User login
Simultaneous integrated boost using stereotactic radiosurgery for resected brain metastases: rationale, dosimetric parameters, and preliminary clinical outcomes
Click on the PDF icon at the top of this introduction to read the full article.
Click on the PDF icon at the top of this introduction to read the full article.
Click on the PDF icon at the top of this introduction to read the full article.
Comparison of antiemetic efficacy and safety of palonosetron vs ondansetron in the prevention of chemotherapy-induced nausea and vomiting in children
Background Chemotherapy-induced nausea and vomiting (CINV) in children is a major side effect despite the use of combination antiemetic drugs.
Objective To compare the efficacy and safety profile of palonosetron, a second-generation 5-hydroxytryptamine-3 (5-HT3) receptor antagonist, with ondansetron in the prevention of CINV in children.
Methods A prospective, randomized, crossover study was conducted in patients aged 2-18 years. 160 chemotherapy cycles, consisting of chemotherapy drugs with moderate- and high-emetogenic potential, were studied. The study group received a single dose of intravenous (IV) palonosetron 5 mcg/kg, and the standard group received IV ondansetron 5 mg/m2 every 8 hours while receiving chemotherapy. The patients were observed for vomiting, use of rescue antiemetic medications, and nausea from Day 1 0-72 hours after completion of each chemotherapy cycle. All adverse events during the study period were recorded.
Results The overall percentage of patients with complete response (CR) in the palonosetron and ondansetron groups were 60% and 56.2%, respectively (P = .631). The CR rates in the palonosetron and ondansetron groups were 75% and 70%, respectively, in the acute phase (P = .479), and 68.8% and 65%, respectively, in the delayed phase (P = .614). There was no statistically significant difference in the CR rates cross both groups.
Conclusion A single dose of palonosetron is noninferior to ondansetron in the prevention of CINV in children and can be considered as an alternative antiemetic drug. There was no significant difference in adverse effects between the palonosetron and ondansetron group.
Click on the PDF icon at the top of this introduction to read the full article.
Background Chemotherapy-induced nausea and vomiting (CINV) in children is a major side effect despite the use of combination antiemetic drugs.
Objective To compare the efficacy and safety profile of palonosetron, a second-generation 5-hydroxytryptamine-3 (5-HT3) receptor antagonist, with ondansetron in the prevention of CINV in children.
Methods A prospective, randomized, crossover study was conducted in patients aged 2-18 years. 160 chemotherapy cycles, consisting of chemotherapy drugs with moderate- and high-emetogenic potential, were studied. The study group received a single dose of intravenous (IV) palonosetron 5 mcg/kg, and the standard group received IV ondansetron 5 mg/m2 every 8 hours while receiving chemotherapy. The patients were observed for vomiting, use of rescue antiemetic medications, and nausea from Day 1 0-72 hours after completion of each chemotherapy cycle. All adverse events during the study period were recorded.
Results The overall percentage of patients with complete response (CR) in the palonosetron and ondansetron groups were 60% and 56.2%, respectively (P = .631). The CR rates in the palonosetron and ondansetron groups were 75% and 70%, respectively, in the acute phase (P = .479), and 68.8% and 65%, respectively, in the delayed phase (P = .614). There was no statistically significant difference in the CR rates cross both groups.
Conclusion A single dose of palonosetron is noninferior to ondansetron in the prevention of CINV in children and can be considered as an alternative antiemetic drug. There was no significant difference in adverse effects between the palonosetron and ondansetron group.
Click on the PDF icon at the top of this introduction to read the full article.
Background Chemotherapy-induced nausea and vomiting (CINV) in children is a major side effect despite the use of combination antiemetic drugs.
Objective To compare the efficacy and safety profile of palonosetron, a second-generation 5-hydroxytryptamine-3 (5-HT3) receptor antagonist, with ondansetron in the prevention of CINV in children.
Methods A prospective, randomized, crossover study was conducted in patients aged 2-18 years. 160 chemotherapy cycles, consisting of chemotherapy drugs with moderate- and high-emetogenic potential, were studied. The study group received a single dose of intravenous (IV) palonosetron 5 mcg/kg, and the standard group received IV ondansetron 5 mg/m2 every 8 hours while receiving chemotherapy. The patients were observed for vomiting, use of rescue antiemetic medications, and nausea from Day 1 0-72 hours after completion of each chemotherapy cycle. All adverse events during the study period were recorded.
Results The overall percentage of patients with complete response (CR) in the palonosetron and ondansetron groups were 60% and 56.2%, respectively (P = .631). The CR rates in the palonosetron and ondansetron groups were 75% and 70%, respectively, in the acute phase (P = .479), and 68.8% and 65%, respectively, in the delayed phase (P = .614). There was no statistically significant difference in the CR rates cross both groups.
Conclusion A single dose of palonosetron is noninferior to ondansetron in the prevention of CINV in children and can be considered as an alternative antiemetic drug. There was no significant difference in adverse effects between the palonosetron and ondansetron group.
Click on the PDF icon at the top of this introduction to read the full article.
DDW: New scale measures impact of IBD on sexual function in men
WASHINGTON – Almost 40% of men with inflammatory bowel disease said the disease had a negative effect on their libido and almost 30% said that the disease had prevented them from having sex, in a study that used a new scale designed to evaluate sexual dysfunction in men with IBD, Dr. Aoibhlinn O’Toole reported at the annual Digestive Disease Week.
Dr. O’Toole, an IBD fellow at Beth Israel Deaconess Medical Center, Boston, developed the IBD Sexual Dysfunction Scale (IBDSDS) with her associates at Beth Israel Deaconess and Brigham and Women’s Hospital. The results of the study were based on 175 responses to the IBDSDS questionnaire, which were sent to all the adult male patients treated at the IBD clinics at both medical centers. The IBD-specific tool is now being validated.
Because there has been no IBD-specific scale to measure sexual dysfunction in this group of patients, they developed the IBDSDS and conducted the study to evaluate the prevalence of sexual dysfunction in male patients with IBD and identify factors associated with sexual dysfunction. The process of designing the scale included a literature search of generic questionnaires to identify relevant domains of sexual function and the addition of IBD-specific questions related to the effects of symptoms, medications, and surgery on sexual function.
Despite significant issues that can clearly affect sexuality in this group of patients – including perianal disease and the effect of treatment and symptoms on body image, intimacy, and sexual function – the extent and effects of sexual dysfunction in men with IBD is not well known, Dr. O’Toole pointed out.
The 43 questions in the scale include those that pertain to libido, ejaculation, satisfaction, and body image, as well as elements of two validated screening tools, the International Index of Erectile Function (IIEF), the gold standard screening tool for erectile dysfunction; and the Patient Health Questionnaire 9 (PHQ-9), for depression.
The average age of the 175 respondents was 43 years and the average duration of IBD was 14 years; 57% had Crohn’s disease, 33% had had surgery, 6% had chronic pain, 2% used narcotics, 12% had hypertension, and 4% had diabetes. Almost 90% were in a relationship that “could involve sexual activity” and 2% had not been sexually active in the previous year. In addition, 14% said that they felt that IBD had caused a breakup in an existing relationship, and 21% said they had felt hesitant about starting a new relationship because of IBD.
As for the effects of IBD on sexual function, in the last year, 38% felt that IBD had a negative effect on their libido, 27% said IBD prevented them from having sex, and 18% said that IBD caused problems during sex. In addition, 20% said that IBD made them feel guilty about having sex and 30% said they feared having sex; 2% reported having erectile dysfunction.
The use of erectile-enhancing medications were reported by 23% (prescribed mostly by doctors other than the physician treating the IBD) and 5% were taking testosterone to enhance sexual function. While 78% said they were comfortable speaking about sexual function with their gastroenterologist, only 10% said that their gastroenterologist had initiated a discussion about this topic, Dr. O’Toole said.
Based on other analyses of the results, “we found that impaired sexual function was associated with older age, longer duration of disease, active disease, comorbid depression, presence of an ostomy, and diabetes,” she added.
While the thrombotic risks of testosterone are clear, Dr. O’Toole noted that in patients with IBD, the effects of phosphodiesterase-5 (PDE5) inhibitors like sildenafil (Viagra) on the microcirculation within the gastrointestinal tract and whether the effects of these drugs contribute to microscopic ischemia in the GI tract is unclear, she said. Dr. O’Toole had no relevant financial disclosures.
WASHINGTON – Almost 40% of men with inflammatory bowel disease said the disease had a negative effect on their libido and almost 30% said that the disease had prevented them from having sex, in a study that used a new scale designed to evaluate sexual dysfunction in men with IBD, Dr. Aoibhlinn O’Toole reported at the annual Digestive Disease Week.
Dr. O’Toole, an IBD fellow at Beth Israel Deaconess Medical Center, Boston, developed the IBD Sexual Dysfunction Scale (IBDSDS) with her associates at Beth Israel Deaconess and Brigham and Women’s Hospital. The results of the study were based on 175 responses to the IBDSDS questionnaire, which were sent to all the adult male patients treated at the IBD clinics at both medical centers. The IBD-specific tool is now being validated.
Because there has been no IBD-specific scale to measure sexual dysfunction in this group of patients, they developed the IBDSDS and conducted the study to evaluate the prevalence of sexual dysfunction in male patients with IBD and identify factors associated with sexual dysfunction. The process of designing the scale included a literature search of generic questionnaires to identify relevant domains of sexual function and the addition of IBD-specific questions related to the effects of symptoms, medications, and surgery on sexual function.
Despite significant issues that can clearly affect sexuality in this group of patients – including perianal disease and the effect of treatment and symptoms on body image, intimacy, and sexual function – the extent and effects of sexual dysfunction in men with IBD is not well known, Dr. O’Toole pointed out.
The 43 questions in the scale include those that pertain to libido, ejaculation, satisfaction, and body image, as well as elements of two validated screening tools, the International Index of Erectile Function (IIEF), the gold standard screening tool for erectile dysfunction; and the Patient Health Questionnaire 9 (PHQ-9), for depression.
The average age of the 175 respondents was 43 years and the average duration of IBD was 14 years; 57% had Crohn’s disease, 33% had had surgery, 6% had chronic pain, 2% used narcotics, 12% had hypertension, and 4% had diabetes. Almost 90% were in a relationship that “could involve sexual activity” and 2% had not been sexually active in the previous year. In addition, 14% said that they felt that IBD had caused a breakup in an existing relationship, and 21% said they had felt hesitant about starting a new relationship because of IBD.
As for the effects of IBD on sexual function, in the last year, 38% felt that IBD had a negative effect on their libido, 27% said IBD prevented them from having sex, and 18% said that IBD caused problems during sex. In addition, 20% said that IBD made them feel guilty about having sex and 30% said they feared having sex; 2% reported having erectile dysfunction.
The use of erectile-enhancing medications were reported by 23% (prescribed mostly by doctors other than the physician treating the IBD) and 5% were taking testosterone to enhance sexual function. While 78% said they were comfortable speaking about sexual function with their gastroenterologist, only 10% said that their gastroenterologist had initiated a discussion about this topic, Dr. O’Toole said.
Based on other analyses of the results, “we found that impaired sexual function was associated with older age, longer duration of disease, active disease, comorbid depression, presence of an ostomy, and diabetes,” she added.
While the thrombotic risks of testosterone are clear, Dr. O’Toole noted that in patients with IBD, the effects of phosphodiesterase-5 (PDE5) inhibitors like sildenafil (Viagra) on the microcirculation within the gastrointestinal tract and whether the effects of these drugs contribute to microscopic ischemia in the GI tract is unclear, she said. Dr. O’Toole had no relevant financial disclosures.
WASHINGTON – Almost 40% of men with inflammatory bowel disease said the disease had a negative effect on their libido and almost 30% said that the disease had prevented them from having sex, in a study that used a new scale designed to evaluate sexual dysfunction in men with IBD, Dr. Aoibhlinn O’Toole reported at the annual Digestive Disease Week.
Dr. O’Toole, an IBD fellow at Beth Israel Deaconess Medical Center, Boston, developed the IBD Sexual Dysfunction Scale (IBDSDS) with her associates at Beth Israel Deaconess and Brigham and Women’s Hospital. The results of the study were based on 175 responses to the IBDSDS questionnaire, which were sent to all the adult male patients treated at the IBD clinics at both medical centers. The IBD-specific tool is now being validated.
Because there has been no IBD-specific scale to measure sexual dysfunction in this group of patients, they developed the IBDSDS and conducted the study to evaluate the prevalence of sexual dysfunction in male patients with IBD and identify factors associated with sexual dysfunction. The process of designing the scale included a literature search of generic questionnaires to identify relevant domains of sexual function and the addition of IBD-specific questions related to the effects of symptoms, medications, and surgery on sexual function.
Despite significant issues that can clearly affect sexuality in this group of patients – including perianal disease and the effect of treatment and symptoms on body image, intimacy, and sexual function – the extent and effects of sexual dysfunction in men with IBD is not well known, Dr. O’Toole pointed out.
The 43 questions in the scale include those that pertain to libido, ejaculation, satisfaction, and body image, as well as elements of two validated screening tools, the International Index of Erectile Function (IIEF), the gold standard screening tool for erectile dysfunction; and the Patient Health Questionnaire 9 (PHQ-9), for depression.
The average age of the 175 respondents was 43 years and the average duration of IBD was 14 years; 57% had Crohn’s disease, 33% had had surgery, 6% had chronic pain, 2% used narcotics, 12% had hypertension, and 4% had diabetes. Almost 90% were in a relationship that “could involve sexual activity” and 2% had not been sexually active in the previous year. In addition, 14% said that they felt that IBD had caused a breakup in an existing relationship, and 21% said they had felt hesitant about starting a new relationship because of IBD.
As for the effects of IBD on sexual function, in the last year, 38% felt that IBD had a negative effect on their libido, 27% said IBD prevented them from having sex, and 18% said that IBD caused problems during sex. In addition, 20% said that IBD made them feel guilty about having sex and 30% said they feared having sex; 2% reported having erectile dysfunction.
The use of erectile-enhancing medications were reported by 23% (prescribed mostly by doctors other than the physician treating the IBD) and 5% were taking testosterone to enhance sexual function. While 78% said they were comfortable speaking about sexual function with their gastroenterologist, only 10% said that their gastroenterologist had initiated a discussion about this topic, Dr. O’Toole said.
Based on other analyses of the results, “we found that impaired sexual function was associated with older age, longer duration of disease, active disease, comorbid depression, presence of an ostomy, and diabetes,” she added.
While the thrombotic risks of testosterone are clear, Dr. O’Toole noted that in patients with IBD, the effects of phosphodiesterase-5 (PDE5) inhibitors like sildenafil (Viagra) on the microcirculation within the gastrointestinal tract and whether the effects of these drugs contribute to microscopic ischemia in the GI tract is unclear, she said. Dr. O’Toole had no relevant financial disclosures.
AT DDW 2015
Key clinical point: Once validated, a new scale designed to evaluate sexual dysfunction in men with inflammatory bowel disease could provide a useful tool to evaluate the impact the disease has on sexual function in male patients.
Major finding: The negative effects of IBD on sexual dysfunction in men with the disease, reflected in the responses to the IBD-specific questionnaire, included negative effects on libido in 38% and fear of having sex in 30%.
Data source: Results were based on the responses to the questionnaire from 175 male patients treated at the IBD clinics at two Boston medical centers.
Disclosures: Dr. O’Toole had no relevant financial disclosures.
DDW: Budesonide improves dysphagia, histology, and endoscopic findings in EoE
WASHINGTON – Treatment with an oral formulation of budesonide was associated with significant improvements in dysphagia and esophageal eosinophil counts in adolescents and adults with eosinophilic esophagitis, in a study that is also the first to use a recently validated scoring instrument to evaluate medical therapy for this disorder in a randomized trial.
Results of the multicenter, double-blind, randomized study comparing treatment with an oral budesonide suspension to placebo for 12 weeks in almost 100 patients with eosinophilic esophagitis (EoE) were reported in two separate presentations at the annual Digestive Disease Week. One of the investigators, Dr. Evan Dellon of the Center for Gastrointestinal Biology and Disease, at the University of North Carolina, Chapel Hill, said that treatment with this “mucoadherent” formulation of the topical steroid was associated with significant improvements in dysphagia symptoms, as measured with the Dysphagia Symptom Questionnaire (DSQ), and a histologic response rate of 39%, vs. 3% among those on placebo.
“The study not only adds to the evidence that topical budesonide is effective for inducing histologic response in subjects with active EoE, but [also] shows for the first time that symptoms of dysphagia, as measured with a validated symptom instrument, improve concordantly with the histologic and endoscopic findings,” Dr. Dellon said in an interview after the meeting. “Moreover, this study shows that a topical steroid formulation designed specifically for EoE, rather than an asthma formulation that is adapted for esophageal use, will likely be a beneficial and potentially preferred clinical treatment option.”
Another study investigator, Dr. Ikuo Hirano, professor of medicine and director of the gastroenterology and hepatology fellowship program at Northwestern University, Chicago, reported that treatment was also associated with significant improvements in the EoE Endoscopic Reference Score, EREFS, which was designed to classify and grade the severity of five major endoscopic features of EoE: edema, rings, exudates, furrows, and stricture formation. This was the first study to use this validated endoscopic scoring instrument in a randomized controlled trial of a medical therapy in patients with EoE, he said at the meeting.

The study was conducted between 2012 and 2014 at 25 U.S. sites, in patients aged 11-40 years with EoE. Baseline demographic and endoscopic characteristics were similar in the two groups. Their mean age was 21-22 years (41% of those on placebo and 35% of those on budesonide were younger than age 18 years) and 69% were male; most patients had edema, all had dysphagia, and 39%-41% had heartburn. Patients were excluded if they had esophageal stricture on screening endoscopy that did not allow passage of a standard adult diagnostic endoscope.
Patients were randomized to treatment with budesonide suspension, at a dose of 2 mg twice a day (51 patients) or a placebo suspension (42 patients). The primary outcomes were a change in the DSQ score from baseline, and the proportion of patients with a histologic response, defined as at least 6 eosinophils per high-power field (eos/hpf) from all biopsies. The final analysis included 87 patients.
At baseline, the mean peak eosinophil counts were 156/hpf among those on budesonide and 130/hpf among those on placebo; after treatment, the mean peak counts dropped to 39/hpf among those on budesonide (a 65% reduction) and to 113/hpf among those on placebo (a 10% reduction), a statistically significant difference (P < .05), said Dr. Dellon, also with the department of medicine at UNC.
From a mean of about 29 in both groups at baseline, DSQ scores dropped by a mean of 14.3 among the treated patients, vs. 7.5 among those on placebo, which was a statistically significant difference (P = .0096). The other primary endpoint, the histologic response rate, was 39% among treated patients, vs. 3% among those on placebo, also a significant difference (P < .0001).
Adverse events were not different between the two groups, and growth velocity among those under age 18 years and cortisol levels were not different between the two groups, he added. There was one case of esophageal candidiasis in a patient on budesonide.
During his presentation, Dr. Hirano said that there were also significant improvements in EREFS scores from baseline in the proximal and distal esophagus among those treated with budesonide, but not among those on placebo. Based on EREFS scores, oral budesonide “resulted in significant improvement in endoscopic features of edema, exudate, rings, [and] furrows, compared to placebo,” but there was no significant change in strictures, another component of the EREFS, in either the treatment or placebo groups. However, patients with high-grade strictures were not enrolled in the study, he added.
After treatment, proximal, distal, and total EREFS scores correlated with peak eosinophil counts, a highly statistically significant finding.
Dr. Hirano said that the primary endpoints used in most EoE clinical trials to date have focused mostly on assessments of symptoms and histopathology, which have limitations. “Symptoms are difficult to quantify and often intermittent [and] they may improve as a result of changes in eating behavior and food avoidance,” he said. Patient-reported outcome instruments have been recently validated, “but have questionable utility in clinical practice” and histology “has shown limited correlation between degree of esophageal eosinophilia and symptom severity [and does not] assess for modeling, an important determinant of overall disease complications,” he added.
The utility of endoscopy in EoE includes the features that are present in vast majority of patients with EoE, and provides a gross assessment of overall disease activity, “both in terms of inflammatory and fibrostenotic features,” he said.
“Endoscopic outcomes are now emerging as clinically relevant endpoints of therapy of trials of eosinophilic esophagitis that supports and complements” symptom and histologic assessments, Dr. Hirano commented, adding that more studies are need to determine the “relative importance of these individual endoscopic features as well as the appropriate utilization of endoscopic parameters in disease management.”
The study was funded by Meritage Pharma, recently acquired by the Shire group of companies. All authors received research funds to conduct the study, and Dr. Hirano disclosed having worked as a consultant for Meritage. Dr. Dellon’s disclosures included receiving grant and research support from Meritage. Shire is developing the oral budesonide suspension formulation as a treatment for adolescents and adults with EoE.
WASHINGTON – Treatment with an oral formulation of budesonide was associated with significant improvements in dysphagia and esophageal eosinophil counts in adolescents and adults with eosinophilic esophagitis, in a study that is also the first to use a recently validated scoring instrument to evaluate medical therapy for this disorder in a randomized trial.
Results of the multicenter, double-blind, randomized study comparing treatment with an oral budesonide suspension to placebo for 12 weeks in almost 100 patients with eosinophilic esophagitis (EoE) were reported in two separate presentations at the annual Digestive Disease Week. One of the investigators, Dr. Evan Dellon of the Center for Gastrointestinal Biology and Disease, at the University of North Carolina, Chapel Hill, said that treatment with this “mucoadherent” formulation of the topical steroid was associated with significant improvements in dysphagia symptoms, as measured with the Dysphagia Symptom Questionnaire (DSQ), and a histologic response rate of 39%, vs. 3% among those on placebo.
“The study not only adds to the evidence that topical budesonide is effective for inducing histologic response in subjects with active EoE, but [also] shows for the first time that symptoms of dysphagia, as measured with a validated symptom instrument, improve concordantly with the histologic and endoscopic findings,” Dr. Dellon said in an interview after the meeting. “Moreover, this study shows that a topical steroid formulation designed specifically for EoE, rather than an asthma formulation that is adapted for esophageal use, will likely be a beneficial and potentially preferred clinical treatment option.”
Another study investigator, Dr. Ikuo Hirano, professor of medicine and director of the gastroenterology and hepatology fellowship program at Northwestern University, Chicago, reported that treatment was also associated with significant improvements in the EoE Endoscopic Reference Score, EREFS, which was designed to classify and grade the severity of five major endoscopic features of EoE: edema, rings, exudates, furrows, and stricture formation. This was the first study to use this validated endoscopic scoring instrument in a randomized controlled trial of a medical therapy in patients with EoE, he said at the meeting.
The study was conducted between 2012 and 2014 at 25 U.S. sites, in patients aged 11-40 years with EoE. Baseline demographic and endoscopic characteristics were similar in the two groups. Their mean age was 21-22 years (41% of those on placebo and 35% of those on budesonide were younger than age 18 years) and 69% were male; most patients had edema, all had dysphagia, and 39%-41% had heartburn. Patients were excluded if they had esophageal stricture on screening endoscopy that did not allow passage of a standard adult diagnostic endoscope.
Patients were randomized to treatment with budesonide suspension, at a dose of 2 mg twice a day (51 patients) or a placebo suspension (42 patients). The primary outcomes were a change in the DSQ score from baseline, and the proportion of patients with a histologic response, defined as at least 6 eosinophils per high-power field (eos/hpf) from all biopsies. The final analysis included 87 patients.
At baseline, the mean peak eosinophil counts were 156/hpf among those on budesonide and 130/hpf among those on placebo; after treatment, the mean peak counts dropped to 39/hpf among those on budesonide (a 65% reduction) and to 113/hpf among those on placebo (a 10% reduction), a statistically significant difference (P < .05), said Dr. Dellon, also with the department of medicine at UNC.
From a mean of about 29 in both groups at baseline, DSQ scores dropped by a mean of 14.3 among the treated patients, vs. 7.5 among those on placebo, which was a statistically significant difference (P = .0096). The other primary endpoint, the histologic response rate, was 39% among treated patients, vs. 3% among those on placebo, also a significant difference (P < .0001).
Adverse events were not different between the two groups, and growth velocity among those under age 18 years and cortisol levels were not different between the two groups, he added. There was one case of esophageal candidiasis in a patient on budesonide.
During his presentation, Dr. Hirano said that there were also significant improvements in EREFS scores from baseline in the proximal and distal esophagus among those treated with budesonide, but not among those on placebo. Based on EREFS scores, oral budesonide “resulted in significant improvement in endoscopic features of edema, exudate, rings, [and] furrows, compared to placebo,” but there was no significant change in strictures, another component of the EREFS, in either the treatment or placebo groups. However, patients with high-grade strictures were not enrolled in the study, he added.
After treatment, proximal, distal, and total EREFS scores correlated with peak eosinophil counts, a highly statistically significant finding.
Dr. Hirano said that the primary endpoints used in most EoE clinical trials to date have focused mostly on assessments of symptoms and histopathology, which have limitations. “Symptoms are difficult to quantify and often intermittent [and] they may improve as a result of changes in eating behavior and food avoidance,” he said. Patient-reported outcome instruments have been recently validated, “but have questionable utility in clinical practice” and histology “has shown limited correlation between degree of esophageal eosinophilia and symptom severity [and does not] assess for modeling, an important determinant of overall disease complications,” he added.
The utility of endoscopy in EoE includes the features that are present in vast majority of patients with EoE, and provides a gross assessment of overall disease activity, “both in terms of inflammatory and fibrostenotic features,” he said.
“Endoscopic outcomes are now emerging as clinically relevant endpoints of therapy of trials of eosinophilic esophagitis that supports and complements” symptom and histologic assessments, Dr. Hirano commented, adding that more studies are need to determine the “relative importance of these individual endoscopic features as well as the appropriate utilization of endoscopic parameters in disease management.”
The study was funded by Meritage Pharma, recently acquired by the Shire group of companies. All authors received research funds to conduct the study, and Dr. Hirano disclosed having worked as a consultant for Meritage. Dr. Dellon’s disclosures included receiving grant and research support from Meritage. Shire is developing the oral budesonide suspension formulation as a treatment for adolescents and adults with EoE.
WASHINGTON – Treatment with an oral formulation of budesonide was associated with significant improvements in dysphagia and esophageal eosinophil counts in adolescents and adults with eosinophilic esophagitis, in a study that is also the first to use a recently validated scoring instrument to evaluate medical therapy for this disorder in a randomized trial.
Results of the multicenter, double-blind, randomized study comparing treatment with an oral budesonide suspension to placebo for 12 weeks in almost 100 patients with eosinophilic esophagitis (EoE) were reported in two separate presentations at the annual Digestive Disease Week. One of the investigators, Dr. Evan Dellon of the Center for Gastrointestinal Biology and Disease, at the University of North Carolina, Chapel Hill, said that treatment with this “mucoadherent” formulation of the topical steroid was associated with significant improvements in dysphagia symptoms, as measured with the Dysphagia Symptom Questionnaire (DSQ), and a histologic response rate of 39%, vs. 3% among those on placebo.
“The study not only adds to the evidence that topical budesonide is effective for inducing histologic response in subjects with active EoE, but [also] shows for the first time that symptoms of dysphagia, as measured with a validated symptom instrument, improve concordantly with the histologic and endoscopic findings,” Dr. Dellon said in an interview after the meeting. “Moreover, this study shows that a topical steroid formulation designed specifically for EoE, rather than an asthma formulation that is adapted for esophageal use, will likely be a beneficial and potentially preferred clinical treatment option.”
Another study investigator, Dr. Ikuo Hirano, professor of medicine and director of the gastroenterology and hepatology fellowship program at Northwestern University, Chicago, reported that treatment was also associated with significant improvements in the EoE Endoscopic Reference Score, EREFS, which was designed to classify and grade the severity of five major endoscopic features of EoE: edema, rings, exudates, furrows, and stricture formation. This was the first study to use this validated endoscopic scoring instrument in a randomized controlled trial of a medical therapy in patients with EoE, he said at the meeting.
The study was conducted between 2012 and 2014 at 25 U.S. sites, in patients aged 11-40 years with EoE. Baseline demographic and endoscopic characteristics were similar in the two groups. Their mean age was 21-22 years (41% of those on placebo and 35% of those on budesonide were younger than age 18 years) and 69% were male; most patients had edema, all had dysphagia, and 39%-41% had heartburn. Patients were excluded if they had esophageal stricture on screening endoscopy that did not allow passage of a standard adult diagnostic endoscope.
Patients were randomized to treatment with budesonide suspension, at a dose of 2 mg twice a day (51 patients) or a placebo suspension (42 patients). The primary outcomes were a change in the DSQ score from baseline, and the proportion of patients with a histologic response, defined as at least 6 eosinophils per high-power field (eos/hpf) from all biopsies. The final analysis included 87 patients.
At baseline, the mean peak eosinophil counts were 156/hpf among those on budesonide and 130/hpf among those on placebo; after treatment, the mean peak counts dropped to 39/hpf among those on budesonide (a 65% reduction) and to 113/hpf among those on placebo (a 10% reduction), a statistically significant difference (P < .05), said Dr. Dellon, also with the department of medicine at UNC.
From a mean of about 29 in both groups at baseline, DSQ scores dropped by a mean of 14.3 among the treated patients, vs. 7.5 among those on placebo, which was a statistically significant difference (P = .0096). The other primary endpoint, the histologic response rate, was 39% among treated patients, vs. 3% among those on placebo, also a significant difference (P < .0001).
Adverse events were not different between the two groups, and growth velocity among those under age 18 years and cortisol levels were not different between the two groups, he added. There was one case of esophageal candidiasis in a patient on budesonide.
During his presentation, Dr. Hirano said that there were also significant improvements in EREFS scores from baseline in the proximal and distal esophagus among those treated with budesonide, but not among those on placebo. Based on EREFS scores, oral budesonide “resulted in significant improvement in endoscopic features of edema, exudate, rings, [and] furrows, compared to placebo,” but there was no significant change in strictures, another component of the EREFS, in either the treatment or placebo groups. However, patients with high-grade strictures were not enrolled in the study, he added.
After treatment, proximal, distal, and total EREFS scores correlated with peak eosinophil counts, a highly statistically significant finding.
Dr. Hirano said that the primary endpoints used in most EoE clinical trials to date have focused mostly on assessments of symptoms and histopathology, which have limitations. “Symptoms are difficult to quantify and often intermittent [and] they may improve as a result of changes in eating behavior and food avoidance,” he said. Patient-reported outcome instruments have been recently validated, “but have questionable utility in clinical practice” and histology “has shown limited correlation between degree of esophageal eosinophilia and symptom severity [and does not] assess for modeling, an important determinant of overall disease complications,” he added.
The utility of endoscopy in EoE includes the features that are present in vast majority of patients with EoE, and provides a gross assessment of overall disease activity, “both in terms of inflammatory and fibrostenotic features,” he said.
“Endoscopic outcomes are now emerging as clinically relevant endpoints of therapy of trials of eosinophilic esophagitis that supports and complements” symptom and histologic assessments, Dr. Hirano commented, adding that more studies are need to determine the “relative importance of these individual endoscopic features as well as the appropriate utilization of endoscopic parameters in disease management.”
The study was funded by Meritage Pharma, recently acquired by the Shire group of companies. All authors received research funds to conduct the study, and Dr. Hirano disclosed having worked as a consultant for Meritage. Dr. Dellon’s disclosures included receiving grant and research support from Meritage. Shire is developing the oral budesonide suspension formulation as a treatment for adolescents and adults with EoE.
AT DDW 2015
Key clinical point: A mucoadherent oral formulation of budesonide shows promise as an effective treatment for eosinophilic esophagitis (EoE), with a favorable safety profile.
Major finding: Beneficial effects of oral budesonide in a study of adolescents and adults with EoE included a histologic response rate of 39% and significantly improved dysphagia symptoms.
Data source: A randomized, double-blind multicenter U.S. study evaluated the healing effects and response to of oral budesonide vs. placebo in 93 patients with EoE, aged 11-40 years.
Disclosures: The study was funded by Meritage Pharma, recently acquired by the Shire group of companies. All authors received research funds to conduct the study. Dr. Dellon’s disclosures included receiving grant and research support from Meritage. Dr. Hirano disclosed having worked as a consultant for Meritage.

EZH2 inhibitor proves active in rel/ref NHL

LUGANO—The EZH2 inhibitor tazemetostat (EPZ-6438) has shown “meaningful clinical activity” as monotherapy in patients with advanced non-Hodgkin lymphoma (NHL), according to researchers.
In a phase 1 trial, 9 of the 15 evaluable NHL patients achieved an objective response to tazemetostat.
This included 2 ongoing complete responses (CRs), 1 in a patient with diffuse large B-cell lymphoma (DLBCL) and 1 in a patient with follicular lymphoma (FL).
It also included a partial response (PR) in the first treated patient with an EZH2 mutation.
And researchers said the drug was largely well-tolerated, as most adverse events were grade 1 or 2.
“The breadth, depth, and durability of responses seen in NHL patients among multiple histologies continue to impress, as does the safety and tolerability of tazemetostat in this phase 1 study,” said Vincent Ribrag, MD, of Institut Gustave Roussy in Villejuif, France.
“Among the patients in the dose-escalation cohorts, we have seen a noteworthy deepening of responses over time, and, in the first treated patient with an EZH2 tumor mutation, we have seen a partial response, which is very encouraging.”
Dr Ribrag presented these results at the 13th International Conference on Malignant Lymphoma (abstract 145*). The study, which was previously presented at the 26th EORTC-NCI-AACR Symposium on Molecular Targets and Cancer Therapeutics, was sponsored by Epizyme, Inc., the company developing tazemetostat.
The phase 1 trial has enrolled 19 patients with relapsed or refractory B-cell NHL and 26 patients with advanced solid tumors.
Researchers have evaluated 5 cohorts of patients in the dose-escalation portion of the study—100 mg, 200 mg, 400 mg, 800 mg, and 1600 mg—and 2 cohorts—800 mg and 1600 mg—in the dose-expansion phase. All doses of tazemetostat were given twice daily.
The 19 NHL patients had a median age of 61 (range, 24-84) and were heavily pretreated. Eighty-five percent had received 3 or more prior therapies, and 37% had received 5 or more prior therapies.
Thirty-seven percent of patients were refractory to their last prior regimen, and 26% had received a prior autologous hematopoietic stem cell transplant.
Dosing and efficacy
As of June 8, 2015, 15 NHL patients were evaluable for efficacy. Nine had achieved an objective response, including 2 patients with an ongoing CR. All responses were observed between 2 and 10 months on therapy.
Five of the 9 evaluable patients with DLBCL achieved an objective response. One DLBCL patient with a CR remains on study at 18 months of treatment.
Three of 5 evaluable patients with follicular lymphoma (FL) achieved an objective response. One FL patient with a CR remains on study at 13 months, and 1 FL patient with a PR remains on study at 13 months.
The only patient with marginal zone lymphoma achieved a PR and continues on study at 11 months.
One of the 14 patients evaluated for EZH2 status has a specific EZH2 tumor mutation (Y646H). This patient, who had DLBCL that relapsed or was refractory to 6 previous treatment regimens, achieved a PR after 16 weeks of therapy and remains on study.
The recommended phase 2 dose of tazemetostat is 800 mg twice daily.
Adverse events and next steps
All of the 45 enrolled patients were evaluable for safety. Treatment-related adverse events included asthenia (n=10), nausea (n=6), dyspepsia (n=5), thrombocytopenia (n=4), anorexia (n=4), anemia (n=4), vomiting (n=3), constipation (n=2), muscle spasm (n=2), hypertension (n=2), neutropenia (n=2), and elevated transaminase (n=1).
There were 5 grade 3 or higher adverse events related to treatment, including grade 3 anorexia, grade 3 hypertension, grade 3 transaminase elevation, grade 4 thrombocytopenia, and grade 4 neutropenia.
Epizyme plans to report a further update from this trial by the end of this year. The company is now enrolling patients in a phase 2 study of tazemetostat monotherapy in patients with relapsed or refractory NHL, stratified by cell of origin and EZH2 mutation status.
Epizyme is also planning a phase 2 trial of tazemetostat in adults with INI1-deficient solid tumors, a phase 1 study of pediatric patients with INI1-deficient solid tumors, a combination study of tazemetostat with R-CHOP in patients with DLBCL, and a combination study of tazemetostat with a B-cell signaling agent or other emerging targeted therapies for B-cell lymphomas. ![]()
*Information in the abstract differs from that presented at the meeting.
LUGANO—The EZH2 inhibitor tazemetostat (EPZ-6438) has shown “meaningful clinical activity” as monotherapy in patients with advanced non-Hodgkin lymphoma (NHL), according to researchers.
In a phase 1 trial, 9 of the 15 evaluable NHL patients achieved an objective response to tazemetostat.
This included 2 ongoing complete responses (CRs), 1 in a patient with diffuse large B-cell lymphoma (DLBCL) and 1 in a patient with follicular lymphoma (FL).
It also included a partial response (PR) in the first treated patient with an EZH2 mutation.
And researchers said the drug was largely well-tolerated, as most adverse events were grade 1 or 2.
“The breadth, depth, and durability of responses seen in NHL patients among multiple histologies continue to impress, as does the safety and tolerability of tazemetostat in this phase 1 study,” said Vincent Ribrag, MD, of Institut Gustave Roussy in Villejuif, France.
“Among the patients in the dose-escalation cohorts, we have seen a noteworthy deepening of responses over time, and, in the first treated patient with an EZH2 tumor mutation, we have seen a partial response, which is very encouraging.”
Dr Ribrag presented these results at the 13th International Conference on Malignant Lymphoma (abstract 145*). The study, which was previously presented at the 26th EORTC-NCI-AACR Symposium on Molecular Targets and Cancer Therapeutics, was sponsored by Epizyme, Inc., the company developing tazemetostat.
The phase 1 trial has enrolled 19 patients with relapsed or refractory B-cell NHL and 26 patients with advanced solid tumors.
Researchers have evaluated 5 cohorts of patients in the dose-escalation portion of the study—100 mg, 200 mg, 400 mg, 800 mg, and 1600 mg—and 2 cohorts—800 mg and 1600 mg—in the dose-expansion phase. All doses of tazemetostat were given twice daily.
The 19 NHL patients had a median age of 61 (range, 24-84) and were heavily pretreated. Eighty-five percent had received 3 or more prior therapies, and 37% had received 5 or more prior therapies.
Thirty-seven percent of patients were refractory to their last prior regimen, and 26% had received a prior autologous hematopoietic stem cell transplant.
Dosing and efficacy
As of June 8, 2015, 15 NHL patients were evaluable for efficacy. Nine had achieved an objective response, including 2 patients with an ongoing CR. All responses were observed between 2 and 10 months on therapy.
Five of the 9 evaluable patients with DLBCL achieved an objective response. One DLBCL patient with a CR remains on study at 18 months of treatment.
Three of 5 evaluable patients with follicular lymphoma (FL) achieved an objective response. One FL patient with a CR remains on study at 13 months, and 1 FL patient with a PR remains on study at 13 months.
The only patient with marginal zone lymphoma achieved a PR and continues on study at 11 months.
One of the 14 patients evaluated for EZH2 status has a specific EZH2 tumor mutation (Y646H). This patient, who had DLBCL that relapsed or was refractory to 6 previous treatment regimens, achieved a PR after 16 weeks of therapy and remains on study.
The recommended phase 2 dose of tazemetostat is 800 mg twice daily.
Adverse events and next steps
All of the 45 enrolled patients were evaluable for safety. Treatment-related adverse events included asthenia (n=10), nausea (n=6), dyspepsia (n=5), thrombocytopenia (n=4), anorexia (n=4), anemia (n=4), vomiting (n=3), constipation (n=2), muscle spasm (n=2), hypertension (n=2), neutropenia (n=2), and elevated transaminase (n=1).
There were 5 grade 3 or higher adverse events related to treatment, including grade 3 anorexia, grade 3 hypertension, grade 3 transaminase elevation, grade 4 thrombocytopenia, and grade 4 neutropenia.
Epizyme plans to report a further update from this trial by the end of this year. The company is now enrolling patients in a phase 2 study of tazemetostat monotherapy in patients with relapsed or refractory NHL, stratified by cell of origin and EZH2 mutation status.
Epizyme is also planning a phase 2 trial of tazemetostat in adults with INI1-deficient solid tumors, a phase 1 study of pediatric patients with INI1-deficient solid tumors, a combination study of tazemetostat with R-CHOP in patients with DLBCL, and a combination study of tazemetostat with a B-cell signaling agent or other emerging targeted therapies for B-cell lymphomas. ![]()
*Information in the abstract differs from that presented at the meeting.
LUGANO—The EZH2 inhibitor tazemetostat (EPZ-6438) has shown “meaningful clinical activity” as monotherapy in patients with advanced non-Hodgkin lymphoma (NHL), according to researchers.
In a phase 1 trial, 9 of the 15 evaluable NHL patients achieved an objective response to tazemetostat.
This included 2 ongoing complete responses (CRs), 1 in a patient with diffuse large B-cell lymphoma (DLBCL) and 1 in a patient with follicular lymphoma (FL).
It also included a partial response (PR) in the first treated patient with an EZH2 mutation.
And researchers said the drug was largely well-tolerated, as most adverse events were grade 1 or 2.
“The breadth, depth, and durability of responses seen in NHL patients among multiple histologies continue to impress, as does the safety and tolerability of tazemetostat in this phase 1 study,” said Vincent Ribrag, MD, of Institut Gustave Roussy in Villejuif, France.
“Among the patients in the dose-escalation cohorts, we have seen a noteworthy deepening of responses over time, and, in the first treated patient with an EZH2 tumor mutation, we have seen a partial response, which is very encouraging.”
Dr Ribrag presented these results at the 13th International Conference on Malignant Lymphoma (abstract 145*). The study, which was previously presented at the 26th EORTC-NCI-AACR Symposium on Molecular Targets and Cancer Therapeutics, was sponsored by Epizyme, Inc., the company developing tazemetostat.
The phase 1 trial has enrolled 19 patients with relapsed or refractory B-cell NHL and 26 patients with advanced solid tumors.
Researchers have evaluated 5 cohorts of patients in the dose-escalation portion of the study—100 mg, 200 mg, 400 mg, 800 mg, and 1600 mg—and 2 cohorts—800 mg and 1600 mg—in the dose-expansion phase. All doses of tazemetostat were given twice daily.
The 19 NHL patients had a median age of 61 (range, 24-84) and were heavily pretreated. Eighty-five percent had received 3 or more prior therapies, and 37% had received 5 or more prior therapies.
Thirty-seven percent of patients were refractory to their last prior regimen, and 26% had received a prior autologous hematopoietic stem cell transplant.
Dosing and efficacy
As of June 8, 2015, 15 NHL patients were evaluable for efficacy. Nine had achieved an objective response, including 2 patients with an ongoing CR. All responses were observed between 2 and 10 months on therapy.
Five of the 9 evaluable patients with DLBCL achieved an objective response. One DLBCL patient with a CR remains on study at 18 months of treatment.
Three of 5 evaluable patients with follicular lymphoma (FL) achieved an objective response. One FL patient with a CR remains on study at 13 months, and 1 FL patient with a PR remains on study at 13 months.
The only patient with marginal zone lymphoma achieved a PR and continues on study at 11 months.
One of the 14 patients evaluated for EZH2 status has a specific EZH2 tumor mutation (Y646H). This patient, who had DLBCL that relapsed or was refractory to 6 previous treatment regimens, achieved a PR after 16 weeks of therapy and remains on study.
The recommended phase 2 dose of tazemetostat is 800 mg twice daily.
Adverse events and next steps
All of the 45 enrolled patients were evaluable for safety. Treatment-related adverse events included asthenia (n=10), nausea (n=6), dyspepsia (n=5), thrombocytopenia (n=4), anorexia (n=4), anemia (n=4), vomiting (n=3), constipation (n=2), muscle spasm (n=2), hypertension (n=2), neutropenia (n=2), and elevated transaminase (n=1).
There were 5 grade 3 or higher adverse events related to treatment, including grade 3 anorexia, grade 3 hypertension, grade 3 transaminase elevation, grade 4 thrombocytopenia, and grade 4 neutropenia.
Epizyme plans to report a further update from this trial by the end of this year. The company is now enrolling patients in a phase 2 study of tazemetostat monotherapy in patients with relapsed or refractory NHL, stratified by cell of origin and EZH2 mutation status.
Epizyme is also planning a phase 2 trial of tazemetostat in adults with INI1-deficient solid tumors, a phase 1 study of pediatric patients with INI1-deficient solid tumors, a combination study of tazemetostat with R-CHOP in patients with DLBCL, and a combination study of tazemetostat with a B-cell signaling agent or other emerging targeted therapies for B-cell lymphomas. ![]()
*Information in the abstract differs from that presented at the meeting.
Bleomycin can be safely omitted after negative PET2 in HL

Photo by Jens Maus
LUGANO—Results of the RATHL trial indicate that bleomycin can be omitted from ABVD therapy following a negative interim FDG-PET scan in patients with Hodgkin lymphoma.
Progression-free survival (PFS) and overall survival (OS) were the same at 3 years for patients who were PET-negative after 2 cycles of ABVD and then continued therapy with or without bleomycin.
These results were presented at the 13th International Conference on Malignant Lymphoma (13-ICML).
Investigators based the RATHL study on the principles that it’s desirable to de-escalate treatment in the best responders to avoid late toxicity and that PET scans after 2 cycles of ABVD are highly predictive.
The team enrolled 1214 patients from 6 countries, 861 of whom were in the UK. Patients received a PET scan at staging, 2 cycles of ABVD, and then a second PET scan (PET2).
If patients were negative after PET2, they were randomized to receive 4 more cycles of ABVD or AVD and no radiotherapy.
If they were positive after PET2, patients received 4 cycles of BEACOPP-14 or 3 cycles of escalated BEACOPP. These patients then received a third PET scan, and the positive patients went on to receive radiotherapy or a salvage regimen.
The PET3-negative patients received 2 more cycles of BEACOPP-14 or one of escalated BEACOPP without radiotherapy.
Peter W. Johnson, MD, of the University of Southampton in the UK, presented the results of these treatment regimens during the plenary session of 13-ICML as abstract 008.
Patient characteristics
Patients were a median age of 33 (range, 18-79), and 55% were male. They had disease stages of II (41%), III (31%), or IV (28%).
Seventy-four percent of patients had a performance status of 0. Almost half (49%) had an IPS score of 2 to 3, and 18% had an IPS score of 4 or more. Thirty-two percent had bulky disease.
Investigators followed the patients for a median of 34.7 months (range, 1 day to 68.2 months).
Results after PET2
Seventy-seven patients were missing a second PET scan, mostly due to PET protocol violations of having to use the same scanner for the baseline and second scan and the same acquisition time.
“We were very strict on our quality control,” Dr Johnson said, “because we wished to make sure this was reproducible data.”
So the results after 2 cycles of ABVD treatment were based on 1137 patients.
PET-negative patients
More than 80% of patients were PET-negative after 2 cycles. Four hundred and sixty-nine patients were randomized to receive ABVD and 466 to AVD.
The groups were well-balanced in terms of median age, performance status, stage, B symptoms, bulky disease, and IPS score.
There was a significant excess of neutropenic fever (P=0.032) and infection (P=0.040) in those patients continuing on ABVD compared to AVD. And any hematologic toxicity was highly significantly different between the 2 arms (P<0.001).
“So we have demonstrated that continuing with bleomycin beyond cycle 2 is accompanied by significantly more toxicity,” Dr Johnson said.
Ninety-eight percent of patients in both cohorts received at least 6 cycles of therapy post-randomization.
At a median follow-up of 36.3 months, 65% of patients in the ABVD arm and 69% in the AVD arm achieved a complete remission (CR) or unconfirmed CR (CRu).
Fourteen patients died in each of the arms. Seven patients died of their disease in the AVD arm, compared with 1 in the ABVD arm. Slightly more patients died from toxicity in the ABVD arm.
The primary endpoint of PFS showed very little difference between the 2 arms. The 3-year PFS in the intent-to-treat analysis was 85.4% for patients in the ABVD arm and 84.4% for those in the AVD arm.
The investigators observed that the PFS of 85% was somewhat lower than the 95% PFS observed in the literature. So they looked at the association between baseline factors and PFS after negative PET2.
“And what stands out from this is that if you have high-stage disease at presentation, there is a slightly higher chance of treatment failure following a negative PET scan,” Dr Johnson said. “And you can see the trend here, from early stage disease up to advanced-stage disease, the PET scan becomes a less reliable indicator of result.”
The investigators also conducted a subgroup analysis of the PET2-negative patients and found there was no difference in outcome between treatment arms in patients with more advanced disease, with bulky disease, with a high IPS score, or according to the PET score.
“So we have not succeeded in finding any subgroup where it appears to be beneficial to continue bleomycin,” Dr Johnson said.
The OS rate was also the same between the 2 arms, at 97%.
PET2-positive patients
One hundred and seventy-four patients who were positive after the second PET scan received either BEACOPP for 14 days or escalated BEACOPP.
The percentage of patients who experienced grade 3-4 toxicities was largely similar between the 2 regimens, although the patients receiving escalated BEACOPP had more neutropenia (P=0.057), thrombocytopenia (P=0.001), and neutropenic fever (P=0.08).
In terms of efficacy, two-thirds of patients became PET-negative by the third PET scan, and 48% of patients achieved a CR or CRu.
Twenty-one patients died, 8 due to Hodgkin lymphoma.
The PFS was 66.0% in the BEACOPP-14 group and 71.1% in the escalated-BEACOPP group. The 3-year OS was 89.6% in the BEACOPP-14 group and 82.8% in the escalated-BEACOPP group.
For the entire group of 1214 patients, the 3-year PFS was 82.5%, and the OS was 95.4%.
Based on these results, the investigators concluded that it is safe to omit bleomycin and consolidation radiotherapy from subsequent ABVD therapy after a negative interim PET scan. And doing so reduces toxicity, especially dyspnea, thromboembolism, and neutropenic fever.
“[B]y using more selective chemotherapy and much less radiotherapy than we have previously used in our studies, where we’re giving less than 3% of patients consolidation radiotherapy, the results appear to be favorable and an improvement over what we have seen previously,” Dr Johnson said.
Details on lung toxicity in this study were presented separately at 13-ICML as abstract 041. ![]()
Photo by Jens Maus
LUGANO—Results of the RATHL trial indicate that bleomycin can be omitted from ABVD therapy following a negative interim FDG-PET scan in patients with Hodgkin lymphoma.
Progression-free survival (PFS) and overall survival (OS) were the same at 3 years for patients who were PET-negative after 2 cycles of ABVD and then continued therapy with or without bleomycin.
These results were presented at the 13th International Conference on Malignant Lymphoma (13-ICML).
Investigators based the RATHL study on the principles that it’s desirable to de-escalate treatment in the best responders to avoid late toxicity and that PET scans after 2 cycles of ABVD are highly predictive.
The team enrolled 1214 patients from 6 countries, 861 of whom were in the UK. Patients received a PET scan at staging, 2 cycles of ABVD, and then a second PET scan (PET2).
If patients were negative after PET2, they were randomized to receive 4 more cycles of ABVD or AVD and no radiotherapy.
If they were positive after PET2, patients received 4 cycles of BEACOPP-14 or 3 cycles of escalated BEACOPP. These patients then received a third PET scan, and the positive patients went on to receive radiotherapy or a salvage regimen.
The PET3-negative patients received 2 more cycles of BEACOPP-14 or one of escalated BEACOPP without radiotherapy.
Peter W. Johnson, MD, of the University of Southampton in the UK, presented the results of these treatment regimens during the plenary session of 13-ICML as abstract 008.
Patient characteristics
Patients were a median age of 33 (range, 18-79), and 55% were male. They had disease stages of II (41%), III (31%), or IV (28%).
Seventy-four percent of patients had a performance status of 0. Almost half (49%) had an IPS score of 2 to 3, and 18% had an IPS score of 4 or more. Thirty-two percent had bulky disease.
Investigators followed the patients for a median of 34.7 months (range, 1 day to 68.2 months).
Results after PET2
Seventy-seven patients were missing a second PET scan, mostly due to PET protocol violations of having to use the same scanner for the baseline and second scan and the same acquisition time.
“We were very strict on our quality control,” Dr Johnson said, “because we wished to make sure this was reproducible data.”
So the results after 2 cycles of ABVD treatment were based on 1137 patients.
PET-negative patients
More than 80% of patients were PET-negative after 2 cycles. Four hundred and sixty-nine patients were randomized to receive ABVD and 466 to AVD.
The groups were well-balanced in terms of median age, performance status, stage, B symptoms, bulky disease, and IPS score.
There was a significant excess of neutropenic fever (P=0.032) and infection (P=0.040) in those patients continuing on ABVD compared to AVD. And any hematologic toxicity was highly significantly different between the 2 arms (P<0.001).
“So we have demonstrated that continuing with bleomycin beyond cycle 2 is accompanied by significantly more toxicity,” Dr Johnson said.
Ninety-eight percent of patients in both cohorts received at least 6 cycles of therapy post-randomization.
At a median follow-up of 36.3 months, 65% of patients in the ABVD arm and 69% in the AVD arm achieved a complete remission (CR) or unconfirmed CR (CRu).
Fourteen patients died in each of the arms. Seven patients died of their disease in the AVD arm, compared with 1 in the ABVD arm. Slightly more patients died from toxicity in the ABVD arm.
The primary endpoint of PFS showed very little difference between the 2 arms. The 3-year PFS in the intent-to-treat analysis was 85.4% for patients in the ABVD arm and 84.4% for those in the AVD arm.
The investigators observed that the PFS of 85% was somewhat lower than the 95% PFS observed in the literature. So they looked at the association between baseline factors and PFS after negative PET2.
“And what stands out from this is that if you have high-stage disease at presentation, there is a slightly higher chance of treatment failure following a negative PET scan,” Dr Johnson said. “And you can see the trend here, from early stage disease up to advanced-stage disease, the PET scan becomes a less reliable indicator of result.”
The investigators also conducted a subgroup analysis of the PET2-negative patients and found there was no difference in outcome between treatment arms in patients with more advanced disease, with bulky disease, with a high IPS score, or according to the PET score.
“So we have not succeeded in finding any subgroup where it appears to be beneficial to continue bleomycin,” Dr Johnson said.
The OS rate was also the same between the 2 arms, at 97%.
PET2-positive patients
One hundred and seventy-four patients who were positive after the second PET scan received either BEACOPP for 14 days or escalated BEACOPP.
The percentage of patients who experienced grade 3-4 toxicities was largely similar between the 2 regimens, although the patients receiving escalated BEACOPP had more neutropenia (P=0.057), thrombocytopenia (P=0.001), and neutropenic fever (P=0.08).
In terms of efficacy, two-thirds of patients became PET-negative by the third PET scan, and 48% of patients achieved a CR or CRu.
Twenty-one patients died, 8 due to Hodgkin lymphoma.
The PFS was 66.0% in the BEACOPP-14 group and 71.1% in the escalated-BEACOPP group. The 3-year OS was 89.6% in the BEACOPP-14 group and 82.8% in the escalated-BEACOPP group.
For the entire group of 1214 patients, the 3-year PFS was 82.5%, and the OS was 95.4%.
Based on these results, the investigators concluded that it is safe to omit bleomycin and consolidation radiotherapy from subsequent ABVD therapy after a negative interim PET scan. And doing so reduces toxicity, especially dyspnea, thromboembolism, and neutropenic fever.
“[B]y using more selective chemotherapy and much less radiotherapy than we have previously used in our studies, where we’re giving less than 3% of patients consolidation radiotherapy, the results appear to be favorable and an improvement over what we have seen previously,” Dr Johnson said.
Details on lung toxicity in this study were presented separately at 13-ICML as abstract 041. ![]()
Photo by Jens Maus
LUGANO—Results of the RATHL trial indicate that bleomycin can be omitted from ABVD therapy following a negative interim FDG-PET scan in patients with Hodgkin lymphoma.
Progression-free survival (PFS) and overall survival (OS) were the same at 3 years for patients who were PET-negative after 2 cycles of ABVD and then continued therapy with or without bleomycin.
These results were presented at the 13th International Conference on Malignant Lymphoma (13-ICML).
Investigators based the RATHL study on the principles that it’s desirable to de-escalate treatment in the best responders to avoid late toxicity and that PET scans after 2 cycles of ABVD are highly predictive.
The team enrolled 1214 patients from 6 countries, 861 of whom were in the UK. Patients received a PET scan at staging, 2 cycles of ABVD, and then a second PET scan (PET2).
If patients were negative after PET2, they were randomized to receive 4 more cycles of ABVD or AVD and no radiotherapy.
If they were positive after PET2, patients received 4 cycles of BEACOPP-14 or 3 cycles of escalated BEACOPP. These patients then received a third PET scan, and the positive patients went on to receive radiotherapy or a salvage regimen.
The PET3-negative patients received 2 more cycles of BEACOPP-14 or one of escalated BEACOPP without radiotherapy.
Peter W. Johnson, MD, of the University of Southampton in the UK, presented the results of these treatment regimens during the plenary session of 13-ICML as abstract 008.
Patient characteristics
Patients were a median age of 33 (range, 18-79), and 55% were male. They had disease stages of II (41%), III (31%), or IV (28%).
Seventy-four percent of patients had a performance status of 0. Almost half (49%) had an IPS score of 2 to 3, and 18% had an IPS score of 4 or more. Thirty-two percent had bulky disease.
Investigators followed the patients for a median of 34.7 months (range, 1 day to 68.2 months).
Results after PET2
Seventy-seven patients were missing a second PET scan, mostly due to PET protocol violations of having to use the same scanner for the baseline and second scan and the same acquisition time.
“We were very strict on our quality control,” Dr Johnson said, “because we wished to make sure this was reproducible data.”
So the results after 2 cycles of ABVD treatment were based on 1137 patients.
PET-negative patients
More than 80% of patients were PET-negative after 2 cycles. Four hundred and sixty-nine patients were randomized to receive ABVD and 466 to AVD.
The groups were well-balanced in terms of median age, performance status, stage, B symptoms, bulky disease, and IPS score.
There was a significant excess of neutropenic fever (P=0.032) and infection (P=0.040) in those patients continuing on ABVD compared to AVD. And any hematologic toxicity was highly significantly different between the 2 arms (P<0.001).
“So we have demonstrated that continuing with bleomycin beyond cycle 2 is accompanied by significantly more toxicity,” Dr Johnson said.
Ninety-eight percent of patients in both cohorts received at least 6 cycles of therapy post-randomization.
At a median follow-up of 36.3 months, 65% of patients in the ABVD arm and 69% in the AVD arm achieved a complete remission (CR) or unconfirmed CR (CRu).
Fourteen patients died in each of the arms. Seven patients died of their disease in the AVD arm, compared with 1 in the ABVD arm. Slightly more patients died from toxicity in the ABVD arm.
The primary endpoint of PFS showed very little difference between the 2 arms. The 3-year PFS in the intent-to-treat analysis was 85.4% for patients in the ABVD arm and 84.4% for those in the AVD arm.
The investigators observed that the PFS of 85% was somewhat lower than the 95% PFS observed in the literature. So they looked at the association between baseline factors and PFS after negative PET2.
“And what stands out from this is that if you have high-stage disease at presentation, there is a slightly higher chance of treatment failure following a negative PET scan,” Dr Johnson said. “And you can see the trend here, from early stage disease up to advanced-stage disease, the PET scan becomes a less reliable indicator of result.”
The investigators also conducted a subgroup analysis of the PET2-negative patients and found there was no difference in outcome between treatment arms in patients with more advanced disease, with bulky disease, with a high IPS score, or according to the PET score.
“So we have not succeeded in finding any subgroup where it appears to be beneficial to continue bleomycin,” Dr Johnson said.
The OS rate was also the same between the 2 arms, at 97%.
PET2-positive patients
One hundred and seventy-four patients who were positive after the second PET scan received either BEACOPP for 14 days or escalated BEACOPP.
The percentage of patients who experienced grade 3-4 toxicities was largely similar between the 2 regimens, although the patients receiving escalated BEACOPP had more neutropenia (P=0.057), thrombocytopenia (P=0.001), and neutropenic fever (P=0.08).
In terms of efficacy, two-thirds of patients became PET-negative by the third PET scan, and 48% of patients achieved a CR or CRu.
Twenty-one patients died, 8 due to Hodgkin lymphoma.
The PFS was 66.0% in the BEACOPP-14 group and 71.1% in the escalated-BEACOPP group. The 3-year OS was 89.6% in the BEACOPP-14 group and 82.8% in the escalated-BEACOPP group.
For the entire group of 1214 patients, the 3-year PFS was 82.5%, and the OS was 95.4%.
Based on these results, the investigators concluded that it is safe to omit bleomycin and consolidation radiotherapy from subsequent ABVD therapy after a negative interim PET scan. And doing so reduces toxicity, especially dyspnea, thromboembolism, and neutropenic fever.
“[B]y using more selective chemotherapy and much less radiotherapy than we have previously used in our studies, where we’re giving less than 3% of patients consolidation radiotherapy, the results appear to be favorable and an improvement over what we have seen previously,” Dr Johnson said.
Details on lung toxicity in this study were presented separately at 13-ICML as abstract 041. ![]()
Combo shows promise for heavily pretreated MM

Image by Louis Heiser
and Robert Ackland
VIENNA—Combining a novel agent with dexamethasone can produce successful results where other treatments have failed, according to a presentation at the 20th Congress of the European Hematology Association.
Researchers tested low-dose dexamethasone in combination with melflufen, a peptidase-targeted therapy and antiangiogenic compound, in a phase 1/2 study of patients with relapsed or relapsed-refractory multiple myeloma (MM).
The treatment produced an overall response rate of 52%, and, although grade 3/4 hematologic adverse events were common, there were few serious adverse events related to melflufen.
These results were presented at the meeting as abstract P285.* The research was sponsored by Oncopeptides AB, the company developing melflufen.
Drug dosing and patient characteristics
In the phase 1 portion of this study, researchers evaluated 4 dose levels of melflufen—15 mg, 25 mg, 40 mg, and 55 mg—on day 1 with 40 mg of dexamethasone on days 1, 8, and 15 of 21-day cycles in a standard 3+3 design. Eight cycles of therapy were planned, but patients could continue on treatment if they experienced a clinical benefit.
There were no-dose limiting toxicities (DLTs) when melflufen was given at the 3 lower doses. However, 4 of the 6 patients who received the 55 mg dose experienced DLTs of prolonged and severe neutropenia and thrombocytopenia.
So the researchers said the MTD of melflufen, when combined with 40 mg of weekly dexamethasone, was 40 mg every 21 days.
In the ongoing phase 2 portion of the study, 29 patients have received melflufen at the MTD. The median time from the patients’ MM diagnosis to the first dose of melflufen was 5.5 years (range, 1-15), and their median number of prior therapies was 4 (range, 2-11).
Nineteen of the patients were refractory to an immunomodulatory drug (IMiD) or a proteasome inhibitor (PI); 11 were refractory to an alkylator; 10 were refractory to both an IMiD and a PI; and 5 were refractory to an IMiD, a PI, and an alkylator.
Safety data
Among the 29 patients in the phase 2 portion of the study, 22 had treatment-related grade 3-4 adverse events. These included thrombocytopenia (59%), neutropenia (48%), anemia (31%), leukopenia (21%), asthenia (7%), fatigue (7%), hyperglycemia (7%), and pyrexia/fever (7%).
To date, 12 serious adverse events have been reported in 8 of the phase 2 patients. Three events in 3 patients were considered related to melflufen—2 cases of febrile neutropenia and 1 case of pyrexia.
Fifteen patients discontinued therapy, 8 due to adverse events, 6 due to disease progression, and 1 after completing all planned cycles of treatment.
Efficacy data
Twenty-one patients were evaluable for efficacy according to the protocol, meaning they had received 2 or more cycles of therapy and completed response assessments after cycle 2.
Four patients withdrew from treatment after 1 cycle due to rapid disease progression and were included in a second response assessment (n=25). It was too early to evaluate the remaining 4 patients.
Among the 21 protocol-evaluable patients, the overall response rate was 52%, and the clinical benefit rate was 67%. Eleven patients achieved a partial response, 3 had a minimal response, 6 had stable disease, and 1 had progressive disease.
Among all 25 evaluable patients, the overall response rate was 44%, and the clinical benefit rate was 56%.
The median progression-free survival for these patients was 7.6 months (range, 3.4 months to not reached).
The researchers said enrollment in this trial is ongoing, with the goal of reaching 55 patients to further characterize the safety and efficacy of melflufen in heavily pretreated MM patients. ![]()
*Information in the abstract differs from that presented at the meeting.
Image by Louis Heiser
and Robert Ackland
VIENNA—Combining a novel agent with dexamethasone can produce successful results where other treatments have failed, according to a presentation at the 20th Congress of the European Hematology Association.
Researchers tested low-dose dexamethasone in combination with melflufen, a peptidase-targeted therapy and antiangiogenic compound, in a phase 1/2 study of patients with relapsed or relapsed-refractory multiple myeloma (MM).
The treatment produced an overall response rate of 52%, and, although grade 3/4 hematologic adverse events were common, there were few serious adverse events related to melflufen.
These results were presented at the meeting as abstract P285.* The research was sponsored by Oncopeptides AB, the company developing melflufen.
Drug dosing and patient characteristics
In the phase 1 portion of this study, researchers evaluated 4 dose levels of melflufen—15 mg, 25 mg, 40 mg, and 55 mg—on day 1 with 40 mg of dexamethasone on days 1, 8, and 15 of 21-day cycles in a standard 3+3 design. Eight cycles of therapy were planned, but patients could continue on treatment if they experienced a clinical benefit.
There were no-dose limiting toxicities (DLTs) when melflufen was given at the 3 lower doses. However, 4 of the 6 patients who received the 55 mg dose experienced DLTs of prolonged and severe neutropenia and thrombocytopenia.
So the researchers said the MTD of melflufen, when combined with 40 mg of weekly dexamethasone, was 40 mg every 21 days.
In the ongoing phase 2 portion of the study, 29 patients have received melflufen at the MTD. The median time from the patients’ MM diagnosis to the first dose of melflufen was 5.5 years (range, 1-15), and their median number of prior therapies was 4 (range, 2-11).
Nineteen of the patients were refractory to an immunomodulatory drug (IMiD) or a proteasome inhibitor (PI); 11 were refractory to an alkylator; 10 were refractory to both an IMiD and a PI; and 5 were refractory to an IMiD, a PI, and an alkylator.
Safety data
Among the 29 patients in the phase 2 portion of the study, 22 had treatment-related grade 3-4 adverse events. These included thrombocytopenia (59%), neutropenia (48%), anemia (31%), leukopenia (21%), asthenia (7%), fatigue (7%), hyperglycemia (7%), and pyrexia/fever (7%).
To date, 12 serious adverse events have been reported in 8 of the phase 2 patients. Three events in 3 patients were considered related to melflufen—2 cases of febrile neutropenia and 1 case of pyrexia.
Fifteen patients discontinued therapy, 8 due to adverse events, 6 due to disease progression, and 1 after completing all planned cycles of treatment.
Efficacy data
Twenty-one patients were evaluable for efficacy according to the protocol, meaning they had received 2 or more cycles of therapy and completed response assessments after cycle 2.
Four patients withdrew from treatment after 1 cycle due to rapid disease progression and were included in a second response assessment (n=25). It was too early to evaluate the remaining 4 patients.
Among the 21 protocol-evaluable patients, the overall response rate was 52%, and the clinical benefit rate was 67%. Eleven patients achieved a partial response, 3 had a minimal response, 6 had stable disease, and 1 had progressive disease.
Among all 25 evaluable patients, the overall response rate was 44%, and the clinical benefit rate was 56%.
The median progression-free survival for these patients was 7.6 months (range, 3.4 months to not reached).
The researchers said enrollment in this trial is ongoing, with the goal of reaching 55 patients to further characterize the safety and efficacy of melflufen in heavily pretreated MM patients. ![]()
*Information in the abstract differs from that presented at the meeting.
Image by Louis Heiser
and Robert Ackland
VIENNA—Combining a novel agent with dexamethasone can produce successful results where other treatments have failed, according to a presentation at the 20th Congress of the European Hematology Association.
Researchers tested low-dose dexamethasone in combination with melflufen, a peptidase-targeted therapy and antiangiogenic compound, in a phase 1/2 study of patients with relapsed or relapsed-refractory multiple myeloma (MM).
The treatment produced an overall response rate of 52%, and, although grade 3/4 hematologic adverse events were common, there were few serious adverse events related to melflufen.
These results were presented at the meeting as abstract P285.* The research was sponsored by Oncopeptides AB, the company developing melflufen.
Drug dosing and patient characteristics
In the phase 1 portion of this study, researchers evaluated 4 dose levels of melflufen—15 mg, 25 mg, 40 mg, and 55 mg—on day 1 with 40 mg of dexamethasone on days 1, 8, and 15 of 21-day cycles in a standard 3+3 design. Eight cycles of therapy were planned, but patients could continue on treatment if they experienced a clinical benefit.
There were no-dose limiting toxicities (DLTs) when melflufen was given at the 3 lower doses. However, 4 of the 6 patients who received the 55 mg dose experienced DLTs of prolonged and severe neutropenia and thrombocytopenia.
So the researchers said the MTD of melflufen, when combined with 40 mg of weekly dexamethasone, was 40 mg every 21 days.
In the ongoing phase 2 portion of the study, 29 patients have received melflufen at the MTD. The median time from the patients’ MM diagnosis to the first dose of melflufen was 5.5 years (range, 1-15), and their median number of prior therapies was 4 (range, 2-11).
Nineteen of the patients were refractory to an immunomodulatory drug (IMiD) or a proteasome inhibitor (PI); 11 were refractory to an alkylator; 10 were refractory to both an IMiD and a PI; and 5 were refractory to an IMiD, a PI, and an alkylator.
Safety data
Among the 29 patients in the phase 2 portion of the study, 22 had treatment-related grade 3-4 adverse events. These included thrombocytopenia (59%), neutropenia (48%), anemia (31%), leukopenia (21%), asthenia (7%), fatigue (7%), hyperglycemia (7%), and pyrexia/fever (7%).
To date, 12 serious adverse events have been reported in 8 of the phase 2 patients. Three events in 3 patients were considered related to melflufen—2 cases of febrile neutropenia and 1 case of pyrexia.
Fifteen patients discontinued therapy, 8 due to adverse events, 6 due to disease progression, and 1 after completing all planned cycles of treatment.
Efficacy data
Twenty-one patients were evaluable for efficacy according to the protocol, meaning they had received 2 or more cycles of therapy and completed response assessments after cycle 2.
Four patients withdrew from treatment after 1 cycle due to rapid disease progression and were included in a second response assessment (n=25). It was too early to evaluate the remaining 4 patients.
Among the 21 protocol-evaluable patients, the overall response rate was 52%, and the clinical benefit rate was 67%. Eleven patients achieved a partial response, 3 had a minimal response, 6 had stable disease, and 1 had progressive disease.
Among all 25 evaluable patients, the overall response rate was 44%, and the clinical benefit rate was 56%.
The median progression-free survival for these patients was 7.6 months (range, 3.4 months to not reached).
The researchers said enrollment in this trial is ongoing, with the goal of reaching 55 patients to further characterize the safety and efficacy of melflufen in heavily pretreated MM patients. ![]()
*Information in the abstract differs from that presented at the meeting.
FDA approves antiplatelet drug for PCI patients

Photo courtesy of
The Medicines Company
The US Food and Drug Administration (FDA) has approved the intravenous antiplatelet agent cangrelor (Kengreal) for use in adults undergoing percutaneous coronary intervention (PCI).
The drug can now be used to reduce periprocedural thrombotic events in patients who have not been treated with a P2Y12 inhibitor and are not receiving a glycoprotein IIb/IIIa inhibitor.
The FDA’s approval of cangrelor was based on results of the CHAMPION PHOENIX trial.
In this phase 3 trial, researchers compared cangrelor to clopidogrel in 11,145 patients undergoing PCI.
The study’s primary efficacy endpoint was the incidence of death, myocardial infarction, ischemia-driven revascularization, or stent thrombosis.
At 48 hours, 4.7% of patients in the cangrelor arm had met this endpoint, compared to 5.9% of patients in the clopidogrel arm (P=0.005). At 30 days, the incidence was 6.0% in the cangrelor arm and 7.0% in the clopidogrel arm (P=0.03).
The study’s primary safety endpoint was severe bleeding according to GUSTO criteria. At 48 hours, major bleeding had occurred in 0.16% of patients in the cangrelor arm and 0.11% of patients in the clopidogrel arm (P=0.44).
Major bleeding occurred in 4.3% of patients on cangrelor and 2.5% of patients on clopidogrel (P<0.001). And minor bleeding occurred in 11.8% of patients on cangrelor and 8.6% of patients on clopidogrel (P<0.001).
Cangrelor is manufactured by The Medicines Company, which is based in Parsippany, New Jersey. ![]()
Photo courtesy of
The Medicines Company
The US Food and Drug Administration (FDA) has approved the intravenous antiplatelet agent cangrelor (Kengreal) for use in adults undergoing percutaneous coronary intervention (PCI).
The drug can now be used to reduce periprocedural thrombotic events in patients who have not been treated with a P2Y12 inhibitor and are not receiving a glycoprotein IIb/IIIa inhibitor.
The FDA’s approval of cangrelor was based on results of the CHAMPION PHOENIX trial.
In this phase 3 trial, researchers compared cangrelor to clopidogrel in 11,145 patients undergoing PCI.
The study’s primary efficacy endpoint was the incidence of death, myocardial infarction, ischemia-driven revascularization, or stent thrombosis.
At 48 hours, 4.7% of patients in the cangrelor arm had met this endpoint, compared to 5.9% of patients in the clopidogrel arm (P=0.005). At 30 days, the incidence was 6.0% in the cangrelor arm and 7.0% in the clopidogrel arm (P=0.03).
The study’s primary safety endpoint was severe bleeding according to GUSTO criteria. At 48 hours, major bleeding had occurred in 0.16% of patients in the cangrelor arm and 0.11% of patients in the clopidogrel arm (P=0.44).
Major bleeding occurred in 4.3% of patients on cangrelor and 2.5% of patients on clopidogrel (P<0.001). And minor bleeding occurred in 11.8% of patients on cangrelor and 8.6% of patients on clopidogrel (P<0.001).
Cangrelor is manufactured by The Medicines Company, which is based in Parsippany, New Jersey. ![]()
Photo courtesy of
The Medicines Company
The US Food and Drug Administration (FDA) has approved the intravenous antiplatelet agent cangrelor (Kengreal) for use in adults undergoing percutaneous coronary intervention (PCI).
The drug can now be used to reduce periprocedural thrombotic events in patients who have not been treated with a P2Y12 inhibitor and are not receiving a glycoprotein IIb/IIIa inhibitor.
The FDA’s approval of cangrelor was based on results of the CHAMPION PHOENIX trial.
In this phase 3 trial, researchers compared cangrelor to clopidogrel in 11,145 patients undergoing PCI.
The study’s primary efficacy endpoint was the incidence of death, myocardial infarction, ischemia-driven revascularization, or stent thrombosis.
At 48 hours, 4.7% of patients in the cangrelor arm had met this endpoint, compared to 5.9% of patients in the clopidogrel arm (P=0.005). At 30 days, the incidence was 6.0% in the cangrelor arm and 7.0% in the clopidogrel arm (P=0.03).
The study’s primary safety endpoint was severe bleeding according to GUSTO criteria. At 48 hours, major bleeding had occurred in 0.16% of patients in the cangrelor arm and 0.11% of patients in the clopidogrel arm (P=0.44).
Major bleeding occurred in 4.3% of patients on cangrelor and 2.5% of patients on clopidogrel (P<0.001). And minor bleeding occurred in 11.8% of patients on cangrelor and 8.6% of patients on clopidogrel (P<0.001).
Cangrelor is manufactured by The Medicines Company, which is based in Parsippany, New Jersey. ![]()
Perioperative factors influenced open TAAA repair
Open thoracoabdominal aortic aneurysm (TAAA) repair produced respectable early outcomes, although preoperative and intraoperative factors were found to influence risk, according to Dr. Joseph S. Coselli, who presented the results of the study he and his colleagues at the Baylor College of Medicine in Houston performed at the annual meeting of the American Association for Thoracic Surgery.
They analyzed data from 3,309 open TAAA repairs performed between October 1986 and December 2014.
“I have been very fortunate to have spent my entire career at Baylor College of Medicine, the epicenter of aortic surgery in the 1950s, ’60s, and ’70s, as well as to have been mentored by Dr. E. Stanley Crawford, who was arguably the finest aortic surgeon of his era. Since transitioning from Dr. Crawford’s surgical practice to my own surgical practice, we have kept his pioneering spirit alive by developing a multimodal strategy for thoracoabdominal aortic aneurysm repair that is based on the Crawford extent of repair and our evolving investigation. We sought to describe our series of over 3,000 TAAA repairs and to identify predictors of early death and other adverse postoperative outcomes,” said Dr. Coselli.
The median patient age was around 67 years, and the repairs involved acute or subacute aortic dissection in about 5% of the cases. Nearly 31% of the case involved chronic dissection, with nearly 22% emergent or urgent repairs and around 5% ruptured aneurysms. Connective tissue disorders were present in roughly 10% of patients. “Operatively, we tend to reserve surgical adjuncts for use in the most-extensive repairs, namely extents I and II TAAA repair; intercostal or lumbar artery reattachment was used in just over half of the repairs, left heart bypass (LHB) was used in around 45% of patients, cold renal perfusion was performed in 58%. and cerebrospinal fluid drainage (CSFD) was used in 45%,” said Dr. Coselli.
There was substantial atherosclerotic disease in older patients, and in nearly 41% of repairs, a visceral vessel procedure was performed.
Unlike many aortic centers that routinely use deep hypothermic circulatory arrest (HCA) for extensive TAAA repair, Dr. Coselli reserved this approach for a small number of highly complex repairs (1.4%) in which the aorta could not be safely clamped.
Of the more than a thousand most extensive (i.e., Crawford extent II) repairs, intercostal/lumbar artery reattachment was used in the vast majority (88%), LHB in 82%, and CSFD in 61%. They used multivariable analysis to identify predictors of operative (30-day or in-hospital) mortality and adverse event, a composite outcome comprising operative death and permanent (present at discharge) spinal cord deficit, renal failure, or stroke, according to Dr. Coselli.
Their results showed an operative mortality rate of 7.5%, a 30-day death rate of 4.8%, with the adverse event outcome occurring in about 14% of repairs. A video of his presentation is available at the AATS website.
The statistically significant predictors of operative death were rupture; renal insufficiency, symptoms, procedures targeting visceral vessels, increasing age, and increasing clamp time, while extent IV repair (the least extensive form of TAAA repair) was inversely associated with death. Their analysis showed that the significant predictors of adverse event were use of HCA, renal insufficiency, rupture, extent II repair, visceral vessel procedures, urgent or emergent repair, increasing age, and increasing clamp time. In addition, they used multivariable analysis to identify predictors of renal failure and paraplegia.
In the 3,060 early survivors, roughly 7% had a life-altering complication at discharge: Nearly 3% of patients had renal failure necessitating dialysis, slightly more than 1% had a unresolved stroke, and about 4% had unresolved paraplegia or paraparesis. Repair failure, primarily pseudoaneurysm, or patch aneurysm, occurred after nearly 3% of repairs, said Dr. Coselli.
Outcomes differed by extent of repair, with the risk being greatest in extent II repair. Actuarial survival was 63.6% at 5 years, 36.8% at 10 years, and 18.3% at 15 years. Freedom from repair failure was nearly 98% at 5 years, around 95% at 10 years, and 94% at 15 years.
“Along with respectable early outcomes, after repair, patients have acceptable long-term survival, and late repair failure was uncommon. Notably, there are several subgroups of patients that do exceedingly well. Paraplegia in young patients with connective tissue disorders, even in the most-extensive repair (extent II), is remarkably rare – these patients do extremely well across the board,” he concluded.
Dr. Cosselli reported that he is a principal investigator and consultant for Medtronic and W.L. Gore & Assoc., as well as being a principal investigator, consultant, and having various financial relationships with Vascutek.
Open thoracoabdominal aortic aneurysm (TAAA) repair produced respectable early outcomes, although preoperative and intraoperative factors were found to influence risk, according to Dr. Joseph S. Coselli, who presented the results of the study he and his colleagues at the Baylor College of Medicine in Houston performed at the annual meeting of the American Association for Thoracic Surgery.
They analyzed data from 3,309 open TAAA repairs performed between October 1986 and December 2014.
“I have been very fortunate to have spent my entire career at Baylor College of Medicine, the epicenter of aortic surgery in the 1950s, ’60s, and ’70s, as well as to have been mentored by Dr. E. Stanley Crawford, who was arguably the finest aortic surgeon of his era. Since transitioning from Dr. Crawford’s surgical practice to my own surgical practice, we have kept his pioneering spirit alive by developing a multimodal strategy for thoracoabdominal aortic aneurysm repair that is based on the Crawford extent of repair and our evolving investigation. We sought to describe our series of over 3,000 TAAA repairs and to identify predictors of early death and other adverse postoperative outcomes,” said Dr. Coselli.
The median patient age was around 67 years, and the repairs involved acute or subacute aortic dissection in about 5% of the cases. Nearly 31% of the case involved chronic dissection, with nearly 22% emergent or urgent repairs and around 5% ruptured aneurysms. Connective tissue disorders were present in roughly 10% of patients. “Operatively, we tend to reserve surgical adjuncts for use in the most-extensive repairs, namely extents I and II TAAA repair; intercostal or lumbar artery reattachment was used in just over half of the repairs, left heart bypass (LHB) was used in around 45% of patients, cold renal perfusion was performed in 58%. and cerebrospinal fluid drainage (CSFD) was used in 45%,” said Dr. Coselli.
There was substantial atherosclerotic disease in older patients, and in nearly 41% of repairs, a visceral vessel procedure was performed.
Unlike many aortic centers that routinely use deep hypothermic circulatory arrest (HCA) for extensive TAAA repair, Dr. Coselli reserved this approach for a small number of highly complex repairs (1.4%) in which the aorta could not be safely clamped.
Of the more than a thousand most extensive (i.e., Crawford extent II) repairs, intercostal/lumbar artery reattachment was used in the vast majority (88%), LHB in 82%, and CSFD in 61%. They used multivariable analysis to identify predictors of operative (30-day or in-hospital) mortality and adverse event, a composite outcome comprising operative death and permanent (present at discharge) spinal cord deficit, renal failure, or stroke, according to Dr. Coselli.
Their results showed an operative mortality rate of 7.5%, a 30-day death rate of 4.8%, with the adverse event outcome occurring in about 14% of repairs. A video of his presentation is available at the AATS website.
The statistically significant predictors of operative death were rupture; renal insufficiency, symptoms, procedures targeting visceral vessels, increasing age, and increasing clamp time, while extent IV repair (the least extensive form of TAAA repair) was inversely associated with death. Their analysis showed that the significant predictors of adverse event were use of HCA, renal insufficiency, rupture, extent II repair, visceral vessel procedures, urgent or emergent repair, increasing age, and increasing clamp time. In addition, they used multivariable analysis to identify predictors of renal failure and paraplegia.
In the 3,060 early survivors, roughly 7% had a life-altering complication at discharge: Nearly 3% of patients had renal failure necessitating dialysis, slightly more than 1% had a unresolved stroke, and about 4% had unresolved paraplegia or paraparesis. Repair failure, primarily pseudoaneurysm, or patch aneurysm, occurred after nearly 3% of repairs, said Dr. Coselli.
Outcomes differed by extent of repair, with the risk being greatest in extent II repair. Actuarial survival was 63.6% at 5 years, 36.8% at 10 years, and 18.3% at 15 years. Freedom from repair failure was nearly 98% at 5 years, around 95% at 10 years, and 94% at 15 years.
“Along with respectable early outcomes, after repair, patients have acceptable long-term survival, and late repair failure was uncommon. Notably, there are several subgroups of patients that do exceedingly well. Paraplegia in young patients with connective tissue disorders, even in the most-extensive repair (extent II), is remarkably rare – these patients do extremely well across the board,” he concluded.
Dr. Cosselli reported that he is a principal investigator and consultant for Medtronic and W.L. Gore & Assoc., as well as being a principal investigator, consultant, and having various financial relationships with Vascutek.
Open thoracoabdominal aortic aneurysm (TAAA) repair produced respectable early outcomes, although preoperative and intraoperative factors were found to influence risk, according to Dr. Joseph S. Coselli, who presented the results of the study he and his colleagues at the Baylor College of Medicine in Houston performed at the annual meeting of the American Association for Thoracic Surgery.
They analyzed data from 3,309 open TAAA repairs performed between October 1986 and December 2014.
“I have been very fortunate to have spent my entire career at Baylor College of Medicine, the epicenter of aortic surgery in the 1950s, ’60s, and ’70s, as well as to have been mentored by Dr. E. Stanley Crawford, who was arguably the finest aortic surgeon of his era. Since transitioning from Dr. Crawford’s surgical practice to my own surgical practice, we have kept his pioneering spirit alive by developing a multimodal strategy for thoracoabdominal aortic aneurysm repair that is based on the Crawford extent of repair and our evolving investigation. We sought to describe our series of over 3,000 TAAA repairs and to identify predictors of early death and other adverse postoperative outcomes,” said Dr. Coselli.
The median patient age was around 67 years, and the repairs involved acute or subacute aortic dissection in about 5% of the cases. Nearly 31% of the case involved chronic dissection, with nearly 22% emergent or urgent repairs and around 5% ruptured aneurysms. Connective tissue disorders were present in roughly 10% of patients. “Operatively, we tend to reserve surgical adjuncts for use in the most-extensive repairs, namely extents I and II TAAA repair; intercostal or lumbar artery reattachment was used in just over half of the repairs, left heart bypass (LHB) was used in around 45% of patients, cold renal perfusion was performed in 58%. and cerebrospinal fluid drainage (CSFD) was used in 45%,” said Dr. Coselli.
There was substantial atherosclerotic disease in older patients, and in nearly 41% of repairs, a visceral vessel procedure was performed.
Unlike many aortic centers that routinely use deep hypothermic circulatory arrest (HCA) for extensive TAAA repair, Dr. Coselli reserved this approach for a small number of highly complex repairs (1.4%) in which the aorta could not be safely clamped.
Of the more than a thousand most extensive (i.e., Crawford extent II) repairs, intercostal/lumbar artery reattachment was used in the vast majority (88%), LHB in 82%, and CSFD in 61%. They used multivariable analysis to identify predictors of operative (30-day or in-hospital) mortality and adverse event, a composite outcome comprising operative death and permanent (present at discharge) spinal cord deficit, renal failure, or stroke, according to Dr. Coselli.
Their results showed an operative mortality rate of 7.5%, a 30-day death rate of 4.8%, with the adverse event outcome occurring in about 14% of repairs. A video of his presentation is available at the AATS website.
The statistically significant predictors of operative death were rupture; renal insufficiency, symptoms, procedures targeting visceral vessels, increasing age, and increasing clamp time, while extent IV repair (the least extensive form of TAAA repair) was inversely associated with death. Their analysis showed that the significant predictors of adverse event were use of HCA, renal insufficiency, rupture, extent II repair, visceral vessel procedures, urgent or emergent repair, increasing age, and increasing clamp time. In addition, they used multivariable analysis to identify predictors of renal failure and paraplegia.
In the 3,060 early survivors, roughly 7% had a life-altering complication at discharge: Nearly 3% of patients had renal failure necessitating dialysis, slightly more than 1% had a unresolved stroke, and about 4% had unresolved paraplegia or paraparesis. Repair failure, primarily pseudoaneurysm, or patch aneurysm, occurred after nearly 3% of repairs, said Dr. Coselli.
Outcomes differed by extent of repair, with the risk being greatest in extent II repair. Actuarial survival was 63.6% at 5 years, 36.8% at 10 years, and 18.3% at 15 years. Freedom from repair failure was nearly 98% at 5 years, around 95% at 10 years, and 94% at 15 years.
“Along with respectable early outcomes, after repair, patients have acceptable long-term survival, and late repair failure was uncommon. Notably, there are several subgroups of patients that do exceedingly well. Paraplegia in young patients with connective tissue disorders, even in the most-extensive repair (extent II), is remarkably rare – these patients do extremely well across the board,” he concluded.
Dr. Cosselli reported that he is a principal investigator and consultant for Medtronic and W.L. Gore & Assoc., as well as being a principal investigator, consultant, and having various financial relationships with Vascutek.
AT THE AATS ANNUAL MEETING

Weight in America: Abnormal is the new normal
Three-quarters of men and two-thirds of women aged 25 years or older in the United States are either overweight or obese, according to a study published online June 22 in JAMA Internal Medicine.
During 2007-2012, about 40% of men were overweight and 35% were obese. For women, almost 30% were overweight and 37% were obese, Lin Yang, Ph.D., and Dr. Graham A. Colditz of Washington University, St. Louis, reported in a research letter (JAMA Intern. Med. 2015 June 22 [doi:10.1001/jamainternmed.2015.2405]).
Weight-status distributions across racial groups show that non-Hispanic whites were generally less obese than non-Hispanic blacks and Mexican Americans – an effect that was more pronounced among women. About 34% of white women were obese, compared with 57% of black women, with over 17% occupying the heaviest of three obesity levels, according to the investigators’ analysis of the most recent data from the National Health and Nutrition Examination Survey.
Weight groups in the study were defined by body mass index: underweight (< 18.5 kg/m2), normal weight (18.5-24.9), overweight (25.0-29.9), obesity class 1 (30.0-34.9), obesity class 2 (35.0-39.9), and obesity class 3 (≥ 40).
Compared with an earlier study reporting data for 1988-1994, “the greatest increase in the proportion of patients in the obesity class 3 category was among non-Hispanic black women,” Dr. Yang and Dr. Colditz wrote. Health and policy decision-makers should consider “population-based strategies helping to reduce modifiable risk factors such as physical environment interventions, enhancing primary care efforts to prevent and treat obesity, and altering societal norms of behavior,” they added.
The study was funded by the Washington University Transdiscliplinary Research on Energetics and Cancer Center, the Foundation for Barnes-Jewish Hospital, and the Breast Cancer Research Foundation. The investigators did not report any conflicts.
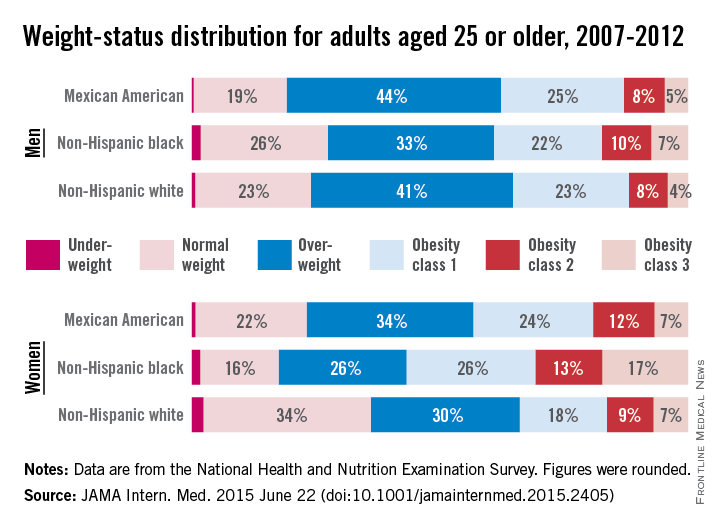
Three-quarters of men and two-thirds of women aged 25 years or older in the United States are either overweight or obese, according to a study published online June 22 in JAMA Internal Medicine.
During 2007-2012, about 40% of men were overweight and 35% were obese. For women, almost 30% were overweight and 37% were obese, Lin Yang, Ph.D., and Dr. Graham A. Colditz of Washington University, St. Louis, reported in a research letter (JAMA Intern. Med. 2015 June 22 [doi:10.1001/jamainternmed.2015.2405]).
Weight-status distributions across racial groups show that non-Hispanic whites were generally less obese than non-Hispanic blacks and Mexican Americans – an effect that was more pronounced among women. About 34% of white women were obese, compared with 57% of black women, with over 17% occupying the heaviest of three obesity levels, according to the investigators’ analysis of the most recent data from the National Health and Nutrition Examination Survey.
Weight groups in the study were defined by body mass index: underweight (< 18.5 kg/m2), normal weight (18.5-24.9), overweight (25.0-29.9), obesity class 1 (30.0-34.9), obesity class 2 (35.0-39.9), and obesity class 3 (≥ 40).
Compared with an earlier study reporting data for 1988-1994, “the greatest increase in the proportion of patients in the obesity class 3 category was among non-Hispanic black women,” Dr. Yang and Dr. Colditz wrote. Health and policy decision-makers should consider “population-based strategies helping to reduce modifiable risk factors such as physical environment interventions, enhancing primary care efforts to prevent and treat obesity, and altering societal norms of behavior,” they added.
The study was funded by the Washington University Transdiscliplinary Research on Energetics and Cancer Center, the Foundation for Barnes-Jewish Hospital, and the Breast Cancer Research Foundation. The investigators did not report any conflicts.
Three-quarters of men and two-thirds of women aged 25 years or older in the United States are either overweight or obese, according to a study published online June 22 in JAMA Internal Medicine.
During 2007-2012, about 40% of men were overweight and 35% were obese. For women, almost 30% were overweight and 37% were obese, Lin Yang, Ph.D., and Dr. Graham A. Colditz of Washington University, St. Louis, reported in a research letter (JAMA Intern. Med. 2015 June 22 [doi:10.1001/jamainternmed.2015.2405]).
Weight-status distributions across racial groups show that non-Hispanic whites were generally less obese than non-Hispanic blacks and Mexican Americans – an effect that was more pronounced among women. About 34% of white women were obese, compared with 57% of black women, with over 17% occupying the heaviest of three obesity levels, according to the investigators’ analysis of the most recent data from the National Health and Nutrition Examination Survey.
Weight groups in the study were defined by body mass index: underweight (< 18.5 kg/m2), normal weight (18.5-24.9), overweight (25.0-29.9), obesity class 1 (30.0-34.9), obesity class 2 (35.0-39.9), and obesity class 3 (≥ 40).
Compared with an earlier study reporting data for 1988-1994, “the greatest increase in the proportion of patients in the obesity class 3 category was among non-Hispanic black women,” Dr. Yang and Dr. Colditz wrote. Health and policy decision-makers should consider “population-based strategies helping to reduce modifiable risk factors such as physical environment interventions, enhancing primary care efforts to prevent and treat obesity, and altering societal norms of behavior,” they added.
The study was funded by the Washington University Transdiscliplinary Research on Energetics and Cancer Center, the Foundation for Barnes-Jewish Hospital, and the Breast Cancer Research Foundation. The investigators did not report any conflicts.
FROM JAMA INTERNAL MEDICINE