User login
Epilepsy has wide-ranging psychosocial impact on youth
The psychosocial impact of epilepsy on children and adolescents is profound, ranging from a sense of vulnerability and disempowerment to discrimination, results from a systematic review of medical literature suggest.
“Children and adolescents perceive that epilepsy forces them to relinquish their sense of privacy, bodily control, normality, freedom, and confidence to participate in school and social activities,” researchers led by Lauren Chong wrote in a study published online Aug. 10 in Pediatrics. “They are overwhelmed by the daily uncertainties attributed to the unpredictable timing and potential harm from seizures, side effects of ongoing treatment, and the impermanence of remission.”

In an effort to describe the perspectives of children and adolescents with epilepsy, Ms. Chong of the Sydney School of Public Health at the University of Sydney, New South Wales, Australia, and her associates searched Medline and other key databases for qualitative primary studies on children’s experience of epilepsy from inception to August 2015 (Pediatrics. 2016;138[3]:e20160658. doi: 10.1542/peds.2016-0658). They used thematic synthesis to analyze their findings. The final analysis included 43 articles involving 951 children and adolescents aged 3-21 years from 21 different countries. Articles written in a language other than English were excluded.
The researchers identified six themes: loss of bodily control such as a sense of being overtaken and alertness to mortality; loss of privacy such as humiliating involuntary function and unwanted special attention; inescapable inferiority and discrimination such as vulnerability to prejudice and inability to achieve academically; therapeutic burden and futility such as financial burden and insurmountable side effects; navigating health care such as unexpected necessity of transition as well as fragmented and inconsistent care; and recontextualizing to regain normality such as distinguishing disease from identity and gaining perspective and maturity.
The researchers observed some differences in experiences and perspectives based on patient age and disease severity. For example, “feelings of loss and abnormality tended to be expressed more strongly by older adolescent patients,” they wrote. “As young adults, they were aware of the potentially serious ramifications of epilepsy on their future, including their independence, school performance, vocation, and relationships. Teenage patients were more frustrated by social limitations on partying, drinking, and sleepovers that differentiated them from their peers.” Patients with more severe disease, meanwhile, “contended with disempowerment and seemed less able to delineate epilepsy from their identity. They seemed more willing to trial therapies that may work and some, on being told they would not achieve remission, chose to disengage from the health care system, deeming further treatment or follow-up to be futile.”
Suggestions for clinical practice based on the analysis include providing access to support groups of other epilepsy sufferers or other children/adolescents with chronic disease; facilitating liaisons between clinicians, families, and school teachers, and delivering coordinated care with psychologists and psychiatrists to address psychosocial aspects of epilepsy.
“Treatment and management should address the psychosocial needs of patients regarding stigma, present lifestyle limitations, and future concerns,” the researchers wrote. “These suggestions may inform strategies for practice and research that may contribute toward the improved [quality of life], therapeutic satisfaction, and health outcomes of children and adolescents with epilepsy.”
Ms. Chong is supported by the University of Sydney Neuroscience Network Research Scholarship. Another coauthor, Allison Tong, PhD, is supported by the National Health and Medical Research Council Fellowship. The researchers reported having no financial disclosures.
The psychosocial impact of epilepsy on children and adolescents is profound, ranging from a sense of vulnerability and disempowerment to discrimination, results from a systematic review of medical literature suggest.
“Children and adolescents perceive that epilepsy forces them to relinquish their sense of privacy, bodily control, normality, freedom, and confidence to participate in school and social activities,” researchers led by Lauren Chong wrote in a study published online Aug. 10 in Pediatrics. “They are overwhelmed by the daily uncertainties attributed to the unpredictable timing and potential harm from seizures, side effects of ongoing treatment, and the impermanence of remission.”
In an effort to describe the perspectives of children and adolescents with epilepsy, Ms. Chong of the Sydney School of Public Health at the University of Sydney, New South Wales, Australia, and her associates searched Medline and other key databases for qualitative primary studies on children’s experience of epilepsy from inception to August 2015 (Pediatrics. 2016;138[3]:e20160658. doi: 10.1542/peds.2016-0658). They used thematic synthesis to analyze their findings. The final analysis included 43 articles involving 951 children and adolescents aged 3-21 years from 21 different countries. Articles written in a language other than English were excluded.
The researchers identified six themes: loss of bodily control such as a sense of being overtaken and alertness to mortality; loss of privacy such as humiliating involuntary function and unwanted special attention; inescapable inferiority and discrimination such as vulnerability to prejudice and inability to achieve academically; therapeutic burden and futility such as financial burden and insurmountable side effects; navigating health care such as unexpected necessity of transition as well as fragmented and inconsistent care; and recontextualizing to regain normality such as distinguishing disease from identity and gaining perspective and maturity.
The researchers observed some differences in experiences and perspectives based on patient age and disease severity. For example, “feelings of loss and abnormality tended to be expressed more strongly by older adolescent patients,” they wrote. “As young adults, they were aware of the potentially serious ramifications of epilepsy on their future, including their independence, school performance, vocation, and relationships. Teenage patients were more frustrated by social limitations on partying, drinking, and sleepovers that differentiated them from their peers.” Patients with more severe disease, meanwhile, “contended with disempowerment and seemed less able to delineate epilepsy from their identity. They seemed more willing to trial therapies that may work and some, on being told they would not achieve remission, chose to disengage from the health care system, deeming further treatment or follow-up to be futile.”
Suggestions for clinical practice based on the analysis include providing access to support groups of other epilepsy sufferers or other children/adolescents with chronic disease; facilitating liaisons between clinicians, families, and school teachers, and delivering coordinated care with psychologists and psychiatrists to address psychosocial aspects of epilepsy.
“Treatment and management should address the psychosocial needs of patients regarding stigma, present lifestyle limitations, and future concerns,” the researchers wrote. “These suggestions may inform strategies for practice and research that may contribute toward the improved [quality of life], therapeutic satisfaction, and health outcomes of children and adolescents with epilepsy.”
Ms. Chong is supported by the University of Sydney Neuroscience Network Research Scholarship. Another coauthor, Allison Tong, PhD, is supported by the National Health and Medical Research Council Fellowship. The researchers reported having no financial disclosures.
The psychosocial impact of epilepsy on children and adolescents is profound, ranging from a sense of vulnerability and disempowerment to discrimination, results from a systematic review of medical literature suggest.
“Children and adolescents perceive that epilepsy forces them to relinquish their sense of privacy, bodily control, normality, freedom, and confidence to participate in school and social activities,” researchers led by Lauren Chong wrote in a study published online Aug. 10 in Pediatrics. “They are overwhelmed by the daily uncertainties attributed to the unpredictable timing and potential harm from seizures, side effects of ongoing treatment, and the impermanence of remission.”
In an effort to describe the perspectives of children and adolescents with epilepsy, Ms. Chong of the Sydney School of Public Health at the University of Sydney, New South Wales, Australia, and her associates searched Medline and other key databases for qualitative primary studies on children’s experience of epilepsy from inception to August 2015 (Pediatrics. 2016;138[3]:e20160658. doi: 10.1542/peds.2016-0658). They used thematic synthesis to analyze their findings. The final analysis included 43 articles involving 951 children and adolescents aged 3-21 years from 21 different countries. Articles written in a language other than English were excluded.
The researchers identified six themes: loss of bodily control such as a sense of being overtaken and alertness to mortality; loss of privacy such as humiliating involuntary function and unwanted special attention; inescapable inferiority and discrimination such as vulnerability to prejudice and inability to achieve academically; therapeutic burden and futility such as financial burden and insurmountable side effects; navigating health care such as unexpected necessity of transition as well as fragmented and inconsistent care; and recontextualizing to regain normality such as distinguishing disease from identity and gaining perspective and maturity.
The researchers observed some differences in experiences and perspectives based on patient age and disease severity. For example, “feelings of loss and abnormality tended to be expressed more strongly by older adolescent patients,” they wrote. “As young adults, they were aware of the potentially serious ramifications of epilepsy on their future, including their independence, school performance, vocation, and relationships. Teenage patients were more frustrated by social limitations on partying, drinking, and sleepovers that differentiated them from their peers.” Patients with more severe disease, meanwhile, “contended with disempowerment and seemed less able to delineate epilepsy from their identity. They seemed more willing to trial therapies that may work and some, on being told they would not achieve remission, chose to disengage from the health care system, deeming further treatment or follow-up to be futile.”
Suggestions for clinical practice based on the analysis include providing access to support groups of other epilepsy sufferers or other children/adolescents with chronic disease; facilitating liaisons between clinicians, families, and school teachers, and delivering coordinated care with psychologists and psychiatrists to address psychosocial aspects of epilepsy.
“Treatment and management should address the psychosocial needs of patients regarding stigma, present lifestyle limitations, and future concerns,” the researchers wrote. “These suggestions may inform strategies for practice and research that may contribute toward the improved [quality of life], therapeutic satisfaction, and health outcomes of children and adolescents with epilepsy.”
Ms. Chong is supported by the University of Sydney Neuroscience Network Research Scholarship. Another coauthor, Allison Tong, PhD, is supported by the National Health and Medical Research Council Fellowship. The researchers reported having no financial disclosures.
FROM PEDIATRICS
Key clinical point: Addressing stigma, future independence, and fear of death may improve the overall well-being of children with epilepsy.
Major finding: Children with epilepsy experience vulnerability, disempowerment, and discrimination.
Data source: A meta-analysis of 43 articles involving 951 children and adolescents with epilepsy aged 3-21 years.
Disclosures: Ms. Chong is supported by the University of Sydney Neuroscience Network Research Scholarship. Another coauthor, Allison Tong, PhD, is supported by the National Health and Medical Research Council Fellowship. The researchers reported having no financial disclosures.
Study evaluates Zika syndrome with joint contractures
Congenital Zika syndrome should be added to the differential diagnosis of congenital infections and arthrogryposis (joint contractures), results from a case series study in Brazil suggest.
“Brain impairment in the presence of microcephaly is the main characteristic of a congenital Zika virus syndrome,” researchers led by Vanessa van der Linden, MD, wrote in a study published online Aug. 9 in the BMJ. “However, little is still known about this condition and its clinical spectrum, which also concerns newborns with a normal head circumference. Two studies have described the association between arthrogryposis and microcephaly in newborns presumed to have congenital Zika virus infection [See Morb Mortal Wkly. Rep. 2016;65:59-62 and Ultrasound Obstet Gynecol. 2016;47:6-7].” The authors went on to note that while arthrogryposis might be considered more of a sign than a specific disease, “it might be associated with several disorders. However, there are no reports in the literature about other congenital infections in humans associated with arthrogryposis.”

Dr. van der Linden, a pediatric neurologist with the Association for Assistance of Disabled Children, Recife, Brazil, and her associates retrospectively evaluated the medical records of seven patients with arthrogryposis associated with congenital infection believed to be caused by Zika virus, during the Brazilian microcephaly epidemic (BMJ. 2016;354:i3899). The main outcomes of interest were clinical, radiologic, and electromyographic findings, and likely collaboration between clinical and primary neurological abnormalities.
The researchers reported that brain images of all seven children revealed characteristics of congenital infection and arthrogryposis. Two children (29%) tested positive for IgM antibody for Zika virus in the cerebrospinal fluid, while arthrogryposis was present in the arms and legs of six children (86%) and in the legs of one child (14%). In addition, hip x-rays showed bilateral dislocation in all seven children and subluxation of the knee associated with genu valgus in three (43%). No evidence of abnormalities was seen on high-definition ultrasonography of the joints, but moderate signs of remodeling of the motor units and a reduced recruitment pattern were found on needle electromyography. Results from brain computed tomography conducted in all seven patients and magnetic resonance imaging conducted in five revealed malformations of cortical development, calcifications predominantly in the cortex and subcortical white matter, reduction in brain volume, ventriculomegaly, and hypoplasia of the brainstem and cerebellum. Spinal MRI conducted in four children showed apparent thinning of the cord and reduced ventral roots.
“Further research is needed with a larger number of cases to study the neurological abnormalities behind arthrogryposis, including histopathology of autopsy samples or tissues from stillborn babies,” the researchers concluded. “As we do not know the potential implications of congenital Zika virus infection as it evolves, children must receive orthopedic follow-up, even those with a standard first orthopedic evaluation, because they could develop musculoskeletal deformities secondary to neurological impairment, central or peripheral, or both, as these occur in patients with cerebral palsy and other chronic encephalopathies.”
The researchers reported having no financial disclosures.
Congenital Zika syndrome should be added to the differential diagnosis of congenital infections and arthrogryposis (joint contractures), results from a case series study in Brazil suggest.
“Brain impairment in the presence of microcephaly is the main characteristic of a congenital Zika virus syndrome,” researchers led by Vanessa van der Linden, MD, wrote in a study published online Aug. 9 in the BMJ. “However, little is still known about this condition and its clinical spectrum, which also concerns newborns with a normal head circumference. Two studies have described the association between arthrogryposis and microcephaly in newborns presumed to have congenital Zika virus infection [See Morb Mortal Wkly. Rep. 2016;65:59-62 and Ultrasound Obstet Gynecol. 2016;47:6-7].” The authors went on to note that while arthrogryposis might be considered more of a sign than a specific disease, “it might be associated with several disorders. However, there are no reports in the literature about other congenital infections in humans associated with arthrogryposis.”
Dr. van der Linden, a pediatric neurologist with the Association for Assistance of Disabled Children, Recife, Brazil, and her associates retrospectively evaluated the medical records of seven patients with arthrogryposis associated with congenital infection believed to be caused by Zika virus, during the Brazilian microcephaly epidemic (BMJ. 2016;354:i3899). The main outcomes of interest were clinical, radiologic, and electromyographic findings, and likely collaboration between clinical and primary neurological abnormalities.
The researchers reported that brain images of all seven children revealed characteristics of congenital infection and arthrogryposis. Two children (29%) tested positive for IgM antibody for Zika virus in the cerebrospinal fluid, while arthrogryposis was present in the arms and legs of six children (86%) and in the legs of one child (14%). In addition, hip x-rays showed bilateral dislocation in all seven children and subluxation of the knee associated with genu valgus in three (43%). No evidence of abnormalities was seen on high-definition ultrasonography of the joints, but moderate signs of remodeling of the motor units and a reduced recruitment pattern were found on needle electromyography. Results from brain computed tomography conducted in all seven patients and magnetic resonance imaging conducted in five revealed malformations of cortical development, calcifications predominantly in the cortex and subcortical white matter, reduction in brain volume, ventriculomegaly, and hypoplasia of the brainstem and cerebellum. Spinal MRI conducted in four children showed apparent thinning of the cord and reduced ventral roots.
“Further research is needed with a larger number of cases to study the neurological abnormalities behind arthrogryposis, including histopathology of autopsy samples or tissues from stillborn babies,” the researchers concluded. “As we do not know the potential implications of congenital Zika virus infection as it evolves, children must receive orthopedic follow-up, even those with a standard first orthopedic evaluation, because they could develop musculoskeletal deformities secondary to neurological impairment, central or peripheral, or both, as these occur in patients with cerebral palsy and other chronic encephalopathies.”
The researchers reported having no financial disclosures.
Congenital Zika syndrome should be added to the differential diagnosis of congenital infections and arthrogryposis (joint contractures), results from a case series study in Brazil suggest.
“Brain impairment in the presence of microcephaly is the main characteristic of a congenital Zika virus syndrome,” researchers led by Vanessa van der Linden, MD, wrote in a study published online Aug. 9 in the BMJ. “However, little is still known about this condition and its clinical spectrum, which also concerns newborns with a normal head circumference. Two studies have described the association between arthrogryposis and microcephaly in newborns presumed to have congenital Zika virus infection [See Morb Mortal Wkly. Rep. 2016;65:59-62 and Ultrasound Obstet Gynecol. 2016;47:6-7].” The authors went on to note that while arthrogryposis might be considered more of a sign than a specific disease, “it might be associated with several disorders. However, there are no reports in the literature about other congenital infections in humans associated with arthrogryposis.”
Dr. van der Linden, a pediatric neurologist with the Association for Assistance of Disabled Children, Recife, Brazil, and her associates retrospectively evaluated the medical records of seven patients with arthrogryposis associated with congenital infection believed to be caused by Zika virus, during the Brazilian microcephaly epidemic (BMJ. 2016;354:i3899). The main outcomes of interest were clinical, radiologic, and electromyographic findings, and likely collaboration between clinical and primary neurological abnormalities.
The researchers reported that brain images of all seven children revealed characteristics of congenital infection and arthrogryposis. Two children (29%) tested positive for IgM antibody for Zika virus in the cerebrospinal fluid, while arthrogryposis was present in the arms and legs of six children (86%) and in the legs of one child (14%). In addition, hip x-rays showed bilateral dislocation in all seven children and subluxation of the knee associated with genu valgus in three (43%). No evidence of abnormalities was seen on high-definition ultrasonography of the joints, but moderate signs of remodeling of the motor units and a reduced recruitment pattern were found on needle electromyography. Results from brain computed tomography conducted in all seven patients and magnetic resonance imaging conducted in five revealed malformations of cortical development, calcifications predominantly in the cortex and subcortical white matter, reduction in brain volume, ventriculomegaly, and hypoplasia of the brainstem and cerebellum. Spinal MRI conducted in four children showed apparent thinning of the cord and reduced ventral roots.
“Further research is needed with a larger number of cases to study the neurological abnormalities behind arthrogryposis, including histopathology of autopsy samples or tissues from stillborn babies,” the researchers concluded. “As we do not know the potential implications of congenital Zika virus infection as it evolves, children must receive orthopedic follow-up, even those with a standard first orthopedic evaluation, because they could develop musculoskeletal deformities secondary to neurological impairment, central or peripheral, or both, as these occur in patients with cerebral palsy and other chronic encephalopathies.”
The researchers reported having no financial disclosures.
FROM BMJ
Key clinical point: The differential diagnosis of congenital infections and arthrogryposis should include congenital Zika syndrome.
Major finding: All seven children revealed characteristics of congenital infection and arthrogryposis. Two children (29%) tested positive for IgM antibody for Zika virus in the cerebrospinal fluid, while arthrogryposis was present in the arms and legs of six children (86%) and in the legs of one child (14%).
Data source: A retrospective case series study of seven children with arthrogryposis associated with congenital infection believed to be caused by Zika virus.
Disclosures: The researchers reported having no financial disclosures.
Subungual Exostosis
Case Report
A 41-year-old man with no dermatologic history presented for a skin examination. During a full-body skin examination, a lesion was identified on the right third toe that was partially visible underneath the nail plate. The patient stated that the lesion had been present for many years and did not appear to be growing but did cause occasional pain. On examination a 1-cm verrucous, hyperkeratotic, tan papule was noted at the distal end of the nail bed causing partial onycholysis (Figure 1). It was not tender to palpation.

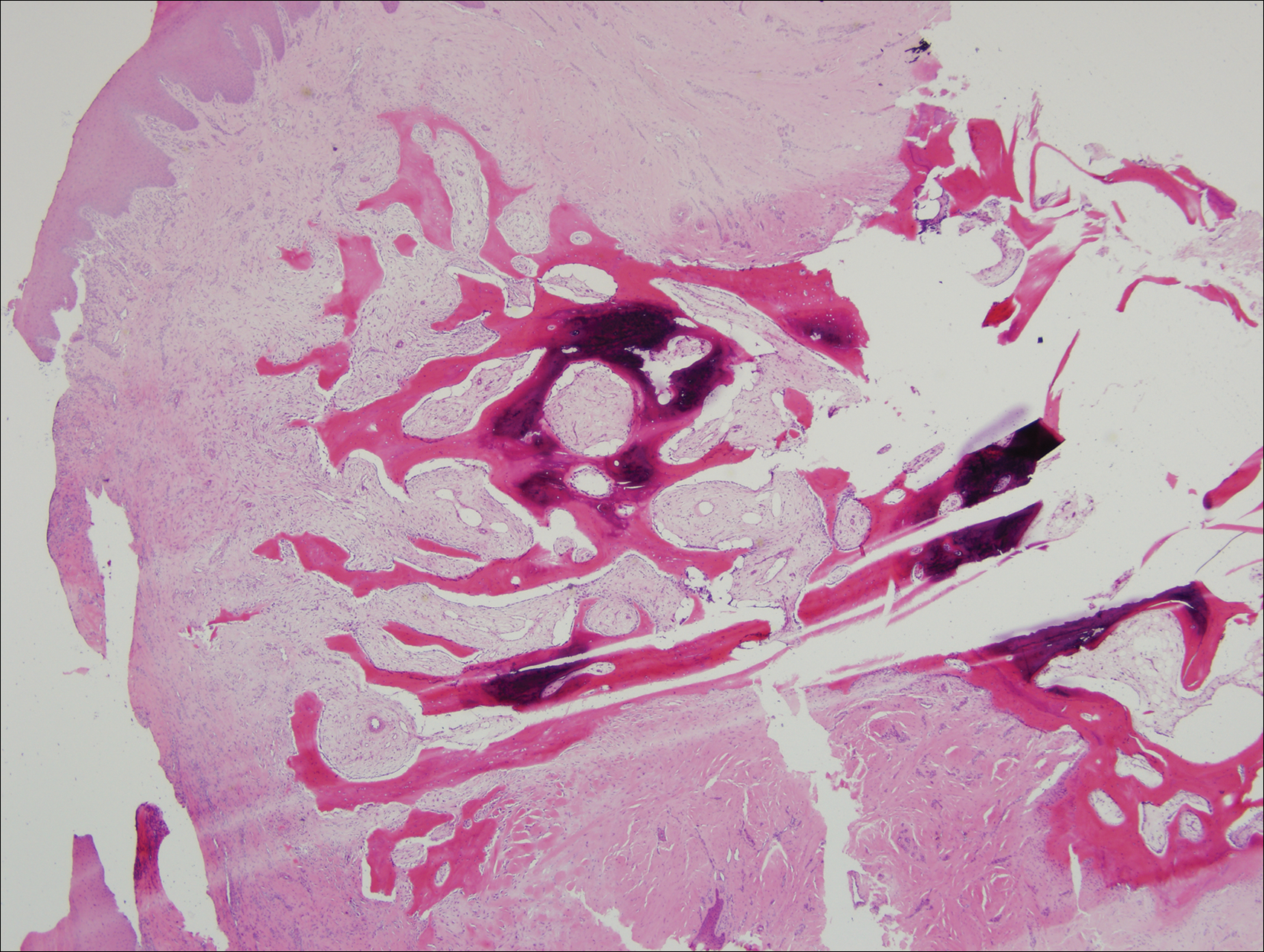
A shave biopsy was obtained of the visible portion of the lesion, which revealed hyperkeratosis, acanthosis, and a population of dermal spindle cells in a myxoid stroma that could not be definitively identified. Special stains were nondiagnostic. The patient was referred to dermatologic surgery for rebiopsy of the lesion after removal of the nail plate. Mature bone was seen embedded in the dermis (Figure 2), and a diagnosis of subungual exostosis was made. Radiography of the digit confirmed a bony excrescence from the tuft of the toe, and the patient was referred to orthopedic surgery for definitive excision. There was no evidence of recurrence at 1-year follow-up.
Comment
Subungual exostosis is an uncommon benign bone tumor located beneath or adjacent to the nail bed on the dorsal aspect of the distal phalanx.1 Although it can occur on any digit, 70% to 80% of cases have arisen on the distal phalanx of the hallux.2 Both sexes are equally susceptible. The majority of lesions occur during the second or third decades of life and usually are asymptomatic unless there is trauma or infection. Growth of the lesion over time can cause lifting or deformity of the nail plate and can cause slight discomfort while walking if located on the great toe.3 Common differential diagnoses include osteochondroma, wart, fibroma, paronychia, myositis ossificans, and pyogenic granuloma.3,4 Diagnosis can be confirmed with radiography, which should be performed prior to any biopsy or invasive procedure. In our patient, initial radiography could have obviated the need for 2 biopsies prior to definitive excision. Histopathologic evaluation typically reveals mature trabecular bone (Figure 2) surrounded by a fibrocartilage cap.
Subungual exostosis begins as an area of proliferating fibrous tissue with cartilaginous metaplasia located beneath or adjacent to the nail bed on the dorsal aspect of the distal phalanx.1 This cartilage undergoes enchondral ossification and is converted to trabecular bone. As the lesion grows and matures, the cartilaginous cap blends imperceptibly with the nail bed and comes into continuity with the underlying distal phalanx.1,3 This process continues until the lesion fuses completely with the distal phalanx.1 Although the cause of subungual exostosis has not been clearly established, chronic irritation, trauma, and chronic infections are considered causative factors of fibrocartilaginous metaplasia.4
The most commonly accepted treatment of subungual exostosis is a localized excision. Partial or total removal of the nail has traditionally be advocated to ensure complete excision of the exostosis, a nail-sparing technique that has been shown to enhance cosmetic results.3 Incomplete excision and incomplete maturation of the lesion have been reported to be responsible for almost 50% of recurrences.3 This high recurrence rate is due to difficulty in ensuring a total excision because the gradual merging of the fibrocartilage cap with the overlying nail bed makes it impossible to develop a cleavage plane5; as a result, it has been suggested that excision should only be attempted after maturation of the tumor so the cleavage plane can fully develop. Other studies claim that delaying treatment can result in elevation and deformity of the nail, pain, and secondary periungual infection.3
Conclusion
Subungual exostosis is a benign bony tumor of the distal phalanx that can cause pain and onycholysis. Radiography of the affected digit is a noninvasive way to confirm the diagnosis and should be part of the initial workup of any suspicious subungual tumor. Once identified, complete removal of the exostosis by excision has been shown to be an effective treatment with few complications.
- Letts M, Davidson D, Nizalik E. Subungual exostosis: diagnosis and treatment in children. J Trauma. 1998;44:346-349.
- Starnes A, Crosby K, Rowe DJ, et al. Subungual exostosis: a simple surgical technique. Dermatol Surg. 2012;38:258-260.
- Lokiec F, Ezra E, Krasin E, et al. A simple and efficient surgical technique for subungual exostosis. J Pediatr Orthop. 2001;21:76-79.
- Turan H, Uslu M, Erdem H. A case of subungual exostosis. Indian J Dermatol Venereol Leprol. 2012;78:186.
- Miller-Breslow A, Dorfman HD. Dupuytren’s (subungual) exostosis. Am J Surg Pathol. 1988;12:368-378.
Case Report
A 41-year-old man with no dermatologic history presented for a skin examination. During a full-body skin examination, a lesion was identified on the right third toe that was partially visible underneath the nail plate. The patient stated that the lesion had been present for many years and did not appear to be growing but did cause occasional pain. On examination a 1-cm verrucous, hyperkeratotic, tan papule was noted at the distal end of the nail bed causing partial onycholysis (Figure 1). It was not tender to palpation.
A shave biopsy was obtained of the visible portion of the lesion, which revealed hyperkeratosis, acanthosis, and a population of dermal spindle cells in a myxoid stroma that could not be definitively identified. Special stains were nondiagnostic. The patient was referred to dermatologic surgery for rebiopsy of the lesion after removal of the nail plate. Mature bone was seen embedded in the dermis (Figure 2), and a diagnosis of subungual exostosis was made. Radiography of the digit confirmed a bony excrescence from the tuft of the toe, and the patient was referred to orthopedic surgery for definitive excision. There was no evidence of recurrence at 1-year follow-up.
Comment
Subungual exostosis is an uncommon benign bone tumor located beneath or adjacent to the nail bed on the dorsal aspect of the distal phalanx.1 Although it can occur on any digit, 70% to 80% of cases have arisen on the distal phalanx of the hallux.2 Both sexes are equally susceptible. The majority of lesions occur during the second or third decades of life and usually are asymptomatic unless there is trauma or infection. Growth of the lesion over time can cause lifting or deformity of the nail plate and can cause slight discomfort while walking if located on the great toe.3 Common differential diagnoses include osteochondroma, wart, fibroma, paronychia, myositis ossificans, and pyogenic granuloma.3,4 Diagnosis can be confirmed with radiography, which should be performed prior to any biopsy or invasive procedure. In our patient, initial radiography could have obviated the need for 2 biopsies prior to definitive excision. Histopathologic evaluation typically reveals mature trabecular bone (Figure 2) surrounded by a fibrocartilage cap.
Subungual exostosis begins as an area of proliferating fibrous tissue with cartilaginous metaplasia located beneath or adjacent to the nail bed on the dorsal aspect of the distal phalanx.1 This cartilage undergoes enchondral ossification and is converted to trabecular bone. As the lesion grows and matures, the cartilaginous cap blends imperceptibly with the nail bed and comes into continuity with the underlying distal phalanx.1,3 This process continues until the lesion fuses completely with the distal phalanx.1 Although the cause of subungual exostosis has not been clearly established, chronic irritation, trauma, and chronic infections are considered causative factors of fibrocartilaginous metaplasia.4
The most commonly accepted treatment of subungual exostosis is a localized excision. Partial or total removal of the nail has traditionally be advocated to ensure complete excision of the exostosis, a nail-sparing technique that has been shown to enhance cosmetic results.3 Incomplete excision and incomplete maturation of the lesion have been reported to be responsible for almost 50% of recurrences.3 This high recurrence rate is due to difficulty in ensuring a total excision because the gradual merging of the fibrocartilage cap with the overlying nail bed makes it impossible to develop a cleavage plane5; as a result, it has been suggested that excision should only be attempted after maturation of the tumor so the cleavage plane can fully develop. Other studies claim that delaying treatment can result in elevation and deformity of the nail, pain, and secondary periungual infection.3
Conclusion
Subungual exostosis is a benign bony tumor of the distal phalanx that can cause pain and onycholysis. Radiography of the affected digit is a noninvasive way to confirm the diagnosis and should be part of the initial workup of any suspicious subungual tumor. Once identified, complete removal of the exostosis by excision has been shown to be an effective treatment with few complications.
Case Report
A 41-year-old man with no dermatologic history presented for a skin examination. During a full-body skin examination, a lesion was identified on the right third toe that was partially visible underneath the nail plate. The patient stated that the lesion had been present for many years and did not appear to be growing but did cause occasional pain. On examination a 1-cm verrucous, hyperkeratotic, tan papule was noted at the distal end of the nail bed causing partial onycholysis (Figure 1). It was not tender to palpation.
A shave biopsy was obtained of the visible portion of the lesion, which revealed hyperkeratosis, acanthosis, and a population of dermal spindle cells in a myxoid stroma that could not be definitively identified. Special stains were nondiagnostic. The patient was referred to dermatologic surgery for rebiopsy of the lesion after removal of the nail plate. Mature bone was seen embedded in the dermis (Figure 2), and a diagnosis of subungual exostosis was made. Radiography of the digit confirmed a bony excrescence from the tuft of the toe, and the patient was referred to orthopedic surgery for definitive excision. There was no evidence of recurrence at 1-year follow-up.
Comment
Subungual exostosis is an uncommon benign bone tumor located beneath or adjacent to the nail bed on the dorsal aspect of the distal phalanx.1 Although it can occur on any digit, 70% to 80% of cases have arisen on the distal phalanx of the hallux.2 Both sexes are equally susceptible. The majority of lesions occur during the second or third decades of life and usually are asymptomatic unless there is trauma or infection. Growth of the lesion over time can cause lifting or deformity of the nail plate and can cause slight discomfort while walking if located on the great toe.3 Common differential diagnoses include osteochondroma, wart, fibroma, paronychia, myositis ossificans, and pyogenic granuloma.3,4 Diagnosis can be confirmed with radiography, which should be performed prior to any biopsy or invasive procedure. In our patient, initial radiography could have obviated the need for 2 biopsies prior to definitive excision. Histopathologic evaluation typically reveals mature trabecular bone (Figure 2) surrounded by a fibrocartilage cap.
Subungual exostosis begins as an area of proliferating fibrous tissue with cartilaginous metaplasia located beneath or adjacent to the nail bed on the dorsal aspect of the distal phalanx.1 This cartilage undergoes enchondral ossification and is converted to trabecular bone. As the lesion grows and matures, the cartilaginous cap blends imperceptibly with the nail bed and comes into continuity with the underlying distal phalanx.1,3 This process continues until the lesion fuses completely with the distal phalanx.1 Although the cause of subungual exostosis has not been clearly established, chronic irritation, trauma, and chronic infections are considered causative factors of fibrocartilaginous metaplasia.4
The most commonly accepted treatment of subungual exostosis is a localized excision. Partial or total removal of the nail has traditionally be advocated to ensure complete excision of the exostosis, a nail-sparing technique that has been shown to enhance cosmetic results.3 Incomplete excision and incomplete maturation of the lesion have been reported to be responsible for almost 50% of recurrences.3 This high recurrence rate is due to difficulty in ensuring a total excision because the gradual merging of the fibrocartilage cap with the overlying nail bed makes it impossible to develop a cleavage plane5; as a result, it has been suggested that excision should only be attempted after maturation of the tumor so the cleavage plane can fully develop. Other studies claim that delaying treatment can result in elevation and deformity of the nail, pain, and secondary periungual infection.3
Conclusion
Subungual exostosis is a benign bony tumor of the distal phalanx that can cause pain and onycholysis. Radiography of the affected digit is a noninvasive way to confirm the diagnosis and should be part of the initial workup of any suspicious subungual tumor. Once identified, complete removal of the exostosis by excision has been shown to be an effective treatment with few complications.
- Letts M, Davidson D, Nizalik E. Subungual exostosis: diagnosis and treatment in children. J Trauma. 1998;44:346-349.
- Starnes A, Crosby K, Rowe DJ, et al. Subungual exostosis: a simple surgical technique. Dermatol Surg. 2012;38:258-260.
- Lokiec F, Ezra E, Krasin E, et al. A simple and efficient surgical technique for subungual exostosis. J Pediatr Orthop. 2001;21:76-79.
- Turan H, Uslu M, Erdem H. A case of subungual exostosis. Indian J Dermatol Venereol Leprol. 2012;78:186.
- Miller-Breslow A, Dorfman HD. Dupuytren’s (subungual) exostosis. Am J Surg Pathol. 1988;12:368-378.
- Letts M, Davidson D, Nizalik E. Subungual exostosis: diagnosis and treatment in children. J Trauma. 1998;44:346-349.
- Starnes A, Crosby K, Rowe DJ, et al. Subungual exostosis: a simple surgical technique. Dermatol Surg. 2012;38:258-260.
- Lokiec F, Ezra E, Krasin E, et al. A simple and efficient surgical technique for subungual exostosis. J Pediatr Orthop. 2001;21:76-79.
- Turan H, Uslu M, Erdem H. A case of subungual exostosis. Indian J Dermatol Venereol Leprol. 2012;78:186.
- Miller-Breslow A, Dorfman HD. Dupuytren’s (subungual) exostosis. Am J Surg Pathol. 1988;12:368-378.
Practice Points
- Subungual exostosis is a benign tumor that is most common on the hallux.
- Plain radiographs can identify an exostosis and should be part of the initial workup of any subungual tumor.
- Surgical excision is an effective and well-tolerated treatment of subungual exostosis.

Two-dose HPV vaccines at younger age are noninferior to standard three-dose vaccine
“The licensed vaccines HPV-16/18 AS04–adjuvanted (Cervarix; GSK Vaccines) and HPV-6/11/16/18 (Gardasil; Merck) were first approved as regimen including three doses (3D) with administration over a 6-month period,” reported Thanyawee Puthanakit, MD, of Chulalongkorn University in Bangkok, and her associates. “Reduced dose schedules could make vaccination easier to implement and more affordable, creating the potential for higher vaccination coverage and improved cervical cancer protection (J Infect Dis. 2016;214:525-36).”

The investigators enrolled girls aged 9-25 years starting in June 2011, from 33 clinical sites in Canada, Germany, Italy, Taiwan, and Thailand. The study lasted through January 2013, during which time 1,447 girls were enrolled and 1,428 were randomized into one of three cohorts: one receiving the two-dose, 6-month regimen; one receiving the two-dose, 12-month regime; and one receiving the three-dose, 6-month regimen. In the former two cohorts, girls aged 9-14 years would receive their doses at 0 months and either 6 or 12 months, depending on the cohort. In the three-dose regimen, girls aged 15-25 years received doses at 0, 1, and 6 months. At enrollment, 550 girls were randomized into the two-dose, 6-month regimen; 415 girls into the two-dose, 12-month regimen; and 482 girls into the three-dose, 6-month regimen. Follow-up occurred at 1 month after they received the final dose for all three cohorts.
Ultimately, 534 girls in the two-dose, 6-month cohort; 394 in the two-dose, 12-month cohort; and 427 in the three-dose, 6-month cohort completed the study through the 1-month follow-up. Serologic testing indicated that girls in both the two-dose cohorts were not immunologically worse off than those who were in the three-dose cohort, with seroconversion differences of 0.00 when comparing HPV-16 and HPV-18 antibodies between any two of the three regimens. Furthermore, geometric mean antibody titer ratios for HPV-16 and HPV-18 were 1.09 (95% confidence interval, 0.97-1.22) and 0.85 (95% CI, 0.76-0.95) for the 6-month two-dose regimen vs. three-dose, and 0.89 (95% CI, 0.79-1.01) and 0.75 (95% CI, 0.67-0.85) for 12-month two-dose regimen vs.three-dose, indicating little statistically significant difference.
“The flexibility around the timing of the second dose, giving the option of annual vaccination over 2 consecutive years, is an added benefit [because] reduced dose schedules of HPV vaccines may facilitate vaccination implementation and reduce cost, allowing for higher vaccination coverage and potentially more girls being protected from cervical cancer,” the investigators noted.
The study was supported by GlaxoSmithKline Biologicals SA. Dr. Puthanakit received a grant from GSK through her institution. Some of her many coauthors disclosed relationships with GSK and/or other pharmaceutical companies.
“The licensed vaccines HPV-16/18 AS04–adjuvanted (Cervarix; GSK Vaccines) and HPV-6/11/16/18 (Gardasil; Merck) were first approved as regimen including three doses (3D) with administration over a 6-month period,” reported Thanyawee Puthanakit, MD, of Chulalongkorn University in Bangkok, and her associates. “Reduced dose schedules could make vaccination easier to implement and more affordable, creating the potential for higher vaccination coverage and improved cervical cancer protection (J Infect Dis. 2016;214:525-36).”
The investigators enrolled girls aged 9-25 years starting in June 2011, from 33 clinical sites in Canada, Germany, Italy, Taiwan, and Thailand. The study lasted through January 2013, during which time 1,447 girls were enrolled and 1,428 were randomized into one of three cohorts: one receiving the two-dose, 6-month regimen; one receiving the two-dose, 12-month regime; and one receiving the three-dose, 6-month regimen. In the former two cohorts, girls aged 9-14 years would receive their doses at 0 months and either 6 or 12 months, depending on the cohort. In the three-dose regimen, girls aged 15-25 years received doses at 0, 1, and 6 months. At enrollment, 550 girls were randomized into the two-dose, 6-month regimen; 415 girls into the two-dose, 12-month regimen; and 482 girls into the three-dose, 6-month regimen. Follow-up occurred at 1 month after they received the final dose for all three cohorts.
Ultimately, 534 girls in the two-dose, 6-month cohort; 394 in the two-dose, 12-month cohort; and 427 in the three-dose, 6-month cohort completed the study through the 1-month follow-up. Serologic testing indicated that girls in both the two-dose cohorts were not immunologically worse off than those who were in the three-dose cohort, with seroconversion differences of 0.00 when comparing HPV-16 and HPV-18 antibodies between any two of the three regimens. Furthermore, geometric mean antibody titer ratios for HPV-16 and HPV-18 were 1.09 (95% confidence interval, 0.97-1.22) and 0.85 (95% CI, 0.76-0.95) for the 6-month two-dose regimen vs. three-dose, and 0.89 (95% CI, 0.79-1.01) and 0.75 (95% CI, 0.67-0.85) for 12-month two-dose regimen vs.three-dose, indicating little statistically significant difference.
“The flexibility around the timing of the second dose, giving the option of annual vaccination over 2 consecutive years, is an added benefit [because] reduced dose schedules of HPV vaccines may facilitate vaccination implementation and reduce cost, allowing for higher vaccination coverage and potentially more girls being protected from cervical cancer,” the investigators noted.
The study was supported by GlaxoSmithKline Biologicals SA. Dr. Puthanakit received a grant from GSK through her institution. Some of her many coauthors disclosed relationships with GSK and/or other pharmaceutical companies.
“The licensed vaccines HPV-16/18 AS04–adjuvanted (Cervarix; GSK Vaccines) and HPV-6/11/16/18 (Gardasil; Merck) were first approved as regimen including three doses (3D) with administration over a 6-month period,” reported Thanyawee Puthanakit, MD, of Chulalongkorn University in Bangkok, and her associates. “Reduced dose schedules could make vaccination easier to implement and more affordable, creating the potential for higher vaccination coverage and improved cervical cancer protection (J Infect Dis. 2016;214:525-36).”
The investigators enrolled girls aged 9-25 years starting in June 2011, from 33 clinical sites in Canada, Germany, Italy, Taiwan, and Thailand. The study lasted through January 2013, during which time 1,447 girls were enrolled and 1,428 were randomized into one of three cohorts: one receiving the two-dose, 6-month regimen; one receiving the two-dose, 12-month regime; and one receiving the three-dose, 6-month regimen. In the former two cohorts, girls aged 9-14 years would receive their doses at 0 months and either 6 or 12 months, depending on the cohort. In the three-dose regimen, girls aged 15-25 years received doses at 0, 1, and 6 months. At enrollment, 550 girls were randomized into the two-dose, 6-month regimen; 415 girls into the two-dose, 12-month regimen; and 482 girls into the three-dose, 6-month regimen. Follow-up occurred at 1 month after they received the final dose for all three cohorts.
Ultimately, 534 girls in the two-dose, 6-month cohort; 394 in the two-dose, 12-month cohort; and 427 in the three-dose, 6-month cohort completed the study through the 1-month follow-up. Serologic testing indicated that girls in both the two-dose cohorts were not immunologically worse off than those who were in the three-dose cohort, with seroconversion differences of 0.00 when comparing HPV-16 and HPV-18 antibodies between any two of the three regimens. Furthermore, geometric mean antibody titer ratios for HPV-16 and HPV-18 were 1.09 (95% confidence interval, 0.97-1.22) and 0.85 (95% CI, 0.76-0.95) for the 6-month two-dose regimen vs. three-dose, and 0.89 (95% CI, 0.79-1.01) and 0.75 (95% CI, 0.67-0.85) for 12-month two-dose regimen vs.three-dose, indicating little statistically significant difference.
“The flexibility around the timing of the second dose, giving the option of annual vaccination over 2 consecutive years, is an added benefit [because] reduced dose schedules of HPV vaccines may facilitate vaccination implementation and reduce cost, allowing for higher vaccination coverage and potentially more girls being protected from cervical cancer,” the investigators noted.
The study was supported by GlaxoSmithKline Biologicals SA. Dr. Puthanakit received a grant from GSK through her institution. Some of her many coauthors disclosed relationships with GSK and/or other pharmaceutical companies.
FROM THE JOURNAL OF INFECTIOUS DISEASES
Key clinical point: Girls receiving 2-dose HPV-16/18 AS04-adjuvanted vaccine at age 9-14 years over a 6- or 12-month timespan appear to be equally protected against HPV than those receiving 3-dose HPV vaccine schedules at age 15-25 years.
Major finding: Geometric mean antibody titer ratios for HPV-16 and HPV-18 were 1.09 (95% CI, 0.97-1.22) and 0.85 (95% CI, 0.76-0.95) for 6-month two-dose regimen vs. three-dose, and 0.89 (95% CI 0.79-1.01) and 0.75 (95% CI, 0.67-0.85) for 12-month two-dose regimen vs. three-dose.
Data source: A randomized, open trial of 1,447 vaccinated girls aged 9-25 years.
Disclosures: Study supported by GlaxoSmithKline Biologicals SA. Dr. Puthanakit received a grant from GSK through her institution. Some of her many coauthors disclosed relationships with GSK and/or other pharmaceutical companies.

Preop G-tubes save money in head and neck cancer resections
SEATTLE – It’s better to place gastrostomy tubes before head and neck cancer surgery rather than after, according to a review of 184 patients.
The 73 patients in the study who got preoperative gastrostomy tubes (G-tubes) were sicker than the 111 who had G-tubes placed after surgery, with significantly higher American Society of Anesthesiologists scores, lower body mass indexes, and greater likelihoods of having both prior radiation and more extensive resections requiring flap reconstructions. They were, overall, a higher-risk population with a greater potential for bad outcomes, which is why tubes were placed preemptively.

Even so, at 6 months, the total average cost for the preop G-tube group was $39,751 versus $48,999 for the postoperative group, a savings of $9,248 per patient. The difference was driven by inpatient savings; the preop group left the hospital an average of 3.2 days sooner than their postop G-tube peers (9.4 days versus 12.6 days; P less than .001). Readmissions and other postdischarge costs were similar between the two groups, as were wound and nonwound complications.
“This data suggests that preoperative placement of G-tubes is associated with lower total health care costs. It appears there’s a potential for health care cost savings if candidates for G-tubes can be identified” before surgery and the tubes placed preoperatively, said investigator Joshua Waltonen, MD, of Wake Forest University, Winston-Salem, N.C.
That’s exactly what Wake Forest is doing now. Physicians there use a scoring system to determine how likely patients are to need G-tubes after surgery. If the risk is high, patients are counseled that putting one in beforehand is a good idea, he said at the International Conference on Head and Neck Cancer, held by the American Head and Neck Society.
The team previously found that risk factors include, among others, supracricoid laryngectomy, prior radiation, flap reconstruction, tracheostomy placement, and preop dysphagia and weight loss (JAMA Otolaryngol Head Neck Surg. 2014 Dec;140[12]:1198-206).
Two factors probably account for the shorter lengths of stay, Dr. Waltonen said. First, patients with preop feeding tubes go into surgery with a nutritional boost, which helps with recovery. Also, with a preop tube, patients don’t have to wait for general surgery to get around to placing one postoperatively.
Both groups were about 60 years old on average. The mean body mass index of the preop group was 23 kg/m2 and 26 kg/m2 in the postop group (P = .009). Almost two-thirds of preop patients had prior radiation versus a quarter of postop patients (P less than .001). Tumor and nodal stages were similar.
There was no outside funding for the work, and Dr. Waltonen had no disclosures.
SEATTLE – It’s better to place gastrostomy tubes before head and neck cancer surgery rather than after, according to a review of 184 patients.
The 73 patients in the study who got preoperative gastrostomy tubes (G-tubes) were sicker than the 111 who had G-tubes placed after surgery, with significantly higher American Society of Anesthesiologists scores, lower body mass indexes, and greater likelihoods of having both prior radiation and more extensive resections requiring flap reconstructions. They were, overall, a higher-risk population with a greater potential for bad outcomes, which is why tubes were placed preemptively.
Even so, at 6 months, the total average cost for the preop G-tube group was $39,751 versus $48,999 for the postoperative group, a savings of $9,248 per patient. The difference was driven by inpatient savings; the preop group left the hospital an average of 3.2 days sooner than their postop G-tube peers (9.4 days versus 12.6 days; P less than .001). Readmissions and other postdischarge costs were similar between the two groups, as were wound and nonwound complications.
“This data suggests that preoperative placement of G-tubes is associated with lower total health care costs. It appears there’s a potential for health care cost savings if candidates for G-tubes can be identified” before surgery and the tubes placed preoperatively, said investigator Joshua Waltonen, MD, of Wake Forest University, Winston-Salem, N.C.
That’s exactly what Wake Forest is doing now. Physicians there use a scoring system to determine how likely patients are to need G-tubes after surgery. If the risk is high, patients are counseled that putting one in beforehand is a good idea, he said at the International Conference on Head and Neck Cancer, held by the American Head and Neck Society.
The team previously found that risk factors include, among others, supracricoid laryngectomy, prior radiation, flap reconstruction, tracheostomy placement, and preop dysphagia and weight loss (JAMA Otolaryngol Head Neck Surg. 2014 Dec;140[12]:1198-206).
Two factors probably account for the shorter lengths of stay, Dr. Waltonen said. First, patients with preop feeding tubes go into surgery with a nutritional boost, which helps with recovery. Also, with a preop tube, patients don’t have to wait for general surgery to get around to placing one postoperatively.
Both groups were about 60 years old on average. The mean body mass index of the preop group was 23 kg/m2 and 26 kg/m2 in the postop group (P = .009). Almost two-thirds of preop patients had prior radiation versus a quarter of postop patients (P less than .001). Tumor and nodal stages were similar.
There was no outside funding for the work, and Dr. Waltonen had no disclosures.
SEATTLE – It’s better to place gastrostomy tubes before head and neck cancer surgery rather than after, according to a review of 184 patients.
The 73 patients in the study who got preoperative gastrostomy tubes (G-tubes) were sicker than the 111 who had G-tubes placed after surgery, with significantly higher American Society of Anesthesiologists scores, lower body mass indexes, and greater likelihoods of having both prior radiation and more extensive resections requiring flap reconstructions. They were, overall, a higher-risk population with a greater potential for bad outcomes, which is why tubes were placed preemptively.
Even so, at 6 months, the total average cost for the preop G-tube group was $39,751 versus $48,999 for the postoperative group, a savings of $9,248 per patient. The difference was driven by inpatient savings; the preop group left the hospital an average of 3.2 days sooner than their postop G-tube peers (9.4 days versus 12.6 days; P less than .001). Readmissions and other postdischarge costs were similar between the two groups, as were wound and nonwound complications.
“This data suggests that preoperative placement of G-tubes is associated with lower total health care costs. It appears there’s a potential for health care cost savings if candidates for G-tubes can be identified” before surgery and the tubes placed preoperatively, said investigator Joshua Waltonen, MD, of Wake Forest University, Winston-Salem, N.C.
That’s exactly what Wake Forest is doing now. Physicians there use a scoring system to determine how likely patients are to need G-tubes after surgery. If the risk is high, patients are counseled that putting one in beforehand is a good idea, he said at the International Conference on Head and Neck Cancer, held by the American Head and Neck Society.
The team previously found that risk factors include, among others, supracricoid laryngectomy, prior radiation, flap reconstruction, tracheostomy placement, and preop dysphagia and weight loss (JAMA Otolaryngol Head Neck Surg. 2014 Dec;140[12]:1198-206).
Two factors probably account for the shorter lengths of stay, Dr. Waltonen said. First, patients with preop feeding tubes go into surgery with a nutritional boost, which helps with recovery. Also, with a preop tube, patients don’t have to wait for general surgery to get around to placing one postoperatively.
Both groups were about 60 years old on average. The mean body mass index of the preop group was 23 kg/m2 and 26 kg/m2 in the postop group (P = .009). Almost two-thirds of preop patients had prior radiation versus a quarter of postop patients (P less than .001). Tumor and nodal stages were similar.
There was no outside funding for the work, and Dr. Waltonen had no disclosures.
AT AHNS 2016
Key clinical point: It’s better to place gastrostomy tubes before head and neck cancer surgery rather than after.
Major finding: At 6 months, the total average cost for the preop G-tube group was $39,751 versus $48,999 for the postop group, a savings of $9,248 per patient.
Data source: Review of 184 patients.
Disclosures: There was no outside funding for the work, and the presenter had no disclosures.

Medicaid expansion leads to better access to care
Low-income adults living in two states that expanded Medicaid enrollment are showing significant increases in outpatient utilization and preventive care, improved health care quality, and reductions in emergency department use, compared with those living in a state that did not expand Medicaid, according to a new study.
The study also found similar improvements in care whether a state expanded traditional Medicaid or increased coverage through a private insurance option.

Benjamin D. Sommers, MD, PhD, of Harvard University, Boston, and his colleagues examined outcomes for nearly 9,000 low-income Medicaid enrollees in Kentucky (where officials expanded traditional Medicaid), Arkansas (where the state used funds to purchase private insurance to expand coverage), and Texas (which did not expand Medicaid) in November and December of 2013, 2014, and 2015. They looked specifically at changes in use of healthcare services, preventive care, and self-reported health (JAMA Intern Med. 2016 Aug 8. doi: 10.1001/jamainternmed.2016.4419).
“By the end of 2015, we found marked increases in coverage and reduced cost-related barriers to care in the expansion states, with associated increases in preventive care, outpatient visits, annual checkups, and chronic disease care, as well as decreased reliance on the [emergency department],” the researchers wrote.
They found that by 2015 there was a 6 percentage point drop in the likelihood of ED visits (P = 0.04), an increase of 0.69 office visits per person in the outpatient setting (P = 0.04), and an increase likelihood of getting a checkup (16.1 percentage points, P less than .001) in Medicaid expansion states. In Medicaid expansion states the share of adults obtaining regular care for chronic conditions increased by 12 percentage points after expansion (P = .008), compared with Texas. Additionally, adults reporting fair or poor quality of care dropped by 7.1 percentage points (P = .03).
One significant difference between the expansion states was changes in glucose monitoring rates for patients with diabetes were lower in Arkansas than Kentucky (–11.6 percentage points, P = .04).
“Of note, we found improvements in receipt of checkups, care for chronic conditions, and quality of care even in areas with primary care shortages, suggesting that while clinician capacity is undoubtedly an important consideration, insurance expansion can have a demonstrable positive impact even in areas with relative shortages, perhaps partially due to increased use of safety net providers,” the researchers added.
The study was supported by a research grant from the Commonwealth Fund and a grant from the Agency for Healthcare Research and Quality. The researchers reported having no financial disclosures.
Whether the premium assistance model proves to be durable and effective remains an open question. On the upside, the findings of Sommers et al suggest that the Arkansas initiative is living up to its promises. Moreover, the waiver seems to have increased the number of insurers participating in the marketplaces and contributed to lower premiums.
But other evidence concerning premium assistance waivers suggests the need for caution in assessing their effectiveness. The Government Accountability Office has questioned whether these waivers are budget neutral – a federal requirement. In this vein, the Congressional Budget Office has estimated that it will cost 50% more per enrollee to cover the expansion population on the exchanges than in the conventional Medicaid program. Nor are premium assistance waivers necessarily sustainable. In Pennsylvania, for instance, a newly elected Democratic governor worked to phase out that state’s existing alternative waiver, which had been negotiated by a prior Republican administration, in favor of a traditional expansion of the Medicaid entitlement.
Frank J. Thompson, PhD, and Joel C. Cantor, ScD, are both at Rutgers University in New Brunswick, N.J. They reported having no financial disclosures. Their comments were excerpted from a commentary in JAMA Internal Medicine (2016 Aug 8. doi: 10.1001/jamainternmed.2016.4422).
Whether the premium assistance model proves to be durable and effective remains an open question. On the upside, the findings of Sommers et al suggest that the Arkansas initiative is living up to its promises. Moreover, the waiver seems to have increased the number of insurers participating in the marketplaces and contributed to lower premiums.
But other evidence concerning premium assistance waivers suggests the need for caution in assessing their effectiveness. The Government Accountability Office has questioned whether these waivers are budget neutral – a federal requirement. In this vein, the Congressional Budget Office has estimated that it will cost 50% more per enrollee to cover the expansion population on the exchanges than in the conventional Medicaid program. Nor are premium assistance waivers necessarily sustainable. In Pennsylvania, for instance, a newly elected Democratic governor worked to phase out that state’s existing alternative waiver, which had been negotiated by a prior Republican administration, in favor of a traditional expansion of the Medicaid entitlement.
Frank J. Thompson, PhD, and Joel C. Cantor, ScD, are both at Rutgers University in New Brunswick, N.J. They reported having no financial disclosures. Their comments were excerpted from a commentary in JAMA Internal Medicine (2016 Aug 8. doi: 10.1001/jamainternmed.2016.4422).
Whether the premium assistance model proves to be durable and effective remains an open question. On the upside, the findings of Sommers et al suggest that the Arkansas initiative is living up to its promises. Moreover, the waiver seems to have increased the number of insurers participating in the marketplaces and contributed to lower premiums.
But other evidence concerning premium assistance waivers suggests the need for caution in assessing their effectiveness. The Government Accountability Office has questioned whether these waivers are budget neutral – a federal requirement. In this vein, the Congressional Budget Office has estimated that it will cost 50% more per enrollee to cover the expansion population on the exchanges than in the conventional Medicaid program. Nor are premium assistance waivers necessarily sustainable. In Pennsylvania, for instance, a newly elected Democratic governor worked to phase out that state’s existing alternative waiver, which had been negotiated by a prior Republican administration, in favor of a traditional expansion of the Medicaid entitlement.
Frank J. Thompson, PhD, and Joel C. Cantor, ScD, are both at Rutgers University in New Brunswick, N.J. They reported having no financial disclosures. Their comments were excerpted from a commentary in JAMA Internal Medicine (2016 Aug 8. doi: 10.1001/jamainternmed.2016.4422).
Low-income adults living in two states that expanded Medicaid enrollment are showing significant increases in outpatient utilization and preventive care, improved health care quality, and reductions in emergency department use, compared with those living in a state that did not expand Medicaid, according to a new study.
The study also found similar improvements in care whether a state expanded traditional Medicaid or increased coverage through a private insurance option.
Benjamin D. Sommers, MD, PhD, of Harvard University, Boston, and his colleagues examined outcomes for nearly 9,000 low-income Medicaid enrollees in Kentucky (where officials expanded traditional Medicaid), Arkansas (where the state used funds to purchase private insurance to expand coverage), and Texas (which did not expand Medicaid) in November and December of 2013, 2014, and 2015. They looked specifically at changes in use of healthcare services, preventive care, and self-reported health (JAMA Intern Med. 2016 Aug 8. doi: 10.1001/jamainternmed.2016.4419).
“By the end of 2015, we found marked increases in coverage and reduced cost-related barriers to care in the expansion states, with associated increases in preventive care, outpatient visits, annual checkups, and chronic disease care, as well as decreased reliance on the [emergency department],” the researchers wrote.
They found that by 2015 there was a 6 percentage point drop in the likelihood of ED visits (P = 0.04), an increase of 0.69 office visits per person in the outpatient setting (P = 0.04), and an increase likelihood of getting a checkup (16.1 percentage points, P less than .001) in Medicaid expansion states. In Medicaid expansion states the share of adults obtaining regular care for chronic conditions increased by 12 percentage points after expansion (P = .008), compared with Texas. Additionally, adults reporting fair or poor quality of care dropped by 7.1 percentage points (P = .03).
One significant difference between the expansion states was changes in glucose monitoring rates for patients with diabetes were lower in Arkansas than Kentucky (–11.6 percentage points, P = .04).
“Of note, we found improvements in receipt of checkups, care for chronic conditions, and quality of care even in areas with primary care shortages, suggesting that while clinician capacity is undoubtedly an important consideration, insurance expansion can have a demonstrable positive impact even in areas with relative shortages, perhaps partially due to increased use of safety net providers,” the researchers added.
The study was supported by a research grant from the Commonwealth Fund and a grant from the Agency for Healthcare Research and Quality. The researchers reported having no financial disclosures.
Low-income adults living in two states that expanded Medicaid enrollment are showing significant increases in outpatient utilization and preventive care, improved health care quality, and reductions in emergency department use, compared with those living in a state that did not expand Medicaid, according to a new study.
The study also found similar improvements in care whether a state expanded traditional Medicaid or increased coverage through a private insurance option.
Benjamin D. Sommers, MD, PhD, of Harvard University, Boston, and his colleagues examined outcomes for nearly 9,000 low-income Medicaid enrollees in Kentucky (where officials expanded traditional Medicaid), Arkansas (where the state used funds to purchase private insurance to expand coverage), and Texas (which did not expand Medicaid) in November and December of 2013, 2014, and 2015. They looked specifically at changes in use of healthcare services, preventive care, and self-reported health (JAMA Intern Med. 2016 Aug 8. doi: 10.1001/jamainternmed.2016.4419).
“By the end of 2015, we found marked increases in coverage and reduced cost-related barriers to care in the expansion states, with associated increases in preventive care, outpatient visits, annual checkups, and chronic disease care, as well as decreased reliance on the [emergency department],” the researchers wrote.
They found that by 2015 there was a 6 percentage point drop in the likelihood of ED visits (P = 0.04), an increase of 0.69 office visits per person in the outpatient setting (P = 0.04), and an increase likelihood of getting a checkup (16.1 percentage points, P less than .001) in Medicaid expansion states. In Medicaid expansion states the share of adults obtaining regular care for chronic conditions increased by 12 percentage points after expansion (P = .008), compared with Texas. Additionally, adults reporting fair or poor quality of care dropped by 7.1 percentage points (P = .03).
One significant difference between the expansion states was changes in glucose monitoring rates for patients with diabetes were lower in Arkansas than Kentucky (–11.6 percentage points, P = .04).
“Of note, we found improvements in receipt of checkups, care for chronic conditions, and quality of care even in areas with primary care shortages, suggesting that while clinician capacity is undoubtedly an important consideration, insurance expansion can have a demonstrable positive impact even in areas with relative shortages, perhaps partially due to increased use of safety net providers,” the researchers added.
The study was supported by a research grant from the Commonwealth Fund and a grant from the Agency for Healthcare Research and Quality. The researchers reported having no financial disclosures.
FROM JAMA INTERNAL MEDICINE
Key clinical point: Medicaid expansion improved self-reported health outcomes and access to care.
Major finding: By 2015 there was a 6 percentage point drop in the likelihood of emergency department visits (P = .04) and an increase of 0.69 outpatient office visits per person (P = .04).
Data source: A differences-in-differences analysis of survey data from Nov. 2013 through Dec. 2015 of 8,676 low-income adults in Kentucky, Arkansas, and Texas.
Disclosures: The study was supported by a research grant from the Commonwealth Fund and a grant from the Agency for Healthcare Research and Quality. The researchers reported having no financial disclosures.

Intraoperative nerve stimulation reduces risk of shoulder pain from neck dissection
SEATTLE – Direct, intraoperative electrical stimulation of the spinal accessory nerve reduced shoulder pain and dysfunction from oncologic neck dissection in a small, randomized trial.
Shoulder problems are common after neck dissection because of traction and compression of the spinal accessory nerve. Although brief electrical stimulation (BES) has been shown before to improve regeneration and recovery of injured peripheral nerves, it hasn’t been shown until now to help patients recover from neck surgery, said investigator Brittany Barber, MD, a fifth-year resident at the University of Alberta, Edmonton.

After neck dissection in 21 patients, the investigators wrapped a small electrode (Automatic Periodic Stimulation [APS] electrode, Medtronic) around the spinal accessory nerve at the base of the skull on the side of the neck with the most extensive nodal burden; the electrode delivered 100-msec pulses at 20 Hz and 3-5 V for an hour, and then the neck was closed. The team compared outcomes with 20 controls who had neck dissections without BES.
At 12 months, the BES group had an 8.4 point drop from baseline on the 100-point Constant Murley Shoulder Outcome Score, while the controls lost a mean of 29.4 points. The Murley score measures shoulder pain, performance of daily tasks, range of motion, and strength; higher scores are better. Similarly, BES patients lost a mean of 16.2 points on the 50-point Neck Dissection Impairment Index, while controls lost 30.1 points, and controls performed markedly worse on nerve conduction studies. In short, BES patients “were less likely to have clinically significant shoulder dysfunction” after surgery, Dr. Barber said at the International Conference on Head and Neck Cancer, held by the American Head and Neck Society.
The APS electrode is a tiny silicone cuff with a metal conductor. The device was originally designed to monitor recurrent laryngeal nerve function during thyroid surgery. “We had [Medtronic] write a software patch” so it could be used for stimulation, she said.
The team is planning a larger, multicenter trial to shore up their findings, and also plans to test the device for hypoglossal nerve preservation after resection.
Transcutaneous nerve stimulation is another option, but it’s a bit uncomfortable and patients often don’t complete their sessions. “Compliance is not as good as with a single intraoperative procedure,” and the results aren’t that great. “We thought this might be a better alternative,” Dr. Barber said.
The two groups were well matched: Mean age was about 60 years and most patients had advanced-stage tumors. There was no difference in preop shoulder problems or risks for poor postop shoulder outcomes, and no difference in the number of level 5 neck dissections or mean number of lymph nodes removed during surgery.
There was no outside funding for the work. Dr. Barber had no disclosures; a coinvestigator was a Medtronic consultant.
SEATTLE – Direct, intraoperative electrical stimulation of the spinal accessory nerve reduced shoulder pain and dysfunction from oncologic neck dissection in a small, randomized trial.
Shoulder problems are common after neck dissection because of traction and compression of the spinal accessory nerve. Although brief electrical stimulation (BES) has been shown before to improve regeneration and recovery of injured peripheral nerves, it hasn’t been shown until now to help patients recover from neck surgery, said investigator Brittany Barber, MD, a fifth-year resident at the University of Alberta, Edmonton.
After neck dissection in 21 patients, the investigators wrapped a small electrode (Automatic Periodic Stimulation [APS] electrode, Medtronic) around the spinal accessory nerve at the base of the skull on the side of the neck with the most extensive nodal burden; the electrode delivered 100-msec pulses at 20 Hz and 3-5 V for an hour, and then the neck was closed. The team compared outcomes with 20 controls who had neck dissections without BES.
At 12 months, the BES group had an 8.4 point drop from baseline on the 100-point Constant Murley Shoulder Outcome Score, while the controls lost a mean of 29.4 points. The Murley score measures shoulder pain, performance of daily tasks, range of motion, and strength; higher scores are better. Similarly, BES patients lost a mean of 16.2 points on the 50-point Neck Dissection Impairment Index, while controls lost 30.1 points, and controls performed markedly worse on nerve conduction studies. In short, BES patients “were less likely to have clinically significant shoulder dysfunction” after surgery, Dr. Barber said at the International Conference on Head and Neck Cancer, held by the American Head and Neck Society.
The APS electrode is a tiny silicone cuff with a metal conductor. The device was originally designed to monitor recurrent laryngeal nerve function during thyroid surgery. “We had [Medtronic] write a software patch” so it could be used for stimulation, she said.
The team is planning a larger, multicenter trial to shore up their findings, and also plans to test the device for hypoglossal nerve preservation after resection.
Transcutaneous nerve stimulation is another option, but it’s a bit uncomfortable and patients often don’t complete their sessions. “Compliance is not as good as with a single intraoperative procedure,” and the results aren’t that great. “We thought this might be a better alternative,” Dr. Barber said.
The two groups were well matched: Mean age was about 60 years and most patients had advanced-stage tumors. There was no difference in preop shoulder problems or risks for poor postop shoulder outcomes, and no difference in the number of level 5 neck dissections or mean number of lymph nodes removed during surgery.
There was no outside funding for the work. Dr. Barber had no disclosures; a coinvestigator was a Medtronic consultant.
SEATTLE – Direct, intraoperative electrical stimulation of the spinal accessory nerve reduced shoulder pain and dysfunction from oncologic neck dissection in a small, randomized trial.
Shoulder problems are common after neck dissection because of traction and compression of the spinal accessory nerve. Although brief electrical stimulation (BES) has been shown before to improve regeneration and recovery of injured peripheral nerves, it hasn’t been shown until now to help patients recover from neck surgery, said investigator Brittany Barber, MD, a fifth-year resident at the University of Alberta, Edmonton.
After neck dissection in 21 patients, the investigators wrapped a small electrode (Automatic Periodic Stimulation [APS] electrode, Medtronic) around the spinal accessory nerve at the base of the skull on the side of the neck with the most extensive nodal burden; the electrode delivered 100-msec pulses at 20 Hz and 3-5 V for an hour, and then the neck was closed. The team compared outcomes with 20 controls who had neck dissections without BES.
At 12 months, the BES group had an 8.4 point drop from baseline on the 100-point Constant Murley Shoulder Outcome Score, while the controls lost a mean of 29.4 points. The Murley score measures shoulder pain, performance of daily tasks, range of motion, and strength; higher scores are better. Similarly, BES patients lost a mean of 16.2 points on the 50-point Neck Dissection Impairment Index, while controls lost 30.1 points, and controls performed markedly worse on nerve conduction studies. In short, BES patients “were less likely to have clinically significant shoulder dysfunction” after surgery, Dr. Barber said at the International Conference on Head and Neck Cancer, held by the American Head and Neck Society.
The APS electrode is a tiny silicone cuff with a metal conductor. The device was originally designed to monitor recurrent laryngeal nerve function during thyroid surgery. “We had [Medtronic] write a software patch” so it could be used for stimulation, she said.
The team is planning a larger, multicenter trial to shore up their findings, and also plans to test the device for hypoglossal nerve preservation after resection.
Transcutaneous nerve stimulation is another option, but it’s a bit uncomfortable and patients often don’t complete their sessions. “Compliance is not as good as with a single intraoperative procedure,” and the results aren’t that great. “We thought this might be a better alternative,” Dr. Barber said.
The two groups were well matched: Mean age was about 60 years and most patients had advanced-stage tumors. There was no difference in preop shoulder problems or risks for poor postop shoulder outcomes, and no difference in the number of level 5 neck dissections or mean number of lymph nodes removed during surgery.
There was no outside funding for the work. Dr. Barber had no disclosures; a coinvestigator was a Medtronic consultant.
AT AHNS 2016
Key clinical point: Direct, intraoperative electrical stimulation of the spinal accessory nerve reduces shoulder pain and dysfunction from oncologic neck dissection.
Major finding: At 12 months, the BES group had an 8.4 point drop from baseline on the 100-point Constant Murley Shoulder Score, while the controls lost a mean of 29.4 points.
Data source: Randomized trial with 41 patients.
Disclosures: There was no outside funding for the work. The presenter had no disclosures; a co-investigator was a Medtronic consultant.

Veteran Suicide Rate Up 32% Since 2001
Veteran suicides increased 32% from 2001 to 2014 according to a new VA report. The report also noted that rates for adult nonveterans also increased by 23% over the same period. However, veterans still account for 18% of all suicides in the U.S.
The report also highlighted a number of positive developments. For example, a previous study, conducted in 2012, estimated that 22 veterans committed suicide per day. That study included information from 3 million records obtained from mortality records in 20 states or data from veterans who used VHA health services. The more recent study, which examines 55 million veteran records from every state from 1979 to 2014, found that an average of 20 veterans per day die by suicide.
“Twenty a day is not that different from 22,” said David J. Shulkin, MD, VA Under Secretary for Health, in an interview. “It is far too high.”
Preventing veteran suicide is a top priority for the VA, and the recent report showed that the VA’s efforts are making an impact. For example, the rate of suicide among veterans who use VA services increased by 8.8% from 2001 to 2014, compared with a 38.6% increase in suicide among veterans who do not use VA services. These services include mental health treatment at VA medical centers, community-based outpatient clinics, and Vet Centers offering readjustment counseling.
In addition, the Veterans Crisis Line, launched in 2007, offers immediate support to veterans experiencing suicidal thoughts. To date, staffers have answered nearly 2.4 million calls and initiated the dispatch of emergency services to callers in crisis more than 62,000 times. The VA announced that it is expanding its Veterans Crisis Line by creating a satellite site in Atlanta, Georgia, and adding 200 additional responders.
“This collaborative effort provides both updated and comprehensive data that allow us to make better informed decisions on how to prevent this national tragedy,” said Dr. Shulkin, in a statement that previewed the survey results. “We as a nation must focus on bringing the number of veteran suicides to zero.”
Veteran suicides increased 32% from 2001 to 2014 according to a new VA report. The report also noted that rates for adult nonveterans also increased by 23% over the same period. However, veterans still account for 18% of all suicides in the U.S.
The report also highlighted a number of positive developments. For example, a previous study, conducted in 2012, estimated that 22 veterans committed suicide per day. That study included information from 3 million records obtained from mortality records in 20 states or data from veterans who used VHA health services. The more recent study, which examines 55 million veteran records from every state from 1979 to 2014, found that an average of 20 veterans per day die by suicide.
“Twenty a day is not that different from 22,” said David J. Shulkin, MD, VA Under Secretary for Health, in an interview. “It is far too high.”
Preventing veteran suicide is a top priority for the VA, and the recent report showed that the VA’s efforts are making an impact. For example, the rate of suicide among veterans who use VA services increased by 8.8% from 2001 to 2014, compared with a 38.6% increase in suicide among veterans who do not use VA services. These services include mental health treatment at VA medical centers, community-based outpatient clinics, and Vet Centers offering readjustment counseling.
In addition, the Veterans Crisis Line, launched in 2007, offers immediate support to veterans experiencing suicidal thoughts. To date, staffers have answered nearly 2.4 million calls and initiated the dispatch of emergency services to callers in crisis more than 62,000 times. The VA announced that it is expanding its Veterans Crisis Line by creating a satellite site in Atlanta, Georgia, and adding 200 additional responders.
“This collaborative effort provides both updated and comprehensive data that allow us to make better informed decisions on how to prevent this national tragedy,” said Dr. Shulkin, in a statement that previewed the survey results. “We as a nation must focus on bringing the number of veteran suicides to zero.”
Veteran suicides increased 32% from 2001 to 2014 according to a new VA report. The report also noted that rates for adult nonveterans also increased by 23% over the same period. However, veterans still account for 18% of all suicides in the U.S.
The report also highlighted a number of positive developments. For example, a previous study, conducted in 2012, estimated that 22 veterans committed suicide per day. That study included information from 3 million records obtained from mortality records in 20 states or data from veterans who used VHA health services. The more recent study, which examines 55 million veteran records from every state from 1979 to 2014, found that an average of 20 veterans per day die by suicide.
“Twenty a day is not that different from 22,” said David J. Shulkin, MD, VA Under Secretary for Health, in an interview. “It is far too high.”
Preventing veteran suicide is a top priority for the VA, and the recent report showed that the VA’s efforts are making an impact. For example, the rate of suicide among veterans who use VA services increased by 8.8% from 2001 to 2014, compared with a 38.6% increase in suicide among veterans who do not use VA services. These services include mental health treatment at VA medical centers, community-based outpatient clinics, and Vet Centers offering readjustment counseling.
In addition, the Veterans Crisis Line, launched in 2007, offers immediate support to veterans experiencing suicidal thoughts. To date, staffers have answered nearly 2.4 million calls and initiated the dispatch of emergency services to callers in crisis more than 62,000 times. The VA announced that it is expanding its Veterans Crisis Line by creating a satellite site in Atlanta, Georgia, and adding 200 additional responders.
“This collaborative effort provides both updated and comprehensive data that allow us to make better informed decisions on how to prevent this national tragedy,” said Dr. Shulkin, in a statement that previewed the survey results. “We as a nation must focus on bringing the number of veteran suicides to zero.”

Practical Tips for Injecting Cutaneous Fillers: Report From the AAD Meeting
In order to achieve optimal treatment results, clinicians must consider the anatomy of the head and neck when injecting cutaneous fillers in these areas. Dr. Anthony Rossi discusses the importance of knowing where and how to place the filler to attain the desired effect and provides practical tips for injecting the lateral cheeks, temple area, and masseter muscle.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
In order to achieve optimal treatment results, clinicians must consider the anatomy of the head and neck when injecting cutaneous fillers in these areas. Dr. Anthony Rossi discusses the importance of knowing where and how to place the filler to attain the desired effect and provides practical tips for injecting the lateral cheeks, temple area, and masseter muscle.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
In order to achieve optimal treatment results, clinicians must consider the anatomy of the head and neck when injecting cutaneous fillers in these areas. Dr. Anthony Rossi discusses the importance of knowing where and how to place the filler to attain the desired effect and provides practical tips for injecting the lateral cheeks, temple area, and masseter muscle.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel

HPV vaccination provides protection for immunocompromised children
A quadrivalent human papillomavirus vaccine provided adequate seroconversion response rates in immunocompromised children, according to Dr. C. Raina MacIntyre, MBBS, PhD, and her associates.
In a clinical trial of 59 immunocompromised children aged 5-18, seroconversion rates for HPV types 6, 11, 16, and 18 were 93.3%, 100%, 100%, and 88.9%, respectively, 7 months after receiving the first dose of vaccine. After 2 years, seroconversion rates for HPV types 6, 11, 16, and 18 were 82.2%, 91.1%, 91.1%, and 68.9%, respectively.

Local adverse events occurred in 16 patients after the first dose, but incidence decreased after the second and third doses. Injection site erythema, pain, and swelling were the most commonly reported adverse events. Minor disease flare occurred in two patients during the follow-up period, and one patient developed a squamous cell oral carcinoma, but the tumor could not be tested for HPV.
The data suggest “that HPV vaccine could be given earlier for immunosuppressed children, who are at higher risk of earlier onset cancers, but long-term follow-up studies are required to determine persistence of immunity,” the investigators said.
Find the full study in Vaccine (doi: 10.1016/j.vaccine.2016.06.049).
A quadrivalent human papillomavirus vaccine provided adequate seroconversion response rates in immunocompromised children, according to Dr. C. Raina MacIntyre, MBBS, PhD, and her associates.
In a clinical trial of 59 immunocompromised children aged 5-18, seroconversion rates for HPV types 6, 11, 16, and 18 were 93.3%, 100%, 100%, and 88.9%, respectively, 7 months after receiving the first dose of vaccine. After 2 years, seroconversion rates for HPV types 6, 11, 16, and 18 were 82.2%, 91.1%, 91.1%, and 68.9%, respectively.
Local adverse events occurred in 16 patients after the first dose, but incidence decreased after the second and third doses. Injection site erythema, pain, and swelling were the most commonly reported adverse events. Minor disease flare occurred in two patients during the follow-up period, and one patient developed a squamous cell oral carcinoma, but the tumor could not be tested for HPV.
The data suggest “that HPV vaccine could be given earlier for immunosuppressed children, who are at higher risk of earlier onset cancers, but long-term follow-up studies are required to determine persistence of immunity,” the investigators said.
Find the full study in Vaccine (doi: 10.1016/j.vaccine.2016.06.049).
A quadrivalent human papillomavirus vaccine provided adequate seroconversion response rates in immunocompromised children, according to Dr. C. Raina MacIntyre, MBBS, PhD, and her associates.
In a clinical trial of 59 immunocompromised children aged 5-18, seroconversion rates for HPV types 6, 11, 16, and 18 were 93.3%, 100%, 100%, and 88.9%, respectively, 7 months after receiving the first dose of vaccine. After 2 years, seroconversion rates for HPV types 6, 11, 16, and 18 were 82.2%, 91.1%, 91.1%, and 68.9%, respectively.
Local adverse events occurred in 16 patients after the first dose, but incidence decreased after the second and third doses. Injection site erythema, pain, and swelling were the most commonly reported adverse events. Minor disease flare occurred in two patients during the follow-up period, and one patient developed a squamous cell oral carcinoma, but the tumor could not be tested for HPV.
The data suggest “that HPV vaccine could be given earlier for immunosuppressed children, who are at higher risk of earlier onset cancers, but long-term follow-up studies are required to determine persistence of immunity,” the investigators said.
Find the full study in Vaccine (doi: 10.1016/j.vaccine.2016.06.049).
FROM VACCINE
