User login
Paid For Being Special

It’s official. I am a “recognized” hospitalist. I’m certified. I’m special.
Although I’ve always felt that HM was special, that it’s a field with its own defined body of knowledge, area of expertise, and dedicated providers, it is now official. It is special; I am special. I got the letter in the mail the other day to prove it.
The correspondence arrived in an important-looking white envelope, with a return address stamped with the “American Board of Internal Medicine” insignia. The letter itself congratulated me on becoming a member of the first class of internists to complete their Maintenance of Certification (MOC) with Recognition of Focused Practice in Hospital Medicine (FPHM). As you’ve no doubt heard, the ABIM developed this MOC process to recognize hospitalists who’ve been in practice for at least three years after their initial certification in internal medicine (IM).
This is the first ABIM certification program that recognizes physician expertise in a field that is not tied directly to either residency or specialty fellowship training. In other words, unlike the cardiology certification exam, which requires a physician to have completed a fellowship training program, the FPHM allows for clinical experience to substitute for fellowship training. While the FPHM does not confer true “specialty status” (like the cardiology certification exam does), it does, as the moniker implies, recognize that we have focused our practice.
Implicit within that is the understanding that this focus brings with it a level of expertise that distinguishes hospitalists from nonhospitalists. This is a massive step forward for HM, as it lends significant credibility to the work we do and helps the public better understand what a hospitalist is and does. Most important, it helps set apart that cadre of true hospitalists who are dedicating their careers to fundamentally improving the care and outcomes of hospitalized patients.
It is this last point that came to mind as I reviewed this month’s cover story on value-based purchasing (see “Value-Based Purchasing Raises the Stakes,” p. 1).
Sticky Yet Crucial Point
One of the sticking points that I’ve heard from some hospitalists is that the FPHM requires a three-year cycle of self-evaluation. For those new to this process, let’s clear up some of the nomenclature. When IM residents graduate, they are eligible to sit for the ABIM certification exam. Upon passage, they are board-certified internists and can choose to enter into the maintenance of certification process. This is a 10-year process whereby diplomates (ABIM-speak for those certified as a specialist, with a diploma in medicine; not to be confused with a diplomat—a person who conducts negotiations and maintains political rest through the tactful handling of delicate situations, something perhaps more appropriate to the bulk of patient situations we encounter) must complete self-evaluation of medical knowledge modules, self-evaluation of practice performance, and ultimately a secure exam. This is where the FPHM differs.
The 10-year cycle for MOC is maintained for FPHM, such that diplomates only recertify every 10 years. However, the self-evaluation must occur every three years to maintain one’s certification. In other words, fail to keep up with the self-evaluation process, and your FPHM is revoked. This is different than the MOC for IM, and it is why some hospitalists are choosing not to enroll in the FPHM. This is a mistake.
Unnecessary Burden?
For many hospitalists, this extra evaluation, especially the practice improvement, is seen as an undue burden. Why is it that hospitalists should have to do more frequent self-evaluation than other specialists? My answer is that this is an important part of what defines our hospitalist specialty—that is, our ability to go beyond the individual patient encounter to fundamentally improve outcomes for the patients under our care. This is not done through “good doctoring.” Hospitalists are not necessarily better doctors than nonhospitalists. Rather, we have embodied a commitment to process and quality improvement within the hospital. This is what our patients need from us. This is what makes us hospitalists. This is what makes us special.
And this brings me back to value-based purchasing.
The Next Phase: Purchasing Value
For those of you, like me, who struggle to comprehend what buying value actually means, take a few minutes to peruse Bryn Nelson’s cover story this month. Not only will it help you understand the healthcare reform bill, it will help you understand the future of our field. I’ve personally witnessed HM traverse three distinct phases.
In the late 1990s and early 2000s, HM growth was driven by the need to improve efficiency. In most ways, this was code for reducing costs. Hospital executives recognized that hospitalists could reduce the overall costs of a patient admission, thus turning the balance of the prospective payment into profit. In other words, the amount of money a hospital receives for a patient stay is most often fixed and determined up front (prospectively), such that more efficiently moving patients through the system equates to more profit (or less loss).
This growth phase was quickly supplanted by the volume phase—a phase that was driven by the relative departure of primary-care physicians and subspecialists from the hospital. Although some of these doctors still admit their own patients, most of them now take advantage of hospitalist programs to focus their own practice to the outpatient or procedural arenas. Effectively, many of the other doctors have left the house, and hospitalists have had to back-fill this patient volume. To a certain degree, we are all still filling this need.
Connect the Dots
However, it is clear that the next HM driver is going to be quality. And it is programs like VBP that will drive it. Essentially, VBP means that hospitals will be competing with each other to be the best. By best, I mean “most able” to achieve pre-determined quality, safety, and patient-satisfaction indicators. By competing, I mean the reimbursement pie is fixed and those who achieve will get more, and those who fall short will get less.
When you consider that as much as 2% of a hospital’s Medicare reimbursement will soon be at risk, we are talking about millions of dollars per hospital per year. To hospitals with a 1% to 2% profit margin, this is the difference between being in or out of business. It also is interestingly close to the amount of support most hospitals give their HM groups; the exact groups that touch the majority of the patients that will determine their VBP outcomes. Connect the dots, and you can see that your hospitalist group—indeed, your paycheck—is very much at risk.
Which brings me back to the FPHM. In a serendipitous turn of events, the FPHM not only recognizes hospitalists as “special,” but, more important, it also gives us the opportunity to simultaneously enhance both our patients’ outcomes and our compensation. If we get this right, the every-three-year improvement projects required to maintain your certification are exactly the type of work you’ll need to be doing to achieve the outcomes your hospital needs to maintain its Medicare payments. In turn, this will ensure your group maintains its hospital support, and you, your paycheck.
It’s the kind of work that will ensure the best possible outcomes for our patients. And in the end, that, more than an ABIM certificate, is what truly makes us special. TH
Dr. Glasheen is associate professor of medicine at the University of Colorado Denver, where he serves as director of the Hospital Medicine Program and the Hospitalist Training Program, and as associate program director of the Internal Medicine Residency Program.
It’s official. I am a “recognized” hospitalist. I’m certified. I’m special.
Although I’ve always felt that HM was special, that it’s a field with its own defined body of knowledge, area of expertise, and dedicated providers, it is now official. It is special; I am special. I got the letter in the mail the other day to prove it.
The correspondence arrived in an important-looking white envelope, with a return address stamped with the “American Board of Internal Medicine” insignia. The letter itself congratulated me on becoming a member of the first class of internists to complete their Maintenance of Certification (MOC) with Recognition of Focused Practice in Hospital Medicine (FPHM). As you’ve no doubt heard, the ABIM developed this MOC process to recognize hospitalists who’ve been in practice for at least three years after their initial certification in internal medicine (IM).
This is the first ABIM certification program that recognizes physician expertise in a field that is not tied directly to either residency or specialty fellowship training. In other words, unlike the cardiology certification exam, which requires a physician to have completed a fellowship training program, the FPHM allows for clinical experience to substitute for fellowship training. While the FPHM does not confer true “specialty status” (like the cardiology certification exam does), it does, as the moniker implies, recognize that we have focused our practice.
Implicit within that is the understanding that this focus brings with it a level of expertise that distinguishes hospitalists from nonhospitalists. This is a massive step forward for HM, as it lends significant credibility to the work we do and helps the public better understand what a hospitalist is and does. Most important, it helps set apart that cadre of true hospitalists who are dedicating their careers to fundamentally improving the care and outcomes of hospitalized patients.
It is this last point that came to mind as I reviewed this month’s cover story on value-based purchasing (see “Value-Based Purchasing Raises the Stakes,” p. 1).
Sticky Yet Crucial Point
One of the sticking points that I’ve heard from some hospitalists is that the FPHM requires a three-year cycle of self-evaluation. For those new to this process, let’s clear up some of the nomenclature. When IM residents graduate, they are eligible to sit for the ABIM certification exam. Upon passage, they are board-certified internists and can choose to enter into the maintenance of certification process. This is a 10-year process whereby diplomates (ABIM-speak for those certified as a specialist, with a diploma in medicine; not to be confused with a diplomat—a person who conducts negotiations and maintains political rest through the tactful handling of delicate situations, something perhaps more appropriate to the bulk of patient situations we encounter) must complete self-evaluation of medical knowledge modules, self-evaluation of practice performance, and ultimately a secure exam. This is where the FPHM differs.
The 10-year cycle for MOC is maintained for FPHM, such that diplomates only recertify every 10 years. However, the self-evaluation must occur every three years to maintain one’s certification. In other words, fail to keep up with the self-evaluation process, and your FPHM is revoked. This is different than the MOC for IM, and it is why some hospitalists are choosing not to enroll in the FPHM. This is a mistake.
Unnecessary Burden?
For many hospitalists, this extra evaluation, especially the practice improvement, is seen as an undue burden. Why is it that hospitalists should have to do more frequent self-evaluation than other specialists? My answer is that this is an important part of what defines our hospitalist specialty—that is, our ability to go beyond the individual patient encounter to fundamentally improve outcomes for the patients under our care. This is not done through “good doctoring.” Hospitalists are not necessarily better doctors than nonhospitalists. Rather, we have embodied a commitment to process and quality improvement within the hospital. This is what our patients need from us. This is what makes us hospitalists. This is what makes us special.
And this brings me back to value-based purchasing.
The Next Phase: Purchasing Value
For those of you, like me, who struggle to comprehend what buying value actually means, take a few minutes to peruse Bryn Nelson’s cover story this month. Not only will it help you understand the healthcare reform bill, it will help you understand the future of our field. I’ve personally witnessed HM traverse three distinct phases.
In the late 1990s and early 2000s, HM growth was driven by the need to improve efficiency. In most ways, this was code for reducing costs. Hospital executives recognized that hospitalists could reduce the overall costs of a patient admission, thus turning the balance of the prospective payment into profit. In other words, the amount of money a hospital receives for a patient stay is most often fixed and determined up front (prospectively), such that more efficiently moving patients through the system equates to more profit (or less loss).
This growth phase was quickly supplanted by the volume phase—a phase that was driven by the relative departure of primary-care physicians and subspecialists from the hospital. Although some of these doctors still admit their own patients, most of them now take advantage of hospitalist programs to focus their own practice to the outpatient or procedural arenas. Effectively, many of the other doctors have left the house, and hospitalists have had to back-fill this patient volume. To a certain degree, we are all still filling this need.
Connect the Dots
However, it is clear that the next HM driver is going to be quality. And it is programs like VBP that will drive it. Essentially, VBP means that hospitals will be competing with each other to be the best. By best, I mean “most able” to achieve pre-determined quality, safety, and patient-satisfaction indicators. By competing, I mean the reimbursement pie is fixed and those who achieve will get more, and those who fall short will get less.
When you consider that as much as 2% of a hospital’s Medicare reimbursement will soon be at risk, we are talking about millions of dollars per hospital per year. To hospitals with a 1% to 2% profit margin, this is the difference between being in or out of business. It also is interestingly close to the amount of support most hospitals give their HM groups; the exact groups that touch the majority of the patients that will determine their VBP outcomes. Connect the dots, and you can see that your hospitalist group—indeed, your paycheck—is very much at risk.
Which brings me back to the FPHM. In a serendipitous turn of events, the FPHM not only recognizes hospitalists as “special,” but, more important, it also gives us the opportunity to simultaneously enhance both our patients’ outcomes and our compensation. If we get this right, the every-three-year improvement projects required to maintain your certification are exactly the type of work you’ll need to be doing to achieve the outcomes your hospital needs to maintain its Medicare payments. In turn, this will ensure your group maintains its hospital support, and you, your paycheck.
It’s the kind of work that will ensure the best possible outcomes for our patients. And in the end, that, more than an ABIM certificate, is what truly makes us special. TH
Dr. Glasheen is associate professor of medicine at the University of Colorado Denver, where he serves as director of the Hospital Medicine Program and the Hospitalist Training Program, and as associate program director of the Internal Medicine Residency Program.
It’s official. I am a “recognized” hospitalist. I’m certified. I’m special.
Although I’ve always felt that HM was special, that it’s a field with its own defined body of knowledge, area of expertise, and dedicated providers, it is now official. It is special; I am special. I got the letter in the mail the other day to prove it.
The correspondence arrived in an important-looking white envelope, with a return address stamped with the “American Board of Internal Medicine” insignia. The letter itself congratulated me on becoming a member of the first class of internists to complete their Maintenance of Certification (MOC) with Recognition of Focused Practice in Hospital Medicine (FPHM). As you’ve no doubt heard, the ABIM developed this MOC process to recognize hospitalists who’ve been in practice for at least three years after their initial certification in internal medicine (IM).
This is the first ABIM certification program that recognizes physician expertise in a field that is not tied directly to either residency or specialty fellowship training. In other words, unlike the cardiology certification exam, which requires a physician to have completed a fellowship training program, the FPHM allows for clinical experience to substitute for fellowship training. While the FPHM does not confer true “specialty status” (like the cardiology certification exam does), it does, as the moniker implies, recognize that we have focused our practice.
Implicit within that is the understanding that this focus brings with it a level of expertise that distinguishes hospitalists from nonhospitalists. This is a massive step forward for HM, as it lends significant credibility to the work we do and helps the public better understand what a hospitalist is and does. Most important, it helps set apart that cadre of true hospitalists who are dedicating their careers to fundamentally improving the care and outcomes of hospitalized patients.
It is this last point that came to mind as I reviewed this month’s cover story on value-based purchasing (see “Value-Based Purchasing Raises the Stakes,” p. 1).
Sticky Yet Crucial Point
One of the sticking points that I’ve heard from some hospitalists is that the FPHM requires a three-year cycle of self-evaluation. For those new to this process, let’s clear up some of the nomenclature. When IM residents graduate, they are eligible to sit for the ABIM certification exam. Upon passage, they are board-certified internists and can choose to enter into the maintenance of certification process. This is a 10-year process whereby diplomates (ABIM-speak for those certified as a specialist, with a diploma in medicine; not to be confused with a diplomat—a person who conducts negotiations and maintains political rest through the tactful handling of delicate situations, something perhaps more appropriate to the bulk of patient situations we encounter) must complete self-evaluation of medical knowledge modules, self-evaluation of practice performance, and ultimately a secure exam. This is where the FPHM differs.
The 10-year cycle for MOC is maintained for FPHM, such that diplomates only recertify every 10 years. However, the self-evaluation must occur every three years to maintain one’s certification. In other words, fail to keep up with the self-evaluation process, and your FPHM is revoked. This is different than the MOC for IM, and it is why some hospitalists are choosing not to enroll in the FPHM. This is a mistake.
Unnecessary Burden?
For many hospitalists, this extra evaluation, especially the practice improvement, is seen as an undue burden. Why is it that hospitalists should have to do more frequent self-evaluation than other specialists? My answer is that this is an important part of what defines our hospitalist specialty—that is, our ability to go beyond the individual patient encounter to fundamentally improve outcomes for the patients under our care. This is not done through “good doctoring.” Hospitalists are not necessarily better doctors than nonhospitalists. Rather, we have embodied a commitment to process and quality improvement within the hospital. This is what our patients need from us. This is what makes us hospitalists. This is what makes us special.
And this brings me back to value-based purchasing.
The Next Phase: Purchasing Value
For those of you, like me, who struggle to comprehend what buying value actually means, take a few minutes to peruse Bryn Nelson’s cover story this month. Not only will it help you understand the healthcare reform bill, it will help you understand the future of our field. I’ve personally witnessed HM traverse three distinct phases.
In the late 1990s and early 2000s, HM growth was driven by the need to improve efficiency. In most ways, this was code for reducing costs. Hospital executives recognized that hospitalists could reduce the overall costs of a patient admission, thus turning the balance of the prospective payment into profit. In other words, the amount of money a hospital receives for a patient stay is most often fixed and determined up front (prospectively), such that more efficiently moving patients through the system equates to more profit (or less loss).
This growth phase was quickly supplanted by the volume phase—a phase that was driven by the relative departure of primary-care physicians and subspecialists from the hospital. Although some of these doctors still admit their own patients, most of them now take advantage of hospitalist programs to focus their own practice to the outpatient or procedural arenas. Effectively, many of the other doctors have left the house, and hospitalists have had to back-fill this patient volume. To a certain degree, we are all still filling this need.
Connect the Dots
However, it is clear that the next HM driver is going to be quality. And it is programs like VBP that will drive it. Essentially, VBP means that hospitals will be competing with each other to be the best. By best, I mean “most able” to achieve pre-determined quality, safety, and patient-satisfaction indicators. By competing, I mean the reimbursement pie is fixed and those who achieve will get more, and those who fall short will get less.
When you consider that as much as 2% of a hospital’s Medicare reimbursement will soon be at risk, we are talking about millions of dollars per hospital per year. To hospitals with a 1% to 2% profit margin, this is the difference between being in or out of business. It also is interestingly close to the amount of support most hospitals give their HM groups; the exact groups that touch the majority of the patients that will determine their VBP outcomes. Connect the dots, and you can see that your hospitalist group—indeed, your paycheck—is very much at risk.
Which brings me back to the FPHM. In a serendipitous turn of events, the FPHM not only recognizes hospitalists as “special,” but, more important, it also gives us the opportunity to simultaneously enhance both our patients’ outcomes and our compensation. If we get this right, the every-three-year improvement projects required to maintain your certification are exactly the type of work you’ll need to be doing to achieve the outcomes your hospital needs to maintain its Medicare payments. In turn, this will ensure your group maintains its hospital support, and you, your paycheck.
It’s the kind of work that will ensure the best possible outcomes for our patients. And in the end, that, more than an ABIM certificate, is what truly makes us special. TH
Dr. Glasheen is associate professor of medicine at the University of Colorado Denver, where he serves as director of the Hospital Medicine Program and the Hospitalist Training Program, and as associate program director of the Internal Medicine Residency Program.
The To-Don’t List, Part 2


A couple of additions to the list that I started last month, in which I mentioned the problems associated with fixed-duration day shifts, a contractual vacation provision, tenure-based salary increases, poor roles for NPs and PAs, and blinded performance reporting. I think most practices would be better off without those things, and this month I’ll add a few more to the list.
I readily admit that there are some relatively rare situations in which the following things might be a good idea. But most hospitalist practices should think about alternatives.
Extra shifts. I think every hospitalist should have, within reason, a chance to work more or less than others in an HM group. And, of course, compensation should match the amount of work. So those who want to work more than the normal, or contractually required, number of shifts should have at it. But I think it is best to avoid categorizing the work into “normal” shifts and “extra” shifts. Essentially, all shifts should be thought of as “normal.”
What is the problem with having an “extra” shift category? It pretty reliably leads to confusion.
This confusion is easiest to illustrate with an example. Consider Dr. Krause, a hospitalist working in a practice with a seven-on/seven-off schedule. However, the first week in July, she works only six days, but she plans to “pay that back” and more when she works a 10-day stretch two months hence. So far, this sounds easy. By the end of September, Dr. Krause will have worked two extra shifts.
But when another hospitalist in Dr. Krause’s group is out sick in August, several hospitalists in the group rearrange their schedules to fill in. In September, Dr. Krause works the two days that she originally was scheduled to be off and trades away three of the consecutive days she was to work in September.
While it will be clear to Dr. Krause that she will be “even” in the number of shifts worked at the end of September, it probably isn’t clear to anyone else. The person who determines payroll will probably have a really hard time figuring out whether Dr. Krause is to be paid extra for “extra” shifts during any two-week pay period.
The most reliable way to figure out if a doctor worked extra shifts is to add up all worked shifts at the end of the year. But that would mean waiting until the end of the year to compensate the doctor for any extra shifts worked. And most docs would find that really unattractive.
It would be easy enough to just add up the shifts worked every pay period (usually two weeks) and compensate for any above the number expected, but that would then require lowering the salary for any pay period in which the doctor works fewer than the expected number. Although it might not be popular, I see this as the best arrangement. That is, just pay per shift so that there is no need to keep track of whether any particular shift is “normal” or “extra.”
Even if this illustration doesn’t convince you how messy it can be to keep track of extra vs. normal shifts, trust me on this one. It causes lots of problems for lots of physician practices. If your practice is among the few that has a clear-cut system that doesn’t confuse those in payroll, then stick with it.
Shift duration symmetry. Rarely is there a reason to keep every shift the same duration.
Let’s consider a common scenario. A small hospitalist group has a schedule that consists of a 12-hour day shift followed by a 12-hour night shift. As patient volume grows, the day-shift doctor(s) often have to stay after their shift to finish the initial care of new referrals, or the night doctor typically starts their shift with several patients in the ED awaiting admission. So the practice makes a good decision and creates an evening shift, which often is referred to as a “swing shift.” And because all existing shifts are 12 hours, the evening shift will be 12 hours, right?
Not so fast.
Why should the evening shift be the same duration as the day shift? Shouldn’t it be however long is necessary? Practices of no more than about 15 FTEs typically require an evening shift of only about four to six hours. It should start an hour or so before the last day doctor should be finishing work; it should continue until the night doctor has resolved the backlog of patients. As the practice volume grows, it will probably be necessary to lengthen the evening shift until it eventually reaches the same length as other shifts. But there is almost never a real workload or patient-care reason that the shift length needs to be the same duration as other shifts when it is first put into place.
While an evening shift should have a clearly defined start time, it will work best if the end of shift time is left loose and is based on just how busy that night it. For example, it might be reasonable to have the evening doctor accept their last new referral no later than a specified time (10 p.m. is the deadline in my hospitalist group). The swing shift can leave after completing the care of that patient and addressing any other issues that came up during the shift. Some nights, that will mean the evening doctor can leave at 10 p.m.; other nights, it might be 11 p.m. or midnight.
While we’re talking about it, there is no clear reason day and night shifts need to be the same length, either. It is fine to make both 12 hours long, but that isn’t the only reasonable option.
Of course, your compensation formula might influence what can be reasonably done with shift lengths. But if a practice compensates the doctors in a way that requires that all shifts be identical in duration, then the compensation method needs another look. TH
Dr. Nelson has been a practicing hospitalist since 1988 and is co-founder and past president of SHM. He is a principal in Nelson Flores Hospital Medicine Consultants, a national hospitalist practice management consulting firm (www.nelsonflores.com). He is course co-director and faculty for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. This column represents his views and is not intended to reflect an official position of SHM.
A couple of additions to the list that I started last month, in which I mentioned the problems associated with fixed-duration day shifts, a contractual vacation provision, tenure-based salary increases, poor roles for NPs and PAs, and blinded performance reporting. I think most practices would be better off without those things, and this month I’ll add a few more to the list.
I readily admit that there are some relatively rare situations in which the following things might be a good idea. But most hospitalist practices should think about alternatives.
Extra shifts. I think every hospitalist should have, within reason, a chance to work more or less than others in an HM group. And, of course, compensation should match the amount of work. So those who want to work more than the normal, or contractually required, number of shifts should have at it. But I think it is best to avoid categorizing the work into “normal” shifts and “extra” shifts. Essentially, all shifts should be thought of as “normal.”
What is the problem with having an “extra” shift category? It pretty reliably leads to confusion.
This confusion is easiest to illustrate with an example. Consider Dr. Krause, a hospitalist working in a practice with a seven-on/seven-off schedule. However, the first week in July, she works only six days, but she plans to “pay that back” and more when she works a 10-day stretch two months hence. So far, this sounds easy. By the end of September, Dr. Krause will have worked two extra shifts.
But when another hospitalist in Dr. Krause’s group is out sick in August, several hospitalists in the group rearrange their schedules to fill in. In September, Dr. Krause works the two days that she originally was scheduled to be off and trades away three of the consecutive days she was to work in September.
While it will be clear to Dr. Krause that she will be “even” in the number of shifts worked at the end of September, it probably isn’t clear to anyone else. The person who determines payroll will probably have a really hard time figuring out whether Dr. Krause is to be paid extra for “extra” shifts during any two-week pay period.
The most reliable way to figure out if a doctor worked extra shifts is to add up all worked shifts at the end of the year. But that would mean waiting until the end of the year to compensate the doctor for any extra shifts worked. And most docs would find that really unattractive.
It would be easy enough to just add up the shifts worked every pay period (usually two weeks) and compensate for any above the number expected, but that would then require lowering the salary for any pay period in which the doctor works fewer than the expected number. Although it might not be popular, I see this as the best arrangement. That is, just pay per shift so that there is no need to keep track of whether any particular shift is “normal” or “extra.”
Even if this illustration doesn’t convince you how messy it can be to keep track of extra vs. normal shifts, trust me on this one. It causes lots of problems for lots of physician practices. If your practice is among the few that has a clear-cut system that doesn’t confuse those in payroll, then stick with it.
Shift duration symmetry. Rarely is there a reason to keep every shift the same duration.
Let’s consider a common scenario. A small hospitalist group has a schedule that consists of a 12-hour day shift followed by a 12-hour night shift. As patient volume grows, the day-shift doctor(s) often have to stay after their shift to finish the initial care of new referrals, or the night doctor typically starts their shift with several patients in the ED awaiting admission. So the practice makes a good decision and creates an evening shift, which often is referred to as a “swing shift.” And because all existing shifts are 12 hours, the evening shift will be 12 hours, right?
Not so fast.
Why should the evening shift be the same duration as the day shift? Shouldn’t it be however long is necessary? Practices of no more than about 15 FTEs typically require an evening shift of only about four to six hours. It should start an hour or so before the last day doctor should be finishing work; it should continue until the night doctor has resolved the backlog of patients. As the practice volume grows, it will probably be necessary to lengthen the evening shift until it eventually reaches the same length as other shifts. But there is almost never a real workload or patient-care reason that the shift length needs to be the same duration as other shifts when it is first put into place.
While an evening shift should have a clearly defined start time, it will work best if the end of shift time is left loose and is based on just how busy that night it. For example, it might be reasonable to have the evening doctor accept their last new referral no later than a specified time (10 p.m. is the deadline in my hospitalist group). The swing shift can leave after completing the care of that patient and addressing any other issues that came up during the shift. Some nights, that will mean the evening doctor can leave at 10 p.m.; other nights, it might be 11 p.m. or midnight.
While we’re talking about it, there is no clear reason day and night shifts need to be the same length, either. It is fine to make both 12 hours long, but that isn’t the only reasonable option.
Of course, your compensation formula might influence what can be reasonably done with shift lengths. But if a practice compensates the doctors in a way that requires that all shifts be identical in duration, then the compensation method needs another look. TH
Dr. Nelson has been a practicing hospitalist since 1988 and is co-founder and past president of SHM. He is a principal in Nelson Flores Hospital Medicine Consultants, a national hospitalist practice management consulting firm (www.nelsonflores.com). He is course co-director and faculty for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. This column represents his views and is not intended to reflect an official position of SHM.
A couple of additions to the list that I started last month, in which I mentioned the problems associated with fixed-duration day shifts, a contractual vacation provision, tenure-based salary increases, poor roles for NPs and PAs, and blinded performance reporting. I think most practices would be better off without those things, and this month I’ll add a few more to the list.
I readily admit that there are some relatively rare situations in which the following things might be a good idea. But most hospitalist practices should think about alternatives.
Extra shifts. I think every hospitalist should have, within reason, a chance to work more or less than others in an HM group. And, of course, compensation should match the amount of work. So those who want to work more than the normal, or contractually required, number of shifts should have at it. But I think it is best to avoid categorizing the work into “normal” shifts and “extra” shifts. Essentially, all shifts should be thought of as “normal.”
What is the problem with having an “extra” shift category? It pretty reliably leads to confusion.
This confusion is easiest to illustrate with an example. Consider Dr. Krause, a hospitalist working in a practice with a seven-on/seven-off schedule. However, the first week in July, she works only six days, but she plans to “pay that back” and more when she works a 10-day stretch two months hence. So far, this sounds easy. By the end of September, Dr. Krause will have worked two extra shifts.
But when another hospitalist in Dr. Krause’s group is out sick in August, several hospitalists in the group rearrange their schedules to fill in. In September, Dr. Krause works the two days that she originally was scheduled to be off and trades away three of the consecutive days she was to work in September.
While it will be clear to Dr. Krause that she will be “even” in the number of shifts worked at the end of September, it probably isn’t clear to anyone else. The person who determines payroll will probably have a really hard time figuring out whether Dr. Krause is to be paid extra for “extra” shifts during any two-week pay period.
The most reliable way to figure out if a doctor worked extra shifts is to add up all worked shifts at the end of the year. But that would mean waiting until the end of the year to compensate the doctor for any extra shifts worked. And most docs would find that really unattractive.
It would be easy enough to just add up the shifts worked every pay period (usually two weeks) and compensate for any above the number expected, but that would then require lowering the salary for any pay period in which the doctor works fewer than the expected number. Although it might not be popular, I see this as the best arrangement. That is, just pay per shift so that there is no need to keep track of whether any particular shift is “normal” or “extra.”
Even if this illustration doesn’t convince you how messy it can be to keep track of extra vs. normal shifts, trust me on this one. It causes lots of problems for lots of physician practices. If your practice is among the few that has a clear-cut system that doesn’t confuse those in payroll, then stick with it.
Shift duration symmetry. Rarely is there a reason to keep every shift the same duration.
Let’s consider a common scenario. A small hospitalist group has a schedule that consists of a 12-hour day shift followed by a 12-hour night shift. As patient volume grows, the day-shift doctor(s) often have to stay after their shift to finish the initial care of new referrals, or the night doctor typically starts their shift with several patients in the ED awaiting admission. So the practice makes a good decision and creates an evening shift, which often is referred to as a “swing shift.” And because all existing shifts are 12 hours, the evening shift will be 12 hours, right?
Not so fast.
Why should the evening shift be the same duration as the day shift? Shouldn’t it be however long is necessary? Practices of no more than about 15 FTEs typically require an evening shift of only about four to six hours. It should start an hour or so before the last day doctor should be finishing work; it should continue until the night doctor has resolved the backlog of patients. As the practice volume grows, it will probably be necessary to lengthen the evening shift until it eventually reaches the same length as other shifts. But there is almost never a real workload or patient-care reason that the shift length needs to be the same duration as other shifts when it is first put into place.
While an evening shift should have a clearly defined start time, it will work best if the end of shift time is left loose and is based on just how busy that night it. For example, it might be reasonable to have the evening doctor accept their last new referral no later than a specified time (10 p.m. is the deadline in my hospitalist group). The swing shift can leave after completing the care of that patient and addressing any other issues that came up during the shift. Some nights, that will mean the evening doctor can leave at 10 p.m.; other nights, it might be 11 p.m. or midnight.
While we’re talking about it, there is no clear reason day and night shifts need to be the same length, either. It is fine to make both 12 hours long, but that isn’t the only reasonable option.
Of course, your compensation formula might influence what can be reasonably done with shift lengths. But if a practice compensates the doctors in a way that requires that all shifts be identical in duration, then the compensation method needs another look. TH
Dr. Nelson has been a practicing hospitalist since 1988 and is co-founder and past president of SHM. He is a principal in Nelson Flores Hospital Medicine Consultants, a national hospitalist practice management consulting firm (www.nelsonflores.com). He is course co-director and faculty for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. This column represents his views and is not intended to reflect an official position of SHM.
CMS Requires “In-Person Encounter” to Initiate Home Health Services

I’ve been told by home health agencies that I have to fill out some additional paperwork to get my patients outpatient services. Can you explain to me what these new rules are all about?
Alicia Farrouk, MD
Evansville, Ind.
Dr. Hospitalist responds: In June 2010, the Affordable Care Act changed the rules regarding physician orders for durable medical equipment and for certifying or recertifying the need for home health services. Last November, the Center for Medicare & Medicaid Services (CMS) published the final rules in the Federal Register.
The new law went into effect Jan. 1, and I suspect that is why you have been asked to adjust the way you fill out your paperwork. The upshot of the change in the law is that providers can no longer use the discharge plan or transfer form as evidence of “certification” of need for home health services. The ordering provider, as a condition for payment for services, must document an in-person encounter within the 90 days prior or 30 days after the initiation of home health services. The documentation must detail the clinical findings supporting the need for home health services.
If you are a hospitalist and discharging the patient from the hospital but will not be following the patient as an outpatient, you must document the name of the primary-care physician (PCP) who will follow the patient’s need for home health services and initiate the order and plan of care. The PCP will then sign the home health certification and document that they reviewed your note and plan for home health services and agree with the plan.
If you are a hospitalist working in a teaching hospital, the resident can fill out the form, but it must list your name (as attending physician) and your NPI number. This new rule applies only to home health services and durable medical equipment (things that can be used over and over again for medical purposes, such as crutches, walkers, wheelchairs, etc.) but does not include drugs or supplemental oxygen.
HM Model Spreads to Surgical Specialists
I have a friend who told me there is a neurologist in the hospital where he works who I understand is calling himself a hospitalist. What gives? I thought hospitalists were all internists or family physicians.
Bill Mulley, MD
Flagstaff, Ariz.
Dr. Hospitalist responds: The vast majority of hospitalists in the U.S. are general internists. There are smaller numbers of family physicians, pediatricians, and medical subspecialists who also work as hospitalists. Although this is the face of HM in America, we are seeing other fields of medicine adopting this model of care.
I know of surgical hospitalists, OB-GYN hospitalists, and yes, even neurohospitalists (see “Generation Next,” October 2010, p. 1). It is hard for some people to get their heads around the notion of a surgeon as a hospitalist because when one thinks of a surgeon, you are thinking of a physician who works in the operating room. But the traditional surgeon also has a clinic where they provide pre- and post-operative care.
Herein lies the difference between traditional surgeons and surgical hospitalists: The surgical hospitalist is, for the most part, only doing work in the hospital—sound familiar? (Think traditional internist vs. internist working as hospitalist.) The traditional general surgeon performs scheduled elective surgeries and typically only does emergency surgeries when they are on call for the hospital. As I understand it, the life of a surgical hospitalist is spending a shift in the hospital waiting for a patient to show up needing emergency surgery.
The hospital CEO today has increasing challenges convincing physicians to take hospital call. Some find themselves paying sizable sums of money for surgeons to take call from home. Some have decided their money is better spent paying for surgical hospitalists to spend nights in the hospital waiting for their pager to go off.
From a patient’s perspective, this seems to be a no-brainer. Having a surgeon in the hospital increases their chances of more timely care. You have to believe the providers in the ED and the medical hospitalist also love having a surgeon in-house, available to provide consults when requested.
I am a bit surprised that we don’t already have a large number of surgical hospitalists in the country. Then again, I have no idea of how many surgeons are working as surgical hospitalists. I am not sure anybody knows that answer.
There is a belief that we are going to see the continued growth of “specialty hospitalists” in the U.S. I believe we are going to see neurohospitalists managing inpatients with stroke and other neurosurgical issues, working side by side with medical hospitalists. I share in the excitement that was pervasive in the early days of the hospitalist movement, even though I’m not sure what we are going to see next.
I never imagined that we would have more than 30,000 hospitalists, as we do today. But while the HM model can help improve care, I will always feel strongly that no system will improve care without the dedication of motivated and compassionate healthcare providers driving the system. TH
I’ve been told by home health agencies that I have to fill out some additional paperwork to get my patients outpatient services. Can you explain to me what these new rules are all about?
Alicia Farrouk, MD
Evansville, Ind.
Dr. Hospitalist responds: In June 2010, the Affordable Care Act changed the rules regarding physician orders for durable medical equipment and for certifying or recertifying the need for home health services. Last November, the Center for Medicare & Medicaid Services (CMS) published the final rules in the Federal Register.
The new law went into effect Jan. 1, and I suspect that is why you have been asked to adjust the way you fill out your paperwork. The upshot of the change in the law is that providers can no longer use the discharge plan or transfer form as evidence of “certification” of need for home health services. The ordering provider, as a condition for payment for services, must document an in-person encounter within the 90 days prior or 30 days after the initiation of home health services. The documentation must detail the clinical findings supporting the need for home health services.
If you are a hospitalist and discharging the patient from the hospital but will not be following the patient as an outpatient, you must document the name of the primary-care physician (PCP) who will follow the patient’s need for home health services and initiate the order and plan of care. The PCP will then sign the home health certification and document that they reviewed your note and plan for home health services and agree with the plan.
If you are a hospitalist working in a teaching hospital, the resident can fill out the form, but it must list your name (as attending physician) and your NPI number. This new rule applies only to home health services and durable medical equipment (things that can be used over and over again for medical purposes, such as crutches, walkers, wheelchairs, etc.) but does not include drugs or supplemental oxygen.
HM Model Spreads to Surgical Specialists
I have a friend who told me there is a neurologist in the hospital where he works who I understand is calling himself a hospitalist. What gives? I thought hospitalists were all internists or family physicians.
Bill Mulley, MD
Flagstaff, Ariz.
Dr. Hospitalist responds: The vast majority of hospitalists in the U.S. are general internists. There are smaller numbers of family physicians, pediatricians, and medical subspecialists who also work as hospitalists. Although this is the face of HM in America, we are seeing other fields of medicine adopting this model of care.
I know of surgical hospitalists, OB-GYN hospitalists, and yes, even neurohospitalists (see “Generation Next,” October 2010, p. 1). It is hard for some people to get their heads around the notion of a surgeon as a hospitalist because when one thinks of a surgeon, you are thinking of a physician who works in the operating room. But the traditional surgeon also has a clinic where they provide pre- and post-operative care.
Herein lies the difference between traditional surgeons and surgical hospitalists: The surgical hospitalist is, for the most part, only doing work in the hospital—sound familiar? (Think traditional internist vs. internist working as hospitalist.) The traditional general surgeon performs scheduled elective surgeries and typically only does emergency surgeries when they are on call for the hospital. As I understand it, the life of a surgical hospitalist is spending a shift in the hospital waiting for a patient to show up needing emergency surgery.
The hospital CEO today has increasing challenges convincing physicians to take hospital call. Some find themselves paying sizable sums of money for surgeons to take call from home. Some have decided their money is better spent paying for surgical hospitalists to spend nights in the hospital waiting for their pager to go off.
From a patient’s perspective, this seems to be a no-brainer. Having a surgeon in the hospital increases their chances of more timely care. You have to believe the providers in the ED and the medical hospitalist also love having a surgeon in-house, available to provide consults when requested.
I am a bit surprised that we don’t already have a large number of surgical hospitalists in the country. Then again, I have no idea of how many surgeons are working as surgical hospitalists. I am not sure anybody knows that answer.
There is a belief that we are going to see the continued growth of “specialty hospitalists” in the U.S. I believe we are going to see neurohospitalists managing inpatients with stroke and other neurosurgical issues, working side by side with medical hospitalists. I share in the excitement that was pervasive in the early days of the hospitalist movement, even though I’m not sure what we are going to see next.
I never imagined that we would have more than 30,000 hospitalists, as we do today. But while the HM model can help improve care, I will always feel strongly that no system will improve care without the dedication of motivated and compassionate healthcare providers driving the system. TH
I’ve been told by home health agencies that I have to fill out some additional paperwork to get my patients outpatient services. Can you explain to me what these new rules are all about?
Alicia Farrouk, MD
Evansville, Ind.
Dr. Hospitalist responds: In June 2010, the Affordable Care Act changed the rules regarding physician orders for durable medical equipment and for certifying or recertifying the need for home health services. Last November, the Center for Medicare & Medicaid Services (CMS) published the final rules in the Federal Register.
The new law went into effect Jan. 1, and I suspect that is why you have been asked to adjust the way you fill out your paperwork. The upshot of the change in the law is that providers can no longer use the discharge plan or transfer form as evidence of “certification” of need for home health services. The ordering provider, as a condition for payment for services, must document an in-person encounter within the 90 days prior or 30 days after the initiation of home health services. The documentation must detail the clinical findings supporting the need for home health services.
If you are a hospitalist and discharging the patient from the hospital but will not be following the patient as an outpatient, you must document the name of the primary-care physician (PCP) who will follow the patient’s need for home health services and initiate the order and plan of care. The PCP will then sign the home health certification and document that they reviewed your note and plan for home health services and agree with the plan.
If you are a hospitalist working in a teaching hospital, the resident can fill out the form, but it must list your name (as attending physician) and your NPI number. This new rule applies only to home health services and durable medical equipment (things that can be used over and over again for medical purposes, such as crutches, walkers, wheelchairs, etc.) but does not include drugs or supplemental oxygen.
HM Model Spreads to Surgical Specialists
I have a friend who told me there is a neurologist in the hospital where he works who I understand is calling himself a hospitalist. What gives? I thought hospitalists were all internists or family physicians.
Bill Mulley, MD
Flagstaff, Ariz.
Dr. Hospitalist responds: The vast majority of hospitalists in the U.S. are general internists. There are smaller numbers of family physicians, pediatricians, and medical subspecialists who also work as hospitalists. Although this is the face of HM in America, we are seeing other fields of medicine adopting this model of care.
I know of surgical hospitalists, OB-GYN hospitalists, and yes, even neurohospitalists (see “Generation Next,” October 2010, p. 1). It is hard for some people to get their heads around the notion of a surgeon as a hospitalist because when one thinks of a surgeon, you are thinking of a physician who works in the operating room. But the traditional surgeon also has a clinic where they provide pre- and post-operative care.
Herein lies the difference between traditional surgeons and surgical hospitalists: The surgical hospitalist is, for the most part, only doing work in the hospital—sound familiar? (Think traditional internist vs. internist working as hospitalist.) The traditional general surgeon performs scheduled elective surgeries and typically only does emergency surgeries when they are on call for the hospital. As I understand it, the life of a surgical hospitalist is spending a shift in the hospital waiting for a patient to show up needing emergency surgery.
The hospital CEO today has increasing challenges convincing physicians to take hospital call. Some find themselves paying sizable sums of money for surgeons to take call from home. Some have decided their money is better spent paying for surgical hospitalists to spend nights in the hospital waiting for their pager to go off.
From a patient’s perspective, this seems to be a no-brainer. Having a surgeon in the hospital increases their chances of more timely care. You have to believe the providers in the ED and the medical hospitalist also love having a surgeon in-house, available to provide consults when requested.
I am a bit surprised that we don’t already have a large number of surgical hospitalists in the country. Then again, I have no idea of how many surgeons are working as surgical hospitalists. I am not sure anybody knows that answer.
There is a belief that we are going to see the continued growth of “specialty hospitalists” in the U.S. I believe we are going to see neurohospitalists managing inpatients with stroke and other neurosurgical issues, working side by side with medical hospitalists. I share in the excitement that was pervasive in the early days of the hospitalist movement, even though I’m not sure what we are going to see next.
I never imagined that we would have more than 30,000 hospitalists, as we do today. But while the HM model can help improve care, I will always feel strongly that no system will improve care without the dedication of motivated and compassionate healthcare providers driving the system. TH
ONLINE EXCLUSIVE: Listen to a dual-hospitalist couple talk about their shared and diverse interests
What to consider when prescribing for patients with substance abuse disorders
Primary Care Management of Patients With Asthma
There has been little improvement in the impact of asthma on patient morbidity and limitations on activity over the past decade, indicating the need for better utilization of existing therapies and improved patient self-management. This CME supplement discusses the role of small-airway inflammation in asthma and its possible relevance in the selection of anti-inflammatory therapy. While anti-inflammatory therapy is the mainstay of treatment for persistent asthma, long-acting ß-agonists (LABAs) are often used inappropriately, which has caused the FDA to take several actions due to safety concerns. While some of these actions have been questioned as inconsistent with current evidence-based guidelines, patient self-management should be reinforced at each patient visit and supported by a written asthma action plan.
There has been little improvement in the impact of asthma on patient morbidity and limitations on activity over the past decade, indicating the need for better utilization of existing therapies and improved patient self-management. This CME supplement discusses the role of small-airway inflammation in asthma and its possible relevance in the selection of anti-inflammatory therapy. While anti-inflammatory therapy is the mainstay of treatment for persistent asthma, long-acting ß-agonists (LABAs) are often used inappropriately, which has caused the FDA to take several actions due to safety concerns. While some of these actions have been questioned as inconsistent with current evidence-based guidelines, patient self-management should be reinforced at each patient visit and supported by a written asthma action plan.
There has been little improvement in the impact of asthma on patient morbidity and limitations on activity over the past decade, indicating the need for better utilization of existing therapies and improved patient self-management. This CME supplement discusses the role of small-airway inflammation in asthma and its possible relevance in the selection of anti-inflammatory therapy. While anti-inflammatory therapy is the mainstay of treatment for persistent asthma, long-acting ß-agonists (LABAs) are often used inappropriately, which has caused the FDA to take several actions due to safety concerns. While some of these actions have been questioned as inconsistent with current evidence-based guidelines, patient self-management should be reinforced at each patient visit and supported by a written asthma action plan.

Insulin treatment for type 2 diabetes: When to start, which to use
Many patients with type 2 diabetes eventually need insulin, as their ability to produce their own insulin from pancreatic beta cells declines progressively.1 The questions remain as to when insulin therapy should be started, and which regimen is the most appropriate.
Guidelines from professional societies differ on these points,2,3 as do individual clinicians. Moreover, antidiabetic treatment is an evolving topic. Many new drugs—oral agents as well as injectable analogues of glucagon-like peptide-1 (GLP1) and insulin formulations—have become available in the last 15 years.
In this paper, I advocate an individualized approach and review the indications for insulin treatment, the available preparations, the pros and cons of each regimen, and how the properties of each type of insulin influence attempts to intensify the regimen.
Coexisting physiologic and medical conditions such as pregnancy and chronic renal failure and drugs such as glucocorticoids may alter insulin requirements. I will not cover these special situations, as they deserve separate, detailed discussions.
WHEN SHOULD INSULIN BE STARTED? TWO VIEWS
Early on, patients can be adequately managed with lifestyle modifications and oral hypoglycemic agents or injections of a GLP1 analogue, either alone or in combination with oral medication. Later, some patients reach a point at which insulin therapy becomes the main treatment, similar to patients with type 1 diabetes.
The American Diabetes Association (ADA), in a consensus statement,2 has called for using insulin early in the disease if lifestyle management and monotherapy with metformin (Glucophage) fail to control glucose or if lifestyle management is not adequate and metformin is contraindicated. The ADA’s goal hemoglobin A1c level is less than 7% for most patients.
The American Association of Clinical Endocrinologists (AACE) and the American College of Endocrinology (ACE), in another consensus statement, use an algorithm stratified by hemoglobin A1c level, in which insulin is mostly reserved for when combination therapy fails.3 Their goal hemoglobin A1c level is 6.5% or less for most patients.
Comment. Both consensus statements make exceptions for patients presenting with very high blood glucose and hemoglobin A1c levels and those who have contraindications to drugs other than insulin. These patients should start insulin immediately, along with lifestyle management.2,3
Both consensus statements give priority to safety. The AACE/ACE statement gives more weight to the risk of hypoglycemia with insulin treatment, whereas the ADA gives more weight to the risk of edema and congestive heart failure with thiazolidinedione drugs (although both insulin and thiazolidinediones cause weight gain) and to adequate validation of treatments in clinical trials.
Ongoing clinical trials may add insight to this issue. For example, the Outcome Reduction With Initial Glargine Intervention (ORIGIN) study is investigating the effects of the long-acting insulin glargine (Lantus) in early diabetes with regard to glycemic control, safety, and cardiovascular outcomes.4 This study is expected to end this year (2011). The safety of alternative treatment options is also under investigation and scrutiny. In the interim, individualized treatment should be considered, as we will see below.
MY VIEW: AN INDIVIDUALIZED APPROACH
The decision to start insulin therapy should be made individually, based on several factors:
- Whether the patient is willing to try it
- The degree of hyperglycemia
- How relevant the potential side effects of insulin are to the patient compared with those of other hypoglycemic agents
- Whether oral hypoglycemic agents with or without GLP1 analogues are expected to provide the desired benefit
- The patient’s work schedule and lifestyle factors
- Cost
- The availability of nurses, diabetes educators, and others to implement and follow the insulin treatment.
Will patients accept insulin?
Factors that affect whether patients comply with a treatment include the number of pills or injections they must take per day, how often they must check their blood glucose, adverse effects, lifestyle limitations caused by the treatment (especially insulin), and cost. Most patients feel better when their glucose levels are under good control, which is a major motivation for initiating and adhering to insulin. The anticipated reduction of diabetic complications further enhances compliance.
Education promotes compliance. Patients need to know that type 2 diabetes tends to progress and that in time their treatment will have to be intensified, with higher doses of their current drugs and new drugs added or substituted, possibly including insulin. This information is best given early, ie, when the diagnosis is made, even if hyperglycemia is mild at that time.
With newer insulin preparations and delivery devices available, more patients are finding insulin treatment acceptable.
The glycemic goal should be individualized
The key issue is glycemic control. If glycemic control is worsening or if the hemoglobin A1c level remains above the goal, then the treatment strategy should be readdressed.
In general, one should try to achieve the best possible glycemic control with the few est adverse effects. Adequate dietary management with a regular meal schedule and predictable carbohydrate intake for each meal helps to avoid or at least minimize the two most important adverse effects of insulin, ie, weight gain and hypoglycemia.
For most patients, I believe a goal hemoglobin A1c level of less than 7% is reasonable.2 For others, a less stringent goal might be more appropriate, such as 7.5%. Several factors affect this decision, including whether the patient is willing to follow a complex insulin regimen (such as a basal-bolus regimen), his or her work schedule, other lifestyle factors, the duration of diabetes, the type or types of insulin used, coexisting medical conditions, the frequency of hypoglycemia, unawareness of hypoglycemia, age, prognosis, life expectancy, and cost.5
If hyperglycemia is severe (Table 1),2 the goal might not be clear when insulin therapy is started. It should become obvious with ongoing follow-up.
Previously untreated patients presenting with severe hyperglycemia are a heterogeneous group. Many of them have had diabetes for a relatively short time and were recently diagnosed. These patients are likely to safely achieve near-normal glycemic control. Some of them might be adequately treated with oral hypoglycemic agents; if insulin is used, transitioning from insulin to oral hypoglycemic agents may be feasible.2
Some untreated patients may have had diabetes for several years and have advanced disease and therefore might be more difficult to treat. Only 21 (57%) of 37 previously untreated patients intensively treated with insulin reached the goal fasting glucose level of less than 126 mg/dL in one study.6 The only way to evaluate the feasibility of achieving near-normal glycemia safely is by following the patient’s progress over time.
The patient’s glycemic goal should be reevaluated periodically and may need to be adjusted over time, based on changes in any of the factors discussed above.
Risk of hypoglycemia
The goal should be looser in difficult-to-treat patients, ie, those with frequent hypoglycemia and decreased awareness of hypoglycemia.
Patients with advanced diabetes whose glucose levels continue to fluctuate widely after lifestyle management and the insulin regimen have been addressed should also have a looser goal. These fluctuations of glucose levels are surrogate markers for the degree of insulin deficiency. Attempting to achieve near-normal glycemic levels in this situation would be associated with a higher risk of hypoglycemia.
A higher risk of hypoglycemia and its complications (eg, falling and accidents, especially among operators of heavy machinery, construction workers, and drivers) is another reason for adopting a relaxed goal of glycemic control.
ADDING BASAL INSULIN TO ORAL HYPOGLYCEMIC THERAPY
When glycemic control worsens or is not adequate despite the use of oral hypoglycemic agents, often the next step is to add basal insulin therapy, ie, once-daily doses of a long-acting insulin.
NPH, detemir, or glargine?
Most often, glargine or detemir (Levemir) insulin is used. Detemir can also be given twice daily if needed. If cost is a concern, neutral protamine Hagedorn (NPH, Humulin N, Novolin N) insulin once daily at bedtime or twice daily is a reasonable alternative.
Costs of basal insulins are $22 to $50 per 1,000-unit vial for NPH, $70 to $90 per 1,000-unit vial for detemir and glargine, and $170 to $200 for a box of five detemir or glargine pens (containing 1,500 units total). Complicating this issue, vials should not be used for more than 1 month, and thus, the cost of vials vs pens depends on dosage.
Detemir vs NPH. In a trial in patients with inadequately controlled type 2 diabetes who had never taken insulin before and who were taking one or more oral hypoglycemic drugs, the addition of detemir insulin once daily or NPH at bedtime resulted in similar improvements in hemoglobin A1c (a decrease of about 1.5%).10
Detemir had several advantages over NPH. First, the incidence of nocturnal hypoglycemia was 50% lower with detemir at bedtime than with NPH at bedtime, and 87% lower with detemir in the morning than with bedtime NPH.10 In another trial,11 the risk of hypoglycemia at any time of day was 47% lower with insulin detemir than with NPH, and the risk of nocturnal hypoglycemia was 55% lower.
The risk of nocturnal hypoglycemia is lower if detemir is taken in the morning than at bedtime, although the total frequency of hypoglycemic episodes is the same.10 Therefore, another decision after starting basal insulin, based on the patient’s glucose trends and frequency of hypoglycemic events, would be whether insulin should be taken in the morning or at bedtime.
The second advantage of detemir is that it causes less weight gain: 0.7 kg at 20 weeks with detemir at bedtime vs 1.6 kg with NPH at bedtime.10
Further, detemir insulin was associated with less within-subject variability in the fasting glucose level than with NPH when these insulins were used in a basal-bolus regimen.12
Hermansen et al11 found that if the dosage of basal insulin was aggressively increased, 70% of patients achieved a hemoglobin A1c target of less than 7% with either NPH or detemir insulin, with fewer hypoglycemic episodes in patients treated with detemir.
Therefore, adding basal insulin to oral therapy is adequate for many patients who are new to insulin. Many patients would need more, such as the addition of insulin before meals.
Glargine vs NPH. Compared with adding NPH, adding glargine to a regimen of oral hypoglycemic agents controls blood glucose levels better and with less fluctuation in glucose levels, a lower risk of hypoglycemia, and less weight gain.13–15 These results were the same when using glargine with either metformin13 or glimeperide (Amaryl).14
Glargine is usually given once daily at bedtime. One study suggested that giving it in the morning is more effective.14
Detemir vs glargine. Studies that compared detemir and glargine revealed more similarities than differences in their clinical benefits.16,17 Both preparations effectively lower glucose levels and improve quality of life.18
Titrating the insulin regimen is a key in achieving adequate glycemic control. This includes teaching patients how to adjust their insulin, for example by increasing the dosage of glargine or detemir by 2 units every 4 to 7 days until adequate glycemic control is achieved, unless hypoglycemia becomes a barrier.
BASAL VS PRANDIAL INSULIN
Once-daily insulin injection is relatively convenient, but it comes with a limitation: it does not adequately control postprandial hyperglycemia. A solution is insulin before meals, ie, prandial insulin.
Kazda et al19 compared three regimens in patients not taking oral hypoglycemic agents: rapid-acting insulin lispro (Humalog) before each meal, a mix of 50% lispro and 50% protamine lispro (Humalog Mix 50/50) (the protamine delays its release) before each meal, and glargine at bedtime. The absolute change in hemoglobin A1c was −0.3% in the glargine group, −1.1% in the lispro group, and −1.2% in the lispro mix group. The glargine group had better control of fasting glucose.
Similar advantages of better glycemic control and fewer nocturnal hypoglycemic episodes were seen in trials of a mixture of 25% lispro and 75% protamine lispro before meals compared with glargine insulin in patients on simultaneous treatment with oral hypoglycemic agents.20,21 Buse et al21 reported that more patients achieved a hemoglobin A1c level below 7% with this lispro mix (47%) than with glargine (40%). The absolute difference in mean hemoglobin A1c between the two groups was minimal, although it reached statistical significance. As expected, weight gain was less in the glargine group.21
Kann et al22 reported that glycemic control was also better with a mixture of 30% aspart and 70% protamine aspart (NovoLog Mix 70/30) twice a day along with metformin than with glargine insulin once a day along with oral glimepiride, a sulfonylurea. Further, in this study, weight gain was noted in the glargine-glimepiride group only.22 Therefore, the advantage of less weight gain has not been always reproducible in glargine studies.
Comment. These studies point to the contribution of postprandial glucose to hemoglobin A1c.23–25 In patients with satisfactory glycemic control, the postprandial glucose level seems to be the major contributor to hemoglobin A1c. When glycemic control worsens, the contribution of fasting glucose to hemoglobin A1c increases.23
Premixed insulins (lispro mix and aspart mix) provide basal coverage and control postprandial hyperglycemia. Therefore, prandial premixed insulin therapy is expected to be superior to basal insulin therapy. Premixed insulin could be considered as a simplified basal-bolus regimen (see below).
The superiority of prandial (rapid-acting) insulin alone over basal insulin therapy, as seen in the study by Kazda et al,19 has not been reproducible in other studies. For example, in one study, once-daily glargine resulted in a similar improvement in hemoglobin A1c, a lower rate of hypoglycemic episodes, and greater patient satisfaction with treatment compared with lispro insulin before meals.26 This issue remains debatable because all the trials have been open-label and thus are subject to limitations.
The main lesson is that either glargine or lispro monotherapy is a reasonable option and results in better glycemic control in patients for whom two oral hypoglycemic agents have failed. Further, both fasting and postprandial hyperglycemia are important to address. In patients with severe hyperglycemia, a combination of prandial and basal insulin may be indicated. One would expect neither basal nor prandial (bolus) insulin to be adequate in this situation.
In conclusion, adding basal insulin to oral hypoglycemic agents is a reasonable option in the advancement of diabetes therapy and has become a common way to introduce insulin. It is simple and less labor-intensive for patients and medical groups than a basal-bolus regimen. Patients usually find it acceptable. The future availability of an easy-to-deliver, safe, and effective prandial insulin may change the current treatment paradigm; several newer prandial insulins are under investigation.
In advanced diabetes, both prandial and fasting glucose levels are crucial to address. Some patients may need to be started on both basal and prandial insulin simultaneously, depending on their degree of hyperglycemia, the duration of diabetes, coexisting medical conditions, and the goal of glycemic control.
BASAL-BOLUS INSULIN REGIMENS
In the advanced stages of type 2 diabetes, as insulin deficiency worsens, patients need to start giving themselves injections of a rapid-acting insulin—regular, lispro, aspart, or glulisine (Apidra) before meals, in addition to once- or twice-daily basal insulin injections. Such a “basal-bolus” regimen could also be used for newly diagnosed patients presenting with severe hyperglycemia. In addition, some patients on basal insulin plus oral hypoglycemic drugs may develop contraindications to their oral drugs. Adding bolus insulin becomes the main option for these patients too.
For others, a basal-bolus regimen might be chosen purely because of cost. For example, a regimen of NPH and regular insulin (multiple daily injections or premixed) would be significantly less expensive than multiple oral hypoglycemic agents.
Currently, only a few classes of oral hypoglycemic drugs are available in generic formulations. For example, generic glimeperide and metformin cost as little as $4 to $12 per month, while the costs of brand-name oral hypoglycemic agents are in the range of $170 to $200 per month. In contrast, premixed NPH plus regular insulin such as Novolin 70/30 and Humulin 70/30 cost between $22 and $70 per vial.
A basal-bolus regimen should provide 50% of the total daily insulin in the form of basal insulin. A regimen of 50% basal and 50% bolus seemed to provide better glycemic control than a regimen of 35% basal and 65% bolus in several studies.27,28
In patients already taking a single daily dose of basal insulin along with oral hypoglycemic agents, the dosage of basal insulin is usually raised gradually until adequate glycemic control is achieved. A main question is when to add prandial insulin. There is no clear cutoff for a basal insulin dosage at which prandial insulin should be added.
In the Treat-to-Target Trial,29 almost 60% of patients achieved a hemoglobin A1c level of 7% or less with the addition of either glargine or NPH insulin (basal insulin only) to oral hypoglycemic agents during 24 weeks of follow-up. As expected, glargine caused less nocturnal hypoglycemia. Fewer than half the patients who achieved a hemoglobin A1c level less than 7% had no documented nocturnal hypoglycemia (33% of glargine-treated patients and 27% of NPH-treated patients).
Type 2 diabetes is progressive1; over time, patients treated with once-daily basal insulin often require multiple daily injections.
Adding prandial to basal insulin clearly results in better glycemic control and less glucose variability.19,20,22,30–33 Two major factors in deciding to start prandial insulin are the degree of hyperglycemia and the patient’s acceptance of multiple daily injections. The higher the blood glucose levels, the sooner prandial insulin should be added, especially if hyperglycemia is influencing the prognosis of a coexisting condition or a diabetic complication (eg, an infected foot ulcer).
Adding prandial insulin should be also considered if the dosage of basal insulin has progressively been increased and the hemoglobin A1c level is not improving, especially if a patient has both inadequate glycemic control and frequent hypoglycemia, or if the morning glucose level is within the desired range (indicating there is no room for a further increase in the basal insulin dose) in association with inadequate control of hemoglobin A1c.
What is the best basal insulin for a basal-bolus regimen?
Glargine and detemir were shown to be equally effective as the basal component of a basal-bolus regimen.34,35 Findings were similar to those of studies comparing NPH, detemir, and glargine added, by themselves, to oral hypoglycemic agents. When possible, either glargine or detemir is favored because of less hypoglycemia and less weight gain than with NPH. Weight gain is the least with detemir.
Adding prandial insulin to a basal regimen
In general, whether to add prandial insulin can be decided on the basis of the patient’s record of blood glucose monitoring. Insulin could be added before breakfast if the pre-lunch glucose level is elevated, or before lunch if the dinnertime blood glucose level is elevated, or before dinner if the bedtime blood glucose level is elevated—or a combination of these. Prandial insulin can be started at a low dose (4–6 units) and increased gradually.
In the case of poor glycemic control on a high dosage of basal insulin, a reasonable first step would be to change the regimen to a basal-bolus regimen (about 50% basal and 50% bolus) with no change or a small decrease in the total daily dosage of insulin to avoid hypoglycemia. For example, in a patient on 80 units of glargine or detemir insulin who has inadequate control, the regimen could be changed to 35 units of either glargine or detemir and 10 to 12 units of lispro, aspart, or glulisine before each meal as the bolus component.
Further adjustments of the insulin dosage can be made according to the results of glucose monitoring before each meal and at bedtime. In all case scenarios, the insulin regimen should be re-evaluated routinely during the advancement of therapy from single daily injection of basal insulin to multiple daily injections. Redistribution of total insulin dosage to 50% basal and 50% bolus (divided into three doses before meals) should be considered for patients who continue to have fluctuations of glucose levels, inadequate control, or frequent hypoglycemia. This ratio seems to provide better control for most patients.27,28
Starting with a basal-bolus regimen
For patients new to insulin who are starting a basal-bolus regimen, a dosage based on total body weight could be considered. The requirements vary significantly based on dietary management, level of physical activity, stress (especially illnesses), use of oral hypoglycemic agents, and degree of hyperglycemia.
A lower dosage of insulin (0.2 units per kg) should be considered for people with mild stress, with milder hyperglycemia, or on treatment with oral hypoglycemic agents. Elderly patients and patients with renal or liver failure are at higher risk of hypoglycemia and should also receive a lower dosage of insulin, at least to start with.
Others could be started on a dosage of 0.3 to 0.5 units/kg. Fifty percent of the calculated dosage could be given as basal insulin and 50% given as bolus (divided into three doses, before meals). Subsequently, the dosage would need to be titrated on the basis of the record of glucose monitoring.
Choosing a prandial insulin
Rapid-acting insulin analogues (lispro, aspart, and glulisine) control postprandial glucose levels better than regular insulin and cause less hypoglycemia. Their pharmacokinetics enable them to be taken within a few minutes of the start of a meal, or even after the meal if the patient forgets to take an injection before the meal.
For example, in one study,36 taking aspart immediately before the meal provided better glycemic control than taking regular insulin 30 minutes before meals. In a basal-bolus regimen, the use of aspart along with detemir resulted in glycemic control similar to that provided by twice-daily NPH and regular insulin, with less hypoglycemia.37
The dosage of prandial insulin can be adjusted according to the amount of carbohydrates in each meal (the insulin-to-carbohydrate ratio), as in patients with type 1 diabetes. This approach was associated with less weight gain.38
IS THERE STILL A ROLE FOR PREMIXED INSULIN PREPARATIONS?
Basal-bolus insulin regimens have gained popularity because the prandial doses can easily be adjusted according to carbohydrate intake, glucose level (on a sliding scale), variations in meal time, missed meals (eg, when having a procedure), and exercise. For example, the dose of prandial insulin can be reduced if the patient expects to exercise within 2 or 3 hours after the meal.
Some patients may not accept giving themselves four or five injections per day with a basal-bolus regimen. They may accept a simpler regimen, ie, giving themselves three injections of a premixed insulin per day, one before each meal.
Compared with a basal-bolus regimen, the possibility of achieving adequate glycemic control using lispro mix (50% lispro, 50% lispro protamine suspension) before meals seemed to depend on the goal of glycemic control. Its use in one study showed similar ability to achieve hemoglobin A1c less than 7.5% compared with a basal-bolus regimen of glargine and lispro. For a goal hemoglobin A1c level of less than 7%, the use of glargine and lispro was superior. The rate of hypoglycemia was similar with both strategies.39 These findings imply that the goal hemoglobin A1c should be more relaxed (< 7.5%) when using lispro mix (50% lispro) three times daily before meals.
Biphasic insulin aspart (a mix of aspart and protamine aspart) given three times daily provided similar improvement in glycemic control with no difference in the frequency of hypoglycemia compared with a basal-bolus regimen of NPH and aspart.40 Further, the use of biphasic insulin aspart seemed to provide better glycemic control with less weight gain compared with premixed human insulin (70% NPH, 30% regular insulin).41
Therefore, simpler premixed insulin regimens remain reasonable options for selected patients who do not accept a more complex insulin regimen (basal-bolus) or cannot adhere to it for any reason, especially if premixed insulin is given before meals three times daily. In fact, recent studies have focused on comparing premixed insulin three times daily with basal-bolus regimens (detemir or glargine as basal insulin along with pre-meal insulin analogue).
Glycemic control is harder to achieve with premixed insulin twice daily, mainly because of a higher frequency of hypoglycemia.42 In Europe, the use of premixed insulin three times daily is a popular option, whereas in the United States, a twice-daily schedule has been more common.
COST VS CONTROL
Newer insulin analogues make insulin treatment safer and more accepted by patients. The availability of several options for insulin regimens allows individualization of the treatment according to the patient’s acceptance, the safety profile, and the cost.
Patient selection and insulin titration are key issues in ensuring the achievement of adequate control with the fewest side effects. Lifestyle management (diet and physical activity) enhances the efficacy of insulin therapy and reduces the chances of side effects, namely fluctuation of glucose levels, hypoglycemic episodes, and weight gain.
Human insulins (NPH and regular) remain the least expensive, especially when using premixed NPH-regular insulin 70/30. Their use should be considered when the cost of medication is a major concern for the patient. A more relaxed goal of glycemic control may be considered in order to avoid hypoglycemia when using those insulin preparations, such as a hemoglobin A1c level less than 7.5% or even in the range of 7.5% to 8.5%, depending on the expected seasonal variation of hemoglobin A1c (which is higher in winter43), individual factors, and whether the premixed insulin is used twice or three times daily.
RE-EVALUATE THE REGIMEN ROUTINELY
The insulin regimen should be re-evaluated routinely. It might need to be changed in response to the dynamic multifactorial process of progression of diabetes, change in stress level, presence or resolution of intercurrent illnesses, risk of hypoglycemia, concerns about weight gain, and cost.
Finally, adjustment of the regimen should be considered in response to improvement of glycemic control related to improvement of dietary management, exercising, weight loss, and medical therapies.
- UK Prospective Diabetes Study 16. Overview of 6 years’ therapy of type II diabetes: a progressive disease. UK Prospective Diabetes Study Group. Diabetes 1995; 44:1249–1258.
- Nathan DM, Buse JB, Davidson MB, et al; American Diabetes Association. Medical management of hyperglycemia in type 2 diabetes: a consensus algorithm for the initiation and adjustment of therapy: a consensus statement of the American Diabetes Association and the European Association for the Study of Diabetes. Diabetes Care 2009; 32:193–203.
- Rodbard HW, Jellinger PS, Davidson JA, et al. Statement by an American Association of Clinical Endocrinologists/American College of Endocrinology consensus panel on type 2 diabetes mellitus: an algorithm for glycemic control. Endocr Pract 2009; 15:540–558.
- ClinicalTrials.gov. The ORIGIN Trial (Outcome Reduction With Initial Glargine Intervention). http://clinicaltrials.gov/ct2/show/NCT00069784. Accessed 2/11/11.
- American Diabetes Association. Standards of medical care in diabetes—2010. Diabetes Care 2010; 33(suppl 1):S11–S61.
- Retnakaran R, Qi Y, Opsteen C, Vivero E, Zinman B. Initial short-term intensive insulin therapy as a strategy for evaluating the preservation of beta-cell function with oral antidiabetic medications: a pilot study with sitagliptin. Diabetes Obes Metab 2010; 12:909–915.
- Zoungas S, Patel A, Chalmers J, et al; ADVANCE Collaborative Group. Severe hypoglycemia and risks of vascular events and death. N Engl J Med 2010; 363:1410–1418.
- Akram K, Pedersen-Bjergaard U, Borch-Johnsen K, Thorsteinsson B. Frequency and risk factors of severe hypoglycemia in insulin-treated type 2 diabetes: a literature survey. J Diabetes Complications 2006; 20:402–408.
- Cryer PE. Chapter 19. Hypoglycemia. In: Jameson JL, editor. Harrison’s Endocrinology. McGraw Hill, 2006:355–363.
- Philis-Tsimikas A, Charpentier G, Clauson P, Ravn GM, Roberts VL, Thorsteinsson B. Comparison of once-daily insulin detemir with NPH insulin added to a regimen of oral antidiabetic drugs in poorly controlled type 2 diabetes. Clin Ther 2006; 28:1569–1581. Erratum in: Clin Ther 2006; 28:1967.
- Hermansen K, Davies M, Derezinski T, Martinez Ravn G, Clauson P, Home P. A 26-week, randomized, parallel, treat-to-target trial comparing insulin detemir with NPH insulin as add-on therapy to oral glucose-lowering drugs in insulin-naive people with type 2 diabetes. Diabetes Care 2006; 29:1269–1274. Erratum in: Diabetes Care 2007; 30:1035.
- Haak T, Tiengo A, Draeger E, Suntum M, Waldhäusl W. Lower within-subject variability of fasting blood glucose and reduced weight gain with insulin detemir compared to NPH insulin in patients with type 2 diabetes. Diabetes Obes Metab 2005; 7:56–64.
- Yki-Järvinen H, Kauppinen-Mäkelin R, Tiikkainen M, et al. Insulin glargine or NPH combined with metformin in type 2 diabetes: the LANMET study. Diabetalogia 2006; 49:442–451.
- Fritsche A, Schweitzer MA, Häring HU; 4001 Study Group. Glimepiride combined with morning insulin glargine, bedtime neutral protamine hagedorn insulin, or bedtime insulin glargine in patients with type 2 diabetes. A randomized, controlled trial. Ann Intern Med 2003; 138:952–959.
- Rosenstock J, Schwartz SL, Clark CM, Park GD, Donley DW, Edwards MB. Basal insulin therapy in type 2 diabetes: 28-week comparison of insulin glargine (HOE 901) and NPH insulin. Diabetes Care 2001; 24:631–636.
- Rosenstock J, Davies M, Home PD, Larsen J, Koenen C, Schernthaner G. A randomised, 52-week, treat-to-target trial comparing insulin detemir with insulin glargine when administered as add-on to glucose-lowering drugs in insulin-naive people with type 2 diabetes. Diabetologia 2008; 51:408–416.
- King AB. Once-daily insulin detemir is comparable to once-daily insulin glargine in providing glycaemic control over 24 h in patients with type 2 diabetes: a double-blind, randomized, crossover study. Diabetes Obes Metab 2009; 11:69–71.
- Swinnen SG, Snoek FJ, Dain MP, DeVries JH, Hoekstra JB, Holleman F. Rationale, design, and baseline data of the insulin glargine (Lantus) versus insulin detemir (Levemir) Treat-To-Target (L2T3) study: a multinational, randomized noninferiority trial of basal insulin initiation in type 2 diabetes. Diabetes Technol Ther 2009; 11:739–743.
- Kazda C, Hülstrunk H, Helsberg K, Langer F, Forst T, Hanefeld M. Prandial insulin substitution with insulin lispro or insulin lispro mid mixture vs. basal therapy with insulin glargine: a randomized controlled trial in patients with type 2 diabetes beginning insulin therapy. J Diabetes Complications 2006; 20:145–152.
- Malone JK, Bai S, Campaigne BN, Reviriego J, Augendre-Ferrante B. Twice-daily pre-mixed insulin rather than basal insulin therapy alone results in better overall glycaemic control in patients with type 2 diabetes. Diabet Med 2005; 22:374–381.
- Buse JB, Wolffenbuttel BH, Herman WH, et al. DURAbility of basal versus lispro mix 75/25 insulin efficacy (DURABLE) trial 24-week results: safety and efficacy of insulin lispro mix 75/25 versus insulin glargine added to oral antihyperglycemic drugs in patients with type 2 diabetes. Diabetes Care 2009; 32:1007–1013.
- Kann PH, Wascher T, Zackova V, et al. Starting insulin therapy in type 2 diabetes: twice-daily biphasic insulin Aspart 30 plus metformin versus once-daily insulin glargine plus glimepiride. Exp Clin Endocrinol Diabetes 2006; 114:527–532.
- Monnier L, Colette C, Monnier L, Colette C. Contributions of fasting and postprandial glucose to hemoglobin A1c. Endocr Pract 2006; 12(suppl 1):42–46.
- Woerle HJ, Pimenta WP, Meyer C, et al. Diagnostic and therapeutic implications of relationships between fasting, 2-hour postchallenge plasma glucose and hemoglobin A1c values. Arch Intern Med 2004; 164:1627–1632.
- Schrot RJ. Targeting plasma glucose: preprandial versus postprandial. Clinical Diabetes 2004; 22:169–172.
- Bretzel RG, Nuber U, Landgraf W, Owens DR, Bradley C, Linn T. Once-daily basal insulin glargine versus thrice-daily prandial insulin lispro in people with type 2 diabetes on oral hypoglycaemic agents (APOLLO): an open randomised controlled trial. Lancet 2008; 371:1073–1084.
- Tamaki M, Shimizu T, Kanazawa A, Fujitani Y, Watada H, Kawamori R, Hirose T. Effects of changes in basal/total daily insulin ratio in type 2 diabetes patients on intensive insulin therapy including insulin glargine (JUN-LAN Study 6). Diabetes Res Clin Pract 2008; 81:e1–e3.
- Yokoyama H, Tada J, Kamikawa F, Kanno S, Yokota Y, Kuramitsu M. Efficacy of conversion from bedtime NPH insulin to morning insulin glargine in type 2 diabetic patients on basal-prandial insulin therapy. Diabetes Res Clin Pract 2006; 73:35–40.
- Riddle MC, Rosenstock J, Gerich J; Insulin Glargine 4002 Study Investigators. The Treat-To-Target trial: randomized addition of glargine or human NPH insulin to oral therapy of type 2 diabetic patients. Diabetes Care 2003; 26:3080–3086.
- Davies M, Sinnassamy P, Storms F, Gomis R; ATLANTUS Study Group. Insulin glargine-based therapy improves glycemic control in patients with type 2 diabetes sub-optimally controlled on premixed insulin therapies. Diabetes Res Clin Pract 2008; 79:368–375.
- Jacober SJ, Scism-Bacon JL, Zagar AJ. A comparison of intensive mixture therapy with basal insulin therapy in insulin-naïve patients with type 2 diabetes receiving oral antidiabetes agents. Diabetes Obes Metab 2006; 8:448–455.
- Hirsch IB, Yuan H, Campaigne BN, Tan MH. Impact of prandial plus basal vs basal insulin on glycemic variability in type 2 diabetic patients. Endocr Pract 2009; 15:343–348.
- Robbins DC, Beisswenger PJ, Ceriello A, et al. Mealtime 50/50 basal + prandial insulin analogue mixture with a basal insulin analogue, both plus metformin, in the achievement of target HbA1c and pre- and postprandial blood glucose levels in patients with type 2 diabetes: a multinational, 24-week, randomized, open-label, parallel-group comparison. Clin Ther 2007; 29:2349–2364.
- Hollander P, Cooper J, Bregnhøj J, Pedersen CB. A 52-week, multinational, open-label, parallel-group, noninferiority, treat-to-target trial comparing insulin detemir with insulin glargine in a basal-bolus regimen with mealtime insulin aspart in patients with type 2 diabetes. Clin Ther 2008; 30:1976–1987.
- Raskin P, Gylvin T, Weng W, Chaykin L. Comparison of insulin detemir and insulin glargine using a basal-bolus regimen in a randomized, controlled clinical study in patients with type 2 diabetes. Diabetes Metab Res Rev 2009; 25:542–548.
- Perriello G, Pampanelli S, Porcellati F, et al. Insulin aspart improves meal time glycaemic control in patients with type 2 diabetes: a randomized, stratified, double-blind and cross-over trial. Diabet Med 2005; 22:606–611.
- Umpierrez GE, Hor T, Smiley D, et al. Comparison of inpatient insulin regimens with detemir plus aspart versus neutral protamine hagedorn plus regular in medical patients with type 2 diabetes. J Clin Endocrinol Metab 2009; 94:564–569.
- Bergenstal RM, Johnson M, Powers MA, et al. Adjust to target in type 2 diabetes: comparison of a simple algorithm with carbohydrate counting for adjustment of mealtime insulin glulisine. Diabetes Care 2008; 31:1305–1310.
- Rosenstock J, Ahmann AJ, Colon G, Scism-Bacon J, Jiang H, Martin S. Advancing insulin therapy in type 2 diabetes previously treated with glargine plus oral agents: prandial premixed (insulin lispro protamine suspension/lispro) versus basal/bolus (glargine/lispro) therapy. Diabetes Care 2008; 31:20–25.
- Ligthelm RJ, Mouritzen U, Lynggaard H, et al. Biphasic insulin aspart given thrice daily is as efficacious as a basal-bolus insulin regimen with four daily injections: a randomised open-label parallel group four months comparison in patients with type 2 diabetes. Exp Clin Endocrinol Diabetes 2006; 114:511–519.
- Velojic-Golubovic M, Mikic D, Pesic M, Dimic D, Radenkovic S, Antic S. Biphasic insulin aspart 30: better glycemic control than with premixed human insulin 30 in obese patients with type 2 diabetes. J Endocrinol Invest 2009; 32:23–27.
- Holman RR, Farmer AJ, Davies MJ, et al; 4-T Study Group. Three-year efficacy of complex insulin regimens in type 2 diabetes. N Engl Med 2009; 361:1736–1747.
- Tseng CL, Brimacombe M, Xie M, et al. Seasonal patterns in monthly hemoglobin A1c values. Am J Epidemiol 2005; 161:565–574.
Many patients with type 2 diabetes eventually need insulin, as their ability to produce their own insulin from pancreatic beta cells declines progressively.1 The questions remain as to when insulin therapy should be started, and which regimen is the most appropriate.
Guidelines from professional societies differ on these points,2,3 as do individual clinicians. Moreover, antidiabetic treatment is an evolving topic. Many new drugs—oral agents as well as injectable analogues of glucagon-like peptide-1 (GLP1) and insulin formulations—have become available in the last 15 years.
In this paper, I advocate an individualized approach and review the indications for insulin treatment, the available preparations, the pros and cons of each regimen, and how the properties of each type of insulin influence attempts to intensify the regimen.
Coexisting physiologic and medical conditions such as pregnancy and chronic renal failure and drugs such as glucocorticoids may alter insulin requirements. I will not cover these special situations, as they deserve separate, detailed discussions.
WHEN SHOULD INSULIN BE STARTED? TWO VIEWS
Early on, patients can be adequately managed with lifestyle modifications and oral hypoglycemic agents or injections of a GLP1 analogue, either alone or in combination with oral medication. Later, some patients reach a point at which insulin therapy becomes the main treatment, similar to patients with type 1 diabetes.
The American Diabetes Association (ADA), in a consensus statement,2 has called for using insulin early in the disease if lifestyle management and monotherapy with metformin (Glucophage) fail to control glucose or if lifestyle management is not adequate and metformin is contraindicated. The ADA’s goal hemoglobin A1c level is less than 7% for most patients.
The American Association of Clinical Endocrinologists (AACE) and the American College of Endocrinology (ACE), in another consensus statement, use an algorithm stratified by hemoglobin A1c level, in which insulin is mostly reserved for when combination therapy fails.3 Their goal hemoglobin A1c level is 6.5% or less for most patients.
Comment. Both consensus statements make exceptions for patients presenting with very high blood glucose and hemoglobin A1c levels and those who have contraindications to drugs other than insulin. These patients should start insulin immediately, along with lifestyle management.2,3
Both consensus statements give priority to safety. The AACE/ACE statement gives more weight to the risk of hypoglycemia with insulin treatment, whereas the ADA gives more weight to the risk of edema and congestive heart failure with thiazolidinedione drugs (although both insulin and thiazolidinediones cause weight gain) and to adequate validation of treatments in clinical trials.
Ongoing clinical trials may add insight to this issue. For example, the Outcome Reduction With Initial Glargine Intervention (ORIGIN) study is investigating the effects of the long-acting insulin glargine (Lantus) in early diabetes with regard to glycemic control, safety, and cardiovascular outcomes.4 This study is expected to end this year (2011). The safety of alternative treatment options is also under investigation and scrutiny. In the interim, individualized treatment should be considered, as we will see below.
MY VIEW: AN INDIVIDUALIZED APPROACH
The decision to start insulin therapy should be made individually, based on several factors:
- Whether the patient is willing to try it
- The degree of hyperglycemia
- How relevant the potential side effects of insulin are to the patient compared with those of other hypoglycemic agents
- Whether oral hypoglycemic agents with or without GLP1 analogues are expected to provide the desired benefit
- The patient’s work schedule and lifestyle factors
- Cost
- The availability of nurses, diabetes educators, and others to implement and follow the insulin treatment.
Will patients accept insulin?
Factors that affect whether patients comply with a treatment include the number of pills or injections they must take per day, how often they must check their blood glucose, adverse effects, lifestyle limitations caused by the treatment (especially insulin), and cost. Most patients feel better when their glucose levels are under good control, which is a major motivation for initiating and adhering to insulin. The anticipated reduction of diabetic complications further enhances compliance.
Education promotes compliance. Patients need to know that type 2 diabetes tends to progress and that in time their treatment will have to be intensified, with higher doses of their current drugs and new drugs added or substituted, possibly including insulin. This information is best given early, ie, when the diagnosis is made, even if hyperglycemia is mild at that time.
With newer insulin preparations and delivery devices available, more patients are finding insulin treatment acceptable.
The glycemic goal should be individualized
The key issue is glycemic control. If glycemic control is worsening or if the hemoglobin A1c level remains above the goal, then the treatment strategy should be readdressed.
In general, one should try to achieve the best possible glycemic control with the few est adverse effects. Adequate dietary management with a regular meal schedule and predictable carbohydrate intake for each meal helps to avoid or at least minimize the two most important adverse effects of insulin, ie, weight gain and hypoglycemia.
For most patients, I believe a goal hemoglobin A1c level of less than 7% is reasonable.2 For others, a less stringent goal might be more appropriate, such as 7.5%. Several factors affect this decision, including whether the patient is willing to follow a complex insulin regimen (such as a basal-bolus regimen), his or her work schedule, other lifestyle factors, the duration of diabetes, the type or types of insulin used, coexisting medical conditions, the frequency of hypoglycemia, unawareness of hypoglycemia, age, prognosis, life expectancy, and cost.5
If hyperglycemia is severe (Table 1),2 the goal might not be clear when insulin therapy is started. It should become obvious with ongoing follow-up.
Previously untreated patients presenting with severe hyperglycemia are a heterogeneous group. Many of them have had diabetes for a relatively short time and were recently diagnosed. These patients are likely to safely achieve near-normal glycemic control. Some of them might be adequately treated with oral hypoglycemic agents; if insulin is used, transitioning from insulin to oral hypoglycemic agents may be feasible.2
Some untreated patients may have had diabetes for several years and have advanced disease and therefore might be more difficult to treat. Only 21 (57%) of 37 previously untreated patients intensively treated with insulin reached the goal fasting glucose level of less than 126 mg/dL in one study.6 The only way to evaluate the feasibility of achieving near-normal glycemia safely is by following the patient’s progress over time.
The patient’s glycemic goal should be reevaluated periodically and may need to be adjusted over time, based on changes in any of the factors discussed above.
Risk of hypoglycemia
The goal should be looser in difficult-to-treat patients, ie, those with frequent hypoglycemia and decreased awareness of hypoglycemia.
Patients with advanced diabetes whose glucose levels continue to fluctuate widely after lifestyle management and the insulin regimen have been addressed should also have a looser goal. These fluctuations of glucose levels are surrogate markers for the degree of insulin deficiency. Attempting to achieve near-normal glycemic levels in this situation would be associated with a higher risk of hypoglycemia.
A higher risk of hypoglycemia and its complications (eg, falling and accidents, especially among operators of heavy machinery, construction workers, and drivers) is another reason for adopting a relaxed goal of glycemic control.
ADDING BASAL INSULIN TO ORAL HYPOGLYCEMIC THERAPY
When glycemic control worsens or is not adequate despite the use of oral hypoglycemic agents, often the next step is to add basal insulin therapy, ie, once-daily doses of a long-acting insulin.
NPH, detemir, or glargine?
Most often, glargine or detemir (Levemir) insulin is used. Detemir can also be given twice daily if needed. If cost is a concern, neutral protamine Hagedorn (NPH, Humulin N, Novolin N) insulin once daily at bedtime or twice daily is a reasonable alternative.
Costs of basal insulins are $22 to $50 per 1,000-unit vial for NPH, $70 to $90 per 1,000-unit vial for detemir and glargine, and $170 to $200 for a box of five detemir or glargine pens (containing 1,500 units total). Complicating this issue, vials should not be used for more than 1 month, and thus, the cost of vials vs pens depends on dosage.
Detemir vs NPH. In a trial in patients with inadequately controlled type 2 diabetes who had never taken insulin before and who were taking one or more oral hypoglycemic drugs, the addition of detemir insulin once daily or NPH at bedtime resulted in similar improvements in hemoglobin A1c (a decrease of about 1.5%).10
Detemir had several advantages over NPH. First, the incidence of nocturnal hypoglycemia was 50% lower with detemir at bedtime than with NPH at bedtime, and 87% lower with detemir in the morning than with bedtime NPH.10 In another trial,11 the risk of hypoglycemia at any time of day was 47% lower with insulin detemir than with NPH, and the risk of nocturnal hypoglycemia was 55% lower.
The risk of nocturnal hypoglycemia is lower if detemir is taken in the morning than at bedtime, although the total frequency of hypoglycemic episodes is the same.10 Therefore, another decision after starting basal insulin, based on the patient’s glucose trends and frequency of hypoglycemic events, would be whether insulin should be taken in the morning or at bedtime.
The second advantage of detemir is that it causes less weight gain: 0.7 kg at 20 weeks with detemir at bedtime vs 1.6 kg with NPH at bedtime.10
Further, detemir insulin was associated with less within-subject variability in the fasting glucose level than with NPH when these insulins were used in a basal-bolus regimen.12
Hermansen et al11 found that if the dosage of basal insulin was aggressively increased, 70% of patients achieved a hemoglobin A1c target of less than 7% with either NPH or detemir insulin, with fewer hypoglycemic episodes in patients treated with detemir.
Therefore, adding basal insulin to oral therapy is adequate for many patients who are new to insulin. Many patients would need more, such as the addition of insulin before meals.
Glargine vs NPH. Compared with adding NPH, adding glargine to a regimen of oral hypoglycemic agents controls blood glucose levels better and with less fluctuation in glucose levels, a lower risk of hypoglycemia, and less weight gain.13–15 These results were the same when using glargine with either metformin13 or glimeperide (Amaryl).14
Glargine is usually given once daily at bedtime. One study suggested that giving it in the morning is more effective.14
Detemir vs glargine. Studies that compared detemir and glargine revealed more similarities than differences in their clinical benefits.16,17 Both preparations effectively lower glucose levels and improve quality of life.18
Titrating the insulin regimen is a key in achieving adequate glycemic control. This includes teaching patients how to adjust their insulin, for example by increasing the dosage of glargine or detemir by 2 units every 4 to 7 days until adequate glycemic control is achieved, unless hypoglycemia becomes a barrier.
BASAL VS PRANDIAL INSULIN
Once-daily insulin injection is relatively convenient, but it comes with a limitation: it does not adequately control postprandial hyperglycemia. A solution is insulin before meals, ie, prandial insulin.
Kazda et al19 compared three regimens in patients not taking oral hypoglycemic agents: rapid-acting insulin lispro (Humalog) before each meal, a mix of 50% lispro and 50% protamine lispro (Humalog Mix 50/50) (the protamine delays its release) before each meal, and glargine at bedtime. The absolute change in hemoglobin A1c was −0.3% in the glargine group, −1.1% in the lispro group, and −1.2% in the lispro mix group. The glargine group had better control of fasting glucose.
Similar advantages of better glycemic control and fewer nocturnal hypoglycemic episodes were seen in trials of a mixture of 25% lispro and 75% protamine lispro before meals compared with glargine insulin in patients on simultaneous treatment with oral hypoglycemic agents.20,21 Buse et al21 reported that more patients achieved a hemoglobin A1c level below 7% with this lispro mix (47%) than with glargine (40%). The absolute difference in mean hemoglobin A1c between the two groups was minimal, although it reached statistical significance. As expected, weight gain was less in the glargine group.21
Kann et al22 reported that glycemic control was also better with a mixture of 30% aspart and 70% protamine aspart (NovoLog Mix 70/30) twice a day along with metformin than with glargine insulin once a day along with oral glimepiride, a sulfonylurea. Further, in this study, weight gain was noted in the glargine-glimepiride group only.22 Therefore, the advantage of less weight gain has not been always reproducible in glargine studies.
Comment. These studies point to the contribution of postprandial glucose to hemoglobin A1c.23–25 In patients with satisfactory glycemic control, the postprandial glucose level seems to be the major contributor to hemoglobin A1c. When glycemic control worsens, the contribution of fasting glucose to hemoglobin A1c increases.23
Premixed insulins (lispro mix and aspart mix) provide basal coverage and control postprandial hyperglycemia. Therefore, prandial premixed insulin therapy is expected to be superior to basal insulin therapy. Premixed insulin could be considered as a simplified basal-bolus regimen (see below).
The superiority of prandial (rapid-acting) insulin alone over basal insulin therapy, as seen in the study by Kazda et al,19 has not been reproducible in other studies. For example, in one study, once-daily glargine resulted in a similar improvement in hemoglobin A1c, a lower rate of hypoglycemic episodes, and greater patient satisfaction with treatment compared with lispro insulin before meals.26 This issue remains debatable because all the trials have been open-label and thus are subject to limitations.
The main lesson is that either glargine or lispro monotherapy is a reasonable option and results in better glycemic control in patients for whom two oral hypoglycemic agents have failed. Further, both fasting and postprandial hyperglycemia are important to address. In patients with severe hyperglycemia, a combination of prandial and basal insulin may be indicated. One would expect neither basal nor prandial (bolus) insulin to be adequate in this situation.
In conclusion, adding basal insulin to oral hypoglycemic agents is a reasonable option in the advancement of diabetes therapy and has become a common way to introduce insulin. It is simple and less labor-intensive for patients and medical groups than a basal-bolus regimen. Patients usually find it acceptable. The future availability of an easy-to-deliver, safe, and effective prandial insulin may change the current treatment paradigm; several newer prandial insulins are under investigation.
In advanced diabetes, both prandial and fasting glucose levels are crucial to address. Some patients may need to be started on both basal and prandial insulin simultaneously, depending on their degree of hyperglycemia, the duration of diabetes, coexisting medical conditions, and the goal of glycemic control.
BASAL-BOLUS INSULIN REGIMENS
In the advanced stages of type 2 diabetes, as insulin deficiency worsens, patients need to start giving themselves injections of a rapid-acting insulin—regular, lispro, aspart, or glulisine (Apidra) before meals, in addition to once- or twice-daily basal insulin injections. Such a “basal-bolus” regimen could also be used for newly diagnosed patients presenting with severe hyperglycemia. In addition, some patients on basal insulin plus oral hypoglycemic drugs may develop contraindications to their oral drugs. Adding bolus insulin becomes the main option for these patients too.
For others, a basal-bolus regimen might be chosen purely because of cost. For example, a regimen of NPH and regular insulin (multiple daily injections or premixed) would be significantly less expensive than multiple oral hypoglycemic agents.
Currently, only a few classes of oral hypoglycemic drugs are available in generic formulations. For example, generic glimeperide and metformin cost as little as $4 to $12 per month, while the costs of brand-name oral hypoglycemic agents are in the range of $170 to $200 per month. In contrast, premixed NPH plus regular insulin such as Novolin 70/30 and Humulin 70/30 cost between $22 and $70 per vial.
A basal-bolus regimen should provide 50% of the total daily insulin in the form of basal insulin. A regimen of 50% basal and 50% bolus seemed to provide better glycemic control than a regimen of 35% basal and 65% bolus in several studies.27,28
In patients already taking a single daily dose of basal insulin along with oral hypoglycemic agents, the dosage of basal insulin is usually raised gradually until adequate glycemic control is achieved. A main question is when to add prandial insulin. There is no clear cutoff for a basal insulin dosage at which prandial insulin should be added.
In the Treat-to-Target Trial,29 almost 60% of patients achieved a hemoglobin A1c level of 7% or less with the addition of either glargine or NPH insulin (basal insulin only) to oral hypoglycemic agents during 24 weeks of follow-up. As expected, glargine caused less nocturnal hypoglycemia. Fewer than half the patients who achieved a hemoglobin A1c level less than 7% had no documented nocturnal hypoglycemia (33% of glargine-treated patients and 27% of NPH-treated patients).
Type 2 diabetes is progressive1; over time, patients treated with once-daily basal insulin often require multiple daily injections.
Adding prandial to basal insulin clearly results in better glycemic control and less glucose variability.19,20,22,30–33 Two major factors in deciding to start prandial insulin are the degree of hyperglycemia and the patient’s acceptance of multiple daily injections. The higher the blood glucose levels, the sooner prandial insulin should be added, especially if hyperglycemia is influencing the prognosis of a coexisting condition or a diabetic complication (eg, an infected foot ulcer).
Adding prandial insulin should be also considered if the dosage of basal insulin has progressively been increased and the hemoglobin A1c level is not improving, especially if a patient has both inadequate glycemic control and frequent hypoglycemia, or if the morning glucose level is within the desired range (indicating there is no room for a further increase in the basal insulin dose) in association with inadequate control of hemoglobin A1c.
What is the best basal insulin for a basal-bolus regimen?
Glargine and detemir were shown to be equally effective as the basal component of a basal-bolus regimen.34,35 Findings were similar to those of studies comparing NPH, detemir, and glargine added, by themselves, to oral hypoglycemic agents. When possible, either glargine or detemir is favored because of less hypoglycemia and less weight gain than with NPH. Weight gain is the least with detemir.
Adding prandial insulin to a basal regimen
In general, whether to add prandial insulin can be decided on the basis of the patient’s record of blood glucose monitoring. Insulin could be added before breakfast if the pre-lunch glucose level is elevated, or before lunch if the dinnertime blood glucose level is elevated, or before dinner if the bedtime blood glucose level is elevated—or a combination of these. Prandial insulin can be started at a low dose (4–6 units) and increased gradually.
In the case of poor glycemic control on a high dosage of basal insulin, a reasonable first step would be to change the regimen to a basal-bolus regimen (about 50% basal and 50% bolus) with no change or a small decrease in the total daily dosage of insulin to avoid hypoglycemia. For example, in a patient on 80 units of glargine or detemir insulin who has inadequate control, the regimen could be changed to 35 units of either glargine or detemir and 10 to 12 units of lispro, aspart, or glulisine before each meal as the bolus component.
Further adjustments of the insulin dosage can be made according to the results of glucose monitoring before each meal and at bedtime. In all case scenarios, the insulin regimen should be re-evaluated routinely during the advancement of therapy from single daily injection of basal insulin to multiple daily injections. Redistribution of total insulin dosage to 50% basal and 50% bolus (divided into three doses before meals) should be considered for patients who continue to have fluctuations of glucose levels, inadequate control, or frequent hypoglycemia. This ratio seems to provide better control for most patients.27,28
Starting with a basal-bolus regimen
For patients new to insulin who are starting a basal-bolus regimen, a dosage based on total body weight could be considered. The requirements vary significantly based on dietary management, level of physical activity, stress (especially illnesses), use of oral hypoglycemic agents, and degree of hyperglycemia.
A lower dosage of insulin (0.2 units per kg) should be considered for people with mild stress, with milder hyperglycemia, or on treatment with oral hypoglycemic agents. Elderly patients and patients with renal or liver failure are at higher risk of hypoglycemia and should also receive a lower dosage of insulin, at least to start with.
Others could be started on a dosage of 0.3 to 0.5 units/kg. Fifty percent of the calculated dosage could be given as basal insulin and 50% given as bolus (divided into three doses, before meals). Subsequently, the dosage would need to be titrated on the basis of the record of glucose monitoring.
Choosing a prandial insulin
Rapid-acting insulin analogues (lispro, aspart, and glulisine) control postprandial glucose levels better than regular insulin and cause less hypoglycemia. Their pharmacokinetics enable them to be taken within a few minutes of the start of a meal, or even after the meal if the patient forgets to take an injection before the meal.
For example, in one study,36 taking aspart immediately before the meal provided better glycemic control than taking regular insulin 30 minutes before meals. In a basal-bolus regimen, the use of aspart along with detemir resulted in glycemic control similar to that provided by twice-daily NPH and regular insulin, with less hypoglycemia.37
The dosage of prandial insulin can be adjusted according to the amount of carbohydrates in each meal (the insulin-to-carbohydrate ratio), as in patients with type 1 diabetes. This approach was associated with less weight gain.38
IS THERE STILL A ROLE FOR PREMIXED INSULIN PREPARATIONS?
Basal-bolus insulin regimens have gained popularity because the prandial doses can easily be adjusted according to carbohydrate intake, glucose level (on a sliding scale), variations in meal time, missed meals (eg, when having a procedure), and exercise. For example, the dose of prandial insulin can be reduced if the patient expects to exercise within 2 or 3 hours after the meal.
Some patients may not accept giving themselves four or five injections per day with a basal-bolus regimen. They may accept a simpler regimen, ie, giving themselves three injections of a premixed insulin per day, one before each meal.
Compared with a basal-bolus regimen, the possibility of achieving adequate glycemic control using lispro mix (50% lispro, 50% lispro protamine suspension) before meals seemed to depend on the goal of glycemic control. Its use in one study showed similar ability to achieve hemoglobin A1c less than 7.5% compared with a basal-bolus regimen of glargine and lispro. For a goal hemoglobin A1c level of less than 7%, the use of glargine and lispro was superior. The rate of hypoglycemia was similar with both strategies.39 These findings imply that the goal hemoglobin A1c should be more relaxed (< 7.5%) when using lispro mix (50% lispro) three times daily before meals.
Biphasic insulin aspart (a mix of aspart and protamine aspart) given three times daily provided similar improvement in glycemic control with no difference in the frequency of hypoglycemia compared with a basal-bolus regimen of NPH and aspart.40 Further, the use of biphasic insulin aspart seemed to provide better glycemic control with less weight gain compared with premixed human insulin (70% NPH, 30% regular insulin).41
Therefore, simpler premixed insulin regimens remain reasonable options for selected patients who do not accept a more complex insulin regimen (basal-bolus) or cannot adhere to it for any reason, especially if premixed insulin is given before meals three times daily. In fact, recent studies have focused on comparing premixed insulin three times daily with basal-bolus regimens (detemir or glargine as basal insulin along with pre-meal insulin analogue).
Glycemic control is harder to achieve with premixed insulin twice daily, mainly because of a higher frequency of hypoglycemia.42 In Europe, the use of premixed insulin three times daily is a popular option, whereas in the United States, a twice-daily schedule has been more common.
COST VS CONTROL
Newer insulin analogues make insulin treatment safer and more accepted by patients. The availability of several options for insulin regimens allows individualization of the treatment according to the patient’s acceptance, the safety profile, and the cost.
Patient selection and insulin titration are key issues in ensuring the achievement of adequate control with the fewest side effects. Lifestyle management (diet and physical activity) enhances the efficacy of insulin therapy and reduces the chances of side effects, namely fluctuation of glucose levels, hypoglycemic episodes, and weight gain.
Human insulins (NPH and regular) remain the least expensive, especially when using premixed NPH-regular insulin 70/30. Their use should be considered when the cost of medication is a major concern for the patient. A more relaxed goal of glycemic control may be considered in order to avoid hypoglycemia when using those insulin preparations, such as a hemoglobin A1c level less than 7.5% or even in the range of 7.5% to 8.5%, depending on the expected seasonal variation of hemoglobin A1c (which is higher in winter43), individual factors, and whether the premixed insulin is used twice or three times daily.
RE-EVALUATE THE REGIMEN ROUTINELY
The insulin regimen should be re-evaluated routinely. It might need to be changed in response to the dynamic multifactorial process of progression of diabetes, change in stress level, presence or resolution of intercurrent illnesses, risk of hypoglycemia, concerns about weight gain, and cost.
Finally, adjustment of the regimen should be considered in response to improvement of glycemic control related to improvement of dietary management, exercising, weight loss, and medical therapies.
Many patients with type 2 diabetes eventually need insulin, as their ability to produce their own insulin from pancreatic beta cells declines progressively.1 The questions remain as to when insulin therapy should be started, and which regimen is the most appropriate.
Guidelines from professional societies differ on these points,2,3 as do individual clinicians. Moreover, antidiabetic treatment is an evolving topic. Many new drugs—oral agents as well as injectable analogues of glucagon-like peptide-1 (GLP1) and insulin formulations—have become available in the last 15 years.
In this paper, I advocate an individualized approach and review the indications for insulin treatment, the available preparations, the pros and cons of each regimen, and how the properties of each type of insulin influence attempts to intensify the regimen.
Coexisting physiologic and medical conditions such as pregnancy and chronic renal failure and drugs such as glucocorticoids may alter insulin requirements. I will not cover these special situations, as they deserve separate, detailed discussions.
WHEN SHOULD INSULIN BE STARTED? TWO VIEWS
Early on, patients can be adequately managed with lifestyle modifications and oral hypoglycemic agents or injections of a GLP1 analogue, either alone or in combination with oral medication. Later, some patients reach a point at which insulin therapy becomes the main treatment, similar to patients with type 1 diabetes.
The American Diabetes Association (ADA), in a consensus statement,2 has called for using insulin early in the disease if lifestyle management and monotherapy with metformin (Glucophage) fail to control glucose or if lifestyle management is not adequate and metformin is contraindicated. The ADA’s goal hemoglobin A1c level is less than 7% for most patients.
The American Association of Clinical Endocrinologists (AACE) and the American College of Endocrinology (ACE), in another consensus statement, use an algorithm stratified by hemoglobin A1c level, in which insulin is mostly reserved for when combination therapy fails.3 Their goal hemoglobin A1c level is 6.5% or less for most patients.
Comment. Both consensus statements make exceptions for patients presenting with very high blood glucose and hemoglobin A1c levels and those who have contraindications to drugs other than insulin. These patients should start insulin immediately, along with lifestyle management.2,3
Both consensus statements give priority to safety. The AACE/ACE statement gives more weight to the risk of hypoglycemia with insulin treatment, whereas the ADA gives more weight to the risk of edema and congestive heart failure with thiazolidinedione drugs (although both insulin and thiazolidinediones cause weight gain) and to adequate validation of treatments in clinical trials.
Ongoing clinical trials may add insight to this issue. For example, the Outcome Reduction With Initial Glargine Intervention (ORIGIN) study is investigating the effects of the long-acting insulin glargine (Lantus) in early diabetes with regard to glycemic control, safety, and cardiovascular outcomes.4 This study is expected to end this year (2011). The safety of alternative treatment options is also under investigation and scrutiny. In the interim, individualized treatment should be considered, as we will see below.
MY VIEW: AN INDIVIDUALIZED APPROACH
The decision to start insulin therapy should be made individually, based on several factors:
- Whether the patient is willing to try it
- The degree of hyperglycemia
- How relevant the potential side effects of insulin are to the patient compared with those of other hypoglycemic agents
- Whether oral hypoglycemic agents with or without GLP1 analogues are expected to provide the desired benefit
- The patient’s work schedule and lifestyle factors
- Cost
- The availability of nurses, diabetes educators, and others to implement and follow the insulin treatment.
Will patients accept insulin?
Factors that affect whether patients comply with a treatment include the number of pills or injections they must take per day, how often they must check their blood glucose, adverse effects, lifestyle limitations caused by the treatment (especially insulin), and cost. Most patients feel better when their glucose levels are under good control, which is a major motivation for initiating and adhering to insulin. The anticipated reduction of diabetic complications further enhances compliance.
Education promotes compliance. Patients need to know that type 2 diabetes tends to progress and that in time their treatment will have to be intensified, with higher doses of their current drugs and new drugs added or substituted, possibly including insulin. This information is best given early, ie, when the diagnosis is made, even if hyperglycemia is mild at that time.
With newer insulin preparations and delivery devices available, more patients are finding insulin treatment acceptable.
The glycemic goal should be individualized
The key issue is glycemic control. If glycemic control is worsening or if the hemoglobin A1c level remains above the goal, then the treatment strategy should be readdressed.
In general, one should try to achieve the best possible glycemic control with the few est adverse effects. Adequate dietary management with a regular meal schedule and predictable carbohydrate intake for each meal helps to avoid or at least minimize the two most important adverse effects of insulin, ie, weight gain and hypoglycemia.
For most patients, I believe a goal hemoglobin A1c level of less than 7% is reasonable.2 For others, a less stringent goal might be more appropriate, such as 7.5%. Several factors affect this decision, including whether the patient is willing to follow a complex insulin regimen (such as a basal-bolus regimen), his or her work schedule, other lifestyle factors, the duration of diabetes, the type or types of insulin used, coexisting medical conditions, the frequency of hypoglycemia, unawareness of hypoglycemia, age, prognosis, life expectancy, and cost.5
If hyperglycemia is severe (Table 1),2 the goal might not be clear when insulin therapy is started. It should become obvious with ongoing follow-up.
Previously untreated patients presenting with severe hyperglycemia are a heterogeneous group. Many of them have had diabetes for a relatively short time and were recently diagnosed. These patients are likely to safely achieve near-normal glycemic control. Some of them might be adequately treated with oral hypoglycemic agents; if insulin is used, transitioning from insulin to oral hypoglycemic agents may be feasible.2
Some untreated patients may have had diabetes for several years and have advanced disease and therefore might be more difficult to treat. Only 21 (57%) of 37 previously untreated patients intensively treated with insulin reached the goal fasting glucose level of less than 126 mg/dL in one study.6 The only way to evaluate the feasibility of achieving near-normal glycemia safely is by following the patient’s progress over time.
The patient’s glycemic goal should be reevaluated periodically and may need to be adjusted over time, based on changes in any of the factors discussed above.
Risk of hypoglycemia
The goal should be looser in difficult-to-treat patients, ie, those with frequent hypoglycemia and decreased awareness of hypoglycemia.
Patients with advanced diabetes whose glucose levels continue to fluctuate widely after lifestyle management and the insulin regimen have been addressed should also have a looser goal. These fluctuations of glucose levels are surrogate markers for the degree of insulin deficiency. Attempting to achieve near-normal glycemic levels in this situation would be associated with a higher risk of hypoglycemia.
A higher risk of hypoglycemia and its complications (eg, falling and accidents, especially among operators of heavy machinery, construction workers, and drivers) is another reason for adopting a relaxed goal of glycemic control.
ADDING BASAL INSULIN TO ORAL HYPOGLYCEMIC THERAPY
When glycemic control worsens or is not adequate despite the use of oral hypoglycemic agents, often the next step is to add basal insulin therapy, ie, once-daily doses of a long-acting insulin.
NPH, detemir, or glargine?
Most often, glargine or detemir (Levemir) insulin is used. Detemir can also be given twice daily if needed. If cost is a concern, neutral protamine Hagedorn (NPH, Humulin N, Novolin N) insulin once daily at bedtime or twice daily is a reasonable alternative.
Costs of basal insulins are $22 to $50 per 1,000-unit vial for NPH, $70 to $90 per 1,000-unit vial for detemir and glargine, and $170 to $200 for a box of five detemir or glargine pens (containing 1,500 units total). Complicating this issue, vials should not be used for more than 1 month, and thus, the cost of vials vs pens depends on dosage.
Detemir vs NPH. In a trial in patients with inadequately controlled type 2 diabetes who had never taken insulin before and who were taking one or more oral hypoglycemic drugs, the addition of detemir insulin once daily or NPH at bedtime resulted in similar improvements in hemoglobin A1c (a decrease of about 1.5%).10
Detemir had several advantages over NPH. First, the incidence of nocturnal hypoglycemia was 50% lower with detemir at bedtime than with NPH at bedtime, and 87% lower with detemir in the morning than with bedtime NPH.10 In another trial,11 the risk of hypoglycemia at any time of day was 47% lower with insulin detemir than with NPH, and the risk of nocturnal hypoglycemia was 55% lower.
The risk of nocturnal hypoglycemia is lower if detemir is taken in the morning than at bedtime, although the total frequency of hypoglycemic episodes is the same.10 Therefore, another decision after starting basal insulin, based on the patient’s glucose trends and frequency of hypoglycemic events, would be whether insulin should be taken in the morning or at bedtime.
The second advantage of detemir is that it causes less weight gain: 0.7 kg at 20 weeks with detemir at bedtime vs 1.6 kg with NPH at bedtime.10
Further, detemir insulin was associated with less within-subject variability in the fasting glucose level than with NPH when these insulins were used in a basal-bolus regimen.12
Hermansen et al11 found that if the dosage of basal insulin was aggressively increased, 70% of patients achieved a hemoglobin A1c target of less than 7% with either NPH or detemir insulin, with fewer hypoglycemic episodes in patients treated with detemir.
Therefore, adding basal insulin to oral therapy is adequate for many patients who are new to insulin. Many patients would need more, such as the addition of insulin before meals.
Glargine vs NPH. Compared with adding NPH, adding glargine to a regimen of oral hypoglycemic agents controls blood glucose levels better and with less fluctuation in glucose levels, a lower risk of hypoglycemia, and less weight gain.13–15 These results were the same when using glargine with either metformin13 or glimeperide (Amaryl).14
Glargine is usually given once daily at bedtime. One study suggested that giving it in the morning is more effective.14
Detemir vs glargine. Studies that compared detemir and glargine revealed more similarities than differences in their clinical benefits.16,17 Both preparations effectively lower glucose levels and improve quality of life.18
Titrating the insulin regimen is a key in achieving adequate glycemic control. This includes teaching patients how to adjust their insulin, for example by increasing the dosage of glargine or detemir by 2 units every 4 to 7 days until adequate glycemic control is achieved, unless hypoglycemia becomes a barrier.
BASAL VS PRANDIAL INSULIN
Once-daily insulin injection is relatively convenient, but it comes with a limitation: it does not adequately control postprandial hyperglycemia. A solution is insulin before meals, ie, prandial insulin.
Kazda et al19 compared three regimens in patients not taking oral hypoglycemic agents: rapid-acting insulin lispro (Humalog) before each meal, a mix of 50% lispro and 50% protamine lispro (Humalog Mix 50/50) (the protamine delays its release) before each meal, and glargine at bedtime. The absolute change in hemoglobin A1c was −0.3% in the glargine group, −1.1% in the lispro group, and −1.2% in the lispro mix group. The glargine group had better control of fasting glucose.
Similar advantages of better glycemic control and fewer nocturnal hypoglycemic episodes were seen in trials of a mixture of 25% lispro and 75% protamine lispro before meals compared with glargine insulin in patients on simultaneous treatment with oral hypoglycemic agents.20,21 Buse et al21 reported that more patients achieved a hemoglobin A1c level below 7% with this lispro mix (47%) than with glargine (40%). The absolute difference in mean hemoglobin A1c between the two groups was minimal, although it reached statistical significance. As expected, weight gain was less in the glargine group.21
Kann et al22 reported that glycemic control was also better with a mixture of 30% aspart and 70% protamine aspart (NovoLog Mix 70/30) twice a day along with metformin than with glargine insulin once a day along with oral glimepiride, a sulfonylurea. Further, in this study, weight gain was noted in the glargine-glimepiride group only.22 Therefore, the advantage of less weight gain has not been always reproducible in glargine studies.
Comment. These studies point to the contribution of postprandial glucose to hemoglobin A1c.23–25 In patients with satisfactory glycemic control, the postprandial glucose level seems to be the major contributor to hemoglobin A1c. When glycemic control worsens, the contribution of fasting glucose to hemoglobin A1c increases.23
Premixed insulins (lispro mix and aspart mix) provide basal coverage and control postprandial hyperglycemia. Therefore, prandial premixed insulin therapy is expected to be superior to basal insulin therapy. Premixed insulin could be considered as a simplified basal-bolus regimen (see below).
The superiority of prandial (rapid-acting) insulin alone over basal insulin therapy, as seen in the study by Kazda et al,19 has not been reproducible in other studies. For example, in one study, once-daily glargine resulted in a similar improvement in hemoglobin A1c, a lower rate of hypoglycemic episodes, and greater patient satisfaction with treatment compared with lispro insulin before meals.26 This issue remains debatable because all the trials have been open-label and thus are subject to limitations.
The main lesson is that either glargine or lispro monotherapy is a reasonable option and results in better glycemic control in patients for whom two oral hypoglycemic agents have failed. Further, both fasting and postprandial hyperglycemia are important to address. In patients with severe hyperglycemia, a combination of prandial and basal insulin may be indicated. One would expect neither basal nor prandial (bolus) insulin to be adequate in this situation.
In conclusion, adding basal insulin to oral hypoglycemic agents is a reasonable option in the advancement of diabetes therapy and has become a common way to introduce insulin. It is simple and less labor-intensive for patients and medical groups than a basal-bolus regimen. Patients usually find it acceptable. The future availability of an easy-to-deliver, safe, and effective prandial insulin may change the current treatment paradigm; several newer prandial insulins are under investigation.
In advanced diabetes, both prandial and fasting glucose levels are crucial to address. Some patients may need to be started on both basal and prandial insulin simultaneously, depending on their degree of hyperglycemia, the duration of diabetes, coexisting medical conditions, and the goal of glycemic control.
BASAL-BOLUS INSULIN REGIMENS
In the advanced stages of type 2 diabetes, as insulin deficiency worsens, patients need to start giving themselves injections of a rapid-acting insulin—regular, lispro, aspart, or glulisine (Apidra) before meals, in addition to once- or twice-daily basal insulin injections. Such a “basal-bolus” regimen could also be used for newly diagnosed patients presenting with severe hyperglycemia. In addition, some patients on basal insulin plus oral hypoglycemic drugs may develop contraindications to their oral drugs. Adding bolus insulin becomes the main option for these patients too.
For others, a basal-bolus regimen might be chosen purely because of cost. For example, a regimen of NPH and regular insulin (multiple daily injections or premixed) would be significantly less expensive than multiple oral hypoglycemic agents.
Currently, only a few classes of oral hypoglycemic drugs are available in generic formulations. For example, generic glimeperide and metformin cost as little as $4 to $12 per month, while the costs of brand-name oral hypoglycemic agents are in the range of $170 to $200 per month. In contrast, premixed NPH plus regular insulin such as Novolin 70/30 and Humulin 70/30 cost between $22 and $70 per vial.
A basal-bolus regimen should provide 50% of the total daily insulin in the form of basal insulin. A regimen of 50% basal and 50% bolus seemed to provide better glycemic control than a regimen of 35% basal and 65% bolus in several studies.27,28
In patients already taking a single daily dose of basal insulin along with oral hypoglycemic agents, the dosage of basal insulin is usually raised gradually until adequate glycemic control is achieved. A main question is when to add prandial insulin. There is no clear cutoff for a basal insulin dosage at which prandial insulin should be added.
In the Treat-to-Target Trial,29 almost 60% of patients achieved a hemoglobin A1c level of 7% or less with the addition of either glargine or NPH insulin (basal insulin only) to oral hypoglycemic agents during 24 weeks of follow-up. As expected, glargine caused less nocturnal hypoglycemia. Fewer than half the patients who achieved a hemoglobin A1c level less than 7% had no documented nocturnal hypoglycemia (33% of glargine-treated patients and 27% of NPH-treated patients).
Type 2 diabetes is progressive1; over time, patients treated with once-daily basal insulin often require multiple daily injections.
Adding prandial to basal insulin clearly results in better glycemic control and less glucose variability.19,20,22,30–33 Two major factors in deciding to start prandial insulin are the degree of hyperglycemia and the patient’s acceptance of multiple daily injections. The higher the blood glucose levels, the sooner prandial insulin should be added, especially if hyperglycemia is influencing the prognosis of a coexisting condition or a diabetic complication (eg, an infected foot ulcer).
Adding prandial insulin should be also considered if the dosage of basal insulin has progressively been increased and the hemoglobin A1c level is not improving, especially if a patient has both inadequate glycemic control and frequent hypoglycemia, or if the morning glucose level is within the desired range (indicating there is no room for a further increase in the basal insulin dose) in association with inadequate control of hemoglobin A1c.
What is the best basal insulin for a basal-bolus regimen?
Glargine and detemir were shown to be equally effective as the basal component of a basal-bolus regimen.34,35 Findings were similar to those of studies comparing NPH, detemir, and glargine added, by themselves, to oral hypoglycemic agents. When possible, either glargine or detemir is favored because of less hypoglycemia and less weight gain than with NPH. Weight gain is the least with detemir.
Adding prandial insulin to a basal regimen
In general, whether to add prandial insulin can be decided on the basis of the patient’s record of blood glucose monitoring. Insulin could be added before breakfast if the pre-lunch glucose level is elevated, or before lunch if the dinnertime blood glucose level is elevated, or before dinner if the bedtime blood glucose level is elevated—or a combination of these. Prandial insulin can be started at a low dose (4–6 units) and increased gradually.
In the case of poor glycemic control on a high dosage of basal insulin, a reasonable first step would be to change the regimen to a basal-bolus regimen (about 50% basal and 50% bolus) with no change or a small decrease in the total daily dosage of insulin to avoid hypoglycemia. For example, in a patient on 80 units of glargine or detemir insulin who has inadequate control, the regimen could be changed to 35 units of either glargine or detemir and 10 to 12 units of lispro, aspart, or glulisine before each meal as the bolus component.
Further adjustments of the insulin dosage can be made according to the results of glucose monitoring before each meal and at bedtime. In all case scenarios, the insulin regimen should be re-evaluated routinely during the advancement of therapy from single daily injection of basal insulin to multiple daily injections. Redistribution of total insulin dosage to 50% basal and 50% bolus (divided into three doses before meals) should be considered for patients who continue to have fluctuations of glucose levels, inadequate control, or frequent hypoglycemia. This ratio seems to provide better control for most patients.27,28
Starting with a basal-bolus regimen
For patients new to insulin who are starting a basal-bolus regimen, a dosage based on total body weight could be considered. The requirements vary significantly based on dietary management, level of physical activity, stress (especially illnesses), use of oral hypoglycemic agents, and degree of hyperglycemia.
A lower dosage of insulin (0.2 units per kg) should be considered for people with mild stress, with milder hyperglycemia, or on treatment with oral hypoglycemic agents. Elderly patients and patients with renal or liver failure are at higher risk of hypoglycemia and should also receive a lower dosage of insulin, at least to start with.
Others could be started on a dosage of 0.3 to 0.5 units/kg. Fifty percent of the calculated dosage could be given as basal insulin and 50% given as bolus (divided into three doses, before meals). Subsequently, the dosage would need to be titrated on the basis of the record of glucose monitoring.
Choosing a prandial insulin
Rapid-acting insulin analogues (lispro, aspart, and glulisine) control postprandial glucose levels better than regular insulin and cause less hypoglycemia. Their pharmacokinetics enable them to be taken within a few minutes of the start of a meal, or even after the meal if the patient forgets to take an injection before the meal.
For example, in one study,36 taking aspart immediately before the meal provided better glycemic control than taking regular insulin 30 minutes before meals. In a basal-bolus regimen, the use of aspart along with detemir resulted in glycemic control similar to that provided by twice-daily NPH and regular insulin, with less hypoglycemia.37
The dosage of prandial insulin can be adjusted according to the amount of carbohydrates in each meal (the insulin-to-carbohydrate ratio), as in patients with type 1 diabetes. This approach was associated with less weight gain.38
IS THERE STILL A ROLE FOR PREMIXED INSULIN PREPARATIONS?
Basal-bolus insulin regimens have gained popularity because the prandial doses can easily be adjusted according to carbohydrate intake, glucose level (on a sliding scale), variations in meal time, missed meals (eg, when having a procedure), and exercise. For example, the dose of prandial insulin can be reduced if the patient expects to exercise within 2 or 3 hours after the meal.
Some patients may not accept giving themselves four or five injections per day with a basal-bolus regimen. They may accept a simpler regimen, ie, giving themselves three injections of a premixed insulin per day, one before each meal.
Compared with a basal-bolus regimen, the possibility of achieving adequate glycemic control using lispro mix (50% lispro, 50% lispro protamine suspension) before meals seemed to depend on the goal of glycemic control. Its use in one study showed similar ability to achieve hemoglobin A1c less than 7.5% compared with a basal-bolus regimen of glargine and lispro. For a goal hemoglobin A1c level of less than 7%, the use of glargine and lispro was superior. The rate of hypoglycemia was similar with both strategies.39 These findings imply that the goal hemoglobin A1c should be more relaxed (< 7.5%) when using lispro mix (50% lispro) three times daily before meals.
Biphasic insulin aspart (a mix of aspart and protamine aspart) given three times daily provided similar improvement in glycemic control with no difference in the frequency of hypoglycemia compared with a basal-bolus regimen of NPH and aspart.40 Further, the use of biphasic insulin aspart seemed to provide better glycemic control with less weight gain compared with premixed human insulin (70% NPH, 30% regular insulin).41
Therefore, simpler premixed insulin regimens remain reasonable options for selected patients who do not accept a more complex insulin regimen (basal-bolus) or cannot adhere to it for any reason, especially if premixed insulin is given before meals three times daily. In fact, recent studies have focused on comparing premixed insulin three times daily with basal-bolus regimens (detemir or glargine as basal insulin along with pre-meal insulin analogue).
Glycemic control is harder to achieve with premixed insulin twice daily, mainly because of a higher frequency of hypoglycemia.42 In Europe, the use of premixed insulin three times daily is a popular option, whereas in the United States, a twice-daily schedule has been more common.
COST VS CONTROL
Newer insulin analogues make insulin treatment safer and more accepted by patients. The availability of several options for insulin regimens allows individualization of the treatment according to the patient’s acceptance, the safety profile, and the cost.
Patient selection and insulin titration are key issues in ensuring the achievement of adequate control with the fewest side effects. Lifestyle management (diet and physical activity) enhances the efficacy of insulin therapy and reduces the chances of side effects, namely fluctuation of glucose levels, hypoglycemic episodes, and weight gain.
Human insulins (NPH and regular) remain the least expensive, especially when using premixed NPH-regular insulin 70/30. Their use should be considered when the cost of medication is a major concern for the patient. A more relaxed goal of glycemic control may be considered in order to avoid hypoglycemia when using those insulin preparations, such as a hemoglobin A1c level less than 7.5% or even in the range of 7.5% to 8.5%, depending on the expected seasonal variation of hemoglobin A1c (which is higher in winter43), individual factors, and whether the premixed insulin is used twice or three times daily.
RE-EVALUATE THE REGIMEN ROUTINELY
The insulin regimen should be re-evaluated routinely. It might need to be changed in response to the dynamic multifactorial process of progression of diabetes, change in stress level, presence or resolution of intercurrent illnesses, risk of hypoglycemia, concerns about weight gain, and cost.
Finally, adjustment of the regimen should be considered in response to improvement of glycemic control related to improvement of dietary management, exercising, weight loss, and medical therapies.
- UK Prospective Diabetes Study 16. Overview of 6 years’ therapy of type II diabetes: a progressive disease. UK Prospective Diabetes Study Group. Diabetes 1995; 44:1249–1258.
- Nathan DM, Buse JB, Davidson MB, et al; American Diabetes Association. Medical management of hyperglycemia in type 2 diabetes: a consensus algorithm for the initiation and adjustment of therapy: a consensus statement of the American Diabetes Association and the European Association for the Study of Diabetes. Diabetes Care 2009; 32:193–203.
- Rodbard HW, Jellinger PS, Davidson JA, et al. Statement by an American Association of Clinical Endocrinologists/American College of Endocrinology consensus panel on type 2 diabetes mellitus: an algorithm for glycemic control. Endocr Pract 2009; 15:540–558.
- ClinicalTrials.gov. The ORIGIN Trial (Outcome Reduction With Initial Glargine Intervention). http://clinicaltrials.gov/ct2/show/NCT00069784. Accessed 2/11/11.
- American Diabetes Association. Standards of medical care in diabetes—2010. Diabetes Care 2010; 33(suppl 1):S11–S61.
- Retnakaran R, Qi Y, Opsteen C, Vivero E, Zinman B. Initial short-term intensive insulin therapy as a strategy for evaluating the preservation of beta-cell function with oral antidiabetic medications: a pilot study with sitagliptin. Diabetes Obes Metab 2010; 12:909–915.
- Zoungas S, Patel A, Chalmers J, et al; ADVANCE Collaborative Group. Severe hypoglycemia and risks of vascular events and death. N Engl J Med 2010; 363:1410–1418.
- Akram K, Pedersen-Bjergaard U, Borch-Johnsen K, Thorsteinsson B. Frequency and risk factors of severe hypoglycemia in insulin-treated type 2 diabetes: a literature survey. J Diabetes Complications 2006; 20:402–408.
- Cryer PE. Chapter 19. Hypoglycemia. In: Jameson JL, editor. Harrison’s Endocrinology. McGraw Hill, 2006:355–363.
- Philis-Tsimikas A, Charpentier G, Clauson P, Ravn GM, Roberts VL, Thorsteinsson B. Comparison of once-daily insulin detemir with NPH insulin added to a regimen of oral antidiabetic drugs in poorly controlled type 2 diabetes. Clin Ther 2006; 28:1569–1581. Erratum in: Clin Ther 2006; 28:1967.
- Hermansen K, Davies M, Derezinski T, Martinez Ravn G, Clauson P, Home P. A 26-week, randomized, parallel, treat-to-target trial comparing insulin detemir with NPH insulin as add-on therapy to oral glucose-lowering drugs in insulin-naive people with type 2 diabetes. Diabetes Care 2006; 29:1269–1274. Erratum in: Diabetes Care 2007; 30:1035.
- Haak T, Tiengo A, Draeger E, Suntum M, Waldhäusl W. Lower within-subject variability of fasting blood glucose and reduced weight gain with insulin detemir compared to NPH insulin in patients with type 2 diabetes. Diabetes Obes Metab 2005; 7:56–64.
- Yki-Järvinen H, Kauppinen-Mäkelin R, Tiikkainen M, et al. Insulin glargine or NPH combined with metformin in type 2 diabetes: the LANMET study. Diabetalogia 2006; 49:442–451.
- Fritsche A, Schweitzer MA, Häring HU; 4001 Study Group. Glimepiride combined with morning insulin glargine, bedtime neutral protamine hagedorn insulin, or bedtime insulin glargine in patients with type 2 diabetes. A randomized, controlled trial. Ann Intern Med 2003; 138:952–959.
- Rosenstock J, Schwartz SL, Clark CM, Park GD, Donley DW, Edwards MB. Basal insulin therapy in type 2 diabetes: 28-week comparison of insulin glargine (HOE 901) and NPH insulin. Diabetes Care 2001; 24:631–636.
- Rosenstock J, Davies M, Home PD, Larsen J, Koenen C, Schernthaner G. A randomised, 52-week, treat-to-target trial comparing insulin detemir with insulin glargine when administered as add-on to glucose-lowering drugs in insulin-naive people with type 2 diabetes. Diabetologia 2008; 51:408–416.
- King AB. Once-daily insulin detemir is comparable to once-daily insulin glargine in providing glycaemic control over 24 h in patients with type 2 diabetes: a double-blind, randomized, crossover study. Diabetes Obes Metab 2009; 11:69–71.
- Swinnen SG, Snoek FJ, Dain MP, DeVries JH, Hoekstra JB, Holleman F. Rationale, design, and baseline data of the insulin glargine (Lantus) versus insulin detemir (Levemir) Treat-To-Target (L2T3) study: a multinational, randomized noninferiority trial of basal insulin initiation in type 2 diabetes. Diabetes Technol Ther 2009; 11:739–743.
- Kazda C, Hülstrunk H, Helsberg K, Langer F, Forst T, Hanefeld M. Prandial insulin substitution with insulin lispro or insulin lispro mid mixture vs. basal therapy with insulin glargine: a randomized controlled trial in patients with type 2 diabetes beginning insulin therapy. J Diabetes Complications 2006; 20:145–152.
- Malone JK, Bai S, Campaigne BN, Reviriego J, Augendre-Ferrante B. Twice-daily pre-mixed insulin rather than basal insulin therapy alone results in better overall glycaemic control in patients with type 2 diabetes. Diabet Med 2005; 22:374–381.
- Buse JB, Wolffenbuttel BH, Herman WH, et al. DURAbility of basal versus lispro mix 75/25 insulin efficacy (DURABLE) trial 24-week results: safety and efficacy of insulin lispro mix 75/25 versus insulin glargine added to oral antihyperglycemic drugs in patients with type 2 diabetes. Diabetes Care 2009; 32:1007–1013.
- Kann PH, Wascher T, Zackova V, et al. Starting insulin therapy in type 2 diabetes: twice-daily biphasic insulin Aspart 30 plus metformin versus once-daily insulin glargine plus glimepiride. Exp Clin Endocrinol Diabetes 2006; 114:527–532.
- Monnier L, Colette C, Monnier L, Colette C. Contributions of fasting and postprandial glucose to hemoglobin A1c. Endocr Pract 2006; 12(suppl 1):42–46.
- Woerle HJ, Pimenta WP, Meyer C, et al. Diagnostic and therapeutic implications of relationships between fasting, 2-hour postchallenge plasma glucose and hemoglobin A1c values. Arch Intern Med 2004; 164:1627–1632.
- Schrot RJ. Targeting plasma glucose: preprandial versus postprandial. Clinical Diabetes 2004; 22:169–172.
- Bretzel RG, Nuber U, Landgraf W, Owens DR, Bradley C, Linn T. Once-daily basal insulin glargine versus thrice-daily prandial insulin lispro in people with type 2 diabetes on oral hypoglycaemic agents (APOLLO): an open randomised controlled trial. Lancet 2008; 371:1073–1084.
- Tamaki M, Shimizu T, Kanazawa A, Fujitani Y, Watada H, Kawamori R, Hirose T. Effects of changes in basal/total daily insulin ratio in type 2 diabetes patients on intensive insulin therapy including insulin glargine (JUN-LAN Study 6). Diabetes Res Clin Pract 2008; 81:e1–e3.
- Yokoyama H, Tada J, Kamikawa F, Kanno S, Yokota Y, Kuramitsu M. Efficacy of conversion from bedtime NPH insulin to morning insulin glargine in type 2 diabetic patients on basal-prandial insulin therapy. Diabetes Res Clin Pract 2006; 73:35–40.
- Riddle MC, Rosenstock J, Gerich J; Insulin Glargine 4002 Study Investigators. The Treat-To-Target trial: randomized addition of glargine or human NPH insulin to oral therapy of type 2 diabetic patients. Diabetes Care 2003; 26:3080–3086.
- Davies M, Sinnassamy P, Storms F, Gomis R; ATLANTUS Study Group. Insulin glargine-based therapy improves glycemic control in patients with type 2 diabetes sub-optimally controlled on premixed insulin therapies. Diabetes Res Clin Pract 2008; 79:368–375.
- Jacober SJ, Scism-Bacon JL, Zagar AJ. A comparison of intensive mixture therapy with basal insulin therapy in insulin-naïve patients with type 2 diabetes receiving oral antidiabetes agents. Diabetes Obes Metab 2006; 8:448–455.
- Hirsch IB, Yuan H, Campaigne BN, Tan MH. Impact of prandial plus basal vs basal insulin on glycemic variability in type 2 diabetic patients. Endocr Pract 2009; 15:343–348.
- Robbins DC, Beisswenger PJ, Ceriello A, et al. Mealtime 50/50 basal + prandial insulin analogue mixture with a basal insulin analogue, both plus metformin, in the achievement of target HbA1c and pre- and postprandial blood glucose levels in patients with type 2 diabetes: a multinational, 24-week, randomized, open-label, parallel-group comparison. Clin Ther 2007; 29:2349–2364.
- Hollander P, Cooper J, Bregnhøj J, Pedersen CB. A 52-week, multinational, open-label, parallel-group, noninferiority, treat-to-target trial comparing insulin detemir with insulin glargine in a basal-bolus regimen with mealtime insulin aspart in patients with type 2 diabetes. Clin Ther 2008; 30:1976–1987.
- Raskin P, Gylvin T, Weng W, Chaykin L. Comparison of insulin detemir and insulin glargine using a basal-bolus regimen in a randomized, controlled clinical study in patients with type 2 diabetes. Diabetes Metab Res Rev 2009; 25:542–548.
- Perriello G, Pampanelli S, Porcellati F, et al. Insulin aspart improves meal time glycaemic control in patients with type 2 diabetes: a randomized, stratified, double-blind and cross-over trial. Diabet Med 2005; 22:606–611.
- Umpierrez GE, Hor T, Smiley D, et al. Comparison of inpatient insulin regimens with detemir plus aspart versus neutral protamine hagedorn plus regular in medical patients with type 2 diabetes. J Clin Endocrinol Metab 2009; 94:564–569.
- Bergenstal RM, Johnson M, Powers MA, et al. Adjust to target in type 2 diabetes: comparison of a simple algorithm with carbohydrate counting for adjustment of mealtime insulin glulisine. Diabetes Care 2008; 31:1305–1310.
- Rosenstock J, Ahmann AJ, Colon G, Scism-Bacon J, Jiang H, Martin S. Advancing insulin therapy in type 2 diabetes previously treated with glargine plus oral agents: prandial premixed (insulin lispro protamine suspension/lispro) versus basal/bolus (glargine/lispro) therapy. Diabetes Care 2008; 31:20–25.
- Ligthelm RJ, Mouritzen U, Lynggaard H, et al. Biphasic insulin aspart given thrice daily is as efficacious as a basal-bolus insulin regimen with four daily injections: a randomised open-label parallel group four months comparison in patients with type 2 diabetes. Exp Clin Endocrinol Diabetes 2006; 114:511–519.
- Velojic-Golubovic M, Mikic D, Pesic M, Dimic D, Radenkovic S, Antic S. Biphasic insulin aspart 30: better glycemic control than with premixed human insulin 30 in obese patients with type 2 diabetes. J Endocrinol Invest 2009; 32:23–27.
- Holman RR, Farmer AJ, Davies MJ, et al; 4-T Study Group. Three-year efficacy of complex insulin regimens in type 2 diabetes. N Engl Med 2009; 361:1736–1747.
- Tseng CL, Brimacombe M, Xie M, et al. Seasonal patterns in monthly hemoglobin A1c values. Am J Epidemiol 2005; 161:565–574.
- UK Prospective Diabetes Study 16. Overview of 6 years’ therapy of type II diabetes: a progressive disease. UK Prospective Diabetes Study Group. Diabetes 1995; 44:1249–1258.
- Nathan DM, Buse JB, Davidson MB, et al; American Diabetes Association. Medical management of hyperglycemia in type 2 diabetes: a consensus algorithm for the initiation and adjustment of therapy: a consensus statement of the American Diabetes Association and the European Association for the Study of Diabetes. Diabetes Care 2009; 32:193–203.
- Rodbard HW, Jellinger PS, Davidson JA, et al. Statement by an American Association of Clinical Endocrinologists/American College of Endocrinology consensus panel on type 2 diabetes mellitus: an algorithm for glycemic control. Endocr Pract 2009; 15:540–558.
- ClinicalTrials.gov. The ORIGIN Trial (Outcome Reduction With Initial Glargine Intervention). http://clinicaltrials.gov/ct2/show/NCT00069784. Accessed 2/11/11.
- American Diabetes Association. Standards of medical care in diabetes—2010. Diabetes Care 2010; 33(suppl 1):S11–S61.
- Retnakaran R, Qi Y, Opsteen C, Vivero E, Zinman B. Initial short-term intensive insulin therapy as a strategy for evaluating the preservation of beta-cell function with oral antidiabetic medications: a pilot study with sitagliptin. Diabetes Obes Metab 2010; 12:909–915.
- Zoungas S, Patel A, Chalmers J, et al; ADVANCE Collaborative Group. Severe hypoglycemia and risks of vascular events and death. N Engl J Med 2010; 363:1410–1418.
- Akram K, Pedersen-Bjergaard U, Borch-Johnsen K, Thorsteinsson B. Frequency and risk factors of severe hypoglycemia in insulin-treated type 2 diabetes: a literature survey. J Diabetes Complications 2006; 20:402–408.
- Cryer PE. Chapter 19. Hypoglycemia. In: Jameson JL, editor. Harrison’s Endocrinology. McGraw Hill, 2006:355–363.
- Philis-Tsimikas A, Charpentier G, Clauson P, Ravn GM, Roberts VL, Thorsteinsson B. Comparison of once-daily insulin detemir with NPH insulin added to a regimen of oral antidiabetic drugs in poorly controlled type 2 diabetes. Clin Ther 2006; 28:1569–1581. Erratum in: Clin Ther 2006; 28:1967.
- Hermansen K, Davies M, Derezinski T, Martinez Ravn G, Clauson P, Home P. A 26-week, randomized, parallel, treat-to-target trial comparing insulin detemir with NPH insulin as add-on therapy to oral glucose-lowering drugs in insulin-naive people with type 2 diabetes. Diabetes Care 2006; 29:1269–1274. Erratum in: Diabetes Care 2007; 30:1035.
- Haak T, Tiengo A, Draeger E, Suntum M, Waldhäusl W. Lower within-subject variability of fasting blood glucose and reduced weight gain with insulin detemir compared to NPH insulin in patients with type 2 diabetes. Diabetes Obes Metab 2005; 7:56–64.
- Yki-Järvinen H, Kauppinen-Mäkelin R, Tiikkainen M, et al. Insulin glargine or NPH combined with metformin in type 2 diabetes: the LANMET study. Diabetalogia 2006; 49:442–451.
- Fritsche A, Schweitzer MA, Häring HU; 4001 Study Group. Glimepiride combined with morning insulin glargine, bedtime neutral protamine hagedorn insulin, or bedtime insulin glargine in patients with type 2 diabetes. A randomized, controlled trial. Ann Intern Med 2003; 138:952–959.
- Rosenstock J, Schwartz SL, Clark CM, Park GD, Donley DW, Edwards MB. Basal insulin therapy in type 2 diabetes: 28-week comparison of insulin glargine (HOE 901) and NPH insulin. Diabetes Care 2001; 24:631–636.
- Rosenstock J, Davies M, Home PD, Larsen J, Koenen C, Schernthaner G. A randomised, 52-week, treat-to-target trial comparing insulin detemir with insulin glargine when administered as add-on to glucose-lowering drugs in insulin-naive people with type 2 diabetes. Diabetologia 2008; 51:408–416.
- King AB. Once-daily insulin detemir is comparable to once-daily insulin glargine in providing glycaemic control over 24 h in patients with type 2 diabetes: a double-blind, randomized, crossover study. Diabetes Obes Metab 2009; 11:69–71.
- Swinnen SG, Snoek FJ, Dain MP, DeVries JH, Hoekstra JB, Holleman F. Rationale, design, and baseline data of the insulin glargine (Lantus) versus insulin detemir (Levemir) Treat-To-Target (L2T3) study: a multinational, randomized noninferiority trial of basal insulin initiation in type 2 diabetes. Diabetes Technol Ther 2009; 11:739–743.
- Kazda C, Hülstrunk H, Helsberg K, Langer F, Forst T, Hanefeld M. Prandial insulin substitution with insulin lispro or insulin lispro mid mixture vs. basal therapy with insulin glargine: a randomized controlled trial in patients with type 2 diabetes beginning insulin therapy. J Diabetes Complications 2006; 20:145–152.
- Malone JK, Bai S, Campaigne BN, Reviriego J, Augendre-Ferrante B. Twice-daily pre-mixed insulin rather than basal insulin therapy alone results in better overall glycaemic control in patients with type 2 diabetes. Diabet Med 2005; 22:374–381.
- Buse JB, Wolffenbuttel BH, Herman WH, et al. DURAbility of basal versus lispro mix 75/25 insulin efficacy (DURABLE) trial 24-week results: safety and efficacy of insulin lispro mix 75/25 versus insulin glargine added to oral antihyperglycemic drugs in patients with type 2 diabetes. Diabetes Care 2009; 32:1007–1013.
- Kann PH, Wascher T, Zackova V, et al. Starting insulin therapy in type 2 diabetes: twice-daily biphasic insulin Aspart 30 plus metformin versus once-daily insulin glargine plus glimepiride. Exp Clin Endocrinol Diabetes 2006; 114:527–532.
- Monnier L, Colette C, Monnier L, Colette C. Contributions of fasting and postprandial glucose to hemoglobin A1c. Endocr Pract 2006; 12(suppl 1):42–46.
- Woerle HJ, Pimenta WP, Meyer C, et al. Diagnostic and therapeutic implications of relationships between fasting, 2-hour postchallenge plasma glucose and hemoglobin A1c values. Arch Intern Med 2004; 164:1627–1632.
- Schrot RJ. Targeting plasma glucose: preprandial versus postprandial. Clinical Diabetes 2004; 22:169–172.
- Bretzel RG, Nuber U, Landgraf W, Owens DR, Bradley C, Linn T. Once-daily basal insulin glargine versus thrice-daily prandial insulin lispro in people with type 2 diabetes on oral hypoglycaemic agents (APOLLO): an open randomised controlled trial. Lancet 2008; 371:1073–1084.
- Tamaki M, Shimizu T, Kanazawa A, Fujitani Y, Watada H, Kawamori R, Hirose T. Effects of changes in basal/total daily insulin ratio in type 2 diabetes patients on intensive insulin therapy including insulin glargine (JUN-LAN Study 6). Diabetes Res Clin Pract 2008; 81:e1–e3.
- Yokoyama H, Tada J, Kamikawa F, Kanno S, Yokota Y, Kuramitsu M. Efficacy of conversion from bedtime NPH insulin to morning insulin glargine in type 2 diabetic patients on basal-prandial insulin therapy. Diabetes Res Clin Pract 2006; 73:35–40.
- Riddle MC, Rosenstock J, Gerich J; Insulin Glargine 4002 Study Investigators. The Treat-To-Target trial: randomized addition of glargine or human NPH insulin to oral therapy of type 2 diabetic patients. Diabetes Care 2003; 26:3080–3086.
- Davies M, Sinnassamy P, Storms F, Gomis R; ATLANTUS Study Group. Insulin glargine-based therapy improves glycemic control in patients with type 2 diabetes sub-optimally controlled on premixed insulin therapies. Diabetes Res Clin Pract 2008; 79:368–375.
- Jacober SJ, Scism-Bacon JL, Zagar AJ. A comparison of intensive mixture therapy with basal insulin therapy in insulin-naïve patients with type 2 diabetes receiving oral antidiabetes agents. Diabetes Obes Metab 2006; 8:448–455.
- Hirsch IB, Yuan H, Campaigne BN, Tan MH. Impact of prandial plus basal vs basal insulin on glycemic variability in type 2 diabetic patients. Endocr Pract 2009; 15:343–348.
- Robbins DC, Beisswenger PJ, Ceriello A, et al. Mealtime 50/50 basal + prandial insulin analogue mixture with a basal insulin analogue, both plus metformin, in the achievement of target HbA1c and pre- and postprandial blood glucose levels in patients with type 2 diabetes: a multinational, 24-week, randomized, open-label, parallel-group comparison. Clin Ther 2007; 29:2349–2364.
- Hollander P, Cooper J, Bregnhøj J, Pedersen CB. A 52-week, multinational, open-label, parallel-group, noninferiority, treat-to-target trial comparing insulin detemir with insulin glargine in a basal-bolus regimen with mealtime insulin aspart in patients with type 2 diabetes. Clin Ther 2008; 30:1976–1987.
- Raskin P, Gylvin T, Weng W, Chaykin L. Comparison of insulin detemir and insulin glargine using a basal-bolus regimen in a randomized, controlled clinical study in patients with type 2 diabetes. Diabetes Metab Res Rev 2009; 25:542–548.
- Perriello G, Pampanelli S, Porcellati F, et al. Insulin aspart improves meal time glycaemic control in patients with type 2 diabetes: a randomized, stratified, double-blind and cross-over trial. Diabet Med 2005; 22:606–611.
- Umpierrez GE, Hor T, Smiley D, et al. Comparison of inpatient insulin regimens with detemir plus aspart versus neutral protamine hagedorn plus regular in medical patients with type 2 diabetes. J Clin Endocrinol Metab 2009; 94:564–569.
- Bergenstal RM, Johnson M, Powers MA, et al. Adjust to target in type 2 diabetes: comparison of a simple algorithm with carbohydrate counting for adjustment of mealtime insulin glulisine. Diabetes Care 2008; 31:1305–1310.
- Rosenstock J, Ahmann AJ, Colon G, Scism-Bacon J, Jiang H, Martin S. Advancing insulin therapy in type 2 diabetes previously treated with glargine plus oral agents: prandial premixed (insulin lispro protamine suspension/lispro) versus basal/bolus (glargine/lispro) therapy. Diabetes Care 2008; 31:20–25.
- Ligthelm RJ, Mouritzen U, Lynggaard H, et al. Biphasic insulin aspart given thrice daily is as efficacious as a basal-bolus insulin regimen with four daily injections: a randomised open-label parallel group four months comparison in patients with type 2 diabetes. Exp Clin Endocrinol Diabetes 2006; 114:511–519.
- Velojic-Golubovic M, Mikic D, Pesic M, Dimic D, Radenkovic S, Antic S. Biphasic insulin aspart 30: better glycemic control than with premixed human insulin 30 in obese patients with type 2 diabetes. J Endocrinol Invest 2009; 32:23–27.
- Holman RR, Farmer AJ, Davies MJ, et al; 4-T Study Group. Three-year efficacy of complex insulin regimens in type 2 diabetes. N Engl Med 2009; 361:1736–1747.
- Tseng CL, Brimacombe M, Xie M, et al. Seasonal patterns in monthly hemoglobin A1c values. Am J Epidemiol 2005; 161:565–574.
KEY POINTS
- Whether to start insulin therapy and which regimen to use depend on a number of factors, including the patient’s acceptance and willingness to adhere to the therapy.
- A common way to start is to add a once-daily dose of a long-acting insulin at bedtime (basal insulin) to the patient’s antidiabetic regimen.
- Basal regimens do not control postprandial hyperglycemia very well. Another option is to take a long-acting (basal) insulin along with a rapid-acting (prandial or bolus) insulin before meals. Multiple formulations of premixed insulins are available and are convenient to use among new users.
- Basal-bolus regimens, which involve injections of rapid-acting insulin before meals and long-acting insulin at bedtime, are gaining popularity. Their cost and the number of injections may affect patient acceptance of this treatment.
A practical guide to prostate cancer diagnosis and management
Prostate cancer screening, diagnosis, and treatment present challenges to internists, urologists, and oncologists. For the internist, there is the ongoing debate about when and how often to screen with prostate-specific antigen (PSA) testing, as well as about how to interpret the results. For urologists and oncologists, there is no consensus on how to treat prostate cancer with the growing array of options, from surgery to cryoablation. Most therapies have not been compared in head-to-head trials, and anxious patients often approach their internist for help in navigating the maze of options.
This review summarizes current American Urological Association (AUA) guidelines,1 as well as current practice patterns at the Glickman Urological and Kidney Institute of Cleveland Clinic regarding screening, diagnosis, risk assessment, treatment, and posttreatment management of prostate cancer. We try to explain the approved and the experimental treatments, outlining what we know about their advantages and disadvantages.
SCREENING: WHEN AND HOW
Screening for prostate cancer should involve both a digital rectal examination (DRE) and measurement of the serum PSA level. But when should screening start?
The AUA recommends annual screening with DRE and serum PSA test starting at age 40 for all men with a life expectancy of more than 10 years.1
The American Cancer Society2 and the American College of Physicians,3 in contrast, recommend that men who choose to undergo screening should begin at age 50, or at age 45 if they are black or have a family history of prostate cancer in a primary relative diagnosed before age 65. They also recommend that screening with PSA and DRE be stopped at age 75, given the low likelihood of death from de novo prostate cancer after this age. The AUA recommends that screening be stopped at age 75, but may be continued beyond age 75 if the patient has a life expectancy of 10 years or more.
Before being screened, patients should understand the benefits and the risks of testing. While a small subset of prostate cancers behave aggressively, the majority are slow-growing and pose minimal risk for the development of fatal disease.
A discussion of the rationale for these guidelines and their differences is beyond the scope of this review. Differences stem from the observation that most men treated for prostate cancer will likely not die from prostate cancer, but rather from another condition.
Digital rectal examination’s role and limitations
The utility of DRE is limited to the detection of nodules, gross asymmetry, and gland fixation. DRE is not highly specific: only 40% to 50% of men who have abnormal findings on DRE have prostate cancer on biopsy.5 Anyone who has an abnormal finding on DRE should undergo prostate biopsy. However, if a rectal mass is palpated or if the prostate is exquisitely sensitive, biopsy is not indicated.
DRE is highly inaccurate for estimating gland volume; it should not be used to gauge cancer risk.
Prostate-specific antigen: Caveats
PSA measurement was introduced as a clinical screening test for prostate cancer in the early 1990s, and it serves as the foundation for early detection.
PSA, a protein involved in seminal coagulation, is produced by the prostate epithelium and is mostly confined within the prostatic ducts. Cancer cells secrete PSA into the bloodstream at increased levels via a disrupted basement membrane in tumor-affected areas of the gland. Elevated PSA can also result from benign prostatic hypertrophy, prostatitis, and prostate biopsy.
PSA levels represent a continuum of prostate cancer risk, and no single PSA value is sensitive and specific enough to predict the presence of cancer.6 Abnormal PSA cutoffs have been defined from 2.5 μg/L to 4 μg/L, and much debate surrounds this topic. Men who present with an elevated PSA (ie, > 2.5 μg/L) should be tested again. If the value remains high, then prostate biopsy should be considered. An elevated PSA level in older men with benign prostatic hypertrophy is not unexpected, and in these patients observation of the PSA value over time may prove valuable to assess the need for biopsy.
A useful adjunct in men with elevated PSA and benign prostatic hypertrophy is the percentage of serum PSA that is free rather than bound.7 PSA produced by prostate cancer binds more avidly with serum proteins (alpha-1 chymotrypsin and alpha-2 macroglobulin), resulting in a lower percentage of free PSA. In men with an elevated PSA (ie, 4.1–10.0 μg/L), the percentage of free PSA provides an indication of whether the elevation is due to benign prostatic hypertrophy or to cancer: the lower the percent free PSA, the more likely an elevated total PSA represents cancer and not benign prostatic hypertrophy. The sensitivity of a free PSA less than 15% to detect prostate cancer is about 85%, and its use as a screening tool is under study.
Much attention has also been given to other PSA indices, namely, the PSA density (the PSA level divided by the prostate volume), the PSA velocity (the rate of increase in the PSA level over time), and the PSA doubling time. While these nuanced PSA measures are useful to predict disease severity and behavior, they are not routinely used in screening.
BIOPSY IS INDICATED IF EITHER TEST IS ABNORMAL
In the past, imaging of the prostate with transrectal ultrasonography was used as a screening tool to detect prostate cancer. Further research showed that only 15% to 20% of hypoechoic lesions detected on ultrasonography contained cancer.8 Because of its low sensitivity and specificity, primary ultrasonographic screening (ie, transrectal ultrasonography alone) is not acceptable for screening or for diagnosis. Its main role is in guiding prostate biopsy.
Biopsy of the prostate with transrectal ultrasonographic guidance is indicated if either the DRE or the PSA level is abnormal. The standard of care is to use an 18-gauge biopsy needle-gun to obtain two to three tissue samples from each of six regions of the prostate, focusing on the outer peripheral zone, specifically the right and left bases, the mid-gland, and the apex.
Pathologic analysis of each tissue core takes into consideration the presence or absence of cancer, the Gleason score, and the percentage of the tissue sample volume that is occupied by cancer.
The Gleason grading system is based on the histologic appearance and reflects the degree of differentiation and aggressiveness of the cancer. The two most prominent tumor grades present are added to give a final Gleason score. For instance, a Gleason grade of 4+3=7 indicates a tumor with predominant Gleason grade 4 disease with a lesser amount of grade 3 disease. The number of positive core samples and the volume of cancer provide information on the severity of the cancer.
If the PSA is high but biopsy is negative
Prostate biopsy misses up to 30% of small cancers. Many of these are clinically insignificant, but about 20% of those missed cancers can be high-risk and thus merit identification. There should be a low threshold for repeating biopsy 1 year later in men who have a persistently high PSA or a rising PSA.
High-grade prostatic intraepithelial neoplasia is a common finding on biopsy. The incidence of de novo prostate cancer at 5 years in men with this finding is 22% to 26%.9 Patients with multifocal high-grade prostatic intraepithelial neoplasia should be monitored with PSA testing and DRE every 6 to 12 months and should be considered for repeat “saturation” biopsy (ie, obtaining as many as 36 core samples).
IF CANCER IS FOUND, HOW RISKY IS IT?
Patients with a new diagnosis of prostate cancer must decide on a treatment plan. This decision is highly individualized, based on the patient’s personal preferences, lifestyle, performance status (ie, his general well-being), disease severity, continence status, and sexual function.
When counseling patients about their disease and the treatment options, we consider three main factors:
- The severity of disease on biopsy
- The patient’s current state of health and performance status
- The patient’s understanding of and willingness to accept the adverse effects of the various treatments.
Pathologic features, the PSA level, and clinical stage determined by DRE are used to predict the severity of disease. Most data on the efficacy of treatments for prostate cancer are based on the incidence of biochemical recurrence, ie, a rise in PSA level after primary therapy. The AUA and the D’Amico risk criteria use biopsy pathology, clinical stage, and the pretreatment PSA level to predict the likelihood of biochemical recurrence (Table 1).10,11
DISCUSSING TREATMENT OPTIONS WITH THE PATIENT
In our practice, we usually do not recommend treatment in men with low-risk or intermediate-risk prostate cancer who have a life expectancy of less than 10 years, as most of them will likely die of a cause other than prostate cancer. For patients with poor baseline performance status, surveillance or radiation therapy may be preferable to surgery. In younger patients, surgery may confer a more durable benefit.
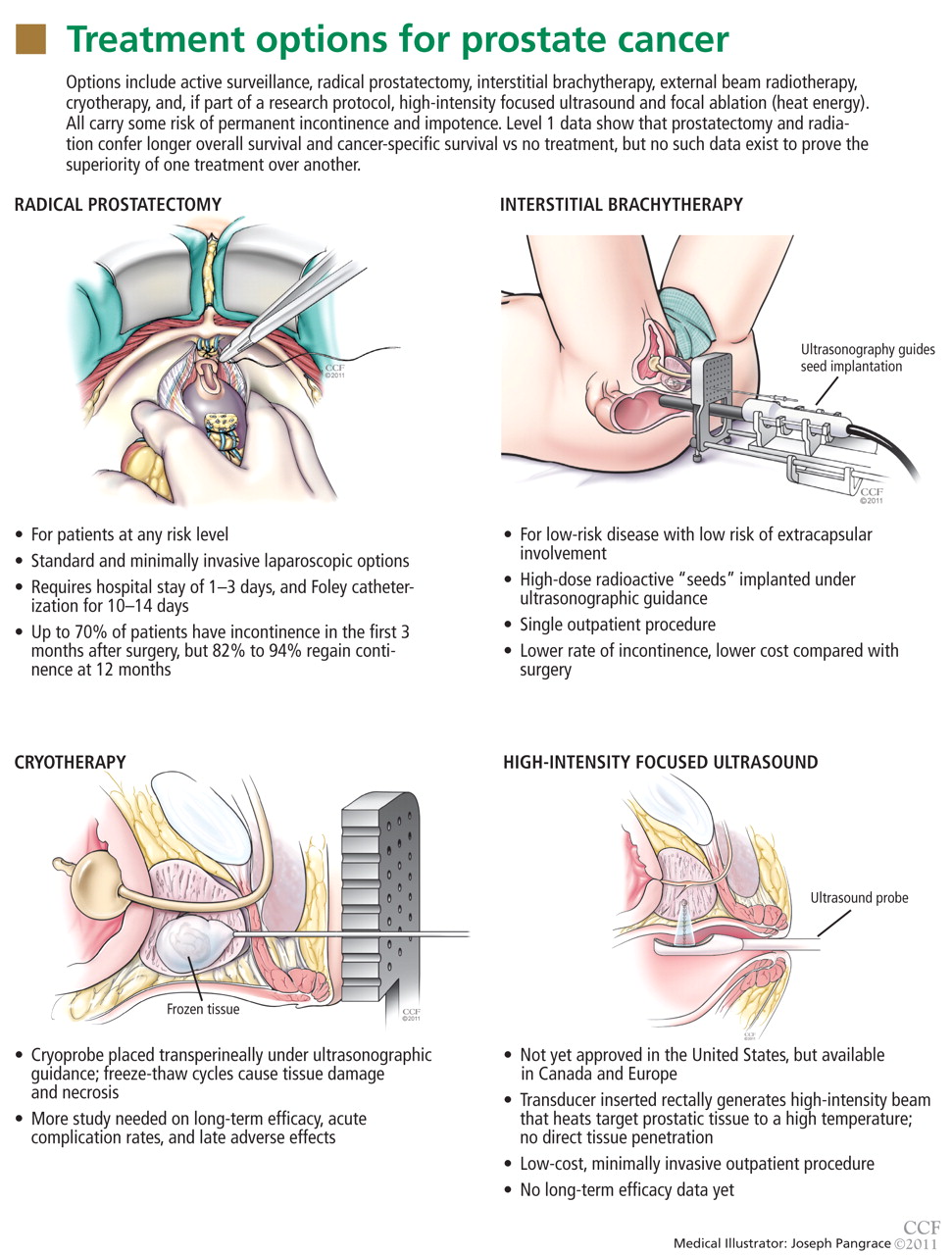
- No prospective, randomized clinical trials have directly compared these treatments
- Prostate cancer progresses slowly
- Definitions of treatment failure used in various studies have been inconsistent
- Clinical studies have been subject to selection bias.
ACTIVE SURVEILLANCE IS ACCEPTABLE FOR LOW-RISK PROSTATE CANCER
Active surveillance is an acceptable option for patients with low-risk prostate cancer (ie, if the Gleason score is ≤ 6, the tumor stage is T1c or T2a, and the PSA level is ≤ 10 μg/L). To rule out high-risk disease before starting a program of surveillance, repeat biopsy is advisable, although optional.
Active surveillance consists of PSA testing and DRE every 6 to 12 months, followed by repeat biopsy if significant changes are noted in either test. Some centers advocate biopsy with transrectal ultrasonographic guidance every year regardless of the PSA or DRE findings.
Whether a change in the PSA level is significant is subjective, but a recent phase 2 study in 453 patients23 on a program of active surveillance used a PSA doubling time of less than 3 years as a criterion for repeat biopsy. Thirty-eight percent of the men had to undergo radiation therapy or surgery within 10 years, and 5 patients (1%) died of prostate cancer. The authors concluded that active surveillance did not put these patients at undue risk, and that this approach prevented overtreatment of clinically insignificant prostate cancer.23
The risks of surveillance include the chance that cancer could progress to an incurable state during the surveillance period, greater anxiety for the patient, and, if prostatectomy becomes necessary, greater technical difficulty due to scarring from repeat biopsies. The benefit is postponement or complete avoidance of the adverse effects of treatment.
Debate continues over the potential dangers of deferred treatment of prostate cancer, but in certain patients it is an acceptable option. Patient education, accurate disease assessment, and compliance with monitoring are critical considerations.
RADICAL PROSTATECTOMY: SEVERAL OPTIONS, EQUIVALENT EFFICACY
Radical prostatectomy is widely used for treating prostate cancer of any risk level. The operation entails removing the prostate and seminal vesicles, as well as the pelvic lymph nodes in patients with intermediate or high-risk cancer.
This procedure was increasingly used in the 1990s with the introduction of PSA screening and nerve-sparing surgical techniques that preserve continence and erectile function.
Radical prostatectomy can be done via a standard open approach or a minimally invasive laparoscopic approach with or without robotic assistance. Open surgery, laparoscopic surgery, and robotic prostatectomy offer equivalent rates of oncologic efficacy, continence, and potency.24 The more experienced the surgeon, the better the outcome is likely to be.
The average biochemical recurrence rate at 5 years after radical prostatectomy is approximately 6% for patients with low-risk cancer, 23% for those with intermediate-risk cancer, and 45% for those with high-risk cancer.25 The rate of death from prostate cancer at 10 years is about 1% for patients with low-risk cancer, 4% for those with intermediate-risk cancer, and 8% for those with high-risk cancer.12
Secondary therapy
Pathologic staging of the surgical specimen after radical prostatectomy yields information that can be beneficial in terms of initiating early secondary therapy.
Patients with node-positive disease should immediately undergo androgen deprivation treatment.26
Evidence of positive surgical margins, seminal vesicle invasion, bladder neck invasion, and extracapsular extension also increase the risk of recurrence. This additional risk can be ascertained via the use of a postoperative nomogram. Patients at high risk of recurrence should be considered for early adjuvant external beam radiotherapy to the surgical field 3 to 6 months after surgery.
Advantages and disadvantages of radical prostatectomy
Advantages of radical prostatectomy include the ability to accurately stage the cancer with the surgical specimen and the ability to remove the pelvic lymph nodes in patients at intermediate and high risk. Another advantage is that postoperative surveillance is straightforward: PSA should become undetectable after surgery, and a measurable increase in PSA represents disease recurrence.
Disadvantages include:
- The risk of surgical complications (reported in 3% to 17% of cases)24
- An average hospital stay of 1 to 3 days (and a typical 3 to 6 weeks before returning to work)
- The need for a Foley catheter for 10 to 14 days
- The risk of incontinence and impotence, which are very distressing to patients.
Postoperative incontinence is typically defined as the need for any type of protective pad for leakage. Up to 70% of patients have incontinence in the first 3 months after surgery, but 82% to 94% of patients regain continence by 12 months.24 A small percentage of patients (3% to 5%) have significant permanent incontinence.
Counseling about postoperative erectile dysfunction
All patients should be counseled about the risk of a postoperative decrease in erectile function, especially those with pre-existing erectile dysfunction. Potency is defined as the ability to have an erection suitable for intercourse (with or without phosphodiesterase type 5 inhibitors) more than 50% of the time. In men with bilateral nerve-sparing open prostatectomy, potency rates at 12 months have been reported between 63% and 81%.13
Data on potency rates vary widely because of differences in how potency was defined, selection bias, and the multifactorial nature of erectile dysfunction. Also, because single-institution, single-surgeon reports and advertisements tend to underestimate rates of impotence after radical prostatectomy by any approach, many patients have false expectations.
INTERSTITIAL BRACHYTHERAPY FOR LOW-RISK CANCERS
Interstitial brachytherapy delivers a localized, high dose (125 to 145 Gy) of radiation to the prostate, with minimal radiation dosing to the bladder, rectum, or other adjacent organs and tissues. “Seeds” or small pellets containing a radioisotope (iodine 125 or palladium 103) are stereotactically implanted through the perineum into the prostate under ultrasonographic guidance. Computerized mapping done before or during surgery helps determine the optimal placement of the seeds, the object being to cover at least 90% of the prostate with 100% of the radiation dose.
In permanent brachytherapy, the implants give off radiation at a low dose rate over weeks to months and are left in place permanently. In temporary brachytherapy, seeds are implanted to deliver a low or high dose rate for a specified period, and then they are removed.
“Implant quality,” ie, delivery of more than 90% of the radiation dose, is a major predictor of success and can depend on both the available instrumentation and the skill of the operator.
Caveats about brachytherapy
The evidence in support of combining androgen deprivation therapy and interstitial brachytherapy is poor, and there is some evidence of increased rates of irritative voiding symptoms,27 so this is generally not recommended.
Interstitial brachytherapy as monotherapy has usually been reserved for patients with low-risk cancer with a low likelihood of extracapsular disease extension or pelvic lymph node involvement. No randomized controlled clinical trial has compared brachytherapy with radical prostatectomy or external beam radiotherapy. One large long-term study reported an 8-year biochemical recurrence rate of 18% in patients with low-risk cancer and 30% in patients with intermediate-risk cancer.28 The long-term efficacy of brachytherapy for intermediate- and high-risk prostate cancer is still under investigation.
Advantages and disadvantages of interstitial brachytherapy
Advantages. Interstitial brachytherapy is done as a single outpatient procedure. It can deliver a targeted high dose of radiation. And it is associated with a lower rate of posttreatment incontinence than radical prostatectomy, and a lower cost.
Disadvantages. There are limited data to support long-term cancer control in intermediate- and high-risk disease. Short-term adverse effects include dysuria, hematuria, urinary urgency, and urinary frequency in up to 80% of patients.29 Voiding symptoms typically peak 1 to 3 months after the procedure and subside after 8 to 12 months. Erectile dysfunction has been reported in 30% to 35% of men at 5 years after the procedure. Other possible adverse effects include urethral stricture, incontinence, recurrent hematuria, rectal bleeding, proctitis, and the development of bladder cancer and other secondary cancers.
EXTERNAL BEAM RADIOTHERAPY
In external beam radiotherapy, radiation is delivered to the prostate and surrounding tissues via an external energy source. Electrons, protons, or neutrons are used, and although each has theoretical advantages over the others, all appear to have similar clinical efficacy.
As with brachytherapy, the object—and the challenge—is to deliver an effective dose of radiation to the tumor while sparing adjacent organs. Intensity-modulated delivery is a radiotherapy technique that delivers more of the radiation dose where we want it to go—and less where we don’t want it to go. For prostate cancer, the target dose with intensity-modulated delivery is typically 75 to 85 Gy, in doses of 2 to 2.25 Gy for 30 to 36 days.
Androgen deprivation therapy before or after external beam radiotherapy augments the effects of the radiotherapy, particularly in patients with high-risk disease.30
The oncologic efficacy of intensity-modulated radiotherapy in patients at low and intermediate risk appears commensurate with that of radical prostatectomy. In one study,31 in low-risk cases, biochemical disease-free survival rates were 85% for radiotherapy vs 93% for prostatectomy; in intermediate-risk cases, 82% for radiotherapy and 87% for prostatectomy; and in high-risk cases, 62% for combined androgen deprivation and radiotherapy vs 38% for prostatectomy.31
Advantages and disadvantages of external beam radiotherapy
Advantages. External beam radiotherapy is noninvasive. It can treat the prostate as well as areas outside the prostate in patients with intermediate- and high-risk disease, and it is proven effective for high-risk cancer when used in combination with androgen deprivation.
Disadvantages. On the other hand, radiotherapy requires a series of daily treatments, which can be inconvenient and burdensome to the patient. Its adverse effects are similar to those of brachytherapy, and it is expensive. Long-term adverse effects include irritative voiding symptoms (frequency, urgency, nocturia), hemorrhagic cystitis, bowel symptoms (pain with defecation, tenesmus, bleeding), and a significantly higher lifetime risk of a secondary malignancy, particularly of the bladder and rectum.32
External beam radiotherapy also induces tissue changes in the pelvis that make salvage surgery more difficult. Patients in whom radiotherapy is ineffective as monotherapy and who require salvage prostatectomy typically have poor outcomes in terms of disease control, continence, and potency.
COMBINED RADIATION THERAPY: BETTER, OR OVERTREATMENT?
Many patients are offered a combination of external beam radiotherapy and interstitial brachytherapy. The rationale is that the combination can boost the dose of radiation to the prostate and at the same time treat cancer that has extended beyond the prostate or to the pelvic lymph nodes.
The radiation dose in the combined approach is 45 to 50 Gy (vs 70 to 80 Gy in monotherapy), thereby minimizing toxicity.
This combination has not been shown to improve overall survival or cancer-specific survival compared with either therapy alone, and it likely constitutes overtreatment.33 Adverse effects of combination therapy include erectile dysfunction, rectal and bladder toxicity, and secondary malignancy.
A serious complication associated more often with the combination of external beam radiotherapy and brachytherapy than other treatments is rectoprostatic fistula, a condition that requires complex reconstructive surgery and often requires permanent urinary and fecal diversion.34
CRYOTHERAPY: MORE STUDY NEEDED
Refinements in cryoablative therapy to destroy prostate tissue have improved the safety and efficacy of this procedure significantly over the past decade. The AUA consensus guidelines recognize cryotherapy as a viable primary cancer monotherapy, but it is most commonly used as a salvage therapy after failure of radiation therapy.
The procedure involves ultrasonographically guided stereotactic placement of cryoprobes into the prostate via a transperineal approach. Argon is pumped through the probes under pressure to initiate ice formation, and repeated freeze-thaw cycles cause tissue damage and necrosis.
Rates of biochemical recurrence at 5 years in patients at low, intermediate, and high risk have been reported at 16%, 27%, and 25%, respectively.35 The presence of viable cancer on biopsy specimens after primary cryoablation has been reported at 15%, compared with 25% after definitive radiation therapy.35
Advantages and disadvantages of cryotherapy
Cryotherapy can destroy cancer tissue in a minimally invasive way. It has no long-term delayed adverse effects, and it is a low-cost and convenient outpatient procedure.
On the other hand, we lack long-term data on its oncologic efficacy, acute complications, and late adverse effects. Acute complications occur in up to 16% of patients and include acute urinary retention requiring prolonged catheterization, hematuria, urethral sloughing, perineal pain, and incontinence.36 Potential late effects include rectoprostatic fistula (< 1%), incontinence (< 5%), persistent hematuria, and chronic pelvic pain.36
Cryoablation therapy appears to have a more significant negative impact on sexual function than does brachytherapy.37
More study of the complications and efficacy of cryotherapy is needed before the procedure can be adopted as routine primary monotherapy.
HIGH-INTENSITY FOCUSED ULTRASOUND: NOT YET FDA-APPROVED
High-intensity focused ultrasound (HIFU) is not yet approved by the US Food and Drug Administration (other than in an approved research protocol) but is used in Canada and in certain countries of Europe and Asia. It involves the insertion of a transducer into the rectum that generates a high-intensity, focused beam that heats target tissue in the prostate to a high temperature. This temperature triggers a heat-shock response that leads to cellular apoptosis and tissue necrosis. The procedure can be done with or without magnetic resonance imaging (MRI) guidance.
Biochemical recurrence rates at 2 years after the procedure have been reported between 23% and 50%, but long-term efficacy data are lacking.38,39
Advantages and disadvantages of ultrasound
HIFU is a minimally invasive, low-cost, outpatient procedure that offers trackless delivery of energy to the prostate: ie, there is no direct mechanical penetration into the tissue.
Complications include rectal-wall injury, fistula, acute urinary retention, hematuria, and urethral stricture.
FOCAL ABLATION: GETTING ATTENTION, BUT STILL UNDER DEVELOPMENT
Focal ablation for prostate cancer has been receiving much attention. This treatment uses heat energy to destroy tumor cells, guided by high-resolution endorectal-coil MRI. The procedure is in the developmental stages and is available only in research protocols.
The procedure has several major hurdles to overcome before becoming acceptable for clinical practice. First, prostate cancer is multifocal, and microscopic tumor foci are likely present that are invisible even to MRI, so ablation of only part of the prostate leaves the rest of the gland at risk of continued or de novo tumor growth.
Second, a wide range of sensitivities and specificities have been reported for endorectal coil MRI for detecting prostate cancer: its sensitivity has ranged from 27% to 100%, and its specificity has ranged from 32% to 99%.40
ANDROGEN DEPRIVATION, AN ADJUVANT THERAPY
Androgen deprivation therapy (medical castration) is not effective as a monotherapy for prostate cancer. A large population-based study in men with localized prostate cancer showed no higher rate of overall survival at 10 years with primary androgen deprivation therapy than with conservative management.41
Androgen deprivation is achieved with a leutinizing hormone-releasing hormone agonist such as leuprolide (Lupron) or goserelin (Zoladex), or an antiandrogen drug such as flutamide or bicalutamide (Casodex), or a combination of each.
Adverse effects include hot flashes, gynecomastia, decreased libido, erectile dysfunction, weight gain, and hyperlipidemia. Long-term effects include osteoporosis and a significantly higher risk of cardiac events, new-onset type 2 diabetes mellitus, and stroke.
Currently, the only recognized role for androgen deprivation therapy in prostate cancer is as an adjunct to external beam radiotherapy or as a treatment of metastatic prostate cancer.
Orchiectomy
The other way to eliminate testicular production of testosterone is surgical castration. Bilateral orchiectomy has advantages over medical androgen deprivation therapy in that it costs less, is highly reliable, and is done as a single treatment on an outpatient basis. Disadvantages include surgery-related morbidity and the irreversible nature of the procedure. The adverse effects are similar to those of androgen deprivation therapy.
POSTTREATMENT MONITORING
The management of patients with recurrent prostate cancer can be complex, and these patients should be referred to a medical or urologic oncologist.42,43
Often, a rise in PSA after primary therapy represents a regrowth of cancer; 30% to 60% of patients with a recurrence have metastasis, and nearly 20% will die from the disease. The average time from documentation of biochemical recurrence to metastatic progression is 8 years. The average time from metastatic progression to death is 5 years.44,45
After radical prostatectomy, the PSA level should be checked every 6 to 12 months for the first 2 years, then annually until the patient’s life expectancy is only 10 years even without prostate cancer. PSA should reach undetectable levels within 4 to 6 weeks after surgery. Biochemical recurrence after surgery is defined as a PSA level of 0.2 μg/L or higher in two serial studies.
After radiation therapy or cryotherapy, monitoring is complicated by the presence of viable prostatic epithelium that continues to produce PSA. During the first 1 to 2 years after radiation therapy, a PSA “bounce” phenomenon is observed whereby PSA levels rise or fluctuate significantly. This bounce should not be mistaken for a recurrence of cancer. The most widely accepted definition of biochemical recurrence is based on the American Society for Therapeutic Radiology and Oncology “Phoenix” criteria, defined as the nadir PSA level plus 2.0 μg/L.46
- Thompson I, Thrasher JB, Aus G, et al; AUA Prostate Cancer Clinical Guideline Update Panel. Guideline for the management of clinically localized prostate cancer: 2007 update. J Urol 2007; 177:2106–2131.
- Brooks DD, Wolf A, Smith RA, Dash C, Guessous I. Prostate cancer screening 2010: updated recommendations from the American Cancer Society. J Natl Med Assoc 2010; 102:423–429.
- US Preventive Services Task Force. Screening for prostate cancer: US Preventive Services Task Force recommendation statement. Ann Intern Med 2008; 149:185–191.
- Okotie OT, Roehl KA, Han M, Loeb S, Gashti SN, Catalona WJ. Characteristics of prostate cancer detected by digital rectal examination only. Urology 2007; 70:1117–1120.
- Philip J, Dutta Roy S, Ballal M, Foster CS, Javlé P. Is a digital rectal examination necessary in the diagnosis and clinical staging of early prostate cancer? BJU Int 2005; 95:969–971.
- Thompson IM, Ankerst DP, Chi C, et al. Assessing prostate cancer risk: results from the Prostate Cancer Prevention Trial. J Natl Cancer Inst 2006; 98:529–534.
- Catalona WJ, Partin AW, Slawin KM, et al. Use of the percentage of free prostate-specific antigen to enhance differentiation of prostate cancer from benign prostatic disease: a prospective multicenter clinical trial. JAMA 1998; 279:1542–1547.
- Terris MK, Freiha FS, McNeal JE, Stamey TA. Efficacy of transrectal ultrasound for identification of clinically undetected prostate cancer. J Urol 1991; 146:78–83.
- Epstein JI, Herawi M. Prostate needle biopsies containing prostatic intraepithelial neoplasia or atypical foci suspicious for carcinoma: implications for patient care. J Urol 2006 Mar; 175( 3 Pt1):820–34.
- D’Amico AV, Whittington R, Malkowicz SB, et al. Biochemical outcome after radical prostatectomy, external beam radiation therapy, or interstitial radiation therapy for clinically localized prostate cancer. JAMA 1998; 280:969–974.
- Greene FL. American Joint Committee on Cancer. American Cancer Society. AJCC cancer staging manual. 6th ed. New York, NY: Springer-Verlag; 2002.
- Stephenson AJ, Kattan MW, Eastham JA, et al. Prostate cancer-specific mortality after radical prostatectomy for patients treated in the prostate-specific antigen era. J Clin Oncol 2009; 27:4300–4305.
- Eastham JA, Scardino PT, Kattan MW. Predicting an optimal outcome after radical prostatectomy: the trifecta nomogram. J Urol 2008; 179:2207–2210.
- Stephenson AJ, Scardino PT, Eastham JA, et al. Preoperative nomogram predicting the 10-year probability of prostate cancer recurrence after radical prostatectomy. J Natl Cancer Inst 2006; 98:715–717.
- Potters L, Roach M, Davis BJ, et al. Postoperative nomogram predicting the 9-year probability of prostate cancer recurrence after permanent prostate brachytherapy using radiation dose as a prognostic variable. Int J Radiat Oncol Biol Phys 2010; 76:1061–1065.
- Zelefsky MJ, Kattan MW, Fearn P, et al. Pretreatment nomogram predicting ten-year biochemical outcome of three-dimensional conformal radiotherapy and intensity-modulated radiotherapy for prostate cancer. Urology 2007; 70:283–287.
- Walz J, Gallina A, Saad F, et al. A nomogram predicting 10-year life expectancy in candidates for radical prostatectomy or radiotherapy for prostate cancer. J Clin Oncol 2007; 25:3576–3581.
- Charlson ME, Pompei P, Ales KL, MacKenzie CR. A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J Chronic Dis 1987; 40:373–383.
- Hall WH, Ramachandran R, Narayan S, Jani AB, Vijayakumar S. An electronic application for rapidly calculating Charlson comorbidity score. BMC Cancer 2004; 4:94.
- Oken MM, Creech RH, Tormey DC, et al. Toxicity and response criteria of the Eastern Cooperative Oncology Group. Am J Clin Oncol 1982; 5:649–655.
- Bill-Axelson A, Holmberg L, Ruutu M, et al; Scandinavian Prostate Cancer Group Study No. 4. Radical prostatectomy versus watchful waiting in early prostate cancer. N Engl J Med 2005; 352:1977–1984.
- Widmark A, Klepp O, Solberg A, et al; Scandinavian Prostate Cancer Group Study 7. Endocrine treatment, with or without radiotherapy, in locally advanced prostate cancer (SPCG-7/SFUO-3): an open randomised phase III trial. Lancet 2009; 373:301–308.
- Krakowsky Y, Loblaw A, Klotz L. Prostate cancer death of men treated with initial active surveillance: clinical and biochemical characteristics. J Urol 2010; 184:131–135.
- Ficarra V, Novara G, Artibani W, et al. Retropubic, laparoscopic, and robot-assisted radical prostatectomy: a systematic review and cumulative analysis of comparative studies. Eur Urol 2009; 55:1037–1063.
- Hernandez DJ, Nielsen ME, Han M, Partin AW. Contemporary evaluation of the D’amico risk classification of prostate cancer. Urology 2007; 70:931–935.
- Messing EM, Manola J, Yao J, et al; Eastern Cooperative Oncology Group study EST 3886. Immediate versus deferred androgen deprivation treatment in patients with node-positive prostate cancer after radical prostatectomy and pelvic lymphadenectomy. Lancet Oncol 2006; 7:472–479.
- Beyer DC, McKeough T, Thomas T. Impact of short course hormonal therapy on overall and cancer specific survival after permanent prostate brachytherapy. Int J Radiat Oncol Biol Phys 2005; 61:1299–1305.
- Zelefsky MJ, Kuban DA, Levy LB, et al. Multi-institutional analysis of long-term outcome for stages T1-T2 prostate cancer treated with permanent seed implantation. Int J Radiat Oncol Biol Phys 2007; 67:327–333.
- Gelblum DY, Potters L, Ashley R, Waldbaum R, Wang XH, Leibel S. Urinary morbidity following ultrasound-guided transperineal prostate seed implantation. Int J Radiat Oncol Biol Phys 1999; 45:59–67.
- Bolla M, Collette L, Blank L, et al. Long-term results with immediate androgen suppression and external irradiation in patients with locally advanced prostate cancer (an EORTC study): a phase III randomised trial. Lancet 2002; 360:103–106.
- Aizer AA, Yu JB, Colberg JW, McKeon AM, Decker RH, Peschel RE. Radical prostatectomy vs intensity-modulated radiation therapy in the management of localized prostate adenocarcinoma. Radiother Oncol 2009; 93:185–191.
- Moon K, Stukenborg GJ, Keim J, Theodorescu D. Cancer incidence after localized therapy for prostate cancer. Cancer 2006; 107:991–998.
- Terakedis BE, Rossi PJ, Liauw SL, Johnstone PA, Jani AB. A surveillance, epidemiology, and end results registry analysis of prostate cancer modality time trends by age. Am J Clin Oncol 2010; 33:619–623.
- Lane BR, Stein DE, Remzi FH, Strong SA, Fazio VW, Angermeier KW. Management of radiotherapy induced rectourethral fistula. J Urol 2006; 175:1382–1387.
- Jones JS, Rewcastle JC, Donnelly BJ, Lugnani FM, Pisters LL, Katz AE. Whole gland primary prostate cryoablation: initial results from the cryo on-line data registry. J Urol 2008; 180:554–558.
- Hubosky SG, Fabrizio MD, Schellhammer PF, Barone BB, Tepera CM, Given RW. Single center experience with third-generation cryosurgery for management of organ-confined prostate cancer: critical evaluation of short-term outcomes, complications, and patient quality of life. J Endourol 2007; 21:1521–1531.
- Malcolm JB, Fabrizio MD, Barone BB, et al. Quality of life after open or robotic prostatectomy, cryoablation or brachytherapy for localized prostate cancer. J Urol 2010; 183:1822–1828.
- Ficarra V, Antoniolli SZ, Novara G, et al. Short-term outcome after high-intensity focused ultrasound in the treatment of patients with high-risk prostate cancer. BJU Int 2006; 98:1193–1198.
- Challacombe BJ, Murphy DG, Zakri R, Cahill DJ. High-intensity focused ultrasound for localized prostate cancer: initial experience with a 2-year follow-up. BJU Int 2009; 104:200–204.
- Bouchelouche K, Turkbey B, Choyke P, Capala J. Imaging prostate cancer: an update on positron emission tomography and magnetic resonance imaging. Curr Urol Rep 2010; 11:180–190.
- Lu-Yao GL, Albertsen PC, Moore DF, et al. Survival following primary androgen deprivation therapy among men with localized prostate cancer. JAMA 2008; 300:173–181.
- Simmons MN, Stephenson AJ, Klein EA. Natural history of biochemical recurrence after radical prostatectomy: risk assessment for secondary therapy. Eur Urol 2007; 51:1175–1184.
- Boukaram C, Hannoun-Levi JM. Management of prostate cancer recurrence after definitive radiation therapy. Cancer Treat Rev 2010; 36:91–100.
- Pound CR, Partin AW, Eisenberger MA, Chan DW, Pearson JD, Walsh PC. Natural history of progression after PSA elevation following radical prostatectomy. JAMA 1999; 281:1591–1597.
- Freedland SJ, Humphreys EB, Mangold LA, et al. Risk of prostate cancer-specific mortality following biochemical recurrence after radical prostatectomy. JAMA 2005; 294:433–439.
- Roach M, Hanks G, Thames H, et al. Defining biochemical failure following radiotherapy with or without hormonal therapy in men with clinically localized prostate cancer: recommendations of the RTOG-ASTRO Phoenix Consensus Conference. Int J Radiat Oncol Biol Phys 2006; 65:965–974.
Prostate cancer screening, diagnosis, and treatment present challenges to internists, urologists, and oncologists. For the internist, there is the ongoing debate about when and how often to screen with prostate-specific antigen (PSA) testing, as well as about how to interpret the results. For urologists and oncologists, there is no consensus on how to treat prostate cancer with the growing array of options, from surgery to cryoablation. Most therapies have not been compared in head-to-head trials, and anxious patients often approach their internist for help in navigating the maze of options.
This review summarizes current American Urological Association (AUA) guidelines,1 as well as current practice patterns at the Glickman Urological and Kidney Institute of Cleveland Clinic regarding screening, diagnosis, risk assessment, treatment, and posttreatment management of prostate cancer. We try to explain the approved and the experimental treatments, outlining what we know about their advantages and disadvantages.
SCREENING: WHEN AND HOW
Screening for prostate cancer should involve both a digital rectal examination (DRE) and measurement of the serum PSA level. But when should screening start?
The AUA recommends annual screening with DRE and serum PSA test starting at age 40 for all men with a life expectancy of more than 10 years.1
The American Cancer Society2 and the American College of Physicians,3 in contrast, recommend that men who choose to undergo screening should begin at age 50, or at age 45 if they are black or have a family history of prostate cancer in a primary relative diagnosed before age 65. They also recommend that screening with PSA and DRE be stopped at age 75, given the low likelihood of death from de novo prostate cancer after this age. The AUA recommends that screening be stopped at age 75, but may be continued beyond age 75 if the patient has a life expectancy of 10 years or more.
Before being screened, patients should understand the benefits and the risks of testing. While a small subset of prostate cancers behave aggressively, the majority are slow-growing and pose minimal risk for the development of fatal disease.
A discussion of the rationale for these guidelines and their differences is beyond the scope of this review. Differences stem from the observation that most men treated for prostate cancer will likely not die from prostate cancer, but rather from another condition.
Digital rectal examination’s role and limitations
The utility of DRE is limited to the detection of nodules, gross asymmetry, and gland fixation. DRE is not highly specific: only 40% to 50% of men who have abnormal findings on DRE have prostate cancer on biopsy.5 Anyone who has an abnormal finding on DRE should undergo prostate biopsy. However, if a rectal mass is palpated or if the prostate is exquisitely sensitive, biopsy is not indicated.
DRE is highly inaccurate for estimating gland volume; it should not be used to gauge cancer risk.
Prostate-specific antigen: Caveats
PSA measurement was introduced as a clinical screening test for prostate cancer in the early 1990s, and it serves as the foundation for early detection.
PSA, a protein involved in seminal coagulation, is produced by the prostate epithelium and is mostly confined within the prostatic ducts. Cancer cells secrete PSA into the bloodstream at increased levels via a disrupted basement membrane in tumor-affected areas of the gland. Elevated PSA can also result from benign prostatic hypertrophy, prostatitis, and prostate biopsy.
PSA levels represent a continuum of prostate cancer risk, and no single PSA value is sensitive and specific enough to predict the presence of cancer.6 Abnormal PSA cutoffs have been defined from 2.5 μg/L to 4 μg/L, and much debate surrounds this topic. Men who present with an elevated PSA (ie, > 2.5 μg/L) should be tested again. If the value remains high, then prostate biopsy should be considered. An elevated PSA level in older men with benign prostatic hypertrophy is not unexpected, and in these patients observation of the PSA value over time may prove valuable to assess the need for biopsy.
A useful adjunct in men with elevated PSA and benign prostatic hypertrophy is the percentage of serum PSA that is free rather than bound.7 PSA produced by prostate cancer binds more avidly with serum proteins (alpha-1 chymotrypsin and alpha-2 macroglobulin), resulting in a lower percentage of free PSA. In men with an elevated PSA (ie, 4.1–10.0 μg/L), the percentage of free PSA provides an indication of whether the elevation is due to benign prostatic hypertrophy or to cancer: the lower the percent free PSA, the more likely an elevated total PSA represents cancer and not benign prostatic hypertrophy. The sensitivity of a free PSA less than 15% to detect prostate cancer is about 85%, and its use as a screening tool is under study.
Much attention has also been given to other PSA indices, namely, the PSA density (the PSA level divided by the prostate volume), the PSA velocity (the rate of increase in the PSA level over time), and the PSA doubling time. While these nuanced PSA measures are useful to predict disease severity and behavior, they are not routinely used in screening.
BIOPSY IS INDICATED IF EITHER TEST IS ABNORMAL
In the past, imaging of the prostate with transrectal ultrasonography was used as a screening tool to detect prostate cancer. Further research showed that only 15% to 20% of hypoechoic lesions detected on ultrasonography contained cancer.8 Because of its low sensitivity and specificity, primary ultrasonographic screening (ie, transrectal ultrasonography alone) is not acceptable for screening or for diagnosis. Its main role is in guiding prostate biopsy.
Biopsy of the prostate with transrectal ultrasonographic guidance is indicated if either the DRE or the PSA level is abnormal. The standard of care is to use an 18-gauge biopsy needle-gun to obtain two to three tissue samples from each of six regions of the prostate, focusing on the outer peripheral zone, specifically the right and left bases, the mid-gland, and the apex.
Pathologic analysis of each tissue core takes into consideration the presence or absence of cancer, the Gleason score, and the percentage of the tissue sample volume that is occupied by cancer.
The Gleason grading system is based on the histologic appearance and reflects the degree of differentiation and aggressiveness of the cancer. The two most prominent tumor grades present are added to give a final Gleason score. For instance, a Gleason grade of 4+3=7 indicates a tumor with predominant Gleason grade 4 disease with a lesser amount of grade 3 disease. The number of positive core samples and the volume of cancer provide information on the severity of the cancer.
If the PSA is high but biopsy is negative
Prostate biopsy misses up to 30% of small cancers. Many of these are clinically insignificant, but about 20% of those missed cancers can be high-risk and thus merit identification. There should be a low threshold for repeating biopsy 1 year later in men who have a persistently high PSA or a rising PSA.
High-grade prostatic intraepithelial neoplasia is a common finding on biopsy. The incidence of de novo prostate cancer at 5 years in men with this finding is 22% to 26%.9 Patients with multifocal high-grade prostatic intraepithelial neoplasia should be monitored with PSA testing and DRE every 6 to 12 months and should be considered for repeat “saturation” biopsy (ie, obtaining as many as 36 core samples).
IF CANCER IS FOUND, HOW RISKY IS IT?
Patients with a new diagnosis of prostate cancer must decide on a treatment plan. This decision is highly individualized, based on the patient’s personal preferences, lifestyle, performance status (ie, his general well-being), disease severity, continence status, and sexual function.
When counseling patients about their disease and the treatment options, we consider three main factors:
- The severity of disease on biopsy
- The patient’s current state of health and performance status
- The patient’s understanding of and willingness to accept the adverse effects of the various treatments.
Pathologic features, the PSA level, and clinical stage determined by DRE are used to predict the severity of disease. Most data on the efficacy of treatments for prostate cancer are based on the incidence of biochemical recurrence, ie, a rise in PSA level after primary therapy. The AUA and the D’Amico risk criteria use biopsy pathology, clinical stage, and the pretreatment PSA level to predict the likelihood of biochemical recurrence (Table 1).10,11
DISCUSSING TREATMENT OPTIONS WITH THE PATIENT
In our practice, we usually do not recommend treatment in men with low-risk or intermediate-risk prostate cancer who have a life expectancy of less than 10 years, as most of them will likely die of a cause other than prostate cancer. For patients with poor baseline performance status, surveillance or radiation therapy may be preferable to surgery. In younger patients, surgery may confer a more durable benefit.
- No prospective, randomized clinical trials have directly compared these treatments
- Prostate cancer progresses slowly
- Definitions of treatment failure used in various studies have been inconsistent
- Clinical studies have been subject to selection bias.
ACTIVE SURVEILLANCE IS ACCEPTABLE FOR LOW-RISK PROSTATE CANCER
Active surveillance is an acceptable option for patients with low-risk prostate cancer (ie, if the Gleason score is ≤ 6, the tumor stage is T1c or T2a, and the PSA level is ≤ 10 μg/L). To rule out high-risk disease before starting a program of surveillance, repeat biopsy is advisable, although optional.
Active surveillance consists of PSA testing and DRE every 6 to 12 months, followed by repeat biopsy if significant changes are noted in either test. Some centers advocate biopsy with transrectal ultrasonographic guidance every year regardless of the PSA or DRE findings.
Whether a change in the PSA level is significant is subjective, but a recent phase 2 study in 453 patients23 on a program of active surveillance used a PSA doubling time of less than 3 years as a criterion for repeat biopsy. Thirty-eight percent of the men had to undergo radiation therapy or surgery within 10 years, and 5 patients (1%) died of prostate cancer. The authors concluded that active surveillance did not put these patients at undue risk, and that this approach prevented overtreatment of clinically insignificant prostate cancer.23
The risks of surveillance include the chance that cancer could progress to an incurable state during the surveillance period, greater anxiety for the patient, and, if prostatectomy becomes necessary, greater technical difficulty due to scarring from repeat biopsies. The benefit is postponement or complete avoidance of the adverse effects of treatment.
Debate continues over the potential dangers of deferred treatment of prostate cancer, but in certain patients it is an acceptable option. Patient education, accurate disease assessment, and compliance with monitoring are critical considerations.
RADICAL PROSTATECTOMY: SEVERAL OPTIONS, EQUIVALENT EFFICACY
Radical prostatectomy is widely used for treating prostate cancer of any risk level. The operation entails removing the prostate and seminal vesicles, as well as the pelvic lymph nodes in patients with intermediate or high-risk cancer.
This procedure was increasingly used in the 1990s with the introduction of PSA screening and nerve-sparing surgical techniques that preserve continence and erectile function.
Radical prostatectomy can be done via a standard open approach or a minimally invasive laparoscopic approach with or without robotic assistance. Open surgery, laparoscopic surgery, and robotic prostatectomy offer equivalent rates of oncologic efficacy, continence, and potency.24 The more experienced the surgeon, the better the outcome is likely to be.
The average biochemical recurrence rate at 5 years after radical prostatectomy is approximately 6% for patients with low-risk cancer, 23% for those with intermediate-risk cancer, and 45% for those with high-risk cancer.25 The rate of death from prostate cancer at 10 years is about 1% for patients with low-risk cancer, 4% for those with intermediate-risk cancer, and 8% for those with high-risk cancer.12
Secondary therapy
Pathologic staging of the surgical specimen after radical prostatectomy yields information that can be beneficial in terms of initiating early secondary therapy.
Patients with node-positive disease should immediately undergo androgen deprivation treatment.26
Evidence of positive surgical margins, seminal vesicle invasion, bladder neck invasion, and extracapsular extension also increase the risk of recurrence. This additional risk can be ascertained via the use of a postoperative nomogram. Patients at high risk of recurrence should be considered for early adjuvant external beam radiotherapy to the surgical field 3 to 6 months after surgery.
Advantages and disadvantages of radical prostatectomy
Advantages of radical prostatectomy include the ability to accurately stage the cancer with the surgical specimen and the ability to remove the pelvic lymph nodes in patients at intermediate and high risk. Another advantage is that postoperative surveillance is straightforward: PSA should become undetectable after surgery, and a measurable increase in PSA represents disease recurrence.
Disadvantages include:
- The risk of surgical complications (reported in 3% to 17% of cases)24
- An average hospital stay of 1 to 3 days (and a typical 3 to 6 weeks before returning to work)
- The need for a Foley catheter for 10 to 14 days
- The risk of incontinence and impotence, which are very distressing to patients.
Postoperative incontinence is typically defined as the need for any type of protective pad for leakage. Up to 70% of patients have incontinence in the first 3 months after surgery, but 82% to 94% of patients regain continence by 12 months.24 A small percentage of patients (3% to 5%) have significant permanent incontinence.
Counseling about postoperative erectile dysfunction
All patients should be counseled about the risk of a postoperative decrease in erectile function, especially those with pre-existing erectile dysfunction. Potency is defined as the ability to have an erection suitable for intercourse (with or without phosphodiesterase type 5 inhibitors) more than 50% of the time. In men with bilateral nerve-sparing open prostatectomy, potency rates at 12 months have been reported between 63% and 81%.13
Data on potency rates vary widely because of differences in how potency was defined, selection bias, and the multifactorial nature of erectile dysfunction. Also, because single-institution, single-surgeon reports and advertisements tend to underestimate rates of impotence after radical prostatectomy by any approach, many patients have false expectations.
INTERSTITIAL BRACHYTHERAPY FOR LOW-RISK CANCERS
Interstitial brachytherapy delivers a localized, high dose (125 to 145 Gy) of radiation to the prostate, with minimal radiation dosing to the bladder, rectum, or other adjacent organs and tissues. “Seeds” or small pellets containing a radioisotope (iodine 125 or palladium 103) are stereotactically implanted through the perineum into the prostate under ultrasonographic guidance. Computerized mapping done before or during surgery helps determine the optimal placement of the seeds, the object being to cover at least 90% of the prostate with 100% of the radiation dose.
In permanent brachytherapy, the implants give off radiation at a low dose rate over weeks to months and are left in place permanently. In temporary brachytherapy, seeds are implanted to deliver a low or high dose rate for a specified period, and then they are removed.
“Implant quality,” ie, delivery of more than 90% of the radiation dose, is a major predictor of success and can depend on both the available instrumentation and the skill of the operator.
Caveats about brachytherapy
The evidence in support of combining androgen deprivation therapy and interstitial brachytherapy is poor, and there is some evidence of increased rates of irritative voiding symptoms,27 so this is generally not recommended.
Interstitial brachytherapy as monotherapy has usually been reserved for patients with low-risk cancer with a low likelihood of extracapsular disease extension or pelvic lymph node involvement. No randomized controlled clinical trial has compared brachytherapy with radical prostatectomy or external beam radiotherapy. One large long-term study reported an 8-year biochemical recurrence rate of 18% in patients with low-risk cancer and 30% in patients with intermediate-risk cancer.28 The long-term efficacy of brachytherapy for intermediate- and high-risk prostate cancer is still under investigation.
Advantages and disadvantages of interstitial brachytherapy
Advantages. Interstitial brachytherapy is done as a single outpatient procedure. It can deliver a targeted high dose of radiation. And it is associated with a lower rate of posttreatment incontinence than radical prostatectomy, and a lower cost.
Disadvantages. There are limited data to support long-term cancer control in intermediate- and high-risk disease. Short-term adverse effects include dysuria, hematuria, urinary urgency, and urinary frequency in up to 80% of patients.29 Voiding symptoms typically peak 1 to 3 months after the procedure and subside after 8 to 12 months. Erectile dysfunction has been reported in 30% to 35% of men at 5 years after the procedure. Other possible adverse effects include urethral stricture, incontinence, recurrent hematuria, rectal bleeding, proctitis, and the development of bladder cancer and other secondary cancers.
EXTERNAL BEAM RADIOTHERAPY
In external beam radiotherapy, radiation is delivered to the prostate and surrounding tissues via an external energy source. Electrons, protons, or neutrons are used, and although each has theoretical advantages over the others, all appear to have similar clinical efficacy.
As with brachytherapy, the object—and the challenge—is to deliver an effective dose of radiation to the tumor while sparing adjacent organs. Intensity-modulated delivery is a radiotherapy technique that delivers more of the radiation dose where we want it to go—and less where we don’t want it to go. For prostate cancer, the target dose with intensity-modulated delivery is typically 75 to 85 Gy, in doses of 2 to 2.25 Gy for 30 to 36 days.
Androgen deprivation therapy before or after external beam radiotherapy augments the effects of the radiotherapy, particularly in patients with high-risk disease.30
The oncologic efficacy of intensity-modulated radiotherapy in patients at low and intermediate risk appears commensurate with that of radical prostatectomy. In one study,31 in low-risk cases, biochemical disease-free survival rates were 85% for radiotherapy vs 93% for prostatectomy; in intermediate-risk cases, 82% for radiotherapy and 87% for prostatectomy; and in high-risk cases, 62% for combined androgen deprivation and radiotherapy vs 38% for prostatectomy.31
Advantages and disadvantages of external beam radiotherapy
Advantages. External beam radiotherapy is noninvasive. It can treat the prostate as well as areas outside the prostate in patients with intermediate- and high-risk disease, and it is proven effective for high-risk cancer when used in combination with androgen deprivation.
Disadvantages. On the other hand, radiotherapy requires a series of daily treatments, which can be inconvenient and burdensome to the patient. Its adverse effects are similar to those of brachytherapy, and it is expensive. Long-term adverse effects include irritative voiding symptoms (frequency, urgency, nocturia), hemorrhagic cystitis, bowel symptoms (pain with defecation, tenesmus, bleeding), and a significantly higher lifetime risk of a secondary malignancy, particularly of the bladder and rectum.32
External beam radiotherapy also induces tissue changes in the pelvis that make salvage surgery more difficult. Patients in whom radiotherapy is ineffective as monotherapy and who require salvage prostatectomy typically have poor outcomes in terms of disease control, continence, and potency.
COMBINED RADIATION THERAPY: BETTER, OR OVERTREATMENT?
Many patients are offered a combination of external beam radiotherapy and interstitial brachytherapy. The rationale is that the combination can boost the dose of radiation to the prostate and at the same time treat cancer that has extended beyond the prostate or to the pelvic lymph nodes.
The radiation dose in the combined approach is 45 to 50 Gy (vs 70 to 80 Gy in monotherapy), thereby minimizing toxicity.
This combination has not been shown to improve overall survival or cancer-specific survival compared with either therapy alone, and it likely constitutes overtreatment.33 Adverse effects of combination therapy include erectile dysfunction, rectal and bladder toxicity, and secondary malignancy.
A serious complication associated more often with the combination of external beam radiotherapy and brachytherapy than other treatments is rectoprostatic fistula, a condition that requires complex reconstructive surgery and often requires permanent urinary and fecal diversion.34
CRYOTHERAPY: MORE STUDY NEEDED
Refinements in cryoablative therapy to destroy prostate tissue have improved the safety and efficacy of this procedure significantly over the past decade. The AUA consensus guidelines recognize cryotherapy as a viable primary cancer monotherapy, but it is most commonly used as a salvage therapy after failure of radiation therapy.
The procedure involves ultrasonographically guided stereotactic placement of cryoprobes into the prostate via a transperineal approach. Argon is pumped through the probes under pressure to initiate ice formation, and repeated freeze-thaw cycles cause tissue damage and necrosis.
Rates of biochemical recurrence at 5 years in patients at low, intermediate, and high risk have been reported at 16%, 27%, and 25%, respectively.35 The presence of viable cancer on biopsy specimens after primary cryoablation has been reported at 15%, compared with 25% after definitive radiation therapy.35
Advantages and disadvantages of cryotherapy
Cryotherapy can destroy cancer tissue in a minimally invasive way. It has no long-term delayed adverse effects, and it is a low-cost and convenient outpatient procedure.
On the other hand, we lack long-term data on its oncologic efficacy, acute complications, and late adverse effects. Acute complications occur in up to 16% of patients and include acute urinary retention requiring prolonged catheterization, hematuria, urethral sloughing, perineal pain, and incontinence.36 Potential late effects include rectoprostatic fistula (< 1%), incontinence (< 5%), persistent hematuria, and chronic pelvic pain.36
Cryoablation therapy appears to have a more significant negative impact on sexual function than does brachytherapy.37
More study of the complications and efficacy of cryotherapy is needed before the procedure can be adopted as routine primary monotherapy.
HIGH-INTENSITY FOCUSED ULTRASOUND: NOT YET FDA-APPROVED
High-intensity focused ultrasound (HIFU) is not yet approved by the US Food and Drug Administration (other than in an approved research protocol) but is used in Canada and in certain countries of Europe and Asia. It involves the insertion of a transducer into the rectum that generates a high-intensity, focused beam that heats target tissue in the prostate to a high temperature. This temperature triggers a heat-shock response that leads to cellular apoptosis and tissue necrosis. The procedure can be done with or without magnetic resonance imaging (MRI) guidance.
Biochemical recurrence rates at 2 years after the procedure have been reported between 23% and 50%, but long-term efficacy data are lacking.38,39
Advantages and disadvantages of ultrasound
HIFU is a minimally invasive, low-cost, outpatient procedure that offers trackless delivery of energy to the prostate: ie, there is no direct mechanical penetration into the tissue.
Complications include rectal-wall injury, fistula, acute urinary retention, hematuria, and urethral stricture.
FOCAL ABLATION: GETTING ATTENTION, BUT STILL UNDER DEVELOPMENT
Focal ablation for prostate cancer has been receiving much attention. This treatment uses heat energy to destroy tumor cells, guided by high-resolution endorectal-coil MRI. The procedure is in the developmental stages and is available only in research protocols.
The procedure has several major hurdles to overcome before becoming acceptable for clinical practice. First, prostate cancer is multifocal, and microscopic tumor foci are likely present that are invisible even to MRI, so ablation of only part of the prostate leaves the rest of the gland at risk of continued or de novo tumor growth.
Second, a wide range of sensitivities and specificities have been reported for endorectal coil MRI for detecting prostate cancer: its sensitivity has ranged from 27% to 100%, and its specificity has ranged from 32% to 99%.40
ANDROGEN DEPRIVATION, AN ADJUVANT THERAPY
Androgen deprivation therapy (medical castration) is not effective as a monotherapy for prostate cancer. A large population-based study in men with localized prostate cancer showed no higher rate of overall survival at 10 years with primary androgen deprivation therapy than with conservative management.41
Androgen deprivation is achieved with a leutinizing hormone-releasing hormone agonist such as leuprolide (Lupron) or goserelin (Zoladex), or an antiandrogen drug such as flutamide or bicalutamide (Casodex), or a combination of each.
Adverse effects include hot flashes, gynecomastia, decreased libido, erectile dysfunction, weight gain, and hyperlipidemia. Long-term effects include osteoporosis and a significantly higher risk of cardiac events, new-onset type 2 diabetes mellitus, and stroke.
Currently, the only recognized role for androgen deprivation therapy in prostate cancer is as an adjunct to external beam radiotherapy or as a treatment of metastatic prostate cancer.
Orchiectomy
The other way to eliminate testicular production of testosterone is surgical castration. Bilateral orchiectomy has advantages over medical androgen deprivation therapy in that it costs less, is highly reliable, and is done as a single treatment on an outpatient basis. Disadvantages include surgery-related morbidity and the irreversible nature of the procedure. The adverse effects are similar to those of androgen deprivation therapy.
POSTTREATMENT MONITORING
The management of patients with recurrent prostate cancer can be complex, and these patients should be referred to a medical or urologic oncologist.42,43
Often, a rise in PSA after primary therapy represents a regrowth of cancer; 30% to 60% of patients with a recurrence have metastasis, and nearly 20% will die from the disease. The average time from documentation of biochemical recurrence to metastatic progression is 8 years. The average time from metastatic progression to death is 5 years.44,45
After radical prostatectomy, the PSA level should be checked every 6 to 12 months for the first 2 years, then annually until the patient’s life expectancy is only 10 years even without prostate cancer. PSA should reach undetectable levels within 4 to 6 weeks after surgery. Biochemical recurrence after surgery is defined as a PSA level of 0.2 μg/L or higher in two serial studies.
After radiation therapy or cryotherapy, monitoring is complicated by the presence of viable prostatic epithelium that continues to produce PSA. During the first 1 to 2 years after radiation therapy, a PSA “bounce” phenomenon is observed whereby PSA levels rise or fluctuate significantly. This bounce should not be mistaken for a recurrence of cancer. The most widely accepted definition of biochemical recurrence is based on the American Society for Therapeutic Radiology and Oncology “Phoenix” criteria, defined as the nadir PSA level plus 2.0 μg/L.46
Prostate cancer screening, diagnosis, and treatment present challenges to internists, urologists, and oncologists. For the internist, there is the ongoing debate about when and how often to screen with prostate-specific antigen (PSA) testing, as well as about how to interpret the results. For urologists and oncologists, there is no consensus on how to treat prostate cancer with the growing array of options, from surgery to cryoablation. Most therapies have not been compared in head-to-head trials, and anxious patients often approach their internist for help in navigating the maze of options.
This review summarizes current American Urological Association (AUA) guidelines,1 as well as current practice patterns at the Glickman Urological and Kidney Institute of Cleveland Clinic regarding screening, diagnosis, risk assessment, treatment, and posttreatment management of prostate cancer. We try to explain the approved and the experimental treatments, outlining what we know about their advantages and disadvantages.
SCREENING: WHEN AND HOW
Screening for prostate cancer should involve both a digital rectal examination (DRE) and measurement of the serum PSA level. But when should screening start?
The AUA recommends annual screening with DRE and serum PSA test starting at age 40 for all men with a life expectancy of more than 10 years.1
The American Cancer Society2 and the American College of Physicians,3 in contrast, recommend that men who choose to undergo screening should begin at age 50, or at age 45 if they are black or have a family history of prostate cancer in a primary relative diagnosed before age 65. They also recommend that screening with PSA and DRE be stopped at age 75, given the low likelihood of death from de novo prostate cancer after this age. The AUA recommends that screening be stopped at age 75, but may be continued beyond age 75 if the patient has a life expectancy of 10 years or more.
Before being screened, patients should understand the benefits and the risks of testing. While a small subset of prostate cancers behave aggressively, the majority are slow-growing and pose minimal risk for the development of fatal disease.
A discussion of the rationale for these guidelines and their differences is beyond the scope of this review. Differences stem from the observation that most men treated for prostate cancer will likely not die from prostate cancer, but rather from another condition.
Digital rectal examination’s role and limitations
The utility of DRE is limited to the detection of nodules, gross asymmetry, and gland fixation. DRE is not highly specific: only 40% to 50% of men who have abnormal findings on DRE have prostate cancer on biopsy.5 Anyone who has an abnormal finding on DRE should undergo prostate biopsy. However, if a rectal mass is palpated or if the prostate is exquisitely sensitive, biopsy is not indicated.
DRE is highly inaccurate for estimating gland volume; it should not be used to gauge cancer risk.
Prostate-specific antigen: Caveats
PSA measurement was introduced as a clinical screening test for prostate cancer in the early 1990s, and it serves as the foundation for early detection.
PSA, a protein involved in seminal coagulation, is produced by the prostate epithelium and is mostly confined within the prostatic ducts. Cancer cells secrete PSA into the bloodstream at increased levels via a disrupted basement membrane in tumor-affected areas of the gland. Elevated PSA can also result from benign prostatic hypertrophy, prostatitis, and prostate biopsy.
PSA levels represent a continuum of prostate cancer risk, and no single PSA value is sensitive and specific enough to predict the presence of cancer.6 Abnormal PSA cutoffs have been defined from 2.5 μg/L to 4 μg/L, and much debate surrounds this topic. Men who present with an elevated PSA (ie, > 2.5 μg/L) should be tested again. If the value remains high, then prostate biopsy should be considered. An elevated PSA level in older men with benign prostatic hypertrophy is not unexpected, and in these patients observation of the PSA value over time may prove valuable to assess the need for biopsy.
A useful adjunct in men with elevated PSA and benign prostatic hypertrophy is the percentage of serum PSA that is free rather than bound.7 PSA produced by prostate cancer binds more avidly with serum proteins (alpha-1 chymotrypsin and alpha-2 macroglobulin), resulting in a lower percentage of free PSA. In men with an elevated PSA (ie, 4.1–10.0 μg/L), the percentage of free PSA provides an indication of whether the elevation is due to benign prostatic hypertrophy or to cancer: the lower the percent free PSA, the more likely an elevated total PSA represents cancer and not benign prostatic hypertrophy. The sensitivity of a free PSA less than 15% to detect prostate cancer is about 85%, and its use as a screening tool is under study.
Much attention has also been given to other PSA indices, namely, the PSA density (the PSA level divided by the prostate volume), the PSA velocity (the rate of increase in the PSA level over time), and the PSA doubling time. While these nuanced PSA measures are useful to predict disease severity and behavior, they are not routinely used in screening.
BIOPSY IS INDICATED IF EITHER TEST IS ABNORMAL
In the past, imaging of the prostate with transrectal ultrasonography was used as a screening tool to detect prostate cancer. Further research showed that only 15% to 20% of hypoechoic lesions detected on ultrasonography contained cancer.8 Because of its low sensitivity and specificity, primary ultrasonographic screening (ie, transrectal ultrasonography alone) is not acceptable for screening or for diagnosis. Its main role is in guiding prostate biopsy.
Biopsy of the prostate with transrectal ultrasonographic guidance is indicated if either the DRE or the PSA level is abnormal. The standard of care is to use an 18-gauge biopsy needle-gun to obtain two to three tissue samples from each of six regions of the prostate, focusing on the outer peripheral zone, specifically the right and left bases, the mid-gland, and the apex.
Pathologic analysis of each tissue core takes into consideration the presence or absence of cancer, the Gleason score, and the percentage of the tissue sample volume that is occupied by cancer.
The Gleason grading system is based on the histologic appearance and reflects the degree of differentiation and aggressiveness of the cancer. The two most prominent tumor grades present are added to give a final Gleason score. For instance, a Gleason grade of 4+3=7 indicates a tumor with predominant Gleason grade 4 disease with a lesser amount of grade 3 disease. The number of positive core samples and the volume of cancer provide information on the severity of the cancer.
If the PSA is high but biopsy is negative
Prostate biopsy misses up to 30% of small cancers. Many of these are clinically insignificant, but about 20% of those missed cancers can be high-risk and thus merit identification. There should be a low threshold for repeating biopsy 1 year later in men who have a persistently high PSA or a rising PSA.
High-grade prostatic intraepithelial neoplasia is a common finding on biopsy. The incidence of de novo prostate cancer at 5 years in men with this finding is 22% to 26%.9 Patients with multifocal high-grade prostatic intraepithelial neoplasia should be monitored with PSA testing and DRE every 6 to 12 months and should be considered for repeat “saturation” biopsy (ie, obtaining as many as 36 core samples).
IF CANCER IS FOUND, HOW RISKY IS IT?
Patients with a new diagnosis of prostate cancer must decide on a treatment plan. This decision is highly individualized, based on the patient’s personal preferences, lifestyle, performance status (ie, his general well-being), disease severity, continence status, and sexual function.
When counseling patients about their disease and the treatment options, we consider three main factors:
- The severity of disease on biopsy
- The patient’s current state of health and performance status
- The patient’s understanding of and willingness to accept the adverse effects of the various treatments.
Pathologic features, the PSA level, and clinical stage determined by DRE are used to predict the severity of disease. Most data on the efficacy of treatments for prostate cancer are based on the incidence of biochemical recurrence, ie, a rise in PSA level after primary therapy. The AUA and the D’Amico risk criteria use biopsy pathology, clinical stage, and the pretreatment PSA level to predict the likelihood of biochemical recurrence (Table 1).10,11
DISCUSSING TREATMENT OPTIONS WITH THE PATIENT
In our practice, we usually do not recommend treatment in men with low-risk or intermediate-risk prostate cancer who have a life expectancy of less than 10 years, as most of them will likely die of a cause other than prostate cancer. For patients with poor baseline performance status, surveillance or radiation therapy may be preferable to surgery. In younger patients, surgery may confer a more durable benefit.
- No prospective, randomized clinical trials have directly compared these treatments
- Prostate cancer progresses slowly
- Definitions of treatment failure used in various studies have been inconsistent
- Clinical studies have been subject to selection bias.
ACTIVE SURVEILLANCE IS ACCEPTABLE FOR LOW-RISK PROSTATE CANCER
Active surveillance is an acceptable option for patients with low-risk prostate cancer (ie, if the Gleason score is ≤ 6, the tumor stage is T1c or T2a, and the PSA level is ≤ 10 μg/L). To rule out high-risk disease before starting a program of surveillance, repeat biopsy is advisable, although optional.
Active surveillance consists of PSA testing and DRE every 6 to 12 months, followed by repeat biopsy if significant changes are noted in either test. Some centers advocate biopsy with transrectal ultrasonographic guidance every year regardless of the PSA or DRE findings.
Whether a change in the PSA level is significant is subjective, but a recent phase 2 study in 453 patients23 on a program of active surveillance used a PSA doubling time of less than 3 years as a criterion for repeat biopsy. Thirty-eight percent of the men had to undergo radiation therapy or surgery within 10 years, and 5 patients (1%) died of prostate cancer. The authors concluded that active surveillance did not put these patients at undue risk, and that this approach prevented overtreatment of clinically insignificant prostate cancer.23
The risks of surveillance include the chance that cancer could progress to an incurable state during the surveillance period, greater anxiety for the patient, and, if prostatectomy becomes necessary, greater technical difficulty due to scarring from repeat biopsies. The benefit is postponement or complete avoidance of the adverse effects of treatment.
Debate continues over the potential dangers of deferred treatment of prostate cancer, but in certain patients it is an acceptable option. Patient education, accurate disease assessment, and compliance with monitoring are critical considerations.
RADICAL PROSTATECTOMY: SEVERAL OPTIONS, EQUIVALENT EFFICACY
Radical prostatectomy is widely used for treating prostate cancer of any risk level. The operation entails removing the prostate and seminal vesicles, as well as the pelvic lymph nodes in patients with intermediate or high-risk cancer.
This procedure was increasingly used in the 1990s with the introduction of PSA screening and nerve-sparing surgical techniques that preserve continence and erectile function.
Radical prostatectomy can be done via a standard open approach or a minimally invasive laparoscopic approach with or without robotic assistance. Open surgery, laparoscopic surgery, and robotic prostatectomy offer equivalent rates of oncologic efficacy, continence, and potency.24 The more experienced the surgeon, the better the outcome is likely to be.
The average biochemical recurrence rate at 5 years after radical prostatectomy is approximately 6% for patients with low-risk cancer, 23% for those with intermediate-risk cancer, and 45% for those with high-risk cancer.25 The rate of death from prostate cancer at 10 years is about 1% for patients with low-risk cancer, 4% for those with intermediate-risk cancer, and 8% for those with high-risk cancer.12
Secondary therapy
Pathologic staging of the surgical specimen after radical prostatectomy yields information that can be beneficial in terms of initiating early secondary therapy.
Patients with node-positive disease should immediately undergo androgen deprivation treatment.26
Evidence of positive surgical margins, seminal vesicle invasion, bladder neck invasion, and extracapsular extension also increase the risk of recurrence. This additional risk can be ascertained via the use of a postoperative nomogram. Patients at high risk of recurrence should be considered for early adjuvant external beam radiotherapy to the surgical field 3 to 6 months after surgery.
Advantages and disadvantages of radical prostatectomy
Advantages of radical prostatectomy include the ability to accurately stage the cancer with the surgical specimen and the ability to remove the pelvic lymph nodes in patients at intermediate and high risk. Another advantage is that postoperative surveillance is straightforward: PSA should become undetectable after surgery, and a measurable increase in PSA represents disease recurrence.
Disadvantages include:
- The risk of surgical complications (reported in 3% to 17% of cases)24
- An average hospital stay of 1 to 3 days (and a typical 3 to 6 weeks before returning to work)
- The need for a Foley catheter for 10 to 14 days
- The risk of incontinence and impotence, which are very distressing to patients.
Postoperative incontinence is typically defined as the need for any type of protective pad for leakage. Up to 70% of patients have incontinence in the first 3 months after surgery, but 82% to 94% of patients regain continence by 12 months.24 A small percentage of patients (3% to 5%) have significant permanent incontinence.
Counseling about postoperative erectile dysfunction
All patients should be counseled about the risk of a postoperative decrease in erectile function, especially those with pre-existing erectile dysfunction. Potency is defined as the ability to have an erection suitable for intercourse (with or without phosphodiesterase type 5 inhibitors) more than 50% of the time. In men with bilateral nerve-sparing open prostatectomy, potency rates at 12 months have been reported between 63% and 81%.13
Data on potency rates vary widely because of differences in how potency was defined, selection bias, and the multifactorial nature of erectile dysfunction. Also, because single-institution, single-surgeon reports and advertisements tend to underestimate rates of impotence after radical prostatectomy by any approach, many patients have false expectations.
INTERSTITIAL BRACHYTHERAPY FOR LOW-RISK CANCERS
Interstitial brachytherapy delivers a localized, high dose (125 to 145 Gy) of radiation to the prostate, with minimal radiation dosing to the bladder, rectum, or other adjacent organs and tissues. “Seeds” or small pellets containing a radioisotope (iodine 125 or palladium 103) are stereotactically implanted through the perineum into the prostate under ultrasonographic guidance. Computerized mapping done before or during surgery helps determine the optimal placement of the seeds, the object being to cover at least 90% of the prostate with 100% of the radiation dose.
In permanent brachytherapy, the implants give off radiation at a low dose rate over weeks to months and are left in place permanently. In temporary brachytherapy, seeds are implanted to deliver a low or high dose rate for a specified period, and then they are removed.
“Implant quality,” ie, delivery of more than 90% of the radiation dose, is a major predictor of success and can depend on both the available instrumentation and the skill of the operator.
Caveats about brachytherapy
The evidence in support of combining androgen deprivation therapy and interstitial brachytherapy is poor, and there is some evidence of increased rates of irritative voiding symptoms,27 so this is generally not recommended.
Interstitial brachytherapy as monotherapy has usually been reserved for patients with low-risk cancer with a low likelihood of extracapsular disease extension or pelvic lymph node involvement. No randomized controlled clinical trial has compared brachytherapy with radical prostatectomy or external beam radiotherapy. One large long-term study reported an 8-year biochemical recurrence rate of 18% in patients with low-risk cancer and 30% in patients with intermediate-risk cancer.28 The long-term efficacy of brachytherapy for intermediate- and high-risk prostate cancer is still under investigation.
Advantages and disadvantages of interstitial brachytherapy
Advantages. Interstitial brachytherapy is done as a single outpatient procedure. It can deliver a targeted high dose of radiation. And it is associated with a lower rate of posttreatment incontinence than radical prostatectomy, and a lower cost.
Disadvantages. There are limited data to support long-term cancer control in intermediate- and high-risk disease. Short-term adverse effects include dysuria, hematuria, urinary urgency, and urinary frequency in up to 80% of patients.29 Voiding symptoms typically peak 1 to 3 months after the procedure and subside after 8 to 12 months. Erectile dysfunction has been reported in 30% to 35% of men at 5 years after the procedure. Other possible adverse effects include urethral stricture, incontinence, recurrent hematuria, rectal bleeding, proctitis, and the development of bladder cancer and other secondary cancers.
EXTERNAL BEAM RADIOTHERAPY
In external beam radiotherapy, radiation is delivered to the prostate and surrounding tissues via an external energy source. Electrons, protons, or neutrons are used, and although each has theoretical advantages over the others, all appear to have similar clinical efficacy.
As with brachytherapy, the object—and the challenge—is to deliver an effective dose of radiation to the tumor while sparing adjacent organs. Intensity-modulated delivery is a radiotherapy technique that delivers more of the radiation dose where we want it to go—and less where we don’t want it to go. For prostate cancer, the target dose with intensity-modulated delivery is typically 75 to 85 Gy, in doses of 2 to 2.25 Gy for 30 to 36 days.
Androgen deprivation therapy before or after external beam radiotherapy augments the effects of the radiotherapy, particularly in patients with high-risk disease.30
The oncologic efficacy of intensity-modulated radiotherapy in patients at low and intermediate risk appears commensurate with that of radical prostatectomy. In one study,31 in low-risk cases, biochemical disease-free survival rates were 85% for radiotherapy vs 93% for prostatectomy; in intermediate-risk cases, 82% for radiotherapy and 87% for prostatectomy; and in high-risk cases, 62% for combined androgen deprivation and radiotherapy vs 38% for prostatectomy.31
Advantages and disadvantages of external beam radiotherapy
Advantages. External beam radiotherapy is noninvasive. It can treat the prostate as well as areas outside the prostate in patients with intermediate- and high-risk disease, and it is proven effective for high-risk cancer when used in combination with androgen deprivation.
Disadvantages. On the other hand, radiotherapy requires a series of daily treatments, which can be inconvenient and burdensome to the patient. Its adverse effects are similar to those of brachytherapy, and it is expensive. Long-term adverse effects include irritative voiding symptoms (frequency, urgency, nocturia), hemorrhagic cystitis, bowel symptoms (pain with defecation, tenesmus, bleeding), and a significantly higher lifetime risk of a secondary malignancy, particularly of the bladder and rectum.32
External beam radiotherapy also induces tissue changes in the pelvis that make salvage surgery more difficult. Patients in whom radiotherapy is ineffective as monotherapy and who require salvage prostatectomy typically have poor outcomes in terms of disease control, continence, and potency.
COMBINED RADIATION THERAPY: BETTER, OR OVERTREATMENT?
Many patients are offered a combination of external beam radiotherapy and interstitial brachytherapy. The rationale is that the combination can boost the dose of radiation to the prostate and at the same time treat cancer that has extended beyond the prostate or to the pelvic lymph nodes.
The radiation dose in the combined approach is 45 to 50 Gy (vs 70 to 80 Gy in monotherapy), thereby minimizing toxicity.
This combination has not been shown to improve overall survival or cancer-specific survival compared with either therapy alone, and it likely constitutes overtreatment.33 Adverse effects of combination therapy include erectile dysfunction, rectal and bladder toxicity, and secondary malignancy.
A serious complication associated more often with the combination of external beam radiotherapy and brachytherapy than other treatments is rectoprostatic fistula, a condition that requires complex reconstructive surgery and often requires permanent urinary and fecal diversion.34
CRYOTHERAPY: MORE STUDY NEEDED
Refinements in cryoablative therapy to destroy prostate tissue have improved the safety and efficacy of this procedure significantly over the past decade. The AUA consensus guidelines recognize cryotherapy as a viable primary cancer monotherapy, but it is most commonly used as a salvage therapy after failure of radiation therapy.
The procedure involves ultrasonographically guided stereotactic placement of cryoprobes into the prostate via a transperineal approach. Argon is pumped through the probes under pressure to initiate ice formation, and repeated freeze-thaw cycles cause tissue damage and necrosis.
Rates of biochemical recurrence at 5 years in patients at low, intermediate, and high risk have been reported at 16%, 27%, and 25%, respectively.35 The presence of viable cancer on biopsy specimens after primary cryoablation has been reported at 15%, compared with 25% after definitive radiation therapy.35
Advantages and disadvantages of cryotherapy
Cryotherapy can destroy cancer tissue in a minimally invasive way. It has no long-term delayed adverse effects, and it is a low-cost and convenient outpatient procedure.
On the other hand, we lack long-term data on its oncologic efficacy, acute complications, and late adverse effects. Acute complications occur in up to 16% of patients and include acute urinary retention requiring prolonged catheterization, hematuria, urethral sloughing, perineal pain, and incontinence.36 Potential late effects include rectoprostatic fistula (< 1%), incontinence (< 5%), persistent hematuria, and chronic pelvic pain.36
Cryoablation therapy appears to have a more significant negative impact on sexual function than does brachytherapy.37
More study of the complications and efficacy of cryotherapy is needed before the procedure can be adopted as routine primary monotherapy.
HIGH-INTENSITY FOCUSED ULTRASOUND: NOT YET FDA-APPROVED
High-intensity focused ultrasound (HIFU) is not yet approved by the US Food and Drug Administration (other than in an approved research protocol) but is used in Canada and in certain countries of Europe and Asia. It involves the insertion of a transducer into the rectum that generates a high-intensity, focused beam that heats target tissue in the prostate to a high temperature. This temperature triggers a heat-shock response that leads to cellular apoptosis and tissue necrosis. The procedure can be done with or without magnetic resonance imaging (MRI) guidance.
Biochemical recurrence rates at 2 years after the procedure have been reported between 23% and 50%, but long-term efficacy data are lacking.38,39
Advantages and disadvantages of ultrasound
HIFU is a minimally invasive, low-cost, outpatient procedure that offers trackless delivery of energy to the prostate: ie, there is no direct mechanical penetration into the tissue.
Complications include rectal-wall injury, fistula, acute urinary retention, hematuria, and urethral stricture.
FOCAL ABLATION: GETTING ATTENTION, BUT STILL UNDER DEVELOPMENT
Focal ablation for prostate cancer has been receiving much attention. This treatment uses heat energy to destroy tumor cells, guided by high-resolution endorectal-coil MRI. The procedure is in the developmental stages and is available only in research protocols.
The procedure has several major hurdles to overcome before becoming acceptable for clinical practice. First, prostate cancer is multifocal, and microscopic tumor foci are likely present that are invisible even to MRI, so ablation of only part of the prostate leaves the rest of the gland at risk of continued or de novo tumor growth.
Second, a wide range of sensitivities and specificities have been reported for endorectal coil MRI for detecting prostate cancer: its sensitivity has ranged from 27% to 100%, and its specificity has ranged from 32% to 99%.40
ANDROGEN DEPRIVATION, AN ADJUVANT THERAPY
Androgen deprivation therapy (medical castration) is not effective as a monotherapy for prostate cancer. A large population-based study in men with localized prostate cancer showed no higher rate of overall survival at 10 years with primary androgen deprivation therapy than with conservative management.41
Androgen deprivation is achieved with a leutinizing hormone-releasing hormone agonist such as leuprolide (Lupron) or goserelin (Zoladex), or an antiandrogen drug such as flutamide or bicalutamide (Casodex), or a combination of each.
Adverse effects include hot flashes, gynecomastia, decreased libido, erectile dysfunction, weight gain, and hyperlipidemia. Long-term effects include osteoporosis and a significantly higher risk of cardiac events, new-onset type 2 diabetes mellitus, and stroke.
Currently, the only recognized role for androgen deprivation therapy in prostate cancer is as an adjunct to external beam radiotherapy or as a treatment of metastatic prostate cancer.
Orchiectomy
The other way to eliminate testicular production of testosterone is surgical castration. Bilateral orchiectomy has advantages over medical androgen deprivation therapy in that it costs less, is highly reliable, and is done as a single treatment on an outpatient basis. Disadvantages include surgery-related morbidity and the irreversible nature of the procedure. The adverse effects are similar to those of androgen deprivation therapy.
POSTTREATMENT MONITORING
The management of patients with recurrent prostate cancer can be complex, and these patients should be referred to a medical or urologic oncologist.42,43
Often, a rise in PSA after primary therapy represents a regrowth of cancer; 30% to 60% of patients with a recurrence have metastasis, and nearly 20% will die from the disease. The average time from documentation of biochemical recurrence to metastatic progression is 8 years. The average time from metastatic progression to death is 5 years.44,45
After radical prostatectomy, the PSA level should be checked every 6 to 12 months for the first 2 years, then annually until the patient’s life expectancy is only 10 years even without prostate cancer. PSA should reach undetectable levels within 4 to 6 weeks after surgery. Biochemical recurrence after surgery is defined as a PSA level of 0.2 μg/L or higher in two serial studies.
After radiation therapy or cryotherapy, monitoring is complicated by the presence of viable prostatic epithelium that continues to produce PSA. During the first 1 to 2 years after radiation therapy, a PSA “bounce” phenomenon is observed whereby PSA levels rise or fluctuate significantly. This bounce should not be mistaken for a recurrence of cancer. The most widely accepted definition of biochemical recurrence is based on the American Society for Therapeutic Radiology and Oncology “Phoenix” criteria, defined as the nadir PSA level plus 2.0 μg/L.46
- Thompson I, Thrasher JB, Aus G, et al; AUA Prostate Cancer Clinical Guideline Update Panel. Guideline for the management of clinically localized prostate cancer: 2007 update. J Urol 2007; 177:2106–2131.
- Brooks DD, Wolf A, Smith RA, Dash C, Guessous I. Prostate cancer screening 2010: updated recommendations from the American Cancer Society. J Natl Med Assoc 2010; 102:423–429.
- US Preventive Services Task Force. Screening for prostate cancer: US Preventive Services Task Force recommendation statement. Ann Intern Med 2008; 149:185–191.
- Okotie OT, Roehl KA, Han M, Loeb S, Gashti SN, Catalona WJ. Characteristics of prostate cancer detected by digital rectal examination only. Urology 2007; 70:1117–1120.
- Philip J, Dutta Roy S, Ballal M, Foster CS, Javlé P. Is a digital rectal examination necessary in the diagnosis and clinical staging of early prostate cancer? BJU Int 2005; 95:969–971.
- Thompson IM, Ankerst DP, Chi C, et al. Assessing prostate cancer risk: results from the Prostate Cancer Prevention Trial. J Natl Cancer Inst 2006; 98:529–534.
- Catalona WJ, Partin AW, Slawin KM, et al. Use of the percentage of free prostate-specific antigen to enhance differentiation of prostate cancer from benign prostatic disease: a prospective multicenter clinical trial. JAMA 1998; 279:1542–1547.
- Terris MK, Freiha FS, McNeal JE, Stamey TA. Efficacy of transrectal ultrasound for identification of clinically undetected prostate cancer. J Urol 1991; 146:78–83.
- Epstein JI, Herawi M. Prostate needle biopsies containing prostatic intraepithelial neoplasia or atypical foci suspicious for carcinoma: implications for patient care. J Urol 2006 Mar; 175( 3 Pt1):820–34.
- D’Amico AV, Whittington R, Malkowicz SB, et al. Biochemical outcome after radical prostatectomy, external beam radiation therapy, or interstitial radiation therapy for clinically localized prostate cancer. JAMA 1998; 280:969–974.
- Greene FL. American Joint Committee on Cancer. American Cancer Society. AJCC cancer staging manual. 6th ed. New York, NY: Springer-Verlag; 2002.
- Stephenson AJ, Kattan MW, Eastham JA, et al. Prostate cancer-specific mortality after radical prostatectomy for patients treated in the prostate-specific antigen era. J Clin Oncol 2009; 27:4300–4305.
- Eastham JA, Scardino PT, Kattan MW. Predicting an optimal outcome after radical prostatectomy: the trifecta nomogram. J Urol 2008; 179:2207–2210.
- Stephenson AJ, Scardino PT, Eastham JA, et al. Preoperative nomogram predicting the 10-year probability of prostate cancer recurrence after radical prostatectomy. J Natl Cancer Inst 2006; 98:715–717.
- Potters L, Roach M, Davis BJ, et al. Postoperative nomogram predicting the 9-year probability of prostate cancer recurrence after permanent prostate brachytherapy using radiation dose as a prognostic variable. Int J Radiat Oncol Biol Phys 2010; 76:1061–1065.
- Zelefsky MJ, Kattan MW, Fearn P, et al. Pretreatment nomogram predicting ten-year biochemical outcome of three-dimensional conformal radiotherapy and intensity-modulated radiotherapy for prostate cancer. Urology 2007; 70:283–287.
- Walz J, Gallina A, Saad F, et al. A nomogram predicting 10-year life expectancy in candidates for radical prostatectomy or radiotherapy for prostate cancer. J Clin Oncol 2007; 25:3576–3581.
- Charlson ME, Pompei P, Ales KL, MacKenzie CR. A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J Chronic Dis 1987; 40:373–383.
- Hall WH, Ramachandran R, Narayan S, Jani AB, Vijayakumar S. An electronic application for rapidly calculating Charlson comorbidity score. BMC Cancer 2004; 4:94.
- Oken MM, Creech RH, Tormey DC, et al. Toxicity and response criteria of the Eastern Cooperative Oncology Group. Am J Clin Oncol 1982; 5:649–655.
- Bill-Axelson A, Holmberg L, Ruutu M, et al; Scandinavian Prostate Cancer Group Study No. 4. Radical prostatectomy versus watchful waiting in early prostate cancer. N Engl J Med 2005; 352:1977–1984.
- Widmark A, Klepp O, Solberg A, et al; Scandinavian Prostate Cancer Group Study 7. Endocrine treatment, with or without radiotherapy, in locally advanced prostate cancer (SPCG-7/SFUO-3): an open randomised phase III trial. Lancet 2009; 373:301–308.
- Krakowsky Y, Loblaw A, Klotz L. Prostate cancer death of men treated with initial active surveillance: clinical and biochemical characteristics. J Urol 2010; 184:131–135.
- Ficarra V, Novara G, Artibani W, et al. Retropubic, laparoscopic, and robot-assisted radical prostatectomy: a systematic review and cumulative analysis of comparative studies. Eur Urol 2009; 55:1037–1063.
- Hernandez DJ, Nielsen ME, Han M, Partin AW. Contemporary evaluation of the D’amico risk classification of prostate cancer. Urology 2007; 70:931–935.
- Messing EM, Manola J, Yao J, et al; Eastern Cooperative Oncology Group study EST 3886. Immediate versus deferred androgen deprivation treatment in patients with node-positive prostate cancer after radical prostatectomy and pelvic lymphadenectomy. Lancet Oncol 2006; 7:472–479.
- Beyer DC, McKeough T, Thomas T. Impact of short course hormonal therapy on overall and cancer specific survival after permanent prostate brachytherapy. Int J Radiat Oncol Biol Phys 2005; 61:1299–1305.
- Zelefsky MJ, Kuban DA, Levy LB, et al. Multi-institutional analysis of long-term outcome for stages T1-T2 prostate cancer treated with permanent seed implantation. Int J Radiat Oncol Biol Phys 2007; 67:327–333.
- Gelblum DY, Potters L, Ashley R, Waldbaum R, Wang XH, Leibel S. Urinary morbidity following ultrasound-guided transperineal prostate seed implantation. Int J Radiat Oncol Biol Phys 1999; 45:59–67.
- Bolla M, Collette L, Blank L, et al. Long-term results with immediate androgen suppression and external irradiation in patients with locally advanced prostate cancer (an EORTC study): a phase III randomised trial. Lancet 2002; 360:103–106.
- Aizer AA, Yu JB, Colberg JW, McKeon AM, Decker RH, Peschel RE. Radical prostatectomy vs intensity-modulated radiation therapy in the management of localized prostate adenocarcinoma. Radiother Oncol 2009; 93:185–191.
- Moon K, Stukenborg GJ, Keim J, Theodorescu D. Cancer incidence after localized therapy for prostate cancer. Cancer 2006; 107:991–998.
- Terakedis BE, Rossi PJ, Liauw SL, Johnstone PA, Jani AB. A surveillance, epidemiology, and end results registry analysis of prostate cancer modality time trends by age. Am J Clin Oncol 2010; 33:619–623.
- Lane BR, Stein DE, Remzi FH, Strong SA, Fazio VW, Angermeier KW. Management of radiotherapy induced rectourethral fistula. J Urol 2006; 175:1382–1387.
- Jones JS, Rewcastle JC, Donnelly BJ, Lugnani FM, Pisters LL, Katz AE. Whole gland primary prostate cryoablation: initial results from the cryo on-line data registry. J Urol 2008; 180:554–558.
- Hubosky SG, Fabrizio MD, Schellhammer PF, Barone BB, Tepera CM, Given RW. Single center experience with third-generation cryosurgery for management of organ-confined prostate cancer: critical evaluation of short-term outcomes, complications, and patient quality of life. J Endourol 2007; 21:1521–1531.
- Malcolm JB, Fabrizio MD, Barone BB, et al. Quality of life after open or robotic prostatectomy, cryoablation or brachytherapy for localized prostate cancer. J Urol 2010; 183:1822–1828.
- Ficarra V, Antoniolli SZ, Novara G, et al. Short-term outcome after high-intensity focused ultrasound in the treatment of patients with high-risk prostate cancer. BJU Int 2006; 98:1193–1198.
- Challacombe BJ, Murphy DG, Zakri R, Cahill DJ. High-intensity focused ultrasound for localized prostate cancer: initial experience with a 2-year follow-up. BJU Int 2009; 104:200–204.
- Bouchelouche K, Turkbey B, Choyke P, Capala J. Imaging prostate cancer: an update on positron emission tomography and magnetic resonance imaging. Curr Urol Rep 2010; 11:180–190.
- Lu-Yao GL, Albertsen PC, Moore DF, et al. Survival following primary androgen deprivation therapy among men with localized prostate cancer. JAMA 2008; 300:173–181.
- Simmons MN, Stephenson AJ, Klein EA. Natural history of biochemical recurrence after radical prostatectomy: risk assessment for secondary therapy. Eur Urol 2007; 51:1175–1184.
- Boukaram C, Hannoun-Levi JM. Management of prostate cancer recurrence after definitive radiation therapy. Cancer Treat Rev 2010; 36:91–100.
- Pound CR, Partin AW, Eisenberger MA, Chan DW, Pearson JD, Walsh PC. Natural history of progression after PSA elevation following radical prostatectomy. JAMA 1999; 281:1591–1597.
- Freedland SJ, Humphreys EB, Mangold LA, et al. Risk of prostate cancer-specific mortality following biochemical recurrence after radical prostatectomy. JAMA 2005; 294:433–439.
- Roach M, Hanks G, Thames H, et al. Defining biochemical failure following radiotherapy with or without hormonal therapy in men with clinically localized prostate cancer: recommendations of the RTOG-ASTRO Phoenix Consensus Conference. Int J Radiat Oncol Biol Phys 2006; 65:965–974.
- Thompson I, Thrasher JB, Aus G, et al; AUA Prostate Cancer Clinical Guideline Update Panel. Guideline for the management of clinically localized prostate cancer: 2007 update. J Urol 2007; 177:2106–2131.
- Brooks DD, Wolf A, Smith RA, Dash C, Guessous I. Prostate cancer screening 2010: updated recommendations from the American Cancer Society. J Natl Med Assoc 2010; 102:423–429.
- US Preventive Services Task Force. Screening for prostate cancer: US Preventive Services Task Force recommendation statement. Ann Intern Med 2008; 149:185–191.
- Okotie OT, Roehl KA, Han M, Loeb S, Gashti SN, Catalona WJ. Characteristics of prostate cancer detected by digital rectal examination only. Urology 2007; 70:1117–1120.
- Philip J, Dutta Roy S, Ballal M, Foster CS, Javlé P. Is a digital rectal examination necessary in the diagnosis and clinical staging of early prostate cancer? BJU Int 2005; 95:969–971.
- Thompson IM, Ankerst DP, Chi C, et al. Assessing prostate cancer risk: results from the Prostate Cancer Prevention Trial. J Natl Cancer Inst 2006; 98:529–534.
- Catalona WJ, Partin AW, Slawin KM, et al. Use of the percentage of free prostate-specific antigen to enhance differentiation of prostate cancer from benign prostatic disease: a prospective multicenter clinical trial. JAMA 1998; 279:1542–1547.
- Terris MK, Freiha FS, McNeal JE, Stamey TA. Efficacy of transrectal ultrasound for identification of clinically undetected prostate cancer. J Urol 1991; 146:78–83.
- Epstein JI, Herawi M. Prostate needle biopsies containing prostatic intraepithelial neoplasia or atypical foci suspicious for carcinoma: implications for patient care. J Urol 2006 Mar; 175( 3 Pt1):820–34.
- D’Amico AV, Whittington R, Malkowicz SB, et al. Biochemical outcome after radical prostatectomy, external beam radiation therapy, or interstitial radiation therapy for clinically localized prostate cancer. JAMA 1998; 280:969–974.
- Greene FL. American Joint Committee on Cancer. American Cancer Society. AJCC cancer staging manual. 6th ed. New York, NY: Springer-Verlag; 2002.
- Stephenson AJ, Kattan MW, Eastham JA, et al. Prostate cancer-specific mortality after radical prostatectomy for patients treated in the prostate-specific antigen era. J Clin Oncol 2009; 27:4300–4305.
- Eastham JA, Scardino PT, Kattan MW. Predicting an optimal outcome after radical prostatectomy: the trifecta nomogram. J Urol 2008; 179:2207–2210.
- Stephenson AJ, Scardino PT, Eastham JA, et al. Preoperative nomogram predicting the 10-year probability of prostate cancer recurrence after radical prostatectomy. J Natl Cancer Inst 2006; 98:715–717.
- Potters L, Roach M, Davis BJ, et al. Postoperative nomogram predicting the 9-year probability of prostate cancer recurrence after permanent prostate brachytherapy using radiation dose as a prognostic variable. Int J Radiat Oncol Biol Phys 2010; 76:1061–1065.
- Zelefsky MJ, Kattan MW, Fearn P, et al. Pretreatment nomogram predicting ten-year biochemical outcome of three-dimensional conformal radiotherapy and intensity-modulated radiotherapy for prostate cancer. Urology 2007; 70:283–287.
- Walz J, Gallina A, Saad F, et al. A nomogram predicting 10-year life expectancy in candidates for radical prostatectomy or radiotherapy for prostate cancer. J Clin Oncol 2007; 25:3576–3581.
- Charlson ME, Pompei P, Ales KL, MacKenzie CR. A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J Chronic Dis 1987; 40:373–383.
- Hall WH, Ramachandran R, Narayan S, Jani AB, Vijayakumar S. An electronic application for rapidly calculating Charlson comorbidity score. BMC Cancer 2004; 4:94.
- Oken MM, Creech RH, Tormey DC, et al. Toxicity and response criteria of the Eastern Cooperative Oncology Group. Am J Clin Oncol 1982; 5:649–655.
- Bill-Axelson A, Holmberg L, Ruutu M, et al; Scandinavian Prostate Cancer Group Study No. 4. Radical prostatectomy versus watchful waiting in early prostate cancer. N Engl J Med 2005; 352:1977–1984.
- Widmark A, Klepp O, Solberg A, et al; Scandinavian Prostate Cancer Group Study 7. Endocrine treatment, with or without radiotherapy, in locally advanced prostate cancer (SPCG-7/SFUO-3): an open randomised phase III trial. Lancet 2009; 373:301–308.
- Krakowsky Y, Loblaw A, Klotz L. Prostate cancer death of men treated with initial active surveillance: clinical and biochemical characteristics. J Urol 2010; 184:131–135.
- Ficarra V, Novara G, Artibani W, et al. Retropubic, laparoscopic, and robot-assisted radical prostatectomy: a systematic review and cumulative analysis of comparative studies. Eur Urol 2009; 55:1037–1063.
- Hernandez DJ, Nielsen ME, Han M, Partin AW. Contemporary evaluation of the D’amico risk classification of prostate cancer. Urology 2007; 70:931–935.
- Messing EM, Manola J, Yao J, et al; Eastern Cooperative Oncology Group study EST 3886. Immediate versus deferred androgen deprivation treatment in patients with node-positive prostate cancer after radical prostatectomy and pelvic lymphadenectomy. Lancet Oncol 2006; 7:472–479.
- Beyer DC, McKeough T, Thomas T. Impact of short course hormonal therapy on overall and cancer specific survival after permanent prostate brachytherapy. Int J Radiat Oncol Biol Phys 2005; 61:1299–1305.
- Zelefsky MJ, Kuban DA, Levy LB, et al. Multi-institutional analysis of long-term outcome for stages T1-T2 prostate cancer treated with permanent seed implantation. Int J Radiat Oncol Biol Phys 2007; 67:327–333.
- Gelblum DY, Potters L, Ashley R, Waldbaum R, Wang XH, Leibel S. Urinary morbidity following ultrasound-guided transperineal prostate seed implantation. Int J Radiat Oncol Biol Phys 1999; 45:59–67.
- Bolla M, Collette L, Blank L, et al. Long-term results with immediate androgen suppression and external irradiation in patients with locally advanced prostate cancer (an EORTC study): a phase III randomised trial. Lancet 2002; 360:103–106.
- Aizer AA, Yu JB, Colberg JW, McKeon AM, Decker RH, Peschel RE. Radical prostatectomy vs intensity-modulated radiation therapy in the management of localized prostate adenocarcinoma. Radiother Oncol 2009; 93:185–191.
- Moon K, Stukenborg GJ, Keim J, Theodorescu D. Cancer incidence after localized therapy for prostate cancer. Cancer 2006; 107:991–998.
- Terakedis BE, Rossi PJ, Liauw SL, Johnstone PA, Jani AB. A surveillance, epidemiology, and end results registry analysis of prostate cancer modality time trends by age. Am J Clin Oncol 2010; 33:619–623.
- Lane BR, Stein DE, Remzi FH, Strong SA, Fazio VW, Angermeier KW. Management of radiotherapy induced rectourethral fistula. J Urol 2006; 175:1382–1387.
- Jones JS, Rewcastle JC, Donnelly BJ, Lugnani FM, Pisters LL, Katz AE. Whole gland primary prostate cryoablation: initial results from the cryo on-line data registry. J Urol 2008; 180:554–558.
- Hubosky SG, Fabrizio MD, Schellhammer PF, Barone BB, Tepera CM, Given RW. Single center experience with third-generation cryosurgery for management of organ-confined prostate cancer: critical evaluation of short-term outcomes, complications, and patient quality of life. J Endourol 2007; 21:1521–1531.
- Malcolm JB, Fabrizio MD, Barone BB, et al. Quality of life after open or robotic prostatectomy, cryoablation or brachytherapy for localized prostate cancer. J Urol 2010; 183:1822–1828.
- Ficarra V, Antoniolli SZ, Novara G, et al. Short-term outcome after high-intensity focused ultrasound in the treatment of patients with high-risk prostate cancer. BJU Int 2006; 98:1193–1198.
- Challacombe BJ, Murphy DG, Zakri R, Cahill DJ. High-intensity focused ultrasound for localized prostate cancer: initial experience with a 2-year follow-up. BJU Int 2009; 104:200–204.
- Bouchelouche K, Turkbey B, Choyke P, Capala J. Imaging prostate cancer: an update on positron emission tomography and magnetic resonance imaging. Curr Urol Rep 2010; 11:180–190.
- Lu-Yao GL, Albertsen PC, Moore DF, et al. Survival following primary androgen deprivation therapy among men with localized prostate cancer. JAMA 2008; 300:173–181.
- Simmons MN, Stephenson AJ, Klein EA. Natural history of biochemical recurrence after radical prostatectomy: risk assessment for secondary therapy. Eur Urol 2007; 51:1175–1184.
- Boukaram C, Hannoun-Levi JM. Management of prostate cancer recurrence after definitive radiation therapy. Cancer Treat Rev 2010; 36:91–100.
- Pound CR, Partin AW, Eisenberger MA, Chan DW, Pearson JD, Walsh PC. Natural history of progression after PSA elevation following radical prostatectomy. JAMA 1999; 281:1591–1597.
- Freedland SJ, Humphreys EB, Mangold LA, et al. Risk of prostate cancer-specific mortality following biochemical recurrence after radical prostatectomy. JAMA 2005; 294:433–439.
- Roach M, Hanks G, Thames H, et al. Defining biochemical failure following radiotherapy with or without hormonal therapy in men with clinically localized prostate cancer: recommendations of the RTOG-ASTRO Phoenix Consensus Conference. Int J Radiat Oncol Biol Phys 2006; 65:965–974.
KEY POINTS
- The AUA recommends annual screening with both digital rectal examination (DRE) and prostate-specific antigen (PSA) testing starting at age 40 for all men whose life expectancy is more than 10 years. Guidelines from other organizations differ somewhat.
- If the DRE is abnormal or if the PSA level is persistently higher than 2.5 μg/L, then biopsy should be considered.
- In low-risk cases, active surveillance may be acceptable in lieu of immediate treatment. Patient education, accurate disease assessment, and compliance with monitoring are critical considerations.
- The most common primary treatments are active surveillance, prostatectomy, interstitial brachytherapy, external beam radiotherapy, and cryotherapy. Newer ablative and focal therapies may offer an advantage in select patients. Which treatment to use is highly patient-dependent.
- Single-institution, single-surgeon reports and advertisements tend to underestimate rates of impotence after prostatectomy, and as a result patients may have false expectations.
Tinnitus: Patients do not have to ‘just live with it’
Unfortunately, physicians often tell patients with tinnitus (the perception of noises in the ear, head, or both without an external acoustic source) to simply “learn to live with it.” This type of advice can result in missing the diagnosis of a potentially serious medical condition or, at the very least, in dismissing the patient’s complaints and hence failing to provide any hope of relief—increasing the negative impact on the patient’s quality of life.
See related patient information
The disabling effects of tinnitus resemble those of chronic pain.1 Specifically, its consequences may include:
- Loss of sleep
- Interference with concentration
- Difficulties functioning at work, at home, and in social relationships
- Negative emotional reactions, including despair, frustration, depression, and suicidal ideation.2,3
Chronic tinnitus affects 42 million Americans and is considered “clinically significant” in 10 million adults, and the numbers are increasing.4–7
Because primary care physicians may serve as the gatekeepers for tinnitus sufferers, as they do for patients with other chronic health issues, it is important that they understand the underlying mechanisms responsible for tinnitus, its impact, and its management options.
The goal of this article is to provide a basic understanding of tinnitus and its treatment so that physicians can provide hope to its sufferers and know when to initiate appropriate referrals for management.
WHAT CAUSES TINNITUS?
The precise cause of tinnitus is unknown. However, substantial evidence indicates that it is the result of plastic changes in the auditory system that cause auditory neurons to become hyperactive and to fire more synchronously.
If the auditory system is injured, eg, if outer hair cells have been lost because of noise exposure or ototoxicity, then neurons that normally have low levels of activity in silence begin to fire at a higher rate and more synchronously. Therefore, reduced neural activity from the peripheral system (ie, the cochlea) may result in increased spontaneous neural activity in the central auditory nervous system.8
Although most investigators of the neurobiology of tinnitus subscribe to this theory, more than one system must be involved, either simultaneously or interactively, since tinnitus has both auditory and nonauditory components.9
Evidence is accumulating that the perception of tinnitus is multimodal and may arise from complex interactions among different sensory and motor systems.10 For example, some patients with tinnitus can modulate its pitch, loudness, or both by forcefully contracting the muscles in the head, neck, or limbs; by moving the eyes in the horizontal or vertical axis; by placing pressure on myofacial trigger points; by moving the face or mouth; or by applying pressure to the temporomandibular joint.11,12 Although somatic tinnitus modulation is not yet well understood, it may reflect the interaction between the auditory system and other sensory systems.
Because the underlying mechanisms of tinnitus are complex and may involve more than the auditory system, a multidisciplinary approach to management should be considered.
RULING OUT HEALTH-THREATENING DISEASE
The complaint of tinnitus should not be taken lightly. True, it may be just a nuisance the patient can learn to ignore. On the other hand, it may negatively affect the patient’s quality of life. Worst of all, it could be a symptom of a potentially health-threatening disease.
Primary care physicians should know the red flags (Table 1) for otologic diseases such as vestibular schwannoma, Meniere disease, cholesteotoma, glomus jugulare tumor, and temporal bone trauma and, if these are present, refer patients to an otolaryngologist for a complete cochleovestibular examination.
At the same time, the physician should avoid heightening the patient’s preoccupation with the tinnitus by creating unnecessary fear about an underlying cause. This may create further anxiety and exacerbate the patient’s perception of tinnitus and emotional reaction to it.13
WHAT IS THE IMPACT OF TINNITUS ON QUALITY OF LIFE?
A quick method is simply to ask, “How much of a problem is your tinnitus?” If the patient considers it a small problem, minimum counseling may suffice (Figure 1). But if the response suggests a greater impact, an in-depth history should be taken (Table 2) to determine the appropriate treatment plan.
Still another option is to use a standardized screening tool. The Tinnitus Handicap Inventory-Screening Version (THI-S)14 consists of 10 questions that screen for the psychosocial consequences of tinnitus (Table 3). For each question, the patient answers “yes” (worth 4 points), “sometimes” (2 points), or “no” (0 points). The possible total score thus ranges from 0 to 40 points; the higher the score, the greater the perceived disability (activity limitation) and handicap (participation restriction). A score of more than 6 points indicates a need for an in-depth evaluation (Table 2). Having the patient complete this tool in the waiting room can save precious time and help identify those in need of referral.
SOME PATIENTS MAY NEED TO SEE ONE OR MORE SPECIALISTS
Patients whose tinnitus is distressing may need referral. Traditionally, the primary care physician refers the patient to an otolaryngologist. However, the complex nature and etiology of tinnitus may necessitate referring the patient to one or more specialists in addition to an otolaryngologist for further assessment and management. The following sections briefly describe what other specialists offer.
AUDIOLOGY: TESTING, SOUND THERAPY
A patient referred to an audiologist may undergo traditional audiologic testing (pure tone and speech thresholds, word recognition), as well as a battery of special psychoacoustic tests. This includes pitch-matching and loudness-matching, evaluation of residual inhibition (suppression of tinnitus after an external masking stimulus has been turned off), and assessing the minimum masking level. These provide a quantitative estimate of the acoustic attributes of the perceived tinnitus. Questionnaires can be used to assess the impact of tinnitus on everyday life and can provide guidance for treatment.15
Real sounds mask the perceived ones
Environmental enrichment devices such as portable machines that generate pleasant sounds (eg, rain, waterfalls, ocean waves), tabletop water fountains, fans, or even televisions or radios can be used to promote relief, provide distraction, and decrease the patient’s awareness of tinnitus.
Hearing aids amplify ambient sounds, reducing the perception of tinnitus.16,17 They also improve communication.
Sound generators, worn in the ear, produce a stable broadband signal (“white noise”). These devices may be used by patients who have normal or near-normal hearing sensitivity and therefore neither benefit from nor require amplification.
Combination instruments are both hearing aids and white-noise generators. These allow patients who have both hearing loss and tinnitus to use a single device.
Music can distract from the tinnitus and help patients relax. Patients may find benefit listening to their preferred music on a personal listening device such as an MP3 or CD player.
Neuromonics Inc. (Bethlehem, PA) makes a sophisticated device for tinnitus treatment. Resembling an MP3 player, it is used with headphones and plays soothing music (baroque or new age) that contains a tinnitus-masking noise. The music is modified to compensate for the patient’s hearing loss, if present. After approximately 2 months of use, the embedded noise is removed to help desensitize the patient to the tinnitus. Results of small trials have been promising.18,19
DENTISTRY: TREATING TINNITUS BY TREATING TMD
Temporomandibular disorder (TMD), involving the temporomandibular joints, the muscles of mastication, and the teeth, is associated with tinnitus.20,21 The prevalence of tinnitus in a Cleveland Clinic study of 109 patients with TMD was 36%.22
There is also an association between cervical muscle disorders and masticatory muscle function. For example, patients who grind their teeth at night must contract the sternocleidomastoid muscles of the neck to stabilize the head during grinding. Correcting cervical posture, changing the sleep position, and controlling conscious parafunctional habits (eg, clenching the teeth, grinding the teeth together) can decrease many of the symptoms of TMD.
The dental examination for tinnitus patients
The dentist looks for a history of TMD symptoms, use of orthotic devices, and head and neck trauma, and performs a clinical examination.
The clinical examination includes mandibular range of motion, auscultation and palpation of the temporomandibular joints, palpation of masticatory and cervical muscles, and cervical range of motion. The intraoral examination includes identifying occlusal attrition patterns, “load testing” of the temporomandibular joints, and identifying premature tooth contacts. Additionally, attempts to restrict jaw opening and lateral movements may modulate the patient’s tinnitus, thus confirming the role of TMD in the patient’s tinnitus.
How tinnitus is treated by managing TMD
Tinnitus can be treated by managing TMD, specifically through the use of dental orthotics (splints, nightguards) to improve abnormal jaw mechanics and tracking.23–25
Tullberg and Ernberg26 treated patients with TMD and tinnitus using a variety of methods, including occlusal splinting, jaw muscle exercises, and relaxation. They reported that 43% of the patients experienced an improvement in their tinnitus after these interventions.
A home exercise program may help patients maintain muscle strength and harmony. Self-help therapies provide patients with a protocol to recognize daytime parafunctional habits and provide suggestions to decrease clenching and other overloading of the masticatory system.
In addition, management of TMD-related tinnitus often involves physical therapy, which can include soft-tissue mobilization, deep heat, ultrasound, low-current electrical stimulation, myofascial trigger-point release techniques, and posture retraining. Occlusal correction procedures (bite correction) can often provide long-term stability to the masticatory system.
NEUROLOGY: LOOKING FOR AN UNDERLYING CONDITION
The comprehensive neurologic evaluation of the tinnitus patient should include a thorough neurologic history, review of systems, examination, and appropriate imaging. The aim is to identify accompanying symptoms or disorders that may help to localize and ultimately diagnose the underlying condition.
Related disorders could manifest with vestibular symptoms (dizziness, imbalance), various pain syndromes including facial pain and headache (tension or migraine),27 or other cranial nerve disorders such as Bell palsy (facial nerve injury)28 or trigeminal neuralgia.
Medical and surgical interventions for tinnitus-associated neurologic conditions
In cases in which there is a treatable underlying neurologic condition, tinnitus-focused interventions should be deferred until treatment has been completed or discontinued.
At that point, other options including various oral medications (eg, antiarrhythmics, anticonvulsants, benzodiazepines, and antidepressants) and anesthetic blocks (eg, intravenous anesthetic-plus-steroid injections)29 may be considered on a case-by-case basis. Results of randomized clinical trials of the aforementioned drugs have not been promising30; however, drugs that affect the emotional status of the patient by reducing anxiety, depression, and sleep disturbance have been shown to be beneficial.31,32
In addition, some experimental surgical treatments (eg, deep brain stimulation, dural grid stimulation)33,34 are being evaluated and show potential for managing tinnitus.
PHYSICAL THERAPY
A preliminary physical therapy evaluation can identify biomechanical problems of the head, neck, and jaw that can contribute to tinnitus.
Subsequent therapy is designed to restore proper cervical and temporomandibular biomechanics and to educate the patient on proper posture, ergonomics, and exercise techniques that together could help minimize these abnormalities and reduce the severity of tinnitus in some patients.11,24–26,35
PSYCHOLOGY: ADDRESSING DEPRESSION, ANXIETY
Tinnitus exacts an emotional toll on its sufferers. Some estimates suggest that 40% to 50% of tinnitus patients experience significant perceived handicap and psychological distress.36 Consequently, many patients respond to the onset of tinnitus with anxiety or depression, or both. Owing to these responses, the chronicity of the condition, and the patient’s perception that tinnitus is uncontrollable, tinnitus can produce notable distress and impairment in quality of life.
When a patient’s responses include both depression and anxiety, the reduction in quality of life and impairment in coping capacities can be significant.37 Sleep problems, poor concentration, social withdrawal, feelings of helplessness, avoidance behaviors, and upset in interpersonal relationships are common signs that quality of life is compromised.
One of the greatest challenges for the primary care physician when treating tinnitus patients is attending to their emotional suffering and disability. Simple screening tools can be useful in quickly assessing a patient’s emotional response to tinnitus and in helping to enter into a conversation with the patient about this topic. These tools include:
- The THI-S (Table 3)14
- The Patient Health Questionnaire-9 (PHQ-9)38
- The Generalized Anxiety Disorder-7 (GAD-7).39
Suicidal ideas need to be addressed
The final question on the PHQ-9 asks about suicidal ideation. This cannot be overlooked when assessing patients with tinnitus. The questionnaire invites the patient to communicate this rather painful topic to the physician in a direct matter.
The physician should be prepared to address suicidal ideas, plans, means, intentions, and safety measures with the patient. This requires that the physician be comfortable conducting these conversations in a direct and forthright manner; it also requires that the physician have reliable referrals to qualified mental health practitioners at the ready to assist the distressed tinnitus patient.
Asking a patient to commit to calling 911 or going to the nearest emergency room if he or she has any impulse toward self-harm is a simple option that many distressed patients may have never considered.
Treatments for depression and anxiety in tinnitus patients
Some patients may already have been seeing a mental health professional before the onset of tinnitus and may elect to discuss treatment with their current provider. However, many need guidance in selecting appropriate treatment. Their options may include:
Psychotropic drugs such as selective serotonin reuptake inhibitors and benzodiazepines, to provide quick relief from debilitating depression and anxiety.
Cognitive behavioral therapy, designed to provide a more active and durable adjustment to tinnitus. It is the most widely validated psychotherapeutic treatment approach to tinnitus.40
- Møller AR. The role of neural plasticity in tinnitus. Prog Brain Res 2007; 166:37–45.
- Dobie RA. Overview: suffering from tinnitus. In:Snow JB, ed. Tinnitus: Theory and Management. Hamilton, Ontario: BC Decker; 2004:1–7.
- Tyler RS, Baker LJ. Difficulties experienced by tinnitus sufferers. J Speech Hear Disord 1983; 48:150–154.
- Henry JA, Dennis KC, Schechter MA. General review of tinnitus: prevalence, mechanisms, effects, and management. J Speech Lang Hear Res 2005; 48:1204–1235.
- Hoffman HJ, Reed GW. Epidemiology of tinnitus. In:Snow JB, editor. Tinnitus: Theory and Management. Hamilton, Ontario: BC Decker; 2004:16–41.
- Hoge CW, McGurk D, Thomas JL, Cox AL, Engel CC, Castro CA. Mild traumatic brain injury in U.S. Soldiers returning from Iraq. N Engl J Med 2008; 358:453–63.
- Rauschecker JP, Leaver AM, Mühlau M. Tuning out the noise: limbicauditory interactions in tinnitus. Neuron 2010; 66:819–826.
- Kaltenbach JA, Zhang J, Finlayson P. Tinnitus as a plastic phenomenon and its possible neural underpinnings in the dorsal cochlear nucleus. Hear Res 2005; 206:200–226.
- Georgiewa P, Klapp BF, Fischer F, et al. An integrative model of developing tinnitus based on recent neurobiological findings. Med Hypotheses 2006; 66:592–600.
- Cacace AT. Expanding the biological basis of tinnitus: crossmodal origins and the role of neuroplasticity. Hear Res 2003; 175:112–132.
- Levine RA. Somatic tinnitus. In:Snow JB, editor. Tinnitus: Theory and Management. Hamilton, Ontario: BC Decker; 2004:108–124.
- Sanchez TG, Kii MA. Modulating tinnitus with visual, muscular, and tactile stimulation. Semin Hear 2008; 29:350–360.
- Schleuning AL, Shi BY, Martin WH. Tinnitus. In:Bailey BJ, Johnson JT, Newlands SD, et al, editors. Head and Neck Surgery—Otolarygnology. 4th ed, vol 2. Philadelphia, PA: Lippincott Williams & Wilkins; 2006:2237–2246.
- Newman CW, Sandridge SA, Bolek L. Development and psychometric adequacy of the screening version of the Tinnitus Handicap Inventory. Otol Neurotol 2008; 29:276–281.
- Newman CW, Sandridge SA. Tinnitus management. In:Montano JJ, Spitzer JB, editors. Adult Audiologic Rehabilitation. San Diego, CA: Plural Publishing Inc; 2009:399–444.
- Kochkin S, Tyler R. Tinnitus treatment and the effectiveness of hearing aids: hearing care professional perceptions. Hearing Review 2008; 15:14–18.
- Sheldrake JB, Jasterboff MM. Role of hearing aids in management of tinnitus. In:Snow JB, editor. Tinnitus: Theory and Management. Hamilton, Ontario: BC Decker; 2004:310–313.
- Davis PB, Paki B, Hanley PJ. Neuromonics Tinnitus Treatment: third clinical trial. Ear Hear 2007; 28:242–259.
- Davis PB, Wilde RA, Steed LG, Hanley PJ. Treatment of tinnitus with a customized acoustic neural stimulus: a controlled clinical study. Ear Nose Throat J 2008; 87:330–339.
- Lam DK, Lawrence HP, Tenenbaum HC. Aural symptoms in temporomandibular disorder patients attending a craniofacial pain unit. J Orofac Pain 2001; 15:146–157.
- Steigerwald DP, Verne SV, Young D. A retrospective evaluation of the impact of temporomandibular joint arthroscopy on the symptoms of headache, neck pain, shoulder pain, dizziness, and tinnitus. Cranio 1996; 14:46–54.
- Kahn K. Multidisciplinary strategies for managing patients with tinnitus. Poster presented at the American Equilibration Society, Chicago, IL, February 24–25, 2010.
- Morgan DH. Tinnitus caused by a temporomandibular disorder. In:Reich GE, Vernon JA, editors. Proceedings of the Fifth International Tinnitus Seminar. Portland, Oregon: American Tinnitus Association; 1996:653–654.
- Wright EF, Bifano SL. Tinnitus improvement through TMD therapy. J Am Dent Assoc 1997; 128:1424–1432.
- Latifpour DH, Grenner J, Sjödahl C. The effect of a new treatment based on somatosensory stimulation in a group of patients with somatically related tinnitus. Int Tinnitus J 2009; 15:94–99.
- Tullberg M, Ernberg M. Long-term effect on tinnitus by treatment of temporomandibular disorders: a two-year follow-up by questionnaire. Acta Odontol Scand 2006; 64:89–96.
- Volcy M, Sheftell FD, Tepper SJ, Rapoport AM, Bigal ME. Tinnitus in migraine: an allodynic symptom secondary to abnormal cortical functioning? Headache 2005; 45:1083–1087.
- Yamamoto E, Nishimura H, Hirono Y. Occurrence of sequelae in Bell’s palsy. Acta Otolaryngol Suppl 1988; 446:93–96.
- Duckert LG, Rees TS. Treatment of tinnitus with intravenous lidocaine: a double-blind randomized trial. Otolaryngol Head Neck Surg 1983; 91:550–555.
- Dobie RA. Clinical trials and drug therapy for tinnitus. In:Snow JB, editor. Tinnitus: Theory and Management. Hamilton, Ontario: BC Decker; 2004:266–277.
- Johnson RM, Brummett R, Schleuning A. Use of alprazolam for relief of tinnitus. A double-blind study. Arch Otolaryngol Head Neck Surg 1993; 119:842–845.
- Brummett R. Drugs for and against tinnitus. The Hearing Journal 1989; 42:34–37.
- Cheung SW, Larson PS. Tinnitus modulation by deep brain stimulation in locus of caudate neurons (area LC). Neuroscience 2010; 169:1768–1778.
- Friedland DR, Gaggl W, Runge-Samuelson C, Ulmer JL, Kopell BH. Feasibility of auditory cortical stimulation for the treatment of tinnitus. Otol Neurotol 2007; 28:1005–1012.
- Simmons R, Dambra C, Lobarinas E, Stocking C, Salvi R. Head, neck, and eye movements that modulate tinnitus. Semin Hear 2008; 29:361–370.
- Bauch CD, Lynn SG, Williams DE, Mellon MW, Weaver AL. Tinnitus impact: three different measurement tools. J Am Acad Audiol 2003; 14:181–187.
- Bartels H, Middel BL, van der Laan BF, Staal MJ, Albers FW. The additive effect of co-occurring anxiety and depression on health status, quality of life and coping strategies in help-seeking tinnitus sufferers. Ear Hear 2008; 29:947–956.
- Kroenke K, Spitzer RL, Williams JB. The PHQ-9: validity of a brief depression severity measure. J Gen Intern Med 2001; 16:606–613.
- Spitzer RL, Kroenke K, Williams JB, Löwe B. A brief measure for assessing generalized anxiety disorder: the GAD-7. Arch Intern Med 2006; 166:1092–1097.
- Andersson G. Psychological aspects of tinnitus and the application of cognitive-behavioral therapy. Clin Psychol Rev 2002; 22:977–990.
- Hesser H, Westin V, Hayes SC, Andersson G. Clients’ in-session acceptance and cognitive defusion behaviors in acceptance-based treatment of tinnitus distress. Behav Res Ther 2009; 47:523–528.
Unfortunately, physicians often tell patients with tinnitus (the perception of noises in the ear, head, or both without an external acoustic source) to simply “learn to live with it.” This type of advice can result in missing the diagnosis of a potentially serious medical condition or, at the very least, in dismissing the patient’s complaints and hence failing to provide any hope of relief—increasing the negative impact on the patient’s quality of life.
See related patient information
The disabling effects of tinnitus resemble those of chronic pain.1 Specifically, its consequences may include:
- Loss of sleep
- Interference with concentration
- Difficulties functioning at work, at home, and in social relationships
- Negative emotional reactions, including despair, frustration, depression, and suicidal ideation.2,3
Chronic tinnitus affects 42 million Americans and is considered “clinically significant” in 10 million adults, and the numbers are increasing.4–7
Because primary care physicians may serve as the gatekeepers for tinnitus sufferers, as they do for patients with other chronic health issues, it is important that they understand the underlying mechanisms responsible for tinnitus, its impact, and its management options.
The goal of this article is to provide a basic understanding of tinnitus and its treatment so that physicians can provide hope to its sufferers and know when to initiate appropriate referrals for management.
WHAT CAUSES TINNITUS?
The precise cause of tinnitus is unknown. However, substantial evidence indicates that it is the result of plastic changes in the auditory system that cause auditory neurons to become hyperactive and to fire more synchronously.
If the auditory system is injured, eg, if outer hair cells have been lost because of noise exposure or ototoxicity, then neurons that normally have low levels of activity in silence begin to fire at a higher rate and more synchronously. Therefore, reduced neural activity from the peripheral system (ie, the cochlea) may result in increased spontaneous neural activity in the central auditory nervous system.8
Although most investigators of the neurobiology of tinnitus subscribe to this theory, more than one system must be involved, either simultaneously or interactively, since tinnitus has both auditory and nonauditory components.9
Evidence is accumulating that the perception of tinnitus is multimodal and may arise from complex interactions among different sensory and motor systems.10 For example, some patients with tinnitus can modulate its pitch, loudness, or both by forcefully contracting the muscles in the head, neck, or limbs; by moving the eyes in the horizontal or vertical axis; by placing pressure on myofacial trigger points; by moving the face or mouth; or by applying pressure to the temporomandibular joint.11,12 Although somatic tinnitus modulation is not yet well understood, it may reflect the interaction between the auditory system and other sensory systems.
Because the underlying mechanisms of tinnitus are complex and may involve more than the auditory system, a multidisciplinary approach to management should be considered.
RULING OUT HEALTH-THREATENING DISEASE
The complaint of tinnitus should not be taken lightly. True, it may be just a nuisance the patient can learn to ignore. On the other hand, it may negatively affect the patient’s quality of life. Worst of all, it could be a symptom of a potentially health-threatening disease.
Primary care physicians should know the red flags (Table 1) for otologic diseases such as vestibular schwannoma, Meniere disease, cholesteotoma, glomus jugulare tumor, and temporal bone trauma and, if these are present, refer patients to an otolaryngologist for a complete cochleovestibular examination.
At the same time, the physician should avoid heightening the patient’s preoccupation with the tinnitus by creating unnecessary fear about an underlying cause. This may create further anxiety and exacerbate the patient’s perception of tinnitus and emotional reaction to it.13
WHAT IS THE IMPACT OF TINNITUS ON QUALITY OF LIFE?
A quick method is simply to ask, “How much of a problem is your tinnitus?” If the patient considers it a small problem, minimum counseling may suffice (Figure 1). But if the response suggests a greater impact, an in-depth history should be taken (Table 2) to determine the appropriate treatment plan.
Still another option is to use a standardized screening tool. The Tinnitus Handicap Inventory-Screening Version (THI-S)14 consists of 10 questions that screen for the psychosocial consequences of tinnitus (Table 3). For each question, the patient answers “yes” (worth 4 points), “sometimes” (2 points), or “no” (0 points). The possible total score thus ranges from 0 to 40 points; the higher the score, the greater the perceived disability (activity limitation) and handicap (participation restriction). A score of more than 6 points indicates a need for an in-depth evaluation (Table 2). Having the patient complete this tool in the waiting room can save precious time and help identify those in need of referral.
SOME PATIENTS MAY NEED TO SEE ONE OR MORE SPECIALISTS
Patients whose tinnitus is distressing may need referral. Traditionally, the primary care physician refers the patient to an otolaryngologist. However, the complex nature and etiology of tinnitus may necessitate referring the patient to one or more specialists in addition to an otolaryngologist for further assessment and management. The following sections briefly describe what other specialists offer.
AUDIOLOGY: TESTING, SOUND THERAPY
A patient referred to an audiologist may undergo traditional audiologic testing (pure tone and speech thresholds, word recognition), as well as a battery of special psychoacoustic tests. This includes pitch-matching and loudness-matching, evaluation of residual inhibition (suppression of tinnitus after an external masking stimulus has been turned off), and assessing the minimum masking level. These provide a quantitative estimate of the acoustic attributes of the perceived tinnitus. Questionnaires can be used to assess the impact of tinnitus on everyday life and can provide guidance for treatment.15
Real sounds mask the perceived ones
Environmental enrichment devices such as portable machines that generate pleasant sounds (eg, rain, waterfalls, ocean waves), tabletop water fountains, fans, or even televisions or radios can be used to promote relief, provide distraction, and decrease the patient’s awareness of tinnitus.
Hearing aids amplify ambient sounds, reducing the perception of tinnitus.16,17 They also improve communication.
Sound generators, worn in the ear, produce a stable broadband signal (“white noise”). These devices may be used by patients who have normal or near-normal hearing sensitivity and therefore neither benefit from nor require amplification.
Combination instruments are both hearing aids and white-noise generators. These allow patients who have both hearing loss and tinnitus to use a single device.
Music can distract from the tinnitus and help patients relax. Patients may find benefit listening to their preferred music on a personal listening device such as an MP3 or CD player.
Neuromonics Inc. (Bethlehem, PA) makes a sophisticated device for tinnitus treatment. Resembling an MP3 player, it is used with headphones and plays soothing music (baroque or new age) that contains a tinnitus-masking noise. The music is modified to compensate for the patient’s hearing loss, if present. After approximately 2 months of use, the embedded noise is removed to help desensitize the patient to the tinnitus. Results of small trials have been promising.18,19
DENTISTRY: TREATING TINNITUS BY TREATING TMD
Temporomandibular disorder (TMD), involving the temporomandibular joints, the muscles of mastication, and the teeth, is associated with tinnitus.20,21 The prevalence of tinnitus in a Cleveland Clinic study of 109 patients with TMD was 36%.22
There is also an association between cervical muscle disorders and masticatory muscle function. For example, patients who grind their teeth at night must contract the sternocleidomastoid muscles of the neck to stabilize the head during grinding. Correcting cervical posture, changing the sleep position, and controlling conscious parafunctional habits (eg, clenching the teeth, grinding the teeth together) can decrease many of the symptoms of TMD.
The dental examination for tinnitus patients
The dentist looks for a history of TMD symptoms, use of orthotic devices, and head and neck trauma, and performs a clinical examination.
The clinical examination includes mandibular range of motion, auscultation and palpation of the temporomandibular joints, palpation of masticatory and cervical muscles, and cervical range of motion. The intraoral examination includes identifying occlusal attrition patterns, “load testing” of the temporomandibular joints, and identifying premature tooth contacts. Additionally, attempts to restrict jaw opening and lateral movements may modulate the patient’s tinnitus, thus confirming the role of TMD in the patient’s tinnitus.
How tinnitus is treated by managing TMD
Tinnitus can be treated by managing TMD, specifically through the use of dental orthotics (splints, nightguards) to improve abnormal jaw mechanics and tracking.23–25
Tullberg and Ernberg26 treated patients with TMD and tinnitus using a variety of methods, including occlusal splinting, jaw muscle exercises, and relaxation. They reported that 43% of the patients experienced an improvement in their tinnitus after these interventions.
A home exercise program may help patients maintain muscle strength and harmony. Self-help therapies provide patients with a protocol to recognize daytime parafunctional habits and provide suggestions to decrease clenching and other overloading of the masticatory system.
In addition, management of TMD-related tinnitus often involves physical therapy, which can include soft-tissue mobilization, deep heat, ultrasound, low-current electrical stimulation, myofascial trigger-point release techniques, and posture retraining. Occlusal correction procedures (bite correction) can often provide long-term stability to the masticatory system.
NEUROLOGY: LOOKING FOR AN UNDERLYING CONDITION
The comprehensive neurologic evaluation of the tinnitus patient should include a thorough neurologic history, review of systems, examination, and appropriate imaging. The aim is to identify accompanying symptoms or disorders that may help to localize and ultimately diagnose the underlying condition.
Related disorders could manifest with vestibular symptoms (dizziness, imbalance), various pain syndromes including facial pain and headache (tension or migraine),27 or other cranial nerve disorders such as Bell palsy (facial nerve injury)28 or trigeminal neuralgia.
Medical and surgical interventions for tinnitus-associated neurologic conditions
In cases in which there is a treatable underlying neurologic condition, tinnitus-focused interventions should be deferred until treatment has been completed or discontinued.
At that point, other options including various oral medications (eg, antiarrhythmics, anticonvulsants, benzodiazepines, and antidepressants) and anesthetic blocks (eg, intravenous anesthetic-plus-steroid injections)29 may be considered on a case-by-case basis. Results of randomized clinical trials of the aforementioned drugs have not been promising30; however, drugs that affect the emotional status of the patient by reducing anxiety, depression, and sleep disturbance have been shown to be beneficial.31,32
In addition, some experimental surgical treatments (eg, deep brain stimulation, dural grid stimulation)33,34 are being evaluated and show potential for managing tinnitus.
PHYSICAL THERAPY
A preliminary physical therapy evaluation can identify biomechanical problems of the head, neck, and jaw that can contribute to tinnitus.
Subsequent therapy is designed to restore proper cervical and temporomandibular biomechanics and to educate the patient on proper posture, ergonomics, and exercise techniques that together could help minimize these abnormalities and reduce the severity of tinnitus in some patients.11,24–26,35
PSYCHOLOGY: ADDRESSING DEPRESSION, ANXIETY
Tinnitus exacts an emotional toll on its sufferers. Some estimates suggest that 40% to 50% of tinnitus patients experience significant perceived handicap and psychological distress.36 Consequently, many patients respond to the onset of tinnitus with anxiety or depression, or both. Owing to these responses, the chronicity of the condition, and the patient’s perception that tinnitus is uncontrollable, tinnitus can produce notable distress and impairment in quality of life.
When a patient’s responses include both depression and anxiety, the reduction in quality of life and impairment in coping capacities can be significant.37 Sleep problems, poor concentration, social withdrawal, feelings of helplessness, avoidance behaviors, and upset in interpersonal relationships are common signs that quality of life is compromised.
One of the greatest challenges for the primary care physician when treating tinnitus patients is attending to their emotional suffering and disability. Simple screening tools can be useful in quickly assessing a patient’s emotional response to tinnitus and in helping to enter into a conversation with the patient about this topic. These tools include:
- The THI-S (Table 3)14
- The Patient Health Questionnaire-9 (PHQ-9)38
- The Generalized Anxiety Disorder-7 (GAD-7).39
Suicidal ideas need to be addressed
The final question on the PHQ-9 asks about suicidal ideation. This cannot be overlooked when assessing patients with tinnitus. The questionnaire invites the patient to communicate this rather painful topic to the physician in a direct matter.
The physician should be prepared to address suicidal ideas, plans, means, intentions, and safety measures with the patient. This requires that the physician be comfortable conducting these conversations in a direct and forthright manner; it also requires that the physician have reliable referrals to qualified mental health practitioners at the ready to assist the distressed tinnitus patient.
Asking a patient to commit to calling 911 or going to the nearest emergency room if he or she has any impulse toward self-harm is a simple option that many distressed patients may have never considered.
Treatments for depression and anxiety in tinnitus patients
Some patients may already have been seeing a mental health professional before the onset of tinnitus and may elect to discuss treatment with their current provider. However, many need guidance in selecting appropriate treatment. Their options may include:
Psychotropic drugs such as selective serotonin reuptake inhibitors and benzodiazepines, to provide quick relief from debilitating depression and anxiety.
Cognitive behavioral therapy, designed to provide a more active and durable adjustment to tinnitus. It is the most widely validated psychotherapeutic treatment approach to tinnitus.40
Unfortunately, physicians often tell patients with tinnitus (the perception of noises in the ear, head, or both without an external acoustic source) to simply “learn to live with it.” This type of advice can result in missing the diagnosis of a potentially serious medical condition or, at the very least, in dismissing the patient’s complaints and hence failing to provide any hope of relief—increasing the negative impact on the patient’s quality of life.
See related patient information
The disabling effects of tinnitus resemble those of chronic pain.1 Specifically, its consequences may include:
- Loss of sleep
- Interference with concentration
- Difficulties functioning at work, at home, and in social relationships
- Negative emotional reactions, including despair, frustration, depression, and suicidal ideation.2,3
Chronic tinnitus affects 42 million Americans and is considered “clinically significant” in 10 million adults, and the numbers are increasing.4–7
Because primary care physicians may serve as the gatekeepers for tinnitus sufferers, as they do for patients with other chronic health issues, it is important that they understand the underlying mechanisms responsible for tinnitus, its impact, and its management options.
The goal of this article is to provide a basic understanding of tinnitus and its treatment so that physicians can provide hope to its sufferers and know when to initiate appropriate referrals for management.
WHAT CAUSES TINNITUS?
The precise cause of tinnitus is unknown. However, substantial evidence indicates that it is the result of plastic changes in the auditory system that cause auditory neurons to become hyperactive and to fire more synchronously.
If the auditory system is injured, eg, if outer hair cells have been lost because of noise exposure or ototoxicity, then neurons that normally have low levels of activity in silence begin to fire at a higher rate and more synchronously. Therefore, reduced neural activity from the peripheral system (ie, the cochlea) may result in increased spontaneous neural activity in the central auditory nervous system.8
Although most investigators of the neurobiology of tinnitus subscribe to this theory, more than one system must be involved, either simultaneously or interactively, since tinnitus has both auditory and nonauditory components.9
Evidence is accumulating that the perception of tinnitus is multimodal and may arise from complex interactions among different sensory and motor systems.10 For example, some patients with tinnitus can modulate its pitch, loudness, or both by forcefully contracting the muscles in the head, neck, or limbs; by moving the eyes in the horizontal or vertical axis; by placing pressure on myofacial trigger points; by moving the face or mouth; or by applying pressure to the temporomandibular joint.11,12 Although somatic tinnitus modulation is not yet well understood, it may reflect the interaction between the auditory system and other sensory systems.
Because the underlying mechanisms of tinnitus are complex and may involve more than the auditory system, a multidisciplinary approach to management should be considered.
RULING OUT HEALTH-THREATENING DISEASE
The complaint of tinnitus should not be taken lightly. True, it may be just a nuisance the patient can learn to ignore. On the other hand, it may negatively affect the patient’s quality of life. Worst of all, it could be a symptom of a potentially health-threatening disease.
Primary care physicians should know the red flags (Table 1) for otologic diseases such as vestibular schwannoma, Meniere disease, cholesteotoma, glomus jugulare tumor, and temporal bone trauma and, if these are present, refer patients to an otolaryngologist for a complete cochleovestibular examination.
At the same time, the physician should avoid heightening the patient’s preoccupation with the tinnitus by creating unnecessary fear about an underlying cause. This may create further anxiety and exacerbate the patient’s perception of tinnitus and emotional reaction to it.13
WHAT IS THE IMPACT OF TINNITUS ON QUALITY OF LIFE?
A quick method is simply to ask, “How much of a problem is your tinnitus?” If the patient considers it a small problem, minimum counseling may suffice (Figure 1). But if the response suggests a greater impact, an in-depth history should be taken (Table 2) to determine the appropriate treatment plan.
Still another option is to use a standardized screening tool. The Tinnitus Handicap Inventory-Screening Version (THI-S)14 consists of 10 questions that screen for the psychosocial consequences of tinnitus (Table 3). For each question, the patient answers “yes” (worth 4 points), “sometimes” (2 points), or “no” (0 points). The possible total score thus ranges from 0 to 40 points; the higher the score, the greater the perceived disability (activity limitation) and handicap (participation restriction). A score of more than 6 points indicates a need for an in-depth evaluation (Table 2). Having the patient complete this tool in the waiting room can save precious time and help identify those in need of referral.
SOME PATIENTS MAY NEED TO SEE ONE OR MORE SPECIALISTS
Patients whose tinnitus is distressing may need referral. Traditionally, the primary care physician refers the patient to an otolaryngologist. However, the complex nature and etiology of tinnitus may necessitate referring the patient to one or more specialists in addition to an otolaryngologist for further assessment and management. The following sections briefly describe what other specialists offer.
AUDIOLOGY: TESTING, SOUND THERAPY
A patient referred to an audiologist may undergo traditional audiologic testing (pure tone and speech thresholds, word recognition), as well as a battery of special psychoacoustic tests. This includes pitch-matching and loudness-matching, evaluation of residual inhibition (suppression of tinnitus after an external masking stimulus has been turned off), and assessing the minimum masking level. These provide a quantitative estimate of the acoustic attributes of the perceived tinnitus. Questionnaires can be used to assess the impact of tinnitus on everyday life and can provide guidance for treatment.15
Real sounds mask the perceived ones
Environmental enrichment devices such as portable machines that generate pleasant sounds (eg, rain, waterfalls, ocean waves), tabletop water fountains, fans, or even televisions or radios can be used to promote relief, provide distraction, and decrease the patient’s awareness of tinnitus.
Hearing aids amplify ambient sounds, reducing the perception of tinnitus.16,17 They also improve communication.
Sound generators, worn in the ear, produce a stable broadband signal (“white noise”). These devices may be used by patients who have normal or near-normal hearing sensitivity and therefore neither benefit from nor require amplification.
Combination instruments are both hearing aids and white-noise generators. These allow patients who have both hearing loss and tinnitus to use a single device.
Music can distract from the tinnitus and help patients relax. Patients may find benefit listening to their preferred music on a personal listening device such as an MP3 or CD player.
Neuromonics Inc. (Bethlehem, PA) makes a sophisticated device for tinnitus treatment. Resembling an MP3 player, it is used with headphones and plays soothing music (baroque or new age) that contains a tinnitus-masking noise. The music is modified to compensate for the patient’s hearing loss, if present. After approximately 2 months of use, the embedded noise is removed to help desensitize the patient to the tinnitus. Results of small trials have been promising.18,19
DENTISTRY: TREATING TINNITUS BY TREATING TMD
Temporomandibular disorder (TMD), involving the temporomandibular joints, the muscles of mastication, and the teeth, is associated with tinnitus.20,21 The prevalence of tinnitus in a Cleveland Clinic study of 109 patients with TMD was 36%.22
There is also an association between cervical muscle disorders and masticatory muscle function. For example, patients who grind their teeth at night must contract the sternocleidomastoid muscles of the neck to stabilize the head during grinding. Correcting cervical posture, changing the sleep position, and controlling conscious parafunctional habits (eg, clenching the teeth, grinding the teeth together) can decrease many of the symptoms of TMD.
The dental examination for tinnitus patients
The dentist looks for a history of TMD symptoms, use of orthotic devices, and head and neck trauma, and performs a clinical examination.
The clinical examination includes mandibular range of motion, auscultation and palpation of the temporomandibular joints, palpation of masticatory and cervical muscles, and cervical range of motion. The intraoral examination includes identifying occlusal attrition patterns, “load testing” of the temporomandibular joints, and identifying premature tooth contacts. Additionally, attempts to restrict jaw opening and lateral movements may modulate the patient’s tinnitus, thus confirming the role of TMD in the patient’s tinnitus.
How tinnitus is treated by managing TMD
Tinnitus can be treated by managing TMD, specifically through the use of dental orthotics (splints, nightguards) to improve abnormal jaw mechanics and tracking.23–25
Tullberg and Ernberg26 treated patients with TMD and tinnitus using a variety of methods, including occlusal splinting, jaw muscle exercises, and relaxation. They reported that 43% of the patients experienced an improvement in their tinnitus after these interventions.
A home exercise program may help patients maintain muscle strength and harmony. Self-help therapies provide patients with a protocol to recognize daytime parafunctional habits and provide suggestions to decrease clenching and other overloading of the masticatory system.
In addition, management of TMD-related tinnitus often involves physical therapy, which can include soft-tissue mobilization, deep heat, ultrasound, low-current electrical stimulation, myofascial trigger-point release techniques, and posture retraining. Occlusal correction procedures (bite correction) can often provide long-term stability to the masticatory system.
NEUROLOGY: LOOKING FOR AN UNDERLYING CONDITION
The comprehensive neurologic evaluation of the tinnitus patient should include a thorough neurologic history, review of systems, examination, and appropriate imaging. The aim is to identify accompanying symptoms or disorders that may help to localize and ultimately diagnose the underlying condition.
Related disorders could manifest with vestibular symptoms (dizziness, imbalance), various pain syndromes including facial pain and headache (tension or migraine),27 or other cranial nerve disorders such as Bell palsy (facial nerve injury)28 or trigeminal neuralgia.
Medical and surgical interventions for tinnitus-associated neurologic conditions
In cases in which there is a treatable underlying neurologic condition, tinnitus-focused interventions should be deferred until treatment has been completed or discontinued.
At that point, other options including various oral medications (eg, antiarrhythmics, anticonvulsants, benzodiazepines, and antidepressants) and anesthetic blocks (eg, intravenous anesthetic-plus-steroid injections)29 may be considered on a case-by-case basis. Results of randomized clinical trials of the aforementioned drugs have not been promising30; however, drugs that affect the emotional status of the patient by reducing anxiety, depression, and sleep disturbance have been shown to be beneficial.31,32
In addition, some experimental surgical treatments (eg, deep brain stimulation, dural grid stimulation)33,34 are being evaluated and show potential for managing tinnitus.
PHYSICAL THERAPY
A preliminary physical therapy evaluation can identify biomechanical problems of the head, neck, and jaw that can contribute to tinnitus.
Subsequent therapy is designed to restore proper cervical and temporomandibular biomechanics and to educate the patient on proper posture, ergonomics, and exercise techniques that together could help minimize these abnormalities and reduce the severity of tinnitus in some patients.11,24–26,35
PSYCHOLOGY: ADDRESSING DEPRESSION, ANXIETY
Tinnitus exacts an emotional toll on its sufferers. Some estimates suggest that 40% to 50% of tinnitus patients experience significant perceived handicap and psychological distress.36 Consequently, many patients respond to the onset of tinnitus with anxiety or depression, or both. Owing to these responses, the chronicity of the condition, and the patient’s perception that tinnitus is uncontrollable, tinnitus can produce notable distress and impairment in quality of life.
When a patient’s responses include both depression and anxiety, the reduction in quality of life and impairment in coping capacities can be significant.37 Sleep problems, poor concentration, social withdrawal, feelings of helplessness, avoidance behaviors, and upset in interpersonal relationships are common signs that quality of life is compromised.
One of the greatest challenges for the primary care physician when treating tinnitus patients is attending to their emotional suffering and disability. Simple screening tools can be useful in quickly assessing a patient’s emotional response to tinnitus and in helping to enter into a conversation with the patient about this topic. These tools include:
- The THI-S (Table 3)14
- The Patient Health Questionnaire-9 (PHQ-9)38
- The Generalized Anxiety Disorder-7 (GAD-7).39
Suicidal ideas need to be addressed
The final question on the PHQ-9 asks about suicidal ideation. This cannot be overlooked when assessing patients with tinnitus. The questionnaire invites the patient to communicate this rather painful topic to the physician in a direct matter.
The physician should be prepared to address suicidal ideas, plans, means, intentions, and safety measures with the patient. This requires that the physician be comfortable conducting these conversations in a direct and forthright manner; it also requires that the physician have reliable referrals to qualified mental health practitioners at the ready to assist the distressed tinnitus patient.
Asking a patient to commit to calling 911 or going to the nearest emergency room if he or she has any impulse toward self-harm is a simple option that many distressed patients may have never considered.
Treatments for depression and anxiety in tinnitus patients
Some patients may already have been seeing a mental health professional before the onset of tinnitus and may elect to discuss treatment with their current provider. However, many need guidance in selecting appropriate treatment. Their options may include:
Psychotropic drugs such as selective serotonin reuptake inhibitors and benzodiazepines, to provide quick relief from debilitating depression and anxiety.
Cognitive behavioral therapy, designed to provide a more active and durable adjustment to tinnitus. It is the most widely validated psychotherapeutic treatment approach to tinnitus.40
- Møller AR. The role of neural plasticity in tinnitus. Prog Brain Res 2007; 166:37–45.
- Dobie RA. Overview: suffering from tinnitus. In:Snow JB, ed. Tinnitus: Theory and Management. Hamilton, Ontario: BC Decker; 2004:1–7.
- Tyler RS, Baker LJ. Difficulties experienced by tinnitus sufferers. J Speech Hear Disord 1983; 48:150–154.
- Henry JA, Dennis KC, Schechter MA. General review of tinnitus: prevalence, mechanisms, effects, and management. J Speech Lang Hear Res 2005; 48:1204–1235.
- Hoffman HJ, Reed GW. Epidemiology of tinnitus. In:Snow JB, editor. Tinnitus: Theory and Management. Hamilton, Ontario: BC Decker; 2004:16–41.
- Hoge CW, McGurk D, Thomas JL, Cox AL, Engel CC, Castro CA. Mild traumatic brain injury in U.S. Soldiers returning from Iraq. N Engl J Med 2008; 358:453–63.
- Rauschecker JP, Leaver AM, Mühlau M. Tuning out the noise: limbicauditory interactions in tinnitus. Neuron 2010; 66:819–826.
- Kaltenbach JA, Zhang J, Finlayson P. Tinnitus as a plastic phenomenon and its possible neural underpinnings in the dorsal cochlear nucleus. Hear Res 2005; 206:200–226.
- Georgiewa P, Klapp BF, Fischer F, et al. An integrative model of developing tinnitus based on recent neurobiological findings. Med Hypotheses 2006; 66:592–600.
- Cacace AT. Expanding the biological basis of tinnitus: crossmodal origins and the role of neuroplasticity. Hear Res 2003; 175:112–132.
- Levine RA. Somatic tinnitus. In:Snow JB, editor. Tinnitus: Theory and Management. Hamilton, Ontario: BC Decker; 2004:108–124.
- Sanchez TG, Kii MA. Modulating tinnitus with visual, muscular, and tactile stimulation. Semin Hear 2008; 29:350–360.
- Schleuning AL, Shi BY, Martin WH. Tinnitus. In:Bailey BJ, Johnson JT, Newlands SD, et al, editors. Head and Neck Surgery—Otolarygnology. 4th ed, vol 2. Philadelphia, PA: Lippincott Williams & Wilkins; 2006:2237–2246.
- Newman CW, Sandridge SA, Bolek L. Development and psychometric adequacy of the screening version of the Tinnitus Handicap Inventory. Otol Neurotol 2008; 29:276–281.
- Newman CW, Sandridge SA. Tinnitus management. In:Montano JJ, Spitzer JB, editors. Adult Audiologic Rehabilitation. San Diego, CA: Plural Publishing Inc; 2009:399–444.
- Kochkin S, Tyler R. Tinnitus treatment and the effectiveness of hearing aids: hearing care professional perceptions. Hearing Review 2008; 15:14–18.
- Sheldrake JB, Jasterboff MM. Role of hearing aids in management of tinnitus. In:Snow JB, editor. Tinnitus: Theory and Management. Hamilton, Ontario: BC Decker; 2004:310–313.
- Davis PB, Paki B, Hanley PJ. Neuromonics Tinnitus Treatment: third clinical trial. Ear Hear 2007; 28:242–259.
- Davis PB, Wilde RA, Steed LG, Hanley PJ. Treatment of tinnitus with a customized acoustic neural stimulus: a controlled clinical study. Ear Nose Throat J 2008; 87:330–339.
- Lam DK, Lawrence HP, Tenenbaum HC. Aural symptoms in temporomandibular disorder patients attending a craniofacial pain unit. J Orofac Pain 2001; 15:146–157.
- Steigerwald DP, Verne SV, Young D. A retrospective evaluation of the impact of temporomandibular joint arthroscopy on the symptoms of headache, neck pain, shoulder pain, dizziness, and tinnitus. Cranio 1996; 14:46–54.
- Kahn K. Multidisciplinary strategies for managing patients with tinnitus. Poster presented at the American Equilibration Society, Chicago, IL, February 24–25, 2010.
- Morgan DH. Tinnitus caused by a temporomandibular disorder. In:Reich GE, Vernon JA, editors. Proceedings of the Fifth International Tinnitus Seminar. Portland, Oregon: American Tinnitus Association; 1996:653–654.
- Wright EF, Bifano SL. Tinnitus improvement through TMD therapy. J Am Dent Assoc 1997; 128:1424–1432.
- Latifpour DH, Grenner J, Sjödahl C. The effect of a new treatment based on somatosensory stimulation in a group of patients with somatically related tinnitus. Int Tinnitus J 2009; 15:94–99.
- Tullberg M, Ernberg M. Long-term effect on tinnitus by treatment of temporomandibular disorders: a two-year follow-up by questionnaire. Acta Odontol Scand 2006; 64:89–96.
- Volcy M, Sheftell FD, Tepper SJ, Rapoport AM, Bigal ME. Tinnitus in migraine: an allodynic symptom secondary to abnormal cortical functioning? Headache 2005; 45:1083–1087.
- Yamamoto E, Nishimura H, Hirono Y. Occurrence of sequelae in Bell’s palsy. Acta Otolaryngol Suppl 1988; 446:93–96.
- Duckert LG, Rees TS. Treatment of tinnitus with intravenous lidocaine: a double-blind randomized trial. Otolaryngol Head Neck Surg 1983; 91:550–555.
- Dobie RA. Clinical trials and drug therapy for tinnitus. In:Snow JB, editor. Tinnitus: Theory and Management. Hamilton, Ontario: BC Decker; 2004:266–277.
- Johnson RM, Brummett R, Schleuning A. Use of alprazolam for relief of tinnitus. A double-blind study. Arch Otolaryngol Head Neck Surg 1993; 119:842–845.
- Brummett R. Drugs for and against tinnitus. The Hearing Journal 1989; 42:34–37.
- Cheung SW, Larson PS. Tinnitus modulation by deep brain stimulation in locus of caudate neurons (area LC). Neuroscience 2010; 169:1768–1778.
- Friedland DR, Gaggl W, Runge-Samuelson C, Ulmer JL, Kopell BH. Feasibility of auditory cortical stimulation for the treatment of tinnitus. Otol Neurotol 2007; 28:1005–1012.
- Simmons R, Dambra C, Lobarinas E, Stocking C, Salvi R. Head, neck, and eye movements that modulate tinnitus. Semin Hear 2008; 29:361–370.
- Bauch CD, Lynn SG, Williams DE, Mellon MW, Weaver AL. Tinnitus impact: three different measurement tools. J Am Acad Audiol 2003; 14:181–187.
- Bartels H, Middel BL, van der Laan BF, Staal MJ, Albers FW. The additive effect of co-occurring anxiety and depression on health status, quality of life and coping strategies in help-seeking tinnitus sufferers. Ear Hear 2008; 29:947–956.
- Kroenke K, Spitzer RL, Williams JB. The PHQ-9: validity of a brief depression severity measure. J Gen Intern Med 2001; 16:606–613.
- Spitzer RL, Kroenke K, Williams JB, Löwe B. A brief measure for assessing generalized anxiety disorder: the GAD-7. Arch Intern Med 2006; 166:1092–1097.
- Andersson G. Psychological aspects of tinnitus and the application of cognitive-behavioral therapy. Clin Psychol Rev 2002; 22:977–990.
- Hesser H, Westin V, Hayes SC, Andersson G. Clients’ in-session acceptance and cognitive defusion behaviors in acceptance-based treatment of tinnitus distress. Behav Res Ther 2009; 47:523–528.
- Møller AR. The role of neural plasticity in tinnitus. Prog Brain Res 2007; 166:37–45.
- Dobie RA. Overview: suffering from tinnitus. In:Snow JB, ed. Tinnitus: Theory and Management. Hamilton, Ontario: BC Decker; 2004:1–7.
- Tyler RS, Baker LJ. Difficulties experienced by tinnitus sufferers. J Speech Hear Disord 1983; 48:150–154.
- Henry JA, Dennis KC, Schechter MA. General review of tinnitus: prevalence, mechanisms, effects, and management. J Speech Lang Hear Res 2005; 48:1204–1235.
- Hoffman HJ, Reed GW. Epidemiology of tinnitus. In:Snow JB, editor. Tinnitus: Theory and Management. Hamilton, Ontario: BC Decker; 2004:16–41.
- Hoge CW, McGurk D, Thomas JL, Cox AL, Engel CC, Castro CA. Mild traumatic brain injury in U.S. Soldiers returning from Iraq. N Engl J Med 2008; 358:453–63.
- Rauschecker JP, Leaver AM, Mühlau M. Tuning out the noise: limbicauditory interactions in tinnitus. Neuron 2010; 66:819–826.
- Kaltenbach JA, Zhang J, Finlayson P. Tinnitus as a plastic phenomenon and its possible neural underpinnings in the dorsal cochlear nucleus. Hear Res 2005; 206:200–226.
- Georgiewa P, Klapp BF, Fischer F, et al. An integrative model of developing tinnitus based on recent neurobiological findings. Med Hypotheses 2006; 66:592–600.
- Cacace AT. Expanding the biological basis of tinnitus: crossmodal origins and the role of neuroplasticity. Hear Res 2003; 175:112–132.
- Levine RA. Somatic tinnitus. In:Snow JB, editor. Tinnitus: Theory and Management. Hamilton, Ontario: BC Decker; 2004:108–124.
- Sanchez TG, Kii MA. Modulating tinnitus with visual, muscular, and tactile stimulation. Semin Hear 2008; 29:350–360.
- Schleuning AL, Shi BY, Martin WH. Tinnitus. In:Bailey BJ, Johnson JT, Newlands SD, et al, editors. Head and Neck Surgery—Otolarygnology. 4th ed, vol 2. Philadelphia, PA: Lippincott Williams & Wilkins; 2006:2237–2246.
- Newman CW, Sandridge SA, Bolek L. Development and psychometric adequacy of the screening version of the Tinnitus Handicap Inventory. Otol Neurotol 2008; 29:276–281.
- Newman CW, Sandridge SA. Tinnitus management. In:Montano JJ, Spitzer JB, editors. Adult Audiologic Rehabilitation. San Diego, CA: Plural Publishing Inc; 2009:399–444.
- Kochkin S, Tyler R. Tinnitus treatment and the effectiveness of hearing aids: hearing care professional perceptions. Hearing Review 2008; 15:14–18.
- Sheldrake JB, Jasterboff MM. Role of hearing aids in management of tinnitus. In:Snow JB, editor. Tinnitus: Theory and Management. Hamilton, Ontario: BC Decker; 2004:310–313.
- Davis PB, Paki B, Hanley PJ. Neuromonics Tinnitus Treatment: third clinical trial. Ear Hear 2007; 28:242–259.
- Davis PB, Wilde RA, Steed LG, Hanley PJ. Treatment of tinnitus with a customized acoustic neural stimulus: a controlled clinical study. Ear Nose Throat J 2008; 87:330–339.
- Lam DK, Lawrence HP, Tenenbaum HC. Aural symptoms in temporomandibular disorder patients attending a craniofacial pain unit. J Orofac Pain 2001; 15:146–157.
- Steigerwald DP, Verne SV, Young D. A retrospective evaluation of the impact of temporomandibular joint arthroscopy on the symptoms of headache, neck pain, shoulder pain, dizziness, and tinnitus. Cranio 1996; 14:46–54.
- Kahn K. Multidisciplinary strategies for managing patients with tinnitus. Poster presented at the American Equilibration Society, Chicago, IL, February 24–25, 2010.
- Morgan DH. Tinnitus caused by a temporomandibular disorder. In:Reich GE, Vernon JA, editors. Proceedings of the Fifth International Tinnitus Seminar. Portland, Oregon: American Tinnitus Association; 1996:653–654.
- Wright EF, Bifano SL. Tinnitus improvement through TMD therapy. J Am Dent Assoc 1997; 128:1424–1432.
- Latifpour DH, Grenner J, Sjödahl C. The effect of a new treatment based on somatosensory stimulation in a group of patients with somatically related tinnitus. Int Tinnitus J 2009; 15:94–99.
- Tullberg M, Ernberg M. Long-term effect on tinnitus by treatment of temporomandibular disorders: a two-year follow-up by questionnaire. Acta Odontol Scand 2006; 64:89–96.
- Volcy M, Sheftell FD, Tepper SJ, Rapoport AM, Bigal ME. Tinnitus in migraine: an allodynic symptom secondary to abnormal cortical functioning? Headache 2005; 45:1083–1087.
- Yamamoto E, Nishimura H, Hirono Y. Occurrence of sequelae in Bell’s palsy. Acta Otolaryngol Suppl 1988; 446:93–96.
- Duckert LG, Rees TS. Treatment of tinnitus with intravenous lidocaine: a double-blind randomized trial. Otolaryngol Head Neck Surg 1983; 91:550–555.
- Dobie RA. Clinical trials and drug therapy for tinnitus. In:Snow JB, editor. Tinnitus: Theory and Management. Hamilton, Ontario: BC Decker; 2004:266–277.
- Johnson RM, Brummett R, Schleuning A. Use of alprazolam for relief of tinnitus. A double-blind study. Arch Otolaryngol Head Neck Surg 1993; 119:842–845.
- Brummett R. Drugs for and against tinnitus. The Hearing Journal 1989; 42:34–37.
- Cheung SW, Larson PS. Tinnitus modulation by deep brain stimulation in locus of caudate neurons (area LC). Neuroscience 2010; 169:1768–1778.
- Friedland DR, Gaggl W, Runge-Samuelson C, Ulmer JL, Kopell BH. Feasibility of auditory cortical stimulation for the treatment of tinnitus. Otol Neurotol 2007; 28:1005–1012.
- Simmons R, Dambra C, Lobarinas E, Stocking C, Salvi R. Head, neck, and eye movements that modulate tinnitus. Semin Hear 2008; 29:361–370.
- Bauch CD, Lynn SG, Williams DE, Mellon MW, Weaver AL. Tinnitus impact: three different measurement tools. J Am Acad Audiol 2003; 14:181–187.
- Bartels H, Middel BL, van der Laan BF, Staal MJ, Albers FW. The additive effect of co-occurring anxiety and depression on health status, quality of life and coping strategies in help-seeking tinnitus sufferers. Ear Hear 2008; 29:947–956.
- Kroenke K, Spitzer RL, Williams JB. The PHQ-9: validity of a brief depression severity measure. J Gen Intern Med 2001; 16:606–613.
- Spitzer RL, Kroenke K, Williams JB, Löwe B. A brief measure for assessing generalized anxiety disorder: the GAD-7. Arch Intern Med 2006; 166:1092–1097.
- Andersson G. Psychological aspects of tinnitus and the application of cognitive-behavioral therapy. Clin Psychol Rev 2002; 22:977–990.
- Hesser H, Westin V, Hayes SC, Andersson G. Clients’ in-session acceptance and cognitive defusion behaviors in acceptance-based treatment of tinnitus distress. Behav Res Ther 2009; 47:523–528.
KEY POINTS
- The first step is to rule out underlying otologic disease.
- Nonotologic interventions range from minimal counseling in the office to referrals to specialists in one or more fields, including audiology, dentistry, neurology, physical therapy, psychology, and psychiatry.
- A simple algorithm can help determine if patient education is all that is required or if referral is needed.
Tinnitus relief: Suggestions for patients
Use sound to:
- Take attention away from your tinnitus
- Improve your sleep
- Improve your concentration
- Improve your relaxation
Two ways of using sound for your tinnitus
- Create a background sound to make the tinnitus less noticeable (eg, fan noise, radio,TV, nature sounds, water sounds)
- Use attention-getting sound to distract you from your tinnitus (lectures, books on tape, talk shows, conversation)
Three steps to determine the best use of sound for your tinnitus
- Identify specific situations when your tinnitus is most bothersome
- Determine which type of sound would be most helpful in each situation
- Determine the best device for presenting the sound in each situation
Obtain and use devices that produce sounds you like
- Background sounds from CDs
- Tabletop devices (eg, sound machines, water fountains)
- Portable listening devices (eg, MP3 player with music)
Protect your ears
- Loud noise can make your tinnitus worse (and damage your hearing)
- Always use earplugs or earmuffs around loud noise
Optimize your lifestyle and minimize tinnitus by
- Getting adequate sleep
- Reducing stress
- Reducing coffee, alcohol, cigarettes, aspirin, salt
- Eating healthy
- Exercising
- Staying busy with meaningful activities
- Becoming aware of your posture
- Taking breaks from work at the computer every 30 minutes to promote proper posture
Become educated about your tinnitus
- Join the American Tinnitus Association (www.ata.org)
- Read The Mindfulness and Acceptance Workbook for Anxiety (JP Forsyth & GH Eifert)
CDs that produce various background sounds
(We offer the following as suggestions, but do not provide a product endorsement.)
- www.sleepmachines.com
- www.binaural.com/bines.html
- www.naturesounds.com
- www.purewhitenoise.com
- www.soundpillow.com
- www.t-gone.com/white-noise
Tabletop devices
This information is provided by your physician and the Cleveland Clinic Journal of Medicine. It is not designed to replace a physician’s medical assessment and judgment.
This page may be reproduced noncommercially to share with patients. Any other reproduction is subject to Cleveland Clinic Journal of Medicine approval. Bulk color reprints are available by calling 216-444-2661.
For patient information on hundreds of health topics, see the Web site, www.clevelandclinic.org/health
Use sound to:
- Take attention away from your tinnitus
- Improve your sleep
- Improve your concentration
- Improve your relaxation
Two ways of using sound for your tinnitus
- Create a background sound to make the tinnitus less noticeable (eg, fan noise, radio,TV, nature sounds, water sounds)
- Use attention-getting sound to distract you from your tinnitus (lectures, books on tape, talk shows, conversation)
Three steps to determine the best use of sound for your tinnitus
- Identify specific situations when your tinnitus is most bothersome
- Determine which type of sound would be most helpful in each situation
- Determine the best device for presenting the sound in each situation
Obtain and use devices that produce sounds you like
- Background sounds from CDs
- Tabletop devices (eg, sound machines, water fountains)
- Portable listening devices (eg, MP3 player with music)
Protect your ears
- Loud noise can make your tinnitus worse (and damage your hearing)
- Always use earplugs or earmuffs around loud noise
Optimize your lifestyle and minimize tinnitus by
- Getting adequate sleep
- Reducing stress
- Reducing coffee, alcohol, cigarettes, aspirin, salt
- Eating healthy
- Exercising
- Staying busy with meaningful activities
- Becoming aware of your posture
- Taking breaks from work at the computer every 30 minutes to promote proper posture
Become educated about your tinnitus
- Join the American Tinnitus Association (www.ata.org)
- Read The Mindfulness and Acceptance Workbook for Anxiety (JP Forsyth & GH Eifert)
CDs that produce various background sounds
(We offer the following as suggestions, but do not provide a product endorsement.)
- www.sleepmachines.com
- www.binaural.com/bines.html
- www.naturesounds.com
- www.purewhitenoise.com
- www.soundpillow.com
- www.t-gone.com/white-noise
Tabletop devices
This information is provided by your physician and the Cleveland Clinic Journal of Medicine. It is not designed to replace a physician’s medical assessment and judgment.
This page may be reproduced noncommercially to share with patients. Any other reproduction is subject to Cleveland Clinic Journal of Medicine approval. Bulk color reprints are available by calling 216-444-2661.
For patient information on hundreds of health topics, see the Web site, www.clevelandclinic.org/health
Use sound to:
- Take attention away from your tinnitus
- Improve your sleep
- Improve your concentration
- Improve your relaxation
Two ways of using sound for your tinnitus
- Create a background sound to make the tinnitus less noticeable (eg, fan noise, radio,TV, nature sounds, water sounds)
- Use attention-getting sound to distract you from your tinnitus (lectures, books on tape, talk shows, conversation)
Three steps to determine the best use of sound for your tinnitus
- Identify specific situations when your tinnitus is most bothersome
- Determine which type of sound would be most helpful in each situation
- Determine the best device for presenting the sound in each situation
Obtain and use devices that produce sounds you like
- Background sounds from CDs
- Tabletop devices (eg, sound machines, water fountains)
- Portable listening devices (eg, MP3 player with music)
Protect your ears
- Loud noise can make your tinnitus worse (and damage your hearing)
- Always use earplugs or earmuffs around loud noise
Optimize your lifestyle and minimize tinnitus by
- Getting adequate sleep
- Reducing stress
- Reducing coffee, alcohol, cigarettes, aspirin, salt
- Eating healthy
- Exercising
- Staying busy with meaningful activities
- Becoming aware of your posture
- Taking breaks from work at the computer every 30 minutes to promote proper posture
Become educated about your tinnitus
- Join the American Tinnitus Association (www.ata.org)
- Read The Mindfulness and Acceptance Workbook for Anxiety (JP Forsyth & GH Eifert)
CDs that produce various background sounds
(We offer the following as suggestions, but do not provide a product endorsement.)
- www.sleepmachines.com
- www.binaural.com/bines.html
- www.naturesounds.com
- www.purewhitenoise.com
- www.soundpillow.com
- www.t-gone.com/white-noise
Tabletop devices
This information is provided by your physician and the Cleveland Clinic Journal of Medicine. It is not designed to replace a physician’s medical assessment and judgment.
This page may be reproduced noncommercially to share with patients. Any other reproduction is subject to Cleveland Clinic Journal of Medicine approval. Bulk color reprints are available by calling 216-444-2661.
For patient information on hundreds of health topics, see the Web site, www.clevelandclinic.org/health