User login
The Official Newspaper of the American Association for Thoracic Surgery
Cognitive decline not seen with lower BP treatment targets
Tighter blood pressure control is not linked to cognitive decline among older adults and may instead be associated with preservation of cognitive function, according to a new analysis.
Further, the cognitive benefits of tighter control are even more pronounced among black patients.
Dr. Hajjar and colleagues report that subjects whose systolic blood pressure (SBP) was maintained at 150 mm Hg or higher during the study period saw significantly greater cognitive decline over 10 years, compared with those treated to levels of 120 mm Hg or lower (JAMA Neurol. 2017 Aug 21; doi: 10.1001/jamaneurol.2017.1863). Furthermore, the investigators noted a differential decrease by blood pressure levels for both cognitive scoring systems, with the greatest decline seen in the group with SBP of 150 mm/Hg or higher and the lowest decrease in the group with 120 mm/Hg or lower (P less than .001 for both).
Black patients saw a greater difference, compared with white patients, between the higher and lower SBP levels in the decrease in cognition. Adjusted differences between the group with 150 mm Hg or higher and those with 120 mm Hg or lower were –0.05 in white patients and –0.08 in black patients for the 3MSE test (P = .03), and –0.07 in white patients and –0.13 in black patients for the DSST (P = .05).
“Almost all guidelines have recommended that target blood pressures be similar for black and white patients,” the investigators wrote in their analysis, adding that “future recommendations for the management of hypertension and cognitive outcomes need to take this racial disparity into consideration.”
The study was funded by the National Institutes on Health and National Institute on Aging. Dr. Hajjar and his colleagues disclosed no conflicts of interest.
Although unanswered questions remain, the data presented by Dr. Hajjar and colleagues add to the existing literature by emphasizing that tight blood pressure control does not appear to lead to poorer cognitive trajectories in older adults and may even be associated with improved cognitive trajectories. An important and unique feature of the data is the diverse population included, with nearly half of the enrollment composed of black individuals. The finding that lower systolic BP was especially protective for black individuals is important, given a noted disparity in rates of dementia among black and white persons. Adding to that the finding that hypertension is more common and more severe in black than in white persons (also supported by the data in this study), and that black persons tend to have more poorly controlled hypertension than do white persons, this outcome points to an important opportunity from a public health standpoint. BP reduction might actually reduce the rates of dementia and reduce the disparities by race with regard to dementia rates; the fact that BP control may require more medications for black than for white patients needs to be considered when monitoring blood pressure levels.
Rebecca F. Gottesman, MD, PhD, of Johns Hopkins University, Baltimore, made these comments in an accompanying editorial (JAMA Neurol. 2017 Aug. 21; doi: 10.1001/jamaneurol.2017.1869). She is an associate editor at JAMA Neurology, and reports no other conflicts of interest.
Although unanswered questions remain, the data presented by Dr. Hajjar and colleagues add to the existing literature by emphasizing that tight blood pressure control does not appear to lead to poorer cognitive trajectories in older adults and may even be associated with improved cognitive trajectories. An important and unique feature of the data is the diverse population included, with nearly half of the enrollment composed of black individuals. The finding that lower systolic BP was especially protective for black individuals is important, given a noted disparity in rates of dementia among black and white persons. Adding to that the finding that hypertension is more common and more severe in black than in white persons (also supported by the data in this study), and that black persons tend to have more poorly controlled hypertension than do white persons, this outcome points to an important opportunity from a public health standpoint. BP reduction might actually reduce the rates of dementia and reduce the disparities by race with regard to dementia rates; the fact that BP control may require more medications for black than for white patients needs to be considered when monitoring blood pressure levels.
Rebecca F. Gottesman, MD, PhD, of Johns Hopkins University, Baltimore, made these comments in an accompanying editorial (JAMA Neurol. 2017 Aug. 21; doi: 10.1001/jamaneurol.2017.1869). She is an associate editor at JAMA Neurology, and reports no other conflicts of interest.
Although unanswered questions remain, the data presented by Dr. Hajjar and colleagues add to the existing literature by emphasizing that tight blood pressure control does not appear to lead to poorer cognitive trajectories in older adults and may even be associated with improved cognitive trajectories. An important and unique feature of the data is the diverse population included, with nearly half of the enrollment composed of black individuals. The finding that lower systolic BP was especially protective for black individuals is important, given a noted disparity in rates of dementia among black and white persons. Adding to that the finding that hypertension is more common and more severe in black than in white persons (also supported by the data in this study), and that black persons tend to have more poorly controlled hypertension than do white persons, this outcome points to an important opportunity from a public health standpoint. BP reduction might actually reduce the rates of dementia and reduce the disparities by race with regard to dementia rates; the fact that BP control may require more medications for black than for white patients needs to be considered when monitoring blood pressure levels.
Rebecca F. Gottesman, MD, PhD, of Johns Hopkins University, Baltimore, made these comments in an accompanying editorial (JAMA Neurol. 2017 Aug. 21; doi: 10.1001/jamaneurol.2017.1869). She is an associate editor at JAMA Neurology, and reports no other conflicts of interest.
Tighter blood pressure control is not linked to cognitive decline among older adults and may instead be associated with preservation of cognitive function, according to a new analysis.
Further, the cognitive benefits of tighter control are even more pronounced among black patients.
Dr. Hajjar and colleagues report that subjects whose systolic blood pressure (SBP) was maintained at 150 mm Hg or higher during the study period saw significantly greater cognitive decline over 10 years, compared with those treated to levels of 120 mm Hg or lower (JAMA Neurol. 2017 Aug 21; doi: 10.1001/jamaneurol.2017.1863). Furthermore, the investigators noted a differential decrease by blood pressure levels for both cognitive scoring systems, with the greatest decline seen in the group with SBP of 150 mm/Hg or higher and the lowest decrease in the group with 120 mm/Hg or lower (P less than .001 for both).
Black patients saw a greater difference, compared with white patients, between the higher and lower SBP levels in the decrease in cognition. Adjusted differences between the group with 150 mm Hg or higher and those with 120 mm Hg or lower were –0.05 in white patients and –0.08 in black patients for the 3MSE test (P = .03), and –0.07 in white patients and –0.13 in black patients for the DSST (P = .05).
“Almost all guidelines have recommended that target blood pressures be similar for black and white patients,” the investigators wrote in their analysis, adding that “future recommendations for the management of hypertension and cognitive outcomes need to take this racial disparity into consideration.”
The study was funded by the National Institutes on Health and National Institute on Aging. Dr. Hajjar and his colleagues disclosed no conflicts of interest.
Tighter blood pressure control is not linked to cognitive decline among older adults and may instead be associated with preservation of cognitive function, according to a new analysis.
Further, the cognitive benefits of tighter control are even more pronounced among black patients.
Dr. Hajjar and colleagues report that subjects whose systolic blood pressure (SBP) was maintained at 150 mm Hg or higher during the study period saw significantly greater cognitive decline over 10 years, compared with those treated to levels of 120 mm Hg or lower (JAMA Neurol. 2017 Aug 21; doi: 10.1001/jamaneurol.2017.1863). Furthermore, the investigators noted a differential decrease by blood pressure levels for both cognitive scoring systems, with the greatest decline seen in the group with SBP of 150 mm/Hg or higher and the lowest decrease in the group with 120 mm/Hg or lower (P less than .001 for both).
Black patients saw a greater difference, compared with white patients, between the higher and lower SBP levels in the decrease in cognition. Adjusted differences between the group with 150 mm Hg or higher and those with 120 mm Hg or lower were –0.05 in white patients and –0.08 in black patients for the 3MSE test (P = .03), and –0.07 in white patients and –0.13 in black patients for the DSST (P = .05).
“Almost all guidelines have recommended that target blood pressures be similar for black and white patients,” the investigators wrote in their analysis, adding that “future recommendations for the management of hypertension and cognitive outcomes need to take this racial disparity into consideration.”
The study was funded by the National Institutes on Health and National Institute on Aging. Dr. Hajjar and his colleagues disclosed no conflicts of interest.
FROM JAMA NEUROLOGY
Key clinical point: Treating to more aggressive blood pressure targets does not promote cognitive decline and may help stem it, particularly among black patients.
Major finding: Black patients saw significantly greater decline in cognition over time associated with systolic BP control to 150 mm Hg vs. 120 mm Hg.
Data source: A cohort of 1,700 hypertension-treated patients aged 70-79, about half of them black, drawn from a 10-year observational study of 3,000 patients.
Disclosures: Both the larger cohort and this study were funded by the National Institutes of Health and the National Institute on Aging. None of the investigators declared conflicts of interest.
Cancer screening in elderly: When to just say no
ESTES PARK, COLO. – A simple walking speed measurement over a 20-foot distance is an invaluable guide to physiologic age as part of individualized decision making about when to stop cancer screening in elderly patients, according to Jeff Wallace, MD, professor of geriatric medicine at the University of Colorado at Denver.
“If you have one measurement to assess ‘am I aging well?’ it’s your gait speed. A lot of us in geriatrics are advocating evaluation of gait speed in all patients as a fifth vital sign. It’s probably more useful than blood pressure in some of the older adults coming into our clinics,” he said at a conference on internal medicine sponsored by the University of Colorado.
Dr. Wallace also gave a shout-out to the ePrognosis cancer-screening decision tool, available free at www.eprognosis.org, as an aid in shared decision-making conversations regarding when to stop cancer screening. This tool, developed by researchers at the University of California, San Francisco, allows physicians to plug key individual patient characteristics into its model, including comorbid conditions, functional status, and body mass index, and then spits out data-driven estimated benefits and harms a patient can expect from advanced-age screening for colon or breast cancer.
Of course, guidelines as to when to stop screening for various cancers are available from the U.S. Preventive Services Task Force, the American Cancer Society, and specialty societies. However, it’s important that nongeriatricians understand the serious limitations of those guidelines.
“We’re not guidelines followers in the geriatrics world because the guidelines don’t apply to most of our patients,” he explained. “We hate guidelines in geriatrics because few studies – and no lung cancer or breast cancer trials – enroll patients over age 75 with comorbid conditions. Also, most of these guidelines do not incorporate patient preferences, which probably should be a primary goal. So we’re left extrapolating.“
Regrettably, though, “it turns out most Americans are drinking the Kool-Aid when it comes to patient preferences. It’s amazing how much cancer screening is going on in this country. We’re doing a lot more than we should,” said Dr. Wallace.
All of that is clearly overscreening. Experts unanimously agree that if someone is not going to live for 10 years, that person is not likely to benefit from cancer screening. The one exception is lung cancer screening of high-risk patients, where there are data to show that annual low-dose CT screening is beneficial in those with even a 5-year life expectancy.
As part of the Choosing Wisely program, the American Geriatric Society has advocated that physicians “don’t recommend screening for breast, colorectal, prostate, or lung cancer without considering life expectancy and the risks of testing, overdiagnosis, and overtreatment.”
That’s where gait speed and ePrognosis come in handy in discussions with patients regarding what they can realistically expect from cancer screening at an advanced age.
The importance of gait speed was highlighted in a pooled analysis of nine cohort studies totaling more than 34,000 community-dwelling adults aged 65 years and older with 6-21 years of follow-up. Investigators at the University of Pittsburgh identified a strong relationship between gait speed and survival. Every 0.1-m/sec made a significant difference (JAMA. 2011 Jan 5;305[1]:50-8).
A gait speed evaluation is simple: The patient is asked to walk 20 feet at a normal speed, not racing. For men age 75, the Pittsburgh investigators found, gait speed predicted 10-year survival across a range of 19%-87%. The median speed was 0.8 m/sec, or about 1.8 mph, so a middle-of-the-pack walker ought to stop all cancer screening by age 75. A fast-walking older man won’t reach a 10-year remaining life expectancy until he’s in his early to mid-80s; a slow walker reaches that life expectancy as early as his late 60s, depending upon just how slow he walks. A woman at age 80 with an average gait speed has roughly 10 years of remaining life, factoring in plus or minus 5 years from that landmark depending upon whether she is a faster- or slower-than-average walker, Dr. Wallace explained.
The U.S. Preventive Services Task Force currently recommends colon cancer screening routinely for 50- to 75-year-olds, declaring in accord with other groups that this strategy has a high certainty of substantial net benefit. But the USPSTF also recommends selective screening for those aged 76-85, with a weaker C recommendation (JAMA. 2016 Jun 21;315[23]:2564-75).
What are the practical implications of that recommendation for selective screening after age 75?
Investigators at Harvard Medical School and the University of Oslo recently took a closer look. Their population-based, prospective, observational study included 1,355,692 Medicare beneficiaries aged 70-79 years at average risk for colorectal cancer who had not had a colonoscopy within the previous 5 years.
The investigators demonstrated that the benefit of screening colonoscopy decreased with age. For patients aged 70-74, the 8-year risk of colorectal cancer was 2.19% in those who were screened, compared with 2.62% in those who weren’t, for an absolute 0.43% difference. The number needed to be screened to detect one additional case of colorectal cancer was 283. Among those aged 75-79, the number needed to be screened climbed to 714 (Ann Intern Med. 2017 Jan 3;166[1]18-26).
Moreover, the risk of colonoscopy-related adverse events also climbed with age. These included perforations, falls while racing to the bathroom during the preprocedural bowel prep, and the humiliation of fecal incontinence. The excess 30-day risk for any adverse event in the colonoscopy group was 5.6 events per 1,000 patients aged 70-74 and 10.3 per 1,000 in 75- to 79-year-olds.
In a similar vein, Mara A. Schonberg, MD, of Harvard Medical School, Boston, has shed light on the risks and benefits of biannual mammographic screening for breast cancer in 70- to 79-year-olds, a practice recommended in American Cancer Society guidelines for women who are in overall good health and have at least a 10-year life expectancy.
She estimated that 2 women per 1,000 screened would avoid death due to breast cancer, for a number needed to screen of 500. But roughly 200 of those 1,000 women would experience a false-positive mammogram, and 20-40 of those false-positive imaging studies would result in a breast biopsy. Also, roughly 30% of the screen-detected cancers would not otherwise become apparent in an older woman’s lifetime, yet nearly all of the malignancies would undergo breast cancer therapy (J Am Geriatr Soc. 2016 Dec;64[12]:2413-8).
Dr. Schonberg’s research speaks to Dr. Wallace.
“It’s breast cancer therapy: It’s procedures; it’s medicalizing the patient’s whole life and creating a high degree of angst when she’s 75 or 80,” he said.
As to when to ‘just say no’ to cancer screening, Dr. Wallace said his answer is after age 65 for cervical cancer screening in women with at least two normal screens in the past 10 years or a prior total hysterectomy for a benign indication. All of the guidelines agree on that, although the American Congress of Obstetricians and Gynecologists recommends in addition that women with cervical intraepithelial neoplasia 2 be screened for the next 20 years.
For prostate cancer, Dr. Wallace recommends his colleagues just say no to screening at age 70 and above because harm is more likely than benefit to ensue.
“I don’t know about you, but I have a ton of patients over age 70 asking me for PSAs. That’s one place I won’t do any screening. I tell them I know you’re in great shape for 76 and you think it’s a good idea, but I think it’s bad medicine and I won’t do it. Even the American Urological Association says don’t do it after age 70,” he said.
For prostate cancer screening at age 55-69, however, patient preference rules the day, he added.
He draws the line at any cancer screening in patients aged 90 or over. Mean survival at age 90 is another 4-5 years. Only 11% of 90-year-old women will reach 100.
“Everybody has to die eventually,” he mused.
Dr. Wallace reported having no financial conflicts regarding his presentation.
ESTES PARK, COLO. – A simple walking speed measurement over a 20-foot distance is an invaluable guide to physiologic age as part of individualized decision making about when to stop cancer screening in elderly patients, according to Jeff Wallace, MD, professor of geriatric medicine at the University of Colorado at Denver.
“If you have one measurement to assess ‘am I aging well?’ it’s your gait speed. A lot of us in geriatrics are advocating evaluation of gait speed in all patients as a fifth vital sign. It’s probably more useful than blood pressure in some of the older adults coming into our clinics,” he said at a conference on internal medicine sponsored by the University of Colorado.
Dr. Wallace also gave a shout-out to the ePrognosis cancer-screening decision tool, available free at www.eprognosis.org, as an aid in shared decision-making conversations regarding when to stop cancer screening. This tool, developed by researchers at the University of California, San Francisco, allows physicians to plug key individual patient characteristics into its model, including comorbid conditions, functional status, and body mass index, and then spits out data-driven estimated benefits and harms a patient can expect from advanced-age screening for colon or breast cancer.
Of course, guidelines as to when to stop screening for various cancers are available from the U.S. Preventive Services Task Force, the American Cancer Society, and specialty societies. However, it’s important that nongeriatricians understand the serious limitations of those guidelines.
“We’re not guidelines followers in the geriatrics world because the guidelines don’t apply to most of our patients,” he explained. “We hate guidelines in geriatrics because few studies – and no lung cancer or breast cancer trials – enroll patients over age 75 with comorbid conditions. Also, most of these guidelines do not incorporate patient preferences, which probably should be a primary goal. So we’re left extrapolating.“
Regrettably, though, “it turns out most Americans are drinking the Kool-Aid when it comes to patient preferences. It’s amazing how much cancer screening is going on in this country. We’re doing a lot more than we should,” said Dr. Wallace.
All of that is clearly overscreening. Experts unanimously agree that if someone is not going to live for 10 years, that person is not likely to benefit from cancer screening. The one exception is lung cancer screening of high-risk patients, where there are data to show that annual low-dose CT screening is beneficial in those with even a 5-year life expectancy.
As part of the Choosing Wisely program, the American Geriatric Society has advocated that physicians “don’t recommend screening for breast, colorectal, prostate, or lung cancer without considering life expectancy and the risks of testing, overdiagnosis, and overtreatment.”
That’s where gait speed and ePrognosis come in handy in discussions with patients regarding what they can realistically expect from cancer screening at an advanced age.
The importance of gait speed was highlighted in a pooled analysis of nine cohort studies totaling more than 34,000 community-dwelling adults aged 65 years and older with 6-21 years of follow-up. Investigators at the University of Pittsburgh identified a strong relationship between gait speed and survival. Every 0.1-m/sec made a significant difference (JAMA. 2011 Jan 5;305[1]:50-8).
A gait speed evaluation is simple: The patient is asked to walk 20 feet at a normal speed, not racing. For men age 75, the Pittsburgh investigators found, gait speed predicted 10-year survival across a range of 19%-87%. The median speed was 0.8 m/sec, or about 1.8 mph, so a middle-of-the-pack walker ought to stop all cancer screening by age 75. A fast-walking older man won’t reach a 10-year remaining life expectancy until he’s in his early to mid-80s; a slow walker reaches that life expectancy as early as his late 60s, depending upon just how slow he walks. A woman at age 80 with an average gait speed has roughly 10 years of remaining life, factoring in plus or minus 5 years from that landmark depending upon whether she is a faster- or slower-than-average walker, Dr. Wallace explained.
The U.S. Preventive Services Task Force currently recommends colon cancer screening routinely for 50- to 75-year-olds, declaring in accord with other groups that this strategy has a high certainty of substantial net benefit. But the USPSTF also recommends selective screening for those aged 76-85, with a weaker C recommendation (JAMA. 2016 Jun 21;315[23]:2564-75).
What are the practical implications of that recommendation for selective screening after age 75?
Investigators at Harvard Medical School and the University of Oslo recently took a closer look. Their population-based, prospective, observational study included 1,355,692 Medicare beneficiaries aged 70-79 years at average risk for colorectal cancer who had not had a colonoscopy within the previous 5 years.
The investigators demonstrated that the benefit of screening colonoscopy decreased with age. For patients aged 70-74, the 8-year risk of colorectal cancer was 2.19% in those who were screened, compared with 2.62% in those who weren’t, for an absolute 0.43% difference. The number needed to be screened to detect one additional case of colorectal cancer was 283. Among those aged 75-79, the number needed to be screened climbed to 714 (Ann Intern Med. 2017 Jan 3;166[1]18-26).
Moreover, the risk of colonoscopy-related adverse events also climbed with age. These included perforations, falls while racing to the bathroom during the preprocedural bowel prep, and the humiliation of fecal incontinence. The excess 30-day risk for any adverse event in the colonoscopy group was 5.6 events per 1,000 patients aged 70-74 and 10.3 per 1,000 in 75- to 79-year-olds.
In a similar vein, Mara A. Schonberg, MD, of Harvard Medical School, Boston, has shed light on the risks and benefits of biannual mammographic screening for breast cancer in 70- to 79-year-olds, a practice recommended in American Cancer Society guidelines for women who are in overall good health and have at least a 10-year life expectancy.
She estimated that 2 women per 1,000 screened would avoid death due to breast cancer, for a number needed to screen of 500. But roughly 200 of those 1,000 women would experience a false-positive mammogram, and 20-40 of those false-positive imaging studies would result in a breast biopsy. Also, roughly 30% of the screen-detected cancers would not otherwise become apparent in an older woman’s lifetime, yet nearly all of the malignancies would undergo breast cancer therapy (J Am Geriatr Soc. 2016 Dec;64[12]:2413-8).
Dr. Schonberg’s research speaks to Dr. Wallace.
“It’s breast cancer therapy: It’s procedures; it’s medicalizing the patient’s whole life and creating a high degree of angst when she’s 75 or 80,” he said.
As to when to ‘just say no’ to cancer screening, Dr. Wallace said his answer is after age 65 for cervical cancer screening in women with at least two normal screens in the past 10 years or a prior total hysterectomy for a benign indication. All of the guidelines agree on that, although the American Congress of Obstetricians and Gynecologists recommends in addition that women with cervical intraepithelial neoplasia 2 be screened for the next 20 years.
For prostate cancer, Dr. Wallace recommends his colleagues just say no to screening at age 70 and above because harm is more likely than benefit to ensue.
“I don’t know about you, but I have a ton of patients over age 70 asking me for PSAs. That’s one place I won’t do any screening. I tell them I know you’re in great shape for 76 and you think it’s a good idea, but I think it’s bad medicine and I won’t do it. Even the American Urological Association says don’t do it after age 70,” he said.
For prostate cancer screening at age 55-69, however, patient preference rules the day, he added.
He draws the line at any cancer screening in patients aged 90 or over. Mean survival at age 90 is another 4-5 years. Only 11% of 90-year-old women will reach 100.
“Everybody has to die eventually,” he mused.
Dr. Wallace reported having no financial conflicts regarding his presentation.
ESTES PARK, COLO. – A simple walking speed measurement over a 20-foot distance is an invaluable guide to physiologic age as part of individualized decision making about when to stop cancer screening in elderly patients, according to Jeff Wallace, MD, professor of geriatric medicine at the University of Colorado at Denver.
“If you have one measurement to assess ‘am I aging well?’ it’s your gait speed. A lot of us in geriatrics are advocating evaluation of gait speed in all patients as a fifth vital sign. It’s probably more useful than blood pressure in some of the older adults coming into our clinics,” he said at a conference on internal medicine sponsored by the University of Colorado.
Dr. Wallace also gave a shout-out to the ePrognosis cancer-screening decision tool, available free at www.eprognosis.org, as an aid in shared decision-making conversations regarding when to stop cancer screening. This tool, developed by researchers at the University of California, San Francisco, allows physicians to plug key individual patient characteristics into its model, including comorbid conditions, functional status, and body mass index, and then spits out data-driven estimated benefits and harms a patient can expect from advanced-age screening for colon or breast cancer.
Of course, guidelines as to when to stop screening for various cancers are available from the U.S. Preventive Services Task Force, the American Cancer Society, and specialty societies. However, it’s important that nongeriatricians understand the serious limitations of those guidelines.
“We’re not guidelines followers in the geriatrics world because the guidelines don’t apply to most of our patients,” he explained. “We hate guidelines in geriatrics because few studies – and no lung cancer or breast cancer trials – enroll patients over age 75 with comorbid conditions. Also, most of these guidelines do not incorporate patient preferences, which probably should be a primary goal. So we’re left extrapolating.“
Regrettably, though, “it turns out most Americans are drinking the Kool-Aid when it comes to patient preferences. It’s amazing how much cancer screening is going on in this country. We’re doing a lot more than we should,” said Dr. Wallace.
All of that is clearly overscreening. Experts unanimously agree that if someone is not going to live for 10 years, that person is not likely to benefit from cancer screening. The one exception is lung cancer screening of high-risk patients, where there are data to show that annual low-dose CT screening is beneficial in those with even a 5-year life expectancy.
As part of the Choosing Wisely program, the American Geriatric Society has advocated that physicians “don’t recommend screening for breast, colorectal, prostate, or lung cancer without considering life expectancy and the risks of testing, overdiagnosis, and overtreatment.”
That’s where gait speed and ePrognosis come in handy in discussions with patients regarding what they can realistically expect from cancer screening at an advanced age.
The importance of gait speed was highlighted in a pooled analysis of nine cohort studies totaling more than 34,000 community-dwelling adults aged 65 years and older with 6-21 years of follow-up. Investigators at the University of Pittsburgh identified a strong relationship between gait speed and survival. Every 0.1-m/sec made a significant difference (JAMA. 2011 Jan 5;305[1]:50-8).
A gait speed evaluation is simple: The patient is asked to walk 20 feet at a normal speed, not racing. For men age 75, the Pittsburgh investigators found, gait speed predicted 10-year survival across a range of 19%-87%. The median speed was 0.8 m/sec, or about 1.8 mph, so a middle-of-the-pack walker ought to stop all cancer screening by age 75. A fast-walking older man won’t reach a 10-year remaining life expectancy until he’s in his early to mid-80s; a slow walker reaches that life expectancy as early as his late 60s, depending upon just how slow he walks. A woman at age 80 with an average gait speed has roughly 10 years of remaining life, factoring in plus or minus 5 years from that landmark depending upon whether she is a faster- or slower-than-average walker, Dr. Wallace explained.
The U.S. Preventive Services Task Force currently recommends colon cancer screening routinely for 50- to 75-year-olds, declaring in accord with other groups that this strategy has a high certainty of substantial net benefit. But the USPSTF also recommends selective screening for those aged 76-85, with a weaker C recommendation (JAMA. 2016 Jun 21;315[23]:2564-75).
What are the practical implications of that recommendation for selective screening after age 75?
Investigators at Harvard Medical School and the University of Oslo recently took a closer look. Their population-based, prospective, observational study included 1,355,692 Medicare beneficiaries aged 70-79 years at average risk for colorectal cancer who had not had a colonoscopy within the previous 5 years.
The investigators demonstrated that the benefit of screening colonoscopy decreased with age. For patients aged 70-74, the 8-year risk of colorectal cancer was 2.19% in those who were screened, compared with 2.62% in those who weren’t, for an absolute 0.43% difference. The number needed to be screened to detect one additional case of colorectal cancer was 283. Among those aged 75-79, the number needed to be screened climbed to 714 (Ann Intern Med. 2017 Jan 3;166[1]18-26).
Moreover, the risk of colonoscopy-related adverse events also climbed with age. These included perforations, falls while racing to the bathroom during the preprocedural bowel prep, and the humiliation of fecal incontinence. The excess 30-day risk for any adverse event in the colonoscopy group was 5.6 events per 1,000 patients aged 70-74 and 10.3 per 1,000 in 75- to 79-year-olds.
In a similar vein, Mara A. Schonberg, MD, of Harvard Medical School, Boston, has shed light on the risks and benefits of biannual mammographic screening for breast cancer in 70- to 79-year-olds, a practice recommended in American Cancer Society guidelines for women who are in overall good health and have at least a 10-year life expectancy.
She estimated that 2 women per 1,000 screened would avoid death due to breast cancer, for a number needed to screen of 500. But roughly 200 of those 1,000 women would experience a false-positive mammogram, and 20-40 of those false-positive imaging studies would result in a breast biopsy. Also, roughly 30% of the screen-detected cancers would not otherwise become apparent in an older woman’s lifetime, yet nearly all of the malignancies would undergo breast cancer therapy (J Am Geriatr Soc. 2016 Dec;64[12]:2413-8).
Dr. Schonberg’s research speaks to Dr. Wallace.
“It’s breast cancer therapy: It’s procedures; it’s medicalizing the patient’s whole life and creating a high degree of angst when she’s 75 or 80,” he said.
As to when to ‘just say no’ to cancer screening, Dr. Wallace said his answer is after age 65 for cervical cancer screening in women with at least two normal screens in the past 10 years or a prior total hysterectomy for a benign indication. All of the guidelines agree on that, although the American Congress of Obstetricians and Gynecologists recommends in addition that women with cervical intraepithelial neoplasia 2 be screened for the next 20 years.
For prostate cancer, Dr. Wallace recommends his colleagues just say no to screening at age 70 and above because harm is more likely than benefit to ensue.
“I don’t know about you, but I have a ton of patients over age 70 asking me for PSAs. That’s one place I won’t do any screening. I tell them I know you’re in great shape for 76 and you think it’s a good idea, but I think it’s bad medicine and I won’t do it. Even the American Urological Association says don’t do it after age 70,” he said.
For prostate cancer screening at age 55-69, however, patient preference rules the day, he added.
He draws the line at any cancer screening in patients aged 90 or over. Mean survival at age 90 is another 4-5 years. Only 11% of 90-year-old women will reach 100.
“Everybody has to die eventually,” he mused.
Dr. Wallace reported having no financial conflicts regarding his presentation.
EXPERT ANALYSIS FROM THE ANNUAL INTERNAL MEDICINE PROGRAM
Cerebral NIRS may be flawed for assessing infant brains after stage 1 palliation of HLHS
The regional oxygenation index (rSO2) based on near infrared spectroscopy (NIRS) measurement is frequently used to assess the adequacy of oxygen delivery after stage 1 palliation of hypoplastic left heart syndrome (HLHS). However, a recent study showed that cerebral rSO2 has low sensitivity and should not be considered reassuring even at rSO2 of 50 or greater. In addition, values below 30 were not found to be sensitive for detecting compromised oxygen delivery, according to a report published online in the Journal of Thoracic and Cardiovascular Surgery.
Erin Rescoe, MD, of Boston Children’s Hospital, and her colleagues at Harvard Medical School, Boston, performed a retrospective study of 73 neonates assessed with cerebral venous oxyhemoglobin saturation (ScvO2) measured by co-oximetry from the internal jugular vein, which is considered the preferred method for assessing the adequacy of tissue oxygen delivery, compared with cerebral rSO2 after stage 1 palliation of HLHS (doi: 10.1016/j.jtcvs.2017.03.154).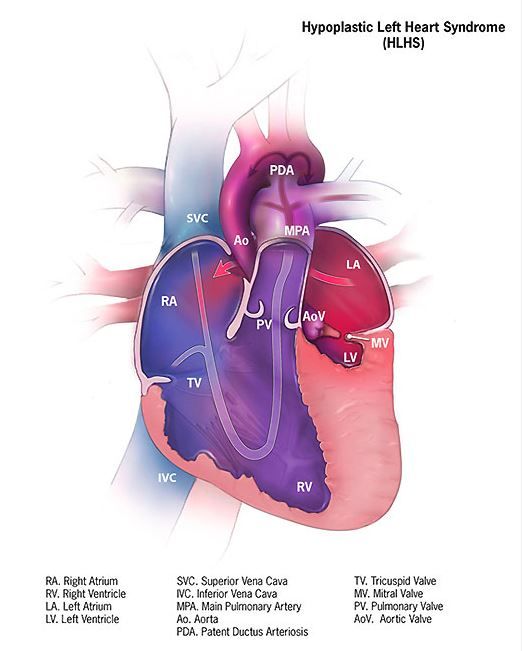
To determine the suggested benefit of NIRS as an effective trend monitor, the researchers used their interpolated data to examine changes in rSO2 and changes in ScvO2 at hourly intervals and compared these values.Of particular concern is the result showing that, in all instances where ScvO2 was less than 30%, rSO2 was greater than 30%. In terms of the sensitivity (the true positive rate) and specificity (the true negative rate) of using NIRS, time-matched pairs of rSO2 and ScvO2 showed that the receiver operating characteristic curves for rSO2 as a diagnostic test to detect ScvO2 less than 30%, less than 40%, and less than 50% were 0.82, 0.84, and 0.87, respectively, showing good specificity, with a value of rSO2 less than 30% indicating that ScvO2 will be less than 30% 99% of the time.
“However, the sensitivity of rSO2 in the range of clinical interest in detecting ScvO2 less than 30% is extremely low,” according to the researchers. Thus, NIRS is likely to produce false negatives, missing patients with clinically low postoperative oxygen saturation.
In fact, rSO2 was less than 30% less than 1% of the time that ScvO2 was less than 30%. Similar results were seen in comparing values at the less than 40% mark (equivalent less than 1% of the time). Better results showed at the less than 50% mark, with equivalence seen 46% of the time.
NIRS measures a composite of arterial and venous blood, according to Dr. Rescoe and her colleagues. Therefore, to do a more direct comparison, they adjusted their NIRS results by calculating an rSO2-based ScvO2 designed to remove arterial contamination from the rSO2 signal: rSO2-based ScvO2 = (rSO2 arterial oxygen saturation x 0.3)/0.7.
This significantly improved the sensitivity of rSO2 to detect ScvO2 at less than 30% to 6.5%, to 29% for rSO2 at less than 40%, and 77.4% for rSO2 less than 50%.
The researchers “were surprised by the extremely low sensitivity of cerebral NIRS to detect even the most severe aberrations in DO2” (i.e., ScvO2 less than 30%, which has been found to be associated with poor outcomes).
“Cerebral rSO2 in isolation should not be used to detect low ScvO2, because its sensitivity is low, although correction of rSO2 for arterial contamination significantly improves sensitivity. Cerebral rSO2 of 50 or greater should not be considered reassuring with regard to ScvO2, although values less than 30 are specific for low ScvO2,” the researchers concluded.
The study was sponsored by the Gerber Foundation, the Hess Family Philanthropic Fund, and Boston Children’s Hospital Heart Center Strategic Investment Fund. The authors disclosed that they had no financial conflicts.
The use of postoperative cerebral venous oxygen saturation monitoring (ScvO2) through an internal jugular vein catheter allows better monitoring of circulation, which may lead to better outcomes, but it is invasive and challenging. NIRS, being noninvasive, has proved attractive, but clinical interpretation in terms of both absolute values and trends is difficult, Edward Buratto, MBBS, and his colleagues noted in their invited commentary (doi: 10.1016/j.jtcvs.2017.04.061).
Dr. Rescoe and her colleagues have analyzed the correlation of NIRS-derived data with ScvO2 measured by co-oximetry from the internal jugular vein in 73 neonates after stage 1 palliation for hypoplastic left heart syndrome. They demonstrated that cerebral rSO2 correlated poorly with low ScvO2, and they suggest that cerebral rSO2 not be used in isolation. This problem was somewhat ameliorated by correction of the signal for arterial contamination. NIRS appears to be too valuable a tool to be simply discarded, they said, suggesting that a perioperative risk assessment that would include multisite NIRS and hemodynamic monitoring might still allow early determination of low-cardiac output.
“Two numbers are better than one,” wrote Dr. Buratto and his colleagues. “Whether the NIRS technology will add any useful information to a simple bedside assessment by an astute clinician is yet to be seen.”
Edward Buratto, MBBS, Steve Horton, PhD, and Igor E. Konstantinov, MD, are from the Department of Cardiothoracic Surgery, The Royal Children’s Hospital; the Department of Pediatrics, University of Melbourne; and Murdoch Children’s Research Institute, Melbourne. They reported having no financial conflicts of interest.
The use of postoperative cerebral venous oxygen saturation monitoring (ScvO2) through an internal jugular vein catheter allows better monitoring of circulation, which may lead to better outcomes, but it is invasive and challenging. NIRS, being noninvasive, has proved attractive, but clinical interpretation in terms of both absolute values and trends is difficult, Edward Buratto, MBBS, and his colleagues noted in their invited commentary (doi: 10.1016/j.jtcvs.2017.04.061).
Dr. Rescoe and her colleagues have analyzed the correlation of NIRS-derived data with ScvO2 measured by co-oximetry from the internal jugular vein in 73 neonates after stage 1 palliation for hypoplastic left heart syndrome. They demonstrated that cerebral rSO2 correlated poorly with low ScvO2, and they suggest that cerebral rSO2 not be used in isolation. This problem was somewhat ameliorated by correction of the signal for arterial contamination. NIRS appears to be too valuable a tool to be simply discarded, they said, suggesting that a perioperative risk assessment that would include multisite NIRS and hemodynamic monitoring might still allow early determination of low-cardiac output.
“Two numbers are better than one,” wrote Dr. Buratto and his colleagues. “Whether the NIRS technology will add any useful information to a simple bedside assessment by an astute clinician is yet to be seen.”
Edward Buratto, MBBS, Steve Horton, PhD, and Igor E. Konstantinov, MD, are from the Department of Cardiothoracic Surgery, The Royal Children’s Hospital; the Department of Pediatrics, University of Melbourne; and Murdoch Children’s Research Institute, Melbourne. They reported having no financial conflicts of interest.
The use of postoperative cerebral venous oxygen saturation monitoring (ScvO2) through an internal jugular vein catheter allows better monitoring of circulation, which may lead to better outcomes, but it is invasive and challenging. NIRS, being noninvasive, has proved attractive, but clinical interpretation in terms of both absolute values and trends is difficult, Edward Buratto, MBBS, and his colleagues noted in their invited commentary (doi: 10.1016/j.jtcvs.2017.04.061).
Dr. Rescoe and her colleagues have analyzed the correlation of NIRS-derived data with ScvO2 measured by co-oximetry from the internal jugular vein in 73 neonates after stage 1 palliation for hypoplastic left heart syndrome. They demonstrated that cerebral rSO2 correlated poorly with low ScvO2, and they suggest that cerebral rSO2 not be used in isolation. This problem was somewhat ameliorated by correction of the signal for arterial contamination. NIRS appears to be too valuable a tool to be simply discarded, they said, suggesting that a perioperative risk assessment that would include multisite NIRS and hemodynamic monitoring might still allow early determination of low-cardiac output.
“Two numbers are better than one,” wrote Dr. Buratto and his colleagues. “Whether the NIRS technology will add any useful information to a simple bedside assessment by an astute clinician is yet to be seen.”
Edward Buratto, MBBS, Steve Horton, PhD, and Igor E. Konstantinov, MD, are from the Department of Cardiothoracic Surgery, The Royal Children’s Hospital; the Department of Pediatrics, University of Melbourne; and Murdoch Children’s Research Institute, Melbourne. They reported having no financial conflicts of interest.
The regional oxygenation index (rSO2) based on near infrared spectroscopy (NIRS) measurement is frequently used to assess the adequacy of oxygen delivery after stage 1 palliation of hypoplastic left heart syndrome (HLHS). However, a recent study showed that cerebral rSO2 has low sensitivity and should not be considered reassuring even at rSO2 of 50 or greater. In addition, values below 30 were not found to be sensitive for detecting compromised oxygen delivery, according to a report published online in the Journal of Thoracic and Cardiovascular Surgery.
Erin Rescoe, MD, of Boston Children’s Hospital, and her colleagues at Harvard Medical School, Boston, performed a retrospective study of 73 neonates assessed with cerebral venous oxyhemoglobin saturation (ScvO2) measured by co-oximetry from the internal jugular vein, which is considered the preferred method for assessing the adequacy of tissue oxygen delivery, compared with cerebral rSO2 after stage 1 palliation of HLHS (doi: 10.1016/j.jtcvs.2017.03.154).
To determine the suggested benefit of NIRS as an effective trend monitor, the researchers used their interpolated data to examine changes in rSO2 and changes in ScvO2 at hourly intervals and compared these values.Of particular concern is the result showing that, in all instances where ScvO2 was less than 30%, rSO2 was greater than 30%. In terms of the sensitivity (the true positive rate) and specificity (the true negative rate) of using NIRS, time-matched pairs of rSO2 and ScvO2 showed that the receiver operating characteristic curves for rSO2 as a diagnostic test to detect ScvO2 less than 30%, less than 40%, and less than 50% were 0.82, 0.84, and 0.87, respectively, showing good specificity, with a value of rSO2 less than 30% indicating that ScvO2 will be less than 30% 99% of the time.
“However, the sensitivity of rSO2 in the range of clinical interest in detecting ScvO2 less than 30% is extremely low,” according to the researchers. Thus, NIRS is likely to produce false negatives, missing patients with clinically low postoperative oxygen saturation.
In fact, rSO2 was less than 30% less than 1% of the time that ScvO2 was less than 30%. Similar results were seen in comparing values at the less than 40% mark (equivalent less than 1% of the time). Better results showed at the less than 50% mark, with equivalence seen 46% of the time.
NIRS measures a composite of arterial and venous blood, according to Dr. Rescoe and her colleagues. Therefore, to do a more direct comparison, they adjusted their NIRS results by calculating an rSO2-based ScvO2 designed to remove arterial contamination from the rSO2 signal: rSO2-based ScvO2 = (rSO2 arterial oxygen saturation x 0.3)/0.7.
This significantly improved the sensitivity of rSO2 to detect ScvO2 at less than 30% to 6.5%, to 29% for rSO2 at less than 40%, and 77.4% for rSO2 less than 50%.
The researchers “were surprised by the extremely low sensitivity of cerebral NIRS to detect even the most severe aberrations in DO2” (i.e., ScvO2 less than 30%, which has been found to be associated with poor outcomes).
“Cerebral rSO2 in isolation should not be used to detect low ScvO2, because its sensitivity is low, although correction of rSO2 for arterial contamination significantly improves sensitivity. Cerebral rSO2 of 50 or greater should not be considered reassuring with regard to ScvO2, although values less than 30 are specific for low ScvO2,” the researchers concluded.
The study was sponsored by the Gerber Foundation, the Hess Family Philanthropic Fund, and Boston Children’s Hospital Heart Center Strategic Investment Fund. The authors disclosed that they had no financial conflicts.
The regional oxygenation index (rSO2) based on near infrared spectroscopy (NIRS) measurement is frequently used to assess the adequacy of oxygen delivery after stage 1 palliation of hypoplastic left heart syndrome (HLHS). However, a recent study showed that cerebral rSO2 has low sensitivity and should not be considered reassuring even at rSO2 of 50 or greater. In addition, values below 30 were not found to be sensitive for detecting compromised oxygen delivery, according to a report published online in the Journal of Thoracic and Cardiovascular Surgery.
Erin Rescoe, MD, of Boston Children’s Hospital, and her colleagues at Harvard Medical School, Boston, performed a retrospective study of 73 neonates assessed with cerebral venous oxyhemoglobin saturation (ScvO2) measured by co-oximetry from the internal jugular vein, which is considered the preferred method for assessing the adequacy of tissue oxygen delivery, compared with cerebral rSO2 after stage 1 palliation of HLHS (doi: 10.1016/j.jtcvs.2017.03.154).
To determine the suggested benefit of NIRS as an effective trend monitor, the researchers used their interpolated data to examine changes in rSO2 and changes in ScvO2 at hourly intervals and compared these values.Of particular concern is the result showing that, in all instances where ScvO2 was less than 30%, rSO2 was greater than 30%. In terms of the sensitivity (the true positive rate) and specificity (the true negative rate) of using NIRS, time-matched pairs of rSO2 and ScvO2 showed that the receiver operating characteristic curves for rSO2 as a diagnostic test to detect ScvO2 less than 30%, less than 40%, and less than 50% were 0.82, 0.84, and 0.87, respectively, showing good specificity, with a value of rSO2 less than 30% indicating that ScvO2 will be less than 30% 99% of the time.
“However, the sensitivity of rSO2 in the range of clinical interest in detecting ScvO2 less than 30% is extremely low,” according to the researchers. Thus, NIRS is likely to produce false negatives, missing patients with clinically low postoperative oxygen saturation.
In fact, rSO2 was less than 30% less than 1% of the time that ScvO2 was less than 30%. Similar results were seen in comparing values at the less than 40% mark (equivalent less than 1% of the time). Better results showed at the less than 50% mark, with equivalence seen 46% of the time.
NIRS measures a composite of arterial and venous blood, according to Dr. Rescoe and her colleagues. Therefore, to do a more direct comparison, they adjusted their NIRS results by calculating an rSO2-based ScvO2 designed to remove arterial contamination from the rSO2 signal: rSO2-based ScvO2 = (rSO2 arterial oxygen saturation x 0.3)/0.7.
This significantly improved the sensitivity of rSO2 to detect ScvO2 at less than 30% to 6.5%, to 29% for rSO2 at less than 40%, and 77.4% for rSO2 less than 50%.
The researchers “were surprised by the extremely low sensitivity of cerebral NIRS to detect even the most severe aberrations in DO2” (i.e., ScvO2 less than 30%, which has been found to be associated with poor outcomes).
“Cerebral rSO2 in isolation should not be used to detect low ScvO2, because its sensitivity is low, although correction of rSO2 for arterial contamination significantly improves sensitivity. Cerebral rSO2 of 50 or greater should not be considered reassuring with regard to ScvO2, although values less than 30 are specific for low ScvO2,” the researchers concluded.
The study was sponsored by the Gerber Foundation, the Hess Family Philanthropic Fund, and Boston Children’s Hospital Heart Center Strategic Investment Fund. The authors disclosed that they had no financial conflicts.
FROM THE JOURNAL OF THORACIC AND CARDIOVASCULAR SURGERY
Key clinical point:
Major finding: In terms of sensitivity, rSO2 was less than 30% less than 1% of the time that ScvO2 was less than 30%.
Data source: A retrospective single institution study of 73 neonates assessed after stage 1 palliation
Disclosures: The study was sponsored by the Gerber Foundation, the Hess Family Philanthropic Fund, and Boston Children’s Hospital Heart Center Strategic Investment Fund. The authors disclosed that they had no financial conflicts.
Sinus of Valsalva preserved in aortic valve replacement
The sinus of Valsalva segment can be preserved during aortic valve replacement irrespective of the type of valve pathology, according to a recent study by Rita Karianna Milewski, MD, and her colleagues at the Hospital of the University of Pennsylvania, Philadelphia.
Severe aortic root dilation coupled to aortic valve disease requires root replacement in patients with a tricuspid or bicuspid aortic valve. Commonly, an aortic valve replacement and supracoronary ascending aorta replacement (AVRSCAAR) procedure has been used for patients who have a mild to moderately dilated sinus segment. One advantage of the procedure is that it retains the sinus of Valsalva (SOV) and preserves the intact coronary ostia.
However, the long-term behavior and risk of aortic events for the retained SOV in both BAV and TAV patients remains unclear, according to Dr. Milewski and her colleagues.
Previous researchers have suggested that patients with BAV and TAV have different rates of complications of the remaining aorta and dilation of the proximal aorta and retained sinus segment. In addition, it has been suggested that the cause of aortic dilation is different in patients with aortic stenosis (AS) and aortic insufficiency (AI) and is based on TAV and BAV morphology, histology, and hemodynamic flow patterns.
However, in the August issue of the Journal of Thoracic and Cardiovascular Surgery, Dr. Milewski and her colleagues reported on their study showing that, in patients with nonaneurysmal SOV undergoing AVRSCAAR, the sinus of Valsalva segment can be preserved regardless of the type of valvular pathology (aortic stenosis vs. aortic insufficiency) or valvular morphology (BAV vs. TAV).
The researchers retrospectively reviewed a prospectively maintained institutional database to stratify all patients by BAV or TAV valvular pathology with concomitant ascending aortic aneurysm who underwent an elective AVRSCAAR from 2002 to 2015 (J Thorac Cardiovasc Surg. 2017;154:421-32).
The distribution of the 428 patients meeting inclusion criteria by subgroups was: BAV group (254 patients: BAV-AS = 178; BAV-AI = 76); TAV group (174 patients: TAV-AS = 61; TAV-AI =113). Preoperative sinus of Valsalva dimensions were divided into 3 subgroups (less than 40 mm, 40-45 mm, and greater than 45 mm).
The mean patient age for patients with BAV and TAV was 59 years and 72 years (P less than .001), respectively (with 78% with BAV being men and 57% with TAV being men). There was a significantly higher subpopulation of AS in the BAV cohort vs. TAV-AS (70% vs. 35%; P less than .001).
With regard to SOV sizing, there was no significant difference in mean preoperative aortic root diameters between BAV and TAV cohorts for the AS or AI subpopulations.
In-hospital/30-day mortality was significantly higher in patients with TAV (5.2%) than in patients with BAV (1.6%, P = .033). In addition, the incidence of transient ischemic attack/stroke was significantly higher in the TAV group (3.4%) vs. the BAV group (0.8%, P = .04).
Valvular morphology and pathology at baseline, preoperative SOV diameter, postoperative time course, and interaction effect of preoperative SOV diameters and postoperative time course were used as covariates to assess outcomes. Within-subject and within–stratified subgroup comparison failed to show main effects across the follow-up times on postoperative SOV size patterns (P = .935), implying that the SOV trends were stable and sustained (discharge to greater than or equal to 10 years) irrespective of valvular morphology and pathology (BAV-AI, BAV-AS, TAV-AI, and TAV-AS).
Preoperative SOV dimensions significantly affected the retained postoperative sinus dimensions (P less than .001), according to Dr. Milewski and her colleagues.
The data indicated that an initial and pronounced postoperative decrease in SOV dimensions occurs with AVRSCAAR independently of aortic valve morphology, aortic valve pathology, and age, they added.
The 10-year freedom from aortic reoperation rates were 97% and 95% in the BAV and TAV subgroups, respectively. The BAV group had significantly improved reoperation-free survival, compared with the TAV group (P less than .001), while the type of valvular pathology within each group did not show a significant survival difference.
“Irrespective of the aortic valve morphology or valve pathology, in patients with mild to moderate aortic root dilatation (less than 45 mm), preservation of the SOV segment in the context of an AVRSCAAR procedure is justified. Continued further follow-up will be important to understand the long-term outcomes of sinus preservation, especially in the younger population with BAVs,” the researchers concluded.
The authors reported having no financial conflicts to disclose.
With regard to the question, ‘‘Is it necessary to replace the sinuses of Valsalva in the setting of bicuspid aortic valve aortopathy?’’, the researchers “leverage their enormous institutional experience to find an answer. The results suggest that this answer is ‘no.’ At least not in all cases,” Thoralf M. Sundt, MD, wrote in his invited commentary on the paper (J Thorac Cardiovasc Surg. 2017;154:419-20).
“The findings of this study argue for us to take a step back and ask how much really needs be done,” he added. And although “it is hard to ask a surgeon to do less rather than more; however, the balance of judgment has to be between the operative risk of the more aggressive approach and the natural history of the disease. In other words, what does it ‘cost’ to be aggressive, and what do we gain?” he asked.
Bicuspid aortic valve aortopathy, it would appear, is not cancer after all. Regardless of theoretic arguments that are based on embryology and the migration of neural crest cells, it does not appear to require resection to ‘clean margins,’ even if we believe that the operative risk ‘in our hands’ is low,” concluded Dr. Sundt.
Thoralf M. Sundt, MD, is at Harvard Medical School, Boston. He reported having no disclosures.
With regard to the question, ‘‘Is it necessary to replace the sinuses of Valsalva in the setting of bicuspid aortic valve aortopathy?’’, the researchers “leverage their enormous institutional experience to find an answer. The results suggest that this answer is ‘no.’ At least not in all cases,” Thoralf M. Sundt, MD, wrote in his invited commentary on the paper (J Thorac Cardiovasc Surg. 2017;154:419-20).
“The findings of this study argue for us to take a step back and ask how much really needs be done,” he added. And although “it is hard to ask a surgeon to do less rather than more; however, the balance of judgment has to be between the operative risk of the more aggressive approach and the natural history of the disease. In other words, what does it ‘cost’ to be aggressive, and what do we gain?” he asked.
Bicuspid aortic valve aortopathy, it would appear, is not cancer after all. Regardless of theoretic arguments that are based on embryology and the migration of neural crest cells, it does not appear to require resection to ‘clean margins,’ even if we believe that the operative risk ‘in our hands’ is low,” concluded Dr. Sundt.
Thoralf M. Sundt, MD, is at Harvard Medical School, Boston. He reported having no disclosures.
With regard to the question, ‘‘Is it necessary to replace the sinuses of Valsalva in the setting of bicuspid aortic valve aortopathy?’’, the researchers “leverage their enormous institutional experience to find an answer. The results suggest that this answer is ‘no.’ At least not in all cases,” Thoralf M. Sundt, MD, wrote in his invited commentary on the paper (J Thorac Cardiovasc Surg. 2017;154:419-20).
“The findings of this study argue for us to take a step back and ask how much really needs be done,” he added. And although “it is hard to ask a surgeon to do less rather than more; however, the balance of judgment has to be between the operative risk of the more aggressive approach and the natural history of the disease. In other words, what does it ‘cost’ to be aggressive, and what do we gain?” he asked.
Bicuspid aortic valve aortopathy, it would appear, is not cancer after all. Regardless of theoretic arguments that are based on embryology and the migration of neural crest cells, it does not appear to require resection to ‘clean margins,’ even if we believe that the operative risk ‘in our hands’ is low,” concluded Dr. Sundt.
Thoralf M. Sundt, MD, is at Harvard Medical School, Boston. He reported having no disclosures.
The sinus of Valsalva segment can be preserved during aortic valve replacement irrespective of the type of valve pathology, according to a recent study by Rita Karianna Milewski, MD, and her colleagues at the Hospital of the University of Pennsylvania, Philadelphia.
Severe aortic root dilation coupled to aortic valve disease requires root replacement in patients with a tricuspid or bicuspid aortic valve. Commonly, an aortic valve replacement and supracoronary ascending aorta replacement (AVRSCAAR) procedure has been used for patients who have a mild to moderately dilated sinus segment. One advantage of the procedure is that it retains the sinus of Valsalva (SOV) and preserves the intact coronary ostia.
However, the long-term behavior and risk of aortic events for the retained SOV in both BAV and TAV patients remains unclear, according to Dr. Milewski and her colleagues.
Previous researchers have suggested that patients with BAV and TAV have different rates of complications of the remaining aorta and dilation of the proximal aorta and retained sinus segment. In addition, it has been suggested that the cause of aortic dilation is different in patients with aortic stenosis (AS) and aortic insufficiency (AI) and is based on TAV and BAV morphology, histology, and hemodynamic flow patterns.
However, in the August issue of the Journal of Thoracic and Cardiovascular Surgery, Dr. Milewski and her colleagues reported on their study showing that, in patients with nonaneurysmal SOV undergoing AVRSCAAR, the sinus of Valsalva segment can be preserved regardless of the type of valvular pathology (aortic stenosis vs. aortic insufficiency) or valvular morphology (BAV vs. TAV).
The researchers retrospectively reviewed a prospectively maintained institutional database to stratify all patients by BAV or TAV valvular pathology with concomitant ascending aortic aneurysm who underwent an elective AVRSCAAR from 2002 to 2015 (J Thorac Cardiovasc Surg. 2017;154:421-32).
The distribution of the 428 patients meeting inclusion criteria by subgroups was: BAV group (254 patients: BAV-AS = 178; BAV-AI = 76); TAV group (174 patients: TAV-AS = 61; TAV-AI =113). Preoperative sinus of Valsalva dimensions were divided into 3 subgroups (less than 40 mm, 40-45 mm, and greater than 45 mm).
The mean patient age for patients with BAV and TAV was 59 years and 72 years (P less than .001), respectively (with 78% with BAV being men and 57% with TAV being men). There was a significantly higher subpopulation of AS in the BAV cohort vs. TAV-AS (70% vs. 35%; P less than .001).
With regard to SOV sizing, there was no significant difference in mean preoperative aortic root diameters between BAV and TAV cohorts for the AS or AI subpopulations.
In-hospital/30-day mortality was significantly higher in patients with TAV (5.2%) than in patients with BAV (1.6%, P = .033). In addition, the incidence of transient ischemic attack/stroke was significantly higher in the TAV group (3.4%) vs. the BAV group (0.8%, P = .04).
Valvular morphology and pathology at baseline, preoperative SOV diameter, postoperative time course, and interaction effect of preoperative SOV diameters and postoperative time course were used as covariates to assess outcomes. Within-subject and within–stratified subgroup comparison failed to show main effects across the follow-up times on postoperative SOV size patterns (P = .935), implying that the SOV trends were stable and sustained (discharge to greater than or equal to 10 years) irrespective of valvular morphology and pathology (BAV-AI, BAV-AS, TAV-AI, and TAV-AS).
Preoperative SOV dimensions significantly affected the retained postoperative sinus dimensions (P less than .001), according to Dr. Milewski and her colleagues.
The data indicated that an initial and pronounced postoperative decrease in SOV dimensions occurs with AVRSCAAR independently of aortic valve morphology, aortic valve pathology, and age, they added.
The 10-year freedom from aortic reoperation rates were 97% and 95% in the BAV and TAV subgroups, respectively. The BAV group had significantly improved reoperation-free survival, compared with the TAV group (P less than .001), while the type of valvular pathology within each group did not show a significant survival difference.
“Irrespective of the aortic valve morphology or valve pathology, in patients with mild to moderate aortic root dilatation (less than 45 mm), preservation of the SOV segment in the context of an AVRSCAAR procedure is justified. Continued further follow-up will be important to understand the long-term outcomes of sinus preservation, especially in the younger population with BAVs,” the researchers concluded.
The authors reported having no financial conflicts to disclose.
The sinus of Valsalva segment can be preserved during aortic valve replacement irrespective of the type of valve pathology, according to a recent study by Rita Karianna Milewski, MD, and her colleagues at the Hospital of the University of Pennsylvania, Philadelphia.
Severe aortic root dilation coupled to aortic valve disease requires root replacement in patients with a tricuspid or bicuspid aortic valve. Commonly, an aortic valve replacement and supracoronary ascending aorta replacement (AVRSCAAR) procedure has been used for patients who have a mild to moderately dilated sinus segment. One advantage of the procedure is that it retains the sinus of Valsalva (SOV) and preserves the intact coronary ostia.
However, the long-term behavior and risk of aortic events for the retained SOV in both BAV and TAV patients remains unclear, according to Dr. Milewski and her colleagues.
Previous researchers have suggested that patients with BAV and TAV have different rates of complications of the remaining aorta and dilation of the proximal aorta and retained sinus segment. In addition, it has been suggested that the cause of aortic dilation is different in patients with aortic stenosis (AS) and aortic insufficiency (AI) and is based on TAV and BAV morphology, histology, and hemodynamic flow patterns.
However, in the August issue of the Journal of Thoracic and Cardiovascular Surgery, Dr. Milewski and her colleagues reported on their study showing that, in patients with nonaneurysmal SOV undergoing AVRSCAAR, the sinus of Valsalva segment can be preserved regardless of the type of valvular pathology (aortic stenosis vs. aortic insufficiency) or valvular morphology (BAV vs. TAV).
The researchers retrospectively reviewed a prospectively maintained institutional database to stratify all patients by BAV or TAV valvular pathology with concomitant ascending aortic aneurysm who underwent an elective AVRSCAAR from 2002 to 2015 (J Thorac Cardiovasc Surg. 2017;154:421-32).
The distribution of the 428 patients meeting inclusion criteria by subgroups was: BAV group (254 patients: BAV-AS = 178; BAV-AI = 76); TAV group (174 patients: TAV-AS = 61; TAV-AI =113). Preoperative sinus of Valsalva dimensions were divided into 3 subgroups (less than 40 mm, 40-45 mm, and greater than 45 mm).
The mean patient age for patients with BAV and TAV was 59 years and 72 years (P less than .001), respectively (with 78% with BAV being men and 57% with TAV being men). There was a significantly higher subpopulation of AS in the BAV cohort vs. TAV-AS (70% vs. 35%; P less than .001).
With regard to SOV sizing, there was no significant difference in mean preoperative aortic root diameters between BAV and TAV cohorts for the AS or AI subpopulations.
In-hospital/30-day mortality was significantly higher in patients with TAV (5.2%) than in patients with BAV (1.6%, P = .033). In addition, the incidence of transient ischemic attack/stroke was significantly higher in the TAV group (3.4%) vs. the BAV group (0.8%, P = .04).
Valvular morphology and pathology at baseline, preoperative SOV diameter, postoperative time course, and interaction effect of preoperative SOV diameters and postoperative time course were used as covariates to assess outcomes. Within-subject and within–stratified subgroup comparison failed to show main effects across the follow-up times on postoperative SOV size patterns (P = .935), implying that the SOV trends were stable and sustained (discharge to greater than or equal to 10 years) irrespective of valvular morphology and pathology (BAV-AI, BAV-AS, TAV-AI, and TAV-AS).
Preoperative SOV dimensions significantly affected the retained postoperative sinus dimensions (P less than .001), according to Dr. Milewski and her colleagues.
The data indicated that an initial and pronounced postoperative decrease in SOV dimensions occurs with AVRSCAAR independently of aortic valve morphology, aortic valve pathology, and age, they added.
The 10-year freedom from aortic reoperation rates were 97% and 95% in the BAV and TAV subgroups, respectively. The BAV group had significantly improved reoperation-free survival, compared with the TAV group (P less than .001), while the type of valvular pathology within each group did not show a significant survival difference.
“Irrespective of the aortic valve morphology or valve pathology, in patients with mild to moderate aortic root dilatation (less than 45 mm), preservation of the SOV segment in the context of an AVRSCAAR procedure is justified. Continued further follow-up will be important to understand the long-term outcomes of sinus preservation, especially in the younger population with BAVs,” the researchers concluded.
The authors reported having no financial conflicts to disclose.
FROM THE JOURNAL OF THORACIC AND CARDIOVASCULAR SURGERY
Key clinical point:
Major finding: The 10-year freedom from aortic reoperation rates were 97% and 95% in the BAV and TAV subgroups, respectively.
Data source: A retrospective review of 428 patients in a prospectively maintained database who met study inclusion criteria and were operated on between 2002 and 2015.
Disclosures: The authors reported having no financial conflicts to disclose.

Five-year outcomes favor on- versus off-pump CABG
Compared with adults who underwent off-pump coronary-artery bypass grafting surgery, those who underwent on-pump CABG had significantly lower rates of mortality and major adverse cardiovascular events at 5 years, results from a large randomized trial demonstrated.
“Given the results, it appears that innovative surgical approaches – such as the more technically demanding off-pump procedure – may not always provide superior clinical outcomes,” researchers led by A. Laurie Shroyer, PhD, wrote (N Engl J Med. 2017 Aug 17;377:623-32). “Additional long-term follow-up, evaluating these same outcomes rigorously at 10 years after CABG, appears to be warranted. Future research may identify the risk factors of the patients and the cardiac surgical processes of care that affect longer-term outcomes of coronary revascularization procedures, with the goal of increasing the rate of long-term event-free survival.”
Dr. Shroyer, of the Northport (N.Y.) VA Medical Center, and her associates conduced a 5-year follow-up study of patients who had participated in the original Randomized On/Off Bypass (ROOBY) trial, which compared the effectiveness of the two surgical approaches (N Engl J Med 2009 Nov 5;361:1827-37). During February 2002–June 2007, 2,203 patients at 18 medical centers were randomly assigned to either on-pump or off-pump CABG, with 1-year assessments completed by May 2008. The primary outcomes were the rates mortality and major adverse cardiovascular events at 5 years, while the secondary 5-year outcomes included death from cardiac causes, repeat revascularization, and nonfatal myocardial infarction.
The mean age of patients was 63 years, nearly all were male, 46% were between the ages of 55 and 64, and about 21% had chronic obstructive pulmonary disease. The researchers found that at 5 years, the rate of death was 15.2% in the off-pump group, compared with 11.9% in the on-pump group, which translated into a relative risk of 1.28 (P = .02). In addition, the rate of major cardiovascular events at 5 years was 31% in the off-pump group, compared with 27.1% in the on-pump group, which translated into a relative risk of 1.14 (P = .046). None of the secondary outcomes at 5 years met the prespecified threshold of a P value of .01 or less for statistical significance, when the off-pump and on-pump groups were compared. This included the rates of nonfatal myocardial infarction (12.1% vs. 9.6%, respectively; P = .05); death from cardiac causes (6.3% vs. 5.3%; P = .29); repeat vascularization (13.1% vs. 11.9%; P = .39), and repeat CABG (1.4% vs. 0.5%; P = .02).
“In combination with findings from other randomized trials and a 2012 Cochrane systematic review [Cochrane Database Syst Rev. 2012;14:CD007224], the 5-year outcomes in our study support the conclusion that off-pump CABG does not offer any substantial advantages over on-pump CABG except possibly in unusual situations such as, for example, in patients with an extensively calcified (porcelain) aorta, in whom the off-pump technique may result in less manipulation of the aorta, potentially decreasing the risk of aortic emboli or stroke,” the researchers wrote. “In light of the low rates of use of off-pump CABG in the United States, the findings in our trial may provide more of a real-world experience than those in the CORONARY and GOPCABE trials, which required surgeons with a very high volume of experience with off-pump procedures, as compared with the ROOBY trial and with most other surgeons who are based in the United States.”
They acknowledged certain limitations of the study, including the fact that the study population comprised mostly males who had multiple coexisting conditions, “so the findings may not be applicable to female patients or to patients who are not veterans.”
The study was supported by a grant from the Department of Veterans Affairs. Dr. Shroyer reported having received grants from the VA Cooperative Studies Program during the conduct of the study. Her coauthors reported having no financial disclosures.

Compared with adults who underwent off-pump coronary-artery bypass grafting surgery, those who underwent on-pump CABG had significantly lower rates of mortality and major adverse cardiovascular events at 5 years, results from a large randomized trial demonstrated.
“Given the results, it appears that innovative surgical approaches – such as the more technically demanding off-pump procedure – may not always provide superior clinical outcomes,” researchers led by A. Laurie Shroyer, PhD, wrote (N Engl J Med. 2017 Aug 17;377:623-32). “Additional long-term follow-up, evaluating these same outcomes rigorously at 10 years after CABG, appears to be warranted. Future research may identify the risk factors of the patients and the cardiac surgical processes of care that affect longer-term outcomes of coronary revascularization procedures, with the goal of increasing the rate of long-term event-free survival.”
Dr. Shroyer, of the Northport (N.Y.) VA Medical Center, and her associates conduced a 5-year follow-up study of patients who had participated in the original Randomized On/Off Bypass (ROOBY) trial, which compared the effectiveness of the two surgical approaches (N Engl J Med 2009 Nov 5;361:1827-37). During February 2002–June 2007, 2,203 patients at 18 medical centers were randomly assigned to either on-pump or off-pump CABG, with 1-year assessments completed by May 2008. The primary outcomes were the rates mortality and major adverse cardiovascular events at 5 years, while the secondary 5-year outcomes included death from cardiac causes, repeat revascularization, and nonfatal myocardial infarction.
The mean age of patients was 63 years, nearly all were male, 46% were between the ages of 55 and 64, and about 21% had chronic obstructive pulmonary disease. The researchers found that at 5 years, the rate of death was 15.2% in the off-pump group, compared with 11.9% in the on-pump group, which translated into a relative risk of 1.28 (P = .02). In addition, the rate of major cardiovascular events at 5 years was 31% in the off-pump group, compared with 27.1% in the on-pump group, which translated into a relative risk of 1.14 (P = .046). None of the secondary outcomes at 5 years met the prespecified threshold of a P value of .01 or less for statistical significance, when the off-pump and on-pump groups were compared. This included the rates of nonfatal myocardial infarction (12.1% vs. 9.6%, respectively; P = .05); death from cardiac causes (6.3% vs. 5.3%; P = .29); repeat vascularization (13.1% vs. 11.9%; P = .39), and repeat CABG (1.4% vs. 0.5%; P = .02).
“In combination with findings from other randomized trials and a 2012 Cochrane systematic review [Cochrane Database Syst Rev. 2012;14:CD007224], the 5-year outcomes in our study support the conclusion that off-pump CABG does not offer any substantial advantages over on-pump CABG except possibly in unusual situations such as, for example, in patients with an extensively calcified (porcelain) aorta, in whom the off-pump technique may result in less manipulation of the aorta, potentially decreasing the risk of aortic emboli or stroke,” the researchers wrote. “In light of the low rates of use of off-pump CABG in the United States, the findings in our trial may provide more of a real-world experience than those in the CORONARY and GOPCABE trials, which required surgeons with a very high volume of experience with off-pump procedures, as compared with the ROOBY trial and with most other surgeons who are based in the United States.”
They acknowledged certain limitations of the study, including the fact that the study population comprised mostly males who had multiple coexisting conditions, “so the findings may not be applicable to female patients or to patients who are not veterans.”
The study was supported by a grant from the Department of Veterans Affairs. Dr. Shroyer reported having received grants from the VA Cooperative Studies Program during the conduct of the study. Her coauthors reported having no financial disclosures.
Compared with adults who underwent off-pump coronary-artery bypass grafting surgery, those who underwent on-pump CABG had significantly lower rates of mortality and major adverse cardiovascular events at 5 years, results from a large randomized trial demonstrated.
“Given the results, it appears that innovative surgical approaches – such as the more technically demanding off-pump procedure – may not always provide superior clinical outcomes,” researchers led by A. Laurie Shroyer, PhD, wrote (N Engl J Med. 2017 Aug 17;377:623-32). “Additional long-term follow-up, evaluating these same outcomes rigorously at 10 years after CABG, appears to be warranted. Future research may identify the risk factors of the patients and the cardiac surgical processes of care that affect longer-term outcomes of coronary revascularization procedures, with the goal of increasing the rate of long-term event-free survival.”
Dr. Shroyer, of the Northport (N.Y.) VA Medical Center, and her associates conduced a 5-year follow-up study of patients who had participated in the original Randomized On/Off Bypass (ROOBY) trial, which compared the effectiveness of the two surgical approaches (N Engl J Med 2009 Nov 5;361:1827-37). During February 2002–June 2007, 2,203 patients at 18 medical centers were randomly assigned to either on-pump or off-pump CABG, with 1-year assessments completed by May 2008. The primary outcomes were the rates mortality and major adverse cardiovascular events at 5 years, while the secondary 5-year outcomes included death from cardiac causes, repeat revascularization, and nonfatal myocardial infarction.
The mean age of patients was 63 years, nearly all were male, 46% were between the ages of 55 and 64, and about 21% had chronic obstructive pulmonary disease. The researchers found that at 5 years, the rate of death was 15.2% in the off-pump group, compared with 11.9% in the on-pump group, which translated into a relative risk of 1.28 (P = .02). In addition, the rate of major cardiovascular events at 5 years was 31% in the off-pump group, compared with 27.1% in the on-pump group, which translated into a relative risk of 1.14 (P = .046). None of the secondary outcomes at 5 years met the prespecified threshold of a P value of .01 or less for statistical significance, when the off-pump and on-pump groups were compared. This included the rates of nonfatal myocardial infarction (12.1% vs. 9.6%, respectively; P = .05); death from cardiac causes (6.3% vs. 5.3%; P = .29); repeat vascularization (13.1% vs. 11.9%; P = .39), and repeat CABG (1.4% vs. 0.5%; P = .02).
“In combination with findings from other randomized trials and a 2012 Cochrane systematic review [Cochrane Database Syst Rev. 2012;14:CD007224], the 5-year outcomes in our study support the conclusion that off-pump CABG does not offer any substantial advantages over on-pump CABG except possibly in unusual situations such as, for example, in patients with an extensively calcified (porcelain) aorta, in whom the off-pump technique may result in less manipulation of the aorta, potentially decreasing the risk of aortic emboli or stroke,” the researchers wrote. “In light of the low rates of use of off-pump CABG in the United States, the findings in our trial may provide more of a real-world experience than those in the CORONARY and GOPCABE trials, which required surgeons with a very high volume of experience with off-pump procedures, as compared with the ROOBY trial and with most other surgeons who are based in the United States.”
They acknowledged certain limitations of the study, including the fact that the study population comprised mostly males who had multiple coexisting conditions, “so the findings may not be applicable to female patients or to patients who are not veterans.”
The study was supported by a grant from the Department of Veterans Affairs. Dr. Shroyer reported having received grants from the VA Cooperative Studies Program during the conduct of the study. Her coauthors reported having no financial disclosures.
FROM THE NEW ENGLAND JOURNAL OF MEDICINE
Key clinical point:
Major finding: At 5 years, the rate of death was 15.2% in the off-pump group, compared with 11.9% in the on-pump group, which translated into a relative risk of 1.28 (P = .02).
Data source: A 5-year follow-up study of 2,203 patients who had participated in the original Randomized On/Off Bypass (ROOBY) trial.
Disclosures: The study was supported by a grant from the Department of Veterans Affairs. Dr. Shroyer reported having received grants from the Department of Veterans Affairs Cooperative Studies Program during the study. The other coauthors reported having no financial disclosures.

CBO: End of ACA subsidies would mean short-term exit of insurers
Terminating the Affordable Care Act’s cost-sharing reduction payments to insurers would cause a short-term exit by insurers from the individual insurance marketplaces, but the availability of plans is expected to rebound, according to the Congressional Budget Office.
In a new analysis requested by Democratic leadership in the House of Representatives, CBO and staff from the congressional Joint Committee on Taxation (JCT) examined what would happen if the Trump administration announced by the end of August that it would cease to make cost-sharing reduction payments at the end of 2017.
However, insurers would be on the hook to cover the payments no longer provided by the government, which means that “participating insurers would raise premiums of ‘silver’ plans to recover the costs.”
Gross premiums for silver plans “would be 20% higher in 2018 and 25% by 2020,” pushing higher premium tax credits and increasing the federal deficit by $194 billion from 2017 through 2026,” the report states. “Most people would pay net premiums (after accounting for premium tax credits) for nongroup insurance throughout the next decade that were similar to or less than what they would pay otherwise.”
The percentage of people facing a “slight increases” would be higher during the next 2 years, they pointed out.
The number of uninsured would be slightly higher in 2018 (about 1 million more uninsured) but then would be slightly lower starting in 2020 (about 1 million less each year).
Should the administration end cost-sharing reduction payments in 2017, those eligible for tax credits who have annual incomes 200%-400% of the federal poverty level would use their subsidies to purchase either gold or bronze plans, with silver plans going almost exclusively to people eligible for cost-sharing reductions (100%-200% of the poverty line).
Terminating the Affordable Care Act’s cost-sharing reduction payments to insurers would cause a short-term exit by insurers from the individual insurance marketplaces, but the availability of plans is expected to rebound, according to the Congressional Budget Office.
In a new analysis requested by Democratic leadership in the House of Representatives, CBO and staff from the congressional Joint Committee on Taxation (JCT) examined what would happen if the Trump administration announced by the end of August that it would cease to make cost-sharing reduction payments at the end of 2017.
However, insurers would be on the hook to cover the payments no longer provided by the government, which means that “participating insurers would raise premiums of ‘silver’ plans to recover the costs.”
Gross premiums for silver plans “would be 20% higher in 2018 and 25% by 2020,” pushing higher premium tax credits and increasing the federal deficit by $194 billion from 2017 through 2026,” the report states. “Most people would pay net premiums (after accounting for premium tax credits) for nongroup insurance throughout the next decade that were similar to or less than what they would pay otherwise.”
The percentage of people facing a “slight increases” would be higher during the next 2 years, they pointed out.
The number of uninsured would be slightly higher in 2018 (about 1 million more uninsured) but then would be slightly lower starting in 2020 (about 1 million less each year).
Should the administration end cost-sharing reduction payments in 2017, those eligible for tax credits who have annual incomes 200%-400% of the federal poverty level would use their subsidies to purchase either gold or bronze plans, with silver plans going almost exclusively to people eligible for cost-sharing reductions (100%-200% of the poverty line).
Terminating the Affordable Care Act’s cost-sharing reduction payments to insurers would cause a short-term exit by insurers from the individual insurance marketplaces, but the availability of plans is expected to rebound, according to the Congressional Budget Office.
In a new analysis requested by Democratic leadership in the House of Representatives, CBO and staff from the congressional Joint Committee on Taxation (JCT) examined what would happen if the Trump administration announced by the end of August that it would cease to make cost-sharing reduction payments at the end of 2017.
However, insurers would be on the hook to cover the payments no longer provided by the government, which means that “participating insurers would raise premiums of ‘silver’ plans to recover the costs.”
Gross premiums for silver plans “would be 20% higher in 2018 and 25% by 2020,” pushing higher premium tax credits and increasing the federal deficit by $194 billion from 2017 through 2026,” the report states. “Most people would pay net premiums (after accounting for premium tax credits) for nongroup insurance throughout the next decade that were similar to or less than what they would pay otherwise.”
The percentage of people facing a “slight increases” would be higher during the next 2 years, they pointed out.
The number of uninsured would be slightly higher in 2018 (about 1 million more uninsured) but then would be slightly lower starting in 2020 (about 1 million less each year).
Should the administration end cost-sharing reduction payments in 2017, those eligible for tax credits who have annual incomes 200%-400% of the federal poverty level would use their subsidies to purchase either gold or bronze plans, with silver plans going almost exclusively to people eligible for cost-sharing reductions (100%-200% of the poverty line).
Physicians express mixed views on new FDA tobacco plan
Physicians associations are expressing mixed opinions about the Food and Drug Administration’s new plan for regulating tobacco products, such as flavored cigars, hookah tobacco, and e-cigarettes.
As part of the new plan, announced July 28, the FDA will relax previous application deadlines set for makers of newer tobacco products. The agency will also seek more public input on the role of flavors in tobacco products before moving forward with specific regulations.

“The delay outlined in [FDA Commissioner Scott Gottlieb’s] vision will cost the American public continued death and disease as a result of tobacco use,” Enid Neptune, MD, vice chair of the ATS Tobacco Action Committee said in the statement. “In short, Dr. Gottlieb’s announcement of the FDA’s new vision for regulating tobacco products is long on delay and short on action. The health of the American public, and particularly today’s youth, will suffer as a result of the FDA’s failure to act.”
The American College of Chest Physicians, meanwhile, applauded the FDA’s plan and expressed its support of the actions outlined.
“We welcome opportunities and actions that reduce tobacco use, addiction, and tobacco-related disease and death,” said Gerard Silvestri, MD, president for the college, in a statement. “We support the actions proposed by the FDA, which are likely to improve public health and reduce the burden of disease on patients and our country.”
As part of the FDA’s revised plan, the agency intends to begin a public dialogue about lowering nicotine levels in combustible cigarettes to nonaddictive levels through “achievable product standards.” The agency also plans to issue an advance notice of proposed rule making to seek input on the potential public health benefits and possible adverse effects of lowering nicotine in cigarettes.
Under revised time lines, applications for newly regulated combustible products, such as cigars, pipe tobacco, and hookah tobacco, must be submitted by makers to the FDA by Aug. 8, 2021, and applications for noncombustible products, such as e-cigarettes, must be submitted by Aug. 8, 2022. Manufacturers can continue to market their products while the agency reviews their product applications. The time frames push back previous deadlines that were established in a May 2016 final rule by the FDA. In the prior rule, manufacturers of all new tobacco products had 12-24 months to prepare and send applications for marketing authorization to the FDA and a 12-month continued compliance period after those dates in which to obtain FDA authorization.

“This comprehensive plan and sweeping approach to tobacco and nicotine allows the FDA to apply the powerful tools given by Congress to achieve the most significant public health impact,” Mitch Zeller, director of the FDA’s Center for Tobacco Products said in a statement. “Public input on these complex issues will help ensure the agency has the proper science-based policies in place to meaningfully reduce the harms caused by tobacco use.”
However, the ATS said that many of the issues raised in the FDA’s revised plan have already been discussed at length in the scientific literature and with the public.
“Scientific literature documenting the role cigars play in tobacco-related disease is extensive,” said Harold J. Farber, MD, chair of the ATS Tobacco Action Committee. “The FDA sought and received extensive public and industry input regarding exempting cigars during the proposed deeming rule. The FDA provided an extensive rational for why premium cigars should be regulated in its final deeming rule.”
In addition, the role of flavoring agents in tobacco products has also been discussed by the FDA, Dr. Neptune added. The agency previously sought, and received, extensive scientific, industry, and public input on the role of flavoring agents in tobacco products, she said. In addition, multiple reports have been issued on the role of flavoring agents, showing that flavoring agents increase tobacco initiation and make tobacco cessation harder, she noted.
“While more scientific information is always welcomed, Commissioner Gottlieb’s call for a new public discussion seeks to hide or ignore the extensive public discussion that has already occurred,” Dr. Neptune said. “In short, Commissioner Gottlieb has more than enough information to take action on flavored nicotine products today.”
[email protected]
On Twitter @legal_med

Physicians associations are expressing mixed opinions about the Food and Drug Administration’s new plan for regulating tobacco products, such as flavored cigars, hookah tobacco, and e-cigarettes.
As part of the new plan, announced July 28, the FDA will relax previous application deadlines set for makers of newer tobacco products. The agency will also seek more public input on the role of flavors in tobacco products before moving forward with specific regulations.
“The delay outlined in [FDA Commissioner Scott Gottlieb’s] vision will cost the American public continued death and disease as a result of tobacco use,” Enid Neptune, MD, vice chair of the ATS Tobacco Action Committee said in the statement. “In short, Dr. Gottlieb’s announcement of the FDA’s new vision for regulating tobacco products is long on delay and short on action. The health of the American public, and particularly today’s youth, will suffer as a result of the FDA’s failure to act.”
The American College of Chest Physicians, meanwhile, applauded the FDA’s plan and expressed its support of the actions outlined.
“We welcome opportunities and actions that reduce tobacco use, addiction, and tobacco-related disease and death,” said Gerard Silvestri, MD, president for the college, in a statement. “We support the actions proposed by the FDA, which are likely to improve public health and reduce the burden of disease on patients and our country.”
As part of the FDA’s revised plan, the agency intends to begin a public dialogue about lowering nicotine levels in combustible cigarettes to nonaddictive levels through “achievable product standards.” The agency also plans to issue an advance notice of proposed rule making to seek input on the potential public health benefits and possible adverse effects of lowering nicotine in cigarettes.
Under revised time lines, applications for newly regulated combustible products, such as cigars, pipe tobacco, and hookah tobacco, must be submitted by makers to the FDA by Aug. 8, 2021, and applications for noncombustible products, such as e-cigarettes, must be submitted by Aug. 8, 2022. Manufacturers can continue to market their products while the agency reviews their product applications. The time frames push back previous deadlines that were established in a May 2016 final rule by the FDA. In the prior rule, manufacturers of all new tobacco products had 12-24 months to prepare and send applications for marketing authorization to the FDA and a 12-month continued compliance period after those dates in which to obtain FDA authorization.
“This comprehensive plan and sweeping approach to tobacco and nicotine allows the FDA to apply the powerful tools given by Congress to achieve the most significant public health impact,” Mitch Zeller, director of the FDA’s Center for Tobacco Products said in a statement. “Public input on these complex issues will help ensure the agency has the proper science-based policies in place to meaningfully reduce the harms caused by tobacco use.”
However, the ATS said that many of the issues raised in the FDA’s revised plan have already been discussed at length in the scientific literature and with the public.
“Scientific literature documenting the role cigars play in tobacco-related disease is extensive,” said Harold J. Farber, MD, chair of the ATS Tobacco Action Committee. “The FDA sought and received extensive public and industry input regarding exempting cigars during the proposed deeming rule. The FDA provided an extensive rational for why premium cigars should be regulated in its final deeming rule.”
In addition, the role of flavoring agents in tobacco products has also been discussed by the FDA, Dr. Neptune added. The agency previously sought, and received, extensive scientific, industry, and public input on the role of flavoring agents in tobacco products, she said. In addition, multiple reports have been issued on the role of flavoring agents, showing that flavoring agents increase tobacco initiation and make tobacco cessation harder, she noted.
“While more scientific information is always welcomed, Commissioner Gottlieb’s call for a new public discussion seeks to hide or ignore the extensive public discussion that has already occurred,” Dr. Neptune said. “In short, Commissioner Gottlieb has more than enough information to take action on flavored nicotine products today.”
[email protected]
On Twitter @legal_med
Physicians associations are expressing mixed opinions about the Food and Drug Administration’s new plan for regulating tobacco products, such as flavored cigars, hookah tobacco, and e-cigarettes.
As part of the new plan, announced July 28, the FDA will relax previous application deadlines set for makers of newer tobacco products. The agency will also seek more public input on the role of flavors in tobacco products before moving forward with specific regulations.
“The delay outlined in [FDA Commissioner Scott Gottlieb’s] vision will cost the American public continued death and disease as a result of tobacco use,” Enid Neptune, MD, vice chair of the ATS Tobacco Action Committee said in the statement. “In short, Dr. Gottlieb’s announcement of the FDA’s new vision for regulating tobacco products is long on delay and short on action. The health of the American public, and particularly today’s youth, will suffer as a result of the FDA’s failure to act.”
The American College of Chest Physicians, meanwhile, applauded the FDA’s plan and expressed its support of the actions outlined.
“We welcome opportunities and actions that reduce tobacco use, addiction, and tobacco-related disease and death,” said Gerard Silvestri, MD, president for the college, in a statement. “We support the actions proposed by the FDA, which are likely to improve public health and reduce the burden of disease on patients and our country.”
As part of the FDA’s revised plan, the agency intends to begin a public dialogue about lowering nicotine levels in combustible cigarettes to nonaddictive levels through “achievable product standards.” The agency also plans to issue an advance notice of proposed rule making to seek input on the potential public health benefits and possible adverse effects of lowering nicotine in cigarettes.
Under revised time lines, applications for newly regulated combustible products, such as cigars, pipe tobacco, and hookah tobacco, must be submitted by makers to the FDA by Aug. 8, 2021, and applications for noncombustible products, such as e-cigarettes, must be submitted by Aug. 8, 2022. Manufacturers can continue to market their products while the agency reviews their product applications. The time frames push back previous deadlines that were established in a May 2016 final rule by the FDA. In the prior rule, manufacturers of all new tobacco products had 12-24 months to prepare and send applications for marketing authorization to the FDA and a 12-month continued compliance period after those dates in which to obtain FDA authorization.
“This comprehensive plan and sweeping approach to tobacco and nicotine allows the FDA to apply the powerful tools given by Congress to achieve the most significant public health impact,” Mitch Zeller, director of the FDA’s Center for Tobacco Products said in a statement. “Public input on these complex issues will help ensure the agency has the proper science-based policies in place to meaningfully reduce the harms caused by tobacco use.”
However, the ATS said that many of the issues raised in the FDA’s revised plan have already been discussed at length in the scientific literature and with the public.
“Scientific literature documenting the role cigars play in tobacco-related disease is extensive,” said Harold J. Farber, MD, chair of the ATS Tobacco Action Committee. “The FDA sought and received extensive public and industry input regarding exempting cigars during the proposed deeming rule. The FDA provided an extensive rational for why premium cigars should be regulated in its final deeming rule.”
In addition, the role of flavoring agents in tobacco products has also been discussed by the FDA, Dr. Neptune added. The agency previously sought, and received, extensive scientific, industry, and public input on the role of flavoring agents in tobacco products, she said. In addition, multiple reports have been issued on the role of flavoring agents, showing that flavoring agents increase tobacco initiation and make tobacco cessation harder, she noted.
“While more scientific information is always welcomed, Commissioner Gottlieb’s call for a new public discussion seeks to hide or ignore the extensive public discussion that has already occurred,” Dr. Neptune said. “In short, Commissioner Gottlieb has more than enough information to take action on flavored nicotine products today.”
[email protected]
On Twitter @legal_med
New findings from first all-female TAVR registry
Paris – A history of pregnancy did not protect against adverse outcomes at 1 year in the Women’s International Transcatheter Aortic Valve Implantation Registry (WIN-TAVI), even though it did within the first 30 days, Alaide Chieffo, MD, reported at the annual congress of the European Association of Percutaneous Cardiovascular Interventions.
One year ago, at EuroPCR 2016, she reported that in WIN-TAVI, a history of pregnancy – albeit typically more than half a century previously – was independently associated with a 43% reduction in the Valve Academic Research Consortium-2 (VARC-2) 30-day composite endpoint, including death, stroke, major vascular complications, life-threatening bleeding, stage 2 or 3 acute kidney injury, coronary artery obstruction, or repeat transcatheter aortic valve replacement (TAVR) done because of valve-related dysfunction. Those early findings, first reported in this publication, were later published (JACC Cardiovasc Interv. 2016 Aug 8;9[15]:1589-600).
At 1 year of follow-up, however, the rate of the VARC-2 composite endpoint was no longer significantly different in women with or without a history of pregnancy. Nor was a history of pregnancy associated with a significantly reduced risk of the secondary endpoint of death or stroke: The 27% reduction in risk of this secondary endpoint in women with a history of pregnancy, compared with that of nulliparous women, didn’t achieve statistical significance in multivariate analysis, according to Dr. Chieffo of the San Raffaele Scientific Institute in Milan.
She speculated that pregnancy earlier in life provided strong protection against poor 30-day outcomes and a similar trend – albeit not statistically significant – at 1 year because women without children may have less family support.
“They are old women, left alone, without the family taking care of them. This is socially important, I think, because we are investing quite a lot of money in a procedure, and then maybe we’re adding adverse events because these patients are not properly taken care of when they are out of the hospital,” the interventional cardiologist said.
Neither of the other two female-specific characteristics evaluated in WIN-TAVI – having a history of osteoporosis or age at menopause – turned out to be related to the risk of bad outcomes at 1 year, she added.
WIN-TAVI is the first all-female registry of patients undergoing TAVR for severe aortic stenosis. The prospective, observational registry includes 1,019 women treated at 19 highly experienced European and North American TAVR centers. They averaged 82.5 years of age with a mean Society of Thoracic Surgeons score of 8.3%, putting them at intermediate or high surgical risk. A percutaneous transfemoral approach was used in 91% of cases. TAVR was performed under conscious sedation in 28% of the women and under local anesthesia in another 37%. Of the women in the registry, 42% received a newer-generation device.
In addition to the lack of significant impact of prior pregnancy on 1-year outcomes, another noteworthy finding at 1 year of follow-up was that preprocedural atrial fibrillation was independently associated with a 58% increase in the risk of death or stroke (P = .02). Prior percutaneous coronary intervention and EuroSCORE (European System for Cardiac Operative Risk Evaluation) were the only other independent predictors.
This observation suggests the need for a women-only randomized trial of TAVR versus surgical aortic valve replacement in women with intermediate surgical risk, Dr. Chieffo suggested. It will be important to learn whether the ability to surgically ablate preoperative atrial fibrillation in women during surgical valve replacement results in a lower 1-year risk of death or stroke than is achieved with TAVR.
Overall, the 1-year clinical outcomes seen in WIN-TAVI are “very good,” she noted. The VARC-2 composite endpoint occurred in 16.5% of women, all-cause mortality in 12.5%, cardiovascular mortality in 10.8%, and stroke in 2.2%. Only 3.2% of women were hospitalized for heart failure or valve-related symptoms. A new pacemaker was implanted in 12.7% of participants. At baseline 74% of women were New York Heart Association functional class III or IV; at 1 year, only 8.1% were. Moderate paravalvular aortic regurgitation was present in 6% of patients at 6 months and in 9.7% at 1 year
The WIN-TAVI registry is entirely self-funded. Dr. Chieffo reported having no financial conflicts regarding her presentation.
Paris – A history of pregnancy did not protect against adverse outcomes at 1 year in the Women’s International Transcatheter Aortic Valve Implantation Registry (WIN-TAVI), even though it did within the first 30 days, Alaide Chieffo, MD, reported at the annual congress of the European Association of Percutaneous Cardiovascular Interventions.
One year ago, at EuroPCR 2016, she reported that in WIN-TAVI, a history of pregnancy – albeit typically more than half a century previously – was independently associated with a 43% reduction in the Valve Academic Research Consortium-2 (VARC-2) 30-day composite endpoint, including death, stroke, major vascular complications, life-threatening bleeding, stage 2 or 3 acute kidney injury, coronary artery obstruction, or repeat transcatheter aortic valve replacement (TAVR) done because of valve-related dysfunction. Those early findings, first reported in this publication, were later published (JACC Cardiovasc Interv. 2016 Aug 8;9[15]:1589-600).
At 1 year of follow-up, however, the rate of the VARC-2 composite endpoint was no longer significantly different in women with or without a history of pregnancy. Nor was a history of pregnancy associated with a significantly reduced risk of the secondary endpoint of death or stroke: The 27% reduction in risk of this secondary endpoint in women with a history of pregnancy, compared with that of nulliparous women, didn’t achieve statistical significance in multivariate analysis, according to Dr. Chieffo of the San Raffaele Scientific Institute in Milan.
She speculated that pregnancy earlier in life provided strong protection against poor 30-day outcomes and a similar trend – albeit not statistically significant – at 1 year because women without children may have less family support.
“They are old women, left alone, without the family taking care of them. This is socially important, I think, because we are investing quite a lot of money in a procedure, and then maybe we’re adding adverse events because these patients are not properly taken care of when they are out of the hospital,” the interventional cardiologist said.
Neither of the other two female-specific characteristics evaluated in WIN-TAVI – having a history of osteoporosis or age at menopause – turned out to be related to the risk of bad outcomes at 1 year, she added.
WIN-TAVI is the first all-female registry of patients undergoing TAVR for severe aortic stenosis. The prospective, observational registry includes 1,019 women treated at 19 highly experienced European and North American TAVR centers. They averaged 82.5 years of age with a mean Society of Thoracic Surgeons score of 8.3%, putting them at intermediate or high surgical risk. A percutaneous transfemoral approach was used in 91% of cases. TAVR was performed under conscious sedation in 28% of the women and under local anesthesia in another 37%. Of the women in the registry, 42% received a newer-generation device.
In addition to the lack of significant impact of prior pregnancy on 1-year outcomes, another noteworthy finding at 1 year of follow-up was that preprocedural atrial fibrillation was independently associated with a 58% increase in the risk of death or stroke (P = .02). Prior percutaneous coronary intervention and EuroSCORE (European System for Cardiac Operative Risk Evaluation) were the only other independent predictors.
This observation suggests the need for a women-only randomized trial of TAVR versus surgical aortic valve replacement in women with intermediate surgical risk, Dr. Chieffo suggested. It will be important to learn whether the ability to surgically ablate preoperative atrial fibrillation in women during surgical valve replacement results in a lower 1-year risk of death or stroke than is achieved with TAVR.
Overall, the 1-year clinical outcomes seen in WIN-TAVI are “very good,” she noted. The VARC-2 composite endpoint occurred in 16.5% of women, all-cause mortality in 12.5%, cardiovascular mortality in 10.8%, and stroke in 2.2%. Only 3.2% of women were hospitalized for heart failure or valve-related symptoms. A new pacemaker was implanted in 12.7% of participants. At baseline 74% of women were New York Heart Association functional class III or IV; at 1 year, only 8.1% were. Moderate paravalvular aortic regurgitation was present in 6% of patients at 6 months and in 9.7% at 1 year
The WIN-TAVI registry is entirely self-funded. Dr. Chieffo reported having no financial conflicts regarding her presentation.
Paris – A history of pregnancy did not protect against adverse outcomes at 1 year in the Women’s International Transcatheter Aortic Valve Implantation Registry (WIN-TAVI), even though it did within the first 30 days, Alaide Chieffo, MD, reported at the annual congress of the European Association of Percutaneous Cardiovascular Interventions.
One year ago, at EuroPCR 2016, she reported that in WIN-TAVI, a history of pregnancy – albeit typically more than half a century previously – was independently associated with a 43% reduction in the Valve Academic Research Consortium-2 (VARC-2) 30-day composite endpoint, including death, stroke, major vascular complications, life-threatening bleeding, stage 2 or 3 acute kidney injury, coronary artery obstruction, or repeat transcatheter aortic valve replacement (TAVR) done because of valve-related dysfunction. Those early findings, first reported in this publication, were later published (JACC Cardiovasc Interv. 2016 Aug 8;9[15]:1589-600).
At 1 year of follow-up, however, the rate of the VARC-2 composite endpoint was no longer significantly different in women with or without a history of pregnancy. Nor was a history of pregnancy associated with a significantly reduced risk of the secondary endpoint of death or stroke: The 27% reduction in risk of this secondary endpoint in women with a history of pregnancy, compared with that of nulliparous women, didn’t achieve statistical significance in multivariate analysis, according to Dr. Chieffo of the San Raffaele Scientific Institute in Milan.
She speculated that pregnancy earlier in life provided strong protection against poor 30-day outcomes and a similar trend – albeit not statistically significant – at 1 year because women without children may have less family support.
“They are old women, left alone, without the family taking care of them. This is socially important, I think, because we are investing quite a lot of money in a procedure, and then maybe we’re adding adverse events because these patients are not properly taken care of when they are out of the hospital,” the interventional cardiologist said.
Neither of the other two female-specific characteristics evaluated in WIN-TAVI – having a history of osteoporosis or age at menopause – turned out to be related to the risk of bad outcomes at 1 year, she added.
WIN-TAVI is the first all-female registry of patients undergoing TAVR for severe aortic stenosis. The prospective, observational registry includes 1,019 women treated at 19 highly experienced European and North American TAVR centers. They averaged 82.5 years of age with a mean Society of Thoracic Surgeons score of 8.3%, putting them at intermediate or high surgical risk. A percutaneous transfemoral approach was used in 91% of cases. TAVR was performed under conscious sedation in 28% of the women and under local anesthesia in another 37%. Of the women in the registry, 42% received a newer-generation device.
In addition to the lack of significant impact of prior pregnancy on 1-year outcomes, another noteworthy finding at 1 year of follow-up was that preprocedural atrial fibrillation was independently associated with a 58% increase in the risk of death or stroke (P = .02). Prior percutaneous coronary intervention and EuroSCORE (European System for Cardiac Operative Risk Evaluation) were the only other independent predictors.
This observation suggests the need for a women-only randomized trial of TAVR versus surgical aortic valve replacement in women with intermediate surgical risk, Dr. Chieffo suggested. It will be important to learn whether the ability to surgically ablate preoperative atrial fibrillation in women during surgical valve replacement results in a lower 1-year risk of death or stroke than is achieved with TAVR.
Overall, the 1-year clinical outcomes seen in WIN-TAVI are “very good,” she noted. The VARC-2 composite endpoint occurred in 16.5% of women, all-cause mortality in 12.5%, cardiovascular mortality in 10.8%, and stroke in 2.2%. Only 3.2% of women were hospitalized for heart failure or valve-related symptoms. A new pacemaker was implanted in 12.7% of participants. At baseline 74% of women were New York Heart Association functional class III or IV; at 1 year, only 8.1% were. Moderate paravalvular aortic regurgitation was present in 6% of patients at 6 months and in 9.7% at 1 year
The WIN-TAVI registry is entirely self-funded. Dr. Chieffo reported having no financial conflicts regarding her presentation.
AT EuroPCR
Key clinical point:
Major finding: Prior pregnancy didn’t protect women against death or stroke at 1 year post TAVR.
Data source: WIN-TAVI, a prospective, multicenter, observational registry includes 1,019 women who underwent TAVR.
Disclosures: WIN-TAVI is entirely self-funded. The presenter reported having no financial conflicts.
New-onset AF after aortic valve replacement did not affect long-term survival
New-onset atrial fibrillation after aortic valve replacement was not an independent risk factor for decreased long-term survival, according to the results of a single-center, retrospective study reported by Ben M. Swinkels, MD, of St Antonius Hospital, Nieuwegein, and his colleagues in the Netherlands.
Key to this success, however, is restoring normal sinus rhythm before hospital discharge, they said.
In this retrospective, longitudinal cohort study, 569 consecutive patients with no history of AF who underwent AVR with or without concomitant coronary artery bypass grafting during 1990-1993 were followed for a mean of 17.8 years (J Thorac Cardiovasc Surg. 2017;154:492-8).
Thirty-day and long-term survival rates were determined in the 241 patients (42%) with and the 328 patients (58%) without new-onset postoperative atrial fibrillation (POAF), which was defined as electrocardiographically documented AF lasting for at least several hours, and occurring after AVR while the patient was still admitted. Standard therapy to prevent new onset POAF was the use of sotalol in patients who were not on beta-blocker therapy, and continuation of beta-blocker therapy for those who were already on it.
There were no significant differences between the two groups in demographic characteristics. There were also no significant differences between the two groups in operative characteristics, postoperative in-hospital adverse events, and postoperative hospital lengths of stay until discharge home, except for mechanical ventilation time, which was significantly longer in the patients with new-onset POAF (P = .011).
Thirty-day mortality was 1.2% in the patients with POAF, and 2.7% in those without, a nonsignificant difference. There was no statistically significant difference between the two survival curves and the Kaplan-Meier overall cumulative survival rates at 15 years of follow-up in the patients with new-onset POAF vs. those without were not statistically different (41.5% vs. 41.3%, respectively).
In addition, the 18-year probability of long-term first adverse events, including recurrent AF, transient ischemic attack, ischemic or hemorrhagic stroke, peripheral venous thromboembolism, or major or minor bleeding was not significantly different between the two groups.
“New-onset POAF after AVR does not affect long-term survival when treatment is aimed to restore sinus rhythm before the patient is discharged home. Future studies with a prospective, randomized design should be done to confirm this finding in patients undergoing different kinds of cardiac surgery,” the researchers concluded.
The study was funded by the authors’ home institution; the authors reported they had nothing to disclose.
The incidence of atrial fibrillation after valve surgery has been described to be as high as 50%, Manuel J. Antunes, MD, said in an editorial commentary. “The adverse effect on long-term survival may not be related to the short-lived new-onset AF but rather to the underlying pathology associated to the arrhythmia, especially pathology that affects the myocardium, principally in atherosclerotic coronary artery disease,” he wrote. “It is not survival alone, however, that should be cause for concern; AF, even in episodes of limited duration, may result in transient ischemic attacks, ischemic, or hemorrhagic strokes, and peripheral thromboembolism, which is why affected patients should immediately be anticoagulated.”
This study, however, is at odds with previously published studies, with opposite conclusions, according to Dr. Antunes. Swinkels and his colleagues suggest that one of the reasons for the discrepancy was the homogeneous character of their series, which consisted almost entirely of patients who had isolated AVR. Dr. Antunes also adds that another important aspect to consider is that the antiarrhythmic drugs used prophylactically or therapeutically for this patient cohort (treated during 1990-1993) are no longer used or have been replaced by new and more efficacious pharmacologic agents.

Manuel J. Antunes, MD, of the University Hospital and Faculty of Medicine, Coimbra, Portugal, made these remarks in an invited editorial (J Thorac Cardiovasc Surg. 2017;154:490-1). He reported having nothing to disclose.
The incidence of atrial fibrillation after valve surgery has been described to be as high as 50%, Manuel J. Antunes, MD, said in an editorial commentary. “The adverse effect on long-term survival may not be related to the short-lived new-onset AF but rather to the underlying pathology associated to the arrhythmia, especially pathology that affects the myocardium, principally in atherosclerotic coronary artery disease,” he wrote. “It is not survival alone, however, that should be cause for concern; AF, even in episodes of limited duration, may result in transient ischemic attacks, ischemic, or hemorrhagic strokes, and peripheral thromboembolism, which is why affected patients should immediately be anticoagulated.”
This study, however, is at odds with previously published studies, with opposite conclusions, according to Dr. Antunes. Swinkels and his colleagues suggest that one of the reasons for the discrepancy was the homogeneous character of their series, which consisted almost entirely of patients who had isolated AVR. Dr. Antunes also adds that another important aspect to consider is that the antiarrhythmic drugs used prophylactically or therapeutically for this patient cohort (treated during 1990-1993) are no longer used or have been replaced by new and more efficacious pharmacologic agents.
Manuel J. Antunes, MD, of the University Hospital and Faculty of Medicine, Coimbra, Portugal, made these remarks in an invited editorial (J Thorac Cardiovasc Surg. 2017;154:490-1). He reported having nothing to disclose.
The incidence of atrial fibrillation after valve surgery has been described to be as high as 50%, Manuel J. Antunes, MD, said in an editorial commentary. “The adverse effect on long-term survival may not be related to the short-lived new-onset AF but rather to the underlying pathology associated to the arrhythmia, especially pathology that affects the myocardium, principally in atherosclerotic coronary artery disease,” he wrote. “It is not survival alone, however, that should be cause for concern; AF, even in episodes of limited duration, may result in transient ischemic attacks, ischemic, or hemorrhagic strokes, and peripheral thromboembolism, which is why affected patients should immediately be anticoagulated.”
This study, however, is at odds with previously published studies, with opposite conclusions, according to Dr. Antunes. Swinkels and his colleagues suggest that one of the reasons for the discrepancy was the homogeneous character of their series, which consisted almost entirely of patients who had isolated AVR. Dr. Antunes also adds that another important aspect to consider is that the antiarrhythmic drugs used prophylactically or therapeutically for this patient cohort (treated during 1990-1993) are no longer used or have been replaced by new and more efficacious pharmacologic agents.
Manuel J. Antunes, MD, of the University Hospital and Faculty of Medicine, Coimbra, Portugal, made these remarks in an invited editorial (J Thorac Cardiovasc Surg. 2017;154:490-1). He reported having nothing to disclose.
New-onset atrial fibrillation after aortic valve replacement was not an independent risk factor for decreased long-term survival, according to the results of a single-center, retrospective study reported by Ben M. Swinkels, MD, of St Antonius Hospital, Nieuwegein, and his colleagues in the Netherlands.
Key to this success, however, is restoring normal sinus rhythm before hospital discharge, they said.
In this retrospective, longitudinal cohort study, 569 consecutive patients with no history of AF who underwent AVR with or without concomitant coronary artery bypass grafting during 1990-1993 were followed for a mean of 17.8 years (J Thorac Cardiovasc Surg. 2017;154:492-8).
Thirty-day and long-term survival rates were determined in the 241 patients (42%) with and the 328 patients (58%) without new-onset postoperative atrial fibrillation (POAF), which was defined as electrocardiographically documented AF lasting for at least several hours, and occurring after AVR while the patient was still admitted. Standard therapy to prevent new onset POAF was the use of sotalol in patients who were not on beta-blocker therapy, and continuation of beta-blocker therapy for those who were already on it.
There were no significant differences between the two groups in demographic characteristics. There were also no significant differences between the two groups in operative characteristics, postoperative in-hospital adverse events, and postoperative hospital lengths of stay until discharge home, except for mechanical ventilation time, which was significantly longer in the patients with new-onset POAF (P = .011).
Thirty-day mortality was 1.2% in the patients with POAF, and 2.7% in those without, a nonsignificant difference. There was no statistically significant difference between the two survival curves and the Kaplan-Meier overall cumulative survival rates at 15 years of follow-up in the patients with new-onset POAF vs. those without were not statistically different (41.5% vs. 41.3%, respectively).
In addition, the 18-year probability of long-term first adverse events, including recurrent AF, transient ischemic attack, ischemic or hemorrhagic stroke, peripheral venous thromboembolism, or major or minor bleeding was not significantly different between the two groups.
“New-onset POAF after AVR does not affect long-term survival when treatment is aimed to restore sinus rhythm before the patient is discharged home. Future studies with a prospective, randomized design should be done to confirm this finding in patients undergoing different kinds of cardiac surgery,” the researchers concluded.
The study was funded by the authors’ home institution; the authors reported they had nothing to disclose.
New-onset atrial fibrillation after aortic valve replacement was not an independent risk factor for decreased long-term survival, according to the results of a single-center, retrospective study reported by Ben M. Swinkels, MD, of St Antonius Hospital, Nieuwegein, and his colleagues in the Netherlands.
Key to this success, however, is restoring normal sinus rhythm before hospital discharge, they said.
In this retrospective, longitudinal cohort study, 569 consecutive patients with no history of AF who underwent AVR with or without concomitant coronary artery bypass grafting during 1990-1993 were followed for a mean of 17.8 years (J Thorac Cardiovasc Surg. 2017;154:492-8).
Thirty-day and long-term survival rates were determined in the 241 patients (42%) with and the 328 patients (58%) without new-onset postoperative atrial fibrillation (POAF), which was defined as electrocardiographically documented AF lasting for at least several hours, and occurring after AVR while the patient was still admitted. Standard therapy to prevent new onset POAF was the use of sotalol in patients who were not on beta-blocker therapy, and continuation of beta-blocker therapy for those who were already on it.
There were no significant differences between the two groups in demographic characteristics. There were also no significant differences between the two groups in operative characteristics, postoperative in-hospital adverse events, and postoperative hospital lengths of stay until discharge home, except for mechanical ventilation time, which was significantly longer in the patients with new-onset POAF (P = .011).
Thirty-day mortality was 1.2% in the patients with POAF, and 2.7% in those without, a nonsignificant difference. There was no statistically significant difference between the two survival curves and the Kaplan-Meier overall cumulative survival rates at 15 years of follow-up in the patients with new-onset POAF vs. those without were not statistically different (41.5% vs. 41.3%, respectively).
In addition, the 18-year probability of long-term first adverse events, including recurrent AF, transient ischemic attack, ischemic or hemorrhagic stroke, peripheral venous thromboembolism, or major or minor bleeding was not significantly different between the two groups.
“New-onset POAF after AVR does not affect long-term survival when treatment is aimed to restore sinus rhythm before the patient is discharged home. Future studies with a prospective, randomized design should be done to confirm this finding in patients undergoing different kinds of cardiac surgery,” the researchers concluded.
The study was funded by the authors’ home institution; the authors reported they had nothing to disclose.
FROM THE JOURNAL OF THORACIC AND CARDIOVASCULAR SURGERY
Key clinical point:
Major finding: Cumulative 15-year survival rates were similar in the patients with new-onset postop AF (41.5%) to those without (41.3%).
Data source: A retrospective longitudinal cohort study of 569 consecutive patients without a history of AF who were followed for a mean of 17.8 years after AVR with or without concomitant CABG.
Disclosures: The study was funded by the authors’ home institution and the authors reported they had nothing to disclose.

Say ‘Aloha’ to the best health care
It probably should come as no surprise that Hawaii, which has been named the healthiest state for 5 consecutive years, is now being honored for having the best health care by personal finance website WalletHub.
The state’s high scores in two of the three broad dimensions of health care – first in outcomes and third in cost – used in the WalletHub analysis allowed it to overcome its ranking of 42nd in the third dimension, access, and finish ahead of Iowa and Minnesota, which tied for second. New Hampshire earned a fourth-place finish and the District of Columbia was fifth, courtesy of its first-place finish in the cost dimension, WalletHub reported. Maine, which finished 14th overall, was No. 1 in access.
The state in 51st place is Louisiana, which placed in the top 5 in both cancer and heart disease rates. Mississippi was credited with the 50th-best health care system, just behind Alaska (49), Arkansas (48), North Carolina (47), and Georgia (46). The lowest ranking in each dimension went to Alaska (cost), Texas (access), and Mississippi (outcomes), according to WalletHub’s analysts.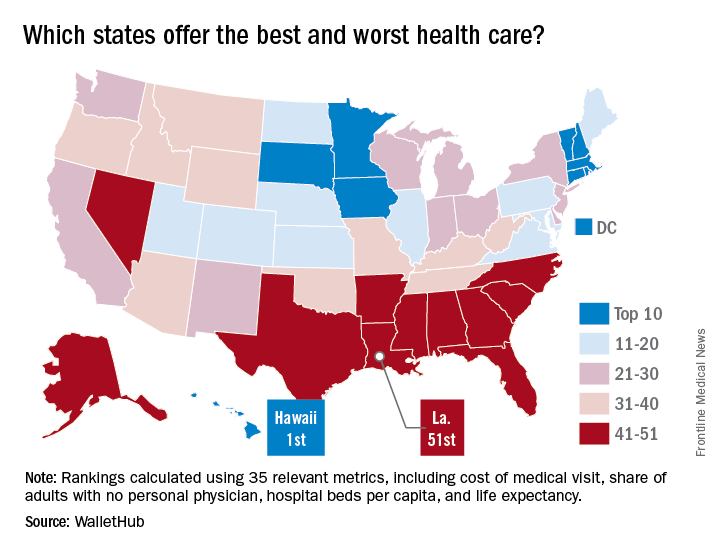
A closer look at some of the individual metrics shows that the District of Columbia has the most physicians per capita and Idaho has the fewest, Medicare acceptance is highest among physicians in North Dakota and lowest in Hawaii, and infant mortality is lowest in New Hampshire and highest in Mississippi, according to the WalletHub analysis, which was based on data from 19 sources, including the Centers for Medicare & Medicaid Services, the Association of American Medical Colleges, and the Social Science Research Council.
It probably should come as no surprise that Hawaii, which has been named the healthiest state for 5 consecutive years, is now being honored for having the best health care by personal finance website WalletHub.
The state’s high scores in two of the three broad dimensions of health care – first in outcomes and third in cost – used in the WalletHub analysis allowed it to overcome its ranking of 42nd in the third dimension, access, and finish ahead of Iowa and Minnesota, which tied for second. New Hampshire earned a fourth-place finish and the District of Columbia was fifth, courtesy of its first-place finish in the cost dimension, WalletHub reported. Maine, which finished 14th overall, was No. 1 in access.
The state in 51st place is Louisiana, which placed in the top 5 in both cancer and heart disease rates. Mississippi was credited with the 50th-best health care system, just behind Alaska (49), Arkansas (48), North Carolina (47), and Georgia (46). The lowest ranking in each dimension went to Alaska (cost), Texas (access), and Mississippi (outcomes), according to WalletHub’s analysts.
A closer look at some of the individual metrics shows that the District of Columbia has the most physicians per capita and Idaho has the fewest, Medicare acceptance is highest among physicians in North Dakota and lowest in Hawaii, and infant mortality is lowest in New Hampshire and highest in Mississippi, according to the WalletHub analysis, which was based on data from 19 sources, including the Centers for Medicare & Medicaid Services, the Association of American Medical Colleges, and the Social Science Research Council.
It probably should come as no surprise that Hawaii, which has been named the healthiest state for 5 consecutive years, is now being honored for having the best health care by personal finance website WalletHub.
The state’s high scores in two of the three broad dimensions of health care – first in outcomes and third in cost – used in the WalletHub analysis allowed it to overcome its ranking of 42nd in the third dimension, access, and finish ahead of Iowa and Minnesota, which tied for second. New Hampshire earned a fourth-place finish and the District of Columbia was fifth, courtesy of its first-place finish in the cost dimension, WalletHub reported. Maine, which finished 14th overall, was No. 1 in access.
The state in 51st place is Louisiana, which placed in the top 5 in both cancer and heart disease rates. Mississippi was credited with the 50th-best health care system, just behind Alaska (49), Arkansas (48), North Carolina (47), and Georgia (46). The lowest ranking in each dimension went to Alaska (cost), Texas (access), and Mississippi (outcomes), according to WalletHub’s analysts.
A closer look at some of the individual metrics shows that the District of Columbia has the most physicians per capita and Idaho has the fewest, Medicare acceptance is highest among physicians in North Dakota and lowest in Hawaii, and infant mortality is lowest in New Hampshire and highest in Mississippi, according to the WalletHub analysis, which was based on data from 19 sources, including the Centers for Medicare & Medicaid Services, the Association of American Medical Colleges, and the Social Science Research Council.