User login
Readmission Penalties for COPD Diagnoses Slated for 2014
Next October, when COPD is added to the list of diagnoses for which hospital readmissions penalties are calculated, hospitalists will need to pay closer attention to comorbidities, home environments, socio-economic status, and other factors that can contribute to COPD readmissions.
This was a central theme at a recent conference on COPD and hospital readmissions sponsored by the COPD Foundation in Washington, D.C. The meeting brought together pulmonologists, policy makers, healthcare quality-improvement experts, and representatives from four national, patient-care transitions programs: the Care Transitions Program of the University of Colorado School of Medicine in Denver; Project RED (Re-Engineered Discharge) at Boston University Medical Center; the Transitional Care Model of the University of Pennsylvania in Philadelphia; and SHM's Project BOOST.
"This summit reinforces what has already been said, that there needs to be a comprehensive approach to COPD patients, not just managing the disease," said one of the conference’s key speakers, Mark Williams, MD, MHM, professor and chief of the division of hospital medicine at Northwestern University Feinberg School of Medicine in Chicago and principal investigator of Project BOOST. "Similar to heart failure, there needs to be support for the patient at home."
COPD is the third-leading cause of death in the U.S., with an estimated 15 million diagnosed patients and many more undiagnosed. One-fifth of hospitalized COPD patients are readmitted within 30 days, according to data from the Agency for Healthcare Research and Quality [PDF]. Many simultaneously present with heart disease, pneumonia, diabetes, or other comorbidities, and 62% of hospitalized COPD patients are readmitted for a condition other than COPD, says Brian Carlin, MD, senior staff physician at Allegheny General Hospital in Pittsburgh, Pa.
Preventing readmissions underscores the need for a patient-centered approach, says conference co-chair Jerry Krishnan, MD, PhD, professor of medicine and public health associate vice president for population health sciences at the University of Illinois Hospital and Health System in Chicago. "There's a tremendous amount of interest among physicians about the quality of care and health outcomes for these patients and conflicting evidence about what actually works," Dr. Krishnan says. "What works in one setting is unlikely to work in another setting."
Other physicians at the conference discussed ways hospitalists could help reduce COPD-related readmissions. Guidelines for non-pharmacologic interventions emphasize access to smoking cessation programs, immunizations for influenza, and pulmonary rehabilitation, says Byron Thomashow, MD, clinical professor of medicine at Columbia University Medical Center in New York City. "I also encourage all of my patients to exercise," he says.
Visit our website for more information on patient care and COPD.
Next October, when COPD is added to the list of diagnoses for which hospital readmissions penalties are calculated, hospitalists will need to pay closer attention to comorbidities, home environments, socio-economic status, and other factors that can contribute to COPD readmissions.
This was a central theme at a recent conference on COPD and hospital readmissions sponsored by the COPD Foundation in Washington, D.C. The meeting brought together pulmonologists, policy makers, healthcare quality-improvement experts, and representatives from four national, patient-care transitions programs: the Care Transitions Program of the University of Colorado School of Medicine in Denver; Project RED (Re-Engineered Discharge) at Boston University Medical Center; the Transitional Care Model of the University of Pennsylvania in Philadelphia; and SHM's Project BOOST.
"This summit reinforces what has already been said, that there needs to be a comprehensive approach to COPD patients, not just managing the disease," said one of the conference’s key speakers, Mark Williams, MD, MHM, professor and chief of the division of hospital medicine at Northwestern University Feinberg School of Medicine in Chicago and principal investigator of Project BOOST. "Similar to heart failure, there needs to be support for the patient at home."
COPD is the third-leading cause of death in the U.S., with an estimated 15 million diagnosed patients and many more undiagnosed. One-fifth of hospitalized COPD patients are readmitted within 30 days, according to data from the Agency for Healthcare Research and Quality [PDF]. Many simultaneously present with heart disease, pneumonia, diabetes, or other comorbidities, and 62% of hospitalized COPD patients are readmitted for a condition other than COPD, says Brian Carlin, MD, senior staff physician at Allegheny General Hospital in Pittsburgh, Pa.
Preventing readmissions underscores the need for a patient-centered approach, says conference co-chair Jerry Krishnan, MD, PhD, professor of medicine and public health associate vice president for population health sciences at the University of Illinois Hospital and Health System in Chicago. "There's a tremendous amount of interest among physicians about the quality of care and health outcomes for these patients and conflicting evidence about what actually works," Dr. Krishnan says. "What works in one setting is unlikely to work in another setting."
Other physicians at the conference discussed ways hospitalists could help reduce COPD-related readmissions. Guidelines for non-pharmacologic interventions emphasize access to smoking cessation programs, immunizations for influenza, and pulmonary rehabilitation, says Byron Thomashow, MD, clinical professor of medicine at Columbia University Medical Center in New York City. "I also encourage all of my patients to exercise," he says.
Visit our website for more information on patient care and COPD.
Next October, when COPD is added to the list of diagnoses for which hospital readmissions penalties are calculated, hospitalists will need to pay closer attention to comorbidities, home environments, socio-economic status, and other factors that can contribute to COPD readmissions.
This was a central theme at a recent conference on COPD and hospital readmissions sponsored by the COPD Foundation in Washington, D.C. The meeting brought together pulmonologists, policy makers, healthcare quality-improvement experts, and representatives from four national, patient-care transitions programs: the Care Transitions Program of the University of Colorado School of Medicine in Denver; Project RED (Re-Engineered Discharge) at Boston University Medical Center; the Transitional Care Model of the University of Pennsylvania in Philadelphia; and SHM's Project BOOST.
"This summit reinforces what has already been said, that there needs to be a comprehensive approach to COPD patients, not just managing the disease," said one of the conference’s key speakers, Mark Williams, MD, MHM, professor and chief of the division of hospital medicine at Northwestern University Feinberg School of Medicine in Chicago and principal investigator of Project BOOST. "Similar to heart failure, there needs to be support for the patient at home."
COPD is the third-leading cause of death in the U.S., with an estimated 15 million diagnosed patients and many more undiagnosed. One-fifth of hospitalized COPD patients are readmitted within 30 days, according to data from the Agency for Healthcare Research and Quality [PDF]. Many simultaneously present with heart disease, pneumonia, diabetes, or other comorbidities, and 62% of hospitalized COPD patients are readmitted for a condition other than COPD, says Brian Carlin, MD, senior staff physician at Allegheny General Hospital in Pittsburgh, Pa.
Preventing readmissions underscores the need for a patient-centered approach, says conference co-chair Jerry Krishnan, MD, PhD, professor of medicine and public health associate vice president for population health sciences at the University of Illinois Hospital and Health System in Chicago. "There's a tremendous amount of interest among physicians about the quality of care and health outcomes for these patients and conflicting evidence about what actually works," Dr. Krishnan says. "What works in one setting is unlikely to work in another setting."
Other physicians at the conference discussed ways hospitalists could help reduce COPD-related readmissions. Guidelines for non-pharmacologic interventions emphasize access to smoking cessation programs, immunizations for influenza, and pulmonary rehabilitation, says Byron Thomashow, MD, clinical professor of medicine at Columbia University Medical Center in New York City. "I also encourage all of my patients to exercise," he says.
Visit our website for more information on patient care and COPD.
Urolithiasis in a Patient With HIV Receiving Atazanavir
HIV Research Has Women to Thank; What the Affordable Care Act Means for the IHS; Making It Easier to Get the Right Health Care; Job Training for Veterans With Disabilities
Recognizing Posttraumatic Stress Disorder

Center for Health Equity Research and Promotion
Gout cases jump sevenfold in half-century
SAN DIEGO – The number of Americans with gout has climbed sevenfold during the last 50 years, according to Dr. Eswar Krishnan.
The population burden of illness imposed by gout has risen both in men and women across all age groups, but most strikingly so in men older than 65 years, said Dr. Krishnan, director of clinical epidemiology in the division of immunology and rheumatology at Stanford (Calif.) University.
He turned to National Health and Nutrition Examination Survey (NHANES) data to gain a more precise picture of U.S. trends in gout prevalence over time than has previously been available. He accomplished this by comparing age- and sex-specific rates from the 1959-1962 and the 2009-2010 editions of the long-running Centers for Disease Control and Prevention–sponsored surveys.

The unadjusted population-based prevalence of self-reported gout jumped from 6 cases per 1,000 during 1959-1962 to 26 per 1,000 in 2009-2010. The estimated number of gout cases climbed from 1.1 million in 1960 to 8.1 million in 2010. Yet the proportion of gout patients who were women remained steady at 31% over time.
The mean age of Americans with gout rose over the half-century from 54 to 61 years among men and from 55 to 65 years among women, he reported at the annual meeting of the American College of Rheumatology.
Statistical analysis indicated that the increase in gout cases among women during the last 50 years could be accounted for entirely by the much-discussed societal growth in abdominal obesity. In contrast, the explanation for the increased prevalence of gout in men was multifactorial. The bulk of the increase was associated with an increased life span and the graying of America, coupled with higher rates of hypertension, diabetes, and abdominal obesity.
However, an immeasurable portion of the increase in gout during the past half-century is probably due to increased awareness of the disease among the U.S. population, Dr. Krishnan added.
NHANES is sponsored by the Centers for Disease Control and Prevention. Dr. Krishnan reported having received research grants from Takeda, which markets gout medication.
SAN DIEGO – The number of Americans with gout has climbed sevenfold during the last 50 years, according to Dr. Eswar Krishnan.
The population burden of illness imposed by gout has risen both in men and women across all age groups, but most strikingly so in men older than 65 years, said Dr. Krishnan, director of clinical epidemiology in the division of immunology and rheumatology at Stanford (Calif.) University.
He turned to National Health and Nutrition Examination Survey (NHANES) data to gain a more precise picture of U.S. trends in gout prevalence over time than has previously been available. He accomplished this by comparing age- and sex-specific rates from the 1959-1962 and the 2009-2010 editions of the long-running Centers for Disease Control and Prevention–sponsored surveys.
The unadjusted population-based prevalence of self-reported gout jumped from 6 cases per 1,000 during 1959-1962 to 26 per 1,000 in 2009-2010. The estimated number of gout cases climbed from 1.1 million in 1960 to 8.1 million in 2010. Yet the proportion of gout patients who were women remained steady at 31% over time.
The mean age of Americans with gout rose over the half-century from 54 to 61 years among men and from 55 to 65 years among women, he reported at the annual meeting of the American College of Rheumatology.
Statistical analysis indicated that the increase in gout cases among women during the last 50 years could be accounted for entirely by the much-discussed societal growth in abdominal obesity. In contrast, the explanation for the increased prevalence of gout in men was multifactorial. The bulk of the increase was associated with an increased life span and the graying of America, coupled with higher rates of hypertension, diabetes, and abdominal obesity.
However, an immeasurable portion of the increase in gout during the past half-century is probably due to increased awareness of the disease among the U.S. population, Dr. Krishnan added.
NHANES is sponsored by the Centers for Disease Control and Prevention. Dr. Krishnan reported having received research grants from Takeda, which markets gout medication.
SAN DIEGO – The number of Americans with gout has climbed sevenfold during the last 50 years, according to Dr. Eswar Krishnan.
The population burden of illness imposed by gout has risen both in men and women across all age groups, but most strikingly so in men older than 65 years, said Dr. Krishnan, director of clinical epidemiology in the division of immunology and rheumatology at Stanford (Calif.) University.
He turned to National Health and Nutrition Examination Survey (NHANES) data to gain a more precise picture of U.S. trends in gout prevalence over time than has previously been available. He accomplished this by comparing age- and sex-specific rates from the 1959-1962 and the 2009-2010 editions of the long-running Centers for Disease Control and Prevention–sponsored surveys.
The unadjusted population-based prevalence of self-reported gout jumped from 6 cases per 1,000 during 1959-1962 to 26 per 1,000 in 2009-2010. The estimated number of gout cases climbed from 1.1 million in 1960 to 8.1 million in 2010. Yet the proportion of gout patients who were women remained steady at 31% over time.
The mean age of Americans with gout rose over the half-century from 54 to 61 years among men and from 55 to 65 years among women, he reported at the annual meeting of the American College of Rheumatology.
Statistical analysis indicated that the increase in gout cases among women during the last 50 years could be accounted for entirely by the much-discussed societal growth in abdominal obesity. In contrast, the explanation for the increased prevalence of gout in men was multifactorial. The bulk of the increase was associated with an increased life span and the graying of America, coupled with higher rates of hypertension, diabetes, and abdominal obesity.
However, an immeasurable portion of the increase in gout during the past half-century is probably due to increased awareness of the disease among the U.S. population, Dr. Krishnan added.
NHANES is sponsored by the Centers for Disease Control and Prevention. Dr. Krishnan reported having received research grants from Takeda, which markets gout medication.
AT THE ACR ANNUAL MEETING
Major finding: The estimated number of Americans with gout in the United States increased more than sevenfold from 1.1 million in 1960 to 8.1 million in 2010.
Data source: The National Health and Nutrition Examination Survey is a program of periodic, large, government-funded, national cross-sectional surveys involving a representative sample of the U.S. population.
Disclosures: The National Health and Nutrition Examination Survey is sponsored by the Centers for Disease Control and Prevention. The presenter reported receiving research grants from Takeda, which markets gout medication.

What is UnitedHealthcare doing?
A month ago, all five physicians in our practice received notice that we would no longer be covered under UnitedHealthcare Medicare Advantage plans. No reason was given, nor had we been given any kind of advanced notice that this was even a possibility. This was based on our business tax ID number, by the way, not on any individual doctor’s credentials. Very quickly it became evident that this was part of a 20%-30% reduction in their physician panels in multiple states, including Rhode Island, Connecticut, New York, New Jersey, Florida, Indiana, and Ohio.
What hasn’t been so easy to figure out is why. The insurance giant has not been forthcoming about the decision. In an advertisement in the Providence Journal, they cited "severe funding reductions for Medicare Advantage Plans."
Medicare Advantage Plans are Medicare plans that are administered by private insurance companies. They contract with the government to administer Medicare, and patients also pay a premium, making it profitable for insurers. These plans, however, are more expensive for the federal government, and in an effort to curtail the burgeoning cost of health care, "companies that don’t use 80% to 85% of revenues on care are forced to issue rebates to members for the difference," according to financial services company The Motley Fool.
In addition, there have been proposed rate cuts to Medicare Advantage Plans, in part to offset the cost of expanding Medicaid as the Affordable Care Act mandates. The Associated Press reported that UnitedHealthcare stock did not perform as expected in the third quarter of 2013. UnitedHealthcare blamed this on the rate cuts that the federal government imposed on Medicare.
So perhaps the Medicare Advantage Plans are not as profitable for the company as they once were, as the aforementioned advertisement in the Providence Journal implied. That does not explain the reduction of 20%-30% of their providers, though.
In a statement to the Hartford Courant, Dennis O’Brien, regional president of UnitedHealthcare Networks, had this to say: "We are assessing our network in Connecticut to help us provide higher quality and more affordable health care coverage for Medicare beneficiaries."
That explains nothing at all. It implies that the physicians they removed from their roster were of inferior quality and were costing them more money. And yet they have not given any explanation for what these "higher quality and more affordable" standards are. Furthermore, if quality and cost were the real issue, why would we be appropriate for UnitedHealthcare commercial patients but not for Medicare patients?
There has been a lot of speculation about why UnitedHealthcare is doing this, but until the company is more forthcoming, or is forced to account for its behavior (by subscribers or by politicians), we won’t really know.
In the meantime, the company’s unilateral decision will leave thousands of patients across states with interrupted medical care. It will take time for these patients to find new doctors, establish care, and build rapport.
If there is anything that’s become clearer to me from this debacle, it is this: We doctors hold ourselves accountable to our patients, but UnitedHealthcare, and maybe other private insurers as well, is accountable only to its shareholders.
In the debate over universal health care, health care is repeatedly referred to as a commodity that is malleable according to market forces. But this is a false equivalence, is it not? Chief Justice John Roberts’ preference for broccoli may be subject to supply and demand, but your right to health care should not be. That narrative needs to be reframed if people’s health and well-being are ever to trump the investors’ bottom line.
Dr. Chan practices rheumatology in Pawtucket, R.I.
A month ago, all five physicians in our practice received notice that we would no longer be covered under UnitedHealthcare Medicare Advantage plans. No reason was given, nor had we been given any kind of advanced notice that this was even a possibility. This was based on our business tax ID number, by the way, not on any individual doctor’s credentials. Very quickly it became evident that this was part of a 20%-30% reduction in their physician panels in multiple states, including Rhode Island, Connecticut, New York, New Jersey, Florida, Indiana, and Ohio.
What hasn’t been so easy to figure out is why. The insurance giant has not been forthcoming about the decision. In an advertisement in the Providence Journal, they cited "severe funding reductions for Medicare Advantage Plans."
Medicare Advantage Plans are Medicare plans that are administered by private insurance companies. They contract with the government to administer Medicare, and patients also pay a premium, making it profitable for insurers. These plans, however, are more expensive for the federal government, and in an effort to curtail the burgeoning cost of health care, "companies that don’t use 80% to 85% of revenues on care are forced to issue rebates to members for the difference," according to financial services company The Motley Fool.
In addition, there have been proposed rate cuts to Medicare Advantage Plans, in part to offset the cost of expanding Medicaid as the Affordable Care Act mandates. The Associated Press reported that UnitedHealthcare stock did not perform as expected in the third quarter of 2013. UnitedHealthcare blamed this on the rate cuts that the federal government imposed on Medicare.
So perhaps the Medicare Advantage Plans are not as profitable for the company as they once were, as the aforementioned advertisement in the Providence Journal implied. That does not explain the reduction of 20%-30% of their providers, though.
In a statement to the Hartford Courant, Dennis O’Brien, regional president of UnitedHealthcare Networks, had this to say: "We are assessing our network in Connecticut to help us provide higher quality and more affordable health care coverage for Medicare beneficiaries."
That explains nothing at all. It implies that the physicians they removed from their roster were of inferior quality and were costing them more money. And yet they have not given any explanation for what these "higher quality and more affordable" standards are. Furthermore, if quality and cost were the real issue, why would we be appropriate for UnitedHealthcare commercial patients but not for Medicare patients?
There has been a lot of speculation about why UnitedHealthcare is doing this, but until the company is more forthcoming, or is forced to account for its behavior (by subscribers or by politicians), we won’t really know.
In the meantime, the company’s unilateral decision will leave thousands of patients across states with interrupted medical care. It will take time for these patients to find new doctors, establish care, and build rapport.
If there is anything that’s become clearer to me from this debacle, it is this: We doctors hold ourselves accountable to our patients, but UnitedHealthcare, and maybe other private insurers as well, is accountable only to its shareholders.
In the debate over universal health care, health care is repeatedly referred to as a commodity that is malleable according to market forces. But this is a false equivalence, is it not? Chief Justice John Roberts’ preference for broccoli may be subject to supply and demand, but your right to health care should not be. That narrative needs to be reframed if people’s health and well-being are ever to trump the investors’ bottom line.
Dr. Chan practices rheumatology in Pawtucket, R.I.
A month ago, all five physicians in our practice received notice that we would no longer be covered under UnitedHealthcare Medicare Advantage plans. No reason was given, nor had we been given any kind of advanced notice that this was even a possibility. This was based on our business tax ID number, by the way, not on any individual doctor’s credentials. Very quickly it became evident that this was part of a 20%-30% reduction in their physician panels in multiple states, including Rhode Island, Connecticut, New York, New Jersey, Florida, Indiana, and Ohio.
What hasn’t been so easy to figure out is why. The insurance giant has not been forthcoming about the decision. In an advertisement in the Providence Journal, they cited "severe funding reductions for Medicare Advantage Plans."
Medicare Advantage Plans are Medicare plans that are administered by private insurance companies. They contract with the government to administer Medicare, and patients also pay a premium, making it profitable for insurers. These plans, however, are more expensive for the federal government, and in an effort to curtail the burgeoning cost of health care, "companies that don’t use 80% to 85% of revenues on care are forced to issue rebates to members for the difference," according to financial services company The Motley Fool.
In addition, there have been proposed rate cuts to Medicare Advantage Plans, in part to offset the cost of expanding Medicaid as the Affordable Care Act mandates. The Associated Press reported that UnitedHealthcare stock did not perform as expected in the third quarter of 2013. UnitedHealthcare blamed this on the rate cuts that the federal government imposed on Medicare.
So perhaps the Medicare Advantage Plans are not as profitable for the company as they once were, as the aforementioned advertisement in the Providence Journal implied. That does not explain the reduction of 20%-30% of their providers, though.
In a statement to the Hartford Courant, Dennis O’Brien, regional president of UnitedHealthcare Networks, had this to say: "We are assessing our network in Connecticut to help us provide higher quality and more affordable health care coverage for Medicare beneficiaries."
That explains nothing at all. It implies that the physicians they removed from their roster were of inferior quality and were costing them more money. And yet they have not given any explanation for what these "higher quality and more affordable" standards are. Furthermore, if quality and cost were the real issue, why would we be appropriate for UnitedHealthcare commercial patients but not for Medicare patients?
There has been a lot of speculation about why UnitedHealthcare is doing this, but until the company is more forthcoming, or is forced to account for its behavior (by subscribers or by politicians), we won’t really know.
In the meantime, the company’s unilateral decision will leave thousands of patients across states with interrupted medical care. It will take time for these patients to find new doctors, establish care, and build rapport.
If there is anything that’s become clearer to me from this debacle, it is this: We doctors hold ourselves accountable to our patients, but UnitedHealthcare, and maybe other private insurers as well, is accountable only to its shareholders.
In the debate over universal health care, health care is repeatedly referred to as a commodity that is malleable according to market forces. But this is a false equivalence, is it not? Chief Justice John Roberts’ preference for broccoli may be subject to supply and demand, but your right to health care should not be. That narrative needs to be reframed if people’s health and well-being are ever to trump the investors’ bottom line.
Dr. Chan practices rheumatology in Pawtucket, R.I.

CDC finds cluster of newborns with late VKDB

Photo by Bertrand Devouard
The Centers for Disease Control and Prevention (CDC) has identified a
small group of newborns in Tennessee with late vitamin K deficiency
bleeding (VKDB).
The agency reported 4 cases of late VKDB, a
serious but preventable bleeding disorder that can cause intracranial
hemorrhage, neurological deficits, and death.
In each case, the newborn’s parents
declined a vitamin K injection at birth, mainly because they were
uninformed about the risk of late VKBD.
Preliminary findings of the CDC’s investigation, in collaboration with the Tennessee Department of Health, appear in the current issue of the Morbidity and Mortality Weekly Report.
“Not giving vitamin K at birth is an emerging trend that can have devastating outcomes for infants and their families,” said CDC Director Tom Frieden, MD. “Ensuring that every newborn receives a vitamin K injection at birth is critical to protect infants.”
Between February and September of this year, 4 cases of late VKDB were diagnosed at a hospital in Nashville, Tennessee.
Three of the infants experienced intracranial hemorrhage, and the fourth had gastrointestinal bleeding. None of the patients had received a vitamin K injection at birth.
Fortunately, all of the infants survived. The patient with gastrointestinal bleeding has made a full recovery. And the 3 infants with intracranial hemorrhage are being followed by neurologists.
One patient has an apparent gross motor deficit, but it seems the others do not. However, all of the patients are still less than 1 year of age, so the full impact of VKDB might only become apparent with time.
The infants’ parents said they declined vitamin K prophylaxis for a number of reasons, including concern about an increased risk of leukemia, the belief that the injection was unnecessary, and a desire to minimize the newborn’s exposure to “toxins.”
Concern about the increased risk of leukemia associated with vitamin K prophylaxis was initially generated by a report published in 1992, but the finding has not been replicated in subsequent studies.
In all cases, parents were uninformed or insufficiently informed about the risk of late VKDB. Most parents only learned about the possibility of late VKDB after their infants developed the condition.
These findings illustrate the importance of educating parents about vitamin K prophylaxis, said Lauren Marcewicz, MD, of the CDC’s National Center on Birth Defects and Developmental Disabilities.
A vitamin K injection at birth has been standard practice in the US since it was first recommended as prophylaxis for late VKDB by the American Academy of Pediatrics in 1961.
The late form of VKDB can develop in infants 2 weeks to 6 months of age who did not receive a vitamin K injection and do not have enough vitamin K-dependent proteins in their bodies to allow normal blood clotting. If untreated, this can cause intracranial hemorrhage, which may lead to neurological problems and can be fatal.
The risk for developing late VKDB has been estimated at 81 times greater among infants who do not receive a vitamin K injection at birth than in infants who do receive it.
The CDC said it is currently working with the Tennessee Department of Health to determine if other cases of late VKDB occurred in the state in recent years.
In addition, a case-control study is underway to assess whether any additional risk factors might contribute to the development of late VKDB in children who do not receive vitamin K prophylaxis. ![]()
Photo by Bertrand Devouard
The Centers for Disease Control and Prevention (CDC) has identified a
small group of newborns in Tennessee with late vitamin K deficiency
bleeding (VKDB).
The agency reported 4 cases of late VKDB, a
serious but preventable bleeding disorder that can cause intracranial
hemorrhage, neurological deficits, and death.
In each case, the newborn’s parents
declined a vitamin K injection at birth, mainly because they were
uninformed about the risk of late VKBD.
Preliminary findings of the CDC’s investigation, in collaboration with the Tennessee Department of Health, appear in the current issue of the Morbidity and Mortality Weekly Report.
“Not giving vitamin K at birth is an emerging trend that can have devastating outcomes for infants and their families,” said CDC Director Tom Frieden, MD. “Ensuring that every newborn receives a vitamin K injection at birth is critical to protect infants.”
Between February and September of this year, 4 cases of late VKDB were diagnosed at a hospital in Nashville, Tennessee.
Three of the infants experienced intracranial hemorrhage, and the fourth had gastrointestinal bleeding. None of the patients had received a vitamin K injection at birth.
Fortunately, all of the infants survived. The patient with gastrointestinal bleeding has made a full recovery. And the 3 infants with intracranial hemorrhage are being followed by neurologists.
One patient has an apparent gross motor deficit, but it seems the others do not. However, all of the patients are still less than 1 year of age, so the full impact of VKDB might only become apparent with time.
The infants’ parents said they declined vitamin K prophylaxis for a number of reasons, including concern about an increased risk of leukemia, the belief that the injection was unnecessary, and a desire to minimize the newborn’s exposure to “toxins.”
Concern about the increased risk of leukemia associated with vitamin K prophylaxis was initially generated by a report published in 1992, but the finding has not been replicated in subsequent studies.
In all cases, parents were uninformed or insufficiently informed about the risk of late VKDB. Most parents only learned about the possibility of late VKDB after their infants developed the condition.
These findings illustrate the importance of educating parents about vitamin K prophylaxis, said Lauren Marcewicz, MD, of the CDC’s National Center on Birth Defects and Developmental Disabilities.
A vitamin K injection at birth has been standard practice in the US since it was first recommended as prophylaxis for late VKDB by the American Academy of Pediatrics in 1961.
The late form of VKDB can develop in infants 2 weeks to 6 months of age who did not receive a vitamin K injection and do not have enough vitamin K-dependent proteins in their bodies to allow normal blood clotting. If untreated, this can cause intracranial hemorrhage, which may lead to neurological problems and can be fatal.
The risk for developing late VKDB has been estimated at 81 times greater among infants who do not receive a vitamin K injection at birth than in infants who do receive it.
The CDC said it is currently working with the Tennessee Department of Health to determine if other cases of late VKDB occurred in the state in recent years.
In addition, a case-control study is underway to assess whether any additional risk factors might contribute to the development of late VKDB in children who do not receive vitamin K prophylaxis. ![]()
Photo by Bertrand Devouard
The Centers for Disease Control and Prevention (CDC) has identified a
small group of newborns in Tennessee with late vitamin K deficiency
bleeding (VKDB).
The agency reported 4 cases of late VKDB, a
serious but preventable bleeding disorder that can cause intracranial
hemorrhage, neurological deficits, and death.
In each case, the newborn’s parents
declined a vitamin K injection at birth, mainly because they were
uninformed about the risk of late VKBD.
Preliminary findings of the CDC’s investigation, in collaboration with the Tennessee Department of Health, appear in the current issue of the Morbidity and Mortality Weekly Report.
“Not giving vitamin K at birth is an emerging trend that can have devastating outcomes for infants and their families,” said CDC Director Tom Frieden, MD. “Ensuring that every newborn receives a vitamin K injection at birth is critical to protect infants.”
Between February and September of this year, 4 cases of late VKDB were diagnosed at a hospital in Nashville, Tennessee.
Three of the infants experienced intracranial hemorrhage, and the fourth had gastrointestinal bleeding. None of the patients had received a vitamin K injection at birth.
Fortunately, all of the infants survived. The patient with gastrointestinal bleeding has made a full recovery. And the 3 infants with intracranial hemorrhage are being followed by neurologists.
One patient has an apparent gross motor deficit, but it seems the others do not. However, all of the patients are still less than 1 year of age, so the full impact of VKDB might only become apparent with time.
The infants’ parents said they declined vitamin K prophylaxis for a number of reasons, including concern about an increased risk of leukemia, the belief that the injection was unnecessary, and a desire to minimize the newborn’s exposure to “toxins.”
Concern about the increased risk of leukemia associated with vitamin K prophylaxis was initially generated by a report published in 1992, but the finding has not been replicated in subsequent studies.
In all cases, parents were uninformed or insufficiently informed about the risk of late VKDB. Most parents only learned about the possibility of late VKDB after their infants developed the condition.
These findings illustrate the importance of educating parents about vitamin K prophylaxis, said Lauren Marcewicz, MD, of the CDC’s National Center on Birth Defects and Developmental Disabilities.
A vitamin K injection at birth has been standard practice in the US since it was first recommended as prophylaxis for late VKDB by the American Academy of Pediatrics in 1961.
The late form of VKDB can develop in infants 2 weeks to 6 months of age who did not receive a vitamin K injection and do not have enough vitamin K-dependent proteins in their bodies to allow normal blood clotting. If untreated, this can cause intracranial hemorrhage, which may lead to neurological problems and can be fatal.
The risk for developing late VKDB has been estimated at 81 times greater among infants who do not receive a vitamin K injection at birth than in infants who do receive it.
The CDC said it is currently working with the Tennessee Department of Health to determine if other cases of late VKDB occurred in the state in recent years.
In addition, a case-control study is underway to assess whether any additional risk factors might contribute to the development of late VKDB in children who do not receive vitamin K prophylaxis. ![]()
Evaluating an Academic Hospitalist Service
Improving quality while reducing costs remains important for hospitals across the United States, including the approximately 150 hospitals that are part of the Veterans Affairs (VA) healthcare system.[1, 2] The field of hospital medicine has grown rapidly, leading to predictions that the majority of inpatient care in the United States eventually will be delivered by hospitalists.[3, 4] In 2010, 57% of US hospitals had hospitalists on staff, including 87% of hospitals with 200 beds,[5] and nearly 80% of VA hospitals.[6]
The demand for hospitalists within teaching hospitals has grown in part as a response to the mandate to reduce residency work hours.[7] Furthermore, previous research has found that hospitalist care is associated with modest reductions in length of stay (LOS) and weak but inconsistent differences in quality.[8] The educational effect of hospitalists has been far less examined. The limited number of studies published to date suggests that hospitalists may improve resident learning and house‐officer satisfaction in academic medical centers and community teaching hospitals[9, 10, 11] and provide positive experiences for medical students12,13; however, Wachter et al reported no significant changes in clinical outcomes or patient, faculty, and house‐staff satisfaction in a newly designed hospital medicine service in San Francisco.[14] Additionally, whether using hospitalists influences nurse‐physician communication[15] is unknown.
Recognizing the limited and sometimes conflicting evidence about the hospitalist model, we report the results of a 3‐year quasi‐experimental evaluation of the experience at our medical center with academic hospitalists. As part of a VA Systems Redesign Improvement Capability Grantknown as the Hospital Outcomes Program of Excellence (HOPE) Initiativewe created a hospitalist‐based medicine team focused on quality improvement, medical education, and patient outcomes.
METHODS
Setting and Design
The main hospital of the VA Ann Arbor Healthcare System, located in Ann Arbor, Michigan, operates 105 acute‐care beds and 40 extended‐care beds. At the time of this evaluation, the medicine service consisted of 4 internal medicine teamsGold, Silver, Burgundy, and Yelloweach of which was responsible for admitting patients on a rotating basis every fourth day, with limited numbers of admissions occurring between each team's primary admitting day. Each team is led by an attending physician, a board‐certified (or board‐eligible) general internist or subspecialist who is also a faculty member at the University of Michigan Medical School. Each team has a senior medical resident, 2 to 3 interns, and 3 to 5 medical students (mostly third‐year students). In total, there are approximately 50 senior medical residents, 60 interns, and 170 medical students who rotate through the medicine service each year. Traditional rounding involves the medical students and interns receiving sign‐out from the overnight team in the morning, then pre‐rounding on each patient by obtaining an interval history, performing an exam, and checking any test results. A tentative plan of care is formed with the senior medical resident, usually by discussing each patient very quickly in the team room. Attending rounds are then conducted, with the physician team visiting each patient one by one to review and plan all aspects of care in detail. When time allows, small segments of teaching may occur during these attending work rounds. This system had been in place for >20 years.
Resulting in part from a grant received from the VA Systems Redesign Central Office (ie, the HOPE Initiative), the Gold team was modified in July 2009 and an academic hospitalist (S.S.) was assigned to head this team. Specific hospitalists were selected by the Associate Chief of Medicine (S.S.) and the Chief of Medicine (R.H.M.) to serve as Gold team attendings on a regular basis. The other teams continued to be overseen by the Chief of Medicine, and the Gold team remained within the medicine service. Characteristics of the Gold and nonGold team attendings can be found in Table 1. The 3 other teams initially were noninterventional concurrent control groups. However, during the second year of the evaluation, the Silver team adopted some of the initiatives as a result of the preliminary findings observed on Gold. Specifically, in the second year of the evaluation, approximately 42% of attendings on the Silver team were from the Gold team. This increased in the third year to 67% of coverage by Gold team attendings on the Silver team. The evaluation of the Gold team ended in June 2012.
| Characteristic | Gold Team | Non‐Gold Teams |
|---|---|---|
| Total number of attendings | 14 | 57 |
| Sex, % | ||
| Male | 79 | 58 |
| Female | 21 | 42 |
| Median years postresidency (range) | 10 (130) | 7 (141) |
| Subspecialists, % | 14 | 40 |
| Median days on service per year (range) | 53 (574) | 30 (592) |
The clinical interventions implemented on the Gold team were quality‐improvement work and were therefore exempt from institutional review board review. Human subjects' approval was, however, received to conduct interviews as part of a qualitative assessment.
Clinical Interventions
Several interventions involving the clinical care delivered were introduced on the Gold team, with a focus on improving communication among healthcare workers (Table 2).
| Clinical Interventions | Educational Interventions |
|---|---|
| Modified structure of attending rounds | Modified structure of attending rounds |
| Circle of Concern rounds | Attending reading list |
| Clinical Care Coordinator | Nifty Fifty reading list for learners |
| Regular attending team meetings | Website to provide expectations to learners |
| Two‐month per year commitment by attendings |
Structure of Attending Rounds
The structure of morning rounds was modified on the Gold team. Similar to the traditional structure, medical students and interns on the Gold team receive sign‐out from the overnight team in the morning. However, interns and students may or may not conduct pre‐rounds on each patient. The majority of time between sign‐out and the arrival of the attending physician is spent on work rounds. The senior resident leads rounds with the interns and students, discussing each patient while focusing on overnight events and current symptoms, new physical‐examination findings, and laboratory and test data. The plan of care to be presented to the attending is then formulated with the senior resident. The attending physician then leads Circle of Concern rounds with an expanded team, including a charge nurse, a clinical pharmacist, and a nurse Clinical Care Coordinator. Attending rounds tend to use an E‐AP format: significant Events overnight are discussed, followed by an Assessment & Plan by problem for the top active problems. Using this model, the attendings are able to focus more on teaching and discussing the patient plan than in the traditional model (in which the learner presents the details of the subjective, objective, laboratory, and radiographic data, with limited time left for the assessment and plan for each problem).
Circle of Concern Rounds
Suzanne Gordon described the Circle of Concern in her book Nursing Against the Odds.[16] From her observations, she noted that physicians typically form a circle to discuss patient care during rounds. The circle expands when another physician joins the group; however, the circle does not similarly expand to include nurses when they approach the group. Instead, nurses typically remain on the periphery, listening silently or trying to communicate to physicians' backs.[16] Thus, to promote nurse‐physician communication, Circle of Concern rounds were formally introduced on the Gold team. Each morning, the charge nurse rounds with the team and is encouraged to bring up nursing concerns. The inpatient clinical pharmacist is also included 2 to 3 times per week to help provide education to residents and students and perform medication reconciliation.
Clinical Care Coordinator
The role of the nurse Clinical Care Coordinatoralso introduced on the Gold teamis to provide continuity of patient care, facilitate interdisciplinary communication, facilitate patient discharge, ensure appropriate appointments are scheduled, communicate with the ambulatory care service to ensure proper transition between inpatient and outpatient care, and help educate residents and students on VA procedures and resources.
Regular Gold Team Meetings
All Gold team attendings are expected to dedicate 2 months per year to inpatient service (divided into half‐month blocks), instead of the average 1 month per year for attendings on the other teams. The Gold team attendings, unlike the other teams, also attend bimonthly meetings to discuss strategies for running the team.
Educational Interventions
Given the high number of learners on the medicine service, we wanted to enhance the educational experience for our learners. We thus implemented various interventions, in addition to the change in the structure of rounds, as described below.
Reading List for Learners: The Nifty Fifty
Because reading about clinical medicine is an integral part of medical education, we make explicit our expectation that residents and students read something clinically relevant every day. To promote this, we have provided a Nifty Fifty reading list of key articles. The PDF of each article is provided, along with a brief summary highlighting key points.
Reading List for Gold Attendings and Support Staff
To promote a common understanding of leadership techniques, management books are provided to Gold attending physicians and other members of the team (eg, Care Coordinator, nurse researcher, systems redesign engineer). One book is discussed at each Gold team meeting (Table 3), with participants taking turns leading the discussion.
| Book Title | Author(s) |
|---|---|
| The One Minute Manager | Ken Blanchard and Spencer Johnson |
| Good to Great | Jim Collins |
| Good to Great and the Social Sectors | Jim Collins |
| The Checklist Manifesto: How to Get Things Right | Atul Gawande |
| The Five Dysfunctions of a Team: A Leadership Fable | Patrick Lencioni |
| Getting to Yes: Negotiating Agreement Without Giving In | Roger Fisher, William Ury, and Bruce Patton |
| The Effective Executive: The Definitive Guide to Getting the Right Things Done | Peter Drucker |
| A Sense of Urgency | John Kotter |
| The Power of Positive Deviance: How Unlikely Innovators Solve the World's Toughest Problems | Richard Pascale, Jerry Sternin, and Monique Sternin |
| On the Mend: Revolutionizing Healthcare to Save Lives and Transform the Industry | John Toussaint and Roger Gerard |
| Outliers: The Story of Success | Malcolm Gladwell |
| Nursing Against the Odds: How Health Care Cost Cutting, Media Stereotypes, and Medical Hubris Undermine Nurses and Patient Care | Suzanne Gordon |
| How the Mighty Fall and Why Some Companies Never Give In | Jim Collins |
| What the Best College Teachers Do | Ken Bain |
| The Creative Destruction of Medicine | Eric Topol |
| What Got You Here Won't Get You There: How Successful People Become Even More Successful! | Marshall Goldsmith |
Website
A HOPE Initiative website was created (
Qualitative Assessment
To evaluate our efforts, we conducted a thorough qualitative assessment during the third year of the program. A total of 35 semistructured qualitative interviews were conducted with patients and staff from all levels of the organization, including senior leadership. The qualitative assessment was led by research staff from the Center for Clinical Management Research, who were minimally involved in the redesign effort and could provide an unbiased view of the initiative. Field notes from the semistructured interviews were analyzed, with themes developed using a descriptive approach and through discussion by a multidisciplinary team, which included building team consensus on findings that were supported by clear evidence in the data.[17]
Quantitative Outcome Measures
Clinical Outcomes
To determine if our communication and educational interventions had an impact on patient care, we used hospital administrative data to evaluate admission rates, LOS, and readmission rates for all 4 of the medicine teams. Additional clinical measures were assessed as needed. For example, we monitored the impact of the clinical pharmacist during a 4‐week pilot study by asking the Clinical Care Coordinator to track the proportion of patient encounters (n=170) in which the clinical pharmacist changed management or provided education to team members. Additionally, 2 staff surveys were conducted. The first survey focused on healthcare‐worker communication and was given to inpatient nurses and physicians (including attendings, residents, and medical students) who were recently on an inpatient medical service rotation. The survey included questions from previously validated communication measures,[18, 19, 20] as well as study‐specific questions. The second survey evaluated the new role of the Clinical Care Coordinator (Appendix). Both physicians and nurses who interacted with the Gold team's Clinical Care Coordinator were asked to complete this survey.
Educational Outcomes
To assess the educational interventions, we used learner evaluations of attendings, by both residents and medical students, and standardized internal medicine National Board of Medical Examiners Subject Examination (or shelf) scores for third‐year medical students. A separate evaluation of medical student perceptions of the rounding structure introduced on the Gold team using survey design has already been published.[21]
Statistical Analyses
Data from all sources were analyzed using SAS 9.3 (SAS Institute, Inc., Cary, NC). Outliers for the LOS variable were removed from the analysis. Means and frequency distributions were examined for all variables. Student t tests and [2] tests of independence were used to compare data between groups. Multivariable linear regression models controlling for time (preintervention vs postintervention) were used to assess the effect of the HOPE Initiative on patient LOS and readmission rates. In all cases, 2‐tailed P values of 0.05 or less were considered statistically significant.
Role of the Funding Source
The VA Office of Systems Redesign provided funding but was not involved in the design or conduct of the study, data analysis, or preparation of the manuscript.
RESULTS
Clinical Outcomes
Patient Outcomes
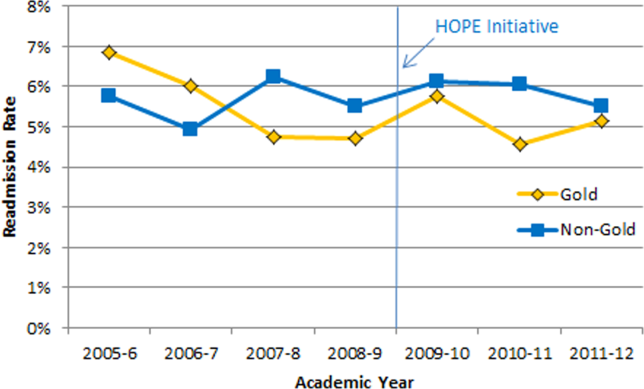
Our multivariable linear regression analysis, controlling for time, showed a significant reduction in LOS of approximately 0.3 days on all teams after the HOPE Initiative began (P=0.004). There were no significant differences between the Gold and non‐Gold teams in the multivariate models when controlling for time for any of the patient‐outcome measures. The number of admissions increased for all 4 medical teams (Figure 1), but, as shown in Figures 2 and 3, the readmission rates for all teams remained relatively stable over this same period of time.


Clinical Pharmacist on Gold Team Rounds
The inpatient clinical pharmacist changed the management plan for 22% of the patients seen on rounds. Contributions from the clinical pharmacist included adjusting the dosing of ordered medication and correcting medication reconciliation. Education and pharmaceutical information was provided to the team in another 6% of the 170 consecutive patient encounters evaluated.
Perception of Circle of Concern Rounds
Circle of Concern rounds were generally well‐received by both nurses and physicians. In a healthcare‐worker communication survey, completed by 38 physicians (62% response rate) and 48 nurses (54% response rate), the majority of both physicians (83%) and nurses (68%) felt Circle of Concern rounds improved communication.
Nurse Perception of Communication
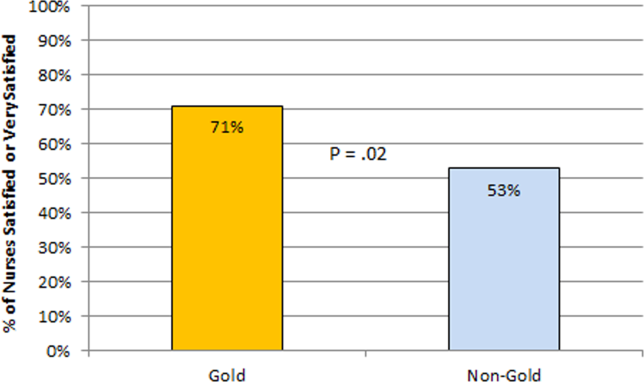
The healthcare‐worker communication survey asked inpatient nurses to rate communication between nurses and physicians on each of the 4 medicine teams. Significantly more nurses were satisfied with communication with the Gold team (71%) compared with the other 3 medicine teams (53%; P=0.02) (Figure 4).
Perception of the Clinical Care Coordinator
In total, 20 physicians (87% response rate) and 10 nurses (56% response rate) completed the Clinical Care Coordinator survey. The physician results were overwhelmingly positive: 100% were satisfied or very satisfied with the role; 100% felt each team should have a Clinical Care Coordinator; and 100% agreed or strongly agreed that the Clinical Care Coordinator ensures that appropriate follow‐up is arranged, provides continuity of care, assists with interdisciplinary communication, and helps facilitate discharge. The majority of nurses was also satisfied or very satisfied with the Clinical Care Coordinator role and felt each team should have one.
Educational Outcomes
House Officer Evaluation of Attendings
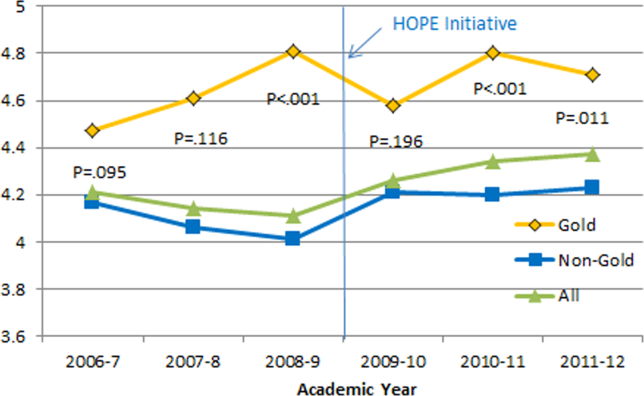
Monthly evaluations of attending physicians by house officers (Figure 5) revealed that prior to the HOPE Initiative, little differences were observed between teams, as would be expected because attending assignment was largely random. After the intervention date of July 2009, however, significant differences were noted, with Gold team attendings receiving significantly higher teaching evaluations immediately after the introduction of the HOPE Initiative. Although ratings for Gold attendings remained more favorable, the difference was no longer statistically significant in the second and third year of the initiative, likely due to Gold attendings serving on other medicine teams, which contributed to an improvement in ratings of all attendings.
Medical Student Evaluation of Attendings
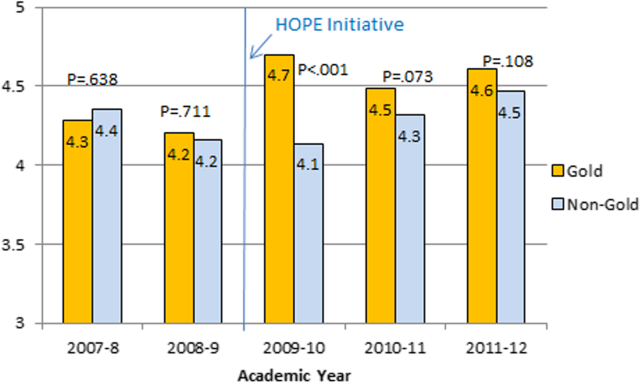
Monthly evaluations of attending physicians by third‐year medical students (Figure 6) revealed differences between the Gold attendings and all others, with the attendings that joined the Gold team in 2009 receiving higher teaching evaluations even before the HOPE Initiative started. However, this difference remained statistically significant in years 2 and 3 postinitiative, despite the addition of 4 new junior attendings.
Medical Student Medicine Shelf Scores
The national average on the shelf exam, which reflects learning after the internal medicine third‐year clerkship, has ranged from 75 to 78 for the past several years, with University of Michigan students averaging significantly higher scores prior to and after the HOPE Initiative. However, following the HOPE Initiative, third‐year medical students on the Gold team scored significantly higher on the shelf exam compared with their colleagues on the non‐Gold teams (84 vs 82; P=0.006). This difference in the shelf exam scores, although small, is statistically significant. It represents a measurable improvement in shelf scores in our system and demonstrates the potential educational benefit for the students. Over this same time period, scores on the United States Medical Licensing Exam, given to medical students at the beginning of their third year, remained stable (233 preHOPE Initiative; 234 postHOPE Initiative).
Qualitative Assessment
Qualitative data collected as part of our evaluation of the HOPE Initiative also suggested that nurse‐physician communication had improved since the start of the project. In particular, they reported positively on the Gold team in general, the Circle of Concern rounds, and the Clinical Care Coordinator (Table 4).
| Staff Type | Statement1 |
|---|---|
| |
| Nurse | [Gold is] above and beyond other [teams]. Other teams don't run as smoothly. |
| Nurse | There has been a difference in communication [on Gold]. You can tell the difference in how they communicate with staff. We know the Clinical Care Coordinator or charge nurse is rounding with that team, so there is more communication. |
| Nurse | The most important thing that has improved communication is the Circle of Concern rounds. |
| Physician | [The Gold Clinical Care Coordinator] expedites care, not only what to do but who to call. She can convey the urgency. On rounds she is able to break off, put in an order, place a call, talk to a patient. Things that we would do at 11 AM she gets to at 9 AM. A couple of hours may not seem like much, but sometimes it can make the difference between things happening that day instead of the next. |
| Physician | The Clinical Care Coordinator is completely indispensable. Major benefit to providing care to Veterans. |
| Physician | I like to think Gold has lifted all of the teams to a higher level. |
| Medical student | It may be due to personalities vs the Gold [team] itself, but there is more emphasis on best practices. Are we following guidelines even if it is not related to the primary reason for admission? |
| Medical student | Gold is very collegial and nurses/physicians know one another by name. Physicians request rather than order; this sets a good example to me on how to approach the nurses. |
| Chief resident | [Gold attendings] encourage senior residents to take charge and run the team, although the attending is there for back‐up and support. This provides great learning for the residents. Interns and medical students also are affected because they have to step up their game as well. |
DISCUSSION
Within academic medical centers, hospitalists are expected to care for patients, teach, and help improve the quality and efficiency of hospital‐based care.[7] The Department of Veterans Affairs runs the largest integrated healthcare system in the United States, with approximately 80% of VA hospitals having hospital medicine programs. Overall, one‐third of US residents perform part of their residency training at a VA hospital.[22, 23] Thus, the effects of a system‐wide change at a VA hospital may have implications throughout the country. We studied one such intervention. Our primary findings are that we were able to improve communication and learner education with minimal effects on patient outcomes. While overall LOS decreased slightly postintervention, after taking into account secular trends, readmission rates did not.
We are not the first to evaluate a hospital medicine team using a quasi‐experimental design. For example, Meltzer and colleagues evaluated a hospitalist program at the University of Chicago Medical Center and found that, by the second year of operation, hospitalist care was associated with significantly shorter LOS (0.49 days), reduced costs, and decreased mortality.[24] Auerbach also evaluated a newly created hospital medicine service, finding decreased LOS (0.61 days), lower costs, and lower risk of mortality by the second year of the program.[25]
Improving nurse‐physician communication is considered important for avoiding medical error,[26] yet there has been limited empirical study of methods to improve communication within the medical profession.[27] Based both on our surveys and qualitative interviews, healthcare‐worker communication appeared to improve on the Gold team during the study. A key component of this improvement is likely related to instituting Circle of Concern rounds, in which nurses joined the medical team during attending rounds. Such an intervention likely helped to address organizational silence[28] and enhance the psychological safety of the nursing staff, because the attending physician was proactive about soliciting the input of nurses during rounds.[29] Such leader inclusivenesswords and deeds exhibited by leaders that invite and appreciate others' contributionscan aid interdisciplinary teams in overcoming the negative effects of status differences, thereby promoting collaboration.[29] The inclusion of nurses on rounds is also relationship‐building, which Gotlib Conn and colleagues found was important to improved interprofessional communication and collaboration.[30] In the future, using a tool such as the Teamwork Effectiveness Assessment Module (TEAM) developed by the American Board of Internal Medicine[31] could provide further evaluation of the impact on interprofessional teamwork and communication.
The focus on learner education, though evaluated in prior studies, is also novel. One previous survey of medical students showed that engaging students in substantive discussions is associated with greater student satisfaction.[32] Another survey of medical students found that attendings who were enthusiastic about teaching, inspired confidence in knowledge and skills, provided useful feedback, and encouraged increased student responsibility were viewed as more effective teachers.[33] No previous study that we are aware of, however, has looked at actual educational outcomes, such as shelf scores. The National Board of Medical Examiners reports that the Medicine subject exam is scaled to have a mean of 70 and a standard deviation of 8.[34] Thus, a mean increase in score of 2 points is small, but not trivial. This shows improvement in a hard educational outcome. Additionally, 2 points, although small in the context of total score and standard deviation, may make a substantial difference to an individual student in terms of overall grade, and, thus, residency applications. Our finding that third‐year medical students on the Gold team performed significantly better than University of Michigan third‐year medical students on other teams is an intriguing finding that warrants confirmation. On the other hand, this finding is consistent with a previous report evaluating learner satisfaction in which Bodnar et al found improved ratings of quantity and quality of teaching on teams with a nontraditional structure (Gold team).[21] Moreover, despite relatively few studies, the reason underlying the educational benefit of hospitalists should surprise few. The hospitalist model ensures that learners are supervised by physicians who are experts in the care of hospitalized patients.[35] Hospitalists hired at teaching hospitals to work on services with learners are generally chosen because they possess superior educational skills.[7]
Our findings should be interpreted in the context of the following limitations. First, our study focused on a single academically affiliated VA hospital. As other VA hospitals are pursuing a similar approach (eg, the Houston and Detroit VA medical centers), replicating our results will be important. Second, the VA system, although the largest integrated healthcare system in the United States, has unique characteristicssuch as an integrated electronic health record and predominantly male patient populationthat may make generalizations to the larger US healthcare system challenging. Third, there was a slightly lower response rate among nurses on a few of the surveys to evaluate our efforts; however, this rate of response is standard at our facility. Finally, our evaluation lacks an empirical measure of healthcare‐worker communication, such as incident reports.
Despite these limitations, our results have important implications. Using both quantitative and qualitative assessment, we found that academic hospitalists have the ability to improve healthcare‐worker communication and enhance learner education without increasing LOS. These findings are directly applicable to VA medical centers and potentially applicable to other academic medical centers.
Acknowledgments
The authors thank Milisa Manojlovich, PhD, RN, Edward Kennedy, MS, and Andrew Hickner, MSI, for help with preparation of this manuscript.
Disclosures: This work was funded by a US Department of Veterans Affairs, Office of Systems Redesign Improvement Capability grant. The findings and conclusions in this report are those of the authors and do not necessarily represent the position or policy of the Department of Veterans Affairs. Dr. Saint reports receiving travel reimbursement for giving invited talks at the Society of Hospital Medicine's National Meeting, as well as serving on the advisory boards of Doximity and Jvion.
APPENDIX
Survey to Evaluate the Care Coordinator Position
| Yes | No | Not Sure | |
| Q1. Are you familiar with the role of the Care Coordinator on the Gold Service (Susan Lee)? | 1 | 2 | 3 |
Please indicate how much you agree or disagree with the statements below.
| Strongly Agree | Agree | Neutral | Disagree | Strongly Disagree | Don't Know | |
| Q2. The Care Coordinator ensures that appropriate primary care follow‐up and any other appropriate services are arranged. | 1 | 2 | 3 | 4 | 5 | 9 |
| Q3. The Care Coordinator provides continuity of patient care on the Gold Service. | 1 | 2 | 3 | 4 | 5 | 9 |
| Q4. The Care Coordinator helps educate House Officers and Medical Students on VA processes (e.g., CPRS). | 1 | 2 | 3 | 4 | 5 | 9 |
| Q5. The Care Coordinator assists with interdisciplinary communication between the medical team and other services (e.g., nursing, ambulatory care, pharmacy, social work) | 1 | 2 | 3 | 4 | 5 | 9 |
| Q6. The Care Coordinator helps facilitate patient discharge. | 1 | 2 | 3 | 4 | 5 | 9 |
| Q7. The Care Coordinator initiates communication with the ambulatory care teams to coordinate care. | 1 | 2 | 3 | 4 | 5 | 9 |
| Yes | No | |
| Q8. Are you a physician (attending or resident), or medical student who has been on more than one medical team at the VA (Gold, Silver, Burgundy, or Yellow)? | 1 | 2 |
If no, please skip to Q13
If yes, comparing your experience on the Gold Service (with the Care Coordinator) to your experience on any of the other services (Silver, Burgundy, or Yellow):
| Not at All | Very Little | Somewhat | To a Great Extent | |
| Q9. To what extent does the presence of a Care Coordinator affect patient care? | 1 | 2 | 3 | 4 |
| Q10. To what extent does the presence of a Care Coordinator improve patient flow? | 1 | 2 | 3 | 4 |
| Q11. To what extent does the presence of a Care Coordinator assist with education? | 1 | 2 | 3 | 4 |
| Q12. To what extent does the presence of a Care Coordinator contribute to attending rounds? | 1 | 2 | 3 | 4 |
| Yes | No | |
| Q13. Do you work [as a nurse] in ambulatory care? | 1 | 2 |
If no, please skip to Q17.
If yes, comparing your experience with the Gold Service (with the Care Coordinator) to the other services (Silver, Burgundy, or Yellow):
| Not at All | Very Little | Somewhat | To a Great Extent | |
| Q14. To what extent does the presence of a Care Coordinator improve coordination of care between inpatient and outpatient services? | 1 | 2 | 3 | 4 |
| Q15. To what extent does the presence of a Care Coordinator help identify high risk patients who require follow‐up? | 1 | 2 | 3 | 4 |
| Q16. To what extent does the presence of a Care Coordinator ensure follow‐up appointments are scheduled? | 1 | 2 | 3 | 4 |
| Yes | No | Not Sure | |
| Q17. Do you think each medical team should have a Care Coordinator? | 1 | 2 | 3 |
| Q18. Are there any additional tasks or duties you think would improve the effectiveness of the Care Coordinator? |
| Very Satisfied | Satisfied | Neutral | Dissatisfied | Very Dissatisfied | |
| Q19. Overall how satisfied are you with the role of the Care Coordinator on the Gold Service? | 1 | 2 | 3 | 4 | 5 |
| Q20. Do you have any other comments about the role of the Care Coordinator? |
| Q21. What is your position? |
| 1. Physician (attending or resident) or medical student |
| 2. Nurse (inpatient or ambulatory care) |
- Kohn LT, Corrigan JM, Donaldson MS, eds. To Err Is Human: Building a Safer Health System. Washington, D.C.: National Academies Press; 2000.
- Institute of Medicine of the National Academies. Crossing the Quality Chasm: A New Health System for the 21st Century. Washington, D.C.: National Academies Press; 2001.
- , , , . Growth in the care of older patients by hospitalists in the United States. N Engl J Med. 2009;360(11):1102–1112.
- . Growth in care provided by hospitalists. N Engl J Med. 2009;360(26):2789–2791.
- American Hospital Association. AHA Annual Survey of Hospitals, 2010. Chicago, IL: Health Forum, LLC; 2010.
- , , , . Preventing hospital‐acquired infections: a national survey of practices reported by U.S. hospitals in 2005 and 2009. J Gen Intern Med. 2012;27(7):773–779.
- , . Hospitalists in teaching hospitals: opportunities but not without danger. J Gen Intern Med. 2004;19(4):392–393.
- , . Do hospitalist physicians improve the quality of inpatient care delivery? A systematic review of process, efficiency and outcome measures. BMC Med. 2011;9:58.
- , , , . Effect of hospitalist attending physicians on trainee educational experiences: a systematic review. J Hosp Med. 2009;4(8):490–498.
- , , , , , . Resident satisfaction on an academic hospitalist service: time to teach. Am J Med. 2002;112(7):597–601.
- , , , et al. The positive impact of initiation of hospitalist clinician educators. J Gen Intern Med. 2004;19(4):293–301.
- , . Third‐year medical students' evaluation of hospitalist and nonhospitalist faculty during the inpatient portion of their pediatrics clerkships. J Hosp Med. 2007;2(1):17–22.
- , , , . Medical student evaluation of the quality of hospitalist and nonhospitalist teaching faculty on inpatient medicine rotations. Acad Med. 2004;79(1):78–82.
- , , , , . Reorganizing an academic medical service: impact on cost, quality, patient satisfaction, and education. JAMA. 1998;279(19):1560–1565.
- . Nurse/physician communication through a sensemaking lens: shifting the paradigm to improve patient safety. Med Care. 2010;48(11):941–946.
- . Nursing Against the Odds: How Health Care Cost Cutting, Media Stereotypes, and Medical Hubris Undermine Nurses and Patient Care. Ithaca, NY: Cornell University Press; 2005.
- . Focus on research methods: whatever happened to qualitative description? Res Nurs Health. 2000;23:334–340.
- , , , , . Organizational assessment in intensive care units (ICUs): construct development, reliability, and validity of the ICU nurse‐physician questionnaire. Med Care. 1991;29(8):709–726.
- . Development of an instrument to measure collaboration and satisfaction about care decisions. J Adv Nurs. 1994;20(1):176–182.
- . Development of the practice environment scale of the Nursing Work Index. Res Nurs Health. 2002;25(3):176–188.
- , , . Does the structure of inpatient rounds affect medical student education? Int J Med Educ. 2013;4:96–100.
- U.S. Department of Veterans Affairs, Office of Academic Affiliations. Medical and Dental Education Program. Available at: http://www.va. gov/oaa/GME_default.asp. Published 2012. Accessed May 08, 2013.
- , . Graduate medical education, 2011–2012. JAMA. 2012;308(21):2264–2279.
- , , , et al. Effects of physician experience on costs and outcomes on an academic general medicine service: results of a trial of hospitalists. Ann Intern Med. 2002;137(11):866–874.
- , , , , , . Implementation of a voluntary hospitalist service at a community teaching hospital: improved clinical efficiency and patient outcomes. Ann Intern Med. 2002;137(11):859–865.
- , , . Communication failures: an insidious contributor to medical mishaps. Acad Med. 2004;79(2):186–194.
- , , . ‘It depends': medical residents' perspectives on working with nurses. Am J Nurs. 2009;109(7):34–44.
- , . Organizational silence: a barrier to change and development in a pluralistic world. Acad Manage Rev. 2000;25(4):706–725.
- , . Making it safe: the effects of leader inclusiveness and professional status on psychological safety and improvement efforts in health care teams. J Organiz Behav. 2006;27:941–966.
- , , , , . Interprofessional communication with hospitalist and consultant physicians in general internal medicine: a qualitative study. BMC Health Serv Res. 2012;12:437.
- , , , , , . A new tool to give hospitalists feedback to improve interprofessional teamwork and advance patient care. Health Aff (Millwood). 2012;31(11):2485–2492.
- , , , , , . Impact of instructional practices on student satisfaction with attendings' teaching in the inpatient component of internal medicine clerkships. J Gen Intern Med. 2006;21(1):7–12.
- , . Medical students' perceptions of the elements of effective inpatient teaching by attending physicians and housestaff. J Gen Intern Med. 2005;20(7):635–639.
- National Board of Medical Examiners Subject Examination Program. Internal Medicine Advanced Clinical Examination, score interpretation guide. Available at: http://www.nbme.org/PDF/SampleScoreReports/Internal_Medicine_ACE_Score_Report.pdf. Published 2011. Accessed September 13, 2013.
- . The impact of hospitalists on medical education and the academic health system. Ann Intern Med. 1999;130(4 part 2):364–367.
Improving quality while reducing costs remains important for hospitals across the United States, including the approximately 150 hospitals that are part of the Veterans Affairs (VA) healthcare system.[1, 2] The field of hospital medicine has grown rapidly, leading to predictions that the majority of inpatient care in the United States eventually will be delivered by hospitalists.[3, 4] In 2010, 57% of US hospitals had hospitalists on staff, including 87% of hospitals with 200 beds,[5] and nearly 80% of VA hospitals.[6]
The demand for hospitalists within teaching hospitals has grown in part as a response to the mandate to reduce residency work hours.[7] Furthermore, previous research has found that hospitalist care is associated with modest reductions in length of stay (LOS) and weak but inconsistent differences in quality.[8] The educational effect of hospitalists has been far less examined. The limited number of studies published to date suggests that hospitalists may improve resident learning and house‐officer satisfaction in academic medical centers and community teaching hospitals[9, 10, 11] and provide positive experiences for medical students12,13; however, Wachter et al reported no significant changes in clinical outcomes or patient, faculty, and house‐staff satisfaction in a newly designed hospital medicine service in San Francisco.[14] Additionally, whether using hospitalists influences nurse‐physician communication[15] is unknown.
Recognizing the limited and sometimes conflicting evidence about the hospitalist model, we report the results of a 3‐year quasi‐experimental evaluation of the experience at our medical center with academic hospitalists. As part of a VA Systems Redesign Improvement Capability Grantknown as the Hospital Outcomes Program of Excellence (HOPE) Initiativewe created a hospitalist‐based medicine team focused on quality improvement, medical education, and patient outcomes.
METHODS
Setting and Design
The main hospital of the VA Ann Arbor Healthcare System, located in Ann Arbor, Michigan, operates 105 acute‐care beds and 40 extended‐care beds. At the time of this evaluation, the medicine service consisted of 4 internal medicine teamsGold, Silver, Burgundy, and Yelloweach of which was responsible for admitting patients on a rotating basis every fourth day, with limited numbers of admissions occurring between each team's primary admitting day. Each team is led by an attending physician, a board‐certified (or board‐eligible) general internist or subspecialist who is also a faculty member at the University of Michigan Medical School. Each team has a senior medical resident, 2 to 3 interns, and 3 to 5 medical students (mostly third‐year students). In total, there are approximately 50 senior medical residents, 60 interns, and 170 medical students who rotate through the medicine service each year. Traditional rounding involves the medical students and interns receiving sign‐out from the overnight team in the morning, then pre‐rounding on each patient by obtaining an interval history, performing an exam, and checking any test results. A tentative plan of care is formed with the senior medical resident, usually by discussing each patient very quickly in the team room. Attending rounds are then conducted, with the physician team visiting each patient one by one to review and plan all aspects of care in detail. When time allows, small segments of teaching may occur during these attending work rounds. This system had been in place for >20 years.
Resulting in part from a grant received from the VA Systems Redesign Central Office (ie, the HOPE Initiative), the Gold team was modified in July 2009 and an academic hospitalist (S.S.) was assigned to head this team. Specific hospitalists were selected by the Associate Chief of Medicine (S.S.) and the Chief of Medicine (R.H.M.) to serve as Gold team attendings on a regular basis. The other teams continued to be overseen by the Chief of Medicine, and the Gold team remained within the medicine service. Characteristics of the Gold and nonGold team attendings can be found in Table 1. The 3 other teams initially were noninterventional concurrent control groups. However, during the second year of the evaluation, the Silver team adopted some of the initiatives as a result of the preliminary findings observed on Gold. Specifically, in the second year of the evaluation, approximately 42% of attendings on the Silver team were from the Gold team. This increased in the third year to 67% of coverage by Gold team attendings on the Silver team. The evaluation of the Gold team ended in June 2012.
| Characteristic | Gold Team | Non‐Gold Teams |
|---|---|---|
| Total number of attendings | 14 | 57 |
| Sex, % | ||
| Male | 79 | 58 |
| Female | 21 | 42 |
| Median years postresidency (range) | 10 (130) | 7 (141) |
| Subspecialists, % | 14 | 40 |
| Median days on service per year (range) | 53 (574) | 30 (592) |
The clinical interventions implemented on the Gold team were quality‐improvement work and were therefore exempt from institutional review board review. Human subjects' approval was, however, received to conduct interviews as part of a qualitative assessment.
Clinical Interventions
Several interventions involving the clinical care delivered were introduced on the Gold team, with a focus on improving communication among healthcare workers (Table 2).
| Clinical Interventions | Educational Interventions |
|---|---|
| Modified structure of attending rounds | Modified structure of attending rounds |
| Circle of Concern rounds | Attending reading list |
| Clinical Care Coordinator | Nifty Fifty reading list for learners |
| Regular attending team meetings | Website to provide expectations to learners |
| Two‐month per year commitment by attendings |
Structure of Attending Rounds
The structure of morning rounds was modified on the Gold team. Similar to the traditional structure, medical students and interns on the Gold team receive sign‐out from the overnight team in the morning. However, interns and students may or may not conduct pre‐rounds on each patient. The majority of time between sign‐out and the arrival of the attending physician is spent on work rounds. The senior resident leads rounds with the interns and students, discussing each patient while focusing on overnight events and current symptoms, new physical‐examination findings, and laboratory and test data. The plan of care to be presented to the attending is then formulated with the senior resident. The attending physician then leads Circle of Concern rounds with an expanded team, including a charge nurse, a clinical pharmacist, and a nurse Clinical Care Coordinator. Attending rounds tend to use an E‐AP format: significant Events overnight are discussed, followed by an Assessment & Plan by problem for the top active problems. Using this model, the attendings are able to focus more on teaching and discussing the patient plan than in the traditional model (in which the learner presents the details of the subjective, objective, laboratory, and radiographic data, with limited time left for the assessment and plan for each problem).
Circle of Concern Rounds
Suzanne Gordon described the Circle of Concern in her book Nursing Against the Odds.[16] From her observations, she noted that physicians typically form a circle to discuss patient care during rounds. The circle expands when another physician joins the group; however, the circle does not similarly expand to include nurses when they approach the group. Instead, nurses typically remain on the periphery, listening silently or trying to communicate to physicians' backs.[16] Thus, to promote nurse‐physician communication, Circle of Concern rounds were formally introduced on the Gold team. Each morning, the charge nurse rounds with the team and is encouraged to bring up nursing concerns. The inpatient clinical pharmacist is also included 2 to 3 times per week to help provide education to residents and students and perform medication reconciliation.
Clinical Care Coordinator
The role of the nurse Clinical Care Coordinatoralso introduced on the Gold teamis to provide continuity of patient care, facilitate interdisciplinary communication, facilitate patient discharge, ensure appropriate appointments are scheduled, communicate with the ambulatory care service to ensure proper transition between inpatient and outpatient care, and help educate residents and students on VA procedures and resources.
Regular Gold Team Meetings
All Gold team attendings are expected to dedicate 2 months per year to inpatient service (divided into half‐month blocks), instead of the average 1 month per year for attendings on the other teams. The Gold team attendings, unlike the other teams, also attend bimonthly meetings to discuss strategies for running the team.
Educational Interventions
Given the high number of learners on the medicine service, we wanted to enhance the educational experience for our learners. We thus implemented various interventions, in addition to the change in the structure of rounds, as described below.
Reading List for Learners: The Nifty Fifty
Because reading about clinical medicine is an integral part of medical education, we make explicit our expectation that residents and students read something clinically relevant every day. To promote this, we have provided a Nifty Fifty reading list of key articles. The PDF of each article is provided, along with a brief summary highlighting key points.
Reading List for Gold Attendings and Support Staff
To promote a common understanding of leadership techniques, management books are provided to Gold attending physicians and other members of the team (eg, Care Coordinator, nurse researcher, systems redesign engineer). One book is discussed at each Gold team meeting (Table 3), with participants taking turns leading the discussion.
| Book Title | Author(s) |
|---|---|
| The One Minute Manager | Ken Blanchard and Spencer Johnson |
| Good to Great | Jim Collins |
| Good to Great and the Social Sectors | Jim Collins |
| The Checklist Manifesto: How to Get Things Right | Atul Gawande |
| The Five Dysfunctions of a Team: A Leadership Fable | Patrick Lencioni |
| Getting to Yes: Negotiating Agreement Without Giving In | Roger Fisher, William Ury, and Bruce Patton |
| The Effective Executive: The Definitive Guide to Getting the Right Things Done | Peter Drucker |
| A Sense of Urgency | John Kotter |
| The Power of Positive Deviance: How Unlikely Innovators Solve the World's Toughest Problems | Richard Pascale, Jerry Sternin, and Monique Sternin |
| On the Mend: Revolutionizing Healthcare to Save Lives and Transform the Industry | John Toussaint and Roger Gerard |
| Outliers: The Story of Success | Malcolm Gladwell |
| Nursing Against the Odds: How Health Care Cost Cutting, Media Stereotypes, and Medical Hubris Undermine Nurses and Patient Care | Suzanne Gordon |
| How the Mighty Fall and Why Some Companies Never Give In | Jim Collins |
| What the Best College Teachers Do | Ken Bain |
| The Creative Destruction of Medicine | Eric Topol |
| What Got You Here Won't Get You There: How Successful People Become Even More Successful! | Marshall Goldsmith |
Website
A HOPE Initiative website was created (
Qualitative Assessment
To evaluate our efforts, we conducted a thorough qualitative assessment during the third year of the program. A total of 35 semistructured qualitative interviews were conducted with patients and staff from all levels of the organization, including senior leadership. The qualitative assessment was led by research staff from the Center for Clinical Management Research, who were minimally involved in the redesign effort and could provide an unbiased view of the initiative. Field notes from the semistructured interviews were analyzed, with themes developed using a descriptive approach and through discussion by a multidisciplinary team, which included building team consensus on findings that were supported by clear evidence in the data.[17]
Quantitative Outcome Measures
Clinical Outcomes
To determine if our communication and educational interventions had an impact on patient care, we used hospital administrative data to evaluate admission rates, LOS, and readmission rates for all 4 of the medicine teams. Additional clinical measures were assessed as needed. For example, we monitored the impact of the clinical pharmacist during a 4‐week pilot study by asking the Clinical Care Coordinator to track the proportion of patient encounters (n=170) in which the clinical pharmacist changed management or provided education to team members. Additionally, 2 staff surveys were conducted. The first survey focused on healthcare‐worker communication and was given to inpatient nurses and physicians (including attendings, residents, and medical students) who were recently on an inpatient medical service rotation. The survey included questions from previously validated communication measures,[18, 19, 20] as well as study‐specific questions. The second survey evaluated the new role of the Clinical Care Coordinator (Appendix). Both physicians and nurses who interacted with the Gold team's Clinical Care Coordinator were asked to complete this survey.
Educational Outcomes
To assess the educational interventions, we used learner evaluations of attendings, by both residents and medical students, and standardized internal medicine National Board of Medical Examiners Subject Examination (or shelf) scores for third‐year medical students. A separate evaluation of medical student perceptions of the rounding structure introduced on the Gold team using survey design has already been published.[21]
Statistical Analyses
Data from all sources were analyzed using SAS 9.3 (SAS Institute, Inc., Cary, NC). Outliers for the LOS variable were removed from the analysis. Means and frequency distributions were examined for all variables. Student t tests and [2] tests of independence were used to compare data between groups. Multivariable linear regression models controlling for time (preintervention vs postintervention) were used to assess the effect of the HOPE Initiative on patient LOS and readmission rates. In all cases, 2‐tailed P values of 0.05 or less were considered statistically significant.
Role of the Funding Source
The VA Office of Systems Redesign provided funding but was not involved in the design or conduct of the study, data analysis, or preparation of the manuscript.
RESULTS
Clinical Outcomes
Patient Outcomes
Our multivariable linear regression analysis, controlling for time, showed a significant reduction in LOS of approximately 0.3 days on all teams after the HOPE Initiative began (P=0.004). There were no significant differences between the Gold and non‐Gold teams in the multivariate models when controlling for time for any of the patient‐outcome measures. The number of admissions increased for all 4 medical teams (Figure 1), but, as shown in Figures 2 and 3, the readmission rates for all teams remained relatively stable over this same period of time.
Clinical Pharmacist on Gold Team Rounds
The inpatient clinical pharmacist changed the management plan for 22% of the patients seen on rounds. Contributions from the clinical pharmacist included adjusting the dosing of ordered medication and correcting medication reconciliation. Education and pharmaceutical information was provided to the team in another 6% of the 170 consecutive patient encounters evaluated.
Perception of Circle of Concern Rounds
Circle of Concern rounds were generally well‐received by both nurses and physicians. In a healthcare‐worker communication survey, completed by 38 physicians (62% response rate) and 48 nurses (54% response rate), the majority of both physicians (83%) and nurses (68%) felt Circle of Concern rounds improved communication.
Nurse Perception of Communication
The healthcare‐worker communication survey asked inpatient nurses to rate communication between nurses and physicians on each of the 4 medicine teams. Significantly more nurses were satisfied with communication with the Gold team (71%) compared with the other 3 medicine teams (53%; P=0.02) (Figure 4).
Perception of the Clinical Care Coordinator
In total, 20 physicians (87% response rate) and 10 nurses (56% response rate) completed the Clinical Care Coordinator survey. The physician results were overwhelmingly positive: 100% were satisfied or very satisfied with the role; 100% felt each team should have a Clinical Care Coordinator; and 100% agreed or strongly agreed that the Clinical Care Coordinator ensures that appropriate follow‐up is arranged, provides continuity of care, assists with interdisciplinary communication, and helps facilitate discharge. The majority of nurses was also satisfied or very satisfied with the Clinical Care Coordinator role and felt each team should have one.
Educational Outcomes
House Officer Evaluation of Attendings
Monthly evaluations of attending physicians by house officers (Figure 5) revealed that prior to the HOPE Initiative, little differences were observed between teams, as would be expected because attending assignment was largely random. After the intervention date of July 2009, however, significant differences were noted, with Gold team attendings receiving significantly higher teaching evaluations immediately after the introduction of the HOPE Initiative. Although ratings for Gold attendings remained more favorable, the difference was no longer statistically significant in the second and third year of the initiative, likely due to Gold attendings serving on other medicine teams, which contributed to an improvement in ratings of all attendings.
Medical Student Evaluation of Attendings
Monthly evaluations of attending physicians by third‐year medical students (Figure 6) revealed differences between the Gold attendings and all others, with the attendings that joined the Gold team in 2009 receiving higher teaching evaluations even before the HOPE Initiative started. However, this difference remained statistically significant in years 2 and 3 postinitiative, despite the addition of 4 new junior attendings.
Medical Student Medicine Shelf Scores
The national average on the shelf exam, which reflects learning after the internal medicine third‐year clerkship, has ranged from 75 to 78 for the past several years, with University of Michigan students averaging significantly higher scores prior to and after the HOPE Initiative. However, following the HOPE Initiative, third‐year medical students on the Gold team scored significantly higher on the shelf exam compared with their colleagues on the non‐Gold teams (84 vs 82; P=0.006). This difference in the shelf exam scores, although small, is statistically significant. It represents a measurable improvement in shelf scores in our system and demonstrates the potential educational benefit for the students. Over this same time period, scores on the United States Medical Licensing Exam, given to medical students at the beginning of their third year, remained stable (233 preHOPE Initiative; 234 postHOPE Initiative).
Qualitative Assessment
Qualitative data collected as part of our evaluation of the HOPE Initiative also suggested that nurse‐physician communication had improved since the start of the project. In particular, they reported positively on the Gold team in general, the Circle of Concern rounds, and the Clinical Care Coordinator (Table 4).
| Staff Type | Statement1 |
|---|---|
| |
| Nurse | [Gold is] above and beyond other [teams]. Other teams don't run as smoothly. |
| Nurse | There has been a difference in communication [on Gold]. You can tell the difference in how they communicate with staff. We know the Clinical Care Coordinator or charge nurse is rounding with that team, so there is more communication. |
| Nurse | The most important thing that has improved communication is the Circle of Concern rounds. |
| Physician | [The Gold Clinical Care Coordinator] expedites care, not only what to do but who to call. She can convey the urgency. On rounds she is able to break off, put in an order, place a call, talk to a patient. Things that we would do at 11 AM she gets to at 9 AM. A couple of hours may not seem like much, but sometimes it can make the difference between things happening that day instead of the next. |
| Physician | The Clinical Care Coordinator is completely indispensable. Major benefit to providing care to Veterans. |
| Physician | I like to think Gold has lifted all of the teams to a higher level. |
| Medical student | It may be due to personalities vs the Gold [team] itself, but there is more emphasis on best practices. Are we following guidelines even if it is not related to the primary reason for admission? |
| Medical student | Gold is very collegial and nurses/physicians know one another by name. Physicians request rather than order; this sets a good example to me on how to approach the nurses. |
| Chief resident | [Gold attendings] encourage senior residents to take charge and run the team, although the attending is there for back‐up and support. This provides great learning for the residents. Interns and medical students also are affected because they have to step up their game as well. |
DISCUSSION
Within academic medical centers, hospitalists are expected to care for patients, teach, and help improve the quality and efficiency of hospital‐based care.[7] The Department of Veterans Affairs runs the largest integrated healthcare system in the United States, with approximately 80% of VA hospitals having hospital medicine programs. Overall, one‐third of US residents perform part of their residency training at a VA hospital.[22, 23] Thus, the effects of a system‐wide change at a VA hospital may have implications throughout the country. We studied one such intervention. Our primary findings are that we were able to improve communication and learner education with minimal effects on patient outcomes. While overall LOS decreased slightly postintervention, after taking into account secular trends, readmission rates did not.
We are not the first to evaluate a hospital medicine team using a quasi‐experimental design. For example, Meltzer and colleagues evaluated a hospitalist program at the University of Chicago Medical Center and found that, by the second year of operation, hospitalist care was associated with significantly shorter LOS (0.49 days), reduced costs, and decreased mortality.[24] Auerbach also evaluated a newly created hospital medicine service, finding decreased LOS (0.61 days), lower costs, and lower risk of mortality by the second year of the program.[25]
Improving nurse‐physician communication is considered important for avoiding medical error,[26] yet there has been limited empirical study of methods to improve communication within the medical profession.[27] Based both on our surveys and qualitative interviews, healthcare‐worker communication appeared to improve on the Gold team during the study. A key component of this improvement is likely related to instituting Circle of Concern rounds, in which nurses joined the medical team during attending rounds. Such an intervention likely helped to address organizational silence[28] and enhance the psychological safety of the nursing staff, because the attending physician was proactive about soliciting the input of nurses during rounds.[29] Such leader inclusivenesswords and deeds exhibited by leaders that invite and appreciate others' contributionscan aid interdisciplinary teams in overcoming the negative effects of status differences, thereby promoting collaboration.[29] The inclusion of nurses on rounds is also relationship‐building, which Gotlib Conn and colleagues found was important to improved interprofessional communication and collaboration.[30] In the future, using a tool such as the Teamwork Effectiveness Assessment Module (TEAM) developed by the American Board of Internal Medicine[31] could provide further evaluation of the impact on interprofessional teamwork and communication.
The focus on learner education, though evaluated in prior studies, is also novel. One previous survey of medical students showed that engaging students in substantive discussions is associated with greater student satisfaction.[32] Another survey of medical students found that attendings who were enthusiastic about teaching, inspired confidence in knowledge and skills, provided useful feedback, and encouraged increased student responsibility were viewed as more effective teachers.[33] No previous study that we are aware of, however, has looked at actual educational outcomes, such as shelf scores. The National Board of Medical Examiners reports that the Medicine subject exam is scaled to have a mean of 70 and a standard deviation of 8.[34] Thus, a mean increase in score of 2 points is small, but not trivial. This shows improvement in a hard educational outcome. Additionally, 2 points, although small in the context of total score and standard deviation, may make a substantial difference to an individual student in terms of overall grade, and, thus, residency applications. Our finding that third‐year medical students on the Gold team performed significantly better than University of Michigan third‐year medical students on other teams is an intriguing finding that warrants confirmation. On the other hand, this finding is consistent with a previous report evaluating learner satisfaction in which Bodnar et al found improved ratings of quantity and quality of teaching on teams with a nontraditional structure (Gold team).[21] Moreover, despite relatively few studies, the reason underlying the educational benefit of hospitalists should surprise few. The hospitalist model ensures that learners are supervised by physicians who are experts in the care of hospitalized patients.[35] Hospitalists hired at teaching hospitals to work on services with learners are generally chosen because they possess superior educational skills.[7]
Our findings should be interpreted in the context of the following limitations. First, our study focused on a single academically affiliated VA hospital. As other VA hospitals are pursuing a similar approach (eg, the Houston and Detroit VA medical centers), replicating our results will be important. Second, the VA system, although the largest integrated healthcare system in the United States, has unique characteristicssuch as an integrated electronic health record and predominantly male patient populationthat may make generalizations to the larger US healthcare system challenging. Third, there was a slightly lower response rate among nurses on a few of the surveys to evaluate our efforts; however, this rate of response is standard at our facility. Finally, our evaluation lacks an empirical measure of healthcare‐worker communication, such as incident reports.
Despite these limitations, our results have important implications. Using both quantitative and qualitative assessment, we found that academic hospitalists have the ability to improve healthcare‐worker communication and enhance learner education without increasing LOS. These findings are directly applicable to VA medical centers and potentially applicable to other academic medical centers.
Acknowledgments
The authors thank Milisa Manojlovich, PhD, RN, Edward Kennedy, MS, and Andrew Hickner, MSI, for help with preparation of this manuscript.
Disclosures: This work was funded by a US Department of Veterans Affairs, Office of Systems Redesign Improvement Capability grant. The findings and conclusions in this report are those of the authors and do not necessarily represent the position or policy of the Department of Veterans Affairs. Dr. Saint reports receiving travel reimbursement for giving invited talks at the Society of Hospital Medicine's National Meeting, as well as serving on the advisory boards of Doximity and Jvion.
APPENDIX
Survey to Evaluate the Care Coordinator Position
| Yes | No | Not Sure | |
| Q1. Are you familiar with the role of the Care Coordinator on the Gold Service (Susan Lee)? | 1 | 2 | 3 |
Please indicate how much you agree or disagree with the statements below.
| Strongly Agree | Agree | Neutral | Disagree | Strongly Disagree | Don't Know | |
| Q2. The Care Coordinator ensures that appropriate primary care follow‐up and any other appropriate services are arranged. | 1 | 2 | 3 | 4 | 5 | 9 |
| Q3. The Care Coordinator provides continuity of patient care on the Gold Service. | 1 | 2 | 3 | 4 | 5 | 9 |
| Q4. The Care Coordinator helps educate House Officers and Medical Students on VA processes (e.g., CPRS). | 1 | 2 | 3 | 4 | 5 | 9 |
| Q5. The Care Coordinator assists with interdisciplinary communication between the medical team and other services (e.g., nursing, ambulatory care, pharmacy, social work) | 1 | 2 | 3 | 4 | 5 | 9 |
| Q6. The Care Coordinator helps facilitate patient discharge. | 1 | 2 | 3 | 4 | 5 | 9 |
| Q7. The Care Coordinator initiates communication with the ambulatory care teams to coordinate care. | 1 | 2 | 3 | 4 | 5 | 9 |
| Yes | No | |
| Q8. Are you a physician (attending or resident), or medical student who has been on more than one medical team at the VA (Gold, Silver, Burgundy, or Yellow)? | 1 | 2 |
If no, please skip to Q13
If yes, comparing your experience on the Gold Service (with the Care Coordinator) to your experience on any of the other services (Silver, Burgundy, or Yellow):
| Not at All | Very Little | Somewhat | To a Great Extent | |
| Q9. To what extent does the presence of a Care Coordinator affect patient care? | 1 | 2 | 3 | 4 |
| Q10. To what extent does the presence of a Care Coordinator improve patient flow? | 1 | 2 | 3 | 4 |
| Q11. To what extent does the presence of a Care Coordinator assist with education? | 1 | 2 | 3 | 4 |
| Q12. To what extent does the presence of a Care Coordinator contribute to attending rounds? | 1 | 2 | 3 | 4 |
| Yes | No | |
| Q13. Do you work [as a nurse] in ambulatory care? | 1 | 2 |
If no, please skip to Q17.
If yes, comparing your experience with the Gold Service (with the Care Coordinator) to the other services (Silver, Burgundy, or Yellow):
| Not at All | Very Little | Somewhat | To a Great Extent | |
| Q14. To what extent does the presence of a Care Coordinator improve coordination of care between inpatient and outpatient services? | 1 | 2 | 3 | 4 |
| Q15. To what extent does the presence of a Care Coordinator help identify high risk patients who require follow‐up? | 1 | 2 | 3 | 4 |
| Q16. To what extent does the presence of a Care Coordinator ensure follow‐up appointments are scheduled? | 1 | 2 | 3 | 4 |
| Yes | No | Not Sure | |
| Q17. Do you think each medical team should have a Care Coordinator? | 1 | 2 | 3 |
| Q18. Are there any additional tasks or duties you think would improve the effectiveness of the Care Coordinator? |
| Very Satisfied | Satisfied | Neutral | Dissatisfied | Very Dissatisfied | |
| Q19. Overall how satisfied are you with the role of the Care Coordinator on the Gold Service? | 1 | 2 | 3 | 4 | 5 |
| Q20. Do you have any other comments about the role of the Care Coordinator? |
| Q21. What is your position? |
| 1. Physician (attending or resident) or medical student |
| 2. Nurse (inpatient or ambulatory care) |
Improving quality while reducing costs remains important for hospitals across the United States, including the approximately 150 hospitals that are part of the Veterans Affairs (VA) healthcare system.[1, 2] The field of hospital medicine has grown rapidly, leading to predictions that the majority of inpatient care in the United States eventually will be delivered by hospitalists.[3, 4] In 2010, 57% of US hospitals had hospitalists on staff, including 87% of hospitals with 200 beds,[5] and nearly 80% of VA hospitals.[6]
The demand for hospitalists within teaching hospitals has grown in part as a response to the mandate to reduce residency work hours.[7] Furthermore, previous research has found that hospitalist care is associated with modest reductions in length of stay (LOS) and weak but inconsistent differences in quality.[8] The educational effect of hospitalists has been far less examined. The limited number of studies published to date suggests that hospitalists may improve resident learning and house‐officer satisfaction in academic medical centers and community teaching hospitals[9, 10, 11] and provide positive experiences for medical students12,13; however, Wachter et al reported no significant changes in clinical outcomes or patient, faculty, and house‐staff satisfaction in a newly designed hospital medicine service in San Francisco.[14] Additionally, whether using hospitalists influences nurse‐physician communication[15] is unknown.
Recognizing the limited and sometimes conflicting evidence about the hospitalist model, we report the results of a 3‐year quasi‐experimental evaluation of the experience at our medical center with academic hospitalists. As part of a VA Systems Redesign Improvement Capability Grantknown as the Hospital Outcomes Program of Excellence (HOPE) Initiativewe created a hospitalist‐based medicine team focused on quality improvement, medical education, and patient outcomes.
METHODS
Setting and Design
The main hospital of the VA Ann Arbor Healthcare System, located in Ann Arbor, Michigan, operates 105 acute‐care beds and 40 extended‐care beds. At the time of this evaluation, the medicine service consisted of 4 internal medicine teamsGold, Silver, Burgundy, and Yelloweach of which was responsible for admitting patients on a rotating basis every fourth day, with limited numbers of admissions occurring between each team's primary admitting day. Each team is led by an attending physician, a board‐certified (or board‐eligible) general internist or subspecialist who is also a faculty member at the University of Michigan Medical School. Each team has a senior medical resident, 2 to 3 interns, and 3 to 5 medical students (mostly third‐year students). In total, there are approximately 50 senior medical residents, 60 interns, and 170 medical students who rotate through the medicine service each year. Traditional rounding involves the medical students and interns receiving sign‐out from the overnight team in the morning, then pre‐rounding on each patient by obtaining an interval history, performing an exam, and checking any test results. A tentative plan of care is formed with the senior medical resident, usually by discussing each patient very quickly in the team room. Attending rounds are then conducted, with the physician team visiting each patient one by one to review and plan all aspects of care in detail. When time allows, small segments of teaching may occur during these attending work rounds. This system had been in place for >20 years.
Resulting in part from a grant received from the VA Systems Redesign Central Office (ie, the HOPE Initiative), the Gold team was modified in July 2009 and an academic hospitalist (S.S.) was assigned to head this team. Specific hospitalists were selected by the Associate Chief of Medicine (S.S.) and the Chief of Medicine (R.H.M.) to serve as Gold team attendings on a regular basis. The other teams continued to be overseen by the Chief of Medicine, and the Gold team remained within the medicine service. Characteristics of the Gold and nonGold team attendings can be found in Table 1. The 3 other teams initially were noninterventional concurrent control groups. However, during the second year of the evaluation, the Silver team adopted some of the initiatives as a result of the preliminary findings observed on Gold. Specifically, in the second year of the evaluation, approximately 42% of attendings on the Silver team were from the Gold team. This increased in the third year to 67% of coverage by Gold team attendings on the Silver team. The evaluation of the Gold team ended in June 2012.
| Characteristic | Gold Team | Non‐Gold Teams |
|---|---|---|
| Total number of attendings | 14 | 57 |
| Sex, % | ||
| Male | 79 | 58 |
| Female | 21 | 42 |
| Median years postresidency (range) | 10 (130) | 7 (141) |
| Subspecialists, % | 14 | 40 |
| Median days on service per year (range) | 53 (574) | 30 (592) |
The clinical interventions implemented on the Gold team were quality‐improvement work and were therefore exempt from institutional review board review. Human subjects' approval was, however, received to conduct interviews as part of a qualitative assessment.
Clinical Interventions
Several interventions involving the clinical care delivered were introduced on the Gold team, with a focus on improving communication among healthcare workers (Table 2).
| Clinical Interventions | Educational Interventions |
|---|---|
| Modified structure of attending rounds | Modified structure of attending rounds |
| Circle of Concern rounds | Attending reading list |
| Clinical Care Coordinator | Nifty Fifty reading list for learners |
| Regular attending team meetings | Website to provide expectations to learners |
| Two‐month per year commitment by attendings |
Structure of Attending Rounds
The structure of morning rounds was modified on the Gold team. Similar to the traditional structure, medical students and interns on the Gold team receive sign‐out from the overnight team in the morning. However, interns and students may or may not conduct pre‐rounds on each patient. The majority of time between sign‐out and the arrival of the attending physician is spent on work rounds. The senior resident leads rounds with the interns and students, discussing each patient while focusing on overnight events and current symptoms, new physical‐examination findings, and laboratory and test data. The plan of care to be presented to the attending is then formulated with the senior resident. The attending physician then leads Circle of Concern rounds with an expanded team, including a charge nurse, a clinical pharmacist, and a nurse Clinical Care Coordinator. Attending rounds tend to use an E‐AP format: significant Events overnight are discussed, followed by an Assessment & Plan by problem for the top active problems. Using this model, the attendings are able to focus more on teaching and discussing the patient plan than in the traditional model (in which the learner presents the details of the subjective, objective, laboratory, and radiographic data, with limited time left for the assessment and plan for each problem).
Circle of Concern Rounds
Suzanne Gordon described the Circle of Concern in her book Nursing Against the Odds.[16] From her observations, she noted that physicians typically form a circle to discuss patient care during rounds. The circle expands when another physician joins the group; however, the circle does not similarly expand to include nurses when they approach the group. Instead, nurses typically remain on the periphery, listening silently or trying to communicate to physicians' backs.[16] Thus, to promote nurse‐physician communication, Circle of Concern rounds were formally introduced on the Gold team. Each morning, the charge nurse rounds with the team and is encouraged to bring up nursing concerns. The inpatient clinical pharmacist is also included 2 to 3 times per week to help provide education to residents and students and perform medication reconciliation.
Clinical Care Coordinator
The role of the nurse Clinical Care Coordinatoralso introduced on the Gold teamis to provide continuity of patient care, facilitate interdisciplinary communication, facilitate patient discharge, ensure appropriate appointments are scheduled, communicate with the ambulatory care service to ensure proper transition between inpatient and outpatient care, and help educate residents and students on VA procedures and resources.
Regular Gold Team Meetings
All Gold team attendings are expected to dedicate 2 months per year to inpatient service (divided into half‐month blocks), instead of the average 1 month per year for attendings on the other teams. The Gold team attendings, unlike the other teams, also attend bimonthly meetings to discuss strategies for running the team.
Educational Interventions
Given the high number of learners on the medicine service, we wanted to enhance the educational experience for our learners. We thus implemented various interventions, in addition to the change in the structure of rounds, as described below.
Reading List for Learners: The Nifty Fifty
Because reading about clinical medicine is an integral part of medical education, we make explicit our expectation that residents and students read something clinically relevant every day. To promote this, we have provided a Nifty Fifty reading list of key articles. The PDF of each article is provided, along with a brief summary highlighting key points.
Reading List for Gold Attendings and Support Staff
To promote a common understanding of leadership techniques, management books are provided to Gold attending physicians and other members of the team (eg, Care Coordinator, nurse researcher, systems redesign engineer). One book is discussed at each Gold team meeting (Table 3), with participants taking turns leading the discussion.
| Book Title | Author(s) |
|---|---|
| The One Minute Manager | Ken Blanchard and Spencer Johnson |
| Good to Great | Jim Collins |
| Good to Great and the Social Sectors | Jim Collins |
| The Checklist Manifesto: How to Get Things Right | Atul Gawande |
| The Five Dysfunctions of a Team: A Leadership Fable | Patrick Lencioni |
| Getting to Yes: Negotiating Agreement Without Giving In | Roger Fisher, William Ury, and Bruce Patton |
| The Effective Executive: The Definitive Guide to Getting the Right Things Done | Peter Drucker |
| A Sense of Urgency | John Kotter |
| The Power of Positive Deviance: How Unlikely Innovators Solve the World's Toughest Problems | Richard Pascale, Jerry Sternin, and Monique Sternin |
| On the Mend: Revolutionizing Healthcare to Save Lives and Transform the Industry | John Toussaint and Roger Gerard |
| Outliers: The Story of Success | Malcolm Gladwell |
| Nursing Against the Odds: How Health Care Cost Cutting, Media Stereotypes, and Medical Hubris Undermine Nurses and Patient Care | Suzanne Gordon |
| How the Mighty Fall and Why Some Companies Never Give In | Jim Collins |
| What the Best College Teachers Do | Ken Bain |
| The Creative Destruction of Medicine | Eric Topol |
| What Got You Here Won't Get You There: How Successful People Become Even More Successful! | Marshall Goldsmith |
Website
A HOPE Initiative website was created (
Qualitative Assessment
To evaluate our efforts, we conducted a thorough qualitative assessment during the third year of the program. A total of 35 semistructured qualitative interviews were conducted with patients and staff from all levels of the organization, including senior leadership. The qualitative assessment was led by research staff from the Center for Clinical Management Research, who were minimally involved in the redesign effort and could provide an unbiased view of the initiative. Field notes from the semistructured interviews were analyzed, with themes developed using a descriptive approach and through discussion by a multidisciplinary team, which included building team consensus on findings that were supported by clear evidence in the data.[17]
Quantitative Outcome Measures
Clinical Outcomes
To determine if our communication and educational interventions had an impact on patient care, we used hospital administrative data to evaluate admission rates, LOS, and readmission rates for all 4 of the medicine teams. Additional clinical measures were assessed as needed. For example, we monitored the impact of the clinical pharmacist during a 4‐week pilot study by asking the Clinical Care Coordinator to track the proportion of patient encounters (n=170) in which the clinical pharmacist changed management or provided education to team members. Additionally, 2 staff surveys were conducted. The first survey focused on healthcare‐worker communication and was given to inpatient nurses and physicians (including attendings, residents, and medical students) who were recently on an inpatient medical service rotation. The survey included questions from previously validated communication measures,[18, 19, 20] as well as study‐specific questions. The second survey evaluated the new role of the Clinical Care Coordinator (Appendix). Both physicians and nurses who interacted with the Gold team's Clinical Care Coordinator were asked to complete this survey.
Educational Outcomes
To assess the educational interventions, we used learner evaluations of attendings, by both residents and medical students, and standardized internal medicine National Board of Medical Examiners Subject Examination (or shelf) scores for third‐year medical students. A separate evaluation of medical student perceptions of the rounding structure introduced on the Gold team using survey design has already been published.[21]
Statistical Analyses
Data from all sources were analyzed using SAS 9.3 (SAS Institute, Inc., Cary, NC). Outliers for the LOS variable were removed from the analysis. Means and frequency distributions were examined for all variables. Student t tests and [2] tests of independence were used to compare data between groups. Multivariable linear regression models controlling for time (preintervention vs postintervention) were used to assess the effect of the HOPE Initiative on patient LOS and readmission rates. In all cases, 2‐tailed P values of 0.05 or less were considered statistically significant.
Role of the Funding Source
The VA Office of Systems Redesign provided funding but was not involved in the design or conduct of the study, data analysis, or preparation of the manuscript.
RESULTS
Clinical Outcomes
Patient Outcomes
Our multivariable linear regression analysis, controlling for time, showed a significant reduction in LOS of approximately 0.3 days on all teams after the HOPE Initiative began (P=0.004). There were no significant differences between the Gold and non‐Gold teams in the multivariate models when controlling for time for any of the patient‐outcome measures. The number of admissions increased for all 4 medical teams (Figure 1), but, as shown in Figures 2 and 3, the readmission rates for all teams remained relatively stable over this same period of time.
Clinical Pharmacist on Gold Team Rounds
The inpatient clinical pharmacist changed the management plan for 22% of the patients seen on rounds. Contributions from the clinical pharmacist included adjusting the dosing of ordered medication and correcting medication reconciliation. Education and pharmaceutical information was provided to the team in another 6% of the 170 consecutive patient encounters evaluated.
Perception of Circle of Concern Rounds
Circle of Concern rounds were generally well‐received by both nurses and physicians. In a healthcare‐worker communication survey, completed by 38 physicians (62% response rate) and 48 nurses (54% response rate), the majority of both physicians (83%) and nurses (68%) felt Circle of Concern rounds improved communication.
Nurse Perception of Communication
The healthcare‐worker communication survey asked inpatient nurses to rate communication between nurses and physicians on each of the 4 medicine teams. Significantly more nurses were satisfied with communication with the Gold team (71%) compared with the other 3 medicine teams (53%; P=0.02) (Figure 4).
Perception of the Clinical Care Coordinator
In total, 20 physicians (87% response rate) and 10 nurses (56% response rate) completed the Clinical Care Coordinator survey. The physician results were overwhelmingly positive: 100% were satisfied or very satisfied with the role; 100% felt each team should have a Clinical Care Coordinator; and 100% agreed or strongly agreed that the Clinical Care Coordinator ensures that appropriate follow‐up is arranged, provides continuity of care, assists with interdisciplinary communication, and helps facilitate discharge. The majority of nurses was also satisfied or very satisfied with the Clinical Care Coordinator role and felt each team should have one.
Educational Outcomes
House Officer Evaluation of Attendings
Monthly evaluations of attending physicians by house officers (Figure 5) revealed that prior to the HOPE Initiative, little differences were observed between teams, as would be expected because attending assignment was largely random. After the intervention date of July 2009, however, significant differences were noted, with Gold team attendings receiving significantly higher teaching evaluations immediately after the introduction of the HOPE Initiative. Although ratings for Gold attendings remained more favorable, the difference was no longer statistically significant in the second and third year of the initiative, likely due to Gold attendings serving on other medicine teams, which contributed to an improvement in ratings of all attendings.
Medical Student Evaluation of Attendings
Monthly evaluations of attending physicians by third‐year medical students (Figure 6) revealed differences between the Gold attendings and all others, with the attendings that joined the Gold team in 2009 receiving higher teaching evaluations even before the HOPE Initiative started. However, this difference remained statistically significant in years 2 and 3 postinitiative, despite the addition of 4 new junior attendings.
Medical Student Medicine Shelf Scores
The national average on the shelf exam, which reflects learning after the internal medicine third‐year clerkship, has ranged from 75 to 78 for the past several years, with University of Michigan students averaging significantly higher scores prior to and after the HOPE Initiative. However, following the HOPE Initiative, third‐year medical students on the Gold team scored significantly higher on the shelf exam compared with their colleagues on the non‐Gold teams (84 vs 82; P=0.006). This difference in the shelf exam scores, although small, is statistically significant. It represents a measurable improvement in shelf scores in our system and demonstrates the potential educational benefit for the students. Over this same time period, scores on the United States Medical Licensing Exam, given to medical students at the beginning of their third year, remained stable (233 preHOPE Initiative; 234 postHOPE Initiative).
Qualitative Assessment
Qualitative data collected as part of our evaluation of the HOPE Initiative also suggested that nurse‐physician communication had improved since the start of the project. In particular, they reported positively on the Gold team in general, the Circle of Concern rounds, and the Clinical Care Coordinator (Table 4).
| Staff Type | Statement1 |
|---|---|
| |
| Nurse | [Gold is] above and beyond other [teams]. Other teams don't run as smoothly. |
| Nurse | There has been a difference in communication [on Gold]. You can tell the difference in how they communicate with staff. We know the Clinical Care Coordinator or charge nurse is rounding with that team, so there is more communication. |
| Nurse | The most important thing that has improved communication is the Circle of Concern rounds. |
| Physician | [The Gold Clinical Care Coordinator] expedites care, not only what to do but who to call. She can convey the urgency. On rounds she is able to break off, put in an order, place a call, talk to a patient. Things that we would do at 11 AM she gets to at 9 AM. A couple of hours may not seem like much, but sometimes it can make the difference between things happening that day instead of the next. |
| Physician | The Clinical Care Coordinator is completely indispensable. Major benefit to providing care to Veterans. |
| Physician | I like to think Gold has lifted all of the teams to a higher level. |
| Medical student | It may be due to personalities vs the Gold [team] itself, but there is more emphasis on best practices. Are we following guidelines even if it is not related to the primary reason for admission? |
| Medical student | Gold is very collegial and nurses/physicians know one another by name. Physicians request rather than order; this sets a good example to me on how to approach the nurses. |
| Chief resident | [Gold attendings] encourage senior residents to take charge and run the team, although the attending is there for back‐up and support. This provides great learning for the residents. Interns and medical students also are affected because they have to step up their game as well. |
DISCUSSION
Within academic medical centers, hospitalists are expected to care for patients, teach, and help improve the quality and efficiency of hospital‐based care.[7] The Department of Veterans Affairs runs the largest integrated healthcare system in the United States, with approximately 80% of VA hospitals having hospital medicine programs. Overall, one‐third of US residents perform part of their residency training at a VA hospital.[22, 23] Thus, the effects of a system‐wide change at a VA hospital may have implications throughout the country. We studied one such intervention. Our primary findings are that we were able to improve communication and learner education with minimal effects on patient outcomes. While overall LOS decreased slightly postintervention, after taking into account secular trends, readmission rates did not.
We are not the first to evaluate a hospital medicine team using a quasi‐experimental design. For example, Meltzer and colleagues evaluated a hospitalist program at the University of Chicago Medical Center and found that, by the second year of operation, hospitalist care was associated with significantly shorter LOS (0.49 days), reduced costs, and decreased mortality.[24] Auerbach also evaluated a newly created hospital medicine service, finding decreased LOS (0.61 days), lower costs, and lower risk of mortality by the second year of the program.[25]
Improving nurse‐physician communication is considered important for avoiding medical error,[26] yet there has been limited empirical study of methods to improve communication within the medical profession.[27] Based both on our surveys and qualitative interviews, healthcare‐worker communication appeared to improve on the Gold team during the study. A key component of this improvement is likely related to instituting Circle of Concern rounds, in which nurses joined the medical team during attending rounds. Such an intervention likely helped to address organizational silence[28] and enhance the psychological safety of the nursing staff, because the attending physician was proactive about soliciting the input of nurses during rounds.[29] Such leader inclusivenesswords and deeds exhibited by leaders that invite and appreciate others' contributionscan aid interdisciplinary teams in overcoming the negative effects of status differences, thereby promoting collaboration.[29] The inclusion of nurses on rounds is also relationship‐building, which Gotlib Conn and colleagues found was important to improved interprofessional communication and collaboration.[30] In the future, using a tool such as the Teamwork Effectiveness Assessment Module (TEAM) developed by the American Board of Internal Medicine[31] could provide further evaluation of the impact on interprofessional teamwork and communication.
The focus on learner education, though evaluated in prior studies, is also novel. One previous survey of medical students showed that engaging students in substantive discussions is associated with greater student satisfaction.[32] Another survey of medical students found that attendings who were enthusiastic about teaching, inspired confidence in knowledge and skills, provided useful feedback, and encouraged increased student responsibility were viewed as more effective teachers.[33] No previous study that we are aware of, however, has looked at actual educational outcomes, such as shelf scores. The National Board of Medical Examiners reports that the Medicine subject exam is scaled to have a mean of 70 and a standard deviation of 8.[34] Thus, a mean increase in score of 2 points is small, but not trivial. This shows improvement in a hard educational outcome. Additionally, 2 points, although small in the context of total score and standard deviation, may make a substantial difference to an individual student in terms of overall grade, and, thus, residency applications. Our finding that third‐year medical students on the Gold team performed significantly better than University of Michigan third‐year medical students on other teams is an intriguing finding that warrants confirmation. On the other hand, this finding is consistent with a previous report evaluating learner satisfaction in which Bodnar et al found improved ratings of quantity and quality of teaching on teams with a nontraditional structure (Gold team).[21] Moreover, despite relatively few studies, the reason underlying the educational benefit of hospitalists should surprise few. The hospitalist model ensures that learners are supervised by physicians who are experts in the care of hospitalized patients.[35] Hospitalists hired at teaching hospitals to work on services with learners are generally chosen because they possess superior educational skills.[7]
Our findings should be interpreted in the context of the following limitations. First, our study focused on a single academically affiliated VA hospital. As other VA hospitals are pursuing a similar approach (eg, the Houston and Detroit VA medical centers), replicating our results will be important. Second, the VA system, although the largest integrated healthcare system in the United States, has unique characteristicssuch as an integrated electronic health record and predominantly male patient populationthat may make generalizations to the larger US healthcare system challenging. Third, there was a slightly lower response rate among nurses on a few of the surveys to evaluate our efforts; however, this rate of response is standard at our facility. Finally, our evaluation lacks an empirical measure of healthcare‐worker communication, such as incident reports.
Despite these limitations, our results have important implications. Using both quantitative and qualitative assessment, we found that academic hospitalists have the ability to improve healthcare‐worker communication and enhance learner education without increasing LOS. These findings are directly applicable to VA medical centers and potentially applicable to other academic medical centers.
Acknowledgments
The authors thank Milisa Manojlovich, PhD, RN, Edward Kennedy, MS, and Andrew Hickner, MSI, for help with preparation of this manuscript.
Disclosures: This work was funded by a US Department of Veterans Affairs, Office of Systems Redesign Improvement Capability grant. The findings and conclusions in this report are those of the authors and do not necessarily represent the position or policy of the Department of Veterans Affairs. Dr. Saint reports receiving travel reimbursement for giving invited talks at the Society of Hospital Medicine's National Meeting, as well as serving on the advisory boards of Doximity and Jvion.
APPENDIX
Survey to Evaluate the Care Coordinator Position
| Yes | No | Not Sure | |
| Q1. Are you familiar with the role of the Care Coordinator on the Gold Service (Susan Lee)? | 1 | 2 | 3 |
Please indicate how much you agree or disagree with the statements below.
| Strongly Agree | Agree | Neutral | Disagree | Strongly Disagree | Don't Know | |
| Q2. The Care Coordinator ensures that appropriate primary care follow‐up and any other appropriate services are arranged. | 1 | 2 | 3 | 4 | 5 | 9 |
| Q3. The Care Coordinator provides continuity of patient care on the Gold Service. | 1 | 2 | 3 | 4 | 5 | 9 |
| Q4. The Care Coordinator helps educate House Officers and Medical Students on VA processes (e.g., CPRS). | 1 | 2 | 3 | 4 | 5 | 9 |
| Q5. The Care Coordinator assists with interdisciplinary communication between the medical team and other services (e.g., nursing, ambulatory care, pharmacy, social work) | 1 | 2 | 3 | 4 | 5 | 9 |
| Q6. The Care Coordinator helps facilitate patient discharge. | 1 | 2 | 3 | 4 | 5 | 9 |
| Q7. The Care Coordinator initiates communication with the ambulatory care teams to coordinate care. | 1 | 2 | 3 | 4 | 5 | 9 |
| Yes | No | |
| Q8. Are you a physician (attending or resident), or medical student who has been on more than one medical team at the VA (Gold, Silver, Burgundy, or Yellow)? | 1 | 2 |
If no, please skip to Q13
If yes, comparing your experience on the Gold Service (with the Care Coordinator) to your experience on any of the other services (Silver, Burgundy, or Yellow):
| Not at All | Very Little | Somewhat | To a Great Extent | |
| Q9. To what extent does the presence of a Care Coordinator affect patient care? | 1 | 2 | 3 | 4 |
| Q10. To what extent does the presence of a Care Coordinator improve patient flow? | 1 | 2 | 3 | 4 |
| Q11. To what extent does the presence of a Care Coordinator assist with education? | 1 | 2 | 3 | 4 |
| Q12. To what extent does the presence of a Care Coordinator contribute to attending rounds? | 1 | 2 | 3 | 4 |
| Yes | No | |
| Q13. Do you work [as a nurse] in ambulatory care? | 1 | 2 |
If no, please skip to Q17.
If yes, comparing your experience with the Gold Service (with the Care Coordinator) to the other services (Silver, Burgundy, or Yellow):
| Not at All | Very Little | Somewhat | To a Great Extent | |
| Q14. To what extent does the presence of a Care Coordinator improve coordination of care between inpatient and outpatient services? | 1 | 2 | 3 | 4 |
| Q15. To what extent does the presence of a Care Coordinator help identify high risk patients who require follow‐up? | 1 | 2 | 3 | 4 |
| Q16. To what extent does the presence of a Care Coordinator ensure follow‐up appointments are scheduled? | 1 | 2 | 3 | 4 |
| Yes | No | Not Sure | |
| Q17. Do you think each medical team should have a Care Coordinator? | 1 | 2 | 3 |
| Q18. Are there any additional tasks or duties you think would improve the effectiveness of the Care Coordinator? |
| Very Satisfied | Satisfied | Neutral | Dissatisfied | Very Dissatisfied | |
| Q19. Overall how satisfied are you with the role of the Care Coordinator on the Gold Service? | 1 | 2 | 3 | 4 | 5 |
| Q20. Do you have any other comments about the role of the Care Coordinator? |
| Q21. What is your position? |
| 1. Physician (attending or resident) or medical student |
| 2. Nurse (inpatient or ambulatory care) |
- Kohn LT, Corrigan JM, Donaldson MS, eds. To Err Is Human: Building a Safer Health System. Washington, D.C.: National Academies Press; 2000.
- Institute of Medicine of the National Academies. Crossing the Quality Chasm: A New Health System for the 21st Century. Washington, D.C.: National Academies Press; 2001.
- , , , . Growth in the care of older patients by hospitalists in the United States. N Engl J Med. 2009;360(11):1102–1112.
- . Growth in care provided by hospitalists. N Engl J Med. 2009;360(26):2789–2791.
- American Hospital Association. AHA Annual Survey of Hospitals, 2010. Chicago, IL: Health Forum, LLC; 2010.
- , , , . Preventing hospital‐acquired infections: a national survey of practices reported by U.S. hospitals in 2005 and 2009. J Gen Intern Med. 2012;27(7):773–779.
- , . Hospitalists in teaching hospitals: opportunities but not without danger. J Gen Intern Med. 2004;19(4):392–393.
- , . Do hospitalist physicians improve the quality of inpatient care delivery? A systematic review of process, efficiency and outcome measures. BMC Med. 2011;9:58.
- , , , . Effect of hospitalist attending physicians on trainee educational experiences: a systematic review. J Hosp Med. 2009;4(8):490–498.
- , , , , , . Resident satisfaction on an academic hospitalist service: time to teach. Am J Med. 2002;112(7):597–601.
- , , , et al. The positive impact of initiation of hospitalist clinician educators. J Gen Intern Med. 2004;19(4):293–301.
- , . Third‐year medical students' evaluation of hospitalist and nonhospitalist faculty during the inpatient portion of their pediatrics clerkships. J Hosp Med. 2007;2(1):17–22.
- , , , . Medical student evaluation of the quality of hospitalist and nonhospitalist teaching faculty on inpatient medicine rotations. Acad Med. 2004;79(1):78–82.
- , , , , . Reorganizing an academic medical service: impact on cost, quality, patient satisfaction, and education. JAMA. 1998;279(19):1560–1565.
- . Nurse/physician communication through a sensemaking lens: shifting the paradigm to improve patient safety. Med Care. 2010;48(11):941–946.
- . Nursing Against the Odds: How Health Care Cost Cutting, Media Stereotypes, and Medical Hubris Undermine Nurses and Patient Care. Ithaca, NY: Cornell University Press; 2005.
- . Focus on research methods: whatever happened to qualitative description? Res Nurs Health. 2000;23:334–340.
- , , , , . Organizational assessment in intensive care units (ICUs): construct development, reliability, and validity of the ICU nurse‐physician questionnaire. Med Care. 1991;29(8):709–726.
- . Development of an instrument to measure collaboration and satisfaction about care decisions. J Adv Nurs. 1994;20(1):176–182.
- . Development of the practice environment scale of the Nursing Work Index. Res Nurs Health. 2002;25(3):176–188.
- , , . Does the structure of inpatient rounds affect medical student education? Int J Med Educ. 2013;4:96–100.
- U.S. Department of Veterans Affairs, Office of Academic Affiliations. Medical and Dental Education Program. Available at: http://www.va. gov/oaa/GME_default.asp. Published 2012. Accessed May 08, 2013.
- , . Graduate medical education, 2011–2012. JAMA. 2012;308(21):2264–2279.
- , , , et al. Effects of physician experience on costs and outcomes on an academic general medicine service: results of a trial of hospitalists. Ann Intern Med. 2002;137(11):866–874.
- , , , , , . Implementation of a voluntary hospitalist service at a community teaching hospital: improved clinical efficiency and patient outcomes. Ann Intern Med. 2002;137(11):859–865.
- , , . Communication failures: an insidious contributor to medical mishaps. Acad Med. 2004;79(2):186–194.
- , , . ‘It depends': medical residents' perspectives on working with nurses. Am J Nurs. 2009;109(7):34–44.
- , . Organizational silence: a barrier to change and development in a pluralistic world. Acad Manage Rev. 2000;25(4):706–725.
- , . Making it safe: the effects of leader inclusiveness and professional status on psychological safety and improvement efforts in health care teams. J Organiz Behav. 2006;27:941–966.
- , , , , . Interprofessional communication with hospitalist and consultant physicians in general internal medicine: a qualitative study. BMC Health Serv Res. 2012;12:437.
- , , , , , . A new tool to give hospitalists feedback to improve interprofessional teamwork and advance patient care. Health Aff (Millwood). 2012;31(11):2485–2492.
- , , , , , . Impact of instructional practices on student satisfaction with attendings' teaching in the inpatient component of internal medicine clerkships. J Gen Intern Med. 2006;21(1):7–12.
- , . Medical students' perceptions of the elements of effective inpatient teaching by attending physicians and housestaff. J Gen Intern Med. 2005;20(7):635–639.
- National Board of Medical Examiners Subject Examination Program. Internal Medicine Advanced Clinical Examination, score interpretation guide. Available at: http://www.nbme.org/PDF/SampleScoreReports/Internal_Medicine_ACE_Score_Report.pdf. Published 2011. Accessed September 13, 2013.
- . The impact of hospitalists on medical education and the academic health system. Ann Intern Med. 1999;130(4 part 2):364–367.
- Kohn LT, Corrigan JM, Donaldson MS, eds. To Err Is Human: Building a Safer Health System. Washington, D.C.: National Academies Press; 2000.
- Institute of Medicine of the National Academies. Crossing the Quality Chasm: A New Health System for the 21st Century. Washington, D.C.: National Academies Press; 2001.
- , , , . Growth in the care of older patients by hospitalists in the United States. N Engl J Med. 2009;360(11):1102–1112.
- . Growth in care provided by hospitalists. N Engl J Med. 2009;360(26):2789–2791.
- American Hospital Association. AHA Annual Survey of Hospitals, 2010. Chicago, IL: Health Forum, LLC; 2010.
- , , , . Preventing hospital‐acquired infections: a national survey of practices reported by U.S. hospitals in 2005 and 2009. J Gen Intern Med. 2012;27(7):773–779.
- , . Hospitalists in teaching hospitals: opportunities but not without danger. J Gen Intern Med. 2004;19(4):392–393.
- , . Do hospitalist physicians improve the quality of inpatient care delivery? A systematic review of process, efficiency and outcome measures. BMC Med. 2011;9:58.
- , , , . Effect of hospitalist attending physicians on trainee educational experiences: a systematic review. J Hosp Med. 2009;4(8):490–498.
- , , , , , . Resident satisfaction on an academic hospitalist service: time to teach. Am J Med. 2002;112(7):597–601.
- , , , et al. The positive impact of initiation of hospitalist clinician educators. J Gen Intern Med. 2004;19(4):293–301.
- , . Third‐year medical students' evaluation of hospitalist and nonhospitalist faculty during the inpatient portion of their pediatrics clerkships. J Hosp Med. 2007;2(1):17–22.
- , , , . Medical student evaluation of the quality of hospitalist and nonhospitalist teaching faculty on inpatient medicine rotations. Acad Med. 2004;79(1):78–82.
- , , , , . Reorganizing an academic medical service: impact on cost, quality, patient satisfaction, and education. JAMA. 1998;279(19):1560–1565.
- . Nurse/physician communication through a sensemaking lens: shifting the paradigm to improve patient safety. Med Care. 2010;48(11):941–946.
- . Nursing Against the Odds: How Health Care Cost Cutting, Media Stereotypes, and Medical Hubris Undermine Nurses and Patient Care. Ithaca, NY: Cornell University Press; 2005.
- . Focus on research methods: whatever happened to qualitative description? Res Nurs Health. 2000;23:334–340.
- , , , , . Organizational assessment in intensive care units (ICUs): construct development, reliability, and validity of the ICU nurse‐physician questionnaire. Med Care. 1991;29(8):709–726.
- . Development of an instrument to measure collaboration and satisfaction about care decisions. J Adv Nurs. 1994;20(1):176–182.
- . Development of the practice environment scale of the Nursing Work Index. Res Nurs Health. 2002;25(3):176–188.
- , , . Does the structure of inpatient rounds affect medical student education? Int J Med Educ. 2013;4:96–100.
- U.S. Department of Veterans Affairs, Office of Academic Affiliations. Medical and Dental Education Program. Available at: http://www.va. gov/oaa/GME_default.asp. Published 2012. Accessed May 08, 2013.
- , . Graduate medical education, 2011–2012. JAMA. 2012;308(21):2264–2279.
- , , , et al. Effects of physician experience on costs and outcomes on an academic general medicine service: results of a trial of hospitalists. Ann Intern Med. 2002;137(11):866–874.
- , , , , , . Implementation of a voluntary hospitalist service at a community teaching hospital: improved clinical efficiency and patient outcomes. Ann Intern Med. 2002;137(11):859–865.
- , , . Communication failures: an insidious contributor to medical mishaps. Acad Med. 2004;79(2):186–194.
- , , . ‘It depends': medical residents' perspectives on working with nurses. Am J Nurs. 2009;109(7):34–44.
- , . Organizational silence: a barrier to change and development in a pluralistic world. Acad Manage Rev. 2000;25(4):706–725.
- , . Making it safe: the effects of leader inclusiveness and professional status on psychological safety and improvement efforts in health care teams. J Organiz Behav. 2006;27:941–966.
- , , , , . Interprofessional communication with hospitalist and consultant physicians in general internal medicine: a qualitative study. BMC Health Serv Res. 2012;12:437.
- , , , , , . A new tool to give hospitalists feedback to improve interprofessional teamwork and advance patient care. Health Aff (Millwood). 2012;31(11):2485–2492.
- , , , , , . Impact of instructional practices on student satisfaction with attendings' teaching in the inpatient component of internal medicine clerkships. J Gen Intern Med. 2006;21(1):7–12.
- , . Medical students' perceptions of the elements of effective inpatient teaching by attending physicians and housestaff. J Gen Intern Med. 2005;20(7):635–639.
- National Board of Medical Examiners Subject Examination Program. Internal Medicine Advanced Clinical Examination, score interpretation guide. Available at: http://www.nbme.org/PDF/SampleScoreReports/Internal_Medicine_ACE_Score_Report.pdf. Published 2011. Accessed September 13, 2013.
- . The impact of hospitalists on medical education and the academic health system. Ann Intern Med. 1999;130(4 part 2):364–367.
© 2013 Society of The Authors. Journal of Hospital Medicine published by Wiley Periodicals, Inc. on behalf of Society of Hospital Medicine.
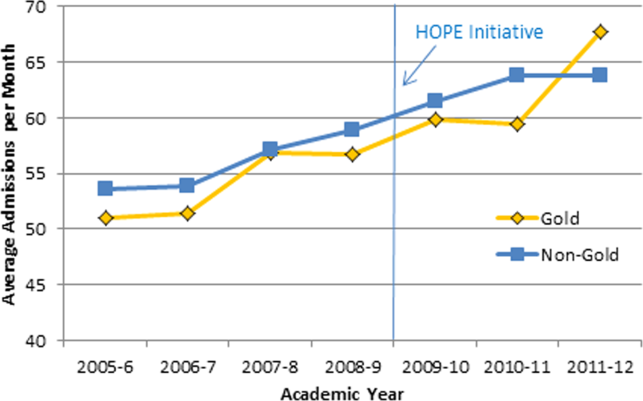
Pediatrics Preoperative Evaluation
Pediatric hospitalists are increasingly following their adult counterparts' lead in participating in comanagement programs with surgeons. In the 20112012 Society of Hospital Medicine survey of hospitalist practice models, 94% of adult hospitalists and 72% of pediatric hospitalists reported comanaging surgical patients.[1] Adult patients comanaged postoperatively have shown equivalent clinical outcomes with strong endorsement from nurses and surgeons in 1 study[2] and reduced morbidity, mortality, and length of stay in other studies.[3, 4]
One of the drivers of pediatric hospitalists comanaging surgical patients may be the increased complexity of hospitalized children.[5, 6, 7, 8] Two pediatric studies have assessed hospitalistsurgeon comanagement of medically complex children in the postoperative period. One study evaluating 14 patients undergoing spinal fusion surgery for neuromuscular scoliosis showed an association between pediatric hospitalist comanagement and a decreased length of stay, with decreased variability in postoperative length of stay.[9] A study of 207 medically complex children undergoing spinal fusion surgery for neuromuscular scoliosis suggested an association between comanagement and reduced laboratory studies and parenteral nutrition but an initial increase in costs.[10]
Pediatric hospitalist programs have also followed adult programs' lead in evaluating surgical patients preoperatively. Studies of preoperative medical evaluations for adult surgical patients have reported mixed results, with improved use of recommended medical therapies, length of stay, and mortality postoperatively in 1 study,[11] whereas other studies have reported longer lengths of stay and higher costs.[12, 13] One adult study described a protocol‐based approach in which hospitalists coordinated pulmonary and cardiac evaluations for high‐risk spine patients but did not report any outcomes.[14] A pediatric study from the Netherlands described a multidisciplinary team approach to these patients, including both preoperative and postoperative evaluation, but did not include a hospitalist or general pediatrician nor present data on outcomes.[15]
In 2009, we began a hospitalist preoperative evaluation program for patients with neuromuscular scoliosis in anticipation of spinal fusion surgery. This program was established by the hospital administration in response to 2 sentinel events. Hospitalists, who had already begun comanaging surgical patients postoperatively, were required to see patients with neuromuscular scoliosis preoperatively. Hospitalists were felt to be knowledgeable about postoperative complications of spinal fusion surgery and were thought to perhaps be able to prevent certain postoperative complications.
In the current study, we sought to evaluate certain outcomes associated with this preoperative program. We hypothesized that evaluations for more complex patients would be more likely to be associated with preoperative changes. We evaluated how frequently hospitalists make recommendations for changes in patients' medical regimens or request further diagnostic evaluations and if any clinical characteristics were associated with hospitalists making these recommendations.
METHODS
Setting/Program Structure
We conducted a retrospective chart review of all 214 patients with the diagnosis of neuromuscular scoliosis who were seen for a preoperative evaluation by a pediatric hospitalist at our institution from November 2009 through September 2012. Nemours/AI duPont Hospital for Children is a 200‐bed freestanding children's hospital with 11 pediatric orthopedic surgeons, 5 of whom perform spinal fusion surgery on patients with neuromuscular scoliosis. Our hospitalist group consists of 6 hospitalists, all of whom rotate on the medically complex comanagement service for 1 week at a time. The hospitalist who was assigned to the medically complex comanagement service for the week saw both postoperative patients and an average of 1 to 2 preoperative patients that week. All patients with neuromuscular scoliosis who were scheduled for spinal fusion surgery were seen preoperatively by a hospitalist. These patients included any with an underlying diagnosis of cerebral palsy, myopathy, skeletal dysplasia, or syndrome such as neurofibromatosis. Patients who were scheduled for spinal fusion surgery were referred to the hospitalists via the orthopedic scheduling department or perioperative services. These patients were typically seen in the general pediatrics outpatient area or in the outpatient orthopedics area of the hospital 1 to 2 months prior to surgery. The goal of the preoperative visit was to ensure patients were evaluated thoroughly before surgery. Hospitalists were given authority to delay or even cancel surgery, though in no case in this study was surgery cancelled. Hospitalists were responsible for following up on consultations and further studies obtained before surgery. Patients with a Cobb angle of more than 90 were by policy referred to pulmonology and cardiology for a preoperative evaluation. Further testing in those domains, such as pulmonary function testing or echocardiograms, was at the discretion of the appropriate specialist.
Study Procedure
After receiving approval from the hospital institutional review board, we performed a case series study. Three investigators (D.R., S.C., and D.P.) reviewed the preoperative visit note for each patient. We identified all patients who had spinal fusion surgery for neuromuscular scoliosis via International Classification of Diseases, 9th Revision (ICD‐9) codes, including that for neuromuscular scoliosis, and reviewed the patients' charts for preoperative visits. We used the preoperative note from the hospitalist as the definitive source for clinical information about the patient such as underlying diagnosis or etiology of the neuromuscular scoliosis. We used a structured data abstraction form to collect data regarding patient demographics, date of visit, time to surgery, type of surgery, number of standing daily (not as‐needed) preoperative prescription medications, and dependence on medical technology. We defined seizure disorder as present when a patient was taking standing prescription medication for seizures or had been recommended to take standing medication for seizures.
We recorded patient comorbidities related to the gastrointestinal, cardiac, and pulmonary systems. Prior to chart review, we agreed on standard definitions for significant problems in these arenas. We defined a significant problem as one in which a standing prescription medication was required, medical technology was required, or a subspecialist was consulted on a regular basis. To establish inter‐rater reliability using this definition, the 3 investigators independently reviewed an initial series of 5 charts. Inter‐rater reliability was established at 90%.
Main Outcome Measures
We recorded whether the hospitalist made any preoperative recommendations. Recommendations were categorized as: change in medication, changes in nutrition, laboratory or imaging studies, other diagnostic tests, or subspecialty referral. We defined a medication change as any change that involved a new prescription medication to be used on a standing basis, a change in dosing to a standing prescription medication, or the discontinuing of a standing prescription medication. We did not include changes in medications used on an as‐needed basis. We also recorded whether the hospitalist made any recommendations regarding further preoperative evaluation such as laboratory studies, imaging studies, other studies, or consultation with a subspecialist. We did not include laboratory studies that are routinely obtained preoperatively such as coagulation studies or blood count. We then recorded whether the hospitalist contacted a subspecialist or requested that an evaluation be done by that subspecialist prior to surgery.
Analysis
We used Stata 12 software (StataCorp, College Station, TX) to conduct all analyses. We used frequencies to describe categorical variables. Linear variables were not normally distributed and were therefore described using median and interquartile range. We calculated the simple, unadjusted odds ratio (OR) (95% confidence interval [CI]) of the hospitalist making a recommendation during the preoperative visit based on each variable. We defined statistical significance as a P value <0.05.
RESULTS
Overall, 214 patients were included in our study. Typical patients included those with cerebral palsy scheduled to undergo posterior spinal fusion surgery. Many had significant comorbidities, including seizures and gastrointestinal (GI) disease, and were dependent on medical technology.
Regarding hospitalist recommendations, overall 155 patients (72%) received at least 1 recommendation. Types of recommendations are listed in Table 1. The most common type of recommendation regarding the patient's current regimen was medication change (82 patients, 38%). Recommendations for changes in nutrition were made in 46 patients (21%). Subspecialist input was elicited in 76 patients (36%); a subspecialist appointment was suggested most commonly (36 patients, 17%), whereas a telephone consultation occurred in 15 patients (7%). Hospitalists also frequently requested further diagnostic evaluation, especially laboratory studies (41 patients, 19%). Imaging studies were requested less frequently (11 patients, 5.1%) as were other studies such as electrocardiograms and pulmonary function tests (6 patients, 2.8%, each). No patient received a preoperative hospitalist recommendation to cancel or postpone surgery.
| Type of Recommendation | n (%) |
|---|---|
| |
| Changes in regimen | |
| Medication change (start new, discontinue, change dose) | 82 (38%) |
| Nutrition modification | 46 (21%) |
| Further diagnostic evaluation | |
| Laboratory studies | 41 (19%) |
| Imaging studies | 11 (5%) |
| Pulmonary function tests | 6 (3%) |
| Electrocardiograms | 6 (3%) |
| Referral to or contacted subspecialist | 76 (36%) |
Certain patient characteristics were associated with a statistically significant increase in likelihood of a preoperative intervention by the pediatric hospitalist (Table 2). These included type of surgery (OR: 2.70, 95% CI: 1.22‐5.97 for posterior spinal fusion), number of preoperative prescription medications (OR: 1.19, 95% CI: 1.06‐1.34), and nonambulatory status (OR: 2.02, 95% CI: 1.09‐3.74). Underlying disease also showed a statistically significant association with recommendations being made; patients were more likely to receive recommendations if they had cerebral palsy (OR: 2.01, 95% CI: 1.03‐3.92), spina bifida (OR: 2.33, 95% CI: 1.90‐3.48), and neuropathy (all had recommendations). An underlying diagnosis of skeletal dysplasia was statistically significantly associated with a decreased rate of recommendations being made (OR: 0.29, 95% CI: 0.14‐0.61). Patients with seizures (OR: 2.68, 95% CI: 1.29‐5.57) or GI comorbidity were more likely to receive a preoperative recommendation made by the hospitalist (OR: 3.35, 95% CI: 1.74‐6.45), but patients with cardiac and pulmonary comorbidities were not.
| Characteristics | Number (%) or Median (IQR) | Recommendations? | ||
|---|---|---|---|---|
| Yes, n=155 | No, n=59 | Odds of Recommendation, OR (95% CI) | ||
| ||||
| Demographics | ||||
| Gender, female | 106 (50%) | 77 (60%) | 29 (49%) | 0.97 (0.53‐1.78) |
| Age, y | 13 (1016) | 13 (1016) | 12 (1016) | 1.05 (0.98‐1.12) |
| Year of visit | ||||
| 2009 | 41 (19%) | 32 (21%) | 9 (15%) | Ref |
| 2010 | 65 (30%) | 47 (30%) | 18 (30%) | 0.73 (0.29‐1.84) |
| 2011 | 64 (30%) | 43 (28%) | 21 (36%) | 0.58 (0.23‐1.42) |
| 2012 | 44 (21%) | 33 (21%) | 11 (19%) | 0.84 (0.31‐2.31) |
| Days from visit to surgery | 34 (1445) | 35 (1747) | 27 (841) | 1.02 (1.001.03) |
| Type of surgerya | ||||
| PSF | 184 (86%) | 139 (90%) | 45 (76%) | 2.70 (1.22‐5.97) |
| Growing rod | 9 (4.7%) | 6 (4%) | 3 (5%) | 0.75 (0.18‐3.11) |
| Cervical fusion | 17 (7.9%) | 9 6%) | 8 (13%) | 0.39 (0.14‐1.07) |
| Halo, then PSF | 4 (1.9%) | 1 (0.6%) | 3 (5%) | 0.12 (0.01‐1.19) |
| Underlying diseasea | ||||
| Cerebral palsy | 78 (36%) | 63 (41%) | 15 (25%) | 2.01 (1.03‐3.92) |
| Neuropathy | 4 (2%) | 4 (3%) | 0 (0%) | All had recommendations |
| Myopathy | 19 (9%) | 16 (10%) | 3 (5%) | 2.14 (0.60‐7.66) |
| Metabolic disorder | 6 (3%) | 4 (3%) | 2 (3%) | 0.75 (0.13‐4.23) |
| Skeletal dysplasia | 38 (18%) | 19 (12%) | 19 (32%) | 0.29 (0.14‐0.61) |
| Spina bifida | 7 (3%) | 6 (4%) | 1 (2%) | 2.33 (1.90‐3.48) |
| Genetic disorder (including osteogenesis imperfecta) | 40 (19%) | 28 (18%) | 12 (20%) | 0.86 (0.41‐1.84) |
| Other | 22 (10%) | 15 (10%) | 7 (12%) | 0.79 (0.31‐2.06) |
| Number of preoperative prescription medications | 2 (15) | 3 (15) | 1 (03) | 1.19 (1.06‐1.34) |
| Institutionalized | 9 (4.2%) | 6 (4%) | 3 (5%) | 0.75 (0.18‐3.11) |
| Nonambulatory | 114 (54%) | 90 (59%) | 24 (41%) | 2.02 (1.09‐3.74) |
| Dependence on technologya | ||||
| Feeding tube | 89 (41.6%) | 66 (43%) | 23 (39%) | 1.16 (0.63‐2.14) |
| Baclofen pump | 20 (9.3%) | 18 (12%) | 2 (3%) | 3.74 (0.84‐16.67) |
| Ventriculoperitoneal shunt | 24 (11.2%) | 18 (12%) | 6 (10%) | 1.16 (0.44‐3.08) |
| Vagal nerve stimulator/deep brain stimulator | 8 (3.7%) | 6 (4%) | 2 (3%) | 1.15 (0.22‐5.85) |
| Tracheostomy | 13 (6.1%) | 9 (6%) | 4 (7%) | 0.85 (0.25‐2.86) |
| Home mechanical ventilation (not BiPAP) | 6 (2.8%) | 5 (3%) | 1 (2%) | 1.93 (0.22‐16.90) |
| Home oxygen, BiPAP, or CPAP | 25 (11.7%) | 22 (14%) | 3 (5%) | 3.09 (0.89‐10.73) |
| Seizure disorder | 70 (33%) | 59 (38%) | 11 (19%) | 2.68 (1.29‐5.57) |
| Significant GI comorbidity | 102 (48%) | 86 (55%) | 16 (27%) | 3.35 (1.74‐6.45) |
| Significant cardiac comorbidity | 37 (17.3%) | 26 (17%) | 11 (19%) | 0.88 (0.40‐1.92) |
| Significant pulmonary comorbidity | 78 (36.4%) | 57 (37%) | 21 (36%) | 1.05 (0.56‐1.97) |
DISCUSSION
This is the first large study to examine the role of the pediatric hospitalist in preoperative evaluation of complex surgical patients. Our program developed as an evolution of a postoperative program that we have described previously.[10] The postoperative component of our comanagement program began in 2003, and the preoperative aspect was added in 2009. We believe that the preoperative component to our program contributed in some degree to the decrease in utilization of certain aspects of postoperative care over time such as parenteral nutrition. This change may have occurred because of improved bowel management perioperatively, for instance. Although the preoperative hospitalist evaluation program was instituted by our hospital administration, we felt a preoperative hospitalist evaluation represented a standardized, comprehensive way to evaluate patients before surgery. By 2009, the hospitalists at our hospital had already developed some expertise in managing patients after undergoing spinal fusion surgery.
The fact that hospitalists made recommendations for changes in medications, nutritional management, or diagnostic tests at such a high rate (72%) is interesting. We were not surprised by this finding based on anecdotal evidence because we feel that many of these patients may receive somewhat fragmented care because they often see multiple medical specialists. The high rate of interventions noted in our study may result from the fact that hospitalists who comanage these patients frequently after spinal fusion surgery were attempting to prevent postoperative complications that they see after this type of surgery. Many pediatric hospitalists have developed significant experience in caring for medically complex children and thus may feel more comfortable making preoperative recommendations than other general pediatricians.
We were not surprised to find that hospitalists made preoperative recommendations more frequently in children who had seizures, significant GI comorbidity, and who were nonambulatory. We also noted a statistically significant increased rate of recommendations when patients were on more preoperative medications. We believe that these variables suggest a population that is more medically complex. The importance of selecting medically complex patients for hospitalist comanagement has been noted previously.[16] Therefore, comanagement programs looking to maximize patient benefit for a preoperative hospitalist evaluation program might limit these visits to those who are most medically complex. We found a particularly low yield in evaluation of patients with skeletal dysplasia for example and may discontinue seeing these patients preoperatively.
We found the lack of statistically significant change in rate of hospitalist recommendations among patients with cardiac and pulmonary comorbidities interesting. Whether this was related to the mandatory preoperative pulmonology and cardiology visits is not certain. We hope to study the impact of these preoperative visits in the future as we continue to evaluate our perioperative program.
Several limitations of this study deserve note. This study was performed at 1 institution with 1 group of hospitalists and 1 group of orthopedic surgeons. Two of the study authors (D.R. and D.P.) were among the hospitalists involved with the clinical program. The study was retrospective and nonrandomized. We did not contact primary care physicians as a rule for further information about these patients. In this study, we did not specifically study the impact of hospitalist preoperative evaluations on postoperative outcomes, although the preoperative component represented an important aspect of the more systematic intervention described elsewhere.[10]
CONCLUSIONS
A preoperative program for pediatric hospitalists to see children in anticipation of spinal surgery for neuromuscular scoliosis leads to a high rate of recommendations for changes in medical management or diagnostic evaluation. Certain patient characteristics are more highly associated with hospitalists making these recommendations prior to surgery.
- 2012 State of Hospital Medicine Report, Society of Hospital Medicine. Further information available at: http://www.hospitalmedicine.org/survey.
- , , , et al.; Hospitalist‐Orthopedic Team Trial Investigators. Medical and surgical comanagement after elective hip and knee arthroplasty: a randomized, controlled trial. Ann Intern Med. 2004;141(1):28–38.
- , , , et al. Outcomes for older patients with hip fractures: the impact of orthopedic and geriatric medicine cocare. J Orthop Trauma. 2006;20(3):172–178, discussion 179–180.
- , , , et al. Effects of a hospitalist model on elderly patients with hip fracture. Arch Intern Med. 2005;165(7):796–801.
- , , . Hospitalist care of the medically complex child. Pediatr Clin North Am. 2005;52(4):1165–1167.
- , , , et al. Increasing prevalence of medically complex children in US hospitals. Pediatrics. 2010;126(4):638–646.
- , , , et al. Children with complex chronic conditions in inpatient hospital settings in the United States. Pediatrics. 2010;126(4):647–655.
- , , , et al. Children with medical complexity: an emerging population for clinical and research initiatives. Pediatrics. 2011;127(3):529–538.
- , , , et al. Pediatric hospitalist comanagement of spinal fusion surgery patients. J Hosp Med. 2007;2:23–30.
- , , , et al. Outcomes and costs associated with hospitalist comanagement of medically complex children undergoing spinal fusion surgery. Hosp Pediatr. 2013;3(3):233–241.
- , , , et al. Perioperative processes and outcomes after implementation of a hospitalist‐run preoperative clinic. J Hosp Med. 2012 7:697–701.
- , , , , . Outcomes and processes of care related to preoperative medical consultation. Arch Intern Med. 2010;170(15):1365–1374.
- , , , et al. Opportunity missed: medical consultation, resource use, and quality of care of patients undergoing major surgery. Arch Intern Med. 2007;167(21):2338–2344.
- , , , et al. Standardizing care for high‐risk patients in spine surgery: the Northwestern High‐Risk Spine Protocol. Spine. 2010;35(25):2232–2238.
- , , , . Neuromuscular scoliosis: clinical evaluation pre‐ and postoperative. J Pediatr Orthop. 2000;9:217–220.
- . Just because you can, doesn't mean that you should: a call for the rational application of hospitalist comanagement. J Hosp Med. 2008:3:398–402.
Pediatric hospitalists are increasingly following their adult counterparts' lead in participating in comanagement programs with surgeons. In the 20112012 Society of Hospital Medicine survey of hospitalist practice models, 94% of adult hospitalists and 72% of pediatric hospitalists reported comanaging surgical patients.[1] Adult patients comanaged postoperatively have shown equivalent clinical outcomes with strong endorsement from nurses and surgeons in 1 study[2] and reduced morbidity, mortality, and length of stay in other studies.[3, 4]
One of the drivers of pediatric hospitalists comanaging surgical patients may be the increased complexity of hospitalized children.[5, 6, 7, 8] Two pediatric studies have assessed hospitalistsurgeon comanagement of medically complex children in the postoperative period. One study evaluating 14 patients undergoing spinal fusion surgery for neuromuscular scoliosis showed an association between pediatric hospitalist comanagement and a decreased length of stay, with decreased variability in postoperative length of stay.[9] A study of 207 medically complex children undergoing spinal fusion surgery for neuromuscular scoliosis suggested an association between comanagement and reduced laboratory studies and parenteral nutrition but an initial increase in costs.[10]
Pediatric hospitalist programs have also followed adult programs' lead in evaluating surgical patients preoperatively. Studies of preoperative medical evaluations for adult surgical patients have reported mixed results, with improved use of recommended medical therapies, length of stay, and mortality postoperatively in 1 study,[11] whereas other studies have reported longer lengths of stay and higher costs.[12, 13] One adult study described a protocol‐based approach in which hospitalists coordinated pulmonary and cardiac evaluations for high‐risk spine patients but did not report any outcomes.[14] A pediatric study from the Netherlands described a multidisciplinary team approach to these patients, including both preoperative and postoperative evaluation, but did not include a hospitalist or general pediatrician nor present data on outcomes.[15]
In 2009, we began a hospitalist preoperative evaluation program for patients with neuromuscular scoliosis in anticipation of spinal fusion surgery. This program was established by the hospital administration in response to 2 sentinel events. Hospitalists, who had already begun comanaging surgical patients postoperatively, were required to see patients with neuromuscular scoliosis preoperatively. Hospitalists were felt to be knowledgeable about postoperative complications of spinal fusion surgery and were thought to perhaps be able to prevent certain postoperative complications.
In the current study, we sought to evaluate certain outcomes associated with this preoperative program. We hypothesized that evaluations for more complex patients would be more likely to be associated with preoperative changes. We evaluated how frequently hospitalists make recommendations for changes in patients' medical regimens or request further diagnostic evaluations and if any clinical characteristics were associated with hospitalists making these recommendations.
METHODS
Setting/Program Structure
We conducted a retrospective chart review of all 214 patients with the diagnosis of neuromuscular scoliosis who were seen for a preoperative evaluation by a pediatric hospitalist at our institution from November 2009 through September 2012. Nemours/AI duPont Hospital for Children is a 200‐bed freestanding children's hospital with 11 pediatric orthopedic surgeons, 5 of whom perform spinal fusion surgery on patients with neuromuscular scoliosis. Our hospitalist group consists of 6 hospitalists, all of whom rotate on the medically complex comanagement service for 1 week at a time. The hospitalist who was assigned to the medically complex comanagement service for the week saw both postoperative patients and an average of 1 to 2 preoperative patients that week. All patients with neuromuscular scoliosis who were scheduled for spinal fusion surgery were seen preoperatively by a hospitalist. These patients included any with an underlying diagnosis of cerebral palsy, myopathy, skeletal dysplasia, or syndrome such as neurofibromatosis. Patients who were scheduled for spinal fusion surgery were referred to the hospitalists via the orthopedic scheduling department or perioperative services. These patients were typically seen in the general pediatrics outpatient area or in the outpatient orthopedics area of the hospital 1 to 2 months prior to surgery. The goal of the preoperative visit was to ensure patients were evaluated thoroughly before surgery. Hospitalists were given authority to delay or even cancel surgery, though in no case in this study was surgery cancelled. Hospitalists were responsible for following up on consultations and further studies obtained before surgery. Patients with a Cobb angle of more than 90 were by policy referred to pulmonology and cardiology for a preoperative evaluation. Further testing in those domains, such as pulmonary function testing or echocardiograms, was at the discretion of the appropriate specialist.
Study Procedure
After receiving approval from the hospital institutional review board, we performed a case series study. Three investigators (D.R., S.C., and D.P.) reviewed the preoperative visit note for each patient. We identified all patients who had spinal fusion surgery for neuromuscular scoliosis via International Classification of Diseases, 9th Revision (ICD‐9) codes, including that for neuromuscular scoliosis, and reviewed the patients' charts for preoperative visits. We used the preoperative note from the hospitalist as the definitive source for clinical information about the patient such as underlying diagnosis or etiology of the neuromuscular scoliosis. We used a structured data abstraction form to collect data regarding patient demographics, date of visit, time to surgery, type of surgery, number of standing daily (not as‐needed) preoperative prescription medications, and dependence on medical technology. We defined seizure disorder as present when a patient was taking standing prescription medication for seizures or had been recommended to take standing medication for seizures.
We recorded patient comorbidities related to the gastrointestinal, cardiac, and pulmonary systems. Prior to chart review, we agreed on standard definitions for significant problems in these arenas. We defined a significant problem as one in which a standing prescription medication was required, medical technology was required, or a subspecialist was consulted on a regular basis. To establish inter‐rater reliability using this definition, the 3 investigators independently reviewed an initial series of 5 charts. Inter‐rater reliability was established at 90%.
Main Outcome Measures
We recorded whether the hospitalist made any preoperative recommendations. Recommendations were categorized as: change in medication, changes in nutrition, laboratory or imaging studies, other diagnostic tests, or subspecialty referral. We defined a medication change as any change that involved a new prescription medication to be used on a standing basis, a change in dosing to a standing prescription medication, or the discontinuing of a standing prescription medication. We did not include changes in medications used on an as‐needed basis. We also recorded whether the hospitalist made any recommendations regarding further preoperative evaluation such as laboratory studies, imaging studies, other studies, or consultation with a subspecialist. We did not include laboratory studies that are routinely obtained preoperatively such as coagulation studies or blood count. We then recorded whether the hospitalist contacted a subspecialist or requested that an evaluation be done by that subspecialist prior to surgery.
Analysis
We used Stata 12 software (StataCorp, College Station, TX) to conduct all analyses. We used frequencies to describe categorical variables. Linear variables were not normally distributed and were therefore described using median and interquartile range. We calculated the simple, unadjusted odds ratio (OR) (95% confidence interval [CI]) of the hospitalist making a recommendation during the preoperative visit based on each variable. We defined statistical significance as a P value <0.05.
RESULTS
Overall, 214 patients were included in our study. Typical patients included those with cerebral palsy scheduled to undergo posterior spinal fusion surgery. Many had significant comorbidities, including seizures and gastrointestinal (GI) disease, and were dependent on medical technology.
Regarding hospitalist recommendations, overall 155 patients (72%) received at least 1 recommendation. Types of recommendations are listed in Table 1. The most common type of recommendation regarding the patient's current regimen was medication change (82 patients, 38%). Recommendations for changes in nutrition were made in 46 patients (21%). Subspecialist input was elicited in 76 patients (36%); a subspecialist appointment was suggested most commonly (36 patients, 17%), whereas a telephone consultation occurred in 15 patients (7%). Hospitalists also frequently requested further diagnostic evaluation, especially laboratory studies (41 patients, 19%). Imaging studies were requested less frequently (11 patients, 5.1%) as were other studies such as electrocardiograms and pulmonary function tests (6 patients, 2.8%, each). No patient received a preoperative hospitalist recommendation to cancel or postpone surgery.
| Type of Recommendation | n (%) |
|---|---|
| |
| Changes in regimen | |
| Medication change (start new, discontinue, change dose) | 82 (38%) |
| Nutrition modification | 46 (21%) |
| Further diagnostic evaluation | |
| Laboratory studies | 41 (19%) |
| Imaging studies | 11 (5%) |
| Pulmonary function tests | 6 (3%) |
| Electrocardiograms | 6 (3%) |
| Referral to or contacted subspecialist | 76 (36%) |
Certain patient characteristics were associated with a statistically significant increase in likelihood of a preoperative intervention by the pediatric hospitalist (Table 2). These included type of surgery (OR: 2.70, 95% CI: 1.22‐5.97 for posterior spinal fusion), number of preoperative prescription medications (OR: 1.19, 95% CI: 1.06‐1.34), and nonambulatory status (OR: 2.02, 95% CI: 1.09‐3.74). Underlying disease also showed a statistically significant association with recommendations being made; patients were more likely to receive recommendations if they had cerebral palsy (OR: 2.01, 95% CI: 1.03‐3.92), spina bifida (OR: 2.33, 95% CI: 1.90‐3.48), and neuropathy (all had recommendations). An underlying diagnosis of skeletal dysplasia was statistically significantly associated with a decreased rate of recommendations being made (OR: 0.29, 95% CI: 0.14‐0.61). Patients with seizures (OR: 2.68, 95% CI: 1.29‐5.57) or GI comorbidity were more likely to receive a preoperative recommendation made by the hospitalist (OR: 3.35, 95% CI: 1.74‐6.45), but patients with cardiac and pulmonary comorbidities were not.
| Characteristics | Number (%) or Median (IQR) | Recommendations? | ||
|---|---|---|---|---|
| Yes, n=155 | No, n=59 | Odds of Recommendation, OR (95% CI) | ||
| ||||
| Demographics | ||||
| Gender, female | 106 (50%) | 77 (60%) | 29 (49%) | 0.97 (0.53‐1.78) |
| Age, y | 13 (1016) | 13 (1016) | 12 (1016) | 1.05 (0.98‐1.12) |
| Year of visit | ||||
| 2009 | 41 (19%) | 32 (21%) | 9 (15%) | Ref |
| 2010 | 65 (30%) | 47 (30%) | 18 (30%) | 0.73 (0.29‐1.84) |
| 2011 | 64 (30%) | 43 (28%) | 21 (36%) | 0.58 (0.23‐1.42) |
| 2012 | 44 (21%) | 33 (21%) | 11 (19%) | 0.84 (0.31‐2.31) |
| Days from visit to surgery | 34 (1445) | 35 (1747) | 27 (841) | 1.02 (1.001.03) |
| Type of surgerya | ||||
| PSF | 184 (86%) | 139 (90%) | 45 (76%) | 2.70 (1.22‐5.97) |
| Growing rod | 9 (4.7%) | 6 (4%) | 3 (5%) | 0.75 (0.18‐3.11) |
| Cervical fusion | 17 (7.9%) | 9 6%) | 8 (13%) | 0.39 (0.14‐1.07) |
| Halo, then PSF | 4 (1.9%) | 1 (0.6%) | 3 (5%) | 0.12 (0.01‐1.19) |
| Underlying diseasea | ||||
| Cerebral palsy | 78 (36%) | 63 (41%) | 15 (25%) | 2.01 (1.03‐3.92) |
| Neuropathy | 4 (2%) | 4 (3%) | 0 (0%) | All had recommendations |
| Myopathy | 19 (9%) | 16 (10%) | 3 (5%) | 2.14 (0.60‐7.66) |
| Metabolic disorder | 6 (3%) | 4 (3%) | 2 (3%) | 0.75 (0.13‐4.23) |
| Skeletal dysplasia | 38 (18%) | 19 (12%) | 19 (32%) | 0.29 (0.14‐0.61) |
| Spina bifida | 7 (3%) | 6 (4%) | 1 (2%) | 2.33 (1.90‐3.48) |
| Genetic disorder (including osteogenesis imperfecta) | 40 (19%) | 28 (18%) | 12 (20%) | 0.86 (0.41‐1.84) |
| Other | 22 (10%) | 15 (10%) | 7 (12%) | 0.79 (0.31‐2.06) |
| Number of preoperative prescription medications | 2 (15) | 3 (15) | 1 (03) | 1.19 (1.06‐1.34) |
| Institutionalized | 9 (4.2%) | 6 (4%) | 3 (5%) | 0.75 (0.18‐3.11) |
| Nonambulatory | 114 (54%) | 90 (59%) | 24 (41%) | 2.02 (1.09‐3.74) |
| Dependence on technologya | ||||
| Feeding tube | 89 (41.6%) | 66 (43%) | 23 (39%) | 1.16 (0.63‐2.14) |
| Baclofen pump | 20 (9.3%) | 18 (12%) | 2 (3%) | 3.74 (0.84‐16.67) |
| Ventriculoperitoneal shunt | 24 (11.2%) | 18 (12%) | 6 (10%) | 1.16 (0.44‐3.08) |
| Vagal nerve stimulator/deep brain stimulator | 8 (3.7%) | 6 (4%) | 2 (3%) | 1.15 (0.22‐5.85) |
| Tracheostomy | 13 (6.1%) | 9 (6%) | 4 (7%) | 0.85 (0.25‐2.86) |
| Home mechanical ventilation (not BiPAP) | 6 (2.8%) | 5 (3%) | 1 (2%) | 1.93 (0.22‐16.90) |
| Home oxygen, BiPAP, or CPAP | 25 (11.7%) | 22 (14%) | 3 (5%) | 3.09 (0.89‐10.73) |
| Seizure disorder | 70 (33%) | 59 (38%) | 11 (19%) | 2.68 (1.29‐5.57) |
| Significant GI comorbidity | 102 (48%) | 86 (55%) | 16 (27%) | 3.35 (1.74‐6.45) |
| Significant cardiac comorbidity | 37 (17.3%) | 26 (17%) | 11 (19%) | 0.88 (0.40‐1.92) |
| Significant pulmonary comorbidity | 78 (36.4%) | 57 (37%) | 21 (36%) | 1.05 (0.56‐1.97) |
DISCUSSION
This is the first large study to examine the role of the pediatric hospitalist in preoperative evaluation of complex surgical patients. Our program developed as an evolution of a postoperative program that we have described previously.[10] The postoperative component of our comanagement program began in 2003, and the preoperative aspect was added in 2009. We believe that the preoperative component to our program contributed in some degree to the decrease in utilization of certain aspects of postoperative care over time such as parenteral nutrition. This change may have occurred because of improved bowel management perioperatively, for instance. Although the preoperative hospitalist evaluation program was instituted by our hospital administration, we felt a preoperative hospitalist evaluation represented a standardized, comprehensive way to evaluate patients before surgery. By 2009, the hospitalists at our hospital had already developed some expertise in managing patients after undergoing spinal fusion surgery.
The fact that hospitalists made recommendations for changes in medications, nutritional management, or diagnostic tests at such a high rate (72%) is interesting. We were not surprised by this finding based on anecdotal evidence because we feel that many of these patients may receive somewhat fragmented care because they often see multiple medical specialists. The high rate of interventions noted in our study may result from the fact that hospitalists who comanage these patients frequently after spinal fusion surgery were attempting to prevent postoperative complications that they see after this type of surgery. Many pediatric hospitalists have developed significant experience in caring for medically complex children and thus may feel more comfortable making preoperative recommendations than other general pediatricians.
We were not surprised to find that hospitalists made preoperative recommendations more frequently in children who had seizures, significant GI comorbidity, and who were nonambulatory. We also noted a statistically significant increased rate of recommendations when patients were on more preoperative medications. We believe that these variables suggest a population that is more medically complex. The importance of selecting medically complex patients for hospitalist comanagement has been noted previously.[16] Therefore, comanagement programs looking to maximize patient benefit for a preoperative hospitalist evaluation program might limit these visits to those who are most medically complex. We found a particularly low yield in evaluation of patients with skeletal dysplasia for example and may discontinue seeing these patients preoperatively.
We found the lack of statistically significant change in rate of hospitalist recommendations among patients with cardiac and pulmonary comorbidities interesting. Whether this was related to the mandatory preoperative pulmonology and cardiology visits is not certain. We hope to study the impact of these preoperative visits in the future as we continue to evaluate our perioperative program.
Several limitations of this study deserve note. This study was performed at 1 institution with 1 group of hospitalists and 1 group of orthopedic surgeons. Two of the study authors (D.R. and D.P.) were among the hospitalists involved with the clinical program. The study was retrospective and nonrandomized. We did not contact primary care physicians as a rule for further information about these patients. In this study, we did not specifically study the impact of hospitalist preoperative evaluations on postoperative outcomes, although the preoperative component represented an important aspect of the more systematic intervention described elsewhere.[10]
CONCLUSIONS
A preoperative program for pediatric hospitalists to see children in anticipation of spinal surgery for neuromuscular scoliosis leads to a high rate of recommendations for changes in medical management or diagnostic evaluation. Certain patient characteristics are more highly associated with hospitalists making these recommendations prior to surgery.
Pediatric hospitalists are increasingly following their adult counterparts' lead in participating in comanagement programs with surgeons. In the 20112012 Society of Hospital Medicine survey of hospitalist practice models, 94% of adult hospitalists and 72% of pediatric hospitalists reported comanaging surgical patients.[1] Adult patients comanaged postoperatively have shown equivalent clinical outcomes with strong endorsement from nurses and surgeons in 1 study[2] and reduced morbidity, mortality, and length of stay in other studies.[3, 4]
One of the drivers of pediatric hospitalists comanaging surgical patients may be the increased complexity of hospitalized children.[5, 6, 7, 8] Two pediatric studies have assessed hospitalistsurgeon comanagement of medically complex children in the postoperative period. One study evaluating 14 patients undergoing spinal fusion surgery for neuromuscular scoliosis showed an association between pediatric hospitalist comanagement and a decreased length of stay, with decreased variability in postoperative length of stay.[9] A study of 207 medically complex children undergoing spinal fusion surgery for neuromuscular scoliosis suggested an association between comanagement and reduced laboratory studies and parenteral nutrition but an initial increase in costs.[10]
Pediatric hospitalist programs have also followed adult programs' lead in evaluating surgical patients preoperatively. Studies of preoperative medical evaluations for adult surgical patients have reported mixed results, with improved use of recommended medical therapies, length of stay, and mortality postoperatively in 1 study,[11] whereas other studies have reported longer lengths of stay and higher costs.[12, 13] One adult study described a protocol‐based approach in which hospitalists coordinated pulmonary and cardiac evaluations for high‐risk spine patients but did not report any outcomes.[14] A pediatric study from the Netherlands described a multidisciplinary team approach to these patients, including both preoperative and postoperative evaluation, but did not include a hospitalist or general pediatrician nor present data on outcomes.[15]
In 2009, we began a hospitalist preoperative evaluation program for patients with neuromuscular scoliosis in anticipation of spinal fusion surgery. This program was established by the hospital administration in response to 2 sentinel events. Hospitalists, who had already begun comanaging surgical patients postoperatively, were required to see patients with neuromuscular scoliosis preoperatively. Hospitalists were felt to be knowledgeable about postoperative complications of spinal fusion surgery and were thought to perhaps be able to prevent certain postoperative complications.
In the current study, we sought to evaluate certain outcomes associated with this preoperative program. We hypothesized that evaluations for more complex patients would be more likely to be associated with preoperative changes. We evaluated how frequently hospitalists make recommendations for changes in patients' medical regimens or request further diagnostic evaluations and if any clinical characteristics were associated with hospitalists making these recommendations.
METHODS
Setting/Program Structure
We conducted a retrospective chart review of all 214 patients with the diagnosis of neuromuscular scoliosis who were seen for a preoperative evaluation by a pediatric hospitalist at our institution from November 2009 through September 2012. Nemours/AI duPont Hospital for Children is a 200‐bed freestanding children's hospital with 11 pediatric orthopedic surgeons, 5 of whom perform spinal fusion surgery on patients with neuromuscular scoliosis. Our hospitalist group consists of 6 hospitalists, all of whom rotate on the medically complex comanagement service for 1 week at a time. The hospitalist who was assigned to the medically complex comanagement service for the week saw both postoperative patients and an average of 1 to 2 preoperative patients that week. All patients with neuromuscular scoliosis who were scheduled for spinal fusion surgery were seen preoperatively by a hospitalist. These patients included any with an underlying diagnosis of cerebral palsy, myopathy, skeletal dysplasia, or syndrome such as neurofibromatosis. Patients who were scheduled for spinal fusion surgery were referred to the hospitalists via the orthopedic scheduling department or perioperative services. These patients were typically seen in the general pediatrics outpatient area or in the outpatient orthopedics area of the hospital 1 to 2 months prior to surgery. The goal of the preoperative visit was to ensure patients were evaluated thoroughly before surgery. Hospitalists were given authority to delay or even cancel surgery, though in no case in this study was surgery cancelled. Hospitalists were responsible for following up on consultations and further studies obtained before surgery. Patients with a Cobb angle of more than 90 were by policy referred to pulmonology and cardiology for a preoperative evaluation. Further testing in those domains, such as pulmonary function testing or echocardiograms, was at the discretion of the appropriate specialist.
Study Procedure
After receiving approval from the hospital institutional review board, we performed a case series study. Three investigators (D.R., S.C., and D.P.) reviewed the preoperative visit note for each patient. We identified all patients who had spinal fusion surgery for neuromuscular scoliosis via International Classification of Diseases, 9th Revision (ICD‐9) codes, including that for neuromuscular scoliosis, and reviewed the patients' charts for preoperative visits. We used the preoperative note from the hospitalist as the definitive source for clinical information about the patient such as underlying diagnosis or etiology of the neuromuscular scoliosis. We used a structured data abstraction form to collect data regarding patient demographics, date of visit, time to surgery, type of surgery, number of standing daily (not as‐needed) preoperative prescription medications, and dependence on medical technology. We defined seizure disorder as present when a patient was taking standing prescription medication for seizures or had been recommended to take standing medication for seizures.
We recorded patient comorbidities related to the gastrointestinal, cardiac, and pulmonary systems. Prior to chart review, we agreed on standard definitions for significant problems in these arenas. We defined a significant problem as one in which a standing prescription medication was required, medical technology was required, or a subspecialist was consulted on a regular basis. To establish inter‐rater reliability using this definition, the 3 investigators independently reviewed an initial series of 5 charts. Inter‐rater reliability was established at 90%.
Main Outcome Measures
We recorded whether the hospitalist made any preoperative recommendations. Recommendations were categorized as: change in medication, changes in nutrition, laboratory or imaging studies, other diagnostic tests, or subspecialty referral. We defined a medication change as any change that involved a new prescription medication to be used on a standing basis, a change in dosing to a standing prescription medication, or the discontinuing of a standing prescription medication. We did not include changes in medications used on an as‐needed basis. We also recorded whether the hospitalist made any recommendations regarding further preoperative evaluation such as laboratory studies, imaging studies, other studies, or consultation with a subspecialist. We did not include laboratory studies that are routinely obtained preoperatively such as coagulation studies or blood count. We then recorded whether the hospitalist contacted a subspecialist or requested that an evaluation be done by that subspecialist prior to surgery.
Analysis
We used Stata 12 software (StataCorp, College Station, TX) to conduct all analyses. We used frequencies to describe categorical variables. Linear variables were not normally distributed and were therefore described using median and interquartile range. We calculated the simple, unadjusted odds ratio (OR) (95% confidence interval [CI]) of the hospitalist making a recommendation during the preoperative visit based on each variable. We defined statistical significance as a P value <0.05.
RESULTS
Overall, 214 patients were included in our study. Typical patients included those with cerebral palsy scheduled to undergo posterior spinal fusion surgery. Many had significant comorbidities, including seizures and gastrointestinal (GI) disease, and were dependent on medical technology.
Regarding hospitalist recommendations, overall 155 patients (72%) received at least 1 recommendation. Types of recommendations are listed in Table 1. The most common type of recommendation regarding the patient's current regimen was medication change (82 patients, 38%). Recommendations for changes in nutrition were made in 46 patients (21%). Subspecialist input was elicited in 76 patients (36%); a subspecialist appointment was suggested most commonly (36 patients, 17%), whereas a telephone consultation occurred in 15 patients (7%). Hospitalists also frequently requested further diagnostic evaluation, especially laboratory studies (41 patients, 19%). Imaging studies were requested less frequently (11 patients, 5.1%) as were other studies such as electrocardiograms and pulmonary function tests (6 patients, 2.8%, each). No patient received a preoperative hospitalist recommendation to cancel or postpone surgery.
| Type of Recommendation | n (%) |
|---|---|
| |
| Changes in regimen | |
| Medication change (start new, discontinue, change dose) | 82 (38%) |
| Nutrition modification | 46 (21%) |
| Further diagnostic evaluation | |
| Laboratory studies | 41 (19%) |
| Imaging studies | 11 (5%) |
| Pulmonary function tests | 6 (3%) |
| Electrocardiograms | 6 (3%) |
| Referral to or contacted subspecialist | 76 (36%) |
Certain patient characteristics were associated with a statistically significant increase in likelihood of a preoperative intervention by the pediatric hospitalist (Table 2). These included type of surgery (OR: 2.70, 95% CI: 1.22‐5.97 for posterior spinal fusion), number of preoperative prescription medications (OR: 1.19, 95% CI: 1.06‐1.34), and nonambulatory status (OR: 2.02, 95% CI: 1.09‐3.74). Underlying disease also showed a statistically significant association with recommendations being made; patients were more likely to receive recommendations if they had cerebral palsy (OR: 2.01, 95% CI: 1.03‐3.92), spina bifida (OR: 2.33, 95% CI: 1.90‐3.48), and neuropathy (all had recommendations). An underlying diagnosis of skeletal dysplasia was statistically significantly associated with a decreased rate of recommendations being made (OR: 0.29, 95% CI: 0.14‐0.61). Patients with seizures (OR: 2.68, 95% CI: 1.29‐5.57) or GI comorbidity were more likely to receive a preoperative recommendation made by the hospitalist (OR: 3.35, 95% CI: 1.74‐6.45), but patients with cardiac and pulmonary comorbidities were not.
| Characteristics | Number (%) or Median (IQR) | Recommendations? | ||
|---|---|---|---|---|
| Yes, n=155 | No, n=59 | Odds of Recommendation, OR (95% CI) | ||
| ||||
| Demographics | ||||
| Gender, female | 106 (50%) | 77 (60%) | 29 (49%) | 0.97 (0.53‐1.78) |
| Age, y | 13 (1016) | 13 (1016) | 12 (1016) | 1.05 (0.98‐1.12) |
| Year of visit | ||||
| 2009 | 41 (19%) | 32 (21%) | 9 (15%) | Ref |
| 2010 | 65 (30%) | 47 (30%) | 18 (30%) | 0.73 (0.29‐1.84) |
| 2011 | 64 (30%) | 43 (28%) | 21 (36%) | 0.58 (0.23‐1.42) |
| 2012 | 44 (21%) | 33 (21%) | 11 (19%) | 0.84 (0.31‐2.31) |
| Days from visit to surgery | 34 (1445) | 35 (1747) | 27 (841) | 1.02 (1.001.03) |
| Type of surgerya | ||||
| PSF | 184 (86%) | 139 (90%) | 45 (76%) | 2.70 (1.22‐5.97) |
| Growing rod | 9 (4.7%) | 6 (4%) | 3 (5%) | 0.75 (0.18‐3.11) |
| Cervical fusion | 17 (7.9%) | 9 6%) | 8 (13%) | 0.39 (0.14‐1.07) |
| Halo, then PSF | 4 (1.9%) | 1 (0.6%) | 3 (5%) | 0.12 (0.01‐1.19) |
| Underlying diseasea | ||||
| Cerebral palsy | 78 (36%) | 63 (41%) | 15 (25%) | 2.01 (1.03‐3.92) |
| Neuropathy | 4 (2%) | 4 (3%) | 0 (0%) | All had recommendations |
| Myopathy | 19 (9%) | 16 (10%) | 3 (5%) | 2.14 (0.60‐7.66) |
| Metabolic disorder | 6 (3%) | 4 (3%) | 2 (3%) | 0.75 (0.13‐4.23) |
| Skeletal dysplasia | 38 (18%) | 19 (12%) | 19 (32%) | 0.29 (0.14‐0.61) |
| Spina bifida | 7 (3%) | 6 (4%) | 1 (2%) | 2.33 (1.90‐3.48) |
| Genetic disorder (including osteogenesis imperfecta) | 40 (19%) | 28 (18%) | 12 (20%) | 0.86 (0.41‐1.84) |
| Other | 22 (10%) | 15 (10%) | 7 (12%) | 0.79 (0.31‐2.06) |
| Number of preoperative prescription medications | 2 (15) | 3 (15) | 1 (03) | 1.19 (1.06‐1.34) |
| Institutionalized | 9 (4.2%) | 6 (4%) | 3 (5%) | 0.75 (0.18‐3.11) |
| Nonambulatory | 114 (54%) | 90 (59%) | 24 (41%) | 2.02 (1.09‐3.74) |
| Dependence on technologya | ||||
| Feeding tube | 89 (41.6%) | 66 (43%) | 23 (39%) | 1.16 (0.63‐2.14) |
| Baclofen pump | 20 (9.3%) | 18 (12%) | 2 (3%) | 3.74 (0.84‐16.67) |
| Ventriculoperitoneal shunt | 24 (11.2%) | 18 (12%) | 6 (10%) | 1.16 (0.44‐3.08) |
| Vagal nerve stimulator/deep brain stimulator | 8 (3.7%) | 6 (4%) | 2 (3%) | 1.15 (0.22‐5.85) |
| Tracheostomy | 13 (6.1%) | 9 (6%) | 4 (7%) | 0.85 (0.25‐2.86) |
| Home mechanical ventilation (not BiPAP) | 6 (2.8%) | 5 (3%) | 1 (2%) | 1.93 (0.22‐16.90) |
| Home oxygen, BiPAP, or CPAP | 25 (11.7%) | 22 (14%) | 3 (5%) | 3.09 (0.89‐10.73) |
| Seizure disorder | 70 (33%) | 59 (38%) | 11 (19%) | 2.68 (1.29‐5.57) |
| Significant GI comorbidity | 102 (48%) | 86 (55%) | 16 (27%) | 3.35 (1.74‐6.45) |
| Significant cardiac comorbidity | 37 (17.3%) | 26 (17%) | 11 (19%) | 0.88 (0.40‐1.92) |
| Significant pulmonary comorbidity | 78 (36.4%) | 57 (37%) | 21 (36%) | 1.05 (0.56‐1.97) |
DISCUSSION
This is the first large study to examine the role of the pediatric hospitalist in preoperative evaluation of complex surgical patients. Our program developed as an evolution of a postoperative program that we have described previously.[10] The postoperative component of our comanagement program began in 2003, and the preoperative aspect was added in 2009. We believe that the preoperative component to our program contributed in some degree to the decrease in utilization of certain aspects of postoperative care over time such as parenteral nutrition. This change may have occurred because of improved bowel management perioperatively, for instance. Although the preoperative hospitalist evaluation program was instituted by our hospital administration, we felt a preoperative hospitalist evaluation represented a standardized, comprehensive way to evaluate patients before surgery. By 2009, the hospitalists at our hospital had already developed some expertise in managing patients after undergoing spinal fusion surgery.
The fact that hospitalists made recommendations for changes in medications, nutritional management, or diagnostic tests at such a high rate (72%) is interesting. We were not surprised by this finding based on anecdotal evidence because we feel that many of these patients may receive somewhat fragmented care because they often see multiple medical specialists. The high rate of interventions noted in our study may result from the fact that hospitalists who comanage these patients frequently after spinal fusion surgery were attempting to prevent postoperative complications that they see after this type of surgery. Many pediatric hospitalists have developed significant experience in caring for medically complex children and thus may feel more comfortable making preoperative recommendations than other general pediatricians.
We were not surprised to find that hospitalists made preoperative recommendations more frequently in children who had seizures, significant GI comorbidity, and who were nonambulatory. We also noted a statistically significant increased rate of recommendations when patients were on more preoperative medications. We believe that these variables suggest a population that is more medically complex. The importance of selecting medically complex patients for hospitalist comanagement has been noted previously.[16] Therefore, comanagement programs looking to maximize patient benefit for a preoperative hospitalist evaluation program might limit these visits to those who are most medically complex. We found a particularly low yield in evaluation of patients with skeletal dysplasia for example and may discontinue seeing these patients preoperatively.
We found the lack of statistically significant change in rate of hospitalist recommendations among patients with cardiac and pulmonary comorbidities interesting. Whether this was related to the mandatory preoperative pulmonology and cardiology visits is not certain. We hope to study the impact of these preoperative visits in the future as we continue to evaluate our perioperative program.
Several limitations of this study deserve note. This study was performed at 1 institution with 1 group of hospitalists and 1 group of orthopedic surgeons. Two of the study authors (D.R. and D.P.) were among the hospitalists involved with the clinical program. The study was retrospective and nonrandomized. We did not contact primary care physicians as a rule for further information about these patients. In this study, we did not specifically study the impact of hospitalist preoperative evaluations on postoperative outcomes, although the preoperative component represented an important aspect of the more systematic intervention described elsewhere.[10]
CONCLUSIONS
A preoperative program for pediatric hospitalists to see children in anticipation of spinal surgery for neuromuscular scoliosis leads to a high rate of recommendations for changes in medical management or diagnostic evaluation. Certain patient characteristics are more highly associated with hospitalists making these recommendations prior to surgery.
- 2012 State of Hospital Medicine Report, Society of Hospital Medicine. Further information available at: http://www.hospitalmedicine.org/survey.
- , , , et al.; Hospitalist‐Orthopedic Team Trial Investigators. Medical and surgical comanagement after elective hip and knee arthroplasty: a randomized, controlled trial. Ann Intern Med. 2004;141(1):28–38.
- , , , et al. Outcomes for older patients with hip fractures: the impact of orthopedic and geriatric medicine cocare. J Orthop Trauma. 2006;20(3):172–178, discussion 179–180.
- , , , et al. Effects of a hospitalist model on elderly patients with hip fracture. Arch Intern Med. 2005;165(7):796–801.
- , , . Hospitalist care of the medically complex child. Pediatr Clin North Am. 2005;52(4):1165–1167.
- , , , et al. Increasing prevalence of medically complex children in US hospitals. Pediatrics. 2010;126(4):638–646.
- , , , et al. Children with complex chronic conditions in inpatient hospital settings in the United States. Pediatrics. 2010;126(4):647–655.
- , , , et al. Children with medical complexity: an emerging population for clinical and research initiatives. Pediatrics. 2011;127(3):529–538.
- , , , et al. Pediatric hospitalist comanagement of spinal fusion surgery patients. J Hosp Med. 2007;2:23–30.
- , , , et al. Outcomes and costs associated with hospitalist comanagement of medically complex children undergoing spinal fusion surgery. Hosp Pediatr. 2013;3(3):233–241.
- , , , et al. Perioperative processes and outcomes after implementation of a hospitalist‐run preoperative clinic. J Hosp Med. 2012 7:697–701.
- , , , , . Outcomes and processes of care related to preoperative medical consultation. Arch Intern Med. 2010;170(15):1365–1374.
- , , , et al. Opportunity missed: medical consultation, resource use, and quality of care of patients undergoing major surgery. Arch Intern Med. 2007;167(21):2338–2344.
- , , , et al. Standardizing care for high‐risk patients in spine surgery: the Northwestern High‐Risk Spine Protocol. Spine. 2010;35(25):2232–2238.
- , , , . Neuromuscular scoliosis: clinical evaluation pre‐ and postoperative. J Pediatr Orthop. 2000;9:217–220.
- . Just because you can, doesn't mean that you should: a call for the rational application of hospitalist comanagement. J Hosp Med. 2008:3:398–402.
- 2012 State of Hospital Medicine Report, Society of Hospital Medicine. Further information available at: http://www.hospitalmedicine.org/survey.
- , , , et al.; Hospitalist‐Orthopedic Team Trial Investigators. Medical and surgical comanagement after elective hip and knee arthroplasty: a randomized, controlled trial. Ann Intern Med. 2004;141(1):28–38.
- , , , et al. Outcomes for older patients with hip fractures: the impact of orthopedic and geriatric medicine cocare. J Orthop Trauma. 2006;20(3):172–178, discussion 179–180.
- , , , et al. Effects of a hospitalist model on elderly patients with hip fracture. Arch Intern Med. 2005;165(7):796–801.
- , , . Hospitalist care of the medically complex child. Pediatr Clin North Am. 2005;52(4):1165–1167.
- , , , et al. Increasing prevalence of medically complex children in US hospitals. Pediatrics. 2010;126(4):638–646.
- , , , et al. Children with complex chronic conditions in inpatient hospital settings in the United States. Pediatrics. 2010;126(4):647–655.
- , , , et al. Children with medical complexity: an emerging population for clinical and research initiatives. Pediatrics. 2011;127(3):529–538.
- , , , et al. Pediatric hospitalist comanagement of spinal fusion surgery patients. J Hosp Med. 2007;2:23–30.
- , , , et al. Outcomes and costs associated with hospitalist comanagement of medically complex children undergoing spinal fusion surgery. Hosp Pediatr. 2013;3(3):233–241.
- , , , et al. Perioperative processes and outcomes after implementation of a hospitalist‐run preoperative clinic. J Hosp Med. 2012 7:697–701.
- , , , , . Outcomes and processes of care related to preoperative medical consultation. Arch Intern Med. 2010;170(15):1365–1374.
- , , , et al. Opportunity missed: medical consultation, resource use, and quality of care of patients undergoing major surgery. Arch Intern Med. 2007;167(21):2338–2344.
- , , , et al. Standardizing care for high‐risk patients in spine surgery: the Northwestern High‐Risk Spine Protocol. Spine. 2010;35(25):2232–2238.
- , , , . Neuromuscular scoliosis: clinical evaluation pre‐ and postoperative. J Pediatr Orthop. 2000;9:217–220.
- . Just because you can, doesn't mean that you should: a call for the rational application of hospitalist comanagement. J Hosp Med. 2008:3:398–402.
© 2013 Society of Hospital Medicine