User login
More Children Than Estimated Have Fetal Alcohol Problems
A study of first graders showed that a significant number of subjects had fetal alcohol spectrum disorders (FASD)—“conservative” rates, National Institute on Alcohol Abuse and Alcoholism (NIAAA) researchers say, ranging from 1% - 5%.
Fetal alcohol spectrum disorders cover a range of health effects that are caused by prenatal alcohol exposure, including growth deficiencies, facial abnormalities, and organ damage, as well as neurobiological deficits that contribute to challenges throughout the life of those affected.
Prenatal alcohol exposure is a “leading preventable cause of developmental disabilities worldwide,” said George Koob, PhD, director of the NIAAA. But determining the prevalence in the US is complex, he notes, because of difficulties in identifying children who have been exposed before birth and also because previous FASD estimates were based on smaller studies.
The study conducted by the Collaboration on Fetal Alcohol Spectrum Disorders Prevalence consortium, collected data between 2010 -2016 on 6,639 children in 4 communities located in the Midwest, Rocky Mountain, Southeast, and Pacific Southwest communities. These sites were selected to be more reflective of US community populations than in previous studies.
Their findings suggest that many children are undiagnosed or misdiagnosed, the researchers say. Of 222 children diagnosed with FASD in the study, for example, only 2 had been previously diagnosed with FASD, although many parents and guardians were aware of the children’s learning and behavioral challenges.
The study’s comprehensive approach may give a truer picture of the prevalence of FASD in the U.S. And, says Christina Chambers, PhD, a co-leader of the investigation, it further highlights the “public health burden of FASD.”
A study of first graders showed that a significant number of subjects had fetal alcohol spectrum disorders (FASD)—“conservative” rates, National Institute on Alcohol Abuse and Alcoholism (NIAAA) researchers say, ranging from 1% - 5%.
Fetal alcohol spectrum disorders cover a range of health effects that are caused by prenatal alcohol exposure, including growth deficiencies, facial abnormalities, and organ damage, as well as neurobiological deficits that contribute to challenges throughout the life of those affected.
Prenatal alcohol exposure is a “leading preventable cause of developmental disabilities worldwide,” said George Koob, PhD, director of the NIAAA. But determining the prevalence in the US is complex, he notes, because of difficulties in identifying children who have been exposed before birth and also because previous FASD estimates were based on smaller studies.
The study conducted by the Collaboration on Fetal Alcohol Spectrum Disorders Prevalence consortium, collected data between 2010 -2016 on 6,639 children in 4 communities located in the Midwest, Rocky Mountain, Southeast, and Pacific Southwest communities. These sites were selected to be more reflective of US community populations than in previous studies.
Their findings suggest that many children are undiagnosed or misdiagnosed, the researchers say. Of 222 children diagnosed with FASD in the study, for example, only 2 had been previously diagnosed with FASD, although many parents and guardians were aware of the children’s learning and behavioral challenges.
The study’s comprehensive approach may give a truer picture of the prevalence of FASD in the U.S. And, says Christina Chambers, PhD, a co-leader of the investigation, it further highlights the “public health burden of FASD.”
A study of first graders showed that a significant number of subjects had fetal alcohol spectrum disorders (FASD)—“conservative” rates, National Institute on Alcohol Abuse and Alcoholism (NIAAA) researchers say, ranging from 1% - 5%.
Fetal alcohol spectrum disorders cover a range of health effects that are caused by prenatal alcohol exposure, including growth deficiencies, facial abnormalities, and organ damage, as well as neurobiological deficits that contribute to challenges throughout the life of those affected.
Prenatal alcohol exposure is a “leading preventable cause of developmental disabilities worldwide,” said George Koob, PhD, director of the NIAAA. But determining the prevalence in the US is complex, he notes, because of difficulties in identifying children who have been exposed before birth and also because previous FASD estimates were based on smaller studies.
The study conducted by the Collaboration on Fetal Alcohol Spectrum Disorders Prevalence consortium, collected data between 2010 -2016 on 6,639 children in 4 communities located in the Midwest, Rocky Mountain, Southeast, and Pacific Southwest communities. These sites were selected to be more reflective of US community populations than in previous studies.
Their findings suggest that many children are undiagnosed or misdiagnosed, the researchers say. Of 222 children diagnosed with FASD in the study, for example, only 2 had been previously diagnosed with FASD, although many parents and guardians were aware of the children’s learning and behavioral challenges.
The study’s comprehensive approach may give a truer picture of the prevalence of FASD in the U.S. And, says Christina Chambers, PhD, a co-leader of the investigation, it further highlights the “public health burden of FASD.”
GPS consolidation may prolong PFS after ASCT

LISBON—Post-transplant therapy including galinpepimut-S (GPS) may prolong progression-free survival (PFS) in patients with high-risk multiple myeloma (MM), according to new research.
In a phase 2 trial, MM patients who received GPS and lenalidomide or bortezomib after autologous stem cell transplant (ASCT) had a median PFS of 23.6 months.
“Currently, post-transplant maintenance therapies for these difficult-to-treat patients are seemingly limited, with PFS rarely exceeding 12 to 14 months,” said Guenther Koehne, MD, PhD, from Miami Cancer Institute of Baptist Health South Florida.
Dr Koehne presented results observed with lenalidomide/bortezomib maintenance plus GPS consolidation at the 44th Annual Meeting of the EBMT (abstract OS4-6).
The trial was supported by the Leo A. Guthart and Kathryn Medina Research Fund and SELLAS Life Sciences Group, the company developing GPS.
The study enrolled 19 MM patients. Fifteen of them had high-risk cytogenetics at diagnosis, and 18 were at least minimal residual disease-positive after ASCT.
The goal of GPS therapy was to stimulate an immune response to prevent or delay MM progression. GPS is a cancer immunotherapeutic consisting of 4 modified peptide chains that induce an innate immune response against the WT1 antigen.
Patients began receiving GPS within 22 days of ASCT. They received 6 doses, administered subcutaneously with the oil emulsifier montanide every 2 weeks. Injection sites were pre-stimulated with granulocyte-macrophage colony-stimulating factor (70 μg) on days -2 (± 1 day) and 0 of each GPS vaccination.
The patients underwent clinical, immune response, and correlative assessment 2 to 4 weeks after the 6th GPS dose. Then, they received 6 additional monthly doses of GPS as well as lenalidomide (n=18) or bortezomib (n=1) maintenance, starting on day 100 post-ASCT. They underwent clinical, immune response, and correlative assessment again, 2 to 4 weeks after the 12th GPS dose.
Results
Dr Koehne said GPS stimulated time-dependent CD4+ or CD8+ T-cell immune responses specific for all 4 WT1 peptides within GPS, 2 of which are heteroclitic.
Immune responses were confirmed in up to 91% of patients, with multivalent immune responses in up to 64% of patients. And 75% of patients had multifunctional cross-epitope T-cell reactivity to antigenic epitopes against which the hosts were not specifically immunized, in a pattern akin to epitope spreading.
Dr Koehne also said immune responses were linked to clinical activity. In patients who received all 12 doses of GPS (n=12), there was a “strong and bidirectional association” between clinical benefit—defined as complete response (CR) or very good partial response (VGPR)—and frequency of CD4/CD8 immune responses.
Of those patients who had achieved CR/VGPR upon completion of GPS treatment, 100% (n=11) had CD4 immune responses and 81.8% (n=9) had CD8 immune responses.
Among patients who maintained immune response positivity, the CR/VGPR rate was 54.6% if CD4 immune response positivity to any of the 4 native GPS peptides was maintained and 44.0% if CD8 immune response positivity to any of the 4 native GPS peptides was maintained.
The PFS was 81% at 12 months and 62% at 18 months. The median PFS was 23.6 months (range, 15.2 to not reached).
The overall survival was 88% at 18 months, and the median overall survival was not reached.
LISBON—Post-transplant therapy including galinpepimut-S (GPS) may prolong progression-free survival (PFS) in patients with high-risk multiple myeloma (MM), according to new research.
In a phase 2 trial, MM patients who received GPS and lenalidomide or bortezomib after autologous stem cell transplant (ASCT) had a median PFS of 23.6 months.
“Currently, post-transplant maintenance therapies for these difficult-to-treat patients are seemingly limited, with PFS rarely exceeding 12 to 14 months,” said Guenther Koehne, MD, PhD, from Miami Cancer Institute of Baptist Health South Florida.
Dr Koehne presented results observed with lenalidomide/bortezomib maintenance plus GPS consolidation at the 44th Annual Meeting of the EBMT (abstract OS4-6).
The trial was supported by the Leo A. Guthart and Kathryn Medina Research Fund and SELLAS Life Sciences Group, the company developing GPS.
The study enrolled 19 MM patients. Fifteen of them had high-risk cytogenetics at diagnosis, and 18 were at least minimal residual disease-positive after ASCT.
The goal of GPS therapy was to stimulate an immune response to prevent or delay MM progression. GPS is a cancer immunotherapeutic consisting of 4 modified peptide chains that induce an innate immune response against the WT1 antigen.
Patients began receiving GPS within 22 days of ASCT. They received 6 doses, administered subcutaneously with the oil emulsifier montanide every 2 weeks. Injection sites were pre-stimulated with granulocyte-macrophage colony-stimulating factor (70 μg) on days -2 (± 1 day) and 0 of each GPS vaccination.
The patients underwent clinical, immune response, and correlative assessment 2 to 4 weeks after the 6th GPS dose. Then, they received 6 additional monthly doses of GPS as well as lenalidomide (n=18) or bortezomib (n=1) maintenance, starting on day 100 post-ASCT. They underwent clinical, immune response, and correlative assessment again, 2 to 4 weeks after the 12th GPS dose.
Results
Dr Koehne said GPS stimulated time-dependent CD4+ or CD8+ T-cell immune responses specific for all 4 WT1 peptides within GPS, 2 of which are heteroclitic.
Immune responses were confirmed in up to 91% of patients, with multivalent immune responses in up to 64% of patients. And 75% of patients had multifunctional cross-epitope T-cell reactivity to antigenic epitopes against which the hosts were not specifically immunized, in a pattern akin to epitope spreading.
Dr Koehne also said immune responses were linked to clinical activity. In patients who received all 12 doses of GPS (n=12), there was a “strong and bidirectional association” between clinical benefit—defined as complete response (CR) or very good partial response (VGPR)—and frequency of CD4/CD8 immune responses.
Of those patients who had achieved CR/VGPR upon completion of GPS treatment, 100% (n=11) had CD4 immune responses and 81.8% (n=9) had CD8 immune responses.
Among patients who maintained immune response positivity, the CR/VGPR rate was 54.6% if CD4 immune response positivity to any of the 4 native GPS peptides was maintained and 44.0% if CD8 immune response positivity to any of the 4 native GPS peptides was maintained.
The PFS was 81% at 12 months and 62% at 18 months. The median PFS was 23.6 months (range, 15.2 to not reached).
The overall survival was 88% at 18 months, and the median overall survival was not reached.
LISBON—Post-transplant therapy including galinpepimut-S (GPS) may prolong progression-free survival (PFS) in patients with high-risk multiple myeloma (MM), according to new research.
In a phase 2 trial, MM patients who received GPS and lenalidomide or bortezomib after autologous stem cell transplant (ASCT) had a median PFS of 23.6 months.
“Currently, post-transplant maintenance therapies for these difficult-to-treat patients are seemingly limited, with PFS rarely exceeding 12 to 14 months,” said Guenther Koehne, MD, PhD, from Miami Cancer Institute of Baptist Health South Florida.
Dr Koehne presented results observed with lenalidomide/bortezomib maintenance plus GPS consolidation at the 44th Annual Meeting of the EBMT (abstract OS4-6).
The trial was supported by the Leo A. Guthart and Kathryn Medina Research Fund and SELLAS Life Sciences Group, the company developing GPS.
The study enrolled 19 MM patients. Fifteen of them had high-risk cytogenetics at diagnosis, and 18 were at least minimal residual disease-positive after ASCT.
The goal of GPS therapy was to stimulate an immune response to prevent or delay MM progression. GPS is a cancer immunotherapeutic consisting of 4 modified peptide chains that induce an innate immune response against the WT1 antigen.
Patients began receiving GPS within 22 days of ASCT. They received 6 doses, administered subcutaneously with the oil emulsifier montanide every 2 weeks. Injection sites were pre-stimulated with granulocyte-macrophage colony-stimulating factor (70 μg) on days -2 (± 1 day) and 0 of each GPS vaccination.
The patients underwent clinical, immune response, and correlative assessment 2 to 4 weeks after the 6th GPS dose. Then, they received 6 additional monthly doses of GPS as well as lenalidomide (n=18) or bortezomib (n=1) maintenance, starting on day 100 post-ASCT. They underwent clinical, immune response, and correlative assessment again, 2 to 4 weeks after the 12th GPS dose.
Results
Dr Koehne said GPS stimulated time-dependent CD4+ or CD8+ T-cell immune responses specific for all 4 WT1 peptides within GPS, 2 of which are heteroclitic.
Immune responses were confirmed in up to 91% of patients, with multivalent immune responses in up to 64% of patients. And 75% of patients had multifunctional cross-epitope T-cell reactivity to antigenic epitopes against which the hosts were not specifically immunized, in a pattern akin to epitope spreading.
Dr Koehne also said immune responses were linked to clinical activity. In patients who received all 12 doses of GPS (n=12), there was a “strong and bidirectional association” between clinical benefit—defined as complete response (CR) or very good partial response (VGPR)—and frequency of CD4/CD8 immune responses.
Of those patients who had achieved CR/VGPR upon completion of GPS treatment, 100% (n=11) had CD4 immune responses and 81.8% (n=9) had CD8 immune responses.
Among patients who maintained immune response positivity, the CR/VGPR rate was 54.6% if CD4 immune response positivity to any of the 4 native GPS peptides was maintained and 44.0% if CD8 immune response positivity to any of the 4 native GPS peptides was maintained.
The PFS was 81% at 12 months and 62% at 18 months. The median PFS was 23.6 months (range, 15.2 to not reached).
The overall survival was 88% at 18 months, and the median overall survival was not reached.
Antibody protects mice from malaria infection

A human antibody can protect mice from infection with the malaria parasite Plasmodium falciparum, according to research published in Nature Medicine.
Researchers isolated the antibody, CIS43, from the blood of a volunteer who had received the PfSPZ Vaccine (Sanaria Inc.), an experimental vaccine made from whole, weakened malaria parasites.
The volunteer was later exposed to infectious malaria-carrying mosquitoes under carefully controlled conditions and did not become infected.
Researchers tested CIS43 in 2 different mouse models and found the antibody provided “high-level” protection from malaria infection.
In fact, CIS43 protects against malaria better than any antibody that has been described before, according to study author Marie Pancera, PhD, of Fred Hutchinson Cancer Research Center in Seattle, Washington.
She and her colleagues found that CIS43 works by binding to an epitope located between the N terminus and central repeat domains of PfCP (P falciparum circumsporozoite protein).
This epitope is conserved across 99.8% of all known P falciparum strains, which, according to the researchers, makes it an attractive target for next-generation vaccines designed to elicit production of CIS43.
Researchers at the National Institute of Allergy and Infectious Diseases Vaccine Research Center are planning to conduct clinical trials of CIS43 next year.
A human antibody can protect mice from infection with the malaria parasite Plasmodium falciparum, according to research published in Nature Medicine.
Researchers isolated the antibody, CIS43, from the blood of a volunteer who had received the PfSPZ Vaccine (Sanaria Inc.), an experimental vaccine made from whole, weakened malaria parasites.
The volunteer was later exposed to infectious malaria-carrying mosquitoes under carefully controlled conditions and did not become infected.
Researchers tested CIS43 in 2 different mouse models and found the antibody provided “high-level” protection from malaria infection.
In fact, CIS43 protects against malaria better than any antibody that has been described before, according to study author Marie Pancera, PhD, of Fred Hutchinson Cancer Research Center in Seattle, Washington.
She and her colleagues found that CIS43 works by binding to an epitope located between the N terminus and central repeat domains of PfCP (P falciparum circumsporozoite protein).
This epitope is conserved across 99.8% of all known P falciparum strains, which, according to the researchers, makes it an attractive target for next-generation vaccines designed to elicit production of CIS43.
Researchers at the National Institute of Allergy and Infectious Diseases Vaccine Research Center are planning to conduct clinical trials of CIS43 next year.
A human antibody can protect mice from infection with the malaria parasite Plasmodium falciparum, according to research published in Nature Medicine.
Researchers isolated the antibody, CIS43, from the blood of a volunteer who had received the PfSPZ Vaccine (Sanaria Inc.), an experimental vaccine made from whole, weakened malaria parasites.
The volunteer was later exposed to infectious malaria-carrying mosquitoes under carefully controlled conditions and did not become infected.
Researchers tested CIS43 in 2 different mouse models and found the antibody provided “high-level” protection from malaria infection.
In fact, CIS43 protects against malaria better than any antibody that has been described before, according to study author Marie Pancera, PhD, of Fred Hutchinson Cancer Research Center in Seattle, Washington.
She and her colleagues found that CIS43 works by binding to an epitope located between the N terminus and central repeat domains of PfCP (P falciparum circumsporozoite protein).
This epitope is conserved across 99.8% of all known P falciparum strains, which, according to the researchers, makes it an attractive target for next-generation vaccines designed to elicit production of CIS43.
Researchers at the National Institute of Allergy and Infectious Diseases Vaccine Research Center are planning to conduct clinical trials of CIS43 next year.
EHRA releases new guide for NOAC use

The European Heart Rhythm Association (EHRA) has released a new version of its “practical guide” for the use of non-vitamin K antagonist oral anticoagulants (NOACs) in patients with atrial fibrillation.
The guide, now in its third edition, gives concrete advice on how to use NOACs in specific clinical situations.
It was published in European Heart Journal and presented at EHRA 2018 in Barcelona, Spain.
The 2018 edition of the guide has several new chapters.
One chapter summarizes the correct dosing of NOACs in conditions other than atrial fibrillation, such as for the prevention of deep vein thrombosis and treatment of venous thromboembolism.
“The dosing for each condition is different, which may lead to confusion, so we have outlined this clearly,” said author Hein Heidbüchel, MD, PhD, of Hasselt University in Hasselt, Belgium.
Another chapter outlines how to use NOACs in particular groups of patients, including those with very low body weight, the very obese, athletes, frail patients in whom there is concern about bleeding, and patients with cognitive impairment who may forget to take their pills.
The guide also includes updated advice on the combined use of antiplatelet agents and NOACs in patients with coronary artery disease, particularly those with an acute coronary syndrome or patients scheduled for percutaneous coronary intervention with stenting.
“We provide guidance around which and how many antiplatelets, for how long, with which NOAC, and at what dose of that NOAC,” Dr Heidbüchel said.
In addition, the guide now includes more scientific evidence on the use of anticoagulants around cardioversion. The document gives detailed advice on what to do in patients on long-term NOAC treatment who need cardioversion, as compared to patients newly diagnosed with atrial fibrillation and started on a NOAC before cardioversion.
Since the previous edition of the guide was published, the first NOAC reversal agent has received market approval. Therefore, the new edition includes advice on how to use this agent, idarucizumab—which reverses the anticoagulant effect of dabigatran—when there is acute bleeding, when urgent surgery is required, or when the patient has a stroke.
The guide also includes advice on andexanet alfa, another reversal agent expected to receive market approval, with the caveat that the instructions on the label should be followed.
Additionally, the guide describes scenarios in which physicians might want to know the NOAC plasma level. One scenario concerns patients undergoing major surgery in whom it is unclear—for example, because of other drugs or renal dysfunction—whether the usual practice of stopping the NOAC 48 hours in advance is sufficient. The plasma level of the NOAC could be measured just before surgery to confirm the anticoagulant effect has waned.
Finally, the chapter on drug-drug interactions has been expanded with anticancer and antiepileptic drugs.
“While this is mostly based on potential pharmacokinetic interactions and case reports, it is the first of its kind,” said author Jan Steffel, MD, of University Heart Center Zurich in Switzerland.
“This is likely to be adapted and become more complete over the years as our experience increases at this new frontier.”
EHRA received unconditional grants from Pfizer/BMS, Daiichi-Sankyo, Boehringer-Ingelheim, and Bayer.
The European Heart Rhythm Association (EHRA) has released a new version of its “practical guide” for the use of non-vitamin K antagonist oral anticoagulants (NOACs) in patients with atrial fibrillation.
The guide, now in its third edition, gives concrete advice on how to use NOACs in specific clinical situations.
It was published in European Heart Journal and presented at EHRA 2018 in Barcelona, Spain.
The 2018 edition of the guide has several new chapters.
One chapter summarizes the correct dosing of NOACs in conditions other than atrial fibrillation, such as for the prevention of deep vein thrombosis and treatment of venous thromboembolism.
“The dosing for each condition is different, which may lead to confusion, so we have outlined this clearly,” said author Hein Heidbüchel, MD, PhD, of Hasselt University in Hasselt, Belgium.
Another chapter outlines how to use NOACs in particular groups of patients, including those with very low body weight, the very obese, athletes, frail patients in whom there is concern about bleeding, and patients with cognitive impairment who may forget to take their pills.
The guide also includes updated advice on the combined use of antiplatelet agents and NOACs in patients with coronary artery disease, particularly those with an acute coronary syndrome or patients scheduled for percutaneous coronary intervention with stenting.
“We provide guidance around which and how many antiplatelets, for how long, with which NOAC, and at what dose of that NOAC,” Dr Heidbüchel said.
In addition, the guide now includes more scientific evidence on the use of anticoagulants around cardioversion. The document gives detailed advice on what to do in patients on long-term NOAC treatment who need cardioversion, as compared to patients newly diagnosed with atrial fibrillation and started on a NOAC before cardioversion.
Since the previous edition of the guide was published, the first NOAC reversal agent has received market approval. Therefore, the new edition includes advice on how to use this agent, idarucizumab—which reverses the anticoagulant effect of dabigatran—when there is acute bleeding, when urgent surgery is required, or when the patient has a stroke.
The guide also includes advice on andexanet alfa, another reversal agent expected to receive market approval, with the caveat that the instructions on the label should be followed.
Additionally, the guide describes scenarios in which physicians might want to know the NOAC plasma level. One scenario concerns patients undergoing major surgery in whom it is unclear—for example, because of other drugs or renal dysfunction—whether the usual practice of stopping the NOAC 48 hours in advance is sufficient. The plasma level of the NOAC could be measured just before surgery to confirm the anticoagulant effect has waned.
Finally, the chapter on drug-drug interactions has been expanded with anticancer and antiepileptic drugs.
“While this is mostly based on potential pharmacokinetic interactions and case reports, it is the first of its kind,” said author Jan Steffel, MD, of University Heart Center Zurich in Switzerland.
“This is likely to be adapted and become more complete over the years as our experience increases at this new frontier.”
EHRA received unconditional grants from Pfizer/BMS, Daiichi-Sankyo, Boehringer-Ingelheim, and Bayer.
The European Heart Rhythm Association (EHRA) has released a new version of its “practical guide” for the use of non-vitamin K antagonist oral anticoagulants (NOACs) in patients with atrial fibrillation.
The guide, now in its third edition, gives concrete advice on how to use NOACs in specific clinical situations.
It was published in European Heart Journal and presented at EHRA 2018 in Barcelona, Spain.
The 2018 edition of the guide has several new chapters.
One chapter summarizes the correct dosing of NOACs in conditions other than atrial fibrillation, such as for the prevention of deep vein thrombosis and treatment of venous thromboembolism.
“The dosing for each condition is different, which may lead to confusion, so we have outlined this clearly,” said author Hein Heidbüchel, MD, PhD, of Hasselt University in Hasselt, Belgium.
Another chapter outlines how to use NOACs in particular groups of patients, including those with very low body weight, the very obese, athletes, frail patients in whom there is concern about bleeding, and patients with cognitive impairment who may forget to take their pills.
The guide also includes updated advice on the combined use of antiplatelet agents and NOACs in patients with coronary artery disease, particularly those with an acute coronary syndrome or patients scheduled for percutaneous coronary intervention with stenting.
“We provide guidance around which and how many antiplatelets, for how long, with which NOAC, and at what dose of that NOAC,” Dr Heidbüchel said.
In addition, the guide now includes more scientific evidence on the use of anticoagulants around cardioversion. The document gives detailed advice on what to do in patients on long-term NOAC treatment who need cardioversion, as compared to patients newly diagnosed with atrial fibrillation and started on a NOAC before cardioversion.
Since the previous edition of the guide was published, the first NOAC reversal agent has received market approval. Therefore, the new edition includes advice on how to use this agent, idarucizumab—which reverses the anticoagulant effect of dabigatran—when there is acute bleeding, when urgent surgery is required, or when the patient has a stroke.
The guide also includes advice on andexanet alfa, another reversal agent expected to receive market approval, with the caveat that the instructions on the label should be followed.
Additionally, the guide describes scenarios in which physicians might want to know the NOAC plasma level. One scenario concerns patients undergoing major surgery in whom it is unclear—for example, because of other drugs or renal dysfunction—whether the usual practice of stopping the NOAC 48 hours in advance is sufficient. The plasma level of the NOAC could be measured just before surgery to confirm the anticoagulant effect has waned.
Finally, the chapter on drug-drug interactions has been expanded with anticancer and antiepileptic drugs.
“While this is mostly based on potential pharmacokinetic interactions and case reports, it is the first of its kind,” said author Jan Steffel, MD, of University Heart Center Zurich in Switzerland.
“This is likely to be adapted and become more complete over the years as our experience increases at this new frontier.”
EHRA received unconditional grants from Pfizer/BMS, Daiichi-Sankyo, Boehringer-Ingelheim, and Bayer.
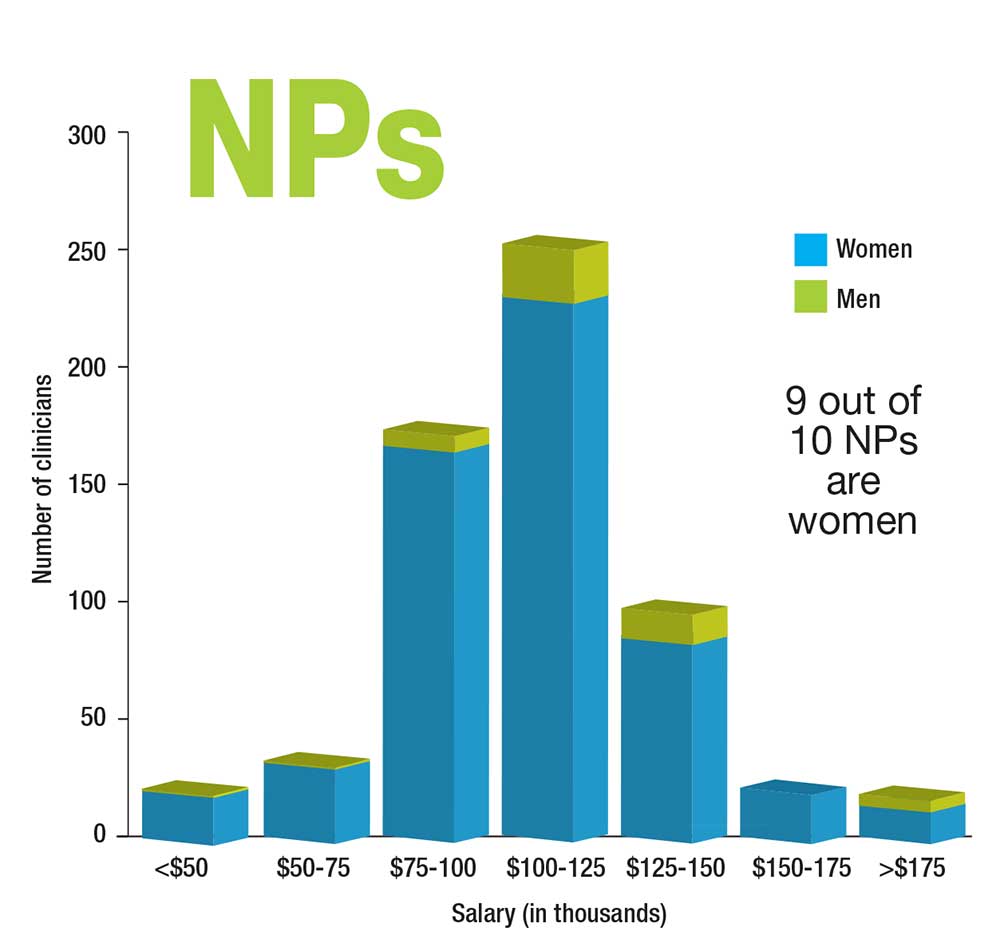
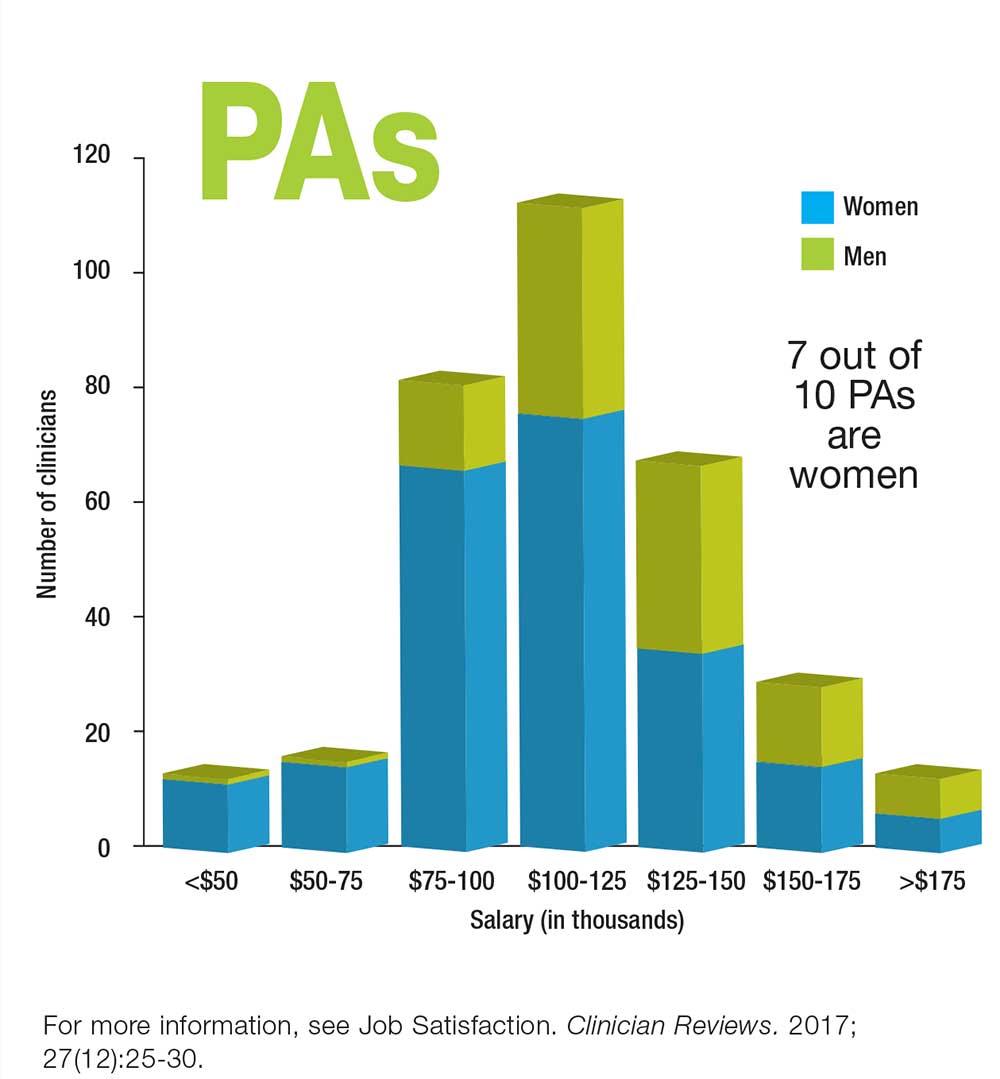
Who Makes More: Male or Female Clinicians?
Fulvestrant plus neratinib reversed treatment-acquired HER2 mutations in metastatic ER+ breast cancer
Dual therapy with fulvestrant and the irreversible HER2 kinase inhibitor neratinib reversed treatment-acquired hormone resistance in metastatic estrogen receptor (ER)–positive breast cancer cells.
Elaine Mardis, PhD, a spokesperson for the American Association of Cancer Research, hailed the research by Utthara Nayar, PhD, and colleagues as “groundbreaking and unexpected” during a briefing held in advance of the annual meeting of the American Association for Cancer Research. The lab experiments were part of a whole-exome sequencing study of metastatic ER-positive tumor biopsies from 168 patients, 12 of whom had acquired the HER2 mutations, said Dr. Nayar of the Dana-Farber Cancer Institute, Boston.
The findings have prompted a phase 2 trial of the combination, which is now recruiting patients, Dr. Nayar said. The 5-year study seeks 152 women with inoperable locally advanced or metastatic ER-positive breast cancer with a confirmed HER2-positive mutation. Patients will be randomized to the combination of neratinib and fulvestrant or to neratinib alone. The primary outcome is progression-free survival.
“We also hope to be able to develop upfront combinations to preempt the resistance and lead to more durable responses,” Dr. Nayar said.
All of the 168 patients who contributed metastatic tumor biopsy samples to the study had developed resistance to estrogen receptor treatments, including aromatase inhibitors, tamoxifen, and fulvestrant. Of these biopsies, 12 had HER2 mutations, 8 of which had been previously characterized as activating.
Dr. Nayar and colleagues examined the untreated primary tumors in five of these patients; there was no mutation in four, suggesting that the mutations were a response to treatment. “In these 80%, the mutations were acquired as tumors were exposed to treatment and not present in the original tumor,” Dr. Nayar said.
These acquired HER2 mutations were mutually exclusive with ER mutations, which suggested a different mechanism of resistance to ER-directed therapies, she noted in her abstract. The mutations conferred resistance to tamoxifen, fulvestrant, and palbociclib.
However, the combination of fulvestrant and neratinib, an irreversible HER2 kinase inhibitor, overcame resistance in these cells.
In addition to pioneering a potentially important therapy for treatment-resistant metastatic breast cancer, the study highlights the importance of gene sequencing metastatic tumors, said Nikhil Wagle, MD, Dr. Nayar’s colleague and deputy director of the Center for Cancer Precision Medicine at Dana-Farber.
“Our study highlights how important it is to profile resistant metastatic tumors since these tumors may harbor targetable mechanisms of resistance that were not present in the original tumor biopsy,” Dr. Wagle noted in a press statement. “Repeated sequencing of tumors can pinpoint new genetic changes that cause resistance to therapies. This in turn can enable physicians to personalize therapy depending on the specific genetic changes in a patient’s tumor over time.”
The study was supported by the Department of Defense, the National Cancer Institute, the Susan G. Komen Foundation, the Dana-Farber Cancer Center, and a number of other private funders. Dr. Wagle is a stockholder in Foundation Medicine. Dr. Nayar had no financial disclosure.
SOURCE: Nayer U et al. AACR 2018, Abstract 4952
Dual therapy with fulvestrant and the irreversible HER2 kinase inhibitor neratinib reversed treatment-acquired hormone resistance in metastatic estrogen receptor (ER)–positive breast cancer cells.
Elaine Mardis, PhD, a spokesperson for the American Association of Cancer Research, hailed the research by Utthara Nayar, PhD, and colleagues as “groundbreaking and unexpected” during a briefing held in advance of the annual meeting of the American Association for Cancer Research. The lab experiments were part of a whole-exome sequencing study of metastatic ER-positive tumor biopsies from 168 patients, 12 of whom had acquired the HER2 mutations, said Dr. Nayar of the Dana-Farber Cancer Institute, Boston.
The findings have prompted a phase 2 trial of the combination, which is now recruiting patients, Dr. Nayar said. The 5-year study seeks 152 women with inoperable locally advanced or metastatic ER-positive breast cancer with a confirmed HER2-positive mutation. Patients will be randomized to the combination of neratinib and fulvestrant or to neratinib alone. The primary outcome is progression-free survival.
“We also hope to be able to develop upfront combinations to preempt the resistance and lead to more durable responses,” Dr. Nayar said.
All of the 168 patients who contributed metastatic tumor biopsy samples to the study had developed resistance to estrogen receptor treatments, including aromatase inhibitors, tamoxifen, and fulvestrant. Of these biopsies, 12 had HER2 mutations, 8 of which had been previously characterized as activating.
Dr. Nayar and colleagues examined the untreated primary tumors in five of these patients; there was no mutation in four, suggesting that the mutations were a response to treatment. “In these 80%, the mutations were acquired as tumors were exposed to treatment and not present in the original tumor,” Dr. Nayar said.
These acquired HER2 mutations were mutually exclusive with ER mutations, which suggested a different mechanism of resistance to ER-directed therapies, she noted in her abstract. The mutations conferred resistance to tamoxifen, fulvestrant, and palbociclib.
However, the combination of fulvestrant and neratinib, an irreversible HER2 kinase inhibitor, overcame resistance in these cells.
In addition to pioneering a potentially important therapy for treatment-resistant metastatic breast cancer, the study highlights the importance of gene sequencing metastatic tumors, said Nikhil Wagle, MD, Dr. Nayar’s colleague and deputy director of the Center for Cancer Precision Medicine at Dana-Farber.
“Our study highlights how important it is to profile resistant metastatic tumors since these tumors may harbor targetable mechanisms of resistance that were not present in the original tumor biopsy,” Dr. Wagle noted in a press statement. “Repeated sequencing of tumors can pinpoint new genetic changes that cause resistance to therapies. This in turn can enable physicians to personalize therapy depending on the specific genetic changes in a patient’s tumor over time.”
The study was supported by the Department of Defense, the National Cancer Institute, the Susan G. Komen Foundation, the Dana-Farber Cancer Center, and a number of other private funders. Dr. Wagle is a stockholder in Foundation Medicine. Dr. Nayar had no financial disclosure.
SOURCE: Nayer U et al. AACR 2018, Abstract 4952
Dual therapy with fulvestrant and the irreversible HER2 kinase inhibitor neratinib reversed treatment-acquired hormone resistance in metastatic estrogen receptor (ER)–positive breast cancer cells.
Elaine Mardis, PhD, a spokesperson for the American Association of Cancer Research, hailed the research by Utthara Nayar, PhD, and colleagues as “groundbreaking and unexpected” during a briefing held in advance of the annual meeting of the American Association for Cancer Research. The lab experiments were part of a whole-exome sequencing study of metastatic ER-positive tumor biopsies from 168 patients, 12 of whom had acquired the HER2 mutations, said Dr. Nayar of the Dana-Farber Cancer Institute, Boston.
The findings have prompted a phase 2 trial of the combination, which is now recruiting patients, Dr. Nayar said. The 5-year study seeks 152 women with inoperable locally advanced or metastatic ER-positive breast cancer with a confirmed HER2-positive mutation. Patients will be randomized to the combination of neratinib and fulvestrant or to neratinib alone. The primary outcome is progression-free survival.
“We also hope to be able to develop upfront combinations to preempt the resistance and lead to more durable responses,” Dr. Nayar said.
All of the 168 patients who contributed metastatic tumor biopsy samples to the study had developed resistance to estrogen receptor treatments, including aromatase inhibitors, tamoxifen, and fulvestrant. Of these biopsies, 12 had HER2 mutations, 8 of which had been previously characterized as activating.
Dr. Nayar and colleagues examined the untreated primary tumors in five of these patients; there was no mutation in four, suggesting that the mutations were a response to treatment. “In these 80%, the mutations were acquired as tumors were exposed to treatment and not present in the original tumor,” Dr. Nayar said.
These acquired HER2 mutations were mutually exclusive with ER mutations, which suggested a different mechanism of resistance to ER-directed therapies, she noted in her abstract. The mutations conferred resistance to tamoxifen, fulvestrant, and palbociclib.
However, the combination of fulvestrant and neratinib, an irreversible HER2 kinase inhibitor, overcame resistance in these cells.
In addition to pioneering a potentially important therapy for treatment-resistant metastatic breast cancer, the study highlights the importance of gene sequencing metastatic tumors, said Nikhil Wagle, MD, Dr. Nayar’s colleague and deputy director of the Center for Cancer Precision Medicine at Dana-Farber.
“Our study highlights how important it is to profile resistant metastatic tumors since these tumors may harbor targetable mechanisms of resistance that were not present in the original tumor biopsy,” Dr. Wagle noted in a press statement. “Repeated sequencing of tumors can pinpoint new genetic changes that cause resistance to therapies. This in turn can enable physicians to personalize therapy depending on the specific genetic changes in a patient’s tumor over time.”
The study was supported by the Department of Defense, the National Cancer Institute, the Susan G. Komen Foundation, the Dana-Farber Cancer Center, and a number of other private funders. Dr. Wagle is a stockholder in Foundation Medicine. Dr. Nayar had no financial disclosure.
SOURCE: Nayer U et al. AACR 2018, Abstract 4952
FROM THE AACR 2018 ANNUAL MEETING
Key clinical point: The combination of fulvestrant and neratinib reversed acquired HER2 mutations in ER+ metastatic breast cancer cells.
Major finding: Of 168 biopsies, 12 had acquired HER2 mutations after hormone treatment; these mutations were reversed with the dual therapy.
Study details: The exome sequencing study comprised 168 biopsies, and the in vitro study comprised 12.
Disclosures: The study was supported by the Department of Defense, the National Cancer Institute, the Susan G. Komen Foundation, the Dana-Farber Cancer Institute, and other private funders. Dr. Wagle is a stockholder in Foundation Medicine. Dr. Nayar had no financial disclosure.
Source: Nayar U et al. AACR 2018, Abstract 4952
Arthritis limits physical activity the most in the South
“Physical activity is a proven strategy for managing arthritis symptoms,” but 35% of Americans with arthritis do not participate in any such activities or exercise, according to investigators who analyzed data from a national survey of more than 440,000 adults.
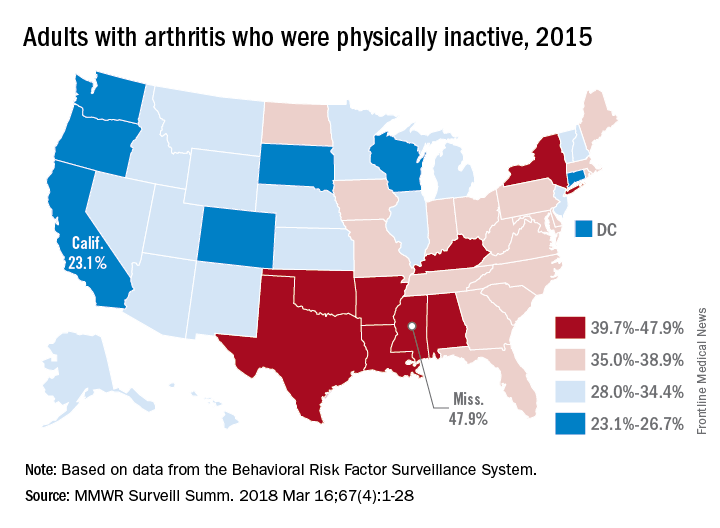
The low rates of inactivity in the western half of the country were topped by California’s 23.1% and South Dakota’s 23.4%, with Oregon (24.0%) and Wisconsin (24.6%) not too far behind, Dr. Barbour and his associates said based on data for 441,456 adults aged 18 years and older who were interviewed for the Behavioral Risk Factor Surveillance System.
Overall prevalence rates show that arthritis has the greatest effect in southern states, which, in addition to high inactivity, had more arthritis-attributable severe joint pain, more arthritis-attributable social participation restriction, and less leisure-time walking among adults with arthritis. This information, the investigators suggested, may help public health professionals “to better understand and target evidence-based nonpharmaceutical interventions, such as arthritis self-management education and physical activity.”
SOURCE: Barbour KE et al. MMWR Surveill Summ. 2018 Mar 16;67(4):1-28.
“Physical activity is a proven strategy for managing arthritis symptoms,” but 35% of Americans with arthritis do not participate in any such activities or exercise, according to investigators who analyzed data from a national survey of more than 440,000 adults.
The low rates of inactivity in the western half of the country were topped by California’s 23.1% and South Dakota’s 23.4%, with Oregon (24.0%) and Wisconsin (24.6%) not too far behind, Dr. Barbour and his associates said based on data for 441,456 adults aged 18 years and older who were interviewed for the Behavioral Risk Factor Surveillance System.
Overall prevalence rates show that arthritis has the greatest effect in southern states, which, in addition to high inactivity, had more arthritis-attributable severe joint pain, more arthritis-attributable social participation restriction, and less leisure-time walking among adults with arthritis. This information, the investigators suggested, may help public health professionals “to better understand and target evidence-based nonpharmaceutical interventions, such as arthritis self-management education and physical activity.”
SOURCE: Barbour KE et al. MMWR Surveill Summ. 2018 Mar 16;67(4):1-28.
“Physical activity is a proven strategy for managing arthritis symptoms,” but 35% of Americans with arthritis do not participate in any such activities or exercise, according to investigators who analyzed data from a national survey of more than 440,000 adults.
The low rates of inactivity in the western half of the country were topped by California’s 23.1% and South Dakota’s 23.4%, with Oregon (24.0%) and Wisconsin (24.6%) not too far behind, Dr. Barbour and his associates said based on data for 441,456 adults aged 18 years and older who were interviewed for the Behavioral Risk Factor Surveillance System.
Overall prevalence rates show that arthritis has the greatest effect in southern states, which, in addition to high inactivity, had more arthritis-attributable severe joint pain, more arthritis-attributable social participation restriction, and less leisure-time walking among adults with arthritis. This information, the investigators suggested, may help public health professionals “to better understand and target evidence-based nonpharmaceutical interventions, such as arthritis self-management education and physical activity.”
SOURCE: Barbour KE et al. MMWR Surveill Summ. 2018 Mar 16;67(4):1-28.
FROM MMWR SURVEILLANCE SUMMARIES
Low vitamin B12 tied to worsening mobility, cognition in early Parkinson’s
suggesting that it may be worthwhile to examine the correction of low levels as a means of slowing disease progression.
Investigators led by Chadwick W. Christine, MD, of the department of neurology at the University of California, San Francisco, sought to understand what contributes to considerable variation in the progression of PD by building on previous research that revealed low serum vitamin B12 levels are common in patients with moderately advanced PD and are associated with neuropathy and cognitive impairment.
They measured serum methylmalonic acid, homocysteine, and holotranscobalamin in addition to B12 because of the limited sensitivity of serum B12 testing alone to detect B12 deficiency. At baseline, 13% of 680 patients had borderline-low B12 levels (less than 184 pmol/L [250 pg/mL]), and 5% had deficient B12 levels (less than 157 pmol/L or 212 pg/mL). Homocysteine was moderately elevated (greater than 15 mmol/L) in 7% of subjects, and 14% of patients with borderline-low B12 also had elevated homocysteine, the investigators reported in Movement Disorders.
Low B12 at baseline predicted greater worsening of mobility in terms of a higher ambulatory capacity score, calculated by adding individual items of the Unified Parkinson’s Disease Rating Scale (UPDRS): falling, freezing when walking, walking, gait, and postural stability. Participants in the low- B12 tertile (less than 234 pmol/L or 317 pg/ mL) developed greater morbidity as assessed by greater annualized worsening of the ambulatory capacity score. For example, those in the low-B12 tertile had annualized change of 1.53, compared with 0.77 in the upper tertile. The worsening score was mostly attributed to poorer gait and postural instability.
To give context to these figures, the researchers pointed to an analysis of the NET-PD LS1 cohort that found a mean ambulatory capacity score of 2.17 among patients who fell and a score of 1.4 for those who did not fall. “Thus, we consider the magnitude of difference to be clinically relevant, particularly given that components of gait dysfunction that develop in PD may not respond to dopaminergic treatments or [deep brain stimulation],” they wrote.
Elevated homocysteine also predicted greater cognitive decline. Baseline elevated homocysteine was associated with lower baseline Mini Mental State Examination (MMSE), as well as greater annualized decline in MMSE (–1.96 vs. 0.06; P = .001).
Of the 456 subjects who continued in the study for 9-24 months and had a second blood sample available, 226 had an increase of more than 20% in B12 levels, 210 stayed within 20% of the original B12 measurement, and 19 had a decrease greater than 20%.
Overall, there was a mean annualized increase in B12 of 52.6 pmol/L, a mean annualized decrease of homocysteine of 0.83 mmol/L, and a mean annualized increase of holotranscobalamin of 14.7 pmol/L.
“These findings are consistent with improved nutritional status during the course of the study, likely attributed to subjects starting the optional [multivitamin] after the baseline visit and/or subjects changing their diets,” the research team said.
While the improvement in B12 status did not lead to statistically significant improvements in UPDRS scores, the researchers said there was a trend toward improvement, which provides “support for a disease-modifying effect of B12,” they wrote.
The researchers speculated that their findings of a link between low B12 levels and worse outcomes could be attributed to an independent (comorbid) effect on the central and peripheral nervous systems, a direct effect on PD pathogenesis, or alternatively, that low B12 may be a marker of an unknown associated factor.
“Given that low B12 status is associated with neurological and other medical morbidities and is readily treated, great care would be needed to design an ethically acceptable randomized, prospective study to evaluate the effect of B12 supplementation on PD progression, given that serum measurements collected as part of a prospective study in unsupplemented patients would likely reveal some subjects with B12 deficiency,” they concluded.
The authors declared no relevant disclosures. The study was supported by a grant from the Michael J. Fox Foundation for Parkinson’s Research, as well as privately donated grants.
SOURCE: Christine C et al. Movement Dis. 2018 Mar 6. doi: 10.1002/mds.27301.
The course of PD can be quite variable, and it is difficult for clinicians to predict what will happen to an individual person with PD, but identifying prognostic factors ought to help practitioners answer their patients’ questions and potentially improve the understanding of mechanisms underlying the disease pathogenesis.
If vitamin B12 is related to the progression of PD as suggested in the study by Christine et al., its replacement may slow the decline of the disease. But there are several issues that need to be addressed in the context of their findings.
First, what constitutes a low vitamin B12 level is not a simple issue. If the evaluation is limited to measurement of vitamin B12 concentration, the diagnosis of genuine deficiency is unreliable. Most experts agree that combined measurement of vitamin B12 with determination of homocysteine levels is necessary and while Christine et al. measured both levels, their statistical analysis and subsequent conclusions are exclusively based on the levels of the vitamin.
Moreover, 34 patients in the study were classified as having “borderline-low” vitamin B12 levels, and 14 had both borderline-low B12 level and high homocysteine concentration. This brings into question whether the researchers identified PD patients who actually had low B12 levels.
The design of the DATATOP trial could also introduce some bias into the findings. At the time of publication, the study was criticized for disregarding the symptomatic effect of selegiline and for a lack of objective definition of criteria for the trial’s primary endpoint – introduction of levodopa.
This could have led to the termination of individuals at different stages of the disease, introducing a potential bias in the sample of patients who remained in the study for enough time to undergo subsequent determination of B12 levels.
The findings in the current study are also in contrast to previous research, and the underlying mechanism of vitamin B12 in PD is also unclear.
Nevertheless, the results of the study by Dr. Christine and his colleagues are intriguing and further investigations to address this hypothesis are warranted.
Francisco Cardoso, MD, PhD, is with the movement disorders unit within the neurology service at the Federal University of Minas Gerais, Belo Horizonte, Brazil. His comments are derived from an editorial accompanying the study by Dr. Christine and colleagues (Movement Dis. 2018 Mar 6. doi: 10.1002/mds.27366). He had no relevant disclosures.
The course of PD can be quite variable, and it is difficult for clinicians to predict what will happen to an individual person with PD, but identifying prognostic factors ought to help practitioners answer their patients’ questions and potentially improve the understanding of mechanisms underlying the disease pathogenesis.
If vitamin B12 is related to the progression of PD as suggested in the study by Christine et al., its replacement may slow the decline of the disease. But there are several issues that need to be addressed in the context of their findings.
First, what constitutes a low vitamin B12 level is not a simple issue. If the evaluation is limited to measurement of vitamin B12 concentration, the diagnosis of genuine deficiency is unreliable. Most experts agree that combined measurement of vitamin B12 with determination of homocysteine levels is necessary and while Christine et al. measured both levels, their statistical analysis and subsequent conclusions are exclusively based on the levels of the vitamin.
Moreover, 34 patients in the study were classified as having “borderline-low” vitamin B12 levels, and 14 had both borderline-low B12 level and high homocysteine concentration. This brings into question whether the researchers identified PD patients who actually had low B12 levels.
The design of the DATATOP trial could also introduce some bias into the findings. At the time of publication, the study was criticized for disregarding the symptomatic effect of selegiline and for a lack of objective definition of criteria for the trial’s primary endpoint – introduction of levodopa.
This could have led to the termination of individuals at different stages of the disease, introducing a potential bias in the sample of patients who remained in the study for enough time to undergo subsequent determination of B12 levels.
The findings in the current study are also in contrast to previous research, and the underlying mechanism of vitamin B12 in PD is also unclear.
Nevertheless, the results of the study by Dr. Christine and his colleagues are intriguing and further investigations to address this hypothesis are warranted.
Francisco Cardoso, MD, PhD, is with the movement disorders unit within the neurology service at the Federal University of Minas Gerais, Belo Horizonte, Brazil. His comments are derived from an editorial accompanying the study by Dr. Christine and colleagues (Movement Dis. 2018 Mar 6. doi: 10.1002/mds.27366). He had no relevant disclosures.
The course of PD can be quite variable, and it is difficult for clinicians to predict what will happen to an individual person with PD, but identifying prognostic factors ought to help practitioners answer their patients’ questions and potentially improve the understanding of mechanisms underlying the disease pathogenesis.
If vitamin B12 is related to the progression of PD as suggested in the study by Christine et al., its replacement may slow the decline of the disease. But there are several issues that need to be addressed in the context of their findings.
First, what constitutes a low vitamin B12 level is not a simple issue. If the evaluation is limited to measurement of vitamin B12 concentration, the diagnosis of genuine deficiency is unreliable. Most experts agree that combined measurement of vitamin B12 with determination of homocysteine levels is necessary and while Christine et al. measured both levels, their statistical analysis and subsequent conclusions are exclusively based on the levels of the vitamin.
Moreover, 34 patients in the study were classified as having “borderline-low” vitamin B12 levels, and 14 had both borderline-low B12 level and high homocysteine concentration. This brings into question whether the researchers identified PD patients who actually had low B12 levels.
The design of the DATATOP trial could also introduce some bias into the findings. At the time of publication, the study was criticized for disregarding the symptomatic effect of selegiline and for a lack of objective definition of criteria for the trial’s primary endpoint – introduction of levodopa.
This could have led to the termination of individuals at different stages of the disease, introducing a potential bias in the sample of patients who remained in the study for enough time to undergo subsequent determination of B12 levels.
The findings in the current study are also in contrast to previous research, and the underlying mechanism of vitamin B12 in PD is also unclear.
Nevertheless, the results of the study by Dr. Christine and his colleagues are intriguing and further investigations to address this hypothesis are warranted.
Francisco Cardoso, MD, PhD, is with the movement disorders unit within the neurology service at the Federal University of Minas Gerais, Belo Horizonte, Brazil. His comments are derived from an editorial accompanying the study by Dr. Christine and colleagues (Movement Dis. 2018 Mar 6. doi: 10.1002/mds.27366). He had no relevant disclosures.
suggesting that it may be worthwhile to examine the correction of low levels as a means of slowing disease progression.
Investigators led by Chadwick W. Christine, MD, of the department of neurology at the University of California, San Francisco, sought to understand what contributes to considerable variation in the progression of PD by building on previous research that revealed low serum vitamin B12 levels are common in patients with moderately advanced PD and are associated with neuropathy and cognitive impairment.
They measured serum methylmalonic acid, homocysteine, and holotranscobalamin in addition to B12 because of the limited sensitivity of serum B12 testing alone to detect B12 deficiency. At baseline, 13% of 680 patients had borderline-low B12 levels (less than 184 pmol/L [250 pg/mL]), and 5% had deficient B12 levels (less than 157 pmol/L or 212 pg/mL). Homocysteine was moderately elevated (greater than 15 mmol/L) in 7% of subjects, and 14% of patients with borderline-low B12 also had elevated homocysteine, the investigators reported in Movement Disorders.
Low B12 at baseline predicted greater worsening of mobility in terms of a higher ambulatory capacity score, calculated by adding individual items of the Unified Parkinson’s Disease Rating Scale (UPDRS): falling, freezing when walking, walking, gait, and postural stability. Participants in the low- B12 tertile (less than 234 pmol/L or 317 pg/ mL) developed greater morbidity as assessed by greater annualized worsening of the ambulatory capacity score. For example, those in the low-B12 tertile had annualized change of 1.53, compared with 0.77 in the upper tertile. The worsening score was mostly attributed to poorer gait and postural instability.
To give context to these figures, the researchers pointed to an analysis of the NET-PD LS1 cohort that found a mean ambulatory capacity score of 2.17 among patients who fell and a score of 1.4 for those who did not fall. “Thus, we consider the magnitude of difference to be clinically relevant, particularly given that components of gait dysfunction that develop in PD may not respond to dopaminergic treatments or [deep brain stimulation],” they wrote.
Elevated homocysteine also predicted greater cognitive decline. Baseline elevated homocysteine was associated with lower baseline Mini Mental State Examination (MMSE), as well as greater annualized decline in MMSE (–1.96 vs. 0.06; P = .001).
Of the 456 subjects who continued in the study for 9-24 months and had a second blood sample available, 226 had an increase of more than 20% in B12 levels, 210 stayed within 20% of the original B12 measurement, and 19 had a decrease greater than 20%.
Overall, there was a mean annualized increase in B12 of 52.6 pmol/L, a mean annualized decrease of homocysteine of 0.83 mmol/L, and a mean annualized increase of holotranscobalamin of 14.7 pmol/L.
“These findings are consistent with improved nutritional status during the course of the study, likely attributed to subjects starting the optional [multivitamin] after the baseline visit and/or subjects changing their diets,” the research team said.
While the improvement in B12 status did not lead to statistically significant improvements in UPDRS scores, the researchers said there was a trend toward improvement, which provides “support for a disease-modifying effect of B12,” they wrote.
The researchers speculated that their findings of a link between low B12 levels and worse outcomes could be attributed to an independent (comorbid) effect on the central and peripheral nervous systems, a direct effect on PD pathogenesis, or alternatively, that low B12 may be a marker of an unknown associated factor.
“Given that low B12 status is associated with neurological and other medical morbidities and is readily treated, great care would be needed to design an ethically acceptable randomized, prospective study to evaluate the effect of B12 supplementation on PD progression, given that serum measurements collected as part of a prospective study in unsupplemented patients would likely reveal some subjects with B12 deficiency,” they concluded.
The authors declared no relevant disclosures. The study was supported by a grant from the Michael J. Fox Foundation for Parkinson’s Research, as well as privately donated grants.
SOURCE: Christine C et al. Movement Dis. 2018 Mar 6. doi: 10.1002/mds.27301.
suggesting that it may be worthwhile to examine the correction of low levels as a means of slowing disease progression.
Investigators led by Chadwick W. Christine, MD, of the department of neurology at the University of California, San Francisco, sought to understand what contributes to considerable variation in the progression of PD by building on previous research that revealed low serum vitamin B12 levels are common in patients with moderately advanced PD and are associated with neuropathy and cognitive impairment.
They measured serum methylmalonic acid, homocysteine, and holotranscobalamin in addition to B12 because of the limited sensitivity of serum B12 testing alone to detect B12 deficiency. At baseline, 13% of 680 patients had borderline-low B12 levels (less than 184 pmol/L [250 pg/mL]), and 5% had deficient B12 levels (less than 157 pmol/L or 212 pg/mL). Homocysteine was moderately elevated (greater than 15 mmol/L) in 7% of subjects, and 14% of patients with borderline-low B12 also had elevated homocysteine, the investigators reported in Movement Disorders.
Low B12 at baseline predicted greater worsening of mobility in terms of a higher ambulatory capacity score, calculated by adding individual items of the Unified Parkinson’s Disease Rating Scale (UPDRS): falling, freezing when walking, walking, gait, and postural stability. Participants in the low- B12 tertile (less than 234 pmol/L or 317 pg/ mL) developed greater morbidity as assessed by greater annualized worsening of the ambulatory capacity score. For example, those in the low-B12 tertile had annualized change of 1.53, compared with 0.77 in the upper tertile. The worsening score was mostly attributed to poorer gait and postural instability.
To give context to these figures, the researchers pointed to an analysis of the NET-PD LS1 cohort that found a mean ambulatory capacity score of 2.17 among patients who fell and a score of 1.4 for those who did not fall. “Thus, we consider the magnitude of difference to be clinically relevant, particularly given that components of gait dysfunction that develop in PD may not respond to dopaminergic treatments or [deep brain stimulation],” they wrote.
Elevated homocysteine also predicted greater cognitive decline. Baseline elevated homocysteine was associated with lower baseline Mini Mental State Examination (MMSE), as well as greater annualized decline in MMSE (–1.96 vs. 0.06; P = .001).
Of the 456 subjects who continued in the study for 9-24 months and had a second blood sample available, 226 had an increase of more than 20% in B12 levels, 210 stayed within 20% of the original B12 measurement, and 19 had a decrease greater than 20%.
Overall, there was a mean annualized increase in B12 of 52.6 pmol/L, a mean annualized decrease of homocysteine of 0.83 mmol/L, and a mean annualized increase of holotranscobalamin of 14.7 pmol/L.
“These findings are consistent with improved nutritional status during the course of the study, likely attributed to subjects starting the optional [multivitamin] after the baseline visit and/or subjects changing their diets,” the research team said.
While the improvement in B12 status did not lead to statistically significant improvements in UPDRS scores, the researchers said there was a trend toward improvement, which provides “support for a disease-modifying effect of B12,” they wrote.
The researchers speculated that their findings of a link between low B12 levels and worse outcomes could be attributed to an independent (comorbid) effect on the central and peripheral nervous systems, a direct effect on PD pathogenesis, or alternatively, that low B12 may be a marker of an unknown associated factor.
“Given that low B12 status is associated with neurological and other medical morbidities and is readily treated, great care would be needed to design an ethically acceptable randomized, prospective study to evaluate the effect of B12 supplementation on PD progression, given that serum measurements collected as part of a prospective study in unsupplemented patients would likely reveal some subjects with B12 deficiency,” they concluded.
The authors declared no relevant disclosures. The study was supported by a grant from the Michael J. Fox Foundation for Parkinson’s Research, as well as privately donated grants.
SOURCE: Christine C et al. Movement Dis. 2018 Mar 6. doi: 10.1002/mds.27301.
FROM MOVEMENT DISORDERS
Key clinical point: Prevention or early correction of low B12 may potentially be a therapeutic target to slow progression in early Parkinson’s disease.
Main finding: Participants in the lowest B12 tertile developed greater morbidity with an annualized worsening of the ambulatory capacity score of 1.53, compared with 0.77 in patients in the upper tertile.
Study details: Analysis of vitamin B12 in 680 baseline and 456 follow-up serum samples of patients with PD participating in the double-blind, randomized DATATOP trial.
Disclosures: The authors declared no relevant disclosures. The study was supported by a grant from the Michael J. Fox Foundation for Parkinson’s Research, as well as privately donated grants.
Source: Christine C et al. Movement Dis. 2018 Mar 6. doi: 10.1002/mds.27301.
Docs worry there’s ‘nowhere to send’ new and expectant moms with depression
Lawmakers in California will begin debate next month on a bill that would require doctors to screen new moms for mental health problems – once while they’re pregnant and again after they give birth.
But many obstetricians and pediatricians bristle at the idea, saying they are afraid to screen new moms for depression and anxiety.
“What are you going to do with those people who screen positive?” asked Laura L. Sirott, MD, an ob.gyn. who practices in Pasadena. “Some providers have nowhere to send them.”
Nationally, depression affects up to one in seven women during or after pregnancy, according to the American Psychological Association.
And, of women who screen positive for the condition, 78% don’t get mental health treatment, according to a 2015 research review published in the journal Obstetrics & Gynecology.
Dr. Sirott said her patients give a range of reasons why they don’t take her up on a referral to a psychologist: “ ‘Oh, they don’t take my insurance.’ Or ‘my insurance pays for three visits.’ ‘I can’t take time off work to go to those visits.’ ‘It’s a 3-month wait to get in to that person.’ ”
She said it’s also hard to find a psychiatrist who is willing to treat them and who is trained in the complexities of prescribing medications to pregnant or breastfeeding women, especially in rural areas.
“So it’s very frustrating,” Dr. Sirott said, “to ask patients about a problem and then not have any way to solve that problem.”
Moms are frustrated, too. After the baby comes, no one asks about the baby’s mother anymore.
Wendy Root Askew struggled for years to get pregnant, and when she finally did, her anxiety got worse. She couldn’t stop worrying that something would go wrong.
“And then, after I had my son, I would have these dreams where someone would come to the door and they would say, ‘Well, you know, we’re just going to wait 2 weeks to see if you get to keep your baby or not,’ ” Ms. Root Askew said. “And it really impacted my ability to bond with him.”
She likes California’s bill, AB 2193, because it goes beyond mandated screening. It would require health insurance companies to set up case management programs to help moms find a therapist, and connect obstetricians or pediatricians to a psychiatric specialist.
“Just like we have case-management programs for patients who have diabetes or sleep issues or back pain, a case-management program requires the insurance company to take some ownership of making sure their patients are getting the treatment they need to be healthy,” said Ms. Root Askew, who is now advocating for the bill on behalf of the group 2020 Mom.
Health insurance companies haven’t taken a position on the legislation. It’s unclear how much it would cost them to comply, because some already have infrastructure in place for case-management programs, and some do not. But there is consensus among insurers and health advocates that such programs save money in the long run.
“The sooner that you can get good treatment for a mom, the less expensive that condition will be to manage over the course of the woman’s life and over the course of that child’s life,” Ms. Root Askew said.
Some doctors still have their objections. Under the bill, they could be disciplined for not screening. Some have said they worry about how much time it would take.
The health care system, and the incentives, aren’t set up for this sort of screening, Dr. Sirott said.
“Currently, I get $6 for screening a patient,” she said. “By the time I put it on a piece of paper and print it, it’s not worth it.”
It’s not clear whether the direct and indirect costs of screening would be worth it to the patients, either. Four other states – Illinois, Massachusetts, New Jersey, and West Virginia – have tried mandated screening, and it did not result in more women getting treatment, according to a 2015 study published in Psychiatric Services.
Even with California’s extra requirement that insurance companies facilitate care, women could still face high copays or limits on the number of therapy sessions. Or, a new mother might be so overwhelmed with care for her newborn that it would be difficult to add anything to her busy schedule.
What does seem to work, according to the study of mandated screening in other states, is when nurses or mental health providers visit new moms at home.
“Despite abundant goodwill, there is no evidence that state policies are addressing this great need,” the study’s authors report.
Supporters of California’s proposed bill, however, say doctors need to start somewhere. Screening is the first step in recognizing the full scope of the problem, said Nirmaljit Dhami, MD, a Mountain View, Calif., psychiatrist. Women should be screened on an ongoing basis throughout pregnancy and for a year after birth, Dr. Dhami said, not just once or twice as the bill requires.
“I often tell doctors that if you don’t know that somebody is suicidal, it doesn’t mean that their suicidality will go away,” she said. “If you don’t ask, the risk is the same.”
This story is part of a partnership that includes KQED, NPR, and Kaiser Health News. KHN’s coverage of women’s health care issues is supported in part by The David and Lucile Packard Foundation. KHN is a nonprofit news service covering health issues. It is an editorially independent program of the Kaiser Family Foundation that is not affiliated with Kaiser Permanente.
Lawmakers in California will begin debate next month on a bill that would require doctors to screen new moms for mental health problems – once while they’re pregnant and again after they give birth.
But many obstetricians and pediatricians bristle at the idea, saying they are afraid to screen new moms for depression and anxiety.
“What are you going to do with those people who screen positive?” asked Laura L. Sirott, MD, an ob.gyn. who practices in Pasadena. “Some providers have nowhere to send them.”
Nationally, depression affects up to one in seven women during or after pregnancy, according to the American Psychological Association.
And, of women who screen positive for the condition, 78% don’t get mental health treatment, according to a 2015 research review published in the journal Obstetrics & Gynecology.
Dr. Sirott said her patients give a range of reasons why they don’t take her up on a referral to a psychologist: “ ‘Oh, they don’t take my insurance.’ Or ‘my insurance pays for three visits.’ ‘I can’t take time off work to go to those visits.’ ‘It’s a 3-month wait to get in to that person.’ ”
She said it’s also hard to find a psychiatrist who is willing to treat them and who is trained in the complexities of prescribing medications to pregnant or breastfeeding women, especially in rural areas.
“So it’s very frustrating,” Dr. Sirott said, “to ask patients about a problem and then not have any way to solve that problem.”
Moms are frustrated, too. After the baby comes, no one asks about the baby’s mother anymore.
Wendy Root Askew struggled for years to get pregnant, and when she finally did, her anxiety got worse. She couldn’t stop worrying that something would go wrong.
“And then, after I had my son, I would have these dreams where someone would come to the door and they would say, ‘Well, you know, we’re just going to wait 2 weeks to see if you get to keep your baby or not,’ ” Ms. Root Askew said. “And it really impacted my ability to bond with him.”
She likes California’s bill, AB 2193, because it goes beyond mandated screening. It would require health insurance companies to set up case management programs to help moms find a therapist, and connect obstetricians or pediatricians to a psychiatric specialist.
“Just like we have case-management programs for patients who have diabetes or sleep issues or back pain, a case-management program requires the insurance company to take some ownership of making sure their patients are getting the treatment they need to be healthy,” said Ms. Root Askew, who is now advocating for the bill on behalf of the group 2020 Mom.
Health insurance companies haven’t taken a position on the legislation. It’s unclear how much it would cost them to comply, because some already have infrastructure in place for case-management programs, and some do not. But there is consensus among insurers and health advocates that such programs save money in the long run.
“The sooner that you can get good treatment for a mom, the less expensive that condition will be to manage over the course of the woman’s life and over the course of that child’s life,” Ms. Root Askew said.
Some doctors still have their objections. Under the bill, they could be disciplined for not screening. Some have said they worry about how much time it would take.
The health care system, and the incentives, aren’t set up for this sort of screening, Dr. Sirott said.
“Currently, I get $6 for screening a patient,” she said. “By the time I put it on a piece of paper and print it, it’s not worth it.”
It’s not clear whether the direct and indirect costs of screening would be worth it to the patients, either. Four other states – Illinois, Massachusetts, New Jersey, and West Virginia – have tried mandated screening, and it did not result in more women getting treatment, according to a 2015 study published in Psychiatric Services.
Even with California’s extra requirement that insurance companies facilitate care, women could still face high copays or limits on the number of therapy sessions. Or, a new mother might be so overwhelmed with care for her newborn that it would be difficult to add anything to her busy schedule.
What does seem to work, according to the study of mandated screening in other states, is when nurses or mental health providers visit new moms at home.
“Despite abundant goodwill, there is no evidence that state policies are addressing this great need,” the study’s authors report.
Supporters of California’s proposed bill, however, say doctors need to start somewhere. Screening is the first step in recognizing the full scope of the problem, said Nirmaljit Dhami, MD, a Mountain View, Calif., psychiatrist. Women should be screened on an ongoing basis throughout pregnancy and for a year after birth, Dr. Dhami said, not just once or twice as the bill requires.
“I often tell doctors that if you don’t know that somebody is suicidal, it doesn’t mean that their suicidality will go away,” she said. “If you don’t ask, the risk is the same.”
This story is part of a partnership that includes KQED, NPR, and Kaiser Health News. KHN’s coverage of women’s health care issues is supported in part by The David and Lucile Packard Foundation. KHN is a nonprofit news service covering health issues. It is an editorially independent program of the Kaiser Family Foundation that is not affiliated with Kaiser Permanente.
Lawmakers in California will begin debate next month on a bill that would require doctors to screen new moms for mental health problems – once while they’re pregnant and again after they give birth.
But many obstetricians and pediatricians bristle at the idea, saying they are afraid to screen new moms for depression and anxiety.
“What are you going to do with those people who screen positive?” asked Laura L. Sirott, MD, an ob.gyn. who practices in Pasadena. “Some providers have nowhere to send them.”
Nationally, depression affects up to one in seven women during or after pregnancy, according to the American Psychological Association.
And, of women who screen positive for the condition, 78% don’t get mental health treatment, according to a 2015 research review published in the journal Obstetrics & Gynecology.
Dr. Sirott said her patients give a range of reasons why they don’t take her up on a referral to a psychologist: “ ‘Oh, they don’t take my insurance.’ Or ‘my insurance pays for three visits.’ ‘I can’t take time off work to go to those visits.’ ‘It’s a 3-month wait to get in to that person.’ ”
She said it’s also hard to find a psychiatrist who is willing to treat them and who is trained in the complexities of prescribing medications to pregnant or breastfeeding women, especially in rural areas.
“So it’s very frustrating,” Dr. Sirott said, “to ask patients about a problem and then not have any way to solve that problem.”
Moms are frustrated, too. After the baby comes, no one asks about the baby’s mother anymore.
Wendy Root Askew struggled for years to get pregnant, and when she finally did, her anxiety got worse. She couldn’t stop worrying that something would go wrong.
“And then, after I had my son, I would have these dreams where someone would come to the door and they would say, ‘Well, you know, we’re just going to wait 2 weeks to see if you get to keep your baby or not,’ ” Ms. Root Askew said. “And it really impacted my ability to bond with him.”
She likes California’s bill, AB 2193, because it goes beyond mandated screening. It would require health insurance companies to set up case management programs to help moms find a therapist, and connect obstetricians or pediatricians to a psychiatric specialist.
“Just like we have case-management programs for patients who have diabetes or sleep issues or back pain, a case-management program requires the insurance company to take some ownership of making sure their patients are getting the treatment they need to be healthy,” said Ms. Root Askew, who is now advocating for the bill on behalf of the group 2020 Mom.
Health insurance companies haven’t taken a position on the legislation. It’s unclear how much it would cost them to comply, because some already have infrastructure in place for case-management programs, and some do not. But there is consensus among insurers and health advocates that such programs save money in the long run.
“The sooner that you can get good treatment for a mom, the less expensive that condition will be to manage over the course of the woman’s life and over the course of that child’s life,” Ms. Root Askew said.
Some doctors still have their objections. Under the bill, they could be disciplined for not screening. Some have said they worry about how much time it would take.
The health care system, and the incentives, aren’t set up for this sort of screening, Dr. Sirott said.
“Currently, I get $6 for screening a patient,” she said. “By the time I put it on a piece of paper and print it, it’s not worth it.”
It’s not clear whether the direct and indirect costs of screening would be worth it to the patients, either. Four other states – Illinois, Massachusetts, New Jersey, and West Virginia – have tried mandated screening, and it did not result in more women getting treatment, according to a 2015 study published in Psychiatric Services.
Even with California’s extra requirement that insurance companies facilitate care, women could still face high copays or limits on the number of therapy sessions. Or, a new mother might be so overwhelmed with care for her newborn that it would be difficult to add anything to her busy schedule.
What does seem to work, according to the study of mandated screening in other states, is when nurses or mental health providers visit new moms at home.
“Despite abundant goodwill, there is no evidence that state policies are addressing this great need,” the study’s authors report.
Supporters of California’s proposed bill, however, say doctors need to start somewhere. Screening is the first step in recognizing the full scope of the problem, said Nirmaljit Dhami, MD, a Mountain View, Calif., psychiatrist. Women should be screened on an ongoing basis throughout pregnancy and for a year after birth, Dr. Dhami said, not just once or twice as the bill requires.
“I often tell doctors that if you don’t know that somebody is suicidal, it doesn’t mean that their suicidality will go away,” she said. “If you don’t ask, the risk is the same.”
This story is part of a partnership that includes KQED, NPR, and Kaiser Health News. KHN’s coverage of women’s health care issues is supported in part by The David and Lucile Packard Foundation. KHN is a nonprofit news service covering health issues. It is an editorially independent program of the Kaiser Family Foundation that is not affiliated with Kaiser Permanente.
VIDEO: Researchers closing in on the elusive ‘male pill’
CHICAGO –
It blocks gonadotropin signaling and testosterone production in the testes. When capsules ranging in dose from 100 mg to 400 mg were given once daily to 100 men in a randomized, placebo controlled trial, the drop in testosterone was more than sufficient to block sperm production. Testosterone levels jumped back up to normal after the end of the 28-day trial, all without inducing liver toxicity or other serious problems.
“We are very excited [about] the results. It’s a big step forward in the development of the male pill. Our last great advance in male contraception was over 300 years ago with the development of the condom,” said senior investigator Stephanie Page, MD, PhD, head of the division of metabolism, endocrinology, and nutrition at the University of Washington, Seattle.
Some men reported a drop in libido that resolved by the end of the study. There was also mild weight gain and small reductions in HDL cholesterol. A few tweaks to the formulation or dosing might fix those problems. “Overall, we were very encouraged about the safety profile,” Dr. Page said.

She explained the work, its promise, and the next steps in a video interview at the Endocrine Society’s annual meeting. The National Institutes of Health is funding development. Dr. Page didn’t have any relevant disclosures.
SOURCE: Page S et al. ENDO 2018, Abstract OR15-2.
CHICAGO –
It blocks gonadotropin signaling and testosterone production in the testes. When capsules ranging in dose from 100 mg to 400 mg were given once daily to 100 men in a randomized, placebo controlled trial, the drop in testosterone was more than sufficient to block sperm production. Testosterone levels jumped back up to normal after the end of the 28-day trial, all without inducing liver toxicity or other serious problems.
“We are very excited [about] the results. It’s a big step forward in the development of the male pill. Our last great advance in male contraception was over 300 years ago with the development of the condom,” said senior investigator Stephanie Page, MD, PhD, head of the division of metabolism, endocrinology, and nutrition at the University of Washington, Seattle.
Some men reported a drop in libido that resolved by the end of the study. There was also mild weight gain and small reductions in HDL cholesterol. A few tweaks to the formulation or dosing might fix those problems. “Overall, we were very encouraged about the safety profile,” Dr. Page said.
She explained the work, its promise, and the next steps in a video interview at the Endocrine Society’s annual meeting. The National Institutes of Health is funding development. Dr. Page didn’t have any relevant disclosures.
SOURCE: Page S et al. ENDO 2018, Abstract OR15-2.
CHICAGO –
It blocks gonadotropin signaling and testosterone production in the testes. When capsules ranging in dose from 100 mg to 400 mg were given once daily to 100 men in a randomized, placebo controlled trial, the drop in testosterone was more than sufficient to block sperm production. Testosterone levels jumped back up to normal after the end of the 28-day trial, all without inducing liver toxicity or other serious problems.
“We are very excited [about] the results. It’s a big step forward in the development of the male pill. Our last great advance in male contraception was over 300 years ago with the development of the condom,” said senior investigator Stephanie Page, MD, PhD, head of the division of metabolism, endocrinology, and nutrition at the University of Washington, Seattle.
Some men reported a drop in libido that resolved by the end of the study. There was also mild weight gain and small reductions in HDL cholesterol. A few tweaks to the formulation or dosing might fix those problems. “Overall, we were very encouraged about the safety profile,” Dr. Page said.
She explained the work, its promise, and the next steps in a video interview at the Endocrine Society’s annual meeting. The National Institutes of Health is funding development. Dr. Page didn’t have any relevant disclosures.
SOURCE: Page S et al. ENDO 2018, Abstract OR15-2.
REPORTING FROM ENDO 2018
