User login
Clinical Edge Journal Scan Commentary: EPI September 2021

Our first study comes out of Sheffield, UK, and Halle, Germany, and looks at the correlation between sarcopenia and EPI (Jalal et al). Notably sarcopenia, or reduction in muscle mass, is a known complication of malnutrition and conditions like EPI. It has traditionally been difficult to diagnose because traditional methods have suffered from low accuracy (i.e., mid-arm circumference). In recent years, commercially available software has been developed to digitally assess skeletal muscle mass on axial CT imaging. Digital imaging allows for granular assessments of metrics such as myosteatosis and sacropenic obesity, both of which remained relatively elusive metrics in prior ways of assessing sarcopenia.
In this study, researchers postulate that, since CT scans are recently performed in the evaluation of those patients with suspected pancreatic pathology, it would be natural to assess for sarcopenia on said CT imaging. Identifying sarcopenia might allow clinicians to identify those patients with or at risk for EPI.
Patients referred to EUS for suspected pancreatic pathology were included in the study (except those found to have pancreatic cancer). This prospective study included 102 patients with suspected or proven benign pancreatic pathology, chronic pancreatitis, or recurrent pancreatic type pain. Fecal elastase testing was used to determine those with EPI, and digital CT analysis was used to recognize patients with sarcopenia.
Overall, EPI was present in 45.1% of patients. The prevalence of sarcopenia (67.4% vs. 37.55%; P < .003), myosteatosis (52.2% vs. 10.7%; P = .046), and sarcopenic obesity (66.7% vs. 24.3%; P = .002) was significantly higher in patients with vs without EPI. Sarcopenia (odds ratio [OR], 4.8; P = .02) was strongly associated with EPI. The authors conclude that digital skeletal mass analysis can be performed on patients already undergoing CT scans for suspected pancreatic pathology for possible further diagnosis, risk assessment and to better inform clinical management.
Another notable study came out of Baylor College of Medicine that looked at the clinical significance of fatty pancreas (FP) (Krill et al). Diffuse echogenicity of the pancreas is a common finding on endoscopic ultrasound (EUS), but of unknown clinical significance. Krill’s group aimed to determine if diffuse fatty infiltration of the pancreas had any clinical implication on pancreatic function. They conducted a retrospective case-control study comparing adult patients with diffuse echogenicity of the pancreas to those without known pancreatic disease with chronic diarrhea. Notably, the incidence of EPI (47% vs. 6%) and chronic pancreatitis (18% vs. 0%) was significantly higher (both P < .001) in the fatty pancreas group vs. the control group.
The authors conclude “Our findings suggest that FP may not merely be a benign sonographic finding, but rather imply underlying parenchymal dysfunction, such as that seen when fat deposition occurs in the liver (i.e., nonalcoholic fatty liver disease).” Additionally the paper states that recent literature has found an association between fatty pancreas and increasing body mass index (BMI), hyperlipidemia, insulin resistance, and metabolic syndrome. Perhaps we will further appreciate the likely prominent and under-appreciated role of metabolic syndrome in the development of acute and chronic pancreatitis.
References:
Jalal M, Rosendahl J, Campbell JA, Vinayagam R, Al-Mukhtar A, Hopper AD. Identification of “digital sarcopenia” can aid the detection of pancreatic exocrine insufficiency and malnutrition assessment in patients with suspected pancreatic pathology. Dig Dis 2021 (Jun 8), (in press).
Krill JT, Szafron D, Elhanafi S, et al. Endoscopic ultrasound finding of diffuse echogenicity in the pancreas, is it relevant? Dig Dis Sci 2021 (Aug 4), (in press).
Our first study comes out of Sheffield, UK, and Halle, Germany, and looks at the correlation between sarcopenia and EPI (Jalal et al). Notably sarcopenia, or reduction in muscle mass, is a known complication of malnutrition and conditions like EPI. It has traditionally been difficult to diagnose because traditional methods have suffered from low accuracy (i.e., mid-arm circumference). In recent years, commercially available software has been developed to digitally assess skeletal muscle mass on axial CT imaging. Digital imaging allows for granular assessments of metrics such as myosteatosis and sacropenic obesity, both of which remained relatively elusive metrics in prior ways of assessing sarcopenia.
In this study, researchers postulate that, since CT scans are recently performed in the evaluation of those patients with suspected pancreatic pathology, it would be natural to assess for sarcopenia on said CT imaging. Identifying sarcopenia might allow clinicians to identify those patients with or at risk for EPI.
Patients referred to EUS for suspected pancreatic pathology were included in the study (except those found to have pancreatic cancer). This prospective study included 102 patients with suspected or proven benign pancreatic pathology, chronic pancreatitis, or recurrent pancreatic type pain. Fecal elastase testing was used to determine those with EPI, and digital CT analysis was used to recognize patients with sarcopenia.
Overall, EPI was present in 45.1% of patients. The prevalence of sarcopenia (67.4% vs. 37.55%; P < .003), myosteatosis (52.2% vs. 10.7%; P = .046), and sarcopenic obesity (66.7% vs. 24.3%; P = .002) was significantly higher in patients with vs without EPI. Sarcopenia (odds ratio [OR], 4.8; P = .02) was strongly associated with EPI. The authors conclude that digital skeletal mass analysis can be performed on patients already undergoing CT scans for suspected pancreatic pathology for possible further diagnosis, risk assessment and to better inform clinical management.
Another notable study came out of Baylor College of Medicine that looked at the clinical significance of fatty pancreas (FP) (Krill et al). Diffuse echogenicity of the pancreas is a common finding on endoscopic ultrasound (EUS), but of unknown clinical significance. Krill’s group aimed to determine if diffuse fatty infiltration of the pancreas had any clinical implication on pancreatic function. They conducted a retrospective case-control study comparing adult patients with diffuse echogenicity of the pancreas to those without known pancreatic disease with chronic diarrhea. Notably, the incidence of EPI (47% vs. 6%) and chronic pancreatitis (18% vs. 0%) was significantly higher (both P < .001) in the fatty pancreas group vs. the control group.
The authors conclude “Our findings suggest that FP may not merely be a benign sonographic finding, but rather imply underlying parenchymal dysfunction, such as that seen when fat deposition occurs in the liver (i.e., nonalcoholic fatty liver disease).” Additionally the paper states that recent literature has found an association between fatty pancreas and increasing body mass index (BMI), hyperlipidemia, insulin resistance, and metabolic syndrome. Perhaps we will further appreciate the likely prominent and under-appreciated role of metabolic syndrome in the development of acute and chronic pancreatitis.
References:
Jalal M, Rosendahl J, Campbell JA, Vinayagam R, Al-Mukhtar A, Hopper AD. Identification of “digital sarcopenia” can aid the detection of pancreatic exocrine insufficiency and malnutrition assessment in patients with suspected pancreatic pathology. Dig Dis 2021 (Jun 8), (in press).
Krill JT, Szafron D, Elhanafi S, et al. Endoscopic ultrasound finding of diffuse echogenicity in the pancreas, is it relevant? Dig Dis Sci 2021 (Aug 4), (in press).
Our first study comes out of Sheffield, UK, and Halle, Germany, and looks at the correlation between sarcopenia and EPI (Jalal et al). Notably sarcopenia, or reduction in muscle mass, is a known complication of malnutrition and conditions like EPI. It has traditionally been difficult to diagnose because traditional methods have suffered from low accuracy (i.e., mid-arm circumference). In recent years, commercially available software has been developed to digitally assess skeletal muscle mass on axial CT imaging. Digital imaging allows for granular assessments of metrics such as myosteatosis and sacropenic obesity, both of which remained relatively elusive metrics in prior ways of assessing sarcopenia.
In this study, researchers postulate that, since CT scans are recently performed in the evaluation of those patients with suspected pancreatic pathology, it would be natural to assess for sarcopenia on said CT imaging. Identifying sarcopenia might allow clinicians to identify those patients with or at risk for EPI.
Patients referred to EUS for suspected pancreatic pathology were included in the study (except those found to have pancreatic cancer). This prospective study included 102 patients with suspected or proven benign pancreatic pathology, chronic pancreatitis, or recurrent pancreatic type pain. Fecal elastase testing was used to determine those with EPI, and digital CT analysis was used to recognize patients with sarcopenia.
Overall, EPI was present in 45.1% of patients. The prevalence of sarcopenia (67.4% vs. 37.55%; P < .003), myosteatosis (52.2% vs. 10.7%; P = .046), and sarcopenic obesity (66.7% vs. 24.3%; P = .002) was significantly higher in patients with vs without EPI. Sarcopenia (odds ratio [OR], 4.8; P = .02) was strongly associated with EPI. The authors conclude that digital skeletal mass analysis can be performed on patients already undergoing CT scans for suspected pancreatic pathology for possible further diagnosis, risk assessment and to better inform clinical management.
Another notable study came out of Baylor College of Medicine that looked at the clinical significance of fatty pancreas (FP) (Krill et al). Diffuse echogenicity of the pancreas is a common finding on endoscopic ultrasound (EUS), but of unknown clinical significance. Krill’s group aimed to determine if diffuse fatty infiltration of the pancreas had any clinical implication on pancreatic function. They conducted a retrospective case-control study comparing adult patients with diffuse echogenicity of the pancreas to those without known pancreatic disease with chronic diarrhea. Notably, the incidence of EPI (47% vs. 6%) and chronic pancreatitis (18% vs. 0%) was significantly higher (both P < .001) in the fatty pancreas group vs. the control group.
The authors conclude “Our findings suggest that FP may not merely be a benign sonographic finding, but rather imply underlying parenchymal dysfunction, such as that seen when fat deposition occurs in the liver (i.e., nonalcoholic fatty liver disease).” Additionally the paper states that recent literature has found an association between fatty pancreas and increasing body mass index (BMI), hyperlipidemia, insulin resistance, and metabolic syndrome. Perhaps we will further appreciate the likely prominent and under-appreciated role of metabolic syndrome in the development of acute and chronic pancreatitis.
References:
Jalal M, Rosendahl J, Campbell JA, Vinayagam R, Al-Mukhtar A, Hopper AD. Identification of “digital sarcopenia” can aid the detection of pancreatic exocrine insufficiency and malnutrition assessment in patients with suspected pancreatic pathology. Dig Dis 2021 (Jun 8), (in press).
Krill JT, Szafron D, Elhanafi S, et al. Endoscopic ultrasound finding of diffuse echogenicity in the pancreas, is it relevant? Dig Dis Sci 2021 (Aug 4), (in press).
Clinical Edge Journal Scan Commentary: PsA September 2021

Identifying risk factors for onset of Psoriatic Arthritis (PsA) is a major unmet need. Comparing potential risk factors for the diagnosis of PsA, rheumatoid arthritis (RA), and ankylosing spondylitis (AS) is of interest. Such studies may help us identify shared and unique risk factors of onset of chronic inflammatory arthritis. Meer E et al compared potential risk factors for the diagnosis of PsA, psoriasis, RA, and AS. They conducted four parallel case-control studies using data collected between 1994 and 2015 in The Health Improvement Network, an anonymized longitudinal patient dataset collected at primary care clinics throughout the United Kingdom. PsA was associated with obesity, pharyngitis, skin infections, moderate alcohol intake, gout, and uveitis. As expected, PsA and AS were associated with uveitis. Interestingly, PsA and RA were associated with preceding gout. Smoking was a risk factor for all disease and statin use was inversely associated with all 4 diseases. This study has identified potential risk factors for inflammatory diseases including PsA and may help in early identification as well as risk mitigation.
Most patients develop psoriatic arthritis (PsA) after or simultaneously with cutaneous psoriasis. The mechanisms underlying progression from cutaneous psoriasis to arthritis psoriasis are currently unclear. An important question is whether modern targeted treatment of cutaneous psoriasis reduces the risk of developing PsA. To address this, Acosta Felquer ML et al conducted a retrospective cohort study to compare the incidence of PsA in 1719 patients with psoriasis (14,721 patient/years of follow up) grouped according to different treatments for their skin psoriasis: topicals, phototherapy or no treatment (n= 1387), conventional disease-modifying antirheumatic drugs (cDMARDs) or biological DMARDs (bDMARDs). During follow-up, 239 patients (14%) developed PsA. The risk of developing PsA in patients treated with bDMARDs was significantly lower (incidence rate ratio (IRR)=0.26; 95% CI 0.03 to 0.94), compared with topicals, but not compared with cDMARDs (IRR=0.35; 95% CI 0.035 to 1.96). Male sex, nail involvement and higher body mass index were associated with increased risk of developing PsA, while bDMARD use was protective. Thus, this study provides some evidence that systemic treatment might ‘protect’ against development if PsA. Appropriately designed prospective studies are required.
One important clinical question is whether patients with oligoarthritis (involvement of <5 joints) progress to polyarthritis. In an observational study Gladman DD et al reported that in 407 patients evaluated within 12 months of diagnosis, 192 (47%) presented with oligoarthritis. More patients with polyarthritis presented with dactylitis, enthesitis, higher HAQ and lower SF-36 scores. Of the 192 patients with oligoarthritis, 75 (39%) progressed to polyarthritis. Lower SF-36 mental component summary score was the predictor for progressing to polyarthritis. Thus, except for the burden of musculoskeletal involvement, oligoarticular PsA resembles polyarticular PsA and therefore the two PsA subclasses should simply be classified together as peripheral arthritis.
Identifying risk factors for onset of Psoriatic Arthritis (PsA) is a major unmet need. Comparing potential risk factors for the diagnosis of PsA, rheumatoid arthritis (RA), and ankylosing spondylitis (AS) is of interest. Such studies may help us identify shared and unique risk factors of onset of chronic inflammatory arthritis. Meer E et al compared potential risk factors for the diagnosis of PsA, psoriasis, RA, and AS. They conducted four parallel case-control studies using data collected between 1994 and 2015 in The Health Improvement Network, an anonymized longitudinal patient dataset collected at primary care clinics throughout the United Kingdom. PsA was associated with obesity, pharyngitis, skin infections, moderate alcohol intake, gout, and uveitis. As expected, PsA and AS were associated with uveitis. Interestingly, PsA and RA were associated with preceding gout. Smoking was a risk factor for all disease and statin use was inversely associated with all 4 diseases. This study has identified potential risk factors for inflammatory diseases including PsA and may help in early identification as well as risk mitigation.
Most patients develop psoriatic arthritis (PsA) after or simultaneously with cutaneous psoriasis. The mechanisms underlying progression from cutaneous psoriasis to arthritis psoriasis are currently unclear. An important question is whether modern targeted treatment of cutaneous psoriasis reduces the risk of developing PsA. To address this, Acosta Felquer ML et al conducted a retrospective cohort study to compare the incidence of PsA in 1719 patients with psoriasis (14,721 patient/years of follow up) grouped according to different treatments for their skin psoriasis: topicals, phototherapy or no treatment (n= 1387), conventional disease-modifying antirheumatic drugs (cDMARDs) or biological DMARDs (bDMARDs). During follow-up, 239 patients (14%) developed PsA. The risk of developing PsA in patients treated with bDMARDs was significantly lower (incidence rate ratio (IRR)=0.26; 95% CI 0.03 to 0.94), compared with topicals, but not compared with cDMARDs (IRR=0.35; 95% CI 0.035 to 1.96). Male sex, nail involvement and higher body mass index were associated with increased risk of developing PsA, while bDMARD use was protective. Thus, this study provides some evidence that systemic treatment might ‘protect’ against development if PsA. Appropriately designed prospective studies are required.
One important clinical question is whether patients with oligoarthritis (involvement of <5 joints) progress to polyarthritis. In an observational study Gladman DD et al reported that in 407 patients evaluated within 12 months of diagnosis, 192 (47%) presented with oligoarthritis. More patients with polyarthritis presented with dactylitis, enthesitis, higher HAQ and lower SF-36 scores. Of the 192 patients with oligoarthritis, 75 (39%) progressed to polyarthritis. Lower SF-36 mental component summary score was the predictor for progressing to polyarthritis. Thus, except for the burden of musculoskeletal involvement, oligoarticular PsA resembles polyarticular PsA and therefore the two PsA subclasses should simply be classified together as peripheral arthritis.
Identifying risk factors for onset of Psoriatic Arthritis (PsA) is a major unmet need. Comparing potential risk factors for the diagnosis of PsA, rheumatoid arthritis (RA), and ankylosing spondylitis (AS) is of interest. Such studies may help us identify shared and unique risk factors of onset of chronic inflammatory arthritis. Meer E et al compared potential risk factors for the diagnosis of PsA, psoriasis, RA, and AS. They conducted four parallel case-control studies using data collected between 1994 and 2015 in The Health Improvement Network, an anonymized longitudinal patient dataset collected at primary care clinics throughout the United Kingdom. PsA was associated with obesity, pharyngitis, skin infections, moderate alcohol intake, gout, and uveitis. As expected, PsA and AS were associated with uveitis. Interestingly, PsA and RA were associated with preceding gout. Smoking was a risk factor for all disease and statin use was inversely associated with all 4 diseases. This study has identified potential risk factors for inflammatory diseases including PsA and may help in early identification as well as risk mitigation.
Most patients develop psoriatic arthritis (PsA) after or simultaneously with cutaneous psoriasis. The mechanisms underlying progression from cutaneous psoriasis to arthritis psoriasis are currently unclear. An important question is whether modern targeted treatment of cutaneous psoriasis reduces the risk of developing PsA. To address this, Acosta Felquer ML et al conducted a retrospective cohort study to compare the incidence of PsA in 1719 patients with psoriasis (14,721 patient/years of follow up) grouped according to different treatments for their skin psoriasis: topicals, phototherapy or no treatment (n= 1387), conventional disease-modifying antirheumatic drugs (cDMARDs) or biological DMARDs (bDMARDs). During follow-up, 239 patients (14%) developed PsA. The risk of developing PsA in patients treated with bDMARDs was significantly lower (incidence rate ratio (IRR)=0.26; 95% CI 0.03 to 0.94), compared with topicals, but not compared with cDMARDs (IRR=0.35; 95% CI 0.035 to 1.96). Male sex, nail involvement and higher body mass index were associated with increased risk of developing PsA, while bDMARD use was protective. Thus, this study provides some evidence that systemic treatment might ‘protect’ against development if PsA. Appropriately designed prospective studies are required.
One important clinical question is whether patients with oligoarthritis (involvement of <5 joints) progress to polyarthritis. In an observational study Gladman DD et al reported that in 407 patients evaluated within 12 months of diagnosis, 192 (47%) presented with oligoarthritis. More patients with polyarthritis presented with dactylitis, enthesitis, higher HAQ and lower SF-36 scores. Of the 192 patients with oligoarthritis, 75 (39%) progressed to polyarthritis. Lower SF-36 mental component summary score was the predictor for progressing to polyarthritis. Thus, except for the burden of musculoskeletal involvement, oligoarticular PsA resembles polyarticular PsA and therefore the two PsA subclasses should simply be classified together as peripheral arthritis.
Clinical Edge Journal Scan Commentary: Uterine Fibroid September 2021

Chiuve et al published a large cohort study in the Journal of Epidemiology and Community Health that evaluated the association between uterine fibroids and diagnosed depression, anxiety and self-directed violence. Women aged 18-50 years with diagnosed uterine fibroids (n=313,754) were identified in the Optum Clinformatics commercial insurance claims database and matched 1:2 on age and calendar time to women without (n=627,539). After adjusting for confounders, women with uterine fibroids had a higher rate of depression, anxiety and self-directed violence then women not diagnosed with fibroids. Among women with pain symptoms and heavy menstrual bleeding, the hazard ratio comparing women with fibroids to women without was 1.21 for depression, 1.18 for anxiety and 1.68 for self-directed violence. Among women with fibroids, those who underwent hysterectomy had higher rates of depression, anxiety and self-directed violence.
A third study by Wesselink et al in Human Reproduction examined ambient air pollution exposure and the risk of developing uterine fibroids. This was a prospective cohort study of 21,998 premenopausal Black women in 56 US metropolitan areas from 1997 to 2011. During the follow up, 28.4% of participants (n=6238) reported uterine fibroid diagnosis by ultrasound or surgery. Increased ozone concentrations were associated with an increased risk of being diagnosed with uterine fibroids, with a stronger association among women less than 35 years of age and parous women. Other pollutants, specifically particulate matter <2.5 microns and nitrogen dioxide, were not associated with an increased risk of uterine fibroids.
Chiuve et al published a large cohort study in the Journal of Epidemiology and Community Health that evaluated the association between uterine fibroids and diagnosed depression, anxiety and self-directed violence. Women aged 18-50 years with diagnosed uterine fibroids (n=313,754) were identified in the Optum Clinformatics commercial insurance claims database and matched 1:2 on age and calendar time to women without (n=627,539). After adjusting for confounders, women with uterine fibroids had a higher rate of depression, anxiety and self-directed violence then women not diagnosed with fibroids. Among women with pain symptoms and heavy menstrual bleeding, the hazard ratio comparing women with fibroids to women without was 1.21 for depression, 1.18 for anxiety and 1.68 for self-directed violence. Among women with fibroids, those who underwent hysterectomy had higher rates of depression, anxiety and self-directed violence.
A third study by Wesselink et al in Human Reproduction examined ambient air pollution exposure and the risk of developing uterine fibroids. This was a prospective cohort study of 21,998 premenopausal Black women in 56 US metropolitan areas from 1997 to 2011. During the follow up, 28.4% of participants (n=6238) reported uterine fibroid diagnosis by ultrasound or surgery. Increased ozone concentrations were associated with an increased risk of being diagnosed with uterine fibroids, with a stronger association among women less than 35 years of age and parous women. Other pollutants, specifically particulate matter <2.5 microns and nitrogen dioxide, were not associated with an increased risk of uterine fibroids.
Chiuve et al published a large cohort study in the Journal of Epidemiology and Community Health that evaluated the association between uterine fibroids and diagnosed depression, anxiety and self-directed violence. Women aged 18-50 years with diagnosed uterine fibroids (n=313,754) were identified in the Optum Clinformatics commercial insurance claims database and matched 1:2 on age and calendar time to women without (n=627,539). After adjusting for confounders, women with uterine fibroids had a higher rate of depression, anxiety and self-directed violence then women not diagnosed with fibroids. Among women with pain symptoms and heavy menstrual bleeding, the hazard ratio comparing women with fibroids to women without was 1.21 for depression, 1.18 for anxiety and 1.68 for self-directed violence. Among women with fibroids, those who underwent hysterectomy had higher rates of depression, anxiety and self-directed violence.
A third study by Wesselink et al in Human Reproduction examined ambient air pollution exposure and the risk of developing uterine fibroids. This was a prospective cohort study of 21,998 premenopausal Black women in 56 US metropolitan areas from 1997 to 2011. During the follow up, 28.4% of participants (n=6238) reported uterine fibroid diagnosis by ultrasound or surgery. Increased ozone concentrations were associated with an increased risk of being diagnosed with uterine fibroids, with a stronger association among women less than 35 years of age and parous women. Other pollutants, specifically particulate matter <2.5 microns and nitrogen dioxide, were not associated with an increased risk of uterine fibroids.
Clinical Edge Journal Scan Commentary: HCC September 2021

Patients with hepatocellular carcinoma (HCC) that has not spread outside the liver have several treatment options available. This month we will review articles that analyze outcomes after liver transplantation, liver resection, as well as radiofrequency ablation.
In HCC patients within the Milan criteria, the 5-year overall survival rate after transplant is about 70%, and the 5-year HCC recurrence rate is about 10%. Patients with tumors beyond the Milan criteria are frequently down staged with locoregional therapies to fall within the Milan criteria. The incidence of HCC recurrence in these patients is around 15.5% at 5 years. In this study, Lee et al demonstrated that statin use substantially reduced the risk of HCC recurrence. In this retrospective analysis of a longitudinal cohort of 430 patients transplanted between September 1995 and December 2019, 323 patients (75.1%) were statin non-users and 107 (24.9%) were statin users. Statin use was defined as at least 90 days of statin therapy, prescribed according to the treatment guidelines for dyslipidemia for primary or secondary prevention of CVD. At a median follow-up of 64.9 months, HCC recurred in 79 patients (18.4%), including 72 (22.3%) in the statin non-user group and 7 (6.5%) in the statin user group. Of those, 61 (77.2%) patients had HCC recurrence that initially presented at extrahepatic site regardless of the presence of intrahepatic tumors. Sixty-three patients (79.7%) had recurrence within 2 years of liver transplantation. The cumulative incidence of HCC recurrence at 2 and 5 years was 18.9% and 22.3% in the statin non-user group, and 3.8% and 5.7% in the statin user group, respectively (P < 0.001).
Liang et al evaluated the importance of tumor size in predicting the likelihood of HCC recurrence following surgical resection. In this retrospective study, a total of 813 cirrhotic patients who underwent curative-intent hepatectomy for solitary HCC without macrovascular invasion between 2001 and 2014 were evaluated. Overall, 464 patients had tumor size ≤ 5 cm, and 349 had tumor size > 5 cm. The 5-year RFS and OS rates were 38.3% and 61.5% in the ≤ 5 cm group, compared with 25.1% and 59.9% in the > 5 cm group. Long-term survival outcomes were significantly worse as tumor size increased. Multivariate analysis indicated that tumor size > 5 cm was an independent risk factor for tumor recurrence and long-term survival.
Finally, Sulaiman et al reported the survival rate of the early and intermediate stage HCC patients who underwent radiofrequency ablation (RFA). In this retrospective analysis, patients with BCLC A and B HCC who underwent RFA treatments between January 2015 to December 2017 were evaluated. Out of 62 patients 46 (74.2%) were reported to have RFA as their only first line of treatment, while 12 (25.8%) were reported to have a combination of RFA and other therapeutic modalities. At a mean follow up of 27 months, the survival rate at 12 and 36 months in patients who received RFA was 82.3% and 57.8%, respectively. A relatively high 36-month survival rate was seen in patients who had a response to RFA compared to the non-response group (100% vs 44.8%, P = 0.021). In terms of prognosis, BCLC staging of liver cancer and response after RFA were significantly associated with survival.
Patients with hepatocellular carcinoma (HCC) that has not spread outside the liver have several treatment options available. This month we will review articles that analyze outcomes after liver transplantation, liver resection, as well as radiofrequency ablation.
In HCC patients within the Milan criteria, the 5-year overall survival rate after transplant is about 70%, and the 5-year HCC recurrence rate is about 10%. Patients with tumors beyond the Milan criteria are frequently down staged with locoregional therapies to fall within the Milan criteria. The incidence of HCC recurrence in these patients is around 15.5% at 5 years. In this study, Lee et al demonstrated that statin use substantially reduced the risk of HCC recurrence. In this retrospective analysis of a longitudinal cohort of 430 patients transplanted between September 1995 and December 2019, 323 patients (75.1%) were statin non-users and 107 (24.9%) were statin users. Statin use was defined as at least 90 days of statin therapy, prescribed according to the treatment guidelines for dyslipidemia for primary or secondary prevention of CVD. At a median follow-up of 64.9 months, HCC recurred in 79 patients (18.4%), including 72 (22.3%) in the statin non-user group and 7 (6.5%) in the statin user group. Of those, 61 (77.2%) patients had HCC recurrence that initially presented at extrahepatic site regardless of the presence of intrahepatic tumors. Sixty-three patients (79.7%) had recurrence within 2 years of liver transplantation. The cumulative incidence of HCC recurrence at 2 and 5 years was 18.9% and 22.3% in the statin non-user group, and 3.8% and 5.7% in the statin user group, respectively (P < 0.001).
Liang et al evaluated the importance of tumor size in predicting the likelihood of HCC recurrence following surgical resection. In this retrospective study, a total of 813 cirrhotic patients who underwent curative-intent hepatectomy for solitary HCC without macrovascular invasion between 2001 and 2014 were evaluated. Overall, 464 patients had tumor size ≤ 5 cm, and 349 had tumor size > 5 cm. The 5-year RFS and OS rates were 38.3% and 61.5% in the ≤ 5 cm group, compared with 25.1% and 59.9% in the > 5 cm group. Long-term survival outcomes were significantly worse as tumor size increased. Multivariate analysis indicated that tumor size > 5 cm was an independent risk factor for tumor recurrence and long-term survival.
Finally, Sulaiman et al reported the survival rate of the early and intermediate stage HCC patients who underwent radiofrequency ablation (RFA). In this retrospective analysis, patients with BCLC A and B HCC who underwent RFA treatments between January 2015 to December 2017 were evaluated. Out of 62 patients 46 (74.2%) were reported to have RFA as their only first line of treatment, while 12 (25.8%) were reported to have a combination of RFA and other therapeutic modalities. At a mean follow up of 27 months, the survival rate at 12 and 36 months in patients who received RFA was 82.3% and 57.8%, respectively. A relatively high 36-month survival rate was seen in patients who had a response to RFA compared to the non-response group (100% vs 44.8%, P = 0.021). In terms of prognosis, BCLC staging of liver cancer and response after RFA were significantly associated with survival.
Patients with hepatocellular carcinoma (HCC) that has not spread outside the liver have several treatment options available. This month we will review articles that analyze outcomes after liver transplantation, liver resection, as well as radiofrequency ablation.
In HCC patients within the Milan criteria, the 5-year overall survival rate after transplant is about 70%, and the 5-year HCC recurrence rate is about 10%. Patients with tumors beyond the Milan criteria are frequently down staged with locoregional therapies to fall within the Milan criteria. The incidence of HCC recurrence in these patients is around 15.5% at 5 years. In this study, Lee et al demonstrated that statin use substantially reduced the risk of HCC recurrence. In this retrospective analysis of a longitudinal cohort of 430 patients transplanted between September 1995 and December 2019, 323 patients (75.1%) were statin non-users and 107 (24.9%) were statin users. Statin use was defined as at least 90 days of statin therapy, prescribed according to the treatment guidelines for dyslipidemia for primary or secondary prevention of CVD. At a median follow-up of 64.9 months, HCC recurred in 79 patients (18.4%), including 72 (22.3%) in the statin non-user group and 7 (6.5%) in the statin user group. Of those, 61 (77.2%) patients had HCC recurrence that initially presented at extrahepatic site regardless of the presence of intrahepatic tumors. Sixty-three patients (79.7%) had recurrence within 2 years of liver transplantation. The cumulative incidence of HCC recurrence at 2 and 5 years was 18.9% and 22.3% in the statin non-user group, and 3.8% and 5.7% in the statin user group, respectively (P < 0.001).
Liang et al evaluated the importance of tumor size in predicting the likelihood of HCC recurrence following surgical resection. In this retrospective study, a total of 813 cirrhotic patients who underwent curative-intent hepatectomy for solitary HCC without macrovascular invasion between 2001 and 2014 were evaluated. Overall, 464 patients had tumor size ≤ 5 cm, and 349 had tumor size > 5 cm. The 5-year RFS and OS rates were 38.3% and 61.5% in the ≤ 5 cm group, compared with 25.1% and 59.9% in the > 5 cm group. Long-term survival outcomes were significantly worse as tumor size increased. Multivariate analysis indicated that tumor size > 5 cm was an independent risk factor for tumor recurrence and long-term survival.
Finally, Sulaiman et al reported the survival rate of the early and intermediate stage HCC patients who underwent radiofrequency ablation (RFA). In this retrospective analysis, patients with BCLC A and B HCC who underwent RFA treatments between January 2015 to December 2017 were evaluated. Out of 62 patients 46 (74.2%) were reported to have RFA as their only first line of treatment, while 12 (25.8%) were reported to have a combination of RFA and other therapeutic modalities. At a mean follow up of 27 months, the survival rate at 12 and 36 months in patients who received RFA was 82.3% and 57.8%, respectively. A relatively high 36-month survival rate was seen in patients who had a response to RFA compared to the non-response group (100% vs 44.8%, P = 0.021). In terms of prognosis, BCLC staging of liver cancer and response after RFA were significantly associated with survival.
Children and COVID: Weekly cases top 200,000, vaccinations down
Weekly pediatric cases of COVID-19 exceeded 200,000 for just the second time during the pandemic, while new vaccinations in children continued to decline.
The weekly count has now increased for 9 consecutive weeks, during which time it has risen by over 2,300%, the American Academy of Pediatrics and the Children’s Hospital Association said in their weekly COVID-19 report. Total cases in children number almost 4.8 million since the pandemic started.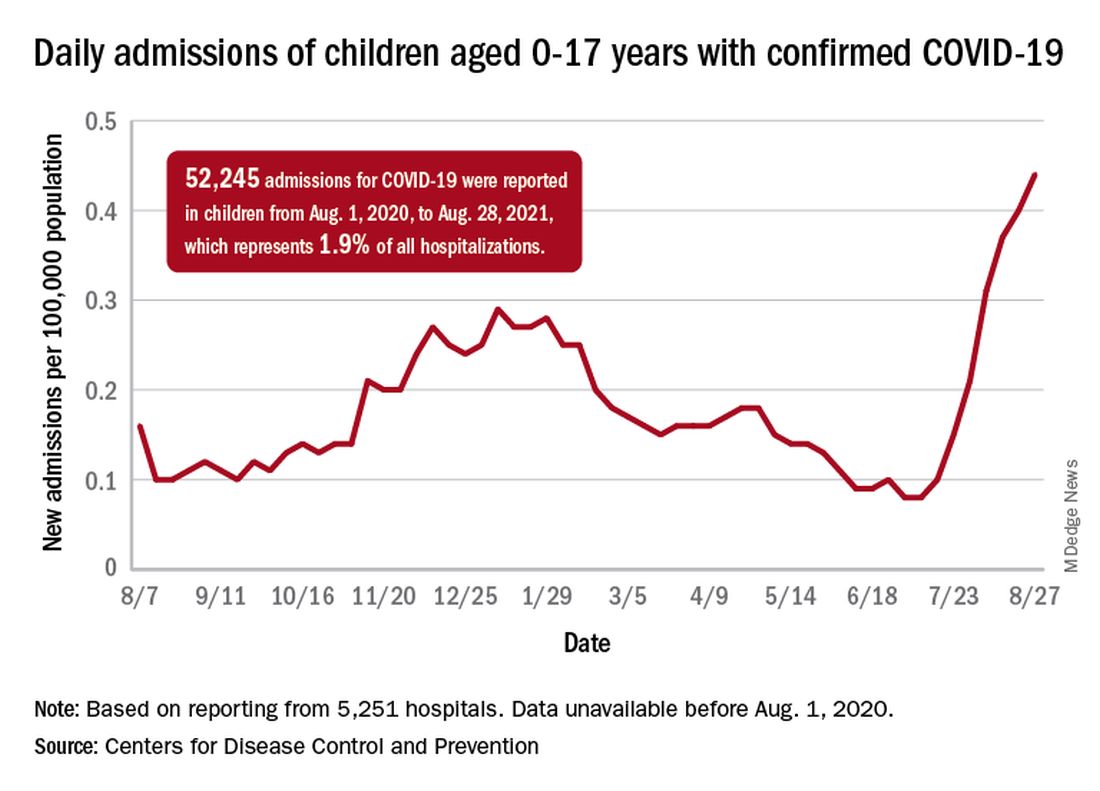
Vaccinations in children are following a different trend. Vaccine initiation has dropped 3 weeks in a row for both of the eligible age groups: First doses administered were down by 29% among 12- to 15-year-olds over that span and by 32% in 16- to 17-year-olds, according to data from the Centers for Disease Control and Prevention.
Since vaccination for children aged 12-15 years started in May, 49% had received at least one dose, and just over 36% were fully vaccinated as of Aug. 30. Among children aged 16-17 years, who have been eligible since December, 57.5% had gotten at least one dose of the vaccine and 46% have completed the two-dose regimen. The total number of children with at least one dose, including those under age 12 who are involved in clinical trials, was about 12 million, the CDC said on its COVID Data Tracker.
Hospitalizations are higher than ever
The recent rise in new child cases has been accompanied by an unprecedented increase in hospitalizations. The daily rate in children aged 0-17 years, which did not surpass 0.30 new admissions per 100,000 population during the worst of the winter surge, had risen to 0.45 per 100,000 by Aug. 26. Since July 4, when the new-admission rate was at its low point of 0.07 per 100,000, hospitalizations in children have jumped by 543%, based on data reported to the CDC by 5,251 hospitals.
A total of 52,245 children were admitted with confirmed COVID-19 from Aug. 1, 2020, when the CDC dataset begins, to Aug. 28, 2021. Those children represent 1.9% of all COVID admissions (2.7 million) in the United States over that period, the CDC said.
Total COVID-related deaths in children are up to 425 in the 48 jurisdictions (45 states, New York City, Puerto Rico, and Guam) that provide mortality data by age, the AAP and the CHA said.
Record-high numbers for the previous 2 reporting weeks – 23 deaths during Aug. 20-26 and 24 deaths during Aug. 13-19, when the previous weekly high was 16 – at least partially reflect the recent addition of South Carolina and New Mexico to the AAP/CHA database, as the two states just started reporting age-related data.
Weekly pediatric cases of COVID-19 exceeded 200,000 for just the second time during the pandemic, while new vaccinations in children continued to decline.
The weekly count has now increased for 9 consecutive weeks, during which time it has risen by over 2,300%, the American Academy of Pediatrics and the Children’s Hospital Association said in their weekly COVID-19 report. Total cases in children number almost 4.8 million since the pandemic started.
Vaccinations in children are following a different trend. Vaccine initiation has dropped 3 weeks in a row for both of the eligible age groups: First doses administered were down by 29% among 12- to 15-year-olds over that span and by 32% in 16- to 17-year-olds, according to data from the Centers for Disease Control and Prevention.
Since vaccination for children aged 12-15 years started in May, 49% had received at least one dose, and just over 36% were fully vaccinated as of Aug. 30. Among children aged 16-17 years, who have been eligible since December, 57.5% had gotten at least one dose of the vaccine and 46% have completed the two-dose regimen. The total number of children with at least one dose, including those under age 12 who are involved in clinical trials, was about 12 million, the CDC said on its COVID Data Tracker.
Hospitalizations are higher than ever
The recent rise in new child cases has been accompanied by an unprecedented increase in hospitalizations. The daily rate in children aged 0-17 years, which did not surpass 0.30 new admissions per 100,000 population during the worst of the winter surge, had risen to 0.45 per 100,000 by Aug. 26. Since July 4, when the new-admission rate was at its low point of 0.07 per 100,000, hospitalizations in children have jumped by 543%, based on data reported to the CDC by 5,251 hospitals.
A total of 52,245 children were admitted with confirmed COVID-19 from Aug. 1, 2020, when the CDC dataset begins, to Aug. 28, 2021. Those children represent 1.9% of all COVID admissions (2.7 million) in the United States over that period, the CDC said.
Total COVID-related deaths in children are up to 425 in the 48 jurisdictions (45 states, New York City, Puerto Rico, and Guam) that provide mortality data by age, the AAP and the CHA said.
Record-high numbers for the previous 2 reporting weeks – 23 deaths during Aug. 20-26 and 24 deaths during Aug. 13-19, when the previous weekly high was 16 – at least partially reflect the recent addition of South Carolina and New Mexico to the AAP/CHA database, as the two states just started reporting age-related data.
Weekly pediatric cases of COVID-19 exceeded 200,000 for just the second time during the pandemic, while new vaccinations in children continued to decline.
The weekly count has now increased for 9 consecutive weeks, during which time it has risen by over 2,300%, the American Academy of Pediatrics and the Children’s Hospital Association said in their weekly COVID-19 report. Total cases in children number almost 4.8 million since the pandemic started.
Vaccinations in children are following a different trend. Vaccine initiation has dropped 3 weeks in a row for both of the eligible age groups: First doses administered were down by 29% among 12- to 15-year-olds over that span and by 32% in 16- to 17-year-olds, according to data from the Centers for Disease Control and Prevention.
Since vaccination for children aged 12-15 years started in May, 49% had received at least one dose, and just over 36% were fully vaccinated as of Aug. 30. Among children aged 16-17 years, who have been eligible since December, 57.5% had gotten at least one dose of the vaccine and 46% have completed the two-dose regimen. The total number of children with at least one dose, including those under age 12 who are involved in clinical trials, was about 12 million, the CDC said on its COVID Data Tracker.
Hospitalizations are higher than ever
The recent rise in new child cases has been accompanied by an unprecedented increase in hospitalizations. The daily rate in children aged 0-17 years, which did not surpass 0.30 new admissions per 100,000 population during the worst of the winter surge, had risen to 0.45 per 100,000 by Aug. 26. Since July 4, when the new-admission rate was at its low point of 0.07 per 100,000, hospitalizations in children have jumped by 543%, based on data reported to the CDC by 5,251 hospitals.
A total of 52,245 children were admitted with confirmed COVID-19 from Aug. 1, 2020, when the CDC dataset begins, to Aug. 28, 2021. Those children represent 1.9% of all COVID admissions (2.7 million) in the United States over that period, the CDC said.
Total COVID-related deaths in children are up to 425 in the 48 jurisdictions (45 states, New York City, Puerto Rico, and Guam) that provide mortality data by age, the AAP and the CHA said.
Record-high numbers for the previous 2 reporting weeks – 23 deaths during Aug. 20-26 and 24 deaths during Aug. 13-19, when the previous weekly high was 16 – at least partially reflect the recent addition of South Carolina and New Mexico to the AAP/CHA database, as the two states just started reporting age-related data.
Clinical Edge Journal Scan Commentary: Breast Cancer September 2021

Metastatic triple-negative breast cancer (TNBC) is a heterogeneous, biologically complex subtype, with continuing efforts to identify therapeutic targets. The PI3K/AKT signaling pathway plays a key role in cell proliferation, survival, invasion, and metabolism. In the phase II LOTUS trial (Dent et al) including 124 patients with advanced TNBC (no prior therapy for advanced disease), addition of the oral AKT inhibitor, ipatasertib, to paclitaxel led to a numerical improvement in OS that was not statistically significant. The median OS was 25.8 vs 16.9 months for the ipatasertib-paclitaxel vs placebo-paclitaxel, respectively (HR 0.80, 95% CI 0.50-1.28). Findings from cohort A of the phase III IPATunity130 trial showed that ipatasertib-paclitaxel did not lead to a statistically significant improvement in PFS vs placebo-paclitaxel in patients with PIK3CA/AKT1/PTEN-altered advanced TNBC in the first-line metastatic setting (mPFS 7.4 vs 6.1 months, respectively; HR 1.02, p=0.9237). These findings support further investigation into predictors of response and other molecular markers that may play a role in the diversity of mTNBC.
Endocrine therapy resistance remains a significant challenge in advanced HR+/HER2- breast cancer, and initial studies with the oral histone deacetylase inhibitor, etinostat, showed promise in this space. Unfortunately, these findings were not upheld in the phase III E2112 trial (Connolly et al), which failed to show an improvement in PFS or OS with exemestane-etinostat (EE) compared to exemestane-placebo (EP) among patients who had progressed on prior non-steroidal AI. Median PFS was 3.3 vs 3.1 months (HR 0.87; p=0.30) and median OS was 23.4 vs 21.7 months (HR 0.99; p=0.94) for the EE vs EP arms, respectively. The combination of an alternative HDAC inhibitor, tucidinostat, has been approved in China in combination with exemestane based on PFS benefit (3.6 months) in the phase III ACE trial. There are notable difference between E2112 and ACE trials, including patient population and design, and importantly OS has not been reported for the latter. The relatively short mPFS and low response rate (5-6%) in E2112 argues for more efficacious therapeutics. There is also value in correlative studies to help further elucidate if there is a role for HDAC inhibitors in this space.
Although adjuvant endocrine therapy has had a significantly beneficial effect on outcomes in early-stage HR+ breast cancer, late recurrences are characteristic of the luminal subtype, and have led to trials investigating extended adjuvant endocrine therapy. The phase III SALSA trial included 3484 women with early HR+ breast cancer who had received 5 years of adjuvant endocrine therapy with randomization to anastrozole for an additional 2 vs 5 years (comparing total of 7 vs 10 years). There was no significant difference in disease-free survival (DFS) at 8 years (73.6% vs 73.9% in the 2 vs 5-year groups, respectively; HR 0.99, p=0.90). Additionally, there was a lower risk of bone fracture in the 2 vs 5-year group (4.7% vs 6.3%; HR 1.35). It is essential to balance modest benefits with toxicities of prolonged AI use, and valuable to identify high-risk patients who may benefit from extended adjuvant endocrine therapy.
References:
Chan A, Moy B, Mansi J, et al; ExteNET Study Group. Final efficacy results of neratinib in HER2-positive hormone receptor-positive early-stage breast cancer from the phase III ExteNET trial. Clin Breast Cancer. 2021;21(1):80-91.e7.
von Minckwitz G, Huang CS, Mano MS, et al; KATHERINE Investigators. Trastuzumab emtansine for residual invasive HER2-positive breast cancer. N Engl J Med. 2019;380(7):617-628.
Dent R, Kim SB, Oliveira M, et al. Double-blind placebo-controlled randomized phase III trial evaluating first-line ipatasertib combined with paclitaxel for PIK3CA/AKT1/PTEN-altered locally advanced unresectable or metastatic triple-negative breast cancer: primary results from IPATunity130 cohort A. Presented at: 2020 San Antonio Breast Cancer Symposium; December 8-11, 2020; Virtual. Oral GS3-04.
Jiang Z, Li W, Hu X, et al. Tucidinostat plus exemestane for postmenopausal patients with advanced, hormone receptor-positive breast cancer (ACE): a randomised, double-blind, placebo-controlled, phase 3 trial. Lancet Oncol. 2019;20(6):806-815.
Mamounas EP, Bandos H, Lembersky BC, et al. Use of letrozole after aromatase inhibitor-based therapy in postmenopausal breast cancer (NRG Oncology/NSABP B-42): a randomised, double-blind, placebo-controlled, phase 3 trial. Lancet Oncol. 2019;20(1):88-99.
Metastatic triple-negative breast cancer (TNBC) is a heterogeneous, biologically complex subtype, with continuing efforts to identify therapeutic targets. The PI3K/AKT signaling pathway plays a key role in cell proliferation, survival, invasion, and metabolism. In the phase II LOTUS trial (Dent et al) including 124 patients with advanced TNBC (no prior therapy for advanced disease), addition of the oral AKT inhibitor, ipatasertib, to paclitaxel led to a numerical improvement in OS that was not statistically significant. The median OS was 25.8 vs 16.9 months for the ipatasertib-paclitaxel vs placebo-paclitaxel, respectively (HR 0.80, 95% CI 0.50-1.28). Findings from cohort A of the phase III IPATunity130 trial showed that ipatasertib-paclitaxel did not lead to a statistically significant improvement in PFS vs placebo-paclitaxel in patients with PIK3CA/AKT1/PTEN-altered advanced TNBC in the first-line metastatic setting (mPFS 7.4 vs 6.1 months, respectively; HR 1.02, p=0.9237). These findings support further investigation into predictors of response and other molecular markers that may play a role in the diversity of mTNBC.
Endocrine therapy resistance remains a significant challenge in advanced HR+/HER2- breast cancer, and initial studies with the oral histone deacetylase inhibitor, etinostat, showed promise in this space. Unfortunately, these findings were not upheld in the phase III E2112 trial (Connolly et al), which failed to show an improvement in PFS or OS with exemestane-etinostat (EE) compared to exemestane-placebo (EP) among patients who had progressed on prior non-steroidal AI. Median PFS was 3.3 vs 3.1 months (HR 0.87; p=0.30) and median OS was 23.4 vs 21.7 months (HR 0.99; p=0.94) for the EE vs EP arms, respectively. The combination of an alternative HDAC inhibitor, tucidinostat, has been approved in China in combination with exemestane based on PFS benefit (3.6 months) in the phase III ACE trial. There are notable difference between E2112 and ACE trials, including patient population and design, and importantly OS has not been reported for the latter. The relatively short mPFS and low response rate (5-6%) in E2112 argues for more efficacious therapeutics. There is also value in correlative studies to help further elucidate if there is a role for HDAC inhibitors in this space.
Although adjuvant endocrine therapy has had a significantly beneficial effect on outcomes in early-stage HR+ breast cancer, late recurrences are characteristic of the luminal subtype, and have led to trials investigating extended adjuvant endocrine therapy. The phase III SALSA trial included 3484 women with early HR+ breast cancer who had received 5 years of adjuvant endocrine therapy with randomization to anastrozole for an additional 2 vs 5 years (comparing total of 7 vs 10 years). There was no significant difference in disease-free survival (DFS) at 8 years (73.6% vs 73.9% in the 2 vs 5-year groups, respectively; HR 0.99, p=0.90). Additionally, there was a lower risk of bone fracture in the 2 vs 5-year group (4.7% vs 6.3%; HR 1.35). It is essential to balance modest benefits with toxicities of prolonged AI use, and valuable to identify high-risk patients who may benefit from extended adjuvant endocrine therapy.
References:
Chan A, Moy B, Mansi J, et al; ExteNET Study Group. Final efficacy results of neratinib in HER2-positive hormone receptor-positive early-stage breast cancer from the phase III ExteNET trial. Clin Breast Cancer. 2021;21(1):80-91.e7.
von Minckwitz G, Huang CS, Mano MS, et al; KATHERINE Investigators. Trastuzumab emtansine for residual invasive HER2-positive breast cancer. N Engl J Med. 2019;380(7):617-628.
Dent R, Kim SB, Oliveira M, et al. Double-blind placebo-controlled randomized phase III trial evaluating first-line ipatasertib combined with paclitaxel for PIK3CA/AKT1/PTEN-altered locally advanced unresectable or metastatic triple-negative breast cancer: primary results from IPATunity130 cohort A. Presented at: 2020 San Antonio Breast Cancer Symposium; December 8-11, 2020; Virtual. Oral GS3-04.
Jiang Z, Li W, Hu X, et al. Tucidinostat plus exemestane for postmenopausal patients with advanced, hormone receptor-positive breast cancer (ACE): a randomised, double-blind, placebo-controlled, phase 3 trial. Lancet Oncol. 2019;20(6):806-815.
Mamounas EP, Bandos H, Lembersky BC, et al. Use of letrozole after aromatase inhibitor-based therapy in postmenopausal breast cancer (NRG Oncology/NSABP B-42): a randomised, double-blind, placebo-controlled, phase 3 trial. Lancet Oncol. 2019;20(1):88-99.
Metastatic triple-negative breast cancer (TNBC) is a heterogeneous, biologically complex subtype, with continuing efforts to identify therapeutic targets. The PI3K/AKT signaling pathway plays a key role in cell proliferation, survival, invasion, and metabolism. In the phase II LOTUS trial (Dent et al) including 124 patients with advanced TNBC (no prior therapy for advanced disease), addition of the oral AKT inhibitor, ipatasertib, to paclitaxel led to a numerical improvement in OS that was not statistically significant. The median OS was 25.8 vs 16.9 months for the ipatasertib-paclitaxel vs placebo-paclitaxel, respectively (HR 0.80, 95% CI 0.50-1.28). Findings from cohort A of the phase III IPATunity130 trial showed that ipatasertib-paclitaxel did not lead to a statistically significant improvement in PFS vs placebo-paclitaxel in patients with PIK3CA/AKT1/PTEN-altered advanced TNBC in the first-line metastatic setting (mPFS 7.4 vs 6.1 months, respectively; HR 1.02, p=0.9237). These findings support further investigation into predictors of response and other molecular markers that may play a role in the diversity of mTNBC.
Endocrine therapy resistance remains a significant challenge in advanced HR+/HER2- breast cancer, and initial studies with the oral histone deacetylase inhibitor, etinostat, showed promise in this space. Unfortunately, these findings were not upheld in the phase III E2112 trial (Connolly et al), which failed to show an improvement in PFS or OS with exemestane-etinostat (EE) compared to exemestane-placebo (EP) among patients who had progressed on prior non-steroidal AI. Median PFS was 3.3 vs 3.1 months (HR 0.87; p=0.30) and median OS was 23.4 vs 21.7 months (HR 0.99; p=0.94) for the EE vs EP arms, respectively. The combination of an alternative HDAC inhibitor, tucidinostat, has been approved in China in combination with exemestane based on PFS benefit (3.6 months) in the phase III ACE trial. There are notable difference between E2112 and ACE trials, including patient population and design, and importantly OS has not been reported for the latter. The relatively short mPFS and low response rate (5-6%) in E2112 argues for more efficacious therapeutics. There is also value in correlative studies to help further elucidate if there is a role for HDAC inhibitors in this space.
Although adjuvant endocrine therapy has had a significantly beneficial effect on outcomes in early-stage HR+ breast cancer, late recurrences are characteristic of the luminal subtype, and have led to trials investigating extended adjuvant endocrine therapy. The phase III SALSA trial included 3484 women with early HR+ breast cancer who had received 5 years of adjuvant endocrine therapy with randomization to anastrozole for an additional 2 vs 5 years (comparing total of 7 vs 10 years). There was no significant difference in disease-free survival (DFS) at 8 years (73.6% vs 73.9% in the 2 vs 5-year groups, respectively; HR 0.99, p=0.90). Additionally, there was a lower risk of bone fracture in the 2 vs 5-year group (4.7% vs 6.3%; HR 1.35). It is essential to balance modest benefits with toxicities of prolonged AI use, and valuable to identify high-risk patients who may benefit from extended adjuvant endocrine therapy.
References:
Chan A, Moy B, Mansi J, et al; ExteNET Study Group. Final efficacy results of neratinib in HER2-positive hormone receptor-positive early-stage breast cancer from the phase III ExteNET trial. Clin Breast Cancer. 2021;21(1):80-91.e7.
von Minckwitz G, Huang CS, Mano MS, et al; KATHERINE Investigators. Trastuzumab emtansine for residual invasive HER2-positive breast cancer. N Engl J Med. 2019;380(7):617-628.
Dent R, Kim SB, Oliveira M, et al. Double-blind placebo-controlled randomized phase III trial evaluating first-line ipatasertib combined with paclitaxel for PIK3CA/AKT1/PTEN-altered locally advanced unresectable or metastatic triple-negative breast cancer: primary results from IPATunity130 cohort A. Presented at: 2020 San Antonio Breast Cancer Symposium; December 8-11, 2020; Virtual. Oral GS3-04.
Jiang Z, Li W, Hu X, et al. Tucidinostat plus exemestane for postmenopausal patients with advanced, hormone receptor-positive breast cancer (ACE): a randomised, double-blind, placebo-controlled, phase 3 trial. Lancet Oncol. 2019;20(6):806-815.
Mamounas EP, Bandos H, Lembersky BC, et al. Use of letrozole after aromatase inhibitor-based therapy in postmenopausal breast cancer (NRG Oncology/NSABP B-42): a randomised, double-blind, placebo-controlled, phase 3 trial. Lancet Oncol. 2019;20(1):88-99.
TNBC: Statin use is linked to survival benefit
Key clinical point: Initiation of statin treatment within 12 months of diagnosis improves survival in women with stage I-III triple-negative breast cancer (TNBC).
Major finding: Statin treatment was initiated in 2,281 patients within 12 months of diagnosis. In 1,534 patients with TNBC, statin use was associated with a significant improvement in breast cancer-specific survival (standardized hazard ratio [HR], 0.42; P = 0.022) and overall survival (HR, 0.70; P = 0.046). No significant association was observed between statin use and survival in patients without TNBC.
Study details: retrospective study of 23,192 patients with stage I-III breast cancer from the Surveillance, Epidemiology, and End Results-Medicare and Texas Cancer Registry-Medicare database between 2008 and 2015.
Disclosures: The study was supported by National Institutes of Health and Cancer Prevention Research Institute of Texas. The authors received grants, research funding, and personal fees outside this work.
Source: Nowakowska MK et al. Cancer. 2021 Aug 3. doi: 10.1002/cncr.33797.
Key clinical point: Initiation of statin treatment within 12 months of diagnosis improves survival in women with stage I-III triple-negative breast cancer (TNBC).
Major finding: Statin treatment was initiated in 2,281 patients within 12 months of diagnosis. In 1,534 patients with TNBC, statin use was associated with a significant improvement in breast cancer-specific survival (standardized hazard ratio [HR], 0.42; P = 0.022) and overall survival (HR, 0.70; P = 0.046). No significant association was observed between statin use and survival in patients without TNBC.
Study details: retrospective study of 23,192 patients with stage I-III breast cancer from the Surveillance, Epidemiology, and End Results-Medicare and Texas Cancer Registry-Medicare database between 2008 and 2015.
Disclosures: The study was supported by National Institutes of Health and Cancer Prevention Research Institute of Texas. The authors received grants, research funding, and personal fees outside this work.
Source: Nowakowska MK et al. Cancer. 2021 Aug 3. doi: 10.1002/cncr.33797.
Key clinical point: Initiation of statin treatment within 12 months of diagnosis improves survival in women with stage I-III triple-negative breast cancer (TNBC).
Major finding: Statin treatment was initiated in 2,281 patients within 12 months of diagnosis. In 1,534 patients with TNBC, statin use was associated with a significant improvement in breast cancer-specific survival (standardized hazard ratio [HR], 0.42; P = 0.022) and overall survival (HR, 0.70; P = 0.046). No significant association was observed between statin use and survival in patients without TNBC.
Study details: retrospective study of 23,192 patients with stage I-III breast cancer from the Surveillance, Epidemiology, and End Results-Medicare and Texas Cancer Registry-Medicare database between 2008 and 2015.
Disclosures: The study was supported by National Institutes of Health and Cancer Prevention Research Institute of Texas. The authors received grants, research funding, and personal fees outside this work.
Source: Nowakowska MK et al. Cancer. 2021 Aug 3. doi: 10.1002/cncr.33797.
Treatment trends in HR-positive, HER-negative breast cancer
Key clinical point: A survey-based study shows higher chemotherapy use in patients with hormone receptor (HR)-positive, human epidermal growth factor receptor 2 (HER2)-negative advanced breast cancer with poor prognostic factors.
Major finding: At least 1 poor prognostic factor was reported in 63% of patients, with varying degrees of overlap between factors. The ability of patients to maintain usual activities was more common in patients without poor prognostic factors. Chemotherapy was prescribed more frequently in patients with poor prognostic factors, whereas endocrine therapy and nonopioid analgesic were more common in patients without poor prognostic factors.
Study details: Real-world data were derived from a large multinational Adelphi Real World Disease Specific Programme survey of 410 oncologists and 2,259 patients with HR-positive, HER-negative advanced breast cancer.
Disclosures: This study was supported by Eli Lilly and Company Ltd, Windlesham, UK. The authors were employees of or received consulting/advisory fees and/or honoraria from Eli Lilly and Company.
Source: Davie A et al. ESMO Open. 2021;6(4):10226 doi: 10.1016/j.esmoop.2021.100226.
Key clinical point: A survey-based study shows higher chemotherapy use in patients with hormone receptor (HR)-positive, human epidermal growth factor receptor 2 (HER2)-negative advanced breast cancer with poor prognostic factors.
Major finding: At least 1 poor prognostic factor was reported in 63% of patients, with varying degrees of overlap between factors. The ability of patients to maintain usual activities was more common in patients without poor prognostic factors. Chemotherapy was prescribed more frequently in patients with poor prognostic factors, whereas endocrine therapy and nonopioid analgesic were more common in patients without poor prognostic factors.
Study details: Real-world data were derived from a large multinational Adelphi Real World Disease Specific Programme survey of 410 oncologists and 2,259 patients with HR-positive, HER-negative advanced breast cancer.
Disclosures: This study was supported by Eli Lilly and Company Ltd, Windlesham, UK. The authors were employees of or received consulting/advisory fees and/or honoraria from Eli Lilly and Company.
Source: Davie A et al. ESMO Open. 2021;6(4):10226 doi: 10.1016/j.esmoop.2021.100226.
Key clinical point: A survey-based study shows higher chemotherapy use in patients with hormone receptor (HR)-positive, human epidermal growth factor receptor 2 (HER2)-negative advanced breast cancer with poor prognostic factors.
Major finding: At least 1 poor prognostic factor was reported in 63% of patients, with varying degrees of overlap between factors. The ability of patients to maintain usual activities was more common in patients without poor prognostic factors. Chemotherapy was prescribed more frequently in patients with poor prognostic factors, whereas endocrine therapy and nonopioid analgesic were more common in patients without poor prognostic factors.
Study details: Real-world data were derived from a large multinational Adelphi Real World Disease Specific Programme survey of 410 oncologists and 2,259 patients with HR-positive, HER-negative advanced breast cancer.
Disclosures: This study was supported by Eli Lilly and Company Ltd, Windlesham, UK. The authors were employees of or received consulting/advisory fees and/or honoraria from Eli Lilly and Company.
Source: Davie A et al. ESMO Open. 2021;6(4):10226 doi: 10.1016/j.esmoop.2021.100226.
High risk for late-onset breast cancer in genetically predisposed women
Key clinical point: Women aged 65 years and above with pathogenic variants (PVs) in BRCA1/2, checkpoint kinase 2 (CHEK2), and partner and localizer of the BRCA2 (PALB2) genes are at an increased risk for breast cancer.
Major finding: The rate of PVs was 3.18% in women with breast cancer and 1.48% in those without. PVs in BRCA1 (odds ratio [OR], 3.37), BRCA2 (OR, 2.64), PALB2 (OR, 3.09), and CHEK2 (OR, 2.13) and were associated with moderate risk for breast cancer. The remaining lifetime risk was 18.4%, 18.7%, 15.9%, and 14.9% for BRCA1, BRCA2, PALB2, and CHEK2 PVs
Study details: This was a population-based study of 13,762 women with breast cancer (age, 65 years and above) and matched 12,945 women without cancer who were tested for PVs in germline predisposition genes.
Disclosures: The study was supported by the National Institutes of Health and Breast Cancer Research Foundation. The authors declared receiving grants, research funding, speaker/personal fees, and/or travel/accommodation/expenses and/or employment and stock ownership.
Source: Boddicker NJ et al. J Clin Oncol. 2021 Jul 22 (in press). doi: 10.1200/JCO.21.00531.
Key clinical point: Women aged 65 years and above with pathogenic variants (PVs) in BRCA1/2, checkpoint kinase 2 (CHEK2), and partner and localizer of the BRCA2 (PALB2) genes are at an increased risk for breast cancer.
Major finding: The rate of PVs was 3.18% in women with breast cancer and 1.48% in those without. PVs in BRCA1 (odds ratio [OR], 3.37), BRCA2 (OR, 2.64), PALB2 (OR, 3.09), and CHEK2 (OR, 2.13) and were associated with moderate risk for breast cancer. The remaining lifetime risk was 18.4%, 18.7%, 15.9%, and 14.9% for BRCA1, BRCA2, PALB2, and CHEK2 PVs
Study details: This was a population-based study of 13,762 women with breast cancer (age, 65 years and above) and matched 12,945 women without cancer who were tested for PVs in germline predisposition genes.
Disclosures: The study was supported by the National Institutes of Health and Breast Cancer Research Foundation. The authors declared receiving grants, research funding, speaker/personal fees, and/or travel/accommodation/expenses and/or employment and stock ownership.
Source: Boddicker NJ et al. J Clin Oncol. 2021 Jul 22 (in press). doi: 10.1200/JCO.21.00531.
Key clinical point: Women aged 65 years and above with pathogenic variants (PVs) in BRCA1/2, checkpoint kinase 2 (CHEK2), and partner and localizer of the BRCA2 (PALB2) genes are at an increased risk for breast cancer.
Major finding: The rate of PVs was 3.18% in women with breast cancer and 1.48% in those without. PVs in BRCA1 (odds ratio [OR], 3.37), BRCA2 (OR, 2.64), PALB2 (OR, 3.09), and CHEK2 (OR, 2.13) and were associated with moderate risk for breast cancer. The remaining lifetime risk was 18.4%, 18.7%, 15.9%, and 14.9% for BRCA1, BRCA2, PALB2, and CHEK2 PVs
Study details: This was a population-based study of 13,762 women with breast cancer (age, 65 years and above) and matched 12,945 women without cancer who were tested for PVs in germline predisposition genes.
Disclosures: The study was supported by the National Institutes of Health and Breast Cancer Research Foundation. The authors declared receiving grants, research funding, speaker/personal fees, and/or travel/accommodation/expenses and/or employment and stock ownership.
Source: Boddicker NJ et al. J Clin Oncol. 2021 Jul 22 (in press). doi: 10.1200/JCO.21.00531.
Targeted early breast screening for women with familial risk is linked to survival benefit
Key clinical point: Targeted breast screening in women aged 30-60 years at an increased familial risk is associated with good long-term survival.
Major finding: A total of 649 breast cancers were detected during the follow-up of 129,119 person-years. Breast cancer-specific survival at 10 years was 91.3%, which was higher than the previously reported survival in women presenting with primary breast cancer. Moreover, 10-year survival for women diagnosed at age 40 years and below was 93.8%.
Study details: This was a retrospective study of women who were offered enhanced screening with annual mammography starting at age 35 years or 5 years younger than the youngest affected relative, with the upper age limit of 50 years for women at moderate risk and 60 years for those at high risk.
Disclosures: This work was supported by the National Institute for Health Research and Prevent Breast Cancer. Dr. DG Evans received consulting fees from companies. The other authors declared no conflict of interests.
Source: Evans DG et al. Breast Cancer Res Treat. 2021 Jul 26 (in press). doi: 10.1007/s10549-021-06333-1.
Key clinical point: Targeted breast screening in women aged 30-60 years at an increased familial risk is associated with good long-term survival.
Major finding: A total of 649 breast cancers were detected during the follow-up of 129,119 person-years. Breast cancer-specific survival at 10 years was 91.3%, which was higher than the previously reported survival in women presenting with primary breast cancer. Moreover, 10-year survival for women diagnosed at age 40 years and below was 93.8%.
Study details: This was a retrospective study of women who were offered enhanced screening with annual mammography starting at age 35 years or 5 years younger than the youngest affected relative, with the upper age limit of 50 years for women at moderate risk and 60 years for those at high risk.
Disclosures: This work was supported by the National Institute for Health Research and Prevent Breast Cancer. Dr. DG Evans received consulting fees from companies. The other authors declared no conflict of interests.
Source: Evans DG et al. Breast Cancer Res Treat. 2021 Jul 26 (in press). doi: 10.1007/s10549-021-06333-1.
Key clinical point: Targeted breast screening in women aged 30-60 years at an increased familial risk is associated with good long-term survival.
Major finding: A total of 649 breast cancers were detected during the follow-up of 129,119 person-years. Breast cancer-specific survival at 10 years was 91.3%, which was higher than the previously reported survival in women presenting with primary breast cancer. Moreover, 10-year survival for women diagnosed at age 40 years and below was 93.8%.
Study details: This was a retrospective study of women who were offered enhanced screening with annual mammography starting at age 35 years or 5 years younger than the youngest affected relative, with the upper age limit of 50 years for women at moderate risk and 60 years for those at high risk.
Disclosures: This work was supported by the National Institute for Health Research and Prevent Breast Cancer. Dr. DG Evans received consulting fees from companies. The other authors declared no conflict of interests.
Source: Evans DG et al. Breast Cancer Res Treat. 2021 Jul 26 (in press). doi: 10.1007/s10549-021-06333-1.