User login
The Official Newspaper of the American Association for Thoracic Surgery
ACA lawsuits progress through the courts
While Republican efforts to repeal and/or replace the Affordable Care Act are likely to resurface after the congressional summer recess, lawsuits challenging the health law continue to wind their way through the courts.
Judges recently ruled in three ACA cases regarding the contraceptive mandate, risk corridors program, and cost-sharing reduction payments.
Real Alternatives Inc. v. HHS
Secular groups are not entitled to a religious exemption to the ACA’s contraceptive mandate and must offer plans to employees that cover birth control, the United States Court of Appeals for the Third Circuit ruled in an Aug. 4 opinion.

But a majority of appeal judges disagreed, concluding that Real Alternatives is not similar to a religious denomination or one of its nontheistic counterparts, “not in structure, not in aim, not in purpose, and not in function.”
“We do not doubt that Real Alternative’s stance on contraceptives is grounded in sincerely-held moral values, but religion is not generally confined to one question or one moral teaching, it has a broader scope,” Judge Marjorie O. Rendell wrote in the majority opinion. “Real Alternatives is functionally similar not to a church, but to the countless nonreligious nonprofit organizations that take morally informed positions on some discrete set of issues ... While commitment to an anti-abortion platform may be important to the people who hold them, that commitment is not a religion in any legally or theologically accepted sense; and organizations do not become quasi-churches for equal-protection purposes merely by espousing a commitment of that sort.”
Molina Healthcare v. HHS
The federal Heath & Human Services department may have to dish out millions to marketplace insurers after a recent decision by the U.S. Court of Federal Claims. In an Aug. 4 opinion, a federal claims judge ruled the federal government owes Long Beach, Calif.–based insurer Molina Healthcare $52 million in risk corridor payments under the ACA.
The decision stems from a lawsuit by Molina and dozens of other insurers against HHS over the ACA’s risk corridor program. The program requires HHS to collect funds from excessively profitable insurers that offer qualified health plans (QHP) under the exchanges, while paying out funds to QHP insurers with excessive losses. Collections from profitable insurers under the program fell short in 2014 and again in 2015, resulting in HHS paying about 12 cents on the dollar in payments to insurers.
Insurers allege they’ve been shortchanged and that the government must reimburse them full payments for 2014 and 2015. Under the Obama administration, the Department of Justice requested to dismiss the cases, arguing that riders attached to appropriations bills in 2015 and 2016 barred it from making full risk corridor payments.
In his decision, Judge Thomas Wheeler said the ACA mandates that HHS pay insurers what they are owed under the risk corridor program, regardless of the riders.
“The undisputed facts show the government entered into an implied-in-fact contract with Molina and subsequently breached the contract when it failed to make full risk corridor payments,” Judge Wheeler wrote. “Importantly, Molina prevails on its argument of breach of an implied-in-fact contract regardless of the government’s appropriation law defenses – later appropriation restrictions cannot erase a previously created contractual obligation ...The government is liable for its breach of a statutory and contractual obligation to make full annual payments to insurers who participated in the risk corridor program.”
Judge Wheeler ruled similarly in February when he concluded the federal government owes Portland, Ore.–based Moda Health $214 million in risk corridor payments.
The issue is far from over. More than 25 lawsuits have been filed in the Court of Federal Claims by insurers seeking risk corridor money. Several of the cases have moved onto federal appeals courts, while other cases have been dismissed. Analysts say the issue is likely to reach the U.S. Supreme Court. It’s unclear where the Trump administration would get the funds to reimburse insurers if the payback rulings stand. About $19.3 billion in risk corridor payments are at stake for 2014 and 2015 and an estimated $3 billion is in play for 2016, the final risk corridor year.
House v. Price
A U.S. appeals court has allowed 16 states to intervene in a lawsuit over whether subsidy payments made to insurers under the ACA are legal. The decision comes as President Trump recently threatened to cut off the cost sharing reduction (CSR) payments to marketplace insurers, calling them a “bailout.”
On Aug. 1, the U.S. Court of Appeals for the District of Columbia Circuit granted a motion by 18 attorneys general to enter the lawsuit. The attorneys general represent California, New York, Connecticut, Delaware, Hawaii, Illinois, Iowa, Kentucky, Maryland, Massachusetts, Minnesota, New Mexico, North Carolina, Pennsylvania, Vermont, Virginia, Washington, and the District of Columbia.
Under the ACA, the federal government provides CSR payments to insurers to offset the costs for providing discount plans to patients who earn up to 200% of the federal poverty level. Plans on the individual exchanges are required to cover a package of essential benefits with pricing limitations to ensure that out-of-pocket costs are low enough for low-income patients.
Republican members of the House of Representatives sued the HHS over the CSR payments under the Obama administration, claiming the funding was illegal because it was never appropriated by Congress. A court ruled in favor of the House in 2016, but an appeal filed by the Obama administration allowed the CSR payments to continue. President Trump has not indicated whether he plans to drop the appeal or carry on the case. But if he fails to continue the suit, the move would immediately end the CSR payments.
On July 29, President Trump tweeted, “If a new HealthCare Bill is not approved quickly, BAILOUTS for Insurance Companies and BAILOUTS for Members of Congress will end very soon!”
The state attorneys general are ready to defend the ACA and the cost sharing reduction payments, California Attorney General Xavier Becerra said in a statement.
“If Donald Trump won’t defend these vital subsidies for American families, then we will,” Mr. Becerra said in the statement. “This ruling gives my fellow attorneys general and me the ability to stand up for the millions of families who otherwise would lack access to affordable health care. It’s time Americans knew we were working for them, not against them.”
[email protected]
On Twitter @legal_med
While Republican efforts to repeal and/or replace the Affordable Care Act are likely to resurface after the congressional summer recess, lawsuits challenging the health law continue to wind their way through the courts.
Judges recently ruled in three ACA cases regarding the contraceptive mandate, risk corridors program, and cost-sharing reduction payments.
Real Alternatives Inc. v. HHS
Secular groups are not entitled to a religious exemption to the ACA’s contraceptive mandate and must offer plans to employees that cover birth control, the United States Court of Appeals for the Third Circuit ruled in an Aug. 4 opinion.
But a majority of appeal judges disagreed, concluding that Real Alternatives is not similar to a religious denomination or one of its nontheistic counterparts, “not in structure, not in aim, not in purpose, and not in function.”
“We do not doubt that Real Alternative’s stance on contraceptives is grounded in sincerely-held moral values, but religion is not generally confined to one question or one moral teaching, it has a broader scope,” Judge Marjorie O. Rendell wrote in the majority opinion. “Real Alternatives is functionally similar not to a church, but to the countless nonreligious nonprofit organizations that take morally informed positions on some discrete set of issues ... While commitment to an anti-abortion platform may be important to the people who hold them, that commitment is not a religion in any legally or theologically accepted sense; and organizations do not become quasi-churches for equal-protection purposes merely by espousing a commitment of that sort.”
Molina Healthcare v. HHS
The federal Heath & Human Services department may have to dish out millions to marketplace insurers after a recent decision by the U.S. Court of Federal Claims. In an Aug. 4 opinion, a federal claims judge ruled the federal government owes Long Beach, Calif.–based insurer Molina Healthcare $52 million in risk corridor payments under the ACA.
The decision stems from a lawsuit by Molina and dozens of other insurers against HHS over the ACA’s risk corridor program. The program requires HHS to collect funds from excessively profitable insurers that offer qualified health plans (QHP) under the exchanges, while paying out funds to QHP insurers with excessive losses. Collections from profitable insurers under the program fell short in 2014 and again in 2015, resulting in HHS paying about 12 cents on the dollar in payments to insurers.
Insurers allege they’ve been shortchanged and that the government must reimburse them full payments for 2014 and 2015. Under the Obama administration, the Department of Justice requested to dismiss the cases, arguing that riders attached to appropriations bills in 2015 and 2016 barred it from making full risk corridor payments.
In his decision, Judge Thomas Wheeler said the ACA mandates that HHS pay insurers what they are owed under the risk corridor program, regardless of the riders.
“The undisputed facts show the government entered into an implied-in-fact contract with Molina and subsequently breached the contract when it failed to make full risk corridor payments,” Judge Wheeler wrote. “Importantly, Molina prevails on its argument of breach of an implied-in-fact contract regardless of the government’s appropriation law defenses – later appropriation restrictions cannot erase a previously created contractual obligation ...The government is liable for its breach of a statutory and contractual obligation to make full annual payments to insurers who participated in the risk corridor program.”
Judge Wheeler ruled similarly in February when he concluded the federal government owes Portland, Ore.–based Moda Health $214 million in risk corridor payments.
The issue is far from over. More than 25 lawsuits have been filed in the Court of Federal Claims by insurers seeking risk corridor money. Several of the cases have moved onto federal appeals courts, while other cases have been dismissed. Analysts say the issue is likely to reach the U.S. Supreme Court. It’s unclear where the Trump administration would get the funds to reimburse insurers if the payback rulings stand. About $19.3 billion in risk corridor payments are at stake for 2014 and 2015 and an estimated $3 billion is in play for 2016, the final risk corridor year.
House v. Price
A U.S. appeals court has allowed 16 states to intervene in a lawsuit over whether subsidy payments made to insurers under the ACA are legal. The decision comes as President Trump recently threatened to cut off the cost sharing reduction (CSR) payments to marketplace insurers, calling them a “bailout.”
On Aug. 1, the U.S. Court of Appeals for the District of Columbia Circuit granted a motion by 18 attorneys general to enter the lawsuit. The attorneys general represent California, New York, Connecticut, Delaware, Hawaii, Illinois, Iowa, Kentucky, Maryland, Massachusetts, Minnesota, New Mexico, North Carolina, Pennsylvania, Vermont, Virginia, Washington, and the District of Columbia.
Under the ACA, the federal government provides CSR payments to insurers to offset the costs for providing discount plans to patients who earn up to 200% of the federal poverty level. Plans on the individual exchanges are required to cover a package of essential benefits with pricing limitations to ensure that out-of-pocket costs are low enough for low-income patients.
Republican members of the House of Representatives sued the HHS over the CSR payments under the Obama administration, claiming the funding was illegal because it was never appropriated by Congress. A court ruled in favor of the House in 2016, but an appeal filed by the Obama administration allowed the CSR payments to continue. President Trump has not indicated whether he plans to drop the appeal or carry on the case. But if he fails to continue the suit, the move would immediately end the CSR payments.
On July 29, President Trump tweeted, “If a new HealthCare Bill is not approved quickly, BAILOUTS for Insurance Companies and BAILOUTS for Members of Congress will end very soon!”
The state attorneys general are ready to defend the ACA and the cost sharing reduction payments, California Attorney General Xavier Becerra said in a statement.
“If Donald Trump won’t defend these vital subsidies for American families, then we will,” Mr. Becerra said in the statement. “This ruling gives my fellow attorneys general and me the ability to stand up for the millions of families who otherwise would lack access to affordable health care. It’s time Americans knew we were working for them, not against them.”
[email protected]
On Twitter @legal_med
While Republican efforts to repeal and/or replace the Affordable Care Act are likely to resurface after the congressional summer recess, lawsuits challenging the health law continue to wind their way through the courts.
Judges recently ruled in three ACA cases regarding the contraceptive mandate, risk corridors program, and cost-sharing reduction payments.
Real Alternatives Inc. v. HHS
Secular groups are not entitled to a religious exemption to the ACA’s contraceptive mandate and must offer plans to employees that cover birth control, the United States Court of Appeals for the Third Circuit ruled in an Aug. 4 opinion.
But a majority of appeal judges disagreed, concluding that Real Alternatives is not similar to a religious denomination or one of its nontheistic counterparts, “not in structure, not in aim, not in purpose, and not in function.”
“We do not doubt that Real Alternative’s stance on contraceptives is grounded in sincerely-held moral values, but religion is not generally confined to one question or one moral teaching, it has a broader scope,” Judge Marjorie O. Rendell wrote in the majority opinion. “Real Alternatives is functionally similar not to a church, but to the countless nonreligious nonprofit organizations that take morally informed positions on some discrete set of issues ... While commitment to an anti-abortion platform may be important to the people who hold them, that commitment is not a religion in any legally or theologically accepted sense; and organizations do not become quasi-churches for equal-protection purposes merely by espousing a commitment of that sort.”
Molina Healthcare v. HHS
The federal Heath & Human Services department may have to dish out millions to marketplace insurers after a recent decision by the U.S. Court of Federal Claims. In an Aug. 4 opinion, a federal claims judge ruled the federal government owes Long Beach, Calif.–based insurer Molina Healthcare $52 million in risk corridor payments under the ACA.
The decision stems from a lawsuit by Molina and dozens of other insurers against HHS over the ACA’s risk corridor program. The program requires HHS to collect funds from excessively profitable insurers that offer qualified health plans (QHP) under the exchanges, while paying out funds to QHP insurers with excessive losses. Collections from profitable insurers under the program fell short in 2014 and again in 2015, resulting in HHS paying about 12 cents on the dollar in payments to insurers.
Insurers allege they’ve been shortchanged and that the government must reimburse them full payments for 2014 and 2015. Under the Obama administration, the Department of Justice requested to dismiss the cases, arguing that riders attached to appropriations bills in 2015 and 2016 barred it from making full risk corridor payments.
In his decision, Judge Thomas Wheeler said the ACA mandates that HHS pay insurers what they are owed under the risk corridor program, regardless of the riders.
“The undisputed facts show the government entered into an implied-in-fact contract with Molina and subsequently breached the contract when it failed to make full risk corridor payments,” Judge Wheeler wrote. “Importantly, Molina prevails on its argument of breach of an implied-in-fact contract regardless of the government’s appropriation law defenses – later appropriation restrictions cannot erase a previously created contractual obligation ...The government is liable for its breach of a statutory and contractual obligation to make full annual payments to insurers who participated in the risk corridor program.”
Judge Wheeler ruled similarly in February when he concluded the federal government owes Portland, Ore.–based Moda Health $214 million in risk corridor payments.
The issue is far from over. More than 25 lawsuits have been filed in the Court of Federal Claims by insurers seeking risk corridor money. Several of the cases have moved onto federal appeals courts, while other cases have been dismissed. Analysts say the issue is likely to reach the U.S. Supreme Court. It’s unclear where the Trump administration would get the funds to reimburse insurers if the payback rulings stand. About $19.3 billion in risk corridor payments are at stake for 2014 and 2015 and an estimated $3 billion is in play for 2016, the final risk corridor year.
House v. Price
A U.S. appeals court has allowed 16 states to intervene in a lawsuit over whether subsidy payments made to insurers under the ACA are legal. The decision comes as President Trump recently threatened to cut off the cost sharing reduction (CSR) payments to marketplace insurers, calling them a “bailout.”
On Aug. 1, the U.S. Court of Appeals for the District of Columbia Circuit granted a motion by 18 attorneys general to enter the lawsuit. The attorneys general represent California, New York, Connecticut, Delaware, Hawaii, Illinois, Iowa, Kentucky, Maryland, Massachusetts, Minnesota, New Mexico, North Carolina, Pennsylvania, Vermont, Virginia, Washington, and the District of Columbia.
Under the ACA, the federal government provides CSR payments to insurers to offset the costs for providing discount plans to patients who earn up to 200% of the federal poverty level. Plans on the individual exchanges are required to cover a package of essential benefits with pricing limitations to ensure that out-of-pocket costs are low enough for low-income patients.
Republican members of the House of Representatives sued the HHS over the CSR payments under the Obama administration, claiming the funding was illegal because it was never appropriated by Congress. A court ruled in favor of the House in 2016, but an appeal filed by the Obama administration allowed the CSR payments to continue. President Trump has not indicated whether he plans to drop the appeal or carry on the case. But if he fails to continue the suit, the move would immediately end the CSR payments.
On July 29, President Trump tweeted, “If a new HealthCare Bill is not approved quickly, BAILOUTS for Insurance Companies and BAILOUTS for Members of Congress will end very soon!”
The state attorneys general are ready to defend the ACA and the cost sharing reduction payments, California Attorney General Xavier Becerra said in a statement.
“If Donald Trump won’t defend these vital subsidies for American families, then we will,” Mr. Becerra said in the statement. “This ruling gives my fellow attorneys general and me the ability to stand up for the millions of families who otherwise would lack access to affordable health care. It’s time Americans knew we were working for them, not against them.”
[email protected]
On Twitter @legal_med

Preop atrial fib in CABG patients spells trouble
COLORADO SPRINGS – Preoperative atrial fibrillation is present in more than 10% of patients undergoing isolated coronary artery bypass graft (CABG) surgery, and if not subjected to concomitant surgical ablation it’s associated with increased perioperative and long-term major morbidity and mortality, S. Chris Malaisrie, MD, reported at the annual meeting of the Western Thoracic Surgical Association.
The increased early and late risks posed by preoperative atrial fibrillation (AF) that go unaddressed remain significant even after adjusting for the numerous comorbid conditions more prevalent in CABG patients with preoperative AF than in those without the arrhythmia, added Dr. Malaisrie, a cardiac surgeon at Northwestern University in Chicago.

The unadjusted operative mortality rate was 1.8% in the no-AF group and 4.0% in patients with preoperative AF. Unadjusted in-hospital rates of permanent stroke, prolonged ventilation, reoperation, and new renal failure were also significantly higher in the preoperative AF group.
Not surprisingly, the preoperative AF group was older. They also had significantly higher baseline rates of numerous comorbid conditions, including diabetes, peripheral vascular disease, renal failure, and prior stroke, as well as a lower mean left ventricular ejection fraction. However, after adjustment for the many comorbidities in multivariate regression analysis, the risks of all in-hospital adverse outcomes remained significantly higher in the preoperative AF group. For example, their adjusted risk of operative mortality was 1.5-fold greater than in the no-AF patients.
In the long-term follow-up analysis, the unadjusted risk of mortality in the first 5 years after CABG was 2.5-fold greater in the preoperative AF group. Their 5-year risk of stroke or systemic embolization was 1.5-fold greater, too. Upon adjustment for potentially confounding comorbid conditions, preoperative AF was associated with a 1.5-fold increased 5-year risk of mortality and a 1.2-fold increase in stroke or systemic embolism.
In an effort to identify a particularly high-risk group of CABG patients with preoperative AF, Dr. Malaisrie and his coinvestigators stratified the group’s long-term stroke and mortality risks by their CHA2DS2-VASc score at the time of surgery. The results were revealing: the unadjusted 5-year risk of stroke or systemic embolization was 7.9% in those with a CHA2DS2-VASc score of 1-3, 12.2% with a score of 4-6, and 15.4% with a score of 7-9. The 5-year survival rate was 74.8% with a score of 1-3, 56.5% with a score of 4-6, and 41.2% with a score of 7-9.
“That’s really a striking finding,” Dr. Malaisrie observed. “When you consider a patient who’s, say, 72-75 years old, who is undergoing isolated CABG with preoperative atrial fibrillation and who has a high CHA2DS2-VASc score of 7-9, 5-year survival is only 41%, with a 15% risk of stroke or systemic embolization.”
Discussant William T. Caine, MD, found the study results unsettling.
“I was surprised to see that in this day and age, fully two-thirds of the patients who had preoperative atrial fibrillation had no attempt at any ablation procedure to treat their atrial fibrillation,” declared Dr. Caine of Intermountain Medical Center in Salt Lake City.
In reply, Dr. Malaisrie noted that other, smaller studies have also found that only about 30% of CABG patients with preoperative AF undergo surgical AF ablation through a maze procedure or some other method.
“Probably most of us in this room would go ahead and perform surgical ablation, but the STS database represents all isolated CABG procedures done throughout the United States,” Dr. Malaisrie said. “I think this dataset should help convince the other 70% of surgeons out there that there is a high cost for preoperative AF – in particular, in patients with very high CHA2DS2-VASc scores. If you can identify a group of patients at increased risk for stroke and mortality, you’d certainly want to bend their survival curve.”
The maze procedure has been convincingly shown to be very safe, with no associated increased risk of perioperative morbidity and mortality. The downside is cost. But while it’s true that adding surgical ablation to an isolated CABG procedure boosts OR time and procedural costs, a successful ablation is likely to pay dividends through reduced downstream rates of major morbidity and mortality.
“I look forward to the second part of our analysis, where we’ll look at the comparative data for the patients who did in fact have surgical ablation. That dataset is pending from the Duke Clinical Research Institute,” according to Dr. Malaisrie.
He cited as study limitations the inability to complete linkage to the Medicare database in about 37% of CABG patients in the STS database, or more than 200,000 people. Also, the Medicare database is an administrative dataset reliant upon medical record coding. The mortality data are probably quite accurate, but the stroke and systemic embolization rates cited in this analysis likely underestimate the true rates.
He reported serving as a consultant to Edwards Lifesciences, Abbott Vascular, and Baxter, and serving on speakers’ bureaus for Bolton and Abiomed. However, the STS analysis was funded exclusively by philanthropy.
COLORADO SPRINGS – Preoperative atrial fibrillation is present in more than 10% of patients undergoing isolated coronary artery bypass graft (CABG) surgery, and if not subjected to concomitant surgical ablation it’s associated with increased perioperative and long-term major morbidity and mortality, S. Chris Malaisrie, MD, reported at the annual meeting of the Western Thoracic Surgical Association.
The increased early and late risks posed by preoperative atrial fibrillation (AF) that go unaddressed remain significant even after adjusting for the numerous comorbid conditions more prevalent in CABG patients with preoperative AF than in those without the arrhythmia, added Dr. Malaisrie, a cardiac surgeon at Northwestern University in Chicago.
The unadjusted operative mortality rate was 1.8% in the no-AF group and 4.0% in patients with preoperative AF. Unadjusted in-hospital rates of permanent stroke, prolonged ventilation, reoperation, and new renal failure were also significantly higher in the preoperative AF group.
Not surprisingly, the preoperative AF group was older. They also had significantly higher baseline rates of numerous comorbid conditions, including diabetes, peripheral vascular disease, renal failure, and prior stroke, as well as a lower mean left ventricular ejection fraction. However, after adjustment for the many comorbidities in multivariate regression analysis, the risks of all in-hospital adverse outcomes remained significantly higher in the preoperative AF group. For example, their adjusted risk of operative mortality was 1.5-fold greater than in the no-AF patients.
In the long-term follow-up analysis, the unadjusted risk of mortality in the first 5 years after CABG was 2.5-fold greater in the preoperative AF group. Their 5-year risk of stroke or systemic embolization was 1.5-fold greater, too. Upon adjustment for potentially confounding comorbid conditions, preoperative AF was associated with a 1.5-fold increased 5-year risk of mortality and a 1.2-fold increase in stroke or systemic embolism.
In an effort to identify a particularly high-risk group of CABG patients with preoperative AF, Dr. Malaisrie and his coinvestigators stratified the group’s long-term stroke and mortality risks by their CHA2DS2-VASc score at the time of surgery. The results were revealing: the unadjusted 5-year risk of stroke or systemic embolization was 7.9% in those with a CHA2DS2-VASc score of 1-3, 12.2% with a score of 4-6, and 15.4% with a score of 7-9. The 5-year survival rate was 74.8% with a score of 1-3, 56.5% with a score of 4-6, and 41.2% with a score of 7-9.
“That’s really a striking finding,” Dr. Malaisrie observed. “When you consider a patient who’s, say, 72-75 years old, who is undergoing isolated CABG with preoperative atrial fibrillation and who has a high CHA2DS2-VASc score of 7-9, 5-year survival is only 41%, with a 15% risk of stroke or systemic embolization.”
Discussant William T. Caine, MD, found the study results unsettling.
“I was surprised to see that in this day and age, fully two-thirds of the patients who had preoperative atrial fibrillation had no attempt at any ablation procedure to treat their atrial fibrillation,” declared Dr. Caine of Intermountain Medical Center in Salt Lake City.
In reply, Dr. Malaisrie noted that other, smaller studies have also found that only about 30% of CABG patients with preoperative AF undergo surgical AF ablation through a maze procedure or some other method.
“Probably most of us in this room would go ahead and perform surgical ablation, but the STS database represents all isolated CABG procedures done throughout the United States,” Dr. Malaisrie said. “I think this dataset should help convince the other 70% of surgeons out there that there is a high cost for preoperative AF – in particular, in patients with very high CHA2DS2-VASc scores. If you can identify a group of patients at increased risk for stroke and mortality, you’d certainly want to bend their survival curve.”
The maze procedure has been convincingly shown to be very safe, with no associated increased risk of perioperative morbidity and mortality. The downside is cost. But while it’s true that adding surgical ablation to an isolated CABG procedure boosts OR time and procedural costs, a successful ablation is likely to pay dividends through reduced downstream rates of major morbidity and mortality.
“I look forward to the second part of our analysis, where we’ll look at the comparative data for the patients who did in fact have surgical ablation. That dataset is pending from the Duke Clinical Research Institute,” according to Dr. Malaisrie.
He cited as study limitations the inability to complete linkage to the Medicare database in about 37% of CABG patients in the STS database, or more than 200,000 people. Also, the Medicare database is an administrative dataset reliant upon medical record coding. The mortality data are probably quite accurate, but the stroke and systemic embolization rates cited in this analysis likely underestimate the true rates.
He reported serving as a consultant to Edwards Lifesciences, Abbott Vascular, and Baxter, and serving on speakers’ bureaus for Bolton and Abiomed. However, the STS analysis was funded exclusively by philanthropy.
COLORADO SPRINGS – Preoperative atrial fibrillation is present in more than 10% of patients undergoing isolated coronary artery bypass graft (CABG) surgery, and if not subjected to concomitant surgical ablation it’s associated with increased perioperative and long-term major morbidity and mortality, S. Chris Malaisrie, MD, reported at the annual meeting of the Western Thoracic Surgical Association.
The increased early and late risks posed by preoperative atrial fibrillation (AF) that go unaddressed remain significant even after adjusting for the numerous comorbid conditions more prevalent in CABG patients with preoperative AF than in those without the arrhythmia, added Dr. Malaisrie, a cardiac surgeon at Northwestern University in Chicago.
The unadjusted operative mortality rate was 1.8% in the no-AF group and 4.0% in patients with preoperative AF. Unadjusted in-hospital rates of permanent stroke, prolonged ventilation, reoperation, and new renal failure were also significantly higher in the preoperative AF group.
Not surprisingly, the preoperative AF group was older. They also had significantly higher baseline rates of numerous comorbid conditions, including diabetes, peripheral vascular disease, renal failure, and prior stroke, as well as a lower mean left ventricular ejection fraction. However, after adjustment for the many comorbidities in multivariate regression analysis, the risks of all in-hospital adverse outcomes remained significantly higher in the preoperative AF group. For example, their adjusted risk of operative mortality was 1.5-fold greater than in the no-AF patients.
In the long-term follow-up analysis, the unadjusted risk of mortality in the first 5 years after CABG was 2.5-fold greater in the preoperative AF group. Their 5-year risk of stroke or systemic embolization was 1.5-fold greater, too. Upon adjustment for potentially confounding comorbid conditions, preoperative AF was associated with a 1.5-fold increased 5-year risk of mortality and a 1.2-fold increase in stroke or systemic embolism.
In an effort to identify a particularly high-risk group of CABG patients with preoperative AF, Dr. Malaisrie and his coinvestigators stratified the group’s long-term stroke and mortality risks by their CHA2DS2-VASc score at the time of surgery. The results were revealing: the unadjusted 5-year risk of stroke or systemic embolization was 7.9% in those with a CHA2DS2-VASc score of 1-3, 12.2% with a score of 4-6, and 15.4% with a score of 7-9. The 5-year survival rate was 74.8% with a score of 1-3, 56.5% with a score of 4-6, and 41.2% with a score of 7-9.
“That’s really a striking finding,” Dr. Malaisrie observed. “When you consider a patient who’s, say, 72-75 years old, who is undergoing isolated CABG with preoperative atrial fibrillation and who has a high CHA2DS2-VASc score of 7-9, 5-year survival is only 41%, with a 15% risk of stroke or systemic embolization.”
Discussant William T. Caine, MD, found the study results unsettling.
“I was surprised to see that in this day and age, fully two-thirds of the patients who had preoperative atrial fibrillation had no attempt at any ablation procedure to treat their atrial fibrillation,” declared Dr. Caine of Intermountain Medical Center in Salt Lake City.
In reply, Dr. Malaisrie noted that other, smaller studies have also found that only about 30% of CABG patients with preoperative AF undergo surgical AF ablation through a maze procedure or some other method.
“Probably most of us in this room would go ahead and perform surgical ablation, but the STS database represents all isolated CABG procedures done throughout the United States,” Dr. Malaisrie said. “I think this dataset should help convince the other 70% of surgeons out there that there is a high cost for preoperative AF – in particular, in patients with very high CHA2DS2-VASc scores. If you can identify a group of patients at increased risk for stroke and mortality, you’d certainly want to bend their survival curve.”
The maze procedure has been convincingly shown to be very safe, with no associated increased risk of perioperative morbidity and mortality. The downside is cost. But while it’s true that adding surgical ablation to an isolated CABG procedure boosts OR time and procedural costs, a successful ablation is likely to pay dividends through reduced downstream rates of major morbidity and mortality.
“I look forward to the second part of our analysis, where we’ll look at the comparative data for the patients who did in fact have surgical ablation. That dataset is pending from the Duke Clinical Research Institute,” according to Dr. Malaisrie.
He cited as study limitations the inability to complete linkage to the Medicare database in about 37% of CABG patients in the STS database, or more than 200,000 people. Also, the Medicare database is an administrative dataset reliant upon medical record coding. The mortality data are probably quite accurate, but the stroke and systemic embolization rates cited in this analysis likely underestimate the true rates.
He reported serving as a consultant to Edwards Lifesciences, Abbott Vascular, and Baxter, and serving on speakers’ bureaus for Bolton and Abiomed. However, the STS analysis was funded exclusively by philanthropy.
AT THE WTSA ANNUAL MEETING
Key clinical point:
Major finding: Preoperative AF in patients undergoing isolated CABG was tied to an adjusted 45% greater 5-year mortality and 25% increase in stroke and systemic embolization risk, compared with CABG patients without the preoperative arrhythmia.
Data source: This retrospective study compared perioperative and long-term morbidity and mortality in nearly 350,000 patients in the Society of Thoracic Surgeons database who underwent isolated CABG, including more than 24,000 who had preoperative atrial fibrillation that wasn’t addressed surgically.
Disclosures: The study presenter reported serving as a consultant to Edwards Lifesciences, Abbott Vascular, and Baxter, and serving on speakers’ bureaus for Bolton and Abiomed. However, the STS analysis was funded exclusively by philanthropy.
First trial of TAVR vs. SAVR in low-risk patients
PARIS – Five-year hemodynamic results of the first randomized trial of transcatheter versus surgical aortic valve replacement in low-surgical-risk patients with severe aortic stenosis showed continued superior valve performance in the TAVR group, Lars Sondergaard, MD, reported at the annual congress of the European Association of Percutaneous Cardiovascular Interventions.
“The durability results are very encouraging. We can’t see that the TAVR patients are doing worse. So I think this is setting the scene to try to move forward in patients at low risk and also in younger patients,” declared Dr. Sondergaard, professor of cardiology at the University of Copenhagen.
He presented an update from the Nordic Aortic Valve Intervention (NOTION) trial, a prospective, multicenter, randomized, all-comers clinical trial in which 280 patients with symptomatic severe aortic stenosis at low surgical risk were assigned to surgical aortic valve replacement (SAVR) or to TAVR with the self-expanding CoreValve. Their mean age was 79 years, with an average Society of Thoracic Surgeons projected risk of mortality score of 3%. Eighty-two percent of participants had an STS score below 4%. Roughly 40% of TAVR patients got the first-generation CoreValve in the 26-mm size, 40% received the 29-mm version, and the rest got the 31-mm CoreValve.

Among patients in the lowest-surgical-risk and youngest subgroup – those aged 70-75 with a Society of Thoracic Surgeons risk score below 4% – the composite primary endpoint rate at 4 years was 15.6% with TAVR compared with 27.2% with SAVR. However, only 62 NOTION participants fell into this category, so the between-group difference, while sizable, didn’t achieve statistical significance, according to Dr. Sondergaard.
There was a trade-off between the two valve replacement strategies with regard to procedural complications. The rate of new-onset atrial fibrillation was far higher in the SAVR group: 59.4% at 1 year and 60.2% at 4 years of follow-up, compared with 21.2% and 24.5% at 1 and 4 years, respectively, in the TAVR group.
On the other hand, 38% of the TAVR patients got a new pacemaker within the first year of follow-up, compared with only 2.4% in the SAVR group. At 4 years, 43.7% of the TAVR group had a pacemaker, versus 9% of the SAVR group.
Turning to the hemodynamic data, the cardiologist noted that the effective orifice area in the TAVR group went from 0.71 cm2 at baseline to 1.66 at 1 year and remained steady thereafter at 1.67 cm2 through 5 years. The TAVR group’s mean gradient improved from 45.4 mm Hg at baseline to 8.6 mm Hg at 1 year and 7.9 mm Hg at 5 years. These outcomes were significantly better than in the SAVR group, where the effective orifice area went from 0.74 cm2 at baseline to 1.32 at 1 year and 1.24 cm2 at 5 years, while the mean gradient fell from 44.9 mm Hg to 12.5 at 1 year and 13.6 mm Hg at 5 years.
Moderate hemodynamic structural valve deterioration was significantly more common in the SAVR group: 20.7% at 5 years, compared with 2.9% in the TAVR patients. The opposite was true with regard to moderate paravalvular leak, which occurred in 20.9% of the TAVI group but only 1.5% of SAVR patients.
Late complications were rare following either procedure. There were no cases of valve thrombosis through 5 years. The incidence of endocarditis at 5 years was 4.3% in the TAVR patients and similar at 5.9% in the SAVR group.
Discussant Samer Mansour, MD, of the University of Montreal, remarked that the rate of new pacemaker implantation following TAVR seemed extraordinarily high.
“This was early days,” Dr. Sondergaard explained. “We had a lower threshold for putting in a pacemaker and we put the valves in a little deeper.”
About half of new pacemaker recipients didn’t use the device after the first year, he added. Also, neither getting a new pacemaker nor moderate paravalvular leak was associated with increased mortality in the TAVR group.
Dr. Mansour observed that subtle but real differences in mortality probably wouldn’t show up in a 280-patient trial. Dr. Sondergaard concurred.
“We designed the NOTION trial in 2008-2009. Knowing what we know now, we should have had a larger study, but at that time TAVR volume wasn’t that big and it wasn’t realistic as a Nordic trial to include 1,000 patients. This was the best we could do,” he said.
Follow-up in the NOTION study will continue out to 10 years.
The study is funded by Medtronic. Dr. Sondergaard reported serving as a consultant to and receiving research grant support from the company.
PARIS – Five-year hemodynamic results of the first randomized trial of transcatheter versus surgical aortic valve replacement in low-surgical-risk patients with severe aortic stenosis showed continued superior valve performance in the TAVR group, Lars Sondergaard, MD, reported at the annual congress of the European Association of Percutaneous Cardiovascular Interventions.
“The durability results are very encouraging. We can’t see that the TAVR patients are doing worse. So I think this is setting the scene to try to move forward in patients at low risk and also in younger patients,” declared Dr. Sondergaard, professor of cardiology at the University of Copenhagen.
He presented an update from the Nordic Aortic Valve Intervention (NOTION) trial, a prospective, multicenter, randomized, all-comers clinical trial in which 280 patients with symptomatic severe aortic stenosis at low surgical risk were assigned to surgical aortic valve replacement (SAVR) or to TAVR with the self-expanding CoreValve. Their mean age was 79 years, with an average Society of Thoracic Surgeons projected risk of mortality score of 3%. Eighty-two percent of participants had an STS score below 4%. Roughly 40% of TAVR patients got the first-generation CoreValve in the 26-mm size, 40% received the 29-mm version, and the rest got the 31-mm CoreValve.
Among patients in the lowest-surgical-risk and youngest subgroup – those aged 70-75 with a Society of Thoracic Surgeons risk score below 4% – the composite primary endpoint rate at 4 years was 15.6% with TAVR compared with 27.2% with SAVR. However, only 62 NOTION participants fell into this category, so the between-group difference, while sizable, didn’t achieve statistical significance, according to Dr. Sondergaard.
There was a trade-off between the two valve replacement strategies with regard to procedural complications. The rate of new-onset atrial fibrillation was far higher in the SAVR group: 59.4% at 1 year and 60.2% at 4 years of follow-up, compared with 21.2% and 24.5% at 1 and 4 years, respectively, in the TAVR group.
On the other hand, 38% of the TAVR patients got a new pacemaker within the first year of follow-up, compared with only 2.4% in the SAVR group. At 4 years, 43.7% of the TAVR group had a pacemaker, versus 9% of the SAVR group.
Turning to the hemodynamic data, the cardiologist noted that the effective orifice area in the TAVR group went from 0.71 cm2 at baseline to 1.66 at 1 year and remained steady thereafter at 1.67 cm2 through 5 years. The TAVR group’s mean gradient improved from 45.4 mm Hg at baseline to 8.6 mm Hg at 1 year and 7.9 mm Hg at 5 years. These outcomes were significantly better than in the SAVR group, where the effective orifice area went from 0.74 cm2 at baseline to 1.32 at 1 year and 1.24 cm2 at 5 years, while the mean gradient fell from 44.9 mm Hg to 12.5 at 1 year and 13.6 mm Hg at 5 years.
Moderate hemodynamic structural valve deterioration was significantly more common in the SAVR group: 20.7% at 5 years, compared with 2.9% in the TAVR patients. The opposite was true with regard to moderate paravalvular leak, which occurred in 20.9% of the TAVI group but only 1.5% of SAVR patients.
Late complications were rare following either procedure. There were no cases of valve thrombosis through 5 years. The incidence of endocarditis at 5 years was 4.3% in the TAVR patients and similar at 5.9% in the SAVR group.
Discussant Samer Mansour, MD, of the University of Montreal, remarked that the rate of new pacemaker implantation following TAVR seemed extraordinarily high.
“This was early days,” Dr. Sondergaard explained. “We had a lower threshold for putting in a pacemaker and we put the valves in a little deeper.”
About half of new pacemaker recipients didn’t use the device after the first year, he added. Also, neither getting a new pacemaker nor moderate paravalvular leak was associated with increased mortality in the TAVR group.
Dr. Mansour observed that subtle but real differences in mortality probably wouldn’t show up in a 280-patient trial. Dr. Sondergaard concurred.
“We designed the NOTION trial in 2008-2009. Knowing what we know now, we should have had a larger study, but at that time TAVR volume wasn’t that big and it wasn’t realistic as a Nordic trial to include 1,000 patients. This was the best we could do,” he said.
Follow-up in the NOTION study will continue out to 10 years.
The study is funded by Medtronic. Dr. Sondergaard reported serving as a consultant to and receiving research grant support from the company.
PARIS – Five-year hemodynamic results of the first randomized trial of transcatheter versus surgical aortic valve replacement in low-surgical-risk patients with severe aortic stenosis showed continued superior valve performance in the TAVR group, Lars Sondergaard, MD, reported at the annual congress of the European Association of Percutaneous Cardiovascular Interventions.
“The durability results are very encouraging. We can’t see that the TAVR patients are doing worse. So I think this is setting the scene to try to move forward in patients at low risk and also in younger patients,” declared Dr. Sondergaard, professor of cardiology at the University of Copenhagen.
He presented an update from the Nordic Aortic Valve Intervention (NOTION) trial, a prospective, multicenter, randomized, all-comers clinical trial in which 280 patients with symptomatic severe aortic stenosis at low surgical risk were assigned to surgical aortic valve replacement (SAVR) or to TAVR with the self-expanding CoreValve. Their mean age was 79 years, with an average Society of Thoracic Surgeons projected risk of mortality score of 3%. Eighty-two percent of participants had an STS score below 4%. Roughly 40% of TAVR patients got the first-generation CoreValve in the 26-mm size, 40% received the 29-mm version, and the rest got the 31-mm CoreValve.
Among patients in the lowest-surgical-risk and youngest subgroup – those aged 70-75 with a Society of Thoracic Surgeons risk score below 4% – the composite primary endpoint rate at 4 years was 15.6% with TAVR compared with 27.2% with SAVR. However, only 62 NOTION participants fell into this category, so the between-group difference, while sizable, didn’t achieve statistical significance, according to Dr. Sondergaard.
There was a trade-off between the two valve replacement strategies with regard to procedural complications. The rate of new-onset atrial fibrillation was far higher in the SAVR group: 59.4% at 1 year and 60.2% at 4 years of follow-up, compared with 21.2% and 24.5% at 1 and 4 years, respectively, in the TAVR group.
On the other hand, 38% of the TAVR patients got a new pacemaker within the first year of follow-up, compared with only 2.4% in the SAVR group. At 4 years, 43.7% of the TAVR group had a pacemaker, versus 9% of the SAVR group.
Turning to the hemodynamic data, the cardiologist noted that the effective orifice area in the TAVR group went from 0.71 cm2 at baseline to 1.66 at 1 year and remained steady thereafter at 1.67 cm2 through 5 years. The TAVR group’s mean gradient improved from 45.4 mm Hg at baseline to 8.6 mm Hg at 1 year and 7.9 mm Hg at 5 years. These outcomes were significantly better than in the SAVR group, where the effective orifice area went from 0.74 cm2 at baseline to 1.32 at 1 year and 1.24 cm2 at 5 years, while the mean gradient fell from 44.9 mm Hg to 12.5 at 1 year and 13.6 mm Hg at 5 years.
Moderate hemodynamic structural valve deterioration was significantly more common in the SAVR group: 20.7% at 5 years, compared with 2.9% in the TAVR patients. The opposite was true with regard to moderate paravalvular leak, which occurred in 20.9% of the TAVI group but only 1.5% of SAVR patients.
Late complications were rare following either procedure. There were no cases of valve thrombosis through 5 years. The incidence of endocarditis at 5 years was 4.3% in the TAVR patients and similar at 5.9% in the SAVR group.
Discussant Samer Mansour, MD, of the University of Montreal, remarked that the rate of new pacemaker implantation following TAVR seemed extraordinarily high.
“This was early days,” Dr. Sondergaard explained. “We had a lower threshold for putting in a pacemaker and we put the valves in a little deeper.”
About half of new pacemaker recipients didn’t use the device after the first year, he added. Also, neither getting a new pacemaker nor moderate paravalvular leak was associated with increased mortality in the TAVR group.
Dr. Mansour observed that subtle but real differences in mortality probably wouldn’t show up in a 280-patient trial. Dr. Sondergaard concurred.
“We designed the NOTION trial in 2008-2009. Knowing what we know now, we should have had a larger study, but at that time TAVR volume wasn’t that big and it wasn’t realistic as a Nordic trial to include 1,000 patients. This was the best we could do,” he said.
Follow-up in the NOTION study will continue out to 10 years.
The study is funded by Medtronic. Dr. Sondergaard reported serving as a consultant to and receiving research grant support from the company.
AT EuroPCR
Key clinical point:
Major finding: At 4 years of follow-up, the composite endpoint of all-cause mortality, MI, or stroke occurred in 29% of low-surgical-risk patients with severe aortic stenosis who were randomized to transcatheter aortic valve replacement (TAVR) and 30% of those who underwent surgical valve replacement.
Data source: NOTION, a prospective multicenter randomized trial in which 280 Nordic patients with symptomatic severe aortic stenosis at low surgical risk were assigned to surgical aortic valve replacement (SAVR) or to TAVR with the self-expanding CoreValve.
Disclosures: The study is funded by Medtronic. The presenter reported serving as a consultant to and receiving research grant support from the company.
Childhood poverty sets stage for adult heart disease
Children from the poorest families show signs of thicker carotid artery walls that may raise their risk for heart attack and stroke as adults, according to data from a longitudinal study of more than 1,000 families in Australia.
“Understanding when associations between SEP [socioeconomic position] and CVD [cardiovascular disease] first appear may help address the increasing social gradients in CVD outcomes and risk factors,” wrote Richard S. Liu, MD, of the Murdoch Children’s Research Institute, Parkville, Australia, and colleagues.
The researchers reviewed data from 1,477 families in Australia. Socioeconomic position of the children’s families was measured biennially at age 0-1 year and onward, and the researchers used imaging to measure the right carotid arteries of children between age 11 and 12 years. Overall, children in the lowest socioeconomic quartile at age 11-12 years were 46% more likely than those in the highest quartile to have thicker carotid arteries (defined as greater than the 75th percentile).
“In univariable analyses, each quartile increment higher of family SEP was associated with a 3.7-micrometer thicker carotid intima-media thickness [IMT],” and the association remained significant in a multivariate analysis controlling for cardiovascular risk factors including secondhand smoke, body weight, and blood pressure, the researchers wrote.
The socioeconomic status of the family had a greater impact than that of the neighborhood, they noted.
In addition, low socioeconomic status of a child’s family at age 2-3 years was associated with thickness in carotid artery measurements at age 11-12 years.
The study findings were limited by several factors, including a lack of data on the clinical consequences of increased carotid thickness in children, as well as the need for investigation of other signs of subclinical atherosclerosis, the researchers said. However, “consistent evidence showed an association between SEP from early life and midchildhood carotid IMT,” and additional research is needed to explore the impact of household factors on childhood health, they emphasized.
The findings were published online Aug. 9 in the Journal of the American Heart Association (J Am Heart Assoc. 2017;6:e0059255).
The study was funded by the National Health and Medical Research Council of Australia and several research institutions. The researchers had no financial conflicts to disclose.
Children from the poorest families show signs of thicker carotid artery walls that may raise their risk for heart attack and stroke as adults, according to data from a longitudinal study of more than 1,000 families in Australia.
“Understanding when associations between SEP [socioeconomic position] and CVD [cardiovascular disease] first appear may help address the increasing social gradients in CVD outcomes and risk factors,” wrote Richard S. Liu, MD, of the Murdoch Children’s Research Institute, Parkville, Australia, and colleagues.
The researchers reviewed data from 1,477 families in Australia. Socioeconomic position of the children’s families was measured biennially at age 0-1 year and onward, and the researchers used imaging to measure the right carotid arteries of children between age 11 and 12 years. Overall, children in the lowest socioeconomic quartile at age 11-12 years were 46% more likely than those in the highest quartile to have thicker carotid arteries (defined as greater than the 75th percentile).
“In univariable analyses, each quartile increment higher of family SEP was associated with a 3.7-micrometer thicker carotid intima-media thickness [IMT],” and the association remained significant in a multivariate analysis controlling for cardiovascular risk factors including secondhand smoke, body weight, and blood pressure, the researchers wrote.
The socioeconomic status of the family had a greater impact than that of the neighborhood, they noted.
In addition, low socioeconomic status of a child’s family at age 2-3 years was associated with thickness in carotid artery measurements at age 11-12 years.
The study findings were limited by several factors, including a lack of data on the clinical consequences of increased carotid thickness in children, as well as the need for investigation of other signs of subclinical atherosclerosis, the researchers said. However, “consistent evidence showed an association between SEP from early life and midchildhood carotid IMT,” and additional research is needed to explore the impact of household factors on childhood health, they emphasized.
The findings were published online Aug. 9 in the Journal of the American Heart Association (J Am Heart Assoc. 2017;6:e0059255).
The study was funded by the National Health and Medical Research Council of Australia and several research institutions. The researchers had no financial conflicts to disclose.
Children from the poorest families show signs of thicker carotid artery walls that may raise their risk for heart attack and stroke as adults, according to data from a longitudinal study of more than 1,000 families in Australia.
“Understanding when associations between SEP [socioeconomic position] and CVD [cardiovascular disease] first appear may help address the increasing social gradients in CVD outcomes and risk factors,” wrote Richard S. Liu, MD, of the Murdoch Children’s Research Institute, Parkville, Australia, and colleagues.
The researchers reviewed data from 1,477 families in Australia. Socioeconomic position of the children’s families was measured biennially at age 0-1 year and onward, and the researchers used imaging to measure the right carotid arteries of children between age 11 and 12 years. Overall, children in the lowest socioeconomic quartile at age 11-12 years were 46% more likely than those in the highest quartile to have thicker carotid arteries (defined as greater than the 75th percentile).
“In univariable analyses, each quartile increment higher of family SEP was associated with a 3.7-micrometer thicker carotid intima-media thickness [IMT],” and the association remained significant in a multivariate analysis controlling for cardiovascular risk factors including secondhand smoke, body weight, and blood pressure, the researchers wrote.
The socioeconomic status of the family had a greater impact than that of the neighborhood, they noted.
In addition, low socioeconomic status of a child’s family at age 2-3 years was associated with thickness in carotid artery measurements at age 11-12 years.
The study findings were limited by several factors, including a lack of data on the clinical consequences of increased carotid thickness in children, as well as the need for investigation of other signs of subclinical atherosclerosis, the researchers said. However, “consistent evidence showed an association between SEP from early life and midchildhood carotid IMT,” and additional research is needed to explore the impact of household factors on childhood health, they emphasized.
The findings were published online Aug. 9 in the Journal of the American Heart Association (J Am Heart Assoc. 2017;6:e0059255).
The study was funded by the National Health and Medical Research Council of Australia and several research institutions. The researchers had no financial conflicts to disclose.
FROM THE JOURNAL OF THE AMERICAN HEART ASSOCIATION
Key clinical point: Low socioeconomic status of families was significantly linked with thicker carotid arteries in children at age 11-12 years, which could increase the risk of stroke in adulthood.
Major finding: Children in the lowest socioeconomic group at age 11-12 years were 46% more likely to have carotid intima-media thickness at a level above the 75th percentile.
Data source: A longitudinal study of children from 1,477 families in Australia.
Disclosures: The study was funded by the National Health and Medical Research Council of Australia and several research institutions. The researchers had no financial conflicts to disclose.
Award for best hospital goes to … the Mayo Clinic
For the second consecutive year, the Mayo Clinic was named the top hospital in the country by U.S. News & World Report.
Also for the second consecutive year, the Cleveland Clinic is ranked second, while Johns Hopkins Hospital in Baltimore and Massachusetts General Hospital in Boston finished third and fourth – switching their places from last year’s ranking – and UCSF Medical Center in San Francisco is fifth after ranking seventh last year, according to the 2017-2018 Best Hospitals ranking.
The Mayo Clinic is nationally ranked in 15 of the 16 specialties included in the overall process, which started with 4,658 community inpatient hospitals and finished with 152 ranking nationally in at least one specialty and 20 earning Honor Roll status with high rankings in multiple specialties. The specialties used in the ranking process include 12 that are data driven – cancer; cardiology and heart surgery; diabetes and endocrinology; otolaryngology; gastroenterology and gastrointestinal surgery; geriatrics; gynecology; nephrology; neurology and neurosurgery; orthopedics; pulmonology; and urology – and four rated by reputation only – ophthalmology; psychiatry; rehabilitation; and rheumatology.
The research organization RTI International conducted the physician survey and produced the Best Hospitals methodology and national rankings under contract with U.S. News. The launch of this year’s edition of Best Hospitals is sponsored by Fidelity Investments.
For the second consecutive year, the Mayo Clinic was named the top hospital in the country by U.S. News & World Report.
Also for the second consecutive year, the Cleveland Clinic is ranked second, while Johns Hopkins Hospital in Baltimore and Massachusetts General Hospital in Boston finished third and fourth – switching their places from last year’s ranking – and UCSF Medical Center in San Francisco is fifth after ranking seventh last year, according to the 2017-2018 Best Hospitals ranking.
The Mayo Clinic is nationally ranked in 15 of the 16 specialties included in the overall process, which started with 4,658 community inpatient hospitals and finished with 152 ranking nationally in at least one specialty and 20 earning Honor Roll status with high rankings in multiple specialties. The specialties used in the ranking process include 12 that are data driven – cancer; cardiology and heart surgery; diabetes and endocrinology; otolaryngology; gastroenterology and gastrointestinal surgery; geriatrics; gynecology; nephrology; neurology and neurosurgery; orthopedics; pulmonology; and urology – and four rated by reputation only – ophthalmology; psychiatry; rehabilitation; and rheumatology.
The research organization RTI International conducted the physician survey and produced the Best Hospitals methodology and national rankings under contract with U.S. News. The launch of this year’s edition of Best Hospitals is sponsored by Fidelity Investments.
For the second consecutive year, the Mayo Clinic was named the top hospital in the country by U.S. News & World Report.
Also for the second consecutive year, the Cleveland Clinic is ranked second, while Johns Hopkins Hospital in Baltimore and Massachusetts General Hospital in Boston finished third and fourth – switching their places from last year’s ranking – and UCSF Medical Center in San Francisco is fifth after ranking seventh last year, according to the 2017-2018 Best Hospitals ranking.
The Mayo Clinic is nationally ranked in 15 of the 16 specialties included in the overall process, which started with 4,658 community inpatient hospitals and finished with 152 ranking nationally in at least one specialty and 20 earning Honor Roll status with high rankings in multiple specialties. The specialties used in the ranking process include 12 that are data driven – cancer; cardiology and heart surgery; diabetes and endocrinology; otolaryngology; gastroenterology and gastrointestinal surgery; geriatrics; gynecology; nephrology; neurology and neurosurgery; orthopedics; pulmonology; and urology – and four rated by reputation only – ophthalmology; psychiatry; rehabilitation; and rheumatology.
The research organization RTI International conducted the physician survey and produced the Best Hospitals methodology and national rankings under contract with U.S. News. The launch of this year’s edition of Best Hospitals is sponsored by Fidelity Investments.
ACA: Five tactics could lead to implosion
With legislative efforts to repeal and/or replace the Affordable Care Act shelved for now, President Trump has tweeted that he wants to “let ObamaCare implode, then deal.” But just what can – and is – his administration doing to foster an implosion? Policy experts help us count the ways:
1. Lax enforcement of the individual mandate
Shortly after he took office, President Trump issued an executive order aimed at “minimizing the economic burden” of the ACA. The order directed all federal agencies to take legal steps to waive, defer, grant exemptions from, or delay the implementation of any ACA provision or requirement that would impose a fiscal burden on states, patients, providers, or health insurers.
As a result, the Internal Revenue Service announced that it would not reject tax returns that do not indicate whether the taxpayer has health insurance. That question is included to determine whether taxpayers will incur a financial penalty under the individual mandate.

“What the Trump administration has done has weakened it even further by effectively saying that they will not enforce the mandate if anyone challenges it,” said Dr. Forman, a practicing radiologist and operational chief for radiology at Yale New Haven Hospital. “So if an individual claims that they shouldn’t have to face the mandate for religious reasons or other objections, that they would be allowed out. By encouraging that, you’re basically weakening the mandate even more, [which] hurts the exchanges and ultimately drives up prices.”
2. Little advertising, outreach
The Trump administration canceled advertising and outreach efforts in the final week of the 2017 open enrollment period. As many as half a million people missed out on enrolling in a health insurance plan as a result, Joshua Peck, former chief marketing officer for healthcare.gov, estimated in a recent blog post.
In the past, the federal government has played a significant role in informing the public about marketplace coverage, their rights and responsibilities under the ACA, and the process of enrollment, said Sarah Lueck, a senior policy analyst for the Center on Budget and Policy Priorities, a nonpartisan research and policy institute. The last week of enrollment is known as a critical time to enroll patients, she said. In 2016 for example, about 700,000 people enrolled during the final week. It’s often the healthiest patients who wait until the last minute, Ms. Lueck added.

“One way you discourage healthy people from enrolling is by pulling back on advertising at the very moment they may be paying attention,” she said in an interview. “It sends a bad signal. Now as the next enrollment period is about to come up in November, it raises a concern about – what are the plans for outreach?”
Without sufficient promotion, the number of patients who learn about the ACA and enroll could drop off, and the percentage of sicker enrollees in the marketplace could rise, according to analysts. The Trump administration has not said whether it plans to advertise or promote enrollment during the upcoming November enrollment period. The Centers for Medicare & Medicaid Services recently shortened open enrollment from the previous 3 months to 45 days.
In a final rule issued in April, the CMS stated the change will “improve individual market risk pools by reducing opportunities for adverse selection ... and will encourage healthier individuals who might have previously enrolled in partial year coverage after December 15th to instead enroll in coverage for the full year.”
3. Highlight what’s “wrong” with the ACA
In addition to pulling positive advertisements about ACA, the Trump administration has also launched a campaign that criticizes the law.
Since January, the Department of Health & Human Services has published more than 20 videos featuring stories about how the ACA has harmed patients. The HHS has also used its Twitter account to advocate repeal and replacement of the ACA. Sen. Ron Wyden (D-Ore.), ranking member of the Finance Committee, and other legislators have raised concerns that the HHS is misusing federal resources to advance partisan legislation by funding the messages.
“It’s not just pulling advertisements and going dark and not telling people [information], but it’s also putting things out there that talk about people who don’t like the law,” Ms. Lueck said. “It’s counterproductive propaganda if you’re coming from the perspective of wanting people to sign up for coverage. The agencies that have been very engaged in trying to get people through the process and covered, are now working in cross purposes with that.”
Ms. Lueck said that the federal government is also putting a negative spin on the current participation of marketplace insurers and the future of the exchanges. On Aug. 2, the CMS released a map on projected insurer participation in the ACA’s 2018 health insurance exchanges. The map shows that 19 counties are projected to have no insurers in 2018, meaning that patients in those counties could be without marketplace options.
“For 2018, at least 13,008 Americans currently enrolled for health coverage on the exchanges live in the counties projected to be without coverage in 2018,” according to the CMS announcement. “In addition to overall issuer participation, increasing rates have also been a concern for the health insurance exchanges. ... A number of insurers in several states requested rate increases of 30% or more. Consumers in the 39 healthcare.gov states have already seen their premiums increase more than 100% since 2013.”
Unmentioned however, is that the number of potential “bare counties” has dropped in half from about a month ago. A similar map by the Kaiser Family Foundation shows that in June, 44 counties were at risk of having no marketplace insurer in 2018, a number that fell to 17 counties as of Aug. 4, according to Kaiser’s most recent map.
Kristine Grow, senior vice president of communications for America’s Health Insurance Plans (AHIP), noted that based on CMS’ projections thus far, the overall percentage of enrollees without an insurer for 2018 is 0.15%.

“We’re talking pretty small numbers, that’s about 15,000 people out of 10 million or so who get their coverage through an exchange,” Ms. Grow said in an interview. “It’s important for those people to have options, so the health plans have been working very hard to try to get into those counties.”
4. Work for Medicaid recipients
Potential work requirements for Medicaid beneficiaries may harm the Medicaid expansions that were part of the ACA.
On March 14, the HHS sent a letter to 50 U.S. governors encouraging states to come up with innovative ideas for their Medicaid programs, including the possibility of work requirements. The letter included specific suggestions, such as introducing plans that include health savings account–like features, encouraging Medicaid patients to secure employer-provided insurance, and requiring small premiums or other contributions from patients to encourage personal responsibility. The letter noted that the HHS would be open to states proposing work requirements for some Medicaid recipients, an approach that has “produced proven results for Americans enrolled in other federal, state, and local programs.”
Four states – Arizona, Indiana, Kentucky, and Pennsylvania – have formally submitted waiver requests to the HHS that would require work as an eligibility condition. To date, none has been approved. Arkansas also recently announced that it would seek changes to its waiver, including a work requirement.
Imposing work requirements would hurt access to Medicaid for patients who need health assistance, but who cannot work, Dr. Forman said. Under the ACA, 31 states and the District of Columbia have expanded their Medicaid coverage to people previously uncovered. Dr. Forman stresses that the bulk of Medicaid funding is spent on elderly, disabled, and mentally ill patients.
5. Withhold cost sharing reduction payments
For months, President Trump has threatened to stop making cost saving reduction (CSR) payments to insurers in the marketplace, a move that analysts say would raise premiums and cause insurers to exit the marketplaces. Most recently, the President on July 29 tweeted, “If a new HealthCare Bill is not approved quickly, BAILOUTS for Insurance Companies and BAILOUTS for Members of Congress will end very soon!”
Under the ACA, the federal government provides CSR payments to insurers to offset the costs for providing discount plans to patients who earn up to 200% of the federal poverty level. Plans on the individual exchanges are required to cover a package of essential benefits with pricing limitations to ensure that out-of-pocket costs are low enough for poorer patients. Because insurers lose money on these plans, the ACA provides about $7 billion to insurers through CSR payments.
Republican members of the House of Representatives sued the HHS over the CSR payments under the Obama administration, claiming the funding was illegal because it was never appropriated by Congress. A court ruled in favor of the House in 2016, but an appeal filed by the Obama administration allowed the CSR payments to continue.
President Trump has not indicated whether he plans to drop the appeal or carry on the case. But if he fails to continue the suit, the move would immediately end the CSR payments.
“If the funding for the CSR benefits goes away, premiums will go up, taxpayer dollars will go up, and choices will go down,” Ms. Grow of AHIP said in an interview. “The benefits as we understand them are still required to be offered on the exchanges. In order to cover those benefits, the premiums for everybody in the individual market will have to go up, and they will go up by about 20%.”
While the federal government would save money by ending the CSR payments, it would face increased costs for tax credits that subsidize premiums for marketplace enrollees with incomes that are 100% to 400% of the poverty level, according to an analysis by the Kaiser Family Foundation.
Following President Trump’s most recent threat to stop the CSR payments, AHIP issued a joint statement with the American Academy of Family Physicians, the American Medical Association, and several others underscoring the importance of the payments.
“Cost-sharing reductions are used to help those who need it most – low- and moderate-income consumers,” the associations said in the Aug. 2 statement. “Without these funds, consumers’ access to care is jeopardized, their premiums will increase dramatically, and they will be left with even fewer coverage options ... As medical professionals, insurers providing health care services and coverage to hundreds of millions of Americans, and business leaders concerned with maintaining a stable health insurance marketplace for consumers, we believe it is imperative that the administration fund the cost-sharing reduction program.”
[email protected]
On Twitter @legal_med
With legislative efforts to repeal and/or replace the Affordable Care Act shelved for now, President Trump has tweeted that he wants to “let ObamaCare implode, then deal.” But just what can – and is – his administration doing to foster an implosion? Policy experts help us count the ways:
1. Lax enforcement of the individual mandate
Shortly after he took office, President Trump issued an executive order aimed at “minimizing the economic burden” of the ACA. The order directed all federal agencies to take legal steps to waive, defer, grant exemptions from, or delay the implementation of any ACA provision or requirement that would impose a fiscal burden on states, patients, providers, or health insurers.
As a result, the Internal Revenue Service announced that it would not reject tax returns that do not indicate whether the taxpayer has health insurance. That question is included to determine whether taxpayers will incur a financial penalty under the individual mandate.
“What the Trump administration has done has weakened it even further by effectively saying that they will not enforce the mandate if anyone challenges it,” said Dr. Forman, a practicing radiologist and operational chief for radiology at Yale New Haven Hospital. “So if an individual claims that they shouldn’t have to face the mandate for religious reasons or other objections, that they would be allowed out. By encouraging that, you’re basically weakening the mandate even more, [which] hurts the exchanges and ultimately drives up prices.”
2. Little advertising, outreach
The Trump administration canceled advertising and outreach efforts in the final week of the 2017 open enrollment period. As many as half a million people missed out on enrolling in a health insurance plan as a result, Joshua Peck, former chief marketing officer for healthcare.gov, estimated in a recent blog post.
In the past, the federal government has played a significant role in informing the public about marketplace coverage, their rights and responsibilities under the ACA, and the process of enrollment, said Sarah Lueck, a senior policy analyst for the Center on Budget and Policy Priorities, a nonpartisan research and policy institute. The last week of enrollment is known as a critical time to enroll patients, she said. In 2016 for example, about 700,000 people enrolled during the final week. It’s often the healthiest patients who wait until the last minute, Ms. Lueck added.
“One way you discourage healthy people from enrolling is by pulling back on advertising at the very moment they may be paying attention,” she said in an interview. “It sends a bad signal. Now as the next enrollment period is about to come up in November, it raises a concern about – what are the plans for outreach?”
Without sufficient promotion, the number of patients who learn about the ACA and enroll could drop off, and the percentage of sicker enrollees in the marketplace could rise, according to analysts. The Trump administration has not said whether it plans to advertise or promote enrollment during the upcoming November enrollment period. The Centers for Medicare & Medicaid Services recently shortened open enrollment from the previous 3 months to 45 days.
In a final rule issued in April, the CMS stated the change will “improve individual market risk pools by reducing opportunities for adverse selection ... and will encourage healthier individuals who might have previously enrolled in partial year coverage after December 15th to instead enroll in coverage for the full year.”
3. Highlight what’s “wrong” with the ACA
In addition to pulling positive advertisements about ACA, the Trump administration has also launched a campaign that criticizes the law.
Since January, the Department of Health & Human Services has published more than 20 videos featuring stories about how the ACA has harmed patients. The HHS has also used its Twitter account to advocate repeal and replacement of the ACA. Sen. Ron Wyden (D-Ore.), ranking member of the Finance Committee, and other legislators have raised concerns that the HHS is misusing federal resources to advance partisan legislation by funding the messages.
“It’s not just pulling advertisements and going dark and not telling people [information], but it’s also putting things out there that talk about people who don’t like the law,” Ms. Lueck said. “It’s counterproductive propaganda if you’re coming from the perspective of wanting people to sign up for coverage. The agencies that have been very engaged in trying to get people through the process and covered, are now working in cross purposes with that.”
Ms. Lueck said that the federal government is also putting a negative spin on the current participation of marketplace insurers and the future of the exchanges. On Aug. 2, the CMS released a map on projected insurer participation in the ACA’s 2018 health insurance exchanges. The map shows that 19 counties are projected to have no insurers in 2018, meaning that patients in those counties could be without marketplace options.
“For 2018, at least 13,008 Americans currently enrolled for health coverage on the exchanges live in the counties projected to be without coverage in 2018,” according to the CMS announcement. “In addition to overall issuer participation, increasing rates have also been a concern for the health insurance exchanges. ... A number of insurers in several states requested rate increases of 30% or more. Consumers in the 39 healthcare.gov states have already seen their premiums increase more than 100% since 2013.”
Unmentioned however, is that the number of potential “bare counties” has dropped in half from about a month ago. A similar map by the Kaiser Family Foundation shows that in June, 44 counties were at risk of having no marketplace insurer in 2018, a number that fell to 17 counties as of Aug. 4, according to Kaiser’s most recent map.
Kristine Grow, senior vice president of communications for America’s Health Insurance Plans (AHIP), noted that based on CMS’ projections thus far, the overall percentage of enrollees without an insurer for 2018 is 0.15%.
“We’re talking pretty small numbers, that’s about 15,000 people out of 10 million or so who get their coverage through an exchange,” Ms. Grow said in an interview. “It’s important for those people to have options, so the health plans have been working very hard to try to get into those counties.”
4. Work for Medicaid recipients
Potential work requirements for Medicaid beneficiaries may harm the Medicaid expansions that were part of the ACA.
On March 14, the HHS sent a letter to 50 U.S. governors encouraging states to come up with innovative ideas for their Medicaid programs, including the possibility of work requirements. The letter included specific suggestions, such as introducing plans that include health savings account–like features, encouraging Medicaid patients to secure employer-provided insurance, and requiring small premiums or other contributions from patients to encourage personal responsibility. The letter noted that the HHS would be open to states proposing work requirements for some Medicaid recipients, an approach that has “produced proven results for Americans enrolled in other federal, state, and local programs.”
Four states – Arizona, Indiana, Kentucky, and Pennsylvania – have formally submitted waiver requests to the HHS that would require work as an eligibility condition. To date, none has been approved. Arkansas also recently announced that it would seek changes to its waiver, including a work requirement.
Imposing work requirements would hurt access to Medicaid for patients who need health assistance, but who cannot work, Dr. Forman said. Under the ACA, 31 states and the District of Columbia have expanded their Medicaid coverage to people previously uncovered. Dr. Forman stresses that the bulk of Medicaid funding is spent on elderly, disabled, and mentally ill patients.
5. Withhold cost sharing reduction payments
For months, President Trump has threatened to stop making cost saving reduction (CSR) payments to insurers in the marketplace, a move that analysts say would raise premiums and cause insurers to exit the marketplaces. Most recently, the President on July 29 tweeted, “If a new HealthCare Bill is not approved quickly, BAILOUTS for Insurance Companies and BAILOUTS for Members of Congress will end very soon!”
Under the ACA, the federal government provides CSR payments to insurers to offset the costs for providing discount plans to patients who earn up to 200% of the federal poverty level. Plans on the individual exchanges are required to cover a package of essential benefits with pricing limitations to ensure that out-of-pocket costs are low enough for poorer patients. Because insurers lose money on these plans, the ACA provides about $7 billion to insurers through CSR payments.
Republican members of the House of Representatives sued the HHS over the CSR payments under the Obama administration, claiming the funding was illegal because it was never appropriated by Congress. A court ruled in favor of the House in 2016, but an appeal filed by the Obama administration allowed the CSR payments to continue.
President Trump has not indicated whether he plans to drop the appeal or carry on the case. But if he fails to continue the suit, the move would immediately end the CSR payments.
“If the funding for the CSR benefits goes away, premiums will go up, taxpayer dollars will go up, and choices will go down,” Ms. Grow of AHIP said in an interview. “The benefits as we understand them are still required to be offered on the exchanges. In order to cover those benefits, the premiums for everybody in the individual market will have to go up, and they will go up by about 20%.”
While the federal government would save money by ending the CSR payments, it would face increased costs for tax credits that subsidize premiums for marketplace enrollees with incomes that are 100% to 400% of the poverty level, according to an analysis by the Kaiser Family Foundation.
Following President Trump’s most recent threat to stop the CSR payments, AHIP issued a joint statement with the American Academy of Family Physicians, the American Medical Association, and several others underscoring the importance of the payments.
“Cost-sharing reductions are used to help those who need it most – low- and moderate-income consumers,” the associations said in the Aug. 2 statement. “Without these funds, consumers’ access to care is jeopardized, their premiums will increase dramatically, and they will be left with even fewer coverage options ... As medical professionals, insurers providing health care services and coverage to hundreds of millions of Americans, and business leaders concerned with maintaining a stable health insurance marketplace for consumers, we believe it is imperative that the administration fund the cost-sharing reduction program.”
[email protected]
On Twitter @legal_med
With legislative efforts to repeal and/or replace the Affordable Care Act shelved for now, President Trump has tweeted that he wants to “let ObamaCare implode, then deal.” But just what can – and is – his administration doing to foster an implosion? Policy experts help us count the ways:
1. Lax enforcement of the individual mandate
Shortly after he took office, President Trump issued an executive order aimed at “minimizing the economic burden” of the ACA. The order directed all federal agencies to take legal steps to waive, defer, grant exemptions from, or delay the implementation of any ACA provision or requirement that would impose a fiscal burden on states, patients, providers, or health insurers.
As a result, the Internal Revenue Service announced that it would not reject tax returns that do not indicate whether the taxpayer has health insurance. That question is included to determine whether taxpayers will incur a financial penalty under the individual mandate.
“What the Trump administration has done has weakened it even further by effectively saying that they will not enforce the mandate if anyone challenges it,” said Dr. Forman, a practicing radiologist and operational chief for radiology at Yale New Haven Hospital. “So if an individual claims that they shouldn’t have to face the mandate for religious reasons or other objections, that they would be allowed out. By encouraging that, you’re basically weakening the mandate even more, [which] hurts the exchanges and ultimately drives up prices.”
2. Little advertising, outreach
The Trump administration canceled advertising and outreach efforts in the final week of the 2017 open enrollment period. As many as half a million people missed out on enrolling in a health insurance plan as a result, Joshua Peck, former chief marketing officer for healthcare.gov, estimated in a recent blog post.
In the past, the federal government has played a significant role in informing the public about marketplace coverage, their rights and responsibilities under the ACA, and the process of enrollment, said Sarah Lueck, a senior policy analyst for the Center on Budget and Policy Priorities, a nonpartisan research and policy institute. The last week of enrollment is known as a critical time to enroll patients, she said. In 2016 for example, about 700,000 people enrolled during the final week. It’s often the healthiest patients who wait until the last minute, Ms. Lueck added.
“One way you discourage healthy people from enrolling is by pulling back on advertising at the very moment they may be paying attention,” she said in an interview. “It sends a bad signal. Now as the next enrollment period is about to come up in November, it raises a concern about – what are the plans for outreach?”
Without sufficient promotion, the number of patients who learn about the ACA and enroll could drop off, and the percentage of sicker enrollees in the marketplace could rise, according to analysts. The Trump administration has not said whether it plans to advertise or promote enrollment during the upcoming November enrollment period. The Centers for Medicare & Medicaid Services recently shortened open enrollment from the previous 3 months to 45 days.
In a final rule issued in April, the CMS stated the change will “improve individual market risk pools by reducing opportunities for adverse selection ... and will encourage healthier individuals who might have previously enrolled in partial year coverage after December 15th to instead enroll in coverage for the full year.”
3. Highlight what’s “wrong” with the ACA
In addition to pulling positive advertisements about ACA, the Trump administration has also launched a campaign that criticizes the law.
Since January, the Department of Health & Human Services has published more than 20 videos featuring stories about how the ACA has harmed patients. The HHS has also used its Twitter account to advocate repeal and replacement of the ACA. Sen. Ron Wyden (D-Ore.), ranking member of the Finance Committee, and other legislators have raised concerns that the HHS is misusing federal resources to advance partisan legislation by funding the messages.
“It’s not just pulling advertisements and going dark and not telling people [information], but it’s also putting things out there that talk about people who don’t like the law,” Ms. Lueck said. “It’s counterproductive propaganda if you’re coming from the perspective of wanting people to sign up for coverage. The agencies that have been very engaged in trying to get people through the process and covered, are now working in cross purposes with that.”
Ms. Lueck said that the federal government is also putting a negative spin on the current participation of marketplace insurers and the future of the exchanges. On Aug. 2, the CMS released a map on projected insurer participation in the ACA’s 2018 health insurance exchanges. The map shows that 19 counties are projected to have no insurers in 2018, meaning that patients in those counties could be without marketplace options.
“For 2018, at least 13,008 Americans currently enrolled for health coverage on the exchanges live in the counties projected to be without coverage in 2018,” according to the CMS announcement. “In addition to overall issuer participation, increasing rates have also been a concern for the health insurance exchanges. ... A number of insurers in several states requested rate increases of 30% or more. Consumers in the 39 healthcare.gov states have already seen their premiums increase more than 100% since 2013.”
Unmentioned however, is that the number of potential “bare counties” has dropped in half from about a month ago. A similar map by the Kaiser Family Foundation shows that in June, 44 counties were at risk of having no marketplace insurer in 2018, a number that fell to 17 counties as of Aug. 4, according to Kaiser’s most recent map.
Kristine Grow, senior vice president of communications for America’s Health Insurance Plans (AHIP), noted that based on CMS’ projections thus far, the overall percentage of enrollees without an insurer for 2018 is 0.15%.
“We’re talking pretty small numbers, that’s about 15,000 people out of 10 million or so who get their coverage through an exchange,” Ms. Grow said in an interview. “It’s important for those people to have options, so the health plans have been working very hard to try to get into those counties.”
4. Work for Medicaid recipients
Potential work requirements for Medicaid beneficiaries may harm the Medicaid expansions that were part of the ACA.
On March 14, the HHS sent a letter to 50 U.S. governors encouraging states to come up with innovative ideas for their Medicaid programs, including the possibility of work requirements. The letter included specific suggestions, such as introducing plans that include health savings account–like features, encouraging Medicaid patients to secure employer-provided insurance, and requiring small premiums or other contributions from patients to encourage personal responsibility. The letter noted that the HHS would be open to states proposing work requirements for some Medicaid recipients, an approach that has “produced proven results for Americans enrolled in other federal, state, and local programs.”
Four states – Arizona, Indiana, Kentucky, and Pennsylvania – have formally submitted waiver requests to the HHS that would require work as an eligibility condition. To date, none has been approved. Arkansas also recently announced that it would seek changes to its waiver, including a work requirement.
Imposing work requirements would hurt access to Medicaid for patients who need health assistance, but who cannot work, Dr. Forman said. Under the ACA, 31 states and the District of Columbia have expanded their Medicaid coverage to people previously uncovered. Dr. Forman stresses that the bulk of Medicaid funding is spent on elderly, disabled, and mentally ill patients.
5. Withhold cost sharing reduction payments
For months, President Trump has threatened to stop making cost saving reduction (CSR) payments to insurers in the marketplace, a move that analysts say would raise premiums and cause insurers to exit the marketplaces. Most recently, the President on July 29 tweeted, “If a new HealthCare Bill is not approved quickly, BAILOUTS for Insurance Companies and BAILOUTS for Members of Congress will end very soon!”
Under the ACA, the federal government provides CSR payments to insurers to offset the costs for providing discount plans to patients who earn up to 200% of the federal poverty level. Plans on the individual exchanges are required to cover a package of essential benefits with pricing limitations to ensure that out-of-pocket costs are low enough for poorer patients. Because insurers lose money on these plans, the ACA provides about $7 billion to insurers through CSR payments.
Republican members of the House of Representatives sued the HHS over the CSR payments under the Obama administration, claiming the funding was illegal because it was never appropriated by Congress. A court ruled in favor of the House in 2016, but an appeal filed by the Obama administration allowed the CSR payments to continue.
President Trump has not indicated whether he plans to drop the appeal or carry on the case. But if he fails to continue the suit, the move would immediately end the CSR payments.
“If the funding for the CSR benefits goes away, premiums will go up, taxpayer dollars will go up, and choices will go down,” Ms. Grow of AHIP said in an interview. “The benefits as we understand them are still required to be offered on the exchanges. In order to cover those benefits, the premiums for everybody in the individual market will have to go up, and they will go up by about 20%.”
While the federal government would save money by ending the CSR payments, it would face increased costs for tax credits that subsidize premiums for marketplace enrollees with incomes that are 100% to 400% of the poverty level, according to an analysis by the Kaiser Family Foundation.
Following President Trump’s most recent threat to stop the CSR payments, AHIP issued a joint statement with the American Academy of Family Physicians, the American Medical Association, and several others underscoring the importance of the payments.
“Cost-sharing reductions are used to help those who need it most – low- and moderate-income consumers,” the associations said in the Aug. 2 statement. “Without these funds, consumers’ access to care is jeopardized, their premiums will increase dramatically, and they will be left with even fewer coverage options ... As medical professionals, insurers providing health care services and coverage to hundreds of millions of Americans, and business leaders concerned with maintaining a stable health insurance marketplace for consumers, we believe it is imperative that the administration fund the cost-sharing reduction program.”
[email protected]
On Twitter @legal_med
Wide variability found in invasive mediastinal staging rates for lung cancer
COLORADO SPRINGS – Significant variability exists between hospitals in Washington state in their rates of invasive mediastinal staging for lung cancer, Farhood Farjah, MD, reported at the annual meeting of the Western Thoracic Surgical Association.
“We found evidence of a fivefold variation in hospital-level rates of invasive mediastinal staging not explained by chance or case mix,” according to Dr. Farjah of the University of Washington, Seattle.

“This has led to substantial concerns about quality of thoracic surgical care in the community at large,” he noted.
The Washington study is the first to show hospital-by-hospital variation in rates of invasive mediastinal staging.
Invasive mediastinal staging for lung cancer is considered important because imaging is known to have a substantial false-negative rate, and staging results have a profound impact on treatment recommendations, which can range from surgery alone to additional chemoradiation therapy.
Yet the meaning of the hospital-level huge variability in practice observed in the Washington study remains unclear.
“Our understanding of the underutilization of invasive mediastinal staging is further complicated by the fact that patterns of invasive mediastinal staging are highly variable across hospitals staffed by at least one board-certified thoracic surgeon with a noncardiac practice,” Dr. Farjah explained. “This variability could be a marker of poor-quality care. However, because the guidelines are not supported by level 1 evidence, it’s equally plausible that this variability might represent uncertainty or even disagreement with the practice guidelines – and specifically about the appropriate indication for invasive staging.”
He presented a retrospective cohort study of 406 patients whose non–small cell lung cancer was resected during July 2011–December 2013 at one of five Washington hospitals, each with at least one board-certified thoracic surgeon with a noncardiac practice on staff. The four participating community hospitals and one academic medical center were involved in a National Cancer Institute–funded, physician-led quality improvement initiative.
Overall, 66% of the 406 patients underwent any form of invasive mediastinal staging: 85% by mediastinoscopy only; 12% by mediastinoscopy plus endobronchial ultrasound-guided nodal aspiration (EBUS); 3% by EBUS only; and the remaining handful by mediastinoscopy, EBUS, and esophageal ultrasound-guided nodal aspiration. The invasive staging was performed at the time of resection in 64% of cases. A median of three nodal stations were sampled.
After statistical adjustment for random variation and between-hospital differences in clinical stage, rates of invasive staging were all over the map. While an overall mean of 66% of the lung cancer patients underwent invasive mediastinal staging, the rates at the five hospitals were 94%, 84%, 31%, 80%, and 17%.
Dr. Farjah and his coinvestigators are now conducting provider interviews and focus groups in an effort to understand what drove the participating surgeons’ wide variability in performing invasive mediastinal staging.
Discussant Jane Yanagawa, MD, of the University of California, Los Angeles, commented, “I think this is a really interesting study because, historically, lower rates of mediastinoscopy are assumed to be a reflection of low-quality care – and you suggest that might not be the case, that it might be more complicated than that.”
Dr. Yanagawa sketched one fairly common scenario that might represent a surgeon’s reasonable avoidance of guideline-recommended invasive mediastinal staging: a patient who by all preoperative imaging appears to have stage IA lung cancer and wishes to avoid the morbidity, time, and cost of needle biopsy, instead choosing to go straight to the operating room for a diagnosis by wedge resection, followed by a completion lobectomy based upon the frozen section results. Could such a pathway account for the variability seen in the Washington study?
“I think it could have,” Dr. Farjah replied. “I would say that’s probably one driver of variability.”
As for the generalizability of the findings of a five-hospital study carried out in a single state, Dr. Farjah said he thinks the results are applicable to any academic or community hospital with at least one board-certified thoracic surgeon with a noncardiac practice.
He reported having no financial conflicts of interest regarding the study.
M. Patricia Rivera, MD, FCCP, comments: Staging of lung cancer is essential to select the best treatment strategy for a given patient. However, despite multiple guideline recommendations

M. Patricia Rivera, MD, FCCP, comments: Staging of lung cancer is essential to select the best treatment strategy for a given patient. However, despite multiple guideline recommendations
M. Patricia Rivera, MD, FCCP, comments: Staging of lung cancer is essential to select the best treatment strategy for a given patient. However, despite multiple guideline recommendations
COLORADO SPRINGS – Significant variability exists between hospitals in Washington state in their rates of invasive mediastinal staging for lung cancer, Farhood Farjah, MD, reported at the annual meeting of the Western Thoracic Surgical Association.
“We found evidence of a fivefold variation in hospital-level rates of invasive mediastinal staging not explained by chance or case mix,” according to Dr. Farjah of the University of Washington, Seattle.
“This has led to substantial concerns about quality of thoracic surgical care in the community at large,” he noted.
The Washington study is the first to show hospital-by-hospital variation in rates of invasive mediastinal staging.
Invasive mediastinal staging for lung cancer is considered important because imaging is known to have a substantial false-negative rate, and staging results have a profound impact on treatment recommendations, which can range from surgery alone to additional chemoradiation therapy.
Yet the meaning of the hospital-level huge variability in practice observed in the Washington study remains unclear.
“Our understanding of the underutilization of invasive mediastinal staging is further complicated by the fact that patterns of invasive mediastinal staging are highly variable across hospitals staffed by at least one board-certified thoracic surgeon with a noncardiac practice,” Dr. Farjah explained. “This variability could be a marker of poor-quality care. However, because the guidelines are not supported by level 1 evidence, it’s equally plausible that this variability might represent uncertainty or even disagreement with the practice guidelines – and specifically about the appropriate indication for invasive staging.”
He presented a retrospective cohort study of 406 patients whose non–small cell lung cancer was resected during July 2011–December 2013 at one of five Washington hospitals, each with at least one board-certified thoracic surgeon with a noncardiac practice on staff. The four participating community hospitals and one academic medical center were involved in a National Cancer Institute–funded, physician-led quality improvement initiative.
Overall, 66% of the 406 patients underwent any form of invasive mediastinal staging: 85% by mediastinoscopy only; 12% by mediastinoscopy plus endobronchial ultrasound-guided nodal aspiration (EBUS); 3% by EBUS only; and the remaining handful by mediastinoscopy, EBUS, and esophageal ultrasound-guided nodal aspiration. The invasive staging was performed at the time of resection in 64% of cases. A median of three nodal stations were sampled.
After statistical adjustment for random variation and between-hospital differences in clinical stage, rates of invasive staging were all over the map. While an overall mean of 66% of the lung cancer patients underwent invasive mediastinal staging, the rates at the five hospitals were 94%, 84%, 31%, 80%, and 17%.
Dr. Farjah and his coinvestigators are now conducting provider interviews and focus groups in an effort to understand what drove the participating surgeons’ wide variability in performing invasive mediastinal staging.
Discussant Jane Yanagawa, MD, of the University of California, Los Angeles, commented, “I think this is a really interesting study because, historically, lower rates of mediastinoscopy are assumed to be a reflection of low-quality care – and you suggest that might not be the case, that it might be more complicated than that.”
Dr. Yanagawa sketched one fairly common scenario that might represent a surgeon’s reasonable avoidance of guideline-recommended invasive mediastinal staging: a patient who by all preoperative imaging appears to have stage IA lung cancer and wishes to avoid the morbidity, time, and cost of needle biopsy, instead choosing to go straight to the operating room for a diagnosis by wedge resection, followed by a completion lobectomy based upon the frozen section results. Could such a pathway account for the variability seen in the Washington study?
“I think it could have,” Dr. Farjah replied. “I would say that’s probably one driver of variability.”
As for the generalizability of the findings of a five-hospital study carried out in a single state, Dr. Farjah said he thinks the results are applicable to any academic or community hospital with at least one board-certified thoracic surgeon with a noncardiac practice.
He reported having no financial conflicts of interest regarding the study.
COLORADO SPRINGS – Significant variability exists between hospitals in Washington state in their rates of invasive mediastinal staging for lung cancer, Farhood Farjah, MD, reported at the annual meeting of the Western Thoracic Surgical Association.
“We found evidence of a fivefold variation in hospital-level rates of invasive mediastinal staging not explained by chance or case mix,” according to Dr. Farjah of the University of Washington, Seattle.
“This has led to substantial concerns about quality of thoracic surgical care in the community at large,” he noted.
The Washington study is the first to show hospital-by-hospital variation in rates of invasive mediastinal staging.
Invasive mediastinal staging for lung cancer is considered important because imaging is known to have a substantial false-negative rate, and staging results have a profound impact on treatment recommendations, which can range from surgery alone to additional chemoradiation therapy.
Yet the meaning of the hospital-level huge variability in practice observed in the Washington study remains unclear.
“Our understanding of the underutilization of invasive mediastinal staging is further complicated by the fact that patterns of invasive mediastinal staging are highly variable across hospitals staffed by at least one board-certified thoracic surgeon with a noncardiac practice,” Dr. Farjah explained. “This variability could be a marker of poor-quality care. However, because the guidelines are not supported by level 1 evidence, it’s equally plausible that this variability might represent uncertainty or even disagreement with the practice guidelines – and specifically about the appropriate indication for invasive staging.”
He presented a retrospective cohort study of 406 patients whose non–small cell lung cancer was resected during July 2011–December 2013 at one of five Washington hospitals, each with at least one board-certified thoracic surgeon with a noncardiac practice on staff. The four participating community hospitals and one academic medical center were involved in a National Cancer Institute–funded, physician-led quality improvement initiative.
Overall, 66% of the 406 patients underwent any form of invasive mediastinal staging: 85% by mediastinoscopy only; 12% by mediastinoscopy plus endobronchial ultrasound-guided nodal aspiration (EBUS); 3% by EBUS only; and the remaining handful by mediastinoscopy, EBUS, and esophageal ultrasound-guided nodal aspiration. The invasive staging was performed at the time of resection in 64% of cases. A median of three nodal stations were sampled.
After statistical adjustment for random variation and between-hospital differences in clinical stage, rates of invasive staging were all over the map. While an overall mean of 66% of the lung cancer patients underwent invasive mediastinal staging, the rates at the five hospitals were 94%, 84%, 31%, 80%, and 17%.
Dr. Farjah and his coinvestigators are now conducting provider interviews and focus groups in an effort to understand what drove the participating surgeons’ wide variability in performing invasive mediastinal staging.
Discussant Jane Yanagawa, MD, of the University of California, Los Angeles, commented, “I think this is a really interesting study because, historically, lower rates of mediastinoscopy are assumed to be a reflection of low-quality care – and you suggest that might not be the case, that it might be more complicated than that.”
Dr. Yanagawa sketched one fairly common scenario that might represent a surgeon’s reasonable avoidance of guideline-recommended invasive mediastinal staging: a patient who by all preoperative imaging appears to have stage IA lung cancer and wishes to avoid the morbidity, time, and cost of needle biopsy, instead choosing to go straight to the operating room for a diagnosis by wedge resection, followed by a completion lobectomy based upon the frozen section results. Could such a pathway account for the variability seen in the Washington study?
“I think it could have,” Dr. Farjah replied. “I would say that’s probably one driver of variability.”
As for the generalizability of the findings of a five-hospital study carried out in a single state, Dr. Farjah said he thinks the results are applicable to any academic or community hospital with at least one board-certified thoracic surgeon with a noncardiac practice.
He reported having no financial conflicts of interest regarding the study.
AT THE WTSA ANNUAL MEETING
Key clinical point:
Major finding: Rates of invasive mediastinal staging after adjustment for clinical stage ranged from a low of 17% at one hospital to as high as 94% at another.
Data source: This retrospective cohort study included 406 patients.
Disclosures: Dr. Farjah reported having no financial conflicts of interest.
TAVR for failed surgical valves: the VIVA study
PARIS – Transcatheter aortic valve replacement using the self-expanding Evolut R device in high-surgical-risk patients with failing surgical aortic bioprostheses showed promising 30-day safety and effectiveness results in the ongoing VIVA study, Ran Kornowski, MD, reported at the annual congress of the European Association of Percutaneous Cardiovascular Interventions.
“We had a lot of patients with small, failing valves in this study. Despite this, our valve gradients postprocedure were very, very low. This means to me that this platform is very well suited to deal with valve-in-valve procedures in general and with small bioprosthetic valves in particular,” observed Dr. Kornowski, chairman of the department of cardiology at Rabin Medical Center in Petah Tikva, Israel, and president of the Israel Heart Society.

The participants’ last surgical aortic valve replacement had been a mean of 9.3 years earlier. Seventy-one percent of subjects were New York Heart Association class III or IV. The mode of bioprosthetic failure was stenosis in 56% of cases, regurgitation in 23%, and both in the remainder. Ninety-three percent of their failing biosprothetic valves were stented devices. Forty-one percent of the devices were up to 21 mm and another 33% were more than 21 but less than 25 mm.
TAVR procedural access was by the iliofemoral route in 97% of cases. Local anesthesia was used in 42% of cases and conscious sedation in 35%. Fourteen percent of patients underwent preimplantation valvuloplasty; 21% postimplantation valvuloplasty. The procedural success rate was 98.5%.
The primary safety endpoint was 30-day cardiovascular mortality. The 2.0% rate was far lower than the prespecified cutoff which defined a positive outcome as less than a 10% rate in this high-surgical-risk population.
Other key 30-day outcomes:
• All-cause mortality occurred in 2.5% of patients.
• The 30-day stroke rate was 3%, with no disabling strokes.
• Major vascular complications occurred in 6.5% of the VIVA patients.
• Major bleeding occurred in 7%, minor bleeding in 7.9%. There were no cases of life-threatening bleeding.
• The incidence of Stage I acute kidney injury was rare, at 0.5%.
• Seven percent of patients received a permanent pacemaker.
• Eighty-seven percent of patients had no postprocedure paravalvular regurgitation (PVR), 11.4 had mild PVR, and 1.5% had moderate PVR.
• NYHA classification improved from baseline to 30 days in 81% of patients. At 30 days, 93% of participants were NYHA class I or II.
Turning to echocardiographic findings, the mean gradient improved from a mean baseline of 31.8 mm Hg to 12.6 mm Hg, while the effective orifice area rose from 1.0 to 1.5 cm2. The magnitude of both improvements was greater for patients with stenosis as their mode of valve failure.
“With the Evolut R, we aim for higher implantations – not more than about 4 mm below the ring – because going deeper could bring about higher gradients and functional deterioration later on,” the cardiologist explained.
The 1-year primary efficacy endpoint – lack of significant aortic stenosis as defined by a mean gradient less than 40 mm Hg – will be reported soon. The VIVA study is sponsored by Medtronic. Dr. Kornowski reported serving as a consultant to the company.
PARIS – Transcatheter aortic valve replacement using the self-expanding Evolut R device in high-surgical-risk patients with failing surgical aortic bioprostheses showed promising 30-day safety and effectiveness results in the ongoing VIVA study, Ran Kornowski, MD, reported at the annual congress of the European Association of Percutaneous Cardiovascular Interventions.
“We had a lot of patients with small, failing valves in this study. Despite this, our valve gradients postprocedure were very, very low. This means to me that this platform is very well suited to deal with valve-in-valve procedures in general and with small bioprosthetic valves in particular,” observed Dr. Kornowski, chairman of the department of cardiology at Rabin Medical Center in Petah Tikva, Israel, and president of the Israel Heart Society.
The participants’ last surgical aortic valve replacement had been a mean of 9.3 years earlier. Seventy-one percent of subjects were New York Heart Association class III or IV. The mode of bioprosthetic failure was stenosis in 56% of cases, regurgitation in 23%, and both in the remainder. Ninety-three percent of their failing biosprothetic valves were stented devices. Forty-one percent of the devices were up to 21 mm and another 33% were more than 21 but less than 25 mm.
TAVR procedural access was by the iliofemoral route in 97% of cases. Local anesthesia was used in 42% of cases and conscious sedation in 35%. Fourteen percent of patients underwent preimplantation valvuloplasty; 21% postimplantation valvuloplasty. The procedural success rate was 98.5%.
The primary safety endpoint was 30-day cardiovascular mortality. The 2.0% rate was far lower than the prespecified cutoff which defined a positive outcome as less than a 10% rate in this high-surgical-risk population.
Other key 30-day outcomes:
• All-cause mortality occurred in 2.5% of patients.
• The 30-day stroke rate was 3%, with no disabling strokes.
• Major vascular complications occurred in 6.5% of the VIVA patients.
• Major bleeding occurred in 7%, minor bleeding in 7.9%. There were no cases of life-threatening bleeding.
• The incidence of Stage I acute kidney injury was rare, at 0.5%.
• Seven percent of patients received a permanent pacemaker.
• Eighty-seven percent of patients had no postprocedure paravalvular regurgitation (PVR), 11.4 had mild PVR, and 1.5% had moderate PVR.
• NYHA classification improved from baseline to 30 days in 81% of patients. At 30 days, 93% of participants were NYHA class I or II.
Turning to echocardiographic findings, the mean gradient improved from a mean baseline of 31.8 mm Hg to 12.6 mm Hg, while the effective orifice area rose from 1.0 to 1.5 cm2. The magnitude of both improvements was greater for patients with stenosis as their mode of valve failure.
“With the Evolut R, we aim for higher implantations – not more than about 4 mm below the ring – because going deeper could bring about higher gradients and functional deterioration later on,” the cardiologist explained.
The 1-year primary efficacy endpoint – lack of significant aortic stenosis as defined by a mean gradient less than 40 mm Hg – will be reported soon. The VIVA study is sponsored by Medtronic. Dr. Kornowski reported serving as a consultant to the company.
PARIS – Transcatheter aortic valve replacement using the self-expanding Evolut R device in high-surgical-risk patients with failing surgical aortic bioprostheses showed promising 30-day safety and effectiveness results in the ongoing VIVA study, Ran Kornowski, MD, reported at the annual congress of the European Association of Percutaneous Cardiovascular Interventions.
“We had a lot of patients with small, failing valves in this study. Despite this, our valve gradients postprocedure were very, very low. This means to me that this platform is very well suited to deal with valve-in-valve procedures in general and with small bioprosthetic valves in particular,” observed Dr. Kornowski, chairman of the department of cardiology at Rabin Medical Center in Petah Tikva, Israel, and president of the Israel Heart Society.
The participants’ last surgical aortic valve replacement had been a mean of 9.3 years earlier. Seventy-one percent of subjects were New York Heart Association class III or IV. The mode of bioprosthetic failure was stenosis in 56% of cases, regurgitation in 23%, and both in the remainder. Ninety-three percent of their failing biosprothetic valves were stented devices. Forty-one percent of the devices were up to 21 mm and another 33% were more than 21 but less than 25 mm.
TAVR procedural access was by the iliofemoral route in 97% of cases. Local anesthesia was used in 42% of cases and conscious sedation in 35%. Fourteen percent of patients underwent preimplantation valvuloplasty; 21% postimplantation valvuloplasty. The procedural success rate was 98.5%.
The primary safety endpoint was 30-day cardiovascular mortality. The 2.0% rate was far lower than the prespecified cutoff which defined a positive outcome as less than a 10% rate in this high-surgical-risk population.
Other key 30-day outcomes:
• All-cause mortality occurred in 2.5% of patients.
• The 30-day stroke rate was 3%, with no disabling strokes.
• Major vascular complications occurred in 6.5% of the VIVA patients.
• Major bleeding occurred in 7%, minor bleeding in 7.9%. There were no cases of life-threatening bleeding.
• The incidence of Stage I acute kidney injury was rare, at 0.5%.
• Seven percent of patients received a permanent pacemaker.
• Eighty-seven percent of patients had no postprocedure paravalvular regurgitation (PVR), 11.4 had mild PVR, and 1.5% had moderate PVR.
• NYHA classification improved from baseline to 30 days in 81% of patients. At 30 days, 93% of participants were NYHA class I or II.
Turning to echocardiographic findings, the mean gradient improved from a mean baseline of 31.8 mm Hg to 12.6 mm Hg, while the effective orifice area rose from 1.0 to 1.5 cm2. The magnitude of both improvements was greater for patients with stenosis as their mode of valve failure.
“With the Evolut R, we aim for higher implantations – not more than about 4 mm below the ring – because going deeper could bring about higher gradients and functional deterioration later on,” the cardiologist explained.
The 1-year primary efficacy endpoint – lack of significant aortic stenosis as defined by a mean gradient less than 40 mm Hg – will be reported soon. The VIVA study is sponsored by Medtronic. Dr. Kornowski reported serving as a consultant to the company.
AT EuroPCR
Key clinical point:
Major finding: The 30-day cardiovascular mortality rate after transcatheter aortic valve replacement via a valve-in-valve procedure in patients with a failing surgically implanted bioprosthesis was 2%, compared with a projected rate of at least 10% with redo surgery.
Data source: VIVA, a prospective observational registry of 202 high-surgical-risk patients at 23 centers in four countries who underwent valve-in-valve transcatheter aortic valve replacement because of a failing surgically implanted aortic bioprosthesis.
Disclosures: VIVA is sponsored by Medtronic. The presenter reported serving as a consultant to the company.
Bailout stenting for coronary bifurcations brings ‘unacceptable’ hazards
PARIS – Bailout stenting during percutaneous coronary intervention for coronary bifurcations doubled the risk of major adverse cardiovascular events in the world’s largest registry of patients with these often-challenging lesions treated using bioactive stents, Marco Zimarino, MD, reported at the annual congress of the European Association of Percutaneous Cardiovascular Interventions.
Indeed, resort to bailout stenting stood out as the major potentially modifiable risk factor for adverse outcomes among the 4,306 participants in the P2BiTO registry, an international collaboration supported by members of the EuroBifurcation Club. Most of the other independent risk factors identified in a multivariate regression analysis of the P2BiTO database were beyond operator control, including diabetes, advanced age, and presentation with an acute coronary syndrome, according to Dr. Zimarino of the University of Chieti (Italy).

Bailout stenting is largely avoidable through meticulous procedural planning, the interventional cardiologist added.
“Careful planning is always mandatory because bailout stenting is associated with an unacceptably higher risk of both in-hospital and 1-year adverse outcomes,” Dr. Zimarino emphasized. “It’s much better to leave a degraded side branch instead of using bailout stenting to get an excellent angiographic outcome that’s a predictor of a worse clinical outcome.”
Conventional wisdom holds that single stenting of either the main artery or a side branch in a patient with coronary bifurcation is safer than double stenting of both. However, that wasn’t really borne out in the P2BiTO registry provided the operator’s plan was for double stenting. The difference in 1-year major adverse cardiovascular events (MACE) between patients treated using a single- or double-stenting strategy wasn’t statistically significant, provided bailout stenting wasn’t utilized. If bailout stenting was employed, though, the risk of MACE was 2.2-fold greater than if the cardiologist stuck with the plan.
Ninety-eight percent of patients in the P2BiTO registry received drug-eluting stents. The other 2% got the Absorb bioabsorbable vascular scaffold. The percutaneous coronary intervention access site, treatment strategy, choice of stent, and duration of dual-antiplatelet therapy were left up to the operator’s discretion.
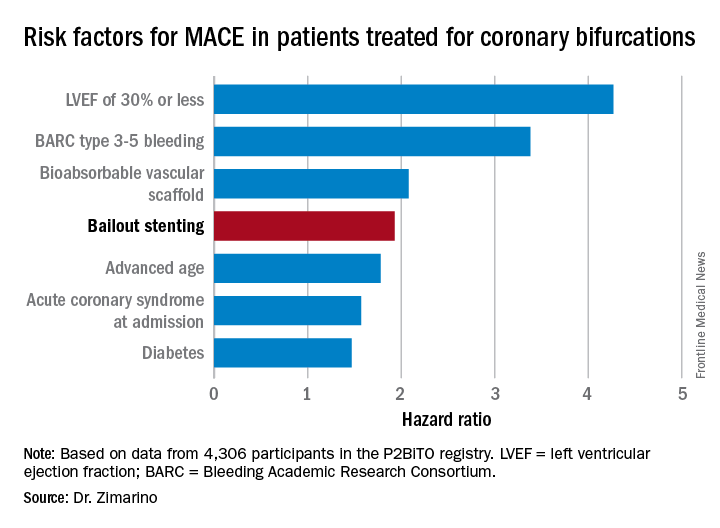
The risk of MACE was reduced by 39% in patients on dual-antiplatelet therapy for 6-12 months, compared with less than 6 months.
Discussant Graham Cassel, MD, director of the heart transplant unit at Milpark Hospital in Johannesburg, commented, “The message comes through very clearly that, if you plan your procedure well, the chance of bailout is far less – and if you do have to bail out, the results are uniformly bad. If you can avoid putting in two or three stents, that’s beneficial.”
Dr. Zimarino reported having no financial conflicts of interest regarding his presentation.

PARIS – Bailout stenting during percutaneous coronary intervention for coronary bifurcations doubled the risk of major adverse cardiovascular events in the world’s largest registry of patients with these often-challenging lesions treated using bioactive stents, Marco Zimarino, MD, reported at the annual congress of the European Association of Percutaneous Cardiovascular Interventions.
Indeed, resort to bailout stenting stood out as the major potentially modifiable risk factor for adverse outcomes among the 4,306 participants in the P2BiTO registry, an international collaboration supported by members of the EuroBifurcation Club. Most of the other independent risk factors identified in a multivariate regression analysis of the P2BiTO database were beyond operator control, including diabetes, advanced age, and presentation with an acute coronary syndrome, according to Dr. Zimarino of the University of Chieti (Italy).
Bailout stenting is largely avoidable through meticulous procedural planning, the interventional cardiologist added.
“Careful planning is always mandatory because bailout stenting is associated with an unacceptably higher risk of both in-hospital and 1-year adverse outcomes,” Dr. Zimarino emphasized. “It’s much better to leave a degraded side branch instead of using bailout stenting to get an excellent angiographic outcome that’s a predictor of a worse clinical outcome.”
Conventional wisdom holds that single stenting of either the main artery or a side branch in a patient with coronary bifurcation is safer than double stenting of both. However, that wasn’t really borne out in the P2BiTO registry provided the operator’s plan was for double stenting. The difference in 1-year major adverse cardiovascular events (MACE) between patients treated using a single- or double-stenting strategy wasn’t statistically significant, provided bailout stenting wasn’t utilized. If bailout stenting was employed, though, the risk of MACE was 2.2-fold greater than if the cardiologist stuck with the plan.
Ninety-eight percent of patients in the P2BiTO registry received drug-eluting stents. The other 2% got the Absorb bioabsorbable vascular scaffold. The percutaneous coronary intervention access site, treatment strategy, choice of stent, and duration of dual-antiplatelet therapy were left up to the operator’s discretion.
The risk of MACE was reduced by 39% in patients on dual-antiplatelet therapy for 6-12 months, compared with less than 6 months.
Discussant Graham Cassel, MD, director of the heart transplant unit at Milpark Hospital in Johannesburg, commented, “The message comes through very clearly that, if you plan your procedure well, the chance of bailout is far less – and if you do have to bail out, the results are uniformly bad. If you can avoid putting in two or three stents, that’s beneficial.”
Dr. Zimarino reported having no financial conflicts of interest regarding his presentation.
PARIS – Bailout stenting during percutaneous coronary intervention for coronary bifurcations doubled the risk of major adverse cardiovascular events in the world’s largest registry of patients with these often-challenging lesions treated using bioactive stents, Marco Zimarino, MD, reported at the annual congress of the European Association of Percutaneous Cardiovascular Interventions.
Indeed, resort to bailout stenting stood out as the major potentially modifiable risk factor for adverse outcomes among the 4,306 participants in the P2BiTO registry, an international collaboration supported by members of the EuroBifurcation Club. Most of the other independent risk factors identified in a multivariate regression analysis of the P2BiTO database were beyond operator control, including diabetes, advanced age, and presentation with an acute coronary syndrome, according to Dr. Zimarino of the University of Chieti (Italy).
Bailout stenting is largely avoidable through meticulous procedural planning, the interventional cardiologist added.
“Careful planning is always mandatory because bailout stenting is associated with an unacceptably higher risk of both in-hospital and 1-year adverse outcomes,” Dr. Zimarino emphasized. “It’s much better to leave a degraded side branch instead of using bailout stenting to get an excellent angiographic outcome that’s a predictor of a worse clinical outcome.”
Conventional wisdom holds that single stenting of either the main artery or a side branch in a patient with coronary bifurcation is safer than double stenting of both. However, that wasn’t really borne out in the P2BiTO registry provided the operator’s plan was for double stenting. The difference in 1-year major adverse cardiovascular events (MACE) between patients treated using a single- or double-stenting strategy wasn’t statistically significant, provided bailout stenting wasn’t utilized. If bailout stenting was employed, though, the risk of MACE was 2.2-fold greater than if the cardiologist stuck with the plan.
Ninety-eight percent of patients in the P2BiTO registry received drug-eluting stents. The other 2% got the Absorb bioabsorbable vascular scaffold. The percutaneous coronary intervention access site, treatment strategy, choice of stent, and duration of dual-antiplatelet therapy were left up to the operator’s discretion.
The risk of MACE was reduced by 39% in patients on dual-antiplatelet therapy for 6-12 months, compared with less than 6 months.
Discussant Graham Cassel, MD, director of the heart transplant unit at Milpark Hospital in Johannesburg, commented, “The message comes through very clearly that, if you plan your procedure well, the chance of bailout is far less – and if you do have to bail out, the results are uniformly bad. If you can avoid putting in two or three stents, that’s beneficial.”
Dr. Zimarino reported having no financial conflicts of interest regarding his presentation.
AT EUROPCR
Key clinical point:
Major finding: Bailout stenting during PCI for coronary bifurcations doubles the risk of major adverse cardiovascular events.
Data source: The P2BiTO registry includes 4,306 patients who received one or more drug-eluting stents or bioabsorbable vascular scaffolds for treatment of coronary bifurcations.
Disclosures: The study presenter reported having no financial conflicts of interest.
Revascularization of CTOs improves health status more than medical therapy
PARIS – The first randomized clinical trial to evaluate quality of life and clinical symptoms as the primary efficacy outcome in patients with coronary chronic total occlusion (CTO) showed a clear advantage for percutaneous revascularization over optimal medical therapy.
At 12 months’ follow-up in the 26-site, 396-patient EuroCTO trial, patients randomized to PCI with drug-eluting stents had significantly less angina and physical limitations coupled with greater improvement in quality of life than the optimal medical therapy (OMT) group on subscales of the Seattle Angina Questionnaire. On the angina frequency subscale, for example, the PCI group improved from a mean baseline score of 77.2 to 91.4 at 12 months, a significantly better result than the OMT group improvement from 80.6 to 87.5.
The PCI group also experienced greater mobility, better activity status, and less pain and discomfort as assessed by the EuroQOL five dimensions questionnaire (EQ-5D), Gerald S. Werner, MD, reported at the annual congress of the European Association of Percutaneous Cardiovascular Interventions.
“PCI of a CTO should be considered as a primary option in symptomatic patients. It is a safe and effective treatment option in expert hands,” said Dr. Werner, director of cardiology and nonsurgical intensive care at the Darmstadt (Ger.) Clinic.
He emphasized the point about “expert hands,” drawing attention to the stellar 86.3% successful revascularization rate in the EuroCTO trial, even though these were often complex procedures. Indeed, in 36% of the CTO PCIs, a retrograde approach was used.
“CTO is a special field. Just like not everybody in every hospital will do a transcatheter aortic valve replacement, not everybody should do a CTO. It can be done safely and to the benefit of the patient, but it needs to be done by someone with expertise,” the cardiologist said.
Study participants were evenly split between those with single- and multivessel disease. Patients with additional nonocclusive disease had those lesions treated by PCI before the 2:1 randomization to CTO PCI or OMT.
The periprocedural complication rate was low at 2.9%, a figure that included a 1.5% incidence of pericardial tamponade as well as vascular repairs. There were no periprocedural MIs or deaths. The 1-year major adverse cardiac event rate was roughly 6% in both study arms.
The PCI group received 6-12 months of dual-antiplatelet therapy with clopidogrel and aspirin. So did roughly 40% of the OMT group because of prior PCI.
Both study arms had comparably high rates of guideline-directed medical therapy, including statins, beta-blockers, and ACE inhibitors. However, the PCI group made significantly less use of nitrates than the OMT group during follow-up, reflecting their greater reduction in angina frequency. The crossover rate from OMT to PCI because of ongoing angina was 7.3%.
The long-term safety and durability of the two treatment strategies will be assessed at 3 years of follow-up.
The EuroCTO trial was originally planned for 600 patients. The investigators eventually settled for less because of slow enrollment. Many interventionalists who are skilled in treating CTOs proved reluctant to randomize the patients.
Dr. Werner contrasted the positive EuroCTO findings regarding clinical symptoms and quality of life to the negative results of the Korean DECISION CTO trial presented at the 2017 meeting of the American College of Cardiology. DECISION CTO found that PCI plus OMT wasn’t superior to OMT alone in reducing MI and other major adverse cardiac events in patients with at least one CTO. In Dr. Werner’s view, the Korean investigators chose the wrong endpoint.
“The quality of life improvement we’ve shown after PCI in EuroCTO is a valid clinical goal in treating stable coronary artery disease. I don’t think we can aim at improving prognosis,” according to Dr. Werner.
The impetus for EuroCTO was a recognition that CTOs are common and seriously undertreated. CTOs account for 16%-18% of all coronary lesions in patients with stable coronary artery disease, yet U.S. national data indicate only 5% of PCIs are performed to treat CTOs.
The EuroCTO trial was sponsored by the Euro CTO Club and supported by research grants from Biosensors and Asahi.
PARIS – The first randomized clinical trial to evaluate quality of life and clinical symptoms as the primary efficacy outcome in patients with coronary chronic total occlusion (CTO) showed a clear advantage for percutaneous revascularization over optimal medical therapy.
At 12 months’ follow-up in the 26-site, 396-patient EuroCTO trial, patients randomized to PCI with drug-eluting stents had significantly less angina and physical limitations coupled with greater improvement in quality of life than the optimal medical therapy (OMT) group on subscales of the Seattle Angina Questionnaire. On the angina frequency subscale, for example, the PCI group improved from a mean baseline score of 77.2 to 91.4 at 12 months, a significantly better result than the OMT group improvement from 80.6 to 87.5.
The PCI group also experienced greater mobility, better activity status, and less pain and discomfort as assessed by the EuroQOL five dimensions questionnaire (EQ-5D), Gerald S. Werner, MD, reported at the annual congress of the European Association of Percutaneous Cardiovascular Interventions.
“PCI of a CTO should be considered as a primary option in symptomatic patients. It is a safe and effective treatment option in expert hands,” said Dr. Werner, director of cardiology and nonsurgical intensive care at the Darmstadt (Ger.) Clinic.
He emphasized the point about “expert hands,” drawing attention to the stellar 86.3% successful revascularization rate in the EuroCTO trial, even though these were often complex procedures. Indeed, in 36% of the CTO PCIs, a retrograde approach was used.
“CTO is a special field. Just like not everybody in every hospital will do a transcatheter aortic valve replacement, not everybody should do a CTO. It can be done safely and to the benefit of the patient, but it needs to be done by someone with expertise,” the cardiologist said.
Study participants were evenly split between those with single- and multivessel disease. Patients with additional nonocclusive disease had those lesions treated by PCI before the 2:1 randomization to CTO PCI or OMT.
The periprocedural complication rate was low at 2.9%, a figure that included a 1.5% incidence of pericardial tamponade as well as vascular repairs. There were no periprocedural MIs or deaths. The 1-year major adverse cardiac event rate was roughly 6% in both study arms.
The PCI group received 6-12 months of dual-antiplatelet therapy with clopidogrel and aspirin. So did roughly 40% of the OMT group because of prior PCI.
Both study arms had comparably high rates of guideline-directed medical therapy, including statins, beta-blockers, and ACE inhibitors. However, the PCI group made significantly less use of nitrates than the OMT group during follow-up, reflecting their greater reduction in angina frequency. The crossover rate from OMT to PCI because of ongoing angina was 7.3%.
The long-term safety and durability of the two treatment strategies will be assessed at 3 years of follow-up.
The EuroCTO trial was originally planned for 600 patients. The investigators eventually settled for less because of slow enrollment. Many interventionalists who are skilled in treating CTOs proved reluctant to randomize the patients.
Dr. Werner contrasted the positive EuroCTO findings regarding clinical symptoms and quality of life to the negative results of the Korean DECISION CTO trial presented at the 2017 meeting of the American College of Cardiology. DECISION CTO found that PCI plus OMT wasn’t superior to OMT alone in reducing MI and other major adverse cardiac events in patients with at least one CTO. In Dr. Werner’s view, the Korean investigators chose the wrong endpoint.
“The quality of life improvement we’ve shown after PCI in EuroCTO is a valid clinical goal in treating stable coronary artery disease. I don’t think we can aim at improving prognosis,” according to Dr. Werner.
The impetus for EuroCTO was a recognition that CTOs are common and seriously undertreated. CTOs account for 16%-18% of all coronary lesions in patients with stable coronary artery disease, yet U.S. national data indicate only 5% of PCIs are performed to treat CTOs.
The EuroCTO trial was sponsored by the Euro CTO Club and supported by research grants from Biosensors and Asahi.
PARIS – The first randomized clinical trial to evaluate quality of life and clinical symptoms as the primary efficacy outcome in patients with coronary chronic total occlusion (CTO) showed a clear advantage for percutaneous revascularization over optimal medical therapy.
At 12 months’ follow-up in the 26-site, 396-patient EuroCTO trial, patients randomized to PCI with drug-eluting stents had significantly less angina and physical limitations coupled with greater improvement in quality of life than the optimal medical therapy (OMT) group on subscales of the Seattle Angina Questionnaire. On the angina frequency subscale, for example, the PCI group improved from a mean baseline score of 77.2 to 91.4 at 12 months, a significantly better result than the OMT group improvement from 80.6 to 87.5.
The PCI group also experienced greater mobility, better activity status, and less pain and discomfort as assessed by the EuroQOL five dimensions questionnaire (EQ-5D), Gerald S. Werner, MD, reported at the annual congress of the European Association of Percutaneous Cardiovascular Interventions.
“PCI of a CTO should be considered as a primary option in symptomatic patients. It is a safe and effective treatment option in expert hands,” said Dr. Werner, director of cardiology and nonsurgical intensive care at the Darmstadt (Ger.) Clinic.
He emphasized the point about “expert hands,” drawing attention to the stellar 86.3% successful revascularization rate in the EuroCTO trial, even though these were often complex procedures. Indeed, in 36% of the CTO PCIs, a retrograde approach was used.
“CTO is a special field. Just like not everybody in every hospital will do a transcatheter aortic valve replacement, not everybody should do a CTO. It can be done safely and to the benefit of the patient, but it needs to be done by someone with expertise,” the cardiologist said.
Study participants were evenly split between those with single- and multivessel disease. Patients with additional nonocclusive disease had those lesions treated by PCI before the 2:1 randomization to CTO PCI or OMT.
The periprocedural complication rate was low at 2.9%, a figure that included a 1.5% incidence of pericardial tamponade as well as vascular repairs. There were no periprocedural MIs or deaths. The 1-year major adverse cardiac event rate was roughly 6% in both study arms.
The PCI group received 6-12 months of dual-antiplatelet therapy with clopidogrel and aspirin. So did roughly 40% of the OMT group because of prior PCI.
Both study arms had comparably high rates of guideline-directed medical therapy, including statins, beta-blockers, and ACE inhibitors. However, the PCI group made significantly less use of nitrates than the OMT group during follow-up, reflecting their greater reduction in angina frequency. The crossover rate from OMT to PCI because of ongoing angina was 7.3%.
The long-term safety and durability of the two treatment strategies will be assessed at 3 years of follow-up.
The EuroCTO trial was originally planned for 600 patients. The investigators eventually settled for less because of slow enrollment. Many interventionalists who are skilled in treating CTOs proved reluctant to randomize the patients.
Dr. Werner contrasted the positive EuroCTO findings regarding clinical symptoms and quality of life to the negative results of the Korean DECISION CTO trial presented at the 2017 meeting of the American College of Cardiology. DECISION CTO found that PCI plus OMT wasn’t superior to OMT alone in reducing MI and other major adverse cardiac events in patients with at least one CTO. In Dr. Werner’s view, the Korean investigators chose the wrong endpoint.
“The quality of life improvement we’ve shown after PCI in EuroCTO is a valid clinical goal in treating stable coronary artery disease. I don’t think we can aim at improving prognosis,” according to Dr. Werner.
The impetus for EuroCTO was a recognition that CTOs are common and seriously undertreated. CTOs account for 16%-18% of all coronary lesions in patients with stable coronary artery disease, yet U.S. national data indicate only 5% of PCIs are performed to treat CTOs.
The EuroCTO trial was sponsored by the Euro CTO Club and supported by research grants from Biosensors and Asahi.
AT EUROPCR
Key clinical point:
Major finding: Patients whose chronic total occlusions were treated by PCI rather than optimal medical therapy experienced significantly less angina and greater improvement in quality of life during 12 months of follow-up.
Data source: EuroCTO, a prospective, 26-site study in which 396 patients with coronary chronic total occlusions were randomized 2:1 to PCI or optimal medical therapy.
Disclosures: EuroCTO was sponsored by the Euro CTO Club and supported by research grants from Biosensors and Asahi.