical trials at three hospitals, found that expansion of 10 common medical abbreviations and acronyms in patient health records significantly increased overall comprehension.
Corresponding author Lisa Grossman Liu, PhD, MD, of Columbia University, New York, told this news organization that “comprehension of abbreviations was much lower than we expected and much lower than the clinicians who participated in this study expected.”
This discovery is particularly relevant in this era of digital care, where providers are now communicating with patients electronically more than ever before – and are required by rules emanating from the 21st Century Cures Act to provide online access to electronic health records.
Using elongated terms
Although the study found that expansion of medical abbreviations and acronyms can improve patient understanding, identifying all of the medical abbreviations that exist is difficult because the terms vary by specialty and geography. The fact that many abbreviations and acronyms have multiple meanings complicates matters even more. For example, the abbreviation PA has 128 possible meanings, Dr. Grossman Liu pointed out.
Technology, fortunately, has advanced in the last few years and is on the cusp of providing a solution. Artificial intelligence systems could help to develop large compendiums of abbreviations and acronyms and then machine learning could elongate the words.
“We’re almost to the point where we have these automated systems that can actually expand abbreviations pretty well and with a great degree of accuracy and ... where those can actually be used in medicine to help with patient communication,” Dr. Grossman Liu said.
Such intervention, however, is not a cure-all.
“There are abbreviations that are really hard to understand even after you expand them, such as MI for myocardial infarction, which is really a tough term all around. It means heart attack. So even if you tell patients, MI means myocardial infarction, they’re still not going to understand it,” Dr. Grossman Liu said.
On the flip side, patients are likely to understand some abbreviations such as hrs, which stands for hours, without elongating the words.
Moving from in-person to online communication
A look at the evolution of clinical documentation explains how this abbreviation problem came to fruition. Prior to this digital age where providers communicate with patients through portals, secure messaging, and other electronic methods, patients and providers would talk face to face. Now, however, electronic written communication is becoming the norm.
“We are not only seeing direct written communication through things like messaging systems or email, but also patients are now reading their medical records online and you can consider that as a form of communication,” Dr. Grossman Liu said. “It’s really interesting that the electronic health record itself has essentially become a medium for communication between patients and providers when previously it was only a way for providers to communicate with themselves and document patient care. So, clinicians use abbreviations because they aren’t intending for patients to see the records.”
Requiring physicians to use complete words in clinical documentation now that electronic records are relied on for patient communication, however, is not a practical solution.
“Abbreviations are so commonly used because they are more efficient to read and more efficient to write. We really shouldn’t be putting the onus on providers to spell out all the abbreviations in their notes. That’s realistically not going to work, because it compromises clinical efficiency,” Dr. Grossman Liu said.
While physicians should not be forced to use complete words in documentation, they should be wary of patients’ unfamiliarity with abbreviations as they communicate in person.
“I use terms like ED constantly when I talk to patients, and it turns out that only 67% of patients understand what you’re talking about when you say ED in reference to the emergency department. So it’s important to be mindful of that,” Dr. Grossman Liu concluded.
A version of this article first appeared on Medscape.com.
MI. HTN. hx. Although these abbreviations might make it easier for physicians and other health care professionals to create and consume clinical documentation, the shorthand confuses patients, according to a study published in JAMA Network Open.
Researchers, who conducted clinical trials at three hospitals, found that expansion of 10 common medical abbreviations and acronyms in patient health records significantly increased overall comprehension.
Corresponding author Lisa Grossman Liu, PhD, MD, of Columbia University, New York, told this news organization that “comprehension of abbreviations was much lower than we expected and much lower than the clinicians who participated in this study expected.”
This discovery is particularly relevant in this era of digital care, where providers are now communicating with patients electronically more than ever before – and are required by rules emanating from the 21st Century Cures Act to provide online access to electronic health records.
Using elongated terms
Although the study found that expansion of medical abbreviations and acronyms can improve patient understanding, identifying all of the medical abbreviations that exist is difficult because the terms vary by specialty and geography. The fact that many abbreviations and acronyms have multiple meanings complicates matters even more. For example, the abbreviation PA has 128 possible meanings, Dr. Grossman Liu pointed out.
Technology, fortunately, has advanced in the last few years and is on the cusp of providing a solution. Artificial intelligence systems could help to develop large compendiums of abbreviations and acronyms and then machine learning could elongate the words.
“We’re almost to the point where we have these automated systems that can actually expand abbreviations pretty well and with a great degree of accuracy and ... where those can actually be used in medicine to help with patient communication,” Dr. Grossman Liu said.
Such intervention, however, is not a cure-all.
“There are abbreviations that are really hard to understand even after you expand them, such as MI for myocardial infarction, which is really a tough term all around. It means heart attack. So even if you tell patients, MI means myocardial infarction, they’re still not going to understand it,” Dr. Grossman Liu said.
On the flip side, patients are likely to understand some abbreviations such as hrs, which stands for hours, without elongating the words.
Moving from in-person to online communication
A look at the evolution of clinical documentation explains how this abbreviation problem came to fruition. Prior to this digital age where providers communicate with patients through portals, secure messaging, and other electronic methods, patients and providers would talk face to face. Now, however, electronic written communication is becoming the norm.
“We are not only seeing direct written communication through things like messaging systems or email, but also patients are now reading their medical records online and you can consider that as a form of communication,” Dr. Grossman Liu said. “It’s really interesting that the electronic health record itself has essentially become a medium for communication between patients and providers when previously it was only a way for providers to communicate with themselves and document patient care. So, clinicians use abbreviations because they aren’t intending for patients to see the records.”
Requiring physicians to use complete words in clinical documentation now that electronic records are relied on for patient communication, however, is not a practical solution.
“Abbreviations are so commonly used because they are more efficient to read and more efficient to write. We really shouldn’t be putting the onus on providers to spell out all the abbreviations in their notes. That’s realistically not going to work, because it compromises clinical efficiency,” Dr. Grossman Liu said.
While physicians should not be forced to use complete words in documentation, they should be wary of patients’ unfamiliarity with abbreviations as they communicate in person.
“I use terms like ED constantly when I talk to patients, and it turns out that only 67% of patients understand what you’re talking about when you say ED in reference to the emergency department. So it’s important to be mindful of that,” Dr. Grossman Liu concluded.
A version of this article first appeared on Medscape.com.
MI. HTN. hx. Although these abbreviations might make it easier for physicians and other health care professionals to create and consume clinical documentation, the shorthand confuses patients, according to a study published in JAMA Network Open.
Researchers, who conducted clinical trials at three hospitals, found that expansion of 10 common medical abbreviations and acronyms in patient health records significantly increased overall comprehension.
Corresponding author Lisa Grossman Liu, PhD, MD, of Columbia University, New York, told this news organization that “comprehension of abbreviations was much lower than we expected and much lower than the clinicians who participated in this study expected.”
This discovery is particularly relevant in this era of digital care, where providers are now communicating with patients electronically more than ever before – and are required by rules emanating from the 21st Century Cures Act to provide online access to electronic health records.
Using elongated terms
Although the study found that expansion of medical abbreviations and acronyms can improve patient understanding, identifying all of the medical abbreviations that exist is difficult because the terms vary by specialty and geography. The fact that many abbreviations and acronyms have multiple meanings complicates matters even more. For example, the abbreviation PA has 128 possible meanings, Dr. Grossman Liu pointed out.
Technology, fortunately, has advanced in the last few years and is on the cusp of providing a solution. Artificial intelligence systems could help to develop large compendiums of abbreviations and acronyms and then machine learning could elongate the words.
“We’re almost to the point where we have these automated systems that can actually expand abbreviations pretty well and with a great degree of accuracy and ... where those can actually be used in medicine to help with patient communication,” Dr. Grossman Liu said.
Such intervention, however, is not a cure-all.
“There are abbreviations that are really hard to understand even after you expand them, such as MI for myocardial infarction, which is really a tough term all around. It means heart attack. So even if you tell patients, MI means myocardial infarction, they’re still not going to understand it,” Dr. Grossman Liu said.
On the flip side, patients are likely to understand some abbreviations such as hrs, which stands for hours, without elongating the words.
Moving from in-person to online communication
A look at the evolution of clinical documentation explains how this abbreviation problem came to fruition. Prior to this digital age where providers communicate with patients through portals, secure messaging, and other electronic methods, patients and providers would talk face to face. Now, however, electronic written communication is becoming the norm.
“We are not only seeing direct written communication through things like messaging systems or email, but also patients are now reading their medical records online and you can consider that as a form of communication,” Dr. Grossman Liu said. “It’s really interesting that the electronic health record itself has essentially become a medium for communication between patients and providers when previously it was only a way for providers to communicate with themselves and document patient care. So, clinicians use abbreviations because they aren’t intending for patients to see the records.”
Requiring physicians to use complete words in clinical documentation now that electronic records are relied on for patient communication, however, is not a practical solution.
“Abbreviations are so commonly used because they are more efficient to read and more efficient to write. We really shouldn’t be putting the onus on providers to spell out all the abbreviations in their notes. That’s realistically not going to work, because it compromises clinical efficiency,” Dr. Grossman Liu said.
While physicians should not be forced to use complete words in documentation, they should be wary of patients’ unfamiliarity with abbreviations as they communicate in person.
“I use terms like ED constantly when I talk to patients, and it turns out that only 67% of patients understand what you’re talking about when you say ED in reference to the emergency department. So it’s important to be mindful of that,” Dr. Grossman Liu concluded.
A version of this article first appeared on Medscape.com.
FROM JAMA NETWORK OPEN
COVID drove telehealth forward in high gear: Now what?
Before the pandemic hit in 2019, Pooja Aysola, MD, considered herself lucky because she could tap into telehealth for neurology consults in her work as an emergency department physician.
“We would wheel in a computer screen with a neurologist on board every time we had a suspected stroke patient. And I was able to talk directly to the neurologist about my patient’s symptoms. And it was great,” Dr. Aysola said.
The pandemic, however, prompted the need for telehealth in many situations beyond specialty care. As such, investment exploded over the past few years.
“We’re seeing telehealth across all specialties ... more than half of clinicians are now saying that they do believe that virtual visits will surpass in-person visits for primary care needs,” said Dr. Aysola, who also serves as senior director, clinical operations at Wheel, a Texas-based telehealth company.
Dr. Aysola spoke during an American Telemedicine Association conference panel addressing how COVID prompted an uptick in telehealth investment and utilization and how such virtual care is likely to evolve moving forward.
Nathaniel Lacktman, a partner at law firm Foley & Lardner, agreed with Dr. Aysola’s assessment of the market.
“The appetite for virtual care has become voracious,” said Mr. Lacktman, who chairs the firm’s telemedicine and digital health team. “It reminds me in some ways of taking my kids out to dinner and saying, ‘Try this new food.’ They’re like, ‘No, I won’t like it.’ They finally get a little taste and they’re like, ‘This is amazing.’”
While there is no doubt that stakeholders – from innovators to investors to providers to patients – will want more than just a taste of telehealth in the future, panelists addressed if this undeniable demand for virtual care was simply a short-term response to the pandemic or if there is a long-term desire to fundamentally change how care is delivered.
Expanding on the pandemic-driven ‘sandbox’
While the uptick in telehealth investment and utilization is not expected to continue at such jarring rates in the future, the panelists pointed out that innovation will proceed but perhaps at a different pace.
“The last 3 years have been a sandbox during which the industry was able to experiment,” said Mr. Lacktman. “What we’re going to see more of even post pandemic is building upon that experimental sandbox and creating models that aren’t just high growth and really quick but that are sustainable and meaningful.”
As such, patients and providers won’t be looking for telehealth to simply provide access to care but to provide a full scope of services while also improving quality.
Rachel Stillman, vice president of 7wireVentures, a Chicago-based venture capital firm, also expects interest in telehealth to continue but at a less frenetic pace. In 2021, the industry witnessed nearly $31 billion of venture financing directed towards digital health companies, she said.
“Now, Q1 2022 has had a little bit of a slower start. But with that said, we still have invested $6 billion in early stage companies. So ... we’re seeing some initial signs perhaps of – I don’t want to call it a slowdown – but increased discipline,” Ms. Stillman said.
Start-up companies will need to carefully position themselves for success in this post pandemic environment. “Ultimately, it really goes down to making sure your fundamentals are strong ... and having a really compelling [return on investment] case for your health plan, your self-insured employer, your health system, or your ultimate buyer,” Ms. Stillman said.
Two models are coming into play as innovation continues, she added. One is a traditional care delivery model whereby a start-up organization is building their own provider network specialized for the conditions or patient populations they are serving.
“Conversely, there are new entrants that are thinking about how they can leverage their insightful and strong technology foundations and platforms for existing provider networks that could benefit from a telemedicine partner,” Ms. Stillman pointed out.
Dr. Aysola added that companies are moving forward strategically to achieve post pandemic success. Some telehealth start-ups, for instance, are “capturing some of the low-hanging fruit, the simple UTIs, the really easy things to treat,” Dr. Aysola said.
Others are addressing the clinician’s experience. “Over 50% of clinicians have thought about leaving their jobs at some point during the pandemic. And so it’s becoming really clear that focusing on the clinician and the clinician’s needs are just imperative to [creating a] winning model post-pandemic,” Dr. Aysola said.
Adapting to the new normal
Health care provider organizations also need to adjust to post pandemic realities. “We work with a number of hospital systems, and it’s astounding how slow they are compared to the start-ups because there’s a lot more constituents; there’s bureaucracy,” Mr. Lacktman said. As a result, “the hospitals are in a more uncomfortable position post pandemic than the start-ups.”
To move forward successfully, these organizations, which are typically risk averse, need to create alignment among legal, compliance, and clinical leaders, Mr. Lacktman advised.
One of the first decisions that these teams need to make is whether they should proceed on their own or enter into a partnership with a start-up or pursue a merger and acquisition. In addition, some health systems, hospitals, and health plans are even opting to establish their own venture funds.
“Building your own venture fund or even investing ... in companies directly or in other venture funds [are strategies] that health systems might be able to leverage both to accelerate partnerships and also really be on top of key trends,” Ms. Stillman said.
No matter how health care systems invest in and implement telemedicine technologies, though, the need to move quickly is paramount.
Traditional health care systems “don’t always have the luxury of time. Things have to be done pretty quickly in order to remain competitive,” Dr. Aysola concluded. “We’ve found that companies can launch a virtual care offering in a matter of weeks. When in reality, if a traditional health care system were to try to launch it on their own, it could take upwards of 15 months.”
A version of this article first appeared on Medscape.com.
Before the pandemic hit in 2019, Pooja Aysola, MD, considered herself lucky because she could tap into telehealth for neurology consults in her work as an emergency department physician.
“We would wheel in a computer screen with a neurologist on board every time we had a suspected stroke patient. And I was able to talk directly to the neurologist about my patient’s symptoms. And it was great,” Dr. Aysola said.
The pandemic, however, prompted the need for telehealth in many situations beyond specialty care. As such, investment exploded over the past few years.
“We’re seeing telehealth across all specialties ... more than half of clinicians are now saying that they do believe that virtual visits will surpass in-person visits for primary care needs,” said Dr. Aysola, who also serves as senior director, clinical operations at Wheel, a Texas-based telehealth company.
Dr. Aysola spoke during an American Telemedicine Association conference panel addressing how COVID prompted an uptick in telehealth investment and utilization and how such virtual care is likely to evolve moving forward.
Nathaniel Lacktman, a partner at law firm Foley & Lardner, agreed with Dr. Aysola’s assessment of the market.
“The appetite for virtual care has become voracious,” said Mr. Lacktman, who chairs the firm’s telemedicine and digital health team. “It reminds me in some ways of taking my kids out to dinner and saying, ‘Try this new food.’ They’re like, ‘No, I won’t like it.’ They finally get a little taste and they’re like, ‘This is amazing.’”
While there is no doubt that stakeholders – from innovators to investors to providers to patients – will want more than just a taste of telehealth in the future, panelists addressed if this undeniable demand for virtual care was simply a short-term response to the pandemic or if there is a long-term desire to fundamentally change how care is delivered.
Expanding on the pandemic-driven ‘sandbox’
While the uptick in telehealth investment and utilization is not expected to continue at such jarring rates in the future, the panelists pointed out that innovation will proceed but perhaps at a different pace.
“The last 3 years have been a sandbox during which the industry was able to experiment,” said Mr. Lacktman. “What we’re going to see more of even post pandemic is building upon that experimental sandbox and creating models that aren’t just high growth and really quick but that are sustainable and meaningful.”
As such, patients and providers won’t be looking for telehealth to simply provide access to care but to provide a full scope of services while also improving quality.
Rachel Stillman, vice president of 7wireVentures, a Chicago-based venture capital firm, also expects interest in telehealth to continue but at a less frenetic pace. In 2021, the industry witnessed nearly $31 billion of venture financing directed towards digital health companies, she said.
“Now, Q1 2022 has had a little bit of a slower start. But with that said, we still have invested $6 billion in early stage companies. So ... we’re seeing some initial signs perhaps of – I don’t want to call it a slowdown – but increased discipline,” Ms. Stillman said.
Start-up companies will need to carefully position themselves for success in this post pandemic environment. “Ultimately, it really goes down to making sure your fundamentals are strong ... and having a really compelling [return on investment] case for your health plan, your self-insured employer, your health system, or your ultimate buyer,” Ms. Stillman said.
Two models are coming into play as innovation continues, she added. One is a traditional care delivery model whereby a start-up organization is building their own provider network specialized for the conditions or patient populations they are serving.
“Conversely, there are new entrants that are thinking about how they can leverage their insightful and strong technology foundations and platforms for existing provider networks that could benefit from a telemedicine partner,” Ms. Stillman pointed out.
Dr. Aysola added that companies are moving forward strategically to achieve post pandemic success. Some telehealth start-ups, for instance, are “capturing some of the low-hanging fruit, the simple UTIs, the really easy things to treat,” Dr. Aysola said.
Others are addressing the clinician’s experience. “Over 50% of clinicians have thought about leaving their jobs at some point during the pandemic. And so it’s becoming really clear that focusing on the clinician and the clinician’s needs are just imperative to [creating a] winning model post-pandemic,” Dr. Aysola said.
Adapting to the new normal
Health care provider organizations also need to adjust to post pandemic realities. “We work with a number of hospital systems, and it’s astounding how slow they are compared to the start-ups because there’s a lot more constituents; there’s bureaucracy,” Mr. Lacktman said. As a result, “the hospitals are in a more uncomfortable position post pandemic than the start-ups.”
To move forward successfully, these organizations, which are typically risk averse, need to create alignment among legal, compliance, and clinical leaders, Mr. Lacktman advised.
One of the first decisions that these teams need to make is whether they should proceed on their own or enter into a partnership with a start-up or pursue a merger and acquisition. In addition, some health systems, hospitals, and health plans are even opting to establish their own venture funds.
“Building your own venture fund or even investing ... in companies directly or in other venture funds [are strategies] that health systems might be able to leverage both to accelerate partnerships and also really be on top of key trends,” Ms. Stillman said.
No matter how health care systems invest in and implement telemedicine technologies, though, the need to move quickly is paramount.
Traditional health care systems “don’t always have the luxury of time. Things have to be done pretty quickly in order to remain competitive,” Dr. Aysola concluded. “We’ve found that companies can launch a virtual care offering in a matter of weeks. When in reality, if a traditional health care system were to try to launch it on their own, it could take upwards of 15 months.”
A version of this article first appeared on Medscape.com.
Before the pandemic hit in 2019, Pooja Aysola, MD, considered herself lucky because she could tap into telehealth for neurology consults in her work as an emergency department physician.
“We would wheel in a computer screen with a neurologist on board every time we had a suspected stroke patient. And I was able to talk directly to the neurologist about my patient’s symptoms. And it was great,” Dr. Aysola said.
The pandemic, however, prompted the need for telehealth in many situations beyond specialty care. As such, investment exploded over the past few years.
“We’re seeing telehealth across all specialties ... more than half of clinicians are now saying that they do believe that virtual visits will surpass in-person visits for primary care needs,” said Dr. Aysola, who also serves as senior director, clinical operations at Wheel, a Texas-based telehealth company.
Dr. Aysola spoke during an American Telemedicine Association conference panel addressing how COVID prompted an uptick in telehealth investment and utilization and how such virtual care is likely to evolve moving forward.
Nathaniel Lacktman, a partner at law firm Foley & Lardner, agreed with Dr. Aysola’s assessment of the market.
“The appetite for virtual care has become voracious,” said Mr. Lacktman, who chairs the firm’s telemedicine and digital health team. “It reminds me in some ways of taking my kids out to dinner and saying, ‘Try this new food.’ They’re like, ‘No, I won’t like it.’ They finally get a little taste and they’re like, ‘This is amazing.’”
While there is no doubt that stakeholders – from innovators to investors to providers to patients – will want more than just a taste of telehealth in the future, panelists addressed if this undeniable demand for virtual care was simply a short-term response to the pandemic or if there is a long-term desire to fundamentally change how care is delivered.
Expanding on the pandemic-driven ‘sandbox’
While the uptick in telehealth investment and utilization is not expected to continue at such jarring rates in the future, the panelists pointed out that innovation will proceed but perhaps at a different pace.
“The last 3 years have been a sandbox during which the industry was able to experiment,” said Mr. Lacktman. “What we’re going to see more of even post pandemic is building upon that experimental sandbox and creating models that aren’t just high growth and really quick but that are sustainable and meaningful.”
As such, patients and providers won’t be looking for telehealth to simply provide access to care but to provide a full scope of services while also improving quality.
Rachel Stillman, vice president of 7wireVentures, a Chicago-based venture capital firm, also expects interest in telehealth to continue but at a less frenetic pace. In 2021, the industry witnessed nearly $31 billion of venture financing directed towards digital health companies, she said.
“Now, Q1 2022 has had a little bit of a slower start. But with that said, we still have invested $6 billion in early stage companies. So ... we’re seeing some initial signs perhaps of – I don’t want to call it a slowdown – but increased discipline,” Ms. Stillman said.
Start-up companies will need to carefully position themselves for success in this post pandemic environment. “Ultimately, it really goes down to making sure your fundamentals are strong ... and having a really compelling [return on investment] case for your health plan, your self-insured employer, your health system, or your ultimate buyer,” Ms. Stillman said.
Two models are coming into play as innovation continues, she added. One is a traditional care delivery model whereby a start-up organization is building their own provider network specialized for the conditions or patient populations they are serving.
“Conversely, there are new entrants that are thinking about how they can leverage their insightful and strong technology foundations and platforms for existing provider networks that could benefit from a telemedicine partner,” Ms. Stillman pointed out.
Dr. Aysola added that companies are moving forward strategically to achieve post pandemic success. Some telehealth start-ups, for instance, are “capturing some of the low-hanging fruit, the simple UTIs, the really easy things to treat,” Dr. Aysola said.
Others are addressing the clinician’s experience. “Over 50% of clinicians have thought about leaving their jobs at some point during the pandemic. And so it’s becoming really clear that focusing on the clinician and the clinician’s needs are just imperative to [creating a] winning model post-pandemic,” Dr. Aysola said.
Adapting to the new normal
Health care provider organizations also need to adjust to post pandemic realities. “We work with a number of hospital systems, and it’s astounding how slow they are compared to the start-ups because there’s a lot more constituents; there’s bureaucracy,” Mr. Lacktman said. As a result, “the hospitals are in a more uncomfortable position post pandemic than the start-ups.”
To move forward successfully, these organizations, which are typically risk averse, need to create alignment among legal, compliance, and clinical leaders, Mr. Lacktman advised.
One of the first decisions that these teams need to make is whether they should proceed on their own or enter into a partnership with a start-up or pursue a merger and acquisition. In addition, some health systems, hospitals, and health plans are even opting to establish their own venture funds.
“Building your own venture fund or even investing ... in companies directly or in other venture funds [are strategies] that health systems might be able to leverage both to accelerate partnerships and also really be on top of key trends,” Ms. Stillman said.
No matter how health care systems invest in and implement telemedicine technologies, though, the need to move quickly is paramount.
Traditional health care systems “don’t always have the luxury of time. Things have to be done pretty quickly in order to remain competitive,” Dr. Aysola concluded. “We’ve found that companies can launch a virtual care offering in a matter of weeks. When in reality, if a traditional health care system were to try to launch it on their own, it could take upwards of 15 months.”
A version of this article first appeared on Medscape.com.
Stroke in the young: Cancer in disguise?
The data were presented by Jamie Verhoeven, MD, Radboud University Medical Centre, the Netherlands, at the recent European Stroke Organisation Conference 2022.
Dr. Verhoeven noted that 10% of all stroke cases occur in individuals younger than 50 years. During the past few decades, the incidence of stroke in the young has steadily increased, whereas the incidence of stroke in older adults has stabilized or decreased.
“Stroke in the young differs from stroke in older patients, and one of the major differences is that stroke in the young has a higher proportion of cryptogenic stroke, with no clear cause found in over one-third of patients,” she said.
Also, having an active cancer is known to be a risk factor for thrombosis. This association is strongest in venous thrombosis and has been less well investigated in arterial thrombosis, Dr. Verhoeven reported.
Her group aimed to investigate whether in some patients with cryptogenic stroke, this may be the first manifestation of an underlying cancer. “If this hypothesis is true, then it would be more obvious in young patients who have a higher incidence of cryptogenic stroke,” she said.
They performed a population-based observational cohort study using diagnostic ICD codes from the national Hospital Discharge Registry in the Netherlands and the Dutch Population Registry from 1998 to 2019.
Patients with a history of cancer before their first stroke and those with central nervous system cancers at the time of stroke or nonmelanoma skin cancers (which have been shown to have no systemic effects) were excluded.
Reference data came from the Netherlands Comprehensive Cancer Organisation, which collects data on all cancer diagnoses in the country.
The researchers identified 27,616 young stroke patients (age range, 15-49 years; median age, 45 years) and 362,782 older stroke patients (age range, 50 years and older; median age, 76 years).
The cumulative incidence of any cancer at 10 years was 3.7% in the younger group and 8.5% in the older group.
The data were compared with matched peers from the general population. The main outcome measures were cumulative incidence of first-ever cancer after stroke (stratified by stroke subtype, age and sex) and standardized incidence rates.
Results showed that the risk for cancer was higher in the younger age group than in the matched general population.
In this age group, the 1-year risk of any new cancer was 2.6 times higher (95% confidence interval, 2.2-3.1) after ischemic stroke and 5.4 times (95% CI, 3.8-7.3) after intracerebral hemorrhage than in matched peers from the general population.
In contrast, in stroke patients older than 50 years, the 1-year risk for any new cancer was 1.2 times higher than the general population after either ischemic or hemorrhagic stroke.
“The younger patients have a higher risk increase of cancer than older patients, and this risk increase is most evident in the first 1 to 2 years after stroke but remains statistically significant for up to 5 to 8 years later,” Dr. Verhoeven said.
The cancers that were most involved in this risk increase were those of the lower respiratory tract, hematologic cancers, and gastrointestinal cancers.
The main strength of this study was the use of national databases that allowed for a very large sample size, but this brings with it the danger of misclassification of events and the lack of clinical data, Dr. Verhoeven noted.
“Young stroke patients are at increased risk of developing a new cancer in the years following their stroke compared to peers from the general population, but this risk is only marginally increased in the older stroke population,” she concluded.
She pointed out that it is not possible to confirm any causal relation from this study design, but a clear association has been shown.
“We need more studies into this field. We need a large clinical dataset to examine which clinical phenotypes are associated with possible underlying cancers to identify which patients are most at risk. We are already working on this,” she said. “Then it remains to be investigated whether screening for an underlying cancer should be added to the diagnostic workup in young stroke patients.”
Commenting on the study after the presentation, William Whiteley, BM, PhD, a clinical epidemiologist at the University of Edinburgh, Scotland, and a consultant neurologist in NHS Lothian, said it was difficult to know whether the link shown between stroke and cancer was causal, but the effect size in this study was “quite large.”
He pointed out that the associations with bowel and lung cancer could be due to shared risk factors, such as smoking, but he said the finding on a link with hematologic cancers is “interesting.”
Noting that there are links between hematologic cancers and thrombotic events, he said: “People have wondered if that is because of clonal expansion, which has been shown to increase the risk of atherosclerosis, so the question is whether this is some kind of common risk factor here.”
Dr. Verhoeven said she did not believe that shared risk factors fully explained the difference in increased risks between young and older patients.
“It does not fully explain why the risk of cancer is specifically higher in the first 1 to 2 years after the stroke diagnosis. I would think if it was just shared risk factors, the risk increase should remain relatively stable, or even increase due to the build-up of exposure to risk factors over the years,” she said.
Dr. Whiteley said that data like these are “really useful in trying to estimate these associations and it gives us some hypotheses to investigate in smaller mechanistic studies.”
Asked whether these data justify screening younger cryptogenic stroke patients more systematically for cancer, Dr. Whiteley replied: “I think we need some absolute risk estimates for that; for example, what proportion of younger patients would be at risk over the next few years when that screening would make a difference.”
Dr. Verhoeven reports no disclosures.
A version of this article first appeared on Medscape.com.
The data were presented by Jamie Verhoeven, MD, Radboud University Medical Centre, the Netherlands, at the recent European Stroke Organisation Conference 2022.
Dr. Verhoeven noted that 10% of all stroke cases occur in individuals younger than 50 years. During the past few decades, the incidence of stroke in the young has steadily increased, whereas the incidence of stroke in older adults has stabilized or decreased.
“Stroke in the young differs from stroke in older patients, and one of the major differences is that stroke in the young has a higher proportion of cryptogenic stroke, with no clear cause found in over one-third of patients,” she said.
Also, having an active cancer is known to be a risk factor for thrombosis. This association is strongest in venous thrombosis and has been less well investigated in arterial thrombosis, Dr. Verhoeven reported.
Her group aimed to investigate whether in some patients with cryptogenic stroke, this may be the first manifestation of an underlying cancer. “If this hypothesis is true, then it would be more obvious in young patients who have a higher incidence of cryptogenic stroke,” she said.
They performed a population-based observational cohort study using diagnostic ICD codes from the national Hospital Discharge Registry in the Netherlands and the Dutch Population Registry from 1998 to 2019.
Patients with a history of cancer before their first stroke and those with central nervous system cancers at the time of stroke or nonmelanoma skin cancers (which have been shown to have no systemic effects) were excluded.
Reference data came from the Netherlands Comprehensive Cancer Organisation, which collects data on all cancer diagnoses in the country.
The researchers identified 27,616 young stroke patients (age range, 15-49 years; median age, 45 years) and 362,782 older stroke patients (age range, 50 years and older; median age, 76 years).
The cumulative incidence of any cancer at 10 years was 3.7% in the younger group and 8.5% in the older group.
The data were compared with matched peers from the general population. The main outcome measures were cumulative incidence of first-ever cancer after stroke (stratified by stroke subtype, age and sex) and standardized incidence rates.
Results showed that the risk for cancer was higher in the younger age group than in the matched general population.
In this age group, the 1-year risk of any new cancer was 2.6 times higher (95% confidence interval, 2.2-3.1) after ischemic stroke and 5.4 times (95% CI, 3.8-7.3) after intracerebral hemorrhage than in matched peers from the general population.
In contrast, in stroke patients older than 50 years, the 1-year risk for any new cancer was 1.2 times higher than the general population after either ischemic or hemorrhagic stroke.
“The younger patients have a higher risk increase of cancer than older patients, and this risk increase is most evident in the first 1 to 2 years after stroke but remains statistically significant for up to 5 to 8 years later,” Dr. Verhoeven said.
The cancers that were most involved in this risk increase were those of the lower respiratory tract, hematologic cancers, and gastrointestinal cancers.
The main strength of this study was the use of national databases that allowed for a very large sample size, but this brings with it the danger of misclassification of events and the lack of clinical data, Dr. Verhoeven noted.
“Young stroke patients are at increased risk of developing a new cancer in the years following their stroke compared to peers from the general population, but this risk is only marginally increased in the older stroke population,” she concluded.
She pointed out that it is not possible to confirm any causal relation from this study design, but a clear association has been shown.
“We need more studies into this field. We need a large clinical dataset to examine which clinical phenotypes are associated with possible underlying cancers to identify which patients are most at risk. We are already working on this,” she said. “Then it remains to be investigated whether screening for an underlying cancer should be added to the diagnostic workup in young stroke patients.”
Commenting on the study after the presentation, William Whiteley, BM, PhD, a clinical epidemiologist at the University of Edinburgh, Scotland, and a consultant neurologist in NHS Lothian, said it was difficult to know whether the link shown between stroke and cancer was causal, but the effect size in this study was “quite large.”
He pointed out that the associations with bowel and lung cancer could be due to shared risk factors, such as smoking, but he said the finding on a link with hematologic cancers is “interesting.”
Noting that there are links between hematologic cancers and thrombotic events, he said: “People have wondered if that is because of clonal expansion, which has been shown to increase the risk of atherosclerosis, so the question is whether this is some kind of common risk factor here.”
Dr. Verhoeven said she did not believe that shared risk factors fully explained the difference in increased risks between young and older patients.
“It does not fully explain why the risk of cancer is specifically higher in the first 1 to 2 years after the stroke diagnosis. I would think if it was just shared risk factors, the risk increase should remain relatively stable, or even increase due to the build-up of exposure to risk factors over the years,” she said.
Dr. Whiteley said that data like these are “really useful in trying to estimate these associations and it gives us some hypotheses to investigate in smaller mechanistic studies.”
Asked whether these data justify screening younger cryptogenic stroke patients more systematically for cancer, Dr. Whiteley replied: “I think we need some absolute risk estimates for that; for example, what proportion of younger patients would be at risk over the next few years when that screening would make a difference.”
Dr. Verhoeven reports no disclosures.
A version of this article first appeared on Medscape.com.
The data were presented by Jamie Verhoeven, MD, Radboud University Medical Centre, the Netherlands, at the recent European Stroke Organisation Conference 2022.
Dr. Verhoeven noted that 10% of all stroke cases occur in individuals younger than 50 years. During the past few decades, the incidence of stroke in the young has steadily increased, whereas the incidence of stroke in older adults has stabilized or decreased.
“Stroke in the young differs from stroke in older patients, and one of the major differences is that stroke in the young has a higher proportion of cryptogenic stroke, with no clear cause found in over one-third of patients,” she said.
Also, having an active cancer is known to be a risk factor for thrombosis. This association is strongest in venous thrombosis and has been less well investigated in arterial thrombosis, Dr. Verhoeven reported.
Her group aimed to investigate whether in some patients with cryptogenic stroke, this may be the first manifestation of an underlying cancer. “If this hypothesis is true, then it would be more obvious in young patients who have a higher incidence of cryptogenic stroke,” she said.
They performed a population-based observational cohort study using diagnostic ICD codes from the national Hospital Discharge Registry in the Netherlands and the Dutch Population Registry from 1998 to 2019.
Patients with a history of cancer before their first stroke and those with central nervous system cancers at the time of stroke or nonmelanoma skin cancers (which have been shown to have no systemic effects) were excluded.
Reference data came from the Netherlands Comprehensive Cancer Organisation, which collects data on all cancer diagnoses in the country.
The researchers identified 27,616 young stroke patients (age range, 15-49 years; median age, 45 years) and 362,782 older stroke patients (age range, 50 years and older; median age, 76 years).
The cumulative incidence of any cancer at 10 years was 3.7% in the younger group and 8.5% in the older group.
The data were compared with matched peers from the general population. The main outcome measures were cumulative incidence of first-ever cancer after stroke (stratified by stroke subtype, age and sex) and standardized incidence rates.
Results showed that the risk for cancer was higher in the younger age group than in the matched general population.
In this age group, the 1-year risk of any new cancer was 2.6 times higher (95% confidence interval, 2.2-3.1) after ischemic stroke and 5.4 times (95% CI, 3.8-7.3) after intracerebral hemorrhage than in matched peers from the general population.
In contrast, in stroke patients older than 50 years, the 1-year risk for any new cancer was 1.2 times higher than the general population after either ischemic or hemorrhagic stroke.
“The younger patients have a higher risk increase of cancer than older patients, and this risk increase is most evident in the first 1 to 2 years after stroke but remains statistically significant for up to 5 to 8 years later,” Dr. Verhoeven said.
The cancers that were most involved in this risk increase were those of the lower respiratory tract, hematologic cancers, and gastrointestinal cancers.
The main strength of this study was the use of national databases that allowed for a very large sample size, but this brings with it the danger of misclassification of events and the lack of clinical data, Dr. Verhoeven noted.
“Young stroke patients are at increased risk of developing a new cancer in the years following their stroke compared to peers from the general population, but this risk is only marginally increased in the older stroke population,” she concluded.
She pointed out that it is not possible to confirm any causal relation from this study design, but a clear association has been shown.
“We need more studies into this field. We need a large clinical dataset to examine which clinical phenotypes are associated with possible underlying cancers to identify which patients are most at risk. We are already working on this,” she said. “Then it remains to be investigated whether screening for an underlying cancer should be added to the diagnostic workup in young stroke patients.”
Commenting on the study after the presentation, William Whiteley, BM, PhD, a clinical epidemiologist at the University of Edinburgh, Scotland, and a consultant neurologist in NHS Lothian, said it was difficult to know whether the link shown between stroke and cancer was causal, but the effect size in this study was “quite large.”
He pointed out that the associations with bowel and lung cancer could be due to shared risk factors, such as smoking, but he said the finding on a link with hematologic cancers is “interesting.”
Noting that there are links between hematologic cancers and thrombotic events, he said: “People have wondered if that is because of clonal expansion, which has been shown to increase the risk of atherosclerosis, so the question is whether this is some kind of common risk factor here.”
Dr. Verhoeven said she did not believe that shared risk factors fully explained the difference in increased risks between young and older patients.
“It does not fully explain why the risk of cancer is specifically higher in the first 1 to 2 years after the stroke diagnosis. I would think if it was just shared risk factors, the risk increase should remain relatively stable, or even increase due to the build-up of exposure to risk factors over the years,” she said.
Dr. Whiteley said that data like these are “really useful in trying to estimate these associations and it gives us some hypotheses to investigate in smaller mechanistic studies.”
Asked whether these data justify screening younger cryptogenic stroke patients more systematically for cancer, Dr. Whiteley replied: “I think we need some absolute risk estimates for that; for example, what proportion of younger patients would be at risk over the next few years when that screening would make a difference.”
Dr. Verhoeven reports no disclosures.
A version of this article first appeared on Medscape.com.
FROM ESOC 2022
Move away from the screen ...
“Go outside and play!”
How often have you said that to your kids (or grandkids)? For that matter, how often did you hear it when you were a kid?
A lot, if memory serves me correctly. Some of it was just my mom wanting me out of the house, some of it an innate realization on her part that too much time spent planted in front of the TV was bad for you. (When I was a kid, Brady Bunch reruns kicked off my summer day at 8:00 a.m.).

The idea that too much time in front of a screen can be bad is nothing new. Regrettably, some of this ancient wisdom has been lost in the eons since I was a kid.
Does this surprise you?
Humans, like all primates, are a social species. We’ve benefited from the combined power of our minds to leave caves, harness nature, and build civilizations. But this has a cost, and perhaps the social media screen has been a tipping point for mental health.
I’m not knocking the basic idea. Share a joke with a friend, see pictures of the new baby, hear out about a new job. That’s fine. The trouble is that it’s gone beyond that. A lot of it is perfectly innocuous ... but a lot isn’t.
As it’s evolved, social media has also become the home of anger. Political and otherwise. It’s so much easier to post memes making fun of other people and their viewpoints than to speak to them in person. Trolls and bots lurk everywhere to get you riled up – things you wouldn’t be encountering if you were talking to your neighbor at the fence or a friend on the phone.
Recent trends on TikTok included students bragging about things they’d stolen from their high schools and people boasting of having “ripped off” Six Flags amusement parks with an annual membership loophole (the latter resulted in park management canceling the plan). How do such things benefit anyone (beyond those posting them getting clicks)?
I’m pretty sure they do nothing to make you feel good, or happy, or positive in any way. And that’s not even counting the political nastiness, cheap shots, and conspiracy theories that drown out rational thought.
Unfortunately, social media in today’s forms is addictive. Seeing one good thing from a friend gives you a dopamine boost, and this drives you to overlook all the bad things the screen does. Like the meth addict who lives for the high, and ignores all the negative aspects – loss of money, family, a home, teeth – that it brings.
So it’s not a surprise that walking away from it for a week made people happier and gave them time to do things that were more important than staring at a screen. Though I do wonder how many of the subjects ended up going back to it, forgetting about the benefits they’d just experienced.
When Frank Zappa released “I’m the Slime” in 1973, it was about television. But today the song is far closer to describing what social media has become than he could have ever imagined. (He died in 1993, never knowing how accurate he’d become).
We encourage our patients to exercise. The benefits of doing so are beyond question. But maybe it’s time to point out not only the good things that come from exercise, but also those that come from turning off the screen in order to do so.
As my mother said: “Go outside and play!”
It’s good for the body and sanity, and both are important.
Dr. Block has a solo neurology practice in Scottsdale, Ariz.
“Go outside and play!”
How often have you said that to your kids (or grandkids)? For that matter, how often did you hear it when you were a kid?
A lot, if memory serves me correctly. Some of it was just my mom wanting me out of the house, some of it an innate realization on her part that too much time spent planted in front of the TV was bad for you. (When I was a kid, Brady Bunch reruns kicked off my summer day at 8:00 a.m.).
The idea that too much time in front of a screen can be bad is nothing new. Regrettably, some of this ancient wisdom has been lost in the eons since I was a kid.
Does this surprise you?
Humans, like all primates, are a social species. We’ve benefited from the combined power of our minds to leave caves, harness nature, and build civilizations. But this has a cost, and perhaps the social media screen has been a tipping point for mental health.
I’m not knocking the basic idea. Share a joke with a friend, see pictures of the new baby, hear out about a new job. That’s fine. The trouble is that it’s gone beyond that. A lot of it is perfectly innocuous ... but a lot isn’t.
As it’s evolved, social media has also become the home of anger. Political and otherwise. It’s so much easier to post memes making fun of other people and their viewpoints than to speak to them in person. Trolls and bots lurk everywhere to get you riled up – things you wouldn’t be encountering if you were talking to your neighbor at the fence or a friend on the phone.
Recent trends on TikTok included students bragging about things they’d stolen from their high schools and people boasting of having “ripped off” Six Flags amusement parks with an annual membership loophole (the latter resulted in park management canceling the plan). How do such things benefit anyone (beyond those posting them getting clicks)?
I’m pretty sure they do nothing to make you feel good, or happy, or positive in any way. And that’s not even counting the political nastiness, cheap shots, and conspiracy theories that drown out rational thought.
Unfortunately, social media in today’s forms is addictive. Seeing one good thing from a friend gives you a dopamine boost, and this drives you to overlook all the bad things the screen does. Like the meth addict who lives for the high, and ignores all the negative aspects – loss of money, family, a home, teeth – that it brings.
So it’s not a surprise that walking away from it for a week made people happier and gave them time to do things that were more important than staring at a screen. Though I do wonder how many of the subjects ended up going back to it, forgetting about the benefits they’d just experienced.
When Frank Zappa released “I’m the Slime” in 1973, it was about television. But today the song is far closer to describing what social media has become than he could have ever imagined. (He died in 1993, never knowing how accurate he’d become).
We encourage our patients to exercise. The benefits of doing so are beyond question. But maybe it’s time to point out not only the good things that come from exercise, but also those that come from turning off the screen in order to do so.
As my mother said: “Go outside and play!”
It’s good for the body and sanity, and both are important.
Dr. Block has a solo neurology practice in Scottsdale, Ariz.
“Go outside and play!”
How often have you said that to your kids (or grandkids)? For that matter, how often did you hear it when you were a kid?
A lot, if memory serves me correctly. Some of it was just my mom wanting me out of the house, some of it an innate realization on her part that too much time spent planted in front of the TV was bad for you. (When I was a kid, Brady Bunch reruns kicked off my summer day at 8:00 a.m.).
The idea that too much time in front of a screen can be bad is nothing new. Regrettably, some of this ancient wisdom has been lost in the eons since I was a kid.
Does this surprise you?
Humans, like all primates, are a social species. We’ve benefited from the combined power of our minds to leave caves, harness nature, and build civilizations. But this has a cost, and perhaps the social media screen has been a tipping point for mental health.
I’m not knocking the basic idea. Share a joke with a friend, see pictures of the new baby, hear out about a new job. That’s fine. The trouble is that it’s gone beyond that. A lot of it is perfectly innocuous ... but a lot isn’t.
As it’s evolved, social media has also become the home of anger. Political and otherwise. It’s so much easier to post memes making fun of other people and their viewpoints than to speak to them in person. Trolls and bots lurk everywhere to get you riled up – things you wouldn’t be encountering if you were talking to your neighbor at the fence or a friend on the phone.
Recent trends on TikTok included students bragging about things they’d stolen from their high schools and people boasting of having “ripped off” Six Flags amusement parks with an annual membership loophole (the latter resulted in park management canceling the plan). How do such things benefit anyone (beyond those posting them getting clicks)?
I’m pretty sure they do nothing to make you feel good, or happy, or positive in any way. And that’s not even counting the political nastiness, cheap shots, and conspiracy theories that drown out rational thought.
Unfortunately, social media in today’s forms is addictive. Seeing one good thing from a friend gives you a dopamine boost, and this drives you to overlook all the bad things the screen does. Like the meth addict who lives for the high, and ignores all the negative aspects – loss of money, family, a home, teeth – that it brings.
So it’s not a surprise that walking away from it for a week made people happier and gave them time to do things that were more important than staring at a screen. Though I do wonder how many of the subjects ended up going back to it, forgetting about the benefits they’d just experienced.
When Frank Zappa released “I’m the Slime” in 1973, it was about television. But today the song is far closer to describing what social media has become than he could have ever imagined. (He died in 1993, never knowing how accurate he’d become).
We encourage our patients to exercise. The benefits of doing so are beyond question. But maybe it’s time to point out not only the good things that come from exercise, but also those that come from turning off the screen in order to do so.
As my mother said: “Go outside and play!”
It’s good for the body and sanity, and both are important.
Dr. Block has a solo neurology practice in Scottsdale, Ariz.
Neuropsychiatric risks of COVID-19: New data
The neuropsychiatric ramifications of severe COVID-19 infection appear to be no different than for other severe acute respiratory infections (SARI).
This suggests that disease severity, rather than pathogen, is the most relevant factor in new-onset neuropsychiatric illness, the investigators note.
The risk of new-onset neuropsychological illness after severe COVID-19 infection are “substantial, but similar to those after other severe respiratory infections,” study investigator Peter Watkinson, MD, Nuffield Department of Clinical Neurosciences, University of Oxford, and John Radcliffe Hospital, Oxford, England, told this news organization.

The study was published online in JAMA Psychiatry.
Significant mental health burden
Research has shown a significant burden of neuropsychological illness after severe COVID-19 infection. However, it’s unclear how this risk compares to SARI.
To investigate, Dr. Watkinson and colleagues evaluated electronic health record data on more than 8.3 million adults, including 16,679 (0.02%) who survived a hospital admission for SARI and 32,525 (0.03%) who survived a hospital stay for COVID-19.
Compared with the remaining population, risks of new anxiety disorder, dementia, psychotic disorder, depression, and bipolar disorder diagnoses were significantly and similarly increased in adults surviving hospitalization for either COVID-19 or SARI.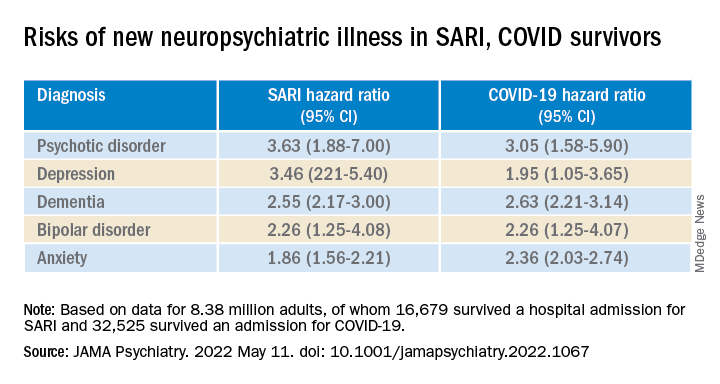
Compared with the wider population, survivors of severe SARI or COVID-19 were also at increased risk of starting treatment with antidepressants, hypnotics/anxiolytics, or antipsychotics.
When comparing survivors of SARI hospitalization to survivors of COVID-19 hospitalization, no significant differences were observed in the postdischarge rates of new-onset anxiety disorder, dementia, depression, or bipolar affective disorder.
The SARI and COVID groups also did not differ in terms of their postdischarge risks of antidepressant or hypnotic/anxiolytic use, but the COVID survivors had a 20% lower risk of starting an antipsychotic.
“In this cohort study, SARI were found to be associated with significant postacute neuropsychiatric morbidity, for which COVID-19 is not distinctly different,” Dr. Watkinson and colleagues write.
“These results may help refine our understanding of the post–severe COVID-19 phenotype and may inform post-discharge support for patients requiring hospital-based and intensive care for SARI regardless of causative pathogen,” they write.
Caveats, cautionary notes
Kevin McConway, PhD, emeritus professor of applied statistics at the Open University in Milton Keynes, England, described the study as “impressive.” However, he pointed out that the study’s observational design is a limitation.
“One can never be absolutely certain about the interpretation of findings of an observational study. What the research can’t tell us is what caused the increased psychiatric risks for people hospitalized with COVID-19 or some other serious respiratory disease,” Dr. McConway said.
“It can’t tell us what might happen in the future, when, we all hope, many fewer are being hospitalized with COVID-19 than was the case in those first two waves, and the current backlog of provision of some health services has decreased,” he added.
“So we can’t just say that, in general, serious COVID-19 has much the same neuropsychiatric consequences as other very serious respiratory illness. Maybe it does, maybe it doesn’t,” Dr. McConway cautioned.
Max Taquet, PhD, with the University of Oxford, noted that the study is limited to hospitalized adult patients, leaving open the question of risk in nonhospitalized individuals – which is the overwhelming majority of patients with COVID-19 – or in children.
Whether the neuropsychiatric risks have remained the same since the emergence of the Omicron variant also remains “an open question since all patients in this study were diagnosed before July 2021,” Dr. Taquet said in statement.
The study was funded by the Wellcome Trust, the John Fell Oxford University Press Research Fund, the Oxford Wellcome Institutional Strategic Support Fund and Cancer Research UK, through the Cancer Research UK Oxford Centre. Dr. Watkinson disclosed grants from the National Institute for Health Research and Sensyne Health outside the submitted work; and serving as chief medical officer for Sensyne Health prior to this work, as well as holding shares in the company. Dr. McConway is a trustee of the UK Science Media Centre and a member of its advisory committee. His comments were provided in his capacity as an independent professional statistician. Dr. Taquet has worked on similar studies trying to identify, quantify, and specify the neurological and psychiatric consequences of COVID-19.
A version of this article first appeared on Medscape.com.
The neuropsychiatric ramifications of severe COVID-19 infection appear to be no different than for other severe acute respiratory infections (SARI).
This suggests that disease severity, rather than pathogen, is the most relevant factor in new-onset neuropsychiatric illness, the investigators note.
The risk of new-onset neuropsychological illness after severe COVID-19 infection are “substantial, but similar to those after other severe respiratory infections,” study investigator Peter Watkinson, MD, Nuffield Department of Clinical Neurosciences, University of Oxford, and John Radcliffe Hospital, Oxford, England, told this news organization.
The study was published online in JAMA Psychiatry.
Significant mental health burden
Research has shown a significant burden of neuropsychological illness after severe COVID-19 infection. However, it’s unclear how this risk compares to SARI.
To investigate, Dr. Watkinson and colleagues evaluated electronic health record data on more than 8.3 million adults, including 16,679 (0.02%) who survived a hospital admission for SARI and 32,525 (0.03%) who survived a hospital stay for COVID-19.
Compared with the remaining population, risks of new anxiety disorder, dementia, psychotic disorder, depression, and bipolar disorder diagnoses were significantly and similarly increased in adults surviving hospitalization for either COVID-19 or SARI.
Compared with the wider population, survivors of severe SARI or COVID-19 were also at increased risk of starting treatment with antidepressants, hypnotics/anxiolytics, or antipsychotics.
When comparing survivors of SARI hospitalization to survivors of COVID-19 hospitalization, no significant differences were observed in the postdischarge rates of new-onset anxiety disorder, dementia, depression, or bipolar affective disorder.
The SARI and COVID groups also did not differ in terms of their postdischarge risks of antidepressant or hypnotic/anxiolytic use, but the COVID survivors had a 20% lower risk of starting an antipsychotic.
“In this cohort study, SARI were found to be associated with significant postacute neuropsychiatric morbidity, for which COVID-19 is not distinctly different,” Dr. Watkinson and colleagues write.
“These results may help refine our understanding of the post–severe COVID-19 phenotype and may inform post-discharge support for patients requiring hospital-based and intensive care for SARI regardless of causative pathogen,” they write.
Caveats, cautionary notes
Kevin McConway, PhD, emeritus professor of applied statistics at the Open University in Milton Keynes, England, described the study as “impressive.” However, he pointed out that the study’s observational design is a limitation.
“One can never be absolutely certain about the interpretation of findings of an observational study. What the research can’t tell us is what caused the increased psychiatric risks for people hospitalized with COVID-19 or some other serious respiratory disease,” Dr. McConway said.
“It can’t tell us what might happen in the future, when, we all hope, many fewer are being hospitalized with COVID-19 than was the case in those first two waves, and the current backlog of provision of some health services has decreased,” he added.
“So we can’t just say that, in general, serious COVID-19 has much the same neuropsychiatric consequences as other very serious respiratory illness. Maybe it does, maybe it doesn’t,” Dr. McConway cautioned.
Max Taquet, PhD, with the University of Oxford, noted that the study is limited to hospitalized adult patients, leaving open the question of risk in nonhospitalized individuals – which is the overwhelming majority of patients with COVID-19 – or in children.
Whether the neuropsychiatric risks have remained the same since the emergence of the Omicron variant also remains “an open question since all patients in this study were diagnosed before July 2021,” Dr. Taquet said in statement.
The study was funded by the Wellcome Trust, the John Fell Oxford University Press Research Fund, the Oxford Wellcome Institutional Strategic Support Fund and Cancer Research UK, through the Cancer Research UK Oxford Centre. Dr. Watkinson disclosed grants from the National Institute for Health Research and Sensyne Health outside the submitted work; and serving as chief medical officer for Sensyne Health prior to this work, as well as holding shares in the company. Dr. McConway is a trustee of the UK Science Media Centre and a member of its advisory committee. His comments were provided in his capacity as an independent professional statistician. Dr. Taquet has worked on similar studies trying to identify, quantify, and specify the neurological and psychiatric consequences of COVID-19.
A version of this article first appeared on Medscape.com.
The neuropsychiatric ramifications of severe COVID-19 infection appear to be no different than for other severe acute respiratory infections (SARI).
This suggests that disease severity, rather than pathogen, is the most relevant factor in new-onset neuropsychiatric illness, the investigators note.
The risk of new-onset neuropsychological illness after severe COVID-19 infection are “substantial, but similar to those after other severe respiratory infections,” study investigator Peter Watkinson, MD, Nuffield Department of Clinical Neurosciences, University of Oxford, and John Radcliffe Hospital, Oxford, England, told this news organization.
The study was published online in JAMA Psychiatry.
Significant mental health burden
Research has shown a significant burden of neuropsychological illness after severe COVID-19 infection. However, it’s unclear how this risk compares to SARI.
To investigate, Dr. Watkinson and colleagues evaluated electronic health record data on more than 8.3 million adults, including 16,679 (0.02%) who survived a hospital admission for SARI and 32,525 (0.03%) who survived a hospital stay for COVID-19.
Compared with the remaining population, risks of new anxiety disorder, dementia, psychotic disorder, depression, and bipolar disorder diagnoses were significantly and similarly increased in adults surviving hospitalization for either COVID-19 or SARI.
Compared with the wider population, survivors of severe SARI or COVID-19 were also at increased risk of starting treatment with antidepressants, hypnotics/anxiolytics, or antipsychotics.
When comparing survivors of SARI hospitalization to survivors of COVID-19 hospitalization, no significant differences were observed in the postdischarge rates of new-onset anxiety disorder, dementia, depression, or bipolar affective disorder.
The SARI and COVID groups also did not differ in terms of their postdischarge risks of antidepressant or hypnotic/anxiolytic use, but the COVID survivors had a 20% lower risk of starting an antipsychotic.
“In this cohort study, SARI were found to be associated with significant postacute neuropsychiatric morbidity, for which COVID-19 is not distinctly different,” Dr. Watkinson and colleagues write.
“These results may help refine our understanding of the post–severe COVID-19 phenotype and may inform post-discharge support for patients requiring hospital-based and intensive care for SARI regardless of causative pathogen,” they write.
Caveats, cautionary notes
Kevin McConway, PhD, emeritus professor of applied statistics at the Open University in Milton Keynes, England, described the study as “impressive.” However, he pointed out that the study’s observational design is a limitation.
“One can never be absolutely certain about the interpretation of findings of an observational study. What the research can’t tell us is what caused the increased psychiatric risks for people hospitalized with COVID-19 or some other serious respiratory disease,” Dr. McConway said.
“It can’t tell us what might happen in the future, when, we all hope, many fewer are being hospitalized with COVID-19 than was the case in those first two waves, and the current backlog of provision of some health services has decreased,” he added.
“So we can’t just say that, in general, serious COVID-19 has much the same neuropsychiatric consequences as other very serious respiratory illness. Maybe it does, maybe it doesn’t,” Dr. McConway cautioned.
Max Taquet, PhD, with the University of Oxford, noted that the study is limited to hospitalized adult patients, leaving open the question of risk in nonhospitalized individuals – which is the overwhelming majority of patients with COVID-19 – or in children.
Whether the neuropsychiatric risks have remained the same since the emergence of the Omicron variant also remains “an open question since all patients in this study were diagnosed before July 2021,” Dr. Taquet said in statement.
The study was funded by the Wellcome Trust, the John Fell Oxford University Press Research Fund, the Oxford Wellcome Institutional Strategic Support Fund and Cancer Research UK, through the Cancer Research UK Oxford Centre. Dr. Watkinson disclosed grants from the National Institute for Health Research and Sensyne Health outside the submitted work; and serving as chief medical officer for Sensyne Health prior to this work, as well as holding shares in the company. Dr. McConway is a trustee of the UK Science Media Centre and a member of its advisory committee. His comments were provided in his capacity as an independent professional statistician. Dr. Taquet has worked on similar studies trying to identify, quantify, and specify the neurological and psychiatric consequences of COVID-19.
A version of this article first appeared on Medscape.com.