User login
Hospitalist-Led Teams Vital to Improved ED Care
Hospitalist-led teams in the ED help reduce diversions, improve patient flow, and provide more timely care to boarded patients, according to a study in the Journal of Hospital Medicine (JHM).
The single-center study, "Hospitalist-Led Medicine Emergency Department Team: Associations with Throughput, Timeliness of Patient Care, and Satisfaction," found a reduction in diversions due to medicine bed capacity of 27% (4.5% to 3%, P=<0.01). Boarded patients were rounded a mean of 2 hours and 9 minutes earlier with hospitalist-led teams; length of stay (LOS) in the ED, LOS in the hospital, and 48-hour returns were unchanged. The study, which took place at 477-bed Denver Health Medical Center (DHMC), assigned a hospitalist and an allied health provider to the ED during dayshifts. At night, ED coverage was rolled into the existing hospitalist duties.
Lead author Smitha R. Chadaga, MD, who works in DHMC's Department of Medicine, believes the study could spur more HM groups to consider dedicating a staffer to the ED. The team in Denver was created to care for medicine patients in the ED awaiting inpatient beds, and to work with nursing supervisors to improve bed management.
"There are numerous places that hospitalists can impact hospital flow, whether it's helping with bed management, providing consultative services to the ED, or caring for boarded patients," Dr. Chadaga says. "Knowing the ins and outs of inpatient medicine really lends itself well to some areas that hospitalists might not have thought about before."
Dr. Chadaga says the research is broadly applicable because HM groups can implement its different features. For example, adding a consultative phone service can help ED physicians determine whether a patient needs to be admitted and could improve patient flow.
Hospitalist-led teams in the ED help reduce diversions, improve patient flow, and provide more timely care to boarded patients, according to a study in the Journal of Hospital Medicine (JHM).
The single-center study, "Hospitalist-Led Medicine Emergency Department Team: Associations with Throughput, Timeliness of Patient Care, and Satisfaction," found a reduction in diversions due to medicine bed capacity of 27% (4.5% to 3%, P=<0.01). Boarded patients were rounded a mean of 2 hours and 9 minutes earlier with hospitalist-led teams; length of stay (LOS) in the ED, LOS in the hospital, and 48-hour returns were unchanged. The study, which took place at 477-bed Denver Health Medical Center (DHMC), assigned a hospitalist and an allied health provider to the ED during dayshifts. At night, ED coverage was rolled into the existing hospitalist duties.
Lead author Smitha R. Chadaga, MD, who works in DHMC's Department of Medicine, believes the study could spur more HM groups to consider dedicating a staffer to the ED. The team in Denver was created to care for medicine patients in the ED awaiting inpatient beds, and to work with nursing supervisors to improve bed management.
"There are numerous places that hospitalists can impact hospital flow, whether it's helping with bed management, providing consultative services to the ED, or caring for boarded patients," Dr. Chadaga says. "Knowing the ins and outs of inpatient medicine really lends itself well to some areas that hospitalists might not have thought about before."
Dr. Chadaga says the research is broadly applicable because HM groups can implement its different features. For example, adding a consultative phone service can help ED physicians determine whether a patient needs to be admitted and could improve patient flow.
Hospitalist-led teams in the ED help reduce diversions, improve patient flow, and provide more timely care to boarded patients, according to a study in the Journal of Hospital Medicine (JHM).
The single-center study, "Hospitalist-Led Medicine Emergency Department Team: Associations with Throughput, Timeliness of Patient Care, and Satisfaction," found a reduction in diversions due to medicine bed capacity of 27% (4.5% to 3%, P=<0.01). Boarded patients were rounded a mean of 2 hours and 9 minutes earlier with hospitalist-led teams; length of stay (LOS) in the ED, LOS in the hospital, and 48-hour returns were unchanged. The study, which took place at 477-bed Denver Health Medical Center (DHMC), assigned a hospitalist and an allied health provider to the ED during dayshifts. At night, ED coverage was rolled into the existing hospitalist duties.
Lead author Smitha R. Chadaga, MD, who works in DHMC's Department of Medicine, believes the study could spur more HM groups to consider dedicating a staffer to the ED. The team in Denver was created to care for medicine patients in the ED awaiting inpatient beds, and to work with nursing supervisors to improve bed management.
"There are numerous places that hospitalists can impact hospital flow, whether it's helping with bed management, providing consultative services to the ED, or caring for boarded patients," Dr. Chadaga says. "Knowing the ins and outs of inpatient medicine really lends itself well to some areas that hospitalists might not have thought about before."
Dr. Chadaga says the research is broadly applicable because HM groups can implement its different features. For example, adding a consultative phone service can help ED physicians determine whether a patient needs to be admitted and could improve patient flow.
High-Tech Connections Give Hospitalists Broad Access to Medical Records
U.S. News and World Report recently named its 156 "most connected" U.S. hospitals, singled out for their combination of high quality and early adoption of information technology. But what does "most connected" really mean for hospitalists working on the wards?
"I've been in hospital medicine for a few years, and I can still remember the old days of going down to the medical records room and pulling a chart off the shelf," says hospitalist Kristian Feterik, MD, clinical assistant professor of medicine at the University of Pittsburgh Medical Center (UPMC) in Pittsburgh, which is on the U.S. News list. "The transition from paper to electronic medical records has just been tremendous. We're almost 100% paperless here."
Going paperless means hospitalists and other clinicians can access medical records anywhere in the hospital or at home using multiple interfaces, including their own tablet, Dr. Feterik says. "We're now piloting an application for smartphones that would notify us of pending tests. Plus, the applications support access to radiology studies, for example, without having to re-enter patient identification numbers once you're in the patient's record."
UPMC clinicians have access to a number of applications, some still in beta testing.
But technology also has its downside. "We need to be mindful about how we write our orders, because it's so easy to order things electronically," Dr. Feterik adds. "I stress to the residents: You need to take a moment and think, 'Why are you ordering this test?'"
U.S. News and World Report recently named its 156 "most connected" U.S. hospitals, singled out for their combination of high quality and early adoption of information technology. But what does "most connected" really mean for hospitalists working on the wards?
"I've been in hospital medicine for a few years, and I can still remember the old days of going down to the medical records room and pulling a chart off the shelf," says hospitalist Kristian Feterik, MD, clinical assistant professor of medicine at the University of Pittsburgh Medical Center (UPMC) in Pittsburgh, which is on the U.S. News list. "The transition from paper to electronic medical records has just been tremendous. We're almost 100% paperless here."
Going paperless means hospitalists and other clinicians can access medical records anywhere in the hospital or at home using multiple interfaces, including their own tablet, Dr. Feterik says. "We're now piloting an application for smartphones that would notify us of pending tests. Plus, the applications support access to radiology studies, for example, without having to re-enter patient identification numbers once you're in the patient's record."
UPMC clinicians have access to a number of applications, some still in beta testing.
But technology also has its downside. "We need to be mindful about how we write our orders, because it's so easy to order things electronically," Dr. Feterik adds. "I stress to the residents: You need to take a moment and think, 'Why are you ordering this test?'"
U.S. News and World Report recently named its 156 "most connected" U.S. hospitals, singled out for their combination of high quality and early adoption of information technology. But what does "most connected" really mean for hospitalists working on the wards?
"I've been in hospital medicine for a few years, and I can still remember the old days of going down to the medical records room and pulling a chart off the shelf," says hospitalist Kristian Feterik, MD, clinical assistant professor of medicine at the University of Pittsburgh Medical Center (UPMC) in Pittsburgh, which is on the U.S. News list. "The transition from paper to electronic medical records has just been tremendous. We're almost 100% paperless here."
Going paperless means hospitalists and other clinicians can access medical records anywhere in the hospital or at home using multiple interfaces, including their own tablet, Dr. Feterik says. "We're now piloting an application for smartphones that would notify us of pending tests. Plus, the applications support access to radiology studies, for example, without having to re-enter patient identification numbers once you're in the patient's record."
UPMC clinicians have access to a number of applications, some still in beta testing.
But technology also has its downside. "We need to be mindful about how we write our orders, because it's so easy to order things electronically," Dr. Feterik adds. "I stress to the residents: You need to take a moment and think, 'Why are you ordering this test?'"
Anti-Inflammatory Diet Anyone?
I’ve known Mr. G. for about a year now. When he first presented to me he’d had about 6 months of hand swelling and pain, and by the time I met him he had fusiform swelling of all his PIPs. There was no doubt that he had rheumatoid arthritis.
But we had a problem, sort of. Mr. G. had a history of drug and alcohol abuse but had turned his life around. Now that he was the model of an upright citizen, he had no interest in becoming dependent on more Western medicine.
Before he saw me, he had consulted a naturopath, who recommended that he follow an anti-inflammatory diet. After my admonitions about joint damage and internal organ involvement, I ultimately agreed to let him try the diet, but only if he agreed to regular follow-up with me.
I saw him for follow-up 6 weeks later – he had followed the diet to the letter, and, contrary to my expectations, his joints were about 50% better. In broad strokes, the anti-inflammatory diet is based on the premise that the intake of fruit and vegetables as well as whole wheat is inversely associated with the risk of inflammation, for which there is support in the literature (Int. J. Vitam. Nutr. Res. 2008;78:293-8). Some variations on the diet include using organic sources as much as possible, staying away from sugar and artificial sweeteners, and avoiding tomatoes, potatoes, and eggplant.
Now of course we as doctors are not satisfied with 50% better. Our patients want to be completely pain free, and we twist ourselves into knots trying to help them achieve that. But Mr. G. was content with the state his hands were in. He felt healthy and his discomfort was manageable. He said he could live with this state of affairs.
This got me thinking about naturopathic medicine. What is it, and how does it differ from our usual advice?
In the process of answering those questions, I got to meet with Celeste Ruland, N.D., a naturopathic doctor and personal trainer. Here’s what I learned from our conversation and my own research:
Naturopathic medicine is a 4-year graduate program. Just like students of allopathic medicine, students of naturopathic medicine study anatomy, physiology, biochemistry, microbiology, pharmacology, and other basic sciences. Students of naturopathic medicine have an organ system–based curriculum. In addition, they study Chinese medicine, herbal medicine, manipulation, and homeopathy. To practice, naturopaths have to meet licensing requirements.
The philosophy, I gathered from speaking to Dr. Ruland, is to treat illness and prevent it, using the "mind/body balance."
"Where are they out of balance, and what is the best way to balance them?" she asked. "The key is to empower the patient to stay well." While prescribing remedies such as homeopathy is sometimes part of the solution, the larger part involves altering the patient’s diet, lifestyle, and environment to restore the mind/body equilibrium.
This may sound like excessive tree-huggery, but I do think there is some value to this. After all, how often do we preach lifestyle modification? It is a very mainstream concept. Recently, Dr. Dean Ornish published a piece in the New York Times about how to eat healthily. How much evidence is there that viscosupplementation works? How much evidence is there that acupuncture works? If something does not harm the patient and could be potentially helpful, I certainly have no objections. I can’t embrace the concepts of naturopathic medicine to the exclusion of Western medicine, of course, but I see a place for it in conjunction with allopathic medicine.
In addition, I kind of like the idea that there are health care providers who don’t have the same constraints that those of us who take insurance do. These providers can spend way more time counseling patients on good sleep hygiene and avoiding highly processed foods, on exercise and stress-reduction – conversations that we would love to have with our patients but don’t have time for.
Epilogue: About 8 months after his diagnosis, Mr. G developed serositis. We managed to treat it – grudgingly on his part – with steroids, but our agreement, after all, was that when the time came he would trust me with my Western medicine. He is now on a biologic DMARD and is doing very well, much better than the initial 50% improvement that had him so satisfied.
Dr. Chan practices rheumatology in Pawtucket, R.I.
I’ve known Mr. G. for about a year now. When he first presented to me he’d had about 6 months of hand swelling and pain, and by the time I met him he had fusiform swelling of all his PIPs. There was no doubt that he had rheumatoid arthritis.
But we had a problem, sort of. Mr. G. had a history of drug and alcohol abuse but had turned his life around. Now that he was the model of an upright citizen, he had no interest in becoming dependent on more Western medicine.
Before he saw me, he had consulted a naturopath, who recommended that he follow an anti-inflammatory diet. After my admonitions about joint damage and internal organ involvement, I ultimately agreed to let him try the diet, but only if he agreed to regular follow-up with me.
I saw him for follow-up 6 weeks later – he had followed the diet to the letter, and, contrary to my expectations, his joints were about 50% better. In broad strokes, the anti-inflammatory diet is based on the premise that the intake of fruit and vegetables as well as whole wheat is inversely associated with the risk of inflammation, for which there is support in the literature (Int. J. Vitam. Nutr. Res. 2008;78:293-8). Some variations on the diet include using organic sources as much as possible, staying away from sugar and artificial sweeteners, and avoiding tomatoes, potatoes, and eggplant.
Now of course we as doctors are not satisfied with 50% better. Our patients want to be completely pain free, and we twist ourselves into knots trying to help them achieve that. But Mr. G. was content with the state his hands were in. He felt healthy and his discomfort was manageable. He said he could live with this state of affairs.
This got me thinking about naturopathic medicine. What is it, and how does it differ from our usual advice?
In the process of answering those questions, I got to meet with Celeste Ruland, N.D., a naturopathic doctor and personal trainer. Here’s what I learned from our conversation and my own research:
Naturopathic medicine is a 4-year graduate program. Just like students of allopathic medicine, students of naturopathic medicine study anatomy, physiology, biochemistry, microbiology, pharmacology, and other basic sciences. Students of naturopathic medicine have an organ system–based curriculum. In addition, they study Chinese medicine, herbal medicine, manipulation, and homeopathy. To practice, naturopaths have to meet licensing requirements.
The philosophy, I gathered from speaking to Dr. Ruland, is to treat illness and prevent it, using the "mind/body balance."
"Where are they out of balance, and what is the best way to balance them?" she asked. "The key is to empower the patient to stay well." While prescribing remedies such as homeopathy is sometimes part of the solution, the larger part involves altering the patient’s diet, lifestyle, and environment to restore the mind/body equilibrium.
This may sound like excessive tree-huggery, but I do think there is some value to this. After all, how often do we preach lifestyle modification? It is a very mainstream concept. Recently, Dr. Dean Ornish published a piece in the New York Times about how to eat healthily. How much evidence is there that viscosupplementation works? How much evidence is there that acupuncture works? If something does not harm the patient and could be potentially helpful, I certainly have no objections. I can’t embrace the concepts of naturopathic medicine to the exclusion of Western medicine, of course, but I see a place for it in conjunction with allopathic medicine.
In addition, I kind of like the idea that there are health care providers who don’t have the same constraints that those of us who take insurance do. These providers can spend way more time counseling patients on good sleep hygiene and avoiding highly processed foods, on exercise and stress-reduction – conversations that we would love to have with our patients but don’t have time for.
Epilogue: About 8 months after his diagnosis, Mr. G developed serositis. We managed to treat it – grudgingly on his part – with steroids, but our agreement, after all, was that when the time came he would trust me with my Western medicine. He is now on a biologic DMARD and is doing very well, much better than the initial 50% improvement that had him so satisfied.
Dr. Chan practices rheumatology in Pawtucket, R.I.
I’ve known Mr. G. for about a year now. When he first presented to me he’d had about 6 months of hand swelling and pain, and by the time I met him he had fusiform swelling of all his PIPs. There was no doubt that he had rheumatoid arthritis.
But we had a problem, sort of. Mr. G. had a history of drug and alcohol abuse but had turned his life around. Now that he was the model of an upright citizen, he had no interest in becoming dependent on more Western medicine.
Before he saw me, he had consulted a naturopath, who recommended that he follow an anti-inflammatory diet. After my admonitions about joint damage and internal organ involvement, I ultimately agreed to let him try the diet, but only if he agreed to regular follow-up with me.
I saw him for follow-up 6 weeks later – he had followed the diet to the letter, and, contrary to my expectations, his joints were about 50% better. In broad strokes, the anti-inflammatory diet is based on the premise that the intake of fruit and vegetables as well as whole wheat is inversely associated with the risk of inflammation, for which there is support in the literature (Int. J. Vitam. Nutr. Res. 2008;78:293-8). Some variations on the diet include using organic sources as much as possible, staying away from sugar and artificial sweeteners, and avoiding tomatoes, potatoes, and eggplant.
Now of course we as doctors are not satisfied with 50% better. Our patients want to be completely pain free, and we twist ourselves into knots trying to help them achieve that. But Mr. G. was content with the state his hands were in. He felt healthy and his discomfort was manageable. He said he could live with this state of affairs.
This got me thinking about naturopathic medicine. What is it, and how does it differ from our usual advice?
In the process of answering those questions, I got to meet with Celeste Ruland, N.D., a naturopathic doctor and personal trainer. Here’s what I learned from our conversation and my own research:
Naturopathic medicine is a 4-year graduate program. Just like students of allopathic medicine, students of naturopathic medicine study anatomy, physiology, biochemistry, microbiology, pharmacology, and other basic sciences. Students of naturopathic medicine have an organ system–based curriculum. In addition, they study Chinese medicine, herbal medicine, manipulation, and homeopathy. To practice, naturopaths have to meet licensing requirements.
The philosophy, I gathered from speaking to Dr. Ruland, is to treat illness and prevent it, using the "mind/body balance."
"Where are they out of balance, and what is the best way to balance them?" she asked. "The key is to empower the patient to stay well." While prescribing remedies such as homeopathy is sometimes part of the solution, the larger part involves altering the patient’s diet, lifestyle, and environment to restore the mind/body equilibrium.
This may sound like excessive tree-huggery, but I do think there is some value to this. After all, how often do we preach lifestyle modification? It is a very mainstream concept. Recently, Dr. Dean Ornish published a piece in the New York Times about how to eat healthily. How much evidence is there that viscosupplementation works? How much evidence is there that acupuncture works? If something does not harm the patient and could be potentially helpful, I certainly have no objections. I can’t embrace the concepts of naturopathic medicine to the exclusion of Western medicine, of course, but I see a place for it in conjunction with allopathic medicine.
In addition, I kind of like the idea that there are health care providers who don’t have the same constraints that those of us who take insurance do. These providers can spend way more time counseling patients on good sleep hygiene and avoiding highly processed foods, on exercise and stress-reduction – conversations that we would love to have with our patients but don’t have time for.
Epilogue: About 8 months after his diagnosis, Mr. G developed serositis. We managed to treat it – grudgingly on his part – with steroids, but our agreement, after all, was that when the time came he would trust me with my Western medicine. He is now on a biologic DMARD and is doing very well, much better than the initial 50% improvement that had him so satisfied.
Dr. Chan practices rheumatology in Pawtucket, R.I.
On a Scale of 1-10
When my wife was hospitalized for back surgery, I learned more about the new information revolution in health care that provides formerly unattainable precision. This investigative report includes suggestions for how we, in the outpatient world, can implement these advances.
At a 3-hour preop marathon, my wife was interviewed by several people, including two nurses. The neurosurgery nurse practitioner asked my wife how much pain she was experiencing.
"It depends on my position," my wife answered. "If I’m sitting, it’s not that painful."
"But when it does hurt?"
"Well, it isn’t that bad."
"On a scale of 1-10?"
"Four."
Later on the anesthesia nurse asked her many questions. One was, "How much pain are you in, on a scale of 1-10?"
"It depends," began my wife, a slow learner.
"On a scale of 1-10?"
"Four."
Things went smoothly after that until the final question, "Do you feel safe at home?"
I had kept my mouth shut until then, but at that point, I got clarification that she was, indeed, asking whether my wife feared being abused after discharge. Not an unfair question, though I did wonder whether someone who really wanted to know would ask the question while a potential abuser looked on.
On the morning of surgery a clerk asked my wife again how much pain she was in, on a scale of one 1-10. In the recovery room they asked her again, several times.
Once my wife reached the ward, each nurse asked, once per shift, how much pain she had, on a scale of 1-10. At first, she tried to explain through her opiate stupor, what she was feeling.
"On a scale of 1-10," came the polite but insistent request. I doubt whether my wife remembered 5 minutes later what number she had given, which had in any case been duly noted and entered into the computer.
Ditto the aides. Ditto the physical therapist. Ditto the occupational therapist. At each visit.
Back home the visiting nurse’s aid called to visit and set up services. Before the nurse came, I said to my wife, "Let’s practice."
"Practice what?"
"Saying ‘four’ "
"Why four?"
"Because she’s going to ask you how much pain you’re having, on a scale of 1-10."
"But it isn’t four."
"Okay, say three."
The nurse came. Her first question was, "How much pain are you having, on a scale of 1-10?"
My wife tried again to give a nuanced answer. But eventually she did say, "Four."
The nurse asked my wife whether she was depressed. "Starting last month, they’re making us ask that."
My wife laughed. "I feel wonderful!" she said. "I don’t look depressed, do I?"
"I need a ‘yes’ or ‘no,’ " said the nurse.
"No," said my wife.
"Thank you," said the nurse, wearily. "I have a 30-page form to fill out for every case."
All of the "yes" and "no" replies, and all the numbers from 1-10, will be recorded and filed in the great information repository in the sky.
We can easily apply this method to our own practices.
Consider:
"Mr. Smith, how is your eczema?"
"Doing better, Doc, thanks."
"Great. How much does it itch, on a scale of 1-10?"
"Well, it’s worse at night."
"On a scale of 1-10, please."
"At night, or when I’m working?"
"On a scale of 1-10."
"Two."
"Excellent. How regular have you been with the application?"
"Pretty regular."
"On a scale of 1-10."
"What?"
"How happy are you with the service you received in this office?"
"Well, pretty happy, I guess."
"On a scale of 1-5, with five being ‘Very happy.’ "
"I suppose three."
"How likely are you to use our services again, or to refer a friend, on a scale of 1-6, with six being, ‘You bet!’ and one being, ‘No way, Jose!’?"
"Look, I think that’s enough."
"Just a few more questions, Mr. Smith. Mr. Smith, why are you staring at me like that? Mr. Smith, please get your hands off my neck. What? How much ... do I want ... you to stop ... throttling me? A lot! What? On a scale of 1-10? 10! 10!"
Dr. Rockoff practices dermatology in Brookline, Mass. To respond to this column, e-mail him at our editorial offices at [email protected].
When my wife was hospitalized for back surgery, I learned more about the new information revolution in health care that provides formerly unattainable precision. This investigative report includes suggestions for how we, in the outpatient world, can implement these advances.
At a 3-hour preop marathon, my wife was interviewed by several people, including two nurses. The neurosurgery nurse practitioner asked my wife how much pain she was experiencing.
"It depends on my position," my wife answered. "If I’m sitting, it’s not that painful."
"But when it does hurt?"
"Well, it isn’t that bad."
"On a scale of 1-10?"
"Four."
Later on the anesthesia nurse asked her many questions. One was, "How much pain are you in, on a scale of 1-10?"
"It depends," began my wife, a slow learner.
"On a scale of 1-10?"
"Four."
Things went smoothly after that until the final question, "Do you feel safe at home?"
I had kept my mouth shut until then, but at that point, I got clarification that she was, indeed, asking whether my wife feared being abused after discharge. Not an unfair question, though I did wonder whether someone who really wanted to know would ask the question while a potential abuser looked on.
On the morning of surgery a clerk asked my wife again how much pain she was in, on a scale of one 1-10. In the recovery room they asked her again, several times.
Once my wife reached the ward, each nurse asked, once per shift, how much pain she had, on a scale of 1-10. At first, she tried to explain through her opiate stupor, what she was feeling.
"On a scale of 1-10," came the polite but insistent request. I doubt whether my wife remembered 5 minutes later what number she had given, which had in any case been duly noted and entered into the computer.
Ditto the aides. Ditto the physical therapist. Ditto the occupational therapist. At each visit.
Back home the visiting nurse’s aid called to visit and set up services. Before the nurse came, I said to my wife, "Let’s practice."
"Practice what?"
"Saying ‘four’ "
"Why four?"
"Because she’s going to ask you how much pain you’re having, on a scale of 1-10."
"But it isn’t four."
"Okay, say three."
The nurse came. Her first question was, "How much pain are you having, on a scale of 1-10?"
My wife tried again to give a nuanced answer. But eventually she did say, "Four."
The nurse asked my wife whether she was depressed. "Starting last month, they’re making us ask that."
My wife laughed. "I feel wonderful!" she said. "I don’t look depressed, do I?"
"I need a ‘yes’ or ‘no,’ " said the nurse.
"No," said my wife.
"Thank you," said the nurse, wearily. "I have a 30-page form to fill out for every case."
All of the "yes" and "no" replies, and all the numbers from 1-10, will be recorded and filed in the great information repository in the sky.
We can easily apply this method to our own practices.
Consider:
"Mr. Smith, how is your eczema?"
"Doing better, Doc, thanks."
"Great. How much does it itch, on a scale of 1-10?"
"Well, it’s worse at night."
"On a scale of 1-10, please."
"At night, or when I’m working?"
"On a scale of 1-10."
"Two."
"Excellent. How regular have you been with the application?"
"Pretty regular."
"On a scale of 1-10."
"What?"
"How happy are you with the service you received in this office?"
"Well, pretty happy, I guess."
"On a scale of 1-5, with five being ‘Very happy.’ "
"I suppose three."
"How likely are you to use our services again, or to refer a friend, on a scale of 1-6, with six being, ‘You bet!’ and one being, ‘No way, Jose!’?"
"Look, I think that’s enough."
"Just a few more questions, Mr. Smith. Mr. Smith, why are you staring at me like that? Mr. Smith, please get your hands off my neck. What? How much ... do I want ... you to stop ... throttling me? A lot! What? On a scale of 1-10? 10! 10!"
Dr. Rockoff practices dermatology in Brookline, Mass. To respond to this column, e-mail him at our editorial offices at [email protected].
When my wife was hospitalized for back surgery, I learned more about the new information revolution in health care that provides formerly unattainable precision. This investigative report includes suggestions for how we, in the outpatient world, can implement these advances.
At a 3-hour preop marathon, my wife was interviewed by several people, including two nurses. The neurosurgery nurse practitioner asked my wife how much pain she was experiencing.
"It depends on my position," my wife answered. "If I’m sitting, it’s not that painful."
"But when it does hurt?"
"Well, it isn’t that bad."
"On a scale of 1-10?"
"Four."
Later on the anesthesia nurse asked her many questions. One was, "How much pain are you in, on a scale of 1-10?"
"It depends," began my wife, a slow learner.
"On a scale of 1-10?"
"Four."
Things went smoothly after that until the final question, "Do you feel safe at home?"
I had kept my mouth shut until then, but at that point, I got clarification that she was, indeed, asking whether my wife feared being abused after discharge. Not an unfair question, though I did wonder whether someone who really wanted to know would ask the question while a potential abuser looked on.
On the morning of surgery a clerk asked my wife again how much pain she was in, on a scale of one 1-10. In the recovery room they asked her again, several times.
Once my wife reached the ward, each nurse asked, once per shift, how much pain she had, on a scale of 1-10. At first, she tried to explain through her opiate stupor, what she was feeling.
"On a scale of 1-10," came the polite but insistent request. I doubt whether my wife remembered 5 minutes later what number she had given, which had in any case been duly noted and entered into the computer.
Ditto the aides. Ditto the physical therapist. Ditto the occupational therapist. At each visit.
Back home the visiting nurse’s aid called to visit and set up services. Before the nurse came, I said to my wife, "Let’s practice."
"Practice what?"
"Saying ‘four’ "
"Why four?"
"Because she’s going to ask you how much pain you’re having, on a scale of 1-10."
"But it isn’t four."
"Okay, say three."
The nurse came. Her first question was, "How much pain are you having, on a scale of 1-10?"
My wife tried again to give a nuanced answer. But eventually she did say, "Four."
The nurse asked my wife whether she was depressed. "Starting last month, they’re making us ask that."
My wife laughed. "I feel wonderful!" she said. "I don’t look depressed, do I?"
"I need a ‘yes’ or ‘no,’ " said the nurse.
"No," said my wife.
"Thank you," said the nurse, wearily. "I have a 30-page form to fill out for every case."
All of the "yes" and "no" replies, and all the numbers from 1-10, will be recorded and filed in the great information repository in the sky.
We can easily apply this method to our own practices.
Consider:
"Mr. Smith, how is your eczema?"
"Doing better, Doc, thanks."
"Great. How much does it itch, on a scale of 1-10?"
"Well, it’s worse at night."
"On a scale of 1-10, please."
"At night, or when I’m working?"
"On a scale of 1-10."
"Two."
"Excellent. How regular have you been with the application?"
"Pretty regular."
"On a scale of 1-10."
"What?"
"How happy are you with the service you received in this office?"
"Well, pretty happy, I guess."
"On a scale of 1-5, with five being ‘Very happy.’ "
"I suppose three."
"How likely are you to use our services again, or to refer a friend, on a scale of 1-6, with six being, ‘You bet!’ and one being, ‘No way, Jose!’?"
"Look, I think that’s enough."
"Just a few more questions, Mr. Smith. Mr. Smith, why are you staring at me like that? Mr. Smith, please get your hands off my neck. What? How much ... do I want ... you to stop ... throttling me? A lot! What? On a scale of 1-10? 10! 10!"
Dr. Rockoff practices dermatology in Brookline, Mass. To respond to this column, e-mail him at our editorial offices at [email protected].

Dr. Minuchin and the Ashtray: A History Lesson
A pod of family psychiatrists is sitting around and chatting about the state of family psychiatry. They are preparing for a plenary at the Group for the Advancement of Psychiatry with the goal of showing how far family psychiatry has come since the first psychiatrists embraced the paradigm of systemic thinking. They also debate why family psychiatry is ignored in current practice, especially since the evidence shows that family treatment dramatically improves recovery rates for many illnesses.
When family therapy had its first wave of popularity, the charismatic leaders were out front wowing the crowds. Dr. Sal Minuchin’s sessions were heavily focused on structure and boundary making, and involved much chair rearranging and pulling family members, especially children, out from between the couple dyad and into their own space and chairs in the room. One of his most famous tapes involved putting an ashtray between the chairs of two family members to literally increase the distance between them!
Jay Haley, Ph.D., delivered strategic barbed arrows that pierced the hearts of the family members. Virginia Satir demonstrated the theater of families, sculpting organic shapes that pulsed with the gestalt of the family. There was much smoking of cigarettes during the sessions, by both the family psychiatrists and the family members. Psychiatry was exciting. The possibilities for change were endless. It was the 1960s.
Unfortunately, in those early days, family therapy was oversold as the sole treatment for schizophrenia and other mental illnesses. As a result, families have felt blamed by the negative attention and are still hesitant to engage in traditional family therapy. Nevertheless, quiet pioneers, like Carol M. Anderson, Ph.D., continue to research and practice a measured educational and collaborative approach aimed at involving families in mental health treatment. Indeed, current American Psychiatric Association guidelines for many psychiatric illnesses recommend that families be brought into the treatment process.
Family research has become much more sophisticated, with Dr. Minuchin’s early research on asthma and "psychosomatic families" being refined by teams led by Betsy Wood in New York, and Dr. Fred Wamboldt and Dr. Marianne Z. Wamboldt in Denver. Family research covers a broad territory, from studies on the impact of care giving on the caregiver’s immune function, to the role of expressed emotion in the outcome of illnesses – medical and psychiatric – to the efficacy of family treatments.
However, the Big Question still remains: Which model is the best? Structural? Strategic? Experiential?
While the arguments among devotees continue, studious researchers are quietly extracting the common factors found in the original family therapy models. These common factors are defined as the variables associated with positive clinical outcomes and are shared by several or all approaches. Andrew Christensen, Ph.D., suggests five principles that evidence-based couple interventions share: a systemic rather than an individual orientation of problems; modification of emotion-driven dysfunctional behaviors by teaching partners constructive ways to deal with differences, problems, and emotions; making both partners aware of avoided, emotion-based, private behaviors of each other, and making these internal experiences accessible to each other; enhancement of constructive communication in speaking and listening; and emphasis on strengths and positive behaviors (Enhancing Couples, Cambridge, Mass.: Hogrefe Publishing, 2009).
For couples and family therapies, common factors are conceptualizing the problems in relational terms, disrupting relational patterns, expanding treatment to include family members of the identified patient and an expanded therapeutic alliance (Common Factors in Couple and Family Therapy: The Overlooked Foundation for Effective Practice, New York: Guilford Press, 2009). Relational patterns have cognitive, behavioral, and affective domains, all of which can be targets of intervention. The therapeutic alliance is with the relationship and the family, rather than with the individual family members.
Patients, families, and psychiatrists all demand treatments that have been shown to work well. Family psychiatry has moved from theatrical showmanship to evidence-based treatments. Within a broad range of family interventions are different levels of family involvement. Family inclusion is the easiest intervention – simply involving the family members as historians, supporters, and allies in treatment.
Second, family psychoeducation has amassed a substantial evidence base showing its efficacy in the treatment of schizophrenia, bipolar disorder, and many medical illnesses, such as diabetes.
Last, but certainly not least, are the family systemic therapies, which in a meta-analysis of family systems therapies, were defined as "any couple, family, group, multifamily group, or individual focused therapeutic intervention that refers to either one of the following systems-oriented authors (Tom Andersen, Dr. Ivan Böszörményi-Nagy, Steve de Shazer, Jay Haley, Ph.D., Dr. Minuchin, Ms. Satir, Dr. Mara Selvini Palazzoli, Dr. Helm Stierlin, Paul Watzlawick, Ph.D., Michael White, Gerald H. Zuk, Ph.D.) or specified the intervention by use of at least one of the following terms: systemic, structural, strategic, triadic, Milan, functional, solution focused, narrative, resource/strength oriented, McMaster model" (Fam. Process 2010;49:457-85).
Family systems therapy has come a long way from the early days. We are very clear that for serious mental illness, family therapy alone is not enough, but neither are medications. Combination treatment produces symptom reduction AND good quality of life.
However, most psychotherapies – of the individual and family variety – are delivered by non-psychiatrists. Psychiatry is in danger of losing itself, as primary care physicians prescribe medications and refer patients to psychotherapists who are often co-located in their offices. Psychiatrists, however, are still the only professionals who have the potential to see the whole person and oversee the entire treatment: medications, individual, and family interventions.
It is to our advantage to be knowledgeable about all psychotherapeutic interventions AND to use them. We must make family therapy more visible and easier to teach in residencies. Psychiatrists have been reluctant to identify themselves as family psychiatrists because our enthusiastic charismatic leaders took the promise of family therapy too far. We hope that the solid family research now available will encourage all psychiatrists to learn and implement family interventions.
Dr. Minuchin and the ashtray, however, remain potent symbols of how creativity and genius created a new paradigm in psychiatry.
Dr. Heru is with the department of psychiatry at the University of Colorado, Denver. She has been a member of the Association of Family Psychiatrists since 2002 and currently serves as the organization’s treasurer. In addition, she is the coauthor of two books on working with families and is the author of numerous articles on this topic.
A pod of family psychiatrists is sitting around and chatting about the state of family psychiatry. They are preparing for a plenary at the Group for the Advancement of Psychiatry with the goal of showing how far family psychiatry has come since the first psychiatrists embraced the paradigm of systemic thinking. They also debate why family psychiatry is ignored in current practice, especially since the evidence shows that family treatment dramatically improves recovery rates for many illnesses.
When family therapy had its first wave of popularity, the charismatic leaders were out front wowing the crowds. Dr. Sal Minuchin’s sessions were heavily focused on structure and boundary making, and involved much chair rearranging and pulling family members, especially children, out from between the couple dyad and into their own space and chairs in the room. One of his most famous tapes involved putting an ashtray between the chairs of two family members to literally increase the distance between them!
Jay Haley, Ph.D., delivered strategic barbed arrows that pierced the hearts of the family members. Virginia Satir demonstrated the theater of families, sculpting organic shapes that pulsed with the gestalt of the family. There was much smoking of cigarettes during the sessions, by both the family psychiatrists and the family members. Psychiatry was exciting. The possibilities for change were endless. It was the 1960s.
Unfortunately, in those early days, family therapy was oversold as the sole treatment for schizophrenia and other mental illnesses. As a result, families have felt blamed by the negative attention and are still hesitant to engage in traditional family therapy. Nevertheless, quiet pioneers, like Carol M. Anderson, Ph.D., continue to research and practice a measured educational and collaborative approach aimed at involving families in mental health treatment. Indeed, current American Psychiatric Association guidelines for many psychiatric illnesses recommend that families be brought into the treatment process.
Family research has become much more sophisticated, with Dr. Minuchin’s early research on asthma and "psychosomatic families" being refined by teams led by Betsy Wood in New York, and Dr. Fred Wamboldt and Dr. Marianne Z. Wamboldt in Denver. Family research covers a broad territory, from studies on the impact of care giving on the caregiver’s immune function, to the role of expressed emotion in the outcome of illnesses – medical and psychiatric – to the efficacy of family treatments.
However, the Big Question still remains: Which model is the best? Structural? Strategic? Experiential?
While the arguments among devotees continue, studious researchers are quietly extracting the common factors found in the original family therapy models. These common factors are defined as the variables associated with positive clinical outcomes and are shared by several or all approaches. Andrew Christensen, Ph.D., suggests five principles that evidence-based couple interventions share: a systemic rather than an individual orientation of problems; modification of emotion-driven dysfunctional behaviors by teaching partners constructive ways to deal with differences, problems, and emotions; making both partners aware of avoided, emotion-based, private behaviors of each other, and making these internal experiences accessible to each other; enhancement of constructive communication in speaking and listening; and emphasis on strengths and positive behaviors (Enhancing Couples, Cambridge, Mass.: Hogrefe Publishing, 2009).
For couples and family therapies, common factors are conceptualizing the problems in relational terms, disrupting relational patterns, expanding treatment to include family members of the identified patient and an expanded therapeutic alliance (Common Factors in Couple and Family Therapy: The Overlooked Foundation for Effective Practice, New York: Guilford Press, 2009). Relational patterns have cognitive, behavioral, and affective domains, all of which can be targets of intervention. The therapeutic alliance is with the relationship and the family, rather than with the individual family members.
Patients, families, and psychiatrists all demand treatments that have been shown to work well. Family psychiatry has moved from theatrical showmanship to evidence-based treatments. Within a broad range of family interventions are different levels of family involvement. Family inclusion is the easiest intervention – simply involving the family members as historians, supporters, and allies in treatment.
Second, family psychoeducation has amassed a substantial evidence base showing its efficacy in the treatment of schizophrenia, bipolar disorder, and many medical illnesses, such as diabetes.
Last, but certainly not least, are the family systemic therapies, which in a meta-analysis of family systems therapies, were defined as "any couple, family, group, multifamily group, or individual focused therapeutic intervention that refers to either one of the following systems-oriented authors (Tom Andersen, Dr. Ivan Böszörményi-Nagy, Steve de Shazer, Jay Haley, Ph.D., Dr. Minuchin, Ms. Satir, Dr. Mara Selvini Palazzoli, Dr. Helm Stierlin, Paul Watzlawick, Ph.D., Michael White, Gerald H. Zuk, Ph.D.) or specified the intervention by use of at least one of the following terms: systemic, structural, strategic, triadic, Milan, functional, solution focused, narrative, resource/strength oriented, McMaster model" (Fam. Process 2010;49:457-85).
Family systems therapy has come a long way from the early days. We are very clear that for serious mental illness, family therapy alone is not enough, but neither are medications. Combination treatment produces symptom reduction AND good quality of life.
However, most psychotherapies – of the individual and family variety – are delivered by non-psychiatrists. Psychiatry is in danger of losing itself, as primary care physicians prescribe medications and refer patients to psychotherapists who are often co-located in their offices. Psychiatrists, however, are still the only professionals who have the potential to see the whole person and oversee the entire treatment: medications, individual, and family interventions.
It is to our advantage to be knowledgeable about all psychotherapeutic interventions AND to use them. We must make family therapy more visible and easier to teach in residencies. Psychiatrists have been reluctant to identify themselves as family psychiatrists because our enthusiastic charismatic leaders took the promise of family therapy too far. We hope that the solid family research now available will encourage all psychiatrists to learn and implement family interventions.
Dr. Minuchin and the ashtray, however, remain potent symbols of how creativity and genius created a new paradigm in psychiatry.
Dr. Heru is with the department of psychiatry at the University of Colorado, Denver. She has been a member of the Association of Family Psychiatrists since 2002 and currently serves as the organization’s treasurer. In addition, she is the coauthor of two books on working with families and is the author of numerous articles on this topic.
A pod of family psychiatrists is sitting around and chatting about the state of family psychiatry. They are preparing for a plenary at the Group for the Advancement of Psychiatry with the goal of showing how far family psychiatry has come since the first psychiatrists embraced the paradigm of systemic thinking. They also debate why family psychiatry is ignored in current practice, especially since the evidence shows that family treatment dramatically improves recovery rates for many illnesses.
When family therapy had its first wave of popularity, the charismatic leaders were out front wowing the crowds. Dr. Sal Minuchin’s sessions were heavily focused on structure and boundary making, and involved much chair rearranging and pulling family members, especially children, out from between the couple dyad and into their own space and chairs in the room. One of his most famous tapes involved putting an ashtray between the chairs of two family members to literally increase the distance between them!
Jay Haley, Ph.D., delivered strategic barbed arrows that pierced the hearts of the family members. Virginia Satir demonstrated the theater of families, sculpting organic shapes that pulsed with the gestalt of the family. There was much smoking of cigarettes during the sessions, by both the family psychiatrists and the family members. Psychiatry was exciting. The possibilities for change were endless. It was the 1960s.
Unfortunately, in those early days, family therapy was oversold as the sole treatment for schizophrenia and other mental illnesses. As a result, families have felt blamed by the negative attention and are still hesitant to engage in traditional family therapy. Nevertheless, quiet pioneers, like Carol M. Anderson, Ph.D., continue to research and practice a measured educational and collaborative approach aimed at involving families in mental health treatment. Indeed, current American Psychiatric Association guidelines for many psychiatric illnesses recommend that families be brought into the treatment process.
Family research has become much more sophisticated, with Dr. Minuchin’s early research on asthma and "psychosomatic families" being refined by teams led by Betsy Wood in New York, and Dr. Fred Wamboldt and Dr. Marianne Z. Wamboldt in Denver. Family research covers a broad territory, from studies on the impact of care giving on the caregiver’s immune function, to the role of expressed emotion in the outcome of illnesses – medical and psychiatric – to the efficacy of family treatments.
However, the Big Question still remains: Which model is the best? Structural? Strategic? Experiential?
While the arguments among devotees continue, studious researchers are quietly extracting the common factors found in the original family therapy models. These common factors are defined as the variables associated with positive clinical outcomes and are shared by several or all approaches. Andrew Christensen, Ph.D., suggests five principles that evidence-based couple interventions share: a systemic rather than an individual orientation of problems; modification of emotion-driven dysfunctional behaviors by teaching partners constructive ways to deal with differences, problems, and emotions; making both partners aware of avoided, emotion-based, private behaviors of each other, and making these internal experiences accessible to each other; enhancement of constructive communication in speaking and listening; and emphasis on strengths and positive behaviors (Enhancing Couples, Cambridge, Mass.: Hogrefe Publishing, 2009).
For couples and family therapies, common factors are conceptualizing the problems in relational terms, disrupting relational patterns, expanding treatment to include family members of the identified patient and an expanded therapeutic alliance (Common Factors in Couple and Family Therapy: The Overlooked Foundation for Effective Practice, New York: Guilford Press, 2009). Relational patterns have cognitive, behavioral, and affective domains, all of which can be targets of intervention. The therapeutic alliance is with the relationship and the family, rather than with the individual family members.
Patients, families, and psychiatrists all demand treatments that have been shown to work well. Family psychiatry has moved from theatrical showmanship to evidence-based treatments. Within a broad range of family interventions are different levels of family involvement. Family inclusion is the easiest intervention – simply involving the family members as historians, supporters, and allies in treatment.
Second, family psychoeducation has amassed a substantial evidence base showing its efficacy in the treatment of schizophrenia, bipolar disorder, and many medical illnesses, such as diabetes.
Last, but certainly not least, are the family systemic therapies, which in a meta-analysis of family systems therapies, were defined as "any couple, family, group, multifamily group, or individual focused therapeutic intervention that refers to either one of the following systems-oriented authors (Tom Andersen, Dr. Ivan Böszörményi-Nagy, Steve de Shazer, Jay Haley, Ph.D., Dr. Minuchin, Ms. Satir, Dr. Mara Selvini Palazzoli, Dr. Helm Stierlin, Paul Watzlawick, Ph.D., Michael White, Gerald H. Zuk, Ph.D.) or specified the intervention by use of at least one of the following terms: systemic, structural, strategic, triadic, Milan, functional, solution focused, narrative, resource/strength oriented, McMaster model" (Fam. Process 2010;49:457-85).
Family systems therapy has come a long way from the early days. We are very clear that for serious mental illness, family therapy alone is not enough, but neither are medications. Combination treatment produces symptom reduction AND good quality of life.
However, most psychotherapies – of the individual and family variety – are delivered by non-psychiatrists. Psychiatry is in danger of losing itself, as primary care physicians prescribe medications and refer patients to psychotherapists who are often co-located in their offices. Psychiatrists, however, are still the only professionals who have the potential to see the whole person and oversee the entire treatment: medications, individual, and family interventions.
It is to our advantage to be knowledgeable about all psychotherapeutic interventions AND to use them. We must make family therapy more visible and easier to teach in residencies. Psychiatrists have been reluctant to identify themselves as family psychiatrists because our enthusiastic charismatic leaders took the promise of family therapy too far. We hope that the solid family research now available will encourage all psychiatrists to learn and implement family interventions.
Dr. Minuchin and the ashtray, however, remain potent symbols of how creativity and genius created a new paradigm in psychiatry.
Dr. Heru is with the department of psychiatry at the University of Colorado, Denver. She has been a member of the Association of Family Psychiatrists since 2002 and currently serves as the organization’s treasurer. In addition, she is the coauthor of two books on working with families and is the author of numerous articles on this topic.
CCR7 Predicts Cervical Metastasis in Oral Cancer
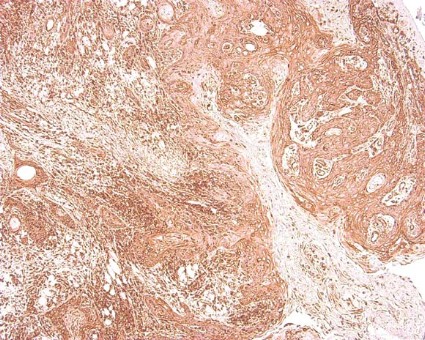
WASHINGTON – Chemokine receptor CCR7 expression is a significant predictor of cervical metastases in patients with squamous cell carcinoma in the oral cavity, based on data from 60 adults.
Metastatic spread of squamous cell carcinoma (SCC) is common, but the mechanisms behind the spread remain unclear, said Dr. Levi G. Ledgerwood of the University of California, Davis. "There has been a great deal of work that has looked at lymphocyte entry into lymphatics," he said at the annual meeting of the American Academy of Otolaryngology-Head and Neck Surgery Foundation.
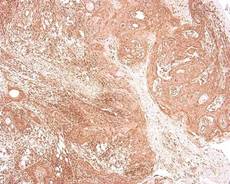
Recent research has focused on the chemokine receptor CCR7, a cell-surface molecule that is required for T-cell entry from the bloodstream and peripheral tissues into lymphatics, he noted. Data from previous studies suggest that CCR7 might play a role in various cancers in the metastases of the lymph nodes.
Dr. Ledgerwood and his colleagues reviewed tissue samples from primary tumors in 60 oral SCC patients who underwent surgical resection at a single center between 2006 and 2011. The study included 30 samples from patients with metastases and 30 samples from patients without metastases. There were no significant demographic differences between the groups, although each group had more male than female patients, Dr. Ledgerwood noted. A total of 30 patients were node positive, and 30 were node negative.
Overall, patients with cervical metastases showed significantly higher CCR7 expression than those without cervical metastases (P less than .001). A total of 97% of node-positive patients were positive for CCR7 expression, but only 43% of patients without cervical metastases were positive for CCR7.
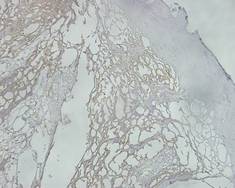
When the lymph nodes of the samples from metastatic cancer patients were examined, all 30 node-positive patients showed expression of CCR7, Dr. Ledgerwood added.
Although the study was limited by its small size, the results suggest a possible role for CCR7 in T-cell access to lymphatics, said Dr. Ledgerwood.
"This is a preliminary study, but we feel that this receptor could provide a very interesting target for future drug therapies and could also help in predicting the behavior of tumors," he said.
Dr. Ledgerwood had no financial conflicts to disclose.
WASHINGTON – Chemokine receptor CCR7 expression is a significant predictor of cervical metastases in patients with squamous cell carcinoma in the oral cavity, based on data from 60 adults.
Metastatic spread of squamous cell carcinoma (SCC) is common, but the mechanisms behind the spread remain unclear, said Dr. Levi G. Ledgerwood of the University of California, Davis. "There has been a great deal of work that has looked at lymphocyte entry into lymphatics," he said at the annual meeting of the American Academy of Otolaryngology-Head and Neck Surgery Foundation.
Recent research has focused on the chemokine receptor CCR7, a cell-surface molecule that is required for T-cell entry from the bloodstream and peripheral tissues into lymphatics, he noted. Data from previous studies suggest that CCR7 might play a role in various cancers in the metastases of the lymph nodes.
Dr. Ledgerwood and his colleagues reviewed tissue samples from primary tumors in 60 oral SCC patients who underwent surgical resection at a single center between 2006 and 2011. The study included 30 samples from patients with metastases and 30 samples from patients without metastases. There were no significant demographic differences between the groups, although each group had more male than female patients, Dr. Ledgerwood noted. A total of 30 patients were node positive, and 30 were node negative.
Overall, patients with cervical metastases showed significantly higher CCR7 expression than those without cervical metastases (P less than .001). A total of 97% of node-positive patients were positive for CCR7 expression, but only 43% of patients without cervical metastases were positive for CCR7.
When the lymph nodes of the samples from metastatic cancer patients were examined, all 30 node-positive patients showed expression of CCR7, Dr. Ledgerwood added.
Although the study was limited by its small size, the results suggest a possible role for CCR7 in T-cell access to lymphatics, said Dr. Ledgerwood.
"This is a preliminary study, but we feel that this receptor could provide a very interesting target for future drug therapies and could also help in predicting the behavior of tumors," he said.
Dr. Ledgerwood had no financial conflicts to disclose.
WASHINGTON – Chemokine receptor CCR7 expression is a significant predictor of cervical metastases in patients with squamous cell carcinoma in the oral cavity, based on data from 60 adults.
Metastatic spread of squamous cell carcinoma (SCC) is common, but the mechanisms behind the spread remain unclear, said Dr. Levi G. Ledgerwood of the University of California, Davis. "There has been a great deal of work that has looked at lymphocyte entry into lymphatics," he said at the annual meeting of the American Academy of Otolaryngology-Head and Neck Surgery Foundation.
Recent research has focused on the chemokine receptor CCR7, a cell-surface molecule that is required for T-cell entry from the bloodstream and peripheral tissues into lymphatics, he noted. Data from previous studies suggest that CCR7 might play a role in various cancers in the metastases of the lymph nodes.
Dr. Ledgerwood and his colleagues reviewed tissue samples from primary tumors in 60 oral SCC patients who underwent surgical resection at a single center between 2006 and 2011. The study included 30 samples from patients with metastases and 30 samples from patients without metastases. There were no significant demographic differences between the groups, although each group had more male than female patients, Dr. Ledgerwood noted. A total of 30 patients were node positive, and 30 were node negative.
Overall, patients with cervical metastases showed significantly higher CCR7 expression than those without cervical metastases (P less than .001). A total of 97% of node-positive patients were positive for CCR7 expression, but only 43% of patients without cervical metastases were positive for CCR7.
When the lymph nodes of the samples from metastatic cancer patients were examined, all 30 node-positive patients showed expression of CCR7, Dr. Ledgerwood added.
Although the study was limited by its small size, the results suggest a possible role for CCR7 in T-cell access to lymphatics, said Dr. Ledgerwood.
"This is a preliminary study, but we feel that this receptor could provide a very interesting target for future drug therapies and could also help in predicting the behavior of tumors," he said.
Dr. Ledgerwood had no financial conflicts to disclose.
AT THE ANNUAL MEETING OF THE AMERICAN ACADEMY OF OTOLARYNGOLOGY-HEAD AND NECK SURGERY FOUNDATION
Open Surgery Tied to Small-Bowel Obstruction Risk
The risk of developing a small-bowel obstruction after open surgery is about fourfold higher when compared with laparoscopic surgery in nine commonly performed abdominal and pelvic procedures, including cholecystectomy, hysterectomy, and appendectomy, investigators reported.
Other factors such as patient age, , prior abdominal surgery, and comorbidities also contributed to the risk of SBO, the study showed. However, laparoscopy "exceeded other risk factors in reduction of the risk of SBO for most of the surgical procedures," wrote Dr. Eva Angenete and her colleagues (Arch. Surg. 2012;147:359-65).
"This study shows that, beyond important factors such as age, previous abdominal surgery, and comorbidity, the surgical technique is the most important factor related to SBO," the authors wrote. "Compared with laparoscopic surgery, open surgery seems to increase the risk of SBO at least four times."
It’s likely that the study results will hold up to further scrutiny because the study was population based and the sample size – 108,141 patients – is large, the authors said.
Still, laparoscopic surgery did not seem to reduce the incidence of SBO in some groups, including hysterectomy patients. "One hypothesis is that this result may be related to a limited dissection in the pelvis," but the small number of laparoscopic hysterectomy patients included in the study could have affected the study’s results, the authors wrote. In addition, there were no clear risk factors for SBO in patients undergoing bariatric surgery, they wrote.
The investigators used the Inpatient Register of the Swedish National Board of Health and Welfare to analyze the risk of SBO in nine procedures, including cholecystectomy, hysterectomy, salpingo-oophorectomy, bowel resection, anterior resection, abdominoperineal resection, rectopexy, appendectomy, and bariatric surgery performed from 2002 to 2004. The database included information on demographic characteristics, comorbidities, previous abdominal surgery, and deaths.
The rate of SBO was lowest after cholecystectomy, occurring in just 0.4% of all cases, and was highest, at 13.9%, in abdominoperineal resection patients. For most surgical procedures, patients who had SBO were older on average. SBO was also more common in patients with previous abdominal surgery.
In those who underwent cholecystectomy, bowel resection, or appendectomy, a higher level of comorbidity was associated with a greater incidence of SBO, the authors said. In the group of complicated cholecystectomy patients as well as the group of anterior resection patients, SBO was more common among men.
SBO was linked with an increased risk of death within 5 years, the study found.
"The aim of this study was to identify the incidence and risk factors for mechanical SBO after a number of common abdominal and pelvic procedures," the authors wrote. "Small-bowel obstruction is a substantial health care challenge, and correctly identified risk factors can provide improved tools to reduce the risk of SBO after an abdominal surgical procedure."
"The safety and the short-term benefits of laparoscopy are already known, and it is possible that laparoscopy should be regarded as the preferred technique in an attempt to further reduce the complications of surgery," the authors concluded.
The project was supported by grants from the Swedish Cancer Foundation, the Swedish Medical Association, the Gothenburg Medical Association, the Assar Gabrielsson Foundation, the Magn Berwall’s Foundation, and the Swedish Research Council. None of the funding sources had any role in the study or the preparation of the manuscript. The authors reported no financial conflicts of interest.
Replacing open abdominal surgery with laparoscopy when possible may offer an opportunity for improved quality of life and decreased morbidity for many patients, along with health care system cost savings, said Dr. Luke M. Funk and Dr. Stanley W. Ashley in an invited critique accompanying the study on small-bowel obstruction (SBO) risk (Arch Surg. 2012;147:365 [doi:10.1001/archsurg.2012.157]).
The finding that SBO risk was lower with laparoscopy even after accounting for patient factors such as age, comorbidities, and previous surgery, has important implications for both the quality and cost of surgical care, Dr. Funk and Dr. Ashley said in their commentary.
"For surgeons, it highlights another potential benefit of minimally invasive surgery and challenges us to continue to offer less invasive procedures whenever they are feasible," they wrote. "For payers and health care policy leaders, it suggests that substantial cost savings could be achieved if open surgery [were] replaced with laparoscopic surgery more often."
Inpatient expenses on adhesiolysis-related complications exceed $2 billion in the United States, they added.
However, to fully realize the benefits of laparoscopy, newer payment models such as bundled or episode-based payments would need to account for the higher initial cost of laparoscopy but lower long-term costs related to shorter hospitalizations, lower complication rates, fewer readmissions, and fewer reoperations, the two surgeons said.
Still, the study’s authors "have provided strong evidence that minimal invasion often results in maximal benefit," Dr. Funk and Dr. Ashley wrote.
Dr. Funk is a general surgeon at Brigham and Women’s Hospital in Boston. Dr. Ashley is vice chairman of the department of surgery at Brigham and Women’s.
Replacing open abdominal surgery with laparoscopy when possible may offer an opportunity for improved quality of life and decreased morbidity for many patients, along with health care system cost savings, said Dr. Luke M. Funk and Dr. Stanley W. Ashley in an invited critique accompanying the study on small-bowel obstruction (SBO) risk (Arch Surg. 2012;147:365 [doi:10.1001/archsurg.2012.157]).
The finding that SBO risk was lower with laparoscopy even after accounting for patient factors such as age, comorbidities, and previous surgery, has important implications for both the quality and cost of surgical care, Dr. Funk and Dr. Ashley said in their commentary.
"For surgeons, it highlights another potential benefit of minimally invasive surgery and challenges us to continue to offer less invasive procedures whenever they are feasible," they wrote. "For payers and health care policy leaders, it suggests that substantial cost savings could be achieved if open surgery [were] replaced with laparoscopic surgery more often."
Inpatient expenses on adhesiolysis-related complications exceed $2 billion in the United States, they added.
However, to fully realize the benefits of laparoscopy, newer payment models such as bundled or episode-based payments would need to account for the higher initial cost of laparoscopy but lower long-term costs related to shorter hospitalizations, lower complication rates, fewer readmissions, and fewer reoperations, the two surgeons said.
Still, the study’s authors "have provided strong evidence that minimal invasion often results in maximal benefit," Dr. Funk and Dr. Ashley wrote.
Dr. Funk is a general surgeon at Brigham and Women’s Hospital in Boston. Dr. Ashley is vice chairman of the department of surgery at Brigham and Women’s.
Replacing open abdominal surgery with laparoscopy when possible may offer an opportunity for improved quality of life and decreased morbidity for many patients, along with health care system cost savings, said Dr. Luke M. Funk and Dr. Stanley W. Ashley in an invited critique accompanying the study on small-bowel obstruction (SBO) risk (Arch Surg. 2012;147:365 [doi:10.1001/archsurg.2012.157]).
The finding that SBO risk was lower with laparoscopy even after accounting for patient factors such as age, comorbidities, and previous surgery, has important implications for both the quality and cost of surgical care, Dr. Funk and Dr. Ashley said in their commentary.
"For surgeons, it highlights another potential benefit of minimally invasive surgery and challenges us to continue to offer less invasive procedures whenever they are feasible," they wrote. "For payers and health care policy leaders, it suggests that substantial cost savings could be achieved if open surgery [were] replaced with laparoscopic surgery more often."
Inpatient expenses on adhesiolysis-related complications exceed $2 billion in the United States, they added.
However, to fully realize the benefits of laparoscopy, newer payment models such as bundled or episode-based payments would need to account for the higher initial cost of laparoscopy but lower long-term costs related to shorter hospitalizations, lower complication rates, fewer readmissions, and fewer reoperations, the two surgeons said.
Still, the study’s authors "have provided strong evidence that minimal invasion often results in maximal benefit," Dr. Funk and Dr. Ashley wrote.
Dr. Funk is a general surgeon at Brigham and Women’s Hospital in Boston. Dr. Ashley is vice chairman of the department of surgery at Brigham and Women’s.
The risk of developing a small-bowel obstruction after open surgery is about fourfold higher when compared with laparoscopic surgery in nine commonly performed abdominal and pelvic procedures, including cholecystectomy, hysterectomy, and appendectomy, investigators reported.
Other factors such as patient age, , prior abdominal surgery, and comorbidities also contributed to the risk of SBO, the study showed. However, laparoscopy "exceeded other risk factors in reduction of the risk of SBO for most of the surgical procedures," wrote Dr. Eva Angenete and her colleagues (Arch. Surg. 2012;147:359-65).
"This study shows that, beyond important factors such as age, previous abdominal surgery, and comorbidity, the surgical technique is the most important factor related to SBO," the authors wrote. "Compared with laparoscopic surgery, open surgery seems to increase the risk of SBO at least four times."
It’s likely that the study results will hold up to further scrutiny because the study was population based and the sample size – 108,141 patients – is large, the authors said.
Still, laparoscopic surgery did not seem to reduce the incidence of SBO in some groups, including hysterectomy patients. "One hypothesis is that this result may be related to a limited dissection in the pelvis," but the small number of laparoscopic hysterectomy patients included in the study could have affected the study’s results, the authors wrote. In addition, there were no clear risk factors for SBO in patients undergoing bariatric surgery, they wrote.
The investigators used the Inpatient Register of the Swedish National Board of Health and Welfare to analyze the risk of SBO in nine procedures, including cholecystectomy, hysterectomy, salpingo-oophorectomy, bowel resection, anterior resection, abdominoperineal resection, rectopexy, appendectomy, and bariatric surgery performed from 2002 to 2004. The database included information on demographic characteristics, comorbidities, previous abdominal surgery, and deaths.
The rate of SBO was lowest after cholecystectomy, occurring in just 0.4% of all cases, and was highest, at 13.9%, in abdominoperineal resection patients. For most surgical procedures, patients who had SBO were older on average. SBO was also more common in patients with previous abdominal surgery.
In those who underwent cholecystectomy, bowel resection, or appendectomy, a higher level of comorbidity was associated with a greater incidence of SBO, the authors said. In the group of complicated cholecystectomy patients as well as the group of anterior resection patients, SBO was more common among men.
SBO was linked with an increased risk of death within 5 years, the study found.
"The aim of this study was to identify the incidence and risk factors for mechanical SBO after a number of common abdominal and pelvic procedures," the authors wrote. "Small-bowel obstruction is a substantial health care challenge, and correctly identified risk factors can provide improved tools to reduce the risk of SBO after an abdominal surgical procedure."
"The safety and the short-term benefits of laparoscopy are already known, and it is possible that laparoscopy should be regarded as the preferred technique in an attempt to further reduce the complications of surgery," the authors concluded.
The project was supported by grants from the Swedish Cancer Foundation, the Swedish Medical Association, the Gothenburg Medical Association, the Assar Gabrielsson Foundation, the Magn Berwall’s Foundation, and the Swedish Research Council. None of the funding sources had any role in the study or the preparation of the manuscript. The authors reported no financial conflicts of interest.
The risk of developing a small-bowel obstruction after open surgery is about fourfold higher when compared with laparoscopic surgery in nine commonly performed abdominal and pelvic procedures, including cholecystectomy, hysterectomy, and appendectomy, investigators reported.
Other factors such as patient age, , prior abdominal surgery, and comorbidities also contributed to the risk of SBO, the study showed. However, laparoscopy "exceeded other risk factors in reduction of the risk of SBO for most of the surgical procedures," wrote Dr. Eva Angenete and her colleagues (Arch. Surg. 2012;147:359-65).
"This study shows that, beyond important factors such as age, previous abdominal surgery, and comorbidity, the surgical technique is the most important factor related to SBO," the authors wrote. "Compared with laparoscopic surgery, open surgery seems to increase the risk of SBO at least four times."
It’s likely that the study results will hold up to further scrutiny because the study was population based and the sample size – 108,141 patients – is large, the authors said.
Still, laparoscopic surgery did not seem to reduce the incidence of SBO in some groups, including hysterectomy patients. "One hypothesis is that this result may be related to a limited dissection in the pelvis," but the small number of laparoscopic hysterectomy patients included in the study could have affected the study’s results, the authors wrote. In addition, there were no clear risk factors for SBO in patients undergoing bariatric surgery, they wrote.
The investigators used the Inpatient Register of the Swedish National Board of Health and Welfare to analyze the risk of SBO in nine procedures, including cholecystectomy, hysterectomy, salpingo-oophorectomy, bowel resection, anterior resection, abdominoperineal resection, rectopexy, appendectomy, and bariatric surgery performed from 2002 to 2004. The database included information on demographic characteristics, comorbidities, previous abdominal surgery, and deaths.
The rate of SBO was lowest after cholecystectomy, occurring in just 0.4% of all cases, and was highest, at 13.9%, in abdominoperineal resection patients. For most surgical procedures, patients who had SBO were older on average. SBO was also more common in patients with previous abdominal surgery.
In those who underwent cholecystectomy, bowel resection, or appendectomy, a higher level of comorbidity was associated with a greater incidence of SBO, the authors said. In the group of complicated cholecystectomy patients as well as the group of anterior resection patients, SBO was more common among men.
SBO was linked with an increased risk of death within 5 years, the study found.
"The aim of this study was to identify the incidence and risk factors for mechanical SBO after a number of common abdominal and pelvic procedures," the authors wrote. "Small-bowel obstruction is a substantial health care challenge, and correctly identified risk factors can provide improved tools to reduce the risk of SBO after an abdominal surgical procedure."
"The safety and the short-term benefits of laparoscopy are already known, and it is possible that laparoscopy should be regarded as the preferred technique in an attempt to further reduce the complications of surgery," the authors concluded.
The project was supported by grants from the Swedish Cancer Foundation, the Swedish Medical Association, the Gothenburg Medical Association, the Assar Gabrielsson Foundation, the Magn Berwall’s Foundation, and the Swedish Research Council. None of the funding sources had any role in the study or the preparation of the manuscript. The authors reported no financial conflicts of interest.
Major Finding: The risk of small-bowel obstruction is four times higher in patients who undergo open surgery than in patients who undergo laparoscopy for nine commonly performed procedures.
Data Source: Data were analyzed from 108,141 cases between 2002 and 2004 from the Inpatient Register of the Swedish National Board of Health and Welfare.
Disclosures: The project was supported by grants from the Swedish Cancer Foundation, the Swedish Medical Association, the Gothenburg Medical Association, the Assar Gabrielsson Foundation, the Magn Berwall’s Foundation, and the Swedish Research Council. None of the funding sources had any role in the study or the preparation of the manuscript. The authors reported no financial conflicts of interest.
Panel Backs Approval of Second Biologic for Ulcerative Colitis
SILVER SPRING, MD. – The approval of a second anti-tumor necrosis factor treatment option for ulcerative colitis is likely, now that the majority of a Food and Drug Administration advisory panel has recommended approval of adalimumab for treating people with moderately to severely active disease.
At a meeting on Aug. 28, the FDA’s Gastrointestinal Drugs Advisory Committee voted 15-2 that the expected benefits of adalimumab – a subcutaneously administered tumor necrosis factor (TNF) blocker – outweighed its potential risks as a treatment for patients with moderately to severely active ulcerative colitis (UC) who have not had an adequate response with conventional treatments. The panel’s recommendation for approval was based on the results of two studies comparing adalimumab against placebo in such patients. But their support for approval came with caveats. While most of the panel agreed that the dose used in the studies had been shown to be clinically effective, they agreed that the optimal dose for treating UC had not yet been determined and that post-approval studies were needed to address dosing, subpopulations of patients who may benefit most from treatment, and long-term safety.
Panel members voting in favor of approval cited the need for more treatments and for a subcutaneous TNF blocker for these patients, as well as its potential steroid-sparing effects. And although the differences in clinical remission rates between placebo and treatment at 8 weeks and at 1 year were less than 10% – one of the main issues raised by FDA reviewers – most of the panel members said that these differences still represented a clinically meaningful benefit. Infliximab (Remicade), an intravenous TNF blocker, is approved for treating UC and Crohn’s disease in pediatric and adult patients.
Like other panelists, Dr. Andelka LoSavio of the department of gastroenterology and nutrition, Loyola University, Maywood, Ill., said that the outstanding issues should not hold up approval of adalimumab for UC. "Once the drug is on the marketplace, we will have more insight into subpopulations where the drug may be more effective," which was the case with Crohn’s disease and adalimumab.
Although the remission rates in the studies were low, these are difficult-to-treat patients, and the responses were statistically significant, with evidence of a steroid-sparing effect, said panelist Dr. Marc Wishingrad, a gastroenterologist who practices in Santa Monica, Calif. "So it seems to me in a global sense that there is enough benefit here, that overall I would recommend that this drug be approved for this indication," he added.
Panelists supported the manufacturer’s recommendation that if a patient does not respond after 8 weeks of treatment, that treatment should be stopped.
The two statisticians on the panel did not support approval, voting no on the risk-benefit question for reasons that included the modest effects on clinical remission rates, uncertain durability of these effects, inadequate long-term data, missing data, and uncertainties about the dose.
Adalimumab – marketed as Humira by Abbott Laboratories – was first approved in 2002 for treating moderate to severe rheumatoid arthritis in adults, and was approved in 2007 for treating moderate to severe Crohn’s disease. It has also been approved for psoriasis, ankylosing spondylitis, and juvenile idiopathic arthritis indications.
The recommended dosing schedule for UC is one 160-mg starting dose, followed by 80 mg on day 15, and then 40 mg every other week starting at day 29, continuing treatment only in people who have responded within the first 8 weeks.
Abbott filed for approval in January 2011, but the FDA raised questions about whether a higher dose would be more effective and about the strength of the results in the two pivotal trials, including whether the differences in clinical remission rates at 8 and 52 weeks between placebo and treatment were clinically meaningful. The company resubmitted the application for approval, with a slightly different proposed indication: reducing the signs and symptoms, and achieving (instead of inducing and maintaining induction of) clinical remission in adults with moderately to severely active UC, who have had an inadequate response to conventional therapy.
The two double-blind, placebo-controlled, phase III studies compared adalimumab against placebo in 1,094 treatment-refractory patients with moderately to severely active UC with a total Mayo score of 6 to 12 points, and an endoscopy sub-score of 2 or 3, despite current or previous steroid and/or immunosuppressant therapy. In one 8-week study, which did not include patients who had previously been treated with a TNF blocker, the clinical remission rate at 8 weeks was 18.5% among those on adalimumab vs. 9.2% in those on placebo, a 9.3% difference that was significant.
In the second study, which followed patients for 1 year and included some who had been treated with infliximab (40%), the clinical remission rate at 8 weeks was 16.5% among those on adalimumab, vs. 9.3% among those on placebo, a 7.2% difference that was statistically significant. At 52 weeks, the remission rate was 17.3% among those on adalimumab, vs. 8.5% among those on placebo, an 8.8% difference that also was statistically significant.
In different votes, the panel nearly unanimously agreed that the 8 week and 52 week clinical remission rates in the studies represented "clinically meaningful benefits."
However, in the second study, 8.5% of the patients on adalimumab were in clinical remission at both weeks 8 and 52, vs. 4.1% among those on placebo. The panel was less unanimous about whether the 4.4% difference between the two groups represented a clinically meaningful benefit of treatment, voting 10-6 with 1 abstention on this question.
Other findings in the 52-week study included a higher steroid discontinuation rate among those on adalimumab, a secondary endpoint: About 13% of those on adalimumab were able to go off steroid treatment before the 52nd week of treatment and had achieved a clinical remission, compared with 5.7% of those on placebo, a statistically significant difference. In addition, the patients on azathioprine or 6-MP at baseline in this study did not appear to benefit from adalimumab: In this subgroup, the remission rate at week 8 among those on adalimumab (12.9%) was similar to the rate among those on placebo (15%). But for those who were not on the immunomodulatory drugs at baseline, the remission rate was nearly 19% among those on adalimumab vs. 6.6% of those on placebo, the FDA reviewer pointed out. In the studies, the safety profile of adalimumab was similar to the placebo, other than a higher rate of injection site reactions among those on adalimumab, and no new safety signals for adalimumab were identified in the trials, according to Abbott.
If the FDA grants approval, adalimumab will be the only self-administered biologic therapy available for patients with UC, the company pointed out. In April 2012, adalimumab was approved in the European Union for treating adults with moderately to severely active UC who have had an inadequate response to conventional therapy, based on the same data submitted to the FDA for the UC indication, according to Abbott.
The company is planning an international registry of patients with UC treated with adalimumab in typical clinical settings to collect long-term safety data, which will include patients in the EU, and, if approved, in the United States. The FDA usually follows the recommendations of its advisory panels, which are not binding. The company expects a decision on approval by the end of the year, according to an Abbott spokesperson.
Panelists have been cleared of potential conflicts of interest related to the topic of the meeting. Occasionally, a panelist may be given a waiver, but not at this meeting.
SILVER SPRING, MD. – The approval of a second anti-tumor necrosis factor treatment option for ulcerative colitis is likely, now that the majority of a Food and Drug Administration advisory panel has recommended approval of adalimumab for treating people with moderately to severely active disease.
At a meeting on Aug. 28, the FDA’s Gastrointestinal Drugs Advisory Committee voted 15-2 that the expected benefits of adalimumab – a subcutaneously administered tumor necrosis factor (TNF) blocker – outweighed its potential risks as a treatment for patients with moderately to severely active ulcerative colitis (UC) who have not had an adequate response with conventional treatments. The panel’s recommendation for approval was based on the results of two studies comparing adalimumab against placebo in such patients. But their support for approval came with caveats. While most of the panel agreed that the dose used in the studies had been shown to be clinically effective, they agreed that the optimal dose for treating UC had not yet been determined and that post-approval studies were needed to address dosing, subpopulations of patients who may benefit most from treatment, and long-term safety.
Panel members voting in favor of approval cited the need for more treatments and for a subcutaneous TNF blocker for these patients, as well as its potential steroid-sparing effects. And although the differences in clinical remission rates between placebo and treatment at 8 weeks and at 1 year were less than 10% – one of the main issues raised by FDA reviewers – most of the panel members said that these differences still represented a clinically meaningful benefit. Infliximab (Remicade), an intravenous TNF blocker, is approved for treating UC and Crohn’s disease in pediatric and adult patients.
Like other panelists, Dr. Andelka LoSavio of the department of gastroenterology and nutrition, Loyola University, Maywood, Ill., said that the outstanding issues should not hold up approval of adalimumab for UC. "Once the drug is on the marketplace, we will have more insight into subpopulations where the drug may be more effective," which was the case with Crohn’s disease and adalimumab.
Although the remission rates in the studies were low, these are difficult-to-treat patients, and the responses were statistically significant, with evidence of a steroid-sparing effect, said panelist Dr. Marc Wishingrad, a gastroenterologist who practices in Santa Monica, Calif. "So it seems to me in a global sense that there is enough benefit here, that overall I would recommend that this drug be approved for this indication," he added.
Panelists supported the manufacturer’s recommendation that if a patient does not respond after 8 weeks of treatment, that treatment should be stopped.
The two statisticians on the panel did not support approval, voting no on the risk-benefit question for reasons that included the modest effects on clinical remission rates, uncertain durability of these effects, inadequate long-term data, missing data, and uncertainties about the dose.
Adalimumab – marketed as Humira by Abbott Laboratories – was first approved in 2002 for treating moderate to severe rheumatoid arthritis in adults, and was approved in 2007 for treating moderate to severe Crohn’s disease. It has also been approved for psoriasis, ankylosing spondylitis, and juvenile idiopathic arthritis indications.
The recommended dosing schedule for UC is one 160-mg starting dose, followed by 80 mg on day 15, and then 40 mg every other week starting at day 29, continuing treatment only in people who have responded within the first 8 weeks.
Abbott filed for approval in January 2011, but the FDA raised questions about whether a higher dose would be more effective and about the strength of the results in the two pivotal trials, including whether the differences in clinical remission rates at 8 and 52 weeks between placebo and treatment were clinically meaningful. The company resubmitted the application for approval, with a slightly different proposed indication: reducing the signs and symptoms, and achieving (instead of inducing and maintaining induction of) clinical remission in adults with moderately to severely active UC, who have had an inadequate response to conventional therapy.
The two double-blind, placebo-controlled, phase III studies compared adalimumab against placebo in 1,094 treatment-refractory patients with moderately to severely active UC with a total Mayo score of 6 to 12 points, and an endoscopy sub-score of 2 or 3, despite current or previous steroid and/or immunosuppressant therapy. In one 8-week study, which did not include patients who had previously been treated with a TNF blocker, the clinical remission rate at 8 weeks was 18.5% among those on adalimumab vs. 9.2% in those on placebo, a 9.3% difference that was significant.
In the second study, which followed patients for 1 year and included some who had been treated with infliximab (40%), the clinical remission rate at 8 weeks was 16.5% among those on adalimumab, vs. 9.3% among those on placebo, a 7.2% difference that was statistically significant. At 52 weeks, the remission rate was 17.3% among those on adalimumab, vs. 8.5% among those on placebo, an 8.8% difference that also was statistically significant.
In different votes, the panel nearly unanimously agreed that the 8 week and 52 week clinical remission rates in the studies represented "clinically meaningful benefits."
However, in the second study, 8.5% of the patients on adalimumab were in clinical remission at both weeks 8 and 52, vs. 4.1% among those on placebo. The panel was less unanimous about whether the 4.4% difference between the two groups represented a clinically meaningful benefit of treatment, voting 10-6 with 1 abstention on this question.
Other findings in the 52-week study included a higher steroid discontinuation rate among those on adalimumab, a secondary endpoint: About 13% of those on adalimumab were able to go off steroid treatment before the 52nd week of treatment and had achieved a clinical remission, compared with 5.7% of those on placebo, a statistically significant difference. In addition, the patients on azathioprine or 6-MP at baseline in this study did not appear to benefit from adalimumab: In this subgroup, the remission rate at week 8 among those on adalimumab (12.9%) was similar to the rate among those on placebo (15%). But for those who were not on the immunomodulatory drugs at baseline, the remission rate was nearly 19% among those on adalimumab vs. 6.6% of those on placebo, the FDA reviewer pointed out. In the studies, the safety profile of adalimumab was similar to the placebo, other than a higher rate of injection site reactions among those on adalimumab, and no new safety signals for adalimumab were identified in the trials, according to Abbott.
If the FDA grants approval, adalimumab will be the only self-administered biologic therapy available for patients with UC, the company pointed out. In April 2012, adalimumab was approved in the European Union for treating adults with moderately to severely active UC who have had an inadequate response to conventional therapy, based on the same data submitted to the FDA for the UC indication, according to Abbott.
The company is planning an international registry of patients with UC treated with adalimumab in typical clinical settings to collect long-term safety data, which will include patients in the EU, and, if approved, in the United States. The FDA usually follows the recommendations of its advisory panels, which are not binding. The company expects a decision on approval by the end of the year, according to an Abbott spokesperson.
Panelists have been cleared of potential conflicts of interest related to the topic of the meeting. Occasionally, a panelist may be given a waiver, but not at this meeting.
SILVER SPRING, MD. – The approval of a second anti-tumor necrosis factor treatment option for ulcerative colitis is likely, now that the majority of a Food and Drug Administration advisory panel has recommended approval of adalimumab for treating people with moderately to severely active disease.
At a meeting on Aug. 28, the FDA’s Gastrointestinal Drugs Advisory Committee voted 15-2 that the expected benefits of adalimumab – a subcutaneously administered tumor necrosis factor (TNF) blocker – outweighed its potential risks as a treatment for patients with moderately to severely active ulcerative colitis (UC) who have not had an adequate response with conventional treatments. The panel’s recommendation for approval was based on the results of two studies comparing adalimumab against placebo in such patients. But their support for approval came with caveats. While most of the panel agreed that the dose used in the studies had been shown to be clinically effective, they agreed that the optimal dose for treating UC had not yet been determined and that post-approval studies were needed to address dosing, subpopulations of patients who may benefit most from treatment, and long-term safety.
Panel members voting in favor of approval cited the need for more treatments and for a subcutaneous TNF blocker for these patients, as well as its potential steroid-sparing effects. And although the differences in clinical remission rates between placebo and treatment at 8 weeks and at 1 year were less than 10% – one of the main issues raised by FDA reviewers – most of the panel members said that these differences still represented a clinically meaningful benefit. Infliximab (Remicade), an intravenous TNF blocker, is approved for treating UC and Crohn’s disease in pediatric and adult patients.
Like other panelists, Dr. Andelka LoSavio of the department of gastroenterology and nutrition, Loyola University, Maywood, Ill., said that the outstanding issues should not hold up approval of adalimumab for UC. "Once the drug is on the marketplace, we will have more insight into subpopulations where the drug may be more effective," which was the case with Crohn’s disease and adalimumab.
Although the remission rates in the studies were low, these are difficult-to-treat patients, and the responses were statistically significant, with evidence of a steroid-sparing effect, said panelist Dr. Marc Wishingrad, a gastroenterologist who practices in Santa Monica, Calif. "So it seems to me in a global sense that there is enough benefit here, that overall I would recommend that this drug be approved for this indication," he added.
Panelists supported the manufacturer’s recommendation that if a patient does not respond after 8 weeks of treatment, that treatment should be stopped.
The two statisticians on the panel did not support approval, voting no on the risk-benefit question for reasons that included the modest effects on clinical remission rates, uncertain durability of these effects, inadequate long-term data, missing data, and uncertainties about the dose.
Adalimumab – marketed as Humira by Abbott Laboratories – was first approved in 2002 for treating moderate to severe rheumatoid arthritis in adults, and was approved in 2007 for treating moderate to severe Crohn’s disease. It has also been approved for psoriasis, ankylosing spondylitis, and juvenile idiopathic arthritis indications.
The recommended dosing schedule for UC is one 160-mg starting dose, followed by 80 mg on day 15, and then 40 mg every other week starting at day 29, continuing treatment only in people who have responded within the first 8 weeks.
Abbott filed for approval in January 2011, but the FDA raised questions about whether a higher dose would be more effective and about the strength of the results in the two pivotal trials, including whether the differences in clinical remission rates at 8 and 52 weeks between placebo and treatment were clinically meaningful. The company resubmitted the application for approval, with a slightly different proposed indication: reducing the signs and symptoms, and achieving (instead of inducing and maintaining induction of) clinical remission in adults with moderately to severely active UC, who have had an inadequate response to conventional therapy.
The two double-blind, placebo-controlled, phase III studies compared adalimumab against placebo in 1,094 treatment-refractory patients with moderately to severely active UC with a total Mayo score of 6 to 12 points, and an endoscopy sub-score of 2 or 3, despite current or previous steroid and/or immunosuppressant therapy. In one 8-week study, which did not include patients who had previously been treated with a TNF blocker, the clinical remission rate at 8 weeks was 18.5% among those on adalimumab vs. 9.2% in those on placebo, a 9.3% difference that was significant.
In the second study, which followed patients for 1 year and included some who had been treated with infliximab (40%), the clinical remission rate at 8 weeks was 16.5% among those on adalimumab, vs. 9.3% among those on placebo, a 7.2% difference that was statistically significant. At 52 weeks, the remission rate was 17.3% among those on adalimumab, vs. 8.5% among those on placebo, an 8.8% difference that also was statistically significant.
In different votes, the panel nearly unanimously agreed that the 8 week and 52 week clinical remission rates in the studies represented "clinically meaningful benefits."
However, in the second study, 8.5% of the patients on adalimumab were in clinical remission at both weeks 8 and 52, vs. 4.1% among those on placebo. The panel was less unanimous about whether the 4.4% difference between the two groups represented a clinically meaningful benefit of treatment, voting 10-6 with 1 abstention on this question.
Other findings in the 52-week study included a higher steroid discontinuation rate among those on adalimumab, a secondary endpoint: About 13% of those on adalimumab were able to go off steroid treatment before the 52nd week of treatment and had achieved a clinical remission, compared with 5.7% of those on placebo, a statistically significant difference. In addition, the patients on azathioprine or 6-MP at baseline in this study did not appear to benefit from adalimumab: In this subgroup, the remission rate at week 8 among those on adalimumab (12.9%) was similar to the rate among those on placebo (15%). But for those who were not on the immunomodulatory drugs at baseline, the remission rate was nearly 19% among those on adalimumab vs. 6.6% of those on placebo, the FDA reviewer pointed out. In the studies, the safety profile of adalimumab was similar to the placebo, other than a higher rate of injection site reactions among those on adalimumab, and no new safety signals for adalimumab were identified in the trials, according to Abbott.
If the FDA grants approval, adalimumab will be the only self-administered biologic therapy available for patients with UC, the company pointed out. In April 2012, adalimumab was approved in the European Union for treating adults with moderately to severely active UC who have had an inadequate response to conventional therapy, based on the same data submitted to the FDA for the UC indication, according to Abbott.
The company is planning an international registry of patients with UC treated with adalimumab in typical clinical settings to collect long-term safety data, which will include patients in the EU, and, if approved, in the United States. The FDA usually follows the recommendations of its advisory panels, which are not binding. The company expects a decision on approval by the end of the year, according to an Abbott spokesperson.
Panelists have been cleared of potential conflicts of interest related to the topic of the meeting. Occasionally, a panelist may be given a waiver, but not at this meeting.
Topical Pain Relievers: FDA Issues Burn Warning
Rare cases of chemical burns caused by over-the-counter topical muscle and joint pain relievers has prompted the Food and Drug Administration to issue an advisory about the use of the products, with recommendations for both consumers and health professionals.
The single- or combination-ingredient products contain menthol, methyl salicylate, or capsaicin. The products included in the advisory are marketed under various names, including Bengay, Capzasin, Flexall, Icy Hot, and Mentholatum, according to the FDA communication.

Injuries prompting the advisory have ranged from first- to third-degree chemical burns, some of which required hospitalization. "In many cases, the burns occurred after only one application of the OTC muscle and joint pain reliever, with severe burning or blistering occurring within 24 hours of the first application," according to the FDA statement.
There were 43 reports of burns caused by application of these OTC products (in patch, balm, and cream formulations) identified in a search of the FDA’s Adverse Event Reporting System from 1969 to April 2011, the National Electronic Injury Surveillance System – Cooperative Adverse Drug Event Surveillance database from 2004 to 2010, and a 1987 report in the medical literature. The literature report described a patient who developed full-thickness skin and muscle necrosis and persistent interstitial nephritis after topical application of methyl salicylate and menthol, followed by the use of a heating pad (Cutis 1987;39:442-4).
Most of the second- and third-degree burns were associated with products that contain menthol as the single active ingredient and with products that contain a combination of menthol (concentration greater than 3%) and methyl salicylate (concentration greater than 10%). Only a few cases involved a product that contained capsaicin.
The advisory noted that health care professionals should counsel patients on how to safely use the products and on when they are recommended and to advise patients to stop using the products if they develop pain, swelling, or blistering at the application site. Consumers are advised to seek medical attention if they develop any of these effects – and to avoid tightly bandaging or applying heat to the application sites.
Currently, a warning about the risk of serious buns is not required on the label of these products.
Serious adverse reactions associated with these products should be reported to the FDA’s MedWatch program at 800-332-1088 or www.fda.gov/medwatch/.
Rare cases of chemical burns caused by over-the-counter topical muscle and joint pain relievers has prompted the Food and Drug Administration to issue an advisory about the use of the products, with recommendations for both consumers and health professionals.
The single- or combination-ingredient products contain menthol, methyl salicylate, or capsaicin. The products included in the advisory are marketed under various names, including Bengay, Capzasin, Flexall, Icy Hot, and Mentholatum, according to the FDA communication.
Injuries prompting the advisory have ranged from first- to third-degree chemical burns, some of which required hospitalization. "In many cases, the burns occurred after only one application of the OTC muscle and joint pain reliever, with severe burning or blistering occurring within 24 hours of the first application," according to the FDA statement.
There were 43 reports of burns caused by application of these OTC products (in patch, balm, and cream formulations) identified in a search of the FDA’s Adverse Event Reporting System from 1969 to April 2011, the National Electronic Injury Surveillance System – Cooperative Adverse Drug Event Surveillance database from 2004 to 2010, and a 1987 report in the medical literature. The literature report described a patient who developed full-thickness skin and muscle necrosis and persistent interstitial nephritis after topical application of methyl salicylate and menthol, followed by the use of a heating pad (Cutis 1987;39:442-4).
Most of the second- and third-degree burns were associated with products that contain menthol as the single active ingredient and with products that contain a combination of menthol (concentration greater than 3%) and methyl salicylate (concentration greater than 10%). Only a few cases involved a product that contained capsaicin.
The advisory noted that health care professionals should counsel patients on how to safely use the products and on when they are recommended and to advise patients to stop using the products if they develop pain, swelling, or blistering at the application site. Consumers are advised to seek medical attention if they develop any of these effects – and to avoid tightly bandaging or applying heat to the application sites.
Currently, a warning about the risk of serious buns is not required on the label of these products.
Serious adverse reactions associated with these products should be reported to the FDA’s MedWatch program at 800-332-1088 or www.fda.gov/medwatch/.
Rare cases of chemical burns caused by over-the-counter topical muscle and joint pain relievers has prompted the Food and Drug Administration to issue an advisory about the use of the products, with recommendations for both consumers and health professionals.
The single- or combination-ingredient products contain menthol, methyl salicylate, or capsaicin. The products included in the advisory are marketed under various names, including Bengay, Capzasin, Flexall, Icy Hot, and Mentholatum, according to the FDA communication.
Injuries prompting the advisory have ranged from first- to third-degree chemical burns, some of which required hospitalization. "In many cases, the burns occurred after only one application of the OTC muscle and joint pain reliever, with severe burning or blistering occurring within 24 hours of the first application," according to the FDA statement.
There were 43 reports of burns caused by application of these OTC products (in patch, balm, and cream formulations) identified in a search of the FDA’s Adverse Event Reporting System from 1969 to April 2011, the National Electronic Injury Surveillance System – Cooperative Adverse Drug Event Surveillance database from 2004 to 2010, and a 1987 report in the medical literature. The literature report described a patient who developed full-thickness skin and muscle necrosis and persistent interstitial nephritis after topical application of methyl salicylate and menthol, followed by the use of a heating pad (Cutis 1987;39:442-4).
Most of the second- and third-degree burns were associated with products that contain menthol as the single active ingredient and with products that contain a combination of menthol (concentration greater than 3%) and methyl salicylate (concentration greater than 10%). Only a few cases involved a product that contained capsaicin.
The advisory noted that health care professionals should counsel patients on how to safely use the products and on when they are recommended and to advise patients to stop using the products if they develop pain, swelling, or blistering at the application site. Consumers are advised to seek medical attention if they develop any of these effects – and to avoid tightly bandaging or applying heat to the application sites.
Currently, a warning about the risk of serious buns is not required on the label of these products.
Serious adverse reactions associated with these products should be reported to the FDA’s MedWatch program at 800-332-1088 or www.fda.gov/medwatch/.

Report: Hospitalists Can Trim Wasteful Healthcare Spending
An author of a report that estimates the national cost of unnecessary or wasteful healthcare at $750 billion per year hopes its findings will serve as a platform for hospitalists to spearhead improvements in healthcare delivery in the U.S.
The Institute of Medicine report, "Best Care at Lower Cost: The Path to Continuously Learning Health Care in America" [PDF], offers 10 broad recommendations that include reforming payment, adopting digital infrastructure, and simplifying transitional care. The paper was published earlier this month by a national committee of healthcare leaders, including Gary Kaplan, MD, FACP, FACMPE, FACPE, chairman and chief executive officer of Virginia Mason Health System in Seattle.
"The hospitalist is in a very unique position," Dr. Kaplan says. "They really are at the nexus of what we see as several of our key recommendations going forward."
In particular, Dr. Kaplan notes that healthcare delivery organizations should develop, implement, and fine-tune their "systems, engineering tools and process-improvement methods." Making such changes would help to "eliminate inefficiencies, remove unnecessary burdens on clinicians and staff, enhance patient experience, and improve patient health outcomes," he says.
"The hospitalists and the care teams with which the hospitalist connects are very critical to streamlining operations," Dr. Kaplan adds.
Many of the report's complaints about unnecessary testing, poor communication, and inefficient care delivery dovetail with the quality initiatives and practice-management improvements HM groups already push, Dr. Kaplan adds. To advance healthcare delivery's evolution, hospitalists should view the task of reform as an opportunity, not a challenge.
"There are very powerful opportunities for the hospitalist now to have great impact," he says. "To not just be the passive participants in a broken and dysfunctional system, but in many ways, [to be] one of the architects of an improved care system going forward."
An author of a report that estimates the national cost of unnecessary or wasteful healthcare at $750 billion per year hopes its findings will serve as a platform for hospitalists to spearhead improvements in healthcare delivery in the U.S.
The Institute of Medicine report, "Best Care at Lower Cost: The Path to Continuously Learning Health Care in America" [PDF], offers 10 broad recommendations that include reforming payment, adopting digital infrastructure, and simplifying transitional care. The paper was published earlier this month by a national committee of healthcare leaders, including Gary Kaplan, MD, FACP, FACMPE, FACPE, chairman and chief executive officer of Virginia Mason Health System in Seattle.
"The hospitalist is in a very unique position," Dr. Kaplan says. "They really are at the nexus of what we see as several of our key recommendations going forward."
In particular, Dr. Kaplan notes that healthcare delivery organizations should develop, implement, and fine-tune their "systems, engineering tools and process-improvement methods." Making such changes would help to "eliminate inefficiencies, remove unnecessary burdens on clinicians and staff, enhance patient experience, and improve patient health outcomes," he says.
"The hospitalists and the care teams with which the hospitalist connects are very critical to streamlining operations," Dr. Kaplan adds.
Many of the report's complaints about unnecessary testing, poor communication, and inefficient care delivery dovetail with the quality initiatives and practice-management improvements HM groups already push, Dr. Kaplan adds. To advance healthcare delivery's evolution, hospitalists should view the task of reform as an opportunity, not a challenge.
"There are very powerful opportunities for the hospitalist now to have great impact," he says. "To not just be the passive participants in a broken and dysfunctional system, but in many ways, [to be] one of the architects of an improved care system going forward."
An author of a report that estimates the national cost of unnecessary or wasteful healthcare at $750 billion per year hopes its findings will serve as a platform for hospitalists to spearhead improvements in healthcare delivery in the U.S.
The Institute of Medicine report, "Best Care at Lower Cost: The Path to Continuously Learning Health Care in America" [PDF], offers 10 broad recommendations that include reforming payment, adopting digital infrastructure, and simplifying transitional care. The paper was published earlier this month by a national committee of healthcare leaders, including Gary Kaplan, MD, FACP, FACMPE, FACPE, chairman and chief executive officer of Virginia Mason Health System in Seattle.
"The hospitalist is in a very unique position," Dr. Kaplan says. "They really are at the nexus of what we see as several of our key recommendations going forward."
In particular, Dr. Kaplan notes that healthcare delivery organizations should develop, implement, and fine-tune their "systems, engineering tools and process-improvement methods." Making such changes would help to "eliminate inefficiencies, remove unnecessary burdens on clinicians and staff, enhance patient experience, and improve patient health outcomes," he says.
"The hospitalists and the care teams with which the hospitalist connects are very critical to streamlining operations," Dr. Kaplan adds.
Many of the report's complaints about unnecessary testing, poor communication, and inefficient care delivery dovetail with the quality initiatives and practice-management improvements HM groups already push, Dr. Kaplan adds. To advance healthcare delivery's evolution, hospitalists should view the task of reform as an opportunity, not a challenge.
"There are very powerful opportunities for the hospitalist now to have great impact," he says. "To not just be the passive participants in a broken and dysfunctional system, but in many ways, [to be] one of the architects of an improved care system going forward."