User login
Surgeon, primary care collaboration needed to catch hyperparathyroidism
A report from the University of Alabama at Birmingham provides further evidence that hyperparathyroidism is often missed in the United States health care system.
Investigators reviewed the electronic health records for 682,704 patients at the university from 2011 to 2015 and identified hypercalcemia (serum calcium greater than 10.5 mg/dL) – usually the first indication of disease – in 10,432 patients. The next step should have been a parathyroid hormone (PTH) measurement, but PTH was measured in only 3,200 patients (31%), and it usually took multiple abnormal calcium levels before PTH was checked, reported Courtney Balentine, MD, and her colleagues at the University of Alabama at Birmingham.
In addition, 592 of 2,666 patients (22%) with both elevated calcium and PTH levels were referred to surgeons for a parathyroidectomy consult, although parathyroidectomy is a low-risk outpatient procedure that cures up to 95% of patients, and surgeons are best suited to discuss the risks and benefits of the procedure with patients, investigators said (Ann Surg. 2017 Jul 3. doi: 10.1097/SLA.0000000000002370).
Underdiagnosis and treatment of hyperparathyroidism can lead to fractures, kidney stones, depression, cognitive impairment, hypertension, stroke, and myocardial infarction.
The investigators plan to meet with primary care doctors to hear how they think the problem should be addressed. Alerts and automatic referrals are also being considered for the EHR. “The combination of systems changes and stakeholder engagement is more likely to succeed than focusing on one component to the exclusion of others,” Dr. Balentine and colleagues said.
The issue could be that primary care physicians are just too overwhelmed to notice or be concerned about an isolated abnormal calcium level in an otherwise routine assessment. Or perhaps they assume surgeons come into play only if there are kidney stones, bone changes, or other obvious signs of trouble, they said.
The team has started to look at charts to get a better understanding of what’s going wrong. “I have been a little bit flabbergasted by how many excuses there are for either not checking a PTH or not referring once the diagnosis is there. … ‘This patient probably would not benefit from the surgery; the risk is too high; he or she does not want X, Y, or Z.’ I think if they just refer [patients to surgeons] to have the conversation, we might very well agree with them, but at least we [could] have the conversation with the patient, and I think [that] would make more sense,” Dr. Balentine said in a transcript of a question and answer session that was published with the report.
“Indeed, the recent American Association of Endocrine Surgery guidelines emphasize the importance of referring patients to surgical experts for discussion of treatment options,” the investigators said in the report.
It’s possible that elevated calcium and PTH levels were evaluated and treated at other institutions and so were not captured by the analysis. “Our mean follow-up was 16 months, however, which suggests that most patients were seen in the UAB system long enough to undergo appropriate evaluation and referral.” Also, patients with “two or more abnormal calcium values had similarly low rates of surgical referral, which suggests that loss to follow-up is unlikely to explain our findings,” they said.
The mean age of the cohort was 54 years; 56% of the patients were white, and 61% were women.
The work was supported by the Agency for Healthcare Research and Quality. The authors reported no conflicts of interest.
A report from the University of Alabama at Birmingham provides further evidence that hyperparathyroidism is often missed in the United States health care system.
Investigators reviewed the electronic health records for 682,704 patients at the university from 2011 to 2015 and identified hypercalcemia (serum calcium greater than 10.5 mg/dL) – usually the first indication of disease – in 10,432 patients. The next step should have been a parathyroid hormone (PTH) measurement, but PTH was measured in only 3,200 patients (31%), and it usually took multiple abnormal calcium levels before PTH was checked, reported Courtney Balentine, MD, and her colleagues at the University of Alabama at Birmingham.
In addition, 592 of 2,666 patients (22%) with both elevated calcium and PTH levels were referred to surgeons for a parathyroidectomy consult, although parathyroidectomy is a low-risk outpatient procedure that cures up to 95% of patients, and surgeons are best suited to discuss the risks and benefits of the procedure with patients, investigators said (Ann Surg. 2017 Jul 3. doi: 10.1097/SLA.0000000000002370).
Underdiagnosis and treatment of hyperparathyroidism can lead to fractures, kidney stones, depression, cognitive impairment, hypertension, stroke, and myocardial infarction.
The investigators plan to meet with primary care doctors to hear how they think the problem should be addressed. Alerts and automatic referrals are also being considered for the EHR. “The combination of systems changes and stakeholder engagement is more likely to succeed than focusing on one component to the exclusion of others,” Dr. Balentine and colleagues said.
The issue could be that primary care physicians are just too overwhelmed to notice or be concerned about an isolated abnormal calcium level in an otherwise routine assessment. Or perhaps they assume surgeons come into play only if there are kidney stones, bone changes, or other obvious signs of trouble, they said.
The team has started to look at charts to get a better understanding of what’s going wrong. “I have been a little bit flabbergasted by how many excuses there are for either not checking a PTH or not referring once the diagnosis is there. … ‘This patient probably would not benefit from the surgery; the risk is too high; he or she does not want X, Y, or Z.’ I think if they just refer [patients to surgeons] to have the conversation, we might very well agree with them, but at least we [could] have the conversation with the patient, and I think [that] would make more sense,” Dr. Balentine said in a transcript of a question and answer session that was published with the report.
“Indeed, the recent American Association of Endocrine Surgery guidelines emphasize the importance of referring patients to surgical experts for discussion of treatment options,” the investigators said in the report.
It’s possible that elevated calcium and PTH levels were evaluated and treated at other institutions and so were not captured by the analysis. “Our mean follow-up was 16 months, however, which suggests that most patients were seen in the UAB system long enough to undergo appropriate evaluation and referral.” Also, patients with “two or more abnormal calcium values had similarly low rates of surgical referral, which suggests that loss to follow-up is unlikely to explain our findings,” they said.
The mean age of the cohort was 54 years; 56% of the patients were white, and 61% were women.
The work was supported by the Agency for Healthcare Research and Quality. The authors reported no conflicts of interest.
A report from the University of Alabama at Birmingham provides further evidence that hyperparathyroidism is often missed in the United States health care system.
Investigators reviewed the electronic health records for 682,704 patients at the university from 2011 to 2015 and identified hypercalcemia (serum calcium greater than 10.5 mg/dL) – usually the first indication of disease – in 10,432 patients. The next step should have been a parathyroid hormone (PTH) measurement, but PTH was measured in only 3,200 patients (31%), and it usually took multiple abnormal calcium levels before PTH was checked, reported Courtney Balentine, MD, and her colleagues at the University of Alabama at Birmingham.
In addition, 592 of 2,666 patients (22%) with both elevated calcium and PTH levels were referred to surgeons for a parathyroidectomy consult, although parathyroidectomy is a low-risk outpatient procedure that cures up to 95% of patients, and surgeons are best suited to discuss the risks and benefits of the procedure with patients, investigators said (Ann Surg. 2017 Jul 3. doi: 10.1097/SLA.0000000000002370).
Underdiagnosis and treatment of hyperparathyroidism can lead to fractures, kidney stones, depression, cognitive impairment, hypertension, stroke, and myocardial infarction.
The investigators plan to meet with primary care doctors to hear how they think the problem should be addressed. Alerts and automatic referrals are also being considered for the EHR. “The combination of systems changes and stakeholder engagement is more likely to succeed than focusing on one component to the exclusion of others,” Dr. Balentine and colleagues said.
The issue could be that primary care physicians are just too overwhelmed to notice or be concerned about an isolated abnormal calcium level in an otherwise routine assessment. Or perhaps they assume surgeons come into play only if there are kidney stones, bone changes, or other obvious signs of trouble, they said.
The team has started to look at charts to get a better understanding of what’s going wrong. “I have been a little bit flabbergasted by how many excuses there are for either not checking a PTH or not referring once the diagnosis is there. … ‘This patient probably would not benefit from the surgery; the risk is too high; he or she does not want X, Y, or Z.’ I think if they just refer [patients to surgeons] to have the conversation, we might very well agree with them, but at least we [could] have the conversation with the patient, and I think [that] would make more sense,” Dr. Balentine said in a transcript of a question and answer session that was published with the report.
“Indeed, the recent American Association of Endocrine Surgery guidelines emphasize the importance of referring patients to surgical experts for discussion of treatment options,” the investigators said in the report.
It’s possible that elevated calcium and PTH levels were evaluated and treated at other institutions and so were not captured by the analysis. “Our mean follow-up was 16 months, however, which suggests that most patients were seen in the UAB system long enough to undergo appropriate evaluation and referral.” Also, patients with “two or more abnormal calcium values had similarly low rates of surgical referral, which suggests that loss to follow-up is unlikely to explain our findings,” they said.
The mean age of the cohort was 54 years; 56% of the patients were white, and 61% were women.
The work was supported by the Agency for Healthcare Research and Quality. The authors reported no conflicts of interest.
FROM ANNALS OF SURGERY
Key clinical point:
Major finding: Just 31% of patients with a finding of hypercalcemia went on to have their parathyroid hormone levels checked.
Data source: Electronic health record review of 682,704 patients at a large American university.
Disclosures: The work was supported by the Agency for Healthcare Research and Quality. The authors reported no conflicts of interest.
Intense exercise reduces hypoglycemia awareness in type 1 diabetes
A single 15-minute session of high-intensity exercise masked symptoms of subsequent hypoglycemia in patients with type 1 diabetes and normal hypoglycemia awareness, according to Dutch investigators.
Twenty patients with type 1 diabetes – 10 with normal hypoglycemia awareness and 10 with impaired awareness – and 10 healthy subjects were asked to push themselves as hard as they could for 30-second bursts during 15 minutes of stationary bicycling and to go at an easier pace in between, reported Hanne Rooijackers, MD, of the Radboud University Medical Center, Nijmegen, the Netherlands, and colleagues.
The subjects had intravenous cannulae in both forearms, one for blood draws and the other for glucose and insulin administration. All three groups were kept euglycemic during exercise, but then were subjected to hyperinsulinemic-hypoglycemic clamps afterwards. Plasma glucose levels were allowed to fall to 2.6 mmol/L over about 35 min., and were kept there for another 60 min. Trembling, palpitations, anxiety, and other symptoms were serially assessed while patients were hypoglycemic, along with cognitive function and levels of hormones involved with hypoglycemic defense.
For comparison, the subjects all had clamps applied and hypoglycemia symptoms and physiologic responses assessed after a 15-minute session of rest at least 2 weeks apart from the exercise session.
The healthy subjects had a peak of about 20 points on a composite score of hypoglycemia symptoms during rest; exercise reduced the peak score only a small amount to about 18 points. Diabetic patients with normal hypoglycemia awareness hit a peak symptom score of 31 points during rest, which fell substantially after exercise to 22 points. Exercise, meanwhile, had no effect on diabetic patients with impaired awareness; after both rest and exercise, they had a peak composite symptom score of about 11 points, Dr. Rooijackers and colleagues reported (Diabetes. 2017 Jul;66[7]:1990-8).
High-intensity interval training (HIIT) did not affect hypoglycemic awareness in patients with impaired awareness probably because of “a ‘floor’ effect, in that symptom responses could not be further suppressed than they already were,” the investigators speculated.
Regular exercise is recommended for patients with type 1 diabetes, and, like others, they are turning to HIIT – short bursts of intense exercise broken up by brief periods of rest or lower intensity movement – because it appears to deliver the benefits for more moderate exercise in less time.
The findings suggest, however, that high-intensity exercise might increase the risk of severe hypoglycemia in type 1 patients by reducing awareness of its symptoms and blunting hormonal defenses.
The team suspects elevated lactate levels account for the findings. Exercise increases plasma lactate levels, and as blood glucose levels fall, the brain uses lactate as an alternative fuel, which likely blunts the effects of hypoglycemia. Plasma lactate spiked in the study subjects about 15 minutes after exercise.
Participants presented early in the morning after fasting overnight and abstaining from strenuous exercise for 2 days. They were in their mid-20s on average, normal weight, and fairly well balanced between men and women. Patients with type 1 diabetes were eligible for the study if they had hemoglobin A1c levels below 9% and no vascular complications beyond retinopathy. Their duration of diabetes was about 10 years.
The work was funded by the Dutch Diabetes Research Foundation and the European Foundation for the Study of Diabetes. The authors had no conflicts of interest.
A single 15-minute session of high-intensity exercise masked symptoms of subsequent hypoglycemia in patients with type 1 diabetes and normal hypoglycemia awareness, according to Dutch investigators.
Twenty patients with type 1 diabetes – 10 with normal hypoglycemia awareness and 10 with impaired awareness – and 10 healthy subjects were asked to push themselves as hard as they could for 30-second bursts during 15 minutes of stationary bicycling and to go at an easier pace in between, reported Hanne Rooijackers, MD, of the Radboud University Medical Center, Nijmegen, the Netherlands, and colleagues.
The subjects had intravenous cannulae in both forearms, one for blood draws and the other for glucose and insulin administration. All three groups were kept euglycemic during exercise, but then were subjected to hyperinsulinemic-hypoglycemic clamps afterwards. Plasma glucose levels were allowed to fall to 2.6 mmol/L over about 35 min., and were kept there for another 60 min. Trembling, palpitations, anxiety, and other symptoms were serially assessed while patients were hypoglycemic, along with cognitive function and levels of hormones involved with hypoglycemic defense.
For comparison, the subjects all had clamps applied and hypoglycemia symptoms and physiologic responses assessed after a 15-minute session of rest at least 2 weeks apart from the exercise session.
The healthy subjects had a peak of about 20 points on a composite score of hypoglycemia symptoms during rest; exercise reduced the peak score only a small amount to about 18 points. Diabetic patients with normal hypoglycemia awareness hit a peak symptom score of 31 points during rest, which fell substantially after exercise to 22 points. Exercise, meanwhile, had no effect on diabetic patients with impaired awareness; after both rest and exercise, they had a peak composite symptom score of about 11 points, Dr. Rooijackers and colleagues reported (Diabetes. 2017 Jul;66[7]:1990-8).
High-intensity interval training (HIIT) did not affect hypoglycemic awareness in patients with impaired awareness probably because of “a ‘floor’ effect, in that symptom responses could not be further suppressed than they already were,” the investigators speculated.
Regular exercise is recommended for patients with type 1 diabetes, and, like others, they are turning to HIIT – short bursts of intense exercise broken up by brief periods of rest or lower intensity movement – because it appears to deliver the benefits for more moderate exercise in less time.
The findings suggest, however, that high-intensity exercise might increase the risk of severe hypoglycemia in type 1 patients by reducing awareness of its symptoms and blunting hormonal defenses.
The team suspects elevated lactate levels account for the findings. Exercise increases plasma lactate levels, and as blood glucose levels fall, the brain uses lactate as an alternative fuel, which likely blunts the effects of hypoglycemia. Plasma lactate spiked in the study subjects about 15 minutes after exercise.
Participants presented early in the morning after fasting overnight and abstaining from strenuous exercise for 2 days. They were in their mid-20s on average, normal weight, and fairly well balanced between men and women. Patients with type 1 diabetes were eligible for the study if they had hemoglobin A1c levels below 9% and no vascular complications beyond retinopathy. Their duration of diabetes was about 10 years.
The work was funded by the Dutch Diabetes Research Foundation and the European Foundation for the Study of Diabetes. The authors had no conflicts of interest.
A single 15-minute session of high-intensity exercise masked symptoms of subsequent hypoglycemia in patients with type 1 diabetes and normal hypoglycemia awareness, according to Dutch investigators.
Twenty patients with type 1 diabetes – 10 with normal hypoglycemia awareness and 10 with impaired awareness – and 10 healthy subjects were asked to push themselves as hard as they could for 30-second bursts during 15 minutes of stationary bicycling and to go at an easier pace in between, reported Hanne Rooijackers, MD, of the Radboud University Medical Center, Nijmegen, the Netherlands, and colleagues.
The subjects had intravenous cannulae in both forearms, one for blood draws and the other for glucose and insulin administration. All three groups were kept euglycemic during exercise, but then were subjected to hyperinsulinemic-hypoglycemic clamps afterwards. Plasma glucose levels were allowed to fall to 2.6 mmol/L over about 35 min., and were kept there for another 60 min. Trembling, palpitations, anxiety, and other symptoms were serially assessed while patients were hypoglycemic, along with cognitive function and levels of hormones involved with hypoglycemic defense.
For comparison, the subjects all had clamps applied and hypoglycemia symptoms and physiologic responses assessed after a 15-minute session of rest at least 2 weeks apart from the exercise session.
The healthy subjects had a peak of about 20 points on a composite score of hypoglycemia symptoms during rest; exercise reduced the peak score only a small amount to about 18 points. Diabetic patients with normal hypoglycemia awareness hit a peak symptom score of 31 points during rest, which fell substantially after exercise to 22 points. Exercise, meanwhile, had no effect on diabetic patients with impaired awareness; after both rest and exercise, they had a peak composite symptom score of about 11 points, Dr. Rooijackers and colleagues reported (Diabetes. 2017 Jul;66[7]:1990-8).
High-intensity interval training (HIIT) did not affect hypoglycemic awareness in patients with impaired awareness probably because of “a ‘floor’ effect, in that symptom responses could not be further suppressed than they already were,” the investigators speculated.
Regular exercise is recommended for patients with type 1 diabetes, and, like others, they are turning to HIIT – short bursts of intense exercise broken up by brief periods of rest or lower intensity movement – because it appears to deliver the benefits for more moderate exercise in less time.
The findings suggest, however, that high-intensity exercise might increase the risk of severe hypoglycemia in type 1 patients by reducing awareness of its symptoms and blunting hormonal defenses.
The team suspects elevated lactate levels account for the findings. Exercise increases plasma lactate levels, and as blood glucose levels fall, the brain uses lactate as an alternative fuel, which likely blunts the effects of hypoglycemia. Plasma lactate spiked in the study subjects about 15 minutes after exercise.
Participants presented early in the morning after fasting overnight and abstaining from strenuous exercise for 2 days. They were in their mid-20s on average, normal weight, and fairly well balanced between men and women. Patients with type 1 diabetes were eligible for the study if they had hemoglobin A1c levels below 9% and no vascular complications beyond retinopathy. Their duration of diabetes was about 10 years.
The work was funded by the Dutch Diabetes Research Foundation and the European Foundation for the Study of Diabetes. The authors had no conflicts of interest.
FROM DIABETES
Key clinical point:
Major finding: Subjects without diabetes hit a peak of about 20 points on a composite score of hypoglycemia symptoms during rest; exercise reduced the peak score only a small amount to about 18 points. Diabetic patients with normal hypoglycemia awareness hit a peak symptom score of 31 points during rest, which fell substantially after exercise to 22 points.
Data source: Hyperinsulinemic-hypoglycemic clamp experiments in 30 patients.
Disclosures: The work was funded by the Dutch Diabetes Research Foundation and the European Foundation for the Study of Diabetes. The authors had no conflicts of interest.
CABG with arterial grafts provides excellent outcomes for CTO
PARIS – Eighty-eight percent of chronic total occlusions (CTOs) in a large series of patients undergoing coronary artery bypass graft surgery were successfully bypassed using arterial conduits with durable patency.
“Bypass graft surgery using arterial grafts is an acceptable modality of treatment for patients with CTOs and perhaps can be a benchmark against which PCI [percutaneous coronary intervention] for CTOs should be measured,” Teresa May Kieser, MD, said at the annual congress of the European Association of Percutaneous Cardiovascular Interventions.

“We have previously shown in another paper that arterial grafting mitigates the adverse effect of incomplete revascularization,” said Dr. Kieser, a cardiothoracic surgeon at the University of Calgary (Alt.).
In recent years, treatment of CTOs has increasingly drawn the attention of interventional cardiologists. Dr. Kieser presented what she thinks is the first study of coronary artery bypass graft (CABG) surgery for management of CTOs. It included 1,333 consecutive CABG patients with a total of 3,906 bypasses, a whopping 98% of which were arterial grafts, with a mean of 2.9 grafts per patient. Eleven percent of the CABGs were done emergently, 48% urgently, and 41% electively.
The key epidemiologic finding to emerge from the study is that CTOs are quite common in CABG patients. In this series, 47% of CABG patients had a mean of 1.35 chronically occluded coronary arteries.
Of 843 CTOs in three major territories, 88% were able to be bypassed. All of the 246 CTOs in the left anterior descending coronary artery were able to be bypassed, as were 84% of 415 CTOs in the right coronary artery and 85% in the circumflex system.
The CTO group as a whole had significantly greater impairment of left ventricular function. Thirty-seven percent of them had an ejection fraction of 30%-50%, compared with 22% of the non-CTO patients. The 10% prevalence of an left ventricular ejection fraction (LVEF) below 30% in the CTO group was twice that of the non-CTO group. The CTO group was also significantly more likely to undergo incomplete revascularization, by a margin of 21% versus 5.7%.
Operative mortality was 3.7% overall and just 0.55% in the elective CABG patients. In a multivariate logistic regression analysis controlled for surgical urgency, incomplete revascularization, and EuroSCORE risk, operative mortality didn’t differ significantly between the CTO and non-CTO groups.
However, in the presence of CTOs, incomplete revascularization was associated with an 11.6% operative mortality, compared with a 2.8% rate in fully revascularized CTO patients.
A total of 110 patients with bypassed CTOs underwent symptom-driven follow-up coronary angiography at a median of 3.6 years after CABG. Reassuringly, CTO graft patency was noted in 95% of the LAD grafts, 92% of the right coronary artery grafts, and 79% of the circumflex grafts.
Dr. Kieser’s audience of interventional cardiologists was clearly bowled over by her results, not only the high rate of successful surgical bypass of CTOs, but also by her use of arterial grafts 98% of the time.
“This is my personal practice,” she explained. “I just believe in arterial grafting so much. They perform best in CTO arteries because of their lack of competitive flow.”
Session chair Oliver Gämperli, MD, of University Hospital Zurich, commented, “We are very concerned about patency rates, and you showed us fantastic patency rates. This is much better than what we’re used to with saphenous vein grafts. I think we need to talk to our surgeons and try to get them to do more arterial grafts of CTOs.”
It’s worth noting that in the CTO subgroup from the landmark randomized SYNTAX trial, the complete revascularization rate was only about 50% in the PCI group, compared with nearly 65% in the CABG group, he added.
Asked why a cardiac surgeon wouldn’t bypass a CTO, Dr. Kieser rattled off several technical reasons, including a vessel size of less than 1 mm, diffuse disease, extensive scar, or an inaccessible location. But that’s not the whole story, she added. She has heard surgical colleagues say, “The patient doesn’t need that artery, he’s learned to live without it.” That burns her up.
“Patients need every artery in the heart, and the one with a CTO is the best one for an arterial graft because it almost cannot fail, especially to the left anterior descending artery. I think we have to change the mentality of the surgeons to ‘If it can be done, it should be done,’ ” Dr. Kieser said.
She reported having no financial conflicts of interest regarding her study.
PARIS – Eighty-eight percent of chronic total occlusions (CTOs) in a large series of patients undergoing coronary artery bypass graft surgery were successfully bypassed using arterial conduits with durable patency.
“Bypass graft surgery using arterial grafts is an acceptable modality of treatment for patients with CTOs and perhaps can be a benchmark against which PCI [percutaneous coronary intervention] for CTOs should be measured,” Teresa May Kieser, MD, said at the annual congress of the European Association of Percutaneous Cardiovascular Interventions.
“We have previously shown in another paper that arterial grafting mitigates the adverse effect of incomplete revascularization,” said Dr. Kieser, a cardiothoracic surgeon at the University of Calgary (Alt.).
In recent years, treatment of CTOs has increasingly drawn the attention of interventional cardiologists. Dr. Kieser presented what she thinks is the first study of coronary artery bypass graft (CABG) surgery for management of CTOs. It included 1,333 consecutive CABG patients with a total of 3,906 bypasses, a whopping 98% of which were arterial grafts, with a mean of 2.9 grafts per patient. Eleven percent of the CABGs were done emergently, 48% urgently, and 41% electively.
The key epidemiologic finding to emerge from the study is that CTOs are quite common in CABG patients. In this series, 47% of CABG patients had a mean of 1.35 chronically occluded coronary arteries.
Of 843 CTOs in three major territories, 88% were able to be bypassed. All of the 246 CTOs in the left anterior descending coronary artery were able to be bypassed, as were 84% of 415 CTOs in the right coronary artery and 85% in the circumflex system.
The CTO group as a whole had significantly greater impairment of left ventricular function. Thirty-seven percent of them had an ejection fraction of 30%-50%, compared with 22% of the non-CTO patients. The 10% prevalence of an left ventricular ejection fraction (LVEF) below 30% in the CTO group was twice that of the non-CTO group. The CTO group was also significantly more likely to undergo incomplete revascularization, by a margin of 21% versus 5.7%.
Operative mortality was 3.7% overall and just 0.55% in the elective CABG patients. In a multivariate logistic regression analysis controlled for surgical urgency, incomplete revascularization, and EuroSCORE risk, operative mortality didn’t differ significantly between the CTO and non-CTO groups.
However, in the presence of CTOs, incomplete revascularization was associated with an 11.6% operative mortality, compared with a 2.8% rate in fully revascularized CTO patients.
A total of 110 patients with bypassed CTOs underwent symptom-driven follow-up coronary angiography at a median of 3.6 years after CABG. Reassuringly, CTO graft patency was noted in 95% of the LAD grafts, 92% of the right coronary artery grafts, and 79% of the circumflex grafts.
Dr. Kieser’s audience of interventional cardiologists was clearly bowled over by her results, not only the high rate of successful surgical bypass of CTOs, but also by her use of arterial grafts 98% of the time.
“This is my personal practice,” she explained. “I just believe in arterial grafting so much. They perform best in CTO arteries because of their lack of competitive flow.”
Session chair Oliver Gämperli, MD, of University Hospital Zurich, commented, “We are very concerned about patency rates, and you showed us fantastic patency rates. This is much better than what we’re used to with saphenous vein grafts. I think we need to talk to our surgeons and try to get them to do more arterial grafts of CTOs.”
It’s worth noting that in the CTO subgroup from the landmark randomized SYNTAX trial, the complete revascularization rate was only about 50% in the PCI group, compared with nearly 65% in the CABG group, he added.
Asked why a cardiac surgeon wouldn’t bypass a CTO, Dr. Kieser rattled off several technical reasons, including a vessel size of less than 1 mm, diffuse disease, extensive scar, or an inaccessible location. But that’s not the whole story, she added. She has heard surgical colleagues say, “The patient doesn’t need that artery, he’s learned to live without it.” That burns her up.
“Patients need every artery in the heart, and the one with a CTO is the best one for an arterial graft because it almost cannot fail, especially to the left anterior descending artery. I think we have to change the mentality of the surgeons to ‘If it can be done, it should be done,’ ” Dr. Kieser said.
She reported having no financial conflicts of interest regarding her study.
PARIS – Eighty-eight percent of chronic total occlusions (CTOs) in a large series of patients undergoing coronary artery bypass graft surgery were successfully bypassed using arterial conduits with durable patency.
“Bypass graft surgery using arterial grafts is an acceptable modality of treatment for patients with CTOs and perhaps can be a benchmark against which PCI [percutaneous coronary intervention] for CTOs should be measured,” Teresa May Kieser, MD, said at the annual congress of the European Association of Percutaneous Cardiovascular Interventions.
“We have previously shown in another paper that arterial grafting mitigates the adverse effect of incomplete revascularization,” said Dr. Kieser, a cardiothoracic surgeon at the University of Calgary (Alt.).
In recent years, treatment of CTOs has increasingly drawn the attention of interventional cardiologists. Dr. Kieser presented what she thinks is the first study of coronary artery bypass graft (CABG) surgery for management of CTOs. It included 1,333 consecutive CABG patients with a total of 3,906 bypasses, a whopping 98% of which were arterial grafts, with a mean of 2.9 grafts per patient. Eleven percent of the CABGs were done emergently, 48% urgently, and 41% electively.
The key epidemiologic finding to emerge from the study is that CTOs are quite common in CABG patients. In this series, 47% of CABG patients had a mean of 1.35 chronically occluded coronary arteries.
Of 843 CTOs in three major territories, 88% were able to be bypassed. All of the 246 CTOs in the left anterior descending coronary artery were able to be bypassed, as were 84% of 415 CTOs in the right coronary artery and 85% in the circumflex system.
The CTO group as a whole had significantly greater impairment of left ventricular function. Thirty-seven percent of them had an ejection fraction of 30%-50%, compared with 22% of the non-CTO patients. The 10% prevalence of an left ventricular ejection fraction (LVEF) below 30% in the CTO group was twice that of the non-CTO group. The CTO group was also significantly more likely to undergo incomplete revascularization, by a margin of 21% versus 5.7%.
Operative mortality was 3.7% overall and just 0.55% in the elective CABG patients. In a multivariate logistic regression analysis controlled for surgical urgency, incomplete revascularization, and EuroSCORE risk, operative mortality didn’t differ significantly between the CTO and non-CTO groups.
However, in the presence of CTOs, incomplete revascularization was associated with an 11.6% operative mortality, compared with a 2.8% rate in fully revascularized CTO patients.
A total of 110 patients with bypassed CTOs underwent symptom-driven follow-up coronary angiography at a median of 3.6 years after CABG. Reassuringly, CTO graft patency was noted in 95% of the LAD grafts, 92% of the right coronary artery grafts, and 79% of the circumflex grafts.
Dr. Kieser’s audience of interventional cardiologists was clearly bowled over by her results, not only the high rate of successful surgical bypass of CTOs, but also by her use of arterial grafts 98% of the time.
“This is my personal practice,” she explained. “I just believe in arterial grafting so much. They perform best in CTO arteries because of their lack of competitive flow.”
Session chair Oliver Gämperli, MD, of University Hospital Zurich, commented, “We are very concerned about patency rates, and you showed us fantastic patency rates. This is much better than what we’re used to with saphenous vein grafts. I think we need to talk to our surgeons and try to get them to do more arterial grafts of CTOs.”
It’s worth noting that in the CTO subgroup from the landmark randomized SYNTAX trial, the complete revascularization rate was only about 50% in the PCI group, compared with nearly 65% in the CABG group, he added.
Asked why a cardiac surgeon wouldn’t bypass a CTO, Dr. Kieser rattled off several technical reasons, including a vessel size of less than 1 mm, diffuse disease, extensive scar, or an inaccessible location. But that’s not the whole story, she added. She has heard surgical colleagues say, “The patient doesn’t need that artery, he’s learned to live without it.” That burns her up.
“Patients need every artery in the heart, and the one with a CTO is the best one for an arterial graft because it almost cannot fail, especially to the left anterior descending artery. I think we have to change the mentality of the surgeons to ‘If it can be done, it should be done,’ ” Dr. Kieser said.
She reported having no financial conflicts of interest regarding her study.
AT EUROPCR
Key clinical point:
Major finding: Chronic total occlusions were present in 47% of 1,333 consecutive CABG patients, and 88% of the CTOs were successfully bypassed using arterial conduits.
Data source: A retrospective observational study of 1,333 consecutive CABG patients, 47% of whom had one or more chronic total occlusions.
Disclosures: The study presenter reported having no financial conflicts.
Plasma biomarker distinguishes ARDS, acute heart failure
WASHINGTON – Plasma levels of an interleukin-33 receptor that’s involved in inflammation regulation appeared able to discriminate between acute respiratory distress syndrome and acute decompensated heart failure in an analysis with 72 patients.
In a second study, high plasma levels of the same interleukin-33 receptor, known as soluble suppressor of tumorgenicity 2 (sST2), identified acute respiratory distress syndrome (ARDS) patients who were sicker and more responsive to conservative fluid management, Sean D. Levy, MD, said at an international conference of the American Thoracic Society.

In order to assess the ability of sST2 to reliably distinguish patients with ARDS from those with acute decompensated heart failure, he and his associates selected 72 patients seen at the Massachusetts General Hospital in Boston with an initial diagnosis of acute decompensated heart failure accompanied by bilateral lung infiltrates and acute hypoxemia respiratory failure requiring endotracheal intubation and mechanical ventilation. The investigators measured the sST2 level in a plasma specimen from each patient. In addition, after each patient either left the hospital or died, their case underwent review by two critical care physicians who retrospectively rediagnosed the patients as either having ARDS or acute decompensated heart failure. This divided the cohort into 30 patients with ARDS and 42 with true acute heart failure. The two subgroups matched up fairly closely for most clinical measures and comorbidities, but APACHE III (Acute Physiology and Chronic Health Evaluation III) scores averaged significantly higher in the ARDS patients.
The plasma levels of sST2 showed a dramatic split between the two subgroups. The 30 patients retrospectively diagnosed with ARDS had an average level of 386 ng/mL with an interquartile range of 318-611 ng/mL. The 42 acute decompensated heart failure patients averaged a sST2 level of 148 ng/mL, with an interquartile range of 84-225 ng/mL. The area under the receiver operator curve for discriminating between ARDS and acute heart failure using a cutpoint of 271 mg/mL was 0.86, showing “good” discrimination, Dr. Levy said. This cutpoint had a sensitivity of 83% and specificity of 88% for correctly distinguishing between ARDS and acute heart failure.
In a second analysis, Dr. Levy and his associates looked at the ability of sST2 levels to separate out patients with acute lung injury who had a more robust response to either the conservative or liberal fluid-management strategies tested in the Fluid and Catheter Treatment Trial (FACTT), run by the National Heart, Lung, and Blood Institute’s ARDS Clinical Trials Network. The primary outcome of FACTT was death from any cause 60 days after entry, and this showed no significant difference between conservative (restricted fluids and increased urine output) and liberal (the reverse) fluid management strategies in acute lung injury patients (N Engl J Med. 2006 Jun 15;354[14]:2564-75). From among the 1,001 patients enrolled in FACTT, 826 had specimens available for measuring sST2 (Crit Care Med. 2013 Nov;41[11]:2521-31),
The researchers applied the sST2 cut point they derived in the first analysis to the FACTT cohort and identified 133 (16%) patients with a low sST2 level and 693 (84%) with a high level. The patients with high sST2 were sicker, with significantly higher APACHE III scores, worse acidemia, and worse renal function.
Patients with high sST2 levels had a significant increase in ventilator-free days on conservative fluid management, compared with liberal management, while the two management strategies produced virtually identical results in the patients with low levels of sST2. Patients with high sST2 also had a significantly quicker time to extubation on a conservative strategy compared with the liberal strategy, and again this correlation did not exist among patients with low sST2. However, as in the overall trial a conservative strategy had no discernible impact on 60-day mortality, compared with the liberal strategy, even in the subgroup with high sST2.
Dr. Levy had no disclosures.
[email protected]
On Twitter @mitchelzoler
WASHINGTON – Plasma levels of an interleukin-33 receptor that’s involved in inflammation regulation appeared able to discriminate between acute respiratory distress syndrome and acute decompensated heart failure in an analysis with 72 patients.
In a second study, high plasma levels of the same interleukin-33 receptor, known as soluble suppressor of tumorgenicity 2 (sST2), identified acute respiratory distress syndrome (ARDS) patients who were sicker and more responsive to conservative fluid management, Sean D. Levy, MD, said at an international conference of the American Thoracic Society.
In order to assess the ability of sST2 to reliably distinguish patients with ARDS from those with acute decompensated heart failure, he and his associates selected 72 patients seen at the Massachusetts General Hospital in Boston with an initial diagnosis of acute decompensated heart failure accompanied by bilateral lung infiltrates and acute hypoxemia respiratory failure requiring endotracheal intubation and mechanical ventilation. The investigators measured the sST2 level in a plasma specimen from each patient. In addition, after each patient either left the hospital or died, their case underwent review by two critical care physicians who retrospectively rediagnosed the patients as either having ARDS or acute decompensated heart failure. This divided the cohort into 30 patients with ARDS and 42 with true acute heart failure. The two subgroups matched up fairly closely for most clinical measures and comorbidities, but APACHE III (Acute Physiology and Chronic Health Evaluation III) scores averaged significantly higher in the ARDS patients.
The plasma levels of sST2 showed a dramatic split between the two subgroups. The 30 patients retrospectively diagnosed with ARDS had an average level of 386 ng/mL with an interquartile range of 318-611 ng/mL. The 42 acute decompensated heart failure patients averaged a sST2 level of 148 ng/mL, with an interquartile range of 84-225 ng/mL. The area under the receiver operator curve for discriminating between ARDS and acute heart failure using a cutpoint of 271 mg/mL was 0.86, showing “good” discrimination, Dr. Levy said. This cutpoint had a sensitivity of 83% and specificity of 88% for correctly distinguishing between ARDS and acute heart failure.
In a second analysis, Dr. Levy and his associates looked at the ability of sST2 levels to separate out patients with acute lung injury who had a more robust response to either the conservative or liberal fluid-management strategies tested in the Fluid and Catheter Treatment Trial (FACTT), run by the National Heart, Lung, and Blood Institute’s ARDS Clinical Trials Network. The primary outcome of FACTT was death from any cause 60 days after entry, and this showed no significant difference between conservative (restricted fluids and increased urine output) and liberal (the reverse) fluid management strategies in acute lung injury patients (N Engl J Med. 2006 Jun 15;354[14]:2564-75). From among the 1,001 patients enrolled in FACTT, 826 had specimens available for measuring sST2 (Crit Care Med. 2013 Nov;41[11]:2521-31),
The researchers applied the sST2 cut point they derived in the first analysis to the FACTT cohort and identified 133 (16%) patients with a low sST2 level and 693 (84%) with a high level. The patients with high sST2 were sicker, with significantly higher APACHE III scores, worse acidemia, and worse renal function.
Patients with high sST2 levels had a significant increase in ventilator-free days on conservative fluid management, compared with liberal management, while the two management strategies produced virtually identical results in the patients with low levels of sST2. Patients with high sST2 also had a significantly quicker time to extubation on a conservative strategy compared with the liberal strategy, and again this correlation did not exist among patients with low sST2. However, as in the overall trial a conservative strategy had no discernible impact on 60-day mortality, compared with the liberal strategy, even in the subgroup with high sST2.
Dr. Levy had no disclosures.
[email protected]
On Twitter @mitchelzoler
WASHINGTON – Plasma levels of an interleukin-33 receptor that’s involved in inflammation regulation appeared able to discriminate between acute respiratory distress syndrome and acute decompensated heart failure in an analysis with 72 patients.
In a second study, high plasma levels of the same interleukin-33 receptor, known as soluble suppressor of tumorgenicity 2 (sST2), identified acute respiratory distress syndrome (ARDS) patients who were sicker and more responsive to conservative fluid management, Sean D. Levy, MD, said at an international conference of the American Thoracic Society.
In order to assess the ability of sST2 to reliably distinguish patients with ARDS from those with acute decompensated heart failure, he and his associates selected 72 patients seen at the Massachusetts General Hospital in Boston with an initial diagnosis of acute decompensated heart failure accompanied by bilateral lung infiltrates and acute hypoxemia respiratory failure requiring endotracheal intubation and mechanical ventilation. The investigators measured the sST2 level in a plasma specimen from each patient. In addition, after each patient either left the hospital or died, their case underwent review by two critical care physicians who retrospectively rediagnosed the patients as either having ARDS or acute decompensated heart failure. This divided the cohort into 30 patients with ARDS and 42 with true acute heart failure. The two subgroups matched up fairly closely for most clinical measures and comorbidities, but APACHE III (Acute Physiology and Chronic Health Evaluation III) scores averaged significantly higher in the ARDS patients.
The plasma levels of sST2 showed a dramatic split between the two subgroups. The 30 patients retrospectively diagnosed with ARDS had an average level of 386 ng/mL with an interquartile range of 318-611 ng/mL. The 42 acute decompensated heart failure patients averaged a sST2 level of 148 ng/mL, with an interquartile range of 84-225 ng/mL. The area under the receiver operator curve for discriminating between ARDS and acute heart failure using a cutpoint of 271 mg/mL was 0.86, showing “good” discrimination, Dr. Levy said. This cutpoint had a sensitivity of 83% and specificity of 88% for correctly distinguishing between ARDS and acute heart failure.
In a second analysis, Dr. Levy and his associates looked at the ability of sST2 levels to separate out patients with acute lung injury who had a more robust response to either the conservative or liberal fluid-management strategies tested in the Fluid and Catheter Treatment Trial (FACTT), run by the National Heart, Lung, and Blood Institute’s ARDS Clinical Trials Network. The primary outcome of FACTT was death from any cause 60 days after entry, and this showed no significant difference between conservative (restricted fluids and increased urine output) and liberal (the reverse) fluid management strategies in acute lung injury patients (N Engl J Med. 2006 Jun 15;354[14]:2564-75). From among the 1,001 patients enrolled in FACTT, 826 had specimens available for measuring sST2 (Crit Care Med. 2013 Nov;41[11]:2521-31),
The researchers applied the sST2 cut point they derived in the first analysis to the FACTT cohort and identified 133 (16%) patients with a low sST2 level and 693 (84%) with a high level. The patients with high sST2 were sicker, with significantly higher APACHE III scores, worse acidemia, and worse renal function.
Patients with high sST2 levels had a significant increase in ventilator-free days on conservative fluid management, compared with liberal management, while the two management strategies produced virtually identical results in the patients with low levels of sST2. Patients with high sST2 also had a significantly quicker time to extubation on a conservative strategy compared with the liberal strategy, and again this correlation did not exist among patients with low sST2. However, as in the overall trial a conservative strategy had no discernible impact on 60-day mortality, compared with the liberal strategy, even in the subgroup with high sST2.
Dr. Levy had no disclosures.
[email protected]
On Twitter @mitchelzoler
AT ATS 2017
Key clinical point:
Major finding: An sST2 cutpoint of 271 ng/mL discriminated between ARDS and acute heart failure with 83% sensitivity and 88% specificity.
Data source: Review of 72 patients admitted for acute decompensated heart failure at one U.S. center.
Disclosures: Dr. Levy had no disclosures.
PD-1 inhibitors treat resistant gray zone lymphoma

Three case reports published in The New England Journal of Medicine describe the successful use of PD-1 inhibitors in gray zone lymphoma.
Two patients who had failed treatment with DA-EPOCH-R (dose-adjusted etoposide, doxorubicin, and cyclophosphamide with vincristine, prednisone, and rituximab) ultimately responded to treatment with pembrolizumab.
Another patient—who had previously received 2 chemotherapy regimens, monotherapy with brentuximab vedotin, and radiation—responded to treatment with nivolumab.
Pembrolizumab treatment
An 18-year-old woman with mediastinal gray-zone lymphoma initially had a partial response to DA-EPOCH-R. However, she progressed 6 weeks after salvage radiotherapy.
She went on to receive pembrolizumab, had a complete metabolic response, and proceeded to allogeneic transplant after 235 days of treatment.
A 76-year-old man with mediastinal gray-zone lymphoma also had a partial response to DA-EPOCH-R but later progressed.
He proceeded to pembrolizumab and had a complete metabolic response. He was still in remission on day 381 of treatment.
Nivolumab treatment
The patient who received nivolumab is Bobbie Flexer, an 80-year-old retired mathematics professor.
“For me, trying nivolumab was a binary choice: I could try the drug or I could give up,” Flexer said.
She had initially achieved a complete metabolic response to DA-EPOCH-R, but her disease progressed after 6 cycles of treatment.
“Given Bobbie’s age and her resistance to chemotherapy, it was difficult to simply increase her dose,” said Flexer’s oncologist, Manali Kamdar, MD, of the University of Colorado School of Medicine in Aurora.
“Bobbie’s tumor biopsy expressed a protein called CD30, and so we started her on brentuximab, which targets these CD30 cells. Unfortunately, Bobbie’s disease progressed through multiple cycles of brentuximab. Subsequently, we switched her to another combined chemotherapy—namely, gemcitabine with oxaliplatin [plus rituximab].”
When that regimen and mediastinal radiation both proved unsuccessful, Dr Kamdar started Flexer on nivolumab.
“Within one dose, she was in less pain, and she looked much better,” Dr Kamdar said.
A PET scan after 6 doses showed that Flexer’s disease was in complete remission, and she was still in remission on day 161 of treatment.
She did experience adverse effects, including 2 bouts of pneumonitis, which were successfully treated with prednisone.
Flexer also experienced an uptick in pancreas enzymes that caused high blood glucose levels. She is learning to treat that side effect with insulin. And dietitians helped her manage expected gut-related side effects of nivolumab.
To Dr Kamdar, Flexer’s case was striking enough to warrant submitting a report to NEJM.
Coincidentally, the journal had just received 2 similar case reports from the National Institutes of Health, in which researchers had used pembrolizumab to target gray zone lymphoma in a nearly identical way.
Together, these cases suggest a new strategy for treating gray zone lymphoma. ![]()
Three case reports published in The New England Journal of Medicine describe the successful use of PD-1 inhibitors in gray zone lymphoma.
Two patients who had failed treatment with DA-EPOCH-R (dose-adjusted etoposide, doxorubicin, and cyclophosphamide with vincristine, prednisone, and rituximab) ultimately responded to treatment with pembrolizumab.
Another patient—who had previously received 2 chemotherapy regimens, monotherapy with brentuximab vedotin, and radiation—responded to treatment with nivolumab.
Pembrolizumab treatment
An 18-year-old woman with mediastinal gray-zone lymphoma initially had a partial response to DA-EPOCH-R. However, she progressed 6 weeks after salvage radiotherapy.
She went on to receive pembrolizumab, had a complete metabolic response, and proceeded to allogeneic transplant after 235 days of treatment.
A 76-year-old man with mediastinal gray-zone lymphoma also had a partial response to DA-EPOCH-R but later progressed.
He proceeded to pembrolizumab and had a complete metabolic response. He was still in remission on day 381 of treatment.
Nivolumab treatment
The patient who received nivolumab is Bobbie Flexer, an 80-year-old retired mathematics professor.
“For me, trying nivolumab was a binary choice: I could try the drug or I could give up,” Flexer said.
She had initially achieved a complete metabolic response to DA-EPOCH-R, but her disease progressed after 6 cycles of treatment.
“Given Bobbie’s age and her resistance to chemotherapy, it was difficult to simply increase her dose,” said Flexer’s oncologist, Manali Kamdar, MD, of the University of Colorado School of Medicine in Aurora.
“Bobbie’s tumor biopsy expressed a protein called CD30, and so we started her on brentuximab, which targets these CD30 cells. Unfortunately, Bobbie’s disease progressed through multiple cycles of brentuximab. Subsequently, we switched her to another combined chemotherapy—namely, gemcitabine with oxaliplatin [plus rituximab].”
When that regimen and mediastinal radiation both proved unsuccessful, Dr Kamdar started Flexer on nivolumab.
“Within one dose, she was in less pain, and she looked much better,” Dr Kamdar said.
A PET scan after 6 doses showed that Flexer’s disease was in complete remission, and she was still in remission on day 161 of treatment.
She did experience adverse effects, including 2 bouts of pneumonitis, which were successfully treated with prednisone.
Flexer also experienced an uptick in pancreas enzymes that caused high blood glucose levels. She is learning to treat that side effect with insulin. And dietitians helped her manage expected gut-related side effects of nivolumab.
To Dr Kamdar, Flexer’s case was striking enough to warrant submitting a report to NEJM.
Coincidentally, the journal had just received 2 similar case reports from the National Institutes of Health, in which researchers had used pembrolizumab to target gray zone lymphoma in a nearly identical way.
Together, these cases suggest a new strategy for treating gray zone lymphoma. ![]()
Three case reports published in The New England Journal of Medicine describe the successful use of PD-1 inhibitors in gray zone lymphoma.
Two patients who had failed treatment with DA-EPOCH-R (dose-adjusted etoposide, doxorubicin, and cyclophosphamide with vincristine, prednisone, and rituximab) ultimately responded to treatment with pembrolizumab.
Another patient—who had previously received 2 chemotherapy regimens, monotherapy with brentuximab vedotin, and radiation—responded to treatment with nivolumab.
Pembrolizumab treatment
An 18-year-old woman with mediastinal gray-zone lymphoma initially had a partial response to DA-EPOCH-R. However, she progressed 6 weeks after salvage radiotherapy.
She went on to receive pembrolizumab, had a complete metabolic response, and proceeded to allogeneic transplant after 235 days of treatment.
A 76-year-old man with mediastinal gray-zone lymphoma also had a partial response to DA-EPOCH-R but later progressed.
He proceeded to pembrolizumab and had a complete metabolic response. He was still in remission on day 381 of treatment.
Nivolumab treatment
The patient who received nivolumab is Bobbie Flexer, an 80-year-old retired mathematics professor.
“For me, trying nivolumab was a binary choice: I could try the drug or I could give up,” Flexer said.
She had initially achieved a complete metabolic response to DA-EPOCH-R, but her disease progressed after 6 cycles of treatment.
“Given Bobbie’s age and her resistance to chemotherapy, it was difficult to simply increase her dose,” said Flexer’s oncologist, Manali Kamdar, MD, of the University of Colorado School of Medicine in Aurora.
“Bobbie’s tumor biopsy expressed a protein called CD30, and so we started her on brentuximab, which targets these CD30 cells. Unfortunately, Bobbie’s disease progressed through multiple cycles of brentuximab. Subsequently, we switched her to another combined chemotherapy—namely, gemcitabine with oxaliplatin [plus rituximab].”
When that regimen and mediastinal radiation both proved unsuccessful, Dr Kamdar started Flexer on nivolumab.
“Within one dose, she was in less pain, and she looked much better,” Dr Kamdar said.
A PET scan after 6 doses showed that Flexer’s disease was in complete remission, and she was still in remission on day 161 of treatment.
She did experience adverse effects, including 2 bouts of pneumonitis, which were successfully treated with prednisone.
Flexer also experienced an uptick in pancreas enzymes that caused high blood glucose levels. She is learning to treat that side effect with insulin. And dietitians helped her manage expected gut-related side effects of nivolumab.
To Dr Kamdar, Flexer’s case was striking enough to warrant submitting a report to NEJM.
Coincidentally, the journal had just received 2 similar case reports from the National Institutes of Health, in which researchers had used pembrolizumab to target gray zone lymphoma in a nearly identical way.
Together, these cases suggest a new strategy for treating gray zone lymphoma. ![]()
Vancomycin research reveals reasons for readmissions and prolonged stays
NEW ORLEANS – Approximately 20% of patients treated with vancomycin for an acute bacterial skin and skin structure infection remained in the hospital 8 days or longer, and about 7% experienced a readmission within 30 days, a retrospective study of 507 patients in the Geisinger Health System database showed.
“We found, for those who had a readmission, the major drivers were those who are your ‘health care frequent flyers’ – those who were admitted in the past 6 months,” said Thomas Lodise, PharmD, PhD, professor of pharmacy practice at Albany (N.Y.) College of Pharmacy and Health Sciences. “So, patients with a previous hospitalization are more likely to be treated again for all-cause admission within 30 days of discharge.” In addition, people with a lower-extremity abscess, particularly older patients with diabetes, and those with a traumatic wound were also more likely to return within 30 days.

Identifying the population at highest readmission risk could become more important soon. “Even though hospitals are not penalized for skin infection readmissions, there is some talk of adding that to the Medicare penalty,” Dr. Lodise said.
“It’s under review now by Medicare,” said Kenneth LaPensee, PhD, a consultant for Paratek Pharmaceuticals, King of Prussia, Pa., a firm developing an antibiotic to treat patients with an acute bacterial skin and skin structure infection (ABSSSI).
Dr. Lodise, Dr. LaPensee, and their colleagues studied adults hospitalized for an ABSSSI primary diagnosis based on ICD-9 codes and treated with at least 2 days of vancomycin. Participants were seen within the integrated Geisinger Health System between 2010 and 2015.
A total 6.9% of patients were readmitted within 30 days or had repeat emergency department visits. That group included more people with a body mass index of 36 kg/m2 or greater – 8.4%, compared with 6.2% of those with a BMI of less than 36. Other factors associated with readmission included smoking or a history of smoking (9.8% vs. 2.7% for nonsmokers) and a history of ABSSSI not requiring hospitalization vs. no prior history of ABSSSI, 22.2% vs. 6.6%, respectively.
In addition, those with a prior hospital admission not related to skin and skin structure infection were at higher risk, 8.8%, compared with 6.3% for those with no prior hospital admission. A prior hospital outpatient visit was likewise associated with a higher risk for readmission, 12.0%, compared with 5.4% without such a history.
Greater disease severity did not appear to correlate with a higher risk of 30-day readmission in the study. The researchers compared the groups by both Eron classification and the Charlson Comorbidity Index disease severity measures.
“People with more comorbidities had higher readmission rates, but it wasn’t statistically significant,” Dr. Lodise said. Also, “we saw some signaling – like with older age and some differences with race – [that] nonwhites were more likely to get readmitted. A total 6.7% of readmissions were among people older than 65 years, compared with 7.2% of younger people.” Advanced age was a factor in the bivariate analysis, but not in the logistic regression, Dr. LaPensee said.
“We’re going to repeat this in a larger data set. We’re planning for 10,000 patients,” Dr. Lodise said. “In our next cohort, we’ll be able to delineate more patient covariates.” An unanswered question is whether treatment with an agent other than vancomycin could improve readmission rates.
Using the same Geisinger database, the investigators also examined prolonged length of stay for patients with ABSSSIs treated with vancomycin. Almost one-fifth, 19.9%, met their definition of a prolonged stay of 8 days or longer.
The average length of stay was 7 days. “We were a bit surprised. We anticipated it being closer to 4 or 5 days,” Dr. Lodise said. “Then we wanted to find out who are these patients with these prolonged lengths of stay?
“The interesting thing was, things you think would be predictive, like increased age or high BMI [body mass index], were not,” Dr. Lodise said. “But what we did find is being elderly with diabetes and having a lower-extremity infection or a lower-extremity infection with an abscess – this was the group at greatest risk for a prolonged length of stay.” Those findings make sense, he added, because those patients tend to be slow responders, and because intravenous vancomycin has no oral, step-down formulation.
Unlike the readmission risk factors, Eron disease severity “was … very predictive of a prolonged length of stay,” Dr. Lodise said.
“These are really correlated – those patients with longer length of stay are more likely to get readmitted,” Dr. Lodise said. “In these more-difficult-to-treat patient populations, they really need more attention [to figure out] what is going on with them, why they keep coming back to the hospital, or why are they staying in so long.”
Dr. Lodise is a consultant for Paratek Pharmaceuticals, the study sponsor. Dr. LaPensee is a Paratek employee.
NEW ORLEANS – Approximately 20% of patients treated with vancomycin for an acute bacterial skin and skin structure infection remained in the hospital 8 days or longer, and about 7% experienced a readmission within 30 days, a retrospective study of 507 patients in the Geisinger Health System database showed.
“We found, for those who had a readmission, the major drivers were those who are your ‘health care frequent flyers’ – those who were admitted in the past 6 months,” said Thomas Lodise, PharmD, PhD, professor of pharmacy practice at Albany (N.Y.) College of Pharmacy and Health Sciences. “So, patients with a previous hospitalization are more likely to be treated again for all-cause admission within 30 days of discharge.” In addition, people with a lower-extremity abscess, particularly older patients with diabetes, and those with a traumatic wound were also more likely to return within 30 days.
Identifying the population at highest readmission risk could become more important soon. “Even though hospitals are not penalized for skin infection readmissions, there is some talk of adding that to the Medicare penalty,” Dr. Lodise said.
“It’s under review now by Medicare,” said Kenneth LaPensee, PhD, a consultant for Paratek Pharmaceuticals, King of Prussia, Pa., a firm developing an antibiotic to treat patients with an acute bacterial skin and skin structure infection (ABSSSI).
Dr. Lodise, Dr. LaPensee, and their colleagues studied adults hospitalized for an ABSSSI primary diagnosis based on ICD-9 codes and treated with at least 2 days of vancomycin. Participants were seen within the integrated Geisinger Health System between 2010 and 2015.
A total 6.9% of patients were readmitted within 30 days or had repeat emergency department visits. That group included more people with a body mass index of 36 kg/m2 or greater – 8.4%, compared with 6.2% of those with a BMI of less than 36. Other factors associated with readmission included smoking or a history of smoking (9.8% vs. 2.7% for nonsmokers) and a history of ABSSSI not requiring hospitalization vs. no prior history of ABSSSI, 22.2% vs. 6.6%, respectively.
In addition, those with a prior hospital admission not related to skin and skin structure infection were at higher risk, 8.8%, compared with 6.3% for those with no prior hospital admission. A prior hospital outpatient visit was likewise associated with a higher risk for readmission, 12.0%, compared with 5.4% without such a history.
Greater disease severity did not appear to correlate with a higher risk of 30-day readmission in the study. The researchers compared the groups by both Eron classification and the Charlson Comorbidity Index disease severity measures.
“People with more comorbidities had higher readmission rates, but it wasn’t statistically significant,” Dr. Lodise said. Also, “we saw some signaling – like with older age and some differences with race – [that] nonwhites were more likely to get readmitted. A total 6.7% of readmissions were among people older than 65 years, compared with 7.2% of younger people.” Advanced age was a factor in the bivariate analysis, but not in the logistic regression, Dr. LaPensee said.
“We’re going to repeat this in a larger data set. We’re planning for 10,000 patients,” Dr. Lodise said. “In our next cohort, we’ll be able to delineate more patient covariates.” An unanswered question is whether treatment with an agent other than vancomycin could improve readmission rates.
Using the same Geisinger database, the investigators also examined prolonged length of stay for patients with ABSSSIs treated with vancomycin. Almost one-fifth, 19.9%, met their definition of a prolonged stay of 8 days or longer.
The average length of stay was 7 days. “We were a bit surprised. We anticipated it being closer to 4 or 5 days,” Dr. Lodise said. “Then we wanted to find out who are these patients with these prolonged lengths of stay?
“The interesting thing was, things you think would be predictive, like increased age or high BMI [body mass index], were not,” Dr. Lodise said. “But what we did find is being elderly with diabetes and having a lower-extremity infection or a lower-extremity infection with an abscess – this was the group at greatest risk for a prolonged length of stay.” Those findings make sense, he added, because those patients tend to be slow responders, and because intravenous vancomycin has no oral, step-down formulation.
Unlike the readmission risk factors, Eron disease severity “was … very predictive of a prolonged length of stay,” Dr. Lodise said.
“These are really correlated – those patients with longer length of stay are more likely to get readmitted,” Dr. Lodise said. “In these more-difficult-to-treat patient populations, they really need more attention [to figure out] what is going on with them, why they keep coming back to the hospital, or why are they staying in so long.”
Dr. Lodise is a consultant for Paratek Pharmaceuticals, the study sponsor. Dr. LaPensee is a Paratek employee.
NEW ORLEANS – Approximately 20% of patients treated with vancomycin for an acute bacterial skin and skin structure infection remained in the hospital 8 days or longer, and about 7% experienced a readmission within 30 days, a retrospective study of 507 patients in the Geisinger Health System database showed.
“We found, for those who had a readmission, the major drivers were those who are your ‘health care frequent flyers’ – those who were admitted in the past 6 months,” said Thomas Lodise, PharmD, PhD, professor of pharmacy practice at Albany (N.Y.) College of Pharmacy and Health Sciences. “So, patients with a previous hospitalization are more likely to be treated again for all-cause admission within 30 days of discharge.” In addition, people with a lower-extremity abscess, particularly older patients with diabetes, and those with a traumatic wound were also more likely to return within 30 days.
Identifying the population at highest readmission risk could become more important soon. “Even though hospitals are not penalized for skin infection readmissions, there is some talk of adding that to the Medicare penalty,” Dr. Lodise said.
“It’s under review now by Medicare,” said Kenneth LaPensee, PhD, a consultant for Paratek Pharmaceuticals, King of Prussia, Pa., a firm developing an antibiotic to treat patients with an acute bacterial skin and skin structure infection (ABSSSI).
Dr. Lodise, Dr. LaPensee, and their colleagues studied adults hospitalized for an ABSSSI primary diagnosis based on ICD-9 codes and treated with at least 2 days of vancomycin. Participants were seen within the integrated Geisinger Health System between 2010 and 2015.
A total 6.9% of patients were readmitted within 30 days or had repeat emergency department visits. That group included more people with a body mass index of 36 kg/m2 or greater – 8.4%, compared with 6.2% of those with a BMI of less than 36. Other factors associated with readmission included smoking or a history of smoking (9.8% vs. 2.7% for nonsmokers) and a history of ABSSSI not requiring hospitalization vs. no prior history of ABSSSI, 22.2% vs. 6.6%, respectively.
In addition, those with a prior hospital admission not related to skin and skin structure infection were at higher risk, 8.8%, compared with 6.3% for those with no prior hospital admission. A prior hospital outpatient visit was likewise associated with a higher risk for readmission, 12.0%, compared with 5.4% without such a history.
Greater disease severity did not appear to correlate with a higher risk of 30-day readmission in the study. The researchers compared the groups by both Eron classification and the Charlson Comorbidity Index disease severity measures.
“People with more comorbidities had higher readmission rates, but it wasn’t statistically significant,” Dr. Lodise said. Also, “we saw some signaling – like with older age and some differences with race – [that] nonwhites were more likely to get readmitted. A total 6.7% of readmissions were among people older than 65 years, compared with 7.2% of younger people.” Advanced age was a factor in the bivariate analysis, but not in the logistic regression, Dr. LaPensee said.
“We’re going to repeat this in a larger data set. We’re planning for 10,000 patients,” Dr. Lodise said. “In our next cohort, we’ll be able to delineate more patient covariates.” An unanswered question is whether treatment with an agent other than vancomycin could improve readmission rates.
Using the same Geisinger database, the investigators also examined prolonged length of stay for patients with ABSSSIs treated with vancomycin. Almost one-fifth, 19.9%, met their definition of a prolonged stay of 8 days or longer.
The average length of stay was 7 days. “We were a bit surprised. We anticipated it being closer to 4 or 5 days,” Dr. Lodise said. “Then we wanted to find out who are these patients with these prolonged lengths of stay?
“The interesting thing was, things you think would be predictive, like increased age or high BMI [body mass index], were not,” Dr. Lodise said. “But what we did find is being elderly with diabetes and having a lower-extremity infection or a lower-extremity infection with an abscess – this was the group at greatest risk for a prolonged length of stay.” Those findings make sense, he added, because those patients tend to be slow responders, and because intravenous vancomycin has no oral, step-down formulation.
Unlike the readmission risk factors, Eron disease severity “was … very predictive of a prolonged length of stay,” Dr. Lodise said.
“These are really correlated – those patients with longer length of stay are more likely to get readmitted,” Dr. Lodise said. “In these more-difficult-to-treat patient populations, they really need more attention [to figure out] what is going on with them, why they keep coming back to the hospital, or why are they staying in so long.”
Dr. Lodise is a consultant for Paratek Pharmaceuticals, the study sponsor. Dr. LaPensee is a Paratek employee.
AT ASM MICROBE 2017
Key clinical point: Older patients with diabetes and lower-extremity abscesses are at particularly high risk for readmissions and prolonged length of hospital stay.
Major finding: Approximately 20% of patients treated with vancomycin for an acute bacterial skin and skin structure infection remained in the hospital 8 days or longer.
Data source: A review of 507 Geisinger Health System patients with acute bacterial skin and skin structure infections treated with at least 2 days of vancomycin.
Disclosures: Dr. Lodise is a consultant for Paratek Pharmaceuticals, the study sponsor. Dr. LaPensee is a Paratek employee.
Ixekizumab helps PsA patients who failed a TNFi
MADRID – The anti–interleukin-17 drug ixekizumab, already on the U.S. market for treating psoriasis, showed efficacy and safety for treating psoriatic arthritis in patients who previously failed to respond to or tolerate a tumor necrosis factor inhibitor in a pivotal, phase 3 trial with 363 patients.
Treatment of patients with psoriatic arthritis (PsA) with ixekizumab (Taltz) led to improvements, compared with placebo, in arthritis, physical function, and psoriasis. These patients were unresponsive to or intolerant of a tumor necrosis factor inhibitor (TNFi) at rates similar to previously reported response rates for PsA patients who were TNFi naive, Peter Nash, MD, said at the European Congress of Rheumatology.
A published report with the data presented by Dr. Nash also recently appeared (Lancet. 2017;389[10086]:2317-27).

Based in part on the results from this trial, as well as results from a companion phase 3 trial that enrolled PsA patients naive to a TNFi (Ann Rheum Dis. 2017 Jan; 6[1]:79-87), the company that markets ixekizumab, Eli Lilly, filed an application with the Food and Drug Administration in early 2017 to have a new label indication for PsA, said a company spokeswoman.
“At least half of PsA patients don’t get at least a 20% improvement [an ACR20 response] on a TNFi, and so they are looking for something else,” explained Mark C. Genovese, MD, professor of medicine and director of the Rheumatology Clinic at Stanford (Calif.) University and a coinvestigator on the trial reported by Dr. Nash. “There is pent up demand” for an alternative to a TNFi for treating PsA, Dr. Genovese said in an interview.

The finding also sets ixekizumab apart from secukinumab (Cosentyx), another interleukin-17 inhibitor that already has FDA approval for treating PsA but that has not been specifically tested in PsA patients who failed or didn’t tolerate a TNFi, he noted.
The SPIRIT-P2 results also showed superior outcomes for patients treated with an ixekizumab injection once every 2 or 4 weeks, compared with placebo, by several secondary measures, including ACR50 and ACR70 rates and minimal disease activity. The ACR70 rate after 24 weeks on treatment was 23% with a dose of ixekizumab every 4 weeks and none with placebo. Minimal disease activity was reached by about a quarter of patients on either dosage of the active drug and by 3% of patients on placebo.
Despite the apparent role for ixekizumab when TNFi treatment fails, the TNFi drug class remains the clear first-line choice for PsA patients who are starting a biological drug for the first time. Not only do the TNFis have a much longer and more extensive track record but they also generally receive better insurance coverage that minimizes out-of-pocket expenses for patients, Dr. Genovese said.
SPIRIT-P2 was sponsored by Eli Lilly, the company that markets ixekizumab. Dr. Nash has been a speaker for or consultant to and has received research funding from Eli Lily and for several other companies. Dr. Genovese has been a consultant to and has received research funding from Eli Lilly, AbbVie, Astellas, Galapagos, Pfizer, and Vertex.
[email protected]
On Twitter @mitchelzoler
MADRID – The anti–interleukin-17 drug ixekizumab, already on the U.S. market for treating psoriasis, showed efficacy and safety for treating psoriatic arthritis in patients who previously failed to respond to or tolerate a tumor necrosis factor inhibitor in a pivotal, phase 3 trial with 363 patients.
Treatment of patients with psoriatic arthritis (PsA) with ixekizumab (Taltz) led to improvements, compared with placebo, in arthritis, physical function, and psoriasis. These patients were unresponsive to or intolerant of a tumor necrosis factor inhibitor (TNFi) at rates similar to previously reported response rates for PsA patients who were TNFi naive, Peter Nash, MD, said at the European Congress of Rheumatology.
A published report with the data presented by Dr. Nash also recently appeared (Lancet. 2017;389[10086]:2317-27).
Based in part on the results from this trial, as well as results from a companion phase 3 trial that enrolled PsA patients naive to a TNFi (Ann Rheum Dis. 2017 Jan; 6[1]:79-87), the company that markets ixekizumab, Eli Lilly, filed an application with the Food and Drug Administration in early 2017 to have a new label indication for PsA, said a company spokeswoman.
“At least half of PsA patients don’t get at least a 20% improvement [an ACR20 response] on a TNFi, and so they are looking for something else,” explained Mark C. Genovese, MD, professor of medicine and director of the Rheumatology Clinic at Stanford (Calif.) University and a coinvestigator on the trial reported by Dr. Nash. “There is pent up demand” for an alternative to a TNFi for treating PsA, Dr. Genovese said in an interview.
The finding also sets ixekizumab apart from secukinumab (Cosentyx), another interleukin-17 inhibitor that already has FDA approval for treating PsA but that has not been specifically tested in PsA patients who failed or didn’t tolerate a TNFi, he noted.
The SPIRIT-P2 results also showed superior outcomes for patients treated with an ixekizumab injection once every 2 or 4 weeks, compared with placebo, by several secondary measures, including ACR50 and ACR70 rates and minimal disease activity. The ACR70 rate after 24 weeks on treatment was 23% with a dose of ixekizumab every 4 weeks and none with placebo. Minimal disease activity was reached by about a quarter of patients on either dosage of the active drug and by 3% of patients on placebo.
Despite the apparent role for ixekizumab when TNFi treatment fails, the TNFi drug class remains the clear first-line choice for PsA patients who are starting a biological drug for the first time. Not only do the TNFis have a much longer and more extensive track record but they also generally receive better insurance coverage that minimizes out-of-pocket expenses for patients, Dr. Genovese said.
SPIRIT-P2 was sponsored by Eli Lilly, the company that markets ixekizumab. Dr. Nash has been a speaker for or consultant to and has received research funding from Eli Lily and for several other companies. Dr. Genovese has been a consultant to and has received research funding from Eli Lilly, AbbVie, Astellas, Galapagos, Pfizer, and Vertex.
[email protected]
On Twitter @mitchelzoler
MADRID – The anti–interleukin-17 drug ixekizumab, already on the U.S. market for treating psoriasis, showed efficacy and safety for treating psoriatic arthritis in patients who previously failed to respond to or tolerate a tumor necrosis factor inhibitor in a pivotal, phase 3 trial with 363 patients.
Treatment of patients with psoriatic arthritis (PsA) with ixekizumab (Taltz) led to improvements, compared with placebo, in arthritis, physical function, and psoriasis. These patients were unresponsive to or intolerant of a tumor necrosis factor inhibitor (TNFi) at rates similar to previously reported response rates for PsA patients who were TNFi naive, Peter Nash, MD, said at the European Congress of Rheumatology.
A published report with the data presented by Dr. Nash also recently appeared (Lancet. 2017;389[10086]:2317-27).
Based in part on the results from this trial, as well as results from a companion phase 3 trial that enrolled PsA patients naive to a TNFi (Ann Rheum Dis. 2017 Jan; 6[1]:79-87), the company that markets ixekizumab, Eli Lilly, filed an application with the Food and Drug Administration in early 2017 to have a new label indication for PsA, said a company spokeswoman.
“At least half of PsA patients don’t get at least a 20% improvement [an ACR20 response] on a TNFi, and so they are looking for something else,” explained Mark C. Genovese, MD, professor of medicine and director of the Rheumatology Clinic at Stanford (Calif.) University and a coinvestigator on the trial reported by Dr. Nash. “There is pent up demand” for an alternative to a TNFi for treating PsA, Dr. Genovese said in an interview.
The finding also sets ixekizumab apart from secukinumab (Cosentyx), another interleukin-17 inhibitor that already has FDA approval for treating PsA but that has not been specifically tested in PsA patients who failed or didn’t tolerate a TNFi, he noted.
The SPIRIT-P2 results also showed superior outcomes for patients treated with an ixekizumab injection once every 2 or 4 weeks, compared with placebo, by several secondary measures, including ACR50 and ACR70 rates and minimal disease activity. The ACR70 rate after 24 weeks on treatment was 23% with a dose of ixekizumab every 4 weeks and none with placebo. Minimal disease activity was reached by about a quarter of patients on either dosage of the active drug and by 3% of patients on placebo.
Despite the apparent role for ixekizumab when TNFi treatment fails, the TNFi drug class remains the clear first-line choice for PsA patients who are starting a biological drug for the first time. Not only do the TNFis have a much longer and more extensive track record but they also generally receive better insurance coverage that minimizes out-of-pocket expenses for patients, Dr. Genovese said.
SPIRIT-P2 was sponsored by Eli Lilly, the company that markets ixekizumab. Dr. Nash has been a speaker for or consultant to and has received research funding from Eli Lily and for several other companies. Dr. Genovese has been a consultant to and has received research funding from Eli Lilly, AbbVie, Astellas, Galapagos, Pfizer, and Vertex.
[email protected]
On Twitter @mitchelzoler
AT THE EULAR 2017 CONGRESS
Key clinical point:
Major finding: The ACR20 rate after 24 weeks of treatment was 53% with monthly ixekizumab and 20% on placebo.
Data source: The SPIRIT-P2 trial, a phase 3 multicenter trial with 363 patients.
Disclosures: SPIRIT-P2 was sponsored by Eli Lilly, the company that markets ixekizumab (Taltz). Dr. Nash has been a speaker for or consultant to and has received research funding from Eli Lily and for several other companies. Dr. Genovese has been a consultant to and has received research funding from Eli Lilly, AbbVie, Astellas, Galapagos, Pfizer, and Vertex.
Subsequent squamous cell carcinoma risk higher in HIV patients with low CD4 count
HIV-infected individuals who have experienced a nonmelanoma skin cancer may be at significantly greater risk of subsequent new squamous cell carcinoma if they have a lower CD4 cell count, a new study suggests.
In a study published online July 12 in JAMA Dermatology, researchers reported the results of a retrospective cohort study using medical record data from 455 HIV-infected and 1,952 HIV-uninfected patients who had previously been diagnosed with at least one nonmelanoma skin cancer.
Patients with CD4 cell counts below 200 cells/mcL had a 44% greater risk of a subsequent nonmelanoma skin cancer, compared with uninfected individuals (95% confidence interval, 1.10-1.88), while those with a viral load greater than 10,000 copies/mL had a 31% greater risk (95% CI, 1.00-1.72), after adjusting for age, sex, smoking status, and obesity.
The increase in nonmelanoma skin cancer risk was largely accounted for by an increased risk of squamous cell carcinoma (SCC). Among patients with lower CD4 cell counts and those with higher viral loads, the risk of SCC was more than twofold greater than among uninfected individuals. In contrast, while there was a trend toward a higher risk of basal cell carcinoma in those two groups, it did not reach significance (JAMA Dermatol. 2017 Jul 12. doi: 10.1001/jamadermatol.2017.1716).
Overall, HIV-infected individuals had a significant 15% increase in the risk of subsequent nonmelanoma skin cancer over an average follow-up period of 5 years, compared with uninfected individuals.
“This study addresses key questions regarding subsequent NMSC [nonmelanoma skin cancer] risk among a high-risk subgroup of HIV-infected population who, by virtue of having had a pathologically validated skin cancer, are at increased risk of subsequent NMSCs,” wrote Maryam M. Asgari, MD, of Massachusetts General Hospital, Boston, and her coauthors. “Specifically, it was previously not known precisely which NMSC subtype is increased in high-risk persons with HIV and whether biomarkers of HIV infections, such as degree of immune dysfunction, are associated with subsequent skin cancer risk.”
While the study wasn’t able to control for known skin cancer risk factors such as skin type, the patients were all non-Hispanic white, which the authors said selected for individuals with fair skin and some sun-exposure history.
The findings could have implications for skin cancer screening among individuals with HIV infection, with the authors suggesting more targeted monitoring for SCC among individuals with low CD4 counts or high viral loads.
“Our findings support immune dysfunction as a risk factor for SCCs and dovetail with SCC risk data from iatrogenic immunodeficiency states, such as organ transplantation and autoimmune diseases.”
The study was partly supported by Kaiser Permanente Northern California, and one author was supported by a grant from the National Cancer Institute. Two authors had previously served as investigators on studies funded by the pharmaceutical industry, one author declared research funding from the pharmaceutical industry, and one declared shares in two medical companies.
HIV-infected individuals who have experienced a nonmelanoma skin cancer may be at significantly greater risk of subsequent new squamous cell carcinoma if they have a lower CD4 cell count, a new study suggests.
In a study published online July 12 in JAMA Dermatology, researchers reported the results of a retrospective cohort study using medical record data from 455 HIV-infected and 1,952 HIV-uninfected patients who had previously been diagnosed with at least one nonmelanoma skin cancer.
Patients with CD4 cell counts below 200 cells/mcL had a 44% greater risk of a subsequent nonmelanoma skin cancer, compared with uninfected individuals (95% confidence interval, 1.10-1.88), while those with a viral load greater than 10,000 copies/mL had a 31% greater risk (95% CI, 1.00-1.72), after adjusting for age, sex, smoking status, and obesity.
The increase in nonmelanoma skin cancer risk was largely accounted for by an increased risk of squamous cell carcinoma (SCC). Among patients with lower CD4 cell counts and those with higher viral loads, the risk of SCC was more than twofold greater than among uninfected individuals. In contrast, while there was a trend toward a higher risk of basal cell carcinoma in those two groups, it did not reach significance (JAMA Dermatol. 2017 Jul 12. doi: 10.1001/jamadermatol.2017.1716).
Overall, HIV-infected individuals had a significant 15% increase in the risk of subsequent nonmelanoma skin cancer over an average follow-up period of 5 years, compared with uninfected individuals.
“This study addresses key questions regarding subsequent NMSC [nonmelanoma skin cancer] risk among a high-risk subgroup of HIV-infected population who, by virtue of having had a pathologically validated skin cancer, are at increased risk of subsequent NMSCs,” wrote Maryam M. Asgari, MD, of Massachusetts General Hospital, Boston, and her coauthors. “Specifically, it was previously not known precisely which NMSC subtype is increased in high-risk persons with HIV and whether biomarkers of HIV infections, such as degree of immune dysfunction, are associated with subsequent skin cancer risk.”
While the study wasn’t able to control for known skin cancer risk factors such as skin type, the patients were all non-Hispanic white, which the authors said selected for individuals with fair skin and some sun-exposure history.
The findings could have implications for skin cancer screening among individuals with HIV infection, with the authors suggesting more targeted monitoring for SCC among individuals with low CD4 counts or high viral loads.
“Our findings support immune dysfunction as a risk factor for SCCs and dovetail with SCC risk data from iatrogenic immunodeficiency states, such as organ transplantation and autoimmune diseases.”
The study was partly supported by Kaiser Permanente Northern California, and one author was supported by a grant from the National Cancer Institute. Two authors had previously served as investigators on studies funded by the pharmaceutical industry, one author declared research funding from the pharmaceutical industry, and one declared shares in two medical companies.
HIV-infected individuals who have experienced a nonmelanoma skin cancer may be at significantly greater risk of subsequent new squamous cell carcinoma if they have a lower CD4 cell count, a new study suggests.
In a study published online July 12 in JAMA Dermatology, researchers reported the results of a retrospective cohort study using medical record data from 455 HIV-infected and 1,952 HIV-uninfected patients who had previously been diagnosed with at least one nonmelanoma skin cancer.
Patients with CD4 cell counts below 200 cells/mcL had a 44% greater risk of a subsequent nonmelanoma skin cancer, compared with uninfected individuals (95% confidence interval, 1.10-1.88), while those with a viral load greater than 10,000 copies/mL had a 31% greater risk (95% CI, 1.00-1.72), after adjusting for age, sex, smoking status, and obesity.
The increase in nonmelanoma skin cancer risk was largely accounted for by an increased risk of squamous cell carcinoma (SCC). Among patients with lower CD4 cell counts and those with higher viral loads, the risk of SCC was more than twofold greater than among uninfected individuals. In contrast, while there was a trend toward a higher risk of basal cell carcinoma in those two groups, it did not reach significance (JAMA Dermatol. 2017 Jul 12. doi: 10.1001/jamadermatol.2017.1716).
Overall, HIV-infected individuals had a significant 15% increase in the risk of subsequent nonmelanoma skin cancer over an average follow-up period of 5 years, compared with uninfected individuals.
“This study addresses key questions regarding subsequent NMSC [nonmelanoma skin cancer] risk among a high-risk subgroup of HIV-infected population who, by virtue of having had a pathologically validated skin cancer, are at increased risk of subsequent NMSCs,” wrote Maryam M. Asgari, MD, of Massachusetts General Hospital, Boston, and her coauthors. “Specifically, it was previously not known precisely which NMSC subtype is increased in high-risk persons with HIV and whether biomarkers of HIV infections, such as degree of immune dysfunction, are associated with subsequent skin cancer risk.”
While the study wasn’t able to control for known skin cancer risk factors such as skin type, the patients were all non-Hispanic white, which the authors said selected for individuals with fair skin and some sun-exposure history.
The findings could have implications for skin cancer screening among individuals with HIV infection, with the authors suggesting more targeted monitoring for SCC among individuals with low CD4 counts or high viral loads.
“Our findings support immune dysfunction as a risk factor for SCCs and dovetail with SCC risk data from iatrogenic immunodeficiency states, such as organ transplantation and autoimmune diseases.”
The study was partly supported by Kaiser Permanente Northern California, and one author was supported by a grant from the National Cancer Institute. Two authors had previously served as investigators on studies funded by the pharmaceutical industry, one author declared research funding from the pharmaceutical industry, and one declared shares in two medical companies.
FROM JAMA DERMATOLOGY
Key clinical point: HIV-infected people who have had a previous nonmelanoma skin cancer are at significantly higher risk of subsequent SCC if they have a lower CD4 count or higher viral load.
Major finding: HIV-infected people with a low CD4 cell count or high viral load have a greater than twofold increased risk of subsequent SCC after a primary nonmelanoma skin cancer than do uninfected people who have had a previous nonmelanoma skin cancer.
Data source: A retrospective cohort study in 455 HIV-infected and 1,945 HIV-uninfected patients.
Disclosures: The study was partly supported by Kaiser Permanente, Northern California, and one author was supported by a grant from the National Cancer Institute. Two authors had previously served as investigators on studies funded by the pharmaceutical industry, one author declared research funding from the pharmaceutical industry, and one declared shares in two medical companies.
Venetoclax-HMA combo promising for AML in patients 65+
MADRID – A combination of the BCL-2 inhibitor venetoclax with a hypomethylating agent may produce high overall response rates among older patients with newly diagnosed acute myeloid leukemia (AML), early data showed.
Among 100 patients age 65 years and older with previously untreated AML, the combination of venetoclax with either decitabine or azacitidine was associated with a 69% overall responses rate, reported Keith W. Pratz, MD, of Johns Hopkins University in Baltimore.

The standard AML induction regimen of cytarabine and an anthracycline with or without cladribine is generally too toxic for patients in their mid-60s or older. For these patients, there are few good therapeutic options, Dr. Pratz said.
Venetoclax has shown good single-agent activity against relapsed/refractory AML and, as reported in a phase 1b study at the 2016 annual meeting of the American Society of Clinical Oncology, induced a combined rate of complete remission (CR) and CR with incomplete marrow recovery (CRi) of 60% when given in escalating doses with a hypomethylating agent.
Dr. Pratz reported on response rates and safety from an expansion cohort of patients 65 years and older treated in that phase 1b study. The patients were treated with either decitabine or azacitidine plus venetoclax at a dose of either 400 mg or 800 mg.
Decitabine was dosed at 20 mg/m2 intravenously on days 1-5 of a 28-day cycle. Azacitidine was dosed at 75 mg/m2 subcutaneously on days 1-7 of every cycle.
The ORRs for each arm were as follows:
- Decitabine plus venetoclax 400 mg: 76% (44% CR, 32% CRi).
- Decitabine plus venetoclax 800 mg: 68% (36% CR, 32% CRi).
- Azacitadine plus venetoclax 400 mg: 72% (28% CR, 44% CRi).
- Azacitadine plus venetoclax 800 mg: 56%: (28% CR, 28% CRi, PR 1% [numbers rounded up]).
The combined CR/CRi rate was 60% among patients with poor-risk cytogenetics and 78% among patients with intermediate-risk disease. In addition, the combination was effective among patients with both primary de novo AML (68%) and secondary AML (related to myelodysplasia or myeloproliferative neoplasms or previous therapy; 73%).
Overall survival after a median of 9 months since the first dose of the study drug was estimated to be 79% at 6 months and 70% at 12 months, with the median not reached.
Treatment-related adverse events were similar between the decitabine- and azacitidine-containing arms at the given dose of venetoclax. Grade 3 or 4 treatment-related adverse events included thrombocytopenia in 56% of patients on the 400-mg dose of venetoclax and in 32% of those on the 800-mg dose. Grade 3/4 febrile neutropenia occurred in 48% and 30%, respectively, and neutropenia in 40% and 32%.
A phase 3 study of venetoclax at the 400-mg dose with azacitidine has been initiated. NCT02993523 is currently enrolling patients, Dr. Pratz said.
The study was supported by Abbvie and Genentech. Dr. Pratz disclosed research funding from Abbvie and other companies.
MADRID – A combination of the BCL-2 inhibitor venetoclax with a hypomethylating agent may produce high overall response rates among older patients with newly diagnosed acute myeloid leukemia (AML), early data showed.
Among 100 patients age 65 years and older with previously untreated AML, the combination of venetoclax with either decitabine or azacitidine was associated with a 69% overall responses rate, reported Keith W. Pratz, MD, of Johns Hopkins University in Baltimore.
The standard AML induction regimen of cytarabine and an anthracycline with or without cladribine is generally too toxic for patients in their mid-60s or older. For these patients, there are few good therapeutic options, Dr. Pratz said.
Venetoclax has shown good single-agent activity against relapsed/refractory AML and, as reported in a phase 1b study at the 2016 annual meeting of the American Society of Clinical Oncology, induced a combined rate of complete remission (CR) and CR with incomplete marrow recovery (CRi) of 60% when given in escalating doses with a hypomethylating agent.
Dr. Pratz reported on response rates and safety from an expansion cohort of patients 65 years and older treated in that phase 1b study. The patients were treated with either decitabine or azacitidine plus venetoclax at a dose of either 400 mg or 800 mg.
Decitabine was dosed at 20 mg/m2 intravenously on days 1-5 of a 28-day cycle. Azacitidine was dosed at 75 mg/m2 subcutaneously on days 1-7 of every cycle.
The ORRs for each arm were as follows:
- Decitabine plus venetoclax 400 mg: 76% (44% CR, 32% CRi).
- Decitabine plus venetoclax 800 mg: 68% (36% CR, 32% CRi).
- Azacitadine plus venetoclax 400 mg: 72% (28% CR, 44% CRi).
- Azacitadine plus venetoclax 800 mg: 56%: (28% CR, 28% CRi, PR 1% [numbers rounded up]).
The combined CR/CRi rate was 60% among patients with poor-risk cytogenetics and 78% among patients with intermediate-risk disease. In addition, the combination was effective among patients with both primary de novo AML (68%) and secondary AML (related to myelodysplasia or myeloproliferative neoplasms or previous therapy; 73%).
Overall survival after a median of 9 months since the first dose of the study drug was estimated to be 79% at 6 months and 70% at 12 months, with the median not reached.
Treatment-related adverse events were similar between the decitabine- and azacitidine-containing arms at the given dose of venetoclax. Grade 3 or 4 treatment-related adverse events included thrombocytopenia in 56% of patients on the 400-mg dose of venetoclax and in 32% of those on the 800-mg dose. Grade 3/4 febrile neutropenia occurred in 48% and 30%, respectively, and neutropenia in 40% and 32%.
A phase 3 study of venetoclax at the 400-mg dose with azacitidine has been initiated. NCT02993523 is currently enrolling patients, Dr. Pratz said.
The study was supported by Abbvie and Genentech. Dr. Pratz disclosed research funding from Abbvie and other companies.
MADRID – A combination of the BCL-2 inhibitor venetoclax with a hypomethylating agent may produce high overall response rates among older patients with newly diagnosed acute myeloid leukemia (AML), early data showed.
Among 100 patients age 65 years and older with previously untreated AML, the combination of venetoclax with either decitabine or azacitidine was associated with a 69% overall responses rate, reported Keith W. Pratz, MD, of Johns Hopkins University in Baltimore.
The standard AML induction regimen of cytarabine and an anthracycline with or without cladribine is generally too toxic for patients in their mid-60s or older. For these patients, there are few good therapeutic options, Dr. Pratz said.
Venetoclax has shown good single-agent activity against relapsed/refractory AML and, as reported in a phase 1b study at the 2016 annual meeting of the American Society of Clinical Oncology, induced a combined rate of complete remission (CR) and CR with incomplete marrow recovery (CRi) of 60% when given in escalating doses with a hypomethylating agent.
Dr. Pratz reported on response rates and safety from an expansion cohort of patients 65 years and older treated in that phase 1b study. The patients were treated with either decitabine or azacitidine plus venetoclax at a dose of either 400 mg or 800 mg.
Decitabine was dosed at 20 mg/m2 intravenously on days 1-5 of a 28-day cycle. Azacitidine was dosed at 75 mg/m2 subcutaneously on days 1-7 of every cycle.
The ORRs for each arm were as follows:
- Decitabine plus venetoclax 400 mg: 76% (44% CR, 32% CRi).
- Decitabine plus venetoclax 800 mg: 68% (36% CR, 32% CRi).
- Azacitadine plus venetoclax 400 mg: 72% (28% CR, 44% CRi).
- Azacitadine plus venetoclax 800 mg: 56%: (28% CR, 28% CRi, PR 1% [numbers rounded up]).
The combined CR/CRi rate was 60% among patients with poor-risk cytogenetics and 78% among patients with intermediate-risk disease. In addition, the combination was effective among patients with both primary de novo AML (68%) and secondary AML (related to myelodysplasia or myeloproliferative neoplasms or previous therapy; 73%).
Overall survival after a median of 9 months since the first dose of the study drug was estimated to be 79% at 6 months and 70% at 12 months, with the median not reached.
Treatment-related adverse events were similar between the decitabine- and azacitidine-containing arms at the given dose of venetoclax. Grade 3 or 4 treatment-related adverse events included thrombocytopenia in 56% of patients on the 400-mg dose of venetoclax and in 32% of those on the 800-mg dose. Grade 3/4 febrile neutropenia occurred in 48% and 30%, respectively, and neutropenia in 40% and 32%.
A phase 3 study of venetoclax at the 400-mg dose with azacitidine has been initiated. NCT02993523 is currently enrolling patients, Dr. Pratz said.
The study was supported by Abbvie and Genentech. Dr. Pratz disclosed research funding from Abbvie and other companies.
AT EHA 2017
Key clinical point: Induction therapy options are limited for patients 65 years and older with acute myeloid leukemia.
Major finding: Venetoclax and a hypomethylating agent were associated with a 69% overall response rate.
Data source: The expansion portion of a phase 1b trial of venetoclax plus decitabine or azacitidine in 100 patients 65 years and older with de novo AML.
Disclosures: The study was supported by Abbvie and Genentech. Dr. Pratz disclosed research funding from Abbvie and other companies.
Substance use treatment cost $34 billion in 2014
Total spending on the treatment of substance use disorder reached $34 billion in 2014, with outpatient care taking the largest share, according to the National Center for Health Statistics.
That $34 billion represents an increase of 273% from the $9.1 billion spent in 1986 and a considerable shift in the distribution of spending over the last 30 years. In 1986, the largest share of spending – 50%, or $4.6 billion – for substance use disorder went toward inpatient care and only $2.4 billion (27%) was used for outpatient care. In 2014, outpatient treatment of substance use disorder had a 40% share ($13.6 billion) of all spending, and inpatient care was down to 19% ($6.4 billion), the NCHS reported in “Health, United States, 2016.”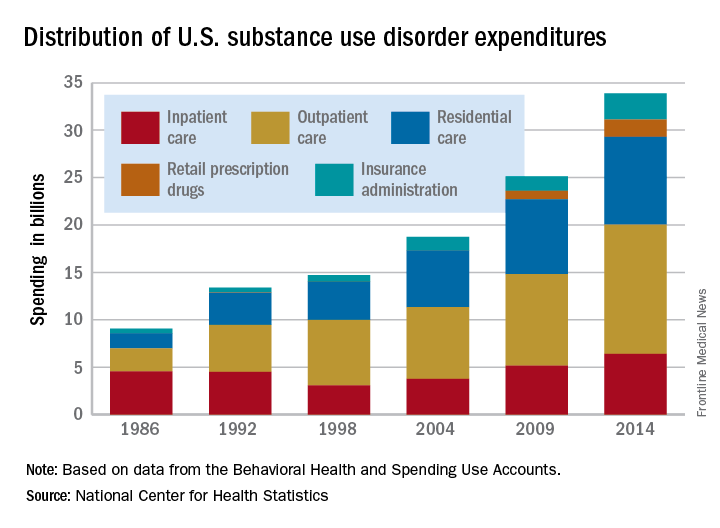
Since methadone is not considered a retail drug by SAMHSA, it is classified under specialty substance use disorder treatment centers, which are included in the estimate for outpatient care, the NCHS noted.
Total spending on the treatment of substance use disorder reached $34 billion in 2014, with outpatient care taking the largest share, according to the National Center for Health Statistics.
That $34 billion represents an increase of 273% from the $9.1 billion spent in 1986 and a considerable shift in the distribution of spending over the last 30 years. In 1986, the largest share of spending – 50%, or $4.6 billion – for substance use disorder went toward inpatient care and only $2.4 billion (27%) was used for outpatient care. In 2014, outpatient treatment of substance use disorder had a 40% share ($13.6 billion) of all spending, and inpatient care was down to 19% ($6.4 billion), the NCHS reported in “Health, United States, 2016.”
Since methadone is not considered a retail drug by SAMHSA, it is classified under specialty substance use disorder treatment centers, which are included in the estimate for outpatient care, the NCHS noted.
Total spending on the treatment of substance use disorder reached $34 billion in 2014, with outpatient care taking the largest share, according to the National Center for Health Statistics.
That $34 billion represents an increase of 273% from the $9.1 billion spent in 1986 and a considerable shift in the distribution of spending over the last 30 years. In 1986, the largest share of spending – 50%, or $4.6 billion – for substance use disorder went toward inpatient care and only $2.4 billion (27%) was used for outpatient care. In 2014, outpatient treatment of substance use disorder had a 40% share ($13.6 billion) of all spending, and inpatient care was down to 19% ($6.4 billion), the NCHS reported in “Health, United States, 2016.”
Since methadone is not considered a retail drug by SAMHSA, it is classified under specialty substance use disorder treatment centers, which are included in the estimate for outpatient care, the NCHS noted.