User login
VIDEO: Making the most of MACRA reimbursement methods
BOSTON – “There’s a hunger out there” among physicians to participate in novel practice models made possible by value-based care, according to Lawrence R. Kosinski, MD, MBA, AGAF, clinical private practice councilor on the American Gastroenterological Association governing board.
In this video interview, conducted during the 2017 AGA Tech Summit, Dr. Kosinski explained how physicians can leverage the reimbursement methods of the recent MACRA legislation in their practices. He discusses how, in his own practice, he and his colleagues created an alternative payment model that uses a proprietary patient portal, SonarMD, to help physicians improve the management of chronic diseases such as inflammatory bowel disease at a lower cost and with markedly improved patient satisfaction.
“We look forward very much to the success of this project going forward, and the AGA will continue to be an integral part of the development of Project Sonar,” he said.
Dr. Kosinski is president of SonarMD.
BOSTON – “There’s a hunger out there” among physicians to participate in novel practice models made possible by value-based care, according to Lawrence R. Kosinski, MD, MBA, AGAF, clinical private practice councilor on the American Gastroenterological Association governing board.
In this video interview, conducted during the 2017 AGA Tech Summit, Dr. Kosinski explained how physicians can leverage the reimbursement methods of the recent MACRA legislation in their practices. He discusses how, in his own practice, he and his colleagues created an alternative payment model that uses a proprietary patient portal, SonarMD, to help physicians improve the management of chronic diseases such as inflammatory bowel disease at a lower cost and with markedly improved patient satisfaction.
“We look forward very much to the success of this project going forward, and the AGA will continue to be an integral part of the development of Project Sonar,” he said.
Dr. Kosinski is president of SonarMD.
BOSTON – “There’s a hunger out there” among physicians to participate in novel practice models made possible by value-based care, according to Lawrence R. Kosinski, MD, MBA, AGAF, clinical private practice councilor on the American Gastroenterological Association governing board.
In this video interview, conducted during the 2017 AGA Tech Summit, Dr. Kosinski explained how physicians can leverage the reimbursement methods of the recent MACRA legislation in their practices. He discusses how, in his own practice, he and his colleagues created an alternative payment model that uses a proprietary patient portal, SonarMD, to help physicians improve the management of chronic diseases such as inflammatory bowel disease at a lower cost and with markedly improved patient satisfaction.
“We look forward very much to the success of this project going forward, and the AGA will continue to be an integral part of the development of Project Sonar,” he said.
Dr. Kosinski is president of SonarMD.
FROM THE 2017 AGA TECH SUMMIT

CMS market stabilization efforts useless without subsidies
New final regulations designed to bring stability to the individual health insurance market may not matter if the White House follows through on a threat to kill subsidies paid to insurers to help reduce deductibles and other out-of-pocket costs for low-income patients.
The final rule from the Centers for Medicare & Medicaid Services grants a number of wishes sought by the insurance industry to help bring a level of predictability and flexibility when designing plans for the individual market. Specifically, it does the following:
• Shortens the open enrollment period for the 2018 plan year to 6 weeks running from Nov. 1 to Dec. 15, so that open enrollment closely aligns with Medicare and other private insurance.
• Requires individuals to submit documentation when seeking coverage through a special enrollment period.
• Allows insurers to collect past-due premiums before issuing coverage for a future year.
• Provides more actuarial flexibility to allow for different plan designs.
• Returns network adequacy oversight to states.
The new rules are not expected to alter the existing market dynamic, according to Kelly Brantley, vice president at Avalere Health. 
“I would say the rule is nominally helpful, but it’s really unlikely to persuade anyone, particularly those insurers who are already on their way out. I don’t think this a game-changer for them,” she said in an interview.
The American Medical Association, in comments to the CMS when the rule was proposed as a draft, said that if finalized, the rule “would raise premiums, out-of-pocket costs, or both for millions of moderate-income families and would make it more difficult for eligible individuals to enroll in health coverage and access needed care.”
The potential impact of these regulatory changes could be moot if President Trump makes good on his threat to withhold cost-sharing subsidies to insurers. The subsides already are the subject of a lawsuit brought by the House of Representatives against the Obama administration; they continue to be paid while the suit makes its way through the judicial process. President Trump has threatened to cut off the subsidies in an effort to force Congressional Democrats to the negotiating table regarding the repeal and replacement of the Affordable Care Act.
“My take on this is that the [market stabilization] rule as written is not likely to shift the market, really, in terms of access,” Ms. Brantley said. “The bigger question is whether the cost-sharing reductions are going to be paid. I think that has a bigger likelihood of influencing issuer participation and robustness of the market in 2018.”
Even with the changes made by the market stabilization rule, “there is still too much instability and uncertainty in this market,” Marilyn Tavenner, president and CEO of the industry group America’s Health Insurance Plans, said in a statement. “Most urgently, health plans and the consumers they serve need to know that funding for cost-sharing reduction subsidies will continue uninterrupted.”
Ms. Tavenner noted that without the subsidies, more plans are likely to drop out of the health insurance exchanges, leading to premium increases, and “doctors and hospitals will see even greater strains on their ability to care for people.”
The AMA, in an April 12 letter to President Trump, cosigned by America’s Health Insurance Plans, the American Academy of Family Physicians, the American Hospital Association, the Federation of American Hospitals, the American Benefits Council, the Blue Cross Blue Shield Association, and the U.S. Chamber of Commerce, stated that the “most critical action to help stabilize the individual market for 2017 and 2018 is to remove uncertainty about continued funding for cost sharing reductions.”
Ms. Brantley added that if the subsides were cut, “it makes it more challenging to bring any kind of money back into the system at a later point. I think it would be hard for those cost-sharing reductions to go away at this point and then ever come back, but I do think that it’s a possibility that that could happen.”
The CMS released the final rule April 13, 2017, and it is scheduled for publication in the Federal Register on April 18, 2017.
New final regulations designed to bring stability to the individual health insurance market may not matter if the White House follows through on a threat to kill subsidies paid to insurers to help reduce deductibles and other out-of-pocket costs for low-income patients.
The final rule from the Centers for Medicare & Medicaid Services grants a number of wishes sought by the insurance industry to help bring a level of predictability and flexibility when designing plans for the individual market. Specifically, it does the following:
• Shortens the open enrollment period for the 2018 plan year to 6 weeks running from Nov. 1 to Dec. 15, so that open enrollment closely aligns with Medicare and other private insurance.
• Requires individuals to submit documentation when seeking coverage through a special enrollment period.
• Allows insurers to collect past-due premiums before issuing coverage for a future year.
• Provides more actuarial flexibility to allow for different plan designs.
• Returns network adequacy oversight to states.
The new rules are not expected to alter the existing market dynamic, according to Kelly Brantley, vice president at Avalere Health.
“I would say the rule is nominally helpful, but it’s really unlikely to persuade anyone, particularly those insurers who are already on their way out. I don’t think this a game-changer for them,” she said in an interview.
The American Medical Association, in comments to the CMS when the rule was proposed as a draft, said that if finalized, the rule “would raise premiums, out-of-pocket costs, or both for millions of moderate-income families and would make it more difficult for eligible individuals to enroll in health coverage and access needed care.”
The potential impact of these regulatory changes could be moot if President Trump makes good on his threat to withhold cost-sharing subsidies to insurers. The subsides already are the subject of a lawsuit brought by the House of Representatives against the Obama administration; they continue to be paid while the suit makes its way through the judicial process. President Trump has threatened to cut off the subsidies in an effort to force Congressional Democrats to the negotiating table regarding the repeal and replacement of the Affordable Care Act.
“My take on this is that the [market stabilization] rule as written is not likely to shift the market, really, in terms of access,” Ms. Brantley said. “The bigger question is whether the cost-sharing reductions are going to be paid. I think that has a bigger likelihood of influencing issuer participation and robustness of the market in 2018.”
Even with the changes made by the market stabilization rule, “there is still too much instability and uncertainty in this market,” Marilyn Tavenner, president and CEO of the industry group America’s Health Insurance Plans, said in a statement. “Most urgently, health plans and the consumers they serve need to know that funding for cost-sharing reduction subsidies will continue uninterrupted.”
Ms. Tavenner noted that without the subsidies, more plans are likely to drop out of the health insurance exchanges, leading to premium increases, and “doctors and hospitals will see even greater strains on their ability to care for people.”
The AMA, in an April 12 letter to President Trump, cosigned by America’s Health Insurance Plans, the American Academy of Family Physicians, the American Hospital Association, the Federation of American Hospitals, the American Benefits Council, the Blue Cross Blue Shield Association, and the U.S. Chamber of Commerce, stated that the “most critical action to help stabilize the individual market for 2017 and 2018 is to remove uncertainty about continued funding for cost sharing reductions.”
Ms. Brantley added that if the subsides were cut, “it makes it more challenging to bring any kind of money back into the system at a later point. I think it would be hard for those cost-sharing reductions to go away at this point and then ever come back, but I do think that it’s a possibility that that could happen.”
The CMS released the final rule April 13, 2017, and it is scheduled for publication in the Federal Register on April 18, 2017.
New final regulations designed to bring stability to the individual health insurance market may not matter if the White House follows through on a threat to kill subsidies paid to insurers to help reduce deductibles and other out-of-pocket costs for low-income patients.
The final rule from the Centers for Medicare & Medicaid Services grants a number of wishes sought by the insurance industry to help bring a level of predictability and flexibility when designing plans for the individual market. Specifically, it does the following:
• Shortens the open enrollment period for the 2018 plan year to 6 weeks running from Nov. 1 to Dec. 15, so that open enrollment closely aligns with Medicare and other private insurance.
• Requires individuals to submit documentation when seeking coverage through a special enrollment period.
• Allows insurers to collect past-due premiums before issuing coverage for a future year.
• Provides more actuarial flexibility to allow for different plan designs.
• Returns network adequacy oversight to states.
The new rules are not expected to alter the existing market dynamic, according to Kelly Brantley, vice president at Avalere Health.
“I would say the rule is nominally helpful, but it’s really unlikely to persuade anyone, particularly those insurers who are already on their way out. I don’t think this a game-changer for them,” she said in an interview.
The American Medical Association, in comments to the CMS when the rule was proposed as a draft, said that if finalized, the rule “would raise premiums, out-of-pocket costs, or both for millions of moderate-income families and would make it more difficult for eligible individuals to enroll in health coverage and access needed care.”
The potential impact of these regulatory changes could be moot if President Trump makes good on his threat to withhold cost-sharing subsidies to insurers. The subsides already are the subject of a lawsuit brought by the House of Representatives against the Obama administration; they continue to be paid while the suit makes its way through the judicial process. President Trump has threatened to cut off the subsidies in an effort to force Congressional Democrats to the negotiating table regarding the repeal and replacement of the Affordable Care Act.
“My take on this is that the [market stabilization] rule as written is not likely to shift the market, really, in terms of access,” Ms. Brantley said. “The bigger question is whether the cost-sharing reductions are going to be paid. I think that has a bigger likelihood of influencing issuer participation and robustness of the market in 2018.”
Even with the changes made by the market stabilization rule, “there is still too much instability and uncertainty in this market,” Marilyn Tavenner, president and CEO of the industry group America’s Health Insurance Plans, said in a statement. “Most urgently, health plans and the consumers they serve need to know that funding for cost-sharing reduction subsidies will continue uninterrupted.”
Ms. Tavenner noted that without the subsidies, more plans are likely to drop out of the health insurance exchanges, leading to premium increases, and “doctors and hospitals will see even greater strains on their ability to care for people.”
The AMA, in an April 12 letter to President Trump, cosigned by America’s Health Insurance Plans, the American Academy of Family Physicians, the American Hospital Association, the Federation of American Hospitals, the American Benefits Council, the Blue Cross Blue Shield Association, and the U.S. Chamber of Commerce, stated that the “most critical action to help stabilize the individual market for 2017 and 2018 is to remove uncertainty about continued funding for cost sharing reductions.”
Ms. Brantley added that if the subsides were cut, “it makes it more challenging to bring any kind of money back into the system at a later point. I think it would be hard for those cost-sharing reductions to go away at this point and then ever come back, but I do think that it’s a possibility that that could happen.”
The CMS released the final rule April 13, 2017, and it is scheduled for publication in the Federal Register on April 18, 2017.

Palbociclib/fulvestrant works in Asians with HR+/HER2– breast cancer too
Among Asian women with hormone receptor–positive/human epidermal growth factor receptor-2 (HER2)–negative metastatic breast cancer that is resistant to endocrine therapy, a combination of palbociclib (Ibrance) and fulvestrant (Faslodex) was associated with a significant improvement in progression-free survival (PFS), reported investigators from the PALOMA-3 trial.
A preplanned subgroup analysis of 102 pre- and postmenopausal women from Japan, South Korea, and Taiwan who were enrolled in the trial showed that median PFS for 71 women assigned to palbociclib and fulvestrant had not been reached at the trial end. In contrast, median PFS among 31 patients assigned to placebo and fulvestrant was 5.8 months (hazard ratio, 0.485; P = .0065), reported Hiroji Iwata, MD, PhD, of the Aichi Cancer Center Hospital in Nagoya, Japan, and his colleagues.
“Overall, palbociclib plus fulvestrant seems to be a reasonable treatment option in Asians with HR-positive/HER2-negative metastatic breast cancer that has progressed on prior endocrine therapy,” they wrote in the Journal of Global Oncology (2017 Apr 11. doi: 10.1200/JGO.2016.008318).
PALOMA-3 was a multinational randomized double-blind, placebo-controlled phase III trial comparing a combination of fulvestrant, a selective estrogen receptor downregulator, and palbociclib, a small-molecule inhibitor of cyclin-dependent kinases 4 and 6 (CDK4/6) with fulvestrant plus placebo in 521 women with HR-positive/HER2-negative advanced breast cancer.
The trial was halted early for efficacy of the combination. The final overall analysis, published in April 2016 in The Lancet Oncology, showed that the combination significantly improved PFS, compared with fulvestrant and placebo, regardless of the patients’ degree of endocrine resistance, level of hormone receptor expression level, or PIK3CA mutational status.
Dr. Iwata and his associates noted that breast cancer is generally diagnosed at a younger age among Asian women (median, 45-50 years vs. 55-60 years among Western women) and that differences in genetic backgrounds may influence drug metabolism, resulting in potential differences in efficacy and adverse event profiles.
Among patients treated with palbociclib, the most common grade 3 or higher adverse events were neutropenia in 92%, compared with none in the placebo arm, and leukopenia in 29% vs. 0%. In contrast, grade 3/4 neutropenia occurred in 58% of non-Asian patients treated with the combination and 0.7% of non-Asian controls. Leukopenia rates were similar between Asian and non-Asian populations, however.
Comparisons of mean trough concentrations across subgroups showed that palbociclib exposures among Asians and non-Asians were similar. Patient reported outcomes were also similar between the groups, except for significantly more dyspnea among patients who received palbociclib (P = .05).
“This study adds to the limited body of literature assessing a CDK4/6 inhibitor in Asians and represents the largest patient experience with palbociclib in Asians. The present findings show that palbociclib plus fulvestrant improved PFS in Asians with HR-positive/HER2-negative [metastatic breast cancer] who experienced progression on prior endocrine therapy and that the safety profile of palbociclib plus fulvestrant in Asians was generally consistent with that observed in non-Asians. Together, these findings suggest that palbociclib is beneficial in patients who have not previously received endocrine therapy and in Asians and non-Asians who experienced relapse or progression during prior endocrine therapy,” they wrote.
The PALOMA-3 trial was supported by Pfizer. Dr. Iwata disclosed consultations with Chugai Pharma, Eisai, and AstraZeneca. Several coauthors are Pfizer employees and shareholders.
Taking into account all caveats inherent to analyses of subpopulations of large clinical trials (for example, invariably small sample size and multiplicity of testing), the data presented by Iwata et al. support the clinically meaningful efficacy of palbociclib for the end point of progression-free survival (PFS) in Asians. However, this report and others indicate that Asians have a higher risk of adverse events (including grade 3 and 4 neutropenia) despite preserved patient-reported outcomes and quality of life. The reasons for this have yet to be elucidated. In light of growing evidence of interethnic pharmacogenomic and safety discrepancies between Asian and non-Asian populations observed in recently published clinical trials and observational studies, there is a clear need for enhanced enrollment of Asian patients and other ethnic groups into clinical trials of new agents for the treatment of metastatic breast cancer.
Ricardo L.B. Costa, MD, and William J. Gradishar, MD, are with the Feinberg School of Medicine and Robert H. Lurie Comprehensive Cancer Center of Northwestern University, Chicago. These comments are excerpted from an editorial accompanying the report by Dr. Iwata and his coauthors (J Glob Oncol. 2017 Apr 11. doi: 10.1200/JGO.2017.009936).
Taking into account all caveats inherent to analyses of subpopulations of large clinical trials (for example, invariably small sample size and multiplicity of testing), the data presented by Iwata et al. support the clinically meaningful efficacy of palbociclib for the end point of progression-free survival (PFS) in Asians. However, this report and others indicate that Asians have a higher risk of adverse events (including grade 3 and 4 neutropenia) despite preserved patient-reported outcomes and quality of life. The reasons for this have yet to be elucidated. In light of growing evidence of interethnic pharmacogenomic and safety discrepancies between Asian and non-Asian populations observed in recently published clinical trials and observational studies, there is a clear need for enhanced enrollment of Asian patients and other ethnic groups into clinical trials of new agents for the treatment of metastatic breast cancer.
Ricardo L.B. Costa, MD, and William J. Gradishar, MD, are with the Feinberg School of Medicine and Robert H. Lurie Comprehensive Cancer Center of Northwestern University, Chicago. These comments are excerpted from an editorial accompanying the report by Dr. Iwata and his coauthors (J Glob Oncol. 2017 Apr 11. doi: 10.1200/JGO.2017.009936).
Taking into account all caveats inherent to analyses of subpopulations of large clinical trials (for example, invariably small sample size and multiplicity of testing), the data presented by Iwata et al. support the clinically meaningful efficacy of palbociclib for the end point of progression-free survival (PFS) in Asians. However, this report and others indicate that Asians have a higher risk of adverse events (including grade 3 and 4 neutropenia) despite preserved patient-reported outcomes and quality of life. The reasons for this have yet to be elucidated. In light of growing evidence of interethnic pharmacogenomic and safety discrepancies between Asian and non-Asian populations observed in recently published clinical trials and observational studies, there is a clear need for enhanced enrollment of Asian patients and other ethnic groups into clinical trials of new agents for the treatment of metastatic breast cancer.
Ricardo L.B. Costa, MD, and William J. Gradishar, MD, are with the Feinberg School of Medicine and Robert H. Lurie Comprehensive Cancer Center of Northwestern University, Chicago. These comments are excerpted from an editorial accompanying the report by Dr. Iwata and his coauthors (J Glob Oncol. 2017 Apr 11. doi: 10.1200/JGO.2017.009936).
Among Asian women with hormone receptor–positive/human epidermal growth factor receptor-2 (HER2)–negative metastatic breast cancer that is resistant to endocrine therapy, a combination of palbociclib (Ibrance) and fulvestrant (Faslodex) was associated with a significant improvement in progression-free survival (PFS), reported investigators from the PALOMA-3 trial.
A preplanned subgroup analysis of 102 pre- and postmenopausal women from Japan, South Korea, and Taiwan who were enrolled in the trial showed that median PFS for 71 women assigned to palbociclib and fulvestrant had not been reached at the trial end. In contrast, median PFS among 31 patients assigned to placebo and fulvestrant was 5.8 months (hazard ratio, 0.485; P = .0065), reported Hiroji Iwata, MD, PhD, of the Aichi Cancer Center Hospital in Nagoya, Japan, and his colleagues.
“Overall, palbociclib plus fulvestrant seems to be a reasonable treatment option in Asians with HR-positive/HER2-negative metastatic breast cancer that has progressed on prior endocrine therapy,” they wrote in the Journal of Global Oncology (2017 Apr 11. doi: 10.1200/JGO.2016.008318).
PALOMA-3 was a multinational randomized double-blind, placebo-controlled phase III trial comparing a combination of fulvestrant, a selective estrogen receptor downregulator, and palbociclib, a small-molecule inhibitor of cyclin-dependent kinases 4 and 6 (CDK4/6) with fulvestrant plus placebo in 521 women with HR-positive/HER2-negative advanced breast cancer.
The trial was halted early for efficacy of the combination. The final overall analysis, published in April 2016 in The Lancet Oncology, showed that the combination significantly improved PFS, compared with fulvestrant and placebo, regardless of the patients’ degree of endocrine resistance, level of hormone receptor expression level, or PIK3CA mutational status.
Dr. Iwata and his associates noted that breast cancer is generally diagnosed at a younger age among Asian women (median, 45-50 years vs. 55-60 years among Western women) and that differences in genetic backgrounds may influence drug metabolism, resulting in potential differences in efficacy and adverse event profiles.
Among patients treated with palbociclib, the most common grade 3 or higher adverse events were neutropenia in 92%, compared with none in the placebo arm, and leukopenia in 29% vs. 0%. In contrast, grade 3/4 neutropenia occurred in 58% of non-Asian patients treated with the combination and 0.7% of non-Asian controls. Leukopenia rates were similar between Asian and non-Asian populations, however.
Comparisons of mean trough concentrations across subgroups showed that palbociclib exposures among Asians and non-Asians were similar. Patient reported outcomes were also similar between the groups, except for significantly more dyspnea among patients who received palbociclib (P = .05).
“This study adds to the limited body of literature assessing a CDK4/6 inhibitor in Asians and represents the largest patient experience with palbociclib in Asians. The present findings show that palbociclib plus fulvestrant improved PFS in Asians with HR-positive/HER2-negative [metastatic breast cancer] who experienced progression on prior endocrine therapy and that the safety profile of palbociclib plus fulvestrant in Asians was generally consistent with that observed in non-Asians. Together, these findings suggest that palbociclib is beneficial in patients who have not previously received endocrine therapy and in Asians and non-Asians who experienced relapse or progression during prior endocrine therapy,” they wrote.
The PALOMA-3 trial was supported by Pfizer. Dr. Iwata disclosed consultations with Chugai Pharma, Eisai, and AstraZeneca. Several coauthors are Pfizer employees and shareholders.
Among Asian women with hormone receptor–positive/human epidermal growth factor receptor-2 (HER2)–negative metastatic breast cancer that is resistant to endocrine therapy, a combination of palbociclib (Ibrance) and fulvestrant (Faslodex) was associated with a significant improvement in progression-free survival (PFS), reported investigators from the PALOMA-3 trial.
A preplanned subgroup analysis of 102 pre- and postmenopausal women from Japan, South Korea, and Taiwan who were enrolled in the trial showed that median PFS for 71 women assigned to palbociclib and fulvestrant had not been reached at the trial end. In contrast, median PFS among 31 patients assigned to placebo and fulvestrant was 5.8 months (hazard ratio, 0.485; P = .0065), reported Hiroji Iwata, MD, PhD, of the Aichi Cancer Center Hospital in Nagoya, Japan, and his colleagues.
“Overall, palbociclib plus fulvestrant seems to be a reasonable treatment option in Asians with HR-positive/HER2-negative metastatic breast cancer that has progressed on prior endocrine therapy,” they wrote in the Journal of Global Oncology (2017 Apr 11. doi: 10.1200/JGO.2016.008318).
PALOMA-3 was a multinational randomized double-blind, placebo-controlled phase III trial comparing a combination of fulvestrant, a selective estrogen receptor downregulator, and palbociclib, a small-molecule inhibitor of cyclin-dependent kinases 4 and 6 (CDK4/6) with fulvestrant plus placebo in 521 women with HR-positive/HER2-negative advanced breast cancer.
The trial was halted early for efficacy of the combination. The final overall analysis, published in April 2016 in The Lancet Oncology, showed that the combination significantly improved PFS, compared with fulvestrant and placebo, regardless of the patients’ degree of endocrine resistance, level of hormone receptor expression level, or PIK3CA mutational status.
Dr. Iwata and his associates noted that breast cancer is generally diagnosed at a younger age among Asian women (median, 45-50 years vs. 55-60 years among Western women) and that differences in genetic backgrounds may influence drug metabolism, resulting in potential differences in efficacy and adverse event profiles.
Among patients treated with palbociclib, the most common grade 3 or higher adverse events were neutropenia in 92%, compared with none in the placebo arm, and leukopenia in 29% vs. 0%. In contrast, grade 3/4 neutropenia occurred in 58% of non-Asian patients treated with the combination and 0.7% of non-Asian controls. Leukopenia rates were similar between Asian and non-Asian populations, however.
Comparisons of mean trough concentrations across subgroups showed that palbociclib exposures among Asians and non-Asians were similar. Patient reported outcomes were also similar between the groups, except for significantly more dyspnea among patients who received palbociclib (P = .05).
“This study adds to the limited body of literature assessing a CDK4/6 inhibitor in Asians and represents the largest patient experience with palbociclib in Asians. The present findings show that palbociclib plus fulvestrant improved PFS in Asians with HR-positive/HER2-negative [metastatic breast cancer] who experienced progression on prior endocrine therapy and that the safety profile of palbociclib plus fulvestrant in Asians was generally consistent with that observed in non-Asians. Together, these findings suggest that palbociclib is beneficial in patients who have not previously received endocrine therapy and in Asians and non-Asians who experienced relapse or progression during prior endocrine therapy,” they wrote.
The PALOMA-3 trial was supported by Pfizer. Dr. Iwata disclosed consultations with Chugai Pharma, Eisai, and AstraZeneca. Several coauthors are Pfizer employees and shareholders.
FROM THE JOURNAL OF GLOBAL ONCOLOGY
Key clinical point: Asian patients with HR+/HER2– metastatic breast cancer derive the same benefits from palbociclib and fulvestrant as non-Asian patients.
Major finding: Median PFS was 5.8 months for patients treated with fulvestrant plus placebo, vs. not reached for patients treated with fulvestrant plus palbociclib.
Data source: Subanalysis of data on 102 Asian patients in the PALOMA-3 randomized, double-blind, placebo-controlled trial.
Disclosures: The PALOMA-3 trial was supported by Pfizer. Dr. Iwata disclosed consultations with Chugai Pharma, Eisai, and AstraZeneca. Several coauthors are Pfizer employees and shareholders.
Preparing for pancreatic cancer ‘tsunami’ ahead
ORLANDO – Overall cancer death rates are dropping dramatically, but pancreatic cancer mortality remains high.
“By 2020 we expect [pancreatic cancer] to be the second most common cause of cancer-related death, exceeded only by lung cancer, and if lung cancer deaths continue to fall – which we expect that they will – it will be the most common cause of cancer-related death,” Margaret A. Tempero, MD, said at the annual conference of the National Comprehensive Cancer Network.
Further, as the population ages there will be an increasing number of patients presenting with pancreatic cancer, said Dr. Tempero of the University of California, San Francisco.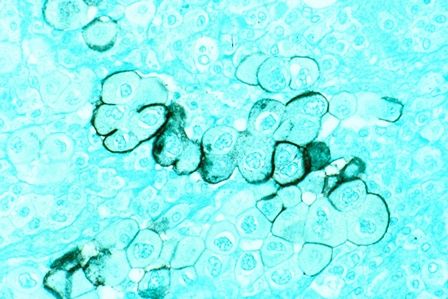
Currently, 80% of pancreatic cancer patients are diagnosed with disease that is not amenable to resection, and 80% of those who have resection and adjuvant therapy experience relapse. The overall survival rate is only about 9%.
“This is really, really an aggressive malignancy,” Dr. Tempero said, noting that the survival among those with metastases who do not receive treatment is only about 3 months.
There are no early symptoms that direct attention to the pancreas. Additionally, some patients experience very early invasion and metastases; in fact, up to two-thirds of patients with lesions only 1 cm in size will already have lymph node metastasis, she said.
The disease tends to be chemoresistant, although this may be changing with treatment advances, but it is characterized by “a lot of desmoplastic stroma, so there’s a lot of microenvironment that’s perturbed around the malignancy,” making it difficult for drugs to permeate the stroma.
“That’s something we’re actively working on – ways that we can actually change the stroma so that we can get more drug into the cancer,” she said.
Another challenge is the disease’s “habit of elaborating a lot of cytokines that disable the person with the disease,” which can lead to frailty that makes it difficult to deliver potentially effective therapies that are well tolerated in patients with other types of cancer, she noted.
An important question is whether pancreatic cancer is diagnosed too late or metastasizes too early, and there is evidence to support both possibilities.
“Either way ... we need to work on better treatment,” she said.
Resectable/borderline resectable disease
One noteworthy recent advance for patients with resectable/borderline resectable disease is the addition of capecitabine to gemcitabine for adjuvant therapy. In the ESPAC 4 study published in March in the Lancet, the combination of gemcitabine and capecitabine showed a clear benefit over gemcitabine alone.
“So that has now entered [the NCCN] guidelines as an important option for adjuvant therapy,” said Dr. Tempero, chair of the NCCN pancreatic cancer guidelines panel.
Ongoing trials are also looking at the FOLFIRINOX (irinotecan plus 5-fluorouracil plus leucovorin plus oxaliplatin) and gemcitabine/nanoparticle albumin-bound paclitaxel (nab-P) regimens in the adjuvant setting. These have previously shown some efficacy in the metastatic setting.
“So we really wanted to get these therapies into the adjuvant setting as soon as we could,” she said.
In the ACCORD trial, FOLFIRINOX is being compared with gemcitabine in the postoperative adjuvant setting, and the APACT trial comparing gemcitabine/nab-P to gemcitabine monotherapy completed accrual last year.
“I’m pretty sure that we’ll have enough events on the APACT study by the end of this year, and hopefully we can present that data in the spring. I’m hoping it will be a positive trial for us,” she said.
Neoadjuvant therapy – a successful strategy used in many other malignancies – is also being looked at for pancreatic cancer.
A pilot study (A021101) completed last year suggested that chemotherapy (FOLFIRINOX for 2 months) and chemoradiation (capecitabine and radiation at 50.4 Gy) followed by surgical resection and adjuvant chemotherapy (gemcitabine for 2 months) provided some benefit in patients with borderline resectable pancreatic cancer. This trial led to another ongoing study (S1505) in which patients with borderline resectable disease will be treated with 4 months of FOLFIRINOX prior to resection, followed by chemoradiation and surgery or FOLFIRINOX and surgery, and patients with resectable disease will undergo resection followed by FOLFIRINOX and surgery or gemcitabine/nab-P and surgery.
“The goal is not to compare the two regimens; the goal is to identify the benchmarks that we get with these regimens. In other words, if you’re going to give FOLFIRINOX, what pathologic complete response rate can you expect? What will your R1 resection rate be? With gemcitabine and nab-paclitaxel, the same thing, because if you want to continue to build on these regimens in the neoadjuvant setting you need to know what you’re likely to get so you can make clinical trial assumptions when you add new drugs.
“Once we have these benchmarking data we can really sail in the neoadjuvant setting. It’s a great window-of-opportunity setting for new drugs, because you’re getting serial tissue,” Dr. Tempero said, explaining that in addition to resection of tissue, there is opportunity to get biopsies ahead of time and look at the effects of the drug.
Locally advanced disease
For locally advanced disease, studies have failed to show a benefit of adding radiation after chemotherapy, but radiation oncologists who argue that, “when your therapy gets better, my therapy gets better,” have a valid point, Dr. Tempero said.
For that reason, the Radiation Therapy Oncology group launched a trial to look at gemcitabine/nab-P with and without radiation, but had difficulty with enrollment due to resistance among some physicians who are opposed to radiation in this setting .
“So I don’t know that we will ever answer this question in locally advanced disease. What I can say ... is, in my mind, in locally advanced disease, the most important component is the chemotherapy,” she said.
Metastatic disease
When it comes to trials involving pancreatic cancer patients with metastatic disease, it is important to understand – and to convey to policymakers – that the goal is not only to provide better care in these patients who are at the end of their life, but also to identify strategies that can be used in the adjuvant and neoadjuvant settings, as this is part of the “overall mission of helping patients to feel better and live longer and be cured,” Dr. Tempero said.
One regimen currently used in the metastatic setting is FOLFIRINOX, which was shown in the Prodige 4-ACCORD 11 trial to be superior to gemcitabine monotherapy for survival (hazard ratio, 0.57).
“This is the first time we ever saw a hazard ratio below 0.6 in this disease,” she said, adding that for some patients this means “they can get tremendous benefit, they can come off chemotherapy and have a chemotherapy holiday,” she said.
That said, it’s a tough regimen, she added, explaining that it has dominating toxicities of myelosuppression, diarrhea, and neuropathy that can be irreversible.
Frail patients may not be able to tolerate the regimen, but modifications to the regimen may help. For example, the 5-fluorourasil bolus is often omitted, and doses are sometimes reduced. Chemotherapy holidays can also be of benefit.
Another regimen for the metastatic setting involves the use of nab-P plus gemcitabine, which was shown in a phase III trial to improve survival (HR for death, 0.72).
The results aren’t quite as dramatic as those seen with FOLFIRINOX, but the regimen is slightly easier to manage, Dr. Tempero said, adding: “It’s still not a walk in the park.”
Myelosuppression, arthralgias, and neuropathy still occur, she explained.
Gemcitabine/capecitabine, which has been shown to improve progression-free survival, can also be used, and may be preferable in elderly patients who aren’t fit enough for the other regimens, she said.
“When I select treatment, I really sit down with the patient, and I look at their comorbidities and let them review the toxicities. They decide,” she said, explaining that she provides recommendations based on their concerns and input. “We do have a conversation and we talk about the goals of treatment, we talk about the toxicities.”
Future efforts for metastatic disease should build upon both FOLFIRINOX and gemcitabine/nab-P, she said.
However, because of the difficulty with administering FOLFIRINOX, only two of the 54 open phase I-III trials ongoing in the United States for metastatic disease incorporate the regimen.
Other treatment options include gemcitabine/cisplatin, GTX (gemcitabine/docetaxel/capecitabine), and gemcitabine/erlotinib. The former remains in the NCCN guidelines, primarily for those with hereditary forms of pancreatic cancer, and in particular for those in the DNA repair pathway (BRCA patients, for example).
“We actually have trials now focusing on just BRCA-related pancreatic cancer,” she said, noting that these patients are “exquisitely sensitive to cisplatin and don’t need a harsh regimen like FOLFIRINOX to get the same benefit.
GTX is a very active regimen, although it has never been compared with gemcitabine monotherapy in a randomized trial. However, because of its clear activity it remains in the NCCN guidelines as an option.
Gemcitabine/erlotinib also remains in the guidelines because of a tiny trial that showed a small benefit, but it is not a preferred combination, she said.
Future therapies
Efforts going forward are focusing on finding drugs that inactivate activated RAS, which is “a really big driver” in many cancers, as well as on addressing the microenvironment (such as the desmoplastic stroma that may help encourage invasion of metastases and/or impede drug delivery to the cancer), Dr. Tempero said.
“So there is a lot of interest right now in various forms of immunotherapy or in stromal remodeling so we can see what impact that has on the progression of this disease,” she said, noting that new agents in registration trials include ibrutinib, laparib, PEGPH20, and insulinlike growth factor 1 (IGF-1) inhibitors, and those in planning stages include chemokine (C-C motif) receptor 2 (CCR2) inhibitors and palbociclib.
“And I think we have opportunities in the maintenance setting and in the neoadjuvant setting to do window-of-opportunity trials where we can test new concepts, where we can get pharmacodynamic and biologic data to understand what these new agents are doing,” she said.
Collaborative effort to identify patients at risk
Population-level screening strategies for pancreatic cancer aren’t feasible because of the relatively low incidence of the disease, but efforts are underway to identify and screen high-risk groups.
“We actually have some tests that you could screen with, but they’re not perfect, and with a disease that occurs at the rate that [pancreatic cancer] does, you can’t screen the whole population, because you will find false positives, and you will cause unnecessary procedures more than you’ll find the cancer, Dr. Tempero said during a meeting with press at the NCCN annual conference.
Instead, it is important to identify and screen only those at high risk, she added.
Such a group might include patients with new-onset diabetes who experience weight loss.
New-onset diabetes can be caused by pancreatic cancer, and weight loss with diabetes is unexpected and should raise a red flag, Dr. Temepero explained, adding that an education gap among community physicians means these patients are sometimes cheered for the weight loss instead – and then they end up in the pancreatic disease clinic with metastatic disease 2 years later.
In an effort to better define and characterize this and other high-risk groups, the National Institute for Diabetes and Digestive and Kidney Diseases and the National Cancer Institute are working together to fund a network of institutions that will develop high-risk cohorts and begin deploying screening strategies. The effort is partly in response to the Recalcitrant Cancer Act passed in 2012 to “force more attention on funding pancreatic cancer research through the branches of the NIH,” she explained.
In this particular high-risk group, the institutions will look at the character of diabetes and the clinical correlates with pancreatic cancer.
“Once we hone in on these, we can use those – what we hope are – early-detection biomarkers, and if those are positive, then we would ask the patient to have a CT scan to look for pancreatic cancer,” she said.
Dr. Tempero reported serving as a scientific advisor and/or receiving grant/research support, consulting fees, and/or honoraria from Celgene Corporation, Champion Oncology, Cornerstone Pharmaceuticals, Eli Lilly, EMD Serono, Gilead Sciences, Halozyme Therapeutics, MCS Biotech Resources, NeoHealth, Novocure, Opsona Therapeutics, Pfizer, Portola Pharmaceuticals, and Threshold Pharmaceuticals.
ORLANDO – Overall cancer death rates are dropping dramatically, but pancreatic cancer mortality remains high.
“By 2020 we expect [pancreatic cancer] to be the second most common cause of cancer-related death, exceeded only by lung cancer, and if lung cancer deaths continue to fall – which we expect that they will – it will be the most common cause of cancer-related death,” Margaret A. Tempero, MD, said at the annual conference of the National Comprehensive Cancer Network.
Further, as the population ages there will be an increasing number of patients presenting with pancreatic cancer, said Dr. Tempero of the University of California, San Francisco.
Currently, 80% of pancreatic cancer patients are diagnosed with disease that is not amenable to resection, and 80% of those who have resection and adjuvant therapy experience relapse. The overall survival rate is only about 9%.
“This is really, really an aggressive malignancy,” Dr. Tempero said, noting that the survival among those with metastases who do not receive treatment is only about 3 months.
There are no early symptoms that direct attention to the pancreas. Additionally, some patients experience very early invasion and metastases; in fact, up to two-thirds of patients with lesions only 1 cm in size will already have lymph node metastasis, she said.
The disease tends to be chemoresistant, although this may be changing with treatment advances, but it is characterized by “a lot of desmoplastic stroma, so there’s a lot of microenvironment that’s perturbed around the malignancy,” making it difficult for drugs to permeate the stroma.
“That’s something we’re actively working on – ways that we can actually change the stroma so that we can get more drug into the cancer,” she said.
Another challenge is the disease’s “habit of elaborating a lot of cytokines that disable the person with the disease,” which can lead to frailty that makes it difficult to deliver potentially effective therapies that are well tolerated in patients with other types of cancer, she noted.
An important question is whether pancreatic cancer is diagnosed too late or metastasizes too early, and there is evidence to support both possibilities.
“Either way ... we need to work on better treatment,” she said.
Resectable/borderline resectable disease
One noteworthy recent advance for patients with resectable/borderline resectable disease is the addition of capecitabine to gemcitabine for adjuvant therapy. In the ESPAC 4 study published in March in the Lancet, the combination of gemcitabine and capecitabine showed a clear benefit over gemcitabine alone.
“So that has now entered [the NCCN] guidelines as an important option for adjuvant therapy,” said Dr. Tempero, chair of the NCCN pancreatic cancer guidelines panel.
Ongoing trials are also looking at the FOLFIRINOX (irinotecan plus 5-fluorouracil plus leucovorin plus oxaliplatin) and gemcitabine/nanoparticle albumin-bound paclitaxel (nab-P) regimens in the adjuvant setting. These have previously shown some efficacy in the metastatic setting.
“So we really wanted to get these therapies into the adjuvant setting as soon as we could,” she said.
In the ACCORD trial, FOLFIRINOX is being compared with gemcitabine in the postoperative adjuvant setting, and the APACT trial comparing gemcitabine/nab-P to gemcitabine monotherapy completed accrual last year.
“I’m pretty sure that we’ll have enough events on the APACT study by the end of this year, and hopefully we can present that data in the spring. I’m hoping it will be a positive trial for us,” she said.
Neoadjuvant therapy – a successful strategy used in many other malignancies – is also being looked at for pancreatic cancer.
A pilot study (A021101) completed last year suggested that chemotherapy (FOLFIRINOX for 2 months) and chemoradiation (capecitabine and radiation at 50.4 Gy) followed by surgical resection and adjuvant chemotherapy (gemcitabine for 2 months) provided some benefit in patients with borderline resectable pancreatic cancer. This trial led to another ongoing study (S1505) in which patients with borderline resectable disease will be treated with 4 months of FOLFIRINOX prior to resection, followed by chemoradiation and surgery or FOLFIRINOX and surgery, and patients with resectable disease will undergo resection followed by FOLFIRINOX and surgery or gemcitabine/nab-P and surgery.
“The goal is not to compare the two regimens; the goal is to identify the benchmarks that we get with these regimens. In other words, if you’re going to give FOLFIRINOX, what pathologic complete response rate can you expect? What will your R1 resection rate be? With gemcitabine and nab-paclitaxel, the same thing, because if you want to continue to build on these regimens in the neoadjuvant setting you need to know what you’re likely to get so you can make clinical trial assumptions when you add new drugs.
“Once we have these benchmarking data we can really sail in the neoadjuvant setting. It’s a great window-of-opportunity setting for new drugs, because you’re getting serial tissue,” Dr. Tempero said, explaining that in addition to resection of tissue, there is opportunity to get biopsies ahead of time and look at the effects of the drug.
Locally advanced disease
For locally advanced disease, studies have failed to show a benefit of adding radiation after chemotherapy, but radiation oncologists who argue that, “when your therapy gets better, my therapy gets better,” have a valid point, Dr. Tempero said.
For that reason, the Radiation Therapy Oncology group launched a trial to look at gemcitabine/nab-P with and without radiation, but had difficulty with enrollment due to resistance among some physicians who are opposed to radiation in this setting .
“So I don’t know that we will ever answer this question in locally advanced disease. What I can say ... is, in my mind, in locally advanced disease, the most important component is the chemotherapy,” she said.
Metastatic disease
When it comes to trials involving pancreatic cancer patients with metastatic disease, it is important to understand – and to convey to policymakers – that the goal is not only to provide better care in these patients who are at the end of their life, but also to identify strategies that can be used in the adjuvant and neoadjuvant settings, as this is part of the “overall mission of helping patients to feel better and live longer and be cured,” Dr. Tempero said.
One regimen currently used in the metastatic setting is FOLFIRINOX, which was shown in the Prodige 4-ACCORD 11 trial to be superior to gemcitabine monotherapy for survival (hazard ratio, 0.57).
“This is the first time we ever saw a hazard ratio below 0.6 in this disease,” she said, adding that for some patients this means “they can get tremendous benefit, they can come off chemotherapy and have a chemotherapy holiday,” she said.
That said, it’s a tough regimen, she added, explaining that it has dominating toxicities of myelosuppression, diarrhea, and neuropathy that can be irreversible.
Frail patients may not be able to tolerate the regimen, but modifications to the regimen may help. For example, the 5-fluorourasil bolus is often omitted, and doses are sometimes reduced. Chemotherapy holidays can also be of benefit.
Another regimen for the metastatic setting involves the use of nab-P plus gemcitabine, which was shown in a phase III trial to improve survival (HR for death, 0.72).
The results aren’t quite as dramatic as those seen with FOLFIRINOX, but the regimen is slightly easier to manage, Dr. Tempero said, adding: “It’s still not a walk in the park.”
Myelosuppression, arthralgias, and neuropathy still occur, she explained.
Gemcitabine/capecitabine, which has been shown to improve progression-free survival, can also be used, and may be preferable in elderly patients who aren’t fit enough for the other regimens, she said.
“When I select treatment, I really sit down with the patient, and I look at their comorbidities and let them review the toxicities. They decide,” she said, explaining that she provides recommendations based on their concerns and input. “We do have a conversation and we talk about the goals of treatment, we talk about the toxicities.”
Future efforts for metastatic disease should build upon both FOLFIRINOX and gemcitabine/nab-P, she said.
However, because of the difficulty with administering FOLFIRINOX, only two of the 54 open phase I-III trials ongoing in the United States for metastatic disease incorporate the regimen.
Other treatment options include gemcitabine/cisplatin, GTX (gemcitabine/docetaxel/capecitabine), and gemcitabine/erlotinib. The former remains in the NCCN guidelines, primarily for those with hereditary forms of pancreatic cancer, and in particular for those in the DNA repair pathway (BRCA patients, for example).
“We actually have trials now focusing on just BRCA-related pancreatic cancer,” she said, noting that these patients are “exquisitely sensitive to cisplatin and don’t need a harsh regimen like FOLFIRINOX to get the same benefit.
GTX is a very active regimen, although it has never been compared with gemcitabine monotherapy in a randomized trial. However, because of its clear activity it remains in the NCCN guidelines as an option.
Gemcitabine/erlotinib also remains in the guidelines because of a tiny trial that showed a small benefit, but it is not a preferred combination, she said.
Future therapies
Efforts going forward are focusing on finding drugs that inactivate activated RAS, which is “a really big driver” in many cancers, as well as on addressing the microenvironment (such as the desmoplastic stroma that may help encourage invasion of metastases and/or impede drug delivery to the cancer), Dr. Tempero said.
“So there is a lot of interest right now in various forms of immunotherapy or in stromal remodeling so we can see what impact that has on the progression of this disease,” she said, noting that new agents in registration trials include ibrutinib, laparib, PEGPH20, and insulinlike growth factor 1 (IGF-1) inhibitors, and those in planning stages include chemokine (C-C motif) receptor 2 (CCR2) inhibitors and palbociclib.
“And I think we have opportunities in the maintenance setting and in the neoadjuvant setting to do window-of-opportunity trials where we can test new concepts, where we can get pharmacodynamic and biologic data to understand what these new agents are doing,” she said.
Collaborative effort to identify patients at risk
Population-level screening strategies for pancreatic cancer aren’t feasible because of the relatively low incidence of the disease, but efforts are underway to identify and screen high-risk groups.
“We actually have some tests that you could screen with, but they’re not perfect, and with a disease that occurs at the rate that [pancreatic cancer] does, you can’t screen the whole population, because you will find false positives, and you will cause unnecessary procedures more than you’ll find the cancer, Dr. Tempero said during a meeting with press at the NCCN annual conference.
Instead, it is important to identify and screen only those at high risk, she added.
Such a group might include patients with new-onset diabetes who experience weight loss.
New-onset diabetes can be caused by pancreatic cancer, and weight loss with diabetes is unexpected and should raise a red flag, Dr. Temepero explained, adding that an education gap among community physicians means these patients are sometimes cheered for the weight loss instead – and then they end up in the pancreatic disease clinic with metastatic disease 2 years later.
In an effort to better define and characterize this and other high-risk groups, the National Institute for Diabetes and Digestive and Kidney Diseases and the National Cancer Institute are working together to fund a network of institutions that will develop high-risk cohorts and begin deploying screening strategies. The effort is partly in response to the Recalcitrant Cancer Act passed in 2012 to “force more attention on funding pancreatic cancer research through the branches of the NIH,” she explained.
In this particular high-risk group, the institutions will look at the character of diabetes and the clinical correlates with pancreatic cancer.
“Once we hone in on these, we can use those – what we hope are – early-detection biomarkers, and if those are positive, then we would ask the patient to have a CT scan to look for pancreatic cancer,” she said.
Dr. Tempero reported serving as a scientific advisor and/or receiving grant/research support, consulting fees, and/or honoraria from Celgene Corporation, Champion Oncology, Cornerstone Pharmaceuticals, Eli Lilly, EMD Serono, Gilead Sciences, Halozyme Therapeutics, MCS Biotech Resources, NeoHealth, Novocure, Opsona Therapeutics, Pfizer, Portola Pharmaceuticals, and Threshold Pharmaceuticals.
ORLANDO – Overall cancer death rates are dropping dramatically, but pancreatic cancer mortality remains high.
“By 2020 we expect [pancreatic cancer] to be the second most common cause of cancer-related death, exceeded only by lung cancer, and if lung cancer deaths continue to fall – which we expect that they will – it will be the most common cause of cancer-related death,” Margaret A. Tempero, MD, said at the annual conference of the National Comprehensive Cancer Network.
Further, as the population ages there will be an increasing number of patients presenting with pancreatic cancer, said Dr. Tempero of the University of California, San Francisco.
Currently, 80% of pancreatic cancer patients are diagnosed with disease that is not amenable to resection, and 80% of those who have resection and adjuvant therapy experience relapse. The overall survival rate is only about 9%.
“This is really, really an aggressive malignancy,” Dr. Tempero said, noting that the survival among those with metastases who do not receive treatment is only about 3 months.
There are no early symptoms that direct attention to the pancreas. Additionally, some patients experience very early invasion and metastases; in fact, up to two-thirds of patients with lesions only 1 cm in size will already have lymph node metastasis, she said.
The disease tends to be chemoresistant, although this may be changing with treatment advances, but it is characterized by “a lot of desmoplastic stroma, so there’s a lot of microenvironment that’s perturbed around the malignancy,” making it difficult for drugs to permeate the stroma.
“That’s something we’re actively working on – ways that we can actually change the stroma so that we can get more drug into the cancer,” she said.
Another challenge is the disease’s “habit of elaborating a lot of cytokines that disable the person with the disease,” which can lead to frailty that makes it difficult to deliver potentially effective therapies that are well tolerated in patients with other types of cancer, she noted.
An important question is whether pancreatic cancer is diagnosed too late or metastasizes too early, and there is evidence to support both possibilities.
“Either way ... we need to work on better treatment,” she said.
Resectable/borderline resectable disease
One noteworthy recent advance for patients with resectable/borderline resectable disease is the addition of capecitabine to gemcitabine for adjuvant therapy. In the ESPAC 4 study published in March in the Lancet, the combination of gemcitabine and capecitabine showed a clear benefit over gemcitabine alone.
“So that has now entered [the NCCN] guidelines as an important option for adjuvant therapy,” said Dr. Tempero, chair of the NCCN pancreatic cancer guidelines panel.
Ongoing trials are also looking at the FOLFIRINOX (irinotecan plus 5-fluorouracil plus leucovorin plus oxaliplatin) and gemcitabine/nanoparticle albumin-bound paclitaxel (nab-P) regimens in the adjuvant setting. These have previously shown some efficacy in the metastatic setting.
“So we really wanted to get these therapies into the adjuvant setting as soon as we could,” she said.
In the ACCORD trial, FOLFIRINOX is being compared with gemcitabine in the postoperative adjuvant setting, and the APACT trial comparing gemcitabine/nab-P to gemcitabine monotherapy completed accrual last year.
“I’m pretty sure that we’ll have enough events on the APACT study by the end of this year, and hopefully we can present that data in the spring. I’m hoping it will be a positive trial for us,” she said.
Neoadjuvant therapy – a successful strategy used in many other malignancies – is also being looked at for pancreatic cancer.
A pilot study (A021101) completed last year suggested that chemotherapy (FOLFIRINOX for 2 months) and chemoradiation (capecitabine and radiation at 50.4 Gy) followed by surgical resection and adjuvant chemotherapy (gemcitabine for 2 months) provided some benefit in patients with borderline resectable pancreatic cancer. This trial led to another ongoing study (S1505) in which patients with borderline resectable disease will be treated with 4 months of FOLFIRINOX prior to resection, followed by chemoradiation and surgery or FOLFIRINOX and surgery, and patients with resectable disease will undergo resection followed by FOLFIRINOX and surgery or gemcitabine/nab-P and surgery.
“The goal is not to compare the two regimens; the goal is to identify the benchmarks that we get with these regimens. In other words, if you’re going to give FOLFIRINOX, what pathologic complete response rate can you expect? What will your R1 resection rate be? With gemcitabine and nab-paclitaxel, the same thing, because if you want to continue to build on these regimens in the neoadjuvant setting you need to know what you’re likely to get so you can make clinical trial assumptions when you add new drugs.
“Once we have these benchmarking data we can really sail in the neoadjuvant setting. It’s a great window-of-opportunity setting for new drugs, because you’re getting serial tissue,” Dr. Tempero said, explaining that in addition to resection of tissue, there is opportunity to get biopsies ahead of time and look at the effects of the drug.
Locally advanced disease
For locally advanced disease, studies have failed to show a benefit of adding radiation after chemotherapy, but radiation oncologists who argue that, “when your therapy gets better, my therapy gets better,” have a valid point, Dr. Tempero said.
For that reason, the Radiation Therapy Oncology group launched a trial to look at gemcitabine/nab-P with and without radiation, but had difficulty with enrollment due to resistance among some physicians who are opposed to radiation in this setting .
“So I don’t know that we will ever answer this question in locally advanced disease. What I can say ... is, in my mind, in locally advanced disease, the most important component is the chemotherapy,” she said.
Metastatic disease
When it comes to trials involving pancreatic cancer patients with metastatic disease, it is important to understand – and to convey to policymakers – that the goal is not only to provide better care in these patients who are at the end of their life, but also to identify strategies that can be used in the adjuvant and neoadjuvant settings, as this is part of the “overall mission of helping patients to feel better and live longer and be cured,” Dr. Tempero said.
One regimen currently used in the metastatic setting is FOLFIRINOX, which was shown in the Prodige 4-ACCORD 11 trial to be superior to gemcitabine monotherapy for survival (hazard ratio, 0.57).
“This is the first time we ever saw a hazard ratio below 0.6 in this disease,” she said, adding that for some patients this means “they can get tremendous benefit, they can come off chemotherapy and have a chemotherapy holiday,” she said.
That said, it’s a tough regimen, she added, explaining that it has dominating toxicities of myelosuppression, diarrhea, and neuropathy that can be irreversible.
Frail patients may not be able to tolerate the regimen, but modifications to the regimen may help. For example, the 5-fluorourasil bolus is often omitted, and doses are sometimes reduced. Chemotherapy holidays can also be of benefit.
Another regimen for the metastatic setting involves the use of nab-P plus gemcitabine, which was shown in a phase III trial to improve survival (HR for death, 0.72).
The results aren’t quite as dramatic as those seen with FOLFIRINOX, but the regimen is slightly easier to manage, Dr. Tempero said, adding: “It’s still not a walk in the park.”
Myelosuppression, arthralgias, and neuropathy still occur, she explained.
Gemcitabine/capecitabine, which has been shown to improve progression-free survival, can also be used, and may be preferable in elderly patients who aren’t fit enough for the other regimens, she said.
“When I select treatment, I really sit down with the patient, and I look at their comorbidities and let them review the toxicities. They decide,” she said, explaining that she provides recommendations based on their concerns and input. “We do have a conversation and we talk about the goals of treatment, we talk about the toxicities.”
Future efforts for metastatic disease should build upon both FOLFIRINOX and gemcitabine/nab-P, she said.
However, because of the difficulty with administering FOLFIRINOX, only two of the 54 open phase I-III trials ongoing in the United States for metastatic disease incorporate the regimen.
Other treatment options include gemcitabine/cisplatin, GTX (gemcitabine/docetaxel/capecitabine), and gemcitabine/erlotinib. The former remains in the NCCN guidelines, primarily for those with hereditary forms of pancreatic cancer, and in particular for those in the DNA repair pathway (BRCA patients, for example).
“We actually have trials now focusing on just BRCA-related pancreatic cancer,” she said, noting that these patients are “exquisitely sensitive to cisplatin and don’t need a harsh regimen like FOLFIRINOX to get the same benefit.
GTX is a very active regimen, although it has never been compared with gemcitabine monotherapy in a randomized trial. However, because of its clear activity it remains in the NCCN guidelines as an option.
Gemcitabine/erlotinib also remains in the guidelines because of a tiny trial that showed a small benefit, but it is not a preferred combination, she said.
Future therapies
Efforts going forward are focusing on finding drugs that inactivate activated RAS, which is “a really big driver” in many cancers, as well as on addressing the microenvironment (such as the desmoplastic stroma that may help encourage invasion of metastases and/or impede drug delivery to the cancer), Dr. Tempero said.
“So there is a lot of interest right now in various forms of immunotherapy or in stromal remodeling so we can see what impact that has on the progression of this disease,” she said, noting that new agents in registration trials include ibrutinib, laparib, PEGPH20, and insulinlike growth factor 1 (IGF-1) inhibitors, and those in planning stages include chemokine (C-C motif) receptor 2 (CCR2) inhibitors and palbociclib.
“And I think we have opportunities in the maintenance setting and in the neoadjuvant setting to do window-of-opportunity trials where we can test new concepts, where we can get pharmacodynamic and biologic data to understand what these new agents are doing,” she said.
Collaborative effort to identify patients at risk
Population-level screening strategies for pancreatic cancer aren’t feasible because of the relatively low incidence of the disease, but efforts are underway to identify and screen high-risk groups.
“We actually have some tests that you could screen with, but they’re not perfect, and with a disease that occurs at the rate that [pancreatic cancer] does, you can’t screen the whole population, because you will find false positives, and you will cause unnecessary procedures more than you’ll find the cancer, Dr. Tempero said during a meeting with press at the NCCN annual conference.
Instead, it is important to identify and screen only those at high risk, she added.
Such a group might include patients with new-onset diabetes who experience weight loss.
New-onset diabetes can be caused by pancreatic cancer, and weight loss with diabetes is unexpected and should raise a red flag, Dr. Temepero explained, adding that an education gap among community physicians means these patients are sometimes cheered for the weight loss instead – and then they end up in the pancreatic disease clinic with metastatic disease 2 years later.
In an effort to better define and characterize this and other high-risk groups, the National Institute for Diabetes and Digestive and Kidney Diseases and the National Cancer Institute are working together to fund a network of institutions that will develop high-risk cohorts and begin deploying screening strategies. The effort is partly in response to the Recalcitrant Cancer Act passed in 2012 to “force more attention on funding pancreatic cancer research through the branches of the NIH,” she explained.
In this particular high-risk group, the institutions will look at the character of diabetes and the clinical correlates with pancreatic cancer.
“Once we hone in on these, we can use those – what we hope are – early-detection biomarkers, and if those are positive, then we would ask the patient to have a CT scan to look for pancreatic cancer,” she said.
Dr. Tempero reported serving as a scientific advisor and/or receiving grant/research support, consulting fees, and/or honoraria from Celgene Corporation, Champion Oncology, Cornerstone Pharmaceuticals, Eli Lilly, EMD Serono, Gilead Sciences, Halozyme Therapeutics, MCS Biotech Resources, NeoHealth, Novocure, Opsona Therapeutics, Pfizer, Portola Pharmaceuticals, and Threshold Pharmaceuticals.
AT THE NCCN ANNUAL CONFERENCE
Key clinical point:
Disclosures: Dr. Tempero reported serving as a scientific advisor and/or receiving grant/research support, consulting fees, and/or honoraria from Celgene Corporation, Champion Oncology, Cornerstone Pharmaceuticals, Eli Lilly, EMD Serono, Gilead Sciences, Halozyme Therapeutics, MCS Biotech Resources, NeoHealth, Novocure, Opsona Therapeutics, Pfizer, Portola Pharmaceuticals, and Threshold Pharmaceuticals.
Expanded drug combinations produce best myeloma induction
NEW YORK – Optimal induction therapy for patients with multiple myeloma requires all the therapeutic tools currently available for combination therapy, which means using four agents followed by autologous stem cell transplantation, Paul G. Richardson, MD, said at a conference held by Imedex.
He suggested that a rational combination regimen for induction therapy of multiple myeloma would include a second- or third-generation immunomodulator such as lenalidomide (Revlimid) or pomalidomide (Pomalyst); a proteasome inhibitor such as bortezomib (Velcade), carfilzomib (Kyprolis), or ixazomib (Ninlaro); plus standard dexamethasone to form a contemporary backbone regimen for inducing remission in patients with multiple myeloma.

“Therapeutic parsimony is not recommended. You need a combination” of all available drug classes, suggested Dr. Richardson, professor of medicine at Harvard Medical School and clinical program leader of the Multiple Myeloma Center at the Dana-Farber Cancer Institute in Boston.
“It isn’t rational to limit the treatment choices. We need to bring them all together,” he said. The “most rational” combination melds an immunomodulator, proteasome inhibitor, plus a monoclonal antibody that he called a “true game changer. Add the antibody on top of the three-drug platform” of an immunomodulator, proteasome inhibitor, and dexamethasone. Dr. Richardson conceded, however, that a concern with such combinations is how to manage the toxicity that would likely result.
He cited several recent examples of demonstrated superior efficacy in the form of more complete responses from combined regimens, followed by autologous stem cell transplantation.
For example, a recent report from a French-led group compared the efficacy of a combination of an immunomodulator, proteasome inhibitor, and dexamethasone against the same combination, followed by autologous stem cell transplantation (N Engl J Med. 2017 Apr 6;376[14]:1311-20). The combined regimen plus transplant resulted in a 59% complete response rate, “the best response rate we’ve ever seen” in multiple myeloma, Dr. Richardson noted, compared with a 48% complete response rate in patients who did not undergo a stem cell transplant.
Another speaker at the meeting, Ruben Niesvizky, MD, suggested a more cautious approach to using the monoclonal antibody daratumumab for induction. He cited the published experience in adding the antibody to pared-down backbone therapy in the setting of relapsed or relapsed and refractory disease, such as a proteasome inhibitor plus dexamethasone (N Engl J Med. 2016 Aug 25;375[8]:754-66) or an immunomodulator plus dexamethasone (N Engl J Med. 2016 Oct 6;375[14]:1319-31).
Adding a monoclonal antibody such as daratumumab to combination therapy is the “wave of the future,” said Dr. Niesvizky, professor of medicine and director of the Multiple Myeloma Center at New York Presbyterian Hospital/Weill Cornell Medical Center. It provides treatment that reduces disease-related complications and achieves effective and extended disease control with improved overall survival, while being well tolerated and facilitating stem cell collection.
Dr. Richardson has been a consultant to Celgene, Genmab, Janssen, Novartis, Oncopeptides AB, and Takeda and has received research funding from Celgene and Takeda. Dr. Niesvizky has been a consultant to Amgen, Bristol-Myers Squibb, Celgene, Janssen, and Takeda and has received research support from Amgen, Bristol-Myers Squibb, Celgene, and Takeda.
[email protected]
On Twitter @mitchelzoler
NEW YORK – Optimal induction therapy for patients with multiple myeloma requires all the therapeutic tools currently available for combination therapy, which means using four agents followed by autologous stem cell transplantation, Paul G. Richardson, MD, said at a conference held by Imedex.
He suggested that a rational combination regimen for induction therapy of multiple myeloma would include a second- or third-generation immunomodulator such as lenalidomide (Revlimid) or pomalidomide (Pomalyst); a proteasome inhibitor such as bortezomib (Velcade), carfilzomib (Kyprolis), or ixazomib (Ninlaro); plus standard dexamethasone to form a contemporary backbone regimen for inducing remission in patients with multiple myeloma.
“Therapeutic parsimony is not recommended. You need a combination” of all available drug classes, suggested Dr. Richardson, professor of medicine at Harvard Medical School and clinical program leader of the Multiple Myeloma Center at the Dana-Farber Cancer Institute in Boston.
“It isn’t rational to limit the treatment choices. We need to bring them all together,” he said. The “most rational” combination melds an immunomodulator, proteasome inhibitor, plus a monoclonal antibody that he called a “true game changer. Add the antibody on top of the three-drug platform” of an immunomodulator, proteasome inhibitor, and dexamethasone. Dr. Richardson conceded, however, that a concern with such combinations is how to manage the toxicity that would likely result.
He cited several recent examples of demonstrated superior efficacy in the form of more complete responses from combined regimens, followed by autologous stem cell transplantation.
For example, a recent report from a French-led group compared the efficacy of a combination of an immunomodulator, proteasome inhibitor, and dexamethasone against the same combination, followed by autologous stem cell transplantation (N Engl J Med. 2017 Apr 6;376[14]:1311-20). The combined regimen plus transplant resulted in a 59% complete response rate, “the best response rate we’ve ever seen” in multiple myeloma, Dr. Richardson noted, compared with a 48% complete response rate in patients who did not undergo a stem cell transplant.
Another speaker at the meeting, Ruben Niesvizky, MD, suggested a more cautious approach to using the monoclonal antibody daratumumab for induction. He cited the published experience in adding the antibody to pared-down backbone therapy in the setting of relapsed or relapsed and refractory disease, such as a proteasome inhibitor plus dexamethasone (N Engl J Med. 2016 Aug 25;375[8]:754-66) or an immunomodulator plus dexamethasone (N Engl J Med. 2016 Oct 6;375[14]:1319-31).
Adding a monoclonal antibody such as daratumumab to combination therapy is the “wave of the future,” said Dr. Niesvizky, professor of medicine and director of the Multiple Myeloma Center at New York Presbyterian Hospital/Weill Cornell Medical Center. It provides treatment that reduces disease-related complications and achieves effective and extended disease control with improved overall survival, while being well tolerated and facilitating stem cell collection.
Dr. Richardson has been a consultant to Celgene, Genmab, Janssen, Novartis, Oncopeptides AB, and Takeda and has received research funding from Celgene and Takeda. Dr. Niesvizky has been a consultant to Amgen, Bristol-Myers Squibb, Celgene, Janssen, and Takeda and has received research support from Amgen, Bristol-Myers Squibb, Celgene, and Takeda.
[email protected]
On Twitter @mitchelzoler
NEW YORK – Optimal induction therapy for patients with multiple myeloma requires all the therapeutic tools currently available for combination therapy, which means using four agents followed by autologous stem cell transplantation, Paul G. Richardson, MD, said at a conference held by Imedex.
He suggested that a rational combination regimen for induction therapy of multiple myeloma would include a second- or third-generation immunomodulator such as lenalidomide (Revlimid) or pomalidomide (Pomalyst); a proteasome inhibitor such as bortezomib (Velcade), carfilzomib (Kyprolis), or ixazomib (Ninlaro); plus standard dexamethasone to form a contemporary backbone regimen for inducing remission in patients with multiple myeloma.
“Therapeutic parsimony is not recommended. You need a combination” of all available drug classes, suggested Dr. Richardson, professor of medicine at Harvard Medical School and clinical program leader of the Multiple Myeloma Center at the Dana-Farber Cancer Institute in Boston.
“It isn’t rational to limit the treatment choices. We need to bring them all together,” he said. The “most rational” combination melds an immunomodulator, proteasome inhibitor, plus a monoclonal antibody that he called a “true game changer. Add the antibody on top of the three-drug platform” of an immunomodulator, proteasome inhibitor, and dexamethasone. Dr. Richardson conceded, however, that a concern with such combinations is how to manage the toxicity that would likely result.
He cited several recent examples of demonstrated superior efficacy in the form of more complete responses from combined regimens, followed by autologous stem cell transplantation.
For example, a recent report from a French-led group compared the efficacy of a combination of an immunomodulator, proteasome inhibitor, and dexamethasone against the same combination, followed by autologous stem cell transplantation (N Engl J Med. 2017 Apr 6;376[14]:1311-20). The combined regimen plus transplant resulted in a 59% complete response rate, “the best response rate we’ve ever seen” in multiple myeloma, Dr. Richardson noted, compared with a 48% complete response rate in patients who did not undergo a stem cell transplant.
Another speaker at the meeting, Ruben Niesvizky, MD, suggested a more cautious approach to using the monoclonal antibody daratumumab for induction. He cited the published experience in adding the antibody to pared-down backbone therapy in the setting of relapsed or relapsed and refractory disease, such as a proteasome inhibitor plus dexamethasone (N Engl J Med. 2016 Aug 25;375[8]:754-66) or an immunomodulator plus dexamethasone (N Engl J Med. 2016 Oct 6;375[14]:1319-31).
Adding a monoclonal antibody such as daratumumab to combination therapy is the “wave of the future,” said Dr. Niesvizky, professor of medicine and director of the Multiple Myeloma Center at New York Presbyterian Hospital/Weill Cornell Medical Center. It provides treatment that reduces disease-related complications and achieves effective and extended disease control with improved overall survival, while being well tolerated and facilitating stem cell collection.
Dr. Richardson has been a consultant to Celgene, Genmab, Janssen, Novartis, Oncopeptides AB, and Takeda and has received research funding from Celgene and Takeda. Dr. Niesvizky has been a consultant to Amgen, Bristol-Myers Squibb, Celgene, Janssen, and Takeda and has received research support from Amgen, Bristol-Myers Squibb, Celgene, and Takeda.
[email protected]
On Twitter @mitchelzoler
EXPERT ANALYSIS FROM A MEETING ON HEMATOLOGIC MALIGNANCIES
FDA sends baricitinib application back for revision
, according to a statement from manufacturer Eli Lilly.
The FDA complete response letter cited the need for additional data to determine the most appropriate doses for the once-daily oral medication and to suss out safety concerns across treatment arms.

In the recently published RA-BEAM trial, a manufacturer-sponsored, international, randomized, double-blind, phase III clinical trial involving 1,305 adults with moderate to severe active RA, 70% of patients taking baricitinib plus background therapy with methotrexate met the primary efficacy end point – the proportion of patients at week 12 who showed an ACR 20 response – compared with 40% for placebo (N Engl J Med. 2017;376:652-62).
[email protected]
On Twitter @denisefulton
, according to a statement from manufacturer Eli Lilly.
The FDA complete response letter cited the need for additional data to determine the most appropriate doses for the once-daily oral medication and to suss out safety concerns across treatment arms.
In the recently published RA-BEAM trial, a manufacturer-sponsored, international, randomized, double-blind, phase III clinical trial involving 1,305 adults with moderate to severe active RA, 70% of patients taking baricitinib plus background therapy with methotrexate met the primary efficacy end point – the proportion of patients at week 12 who showed an ACR 20 response – compared with 40% for placebo (N Engl J Med. 2017;376:652-62).
[email protected]
On Twitter @denisefulton
, according to a statement from manufacturer Eli Lilly.
The FDA complete response letter cited the need for additional data to determine the most appropriate doses for the once-daily oral medication and to suss out safety concerns across treatment arms.
In the recently published RA-BEAM trial, a manufacturer-sponsored, international, randomized, double-blind, phase III clinical trial involving 1,305 adults with moderate to severe active RA, 70% of patients taking baricitinib plus background therapy with methotrexate met the primary efficacy end point – the proportion of patients at week 12 who showed an ACR 20 response – compared with 40% for placebo (N Engl J Med. 2017;376:652-62).
[email protected]
On Twitter @denisefulton
Racial disparities in ovarian cancer care persist until death
Even at the end of life, nonwhite patients with ovarian cancer are more likely to receive suboptimal care.
That’s the finding of investigators who looked at Medicare-enrolled patients with end-stage ovarian cancer in Texas. They found that compared with white patients, nonwhites were less likely to be enrolled in or die in hospice, more likely to be admitted to an intensive care unit, more likely to have an emergency department visit, and more likely to be subjected to some kind of putatively life-extending intervention.
“More investigation is needed to determine not only how to best reduce the overall number of patients with ovarian cancer who receive aggressive and invasive care but also how to lessen the disparity of who receives more aggressive and invasive care. With regard to end-of-life care for patients with ovarian cancer, less may be more,” wrote Jolyn S. Taylor, MD, MPH, of the University of Texas MD Anderson Cancer Center in Houston, and colleagues (J Clin Oncol. 2017 April 7 doi: 10.1200/JCO.2016.70.2894).
Quality-of-care recommendations from the American Society of Clinical Oncology Quality Oncology Practice Initiative, Physician Consortium for Performance Improvement, and National Quality Forum call on clinicians to recognize that excessive or aggressive end-of-life interventions can have a negative effect on the quality of life for patients with limited life expectancy, the authors noted.
“Although changes have occurred over the last decade leading to increased hospice use by patients with ovarian cancer before death, many patients still receive intensive and invasive care in the last month of life. Similar to other disease sites, patients of minority race and ethnicity and lower socioeconomic status who have ovarian cancer have been reported to have less hospice use and more intensive end-of-life care,” the researchers wrote.
To see whether these disparities still existed, the investigators examined Texas Cancer Registry–Medicare data on patients who died from ovarian cancer from 2000 to 2012 who had least 13 months of continuous Medicare coverage before their deaths. They looked for specific measures of end-of-life care quality, including chemotherapy use within 2 weeks of death, ICU admission in the last month of life, and emergency department visits, hospital admissions, or invasive or life-extending procedures, all during the last 30 days of a patient’s life.
Of the 3,666 patients studied, 2,819 (77%) were white, 553 (15%) were Hispanic, 256 (7%) were black, and 38 (1%) were classified as “other.”
In multivariate regression models adjusted for year of death, age at death, time from diagnosis to death, Charlson comorbidity index score, disease stage at diagnosis, educational and poverty level by census tract, and geography (rural versus urban), the researchers found that both black and Hispanic patients were significantly less likely than were white patients to enroll in and die in hospice, with odds ratios (OR) of 0.66 for black patients (P = .004), and 0.76 for Hispanics (P = .01).
Black but not Hispanic patients were more likely to have had more than one emergency department visit within 30 days of death (OR 2.20, P less than .001), or a life-extending procedure (OR 2.13, P less than .001). Hispanic but not black patients were more likely to have been admitted to an ICU within a month of death (OR 1.37, P = .02).
The study was supported by grants from the Cancer Prevention & Research Institute of Texas, National Institutes of Health, National Cancer Institute, and Duncan Family Institute.
Even at the end of life, nonwhite patients with ovarian cancer are more likely to receive suboptimal care.
That’s the finding of investigators who looked at Medicare-enrolled patients with end-stage ovarian cancer in Texas. They found that compared with white patients, nonwhites were less likely to be enrolled in or die in hospice, more likely to be admitted to an intensive care unit, more likely to have an emergency department visit, and more likely to be subjected to some kind of putatively life-extending intervention.
“More investigation is needed to determine not only how to best reduce the overall number of patients with ovarian cancer who receive aggressive and invasive care but also how to lessen the disparity of who receives more aggressive and invasive care. With regard to end-of-life care for patients with ovarian cancer, less may be more,” wrote Jolyn S. Taylor, MD, MPH, of the University of Texas MD Anderson Cancer Center in Houston, and colleagues (J Clin Oncol. 2017 April 7 doi: 10.1200/JCO.2016.70.2894).
Quality-of-care recommendations from the American Society of Clinical Oncology Quality Oncology Practice Initiative, Physician Consortium for Performance Improvement, and National Quality Forum call on clinicians to recognize that excessive or aggressive end-of-life interventions can have a negative effect on the quality of life for patients with limited life expectancy, the authors noted.
“Although changes have occurred over the last decade leading to increased hospice use by patients with ovarian cancer before death, many patients still receive intensive and invasive care in the last month of life. Similar to other disease sites, patients of minority race and ethnicity and lower socioeconomic status who have ovarian cancer have been reported to have less hospice use and more intensive end-of-life care,” the researchers wrote.
To see whether these disparities still existed, the investigators examined Texas Cancer Registry–Medicare data on patients who died from ovarian cancer from 2000 to 2012 who had least 13 months of continuous Medicare coverage before their deaths. They looked for specific measures of end-of-life care quality, including chemotherapy use within 2 weeks of death, ICU admission in the last month of life, and emergency department visits, hospital admissions, or invasive or life-extending procedures, all during the last 30 days of a patient’s life.
Of the 3,666 patients studied, 2,819 (77%) were white, 553 (15%) were Hispanic, 256 (7%) were black, and 38 (1%) were classified as “other.”
In multivariate regression models adjusted for year of death, age at death, time from diagnosis to death, Charlson comorbidity index score, disease stage at diagnosis, educational and poverty level by census tract, and geography (rural versus urban), the researchers found that both black and Hispanic patients were significantly less likely than were white patients to enroll in and die in hospice, with odds ratios (OR) of 0.66 for black patients (P = .004), and 0.76 for Hispanics (P = .01).
Black but not Hispanic patients were more likely to have had more than one emergency department visit within 30 days of death (OR 2.20, P less than .001), or a life-extending procedure (OR 2.13, P less than .001). Hispanic but not black patients were more likely to have been admitted to an ICU within a month of death (OR 1.37, P = .02).
The study was supported by grants from the Cancer Prevention & Research Institute of Texas, National Institutes of Health, National Cancer Institute, and Duncan Family Institute.
Even at the end of life, nonwhite patients with ovarian cancer are more likely to receive suboptimal care.
That’s the finding of investigators who looked at Medicare-enrolled patients with end-stage ovarian cancer in Texas. They found that compared with white patients, nonwhites were less likely to be enrolled in or die in hospice, more likely to be admitted to an intensive care unit, more likely to have an emergency department visit, and more likely to be subjected to some kind of putatively life-extending intervention.
“More investigation is needed to determine not only how to best reduce the overall number of patients with ovarian cancer who receive aggressive and invasive care but also how to lessen the disparity of who receives more aggressive and invasive care. With regard to end-of-life care for patients with ovarian cancer, less may be more,” wrote Jolyn S. Taylor, MD, MPH, of the University of Texas MD Anderson Cancer Center in Houston, and colleagues (J Clin Oncol. 2017 April 7 doi: 10.1200/JCO.2016.70.2894).
Quality-of-care recommendations from the American Society of Clinical Oncology Quality Oncology Practice Initiative, Physician Consortium for Performance Improvement, and National Quality Forum call on clinicians to recognize that excessive or aggressive end-of-life interventions can have a negative effect on the quality of life for patients with limited life expectancy, the authors noted.
“Although changes have occurred over the last decade leading to increased hospice use by patients with ovarian cancer before death, many patients still receive intensive and invasive care in the last month of life. Similar to other disease sites, patients of minority race and ethnicity and lower socioeconomic status who have ovarian cancer have been reported to have less hospice use and more intensive end-of-life care,” the researchers wrote.
To see whether these disparities still existed, the investigators examined Texas Cancer Registry–Medicare data on patients who died from ovarian cancer from 2000 to 2012 who had least 13 months of continuous Medicare coverage before their deaths. They looked for specific measures of end-of-life care quality, including chemotherapy use within 2 weeks of death, ICU admission in the last month of life, and emergency department visits, hospital admissions, or invasive or life-extending procedures, all during the last 30 days of a patient’s life.
Of the 3,666 patients studied, 2,819 (77%) were white, 553 (15%) were Hispanic, 256 (7%) were black, and 38 (1%) were classified as “other.”
In multivariate regression models adjusted for year of death, age at death, time from diagnosis to death, Charlson comorbidity index score, disease stage at diagnosis, educational and poverty level by census tract, and geography (rural versus urban), the researchers found that both black and Hispanic patients were significantly less likely than were white patients to enroll in and die in hospice, with odds ratios (OR) of 0.66 for black patients (P = .004), and 0.76 for Hispanics (P = .01).
Black but not Hispanic patients were more likely to have had more than one emergency department visit within 30 days of death (OR 2.20, P less than .001), or a life-extending procedure (OR 2.13, P less than .001). Hispanic but not black patients were more likely to have been admitted to an ICU within a month of death (OR 1.37, P = .02).
The study was supported by grants from the Cancer Prevention & Research Institute of Texas, National Institutes of Health, National Cancer Institute, and Duncan Family Institute.
FROM JOURNAL OF CLINICAL ONCOLOGY
Key clinical point: Nonwhite patients with ovarian cancer are more likely to receive suboptimal care at the end of life.
Major finding: Black and Hispanic women with ovarian cancer were significantly less likely than were whites to enroll in and die in hospice, more likely to be admitted to an intensive care unit, more likely to have an emergency department visit, and more likely to be subjected to some kind of putatively life-extending intervention.
Data source: Retrospective analysis of Texas Cancer Registry–Medicare data on 3,666 patients.
Disclosures: The study was supported by grants from the Cancer Prevention & Research Institute of Texas, National Institutes of Health, National Cancer Institute, and Duncan Family Institute.
Where are they now? Two Shark Tank innovators share their tales of success
BOSTON – Two gastroenterology innovators spoke at the 2017 AGA Tech Summit, which is sponsored by the AGA Center for Innovation and Technology, to share how their past participation in the AGA Shark Tank panel is helping them succeed.
Single-use endoscopes
For Invendo Medical GmbH Chief Commercial Officer John Cifarelli, who appeared before the panel during the 2015 Tech Summit, having Shark Tank experts suggest that he and his collaborators keep in mind physician practice habits when bringing their single-use endoscope technology to market was key to their ultimate product designs.

Another Shark Tank panel suggestion Mr. Cifarelli said he and his team included was the use of high definition (HD) optics to enhance diagnosis. “The panel told me that physicians have become accustomed to the clarity of HD technology and would have trouble accepting anything less.”
The timing of his appearance before the panel was perfect, since Mr. Cifarelli and his team were still at the conceptual stage with the device. “We had just gone from a company that was making an inverted sleeve colonoscope to be used without sedation, to a company that provides full-platform HD conventional GI endoscopes that are sterile and single use, so we were able to incorporate the panel’s advice into our designs,” he said.
Rather than create a separate, stand-alone, hand-held device as planned, Invendo instead is manufacturing the InvendoscopeTM, a hand-held, HD optics, sterile, single-use device that can be used either attached to or detached from the endoscope – the first such device of its kind, he said. The Invendoscope recently received its CE mark and is expected to come to market later this year.
Mr. Cifarelli said his company is also at work on an HD, single-use, sterile gastroscope and duodenoscope, both of which he expects will be introduced by early 2018.
Technology IDs progression risk in Barrett’s
Appearing before the 2015 panel gave Cernostics CEO Mike Hoerres a comprehensive perspective that subsequently has served his collaborators and him well. The company was just issued two patents on the TissueCypherTM Image Analysis Platform, a tissue systems biology approach that evaluates protein expression in the context of tissue structure when analyzing biopsies from patients with Barrett’s esophagus. The assay technology simultaneously and objectively extracts high-dimensional biomarker expression and morphology data to evaluate multiple tumor, immune, and other stromal processes in a single tissue section.

Since then, quite a lot has happened for Cernostics and TissueCypherTM, including publication of two validation studies in 2016 demonstrating TissueCypherTM’s ability to predict progression to high-grade dysplasia or cancer, which are otherwise missed by standard histology. The company also received a $1.2 million grant from the National Institutes of Health for a phase II SBIR study that is being conducted with the Cleveland Clinic and the University of Pittsburgh Medical Center.
“We have shown that TissueCypherTM can identify who is 10 times more likely to progress to esophageal cancer within 5 years of biopsy vs. low-risk patients – something that is currently difficult to determine by standard pathology. This test could enable early intervention to prevent cancer in high-risk patients, and may spare low-risk patients frequent and unnecessary endoscopies and treatments,” Mr. Hoerres said in the interview.
Currently, about 3-4 million people in the U.S. are part of active surveillance programs for Barrett’s esophagus. “If the promise of the technology to decrease the utilization of endoscopy in patients who are unlikely to progress to dysplastic Barrett’s is realized, there will likely be significant savings in the care of these patients,” Dr. Michael L. Kochman, executive committee chair of the AGA Center for GI Innovation and Technology, said in an interview.
[email protected]
On Twitter @whitneymcknight
BOSTON – Two gastroenterology innovators spoke at the 2017 AGA Tech Summit, which is sponsored by the AGA Center for Innovation and Technology, to share how their past participation in the AGA Shark Tank panel is helping them succeed.
Single-use endoscopes
For Invendo Medical GmbH Chief Commercial Officer John Cifarelli, who appeared before the panel during the 2015 Tech Summit, having Shark Tank experts suggest that he and his collaborators keep in mind physician practice habits when bringing their single-use endoscope technology to market was key to their ultimate product designs.
Another Shark Tank panel suggestion Mr. Cifarelli said he and his team included was the use of high definition (HD) optics to enhance diagnosis. “The panel told me that physicians have become accustomed to the clarity of HD technology and would have trouble accepting anything less.”
The timing of his appearance before the panel was perfect, since Mr. Cifarelli and his team were still at the conceptual stage with the device. “We had just gone from a company that was making an inverted sleeve colonoscope to be used without sedation, to a company that provides full-platform HD conventional GI endoscopes that are sterile and single use, so we were able to incorporate the panel’s advice into our designs,” he said.
Rather than create a separate, stand-alone, hand-held device as planned, Invendo instead is manufacturing the InvendoscopeTM, a hand-held, HD optics, sterile, single-use device that can be used either attached to or detached from the endoscope – the first such device of its kind, he said. The Invendoscope recently received its CE mark and is expected to come to market later this year.
Mr. Cifarelli said his company is also at work on an HD, single-use, sterile gastroscope and duodenoscope, both of which he expects will be introduced by early 2018.
Technology IDs progression risk in Barrett’s
Appearing before the 2015 panel gave Cernostics CEO Mike Hoerres a comprehensive perspective that subsequently has served his collaborators and him well. The company was just issued two patents on the TissueCypherTM Image Analysis Platform, a tissue systems biology approach that evaluates protein expression in the context of tissue structure when analyzing biopsies from patients with Barrett’s esophagus. The assay technology simultaneously and objectively extracts high-dimensional biomarker expression and morphology data to evaluate multiple tumor, immune, and other stromal processes in a single tissue section.
Since then, quite a lot has happened for Cernostics and TissueCypherTM, including publication of two validation studies in 2016 demonstrating TissueCypherTM’s ability to predict progression to high-grade dysplasia or cancer, which are otherwise missed by standard histology. The company also received a $1.2 million grant from the National Institutes of Health for a phase II SBIR study that is being conducted with the Cleveland Clinic and the University of Pittsburgh Medical Center.
“We have shown that TissueCypherTM can identify who is 10 times more likely to progress to esophageal cancer within 5 years of biopsy vs. low-risk patients – something that is currently difficult to determine by standard pathology. This test could enable early intervention to prevent cancer in high-risk patients, and may spare low-risk patients frequent and unnecessary endoscopies and treatments,” Mr. Hoerres said in the interview.
Currently, about 3-4 million people in the U.S. are part of active surveillance programs for Barrett’s esophagus. “If the promise of the technology to decrease the utilization of endoscopy in patients who are unlikely to progress to dysplastic Barrett’s is realized, there will likely be significant savings in the care of these patients,” Dr. Michael L. Kochman, executive committee chair of the AGA Center for GI Innovation and Technology, said in an interview.
[email protected]
On Twitter @whitneymcknight
BOSTON – Two gastroenterology innovators spoke at the 2017 AGA Tech Summit, which is sponsored by the AGA Center for Innovation and Technology, to share how their past participation in the AGA Shark Tank panel is helping them succeed.
Single-use endoscopes
For Invendo Medical GmbH Chief Commercial Officer John Cifarelli, who appeared before the panel during the 2015 Tech Summit, having Shark Tank experts suggest that he and his collaborators keep in mind physician practice habits when bringing their single-use endoscope technology to market was key to their ultimate product designs.
Another Shark Tank panel suggestion Mr. Cifarelli said he and his team included was the use of high definition (HD) optics to enhance diagnosis. “The panel told me that physicians have become accustomed to the clarity of HD technology and would have trouble accepting anything less.”
The timing of his appearance before the panel was perfect, since Mr. Cifarelli and his team were still at the conceptual stage with the device. “We had just gone from a company that was making an inverted sleeve colonoscope to be used without sedation, to a company that provides full-platform HD conventional GI endoscopes that are sterile and single use, so we were able to incorporate the panel’s advice into our designs,” he said.
Rather than create a separate, stand-alone, hand-held device as planned, Invendo instead is manufacturing the InvendoscopeTM, a hand-held, HD optics, sterile, single-use device that can be used either attached to or detached from the endoscope – the first such device of its kind, he said. The Invendoscope recently received its CE mark and is expected to come to market later this year.
Mr. Cifarelli said his company is also at work on an HD, single-use, sterile gastroscope and duodenoscope, both of which he expects will be introduced by early 2018.
Technology IDs progression risk in Barrett’s
Appearing before the 2015 panel gave Cernostics CEO Mike Hoerres a comprehensive perspective that subsequently has served his collaborators and him well. The company was just issued two patents on the TissueCypherTM Image Analysis Platform, a tissue systems biology approach that evaluates protein expression in the context of tissue structure when analyzing biopsies from patients with Barrett’s esophagus. The assay technology simultaneously and objectively extracts high-dimensional biomarker expression and morphology data to evaluate multiple tumor, immune, and other stromal processes in a single tissue section.
Since then, quite a lot has happened for Cernostics and TissueCypherTM, including publication of two validation studies in 2016 demonstrating TissueCypherTM’s ability to predict progression to high-grade dysplasia or cancer, which are otherwise missed by standard histology. The company also received a $1.2 million grant from the National Institutes of Health for a phase II SBIR study that is being conducted with the Cleveland Clinic and the University of Pittsburgh Medical Center.
“We have shown that TissueCypherTM can identify who is 10 times more likely to progress to esophageal cancer within 5 years of biopsy vs. low-risk patients – something that is currently difficult to determine by standard pathology. This test could enable early intervention to prevent cancer in high-risk patients, and may spare low-risk patients frequent and unnecessary endoscopies and treatments,” Mr. Hoerres said in the interview.
Currently, about 3-4 million people in the U.S. are part of active surveillance programs for Barrett’s esophagus. “If the promise of the technology to decrease the utilization of endoscopy in patients who are unlikely to progress to dysplastic Barrett’s is realized, there will likely be significant savings in the care of these patients,” Dr. Michael L. Kochman, executive committee chair of the AGA Center for GI Innovation and Technology, said in an interview.
[email protected]
On Twitter @whitneymcknight
FROM THE 2017 AGA TECH SUMMIT
Study shows no adverse events with long-term denosumab in postmenopausal women
Extended follow-up of postmenopausal women taking denosumab for high-risk osteoporosis in the FREEDOM trial showed no increasing rates of either common adverse events or specific adverse events identified in the original study.
“This analysis provides reassuring information regarding safety and tolerability of both short-term and longer-term treatment with denosumab,” said Nelson B. Watts, MD, of Mercy Health, Cincinnati, and his associates.
The average age of the women was 72.3 years, and about 23% had vertebral fractures at baseline. The specific, infrequent adverse events that occurred more commonly in the denosumab group than the placebo group in the original trial were malignancy, eczema/dermatitis, pancreatitis, endocarditis, delayed fracture healing, infections, opportunistic infections, and cellulitis or erysipelas. The more common adverse events associated with the active treatment, and currently listed in the prescribing information for denosumab, were back pain, pain in the extremities, musculoskeletal pain, hypercholesterolemia, and cystitis, the investigators reported (J Bone Mineral Res. 2017 Apr 3. doi: 10.1002/jbmr.3119).
“We found no evidence for a relationship between treatment with denosumab and increasing rates of either low-frequency adverse events or common adverse events in patients who were assigned to placebo in the [original] trial and received 3 years of denosumab in the extension study, and no indication of increased incidence of low-frequency adverse events and common adverse events in patients receiving denosumab in years 4-6, compared with years 1-3,” Dr. Watts and his associates wrote.
This study was funded by Amgen, maker of denosumab (Prolia). Dr. Watts reported ties to Amgen, Shire, AbbVie, Merck, Radius, Sanofi, and Osteodynamics; his associates reported ties to numerous industry sources.
Extended follow-up of postmenopausal women taking denosumab for high-risk osteoporosis in the FREEDOM trial showed no increasing rates of either common adverse events or specific adverse events identified in the original study.
“This analysis provides reassuring information regarding safety and tolerability of both short-term and longer-term treatment with denosumab,” said Nelson B. Watts, MD, of Mercy Health, Cincinnati, and his associates.
The average age of the women was 72.3 years, and about 23% had vertebral fractures at baseline. The specific, infrequent adverse events that occurred more commonly in the denosumab group than the placebo group in the original trial were malignancy, eczema/dermatitis, pancreatitis, endocarditis, delayed fracture healing, infections, opportunistic infections, and cellulitis or erysipelas. The more common adverse events associated with the active treatment, and currently listed in the prescribing information for denosumab, were back pain, pain in the extremities, musculoskeletal pain, hypercholesterolemia, and cystitis, the investigators reported (J Bone Mineral Res. 2017 Apr 3. doi: 10.1002/jbmr.3119).
“We found no evidence for a relationship between treatment with denosumab and increasing rates of either low-frequency adverse events or common adverse events in patients who were assigned to placebo in the [original] trial and received 3 years of denosumab in the extension study, and no indication of increased incidence of low-frequency adverse events and common adverse events in patients receiving denosumab in years 4-6, compared with years 1-3,” Dr. Watts and his associates wrote.
This study was funded by Amgen, maker of denosumab (Prolia). Dr. Watts reported ties to Amgen, Shire, AbbVie, Merck, Radius, Sanofi, and Osteodynamics; his associates reported ties to numerous industry sources.
Extended follow-up of postmenopausal women taking denosumab for high-risk osteoporosis in the FREEDOM trial showed no increasing rates of either common adverse events or specific adverse events identified in the original study.
“This analysis provides reassuring information regarding safety and tolerability of both short-term and longer-term treatment with denosumab,” said Nelson B. Watts, MD, of Mercy Health, Cincinnati, and his associates.
The average age of the women was 72.3 years, and about 23% had vertebral fractures at baseline. The specific, infrequent adverse events that occurred more commonly in the denosumab group than the placebo group in the original trial were malignancy, eczema/dermatitis, pancreatitis, endocarditis, delayed fracture healing, infections, opportunistic infections, and cellulitis or erysipelas. The more common adverse events associated with the active treatment, and currently listed in the prescribing information for denosumab, were back pain, pain in the extremities, musculoskeletal pain, hypercholesterolemia, and cystitis, the investigators reported (J Bone Mineral Res. 2017 Apr 3. doi: 10.1002/jbmr.3119).
“We found no evidence for a relationship between treatment with denosumab and increasing rates of either low-frequency adverse events or common adverse events in patients who were assigned to placebo in the [original] trial and received 3 years of denosumab in the extension study, and no indication of increased incidence of low-frequency adverse events and common adverse events in patients receiving denosumab in years 4-6, compared with years 1-3,” Dr. Watts and his associates wrote.
This study was funded by Amgen, maker of denosumab (Prolia). Dr. Watts reported ties to Amgen, Shire, AbbVie, Merck, Radius, Sanofi, and Osteodynamics; his associates reported ties to numerous industry sources.
FROM THE JOURNAL OF BONE AND MINERAL RESEARCH
Key clinical point: Denosumab, taken long term, is not linked with any adverse events.
Major finding: Extended follow-up of postmenopausal women taking denosumab for high-risk osteoporosis showed no increasing rates of either common adverse events or of specific adverse events identified in the original trial.
Data source: Extended (6-year) follow-up of 4,550 women in the international phase III randomized, double-blind FREEDOM trial.
Disclosures: This study was funded by Amgen, maker of denosumab. Dr. Watts reported ties to Amgen, Shire, AbbVie, Merck, Radius, Sanofi, and Osteodynamics; his associates reported ties to numerous industry sources.
Neurokinin receptor antagonist nearly halves hot flashes
ORLANDO – A novel antagonist of a neurokinin pathway effectively reduced hot flashes in postmenopausal women, according to results of a phase II trial.
The neurokinin 3 receptor (NK3R) antagonist, termed MLE4901, cut the number of hot flashes nearly in half compared to the effect of a placebo, and also improved overall menopause-related quality of life symptoms.
The medication has the potential to fulfill an unmet clinical need, since 70% of women experience hot flashes and the median duration of symptoms is more than 7 years, Julia K. Prague, MD, said at the annual meeting of the Endocrine Society.
The study results were published concurrently with Dr. Prague’s presentation (Lancet. 2017 Apr 3. doi: 10.1016/S0140-6736[17]30823-1).
Evidence from postmortem studies of postmenopausal women, said Dr. Prague, pointed to NKB (neurokinin B)/NK3R signaling as playing a role in hot flashes. The brains of these women showed hypertrophy of NKB neurons and increased neuronal activity, as well as increased NKB gene expression. The same effects were seen in monkeys whose ovaries had been removed, and the effect was reversed when the monkeys were given estrogen. 
Also, previous work has shown that administering NKB to premenopausal women gave them hot flashes (Sci Rep. 2015 Feb 6;5:8466). The preclinical work laid the groundwork for the hypothesis that taking an oral NK3R antagonist could mitigate hot flashes in menopausal women.
The randomized, placebo-controlled, double-blind 2-way crossover study enrolled 37 healthy women aged 40-62 who were at least 12 months out from their last menses. To qualify for enrollment, they needed to be experiencing at least seven hot flashes per 24 hours; the actual mean total number in the study group was 13 per 24 hours and 85 per week. A total of 28 women completed the full protocol.
The mean age of the women was 55 years, and the mean body mass index was 25.8 kg/m2. Three quarters of the women were white.
The women had an initial 2-week baseline period, during which they kept a symptom diary, and then were randomized to receive either an oral NK3R antagonist or a placebo twice daily. Then, each patient went through a 2-week washout period, after which they were crossed over to the other arm of the study. Finally, patients were monitored for a further 2 weeks after taking the study drug.
The NK3R antagonist, said Dr. Prague, “significantly reduced the total weekly number of hot [flashes] compared to placebo in the fourth week of treatment.” Patients taking placebo experienced 49.01 hot flashes per week (range, 40.81-58.86), while those taking the NK3R antagonist had 19.35 (range, 15.99-23.42, P less than .0001). This amounted to a 45% reduction in number of hot flashes compared to placebo.
Dr. Prague, a clinical research fellow at Imperial College, London, said that the treatment effect size seen was similar regardless of whether patients received the active study drug or placebo first.
Using the Menopause-Related Quality of Life questionnaire, Dr. Prague and her colleagues determined that when women were taking the NK3R antagonist, in addition to a significant reduction in vasomotor symptoms, menopause-related psychosocial symptoms were reduced by 15% (P = .0083) and physical symptoms by 19% (P = .0002). As expected for the nonhormonal medication, she said, sexual symptoms were reduced by a nonsignificant 8% (P = .24).
A subset of patients received more intensive study, with external validation of hot flashes and a series of 3-day-long stays during which an intravenous catheter was placed for blood sampling every 10 minutes.
Data from this group of patients showed that, while the NK3R antagonist did not significantly affect the number of luteinizing hormone pulses detected compared with placebo (P = .41), it did increase the mean amplitude of each pulse (P = .0243). Also, the active drug made the luteinizing hormone pulses more orderly (P = .0006 compared to placebo).
The NK3R antagonist was well tolerated. Though no serious adverse events were seen, three patients taking the NK3R antagonist did have a transient and asymptomatic elevation of transaminases without hyperbilirubinemia at 28 days after starting treatment. The elevation resolved for all patients within 90 days of stopping the medication.
The novel drug could represent “a potentially practice-changing therapeutic,” said Dr. Prague, since it “significantly relieves hot [flash] symptoms without the need for estrogen exposure.” She added that planning is underway for longer studies involving more patients.
The study was supported by AstraZeneca and Millendo Therapeutics, which are involved with manufacturing MLE4901.
[email protected]
On Twitter @karioakes
ORLANDO – A novel antagonist of a neurokinin pathway effectively reduced hot flashes in postmenopausal women, according to results of a phase II trial.
The neurokinin 3 receptor (NK3R) antagonist, termed MLE4901, cut the number of hot flashes nearly in half compared to the effect of a placebo, and also improved overall menopause-related quality of life symptoms.
The medication has the potential to fulfill an unmet clinical need, since 70% of women experience hot flashes and the median duration of symptoms is more than 7 years, Julia K. Prague, MD, said at the annual meeting of the Endocrine Society.
The study results were published concurrently with Dr. Prague’s presentation (Lancet. 2017 Apr 3. doi: 10.1016/S0140-6736[17]30823-1).
Evidence from postmortem studies of postmenopausal women, said Dr. Prague, pointed to NKB (neurokinin B)/NK3R signaling as playing a role in hot flashes. The brains of these women showed hypertrophy of NKB neurons and increased neuronal activity, as well as increased NKB gene expression. The same effects were seen in monkeys whose ovaries had been removed, and the effect was reversed when the monkeys were given estrogen.
Also, previous work has shown that administering NKB to premenopausal women gave them hot flashes (Sci Rep. 2015 Feb 6;5:8466). The preclinical work laid the groundwork for the hypothesis that taking an oral NK3R antagonist could mitigate hot flashes in menopausal women.
The randomized, placebo-controlled, double-blind 2-way crossover study enrolled 37 healthy women aged 40-62 who were at least 12 months out from their last menses. To qualify for enrollment, they needed to be experiencing at least seven hot flashes per 24 hours; the actual mean total number in the study group was 13 per 24 hours and 85 per week. A total of 28 women completed the full protocol.
The mean age of the women was 55 years, and the mean body mass index was 25.8 kg/m2. Three quarters of the women were white.
The women had an initial 2-week baseline period, during which they kept a symptom diary, and then were randomized to receive either an oral NK3R antagonist or a placebo twice daily. Then, each patient went through a 2-week washout period, after which they were crossed over to the other arm of the study. Finally, patients were monitored for a further 2 weeks after taking the study drug.
The NK3R antagonist, said Dr. Prague, “significantly reduced the total weekly number of hot [flashes] compared to placebo in the fourth week of treatment.” Patients taking placebo experienced 49.01 hot flashes per week (range, 40.81-58.86), while those taking the NK3R antagonist had 19.35 (range, 15.99-23.42, P less than .0001). This amounted to a 45% reduction in number of hot flashes compared to placebo.
Dr. Prague, a clinical research fellow at Imperial College, London, said that the treatment effect size seen was similar regardless of whether patients received the active study drug or placebo first.
Using the Menopause-Related Quality of Life questionnaire, Dr. Prague and her colleagues determined that when women were taking the NK3R antagonist, in addition to a significant reduction in vasomotor symptoms, menopause-related psychosocial symptoms were reduced by 15% (P = .0083) and physical symptoms by 19% (P = .0002). As expected for the nonhormonal medication, she said, sexual symptoms were reduced by a nonsignificant 8% (P = .24).
A subset of patients received more intensive study, with external validation of hot flashes and a series of 3-day-long stays during which an intravenous catheter was placed for blood sampling every 10 minutes.
Data from this group of patients showed that, while the NK3R antagonist did not significantly affect the number of luteinizing hormone pulses detected compared with placebo (P = .41), it did increase the mean amplitude of each pulse (P = .0243). Also, the active drug made the luteinizing hormone pulses more orderly (P = .0006 compared to placebo).
The NK3R antagonist was well tolerated. Though no serious adverse events were seen, three patients taking the NK3R antagonist did have a transient and asymptomatic elevation of transaminases without hyperbilirubinemia at 28 days after starting treatment. The elevation resolved for all patients within 90 days of stopping the medication.
The novel drug could represent “a potentially practice-changing therapeutic,” said Dr. Prague, since it “significantly relieves hot [flash] symptoms without the need for estrogen exposure.” She added that planning is underway for longer studies involving more patients.
The study was supported by AstraZeneca and Millendo Therapeutics, which are involved with manufacturing MLE4901.
[email protected]
On Twitter @karioakes
ORLANDO – A novel antagonist of a neurokinin pathway effectively reduced hot flashes in postmenopausal women, according to results of a phase II trial.
The neurokinin 3 receptor (NK3R) antagonist, termed MLE4901, cut the number of hot flashes nearly in half compared to the effect of a placebo, and also improved overall menopause-related quality of life symptoms.
The medication has the potential to fulfill an unmet clinical need, since 70% of women experience hot flashes and the median duration of symptoms is more than 7 years, Julia K. Prague, MD, said at the annual meeting of the Endocrine Society.
The study results were published concurrently with Dr. Prague’s presentation (Lancet. 2017 Apr 3. doi: 10.1016/S0140-6736[17]30823-1).
Evidence from postmortem studies of postmenopausal women, said Dr. Prague, pointed to NKB (neurokinin B)/NK3R signaling as playing a role in hot flashes. The brains of these women showed hypertrophy of NKB neurons and increased neuronal activity, as well as increased NKB gene expression. The same effects were seen in monkeys whose ovaries had been removed, and the effect was reversed when the monkeys were given estrogen.
Also, previous work has shown that administering NKB to premenopausal women gave them hot flashes (Sci Rep. 2015 Feb 6;5:8466). The preclinical work laid the groundwork for the hypothesis that taking an oral NK3R antagonist could mitigate hot flashes in menopausal women.
The randomized, placebo-controlled, double-blind 2-way crossover study enrolled 37 healthy women aged 40-62 who were at least 12 months out from their last menses. To qualify for enrollment, they needed to be experiencing at least seven hot flashes per 24 hours; the actual mean total number in the study group was 13 per 24 hours and 85 per week. A total of 28 women completed the full protocol.
The mean age of the women was 55 years, and the mean body mass index was 25.8 kg/m2. Three quarters of the women were white.
The women had an initial 2-week baseline period, during which they kept a symptom diary, and then were randomized to receive either an oral NK3R antagonist or a placebo twice daily. Then, each patient went through a 2-week washout period, after which they were crossed over to the other arm of the study. Finally, patients were monitored for a further 2 weeks after taking the study drug.
The NK3R antagonist, said Dr. Prague, “significantly reduced the total weekly number of hot [flashes] compared to placebo in the fourth week of treatment.” Patients taking placebo experienced 49.01 hot flashes per week (range, 40.81-58.86), while those taking the NK3R antagonist had 19.35 (range, 15.99-23.42, P less than .0001). This amounted to a 45% reduction in number of hot flashes compared to placebo.
Dr. Prague, a clinical research fellow at Imperial College, London, said that the treatment effect size seen was similar regardless of whether patients received the active study drug or placebo first.
Using the Menopause-Related Quality of Life questionnaire, Dr. Prague and her colleagues determined that when women were taking the NK3R antagonist, in addition to a significant reduction in vasomotor symptoms, menopause-related psychosocial symptoms were reduced by 15% (P = .0083) and physical symptoms by 19% (P = .0002). As expected for the nonhormonal medication, she said, sexual symptoms were reduced by a nonsignificant 8% (P = .24).
A subset of patients received more intensive study, with external validation of hot flashes and a series of 3-day-long stays during which an intravenous catheter was placed for blood sampling every 10 minutes.
Data from this group of patients showed that, while the NK3R antagonist did not significantly affect the number of luteinizing hormone pulses detected compared with placebo (P = .41), it did increase the mean amplitude of each pulse (P = .0243). Also, the active drug made the luteinizing hormone pulses more orderly (P = .0006 compared to placebo).
The NK3R antagonist was well tolerated. Though no serious adverse events were seen, three patients taking the NK3R antagonist did have a transient and asymptomatic elevation of transaminases without hyperbilirubinemia at 28 days after starting treatment. The elevation resolved for all patients within 90 days of stopping the medication.
The novel drug could represent “a potentially practice-changing therapeutic,” said Dr. Prague, since it “significantly relieves hot [flash] symptoms without the need for estrogen exposure.” She added that planning is underway for longer studies involving more patients.
The study was supported by AstraZeneca and Millendo Therapeutics, which are involved with manufacturing MLE4901.
[email protected]
On Twitter @karioakes
AT ENDO 2017
Key clinical point:
Major finding: The neurokinin 3 receptor antagonist reduced hot flashes from a mean of 85 per week at baseline to a mean of 49 per week.
Data source: Phase II randomized, double-blind, placebo-controlled two-way crossover study of 37 postmenopausal women with moderate to severe hot flashes.
Disclosures: The study was funded by AstraZeneca and Millendo Therapeutics, which are involved with the manufacture of the medicine, termed MLE4901.