User login
Transfusion linked to bad outcomes in percutaneous peripheral vascular interventions
CHICAGO – Periprocedural blood transfusion rates vary greatly among hospitals performing similar percutaneous interventions for peripheral arterial disease, but these rates can be markedly reduced via a focused quality improvement program.
That’s been the lesson learned in Michigan, where blood transfusion rates dropped by 52% statewide at the 44 hospitals participating in the Blue Cross Blue Shield of Michigan Cardiovascular Consortium Vascular Intervention Collaborative (BMC2 PCI-VIC), Dr. Peter K. Henke reported at the American Heart Association scientific sessions.

That’s good news because periprocedural blood transfusions in patients undergoing percutaneous interventions for peripheral arterial disease (PAD) are associated with startlingly high major morbidity and mortality rates. Indeed, among 18,127 patients undergoing nonhybrid percutaneous interventions for PAD in the BMC2 PCI-VIC registry, periprocedural blood transfusion was an independent predictor of a 25-fold increased risk of MI, a 12.7-fold increase in in-hospital mortality, a 6-fold increased risk of TIA/stroke, and a 49-fold increase in vascular access complications in a logistic regression analysis adjusted for patient demographics, comorbid disease states, and periprocedural medications, according to Dr. Henke, professor of vascular surgery at the University of Michigan, Ann Arbor.
That being said, he was quick to add that he believes these associations largely reflect correlation, not causality. Transfusion recipients were significantly older and sicker than nontransfused patients undergoing the same percutaneous peripheral vascular interventions. They were far more likely to have critical limb ischemia and undergo an urgent or emergent procedure. Of note, as statewide transfusion rates fell from about 6.6% to 3.2% in response to the quality improvement program, crude in-hospital mortality didn’t change significantly, again suggesting a noncausal relationship.
The quality improvement project was undertaken in response to the observation that periprocedural transfusion rates varied institutionally across the state from 0% to 14% for patients undergoing the same percutaneous interventions for PAD. That was a red flag indicating an opportunity for improved practice.
“The median nadir hemoglobin varied within a rather narrow range of 6.8-8.5 g/dL, yet the transfusion rates were quite wide ranging,” the surgeon observed.
Over a 2-year period, the BMC2 PCI-VIC quality improvement team made repeated site visits to the hospitals with the lowest transfusion rates. They performed detailed analysis of peripheral vascular procedure processes, protocols, and order sets in order to identify best practices. Those best practices were then shared at meetings with representatives of all the participating hospitals. Feedback was provided. And transfusion rates began dropping.
Analysis of the 18,000-plus patients enrolled in the registry led to identification of a specific set of risk factors for blood transfusions, most of which occurred after patients had left the catheterization lab. These risk factors included low creatinine clearance, preprocedural anemia, chronic obstructive pulmonary disease, use of warfarin, cerebrovascular disease, critical limb ischemia, and urgent or emergent procedures.
This was the largest-ever study focused on transfusion in patients undergoing endovascular procedures for PAD, according to Dr. Henke. He noted that the results are consistent with a recent report by other investigators regarding the implications of periprocedural blood transfusion in patients undergoing percutaneous coronary intervention. In more than 2.2 million patients who underwent PCI in 2009-2013, transfusion rates varied institutionally from 0% to 13%. Transfusion was associated with 4.6-fold in-hospital mortality, a 3.6-fold increase in acute MI, and a 7.7-fold increased risk of stroke (JAMA 2014;311:836-43).
Dr. Henke reported no financial conflicts of interest regarding the PAD transfusion study, which was funded by Blue Cross Blue Shield of Michigan and the Blue Care Network.
CHICAGO – Periprocedural blood transfusion rates vary greatly among hospitals performing similar percutaneous interventions for peripheral arterial disease, but these rates can be markedly reduced via a focused quality improvement program.
That’s been the lesson learned in Michigan, where blood transfusion rates dropped by 52% statewide at the 44 hospitals participating in the Blue Cross Blue Shield of Michigan Cardiovascular Consortium Vascular Intervention Collaborative (BMC2 PCI-VIC), Dr. Peter K. Henke reported at the American Heart Association scientific sessions.
That’s good news because periprocedural blood transfusions in patients undergoing percutaneous interventions for peripheral arterial disease (PAD) are associated with startlingly high major morbidity and mortality rates. Indeed, among 18,127 patients undergoing nonhybrid percutaneous interventions for PAD in the BMC2 PCI-VIC registry, periprocedural blood transfusion was an independent predictor of a 25-fold increased risk of MI, a 12.7-fold increase in in-hospital mortality, a 6-fold increased risk of TIA/stroke, and a 49-fold increase in vascular access complications in a logistic regression analysis adjusted for patient demographics, comorbid disease states, and periprocedural medications, according to Dr. Henke, professor of vascular surgery at the University of Michigan, Ann Arbor.
That being said, he was quick to add that he believes these associations largely reflect correlation, not causality. Transfusion recipients were significantly older and sicker than nontransfused patients undergoing the same percutaneous peripheral vascular interventions. They were far more likely to have critical limb ischemia and undergo an urgent or emergent procedure. Of note, as statewide transfusion rates fell from about 6.6% to 3.2% in response to the quality improvement program, crude in-hospital mortality didn’t change significantly, again suggesting a noncausal relationship.
The quality improvement project was undertaken in response to the observation that periprocedural transfusion rates varied institutionally across the state from 0% to 14% for patients undergoing the same percutaneous interventions for PAD. That was a red flag indicating an opportunity for improved practice.
“The median nadir hemoglobin varied within a rather narrow range of 6.8-8.5 g/dL, yet the transfusion rates were quite wide ranging,” the surgeon observed.
Over a 2-year period, the BMC2 PCI-VIC quality improvement team made repeated site visits to the hospitals with the lowest transfusion rates. They performed detailed analysis of peripheral vascular procedure processes, protocols, and order sets in order to identify best practices. Those best practices were then shared at meetings with representatives of all the participating hospitals. Feedback was provided. And transfusion rates began dropping.
Analysis of the 18,000-plus patients enrolled in the registry led to identification of a specific set of risk factors for blood transfusions, most of which occurred after patients had left the catheterization lab. These risk factors included low creatinine clearance, preprocedural anemia, chronic obstructive pulmonary disease, use of warfarin, cerebrovascular disease, critical limb ischemia, and urgent or emergent procedures.
This was the largest-ever study focused on transfusion in patients undergoing endovascular procedures for PAD, according to Dr. Henke. He noted that the results are consistent with a recent report by other investigators regarding the implications of periprocedural blood transfusion in patients undergoing percutaneous coronary intervention. In more than 2.2 million patients who underwent PCI in 2009-2013, transfusion rates varied institutionally from 0% to 13%. Transfusion was associated with 4.6-fold in-hospital mortality, a 3.6-fold increase in acute MI, and a 7.7-fold increased risk of stroke (JAMA 2014;311:836-43).
Dr. Henke reported no financial conflicts of interest regarding the PAD transfusion study, which was funded by Blue Cross Blue Shield of Michigan and the Blue Care Network.
CHICAGO – Periprocedural blood transfusion rates vary greatly among hospitals performing similar percutaneous interventions for peripheral arterial disease, but these rates can be markedly reduced via a focused quality improvement program.
That’s been the lesson learned in Michigan, where blood transfusion rates dropped by 52% statewide at the 44 hospitals participating in the Blue Cross Blue Shield of Michigan Cardiovascular Consortium Vascular Intervention Collaborative (BMC2 PCI-VIC), Dr. Peter K. Henke reported at the American Heart Association scientific sessions.
That’s good news because periprocedural blood transfusions in patients undergoing percutaneous interventions for peripheral arterial disease (PAD) are associated with startlingly high major morbidity and mortality rates. Indeed, among 18,127 patients undergoing nonhybrid percutaneous interventions for PAD in the BMC2 PCI-VIC registry, periprocedural blood transfusion was an independent predictor of a 25-fold increased risk of MI, a 12.7-fold increase in in-hospital mortality, a 6-fold increased risk of TIA/stroke, and a 49-fold increase in vascular access complications in a logistic regression analysis adjusted for patient demographics, comorbid disease states, and periprocedural medications, according to Dr. Henke, professor of vascular surgery at the University of Michigan, Ann Arbor.
That being said, he was quick to add that he believes these associations largely reflect correlation, not causality. Transfusion recipients were significantly older and sicker than nontransfused patients undergoing the same percutaneous peripheral vascular interventions. They were far more likely to have critical limb ischemia and undergo an urgent or emergent procedure. Of note, as statewide transfusion rates fell from about 6.6% to 3.2% in response to the quality improvement program, crude in-hospital mortality didn’t change significantly, again suggesting a noncausal relationship.
The quality improvement project was undertaken in response to the observation that periprocedural transfusion rates varied institutionally across the state from 0% to 14% for patients undergoing the same percutaneous interventions for PAD. That was a red flag indicating an opportunity for improved practice.
“The median nadir hemoglobin varied within a rather narrow range of 6.8-8.5 g/dL, yet the transfusion rates were quite wide ranging,” the surgeon observed.
Over a 2-year period, the BMC2 PCI-VIC quality improvement team made repeated site visits to the hospitals with the lowest transfusion rates. They performed detailed analysis of peripheral vascular procedure processes, protocols, and order sets in order to identify best practices. Those best practices were then shared at meetings with representatives of all the participating hospitals. Feedback was provided. And transfusion rates began dropping.
Analysis of the 18,000-plus patients enrolled in the registry led to identification of a specific set of risk factors for blood transfusions, most of which occurred after patients had left the catheterization lab. These risk factors included low creatinine clearance, preprocedural anemia, chronic obstructive pulmonary disease, use of warfarin, cerebrovascular disease, critical limb ischemia, and urgent or emergent procedures.
This was the largest-ever study focused on transfusion in patients undergoing endovascular procedures for PAD, according to Dr. Henke. He noted that the results are consistent with a recent report by other investigators regarding the implications of periprocedural blood transfusion in patients undergoing percutaneous coronary intervention. In more than 2.2 million patients who underwent PCI in 2009-2013, transfusion rates varied institutionally from 0% to 13%. Transfusion was associated with 4.6-fold in-hospital mortality, a 3.6-fold increase in acute MI, and a 7.7-fold increased risk of stroke (JAMA 2014;311:836-43).
Dr. Henke reported no financial conflicts of interest regarding the PAD transfusion study, which was funded by Blue Cross Blue Shield of Michigan and the Blue Care Network.
AT THE AHA SCIENTIFIC SESSIONS
Key clinical point: High institutional blood transfusion rates in conjunction with percutaneous interventions for peripheral arterial disease can be sharply and safely lowered through a focused quality improvement program.
Major finding: The average periprocedural transfusion rate at 44 Michigan hospitals fell from 6.6% to 3.2% in response to the performance improvement program.
Data source: A retrospective analysis of prospectively gathered data on 18,127 Michigan patients who underwent nonhybrid percutaneous interventions for peripheral arterial disease.
Disclosures: The study was funded by Blue Cross Blue Shield of Michigan and the Blue Care Network. The presenter reported having no financial conflicts.

Imaging reveals how HSPCs interact with niche

(green) in a zebrafish
Boston Children’s Hospital
Using a zebrafish model and enhanced imaging, a group of researchers discovered how hematopoietic stem and progenitor cells (HSPCs) interact with their niche.
Subsequent imaging in mice showed that HSPCs behaved the same way in mammals, which suggests similar results might be observed in humans.
In fact, the researchers are already using the results of this study to inform research on hematopoietic stem cell transplants.
“The same process occurs during a bone marrow transplant as occurs in the body naturally,” said senior study investigator Leonard Zon, MD, of Boston Children’s Hospital in Massachusetts.
“Our direct visualization gives us a series of steps to target, and, in theory, we can look for drugs that affect every step of that process.”
He and his colleagues described this research in a paper published in Cell, as well as in two animations on YouTube, one that’s general and one more technical.
“Stem cell and bone marrow transplants are still very much a black box,” said study author Owen Tamplin, PhD, also of Boston Children’s Hospital.
“Cells are introduced into a patient, and, later on, we can measure recovery of their blood system, but what happens in between can’t be seen. Now, we have a system where we can actually watch that middle step.”
The researchers already knew that HSPCs bud off from cells in the aorta, then circulate in the body until they find a niche where they’re prepped for creating blood.
With the current study, the team observed how this niche forms, using time-lapse imaging of naturally transparent zebrafish embryos and a genetic modification that tagged the HSPCs green.
On arrival in its niche (in the tail in zebrafish), the newborn HSPC attaches itself to the blood vessel wall. There, chemical signals prompt it to squeeze itself through the wall and into a space just outside the blood vessel. Other cells begin to interact with the HSPC, and nearby endothelial cells wrap themselves around it.
“We think that is the beginning of making a stem cell happy in its niche, like a mother cuddling a baby,” Dr Zon said.
As the HSPC is being “cuddled,” it’s brought into contact with a nearby stromal cell that helps keep it attached.
The “cuddling” was reconstructed from confocal and electron microscopy images of the zebrafish taken during this stage. Through a series of image slices, the researchers were able to reassemble the whole 3D structure—HSPC, cuddling endothelial cells, and stromal cells.
“Nobody’s ever visualized live how a stem cell interacts with its niche,” Dr Zon said. “This is the first time we get a very high-resolution view of the process.”
Next, the cuddled HSPC begins dividing. One daughter cell leaves the niche, while the other stays. Eventually, all the HSPCs leave and begin colonizing their future site of blood production. (In zebrafish, this is in the kidney, which is similar to mammalian bone marrow.)
Additional imaging in mice revealed evidence that HSPCs go through much the same process in mammals, which makes it likely in humans too.
These detailed observations are already informing the Zon lab’s attempt to improve stem cell transplants. By conducting a chemical screen in large numbers of zebrafish embryos, the researchers found that the compound lycorine promotes interaction between the HSPC and its niche, leading to greater numbers of HSPCs in the adult fish. ![]()
(green) in a zebrafish
Boston Children’s Hospital
Using a zebrafish model and enhanced imaging, a group of researchers discovered how hematopoietic stem and progenitor cells (HSPCs) interact with their niche.
Subsequent imaging in mice showed that HSPCs behaved the same way in mammals, which suggests similar results might be observed in humans.
In fact, the researchers are already using the results of this study to inform research on hematopoietic stem cell transplants.
“The same process occurs during a bone marrow transplant as occurs in the body naturally,” said senior study investigator Leonard Zon, MD, of Boston Children’s Hospital in Massachusetts.
“Our direct visualization gives us a series of steps to target, and, in theory, we can look for drugs that affect every step of that process.”
He and his colleagues described this research in a paper published in Cell, as well as in two animations on YouTube, one that’s general and one more technical.
“Stem cell and bone marrow transplants are still very much a black box,” said study author Owen Tamplin, PhD, also of Boston Children’s Hospital.
“Cells are introduced into a patient, and, later on, we can measure recovery of their blood system, but what happens in between can’t be seen. Now, we have a system where we can actually watch that middle step.”
The researchers already knew that HSPCs bud off from cells in the aorta, then circulate in the body until they find a niche where they’re prepped for creating blood.
With the current study, the team observed how this niche forms, using time-lapse imaging of naturally transparent zebrafish embryos and a genetic modification that tagged the HSPCs green.
On arrival in its niche (in the tail in zebrafish), the newborn HSPC attaches itself to the blood vessel wall. There, chemical signals prompt it to squeeze itself through the wall and into a space just outside the blood vessel. Other cells begin to interact with the HSPC, and nearby endothelial cells wrap themselves around it.
“We think that is the beginning of making a stem cell happy in its niche, like a mother cuddling a baby,” Dr Zon said.
As the HSPC is being “cuddled,” it’s brought into contact with a nearby stromal cell that helps keep it attached.
The “cuddling” was reconstructed from confocal and electron microscopy images of the zebrafish taken during this stage. Through a series of image slices, the researchers were able to reassemble the whole 3D structure—HSPC, cuddling endothelial cells, and stromal cells.
“Nobody’s ever visualized live how a stem cell interacts with its niche,” Dr Zon said. “This is the first time we get a very high-resolution view of the process.”
Next, the cuddled HSPC begins dividing. One daughter cell leaves the niche, while the other stays. Eventually, all the HSPCs leave and begin colonizing their future site of blood production. (In zebrafish, this is in the kidney, which is similar to mammalian bone marrow.)
Additional imaging in mice revealed evidence that HSPCs go through much the same process in mammals, which makes it likely in humans too.
These detailed observations are already informing the Zon lab’s attempt to improve stem cell transplants. By conducting a chemical screen in large numbers of zebrafish embryos, the researchers found that the compound lycorine promotes interaction between the HSPC and its niche, leading to greater numbers of HSPCs in the adult fish. ![]()
(green) in a zebrafish
Boston Children’s Hospital
Using a zebrafish model and enhanced imaging, a group of researchers discovered how hematopoietic stem and progenitor cells (HSPCs) interact with their niche.
Subsequent imaging in mice showed that HSPCs behaved the same way in mammals, which suggests similar results might be observed in humans.
In fact, the researchers are already using the results of this study to inform research on hematopoietic stem cell transplants.
“The same process occurs during a bone marrow transplant as occurs in the body naturally,” said senior study investigator Leonard Zon, MD, of Boston Children’s Hospital in Massachusetts.
“Our direct visualization gives us a series of steps to target, and, in theory, we can look for drugs that affect every step of that process.”
He and his colleagues described this research in a paper published in Cell, as well as in two animations on YouTube, one that’s general and one more technical.
“Stem cell and bone marrow transplants are still very much a black box,” said study author Owen Tamplin, PhD, also of Boston Children’s Hospital.
“Cells are introduced into a patient, and, later on, we can measure recovery of their blood system, but what happens in between can’t be seen. Now, we have a system where we can actually watch that middle step.”
The researchers already knew that HSPCs bud off from cells in the aorta, then circulate in the body until they find a niche where they’re prepped for creating blood.
With the current study, the team observed how this niche forms, using time-lapse imaging of naturally transparent zebrafish embryos and a genetic modification that tagged the HSPCs green.
On arrival in its niche (in the tail in zebrafish), the newborn HSPC attaches itself to the blood vessel wall. There, chemical signals prompt it to squeeze itself through the wall and into a space just outside the blood vessel. Other cells begin to interact with the HSPC, and nearby endothelial cells wrap themselves around it.
“We think that is the beginning of making a stem cell happy in its niche, like a mother cuddling a baby,” Dr Zon said.
As the HSPC is being “cuddled,” it’s brought into contact with a nearby stromal cell that helps keep it attached.
The “cuddling” was reconstructed from confocal and electron microscopy images of the zebrafish taken during this stage. Through a series of image slices, the researchers were able to reassemble the whole 3D structure—HSPC, cuddling endothelial cells, and stromal cells.
“Nobody’s ever visualized live how a stem cell interacts with its niche,” Dr Zon said. “This is the first time we get a very high-resolution view of the process.”
Next, the cuddled HSPC begins dividing. One daughter cell leaves the niche, while the other stays. Eventually, all the HSPCs leave and begin colonizing their future site of blood production. (In zebrafish, this is in the kidney, which is similar to mammalian bone marrow.)
Additional imaging in mice revealed evidence that HSPCs go through much the same process in mammals, which makes it likely in humans too.
These detailed observations are already informing the Zon lab’s attempt to improve stem cell transplants. By conducting a chemical screen in large numbers of zebrafish embryos, the researchers found that the compound lycorine promotes interaction between the HSPC and its niche, leading to greater numbers of HSPCs in the adult fish. ![]()
IPT doesn’t seem to benefit children with anemia

one of the trials took place
Credit: Gabrielle Tenenbaum
Intermittent preventive antimalarial treatment (IPT) does not provide much benefit for anemic children living in malaria-endemic regions, results of a review indicate.
Researchers reviewed 6 randomized, controlled trials and found that IPT, doses of antimalarial drugs given at regular intervals in case children had contracted malaria, did lead to an improvement in hemoglobin levels.
But this did not translate to a reduction in the incidence of anemia or the rate of death and hospitalization compared to children who received placebo.
“While we did note small benefits in hemoglobin levels when treating anemic children with IPT, there was no detectable effect on the number of deaths or hospital admissions,” said review author Mwaka Athuman, of Ifakara Health Institute in Dodoma, Tanzania, Africa.
“However, 3 of the trials were carried out in areas where malaria transmission was low, so any estimate of the protective effect of IPT would be expected to be modest. The summary of the evidence will assist people forming policy guidance as to whether IPT is worthwhile and provide a basis for researchers to consider whether additional studies are needed.”
The researchers reported these findings in the Cochrane Database of Systematic Reviews.
The team reviewed 6 trials that included a total of 3847 children with anemia. Three trials were conducted in areas of low malaria endemicity and 3 in areas of moderate-to-high endemicity.
In all trials, there was a group of children who received IPT and a control group receiving placebo. In some trials, children also received iron supplements, and this was taken into consideration when the researchers analyzed the data.
Data from 4 of the trials showed that IPT did increase the mean change in hemoglobin levels from baseline to follow-up at 12 weeks—on average, by 0.32 g/dL. The reviewers dubbed this moderate-quality evidence.
Results from the same 4 trials showed that the mean hemoglobin at 12 weeks’ follow-up was, on average, 0.35 g/dL higher in the IPT group than in the placebo group. This was considered low-quality evidence.
Regardless of improvements in hemoglobin, there was no significant difference in the number of children who had anemia at 12 weeks. The median risk of anemia across 4 trials was 579 per 1000 in the placebo group and 561 per 1000 in the IPT group. This was considered moderate-quality evidence.
Similarly, there was no significant difference in the rate of death and hospitalization at 6 months between children who received IPT and those who received placebo.
The median risk of both events combined was 34 per 1000 in the placebo group and 31 per 1000 in the IPT group. This was based on data from 3 trials and was considered moderate-quality evidence.
For all of these outcomes, there was no significant difference between children who received iron and those who did not, and there was no difference between children living in regions of low malaria endemicity and those living in regions of moderate-to-high malaria endemicity. ![]()
one of the trials took place
Credit: Gabrielle Tenenbaum
Intermittent preventive antimalarial treatment (IPT) does not provide much benefit for anemic children living in malaria-endemic regions, results of a review indicate.
Researchers reviewed 6 randomized, controlled trials and found that IPT, doses of antimalarial drugs given at regular intervals in case children had contracted malaria, did lead to an improvement in hemoglobin levels.
But this did not translate to a reduction in the incidence of anemia or the rate of death and hospitalization compared to children who received placebo.
“While we did note small benefits in hemoglobin levels when treating anemic children with IPT, there was no detectable effect on the number of deaths or hospital admissions,” said review author Mwaka Athuman, of Ifakara Health Institute in Dodoma, Tanzania, Africa.
“However, 3 of the trials were carried out in areas where malaria transmission was low, so any estimate of the protective effect of IPT would be expected to be modest. The summary of the evidence will assist people forming policy guidance as to whether IPT is worthwhile and provide a basis for researchers to consider whether additional studies are needed.”
The researchers reported these findings in the Cochrane Database of Systematic Reviews.
The team reviewed 6 trials that included a total of 3847 children with anemia. Three trials were conducted in areas of low malaria endemicity and 3 in areas of moderate-to-high endemicity.
In all trials, there was a group of children who received IPT and a control group receiving placebo. In some trials, children also received iron supplements, and this was taken into consideration when the researchers analyzed the data.
Data from 4 of the trials showed that IPT did increase the mean change in hemoglobin levels from baseline to follow-up at 12 weeks—on average, by 0.32 g/dL. The reviewers dubbed this moderate-quality evidence.
Results from the same 4 trials showed that the mean hemoglobin at 12 weeks’ follow-up was, on average, 0.35 g/dL higher in the IPT group than in the placebo group. This was considered low-quality evidence.
Regardless of improvements in hemoglobin, there was no significant difference in the number of children who had anemia at 12 weeks. The median risk of anemia across 4 trials was 579 per 1000 in the placebo group and 561 per 1000 in the IPT group. This was considered moderate-quality evidence.
Similarly, there was no significant difference in the rate of death and hospitalization at 6 months between children who received IPT and those who received placebo.
The median risk of both events combined was 34 per 1000 in the placebo group and 31 per 1000 in the IPT group. This was based on data from 3 trials and was considered moderate-quality evidence.
For all of these outcomes, there was no significant difference between children who received iron and those who did not, and there was no difference between children living in regions of low malaria endemicity and those living in regions of moderate-to-high malaria endemicity. ![]()
one of the trials took place
Credit: Gabrielle Tenenbaum
Intermittent preventive antimalarial treatment (IPT) does not provide much benefit for anemic children living in malaria-endemic regions, results of a review indicate.
Researchers reviewed 6 randomized, controlled trials and found that IPT, doses of antimalarial drugs given at regular intervals in case children had contracted malaria, did lead to an improvement in hemoglobin levels.
But this did not translate to a reduction in the incidence of anemia or the rate of death and hospitalization compared to children who received placebo.
“While we did note small benefits in hemoglobin levels when treating anemic children with IPT, there was no detectable effect on the number of deaths or hospital admissions,” said review author Mwaka Athuman, of Ifakara Health Institute in Dodoma, Tanzania, Africa.
“However, 3 of the trials were carried out in areas where malaria transmission was low, so any estimate of the protective effect of IPT would be expected to be modest. The summary of the evidence will assist people forming policy guidance as to whether IPT is worthwhile and provide a basis for researchers to consider whether additional studies are needed.”
The researchers reported these findings in the Cochrane Database of Systematic Reviews.
The team reviewed 6 trials that included a total of 3847 children with anemia. Three trials were conducted in areas of low malaria endemicity and 3 in areas of moderate-to-high endemicity.
In all trials, there was a group of children who received IPT and a control group receiving placebo. In some trials, children also received iron supplements, and this was taken into consideration when the researchers analyzed the data.
Data from 4 of the trials showed that IPT did increase the mean change in hemoglobin levels from baseline to follow-up at 12 weeks—on average, by 0.32 g/dL. The reviewers dubbed this moderate-quality evidence.
Results from the same 4 trials showed that the mean hemoglobin at 12 weeks’ follow-up was, on average, 0.35 g/dL higher in the IPT group than in the placebo group. This was considered low-quality evidence.
Regardless of improvements in hemoglobin, there was no significant difference in the number of children who had anemia at 12 weeks. The median risk of anemia across 4 trials was 579 per 1000 in the placebo group and 561 per 1000 in the IPT group. This was considered moderate-quality evidence.
Similarly, there was no significant difference in the rate of death and hospitalization at 6 months between children who received IPT and those who received placebo.
The median risk of both events combined was 34 per 1000 in the placebo group and 31 per 1000 in the IPT group. This was based on data from 3 trials and was considered moderate-quality evidence.
For all of these outcomes, there was no significant difference between children who received iron and those who did not, and there was no difference between children living in regions of low malaria endemicity and those living in regions of moderate-to-high malaria endemicity. ![]()
Investigation of simulated saline continues
Credit: FDA
The US Food and Drug Administration (FDA) and the Centers for Disease Control and Prevention (CDC) are still investigating multiple instances of Wallcur’s simulated intravenous (IV) saline products being administered to patients.
So far, more than 40 patients have received infusions of Wallcur’s simulated IV saline solution, Practi-0.9% sodium chloride solution, which is intended for training purposes only. The product is not sterile and should not be injected in humans or animals.
There have been many adverse events associated with the infusions, including fever, chills, tremors, and headache. Some patients were hospitalized, and there has been 1 death, although it’s not clear if this death is directly related to the product.
Adverse events have been reported in 7 states: Florida, Georgia, Idaho, Louisiana, North Carolina, New York, and Colorado.
The FDA, in partnership with the CDC, has collected samples of Wallcur Practi 0.9% sodium chloride solution from clinics and distributors. These products are being tested to determine if they caused the adverse events observed in patients.
In addition, Wallcur has initiated a voluntary recall of Practi-0.9% sodium chloride IV solutions.
Most medical facilities that received the product said they were unaware that the IV solution bags were simulation products. However, at least one clinic recognized the Wallcur product was a simulation product upon receipt and returned it to the distributor.
The FDA said it is working with distributors who sold the simulated IV products and clinics that purchased and administered the products from Wallcur to determine how these products entered the supply chain and were administered to patients.
While Sodium Chloride 0.9% Injection (normal saline) has been in short supply, the FDA has been working with manufacturers to end the shortage.
The FDA has allowed the temporary distribution of additional IV normal saline from alternate sources: Fresenius Kabi USA, Baxter Healthcare Corp., and B. Braun Medical Inc. Currently, normal saline is available from several manufacturers, as posted on the FDA’s website.
FDA recommendations
The FDA is encouraging healthcare providers to ensure IV solution simulation products are removed from office inventory to eliminate the possible injection of Wallcur simulated products into patients.
Providers should visually inspect all current IV saline solution bags to ensure none of the bags are labeled “Wallcur,” “Practi-products,” “For clinical simulation,” or “Not for use in human or animal patients.”
If you have products labeled with any of these words or suspect you may have received other products intended for training purposes, separate simulation products from existing inventory, and contact your distributor for directions on how to return these products.
If you have received Wallcur Practi-products by mistake, please contact the distributor, or Wallcur, LLC of San Diego for return instructions.
Consider reviewing your office procedures and make sure there are procedures in place to visually inspect all future shipments of normal saline products to ensure they are for clinical use.
If you suspect that any Wallcur training IV products may have been administered to a patient, whether or not the incident has resulted in an adverse event:
- Evaluate all potentially exposed patients with new or ongoing symptoms
- Use appropriate treatment
- Report suspected cases to the state health department
- Report any adverse events following the use of these products to the FDA’s MedWatch program online or at 1-800-332-1088.
Patients who believe they received an injection of Wallcur simulated IV solution should contact their healthcare provider.
Patients who received simulated IV saline experienced fever, chills, muscle aches, and headaches almost immediately upon injection, and some required hospitalization. In most reported cases, these signs and symptoms were immediately recognized, and patients received appropriate medical attention.
Wholesalers, distributors, and suppliers of IV saline products should inspect their inventory to ensure they are not distributing simulated products as clinical-use products.
If you suspect you may have distributed Wallcur simulated IV solution to clients by mistake, immediately attempt to recall the products and warn clients of the potential risks. You should also contact Wallcur and your distributor and file a report with the FDA’s MedWatch program. ![]()
Credit: FDA
The US Food and Drug Administration (FDA) and the Centers for Disease Control and Prevention (CDC) are still investigating multiple instances of Wallcur’s simulated intravenous (IV) saline products being administered to patients.
So far, more than 40 patients have received infusions of Wallcur’s simulated IV saline solution, Practi-0.9% sodium chloride solution, which is intended for training purposes only. The product is not sterile and should not be injected in humans or animals.
There have been many adverse events associated with the infusions, including fever, chills, tremors, and headache. Some patients were hospitalized, and there has been 1 death, although it’s not clear if this death is directly related to the product.
Adverse events have been reported in 7 states: Florida, Georgia, Idaho, Louisiana, North Carolina, New York, and Colorado.
The FDA, in partnership with the CDC, has collected samples of Wallcur Practi 0.9% sodium chloride solution from clinics and distributors. These products are being tested to determine if they caused the adverse events observed in patients.
In addition, Wallcur has initiated a voluntary recall of Practi-0.9% sodium chloride IV solutions.
Most medical facilities that received the product said they were unaware that the IV solution bags were simulation products. However, at least one clinic recognized the Wallcur product was a simulation product upon receipt and returned it to the distributor.
The FDA said it is working with distributors who sold the simulated IV products and clinics that purchased and administered the products from Wallcur to determine how these products entered the supply chain and were administered to patients.
While Sodium Chloride 0.9% Injection (normal saline) has been in short supply, the FDA has been working with manufacturers to end the shortage.
The FDA has allowed the temporary distribution of additional IV normal saline from alternate sources: Fresenius Kabi USA, Baxter Healthcare Corp., and B. Braun Medical Inc. Currently, normal saline is available from several manufacturers, as posted on the FDA’s website.
FDA recommendations
The FDA is encouraging healthcare providers to ensure IV solution simulation products are removed from office inventory to eliminate the possible injection of Wallcur simulated products into patients.
Providers should visually inspect all current IV saline solution bags to ensure none of the bags are labeled “Wallcur,” “Practi-products,” “For clinical simulation,” or “Not for use in human or animal patients.”
If you have products labeled with any of these words or suspect you may have received other products intended for training purposes, separate simulation products from existing inventory, and contact your distributor for directions on how to return these products.
If you have received Wallcur Practi-products by mistake, please contact the distributor, or Wallcur, LLC of San Diego for return instructions.
Consider reviewing your office procedures and make sure there are procedures in place to visually inspect all future shipments of normal saline products to ensure they are for clinical use.
If you suspect that any Wallcur training IV products may have been administered to a patient, whether or not the incident has resulted in an adverse event:
- Evaluate all potentially exposed patients with new or ongoing symptoms
- Use appropriate treatment
- Report suspected cases to the state health department
- Report any adverse events following the use of these products to the FDA’s MedWatch program online or at 1-800-332-1088.
Patients who believe they received an injection of Wallcur simulated IV solution should contact their healthcare provider.
Patients who received simulated IV saline experienced fever, chills, muscle aches, and headaches almost immediately upon injection, and some required hospitalization. In most reported cases, these signs and symptoms were immediately recognized, and patients received appropriate medical attention.
Wholesalers, distributors, and suppliers of IV saline products should inspect their inventory to ensure they are not distributing simulated products as clinical-use products.
If you suspect you may have distributed Wallcur simulated IV solution to clients by mistake, immediately attempt to recall the products and warn clients of the potential risks. You should also contact Wallcur and your distributor and file a report with the FDA’s MedWatch program. ![]()
Credit: FDA
The US Food and Drug Administration (FDA) and the Centers for Disease Control and Prevention (CDC) are still investigating multiple instances of Wallcur’s simulated intravenous (IV) saline products being administered to patients.
So far, more than 40 patients have received infusions of Wallcur’s simulated IV saline solution, Practi-0.9% sodium chloride solution, which is intended for training purposes only. The product is not sterile and should not be injected in humans or animals.
There have been many adverse events associated with the infusions, including fever, chills, tremors, and headache. Some patients were hospitalized, and there has been 1 death, although it’s not clear if this death is directly related to the product.
Adverse events have been reported in 7 states: Florida, Georgia, Idaho, Louisiana, North Carolina, New York, and Colorado.
The FDA, in partnership with the CDC, has collected samples of Wallcur Practi 0.9% sodium chloride solution from clinics and distributors. These products are being tested to determine if they caused the adverse events observed in patients.
In addition, Wallcur has initiated a voluntary recall of Practi-0.9% sodium chloride IV solutions.
Most medical facilities that received the product said they were unaware that the IV solution bags were simulation products. However, at least one clinic recognized the Wallcur product was a simulation product upon receipt and returned it to the distributor.
The FDA said it is working with distributors who sold the simulated IV products and clinics that purchased and administered the products from Wallcur to determine how these products entered the supply chain and were administered to patients.
While Sodium Chloride 0.9% Injection (normal saline) has been in short supply, the FDA has been working with manufacturers to end the shortage.
The FDA has allowed the temporary distribution of additional IV normal saline from alternate sources: Fresenius Kabi USA, Baxter Healthcare Corp., and B. Braun Medical Inc. Currently, normal saline is available from several manufacturers, as posted on the FDA’s website.
FDA recommendations
The FDA is encouraging healthcare providers to ensure IV solution simulation products are removed from office inventory to eliminate the possible injection of Wallcur simulated products into patients.
Providers should visually inspect all current IV saline solution bags to ensure none of the bags are labeled “Wallcur,” “Practi-products,” “For clinical simulation,” or “Not for use in human or animal patients.”
If you have products labeled with any of these words or suspect you may have received other products intended for training purposes, separate simulation products from existing inventory, and contact your distributor for directions on how to return these products.
If you have received Wallcur Practi-products by mistake, please contact the distributor, or Wallcur, LLC of San Diego for return instructions.
Consider reviewing your office procedures and make sure there are procedures in place to visually inspect all future shipments of normal saline products to ensure they are for clinical use.
If you suspect that any Wallcur training IV products may have been administered to a patient, whether or not the incident has resulted in an adverse event:
- Evaluate all potentially exposed patients with new or ongoing symptoms
- Use appropriate treatment
- Report suspected cases to the state health department
- Report any adverse events following the use of these products to the FDA’s MedWatch program online or at 1-800-332-1088.
Patients who believe they received an injection of Wallcur simulated IV solution should contact their healthcare provider.
Patients who received simulated IV saline experienced fever, chills, muscle aches, and headaches almost immediately upon injection, and some required hospitalization. In most reported cases, these signs and symptoms were immediately recognized, and patients received appropriate medical attention.
Wholesalers, distributors, and suppliers of IV saline products should inspect their inventory to ensure they are not distributing simulated products as clinical-use products.
If you suspect you may have distributed Wallcur simulated IV solution to clients by mistake, immediately attempt to recall the products and warn clients of the potential risks. You should also contact Wallcur and your distributor and file a report with the FDA’s MedWatch program. ![]()
Platelet transfusions may increase risk of death
![]()
Platelet transfusions may increase the risk of death in patients with platelet consumptive disorders, results of a large study suggest.
Investigators observed a 2-fold increase in the risk of death among patients with thrombotic thrombocytopenic purpura (TTP) who received platelet transfusions and a 5-fold increase among transfused patients with heparin-induced thrombocytopenia (HIT).
There was no increased risk among patients with immune thrombocytopenia (ITP), however.
Aaron Tobian, MD, PhD, of the Johns Hopkins University School of Medicine in Baltimore, Maryland, and his colleagues reported these results in Blood. They were previously presented at the 2014 AABB Annual Meeting.
“Because these conditions are so rare, they’re difficult to study,” Dr Tobian noted. “There was some suggestion that transfusion may be harmful in these conditions, but it really was not known until now.”
“Our study is the first one to show that platelet transfusions are frequently administered to patients with ITP, HIT, and TTP, and that they’re associated with higher odds of arterial blood clots and mortality in TTP and HIT.”
For this study, Dr Tobian and his colleagues analyzed data from the Nationwide Inpatient Sample, a federal database that contains billing records for about 20% of all patients treated and discharged at about 1000 US community hospitals in 47 states.
The database contains information on about 8 million inpatient hospitalizations per year nationwide. The study covered the years 2007 to 2011.
During that time, there were 79,980 hospital admissions for ITP, 10,624 for TTP, and 6332 for HIT. Platelet transfusions were reported in 10.1% of hospitalizations for TTP, 7.1% for HIT, and 25.8% for ITP.
“Our analysis found no significantly increased risks from platelet transfusions in ITP,” said study author Ruchika Goel, MD, also of Johns Hopkins.
“But in TTP, a platelet transfusion increased the odds of a potentially lethal arterial blood clot more than 5-fold and doubled the odds of a heart attack.”
Specifically, in an age- and gender-adjusted analysis, the odds ratio (OR) for arterial thrombosis was 5.8, and the OR for acute myocardial infarction (AMI) was 2.0 in TTP patients who received platelet transfusions. The OR for stroke was 1.6, and the OR for venous thrombosis was 1.1.
Similarly, HIT patients had an increased risk of arterial thrombosis (OR=3.4) and AMI (OR=1.9) if they received a platelet transfusion. But they did not have an increased risk of venous thrombosis (OR=0.8) or stroke (OR=0.5).
Platelet transfusions among ITP patients were not significantly associated with venous thrombosis (OR=1.3), arterial thrombosis (OR=0.3), AMI (OR=1.3), or stroke (OR=1.3) after adjustment for age and gender.
The all-cause, in-hospital mortality rates were 8.8% for TTP patients, 3.4% for HIT patients, and 1.4% for ITP patients.
Patients with TTP and HIT had a significantly increased risk of all-cause mortality if they received platelet transfusions, with age- and gender-adjusted ORs of 2.0 and 5.2, respectively. But platelet transfusions were not significantly associated with mortality in ITP patients, with an OR of 1.1.
The investigators said they were surprised at the prevalence of platelet transfusions in this patient population, in spite of some practitioners’ concerns about the risks.
But Dr Tobian noted that, in some cases, doctors may not know a patient has a platelet disorder until they see the potentially deadly reaction to the transfusion. And in other cases, the transfusion may be used as a last resort.
He and his colleagues believe that, for patients with HIT and TTP, platelet transfusions should be reserved “only for severe, life-threatening bleeding refractory to other therapies or major surgery.” ![]()
![]()
Platelet transfusions may increase the risk of death in patients with platelet consumptive disorders, results of a large study suggest.
Investigators observed a 2-fold increase in the risk of death among patients with thrombotic thrombocytopenic purpura (TTP) who received platelet transfusions and a 5-fold increase among transfused patients with heparin-induced thrombocytopenia (HIT).
There was no increased risk among patients with immune thrombocytopenia (ITP), however.
Aaron Tobian, MD, PhD, of the Johns Hopkins University School of Medicine in Baltimore, Maryland, and his colleagues reported these results in Blood. They were previously presented at the 2014 AABB Annual Meeting.
“Because these conditions are so rare, they’re difficult to study,” Dr Tobian noted. “There was some suggestion that transfusion may be harmful in these conditions, but it really was not known until now.”
“Our study is the first one to show that platelet transfusions are frequently administered to patients with ITP, HIT, and TTP, and that they’re associated with higher odds of arterial blood clots and mortality in TTP and HIT.”
For this study, Dr Tobian and his colleagues analyzed data from the Nationwide Inpatient Sample, a federal database that contains billing records for about 20% of all patients treated and discharged at about 1000 US community hospitals in 47 states.
The database contains information on about 8 million inpatient hospitalizations per year nationwide. The study covered the years 2007 to 2011.
During that time, there were 79,980 hospital admissions for ITP, 10,624 for TTP, and 6332 for HIT. Platelet transfusions were reported in 10.1% of hospitalizations for TTP, 7.1% for HIT, and 25.8% for ITP.
“Our analysis found no significantly increased risks from platelet transfusions in ITP,” said study author Ruchika Goel, MD, also of Johns Hopkins.
“But in TTP, a platelet transfusion increased the odds of a potentially lethal arterial blood clot more than 5-fold and doubled the odds of a heart attack.”
Specifically, in an age- and gender-adjusted analysis, the odds ratio (OR) for arterial thrombosis was 5.8, and the OR for acute myocardial infarction (AMI) was 2.0 in TTP patients who received platelet transfusions. The OR for stroke was 1.6, and the OR for venous thrombosis was 1.1.
Similarly, HIT patients had an increased risk of arterial thrombosis (OR=3.4) and AMI (OR=1.9) if they received a platelet transfusion. But they did not have an increased risk of venous thrombosis (OR=0.8) or stroke (OR=0.5).
Platelet transfusions among ITP patients were not significantly associated with venous thrombosis (OR=1.3), arterial thrombosis (OR=0.3), AMI (OR=1.3), or stroke (OR=1.3) after adjustment for age and gender.
The all-cause, in-hospital mortality rates were 8.8% for TTP patients, 3.4% for HIT patients, and 1.4% for ITP patients.
Patients with TTP and HIT had a significantly increased risk of all-cause mortality if they received platelet transfusions, with age- and gender-adjusted ORs of 2.0 and 5.2, respectively. But platelet transfusions were not significantly associated with mortality in ITP patients, with an OR of 1.1.
The investigators said they were surprised at the prevalence of platelet transfusions in this patient population, in spite of some practitioners’ concerns about the risks.
But Dr Tobian noted that, in some cases, doctors may not know a patient has a platelet disorder until they see the potentially deadly reaction to the transfusion. And in other cases, the transfusion may be used as a last resort.
He and his colleagues believe that, for patients with HIT and TTP, platelet transfusions should be reserved “only for severe, life-threatening bleeding refractory to other therapies or major surgery.” ![]()
![]()
Platelet transfusions may increase the risk of death in patients with platelet consumptive disorders, results of a large study suggest.
Investigators observed a 2-fold increase in the risk of death among patients with thrombotic thrombocytopenic purpura (TTP) who received platelet transfusions and a 5-fold increase among transfused patients with heparin-induced thrombocytopenia (HIT).
There was no increased risk among patients with immune thrombocytopenia (ITP), however.
Aaron Tobian, MD, PhD, of the Johns Hopkins University School of Medicine in Baltimore, Maryland, and his colleagues reported these results in Blood. They were previously presented at the 2014 AABB Annual Meeting.
“Because these conditions are so rare, they’re difficult to study,” Dr Tobian noted. “There was some suggestion that transfusion may be harmful in these conditions, but it really was not known until now.”
“Our study is the first one to show that platelet transfusions are frequently administered to patients with ITP, HIT, and TTP, and that they’re associated with higher odds of arterial blood clots and mortality in TTP and HIT.”
For this study, Dr Tobian and his colleagues analyzed data from the Nationwide Inpatient Sample, a federal database that contains billing records for about 20% of all patients treated and discharged at about 1000 US community hospitals in 47 states.
The database contains information on about 8 million inpatient hospitalizations per year nationwide. The study covered the years 2007 to 2011.
During that time, there were 79,980 hospital admissions for ITP, 10,624 for TTP, and 6332 for HIT. Platelet transfusions were reported in 10.1% of hospitalizations for TTP, 7.1% for HIT, and 25.8% for ITP.
“Our analysis found no significantly increased risks from platelet transfusions in ITP,” said study author Ruchika Goel, MD, also of Johns Hopkins.
“But in TTP, a platelet transfusion increased the odds of a potentially lethal arterial blood clot more than 5-fold and doubled the odds of a heart attack.”
Specifically, in an age- and gender-adjusted analysis, the odds ratio (OR) for arterial thrombosis was 5.8, and the OR for acute myocardial infarction (AMI) was 2.0 in TTP patients who received platelet transfusions. The OR for stroke was 1.6, and the OR for venous thrombosis was 1.1.
Similarly, HIT patients had an increased risk of arterial thrombosis (OR=3.4) and AMI (OR=1.9) if they received a platelet transfusion. But they did not have an increased risk of venous thrombosis (OR=0.8) or stroke (OR=0.5).
Platelet transfusions among ITP patients were not significantly associated with venous thrombosis (OR=1.3), arterial thrombosis (OR=0.3), AMI (OR=1.3), or stroke (OR=1.3) after adjustment for age and gender.
The all-cause, in-hospital mortality rates were 8.8% for TTP patients, 3.4% for HIT patients, and 1.4% for ITP patients.
Patients with TTP and HIT had a significantly increased risk of all-cause mortality if they received platelet transfusions, with age- and gender-adjusted ORs of 2.0 and 5.2, respectively. But platelet transfusions were not significantly associated with mortality in ITP patients, with an OR of 1.1.
The investigators said they were surprised at the prevalence of platelet transfusions in this patient population, in spite of some practitioners’ concerns about the risks.
But Dr Tobian noted that, in some cases, doctors may not know a patient has a platelet disorder until they see the potentially deadly reaction to the transfusion. And in other cases, the transfusion may be used as a last resort.
He and his colleagues believe that, for patients with HIT and TTP, platelet transfusions should be reserved “only for severe, life-threatening bleeding refractory to other therapies or major surgery.” ![]()
Adults with eczema face increased risk of fracture and bone or joint injuries
Eczema in adulthood is directly associated with an increase in incidence of injuries that cause physical limitations, particularly fracture, bone, and joint injuries, according to the results of a prospective study published online in JAMA Dermatology.
“The risk of bone fracture and other injury causing limitation in adults with eczema has been largely unexplored,” noted Dr. Nitin Garg and Dr. Jonathan I. Silverberg of Northwestern University in Chicago.
“Patients with eczema may be at risk of fracture given their use of systemic corticosteroids, which may decrease bone mineral density [and] therefore, studies describing the prevalence of fracture among adults with eczema are needed,” they added (JAMA Dermatol. 2015;151:33-41 [doi:10.1001/jamadermatol.2014.2098]).

Dr. Garg and Dr. Silverberg used data from the 2012 National Health Interview Survey, which was conducted by the National Center for Health Statistics, to create their prospective, questionnaire-based study. The final analysis included 34,500 adults aged 18-85 years. They controlled for factors such as age, sex, race, Hispanic origin, household income, highest level of household education, family structure, and whether or not the subject was born in the United States.
The prevalence of self-reported eczema or skin allergy was 7.2%, the prevalence of any limitation-causing injury was 2.0%, and any limitation-causing injury in the past 12 months among adults was 7.2%. A fracture and bone or joint injury (FBJI) causing limitation was reported by 1.5% of the study population and other types of injury causing limitation were reported by 0.6%. The prevalence of FBJI causing limitation increased gradually with age, to peak in subjects aged 50-69 years, decreasing thereafter.
In a logistic regression analysis, adults with eczema had a 44% increased risk of any injury causing limitation (adjusted odds ratio, 1.44), and a 67% increased risk of FBJI (aOR, 1.67).
Adults with eczema who also reported experiencing fatigue (aOR, 1.59; 95% CI, 1.16-2.19), daytime sleepiness (aOR, 1.81), or insomnia (aOR, 1.74) had higher rates of FBJI than individuals with sleep symptoms but no eczema. Adults with both eczema and psychiatric or behavioral disorders also were more likely to experience FBJI than individuals suffering from eczema alone, or individuals suffering from psychiatric and behavioral disorders, but not eczema.
“Taken together, these data suggest that adult eczema is a previously unrecognized risk factor for fracture and other injury, emphasizing the importance of developing safer and more effective clinical interventions for itch and sleep problems in eczema, as well as preventive measures for injury risk reduction in eczema,” wrote Dr. Garg and Dr. Silverberg. The authors reported no relevant financial disclosures.
Eczema in adulthood is directly associated with an increase in incidence of injuries that cause physical limitations, particularly fracture, bone, and joint injuries, according to the results of a prospective study published online in JAMA Dermatology.
“The risk of bone fracture and other injury causing limitation in adults with eczema has been largely unexplored,” noted Dr. Nitin Garg and Dr. Jonathan I. Silverberg of Northwestern University in Chicago.
“Patients with eczema may be at risk of fracture given their use of systemic corticosteroids, which may decrease bone mineral density [and] therefore, studies describing the prevalence of fracture among adults with eczema are needed,” they added (JAMA Dermatol. 2015;151:33-41 [doi:10.1001/jamadermatol.2014.2098]).
Dr. Garg and Dr. Silverberg used data from the 2012 National Health Interview Survey, which was conducted by the National Center for Health Statistics, to create their prospective, questionnaire-based study. The final analysis included 34,500 adults aged 18-85 years. They controlled for factors such as age, sex, race, Hispanic origin, household income, highest level of household education, family structure, and whether or not the subject was born in the United States.
The prevalence of self-reported eczema or skin allergy was 7.2%, the prevalence of any limitation-causing injury was 2.0%, and any limitation-causing injury in the past 12 months among adults was 7.2%. A fracture and bone or joint injury (FBJI) causing limitation was reported by 1.5% of the study population and other types of injury causing limitation were reported by 0.6%. The prevalence of FBJI causing limitation increased gradually with age, to peak in subjects aged 50-69 years, decreasing thereafter.
In a logistic regression analysis, adults with eczema had a 44% increased risk of any injury causing limitation (adjusted odds ratio, 1.44), and a 67% increased risk of FBJI (aOR, 1.67).
Adults with eczema who also reported experiencing fatigue (aOR, 1.59; 95% CI, 1.16-2.19), daytime sleepiness (aOR, 1.81), or insomnia (aOR, 1.74) had higher rates of FBJI than individuals with sleep symptoms but no eczema. Adults with both eczema and psychiatric or behavioral disorders also were more likely to experience FBJI than individuals suffering from eczema alone, or individuals suffering from psychiatric and behavioral disorders, but not eczema.
“Taken together, these data suggest that adult eczema is a previously unrecognized risk factor for fracture and other injury, emphasizing the importance of developing safer and more effective clinical interventions for itch and sleep problems in eczema, as well as preventive measures for injury risk reduction in eczema,” wrote Dr. Garg and Dr. Silverberg. The authors reported no relevant financial disclosures.
Eczema in adulthood is directly associated with an increase in incidence of injuries that cause physical limitations, particularly fracture, bone, and joint injuries, according to the results of a prospective study published online in JAMA Dermatology.
“The risk of bone fracture and other injury causing limitation in adults with eczema has been largely unexplored,” noted Dr. Nitin Garg and Dr. Jonathan I. Silverberg of Northwestern University in Chicago.
“Patients with eczema may be at risk of fracture given their use of systemic corticosteroids, which may decrease bone mineral density [and] therefore, studies describing the prevalence of fracture among adults with eczema are needed,” they added (JAMA Dermatol. 2015;151:33-41 [doi:10.1001/jamadermatol.2014.2098]).
Dr. Garg and Dr. Silverberg used data from the 2012 National Health Interview Survey, which was conducted by the National Center for Health Statistics, to create their prospective, questionnaire-based study. The final analysis included 34,500 adults aged 18-85 years. They controlled for factors such as age, sex, race, Hispanic origin, household income, highest level of household education, family structure, and whether or not the subject was born in the United States.
The prevalence of self-reported eczema or skin allergy was 7.2%, the prevalence of any limitation-causing injury was 2.0%, and any limitation-causing injury in the past 12 months among adults was 7.2%. A fracture and bone or joint injury (FBJI) causing limitation was reported by 1.5% of the study population and other types of injury causing limitation were reported by 0.6%. The prevalence of FBJI causing limitation increased gradually with age, to peak in subjects aged 50-69 years, decreasing thereafter.
In a logistic regression analysis, adults with eczema had a 44% increased risk of any injury causing limitation (adjusted odds ratio, 1.44), and a 67% increased risk of FBJI (aOR, 1.67).
Adults with eczema who also reported experiencing fatigue (aOR, 1.59; 95% CI, 1.16-2.19), daytime sleepiness (aOR, 1.81), or insomnia (aOR, 1.74) had higher rates of FBJI than individuals with sleep symptoms but no eczema. Adults with both eczema and psychiatric or behavioral disorders also were more likely to experience FBJI than individuals suffering from eczema alone, or individuals suffering from psychiatric and behavioral disorders, but not eczema.
“Taken together, these data suggest that adult eczema is a previously unrecognized risk factor for fracture and other injury, emphasizing the importance of developing safer and more effective clinical interventions for itch and sleep problems in eczema, as well as preventive measures for injury risk reduction in eczema,” wrote Dr. Garg and Dr. Silverberg. The authors reported no relevant financial disclosures.
FROM JAMA DERMATOLOGY
Key clinical point: Eczema in adulthood is associated with an increased risk of limitation-causing injuries.
Major finding: Adults with eczema had a 67% increased risk of fracture and bone or joint injury (FBJI) causing limitation (aOR 1.67).
Data source: Prospective, questionnaire-based, cohort study of 34,500 adults aged 18-85 years from the 2012 National Health Interview Survey.
Disclosures: The authors reported no financial conflicts of interest.

MEK inhibitors can induce skin eruptions with distinctive duskiness
Case reports of unusual drug hypersensitivity to MEK inhibitors, involving skin eruptions with distinctive central duskiness, have been described online in JAMA Dermatology.
Three patients who were receiving different MEK inhibitors (selumetinib, cobimetinib, and trametinib) developed grade 2 or 3 eruptions, all associated with unique duskiness, reported Dr. Urvi Patel and associates at Washington University, St. Louis.
A 60-year-old man with pancreatic cancer who was receiving selumetinib as part of a clinical trial presented with a grade 2 generalized eruption and pruritus 12 days after initiating therapy. He had diffuse targetoid patches with central duskiness. Selumetinib and other study drugs were withheld, the patient was given topical corticosteroid treatment, and the eruption completely resolved after 4 weeks. The patient did not restart the study drugs because of an elevated alkaline phosphatase level and fatigue.
A woman in her 40s who was receiving cobimetinib and other medication for metastatic melanoma developed grade 2 coalescing urticarial patches with surrounding duskiness on day 28 of treatment. Histopathologic examination showed a superficial perivascular lymphocytic infiltrate with rare eosinophils. After treatment was halted for 7 days and a regimen of oral prednisone was started, cobimetinib therapy was reinstituted at a lower dose. There was no recurrence of the eruption 1 year after cobimetinib therapy was restarted, Dr. Patel and associates reported (JAMA Dermatol. 2015 Jan. 14 [doi:10.1001/jamadermatol.2014.3207]).
The third patient, a woman in her 50s with metastatic melanoma, developed a grade 3 eruption 7 weeks into trametinib treatment together with another drug. The worsening urticarial patches and plaques had surrounding diffuse duskiness. After trametinib treatment was withheld for a week, and a regimen of oral prednisone was begun, trametinib therapy was restarted and the eruption did not return.
“As shown in our patients, successful treatment of this MEK inhibitor–associated cutaneous eruption can include a drug holiday and oral corticosteroid therapy, with reinstitution of the drug at a lower dose without recurrence,” Dr. Patel and his associates wrote.
MEK inhibitors target the mitogen-activated protein kinase pathway. Trametinib has been approved for treating advanced melanoma, and more than a dozen other MEK inhibitors are in clinical trials (including selumetinib and cobimetinib) for treatment of melanoma and other solid-organ malignant neoplasms, including pancreatic, hepatocellular, colorectal, and non–small cell lung cancer, the authors noted.
On Twitter @nikolaideslaura
Case reports of unusual drug hypersensitivity to MEK inhibitors, involving skin eruptions with distinctive central duskiness, have been described online in JAMA Dermatology.
Three patients who were receiving different MEK inhibitors (selumetinib, cobimetinib, and trametinib) developed grade 2 or 3 eruptions, all associated with unique duskiness, reported Dr. Urvi Patel and associates at Washington University, St. Louis.
A 60-year-old man with pancreatic cancer who was receiving selumetinib as part of a clinical trial presented with a grade 2 generalized eruption and pruritus 12 days after initiating therapy. He had diffuse targetoid patches with central duskiness. Selumetinib and other study drugs were withheld, the patient was given topical corticosteroid treatment, and the eruption completely resolved after 4 weeks. The patient did not restart the study drugs because of an elevated alkaline phosphatase level and fatigue.
A woman in her 40s who was receiving cobimetinib and other medication for metastatic melanoma developed grade 2 coalescing urticarial patches with surrounding duskiness on day 28 of treatment. Histopathologic examination showed a superficial perivascular lymphocytic infiltrate with rare eosinophils. After treatment was halted for 7 days and a regimen of oral prednisone was started, cobimetinib therapy was reinstituted at a lower dose. There was no recurrence of the eruption 1 year after cobimetinib therapy was restarted, Dr. Patel and associates reported (JAMA Dermatol. 2015 Jan. 14 [doi:10.1001/jamadermatol.2014.3207]).
The third patient, a woman in her 50s with metastatic melanoma, developed a grade 3 eruption 7 weeks into trametinib treatment together with another drug. The worsening urticarial patches and plaques had surrounding diffuse duskiness. After trametinib treatment was withheld for a week, and a regimen of oral prednisone was begun, trametinib therapy was restarted and the eruption did not return.
“As shown in our patients, successful treatment of this MEK inhibitor–associated cutaneous eruption can include a drug holiday and oral corticosteroid therapy, with reinstitution of the drug at a lower dose without recurrence,” Dr. Patel and his associates wrote.
MEK inhibitors target the mitogen-activated protein kinase pathway. Trametinib has been approved for treating advanced melanoma, and more than a dozen other MEK inhibitors are in clinical trials (including selumetinib and cobimetinib) for treatment of melanoma and other solid-organ malignant neoplasms, including pancreatic, hepatocellular, colorectal, and non–small cell lung cancer, the authors noted.
On Twitter @nikolaideslaura
Case reports of unusual drug hypersensitivity to MEK inhibitors, involving skin eruptions with distinctive central duskiness, have been described online in JAMA Dermatology.
Three patients who were receiving different MEK inhibitors (selumetinib, cobimetinib, and trametinib) developed grade 2 or 3 eruptions, all associated with unique duskiness, reported Dr. Urvi Patel and associates at Washington University, St. Louis.
A 60-year-old man with pancreatic cancer who was receiving selumetinib as part of a clinical trial presented with a grade 2 generalized eruption and pruritus 12 days after initiating therapy. He had diffuse targetoid patches with central duskiness. Selumetinib and other study drugs were withheld, the patient was given topical corticosteroid treatment, and the eruption completely resolved after 4 weeks. The patient did not restart the study drugs because of an elevated alkaline phosphatase level and fatigue.
A woman in her 40s who was receiving cobimetinib and other medication for metastatic melanoma developed grade 2 coalescing urticarial patches with surrounding duskiness on day 28 of treatment. Histopathologic examination showed a superficial perivascular lymphocytic infiltrate with rare eosinophils. After treatment was halted for 7 days and a regimen of oral prednisone was started, cobimetinib therapy was reinstituted at a lower dose. There was no recurrence of the eruption 1 year after cobimetinib therapy was restarted, Dr. Patel and associates reported (JAMA Dermatol. 2015 Jan. 14 [doi:10.1001/jamadermatol.2014.3207]).
The third patient, a woman in her 50s with metastatic melanoma, developed a grade 3 eruption 7 weeks into trametinib treatment together with another drug. The worsening urticarial patches and plaques had surrounding diffuse duskiness. After trametinib treatment was withheld for a week, and a regimen of oral prednisone was begun, trametinib therapy was restarted and the eruption did not return.
“As shown in our patients, successful treatment of this MEK inhibitor–associated cutaneous eruption can include a drug holiday and oral corticosteroid therapy, with reinstitution of the drug at a lower dose without recurrence,” Dr. Patel and his associates wrote.
MEK inhibitors target the mitogen-activated protein kinase pathway. Trametinib has been approved for treating advanced melanoma, and more than a dozen other MEK inhibitors are in clinical trials (including selumetinib and cobimetinib) for treatment of melanoma and other solid-organ malignant neoplasms, including pancreatic, hepatocellular, colorectal, and non–small cell lung cancer, the authors noted.
On Twitter @nikolaideslaura
FROM JAMA DERMATOLOGY
Key clinical point: This MEK inhibitor–associated cutaneous eruption can be treated with a drug holiday and oral corticosteroid treatment, restarting the drug at a lower dose without recurrence.
Major finding: Three patients who were receiving different MEK inhibitors (selumetinib, cobimetinib, and trametinib) developed grade 2 or 3 eruptions, all associated with unique duskiness.
Data source: Three case studies of patients receiving different MEK inhibitors.
Disclosures: Dr. Lynn Cornelius has received a research grant from Genentech and is a clinical subinvestigator for GlaxoSmithKline. Dr. Milan J. Anadkat has received honoraria as a speaker and/or consultant from AstraZeneca, Bristol-Myers Squibb, Eisai, ImClone, and Therakos. No other disclosures were reported.
Real-world data with rivaroxaban similar to trial data

Credit: CDC
A post-marketing study in patients with non-valvular atrial fibrillation (NVAF) suggests that rates and patterns of major bleeding associated with the use of rivaroxaban in routine clinical practice are generally consistent with those observed in a previous phase 3 trial.
The new study, which included more than 27,000 patients, showed a low rate of major bleeding. And gastrointestinal bleeding was more common than intracranial hemorrhage.
While the results are not intended for a direct comparison, the researchers said these data are generally consistent with data from the ROCKET-AF trial.
The results, published in Clinical Cardiology, are the initial findings from an ongoing, 5-year, observational study of patients using rivaroxaban daily over the course of their lives.
“These findings reaffirm the safety profile of Xarelto [rivaroxaban],” said study author W. Frank Peacock, MD, of the Baylor College of Medicine in Houston, Texas.
“We anticipate future findings from this 5-year observational study will continue to provide real-world information about the use of Xarelto in routine clinical practice.”
Dr Peacock and his colleagues analyzed data from January 1, 2013, to March 31, 2014, evaluating major bleeding in 27,467 NVAF patients treated with rivaroxaban in a real-world, clinical setting.
There were a total of 496 major bleeding events in 478 patients. So the incidence of major bleeding was 2.86 per 100 person-years, which was generally consistent with the rate reported in the ROCKET-AF trial.
Most bleeds were gastrointestinal (88.5%), followed by intracranial (7.5%). Fourteen patients each experienced 2 major bleeding events, and 2 patients each experienced 3 events.
Major bleeding was more likely in females and older patients. The incidence of major bleeding was 2.68 for males and 2.99 for females. The mean age of patients with major bleeding was 78.4, compared to 75.7 for those without major bleeding.
Comorbidities tended to be more prevalent among patients who experienced major bleeding. The most common were hypertension (95.6% vs 75.8%), coronary heart disease (64.2% vs 36.7%), heart failure (48.5% vs 23.7%), and renal disease (38.7% vs 16.7%).
Patients with major bleeding were less likely to be on medications such as statins, proton pump inhibitors, and amiodarone—29.1% vs 36.6%.
Fourteen patients died while in the hospital for major bleeding, for a fatal bleeding rate of 0.08 per 100 person-years. None of these patients had multiple bleeding events.
Fatal bleeding events included intracranial hemorrhage with intracerebral bleeding (n=7), gastrointestinal hemorrhage not otherwise specified (n=3), blood in the stool (n=2), subdural hemorrhage (n=1), and intracranial hemorrhage not otherwise specified (n=1).
Patients’ mean age at death was 82.4 years, and the mean time from hospitalization for the bleeding event to death was 3.9 days.
This ongoing study is funded by Janssen Scientific Affairs, LLC, and Bayer Healthcare, the companies developing rivaroxaban. ![]()
Credit: CDC
A post-marketing study in patients with non-valvular atrial fibrillation (NVAF) suggests that rates and patterns of major bleeding associated with the use of rivaroxaban in routine clinical practice are generally consistent with those observed in a previous phase 3 trial.
The new study, which included more than 27,000 patients, showed a low rate of major bleeding. And gastrointestinal bleeding was more common than intracranial hemorrhage.
While the results are not intended for a direct comparison, the researchers said these data are generally consistent with data from the ROCKET-AF trial.
The results, published in Clinical Cardiology, are the initial findings from an ongoing, 5-year, observational study of patients using rivaroxaban daily over the course of their lives.
“These findings reaffirm the safety profile of Xarelto [rivaroxaban],” said study author W. Frank Peacock, MD, of the Baylor College of Medicine in Houston, Texas.
“We anticipate future findings from this 5-year observational study will continue to provide real-world information about the use of Xarelto in routine clinical practice.”
Dr Peacock and his colleagues analyzed data from January 1, 2013, to March 31, 2014, evaluating major bleeding in 27,467 NVAF patients treated with rivaroxaban in a real-world, clinical setting.
There were a total of 496 major bleeding events in 478 patients. So the incidence of major bleeding was 2.86 per 100 person-years, which was generally consistent with the rate reported in the ROCKET-AF trial.
Most bleeds were gastrointestinal (88.5%), followed by intracranial (7.5%). Fourteen patients each experienced 2 major bleeding events, and 2 patients each experienced 3 events.
Major bleeding was more likely in females and older patients. The incidence of major bleeding was 2.68 for males and 2.99 for females. The mean age of patients with major bleeding was 78.4, compared to 75.7 for those without major bleeding.
Comorbidities tended to be more prevalent among patients who experienced major bleeding. The most common were hypertension (95.6% vs 75.8%), coronary heart disease (64.2% vs 36.7%), heart failure (48.5% vs 23.7%), and renal disease (38.7% vs 16.7%).
Patients with major bleeding were less likely to be on medications such as statins, proton pump inhibitors, and amiodarone—29.1% vs 36.6%.
Fourteen patients died while in the hospital for major bleeding, for a fatal bleeding rate of 0.08 per 100 person-years. None of these patients had multiple bleeding events.
Fatal bleeding events included intracranial hemorrhage with intracerebral bleeding (n=7), gastrointestinal hemorrhage not otherwise specified (n=3), blood in the stool (n=2), subdural hemorrhage (n=1), and intracranial hemorrhage not otherwise specified (n=1).
Patients’ mean age at death was 82.4 years, and the mean time from hospitalization for the bleeding event to death was 3.9 days.
This ongoing study is funded by Janssen Scientific Affairs, LLC, and Bayer Healthcare, the companies developing rivaroxaban. ![]()
Credit: CDC
A post-marketing study in patients with non-valvular atrial fibrillation (NVAF) suggests that rates and patterns of major bleeding associated with the use of rivaroxaban in routine clinical practice are generally consistent with those observed in a previous phase 3 trial.
The new study, which included more than 27,000 patients, showed a low rate of major bleeding. And gastrointestinal bleeding was more common than intracranial hemorrhage.
While the results are not intended for a direct comparison, the researchers said these data are generally consistent with data from the ROCKET-AF trial.
The results, published in Clinical Cardiology, are the initial findings from an ongoing, 5-year, observational study of patients using rivaroxaban daily over the course of their lives.
“These findings reaffirm the safety profile of Xarelto [rivaroxaban],” said study author W. Frank Peacock, MD, of the Baylor College of Medicine in Houston, Texas.
“We anticipate future findings from this 5-year observational study will continue to provide real-world information about the use of Xarelto in routine clinical practice.”
Dr Peacock and his colleagues analyzed data from January 1, 2013, to March 31, 2014, evaluating major bleeding in 27,467 NVAF patients treated with rivaroxaban in a real-world, clinical setting.
There were a total of 496 major bleeding events in 478 patients. So the incidence of major bleeding was 2.86 per 100 person-years, which was generally consistent with the rate reported in the ROCKET-AF trial.
Most bleeds were gastrointestinal (88.5%), followed by intracranial (7.5%). Fourteen patients each experienced 2 major bleeding events, and 2 patients each experienced 3 events.
Major bleeding was more likely in females and older patients. The incidence of major bleeding was 2.68 for males and 2.99 for females. The mean age of patients with major bleeding was 78.4, compared to 75.7 for those without major bleeding.
Comorbidities tended to be more prevalent among patients who experienced major bleeding. The most common were hypertension (95.6% vs 75.8%), coronary heart disease (64.2% vs 36.7%), heart failure (48.5% vs 23.7%), and renal disease (38.7% vs 16.7%).
Patients with major bleeding were less likely to be on medications such as statins, proton pump inhibitors, and amiodarone—29.1% vs 36.6%.
Fourteen patients died while in the hospital for major bleeding, for a fatal bleeding rate of 0.08 per 100 person-years. None of these patients had multiple bleeding events.
Fatal bleeding events included intracranial hemorrhage with intracerebral bleeding (n=7), gastrointestinal hemorrhage not otherwise specified (n=3), blood in the stool (n=2), subdural hemorrhage (n=1), and intracranial hemorrhage not otherwise specified (n=1).
Patients’ mean age at death was 82.4 years, and the mean time from hospitalization for the bleeding event to death was 3.9 days.
This ongoing study is funded by Janssen Scientific Affairs, LLC, and Bayer Healthcare, the companies developing rivaroxaban. ![]()
CDC report shows big drop in rate of CLABSIs

through a central line
Credit: Rhoda Baer
Healthcare-associated infections (HAIs) are on the decline in the US, according to a report by the Centers for Disease Control and Prevention (CDC).
The data show that most types of HAIs have decreased in recent years, with a particularly large decrease in the rate of central line-associated bloodstream infections (CLABSIs).
The National and State Healthcare-associated Infection Progress Report is a snapshot of how each state and the country are doing in eliminating the infections that hospitals are required to report to the CDC.
The report summarizes data submitted to the CDC’s National Healthcare Safety Network, the nation’s HAI tracking system, which is used by more than 14,500 healthcare facilities across all 50 states, Washington, DC, and Puerto Rico.
“Hospitals have made real progress to reduce some types of healthcare-associated infections; it can be done,” said CDC Director Tom Frieden, MD.
“The key is for every hospital to have rigorous infection control programs to protect patients and healthcare workers, and for health care facilities and others to work together to reduce the many types of infections that haven’t decreased enough.”
On the national level, the report showed a 46% decrease in CLABSIs between 2008 and 2013. It also revealed a 19% decrease in surgical site infections related to the 10 procedures tracked in the report between 2008 and 2013.
There was an 8% decrease in methicillin-resistant Staphylococcus aureus (MRSA) bloodstream infections between 2011 and 2013 and a 10% decrease in Clostridium difficile infections between 2011 and 2013.
However, there was a 6% increase in catheter-associated urinary tract infections since 2009.
Not all states reported or had enough data to calculate valid infection information on every infection in the report. But the CDC compared the number of infections reported to a national baseline.
And they found that 26 states performed better than the nation on at least 2 of the infection types. Sixteen states performed better than the nation on 3 or more infections, including 6 states performing better on 4 infections.
But 19 states performed worse than the nation on 2 infections, with 8 states performing worse on at least 3 infections.
The national baseline for HAIs will be reset at the end of 2015. Starting in 2016, HAI prevention progress from 2016 to 2020 will be measured in comparison to infection data from 2015. ![]()
through a central line
Credit: Rhoda Baer
Healthcare-associated infections (HAIs) are on the decline in the US, according to a report by the Centers for Disease Control and Prevention (CDC).
The data show that most types of HAIs have decreased in recent years, with a particularly large decrease in the rate of central line-associated bloodstream infections (CLABSIs).
The National and State Healthcare-associated Infection Progress Report is a snapshot of how each state and the country are doing in eliminating the infections that hospitals are required to report to the CDC.
The report summarizes data submitted to the CDC’s National Healthcare Safety Network, the nation’s HAI tracking system, which is used by more than 14,500 healthcare facilities across all 50 states, Washington, DC, and Puerto Rico.
“Hospitals have made real progress to reduce some types of healthcare-associated infections; it can be done,” said CDC Director Tom Frieden, MD.
“The key is for every hospital to have rigorous infection control programs to protect patients and healthcare workers, and for health care facilities and others to work together to reduce the many types of infections that haven’t decreased enough.”
On the national level, the report showed a 46% decrease in CLABSIs between 2008 and 2013. It also revealed a 19% decrease in surgical site infections related to the 10 procedures tracked in the report between 2008 and 2013.
There was an 8% decrease in methicillin-resistant Staphylococcus aureus (MRSA) bloodstream infections between 2011 and 2013 and a 10% decrease in Clostridium difficile infections between 2011 and 2013.
However, there was a 6% increase in catheter-associated urinary tract infections since 2009.
Not all states reported or had enough data to calculate valid infection information on every infection in the report. But the CDC compared the number of infections reported to a national baseline.
And they found that 26 states performed better than the nation on at least 2 of the infection types. Sixteen states performed better than the nation on 3 or more infections, including 6 states performing better on 4 infections.
But 19 states performed worse than the nation on 2 infections, with 8 states performing worse on at least 3 infections.
The national baseline for HAIs will be reset at the end of 2015. Starting in 2016, HAI prevention progress from 2016 to 2020 will be measured in comparison to infection data from 2015. ![]()
through a central line
Credit: Rhoda Baer
Healthcare-associated infections (HAIs) are on the decline in the US, according to a report by the Centers for Disease Control and Prevention (CDC).
The data show that most types of HAIs have decreased in recent years, with a particularly large decrease in the rate of central line-associated bloodstream infections (CLABSIs).
The National and State Healthcare-associated Infection Progress Report is a snapshot of how each state and the country are doing in eliminating the infections that hospitals are required to report to the CDC.
The report summarizes data submitted to the CDC’s National Healthcare Safety Network, the nation’s HAI tracking system, which is used by more than 14,500 healthcare facilities across all 50 states, Washington, DC, and Puerto Rico.
“Hospitals have made real progress to reduce some types of healthcare-associated infections; it can be done,” said CDC Director Tom Frieden, MD.
“The key is for every hospital to have rigorous infection control programs to protect patients and healthcare workers, and for health care facilities and others to work together to reduce the many types of infections that haven’t decreased enough.”
On the national level, the report showed a 46% decrease in CLABSIs between 2008 and 2013. It also revealed a 19% decrease in surgical site infections related to the 10 procedures tracked in the report between 2008 and 2013.
There was an 8% decrease in methicillin-resistant Staphylococcus aureus (MRSA) bloodstream infections between 2011 and 2013 and a 10% decrease in Clostridium difficile infections between 2011 and 2013.
However, there was a 6% increase in catheter-associated urinary tract infections since 2009.
Not all states reported or had enough data to calculate valid infection information on every infection in the report. But the CDC compared the number of infections reported to a national baseline.
And they found that 26 states performed better than the nation on at least 2 of the infection types. Sixteen states performed better than the nation on 3 or more infections, including 6 states performing better on 4 infections.
But 19 states performed worse than the nation on 2 infections, with 8 states performing worse on at least 3 infections.
The national baseline for HAIs will be reset at the end of 2015. Starting in 2016, HAI prevention progress from 2016 to 2020 will be measured in comparison to infection data from 2015. ![]()
Iron overload aids potentially deadly bacteria
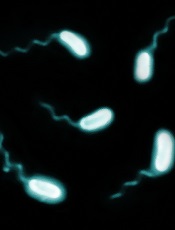
Credit: Paul A. Gulig
Researchers say they’ve determined why patients with hereditary hemochromatosis are so vulnerable to severe illness from Vibrio vulnificus infection.
Patients with hereditary hemochromatosis have a deficiency of the iron-regulating hormone hepcidin and therefore develop excess iron in their blood and tissue, providing prime growth conditions for Vibrio vulnificus.
The researchers also showed that minihepcidin, a medicinal form of the hormone hepcidin that lowers iron levels in blood, could cure the infection by restricting bacterial growth.
The findings appear in Cell Host and Microbe.
“This is the first time that the association of hepcidin deficiency and susceptibility to Vibrio vulnificus infection was tested,” said study author Yonca Bulut, MD, of the David Geffen School of Medicine at UCLA in Los Angeles.
“The dramatic effectiveness of the new treatment, even after the infection was established, was impressive.”
To conduct this study, Dr Bulut and her colleagues compared the fatality of Vibrio vulnificus infection in healthy mice with mice that lacked hepcidin, modeling human hereditary hemochromatosis.
The infection was much more lethal in hepcidin-deficient mice because their bodies could not decrease iron levels in the blood in response to infection, a process mediated by hepcidin in healthy mice.
Giving minihepcidin to hepcidin-deficient mice prevented infection if the hormone was given before Vibrio vulnificus was introduced. And mice given minihepcidin 3 hours after the bacterium was introduced were cured of any infection.
“We found that hepcidin is required for resistance to a Vibrio vulnificus infection,” said study author Joao Arezes, a graduate student from the University of Porto in Portugal.
“The development of the treatment tested in mouse models could reduce the high mortality rate of this disease.”
The next stage of this research is to investigate why Vibrio vulnificus bacteria become so lethal when iron levels are high, and to learn which other microbes respond similarly to excess iron. ![]()
Credit: Paul A. Gulig
Researchers say they’ve determined why patients with hereditary hemochromatosis are so vulnerable to severe illness from Vibrio vulnificus infection.
Patients with hereditary hemochromatosis have a deficiency of the iron-regulating hormone hepcidin and therefore develop excess iron in their blood and tissue, providing prime growth conditions for Vibrio vulnificus.
The researchers also showed that minihepcidin, a medicinal form of the hormone hepcidin that lowers iron levels in blood, could cure the infection by restricting bacterial growth.
The findings appear in Cell Host and Microbe.
“This is the first time that the association of hepcidin deficiency and susceptibility to Vibrio vulnificus infection was tested,” said study author Yonca Bulut, MD, of the David Geffen School of Medicine at UCLA in Los Angeles.
“The dramatic effectiveness of the new treatment, even after the infection was established, was impressive.”
To conduct this study, Dr Bulut and her colleagues compared the fatality of Vibrio vulnificus infection in healthy mice with mice that lacked hepcidin, modeling human hereditary hemochromatosis.
The infection was much more lethal in hepcidin-deficient mice because their bodies could not decrease iron levels in the blood in response to infection, a process mediated by hepcidin in healthy mice.
Giving minihepcidin to hepcidin-deficient mice prevented infection if the hormone was given before Vibrio vulnificus was introduced. And mice given minihepcidin 3 hours after the bacterium was introduced were cured of any infection.
“We found that hepcidin is required for resistance to a Vibrio vulnificus infection,” said study author Joao Arezes, a graduate student from the University of Porto in Portugal.
“The development of the treatment tested in mouse models could reduce the high mortality rate of this disease.”
The next stage of this research is to investigate why Vibrio vulnificus bacteria become so lethal when iron levels are high, and to learn which other microbes respond similarly to excess iron. ![]()
Credit: Paul A. Gulig
Researchers say they’ve determined why patients with hereditary hemochromatosis are so vulnerable to severe illness from Vibrio vulnificus infection.
Patients with hereditary hemochromatosis have a deficiency of the iron-regulating hormone hepcidin and therefore develop excess iron in their blood and tissue, providing prime growth conditions for Vibrio vulnificus.
The researchers also showed that minihepcidin, a medicinal form of the hormone hepcidin that lowers iron levels in blood, could cure the infection by restricting bacterial growth.
The findings appear in Cell Host and Microbe.
“This is the first time that the association of hepcidin deficiency and susceptibility to Vibrio vulnificus infection was tested,” said study author Yonca Bulut, MD, of the David Geffen School of Medicine at UCLA in Los Angeles.
“The dramatic effectiveness of the new treatment, even after the infection was established, was impressive.”
To conduct this study, Dr Bulut and her colleagues compared the fatality of Vibrio vulnificus infection in healthy mice with mice that lacked hepcidin, modeling human hereditary hemochromatosis.
The infection was much more lethal in hepcidin-deficient mice because their bodies could not decrease iron levels in the blood in response to infection, a process mediated by hepcidin in healthy mice.
Giving minihepcidin to hepcidin-deficient mice prevented infection if the hormone was given before Vibrio vulnificus was introduced. And mice given minihepcidin 3 hours after the bacterium was introduced were cured of any infection.
“We found that hepcidin is required for resistance to a Vibrio vulnificus infection,” said study author Joao Arezes, a graduate student from the University of Porto in Portugal.
“The development of the treatment tested in mouse models could reduce the high mortality rate of this disease.”
The next stage of this research is to investigate why Vibrio vulnificus bacteria become so lethal when iron levels are high, and to learn which other microbes respond similarly to excess iron.