User login
Acute Limb Arterial Ischemia
Acute limb ischemia (ALI) is an emergent medical condition that is characterized by a precipitous decrease in limb perfusion that threatens the viability of the affected limb, and symptoms that have been present for 14 days or less.1-5 The incidence of lower extremity ALI in the US is nine to 16 cases per 100,000 persons per year, and one to three cases per 100,000 persons per year for upper extremity ALI.3 Symptoms suggestive of this condition classically include pain in the effected limb at rest, loss of sensation, impaired motor function, and cyanosis/pallor. Irreparable damage can occur in as quickly as 4 to 6 hours with complete arterial occlusion. A majority of ALI is caused by thrombosis, with the remainder of cases caused by embolism, 85% and 15% respectively.1-6 If not addressed promptly, this condition carries a high degree of morbidity (ie, limb loss) and mortality. Immediate initiation of anticoagulation therapy and vascular surgery consultation are mainstays of ED management. Time-to-treatment is a predictor of success and is an area where the emergency physician (EP) can make a significant difference in patient outcomes.7 Although vascular interruption via traumatic mechanism is not addressed in this review, it should remain a consideration in relation to the historical features of each case.
Presentation
Traditionally, symptoms of ALI can be remembered as the “six Ps”: pain, pallor, paresthesia, paralysis, pulselessness, and poikilothermia. Note that ALI represents a spectrum of disease, and the presenting features depend heavily on the level and degree of obstruction. Pain, however, is most frequently the first presenting symptom of patients with ALI.1-6 Pain will occur in muscle groups distal to the occlusion. Obstruction of the aortoiliac region might produce pain in the buttocks, thigh, and hip, whereas occlusion of the femoral artery may produce pain in the calf. Single-level disease will often produce claudication, but multilevel disease may present as a nonhealing ulcer or with focal gangrene. The differential diagnosis of ALI includes direct arterial injury, vasospasm, compartment syndrome, chronic peripheral artery disease, stroke, spinal cord injury, vasculitis, muscular trauma, and radiculopathy.3,5
Etiology
As stated previously, ALI is a result of either thrombotic or embolic phenomena that either partially or completely occludes a vessel such that adequate perfusion is no longer achieved. Consequently, there is a decrease in the metabolism of the tissue supplied in those territories, which can rapidly progress to necrosis. Thrombosis is the most common cause of ALI, accounting for approximately 85%.2,3Typically, thrombosis presents in the setting of pre-existing peripheral artery disease (PAD).8 As PAD worsens, damage to the arterial endothelium triggers platelet activation, and accumulation in a manner conceptually similar to thrombosis in myocardial infarction.9 Hypercoagulable states increase the risk of thrombi development.10 Symptoms of thrombosis are often more insidious in onset when compared to embolism, and signs/symptoms of prior claudication are almost always present. Consequently, there is a greater chance that collateral circulation has developed over time.2,6,11,12
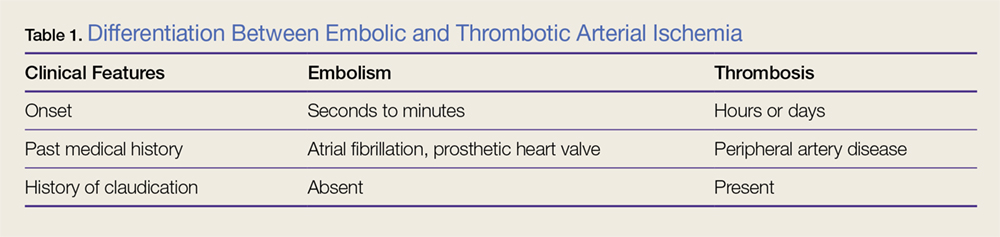
By contrast, ALI caused by embolism is more acute in onset, and is often more emergent due to complete occlusion without chance of collateral vessel development.1,3,6,12 See Table 1 for differences in risk factors and presentation between thrombotic and embolic occlusion.
Historical Features
Information should be obtained systematically in all presentations and should include time of symptom onset, duration, severity, and location; however, special attention should be paid to the evolution of symptoms over time. One historical pearl that should raise suspicion of embolism vs thrombus is a patient history with a specific time of symptom onset. Specific questioning about history of claudication, including description of typical symptoms, is critical. A full list of other medical comorbidities should be obtained. This may reveal risk factors for thrombotic and embolic disease.1,3-5 This also may alter available treatment options.7,8,12,13 At presentation, the EP should obtain a list of the patient’s current medications, and special attention should be given to prothrombotic medications and medications that may interact with anticoagulants.
Physical Examination
On physical examination, the EP should pay particular attention to both the external appearance and temperature of the skin of the patient’s affected extremity. The presence or absence of peripheral pulses is an important feature when assessing for ALI; however, the presence of peripheral pulses does not exclude ALI from the differential.
Precise evaluation of sensation is important to attempt to quantify the extent of injury, localize a possible obstruction, and differentiate ALI from other possible causes of sensation deficits. Though not referenced in the six Ps, the patient’s limb may also appear mottled or marbled. Embolic phenomena occur at sites of vascular bifurcation. In a patient with aortic embolism, femoral pulses will be absent with bilateral mottling and paralysis of the lower extremities. Iliac artery embolism will produce the same symptoms, except unilateral. Femoral artery embolism will yield coolness and mottling distal to the inguinal ligament. Similarly, popliteal artery embolism will produce those same findings, except distal to the knee with preserved femoral pulses.
Diagnosis and Evaluation
After the history and physical examination are completed, further diagnostic methodologies should be considered, including laboratory evaluation and additional imaging studies.
Imaging Studies
Doppler ultrasound examination to assess for pulses on the affected limb should be performed immediately. Bedside continuous-wave Doppler may be used to differentiate arterial vs venous signal.6,14-16 An ankle brachial index may be calculated through either direct auscultation of pulses or Doppler signal. A ratio of less than 0.9 is suggestive of ischemia, while a ratio of less than 0.5 is considered critical ischemia.2
Laboratory Evaluation
Laboratory evaluation of hematocrit, coagulation studies, renal function, electrolyte levels, lactate, and creatinine kinase should be completed.1,5 An electrocardiogram and bedside/formal echocardiogram may be considered if embolism is suspected.1,6,17
Imaging
Angiography is currently the gold standard imaging modality to diagnose ALI.16 However, other imaging modalities exist that expose the patient to less radiation and are generally preferred by patients.18 Duplex ultrasonography is the least invasive imaging modality, with a reported sensitivity of 88% and specificity of 96% for the detection of greater than 50% stenosis.6,19 Contrast-enhanced magnetic resonance angiography (MRA) of the lower extremity is also relatively noninvasive, but is more limited in its application. It carries a reported sensitivity of 95% and a specificity of 97% for detection of stenosis of greater than 50%.6,19 An MRA without contrast may be considered for patients with an estimated glomerular filtration rate of less than 30 mL/min/1.73 m2 and who are not on dialysis, but the diagnostic efficacy is reduced.16 Finally, the sensitivity and specificity of computed tomography angiography (CTA) to detect aortoiliac stenosis of greater than 50% is 96% and 98% respectively.6,18,19 Other studies demonstrated similar results for other arterial locations in the lower extremities.18,19 A principal advantage of CTA is that direct visualization of calcifications, clips, stents, and prior bypasses is possible without the limitations of MRA.16 The American College of Radiology (ACR) lists ultrasound duplex Doppler and noncontrast MRA of the lower extremity as “may be appropriate.”16 In contrast, the ACR classifies MRA with contrast, CTA with contrast, and angiography of the lower extremity as “usually appropriate.”16 Selecting the optimal imaging study for a patient may require involvement of a facility’s radiology department and/or a vascular surgeon.14,15
Management in the ED
Even before the definitive diagnosis of ALI is made, steps can be taken to minimize and/or slow progression of injury. Placing the affected limb in a dependent position and providing intravenous (IV) fluid hydration will maximize perfusion.1,3,5 Even with consideration of the diagnostic modalities previously described, ALI is often considered a clinical diagnosis. Since time is critical, early consultation with vascular surgery services is imperative if ALI is suspected.
Intravenous Fluid Therapy
Suspected ALI should be treated in the ED with an IV heparin bolus, followed by constant IV infusion. Heparin prevents proximal and distal propagation of the thrombus.1,3,5,6,15,17,20 Additionally, it helps maintain the microcirculation surrounding the affected area.6 A heparin bolus dose of 100 U/kg followed by a continuous infusion of heparin 1,000 U/h is the recommended standard.1,3,5,6,15 A goal partial thromboplastin time of 60 to 100 seconds, or an international normalized ratio of 2 to 3 is desirable.8,21
Staging: The Rutherford Classification System
Once immediate therapies are started, the stage of PAD should be determined using the Rutherford classification system in collaboration with vascular surgery services; this will further guide treatment and disposition.
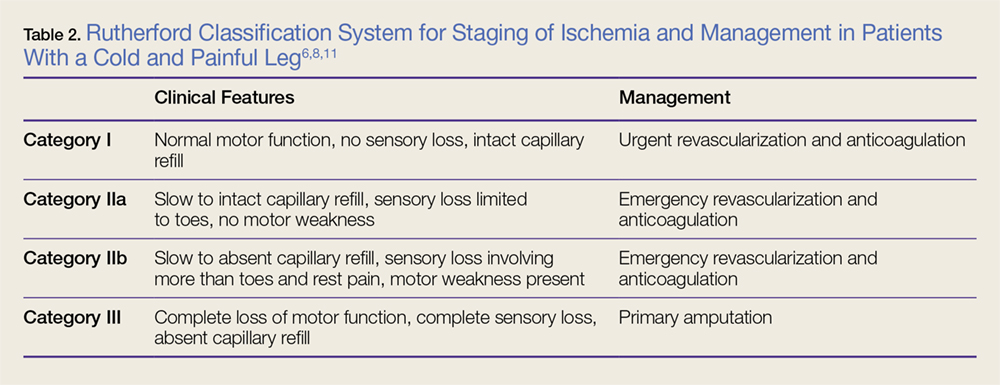
Category I. In category I ALI, the affected limb is considered viable and not immediately threatened.
Category IIa. The limb is considered to be marginally threatened and salvageable.
Category IIb. An ALI classified as a category IIb is the most urgent type in which the limb is immediately threatened.
Category III. The limb is classified as having irreversible damage.2,3,17,22
(See Table 2 for a more detailed summary of the Rutherford classification system.)
Treatment
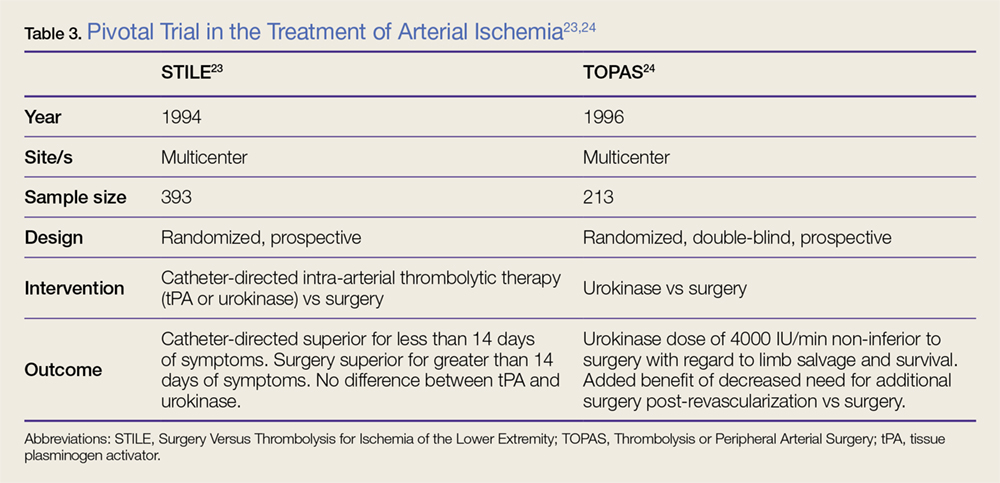
Definitive treatment decisions should be made in consultation with vascular surgery services. The results of three clinical trials developed the foundation for management of ALI: the Thrombolysis or Peripheral Arterial Surgery (TOPAS) trial, Surgery Versus Thrombolysis for Ischemia of the Lower Extremity (STILE) trial, and Rutherford trial.22-24 Table 3 provides a summary of the treatment techniques utilized, which include mechanical recanalization with percutaneous aspiration thrombectomy, percutaneous mechanical thrombectomy,6,12,25-28 pharmacological recanalization via catheter-directed thrombolysis,6,8,12,20,23-28 and/or surgical management via thrombectomy or embolectomy.6,11,23,24,27
Complications
The complications of treating ALI can be stratified into three subsets: pharmacologic, mechanical, and reperfusion injury-related. Medical treatment with heparin is not without risk. Intracranial hemorrhage, major bleeding at other sites, and compartment syndrome secondary to bleeding can all occur. Treatment may also cause distal embolization and lead to mechanical occlusion of another site. Finally, reperfusion injury predisposes the patient to a host of new problems. Reperfusion injury occurs when fresh blood enters a previously ischemic zone. When this occurs, oxygen free radicals, inflammatory mediators, and catabolism byproducts mix with the blood. This process can damage surrounding epithelial cells and lead to increased interstitial permeability. As a result, compartment syndrome may also develop via this mechanism.1,3,5,6 The anterior compartment of the lower extremity is most at risk. As such, assessment of peroneal nerve activity via dorsiflexion of the foot and sensation testing is important after the initiation of treatment.6 Systemic distribution of these harmful byproducts can also cause arrhythmias, renal failure, and systemic acadisos.1,3,5,6 It is important for physicians and staff to monitor the patient closely for the development of these complications and be prepared to intervene.
Opportunities for Improvement
In a condition where minutes matter, expedient action is critical. Time-to-recognition, imaging, consultation, and intervention all are potential sources of delay. Two recent studies have investigated the treatment timeline of ALI. The first study showed that the greatest source of delay is time from symptom onset to presentation in the ED; an average of 11.35 hours. The second largest source of delay was time from recognition of ALI to imaging, with an average delay of 4.75 hours. The average ED evaluation time was 40 minutes, and the average total time to intervention was 10.2 hours. While time-to-symptom presentation may represent a failure of public health, time-to-imaging was identified as an area of unacceptable delay by the authors.29 A second study examined the effect of pre-hospital care on the time-to-treatment. Persons who were transported via emergency medical services (EMS) arrived to the hospital at a median time of 5 hours after symptom onset, were seen by a physician at a median time of 51 minutes, and had revascularization at a median time of 23 hours. Those not transported by EMS arrived to the hospital at a median time of 48 hours after symptom onset, were seen by a physician at a median time of 80 minutes, and had revascularization at a median time of 93 hours. As a secondary goal, the study examined the effect of heparinization in the ED and showed that treatment with heparin was associated with a favorable outcome.30 While the total treatment times in each study vary widely, they share several important commonalities and reinforce expedient management as an important goal.
Outcomes
Advances in the treatment of this condition began in the 1970s, with an explosion of new techniques and data in the past several years. Still, ALI is a high morbidity and high mortality condition. Rates of limb loss are approximately 30% for all cases, and it is a fatal condition for as many as one-in-five. As discussed earlier, the patients who are most likely to experience ALI typically have several medical comorbidities. Perhaps unsurprisingly, ALI portends a poor prognosis even if the limb is salvaged. Approximately 15% to 20% of patients with ALI will die within 1 year of diagnosis.3,4,6,12
Conclusion
Acute limb ischemia is a rare condition, but a true medical emergency. Prompt recognition of the signs and symptoms of ALI are critical for optimizing patient outcomes. A high index of clinical suspicion in patients with risk factors may lead to early diagnosis. Early vascular surgery consultation and early IV heparin treatment are important aspects of care. Prompt imaging and staging guide further management. Special care should be paid to possible post-treatment complications and to the investigation of contributing factors. The EP has a great opportunity to positively impact care with expeditious management. Early diagnosis, targeted history and physical examination, prompt treatment, collaboration with specialists, and prevention and treatment of life-threatening complications are all hallmarks of emergency medicine.
1. Braun R, Lin M. Acute limb ischemia: a case report and literature review. J Emerg Med. 2015;49(6):1011-1017. doi:10.1016/j.jemermed.2015.03.008.
2. Callum K, Bradbury A. ABC of arterial and venous disease: acute limb ischaemia. BMJ. 2000;320(7237):764-767.
3. Creager MA, Kaufman JA, Conte MS. Clinical practice. Acute limb ischemia. N Engl J Med. 2012;366(23):2198-2206. doi:10.1056/NEJMcp1006054.
4. Purushottam B, Gujja K, Zalewski A, Krishnan P. Acute limb ischemia. Interv Cardiol Clin. 2014;3(4):557-572.
5. Santistevan JR. Acute limb ischemia: an emergency medicine approach. Emerg Med Clin North Am. 2017;35(4):889-909. doi:10.1016/j.emc.2017.07.006.
6. Acar RD, Sahin M, Kirma C. One of the most urgent vascular circumstances: acute limb ischemia. SAGE Open Med. 2013;1:2050312113516110. doi:10.1177/2050312113516110.
7. Abou-Zamzam AM Jr, Gomez NR, Molkara A, et al. A prospective analysis of critical limb ischemia: factors leading to major primary amputation versus revascularization. Ann Vasc Surg. 2007;21(4):458-463.
8. Gerhard-Herman MD, Gornik HL, Barrett C, et al. 2016 AHA/ACC guideline on the management of patients with lower extremity peripheral artery disease: executive summary: a report of the American College of Cardiology/American Heart Association Task Force on clinical practice guidelines. J Am Coll Cardiol. 2017;69(11):1465-1508.
9. Rajagopalan S, Mckay I, Ford I, Bachoo P, Greaves M, Brittenden J. Platelet activation increases with the severity of peripheral arterial disease: implications for clinical management. J Vasc Surg. 2007;46(3):485-490.
10. Deitcher SR, Carman TL, Sheikh MA, Gomes M. Hypercoagulable syndromes: evaluation and management strategies for acute limb ischemia. Semin Vasc Surg. 2001;14(2):74-85.
11. Blaisdell FW, Steele M, Allen RE. Management of acute lower extremity arterial ischemia due to embolism and thrombosis. Surgery. 1978;84(6):822-834.
12. Byrne RM, Taha AG, Avgerinos E, Marone LK, Makaroun MS, Chaer RA. Contemporary outcomes of endovascular interventions for acute limb ischemia. J Vasc Surg. 2014;59(4):988-995.
13. Soden PA, Zettervall SL, Curran T, et al. Regional variation in patient selection and treatment for lower extremity vascular disease in the Vascular Quality Initiative. J Vasc Surg. 2017;65(1):108-118. doi:10.1016/j.jvs.2016.06.105.
14. Aboyans V, Björck M, Brodmann M, et al; ESC Scientific Document Group. Questions and answers on diagnosis and management of patients with Peripheral Arterial Diseases: a companion document of the 2017 ESC Guidelines for the Diagnosis and Treatment of Peripheral Arterial Diseases, in collaboration with the European Society for Vascular Surgery (ESVS): Endorsed by: the European Stroke Organisation (ESO)The Task Force for the Diagnosis and Treatment of Peripheral Arterial Diseases of the European Society of Cardiology (ESC) and of the European Society for Vascular Surgery (ESVS). Eur Heart J. 2017. doi:10.1093/eurheartj/ehx499. [Epub ahead of print]
15. Authors/Task Force Members, Aboyans V, Ricco JB, et al. 2017 ESC guidelines on the diagnosis and treatment of peripheral arterial diseases, in collaboration with the European Society for Vascular Surgery (ESVS). Eur J Vasc Endovasc Surg. 2017. doi:10.1016/j.ejvs.2017.07.018. [Epub ahead of print]
16. Expert Panel on Vascular Imaging: Weiss CR, Azene EM, Majdalany BS, et al. ACR Appropriateness Criteria® sudden onset of cold, painful leg. J Am Coll Radiol. 2017;14(5S):S307-S313. doi:10.1016/j.jacr.2017.02.015.
17. Dieter RS, Dieter RA Jr, Dieter RA 3rd, Nanjundappa A. Critical Limb Ischemia: Acute and Chronic. New York, NY: Springer; 2016.
18. Met R, Bipat S, Legemate DA, Reekers JA, Koelemay MJ. Diagnostic performance of computed tomography angiography in peripheral arterial disease: a systematic review and meta-analysis. JAMA. 2009;301(4):415-424.
19. Collins R, Burch J, Cranny G, et al. Duplex ultrasonography, magnetic resonance angiography, and computed tomography angiography for diagnosis and assessment of symptomatic, lower limb peripheral arterial disease: systematic review. BMJ. 2007;334(7606):1257.
20. Giannini D, Balbarini A. Thrombolytic therapy in peripheral arterial disease. Curr Drug Targets Cardiovasc Haematol Disord. 2004;4(3):249-258.
21. Kearon C, Kahn SR, Agnelli G, Goldhaber S, Raskob GE, Comerota AJ. Antithrombotic therapy for venous thromboembolic disease: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines (8th Edition). Chest. 2008;133(6 Suppl):454S-545S. doi:10.1378/chest.08-0658.
22. Rutherford RB, Baker JD, Ernst C, et al. Recommended standards for reports dealing with lower extremity ischemia: revised version. J Vasc Surg. 1997;26(3):517-538.
23. Ouriel K, Veith FJ, Sasahara AA. Thrombolysis or peripheral arterial surgery: phase I results. TOPAS Investigators. J Vasc Surg. 1996;23(1):64-73; discussion 74-75.
24. Results of a prospective randomized trial evaluating surgery versus thrombolysis for ischemia of the lower extremity. The STILE trial. Ann Surg. 1994;220(3):251-266; discussion 266-268.
25. Kashyap VS, Gilani R, Bena JF, Bannazadeh M, Sarac TP. Endovascular therapy for acute limb ischemia. J Vasc Surg. 2011;53(2):340-346. doi:10.1016/j.jvs.2010.08.064.
26. Patel NH, Krishnamurthy VN, Kim S, et al. Quality improvement guidelines for percutaneous management of acute lower-extremity ischemia. J Vasc Interv Radiol. 2013;24(1):3-15.
27. Taha AG, Byrne RM, Avgerinos ED, Marone LK, Makaroun MS, Chaer RA. Comparative effectiveness of endovascular versus surgical revascularization for acute lower extremity ischemia. J Vasc Surg. 2015;61(1):147-154. doi:10.1016/j.jvs.2014.06.109.
28. Zeller T, Tepe G. Treatment of acute limb ischemia with focus on endovascular techniques. Vasa. 2009;38(2):123-133. doi: 10.1024/0301-1526.38.2.123.
29. Normahani P, Standfield NJ, Jaffer U. Sources of delay in the acute limb ischemia patient pathway. Ann Vasc Surg. 2017;38:279-285. doi:10.1016/j.avsg.2016.05.118.
30. Langenskiöld M, Smidfelt K, Karlsson A, Bohm C, Herlitz J, Nordanstig J. Weak links in the early chain of care of acute lower limb ischaemia in terms of recognition and emergency management. Eur J Vasc Endovasc Surg. 2017;54(2):235-240. doi:10.1016/j.ejvs.2017.04.010.
Acute limb ischemia (ALI) is an emergent medical condition that is characterized by a precipitous decrease in limb perfusion that threatens the viability of the affected limb, and symptoms that have been present for 14 days or less.1-5 The incidence of lower extremity ALI in the US is nine to 16 cases per 100,000 persons per year, and one to three cases per 100,000 persons per year for upper extremity ALI.3 Symptoms suggestive of this condition classically include pain in the effected limb at rest, loss of sensation, impaired motor function, and cyanosis/pallor. Irreparable damage can occur in as quickly as 4 to 6 hours with complete arterial occlusion. A majority of ALI is caused by thrombosis, with the remainder of cases caused by embolism, 85% and 15% respectively.1-6 If not addressed promptly, this condition carries a high degree of morbidity (ie, limb loss) and mortality. Immediate initiation of anticoagulation therapy and vascular surgery consultation are mainstays of ED management. Time-to-treatment is a predictor of success and is an area where the emergency physician (EP) can make a significant difference in patient outcomes.7 Although vascular interruption via traumatic mechanism is not addressed in this review, it should remain a consideration in relation to the historical features of each case.
Presentation
Traditionally, symptoms of ALI can be remembered as the “six Ps”: pain, pallor, paresthesia, paralysis, pulselessness, and poikilothermia. Note that ALI represents a spectrum of disease, and the presenting features depend heavily on the level and degree of obstruction. Pain, however, is most frequently the first presenting symptom of patients with ALI.1-6 Pain will occur in muscle groups distal to the occlusion. Obstruction of the aortoiliac region might produce pain in the buttocks, thigh, and hip, whereas occlusion of the femoral artery may produce pain in the calf. Single-level disease will often produce claudication, but multilevel disease may present as a nonhealing ulcer or with focal gangrene. The differential diagnosis of ALI includes direct arterial injury, vasospasm, compartment syndrome, chronic peripheral artery disease, stroke, spinal cord injury, vasculitis, muscular trauma, and radiculopathy.3,5
Etiology
As stated previously, ALI is a result of either thrombotic or embolic phenomena that either partially or completely occludes a vessel such that adequate perfusion is no longer achieved. Consequently, there is a decrease in the metabolism of the tissue supplied in those territories, which can rapidly progress to necrosis. Thrombosis is the most common cause of ALI, accounting for approximately 85%.2,3Typically, thrombosis presents in the setting of pre-existing peripheral artery disease (PAD).8 As PAD worsens, damage to the arterial endothelium triggers platelet activation, and accumulation in a manner conceptually similar to thrombosis in myocardial infarction.9 Hypercoagulable states increase the risk of thrombi development.10 Symptoms of thrombosis are often more insidious in onset when compared to embolism, and signs/symptoms of prior claudication are almost always present. Consequently, there is a greater chance that collateral circulation has developed over time.2,6,11,12
By contrast, ALI caused by embolism is more acute in onset, and is often more emergent due to complete occlusion without chance of collateral vessel development.1,3,6,12 See Table 1 for differences in risk factors and presentation between thrombotic and embolic occlusion.
Historical Features
Information should be obtained systematically in all presentations and should include time of symptom onset, duration, severity, and location; however, special attention should be paid to the evolution of symptoms over time. One historical pearl that should raise suspicion of embolism vs thrombus is a patient history with a specific time of symptom onset. Specific questioning about history of claudication, including description of typical symptoms, is critical. A full list of other medical comorbidities should be obtained. This may reveal risk factors for thrombotic and embolic disease.1,3-5 This also may alter available treatment options.7,8,12,13 At presentation, the EP should obtain a list of the patient’s current medications, and special attention should be given to prothrombotic medications and medications that may interact with anticoagulants.
Physical Examination
On physical examination, the EP should pay particular attention to both the external appearance and temperature of the skin of the patient’s affected extremity. The presence or absence of peripheral pulses is an important feature when assessing for ALI; however, the presence of peripheral pulses does not exclude ALI from the differential.
Precise evaluation of sensation is important to attempt to quantify the extent of injury, localize a possible obstruction, and differentiate ALI from other possible causes of sensation deficits. Though not referenced in the six Ps, the patient’s limb may also appear mottled or marbled. Embolic phenomena occur at sites of vascular bifurcation. In a patient with aortic embolism, femoral pulses will be absent with bilateral mottling and paralysis of the lower extremities. Iliac artery embolism will produce the same symptoms, except unilateral. Femoral artery embolism will yield coolness and mottling distal to the inguinal ligament. Similarly, popliteal artery embolism will produce those same findings, except distal to the knee with preserved femoral pulses.
Diagnosis and Evaluation
After the history and physical examination are completed, further diagnostic methodologies should be considered, including laboratory evaluation and additional imaging studies.
Imaging Studies
Doppler ultrasound examination to assess for pulses on the affected limb should be performed immediately. Bedside continuous-wave Doppler may be used to differentiate arterial vs venous signal.6,14-16 An ankle brachial index may be calculated through either direct auscultation of pulses or Doppler signal. A ratio of less than 0.9 is suggestive of ischemia, while a ratio of less than 0.5 is considered critical ischemia.2
Laboratory Evaluation
Laboratory evaluation of hematocrit, coagulation studies, renal function, electrolyte levels, lactate, and creatinine kinase should be completed.1,5 An electrocardiogram and bedside/formal echocardiogram may be considered if embolism is suspected.1,6,17
Imaging
Angiography is currently the gold standard imaging modality to diagnose ALI.16 However, other imaging modalities exist that expose the patient to less radiation and are generally preferred by patients.18 Duplex ultrasonography is the least invasive imaging modality, with a reported sensitivity of 88% and specificity of 96% for the detection of greater than 50% stenosis.6,19 Contrast-enhanced magnetic resonance angiography (MRA) of the lower extremity is also relatively noninvasive, but is more limited in its application. It carries a reported sensitivity of 95% and a specificity of 97% for detection of stenosis of greater than 50%.6,19 An MRA without contrast may be considered for patients with an estimated glomerular filtration rate of less than 30 mL/min/1.73 m2 and who are not on dialysis, but the diagnostic efficacy is reduced.16 Finally, the sensitivity and specificity of computed tomography angiography (CTA) to detect aortoiliac stenosis of greater than 50% is 96% and 98% respectively.6,18,19 Other studies demonstrated similar results for other arterial locations in the lower extremities.18,19 A principal advantage of CTA is that direct visualization of calcifications, clips, stents, and prior bypasses is possible without the limitations of MRA.16 The American College of Radiology (ACR) lists ultrasound duplex Doppler and noncontrast MRA of the lower extremity as “may be appropriate.”16 In contrast, the ACR classifies MRA with contrast, CTA with contrast, and angiography of the lower extremity as “usually appropriate.”16 Selecting the optimal imaging study for a patient may require involvement of a facility’s radiology department and/or a vascular surgeon.14,15
Management in the ED
Even before the definitive diagnosis of ALI is made, steps can be taken to minimize and/or slow progression of injury. Placing the affected limb in a dependent position and providing intravenous (IV) fluid hydration will maximize perfusion.1,3,5 Even with consideration of the diagnostic modalities previously described, ALI is often considered a clinical diagnosis. Since time is critical, early consultation with vascular surgery services is imperative if ALI is suspected.
Intravenous Fluid Therapy
Suspected ALI should be treated in the ED with an IV heparin bolus, followed by constant IV infusion. Heparin prevents proximal and distal propagation of the thrombus.1,3,5,6,15,17,20 Additionally, it helps maintain the microcirculation surrounding the affected area.6 A heparin bolus dose of 100 U/kg followed by a continuous infusion of heparin 1,000 U/h is the recommended standard.1,3,5,6,15 A goal partial thromboplastin time of 60 to 100 seconds, or an international normalized ratio of 2 to 3 is desirable.8,21
Staging: The Rutherford Classification System
Once immediate therapies are started, the stage of PAD should be determined using the Rutherford classification system in collaboration with vascular surgery services; this will further guide treatment and disposition.
Category I. In category I ALI, the affected limb is considered viable and not immediately threatened.
Category IIa. The limb is considered to be marginally threatened and salvageable.
Category IIb. An ALI classified as a category IIb is the most urgent type in which the limb is immediately threatened.
Category III. The limb is classified as having irreversible damage.2,3,17,22
(See Table 2 for a more detailed summary of the Rutherford classification system.)
Treatment
Definitive treatment decisions should be made in consultation with vascular surgery services. The results of three clinical trials developed the foundation for management of ALI: the Thrombolysis or Peripheral Arterial Surgery (TOPAS) trial, Surgery Versus Thrombolysis for Ischemia of the Lower Extremity (STILE) trial, and Rutherford trial.22-24 Table 3 provides a summary of the treatment techniques utilized, which include mechanical recanalization with percutaneous aspiration thrombectomy, percutaneous mechanical thrombectomy,6,12,25-28 pharmacological recanalization via catheter-directed thrombolysis,6,8,12,20,23-28 and/or surgical management via thrombectomy or embolectomy.6,11,23,24,27
Complications
The complications of treating ALI can be stratified into three subsets: pharmacologic, mechanical, and reperfusion injury-related. Medical treatment with heparin is not without risk. Intracranial hemorrhage, major bleeding at other sites, and compartment syndrome secondary to bleeding can all occur. Treatment may also cause distal embolization and lead to mechanical occlusion of another site. Finally, reperfusion injury predisposes the patient to a host of new problems. Reperfusion injury occurs when fresh blood enters a previously ischemic zone. When this occurs, oxygen free radicals, inflammatory mediators, and catabolism byproducts mix with the blood. This process can damage surrounding epithelial cells and lead to increased interstitial permeability. As a result, compartment syndrome may also develop via this mechanism.1,3,5,6 The anterior compartment of the lower extremity is most at risk. As such, assessment of peroneal nerve activity via dorsiflexion of the foot and sensation testing is important after the initiation of treatment.6 Systemic distribution of these harmful byproducts can also cause arrhythmias, renal failure, and systemic acadisos.1,3,5,6 It is important for physicians and staff to monitor the patient closely for the development of these complications and be prepared to intervene.
Opportunities for Improvement
In a condition where minutes matter, expedient action is critical. Time-to-recognition, imaging, consultation, and intervention all are potential sources of delay. Two recent studies have investigated the treatment timeline of ALI. The first study showed that the greatest source of delay is time from symptom onset to presentation in the ED; an average of 11.35 hours. The second largest source of delay was time from recognition of ALI to imaging, with an average delay of 4.75 hours. The average ED evaluation time was 40 minutes, and the average total time to intervention was 10.2 hours. While time-to-symptom presentation may represent a failure of public health, time-to-imaging was identified as an area of unacceptable delay by the authors.29 A second study examined the effect of pre-hospital care on the time-to-treatment. Persons who were transported via emergency medical services (EMS) arrived to the hospital at a median time of 5 hours after symptom onset, were seen by a physician at a median time of 51 minutes, and had revascularization at a median time of 23 hours. Those not transported by EMS arrived to the hospital at a median time of 48 hours after symptom onset, were seen by a physician at a median time of 80 minutes, and had revascularization at a median time of 93 hours. As a secondary goal, the study examined the effect of heparinization in the ED and showed that treatment with heparin was associated with a favorable outcome.30 While the total treatment times in each study vary widely, they share several important commonalities and reinforce expedient management as an important goal.
Outcomes
Advances in the treatment of this condition began in the 1970s, with an explosion of new techniques and data in the past several years. Still, ALI is a high morbidity and high mortality condition. Rates of limb loss are approximately 30% for all cases, and it is a fatal condition for as many as one-in-five. As discussed earlier, the patients who are most likely to experience ALI typically have several medical comorbidities. Perhaps unsurprisingly, ALI portends a poor prognosis even if the limb is salvaged. Approximately 15% to 20% of patients with ALI will die within 1 year of diagnosis.3,4,6,12
Conclusion
Acute limb ischemia is a rare condition, but a true medical emergency. Prompt recognition of the signs and symptoms of ALI are critical for optimizing patient outcomes. A high index of clinical suspicion in patients with risk factors may lead to early diagnosis. Early vascular surgery consultation and early IV heparin treatment are important aspects of care. Prompt imaging and staging guide further management. Special care should be paid to possible post-treatment complications and to the investigation of contributing factors. The EP has a great opportunity to positively impact care with expeditious management. Early diagnosis, targeted history and physical examination, prompt treatment, collaboration with specialists, and prevention and treatment of life-threatening complications are all hallmarks of emergency medicine.
Acute limb ischemia (ALI) is an emergent medical condition that is characterized by a precipitous decrease in limb perfusion that threatens the viability of the affected limb, and symptoms that have been present for 14 days or less.1-5 The incidence of lower extremity ALI in the US is nine to 16 cases per 100,000 persons per year, and one to three cases per 100,000 persons per year for upper extremity ALI.3 Symptoms suggestive of this condition classically include pain in the effected limb at rest, loss of sensation, impaired motor function, and cyanosis/pallor. Irreparable damage can occur in as quickly as 4 to 6 hours with complete arterial occlusion. A majority of ALI is caused by thrombosis, with the remainder of cases caused by embolism, 85% and 15% respectively.1-6 If not addressed promptly, this condition carries a high degree of morbidity (ie, limb loss) and mortality. Immediate initiation of anticoagulation therapy and vascular surgery consultation are mainstays of ED management. Time-to-treatment is a predictor of success and is an area where the emergency physician (EP) can make a significant difference in patient outcomes.7 Although vascular interruption via traumatic mechanism is not addressed in this review, it should remain a consideration in relation to the historical features of each case.
Presentation
Traditionally, symptoms of ALI can be remembered as the “six Ps”: pain, pallor, paresthesia, paralysis, pulselessness, and poikilothermia. Note that ALI represents a spectrum of disease, and the presenting features depend heavily on the level and degree of obstruction. Pain, however, is most frequently the first presenting symptom of patients with ALI.1-6 Pain will occur in muscle groups distal to the occlusion. Obstruction of the aortoiliac region might produce pain in the buttocks, thigh, and hip, whereas occlusion of the femoral artery may produce pain in the calf. Single-level disease will often produce claudication, but multilevel disease may present as a nonhealing ulcer or with focal gangrene. The differential diagnosis of ALI includes direct arterial injury, vasospasm, compartment syndrome, chronic peripheral artery disease, stroke, spinal cord injury, vasculitis, muscular trauma, and radiculopathy.3,5
Etiology
As stated previously, ALI is a result of either thrombotic or embolic phenomena that either partially or completely occludes a vessel such that adequate perfusion is no longer achieved. Consequently, there is a decrease in the metabolism of the tissue supplied in those territories, which can rapidly progress to necrosis. Thrombosis is the most common cause of ALI, accounting for approximately 85%.2,3Typically, thrombosis presents in the setting of pre-existing peripheral artery disease (PAD).8 As PAD worsens, damage to the arterial endothelium triggers platelet activation, and accumulation in a manner conceptually similar to thrombosis in myocardial infarction.9 Hypercoagulable states increase the risk of thrombi development.10 Symptoms of thrombosis are often more insidious in onset when compared to embolism, and signs/symptoms of prior claudication are almost always present. Consequently, there is a greater chance that collateral circulation has developed over time.2,6,11,12
By contrast, ALI caused by embolism is more acute in onset, and is often more emergent due to complete occlusion without chance of collateral vessel development.1,3,6,12 See Table 1 for differences in risk factors and presentation between thrombotic and embolic occlusion.
Historical Features
Information should be obtained systematically in all presentations and should include time of symptom onset, duration, severity, and location; however, special attention should be paid to the evolution of symptoms over time. One historical pearl that should raise suspicion of embolism vs thrombus is a patient history with a specific time of symptom onset. Specific questioning about history of claudication, including description of typical symptoms, is critical. A full list of other medical comorbidities should be obtained. This may reveal risk factors for thrombotic and embolic disease.1,3-5 This also may alter available treatment options.7,8,12,13 At presentation, the EP should obtain a list of the patient’s current medications, and special attention should be given to prothrombotic medications and medications that may interact with anticoagulants.
Physical Examination
On physical examination, the EP should pay particular attention to both the external appearance and temperature of the skin of the patient’s affected extremity. The presence or absence of peripheral pulses is an important feature when assessing for ALI; however, the presence of peripheral pulses does not exclude ALI from the differential.
Precise evaluation of sensation is important to attempt to quantify the extent of injury, localize a possible obstruction, and differentiate ALI from other possible causes of sensation deficits. Though not referenced in the six Ps, the patient’s limb may also appear mottled or marbled. Embolic phenomena occur at sites of vascular bifurcation. In a patient with aortic embolism, femoral pulses will be absent with bilateral mottling and paralysis of the lower extremities. Iliac artery embolism will produce the same symptoms, except unilateral. Femoral artery embolism will yield coolness and mottling distal to the inguinal ligament. Similarly, popliteal artery embolism will produce those same findings, except distal to the knee with preserved femoral pulses.
Diagnosis and Evaluation
After the history and physical examination are completed, further diagnostic methodologies should be considered, including laboratory evaluation and additional imaging studies.
Imaging Studies
Doppler ultrasound examination to assess for pulses on the affected limb should be performed immediately. Bedside continuous-wave Doppler may be used to differentiate arterial vs venous signal.6,14-16 An ankle brachial index may be calculated through either direct auscultation of pulses or Doppler signal. A ratio of less than 0.9 is suggestive of ischemia, while a ratio of less than 0.5 is considered critical ischemia.2
Laboratory Evaluation
Laboratory evaluation of hematocrit, coagulation studies, renal function, electrolyte levels, lactate, and creatinine kinase should be completed.1,5 An electrocardiogram and bedside/formal echocardiogram may be considered if embolism is suspected.1,6,17
Imaging
Angiography is currently the gold standard imaging modality to diagnose ALI.16 However, other imaging modalities exist that expose the patient to less radiation and are generally preferred by patients.18 Duplex ultrasonography is the least invasive imaging modality, with a reported sensitivity of 88% and specificity of 96% for the detection of greater than 50% stenosis.6,19 Contrast-enhanced magnetic resonance angiography (MRA) of the lower extremity is also relatively noninvasive, but is more limited in its application. It carries a reported sensitivity of 95% and a specificity of 97% for detection of stenosis of greater than 50%.6,19 An MRA without contrast may be considered for patients with an estimated glomerular filtration rate of less than 30 mL/min/1.73 m2 and who are not on dialysis, but the diagnostic efficacy is reduced.16 Finally, the sensitivity and specificity of computed tomography angiography (CTA) to detect aortoiliac stenosis of greater than 50% is 96% and 98% respectively.6,18,19 Other studies demonstrated similar results for other arterial locations in the lower extremities.18,19 A principal advantage of CTA is that direct visualization of calcifications, clips, stents, and prior bypasses is possible without the limitations of MRA.16 The American College of Radiology (ACR) lists ultrasound duplex Doppler and noncontrast MRA of the lower extremity as “may be appropriate.”16 In contrast, the ACR classifies MRA with contrast, CTA with contrast, and angiography of the lower extremity as “usually appropriate.”16 Selecting the optimal imaging study for a patient may require involvement of a facility’s radiology department and/or a vascular surgeon.14,15
Management in the ED
Even before the definitive diagnosis of ALI is made, steps can be taken to minimize and/or slow progression of injury. Placing the affected limb in a dependent position and providing intravenous (IV) fluid hydration will maximize perfusion.1,3,5 Even with consideration of the diagnostic modalities previously described, ALI is often considered a clinical diagnosis. Since time is critical, early consultation with vascular surgery services is imperative if ALI is suspected.
Intravenous Fluid Therapy
Suspected ALI should be treated in the ED with an IV heparin bolus, followed by constant IV infusion. Heparin prevents proximal and distal propagation of the thrombus.1,3,5,6,15,17,20 Additionally, it helps maintain the microcirculation surrounding the affected area.6 A heparin bolus dose of 100 U/kg followed by a continuous infusion of heparin 1,000 U/h is the recommended standard.1,3,5,6,15 A goal partial thromboplastin time of 60 to 100 seconds, or an international normalized ratio of 2 to 3 is desirable.8,21
Staging: The Rutherford Classification System
Once immediate therapies are started, the stage of PAD should be determined using the Rutherford classification system in collaboration with vascular surgery services; this will further guide treatment and disposition.
Category I. In category I ALI, the affected limb is considered viable and not immediately threatened.
Category IIa. The limb is considered to be marginally threatened and salvageable.
Category IIb. An ALI classified as a category IIb is the most urgent type in which the limb is immediately threatened.
Category III. The limb is classified as having irreversible damage.2,3,17,22
(See Table 2 for a more detailed summary of the Rutherford classification system.)
Treatment
Definitive treatment decisions should be made in consultation with vascular surgery services. The results of three clinical trials developed the foundation for management of ALI: the Thrombolysis or Peripheral Arterial Surgery (TOPAS) trial, Surgery Versus Thrombolysis for Ischemia of the Lower Extremity (STILE) trial, and Rutherford trial.22-24 Table 3 provides a summary of the treatment techniques utilized, which include mechanical recanalization with percutaneous aspiration thrombectomy, percutaneous mechanical thrombectomy,6,12,25-28 pharmacological recanalization via catheter-directed thrombolysis,6,8,12,20,23-28 and/or surgical management via thrombectomy or embolectomy.6,11,23,24,27
Complications
The complications of treating ALI can be stratified into three subsets: pharmacologic, mechanical, and reperfusion injury-related. Medical treatment with heparin is not without risk. Intracranial hemorrhage, major bleeding at other sites, and compartment syndrome secondary to bleeding can all occur. Treatment may also cause distal embolization and lead to mechanical occlusion of another site. Finally, reperfusion injury predisposes the patient to a host of new problems. Reperfusion injury occurs when fresh blood enters a previously ischemic zone. When this occurs, oxygen free radicals, inflammatory mediators, and catabolism byproducts mix with the blood. This process can damage surrounding epithelial cells and lead to increased interstitial permeability. As a result, compartment syndrome may also develop via this mechanism.1,3,5,6 The anterior compartment of the lower extremity is most at risk. As such, assessment of peroneal nerve activity via dorsiflexion of the foot and sensation testing is important after the initiation of treatment.6 Systemic distribution of these harmful byproducts can also cause arrhythmias, renal failure, and systemic acadisos.1,3,5,6 It is important for physicians and staff to monitor the patient closely for the development of these complications and be prepared to intervene.
Opportunities for Improvement
In a condition where minutes matter, expedient action is critical. Time-to-recognition, imaging, consultation, and intervention all are potential sources of delay. Two recent studies have investigated the treatment timeline of ALI. The first study showed that the greatest source of delay is time from symptom onset to presentation in the ED; an average of 11.35 hours. The second largest source of delay was time from recognition of ALI to imaging, with an average delay of 4.75 hours. The average ED evaluation time was 40 minutes, and the average total time to intervention was 10.2 hours. While time-to-symptom presentation may represent a failure of public health, time-to-imaging was identified as an area of unacceptable delay by the authors.29 A second study examined the effect of pre-hospital care on the time-to-treatment. Persons who were transported via emergency medical services (EMS) arrived to the hospital at a median time of 5 hours after symptom onset, were seen by a physician at a median time of 51 minutes, and had revascularization at a median time of 23 hours. Those not transported by EMS arrived to the hospital at a median time of 48 hours after symptom onset, were seen by a physician at a median time of 80 minutes, and had revascularization at a median time of 93 hours. As a secondary goal, the study examined the effect of heparinization in the ED and showed that treatment with heparin was associated with a favorable outcome.30 While the total treatment times in each study vary widely, they share several important commonalities and reinforce expedient management as an important goal.
Outcomes
Advances in the treatment of this condition began in the 1970s, with an explosion of new techniques and data in the past several years. Still, ALI is a high morbidity and high mortality condition. Rates of limb loss are approximately 30% for all cases, and it is a fatal condition for as many as one-in-five. As discussed earlier, the patients who are most likely to experience ALI typically have several medical comorbidities. Perhaps unsurprisingly, ALI portends a poor prognosis even if the limb is salvaged. Approximately 15% to 20% of patients with ALI will die within 1 year of diagnosis.3,4,6,12
Conclusion
Acute limb ischemia is a rare condition, but a true medical emergency. Prompt recognition of the signs and symptoms of ALI are critical for optimizing patient outcomes. A high index of clinical suspicion in patients with risk factors may lead to early diagnosis. Early vascular surgery consultation and early IV heparin treatment are important aspects of care. Prompt imaging and staging guide further management. Special care should be paid to possible post-treatment complications and to the investigation of contributing factors. The EP has a great opportunity to positively impact care with expeditious management. Early diagnosis, targeted history and physical examination, prompt treatment, collaboration with specialists, and prevention and treatment of life-threatening complications are all hallmarks of emergency medicine.
1. Braun R, Lin M. Acute limb ischemia: a case report and literature review. J Emerg Med. 2015;49(6):1011-1017. doi:10.1016/j.jemermed.2015.03.008.
2. Callum K, Bradbury A. ABC of arterial and venous disease: acute limb ischaemia. BMJ. 2000;320(7237):764-767.
3. Creager MA, Kaufman JA, Conte MS. Clinical practice. Acute limb ischemia. N Engl J Med. 2012;366(23):2198-2206. doi:10.1056/NEJMcp1006054.
4. Purushottam B, Gujja K, Zalewski A, Krishnan P. Acute limb ischemia. Interv Cardiol Clin. 2014;3(4):557-572.
5. Santistevan JR. Acute limb ischemia: an emergency medicine approach. Emerg Med Clin North Am. 2017;35(4):889-909. doi:10.1016/j.emc.2017.07.006.
6. Acar RD, Sahin M, Kirma C. One of the most urgent vascular circumstances: acute limb ischemia. SAGE Open Med. 2013;1:2050312113516110. doi:10.1177/2050312113516110.
7. Abou-Zamzam AM Jr, Gomez NR, Molkara A, et al. A prospective analysis of critical limb ischemia: factors leading to major primary amputation versus revascularization. Ann Vasc Surg. 2007;21(4):458-463.
8. Gerhard-Herman MD, Gornik HL, Barrett C, et al. 2016 AHA/ACC guideline on the management of patients with lower extremity peripheral artery disease: executive summary: a report of the American College of Cardiology/American Heart Association Task Force on clinical practice guidelines. J Am Coll Cardiol. 2017;69(11):1465-1508.
9. Rajagopalan S, Mckay I, Ford I, Bachoo P, Greaves M, Brittenden J. Platelet activation increases with the severity of peripheral arterial disease: implications for clinical management. J Vasc Surg. 2007;46(3):485-490.
10. Deitcher SR, Carman TL, Sheikh MA, Gomes M. Hypercoagulable syndromes: evaluation and management strategies for acute limb ischemia. Semin Vasc Surg. 2001;14(2):74-85.
11. Blaisdell FW, Steele M, Allen RE. Management of acute lower extremity arterial ischemia due to embolism and thrombosis. Surgery. 1978;84(6):822-834.
12. Byrne RM, Taha AG, Avgerinos E, Marone LK, Makaroun MS, Chaer RA. Contemporary outcomes of endovascular interventions for acute limb ischemia. J Vasc Surg. 2014;59(4):988-995.
13. Soden PA, Zettervall SL, Curran T, et al. Regional variation in patient selection and treatment for lower extremity vascular disease in the Vascular Quality Initiative. J Vasc Surg. 2017;65(1):108-118. doi:10.1016/j.jvs.2016.06.105.
14. Aboyans V, Björck M, Brodmann M, et al; ESC Scientific Document Group. Questions and answers on diagnosis and management of patients with Peripheral Arterial Diseases: a companion document of the 2017 ESC Guidelines for the Diagnosis and Treatment of Peripheral Arterial Diseases, in collaboration with the European Society for Vascular Surgery (ESVS): Endorsed by: the European Stroke Organisation (ESO)The Task Force for the Diagnosis and Treatment of Peripheral Arterial Diseases of the European Society of Cardiology (ESC) and of the European Society for Vascular Surgery (ESVS). Eur Heart J. 2017. doi:10.1093/eurheartj/ehx499. [Epub ahead of print]
15. Authors/Task Force Members, Aboyans V, Ricco JB, et al. 2017 ESC guidelines on the diagnosis and treatment of peripheral arterial diseases, in collaboration with the European Society for Vascular Surgery (ESVS). Eur J Vasc Endovasc Surg. 2017. doi:10.1016/j.ejvs.2017.07.018. [Epub ahead of print]
16. Expert Panel on Vascular Imaging: Weiss CR, Azene EM, Majdalany BS, et al. ACR Appropriateness Criteria® sudden onset of cold, painful leg. J Am Coll Radiol. 2017;14(5S):S307-S313. doi:10.1016/j.jacr.2017.02.015.
17. Dieter RS, Dieter RA Jr, Dieter RA 3rd, Nanjundappa A. Critical Limb Ischemia: Acute and Chronic. New York, NY: Springer; 2016.
18. Met R, Bipat S, Legemate DA, Reekers JA, Koelemay MJ. Diagnostic performance of computed tomography angiography in peripheral arterial disease: a systematic review and meta-analysis. JAMA. 2009;301(4):415-424.
19. Collins R, Burch J, Cranny G, et al. Duplex ultrasonography, magnetic resonance angiography, and computed tomography angiography for diagnosis and assessment of symptomatic, lower limb peripheral arterial disease: systematic review. BMJ. 2007;334(7606):1257.
20. Giannini D, Balbarini A. Thrombolytic therapy in peripheral arterial disease. Curr Drug Targets Cardiovasc Haematol Disord. 2004;4(3):249-258.
21. Kearon C, Kahn SR, Agnelli G, Goldhaber S, Raskob GE, Comerota AJ. Antithrombotic therapy for venous thromboembolic disease: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines (8th Edition). Chest. 2008;133(6 Suppl):454S-545S. doi:10.1378/chest.08-0658.
22. Rutherford RB, Baker JD, Ernst C, et al. Recommended standards for reports dealing with lower extremity ischemia: revised version. J Vasc Surg. 1997;26(3):517-538.
23. Ouriel K, Veith FJ, Sasahara AA. Thrombolysis or peripheral arterial surgery: phase I results. TOPAS Investigators. J Vasc Surg. 1996;23(1):64-73; discussion 74-75.
24. Results of a prospective randomized trial evaluating surgery versus thrombolysis for ischemia of the lower extremity. The STILE trial. Ann Surg. 1994;220(3):251-266; discussion 266-268.
25. Kashyap VS, Gilani R, Bena JF, Bannazadeh M, Sarac TP. Endovascular therapy for acute limb ischemia. J Vasc Surg. 2011;53(2):340-346. doi:10.1016/j.jvs.2010.08.064.
26. Patel NH, Krishnamurthy VN, Kim S, et al. Quality improvement guidelines for percutaneous management of acute lower-extremity ischemia. J Vasc Interv Radiol. 2013;24(1):3-15.
27. Taha AG, Byrne RM, Avgerinos ED, Marone LK, Makaroun MS, Chaer RA. Comparative effectiveness of endovascular versus surgical revascularization for acute lower extremity ischemia. J Vasc Surg. 2015;61(1):147-154. doi:10.1016/j.jvs.2014.06.109.
28. Zeller T, Tepe G. Treatment of acute limb ischemia with focus on endovascular techniques. Vasa. 2009;38(2):123-133. doi: 10.1024/0301-1526.38.2.123.
29. Normahani P, Standfield NJ, Jaffer U. Sources of delay in the acute limb ischemia patient pathway. Ann Vasc Surg. 2017;38:279-285. doi:10.1016/j.avsg.2016.05.118.
30. Langenskiöld M, Smidfelt K, Karlsson A, Bohm C, Herlitz J, Nordanstig J. Weak links in the early chain of care of acute lower limb ischaemia in terms of recognition and emergency management. Eur J Vasc Endovasc Surg. 2017;54(2):235-240. doi:10.1016/j.ejvs.2017.04.010.
1. Braun R, Lin M. Acute limb ischemia: a case report and literature review. J Emerg Med. 2015;49(6):1011-1017. doi:10.1016/j.jemermed.2015.03.008.
2. Callum K, Bradbury A. ABC of arterial and venous disease: acute limb ischaemia. BMJ. 2000;320(7237):764-767.
3. Creager MA, Kaufman JA, Conte MS. Clinical practice. Acute limb ischemia. N Engl J Med. 2012;366(23):2198-2206. doi:10.1056/NEJMcp1006054.
4. Purushottam B, Gujja K, Zalewski A, Krishnan P. Acute limb ischemia. Interv Cardiol Clin. 2014;3(4):557-572.
5. Santistevan JR. Acute limb ischemia: an emergency medicine approach. Emerg Med Clin North Am. 2017;35(4):889-909. doi:10.1016/j.emc.2017.07.006.
6. Acar RD, Sahin M, Kirma C. One of the most urgent vascular circumstances: acute limb ischemia. SAGE Open Med. 2013;1:2050312113516110. doi:10.1177/2050312113516110.
7. Abou-Zamzam AM Jr, Gomez NR, Molkara A, et al. A prospective analysis of critical limb ischemia: factors leading to major primary amputation versus revascularization. Ann Vasc Surg. 2007;21(4):458-463.
8. Gerhard-Herman MD, Gornik HL, Barrett C, et al. 2016 AHA/ACC guideline on the management of patients with lower extremity peripheral artery disease: executive summary: a report of the American College of Cardiology/American Heart Association Task Force on clinical practice guidelines. J Am Coll Cardiol. 2017;69(11):1465-1508.
9. Rajagopalan S, Mckay I, Ford I, Bachoo P, Greaves M, Brittenden J. Platelet activation increases with the severity of peripheral arterial disease: implications for clinical management. J Vasc Surg. 2007;46(3):485-490.
10. Deitcher SR, Carman TL, Sheikh MA, Gomes M. Hypercoagulable syndromes: evaluation and management strategies for acute limb ischemia. Semin Vasc Surg. 2001;14(2):74-85.
11. Blaisdell FW, Steele M, Allen RE. Management of acute lower extremity arterial ischemia due to embolism and thrombosis. Surgery. 1978;84(6):822-834.
12. Byrne RM, Taha AG, Avgerinos E, Marone LK, Makaroun MS, Chaer RA. Contemporary outcomes of endovascular interventions for acute limb ischemia. J Vasc Surg. 2014;59(4):988-995.
13. Soden PA, Zettervall SL, Curran T, et al. Regional variation in patient selection and treatment for lower extremity vascular disease in the Vascular Quality Initiative. J Vasc Surg. 2017;65(1):108-118. doi:10.1016/j.jvs.2016.06.105.
14. Aboyans V, Björck M, Brodmann M, et al; ESC Scientific Document Group. Questions and answers on diagnosis and management of patients with Peripheral Arterial Diseases: a companion document of the 2017 ESC Guidelines for the Diagnosis and Treatment of Peripheral Arterial Diseases, in collaboration with the European Society for Vascular Surgery (ESVS): Endorsed by: the European Stroke Organisation (ESO)The Task Force for the Diagnosis and Treatment of Peripheral Arterial Diseases of the European Society of Cardiology (ESC) and of the European Society for Vascular Surgery (ESVS). Eur Heart J. 2017. doi:10.1093/eurheartj/ehx499. [Epub ahead of print]
15. Authors/Task Force Members, Aboyans V, Ricco JB, et al. 2017 ESC guidelines on the diagnosis and treatment of peripheral arterial diseases, in collaboration with the European Society for Vascular Surgery (ESVS). Eur J Vasc Endovasc Surg. 2017. doi:10.1016/j.ejvs.2017.07.018. [Epub ahead of print]
16. Expert Panel on Vascular Imaging: Weiss CR, Azene EM, Majdalany BS, et al. ACR Appropriateness Criteria® sudden onset of cold, painful leg. J Am Coll Radiol. 2017;14(5S):S307-S313. doi:10.1016/j.jacr.2017.02.015.
17. Dieter RS, Dieter RA Jr, Dieter RA 3rd, Nanjundappa A. Critical Limb Ischemia: Acute and Chronic. New York, NY: Springer; 2016.
18. Met R, Bipat S, Legemate DA, Reekers JA, Koelemay MJ. Diagnostic performance of computed tomography angiography in peripheral arterial disease: a systematic review and meta-analysis. JAMA. 2009;301(4):415-424.
19. Collins R, Burch J, Cranny G, et al. Duplex ultrasonography, magnetic resonance angiography, and computed tomography angiography for diagnosis and assessment of symptomatic, lower limb peripheral arterial disease: systematic review. BMJ. 2007;334(7606):1257.
20. Giannini D, Balbarini A. Thrombolytic therapy in peripheral arterial disease. Curr Drug Targets Cardiovasc Haematol Disord. 2004;4(3):249-258.
21. Kearon C, Kahn SR, Agnelli G, Goldhaber S, Raskob GE, Comerota AJ. Antithrombotic therapy for venous thromboembolic disease: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines (8th Edition). Chest. 2008;133(6 Suppl):454S-545S. doi:10.1378/chest.08-0658.
22. Rutherford RB, Baker JD, Ernst C, et al. Recommended standards for reports dealing with lower extremity ischemia: revised version. J Vasc Surg. 1997;26(3):517-538.
23. Ouriel K, Veith FJ, Sasahara AA. Thrombolysis or peripheral arterial surgery: phase I results. TOPAS Investigators. J Vasc Surg. 1996;23(1):64-73; discussion 74-75.
24. Results of a prospective randomized trial evaluating surgery versus thrombolysis for ischemia of the lower extremity. The STILE trial. Ann Surg. 1994;220(3):251-266; discussion 266-268.
25. Kashyap VS, Gilani R, Bena JF, Bannazadeh M, Sarac TP. Endovascular therapy for acute limb ischemia. J Vasc Surg. 2011;53(2):340-346. doi:10.1016/j.jvs.2010.08.064.
26. Patel NH, Krishnamurthy VN, Kim S, et al. Quality improvement guidelines for percutaneous management of acute lower-extremity ischemia. J Vasc Interv Radiol. 2013;24(1):3-15.
27. Taha AG, Byrne RM, Avgerinos ED, Marone LK, Makaroun MS, Chaer RA. Comparative effectiveness of endovascular versus surgical revascularization for acute lower extremity ischemia. J Vasc Surg. 2015;61(1):147-154. doi:10.1016/j.jvs.2014.06.109.
28. Zeller T, Tepe G. Treatment of acute limb ischemia with focus on endovascular techniques. Vasa. 2009;38(2):123-133. doi: 10.1024/0301-1526.38.2.123.
29. Normahani P, Standfield NJ, Jaffer U. Sources of delay in the acute limb ischemia patient pathway. Ann Vasc Surg. 2017;38:279-285. doi:10.1016/j.avsg.2016.05.118.
30. Langenskiöld M, Smidfelt K, Karlsson A, Bohm C, Herlitz J, Nordanstig J. Weak links in the early chain of care of acute lower limb ischaemia in terms of recognition and emergency management. Eur J Vasc Endovasc Surg. 2017;54(2):235-240. doi:10.1016/j.ejvs.2017.04.010.
Early management of patients with acute ischemic stroke
(AIS). Conceptually, early management can be separated into initial triage and decisions about intervention to restore blood flow with thrombolysis or mechanical thrombectomy. If reperfusion therapy is not appropriate, then the focus is on management to minimize further damage from the stroke, decrease the likelihood of recurrence, and lessen secondary problems related to the stroke.

All patients with AIS should receive noncontrast CT to determine if there is evidence of a hemorrhagic stroke and, if such evidence exists, than the patient is not a candidate for thrombolysis. Intravenous alteplase should be considered for patients who present within 3 hours of stroke onset and for selected patients presenting between 3-4.5 hours after stroke onset (for more details, see Table 6 in the guidelines). Selected patients with AIS who present within 6-24 hours of last time they were known to be normal and who have large vessel occlusion in the anterior circulation, may be candidates for mechanical thrombectomy in specialized centers. Patients who are not candidates for acute interventions should then be managed according to early stroke management guidelines.
Early stroke management for patients with AIS admitted to medical floors involves attention to blood pressure, glucose, and antiplatelet therapy. For patients with blood pressure lower than 220/120 mm Hg who did not receive IV alteplase or thrombectomy, treatment of hypertension in the first 48-72 hours after an AIS does not change the outcome. It is reasonable when patients have BP greater than or equal to 220/120 mm Hg, to lower blood pressure by 15% during the first 24 hours after onset of stroke. Starting or restarting antihypertensive therapy during hospitalization in patients with blood pressure higher than 140/90 mm Hg who are neurologically stable improves long-term blood pressure control and is considered a reasonable strategy.
For patients with noncardioembolic AIS, the use of antiplatelet agents rather than oral anticoagulation is recommended. Patients should be treated with aspirin 160 mg-325 mg within 24-48 hours of presentation. In patients unsafe or unable to swallow, rectal or nasogastric administration is recommended. In patients with minor stroke, 21 days of dual-antiplatelet therapy (aspirin and clopidogrel) started within 24 hours can decrease stroke recurrence for the first 90 days after a stroke. This recommendation is based on a single study, the CHANCE trial, in a homogeneous population in China, and its generalizability is not known. If a patient had an AIS while already on aspirin, there is some evidence supporting a decreased risk of major cardiovascular events and recurrent stroke in patients switching to an alternative antiplatelet agent or combination antiplatelet therapy. Because of methodologic issues in the those studies, the guideline concludes that, for those already on aspirin, it is of unclear benefit to increase the dose of aspirin, switch to a different antiplatelet agent, or add a second antiplatelet agent. Switching to warfarin is not beneficial for secondary stroke prevention. High-dose statin therapy should be initiated. For patients with AIS in the setting of atrial fibrillation, oral anticoagulation can be started within 4-14 days after the stroke. One study showed that anticoagulation should not be started before 4 days after the stroke, with a hazard ratio of 0.53 for starting anticoagulation at 4-14 days, compared with less than 4 days.
Hyperglycemia should be controlled to a range of 140-180 mg/dL, because higher values are associated with worse outcomes. Oxygen should be used if needed to maintain oxygen saturation greater than 94%. High-intensity statin therapy should be used, and smoking cessation is strongly encouraged for those who use tobacco, with avoidance of secondhand smoke whenever possible.
Patients should be screened for dysphagia before taking anything per oral, including medications. A nasogastric tube may be considered within the first 7 days, if patients are dysphagic. Oral hygiene protocols may include antibacterial mouth rinse, systematic oral care, and decontamination gel to decrease the risk of pneumonia .
For deep vein thrombosis prophylaxis, intermittent pneumatic compression, in addition to the aspirin that a patient is on is reasonable, and the benefit of prophylactic-dose subcutaneous heparin (unfractionated heparin or low-molecular-weight heparin) in immobile patients with AIS is not well established.
In the poststroke setting, patients should be screened for depression and, if appropriate, treated with antidepressants. Regular skin assessments are recommended with objective scales, and skin friction and pressure should be actively minimized with regular turning, good skin hygiene, and use of specialized mattresses, wheelchair cushions, and seating until mobility returns. Early rehabilitation for hospitalized stroke patients should be provided, but high-dose, very-early mobilization within 24 hours of stroke should not be done because it reduces the odds of a favorable outcome at 3 months.
Completing the diagnostic evaluation for the cause of stroke and decreasing the chance of future strokes should be part of the initial hospitalization. While MRI is more sensitive than is CT for detecting AIS, routine use of MRI in all patients with AIS is not cost effective and therefore is not recommended. For patients with nondisabling AIS in the carotid territory and who are candidates for carotid endarterectomy or stenting, noninvasive imaging of the cervical vessels should be performed within 24 hours of admission, with plans for carotid revascularization between 48 hours and 7 days if indicated. Cardiac monitoring for at least the first 24 hours of admission should be performed, while primarily looking for atrial fibrillation as a cause of stroke. In some patients, prolonged cardiac monitoring may be reasonable. With prolonged cardiac monitoring, atrial fibrillation is newly detected in nearly a quarter of patients with stroke or TIA, but the effect on outcomes is uncertain. Routine use of echocardiography is not recommended but may be done in selected patients. All patients should be screened for diabetes. It is not clear whether screening for thrombophilic states is useful.
All patients should be counseled on stroke, and provided education about it and how it will affect their lives. Following their acute medical stay, all patients will benefit from rehabilitation, with the benefits associated using a program tailored to their needs and outcome goals.
The bottom line
Early management of stroke involves first determining whether someone is a candidate for reperfusion therapy with alteplase or thrombectomy and then, if not, admitting them to a monitored setting to screen for atrial fibrillation and evaluation for carotid stenosis. Patients should be evaluated for both depression and swallowing function, and there should be initiation of deep vein thrombosis prevention, appropriate management of elevated blood pressures, anti-platelet therapy, and statin therapy as well as plans for rehabilitation services.
Reference
Powers WJ et al. on behalf of the American Heart Association Stroke Council. 2018 Guidelines for the early management of patients with acute ischemic stroke: A guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke. 2018 Mar;49(3):e46-e110.
Dr. Skolnik is a professor of family and community medicine at Jefferson Medical College, Philadelphia, and an associate director of the family medicine residency program at Abington (Pa.) Jefferson Health. Dr. Callahan is an attending physician and preceptor in the family medicine residency program at Abington Jefferson Health.
(AIS). Conceptually, early management can be separated into initial triage and decisions about intervention to restore blood flow with thrombolysis or mechanical thrombectomy. If reperfusion therapy is not appropriate, then the focus is on management to minimize further damage from the stroke, decrease the likelihood of recurrence, and lessen secondary problems related to the stroke.
All patients with AIS should receive noncontrast CT to determine if there is evidence of a hemorrhagic stroke and, if such evidence exists, than the patient is not a candidate for thrombolysis. Intravenous alteplase should be considered for patients who present within 3 hours of stroke onset and for selected patients presenting between 3-4.5 hours after stroke onset (for more details, see Table 6 in the guidelines). Selected patients with AIS who present within 6-24 hours of last time they were known to be normal and who have large vessel occlusion in the anterior circulation, may be candidates for mechanical thrombectomy in specialized centers. Patients who are not candidates for acute interventions should then be managed according to early stroke management guidelines.
Early stroke management for patients with AIS admitted to medical floors involves attention to blood pressure, glucose, and antiplatelet therapy. For patients with blood pressure lower than 220/120 mm Hg who did not receive IV alteplase or thrombectomy, treatment of hypertension in the first 48-72 hours after an AIS does not change the outcome. It is reasonable when patients have BP greater than or equal to 220/120 mm Hg, to lower blood pressure by 15% during the first 24 hours after onset of stroke. Starting or restarting antihypertensive therapy during hospitalization in patients with blood pressure higher than 140/90 mm Hg who are neurologically stable improves long-term blood pressure control and is considered a reasonable strategy.
For patients with noncardioembolic AIS, the use of antiplatelet agents rather than oral anticoagulation is recommended. Patients should be treated with aspirin 160 mg-325 mg within 24-48 hours of presentation. In patients unsafe or unable to swallow, rectal or nasogastric administration is recommended. In patients with minor stroke, 21 days of dual-antiplatelet therapy (aspirin and clopidogrel) started within 24 hours can decrease stroke recurrence for the first 90 days after a stroke. This recommendation is based on a single study, the CHANCE trial, in a homogeneous population in China, and its generalizability is not known. If a patient had an AIS while already on aspirin, there is some evidence supporting a decreased risk of major cardiovascular events and recurrent stroke in patients switching to an alternative antiplatelet agent or combination antiplatelet therapy. Because of methodologic issues in the those studies, the guideline concludes that, for those already on aspirin, it is of unclear benefit to increase the dose of aspirin, switch to a different antiplatelet agent, or add a second antiplatelet agent. Switching to warfarin is not beneficial for secondary stroke prevention. High-dose statin therapy should be initiated. For patients with AIS in the setting of atrial fibrillation, oral anticoagulation can be started within 4-14 days after the stroke. One study showed that anticoagulation should not be started before 4 days after the stroke, with a hazard ratio of 0.53 for starting anticoagulation at 4-14 days, compared with less than 4 days.
Hyperglycemia should be controlled to a range of 140-180 mg/dL, because higher values are associated with worse outcomes. Oxygen should be used if needed to maintain oxygen saturation greater than 94%. High-intensity statin therapy should be used, and smoking cessation is strongly encouraged for those who use tobacco, with avoidance of secondhand smoke whenever possible.
Patients should be screened for dysphagia before taking anything per oral, including medications. A nasogastric tube may be considered within the first 7 days, if patients are dysphagic. Oral hygiene protocols may include antibacterial mouth rinse, systematic oral care, and decontamination gel to decrease the risk of pneumonia .
For deep vein thrombosis prophylaxis, intermittent pneumatic compression, in addition to the aspirin that a patient is on is reasonable, and the benefit of prophylactic-dose subcutaneous heparin (unfractionated heparin or low-molecular-weight heparin) in immobile patients with AIS is not well established.
In the poststroke setting, patients should be screened for depression and, if appropriate, treated with antidepressants. Regular skin assessments are recommended with objective scales, and skin friction and pressure should be actively minimized with regular turning, good skin hygiene, and use of specialized mattresses, wheelchair cushions, and seating until mobility returns. Early rehabilitation for hospitalized stroke patients should be provided, but high-dose, very-early mobilization within 24 hours of stroke should not be done because it reduces the odds of a favorable outcome at 3 months.
Completing the diagnostic evaluation for the cause of stroke and decreasing the chance of future strokes should be part of the initial hospitalization. While MRI is more sensitive than is CT for detecting AIS, routine use of MRI in all patients with AIS is not cost effective and therefore is not recommended. For patients with nondisabling AIS in the carotid territory and who are candidates for carotid endarterectomy or stenting, noninvasive imaging of the cervical vessels should be performed within 24 hours of admission, with plans for carotid revascularization between 48 hours and 7 days if indicated. Cardiac monitoring for at least the first 24 hours of admission should be performed, while primarily looking for atrial fibrillation as a cause of stroke. In some patients, prolonged cardiac monitoring may be reasonable. With prolonged cardiac monitoring, atrial fibrillation is newly detected in nearly a quarter of patients with stroke or TIA, but the effect on outcomes is uncertain. Routine use of echocardiography is not recommended but may be done in selected patients. All patients should be screened for diabetes. It is not clear whether screening for thrombophilic states is useful.
All patients should be counseled on stroke, and provided education about it and how it will affect their lives. Following their acute medical stay, all patients will benefit from rehabilitation, with the benefits associated using a program tailored to their needs and outcome goals.
The bottom line
Early management of stroke involves first determining whether someone is a candidate for reperfusion therapy with alteplase or thrombectomy and then, if not, admitting them to a monitored setting to screen for atrial fibrillation and evaluation for carotid stenosis. Patients should be evaluated for both depression and swallowing function, and there should be initiation of deep vein thrombosis prevention, appropriate management of elevated blood pressures, anti-platelet therapy, and statin therapy as well as plans for rehabilitation services.
Reference
Powers WJ et al. on behalf of the American Heart Association Stroke Council. 2018 Guidelines for the early management of patients with acute ischemic stroke: A guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke. 2018 Mar;49(3):e46-e110.
Dr. Skolnik is a professor of family and community medicine at Jefferson Medical College, Philadelphia, and an associate director of the family medicine residency program at Abington (Pa.) Jefferson Health. Dr. Callahan is an attending physician and preceptor in the family medicine residency program at Abington Jefferson Health.
(AIS). Conceptually, early management can be separated into initial triage and decisions about intervention to restore blood flow with thrombolysis or mechanical thrombectomy. If reperfusion therapy is not appropriate, then the focus is on management to minimize further damage from the stroke, decrease the likelihood of recurrence, and lessen secondary problems related to the stroke.
All patients with AIS should receive noncontrast CT to determine if there is evidence of a hemorrhagic stroke and, if such evidence exists, than the patient is not a candidate for thrombolysis. Intravenous alteplase should be considered for patients who present within 3 hours of stroke onset and for selected patients presenting between 3-4.5 hours after stroke onset (for more details, see Table 6 in the guidelines). Selected patients with AIS who present within 6-24 hours of last time they were known to be normal and who have large vessel occlusion in the anterior circulation, may be candidates for mechanical thrombectomy in specialized centers. Patients who are not candidates for acute interventions should then be managed according to early stroke management guidelines.
Early stroke management for patients with AIS admitted to medical floors involves attention to blood pressure, glucose, and antiplatelet therapy. For patients with blood pressure lower than 220/120 mm Hg who did not receive IV alteplase or thrombectomy, treatment of hypertension in the first 48-72 hours after an AIS does not change the outcome. It is reasonable when patients have BP greater than or equal to 220/120 mm Hg, to lower blood pressure by 15% during the first 24 hours after onset of stroke. Starting or restarting antihypertensive therapy during hospitalization in patients with blood pressure higher than 140/90 mm Hg who are neurologically stable improves long-term blood pressure control and is considered a reasonable strategy.
For patients with noncardioembolic AIS, the use of antiplatelet agents rather than oral anticoagulation is recommended. Patients should be treated with aspirin 160 mg-325 mg within 24-48 hours of presentation. In patients unsafe or unable to swallow, rectal or nasogastric administration is recommended. In patients with minor stroke, 21 days of dual-antiplatelet therapy (aspirin and clopidogrel) started within 24 hours can decrease stroke recurrence for the first 90 days after a stroke. This recommendation is based on a single study, the CHANCE trial, in a homogeneous population in China, and its generalizability is not known. If a patient had an AIS while already on aspirin, there is some evidence supporting a decreased risk of major cardiovascular events and recurrent stroke in patients switching to an alternative antiplatelet agent or combination antiplatelet therapy. Because of methodologic issues in the those studies, the guideline concludes that, for those already on aspirin, it is of unclear benefit to increase the dose of aspirin, switch to a different antiplatelet agent, or add a second antiplatelet agent. Switching to warfarin is not beneficial for secondary stroke prevention. High-dose statin therapy should be initiated. For patients with AIS in the setting of atrial fibrillation, oral anticoagulation can be started within 4-14 days after the stroke. One study showed that anticoagulation should not be started before 4 days after the stroke, with a hazard ratio of 0.53 for starting anticoagulation at 4-14 days, compared with less than 4 days.
Hyperglycemia should be controlled to a range of 140-180 mg/dL, because higher values are associated with worse outcomes. Oxygen should be used if needed to maintain oxygen saturation greater than 94%. High-intensity statin therapy should be used, and smoking cessation is strongly encouraged for those who use tobacco, with avoidance of secondhand smoke whenever possible.
Patients should be screened for dysphagia before taking anything per oral, including medications. A nasogastric tube may be considered within the first 7 days, if patients are dysphagic. Oral hygiene protocols may include antibacterial mouth rinse, systematic oral care, and decontamination gel to decrease the risk of pneumonia .
For deep vein thrombosis prophylaxis, intermittent pneumatic compression, in addition to the aspirin that a patient is on is reasonable, and the benefit of prophylactic-dose subcutaneous heparin (unfractionated heparin or low-molecular-weight heparin) in immobile patients with AIS is not well established.
In the poststroke setting, patients should be screened for depression and, if appropriate, treated with antidepressants. Regular skin assessments are recommended with objective scales, and skin friction and pressure should be actively minimized with regular turning, good skin hygiene, and use of specialized mattresses, wheelchair cushions, and seating until mobility returns. Early rehabilitation for hospitalized stroke patients should be provided, but high-dose, very-early mobilization within 24 hours of stroke should not be done because it reduces the odds of a favorable outcome at 3 months.
Completing the diagnostic evaluation for the cause of stroke and decreasing the chance of future strokes should be part of the initial hospitalization. While MRI is more sensitive than is CT for detecting AIS, routine use of MRI in all patients with AIS is not cost effective and therefore is not recommended. For patients with nondisabling AIS in the carotid territory and who are candidates for carotid endarterectomy or stenting, noninvasive imaging of the cervical vessels should be performed within 24 hours of admission, with plans for carotid revascularization between 48 hours and 7 days if indicated. Cardiac monitoring for at least the first 24 hours of admission should be performed, while primarily looking for atrial fibrillation as a cause of stroke. In some patients, prolonged cardiac monitoring may be reasonable. With prolonged cardiac monitoring, atrial fibrillation is newly detected in nearly a quarter of patients with stroke or TIA, but the effect on outcomes is uncertain. Routine use of echocardiography is not recommended but may be done in selected patients. All patients should be screened for diabetes. It is not clear whether screening for thrombophilic states is useful.
All patients should be counseled on stroke, and provided education about it and how it will affect their lives. Following their acute medical stay, all patients will benefit from rehabilitation, with the benefits associated using a program tailored to their needs and outcome goals.
The bottom line
Early management of stroke involves first determining whether someone is a candidate for reperfusion therapy with alteplase or thrombectomy and then, if not, admitting them to a monitored setting to screen for atrial fibrillation and evaluation for carotid stenosis. Patients should be evaluated for both depression and swallowing function, and there should be initiation of deep vein thrombosis prevention, appropriate management of elevated blood pressures, anti-platelet therapy, and statin therapy as well as plans for rehabilitation services.
Reference
Powers WJ et al. on behalf of the American Heart Association Stroke Council. 2018 Guidelines for the early management of patients with acute ischemic stroke: A guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke. 2018 Mar;49(3):e46-e110.
Dr. Skolnik is a professor of family and community medicine at Jefferson Medical College, Philadelphia, and an associate director of the family medicine residency program at Abington (Pa.) Jefferson Health. Dr. Callahan is an attending physician and preceptor in the family medicine residency program at Abington Jefferson Health.
VIDEO: Stem cells may reverse premature menopause, restore fertility
CHICAGO –
Neither of the women had menstruated for about 5 years; both were in premature menopause and wanted desperately to start a family. Estrogen levels began increasing soon after treatment, and night sweats and other symptoms of menopause almost disappeared. After a year, the treated ovary was almost the size of a normal premenopausal ovary. There weren’t any complications or side effects, and both women are now pursuing pregnancy.
The results are “very exciting, very encouraging,” said senior investigator Ayman Al-Hendy, MD, PhD, a gynecology professor at the University of Illinois at Chicago.
“The eggs are there, but they are not active.” Something about the stem cells seems “to activate these eggs to become fertilizable,” he said.
Far more work is planned on the project, and there’s no shortage of volunteers; premature menopause is a devastating diagnosis to young women hoping to start families.

Dr. Al-Hendy explained the procedure and the next steps in a video interview at the Endocrine Society annual meeting.
The work is supported by MD Stem Cells and the National Institutes of Health. Dr. Al-Hendy didn’t have any relevant disclosures.
SOURCE: Al-Hendy A et al. ENDO 2018, Abstract OR33-6.
CHICAGO –
Neither of the women had menstruated for about 5 years; both were in premature menopause and wanted desperately to start a family. Estrogen levels began increasing soon after treatment, and night sweats and other symptoms of menopause almost disappeared. After a year, the treated ovary was almost the size of a normal premenopausal ovary. There weren’t any complications or side effects, and both women are now pursuing pregnancy.
The results are “very exciting, very encouraging,” said senior investigator Ayman Al-Hendy, MD, PhD, a gynecology professor at the University of Illinois at Chicago.
“The eggs are there, but they are not active.” Something about the stem cells seems “to activate these eggs to become fertilizable,” he said.
Far more work is planned on the project, and there’s no shortage of volunteers; premature menopause is a devastating diagnosis to young women hoping to start families.
Dr. Al-Hendy explained the procedure and the next steps in a video interview at the Endocrine Society annual meeting.
The work is supported by MD Stem Cells and the National Institutes of Health. Dr. Al-Hendy didn’t have any relevant disclosures.
SOURCE: Al-Hendy A et al. ENDO 2018, Abstract OR33-6.
CHICAGO –
Neither of the women had menstruated for about 5 years; both were in premature menopause and wanted desperately to start a family. Estrogen levels began increasing soon after treatment, and night sweats and other symptoms of menopause almost disappeared. After a year, the treated ovary was almost the size of a normal premenopausal ovary. There weren’t any complications or side effects, and both women are now pursuing pregnancy.
The results are “very exciting, very encouraging,” said senior investigator Ayman Al-Hendy, MD, PhD, a gynecology professor at the University of Illinois at Chicago.
“The eggs are there, but they are not active.” Something about the stem cells seems “to activate these eggs to become fertilizable,” he said.
Far more work is planned on the project, and there’s no shortage of volunteers; premature menopause is a devastating diagnosis to young women hoping to start families.
Dr. Al-Hendy explained the procedure and the next steps in a video interview at the Endocrine Society annual meeting.
The work is supported by MD Stem Cells and the National Institutes of Health. Dr. Al-Hendy didn’t have any relevant disclosures.
SOURCE: Al-Hendy A et al. ENDO 2018, Abstract OR33-6.
REPORTING FROM ENDO 2018
VIDEO: Fezolinetant drops testosterone levels in PCOS
CHICAGO – currently in development. The proof-of-concept phase 2 trial, which saw no concerning safety signals for the medication, fezolinetant, sets the stage for a larger, and perhaps longer, study to learn more about the neurokinin 3 receptor antagonist’s efficacy against PCOS.
“The primary outcome for this phase 2 trial was to see if we could lower testosterone levels in these PCOS patients,” said Graeme Fraser, PhD, chief scientific officer for Ogeda, discussing the poster he and his colleagues presented at the annual meeting of the Endocrine Society.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
“Testosterone levels decreased: Measured at about 3 hours postdose, which is the approximate pharmacokinetic Cmax [maximum serum concentration], there was … a more than 30% decrease in testosterone levels,” said Dr. Fraser. By week 12, he said, “there was a very consistent decrease of 30% of testosterone levels. So that was quite good; we successfully hit the primary outcome.”
At 12 weeks, the higher dose of fezolinetant decreased testosterone by 0.64 nmol/L, compared with the 0.04 nmol/L seen with placebo (P less than .01).
Fezolinetant downregulates the activity of candy neurons in the hypothalamus, said Dr. Fraser in an interview. In turn, gonadotropin-releasing hormone (GNRH) pulse frequency is reduced, lowering luteinizing hormone (LH) levels. Since LH drives testosterone levels, this drops as well – a beneficial effect in PCOS, with its cardinal symptom of hyperandrogenism.
The double-blind, placebo-controlled study was conducted in Western Europe; 73 participants were randomized into three groups: 27 to a placebo group, 23 to a treatment group given 60 mg of fezolinetant once daily, and 23 to a treatment group given 180 mg of fezolinetant once daily. All groups received treatment for 12 weeks.
A total of 26 patients on placebo, 21 on 60-mg fezolinetant, and 17 on 180-mg fezolinetant completed the study. Patients who completed the study were included in the safety analysis, while all who took the study medication were included in the intent-to-treat analysis for primary and secondary outcome measures.
All participants had PCOS with hyperandrogenism, mean age was about 31 years, and about three quarters of enrollees were white, though local regulations restricted the collection of race and ethnicity data in some cases. One secondary outcome measure of the study was how fezolinetant affected the LH:FSH (follicle-stimulating hormone) ratio. “Patients with PCOS tend to have a very high GNRH [gonadotropin-releasing hormone] pulse frequency, which leads to a very high LH:FSH ratio,” said Dr. Fraser.
At baseline, the LH:FSH ratio was about 3. “With treatment, that ratio normalized to about 1, which is where it is in healthy women,” he said. The decrease in LH:FSH ratio occurred in a dose-dependent fashion and was statistically significant (P less than .001 for 180 mg fezolinetant versus placebo).
Dr. Fraser and his collaborators also tracked anti-müllerian hormone (AMH) levels, ovarian volume, and number of follicles. Although the investigators saw trends toward reduction in AMH levels and toward smaller ovarian volumes, these trends weren’t significant. “It was somewhat ambitious, I guess, to consider we’d hit these endpoints within 12 weeks,” he said. There were no serious drug-related adverse events.
“Most importantly, I would say, we did not get an increase in menses frequency, and, of course, that’s an important marker for fertility,” said Dr. Fraser. “There’s a debate in PCOS about whether this disease is driven by a malfunction in the brain or a malfunction in the ovaries. I guess on face value, perhaps this problem is in the ovaries.”
With the trends toward lower AMH and ovarian volumes, the research team is left wondering what would happen if the duration of therapy were extended. “Perhaps, the system would have been reset, and the frequency would have been restored. … So one thought that we have is to prolong the study in future trials and see if that could lead to an increase in fertility in PCOS,” said Dr. Fraser.
Fezolinetant is also being studied for menopause-related hot flashes in the United States and Europe.
Dr. Fraser is an employee of Ogeda, which sponsored the trial. Ogeda is a wholly owned subsidiary of Astelas.
SOURCE: Fraser G et al. ENDO 2018, Abstract SAT-305-LB.
CHICAGO – currently in development. The proof-of-concept phase 2 trial, which saw no concerning safety signals for the medication, fezolinetant, sets the stage for a larger, and perhaps longer, study to learn more about the neurokinin 3 receptor antagonist’s efficacy against PCOS.
“The primary outcome for this phase 2 trial was to see if we could lower testosterone levels in these PCOS patients,” said Graeme Fraser, PhD, chief scientific officer for Ogeda, discussing the poster he and his colleagues presented at the annual meeting of the Endocrine Society.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
“Testosterone levels decreased: Measured at about 3 hours postdose, which is the approximate pharmacokinetic Cmax [maximum serum concentration], there was … a more than 30% decrease in testosterone levels,” said Dr. Fraser. By week 12, he said, “there was a very consistent decrease of 30% of testosterone levels. So that was quite good; we successfully hit the primary outcome.”
At 12 weeks, the higher dose of fezolinetant decreased testosterone by 0.64 nmol/L, compared with the 0.04 nmol/L seen with placebo (P less than .01).
Fezolinetant downregulates the activity of candy neurons in the hypothalamus, said Dr. Fraser in an interview. In turn, gonadotropin-releasing hormone (GNRH) pulse frequency is reduced, lowering luteinizing hormone (LH) levels. Since LH drives testosterone levels, this drops as well – a beneficial effect in PCOS, with its cardinal symptom of hyperandrogenism.
The double-blind, placebo-controlled study was conducted in Western Europe; 73 participants were randomized into three groups: 27 to a placebo group, 23 to a treatment group given 60 mg of fezolinetant once daily, and 23 to a treatment group given 180 mg of fezolinetant once daily. All groups received treatment for 12 weeks.
A total of 26 patients on placebo, 21 on 60-mg fezolinetant, and 17 on 180-mg fezolinetant completed the study. Patients who completed the study were included in the safety analysis, while all who took the study medication were included in the intent-to-treat analysis for primary and secondary outcome measures.
All participants had PCOS with hyperandrogenism, mean age was about 31 years, and about three quarters of enrollees were white, though local regulations restricted the collection of race and ethnicity data in some cases. One secondary outcome measure of the study was how fezolinetant affected the LH:FSH (follicle-stimulating hormone) ratio. “Patients with PCOS tend to have a very high GNRH [gonadotropin-releasing hormone] pulse frequency, which leads to a very high LH:FSH ratio,” said Dr. Fraser.
At baseline, the LH:FSH ratio was about 3. “With treatment, that ratio normalized to about 1, which is where it is in healthy women,” he said. The decrease in LH:FSH ratio occurred in a dose-dependent fashion and was statistically significant (P less than .001 for 180 mg fezolinetant versus placebo).
Dr. Fraser and his collaborators also tracked anti-müllerian hormone (AMH) levels, ovarian volume, and number of follicles. Although the investigators saw trends toward reduction in AMH levels and toward smaller ovarian volumes, these trends weren’t significant. “It was somewhat ambitious, I guess, to consider we’d hit these endpoints within 12 weeks,” he said. There were no serious drug-related adverse events.
“Most importantly, I would say, we did not get an increase in menses frequency, and, of course, that’s an important marker for fertility,” said Dr. Fraser. “There’s a debate in PCOS about whether this disease is driven by a malfunction in the brain or a malfunction in the ovaries. I guess on face value, perhaps this problem is in the ovaries.”
With the trends toward lower AMH and ovarian volumes, the research team is left wondering what would happen if the duration of therapy were extended. “Perhaps, the system would have been reset, and the frequency would have been restored. … So one thought that we have is to prolong the study in future trials and see if that could lead to an increase in fertility in PCOS,” said Dr. Fraser.
Fezolinetant is also being studied for menopause-related hot flashes in the United States and Europe.
Dr. Fraser is an employee of Ogeda, which sponsored the trial. Ogeda is a wholly owned subsidiary of Astelas.
SOURCE: Fraser G et al. ENDO 2018, Abstract SAT-305-LB.
CHICAGO – currently in development. The proof-of-concept phase 2 trial, which saw no concerning safety signals for the medication, fezolinetant, sets the stage for a larger, and perhaps longer, study to learn more about the neurokinin 3 receptor antagonist’s efficacy against PCOS.
“The primary outcome for this phase 2 trial was to see if we could lower testosterone levels in these PCOS patients,” said Graeme Fraser, PhD, chief scientific officer for Ogeda, discussing the poster he and his colleagues presented at the annual meeting of the Endocrine Society.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
“Testosterone levels decreased: Measured at about 3 hours postdose, which is the approximate pharmacokinetic Cmax [maximum serum concentration], there was … a more than 30% decrease in testosterone levels,” said Dr. Fraser. By week 12, he said, “there was a very consistent decrease of 30% of testosterone levels. So that was quite good; we successfully hit the primary outcome.”
At 12 weeks, the higher dose of fezolinetant decreased testosterone by 0.64 nmol/L, compared with the 0.04 nmol/L seen with placebo (P less than .01).
Fezolinetant downregulates the activity of candy neurons in the hypothalamus, said Dr. Fraser in an interview. In turn, gonadotropin-releasing hormone (GNRH) pulse frequency is reduced, lowering luteinizing hormone (LH) levels. Since LH drives testosterone levels, this drops as well – a beneficial effect in PCOS, with its cardinal symptom of hyperandrogenism.
The double-blind, placebo-controlled study was conducted in Western Europe; 73 participants were randomized into three groups: 27 to a placebo group, 23 to a treatment group given 60 mg of fezolinetant once daily, and 23 to a treatment group given 180 mg of fezolinetant once daily. All groups received treatment for 12 weeks.
A total of 26 patients on placebo, 21 on 60-mg fezolinetant, and 17 on 180-mg fezolinetant completed the study. Patients who completed the study were included in the safety analysis, while all who took the study medication were included in the intent-to-treat analysis for primary and secondary outcome measures.
All participants had PCOS with hyperandrogenism, mean age was about 31 years, and about three quarters of enrollees were white, though local regulations restricted the collection of race and ethnicity data in some cases. One secondary outcome measure of the study was how fezolinetant affected the LH:FSH (follicle-stimulating hormone) ratio. “Patients with PCOS tend to have a very high GNRH [gonadotropin-releasing hormone] pulse frequency, which leads to a very high LH:FSH ratio,” said Dr. Fraser.
At baseline, the LH:FSH ratio was about 3. “With treatment, that ratio normalized to about 1, which is where it is in healthy women,” he said. The decrease in LH:FSH ratio occurred in a dose-dependent fashion and was statistically significant (P less than .001 for 180 mg fezolinetant versus placebo).
Dr. Fraser and his collaborators also tracked anti-müllerian hormone (AMH) levels, ovarian volume, and number of follicles. Although the investigators saw trends toward reduction in AMH levels and toward smaller ovarian volumes, these trends weren’t significant. “It was somewhat ambitious, I guess, to consider we’d hit these endpoints within 12 weeks,” he said. There were no serious drug-related adverse events.
“Most importantly, I would say, we did not get an increase in menses frequency, and, of course, that’s an important marker for fertility,” said Dr. Fraser. “There’s a debate in PCOS about whether this disease is driven by a malfunction in the brain or a malfunction in the ovaries. I guess on face value, perhaps this problem is in the ovaries.”
With the trends toward lower AMH and ovarian volumes, the research team is left wondering what would happen if the duration of therapy were extended. “Perhaps, the system would have been reset, and the frequency would have been restored. … So one thought that we have is to prolong the study in future trials and see if that could lead to an increase in fertility in PCOS,” said Dr. Fraser.
Fezolinetant is also being studied for menopause-related hot flashes in the United States and Europe.
Dr. Fraser is an employee of Ogeda, which sponsored the trial. Ogeda is a wholly owned subsidiary of Astelas.
SOURCE: Fraser G et al. ENDO 2018, Abstract SAT-305-LB.
REPORTING FROM ENDO 2018
Match Day 2018: Ob.gyn. increases positions and matches
compared with 2017, according to the National Resident Matching Program (NRMP).
Ob.gyn. brought 1,336 first-year positions to the Match Day party this year and filled 78.7% of them with U.S. graduates. The overall fill rate of 99.6% is actually down from last year, when the specialty managed to fill all 1,288 positions offered. For all specialties, U.S. graduates filled 58.7% of the record-high 30,232 available spots, and the overall fill rate was 96.1%, the NRMP said in its 2018 Main Residency Match report.
compared with 2017, according to the National Resident Matching Program (NRMP).
Ob.gyn. brought 1,336 first-year positions to the Match Day party this year and filled 78.7% of them with U.S. graduates. The overall fill rate of 99.6% is actually down from last year, when the specialty managed to fill all 1,288 positions offered. For all specialties, U.S. graduates filled 58.7% of the record-high 30,232 available spots, and the overall fill rate was 96.1%, the NRMP said in its 2018 Main Residency Match report.
compared with 2017, according to the National Resident Matching Program (NRMP).
Ob.gyn. brought 1,336 first-year positions to the Match Day party this year and filled 78.7% of them with U.S. graduates. The overall fill rate of 99.6% is actually down from last year, when the specialty managed to fill all 1,288 positions offered. For all specialties, U.S. graduates filled 58.7% of the record-high 30,232 available spots, and the overall fill rate was 96.1%, the NRMP said in its 2018 Main Residency Match report.
Abdominal pain with high transaminases
A 54-year-old woman presents with severe abdominal pain lasting 3 hours. The pain came on suddenly and was 10/10 in severity. It was in her right upper quadrant radiating to her back. She has had a 50-pound weight loss in the past year. Her medications include sertraline, phentermine-topiramate, and simvastatin.
She is evaluated in the emergency department, and labs show the following: aspartate aminotransferase, 450; alanine aminotransferase, 500; alkaline phosphatase, 100; bilirubin, 1.2. She receives morphine for her pain with minimal relief. An ultrasound shows no gallstones and no dilated common bile duct (CBD).
Her pain resolves 3 hours after arriving in the ED. Repeat labs 15 minutes after pain resolution show the following: AST, 900; ALT, 1,000; alk phos, 130; bili, 1.2.
What is the most likely diagnosis?
A. Acetaminophen toxicity.
B. Hepatitis A.
C. Ischemic hepatitis.
D. Simvastatin.
E. Passage of gallstone.
The correct answer in this case is passage of a gallstone.
The patient has had weight loss, which increases the risk of gallstone formation, and the pain pattern is consistent with passage of a gallstone through the common bile duct.
I have seen a number of cases where the diagnosis was missed when the lab pattern is similar to the labs in this case. The high transaminases and the absence of significant alkaline phosphatase elevation can be confusing. We are taught in our medical training that alkaline phosphatase is a lab value that goes up with obstruction, and that transaminases are liver injury labs. What are the data on liver labs in the setting of acute obstruction as seen with the passage of a gallstone?
Frederick Kiechle, MD, and colleagues reported that alkaline phosphatase levels, either alone or in conjunction with bilirubin levels, were not useful in determining the presence of common bile duct stones.1 Ming-Hsun Yang et al. found that normal gamma-glutamyl transferase results had the highest negative predictive value for the presence of a common bile duct stone (97%).2 The sensitivity for ultrasound detection of CBD stone in this study was only 35%.
Keun Soo Ahn and colleagues found that, in patients with symptomatic CBD stones, the average AST was 275, and the average ALT was 317 – about six to seven times the upper limit of normal for these lab tests.3 In the same study, the average alkaline phosphatase was 213, which is about twice the upper limit of normal.
Sometimes, extremely high transaminase elevations can occur with choledocholithiasis. Saroja Bangaru et al. reported on a case series of patients who all had transaminase values greater than 1,000 with symptomatic choledocholithiasis.4 All of the patients had normal or just mildly elevated alkaline phosphatase levels.
Rahul Nathwani, MD, and colleagues also reported on a series of 16 patients with choledocholithiasis and transaminase levels greater than 1,000.5 All patients were symptomatic, and the average alkaline phosphatase levels were 2.5 times the upper limit of normal.
Ala Sharara, MD, et al. looked at 40 patients in a retrospective study of patients found to have choledocholithiasis who presented within 12 hours of pain onset.6 Levels of AST and ALT both significantly correlated with duration of pain (P less than .001), whereas there was no significant correlation with alkaline phosphatase and bilirubin levels.

Pearl: AST and ALT elevations in patients with acute abdominal pain could be due to choledocholithiasis, even if there are minimal or no abnormalities in alkaline phosphatase. Marked elevations (greater than 1,000) can occur.
Dr. Paauw is professor of medicine in the division of general internal medicine at the University of Washington, Seattle, and he serves as third-year medical student clerkship director at the University of Washington. Contact Dr. Paauw at [email protected].
References
1. Am J Emerg Med. 1985 Nov;3(6):556-60.
2. Surg Endosc. 2008 Jul;22(7):1620-4.
3. World J Surg. 2016 Aug;40(8):1925-31.
4. J Clin Gastroenterol. 2017 Sep;51(8):728-33.
5. Am J Gastroenterol. 2005 Feb;100(2):295-8.
6. Clin Gastroenterol Hepatol. 2010 Dec;8(12):1077-82.
A 54-year-old woman presents with severe abdominal pain lasting 3 hours. The pain came on suddenly and was 10/10 in severity. It was in her right upper quadrant radiating to her back. She has had a 50-pound weight loss in the past year. Her medications include sertraline, phentermine-topiramate, and simvastatin.
She is evaluated in the emergency department, and labs show the following: aspartate aminotransferase, 450; alanine aminotransferase, 500; alkaline phosphatase, 100; bilirubin, 1.2. She receives morphine for her pain with minimal relief. An ultrasound shows no gallstones and no dilated common bile duct (CBD).
Her pain resolves 3 hours after arriving in the ED. Repeat labs 15 minutes after pain resolution show the following: AST, 900; ALT, 1,000; alk phos, 130; bili, 1.2.
What is the most likely diagnosis?
A. Acetaminophen toxicity.
B. Hepatitis A.
C. Ischemic hepatitis.
D. Simvastatin.
E. Passage of gallstone.
The correct answer in this case is passage of a gallstone.
The patient has had weight loss, which increases the risk of gallstone formation, and the pain pattern is consistent with passage of a gallstone through the common bile duct.
I have seen a number of cases where the diagnosis was missed when the lab pattern is similar to the labs in this case. The high transaminases and the absence of significant alkaline phosphatase elevation can be confusing. We are taught in our medical training that alkaline phosphatase is a lab value that goes up with obstruction, and that transaminases are liver injury labs. What are the data on liver labs in the setting of acute obstruction as seen with the passage of a gallstone?
Frederick Kiechle, MD, and colleagues reported that alkaline phosphatase levels, either alone or in conjunction with bilirubin levels, were not useful in determining the presence of common bile duct stones.1 Ming-Hsun Yang et al. found that normal gamma-glutamyl transferase results had the highest negative predictive value for the presence of a common bile duct stone (97%).2 The sensitivity for ultrasound detection of CBD stone in this study was only 35%.
Keun Soo Ahn and colleagues found that, in patients with symptomatic CBD stones, the average AST was 275, and the average ALT was 317 – about six to seven times the upper limit of normal for these lab tests.3 In the same study, the average alkaline phosphatase was 213, which is about twice the upper limit of normal.
Sometimes, extremely high transaminase elevations can occur with choledocholithiasis. Saroja Bangaru et al. reported on a case series of patients who all had transaminase values greater than 1,000 with symptomatic choledocholithiasis.4 All of the patients had normal or just mildly elevated alkaline phosphatase levels.
Rahul Nathwani, MD, and colleagues also reported on a series of 16 patients with choledocholithiasis and transaminase levels greater than 1,000.5 All patients were symptomatic, and the average alkaline phosphatase levels were 2.5 times the upper limit of normal.
Ala Sharara, MD, et al. looked at 40 patients in a retrospective study of patients found to have choledocholithiasis who presented within 12 hours of pain onset.6 Levels of AST and ALT both significantly correlated with duration of pain (P less than .001), whereas there was no significant correlation with alkaline phosphatase and bilirubin levels.
Pearl: AST and ALT elevations in patients with acute abdominal pain could be due to choledocholithiasis, even if there are minimal or no abnormalities in alkaline phosphatase. Marked elevations (greater than 1,000) can occur.
Dr. Paauw is professor of medicine in the division of general internal medicine at the University of Washington, Seattle, and he serves as third-year medical student clerkship director at the University of Washington. Contact Dr. Paauw at [email protected].
References
1. Am J Emerg Med. 1985 Nov;3(6):556-60.
2. Surg Endosc. 2008 Jul;22(7):1620-4.
3. World J Surg. 2016 Aug;40(8):1925-31.
4. J Clin Gastroenterol. 2017 Sep;51(8):728-33.
5. Am J Gastroenterol. 2005 Feb;100(2):295-8.
6. Clin Gastroenterol Hepatol. 2010 Dec;8(12):1077-82.
A 54-year-old woman presents with severe abdominal pain lasting 3 hours. The pain came on suddenly and was 10/10 in severity. It was in her right upper quadrant radiating to her back. She has had a 50-pound weight loss in the past year. Her medications include sertraline, phentermine-topiramate, and simvastatin.
She is evaluated in the emergency department, and labs show the following: aspartate aminotransferase, 450; alanine aminotransferase, 500; alkaline phosphatase, 100; bilirubin, 1.2. She receives morphine for her pain with minimal relief. An ultrasound shows no gallstones and no dilated common bile duct (CBD).
Her pain resolves 3 hours after arriving in the ED. Repeat labs 15 minutes after pain resolution show the following: AST, 900; ALT, 1,000; alk phos, 130; bili, 1.2.
What is the most likely diagnosis?
A. Acetaminophen toxicity.
B. Hepatitis A.
C. Ischemic hepatitis.
D. Simvastatin.
E. Passage of gallstone.
The correct answer in this case is passage of a gallstone.
The patient has had weight loss, which increases the risk of gallstone formation, and the pain pattern is consistent with passage of a gallstone through the common bile duct.
I have seen a number of cases where the diagnosis was missed when the lab pattern is similar to the labs in this case. The high transaminases and the absence of significant alkaline phosphatase elevation can be confusing. We are taught in our medical training that alkaline phosphatase is a lab value that goes up with obstruction, and that transaminases are liver injury labs. What are the data on liver labs in the setting of acute obstruction as seen with the passage of a gallstone?
Frederick Kiechle, MD, and colleagues reported that alkaline phosphatase levels, either alone or in conjunction with bilirubin levels, were not useful in determining the presence of common bile duct stones.1 Ming-Hsun Yang et al. found that normal gamma-glutamyl transferase results had the highest negative predictive value for the presence of a common bile duct stone (97%).2 The sensitivity for ultrasound detection of CBD stone in this study was only 35%.
Keun Soo Ahn and colleagues found that, in patients with symptomatic CBD stones, the average AST was 275, and the average ALT was 317 – about six to seven times the upper limit of normal for these lab tests.3 In the same study, the average alkaline phosphatase was 213, which is about twice the upper limit of normal.
Sometimes, extremely high transaminase elevations can occur with choledocholithiasis. Saroja Bangaru et al. reported on a case series of patients who all had transaminase values greater than 1,000 with symptomatic choledocholithiasis.4 All of the patients had normal or just mildly elevated alkaline phosphatase levels.
Rahul Nathwani, MD, and colleagues also reported on a series of 16 patients with choledocholithiasis and transaminase levels greater than 1,000.5 All patients were symptomatic, and the average alkaline phosphatase levels were 2.5 times the upper limit of normal.
Ala Sharara, MD, et al. looked at 40 patients in a retrospective study of patients found to have choledocholithiasis who presented within 12 hours of pain onset.6 Levels of AST and ALT both significantly correlated with duration of pain (P less than .001), whereas there was no significant correlation with alkaline phosphatase and bilirubin levels.
Pearl: AST and ALT elevations in patients with acute abdominal pain could be due to choledocholithiasis, even if there are minimal or no abnormalities in alkaline phosphatase. Marked elevations (greater than 1,000) can occur.
Dr. Paauw is professor of medicine in the division of general internal medicine at the University of Washington, Seattle, and he serves as third-year medical student clerkship director at the University of Washington. Contact Dr. Paauw at [email protected].
References
1. Am J Emerg Med. 1985 Nov;3(6):556-60.
2. Surg Endosc. 2008 Jul;22(7):1620-4.
3. World J Surg. 2016 Aug;40(8):1925-31.
4. J Clin Gastroenterol. 2017 Sep;51(8):728-33.
5. Am J Gastroenterol. 2005 Feb;100(2):295-8.
6. Clin Gastroenterol Hepatol. 2010 Dec;8(12):1077-82.
New tool improves hand-off communications
Transitions of care can be rife with communications issues – and subsequent adverse events. They are also a place where hospitalists can take the lead in making improvements.
“They are the team leaders, typically,” said Ana Pujols McKee, MD, the executive vice president and chief medical officer for The Joint Commission. “The hospitalist really owns this process of the transfer of this accurate information.”
To help, The Joint Commission has issued a new Sentinel Event Alert, which provides seven recommendations to improve the communication failures that can occur when patients are transitioned from one caregiver to another, as well as a Targeted Solutions Tool to put the recommendations into action.
“Every organization is challenged in communicating accurate and timely information regarding patients,” Dr. McKee said. “One of the riskiest transitions that patients go through is when they change levels of care from ICU to med-surg, or from the ER to ICU, OR to ICU, med-surg to home, and home to home care. All of those transitions inherently carry a certain amount of risk and are deeply reliant on the transfer of the right information at the right time to the right person.”
These resources reflect what The Joint Commission has found: “The knowledge that we now have is that one of the defects that occurs in this transitioning is that – I’ll speak of sender and receiver – the information that is sent is always sent from the perspective of what the sender thinks is important, not the information the receiver needs to manage that patient safely.”
The tool uses the principles of Lean Six Sigma and change management, and organizations can use it to identify their opportunities for improvement and develop strategies to address their specific root causes in their organization.
“It’s a self-guided tool,” Dr. McKee said. “Organizations have reduced errors significantly in using this tool. I think if the hospitalist community takes this on, that would really help transform how we do transitions of care.”
Transitions of care can be rife with communications issues – and subsequent adverse events. They are also a place where hospitalists can take the lead in making improvements.
“They are the team leaders, typically,” said Ana Pujols McKee, MD, the executive vice president and chief medical officer for The Joint Commission. “The hospitalist really owns this process of the transfer of this accurate information.”
To help, The Joint Commission has issued a new Sentinel Event Alert, which provides seven recommendations to improve the communication failures that can occur when patients are transitioned from one caregiver to another, as well as a Targeted Solutions Tool to put the recommendations into action.
“Every organization is challenged in communicating accurate and timely information regarding patients,” Dr. McKee said. “One of the riskiest transitions that patients go through is when they change levels of care from ICU to med-surg, or from the ER to ICU, OR to ICU, med-surg to home, and home to home care. All of those transitions inherently carry a certain amount of risk and are deeply reliant on the transfer of the right information at the right time to the right person.”
These resources reflect what The Joint Commission has found: “The knowledge that we now have is that one of the defects that occurs in this transitioning is that – I’ll speak of sender and receiver – the information that is sent is always sent from the perspective of what the sender thinks is important, not the information the receiver needs to manage that patient safely.”
The tool uses the principles of Lean Six Sigma and change management, and organizations can use it to identify their opportunities for improvement and develop strategies to address their specific root causes in their organization.
“It’s a self-guided tool,” Dr. McKee said. “Organizations have reduced errors significantly in using this tool. I think if the hospitalist community takes this on, that would really help transform how we do transitions of care.”
Transitions of care can be rife with communications issues – and subsequent adverse events. They are also a place where hospitalists can take the lead in making improvements.
“They are the team leaders, typically,” said Ana Pujols McKee, MD, the executive vice president and chief medical officer for The Joint Commission. “The hospitalist really owns this process of the transfer of this accurate information.”
To help, The Joint Commission has issued a new Sentinel Event Alert, which provides seven recommendations to improve the communication failures that can occur when patients are transitioned from one caregiver to another, as well as a Targeted Solutions Tool to put the recommendations into action.
“Every organization is challenged in communicating accurate and timely information regarding patients,” Dr. McKee said. “One of the riskiest transitions that patients go through is when they change levels of care from ICU to med-surg, or from the ER to ICU, OR to ICU, med-surg to home, and home to home care. All of those transitions inherently carry a certain amount of risk and are deeply reliant on the transfer of the right information at the right time to the right person.”
These resources reflect what The Joint Commission has found: “The knowledge that we now have is that one of the defects that occurs in this transitioning is that – I’ll speak of sender and receiver – the information that is sent is always sent from the perspective of what the sender thinks is important, not the information the receiver needs to manage that patient safely.”
The tool uses the principles of Lean Six Sigma and change management, and organizations can use it to identify their opportunities for improvement and develop strategies to address their specific root causes in their organization.
“It’s a self-guided tool,” Dr. McKee said. “Organizations have reduced errors significantly in using this tool. I think if the hospitalist community takes this on, that would really help transform how we do transitions of care.”
Popular vaginal dryness products don’t beat placebos
based on data from a randomized trial of more than 300 patients suffering from genitourinary syndrome of menopause (GSM), a constellation of symptoms including pain on vaginal penetration and vaginal dryness.
“Surveys of postmenopausal women demonstrate a preference for effective, nonhormonal therapies, often due to safety concerns,” wrote Caroline M. Mitchell, MD, of Massachusetts General Hospital, Boston, and her colleagues. The report was published in JAMA Internal Medicine. The researchers randomized 302 postmenopausal women with GSM 1:1:1 to a Vagifem 10-microgram estradiol tablet and placebo gel, a placebo tablet and Replens gel, or a placebo tablet and a placebo gel.
The average age of the women was 61 years, 88% were white, and 81% were sexually active.
The primary outcome was a decrease in the most bothersome symptoms reported by the women after 12 weeks of treatment. The most common of these were pain on penetration (60%) and vulvovaginal dryness (21%).
After 12 weeks, the women reported no significant difference in most bothersome symptoms between estradiol or moisturizing gel, compared with placebo products (P = .25 and P = .31, respectively). The average improvement in symptom scores was similar between the estradiol tablet and placebo tablet (P = .64) and between the moisturizer and placebo gels (P = .17).
The study was limited by several factors including the homogenous population and the absence of a head-to-head comparison of treatments, the researchers noted. However, the results suggest that more research is needed about genitourinary syndrome of menopause, but that a nonprescription lubricating gel may be an appropriate estrogen-free choice, and that “treatment choice should be based on individual patient preferences regarding cost and formulation,” they said.
The study was funded by the National Institutes of Health/National Institute on Aging. Dr. Mitchell is a consultant for Symbiomix Therapeutics, and coauthors reported grant support from Bayer and having served on a scientific advisory board for Sermonix.
SOURCE: Mitchell C et al. JAMA Intern Med. 2018 Mar. doi: 10.1001/jamainternmed.2018.0116.
The double-negative finding of the study suggests a potential change in clinical practice as to the value of estrogen for postmenopausal women, Alison J. Huang, MD, and Deborah Grady, MD, wrote in an editorial.
“Based on the results of this study, women and their physicians may want to take this one step further and conclude that postmenopausal women experiencing vulvovaginal symptoms should choose the cheapest moisturizer or lubricant available over the counter – at least until new evidence arises to suggest that there is any benefit to doing otherwise,” they said. The study compared popular active treatments – an estradiol tablet and a nonhormonal moisturizing gel – with placebo and not with each other, which could be considered a limitation, they said. However, the similar effectiveness of the treatments to placebo support a choice of treatments for vulvovaginal symptoms based on cost and patient preference for a particular formulation, they noted (JAMA Intern Med. 2018 Mar. doi: 10.1001/jamainternmed.2018.0094).
Dr. Huang and Dr. Grady are affiliated with the University of California, San Francisco, and the San Francisco Veterans Affairs Health Care System. Dr. Huang disclosed research grants from Pfizer and Astellas Pharma. Dr. Grady has served as a consultant to MenoGeniX.
The double-negative finding of the study suggests a potential change in clinical practice as to the value of estrogen for postmenopausal women, Alison J. Huang, MD, and Deborah Grady, MD, wrote in an editorial.
“Based on the results of this study, women and their physicians may want to take this one step further and conclude that postmenopausal women experiencing vulvovaginal symptoms should choose the cheapest moisturizer or lubricant available over the counter – at least until new evidence arises to suggest that there is any benefit to doing otherwise,” they said. The study compared popular active treatments – an estradiol tablet and a nonhormonal moisturizing gel – with placebo and not with each other, which could be considered a limitation, they said. However, the similar effectiveness of the treatments to placebo support a choice of treatments for vulvovaginal symptoms based on cost and patient preference for a particular formulation, they noted (JAMA Intern Med. 2018 Mar. doi: 10.1001/jamainternmed.2018.0094).
Dr. Huang and Dr. Grady are affiliated with the University of California, San Francisco, and the San Francisco Veterans Affairs Health Care System. Dr. Huang disclosed research grants from Pfizer and Astellas Pharma. Dr. Grady has served as a consultant to MenoGeniX.
The double-negative finding of the study suggests a potential change in clinical practice as to the value of estrogen for postmenopausal women, Alison J. Huang, MD, and Deborah Grady, MD, wrote in an editorial.
“Based on the results of this study, women and their physicians may want to take this one step further and conclude that postmenopausal women experiencing vulvovaginal symptoms should choose the cheapest moisturizer or lubricant available over the counter – at least until new evidence arises to suggest that there is any benefit to doing otherwise,” they said. The study compared popular active treatments – an estradiol tablet and a nonhormonal moisturizing gel – with placebo and not with each other, which could be considered a limitation, they said. However, the similar effectiveness of the treatments to placebo support a choice of treatments for vulvovaginal symptoms based on cost and patient preference for a particular formulation, they noted (JAMA Intern Med. 2018 Mar. doi: 10.1001/jamainternmed.2018.0094).
Dr. Huang and Dr. Grady are affiliated with the University of California, San Francisco, and the San Francisco Veterans Affairs Health Care System. Dr. Huang disclosed research grants from Pfizer and Astellas Pharma. Dr. Grady has served as a consultant to MenoGeniX.
based on data from a randomized trial of more than 300 patients suffering from genitourinary syndrome of menopause (GSM), a constellation of symptoms including pain on vaginal penetration and vaginal dryness.
“Surveys of postmenopausal women demonstrate a preference for effective, nonhormonal therapies, often due to safety concerns,” wrote Caroline M. Mitchell, MD, of Massachusetts General Hospital, Boston, and her colleagues. The report was published in JAMA Internal Medicine. The researchers randomized 302 postmenopausal women with GSM 1:1:1 to a Vagifem 10-microgram estradiol tablet and placebo gel, a placebo tablet and Replens gel, or a placebo tablet and a placebo gel.
The average age of the women was 61 years, 88% were white, and 81% were sexually active.
The primary outcome was a decrease in the most bothersome symptoms reported by the women after 12 weeks of treatment. The most common of these were pain on penetration (60%) and vulvovaginal dryness (21%).
After 12 weeks, the women reported no significant difference in most bothersome symptoms between estradiol or moisturizing gel, compared with placebo products (P = .25 and P = .31, respectively). The average improvement in symptom scores was similar between the estradiol tablet and placebo tablet (P = .64) and between the moisturizer and placebo gels (P = .17).
The study was limited by several factors including the homogenous population and the absence of a head-to-head comparison of treatments, the researchers noted. However, the results suggest that more research is needed about genitourinary syndrome of menopause, but that a nonprescription lubricating gel may be an appropriate estrogen-free choice, and that “treatment choice should be based on individual patient preferences regarding cost and formulation,” they said.
The study was funded by the National Institutes of Health/National Institute on Aging. Dr. Mitchell is a consultant for Symbiomix Therapeutics, and coauthors reported grant support from Bayer and having served on a scientific advisory board for Sermonix.
SOURCE: Mitchell C et al. JAMA Intern Med. 2018 Mar. doi: 10.1001/jamainternmed.2018.0116.
based on data from a randomized trial of more than 300 patients suffering from genitourinary syndrome of menopause (GSM), a constellation of symptoms including pain on vaginal penetration and vaginal dryness.
“Surveys of postmenopausal women demonstrate a preference for effective, nonhormonal therapies, often due to safety concerns,” wrote Caroline M. Mitchell, MD, of Massachusetts General Hospital, Boston, and her colleagues. The report was published in JAMA Internal Medicine. The researchers randomized 302 postmenopausal women with GSM 1:1:1 to a Vagifem 10-microgram estradiol tablet and placebo gel, a placebo tablet and Replens gel, or a placebo tablet and a placebo gel.
The average age of the women was 61 years, 88% were white, and 81% were sexually active.
The primary outcome was a decrease in the most bothersome symptoms reported by the women after 12 weeks of treatment. The most common of these were pain on penetration (60%) and vulvovaginal dryness (21%).
After 12 weeks, the women reported no significant difference in most bothersome symptoms between estradiol or moisturizing gel, compared with placebo products (P = .25 and P = .31, respectively). The average improvement in symptom scores was similar between the estradiol tablet and placebo tablet (P = .64) and between the moisturizer and placebo gels (P = .17).
The study was limited by several factors including the homogenous population and the absence of a head-to-head comparison of treatments, the researchers noted. However, the results suggest that more research is needed about genitourinary syndrome of menopause, but that a nonprescription lubricating gel may be an appropriate estrogen-free choice, and that “treatment choice should be based on individual patient preferences regarding cost and formulation,” they said.
The study was funded by the National Institutes of Health/National Institute on Aging. Dr. Mitchell is a consultant for Symbiomix Therapeutics, and coauthors reported grant support from Bayer and having served on a scientific advisory board for Sermonix.
SOURCE: Mitchell C et al. JAMA Intern Med. 2018 Mar. doi: 10.1001/jamainternmed.2018.0116.
FROM JAMA INTERNAL MEDICINE
Key clinical point: Estradiol tablets had no increased benefit, compared with placebo, for relieving postmenopausal vulvovaginal symptoms.
Major finding: The improvement in vaginal discomfort after 12 weeks was not significantly different between an estradiol tablet and placebo (P = .64) or between a popular vaginal moisturizer and placebo (P = .17).
Study details: The data come from a randomized, clinical trial of 302 postmenopausal women.
Disclosures: The study was funded by the National Institutes of Health/National Institute on Aging. Dr. Mitchell is a consultant for Symbiomix Therapeutics, and coauthors reported grant support from Bayer and having served on a scientific advisory board for Sermonix.
Source: Mitchell C et al. JAMA Intern Med. 2018 Mar. doi: 10.1001/jamainternmed.2018.0116.
How the ADA shapes health care
Question: After many years of diabetes, a 60-year-old office worker develops nephropathy followed by end-stage renal disease, and now requires dialysis. He has opted for peritoneal dialysis rather than hemodialysis, so that he does not have to be away from the workplace for treatment. His diabetes is insulin requiring, and he has occasional hypoglycemic reactions. Although he qualifies for Social Security disability benefits, he prefers to continue working full time. The employer is considering terminating him.
Which of the following is best?
A. The Americans with Disabilities Act prohibits job discrimination against patients with disabilities, so long as they are otherwise qualified for every aspect of the job.
B. Renal insufficiency and diabetes are considered disabilities under the ADA.
C. The employer is obligated to provide full accommodation to enable this employee to continue working.
D. If the accommodations needed for a disabled person are unreasonable, or prove too disruptive or expensive, then the employer is not obligated to provide them.
E. This patient should simply retire and enjoy his SS disability benefits.
Answer: D. Enacted in 1990, the Americans with Disabilities Act seeks to provide clear, strong, consistent, and enforceable standards for ending discrimination against individuals with disabilities.1 The main thrust of the ADA, Title I, is to protect otherwise qualified workers with permanent disabilities from losing their jobs or seeking one, so long as they are qualified to perform the essential (not necessarily all) functions of the job.
In addition, the law prohibits discrimination against people with disabilities from accessing public accommodations (Title III), which include doctors’ offices and health care facilities, as well as restaurants, retail stores, etc. Other areas under the purview of the omnibus ADA include transportation, communications, and access to state and local government programs and services.
The Equal Employment Opportunity Commission (EEOC) enforces Title I of the ADA, the section that deals with job discrimination. Its compliance manual sets out guidelines for determining whether an individual in fact has a disability.
The word “disability” has three components, and the term is not synonymous with “impairment.” However, a disability begins with having an impairment, defined as a physiological disorder affecting one or more of a number of body systems or a mental or psychological disorder.
An example given by the EEOC: If a person cannot find a job because that person has the equivalent of a second-grade education and therefore cannot read, that person does not have an impairment for purposes of the ADA. If, however, that person cannot read because of severe dyslexia, that person has an impairment. Likewise, being overweight is not considered an impairment (unless due to an underlying physical condition, e.g., hypothyroidism), although extreme obesity in excess of 100% ideal body weight is.
Having determined that an impairment exists, the next step in the analysis is to ascertain if the impairment limits one or more “major life activities.” These have classically included activities such as caring for oneself, performing manual tasks, walking, seeing, hearing, speaking, and breathing.
Third, the limitation must be substantial, meaning sufficiently severe, compared with what an average person is capable of doing. According to the EEOC, a mild type 2 diabetes patient on diet treatment alone and no other restriction has an impairment; but the impairment does not substantially limit any of his major life activities. On the other hand, some impairments are so severe that there is no doubt they substantially limit major life activities, e.g., insulin-dependent diabetes, legal blindness, deafness, manic-depressive syndrome, alcoholism, and HIV infection.
There is litigation aplenty over these issues.
In its seminal 1988 case, the U.S. Supreme Court provided the analytical steps listed above in arriving at its holding that, under the ADA, asymptomatic HIV infection is a disability.2 The case involved a dentist who was sued when he declined to treat an HIV-positive female patient in the office, offering instead to treat her in a hospital without any additional charge. A dental office, like a doctor’s office, is recognized as a place of public accommodations, and therefore falls under the protection of Title III of the ADA.
The court first considered whether HIV infection was a physical impairment. Second, it identified the major life activity upon which the plaintiff relied (reproduction and childbearing) and determined whether it constituted a major life activity under the ADA. Third, it tied the two statutory phrases together, and asked whether the impairment substantially limited these major life activities.
The court held that, in light of the immediacy with which the HIV virus begins to damage the infected person’s white blood cells and the severity of the disease, it is an impairment from the moment of infection, even if the patient was asymptomatic. It also ruled that the HIV infection substantially limited her ability to reproduce in two independent ways. First, a woman infected with HIV who tries to conceive a child imposes on the man a significant risk of becoming infected, and second, an infected woman risks infecting her child during gestation and childbirth, i.e., perinatal transmission.
In 2004, a case reached the U.S. Third Circuit Court of Appeals regarding Cathy Fiscus, an employee at a Walmart Sam’s Club warehouse store in Pittsburgh, who faced being terminated after 12 years at her job. A lower U.S. district court had ruled in favor of the company, agreeing with Walmart that the woman’s end-stage renal disease had not left her significantly limited in a major life activity. Ms. Fiscus sought a reasonable accommodation from her employer during the period of her peritoneal dialysis, which required her to self administer the 45-minute dialysis process at the workplace. Walmart initially agreed, but later declined. The appeals court overturned the lower court’s ruling, writing, “A physical impairment that limits an individual’s ability to cleanse and eliminate body waste does impair a major life activity.”3
Not all conditions are covered by the ADA’s definition of disability. The list includes temporary physical or mental impairments, current illegal drug use, predisposition to illness, personality traits, advanced age, and pregnancy, to name a few.
To avoid running afoul of the ADA, an employer is required to make “reasonable accommodations” for the disabled employee. This refers to practices that allow a disabled person to perform the essential functions of the job.
Examples of reasonable accommodations include making existing facilities readily accessible to and usable by individuals with disabilities, restructuring jobs, modifying work schedules, and providing qualified readers or interpreters.
A “qualified individual with a disability” is an individual with a disability who, “with or without reasonable accommodation,” can perform the essential functions of the employment position in question. A person is not a qualified individual with a disability, however, if he or she cannot satisfy the basic attendance requirements of a position.
Employers are not required to offer any and all accommodations, such as those that are disruptive to the business, overly burdensome, or prohibitively expensive. Providing a clean and private area in the workplace for self-administered peritoneal dialysis fluid exchange would likely qualify as a reasonable accommodation that should be offered, absent some compelling reason not to.
The protection given by the ADA may be suspended if the condition poses a direct threat, defined as “a significant risk to the health or safety of others that cannot be eliminated by a modification of policies, practices, or procedures, or by the provision of auxiliary aids or services.”4 The U.S. Supreme Court has noted that this should be assessed by the objective reasonableness of the views of health care professionals.

Dr. Tan is emeritus professor of medicine and a former adjunct professor of law at the University of Hawaii, Honolulu. This article is meant to be educational and does not constitute medical, ethical or legal advice. For additional information, readers may contact the author at [email protected].
References
1. Americans with Disabilities Act of 1990 (ADA), 104 Stat. 327, 42 U. S. C. § 12101 et seq.
2. Bragdon v. Abbott et al. 524 U.S. 624 (1998).
3. Cathy A. Fiscus v. Wal-Mart Stores Inc., 385 F.3d 378 (3d Cir. 2004).
4. 42 U. S. C. § 12182(b)(3).
5. Available at www.kidney.org/atoz/content/employersguide.
Question: After many years of diabetes, a 60-year-old office worker develops nephropathy followed by end-stage renal disease, and now requires dialysis. He has opted for peritoneal dialysis rather than hemodialysis, so that he does not have to be away from the workplace for treatment. His diabetes is insulin requiring, and he has occasional hypoglycemic reactions. Although he qualifies for Social Security disability benefits, he prefers to continue working full time. The employer is considering terminating him.
Which of the following is best?
A. The Americans with Disabilities Act prohibits job discrimination against patients with disabilities, so long as they are otherwise qualified for every aspect of the job.
B. Renal insufficiency and diabetes are considered disabilities under the ADA.
C. The employer is obligated to provide full accommodation to enable this employee to continue working.
D. If the accommodations needed for a disabled person are unreasonable, or prove too disruptive or expensive, then the employer is not obligated to provide them.
E. This patient should simply retire and enjoy his SS disability benefits.
Answer: D. Enacted in 1990, the Americans with Disabilities Act seeks to provide clear, strong, consistent, and enforceable standards for ending discrimination against individuals with disabilities.1 The main thrust of the ADA, Title I, is to protect otherwise qualified workers with permanent disabilities from losing their jobs or seeking one, so long as they are qualified to perform the essential (not necessarily all) functions of the job.
In addition, the law prohibits discrimination against people with disabilities from accessing public accommodations (Title III), which include doctors’ offices and health care facilities, as well as restaurants, retail stores, etc. Other areas under the purview of the omnibus ADA include transportation, communications, and access to state and local government programs and services.
The Equal Employment Opportunity Commission (EEOC) enforces Title I of the ADA, the section that deals with job discrimination. Its compliance manual sets out guidelines for determining whether an individual in fact has a disability.
The word “disability” has three components, and the term is not synonymous with “impairment.” However, a disability begins with having an impairment, defined as a physiological disorder affecting one or more of a number of body systems or a mental or psychological disorder.
An example given by the EEOC: If a person cannot find a job because that person has the equivalent of a second-grade education and therefore cannot read, that person does not have an impairment for purposes of the ADA. If, however, that person cannot read because of severe dyslexia, that person has an impairment. Likewise, being overweight is not considered an impairment (unless due to an underlying physical condition, e.g., hypothyroidism), although extreme obesity in excess of 100% ideal body weight is.
Having determined that an impairment exists, the next step in the analysis is to ascertain if the impairment limits one or more “major life activities.” These have classically included activities such as caring for oneself, performing manual tasks, walking, seeing, hearing, speaking, and breathing.
Third, the limitation must be substantial, meaning sufficiently severe, compared with what an average person is capable of doing. According to the EEOC, a mild type 2 diabetes patient on diet treatment alone and no other restriction has an impairment; but the impairment does not substantially limit any of his major life activities. On the other hand, some impairments are so severe that there is no doubt they substantially limit major life activities, e.g., insulin-dependent diabetes, legal blindness, deafness, manic-depressive syndrome, alcoholism, and HIV infection.
There is litigation aplenty over these issues.
In its seminal 1988 case, the U.S. Supreme Court provided the analytical steps listed above in arriving at its holding that, under the ADA, asymptomatic HIV infection is a disability.2 The case involved a dentist who was sued when he declined to treat an HIV-positive female patient in the office, offering instead to treat her in a hospital without any additional charge. A dental office, like a doctor’s office, is recognized as a place of public accommodations, and therefore falls under the protection of Title III of the ADA.
The court first considered whether HIV infection was a physical impairment. Second, it identified the major life activity upon which the plaintiff relied (reproduction and childbearing) and determined whether it constituted a major life activity under the ADA. Third, it tied the two statutory phrases together, and asked whether the impairment substantially limited these major life activities.
The court held that, in light of the immediacy with which the HIV virus begins to damage the infected person’s white blood cells and the severity of the disease, it is an impairment from the moment of infection, even if the patient was asymptomatic. It also ruled that the HIV infection substantially limited her ability to reproduce in two independent ways. First, a woman infected with HIV who tries to conceive a child imposes on the man a significant risk of becoming infected, and second, an infected woman risks infecting her child during gestation and childbirth, i.e., perinatal transmission.
In 2004, a case reached the U.S. Third Circuit Court of Appeals regarding Cathy Fiscus, an employee at a Walmart Sam’s Club warehouse store in Pittsburgh, who faced being terminated after 12 years at her job. A lower U.S. district court had ruled in favor of the company, agreeing with Walmart that the woman’s end-stage renal disease had not left her significantly limited in a major life activity. Ms. Fiscus sought a reasonable accommodation from her employer during the period of her peritoneal dialysis, which required her to self administer the 45-minute dialysis process at the workplace. Walmart initially agreed, but later declined. The appeals court overturned the lower court’s ruling, writing, “A physical impairment that limits an individual’s ability to cleanse and eliminate body waste does impair a major life activity.”3
Not all conditions are covered by the ADA’s definition of disability. The list includes temporary physical or mental impairments, current illegal drug use, predisposition to illness, personality traits, advanced age, and pregnancy, to name a few.
To avoid running afoul of the ADA, an employer is required to make “reasonable accommodations” for the disabled employee. This refers to practices that allow a disabled person to perform the essential functions of the job.
Examples of reasonable accommodations include making existing facilities readily accessible to and usable by individuals with disabilities, restructuring jobs, modifying work schedules, and providing qualified readers or interpreters.
A “qualified individual with a disability” is an individual with a disability who, “with or without reasonable accommodation,” can perform the essential functions of the employment position in question. A person is not a qualified individual with a disability, however, if he or she cannot satisfy the basic attendance requirements of a position.
Employers are not required to offer any and all accommodations, such as those that are disruptive to the business, overly burdensome, or prohibitively expensive. Providing a clean and private area in the workplace for self-administered peritoneal dialysis fluid exchange would likely qualify as a reasonable accommodation that should be offered, absent some compelling reason not to.
The protection given by the ADA may be suspended if the condition poses a direct threat, defined as “a significant risk to the health or safety of others that cannot be eliminated by a modification of policies, practices, or procedures, or by the provision of auxiliary aids or services.”4 The U.S. Supreme Court has noted that this should be assessed by the objective reasonableness of the views of health care professionals.
Dr. Tan is emeritus professor of medicine and a former adjunct professor of law at the University of Hawaii, Honolulu. This article is meant to be educational and does not constitute medical, ethical or legal advice. For additional information, readers may contact the author at [email protected].
References
1. Americans with Disabilities Act of 1990 (ADA), 104 Stat. 327, 42 U. S. C. § 12101 et seq.
2. Bragdon v. Abbott et al. 524 U.S. 624 (1998).
3. Cathy A. Fiscus v. Wal-Mart Stores Inc., 385 F.3d 378 (3d Cir. 2004).
4. 42 U. S. C. § 12182(b)(3).
5. Available at www.kidney.org/atoz/content/employersguide.
Question: After many years of diabetes, a 60-year-old office worker develops nephropathy followed by end-stage renal disease, and now requires dialysis. He has opted for peritoneal dialysis rather than hemodialysis, so that he does not have to be away from the workplace for treatment. His diabetes is insulin requiring, and he has occasional hypoglycemic reactions. Although he qualifies for Social Security disability benefits, he prefers to continue working full time. The employer is considering terminating him.
Which of the following is best?
A. The Americans with Disabilities Act prohibits job discrimination against patients with disabilities, so long as they are otherwise qualified for every aspect of the job.
B. Renal insufficiency and diabetes are considered disabilities under the ADA.
C. The employer is obligated to provide full accommodation to enable this employee to continue working.
D. If the accommodations needed for a disabled person are unreasonable, or prove too disruptive or expensive, then the employer is not obligated to provide them.
E. This patient should simply retire and enjoy his SS disability benefits.
Answer: D. Enacted in 1990, the Americans with Disabilities Act seeks to provide clear, strong, consistent, and enforceable standards for ending discrimination against individuals with disabilities.1 The main thrust of the ADA, Title I, is to protect otherwise qualified workers with permanent disabilities from losing their jobs or seeking one, so long as they are qualified to perform the essential (not necessarily all) functions of the job.
In addition, the law prohibits discrimination against people with disabilities from accessing public accommodations (Title III), which include doctors’ offices and health care facilities, as well as restaurants, retail stores, etc. Other areas under the purview of the omnibus ADA include transportation, communications, and access to state and local government programs and services.
The Equal Employment Opportunity Commission (EEOC) enforces Title I of the ADA, the section that deals with job discrimination. Its compliance manual sets out guidelines for determining whether an individual in fact has a disability.
The word “disability” has three components, and the term is not synonymous with “impairment.” However, a disability begins with having an impairment, defined as a physiological disorder affecting one or more of a number of body systems or a mental or psychological disorder.
An example given by the EEOC: If a person cannot find a job because that person has the equivalent of a second-grade education and therefore cannot read, that person does not have an impairment for purposes of the ADA. If, however, that person cannot read because of severe dyslexia, that person has an impairment. Likewise, being overweight is not considered an impairment (unless due to an underlying physical condition, e.g., hypothyroidism), although extreme obesity in excess of 100% ideal body weight is.
Having determined that an impairment exists, the next step in the analysis is to ascertain if the impairment limits one or more “major life activities.” These have classically included activities such as caring for oneself, performing manual tasks, walking, seeing, hearing, speaking, and breathing.
Third, the limitation must be substantial, meaning sufficiently severe, compared with what an average person is capable of doing. According to the EEOC, a mild type 2 diabetes patient on diet treatment alone and no other restriction has an impairment; but the impairment does not substantially limit any of his major life activities. On the other hand, some impairments are so severe that there is no doubt they substantially limit major life activities, e.g., insulin-dependent diabetes, legal blindness, deafness, manic-depressive syndrome, alcoholism, and HIV infection.
There is litigation aplenty over these issues.
In its seminal 1988 case, the U.S. Supreme Court provided the analytical steps listed above in arriving at its holding that, under the ADA, asymptomatic HIV infection is a disability.2 The case involved a dentist who was sued when he declined to treat an HIV-positive female patient in the office, offering instead to treat her in a hospital without any additional charge. A dental office, like a doctor’s office, is recognized as a place of public accommodations, and therefore falls under the protection of Title III of the ADA.
The court first considered whether HIV infection was a physical impairment. Second, it identified the major life activity upon which the plaintiff relied (reproduction and childbearing) and determined whether it constituted a major life activity under the ADA. Third, it tied the two statutory phrases together, and asked whether the impairment substantially limited these major life activities.
The court held that, in light of the immediacy with which the HIV virus begins to damage the infected person’s white blood cells and the severity of the disease, it is an impairment from the moment of infection, even if the patient was asymptomatic. It also ruled that the HIV infection substantially limited her ability to reproduce in two independent ways. First, a woman infected with HIV who tries to conceive a child imposes on the man a significant risk of becoming infected, and second, an infected woman risks infecting her child during gestation and childbirth, i.e., perinatal transmission.
In 2004, a case reached the U.S. Third Circuit Court of Appeals regarding Cathy Fiscus, an employee at a Walmart Sam’s Club warehouse store in Pittsburgh, who faced being terminated after 12 years at her job. A lower U.S. district court had ruled in favor of the company, agreeing with Walmart that the woman’s end-stage renal disease had not left her significantly limited in a major life activity. Ms. Fiscus sought a reasonable accommodation from her employer during the period of her peritoneal dialysis, which required her to self administer the 45-minute dialysis process at the workplace. Walmart initially agreed, but later declined. The appeals court overturned the lower court’s ruling, writing, “A physical impairment that limits an individual’s ability to cleanse and eliminate body waste does impair a major life activity.”3
Not all conditions are covered by the ADA’s definition of disability. The list includes temporary physical or mental impairments, current illegal drug use, predisposition to illness, personality traits, advanced age, and pregnancy, to name a few.
To avoid running afoul of the ADA, an employer is required to make “reasonable accommodations” for the disabled employee. This refers to practices that allow a disabled person to perform the essential functions of the job.
Examples of reasonable accommodations include making existing facilities readily accessible to and usable by individuals with disabilities, restructuring jobs, modifying work schedules, and providing qualified readers or interpreters.
A “qualified individual with a disability” is an individual with a disability who, “with or without reasonable accommodation,” can perform the essential functions of the employment position in question. A person is not a qualified individual with a disability, however, if he or she cannot satisfy the basic attendance requirements of a position.
Employers are not required to offer any and all accommodations, such as those that are disruptive to the business, overly burdensome, or prohibitively expensive. Providing a clean and private area in the workplace for self-administered peritoneal dialysis fluid exchange would likely qualify as a reasonable accommodation that should be offered, absent some compelling reason not to.
The protection given by the ADA may be suspended if the condition poses a direct threat, defined as “a significant risk to the health or safety of others that cannot be eliminated by a modification of policies, practices, or procedures, or by the provision of auxiliary aids or services.”4 The U.S. Supreme Court has noted that this should be assessed by the objective reasonableness of the views of health care professionals.
Dr. Tan is emeritus professor of medicine and a former adjunct professor of law at the University of Hawaii, Honolulu. This article is meant to be educational and does not constitute medical, ethical or legal advice. For additional information, readers may contact the author at [email protected].
References
1. Americans with Disabilities Act of 1990 (ADA), 104 Stat. 327, 42 U. S. C. § 12101 et seq.
2. Bragdon v. Abbott et al. 524 U.S. 624 (1998).
3. Cathy A. Fiscus v. Wal-Mart Stores Inc., 385 F.3d 378 (3d Cir. 2004).
4. 42 U. S. C. § 12182(b)(3).
5. Available at www.kidney.org/atoz/content/employersguide.
VAM Registration Now Open
Registration and housing for the 2018 Vascular Annual Meeting are now open. Register today for VAM, June 20 to 23 in Boston, including looking over housing options. Following a full day of postgraduate courses, VESS abstracts, workshops and international programming on Wednesday, June 20, abstract-based scientific sessions will open June 21 and continue to June 23. The Exhibit Hall will be open June 21 to 22.
Registration and housing for the 2018 Vascular Annual Meeting are now open. Register today for VAM, June 20 to 23 in Boston, including looking over housing options. Following a full day of postgraduate courses, VESS abstracts, workshops and international programming on Wednesday, June 20, abstract-based scientific sessions will open June 21 and continue to June 23. The Exhibit Hall will be open June 21 to 22.
Registration and housing for the 2018 Vascular Annual Meeting are now open. Register today for VAM, June 20 to 23 in Boston, including looking over housing options. Following a full day of postgraduate courses, VESS abstracts, workshops and international programming on Wednesday, June 20, abstract-based scientific sessions will open June 21 and continue to June 23. The Exhibit Hall will be open June 21 to 22.