User login
FEVAR radiation injury reexamined
CORONADO, CALIF. – Skin injury following fenestrated endovascular aortic stent grafting is less prevalent than expected, results from a single-center retrospective study showed.
“Radiation-induced skin injury is a serious potential complication of fluoroscopically guided interventions,” Dr. Melissa L. Kirkwood said at the annual meeting of the Western Vascular Society. “These injuries are associated with a threshold radiation dose, above which the severity of injury increases with increasing dose. Instances of these injuries are mostly limited to case reports of coronary interventions, TIPS procedures, and neuroembolizations.”
These radiation-induced skin lesions can be classified as prompt, early, mid-term, or late depending on when they present following the fluoroscopically guided intervention. “The National Cancer Institute has defined four grades of skin injury, with the most frequent being transient erythema, a prompt reaction within the first 24 hours occurring at skin doses as low as 2 Gy,” said Dr. Kirkwood of the division of vascular and endovascular surgery at the University of Texas Southwestern Medical Center, Dallas. “With increasing skin doses, more severe effects present themselves. Atrophy, ulceration, and necrosis are possibilities.”
She went on to note that fenestrated endovascular aneurysm repair often requires high doses of radiation, yet the prevalence of deterministic skin injury following these cases is unknown. In a recent study, Dr. Kirkwood and her associates retrospectively reviewed 61 complex fluoroscopically guided interventions that met substantial radiation dose level (SRDL) criteria, which is defined by the National Council on Radiation and Protection Measurements as a reference air kerma (RAK) greater than or equal to 5 Gy (J. Vasc. Surg. 2014; 60:742-8).
“Despite mean peak skin doses as high as 6.5 Gy, ranging up to 18.5 Gy, we did not detect any skin injuries in this cohort,” Dr. Kirkwood said. “That study, however, was limited by its retrospective design. There was no postoperative protocol in place to ensure that a thorough skin exam was performed on each patient at every follow-up visit. Therefore, we hypothesized that a more thorough postoperative follow-up of patients would detect some skin injury following these cases.”For the current study, she and her associates sought to examine the prevalence of deterministic effects after FEVAR as well as any patient characteristics that may predispose patients to skin injury.
In June 2013, the researchers implemented a new policy regarding the follow-up of FEVAR patients, which involved a full skin exam at postoperative week 2 and 4, and at 3 and 6 months, as well as questioning patients about any skin-related complaints. For the current study, they retrospectively reviewed all FEVARs over a 7-month period after the change in policy and highlighted all the cases that reached a RAK of 5 Gy or greater.
Peak skin dose, a dose index, and simulated skin dose maps were calculated using customized software employing input data from fluoroscopic machine logs. Of 317 cases performed, 22 met or exceeded a RAK of 5 Gy. Of these, 21 were FEVARs and one was an embolization. Dr. Kirkwood reported that the average RAK for all FEVARs was 8 Gy, with a range of 5-11 Gy.
Slightly more than half of patients (52%) had multiple fluoroscopically guided interventions within 6 months of their SRDL event. The average RAK for these patients was 10 Gy (range of 5 - 15). The mean peak skin dose for all FEVARs was 5 Gy (range of 2 - 10 Gy), and the dose index was 0.69. The average peak skin dose for the subset of patients with multiple procedures was 7 Gy (a range of 3 - 9 Gy).
In terms of the follow-up, all 21 FEVAR patients were examined at the 1- or 2-week mark, 81% were examined at 1 month, 52% were examined at 3 months, and 62% were examined at 6 months. No radiation skin injuries were reported. “Based on the published data, we would expect to see all grades of skin injury, especially in the cohort of the 5-10 Gy,” Dr. Kirkwood said.
In the previous study, conducted prior to the new follow-up policy, the dose index for FEVARs was 0.78, “meaning that the peak skin dose that the patient received could be roughly estimated as 78% of the RAK dose displayed on the monitor,” Dr. Kirkwood explained.
“In the current work, the dose index decreased to 60%. This suggests that surgeons in our group have now more appropriately and effectively employed strategies to decrease radiation dose to the patient. However, even when the best operating practice is employed, FEVARs still continue to require high radiation doses in order to complete.”
The present study demonstrated that deterministic skin injuries “are uncommon after FEVAR, even at high RAK levels and regardless of cumulative dose,” she concluded. “Even with more comprehensive patient follow-up, the fact that no skin injuries were reported suggests that skin injuries in this patient cohort are less prevalent than the published guidelines would predict.”
Dr. Kirkwood reported no financial disclosures.
This report is a follow-up of a study by the same group published in the Journal of Vascular Surgery in 2013 (58:715-21) in which they demonstrated that the use of a variety of radiation safety measures including increasing table height, utilizing collimation and angulation, decreasing magnification modes, and maintaining minimal patient-to-detector distance resulted in a 60% reduction in skin dose to their patients when measured as an index of peak skin dose to reference air kerma (PSD/RAK). Unfortunately, skin exposure remained high for FEVAR despite these measures, underscoring the fact that for very complex interventions, even with excellent radiation safety practices, the risk of skin injury remains.
The fact that skin doses as high as 11 Gy did not result in any deterministic injuries is both reassuring and a little surprising. According to the Centers for Disease Control and Prevention, radiation doses of greater than 2 Gy but less than 15 Gy will usually result in erythema within 1-2 days, with a second period of erythema and edema at 2-5 weeks, occasionally resulting in desquamation at 6-7 weeks. Late changes can include mild skin atrophy and some hyperpigmentation. Although complete healing can usually be expected at these doses, squamous skin cancer can still occur, often more than a decade after exposure.
|
Dr. Frank Pomposelli |
So why were no injuries seen? It may be that some were missed since follow-up examinations were not performed in 100% of their patients at any time interval, and it’s not stated whether exams were routinely performed in the first 1-2 days, when I would presume most patients were still hospitalized and the first stage of skin erythema is usually seen. Alternatively, it may be that the surrogate measure of either RAK or the index of PSD/RAK overestimated the true radiation skin dose, which seems highly likely, especially if the time of exposure in any one location was based less on the frequent changes in gantry angle and table position so commonly used in these procedures.
In our hospital, the Massachusetts Department of Public Health regulations require the patient and their physician be notified by letter when the estimated total absorbed radiation dose equals or exceeds 2 Gy. This is based on calculations by our physicist who reviews the details of any case in which the RAK measured equals or exceeds 2 Gy. Like the experiences of the authors, this most commonly occurs with lengthy and complex interventions. In our experience, we have never observed a significant skin injury presumably for the same reason – the exposure in any one location tends to be far less than the total calculated skin dose. Nevertheless, this study should not lull surgeons into a sense of complacency regarding the risk to the patient (and themselves and their staff). As our comfort and expertise with complex interventions increase, it is likely that radiation exposure will continue to increase, placing our patients at increased risk. Understanding the risk of radiation skin injury and how to minimize it is critical for any surgeon performing FEVAR and any other complex intervention utilizing fluoroscopic imaging.
Dr. Frank Pomposelli is an associate professor of surgery at Harvard Medical School. He is also an associate medical editor for Vascular Specialist.
This report is a follow-up of a study by the same group published in the Journal of Vascular Surgery in 2013 (58:715-21) in which they demonstrated that the use of a variety of radiation safety measures including increasing table height, utilizing collimation and angulation, decreasing magnification modes, and maintaining minimal patient-to-detector distance resulted in a 60% reduction in skin dose to their patients when measured as an index of peak skin dose to reference air kerma (PSD/RAK). Unfortunately, skin exposure remained high for FEVAR despite these measures, underscoring the fact that for very complex interventions, even with excellent radiation safety practices, the risk of skin injury remains.
The fact that skin doses as high as 11 Gy did not result in any deterministic injuries is both reassuring and a little surprising. According to the Centers for Disease Control and Prevention, radiation doses of greater than 2 Gy but less than 15 Gy will usually result in erythema within 1-2 days, with a second period of erythema and edema at 2-5 weeks, occasionally resulting in desquamation at 6-7 weeks. Late changes can include mild skin atrophy and some hyperpigmentation. Although complete healing can usually be expected at these doses, squamous skin cancer can still occur, often more than a decade after exposure.
|
|
Dr. Frank Pomposelli |
So why were no injuries seen? It may be that some were missed since follow-up examinations were not performed in 100% of their patients at any time interval, and it’s not stated whether exams were routinely performed in the first 1-2 days, when I would presume most patients were still hospitalized and the first stage of skin erythema is usually seen. Alternatively, it may be that the surrogate measure of either RAK or the index of PSD/RAK overestimated the true radiation skin dose, which seems highly likely, especially if the time of exposure in any one location was based less on the frequent changes in gantry angle and table position so commonly used in these procedures.
In our hospital, the Massachusetts Department of Public Health regulations require the patient and their physician be notified by letter when the estimated total absorbed radiation dose equals or exceeds 2 Gy. This is based on calculations by our physicist who reviews the details of any case in which the RAK measured equals or exceeds 2 Gy. Like the experiences of the authors, this most commonly occurs with lengthy and complex interventions. In our experience, we have never observed a significant skin injury presumably for the same reason – the exposure in any one location tends to be far less than the total calculated skin dose. Nevertheless, this study should not lull surgeons into a sense of complacency regarding the risk to the patient (and themselves and their staff). As our comfort and expertise with complex interventions increase, it is likely that radiation exposure will continue to increase, placing our patients at increased risk. Understanding the risk of radiation skin injury and how to minimize it is critical for any surgeon performing FEVAR and any other complex intervention utilizing fluoroscopic imaging.
Dr. Frank Pomposelli is an associate professor of surgery at Harvard Medical School. He is also an associate medical editor for Vascular Specialist.
This report is a follow-up of a study by the same group published in the Journal of Vascular Surgery in 2013 (58:715-21) in which they demonstrated that the use of a variety of radiation safety measures including increasing table height, utilizing collimation and angulation, decreasing magnification modes, and maintaining minimal patient-to-detector distance resulted in a 60% reduction in skin dose to their patients when measured as an index of peak skin dose to reference air kerma (PSD/RAK). Unfortunately, skin exposure remained high for FEVAR despite these measures, underscoring the fact that for very complex interventions, even with excellent radiation safety practices, the risk of skin injury remains.
The fact that skin doses as high as 11 Gy did not result in any deterministic injuries is both reassuring and a little surprising. According to the Centers for Disease Control and Prevention, radiation doses of greater than 2 Gy but less than 15 Gy will usually result in erythema within 1-2 days, with a second period of erythema and edema at 2-5 weeks, occasionally resulting in desquamation at 6-7 weeks. Late changes can include mild skin atrophy and some hyperpigmentation. Although complete healing can usually be expected at these doses, squamous skin cancer can still occur, often more than a decade after exposure.
|
|
Dr. Frank Pomposelli |
So why were no injuries seen? It may be that some were missed since follow-up examinations were not performed in 100% of their patients at any time interval, and it’s not stated whether exams were routinely performed in the first 1-2 days, when I would presume most patients were still hospitalized and the first stage of skin erythema is usually seen. Alternatively, it may be that the surrogate measure of either RAK or the index of PSD/RAK overestimated the true radiation skin dose, which seems highly likely, especially if the time of exposure in any one location was based less on the frequent changes in gantry angle and table position so commonly used in these procedures.
In our hospital, the Massachusetts Department of Public Health regulations require the patient and their physician be notified by letter when the estimated total absorbed radiation dose equals or exceeds 2 Gy. This is based on calculations by our physicist who reviews the details of any case in which the RAK measured equals or exceeds 2 Gy. Like the experiences of the authors, this most commonly occurs with lengthy and complex interventions. In our experience, we have never observed a significant skin injury presumably for the same reason – the exposure in any one location tends to be far less than the total calculated skin dose. Nevertheless, this study should not lull surgeons into a sense of complacency regarding the risk to the patient (and themselves and their staff). As our comfort and expertise with complex interventions increase, it is likely that radiation exposure will continue to increase, placing our patients at increased risk. Understanding the risk of radiation skin injury and how to minimize it is critical for any surgeon performing FEVAR and any other complex intervention utilizing fluoroscopic imaging.
Dr. Frank Pomposelli is an associate professor of surgery at Harvard Medical School. He is also an associate medical editor for Vascular Specialist.
CORONADO, CALIF. – Skin injury following fenestrated endovascular aortic stent grafting is less prevalent than expected, results from a single-center retrospective study showed.
“Radiation-induced skin injury is a serious potential complication of fluoroscopically guided interventions,” Dr. Melissa L. Kirkwood said at the annual meeting of the Western Vascular Society. “These injuries are associated with a threshold radiation dose, above which the severity of injury increases with increasing dose. Instances of these injuries are mostly limited to case reports of coronary interventions, TIPS procedures, and neuroembolizations.”
These radiation-induced skin lesions can be classified as prompt, early, mid-term, or late depending on when they present following the fluoroscopically guided intervention. “The National Cancer Institute has defined four grades of skin injury, with the most frequent being transient erythema, a prompt reaction within the first 24 hours occurring at skin doses as low as 2 Gy,” said Dr. Kirkwood of the division of vascular and endovascular surgery at the University of Texas Southwestern Medical Center, Dallas. “With increasing skin doses, more severe effects present themselves. Atrophy, ulceration, and necrosis are possibilities.”
She went on to note that fenestrated endovascular aneurysm repair often requires high doses of radiation, yet the prevalence of deterministic skin injury following these cases is unknown. In a recent study, Dr. Kirkwood and her associates retrospectively reviewed 61 complex fluoroscopically guided interventions that met substantial radiation dose level (SRDL) criteria, which is defined by the National Council on Radiation and Protection Measurements as a reference air kerma (RAK) greater than or equal to 5 Gy (J. Vasc. Surg. 2014; 60:742-8).
“Despite mean peak skin doses as high as 6.5 Gy, ranging up to 18.5 Gy, we did not detect any skin injuries in this cohort,” Dr. Kirkwood said. “That study, however, was limited by its retrospective design. There was no postoperative protocol in place to ensure that a thorough skin exam was performed on each patient at every follow-up visit. Therefore, we hypothesized that a more thorough postoperative follow-up of patients would detect some skin injury following these cases.”For the current study, she and her associates sought to examine the prevalence of deterministic effects after FEVAR as well as any patient characteristics that may predispose patients to skin injury.
In June 2013, the researchers implemented a new policy regarding the follow-up of FEVAR patients, which involved a full skin exam at postoperative week 2 and 4, and at 3 and 6 months, as well as questioning patients about any skin-related complaints. For the current study, they retrospectively reviewed all FEVARs over a 7-month period after the change in policy and highlighted all the cases that reached a RAK of 5 Gy or greater.
Peak skin dose, a dose index, and simulated skin dose maps were calculated using customized software employing input data from fluoroscopic machine logs. Of 317 cases performed, 22 met or exceeded a RAK of 5 Gy. Of these, 21 were FEVARs and one was an embolization. Dr. Kirkwood reported that the average RAK for all FEVARs was 8 Gy, with a range of 5-11 Gy.
Slightly more than half of patients (52%) had multiple fluoroscopically guided interventions within 6 months of their SRDL event. The average RAK for these patients was 10 Gy (range of 5 - 15). The mean peak skin dose for all FEVARs was 5 Gy (range of 2 - 10 Gy), and the dose index was 0.69. The average peak skin dose for the subset of patients with multiple procedures was 7 Gy (a range of 3 - 9 Gy).
In terms of the follow-up, all 21 FEVAR patients were examined at the 1- or 2-week mark, 81% were examined at 1 month, 52% were examined at 3 months, and 62% were examined at 6 months. No radiation skin injuries were reported. “Based on the published data, we would expect to see all grades of skin injury, especially in the cohort of the 5-10 Gy,” Dr. Kirkwood said.
In the previous study, conducted prior to the new follow-up policy, the dose index for FEVARs was 0.78, “meaning that the peak skin dose that the patient received could be roughly estimated as 78% of the RAK dose displayed on the monitor,” Dr. Kirkwood explained.
“In the current work, the dose index decreased to 60%. This suggests that surgeons in our group have now more appropriately and effectively employed strategies to decrease radiation dose to the patient. However, even when the best operating practice is employed, FEVARs still continue to require high radiation doses in order to complete.”
The present study demonstrated that deterministic skin injuries “are uncommon after FEVAR, even at high RAK levels and regardless of cumulative dose,” she concluded. “Even with more comprehensive patient follow-up, the fact that no skin injuries were reported suggests that skin injuries in this patient cohort are less prevalent than the published guidelines would predict.”
Dr. Kirkwood reported no financial disclosures.
CORONADO, CALIF. – Skin injury following fenestrated endovascular aortic stent grafting is less prevalent than expected, results from a single-center retrospective study showed.
“Radiation-induced skin injury is a serious potential complication of fluoroscopically guided interventions,” Dr. Melissa L. Kirkwood said at the annual meeting of the Western Vascular Society. “These injuries are associated with a threshold radiation dose, above which the severity of injury increases with increasing dose. Instances of these injuries are mostly limited to case reports of coronary interventions, TIPS procedures, and neuroembolizations.”
These radiation-induced skin lesions can be classified as prompt, early, mid-term, or late depending on when they present following the fluoroscopically guided intervention. “The National Cancer Institute has defined four grades of skin injury, with the most frequent being transient erythema, a prompt reaction within the first 24 hours occurring at skin doses as low as 2 Gy,” said Dr. Kirkwood of the division of vascular and endovascular surgery at the University of Texas Southwestern Medical Center, Dallas. “With increasing skin doses, more severe effects present themselves. Atrophy, ulceration, and necrosis are possibilities.”
She went on to note that fenestrated endovascular aneurysm repair often requires high doses of radiation, yet the prevalence of deterministic skin injury following these cases is unknown. In a recent study, Dr. Kirkwood and her associates retrospectively reviewed 61 complex fluoroscopically guided interventions that met substantial radiation dose level (SRDL) criteria, which is defined by the National Council on Radiation and Protection Measurements as a reference air kerma (RAK) greater than or equal to 5 Gy (J. Vasc. Surg. 2014; 60:742-8).
“Despite mean peak skin doses as high as 6.5 Gy, ranging up to 18.5 Gy, we did not detect any skin injuries in this cohort,” Dr. Kirkwood said. “That study, however, was limited by its retrospective design. There was no postoperative protocol in place to ensure that a thorough skin exam was performed on each patient at every follow-up visit. Therefore, we hypothesized that a more thorough postoperative follow-up of patients would detect some skin injury following these cases.”For the current study, she and her associates sought to examine the prevalence of deterministic effects after FEVAR as well as any patient characteristics that may predispose patients to skin injury.
In June 2013, the researchers implemented a new policy regarding the follow-up of FEVAR patients, which involved a full skin exam at postoperative week 2 and 4, and at 3 and 6 months, as well as questioning patients about any skin-related complaints. For the current study, they retrospectively reviewed all FEVARs over a 7-month period after the change in policy and highlighted all the cases that reached a RAK of 5 Gy or greater.
Peak skin dose, a dose index, and simulated skin dose maps were calculated using customized software employing input data from fluoroscopic machine logs. Of 317 cases performed, 22 met or exceeded a RAK of 5 Gy. Of these, 21 were FEVARs and one was an embolization. Dr. Kirkwood reported that the average RAK for all FEVARs was 8 Gy, with a range of 5-11 Gy.
Slightly more than half of patients (52%) had multiple fluoroscopically guided interventions within 6 months of their SRDL event. The average RAK for these patients was 10 Gy (range of 5 - 15). The mean peak skin dose for all FEVARs was 5 Gy (range of 2 - 10 Gy), and the dose index was 0.69. The average peak skin dose for the subset of patients with multiple procedures was 7 Gy (a range of 3 - 9 Gy).
In terms of the follow-up, all 21 FEVAR patients were examined at the 1- or 2-week mark, 81% were examined at 1 month, 52% were examined at 3 months, and 62% were examined at 6 months. No radiation skin injuries were reported. “Based on the published data, we would expect to see all grades of skin injury, especially in the cohort of the 5-10 Gy,” Dr. Kirkwood said.
In the previous study, conducted prior to the new follow-up policy, the dose index for FEVARs was 0.78, “meaning that the peak skin dose that the patient received could be roughly estimated as 78% of the RAK dose displayed on the monitor,” Dr. Kirkwood explained.
“In the current work, the dose index decreased to 60%. This suggests that surgeons in our group have now more appropriately and effectively employed strategies to decrease radiation dose to the patient. However, even when the best operating practice is employed, FEVARs still continue to require high radiation doses in order to complete.”
The present study demonstrated that deterministic skin injuries “are uncommon after FEVAR, even at high RAK levels and regardless of cumulative dose,” she concluded. “Even with more comprehensive patient follow-up, the fact that no skin injuries were reported suggests that skin injuries in this patient cohort are less prevalent than the published guidelines would predict.”
Dr. Kirkwood reported no financial disclosures.

FDA’s new labeling rule: clinical implications
As reviewed in a previous column, in December 2014, the Food and Drug Administration released the Pregnancy and Lactation Labeling Rule (PLLR), which will go into effect on June 30, 2015. This replaces and addresses the limitations of the system that has been in place for more than 30 years, which ascribed a pregnancy risk category of A,B,C,D, or X to drugs, with the purpose of informing the clinician and patient about the reproductive safety of medications during pregnancy. Though well intentioned, criticisms of this system have been abundant.
The system certainly simplified the interaction between physicians and patients, who presumably would be reassured that the risk of a certain medicine had been quantified by a regulatory body and therefore could be used as a basis for making a decision about whether or not to take a medicine during pregnancy. While the purpose of the labeling system was to provide some overarching guidance about available reproductive safety information of a medicine, it was ultimately used by clinicians and patients either to somehow garner reassurance about a medicine, or to heighten concern about a medicine.

From the outset, the system could not take into account the accruing reproductive safety information regarding compounds across therapeutic categories, and as a result, the risk category could be inadvertently reassuring or even misleading to patients with respect to medicines they might decide to stop or to continue.
With the older labeling system, some medicines are in the same category, despite very different amounts of reproductive safety information available on the drugs. In the 1990s, there were more reproductive safety data available on certain selective serotonin reuptake inhibitors (SSRIs), compared with others, but now the amount of such data available across SSRIs is fairly consistent. Yet SSRI labels have not been updated with the abundance of new reproductive safety information that has become available.
Almost 10 years ago, paroxetine (Paxil) was switched from a category C to D, when first-trimester exposure was linked to an increased risk of birth defects, particularly heart defects. But it was not switched back to category C when data became available that did not support that level of concern. Because of some of its side effects, paroxetine may not be considered by many to be a first-line treatment for major depression, but it certainly would not be absolutely contraindicated during pregnancy as might be presumed by the assignment of a category D label.
Lithium and sodium valproate provide another example of the limitations of the old system, which will be addressed in the new system. While the teratogenicity of both agents has been well described, the absolute risk of malformations with fetal exposure to lithium is approximately 0.05%- 0.1%, but the risk of neural tube defects with sodium valproate is estimated at 8%. Complicating the issue further, in 2013, the FDA announced that sodium valproate had been changed from a category D to X for migraine prevention, but retained the category D classification for other indications.
Placing lithium in category D suggests a relative contraindication and yet discontinuing that medication during pregnancy can put the mother and her baby at risk, given the data supporting the rapid onset of relapse in women who stop mood stabilizers during pregnancy.
For women maintained on lithium for recurrent or brittle bipolar disorder, the drug would certainly not be contraindicated and may afford critical emotional well-being and protection from relapse during pregnancy; the clinical scenario of discontinuation of lithium proximate to or during pregnancy and subsequent relapse of underlying illness is a serious clinical matter frequently demanding urgent intervention.
Still another example of the incomplete informative value of the older system is found in the assignment of atypical antipsychotics into different risk categories. Lurasidone (Latuda), approved in 2010, is in category B, but other atypical antipsychotics are in category C. One might assume that this implies that there are more reproductive safety data available on lurasidone supporting safety, but in fact, reproductive safety data for this molecule are extremely limited, and the absence of adverse event information resulted in a category B. This is a great example of the clinical maxim that incomplete or sparse data is just that; it does not imply safety, it implies that we do not know a lot about the safety of a medication.
If the old system of pregnancy labeling was arbitrary, the PLLR will be more descriptive. Safety information during pregnancy and lactation in the drug label will appear in a section on pregnancy, reformatted to include a risk summary, clinical considerations, and data subsections, as well as a section on lactation, and a section on females and males of reproductive potential.
Ongoing revision of the label as information becomes outdated is a requirement, and manufacturers will be obligated to include information on whether there is a pregnancy registry for the given drug. The goal of the PLLR is thus to provide the patient and clinician with information which addresses both sides of the risk-benefit decision for a given medicine – risks of fetal drug exposure and the risk of untreated illness for the woman and baby, a factor that is not addressed at all with the current system.
Certainly, the new label system will be a charge to industry to establish, support, and encourage enrollment in well-designed pregnancy registries across therapeutic areas to provide ample amounts of good quality data that can then be used by patients along with their physicians to make the most appropriate clinical decisions.
Much of the currently available reproductive safety information on drugs is derived from spontaneous reports, where there has been inconsistent information and variable levels of scrutiny with respect to outcomes assessment, and from small, underpowered cohort studies or large administrative databases. Postmarketing surveillance efforts have been rather modest and have not been a priority for manufacturers in most cases. Hopefully, this will change as pregnancy registries become part of routine postmarketing surveillance.
The new system will not be a panacea, and I expect there will be growing pains, considering the huge challenge of reducing the available data of varying quality into distinct paragraphs. It may also be difficult to synthesize the volume of data and the nuanced differences between certain studies into a paragraph on risk assessment. The task will be simpler for some agents and more challenging for others where the data are less consistent. Questions also remain as to how data will be revised over time.
But despite these challenges, the new system represents a monumental change, and in my mind, will bring a focus to the importance of the issue of quantifying reproductive safety of medications used by women either planning to get pregnant or who are pregnant or breastfeeding, across therapeutic areas. Of particular importance, the new system will hopefully lead to more discussion between physician and patient about what is and is not known about the reproductive safety of a medication, versus a cursory reference to some previously assigned category label.
Our group has shown that when it comes to making decisions about using medication during pregnancy, even when given the same information, women will make different decisions. This is critical since people make personal decisions about the use of these medications in collaboration with their doctors on a case-by-case basis, based on personal preference, available information, and clinical conditions across a spectrum of severity.
As the FDA requirements shift from the arbitrary category label assignment to a more descriptive explanation of risk, based on available data, an important question will be what mechanism will be used by regulators collaborating with industry to update labels with the growing amounts of information on reproductive safety, particularly if there is a commitment from industry to enhance postmarketing surveillance with more pregnancy registries.
Better data can catalyze thoughtful discussions between doctor and patient regarding decisions to use or defer treatment with a given medicine. One might wonder if the new system will open a Pandora’s box. But I believe in this case, opening Pandora’s box would be welcome because it will hopefully lead to a more careful examination of the available information regarding reproductive safety and more informed decisions on the part of patients.
Dr. Cohen is the director of the Center for Women’s Mental Health at Massachusetts General Hospital in Boston, which provides information about reproductive mental health. He has been a consultant to manufacturers of antidepressant medications and is the principal investigator of the National Pregnancy Registry for Atypical Antipsychotics, which receives support from the manufacturers of those drugs. To comment, e-mail him at [email protected]. Scan this QR code or go to obgynnews.com to view similar columns.
As reviewed in a previous column, in December 2014, the Food and Drug Administration released the Pregnancy and Lactation Labeling Rule (PLLR), which will go into effect on June 30, 2015. This replaces and addresses the limitations of the system that has been in place for more than 30 years, which ascribed a pregnancy risk category of A,B,C,D, or X to drugs, with the purpose of informing the clinician and patient about the reproductive safety of medications during pregnancy. Though well intentioned, criticisms of this system have been abundant.
The system certainly simplified the interaction between physicians and patients, who presumably would be reassured that the risk of a certain medicine had been quantified by a regulatory body and therefore could be used as a basis for making a decision about whether or not to take a medicine during pregnancy. While the purpose of the labeling system was to provide some overarching guidance about available reproductive safety information of a medicine, it was ultimately used by clinicians and patients either to somehow garner reassurance about a medicine, or to heighten concern about a medicine.
From the outset, the system could not take into account the accruing reproductive safety information regarding compounds across therapeutic categories, and as a result, the risk category could be inadvertently reassuring or even misleading to patients with respect to medicines they might decide to stop or to continue.
With the older labeling system, some medicines are in the same category, despite very different amounts of reproductive safety information available on the drugs. In the 1990s, there were more reproductive safety data available on certain selective serotonin reuptake inhibitors (SSRIs), compared with others, but now the amount of such data available across SSRIs is fairly consistent. Yet SSRI labels have not been updated with the abundance of new reproductive safety information that has become available.
Almost 10 years ago, paroxetine (Paxil) was switched from a category C to D, when first-trimester exposure was linked to an increased risk of birth defects, particularly heart defects. But it was not switched back to category C when data became available that did not support that level of concern. Because of some of its side effects, paroxetine may not be considered by many to be a first-line treatment for major depression, but it certainly would not be absolutely contraindicated during pregnancy as might be presumed by the assignment of a category D label.
Lithium and sodium valproate provide another example of the limitations of the old system, which will be addressed in the new system. While the teratogenicity of both agents has been well described, the absolute risk of malformations with fetal exposure to lithium is approximately 0.05%- 0.1%, but the risk of neural tube defects with sodium valproate is estimated at 8%. Complicating the issue further, in 2013, the FDA announced that sodium valproate had been changed from a category D to X for migraine prevention, but retained the category D classification for other indications.
Placing lithium in category D suggests a relative contraindication and yet discontinuing that medication during pregnancy can put the mother and her baby at risk, given the data supporting the rapid onset of relapse in women who stop mood stabilizers during pregnancy.
For women maintained on lithium for recurrent or brittle bipolar disorder, the drug would certainly not be contraindicated and may afford critical emotional well-being and protection from relapse during pregnancy; the clinical scenario of discontinuation of lithium proximate to or during pregnancy and subsequent relapse of underlying illness is a serious clinical matter frequently demanding urgent intervention.
Still another example of the incomplete informative value of the older system is found in the assignment of atypical antipsychotics into different risk categories. Lurasidone (Latuda), approved in 2010, is in category B, but other atypical antipsychotics are in category C. One might assume that this implies that there are more reproductive safety data available on lurasidone supporting safety, but in fact, reproductive safety data for this molecule are extremely limited, and the absence of adverse event information resulted in a category B. This is a great example of the clinical maxim that incomplete or sparse data is just that; it does not imply safety, it implies that we do not know a lot about the safety of a medication.
If the old system of pregnancy labeling was arbitrary, the PLLR will be more descriptive. Safety information during pregnancy and lactation in the drug label will appear in a section on pregnancy, reformatted to include a risk summary, clinical considerations, and data subsections, as well as a section on lactation, and a section on females and males of reproductive potential.
Ongoing revision of the label as information becomes outdated is a requirement, and manufacturers will be obligated to include information on whether there is a pregnancy registry for the given drug. The goal of the PLLR is thus to provide the patient and clinician with information which addresses both sides of the risk-benefit decision for a given medicine – risks of fetal drug exposure and the risk of untreated illness for the woman and baby, a factor that is not addressed at all with the current system.
Certainly, the new label system will be a charge to industry to establish, support, and encourage enrollment in well-designed pregnancy registries across therapeutic areas to provide ample amounts of good quality data that can then be used by patients along with their physicians to make the most appropriate clinical decisions.
Much of the currently available reproductive safety information on drugs is derived from spontaneous reports, where there has been inconsistent information and variable levels of scrutiny with respect to outcomes assessment, and from small, underpowered cohort studies or large administrative databases. Postmarketing surveillance efforts have been rather modest and have not been a priority for manufacturers in most cases. Hopefully, this will change as pregnancy registries become part of routine postmarketing surveillance.
The new system will not be a panacea, and I expect there will be growing pains, considering the huge challenge of reducing the available data of varying quality into distinct paragraphs. It may also be difficult to synthesize the volume of data and the nuanced differences between certain studies into a paragraph on risk assessment. The task will be simpler for some agents and more challenging for others where the data are less consistent. Questions also remain as to how data will be revised over time.
But despite these challenges, the new system represents a monumental change, and in my mind, will bring a focus to the importance of the issue of quantifying reproductive safety of medications used by women either planning to get pregnant or who are pregnant or breastfeeding, across therapeutic areas. Of particular importance, the new system will hopefully lead to more discussion between physician and patient about what is and is not known about the reproductive safety of a medication, versus a cursory reference to some previously assigned category label.
Our group has shown that when it comes to making decisions about using medication during pregnancy, even when given the same information, women will make different decisions. This is critical since people make personal decisions about the use of these medications in collaboration with their doctors on a case-by-case basis, based on personal preference, available information, and clinical conditions across a spectrum of severity.
As the FDA requirements shift from the arbitrary category label assignment to a more descriptive explanation of risk, based on available data, an important question will be what mechanism will be used by regulators collaborating with industry to update labels with the growing amounts of information on reproductive safety, particularly if there is a commitment from industry to enhance postmarketing surveillance with more pregnancy registries.
Better data can catalyze thoughtful discussions between doctor and patient regarding decisions to use or defer treatment with a given medicine. One might wonder if the new system will open a Pandora’s box. But I believe in this case, opening Pandora’s box would be welcome because it will hopefully lead to a more careful examination of the available information regarding reproductive safety and more informed decisions on the part of patients.
Dr. Cohen is the director of the Center for Women’s Mental Health at Massachusetts General Hospital in Boston, which provides information about reproductive mental health. He has been a consultant to manufacturers of antidepressant medications and is the principal investigator of the National Pregnancy Registry for Atypical Antipsychotics, which receives support from the manufacturers of those drugs. To comment, e-mail him at [email protected]. Scan this QR code or go to obgynnews.com to view similar columns.
As reviewed in a previous column, in December 2014, the Food and Drug Administration released the Pregnancy and Lactation Labeling Rule (PLLR), which will go into effect on June 30, 2015. This replaces and addresses the limitations of the system that has been in place for more than 30 years, which ascribed a pregnancy risk category of A,B,C,D, or X to drugs, with the purpose of informing the clinician and patient about the reproductive safety of medications during pregnancy. Though well intentioned, criticisms of this system have been abundant.
The system certainly simplified the interaction between physicians and patients, who presumably would be reassured that the risk of a certain medicine had been quantified by a regulatory body and therefore could be used as a basis for making a decision about whether or not to take a medicine during pregnancy. While the purpose of the labeling system was to provide some overarching guidance about available reproductive safety information of a medicine, it was ultimately used by clinicians and patients either to somehow garner reassurance about a medicine, or to heighten concern about a medicine.
From the outset, the system could not take into account the accruing reproductive safety information regarding compounds across therapeutic categories, and as a result, the risk category could be inadvertently reassuring or even misleading to patients with respect to medicines they might decide to stop or to continue.
With the older labeling system, some medicines are in the same category, despite very different amounts of reproductive safety information available on the drugs. In the 1990s, there were more reproductive safety data available on certain selective serotonin reuptake inhibitors (SSRIs), compared with others, but now the amount of such data available across SSRIs is fairly consistent. Yet SSRI labels have not been updated with the abundance of new reproductive safety information that has become available.
Almost 10 years ago, paroxetine (Paxil) was switched from a category C to D, when first-trimester exposure was linked to an increased risk of birth defects, particularly heart defects. But it was not switched back to category C when data became available that did not support that level of concern. Because of some of its side effects, paroxetine may not be considered by many to be a first-line treatment for major depression, but it certainly would not be absolutely contraindicated during pregnancy as might be presumed by the assignment of a category D label.
Lithium and sodium valproate provide another example of the limitations of the old system, which will be addressed in the new system. While the teratogenicity of both agents has been well described, the absolute risk of malformations with fetal exposure to lithium is approximately 0.05%- 0.1%, but the risk of neural tube defects with sodium valproate is estimated at 8%. Complicating the issue further, in 2013, the FDA announced that sodium valproate had been changed from a category D to X for migraine prevention, but retained the category D classification for other indications.
Placing lithium in category D suggests a relative contraindication and yet discontinuing that medication during pregnancy can put the mother and her baby at risk, given the data supporting the rapid onset of relapse in women who stop mood stabilizers during pregnancy.
For women maintained on lithium for recurrent or brittle bipolar disorder, the drug would certainly not be contraindicated and may afford critical emotional well-being and protection from relapse during pregnancy; the clinical scenario of discontinuation of lithium proximate to or during pregnancy and subsequent relapse of underlying illness is a serious clinical matter frequently demanding urgent intervention.
Still another example of the incomplete informative value of the older system is found in the assignment of atypical antipsychotics into different risk categories. Lurasidone (Latuda), approved in 2010, is in category B, but other atypical antipsychotics are in category C. One might assume that this implies that there are more reproductive safety data available on lurasidone supporting safety, but in fact, reproductive safety data for this molecule are extremely limited, and the absence of adverse event information resulted in a category B. This is a great example of the clinical maxim that incomplete or sparse data is just that; it does not imply safety, it implies that we do not know a lot about the safety of a medication.
If the old system of pregnancy labeling was arbitrary, the PLLR will be more descriptive. Safety information during pregnancy and lactation in the drug label will appear in a section on pregnancy, reformatted to include a risk summary, clinical considerations, and data subsections, as well as a section on lactation, and a section on females and males of reproductive potential.
Ongoing revision of the label as information becomes outdated is a requirement, and manufacturers will be obligated to include information on whether there is a pregnancy registry for the given drug. The goal of the PLLR is thus to provide the patient and clinician with information which addresses both sides of the risk-benefit decision for a given medicine – risks of fetal drug exposure and the risk of untreated illness for the woman and baby, a factor that is not addressed at all with the current system.
Certainly, the new label system will be a charge to industry to establish, support, and encourage enrollment in well-designed pregnancy registries across therapeutic areas to provide ample amounts of good quality data that can then be used by patients along with their physicians to make the most appropriate clinical decisions.
Much of the currently available reproductive safety information on drugs is derived from spontaneous reports, where there has been inconsistent information and variable levels of scrutiny with respect to outcomes assessment, and from small, underpowered cohort studies or large administrative databases. Postmarketing surveillance efforts have been rather modest and have not been a priority for manufacturers in most cases. Hopefully, this will change as pregnancy registries become part of routine postmarketing surveillance.
The new system will not be a panacea, and I expect there will be growing pains, considering the huge challenge of reducing the available data of varying quality into distinct paragraphs. It may also be difficult to synthesize the volume of data and the nuanced differences between certain studies into a paragraph on risk assessment. The task will be simpler for some agents and more challenging for others where the data are less consistent. Questions also remain as to how data will be revised over time.
But despite these challenges, the new system represents a monumental change, and in my mind, will bring a focus to the importance of the issue of quantifying reproductive safety of medications used by women either planning to get pregnant or who are pregnant or breastfeeding, across therapeutic areas. Of particular importance, the new system will hopefully lead to more discussion between physician and patient about what is and is not known about the reproductive safety of a medication, versus a cursory reference to some previously assigned category label.
Our group has shown that when it comes to making decisions about using medication during pregnancy, even when given the same information, women will make different decisions. This is critical since people make personal decisions about the use of these medications in collaboration with their doctors on a case-by-case basis, based on personal preference, available information, and clinical conditions across a spectrum of severity.
As the FDA requirements shift from the arbitrary category label assignment to a more descriptive explanation of risk, based on available data, an important question will be what mechanism will be used by regulators collaborating with industry to update labels with the growing amounts of information on reproductive safety, particularly if there is a commitment from industry to enhance postmarketing surveillance with more pregnancy registries.
Better data can catalyze thoughtful discussions between doctor and patient regarding decisions to use or defer treatment with a given medicine. One might wonder if the new system will open a Pandora’s box. But I believe in this case, opening Pandora’s box would be welcome because it will hopefully lead to a more careful examination of the available information regarding reproductive safety and more informed decisions on the part of patients.
Dr. Cohen is the director of the Center for Women’s Mental Health at Massachusetts General Hospital in Boston, which provides information about reproductive mental health. He has been a consultant to manufacturers of antidepressant medications and is the principal investigator of the National Pregnancy Registry for Atypical Antipsychotics, which receives support from the manufacturers of those drugs. To comment, e-mail him at [email protected]. Scan this QR code or go to obgynnews.com to view similar columns.

Why neutrophils have conflicting roles in cancer

Credit: Volker Brinkmann
New research has revealed distinct subpopulations of neutrophils that have conflicting functions when it comes to cancer.
Investigators identified a population of “normal,” high-density neutrophils (HDNs) that have anti-tumor properties and a population of low-density
neutrophils (LDNs) that exhibit pro-tumor activity.
They also found that the ratio of HDNs to LDNs determines whether the neutrophils have a pro- or anti-cancer effect overall.
This suggests we may be able to fight cancers by increasing the proportion of the anti-tumor HDNs while limiting the pro-tumor LDNs, according to Zvika Granot, PhD, of Hebrew University Medical School in Jerusalem, Israel.
“The novel distinction between harmful and beneficial neutrophils opens up new diagnostic and therapeutic opportunities,” Dr Granot said. “We are currently evaluating the effects of boosting the helpful anti-tumor neutrophil population, while limiting the tumor-promoting neutrophil population, on progression of the disease. If successful, this therapeutic strategy may take us closer to developing effective new therapies for cancer.”
Dr Granot and his colleagues described their discovery of LDNs and HDNs in Cell Reports.
The investigators found that LDNs were rare in healthy control subjects, but they accumulated in tumor-bearing mice and in cancer patients. HDNs exhibited cytotoxicity toward cancer cells and retarded tumor growth, but LDNs did not.
LDNs had impaired neutrophil function and immunosuppressive properties. They consisted of immature myeloid-derived suppressor cells and mature cells that were derived from HDNs.
HDNs transformed into LDNs in a TGF-β-dependent fashion, losing their anti-tumor properties and gaining immunosuppressive properties.
In the early stages of cancer development, HDNs prevailed. But as cancer progressed, the LDNs took over, and the overall neutrophil contribution became tumor-promoting.
The investigators noted that the expansion of LDNs was a relatively late event. So although these neutrophils likely contribute to tumor growth and progression, it’s less likely that they contribute to tumor initiation.
Regardless, this research challenges the concept that mature neutrophils are limited in their ability to change. It shows that neutrophils are not a homogeneous population of cells and may consist of multiple subtypes. And it provides a mechanistic explanation for the controversy surrounding neutrophil function in cancer. ![]()
Credit: Volker Brinkmann
New research has revealed distinct subpopulations of neutrophils that have conflicting functions when it comes to cancer.
Investigators identified a population of “normal,” high-density neutrophils (HDNs) that have anti-tumor properties and a population of low-density
neutrophils (LDNs) that exhibit pro-tumor activity.
They also found that the ratio of HDNs to LDNs determines whether the neutrophils have a pro- or anti-cancer effect overall.
This suggests we may be able to fight cancers by increasing the proportion of the anti-tumor HDNs while limiting the pro-tumor LDNs, according to Zvika Granot, PhD, of Hebrew University Medical School in Jerusalem, Israel.
“The novel distinction between harmful and beneficial neutrophils opens up new diagnostic and therapeutic opportunities,” Dr Granot said. “We are currently evaluating the effects of boosting the helpful anti-tumor neutrophil population, while limiting the tumor-promoting neutrophil population, on progression of the disease. If successful, this therapeutic strategy may take us closer to developing effective new therapies for cancer.”
Dr Granot and his colleagues described their discovery of LDNs and HDNs in Cell Reports.
The investigators found that LDNs were rare in healthy control subjects, but they accumulated in tumor-bearing mice and in cancer patients. HDNs exhibited cytotoxicity toward cancer cells and retarded tumor growth, but LDNs did not.
LDNs had impaired neutrophil function and immunosuppressive properties. They consisted of immature myeloid-derived suppressor cells and mature cells that were derived from HDNs.
HDNs transformed into LDNs in a TGF-β-dependent fashion, losing their anti-tumor properties and gaining immunosuppressive properties.
In the early stages of cancer development, HDNs prevailed. But as cancer progressed, the LDNs took over, and the overall neutrophil contribution became tumor-promoting.
The investigators noted that the expansion of LDNs was a relatively late event. So although these neutrophils likely contribute to tumor growth and progression, it’s less likely that they contribute to tumor initiation.
Regardless, this research challenges the concept that mature neutrophils are limited in their ability to change. It shows that neutrophils are not a homogeneous population of cells and may consist of multiple subtypes. And it provides a mechanistic explanation for the controversy surrounding neutrophil function in cancer. ![]()
Credit: Volker Brinkmann
New research has revealed distinct subpopulations of neutrophils that have conflicting functions when it comes to cancer.
Investigators identified a population of “normal,” high-density neutrophils (HDNs) that have anti-tumor properties and a population of low-density
neutrophils (LDNs) that exhibit pro-tumor activity.
They also found that the ratio of HDNs to LDNs determines whether the neutrophils have a pro- or anti-cancer effect overall.
This suggests we may be able to fight cancers by increasing the proportion of the anti-tumor HDNs while limiting the pro-tumor LDNs, according to Zvika Granot, PhD, of Hebrew University Medical School in Jerusalem, Israel.
“The novel distinction between harmful and beneficial neutrophils opens up new diagnostic and therapeutic opportunities,” Dr Granot said. “We are currently evaluating the effects of boosting the helpful anti-tumor neutrophil population, while limiting the tumor-promoting neutrophil population, on progression of the disease. If successful, this therapeutic strategy may take us closer to developing effective new therapies for cancer.”
Dr Granot and his colleagues described their discovery of LDNs and HDNs in Cell Reports.
The investigators found that LDNs were rare in healthy control subjects, but they accumulated in tumor-bearing mice and in cancer patients. HDNs exhibited cytotoxicity toward cancer cells and retarded tumor growth, but LDNs did not.
LDNs had impaired neutrophil function and immunosuppressive properties. They consisted of immature myeloid-derived suppressor cells and mature cells that were derived from HDNs.
HDNs transformed into LDNs in a TGF-β-dependent fashion, losing their anti-tumor properties and gaining immunosuppressive properties.
In the early stages of cancer development, HDNs prevailed. But as cancer progressed, the LDNs took over, and the overall neutrophil contribution became tumor-promoting.
The investigators noted that the expansion of LDNs was a relatively late event. So although these neutrophils likely contribute to tumor growth and progression, it’s less likely that they contribute to tumor initiation.
Regardless, this research challenges the concept that mature neutrophils are limited in their ability to change. It shows that neutrophils are not a homogeneous population of cells and may consist of multiple subtypes. And it provides a mechanistic explanation for the controversy surrounding neutrophil function in cancer. ![]()
Group creates detailed map of proteins in human body
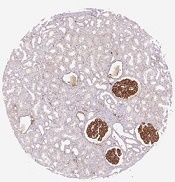
in the renal glomeruli,
the network responsible
for filtering the blood
Credit: Human Protein Atlas
Scientists say they’ve completed the first major analysis based on the Human Protein Atlas, providing a detailed picture of proteins linked to cancer, the number of proteins present in the bloodstream, and all proteins targeted by drugs.
The group described their work in Science.
The Human Protein Atlas, a multinational research project, recently launched an open-source, tissue-based, interactive map of the human proteome.
In the Science article, researchers described how they studied the human proteome. The group analyzed samples representing the 44 major tissues and organs in the human body.
They used 24,028 antibodies, corresponding to 16,975 protein-encoding genes, to produce more than 13 million tissue-based immunohistochemistry images. They complemented this analysis with RNA-sequencing data for 32 of the 44 tissue types.
In this way, the scientists mapped the distribution of proteins in all major tissues and organs in the human body. They identified proteins restricted to certain tissues—such as the brain, heart, or liver—and those present throughout the body.
Almost half of the nearly 17,000 protein-encoding genes are expressed in all the tissues the researchers analyzed. The group also found that 3171 proteins are secreted from cells, and 5570 are located in the membrane systems of cells.
“This is important information for the pharmaceutical industry,” said study author Mathias Uhlén, PhD, a professor at the KTH Royal Institute of Technology in Stockholm, Sweden, and the director of the Human Protein Atlas program.
“We show that 70% of the current targets for approved pharmaceutical drugs are either secreted or membrane-bound proteins. Interestingly, 30% of these protein targets are found in all analyzed tissues and organs. This could help explain some side effects of drugs and, thus, might have consequences for future drug development.” ![]()
in the renal glomeruli,
the network responsible
for filtering the blood
Credit: Human Protein Atlas
Scientists say they’ve completed the first major analysis based on the Human Protein Atlas, providing a detailed picture of proteins linked to cancer, the number of proteins present in the bloodstream, and all proteins targeted by drugs.
The group described their work in Science.
The Human Protein Atlas, a multinational research project, recently launched an open-source, tissue-based, interactive map of the human proteome.
In the Science article, researchers described how they studied the human proteome. The group analyzed samples representing the 44 major tissues and organs in the human body.
They used 24,028 antibodies, corresponding to 16,975 protein-encoding genes, to produce more than 13 million tissue-based immunohistochemistry images. They complemented this analysis with RNA-sequencing data for 32 of the 44 tissue types.
In this way, the scientists mapped the distribution of proteins in all major tissues and organs in the human body. They identified proteins restricted to certain tissues—such as the brain, heart, or liver—and those present throughout the body.
Almost half of the nearly 17,000 protein-encoding genes are expressed in all the tissues the researchers analyzed. The group also found that 3171 proteins are secreted from cells, and 5570 are located in the membrane systems of cells.
“This is important information for the pharmaceutical industry,” said study author Mathias Uhlén, PhD, a professor at the KTH Royal Institute of Technology in Stockholm, Sweden, and the director of the Human Protein Atlas program.
“We show that 70% of the current targets for approved pharmaceutical drugs are either secreted or membrane-bound proteins. Interestingly, 30% of these protein targets are found in all analyzed tissues and organs. This could help explain some side effects of drugs and, thus, might have consequences for future drug development.” ![]()
in the renal glomeruli,
the network responsible
for filtering the blood
Credit: Human Protein Atlas
Scientists say they’ve completed the first major analysis based on the Human Protein Atlas, providing a detailed picture of proteins linked to cancer, the number of proteins present in the bloodstream, and all proteins targeted by drugs.
The group described their work in Science.
The Human Protein Atlas, a multinational research project, recently launched an open-source, tissue-based, interactive map of the human proteome.
In the Science article, researchers described how they studied the human proteome. The group analyzed samples representing the 44 major tissues and organs in the human body.
They used 24,028 antibodies, corresponding to 16,975 protein-encoding genes, to produce more than 13 million tissue-based immunohistochemistry images. They complemented this analysis with RNA-sequencing data for 32 of the 44 tissue types.
In this way, the scientists mapped the distribution of proteins in all major tissues and organs in the human body. They identified proteins restricted to certain tissues—such as the brain, heart, or liver—and those present throughout the body.
Almost half of the nearly 17,000 protein-encoding genes are expressed in all the tissues the researchers analyzed. The group also found that 3171 proteins are secreted from cells, and 5570 are located in the membrane systems of cells.
“This is important information for the pharmaceutical industry,” said study author Mathias Uhlén, PhD, a professor at the KTH Royal Institute of Technology in Stockholm, Sweden, and the director of the Human Protein Atlas program.
“We show that 70% of the current targets for approved pharmaceutical drugs are either secreted or membrane-bound proteins. Interestingly, 30% of these protein targets are found in all analyzed tissues and organs. This could help explain some side effects of drugs and, thus, might have consequences for future drug development.” ![]()
CO2 tells malaria-carrying mosquitoes when to land

working on an experiment
involving a wind tunnel
Credit: Carrie Rosema
House-dwelling, malaria-carrying mosquitoes can detect minute changes in concentrations of exhaled carbon dioxide to determine when humans are present, according to research published in the Journal of Chemical Ecology.
Anopheles gambiae mosquitoes spend much of their adult lives indoors, where they are constantly exposed to human odor, even when people are absent.
But researchers found these mosquitoes respond very weakly to human skin odor alone.
Experiments showed that mosquitoes were more likely to a land on a source of skin odor if carbon dioxide was also present, even at very low levels.
“Responding strongly to human skin odor alone once inside a dwelling where human odor is ubiquitous is a highly inefficient means for the mosquito of locating a feeding site,” said study author Ring Cardé, PhD, of the University of California, Riverside.
“We already know that mosquitoes will readily fly upwind towards human skin odor, but landing, the final stage of host location, which typically takes place indoors, does not occur unless a fluctuating concentration of carbon dioxide indicates that a human host is present.”
Dr Cardé and his colleagues discovered the importance of carbon dioxide in mosquitoes’ landing patterns by studying Anopheles gambiae mosquitoes collected in Cameroon.
The researchers collected skin odor by using pieces of white polyester gauze worn by one of the study authors in a cotton sock for 4 to 6 hours before the experiments began. The team then recorded the mosquitoes’ landing behavior with a video camera equipped with night vision.
The landing behavior “dramatically increased” with the addition of carbon dioxide at a range of concentrations above ambient. This was true even when the carbon dioxide level was just 0.015% above ambient within the assay cage.
These results suggest the mosquitoes use a “sit-and-wait” ambush strategy during which they ignore persistent human odor until a living human is present.
One take-home message from this work is that researchers investigating which human odors mediate host-finding and which compounds are good mosquito repellents need to precisely control exposure to carbon dioxide. A researcher entering an assay room quickly elevates the level of carbon dioxide, thereby altering the mosquitoes’ behavior.
“It also would be useful next to see if mosquitoes’ response to skin odor is similarly affected by carbon dioxide in outdoor situations and how these interactions play out in human dwellings,” Dr Cardé noted. ![]()
working on an experiment
involving a wind tunnel
Credit: Carrie Rosema
House-dwelling, malaria-carrying mosquitoes can detect minute changes in concentrations of exhaled carbon dioxide to determine when humans are present, according to research published in the Journal of Chemical Ecology.
Anopheles gambiae mosquitoes spend much of their adult lives indoors, where they are constantly exposed to human odor, even when people are absent.
But researchers found these mosquitoes respond very weakly to human skin odor alone.
Experiments showed that mosquitoes were more likely to a land on a source of skin odor if carbon dioxide was also present, even at very low levels.
“Responding strongly to human skin odor alone once inside a dwelling where human odor is ubiquitous is a highly inefficient means for the mosquito of locating a feeding site,” said study author Ring Cardé, PhD, of the University of California, Riverside.
“We already know that mosquitoes will readily fly upwind towards human skin odor, but landing, the final stage of host location, which typically takes place indoors, does not occur unless a fluctuating concentration of carbon dioxide indicates that a human host is present.”
Dr Cardé and his colleagues discovered the importance of carbon dioxide in mosquitoes’ landing patterns by studying Anopheles gambiae mosquitoes collected in Cameroon.
The researchers collected skin odor by using pieces of white polyester gauze worn by one of the study authors in a cotton sock for 4 to 6 hours before the experiments began. The team then recorded the mosquitoes’ landing behavior with a video camera equipped with night vision.
The landing behavior “dramatically increased” with the addition of carbon dioxide at a range of concentrations above ambient. This was true even when the carbon dioxide level was just 0.015% above ambient within the assay cage.
These results suggest the mosquitoes use a “sit-and-wait” ambush strategy during which they ignore persistent human odor until a living human is present.
One take-home message from this work is that researchers investigating which human odors mediate host-finding and which compounds are good mosquito repellents need to precisely control exposure to carbon dioxide. A researcher entering an assay room quickly elevates the level of carbon dioxide, thereby altering the mosquitoes’ behavior.
“It also would be useful next to see if mosquitoes’ response to skin odor is similarly affected by carbon dioxide in outdoor situations and how these interactions play out in human dwellings,” Dr Cardé noted. ![]()
working on an experiment
involving a wind tunnel
Credit: Carrie Rosema
House-dwelling, malaria-carrying mosquitoes can detect minute changes in concentrations of exhaled carbon dioxide to determine when humans are present, according to research published in the Journal of Chemical Ecology.
Anopheles gambiae mosquitoes spend much of their adult lives indoors, where they are constantly exposed to human odor, even when people are absent.
But researchers found these mosquitoes respond very weakly to human skin odor alone.
Experiments showed that mosquitoes were more likely to a land on a source of skin odor if carbon dioxide was also present, even at very low levels.
“Responding strongly to human skin odor alone once inside a dwelling where human odor is ubiquitous is a highly inefficient means for the mosquito of locating a feeding site,” said study author Ring Cardé, PhD, of the University of California, Riverside.
“We already know that mosquitoes will readily fly upwind towards human skin odor, but landing, the final stage of host location, which typically takes place indoors, does not occur unless a fluctuating concentration of carbon dioxide indicates that a human host is present.”
Dr Cardé and his colleagues discovered the importance of carbon dioxide in mosquitoes’ landing patterns by studying Anopheles gambiae mosquitoes collected in Cameroon.
The researchers collected skin odor by using pieces of white polyester gauze worn by one of the study authors in a cotton sock for 4 to 6 hours before the experiments began. The team then recorded the mosquitoes’ landing behavior with a video camera equipped with night vision.
The landing behavior “dramatically increased” with the addition of carbon dioxide at a range of concentrations above ambient. This was true even when the carbon dioxide level was just 0.015% above ambient within the assay cage.
These results suggest the mosquitoes use a “sit-and-wait” ambush strategy during which they ignore persistent human odor until a living human is present.
One take-home message from this work is that researchers investigating which human odors mediate host-finding and which compounds are good mosquito repellents need to precisely control exposure to carbon dioxide. A researcher entering an assay room quickly elevates the level of carbon dioxide, thereby altering the mosquitoes’ behavior.
“It also would be useful next to see if mosquitoes’ response to skin odor is similarly affected by carbon dioxide in outdoor situations and how these interactions play out in human dwellings,” Dr Cardé noted. ![]()
Theorem helps pinpoint start of patient recovery

Credit: CDC
The 2500-year-old Pythagorean theorem could be the most effective way to identify the point at which a patient’s health begins to improve, a new study suggests.
Researchers made the discovery while examining receiver operating characteristic (ROC) curves, which are used to measure changes in a patient’s health status.
“It all comes down to choosing a point on a curve to determine when recovery has occurred,” said study author Rob Froud, PhD, of the University of Warwick in Coventry, UK.
“For many chronic conditions, epidemiologists agree that the correct point to choose is that which is closest to the top-left corner of the plot containing the curve. As we stopped to think about it, it struck us as obvious that the way to choose this point was by using Pythagoras’s theorem.”
The theorem states that, in a right-angled triangle, the sum of the squares of the 2 right-angled sides is equal to the square of the hypotenuse (the longer diagonal that joins the 2 right-angled sides).
With this formula (a2+b2=c2), a person can determine the length of the hypotenuse when given the length of the other 2 sides.
“We set about exploring the implications of this and how it might change conclusions in research,” Dr Froud said. “We conducted several experiments using real trial data, and it seems using Pythagoras’s theorem makes a material difference.”
“It helps to identify the point at which a patient has improved with more consistency and accuracy than other methods commonly used. The moral of the story is that, before you throw out the old stuff in the attic, just go through it one last time, as there may be something in there that is still relevant and useful.”
Dr Froud and his colleague Gary Abel, PhD, of the University of Cambridge in the UK, described this research in PLOS ONE. ![]()
Credit: CDC
The 2500-year-old Pythagorean theorem could be the most effective way to identify the point at which a patient’s health begins to improve, a new study suggests.
Researchers made the discovery while examining receiver operating characteristic (ROC) curves, which are used to measure changes in a patient’s health status.
“It all comes down to choosing a point on a curve to determine when recovery has occurred,” said study author Rob Froud, PhD, of the University of Warwick in Coventry, UK.
“For many chronic conditions, epidemiologists agree that the correct point to choose is that which is closest to the top-left corner of the plot containing the curve. As we stopped to think about it, it struck us as obvious that the way to choose this point was by using Pythagoras’s theorem.”
The theorem states that, in a right-angled triangle, the sum of the squares of the 2 right-angled sides is equal to the square of the hypotenuse (the longer diagonal that joins the 2 right-angled sides).
With this formula (a2+b2=c2), a person can determine the length of the hypotenuse when given the length of the other 2 sides.
“We set about exploring the implications of this and how it might change conclusions in research,” Dr Froud said. “We conducted several experiments using real trial data, and it seems using Pythagoras’s theorem makes a material difference.”
“It helps to identify the point at which a patient has improved with more consistency and accuracy than other methods commonly used. The moral of the story is that, before you throw out the old stuff in the attic, just go through it one last time, as there may be something in there that is still relevant and useful.”
Dr Froud and his colleague Gary Abel, PhD, of the University of Cambridge in the UK, described this research in PLOS ONE. ![]()
Credit: CDC
The 2500-year-old Pythagorean theorem could be the most effective way to identify the point at which a patient’s health begins to improve, a new study suggests.
Researchers made the discovery while examining receiver operating characteristic (ROC) curves, which are used to measure changes in a patient’s health status.
“It all comes down to choosing a point on a curve to determine when recovery has occurred,” said study author Rob Froud, PhD, of the University of Warwick in Coventry, UK.
“For many chronic conditions, epidemiologists agree that the correct point to choose is that which is closest to the top-left corner of the plot containing the curve. As we stopped to think about it, it struck us as obvious that the way to choose this point was by using Pythagoras’s theorem.”
The theorem states that, in a right-angled triangle, the sum of the squares of the 2 right-angled sides is equal to the square of the hypotenuse (the longer diagonal that joins the 2 right-angled sides).
With this formula (a2+b2=c2), a person can determine the length of the hypotenuse when given the length of the other 2 sides.
“We set about exploring the implications of this and how it might change conclusions in research,” Dr Froud said. “We conducted several experiments using real trial data, and it seems using Pythagoras’s theorem makes a material difference.”
“It helps to identify the point at which a patient has improved with more consistency and accuracy than other methods commonly used. The moral of the story is that, before you throw out the old stuff in the attic, just go through it one last time, as there may be something in there that is still relevant and useful.”
Dr Froud and his colleague Gary Abel, PhD, of the University of Cambridge in the UK, described this research in PLOS ONE. ![]()
A renowned device innovator honored
In November last year, one of the highly prestigious National Medals of Technology and Innovation was presented to Thomas J. Fogarty, Fogarty Institute for Innovation, for his innovations in minimally invasive medical devices. U.S. President Obama presided at the ceremony and presented the award.
Dr. Fogarty is chairman, director and founder of the Fogarty Institute for Innovation, and has served as a founder, chairman, or board member of over 30 business and research companies. During the past 40 years, he acquired 135 surgical patents, including the Fogarty balloon catheter and the Aneurx Stent Graft, an endovascular device that replaces open surgery for aortic aneurysm.

Along with the recently awarded National Medal of Technology and Innovation, he has received the Jacobson Innovation Award of the American College of Surgeons and the 2000 Lemelson-MIT prize for Invention and Innovation. He was inducted into the Inventors Hall of Fame in 2001.
Surgeon who saved Pope’s life thanked
Dr. Juan Carlos Parodi today is a prominent figure in the world vascular community, one famous for his work in the development of endovascular aortic aneurysm repair (EVAR) several decades ago.
But it was an emergency gall bladder operation many years ago, which he performed in his native Argentina, that caused him to rise to a unique prominence, illustrated in a more recent visit to Vatican City, where he had a 40-minute private audience with Pope Francis.

Dr. Parodi explained: “In 1980 I was called to treat a poor priest with a gangrenous cholecystitis caused by Clostridium. I took care of him without charging him, and after days of dialysis he survived. I forgot the experience until one day I received a call telling me that the poor priest I took care of became the Pope Francis. He invited me to visit him in the Vatican, and I went to visit him last year.
“Pope Francis received me saying: Welcome the surgeon who saved my life coming in the middle of the night to do an operation without asking for any compensation! I told him that as a physician we help people who need us, regardless of the lack of payment capacity. I was honored by being invited by him,” Dr. Parodi added.
Currently, Dr. Parodi is a professor of surgery at the University of Buenos Aires, and chief of vascular surgery at the Sanatorio Trinidad, Buenos Aires.
In November last year, one of the highly prestigious National Medals of Technology and Innovation was presented to Thomas J. Fogarty, Fogarty Institute for Innovation, for his innovations in minimally invasive medical devices. U.S. President Obama presided at the ceremony and presented the award.
Dr. Fogarty is chairman, director and founder of the Fogarty Institute for Innovation, and has served as a founder, chairman, or board member of over 30 business and research companies. During the past 40 years, he acquired 135 surgical patents, including the Fogarty balloon catheter and the Aneurx Stent Graft, an endovascular device that replaces open surgery for aortic aneurysm.
Along with the recently awarded National Medal of Technology and Innovation, he has received the Jacobson Innovation Award of the American College of Surgeons and the 2000 Lemelson-MIT prize for Invention and Innovation. He was inducted into the Inventors Hall of Fame in 2001.
Surgeon who saved Pope’s life thanked
Dr. Juan Carlos Parodi today is a prominent figure in the world vascular community, one famous for his work in the development of endovascular aortic aneurysm repair (EVAR) several decades ago.
But it was an emergency gall bladder operation many years ago, which he performed in his native Argentina, that caused him to rise to a unique prominence, illustrated in a more recent visit to Vatican City, where he had a 40-minute private audience with Pope Francis.
Dr. Parodi explained: “In 1980 I was called to treat a poor priest with a gangrenous cholecystitis caused by Clostridium. I took care of him without charging him, and after days of dialysis he survived. I forgot the experience until one day I received a call telling me that the poor priest I took care of became the Pope Francis. He invited me to visit him in the Vatican, and I went to visit him last year.
“Pope Francis received me saying: Welcome the surgeon who saved my life coming in the middle of the night to do an operation without asking for any compensation! I told him that as a physician we help people who need us, regardless of the lack of payment capacity. I was honored by being invited by him,” Dr. Parodi added.
Currently, Dr. Parodi is a professor of surgery at the University of Buenos Aires, and chief of vascular surgery at the Sanatorio Trinidad, Buenos Aires.
In November last year, one of the highly prestigious National Medals of Technology and Innovation was presented to Thomas J. Fogarty, Fogarty Institute for Innovation, for his innovations in minimally invasive medical devices. U.S. President Obama presided at the ceremony and presented the award.
Dr. Fogarty is chairman, director and founder of the Fogarty Institute for Innovation, and has served as a founder, chairman, or board member of over 30 business and research companies. During the past 40 years, he acquired 135 surgical patents, including the Fogarty balloon catheter and the Aneurx Stent Graft, an endovascular device that replaces open surgery for aortic aneurysm.
Along with the recently awarded National Medal of Technology and Innovation, he has received the Jacobson Innovation Award of the American College of Surgeons and the 2000 Lemelson-MIT prize for Invention and Innovation. He was inducted into the Inventors Hall of Fame in 2001.
Surgeon who saved Pope’s life thanked
Dr. Juan Carlos Parodi today is a prominent figure in the world vascular community, one famous for his work in the development of endovascular aortic aneurysm repair (EVAR) several decades ago.
But it was an emergency gall bladder operation many years ago, which he performed in his native Argentina, that caused him to rise to a unique prominence, illustrated in a more recent visit to Vatican City, where he had a 40-minute private audience with Pope Francis.
Dr. Parodi explained: “In 1980 I was called to treat a poor priest with a gangrenous cholecystitis caused by Clostridium. I took care of him without charging him, and after days of dialysis he survived. I forgot the experience until one day I received a call telling me that the poor priest I took care of became the Pope Francis. He invited me to visit him in the Vatican, and I went to visit him last year.
“Pope Francis received me saying: Welcome the surgeon who saved my life coming in the middle of the night to do an operation without asking for any compensation! I told him that as a physician we help people who need us, regardless of the lack of payment capacity. I was honored by being invited by him,” Dr. Parodi added.
Currently, Dr. Parodi is a professor of surgery at the University of Buenos Aires, and chief of vascular surgery at the Sanatorio Trinidad, Buenos Aires.

Tips on tics
As an experienced clinician who has seen tics and habits in your patients come and go, you may be surprised by the amount of concern parents express about them. At times, it seems, and may be, that the parent’s attention to the habit actually keeps it going! This does not always mean that the child keeps doing the habit to aggravate the parent, as parental correction may amp up the child’s anxiety, which may make the habit worse.
As with other parent concerns, both empathizing with their worry and providing evidence-based information is helpful in relieving their distress.

Habits are complex behaviors done the same way repeatedly. Habits can have a strong protective effect on our lives and be a foundation for success when they ensure that we wash our hands (protection from infection), help us know where the keys are (efficiency), or soothe us to sleep (bedtime routines).
Tics are “involuntary” (meaning often, but not always, suppressible), brief, abrupt, repeated movements usually of the face, head, or neck. More complex, apparently meaningless movements may fall into the category of stereotypies. If they last more than 4 weeks, are driven, and cause marked dysfunction or significant self-injury, they may even qualify as stereotypic movement disorder.
It is good to know that repeated behaviors such as thumb sucking, nail/lip biting, hair twirling, body rocking, self biting, and head banging are relatively common in childhood, and often (but not mostly) disappear after age 4. I like to set the expectation that one habit or tic often evolves to another to reduce panic when this happens. Thumb and hand sucking at a younger developmental age may be replaced by body rocking and head banging, and later by nail biting and finger and foot tapping.
Even in college, habits are common and stress-related such as touching the face; playing with hair, pens, or jewelry; shaking a leg; tapping fingers; or scratching the head. Parents may connect some of these to acne or poor hygiene (a good opening for coaching!) but more importantly they may be accompanied by general distress, anxiety, obsessive-compulsive symptoms, and impulsive aggressive symptoms, which need to be looked for and addressed.
Stereotypies occur in about 20% of typically developing children (called “primary”) and are classified into:
• Common behaviors (such as, rocking, head banging, finger drumming, pencil tapping, hair twisting),
• Head nodding.
• Complex motor movements (such as hand and arm flapping/waving).
Habits – including nail biting, lip chewing, and nose picking – also may be diagnosed as stereotypic movement disorders, although ICD-10 lists includes them as “other specified behavioral and emotional disorders.”
For both conditions, the behavior must not be better accounted for by a compulsion, a tic disorder, part of autism, hair pulling (trichotillomania), or paroxysmal dyskinesias.
So what is the difference between motor stereotypies and tics (and why do you care)? Motor stereotypies begin before 3 years in more than 60%, whereas tics appear later (mean 5-7 years). Stereotypies are more fixed in their pattern, compared with tics that keep shifting form, disappearing, and reappearing. Stereotypies frequently involve the arms, hands, or the entire body, while tics involve the eyes, face, head, and shoulders. Stereotypies are more fixed, rhythmic, and prolonged (most more than 10 seconds) than tics, which are mostly brief, rapid, random, and fluctuating.
One key distinguishing factor is that tics have a premonitory urge and result in a sense of relief after the tic is performed. This also means that they can be suppressed to some extent when the situation requires. While both may occur more during anxiety, excitement, or fatigue, stereotypic movements, unlike tics, also are common when the child is engrossed.
Tics can occur as a side effect of medications such as stimulants and may decrease by lowering the dose, but tics also come and go, so the impact of a medication can be hard to sort out.
One vocal or multiple motor tics occurring many times per day starting before age 18 years and lasting more than 1 year are considered chronic; those occurring less than 1 year are transient. Chronic multiple motor tics accompanied by vocalizations, even sniffing or throat clearing, qualify as Tourette syndrome. The feared component of Tourette of coprolalia (saying bad words or gestures) is fortunately rare. These diagnoses can only be made after ruling out the effects of medication or another neurological condition such as Sydenham’s chorea (resulting from infection via group A beta-hemolytic streptococcus, the bacterium that causes rheumatic fever) or PANDAS (pediatric autoimmune neuropsychiatric disorders associated with streptococcal infections).
The importance of distinguishing tics from stereotypies is in the treatment options, differential diagnosis, and prognosis. Some families (and certainly the kids themselves) do not even notice that they are moving abnormally even though 25% have at least one family member with a similar behavior. But many parents are upset about the potential for teasing and stigmatization. When you ask them directly what they are afraid of, they often admit fearing an underlying diagnosis such as intellectual disability, autism, or Tourette syndrome. The first two are straightforward to rule in or out, but Tourette can be subtle. If parents don’t bring up the possibilities, it is worth telling them directly which underlying conditions can be ruled out.
There are many conditions comorbid with tics including attention-deficit/hyperactivity disorder (ADHD), obsessive compulsive disorder (OCD), learning disorder (LD), behavioral, developmental or social problems, and mood or anxiety disorders. This clearly means that a comprehensive evaluation looking specifically for these conditions is needed when a child has chronic tics. Typically developing children with complex arm or hand movements also are more likely to have ADHD (30%), LD (20%), obsessive-compulsive behaviors (10%), or tics (18%).
Tics and stereotypies may be annoying, but generally are not harmful or progressive, although repeated movements such as skin or nose picking may result in scars or infections, and severe head banging can lead to eye injuries. Frequently repeated motor acts can cause significant muscle pain and fatigue. The most common problems are probably injury to self-esteem or oppositional behavior as a result of repeated (and fruitless) nagging or punishment by parents, even if well-meaning.
Since they occur so often along with comorbid conditions, our job includes determining the most problematic aspect before advising on a treatment. Both tics and stereotypies may be reduced by distraction, but the effect on stereotypies is faster and more certain. You can make this intervention in the office by simply asking how the child can tell when they make the movement and have them plan out what they could do instead. An example might be to shift a hand flapping movement (that makes peers think of autism) into more acceptable fist clenching. Habit reversal training or differential reinforcement based on a functional analysis can be taught by psychologists when this simple suggestion is not effective. When tics are severe, teacher education and school accommodations (504 Plan with extended time, scribe, private location for tic breaks) may be needed.
Medication is not indicated for most tics because most are mild. If ADHD is present, tics may actually be reduced by stimulants or atomoxetine rather than worsened. If the tic is severe and habit reversal training has not been successful, alpha agonists such as clonidine or guanfacine, or typical or atypical neuroleptics may be helpful. Even baclofen, benzodiazepines, anticonvulsants, nicotine, and Botox have been used. These require consultation with a specialist.
As for other chronic medical conditions, tics and persisting stereotypies deserve a comprehensive approach, including repeated education of the parent and child, evaluation for comorbidity, school accommodations, building other strengths and social support, and only rarely pulling out your prescription pad.
Dr. Howard is an assistant professor of pediatrics at The Johns Hopkins University, Baltimore, and creator of CHADIS (www.CHADIS.com). She has no other relevant disclosures. Dr. Howard’s contribution to this publication was as a paid expert to Frontline. E-mail her at [email protected].
As an experienced clinician who has seen tics and habits in your patients come and go, you may be surprised by the amount of concern parents express about them. At times, it seems, and may be, that the parent’s attention to the habit actually keeps it going! This does not always mean that the child keeps doing the habit to aggravate the parent, as parental correction may amp up the child’s anxiety, which may make the habit worse.
As with other parent concerns, both empathizing with their worry and providing evidence-based information is helpful in relieving their distress.
Habits are complex behaviors done the same way repeatedly. Habits can have a strong protective effect on our lives and be a foundation for success when they ensure that we wash our hands (protection from infection), help us know where the keys are (efficiency), or soothe us to sleep (bedtime routines).
Tics are “involuntary” (meaning often, but not always, suppressible), brief, abrupt, repeated movements usually of the face, head, or neck. More complex, apparently meaningless movements may fall into the category of stereotypies. If they last more than 4 weeks, are driven, and cause marked dysfunction or significant self-injury, they may even qualify as stereotypic movement disorder.
It is good to know that repeated behaviors such as thumb sucking, nail/lip biting, hair twirling, body rocking, self biting, and head banging are relatively common in childhood, and often (but not mostly) disappear after age 4. I like to set the expectation that one habit or tic often evolves to another to reduce panic when this happens. Thumb and hand sucking at a younger developmental age may be replaced by body rocking and head banging, and later by nail biting and finger and foot tapping.
Even in college, habits are common and stress-related such as touching the face; playing with hair, pens, or jewelry; shaking a leg; tapping fingers; or scratching the head. Parents may connect some of these to acne or poor hygiene (a good opening for coaching!) but more importantly they may be accompanied by general distress, anxiety, obsessive-compulsive symptoms, and impulsive aggressive symptoms, which need to be looked for and addressed.
Stereotypies occur in about 20% of typically developing children (called “primary”) and are classified into:
• Common behaviors (such as, rocking, head banging, finger drumming, pencil tapping, hair twisting),
• Head nodding.
• Complex motor movements (such as hand and arm flapping/waving).
Habits – including nail biting, lip chewing, and nose picking – also may be diagnosed as stereotypic movement disorders, although ICD-10 lists includes them as “other specified behavioral and emotional disorders.”
For both conditions, the behavior must not be better accounted for by a compulsion, a tic disorder, part of autism, hair pulling (trichotillomania), or paroxysmal dyskinesias.
So what is the difference between motor stereotypies and tics (and why do you care)? Motor stereotypies begin before 3 years in more than 60%, whereas tics appear later (mean 5-7 years). Stereotypies are more fixed in their pattern, compared with tics that keep shifting form, disappearing, and reappearing. Stereotypies frequently involve the arms, hands, or the entire body, while tics involve the eyes, face, head, and shoulders. Stereotypies are more fixed, rhythmic, and prolonged (most more than 10 seconds) than tics, which are mostly brief, rapid, random, and fluctuating.
One key distinguishing factor is that tics have a premonitory urge and result in a sense of relief after the tic is performed. This also means that they can be suppressed to some extent when the situation requires. While both may occur more during anxiety, excitement, or fatigue, stereotypic movements, unlike tics, also are common when the child is engrossed.
Tics can occur as a side effect of medications such as stimulants and may decrease by lowering the dose, but tics also come and go, so the impact of a medication can be hard to sort out.
One vocal or multiple motor tics occurring many times per day starting before age 18 years and lasting more than 1 year are considered chronic; those occurring less than 1 year are transient. Chronic multiple motor tics accompanied by vocalizations, even sniffing or throat clearing, qualify as Tourette syndrome. The feared component of Tourette of coprolalia (saying bad words or gestures) is fortunately rare. These diagnoses can only be made after ruling out the effects of medication or another neurological condition such as Sydenham’s chorea (resulting from infection via group A beta-hemolytic streptococcus, the bacterium that causes rheumatic fever) or PANDAS (pediatric autoimmune neuropsychiatric disorders associated with streptococcal infections).
The importance of distinguishing tics from stereotypies is in the treatment options, differential diagnosis, and prognosis. Some families (and certainly the kids themselves) do not even notice that they are moving abnormally even though 25% have at least one family member with a similar behavior. But many parents are upset about the potential for teasing and stigmatization. When you ask them directly what they are afraid of, they often admit fearing an underlying diagnosis such as intellectual disability, autism, or Tourette syndrome. The first two are straightforward to rule in or out, but Tourette can be subtle. If parents don’t bring up the possibilities, it is worth telling them directly which underlying conditions can be ruled out.
There are many conditions comorbid with tics including attention-deficit/hyperactivity disorder (ADHD), obsessive compulsive disorder (OCD), learning disorder (LD), behavioral, developmental or social problems, and mood or anxiety disorders. This clearly means that a comprehensive evaluation looking specifically for these conditions is needed when a child has chronic tics. Typically developing children with complex arm or hand movements also are more likely to have ADHD (30%), LD (20%), obsessive-compulsive behaviors (10%), or tics (18%).
Tics and stereotypies may be annoying, but generally are not harmful or progressive, although repeated movements such as skin or nose picking may result in scars or infections, and severe head banging can lead to eye injuries. Frequently repeated motor acts can cause significant muscle pain and fatigue. The most common problems are probably injury to self-esteem or oppositional behavior as a result of repeated (and fruitless) nagging or punishment by parents, even if well-meaning.
Since they occur so often along with comorbid conditions, our job includes determining the most problematic aspect before advising on a treatment. Both tics and stereotypies may be reduced by distraction, but the effect on stereotypies is faster and more certain. You can make this intervention in the office by simply asking how the child can tell when they make the movement and have them plan out what they could do instead. An example might be to shift a hand flapping movement (that makes peers think of autism) into more acceptable fist clenching. Habit reversal training or differential reinforcement based on a functional analysis can be taught by psychologists when this simple suggestion is not effective. When tics are severe, teacher education and school accommodations (504 Plan with extended time, scribe, private location for tic breaks) may be needed.
Medication is not indicated for most tics because most are mild. If ADHD is present, tics may actually be reduced by stimulants or atomoxetine rather than worsened. If the tic is severe and habit reversal training has not been successful, alpha agonists such as clonidine or guanfacine, or typical or atypical neuroleptics may be helpful. Even baclofen, benzodiazepines, anticonvulsants, nicotine, and Botox have been used. These require consultation with a specialist.
As for other chronic medical conditions, tics and persisting stereotypies deserve a comprehensive approach, including repeated education of the parent and child, evaluation for comorbidity, school accommodations, building other strengths and social support, and only rarely pulling out your prescription pad.
Dr. Howard is an assistant professor of pediatrics at The Johns Hopkins University, Baltimore, and creator of CHADIS (www.CHADIS.com). She has no other relevant disclosures. Dr. Howard’s contribution to this publication was as a paid expert to Frontline. E-mail her at [email protected].
As an experienced clinician who has seen tics and habits in your patients come and go, you may be surprised by the amount of concern parents express about them. At times, it seems, and may be, that the parent’s attention to the habit actually keeps it going! This does not always mean that the child keeps doing the habit to aggravate the parent, as parental correction may amp up the child’s anxiety, which may make the habit worse.
As with other parent concerns, both empathizing with their worry and providing evidence-based information is helpful in relieving their distress.
Habits are complex behaviors done the same way repeatedly. Habits can have a strong protective effect on our lives and be a foundation for success when they ensure that we wash our hands (protection from infection), help us know where the keys are (efficiency), or soothe us to sleep (bedtime routines).
Tics are “involuntary” (meaning often, but not always, suppressible), brief, abrupt, repeated movements usually of the face, head, or neck. More complex, apparently meaningless movements may fall into the category of stereotypies. If they last more than 4 weeks, are driven, and cause marked dysfunction or significant self-injury, they may even qualify as stereotypic movement disorder.
It is good to know that repeated behaviors such as thumb sucking, nail/lip biting, hair twirling, body rocking, self biting, and head banging are relatively common in childhood, and often (but not mostly) disappear after age 4. I like to set the expectation that one habit or tic often evolves to another to reduce panic when this happens. Thumb and hand sucking at a younger developmental age may be replaced by body rocking and head banging, and later by nail biting and finger and foot tapping.
Even in college, habits are common and stress-related such as touching the face; playing with hair, pens, or jewelry; shaking a leg; tapping fingers; or scratching the head. Parents may connect some of these to acne or poor hygiene (a good opening for coaching!) but more importantly they may be accompanied by general distress, anxiety, obsessive-compulsive symptoms, and impulsive aggressive symptoms, which need to be looked for and addressed.
Stereotypies occur in about 20% of typically developing children (called “primary”) and are classified into:
• Common behaviors (such as, rocking, head banging, finger drumming, pencil tapping, hair twisting),
• Head nodding.
• Complex motor movements (such as hand and arm flapping/waving).
Habits – including nail biting, lip chewing, and nose picking – also may be diagnosed as stereotypic movement disorders, although ICD-10 lists includes them as “other specified behavioral and emotional disorders.”
For both conditions, the behavior must not be better accounted for by a compulsion, a tic disorder, part of autism, hair pulling (trichotillomania), or paroxysmal dyskinesias.
So what is the difference between motor stereotypies and tics (and why do you care)? Motor stereotypies begin before 3 years in more than 60%, whereas tics appear later (mean 5-7 years). Stereotypies are more fixed in their pattern, compared with tics that keep shifting form, disappearing, and reappearing. Stereotypies frequently involve the arms, hands, or the entire body, while tics involve the eyes, face, head, and shoulders. Stereotypies are more fixed, rhythmic, and prolonged (most more than 10 seconds) than tics, which are mostly brief, rapid, random, and fluctuating.
One key distinguishing factor is that tics have a premonitory urge and result in a sense of relief after the tic is performed. This also means that they can be suppressed to some extent when the situation requires. While both may occur more during anxiety, excitement, or fatigue, stereotypic movements, unlike tics, also are common when the child is engrossed.
Tics can occur as a side effect of medications such as stimulants and may decrease by lowering the dose, but tics also come and go, so the impact of a medication can be hard to sort out.
One vocal or multiple motor tics occurring many times per day starting before age 18 years and lasting more than 1 year are considered chronic; those occurring less than 1 year are transient. Chronic multiple motor tics accompanied by vocalizations, even sniffing or throat clearing, qualify as Tourette syndrome. The feared component of Tourette of coprolalia (saying bad words or gestures) is fortunately rare. These diagnoses can only be made after ruling out the effects of medication or another neurological condition such as Sydenham’s chorea (resulting from infection via group A beta-hemolytic streptococcus, the bacterium that causes rheumatic fever) or PANDAS (pediatric autoimmune neuropsychiatric disorders associated with streptococcal infections).
The importance of distinguishing tics from stereotypies is in the treatment options, differential diagnosis, and prognosis. Some families (and certainly the kids themselves) do not even notice that they are moving abnormally even though 25% have at least one family member with a similar behavior. But many parents are upset about the potential for teasing and stigmatization. When you ask them directly what they are afraid of, they often admit fearing an underlying diagnosis such as intellectual disability, autism, or Tourette syndrome. The first two are straightforward to rule in or out, but Tourette can be subtle. If parents don’t bring up the possibilities, it is worth telling them directly which underlying conditions can be ruled out.
There are many conditions comorbid with tics including attention-deficit/hyperactivity disorder (ADHD), obsessive compulsive disorder (OCD), learning disorder (LD), behavioral, developmental or social problems, and mood or anxiety disorders. This clearly means that a comprehensive evaluation looking specifically for these conditions is needed when a child has chronic tics. Typically developing children with complex arm or hand movements also are more likely to have ADHD (30%), LD (20%), obsessive-compulsive behaviors (10%), or tics (18%).
Tics and stereotypies may be annoying, but generally are not harmful or progressive, although repeated movements such as skin or nose picking may result in scars or infections, and severe head banging can lead to eye injuries. Frequently repeated motor acts can cause significant muscle pain and fatigue. The most common problems are probably injury to self-esteem or oppositional behavior as a result of repeated (and fruitless) nagging or punishment by parents, even if well-meaning.
Since they occur so often along with comorbid conditions, our job includes determining the most problematic aspect before advising on a treatment. Both tics and stereotypies may be reduced by distraction, but the effect on stereotypies is faster and more certain. You can make this intervention in the office by simply asking how the child can tell when they make the movement and have them plan out what they could do instead. An example might be to shift a hand flapping movement (that makes peers think of autism) into more acceptable fist clenching. Habit reversal training or differential reinforcement based on a functional analysis can be taught by psychologists when this simple suggestion is not effective. When tics are severe, teacher education and school accommodations (504 Plan with extended time, scribe, private location for tic breaks) may be needed.
Medication is not indicated for most tics because most are mild. If ADHD is present, tics may actually be reduced by stimulants or atomoxetine rather than worsened. If the tic is severe and habit reversal training has not been successful, alpha agonists such as clonidine or guanfacine, or typical or atypical neuroleptics may be helpful. Even baclofen, benzodiazepines, anticonvulsants, nicotine, and Botox have been used. These require consultation with a specialist.
As for other chronic medical conditions, tics and persisting stereotypies deserve a comprehensive approach, including repeated education of the parent and child, evaluation for comorbidity, school accommodations, building other strengths and social support, and only rarely pulling out your prescription pad.
Dr. Howard is an assistant professor of pediatrics at The Johns Hopkins University, Baltimore, and creator of CHADIS (www.CHADIS.com). She has no other relevant disclosures. Dr. Howard’s contribution to this publication was as a paid expert to Frontline. E-mail her at [email protected].

ACOG offers strategies to reduce unintended pregnancy
A new Committee Opinion published by the American College of Obstetricians and Gynecologists (ACOG) in Obstetrics & Gynecology outlines the current barriers women face when attempting to obtain contraception and provides strategies to overcome these barriers.
Unintended pregnancy and abortion rates are higher in the United States than in most other developed countries, says ACOG; the most recent data report that 49% of US pregnancies are unintended.1
The cost of unintended pregnancy
The human cost of unintended pregnancy is high, says ACOG, because women must choose to carry the pregnancy to term and keep the baby, decide for adoption, or undergo abortion. Women and their families struggle with this challenge for medical, ethical, social, legal, and financial reasons. US births from unintended pregnancies resulted in approximately $12.5 billion in government expenditures in 2008. Affordable access to contraceptives would not only improve health but also reduce costs, as each dollar spent on publicly funded contraceptive services saves the US health-care system nearly $6.1
“The most effective way to reduce abortion rates is to prevent unintended pregnancy by improving access to consistent, effective, and affordable contraception,” states the Committee Opinion.1
What are barriers to use?
Major barriers to contraceptive use include lack of knowledge, misperceptions, and exaggerated concerns about safety among patients and health-care professionals, says the Committee.
Patients are concerned that oral contraceptives are linked to major health problems, that intrauterine devices (IUDs) carry a high risk of infection, and that certain contraceptives are abortifacients (although no FDA-approved contraceptive is an abortifacient).
Health-care professionals also may have knowledge deficits: some are uncertain about the risks and benefits of IUDs and lack knowledge about correct patient selection and contraindications.1
What strategies does ACOG support?
One in four American women who obtain contraceptive services seek them at publicly funded family planning clinics, cites ACOG.1 The Affordable Care Act (ACA) provides that all FDA-approved contraceptive methods, sterilization procedures, and patient contraceptive education and counseling are covered for women without cost sharing for all new and revised health plans and Medicaid. However, many employers are now exempt. Women covered by exempted employers and those who remain uninsured will not benefit from ACA coverage. For these women, cost barriers persist and the most effective methods (IUDs, contraceptive implant) likely will be unattainable, says ACOG.1
Insurance companies, clinic systems, or pharmacy and therapeutics committees create additional barriers, including the number of products dispensed at one time. Insurance plans prevent 73% of women from receiving more than a 1 month supply of contraception at a time, yet most women are unable to obtain refills on a timely basis. Some systems require that women “fail” certain contraceptive methods before a more expensive method (IUD, implant) will be covered. ACOG states: “All FDA-approved contraceptive methods should be available to all insured women without cost sharing and without the need to ‘fail’ certain methods first. In the absence of contraindications, patient choice and efficacy should be the principal factors in choosing one method of contraception over another.”1
Additional strategies ACOG supports and recommends to ensure affordable and accessible contraception include:
- Full implementation of the ACA requirement that new and revised private health insurance plans cover all FDA-approved contraceptives without cost sharing, including nonequivalent options from within one method category (levonorgestrel as well as copper IUDs)
- Easily accessible alternative contraceptive coverage for women who receive health insurance through employers and plans exempted from the contraceptive coverage requirement
- Medicaid expansion in all states, an action critical to the ability of low-income women to obtain improved access to contraceptives
- Adequate funding for the federal Title X family planning program and Medicaid family planning services to ensure contraceptive availability for low-income women, including the use of public funds for contraceptive provision at the time of abortion
- Sufficient compensation for contraceptive services by public and private payers to ensure access, including appropriate payment for clinician services and acquisition-cost reimbursement for supplies
- Age-appropriate, medically accurate, comprehensive sexuality education that includes information on abstinence as well as the full range of FDA-approved contraceptives
- Confidential, comprehensive contraceptive care and access to contraceptive methods for adolescents without mandated parental notification or consent, including confidentiality in billing and insurance claims processing procedures
To see all of ACOG’s recommendations, access the full report.
Reference
- Committee on Health Care for Underserved Women; American College of Obstetricians and Gynecologists. Committee Opinion No. 615: Access to Contraception. Obstet Gynecol. 2015;125(1):250–255. https://www.acog.org/-/media/Committee-Opinions/Committee-on-Health-Care-for-Underserved-Women/co615.pdf?dmc=1&ts=20150102T2211197738.
A new Committee Opinion published by the American College of Obstetricians and Gynecologists (ACOG) in Obstetrics & Gynecology outlines the current barriers women face when attempting to obtain contraception and provides strategies to overcome these barriers.
Unintended pregnancy and abortion rates are higher in the United States than in most other developed countries, says ACOG; the most recent data report that 49% of US pregnancies are unintended.1
The cost of unintended pregnancy
The human cost of unintended pregnancy is high, says ACOG, because women must choose to carry the pregnancy to term and keep the baby, decide for adoption, or undergo abortion. Women and their families struggle with this challenge for medical, ethical, social, legal, and financial reasons. US births from unintended pregnancies resulted in approximately $12.5 billion in government expenditures in 2008. Affordable access to contraceptives would not only improve health but also reduce costs, as each dollar spent on publicly funded contraceptive services saves the US health-care system nearly $6.1
“The most effective way to reduce abortion rates is to prevent unintended pregnancy by improving access to consistent, effective, and affordable contraception,” states the Committee Opinion.1
What are barriers to use?
Major barriers to contraceptive use include lack of knowledge, misperceptions, and exaggerated concerns about safety among patients and health-care professionals, says the Committee.
Patients are concerned that oral contraceptives are linked to major health problems, that intrauterine devices (IUDs) carry a high risk of infection, and that certain contraceptives are abortifacients (although no FDA-approved contraceptive is an abortifacient).
Health-care professionals also may have knowledge deficits: some are uncertain about the risks and benefits of IUDs and lack knowledge about correct patient selection and contraindications.1
What strategies does ACOG support?
One in four American women who obtain contraceptive services seek them at publicly funded family planning clinics, cites ACOG.1 The Affordable Care Act (ACA) provides that all FDA-approved contraceptive methods, sterilization procedures, and patient contraceptive education and counseling are covered for women without cost sharing for all new and revised health plans and Medicaid. However, many employers are now exempt. Women covered by exempted employers and those who remain uninsured will not benefit from ACA coverage. For these women, cost barriers persist and the most effective methods (IUDs, contraceptive implant) likely will be unattainable, says ACOG.1
Insurance companies, clinic systems, or pharmacy and therapeutics committees create additional barriers, including the number of products dispensed at one time. Insurance plans prevent 73% of women from receiving more than a 1 month supply of contraception at a time, yet most women are unable to obtain refills on a timely basis. Some systems require that women “fail” certain contraceptive methods before a more expensive method (IUD, implant) will be covered. ACOG states: “All FDA-approved contraceptive methods should be available to all insured women without cost sharing and without the need to ‘fail’ certain methods first. In the absence of contraindications, patient choice and efficacy should be the principal factors in choosing one method of contraception over another.”1
Additional strategies ACOG supports and recommends to ensure affordable and accessible contraception include:
- Full implementation of the ACA requirement that new and revised private health insurance plans cover all FDA-approved contraceptives without cost sharing, including nonequivalent options from within one method category (levonorgestrel as well as copper IUDs)
- Easily accessible alternative contraceptive coverage for women who receive health insurance through employers and plans exempted from the contraceptive coverage requirement
- Medicaid expansion in all states, an action critical to the ability of low-income women to obtain improved access to contraceptives
- Adequate funding for the federal Title X family planning program and Medicaid family planning services to ensure contraceptive availability for low-income women, including the use of public funds for contraceptive provision at the time of abortion
- Sufficient compensation for contraceptive services by public and private payers to ensure access, including appropriate payment for clinician services and acquisition-cost reimbursement for supplies
- Age-appropriate, medically accurate, comprehensive sexuality education that includes information on abstinence as well as the full range of FDA-approved contraceptives
- Confidential, comprehensive contraceptive care and access to contraceptive methods for adolescents without mandated parental notification or consent, including confidentiality in billing and insurance claims processing procedures
To see all of ACOG’s recommendations, access the full report.
A new Committee Opinion published by the American College of Obstetricians and Gynecologists (ACOG) in Obstetrics & Gynecology outlines the current barriers women face when attempting to obtain contraception and provides strategies to overcome these barriers.
Unintended pregnancy and abortion rates are higher in the United States than in most other developed countries, says ACOG; the most recent data report that 49% of US pregnancies are unintended.1
The cost of unintended pregnancy
The human cost of unintended pregnancy is high, says ACOG, because women must choose to carry the pregnancy to term and keep the baby, decide for adoption, or undergo abortion. Women and their families struggle with this challenge for medical, ethical, social, legal, and financial reasons. US births from unintended pregnancies resulted in approximately $12.5 billion in government expenditures in 2008. Affordable access to contraceptives would not only improve health but also reduce costs, as each dollar spent on publicly funded contraceptive services saves the US health-care system nearly $6.1
“The most effective way to reduce abortion rates is to prevent unintended pregnancy by improving access to consistent, effective, and affordable contraception,” states the Committee Opinion.1
What are barriers to use?
Major barriers to contraceptive use include lack of knowledge, misperceptions, and exaggerated concerns about safety among patients and health-care professionals, says the Committee.
Patients are concerned that oral contraceptives are linked to major health problems, that intrauterine devices (IUDs) carry a high risk of infection, and that certain contraceptives are abortifacients (although no FDA-approved contraceptive is an abortifacient).
Health-care professionals also may have knowledge deficits: some are uncertain about the risks and benefits of IUDs and lack knowledge about correct patient selection and contraindications.1
What strategies does ACOG support?
One in four American women who obtain contraceptive services seek them at publicly funded family planning clinics, cites ACOG.1 The Affordable Care Act (ACA) provides that all FDA-approved contraceptive methods, sterilization procedures, and patient contraceptive education and counseling are covered for women without cost sharing for all new and revised health plans and Medicaid. However, many employers are now exempt. Women covered by exempted employers and those who remain uninsured will not benefit from ACA coverage. For these women, cost barriers persist and the most effective methods (IUDs, contraceptive implant) likely will be unattainable, says ACOG.1
Insurance companies, clinic systems, or pharmacy and therapeutics committees create additional barriers, including the number of products dispensed at one time. Insurance plans prevent 73% of women from receiving more than a 1 month supply of contraception at a time, yet most women are unable to obtain refills on a timely basis. Some systems require that women “fail” certain contraceptive methods before a more expensive method (IUD, implant) will be covered. ACOG states: “All FDA-approved contraceptive methods should be available to all insured women without cost sharing and without the need to ‘fail’ certain methods first. In the absence of contraindications, patient choice and efficacy should be the principal factors in choosing one method of contraception over another.”1
Additional strategies ACOG supports and recommends to ensure affordable and accessible contraception include:
- Full implementation of the ACA requirement that new and revised private health insurance plans cover all FDA-approved contraceptives without cost sharing, including nonequivalent options from within one method category (levonorgestrel as well as copper IUDs)
- Easily accessible alternative contraceptive coverage for women who receive health insurance through employers and plans exempted from the contraceptive coverage requirement
- Medicaid expansion in all states, an action critical to the ability of low-income women to obtain improved access to contraceptives
- Adequate funding for the federal Title X family planning program and Medicaid family planning services to ensure contraceptive availability for low-income women, including the use of public funds for contraceptive provision at the time of abortion
- Sufficient compensation for contraceptive services by public and private payers to ensure access, including appropriate payment for clinician services and acquisition-cost reimbursement for supplies
- Age-appropriate, medically accurate, comprehensive sexuality education that includes information on abstinence as well as the full range of FDA-approved contraceptives
- Confidential, comprehensive contraceptive care and access to contraceptive methods for adolescents without mandated parental notification or consent, including confidentiality in billing and insurance claims processing procedures
To see all of ACOG’s recommendations, access the full report.
Reference
- Committee on Health Care for Underserved Women; American College of Obstetricians and Gynecologists. Committee Opinion No. 615: Access to Contraception. Obstet Gynecol. 2015;125(1):250–255. https://www.acog.org/-/media/Committee-Opinions/Committee-on-Health-Care-for-Underserved-Women/co615.pdf?dmc=1&ts=20150102T2211197738.
Reference
- Committee on Health Care for Underserved Women; American College of Obstetricians and Gynecologists. Committee Opinion No. 615: Access to Contraception. Obstet Gynecol. 2015;125(1):250–255. https://www.acog.org/-/media/Committee-Opinions/Committee-on-Health-Care-for-Underserved-Women/co615.pdf?dmc=1&ts=20150102T2211197738.
Antifungal treatment may cause DNA strain type switching in onychomycosis
Although DNA strain type switches are known to be a natural occurrence in patients with onychomycosis, increases in strain type switching that follow treatment failure could be an antifungal-induced response, according to the results of a study published in the British Journal of Dermatology.
“The dermatophyte Trichophyton rubrum is responsible for the majority (~80%) of [onychomycosis] cases, many of which frequently relapse after successful antifungal treatment,” noted the study authors, led by Dr. Aditya K. Gupta of the University of Toronto. Despite several previous studies of various facets related to onychomycosis, “data outlining onychomycosis infections of T. rubrum with DNA strain type, treatments, outcome and geographical location are still warranted,” they added (Br. J. Dermatol. 2015;172:74-80).

Dr. Gupta and his associates examined 50 adults infected with T. rubrum, determined via analysis of toenail specimens from onychomycosis patients in southwest Ontario. The patients were divided into cohorts based on the treatment they received: oral terbinafine, laser, or placebo (no terbinafine and no laser). Typing of DNA strains was done only in culture-positive samples before and after treatment, leaving a study population of six in the terbinafine group, nine in the laser group, and eight in the placebo group.
Half of the terbinafine subjects were prescribed oral terbinafine 250 mg/day for 12 weeks, while the other three received oral terbinafine 250 mg/day pulse therapy at on/off intervals of 2 weeks up to 12 weeks.
The investigators also used three DNA strains known to be common in Europe for comparison and found that six distinct strains, labeled A-F, accounted for 94% of the T. rubrum strains – these strains corresponded to the European ones. However, three other strains (6% of strains) were found that investigators concluded were native to North America.
Strain type switching occurred in five (83%) of the terbinafine subjects, five (56%) of the laser cohort subjects, and two (25%) of those in the placebo cohort. Roughly half of the type switches noted in the terbinafine cohort were associated with mycological cures and were followed by relapse shortly thereafter. Dr. Gupta and his associates also found that all DNA strains in this cohort were susceptible to terbinafine while in vitro. Strain types in the laser and placebo cohorts did not show any signs of intermittent cures.
The patients were sampled at intervals of 0, 12, 24, 36, 48, 60, and 72 weeks of treatment, and T. rubrum DNA strain types were determined at week 0 (n = 6) and week 48 (n = 1) or 72 (n = 5). Patients in the laser cohort were treated at weeks 0, 8, and 16 and sampled at weeks 0, 8, 16, 24, and 48, with T. rubrum DNA strain types determined at week 0 (n = 9) and week 24 (n = 5) or 48 (n = 4). Finally, placebo patients were sampled at the same regularity as those in the laser cohort, with T. rubrum DNA strain types determined at week 0 (n = 8) and week 24 (n = 1) or 48 (n = 7), they reported.
“The T. rubrum DNA strain type switches observed in ongoing infections among all treatment groups could be attributed to microevolution or coinfections of DNA strains,” the researchers noted. “The presence of coinfecting T. rubrum DNA strains that flux with environmental conditions or local niches could account for the DNA strain type switches observed in all treatment groups, where only the relatively stable types are able to propagate in culture,” they added.
Dr. Gupta and his associates did not disclose any source of funding or any relevant conflicts of interest.
Although DNA strain type switches are known to be a natural occurrence in patients with onychomycosis, increases in strain type switching that follow treatment failure could be an antifungal-induced response, according to the results of a study published in the British Journal of Dermatology.
“The dermatophyte Trichophyton rubrum is responsible for the majority (~80%) of [onychomycosis] cases, many of which frequently relapse after successful antifungal treatment,” noted the study authors, led by Dr. Aditya K. Gupta of the University of Toronto. Despite several previous studies of various facets related to onychomycosis, “data outlining onychomycosis infections of T. rubrum with DNA strain type, treatments, outcome and geographical location are still warranted,” they added (Br. J. Dermatol. 2015;172:74-80).
Dr. Gupta and his associates examined 50 adults infected with T. rubrum, determined via analysis of toenail specimens from onychomycosis patients in southwest Ontario. The patients were divided into cohorts based on the treatment they received: oral terbinafine, laser, or placebo (no terbinafine and no laser). Typing of DNA strains was done only in culture-positive samples before and after treatment, leaving a study population of six in the terbinafine group, nine in the laser group, and eight in the placebo group.
Half of the terbinafine subjects were prescribed oral terbinafine 250 mg/day for 12 weeks, while the other three received oral terbinafine 250 mg/day pulse therapy at on/off intervals of 2 weeks up to 12 weeks.
The investigators also used three DNA strains known to be common in Europe for comparison and found that six distinct strains, labeled A-F, accounted for 94% of the T. rubrum strains – these strains corresponded to the European ones. However, three other strains (6% of strains) were found that investigators concluded were native to North America.
Strain type switching occurred in five (83%) of the terbinafine subjects, five (56%) of the laser cohort subjects, and two (25%) of those in the placebo cohort. Roughly half of the type switches noted in the terbinafine cohort were associated with mycological cures and were followed by relapse shortly thereafter. Dr. Gupta and his associates also found that all DNA strains in this cohort were susceptible to terbinafine while in vitro. Strain types in the laser and placebo cohorts did not show any signs of intermittent cures.
The patients were sampled at intervals of 0, 12, 24, 36, 48, 60, and 72 weeks of treatment, and T. rubrum DNA strain types were determined at week 0 (n = 6) and week 48 (n = 1) or 72 (n = 5). Patients in the laser cohort were treated at weeks 0, 8, and 16 and sampled at weeks 0, 8, 16, 24, and 48, with T. rubrum DNA strain types determined at week 0 (n = 9) and week 24 (n = 5) or 48 (n = 4). Finally, placebo patients were sampled at the same regularity as those in the laser cohort, with T. rubrum DNA strain types determined at week 0 (n = 8) and week 24 (n = 1) or 48 (n = 7), they reported.
“The T. rubrum DNA strain type switches observed in ongoing infections among all treatment groups could be attributed to microevolution or coinfections of DNA strains,” the researchers noted. “The presence of coinfecting T. rubrum DNA strains that flux with environmental conditions or local niches could account for the DNA strain type switches observed in all treatment groups, where only the relatively stable types are able to propagate in culture,” they added.
Dr. Gupta and his associates did not disclose any source of funding or any relevant conflicts of interest.
Although DNA strain type switches are known to be a natural occurrence in patients with onychomycosis, increases in strain type switching that follow treatment failure could be an antifungal-induced response, according to the results of a study published in the British Journal of Dermatology.
“The dermatophyte Trichophyton rubrum is responsible for the majority (~80%) of [onychomycosis] cases, many of which frequently relapse after successful antifungal treatment,” noted the study authors, led by Dr. Aditya K. Gupta of the University of Toronto. Despite several previous studies of various facets related to onychomycosis, “data outlining onychomycosis infections of T. rubrum with DNA strain type, treatments, outcome and geographical location are still warranted,” they added (Br. J. Dermatol. 2015;172:74-80).
Dr. Gupta and his associates examined 50 adults infected with T. rubrum, determined via analysis of toenail specimens from onychomycosis patients in southwest Ontario. The patients were divided into cohorts based on the treatment they received: oral terbinafine, laser, or placebo (no terbinafine and no laser). Typing of DNA strains was done only in culture-positive samples before and after treatment, leaving a study population of six in the terbinafine group, nine in the laser group, and eight in the placebo group.
Half of the terbinafine subjects were prescribed oral terbinafine 250 mg/day for 12 weeks, while the other three received oral terbinafine 250 mg/day pulse therapy at on/off intervals of 2 weeks up to 12 weeks.
The investigators also used three DNA strains known to be common in Europe for comparison and found that six distinct strains, labeled A-F, accounted for 94% of the T. rubrum strains – these strains corresponded to the European ones. However, three other strains (6% of strains) were found that investigators concluded were native to North America.
Strain type switching occurred in five (83%) of the terbinafine subjects, five (56%) of the laser cohort subjects, and two (25%) of those in the placebo cohort. Roughly half of the type switches noted in the terbinafine cohort were associated with mycological cures and were followed by relapse shortly thereafter. Dr. Gupta and his associates also found that all DNA strains in this cohort were susceptible to terbinafine while in vitro. Strain types in the laser and placebo cohorts did not show any signs of intermittent cures.
The patients were sampled at intervals of 0, 12, 24, 36, 48, 60, and 72 weeks of treatment, and T. rubrum DNA strain types were determined at week 0 (n = 6) and week 48 (n = 1) or 72 (n = 5). Patients in the laser cohort were treated at weeks 0, 8, and 16 and sampled at weeks 0, 8, 16, 24, and 48, with T. rubrum DNA strain types determined at week 0 (n = 9) and week 24 (n = 5) or 48 (n = 4). Finally, placebo patients were sampled at the same regularity as those in the laser cohort, with T. rubrum DNA strain types determined at week 0 (n = 8) and week 24 (n = 1) or 48 (n = 7), they reported.
“The T. rubrum DNA strain type switches observed in ongoing infections among all treatment groups could be attributed to microevolution or coinfections of DNA strains,” the researchers noted. “The presence of coinfecting T. rubrum DNA strains that flux with environmental conditions or local niches could account for the DNA strain type switches observed in all treatment groups, where only the relatively stable types are able to propagate in culture,” they added.
Dr. Gupta and his associates did not disclose any source of funding or any relevant conflicts of interest.
FROM THE BRITISH JOURNAL OF DERMATOLOGY
Key clinical point: Antifungal treatment of onychomycosis could induce higher rates of DNA strain type switching in certain patients.
Major finding: Strain type switching occurred in 83% of the terbinafine group, 56% of the laser group, and 25% of the placebo group.
Data source: Cohort study of 23 individuals selected from 50 adults with onychomycosis who contributed samples to determine strain types.
Disclosures: The study authors did not disclose any source of funding or any relevant conflicts of interest.
