User login
Report Cites Wide Variation in Prescription Drug Use by Medicare Patients
A recent Dartmouth Atlas Project report that highlights regional differences for prescription drug use among Medicare patients across the U.S. provides insights into best practices related to effective and high-risk prescription drug therapy.
The report [PDF] found geographic disparity in the total use of prescription medications, variations in effective prescription care, dissimilarities in the use of potentially harmful medications, and differences in total spending on prescription drugs.
Lead author Jeffrey Munson, MD, MSCE, says he expected some geographic variation in the use of discretionary medications, but was surprised by the discrepancy in patients' medication usage. For example, in San Angelo, Texas, 91.4% of heart attack survivors in 2008–2009 filled at least one prescription for beta blockers in the year after their discharge, compared with just 62.5% of the same population of patients in Salem, Ore.
"Clearly, there are regions of the country that have figured out how to best handle certain aspects of medication usage," says Dr. Munson, assistant professor at the Dartmouth Institute for Health Policy & Clinical Practice in Lebanon, N.H. "Instead of just looking at regions that are high performing and saying, 'Wow, that seems to be a really high bar they've set, I'm not sure we can achieve it,' I wonder if maybe it's time we look at those regions and say, 'How are you achieving those very high standards, and what about what you do can I do where I live.'"
The Dartmouth Atlas Project report documents geographic variation in healthcare utilization unrelated to outcome and offers an extensive database for comparison by state, county, region, and facility. Dr. Munson says he understands that healthcare reform is pushing hospitalists and other physicians to focus on many new issues, but that medication usage by patients is among the most pressing issues in healthcare.
"I know that everybody is under increasing time pressures," he adds, "but it’s hard to imagine a larger problem than not getting people the drugs they need to prevent really significant clinical outcomes."
Visit our website for more information on medication issues.
A recent Dartmouth Atlas Project report that highlights regional differences for prescription drug use among Medicare patients across the U.S. provides insights into best practices related to effective and high-risk prescription drug therapy.
The report [PDF] found geographic disparity in the total use of prescription medications, variations in effective prescription care, dissimilarities in the use of potentially harmful medications, and differences in total spending on prescription drugs.
Lead author Jeffrey Munson, MD, MSCE, says he expected some geographic variation in the use of discretionary medications, but was surprised by the discrepancy in patients' medication usage. For example, in San Angelo, Texas, 91.4% of heart attack survivors in 2008–2009 filled at least one prescription for beta blockers in the year after their discharge, compared with just 62.5% of the same population of patients in Salem, Ore.
"Clearly, there are regions of the country that have figured out how to best handle certain aspects of medication usage," says Dr. Munson, assistant professor at the Dartmouth Institute for Health Policy & Clinical Practice in Lebanon, N.H. "Instead of just looking at regions that are high performing and saying, 'Wow, that seems to be a really high bar they've set, I'm not sure we can achieve it,' I wonder if maybe it's time we look at those regions and say, 'How are you achieving those very high standards, and what about what you do can I do where I live.'"
The Dartmouth Atlas Project report documents geographic variation in healthcare utilization unrelated to outcome and offers an extensive database for comparison by state, county, region, and facility. Dr. Munson says he understands that healthcare reform is pushing hospitalists and other physicians to focus on many new issues, but that medication usage by patients is among the most pressing issues in healthcare.
"I know that everybody is under increasing time pressures," he adds, "but it’s hard to imagine a larger problem than not getting people the drugs they need to prevent really significant clinical outcomes."
Visit our website for more information on medication issues.
A recent Dartmouth Atlas Project report that highlights regional differences for prescription drug use among Medicare patients across the U.S. provides insights into best practices related to effective and high-risk prescription drug therapy.
The report [PDF] found geographic disparity in the total use of prescription medications, variations in effective prescription care, dissimilarities in the use of potentially harmful medications, and differences in total spending on prescription drugs.
Lead author Jeffrey Munson, MD, MSCE, says he expected some geographic variation in the use of discretionary medications, but was surprised by the discrepancy in patients' medication usage. For example, in San Angelo, Texas, 91.4% of heart attack survivors in 2008–2009 filled at least one prescription for beta blockers in the year after their discharge, compared with just 62.5% of the same population of patients in Salem, Ore.
"Clearly, there are regions of the country that have figured out how to best handle certain aspects of medication usage," says Dr. Munson, assistant professor at the Dartmouth Institute for Health Policy & Clinical Practice in Lebanon, N.H. "Instead of just looking at regions that are high performing and saying, 'Wow, that seems to be a really high bar they've set, I'm not sure we can achieve it,' I wonder if maybe it's time we look at those regions and say, 'How are you achieving those very high standards, and what about what you do can I do where I live.'"
The Dartmouth Atlas Project report documents geographic variation in healthcare utilization unrelated to outcome and offers an extensive database for comparison by state, county, region, and facility. Dr. Munson says he understands that healthcare reform is pushing hospitalists and other physicians to focus on many new issues, but that medication usage by patients is among the most pressing issues in healthcare.
"I know that everybody is under increasing time pressures," he adds, "but it’s hard to imagine a larger problem than not getting people the drugs they need to prevent really significant clinical outcomes."
Visit our website for more information on medication issues.
Risk of Perioperative Morbidity, Post-Op Mortality Higher for Current Smokers
Clinical question: Is there an association between current and past smoking on outcomes among patients having major surgery?
Background: Smoking is associated with adverse postoperative outcomes, but it is not known whether the associations are dose-dependent or limited to patients with smoking-related diseases. Smoking-related effects on postoperative events among patients having major surgery are also not well established.
Study design: Retrospective cohort study.
Setting: Four hundred forty-eight non-VA hospitals across the U.S., Canada, Lebanon, and the United Arab Emirates.
Synopsis: Data from 607,558 adult patients undergoing major surgery were obtained from the American College of Surgeons (ACS) National Surgical Quality Improvement Program (NSQIP) database. After adjusting for confounders (cardiopulmonary diseases and cancer), the effects of current and past smoking (quit >1 year prior) on 30-day postoperative outcomes were measured.
There were 125,192 (21%) current smokers and 78,763 (13%) past smokers. Increased odds of post-op mortality were noted in current smokers only (odds ratio [OR] 1.17; 95% CI, 1.10–1.24). The adjusted odds ratios were higher for arterial and respiratory events among current smokers compared with past smokers (OR 1.65; 95% CI, 1.51–1.81 vs. OR 1.20; CI, 1.09–1.31 for arterial events, respectively) and (OR, 1.45; CI, 1.40–1.51 vs. OR, 1.13; CI, 1.08–1.18, for respiratory events, respectively). No significant effects on venous events were observed.
There was an increased adjusted odds of mortality for current smokers with <10 pack-years, while the effects on arterial and respiratory events increased incrementally with increased pack-years. Smoking was associated with adverse post-op outcomes regardless of smoking-related diseases. Variability in hospital quality or surgical strategies may have confounded the results.
Bottom line: Among patients undergoing major surgery, current but not past smoking was associated with higher mortality; smoking cessation for at least a year prior to surgery may decrease postoperative adverse events.
Citation: Musallam KM, Rosendaal FR, Zaatari G, et al. Smoking and the risk of mortality and vascular and respiratory events in patients undergoing major surgery. JAMA Surg. 2013;148:755-762.
Clinical question: Is there an association between current and past smoking on outcomes among patients having major surgery?
Background: Smoking is associated with adverse postoperative outcomes, but it is not known whether the associations are dose-dependent or limited to patients with smoking-related diseases. Smoking-related effects on postoperative events among patients having major surgery are also not well established.
Study design: Retrospective cohort study.
Setting: Four hundred forty-eight non-VA hospitals across the U.S., Canada, Lebanon, and the United Arab Emirates.
Synopsis: Data from 607,558 adult patients undergoing major surgery were obtained from the American College of Surgeons (ACS) National Surgical Quality Improvement Program (NSQIP) database. After adjusting for confounders (cardiopulmonary diseases and cancer), the effects of current and past smoking (quit >1 year prior) on 30-day postoperative outcomes were measured.
There were 125,192 (21%) current smokers and 78,763 (13%) past smokers. Increased odds of post-op mortality were noted in current smokers only (odds ratio [OR] 1.17; 95% CI, 1.10–1.24). The adjusted odds ratios were higher for arterial and respiratory events among current smokers compared with past smokers (OR 1.65; 95% CI, 1.51–1.81 vs. OR 1.20; CI, 1.09–1.31 for arterial events, respectively) and (OR, 1.45; CI, 1.40–1.51 vs. OR, 1.13; CI, 1.08–1.18, for respiratory events, respectively). No significant effects on venous events were observed.
There was an increased adjusted odds of mortality for current smokers with <10 pack-years, while the effects on arterial and respiratory events increased incrementally with increased pack-years. Smoking was associated with adverse post-op outcomes regardless of smoking-related diseases. Variability in hospital quality or surgical strategies may have confounded the results.
Bottom line: Among patients undergoing major surgery, current but not past smoking was associated with higher mortality; smoking cessation for at least a year prior to surgery may decrease postoperative adverse events.
Citation: Musallam KM, Rosendaal FR, Zaatari G, et al. Smoking and the risk of mortality and vascular and respiratory events in patients undergoing major surgery. JAMA Surg. 2013;148:755-762.
Clinical question: Is there an association between current and past smoking on outcomes among patients having major surgery?
Background: Smoking is associated with adverse postoperative outcomes, but it is not known whether the associations are dose-dependent or limited to patients with smoking-related diseases. Smoking-related effects on postoperative events among patients having major surgery are also not well established.
Study design: Retrospective cohort study.
Setting: Four hundred forty-eight non-VA hospitals across the U.S., Canada, Lebanon, and the United Arab Emirates.
Synopsis: Data from 607,558 adult patients undergoing major surgery were obtained from the American College of Surgeons (ACS) National Surgical Quality Improvement Program (NSQIP) database. After adjusting for confounders (cardiopulmonary diseases and cancer), the effects of current and past smoking (quit >1 year prior) on 30-day postoperative outcomes were measured.
There were 125,192 (21%) current smokers and 78,763 (13%) past smokers. Increased odds of post-op mortality were noted in current smokers only (odds ratio [OR] 1.17; 95% CI, 1.10–1.24). The adjusted odds ratios were higher for arterial and respiratory events among current smokers compared with past smokers (OR 1.65; 95% CI, 1.51–1.81 vs. OR 1.20; CI, 1.09–1.31 for arterial events, respectively) and (OR, 1.45; CI, 1.40–1.51 vs. OR, 1.13; CI, 1.08–1.18, for respiratory events, respectively). No significant effects on venous events were observed.
There was an increased adjusted odds of mortality for current smokers with <10 pack-years, while the effects on arterial and respiratory events increased incrementally with increased pack-years. Smoking was associated with adverse post-op outcomes regardless of smoking-related diseases. Variability in hospital quality or surgical strategies may have confounded the results.
Bottom line: Among patients undergoing major surgery, current but not past smoking was associated with higher mortality; smoking cessation for at least a year prior to surgery may decrease postoperative adverse events.
Citation: Musallam KM, Rosendaal FR, Zaatari G, et al. Smoking and the risk of mortality and vascular and respiratory events in patients undergoing major surgery. JAMA Surg. 2013;148:755-762.
Medical conferences going digital
The medical conferences of the future made a preview appearance at this year’s Transcatheter Cardiovascular Therapeutics annual meeting in San Francisco. Paperless, electronic, interactive, and definitely high tech it was.
Every paid attendee was offered a new Samsung tablet computer, preloaded with pertinent apps and information, to personalize and keep if they wanted or return at the end of the meeting. If attendees preferred to download the apps to their own devices, that was fine too, and many of them did. (I got a loaner through the press room, and found it easy to use.)

Rather than tack the cost of the tablets onto registration fees, the organizers shifted funds from the no-longer-needed bulky printed programs and other materials to pay for the tablets, according to the Cardiovascular Research Foundation, cosponsor of the TCT meeting with the American College of Cardiology. No funds from industry were solicited for the tablets, no advertising appeared on the home screens, and the tablets were not being used to mine for user data of any kind, but the preloaded apps did contain some advertisements.
Paperless medical conferences are not new – many conferences eschew pulp these days, providing materials on zip drives instead of printed programs that attendees can load onto their computers. And apps for the larger medical conferences now are commonplace, too, for those who have their own smartphones or tablets. But this is the first time I’ve seen a conference give out tablets and include interactive social media features, convenient continuing medical education mechanisms, and more.
Through the apps, attendees could navigate the convention center; view abstracts; download speaker slides and disclosures; watch live cases; take notes; contact some faculty; find shuttle buses, hotels, and restaurants; and access exhibition materials. After attending a session, they could log their hours, write a review, and apply for CME credits through the apps. If they were willing to enable certain settings, they could see who else at the meeting was in their vicinity, and communicate with them.

Each of the major sessions I covered included a "digital moderator" in addition to the regular moderator. Instead of standing in line at microphones to ask questions, members of the audience texted comments and questions that appeared on a screen to the side of the main screen showing the presenter’s slides, so everyone could see them in real time. This feature wasn’t as much used as one might fear – doctors were still paying attention to the speaker, not staring down at their devices, for the most part. From what I could see, the digital moderators provided most of the texted comments and questions, though at one session the live moderator noted that audience texts were asking the speaker to comment about stroke risk, so he raised the question.
Keep in mind, the TCT always has been one of the most high-tech conferences happening in a very high-tech specialty, interventional cardiology. The typical setup in their main forum was similar to that in past meetings, a multitasking-palooza featuring a long dais of speakers and multiple video screens, with individual headsets that let you tune into whichever "channel" interests you most at the moment. Screens with live cases flank either end, with the presenter and his or her slides in the middle and screens promoting upcoming sessions and showing the audience texts in between the other screens.
TCT comes to San Francisco regularly because the city has the infrastructure to support these technologic demands, a spokeswoman in their press room told me. Some other locations haven’t been able to handle their needs.
I wondered if the technology will be so appealing that attendees might prefer virtual attendance rather than having to be there. It’s possible, she said, but unlikely. Like most people, these doctors value their face time.
On Twitter @sherryboschert
The medical conferences of the future made a preview appearance at this year’s Transcatheter Cardiovascular Therapeutics annual meeting in San Francisco. Paperless, electronic, interactive, and definitely high tech it was.
Every paid attendee was offered a new Samsung tablet computer, preloaded with pertinent apps and information, to personalize and keep if they wanted or return at the end of the meeting. If attendees preferred to download the apps to their own devices, that was fine too, and many of them did. (I got a loaner through the press room, and found it easy to use.)
Rather than tack the cost of the tablets onto registration fees, the organizers shifted funds from the no-longer-needed bulky printed programs and other materials to pay for the tablets, according to the Cardiovascular Research Foundation, cosponsor of the TCT meeting with the American College of Cardiology. No funds from industry were solicited for the tablets, no advertising appeared on the home screens, and the tablets were not being used to mine for user data of any kind, but the preloaded apps did contain some advertisements.
Paperless medical conferences are not new – many conferences eschew pulp these days, providing materials on zip drives instead of printed programs that attendees can load onto their computers. And apps for the larger medical conferences now are commonplace, too, for those who have their own smartphones or tablets. But this is the first time I’ve seen a conference give out tablets and include interactive social media features, convenient continuing medical education mechanisms, and more.
Through the apps, attendees could navigate the convention center; view abstracts; download speaker slides and disclosures; watch live cases; take notes; contact some faculty; find shuttle buses, hotels, and restaurants; and access exhibition materials. After attending a session, they could log their hours, write a review, and apply for CME credits through the apps. If they were willing to enable certain settings, they could see who else at the meeting was in their vicinity, and communicate with them.
Each of the major sessions I covered included a "digital moderator" in addition to the regular moderator. Instead of standing in line at microphones to ask questions, members of the audience texted comments and questions that appeared on a screen to the side of the main screen showing the presenter’s slides, so everyone could see them in real time. This feature wasn’t as much used as one might fear – doctors were still paying attention to the speaker, not staring down at their devices, for the most part. From what I could see, the digital moderators provided most of the texted comments and questions, though at one session the live moderator noted that audience texts were asking the speaker to comment about stroke risk, so he raised the question.
Keep in mind, the TCT always has been one of the most high-tech conferences happening in a very high-tech specialty, interventional cardiology. The typical setup in their main forum was similar to that in past meetings, a multitasking-palooza featuring a long dais of speakers and multiple video screens, with individual headsets that let you tune into whichever "channel" interests you most at the moment. Screens with live cases flank either end, with the presenter and his or her slides in the middle and screens promoting upcoming sessions and showing the audience texts in between the other screens.
TCT comes to San Francisco regularly because the city has the infrastructure to support these technologic demands, a spokeswoman in their press room told me. Some other locations haven’t been able to handle their needs.
I wondered if the technology will be so appealing that attendees might prefer virtual attendance rather than having to be there. It’s possible, she said, but unlikely. Like most people, these doctors value their face time.
On Twitter @sherryboschert
The medical conferences of the future made a preview appearance at this year’s Transcatheter Cardiovascular Therapeutics annual meeting in San Francisco. Paperless, electronic, interactive, and definitely high tech it was.
Every paid attendee was offered a new Samsung tablet computer, preloaded with pertinent apps and information, to personalize and keep if they wanted or return at the end of the meeting. If attendees preferred to download the apps to their own devices, that was fine too, and many of them did. (I got a loaner through the press room, and found it easy to use.)
Rather than tack the cost of the tablets onto registration fees, the organizers shifted funds from the no-longer-needed bulky printed programs and other materials to pay for the tablets, according to the Cardiovascular Research Foundation, cosponsor of the TCT meeting with the American College of Cardiology. No funds from industry were solicited for the tablets, no advertising appeared on the home screens, and the tablets were not being used to mine for user data of any kind, but the preloaded apps did contain some advertisements.
Paperless medical conferences are not new – many conferences eschew pulp these days, providing materials on zip drives instead of printed programs that attendees can load onto their computers. And apps for the larger medical conferences now are commonplace, too, for those who have their own smartphones or tablets. But this is the first time I’ve seen a conference give out tablets and include interactive social media features, convenient continuing medical education mechanisms, and more.
Through the apps, attendees could navigate the convention center; view abstracts; download speaker slides and disclosures; watch live cases; take notes; contact some faculty; find shuttle buses, hotels, and restaurants; and access exhibition materials. After attending a session, they could log their hours, write a review, and apply for CME credits through the apps. If they were willing to enable certain settings, they could see who else at the meeting was in their vicinity, and communicate with them.
Each of the major sessions I covered included a "digital moderator" in addition to the regular moderator. Instead of standing in line at microphones to ask questions, members of the audience texted comments and questions that appeared on a screen to the side of the main screen showing the presenter’s slides, so everyone could see them in real time. This feature wasn’t as much used as one might fear – doctors were still paying attention to the speaker, not staring down at their devices, for the most part. From what I could see, the digital moderators provided most of the texted comments and questions, though at one session the live moderator noted that audience texts were asking the speaker to comment about stroke risk, so he raised the question.
Keep in mind, the TCT always has been one of the most high-tech conferences happening in a very high-tech specialty, interventional cardiology. The typical setup in their main forum was similar to that in past meetings, a multitasking-palooza featuring a long dais of speakers and multiple video screens, with individual headsets that let you tune into whichever "channel" interests you most at the moment. Screens with live cases flank either end, with the presenter and his or her slides in the middle and screens promoting upcoming sessions and showing the audience texts in between the other screens.
TCT comes to San Francisco regularly because the city has the infrastructure to support these technologic demands, a spokeswoman in their press room told me. Some other locations haven’t been able to handle their needs.
I wondered if the technology will be so appealing that attendees might prefer virtual attendance rather than having to be there. It’s possible, she said, but unlikely. Like most people, these doctors value their face time.
On Twitter @sherryboschert

A rapid-fire update on lasers in dermatologic surgery
If you have 5 minutes and need an update on the latest advancements in lasers in dermatologic surgery, watch our interview with Dr. Elizabeth Tanzi of Washington Institute of Dermatologic Surgery. Dr. Tanzi talks about the new trends in laser treatments, her two favorite laser machines, and shares her thoughts on the future of lasers.
If you have 5 minutes and need an update on the latest advancements in lasers in dermatologic surgery, watch our interview with Dr. Elizabeth Tanzi of Washington Institute of Dermatologic Surgery. Dr. Tanzi talks about the new trends in laser treatments, her two favorite laser machines, and shares her thoughts on the future of lasers.
If you have 5 minutes and need an update on the latest advancements in lasers in dermatologic surgery, watch our interview with Dr. Elizabeth Tanzi of Washington Institute of Dermatologic Surgery. Dr. Tanzi talks about the new trends in laser treatments, her two favorite laser machines, and shares her thoughts on the future of lasers.
Impact of psoriasis on sexual activity
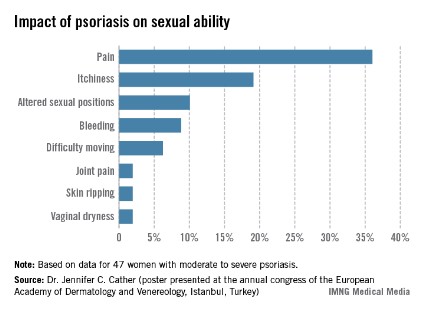
One third of a group of women with psoriasis reported that the pain associated with their condition interfered with their sexual activity, according to findings from a survey presented by Dr. Jennifer C. Cather.
Based on responses from a survey of 60 women with moderate to severe psoriasis, the specific complaints that were the most common ways in which psoriasis interfered with sexual activity were itchiness (19%), the need to adjust sexual position (10%), and bleeding (9%), Dr. Cather reported at the Skin Disease Education Foundation’s annual Las Vegas dermatology seminar. The survey was part of an effort to determine the impact of psoriasis on women’s sexual activity, desires, and relationships.
The data were previously presented in a poster at the annual congress of the European Academy of Dermatology and Venereology (Istanbul.
SDEF and this news organization are owned by Frontline Medical Communications. Dr. Cather disclosed that she is a consultant, speaker, or researcher for AbbVie, Novartis, Leo, Janssen, Amgen, Celgene, Merck, and Pfizer.

One third of a group of women with psoriasis reported that the pain associated with their condition interfered with their sexual activity, according to findings from a survey presented by Dr. Jennifer C. Cather.
Based on responses from a survey of 60 women with moderate to severe psoriasis, the specific complaints that were the most common ways in which psoriasis interfered with sexual activity were itchiness (19%), the need to adjust sexual position (10%), and bleeding (9%), Dr. Cather reported at the Skin Disease Education Foundation’s annual Las Vegas dermatology seminar. The survey was part of an effort to determine the impact of psoriasis on women’s sexual activity, desires, and relationships.
The data were previously presented in a poster at the annual congress of the European Academy of Dermatology and Venereology (Istanbul.
SDEF and this news organization are owned by Frontline Medical Communications. Dr. Cather disclosed that she is a consultant, speaker, or researcher for AbbVie, Novartis, Leo, Janssen, Amgen, Celgene, Merck, and Pfizer.
One third of a group of women with psoriasis reported that the pain associated with their condition interfered with their sexual activity, according to findings from a survey presented by Dr. Jennifer C. Cather.
Based on responses from a survey of 60 women with moderate to severe psoriasis, the specific complaints that were the most common ways in which psoriasis interfered with sexual activity were itchiness (19%), the need to adjust sexual position (10%), and bleeding (9%), Dr. Cather reported at the Skin Disease Education Foundation’s annual Las Vegas dermatology seminar. The survey was part of an effort to determine the impact of psoriasis on women’s sexual activity, desires, and relationships.
The data were previously presented in a poster at the annual congress of the European Academy of Dermatology and Venereology (Istanbul.
SDEF and this news organization are owned by Frontline Medical Communications. Dr. Cather disclosed that she is a consultant, speaker, or researcher for AbbVie, Novartis, Leo, Janssen, Amgen, Celgene, Merck, and Pfizer.
EXPERT ANALYSIS FROM SDEF LAS VEGAS DERMATOLOGY SEMINAR
New and Noteworthy Information—November 2013
In early December 2013, the FDA will formally recommend to the US Department of Health and Human Services (HHS) that hydrocodone combination products be reclassified as Schedule II drugs. The proposed change would tighten the controls on these products, which now are classified as Schedule III. The recommendation follows the US Drug Enforcement Administration’s (DEA) 2009 request for guidance from HHS regarding hydrocodone combination products such as Vicodin. The FDA’s determination is the result of an analysis of the scientific literature, a review of hundreds of public comments on the issue, and several public meetings, according to a statement by Janet Woodcock, MD, Director of the Center for Drug Evaluation and Research. The recommendation will influence the DEA’s final decision on the appropriate scheduling of these products.
Influenza vaccination may reduce patients’ risk of major adverse cardiovascular events, including stroke, according to a meta-analysis published October 23 in JAMA. Researchers conducted a systematic review of randomized clinical trials listed in MEDLINE, EMBASE, and the Cochrane Library Central Register of Controlled Trials that compared influenza vaccine with placebo or control in patients at high risk of cardiovascular disease. Six trials encompassing 6,735 patients were included. Influenza vaccine was associated with a lower risk of composite cardiovascular events (2.9% vs 4.7%) in published trials. A treatment interaction was detected between patients with and without recent acute coronary syndrome. The greatest treatment effect was observed among the highest-risk patients with more active coronary disease, and a larger trial is warranted to assess these findings, said the researchers.
Short sleep duration and poor sleep quality may be associated with greater β-amyloid burden among community-dwelling older adults, according to research published online ahead of print October 21 in JAMA Neurology. Investigators performed a cross-sectional study of 70 adult participants (mean age, 76) in the neuroimaging substudy of the Baltimore Longitudinal Study of Aging. The study’s main outcome measure was β-amyloid burden, measured by carbon 11-labeled Pittsburgh compound B PET distribution volume ratios. After adjustment for potential confounders, the researchers found an association between reports of shorter sleep duration and greater β-amyloid burden, measured by mean cortical distribution volume ratio and precuneus distribution volume ratio. Reports of lower sleep quality were associated with greater β-amyloid burden, measured by precuneus distribution volume ratio.
High blood glucose levels may adversely affect cognition, even among patients without type 2 diabetes or impaired glucose tolerance, researchers reported online ahead of print October 23 in Neurology. The effect may be mediated by structural changes in learning-relevant brain areas, the authors noted. The group tested memory in 141 individuals using the Rey Auditory Verbal Learning Test and acquired peripheral levels of fasting HbA1c, glucose, and insulin. Clinicians performed 3-T MRI scans to assess hippocampal volume and microstructure. Lower HbA1c and glucose levels were significantly associated with better scores in delayed recall, learning ability, and memory consolidation. In multiple regression models, HbA1c remained strongly associated with memory performance. Mediation analyses indicated that beneficial effects of lower HbA1c on memory are partly mediated by hippocampal volume and microstructure.
Among older adults, arterial stiffness may be associated with b-amyloid plaque deposition in the brain, independent of blood pressure and APOE ε4 allele, according to a study published online ahead of print October 16 in Neurology. Investigators studied 91 dementia-free participants between ages 83 and 96. Participants underwent brain MRI and PET imaging with Pittsburgh compound B. The researchers measured resting blood pressure (BP), mean arterial pressure (MAP), and arterial stiffness by pulse wave velocity (PWV) in the central, peripheral, and mixed vascular beds. A total of 44 subjects were β-amyloid positive on PET scan. The investigators found that β-amyloid deposition was associated with mixed PWV, systolic BP, and MAP. One SD increase in brachial ankle PWV resulted in a twofold increase in the odds of being β-amyloid positive.
The FDA has approved Vizamyl (flutemetamol F 18 injection), a radioactive diagnostic drug, for use with PET imaging of the brain in adults being evaluated for Alzheimer’s disease and dementia. Vizamyl attaches to β-amyloid and produces a PET image that is used to evaluate the presence of β-amyloid. The drug’s effectiveness was established in two clinical studies of 384 participants with a range of cognitive function. All participants were injected with Vizamyl and scanned. The images were interpreted by five independent readers masked to all clinical information. A portion of scan results was also confirmed by autopsy. Following the approval of Amyvid (Florbetapir F 18 injection) in 2012, Vizamyl, manufactured by Medi-Physics (Arlington Heights, Illinois), becomes the second diagnostic drug available for visualizing β-amyloid on a PET scan of the brain.
Clostridium perfringens type B, an epsilon toxin-secreting bacillus, may trigger multiple sclerosis (MS), according to research published October 16 in PLOS One. After detecting C. perfringens type B in a woman with MS, investigators tested blood and CSF from patients with MS and controls for antibody reactivity to the epsilon toxin. Levels of epsilon toxin antibodies were 10 times higher in patients with MS, compared with controls. After examining stool samples, the study authors found the human commensal C. perfringens type A in approximately 50% of healthy controls, compared with 23% of patients with MS. C. perfringens epsilon toxin fits mechanistically with nascent MS lesion formation because these lesions are characterized by blood–brain barrier permeability and oligodendrocyte cell death in the absence of an adaptive immune infiltrate, said the researchers.
Chronic cerebrospinal venous insufficiency (CCSVI), which has been proposed as a contributor to multiple sclerosis (MS), occurs rarely in patients with MS and in controls, according to a study published online ahead of print October 8 in Lancet. Researchers performed an assessor-blinded, case-control, multicenter study of 79 people with MS, 55 unaffected siblings, and 43 unrelated healthy volunteers. Catheter venography criteria for CCSVI were positive for 2% of people with MS, 2% of siblings, and 3% of unrelated controls. Greater than 50% narrowing of any major vein was present in 74% of people with MS, 66% of siblings, and 70% of unrelated controls. The Zamboni ultrasound criteria are neither sensitive nor specific for narrowing on catheter venography, and the significance of venous narrowing to MS remains unknown, said the investigators.
Measures of α-synuclein deposition in cutaneous autonomic nerves may be a useful biomarker in patients with Parkinson’s disease, according to research published online ahead of print October 2 in Neurology. Investigators examined 20 patients with Parkinson’s disease and 14 age- and sex-matched control subjects. The researchers performed autonomic testing and skin biopsies at the distal leg, distal thigh, and proximal thigh for all participants. Deposition of α-synuclein and the density of intraepidermal, sudomotor, and pilomotor nerve fibers were measured. The investigators normalized α-synuclein deposition to nerve fiber density. Patients with Parkinson’s disease had greater α-synuclein deposition and higher α-synuclein ratios than controls within pilomotor nerves and sudomotor nerves, but not sensory nerves. Higher α-synuclein ratios correlated with Hoehn and Yahr scores, sympathetic adrenergic function, and parasympathetic function.
Depression may be an independent risk factor for Parkinson’s disease, according to research published October 22 in Neurology. Investigators conducted a retrospective study of 4,634 patients with depression and 18,544 matched controls who were selected from a national health insurance database. Patients were observed for a maximum of 10 years to determine the rates of new-onset Parkinson’s disease. Cox regression was used to identify the predictors of the disease. During the follow-up period, 66 patients with depression and 97 controls were diagnosed with Parkinson’s disease. After adjusting for age and sex, the researchers found that patients with depression were 3.24 times more likely to develop Parkinson’s disease, compared with the control patients. The investigators observed that age and difficult-to-treat depression are independent risk factors for Parkinson’s disease in patients with depression.
The levels of docosahexaenoic acid (DHA) and eicosapentaenoic acid (EPA) in red blood cells may have no association with age-associated cognitive decline, researchers reported in the October 22 issue of Neurology. The investigators conducted a retrospective cohort study of 2,157 women with normal cognition who were followed with annual cognitive testing for a median of 5.9 years. End points were composite cognitive function and performance in seven cognitive domains. After adjustment for demographic, clinical, and behavioral characteristics, the investigators found no significant cross-sectional cognitive differences between women in the high and low DHA and EPA tertiles at the first annual cognitive battery. In addition, no significant differences were found between the high and low DHA and EPA tertiles in the rate of cognitive change over time.
Common psychosocial stressors (eg, divorce, widowhood, work problems, and illness in a relative) may have severe and long-standing physiologic and psychologic consequences such as dementia, according to research published September 30 in BMJ Open. In a prospective longitudinal population study, clinicians performed psychiatric examinations for 800 women born in 1914, 1918, 1922, and 1930. Baseline examinations took place in 1968, and follow-up occurred in 1974, 1980, 1992, 2000, and 2005. During follow-up, 153 women developed dementia. The number of psychosocial stressors in 1968 was associated with higher incidence of dementia and Alzheimer’s disease (AD) between 1968 and 2005 in multivariate Cox regressions. The number of psychosocial stressors in 1968 was also associated with distress in 1968, 1974, 1980, 2000, and 2005 in multivariate logistic regressions.
Aggressive medical management may provide more benefit than percutaneous transluminal angioplasty and stenting (PTAS) for high-risk patients with atherosclerotic intracranial arterial stenosis, according to a study published online ahead of print October 26 in Lancet. Investigators randomized 451 patients with recent transient ischemic attack or stroke to aggressive medical management or aggressive medical management plus stenting with the Wingspan stent. The cumulative probability of stroke or death was smaller in the medical group vs the PTAS group. Beyond 30 days, 10% of patients in the medical group and 10% of patients in the stenting group had a primary end point. The absolute differences in the primary end point rates between the two groups were 7.1% at year 1, 6.5% at year 2 and 9.0% at year 3.
—Erik Greb
Senior Associate Editor
In early December 2013, the FDA will formally recommend to the US Department of Health and Human Services (HHS) that hydrocodone combination products be reclassified as Schedule II drugs. The proposed change would tighten the controls on these products, which now are classified as Schedule III. The recommendation follows the US Drug Enforcement Administration’s (DEA) 2009 request for guidance from HHS regarding hydrocodone combination products such as Vicodin. The FDA’s determination is the result of an analysis of the scientific literature, a review of hundreds of public comments on the issue, and several public meetings, according to a statement by Janet Woodcock, MD, Director of the Center for Drug Evaluation and Research. The recommendation will influence the DEA’s final decision on the appropriate scheduling of these products.
Influenza vaccination may reduce patients’ risk of major adverse cardiovascular events, including stroke, according to a meta-analysis published October 23 in JAMA. Researchers conducted a systematic review of randomized clinical trials listed in MEDLINE, EMBASE, and the Cochrane Library Central Register of Controlled Trials that compared influenza vaccine with placebo or control in patients at high risk of cardiovascular disease. Six trials encompassing 6,735 patients were included. Influenza vaccine was associated with a lower risk of composite cardiovascular events (2.9% vs 4.7%) in published trials. A treatment interaction was detected between patients with and without recent acute coronary syndrome. The greatest treatment effect was observed among the highest-risk patients with more active coronary disease, and a larger trial is warranted to assess these findings, said the researchers.
Short sleep duration and poor sleep quality may be associated with greater β-amyloid burden among community-dwelling older adults, according to research published online ahead of print October 21 in JAMA Neurology. Investigators performed a cross-sectional study of 70 adult participants (mean age, 76) in the neuroimaging substudy of the Baltimore Longitudinal Study of Aging. The study’s main outcome measure was β-amyloid burden, measured by carbon 11-labeled Pittsburgh compound B PET distribution volume ratios. After adjustment for potential confounders, the researchers found an association between reports of shorter sleep duration and greater β-amyloid burden, measured by mean cortical distribution volume ratio and precuneus distribution volume ratio. Reports of lower sleep quality were associated with greater β-amyloid burden, measured by precuneus distribution volume ratio.
High blood glucose levels may adversely affect cognition, even among patients without type 2 diabetes or impaired glucose tolerance, researchers reported online ahead of print October 23 in Neurology. The effect may be mediated by structural changes in learning-relevant brain areas, the authors noted. The group tested memory in 141 individuals using the Rey Auditory Verbal Learning Test and acquired peripheral levels of fasting HbA1c, glucose, and insulin. Clinicians performed 3-T MRI scans to assess hippocampal volume and microstructure. Lower HbA1c and glucose levels were significantly associated with better scores in delayed recall, learning ability, and memory consolidation. In multiple regression models, HbA1c remained strongly associated with memory performance. Mediation analyses indicated that beneficial effects of lower HbA1c on memory are partly mediated by hippocampal volume and microstructure.
Among older adults, arterial stiffness may be associated with b-amyloid plaque deposition in the brain, independent of blood pressure and APOE ε4 allele, according to a study published online ahead of print October 16 in Neurology. Investigators studied 91 dementia-free participants between ages 83 and 96. Participants underwent brain MRI and PET imaging with Pittsburgh compound B. The researchers measured resting blood pressure (BP), mean arterial pressure (MAP), and arterial stiffness by pulse wave velocity (PWV) in the central, peripheral, and mixed vascular beds. A total of 44 subjects were β-amyloid positive on PET scan. The investigators found that β-amyloid deposition was associated with mixed PWV, systolic BP, and MAP. One SD increase in brachial ankle PWV resulted in a twofold increase in the odds of being β-amyloid positive.
The FDA has approved Vizamyl (flutemetamol F 18 injection), a radioactive diagnostic drug, for use with PET imaging of the brain in adults being evaluated for Alzheimer’s disease and dementia. Vizamyl attaches to β-amyloid and produces a PET image that is used to evaluate the presence of β-amyloid. The drug’s effectiveness was established in two clinical studies of 384 participants with a range of cognitive function. All participants were injected with Vizamyl and scanned. The images were interpreted by five independent readers masked to all clinical information. A portion of scan results was also confirmed by autopsy. Following the approval of Amyvid (Florbetapir F 18 injection) in 2012, Vizamyl, manufactured by Medi-Physics (Arlington Heights, Illinois), becomes the second diagnostic drug available for visualizing β-amyloid on a PET scan of the brain.
Clostridium perfringens type B, an epsilon toxin-secreting bacillus, may trigger multiple sclerosis (MS), according to research published October 16 in PLOS One. After detecting C. perfringens type B in a woman with MS, investigators tested blood and CSF from patients with MS and controls for antibody reactivity to the epsilon toxin. Levels of epsilon toxin antibodies were 10 times higher in patients with MS, compared with controls. After examining stool samples, the study authors found the human commensal C. perfringens type A in approximately 50% of healthy controls, compared with 23% of patients with MS. C. perfringens epsilon toxin fits mechanistically with nascent MS lesion formation because these lesions are characterized by blood–brain barrier permeability and oligodendrocyte cell death in the absence of an adaptive immune infiltrate, said the researchers.
Chronic cerebrospinal venous insufficiency (CCSVI), which has been proposed as a contributor to multiple sclerosis (MS), occurs rarely in patients with MS and in controls, according to a study published online ahead of print October 8 in Lancet. Researchers performed an assessor-blinded, case-control, multicenter study of 79 people with MS, 55 unaffected siblings, and 43 unrelated healthy volunteers. Catheter venography criteria for CCSVI were positive for 2% of people with MS, 2% of siblings, and 3% of unrelated controls. Greater than 50% narrowing of any major vein was present in 74% of people with MS, 66% of siblings, and 70% of unrelated controls. The Zamboni ultrasound criteria are neither sensitive nor specific for narrowing on catheter venography, and the significance of venous narrowing to MS remains unknown, said the investigators.
Measures of α-synuclein deposition in cutaneous autonomic nerves may be a useful biomarker in patients with Parkinson’s disease, according to research published online ahead of print October 2 in Neurology. Investigators examined 20 patients with Parkinson’s disease and 14 age- and sex-matched control subjects. The researchers performed autonomic testing and skin biopsies at the distal leg, distal thigh, and proximal thigh for all participants. Deposition of α-synuclein and the density of intraepidermal, sudomotor, and pilomotor nerve fibers were measured. The investigators normalized α-synuclein deposition to nerve fiber density. Patients with Parkinson’s disease had greater α-synuclein deposition and higher α-synuclein ratios than controls within pilomotor nerves and sudomotor nerves, but not sensory nerves. Higher α-synuclein ratios correlated with Hoehn and Yahr scores, sympathetic adrenergic function, and parasympathetic function.
Depression may be an independent risk factor for Parkinson’s disease, according to research published October 22 in Neurology. Investigators conducted a retrospective study of 4,634 patients with depression and 18,544 matched controls who were selected from a national health insurance database. Patients were observed for a maximum of 10 years to determine the rates of new-onset Parkinson’s disease. Cox regression was used to identify the predictors of the disease. During the follow-up period, 66 patients with depression and 97 controls were diagnosed with Parkinson’s disease. After adjusting for age and sex, the researchers found that patients with depression were 3.24 times more likely to develop Parkinson’s disease, compared with the control patients. The investigators observed that age and difficult-to-treat depression are independent risk factors for Parkinson’s disease in patients with depression.
The levels of docosahexaenoic acid (DHA) and eicosapentaenoic acid (EPA) in red blood cells may have no association with age-associated cognitive decline, researchers reported in the October 22 issue of Neurology. The investigators conducted a retrospective cohort study of 2,157 women with normal cognition who were followed with annual cognitive testing for a median of 5.9 years. End points were composite cognitive function and performance in seven cognitive domains. After adjustment for demographic, clinical, and behavioral characteristics, the investigators found no significant cross-sectional cognitive differences between women in the high and low DHA and EPA tertiles at the first annual cognitive battery. In addition, no significant differences were found between the high and low DHA and EPA tertiles in the rate of cognitive change over time.
Common psychosocial stressors (eg, divorce, widowhood, work problems, and illness in a relative) may have severe and long-standing physiologic and psychologic consequences such as dementia, according to research published September 30 in BMJ Open. In a prospective longitudinal population study, clinicians performed psychiatric examinations for 800 women born in 1914, 1918, 1922, and 1930. Baseline examinations took place in 1968, and follow-up occurred in 1974, 1980, 1992, 2000, and 2005. During follow-up, 153 women developed dementia. The number of psychosocial stressors in 1968 was associated with higher incidence of dementia and Alzheimer’s disease (AD) between 1968 and 2005 in multivariate Cox regressions. The number of psychosocial stressors in 1968 was also associated with distress in 1968, 1974, 1980, 2000, and 2005 in multivariate logistic regressions.
Aggressive medical management may provide more benefit than percutaneous transluminal angioplasty and stenting (PTAS) for high-risk patients with atherosclerotic intracranial arterial stenosis, according to a study published online ahead of print October 26 in Lancet. Investigators randomized 451 patients with recent transient ischemic attack or stroke to aggressive medical management or aggressive medical management plus stenting with the Wingspan stent. The cumulative probability of stroke or death was smaller in the medical group vs the PTAS group. Beyond 30 days, 10% of patients in the medical group and 10% of patients in the stenting group had a primary end point. The absolute differences in the primary end point rates between the two groups were 7.1% at year 1, 6.5% at year 2 and 9.0% at year 3.
—Erik Greb
Senior Associate Editor
In early December 2013, the FDA will formally recommend to the US Department of Health and Human Services (HHS) that hydrocodone combination products be reclassified as Schedule II drugs. The proposed change would tighten the controls on these products, which now are classified as Schedule III. The recommendation follows the US Drug Enforcement Administration’s (DEA) 2009 request for guidance from HHS regarding hydrocodone combination products such as Vicodin. The FDA’s determination is the result of an analysis of the scientific literature, a review of hundreds of public comments on the issue, and several public meetings, according to a statement by Janet Woodcock, MD, Director of the Center for Drug Evaluation and Research. The recommendation will influence the DEA’s final decision on the appropriate scheduling of these products.
Influenza vaccination may reduce patients’ risk of major adverse cardiovascular events, including stroke, according to a meta-analysis published October 23 in JAMA. Researchers conducted a systematic review of randomized clinical trials listed in MEDLINE, EMBASE, and the Cochrane Library Central Register of Controlled Trials that compared influenza vaccine with placebo or control in patients at high risk of cardiovascular disease. Six trials encompassing 6,735 patients were included. Influenza vaccine was associated with a lower risk of composite cardiovascular events (2.9% vs 4.7%) in published trials. A treatment interaction was detected between patients with and without recent acute coronary syndrome. The greatest treatment effect was observed among the highest-risk patients with more active coronary disease, and a larger trial is warranted to assess these findings, said the researchers.
Short sleep duration and poor sleep quality may be associated with greater β-amyloid burden among community-dwelling older adults, according to research published online ahead of print October 21 in JAMA Neurology. Investigators performed a cross-sectional study of 70 adult participants (mean age, 76) in the neuroimaging substudy of the Baltimore Longitudinal Study of Aging. The study’s main outcome measure was β-amyloid burden, measured by carbon 11-labeled Pittsburgh compound B PET distribution volume ratios. After adjustment for potential confounders, the researchers found an association between reports of shorter sleep duration and greater β-amyloid burden, measured by mean cortical distribution volume ratio and precuneus distribution volume ratio. Reports of lower sleep quality were associated with greater β-amyloid burden, measured by precuneus distribution volume ratio.
High blood glucose levels may adversely affect cognition, even among patients without type 2 diabetes or impaired glucose tolerance, researchers reported online ahead of print October 23 in Neurology. The effect may be mediated by structural changes in learning-relevant brain areas, the authors noted. The group tested memory in 141 individuals using the Rey Auditory Verbal Learning Test and acquired peripheral levels of fasting HbA1c, glucose, and insulin. Clinicians performed 3-T MRI scans to assess hippocampal volume and microstructure. Lower HbA1c and glucose levels were significantly associated with better scores in delayed recall, learning ability, and memory consolidation. In multiple regression models, HbA1c remained strongly associated with memory performance. Mediation analyses indicated that beneficial effects of lower HbA1c on memory are partly mediated by hippocampal volume and microstructure.
Among older adults, arterial stiffness may be associated with b-amyloid plaque deposition in the brain, independent of blood pressure and APOE ε4 allele, according to a study published online ahead of print October 16 in Neurology. Investigators studied 91 dementia-free participants between ages 83 and 96. Participants underwent brain MRI and PET imaging with Pittsburgh compound B. The researchers measured resting blood pressure (BP), mean arterial pressure (MAP), and arterial stiffness by pulse wave velocity (PWV) in the central, peripheral, and mixed vascular beds. A total of 44 subjects were β-amyloid positive on PET scan. The investigators found that β-amyloid deposition was associated with mixed PWV, systolic BP, and MAP. One SD increase in brachial ankle PWV resulted in a twofold increase in the odds of being β-amyloid positive.
The FDA has approved Vizamyl (flutemetamol F 18 injection), a radioactive diagnostic drug, for use with PET imaging of the brain in adults being evaluated for Alzheimer’s disease and dementia. Vizamyl attaches to β-amyloid and produces a PET image that is used to evaluate the presence of β-amyloid. The drug’s effectiveness was established in two clinical studies of 384 participants with a range of cognitive function. All participants were injected with Vizamyl and scanned. The images were interpreted by five independent readers masked to all clinical information. A portion of scan results was also confirmed by autopsy. Following the approval of Amyvid (Florbetapir F 18 injection) in 2012, Vizamyl, manufactured by Medi-Physics (Arlington Heights, Illinois), becomes the second diagnostic drug available for visualizing β-amyloid on a PET scan of the brain.
Clostridium perfringens type B, an epsilon toxin-secreting bacillus, may trigger multiple sclerosis (MS), according to research published October 16 in PLOS One. After detecting C. perfringens type B in a woman with MS, investigators tested blood and CSF from patients with MS and controls for antibody reactivity to the epsilon toxin. Levels of epsilon toxin antibodies were 10 times higher in patients with MS, compared with controls. After examining stool samples, the study authors found the human commensal C. perfringens type A in approximately 50% of healthy controls, compared with 23% of patients with MS. C. perfringens epsilon toxin fits mechanistically with nascent MS lesion formation because these lesions are characterized by blood–brain barrier permeability and oligodendrocyte cell death in the absence of an adaptive immune infiltrate, said the researchers.
Chronic cerebrospinal venous insufficiency (CCSVI), which has been proposed as a contributor to multiple sclerosis (MS), occurs rarely in patients with MS and in controls, according to a study published online ahead of print October 8 in Lancet. Researchers performed an assessor-blinded, case-control, multicenter study of 79 people with MS, 55 unaffected siblings, and 43 unrelated healthy volunteers. Catheter venography criteria for CCSVI were positive for 2% of people with MS, 2% of siblings, and 3% of unrelated controls. Greater than 50% narrowing of any major vein was present in 74% of people with MS, 66% of siblings, and 70% of unrelated controls. The Zamboni ultrasound criteria are neither sensitive nor specific for narrowing on catheter venography, and the significance of venous narrowing to MS remains unknown, said the investigators.
Measures of α-synuclein deposition in cutaneous autonomic nerves may be a useful biomarker in patients with Parkinson’s disease, according to research published online ahead of print October 2 in Neurology. Investigators examined 20 patients with Parkinson’s disease and 14 age- and sex-matched control subjects. The researchers performed autonomic testing and skin biopsies at the distal leg, distal thigh, and proximal thigh for all participants. Deposition of α-synuclein and the density of intraepidermal, sudomotor, and pilomotor nerve fibers were measured. The investigators normalized α-synuclein deposition to nerve fiber density. Patients with Parkinson’s disease had greater α-synuclein deposition and higher α-synuclein ratios than controls within pilomotor nerves and sudomotor nerves, but not sensory nerves. Higher α-synuclein ratios correlated with Hoehn and Yahr scores, sympathetic adrenergic function, and parasympathetic function.
Depression may be an independent risk factor for Parkinson’s disease, according to research published October 22 in Neurology. Investigators conducted a retrospective study of 4,634 patients with depression and 18,544 matched controls who were selected from a national health insurance database. Patients were observed for a maximum of 10 years to determine the rates of new-onset Parkinson’s disease. Cox regression was used to identify the predictors of the disease. During the follow-up period, 66 patients with depression and 97 controls were diagnosed with Parkinson’s disease. After adjusting for age and sex, the researchers found that patients with depression were 3.24 times more likely to develop Parkinson’s disease, compared with the control patients. The investigators observed that age and difficult-to-treat depression are independent risk factors for Parkinson’s disease in patients with depression.
The levels of docosahexaenoic acid (DHA) and eicosapentaenoic acid (EPA) in red blood cells may have no association with age-associated cognitive decline, researchers reported in the October 22 issue of Neurology. The investigators conducted a retrospective cohort study of 2,157 women with normal cognition who were followed with annual cognitive testing for a median of 5.9 years. End points were composite cognitive function and performance in seven cognitive domains. After adjustment for demographic, clinical, and behavioral characteristics, the investigators found no significant cross-sectional cognitive differences between women in the high and low DHA and EPA tertiles at the first annual cognitive battery. In addition, no significant differences were found between the high and low DHA and EPA tertiles in the rate of cognitive change over time.
Common psychosocial stressors (eg, divorce, widowhood, work problems, and illness in a relative) may have severe and long-standing physiologic and psychologic consequences such as dementia, according to research published September 30 in BMJ Open. In a prospective longitudinal population study, clinicians performed psychiatric examinations for 800 women born in 1914, 1918, 1922, and 1930. Baseline examinations took place in 1968, and follow-up occurred in 1974, 1980, 1992, 2000, and 2005. During follow-up, 153 women developed dementia. The number of psychosocial stressors in 1968 was associated with higher incidence of dementia and Alzheimer’s disease (AD) between 1968 and 2005 in multivariate Cox regressions. The number of psychosocial stressors in 1968 was also associated with distress in 1968, 1974, 1980, 2000, and 2005 in multivariate logistic regressions.
Aggressive medical management may provide more benefit than percutaneous transluminal angioplasty and stenting (PTAS) for high-risk patients with atherosclerotic intracranial arterial stenosis, according to a study published online ahead of print October 26 in Lancet. Investigators randomized 451 patients with recent transient ischemic attack or stroke to aggressive medical management or aggressive medical management plus stenting with the Wingspan stent. The cumulative probability of stroke or death was smaller in the medical group vs the PTAS group. Beyond 30 days, 10% of patients in the medical group and 10% of patients in the stenting group had a primary end point. The absolute differences in the primary end point rates between the two groups were 7.1% at year 1, 6.5% at year 2 and 9.0% at year 3.
—Erik Greb
Senior Associate Editor
Ventricular Assist Device Therapy: A Roundtable Discussion

Topics
- Anticipated Time Horizon For VAD Support
- Incorporating VAD Implantation Earlier In Heart Failure Progression
- Support Structure For VAD Program Success
Faculty/Faculty Disclosures
John B. O’Connell, MD
Thoratec Corporation
Pleasanton, CA
Dr O’Connell discloses that at the time of the roundtable discussion he was a paid consultant for Thoratec Corporation. As of September 30, 2013, he is a full-time employee of Thoratec Corporation. Dr O’Connell also discloses that he is on the Data and Safety Monitoring Committee for Auven Therapeutics.
Walter Dembitsky, MD
Sharp Memorial Hospital
San Diego, CA
Dr Dembitsky discloses that he is a paid consultant and lecturer for, and has received research grants from, Thoratec Corporation.
Ranjit John, MD
University of Minnesota
Minneapolis, MI
Dr John discloses that he is a paid consultant for, and has received research grants from, Thoratec Corporation.
Jaap Lahpor, MD, PhD
University Medical Centre Utrecht
Utrecht, Netherlands
Dr Lahpor discloses that he is a paid consultant and speaker for Thoratec Corporation.
Jonathan D. Rich, MD
Northwestern University
Chicago, IL
Dr Rich discloses that he has received honoraria in the past from Thoratec Corporation.
Welcome to Audiocast #1 of 3. In this audiocast we will discuss the question: When you evaluate a patient for VAD therapy, what time horizon for support do you have in mind?
Welcome to Audiocast #2 of 3. In this audiocast we will answer the question: As patients are supported for longer periods of time, is trying to implant patients earlier in their heart failure progression becoming more important?
Welcome to Audiocast #3 of 3. In this audiocast we will ask the question: As more and more patients are supported for longer periods of time, what types of additional support structure will be required and how are we measuring success?
Topics
- Anticipated Time Horizon For VAD Support
- Incorporating VAD Implantation Earlier In Heart Failure Progression
- Support Structure For VAD Program Success
Faculty/Faculty Disclosures
John B. O’Connell, MD
Thoratec Corporation
Pleasanton, CA
Dr O’Connell discloses that at the time of the roundtable discussion he was a paid consultant for Thoratec Corporation. As of September 30, 2013, he is a full-time employee of Thoratec Corporation. Dr O’Connell also discloses that he is on the Data and Safety Monitoring Committee for Auven Therapeutics.
Walter Dembitsky, MD
Sharp Memorial Hospital
San Diego, CA
Dr Dembitsky discloses that he is a paid consultant and lecturer for, and has received research grants from, Thoratec Corporation.
Ranjit John, MD
University of Minnesota
Minneapolis, MI
Dr John discloses that he is a paid consultant for, and has received research grants from, Thoratec Corporation.
Jaap Lahpor, MD, PhD
University Medical Centre Utrecht
Utrecht, Netherlands
Dr Lahpor discloses that he is a paid consultant and speaker for Thoratec Corporation.
Jonathan D. Rich, MD
Northwestern University
Chicago, IL
Dr Rich discloses that he has received honoraria in the past from Thoratec Corporation.
Welcome to Audiocast #1 of 3. In this audiocast we will discuss the question: When you evaluate a patient for VAD therapy, what time horizon for support do you have in mind?
Welcome to Audiocast #2 of 3. In this audiocast we will answer the question: As patients are supported for longer periods of time, is trying to implant patients earlier in their heart failure progression becoming more important?
Welcome to Audiocast #3 of 3. In this audiocast we will ask the question: As more and more patients are supported for longer periods of time, what types of additional support structure will be required and how are we measuring success?
Topics
- Anticipated Time Horizon For VAD Support
- Incorporating VAD Implantation Earlier In Heart Failure Progression
- Support Structure For VAD Program Success
Faculty/Faculty Disclosures
John B. O’Connell, MD
Thoratec Corporation
Pleasanton, CA
Dr O’Connell discloses that at the time of the roundtable discussion he was a paid consultant for Thoratec Corporation. As of September 30, 2013, he is a full-time employee of Thoratec Corporation. Dr O’Connell also discloses that he is on the Data and Safety Monitoring Committee for Auven Therapeutics.
Walter Dembitsky, MD
Sharp Memorial Hospital
San Diego, CA
Dr Dembitsky discloses that he is a paid consultant and lecturer for, and has received research grants from, Thoratec Corporation.
Ranjit John, MD
University of Minnesota
Minneapolis, MI
Dr John discloses that he is a paid consultant for, and has received research grants from, Thoratec Corporation.
Jaap Lahpor, MD, PhD
University Medical Centre Utrecht
Utrecht, Netherlands
Dr Lahpor discloses that he is a paid consultant and speaker for Thoratec Corporation.
Jonathan D. Rich, MD
Northwestern University
Chicago, IL
Dr Rich discloses that he has received honoraria in the past from Thoratec Corporation.
Welcome to Audiocast #1 of 3. In this audiocast we will discuss the question: When you evaluate a patient for VAD therapy, what time horizon for support do you have in mind?
Welcome to Audiocast #2 of 3. In this audiocast we will answer the question: As patients are supported for longer periods of time, is trying to implant patients earlier in their heart failure progression becoming more important?
Welcome to Audiocast #3 of 3. In this audiocast we will ask the question: As more and more patients are supported for longer periods of time, what types of additional support structure will be required and how are we measuring success?

Doing Everything
We were called to the emergency department to see a young woman, DR, with metastatic endometrial cancer. She had presented with abdominal pain and was found to have evidence of perforation on CT imaging. The CT also demonstrated the unresectable uterus and multiple peritoneal implants. The tumor had not been responsive to the last bout of chemotherapy. DR had been less active, and had lost significant weight over the last several months. A former real estate agent, she hadn’t worked since her diagnosis. She lived with a friend and had a daughter who was very worried about her condition.
I was also worried. After looking at the CT I had told the resident over the phone that operation might not be a great choice. Yes but the family "wants everything done," she replied... CRINGE. "I’ll be over," I said.
Why do we cringe at this statement? Perhaps we feel trapped by a family (or a medical team) who suggests we do everything. There is no out. The die has been cast. This is certainly the case when a non-surgical team has suggested to a family the option of a last-ditch operative intervention. What scares us about the family who wants "everything done"? Often, we don’t think we should be intervening with a surgical operation when the outcome appears dismal. We are concerned with litigation if we don’t try "everything." We fear the communication challenge of speaking with a family with "unrealistic expectations."
But if we take a step back, we might gain some appreciation for the family perspective. Who wouldn’t want everything done to save a loved one, or to prolong our time with a loved one? Who wouldn’t want everything done that might maximize the opportunity for recovery? And who would ever want to do nothing for a loved one in a medical crisis?
I have witnessed (and participated in) two responses to these challenging moments. The first is to acquiesce and perform an operation as a "last-ditch effort." The second is to simply refuse to intervene or even refuse the consult. Neither of these approaches is serves the patient, his or her family, or the health care team (including ourselves). To simply acquiesce puts the patient at increased risk of suffering, gives the family a false notion of hope, and creates moral distress in our team. To simply refuse and walk away leads to patient and family abandonment (with a lack of understanding why operative intervention is not indicated) and leads to conflict within our health care team.
I suggest we enter these situations with the premise that we always do everything and we never do nothing. We do our best to provide treatments to meet the goals and needs of our patients and their loved ones. At times, this may mean a surgical intervention to restore a patient to full premorbid health. At others, this may mean an operation to alleviate suffering, for example, from a malignant bowel obstruction. And sometimes this means not operating as it will only increase or prolong suffering. Yet in the latter situation, there are plenty of appropriate interventions: relieving pain or dyspnea, providing spiritual support, promoting bereavement, and assisting all participants in avoiding complicated grief. These therapies can and should be provided with the same aggressive approach with which we provide operative therapy.
With this approach we are able to reassure our patients and their loved ones that our interests lie in providing the best possible treatments in meeting their goals and needs. And that no matter what, we will find a means to help in some way.
As we sat in the emergency department, we reassured DR that we were there to help and find the best course of action. We admitted our uncertainty with the immediate prognosis with or without operative intervention, but that ultimately she was dying from the cancer. She expressed that she was not ready to die. "I hope we can avoid death as long as possible," I said. "While I am unsure which course of action will prolong your life the most, I am concerned that with operation your death has a higher likelihood of occurring in the midst of a prolonged ICU stay. If we try antibiotic therapy and pain control you might have more of an opportunity to spend time with your daughter and friends." We recommended avoiding operation, focusing on symptom management, and maximizing time with her loved ones.
DR wanted time. She was admitted for antibiotic therapy and aggressive symptom control with a consult to palliative medicine. She stabilized and was able to be transitioned to home hospice with her daughter and friend as caretakers.
This approach is effectively one of risk and benefit, recognition of uncertainty, and adherence to patient values. We recognize the inevitability of death from the beginning of a serious illness and openly discuss with our patients their fears and goals. We join with them in the uncertain future and the hard decisions to come. We work with patients to embrace life-enhancing therapies and to forgo death-avoiding therapies in order to maximize those that work toward patient-centered outcomes. This is a world in which we aggressively do everything to promote health, broadly defined, and ameliorate suffering. We always do everything.
Dr. Weinstein is an ACS Fellow and associate professor of surgery at Thomas Jefferson University in Philadelphia. He is director of the surgical intensive care unit and Executive Medical Co-Director of the Thomas Jefferson University Hospital Center for Critical Care. He is a member of the Palliative Care Task Force of the American College of Surgeons.
We were called to the emergency department to see a young woman, DR, with metastatic endometrial cancer. She had presented with abdominal pain and was found to have evidence of perforation on CT imaging. The CT also demonstrated the unresectable uterus and multiple peritoneal implants. The tumor had not been responsive to the last bout of chemotherapy. DR had been less active, and had lost significant weight over the last several months. A former real estate agent, she hadn’t worked since her diagnosis. She lived with a friend and had a daughter who was very worried about her condition.
I was also worried. After looking at the CT I had told the resident over the phone that operation might not be a great choice. Yes but the family "wants everything done," she replied... CRINGE. "I’ll be over," I said.
Why do we cringe at this statement? Perhaps we feel trapped by a family (or a medical team) who suggests we do everything. There is no out. The die has been cast. This is certainly the case when a non-surgical team has suggested to a family the option of a last-ditch operative intervention. What scares us about the family who wants "everything done"? Often, we don’t think we should be intervening with a surgical operation when the outcome appears dismal. We are concerned with litigation if we don’t try "everything." We fear the communication challenge of speaking with a family with "unrealistic expectations."
But if we take a step back, we might gain some appreciation for the family perspective. Who wouldn’t want everything done to save a loved one, or to prolong our time with a loved one? Who wouldn’t want everything done that might maximize the opportunity for recovery? And who would ever want to do nothing for a loved one in a medical crisis?
I have witnessed (and participated in) two responses to these challenging moments. The first is to acquiesce and perform an operation as a "last-ditch effort." The second is to simply refuse to intervene or even refuse the consult. Neither of these approaches is serves the patient, his or her family, or the health care team (including ourselves). To simply acquiesce puts the patient at increased risk of suffering, gives the family a false notion of hope, and creates moral distress in our team. To simply refuse and walk away leads to patient and family abandonment (with a lack of understanding why operative intervention is not indicated) and leads to conflict within our health care team.
I suggest we enter these situations with the premise that we always do everything and we never do nothing. We do our best to provide treatments to meet the goals and needs of our patients and their loved ones. At times, this may mean a surgical intervention to restore a patient to full premorbid health. At others, this may mean an operation to alleviate suffering, for example, from a malignant bowel obstruction. And sometimes this means not operating as it will only increase or prolong suffering. Yet in the latter situation, there are plenty of appropriate interventions: relieving pain or dyspnea, providing spiritual support, promoting bereavement, and assisting all participants in avoiding complicated grief. These therapies can and should be provided with the same aggressive approach with which we provide operative therapy.
With this approach we are able to reassure our patients and their loved ones that our interests lie in providing the best possible treatments in meeting their goals and needs. And that no matter what, we will find a means to help in some way.
As we sat in the emergency department, we reassured DR that we were there to help and find the best course of action. We admitted our uncertainty with the immediate prognosis with or without operative intervention, but that ultimately she was dying from the cancer. She expressed that she was not ready to die. "I hope we can avoid death as long as possible," I said. "While I am unsure which course of action will prolong your life the most, I am concerned that with operation your death has a higher likelihood of occurring in the midst of a prolonged ICU stay. If we try antibiotic therapy and pain control you might have more of an opportunity to spend time with your daughter and friends." We recommended avoiding operation, focusing on symptom management, and maximizing time with her loved ones.
DR wanted time. She was admitted for antibiotic therapy and aggressive symptom control with a consult to palliative medicine. She stabilized and was able to be transitioned to home hospice with her daughter and friend as caretakers.
This approach is effectively one of risk and benefit, recognition of uncertainty, and adherence to patient values. We recognize the inevitability of death from the beginning of a serious illness and openly discuss with our patients their fears and goals. We join with them in the uncertain future and the hard decisions to come. We work with patients to embrace life-enhancing therapies and to forgo death-avoiding therapies in order to maximize those that work toward patient-centered outcomes. This is a world in which we aggressively do everything to promote health, broadly defined, and ameliorate suffering. We always do everything.
Dr. Weinstein is an ACS Fellow and associate professor of surgery at Thomas Jefferson University in Philadelphia. He is director of the surgical intensive care unit and Executive Medical Co-Director of the Thomas Jefferson University Hospital Center for Critical Care. He is a member of the Palliative Care Task Force of the American College of Surgeons.
We were called to the emergency department to see a young woman, DR, with metastatic endometrial cancer. She had presented with abdominal pain and was found to have evidence of perforation on CT imaging. The CT also demonstrated the unresectable uterus and multiple peritoneal implants. The tumor had not been responsive to the last bout of chemotherapy. DR had been less active, and had lost significant weight over the last several months. A former real estate agent, she hadn’t worked since her diagnosis. She lived with a friend and had a daughter who was very worried about her condition.
I was also worried. After looking at the CT I had told the resident over the phone that operation might not be a great choice. Yes but the family "wants everything done," she replied... CRINGE. "I’ll be over," I said.
Why do we cringe at this statement? Perhaps we feel trapped by a family (or a medical team) who suggests we do everything. There is no out. The die has been cast. This is certainly the case when a non-surgical team has suggested to a family the option of a last-ditch operative intervention. What scares us about the family who wants "everything done"? Often, we don’t think we should be intervening with a surgical operation when the outcome appears dismal. We are concerned with litigation if we don’t try "everything." We fear the communication challenge of speaking with a family with "unrealistic expectations."
But if we take a step back, we might gain some appreciation for the family perspective. Who wouldn’t want everything done to save a loved one, or to prolong our time with a loved one? Who wouldn’t want everything done that might maximize the opportunity for recovery? And who would ever want to do nothing for a loved one in a medical crisis?
I have witnessed (and participated in) two responses to these challenging moments. The first is to acquiesce and perform an operation as a "last-ditch effort." The second is to simply refuse to intervene or even refuse the consult. Neither of these approaches is serves the patient, his or her family, or the health care team (including ourselves). To simply acquiesce puts the patient at increased risk of suffering, gives the family a false notion of hope, and creates moral distress in our team. To simply refuse and walk away leads to patient and family abandonment (with a lack of understanding why operative intervention is not indicated) and leads to conflict within our health care team.
I suggest we enter these situations with the premise that we always do everything and we never do nothing. We do our best to provide treatments to meet the goals and needs of our patients and their loved ones. At times, this may mean a surgical intervention to restore a patient to full premorbid health. At others, this may mean an operation to alleviate suffering, for example, from a malignant bowel obstruction. And sometimes this means not operating as it will only increase or prolong suffering. Yet in the latter situation, there are plenty of appropriate interventions: relieving pain or dyspnea, providing spiritual support, promoting bereavement, and assisting all participants in avoiding complicated grief. These therapies can and should be provided with the same aggressive approach with which we provide operative therapy.
With this approach we are able to reassure our patients and their loved ones that our interests lie in providing the best possible treatments in meeting their goals and needs. And that no matter what, we will find a means to help in some way.
As we sat in the emergency department, we reassured DR that we were there to help and find the best course of action. We admitted our uncertainty with the immediate prognosis with or without operative intervention, but that ultimately she was dying from the cancer. She expressed that she was not ready to die. "I hope we can avoid death as long as possible," I said. "While I am unsure which course of action will prolong your life the most, I am concerned that with operation your death has a higher likelihood of occurring in the midst of a prolonged ICU stay. If we try antibiotic therapy and pain control you might have more of an opportunity to spend time with your daughter and friends." We recommended avoiding operation, focusing on symptom management, and maximizing time with her loved ones.
DR wanted time. She was admitted for antibiotic therapy and aggressive symptom control with a consult to palliative medicine. She stabilized and was able to be transitioned to home hospice with her daughter and friend as caretakers.
This approach is effectively one of risk and benefit, recognition of uncertainty, and adherence to patient values. We recognize the inevitability of death from the beginning of a serious illness and openly discuss with our patients their fears and goals. We join with them in the uncertain future and the hard decisions to come. We work with patients to embrace life-enhancing therapies and to forgo death-avoiding therapies in order to maximize those that work toward patient-centered outcomes. This is a world in which we aggressively do everything to promote health, broadly defined, and ameliorate suffering. We always do everything.
Dr. Weinstein is an ACS Fellow and associate professor of surgery at Thomas Jefferson University in Philadelphia. He is director of the surgical intensive care unit and Executive Medical Co-Director of the Thomas Jefferson University Hospital Center for Critical Care. He is a member of the Palliative Care Task Force of the American College of Surgeons.
EHR Report: Medical legal issues regarding electronic medical records
Electronic health records have led to recent issues appearing in the court system that can potentially convolute physician defense. Both health care attorneys and physicians are grappling with new technology that brings with it the need for close attention to new areas of detail. Certain habits, or lack of habits, can affect the medical-legal environment. Physicians who are aware of these issues can take steps to reduce their exposure.
One of the largest problems seen with EHRs is the failure of physicians to review dictated records. After a note is dictated into the electronic system, health care providers should be encouraged to read it and any accompanying documentation such as prescriptions.
Voice recognition systems are not foolproof and can lead to inaccuracies in the transcription of operative reports, office notes, and prescriptions. When a doctor is deposed and has to explain that what the record says is not really what he or she meant it to say, it decreases his or her credibility with the jury and undermines subsequent testimony. When a physician says that the record is not an accurate representation of what occurred, the jury is left with an impression of carelessness and a failure on the doctor’s part to take the time to ensure patient safety. Taking a few minutes to guarantee the accuracy of the record at the time of creation can save years of explanation after a case has been instituted.
The failure of the physician to review his or her notes can also lead to the veracity of the EHR being called into question. We are aware of at least one case in which an emergency department physician was asked to testify at trial about her interaction with a patient from many years prior. Understandably, the emergency department physician did not have a recollection of the visit and intended to rely on the record. The EHR documented the care that was provided, but the physicians had not signed it. At trial, the doctor was not allowed to testify about what she did for the patient. The rationale was that the doctor did not recall what was done, and her failure to sign the EHR contemporaneously meant that there was no evidence that the EHR was accurate.
A physician should be able to say that his or her custom and practice is to review the EHR before it is finalized and make any updates or addendums as needed. That way, even if there is no signature, the physician has given credence to the accuracy of the records.
Health care providers should be encouraged to use the "free-text" section that is available when it adds to the accuracy of the record. Often, the "drop box" does not provide an adequate selection to describe the history or physical. In anesthesia cases, for instance, the EHR drop box may allow only a description of "awake," "drowsy," or "unresponsive." These choices, while true, do not give an accurate picture of the patient. If a patient in the postanesthesia care unit is technically awake but not properly responsive, that should be documented.
Similarly, in the primary care physician’s office there are times when the general description of how a patient is looking can be informative and integral to the physician formulating an assessment. An example might be the case of a sick child. The child may be curious, playful, and smiling when pulling at the stethoscope. If we are using that information as an important part of our decision as to whether or not that child is seriously ill, then that level of detail should be included in the record. The term "NAD" (no acute distress) does not reflect the level of observation that influenced the decision not to do further testing.
If the drop box is the only source of information utilized, then the true description of the patient is not contained within the records. Sometimes, the most important bits of information cannot be explained utilizing drop boxes.
Another common issue is the failure of EHRs to document when a patient calls the physician’s office but is not actually seen for an appointment. The patient alleges that he or she called the doctor multiple times to report a problem. The HER, however, may not have any record of such a phone call. Physicians need to ensure that they are made aware of these telephone calls and that some type of note is made. The note should not just indicate that a call was made but also should document the physician response and recommendations.
Finally, a new area of concern that has emerged is failure to follow up on a recommendation once it has been made. An ideal situation would be for the EHR or physician office to send a follow-up reminder if an important test is not done. This reminder to the patient should be recorded as well as whether the patient went through with the recommendation and steps the health care provider took to encourage compliance.
This overview does not represent an exhaustive list of EHR issues but rather highlights some common issues along with steps that can be taken to minimize errors, with a goal of increasing overall safety for the patient and decreasing liability for the health care provider.
Mr. Marcoz is a health care attorney in Wilmington, Del., who is shareholder at Marshall Dennehey Warner Coleman & Goggin in the Health Care Liability Practice Group. His areas of practice include medical malpractice and dental insurance defense. Dr. Skolnik is associate director of the family medicine residency program at Abington (Pa.) Memorial Hospital and professor of family and community medicine at Temple University, Philadelphia. He is also editor-in-chief of Redi-Reference Inc., a software company that creates mobile apps.
Electronic health records have led to recent issues appearing in the court system that can potentially convolute physician defense. Both health care attorneys and physicians are grappling with new technology that brings with it the need for close attention to new areas of detail. Certain habits, or lack of habits, can affect the medical-legal environment. Physicians who are aware of these issues can take steps to reduce their exposure.
One of the largest problems seen with EHRs is the failure of physicians to review dictated records. After a note is dictated into the electronic system, health care providers should be encouraged to read it and any accompanying documentation such as prescriptions.
Voice recognition systems are not foolproof and can lead to inaccuracies in the transcription of operative reports, office notes, and prescriptions. When a doctor is deposed and has to explain that what the record says is not really what he or she meant it to say, it decreases his or her credibility with the jury and undermines subsequent testimony. When a physician says that the record is not an accurate representation of what occurred, the jury is left with an impression of carelessness and a failure on the doctor’s part to take the time to ensure patient safety. Taking a few minutes to guarantee the accuracy of the record at the time of creation can save years of explanation after a case has been instituted.
The failure of the physician to review his or her notes can also lead to the veracity of the EHR being called into question. We are aware of at least one case in which an emergency department physician was asked to testify at trial about her interaction with a patient from many years prior. Understandably, the emergency department physician did not have a recollection of the visit and intended to rely on the record. The EHR documented the care that was provided, but the physicians had not signed it. At trial, the doctor was not allowed to testify about what she did for the patient. The rationale was that the doctor did not recall what was done, and her failure to sign the EHR contemporaneously meant that there was no evidence that the EHR was accurate.
A physician should be able to say that his or her custom and practice is to review the EHR before it is finalized and make any updates or addendums as needed. That way, even if there is no signature, the physician has given credence to the accuracy of the records.
Health care providers should be encouraged to use the "free-text" section that is available when it adds to the accuracy of the record. Often, the "drop box" does not provide an adequate selection to describe the history or physical. In anesthesia cases, for instance, the EHR drop box may allow only a description of "awake," "drowsy," or "unresponsive." These choices, while true, do not give an accurate picture of the patient. If a patient in the postanesthesia care unit is technically awake but not properly responsive, that should be documented.
Similarly, in the primary care physician’s office there are times when the general description of how a patient is looking can be informative and integral to the physician formulating an assessment. An example might be the case of a sick child. The child may be curious, playful, and smiling when pulling at the stethoscope. If we are using that information as an important part of our decision as to whether or not that child is seriously ill, then that level of detail should be included in the record. The term "NAD" (no acute distress) does not reflect the level of observation that influenced the decision not to do further testing.
If the drop box is the only source of information utilized, then the true description of the patient is not contained within the records. Sometimes, the most important bits of information cannot be explained utilizing drop boxes.
Another common issue is the failure of EHRs to document when a patient calls the physician’s office but is not actually seen for an appointment. The patient alleges that he or she called the doctor multiple times to report a problem. The HER, however, may not have any record of such a phone call. Physicians need to ensure that they are made aware of these telephone calls and that some type of note is made. The note should not just indicate that a call was made but also should document the physician response and recommendations.
Finally, a new area of concern that has emerged is failure to follow up on a recommendation once it has been made. An ideal situation would be for the EHR or physician office to send a follow-up reminder if an important test is not done. This reminder to the patient should be recorded as well as whether the patient went through with the recommendation and steps the health care provider took to encourage compliance.
This overview does not represent an exhaustive list of EHR issues but rather highlights some common issues along with steps that can be taken to minimize errors, with a goal of increasing overall safety for the patient and decreasing liability for the health care provider.
Mr. Marcoz is a health care attorney in Wilmington, Del., who is shareholder at Marshall Dennehey Warner Coleman & Goggin in the Health Care Liability Practice Group. His areas of practice include medical malpractice and dental insurance defense. Dr. Skolnik is associate director of the family medicine residency program at Abington (Pa.) Memorial Hospital and professor of family and community medicine at Temple University, Philadelphia. He is also editor-in-chief of Redi-Reference Inc., a software company that creates mobile apps.
Electronic health records have led to recent issues appearing in the court system that can potentially convolute physician defense. Both health care attorneys and physicians are grappling with new technology that brings with it the need for close attention to new areas of detail. Certain habits, or lack of habits, can affect the medical-legal environment. Physicians who are aware of these issues can take steps to reduce their exposure.
One of the largest problems seen with EHRs is the failure of physicians to review dictated records. After a note is dictated into the electronic system, health care providers should be encouraged to read it and any accompanying documentation such as prescriptions.
Voice recognition systems are not foolproof and can lead to inaccuracies in the transcription of operative reports, office notes, and prescriptions. When a doctor is deposed and has to explain that what the record says is not really what he or she meant it to say, it decreases his or her credibility with the jury and undermines subsequent testimony. When a physician says that the record is not an accurate representation of what occurred, the jury is left with an impression of carelessness and a failure on the doctor’s part to take the time to ensure patient safety. Taking a few minutes to guarantee the accuracy of the record at the time of creation can save years of explanation after a case has been instituted.
The failure of the physician to review his or her notes can also lead to the veracity of the EHR being called into question. We are aware of at least one case in which an emergency department physician was asked to testify at trial about her interaction with a patient from many years prior. Understandably, the emergency department physician did not have a recollection of the visit and intended to rely on the record. The EHR documented the care that was provided, but the physicians had not signed it. At trial, the doctor was not allowed to testify about what she did for the patient. The rationale was that the doctor did not recall what was done, and her failure to sign the EHR contemporaneously meant that there was no evidence that the EHR was accurate.
A physician should be able to say that his or her custom and practice is to review the EHR before it is finalized and make any updates or addendums as needed. That way, even if there is no signature, the physician has given credence to the accuracy of the records.
Health care providers should be encouraged to use the "free-text" section that is available when it adds to the accuracy of the record. Often, the "drop box" does not provide an adequate selection to describe the history or physical. In anesthesia cases, for instance, the EHR drop box may allow only a description of "awake," "drowsy," or "unresponsive." These choices, while true, do not give an accurate picture of the patient. If a patient in the postanesthesia care unit is technically awake but not properly responsive, that should be documented.
Similarly, in the primary care physician’s office there are times when the general description of how a patient is looking can be informative and integral to the physician formulating an assessment. An example might be the case of a sick child. The child may be curious, playful, and smiling when pulling at the stethoscope. If we are using that information as an important part of our decision as to whether or not that child is seriously ill, then that level of detail should be included in the record. The term "NAD" (no acute distress) does not reflect the level of observation that influenced the decision not to do further testing.
If the drop box is the only source of information utilized, then the true description of the patient is not contained within the records. Sometimes, the most important bits of information cannot be explained utilizing drop boxes.
Another common issue is the failure of EHRs to document when a patient calls the physician’s office but is not actually seen for an appointment. The patient alleges that he or she called the doctor multiple times to report a problem. The HER, however, may not have any record of such a phone call. Physicians need to ensure that they are made aware of these telephone calls and that some type of note is made. The note should not just indicate that a call was made but also should document the physician response and recommendations.
Finally, a new area of concern that has emerged is failure to follow up on a recommendation once it has been made. An ideal situation would be for the EHR or physician office to send a follow-up reminder if an important test is not done. This reminder to the patient should be recorded as well as whether the patient went through with the recommendation and steps the health care provider took to encourage compliance.
This overview does not represent an exhaustive list of EHR issues but rather highlights some common issues along with steps that can be taken to minimize errors, with a goal of increasing overall safety for the patient and decreasing liability for the health care provider.
Mr. Marcoz is a health care attorney in Wilmington, Del., who is shareholder at Marshall Dennehey Warner Coleman & Goggin in the Health Care Liability Practice Group. His areas of practice include medical malpractice and dental insurance defense. Dr. Skolnik is associate director of the family medicine residency program at Abington (Pa.) Memorial Hospital and professor of family and community medicine at Temple University, Philadelphia. He is also editor-in-chief of Redi-Reference Inc., a software company that creates mobile apps.

Observation-Status Patients Are Clinically Heterogeneous, Costly to Hospitals
Clinical question: What are the characteristics of a large cohort of patients under observation status?
Background: The use of observation hospital services has increased significantly. The Centers for Medicare and Medicaid Services (CMS) defines observation status as a “well-defined set of specific, clinically appropriate services,” usually lasting <24 hours and exceeding 48 hours in “only rare and exceptional cases.”
Study design: Retrospective descriptive study.
Setting: University of Wisconsin Hospital and Clinics, a 566-bed tertiary academic medical center.
Synopsis: A total of 43,853 hospitalizations were reviewed during the study period. Of those, 4578 (10.4%) were observation. The mean observation LOS was 33.3 hours, which included 16.5% of patients with LOS >48 hours. Although chest pain was the top observation diagnosis, 1141 distinct observation diagnosis codes were found.
These findings illustrate a significant disparity between the CMS definition for observation stay and the description of observation patients in this cohort, despite using CMS-endorsed InterQual criteria to determine status. While the cost per encounter for observation care was less than inpatient care, reimbursement was insufficient to cover those reduced costs. Ultimately, the net loss of revenue per observation encounter was $331, compared to a net gain in revenue per inpatient encounter of $2,163. This operating loss for hospitals is coupled with the fact that some of this cost is being transferred to patients.
Bottom line: Definitions and reimbursement models for observation status warrant continued research and discussion in the context of our evolving healthcare climate.
Citation: Sheehy AM, Graf B, Gangireddy S, et al. Hospitalized but not admitted: characteristics of patients with “observation status” at an academic medical center [published online ahead of print July 8, 2013]. JAMA Intern Med.
Clinical question: What are the characteristics of a large cohort of patients under observation status?
Background: The use of observation hospital services has increased significantly. The Centers for Medicare and Medicaid Services (CMS) defines observation status as a “well-defined set of specific, clinically appropriate services,” usually lasting <24 hours and exceeding 48 hours in “only rare and exceptional cases.”
Study design: Retrospective descriptive study.
Setting: University of Wisconsin Hospital and Clinics, a 566-bed tertiary academic medical center.
Synopsis: A total of 43,853 hospitalizations were reviewed during the study period. Of those, 4578 (10.4%) were observation. The mean observation LOS was 33.3 hours, which included 16.5% of patients with LOS >48 hours. Although chest pain was the top observation diagnosis, 1141 distinct observation diagnosis codes were found.
These findings illustrate a significant disparity between the CMS definition for observation stay and the description of observation patients in this cohort, despite using CMS-endorsed InterQual criteria to determine status. While the cost per encounter for observation care was less than inpatient care, reimbursement was insufficient to cover those reduced costs. Ultimately, the net loss of revenue per observation encounter was $331, compared to a net gain in revenue per inpatient encounter of $2,163. This operating loss for hospitals is coupled with the fact that some of this cost is being transferred to patients.
Bottom line: Definitions and reimbursement models for observation status warrant continued research and discussion in the context of our evolving healthcare climate.
Citation: Sheehy AM, Graf B, Gangireddy S, et al. Hospitalized but not admitted: characteristics of patients with “observation status” at an academic medical center [published online ahead of print July 8, 2013]. JAMA Intern Med.
Clinical question: What are the characteristics of a large cohort of patients under observation status?
Background: The use of observation hospital services has increased significantly. The Centers for Medicare and Medicaid Services (CMS) defines observation status as a “well-defined set of specific, clinically appropriate services,” usually lasting <24 hours and exceeding 48 hours in “only rare and exceptional cases.”
Study design: Retrospective descriptive study.
Setting: University of Wisconsin Hospital and Clinics, a 566-bed tertiary academic medical center.
Synopsis: A total of 43,853 hospitalizations were reviewed during the study period. Of those, 4578 (10.4%) were observation. The mean observation LOS was 33.3 hours, which included 16.5% of patients with LOS >48 hours. Although chest pain was the top observation diagnosis, 1141 distinct observation diagnosis codes were found.
These findings illustrate a significant disparity between the CMS definition for observation stay and the description of observation patients in this cohort, despite using CMS-endorsed InterQual criteria to determine status. While the cost per encounter for observation care was less than inpatient care, reimbursement was insufficient to cover those reduced costs. Ultimately, the net loss of revenue per observation encounter was $331, compared to a net gain in revenue per inpatient encounter of $2,163. This operating loss for hospitals is coupled with the fact that some of this cost is being transferred to patients.
Bottom line: Definitions and reimbursement models for observation status warrant continued research and discussion in the context of our evolving healthcare climate.
Citation: Sheehy AM, Graf B, Gangireddy S, et al. Hospitalized but not admitted: characteristics of patients with “observation status” at an academic medical center [published online ahead of print July 8, 2013]. JAMA Intern Med.