User login
Attention: New Resident Medical Editors Wanted! (copy 1)
Thoracic Surgery News is seeking 2 new resident associate medical editors for a 1-year appointment for our publication. To apply, you should be a resident in a field of thoracic surgery and willing to review and potentially comment upon articles for our monthly Residents’ Corner section.

In addition, resident medical editors are expected to work with the other editors to contribute 4 to 6 short articles throughout the appointment year, whether it is case studies by themselves or solicited from other thoracic surgeons, news or opinion pieces on resident issues, or summaries of resident-oriented sessions at meetings they attend.
Please send a CV and cover letter indicating your interest to [email protected] Deadline: October 15, 2012
Thoracic Surgery News is seeking 2 new resident associate medical editors for a 1-year appointment for our publication. To apply, you should be a resident in a field of thoracic surgery and willing to review and potentially comment upon articles for our monthly Residents’ Corner section.
In addition, resident medical editors are expected to work with the other editors to contribute 4 to 6 short articles throughout the appointment year, whether it is case studies by themselves or solicited from other thoracic surgeons, news or opinion pieces on resident issues, or summaries of resident-oriented sessions at meetings they attend.
Please send a CV and cover letter indicating your interest to [email protected] Deadline: October 15, 2012
Thoracic Surgery News is seeking 2 new resident associate medical editors for a 1-year appointment for our publication. To apply, you should be a resident in a field of thoracic surgery and willing to review and potentially comment upon articles for our monthly Residents’ Corner section.
In addition, resident medical editors are expected to work with the other editors to contribute 4 to 6 short articles throughout the appointment year, whether it is case studies by themselves or solicited from other thoracic surgeons, news or opinion pieces on resident issues, or summaries of resident-oriented sessions at meetings they attend.
Please send a CV and cover letter indicating your interest to [email protected] Deadline: October 15, 2012
Attention: New Resident Medical Editors Wanted!
Thoracic Surgery News is seeking 2 new resident associate medical editors for a 1-year appointment for our publication. To apply, you should be a resident in a field of thoracic surgery and willing to review and potentially comment upon articles for our monthly Residents’ Corner section.
In addition, resident medical editors are expected to work with the other editors to contribute 4 to 6 short articles throughout the appointment year, whether it is case studies by themselves or solicited from other thoracic surgeons, news or opinion pieces on resident issues, or summaries of resident-oriented sessions at meetings they attend.
Please send a CV and cover letter indicating your interest to [email protected] Deadline: November 15, 2012
Thoracic Surgery News is seeking 2 new resident associate medical editors for a 1-year appointment for our publication. To apply, you should be a resident in a field of thoracic surgery and willing to review and potentially comment upon articles for our monthly Residents’ Corner section.
In addition, resident medical editors are expected to work with the other editors to contribute 4 to 6 short articles throughout the appointment year, whether it is case studies by themselves or solicited from other thoracic surgeons, news or opinion pieces on resident issues, or summaries of resident-oriented sessions at meetings they attend.
Please send a CV and cover letter indicating your interest to [email protected] Deadline: November 15, 2012
Thoracic Surgery News is seeking 2 new resident associate medical editors for a 1-year appointment for our publication. To apply, you should be a resident in a field of thoracic surgery and willing to review and potentially comment upon articles for our monthly Residents’ Corner section.
In addition, resident medical editors are expected to work with the other editors to contribute 4 to 6 short articles throughout the appointment year, whether it is case studies by themselves or solicited from other thoracic surgeons, news or opinion pieces on resident issues, or summaries of resident-oriented sessions at meetings they attend.
Please send a CV and cover letter indicating your interest to [email protected] Deadline: November 15, 2012
PMI After Hip Fracture Surgery
Perioperative myocardial infarction (PMI) often remains unrecognized with higher mortality in the aged.13 Perioperative ischemic symptoms are often masked by analgesia, sedation, and transient and subtle electrocardiographic (ECG) changes. Postoperative troponin measurement is not routinely done for PMI diagnosis. Hip fracture surgery is the most common non‐cardiac surgical procedure in the elderly, with limited data on clinical presentation of PMI.46 Moreover, the elderly are significantly underrepresented in clinical studies.7 We therefore examined the clinical presentation of PMI and its outcomes among elderly patients admitted for hip fracture repair.
METHODS
Study Population
A population‐based, retrospective, case‐control study was conducted of all residents in Olmsted County, Minnesota undergoing surgery for hip fracture repair from January 1, 1988 through December 31, 2002. Primary indication for the surgery was proximal femur (femoral neck or subtrochanteric) fracture. Patients who were 65 years old, had a pathological hip fracture, multiple injuries or fractures, surgery >72 hours after injury (due to higher mortality with delayed surgery),8 nonsurgical management of hip fracture repair, or incomplete data were excluded. All patients provided prior authorization to use their medical records for research, per institutional protocols.9
Criteria for Perioperative Myocardial Infarction and Death
We utilized the universal definition of acute myocardial infarction10 to define PMI within the first 7 days following hip fracture surgery. We included creatine kinase‐MB fraction (CK‐MB) as the biomarker for 1988July 2000, and troponin as the biomarker for August 20002002. Mortality was defined as death from any cause within the first year following hip fracture repair. Deaths were identified through the National Death Index.
Statistical Analysis
For each case of PMI, we identified 2 control patients who were selected at random from the non‐PMI patient population. These controls were matched to cases based on age at the time of surgery (5 years) and gender in 1:2 ratios. Baseline characteristics across PMI and non‐PMI groups were compared using the Kruskal‐Wallis test (for continuous data) and the chi‐square or Fisher's exact tests (for categorical data). Mean values were utilized in place of the missing values for the following variables: preoperative troponin (missing values 88 [17.5%]), CK‐MB (8 [1.6%]), troponin (21 [5.4%]), and postoperative hemoglobin (17 [3.4%]). Univariate predictors of PMI with P 0.2 baseline characteristics were entered into a multivariate, conditional, logistic regression analysis. Rates of outcomes were calculated using the Kaplan‐Meier method, and by a landmark survival curve for those with and without PMI. Cox proportional hazards analysis was utilized for survival analysis at 30 days and 1 year. All statistical tests were 2‐sided, and P values 0.05 were considered significant. All analyses were performed using SAS for UNIX (version 9.1.3; SAS Institute, Inc, Cary, NC).
RESULTS
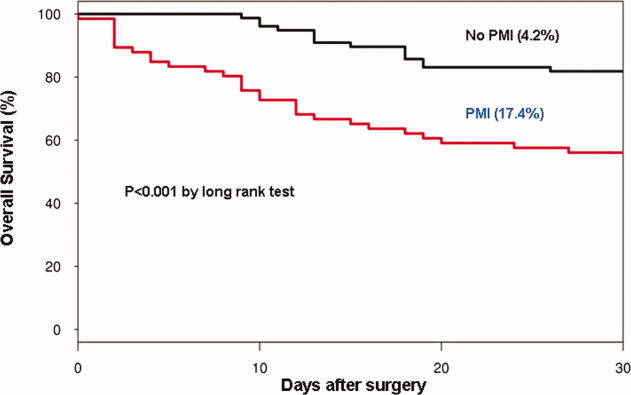
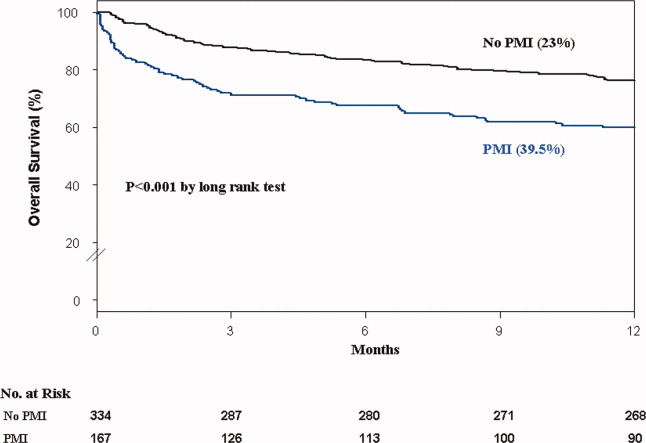
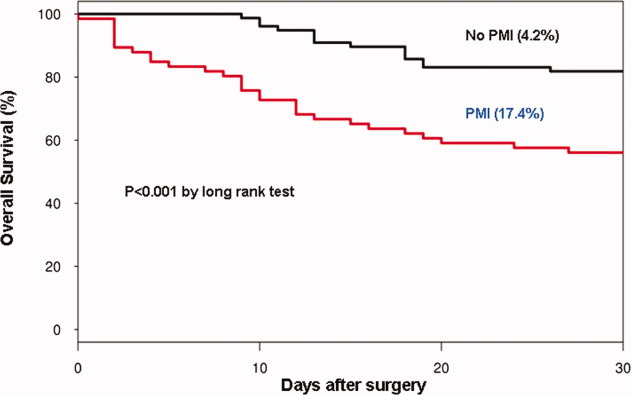
In the cohort of 1212 with hip fracture surgeries, 167 (13.8%) cases of PMI occurred in the first 7 days, of which 153 (92%) occurred within the first 48 hours. A total of 334 controls were matched with 167 cases of PMI. Table 1 summarizes the demographic characteristics of the study participants. Of the patients with PMI, 25.2% experienced symptoms of ischemia; 7% reported chest pain, and 12% reported dyspnea. Only 22.8% of patients with PMI had ECG changes consistent with ischemia. ST elevation MI was present in 7.2% patients. PMI patients had a lower mean hemoglobin compared to the patients without PMI (8.9 mg/dL vs 9.4 mg/dL, P 0.001). Median length of stay (LOS) in the hospital was higher among patients who experienced PMI (11.6 vs 7.4 days, P 0.001). Overall in‐hospital mortality was 5.6%. There were 24 deaths (14.4%) in the PMI group compared to 4 (1.2%) in‐hospital deaths in patients without PMI (P 0.001). A total of 473 (94%) patients survived to discharge. At 30‐day follow‐up, there were 29 (17.4%) deaths in the PMI group and 14 (4.2%) deaths in non‐PMI group. During the follow‐up for 1 year, there were 143 (29%) deaths: PMI 66 (39.5%) and 77 (23%) non‐PMI group (P 0.01).
| Characteristics, n (%) | Patients With PMI | Patients Without PMI | P Value* |
|---|---|---|---|
| (N = 167) | (N = 334) | ||
| |||
| Age mean SD | 85.3 7.4 | 85.2 7.1 | 0.5 |
| Weight (kg) mean SD | 59.98 16.7 | 59.80 13.9 | 0.5 |
| Women | 127 (76.4) | 254 (76) | 0.5 |
| Any symptom of ischemia, n (%) | |||
| Chest/arm pain | 11 (7) | 4 (1) | 0.002 |
| Dyspnea | 20 (12) | 14 (4) | 0.001 |
| Nausea/vomiting | 8 (5) | 6 (2) | 0.08 |
| Diaphoresis | 1 (1) | 1 (0.3) | 1.0 |
| PND | 3 (2) | 1 (0.3) | 0.3 |
| ECG changes, n (%) | |||
| ST‐segment elevation MI | 12 (7.2) | 0 | 0.01 |
| New ECG changes consistent with ischemia | 38 (22.8) | 1(0.3) | 0.01 |
| Biochemical evidence of ischemia, n (%) | |||
| CK‐MB | 147 (88) | 20 (6) | 0.01 |
| Troponin | 52 (33) | 9 (3) | 0.001 |
| Laboratory markers | |||
| Hemoglobin gm/dL mean (SD) | 8.9 1.0 | 9.4 1.2 | 0.001 |
| Postoperative anemia (8.0 gm/dL), n (%) | 22 (13.2) | 37 (11.1) | 0.5 |
| Length of stay (days), mean SD | 11.6 7.7 | 7.4 6.4 | 0.001 |
| In‐hospital outcome | 0.001 | ||
| Dead | 24 (14.4) | 4 (1.2) | |
| Alive | 143 (85.6) | 330 (98.8) | |
| 30‐Day outcome | 0.001 | ||
| Dead | 29 (17.4) | 14 (4.2) | |
| Alive | 138 (82.6) | 320 (95.8) | |
| 1‐Year outcome | 0.001 | ||
| Dead | 66 (39.5) | 77 (23) | |
| Alive | 101 (60.4) | 257 (77) | |
Table 2 describes the risk factors associated with PMI in‐hospital, 30‐day, and 1‐year mortality. Risk factors for PMI were coronary artery disease (CAD) (odds ratio [OR], 3.5; confidence interval [CI], 2.25.6), and serum creatinine >2 mg/dL (OR, 2.4; CI, 1.34.4). Risk factors for in‐hospital mortality were age 8589 (OR, 5.3; CI, 1.617.7), age 90 (OR, 8.9; CI, 2.630.8), PMI (OR 15.1; CI, 4.648.8), male gender (OR 5.8; CI, 2.215.2), dyspnea (OR 5.4; CI, 1.816.9), and hemoglobin 8.0 gm/dL (OR, 3.5; CI, 1.29.9). PMI was a strong predictor for 30‐day mortality (hazard ratio [HR], 4.3; CI, 2.18.9). Risk factors for 1‐year mortality were: age 90 (HR, 2.0; CI, 1.43.1), male gender (HR, 2.1; CI, 1.53.0), and PMI (HR, 1.9; CI, 1.42.7). Figures 1 and 2 describe the Kaplan‐Meier survival curves for patients with and without PMI.
| Unadjusted OR (95% CI) | Adjusted OR (95% CI) | P Value | |
|---|---|---|---|
| |||
| Perioperative myocardial infarction | |||
| Coronary artery disease | 3.0 (2.14.5) | 3.5 (2.25.6) | 0.001 |
| Serum creatinine >2.0 mg/dL | 2.7 (1.64.8) | 2.4 (1.34.4) | 0.003 |
| In‐hospital mortality | |||
| Age 8589 | 1.7 (0.83.7) | 5.3 (1.617.7) | 0.01 |
| Age 90 | 2.2 (1.04.8) | 8.9 (2.630.8) | 0.001 |
| Male gender | 3.0 (1.46.4) | 5.8 (2.215.2) | 0.001 |
| Postoperative anemia (8.0 gm/dL) | 4.2 (1.710.0) | 3.5 (1.29.9) | 0.02 |
| Perioperative myocardial infarction | 14.0 (5.248.0) | 15.1 (4.649.0) | 0.001 |
| 30‐Day mortality | |||
| Perioperative myocardial infarction | 4.1 (2.27.8) | 4.3 (2.18.9) | 0.001 |
| 1‐Year mortality | |||
| Age 8589 | 1.3 (0.81.9) | 1.6 (1.02.4) | 0.03 |
| Age 90 | 1.9 (1.32.9) | 2.0 (1.43.1) | 0.001 |
| Male gender | 1.9 (1.32.6) | 2.1 (1.53.0) | 0.001 |
| Dementia | 2.5 (1.83.6) | 2.7 (1.93.8) | 0.001 |
| Perioperative myocardial infarction | 2.0 (1.52.8) | 1.9 (1.42.7) | 0.001 |
DISCUSSION
We report the high incidence of PMI (13.8%) in the cohort of 1212 elderly patients (mean age 85 years) undergoing hip fracture surgery. Most PMI events (92%) occurred within the first 48 hours of surgery. Most of the events (75%) were asymptomatic. Elderly patients with PMI had an increased hospital LOS by 4.2 days, with high in‐hospital mortality (13.8%), 30‐day mortality (17.4%), and 1‐year mortality (39.5%).
Most of the PMI patients were identified with cardiac biomarkers on the basis of universal definition of MI within the first 48 hours. Although universal definition of MI does not define PMI as a separate type, PMI shares common pathophysiological pathways of Type 1 MI (primary coronary event) and Type 2 MI (myocardial oxygen supplydemand imbalance). Postoperative tachycardia, hemodynamic instability, anemia, and hypoxemia may initiate pathways causing more Type 2 MI. Our study highlights the continued need for active surveillance of clinical symptoms, postoperative ECG monitoring for STT changes, and utilizing cardiac troponin in older postoperative patients to improve diagnostic accuracy of PMI.
The current study has higher asymptomatic PMI events when compared to a study of Devereaux et al.11 The current study had an older population undergoing urgent hip fracture surgery, with a higher burden of CAD (60%) and renal failure (20%) with serum creatinine >2 gm/dL (see Supporting Information, Appendix 1, in the online version of this article). Older age and a higher burden of these risk factors may explain the higher incidence of PMI in the current study. Perioperative liberal use of analgesics in hip fracture surgery may explain more asymptomatic patients.
In light of the recently published FOCUS12 trial, an important finding from our study is that postoperative anemia among elderly (8.0 gm/dL) is associated with a 3.5‐fold increased in‐hospital mortality. It is critical to maintain perioperative hemoglobin above 8.0 gm/dL in very elderly patients, due to asymptomatic presentation of PMI.
In the current study, PMI is associated with a 15‐fold increased risk of in‐hospital death and a 4.3‐fold increased risk of 30‐day mortality in the elderly. Advanced age (85 years) is a well known strong predictor of initial hospital admission and death in elderly patients after outpatient surgery.13 Furthermore, the odds for an in‐hospital death increase by 70% for each 10‐year increase in age.14 Therefore, early detection of silent PMI among at‐risk elderly patients by cardiac biomarkers may help in optimization of cardiac pharmacotherapy known to decrease short‐ and long‐term mortality.
There are limitations inherent to the retrospective design and methodology. Data collection was done through the year 2002. CK was used for the period that spans from 1988 to mid‐2000. Troponin was used from 2000 to 2002. Statin use was not analyzed for lack of significant data. Limited use of beta‐blockers (15%) and angiotensin‐converting‐enzyme (ACE) inhibitors (25%) may also contribute to higher events (see Supporting Information, Appendix 1, in the online version of this article).
CONCLUSIONS
Elderly patients have a higher incidence of PMI and mortality after hip fracture surgery than what guidelines indicate. The majority of the elderly patients with PMI did not experience ischemic symptoms and required cardiac biomarkers for diagnosis. The results of our study support the measurement of troponin in postoperative elderly patients for the diagnosis of PMI to implement in‐hospital preventive strategies to reduce PMI‐associated mortality.
Acknowledgements
The authors gratefully acknowledge the assistance of Ms Dawn Bergen in drafting and editing the manuscript.
Disclosures: This research was supported by funding from AHA grant 03‐30103N‐04, Rochester Epidemiology Project (grant RO1‐AR30582 from the National Institute of Arthritis and Musculoskeletal and Skin Diseases). The project was also supported by the National Center for Research Resources and the National Center for Advancing Translational Sciences, National Institutes of Health, through grant UL1 RR024150. The content is solely the responsibility of the authors and does not necessarily represent the official views of the NIH.
- , , , et al. Impact of age on perioperative complications and length of stay in patients undergoing noncardiac surgery. Ann Intern Med. 2001;134(8):637–643.
- , , , et al. Meta‐analysis: excess mortality after hip fracture among older women and men. Ann Intern Med. 2010;152(6):380–390.
- , , , et al. Body mass index (BMI) and risk of noncardiac postoperative medical complications in elderly hip fracture patients: a population‐based study. J Hosp Med. 2009;4(8):E1–E9.
- . History of the Rochester Epidemiology Project. Mayo Clin Proc. 1996;71(3):266–274.
- , , , . Incidence and mortality of hip fractures in the United States. JAMA. 2009;302(14):1573–1579.
- , , , et al. Body mass index and risk of adverse cardiac events in elderly patients with hip fracture: a population‐based study. J Am Geriatr Soc. 2009;57(3):419–426.
- , , , et al. Acute coronary care in the elderly, part I. Non‐ST‐segment‐elevation acute coronary syndromes: a scientific statement for healthcare professionals from the American Heart Association Council on Clinical Cardiology: in collaboration with the Society of Geriatric Cardiology. Circulation. 2007;115(19):2549–2569.
- , . Hip fracture mortality. A prospective, multifactorial study to predict and minimize death risk. Clin Orthop Relat Res. 1992;280:214–222.
- , , , et al. ACC/AHA/ACP‐ASIM guidelines for the management of patients with chronic stable angina. J Am Coll Cardiol. 1999;33(7):2092–2190.
- , , ; for the Joint ESC/ACCF/AHA/WHF Task Force for the Redefinition of Myocardial Infarction. Universal definition of myocardial infarction. J Am Coll Cardiol. 2007;50(22):2173–2195.
- , , , et al. Characteristics and short‐term prognosis of perioperative myocardial infarction in patients undergoing noncardiac surgery. Ann Intern Med. 2011;154(8):523–528.
- , , , et al. Liberal or restrictive transfusion in high‐risk patients after hip surgery. N Engl J Med. 2011;365(26):2453–2462.
- , , , . Inpatient hospital admission and death after outpatient surgery in elderly patients: importance of patient and system characteristics and location of care. Arch Surg. 2004;139(1):67–72.
- , , , et al. Predictors of hospital mortality in the global registry of acute coronary events. Arch Intern Med. 2003;163(19):2345–2353.
Perioperative myocardial infarction (PMI) often remains unrecognized with higher mortality in the aged.13 Perioperative ischemic symptoms are often masked by analgesia, sedation, and transient and subtle electrocardiographic (ECG) changes. Postoperative troponin measurement is not routinely done for PMI diagnosis. Hip fracture surgery is the most common non‐cardiac surgical procedure in the elderly, with limited data on clinical presentation of PMI.46 Moreover, the elderly are significantly underrepresented in clinical studies.7 We therefore examined the clinical presentation of PMI and its outcomes among elderly patients admitted for hip fracture repair.
METHODS
Study Population
A population‐based, retrospective, case‐control study was conducted of all residents in Olmsted County, Minnesota undergoing surgery for hip fracture repair from January 1, 1988 through December 31, 2002. Primary indication for the surgery was proximal femur (femoral neck or subtrochanteric) fracture. Patients who were 65 years old, had a pathological hip fracture, multiple injuries or fractures, surgery >72 hours after injury (due to higher mortality with delayed surgery),8 nonsurgical management of hip fracture repair, or incomplete data were excluded. All patients provided prior authorization to use their medical records for research, per institutional protocols.9
Criteria for Perioperative Myocardial Infarction and Death
We utilized the universal definition of acute myocardial infarction10 to define PMI within the first 7 days following hip fracture surgery. We included creatine kinase‐MB fraction (CK‐MB) as the biomarker for 1988July 2000, and troponin as the biomarker for August 20002002. Mortality was defined as death from any cause within the first year following hip fracture repair. Deaths were identified through the National Death Index.
Statistical Analysis
For each case of PMI, we identified 2 control patients who were selected at random from the non‐PMI patient population. These controls were matched to cases based on age at the time of surgery (5 years) and gender in 1:2 ratios. Baseline characteristics across PMI and non‐PMI groups were compared using the Kruskal‐Wallis test (for continuous data) and the chi‐square or Fisher's exact tests (for categorical data). Mean values were utilized in place of the missing values for the following variables: preoperative troponin (missing values 88 [17.5%]), CK‐MB (8 [1.6%]), troponin (21 [5.4%]), and postoperative hemoglobin (17 [3.4%]). Univariate predictors of PMI with P 0.2 baseline characteristics were entered into a multivariate, conditional, logistic regression analysis. Rates of outcomes were calculated using the Kaplan‐Meier method, and by a landmark survival curve for those with and without PMI. Cox proportional hazards analysis was utilized for survival analysis at 30 days and 1 year. All statistical tests were 2‐sided, and P values 0.05 were considered significant. All analyses were performed using SAS for UNIX (version 9.1.3; SAS Institute, Inc, Cary, NC).
RESULTS
In the cohort of 1212 with hip fracture surgeries, 167 (13.8%) cases of PMI occurred in the first 7 days, of which 153 (92%) occurred within the first 48 hours. A total of 334 controls were matched with 167 cases of PMI. Table 1 summarizes the demographic characteristics of the study participants. Of the patients with PMI, 25.2% experienced symptoms of ischemia; 7% reported chest pain, and 12% reported dyspnea. Only 22.8% of patients with PMI had ECG changes consistent with ischemia. ST elevation MI was present in 7.2% patients. PMI patients had a lower mean hemoglobin compared to the patients without PMI (8.9 mg/dL vs 9.4 mg/dL, P 0.001). Median length of stay (LOS) in the hospital was higher among patients who experienced PMI (11.6 vs 7.4 days, P 0.001). Overall in‐hospital mortality was 5.6%. There were 24 deaths (14.4%) in the PMI group compared to 4 (1.2%) in‐hospital deaths in patients without PMI (P 0.001). A total of 473 (94%) patients survived to discharge. At 30‐day follow‐up, there were 29 (17.4%) deaths in the PMI group and 14 (4.2%) deaths in non‐PMI group. During the follow‐up for 1 year, there were 143 (29%) deaths: PMI 66 (39.5%) and 77 (23%) non‐PMI group (P 0.01).
| Characteristics, n (%) | Patients With PMI | Patients Without PMI | P Value* |
|---|---|---|---|
| (N = 167) | (N = 334) | ||
| |||
| Age mean SD | 85.3 7.4 | 85.2 7.1 | 0.5 |
| Weight (kg) mean SD | 59.98 16.7 | 59.80 13.9 | 0.5 |
| Women | 127 (76.4) | 254 (76) | 0.5 |
| Any symptom of ischemia, n (%) | |||
| Chest/arm pain | 11 (7) | 4 (1) | 0.002 |
| Dyspnea | 20 (12) | 14 (4) | 0.001 |
| Nausea/vomiting | 8 (5) | 6 (2) | 0.08 |
| Diaphoresis | 1 (1) | 1 (0.3) | 1.0 |
| PND | 3 (2) | 1 (0.3) | 0.3 |
| ECG changes, n (%) | |||
| ST‐segment elevation MI | 12 (7.2) | 0 | 0.01 |
| New ECG changes consistent with ischemia | 38 (22.8) | 1(0.3) | 0.01 |
| Biochemical evidence of ischemia, n (%) | |||
| CK‐MB | 147 (88) | 20 (6) | 0.01 |
| Troponin | 52 (33) | 9 (3) | 0.001 |
| Laboratory markers | |||
| Hemoglobin gm/dL mean (SD) | 8.9 1.0 | 9.4 1.2 | 0.001 |
| Postoperative anemia (8.0 gm/dL), n (%) | 22 (13.2) | 37 (11.1) | 0.5 |
| Length of stay (days), mean SD | 11.6 7.7 | 7.4 6.4 | 0.001 |
| In‐hospital outcome | 0.001 | ||
| Dead | 24 (14.4) | 4 (1.2) | |
| Alive | 143 (85.6) | 330 (98.8) | |
| 30‐Day outcome | 0.001 | ||
| Dead | 29 (17.4) | 14 (4.2) | |
| Alive | 138 (82.6) | 320 (95.8) | |
| 1‐Year outcome | 0.001 | ||
| Dead | 66 (39.5) | 77 (23) | |
| Alive | 101 (60.4) | 257 (77) | |
Table 2 describes the risk factors associated with PMI in‐hospital, 30‐day, and 1‐year mortality. Risk factors for PMI were coronary artery disease (CAD) (odds ratio [OR], 3.5; confidence interval [CI], 2.25.6), and serum creatinine >2 mg/dL (OR, 2.4; CI, 1.34.4). Risk factors for in‐hospital mortality were age 8589 (OR, 5.3; CI, 1.617.7), age 90 (OR, 8.9; CI, 2.630.8), PMI (OR 15.1; CI, 4.648.8), male gender (OR 5.8; CI, 2.215.2), dyspnea (OR 5.4; CI, 1.816.9), and hemoglobin 8.0 gm/dL (OR, 3.5; CI, 1.29.9). PMI was a strong predictor for 30‐day mortality (hazard ratio [HR], 4.3; CI, 2.18.9). Risk factors for 1‐year mortality were: age 90 (HR, 2.0; CI, 1.43.1), male gender (HR, 2.1; CI, 1.53.0), and PMI (HR, 1.9; CI, 1.42.7). Figures 1 and 2 describe the Kaplan‐Meier survival curves for patients with and without PMI.
| Unadjusted OR (95% CI) | Adjusted OR (95% CI) | P Value | |
|---|---|---|---|
| |||
| Perioperative myocardial infarction | |||
| Coronary artery disease | 3.0 (2.14.5) | 3.5 (2.25.6) | 0.001 |
| Serum creatinine >2.0 mg/dL | 2.7 (1.64.8) | 2.4 (1.34.4) | 0.003 |
| In‐hospital mortality | |||
| Age 8589 | 1.7 (0.83.7) | 5.3 (1.617.7) | 0.01 |
| Age 90 | 2.2 (1.04.8) | 8.9 (2.630.8) | 0.001 |
| Male gender | 3.0 (1.46.4) | 5.8 (2.215.2) | 0.001 |
| Postoperative anemia (8.0 gm/dL) | 4.2 (1.710.0) | 3.5 (1.29.9) | 0.02 |
| Perioperative myocardial infarction | 14.0 (5.248.0) | 15.1 (4.649.0) | 0.001 |
| 30‐Day mortality | |||
| Perioperative myocardial infarction | 4.1 (2.27.8) | 4.3 (2.18.9) | 0.001 |
| 1‐Year mortality | |||
| Age 8589 | 1.3 (0.81.9) | 1.6 (1.02.4) | 0.03 |
| Age 90 | 1.9 (1.32.9) | 2.0 (1.43.1) | 0.001 |
| Male gender | 1.9 (1.32.6) | 2.1 (1.53.0) | 0.001 |
| Dementia | 2.5 (1.83.6) | 2.7 (1.93.8) | 0.001 |
| Perioperative myocardial infarction | 2.0 (1.52.8) | 1.9 (1.42.7) | 0.001 |
DISCUSSION
We report the high incidence of PMI (13.8%) in the cohort of 1212 elderly patients (mean age 85 years) undergoing hip fracture surgery. Most PMI events (92%) occurred within the first 48 hours of surgery. Most of the events (75%) were asymptomatic. Elderly patients with PMI had an increased hospital LOS by 4.2 days, with high in‐hospital mortality (13.8%), 30‐day mortality (17.4%), and 1‐year mortality (39.5%).
Most of the PMI patients were identified with cardiac biomarkers on the basis of universal definition of MI within the first 48 hours. Although universal definition of MI does not define PMI as a separate type, PMI shares common pathophysiological pathways of Type 1 MI (primary coronary event) and Type 2 MI (myocardial oxygen supplydemand imbalance). Postoperative tachycardia, hemodynamic instability, anemia, and hypoxemia may initiate pathways causing more Type 2 MI. Our study highlights the continued need for active surveillance of clinical symptoms, postoperative ECG monitoring for STT changes, and utilizing cardiac troponin in older postoperative patients to improve diagnostic accuracy of PMI.
The current study has higher asymptomatic PMI events when compared to a study of Devereaux et al.11 The current study had an older population undergoing urgent hip fracture surgery, with a higher burden of CAD (60%) and renal failure (20%) with serum creatinine >2 gm/dL (see Supporting Information, Appendix 1, in the online version of this article). Older age and a higher burden of these risk factors may explain the higher incidence of PMI in the current study. Perioperative liberal use of analgesics in hip fracture surgery may explain more asymptomatic patients.
In light of the recently published FOCUS12 trial, an important finding from our study is that postoperative anemia among elderly (8.0 gm/dL) is associated with a 3.5‐fold increased in‐hospital mortality. It is critical to maintain perioperative hemoglobin above 8.0 gm/dL in very elderly patients, due to asymptomatic presentation of PMI.
In the current study, PMI is associated with a 15‐fold increased risk of in‐hospital death and a 4.3‐fold increased risk of 30‐day mortality in the elderly. Advanced age (85 years) is a well known strong predictor of initial hospital admission and death in elderly patients after outpatient surgery.13 Furthermore, the odds for an in‐hospital death increase by 70% for each 10‐year increase in age.14 Therefore, early detection of silent PMI among at‐risk elderly patients by cardiac biomarkers may help in optimization of cardiac pharmacotherapy known to decrease short‐ and long‐term mortality.
There are limitations inherent to the retrospective design and methodology. Data collection was done through the year 2002. CK was used for the period that spans from 1988 to mid‐2000. Troponin was used from 2000 to 2002. Statin use was not analyzed for lack of significant data. Limited use of beta‐blockers (15%) and angiotensin‐converting‐enzyme (ACE) inhibitors (25%) may also contribute to higher events (see Supporting Information, Appendix 1, in the online version of this article).
CONCLUSIONS
Elderly patients have a higher incidence of PMI and mortality after hip fracture surgery than what guidelines indicate. The majority of the elderly patients with PMI did not experience ischemic symptoms and required cardiac biomarkers for diagnosis. The results of our study support the measurement of troponin in postoperative elderly patients for the diagnosis of PMI to implement in‐hospital preventive strategies to reduce PMI‐associated mortality.
Acknowledgements
The authors gratefully acknowledge the assistance of Ms Dawn Bergen in drafting and editing the manuscript.
Disclosures: This research was supported by funding from AHA grant 03‐30103N‐04, Rochester Epidemiology Project (grant RO1‐AR30582 from the National Institute of Arthritis and Musculoskeletal and Skin Diseases). The project was also supported by the National Center for Research Resources and the National Center for Advancing Translational Sciences, National Institutes of Health, through grant UL1 RR024150. The content is solely the responsibility of the authors and does not necessarily represent the official views of the NIH.
Perioperative myocardial infarction (PMI) often remains unrecognized with higher mortality in the aged.13 Perioperative ischemic symptoms are often masked by analgesia, sedation, and transient and subtle electrocardiographic (ECG) changes. Postoperative troponin measurement is not routinely done for PMI diagnosis. Hip fracture surgery is the most common non‐cardiac surgical procedure in the elderly, with limited data on clinical presentation of PMI.46 Moreover, the elderly are significantly underrepresented in clinical studies.7 We therefore examined the clinical presentation of PMI and its outcomes among elderly patients admitted for hip fracture repair.
METHODS
Study Population
A population‐based, retrospective, case‐control study was conducted of all residents in Olmsted County, Minnesota undergoing surgery for hip fracture repair from January 1, 1988 through December 31, 2002. Primary indication for the surgery was proximal femur (femoral neck or subtrochanteric) fracture. Patients who were 65 years old, had a pathological hip fracture, multiple injuries or fractures, surgery >72 hours after injury (due to higher mortality with delayed surgery),8 nonsurgical management of hip fracture repair, or incomplete data were excluded. All patients provided prior authorization to use their medical records for research, per institutional protocols.9
Criteria for Perioperative Myocardial Infarction and Death
We utilized the universal definition of acute myocardial infarction10 to define PMI within the first 7 days following hip fracture surgery. We included creatine kinase‐MB fraction (CK‐MB) as the biomarker for 1988July 2000, and troponin as the biomarker for August 20002002. Mortality was defined as death from any cause within the first year following hip fracture repair. Deaths were identified through the National Death Index.
Statistical Analysis
For each case of PMI, we identified 2 control patients who were selected at random from the non‐PMI patient population. These controls were matched to cases based on age at the time of surgery (5 years) and gender in 1:2 ratios. Baseline characteristics across PMI and non‐PMI groups were compared using the Kruskal‐Wallis test (for continuous data) and the chi‐square or Fisher's exact tests (for categorical data). Mean values were utilized in place of the missing values for the following variables: preoperative troponin (missing values 88 [17.5%]), CK‐MB (8 [1.6%]), troponin (21 [5.4%]), and postoperative hemoglobin (17 [3.4%]). Univariate predictors of PMI with P 0.2 baseline characteristics were entered into a multivariate, conditional, logistic regression analysis. Rates of outcomes were calculated using the Kaplan‐Meier method, and by a landmark survival curve for those with and without PMI. Cox proportional hazards analysis was utilized for survival analysis at 30 days and 1 year. All statistical tests were 2‐sided, and P values 0.05 were considered significant. All analyses were performed using SAS for UNIX (version 9.1.3; SAS Institute, Inc, Cary, NC).
RESULTS
In the cohort of 1212 with hip fracture surgeries, 167 (13.8%) cases of PMI occurred in the first 7 days, of which 153 (92%) occurred within the first 48 hours. A total of 334 controls were matched with 167 cases of PMI. Table 1 summarizes the demographic characteristics of the study participants. Of the patients with PMI, 25.2% experienced symptoms of ischemia; 7% reported chest pain, and 12% reported dyspnea. Only 22.8% of patients with PMI had ECG changes consistent with ischemia. ST elevation MI was present in 7.2% patients. PMI patients had a lower mean hemoglobin compared to the patients without PMI (8.9 mg/dL vs 9.4 mg/dL, P 0.001). Median length of stay (LOS) in the hospital was higher among patients who experienced PMI (11.6 vs 7.4 days, P 0.001). Overall in‐hospital mortality was 5.6%. There were 24 deaths (14.4%) in the PMI group compared to 4 (1.2%) in‐hospital deaths in patients without PMI (P 0.001). A total of 473 (94%) patients survived to discharge. At 30‐day follow‐up, there were 29 (17.4%) deaths in the PMI group and 14 (4.2%) deaths in non‐PMI group. During the follow‐up for 1 year, there were 143 (29%) deaths: PMI 66 (39.5%) and 77 (23%) non‐PMI group (P 0.01).
| Characteristics, n (%) | Patients With PMI | Patients Without PMI | P Value* |
|---|---|---|---|
| (N = 167) | (N = 334) | ||
| |||
| Age mean SD | 85.3 7.4 | 85.2 7.1 | 0.5 |
| Weight (kg) mean SD | 59.98 16.7 | 59.80 13.9 | 0.5 |
| Women | 127 (76.4) | 254 (76) | 0.5 |
| Any symptom of ischemia, n (%) | |||
| Chest/arm pain | 11 (7) | 4 (1) | 0.002 |
| Dyspnea | 20 (12) | 14 (4) | 0.001 |
| Nausea/vomiting | 8 (5) | 6 (2) | 0.08 |
| Diaphoresis | 1 (1) | 1 (0.3) | 1.0 |
| PND | 3 (2) | 1 (0.3) | 0.3 |
| ECG changes, n (%) | |||
| ST‐segment elevation MI | 12 (7.2) | 0 | 0.01 |
| New ECG changes consistent with ischemia | 38 (22.8) | 1(0.3) | 0.01 |
| Biochemical evidence of ischemia, n (%) | |||
| CK‐MB | 147 (88) | 20 (6) | 0.01 |
| Troponin | 52 (33) | 9 (3) | 0.001 |
| Laboratory markers | |||
| Hemoglobin gm/dL mean (SD) | 8.9 1.0 | 9.4 1.2 | 0.001 |
| Postoperative anemia (8.0 gm/dL), n (%) | 22 (13.2) | 37 (11.1) | 0.5 |
| Length of stay (days), mean SD | 11.6 7.7 | 7.4 6.4 | 0.001 |
| In‐hospital outcome | 0.001 | ||
| Dead | 24 (14.4) | 4 (1.2) | |
| Alive | 143 (85.6) | 330 (98.8) | |
| 30‐Day outcome | 0.001 | ||
| Dead | 29 (17.4) | 14 (4.2) | |
| Alive | 138 (82.6) | 320 (95.8) | |
| 1‐Year outcome | 0.001 | ||
| Dead | 66 (39.5) | 77 (23) | |
| Alive | 101 (60.4) | 257 (77) | |
Table 2 describes the risk factors associated with PMI in‐hospital, 30‐day, and 1‐year mortality. Risk factors for PMI were coronary artery disease (CAD) (odds ratio [OR], 3.5; confidence interval [CI], 2.25.6), and serum creatinine >2 mg/dL (OR, 2.4; CI, 1.34.4). Risk factors for in‐hospital mortality were age 8589 (OR, 5.3; CI, 1.617.7), age 90 (OR, 8.9; CI, 2.630.8), PMI (OR 15.1; CI, 4.648.8), male gender (OR 5.8; CI, 2.215.2), dyspnea (OR 5.4; CI, 1.816.9), and hemoglobin 8.0 gm/dL (OR, 3.5; CI, 1.29.9). PMI was a strong predictor for 30‐day mortality (hazard ratio [HR], 4.3; CI, 2.18.9). Risk factors for 1‐year mortality were: age 90 (HR, 2.0; CI, 1.43.1), male gender (HR, 2.1; CI, 1.53.0), and PMI (HR, 1.9; CI, 1.42.7). Figures 1 and 2 describe the Kaplan‐Meier survival curves for patients with and without PMI.
| Unadjusted OR (95% CI) | Adjusted OR (95% CI) | P Value | |
|---|---|---|---|
| |||
| Perioperative myocardial infarction | |||
| Coronary artery disease | 3.0 (2.14.5) | 3.5 (2.25.6) | 0.001 |
| Serum creatinine >2.0 mg/dL | 2.7 (1.64.8) | 2.4 (1.34.4) | 0.003 |
| In‐hospital mortality | |||
| Age 8589 | 1.7 (0.83.7) | 5.3 (1.617.7) | 0.01 |
| Age 90 | 2.2 (1.04.8) | 8.9 (2.630.8) | 0.001 |
| Male gender | 3.0 (1.46.4) | 5.8 (2.215.2) | 0.001 |
| Postoperative anemia (8.0 gm/dL) | 4.2 (1.710.0) | 3.5 (1.29.9) | 0.02 |
| Perioperative myocardial infarction | 14.0 (5.248.0) | 15.1 (4.649.0) | 0.001 |
| 30‐Day mortality | |||
| Perioperative myocardial infarction | 4.1 (2.27.8) | 4.3 (2.18.9) | 0.001 |
| 1‐Year mortality | |||
| Age 8589 | 1.3 (0.81.9) | 1.6 (1.02.4) | 0.03 |
| Age 90 | 1.9 (1.32.9) | 2.0 (1.43.1) | 0.001 |
| Male gender | 1.9 (1.32.6) | 2.1 (1.53.0) | 0.001 |
| Dementia | 2.5 (1.83.6) | 2.7 (1.93.8) | 0.001 |
| Perioperative myocardial infarction | 2.0 (1.52.8) | 1.9 (1.42.7) | 0.001 |
DISCUSSION
We report the high incidence of PMI (13.8%) in the cohort of 1212 elderly patients (mean age 85 years) undergoing hip fracture surgery. Most PMI events (92%) occurred within the first 48 hours of surgery. Most of the events (75%) were asymptomatic. Elderly patients with PMI had an increased hospital LOS by 4.2 days, with high in‐hospital mortality (13.8%), 30‐day mortality (17.4%), and 1‐year mortality (39.5%).
Most of the PMI patients were identified with cardiac biomarkers on the basis of universal definition of MI within the first 48 hours. Although universal definition of MI does not define PMI as a separate type, PMI shares common pathophysiological pathways of Type 1 MI (primary coronary event) and Type 2 MI (myocardial oxygen supplydemand imbalance). Postoperative tachycardia, hemodynamic instability, anemia, and hypoxemia may initiate pathways causing more Type 2 MI. Our study highlights the continued need for active surveillance of clinical symptoms, postoperative ECG monitoring for STT changes, and utilizing cardiac troponin in older postoperative patients to improve diagnostic accuracy of PMI.
The current study has higher asymptomatic PMI events when compared to a study of Devereaux et al.11 The current study had an older population undergoing urgent hip fracture surgery, with a higher burden of CAD (60%) and renal failure (20%) with serum creatinine >2 gm/dL (see Supporting Information, Appendix 1, in the online version of this article). Older age and a higher burden of these risk factors may explain the higher incidence of PMI in the current study. Perioperative liberal use of analgesics in hip fracture surgery may explain more asymptomatic patients.
In light of the recently published FOCUS12 trial, an important finding from our study is that postoperative anemia among elderly (8.0 gm/dL) is associated with a 3.5‐fold increased in‐hospital mortality. It is critical to maintain perioperative hemoglobin above 8.0 gm/dL in very elderly patients, due to asymptomatic presentation of PMI.
In the current study, PMI is associated with a 15‐fold increased risk of in‐hospital death and a 4.3‐fold increased risk of 30‐day mortality in the elderly. Advanced age (85 years) is a well known strong predictor of initial hospital admission and death in elderly patients after outpatient surgery.13 Furthermore, the odds for an in‐hospital death increase by 70% for each 10‐year increase in age.14 Therefore, early detection of silent PMI among at‐risk elderly patients by cardiac biomarkers may help in optimization of cardiac pharmacotherapy known to decrease short‐ and long‐term mortality.
There are limitations inherent to the retrospective design and methodology. Data collection was done through the year 2002. CK was used for the period that spans from 1988 to mid‐2000. Troponin was used from 2000 to 2002. Statin use was not analyzed for lack of significant data. Limited use of beta‐blockers (15%) and angiotensin‐converting‐enzyme (ACE) inhibitors (25%) may also contribute to higher events (see Supporting Information, Appendix 1, in the online version of this article).
CONCLUSIONS
Elderly patients have a higher incidence of PMI and mortality after hip fracture surgery than what guidelines indicate. The majority of the elderly patients with PMI did not experience ischemic symptoms and required cardiac biomarkers for diagnosis. The results of our study support the measurement of troponin in postoperative elderly patients for the diagnosis of PMI to implement in‐hospital preventive strategies to reduce PMI‐associated mortality.
Acknowledgements
The authors gratefully acknowledge the assistance of Ms Dawn Bergen in drafting and editing the manuscript.
Disclosures: This research was supported by funding from AHA grant 03‐30103N‐04, Rochester Epidemiology Project (grant RO1‐AR30582 from the National Institute of Arthritis and Musculoskeletal and Skin Diseases). The project was also supported by the National Center for Research Resources and the National Center for Advancing Translational Sciences, National Institutes of Health, through grant UL1 RR024150. The content is solely the responsibility of the authors and does not necessarily represent the official views of the NIH.
- , , , et al. Impact of age on perioperative complications and length of stay in patients undergoing noncardiac surgery. Ann Intern Med. 2001;134(8):637–643.
- , , , et al. Meta‐analysis: excess mortality after hip fracture among older women and men. Ann Intern Med. 2010;152(6):380–390.
- , , , et al. Body mass index (BMI) and risk of noncardiac postoperative medical complications in elderly hip fracture patients: a population‐based study. J Hosp Med. 2009;4(8):E1–E9.
- . History of the Rochester Epidemiology Project. Mayo Clin Proc. 1996;71(3):266–274.
- , , , . Incidence and mortality of hip fractures in the United States. JAMA. 2009;302(14):1573–1579.
- , , , et al. Body mass index and risk of adverse cardiac events in elderly patients with hip fracture: a population‐based study. J Am Geriatr Soc. 2009;57(3):419–426.
- , , , et al. Acute coronary care in the elderly, part I. Non‐ST‐segment‐elevation acute coronary syndromes: a scientific statement for healthcare professionals from the American Heart Association Council on Clinical Cardiology: in collaboration with the Society of Geriatric Cardiology. Circulation. 2007;115(19):2549–2569.
- , . Hip fracture mortality. A prospective, multifactorial study to predict and minimize death risk. Clin Orthop Relat Res. 1992;280:214–222.
- , , , et al. ACC/AHA/ACP‐ASIM guidelines for the management of patients with chronic stable angina. J Am Coll Cardiol. 1999;33(7):2092–2190.
- , , ; for the Joint ESC/ACCF/AHA/WHF Task Force for the Redefinition of Myocardial Infarction. Universal definition of myocardial infarction. J Am Coll Cardiol. 2007;50(22):2173–2195.
- , , , et al. Characteristics and short‐term prognosis of perioperative myocardial infarction in patients undergoing noncardiac surgery. Ann Intern Med. 2011;154(8):523–528.
- , , , et al. Liberal or restrictive transfusion in high‐risk patients after hip surgery. N Engl J Med. 2011;365(26):2453–2462.
- , , , . Inpatient hospital admission and death after outpatient surgery in elderly patients: importance of patient and system characteristics and location of care. Arch Surg. 2004;139(1):67–72.
- , , , et al. Predictors of hospital mortality in the global registry of acute coronary events. Arch Intern Med. 2003;163(19):2345–2353.
- , , , et al. Impact of age on perioperative complications and length of stay in patients undergoing noncardiac surgery. Ann Intern Med. 2001;134(8):637–643.
- , , , et al. Meta‐analysis: excess mortality after hip fracture among older women and men. Ann Intern Med. 2010;152(6):380–390.
- , , , et al. Body mass index (BMI) and risk of noncardiac postoperative medical complications in elderly hip fracture patients: a population‐based study. J Hosp Med. 2009;4(8):E1–E9.
- . History of the Rochester Epidemiology Project. Mayo Clin Proc. 1996;71(3):266–274.
- , , , . Incidence and mortality of hip fractures in the United States. JAMA. 2009;302(14):1573–1579.
- , , , et al. Body mass index and risk of adverse cardiac events in elderly patients with hip fracture: a population‐based study. J Am Geriatr Soc. 2009;57(3):419–426.
- , , , et al. Acute coronary care in the elderly, part I. Non‐ST‐segment‐elevation acute coronary syndromes: a scientific statement for healthcare professionals from the American Heart Association Council on Clinical Cardiology: in collaboration with the Society of Geriatric Cardiology. Circulation. 2007;115(19):2549–2569.
- , . Hip fracture mortality. A prospective, multifactorial study to predict and minimize death risk. Clin Orthop Relat Res. 1992;280:214–222.
- , , , et al. ACC/AHA/ACP‐ASIM guidelines for the management of patients with chronic stable angina. J Am Coll Cardiol. 1999;33(7):2092–2190.
- , , ; for the Joint ESC/ACCF/AHA/WHF Task Force for the Redefinition of Myocardial Infarction. Universal definition of myocardial infarction. J Am Coll Cardiol. 2007;50(22):2173–2195.
- , , , et al. Characteristics and short‐term prognosis of perioperative myocardial infarction in patients undergoing noncardiac surgery. Ann Intern Med. 2011;154(8):523–528.
- , , , et al. Liberal or restrictive transfusion in high‐risk patients after hip surgery. N Engl J Med. 2011;365(26):2453–2462.
- , , , . Inpatient hospital admission and death after outpatient surgery in elderly patients: importance of patient and system characteristics and location of care. Arch Surg. 2004;139(1):67–72.
- , , , et al. Predictors of hospital mortality in the global registry of acute coronary events. Arch Intern Med. 2003;163(19):2345–2353.
Ask-Tell-Ask: Simple Technique Can Help Hospitalists Communicate Difficult Messages
Sometimes a hospitalist is put in the difficult position of communicating information that involves bad news—for instance, a poor prognosis to a patient or clarifying treatment options and goals for care to a family member of a patient with an advanced illness. A workshop at HM12 offered a technique that hospitalists can use to convey such difficult messages.
“Ask-Tell-Ask” is a back-and-forth cycle between the patient and health professional that addresses four essential components: the patient’s perspective, information that needs to be delivered, response to the patient’s emotions, and recommendations by the professional.
—Kristen Schaefer, MD, palliative-care physician, Brigham and Women’s Hospital, Boston
“In the setting of an advanced illness, the patient’s perspective needs to be more fully explored so that we can figure out what information they need and want,” says Kristen Schaefer, MD, a palliative-care physician and director of residency education at Brigham and Women’s Hospital in Boston who spoke at an HM12 workshop. “That communication needs to be multidirectional to promote shared decision-making. All of these communication techniques are based on a better understanding of the patient’s perspective, but with Ask-Tell-Ask, you are clarifying their emotional response to illness, their values and personal goals in life, and how they cope with setbacks.”
Physicians should always start in an open-ended way, asking questions and listening to the response, Dr. Schaefer explains. “Then you can tailor the information you provide to what they have told you. There’s always emotional content around these issues, and you need to clarify that emotion,” she says. “If there is a big emotion in the room, and it hasn’t been addressed, it doesn’t matter what you teach the patient. You’ll never get to the underlying problems.”
Another effective technique, Dr. Schaefer says, is the judicious use of silence. She says healthcare providers can learn to listen more, talk less, and always start with the patient’s perspective as the basis for communication.
“It makes for more satisfying work—and it’s also more effective,” she says.
Larry Beresford is a freelance writer in Oakland, Calif.
Sometimes a hospitalist is put in the difficult position of communicating information that involves bad news—for instance, a poor prognosis to a patient or clarifying treatment options and goals for care to a family member of a patient with an advanced illness. A workshop at HM12 offered a technique that hospitalists can use to convey such difficult messages.
“Ask-Tell-Ask” is a back-and-forth cycle between the patient and health professional that addresses four essential components: the patient’s perspective, information that needs to be delivered, response to the patient’s emotions, and recommendations by the professional.
—Kristen Schaefer, MD, palliative-care physician, Brigham and Women’s Hospital, Boston
“In the setting of an advanced illness, the patient’s perspective needs to be more fully explored so that we can figure out what information they need and want,” says Kristen Schaefer, MD, a palliative-care physician and director of residency education at Brigham and Women’s Hospital in Boston who spoke at an HM12 workshop. “That communication needs to be multidirectional to promote shared decision-making. All of these communication techniques are based on a better understanding of the patient’s perspective, but with Ask-Tell-Ask, you are clarifying their emotional response to illness, their values and personal goals in life, and how they cope with setbacks.”
Physicians should always start in an open-ended way, asking questions and listening to the response, Dr. Schaefer explains. “Then you can tailor the information you provide to what they have told you. There’s always emotional content around these issues, and you need to clarify that emotion,” she says. “If there is a big emotion in the room, and it hasn’t been addressed, it doesn’t matter what you teach the patient. You’ll never get to the underlying problems.”
Another effective technique, Dr. Schaefer says, is the judicious use of silence. She says healthcare providers can learn to listen more, talk less, and always start with the patient’s perspective as the basis for communication.
“It makes for more satisfying work—and it’s also more effective,” she says.
Larry Beresford is a freelance writer in Oakland, Calif.
Sometimes a hospitalist is put in the difficult position of communicating information that involves bad news—for instance, a poor prognosis to a patient or clarifying treatment options and goals for care to a family member of a patient with an advanced illness. A workshop at HM12 offered a technique that hospitalists can use to convey such difficult messages.
“Ask-Tell-Ask” is a back-and-forth cycle between the patient and health professional that addresses four essential components: the patient’s perspective, information that needs to be delivered, response to the patient’s emotions, and recommendations by the professional.
—Kristen Schaefer, MD, palliative-care physician, Brigham and Women’s Hospital, Boston
“In the setting of an advanced illness, the patient’s perspective needs to be more fully explored so that we can figure out what information they need and want,” says Kristen Schaefer, MD, a palliative-care physician and director of residency education at Brigham and Women’s Hospital in Boston who spoke at an HM12 workshop. “That communication needs to be multidirectional to promote shared decision-making. All of these communication techniques are based on a better understanding of the patient’s perspective, but with Ask-Tell-Ask, you are clarifying their emotional response to illness, their values and personal goals in life, and how they cope with setbacks.”
Physicians should always start in an open-ended way, asking questions and listening to the response, Dr. Schaefer explains. “Then you can tailor the information you provide to what they have told you. There’s always emotional content around these issues, and you need to clarify that emotion,” she says. “If there is a big emotion in the room, and it hasn’t been addressed, it doesn’t matter what you teach the patient. You’ll never get to the underlying problems.”
Another effective technique, Dr. Schaefer says, is the judicious use of silence. She says healthcare providers can learn to listen more, talk less, and always start with the patient’s perspective as the basis for communication.
“It makes for more satisfying work—and it’s also more effective,” she says.
Larry Beresford is a freelance writer in Oakland, Calif.
Huber the Tuber
Recently, I had an office visit from a lovely 80-year-old woman, born and raised in Providence, R.I., whose past medical history included pulmonary tuberculosis for which she was sent to a sanatorium – 50 years ago.
Her TB had nothing to do with why she had come to see me. By and large, this is a really healthy patient whose only complaint was a 2-month history of right shoulder pain that turned out to be caused by rotator cuff tendonitis. But I lingered with her, and we chatted for awhile. She used to work at Veterans Affairs, processing claims and grievances so she was familiar with medical terminology and was in general a joy to talk with. And I was captivated by the progress in medicine that she represented.
Now, by the time I went to medical school, we were no longer sending patients to sanatoria. The word was as abstract a concept to me as, say, injecting intramuscular gold to treat rheumatic diseases. By the time I was in training, everyone in the developing world got a BCG vaccine, which prevents severe complications from TB but does not prevent infections. As long as I have been a physician, we have understood transmission well, have known about four-drug regimens, and were aware of drug-resistant TB (I am still floored when I read about XDR-TB, with the X being short for "extensively.")
Needless to say I was fascinated by her story.
When she was originally diagnosed more than half a century ago, this woman did not have the usual symptoms that we associate with active pulmonary tuberculosis. She had not had a cough and certainly did not have "wasting." She simply tripped one day and in doing so coughed up some blood. She was found to have disease in both apices and, subsequently, she spent 14 months in a local sanatorium. She remembers being treated with "PAS and streptomycin" (PAS being p-aminosalicylic acid), and "lots of fresh air."
Although tuberculosis is rare in the USA today, it was "so rampant that cautionary visual messages appeared in myriad public places, from offices to restrooms," according to the National Library of Medicine. "Huber the Tuber" was a mascot developed by TB patient and physician Harry Wilmer (1917-2005). In the educational pamphlet, Huber rides respiratory droplets along with his cohort "Nasty von Sputum, Rusty the Bloodyvitch, and Huey the Long Tuber." That final appellation is supposedly a reference to Sen. Huey Long, according to the NLM. (Can we still anthropomorphize bacteria into corrupt government officials?)
The discovery of Mycobacterium tuberculosis by German bacteriologist Dr. Robert Koch in 1882 led to a revolution of isolating patients, which in turn led to a decrease in transmission. In 1905, the American Sanatorium Association was formed – it still exists today as the American Thoracic Society! When the association started, there were 106 sanatoria in the United States, which provided 9,107 beds for patients. At its peak in 1954, there were 108,457 beds worsening (Am. J. Respir. Crit. Care Med. 2004:169;118-6). From a patient’s journal during time spent in a sanatorium in 1944, we know that there were only two rules for sanatorium residents:
1. Absolute and utter rest of mind and body – no bath, no movement except to toilet once a day, no sitting up except propped by pillows and semireclining, no deep breath. Lead the life of a log, in fact. Don’t try, therefore, to sew, knit, or write, except as occasional relief from reading and sleeping.
2. Eat nourishing food and have plenty of fresh air.
Not everyone got antibiotic treatment, unless their chest x-rays showed worsening. Some patients were treated with an induced pneumothorax, according to the women’s journal. Why this would be is not clear to me.
Then, in 1952, isoniazid was developed, and that was the start of the end of the sanatorium.
In our daily lives, we focus on individual patients, but history informs the current practice of medicine. How wonderful that we can now treat many illnesses that were once considered uniformly fatal. How fortunate are we to call this our profession, one that provides an unambiguous good.
Dr. Chan practices rheumatology in Pawtucket, R.I.
Recently, I had an office visit from a lovely 80-year-old woman, born and raised in Providence, R.I., whose past medical history included pulmonary tuberculosis for which she was sent to a sanatorium – 50 years ago.
Her TB had nothing to do with why she had come to see me. By and large, this is a really healthy patient whose only complaint was a 2-month history of right shoulder pain that turned out to be caused by rotator cuff tendonitis. But I lingered with her, and we chatted for awhile. She used to work at Veterans Affairs, processing claims and grievances so she was familiar with medical terminology and was in general a joy to talk with. And I was captivated by the progress in medicine that she represented.
Now, by the time I went to medical school, we were no longer sending patients to sanatoria. The word was as abstract a concept to me as, say, injecting intramuscular gold to treat rheumatic diseases. By the time I was in training, everyone in the developing world got a BCG vaccine, which prevents severe complications from TB but does not prevent infections. As long as I have been a physician, we have understood transmission well, have known about four-drug regimens, and were aware of drug-resistant TB (I am still floored when I read about XDR-TB, with the X being short for "extensively.")
Needless to say I was fascinated by her story.
When she was originally diagnosed more than half a century ago, this woman did not have the usual symptoms that we associate with active pulmonary tuberculosis. She had not had a cough and certainly did not have "wasting." She simply tripped one day and in doing so coughed up some blood. She was found to have disease in both apices and, subsequently, she spent 14 months in a local sanatorium. She remembers being treated with "PAS and streptomycin" (PAS being p-aminosalicylic acid), and "lots of fresh air."
Although tuberculosis is rare in the USA today, it was "so rampant that cautionary visual messages appeared in myriad public places, from offices to restrooms," according to the National Library of Medicine. "Huber the Tuber" was a mascot developed by TB patient and physician Harry Wilmer (1917-2005). In the educational pamphlet, Huber rides respiratory droplets along with his cohort "Nasty von Sputum, Rusty the Bloodyvitch, and Huey the Long Tuber." That final appellation is supposedly a reference to Sen. Huey Long, according to the NLM. (Can we still anthropomorphize bacteria into corrupt government officials?)
The discovery of Mycobacterium tuberculosis by German bacteriologist Dr. Robert Koch in 1882 led to a revolution of isolating patients, which in turn led to a decrease in transmission. In 1905, the American Sanatorium Association was formed – it still exists today as the American Thoracic Society! When the association started, there were 106 sanatoria in the United States, which provided 9,107 beds for patients. At its peak in 1954, there were 108,457 beds worsening (Am. J. Respir. Crit. Care Med. 2004:169;118-6). From a patient’s journal during time spent in a sanatorium in 1944, we know that there were only two rules for sanatorium residents:
1. Absolute and utter rest of mind and body – no bath, no movement except to toilet once a day, no sitting up except propped by pillows and semireclining, no deep breath. Lead the life of a log, in fact. Don’t try, therefore, to sew, knit, or write, except as occasional relief from reading and sleeping.
2. Eat nourishing food and have plenty of fresh air.
Not everyone got antibiotic treatment, unless their chest x-rays showed worsening. Some patients were treated with an induced pneumothorax, according to the women’s journal. Why this would be is not clear to me.
Then, in 1952, isoniazid was developed, and that was the start of the end of the sanatorium.
In our daily lives, we focus on individual patients, but history informs the current practice of medicine. How wonderful that we can now treat many illnesses that were once considered uniformly fatal. How fortunate are we to call this our profession, one that provides an unambiguous good.
Dr. Chan practices rheumatology in Pawtucket, R.I.
Recently, I had an office visit from a lovely 80-year-old woman, born and raised in Providence, R.I., whose past medical history included pulmonary tuberculosis for which she was sent to a sanatorium – 50 years ago.
Her TB had nothing to do with why she had come to see me. By and large, this is a really healthy patient whose only complaint was a 2-month history of right shoulder pain that turned out to be caused by rotator cuff tendonitis. But I lingered with her, and we chatted for awhile. She used to work at Veterans Affairs, processing claims and grievances so she was familiar with medical terminology and was in general a joy to talk with. And I was captivated by the progress in medicine that she represented.
Now, by the time I went to medical school, we were no longer sending patients to sanatoria. The word was as abstract a concept to me as, say, injecting intramuscular gold to treat rheumatic diseases. By the time I was in training, everyone in the developing world got a BCG vaccine, which prevents severe complications from TB but does not prevent infections. As long as I have been a physician, we have understood transmission well, have known about four-drug regimens, and were aware of drug-resistant TB (I am still floored when I read about XDR-TB, with the X being short for "extensively.")
Needless to say I was fascinated by her story.
When she was originally diagnosed more than half a century ago, this woman did not have the usual symptoms that we associate with active pulmonary tuberculosis. She had not had a cough and certainly did not have "wasting." She simply tripped one day and in doing so coughed up some blood. She was found to have disease in both apices and, subsequently, she spent 14 months in a local sanatorium. She remembers being treated with "PAS and streptomycin" (PAS being p-aminosalicylic acid), and "lots of fresh air."
Although tuberculosis is rare in the USA today, it was "so rampant that cautionary visual messages appeared in myriad public places, from offices to restrooms," according to the National Library of Medicine. "Huber the Tuber" was a mascot developed by TB patient and physician Harry Wilmer (1917-2005). In the educational pamphlet, Huber rides respiratory droplets along with his cohort "Nasty von Sputum, Rusty the Bloodyvitch, and Huey the Long Tuber." That final appellation is supposedly a reference to Sen. Huey Long, according to the NLM. (Can we still anthropomorphize bacteria into corrupt government officials?)
The discovery of Mycobacterium tuberculosis by German bacteriologist Dr. Robert Koch in 1882 led to a revolution of isolating patients, which in turn led to a decrease in transmission. In 1905, the American Sanatorium Association was formed – it still exists today as the American Thoracic Society! When the association started, there were 106 sanatoria in the United States, which provided 9,107 beds for patients. At its peak in 1954, there were 108,457 beds worsening (Am. J. Respir. Crit. Care Med. 2004:169;118-6). From a patient’s journal during time spent in a sanatorium in 1944, we know that there were only two rules for sanatorium residents:
1. Absolute and utter rest of mind and body – no bath, no movement except to toilet once a day, no sitting up except propped by pillows and semireclining, no deep breath. Lead the life of a log, in fact. Don’t try, therefore, to sew, knit, or write, except as occasional relief from reading and sleeping.
2. Eat nourishing food and have plenty of fresh air.
Not everyone got antibiotic treatment, unless their chest x-rays showed worsening. Some patients were treated with an induced pneumothorax, according to the women’s journal. Why this would be is not clear to me.
Then, in 1952, isoniazid was developed, and that was the start of the end of the sanatorium.
In our daily lives, we focus on individual patients, but history informs the current practice of medicine. How wonderful that we can now treat many illnesses that were once considered uniformly fatal. How fortunate are we to call this our profession, one that provides an unambiguous good.
Dr. Chan practices rheumatology in Pawtucket, R.I.
Hospitalists Play Integral Roles in HHS-Funded Innovation Projects
In May and June, U.S. Department of Health and Human Services (HHS) Secretary Kathleen Sebelius in May and June announced 107 healthcare innovations grants to improve coordination of care and reduce costs. The grants, a provision of the Affordable Care Act (ACA), range from $1 million to $30 million. HHS anticipates that the projects will reduce healthcare spending by $254 million over the next three years and provide "new ideas on how to deliver better health, improved care, and lower costs to people enrolled in Medicare, Medicaid and [the] Children's Health Insurance Program (CHIP)."
Hospitalists played key roles in planning and developing several of the projects. Common themes include coordination and integration of services, promotion of community collaborations, integrating behavioral and physical care, and the use of telemedicine—many of the same approaches utilized by SHM's Project BOOST and other national initiatives for preventing unnecessary readmissions.
In Atlanta, Emory University's Center for Critical Care received a $10.7 million grant to deploy 40 nurse practitioners (NPs) and physician assistants (PAs) trained in critical care to underserved and rural ICUs in Georgia. In many of the targeted hospitals, hospitalists manage patients in the ICU, but this program brings an additional layer of staffing and expertise to the care, allowing patients to stay in their beds rather than having to be transferred, says Daniel Owens, MBA, the center’s director of operations and senior administrator of the division of hospital medicine at Emory.
The project will bring NPs and PAs from participating hospitals to Emory for an intensive, six-month, critical-care residency. "If they don't have these folks, we'll help to identify staff for the jobs," he adds.
At Vanderbilt University Medical Center in Nashville, Tenn., a $2.4 million project to reduce rehospitalizations for a high-risk geriatric patients aims to close the gaps in care transitions between hospital, outpatient, post-acute, and extended-care settings, says Vanderbilt hospitalist Eduard Vasilevskis, MD. The project will employ transition advocates or coordinators in the hospital to improve communication at both ends, with evidence-based protocols to improve discharge planning. Long-term care providers will be offered Web-based training and video conferencing.
"The goal is to break the cycle of rehospitalization," says Dr. Vasilevskis, "but if patients need to come back to the hospital, there will be someone involved in their care who is familiar with the settings where they’ve come from."
Beth Israel Deaconess Medical Center (BIDMC) in Boston received $4.9 million for its Post-Acute Care Transitions program (PACT), which links the hospital to six affiliated primary care practices using a bundle of post-acute care interventions, care-transition specialists, and dedicated clinical pharmacists. Nurses remain in contact with patients by telephone for 30 days post-hospital discharge and coordinate the services of extended-care facilities and visiting nurses. Pharmacists perform in-hospital medication reconciliation and patient education, says hospitalist Lauren Doctoroff, MD, FHM. She and Julius Yang, MD, BIDMC medical director of inpatient quality, helped develop the pilot program, which began in August 2011.
"These care-transitions specialists offer us an added level of patient support and a different level of integration focused on risk assessment of such issues as social supports and problems with medical compliance, which can be used by the inpatient team to come up with the most rational and ideal discharge plan," Dr. Doctoroff says. "One of my colleagues said to me, ‘I feel so much better knowing there is this added level of support for patients after discharge.'"
The HHS grants reflect an important recognition that what happens to patients following discharge partly reflects what happens in the hospital but also depends on collaborations with post-acute providers, Dr. Doctoroff says.
"Hospitalists can't do everything, but they need their eye out of the hospital on post-acute providers in order to deliver the best care," she adds.
In May and June, U.S. Department of Health and Human Services (HHS) Secretary Kathleen Sebelius in May and June announced 107 healthcare innovations grants to improve coordination of care and reduce costs. The grants, a provision of the Affordable Care Act (ACA), range from $1 million to $30 million. HHS anticipates that the projects will reduce healthcare spending by $254 million over the next three years and provide "new ideas on how to deliver better health, improved care, and lower costs to people enrolled in Medicare, Medicaid and [the] Children's Health Insurance Program (CHIP)."
Hospitalists played key roles in planning and developing several of the projects. Common themes include coordination and integration of services, promotion of community collaborations, integrating behavioral and physical care, and the use of telemedicine—many of the same approaches utilized by SHM's Project BOOST and other national initiatives for preventing unnecessary readmissions.
In Atlanta, Emory University's Center for Critical Care received a $10.7 million grant to deploy 40 nurse practitioners (NPs) and physician assistants (PAs) trained in critical care to underserved and rural ICUs in Georgia. In many of the targeted hospitals, hospitalists manage patients in the ICU, but this program brings an additional layer of staffing and expertise to the care, allowing patients to stay in their beds rather than having to be transferred, says Daniel Owens, MBA, the center’s director of operations and senior administrator of the division of hospital medicine at Emory.
The project will bring NPs and PAs from participating hospitals to Emory for an intensive, six-month, critical-care residency. "If they don't have these folks, we'll help to identify staff for the jobs," he adds.
At Vanderbilt University Medical Center in Nashville, Tenn., a $2.4 million project to reduce rehospitalizations for a high-risk geriatric patients aims to close the gaps in care transitions between hospital, outpatient, post-acute, and extended-care settings, says Vanderbilt hospitalist Eduard Vasilevskis, MD. The project will employ transition advocates or coordinators in the hospital to improve communication at both ends, with evidence-based protocols to improve discharge planning. Long-term care providers will be offered Web-based training and video conferencing.
"The goal is to break the cycle of rehospitalization," says Dr. Vasilevskis, "but if patients need to come back to the hospital, there will be someone involved in their care who is familiar with the settings where they’ve come from."
Beth Israel Deaconess Medical Center (BIDMC) in Boston received $4.9 million for its Post-Acute Care Transitions program (PACT), which links the hospital to six affiliated primary care practices using a bundle of post-acute care interventions, care-transition specialists, and dedicated clinical pharmacists. Nurses remain in contact with patients by telephone for 30 days post-hospital discharge and coordinate the services of extended-care facilities and visiting nurses. Pharmacists perform in-hospital medication reconciliation and patient education, says hospitalist Lauren Doctoroff, MD, FHM. She and Julius Yang, MD, BIDMC medical director of inpatient quality, helped develop the pilot program, which began in August 2011.
"These care-transitions specialists offer us an added level of patient support and a different level of integration focused on risk assessment of such issues as social supports and problems with medical compliance, which can be used by the inpatient team to come up with the most rational and ideal discharge plan," Dr. Doctoroff says. "One of my colleagues said to me, ‘I feel so much better knowing there is this added level of support for patients after discharge.'"
The HHS grants reflect an important recognition that what happens to patients following discharge partly reflects what happens in the hospital but also depends on collaborations with post-acute providers, Dr. Doctoroff says.
"Hospitalists can't do everything, but they need their eye out of the hospital on post-acute providers in order to deliver the best care," she adds.
In May and June, U.S. Department of Health and Human Services (HHS) Secretary Kathleen Sebelius in May and June announced 107 healthcare innovations grants to improve coordination of care and reduce costs. The grants, a provision of the Affordable Care Act (ACA), range from $1 million to $30 million. HHS anticipates that the projects will reduce healthcare spending by $254 million over the next three years and provide "new ideas on how to deliver better health, improved care, and lower costs to people enrolled in Medicare, Medicaid and [the] Children's Health Insurance Program (CHIP)."
Hospitalists played key roles in planning and developing several of the projects. Common themes include coordination and integration of services, promotion of community collaborations, integrating behavioral and physical care, and the use of telemedicine—many of the same approaches utilized by SHM's Project BOOST and other national initiatives for preventing unnecessary readmissions.
In Atlanta, Emory University's Center for Critical Care received a $10.7 million grant to deploy 40 nurse practitioners (NPs) and physician assistants (PAs) trained in critical care to underserved and rural ICUs in Georgia. In many of the targeted hospitals, hospitalists manage patients in the ICU, but this program brings an additional layer of staffing and expertise to the care, allowing patients to stay in their beds rather than having to be transferred, says Daniel Owens, MBA, the center’s director of operations and senior administrator of the division of hospital medicine at Emory.
The project will bring NPs and PAs from participating hospitals to Emory for an intensive, six-month, critical-care residency. "If they don't have these folks, we'll help to identify staff for the jobs," he adds.
At Vanderbilt University Medical Center in Nashville, Tenn., a $2.4 million project to reduce rehospitalizations for a high-risk geriatric patients aims to close the gaps in care transitions between hospital, outpatient, post-acute, and extended-care settings, says Vanderbilt hospitalist Eduard Vasilevskis, MD. The project will employ transition advocates or coordinators in the hospital to improve communication at both ends, with evidence-based protocols to improve discharge planning. Long-term care providers will be offered Web-based training and video conferencing.
"The goal is to break the cycle of rehospitalization," says Dr. Vasilevskis, "but if patients need to come back to the hospital, there will be someone involved in their care who is familiar with the settings where they’ve come from."
Beth Israel Deaconess Medical Center (BIDMC) in Boston received $4.9 million for its Post-Acute Care Transitions program (PACT), which links the hospital to six affiliated primary care practices using a bundle of post-acute care interventions, care-transition specialists, and dedicated clinical pharmacists. Nurses remain in contact with patients by telephone for 30 days post-hospital discharge and coordinate the services of extended-care facilities and visiting nurses. Pharmacists perform in-hospital medication reconciliation and patient education, says hospitalist Lauren Doctoroff, MD, FHM. She and Julius Yang, MD, BIDMC medical director of inpatient quality, helped develop the pilot program, which began in August 2011.
"These care-transitions specialists offer us an added level of patient support and a different level of integration focused on risk assessment of such issues as social supports and problems with medical compliance, which can be used by the inpatient team to come up with the most rational and ideal discharge plan," Dr. Doctoroff says. "One of my colleagues said to me, ‘I feel so much better knowing there is this added level of support for patients after discharge.'"
The HHS grants reflect an important recognition that what happens to patients following discharge partly reflects what happens in the hospital but also depends on collaborations with post-acute providers, Dr. Doctoroff says.
"Hospitalists can't do everything, but they need their eye out of the hospital on post-acute providers in order to deliver the best care," she adds.
ITL: Physician Reviews of HM-Relevant Research
Clinical question: Does treatment with drotrecogin alfa (activated) reduce mortality in patients with septic shock?
Background: Recombinant human activated protein C, or drotrecogin alfa (activated) (DrotAA), was approved for the treatment of patients with severe sepsis in 2001 on the basis of the Prospective Recombinant Human Activated Protein C Worldwide Evaluation in Severe Sepsis (PROWESS) study. Since approval, conflicting reports about its efficacy have surfaced.
Study design: Double-blind, randomized-controlled trial.
Setting: Multicenter, multinational trial.
Synopsis: This trial enrolled 1,697 patients with septic shock to receive either DrotAA or placebo. At 28 days, 223 of 846 patients (26.4%) in the DrotAA group and 202 of 834 (24.2%) in the placebo group had died (relative risk in the DrotAA group, 1.09; 95% confidence interval, 0.92 to 1.28; P=0.31). At 90 days, there was still no significant difference in mortality. Mortality was also unchanged in patients with severe protein C deficiency at baseline. This lack of mortality benefit with either therapy persisted across all predefined subgroups in this study.
The incidence of non-serious bleeding was more common among patients who received DrotAA than among those in the placebo group (8.6% vs. 4.8%, P=0.002), but the incidence of serious bleeding events was similar in both groups. This study was appropriately powered after adjusting the sample size when aggregate mortality was found to be lower than anticipated.
Bottom line: DrotAA does not significantly reduce mortality at 28 or 90 days in patients with septic shock.
Citation: Ranieri VM, Thompson BT, Barie PS, et al. Drotrecogin alfa (activated) in adults with septic shock. N Engl J Med. 2012;366:2055-2064.
Read more of our physician reviews of recent, HM-relevant literature.
Clinical question: Does treatment with drotrecogin alfa (activated) reduce mortality in patients with septic shock?
Background: Recombinant human activated protein C, or drotrecogin alfa (activated) (DrotAA), was approved for the treatment of patients with severe sepsis in 2001 on the basis of the Prospective Recombinant Human Activated Protein C Worldwide Evaluation in Severe Sepsis (PROWESS) study. Since approval, conflicting reports about its efficacy have surfaced.
Study design: Double-blind, randomized-controlled trial.
Setting: Multicenter, multinational trial.
Synopsis: This trial enrolled 1,697 patients with septic shock to receive either DrotAA or placebo. At 28 days, 223 of 846 patients (26.4%) in the DrotAA group and 202 of 834 (24.2%) in the placebo group had died (relative risk in the DrotAA group, 1.09; 95% confidence interval, 0.92 to 1.28; P=0.31). At 90 days, there was still no significant difference in mortality. Mortality was also unchanged in patients with severe protein C deficiency at baseline. This lack of mortality benefit with either therapy persisted across all predefined subgroups in this study.
The incidence of non-serious bleeding was more common among patients who received DrotAA than among those in the placebo group (8.6% vs. 4.8%, P=0.002), but the incidence of serious bleeding events was similar in both groups. This study was appropriately powered after adjusting the sample size when aggregate mortality was found to be lower than anticipated.
Bottom line: DrotAA does not significantly reduce mortality at 28 or 90 days in patients with septic shock.
Citation: Ranieri VM, Thompson BT, Barie PS, et al. Drotrecogin alfa (activated) in adults with septic shock. N Engl J Med. 2012;366:2055-2064.
Read more of our physician reviews of recent, HM-relevant literature.
Clinical question: Does treatment with drotrecogin alfa (activated) reduce mortality in patients with septic shock?
Background: Recombinant human activated protein C, or drotrecogin alfa (activated) (DrotAA), was approved for the treatment of patients with severe sepsis in 2001 on the basis of the Prospective Recombinant Human Activated Protein C Worldwide Evaluation in Severe Sepsis (PROWESS) study. Since approval, conflicting reports about its efficacy have surfaced.
Study design: Double-blind, randomized-controlled trial.
Setting: Multicenter, multinational trial.
Synopsis: This trial enrolled 1,697 patients with septic shock to receive either DrotAA or placebo. At 28 days, 223 of 846 patients (26.4%) in the DrotAA group and 202 of 834 (24.2%) in the placebo group had died (relative risk in the DrotAA group, 1.09; 95% confidence interval, 0.92 to 1.28; P=0.31). At 90 days, there was still no significant difference in mortality. Mortality was also unchanged in patients with severe protein C deficiency at baseline. This lack of mortality benefit with either therapy persisted across all predefined subgroups in this study.
The incidence of non-serious bleeding was more common among patients who received DrotAA than among those in the placebo group (8.6% vs. 4.8%, P=0.002), but the incidence of serious bleeding events was similar in both groups. This study was appropriately powered after adjusting the sample size when aggregate mortality was found to be lower than anticipated.
Bottom line: DrotAA does not significantly reduce mortality at 28 or 90 days in patients with septic shock.
Citation: Ranieri VM, Thompson BT, Barie PS, et al. Drotrecogin alfa (activated) in adults with septic shock. N Engl J Med. 2012;366:2055-2064.
Read more of our physician reviews of recent, HM-relevant literature.
You Need a Budget
For many years, I chaired the office efficiency course at the American Academy of Dermatology’s annual meeting. Each year, I asked how many participants compiled a yearly budget for their practices. In an audience of 400, the largest affirmative response I ever received was three, and some years there were no raised hands at all.
Why do physicians so vigorously resist an exercise that is so basic to every other business and profession on the planet? Typically, I hear one of two reasons: It’s tedious, or my colleagues seem to be doing just fine without one.
But the days of "doing just fine" are coming to an end. As competition for patients increases, expenses continue their upward spiral, and the government continues its steady encroachment on private practice, physicians who plan ahead will have an advantage.
Budgeting need not be tedious; determine what you need to do yourself and what can be delegated. And now, as the year winds down, is an excellent opportunity to map out your finances.
The first step – the basic gathering of numbers that everyone seems to dread – can be delegated. Ask your accountant to compile the practice’s gross income over the last 12 months, in monthly increments.
Break it down by type of service: office visits, hospital visits, surgery, lab fees, and so on, listing both the amounts billed and collected. This is not only for calculations of collection ratios, but to determine your "seasonality" – which I’ll discuss in greater detail next month. Do the same for expenses, and again break them down by category: salaries, rent/mortgage, business and medical supplies, and so on.
In many cases, the mere collection of this raw data will save money. You might discover, for example, that expenditures for business supplies are unexpectedly high. Perhaps a competing vendor can do better, or perhaps you have an overuse or theft problem.
Once the numbers are accumulated, start extrapolating them into next year. If your income rose by, say, 6% this year, can you expect a similar rise next year? Why or why not? To get a fix on a realistic goal, go through each component of your gross income and decide where the increase could come from. Can you raise prices for office visits or cosmetic procedures, renegotiate at least one third-party contract, or add another exam room in order to see more patients?
Perhaps there is an impending change in your area that you can factor in, such as a competitor who is retiring. If that physician is known for a specific service, and it’s not a service you offer, could you start?
You are, I hope, beginning to see that this exercise is well worth the effort. After you have mapped out income, turn to expenses. Perhaps some of the assumptions that you’ve made on income will affect expenses; for example, adding a new procedure may require the purchase of new equipment. If you have a higher census goal, you may need an additional assistant.
If you’re considering adding an associate, you can determine if he or she will bring in enough revenue to cover salary and expenses by completing two versions of next year’s projected budget – one with the associate and one without.
Once you have prepared your budget, follow it. Your accountant or manager can generate monthly spreadsheets comparing actual financials with projections, and the year-to-date, compared with previous years. There are many parameters to explore.
Look for deviations from predictions and possible reasons for them, such as factors you didn’t (or couldn’t) anticipate. Make a note of them; it will help you with next year’s projections.
A budget can be justified in two major ways: You’ll better understand where your practice is going, and the forces at work to change it. And you’ll become aware of unexpected events while there is still time to influence them, rather than making such discoveries well after the fact – or worse, never finding out at all.
Dr. Eastern practices dermatology and dermatologic surgery in Belleville, N.J.
For many years, I chaired the office efficiency course at the American Academy of Dermatology’s annual meeting. Each year, I asked how many participants compiled a yearly budget for their practices. In an audience of 400, the largest affirmative response I ever received was three, and some years there were no raised hands at all.
Why do physicians so vigorously resist an exercise that is so basic to every other business and profession on the planet? Typically, I hear one of two reasons: It’s tedious, or my colleagues seem to be doing just fine without one.
But the days of "doing just fine" are coming to an end. As competition for patients increases, expenses continue their upward spiral, and the government continues its steady encroachment on private practice, physicians who plan ahead will have an advantage.
Budgeting need not be tedious; determine what you need to do yourself and what can be delegated. And now, as the year winds down, is an excellent opportunity to map out your finances.
The first step – the basic gathering of numbers that everyone seems to dread – can be delegated. Ask your accountant to compile the practice’s gross income over the last 12 months, in monthly increments.
Break it down by type of service: office visits, hospital visits, surgery, lab fees, and so on, listing both the amounts billed and collected. This is not only for calculations of collection ratios, but to determine your "seasonality" – which I’ll discuss in greater detail next month. Do the same for expenses, and again break them down by category: salaries, rent/mortgage, business and medical supplies, and so on.
In many cases, the mere collection of this raw data will save money. You might discover, for example, that expenditures for business supplies are unexpectedly high. Perhaps a competing vendor can do better, or perhaps you have an overuse or theft problem.
Once the numbers are accumulated, start extrapolating them into next year. If your income rose by, say, 6% this year, can you expect a similar rise next year? Why or why not? To get a fix on a realistic goal, go through each component of your gross income and decide where the increase could come from. Can you raise prices for office visits or cosmetic procedures, renegotiate at least one third-party contract, or add another exam room in order to see more patients?
Perhaps there is an impending change in your area that you can factor in, such as a competitor who is retiring. If that physician is known for a specific service, and it’s not a service you offer, could you start?
You are, I hope, beginning to see that this exercise is well worth the effort. After you have mapped out income, turn to expenses. Perhaps some of the assumptions that you’ve made on income will affect expenses; for example, adding a new procedure may require the purchase of new equipment. If you have a higher census goal, you may need an additional assistant.
If you’re considering adding an associate, you can determine if he or she will bring in enough revenue to cover salary and expenses by completing two versions of next year’s projected budget – one with the associate and one without.
Once you have prepared your budget, follow it. Your accountant or manager can generate monthly spreadsheets comparing actual financials with projections, and the year-to-date, compared with previous years. There are many parameters to explore.
Look for deviations from predictions and possible reasons for them, such as factors you didn’t (or couldn’t) anticipate. Make a note of them; it will help you with next year’s projections.
A budget can be justified in two major ways: You’ll better understand where your practice is going, and the forces at work to change it. And you’ll become aware of unexpected events while there is still time to influence them, rather than making such discoveries well after the fact – or worse, never finding out at all.
Dr. Eastern practices dermatology and dermatologic surgery in Belleville, N.J.
For many years, I chaired the office efficiency course at the American Academy of Dermatology’s annual meeting. Each year, I asked how many participants compiled a yearly budget for their practices. In an audience of 400, the largest affirmative response I ever received was three, and some years there were no raised hands at all.
Why do physicians so vigorously resist an exercise that is so basic to every other business and profession on the planet? Typically, I hear one of two reasons: It’s tedious, or my colleagues seem to be doing just fine without one.
But the days of "doing just fine" are coming to an end. As competition for patients increases, expenses continue their upward spiral, and the government continues its steady encroachment on private practice, physicians who plan ahead will have an advantage.
Budgeting need not be tedious; determine what you need to do yourself and what can be delegated. And now, as the year winds down, is an excellent opportunity to map out your finances.
The first step – the basic gathering of numbers that everyone seems to dread – can be delegated. Ask your accountant to compile the practice’s gross income over the last 12 months, in monthly increments.
Break it down by type of service: office visits, hospital visits, surgery, lab fees, and so on, listing both the amounts billed and collected. This is not only for calculations of collection ratios, but to determine your "seasonality" – which I’ll discuss in greater detail next month. Do the same for expenses, and again break them down by category: salaries, rent/mortgage, business and medical supplies, and so on.
In many cases, the mere collection of this raw data will save money. You might discover, for example, that expenditures for business supplies are unexpectedly high. Perhaps a competing vendor can do better, or perhaps you have an overuse or theft problem.
Once the numbers are accumulated, start extrapolating them into next year. If your income rose by, say, 6% this year, can you expect a similar rise next year? Why or why not? To get a fix on a realistic goal, go through each component of your gross income and decide where the increase could come from. Can you raise prices for office visits or cosmetic procedures, renegotiate at least one third-party contract, or add another exam room in order to see more patients?
Perhaps there is an impending change in your area that you can factor in, such as a competitor who is retiring. If that physician is known for a specific service, and it’s not a service you offer, could you start?
You are, I hope, beginning to see that this exercise is well worth the effort. After you have mapped out income, turn to expenses. Perhaps some of the assumptions that you’ve made on income will affect expenses; for example, adding a new procedure may require the purchase of new equipment. If you have a higher census goal, you may need an additional assistant.
If you’re considering adding an associate, you can determine if he or she will bring in enough revenue to cover salary and expenses by completing two versions of next year’s projected budget – one with the associate and one without.
Once you have prepared your budget, follow it. Your accountant or manager can generate monthly spreadsheets comparing actual financials with projections, and the year-to-date, compared with previous years. There are many parameters to explore.
Look for deviations from predictions and possible reasons for them, such as factors you didn’t (or couldn’t) anticipate. Make a note of them; it will help you with next year’s projections.
A budget can be justified in two major ways: You’ll better understand where your practice is going, and the forces at work to change it. And you’ll become aware of unexpected events while there is still time to influence them, rather than making such discoveries well after the fact – or worse, never finding out at all.
Dr. Eastern practices dermatology and dermatologic surgery in Belleville, N.J.

Two Forms of Contraception
Until last month, I had only ever had two positive pregnancy test results in women of child-bearing age taking isotretinoin. Both of the previous reports came in on the same day, one after the other. When I called each patient to give her the results, and asked her to repeat the test, neither was at all perturbed. "If I’m pregnant," laughed one, "it would be another Immaculate Conception."
Both results turned out to be laboratory errors committed by a single technician, who was reported and rebuked. Repeat tests were negative.
Then, last month, I got another positive. Victoria had actually completed her treatment course 6 weeks earlier, and had already obtained a 30-day post-treatment test – which was negative. Then, she had another test done a few weeks later, which was positive.
I called and got her mother, who asked, "Is everything all right?" But Victoria is 19, so I just said I needed her daughter’s cell phone number.
"We had a condom accident," Victoria said when I reached her. We reviewed her case, determining the last day she had actually taken the medication. Her sexual activity had clearly taken place more than 30 days later.
I suggested she contact her gynecologist at once, to be evaluated and to have the pregnancy test repeated, and I faxed a note to that physician with the relevant details. "If pregnancy is confirmed," I told her, "I’m sure you’ll consider many things before you decide what to do. But one thing you don’t have to factor in is your isotretinoin treatment, because it was no longer in your blood when you became pregnant."
A few days later, Victoria came to my office. "I’ve decided to end the pregnancy," she said. "This just isn’t the right time."
I told her I understood. "By the way," I said, "you listed your two methods of contraception as the patch and condoms. So even if the condom failed, it looks like the patch did too."
"No," said Victoria, "I wasn’t on the patch anymore."
"What?!" I exclaimed.
"I ran out a month earlier," she said, "and my regular doctor was out on maternity leave."
"Wasn’t there anyone else in her office who could refill it for you?" I asked.
"I guess so," she said, "but I kept calling and pushing the button for ‘prescription refills,’ and no one ever called back."
I tried my best not to shake my head in disbelief. Victoria is an intelligent young woman. There is no language barrier. We had discussed contraception before she started therapy, and she signed all the right forms. Each month she got a pregnancy test. Each month she went online and answered the contraceptive-related questions before she could get more isotretinoin.
And when she ran out of contraceptive patches, she didn’t get them refilled.
Victoria’s story could have been worse. She might have become pregnant while still taking isotretinoin. She might have been forced to make a decision to terminate a pregnancy she otherwise would have wanted to carry to term.
Victoria’s story speaks for itself. Despite our best efforts, persuasive or bureaucratic, people will sometimes act in ways that they themselves know perfectly well are against their own interests.
The newest iPledge program upgrade includes some changes, some of which are helpful. One novelty, however, is that if "Abstinence" is the first form of contraception, "None" automatically becomes the second – there is a new warning that this is "Not recommended." This means we should not rely on a patient’s self-reported abstinence, but are better off relying on her use of artificial contraception. Perhaps. But perhaps not. Contraception only works if you use it.
Humans have what a psychiatrist I know calls "design flaws." If ever called upon to redesign the species, I’m sure many of us would contribute some good ideas. In the meantime, however, all we can do is try to acknowledge these flaws, and do our best to mitigate their impact.
After all, we have them ourselves.
Dr. Rockoff practices dermatology in Brookline, Mass.
Until last month, I had only ever had two positive pregnancy test results in women of child-bearing age taking isotretinoin. Both of the previous reports came in on the same day, one after the other. When I called each patient to give her the results, and asked her to repeat the test, neither was at all perturbed. "If I’m pregnant," laughed one, "it would be another Immaculate Conception."
Both results turned out to be laboratory errors committed by a single technician, who was reported and rebuked. Repeat tests were negative.
Then, last month, I got another positive. Victoria had actually completed her treatment course 6 weeks earlier, and had already obtained a 30-day post-treatment test – which was negative. Then, she had another test done a few weeks later, which was positive.
I called and got her mother, who asked, "Is everything all right?" But Victoria is 19, so I just said I needed her daughter’s cell phone number.
"We had a condom accident," Victoria said when I reached her. We reviewed her case, determining the last day she had actually taken the medication. Her sexual activity had clearly taken place more than 30 days later.
I suggested she contact her gynecologist at once, to be evaluated and to have the pregnancy test repeated, and I faxed a note to that physician with the relevant details. "If pregnancy is confirmed," I told her, "I’m sure you’ll consider many things before you decide what to do. But one thing you don’t have to factor in is your isotretinoin treatment, because it was no longer in your blood when you became pregnant."
A few days later, Victoria came to my office. "I’ve decided to end the pregnancy," she said. "This just isn’t the right time."
I told her I understood. "By the way," I said, "you listed your two methods of contraception as the patch and condoms. So even if the condom failed, it looks like the patch did too."
"No," said Victoria, "I wasn’t on the patch anymore."
"What?!" I exclaimed.
"I ran out a month earlier," she said, "and my regular doctor was out on maternity leave."
"Wasn’t there anyone else in her office who could refill it for you?" I asked.
"I guess so," she said, "but I kept calling and pushing the button for ‘prescription refills,’ and no one ever called back."
I tried my best not to shake my head in disbelief. Victoria is an intelligent young woman. There is no language barrier. We had discussed contraception before she started therapy, and she signed all the right forms. Each month she got a pregnancy test. Each month she went online and answered the contraceptive-related questions before she could get more isotretinoin.
And when she ran out of contraceptive patches, she didn’t get them refilled.
Victoria’s story could have been worse. She might have become pregnant while still taking isotretinoin. She might have been forced to make a decision to terminate a pregnancy she otherwise would have wanted to carry to term.
Victoria’s story speaks for itself. Despite our best efforts, persuasive or bureaucratic, people will sometimes act in ways that they themselves know perfectly well are against their own interests.
The newest iPledge program upgrade includes some changes, some of which are helpful. One novelty, however, is that if "Abstinence" is the first form of contraception, "None" automatically becomes the second – there is a new warning that this is "Not recommended." This means we should not rely on a patient’s self-reported abstinence, but are better off relying on her use of artificial contraception. Perhaps. But perhaps not. Contraception only works if you use it.
Humans have what a psychiatrist I know calls "design flaws." If ever called upon to redesign the species, I’m sure many of us would contribute some good ideas. In the meantime, however, all we can do is try to acknowledge these flaws, and do our best to mitigate their impact.
After all, we have them ourselves.
Dr. Rockoff practices dermatology in Brookline, Mass.
Until last month, I had only ever had two positive pregnancy test results in women of child-bearing age taking isotretinoin. Both of the previous reports came in on the same day, one after the other. When I called each patient to give her the results, and asked her to repeat the test, neither was at all perturbed. "If I’m pregnant," laughed one, "it would be another Immaculate Conception."
Both results turned out to be laboratory errors committed by a single technician, who was reported and rebuked. Repeat tests were negative.
Then, last month, I got another positive. Victoria had actually completed her treatment course 6 weeks earlier, and had already obtained a 30-day post-treatment test – which was negative. Then, she had another test done a few weeks later, which was positive.
I called and got her mother, who asked, "Is everything all right?" But Victoria is 19, so I just said I needed her daughter’s cell phone number.
"We had a condom accident," Victoria said when I reached her. We reviewed her case, determining the last day she had actually taken the medication. Her sexual activity had clearly taken place more than 30 days later.
I suggested she contact her gynecologist at once, to be evaluated and to have the pregnancy test repeated, and I faxed a note to that physician with the relevant details. "If pregnancy is confirmed," I told her, "I’m sure you’ll consider many things before you decide what to do. But one thing you don’t have to factor in is your isotretinoin treatment, because it was no longer in your blood when you became pregnant."
A few days later, Victoria came to my office. "I’ve decided to end the pregnancy," she said. "This just isn’t the right time."
I told her I understood. "By the way," I said, "you listed your two methods of contraception as the patch and condoms. So even if the condom failed, it looks like the patch did too."
"No," said Victoria, "I wasn’t on the patch anymore."
"What?!" I exclaimed.
"I ran out a month earlier," she said, "and my regular doctor was out on maternity leave."
"Wasn’t there anyone else in her office who could refill it for you?" I asked.
"I guess so," she said, "but I kept calling and pushing the button for ‘prescription refills,’ and no one ever called back."
I tried my best not to shake my head in disbelief. Victoria is an intelligent young woman. There is no language barrier. We had discussed contraception before she started therapy, and she signed all the right forms. Each month she got a pregnancy test. Each month she went online and answered the contraceptive-related questions before she could get more isotretinoin.
And when she ran out of contraceptive patches, she didn’t get them refilled.
Victoria’s story could have been worse. She might have become pregnant while still taking isotretinoin. She might have been forced to make a decision to terminate a pregnancy she otherwise would have wanted to carry to term.
Victoria’s story speaks for itself. Despite our best efforts, persuasive or bureaucratic, people will sometimes act in ways that they themselves know perfectly well are against their own interests.
The newest iPledge program upgrade includes some changes, some of which are helpful. One novelty, however, is that if "Abstinence" is the first form of contraception, "None" automatically becomes the second – there is a new warning that this is "Not recommended." This means we should not rely on a patient’s self-reported abstinence, but are better off relying on her use of artificial contraception. Perhaps. But perhaps not. Contraception only works if you use it.
Humans have what a psychiatrist I know calls "design flaws." If ever called upon to redesign the species, I’m sure many of us would contribute some good ideas. In the meantime, however, all we can do is try to acknowledge these flaws, and do our best to mitigate their impact.
After all, we have them ourselves.
Dr. Rockoff practices dermatology in Brookline, Mass.
