User login
Method may enable eradication of LSCs in AML
Disrupting mitophagy may be a “promising strategy” for eliminating leukemia stem cells (LSCs) in acute myeloid leukemia (AML), according to researchers.
The team found that AML LSCs depend on mitophagy to maintain their “stemness,” but targeting the central metabolic stress regulator AMPK or the mitochondrial dynamics regulator FIS1 can disrupt mitophagy and impair LSC function.
Craig T. Jordan, PhD, of the University of Colorado in Aurora, and his colleagues reported these findings in Cell Stem Cell.
The researchers said in vitro experiments showed that LSCs have elevated levels of FIS1 and “distinct mitochondrial morphology.”
When the team inhibited FIS1 in the AML cell line MOLM-13 and primary AML cells, they observed disruption of mitochondrial dynamics. Experiments in mouse models indicated that FIS1 is required for LSC self-renewal.
Specifically, the researchers said they found that depletion of FIS1 hinders mitophagy and leads to inactivation of GSK3, myeloid differentiation, cell-cycle arrest, and loss of LSC function.
Dr Jordan and his colleagues also found that AMPK is an upstream regulator of FIS1, and targeting AMPK produces similar effects as targeting FIS1—namely, disrupting mitophagy and impairing LSC self-renewal.
The researchers said their findings suggest that mitochondrial stress generated from oncogenic transformation may activate AMPK signaling in LSCs. And the AMPK signaling drives FIS1-mediated mitophagy, which eliminates stressed mitochondria and allows LSCs to thrive.
However, when AMPK or FIS1 is inhibited, the damaged mitochondria are not eliminated. This leads to “GSK3 inhibition and other unknown events” that prompt differentiation and hinder LSC function.
“Leukemia stem cells require AMPK for their survival, but normal hematopoietic cells can do without it,” Dr Jordan noted. “The reason this study is so important is that, so far, nobody’s come up with a good way to kill leukemia stem cells while sparing normal blood-forming cells. If we can translate this concept to patients, the potential for improved therapy is very exciting.”
Disrupting mitophagy may be a “promising strategy” for eliminating leukemia stem cells (LSCs) in acute myeloid leukemia (AML), according to researchers.
The team found that AML LSCs depend on mitophagy to maintain their “stemness,” but targeting the central metabolic stress regulator AMPK or the mitochondrial dynamics regulator FIS1 can disrupt mitophagy and impair LSC function.
Craig T. Jordan, PhD, of the University of Colorado in Aurora, and his colleagues reported these findings in Cell Stem Cell.
The researchers said in vitro experiments showed that LSCs have elevated levels of FIS1 and “distinct mitochondrial morphology.”
When the team inhibited FIS1 in the AML cell line MOLM-13 and primary AML cells, they observed disruption of mitochondrial dynamics. Experiments in mouse models indicated that FIS1 is required for LSC self-renewal.
Specifically, the researchers said they found that depletion of FIS1 hinders mitophagy and leads to inactivation of GSK3, myeloid differentiation, cell-cycle arrest, and loss of LSC function.
Dr Jordan and his colleagues also found that AMPK is an upstream regulator of FIS1, and targeting AMPK produces similar effects as targeting FIS1—namely, disrupting mitophagy and impairing LSC self-renewal.
The researchers said their findings suggest that mitochondrial stress generated from oncogenic transformation may activate AMPK signaling in LSCs. And the AMPK signaling drives FIS1-mediated mitophagy, which eliminates stressed mitochondria and allows LSCs to thrive.
However, when AMPK or FIS1 is inhibited, the damaged mitochondria are not eliminated. This leads to “GSK3 inhibition and other unknown events” that prompt differentiation and hinder LSC function.
“Leukemia stem cells require AMPK for their survival, but normal hematopoietic cells can do without it,” Dr Jordan noted. “The reason this study is so important is that, so far, nobody’s come up with a good way to kill leukemia stem cells while sparing normal blood-forming cells. If we can translate this concept to patients, the potential for improved therapy is very exciting.”
Disrupting mitophagy may be a “promising strategy” for eliminating leukemia stem cells (LSCs) in acute myeloid leukemia (AML), according to researchers.
The team found that AML LSCs depend on mitophagy to maintain their “stemness,” but targeting the central metabolic stress regulator AMPK or the mitochondrial dynamics regulator FIS1 can disrupt mitophagy and impair LSC function.
Craig T. Jordan, PhD, of the University of Colorado in Aurora, and his colleagues reported these findings in Cell Stem Cell.
The researchers said in vitro experiments showed that LSCs have elevated levels of FIS1 and “distinct mitochondrial morphology.”
When the team inhibited FIS1 in the AML cell line MOLM-13 and primary AML cells, they observed disruption of mitochondrial dynamics. Experiments in mouse models indicated that FIS1 is required for LSC self-renewal.
Specifically, the researchers said they found that depletion of FIS1 hinders mitophagy and leads to inactivation of GSK3, myeloid differentiation, cell-cycle arrest, and loss of LSC function.
Dr Jordan and his colleagues also found that AMPK is an upstream regulator of FIS1, and targeting AMPK produces similar effects as targeting FIS1—namely, disrupting mitophagy and impairing LSC self-renewal.
The researchers said their findings suggest that mitochondrial stress generated from oncogenic transformation may activate AMPK signaling in LSCs. And the AMPK signaling drives FIS1-mediated mitophagy, which eliminates stressed mitochondria and allows LSCs to thrive.
However, when AMPK or FIS1 is inhibited, the damaged mitochondria are not eliminated. This leads to “GSK3 inhibition and other unknown events” that prompt differentiation and hinder LSC function.
“Leukemia stem cells require AMPK for their survival, but normal hematopoietic cells can do without it,” Dr Jordan noted. “The reason this study is so important is that, so far, nobody’s come up with a good way to kill leukemia stem cells while sparing normal blood-forming cells. If we can translate this concept to patients, the potential for improved therapy is very exciting.”
Protein ‘atlas’ could aid study, treatment of diseases

New technology has enabled researchers to create a “genomic atlas of the human plasma proteome,” according to an article published in Nature.
The researchers identified nearly 2000 genetic associations with close to 1500 proteins, and they believe these discoveries will improve our understanding of diseases and aid drug development.
“Compared to genes, proteins have been relatively understudied in human blood, even though they are the ‘effectors’ of human biology, are disrupted in many diseases, and are the targets of most medicines,” said study author Adam Butterworth, PhD, of the University of Cambridge in the UK.
“Novel technologies are now allowing us to start addressing this gap in our knowledge.”
Dr Butterworth and his colleagues used an assay called SOMAscan (developed by the company SomaLogic) to measure 3622 proteins in the blood of 3301 people. The team then analyzed the DNA of these individuals to see which regions of their genomes were associated with protein levels.
In this way, the researchers found 1927 significant associations between 1478 proteins and 764 genomic regions. These findings are publicly available via the University of Cambridge website.
The researchers said one way to use this information is to identify biological pathways that cause diseases.
“Thanks to the genomics revolution over the past decade, we’ve been good at finding statistical associations between the genome and disease, but the difficulty has been then identifying the disease-causing genes and pathways,” said study author James Peters, PhD, of the University of Cambridge.
“Now, by combining our database with what we know about associations between genetic variants and disease, we are able to say a lot more about the biology of disease.”
In some cases, the researchers identified multiple genetic variants influencing levels of a protein. By combining these variants into a “score” for that protein, they were able to identify new associations between proteins and disease.
The team also said the proteomic genetic data can be used to aid drug development. In addition to highlighting potential side effects of drugs, the findings can provide insights on protein targets of new and existing drugs.
By linking drugs, proteins, genetic variation, and diseases, the researchers have already suggested existing drugs that could potentially be used to treat different diseases and increased confidence that certain drugs currently in development might be successful in clinical trials.
“Our database is really just a starting point,” said study author Benjamin Sun, an MB/PhD student at the University of Cambridge.
“We’ve given some examples in this study of how it might be used, but now it’s over to the research community to begin using it and finding new applications.”
The research was funded by MSD, National Institute for Health Research, NHS Blood and Transplant, British Heart Foundation, Medical Research Council, UK Research and Innovation, and SomaLogic.
New technology has enabled researchers to create a “genomic atlas of the human plasma proteome,” according to an article published in Nature.
The researchers identified nearly 2000 genetic associations with close to 1500 proteins, and they believe these discoveries will improve our understanding of diseases and aid drug development.
“Compared to genes, proteins have been relatively understudied in human blood, even though they are the ‘effectors’ of human biology, are disrupted in many diseases, and are the targets of most medicines,” said study author Adam Butterworth, PhD, of the University of Cambridge in the UK.
“Novel technologies are now allowing us to start addressing this gap in our knowledge.”
Dr Butterworth and his colleagues used an assay called SOMAscan (developed by the company SomaLogic) to measure 3622 proteins in the blood of 3301 people. The team then analyzed the DNA of these individuals to see which regions of their genomes were associated with protein levels.
In this way, the researchers found 1927 significant associations between 1478 proteins and 764 genomic regions. These findings are publicly available via the University of Cambridge website.
The researchers said one way to use this information is to identify biological pathways that cause diseases.
“Thanks to the genomics revolution over the past decade, we’ve been good at finding statistical associations between the genome and disease, but the difficulty has been then identifying the disease-causing genes and pathways,” said study author James Peters, PhD, of the University of Cambridge.
“Now, by combining our database with what we know about associations between genetic variants and disease, we are able to say a lot more about the biology of disease.”
In some cases, the researchers identified multiple genetic variants influencing levels of a protein. By combining these variants into a “score” for that protein, they were able to identify new associations between proteins and disease.
The team also said the proteomic genetic data can be used to aid drug development. In addition to highlighting potential side effects of drugs, the findings can provide insights on protein targets of new and existing drugs.
By linking drugs, proteins, genetic variation, and diseases, the researchers have already suggested existing drugs that could potentially be used to treat different diseases and increased confidence that certain drugs currently in development might be successful in clinical trials.
“Our database is really just a starting point,” said study author Benjamin Sun, an MB/PhD student at the University of Cambridge.
“We’ve given some examples in this study of how it might be used, but now it’s over to the research community to begin using it and finding new applications.”
The research was funded by MSD, National Institute for Health Research, NHS Blood and Transplant, British Heart Foundation, Medical Research Council, UK Research and Innovation, and SomaLogic.
New technology has enabled researchers to create a “genomic atlas of the human plasma proteome,” according to an article published in Nature.
The researchers identified nearly 2000 genetic associations with close to 1500 proteins, and they believe these discoveries will improve our understanding of diseases and aid drug development.
“Compared to genes, proteins have been relatively understudied in human blood, even though they are the ‘effectors’ of human biology, are disrupted in many diseases, and are the targets of most medicines,” said study author Adam Butterworth, PhD, of the University of Cambridge in the UK.
“Novel technologies are now allowing us to start addressing this gap in our knowledge.”
Dr Butterworth and his colleagues used an assay called SOMAscan (developed by the company SomaLogic) to measure 3622 proteins in the blood of 3301 people. The team then analyzed the DNA of these individuals to see which regions of their genomes were associated with protein levels.
In this way, the researchers found 1927 significant associations between 1478 proteins and 764 genomic regions. These findings are publicly available via the University of Cambridge website.
The researchers said one way to use this information is to identify biological pathways that cause diseases.
“Thanks to the genomics revolution over the past decade, we’ve been good at finding statistical associations between the genome and disease, but the difficulty has been then identifying the disease-causing genes and pathways,” said study author James Peters, PhD, of the University of Cambridge.
“Now, by combining our database with what we know about associations between genetic variants and disease, we are able to say a lot more about the biology of disease.”
In some cases, the researchers identified multiple genetic variants influencing levels of a protein. By combining these variants into a “score” for that protein, they were able to identify new associations between proteins and disease.
The team also said the proteomic genetic data can be used to aid drug development. In addition to highlighting potential side effects of drugs, the findings can provide insights on protein targets of new and existing drugs.
By linking drugs, proteins, genetic variation, and diseases, the researchers have already suggested existing drugs that could potentially be used to treat different diseases and increased confidence that certain drugs currently in development might be successful in clinical trials.
“Our database is really just a starting point,” said study author Benjamin Sun, an MB/PhD student at the University of Cambridge.
“We’ve given some examples in this study of how it might be used, but now it’s over to the research community to begin using it and finding new applications.”
The research was funded by MSD, National Institute for Health Research, NHS Blood and Transplant, British Heart Foundation, Medical Research Council, UK Research and Innovation, and SomaLogic.
Treating substance use disorders: What do you do after withdrawal?
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel

PE is rare in patients presenting to the ED with syncope
Clinical question: What is the prevalence of pulmonary embolism (PE) in patients presenting to the ED with syncope?

Study design: Retrospective, observational study.
Setting: Canada, Denmark, Italy, and the United States, from January 2010 to September 2016.
Synopsis: Longitudinal administrative databases were used to identify patients with ICD codes for syncope at discharge from the ED or hospital. Those with an ICD code for PE were included to calculate the prevalence of PE in this population (primary outcome).
The prevalence of PE in all patients ranged from 0.06% (95% confidence interval, 0.05%-0.06%) to 0.55% (95% CI, 0.50%-0.61%); and in hospitalized patients from 0.15% (95% CI, 0.14%-0.16%) to 2.10% (95% CI, 1.84%-2.39%). This is a much lower than the estimated 17.3% prevalence of PE in patients presenting with syncope estimated by the PESIT study published in the New England Journal of Medicine in 2016. Further definitive research is needed to better characterize prevalence rates.
Limitations of this study include the potential for information bias: The inclusion criteria of patients coded for syncope at discharge likely omits some patients who initially presented with syncope but were coded for a primary diagnosis that caused syncope.
Bottom line: PE in patients presenting to the ED with syncope may be rare.
Citation: Costantino G et al. Prevalence of pulmonary embolism in patients with syncope. JAMA. 2018;178(3):356-62.
Dr. Roy is a hospitalist at Beth Israel Deaconess Medical Center, and instructor in medicine, Harvard Medical School, Boston.
Clinical question: What is the prevalence of pulmonary embolism (PE) in patients presenting to the ED with syncope?
Study design: Retrospective, observational study.
Setting: Canada, Denmark, Italy, and the United States, from January 2010 to September 2016.
Synopsis: Longitudinal administrative databases were used to identify patients with ICD codes for syncope at discharge from the ED or hospital. Those with an ICD code for PE were included to calculate the prevalence of PE in this population (primary outcome).
The prevalence of PE in all patients ranged from 0.06% (95% confidence interval, 0.05%-0.06%) to 0.55% (95% CI, 0.50%-0.61%); and in hospitalized patients from 0.15% (95% CI, 0.14%-0.16%) to 2.10% (95% CI, 1.84%-2.39%). This is a much lower than the estimated 17.3% prevalence of PE in patients presenting with syncope estimated by the PESIT study published in the New England Journal of Medicine in 2016. Further definitive research is needed to better characterize prevalence rates.
Limitations of this study include the potential for information bias: The inclusion criteria of patients coded for syncope at discharge likely omits some patients who initially presented with syncope but were coded for a primary diagnosis that caused syncope.
Bottom line: PE in patients presenting to the ED with syncope may be rare.
Citation: Costantino G et al. Prevalence of pulmonary embolism in patients with syncope. JAMA. 2018;178(3):356-62.
Dr. Roy is a hospitalist at Beth Israel Deaconess Medical Center, and instructor in medicine, Harvard Medical School, Boston.
Clinical question: What is the prevalence of pulmonary embolism (PE) in patients presenting to the ED with syncope?
Study design: Retrospective, observational study.
Setting: Canada, Denmark, Italy, and the United States, from January 2010 to September 2016.
Synopsis: Longitudinal administrative databases were used to identify patients with ICD codes for syncope at discharge from the ED or hospital. Those with an ICD code for PE were included to calculate the prevalence of PE in this population (primary outcome).
The prevalence of PE in all patients ranged from 0.06% (95% confidence interval, 0.05%-0.06%) to 0.55% (95% CI, 0.50%-0.61%); and in hospitalized patients from 0.15% (95% CI, 0.14%-0.16%) to 2.10% (95% CI, 1.84%-2.39%). This is a much lower than the estimated 17.3% prevalence of PE in patients presenting with syncope estimated by the PESIT study published in the New England Journal of Medicine in 2016. Further definitive research is needed to better characterize prevalence rates.
Limitations of this study include the potential for information bias: The inclusion criteria of patients coded for syncope at discharge likely omits some patients who initially presented with syncope but were coded for a primary diagnosis that caused syncope.
Bottom line: PE in patients presenting to the ED with syncope may be rare.
Citation: Costantino G et al. Prevalence of pulmonary embolism in patients with syncope. JAMA. 2018;178(3):356-62.
Dr. Roy is a hospitalist at Beth Israel Deaconess Medical Center, and instructor in medicine, Harvard Medical School, Boston.
Weight gain linked to progression of fibrosis in NAFLD patients
according to recent research published in Clinical Gastroenterology and Hepatology.

Researchers evaluated 40,700 Korean adults (minimum age, 18 years) with NAFLD who underwent health screenings during 2002-2016 with a median 6-year follow-up. Patients were categorized and placed into weight quintiles based on whether they lost weight (quintile 1, 2.3-kg or greater weight loss; quintile 2, 2.2-kg to 0.6-kg weight loss), gained weight (quintile 4, 0.7- to 2.1-kg weight gain; quintile 5, at least 2.2-kg or greater weight gain) or whether their weight remained stable (quintile 3, 0.5-kg weight loss to 0.6-kg weight gain). Researchers followed patients from baseline to fibrosis progression or last visit, calculated as person-years, and used the aspartate aminotransferase to platelet ratio index (APRI) to measure outcomes. They defined body mass index based on criteria specific to Asian populations, with underweight categorized as less than 18.5 kg/m2, normal weight as 18.5-23 kg/m2, overweight as 23-25 kg/m2, and obese as at least 25 kg/m2.
“Our findings from mostly asymptomatic, relatively young individuals with ultrasonographically detected steatosis, possibly reflecting low-risk NAFLD patients, are less likely to be affected by survivor bias and biases related to comorbidities, compared with previous findings from cohorts of high-risk groups that underwent liver biopsy,” Seungho Ryu, MD, PhD, from Kangbuk Samsung Hospital in Seoul, South Korea, and colleagues wrote in the study.
There were 5,454 participants who progressed from a low APRI to an intermediate or high APRI within 275,451.5 person-years, researchers said. Compared with the stable-weight group, hazard ratios for APRI progression in the first weight-change quintile were 0.68 (95% confidence interval, 0.62-0.74) and 0.86 in the second weight-change quintile (95% CI, 0.78-0.94). In the weight-gain groups, an increase in weight was associated with APRI progression in the fourth quintile (HR, 1.17; 95% CI, 1.07-1.28) and fifth quintile (HR, 1.71; 95% CI, 1.58-1.85) groups.
After multivariable adjustment, there was an increase in APRI progression among patients with BMIs between 23 and 24.9 kg/m2 (HR, 1.13; 95% CI, 1.02-1.26), between 25 and 29.9 kg/m2 (HR, 1.41; 95% CI, 1.28-1.55), and greater than or equal to 30 kg/m2 (HR, 2.09; 95% CI, 1.86-2.36) compared with patients with a BMI between 18.5 and 22.9 kg/m2,.
Limitations of the study included the use of ultrasonography in place of liver biopsy for diagnosing NAFLD and the use of APRI to predict fibrosis in individuals with NAFLD, researchers said.
“APRI has demonstrated a reasonable utility as a noninvasive method for the prediction of histologically confirmed advanced fibrosis,” Dr. Ryu and colleagues wrote. “Nonetheless, we acknowledge that there is no currently available longitudinal data to support the use of worsening noninvasive fibrosis markers as an indicator of histological progression of fibrosis stage over time.”
Other limitations included the study’s retrospective design, lack of availability of medication use and dietary intake, and lack of generalization based on a young, healthy population of mostly Korean employees who were employed by companies or local government. However, researchers said clinicians should encourage their patients with NAFLD to maintain a healthy weight to avoid progression of fibrosis.
The authors reported no relevant financial disclosures.
SOURCE: Kim Y et al. Clin Gastroenterol Hepatol. 2018. doi: 10.1016/j.cgh.2018.07.006.
according to recent research published in Clinical Gastroenterology and Hepatology.
Researchers evaluated 40,700 Korean adults (minimum age, 18 years) with NAFLD who underwent health screenings during 2002-2016 with a median 6-year follow-up. Patients were categorized and placed into weight quintiles based on whether they lost weight (quintile 1, 2.3-kg or greater weight loss; quintile 2, 2.2-kg to 0.6-kg weight loss), gained weight (quintile 4, 0.7- to 2.1-kg weight gain; quintile 5, at least 2.2-kg or greater weight gain) or whether their weight remained stable (quintile 3, 0.5-kg weight loss to 0.6-kg weight gain). Researchers followed patients from baseline to fibrosis progression or last visit, calculated as person-years, and used the aspartate aminotransferase to platelet ratio index (APRI) to measure outcomes. They defined body mass index based on criteria specific to Asian populations, with underweight categorized as less than 18.5 kg/m2, normal weight as 18.5-23 kg/m2, overweight as 23-25 kg/m2, and obese as at least 25 kg/m2.
“Our findings from mostly asymptomatic, relatively young individuals with ultrasonographically detected steatosis, possibly reflecting low-risk NAFLD patients, are less likely to be affected by survivor bias and biases related to comorbidities, compared with previous findings from cohorts of high-risk groups that underwent liver biopsy,” Seungho Ryu, MD, PhD, from Kangbuk Samsung Hospital in Seoul, South Korea, and colleagues wrote in the study.
There were 5,454 participants who progressed from a low APRI to an intermediate or high APRI within 275,451.5 person-years, researchers said. Compared with the stable-weight group, hazard ratios for APRI progression in the first weight-change quintile were 0.68 (95% confidence interval, 0.62-0.74) and 0.86 in the second weight-change quintile (95% CI, 0.78-0.94). In the weight-gain groups, an increase in weight was associated with APRI progression in the fourth quintile (HR, 1.17; 95% CI, 1.07-1.28) and fifth quintile (HR, 1.71; 95% CI, 1.58-1.85) groups.
After multivariable adjustment, there was an increase in APRI progression among patients with BMIs between 23 and 24.9 kg/m2 (HR, 1.13; 95% CI, 1.02-1.26), between 25 and 29.9 kg/m2 (HR, 1.41; 95% CI, 1.28-1.55), and greater than or equal to 30 kg/m2 (HR, 2.09; 95% CI, 1.86-2.36) compared with patients with a BMI between 18.5 and 22.9 kg/m2,.
Limitations of the study included the use of ultrasonography in place of liver biopsy for diagnosing NAFLD and the use of APRI to predict fibrosis in individuals with NAFLD, researchers said.
“APRI has demonstrated a reasonable utility as a noninvasive method for the prediction of histologically confirmed advanced fibrosis,” Dr. Ryu and colleagues wrote. “Nonetheless, we acknowledge that there is no currently available longitudinal data to support the use of worsening noninvasive fibrosis markers as an indicator of histological progression of fibrosis stage over time.”
Other limitations included the study’s retrospective design, lack of availability of medication use and dietary intake, and lack of generalization based on a young, healthy population of mostly Korean employees who were employed by companies or local government. However, researchers said clinicians should encourage their patients with NAFLD to maintain a healthy weight to avoid progression of fibrosis.
The authors reported no relevant financial disclosures.
SOURCE: Kim Y et al. Clin Gastroenterol Hepatol. 2018. doi: 10.1016/j.cgh.2018.07.006.
according to recent research published in Clinical Gastroenterology and Hepatology.
Researchers evaluated 40,700 Korean adults (minimum age, 18 years) with NAFLD who underwent health screenings during 2002-2016 with a median 6-year follow-up. Patients were categorized and placed into weight quintiles based on whether they lost weight (quintile 1, 2.3-kg or greater weight loss; quintile 2, 2.2-kg to 0.6-kg weight loss), gained weight (quintile 4, 0.7- to 2.1-kg weight gain; quintile 5, at least 2.2-kg or greater weight gain) or whether their weight remained stable (quintile 3, 0.5-kg weight loss to 0.6-kg weight gain). Researchers followed patients from baseline to fibrosis progression or last visit, calculated as person-years, and used the aspartate aminotransferase to platelet ratio index (APRI) to measure outcomes. They defined body mass index based on criteria specific to Asian populations, with underweight categorized as less than 18.5 kg/m2, normal weight as 18.5-23 kg/m2, overweight as 23-25 kg/m2, and obese as at least 25 kg/m2.
“Our findings from mostly asymptomatic, relatively young individuals with ultrasonographically detected steatosis, possibly reflecting low-risk NAFLD patients, are less likely to be affected by survivor bias and biases related to comorbidities, compared with previous findings from cohorts of high-risk groups that underwent liver biopsy,” Seungho Ryu, MD, PhD, from Kangbuk Samsung Hospital in Seoul, South Korea, and colleagues wrote in the study.
There were 5,454 participants who progressed from a low APRI to an intermediate or high APRI within 275,451.5 person-years, researchers said. Compared with the stable-weight group, hazard ratios for APRI progression in the first weight-change quintile were 0.68 (95% confidence interval, 0.62-0.74) and 0.86 in the second weight-change quintile (95% CI, 0.78-0.94). In the weight-gain groups, an increase in weight was associated with APRI progression in the fourth quintile (HR, 1.17; 95% CI, 1.07-1.28) and fifth quintile (HR, 1.71; 95% CI, 1.58-1.85) groups.
After multivariable adjustment, there was an increase in APRI progression among patients with BMIs between 23 and 24.9 kg/m2 (HR, 1.13; 95% CI, 1.02-1.26), between 25 and 29.9 kg/m2 (HR, 1.41; 95% CI, 1.28-1.55), and greater than or equal to 30 kg/m2 (HR, 2.09; 95% CI, 1.86-2.36) compared with patients with a BMI between 18.5 and 22.9 kg/m2,.
Limitations of the study included the use of ultrasonography in place of liver biopsy for diagnosing NAFLD and the use of APRI to predict fibrosis in individuals with NAFLD, researchers said.
“APRI has demonstrated a reasonable utility as a noninvasive method for the prediction of histologically confirmed advanced fibrosis,” Dr. Ryu and colleagues wrote. “Nonetheless, we acknowledge that there is no currently available longitudinal data to support the use of worsening noninvasive fibrosis markers as an indicator of histological progression of fibrosis stage over time.”
Other limitations included the study’s retrospective design, lack of availability of medication use and dietary intake, and lack of generalization based on a young, healthy population of mostly Korean employees who were employed by companies or local government. However, researchers said clinicians should encourage their patients with NAFLD to maintain a healthy weight to avoid progression of fibrosis.
The authors reported no relevant financial disclosures.
SOURCE: Kim Y et al. Clin Gastroenterol Hepatol. 2018. doi: 10.1016/j.cgh.2018.07.006.
FROM CLINICAL GASTROENTEROLOGY AND HEPATOLOGY
Key clinical point: Obesity and weight gain were linked to progression of fibrosis in adults with NAFLD.
Major finding: Degree of weight change was associated with risk of fibrosis progression; patients who gained weight in quintile 4 and quintile 5 had hazard ratios of 1.17 and 1.71, respectively, when compared with the quintile of patients whose weight remained stable.
Data source: A retrospective study of 40,700 Korean adults with NAFLD who underwent health screenings during 2002-2016 with a median 6-year follow-up.
Disclosures: The authors reported no relevant financial disclosures.
Source: Kim Y et al. Clin Gastroenterol Hepatol. 2018. doi: 10.1016/j.cgh.2018.07.006.
Vadastuximab talirine gives big boost to AML remission
For elderly patients with CD33-positive acute myeloid leukemia (AML), vadastuximab talirine in combination with a hypomethylating agent (HMA) improves remission rates, compared with HMA therapy alone, according to a phase 1 trial.

More than half of the patients treated with combination therapy achieved deep remission, defined as a negative-flow cytometry test for minimal residual disease. Despite these promising results, hematologic toxicity concerns may limit future trials.
“Outcomes for patients with acute myeloid leukemia (AML) remain poor, particularly in older patients,” wrote Amir T. Fathi, MD, of the division of hematology and oncology at Massachusetts General Hospital Cancer Center, Boston, and his coauthors.
Many elderly patients currently receive hypomethylating agents HMAs as a form of low-intensity therapy, but associated remission rates are low. “The development of novel, well-tolerated therapies to enhance the efficacy of HMAs could meaningfully improve the standard of care for older patients with AML,” the investigators wrote in Blood. Vadastuximab talirine is a novel antibody therapy that targets CD33; preclinical data suggested that it could be an effective combination with HMA therapy.
The phase 1 trial involved 53 patients with newly diagnosed, CD33-positive AML and a median age of 75 years. Patients were naive to HMA therapy but could have previously received other low-intensity treatments. HMA therapy was administered first; either azacitidine (75 mg/m2 subcutaneous IV for 7 days) or decitabine (20 mg/m2 IV for 5 days), according to institutional standards. On the last day of HMA therapy, vadastuximab talirine (10 mcg/kg IV) was given. This protocol was repeated in 28-day cycles for up to four cycles. Patients who tolerated the combination and showed a clinical response were eligible to continue therapy.
The composite remission rate (CRc: complete remission and complete remission with incomplete blood count recovery) with combination therapy was 70%. Historically, HMA monotherapies have much lower composite remission rates (decitabine, 17.8%; azacytidine, 27.8%). Of all patients achieving remission, 51% tested negative by flow cytometry for minimal residual disease. Median overall survival was 11.3 months and median relapse-free survival was 7.7 months.
“Nevertheless, the increased response rate with the addition of vadastuximab talirine to HMAs was also associated with increased toxicity when compared to single-agent HMA therapy – indicative of the greater degree of myelosuppression,” the researchers wrote. The most common grade 3 or higher adverse events were thrombocytopenia (57%), febrile neutropenia (49%), anemia (45%), neutropenia (42%), and fatigue (15%).
The investigators stated that “the overall safety profile was similar for patients treated with vadastuximab talirine in combination with azacitidine versus decitabine (with the exception of incidence of febrile neutropenia).”
Following the encouraging results of this phase 1 trial, the CASCADE phase 3 trial was launched to again compare this combination with HMA monotherapy; however, the trial was halted early because of deaths in the combination arm. The investigators cited the need for stricter protocols to ensure safety during future trials.
“With such guidance and precaution, promising combinations for AML, a disease affecting predominantly older and more frail patients, may be more effectively studied so as to enhance our current suboptimal therapeutic options,” they wrote.
Seattle Genetics provided study funding and author compensation.
SOURCE: Fathi AT et al. Blood. 2018 Jul 25. doi: 10.1182/blood-2018-03-841171.
For elderly patients with CD33-positive acute myeloid leukemia (AML), vadastuximab talirine in combination with a hypomethylating agent (HMA) improves remission rates, compared with HMA therapy alone, according to a phase 1 trial.
More than half of the patients treated with combination therapy achieved deep remission, defined as a negative-flow cytometry test for minimal residual disease. Despite these promising results, hematologic toxicity concerns may limit future trials.
“Outcomes for patients with acute myeloid leukemia (AML) remain poor, particularly in older patients,” wrote Amir T. Fathi, MD, of the division of hematology and oncology at Massachusetts General Hospital Cancer Center, Boston, and his coauthors.
Many elderly patients currently receive hypomethylating agents HMAs as a form of low-intensity therapy, but associated remission rates are low. “The development of novel, well-tolerated therapies to enhance the efficacy of HMAs could meaningfully improve the standard of care for older patients with AML,” the investigators wrote in Blood. Vadastuximab talirine is a novel antibody therapy that targets CD33; preclinical data suggested that it could be an effective combination with HMA therapy.
The phase 1 trial involved 53 patients with newly diagnosed, CD33-positive AML and a median age of 75 years. Patients were naive to HMA therapy but could have previously received other low-intensity treatments. HMA therapy was administered first; either azacitidine (75 mg/m2 subcutaneous IV for 7 days) or decitabine (20 mg/m2 IV for 5 days), according to institutional standards. On the last day of HMA therapy, vadastuximab talirine (10 mcg/kg IV) was given. This protocol was repeated in 28-day cycles for up to four cycles. Patients who tolerated the combination and showed a clinical response were eligible to continue therapy.
The composite remission rate (CRc: complete remission and complete remission with incomplete blood count recovery) with combination therapy was 70%. Historically, HMA monotherapies have much lower composite remission rates (decitabine, 17.8%; azacytidine, 27.8%). Of all patients achieving remission, 51% tested negative by flow cytometry for minimal residual disease. Median overall survival was 11.3 months and median relapse-free survival was 7.7 months.
“Nevertheless, the increased response rate with the addition of vadastuximab talirine to HMAs was also associated with increased toxicity when compared to single-agent HMA therapy – indicative of the greater degree of myelosuppression,” the researchers wrote. The most common grade 3 or higher adverse events were thrombocytopenia (57%), febrile neutropenia (49%), anemia (45%), neutropenia (42%), and fatigue (15%).
The investigators stated that “the overall safety profile was similar for patients treated with vadastuximab talirine in combination with azacitidine versus decitabine (with the exception of incidence of febrile neutropenia).”
Following the encouraging results of this phase 1 trial, the CASCADE phase 3 trial was launched to again compare this combination with HMA monotherapy; however, the trial was halted early because of deaths in the combination arm. The investigators cited the need for stricter protocols to ensure safety during future trials.
“With such guidance and precaution, promising combinations for AML, a disease affecting predominantly older and more frail patients, may be more effectively studied so as to enhance our current suboptimal therapeutic options,” they wrote.
Seattle Genetics provided study funding and author compensation.
SOURCE: Fathi AT et al. Blood. 2018 Jul 25. doi: 10.1182/blood-2018-03-841171.
For elderly patients with CD33-positive acute myeloid leukemia (AML), vadastuximab talirine in combination with a hypomethylating agent (HMA) improves remission rates, compared with HMA therapy alone, according to a phase 1 trial.
More than half of the patients treated with combination therapy achieved deep remission, defined as a negative-flow cytometry test for minimal residual disease. Despite these promising results, hematologic toxicity concerns may limit future trials.
“Outcomes for patients with acute myeloid leukemia (AML) remain poor, particularly in older patients,” wrote Amir T. Fathi, MD, of the division of hematology and oncology at Massachusetts General Hospital Cancer Center, Boston, and his coauthors.
Many elderly patients currently receive hypomethylating agents HMAs as a form of low-intensity therapy, but associated remission rates are low. “The development of novel, well-tolerated therapies to enhance the efficacy of HMAs could meaningfully improve the standard of care for older patients with AML,” the investigators wrote in Blood. Vadastuximab talirine is a novel antibody therapy that targets CD33; preclinical data suggested that it could be an effective combination with HMA therapy.
The phase 1 trial involved 53 patients with newly diagnosed, CD33-positive AML and a median age of 75 years. Patients were naive to HMA therapy but could have previously received other low-intensity treatments. HMA therapy was administered first; either azacitidine (75 mg/m2 subcutaneous IV for 7 days) or decitabine (20 mg/m2 IV for 5 days), according to institutional standards. On the last day of HMA therapy, vadastuximab talirine (10 mcg/kg IV) was given. This protocol was repeated in 28-day cycles for up to four cycles. Patients who tolerated the combination and showed a clinical response were eligible to continue therapy.
The composite remission rate (CRc: complete remission and complete remission with incomplete blood count recovery) with combination therapy was 70%. Historically, HMA monotherapies have much lower composite remission rates (decitabine, 17.8%; azacytidine, 27.8%). Of all patients achieving remission, 51% tested negative by flow cytometry for minimal residual disease. Median overall survival was 11.3 months and median relapse-free survival was 7.7 months.
“Nevertheless, the increased response rate with the addition of vadastuximab talirine to HMAs was also associated with increased toxicity when compared to single-agent HMA therapy – indicative of the greater degree of myelosuppression,” the researchers wrote. The most common grade 3 or higher adverse events were thrombocytopenia (57%), febrile neutropenia (49%), anemia (45%), neutropenia (42%), and fatigue (15%).
The investigators stated that “the overall safety profile was similar for patients treated with vadastuximab talirine in combination with azacitidine versus decitabine (with the exception of incidence of febrile neutropenia).”
Following the encouraging results of this phase 1 trial, the CASCADE phase 3 trial was launched to again compare this combination with HMA monotherapy; however, the trial was halted early because of deaths in the combination arm. The investigators cited the need for stricter protocols to ensure safety during future trials.
“With such guidance and precaution, promising combinations for AML, a disease affecting predominantly older and more frail patients, may be more effectively studied so as to enhance our current suboptimal therapeutic options,” they wrote.
Seattle Genetics provided study funding and author compensation.
SOURCE: Fathi AT et al. Blood. 2018 Jul 25. doi: 10.1182/blood-2018-03-841171.
FROM BLOOD
Key clinical point:
Major finding: The composite remission rate in patients treated with vadastuximab talirine and HMA therapy was 70%, compared with 17.8%-27.8% for patients treated with HMA therapy alone historically.
Study details: A prospective, phase 1 trial involving 53 elderly patients with CD33-positive AML at 14 treatment centers.
Disclosures: Seattle Genetics provided study funding and author compensation.
Source: Fathi AT et al. Blood. 2018 Jul 25. doi: 10.1182/blood-2018-03-841171.
Lay health workers improve end-of-life care
Lay health workers (LHWs) can improve documentation of cancer patients’ care preferences in the aftermath of their diagnosis, investigators report.
Physicians, palliative care workers, and other health professionals can help cancer patients understand their prognosis and establish end-of-life care preferences, but busy schedules and professional reluctance often prevent this. Nonclinical, nonprofessional LHWs often are employed to assist with screening and adherence, but little work has been done to use them in end-of-life care, Manali I. Patel, MD, MPH, and her associates wrote in JAMA Oncology.
To investigate their potential in this role, the researchers randomized 213 patients with stage 3 or 4 recurrent cancer to usual care or the LHW intervention, which included a 6-month structured program delivered by a single LHW who was enrolled in a part-time graduate health education program. The LHWs received an 80-hour online skills-based seminar and 4 weeks’ observation training with a palliative care team.
The LHWs helped patients with advanced care planning, including: education about goals of care, establishment of care preferences, establishment of a surrogate decision maker, creation of an advanced directive, and encouragement to discuss the patient’s care with the clinician.
In the intervention arm, 92.4% of patients successfully had their goals of care documented in the electronic health record within 6 months of randomization, compared with 17.6% of the usual care group (P less than .001). They also were more likely to have created an advanced directive (67.6% vs. 25.9%; P less than .001), Dr. Patel, of Stanford (Calif.) University, and her associates reported.
Patient satisfaction was also greater in the intervention arm, as measured by the Consumer Assessment of Health Care Providers & Systems “satisfaction with provider” item (mean score, 9.16 vs. 7.83; P less than .001). At 6 months, with respect to their oncology provider, patients in the intervention arm registered a mean increase in satisfaction score of 1.53 (P less than .001).
Patients who died were more likely to receive hospice care if they were in the LHW group (76.7% vs. 48.3%; P =.002). Those in the LHW group also had lower health care costs during the final 30 days of their lives ($1,048 vs. $23,482; P less than .001).
Overall, the study shows that LHWs may be one mechanism for delivering high-value care and avoiding unnecessary, burdensome late-life treatments, at least in cancer patients.
SOURCE: Patel MI et al. JAMA Oncol. 2018 Jul 26doi:10.1001/jamaoncol.2018.2446.
Lay health workers (LHWs) can improve documentation of cancer patients’ care preferences in the aftermath of their diagnosis, investigators report.
Physicians, palliative care workers, and other health professionals can help cancer patients understand their prognosis and establish end-of-life care preferences, but busy schedules and professional reluctance often prevent this. Nonclinical, nonprofessional LHWs often are employed to assist with screening and adherence, but little work has been done to use them in end-of-life care, Manali I. Patel, MD, MPH, and her associates wrote in JAMA Oncology.
To investigate their potential in this role, the researchers randomized 213 patients with stage 3 or 4 recurrent cancer to usual care or the LHW intervention, which included a 6-month structured program delivered by a single LHW who was enrolled in a part-time graduate health education program. The LHWs received an 80-hour online skills-based seminar and 4 weeks’ observation training with a palliative care team.
The LHWs helped patients with advanced care planning, including: education about goals of care, establishment of care preferences, establishment of a surrogate decision maker, creation of an advanced directive, and encouragement to discuss the patient’s care with the clinician.
In the intervention arm, 92.4% of patients successfully had their goals of care documented in the electronic health record within 6 months of randomization, compared with 17.6% of the usual care group (P less than .001). They also were more likely to have created an advanced directive (67.6% vs. 25.9%; P less than .001), Dr. Patel, of Stanford (Calif.) University, and her associates reported.
Patient satisfaction was also greater in the intervention arm, as measured by the Consumer Assessment of Health Care Providers & Systems “satisfaction with provider” item (mean score, 9.16 vs. 7.83; P less than .001). At 6 months, with respect to their oncology provider, patients in the intervention arm registered a mean increase in satisfaction score of 1.53 (P less than .001).
Patients who died were more likely to receive hospice care if they were in the LHW group (76.7% vs. 48.3%; P =.002). Those in the LHW group also had lower health care costs during the final 30 days of their lives ($1,048 vs. $23,482; P less than .001).
Overall, the study shows that LHWs may be one mechanism for delivering high-value care and avoiding unnecessary, burdensome late-life treatments, at least in cancer patients.
SOURCE: Patel MI et al. JAMA Oncol. 2018 Jul 26doi:10.1001/jamaoncol.2018.2446.
Lay health workers (LHWs) can improve documentation of cancer patients’ care preferences in the aftermath of their diagnosis, investigators report.
Physicians, palliative care workers, and other health professionals can help cancer patients understand their prognosis and establish end-of-life care preferences, but busy schedules and professional reluctance often prevent this. Nonclinical, nonprofessional LHWs often are employed to assist with screening and adherence, but little work has been done to use them in end-of-life care, Manali I. Patel, MD, MPH, and her associates wrote in JAMA Oncology.
To investigate their potential in this role, the researchers randomized 213 patients with stage 3 or 4 recurrent cancer to usual care or the LHW intervention, which included a 6-month structured program delivered by a single LHW who was enrolled in a part-time graduate health education program. The LHWs received an 80-hour online skills-based seminar and 4 weeks’ observation training with a palliative care team.
The LHWs helped patients with advanced care planning, including: education about goals of care, establishment of care preferences, establishment of a surrogate decision maker, creation of an advanced directive, and encouragement to discuss the patient’s care with the clinician.
In the intervention arm, 92.4% of patients successfully had their goals of care documented in the electronic health record within 6 months of randomization, compared with 17.6% of the usual care group (P less than .001). They also were more likely to have created an advanced directive (67.6% vs. 25.9%; P less than .001), Dr. Patel, of Stanford (Calif.) University, and her associates reported.
Patient satisfaction was also greater in the intervention arm, as measured by the Consumer Assessment of Health Care Providers & Systems “satisfaction with provider” item (mean score, 9.16 vs. 7.83; P less than .001). At 6 months, with respect to their oncology provider, patients in the intervention arm registered a mean increase in satisfaction score of 1.53 (P less than .001).
Patients who died were more likely to receive hospice care if they were in the LHW group (76.7% vs. 48.3%; P =.002). Those in the LHW group also had lower health care costs during the final 30 days of their lives ($1,048 vs. $23,482; P less than .001).
Overall, the study shows that LHWs may be one mechanism for delivering high-value care and avoiding unnecessary, burdensome late-life treatments, at least in cancer patients.
SOURCE: Patel MI et al. JAMA Oncol. 2018 Jul 26doi:10.1001/jamaoncol.2018.2446.
FROM JAMA ONCOLOGY
Key clinical point: Lay health workers helped advanced cancer patients document their treatment preferences and reduced end of life costs.
Major finding: 92.4% of patients working with LHWs had their preferences recorded at 6 months, compared with 17.6% of controls.
Study details: Randomized, controlled trial of 213 patients with stage 3 or 4 recurrent cancer.
Disclosures: The study was funded by the Department of Veterans Affairs, the National Institutes of Health, and the California Healthcare Foundation.
Source: Patel MI et al. JAMA Oncology. 2018 Jul 26. doi: 10.1001/jamaoncol.2018.2446.
Asystole Following Nitroglycerin: A Review of Two Cases
Case reports of a 54-year-old man with angina and a 69-year-old woman demonstrate an underreported, self-limiting side effect associated with nitroglycerin.
Nitroglycerin (NTG), or glyceryl trinitrate, was first introduced into the medical community by Murrell,1,2 who reported on anecdotal observations of its antianginal properties by workers within manufacturing plants refining the product for its explosive properties. While the route of administration of NTG has changed from this incidental environmental exposure to the now formulated therapies available, its benefit as an outpatient, abortive treatment for stable angina has been validated beyond early subjective observations in the literature.1-3 In fact, its successful use over the years for angina has produced an expansive pharmacopeia, including its use for undifferentiated chest pain and exacerbation of congestive heart failure.3-5
Despite the extensive history of NTG as a proven vasodilator, emerging uses continue to be explored in equal measure with technological advances.2,6 Though morbidity and mortality reductions are dependent on its use within clinical practice, NTG is not an innocuous drug.5 Most of the reported side effects associated with NTG are well established and include hypotension, tachycardia, flushing, nausea, vomiting, and headache.3,6,7 An often forgotten side effect associated with NTG use is asystole. We present the following two cases to highlight both common uses of NTG as well as this underreported side effect.
Case 1: Nitroglycerin for Stable Anginal Chest Pain
A 54-year-old man with a history of hypertension (HTN), hyperlipidemia (HLP), and gastroesophageal reflux disease (GERD) presented to the ED for evaluation of a 3-hour history of intermittent, retrosternal, left-sided, nonradiating chest “pressure and tightness.” The patient stated that the chest discomfort began at rest but was exacerbated by exertion with episodes lasting 10 to 15 minutes. The patient rated the peak pain associated with these episodes as a “7” on a pain scale of 1 to 10. He further noted that his symptoms abated and he became “pain-free” when at rest.
The patient’s vital signs at presentation were: blood pressure (BP), 156/87 mm Hg; heart rate (HR), 68 beats/min; respiratory rate (RR), 18 beats/min; and temperature (T), 98.4°F. Oxygen saturation was 96% on room air.
The patient, who performed regular BP checks at home, noted that his recent BP readings had been very high. A review of the patient’s systems was positive for shortness of breath and diaphoresis; symptoms were otherwise negative, including any prior episodes. His social history was noncontributory and negative for tobacco, alcohol, or drug use. The patient did report that he had taken an uneventful 6-hour car ride the previous week.
On physical examination, the patient was nontoxic and resting comfortably, without signs of acute distress or pain. Cardiac and pulmonary examinations were normal, and radial pulses were 2+ and symmetric. The abdominal examination was benign and the neurological examination was nonfocal. There was no evidence of peripheral edema or asymmetry of the calves, which were nontender to palpation.
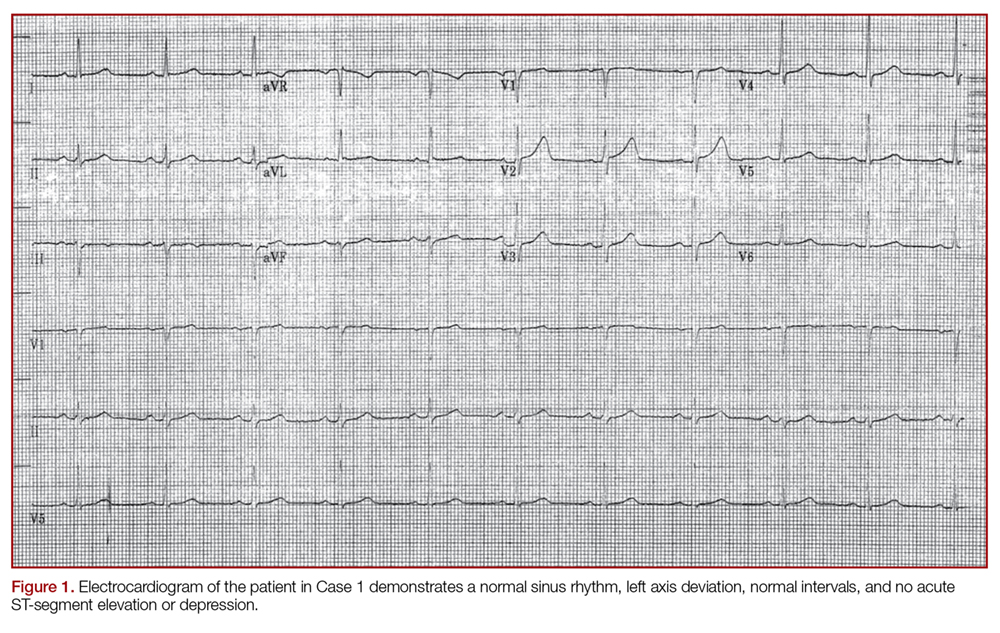
The initial electrocardiogram (ECG) (Figure 1) showed a normal sinus rhythm of 65 beats/min, left axis deviation, and normal intervals; there was no acute ST-segment elevation or depression.
Case 2: Nitroglycerin for Unstable Anginal Chest Pain
A 69-year-old obese woman with a medical history significant for HTN, HLP, and GERD presented to the ED for evaluation of nausea and chest pressure. She described the chest pressure as feeling dull and heavy. She further noted that the discomfort had been occurring intermittently upon exertion, but that this recent episode started while at rest and persisted.
The patient’s vital signs at presentation were: BP, 183/80 mm Hg; HR, 94 beats/min; RR, 20 beats/min; and T, 98.0°F. Oxygen saturation was 92% on room air. On a review of systems, the patient denied any associated symptoms; she likewise denied a history of any recent surgeries, immobilization, active malignancy, or recent travel. Her social history was noncontributory and was negative for tobacco, alcohol, or recreational drug use.
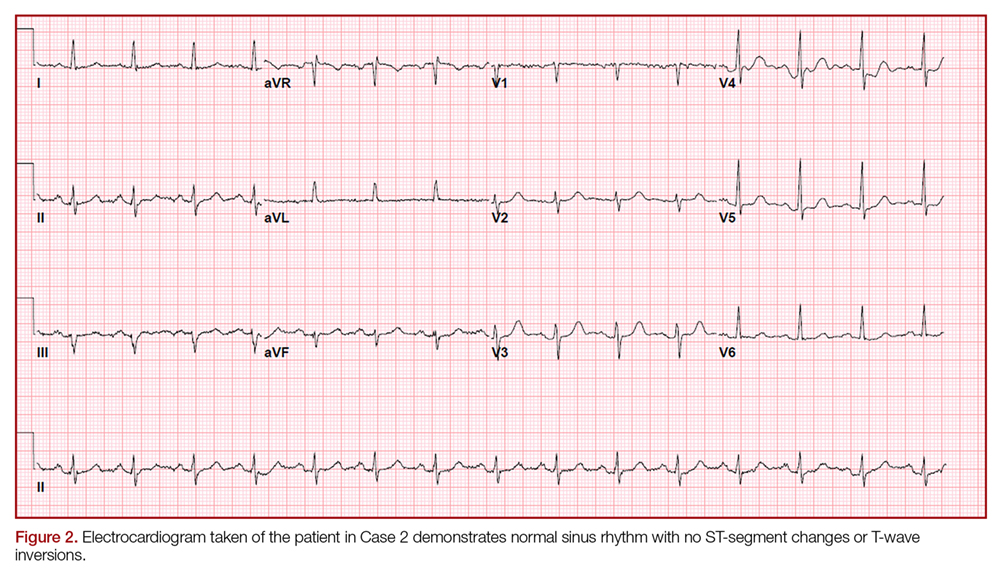
On physical examination the patient was nontoxic and resting comfortably, without signs of acute distress or diaphoresis. The cardiac and pulmonary examinations were normal, and radial pulses were 2+ and symmetric. The patient had trace pedal edema bilaterally, but her calves were symmetric and nontender. The abdomen was benign and the neurological examination was nonfocal. An ECG (Figure 2) showed a normal sinus rhythm with no signs of ischemia (eg, no ST-segment changes or T-wave inversions were present).
Cases 1 and 2: Shared Clinical Course
In both of the two cases presented, ECGs were obtained for the patients upon arrival at the ED. Both patients were placed on telemetry with continuous monitoring, and intravenous (IV) access was obtained. Baseline laboratory evaluation for each of these patients included a complete blood count, basic metabolic panel, and cardiac enzyme measurement. A D-dimer test was also ordered for the patient in Case 1 based on his concerning history and low-pretest probability for a pulmonary embolism (ie, positive pulmonary embolism rule-out criteria). Portable chest X-ray imaging on each of the patients showed no acute pathology, and all of their laboratory results were within normal ranges. Both of the patients in Case 1 and 2 received a 324-mg chewable aspirin and an IV fluid bolus.
Case 1
During evaluation, the patient in Case 1 developed unprovoked chest pain, which he rated as a “7,” for which he was given 400 mcg NTG sublingually (SL). After administration of NTG, the patient reported that his pain reduced to a “4.” Repeat ECG and vital signs remained unchanged. Though Case 1 patient’s pain abated, since it persisted, he was given a second dose of SL NTG. Within 2 minutes of receiving the second dose of NTG, the patient became bradycardic (30 beats/min) with a stable BP and then became unresponsive, converting to asystolic rhythm. Cardiopulmonary resuscitation (CPR) was initiated, with a successful return of vital signs and baseline cognition following 20 seconds of compressions. Despite success following critical interventions, his HR persisted at 30 beats/min with a narrow regular complex, and normal BP. Because of the persistent bradycardia and preceding asystolic rhythm, he was given 0.5 mg of atropine IV, which increased his HR to 80 beats/min. Cardiology service was consulted, and the patient was admitted following an otherwise stable course. Since the cardiologist did not feel emergent cardiac catheterization was indicated, the patient was observed and subsequently discharged home following an uneventful hospitalization, including a normal stress test.
Case 2
The patient in Case 2, had chest pain upon arrival at the ED and was administered SL NTG, with notable improvement in chest pain, but not complete resolution. With serial examinations, including a review of pain scale scores, she was given two subsequent doses of SL NTG. Within 1 minute from receiving the third dose of NTG, the patient complained of lightheadedness and nausea, and became pale and diaphoretic. Telemetry revealed bradycardia, which progressed to junctional escape beats, followed by ventricular escape beats, and then asystole, at which point she became unresponsive and pulseless. Cardiopulmonary resuscitation was initiated, with a return of spontaneous circulation within 15 seconds of intervention; she gradually returned to her baseline with observation. Repeat vital signs were: BP, 155/70 mm Hg; HR, 99 beats/min; RR, 20 breaths/min; and she was afebrile. Oxygen saturation was 99% on 15 liters of oxygen/min, which was weaned prior to hospital admission. A repeat ECG demonstrated a normal sinus rhythm without evidence of ischemia. Cardiology service was consulted and the patient was admitted for further evaluation, including a 3-day inpatient observation, serial cardiac enzymes, thyroid panel, contrast chest computed tomography scan, echocardiogram, and cardiac stress test. All studies were within normal limits, except for an incidental minor pectus excavatum attributed to the quality CPR. In addition, a nuclear medicine perfusion imaging study was obtained, which revealed no evidence of myocardial ischemia or scar, consistent with the patient’s stable course. The patient’s symptoms resolved early in her inpatient stay, and she was discharged home with prescriptions for antihypertensive and antihyperlipidemia agents and instructed to follow-up with her primary care physician.
Discussion
Nitroglycerin is commonly used to treat various symptoms of cardiac origin, namely relief of chest pain due to suspected acute coronary syndromes.2,3The mechanism of action of NTG is predominantly through potent smooth muscle relaxation of the venous and arterial systems, reducing both preload and afterload.2,3 This results in reduced myocardial oxygen demand, potentiating the relief of myocardial ischemia.
Contraindications
Contraindications to NTG include known allergy, pericardial tamponade, restrictive cardiomyopathy, increased intracranial pressure, and concomitant use of phosphodiesterase inhibitors. Moreover, NTG should not be given to treat conditions wherein cardiac output is dependent on venous return, as in the setting of inferior myocardial infarction (MI) with right ventricular involvement. Furthermore, there is no evidence in the literature to support the erroneous use of NTG as a diagnostic therapy, with limited sensitivity yields for conclusive cardiac-associated chest pain.8
Adverse Effects and Events
The common side effects of NTG are well documented and include hypotension, tachycardia, flushing, nausea, vomiting, and headache.7,3,6 Syncope, bradycardia, and cardiac arrest following the administration of NTG are rare events, as evidenced by the paucity of literature describing these complications. Rather, it appears that these side effects are observed only in the setting of myocardial ischemia or MI.3,9-11 Fewer cases of ventricular fibrillation, responsive to defibrillation, and asystole also have been observed.9The exact mechanism for bradycardia without hypotension and subsequent asystole following NTG administration remains elusive, though this response is thought to be associated with the Bezold-Jarisch reflex.
Bezold-Jarisch Reflex
The Bezold-Jarisch reflex is a cardiovascular response consisting of bradycardia and hypotension that is believed to be from stimulation of inhibitory cardiac receptors by stretch, chemical, or pharmacological stimulation.12 The earliest cases of Bezold-Jarisch reflex following NTG occurred in the setting of MI and were attributed to ongoing myocardial ischemia.13 Recent studies have revealed that coronary stenosis without concurrent ischemia is actually not a sensitizing factor, and that bradycardia and asystole following NTG have occurred in patients without evidence of coronary artery disease.9,14 As part of this response, it is theorized that the development of bradycardia is related to vasovagal stimulation, a centrally mediated response to the headache or nausea following NTG administration.10,11,15
Despite these observational studies and after thorough review of the available cases, no unifying factors exist to predict with certainty the patient population in which this response is likely to occur.12,16Based on a literature review, it appears that asystole following NTG is self-limited; however, in most cases, bradycardia was treated with atropine without adverse side effects.12,15,16
Conclusion
The two cases presented involved a middle-aged male patient and an elderly female patient, both of whom had several cardiac risk factors but no evidence of acute ischemia or infarction on ECG or laboratory studies. It is well established that NTG can cause hypotension without bradycardia; however, the development of bradycardia without, or even preceding, hypotension is less recognized. Several mechanisms have been postulated but none fully explain this reaction; moreover, no anticipatory risk factors have been consistently observed. Even though the patients in Case 1 and 2 underwent extensive evaluation, no specific etiology of the observed reaction was identified, though neither patient underwent cardiac catheterization to definitively exclude abnormal coronary artery pathology as a precipitating factor.
These cases illustrate the unpredictable adverse reaction to a common medication used for a ubiquitous complaint. The explanation as to the source for this reaction is lacking, the literature has consistently described the transient and self-limiting effect of asystole following NTG.9,12,14,16Bradycardia, though self-limiting, remains responsive to appropriately dosed atropine when NTG-induced.3,12,16 The authors wish to stress the importance of establishing IV access and being prepared for adverse events whenever administering sublingual nitroglycerin to a patient.
1. Miura T, Nishinaka T, Terada T, Yonezawa K. Vasodilatory effect of nitroglycerin in Japanese subjects with different aldehyde dehydrogenase 2 (ALDH2) genotypes. Chem Biol Interact. 2017;276:40-45. doi:10.1016/j.cbi.2017.03.012.
2. Noonan PK, Williams RL, Benet LZ. Dose dependent pharmacokinetics of nitroglycerin after multiple intravenous infusions in healthy volunteers. J Pharmacokinet Biopharm. 1985;13(2):143-157.
3. Proulx MH, de Montigny L, Ross D, Vacon C, Juste LE, Segal E. Prehospital nitroglycerin in tachycardic chest pain patients: a risk for hypotension or not? Prehosp Emerg Care. 2017;21(1):68-73. doi:10.1080/10903127.2016.1194929.
4. Huis In ‘t Veld MA, Cullen L, Mahler SA, Backus BE, Dezman ZDW, Mattu A. The fast and the furious: low-risk chest pain and the rapid rule-out protocol. West J Emerg Med. 2017;18(3):474-478. doi:10.5811/westjem.2016.12.32676.
5. Pasupathy S, Tavella R, Grover S, et al. Early use of N-acetylcysteine with nitrate therapy in patients undergoing primary percutaneous coronary intervention for ST-segment-elevation myocardial infarction reduces myocardial infarct size (the NACIAM Trial [N-acetylcysteine in Acute Myocardial Infarction]). Circulation. 2017;136(10):894-903. doi:10.1161/CIRCULATIONAHA.117.027575.
6. Turan B, Daşlı T, Erkol A, Erden İ. Effectiveness of sublingual nitroglycerin before puncture compared with conventional intra-carterial nitroglycerin in transradial procedures: a randomized trial. Cardiovasc Revasc Med. 2015;16(7):391-396. doi:10.1016/j.carrev.2015.07.006.
7. Nagy-Grócz G, Bohár Z, Fejes-Szabó A, et al. Nitroglycerin increases serotonin transporter expression in rat spinal cord but anandamide modulated this effect. J Chem Neuroanat. 2017;85:13-20. doi:10.1016/j.jchemneu.2017.06.002.
8. Steele R, McNaughton T, McConahy M, Lam J. Chest pain in emergency department patients: if the pain is relieved by nitroglycerin, is it more likely to be cardiac chest pain? CJEM. 2006;8(3):164-169.
9. Dettorre K, Brywczynski J, McKinney J, Slovis C. Not the nitro? Patient goes into prehospital V-fib arrest following nitroglycerin. JEMS. 2009;34(5):34,36. doi:10.1016/S0197-2510(09)70124-X.
10. Buckley R, Roberts R. Symptomatic bradycardia following the administration of sublingual nitroglycerin. Am J Emerg Med. 1993;11(3):253-255.
11. Takase B, Uehata A, Nishioka T, et al. Different mechanisms of isoproterenol-induced and nitroglycerin-induced syncope during head-up tilt in patients with unexplained syncope: important role of epinephrine in nitroglycerin-induced syncope. J Cardiovasc Electrophysiol. 2001;12(7):791-796.
12. Brandes W, Santiago T, Limacher M. Nitroglycerin-induced hypotension, bradycardia, and asystole: report of a case and review of the literature. Clin Cardiol. 1990;13(10):741-744.
13. Ong EA, Canlas C, Smith W. Nitroglycerin-induced asystole. Arch Intern Med. 1985;145(5):954.
14. Shah SP, Waxman S. Two cases of Bezold-Jarisch reflex induced by intra-arterial nitroglycerin in critical left main coronary artery stenosis. Tex Heart Inst J. 2013;40(4):484-486.
15. Mark AL. The Bezold-Jarisch reflex revisited: clinical implications of inhibitory reflexes originating in the heart. J Am Coll Cardiol. 1983;1(1):90-102.
16. Younas F, Janjua M, Badshah A, DeGregorio M, Patel KC, Cotant JF. Transient complete heart block and isolated ventricular asystole with nitroglycerin. J Cardiovasc Med (Hagerstown). 2012;13(8):533-535. doi:10.2459/JCM.0b013e3283416b8b.
Case reports of a 54-year-old man with angina and a 69-year-old woman demonstrate an underreported, self-limiting side effect associated with nitroglycerin.
Case reports of a 54-year-old man with angina and a 69-year-old woman demonstrate an underreported, self-limiting side effect associated with nitroglycerin.
Nitroglycerin (NTG), or glyceryl trinitrate, was first introduced into the medical community by Murrell,1,2 who reported on anecdotal observations of its antianginal properties by workers within manufacturing plants refining the product for its explosive properties. While the route of administration of NTG has changed from this incidental environmental exposure to the now formulated therapies available, its benefit as an outpatient, abortive treatment for stable angina has been validated beyond early subjective observations in the literature.1-3 In fact, its successful use over the years for angina has produced an expansive pharmacopeia, including its use for undifferentiated chest pain and exacerbation of congestive heart failure.3-5
Despite the extensive history of NTG as a proven vasodilator, emerging uses continue to be explored in equal measure with technological advances.2,6 Though morbidity and mortality reductions are dependent on its use within clinical practice, NTG is not an innocuous drug.5 Most of the reported side effects associated with NTG are well established and include hypotension, tachycardia, flushing, nausea, vomiting, and headache.3,6,7 An often forgotten side effect associated with NTG use is asystole. We present the following two cases to highlight both common uses of NTG as well as this underreported side effect.
Case 1: Nitroglycerin for Stable Anginal Chest Pain
A 54-year-old man with a history of hypertension (HTN), hyperlipidemia (HLP), and gastroesophageal reflux disease (GERD) presented to the ED for evaluation of a 3-hour history of intermittent, retrosternal, left-sided, nonradiating chest “pressure and tightness.” The patient stated that the chest discomfort began at rest but was exacerbated by exertion with episodes lasting 10 to 15 minutes. The patient rated the peak pain associated with these episodes as a “7” on a pain scale of 1 to 10. He further noted that his symptoms abated and he became “pain-free” when at rest.
The patient’s vital signs at presentation were: blood pressure (BP), 156/87 mm Hg; heart rate (HR), 68 beats/min; respiratory rate (RR), 18 beats/min; and temperature (T), 98.4°F. Oxygen saturation was 96% on room air.
The patient, who performed regular BP checks at home, noted that his recent BP readings had been very high. A review of the patient’s systems was positive for shortness of breath and diaphoresis; symptoms were otherwise negative, including any prior episodes. His social history was noncontributory and negative for tobacco, alcohol, or drug use. The patient did report that he had taken an uneventful 6-hour car ride the previous week.
On physical examination, the patient was nontoxic and resting comfortably, without signs of acute distress or pain. Cardiac and pulmonary examinations were normal, and radial pulses were 2+ and symmetric. The abdominal examination was benign and the neurological examination was nonfocal. There was no evidence of peripheral edema or asymmetry of the calves, which were nontender to palpation.
The initial electrocardiogram (ECG) (Figure 1) showed a normal sinus rhythm of 65 beats/min, left axis deviation, and normal intervals; there was no acute ST-segment elevation or depression.
Case 2: Nitroglycerin for Unstable Anginal Chest Pain
A 69-year-old obese woman with a medical history significant for HTN, HLP, and GERD presented to the ED for evaluation of nausea and chest pressure. She described the chest pressure as feeling dull and heavy. She further noted that the discomfort had been occurring intermittently upon exertion, but that this recent episode started while at rest and persisted.
The patient’s vital signs at presentation were: BP, 183/80 mm Hg; HR, 94 beats/min; RR, 20 beats/min; and T, 98.0°F. Oxygen saturation was 92% on room air. On a review of systems, the patient denied any associated symptoms; she likewise denied a history of any recent surgeries, immobilization, active malignancy, or recent travel. Her social history was noncontributory and was negative for tobacco, alcohol, or recreational drug use.
On physical examination the patient was nontoxic and resting comfortably, without signs of acute distress or diaphoresis. The cardiac and pulmonary examinations were normal, and radial pulses were 2+ and symmetric. The patient had trace pedal edema bilaterally, but her calves were symmetric and nontender. The abdomen was benign and the neurological examination was nonfocal. An ECG (Figure 2) showed a normal sinus rhythm with no signs of ischemia (eg, no ST-segment changes or T-wave inversions were present).
Cases 1 and 2: Shared Clinical Course
In both of the two cases presented, ECGs were obtained for the patients upon arrival at the ED. Both patients were placed on telemetry with continuous monitoring, and intravenous (IV) access was obtained. Baseline laboratory evaluation for each of these patients included a complete blood count, basic metabolic panel, and cardiac enzyme measurement. A D-dimer test was also ordered for the patient in Case 1 based on his concerning history and low-pretest probability for a pulmonary embolism (ie, positive pulmonary embolism rule-out criteria). Portable chest X-ray imaging on each of the patients showed no acute pathology, and all of their laboratory results were within normal ranges. Both of the patients in Case 1 and 2 received a 324-mg chewable aspirin and an IV fluid bolus.
Case 1
During evaluation, the patient in Case 1 developed unprovoked chest pain, which he rated as a “7,” for which he was given 400 mcg NTG sublingually (SL). After administration of NTG, the patient reported that his pain reduced to a “4.” Repeat ECG and vital signs remained unchanged. Though Case 1 patient’s pain abated, since it persisted, he was given a second dose of SL NTG. Within 2 minutes of receiving the second dose of NTG, the patient became bradycardic (30 beats/min) with a stable BP and then became unresponsive, converting to asystolic rhythm. Cardiopulmonary resuscitation (CPR) was initiated, with a successful return of vital signs and baseline cognition following 20 seconds of compressions. Despite success following critical interventions, his HR persisted at 30 beats/min with a narrow regular complex, and normal BP. Because of the persistent bradycardia and preceding asystolic rhythm, he was given 0.5 mg of atropine IV, which increased his HR to 80 beats/min. Cardiology service was consulted, and the patient was admitted following an otherwise stable course. Since the cardiologist did not feel emergent cardiac catheterization was indicated, the patient was observed and subsequently discharged home following an uneventful hospitalization, including a normal stress test.
Case 2
The patient in Case 2, had chest pain upon arrival at the ED and was administered SL NTG, with notable improvement in chest pain, but not complete resolution. With serial examinations, including a review of pain scale scores, she was given two subsequent doses of SL NTG. Within 1 minute from receiving the third dose of NTG, the patient complained of lightheadedness and nausea, and became pale and diaphoretic. Telemetry revealed bradycardia, which progressed to junctional escape beats, followed by ventricular escape beats, and then asystole, at which point she became unresponsive and pulseless. Cardiopulmonary resuscitation was initiated, with a return of spontaneous circulation within 15 seconds of intervention; she gradually returned to her baseline with observation. Repeat vital signs were: BP, 155/70 mm Hg; HR, 99 beats/min; RR, 20 breaths/min; and she was afebrile. Oxygen saturation was 99% on 15 liters of oxygen/min, which was weaned prior to hospital admission. A repeat ECG demonstrated a normal sinus rhythm without evidence of ischemia. Cardiology service was consulted and the patient was admitted for further evaluation, including a 3-day inpatient observation, serial cardiac enzymes, thyroid panel, contrast chest computed tomography scan, echocardiogram, and cardiac stress test. All studies were within normal limits, except for an incidental minor pectus excavatum attributed to the quality CPR. In addition, a nuclear medicine perfusion imaging study was obtained, which revealed no evidence of myocardial ischemia or scar, consistent with the patient’s stable course. The patient’s symptoms resolved early in her inpatient stay, and she was discharged home with prescriptions for antihypertensive and antihyperlipidemia agents and instructed to follow-up with her primary care physician.
Discussion
Nitroglycerin is commonly used to treat various symptoms of cardiac origin, namely relief of chest pain due to suspected acute coronary syndromes.2,3The mechanism of action of NTG is predominantly through potent smooth muscle relaxation of the venous and arterial systems, reducing both preload and afterload.2,3 This results in reduced myocardial oxygen demand, potentiating the relief of myocardial ischemia.
Contraindications
Contraindications to NTG include known allergy, pericardial tamponade, restrictive cardiomyopathy, increased intracranial pressure, and concomitant use of phosphodiesterase inhibitors. Moreover, NTG should not be given to treat conditions wherein cardiac output is dependent on venous return, as in the setting of inferior myocardial infarction (MI) with right ventricular involvement. Furthermore, there is no evidence in the literature to support the erroneous use of NTG as a diagnostic therapy, with limited sensitivity yields for conclusive cardiac-associated chest pain.8
Adverse Effects and Events
The common side effects of NTG are well documented and include hypotension, tachycardia, flushing, nausea, vomiting, and headache.7,3,6 Syncope, bradycardia, and cardiac arrest following the administration of NTG are rare events, as evidenced by the paucity of literature describing these complications. Rather, it appears that these side effects are observed only in the setting of myocardial ischemia or MI.3,9-11 Fewer cases of ventricular fibrillation, responsive to defibrillation, and asystole also have been observed.9The exact mechanism for bradycardia without hypotension and subsequent asystole following NTG administration remains elusive, though this response is thought to be associated with the Bezold-Jarisch reflex.
Bezold-Jarisch Reflex
The Bezold-Jarisch reflex is a cardiovascular response consisting of bradycardia and hypotension that is believed to be from stimulation of inhibitory cardiac receptors by stretch, chemical, or pharmacological stimulation.12 The earliest cases of Bezold-Jarisch reflex following NTG occurred in the setting of MI and were attributed to ongoing myocardial ischemia.13 Recent studies have revealed that coronary stenosis without concurrent ischemia is actually not a sensitizing factor, and that bradycardia and asystole following NTG have occurred in patients without evidence of coronary artery disease.9,14 As part of this response, it is theorized that the development of bradycardia is related to vasovagal stimulation, a centrally mediated response to the headache or nausea following NTG administration.10,11,15
Despite these observational studies and after thorough review of the available cases, no unifying factors exist to predict with certainty the patient population in which this response is likely to occur.12,16Based on a literature review, it appears that asystole following NTG is self-limited; however, in most cases, bradycardia was treated with atropine without adverse side effects.12,15,16
Conclusion
The two cases presented involved a middle-aged male patient and an elderly female patient, both of whom had several cardiac risk factors but no evidence of acute ischemia or infarction on ECG or laboratory studies. It is well established that NTG can cause hypotension without bradycardia; however, the development of bradycardia without, or even preceding, hypotension is less recognized. Several mechanisms have been postulated but none fully explain this reaction; moreover, no anticipatory risk factors have been consistently observed. Even though the patients in Case 1 and 2 underwent extensive evaluation, no specific etiology of the observed reaction was identified, though neither patient underwent cardiac catheterization to definitively exclude abnormal coronary artery pathology as a precipitating factor.
These cases illustrate the unpredictable adverse reaction to a common medication used for a ubiquitous complaint. The explanation as to the source for this reaction is lacking, the literature has consistently described the transient and self-limiting effect of asystole following NTG.9,12,14,16Bradycardia, though self-limiting, remains responsive to appropriately dosed atropine when NTG-induced.3,12,16 The authors wish to stress the importance of establishing IV access and being prepared for adverse events whenever administering sublingual nitroglycerin to a patient.
Nitroglycerin (NTG), or glyceryl trinitrate, was first introduced into the medical community by Murrell,1,2 who reported on anecdotal observations of its antianginal properties by workers within manufacturing plants refining the product for its explosive properties. While the route of administration of NTG has changed from this incidental environmental exposure to the now formulated therapies available, its benefit as an outpatient, abortive treatment for stable angina has been validated beyond early subjective observations in the literature.1-3 In fact, its successful use over the years for angina has produced an expansive pharmacopeia, including its use for undifferentiated chest pain and exacerbation of congestive heart failure.3-5
Despite the extensive history of NTG as a proven vasodilator, emerging uses continue to be explored in equal measure with technological advances.2,6 Though morbidity and mortality reductions are dependent on its use within clinical practice, NTG is not an innocuous drug.5 Most of the reported side effects associated with NTG are well established and include hypotension, tachycardia, flushing, nausea, vomiting, and headache.3,6,7 An often forgotten side effect associated with NTG use is asystole. We present the following two cases to highlight both common uses of NTG as well as this underreported side effect.
Case 1: Nitroglycerin for Stable Anginal Chest Pain
A 54-year-old man with a history of hypertension (HTN), hyperlipidemia (HLP), and gastroesophageal reflux disease (GERD) presented to the ED for evaluation of a 3-hour history of intermittent, retrosternal, left-sided, nonradiating chest “pressure and tightness.” The patient stated that the chest discomfort began at rest but was exacerbated by exertion with episodes lasting 10 to 15 minutes. The patient rated the peak pain associated with these episodes as a “7” on a pain scale of 1 to 10. He further noted that his symptoms abated and he became “pain-free” when at rest.
The patient’s vital signs at presentation were: blood pressure (BP), 156/87 mm Hg; heart rate (HR), 68 beats/min; respiratory rate (RR), 18 beats/min; and temperature (T), 98.4°F. Oxygen saturation was 96% on room air.
The patient, who performed regular BP checks at home, noted that his recent BP readings had been very high. A review of the patient’s systems was positive for shortness of breath and diaphoresis; symptoms were otherwise negative, including any prior episodes. His social history was noncontributory and negative for tobacco, alcohol, or drug use. The patient did report that he had taken an uneventful 6-hour car ride the previous week.
On physical examination, the patient was nontoxic and resting comfortably, without signs of acute distress or pain. Cardiac and pulmonary examinations were normal, and radial pulses were 2+ and symmetric. The abdominal examination was benign and the neurological examination was nonfocal. There was no evidence of peripheral edema or asymmetry of the calves, which were nontender to palpation.
The initial electrocardiogram (ECG) (Figure 1) showed a normal sinus rhythm of 65 beats/min, left axis deviation, and normal intervals; there was no acute ST-segment elevation or depression.
Case 2: Nitroglycerin for Unstable Anginal Chest Pain
A 69-year-old obese woman with a medical history significant for HTN, HLP, and GERD presented to the ED for evaluation of nausea and chest pressure. She described the chest pressure as feeling dull and heavy. She further noted that the discomfort had been occurring intermittently upon exertion, but that this recent episode started while at rest and persisted.
The patient’s vital signs at presentation were: BP, 183/80 mm Hg; HR, 94 beats/min; RR, 20 beats/min; and T, 98.0°F. Oxygen saturation was 92% on room air. On a review of systems, the patient denied any associated symptoms; she likewise denied a history of any recent surgeries, immobilization, active malignancy, or recent travel. Her social history was noncontributory and was negative for tobacco, alcohol, or recreational drug use.
On physical examination the patient was nontoxic and resting comfortably, without signs of acute distress or diaphoresis. The cardiac and pulmonary examinations were normal, and radial pulses were 2+ and symmetric. The patient had trace pedal edema bilaterally, but her calves were symmetric and nontender. The abdomen was benign and the neurological examination was nonfocal. An ECG (Figure 2) showed a normal sinus rhythm with no signs of ischemia (eg, no ST-segment changes or T-wave inversions were present).
Cases 1 and 2: Shared Clinical Course
In both of the two cases presented, ECGs were obtained for the patients upon arrival at the ED. Both patients were placed on telemetry with continuous monitoring, and intravenous (IV) access was obtained. Baseline laboratory evaluation for each of these patients included a complete blood count, basic metabolic panel, and cardiac enzyme measurement. A D-dimer test was also ordered for the patient in Case 1 based on his concerning history and low-pretest probability for a pulmonary embolism (ie, positive pulmonary embolism rule-out criteria). Portable chest X-ray imaging on each of the patients showed no acute pathology, and all of their laboratory results were within normal ranges. Both of the patients in Case 1 and 2 received a 324-mg chewable aspirin and an IV fluid bolus.
Case 1
During evaluation, the patient in Case 1 developed unprovoked chest pain, which he rated as a “7,” for which he was given 400 mcg NTG sublingually (SL). After administration of NTG, the patient reported that his pain reduced to a “4.” Repeat ECG and vital signs remained unchanged. Though Case 1 patient’s pain abated, since it persisted, he was given a second dose of SL NTG. Within 2 minutes of receiving the second dose of NTG, the patient became bradycardic (30 beats/min) with a stable BP and then became unresponsive, converting to asystolic rhythm. Cardiopulmonary resuscitation (CPR) was initiated, with a successful return of vital signs and baseline cognition following 20 seconds of compressions. Despite success following critical interventions, his HR persisted at 30 beats/min with a narrow regular complex, and normal BP. Because of the persistent bradycardia and preceding asystolic rhythm, he was given 0.5 mg of atropine IV, which increased his HR to 80 beats/min. Cardiology service was consulted, and the patient was admitted following an otherwise stable course. Since the cardiologist did not feel emergent cardiac catheterization was indicated, the patient was observed and subsequently discharged home following an uneventful hospitalization, including a normal stress test.
Case 2
The patient in Case 2, had chest pain upon arrival at the ED and was administered SL NTG, with notable improvement in chest pain, but not complete resolution. With serial examinations, including a review of pain scale scores, she was given two subsequent doses of SL NTG. Within 1 minute from receiving the third dose of NTG, the patient complained of lightheadedness and nausea, and became pale and diaphoretic. Telemetry revealed bradycardia, which progressed to junctional escape beats, followed by ventricular escape beats, and then asystole, at which point she became unresponsive and pulseless. Cardiopulmonary resuscitation was initiated, with a return of spontaneous circulation within 15 seconds of intervention; she gradually returned to her baseline with observation. Repeat vital signs were: BP, 155/70 mm Hg; HR, 99 beats/min; RR, 20 breaths/min; and she was afebrile. Oxygen saturation was 99% on 15 liters of oxygen/min, which was weaned prior to hospital admission. A repeat ECG demonstrated a normal sinus rhythm without evidence of ischemia. Cardiology service was consulted and the patient was admitted for further evaluation, including a 3-day inpatient observation, serial cardiac enzymes, thyroid panel, contrast chest computed tomography scan, echocardiogram, and cardiac stress test. All studies were within normal limits, except for an incidental minor pectus excavatum attributed to the quality CPR. In addition, a nuclear medicine perfusion imaging study was obtained, which revealed no evidence of myocardial ischemia or scar, consistent with the patient’s stable course. The patient’s symptoms resolved early in her inpatient stay, and she was discharged home with prescriptions for antihypertensive and antihyperlipidemia agents and instructed to follow-up with her primary care physician.
Discussion
Nitroglycerin is commonly used to treat various symptoms of cardiac origin, namely relief of chest pain due to suspected acute coronary syndromes.2,3The mechanism of action of NTG is predominantly through potent smooth muscle relaxation of the venous and arterial systems, reducing both preload and afterload.2,3 This results in reduced myocardial oxygen demand, potentiating the relief of myocardial ischemia.
Contraindications
Contraindications to NTG include known allergy, pericardial tamponade, restrictive cardiomyopathy, increased intracranial pressure, and concomitant use of phosphodiesterase inhibitors. Moreover, NTG should not be given to treat conditions wherein cardiac output is dependent on venous return, as in the setting of inferior myocardial infarction (MI) with right ventricular involvement. Furthermore, there is no evidence in the literature to support the erroneous use of NTG as a diagnostic therapy, with limited sensitivity yields for conclusive cardiac-associated chest pain.8
Adverse Effects and Events
The common side effects of NTG are well documented and include hypotension, tachycardia, flushing, nausea, vomiting, and headache.7,3,6 Syncope, bradycardia, and cardiac arrest following the administration of NTG are rare events, as evidenced by the paucity of literature describing these complications. Rather, it appears that these side effects are observed only in the setting of myocardial ischemia or MI.3,9-11 Fewer cases of ventricular fibrillation, responsive to defibrillation, and asystole also have been observed.9The exact mechanism for bradycardia without hypotension and subsequent asystole following NTG administration remains elusive, though this response is thought to be associated with the Bezold-Jarisch reflex.
Bezold-Jarisch Reflex
The Bezold-Jarisch reflex is a cardiovascular response consisting of bradycardia and hypotension that is believed to be from stimulation of inhibitory cardiac receptors by stretch, chemical, or pharmacological stimulation.12 The earliest cases of Bezold-Jarisch reflex following NTG occurred in the setting of MI and were attributed to ongoing myocardial ischemia.13 Recent studies have revealed that coronary stenosis without concurrent ischemia is actually not a sensitizing factor, and that bradycardia and asystole following NTG have occurred in patients without evidence of coronary artery disease.9,14 As part of this response, it is theorized that the development of bradycardia is related to vasovagal stimulation, a centrally mediated response to the headache or nausea following NTG administration.10,11,15
Despite these observational studies and after thorough review of the available cases, no unifying factors exist to predict with certainty the patient population in which this response is likely to occur.12,16Based on a literature review, it appears that asystole following NTG is self-limited; however, in most cases, bradycardia was treated with atropine without adverse side effects.12,15,16
Conclusion
The two cases presented involved a middle-aged male patient and an elderly female patient, both of whom had several cardiac risk factors but no evidence of acute ischemia or infarction on ECG or laboratory studies. It is well established that NTG can cause hypotension without bradycardia; however, the development of bradycardia without, or even preceding, hypotension is less recognized. Several mechanisms have been postulated but none fully explain this reaction; moreover, no anticipatory risk factors have been consistently observed. Even though the patients in Case 1 and 2 underwent extensive evaluation, no specific etiology of the observed reaction was identified, though neither patient underwent cardiac catheterization to definitively exclude abnormal coronary artery pathology as a precipitating factor.
These cases illustrate the unpredictable adverse reaction to a common medication used for a ubiquitous complaint. The explanation as to the source for this reaction is lacking, the literature has consistently described the transient and self-limiting effect of asystole following NTG.9,12,14,16Bradycardia, though self-limiting, remains responsive to appropriately dosed atropine when NTG-induced.3,12,16 The authors wish to stress the importance of establishing IV access and being prepared for adverse events whenever administering sublingual nitroglycerin to a patient.
1. Miura T, Nishinaka T, Terada T, Yonezawa K. Vasodilatory effect of nitroglycerin in Japanese subjects with different aldehyde dehydrogenase 2 (ALDH2) genotypes. Chem Biol Interact. 2017;276:40-45. doi:10.1016/j.cbi.2017.03.012.
2. Noonan PK, Williams RL, Benet LZ. Dose dependent pharmacokinetics of nitroglycerin after multiple intravenous infusions in healthy volunteers. J Pharmacokinet Biopharm. 1985;13(2):143-157.
3. Proulx MH, de Montigny L, Ross D, Vacon C, Juste LE, Segal E. Prehospital nitroglycerin in tachycardic chest pain patients: a risk for hypotension or not? Prehosp Emerg Care. 2017;21(1):68-73. doi:10.1080/10903127.2016.1194929.
4. Huis In ‘t Veld MA, Cullen L, Mahler SA, Backus BE, Dezman ZDW, Mattu A. The fast and the furious: low-risk chest pain and the rapid rule-out protocol. West J Emerg Med. 2017;18(3):474-478. doi:10.5811/westjem.2016.12.32676.
5. Pasupathy S, Tavella R, Grover S, et al. Early use of N-acetylcysteine with nitrate therapy in patients undergoing primary percutaneous coronary intervention for ST-segment-elevation myocardial infarction reduces myocardial infarct size (the NACIAM Trial [N-acetylcysteine in Acute Myocardial Infarction]). Circulation. 2017;136(10):894-903. doi:10.1161/CIRCULATIONAHA.117.027575.
6. Turan B, Daşlı T, Erkol A, Erden İ. Effectiveness of sublingual nitroglycerin before puncture compared with conventional intra-carterial nitroglycerin in transradial procedures: a randomized trial. Cardiovasc Revasc Med. 2015;16(7):391-396. doi:10.1016/j.carrev.2015.07.006.
7. Nagy-Grócz G, Bohár Z, Fejes-Szabó A, et al. Nitroglycerin increases serotonin transporter expression in rat spinal cord but anandamide modulated this effect. J Chem Neuroanat. 2017;85:13-20. doi:10.1016/j.jchemneu.2017.06.002.
8. Steele R, McNaughton T, McConahy M, Lam J. Chest pain in emergency department patients: if the pain is relieved by nitroglycerin, is it more likely to be cardiac chest pain? CJEM. 2006;8(3):164-169.
9. Dettorre K, Brywczynski J, McKinney J, Slovis C. Not the nitro? Patient goes into prehospital V-fib arrest following nitroglycerin. JEMS. 2009;34(5):34,36. doi:10.1016/S0197-2510(09)70124-X.
10. Buckley R, Roberts R. Symptomatic bradycardia following the administration of sublingual nitroglycerin. Am J Emerg Med. 1993;11(3):253-255.
11. Takase B, Uehata A, Nishioka T, et al. Different mechanisms of isoproterenol-induced and nitroglycerin-induced syncope during head-up tilt in patients with unexplained syncope: important role of epinephrine in nitroglycerin-induced syncope. J Cardiovasc Electrophysiol. 2001;12(7):791-796.
12. Brandes W, Santiago T, Limacher M. Nitroglycerin-induced hypotension, bradycardia, and asystole: report of a case and review of the literature. Clin Cardiol. 1990;13(10):741-744.
13. Ong EA, Canlas C, Smith W. Nitroglycerin-induced asystole. Arch Intern Med. 1985;145(5):954.
14. Shah SP, Waxman S. Two cases of Bezold-Jarisch reflex induced by intra-arterial nitroglycerin in critical left main coronary artery stenosis. Tex Heart Inst J. 2013;40(4):484-486.
15. Mark AL. The Bezold-Jarisch reflex revisited: clinical implications of inhibitory reflexes originating in the heart. J Am Coll Cardiol. 1983;1(1):90-102.
16. Younas F, Janjua M, Badshah A, DeGregorio M, Patel KC, Cotant JF. Transient complete heart block and isolated ventricular asystole with nitroglycerin. J Cardiovasc Med (Hagerstown). 2012;13(8):533-535. doi:10.2459/JCM.0b013e3283416b8b.
1. Miura T, Nishinaka T, Terada T, Yonezawa K. Vasodilatory effect of nitroglycerin in Japanese subjects with different aldehyde dehydrogenase 2 (ALDH2) genotypes. Chem Biol Interact. 2017;276:40-45. doi:10.1016/j.cbi.2017.03.012.
2. Noonan PK, Williams RL, Benet LZ. Dose dependent pharmacokinetics of nitroglycerin after multiple intravenous infusions in healthy volunteers. J Pharmacokinet Biopharm. 1985;13(2):143-157.
3. Proulx MH, de Montigny L, Ross D, Vacon C, Juste LE, Segal E. Prehospital nitroglycerin in tachycardic chest pain patients: a risk for hypotension or not? Prehosp Emerg Care. 2017;21(1):68-73. doi:10.1080/10903127.2016.1194929.
4. Huis In ‘t Veld MA, Cullen L, Mahler SA, Backus BE, Dezman ZDW, Mattu A. The fast and the furious: low-risk chest pain and the rapid rule-out protocol. West J Emerg Med. 2017;18(3):474-478. doi:10.5811/westjem.2016.12.32676.
5. Pasupathy S, Tavella R, Grover S, et al. Early use of N-acetylcysteine with nitrate therapy in patients undergoing primary percutaneous coronary intervention for ST-segment-elevation myocardial infarction reduces myocardial infarct size (the NACIAM Trial [N-acetylcysteine in Acute Myocardial Infarction]). Circulation. 2017;136(10):894-903. doi:10.1161/CIRCULATIONAHA.117.027575.
6. Turan B, Daşlı T, Erkol A, Erden İ. Effectiveness of sublingual nitroglycerin before puncture compared with conventional intra-carterial nitroglycerin in transradial procedures: a randomized trial. Cardiovasc Revasc Med. 2015;16(7):391-396. doi:10.1016/j.carrev.2015.07.006.
7. Nagy-Grócz G, Bohár Z, Fejes-Szabó A, et al. Nitroglycerin increases serotonin transporter expression in rat spinal cord but anandamide modulated this effect. J Chem Neuroanat. 2017;85:13-20. doi:10.1016/j.jchemneu.2017.06.002.
8. Steele R, McNaughton T, McConahy M, Lam J. Chest pain in emergency department patients: if the pain is relieved by nitroglycerin, is it more likely to be cardiac chest pain? CJEM. 2006;8(3):164-169.
9. Dettorre K, Brywczynski J, McKinney J, Slovis C. Not the nitro? Patient goes into prehospital V-fib arrest following nitroglycerin. JEMS. 2009;34(5):34,36. doi:10.1016/S0197-2510(09)70124-X.
10. Buckley R, Roberts R. Symptomatic bradycardia following the administration of sublingual nitroglycerin. Am J Emerg Med. 1993;11(3):253-255.
11. Takase B, Uehata A, Nishioka T, et al. Different mechanisms of isoproterenol-induced and nitroglycerin-induced syncope during head-up tilt in patients with unexplained syncope: important role of epinephrine in nitroglycerin-induced syncope. J Cardiovasc Electrophysiol. 2001;12(7):791-796.
12. Brandes W, Santiago T, Limacher M. Nitroglycerin-induced hypotension, bradycardia, and asystole: report of a case and review of the literature. Clin Cardiol. 1990;13(10):741-744.
13. Ong EA, Canlas C, Smith W. Nitroglycerin-induced asystole. Arch Intern Med. 1985;145(5):954.
14. Shah SP, Waxman S. Two cases of Bezold-Jarisch reflex induced by intra-arterial nitroglycerin in critical left main coronary artery stenosis. Tex Heart Inst J. 2013;40(4):484-486.
15. Mark AL. The Bezold-Jarisch reflex revisited: clinical implications of inhibitory reflexes originating in the heart. J Am Coll Cardiol. 1983;1(1):90-102.
16. Younas F, Janjua M, Badshah A, DeGregorio M, Patel KC, Cotant JF. Transient complete heart block and isolated ventricular asystole with nitroglycerin. J Cardiovasc Med (Hagerstown). 2012;13(8):533-535. doi:10.2459/JCM.0b013e3283416b8b.
Neoadjuvant-treated N2 rectal cancer linked to PCR failure
Orlando – Clinical an analysis of a large, multicenter database has suggested.

In multivariate regression, pretreatment N2 stage was the only variable significantly associated with failure of achieving pathologic complete response, according to Ebram Salama, MD, of Sir Mortimer B. Davis Jewish General Hospital at McGill University, Montreal.
“We should be reconsidering putting these patients in watch-and-wait protocols,” Dr. Salama said in an oral abstract presentation at the American College of Surgeons Quality and Safety Conference.
The analysis included 369 elective cases of cT2-4 N0-2 rectal cancer that were treated with neoadjuvant chemoradiotherapy during 2016 from the American College of Surgeons National Surgical Quality Improvement Program (NSQIP) proctectomy-specific database.
Of those cases, 53 (14.4%) achieved PCR, a proportion consistent with what has been reported previously in medical literature, Dr. Salama noted during his presentation.
The multivariate analysis revealed that pretreatment N2 stage was a negative predictor of PCR with an odds ratio of 0.18 (95% confidence interval, 0.04-0.82; P = .026), according to presented data.
By contrast, Dr. Salama said, there were no significant associations between response and other variables, including pretreatment N1 stage, pretreatment T stage, tumor location, gender, or body mass index.
Dr. Salama acknowledged limitations of this retrospective study, including a lack of data on other variables of interest, such as carcinoembryonic antigen, tumor size, imaging characteristics, molecular markers, and the time interval between chemoradiotherapy and surgery.
“We obviously need more data to evaluate other predictive factors in achieving a complete pathological response,” he said, adding that it’s also unclear whether the results of the present study could be generalized to institutions not participating in ACS NSQIP.
Dr. Salama presented the research on behalf of Nathalie Wong-Chong, MD, also of McGill University. He had no conflicts of interest to report for his presentation.
Orlando – Clinical an analysis of a large, multicenter database has suggested.
In multivariate regression, pretreatment N2 stage was the only variable significantly associated with failure of achieving pathologic complete response, according to Ebram Salama, MD, of Sir Mortimer B. Davis Jewish General Hospital at McGill University, Montreal.
“We should be reconsidering putting these patients in watch-and-wait protocols,” Dr. Salama said in an oral abstract presentation at the American College of Surgeons Quality and Safety Conference.
The analysis included 369 elective cases of cT2-4 N0-2 rectal cancer that were treated with neoadjuvant chemoradiotherapy during 2016 from the American College of Surgeons National Surgical Quality Improvement Program (NSQIP) proctectomy-specific database.
Of those cases, 53 (14.4%) achieved PCR, a proportion consistent with what has been reported previously in medical literature, Dr. Salama noted during his presentation.
The multivariate analysis revealed that pretreatment N2 stage was a negative predictor of PCR with an odds ratio of 0.18 (95% confidence interval, 0.04-0.82; P = .026), according to presented data.
By contrast, Dr. Salama said, there were no significant associations between response and other variables, including pretreatment N1 stage, pretreatment T stage, tumor location, gender, or body mass index.
Dr. Salama acknowledged limitations of this retrospective study, including a lack of data on other variables of interest, such as carcinoembryonic antigen, tumor size, imaging characteristics, molecular markers, and the time interval between chemoradiotherapy and surgery.
“We obviously need more data to evaluate other predictive factors in achieving a complete pathological response,” he said, adding that it’s also unclear whether the results of the present study could be generalized to institutions not participating in ACS NSQIP.
Dr. Salama presented the research on behalf of Nathalie Wong-Chong, MD, also of McGill University. He had no conflicts of interest to report for his presentation.
Orlando – Clinical an analysis of a large, multicenter database has suggested.
In multivariate regression, pretreatment N2 stage was the only variable significantly associated with failure of achieving pathologic complete response, according to Ebram Salama, MD, of Sir Mortimer B. Davis Jewish General Hospital at McGill University, Montreal.
“We should be reconsidering putting these patients in watch-and-wait protocols,” Dr. Salama said in an oral abstract presentation at the American College of Surgeons Quality and Safety Conference.
The analysis included 369 elective cases of cT2-4 N0-2 rectal cancer that were treated with neoadjuvant chemoradiotherapy during 2016 from the American College of Surgeons National Surgical Quality Improvement Program (NSQIP) proctectomy-specific database.
Of those cases, 53 (14.4%) achieved PCR, a proportion consistent with what has been reported previously in medical literature, Dr. Salama noted during his presentation.
The multivariate analysis revealed that pretreatment N2 stage was a negative predictor of PCR with an odds ratio of 0.18 (95% confidence interval, 0.04-0.82; P = .026), according to presented data.
By contrast, Dr. Salama said, there were no significant associations between response and other variables, including pretreatment N1 stage, pretreatment T stage, tumor location, gender, or body mass index.
Dr. Salama acknowledged limitations of this retrospective study, including a lack of data on other variables of interest, such as carcinoembryonic antigen, tumor size, imaging characteristics, molecular markers, and the time interval between chemoradiotherapy and surgery.
“We obviously need more data to evaluate other predictive factors in achieving a complete pathological response,” he said, adding that it’s also unclear whether the results of the present study could be generalized to institutions not participating in ACS NSQIP.
Dr. Salama presented the research on behalf of Nathalie Wong-Chong, MD, also of McGill University. He had no conflicts of interest to report for his presentation.
REPORTING FROM ACSQSC 2018
Key clinical point: N2 disease may be a negative predictor of pathological complete response after neoadjuvant chemoradiotherapy for rectal cancer.
Major finding: Pretreatment N2 stage was a negative predictor of complete pathological response, with an odds ratio of 0.18 (95% confidence interval, 0.04-0.82; P = .026).
Study details: A study of 369 elective cases of cT2-4 N0-2 rectal cancer treated with neoadjuvant chemoradiotherapy from 2016 in the ACS NSQIP proctectomy-specific database.
Disclosures: Dr. Salama had no conflicts of interest to report for his presentation.
PET/CT accurately predicts MCL stage
Bone marrow involvement in mantle cell lymphoma could be assessed using just 18fluorodeoxyglucose (FDG)–PET/CT, according to findings from a small, retrospective study published in Clinical Lymphoma, Myeloma & Leukemia.

Rustain Morgan, MD, of the University of Colorado, Aurora, and his colleagues found that, at a certain threshold of bone marrow voxels in standard uptake value (SUV), there was 100% sensitivity and 80% specificity in determining bone marrow involvement in mantle cell lymphoma (MCL).
Currently, National Comprehensive Cancer Network guidelines call for bone marrow biopsy and whole body FDG PET/CT scan to complete an initial diagnosis of MCL.
“One of the most important factors for correct staging is the identification of bone marrow involvement, occurring in approximately 55% of patients with MCL, which classifies patients as advanced stage. However, accurate analysis of bone marrow involvement can be challenging due to sampling error,” the researchers wrote. “While bone marrow biopsy remains the gold standard, it is not a perfect standard given unilateral variability.”
In previous studies, FDG PET/CT was not considered sensitive enough to detect gastrointestinal or bone marrow involvement. However, these earlier studies used SUV maximum or mean or a visual assessment of the bone marrow activity, compared with hepatic uptake. To address this issue, the researchers developed a new method of examining SUV distribution throughout the pelvic bones by analyzing thousands of bone marrow voxels within the bilateral iliacs.
During the developmental phase, an institutional dataset of 11 patients with MCL was used to define the voxel-based analysis. These patients had undergone both unilateral iliac bone marrow biopsy and FDG PET/CT at the initial diagnosis. Then, FDG PET/CT scans from another 12 patients with MCL from a different institution were used to validate the developmental phase findings. Finally, a control group of 5 people with no known malignancy were referred for FDG PET/CT pulmonary nodule evaluation.
“The hypothesis of the study was that, if the bone marrow was involved by lymphoma, then there would be a small increase in the SUV of each voxel, reflecting involvement by the lymphoma. In order to capture such changes, we analyzed the percent of total voxels in SUV ranging from 0.75 to 1.20, in increments of 0.05, as this is where the greatest divergence was visually identified,” the researchers wrote. “The goal was to identify if a percentage of voxels at a set SUV could detect lymphomatous involvement.”
The researchers identified 10 candidate thresholds in the developmental phase; 4 of these performed better than the others in the validation phase. Using those thresholds, 10 of the 12 patients in the validation cohort could be correctly staged using FDG PET/CT.
Further analysis identified a single threshold that performed best: If greater than 38% of the voxels (averaging 1,734 voxels) demonstrated an SUV of less than 0.95, the sensitivity was 100% and the specificity was 80%.
The researchers acknowledged that the findings are limited because of the study’s small sample size and said the results should be validated in a larger trial.
There was no external funding for the study and the researchers reported having no financial disclosures.
SOURCE: Morgan R et al. Clin Lymphoma Myeloma Leuk. 2018 Jul 4. doi: 10.1016/j.clml.2018.06.024.
Bone marrow involvement in mantle cell lymphoma could be assessed using just 18fluorodeoxyglucose (FDG)–PET/CT, according to findings from a small, retrospective study published in Clinical Lymphoma, Myeloma & Leukemia.
Rustain Morgan, MD, of the University of Colorado, Aurora, and his colleagues found that, at a certain threshold of bone marrow voxels in standard uptake value (SUV), there was 100% sensitivity and 80% specificity in determining bone marrow involvement in mantle cell lymphoma (MCL).
Currently, National Comprehensive Cancer Network guidelines call for bone marrow biopsy and whole body FDG PET/CT scan to complete an initial diagnosis of MCL.
“One of the most important factors for correct staging is the identification of bone marrow involvement, occurring in approximately 55% of patients with MCL, which classifies patients as advanced stage. However, accurate analysis of bone marrow involvement can be challenging due to sampling error,” the researchers wrote. “While bone marrow biopsy remains the gold standard, it is not a perfect standard given unilateral variability.”
In previous studies, FDG PET/CT was not considered sensitive enough to detect gastrointestinal or bone marrow involvement. However, these earlier studies used SUV maximum or mean or a visual assessment of the bone marrow activity, compared with hepatic uptake. To address this issue, the researchers developed a new method of examining SUV distribution throughout the pelvic bones by analyzing thousands of bone marrow voxels within the bilateral iliacs.
During the developmental phase, an institutional dataset of 11 patients with MCL was used to define the voxel-based analysis. These patients had undergone both unilateral iliac bone marrow biopsy and FDG PET/CT at the initial diagnosis. Then, FDG PET/CT scans from another 12 patients with MCL from a different institution were used to validate the developmental phase findings. Finally, a control group of 5 people with no known malignancy were referred for FDG PET/CT pulmonary nodule evaluation.
“The hypothesis of the study was that, if the bone marrow was involved by lymphoma, then there would be a small increase in the SUV of each voxel, reflecting involvement by the lymphoma. In order to capture such changes, we analyzed the percent of total voxels in SUV ranging from 0.75 to 1.20, in increments of 0.05, as this is where the greatest divergence was visually identified,” the researchers wrote. “The goal was to identify if a percentage of voxels at a set SUV could detect lymphomatous involvement.”
The researchers identified 10 candidate thresholds in the developmental phase; 4 of these performed better than the others in the validation phase. Using those thresholds, 10 of the 12 patients in the validation cohort could be correctly staged using FDG PET/CT.
Further analysis identified a single threshold that performed best: If greater than 38% of the voxels (averaging 1,734 voxels) demonstrated an SUV of less than 0.95, the sensitivity was 100% and the specificity was 80%.
The researchers acknowledged that the findings are limited because of the study’s small sample size and said the results should be validated in a larger trial.
There was no external funding for the study and the researchers reported having no financial disclosures.
SOURCE: Morgan R et al. Clin Lymphoma Myeloma Leuk. 2018 Jul 4. doi: 10.1016/j.clml.2018.06.024.
Bone marrow involvement in mantle cell lymphoma could be assessed using just 18fluorodeoxyglucose (FDG)–PET/CT, according to findings from a small, retrospective study published in Clinical Lymphoma, Myeloma & Leukemia.
Rustain Morgan, MD, of the University of Colorado, Aurora, and his colleagues found that, at a certain threshold of bone marrow voxels in standard uptake value (SUV), there was 100% sensitivity and 80% specificity in determining bone marrow involvement in mantle cell lymphoma (MCL).
Currently, National Comprehensive Cancer Network guidelines call for bone marrow biopsy and whole body FDG PET/CT scan to complete an initial diagnosis of MCL.
“One of the most important factors for correct staging is the identification of bone marrow involvement, occurring in approximately 55% of patients with MCL, which classifies patients as advanced stage. However, accurate analysis of bone marrow involvement can be challenging due to sampling error,” the researchers wrote. “While bone marrow biopsy remains the gold standard, it is not a perfect standard given unilateral variability.”
In previous studies, FDG PET/CT was not considered sensitive enough to detect gastrointestinal or bone marrow involvement. However, these earlier studies used SUV maximum or mean or a visual assessment of the bone marrow activity, compared with hepatic uptake. To address this issue, the researchers developed a new method of examining SUV distribution throughout the pelvic bones by analyzing thousands of bone marrow voxels within the bilateral iliacs.
During the developmental phase, an institutional dataset of 11 patients with MCL was used to define the voxel-based analysis. These patients had undergone both unilateral iliac bone marrow biopsy and FDG PET/CT at the initial diagnosis. Then, FDG PET/CT scans from another 12 patients with MCL from a different institution were used to validate the developmental phase findings. Finally, a control group of 5 people with no known malignancy were referred for FDG PET/CT pulmonary nodule evaluation.
“The hypothesis of the study was that, if the bone marrow was involved by lymphoma, then there would be a small increase in the SUV of each voxel, reflecting involvement by the lymphoma. In order to capture such changes, we analyzed the percent of total voxels in SUV ranging from 0.75 to 1.20, in increments of 0.05, as this is where the greatest divergence was visually identified,” the researchers wrote. “The goal was to identify if a percentage of voxels at a set SUV could detect lymphomatous involvement.”
The researchers identified 10 candidate thresholds in the developmental phase; 4 of these performed better than the others in the validation phase. Using those thresholds, 10 of the 12 patients in the validation cohort could be correctly staged using FDG PET/CT.
Further analysis identified a single threshold that performed best: If greater than 38% of the voxels (averaging 1,734 voxels) demonstrated an SUV of less than 0.95, the sensitivity was 100% and the specificity was 80%.
The researchers acknowledged that the findings are limited because of the study’s small sample size and said the results should be validated in a larger trial.
There was no external funding for the study and the researchers reported having no financial disclosures.
SOURCE: Morgan R et al. Clin Lymphoma Myeloma Leuk. 2018 Jul 4. doi: 10.1016/j.clml.2018.06.024.
REPORTING FROM CLINICAL LYMPHOMA, MYELOMA & LEUKEMIA
Key clinical point:
Major finding: If greater than 38% of the voxels demonstrated an standard uptake value of less than 0.95, there was a sensitivity of 100% and a specificity of 80%.
Study details: A retrospective cohort study of 23 patients with mantle cell leukemia and 5 controls.
Disclosures: There was no external funding for the study and the researchers reported having no financial disclosures.
Source: Morgan R et al. Clin Lymphoma Myeloma Leuk. 2018 Jul 4. doi: 10.1016/j.clml.2018.06.024.