User login
Product News: 11 2017
Cyltezo
Boehringer Ingelheim Pharmaceuticals, Inc, announces US Food and Drug Administration approval of the biosimilar Cyltezo (adalimumab-adbm) in a prefilled syringe for the treatment of plaque psoriasis and psoriatic arthritis as well as other chronic inflammatory diseases. Cyltezo is not commercially available at this time. For more information, visit www.boehringer-ingelheim.us.
Facing Forward App
Cutanea Life Sciences, Inc, introduces Facing Forward, a mobile app for patients with acne to track their treatment with Aktipak (erythromycin and benzoyl peroxide) Gel 3%/5%. The app features a camera function for users to take photographs to track their progress, dosing reminders, prescription refill reminders, acne information resources, and a compliance report so that the physician can determine if the patient is using the medication properly. This app is available free through the App Store or Google Play. For more information, visit www.cutanea.com.
Glytone Dark Spot Corrector
Pierre Fabre Dermo Cosmetique USA introduces the Glytone Dark Spot Corrector, a brightening formula with hydroquinone 2% to help reduce the appearance of pigmentation changes due to pregnancy, use of oral contraceptives, skin aging, or photodamage. It also contains glycolic acid to exfoliate dead cells from the skin’s surface and kojic acid to brighten the skin. For more information, visit www.glytone-usa.com.
Loyon
IntraDerm Pharmaceuticals, a division of Sonoma Pharmaceuticals, Inc, announces US commercialization of Loyon to manage and relieve the scaling, erythema, and pruritus associated with various types of dermatoses including seborrhea and seborrheic dermatitis. Loyon is a combination of the dry emollient Cetiol CC and the medical silicone oil dimethicone. It is a fast and effective treatment for scaling associated with seborrheic dermatitis or psoriasis, which impacts patient quality of life.
Stelara
Janssen Biotech, Inc, announces US Food and Drug Administration approval of Stelara (ustekinumab) for the treatment of moderate to severe plaque psoriasis in adolescents (≥12 years of age) who are candidates for phototherapy or systemic therapy. Stelara was first approved for the treatment of plaque psoriasis in adults in 2009. For more information, visit www.stelarahcp.com.
If you would like your product included in Product News, please email a press release to the Editorial Office at [email protected].
Cyltezo
Boehringer Ingelheim Pharmaceuticals, Inc, announces US Food and Drug Administration approval of the biosimilar Cyltezo (adalimumab-adbm) in a prefilled syringe for the treatment of plaque psoriasis and psoriatic arthritis as well as other chronic inflammatory diseases. Cyltezo is not commercially available at this time. For more information, visit www.boehringer-ingelheim.us.
Facing Forward App
Cutanea Life Sciences, Inc, introduces Facing Forward, a mobile app for patients with acne to track their treatment with Aktipak (erythromycin and benzoyl peroxide) Gel 3%/5%. The app features a camera function for users to take photographs to track their progress, dosing reminders, prescription refill reminders, acne information resources, and a compliance report so that the physician can determine if the patient is using the medication properly. This app is available free through the App Store or Google Play. For more information, visit www.cutanea.com.
Glytone Dark Spot Corrector
Pierre Fabre Dermo Cosmetique USA introduces the Glytone Dark Spot Corrector, a brightening formula with hydroquinone 2% to help reduce the appearance of pigmentation changes due to pregnancy, use of oral contraceptives, skin aging, or photodamage. It also contains glycolic acid to exfoliate dead cells from the skin’s surface and kojic acid to brighten the skin. For more information, visit www.glytone-usa.com.
Loyon
IntraDerm Pharmaceuticals, a division of Sonoma Pharmaceuticals, Inc, announces US commercialization of Loyon to manage and relieve the scaling, erythema, and pruritus associated with various types of dermatoses including seborrhea and seborrheic dermatitis. Loyon is a combination of the dry emollient Cetiol CC and the medical silicone oil dimethicone. It is a fast and effective treatment for scaling associated with seborrheic dermatitis or psoriasis, which impacts patient quality of life.
Stelara
Janssen Biotech, Inc, announces US Food and Drug Administration approval of Stelara (ustekinumab) for the treatment of moderate to severe plaque psoriasis in adolescents (≥12 years of age) who are candidates for phototherapy or systemic therapy. Stelara was first approved for the treatment of plaque psoriasis in adults in 2009. For more information, visit www.stelarahcp.com.
If you would like your product included in Product News, please email a press release to the Editorial Office at [email protected].
Cyltezo
Boehringer Ingelheim Pharmaceuticals, Inc, announces US Food and Drug Administration approval of the biosimilar Cyltezo (adalimumab-adbm) in a prefilled syringe for the treatment of plaque psoriasis and psoriatic arthritis as well as other chronic inflammatory diseases. Cyltezo is not commercially available at this time. For more information, visit www.boehringer-ingelheim.us.
Facing Forward App
Cutanea Life Sciences, Inc, introduces Facing Forward, a mobile app for patients with acne to track their treatment with Aktipak (erythromycin and benzoyl peroxide) Gel 3%/5%. The app features a camera function for users to take photographs to track their progress, dosing reminders, prescription refill reminders, acne information resources, and a compliance report so that the physician can determine if the patient is using the medication properly. This app is available free through the App Store or Google Play. For more information, visit www.cutanea.com.
Glytone Dark Spot Corrector
Pierre Fabre Dermo Cosmetique USA introduces the Glytone Dark Spot Corrector, a brightening formula with hydroquinone 2% to help reduce the appearance of pigmentation changes due to pregnancy, use of oral contraceptives, skin aging, or photodamage. It also contains glycolic acid to exfoliate dead cells from the skin’s surface and kojic acid to brighten the skin. For more information, visit www.glytone-usa.com.
Loyon
IntraDerm Pharmaceuticals, a division of Sonoma Pharmaceuticals, Inc, announces US commercialization of Loyon to manage and relieve the scaling, erythema, and pruritus associated with various types of dermatoses including seborrhea and seborrheic dermatitis. Loyon is a combination of the dry emollient Cetiol CC and the medical silicone oil dimethicone. It is a fast and effective treatment for scaling associated with seborrheic dermatitis or psoriasis, which impacts patient quality of life.
Stelara
Janssen Biotech, Inc, announces US Food and Drug Administration approval of Stelara (ustekinumab) for the treatment of moderate to severe plaque psoriasis in adolescents (≥12 years of age) who are candidates for phototherapy or systemic therapy. Stelara was first approved for the treatment of plaque psoriasis in adults in 2009. For more information, visit www.stelarahcp.com.
If you would like your product included in Product News, please email a press release to the Editorial Office at [email protected].

Clinical Pearl: A Simple and Effective Technique for Improving Surgical Closures for the Early-Learning Resident
Practice Gap
For first-year dermatology residents, dermatologic surgeries can present many challenges. Although approximation of wound edges following excision may be intuitive for the experienced surgeon, an early trainee may need some guidance. Infusion of anesthetics can distort the normal skin field or it may be difficult for the patient to remain in the same position for the required period of time; for example, an elderly patient who requires an excision on the posterior aspect of the neck may be unable to assume the same position for the full duration of the procedure. We offer a simple and effective technique for early-learning dermatology residents to improve surgical closures.
The Technique
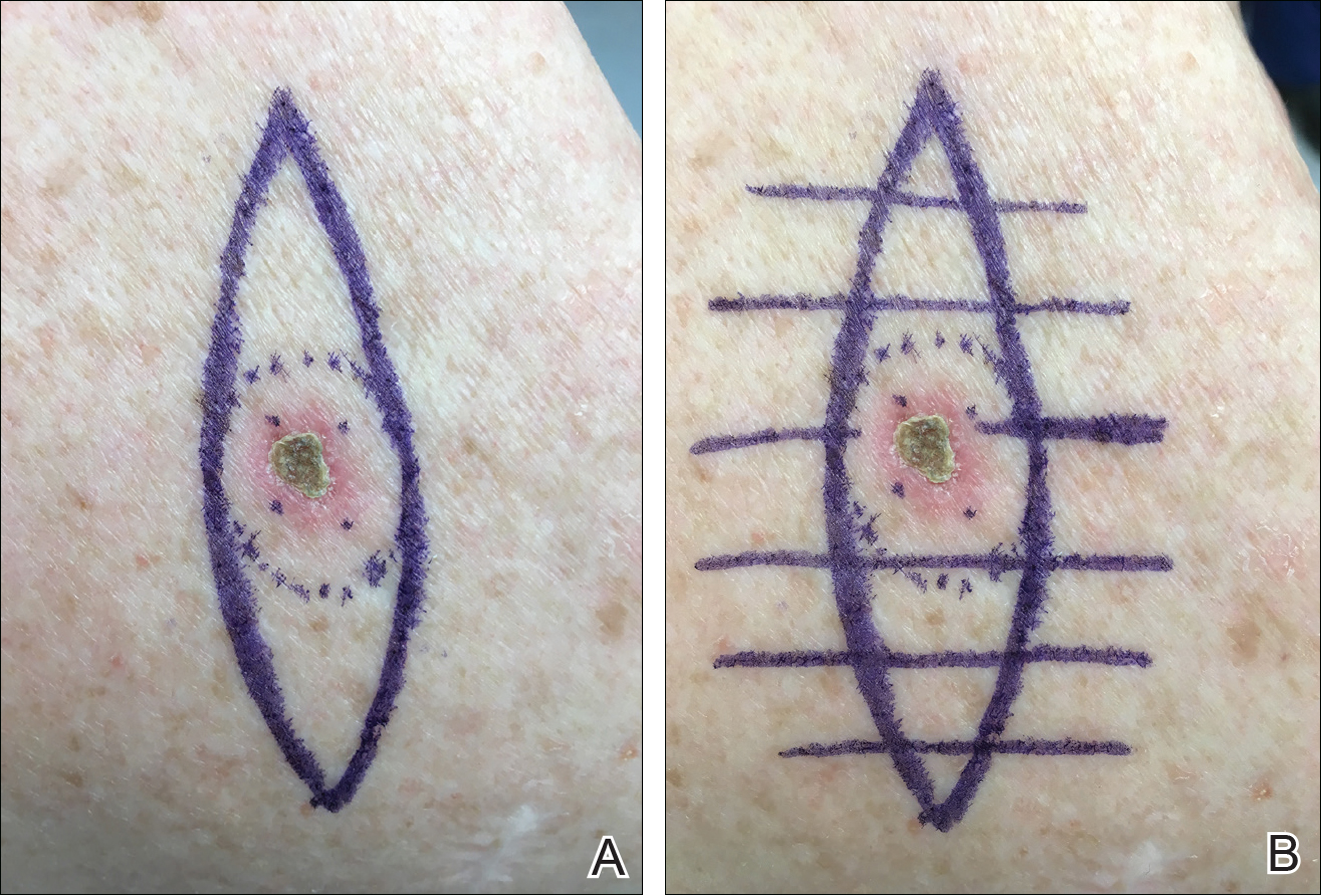
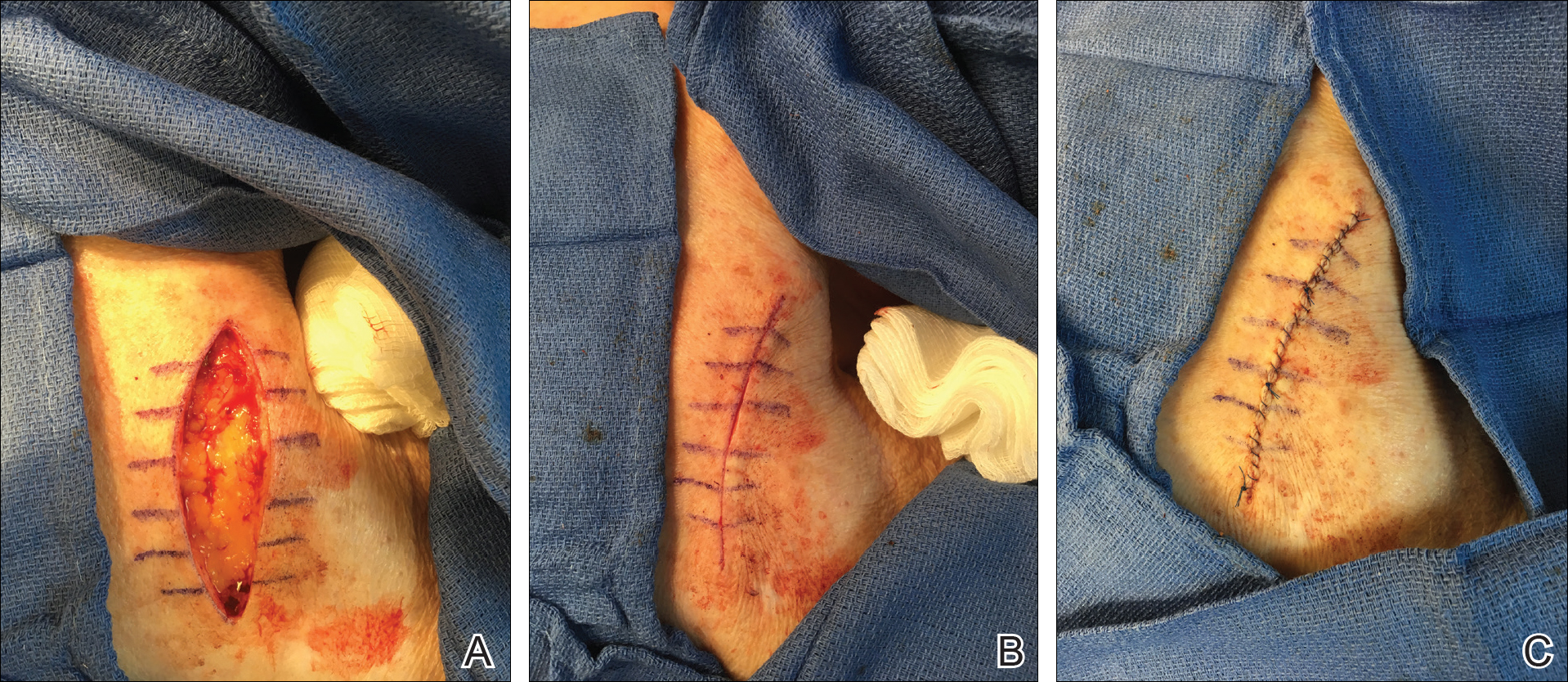
We propose drawing straight lines using a sterile marking pen perpendicular to the fusiform plane laid out for any simple, intermediate, or complex linear closure (Figure 1). These lines can then be used as scaffolding for the surgical closure (Figure 2). We recommend drawing the lines at the time of initial planning when the site of excision is in the normal anatomic position.
Practice Implications
By creating a sketch with perpendicular lines, approximation of skin edges and surgical closures may become easier for the learning resident. Patients also can rest more comfortably during the procedure, and the overall cosmesis, healing, and outcome of the procedure may improve. The addition of a sterile marking pen to the surgical tray may aide in highlighting faded pen markings for easier visualization after cleansing of the surgical site.
Practice Gap
For first-year dermatology residents, dermatologic surgeries can present many challenges. Although approximation of wound edges following excision may be intuitive for the experienced surgeon, an early trainee may need some guidance. Infusion of anesthetics can distort the normal skin field or it may be difficult for the patient to remain in the same position for the required period of time; for example, an elderly patient who requires an excision on the posterior aspect of the neck may be unable to assume the same position for the full duration of the procedure. We offer a simple and effective technique for early-learning dermatology residents to improve surgical closures.
The Technique
We propose drawing straight lines using a sterile marking pen perpendicular to the fusiform plane laid out for any simple, intermediate, or complex linear closure (Figure 1). These lines can then be used as scaffolding for the surgical closure (Figure 2). We recommend drawing the lines at the time of initial planning when the site of excision is in the normal anatomic position.
Practice Implications
By creating a sketch with perpendicular lines, approximation of skin edges and surgical closures may become easier for the learning resident. Patients also can rest more comfortably during the procedure, and the overall cosmesis, healing, and outcome of the procedure may improve. The addition of a sterile marking pen to the surgical tray may aide in highlighting faded pen markings for easier visualization after cleansing of the surgical site.
Practice Gap
For first-year dermatology residents, dermatologic surgeries can present many challenges. Although approximation of wound edges following excision may be intuitive for the experienced surgeon, an early trainee may need some guidance. Infusion of anesthetics can distort the normal skin field or it may be difficult for the patient to remain in the same position for the required period of time; for example, an elderly patient who requires an excision on the posterior aspect of the neck may be unable to assume the same position for the full duration of the procedure. We offer a simple and effective technique for early-learning dermatology residents to improve surgical closures.
The Technique
We propose drawing straight lines using a sterile marking pen perpendicular to the fusiform plane laid out for any simple, intermediate, or complex linear closure (Figure 1). These lines can then be used as scaffolding for the surgical closure (Figure 2). We recommend drawing the lines at the time of initial planning when the site of excision is in the normal anatomic position.
Practice Implications
By creating a sketch with perpendicular lines, approximation of skin edges and surgical closures may become easier for the learning resident. Patients also can rest more comfortably during the procedure, and the overall cosmesis, healing, and outcome of the procedure may improve. The addition of a sterile marking pen to the surgical tray may aide in highlighting faded pen markings for easier visualization after cleansing of the surgical site.
PsA disease activity instruments differ on residual disease
Definitions of low disease activity or remission in patients with psoriatic arthritis that come from validated disease activity instruments identify different levels of residual disease despite having significant overlap. This level of variation between instruments can leave patients with residual disease that can affect their quality of life, researchers reported.
Treatment recommendations from the European League Against Rheumatism (EULAR) and the Group for Research and Assessment of Psoriasis and Psoriatic Arthritis (GRAPPA) advise aiming “for remission or the lowest possible disease activity in all involved domains of the disease,” but they do not specify a target or instrument to be used to define either low disease activity or remission, wrote Laura Coates, MD, of the University of Oxford (England) and her coauthors. To look at the variation produced by existing instruments to measure those states, they applied a variety of scoring indices to a group of 250 psoriatic arthritis patients who were considered by their treating rheumatologist to have quiescent disease.
The investigators tested the Disease Activity Index for Psoriatic Arthritis (DAPSA), minimal disease activity (MDA) criteria, and the Psoriatic Arthritis Disease Activity Score (PASDAS) in the group of patients, who were required to have been on stable treatment for at least 6 months (Ann Rheum Dis. 2017 Oct 28. doi: 10.1136/annrheumdis-2017-211998).
The cut points they used to measure remission included a score of 4 or less for DAPSA and the clinical DAPSA (cDAPSA, which doesn’t use C-reactive protein [CRP]), and a state called very low disease activity (VLDA) in which all seven MDA domain cut points were met. “Near remission” on the PASDAS was a score of 1.9 or less.
Low or minimal disease activity was defined by DAPSA of 14 or less, cDAPSA of 13 or less, or meeting the cut points for a combination of different MDA domains, including one in which any five of the seven cut points are required to be met (“MDA 5/7”), one where both the tender and swollen joint count cut points are required to be met with any three of the remaining five cut points (“MDA joints”), one where the skin domain is required to be met along with four of any of the remaining six (“MDA skin”), and one where both the joint and skin domains need to be met with any two of the remaining four domains (“MDA joints and skin”).
Little is known about whether the disease activity composite scores of the DAPSA and PASDAS reflect the same clinical disease activity on the various MDA disease domain combinations, Dr. Coates and her associates said.
The results of the analysis showed that VLDA and PASDAS were the most stringent scores for remission and that the DAPSA and cDAPSA scores were the least stringent target for remission. For example, in the entire cohort, 107 (43.7%) patients fulfilled DAPSA remission, 113 (45.7%) were in cDAPSA remission, 56 (22.5%) met VLDA criteria, and 37 (19.5%) were in PASDAS “near remission.”
All patients who met VLDA criteria were in DAPSA/cDAPSA remission. Of those patients in DAPSA remission but not in VLDA, 43 of 56 patients did not fulfill one of seven domains, while nine did not fulfill two of seven domains. Domains not fulfilled were skin (n = 33), tender joints (n = 7), swollen joints (n = 1), enthesitis (n = 3), visual analog scale scores (n = 6), or Health Assessment Questionnaire (n = 9).
“Residual skin disease was highest in patients achieving DAPSA or cDAPSA remission … this resulted in a group of patients, seen as in a low disease activity state, with the remaining skin disease impacting their quality of life,” the investigators wrote. This analysis “highlights the need for multiple separate measures for different domains to be assessed if a multidimensional definition is not used to ensure that remission retains face validity for the patients.”
The addition of the inflammatory marker CRP in both remission and low disease activity measures (in DAPSA and PASDAS) did not have added value, suggesting that “the inclusion of CRP is unnecessary [since] a similar proportion of patients have a raised CRP in all definitions. … A target without an inflammatory marker will be more practical in clinical practice,” they said.
However, Dr. Coates and her colleagues stressed that the cut-off for acceptable disease activity is important because a stricter target may encourage the overtreatment of patients, which would result in increased side effects and costs.
“The ideal stringency of a target with assessment of residual disease in the various clinical domains of psoriatic arthritis should be a focus of research,” they wrote.
The original cohort of patients was supported with an unrestricted grant from Pfizer. Dr. Coates did not declare any conflicts, but several of her coauthors declared receiving speaker or consultancy fees from the pharmaceutical industry.
Definitions of low disease activity or remission in patients with psoriatic arthritis that come from validated disease activity instruments identify different levels of residual disease despite having significant overlap. This level of variation between instruments can leave patients with residual disease that can affect their quality of life, researchers reported.
Treatment recommendations from the European League Against Rheumatism (EULAR) and the Group for Research and Assessment of Psoriasis and Psoriatic Arthritis (GRAPPA) advise aiming “for remission or the lowest possible disease activity in all involved domains of the disease,” but they do not specify a target or instrument to be used to define either low disease activity or remission, wrote Laura Coates, MD, of the University of Oxford (England) and her coauthors. To look at the variation produced by existing instruments to measure those states, they applied a variety of scoring indices to a group of 250 psoriatic arthritis patients who were considered by their treating rheumatologist to have quiescent disease.
The investigators tested the Disease Activity Index for Psoriatic Arthritis (DAPSA), minimal disease activity (MDA) criteria, and the Psoriatic Arthritis Disease Activity Score (PASDAS) in the group of patients, who were required to have been on stable treatment for at least 6 months (Ann Rheum Dis. 2017 Oct 28. doi: 10.1136/annrheumdis-2017-211998).
The cut points they used to measure remission included a score of 4 or less for DAPSA and the clinical DAPSA (cDAPSA, which doesn’t use C-reactive protein [CRP]), and a state called very low disease activity (VLDA) in which all seven MDA domain cut points were met. “Near remission” on the PASDAS was a score of 1.9 or less.
Low or minimal disease activity was defined by DAPSA of 14 or less, cDAPSA of 13 or less, or meeting the cut points for a combination of different MDA domains, including one in which any five of the seven cut points are required to be met (“MDA 5/7”), one where both the tender and swollen joint count cut points are required to be met with any three of the remaining five cut points (“MDA joints”), one where the skin domain is required to be met along with four of any of the remaining six (“MDA skin”), and one where both the joint and skin domains need to be met with any two of the remaining four domains (“MDA joints and skin”).
Little is known about whether the disease activity composite scores of the DAPSA and PASDAS reflect the same clinical disease activity on the various MDA disease domain combinations, Dr. Coates and her associates said.
The results of the analysis showed that VLDA and PASDAS were the most stringent scores for remission and that the DAPSA and cDAPSA scores were the least stringent target for remission. For example, in the entire cohort, 107 (43.7%) patients fulfilled DAPSA remission, 113 (45.7%) were in cDAPSA remission, 56 (22.5%) met VLDA criteria, and 37 (19.5%) were in PASDAS “near remission.”
All patients who met VLDA criteria were in DAPSA/cDAPSA remission. Of those patients in DAPSA remission but not in VLDA, 43 of 56 patients did not fulfill one of seven domains, while nine did not fulfill two of seven domains. Domains not fulfilled were skin (n = 33), tender joints (n = 7), swollen joints (n = 1), enthesitis (n = 3), visual analog scale scores (n = 6), or Health Assessment Questionnaire (n = 9).
“Residual skin disease was highest in patients achieving DAPSA or cDAPSA remission … this resulted in a group of patients, seen as in a low disease activity state, with the remaining skin disease impacting their quality of life,” the investigators wrote. This analysis “highlights the need for multiple separate measures for different domains to be assessed if a multidimensional definition is not used to ensure that remission retains face validity for the patients.”
The addition of the inflammatory marker CRP in both remission and low disease activity measures (in DAPSA and PASDAS) did not have added value, suggesting that “the inclusion of CRP is unnecessary [since] a similar proportion of patients have a raised CRP in all definitions. … A target without an inflammatory marker will be more practical in clinical practice,” they said.
However, Dr. Coates and her colleagues stressed that the cut-off for acceptable disease activity is important because a stricter target may encourage the overtreatment of patients, which would result in increased side effects and costs.
“The ideal stringency of a target with assessment of residual disease in the various clinical domains of psoriatic arthritis should be a focus of research,” they wrote.
The original cohort of patients was supported with an unrestricted grant from Pfizer. Dr. Coates did not declare any conflicts, but several of her coauthors declared receiving speaker or consultancy fees from the pharmaceutical industry.
Definitions of low disease activity or remission in patients with psoriatic arthritis that come from validated disease activity instruments identify different levels of residual disease despite having significant overlap. This level of variation between instruments can leave patients with residual disease that can affect their quality of life, researchers reported.
Treatment recommendations from the European League Against Rheumatism (EULAR) and the Group for Research and Assessment of Psoriasis and Psoriatic Arthritis (GRAPPA) advise aiming “for remission or the lowest possible disease activity in all involved domains of the disease,” but they do not specify a target or instrument to be used to define either low disease activity or remission, wrote Laura Coates, MD, of the University of Oxford (England) and her coauthors. To look at the variation produced by existing instruments to measure those states, they applied a variety of scoring indices to a group of 250 psoriatic arthritis patients who were considered by their treating rheumatologist to have quiescent disease.
The investigators tested the Disease Activity Index for Psoriatic Arthritis (DAPSA), minimal disease activity (MDA) criteria, and the Psoriatic Arthritis Disease Activity Score (PASDAS) in the group of patients, who were required to have been on stable treatment for at least 6 months (Ann Rheum Dis. 2017 Oct 28. doi: 10.1136/annrheumdis-2017-211998).
The cut points they used to measure remission included a score of 4 or less for DAPSA and the clinical DAPSA (cDAPSA, which doesn’t use C-reactive protein [CRP]), and a state called very low disease activity (VLDA) in which all seven MDA domain cut points were met. “Near remission” on the PASDAS was a score of 1.9 or less.
Low or minimal disease activity was defined by DAPSA of 14 or less, cDAPSA of 13 or less, or meeting the cut points for a combination of different MDA domains, including one in which any five of the seven cut points are required to be met (“MDA 5/7”), one where both the tender and swollen joint count cut points are required to be met with any three of the remaining five cut points (“MDA joints”), one where the skin domain is required to be met along with four of any of the remaining six (“MDA skin”), and one where both the joint and skin domains need to be met with any two of the remaining four domains (“MDA joints and skin”).
Little is known about whether the disease activity composite scores of the DAPSA and PASDAS reflect the same clinical disease activity on the various MDA disease domain combinations, Dr. Coates and her associates said.
The results of the analysis showed that VLDA and PASDAS were the most stringent scores for remission and that the DAPSA and cDAPSA scores were the least stringent target for remission. For example, in the entire cohort, 107 (43.7%) patients fulfilled DAPSA remission, 113 (45.7%) were in cDAPSA remission, 56 (22.5%) met VLDA criteria, and 37 (19.5%) were in PASDAS “near remission.”
All patients who met VLDA criteria were in DAPSA/cDAPSA remission. Of those patients in DAPSA remission but not in VLDA, 43 of 56 patients did not fulfill one of seven domains, while nine did not fulfill two of seven domains. Domains not fulfilled were skin (n = 33), tender joints (n = 7), swollen joints (n = 1), enthesitis (n = 3), visual analog scale scores (n = 6), or Health Assessment Questionnaire (n = 9).
“Residual skin disease was highest in patients achieving DAPSA or cDAPSA remission … this resulted in a group of patients, seen as in a low disease activity state, with the remaining skin disease impacting their quality of life,” the investigators wrote. This analysis “highlights the need for multiple separate measures for different domains to be assessed if a multidimensional definition is not used to ensure that remission retains face validity for the patients.”
The addition of the inflammatory marker CRP in both remission and low disease activity measures (in DAPSA and PASDAS) did not have added value, suggesting that “the inclusion of CRP is unnecessary [since] a similar proportion of patients have a raised CRP in all definitions. … A target without an inflammatory marker will be more practical in clinical practice,” they said.
However, Dr. Coates and her colleagues stressed that the cut-off for acceptable disease activity is important because a stricter target may encourage the overtreatment of patients, which would result in increased side effects and costs.
“The ideal stringency of a target with assessment of residual disease in the various clinical domains of psoriatic arthritis should be a focus of research,” they wrote.
The original cohort of patients was supported with an unrestricted grant from Pfizer. Dr. Coates did not declare any conflicts, but several of her coauthors declared receiving speaker or consultancy fees from the pharmaceutical industry.
FROM ANNALS OF THE RHEUMATIC DISEASES
Key clinical point:
Major finding: Modified minimal disease activity measures were the most stringent targets for low disease activity in terms of residual disease in joints, skin, and entheses.
Data source: Cross-sectional study of 250 patients with psoriatic arthritis who were considered to be in an “acceptable disease state,” according to their rheumatologist.
Disclosures: The original cohort of patients was supported with an unrestricted grant from Pfizer. Dr. Coates did not declare any conflicts, but several of her coauthors declared receiving speaker or consultancy fees from the pharmaceutical industry.
Morbidly adherent placenta: A multidisciplinary approach
The rate of placenta accreta has been rising, almost certainly as a consequence of the increasing cesarean delivery rate. It is estimated that morbidly adherent placenta (placenta accreta, increta, and percreta) occurs today in approximately 1 in 500 pregnancies. Women who have had prior cesarean deliveries or other uterine surgery, such as myomectomy, are at higher risk.
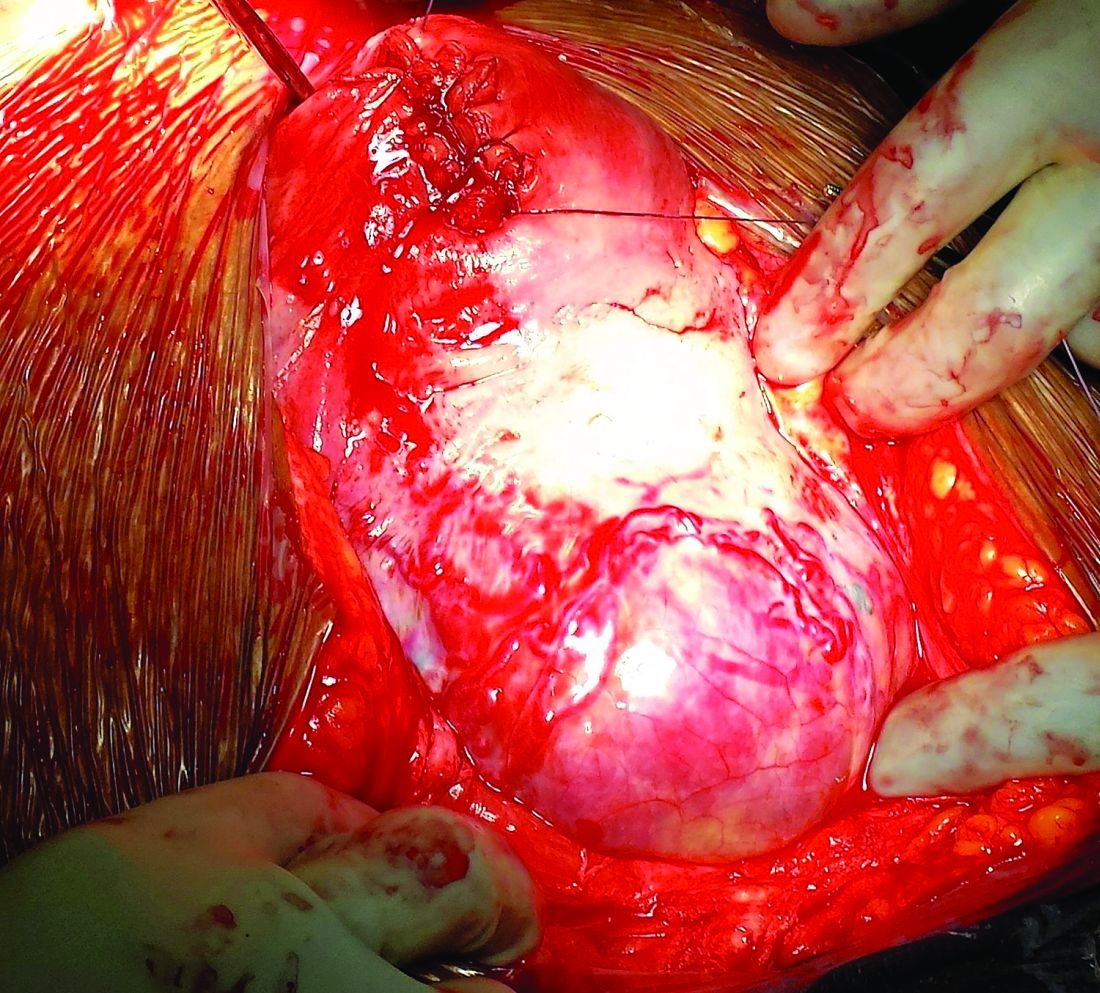
Morbidly adherent placenta (MAP) is associated with significant hemorrhage and morbidity – not only in cases of attempted placental removal, which is usually not advisable, but also in cases of cesarean hysterectomy. Cesarean hysterectomy is technically complex and completely different from other hysterectomies. The abnormal vasculature of MAP requires intricate, stepwise, vessel-by-vessel dissection and not only the uterine artery ligation that is the focus in hysterectomies performed for other indications.
In the last several years, we have demonstrated improved outcomes with such an approach at the University of Maryland, Baltimore. In 2014, we instituted a multidisciplinary complex obstetric surgery program for patients with MAP and others at high risk of intrapartum and postpartum complications. The program brings together obstetric anesthesiologists, the blood bank staff, the neonatal and surgical intensive care unit staff, vascular surgeons, perinatologists, interventional radiologists, urologists, and others.
Since the program was implemented, we have reduced our transfusion rate in patients with MAP by more than 60% while caring for increasing numbers of patients with the condition. We also have reduced the intensive care unit admission rate and improved overall surgical morbidity, including bladder complications. Moreover, our multidisciplinary approach is allowing us to develop more algorithms for management and to selectively take conservative approaches while also allowing us to lay the groundwork for future research.
The patients at risk
Anticipation is important: Identifying patient populations at high risk – and then evaluating individual risks – is essential for the prevention of delivery complications and the reduction of maternal morbidity.
Having had multiple cesarean deliveries – especially in pregnancies involving placenta previa – is one of the most important risk factors for developing MAP. One prospective cohort study of more than 30,000 women in 19 academic centers who had had cesarean deliveries found that, in cases of placenta previa, the risk of placenta accreta went from 3% after one cesarean delivery to 67% after five or more cesarean deliveries (Obstet Gynecol. 2006 Jun;107[6]:1226-32). Placenta accreta was defined in this study as the placenta’s being adherent to the uterine wall without easy separation. This definition included all forms of MAP.
Even without a history of placenta previa, patients who have had multiple cesarean deliveries – and developed consequent myometrial damage and scarring – should be evaluated for placental location during future pregnancies, as should patients who have had a myomectomy. A placenta that is anteriorly located in a patient who had a prior classical cesarean incision should also be thoroughly investigated. Overall, there is a risk of MAP whenever the placenta attaches to an area of uterine scarring.
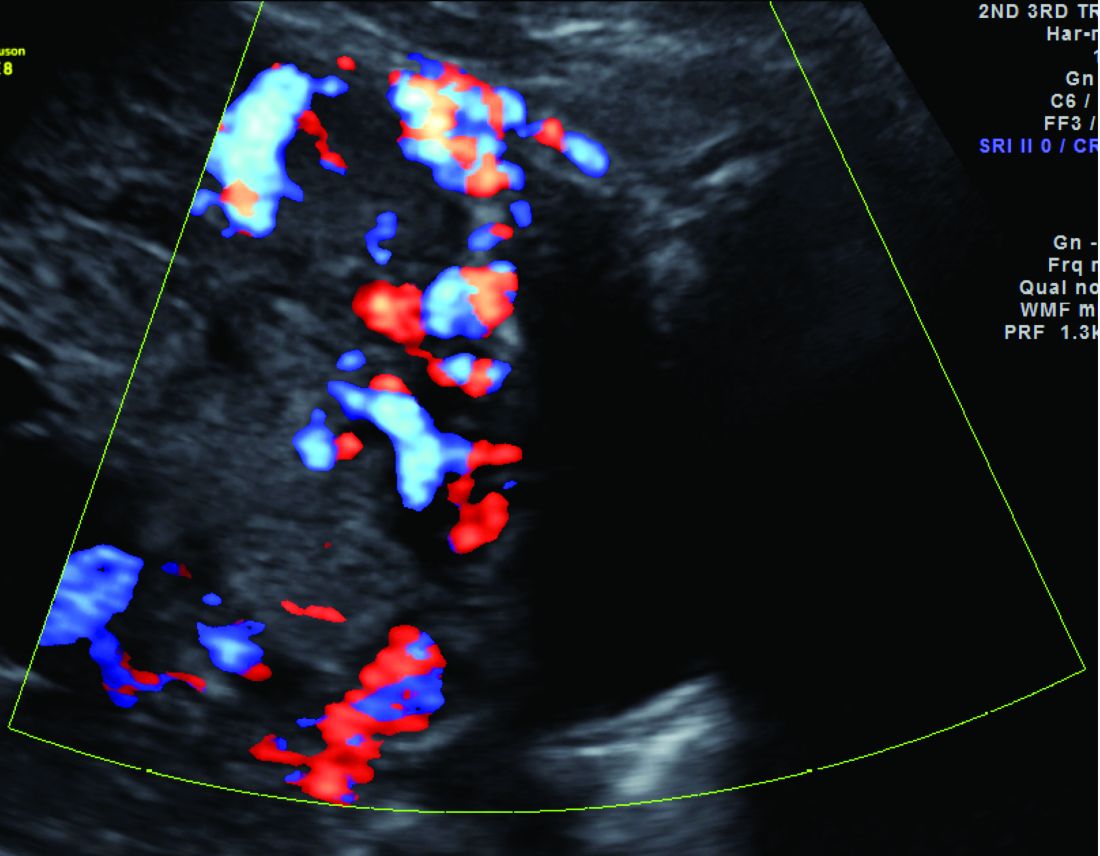
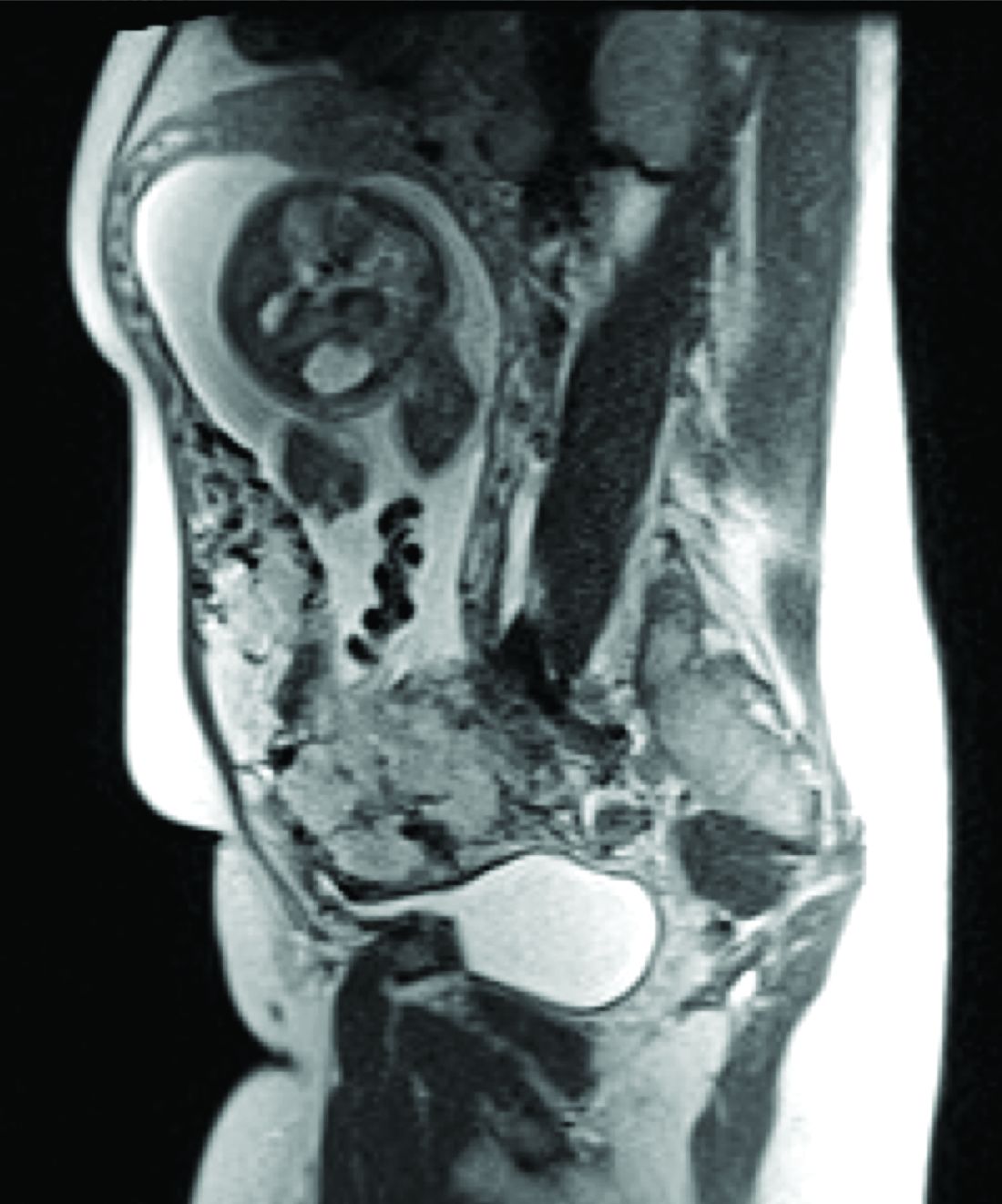
Diagnosis of MAP can be made – as best as is currently possible – by ultrasonography or by MRI, the latter of which is performed in high-risk or ambiguous cases to look more closely at the depth of placental growth.
Our outcomes and process
In our complex obstetric surgery program, we identify and evaluate patients at risk for developing MAP and also prepare comprehensive surgical plans. Each individual’s plan addresses the optimal timing of and conditions for delivery, how the patient and the team should prepare for high-quality perioperative care, and how possible complications and emergency surgery should be handled, such as who should be called in the case of emergency preterm delivery.
Indeed, research has shown that the value of a multidisciplinary approach is greatest when MAP is identified or suspected before delivery. For instance, investigators who analyzed the pregnancies complicated by placenta accreta in Utah over a 12-year period found that cases managed by a multidisciplinary care team had a 50% risk reduction for early morbidities, compared with cases managed with standard obstetric care. The benefits were even greater when placenta accreta (defined in the study to include the spectrum of MAP) was suspected before delivery; this group had a nearly 80% risk reduction with multidisciplinary care (Obstet Gynecol. 2011 Feb;117[2 Pt 1]:331-7).
We recently compared our outcomes before and after the multidisciplinary complex obstetric surgery program was established. For patients with MAP, estimated blood loss has decreased by 40%, and the use of blood products has fallen by 60%-70%, with a corresponding reduction in intensive care unit admission. Moreover, our bladder complication rate fell to 6% after program implementation. This and our reoperation rate, among other outcomes, are lower than published rates from other similar medical centers that use a multidisciplinary approach.
We strive to have two surgeons in the operating room – either two senior surgeons or one senior surgeon and one junior surgeon – as well as a separate “operation supervisor” who monitors blood loss (volume and sources), vital signs, and other clinical points and who is continually thinking about next steps. The operation supervisor is not necessarily a third surgeon but could be an experienced surgical nurse or an obstetric anesthesiologist.
Obstetric anesthesiologists and the blood bank staff have proven to be especially important parts of our multidisciplinary team. At 28-30 weeks’ gestation, each patient has an anesthesia consult and also is tested for blood type and screened for antibodies. Patients also are tested for anemia at this time so that it may be corrected if necessary before surgery.
As determined by our multidisciplinary team, all deliveries are performed under general anesthesia, with early placement of both a central venous catheter and a peripheral arterial line to enable rapid transfusions of blood or fluid. Patients are routinely placed in the dorsal lithotomy position, which enables direct access to the vagina and better assessment of vaginal bleeding. And, when significant blood loss is anticipated, the intensive care unit team prepares a bed, and our surgical colleagues are alerted.
Conservative management
Interest in conservative management – in avoiding hysterectomy when it is deemed to carry much higher risks of hemorrhage or injury to adjacent tissue than leaving the placenta in situ – has resurged in Europe. However, research is still in its infancy regarding the benefits and safety of conservative management, and clear guidance about eligibility and contraindications is still needed (Am J Obstet Gynecol. 2015 Dec;213[6]:755-60).
One patient with the placenta left in situ had an urgent hysterectomy within 2 hours of delivery because of vaginal bleeding, with the total blood loss within an acceptable range and without complications. Another required an urgent hysterectomy 6 weeks after delivery because of severe hemorrhaging. The remaining two had nonurgent hysterectomies at least 6 weeks later, with the total blood loss minimized by the period of recovery and by some spontaneous regression of the placental bulk.
As we have gained more experience with conservative management and spent more time shaping multidisciplinary protocols, it has become clear to us that programs must have in place excellent protocols and strict rules for monitoring and follow-up given the risks of life-threatening hemorrhage and other significant complications when the placenta is left in situ.
A conservative approach also may be preferred by women who desire fertility preservation. Currently, in such cases, we have performed segmental or local resection with uterine repair. We do not yet have any data on subsequent pregnancies.
Research conducted within the growing sphere of complex obstetric surgery should help us to improve decision making and management of MAP. For instance, we need better imaging techniques to more accurately predict MAP and show us the degree of placental invasion. A study published several years ago that blinded sonographers from information about patients’ clinical history and risk factors found significant interobserver variability for the diagnosis of placenta accreta and sensitivity (53.5%) that was significantly lower than previously described (J Ultrasound Med. 2014 Dec;33[12]:2153-8).
Dr. Turan’s stepwise dissection
In addition to a multidisciplinary approach, a meticulous dissection technique can help drive improved outcomes. The morbidly adherent placenta is a hypervascular organ; it recruits a host of blood vessels, largely from the vaginal arteries, superior vesical arteries, and vaginal venous plexus.
Moreover, in most cases, this vascular remodeling exacerbates vascular patterns that are distorted to begin with as a result of the scarring process following previous uterine surgery. Scarred tissue is already hypervascular.
I have found that most of the blood loss during hysterectomy occurs during dissection of the poorly defined interface between the lower uterine segment and the bladder and not during dissection of the uterine artery. Identification of the cleavage plane and ligation of each individual vessel using a bipolar or small hand-held desiccation device are key in reducing blood loss. This can take a significant amount of time but is well worth it.
Managing super morbid obesity
The number of pregnant women who require challenging obstetric surgeries is increasing, and this includes women with super morbid obesity (BMI greater than 50 kg/m2 or weight greater than 350 lb). Cesarean deliveries for these patients have proven to be much more complicated, involving special anesthesia needs, for instance.

In addition to women with placental implantation abnormalities (MAP and placenta previa, for instance) and those with extreme morbid obesity, the complex obstetric surgery program also aims to manage patients with increased risk for surgical morbidities based on previous surgery, patients whose fetuses require ex utero intrapartum treatment, and women who require abdominal cerclage.
Dr. Turan is director of fetal therapy and complex obstetric surgery at the University of Maryland, Baltimore, as well as an associate professor of obstetrics, gynecology, and reproductive sciences. He reported having no relevant financial disclosures.
The rate of placenta accreta has been rising, almost certainly as a consequence of the increasing cesarean delivery rate. It is estimated that morbidly adherent placenta (placenta accreta, increta, and percreta) occurs today in approximately 1 in 500 pregnancies. Women who have had prior cesarean deliveries or other uterine surgery, such as myomectomy, are at higher risk.
Morbidly adherent placenta (MAP) is associated with significant hemorrhage and morbidity – not only in cases of attempted placental removal, which is usually not advisable, but also in cases of cesarean hysterectomy. Cesarean hysterectomy is technically complex and completely different from other hysterectomies. The abnormal vasculature of MAP requires intricate, stepwise, vessel-by-vessel dissection and not only the uterine artery ligation that is the focus in hysterectomies performed for other indications.
In the last several years, we have demonstrated improved outcomes with such an approach at the University of Maryland, Baltimore. In 2014, we instituted a multidisciplinary complex obstetric surgery program for patients with MAP and others at high risk of intrapartum and postpartum complications. The program brings together obstetric anesthesiologists, the blood bank staff, the neonatal and surgical intensive care unit staff, vascular surgeons, perinatologists, interventional radiologists, urologists, and others.
Since the program was implemented, we have reduced our transfusion rate in patients with MAP by more than 60% while caring for increasing numbers of patients with the condition. We also have reduced the intensive care unit admission rate and improved overall surgical morbidity, including bladder complications. Moreover, our multidisciplinary approach is allowing us to develop more algorithms for management and to selectively take conservative approaches while also allowing us to lay the groundwork for future research.
The patients at risk
Anticipation is important: Identifying patient populations at high risk – and then evaluating individual risks – is essential for the prevention of delivery complications and the reduction of maternal morbidity.
Having had multiple cesarean deliveries – especially in pregnancies involving placenta previa – is one of the most important risk factors for developing MAP. One prospective cohort study of more than 30,000 women in 19 academic centers who had had cesarean deliveries found that, in cases of placenta previa, the risk of placenta accreta went from 3% after one cesarean delivery to 67% after five or more cesarean deliveries (Obstet Gynecol. 2006 Jun;107[6]:1226-32). Placenta accreta was defined in this study as the placenta’s being adherent to the uterine wall without easy separation. This definition included all forms of MAP.
Even without a history of placenta previa, patients who have had multiple cesarean deliveries – and developed consequent myometrial damage and scarring – should be evaluated for placental location during future pregnancies, as should patients who have had a myomectomy. A placenta that is anteriorly located in a patient who had a prior classical cesarean incision should also be thoroughly investigated. Overall, there is a risk of MAP whenever the placenta attaches to an area of uterine scarring.
Diagnosis of MAP can be made – as best as is currently possible – by ultrasonography or by MRI, the latter of which is performed in high-risk or ambiguous cases to look more closely at the depth of placental growth.
Our outcomes and process
In our complex obstetric surgery program, we identify and evaluate patients at risk for developing MAP and also prepare comprehensive surgical plans. Each individual’s plan addresses the optimal timing of and conditions for delivery, how the patient and the team should prepare for high-quality perioperative care, and how possible complications and emergency surgery should be handled, such as who should be called in the case of emergency preterm delivery.
Indeed, research has shown that the value of a multidisciplinary approach is greatest when MAP is identified or suspected before delivery. For instance, investigators who analyzed the pregnancies complicated by placenta accreta in Utah over a 12-year period found that cases managed by a multidisciplinary care team had a 50% risk reduction for early morbidities, compared with cases managed with standard obstetric care. The benefits were even greater when placenta accreta (defined in the study to include the spectrum of MAP) was suspected before delivery; this group had a nearly 80% risk reduction with multidisciplinary care (Obstet Gynecol. 2011 Feb;117[2 Pt 1]:331-7).
We recently compared our outcomes before and after the multidisciplinary complex obstetric surgery program was established. For patients with MAP, estimated blood loss has decreased by 40%, and the use of blood products has fallen by 60%-70%, with a corresponding reduction in intensive care unit admission. Moreover, our bladder complication rate fell to 6% after program implementation. This and our reoperation rate, among other outcomes, are lower than published rates from other similar medical centers that use a multidisciplinary approach.
We strive to have two surgeons in the operating room – either two senior surgeons or one senior surgeon and one junior surgeon – as well as a separate “operation supervisor” who monitors blood loss (volume and sources), vital signs, and other clinical points and who is continually thinking about next steps. The operation supervisor is not necessarily a third surgeon but could be an experienced surgical nurse or an obstetric anesthesiologist.
Obstetric anesthesiologists and the blood bank staff have proven to be especially important parts of our multidisciplinary team. At 28-30 weeks’ gestation, each patient has an anesthesia consult and also is tested for blood type and screened for antibodies. Patients also are tested for anemia at this time so that it may be corrected if necessary before surgery.
As determined by our multidisciplinary team, all deliveries are performed under general anesthesia, with early placement of both a central venous catheter and a peripheral arterial line to enable rapid transfusions of blood or fluid. Patients are routinely placed in the dorsal lithotomy position, which enables direct access to the vagina and better assessment of vaginal bleeding. And, when significant blood loss is anticipated, the intensive care unit team prepares a bed, and our surgical colleagues are alerted.
Conservative management
Interest in conservative management – in avoiding hysterectomy when it is deemed to carry much higher risks of hemorrhage or injury to adjacent tissue than leaving the placenta in situ – has resurged in Europe. However, research is still in its infancy regarding the benefits and safety of conservative management, and clear guidance about eligibility and contraindications is still needed (Am J Obstet Gynecol. 2015 Dec;213[6]:755-60).
One patient with the placenta left in situ had an urgent hysterectomy within 2 hours of delivery because of vaginal bleeding, with the total blood loss within an acceptable range and without complications. Another required an urgent hysterectomy 6 weeks after delivery because of severe hemorrhaging. The remaining two had nonurgent hysterectomies at least 6 weeks later, with the total blood loss minimized by the period of recovery and by some spontaneous regression of the placental bulk.
As we have gained more experience with conservative management and spent more time shaping multidisciplinary protocols, it has become clear to us that programs must have in place excellent protocols and strict rules for monitoring and follow-up given the risks of life-threatening hemorrhage and other significant complications when the placenta is left in situ.
A conservative approach also may be preferred by women who desire fertility preservation. Currently, in such cases, we have performed segmental or local resection with uterine repair. We do not yet have any data on subsequent pregnancies.
Research conducted within the growing sphere of complex obstetric surgery should help us to improve decision making and management of MAP. For instance, we need better imaging techniques to more accurately predict MAP and show us the degree of placental invasion. A study published several years ago that blinded sonographers from information about patients’ clinical history and risk factors found significant interobserver variability for the diagnosis of placenta accreta and sensitivity (53.5%) that was significantly lower than previously described (J Ultrasound Med. 2014 Dec;33[12]:2153-8).
Dr. Turan’s stepwise dissection
In addition to a multidisciplinary approach, a meticulous dissection technique can help drive improved outcomes. The morbidly adherent placenta is a hypervascular organ; it recruits a host of blood vessels, largely from the vaginal arteries, superior vesical arteries, and vaginal venous plexus.
Moreover, in most cases, this vascular remodeling exacerbates vascular patterns that are distorted to begin with as a result of the scarring process following previous uterine surgery. Scarred tissue is already hypervascular.
I have found that most of the blood loss during hysterectomy occurs during dissection of the poorly defined interface between the lower uterine segment and the bladder and not during dissection of the uterine artery. Identification of the cleavage plane and ligation of each individual vessel using a bipolar or small hand-held desiccation device are key in reducing blood loss. This can take a significant amount of time but is well worth it.
Managing super morbid obesity
The number of pregnant women who require challenging obstetric surgeries is increasing, and this includes women with super morbid obesity (BMI greater than 50 kg/m2 or weight greater than 350 lb). Cesarean deliveries for these patients have proven to be much more complicated, involving special anesthesia needs, for instance.
In addition to women with placental implantation abnormalities (MAP and placenta previa, for instance) and those with extreme morbid obesity, the complex obstetric surgery program also aims to manage patients with increased risk for surgical morbidities based on previous surgery, patients whose fetuses require ex utero intrapartum treatment, and women who require abdominal cerclage.
Dr. Turan is director of fetal therapy and complex obstetric surgery at the University of Maryland, Baltimore, as well as an associate professor of obstetrics, gynecology, and reproductive sciences. He reported having no relevant financial disclosures.
The rate of placenta accreta has been rising, almost certainly as a consequence of the increasing cesarean delivery rate. It is estimated that morbidly adherent placenta (placenta accreta, increta, and percreta) occurs today in approximately 1 in 500 pregnancies. Women who have had prior cesarean deliveries or other uterine surgery, such as myomectomy, are at higher risk.
Morbidly adherent placenta (MAP) is associated with significant hemorrhage and morbidity – not only in cases of attempted placental removal, which is usually not advisable, but also in cases of cesarean hysterectomy. Cesarean hysterectomy is technically complex and completely different from other hysterectomies. The abnormal vasculature of MAP requires intricate, stepwise, vessel-by-vessel dissection and not only the uterine artery ligation that is the focus in hysterectomies performed for other indications.
In the last several years, we have demonstrated improved outcomes with such an approach at the University of Maryland, Baltimore. In 2014, we instituted a multidisciplinary complex obstetric surgery program for patients with MAP and others at high risk of intrapartum and postpartum complications. The program brings together obstetric anesthesiologists, the blood bank staff, the neonatal and surgical intensive care unit staff, vascular surgeons, perinatologists, interventional radiologists, urologists, and others.
Since the program was implemented, we have reduced our transfusion rate in patients with MAP by more than 60% while caring for increasing numbers of patients with the condition. We also have reduced the intensive care unit admission rate and improved overall surgical morbidity, including bladder complications. Moreover, our multidisciplinary approach is allowing us to develop more algorithms for management and to selectively take conservative approaches while also allowing us to lay the groundwork for future research.
The patients at risk
Anticipation is important: Identifying patient populations at high risk – and then evaluating individual risks – is essential for the prevention of delivery complications and the reduction of maternal morbidity.
Having had multiple cesarean deliveries – especially in pregnancies involving placenta previa – is one of the most important risk factors for developing MAP. One prospective cohort study of more than 30,000 women in 19 academic centers who had had cesarean deliveries found that, in cases of placenta previa, the risk of placenta accreta went from 3% after one cesarean delivery to 67% after five or more cesarean deliveries (Obstet Gynecol. 2006 Jun;107[6]:1226-32). Placenta accreta was defined in this study as the placenta’s being adherent to the uterine wall without easy separation. This definition included all forms of MAP.
Even without a history of placenta previa, patients who have had multiple cesarean deliveries – and developed consequent myometrial damage and scarring – should be evaluated for placental location during future pregnancies, as should patients who have had a myomectomy. A placenta that is anteriorly located in a patient who had a prior classical cesarean incision should also be thoroughly investigated. Overall, there is a risk of MAP whenever the placenta attaches to an area of uterine scarring.
Diagnosis of MAP can be made – as best as is currently possible – by ultrasonography or by MRI, the latter of which is performed in high-risk or ambiguous cases to look more closely at the depth of placental growth.
Our outcomes and process
In our complex obstetric surgery program, we identify and evaluate patients at risk for developing MAP and also prepare comprehensive surgical plans. Each individual’s plan addresses the optimal timing of and conditions for delivery, how the patient and the team should prepare for high-quality perioperative care, and how possible complications and emergency surgery should be handled, such as who should be called in the case of emergency preterm delivery.
Indeed, research has shown that the value of a multidisciplinary approach is greatest when MAP is identified or suspected before delivery. For instance, investigators who analyzed the pregnancies complicated by placenta accreta in Utah over a 12-year period found that cases managed by a multidisciplinary care team had a 50% risk reduction for early morbidities, compared with cases managed with standard obstetric care. The benefits were even greater when placenta accreta (defined in the study to include the spectrum of MAP) was suspected before delivery; this group had a nearly 80% risk reduction with multidisciplinary care (Obstet Gynecol. 2011 Feb;117[2 Pt 1]:331-7).
We recently compared our outcomes before and after the multidisciplinary complex obstetric surgery program was established. For patients with MAP, estimated blood loss has decreased by 40%, and the use of blood products has fallen by 60%-70%, with a corresponding reduction in intensive care unit admission. Moreover, our bladder complication rate fell to 6% after program implementation. This and our reoperation rate, among other outcomes, are lower than published rates from other similar medical centers that use a multidisciplinary approach.
We strive to have two surgeons in the operating room – either two senior surgeons or one senior surgeon and one junior surgeon – as well as a separate “operation supervisor” who monitors blood loss (volume and sources), vital signs, and other clinical points and who is continually thinking about next steps. The operation supervisor is not necessarily a third surgeon but could be an experienced surgical nurse or an obstetric anesthesiologist.
Obstetric anesthesiologists and the blood bank staff have proven to be especially important parts of our multidisciplinary team. At 28-30 weeks’ gestation, each patient has an anesthesia consult and also is tested for blood type and screened for antibodies. Patients also are tested for anemia at this time so that it may be corrected if necessary before surgery.
As determined by our multidisciplinary team, all deliveries are performed under general anesthesia, with early placement of both a central venous catheter and a peripheral arterial line to enable rapid transfusions of blood or fluid. Patients are routinely placed in the dorsal lithotomy position, which enables direct access to the vagina and better assessment of vaginal bleeding. And, when significant blood loss is anticipated, the intensive care unit team prepares a bed, and our surgical colleagues are alerted.
Conservative management
Interest in conservative management – in avoiding hysterectomy when it is deemed to carry much higher risks of hemorrhage or injury to adjacent tissue than leaving the placenta in situ – has resurged in Europe. However, research is still in its infancy regarding the benefits and safety of conservative management, and clear guidance about eligibility and contraindications is still needed (Am J Obstet Gynecol. 2015 Dec;213[6]:755-60).
One patient with the placenta left in situ had an urgent hysterectomy within 2 hours of delivery because of vaginal bleeding, with the total blood loss within an acceptable range and without complications. Another required an urgent hysterectomy 6 weeks after delivery because of severe hemorrhaging. The remaining two had nonurgent hysterectomies at least 6 weeks later, with the total blood loss minimized by the period of recovery and by some spontaneous regression of the placental bulk.
As we have gained more experience with conservative management and spent more time shaping multidisciplinary protocols, it has become clear to us that programs must have in place excellent protocols and strict rules for monitoring and follow-up given the risks of life-threatening hemorrhage and other significant complications when the placenta is left in situ.
A conservative approach also may be preferred by women who desire fertility preservation. Currently, in such cases, we have performed segmental or local resection with uterine repair. We do not yet have any data on subsequent pregnancies.
Research conducted within the growing sphere of complex obstetric surgery should help us to improve decision making and management of MAP. For instance, we need better imaging techniques to more accurately predict MAP and show us the degree of placental invasion. A study published several years ago that blinded sonographers from information about patients’ clinical history and risk factors found significant interobserver variability for the diagnosis of placenta accreta and sensitivity (53.5%) that was significantly lower than previously described (J Ultrasound Med. 2014 Dec;33[12]:2153-8).
Dr. Turan’s stepwise dissection
In addition to a multidisciplinary approach, a meticulous dissection technique can help drive improved outcomes. The morbidly adherent placenta is a hypervascular organ; it recruits a host of blood vessels, largely from the vaginal arteries, superior vesical arteries, and vaginal venous plexus.
Moreover, in most cases, this vascular remodeling exacerbates vascular patterns that are distorted to begin with as a result of the scarring process following previous uterine surgery. Scarred tissue is already hypervascular.
I have found that most of the blood loss during hysterectomy occurs during dissection of the poorly defined interface between the lower uterine segment and the bladder and not during dissection of the uterine artery. Identification of the cleavage plane and ligation of each individual vessel using a bipolar or small hand-held desiccation device are key in reducing blood loss. This can take a significant amount of time but is well worth it.
Managing super morbid obesity
The number of pregnant women who require challenging obstetric surgeries is increasing, and this includes women with super morbid obesity (BMI greater than 50 kg/m2 or weight greater than 350 lb). Cesarean deliveries for these patients have proven to be much more complicated, involving special anesthesia needs, for instance.
In addition to women with placental implantation abnormalities (MAP and placenta previa, for instance) and those with extreme morbid obesity, the complex obstetric surgery program also aims to manage patients with increased risk for surgical morbidities based on previous surgery, patients whose fetuses require ex utero intrapartum treatment, and women who require abdominal cerclage.
Dr. Turan is director of fetal therapy and complex obstetric surgery at the University of Maryland, Baltimore, as well as an associate professor of obstetrics, gynecology, and reproductive sciences. He reported having no relevant financial disclosures.
Multidisciplinary teams offer key to complex deliveries
Medical practice has evolved, and will continue to do so, as we begin pushing for more personalized and better precision health care. Gone are the days of the general practitioner who attempted to treat all conditions in all patients. Health care is now so complex that not only specialists but also so-called superspecialists are needed to manage complicated cases successfully.
One of the biggest challenges, and greatest opportunities, in ob.gyn. is the need to establish a multidisciplinary health team to the address the needs of today’s patients. More than ever, we are working with patients with advanced maternal age having their first pregnancies. More than ever, we are managing patients who have preexisting diabetes and are concurrently overweight or obese. More than ever, our patients are having multiple cesarean deliveries. More than ever, our patients are hoping – perhaps even expecting – to retain their fertility after a complicated delivery. More than ever, a single patient may need the guidance and care of not just an ob.gyn. or maternal-fetal medicine subspecialist but also an endocrinologist, cardiologist, diabetologist, genetic counselor, nutritionist – the list could go on.

The emergence and continued growth of personalized and preventive medicine in the very near future will catalyze fundamental changes at many different levels in health care and health systems. The need to establish multidisciplinary care teams is already apparent in ob.gyn. but is especially necessary in helping patients who experience complicated deliveries that could jeopardize their immediate and long-term health and fertility.
This month, we have invited M. Ozhan Turan, MD, PhD, the director of fetal therapy and complex obstetric surgery at the University of Maryland, Baltimore, to discuss the use of a multidisciplinary team in the management of patients with placenta accreta and other forms of morbidly adherent placenta.
Dr. Reece, who specializes in maternal-fetal medicine, is vice president for medical affairs at the University of Maryland, Baltimore, as well as the John Z. and Akiko K. Bowers Distinguished Professor and dean of the school of medicine. Dr. Reece said he had no relevant financial disclosures. He is the medical editor of this column.
Medical practice has evolved, and will continue to do so, as we begin pushing for more personalized and better precision health care. Gone are the days of the general practitioner who attempted to treat all conditions in all patients. Health care is now so complex that not only specialists but also so-called superspecialists are needed to manage complicated cases successfully.
One of the biggest challenges, and greatest opportunities, in ob.gyn. is the need to establish a multidisciplinary health team to the address the needs of today’s patients. More than ever, we are working with patients with advanced maternal age having their first pregnancies. More than ever, we are managing patients who have preexisting diabetes and are concurrently overweight or obese. More than ever, our patients are having multiple cesarean deliveries. More than ever, our patients are hoping – perhaps even expecting – to retain their fertility after a complicated delivery. More than ever, a single patient may need the guidance and care of not just an ob.gyn. or maternal-fetal medicine subspecialist but also an endocrinologist, cardiologist, diabetologist, genetic counselor, nutritionist – the list could go on.
The emergence and continued growth of personalized and preventive medicine in the very near future will catalyze fundamental changes at many different levels in health care and health systems. The need to establish multidisciplinary care teams is already apparent in ob.gyn. but is especially necessary in helping patients who experience complicated deliveries that could jeopardize their immediate and long-term health and fertility.
This month, we have invited M. Ozhan Turan, MD, PhD, the director of fetal therapy and complex obstetric surgery at the University of Maryland, Baltimore, to discuss the use of a multidisciplinary team in the management of patients with placenta accreta and other forms of morbidly adherent placenta.
Dr. Reece, who specializes in maternal-fetal medicine, is vice president for medical affairs at the University of Maryland, Baltimore, as well as the John Z. and Akiko K. Bowers Distinguished Professor and dean of the school of medicine. Dr. Reece said he had no relevant financial disclosures. He is the medical editor of this column.
Medical practice has evolved, and will continue to do so, as we begin pushing for more personalized and better precision health care. Gone are the days of the general practitioner who attempted to treat all conditions in all patients. Health care is now so complex that not only specialists but also so-called superspecialists are needed to manage complicated cases successfully.
One of the biggest challenges, and greatest opportunities, in ob.gyn. is the need to establish a multidisciplinary health team to the address the needs of today’s patients. More than ever, we are working with patients with advanced maternal age having their first pregnancies. More than ever, we are managing patients who have preexisting diabetes and are concurrently overweight or obese. More than ever, our patients are having multiple cesarean deliveries. More than ever, our patients are hoping – perhaps even expecting – to retain their fertility after a complicated delivery. More than ever, a single patient may need the guidance and care of not just an ob.gyn. or maternal-fetal medicine subspecialist but also an endocrinologist, cardiologist, diabetologist, genetic counselor, nutritionist – the list could go on.
The emergence and continued growth of personalized and preventive medicine in the very near future will catalyze fundamental changes at many different levels in health care and health systems. The need to establish multidisciplinary care teams is already apparent in ob.gyn. but is especially necessary in helping patients who experience complicated deliveries that could jeopardize their immediate and long-term health and fertility.
This month, we have invited M. Ozhan Turan, MD, PhD, the director of fetal therapy and complex obstetric surgery at the University of Maryland, Baltimore, to discuss the use of a multidisciplinary team in the management of patients with placenta accreta and other forms of morbidly adherent placenta.
Dr. Reece, who specializes in maternal-fetal medicine, is vice president for medical affairs at the University of Maryland, Baltimore, as well as the John Z. and Akiko K. Bowers Distinguished Professor and dean of the school of medicine. Dr. Reece said he had no relevant financial disclosures. He is the medical editor of this column.
Strategies to evaluate postmenopausal bleeding
Postmenopausal bleeding is a symptom that can announce the presence of a gynecologic malignancy. In this column, we will discuss the important considerations to make in the work-up of this symptom.
Roughly 10% of women will present for evaluation of postmenopausal bleeding.1 More than a third of these women will have benign pathology, with the incidence of endometrial cancer in this group at only about 5%.2 Other gynecologic malignancies should be considered as well, including cervical, vaginal, vulvar, and more rarely, those of the fallopian tubes or ovaries.

Use of ultrasound
Ultrasound is a commonly performed initial approach to work-up because of its noninvasive nature. Transvaginal ultrasound has a high negative predictive value of 99.4%-100% in ruling out malignancy.3 Among women with postmenopausal bleeding, the risk of cancer is 7.3% if their endometrial lining is 5 mm or greater and less than 0.07% risk if their lining is 4 mm or less. Therefore, this cutoff dimension is typically used to triage patients to additional sampling.
If ultrasound is performed on postmenopausal women who are asymptomatic (no bleeding), then an endometrial stripe of greater than 11 mm is considered justification for further work-up and is associated with a 6.7% risk of endometrial cancer.4 If the ultrasound reveals intracavitary lesions, a sonohysterogram would be preferred to characterize intrauterine pathology. In fact, sonohysterography is superior to transvaginal ultrasound (with a sensitivity of 80% vs. 49%, respectively) in detecting endometrial polypoid lesions.5 Preoperative identification of an intracavitary lesion may assist in selecting the best sampling technique (blind vs. hysteroscopy-guided approach).
Endometrial sampling
If an ultrasound reveals a thickened or unevaluable endometrial stripe or if the clinician chooses to proceed directly with diagnostic confirmation, several options for endometrial sampling exist, including office-based or operative procedures, as well as blind or visually guided ones. Endometrial pipelle biopsy, D&C without hysteroscopy, endometrial lavage, and endometrial brush biopsy all constitute “blind” sampling techniques. Targeted biopsy techniques include hysteroscopy D&C and saline infusion sonohysterography–guided biopsy.
Blind D&C
Although D&C may be considered the gold standard of diagnostic sampling techniques, it should be noted that 60% of these procedures sample less than half of the endometrium.6 When used in conjunction with hysteroscopy, the sensitivity in detecting cancer is high at 97% with a specificity of 93%-100%.7
While some patients are candidates for office-based procedures, D&C often requires regional or general anesthesia and is frequently performed in a hospital-based environment or surgical center. This may be most appropriate for patients who have had failed office attempts at sampling, have multiple medical comorbidities that limit the feasibility of office-based procedures (such as morbid obesity), or have severe cervical stenosis. D&C is associated with an increased risk for uterine perforation, compared with outpatient sampling procedures.
The need to go to the operating room rather than to an ambulatory setting also may increase the costs borne by the patient. The advantages of D&C include the potential for large-volume sampling and the potentially therapeutic nature of the procedure in cases of benign pathology.
Office-based procedures
Office-based sampling techniques include those using a pipelle, those employing an endometrial brush, and those guided by saline infusion sonohysterography. If performed in the office, they require minimal or no cervical dilation, are associated with a lower risk of perforation or adverse reaction to anesthesia, and usually have lower costs for patients.
Endometrial pipelle biopsies are a very effective diagnostic tool when there is global, endometrial pathology; they have a sensitivity of 83% in confirming cancer.8 It is an inexpensive and technically straightforward technique that can be easily performed in an office setting.
However, when the endometrial lining is atrophied, alternative tools may provide superior results. Endometrial brushes have been shown to be 33% more successful in collecting adequate samples,compared with pipelles, because they sample a larger endometrial surface area.9
There is ongoing development of sampling techniques, such as endometrial lavage or the combination of saline infusion sonohysterography and endometrial biopsy.10 However, future studies regarding accuracy, cost, and patient acceptability are needed before these techniques are translated to the clinical setting.
Targeted endometrial sampling
Targeted or visually guided sampling, such as hysteroscopy, has been shown to be very accurate in identifying benign pathology, although the sensitivity of hysteroscopic diagnosis of cancer is significantly lower at approximately 50%.11 Therefore, the benefit of hysteroscopy is in complementing the blind nature of D&C by guiding sampling of intracavitary lesions, should they exist.
Hysteroscopy is safe in endometrial cancer and is not associated with upstaging the cancer from transtubal extirpation of malignant cells.12
The addition of hysteroscopy contributes some cost and equipment to the blind D&C procedure; therefore, it might be best applied in cases where there is known intracavitary pathology or inadequate prior sampling. In well-selected patients, hysteroscopy often can be used in an office setting, which improves the practicality of the procedure. Smaller and, in some cases, disposable equipment aids in the feasibility of adding visual guidance to office sampling.
Optimizing sampling
Postmenopausal women have a higher risk for sampling failure, compared with younger women. Obesity also is a risk for failed sampling.13 Cervical ripening with misoprostol may increase access to the endometrial cavity, and ultrasound guidance may decrease the risk of uterine perforation in a stenotic cervix.
Clinicians should ensure that histology results are concordant with clinical data. Discordant results should be reevaluated. For example, if an ultrasound demonstrates a thickened endometrial stripe, but the sampling reveals “scant atrophic tissue,” then there is unexplained pathology to address. Further work-up, such as more comprehensive sampling with hysteroscopy, should be considered in such cases. Additionally, persistent postmenopausal bleeding, despite a benign endometrial biopsy, should be reevaluated over time to rule out occult disease missed during prior sampling.
Clinicians are now equipped with multiple ways of obtaining clinical data, and patients have options that may decrease barriers to their care. Hysteroscopy does not improve upon D&C in the diagnosis of endometrial cancer, although it may be helpful in distinguishing and treating nonmalignant lesions.
Dr. Cotangco is a resident in the department of obstetrics and gynecology at the University of Illinois, Chicago. Dr. Rossi is an assistant professor in the division of gynecologic oncology at the University of North Carolina, Chapel Hill. They reported having no relevant financial disclosures.
References
1. Acta Obstet Gynecol Scand. 2004 Feb;83(2):203-7.
2. Menopause Int. 2010 Mar;16(1):5-8.
3. Obstet Gynecol. 2009 Aug;114(2 Pt 1):409-11.
4. Ultrasound Obstet Gynecol. 2004 Oct;24(5):558-65.
5. Ultrasound Obstet Gynecol. 2001 Aug;18(2):157-62.
6. Am J Obstet Gynecol. 2009 Jul;201(1):5-11.
7. Obstet Gynecol Clin North Am. 2000 Jun;27(2):235-44.
8. J Reprod Med. 1995 Aug;40(8):553-5.
9. BJOG. 2008 Jul;115(8):1028-36.
10. PLoS Med. 2016 Dec. doi: 10.1371/journal.pmed.1002206.
11. Arch Gynecol Obstet. 2012 Mar;285(3):839-43.
12. Am J Obstet Gynecol. 2012 Jul;207(1):71.e1-5.
13. Gynecol Oncol. 2017 Feb;144(2):324-8.
Postmenopausal bleeding is a symptom that can announce the presence of a gynecologic malignancy. In this column, we will discuss the important considerations to make in the work-up of this symptom.
Roughly 10% of women will present for evaluation of postmenopausal bleeding.1 More than a third of these women will have benign pathology, with the incidence of endometrial cancer in this group at only about 5%.2 Other gynecologic malignancies should be considered as well, including cervical, vaginal, vulvar, and more rarely, those of the fallopian tubes or ovaries.
Use of ultrasound
Ultrasound is a commonly performed initial approach to work-up because of its noninvasive nature. Transvaginal ultrasound has a high negative predictive value of 99.4%-100% in ruling out malignancy.3 Among women with postmenopausal bleeding, the risk of cancer is 7.3% if their endometrial lining is 5 mm or greater and less than 0.07% risk if their lining is 4 mm or less. Therefore, this cutoff dimension is typically used to triage patients to additional sampling.
If ultrasound is performed on postmenopausal women who are asymptomatic (no bleeding), then an endometrial stripe of greater than 11 mm is considered justification for further work-up and is associated with a 6.7% risk of endometrial cancer.4 If the ultrasound reveals intracavitary lesions, a sonohysterogram would be preferred to characterize intrauterine pathology. In fact, sonohysterography is superior to transvaginal ultrasound (with a sensitivity of 80% vs. 49%, respectively) in detecting endometrial polypoid lesions.5 Preoperative identification of an intracavitary lesion may assist in selecting the best sampling technique (blind vs. hysteroscopy-guided approach).
Endometrial sampling
If an ultrasound reveals a thickened or unevaluable endometrial stripe or if the clinician chooses to proceed directly with diagnostic confirmation, several options for endometrial sampling exist, including office-based or operative procedures, as well as blind or visually guided ones. Endometrial pipelle biopsy, D&C without hysteroscopy, endometrial lavage, and endometrial brush biopsy all constitute “blind” sampling techniques. Targeted biopsy techniques include hysteroscopy D&C and saline infusion sonohysterography–guided biopsy.
Blind D&C
Although D&C may be considered the gold standard of diagnostic sampling techniques, it should be noted that 60% of these procedures sample less than half of the endometrium.6 When used in conjunction with hysteroscopy, the sensitivity in detecting cancer is high at 97% with a specificity of 93%-100%.7
While some patients are candidates for office-based procedures, D&C often requires regional or general anesthesia and is frequently performed in a hospital-based environment or surgical center. This may be most appropriate for patients who have had failed office attempts at sampling, have multiple medical comorbidities that limit the feasibility of office-based procedures (such as morbid obesity), or have severe cervical stenosis. D&C is associated with an increased risk for uterine perforation, compared with outpatient sampling procedures.
The need to go to the operating room rather than to an ambulatory setting also may increase the costs borne by the patient. The advantages of D&C include the potential for large-volume sampling and the potentially therapeutic nature of the procedure in cases of benign pathology.
Office-based procedures
Office-based sampling techniques include those using a pipelle, those employing an endometrial brush, and those guided by saline infusion sonohysterography. If performed in the office, they require minimal or no cervical dilation, are associated with a lower risk of perforation or adverse reaction to anesthesia, and usually have lower costs for patients.
Endometrial pipelle biopsies are a very effective diagnostic tool when there is global, endometrial pathology; they have a sensitivity of 83% in confirming cancer.8 It is an inexpensive and technically straightforward technique that can be easily performed in an office setting.
However, when the endometrial lining is atrophied, alternative tools may provide superior results. Endometrial brushes have been shown to be 33% more successful in collecting adequate samples,compared with pipelles, because they sample a larger endometrial surface area.9
There is ongoing development of sampling techniques, such as endometrial lavage or the combination of saline infusion sonohysterography and endometrial biopsy.10 However, future studies regarding accuracy, cost, and patient acceptability are needed before these techniques are translated to the clinical setting.
Targeted endometrial sampling
Targeted or visually guided sampling, such as hysteroscopy, has been shown to be very accurate in identifying benign pathology, although the sensitivity of hysteroscopic diagnosis of cancer is significantly lower at approximately 50%.11 Therefore, the benefit of hysteroscopy is in complementing the blind nature of D&C by guiding sampling of intracavitary lesions, should they exist.
Hysteroscopy is safe in endometrial cancer and is not associated with upstaging the cancer from transtubal extirpation of malignant cells.12
The addition of hysteroscopy contributes some cost and equipment to the blind D&C procedure; therefore, it might be best applied in cases where there is known intracavitary pathology or inadequate prior sampling. In well-selected patients, hysteroscopy often can be used in an office setting, which improves the practicality of the procedure. Smaller and, in some cases, disposable equipment aids in the feasibility of adding visual guidance to office sampling.
Optimizing sampling
Postmenopausal women have a higher risk for sampling failure, compared with younger women. Obesity also is a risk for failed sampling.13 Cervical ripening with misoprostol may increase access to the endometrial cavity, and ultrasound guidance may decrease the risk of uterine perforation in a stenotic cervix.
Clinicians should ensure that histology results are concordant with clinical data. Discordant results should be reevaluated. For example, if an ultrasound demonstrates a thickened endometrial stripe, but the sampling reveals “scant atrophic tissue,” then there is unexplained pathology to address. Further work-up, such as more comprehensive sampling with hysteroscopy, should be considered in such cases. Additionally, persistent postmenopausal bleeding, despite a benign endometrial biopsy, should be reevaluated over time to rule out occult disease missed during prior sampling.
Clinicians are now equipped with multiple ways of obtaining clinical data, and patients have options that may decrease barriers to their care. Hysteroscopy does not improve upon D&C in the diagnosis of endometrial cancer, although it may be helpful in distinguishing and treating nonmalignant lesions.
Dr. Cotangco is a resident in the department of obstetrics and gynecology at the University of Illinois, Chicago. Dr. Rossi is an assistant professor in the division of gynecologic oncology at the University of North Carolina, Chapel Hill. They reported having no relevant financial disclosures.
References
1. Acta Obstet Gynecol Scand. 2004 Feb;83(2):203-7.
2. Menopause Int. 2010 Mar;16(1):5-8.
3. Obstet Gynecol. 2009 Aug;114(2 Pt 1):409-11.
4. Ultrasound Obstet Gynecol. 2004 Oct;24(5):558-65.
5. Ultrasound Obstet Gynecol. 2001 Aug;18(2):157-62.
6. Am J Obstet Gynecol. 2009 Jul;201(1):5-11.
7. Obstet Gynecol Clin North Am. 2000 Jun;27(2):235-44.
8. J Reprod Med. 1995 Aug;40(8):553-5.
9. BJOG. 2008 Jul;115(8):1028-36.
10. PLoS Med. 2016 Dec. doi: 10.1371/journal.pmed.1002206.
11. Arch Gynecol Obstet. 2012 Mar;285(3):839-43.
12. Am J Obstet Gynecol. 2012 Jul;207(1):71.e1-5.
13. Gynecol Oncol. 2017 Feb;144(2):324-8.
Postmenopausal bleeding is a symptom that can announce the presence of a gynecologic malignancy. In this column, we will discuss the important considerations to make in the work-up of this symptom.
Roughly 10% of women will present for evaluation of postmenopausal bleeding.1 More than a third of these women will have benign pathology, with the incidence of endometrial cancer in this group at only about 5%.2 Other gynecologic malignancies should be considered as well, including cervical, vaginal, vulvar, and more rarely, those of the fallopian tubes or ovaries.
Use of ultrasound
Ultrasound is a commonly performed initial approach to work-up because of its noninvasive nature. Transvaginal ultrasound has a high negative predictive value of 99.4%-100% in ruling out malignancy.3 Among women with postmenopausal bleeding, the risk of cancer is 7.3% if their endometrial lining is 5 mm or greater and less than 0.07% risk if their lining is 4 mm or less. Therefore, this cutoff dimension is typically used to triage patients to additional sampling.
If ultrasound is performed on postmenopausal women who are asymptomatic (no bleeding), then an endometrial stripe of greater than 11 mm is considered justification for further work-up and is associated with a 6.7% risk of endometrial cancer.4 If the ultrasound reveals intracavitary lesions, a sonohysterogram would be preferred to characterize intrauterine pathology. In fact, sonohysterography is superior to transvaginal ultrasound (with a sensitivity of 80% vs. 49%, respectively) in detecting endometrial polypoid lesions.5 Preoperative identification of an intracavitary lesion may assist in selecting the best sampling technique (blind vs. hysteroscopy-guided approach).
Endometrial sampling
If an ultrasound reveals a thickened or unevaluable endometrial stripe or if the clinician chooses to proceed directly with diagnostic confirmation, several options for endometrial sampling exist, including office-based or operative procedures, as well as blind or visually guided ones. Endometrial pipelle biopsy, D&C without hysteroscopy, endometrial lavage, and endometrial brush biopsy all constitute “blind” sampling techniques. Targeted biopsy techniques include hysteroscopy D&C and saline infusion sonohysterography–guided biopsy.
Blind D&C
Although D&C may be considered the gold standard of diagnostic sampling techniques, it should be noted that 60% of these procedures sample less than half of the endometrium.6 When used in conjunction with hysteroscopy, the sensitivity in detecting cancer is high at 97% with a specificity of 93%-100%.7
While some patients are candidates for office-based procedures, D&C often requires regional or general anesthesia and is frequently performed in a hospital-based environment or surgical center. This may be most appropriate for patients who have had failed office attempts at sampling, have multiple medical comorbidities that limit the feasibility of office-based procedures (such as morbid obesity), or have severe cervical stenosis. D&C is associated with an increased risk for uterine perforation, compared with outpatient sampling procedures.
The need to go to the operating room rather than to an ambulatory setting also may increase the costs borne by the patient. The advantages of D&C include the potential for large-volume sampling and the potentially therapeutic nature of the procedure in cases of benign pathology.
Office-based procedures
Office-based sampling techniques include those using a pipelle, those employing an endometrial brush, and those guided by saline infusion sonohysterography. If performed in the office, they require minimal or no cervical dilation, are associated with a lower risk of perforation or adverse reaction to anesthesia, and usually have lower costs for patients.
Endometrial pipelle biopsies are a very effective diagnostic tool when there is global, endometrial pathology; they have a sensitivity of 83% in confirming cancer.8 It is an inexpensive and technically straightforward technique that can be easily performed in an office setting.
However, when the endometrial lining is atrophied, alternative tools may provide superior results. Endometrial brushes have been shown to be 33% more successful in collecting adequate samples,compared with pipelles, because they sample a larger endometrial surface area.9
There is ongoing development of sampling techniques, such as endometrial lavage or the combination of saline infusion sonohysterography and endometrial biopsy.10 However, future studies regarding accuracy, cost, and patient acceptability are needed before these techniques are translated to the clinical setting.
Targeted endometrial sampling
Targeted or visually guided sampling, such as hysteroscopy, has been shown to be very accurate in identifying benign pathology, although the sensitivity of hysteroscopic diagnosis of cancer is significantly lower at approximately 50%.11 Therefore, the benefit of hysteroscopy is in complementing the blind nature of D&C by guiding sampling of intracavitary lesions, should they exist.
Hysteroscopy is safe in endometrial cancer and is not associated with upstaging the cancer from transtubal extirpation of malignant cells.12
The addition of hysteroscopy contributes some cost and equipment to the blind D&C procedure; therefore, it might be best applied in cases where there is known intracavitary pathology or inadequate prior sampling. In well-selected patients, hysteroscopy often can be used in an office setting, which improves the practicality of the procedure. Smaller and, in some cases, disposable equipment aids in the feasibility of adding visual guidance to office sampling.
Optimizing sampling
Postmenopausal women have a higher risk for sampling failure, compared with younger women. Obesity also is a risk for failed sampling.13 Cervical ripening with misoprostol may increase access to the endometrial cavity, and ultrasound guidance may decrease the risk of uterine perforation in a stenotic cervix.
Clinicians should ensure that histology results are concordant with clinical data. Discordant results should be reevaluated. For example, if an ultrasound demonstrates a thickened endometrial stripe, but the sampling reveals “scant atrophic tissue,” then there is unexplained pathology to address. Further work-up, such as more comprehensive sampling with hysteroscopy, should be considered in such cases. Additionally, persistent postmenopausal bleeding, despite a benign endometrial biopsy, should be reevaluated over time to rule out occult disease missed during prior sampling.
Clinicians are now equipped with multiple ways of obtaining clinical data, and patients have options that may decrease barriers to their care. Hysteroscopy does not improve upon D&C in the diagnosis of endometrial cancer, although it may be helpful in distinguishing and treating nonmalignant lesions.
Dr. Cotangco is a resident in the department of obstetrics and gynecology at the University of Illinois, Chicago. Dr. Rossi is an assistant professor in the division of gynecologic oncology at the University of North Carolina, Chapel Hill. They reported having no relevant financial disclosures.
References
1. Acta Obstet Gynecol Scand. 2004 Feb;83(2):203-7.
2. Menopause Int. 2010 Mar;16(1):5-8.
3. Obstet Gynecol. 2009 Aug;114(2 Pt 1):409-11.
4. Ultrasound Obstet Gynecol. 2004 Oct;24(5):558-65.
5. Ultrasound Obstet Gynecol. 2001 Aug;18(2):157-62.
6. Am J Obstet Gynecol. 2009 Jul;201(1):5-11.
7. Obstet Gynecol Clin North Am. 2000 Jun;27(2):235-44.
8. J Reprod Med. 1995 Aug;40(8):553-5.
9. BJOG. 2008 Jul;115(8):1028-36.
10. PLoS Med. 2016 Dec. doi: 10.1371/journal.pmed.1002206.
11. Arch Gynecol Obstet. 2012 Mar;285(3):839-43.
12. Am J Obstet Gynecol. 2012 Jul;207(1):71.e1-5.
13. Gynecol Oncol. 2017 Feb;144(2):324-8.
In Lewy body disease, CSF may reveal dementia risk
SAN DIEGO – In patients with Lewy body disease, cerebrospinal fluid biomarkers may predict the extent of Alzheimer’s disease pathology, according to a new postmortem analysis.
In the small prospective study, David Irwin, MD, and his colleagues at the University of Pennsylvania, Philadelphia, found that higher antemortem cerebrospinal fluid (CSF) levels of total tau (t-tau) protein and lower amyloid-beta 1-42 (Abeta 1-42) levels were associated with postmortem evidence of cerebral Alzheimer’s disease and synuclein pathology.

The findings could have prognostic indications because about 40% of LBD patients have enough Abeta 1-42 and tau tangle pathology to have a secondary diagnosis of Alzheimer’s disease, and greater Alzheimer’s disease pathology has been linked to shorter survival. It could also help individualize therapy, as LBD patients with more Alzheimer’s disease character could be expected to respond better to antisynuclein and Alzheimer’s therapies, according to Dr. Irwin, who presented the study at a poster session at the annual meeting of the American Neurological Association.
In fact, the CSF ratio of CSF t-tau/Abeta 1-42 predicted the presence or absence of Alzheimer’s disease pathology with 90% sensitivity and 100% specificity.
If the results from the small study hold up, “we can identify who has Alzheimer’s copathology and who has a more aggressive form of Lewy body disease where it’s reaching the cortex rather than being in the brain stem, and that correlates with memory loss, dementia, and other things that impair the patient’s functioning,” Dr. Irwin said in an interview.
The study was possible because the Udall Center for Parkinson’s Research at the University of Pennsylvania has an active autopsy program and a significant number of Parkinson’s disease patients who have donated their brain for research. “It’s very rare to have autopsy-confirmed samples where we can validate what we’re measuring in the spinal fluid to what is actually accumulating in the brain,” Dr. Irwin said.
The study included 24 patients with autopsy-confirmed LBD who had undergone CSF testing while they were still alive. The researchers calculated ordinal pathology scores of tau tangles, Abeta 1-42 plaques, and alpha-synuclein pathology across seven regions of the brain, producing a global pathology score for each variable. The subjects were then divided into two groups: Lewy body synuclein stages with medium to high Alzheimer’s copathology (SYN+AD, n = 10) and those with low to no Alzheimer’s copathology (SYN-AD, n = 14).
In the CSF, the researchers analyzed associations with t-tau, phosphorylated tau (p-tau), and Abeta 1-42. They found that Abeta 1-42 levels were significantly different between SYN+AD and SYN-AD patients (147.2 pg/mL vs. 231.1 pg/mL, respectively; P = .001), as were CSF t-tau levels (63.9 pg/mL vs. 36.9 pg/mL; P = .02). P-tau was not significantly different (20.2 pg/mL vs. 15.5 pg/mL; P = 0.3), which was a surprise since it “is usually the strongest correlate of tangles in the brain,” Dr. Irwin said.
A ratio of CSF t-tau/Abeta 1-42 higher than 0.30 distinguished between SYN+AD and SYN-AD (area under the curve, 0.92; 95% confidence interval, 0.7-1.0; 90% sensitivity, 100% specificity), while CSF Abeta 1-42 less than 185 pg/mL distinguished neocortical synuclein stage (AUC, 0.92; 95% CI, 0.54-0.94; 77% sensitivity, 82% specificity).
The study was funded by the National Institute of Neurological Disorders and Stroke. Dr. Irwin reported having no financial disclosures.
SAN DIEGO – In patients with Lewy body disease, cerebrospinal fluid biomarkers may predict the extent of Alzheimer’s disease pathology, according to a new postmortem analysis.
In the small prospective study, David Irwin, MD, and his colleagues at the University of Pennsylvania, Philadelphia, found that higher antemortem cerebrospinal fluid (CSF) levels of total tau (t-tau) protein and lower amyloid-beta 1-42 (Abeta 1-42) levels were associated with postmortem evidence of cerebral Alzheimer’s disease and synuclein pathology.
The findings could have prognostic indications because about 40% of LBD patients have enough Abeta 1-42 and tau tangle pathology to have a secondary diagnosis of Alzheimer’s disease, and greater Alzheimer’s disease pathology has been linked to shorter survival. It could also help individualize therapy, as LBD patients with more Alzheimer’s disease character could be expected to respond better to antisynuclein and Alzheimer’s therapies, according to Dr. Irwin, who presented the study at a poster session at the annual meeting of the American Neurological Association.
In fact, the CSF ratio of CSF t-tau/Abeta 1-42 predicted the presence or absence of Alzheimer’s disease pathology with 90% sensitivity and 100% specificity.
If the results from the small study hold up, “we can identify who has Alzheimer’s copathology and who has a more aggressive form of Lewy body disease where it’s reaching the cortex rather than being in the brain stem, and that correlates with memory loss, dementia, and other things that impair the patient’s functioning,” Dr. Irwin said in an interview.
The study was possible because the Udall Center for Parkinson’s Research at the University of Pennsylvania has an active autopsy program and a significant number of Parkinson’s disease patients who have donated their brain for research. “It’s very rare to have autopsy-confirmed samples where we can validate what we’re measuring in the spinal fluid to what is actually accumulating in the brain,” Dr. Irwin said.
The study included 24 patients with autopsy-confirmed LBD who had undergone CSF testing while they were still alive. The researchers calculated ordinal pathology scores of tau tangles, Abeta 1-42 plaques, and alpha-synuclein pathology across seven regions of the brain, producing a global pathology score for each variable. The subjects were then divided into two groups: Lewy body synuclein stages with medium to high Alzheimer’s copathology (SYN+AD, n = 10) and those with low to no Alzheimer’s copathology (SYN-AD, n = 14).
In the CSF, the researchers analyzed associations with t-tau, phosphorylated tau (p-tau), and Abeta 1-42. They found that Abeta 1-42 levels were significantly different between SYN+AD and SYN-AD patients (147.2 pg/mL vs. 231.1 pg/mL, respectively; P = .001), as were CSF t-tau levels (63.9 pg/mL vs. 36.9 pg/mL; P = .02). P-tau was not significantly different (20.2 pg/mL vs. 15.5 pg/mL; P = 0.3), which was a surprise since it “is usually the strongest correlate of tangles in the brain,” Dr. Irwin said.
A ratio of CSF t-tau/Abeta 1-42 higher than 0.30 distinguished between SYN+AD and SYN-AD (area under the curve, 0.92; 95% confidence interval, 0.7-1.0; 90% sensitivity, 100% specificity), while CSF Abeta 1-42 less than 185 pg/mL distinguished neocortical synuclein stage (AUC, 0.92; 95% CI, 0.54-0.94; 77% sensitivity, 82% specificity).
The study was funded by the National Institute of Neurological Disorders and Stroke. Dr. Irwin reported having no financial disclosures.
SAN DIEGO – In patients with Lewy body disease, cerebrospinal fluid biomarkers may predict the extent of Alzheimer’s disease pathology, according to a new postmortem analysis.
In the small prospective study, David Irwin, MD, and his colleagues at the University of Pennsylvania, Philadelphia, found that higher antemortem cerebrospinal fluid (CSF) levels of total tau (t-tau) protein and lower amyloid-beta 1-42 (Abeta 1-42) levels were associated with postmortem evidence of cerebral Alzheimer’s disease and synuclein pathology.
The findings could have prognostic indications because about 40% of LBD patients have enough Abeta 1-42 and tau tangle pathology to have a secondary diagnosis of Alzheimer’s disease, and greater Alzheimer’s disease pathology has been linked to shorter survival. It could also help individualize therapy, as LBD patients with more Alzheimer’s disease character could be expected to respond better to antisynuclein and Alzheimer’s therapies, according to Dr. Irwin, who presented the study at a poster session at the annual meeting of the American Neurological Association.
In fact, the CSF ratio of CSF t-tau/Abeta 1-42 predicted the presence or absence of Alzheimer’s disease pathology with 90% sensitivity and 100% specificity.
If the results from the small study hold up, “we can identify who has Alzheimer’s copathology and who has a more aggressive form of Lewy body disease where it’s reaching the cortex rather than being in the brain stem, and that correlates with memory loss, dementia, and other things that impair the patient’s functioning,” Dr. Irwin said in an interview.
The study was possible because the Udall Center for Parkinson’s Research at the University of Pennsylvania has an active autopsy program and a significant number of Parkinson’s disease patients who have donated their brain for research. “It’s very rare to have autopsy-confirmed samples where we can validate what we’re measuring in the spinal fluid to what is actually accumulating in the brain,” Dr. Irwin said.
The study included 24 patients with autopsy-confirmed LBD who had undergone CSF testing while they were still alive. The researchers calculated ordinal pathology scores of tau tangles, Abeta 1-42 plaques, and alpha-synuclein pathology across seven regions of the brain, producing a global pathology score for each variable. The subjects were then divided into two groups: Lewy body synuclein stages with medium to high Alzheimer’s copathology (SYN+AD, n = 10) and those with low to no Alzheimer’s copathology (SYN-AD, n = 14).
In the CSF, the researchers analyzed associations with t-tau, phosphorylated tau (p-tau), and Abeta 1-42. They found that Abeta 1-42 levels were significantly different between SYN+AD and SYN-AD patients (147.2 pg/mL vs. 231.1 pg/mL, respectively; P = .001), as were CSF t-tau levels (63.9 pg/mL vs. 36.9 pg/mL; P = .02). P-tau was not significantly different (20.2 pg/mL vs. 15.5 pg/mL; P = 0.3), which was a surprise since it “is usually the strongest correlate of tangles in the brain,” Dr. Irwin said.
A ratio of CSF t-tau/Abeta 1-42 higher than 0.30 distinguished between SYN+AD and SYN-AD (area under the curve, 0.92; 95% confidence interval, 0.7-1.0; 90% sensitivity, 100% specificity), while CSF Abeta 1-42 less than 185 pg/mL distinguished neocortical synuclein stage (AUC, 0.92; 95% CI, 0.54-0.94; 77% sensitivity, 82% specificity).
The study was funded by the National Institute of Neurological Disorders and Stroke. Dr. Irwin reported having no financial disclosures.
AT ANA 2017
Key clinical point:
Major finding: A CSF ratio of t-tau/Abeta 1-42 greater than 0.30 predicted the presence or absence of Alzheimer’s disease pathology with 90% sensitivity and 100% specificity.
Data source: Prospective study of 24 patients with Lewy body disease.
Disclosures: The study was funded by the National Institute of Neurological Disorders and Stroke. Dr. Irwin reported having no financial disclosures.
Why VADS is gaining ground in pediatrics
The miniaturization of continuous-flow ventricular assist devices has launched the era of continuous-flow VAD support in pediatric patients, and the trend may accelerate with the introduction of a continuous-flow device designed specifically for small children. In an expert opinion in the Journal of Thoracic and Cardiovascular Surgery, Iki Adachi, MD, of Baylor College of Medicine in Houston, said the emerging science of continuous-flow VADs in children promises to solve problems like device size mismatch, hospital-only VADs, and chronic therapy (J Thorac Cardiovasc Surg. 2017 Oct;154:1358-61). “With ongoing device miniaturization, enthusiasm has been growing among pediatric physicians for the use of continuous-flow VADs in children,” Dr. Adachi said. He noted the introduction of a continuous-flow device for small children, the Infant Jarvik 2015, “may further accelerate the trend.”
Dr. Adachi cited PediMACS reports that stated that more than half of the long-term devices now registered are continuous-flow devices, and that continuous-flow VADs comprised 62% of all durable VAD implants in the third quarter of 2016. “With the encouraging results recorded to date, the use of continuous-flow devices in the pediatric population is rapidly increasing,” he said.
Miniaturization has addressed the problem of size mismatch when using continuous-flow VAD devices in children, he said, noting that use of the Infant Jarvik device may be expanded even further to children as small at 8 kg or less. The PumpKIN trial(Pumps for Kids, Infants, and Neonates), which is evaluating the Infant Jarvik 2015 vs. the Berlin Heart EXCOR, could provide answers on the feasibility of continuous-flow VADs in small children.
“Based on experience with the chronic animal model, I believe that the Infant Jarvik device will properly fit the patients included in the trial,” he said.
Continuous-flow VAD in children also holds potential for managing these patients outside the hospital setting. “Outpatient management of children with continuous-flow VADs has been shown to be feasible,” he said, adding that the PediMACS registry has reported that only 45% of patients have been managed this way. “Nonetheless, with maturation of the pediatric field, outpatient management will become routine rather than the exception,” he said.
Greater use of continuous-flow VADs also may create opportunities to improve the status and suitability for transplantation of children with severe heart failure, he said. He gave as an example his group’s practice at Houston’s Texas Children’s Hospital, which is to deactivate patients on the transplant wait list for 3 months once they start continuous-flow VAD support. “A postoperative ‘grace period’ affords protected opportunities for both physical and psychological recovery,” he said. This timeout of sorts also affords the care team time to assess the myocardium for possible functional recovery.
In patients who are not good candidates for transplantation, durable continuous-flow VADs may provide chronic therapy, and in time, these patients may become suitable transplant candidates, said Dr. Adachi. “Bypassing such an unfavorable period for transplantation with prolonged VAD support may be a reasonable approach,” he said.
Patients with failing single-ventricle circulation also may benefit from VAD support, although the challenges facing this population are more profound than in other groups, Dr. Adachi said. VAD support for single-ventricle disease is sparse, but these patients require careful evaluation of the nature of their condition. “If systolic dysfunction is the predominant cause of circulatory failure, then VAD support for the failing systemic ventricle will likely improve hemodynamics,” said Dr. Adachi. VAD support also could help the patient move through the various stages of palliation.
“Again, the emphasis is not just on simply keeping the patient alive until a donor organ becomes available; rather, attention is refocused on overall health beyond survival, which may eventually affect transplantation candidacy and even post transplantation outcome,” Dr. Adachi concluded.
Dr. Adachi serves as a consultant and proctor for Berlin Heart and HeartWare, and as a consultant for the New England Research Institute related to the PumpKIN trial.
The miniaturization of continuous-flow ventricular assist devices has launched the era of continuous-flow VAD support in pediatric patients, and the trend may accelerate with the introduction of a continuous-flow device designed specifically for small children. In an expert opinion in the Journal of Thoracic and Cardiovascular Surgery, Iki Adachi, MD, of Baylor College of Medicine in Houston, said the emerging science of continuous-flow VADs in children promises to solve problems like device size mismatch, hospital-only VADs, and chronic therapy (J Thorac Cardiovasc Surg. 2017 Oct;154:1358-61). “With ongoing device miniaturization, enthusiasm has been growing among pediatric physicians for the use of continuous-flow VADs in children,” Dr. Adachi said. He noted the introduction of a continuous-flow device for small children, the Infant Jarvik 2015, “may further accelerate the trend.”
Dr. Adachi cited PediMACS reports that stated that more than half of the long-term devices now registered are continuous-flow devices, and that continuous-flow VADs comprised 62% of all durable VAD implants in the third quarter of 2016. “With the encouraging results recorded to date, the use of continuous-flow devices in the pediatric population is rapidly increasing,” he said.
Miniaturization has addressed the problem of size mismatch when using continuous-flow VAD devices in children, he said, noting that use of the Infant Jarvik device may be expanded even further to children as small at 8 kg or less. The PumpKIN trial(Pumps for Kids, Infants, and Neonates), which is evaluating the Infant Jarvik 2015 vs. the Berlin Heart EXCOR, could provide answers on the feasibility of continuous-flow VADs in small children.
“Based on experience with the chronic animal model, I believe that the Infant Jarvik device will properly fit the patients included in the trial,” he said.
Continuous-flow VAD in children also holds potential for managing these patients outside the hospital setting. “Outpatient management of children with continuous-flow VADs has been shown to be feasible,” he said, adding that the PediMACS registry has reported that only 45% of patients have been managed this way. “Nonetheless, with maturation of the pediatric field, outpatient management will become routine rather than the exception,” he said.
Greater use of continuous-flow VADs also may create opportunities to improve the status and suitability for transplantation of children with severe heart failure, he said. He gave as an example his group’s practice at Houston’s Texas Children’s Hospital, which is to deactivate patients on the transplant wait list for 3 months once they start continuous-flow VAD support. “A postoperative ‘grace period’ affords protected opportunities for both physical and psychological recovery,” he said. This timeout of sorts also affords the care team time to assess the myocardium for possible functional recovery.
In patients who are not good candidates for transplantation, durable continuous-flow VADs may provide chronic therapy, and in time, these patients may become suitable transplant candidates, said Dr. Adachi. “Bypassing such an unfavorable period for transplantation with prolonged VAD support may be a reasonable approach,” he said.
Patients with failing single-ventricle circulation also may benefit from VAD support, although the challenges facing this population are more profound than in other groups, Dr. Adachi said. VAD support for single-ventricle disease is sparse, but these patients require careful evaluation of the nature of their condition. “If systolic dysfunction is the predominant cause of circulatory failure, then VAD support for the failing systemic ventricle will likely improve hemodynamics,” said Dr. Adachi. VAD support also could help the patient move through the various stages of palliation.
“Again, the emphasis is not just on simply keeping the patient alive until a donor organ becomes available; rather, attention is refocused on overall health beyond survival, which may eventually affect transplantation candidacy and even post transplantation outcome,” Dr. Adachi concluded.
Dr. Adachi serves as a consultant and proctor for Berlin Heart and HeartWare, and as a consultant for the New England Research Institute related to the PumpKIN trial.
The miniaturization of continuous-flow ventricular assist devices has launched the era of continuous-flow VAD support in pediatric patients, and the trend may accelerate with the introduction of a continuous-flow device designed specifically for small children. In an expert opinion in the Journal of Thoracic and Cardiovascular Surgery, Iki Adachi, MD, of Baylor College of Medicine in Houston, said the emerging science of continuous-flow VADs in children promises to solve problems like device size mismatch, hospital-only VADs, and chronic therapy (J Thorac Cardiovasc Surg. 2017 Oct;154:1358-61). “With ongoing device miniaturization, enthusiasm has been growing among pediatric physicians for the use of continuous-flow VADs in children,” Dr. Adachi said. He noted the introduction of a continuous-flow device for small children, the Infant Jarvik 2015, “may further accelerate the trend.”
Dr. Adachi cited PediMACS reports that stated that more than half of the long-term devices now registered are continuous-flow devices, and that continuous-flow VADs comprised 62% of all durable VAD implants in the third quarter of 2016. “With the encouraging results recorded to date, the use of continuous-flow devices in the pediatric population is rapidly increasing,” he said.
Miniaturization has addressed the problem of size mismatch when using continuous-flow VAD devices in children, he said, noting that use of the Infant Jarvik device may be expanded even further to children as small at 8 kg or less. The PumpKIN trial(Pumps for Kids, Infants, and Neonates), which is evaluating the Infant Jarvik 2015 vs. the Berlin Heart EXCOR, could provide answers on the feasibility of continuous-flow VADs in small children.
“Based on experience with the chronic animal model, I believe that the Infant Jarvik device will properly fit the patients included in the trial,” he said.
Continuous-flow VAD in children also holds potential for managing these patients outside the hospital setting. “Outpatient management of children with continuous-flow VADs has been shown to be feasible,” he said, adding that the PediMACS registry has reported that only 45% of patients have been managed this way. “Nonetheless, with maturation of the pediatric field, outpatient management will become routine rather than the exception,” he said.
Greater use of continuous-flow VADs also may create opportunities to improve the status and suitability for transplantation of children with severe heart failure, he said. He gave as an example his group’s practice at Houston’s Texas Children’s Hospital, which is to deactivate patients on the transplant wait list for 3 months once they start continuous-flow VAD support. “A postoperative ‘grace period’ affords protected opportunities for both physical and psychological recovery,” he said. This timeout of sorts also affords the care team time to assess the myocardium for possible functional recovery.
In patients who are not good candidates for transplantation, durable continuous-flow VADs may provide chronic therapy, and in time, these patients may become suitable transplant candidates, said Dr. Adachi. “Bypassing such an unfavorable period for transplantation with prolonged VAD support may be a reasonable approach,” he said.
Patients with failing single-ventricle circulation also may benefit from VAD support, although the challenges facing this population are more profound than in other groups, Dr. Adachi said. VAD support for single-ventricle disease is sparse, but these patients require careful evaluation of the nature of their condition. “If systolic dysfunction is the predominant cause of circulatory failure, then VAD support for the failing systemic ventricle will likely improve hemodynamics,” said Dr. Adachi. VAD support also could help the patient move through the various stages of palliation.
“Again, the emphasis is not just on simply keeping the patient alive until a donor organ becomes available; rather, attention is refocused on overall health beyond survival, which may eventually affect transplantation candidacy and even post transplantation outcome,” Dr. Adachi concluded.
Dr. Adachi serves as a consultant and proctor for Berlin Heart and HeartWare, and as a consultant for the New England Research Institute related to the PumpKIN trial.
FROM THE JOURNAL OF THORACIC AND CARDIOVASCULAR SURGERY
Key clinical point: Advances in continuous-flow ventricular assist devices (VADs) promise a paradigm shift in pediatrics.
Major finding: Device miniaturization is solving problems such as size mismatch, inpatients on VADs, and chronic therapy.
Data source: Expert opinion drawing on PediMACS reports and published trials of continuous-flow VAD.
Disclosures: Dr. Adachi serves as a consultant and proctor for Berlin Heart and HeartWare and as a consultant for the New England Research Institute related to the PumpKIN trial.
Obesity-Related Cancer Is on the Rise
Overweight and obesity are associated with an increased risk of 13 types of cancer—and those cancers account for about 40% of all cancers diagnosed in 2014, according to the CDC.
The 13 cancers are meningioma, adenocarcinoma of the esophagus, multiple myeloma, kidney, uterine, ovarian, thyroid, breast, liver, gallbladder, upper stomach, pancreas, and colorectal. About 630,000 people were diagnosed with 1 of those cancers in 2014; 2 in 3 cancers were in adults aged 50 to 74 years. In 2013-2014, about 2 of every 3 American adults were overweight or obese.
Related: The Impact of Obesity on Simvastatin for Lowering LDL-C Among Veterans
Overall, the rate of new cancer cases has been on the decline since the 1990s, the report says, but increases in overweight- and obesity-related cancers “are likely slowing this progress.” Obesity-related cancers (not including colorectal cancer, which declined by 23%) increased by 7% between 2005 and 2014, while the rates of nonobesity–related cancers declined 13%.
Health care providers can help, the CDC says, by counseling patients on healthy weight and its role in cancer prevention, referring obese patients to intensive management programs and connecting patients and their families to community services that give them easier access to healthful food. The National Comprehensive Cancer Control Program (https://www.cdc.gov/cancer/ncccp/index.htm) funds cancer coalitions across the U.S., which include strategies to prevent and control overweight and obesity.
Related: The Impact of Obesity on the Recovery of Patients With Cancer
“When people ask me if there’s a cure for cancer, I say, ‘Yes, good health is the best prescription for preventing chronic diseases, including cancer,” said Lisa Richardson, MD, director of CDC’s Division of Cancer Prevention and Control. That means, she says, giving people the information they need to make healthy choices where they live, work, learn, and play.
Overweight and obesity are associated with an increased risk of 13 types of cancer—and those cancers account for about 40% of all cancers diagnosed in 2014, according to the CDC.
The 13 cancers are meningioma, adenocarcinoma of the esophagus, multiple myeloma, kidney, uterine, ovarian, thyroid, breast, liver, gallbladder, upper stomach, pancreas, and colorectal. About 630,000 people were diagnosed with 1 of those cancers in 2014; 2 in 3 cancers were in adults aged 50 to 74 years. In 2013-2014, about 2 of every 3 American adults were overweight or obese.
Related: The Impact of Obesity on Simvastatin for Lowering LDL-C Among Veterans
Overall, the rate of new cancer cases has been on the decline since the 1990s, the report says, but increases in overweight- and obesity-related cancers “are likely slowing this progress.” Obesity-related cancers (not including colorectal cancer, which declined by 23%) increased by 7% between 2005 and 2014, while the rates of nonobesity–related cancers declined 13%.
Health care providers can help, the CDC says, by counseling patients on healthy weight and its role in cancer prevention, referring obese patients to intensive management programs and connecting patients and their families to community services that give them easier access to healthful food. The National Comprehensive Cancer Control Program (https://www.cdc.gov/cancer/ncccp/index.htm) funds cancer coalitions across the U.S., which include strategies to prevent and control overweight and obesity.
Related: The Impact of Obesity on the Recovery of Patients With Cancer
“When people ask me if there’s a cure for cancer, I say, ‘Yes, good health is the best prescription for preventing chronic diseases, including cancer,” said Lisa Richardson, MD, director of CDC’s Division of Cancer Prevention and Control. That means, she says, giving people the information they need to make healthy choices where they live, work, learn, and play.
Overweight and obesity are associated with an increased risk of 13 types of cancer—and those cancers account for about 40% of all cancers diagnosed in 2014, according to the CDC.
The 13 cancers are meningioma, adenocarcinoma of the esophagus, multiple myeloma, kidney, uterine, ovarian, thyroid, breast, liver, gallbladder, upper stomach, pancreas, and colorectal. About 630,000 people were diagnosed with 1 of those cancers in 2014; 2 in 3 cancers were in adults aged 50 to 74 years. In 2013-2014, about 2 of every 3 American adults were overweight or obese.
Related: The Impact of Obesity on Simvastatin for Lowering LDL-C Among Veterans
Overall, the rate of new cancer cases has been on the decline since the 1990s, the report says, but increases in overweight- and obesity-related cancers “are likely slowing this progress.” Obesity-related cancers (not including colorectal cancer, which declined by 23%) increased by 7% between 2005 and 2014, while the rates of nonobesity–related cancers declined 13%.
Health care providers can help, the CDC says, by counseling patients on healthy weight and its role in cancer prevention, referring obese patients to intensive management programs and connecting patients and their families to community services that give them easier access to healthful food. The National Comprehensive Cancer Control Program (https://www.cdc.gov/cancer/ncccp/index.htm) funds cancer coalitions across the U.S., which include strategies to prevent and control overweight and obesity.
Related: The Impact of Obesity on the Recovery of Patients With Cancer
“When people ask me if there’s a cure for cancer, I say, ‘Yes, good health is the best prescription for preventing chronic diseases, including cancer,” said Lisa Richardson, MD, director of CDC’s Division of Cancer Prevention and Control. That means, she says, giving people the information they need to make healthy choices where they live, work, learn, and play.
Team identifies HSCs that rapidly reconstitute hematopoiesis

Researchers say they have identified a subpopulation of hematopoietic stem cells (HSCs) that immediately contributes to long-term, multilineage hematopoietic reconstitution after transplant.
These HSCs were discovered in macaques, but the cells are similar to a subset of HSCs found in humans.
The researchers found the 2 sets of cells behaved identically when tested in vitro.
The team believes their findings will increase the efficiency of future efforts for HSC transplants, gene therapies, and gene editing.
Hans-Peter Kiem, MD, PhD, of the Fred Hutchinson Cancer Research Center in Seattle, Washington, and his colleagues reported these findings in Science Translational Medicine.
The researchers performed HSC transplants in pig-tailed macaques, following hundreds of thousands of cells immediately after transplant and over the course of 7.5 years.
Previous reports had suggested that successive waves of progenitor cells expand and contract to establish the new bone marrow after transplant.
However, Dr Kiem and his colleagues homed in on a distinct group of HSCs that took hold early after transplant and went on to produce all cell lineages that constitute a complete blood system.
“These findings came as a surprise,” Dr Kiem said. “We had thought that there were multiple types of blood stem cells that take on different roles in rebuilding a blood and immune system. This population does it all.”
The population is a subset of CD34+ cells expressing CD90 and lacking CD45RA markers.
“The gold standard target cell population for stem cell gene therapy are cells with the marker CD34,” said study author Stefan Radtke, PhD, of the Fred Hutchinson Cancer Research Center.
“But we used 2 additional markers to further distinguish the population from the other blood stem cells.”
The researchers noted that the CD34+ CD45RA- CD90+ HSCs started repopulating the hematopoietic system within 10 days of being infused in macaques undergoing transplant.
A year later, the researchers found strong molecular traces of the cells, suggesting they were responsible for the ongoing maintenance of the newly transplanted system.
The team also determined the minimum numbers of CD34+ CD45RA- CD90+ HSCs that were necessary for successful transplant (defined as sustained neutrophil and platelet recovery).
And the researchers found similar gene expression profiles between macaque and human CD34+ CD45RA- CD90+ HSCs.
The team therefore believes these findings could have implications for HSC transplants in humans.
The researchers are now working to move their findings into the clinic with the hopes of integrating them in ongoing clinical trials. The team is currently looking for commercial partners. ![]()
Researchers say they have identified a subpopulation of hematopoietic stem cells (HSCs) that immediately contributes to long-term, multilineage hematopoietic reconstitution after transplant.
These HSCs were discovered in macaques, but the cells are similar to a subset of HSCs found in humans.
The researchers found the 2 sets of cells behaved identically when tested in vitro.
The team believes their findings will increase the efficiency of future efforts for HSC transplants, gene therapies, and gene editing.
Hans-Peter Kiem, MD, PhD, of the Fred Hutchinson Cancer Research Center in Seattle, Washington, and his colleagues reported these findings in Science Translational Medicine.
The researchers performed HSC transplants in pig-tailed macaques, following hundreds of thousands of cells immediately after transplant and over the course of 7.5 years.
Previous reports had suggested that successive waves of progenitor cells expand and contract to establish the new bone marrow after transplant.
However, Dr Kiem and his colleagues homed in on a distinct group of HSCs that took hold early after transplant and went on to produce all cell lineages that constitute a complete blood system.
“These findings came as a surprise,” Dr Kiem said. “We had thought that there were multiple types of blood stem cells that take on different roles in rebuilding a blood and immune system. This population does it all.”
The population is a subset of CD34+ cells expressing CD90 and lacking CD45RA markers.
“The gold standard target cell population for stem cell gene therapy are cells with the marker CD34,” said study author Stefan Radtke, PhD, of the Fred Hutchinson Cancer Research Center.
“But we used 2 additional markers to further distinguish the population from the other blood stem cells.”
The researchers noted that the CD34+ CD45RA- CD90+ HSCs started repopulating the hematopoietic system within 10 days of being infused in macaques undergoing transplant.
A year later, the researchers found strong molecular traces of the cells, suggesting they were responsible for the ongoing maintenance of the newly transplanted system.
The team also determined the minimum numbers of CD34+ CD45RA- CD90+ HSCs that were necessary for successful transplant (defined as sustained neutrophil and platelet recovery).
And the researchers found similar gene expression profiles between macaque and human CD34+ CD45RA- CD90+ HSCs.
The team therefore believes these findings could have implications for HSC transplants in humans.
The researchers are now working to move their findings into the clinic with the hopes of integrating them in ongoing clinical trials. The team is currently looking for commercial partners. ![]()
Researchers say they have identified a subpopulation of hematopoietic stem cells (HSCs) that immediately contributes to long-term, multilineage hematopoietic reconstitution after transplant.
These HSCs were discovered in macaques, but the cells are similar to a subset of HSCs found in humans.
The researchers found the 2 sets of cells behaved identically when tested in vitro.
The team believes their findings will increase the efficiency of future efforts for HSC transplants, gene therapies, and gene editing.
Hans-Peter Kiem, MD, PhD, of the Fred Hutchinson Cancer Research Center in Seattle, Washington, and his colleagues reported these findings in Science Translational Medicine.
The researchers performed HSC transplants in pig-tailed macaques, following hundreds of thousands of cells immediately after transplant and over the course of 7.5 years.
Previous reports had suggested that successive waves of progenitor cells expand and contract to establish the new bone marrow after transplant.
However, Dr Kiem and his colleagues homed in on a distinct group of HSCs that took hold early after transplant and went on to produce all cell lineages that constitute a complete blood system.
“These findings came as a surprise,” Dr Kiem said. “We had thought that there were multiple types of blood stem cells that take on different roles in rebuilding a blood and immune system. This population does it all.”
The population is a subset of CD34+ cells expressing CD90 and lacking CD45RA markers.
“The gold standard target cell population for stem cell gene therapy are cells with the marker CD34,” said study author Stefan Radtke, PhD, of the Fred Hutchinson Cancer Research Center.
“But we used 2 additional markers to further distinguish the population from the other blood stem cells.”
The researchers noted that the CD34+ CD45RA- CD90+ HSCs started repopulating the hematopoietic system within 10 days of being infused in macaques undergoing transplant.
A year later, the researchers found strong molecular traces of the cells, suggesting they were responsible for the ongoing maintenance of the newly transplanted system.
The team also determined the minimum numbers of CD34+ CD45RA- CD90+ HSCs that were necessary for successful transplant (defined as sustained neutrophil and platelet recovery).
And the researchers found similar gene expression profiles between macaque and human CD34+ CD45RA- CD90+ HSCs.
The team therefore believes these findings could have implications for HSC transplants in humans.
The researchers are now working to move their findings into the clinic with the hopes of integrating them in ongoing clinical trials. The team is currently looking for commercial partners. ![]()